






Bahasa
Halaman
Hukum


Principle of Surgical OncologyPrinciple of Surgical Oncology
Woramin Riansuwan, M.D.Colorectal Surgery Unit
Division of General SurgeryDepartment of Surgery
Faculty of Medicine Siriraj Hospital

Multidisciplinary TeamMultidisciplinary Team
SurgeonsMedical oncologistsRadiation oncologistsReconstructive SurgeonsPathologistsRadiologistsPrimary Care Physicians

DefinitionsDefinitionsPrimary (or definitive) therapyen bloc resection of tumor with adequate margins of normal tissues and in some cases regional lymph nodesAdjuvant therapyrefers to radiation therapy and systemic therapies, including chemotherapy, immunotherapy, hormonal therapy, and increasingly, biologic therapy.

Goals of TreatmentGoals of Treatment
Primary goal of surgical and radiation therapy: local and regional control
Primary goal of systemic therapies : systemic control by treating distant foci of subclinical disease to prevent recurrence.

Cancer EpidemiologyCancer Epidemiology

Cancer EpidemiologyCancer Epidemiology

Ten most common cancer in Thai maleTen most common cancer in Thai male
2007 Thailand NCI Cancer Registry

Ten most common cancer in Thai femaleTen most common cancer in Thai female
2007 Thailand NCI Cancer Registry

Trends in Cancer Incidence and MortalityTrends in Cancer Incidence and Mortality

Acquired Capabilities of CancerAcquired Capabilities of Cancer
Cell, Vol. 100, 57–70, January 7, 2000,

MetastaticMetastatic ProcessProcess

Three steps of Three steps of TumorigenesisTumorigenesis: initiation, promotion & : initiation, promotion & progressionprogression
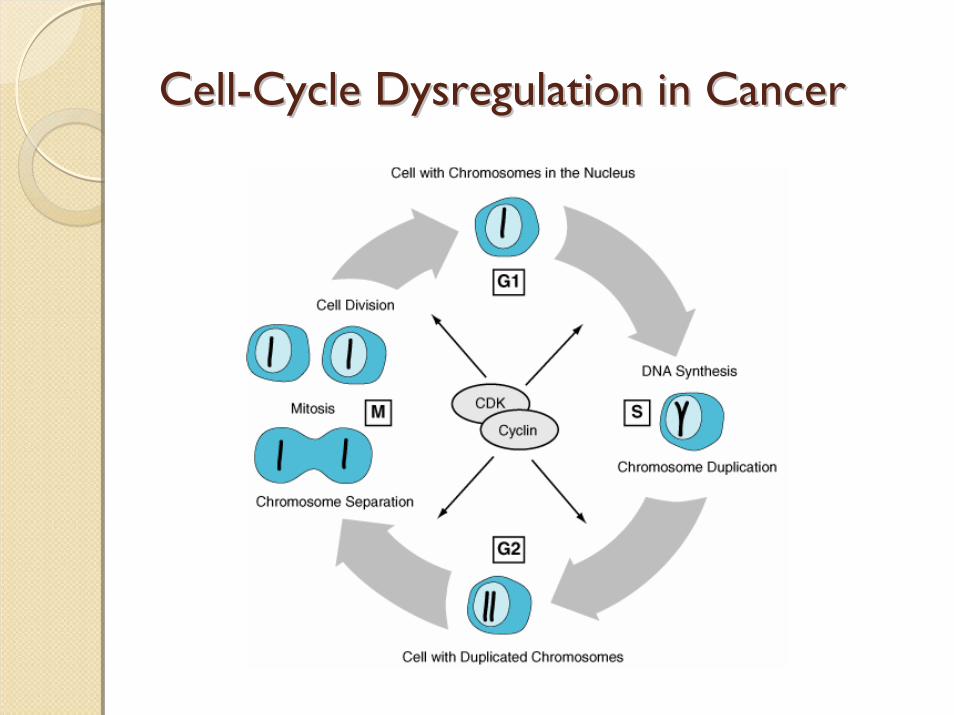
CellCell--Cycle Cycle DysregulationDysregulation in Cancerin Cancer

Cancer EtiologyCancer Etiology
Genes Carcinogens
Cancer

GenesGenes
Oncogenes
Tumor Suppressor Genes

Genes Associated with Hereditary CancerGenes Associated with Hereditary Cancer
Genes Syndrome
APC Familial adenomatous polyposis(FAP)
BMPRIA Juvenile polyposis coli
BRCA1 Breast/ovarian syndrome
BRCA2 Breast/ovarian syndrome
hMLH1; hMSH2; hMSH6; hPMS1; hPMS2
Hereditary nonpolyposiscolorectal cancer

Criteria suggest of Hereditary Cancer Criteria suggest of Hereditary Cancer
Tumor development at a much younger age than usualPresence of bilateral diseasePresence of multiple primary malignanciesPresentation of a cancer in the less affected
sex (e.g., male breast cancer)Clustering of the same cancer type in relativesCancer associated with other conditions such
as mental retardation or pathognomonic skin lesions

CarcinogensCarcinogens
Chemical CarcinogensPhysical CarcinogensViral Carcinogens

IARC Group 1 Chemical CarcinogensIARC Group 1 Chemical CarcinogensChemical Predominant Tumor Type
Aflatoxins Liver cancer
Arsenic Skin cancer
Benzene Leukemia
Benzidine Bladder cancer
Ethylene oxide Leukemia, lymphoma
Estrogen replacement therapy Endometrial cancer, breast cancer
Tamoxifen Endometrial cancer
Tobacco smoke Lung cancer, oral cancer, pharyngeal cancer, laryngeal cancer, esophageal cancer (squamous cell, pancreatic cancer, bladder cancer, liver cancer, renal cell carcinoma, cervical cancer, leukemia)

Selected Viral CarcinogensSelected Viral CarcinogensVirus Predominant Tumor Typeb
Burkitt's lymphomaHodgkin's diseaseImmunosuppression-related lymphomaSinonasal angiocentric T-cell lymphoma
Epstein-Barr virus
Nasopharyngeal carcinomaHepatitis B Hepatocellular carcinoma
Hepatitis C Hepatocellular carcinoma
Kaposi's sarcomaHuman immunodeficiency virus-1
Non-Hodgkin's lymphoma
Cervical cancerHuman papillomavirus types 16 and 18
Anal cancer
Human T-cell lymphotropic viruses Adult T-cell leukemia/lymphoma
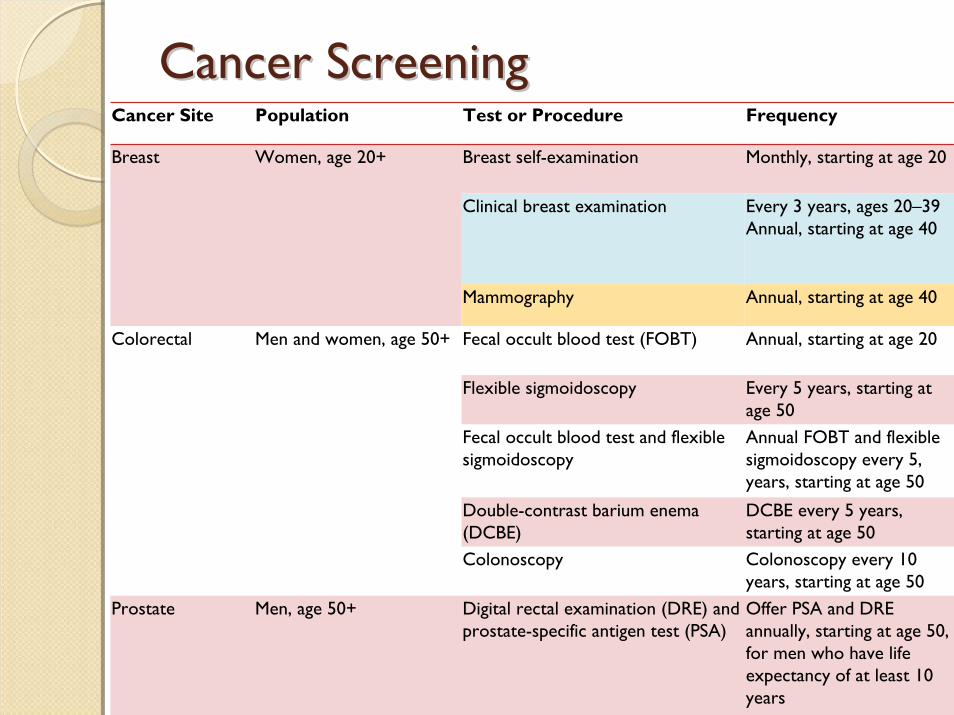
Cancer ScreeningCancer ScreeningCancer Site Population Test or Procedure Frequency
Breast self-examination Monthly, starting at age 20
Clinical breast examination Every 3 years, ages 20–39Annual, starting at age 40
Breast Women, age 20+
Mammography Annual, starting at age 40
Fecal occult blood test (FOBT) Annual, starting at age 20
Flexible sigmoidoscopy Every 5 years, starting at age 50
Fecal occult blood test and flexible sigmoidoscopy
Annual FOBT and flexible sigmoidoscopy every 5, years, starting at age 50
Double-contrast barium enema (DCBE)
DCBE every 5 years, starting at age 50
Colorectal Men and women, age 50+
Colonoscopy Colonoscopy every 10 years, starting at age 50
Prostate Men, age 50+ Digital rectal examination (DRE) and prostate-specific antigen test (PSA)
Offer PSA and DRE annually, starting at age 50, for men who have life expectancy of at least 10 years

Cancer StagingCancer StagingAmerican Joint Committee on Cancer (AJCC) Union Internationale Contre Cancer (International Union Against Cancer, UICC)three components: Primary tumor (T), Nodal metastases (N), Distant metastases (M)Clinical staging (cTNM or TNM), Pathologic staging (pTNM), re-treatment (rTNM) or autopsy staging (aTNM)
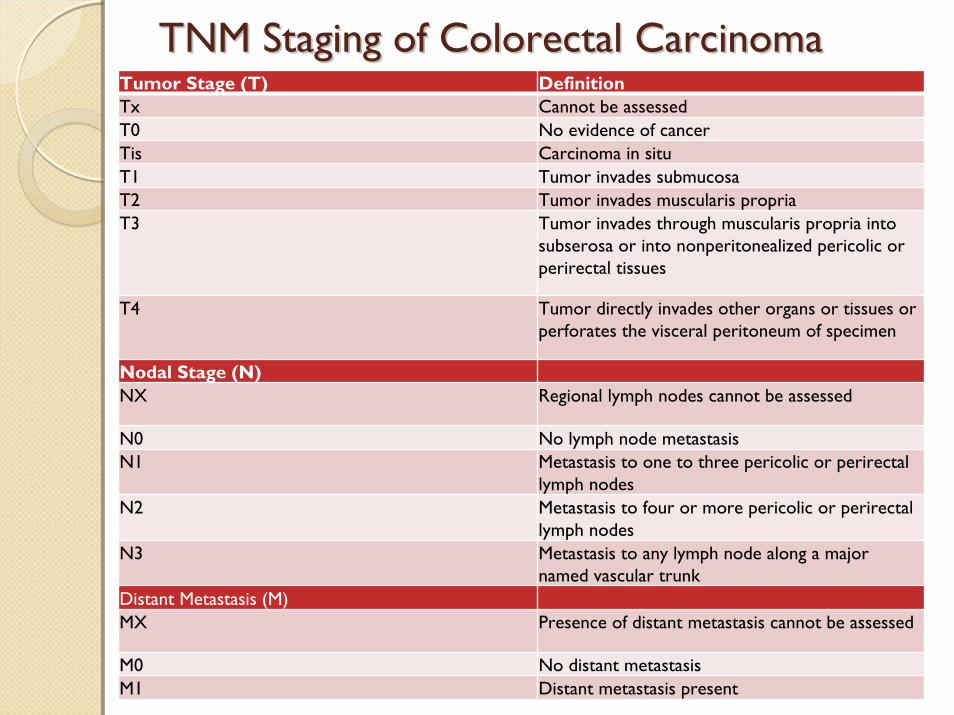
TNM Staging of Colorectal CarcinomaTNM Staging of Colorectal CarcinomaTumor Stage (T) DefinitionTx Cannot be assessedT0 No evidence of cancerTis Carcinoma in situT1 Tumor invades submucosaT2 Tumor invades muscularis propriaT3 Tumor invades through muscularis propria into
subserosa or into nonperitonealized pericolic or perirectal tissues
T4 Tumor directly invades other organs or tissues or perforates the visceral peritoneum of specimen
Nodal Stage (N)NX Regional lymph nodes cannot be assessed
N0 No lymph node metastasisN1 Metastasis to one to three pericolic or perirectal
lymph nodesN2 Metastasis to four or more pericolic or perirectal
lymph nodesN3 Metastasis to any lymph node along a major
named vascular trunkDistant Metastasis (M)MX Presence of distant metastasis cannot be assessed
M0 No distant metastasisM1 Distant metastasis present

TNM Staging of Colorectal Cancer and 5TNM Staging of Colorectal Cancer and 5--Year SurvivalYear Survival
Stage TNM 5-Year Survival
I T1-2, N0, M0 70–95%
II T3-4, N0, M0 54–65%
III Tany, N1-3, M0 39–60%
IV Tany, Nany, M1 0–16%

Tumor MarkersTumor MarkersMarker Cancer Sensitivity Specificity
PSA (4 g/L) Prostate 57–93% 55–68%
CEA Colorectal 40–47% 90%
Breast 45% 81%
Recurrent disease 84% 100%
AFP Hepatocellular 98% 65%
CA 19-9 Pancreatic 78–90% 95%
CA 27-29 Breast 62% 83%
CA 15-3 Breast 57% 87%

Roles of Surgery in CancerRoles of Surgery in Cancer
Prevention of CancerDiagnosis of CancerTreatment of Cancer

Prevention of CancerPrevention of Cancer
Some underlying conditions Congenital or Genetic traits
high incidence of subsequent cancer

Familial Adenomatous Polyposis (FAP)Familial Adenomatous Polyposis (FAP)
50% develop colon cancer by age of 40.By age 70, virtually all develop colon cancerprophylactic proctocolectomy before age 20 to prevent CRC is advised for who carry APC gene

Ulcerative Colitis (UC)Ulcerative Colitis (UC)40% of UC (Pancolitis) die of colon cancer 3% of children with UC develop colon cancer by the age of 10, and 20% develop cancer during each ensuing decadeColectomy is indicated for patients with ulcerative colitis if the chronicity of this disease is well established.
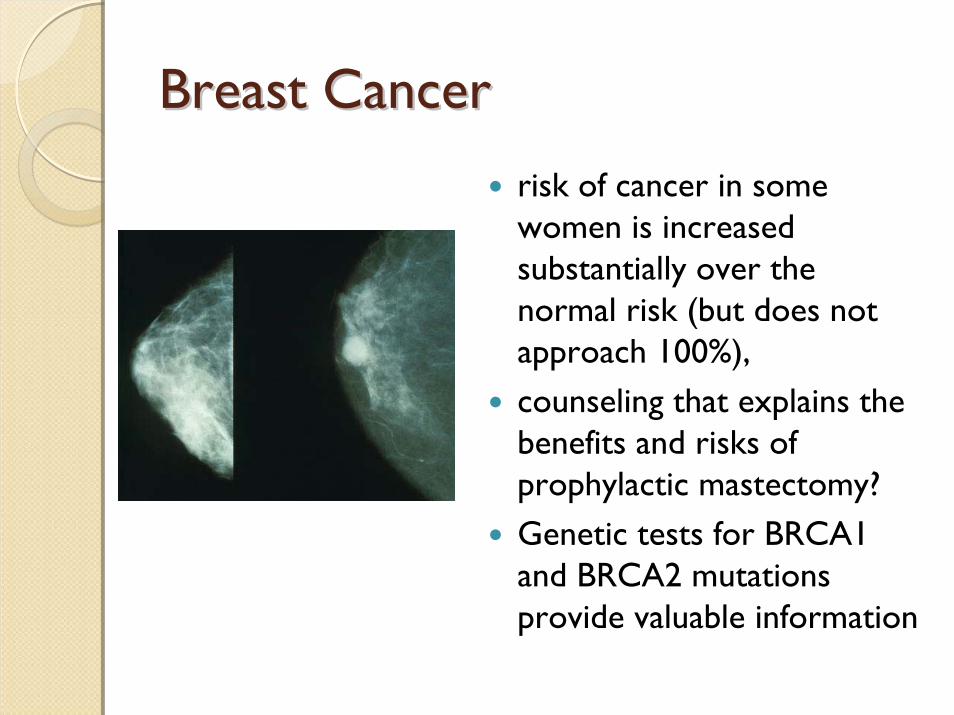
Breast CancerBreast Cancer
risk of cancer in some women is increased substantially over the normal risk (but does not approach 100%),counseling that explains the benefits and risks of prophylactic mastectomy?Genetic tests for BRCA1 and BRCA2 mutations provide valuable information
Diagnosis of CancerDiagnosis of Cancer
Acquisition of tissue for exact histologic diagnosis
Biopsy

BiopsyBiopsy
Aspiration BiopsyNeedle BiopsyIncisional BiopsyExcisional Biopsy

Aspiration BiopsyAspiration Biopsy
Needle BiopsyNeedle Biopsy
A core of tissue is obtained through a specially designed needle introduced into the suspect tissue. The core of tissue provided by needle biopsy is sufficient for the diagnosis of most tumor types. Soft tissue and bony sarcomas often present major difficulties in differentiating benign and reparative lesions from malignancies and often cannot be diagnosed accurately.Needle tract tumor seeding ???

Imaging Guide BiopsyImaging Guide Biopsy
U/S guide biopsy CT guide biopsy
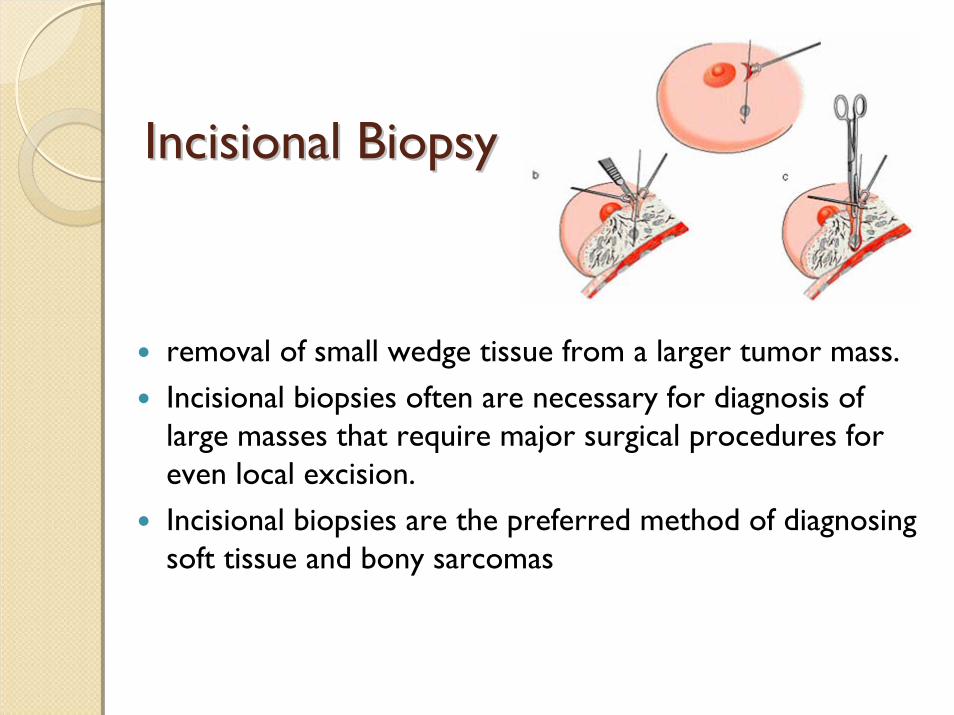
IncisionalIncisional BiopsyBiopsy
removal of small wedge tissue from a larger tumor mass.Incisional biopsies often are necessary for diagnosis of large masses that require major surgical procedures for even local excision.Incisional biopsies are the preferred method of diagnosing soft tissue and bony sarcomas
ExcisionalExcisional BiopsyBiopsy
excision of entire suspected tumor tissue with little or no margin of surrounding normal tissue Excisional biopsy is the procedure of choice for most tumors if it can be performed without contaminating new tissue planes or further compromising the ultimate surgical proceduree.g. Lymph node biopsy

EndoscopicEndoscopic BiopsyBiopsy
Incisional Biopsy Excisional biopsy(Polypectomy)

Principles of Surgical Biopsy (1)Principles of Surgical Biopsy (1)
Needle tracks or scars should be placed carefully so that they can be conveniently removed as part of the subsequent definitive surgical procedure. Care should be taken to avoid contaminating new tissue planes during the biopsy procedure. It is not uncommon to take biopsy samples from several suspected lesions at one time. Care should be taken to avoid using instruments that may have come in contact with tumor when obtaining tissue from a potentially uncontaminated area.

Principles of Surgical Biopsy (2)Principles of Surgical Biopsy (2)Adequate tissue samples must be obtained to meet the needs of the pathologist. mark distinctive areas of the tumor carefully to facilitate subsequent orientation of the specimen by the pathologist. Certain fixatives are best suited to specific types or sizes of tissue..Placement of radiopaque clips during biopsy and staging procedures is sometimes important to delineate areas of known tumor and to guide the subsequent delivery of radiation therapy to these areas.

Treatment of CancerTreatment of Cancer
Curative Resection of Primary CancerCytoreductive SurgeryMetastatic DiseaseOncologic EmergenciesPalliationReconstruction and Rehabilitation

Surgical Challenges in Curative Treatment of Solid TumorsSurgical Challenges in Curative Treatment of Solid Tumors
Identification of patients who cured by local treatment alone;Best balance between local cure vs. morbidity and the QoL of treatmentApply adjuvant treatments which improve the local control and distant metastasis.
cancer type and the site of involvement
Vary in selection of the appropriate local therapy in cancer treatment

Definitive surgical therapy with sufficient Definitive surgical therapy with sufficient margins is sufficient local therapymargins is sufficient local therapy
wide excision of primary melanomas of skin can be cured locally by surgery alone in 90% of cases. The resection of colon cancers with a 5-cm margin from the tumor results in anastomoticrecurrences in fewer than 5% of cases.

Surgery obtain histology confirmation of diagnosisSurgery obtain histology confirmation of diagnosis
primary local therapy is achieved through nonsurgical modality
( e.g. Radiation Therapy)
Long bones Ewing's sarcoma Nasopharyngeal Cancer

Lymphatic mapping & sentinel lymph node biopsyLymphatic mapping & sentinel lymph node biopsy

The magnitude of surgical resection is The magnitude of surgical resection is modified when use of modified when use of NeoadjuvantNeoadjuvant treatmenttreatment
Surgery alone : 5yr survival rates is 10% - 20%
NeoadjuvantRadiation therapy combined with Chemotherapy. :long-term cure rates are now 80%.
Rhabdomyosarcoma

CytoreductiveCytoreductive SurgerySurgery
extensive local spread of cancer precludes the removal of all gross disease by surgerypartial surgical resection of bulk disease in selected cancers improves the ability of other treatment modalities to control unresectableresidual gross disease.cytoreductive surgery is of benefit only when other effective treatments are available to control unresectable. residual disease
Burkitt's lymphoma
Ovarian Cancer

MetastaticMetastatic DiseaseDiseaseSingle site of metastatic disease that can be resected without major morbidity should undergo resectionLimited lung, liver or brain metastases can be cured by surgical resection. Appropriate for cancers that not respond well to systemic chemotherapy.resection of colorectal hepatic metastases, in whom the liver is the only site metastasis can lead to long-term cure in 25%.

OncologicOncologic EmergenciesEmergencies
Exsanguinating HemorrhagePerforationDrainage of AbscessesImpending Destruction of Vital Organs

OncologicOncologic Emergencies: HemorrhageEmergencies: Hemorrhage

OncologicOncologic Emergencies : AEmergencies : Advanced Cancerdvanced Cancer
Non-Surgical Intervention
Endoscopic Therapy
Intervention Radiology
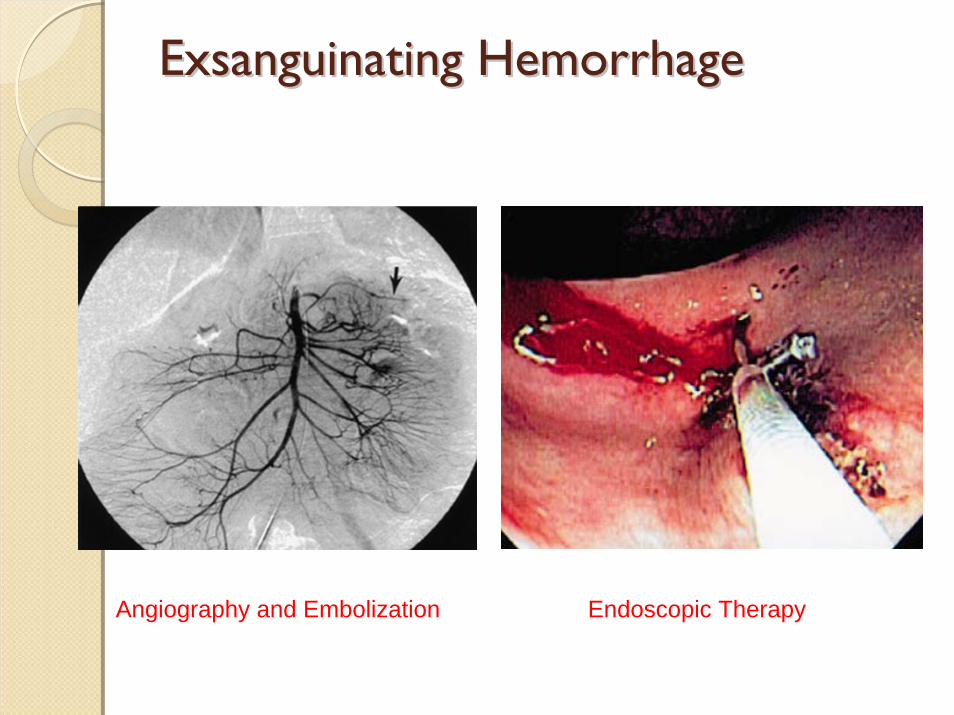
ExsanguinatingExsanguinating HemorrhageHemorrhage
Angiography and Embolization Endoscopic Therapy

Drainage of Abscesses : Drainage of Abscesses : PercutaneousPercutaneous DrainageDrainage

PalliationPalliation
Relief of Pain Relief of Functional Abnormalities(Relieve mechanical problems e.g. intestinal obstruction)
Improve the Quality of Life
Advances Stage : Non Surgical Intervention

Palliation: PainPalliation: Pain
Pain MedicationsNerve BlockEpidural BlockCeliac Ganglion Block: EUS guidePain Clinic
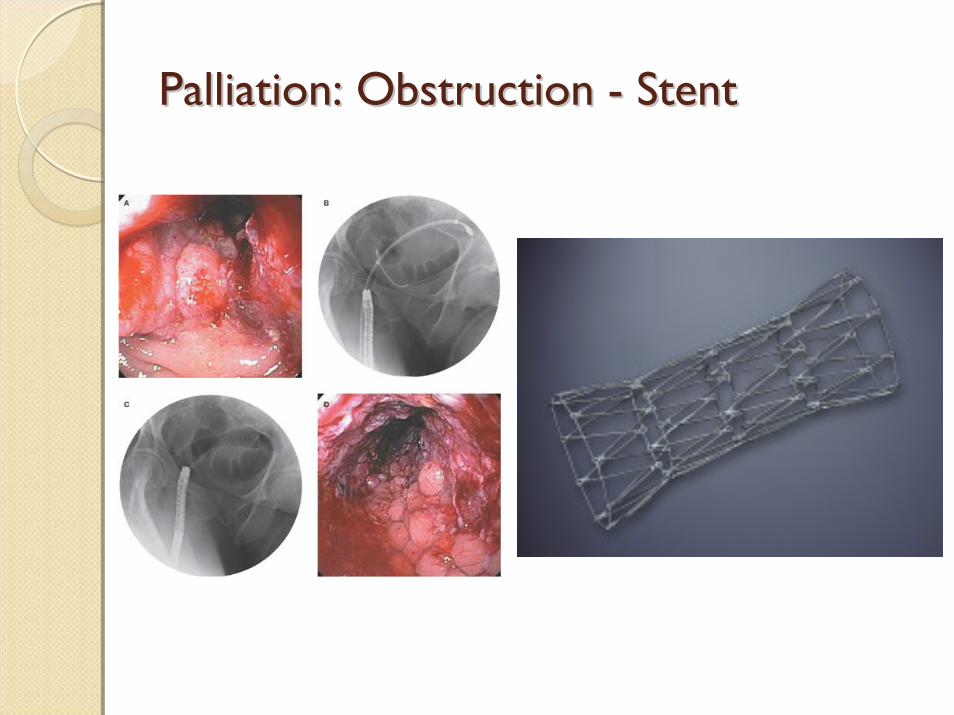
Palliation: Obstruction Palliation: Obstruction -- StentStent

Reconstruction and RehabilitationReconstruction and Rehabilitation
Reconstruction and rehabilitation after definitive TxImprove function and cosmetic appearanceFree flaps using microvascular anastomotic techniques is having a profound impact on the ability to bring fresh tissue to resected or heavily irradiated areas.Lost function (especially of extremities) often can be restored by surgical approaches. Lysis of contractures or muscle transposition to restore muscular function damaged by previous surgery or radiation therapy.

Reconstruction and RehabilitationReconstruction and Rehabilitation

Thank YouThank You
Top Related
Copyright © 2022 FDOKUMEN

