






Bahasa
Halaman
Hukum

http://france.elsevier.com/direct/EURPSY/
European Psychiatry 21 (2006) 143–151
Original article
* CorresponE-mail ad
0924-9338/$doi:10.1016/j
Posttraumatic stress disorder in victims of the March 11 attacks
in Madrid admitted to a hospital emergency room: 6-month follow-upD. Fraguas *, S. Terán, J. Conejo-Galindo, O. Medina, E. Sainz CortónL. Ferrando, R. Gabriel, C. Arango
Department of Psychiatry, Gregorio Marañón General Hospital, Ibiza 43, CP 28009 Madrid, Spain
Abstract
Purpose: To determine the change in prevalence of posttraumatic stress disorder (PTSD) symptoms in victims of the March 11 attacks andtheir relatives, 1 and 6 months after the attacks.
Subjects and methods: Evaluation of PTSD symptoms using the Davidson Trauma Scale (DTS) and General Health Questionnaire (GHQ) ina sample of 56 patients admitted to an emergency room of a general hospital, and assessment of PTSD symptoms in relatives of the patients.
Results: At Month 1, 41.1% of patients (31.3% of males and 54.2% of females) presented with PTSD. At Month 6, this figure was 40.9%(30.4% of males and 52.4% of females). There was a significant improvement in perception of health among females between Month 1 andMonth 6. Relatives presented similar DTS scores at baseline and at 6 months.
Discussion: We verified that rates of PTSD did not vary substantively between the two evaluations. PTSD symptoms positively correlatedwith psychological health involvement. This correlation points out that both PTSD symptoms and subjective general health involvement are partof the psychological response to trauma.
Conclusion: The prevalence of PTSD symptoms was high and remained stable between Month 1 and Month 6, while subjective perception ofhealth improved significantly.© 2006 Elsevier SAS. All rights reserved.
Keywords: Disasters; Mental health; PTSD; Relatives; Terrorist attack
1. Introduction
On March 11, 2004, Madrid experienced the worst terroristattack in its history. Ten bombs exploded on four differentcommuter trains headed to the central station in Madrid. Thedeath toll rose to 192 (177 pronounced dead at the scene, with15 more in the ensuing days). About 2000 people were injured[30].
Three hundred ambulances were deployed that day; 4600blood donations were collected in Madrid and another 2500were sent from the rest of Spain. The emergency numberhandled 14,188 calls [10,13]. The social repercussions of thistragedy and its long-term economic effects are still unknown[3].
ding author.dress: [email protected] (D. Fraguas).
- see front matter © 2006 Elsevier SAS. All rights reserved..eurpsy.2006.03.003
Hospital Gregorio Marañón is the closest hospital to thescene of the attacks, so it was the first to receive the injuredand it treated the greatest number of victims on March 11, i.e. atotal of 325 patients [38]. On March 11, our hospital’s Depart-ment of Psychiatry implemented a plan for attending both thevictims of the attacks and their relatives, as well as follow-upon victims after March 11 [39].
According to the current definition in the DSM-IV, a trau-matic event is one that involves actual or threatened death orserious injury, or a threat to the physical integrity of self orothers, and that involves intense fear, helplessness, or horror[2].
Exposure to a traumatic event is associated with the occur-rence of Posttraumatic Stress Disorder (PTSD). However,PTSD is not an inevitable consequence of a trauma [51]. Theprevalence of PTSD after trauma varies as a function of thestudy population. The National Comorbidity Survey Replica-tion, conducted in the US between 2001 and 2003, obtained a

D. Fraguas et al. / European Psychiatry 21 (2006) 143–151144
PTSD lifetime prevalence of 6.8% [25] and a PTSD 12-monthprevalence of 3.5% [26]. However, a 2003 study of a Europeanpopulation found a PTSD lifetime prevalence of 1.9% (the 12-month prevalence was 0.9%) in the general population [1].
The literature on PTSD shows that more than two-thirds ofthe population can expect to experience a significant traumaticincident during their lifetime, and one out of every 15 indivi-duals experiences a traumatic event each year [6,8,27,31,37].Although the data are limited, a large portion of the world po-pulation is exposed to the threat of terrorism. Epidemiologicaldata on the psychopathologic consequences of terrorist attacksare relatively rare in the medical literature. PTSD is the moststudied psychopathologic consequence and, plausibly, the mostcommon change in individuals exposed to such incidents ordisasters [9,18,20,24,32,33].
The prevalence of PTSD after a terrorist attack varies from12.0% [17] to 36.8% [41]. The terrorist attacks of 11S in NewYork meant a challenge in the studies on PTSD prevalence inthe population affected. The terrorist attacks of March 11th inMadrid have similarities with 11S in New York. Schlenger etal. [40] found a prevalence of PTSD after the attacks in NewYork City metropolitan area of 11.2%, significantly higherthan in Washington DC (2.7%), other major metropolitan areas(3.6%) and the rest of the country (4.0%).
The longitudinal course of PTSD symptoms tends to de-crease with time [45]. However, the different studies on thecourse of PTSD report a wide variation in stability of PTSDsymptoms. Breslau et al. [8] found, in a community sample,that approximately the 26% of PTSD cases remitted by6 months, and 40% by 12 months, and, using a Kaplan–Meiermethod, they estimated that the median time to remission ofPTSD was 24.9 months, although in more than 30% of casesPTSD persisted for more than 60 months. In contrast, a nation-wide longitudinal study conducted in the United States, outsideof New York City, found that only 17% of the sample reportedposttraumatic stress symptoms 2 months after the September11 attacks, and 5.8% at 6 months [46]. Perkonigg et al. [36]reported that more than 50% of a community sample of ado-lescent and young adults with DSM-IV criteria for PTSD atbaseline remained symptomatic for more than 3 years. Northet al. [34] assessed PTSD rates among survivors of the St.Louis flood; they found that 22% of the sample had PTSD at4 months after the end of the flood, and 16% at 16 months.Shalev and Freedman [41] found that 36.8% of patients ad-mitted to an emergency room in Jerusalem subsequent to aterrorist attack met DSM-IV PTSD diagnostic criteria at4 months after the attack. Jehel et al. [23] assessed PTSD invictims of a bomb attack in Paris. They found a PTSD preva-lence of 38.5% at 6 months and 25.0% at 32 months. Themarked discrepancies among the above-mentioned studies asto the course of PTSD are partially attributable to the metho-dological differences in the studies (i.e. different samples, dif-ferent scales used to assess PTSD). Further research on thecourse of PTSD is necessary in light of these discrepancies.
In this perspective, the present study evaluated the preva-lence of PTSD both among victims of the March 11 attacks
and their relatives, 1 and 6 months after the attacks. A priori,our hypothesis was that, after 1 and 6 months, subjects affectedby the March 11 attack would present a high prevalence ofposttraumatic stress symptoms, associated with worsening ofsubjective perception of health. Likewise, we posited that rela-tives would develop posttraumatic stress symptoms, althoughto a lesser extent than victims. We also hoped to identify themost decisive variables associated with the presence of PTSD.
2. Subjects and methods
This study is part of a multicenter investigation on the psy-chological effects of the terrorist attack that took place in Ma-drid on March 11, conducted in four of the city’s hospitals(Hospital Gregorio Marañón, Hospital 12 de Octubre, Hospitalde la Princesa and Hospital Príncipe de Asturias).
Of the 325 patients treated in the emergency room at ourhospital as a consequence of injuries suffered in the March11 attack, we selected a random sample of 56 persons (usinga table of random numbers) and a second random sample toallow substitutions in case some subjects could not be con-tacted.
The size of the sample was determined according to the sta-tistical predictions of the multicenter study.
The study was approved by the Clinical Research EthicsCommittee of the Hospital Gregorio Marañón. All participantssigned an informed consent prior to enrolment in the study.The medical information collected was strictly confidential.
The exclusion criteria were: being under the age of 18 yearsor over the age of 65 years and residing outside of the Com-munity of Madrid.
In order to contact the patients, up to three telephone callswere made at different times and on different days; after threefailed calls, the chosen subject was substituted by the first per-son on the backup list and so on. The calls were made directlyby four of the psychiatrists (DF, ST, JC-G, and OM) authors ofthe study, from the outpatient psychiatric clinic of the hospital.The calls were made following a protocol, so it would be thesame for all selected individuals.
Twenty-four patients from the first sample could not befound and they were replaced with 24 patients from the secondsample. Once located, the patients agreed to participate in thestudy. None of the subjects, once they were contacted, refusedto participate in the study.
Fifty-six individuals participated in the first data collectionbetween Weeks 5 and 8 after the attack, and 44 individualsparticipated in the second data collection 6 months after theattack.
Each person interviewed was given a general questionnairewith socio-demographic variables (age, gender, educational le-vel, occupation, religion), personal history of general and psy-chiatric health, vital traumatic events in the past year, existenceof other victims in his/her surroundings, and habitual use ofcommuter trains.

D. Fraguas et al. / European Psychiatry 21 (2006) 143–151 145
We used the validated Spanish version of the DavidsonTrauma Scale (DTS) [4,11] composed of 17 items, correspond-ing to the 17 symptoms of PTSD per the DSM-IV criteria. Theitems may be categorised as follows: 1–4 and 17 correspondedto Criterion B (Intrusive memories, re-experiencing); 5–11 cor-responded to Criterion C (Avoidance and numbing); and 12–16corresponded to Criterion D (Arousal activation). For eachitem, we scored the frequency and severity of symptoms duringthe previous week. With a maximum score of 136, a cut-offscore of 40 was considered to have predictive diagnostic powerper the DSM-IV criteria. The Davidson Trauma Scale is suffi-ciently accurate for diagnostic assessment [11]. With a highestscore of 40, its sensitivity is 0.92 and its specificity is 0.79,with overall efficiency of 0.83. The Spanish version of the Da-vidson Trauma Scale was previously validated [4].
Likewise, the interviewed patients were given copies of theDavidson Trauma Scale, with instructions to have them com-pleted by any adult family members living with them whowished to participate. The scales, identified with a personalcode, were submitted to us by mail (postage paid).
The self-administered Goldberg General Health Question-naire (GHQ) [22,29] was also used to collect subjectivechanges in perception of psychological health experienced byeach individual, under its various sections: A (somatic symp-toms), B (anxiety/insomnia), C (daily tasks) and D (depres-sion), and to correlate them with the various PTSD criteria.
Patients were classified according to the medical prognosis:“mild” (no life risk and discharge from the emergency room inthe first 24 hours), “intermediate” (no life risk anddischarge > 24 h) and “serious” (life risk).
History of psychiatry disorders (major depression, dysthy-mia, mania, hypomania, panic disorder, agoraphobia, socialphobia, obsessive-compulsive disorder, posttraumatic stressdisorder, generalized anxiety disorder, alcohol dependence/abuse, non-alcohol substance dependence/abuse, schizophreniaand other psychotic disorders) was assessed using the corre-sponding items of the Mini International Neuropsychiatric In-terview (MINI) scale [15,43,44].
The patients completed the scales of the study (DTS, GHQ,MINI, and general questionnaire with socio-demographic vari-ables) in person at the outpatient clinic of our hospital. Theinterviews with the patients were conducted by the four psy-chiatrists.
Statistical analysis: as several subgroups had fewer than 30subjects we decided to use non-parametric tests. The quantita-tive variables were analysed amongst themselves using Spear-man’s rank correlation. The dichotomous variables were eval-uated amongst themselves using the Chi-square test. Theanalysis between the dichotomous variables and the quantita-tive independent variables was done using the Mann–WhitneyU-test. The dichotomous variables and quantitative dependentvariables were analysed with the Wilcoxon Z-test. The Wilcox-on Z-test is a non-parametric test that compares two pairedgroups. It calculates the difference between each set of pairs,and analyses that list of differences. It resembles the mediantest in scope, but it is much more sensitive. In fact, for large
numbers, it is almost as sensitive as the two-sample Student’st-test. For small numbers with unknown distributions this testis even more sensitive than Student’s t-test. The analysis of thequalitative related variables was done with the McNemar test.The McNemar test assesses the significance of the differencebetween two dependent samples when the variable of interest isa dichotomy. It is a non-parametric test that uses matched pairsof labels (A, B). It determines whether the proportion of A- andB-labels is equal for both members. Two multiple regressionanalyses, with PTSD at 1 and 6 months as the dependent vari-ables, were performed to assess what variables would explain asignificant variance at each time. The comparative analysis be-tween the 1st and 6th months was done with the sample of the44 patients who participated both at the 1-month and the 6-month interviews. The probability of making a type I errorwas 0.05. The SPSS 12.0 statistics software package was used[48].
3. Results
3.1. Victims
The characteristics of the sample are summarised in Table 1.There were no statistically significant differences between thedemographic variables of the subjects evaluated at Month 1and Month 6.
We performed an analysis of the data on the 12 subjects lostto follow-up between the two evaluations. Eight patients werelost to follow-up because they could not be located and fourbecause they refused to remain in the study. There were nosignificant differences in the main variables (age, gender, med-ical prognosis, country of origin, GHQ score, DTS score andPTSD prevalence) between those who attended the second visitand those who did not.
3.1.1. DTS resultsThe Davidson Trauma Scale results and the PTSD propor-
tions (determined as DTS > 40), itemised by gender and coun-try of origin, are shown in Table 2. The DTS scores were high-er for women than men; that difference was statisticallysignificant at Month 1, but not at Month 6. Likewise, womenpresented higher PTSD prevalence figures both at Month 1 andMonth 6.
No significant differences in overall Davidson Trauma Scaleresults were found between Month 1 and Month 6.
Patients with a psychiatric history prior to March 11 hadhigher PTSD prevalence at Month 1 than those with no suchhistory (PTSD 76.9% (10/13) vs. 30.2% (13/43), chi-squareP = 0.003). This difference was not significant at Month 6(PTSD 63.6% (7/11) vs. 33.3% (11/33), chi-square P = 0.077).
There was no significant difference between the two evalua-tions in PTSD sub-criteria, although there was a slight decreasein the proportion of re-experiencing and intrusive memoriessymptoms (Criterion B) and hyperarousal (Criterion D), as wellas a slight increase in avoidance symptoms (Criterion C).
Table 1Socio-demographic characteristics of the sample
Month 1 (N = 56) Month 6 (N = 44) StatisticsAge (mean ± S.D.) 38.2 ± 11.4 37.6 ± 10.7 Mann–Whitney n.s.Gender (% Male) 57.1% (N = 32) 52.3% (N = 23) Chi-square n.s.Medical prognosis (% mild) 76.8% (N = 43) 72.7% (N = 32) Chi-square n.s.Country of origin (% Spain) 60.7% (N = 34) 63.6%(N = 28) Chi-square n.s.Education Level
Primary school 25.0%(N = 14) 22.7%(N = 10) Chi-square n.sSecondary or higher 75.0% (N = 42) 77.3%(N = 34) Chi-square n.s
Marital status (% married) 69.6% (N = 39) 72.7%(N = 32) Chi-square n.s.Active workers 75.0% (N = 42) 79.5%(N = 35) Chi-square n.s.Relatives or friends of victims 51.8% (N = 29) 56.8%(N = 25) Chi-square n.s.Use of trains on 3/11 92.9% (N = 52) 90.9% (N = 40) Chi-square n.s.Frequency of use of trains before 3/11
2–3 times a week/daily 82.1% (N = 46) 79.5%(N = 35) Chi-square n.s.Occasionally/never 8.9% (N = 5) 9.1%(N = 4) Chi-square n.s.
Life stressors (past year)One 42.9%(N = 24) 45.5% (N = 20) Chi-square n.s.Two or more 17.9%(N = 10) 16.0%(N = 7) Chi-square n.s.
Psychiatric history before 3/11 23.2% (N = 13) 25.0% (N = 11) Chi-square n.s.
No significant differences were found between Month 1 and Month 6. Chi-square n.s.: P > 0.05. Mann–Whitney n.s.: P > 0.05.
Table 2DTS Scores and prevalence of current posttraumatic stress disorder
Month 1 Month 6 StatisticsDTS (Mean ± S.D.)
Total 38.4 ± 28.5 (N = 56) 36.2 ± 30.1 (N = 44) Wilcoxon 0.193 P = 0.847Male 31.1 ± 24.8 (N = 32) 28.0 ± 27.0 (N = 23) Wilcoxon 0.244 P = 0.808Female 48.1 ± 30.8 (N = 24) 45.1 ± 31.3 (N = 21) Wilcoxon 0.174 P = 0.862Comparison by gender Mann–Whitney P = 0.033 Mann–Whitney P = 0.060
Native 34.4 ± 25.6 (N = 34) 33.6 ± 29.0 (N = 22) Wilcoxon 0.060 P = 0.952Immigrant 44.5 ± 32.3 (N = 22) 40.7 ± 32.3 (N = 16) Wilcoxon 0.517 P = 0.605Comparison by country of origin Mann–Whitney P = 0.279 Mann–Whitney P = 0.442
PTSD (DTS > 40) (%)Total 41.1% (N = 23) 40.9%(N = 18) McNemar P = 1.000Male 31.3%(N = 10) 30.4% (N = 7) McNemar P = 1.000Female 54.2%(N = 13) 52.4%(N = 11) McNemar P = 1.000Native 44.1%(N = 15) 39.3%(N = 11) McNemar P = 1.000Immigrant 36.4%(N = 8) 43.6%(N = 7) McNemar P = 1.000
Symptoms of PTSDCriterion B (intrusive memories) 92.9%(N = 52) 86.4%(N = 38) McNemar P = 0.687Criterion C (avoidance behaviour) 55.4%(N = 31) 56.8% (N = 25) McNemar P = 0.508Criterion D (hyperarousal) 71.4%(N = 40) 63.6%(N = 28) McNemar P = 0.549
Current PTSD denotes symptoms consistent with a diagnosis of PTSD within the 7 days prior to interview. Significant values are indicated in boldface. P valuesare 2-tailed. Intrusive memories and re-experiencing (DMS-IV Criterion B) constituted the most common posttraumatic stress symptom; it was present in 92.9%of patients evaluated at Month 1 and in 86.4% of those evaluated at Month 6.
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151146
We found a high correlation between DTS scores at 1 and6 months (R Spearman 0.683, P < 0.000).
The immigrant population presented results similar to theSpanish population (Table 2).
3.1.2. GHQ resultsThe results of the Goldberg GHQ are shown in Table 3. At
Month 1, the scores were higher than they were at Month 6.This difference was statistically significant. Contrary to thePTSD figures, where there was little variation between Month1 and Month 6, perception of psychological health significantlyimproved over time.
Women scored higher than men; this difference was statis-tically significant only at Month 1. These data allow us to infer
that the improvement observed in the subjective health evalua-tion between Month 1 and Month 6 for the entire sample wasattributable to the change in Goldberg scores for females.
The authors of the questionnaire established a cut-off scoreof 6, after which perception of psychological health conditionis relevant [36,46]. There were no significant differences be-tween the two evaluations. However, at Month 1, 67.9% ofthe sample (56.3% of males and 79.2% of females) obtainedscores greater than 6 on the Goldberg questionnaire. At Month6, the percentage of subjects with a score greater than 6 was45.5% (47.8% of males and 28.7% of females).
Analysed by sub-scales, sub-scale D (depression) was theleast frequently endorsed aspect of general health, while sub-scales A (somatic symptoms) and B (anxiety/insomnia) were
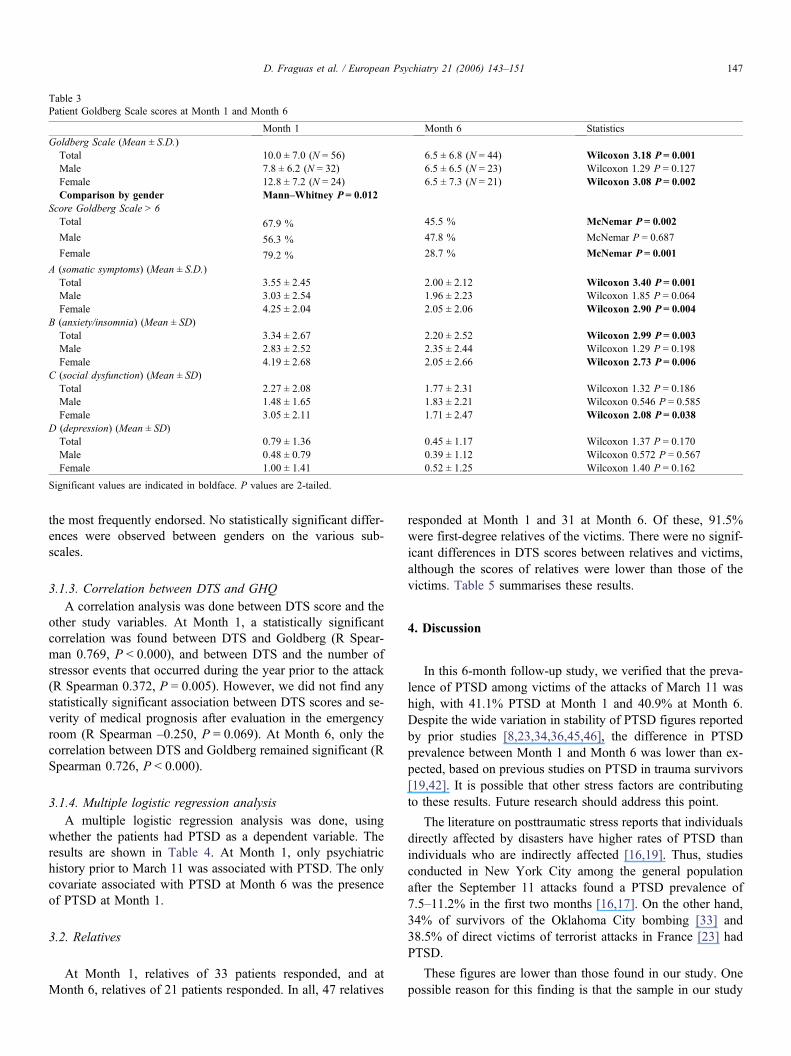
Table 3Patient Goldberg Scale scores at Month 1 and Month 6
Month 1 Month 6 StatisticsGoldberg Scale (Mean ± S.D.)
Total 10.0 ± 7.0 (N = 56) 6.5 ± 6.8 (N = 44) Wilcoxon 3.18 P = 0.001Male 7.8 ± 6.2 (N = 32) 6.5 ± 6.5 (N = 23) Wilcoxon 1.29 P = 0.127Female 12.8 ± 7.2 (N = 24) 6.5 ± 7.3 (N = 21) Wilcoxon 3.08 P = 0.002Comparison by gender Mann–Whitney P = 0.012
Score Goldberg Scale > 6Total 67.9 % 45.5 % McNemar P = 0.002
Male 56.3 % 47.8 % McNemar P = 0.687
Female 79.2 % 28.7 % McNemar P = 0.001
A (somatic symptoms) (Mean ± S.D.)Total 3.55 ± 2.45 2.00 ± 2.12 Wilcoxon 3.40 P = 0.001Male 3.03 ± 2.54 1.96 ± 2.23 Wilcoxon 1.85 P = 0.064Female 4.25 ± 2.04 2.05 ± 2.06 Wilcoxon 2.90 P = 0.004
B (anxiety/insomnia) (Mean ± SD)Total 3.34 ± 2.67 2.20 ± 2.52 Wilcoxon 2.99 P = 0.003Male 2.83 ± 2.52 2.35 ± 2.44 Wilcoxon 1.29 P = 0.198Female 4.19 ± 2.68 2.05 ± 2.66 Wilcoxon 2.73 P = 0.006
C (social dysfunction) (Mean ± SD)Total 2.27 ± 2.08 1.77 ± 2.31 Wilcoxon 1.32 P = 0.186Male 1.48 ± 1.65 1.83 ± 2.21 Wilcoxon 0.546 P = 0.585Female 3.05 ± 2.11 1.71 ± 2.47 Wilcoxon 2.08 P = 0.038
D (depression) (Mean ± SD)Total 0.79 ± 1.36 0.45 ± 1.17 Wilcoxon 1.37 P = 0.170Male 0.48 ± 0.79 0.39 ± 1.12 Wilcoxon 0.572 P = 0.567Female 1.00 ± 1.41 0.52 ± 1.25 Wilcoxon 1.40 P = 0.162
Significant values are indicated in boldface. P values are 2-tailed.
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151 147
the most frequently endorsed. No statistically significant differ-ences were observed between genders on the various sub-scales.
3.1.3. Correlation between DTS and GHQA correlation analysis was done between DTS score and the
other study variables. At Month 1, a statistically significantcorrelation was found between DTS and Goldberg (R Spear-man 0.769, P < 0.000), and between DTS and the number ofstressor events that occurred during the year prior to the attack(R Spearman 0.372, P = 0.005). However, we did not find anystatistically significant association between DTS scores and se-verity of medical prognosis after evaluation in the emergencyroom (R Spearman –0.250, P = 0.069). At Month 6, only thecorrelation between DTS and Goldberg remained significant (RSpearman 0.726, P < 0.000).
3.1.4. Multiple logistic regression analysisA multiple logistic regression analysis was done, using
whether the patients had PTSD as a dependent variable. Theresults are shown in Table 4. At Month 1, only psychiatrichistory prior to March 11 was associated with PTSD. The onlycovariate associated with PTSD at Month 6 was the presenceof PTSD at Month 1.
3.2. Relatives
At Month 1, relatives of 33 patients responded, and atMonth 6, relatives of 21 patients responded. In all, 47 relatives
responded at Month 1 and 31 at Month 6. Of these, 91.5%were first-degree relatives of the victims. There were no signif-icant differences in DTS scores between relatives and victims,although the scores of relatives were lower than those of thevictims. Table 5 summarises these results.
4. Discussion
In this 6-month follow-up study, we verified that the preva-lence of PTSD among victims of the attacks of March 11 washigh, with 41.1% PTSD at Month 1 and 40.9% at Month 6.Despite the wide variation in stability of PTSD figures reportedby prior studies [8,23,34,36,45,46], the difference in PTSDprevalence between Month 1 and Month 6 was lower than ex-pected, based on previous studies on PTSD in trauma survivors[19,42]. It is possible that other stress factors are contributingto these results. Future research should address this point.
The literature on posttraumatic stress reports that individualsdirectly affected by disasters have higher rates of PTSD thanindividuals who are indirectly affected [16,19]. Thus, studiesconducted in New York City among the general populationafter the September 11 attacks found a PTSD prevalence of7.5–11.2% in the first two months [16,17]. On the other hand,34% of survivors of the Oklahoma City bombing [33] and38.5% of direct victims of terrorist attacks in France [23] hadPTSD.
These figures are lower than those found in our study. Onepossible reason for this finding is that the sample in our study
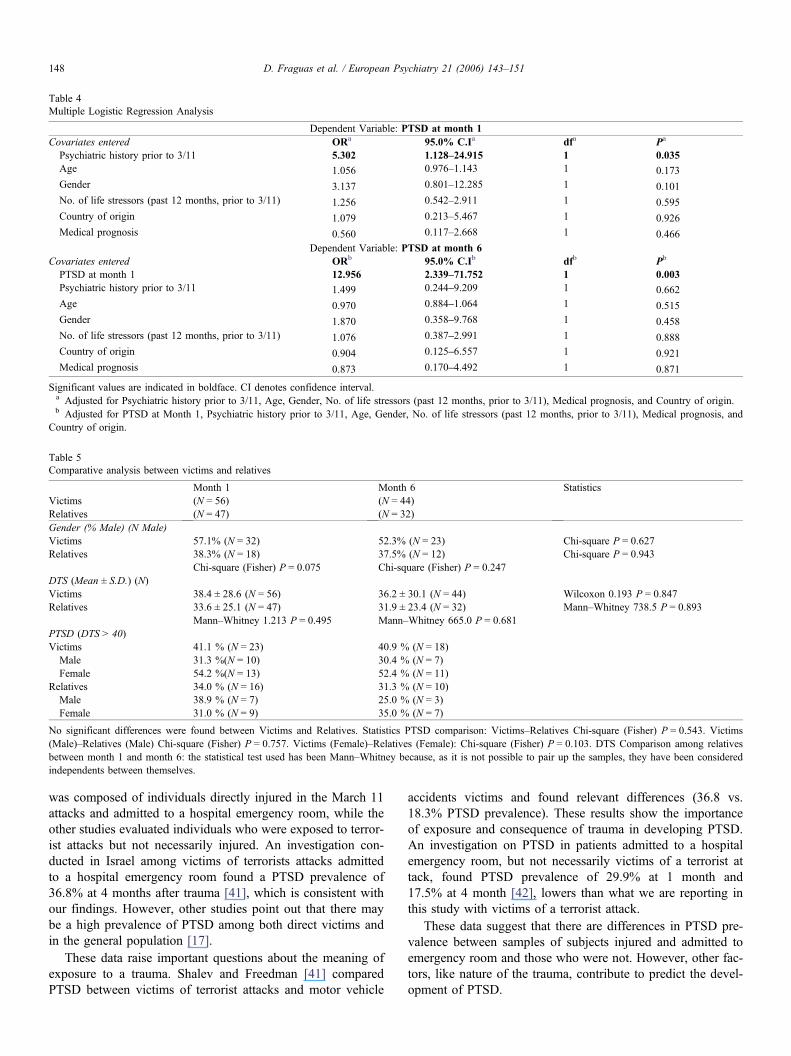
Table 4Multiple Logistic Regression Analysis
Dependent Variable: PTSD at month 1Covariates entered ORa 95.0% C.Ia dfa Pa
Psychiatric history prior to 3/11 5.302 1.128–24.915 1 0.035Age 1.056 0.976–1.143 1 0.173Gender 3.137 0.801–12.285 1 0.101No. of life stressors (past 12 months, prior to 3/11) 1.256 0.542–2.911 1 0.595Country of origin 1.079 0.213–5.467 1 0.926Medical prognosis 0.560 0.117–2.668 1 0.466
Dependent Variable: PTSD at month 6Covariates entered ORb 95.0% C.Ib dfb Pb
PTSD at month 1 12.956 2.339–71.752 1 0.003Psychiatric history prior to 3/11 1.499 0.244–9.209 1 0.662Age 0.970 0.884–1.064 1 0.515Gender 1.870 0.358–9.768 1 0.458No. of life stressors (past 12 months, prior to 3/11) 1.076 0.387–2.991 1 0.888Country of origin 0.904 0.125–6.557 1 0.921Medical prognosis 0.873 0.170–4.492 1 0.871
Significant values are indicated in boldface. CI denotes confidence interval.a Adjusted for Psychiatric history prior to 3/11, Age, Gender, No. of life stressors (past 12 months, prior to 3/11), Medical prognosis, and Country of origin.b Adjusted for PTSD at Month 1, Psychiatric history prior to 3/11, Age, Gender, No. of life stressors (past 12 months, prior to 3/11), Medical prognosis, and
Country of origin.
Table 5Comparative analysis between victims and relatives
Month 1 Month 6 StatisticsVictims (N = 56) (N = 44)Relatives (N = 47) (N = 32)Gender (% Male) (N Male)Victims 57.1% (N = 32) 52.3% (N = 23) Chi-square P = 0.627Relatives 38.3% (N = 18) 37.5% (N = 12) Chi-square P = 0.943
Chi-square (Fisher) P = 0.075 Chi-square (Fisher) P = 0.247DTS (Mean ± S.D.) (N)Victims 38.4 ± 28.6 (N = 56) 36.2 ± 30.1 (N = 44) Wilcoxon 0.193 P = 0.847Relatives 33.6 ± 25.1 (N = 47) 31.9 ± 23.4 (N = 32) Mann–Whitney 738.5 P = 0.893
Mann–Whitney 1.213 P = 0.495 Mann–Whitney 665.0 P = 0.681PTSD (DTS > 40)Victims 41.1 % (N = 23) 40.9 % (N = 18)
Male 31.3 %(N = 10) 30.4 % (N = 7)Female 54.2 %(N = 13) 52.4 % (N = 11)
Relatives 34.0 % (N = 16) 31.3 % (N = 10)Male 38.9 % (N = 7) 25.0 % (N = 3)Female 31.0 % (N = 9) 35.0 % (N = 7)
No significant differences were found between Victims and Relatives. Statistics PTSD comparison: Victims–Relatives Chi-square (Fisher) P = 0.543. Victims(Male)–Relatives (Male) Chi-square (Fisher) P = 0.757. Victims (Female)–Relatives (Female): Chi-square (Fisher) P = 0.103. DTS Comparison among relativesbetween month 1 and month 6: the statistical test used has been Mann–Whitney because, as it is not possible to pair up the samples, they have been consideredindependents between themselves.
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151148
was composed of individuals directly injured in the March 11attacks and admitted to a hospital emergency room, while theother studies evaluated individuals who were exposed to terror-ist attacks but not necessarily injured. An investigation con-ducted in Israel among victims of terrorists attacks admittedto a hospital emergency room found a PTSD prevalence of36.8% at 4 months after trauma [41], which is consistent withour findings. However, other studies point out that there maybe a high prevalence of PTSD among both direct victims andin the general population [17].
These data raise important questions about the meaning ofexposure to a trauma. Shalev and Freedman [41] comparedPTSD between victims of terrorist attacks and motor vehicle
accidents victims and found relevant differences (36.8 vs.18.3% PTSD prevalence). These results show the importanceof exposure and consequence of trauma in developing PTSD.An investigation on PTSD in patients admitted to a hospitalemergency room, but not necessarily victims of a terrorist attack, found PTSD prevalence of 29.9% at 1 month and17.5% at 4 month [42], lowers than what we are reporting inthis study with victims of a terrorist attack.
These data suggest that there are differences in PTSD pre-valence between samples of subjects injured and admitted toemergency room and those who were not. However, other fac-tors, like nature of the trauma, contribute to predict the devel-opment of PTSD.
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151 149
A review of PTSD in the literature shows results that sup-port these concepts, but also it points out that there is no simplerelationship between exposure to a traumatic event and the de-velopment of PTSD, so other factors need to be considered[51].
Posttraumatic stress symptoms positively correlate with per-ception of health problems. This correlation leads us to thinkthat both posttraumatic stress symptoms and subjective healthproblems are part of the psychological response to trauma.These results may also be due to a possible overlap betweenwhat the DTS and GHQ scales assess. However, it is importantto point out that a recent study based on US National Comor-bidity Survey data, shows that, after controlling for sex, healthperceptions, stress, health-related behaviours, insurance cover-age, total trauma exposure, total number of psychiatric diag-noses and neuroticism, PTSD is predictive of poor health [28].
Changes in GHQ results between 1 and 6 months seem toindicate that perception of health problems is linked to an acutestress process, while PTSD is more likely to be a persistentconsequence of trauma.
Assessed at Month 1, posttraumatic stress symptoms corre-lated positively with the number of stressor events that oc-curred during the year prior to the attack, but not in the secondevaluation. Experience of adverse events could be a vulnerabil-ity factor for the acute response to trauma [35,49,50,52].
Also, in the first evaluation, there was a weak, non-signifi-cant correlation between PTSD symptomatology and mildprognosis. This correlation was not maintained at the secondevaluation. We found no similar findings in the reviewed lit-erature. One explanation for this fact is that more severe inju-ries may have received more medical attention and psycholo-gical support than mild injuries. This may also be related to aprimary concern for life-threatening injuries and the possiblesequelae of more severe injuries.
The differences between genders are a notable finding ofthis study. Female subjects seem to have a higher likelihoodof developing PTSD after trauma than male subjects. Theseresults are consistent with those found in other investigations[7,31,53]. However, some studies have not found such differ-ences [12,14].
These discrepancies may be due in part to the social andeconomic circumstances of the samples [53]. However, futureinvestigation is needed to clarify this point.
There were no statistically significant differences betweenvictims and relatives in prevalence of PTSD, although it waslower in relatives than in victims. Likewise, among relativesthere were no relevant differences in PTSD between genders.This result needs further investigation to be understood, butbased on these data we can suggest that women are more likelyto develop PTSD symptoms than men after direct exposure totrauma (victims), and that there is no such difference after in-direct trauma (relatives).
The percentage of relatives with PTSD was higher than thatfound in other study in the general population [31]. The highlevel of involvement among relatives found in our study couldbe a consequence of a selective sample. However, it also sug-
gests that there is an indirectly experienced trauma disorderamong relatives. This question requires future investigation.
Prior studies have found differences in PTSD response be-tween native and immigrant populations [17,19]. Our study didnot find significant differences between natives and immi-grants. However, it is worth mentioning that, although it wasnot significant, immigrants had an increase in PTSD preva-lence between Month 1 and Month 6, while natives had a de-crease in these figures (Table 2). Increased power from a largersample size might have resulted in this non-significant relation-ship reaching statistical significance.
Patients with a psychiatric history before March 11 hadhigher prevalence of PTSD than those with no such history.These results are consistent with prior studies [17,19]. How-ever, this difference was only significant at Month 1, whichmay be due to the small size of our sample.
The high rates of PTSD at 1 and 6 months lead us to thinkabout the implications for health services in the aftermath oflarge-scale trauma. A long-term follow-up of 32 years, con-ducted in Israel among war veterans, points out the importanceof early and maintained health care in order to reduce the psy-chological sequelae of trauma [47]. A prospective study ofposttraumatic stress and depressive reactions among adoles-cents affected by a devastating earthquake in Armenia foundthat psychological treatment, even provided at 18 months afterthe trauma, is effective in reducing PTSD symptoms [21]. Ourhospital designed a plan for attending to both victims and theirrelatives based on the importance of an early and maintainedtreatment [39].
Available data show that there is a large subgroup of pa-tients affected by PTSD who do not seek treatment, mainlybecause they do not believe they have a problem [5]. The re-sults of our study also support the importance of being alert toPTSD symptoms, so they can be correctly diagnosed and trea-ted. They also hold the advisability of offering the patients thechance to receive mental health care.
Some limitations of our study should be noted: First, thelack of information about the victims prior to the attacks limitsthe possibility of drawing causal inferences. Second, this studyis part of a multicenter study and the size of the sample wasdetermined based on the multicenter criteria. Third, the smallsize of the sample may be a cause of possible type II errors.Fourth, the Davidson Trauma Scale is a self-administered scalefor detecting PTSD symptoms, which evaluates symptomaticseverity but was not designed for diagnostic purposes. Fifth,relatives were selected by the patients; therefore other factorsassociated with that selection could not be controlled. Sixth,the results can not be generalised to victims of a terrorist attackwho are not injured and treated in an emergency room. Se-venth, the existence of a psychiatric history prior to March 11was evaluated using the MINI scale, but it is not a scale speci-fically developed for that function.
The randomised patient sampling strategy, the high level ofvictim participation, and the similar socio-demographic charac-teristics between participants and subjects lost to follow-up
[18
[19
[20
[21
[22
[23
[24
[25
[26
[27
[28
[29
[30
[31
[32
[33
[34
[35
[36
[37
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151150
provide reasonable protection against other possible selectionbiases.
Acknowledgements
Supported in part by a grant from the Fondo de Investiga-ción Sanitaria (FIS PIO52160 I.P. E. Sainz Corton).
References
[1] Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, BrysonH, et al. ESEMeD/MHEDEA 2000 Investigators, European Study of theEpidemiology of Mental Disorders (ESEMeD) Project. Prevalence ofmental disorders in Europe: results from the European Study of the Epi-demiology of Mental Disorders (ESEMeD) Project. Acta Psychiatr ScandSuppl 2004(420):21–7.
[2] American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders, 4th ed. Washington, DC: American Psychiatric Press;1994.
[3] Banco de España. In: Los efectos de los atentados del 11 de marzo de2004, según los indicadores coyunturales. Mayo: Boletín Económico;2004. p. 31–8.
[4] Bobes J, Calcedo-Barba A, García M, Francois M, Rico-Villademoros F,González MP, et al. Evaluation of the psychometric properties of theSpanish version of 5 questionnaires for the evaluation of post-traumaticstress syndrome. Actas Esp Psiquiatr 2000;28(4):207–18.
[5] Boscarino JA, Adams RE, Stuber J, Galea S. Disparities in mental healthtreatment following the World Trade Center Disaster: implications formental health care and health services research. J Trauma Stress 2005;18(4):287–97.
[6] Breslau N, Davis GC, Andreski P, Peterson E. Traumatic events andposttraumatic stress disorder in an urban population of young adults.Arch Gen Psychiatry 1991;48(3):216–22.
[7] Breslau N, Davis GC. Posttraumatic stress disorder in an urban popula-tion of young adults: risk factors for chronicity. Am J Psychiatry 1992;149(5):671–5.
[8] Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, Andreski P.Trauma and posttraumatic stress disorder in the community. Arch GenPsychiatry 1998;55(7):626–32.
[9] Corradi J, Fagen PW, Garreton M, editors. Fear at the edge: state terrorand resistance in Latin America. Berkeley, CA: University of CaliforniaPress; 1992.
[10] Clave 20. Revista Interna de SAMUR-Protección Civil “Villa de Ma-drid”. Especial 11 de Marzo. Junio 2004.
[11] Davidson JR, Book SW, Colket JT, Tupler LA, Roth S, David D, et al.Assessment of a new self-rating scale for post-traumatic stress disorder.Psychol Med 1997;27(1):153–60.
[12] Ehlers A, Mayou RA, Bryant B. Psychological predictors of chronicposttraumatic stress disorder after motor vehicle accidents. J AbnormPsychol 1998;107:508–19.
[13] El País. La cifras de la tragedia. 12 de Septiembre. Madrid; 2004: 20.[14] Freedman SA, Gluck N, Tuval-Mashiach R, Brandes D, Peri T,
Shalev AY. Gender differences in responses to traumatic events: a pro-spective study. J Trauma Stress 2002;15(5):407–13.
[15] Ferrando L, Bobes J, Gibert J, Soto M, Soto O. Mini Entrevista Neurop-siquiátrica Internacional. Versión Española. En: Banco de instrumentosbásicos para la práctica de la psiquiatría clínica. 2ª edición. J Bobes et aleds. Ars Médica 2002.
[16] Galea S, Ahern J, Resnick H, Kilpatrick D, Bucuvalas M, Gold J. Psy-chological sequelae of the September 11 terrorist attacks in New YorkCity. N Engl J Med 2002;346:982–7.
[17] Galea S, Resnick H. Posttraumatic stress disorder in the general popula-tion after mass terrorist incidents: considerations about the nature of ex-posure. CNS Spectr 2005;10(2):107–15.
] Galea S, Resnick H, Ahern J, Gold J, Bucuvalas M, Kilpatrick D, et al.Posttraumatic stress disorder in Manhattan, New York City, after theSeptember 11th terrorist attacks. J Urban Health 2002;79(3):340–53.
] Galea S, Vlahov D, Resnick H, Ahern J, Susser E, Gold J, et al. Trendsof probable Post-Traumatic Stress Disorder in New York City after theSeptember 11 Terrorist Attacks. Am J Epidemiol 2003;158:514–24.
] Galea S, Vlahov D, Resnick H, Kilpatrick D, Bucuvalas MJ,Morgan MD, et al. An investigation of the psychological effects of theSeptember 11, 2001, attacks on New York City: developing and imple-menting research in the acute postdisaster period. CNS Spectr 2002;7(8):585–7 (593–6).
] Goenjian AK, Walling D, Steinberg AM, Karayan I, Najarian LM, Py-noos R. A prospective study of posttraumatic stress and depressive reac-tions among treated and untreated adolescents 5 years after a catastrophicdisaster. Am J Psychiatry 2005;162(12):2302–8.
] Goldberg DP, Hillier VF. A scaled version of the General Health Ques-tionnaire. Psychol Med 1979;9(1):139–45.
] Jehel L, Paterniti S, Brunet A, Duchet C, Guelfi JD. Prediction of theoccurrence and intensity of post-traumatic stress disorder in victims32 months after bomb attack. Eur Psychiatry 2003;18(4):172–6.
] Kessler RC. Posttraumatic stress disorder: the burden to the individualand to society. J Clin Psychiatry 2000;61(suppl. 5):4–12.
] Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE.Lifetime prevalence and age-of-onset distributions of DSM-IV disordersin the National Comorbidity Survey Replication. Arch Gen Psychiatry2005;62(6):593–602.
] Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Preva-lence, severity, and comorbidity of 12-month DSM-IV disorders in theNational Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62(6):590–2.
] Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttrau-matic stress disorder in the National Comorbidity Survey. Arch Gen Psy-chiatry 1995;52(12):1048–60.
] Lauterbach D, Vora R, Rakow M. The relationship between posttrau-matic stress disorder and self-reported health problems. Psychosom Med2005;67(6):939–47.
] Lobo A, Pérez Echeverría MJ, Artal J. Validity of the scaled version ofthe General Health Questionnaire (GHQ-28) in a Spanish population.Psychol Med 1986;16(1):135–40.
] Ministerio del Interior. Dirección General de Protección Civil y Emer-gencias. Reflexiones sobre las actuaciones en materia de protección civiltras los atentados terroristas del 11 de marzo de 2004 en Madrid. 30 deJunio 2004. http: www.proteccioncivil.org/informes/infoactua.htm.
] Norris FH. Epidemiology of trauma: frequency and impact of differentpotentially traumatic events on different demographic groups. J ConsultClin Psychol 1992;60(3):409–18.
] Norris FH, Friedman MJ, Watson PJ, Byrne CM, Díaz E, Kaniasty K.60,000 disaster victims speak: part I. An empirical review of the empiri-cal literature, 1981-2001. Psychiatry 2002;65(3):207–39 (Review).
] North CS, Nixon SJ, Shariat S, Mallonee S, McMillen JC,Spitznagel EL, et al. Psychiatric disorders among survivors of the Okla-homa City bombing. JAMA 1999;282(8):755–62 (25).
] North CS, Kawasaki A, Spitznagel EL, Hong BA. The course of PTSD,major depression, substance abuse, and somatization after a natural dis-aster. J Nerv Ment Dis 2004;192(12):823–9.
] Perkonigg A, Kessler RC, Storz S, Wittchen HU. Traumatic events andpost-traumatic stress disorder in the community: prevalence, risk factorsand comorbidity. Acta Psychiatr Scand 2000;101(1):46–59.
] Perkonigg A, Pfister H, Stein MB, Hofler M, Lieb R, Maercker A, et al.Longitudinal course of posttraumatic stress disorder and posttraumaticstress disorder symptoms in a community sample of adolescents andyoung adults. Am J Psychiatry 2005;162(7):1320–7.
] Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, Best CL. Preva-lence of civilian trauma and posttraumatic stress disorder in a representa-tive national sample of women. J Consult Clin Psychol 1993;61(6):984–91.
[38
[39
[40
[41
[42
[43
[44
[45
[46
[47
[48
[49
[50
[51
[52
[53
D. Fraguas et al. / European Psychiatry 21 (2006) 143–151 151
] Rodríguez P, Serra JA. Coordinación general de las actuaciones del 11Men el hospital General Universitario Gregorio Marañón de Madrid. MedClin (Barc) 2005;124(suppl. 1):3–7.
] Sainz Cortón E, Gonzalo Franco S, Gómez Rojo RM. Actuación delHospital General Universitario Gregorio Marañón en los atentados del11 de marzo. Salud Mental. Med Clin (Barc) 2005;124(Suppl. 1):39–41.
] Schlenger WE, Caddell JM, Ebert L, Jordan BK, Rourke KM, Wilson D,et al. Psychological reactions to terrorist attacks: findings from the Na-tional Study of Americans’ Reactions to September 11. JAMA 2002;288(5):581–8.
] Shalev AY, Freedman S. PTSD following terrorist attacks: a prospectiveevaluation. Am J Psychiatry 2005;162:1188–91.
] Shalev AY, Freedman S, Peri T, Brandes D, Sahar T, Orr SP, et al. Pro-spective study of Posttraumatic Stress Disorder and Depression followingTrauma. Am J Psychiatry 1998;155(5):630–7.
] Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E,et al. The Mini-International Neuropsychiatric Interview (MINI): the de-velopment and validation of a structured diagnostic psychiatric interviewfor DSM-IV and ICD-10. J Clin Psychiatry 1998;59(suppl. 20):22–33.
] Sheehan DV, Lecrubier Y, Sheehan KH, Janavs J, Weiller E, KeskinerA, et al. The validity of the Mini International Neuropsychiatric Inter-view (MINI) according to the SCID-P and its reliability. Eur Psychiatry1997;12:232–41.
] Silver RC, Holman EA, McIntosh DN, Poulin M, Gil-Rivas V. Nation-wide longitudinal study of psychological responses to September 11.JAMA 2002;288(10):1235–44.
] Silver RC, Holman EA, McIntosh DN, Poulin M, Gil-Rivas V. Nation-wide longitudinal study of psychological responses to September 11.JAMA 2002;288(10):1235–44.
] Shlosberg A, Strous RD. Long-Term Follow-Up (32 years) of PTSD inIsraeli Yom Kippur War Veterans. J Nerv Ment Dis 2005;193(10):693–6.
] SPSS. SPSS for Windows, version 12.0. Illinois, Chicago, USA: SPSSIns; 2002.
] Yehuda R, Halligan SL, Bierer LM. Relationship of parental trauma ex-posure and PTSD to PTSD, depressive and anxiety disorders in off-spring. J Psychiatr Res 2001;35(5):261–70.
] Yehuda R, Kahana B, Schmeidler J, Southwick SM, Wilson S, Giller EL.Impact of cumulative lifetime trauma and recent stress on current post-traumatic stress disorder symptoms in holocaust survivors. Am J Psy-chiatry 1995;152(12):1815–8.
] Yehuda R, McFarlane AC, Shalev AY. Predicting the development ofPosttraumatic Stress Disorder from the acute response to a traumaticevent. Biol Psychiatry 1998;44:1305–13.
] Yehuda R, Schmeidler J, Wainberg M, Binder-Brynes K, Duvdevani T.Vulnerability to posttraumatic stress disorder in adult offspring of Holo-caust survivors. Am J Psychiatry 1998;155(9):1163–71.
] Weissman MM, Neria Y, Das A, Feder A, Blanco C, Lantigua R, et al.Gender differences in posttraumatic stress disorder among primary carepatients after the World Trade Center attack of September 11, 2001.Gend Med 2005;2(2):76–87.
Top Related
Copyright © 2022 FDOKUMEN

