







Bahasa
Halaman
Hukum


Radiation exposure in bone mineral density assessment
Christopher F. Njeha, *, Thomas Fuerst a, Didier Hans a, Glen M. Blakeb,Harry K. Genant a
aOsteoporosis and Arthritis Research Group, Department of Radiology, University of California, San Francisco, CA, U.S.A.bDepartment of Nuclear Medicine, Guy's Hospital, London, U.K.
Abstract
Osteoporosis is a systematic skeletal disease characterized by low bone mass and microarchitectural deteriorationof bone tissue which leads to diminished biomechanical competence of the skeleton and low-trauma or atraumaticfractures. Due to increased awareness of the impact of osteoporosis on the elderly population, the use of bone
densitometric techniques is becoming more widespread. Considerable progress has been made in the development ofnon-invasive methods for the assessment of the skeleton. While DXA and QCT are commonly used techniques, thepopularity of other approaches such as RA, SXA and QUS is gaining grounds. QCT has an advantage over the
other techniques in its ability to measure the true volumetric density of trabecular or cortical bone. We thereforepresent an overview of these current techniques for bone mineral density (BMD) measurements. In the secondsection we discuss the radiation doses incurred in BMD measurements by patients and methods for reducing patient
and sta� radiation exposure are given. Studies of radiation dose to patient from DXA con®rms that patient dose issmall (0.08±4.6 mSv) compared to that given by many other investigations involving ionizing radiation. Fan beamtechnology with increased resolution has resulted in increase patient dose radiation dose (6.7±31 mSv) but this is stillrelatively small. Carrying vertebral morphometry using DXA also incurs less radiation dose (<60 mSv) than
standard lateral radiographs QCT has radiation dose (25±360 mSv) comparable to simple radiological examinationsuch as chest X-ray but lower than imaging CT. Radiation dose from other techniques such as RA and SXA are inthe same order of magnitude as pencil beam DXA. For pencil beam DXA and SXA systems the time average dose
to sta� from scatter is very low even with the operator sitting as close as 1 m from the patient during measurement.However the scatter dose from fan beam DXA systems is considerable higher and approaches limits set by regulatorbodies for occupational exposure. # 1998 Elsevier Science Ltd. All rights reserved.
1. Osteoporosis and metabolic bone diseases
Osteoporosis is the most common metabolic bone
disorder. It is a systemic skeletal disease characterized
by low bone mass and microarchitectural deterioration
of bone tissue, with a consequent increase in bone fra-
gility and susceptibility to fracture (Anonymous, 1993).
Such fractures can occur in any site but are most com-
mon in the spine, wrist and hip, and all regions of the
skeleton with a high percentage of trabecular bone.
Osteoporosis has frequently been called the silent epi-
demic because it is asymptomatic and not clinically
manifested until a patient su�ers a fracture. The dis-
ease represents a major world-wide public health pro-
blem with an estimated 1.3 million fractures per year
in the U.S.A. In 1995, the estimated medical, nursing
home and social cost of osteoporotic fractures
exceeded $13.8 billion in the United States alone
(NOF, 1997). As life expectancy increases a resulting
increase in osteoporosis-related problems is expected.
Hence, the prevention of osteoporotic fractures with
consequent reductions in health care costs and excess
morbidity and mortality is an important clinical goal.
The susceptibility to fracture depends on a variety of
factors including the propensity to fall, visual acuity,
Applied Radiation and Isotopes 50 (1999) 215±236
0969-8043/98/$19.00 # 1998 Elsevier Science Ltd. All rights reserved.
PII: S0969-8043(98 )00026-8
AppliedRadiation andIsotopes
PERGAMON
* To whom all correspondence should be addressed.

protective response to falling and bone strength(Prudham and Evans, 1981; Kelsey and Ho�man,
1987). However, studies have shown that bone mass isone of the most important determinants of bonestrength and accounts for up to 80% of its variance
(Hodgskinson et al., 1997). Reduced bone mass, whichis readily accessible, is therefore a useful predictor ofincreased fracture risk (Ross et al., 1990). Many pro-
spective studies have shown that a decrease in bonedensity at the spine or hip of one population standarddeviation increases the risk by a factor of two to three
(Cummings et al., 1993). Methods of measuring bonemineral density are pertinent to the detection of lowbone mass (osteopenia), identi®cation of those individ-uals at risk of atraumatic fracture and assessment of
the e�cacy of the prevention and treatment of osteo-porosis. Estimation of spinal bone mineral contentfrom the visual assessment of bone density on conven-
tional radiographs is unreliable if vertebral fracturesare not present, since the subjective assessment is in¯u-enced by radiographic exposure factors, patient size
and ®lm processing techniques (Banks et al., 1995;Masud et al., 1996). Additionally the presence of clini-cal risk factors such as lifestyle, diet and family history
of osteoporosis is relatively ine�ective in predictingosteopenia (Cooper et al., 1991). These factors havenecessitated the need for objective, non-invasivemethods of bone density measurements. Such methods,
ideally, should be accurate, precise (reproducible), sen-sitive, inexpensive and involve a minimal exposure toionizing radiation.
In the past several decades, considerable progresshas been made in the development of methods forassessing the skeleton non-invasively. These include:
radiographic absorptiometry (RA), single photon andsingle X-ray absorptiometry (SPA/SXA), dual photonand dual X-ray absorptiometry (DPA/DXA), spinaland peripheral quantitative computed tomography
(QCT/pQCT), quantitative ultrasound (QUS), andquantitative magnetic resonance (QMR) and magneticresonance microscopy (mMR) (Genant et al., 1996;
Adams, 1997; Blake and Fogelman, 1997; Njeh et al.,1997a). These techniques vary in precision, accuracyand discrimination, and di�er substantially in funda-
mental methodology, clinical and research utility, andgeneral availability. We will limit our discussion tothose techniques that use ionizing radiation.
2. Technical principles of absorptiometry
2.1. Radiographic absorptiometry (RA)
This technique, also known as photo-densitometry,was the ®rst quantitative technique to assess integral(trabecular and cortical) bone mass (Morgan et al.,
1967). In RA, a standardized hand radiograph is takenwith an aluminum step-wedge placed on the ®lm and
analyzed using an optical densitometer. The bone min-eral density (BMD) is determined by comparison withthe de®ned density of the aluminum step-wedge. The
results are expressed in aluminum equivalent values orarbitrary units (Cosman et al., 1991; Matsumoto et al.,1994). RA is a low cost and readily accessible tech-
nique. The attenuation of an X-ray beam in an absorb-ing medium is highly dependent on its compositionand thickness. In RA applications, the variation in the
amount of soft tissue overlying the bone is notaccounted for. Therefore RA is restricted to the appen-dicular bones such as the metacarpals and phalangeswhich are surrounded by a relatively small amount of
soft tissue. The physical factors that in¯uence theradiographic image such as ¯uctuation in beam qual-ity, instability of X-ray source, ®lm response, proces-
sing conditions, radiation scattering and beamhardening e�ects also have adverse e�ects on precisionand accuracy of RA. Hence, RA implementation was
initially characterized by signi®cant precision errors ofabout 9±10% (Morgan et al., 1967). Recently devel-oped computer-assisted methods have reduced oper-
ator errors and improved precision (Matsumoto et al.,1994; Yang et al., 1994) (Trouerbach et al., 1987).Cadaveric studies have demonstrated that RA is accu-rate and suitable for the measurements of the BMD of
phalanges and metacarpals and is used in about 500centers worldwide (Yang et al., 1994). New systems arebecoming available that are entirely self contained and
highly automated.
2.2. Single photon absorptiometry
This was ®rst introduced by Cameron and Sorensonin 1963 (Cameron and Sorenson, 1963). A highly colli-mated photon beam from a single-energy radionuclide
source, such as 125I (photon energy 27.3 keV) or 241Am(60 keV) coupled to a radiation detector (usually asodium iodide crystal mounted on a photomultiplier
tube), is used to measure radiation attenuation at themeasurement site. To correct for overlying soft tissue,the anatomical site at which BMD is being measuredhas to be immersed in a water bath or surrounded by
water bags or water equivalent moldable materials(Adams, 1997). The method overcame the problemsfor RA caused by polychromatic X-rays (temporal and
spatial non-uniformity and beam hardening) and non-uniformity of ®lm sensitivity and development. Theamount of bone mineral in the beam can be derived
from Eq. (1) (Wahner and Fogelman, 1994).
MB � rB ln�I0=II��mBrB ÿ mSrS�
�1�
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236216
Where I0 is the transmitted intensity through soft tis-sue only, Ii is the transmitted intensity through bone
and soft tissue, m is the mass attenuation coe�cientand r is the density, the subscripts B and S refer tobone and soft tissue, respectively.
SPA was a widely used and established bone densitytechnique but it has now been superseded by single X-ray absorptiometry or peripheral dual X-ray absorptio-
metry.
2.3. Dual photon absorptiometry (DPA)
Single photon measurements are not possible at siteswith variable soft tissue thickness and composition (i.e.the axial skeleton, hip or whole body). Dual photonabsorptiometry (DPA) techniques were therefore intro-
duced to overcome the restriction of constant overallthickness of measurement site. This approach uses aradionuclide source, typically 153Gd with photon ener-
gies of 44 and 100 keV (Mazess and Barden, 1987).The simultaneous measurement of gamma radiation at
two di�erent energies allows for the correction of softtissue and fat of the torso without the need for a water
bath. The bone mineral density (g/cm2) can be derivedfrom:
MB � ln�IOL=IIL� ÿ �ln�IOH=IIH��mSL=mSH��mBL ÿ mBH�mSL=mSH�
�2�
Where symbols are as for the single photon case, with
the addition of subscripts L and H for lower andhigher photon energies, respectively. Eq. (2) is knownas the DPA equation.
2.4. Single X-ray absorptiometry (SXA)
Photon absorptiometric techniques are limited inthat the photon source is a radionuclide. This source
decays and requires regular replacement. It also has alow photon ¯uence which causes scanning times to belong and spatial resolution to be poor. These short-
comings have been overcome by the introduction of alow dose X-ray source. The physical principles of SXA
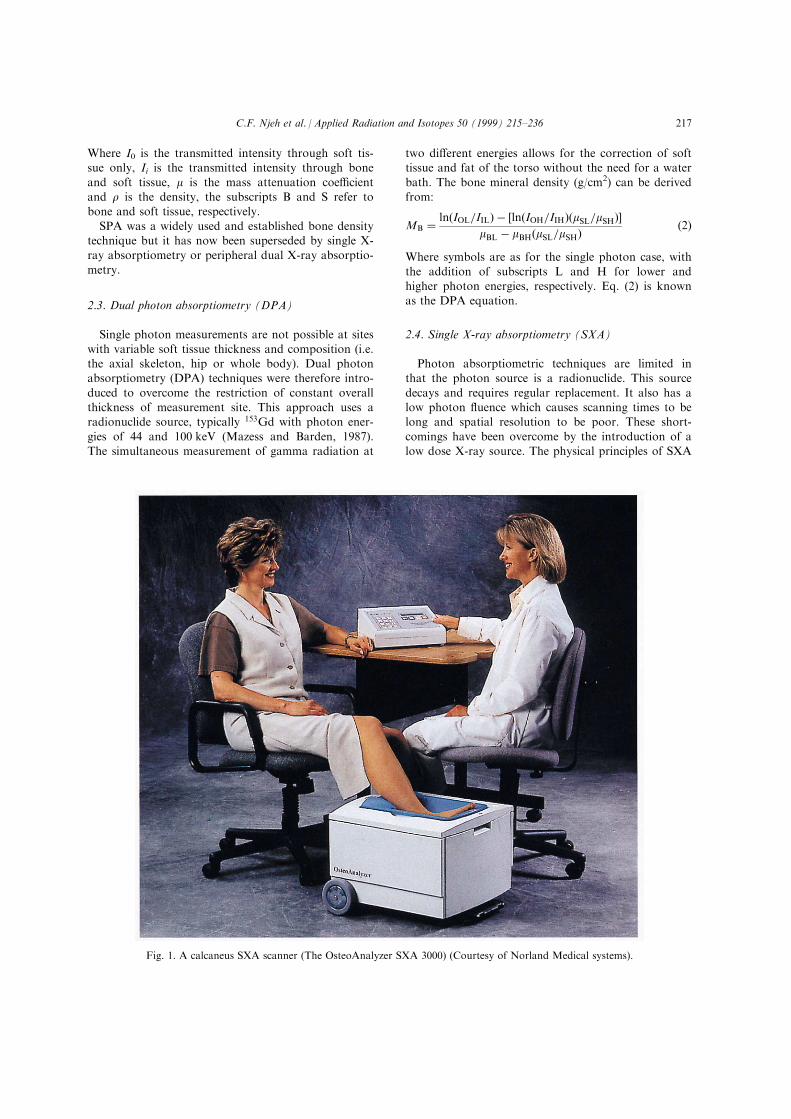
Fig. 1. A calcaneus SXA scanner (The OsteoAnalyzer SXA 3000) (Courtesy of Norland Medical systems).
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 217
are the same as SPA except that the radionuclidesource has been replaced by an X-ray tube (55 kVp,
300 mA). This has imparted better precision andimproved spatial resolution to these systems and hasreduced examination time (Kelly et al., 1994). SXA
makes possible a quantitative assessment of bone min-eral content at peripheral sites of the skeleton (e.g. dis-tal or ultradistal radius and calcaneus) (Fig. 1). SXA
has proven to be a valuable method in the diagnosis ofosteoporosis, providing reasonable precision andexceptionally low radiation exposure. However,
recently peripheral DXA systems have been supple-menting SXA systems, eliminating the need for a waterbath or water bolus.
2.5. Dual X-ray absorptiometry (DXA)
2.5.1. Pencil beam DXADual X-ray absorptiometry (DXA) is based on the
method of X-ray spectrophotometry developed in the1970s. It was introduced commercially as the directsuccessor to DPA in 1987. Similar to DPA the funda-mental physical principle behind DXA is the measure-
ment of the transmission of X-rays with high- andlow-photon energies. The main advantages of an X-ray
system over a DPA radionuclide system are shortened
examination time due to an increased photon ¯uence
of the X-ray tube and greater accuracy and precision
resulting from higher resolution and removal of errors
due to source decay (Kelly et al., 1988). The preferred
anatomic sites for DXA measurement of bone mineral
include the lumbar spine, the proximal femur and the
whole body, but peripheral sites can also be scanned.
Using the dependence of the X-ray attenuation coe�-
cient on atomic number and photon energy, measure-
ment of the transmission factors at two di�erent
energies enables the areal densities (i.e. mass per unit
projected area) of two di�erent types of tissues to be
inferred. In DXA scans these are taken to be bone
mineral (hydoxyapatite) and soft tissue, respectively.
This basic principle can be explained simply using
Eq. (2).
Unlike monoenergetic radionuclide sources, the
bremsstrahlung X-rays consist of a broad spectrum of
photon energies, with beam hardening as a potential
source of error. Two methods of generating dual
energy X-ray spectrum have been implemented using
either K-edge ®lters or kVp switching. K-edge absorp-
tion ®lters made of a rare earth material such as cer-
ium (Ce) and samarium (Sm) are used to split the
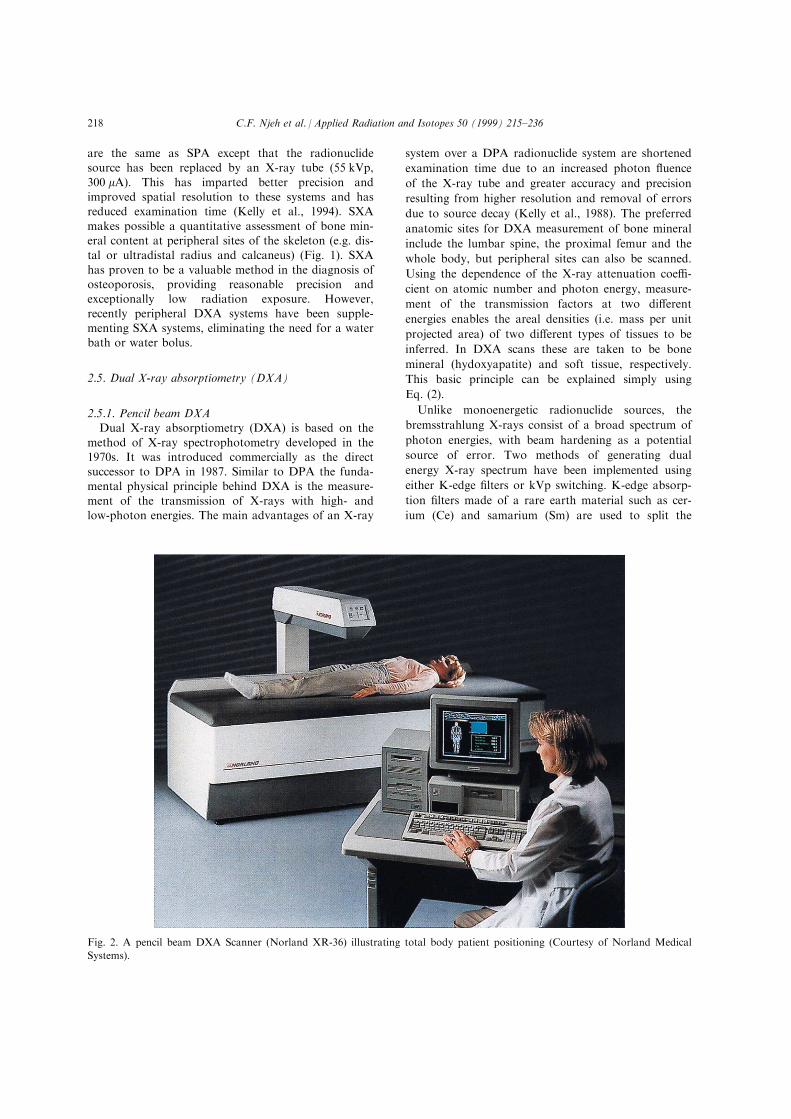
Fig. 2. A pencil beam DXA Scanner (Norland XR-36) illustrating total body patient positioning (Courtesy of Norland Medical
Systems).
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236218
polyenergetic X-ray beam into high and low energy
components that mimic the emissions from 154Gd. The
two components have inherently narrow spectral distri-
bution and hence the problems associated with beam
hardening are minimized. Lunar DPX (Lunar,
Madison) systems have a cerium ®lter and use pulse
height analysis at the detector to discriminate between
high and low energy photons. Norland XR (Atkinson,
Wisconsin) systems use a samarium ®lter and separate
detectors for high and low energy X-rays (Blake and
Fogelman, 1997).
The second way of producing a dual energy X-ray
beam is to switch the high voltage generator between
high and low kVp during alternate half cycles of the
mains supply. Hologic (Waltham, U.S.A.) uses this
method in its QDR series of DXA systems (Wahner
and Fogelman, 1994). The spectra distribution is wider
than with the K-edge ®lter method and the consequent
e�ect of beam hardening is corrected by a rotating
calibration wheel containing bone and soft tissue
equivalent ®lters that measure the attenuation coe�-
cient in Eq. (2) and calibrates the scanned image pixel
by pixel (Blake et al., 1992). Pulse height analysis is
not required, giving the instrument an inherently wide
dynamic range.
First generation DXA systems, such as the Hologic
QDR 1000, Norland XR-36 (Fig. 2) and Lunar DPX
scan patients rectilinearly using a pin hole collimator
producing a pencil beam coupled to a single detector
in the scanning arm. When a DXA scan is analyzedthe basic data process create a pixel-by-pixel map of
BMD over the entire scanned ®eld calculated fromEq. (2). An edge detection algorithm is ®rst used to®nd the bone edges. The total projected area of bone
is then derived by summing the pixels within the boneedges and a reported value of BMD calculated as themean BMD over all the pixels identi®ed as bones.
Finally, bone mineral content (BMC) is derived bymultiplying BMD by projected area.
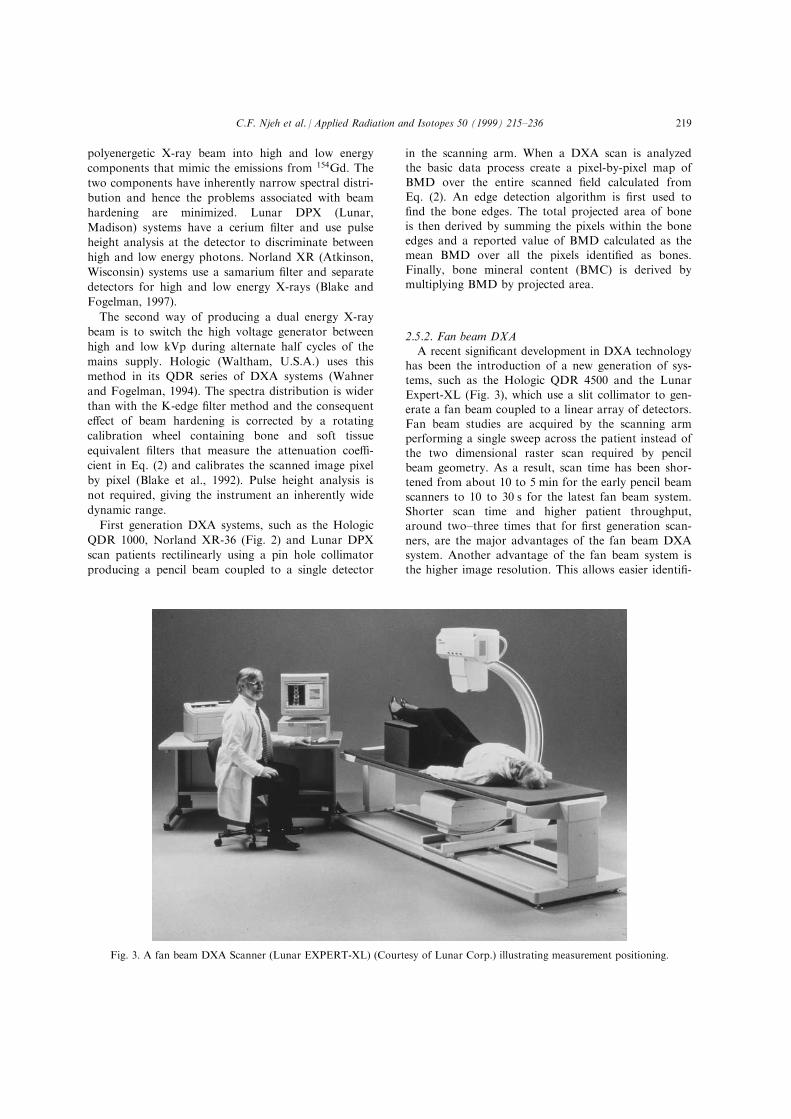
2.5.2. Fan beam DXA
A recent signi®cant development in DXA technologyhas been the introduction of a new generation of sys-tems, such as the Hologic QDR 4500 and the Lunar
Expert-XL (Fig. 3), which use a slit collimator to gen-erate a fan beam coupled to a linear array of detectors.Fan beam studies are acquired by the scanning armperforming a single sweep across the patient instead of
the two dimensional raster scan required by pencilbeam geometry. As a result, scan time has been shor-tened from about 10 to 5 min for the early pencil beam
scanners to 10 to 30 s for the latest fan beam system.Shorter scan time and higher patient throughput,around two±three times that for ®rst generation scan-
ners, are the major advantages of the fan beam DXAsystem. Another advantage of the fan beam system isthe higher image resolution. This allows easier identi®-
Fig. 3. A fan beam DXA Scanner (Lunar EXPERT-XL) (Courtesy of Lunar Corp.) illustrating measurement positioning.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 219

cation of vertebral structure and artifacts resultingfrom degenerative disease.
2.5.3. pDXA
DXA is also employed for measurements of theappendicular skeleton. Most standard DXA densi-tometers allow for highly precise measurement of the
radius or calcaneus using regions of interest like thosederived from SPA and SXA measurements as well asuser-de®ned subregions (Faulkner et al., 1994; Yamada
et al., 1994). Recently peripheral DXA (pDXA) densi-tometers specially designed for the forearm or calca-neus have been introduced and may provide these
measurements at a lower cost (Fig. 4). They have theadvantage compared with SXA systems that they dis-pense with the need for a water bath.
2.6. Quantitative computed tomography (QCT)
2.6.1. Spinal QCTQCT is the only method available with the ability to
determine in three dimensions the true volumetric den-sity (mg/cm3) of trabecular or cortical bone. Generally,spinal QCT is performed on standard clinical CT scan-
ners. An external bone mineral reference phantom isused to calibrate the CT number measurements tobone-equivalent values. Special software is used toanalyze the image and place regions of interest inside
the vertebral bodies. Typically two to four vertebra inthe range of L1±L3 are evaluated. Based on an initiallateral scout image, single 8±10 mm thick sections are
obtained through the mid-plane of each of these ver-tebrae using a low-dose technique and the gantry
angled parallel to the vertebral endplates. In order toimprove precision and reduce acquisition and analysistime, the sagittal location of mid-vertebral slices and
the axial placement of regions of interest can be highlyautomated (GluÈ er et al., 1988; Kalender et al., 1988).Due to the high responsiveness of spinal trabecular
bone, and its importance for vertebral strength, QCThas been principally employed to determine trabecularbone density in the vertebral centrum (Genant et al.,
1982). The two-dimensional QCT methods cannot beused to assess the proximal femur because of the proxi-mal femur's complex architecture and dramatic three-dimensional variation in its density. QCT can be per-
formed in single-energy (SEQCT) or dual-energy(DEQCT) modes, which di�er in accuracy, precisionand radiation (Genant and Boyd, 1977). Although it is
possible to improve accuracy by employing DEQCT,this approach incurs reduced in vivo precision andhigher dose, and thus is recommended only for
research studies that require higher accuracy (VanKuijk et al., 1990). The validity of QCT for measure-ment of vertebral cancellous bone is widely accepted
and it is available at over 4000 centers worldwide.
2.6.2. Peripheral quantitative computed tomography(pQCT)
Special purpose pQCT scanners have been employedfor measurements of BMC and BMD of the peripheralskeleton. Initially, a radionuclide source (usually 125I)
Fig. 4. Peripheral DXA scanner (Lunar PIXI) illustrating forearm measurement position (Courtesy of Lunar Corp.).
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236220
was used. However, state of the art scanners employ
X-ray sources (Genant et al., 1996; Gluer et al., 1997).
pQCT allows for a true volumetric density measure-
ment of appendicular bone without superimposition of
other tissues and provides exact three-dimensional
localization of the target-volume. Ease of use and the
ability to separately assess cortical and trabecular bone
and to measure BMD, BMC, and axial cross-sectional
area make the method an interesting alternative to
SPA or SXA. With the commonly used clinical pQCT
scanner, measurements in the distal radius are per-
formed at only one site with a single axial slice of
2.5 mm thickness located at the level that represents
4% of the ulnar length from the distal radial cortical
endplate. Modern pQCT scanners also incorporate a
multi-slice data acquisition capability covering a larger
volume of bone as compared with the commonly used
single slice technique (Kaisel and RuÈ egsegger, 1991).
The measurement of several slices is potentially more
representative of changes in the distal radius and may
therefore re¯ect the bone status of an individual more
accurately. If studies employing this multi-slice pQCT
technique are successful, they may contribute to more
extensive use of this already promising technique.
2.7. Sites measured
The choice of the optimum skeletal site for the pre-diction of osteoporosis is a subject of great debate.However, the consensus is that sites with higher con-
tents of cancellous (high turnover) bone are more sen-sitive to osteoporotic changes. Longitudinal studiessuggest that most of the skeletal sites currently
measured (spine, femur, radius and calcaneus) are use-ful for predicting the risk of fracture at any site. Thebest assessment of risk at a speci®c site, however is to
measure the BMD at that site (Miller et al., 1996).
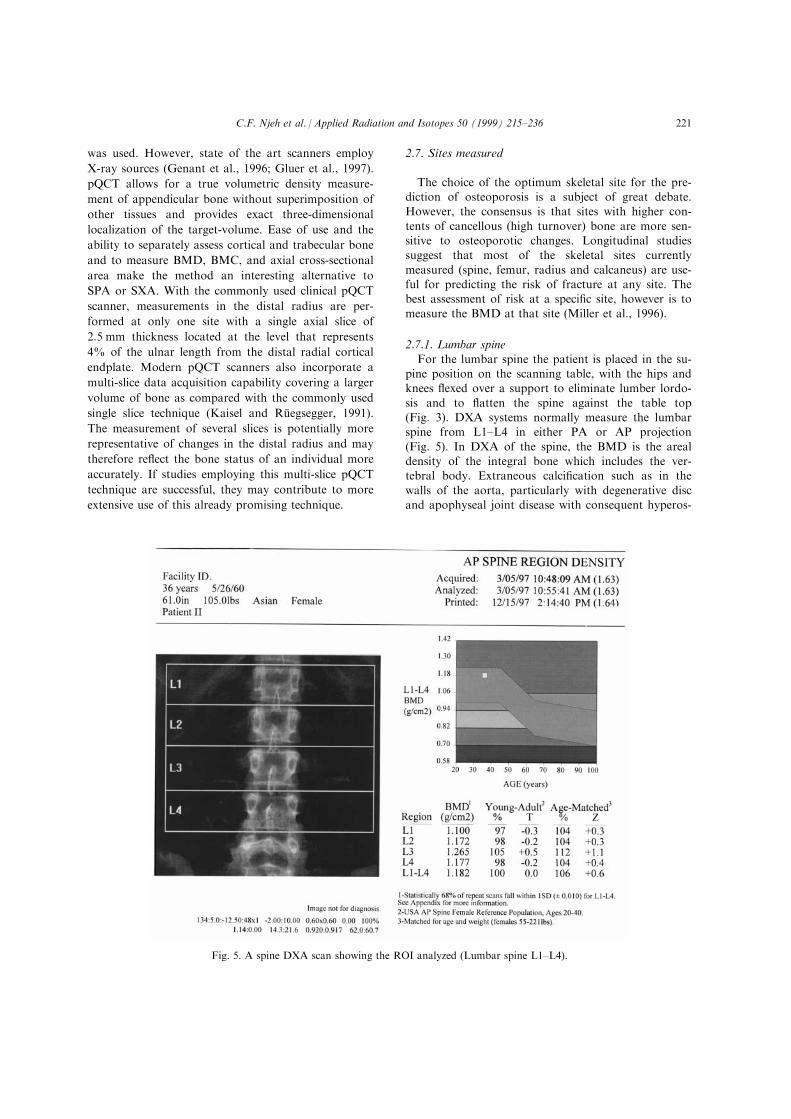
2.7.1. Lumbar spine
For the lumbar spine the patient is placed in the su-pine position on the scanning table, with the hips andknees ¯exed over a support to eliminate lumber lordo-
sis and to ¯atten the spine against the table top(Fig. 3). DXA systems normally measure the lumbarspine from L1±L4 in either PA or AP projection
(Fig. 5). In DXA of the spine, the BMD is the arealdensity of the integral bone which includes the ver-tebral body. Extraneous calci®cation such as in the
walls of the aorta, particularly with degenerative discand apophyseal joint disease with consequent hyperos-
Fig. 5. A spine DXA scan showing the ROI analyzed (Lumbar spine L1±L4).
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 221
tosis, will cause inaccuracies and over estimation of
BMD (Franck et al., 1995). Falsely elevated spinal
BMD on PA-DXA may be caused by other etiologies
such as vertebral wedge (crush fracture), Paget's dis-
ease of bone, sclerotic metastases and vertebral haemo-
globin.
The development of lateral DXA scanning of the
lumbar spine was aimed at reducing the errors intrinsic
in the posteroanterior examination of the lumbar
spine. A lateral examination of the lumbar spine
makes possible an evaluation of the vertebral body
also ensuring almost exclusive measurement of trabecu-
lar bone. Therefore, the correlation between lateral
DXA and quantitative computed tomography (QCT),
both measures of the vertebral body, has been found
to be stronger than that between PA-DXA and QCT
(Yu et al., 1994). However, overlap of the iliac crest at
level L4 and ribs at level L2 may substantially increase
the measured bone density. Nevertheless, the inclusion
of L2 through L4 usually yields the best precision and
diagnostic sensitivity (Rupich et al., 1992; Jergas et al.,
1995).
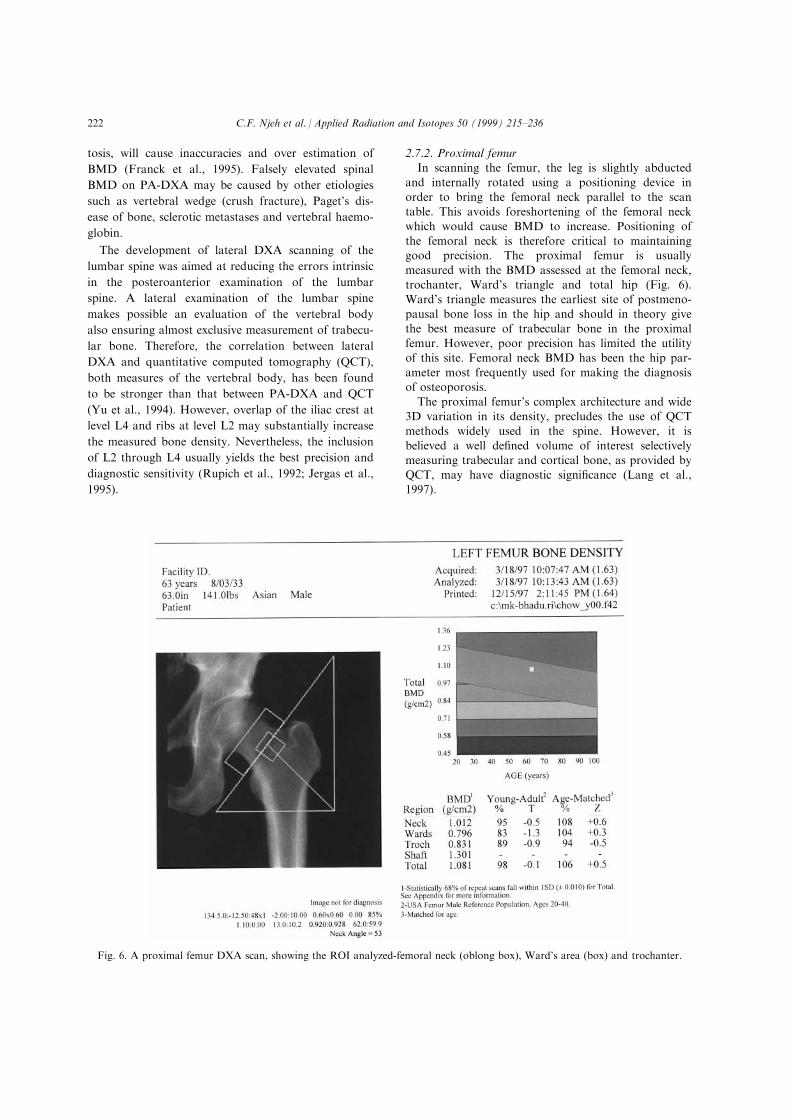
2.7.2. Proximal femur
In scanning the femur, the leg is slightly abducted
and internally rotated using a positioning device in
order to bring the femoral neck parallel to the scan
table. This avoids foreshortening of the femoral neck
which would cause BMD to increase. Positioning of
the femoral neck is therefore critical to maintaininggood precision. The proximal femur is usually
measured with the BMD assessed at the femoral neck,
trochanter, Ward's triangle and total hip (Fig. 6).
Ward's triangle measures the earliest site of postmeno-
pausal bone loss in the hip and should in theory give
the best measure of trabecular bone in the proximal
femur. However, poor precision has limited the utility
of this site. Femoral neck BMD has been the hip par-
ameter most frequently used for making the diagnosisof osteoporosis.
The proximal femur's complex architecture and wide
3D variation in its density, precludes the use of QCT
methods widely used in the spine. However, it is
believed a well de®ned volume of interest selectivelymeasuring trabecular and cortical bone, as provided by
QCT, may have diagnostic signi®cance (Lang et al.,
1997).
Fig. 6. A proximal femur DXA scan, showing the ROI analyzed-femoral neck (oblong box), Ward's area (box) and trochanter.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236222
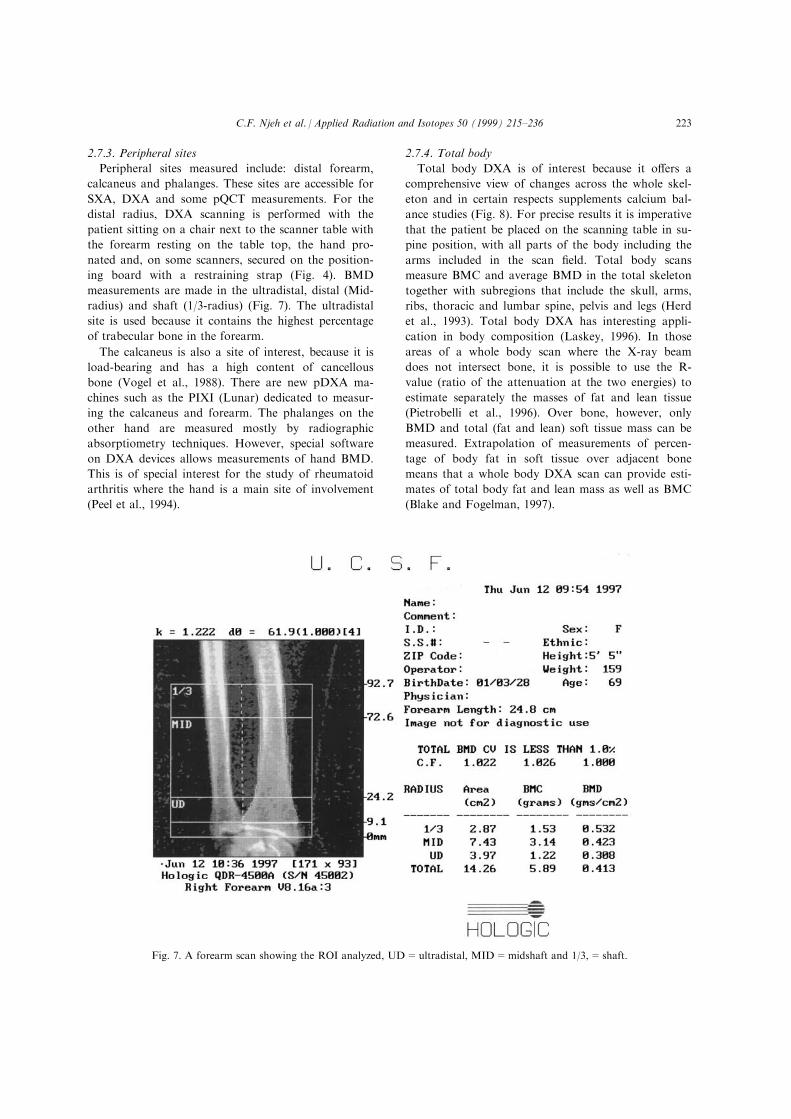
2.7.3. Peripheral sites
Peripheral sites measured include: distal forearm,
calcaneus and phalanges. These sites are accessible for
SXA, DXA and some pQCT measurements. For the
distal radius, DXA scanning is performed with the
patient sitting on a chair next to the scanner table with
the forearm resting on the table top, the hand pro-
nated and, on some scanners, secured on the position-
ing board with a restraining strap (Fig. 4). BMD
measurements are made in the ultradistal, distal (Mid-
radius) and shaft (1/3-radius) (Fig. 7). The ultradistal
site is used because it contains the highest percentage
of trabecular bone in the forearm.
The calcaneus is also a site of interest, because it is
load-bearing and has a high content of cancellous
bone (Vogel et al., 1988). There are new pDXA ma-
chines such as the PIXI (Lunar) dedicated to measur-
ing the calcaneus and forearm. The phalanges on the
other hand are measured mostly by radiographic
absorptiometry techniques. However, special software
on DXA devices allows measurements of hand BMD.
This is of special interest for the study of rheumatoid
arthritis where the hand is a main site of involvement
(Peel et al., 1994).
2.7.4. Total body
Total body DXA is of interest because it o�ers a
comprehensive view of changes across the whole skel-
eton and in certain respects supplements calcium bal-
ance studies (Fig. 8). For precise results it is imperative
that the patient be placed on the scanning table in su-
pine position, with all parts of the body including the
arms included in the scan ®eld. Total body scans
measure BMC and average BMD in the total skeleton
together with subregions that include the skull, arms,
ribs, thoracic and lumbar spine, pelvis and legs (Herd
et al., 1993). Total body DXA has interesting appli-
cation in body composition (Laskey, 1996). In those
areas of a whole body scan where the X-ray beam
does not intersect bone, it is possible to use the R-
value (ratio of the attenuation at the two energies) to
estimate separately the masses of fat and lean tissue
(Pietrobelli et al., 1996). Over bone, however, only
BMD and total (fat and lean) soft tissue mass can be
measured. Extrapolation of measurements of percen-
tage of body fat in soft tissue over adjacent bone
means that a whole body DXA scan can provide esti-
mates of total body fat and lean mass as well as BMC
(Blake and Fogelman, 1997).
Fig. 7. A forearm scan showing the ROI analyzed, UD=ultradistal, MID=midshaft and 1/3,=shaft.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 223
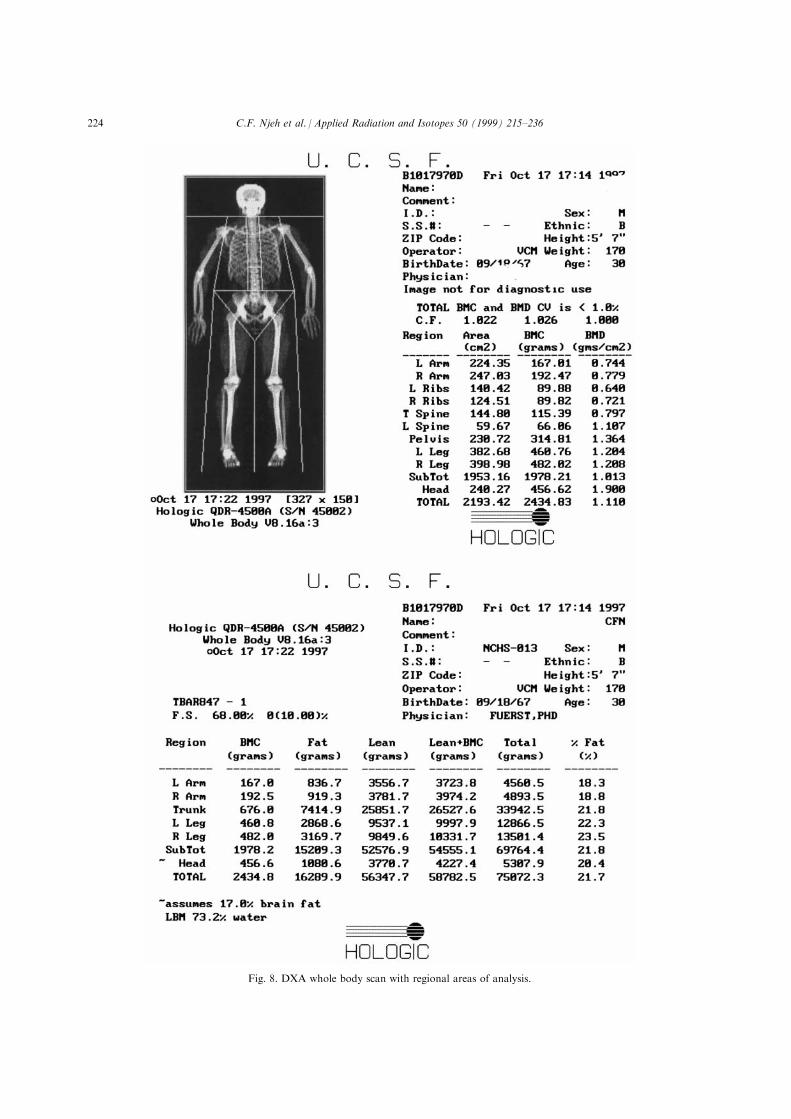
Fig. 8. DXA whole body scan with regional areas of analysis.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236224

2.7.5. Vertebral morphometry
As a result of the relatively high resolution of fan-
beam DXA scanners anatomic details of the examined
region are depicted clearly. Using DXA to obtain lat-
eral images of the lumbar spine allows the scanning
beam Ð in contrast to conventional cone beam radi-
ography Ð to be generally parallel to the vertebral
endplates. This allows a better de®nition of vertebral
dimensions for a morphometric analysis, even though
resolution and signal to noise ratio are both worse
than X-ray. In reference to the DXA approach, this
method has been called morphometric X-ray absorp-
tiometry, or MXA (Steiger et al., 1994). Overlying
structures such as ribs or the iliac crest may have an
adverse e�ect on the morphometric analysis. To
enhance the accuracy of MXA, technical modi®cations
of the X-ray tube and the detector system may provide
images with higher resolution thereby enhancing the
analysis of vertebral deformities. These techniques are
still in the developmental and early clinical evaluation
phase.
3. Radiation dose to the patient
Previous sections have demonstrated the usefulness
of measuring BMD with the absorptiometric technique
in the assessment of bone integrity. Studies of the radi-
ation dose to patients from absorptiometry scans have
con®rmed that patient exposure is small compared to
many other sources of exposure including most radio-
logical investigations involving ionizing radiation
(Kalender, 1992; Lewis et al., 1994; Huda and Morin,
1996; Njeh et al., 1996). Due to the low radiation
doses encountered in BMD measurements, there have
been limited studies on doses incurred in this examin-
ation. In cases where doses have been measured, only
the entrance surface dose (ESD) has been reported
(Table 1). ESD does not permit a direct comparison of
the patient doses associated with absorptiometric and
other radiological examinations. Also, as explained
elsewhere in this volume the radiation hazard to the
patient is often expressed in terms of the e�ective dose
(ED). This is de®ned as the sum of the absorbed doses
Table 1
Manufacturer reported Entrance Skin Dose (ESD) for some of the more common densitometers
Technique Manufacturer Model Site ESD (mGy) Comments
DXA Hologic QDR 1000/1500 AP spine/femur <43 70 and 140 dual output, 43 and 110 keV
Total body <13
QDR 2000 AP spine/femur 192 fan beam mode
lateral spine 237
total body 8
DXA Lunar DPX-L/DPX-IQ AP spine/femur 11$ 76 kVp with cerium ®lter, 38 and 70 keV
Lateral spine 77
total body 0.2
EXPERT-XL Spine/femur-5 mA fast 530 Fan beam
Total body 1.5 mA fast 50
Forearm/hand 120
DXA PIXI Calcaneus/forearm <200
SPA Lunar SP2 forearm 150 7.4 GBq 125I
DXA Norland XR-36 AP spine 0.9±44.4* 100 kVp with samarium ®lter, 80 and 46.8 keV
Femur 1.8±89*
lateral spine 123
Total body 0.4
pDXA Norland pDEXA radius and ulna <25 60 kVp, tin ®lter, 28 and 48 keV
SXA Norland SXA300 calcaneus 13 36 kV, tin ®ltered, 27 keV
DXA Sopha Medical L-XRA AP spine 20 80 kVp with neodymium ®lter, 43 and 70 keV
lateral spine 40
pQCT Stratec XCT 960 Forearm 30 45 kVp, 0.3 mA, 38.5 keV
pDXA Osteometer DX-200 Forearm 55 kVp, 0.3 mA, tin (Sn) ®lter
DXA DMS Challenger Spine/femur <3.3 samarium ®lter, 35 and 75 kev
*The Norland XR-36 has a dynamic ®ltration which compensates for di�erent tissue thickness, so the ESD is dependent on the body
thickness of the patient.$ESD for DPX-IQ is similar to DPX-L, and is also dependent on the tube current, resolution and scan speed used. The ESD is linearly
proportional to these parameters if everything else remains constant.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 225

to each irradiated organ weighted for the radiationtype and the radio-sensitivity of that organ (ICRP,
1991). The ED is equivalent to the uniform wholebody dose that will put the patient at equivalent riskfrom the carcinogenic and genetic e�ects of radiation
(ICRP, 1991). For low doses, as encountered in DXA,the principal risks to patients are the stochastic processof carcinogenesis and genetic e�ects. The following sec-
tions will discuss doses incurred in BMD measure-ments from di�erent techniques.
3.1. Patient doses from DXA
The entrance radiation dose from a DXA examin-
ation is determined by machine dependent parameterssuch as source-detector geometry, focal spot size,source collimation, scan speed, tube current and sourcespectra. The operator can only change the mA and the
scan speed (resolution). However, the mA and scanspeed use can a�ect the precision of BMD measure-ment. E�ective dose from DXA measurements have
been reported in the literature (Pye et al., 1990;Kalender, 1992; Rawling et al., 1992). However, Lewiset al. (1994) presented the ®rst extensive e�ective dose
estimates for Hologic QDR 1000 and QDR 2000 DXAscanners. Similar studies have been reported by Njehet al. (1996) and Bezakova et al. (1997) for Lunar ma-
chines. Due to di�erences in the production of X-raysby these systems, their respective EDs are expected tobe di�erent. Lewis et al. reported the highest ED forthe total body of 3.6 mSv (4.6 mSv including the ovar-
ies) (Table 2). ESDs were found to be proportionate to
the speed of the scanning arm of QDR 1000. Njeh etal. (1996) and Bezakova et al. (1997) observed lowervalues of e�ective dose for a Lunar DPX-L machine
(Table 3). Clinically patients on one visit may receivescans of a number of di�erent regions (generally two
but not more than three) such as the posterior±anter-ior spine, lateral spine, left and right proximal femur,
hand, forearm, calcaneus and total body. The totale�ective dose per visit will therefore be a summationof the regions scanned. For example, a postmenopau-
sal patient undergoing scans of the spine and hip per-formed on a QDR-1000 would receive an e�ective
dose of 0.6 mSv (0.5 spine and 0.1 femur). However, apremenopausal woman scanned on the same scanner
would receive an e�ective dose of 1.9 mSv because ofinclusion of the ovaries. On the other hand, a postme-
nopausal woman and premenopausal woman scannedon a Lunar DPX-L will receive an e�ective dose of0.29 and 0.36 mSv, respectively.In lateral DXA scans, mAs values and therefore sur-
face dose values are increased typically by a factor of
2±4. However, due to the fact that organ doses are sig-ni®cantly lower relative to the ESD for the lateral
beam and that the length of the spine scanned is shor-tened in most cases, e�ective dose values for lateral
scans are comparable to PA projection scans. Lewis etal. (1994) reported EDs of 0.5 and 0.6 mSv for AP andlateral spine, respectively.
DXA measurement, if accompanied by a lateralradiograph, will signi®cantly change the magnitude of
Table 2
Scanning times, entrance surface doses and e�ective doses for postmenopausal women for a pencil beam mode
scans performed on the QDR-1000 (Hologic)
Scan type Scan time (min) Entrance surface dose (mGy) E�ective dose (mSv)
Total Body 17 18 3.6 (4.6)
AP spine (L1±L4) 8 60 0.5 (0.5)
Lateral spine(L2±L4) 20 238 0.6 (0.6)
Proximal femur 6 60 0.1 (1.4)
Distal forearm 6 113 0.07 (0.07)
Values in bracket includes the ovaries, therefore representing premenopausal women. Data from Lewis et al.
(1994).
Table 3
Entrance surface dose (ESD) and e�ective dose (ED) for Lunar DPX-L DXA scanner
E�ective dose (mSv)
Ref. Mode Entrance surface dose (mGy) PA-spine femur
(Njeh et al., 1996) Medium, 0.75 mA 10.25 0.21 0.08 (0.15)
(Bezakova et al., 1997) Medium, 0.75 mA 11.5 0.19 0.023 (0.14)
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236226

the dose involved. For a conventional lateral X-ray®lm examination, Kalender (1992) estimated an ED of
700 mSv for 90 kVp and radiation ®eld height of 25 cm.For larger ®elds, values of 2000 mSv can be expected(Richardson, 1990). Thus an e�ective dose of up to
2000 mSv will result from a DXA scan plus X-ray ®lm.On the other hand, Huda and Morin (1996) estimatedED for 80 kVp AP and lateral X-ray examination to
be in the range of 40±120 and 60±190 mSv, respectively.They assumed an ESD range of 2±4 mSv and an X-raybeam area between 400±600 cm2 at the patient
entrance.The dose associated with DXA BMD measurement
can be considered low or even insigni®cant in compari-son with natural background radiation levels. It is well
below the background value of about 7 mSv per day.
3.2. Patient doses from fan beam DXA
Fan beam DXA scanners were introduced to reducescanning time and increase image resolution. A conse-
quence has been an increase in radiation dose due tothe increase in photon ¯ux required. In the LunarExpert there is an increase in photon ¯ux by using a
higher tube potential (134 instead of 76 kVp) and ahigher tube current (5 instead of 0.75 mA). HologicQDR 4500 operates at 140 and 100 kVp compared to
140 and 70 kVp for QDR 1000. Entrance surface doses
have been reported for both the Lunar Expert, Expert
XL and Hologic QDR 2000 and QDR 4500. Stewart
et al. (1996) reported an ESD of 0.7, 1.1 and 0.12 mSv
for spine/femur, lateral spine and peripheral sites, re-
spectively, for the Lunar Expert-XL. E�ective dose for
these fan beams have been reported in the literature
(Lewis et al., 1994; Njeh et al., 1996; Blake and
Fogelman, 1997) (Table 4 and 5). The fan beam has
led to about a 100 fold increase in dose for the Lunar
and 10 fold increase for the hologic scanner. One of
the reasons for the di�erence in e�ective doses between
the Hologic QDR 4500 and the Expert-XL is that for
the Expert-XL the spine measurements are performed
in the AP direction. Hence the distance to the sensitive
organs such as the stomach is reduced and results in
approximate doubling of ED.
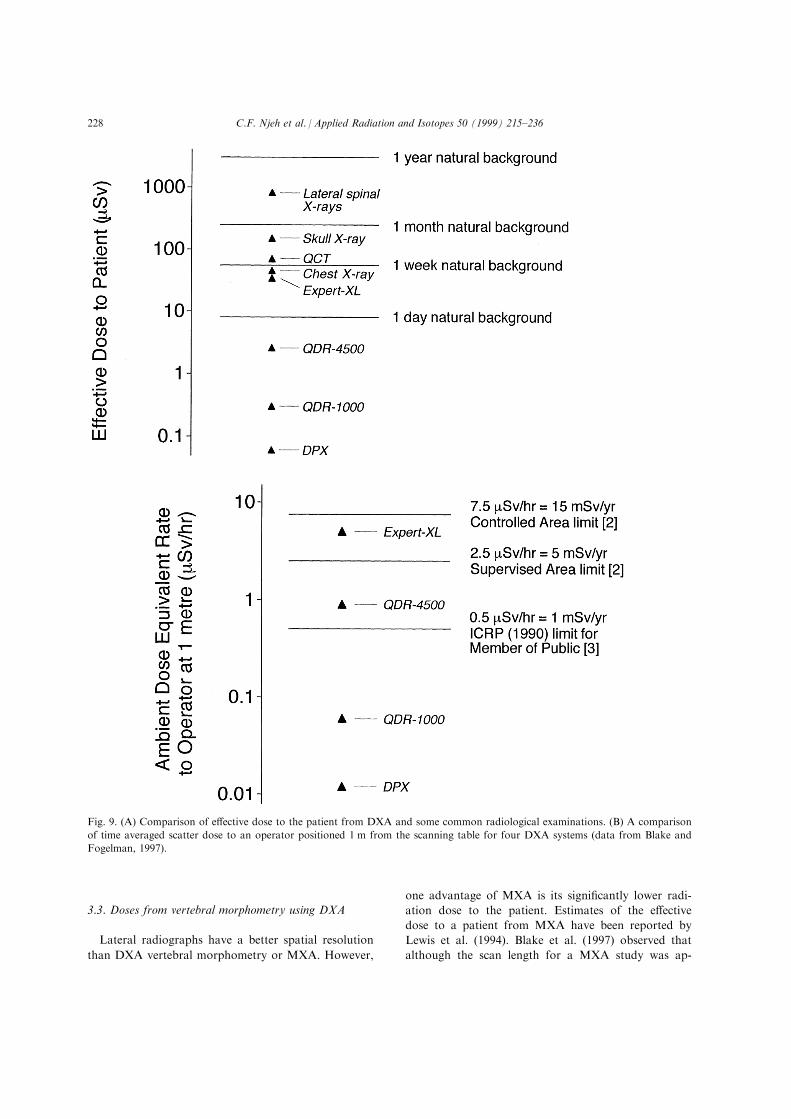
Despite the increases associated with advances in
technology, patient dose from DXA remains very low
when compared with natural background radiation
and from other common radiological procedures
(Fig. 9). For example the mean ED per radiograph for
AP lumbar spine X-ray examination has been quoted
as 690 mSv (Shrimpton et al., 1998) which are about
10 fold higher than fan beam ED. On the other hand
the fan beam DXA EDs are comparable to 17 mSvreported for chest PA X-ray examination (Shrimpton
et al., 1998).
Table 4
Scan times and doses (where values in brackets include the ovaries) for a Hologic QDR-2000 fan beam mode
reported by Lewis et al. (1994)
Scan type Scan time (min) Entrance skin dose (mGy) E�ective dose (mSv)
PA Spine (L1±L4) 0.1 57 0.4 (0.4)
1 138 0.9 (0.9)
2 271 1.8 (1.8)
3 432 2.9 (2.9)
Lateral Spine (L2±L4) 3 684 1.2 (1.2)
6 1390 2.5 (2.5)
Proximal femur 1 138 0.3 (3.0)
2 271 0.6 (5.9)
Total body 6 11 2.7 (3.6)
Table 5
Doses from Fourth Generation (fan beam) DXA scanner
E�ective dose (mSv)
DXA system Mode Entrance surface dose (mGy) PA spine femur Ref.
QDR 4500 Array (1 min) ÿ 6.7 (Patel et al., 1996b)
QDR-4500 ÿ 295 8 ÿ (Starritt et al., 1996)
Expert-XL 5 mA Fast 700 73 (max scan size) ÿ (Stewart et al., 1996)
Expert Medium (40 s) 895 31 4.7 (32.0) (Njeh et al., 1996)
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 227
3.3. Doses from vertebral morphometry using DXA
Lateral radiographs have a better spatial resolution
than DXA vertebral morphometry or MXA. However,
one advantage of MXA is its signi®cantly lower radi-
ation dose to the patient. Estimates of the e�ective
dose to a patient from MXA have been reported by
Lewis et al. (1994). Blake et al. (1997) observed that
although the scan length for a MXA study was ap-
Fig. 9. (A) Comparison of e�ective dose to the patient from DXA and some common radiological examinations. (B) A comparison
of time averaged scatter dose to an operator positioned 1 m from the scanning table for four DXA systems (data from Blake and
Fogelman, 1997).
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236228

proximately 3 times greater than a bone density scanof the lumbar spine, patient dose is approximately 10
times higher (assuming the same scan mA, collimationand scan speed) because of the inclusion of the lungsand breast in the scan ®eld. Table 6 shows that the
highest dose of 51 mSv is incurred from the mediummode using QDR 4500. This is signi®cantly lower thanan approximate dose of 600±800 mSv from lateral
radiographs (combined thoracic and lumbar)(Shrimpton et al., 1998).
3.4. Pediatric doses from DXA
Di�erent diseases such as juvenile rheumatoid arthri-
tis (Falcini et al., 1996) may directly or indirectlydecrease the bone mineral content in children.Therefore, an assessment of bone integrity may assistin the choice of the right therapeutic strategy and best
follow up for patients with diseases a�ecting bonemetabolism. Also, bone mass accrued during childhoodhas been proposed as a determinant of an individual's
susceptibility to osteoporotic fractures in adulthood(Seeman et al., 1993). DXA is presently the mostwidely used technique for the assessment of bone integ-
rity. As previously stated, DXA can also be used tostudy other aspects of body composition such as per-
centage of fat and lean body mass (Laskey, 1996).
Njeh et al. (1997b) assessed the dose incurred from
DXA scanning of a 5-year-old child and a 10-year-old
child using a Lunar DPX-L scanner. They measured
the entrance surface dose and percentage depth doses
for the total body and PA spine scan modes using
lithium borate thermoluminescent dosemeters located
at the surface and distributed throughout various
organ locations in anthropomorphic child phantoms.
The EDs were calculated from the percentage depth
doses, amount of each organ irradiated and tissue
weighting factors (ICRP, 1991). The results are rep-
resented in Table 7. The EDs are more than two
orders of magnitude lower than reported ESDs and
EDs for pediatric chest X-rays. Fewer studies have
reported DXA pediatric dose. Koo et al. (1995)
reported an ESD of 3 mGy for pediatric total body
using the Hologic 1000/W. Faulkner et al. (1993)
reported 10 mGy ESD and e�ective dose equivalent of
2.7 mSv for total body mode using the Hologic QDR-
2000 (fan beam mode). This is similar to adult total
body ED reported by Lewis et al. (1994) for the same
type of scanner. Therefore, one could extrapolate that
similar EDs could be derived for the pediatric mode as
were reported for the adult scanning mode, due to pro-
Table 6
E�ective dose for vertebral morphometry scans performed on DXA bone densitometer and on
conventional radiographs
E�ective dose (mSv)
System Scan mode PA centerline scan MXA scan
QDR-2000 34
QDR-4500 Dual-energy fast 4 (30 s) 20 (5 min)
QDR-4500 Dual-energy medium 10 (90 s) 41 (10 min)
QDR-4500 Dual-energy hi-res 20 (3 min) 20 (10 min)
QDR-4500 Single-energy ÿ 2 (10 s)
Expert-XL 5 mA fast ÿ 38 (40 s)
Lateral Radiograph ÿ ÿ 800
Scan times are given in brackets. For QDR-4500 study requires the acquisition of both a PA
centerline and a lateral morphometry scan. Data from (Blake et al., 1997) and (Rawlings et al.,
1996) for QDR 2000. hi-res=high resolution.
Table 7
E�ective dose for a pediatric scan mode using a lunar DPX-L (Njeh et al., 1997b)
Scan Mode Patient size Age
Scan time
(min) ESD (mGy) ED (mSv)
PA spine 6±16 cm 5 5 6.0 0.28
PA spine 10 6.0 0.20
Total body medium 15±25 kg 5 9 0.12 0.03
total body large 25±35 kg 10 12 0.1 0.02
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 229

portionate reduction in the scan ®eld for the pediatric
mode.Few studies have reported the e�ective doses for
common pediatric radiological examinations. However,ESDs for common pediatric radiological examinationshave been reported (Ruiz et al., 1991; Chapple et al.,
1993; Martin et al., 1994; Kyriou et al., 1996). ESDsare in the range of 50±400 mGy for PA chest X-ray
and 420±1990 mGy for an abdominal X-ray examin-ation. Njeh et al. (1997b) used these ESD values andapplied NRPB-SR279 (Hart et al., 1996) Monte Carlo
data to estimate the EDs. The results are presented inTable 8 which in comparison with Table 7 shows that
doses encountered in DXA are more than two ordersof magnitude less than common radiological examin-ations.
Exposure of children to ionizing radiation givesmore grounds for concern than that for adults, because
for children there is a longer period available for thedelayed e�ects of radiation to manifest. This meansthat the lifetime risk of radiation-induced cancer per
unit dose to the child is likely to be higher than for theadult. The probability of aggregated radiation detri-
ment can be related to ED and for children this is ageand sex related. For a 10-year-old female, the total life-
time risk of radiation-induced cancer is estimated as16�10ÿ2 Svÿ1 compared with 5.9�10ÿ2 Svÿ1 for a30-year-old adult (NRPB, 1993). A pediatric subject
referred for a bone densitometry examination mayreceive a PA spine and total body scan. The total e�ec-
tive dose will then be 0.31 mSv, giving a lifetime risk of5�10ÿ8 for fatal cancer. This is negligible comparedwith the possible bene®ts from the scan. In addition to
carcinogenesis, genetic e�ects are also of concern inthe total body examination because of the irradiation
of the gonads. The estimated dose to the ovaries was0.002 mSv, which is 9% of the total dose. Even thoughthese doses are quite low, good radiological practice
should be implemented.
3.5. Patient doses from QCT
As mentioned earlier, spinal QCT for BMDmeasurement can use standard CT machines or those
with specialized software. As discussed by Jessen et al.(1998) CT has problems with speci®cation of radiation
doses imparted. The main problem is the non-uniform-ity of dose distribution within the patient. This isbecause in most CT examination a number of CT
slices may be contiguous or overlapping. The radiationdose to patients undergoing QCT depends upon the
following factors: (1) scan parameters-kVp, mAs, slicethickness, number and spacing of slices, (2) patientsize, (3) X-ray source/detector geometry; and (4) detec-
tor collimation and calibration. Hence the dose deliv-ered is highly scanner speci®c. The X-ray beam of the
QCT systems has a slice thickness in the range of 8±10 mm; the radiation received by the patient is there-fore limited to a narrow band. BMD assessment using
CT involves in most cases 3-slices.The radiation dose from QCT has been reported
over the years, however, there has been no consistencyin the parameter reported-entrance surface dose, CT
dose index (CTDI), mean depth dose, etc. Banks andStevenson (1986) reported the approximate mean sur-face dose (multislice, 125 kVp, 230 mAs) as 16 mGy.
However, Kalender (1992) reported a surface dose of2.5 mGy for a SOMATOM Plus (80 kVp, 125 mAs).
Note that the scan parameters are di�erent for thesetwo studies. This illustrates the fact that low dosevalues can be achieved via low kVp and low mAs.
Changing from 120 to 80 kVp with ®xed mAs settings,Kalender (1992) was able to measure a dose reduction
of a factor of about 4. QCT BMD examinations arealways accompanied by a lateral scout radiograph
(tomogram) which is required to ensure reproduciblepositioning and involves an additional radiation dose.Kalender (1992) measured an ESD of 0.46 mGy for
lateral scout radiographs. He further estimated the ED
Table 8
Reported mean ESDs per radiograph and calculated EDs using Monte Carlo simulation for two common radiological examination
for comparison with Table 7 (Njeh et al., 1997a,b)
PA chest Abdomen
Ref Age (years) ESD (mGy) ED (mSv) ESD (mGy) ED (mSv)
(Martin et al., 1994) 1±5 50 5.2 470 89.8
(Kyriou et al., 1996) 1±4 70 7.3 420 73.2
(Chapple et al., 1993) 1±5 200 37.8 1200 242
(Martin et al., 1994) 6±10 80 7.9 770 132
(Kyriou et al., 1996) 5±9 60 6.1 670 106
(Ruiz et al., 1991) 6±10 310 43.2 1280 245
(Kyriou et al., 1996) 10±15 80 5.7 1060 125
(Ruiz et al., 1991) 10±14 400 38.8 ÿ ÿ
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236230

from the tomogram and QCT to be 31.9 and 28.6 mSv,respectively. It is worth nothing that his methodologywas very crude. For instance, no depth dose was calcu-lated. A QCT organ dose of 1.5 mSv estimated from
the center of a phantom was assumed for all theorgans. This assumption is not valid since the center ofdi�erent organs/tissue varies and thus the organ dose
also varies. However, he acknowledged the fact thathis results were only accurate to within a factor of 2 to
3.Huda and Morin (1996) estimated the ED for
SEQCT and DEQCT using a GE 9800Q CT scanner.
The estimate, based on the methodology of Shrimptonet al. (1991), reported an e�ective dose of 10.8 mSv for
a GE 9800Q scanner (120 KVp, 400 mAs, 22 slices).By assuming that the e�ective dose was linearly pro-portional to the number of slices and mAs, they calcu-
lated the ED as a function of these parameters. Theyalso scaled the dose by a factor of 0.3 when 80 kVpwas used instead of 120 kVp. When a tomogram
(Scout) and 3 CT images are acquired at 80 kVp, ane�ective dose equivalent in the range of 200±360 mSv is
estimated, depending on mAs used. Similarly, for atomogram and six CT slices associated with the 80 and120 kVp DEQCT an ED of 700±1400 mSv is estimated.
This also represents an over simpli®cation in the e�ec-tive dose estimates. Their values are about 8 times
higher than those reported by Kalender (1992). Thescaling method used may have overestimated the doseconsidering that the radio-sensitive organs are not
located proportionally in the body. However,Karantanas et al. (1991) have also reported an e�ectivedose equivalent of 370 mSv (no details of how EDE
was calculated were given) for 4 slices and a scoutview, using a Siemens Somaton DR2-G. They used
125 kVp, 60 mAs and 2408 tube rotation in the dataacquisition. They reported a computed tomographicdosimetric index (CTDI) of 5 mGy. The QCT BMD
doses are similar in magnitude to other normal radio-logical examination such as abdominal AP X-ray of700 mSv, but lower than normal CT-examinations,
such as 3300 mSv for the lumbar spine (Shrimpton etal., 1998).
The high doses encountered during normal imagingCT examination is necessary in order to obtain the lowcontrast resolution required to separate lesions from
normal tissue and to use CT to its optimal diagnosticpotential. However when measuring high Z material
such as bone, high doses such as those used for ima-ging are generally not necessary. Also the use of alarge region of interest (ROI) to determine mean CT
numbers for these studies allows much lower X-raydoses. Because bone mineral sensitivity goes up anddose goes down at lower kVp, the lowest possible set-
ting is recommended for BMD measurements (Cann,1988).
3.6. Patient dose from other techniques
For other techniques such as RA, PQCT, and SXAno e�ective dose calculations have been reported, onlyentrance surface doses have been reported. Muller et
al. (1989) reported an ESD of 100 mGy for a low dosepQCT. For a SXA DTX-100 (Osteometer A/sRodovre, Denmark), an ESD of 16.6 mGy (40 kVp,
0.2 mA) has been reported (Kelly et al., 1994). Sincevery few radiosensitive organs are irradiated using per-ipheral techniques, the ED is bound to be very low.
For example only a small fraction of these radio-sensi-tive tissues are exposed: skin, red bone marrow andbone surfaces.For superseded techniques such as SPA and DPA at
the most only absorbed doses have been reported.These doses are dependent upon the strength of thesource and the beam characteristics. The peak skin
entrance dose for DPA ranged from 50±150 mGy,while for SPA of the radius it was about 50 mGy(Huddleston, 1988).
3.7. Sta� dose from DXA
In the United Kingdom, the maximum annual dosefor a non-classi®ed worker is 15 mSv, corresponding toa time averaged dose rate in the workplace of
7.5 mSv hÿ1 (IRR, 1985). If the dose rates approachthis limit then the working area is de®ned as aControlled Area and requires environmental monitor-
ing and a written system of work. This includes moni-toring the radiation exposure of sta� members enteringthis area by ways such as TLD batches. At lower dose
rates of up to 5 mSv yearÿ1 (2.5 mSv hÿ1) the lesserSupervised Area requirement applies. In 1990 theInternational Commission on Radiological Protection(ICRP) recommended an annual dose limit of
1 mSv yearÿ1 (equivalent to 0.5 mSv hÿ1 in the workplace) for members of the public (ICRP, 1991).For pencil beam systems such as the Lunar DPX
and the Hologic QPR 1000, a time-averaged dose tosta� from scatter is very low even with the operatorsitting as close as 1 m from the patient without shield-
ing during scanning (Njeh et al., 1996; Patel et al.,1996a). For the Lunar DPX-L scanner, the maximumscattered dose-rate to an operator at 1 m from thepatient for continuous exposure would be less than
1 mSv hÿ1 (Njeh et al., 1996). The typical maximumworkload for this type of scanner is 16 patients perday with two views per patient, with the X-ray beam
on for 4 min per view. Thus, the maximum annualwork-load would be approximately 533 h per year. Theannual dose to the operator at 1 m would therefore be
less than 0.4 mSv per year, which is similar to theNational Radiological Protection Board (U.K.)suggested constraints of 0.3 mSv per year to members
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 231

of the public from a single source (NRPB, 1993).Therefore, no protective screen for the operator, or ad-
ditional protection for the public in adjoining areas isnecessary.Associated with the increase in patient dose and
higher patient throughput with fan beam DXA is agreater occupational hazard to sta� from scatteredradiation (Njeh et al., 1996; Patel et al., 1996a). The
scattered dose from the fan beam systems such as theQDR 4500 and Lunar Expert XL is considerablyhigher and approaches limits set by the regulatory
authorities for occupational exposure. The scattereddose-rate for the Lunar EXPERT Scanner at 1 m fromthe patient is 64 mSv hÿ1 (scan width 180 mm) (Njeh etal., 1996). If one allows for a nominal scan width of
120 mm, the scattered dose rate reduces to 42 mSv hÿ1.Considering a maximum daily beam on time of60 min, the time average dose rate at 1 m would be ap-
proximately 5 mSv hÿ1 (using an 8 h day). On thisbasis, the Controlled Area, as required by IRR 1985(IRR, 1985) would not need to extend beyond 1 m
around the radiation beam. However, in order toensure that the operator receives an annual dose ofless than 1 mSv (the new ICRP proposed limit for
members of the public) (ICRP, 1991), the operatorwould need to have a protective screen or be at least3.5 m from the beam. Thus, in a relatively small room,to achieve doses as low as reasonably achievable, a
protective screen o�ering a small degree of attenuationwould be required. On the other hand, with a reducedscan time and workload, the daily beam-on time could
be as low as 20 min, in which case a protective screenwould not be necessary, provided the operator is atleast 2 m away from the beam. A similar sta� dose
analysis has been made for Hologic QDR 2000plusand QDR 4500 by Patel et al. (1996a) and found to be2.1 and 2.4 mSv/h, respectively. This occupational dosewas found to be similar to that from a 99Tcm MDP
radionuclide bone scan (Fig. 9).
3.8. Sta� dose from other techniques
Similar or lower scattered radiation dose have beenreported for peripheral scanners such SXA. Kelly et al.
(1994) reported the scattered radiation to be less than1 mSv at a distance of 10 cm from all sides of the scan-ner. Scattered dose assessment is important in the
examination of the radius because of the proximity ofsensitive organs such as the breast to the scatteredradiation.
3.9. Reduction of occupational dose
Reduction of occupational exposure can be achievedby making appropriate use of shielding, distance, timeand radiographic method as follows:
. Shielding: When installing a fan beam systemactive precautions to reduce dose to sta� such as use
of a radiation barrier should be considered.. Distance: Apply the inverse square law by having
a scanning room large enough to place the operator at
least 3 m from the patient.. Time: Use of scan modes with shorter scan times
has been observed to approximately halve the dose for
QDR systems (Lewis et al., 1994).. Method: Patel et al. (1996a) have observed that
scanning the patient right hip in preference to the left
can give a three-fold reduction in potential occu-pational dose.
3.10. Dose reduction techniques in DXA applications
To minimize patient doses, as for instance requiredby the U.K. Government Ionizing Radiation
Regulation (IRR) of 1988 (IRR, 1988), the smallestpossible scan width and length should be used. For theLunar Expert a range of collimation widths are avail-
able. Njeh et al. (1996) have been able to show that a60% reduction in e�ective dose can be achieved byusing smaller ®eld sizes. The Lunar DPX-L scanners
have an ``auto scan width'' option which automaticallynarrows the width of the scan path when it locates thepatient's bone mass. Using this facility will reduce thearea exposed and thus the e�ective dose.
For the femur, the greatest contributor to the EDare the ovaries, but since a large number of femalepatients are postmenopausal the radiation hazard of
concern is carcinogenesis, the genetic risk to future o�-spring no longer being a factor. Nevertheless, exclud-ing the ovaries from the calculation results in a greater
than 70% reduction in the ED and a good workingprotocol should exclude the ovaries from the scanning®eld for both femur and AP lumbar spine. This maynot be possible for the fan beam femur scans
The operator should be adequately trained in orderto be able to locate the landmark for proper position-ing. This will avoid repeated starting and terminating
of a scan. Repeat measurements should be justi®ed interms of fast bone losses, borderline bone mineral den-sity and monitoring for treatment e�cacy.
4. Problems with measuring patient and sta� dose from
absorptiometric techniques
Various detectors have been used to measure skin
entrance and depth doses from DXA. These includeionization chambers (Sorenson, 1991; Lewis et al.,1994; Njeh et al., 1997b), proportional counters
(Waker et al., 1992) GM-Tubes (Pye et al., 1990), ther-moluminescent dosimeters (such as LiF and LiBO)(Njeh et al., 1996; Njeh et al., 1997b) and ®lm
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236232

(Bezakova et al., 1997). Lithium borate (Li2B4O7:Mn)TLDs have an improved energy response compared
with lithium ¯uoride (LiF). It also has better tissueequivalence than LiF, with an e�ective atomic numberof 7.4 compared with 7.42 for tissue and 8.14 for LiF.
For the dosimetry of X-rays with energies below100 keV as used in DXA, the di�erence in e�ectiveatomic number between TLDs and tissue leads to a
di�erence in mass attenuation coe�cient and thuserrors in measured dose (Kron, 1994).The physical properties of the DXA machine pose a
number of practical problems with regards to dosim-etry. First, the dose rate during scanning is very lowand multiple scans have been used to increase the radi-ation ¯ux (Njeh et al., 1996) above the detection limit.
This is achievable for ESD but may be problematic fordepth dose as the dose rate drops exponentially. Forinstance, Njeh et al. (1997b) exposed TLDs to 60 and
167 scans for the PA spine and total body, respect-ively, using pediatric mode on a Lunar DPX-L inorder to achieve a measurable dose. For ®rst-gener-
ation DXA, the beam size is small and precise posi-tioning of the detector in relation to the small DXAbeam is required.
The accuracy of the e�ective dose estimates dependsnot only on the accuracy of the measurement of thedose rate at the surface and at depths but also on thecorrect determination of the relative positions, frac-
tions and depths of the individual radiosensitiveorgans/tissue exposed. It is apparent from the abovethat computation of e�ective doses is generally time
consuming and cumbersome. Current computer pro-grams compute EDs for common radiological examin-ation but not for BMD measurements. Huda and
Morin (1996) have suggested a method of estimatingED using ESD, kVp and ®ltration information
.
5. Summary
Osteoporosis is a consequence of decrease in bone
mass and leads to mechanical weakness of the bone.Management of this can be improved by assessment ofbone mass using absorptiometric techniques such asRA, SXA, DXA and QCT. Availability and ease of
use have made DXA the most widely used techniquefor measurements of bone density in clinical trials andepidemiological studies. Studies of radiation dose to
patients from DXA con®rms that patient dose is smallcompared to that given by many other diagnostic in-vestigations involving ionizing radiation. Despite the
increase in dose associated with the development offan beam technology patient dose is still relativelysmall. QCT gives rise to doses which are comparable
to simple radiological examination such as the chestX-ray but lower than imaging CT. Radiation dose
from other techniques such as RA and SXA are of thesame order of magnitude as pencil beam DXA.
References
Adams, J. E., 1997. Single and dual energy X-ray absorptio-
metry. Eur. Radiol. 7 (Suppl. 2), S20±S31.
Anonymous, 1993. Consensus development conference: diag-
nosis, prophylaxis and treatment of osteoporosis. Am. J.
Med. 94, 646±650.
Banks, L. M., Stevenson, J. C., 1986. Modi®ed method of
spinal computed tomography for trabecular bone mineral
measurements. J. Comput. Assist. Tomogr. 10 (3), 463±467.
Banks, L. M., Van Kuijk, C., Genant, H. K., 1995.
Radiographic Technique for Assessing Osteoporotic
Vertebral Deformity. In Vertebral Fracture in Osteoporosis,
pp. 131±147. Radiology Research and Education
Foundation, San Francisco.
Bezakova, E., Collins, P. J., Beddoe, A. H., 1997. Absorbed
dose measurements in dual energy X-ray absorptiometry
(DXA). Br. J. Radiol. 70, 172±179.
Blake, G. M., Fogelman, I., 1997. Technical principles of dual
energy X-ray absorptiometry. Semin. Nucl. Med. 27 (3),
210±228.
Blake, G. M., McKeeney, D. B., Chhaya, S. C., Ryan, P. J.
et al, 1992. Dual energy X-ray absorptiometry: the e�ects
of beam hardening on bone density measurements. Med.
Phys. 19 (2), 459±465.
Blake, G. M., Rea, J. A., Fogelman, I., 1997. Vertebral mor-
phometry studies using dual-energy X-ray absorptiometry.
Semin. Nucl. Med. 27 (3), 276±290.
Cameron, J. R., Sorenson, J. A., 1963. Measurement of bone
mineral in vivo: an improved method. Science 142, 230±232.
Cann, C. E., 1988. Quantitative CT for determination of bone
mineral density: a review. Radiology 166, 509±522.
Chapple, C. L., Faulkner, K., Lee, R. E., Hunter, E. W.,
1993. Radiation doses to paediatric patients undergoing less
common radiological procedures involving ¯uoroscopy. Br.
J. Radiol. 66 (789), 823±827.
Cooper, C., Shah, S., Hand, D. J., Adams, J. et al, 1991.
Screening for vertebral osteoporosis using individual risk
factors. The Multicentre Vertebral Fracture Study Group.
Osteoporos. Int. 2 (1), 48±53.
Cosman, F., Herrington, B., Himmelstein, S., Lindsay, R.,
1991. Radiographic absorptiometry: a simple method for
determination of bone mass. Osteoporosis Int. 2, 34±38.
Cummings, S. R., Black, D. M., Nevitt, M. C., Browner, W.
et al, 1993. Bone density at various sites for prediction of
hip fractures. The Study of Osteoporotic Fractures
Research Group. Lancet 341 (8837), 72±75.
Falcini, F., Trapani, S., Civinini, R., Capone, A. et al, 1996.
The primary role of steroids on the osteoporosis in juvenile
rheumatoid patients evaluated by dual energy X-ray
absorptiometry. J. Endocrinol. Invest. 19 (3), 165±169.
Faulkner, R. A., Bailey, D. A., Drinkwater, D. T., Wilkinson,
A. A. et al, 1993. Regional and total body bone mineral
content, bone mineral density, and total body tissue compo-
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 233
sition in children 8±16 years of age. Calcif. Tissue Int. 53
(1), 7±12.
Faulkner, K. G., McClung, M. R., Schmeer, M. S., Roberts,
L. A. et al, 1994. Densitometry of the radius using single
and dual energy absorptiometry. Calcif. Tissue Int. 54,
208±211.
Franck, H., Munz, M., Scherrer, M., 1995. Evaluation of
dual-energy X-ray absorptiometry bone mineral measure-
ment Ð comparison of a single-beam and fan-beam design:
the e�ect of osteophytic calci®cation on spine bone mineral
density. Calcif. Tissue Int. 56 (3), 192±195.
Genant, H. K., Boyd, D. P., 1977. Quantitative bone mineral
analysis using dual energy computed tomography. Invest.
Radiol. 12, 545±551.
Genant, H. K., Cann, C. E., Ettinger, B., Gordan, G. S.,
1982. Quantitative computed tomography of vertebral
spongiosa: A sensitive method for detecting early bone loss
after oophorectomy. Ann. Int. Med. 97 (5), 699±705.
Genant, H. K., Engelke, K., Fuerst, T., Gluer, C. C. et al,
1996. Noninvasive assessment of bone mineral and struc-
ture: state of the art. J. Bone Miner. Res. 11 (6), 707±730.
Gluer, C. C., Jergas, M., Hans, D., 1997. Peripheral measure-
ment techniques for the assessment of osteoporosis. Semin.
Nucl. Med. 27 (3), 229±247.
GluÈ er, C. C., Reiser, U. J., Davis, C. A., Rutt, B. K. et al,
1988. Vertebral mineral determination by quantitative com-
puted tomography (QCT): Accuracy of single and dual
energy measurements. J. Comput. Assist. Tomogr. 12 (2),
242±258.
Hart, D., Jones, D. G., Wall, B. F., 1996. Coe�cient for
Estimating E�ective Doses from Pediatric X-Ray
Examinations. London, NRPB (HMSO).
Herd, R. J., Blake, G. M., Parker, J. C., Ryan, P. J. et al,
1993. Total body studies in normal British women using
dual energy X-ray absorptiometry. Br. J. Radiol. 66 (784),
303±308.
Hodgskinson, R., Njeh, C. F., Currey, J. D., Langton, C. M.,
1997. The ability of ultrasound velocity to predict the sti�-
ness of cancellous bone in vitro. Bone 21 (2), 183±190.
Huda, W., Morin, R. L., 1996. Patient doses in bone mineral
densitometry. Br. J. Radiol. 69 (821), 422±425.
Huddleston, A. L., 1988. Quantitative Methods in Bone
Densitometry. Kluwer Academic Publisher, Boston.
ICRP, 1977. International Commission on Radiological
Protection, ICRP Publication 26. Pergammon Press,
Oxford.
ICRP, 1991. International Commission on Radiological
Protection, ICRP Publication 60: 1990 recommendations of
the International Commission on Radiological Protection.
Pergammon Press, Oxford.
IRR, 1985. The Ionising Radiation Regulations. HMSO,
London.
IRR, 1988. The Ionising Radiation (protection of Persons
undergoing Medical Examination) Regulations. HMSO,
London.
Jergas, M., Breitenseher, M., GluÈ er, C. C., Black, D., et al.,
1995. Which vertebrae should be assessed using lateral
dual-energy X-ray absorptiometry of the lumbar spine?
Osteoporosis Int., 5, 196±204; in press.
Jessen, K. A., Shrimpton, P. C., Geleijns, J., Panzer, W.,
Tosi, G., 1998. Dosimetry and patient doses in computed
tomography. This volume (Internal Reference).
Kaisel, W., RuÈ egsegger, P., 1991. 3D-QCT at peripheral
measuring sites. Osteoporosis Int. 1, 193.
Kalender, W. A., 1992. E�ective dose values in bone mineral
measurements by photon absorptiometry and computed
tomography. Osteoporos Int. 2 (2), 82±87.
Kalender, W. A., Brestowsky, H., Felsenberg, D., 1988. Bone
mineral measurements: automated determination of the
midvertebral CT section. Radiology 168, 219±221.
Karantanas, A. H., Kalef-Ezra, J. A., Glaros, D. C., 1991.
Quantitative computed tomography for bone mineral
measurement: technical aspects, dosimetry, normal data
and clinical applications. Br. J. Radiol. 64 (760), 298±304.
Kelly, T., Slovick, D., Schoen®eld, D., Neer, R., 1988.
Quantitative digital radiography vs dual photon absorptio-
metry of the lumbar spine. J. Clin. Endocr. Metab. 67,
839±844.
Kelly, T. L., Crane, G., Baran, D. T., 1994. Single X-ray
absorptiometry of the forearm: precision, correlation, and
reference data. Calcif. Tissue Int. 54 (3), 212±218.
Kelsey, J. L., Ho�man, S., 1987. Risk factors for hip fracture
[editorial]. New Engl. J. Med. 316 (7), 404±406.
Koo, W. W., Walters, J., Bush, A. J., 1995. Technical con-
siderations of dual-energy X-ray absorptiometry-based
bone mineral measurements for pediatric studies. J. Bone
Miner. Res. 10 (12), 1998±2004.
Kron, T., 1994. Thermoluminescence dosimetry and its appli-
cations in medicine Ð Part 1: Physics, materials and equip-
ment. Australas. Phys. Eng. Sci. Med. 17 (4), 175±199.
Kyriou, J. C., Fitzgerald, M., Pettett, A., Cook, J. V. et al,
1996. A comparison of doses and techniques between
specialist and non-specialist centres in the diagnostic X-ray
imaging of children. Br. J. Radiol. 69 (821), 437±450.
Lang, T. F., Keyak, J. H., Heitz, M. W., Augat, P. et al,
1997. Volumetric quantitative computed tomography of the
proximal femur: precision and relation to bone strength.
Bone 21 (1), 101±108.
Laskey, M. A., 1996. Dual-energy X-ray absorptiometry and
body composition. Nutrition 12 (1), 45±51.
Lewis, M. K., Blake, G. M., Fogelman, I., 1994. Patient dose
in dual X-ray absorptiometry. Osteoporos. Int. 4 (1), 11±
15.
Martin, C. J., Farquhar, B., Stockdale, E., MacDonald, S.,
1994. A study of the relationship between patient dose and
size in paediatric radiology. Br. J. Radiol. 67 (801), 864±
871.
Masud, T., Mootoosamy, I., McCloskey, E. V., O'Sullivan,
M. P. et al, 1996. Assessment of osteopenia from spine
radiographs using two di�erent methods: the Chingford
Study. Br. J. Radiol. 69 (821), 451±466.
Matsumoto, C., Kushida, K., Yamazaki, K., Imose, K. et al,
1994. Metacarpal bone mass in normal and osteoporotic
Japanese women using computed X-ray densitometry.
Calcif. Tissue Int. 54, 324±329.
Mazess, R. B., Barden, H. S., 1987. Single- and dual photon
absorptiometry for bone measurement in osteoporosis.
Osteoporosis Update, pp. 73±80. Radiology Research and
Education Foundation, San Francisco.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236234
Miller, P. D., Bonnick, S. L., Rosen, C. J., Altman, R. D. et
al, 1996. Clinical utility of bone mass measurements in
adults: consensus of an international panel. The Society for
Clinical Densitometry. Semin. Arthritis Rheum. 25 (6),
361±372.
Morgan, D. B., Spiers, F. W., Pulvertaft, C. N., Fourman, P.,
1967. The amount of bone in the metacarpal and phalanx
according to age and sex. Clin. Radiol. 18, 101±108.
Muller, A., Ruegsegger, E., Ruegsegger, P., 1989. Peripheral
QCT: a low-risk procedure to identify women predisposed
to osteoporosis. Phys. Med. Biol. 34 (6), 741±749.
Njeh, C. F., Apple, K., Temperton, D. H., Boivin, C. M.,
1996. Radiological assessment of a new bone densitometer
Ð the Lunar EXPERT. Br. J. Radiol. 69 (820), 335±340.
Njeh, C. F., Boivin, C. M., Langton, C. M., 1997a. The role
of ultrasound in the assessment of osteoporosis: a review.
Osteoporos. Int. 7 (1), 7±22.
Njeh, C. F., Samat, S. B., Nightingale, A., McNeil, E. A. et
al, 1997b. Radiation dose and in vitro precision in paedia-
tric bone mineral density measurement using dual X-ray
absorptiometry. Br. J. Radiol. 70 (835), 719±727.
NOF, 1997. Boning Up on Osteoporosis: A Guide to
Prevention and Treatment. National Osteoporosis
Foundation, Washington, DC.
NRPB, 1993. Documents of the NRPB, Vol. 4, Occupational,
public and medical Exposure. National Radiological
Protection Board, Chilton.
Patel, R., Blake, G. M., Batchelor, S., Fogelman, I., 1996a.
Occupational dose to the radiographer in dual X-ray
absorptiometry: a comparison of pencil-beam and fan-beam
systems. Br. J. Radiol. 69 (822), 539±543.
Patel, R., Lewis, M. K., Blake, G. M., Batchelor, S., et al.,
1996b. New Generation DXA scanners increase dose to
patients and sta�. In Current Research in Osteoporosis and
Bone Mineral Measurement IV, p. 99. British Institute of
radiology, London.
Peel, N. F., Spittlehouse, A. J., Bax, D. E., Eastell, R., 1994.
Bone mineral density of the hand in rheumatoid arthritis.
Arthritis Rheum. 37 (7), 983±991.
Pietrobelli, A., Formica, C., Wang, Z., Heyms®eld, S. B.,
1996. Dual-energy X-ray absorptiometry body composition
model: review of physical concepts. Am. J. Physiol. 271 (6
Pt 1), E941±E951.
Prudham, D., Evans, J. G., 1981. Factors associated with falls
in the elderly: a community study. Age Ageing 10 (3), 141±
146.
Pye, D. W., Hannan, W. J., Hesp, R., 1990. E�ect dose equiv-
alent in dual X-ray absorptiometry [letter]. Br. J. Radiol. 63
(746), 149.
Rawling, D. J., Faulkner, K., Chapple, C. L., 1992. The in¯u-
ence of scan time on patient dose and precision in bone
mineral densitometry. In Current Research in Osteoporosis
and Bone Mineral Measurement II, pp. 23±24. British
Institute of Radiology, London.
Rawlings, D. J., Warren, H., Faulkner, K., 1996.
Performance and acceptance testing of morphometric soft-
ware. In Current Research in Osteoporosis and Bone Mineral
Measurement, p. 97. British Institute of Radiology,
London.
Richardson, R. B., 1990. Past and revised risk estimates for
cancer induced by irradiation and their in¯uence on dose
limits. Br. J. Radiol. 63 (748), 235±245.
Ross, P. D., Davis, J. W., Vogel, J. M., Wasnich, R. D.,
1990. A critical review of bone mass and the risk of frac-
tures in osteoporosis [see comments]. Calcif. Tissue Int. 46
(3), 149±161.
Ruiz, M. J., Gonzalez, L., Vano, E., Martinez, A., 1991.
Measurement of radiation doses in the most frequent simple
examinations in paediatric radiology and its dependence on
patient age. Br. J. Radiol. 64 (766), 929±933.
Rupich, R. C., Gri�n, M. G., Paci®ci, R., Avioli, L. V. et al,
1992. Lateral dual-energy radiography: artifact error from
rib and pelvic bone. J. Bone Min. Res. 7 (1), 97±101.
Seeman, E., Young, N., Szmukler, G., Tsalamandris, C. et al,
1993. Risk factors for osteoporosis. Osteoporos Int. 3
(Suppl. 1), 40±43.
Shrimpton, P. C., Jones, D. G., Hillier, M. C., Wall, B. F., et
al., 1991. Survey of CT Practice in The U.K. Part 2:
Dosimetric Aspects. London, NRPB, Chilton.
Shrimpton, P. C., Wall, B. F., Hart, D., 1998. Diagnostic
medical exposures in the U.K. Applied Radiation and
Isotopes 50, 261±269.
Sorenson, J. A., 1991. Relationship between patient exposure
and measurement precision in dual-photon absorptiometry
of the spine. Phys. Med. Biol. 36 (2), 169±176.
Starritt, H. C., Elvins, D. M., Ring, F. J., 1996. Radiation
dose and the hologic acclaim X-ray bone densitometer. In
Current Research in Osteoporosis and bone mineral measure-
ment IV, pp. 99±100. British Institute of Radiology,
London.
Steiger, P., Cummings, S. R., Genant, H. K., Weiss, H., 1994.
Morphometric X-ray absorptiometry of the spine: corre-
lation in vivo with morphometric radiography. Osteoporosis
Int. 4, 238±244.
Stewart, S. P., Milner, D., Moore, A. C., Emery, P., et al.,
1996. Preliminary report on the lunar Expert-XL Imaging
densitometer: dosimetry, precision and cross calibration. In
Current Research in Osteoporosis and Bone Mineral
Measurement IV, pp. 101±102. British Institute of
Radiology, London.
Trouerbach, W. T., BirkenhaÈ ger, J. C., Collette, B. J. A.,
Drogendijk, A. C. et al, 1987. A study on the phalanx bone
mineral content in 273 normal pre- and post-menopausal
females (transverse study of age-dependent bone loss). Bone
Mineral 3, 53±62.
van Kuijk, C., Grashuis, J. L., Steenbeek, J. C. M., SchuÈ tte,
H. E. et al, 1990. Evaluation of postprocessing dual-energy
methods in quantitative computed tomography. Part 2.
Practical Aspects. Invest. Radiol. 25, 882±889.
Vogel, J. M., Wasnich, R. D., Ross, P. D., 1988. The clinical
relevance of calcaneus bone mineral measurements: a
review. Bone Miner. 5 (1), 35±58.
Wahner, H. W., Fogelman, I., 1994. The Evaluation of
Osteoporosis: Dual Energy X-Ray Absorptiometry in
Clinical Practice. Martin Dunitz Ltd., London, U.K.
Waker, A. J., Oldroyd, B., Marco, M., 1992. The application
of microdosimetry in clinical bone densitometry using a
dual-photon absorptiometer. Br. J. Radiol. 65 (774), 523±
527.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236 235

Yamada, M., Ito, M., Hayashi, K., Ohki, M. et al, 1994.
Dual energy X-ray absorptiometry of the calcaneus:
Comparison with other techniques to assess bone density
and value in predicting risk of spine fracture. AJR 163 (12),
1435±1440.
Yang, S. O., Hagiwara, S., Engelke, K., Dhillon, M. S. et al,
1994. Radiographic absorptiometry for bone mineral
measurement of the phalanges: precision and accuracy
study. Radiology 192 (3), 857±859.
Yu, W., GluÈ er, C. C., Grampp, S., Jergas, M. et al, 1994.
Spinal bone mineral assessment in postmenopausal women:
a comparison between dual X-ray absorptiometry and
quantitative computed tomography. J. Bone Miner. Res. 9
(Suppl. 1), S406.
C.F. Njeh et al. / Applied Radiation and Isotopes 50 (1999) 215±236236
Top Related
Copyright © 2022 FDOKUMEN

