







Bahasa
Halaman
Hukum


Predictors of Fluoroscopy Time during Percutaneous Nephrolithotomy: Impact of
Postgraduate Urology Trainees and S.T.O.N.E. Nephrolithometry Score
Yasser A. Noureldin1,2
Mohamed A. Elkoushy,1,3
Sero Andonian1
1Division of Urology, McGill University Health Centre, Montreal, Québec, Canada
2Department of Urology, Benha University Hospital, Benha University, Benha, Egypt
3Department of Urology, Suez Canal University, Ismailia, Egypt
Corresponding Author:
Sero Andonian, MD, MSc, FRCS(C), FACS
Assistant Professor of Urology,
McGill University Health Centre
687 Pine Ave. West, Suite S6.92
Montreal, Québec, Canada H3A 1A1
Tel: 514-843-2865; Fax: 514-843-1552
E-mail: [email protected]
Word count:
Abstract: 276
Manuscript: 2323
Key words: Percutaneous nephrolithotomy, Fluoroscopy, Ionizing Radiation, and
Scoring Method.
Acknowledgements: This work was supported by grants from Fonds de la Recherche en
Santé du Québec (FRSQ) to Dr Sero Andonian.
Conflict of Interest: None.
Page 1 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
1
1
ABSTRACT
Objectives: To determine predictors of Fluoroscopy Time (FT) during Percutaneous
Nephrolithotomy (PCNL) and assess the impact of urology Post-Graduate Trainees
(PGTs) and S.T.O.N.E. Nephrolithometry Score.
Methods: A prospective review of patients undergoing PCNL between 2010 and 2013 at
a tertiary health care centre was performed. Patients’ demographics, stone characteristics,
including S.T.O.N.E. Nephrolithometry Score, and operative data were compared among
PGTs. Predictors of FT were determined using univariate and multivariate models.
Results: A total of 103 PCNLs were assisted by 10 PGTs from Post-Graduate Years
(PGY) 4 and 5 [37 (35.9%) and 66 (64.1%) cases, respectively)]. Sixty percent of patients
were males with a mean age of 55.2±1.5 years and a mean BMI of 26.4±0.5 kg/m2. The
mean S.T.O.N.E score was 7.7±0.1, with tubeless PCNL in 53 (51.5%) cases. The mean
FT was 120±5 seconds, mean operative time was 102±3.5 minutes and mean length of
hospital stay was 4.2±0.34 days. The overall stone-free rate was 72.8%. PGY-5 trainees
used significantly less FT than PGY-4 trainees (115±6 vs. 130±7 sec; p=0.04). FT
significantly correlated with the number of involved calyces (r= 0.24, p= 0.02), number
of punctures (r=0.6, p=0.01), number of tracts (r=0.4; p=0.01), and operative time (r=0.4,
p=0.01). In addition, cases with estimated blood loss (EBL) <250 mL were associated
with significantly less FT than those with blood loss >250 mL (109±5.1 vs. 148.2±10.9
sec; p=0.001). On multivariate analysis, the number of punctures, EBL and operative
time were found to be independent predictors for FT. However, there was no correlation
of FT with S.T.O.N.E. Nephrolithometry Score (r=0.16; p=0.1).
Page 2 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
2
2
Conclusions: The number of punctures, EBL and operative time were the only
independent predictors of prolonged FT during PCNL.
Page 3 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
3
3
INTRUDUCTION
Since Percutaneous Nephrolithotomy (PCNL) was introduced in 1976 1, it has
become a widely-accepted option for management of large renal stones due to its high
success rate, low morbidity and early convalescence.2,3
However, it is associated with the
highest radiation exposure among the different endourological procedures.4 Therefore, it
is important to identify factors associated with increased Fluoroscopy Time (FT) and
Effective Radiation Dose (ERD) during PCNL. There are only two previous studies
examining this relationship. While Tepeler et al found that FT was significantly
prolonged in patients with increased stone burden and multiple access tracts, Mancini et
al found that increased Body Mass Index (BMI), stone burden, and multiple access tracts
were associated with increased ERD.5,6
The S.T.O.N.E. Nephrolithometry Score has been
recently described as an objective assessment tool for pre-operative evaluation of
complexity of PCNL. However, previous studies did not examine the impact of
S.T.O.N.E. Nephrolithometry Score on FT.
Recently, significant variations have been shown among different surgeons and
Post-Graduate Trainees (PGTs) in FT during retrograde ureteroscopy.7,8
Yet, the impact
of PGTs on FT has not been evaluated during PCNL. Therefore, the aim of the present
study was to determine predictors of FT during PCNL and assess the impact of urology
PGTs and S.T.O.N.E. Nephrolithometry Score.
Page 4 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
4
4
MATERIALS AND METHODS
Study design and Enrollment:
Approvals from Institutional Research Ethics Board (No. 14-050-GEN) and
Director of Professional Services of McGill University Health Centre were obtained.
Chart and electronic data were reviewed for all patients undergoing PCNL between 2010
and 2013. All PCNLs were performed by a single fellowship-trained endourologist (SA)
with the assistance of PGTs from Post-Graduate Years (PGY) 4 and 5. There are no
endourology clinical fellows at this centre. Therefore, PCNLs are considered to be
cases appropriate for PGY-5 trainees. When PGY-5 trainees were not available,
PGY-4 trainees performed these cases. Therefore, the PGY level was not chosen
according to the difficulty of PCNL cases. PGTs attempted the first puncture
regardless of their level of training and previous PCNL experience. In addition, the
person who was performing the procedure or puncture, whether it is the attending
urologist or the PGT, controlled the foot switch for fluoroscopy. Patients who
underwent second-look PCNL, or PCNL without involvement of any PGT were
excluded. In addition, patients who had their percutaneous access obtained by the
interventional radiologist were also excluded from the study. All PGTs received annual
lectures on Radiation Safety and were instructed to minimize FT intra-operatively.
Procedure:
The attending endourologist was scrubbed throughout every PCNL case. All
patients received broad-spectrum antibiotics peri-operatively. Under the benefit of
general anesthesia, patients underwent flexible cystoscopy to place a 5F ureteral catheter
and secure it to an indwelling 18F Foley urethral catheter. All patients underwent PCNL
Page 5 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
5
5
procedure in the prone position as previously described.9 At the end of the procedure,
patients had antegrade indwelling double-pigtail 6F ureteral stents inserted. For tubeless
cases, the skin was closed with 4-0 absorbable suture and for standard PCNL cases a 20F
council-tip nephrostomy was inserted. The FT was calculated from the beginning to the
end of the procedure including flexible cystoscopy and insertion of the ureteral catheter.
The operative time included both cystoscopy and PCNL procedure. A puncture was
defined as a needle pass through the kidney without necessarily tract dilation. A
tract is when a puncture was dilated.
Outcome measures:
Patient and PGT characteristics were collected prospectively on data sheets that
were filled out by the attending surgeon immediately post-operatively. Variations in FT
were assessed among PGTs, PGY level, presence and degree of hydronephrosis (mild,
moderate, and severe), presence of pre-operative indwelling ureteral stents, presence of
post-operative nephrostomy tube, Estimated Blood Loss (EBL), and site of tract (upper,
mid and lower poles) were compared. In addition, correlation of FT with stone volume
(mm2), Hounsfield Units (HU), number of punctures, number of tracts, tract length,
number of involved calyces and operative time were assessed. Moreover, the impact of
PCNL complexity on FT was determined by comparing the S.T.O.N.E. Nephrolithometry
Score with FT.
S.T.O.N.E. Nephrolithometry Score:
This score is calculated by adding five parameters obtained from the pre-operative
non-contrast computed tomography (NCCT) of the kidney stone. These parameters
include the Stone size (mm2) (1-399=1, 400-799=2, 800-1599=3, and ≥1600=4), Tract
Page 6 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
6
6
length (mm) (≤100=1, >100=2), Obstruction or hydronephrosis (no or mild=1, and
moderate or severe=2), Number of involved calyces (pelvis involvement, one or two
calyces=1, three calyces=2, and staghorn stone=3), and stone Essence or density (HU)
(≤950=1, and >950=2). The total S.T.O.N.E. Nephrolithometry Score ranges from 5-13,
with the score of 5 representing the simplest PCNL and the score of 13 representing the
most complex PCNL.10
All procedures were performed using the OEC 9900 Elite (General Electric) C-
arm unit. FT was obtained from the timer on the C-arm unit and recorded by the
attending urologist on the data sheets. These FTs were confirmed from the radiology
reports. PGTs assisting in the PCNL procedures controlled the foot pedal. Prior to
November 2010, all PCNL cases were performed using Standard Fluoroscopy (SF) with
refresh rates of 30 frames per second. After November 2010, Pulsed Fluoroscopy (PF) at
a refresh rate of 4 frames per second was routinely used. We have previously shown that
Pulsed Fluoroscopy (4 frames per second) resulted in 65% less Fluoroscopy Time than
when Standard Fluoroscopy (30 frames per second) was used during PCNL.11
Therefore,
in order to standardize the FT used in the present study, the Fluoroscopy Times obtained
using SF prior to November 2010 were multiplied by 0.35. 11
Data analysis:
Comparative and descriptive data were presented in terms of numbers,
percentages, means and standard errors of mean. Links between continuous variables
were assessed using the Spearman rank correlation coefficient or the Pearson's
correlation coefficient, whenever appropriate. Categorical variables were compared
using Fisher’s exact test while continuous variables were compared using the Mann-
Page 7 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
7
7
Whitney U-test and Kruskal-Wallis test or independent sample (t) test and one way
ANOVA test, whenever appropriate. Two tailed p-value <0.05 was considered
statistically significant. Univariate and multivariate linear regression analyses were
performed to determine the independent predictors of FT. Statistical analysis was
performed using the Statistical Package of Social Sciences for Windows (SPSS, Chicago,
IL) version 20.
Page 8 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
8
8
RESULTS
Out of 130 PCNL cases, 103 were included in the data analysis. Twenty-seven
cases were excluded; 15 had the access tract performed by interventional radiology, 6 had
second-look PCNLs, and 6 were performed without the assistance of any PGTs. These
103 PCNL cases were assisted by 10 PGTs (coded A to J) from PGY-4 and PGY-5,
including 37 (35.9%) PCNLs assisted by PGY-4 trainees and 66 (64.1%) PCNLs assisted
by PGY-5 trainees. [The median number of cases assisted per PGT was 9 (7-17)]. The
overall stone-free rate was 72.8% after the primary PCNL procedure. Other pre-operative
and demographic data are presented in Table 1.
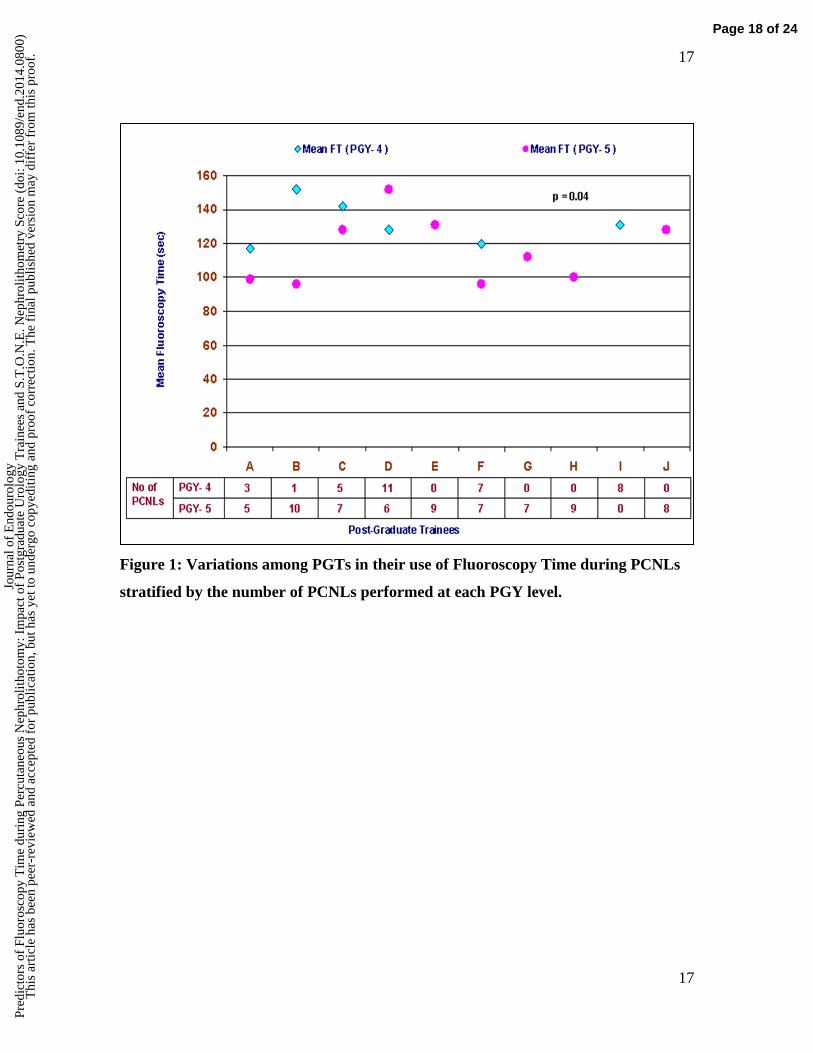
The mean FT (sec) utilized by each PGT from A to J was (106±12.8, 101.3±15,
136±15.6, 136.6±10.5, 130.6±32, 108±8.3, 112.3±8.8, 103.8±15.5, 131.3±19.3, and
128.4±23 sec; p=0.45), respectively. PGY level significantly affected FT, where PGY-5
trainees utilized significantly less FT than PGY-4 trainees (115±6 vs. 130±7 sec; p=0.04)
(Table 2; Figure 1). In addition, there was no significant difference in the mean FT
between PGTs who performed > 9 PCNLs compared to PGTs with ≤ 9 PCNLs
(116±12 vs 119±5, p=0.6). Similarly, there were no significant differences in FT
among PCNL cases performed in 2010, 2011, 2012, and 2013 years with mean FT of
117.7±10.7, 127.7±9, 104.4±6.9, and 128.3±12.5 seconds, respectively (p=0.3).
However, there was a significant correlation between FT and number of involved calyces
(r= 0.24, p= 0.02), number of punctures (r=0.6, p=0.01), number of tracts (r=0.4; p=0.01),
and operative time (r=0.4, p=0.01). Furthermore, PCNLs where the EBL was <250 mL
were associated with significantly lower FT than those with EBL ≥250mL (109±5.1 vs.
148.2±10.9 sec; p=0.001). There was significant correlation between the number of
Page 9 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
9
9
punctures and number of involved calyces (r=0.3; p=0.001), and operative time
(r=0.4; p<0.001). In addition, there was significant correlation between operative
time and S.T.O.N.E. score (r=0.4; p<0.001).
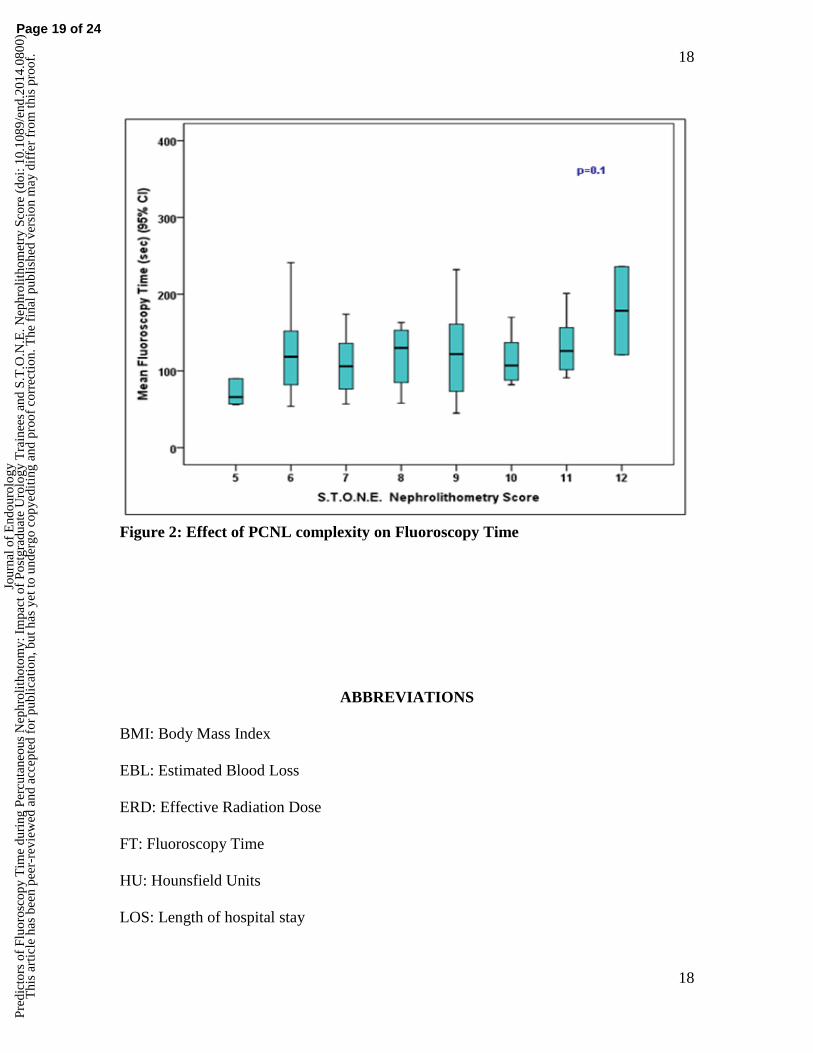
There was no correlation between FT and S.T.O.N.E. Nephrolithometry Score
(r=0.16; p=0.1), stone volume (r=0.07; p=0.5), stone HU (r=0.05; p=0.6), tract length
(r=0.04; p=0.7) and BMI (r=0.001; p=0.1) (Figure 2). There was no association
between FT and stone-free status. The mean FT in stone-free cases was 117±6.2 (sec)
compared with 130±7.9 (sec) in non stone-free cases (p=0.2). Similarly, FT was not
affected by the presence of pre-operative indwelling ureteral stents (p=0.4), presence of
hydronephrosis (p= 0.3), degree of hydronephrosis (p=0.5), involvement of renal pelvis
(p=0.2), (tract site [upper, middle or lower calyx] (p=0.1) or insertion of post-operative
nephrostomy tube (p=0.2).
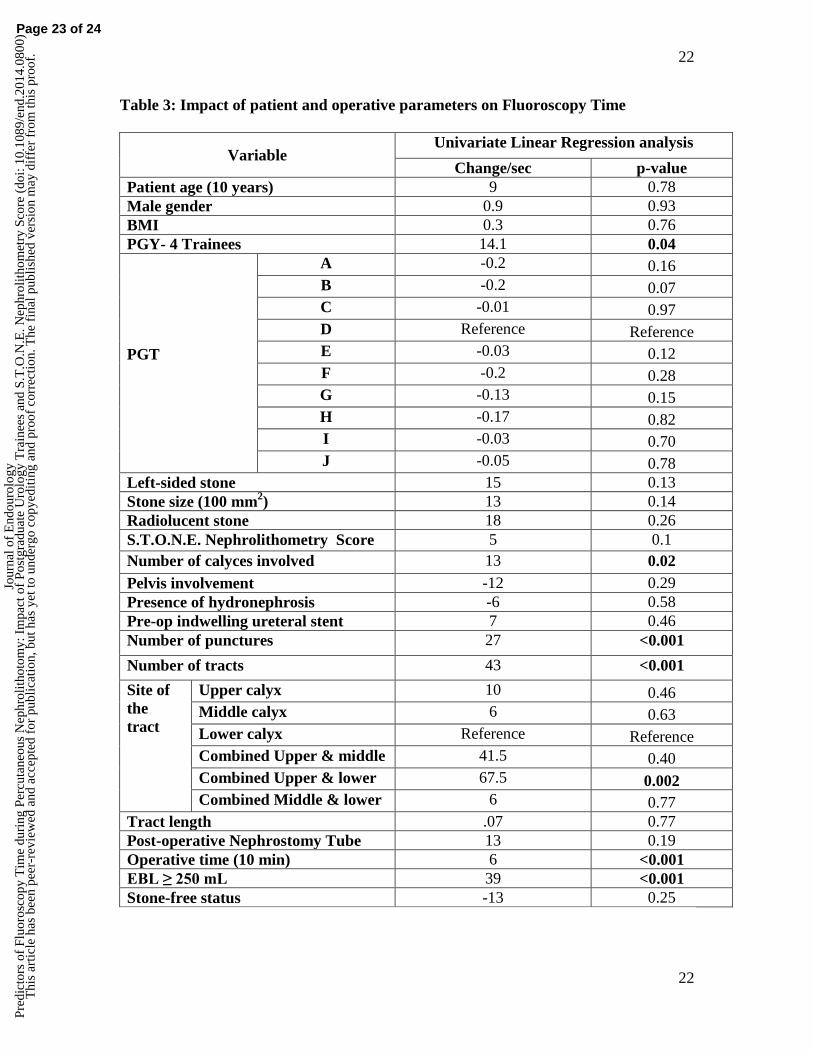
On univariate linear regression analysis, significantly longer FT was associated
with PGY-4 trainees, increased number of involved calyces, increased number of
punctures, increased number of tracts, combined upper and lower tracts, operative time
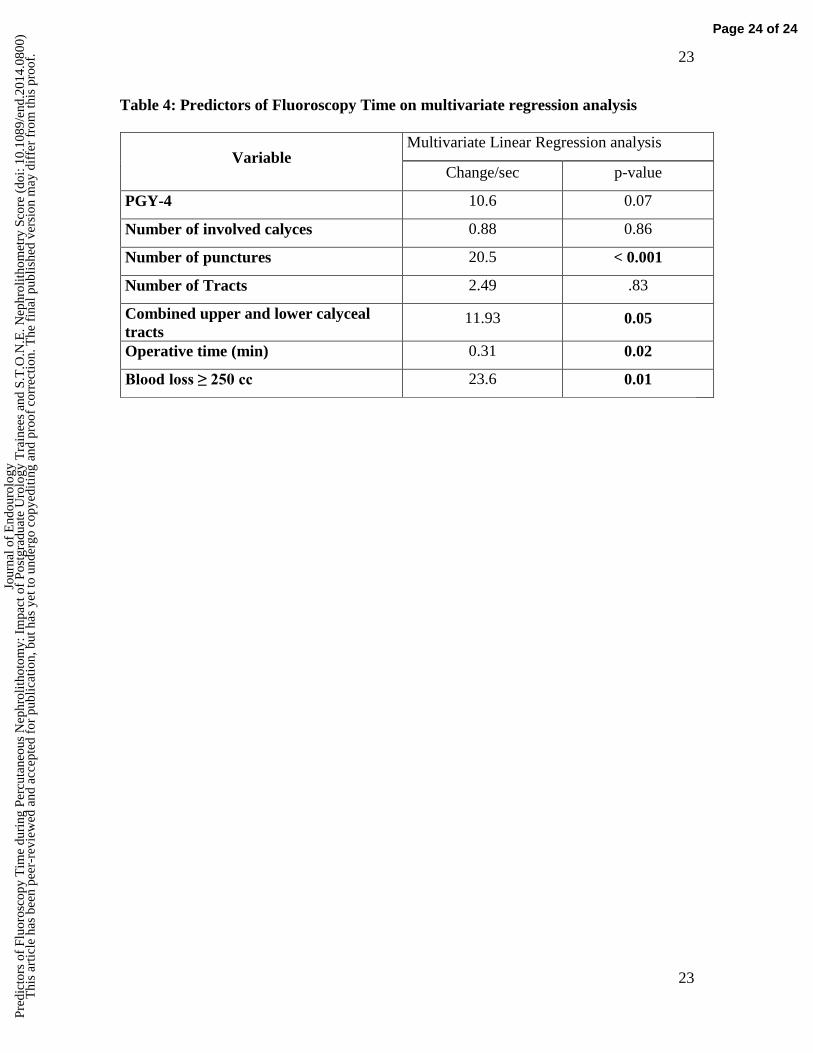
and EBL ≥ 250 mL (Table 3). However, on multivariate linear regression analysis, only
the number of punctures, operative time, and EBL ≥ 250 mL maintained their
significance as independent predictors of FT during PCNL (Table 4).
Page 10 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
10
10
DISCUSSION
Surgeon behavior is one of the important modifiable predictors of FT during
endourological procedures. Previous studies have shown that there were significant
differences in FT among surgeons and PGTs assisting in ureteroscopies.8 Therefore, the
hypothesis for the present study was that there would be significant differences in FT
among PGTs assisting PCNL. Although PGY-5 trainees used significantly less FT than
PGY-4 trainees (115±6 vs. 130±7 sec; p=0.04) (Figure 1), there were no significant
differences among PGTs assisting PCNLs (p=0.45). There could be several theories to
explain the lack of significant differences among PGTs. First, the mean FT in the present
study is 120±5 seconds (2 minutes), which is much shorter than previous modern series
examining FT during PCNL. For example, the study of Tepeler et al had a mean FT of
10.19±6.3 minutes.5
Another study by Mancini et al found mean FT of 7.76±0.9 minutes.6
Therefore, the amount of FT used in the present study was already low with minimal
variations among the different PGTs (Figure 1). Second, all PGTs attended radiation
safety lectures and were advised to minimize intra-operative fluoroscopy as much as
possible. Third, PF at 4 frames per second was used in all cases since November 2010.
PF has been recently shown to decrease FT by 65%.11
Fourth, the median number of
PCNLs assisted by each trainee was only 9, which may not have been enough since 36 to
45 PCNLs are required to achieve competency.12,13
In addition, the median number of
months that PGTs rotated through the endourology site was 3.5 months. Fifth, the
present study was performed prior to acquisition of virtual reality simulator to train
percutaneous renal access. Nonetheless, PGY-5 trainees used significantly less FT than
Page 11 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
11
11
PGY-4 trainees, indicating that the more experienced senior trainees used significantly
less FT during PCNL.
The S.T.O.N.E. Nephrolithometry Score System has been recently devised for
objective assessment PCNL complexity, 10
and it has been shown to correlate with stone-
free status. 10,14
Although FT significantly correlated with the number of involved calyces
(r= 0.24, p= 0.02), there was no correlation between FT and the S.T.O.N.E.
Nephrolithometry Score. Perhaps the lack of correlation has to do the way S.T.O.N.E.
Nephrolithometry Score is calculated. The higher the number of involved calyces, the
higher the N number and thus the higher the S.T.O.N.E. Nephrolithometry Score.
However, it has been previously shown that non-branched stones (lower number of
involved calyces) are associated with significantly higher Effective Radiation Dose when
compared with branched stones (higher number of calyces).6 Therefore, the current
findings of lack of relationship between S.T.O.N.E. Nephrolithometry Score and FT are
congruent with previous published results.
Previous studies have shown that multiple access tracts and large stone burden
were associated with prolonged FT. 5,6
This was not consistent with the current study
where the increase in number of tracts and stone volume were not significantly associated
with prolonged FT on multivariate analysis. This could be due to the relatively short FT
(2 minutes) used in the present study due to several factors including the use of Pulsed
Fluoroscopy at 4 frames per second. Nevertheless, the number of punctures significantly
correlated with FT. This may be explained by the fact that fluoroscopy is mainly used
during percutaneous access rather than tract maturation and stone extraction. Whereas the
number of punctures was not assessed in previous studies, the advantage of the present
Page 12 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
12
12
study is that the number of punctures was recorded prospectively after each procedure.
Patient age, sex, and BMI did not significantly affect the FT, which is consistent with
what has been previously reported. 5,6
In addition, the present study revealed no effect of
stone HU, presence or degree of hydronephrosis, pre-operative indwelling ureteral stent,
tract length, post-operative nephrostomy tube insertion on FT. This is similar to the
previously published study. 5
This study is not without limitations including its retrospective nature, despite the
fact that most of the data were prospectively collected by the attending surgeon
immediately post-operatively on PCNL data sheets. Another limitation is that the
intra-operative blood loss was estimated rather than reporting hemoglobin drop. In
addition, the relatively small number of cases (median of 9 PCNLs) assisted by each PGT
is another limitation since it is estimated that up to 45 PCNLs are required to achieve
competency.12,13
This precluded calculation of the learning curve for PGTs. Another
limitation is the lack of data regarding the different level of involvement of the
attending urologist in each case. Finally, the dose area product was not available to
calculate the effective radiation dose (ERD). Therefore, FT was used as a surrogate for
ERD. Nevertheless, this the first study to report on the effect of S.T.O.N.E.
Nephrolithometry Score and PGTs assisting in PCNLs on FT. In addition, this is the first
study to report the number of punctures as an independent predictor of prolonged FT
during PCNL.
Conclusions
The number of punctures, EBL and operative time were the only
independent predictors of prolonged FT during PCNL.
Page 13 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
13
13
Page 14 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
14
14
REFERENCES
1. Fernstrom I, Johansson B. Percutaneous pyelolithotomy. A new extraction technique.
Scand J Urol Nephrol. 1976; 10(3): 257-259.
2. Preminger GM, Clayman RV, Hardeman SW, et al. Percutaneous nephrostolithotomy
vs. open surgery for renal calculi: A comparative study. JAMA 1985; 254(8):1054–
1058.
3. Brannen GE, Bush WH, Correa RJ, et al. Kidney stone removal: Percutaneous versus
surgical lithotomy. J Urol 1985; 133(1):6–12.
4. Hellawell GO, Mutch SJ, Thevendran G, et al. Radiation exposure and the urologist:
What are the risks? J Urol. 2005; 174(3):948–952.
5. Tepeler A, Binbay M, Yuruk E et al: Factors affecting the fluoroscopic screening
time during percutaneous nephrolithotomy. J Endourol 2009; 23(11): 1825-1829.
6. Mancini JG, Raymundo EM, Lipkin M et al: Factors affecting patient radiation
exposure during percutaneous nephrolithotomy. J Urol 2010; 184(6): 2373.
7. Ngo TC, Macleod LC, Rosenstein DI, et al. Tracking intraoperative fluoroscopy
utilization reduces radiation exposure during ureteroscopy. J Endourol 2011;25:763-
767.
8. Elkoushy MA, Andonian S. Variations among urology trainees in their use of
fluoroscopy during ureteroscopy. J Endourol 2013; 27(1):19-23.
9. Shahrour W, Andonian S. Ambulatory Percutaneous Nephrolithotomy: Initial Series
Urology 2010; 76: 1288–1292.
10. Okhunov Z, Friedlander JI, George AK, et al. S.T.O.N.E. Nephrolithometry: Novel
surgical classification system for kidney calculi. Urology 2013a. 81(6): 1154-1160.
11. Elkoushy MA, Shahrour W, Andonian S. Pulsed fluoroscopy in ureteroscopy and
percutaneous nephrolithotomy Urology 2012; 79 (6): 1230–1235.
12. Ziaee SAM, Sichani MM, Kashi AH, et al. Evaluation of the Learning Curve for
Percutaneous Nephrolithotomy Urol J 2010; 7(4): 226-231.
13. Jang WS, Choi KH, Yang SC, et al. The learning curve for flank percutaneous
nephrolithotomy for kidney calculi: a single surgeon’s experience. Korean J Urol
2011; 52(4):284-288.
Page 15 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.

15
15
14. Okhunov Z, Helmy M, Perez-Lansac A, et al. Interobserver reliability and
reproducibility of S.T.O.N.E. Nephrolithometry for renal calculi. J Endourol 2013b;
27(10):1303-1306.
Page 16 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
16
16
Figure Legends
Page 17 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
17
17
Figure 1: Variations among PGTs in their use of Fluoroscopy Time during PCNLs
stratified by the number of PCNLs performed at each PGY level.
Page 18 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
18
18
Figure 2: Effect of PCNL complexity on Fluoroscopy Time
ABBREVIATIONS
BMI: Body Mass Index
EBL: Estimated Blood Loss
ERD: Effective Radiation Dose
FT: Fluoroscopy Time
HU: Hounsfield Units
LOS: Length of hospital stay
Page 19 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
19
19
N/A: Not Applicable
PCA: Percutaneous access
PCNL: Percutaneous Nephrolithotomy
PCS: Pelvi-Calyceal System
PGTs: Post-Graduate Trainees
PGY: Post-Graduate Year
PF: Pulsed Fluoroscopy
SF: Standard Fluoroscopy
TABLES
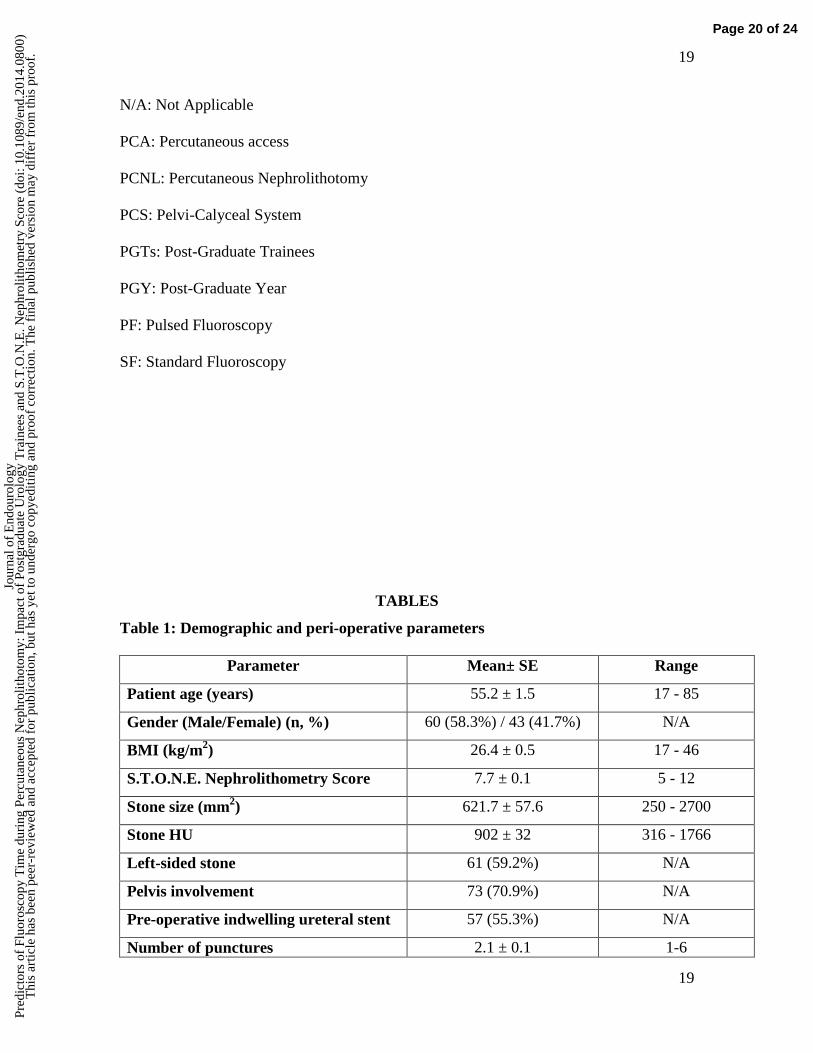
Table 1: Demographic and peri-operative parameters
Parameter Mean± SE Range
Patient age (years) 55.2 ± 1.5 17 - 85
Gender (Male/Female) (n, %) 60 (58.3%) / 43 (41.7%) N/A
BMI (kg/m2) 26.4 ± 0.5 17 - 46
S.T.O.N.E. Nephrolithometry Score 7.7 ± 0.1 5 - 12
Stone size (mm2) 621.7 ± 57.6 250 - 2700
Stone HU 902 ± 32 316 - 1766
Left-sided stone 61 (59.2%) N/A
Pelvis involvement 73 (70.9%) N/A
Pre-operative indwelling ureteral stent 57 (55.3%) N/A
Number of punctures 2.1 ± 0.1 1-6
Page 20 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
20
20
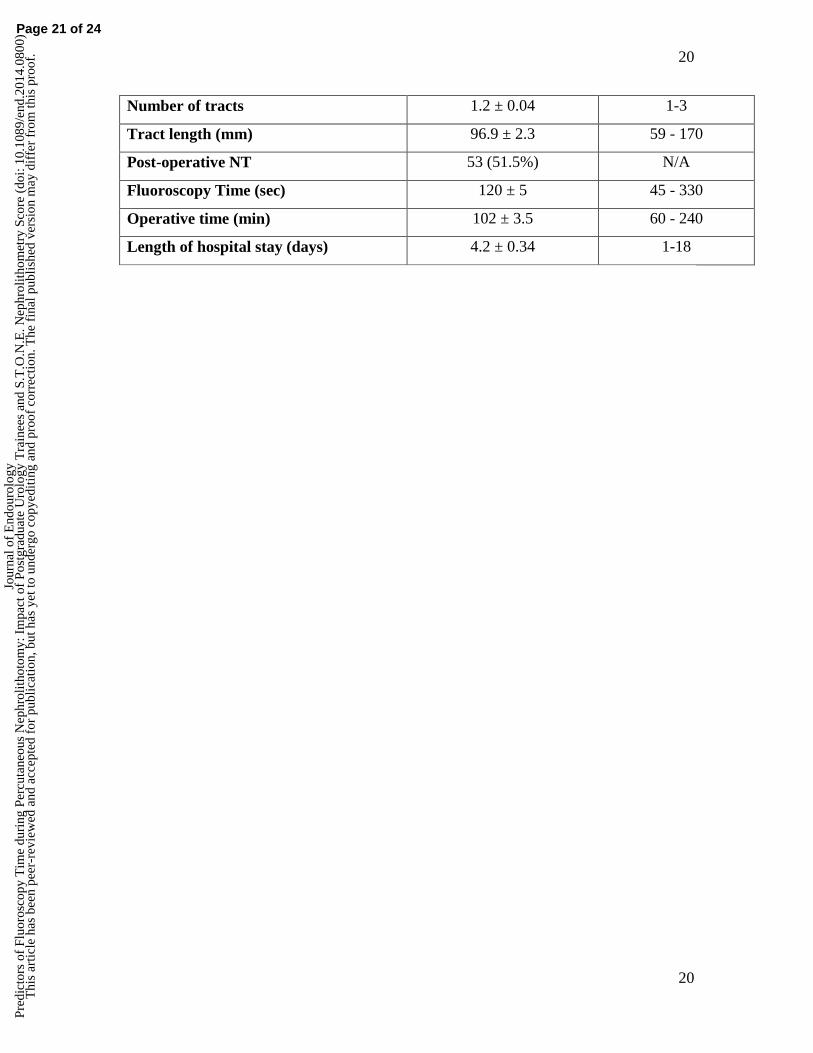
Number of tracts 1.2 ± 0.04 1-3
Tract length (mm) 96.9 ± 2.3 59 - 170
Post-operative NT 53 (51.5%) N/A
Fluoroscopy Time (sec) 120 ± 5 45 - 330
Operative time (min) 102 ± 3.5 60 - 240
Length of hospital stay (days) 4.2 ± 0.34 1-18
Page 21 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
21
21
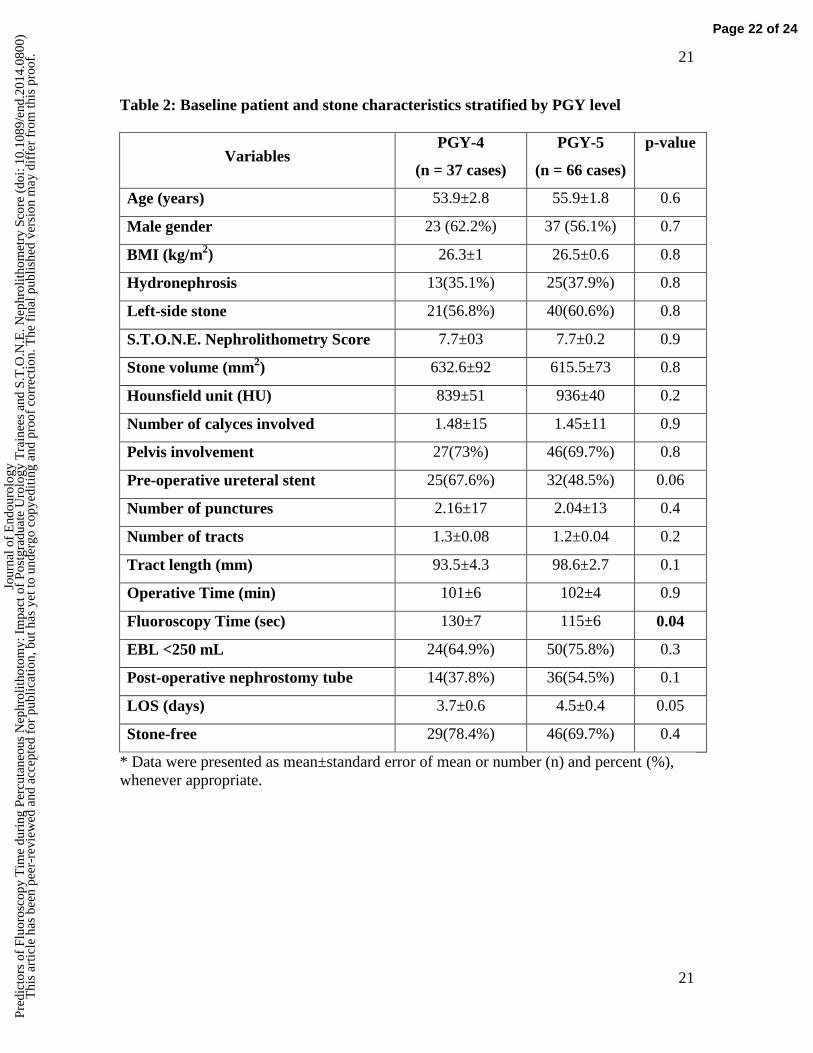
Table 2: Baseline patient and stone characteristics stratified by PGY level
Variables PGY-4
(n = 37 cases)
PGY-5
(n = 66 cases)
p-value
Age (years) 53.9±2.8 55.9±1.8 0.6
Male gender 23 (62.2%) 37 (56.1%) 0.7
BMI (kg/m2) 26.3±1 26.5±0.6 0.8
Hydronephrosis 13(35.1%) 25(37.9%) 0.8
Left-side stone 21(56.8%) 40(60.6%) 0.8
S.T.O.N.E. Nephrolithometry Score 7.7±03 7.7±0.2 0.9
Stone volume (mm2) 632.6±92 615.5±73 0.8
Hounsfield unit (HU) 839±51 936±40 0.2
Number of calyces involved 1.48±15 1.45±11 0.9
Pelvis involvement 27(73%) 46(69.7%) 0.8
Pre-operative ureteral stent 25(67.6%) 32(48.5%) 0.06
Number of punctures 2.16±17 2.04±13 0.4
Number of tracts 1.3±0.08 1.2±0.04 0.2
Tract length (mm) 93.5±4.3 98.6±2.7 0.1
Operative Time (min) 101±6 102±4 0.9
Fluoroscopy Time (sec) 130±7 115±6 0.04
EBL <250 mL 24(64.9%) 50(75.8%) 0.3
Post-operative nephrostomy tube 14(37.8%) 36(54.5%) 0.1
LOS (days) 3.7±0.6 4.5±0.4 0.05
Stone-free 29(78.4%) 46(69.7%) 0.4
* Data were presented as mean±standard error of mean or number (n) and percent (%),
whenever appropriate.
Page 22 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
22
22
Table 3: Impact of patient and operative parameters on Fluoroscopy Time
Variable Univariate Linear Regression analysis
Change/sec p-value
Patient age (10 years) 9 0.78
Male gender 0.9 0.93
BMI 0.3 0.76
PGY- 4 Trainees 14.1 0.04
PGT
A -0.2 0.16
B -0.2 0.07
C -0.01 0.97
D Reference Reference
E -0.03 0.12
F -0.2 0.28
G -0.13 0.15
H -0.17 0.82
I -0.03 0.70
J -0.05 0.78
Left-sided stone 15 0.13
Stone size (100 mm2) 13 0.14
Radiolucent stone 18 0.26
S.T.O.N.E. Nephrolithometry Score 5 0.1
Number of calyces involved 13 0.02
Pelvis involvement -12 0.29
Presence of hydronephrosis -6 0.58
Pre-op indwelling ureteral stent 7 0.46
Number of punctures 27 <0.001
Number of tracts 43 <0.001
Site of
the
tract
Upper calyx 10 0.46
Middle calyx 6 0.63
Lower calyx Reference Reference
Combined Upper & middle 41.5 0.40
Combined Upper & lower 67.5 0.002
Combined Middle & lower 6 0.77
Tract length .07 0.77
Post-operative Nephrostomy Tube 13 0.19
Operative time (10 min) 6 <0.001
EBL ≥ 250 mL 39 <0.001
Stone-free status -13 0.25
Page 23 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
23
23
Table 4: Predictors of Fluoroscopy Time on multivariate regression analysis
Variable Multivariate Linear Regression analysis
Change/sec p-value
PGY-4 10.6 0.07
Number of involved calyces 0.88 0.86
Number of punctures 20.5 < 0.001
Number of Tracts 2.49 .83
Combined upper and lower calyceal
tracts 11.93 0.05
Operative time (min) 0.31 0.02
Blood loss ≥ 250 cc 23.6 0.01
Page 24 of 24
Jour
nal o
f E
ndou
rolo
gyPr
edic
tors
of
Fluo
rosc
opy
Tim
e du
ring
Per
cuta
neou
s N
ephr
olith
otom
y: I
mpa
ct o
f Po
stgr
adua
te U
rolo
gy T
rain
ees
and
S.T
.O.N
.E. N
ephr
olith
omet
ry S
core
(do
i: 10
.108
9/en
d.20
14.0
800)
Thi
s ar
ticle
has
bee
n pe
er-r
evie
wed
and
acc
epte
d fo
r pu
blic
atio
n, b
ut h
as y
et to
und
ergo
cop
yedi
ting
and
proo
f co
rrec
tion.
The
fin
al p
ublis
hed
vers
ion
may
dif
fer
from
this
pro
of.
Top Related
Copyright © 2022 FDOKUMEN

