







Bahasa
Halaman
Hukum

COPYRIGHT AND CITATION CONSIDERATIONS FOR THIS THESIS/ DISSERTATION
o Attribution — You must give appropriate credit, provide a link to the license, and indicate ifchanges were made. You may do so in any reasonable manner, but not in any way thatsuggests the licensor endorses you or your use.
o NonCommercial — You may not use the material for commercial purposes.
o ShareAlike — If you remix, transform, or build upon the material, you must distribute yourcontributions under the same license as the original.
How to cite this thesis
Surname, Initial(s). (2012) Title of the thesis or dissertation. PhD. (Chemistry)/ M.Sc. (Physics)/ M.A. (Philosophy)/M.Com. (Finance) etc. [Unpublished]: University of Johannesburg. Retrieved from: https://ujcontent.uj.ac.za/vital/access/manager/Index?site_name=Research%20Output (Accessed: Date).
Perceived Effectiveness of Complementary Medicine by Mothers of Infants
with Colic in Gauteng
A dissertation submitted to the
Faculty of Health Sciences, University of Johannesburg,
as partial fulfilment for the
Master’s Degree in Technology Homoeopathy
by
Natalie Christina Di Gaspero
(Student Number: 200901633)
Supervisor:
Dr Radmila Razlog M.Tech Hom (TWR) Date
Co-supervisor:
Dr Reshma Patel M. Tech Hom (UJ) Date
i
DECLARATION
I declare that this dissertation is my own, unaided work. It is being submitted for the Degree of
Master of Technology: Homoeopathy at the University of Johannesburg, Johannesburg. It has
not been submitted before for any degree or examination in any other Technikon or University.
Natalie Christina Di Gaspero
day of 2017.
iii
ABSTRACT
Infantile colic is a self-limiting condition that is characterised by spasmodic, excessive and
inconsolable crying without apparent cause. It is defined according to Wessel’s criteria as crying
in a seemingly healthy infant that lasts for more than three hours each day, on more than three
days a week, for a period of more than three weeks. Infantile colic affects infants between the
ages of 2-16 weeks and tends to naturally resolve itself around 16 weeks of age. Infantile colic is
a common, but poorly understood condition that occurs in 10-30% of infants. Research indicates
that there may be various independent aetiologies of colic. Infantile colic is one of the most
common reasons parents take their infants to paediatric healthcare practitioners despite there
being no widely accepted conventional treatment for colic. Due to the recent growth of the
complementary medicine market in South Africa and numerous complementary medicines being
available over-the-counter, parents may turn to complementary medical treatments for their
infants’ colic. There is currently no gold standard treatment for colic and there is limited research
available on the use, safety and effectiveness of complementary medicine in infantile colic.
The aim of this study was to determine the perceived effectiveness of complementary medicine
by mothers of infants with colic in Gauteng, by means of an Infantile Colic Questionnaire.
A quantitative-descriptive design was used whereby data was collected through a randomised
cross-sectional survey to determine the perceived effectiveness of complementary medicine by
mothers of infants with colic in Gauteng. The Infantile Colic Questionnaire was completed on a
voluntary basis as a convenience sample. Participants were recruited from various baby and
health clinics, health shops, antenatal groups and nursery schools. The research sample consisted
of 150 mothers (participants), aged between 18-45 years with a child/children who
suffer/suffered from symptoms of infantile colic and use complementary medicine as a form of
treatment. The survey was completed on a voluntary basis and interested participants were given
an Information Leaflet and Consent Form. Once consent was given, participants completed the
Infantile Colic Questionnaire. All completed surveys were treated as strictly confidential, and
only the researcher, supervisor and statistician had access to the information. No identifying data
was requested or permitted on the survey. Data obtained was statistically analysed with the
assistance of Statkon through frequencies and multiple response analysis.
Majority of participants made use of both complementary medicine and conventional medicine
(73%) for their infant’s colic. The most commonly used complementary products for infantile
colic were individualised homeopathic remedies (58.6%), probiotics (46.7%) and over-the-
iv
counter herbal medicines (44.1%). Participants obtained their information regarding
complementary medicine from complementary medicine practitioners (61.8%), family and
friends (53.9%) and general practitioners (50%). Complementary medicine was chosen as a
modality for treatment due to it being perceived as safe, less harmful and with fewer or no side
effects.
It was evident that most participants weren’t familiar with the term “complementary medicine”
and were therefore confused as to which products are classified as complementary medicines.
Furthermore, for some products the distinction is vague, as the formulations contain both
complementary and conventional medicines, which further contributed to the misunderstanding.
Results from this study, conducted on the perceived effectiveness of complementary medicine by
mothers of infants with colic in Gauteng, indicated that participants perceived complementary
medicine as an effective form of treatment for infantile colic; however, there is uncertainty
whether it works well in conjunction with conventional medicine. Further education is also
needed on complementary medicine due to the misunderstanding of terms, complementary
medicine and conventional medicine.
In conclusion, complementary medicine is perceived to be an effective form of treatment by
mothers of infants with infantile colic; however, further research and larger scale studies should
be conducted to validate this.
v
DEDICATION
Dedicated to my beloved parents, Alfredo and Lesley.
Without you, none of this would be possible. Thank you for all the sacrifices you have made to
provide me with a world of opportunity. Thank you for your unwavering support and
unconditional love, I owe my success to you.
vi
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to those that assisted me in completing this thesis:
Dr Radmila Razlog (Supervisor), thank you for your continuous guidance and for dedicating
your valuable time and patience to my research. Your kindness, positivity and passion for
homeopathy have been inspiring throughout my years of study.
Dr Reshma Patel (Co-Supervisor), thank you for your advice and knowledgeable input.
Your help has been invaluable and I am truly grateful.
To my siblings Daniella, Gabriella and Marco Di Gaspero, thank you for standing by my
side and for always believing in me. I am truly blessed to always have your love and
support. Thank you to Daniella for always proofing my work, your help has been invaluable
and I will always be grateful.
Riccardo De Cecco, thank you for always having confidence in me and for inspiring me to
be the best version of myself. Thank you for your endless love and help throughout the
years.
To my friends, I thank you for your part in my journey. For your friendship, encouragement
and support through the years, I couldn’t have done it without you.
The staff within the Department of Homeopathy, thank you for all your guidance and
knowledgeable input.
Mr Anesu Kuhudzai (Statkon), thank you for your assistance and statistical expertise.
To all the participants who willingly gave up their time to partake in the study.
vii
TABLE OF CONTENTS
DECLARATION ........................................................................................................................... i
AFFIDAVIT .................................................................................................................................. ii
ABSTRACT ................................................................................................................................. iii
DEDICATION ............................................................................................................................... v
ACKNOWLEDGEMENTS ........................................................................................................ vi
TABLE OF CONTENTS ........................................................................................................... vii
LIST OF FIGURES .................................................................................................................... xii
CHAPTER ONE: INTRODUCTION .......................................................................................... 1
1.1 Problem statement ...................................................................................................... 1
1.2 Aim of the study ......................................................................................................... 1
1.3 Importance of the study .............................................................................................. 1
1.4 Delimitations of the study .......................................................................................... 2
1.5 Assumptions ............................................................................................................... 3
1.6 Objectives ................................................................................................................... 3
CHAPTER TWO: LITERATURE REVIEW ............................................................................ 4
2.1 Introduction to infantile colic ..................................................................................... 4
2.1.1 Aetiology of infantile colic......................................................................................... 4
2.1.1.1 Lactose intolerance ..................................................................................................... 4
2.1.1.2 Motility ....................................................................................................................... 5
2.1.1.3 Gastro-oesophageal reflux .......................................................................................... 5
2.1.1.4 Gut Hormones ............................................................................................................ 6
2.1.1.5 Gut Microflora ............................................................................................................ 6
2.1.1.6 Food Hypersensitivity ................................................................................................ 6
2.1.1.7 Psychological factors .................................................................................................. 7
viii
2.1.1.8 Migrainous phenomenon ............................................................................................ 7
2.1.1.9 Melatonin and serotonin ............................................................................................. 7
2.1.1.10 Fourth trimester theory ............................................................................................... 8
2.1.1.11 Gastrointestinal gas .................................................................................................... 8
2.1.1.12 Maternal smoking ....................................................................................................... 8
2.1.2 Physical signs and symptoms ..................................................................................... 8
2.1.3 Diagnosis .................................................................................................................... 9
2.1.4 Differential diagnosis for crying ................................................................................ 9
2.1.4.1 Cardiac causes ............................................................................................................ 9
2.1.4.2 Gastrointestinal causes ............................................................................................. 10
2.1.4.3 Infectious causes ...................................................................................................... 11
2.1.4.4 Trauma ..................................................................................................................... 12
2.1.4.5 Other causes ............................................................................................................. 12
2.2 Treatment approaches............................................................................................... 13
2.2.1 Conventional medicine ............................................................................................. 13
2.2.2 Lifestyle and behavioural adjustments ..................................................................... 15
2.2.3 General complementary medicine for infantile colic ............................................... 16
2.2.3.1 Homeopathy ............................................................................................................. 17
2.2.3.2 Aromatherapy ........................................................................................................... 18
2.2.3.3 Ayurveda .................................................................................................................. 19
2.2.3.4 Phytotherapy ............................................................................................................. 19
2.2.3.5 Unani-Tibb ............................................................................................................... 20
2.2.3.6 Naturopathy .............................................................................................................. 21
2.2.4 Over-the-counter complementary medicine for infantile colic ................................ 21
CHAPTER THREE: METHODOLOGY ................................................................................. 28
3.1 Introduction .............................................................................................................. 28
3.2 Research Sample ...................................................................................................... 28
ix
3.2.1. Inclusion criteria ....................................................................................................... 29
3.2.2. Exclusion criteria ...................................................................................................... 29
3.3. Research Procedure and design ................................................................................ 29
3.4 Reliability and validity measures ............................................................................. 30
3.5 Data collection and analysis ..................................................................................... 30
3.6 Ethics ........................................................................................................................ 30
CHAPTER FOUR: RESULTS ................................................................................................... 32
4.1 Introduction .............................................................................................................. 32
4.1.1 Sample ...................................................................................................................... 32
4.2 General ..................................................................................................................... 32
4.2.1 Age of mother/respondent ........................................................................................ 32
4.2.2 Number of children .................................................................................................. 33
4.2.3 Gender of your child/children .................................................................................. 34
4.2.4 Diagnosis of colic ..................................................................................................... 34
4.2.5 Occurrence of colic .................................................................................................. 35
4.2.6 Antenatal class attendance........................................................................................ 37
4.3 Behaviours ................................................................................................................ 38
4.3.1 Crying ....................................................................................................................... 38
4.3.2 Timing of colic symptoms ........................................................................................ 41
4.3.3 Reasons for discomfort ............................................................................................. 43
4.3.4 Vomiting ................................................................................................................... 44
4.3.5 Sleeping .................................................................................................................... 45
4.4 Feeding ..................................................................................................................... 46
4.5 Burping ..................................................................................................................... 46
4.6 Sucking for comfort ................................................................................................. 47
4.7 Methods to soothe baby ............................................................................................ 47
4.8 Treatment ................................................................................................................. 48
x
4.8.1 Use of complementary medicine .............................................................................. 48
4.8.2 Information about complementary medicine ........................................................... 49
4.8.3 Complementary medicines used for colic ................................................................ 50
4.8.4 Conventional medicines used for colic .................................................................... 51
4.8.5 Perceived effectiveness of complementary medicine for colic ................................ 52
4.8.6 Perceived effectiveness of the combined use of conventional medicine with
complementary medicine ......................................................................................... 53
4.8.7 Awareness of side effects of complementary medicine ........................................... 53
CHAPTER FIVE: DISCUSSION .............................................................................................. 54
5.1 Introduction .............................................................................................................. 54
5.2 General information ................................................................................................. 54
5.3 Crying ....................................................................................................................... 55
5.4 Timing of colic symptoms ........................................................................................ 56
5.5 Reasons for discomfort ............................................................................................. 56
5.6 Vomiting ................................................................................................................... 57
5.7 Sleeping .................................................................................................................... 57
5.8 Feeding and burping ................................................................................................. 57
5.9 Methods to soothe .................................................................................................... 58
5.10 Treatments ................................................................................................................ 59
5.11 Consultation with a complementary medicine practitioner ...................................... 59
5.12 Sources of complementary information ................................................................... 60
5.13 Complementary medicine......................................................................................... 60
5.14 Conventional medicine ............................................................................................. 62
5.15 Statements regarding complementary medicine ...................................................... 63
5.16 Limitations and assumptions .................................................................................... 63
CHAPTER SIX: CONCLUSIONS AND RECOMMENDATIONS ....................................... 65
6.1 Conclusions .............................................................................................................. 65
xi
6.2 Recommendations .................................................................................................... 66
REFERENCES ............................................................................................................................ 68
APPENDIX A ............................................................................................................................... 79
APPENDIX B ............................................................................................................................... 80
APPENDIX C ............................................................................................................................... 81
APPENDIX D ............................................................................................................................... 82
APPENDIX E ............................................................................................................................... 93
APPENDIX F ............................................................................................................................... 97
APPENDIX G .............................................................................................................................. 98
APPENDIX H ............................................................................................................................ 110
APPENDIX I .............................................................................................................................. 111
APPENDIX J.............................................................................................................................. 112
APPENDIX K ............................................................................................................................ 116
APPENDIX L ............................................................................................................................. 118
xii
LIST OF FIGURES
Figure 4.1: Age of respondents in 10 year increments ................................................................. 33
Figure 4.2: Number of children .................................................................................................... 33
Figure 4.3: Gender of child ........................................................................................................... 34
Figure 4.4: Self-diagnosis of colic ................................................................................................ 35
Figure 4.5: Colic diagnosis by a health care practitioner ............................................................. 35
Figure 4.6: Age the colic started ................................................................................................... 36
Figure 4.7: Which child suffered from colic? ............................................................................... 36
Figure 4.8: Antenatal class attendance ......................................................................................... 37
Figure 4 9: Incidence of colic in a day ......................................................................................... 38
Figure 4.10: Duration of colic episode ......................................................................................... 39
Figure 4.11: Ability to soothe the colic baby ............................................................................... 39
Figure 4.12: Duration of crying at any given time ....................................................................... 40
Figure 4.13: Frequency of crying over a period of a week ........................................................... 40
Figure 4.14: Believed reasons for excessive crying ..................................................................... 41
Figure 4.15: Timing of colic symptoms in relation to feeding ..................................................... 42
Figure 4.16: Time of day the colic occurred................................................................................. 42
Figure 4.17: Reasons for discomfort ............................................................................................ 44
Figure 4.18: Vomiting milk after a feed ....................................................................................... 45
Figure 4.19: Reason for sleeping .................................................................................................. 45
Figure 4.20: Feeding methods ...................................................................................................... 46
Figure 4.21: Burping ..................................................................................................................... 47
xiii
Figure 4.22: Use of a dummy or thumb to soothe ........................................................................ 47
Figure 4.23: Methods to soothe baby ........................................................................................... 48
Figure 4.24: Treatment choice for colic ....................................................................................... 49
Figure 4.25: Information sources regarding complementary medicine for colic ......................... 49
Figure 4.26: Complementary medicines used for colic ................................................................ 51
Figure 4.27: Conventional medication used to treat colic ............................................................ 52
Figure 4.28: Perceived effectiveness of complementary medicine for colic ................................ 52
Figure 4.29: Perceived effectiveness of the combined use of conventional medicine with
complementary medicine ............................................................................................................... 53
Figure 4.30: Awareness of side effects of complementary medicine ........................................... 53
Figure J.1:.Number of children suffering from colic ................................................................. 112
Figure J.2.: Sufficiency of the ante-natal class........................................................................... 112
Figure J.3.: Is vomiting normal after a feed? ............................................................................. 113
Figure J.4.: Feeding method changes ......................................................................................... 113
Figure J.5.: Feeding on demand ................................................................................................. 114
Figure J.6.: Increase in feeding hours between 5pm and 12am ................................................. 114
Figure J.7.: Consulted with a complementary medicine practitioner ......................................... 115
1
CHAPTER ONE
INTRODUCTION
1.1 Problem statement
Infantile colic is defined as a behavioural disorder that is characterised by spasmodic, excessive
and inconsolable crying without apparent cause in an otherwise healthy infant. Infantile colic is a
common but poorly understood condition that affects many infants between the ages of 2-16
weeks and is prevalent in both males and females. Infants are classified as having colic if they
cry more than three hours each day, on more than three days a week, for a period of more than
three weeks (Savino, Tarasco, Sorrenti, Lingua, Moja, Gordon et al., 2014b). Infantile colic
occurs in 10-30% of infants making it one of the most common reasons parents take their infants
to paediatric healthcare practitioners. Infantile colic is not only distressing to the infant but on
the family too; and since there is no widely accepted conventional treatment for colic, parents
may turn to complementary medical treatments (Savino & Tarasco, 2010). The recent growth of
the complementary medicine market in South Africa has resulted in complementary medicines
being available in numerous retail outlets where they are obtainable without a prior medical
consultation (Gqaleni, Moodley, Kruger, Ntuli & McLeod, 2016). Despite this, there is currently
no gold standard treatment for colic and there is limited research available on the use, safety and
effectiveness of complementary medicine in infantile colic (Perry, Hunt & Ernst, 2011).
1.2 Aim of the study
The aim of this study was to determine the perceived effectiveness of complementary medicine
by mothers of infants with colic in Gauteng, by means of an Infantile Colic Questionnaire
(Appendix G).
1.3 Importance of the study
There is a growing necessity and demand for complementary medicine in South Africa, despite
conventional medicine being the main source of healthcare (Snyman, 2014). South Africa has
made substantial progress with integrating complementary medicine into the legal framework,
mainly due to the need and increase in demand for medical care (Gqaleni et al., 2016).
In a recent study conducted on the attitudes and perceptions of people in health shops towards
complementary and alternative medicine, it was concluded that complementary medicine is
growing in popularity and that it is used as a form of primary healthcare amongst many South
2
Africans. Out of the respondents, 97.3% (n=554) used vitamins/supplements; 62.3% (n=355)
used herbal preparations; 48.9% (n=278) used homoeopathy; 10.8% (n=61) used Traditional
Chinese Medicine; 10.2% (n=58) used Ayurveda; 6.5% (n=37) used aromatherapy; and 4.3%
(n=24) used Unani-Tibb (Snyman, 2014). In the last few years there has been an influx of
complementary medicine products into the South African market, however the efficacy of some
of these products is unknown (Gqaleni et al., 2016). With limited research available on the use,
safety and effectiveness of complementary medicine in infantile colic, it is important to establish
the use and perceived efficacy of these products (Perry et al., 2011). Not only is it important to
establish which complementary medicines are popular and effective for infantile colic, but also
to identify the effectiveness of these products allowing for further clinical, investigatory and
safety research to be conducted on them.
According to the World Health Organisation (WHO), it is estimated that 80% of the population
in developing countries use traditional or complementary medicine for their primary health
needs. South Africa recognises complementary medicine practitioners through the statutory
council, Allied Health Professions Council of South Africa (AHPCSA), however complementary
medicine is not currently integrated into our national health care system (Embrey, 2013). The
inclusion of complementary medicine into our national health care system will be greatly
beneficial to the population. This process can be facilitated by research conducted on the safety
and efficacy of complementary medicine deeming it important for such research to be conducted.
This can facilitate the growth of complementary medicine as a treatment modality as well as
provide a broader understanding to health care practitioners on the public’s usage and experience
with complementary medicine.
Infantile colic is a common but poorly understood condition (Savino & Tarasco, 2010). The
survey may also provide some additional information on the signs and symptoms of colic, the
prevalence and the assumed causes. This allows for further research to be conducted in this field.
1.4 Delimitations of the study
There were a few factors which may have negatively affected the study:
Numerous participants were unfamiliar with the term “Complementary Medicine” and
which over-the-counter products fell into the complementary medicine category. Thus some
findings may have been affected by this.
A few participants made use of both complementary medicine and conventional medicine
simultaneously that made isolating the efficacy of the complementary medicine difficult. It
3
was assumed by the researcher that the positive effects were due to complementary
medicine.
Participants who had more than one child with colic were conflicted when answering
questions where the answer was different for each child. This resulted in a few questions
having multiple answers.
1.5 Assumptions
For the purpose of the study, the following was assumed:
That the survey was completed honestly and truthfully without bias and prejudice.
That the information that was provided by the participant was a true reflection of the
participant’s use of complementary medicine for colic.
That the infant has/had colic based on their presenting symptoms and not another possible
underlying pathology.
1.6 Objectives
The objectives for this study were:
To provide insight into the use and perceived effectiveness of complementary medicines in
order to develop an approach for the treatment of infantile colic.
To provide valuable information regarding the understanding and use of complementary
medicine in Gauteng.
To provide a better understanding of infantile colic due to limited research being available
on the aetiology and development of infantile colic. This may open up the field for
additional research.
4
CHAPTER TWO
LITERATURE REVIEW
2.1 Introduction to infantile colic
Infantile colic is defined according to Wessel’s criteria as crying in a seemingly healthy infant
that lasts for more than three hours each day, on more than three days a week, for a period of
more than three weeks (Savino & Tarasco, 2010; Savino et al., 2014b) Around the age of 6
weeks, the occurrence of crying intensifies, especially in the late afternoon and evening. Colic
tends to naturally ease around the age of 16 weeks, the definitive reason for this is unknown
(Savino, Ceratto, De Marco & di Montezemolo, 2014a).
Infantile colic is a prevalent condition that occurs in 10-30% of infants. There is no genetic link
for this condition and it affects infants of all socio-economic groups. It is thought to be equally
prevalent in both genders and there have been no reported differences in incidence between
breast-fed and formula-fed infants (Savino, 2007).
Infantile colic is not only distressing to the infant, but on the family too; and since there is no
widely accepted conventional treatment for colic, parents may turn to complementary medical
treatments (Savino & Tarasco, 2010).
2.1.1 Aetiology of infantile colic
The aetiology of infantile colic is not fully understood despite its frequent occurrence. Research
suggests that there may be numerous independent causes of this disorder (Savino et al., 2014b).
As a result of this, many interventions for infantile colic have been investigated. Many theories
exist as to what could cause infantile colic. One possibility stems off the notion of the gut
hypothesis, with hypertonicity and increased formation of intraluminal gas (Marek, 2011).
Allergic theories suggest that food allergies may result in infantile colic. This may occur due to
lactose intolerance, hypermotility, gastro-oesophageal reflux, gut hormones, gut microflora, and
food hypersensitivity. Other theories include the effect of maternal smoking, low birth weight,
infant migraines, neurohormones and the maternal diet of breastfeeding mothers (Savino &
Tarasco, 2010).
2.1.1.1 Lactose intolerance
Recently lactose intolerance has been identified as a possible causative factor for infantile colic.
This is due to a relative lactase deficiency resulting in the failure to break down the lactose in
5
food. Due to this, large amounts of lactose enter the large intestines where it becomes a substrate
for lactobacilli and bifidobacteria. Fermentation occurs resulting in the rapid production of lactic
acid and hydrogen, which causes the intestines to distend creating pain for the infant. A small
study was conducted on the use of a lactase-treated feed for infants with colic however, as a
small sample size was used, it reduced the efficacy of the study. It was noted that there was a
reduction in both crying time and breath hydrogen in infants who had used a lactase-treated feed.
This supported the theory that symptoms could be alleviated by reducing the lactose content of a
lactose-intolerant infant’s feed; however, infants can expect no relief with this form of treatment
if the colic is due to other factors (Savino, 2007).
2.1.1.2 Motility
During the first few weeks of life, there is a delay in the development of the nervous system that
may lead to intestinal hypermotility in infants. The autonomic nervous system (ANS) consisting
of the sympathetic and parasympathetic nervous systems have been investigated to find the cause
of this ‘hypertonia of infancy’, as it was termed, which was thought to be a result of vagotonia.
Vagotonia is when the equilibrium between the sympathetic and parasympathetic nervous system
(ANS) is favoured towards the parasympathetic nervous system. The theory of this over
stimulation of the parasympathetic nervous system was supported by the beneficial effects that
the following conventional and complementary antispasmodic medications had on colic:
dicyclomine, cimetropium bromide, Matricariae recrutaria, Foeniculum vulgare and Melissa
officinalis (Savino, 2007). However, the findings stating, ‘the balance of the autonomic nervous
system is normal in colicky infants’ suggested that the imbalance in the autonomic nervous
system is not associated with infantile colic (Kirjavainen, Jahnukainen, Huhtala, Lehtonen,
Kirjavainen, Korvenranta et al.,2007).
2.1.1.3 Gastro-oesophageal reflux
The relationship between gastro-oesophageal reflux and colic is controversial as the two are
viewed as different clinical conditions. The confusion between the two occurs when gastro-
oesophageal reflux doesn’t present with its typical symptoms but rather the irritability and
excessive crying of colic. Results from studies that examined the role of gastric emptying and
pathological gastro-oesophageal reflux in colicky infants suggested that in the absence of
regurgitation and vomiting, gastro-oesophageal reflux is not a likely cause for infantile
irritability, and pathological gastro-oesophageal reflux is only implicated in a select few colicky
infants. However, most studies emphasise that the link between infantile colic and gastro-
oesophageal reflux is unlikely (Savino, 2007).
6
2.1.1.4 Gut Hormones
The gastrointestinal tract contains numerous hormones responsible for the regulation of intestinal
motility namely vasoactive intestinal peptide, gastrin, motilin and ghrelin. In gastrointestinal
disorders in children, it has been observed that vasoactive intestinal peptide and gastrin levels are
elevated however; this is not true for colic. The only instance that gastrin levels are elevated in
colic infants is when the child is being formula fed and not breastfed. It has been noted that
motilin, which is responsible for promoting gastric emptying and small bowel peristalsis, is
increased in colicky infants. Raised serum levels of ghrelin have also been found in colicky
infants and this hormone is thought to be responsible for abnormal hyperperistalsis and increased
appetite, symptoms which evident of colic (Savino, 2007).
2.1.1.5 Gut Microflora
Lactobacilli are important non-pathogenic bacteria responsible for the development of local and
systemic immune responses. In infants with colic, it was found that not only were there
decreased counts of intestinal lactobacilli in comparison to healthy infants, but that there was an
increased amount of Lactobacillus brevis and Lactobacillus lactis, which are responsible for
abdominal distension and increased intestinal gas. An inadequate balance of lactobacilli in
colicky infants may trigger immaturity in the intestinal barrier, which may result in abnormal
immune responses (Savino, 2007). In a randomised, double blind, placebo controlled trial it was
discovered that the crying and fussing times in the colic infants who were taking Lactobacillus
reuteri was significantly shorter than those who were in the placebo group (Chau, Lau,
Greenberg, Jacobson, Yazdani-Brojeni, Verma, et al., 2015).
2.1.1.6 Food Hypersensitivity
There is increasing evidence that infantile colic is related to food hypersensitivities. Possible
allergens that cause colic are cow’s milk proteins, breast milk or infant formula. In a systematic
review, it was found that hypoallergenic formulas were effective in reducing colic in formula fed
infants. Another study investigated the effects of eliminating cow’s milk from the mothers’ diet
on infantile colic. It was concluded that there was a significant improvement in the infants’ colic
or complete resolution (Savino, 2007). Other additional dietary exclusions that can be made in
the maternal diet are the removal of eggs, wheat, soy, tree nuts, peanuts and fish. After a two
week exclusion period, there should be a substantial improvement in the infants behaviour if the
symptoms are allergy related (Savino & Tarasco, 2010).
7
2.1.1.7 Psychological factors
Infants with colic are often considered to be irritable, hypersensitive and have a difficult
temperament. However, this doesn’t provide an explanation for the excessive crying but does
indicate it as a contributing factor. Many studies are being conducted to examine the importance
of quality infant-parent interactions in relation to excessive crying and irritability in infants. It
has been observed that less than optimal parent-infant interactions are common with severely
colic infants (Savino, 2007).
2.1.1.8 Migrainous phenomenon
Migraines are considered a highly genetic disorder and it is possible that infants may express
migrainous genes early in brain development. This then presents later on in life as a migraine
headache. In a cross-sectional study, it was found that mothers who had migraines were more
than twice as likely to have a child with colic. However if colic is due to migraines, the
pathophysiology is still not understood enough to be able to determine why the infant cries. It is
poorly understood whether the crying is caused due to a headache or abdominal pain due to an
abdominal migraine. The migraine could result in the infant being excessively sensitive to
external stimuli, commonly seen in migraines, and the sensitivity is expressed as crying. Infants
grow and develop at a rapid rate, especially in the first few weeks of life and their visual
perceptual abilities increase drastically within this time. These overwhelming visual senses could
also result in excessive crying and could provide a reason as to why the colic only approximately
starts at 2 weeks of age (Gelfand, 2016).
2.1.1.9 Melatonin and serotonin
Melatonin is a neurohormone produced by the pineal gland, retina and gastrointestinal tract with
the gastrointestinal tract producing 400 times the amount of melatonin produced by the pineal
gland. Melatonin is not only responsible for the day-night cycle but also in relaxing the intestinal
smooth muscles. Serotonin has the opposite effect as it increases the intestinal smooth muscle
contractions. Melatonin and serotonin levels peak in the evening due to the circadian rhythm, the
same time that colic seems to intensify. The production of endogenous melatonin does not occur
until the infant is 12 weeks of age, when colic generally resolves, suggesting that colic may be
due to abnormal circadian melatonin rhythms (Kumral, Tuzun, Yesilirmak, Duman & Ozkan,
2009; Rosen 2007).
8
2.1.1.10 Fourth trimester theory
A popular conventional medical theory as to the cause of infantile colic is a theory termed the
“fourth trimester”. This is a three month period in which the infant has neural regulation
difficulties and the child has to cope with potentially overwhelming sensory stimuli. The way in
which an infant deals with external stimuli varies and there is increasing evidence that the
gastrointestinal tract may be involved in colic via neuroimmune connections (Rosen, 2007).
2.1.1.11 Gastrointestinal gas
Excessive gastrointestinal gas can result in colic in infants and this is due to aerophagia caused
by inconsolable crying or gas production due to fermentation in the intestines. Aerophagia from
crying can result in abdominal distension and flatulence, which causes discomfort for the child
(Wyllie, Hyams & Kay, 2015). The reaction of hydrogen ions and bicarbonate due to bacteria
fermentation in the small intestine results in intraluminal carbon dioxide gas production. This
causes abdominal distension, burping and flatus that are common in colic. The symptoms can
mildly be alleviated by keeping the child in a supine position and choosing the appropriate teat if
bottle feeding (Walker, Goulet & Mieli-Vergani, 2004).
2.1.1.12 Maternal smoking
Studies have revealed a link between infantile colic and exposure to cigarette smoke and its
metabolites. Evidence indicates that maternal smoking causes increased plasma and intestinal
motilin levels. Increased intestinal motilin results in increased gastrointestinal peristalsis, which
causes the abdominal discomfort seen in infantile colic (Kheir, 2012).
2.1.2 Physical signs and symptoms
The physical signs and symptoms of colic include: crying; flushing of the face; drawing up of the
legs; arching of the back; clenched fists; bloated abdomen; abdominal guarding; passing of gas
whilst crying; difficulties passing stool; vomiting after feeding and restless sleep (Renee, 2014).
Infantile colic is often graded as mild, moderate or severe, yet there are no guidelines defining
each grade. Episodes of crying tend to increase at 6 weeks of age, occurring more frequently late
afternoon and evening. Colic tends to spontaneously resolve itself around 3-4 months of age. The
pattern of crying is characteristic of colic and this helps to differentiate it from other more severe
conditions (Savino, 2007).
9
2.1.3 Diagnosis
The diagnosis of infantile colic is made through an extensive medical history of the patient as
well as performing the relevant physical examinations based on the presenting symptoms and
case history. It is important to rule out any other underlying conditions as well as excluding any
feeding disorders. The history taking should include the association between the behaviour of the
infant and the duration and timing of the crying. Evaluation to see if the infant is being fed
correctly, is gaining weight, has a fever or has abnormal stools is important. Common conditions
such as cow’s milk protein allergy and gastro-oesophageal reflux need to be ruled out as well as
other uncommon conditions such as bowel intussusception and infections (Savino et al., 2014a).
2.1.4 Differential diagnosis for crying
Crying in infants and young children is common as this is a form of communication. If the
infant’s crying exceeds the normal range of a maximum of 3 hours a day, it is important to
distinguish the cause (Porter & Kaplan, 2011). Other organic causes of crying other than colic
are as follows:
2.1.4.1 Cardiac causes
Coarctation of the aorta
Localised narrowing of the aortic lumen resulting in hypertension, left ventricular hypertrophy
and decreased blood supply to the abdominal organs and lower extremities. Symptoms
experienced vary in each case but range from a headache, chest pain, fatigue, cold extremities
and leg claudication. In order to diagnose coarctation of the aorta, an echocardiogram, computed
tomography (CT) or magnetic resonance (MR) angiography need to be performed (Porter &
Kaplan, 2011).
Heart failure
Heart failure is a syndrome of ventricular dysfunction. The following signs and symptoms may
be found in infants with heart failure: tachycardia; tachypnoea; dyspnoea with feeding;
diaphoresis; restlessness and irritability. Dyspnoea with feeding results in insufficient food
intake so infants are often undernourished and have poor growth (Halpern & Coelho, 2016;
Porter & Kaplan, 2011).
Supraventricular tachycardia
Supraventricular tachycardia is an abnormal heart rhythm arising from improper electrical
conduction in the upper region of the heart. In an infant, this results in the heart rate being
10
greater than 180 beats per minute. Symptoms include episodic breathlessness, lethargy, feeding
difficulties and rapid precordial pulsations (Herman & Le, 2007; Porter & Kaplan, 2011).
2.1.4.2 Gastrointestinal causes
Constipation
Constipation is defined as a delay or difficulty in passing stool. Stools may be hard or even
large, occurring for a period of more than 2 weeks. Constipation can often result in anal tears or
fissures as well as a distended abdomen. Constipation causes pain and discomfort in the infant
which results in excessive crying (Freedman, Al-Harthy & Thull-Freedman, 2009; Porter &
Kaplan, 2011).
Gastroenteritis
Gastroenteritis is the inflammation of the lining of the stomach and intestines. Symptoms
include nausea, vomiting, diarrhoea, loss of appetite and abdominal pain. Gastroenteritis should
be monitored closely in infants as dehydration occurs easily due to the rapid loss of fluids
(Porter & Kaplan, 2011).
Gastro-oesophageal reflux
Gastro-oesophageal reflux is due to the incompetence of the lower oesophageal sphincter, which
allows the reflux of gastric contents back up into the oesophagus. The infant presents with
recurring fussiness after feeds, regurgitation, poor weight gain and arching of the back
(Freedman et al., 2009; Porter & Kaplan, 2011). Gastro-oesophageal reflux affects numerous
infants however, like colic; it is self-limiting and usually resolves around 6-12 months of age
(Savino, 2007).
Intussusception
Intussusception is telescoping of one portion of the intestine into an adjacent section of
intestines and results in intestinal obstruction and sometimes intestinal ischemia. Intussusception
presents with recurring colicky pain with vomiting (Herman & Le, 2007; Porter & Kaplan,
2011).
Milk protein intolerance
Milk protein intolerance is the inability to digest milk proteins due to a lack of intestinal
enzymes to break it down. This results in abdominal distension, vomiting, diarrhoea, abdominal
cramps, flatulence and insufficient weight gain. Eliminating the allergen should result in relief
of the symptoms (Halpern & Coelho, 2016; Porter & Kaplan, 2011).
11
Volvulus
Volvulus is an intestinal obstruction that impairs the passage of contents through the intestine.
Symptoms include vomiting, obstipation and abdominal colic. Diagnosis is confirmed through
abdominal x-rays (Herman & Le, 2007; Porter & Kaplan, 2011).
2.1.4.3 Infectious causes
Meningitis
Meningitis is the inflammation of the meninges of the brain or spinal cord due to a viral or
bacterial infection. Signs include fever, lethargy, seizures, irritability, high pitched and
inconsolable crying and bulging of the fontanelle. In suspected infantile colic it is important to
rule out neck stiffness and the above mentioned symptoms, through a lumbar puncture, to
eliminate meningitis as a possible cause (Herman & Le, 2007; Porter & Kaplan, 2011).
Otitis media
Otitis media is a bacterial or viral infection of the middle ear. Infants commonly experience the
following symptoms: otalgia, fever, nausea, vomiting and diarrhoea. Diagnosis determined by
performing an otoscopy in which the tympanic membrane is bulging with or without a purulent
discharge. Infants who have otitis media become irritable and have difficulty sleeping,
symptoms common in colic (Herman & Le, 2007; Porter & Kaplan, 2011).
Respiratory infections
Respiratory infections in infants has multiple causes however, the most common ones are
bronchiolitis and pneumonia. Colic infants tend to hold their breath for short periods of time,
making it essential to eliminate any underlying respiratory cause. The infant often presents with
a fever, wheezing, rales, grunting, cyanosis, difficulty breathing when feeding and decreased
breath sounds on auscultation (Freedman et al., 2009; Porter & Kaplan, 2011).
Urinary tract infection
Signs and symptoms of a urinary tract infection in infants are usually non-specific and include
difficulty feeding, diarrhoea, vomiting, failure to thrive, mild jaundice, lethargy, fever and
hypothermia. In some cases infants may present with abdominal pain, foul-smelling urine,
dysuria, increased urinary frequency or urinary retention (Herman & Le, 2007; Porter & Kaplan,
2011).
12
2.1.4.4 Trauma
Corneal abrasion
Corneal abrasion is a superficial injury to the eye that is usually self-limiting. It is most often
caused due to a foreign body in the infant’s eye or due to a superficial corneal scratch from the
infants’ sharp or uncut nails. The infant becomes irritable and cries inconsolably, symptoms
typical of colic (Halpern & Coelho, 2016; Porter & Kaplan, 2011).
Fracture or abuse
Irritability, fussiness and crying may be as a result of child abuse. Signs of abuse include
unexplained bruises and fractures as well as the favouring of a limb. A thorough history and
examination should be performed to rule it out as a possibility (Porter & Kaplan, 2011).
Hair tourniquet
Hair tourniquet occurs when a hair wraps around an appendage, such as a toe, finger or penis,
and there is swelling distal to the hair. A thorough examination needs to be performed to rule
this out as a possible diagnosis (Halpern & Coelho, 2016; Porter & Kaplan, 2011).
Head trauma with intracranial bleeding
The infant will have an inconsolable, high pitched cry with localised swelling on the skull. A
head CT should be performed to eliminate this as a diagnosis (Herman & Le, 2007; Porter &
Kaplan, 2011).
Shaken baby syndrome
Colic, which is not only distressing on the child, but on the parents too, and in some cases it
results in a caregiver ‘shaking the baby’. Shaken baby syndrome occurs due to the brain
rebounding on the skull resulting in bruising, swelling and bleeding of the brain. The child will
present with behavioural changes, inconsolable and high pitched cry, irritability, lethargy,
vomiting, loss of consciousness and convulsions (Porter & Kaplan, 2011).
2.1.4.5 Other causes
Testicular torsion
In boys it is important to examine the penis and scrotum. In testicular torsion the infant will
present with ecchymosis and firmness of the testes. This is a medical emergency and the infant
will be irritable, fussy and crying due to the discomfort (Porter & Kaplan, 2011).
13
Vaccine reaction
It is common for children to experience a mild reaction after a vaccination, especially if a live
vaccine was administered. The child may present with a fever, rash, vomiting and diarrhoea.
The symptoms should not persist longer than 3-7 days (Halpern & Coelho, 2016; Porter &
Kaplan, 2011).
2.2 Treatment approaches
The treatment of infantile colic is aimed at reducing the intensity of crying or eliminating factors
that appear to exacerbate the crying. There is no gold standard treatment for colic and as a result
many treatment options are utilised (Bailey, D'Auria & Haushalter, 2013).
2.2.1 Conventional medicine
Conventional medicine is defined as a health care system compromising of medical doctors and
other healthcare professionals that treat symptoms and diseases with drugs, radiation or surgery.
Commonly it is also referred to as allopathic medicine, mainstream medicine, orthodox medicine
and Western medicine. Conventional medicine makes use of a broad spectrum of medications
including both over-the-counter and prescription medications. Numerous conventional
treatments are available for infantile colic (National Cancer Institute, 2016). In a systematic
review of treatments for infantile colic, it was found that there was little evidence to support
many conventional medicines and that many of them are prohibited due to the reported side
effects. It was found that an integrative approach, combining both conventional and
complementary medicines, to be the most effective (Rosen, 2007).
Some of the following products available for infantile colic include:
Adcock Ingram Muthi Wenyoni
Muthi Wenyoni is an antacid consisting of calcium carbonate and magnesium carbonate, which
helps to relieve dyspepsia by neutralising stomach acid (Resmed, 2016). This medication is
popular amongst South Africans for treating ‘inyoni’ or ‘umphezulu’, a condition which is
associated with diarrhoea and dehydration accompanied with a high pitched cry. The side
effects that could result from the calcium carbonate are constipation, vomiting and loss of
appetite. The magnesium carbonate could cause side effects such as nausea, diarrhoea and
abdominal discomfort (Bland, Rollins, Broeck & Coovadia, 2014).
14
Buscopan®
Hyosine butylbromide is an antispasmodic used in infants over one month of age. Buscopan®
relieves pain by exerting a spasmolytic action on the smooth muscle of the gastrointestinal,
biliary and genitourinary tracts. It is indicated in conditions with gastrointestinal spasms, colic
being one of them (Whittaker, 2010). The side effects that could result from hyosine
butylbromide are urticaria, xerostomia, tachycardia, dyshidrosis, and urinary retention
(Boehringer Ingelheim, 2013).
Colief® Infant Drops
Colief® is a natural product containing the enzyme lactase that aids in the breakdown of lactose
due to lactose intolerance or insufficient lactase production (Colief, 2011). Infants experience
digestive discomfort due to abdominal distension as a result of bacterial fermentation in the
large intestines. Lactase is best given before a feed in order to increase the lactase levels to
match the high levels of lactose in breast milk or cow’s milk based formula (Whittaker, 2010).
Colief® is safe to use and there are no reported side effects. It has been noted that in some cases
the stool may become looser and more frequent; however, if the infant is happy and gaining
weight, there is no need for concern but the number of drops per dose should be reduced
(Colief, 2011).
Nexium®
Nexium® is a scheduled medication for the short-term treatment of gastro-oesophageal reflux
disorder. Nexium® contains esomeprazole magnesium which suppresses the secretion of gastric
acid that may be causing erosive esophagitis. The acid-mediated gastro-oesophageal reflux
could be causing the colic and discomfort in the infant. The infant should not take Nexium® for
longer than a period of six weeks and the safety and effectiveness of it hasn’t been established
in infants less than one month of age (Anderson, 2014). The side effects that could result from
esomeprazole magnesium are headaches, dizziness, xerostomia, abdominal pain,
gastrointestinal disturbances, skin reactions, insomnia, constipation, flatulence and nausea
(AstraZeneca, 2015).
Telament Paediatric Colic Drops®
Telament Paediatric Colic Drops® contains simethicone that is indicated for symptoms
associated with excessive gas accumulation in the gastrointestinal tract such as colic, flatulence
and dyspepsia (Adcock Ingram, 2004a). Simethicone works by dispersing and preventing gas
bubble formation in the intestinal tract. Three double-blind, placebo-controlled studies aimed at
establishing the efficacy of simethicone, all had conflicting results. The first study showed that
15
infants had fewer crying episodes with simethicone whereas the second study showed that the
placebo was more effective. The third study showed neither the simethicone nor placebo as
effective (Whittaker, 2010). The use of simethicone is a widely accepted over-the-counter
medication for infantile colic however studies indicated that there is no benefit on colic
symptoms. If there is any calming effect, it is suspected to be due to the sweet taste (Halpern &
Coelho, 2016). The side effects that could result from Telament Paediatric Colic Drops® are
abdominal distension, diarrhoea, constipation, flatulence and gastro-oesophageal reflux
(Adcock Ingram, 2004a).
2.2.2 Lifestyle and behavioural adjustments
Breastfeeding mothers are often advised to adjust their diet to see if there is any relief in the
infants’ symptoms. Mother’s should avoid cow’s milk and dairy. Bottle fed infants are advised to
use formulas that contain partially hydrolysed whey proteins as well as prebiotic
oligosaccharides (Savino et al., 2014a). Oligosaccharides are found in high concentrations in
breast milk and are minimal in cow’s milk or cow’s milk based formulas. The supplementation
of infant formulas with prebiotic oligosaccharides has been found to increase intestinal
bifidobacteria and promote infant health (Stiverson, Williams, Chen, Adams, Hustead, Price et
al., 2014). This has shown to be an effective form of treatment (Savino et al., 2014a).
Common comforting methods used in colic infants include: increased carrying, swaddling, a crib
vibrator and infant massage. However, most of these comforting methods aren’t always
beneficial. In one study it was found that swaddling is an effective soothing technique and it was
found to be more effective than infant massage in calming colic infants (Evanoo, 2007).
Baby exercises assist with stretching the abdominal muscles while improving circulation to the
muscles. This is achieved by the infant lying on their back, while their legs are gently cycled
around in a bicycle motion. This assists with the movement of the stool or gas along the
gastrointestinal tract which may relieve any discomfort the infant may be experiencing
(Eshelman, 2013).
Behavioural interventions involve advising or counselling parents on how to soothe infants more
effectively and how to not overstimulate them (Savino & Tarasco, 2010).
In an online survey conducted in New Zealand on colic and reflux by parents who had infants
with excessive crying and/or colicky behaviour, it was noted that complementary medicines,
cranial and baby massage and behavioural interventions relieved colic symptoms completely in
16
less than 3% of infants however most of these treatments did not significantly improve the colic
symptoms (Hodge & Murphy, 2014).
Two studies conducted on the implementation of the behavioural intervention, regulation,
entertainment, structure and touch (REST), found a significant reduction in infant crying
(Evanoo, 2007). The intervention is utilised in both the infants and the parents. REST for infants
consists of:
Regulation: manage the state of the infant and as a parent, be able to understand the infants’
cues. Preventing overstimulation in the beginning of the infants’ life is important.
Entertainment: synchronise the infants’ behaviour with external stimuli such as noise or
light.
Structure: it is essential to establish a routine as to create stability in the infants’ day to day
life.
Touch: this aims to provide close skin to skin contact and can incorporate soothing
techniques such as holding the infant or rocking them (Evanoo, 2007).
REST (reassurance, empathy, support and time out) is also implemented in parents as many
parents feel helpless or overwhelmed when their infant cries excessively. This often leads to
frustration and in some cases the parents shake the child which may result in shaken baby
syndrome. REST for parents consists of:
Reassurance: reassure the parent that they are caring for the infant correctly and that colic is
a self-limiting condition.
Empathy: listen to the parent and recognise the challenge of caring for a colic infant.
Support: from health care providers or support groups. Teach the parent the appropriate
response to the infant (REST intervention for the infant)
Time out: explain the importance of the parent taking time to rest and take a break from the
infant each day. Let them know that it is acceptable to allow for someone else to watch the
infant or for the infant to be placed safely in a crib or play area if the parent is feeling
overwhelmed or frustrated (Evanoo, 2007).
2.2.3 General complementary medicine for infantile colic
Complementary medicine (CM) is defined by the World Health Organisation (WHO) as “a broad
set of health care practices that are neither part of that country’s own tradition, nor integrated
into the dominant health care system”. In some countries, the term is often used interchangeably
with traditional and complementary medicine (T&CM), a term that is used globally to describe
17
traditional products, practitioners and practices (WHO, 2016). However, in South Africa,
traditional medicine and complementary medicine are seen as two different modalities.
According to the Medicines Control Council (MCC) of South Africa, complementary medicine
means any substance or mixture that originates from plants, minerals or animal that is intended
to be used to alleviate or prevent illness. To guarantee the safety and efficacy of medicines, the
MCC controls the manufacturing, distribution and sale (MCC, 2016).
Complementary medicine is regulated in South Africa by the MCC whereby the standards are
established by the Medicines Related Substances Act, (Act 101 of 1965) (MCC, 2016). As of
2001, Allied Health Professions Council of South Africa (AHPCSA) regulates practitioners who
practice in the field of complementary medicine. AHPCSA regulates all health professions in
terms of the Allied Health Professions Act, 63 of 1982 (the Act) and includes the following
complementary health disciplines: Ayurveda, Chinese Medicine and Acupuncture, Chiropractic,
Homeopathy, Naturopathy, Osteopathy, Phytotherapy, Therapeutic Aromatherapy, Therapeutic
Massage Therapy, Therapeutic Reflexology and Unani-Tibb (AHPCSA, 2015).
2.2.3.1 Homeopathy
Homeopathy is a holistic, natural, health care system that has been around for more than 200
years. Homeopathy makes use of plant, animal or mineral based remedies aimed at treating each
patient individually in order to stimulate the body’s own healing ability. According to the WHO,
homeopathy is the second largest therapeutic system in the world (WHO, 2016). Homeopathy
focuses on treating the totality of symptoms by not only taking into account the physical
symptoms, but the mental and emotional too, making it a true holistic treatment (School of
Homeopathy, 2012).
The word homeopathy is derived from the Greek words “homoios” which means like and
“pathos”, meaning suffering. The origin of the word leads to one of the main homeopathic
principles “like cures like”, meaning that a crude substance which produces symptoms in a
healthy person can cure similar symptoms in a sick person, if administered as a minimal dose.
The Law of Similars, was developed by the founder of homeopathy, Dr. Samuel Hahnemann. He
also founded the principle, “the minimum dose”. Hahnemann states that the diseased body only
needs small doses of a remedy to bring about a cure. However, the opposite is true in allopathy.
In order to achieve a greater physiological response; the dose needs to be increased. This often
leads to uncomfortable and unnatural side effects. Whereas in homeopathy, the minimum dose is
able to overcome the disease and this is achieved in a gentle and permanent manner. This is
further described in the second aphorism, which is found in the Organon of Medicine: “The
18
highest ideal of cure is rapid, gentle and permanent restoration of the health, or removal and
annihilation of the disease in its whole extent, in the shortest, most reliable, and most harmless
way, on easily comprehensible principles” (De Schepper, 2008). This is the reason that
homeopathy is favoured in the treatment of infantile colic: it is considered to be safe in infants
and it does not have the adverse effects of conventional medicine. There are numerous
homeopathic remedies that can be prescribed to treat colic based on the infant’s individualised
symptoms (Loo, 2008). A similimum research study was conducted to establish the efficacy of
individualised homeopathic remedies in the treatment of colic. Results showed that there was an
improvement in the infant’s colic as well as the infant’s overall temperament and physical health.
However, due to the small sample size additional larger scale studies should be conducted to
further validate this finding (Vermeulen, 2004).
Homeopathic remedies are administered in varying strengths through a process of dilution and
succussion (addition of energy through agitation). This is sub-sequentially referred to as a
potency. Samuel Hahnemann discovered that the therapeutic action of a substance is improved
through a process of potentisation in which a substance is diluted and then succussed or triturated
(School of Homeopathy, 2012). Standardised methods of dilution are achieved through liquid
dilution or trituration. Soluble substances undergo liquid dilution and succussion in a bottle until
the desired potency is reached whereas insoluble substances are combined with lactose powder
and triturated until the desired potency is achieved (Kayne & Kayne, 2007).
There are varying scales of potentisation in which a potency is compounded according to
prescribed ratios. These include the:
Decimal scale (X=1:10) or (D=1:10)
Centesimal scale (C=1:100)
Millesimal scale (M=1:1000)
Quinquagintimillesimal sacale (LM=1:50000) (Kanye & Kanye, 2007).
2.2.3.2 Aromatherapy
Aromatherapy is a natural and holistic therapy that aims at treating the mind, body and spirit
through essential oils. The essential oils assist the body to function at its optimal level. Essential
oils are extracted from the seed, flower, leaves, bark or root of the plants through a process
known as distillation. Aromatherapy doesn’t only heal through smell alone, as the name implies,
but through other therapeutic properties as well. Aromatherapy also has antiviral, antibacterial,
antibiotic, anti-inflammatory and antiseptic effects, whereby the oils are absorbed into the
bloodstream. The aim of the essential oils is to relax the body and improve the circulatory and
19
lymphatic systems throughout the body. Aromatherapy strives to restore equilibrium in the body
so that the body can unlock its natural healing potential (Aroma SA, 2016).
Anethum graveolens is an essential oil found in the seeds of dill, it reduces intestinal spasm and
griping. The carminative volatile oil aids in digestion, passage of gas and stimulates the appetite
(Jana & Shekhawat, 2010). Piminella anisum oil, commonly known as aniseed oil is well known
for its ability to ease colic by reducing flatulence, hiccoughs and nausea. It is also helps with
abdominal distension and facilitates digestion. Foeniculum vulgare oil is commonly known as
fennel, it is indicated for constipation, colic, indigestion and flatulence (Roberts, 2012). The
posology of Anethum graveolens is 0.1g-0.3g, Piminella anisum is 0.3g and Foeniculum vulgare
tincture is 5ml-7.5ml (WHO, 2007).
Lavandula officinalis, commonly known as lavender oil, is an essential oil that has shown to
have no toxicity. It has significant antispasmodic properties and it also relaxes, calms and
alleviates stress (Roberts, 2012). It is frequently used for infantile colic and in a study conducted
on the effectiveness of aromatherapy massage using lavender oil as a treatment for infantile
colic, showed that it was effective in reducing colic symptoms (Çetinkaya & Başbakkal, 2012).
The posology of lavender is 1-4 drops internally (approximately equivalent to 20mg-80mg)
(WHO, 2007)
2.2.3.3 Ayurveda
Ayurveda is an ancient Indian healing technique that promotes a powerful mind-body health
system. The word Ayurveda means science of life, “Ayur” meaning life and “Veda” meaning
science or knowledge. Two main principles define Ayurveda: the mind and body are connected
and; nothing has more power to heal the body other than the mind. Ayurveda aims to promote a
harmonious balance between the physical body, mental state and spirituality. This is achieved by
focusing on lifestyle, diet, exercise, rest, relaxation and herbal treatments (Chopra, 2017).
Anethum graveolens is commonly known as dill and is used in ayurvedic medicine. It treats
abdominal discomfort, colic and stimulates digestion. Anethum graveolens is one of the
ingredients in Gripe Water® which relieves colic pain in infants and helps to expel flatulence in
children (Jana & Shekhawat 2010).
2.2.3.4 Phytotherapy
Phytotherapy or herbalism is the oldest medical practice in the world. It uses herbal medicine
that is derived from plants to treat illnesses. Phytotherapists use individualised treatments to
20
balance and heal the body through herbal extracts (tinctures), syrups, creams, lotions or
ointments (South African Association of Herbal Practitioners, 2011).
Marticaria chamomilla flos and Achillea millefolium are common herbs that are used in infantile
colic. Marticaria chamomilla flos (chamomile) is very useful in young children where there is
irritability, restlessness and colic. There are episodes of colic where only small amounts of
flatulence are passed at a time. The intestines are in constant motion and there is griping in the
lower abdomen. Achillea millefolium (yarrow) is commonly indicated in conditions where there
is inflammation, pains, spasms, flatulence and dyspepsia. It has been used in gastrointestinal
disorders as an antispasmodic and an anti-inflammatory (Saeidnia, Gohari, Mokhber-Dezfuli &
Kiuchi, 2011). It also helps to alleviate pain from abdominal distension and trapped flatus (Jellin,
2015). The posology of Marticaria chamomilla flos in children is 0.6ml-2ml for a single dose
and Achillea millefolium is 5ml three times a day (WHO, 1999; WHO, 2009).
In a systematic review conducted on nutritional supplements and other complementary
medicines for infantile colic, the following was found: three studies on herbal supplements;
namely Foeniculum vulgare (fennel), Matricaria chamomilla (chamomile), Verbena (vervain),
Glycyrrhiza glabra (liquorice) and Melissa officinalis (lemon balm) all significantly improved
the colic symptoms; and reflexology showed a significant decrease in symptoms however there
was no difference between targeted and non-targeted reflexology (Perry et al., 2011).
2.2.3.5 Unani-Tibb
Unani-Tibb is a system of integrative medicine whose key principle is that the body has the
ability to heal itself and that it can maintain optimal health. It is based on the teachings of
Hippocrates and Galen, which was then developed into Unani-Tibb by Ibn Sina. Unani-Tibb
focuses on empowering the patient through knowledge on their body and their disorder.
Treatment is aimed at self-healing through lifestyle changes, herbal medication, hands-on
therapy such as massage, cupping and acupressure or dietary changes (The South African
Society of Integrative Medicine, 2015).
Unani-Tibb has a principle of temperaments which describes each person’s physical,
psychological, emotional and spiritual qualities. There are four categories: Sanguinous, which is
hot and moist; Phlegmatic, which is cold and moist; Melancholic, which is cold and dry; and
lastly Bilious, which is hot and dry. By knowing ones temperament you are able to make positive
lifestyle adjustments to improve your health and quality of life.
21
Colic is associated with the Phlegmatic temperament of cold and moist. This results in an
immature digestive system and difficulty in digesting milk and other foods. In order to correct
this, heat is needed to balance out the digestion and the coldness experienced (Tibb, 2016).
2.2.3.6 Naturopathy
Naturopathy is a natural approach to healing that encourages each person’s inherent-self healing
process. Naturopathy is focused on holistic treatment that minimises the risk of harm and
facilitates the body’s own healing ability. This is achieved through herbal and homeopathic
supplements, dietary and lifestyle adjustments, vitamins and mineral recommendations and
manipulative therapies (The American Association of Naturopathic Practitioners, 2016).
2.2.4 Over-the-counter complementary medicine for infantile colic
Infantile colic is one of the most common reasons parents take their infants to paediatric
healthcare practitioners (Rosen, 2007). Complementary medicine is often promoted in the
treatment of infantile colic however there has been no synthesis of information to provide
practitioners about their uses and benefits (Perry et al., 2011).
The recent growth in the South African complementary medicine market has resulted in
complementary medicines being available for purchase in numerous health shops, pharmacies
and some large supermarket chains. The majority of the medicines are currently unscheduled,
allowing for them to be purchased over-the-counter without a practitioner prescription (Gqaleni
et al., 2016).
The complementary medicine products that are currently available over-the-counter in South
Africa include:
Homeopathy
Aromatherapy
Ayurveda
Traditional Chinese medicine
Herbal preparations (Phytotherapy)
Unani-Tibb
Vitamins, minerals and supplements (Naturopathy) (Snyman, 2014).
Some of the following complementary products that are available over-the-counter for infantile
colic includes:
22
Colic Calm
Colic Calm is a homeopathic preparation that relieves abdominal discomfort, flatulence and
gastroesophageal reflux found in colic. Colic calm contains the following homeopathic remedies:
Matricaria chamomilla (3X) indicated for irritability, restlessness and hypersensitivity to pain;
Foeniculum vulgare (3X) for muscle spasms, indigestion and accumulation of gas; Carum carvi
(3X) indicated for indigestion and as an anti-spasmodic; Mentha piperita (3X) assists with gas
expulsion and gastrointestinal spasms; Zingiber officinale (3X) relieves nausea and promotes
gastric mobility; Melissa officinalis (3X) promotes sleep and reduces flatulence; Aloe socotrina
(3X) assists with diarrhoea, flatulence and abdominal cramping; Prunus spinosa (3X) relaxes
spasms; and Carbo vegetabilis (1X) provides relief from flatulence, abdominal distension
cramping, indigestion and belching. There are no reported side effects; however, due to the
activated charcoal (Carbo vegetabilis) the stool may become darker in colour, although this is
not harmful to the infant (Colic Calm, 2013).
Heel Nux Vomica Homaccord®
Nux Vomica Homaccord® is a homeopathic preparation indicated for functional disorders of the
gastrointestinal and hepatic regions. The main homeopathic remedies are Nux vomica (D2, D30,
D200, D1000), Bryonia cretica (D2, D6, D10, D15, D30, D200, D1000), Lycopodium clavatum
(D3, D200, D1000) and Citrillus colocynthis (D3, D10, D30, D200) which assist with abdominal
cramps, distension, flatulence, indigestion and detoxification. There are no known side effects
(Heel, 2014a).
A cohort study was conducted in four European countries to investigate the efficacy of Nux
Vomica Homaccord® drops on either gastric symptoms or intestinal symptoms. Results
indicated that more than 80% of cases rated the Nux Vomica Homaccord® as either very good or
good. Although the study was not specifically aimed at infantile colic but rather digestive
disorders, constipation and functional liver disturbances; the symptoms from these conditions
may overlap with symptoms found in colic (Heel, 2014a).
Heel Spascupreel®
Spascupreel® is available as homeopathic tablets and ampules indicated for spasms in the
stomach, intestine and gall bladder. Spascupreel® contains the following homeopathic remedies,
which are indicated for gastrointestinal cramps and spasms: Citrullus colocynthis (D4),
Ammonium bromatum (D4), Atropinum sulfuricum (D4), Veratrum album (D6), Magnesium
phosphoricum (D6), Gelsemium sempervirens (D6), Passiflora incarnate (D2), Agaricus (D4),
23
Chamomilla recutita (D3), Cuprum sulfuricum (D6) and Aconitum napellus (D6). There are no
reported side effects (Heel, 2014b).
A study was conducted on the effects of Spascupreel® versus hyoscine butylbromide
(Buscopan®) for gastrointestinal cramps in children younger than 12 years of age, and it was
found that both medications reduced severity of spasms, pain and frequency of crying. In
conclusion, parents who preferred to opt for alternative therapy for their infants/children could
make use of Spascupreel® as an effective and well tolerated option (Muller-Krampe, Oberbaum,
Dipl-Math, & Weiser, 2007).
Heel Viburcol®
Viburcol® is a homeopathic suppository for restless children with or without fever and who have
discomfort due to the pain caused by colic. The homeopathic remedies contained in each
suppository are: Chamomilla recutita (D1), Atropa Belladona (D2), Plantago major (D3),
Pulsatilla pratensis (D2) and Calcium carbonicum (D8), which reduces inflammation, pain,
irritability and fussiness. There are no known side effects or contraindications and Viburcol® is
safe to use from birth (Heel, 2014c).
In a controlled cohort study comparing the effects of Viburcol® with Paracetamol in children
younger than 12 years of age on restlessness and irritability associated with an illness, 93% of
the patients reported the overall efficacy of Viburcol® as either very good or good. Results also
indicated that 87% of children showed a significant improvement in their symptoms after 3 days
of treatment with Viburcol®. The study did not specifically focus on the effects that Viburcol®
has on infantile colic; nevertheless, the positive effects that it has on restlessness and irritability
can assist with colic symptoms (Muller-Krampe, Gottwald & Weiser, 2007).
Bayer Iberogast®
Iberogast® is a herbal product that is used to restore intestinal health and to relieve discomfort in
the stomach and abdomen. Iberogast® (100ml) contains the following herbs that relieves
abdominal cramps and spasms, flatulence, indigestion and restore normal gastrointestinal
motility: Iberis amara (bitter candytuft) (15ml), Angelica archangelica (angelica) (10ml),
Matricaria chamomilla (chamomile) (20ml), Silybum marianum (milk thistle) (10ml), Melissa
officinalis (lemon balm) (10ml), Mentha piperita (peppermint) (5ml), Chelidonium majus
(greater celandine) (10ml), Carum carvi (caraway fruits) (10ml) and Glycyrrhiza glabra
(liquorice) (10ml) (Bayer, 2015). In a study conducted on the safety and efficacy of Iberogast®,
it was found that there are no serious adverse effects. However, hypersensitivity reactions such
24
as pruritus, dyspnoea or skin reactions may occur rarely (Ottillinger, Storr, Malfertheiner &
Allescher, 2012).
Herbal teas
Various herbal teas mainly include Matricaria chamomilla (chamomile), Lavandula angustifolia
(lavender), Foeniculum vulgare (fennel), Anethum graveolens (dill), Pimpinella anisum
(aniseed), Mentha piperita (peppermint), Glycyrrhiza glabra (liquorice) and Achillea millefolium
(yarrow), which are all known for their ability to soothe the digestive tract, relieve colic and
spasmodic pains, relax and calm as well as reduce flatulence, dyspepsia and nausea (Jellin,
2015).
Natura® Magen
Natura® Magen is a homeopathic preparation aiding in soothing the digestive mucosa and is
therefore effective in the treatment of colic, dyspepsia, indigestion, digestive upsets, nausea and
vomiting. The formulation reduces nausea, vomiting, belching and bloating after eating and
decreases cramping, gastric pain and flatulence. Magen contains the following homeopathic
remedies: Anamirta cocculus (D8), Antimonium crudum (D10), Arsenicum iodatum (D6), Atropa
belladonna (D8), Carbo vegetabilis (D30), Cephaelis acuminata (D8), Cinchona succirubra
(D3), Daphne mezereum (D8), Magnesium phosphoricum (D10) and Strychnos nux-vomica (D4).
There are no known side effects (Natura, 2016a).
A randomised, double-blind placebo controlled study was conducted to establish the effect of
Magen on infantile colic. In contrast to the placebo group, Magen was found to be an effective
form of treatment for colic (p=0.0005), with most of the improvement occurring after 3 days of
use. Due to the small sample size of 30 participants, a larger scale study should be conducted to
further validate the product’s efficacy on infantile colic (Pestana-Caldeira, 2010).
Natura® Sedaped
Sedaped is a homeopathic preparation for spasmodic colic, irritability, vomiting and diarrhoea.
The homeopathic mode of action is to reduce spasmodic pains, provide an analgesic action and
relieve nervous hypersensitivity. Sedaped contains the following homeopathic remedies:
Atropium sulphuricum (D10) reducing inflammation and neuralgic pains; Banisteropsis caapi
(D60) reducing hypersensitivity; Cuprum aceticum (D30) for spasmodic abdominal pains;
Gelsemium sempervirens (D8) for inflammation; Magnesium phosphoricum (D10) for spasmodic
colic pains and acts like an analgesic; Veratrum viride (D8) assists with hiccoughs; Verbena
officinalis (D8) works as a general anti-spasmodic; and Zincum metallicum (D10) assists with
25
flatulent colic, hiccoughs and muscular twitches. There are no reported side effects (Natura,
2016b).
Sister Lilian ColicCare
ColicCare is comprised of tissue salts and homeopathic remedies that assist in the treatment of
cramps, muscle spasms and crying. The following remedies reduce the colic symptoms:
Magnesium phosphoricum (D6), Natrum phosphoricum (D6), Chamomilla vulgaris (D6),
Lycopodium clavatum (30CH), Atropa belladonna (30CH), Dioscorea vilossa (30CH) and
Plumbum metallicum (30CH). There are no known adverse effects or contraindications (Sister
Lilian Remedies, 2016).
Tummy Calm®
Tummy Calm® is a homeopathic medication that relieves the symptoms of colic such as
flatulence, bloating and abdominal discomfort. Tummy Calm® contains the following
homeopathic remedies: Calcarea phosphoricum (12X), Carbo vegetabilis (2X), Matricaria
chamomilla (12X), Citrillus colocynthis (12X), Lycopodium clavatum (12X), Moschus
moschiferus (12X), Natrum muriaticum (12X), Silicea terra (12X) and Thuja occidentalis (12X).
The homeopathic remedies are indicated for abdominal distension; abdominal cramping;
diarrhoea; flatulence; belching; hiccoughs; indigestion as well as soothing and calming the
infant. There are no reported side effects however, due to the activated charcoal (Carbo
vegetabilis), the stool may become darker or black in colour. This is not harmful to the infant and
is only temporary (Tummy Calm, 2014).
Himalaya Bonnisan®
Bonnisan® is based on Unani-Tibb and is a herbal formula that relieves muscle spasms, protects
the gastrointestinal mucosa and expels gas through its key ingredients of Anethum graveolens
(0.0018ml per 5ml) oil, Tinospora gulancha (0.5ml per 5ml) and Phyllanthus emblica (0.5ml per
5ml). This formula alleviates the abdominal symptoms of colic. There are no known side effects
if taken as per the prescribed dosage (Himalaya, 2016).
Tibb Bonnycare
Bonnycare is based on Unani-Tibb principles and is a herbal formula that assists with infantile
colic, flatulence and gastrointestinal discomfort. Bonnycare (5ml) contains Anethum graveolens
oil (0.0018ml) and Tinospora cordifolia (1mg) that acts as a carminative and antispasmodic in
colic; Terminalis chebula (0.5mg) is an antibacterial that prevents diarrhoea; Cichorium intybus
(0.5mg) and Emblica officinalis (0.5mg) are antioxidants and normalises the gastrointestinal
flora; Piper longum (0.5mg); and Elletaria cardamomum (0.5mg) supports digestion and
26
provides a carminative effect on the gastrointestinal tract. The combination of these herbs
provides relief from infantile colic. There are no reported adverse reactions (Tibb Health
Sciences, 2011).
Telament Paediatric Gripe Water®
The Gripe Water contains sodium bicarbonate (50mg per 5ml) and Anethum graveolens oil
(2.15mg per 5ml) that is an antispasmodic and antiflatulent. There are no known adverse
reactions however, hypersensitivity to the ingredients due to allergies have been reported in rare
cases (Adcock Ingram, 2014b).
Woodwards Gripe Water®
The Gripe Water contains Anethum graveolens oil (2.3mg per 5ml) and sodium hydrogen
carbonate (52.5mg per 5ml) that relieves abdominal pain and is an antacid and antiflatulent.
There are no reported side effects however, infants who are allergic to the ingredients may
experience hypersensitivity reactions (Woodwards, 2017).
Lennon Behoedmiddel® vir Kinders
Behoedmiddel® is an antacid containing magnesium carbonate and prepared chalk, which helps
to relieve gastro-oesophageal reflux and abdominal discomfort. Possible adverse reactions from
magnesium carbonate are diarrhoea and mucosal irritation and the prepared chalk may cause
constipation (Lennon, 2000).
Probiotics
Various probiotics are available over-the-counter and they are frequently used to reduce colic by
promoting bowel mobility and intestinal health. It is believed that the possible mechanism of
action of the probiotics is that it improves bowel motility and function thus reducing possible
visceral pain. The use of the probiotic, Lactobacillus reuteri, has shown to be more effective in
the treatment of colic than simethicone or placebo (Savino et al., 2014a). A randomised study
consisted on ninety breastfed colic infants who were randomly assigned to receive either the
Lactobacillus reuteri ATCC 55730 or simethicone for 28 days. Results showed that 95% of
participants receiving L. reuteri had a significant decrease in the crying time compared to the 7%
of participants in the simethicone group. L. reuteri improved the colic behaviour within seven
days of treatment (Savino & Tarasco, 2010).
A double-blind, randomised, placebo-controlled study was conducted on the probiotic
Lactobacillus reuteri DSM 17938 (daughter strain of L. reuteri ATCC 55730) in reducing colic
symptoms in breastfed infants. Infants receiving L. reuteri had an improvement in colic
27
symptoms and showed a significant decrease (p=0.045) in crying and fussing time. The results
suggested that L. reuteri may induce changes in the gut microbiota, particularly to the levels of
Escherichia coli. Previous studies have indicated a drastic discrepancy in intestinal microbiota
between colic and non-colic infants suggesting inadequate levels of lactobacilli in colic infants.
The gastrointestinal tracts of infants with colic tend to be colonised with gas forming microbiota
such as Clostridium difficile, Escherichia species and Klebsiella species, which leads to
abdominal discomfort, distension and flatulence (Chau et al., 2015).
In a study conducted on the quantitative differences in lactobacillus species found in breastfed
colic infants compared to non-colic infants, it was found that breastfed colic infants had fewer
lactobacilli. Furthermore a second study was conducted and found that Lactobacillus
acidophilus was less prevalent in colic infants. However, Lactobacillus brevis and Lactobacillus
lactis was found to be more prevalent in colic infants. Results indicated that some strains of
lactobacillus protect against gastrointestinal neuroimmune disruption and reduce pain, whereas
others contribute to ailments or diseases (Rosen, 2007).
In a systematic evaluation conducted on probiotic and synbiotic safety in infants less than two
years of age, it was found that in all 57 clinical trials and eight follow up studies, probiotics and
synbiotics are safe for infants to use (van den Nieuwboer, Claassen, Morelli, Guarner &
Brummer, 2014).
28
CHAPTER THREE
METHODOLOGY
3.1 Introduction
The aim of the quantitative-descriptive design study was to determine the perceived
effectiveness of complementary medicine by mothers of infants with colic in Gauteng, by means
of an Infantile Colic Questionnaire (Appendix G). The survey was completed on a voluntary
basis as a convenience sample. Prior permission was attained from the University of
Johannesburg’s (UJ) Higher Degrees Committee (Appendix A) and the University of
Johannesburg’s Research Ethics Committee (Appendix B) before commencement of the
research.
3.2 Research Sample
The research sample consisted of 150 participants (Wilson Van Voorhis & Morgan, 2007). The
sample consisted of mothers aged between 18-45 years who have/had a child/children with
infantile colic and used complementary medicine as a form of treatment. A search engine was
used to randomly select various places from different regions in Gauteng. Weleda Pharmacies
and Wellness Warehouse were selected as both are popular complementary medicine retailers
meeting inclusion criteria. Schools and baby clinics were also chosen due to its great
accessibility to the required sample group, mothers aged between 18-45 years who have/had
child/children with infantile colic. Various businesses were selected at random to allow for
unsystematic selection outside of the aforementioned sources. Recruitment of participants
occurred through word-of-mouth and advertising flyers (Appendix C), which were placed around
the following baby and health clinics; health shops; nursery schools; and health and beauty
businesses in the Gauteng region, with relevant permission prior (Appendix D):
Weleda Pharmacy in Bryanston
Weleda Pharmacy in Fourways
Wellness Warehouse in Bedfordview
Mary’s Little Lambs Baby Clinic in Edenvale
Bedfordview Mother and Baby Clinic in Bedfordview
Baker Street Pharmacy Clinic in Edenvale
Edenvale Private Nursery School in Edenvale
St Anthony’s College in Mulbarton
29
Hair Related in Edenvale
Wellbean Pilates Studio in Edenvale
New Era Chickens in Modderfontein
3.2.1. Inclusion criteria
Prospective participants needed to meet the following criteria in order to participate in the
research study. Mothers were included who:
Were aged between 18-45 years;
Have/had one or more children who suffer/suffered from symptoms of infantile colic; and
Are using/have used complementary medicine as a form of treatment for infantile colic.
3.2.2. Exclusion criteria
Participants were excluded from the study if:
They have never used or heard of complementary medicine
3.3. Research Procedure and design
A quantitative-descriptive design was used whereby data was collected through a randomised
cross-sectional survey. A total of 152 participants were recruited via an advertisement and word
of mouth. The surveys were distributed at various baby and health clinics; health shops; nursery
schools; and health and beauty businesses in the Gauteng region. Interested participants were
given an Information Leaflet (Appendix E) that explained the purpose and procedure of the
study. All interested prospective participants were given a Consent Form (Appendix F) to
complete and once consent had been given, participants then completed the Infantile Colic
Questionnaire (Appendix G). Participants were required to answer the questionnaire by crossing
the appropriate response box or by a short written response. This allowed for ease of answering
the questions and limited the time it took to complete the survey, which encouraged greater
participation in the study. Participants were provided with a private area to complete the survey
in. The survey took approximately 8-10 minutes to complete. On completion, the survey was
placed into a sealable envelope and placed into a lockable box. All completed surveys were
treated as strictly confidential and only the researcher, supervisor and statistician had access to
the information. No identifying data was requested or permitted on the survey.
The researcher spent several days at each aforementioned place recruiting participants. Staff
members from each place were also recruited for assistance and thoroughly briefed on the
research procedure. A document containing the research procedure was attached to the lockable
30
box (Appendix H). The staff members were requested to provide each interested participant with
a new envelope containing an Information Leaflet, Consent Form and Questionnaire as well as a
clipboard and pen. Participants were guided to the identified private area to complete the survey
in and to allow for privacy. Once completed, staff members collected the envelopes with the
documents inside, ensured the envelope was sealed and placed a ‘completed’ label on the
envelope seal. The lockable box was stored in a safe place within the various places. Staff
members were not permitted to answer any questions pertaining to the survey. The researcher
could be contacted telephonically to answer any queries and to collect the completed surveys.
3.4 Reliability and validity measures
The Infantile Colic Questionnaire is used as a reliable tool in research related to infantile colic
and reflux (Murphy, 2015). Research studies on colic in new-borns have utilised the
questionnaire (Appendix I) (Hodge & Murphy, 2014). Development of a valid and reliable
questionnaire is important as it reduces measurement errors by utilising several steps to test the
questionnaires used for data collection (Radhakrishna, 2007). Prior to the commencement of the
study, five mothers who met the study criteria were asked to participate in a pilot study, pre-
testing the questionnaire. Findings were analysed and changes were made accordingly, with
expert supervisory input from the statistician (Kuhudzai, 2016a). The results recorded were not
utilised during analysis of the study.
3.5 Data collection and analysis
Statistical analysis was prepared with the assistance of Statkon using SPSS Statistics (Statistical
Package for Social Sciences) (version 23). The following tests were utilised:
Frequencies and custom tables
Multiple response analysis for questions where more than one answer can be selected.
Open ended responses (Kuhudzai, 2016b).
Data presented as frequencies and custom tables provided information on infantile colic and the
usage of complementary medicine for infantile colic by mothers in Gauteng (Kuhudzai, 2016b).
3.6 Ethics
This study aimed to uphold and protect the well-being of all participants. It was explained to all
participants that they have the right to anonymity, privacy and confidentiality. The participants
were informed about the requirements, duration and purpose of the study. Each participant was
given an Information Leaflet (Appendix E) as well as a Consent Form (Appendix F), which was
31
signed before the study commenced. The researcher was honest and transparent and was
available to the participants if they had any other questions and concerns about the study. No
identifying information was requested from the participant ensuring anonymity throughout the
study. The completed surveys were placed in a sealable envelope and stored in a lockable box
which only the researcher, supervisor and statistician had access to, ensuring confidentiality.
Completion of the survey took place in a private area, thus ensuring privacy and confidentiality.
The research did not infringe on any human rights, or deceive on any findings. There were no
anticipated risks by participating in this study. It was stressed that this study was voluntary and
that participants had the right to withdraw from the study at any time, up until the questionnaire
had been submitted, for whatever reason and without consequence. Feedback of the results of the
study was provided to the participants who requested it.
Ethical clearance was obtained from the Faculty of Health Sciences, Research Ethics Committee
(REC-01-126-2016) and Higher Degrees Committee (HDC-01-46-2016) prior to the conduction
of the research (Appendix A and B).

32
CHAPTER FOUR
RESULTS
4.1 Introduction
The research study aimed to establish the use and perceived effectiveness of complementary
medicine for infantile colic. A further objective of the study was to gather more information on
infantile colic, which is a poorly understood condition (Savino et al., 2014a). The data was
collected through the Infantile Colic Questionnaire (Appendix G). A pilot study was conducted,
pre-testing the questionnaire. Adjustments were made to questions: 4; 8; 11; 12; 15; and 24 to
allow for easier statistical data collection. Changes were made through expert advisory input
from the statistician (Kuhudzai, 2016a).
Participants of the study consisted of mothers who have/had one or more children who
suffer/suffered from colic and used complementary medicine as a form of treatment. The
participant sample was drawn from various areas within Gauteng, different socioeconomic areas
and different types of clinics/businesses/shops in order to allow for the best data representation
of the area. The chosen data collection areas were selected by using an internet search engine and
through popular areas that were frequently visited by mothers, as recommended by the
community. The survey was conducted between October and December 2016.
4.1.1 Sample
A total of 220 questionnaires were printed and distributed to the various data collection areas in
Gauteng. A total of 157 questionnaires were completed of which only 152 questionnaires were
utilised in the data collection as they were completed correctly and with no missing answers.
4.2 General
4.2.1 Age of mother/respondent
The participants were asked to provide their age as part of the inclusion criteria. The age of the
participants was spread across the age groups of 18-29, 30-39 and 40-45. As seen in Figure 4.1,
majority of the respondents were aged between 30-39 years making up 44.1% (n=67) of the
sample; then 18-29 years at 32.2% (n=49); and 40-45 years at 23.7% (n=36).
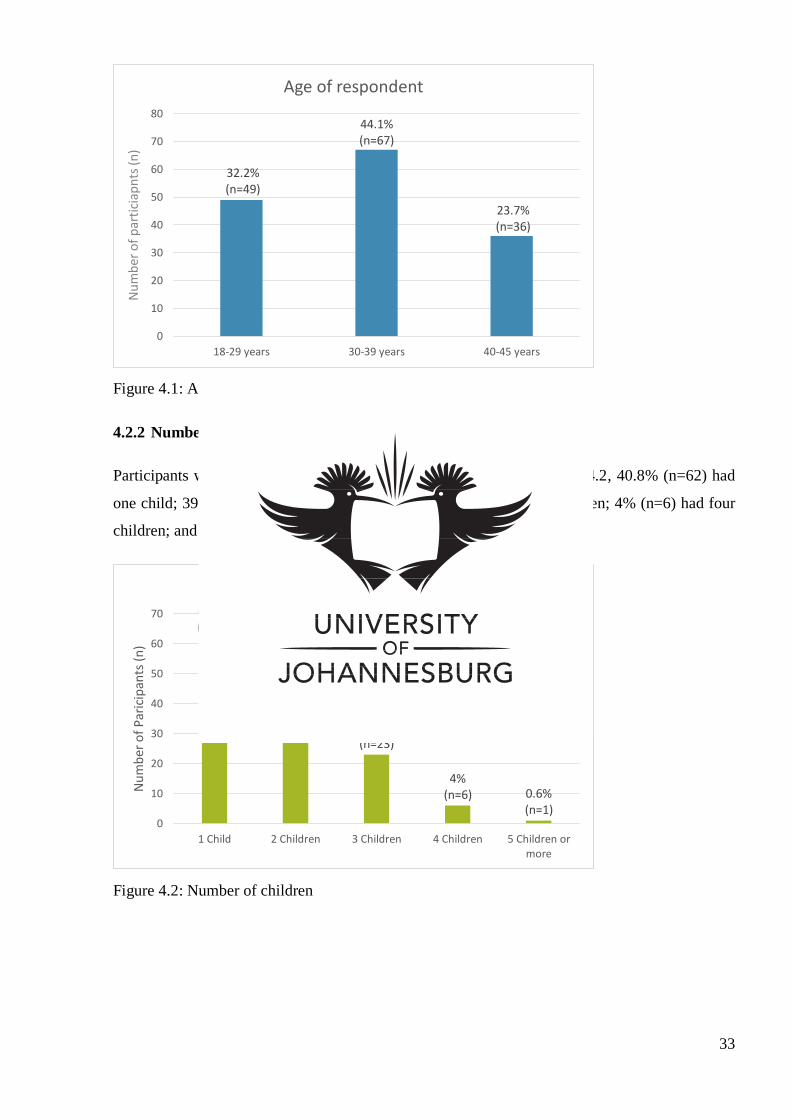
33
Figure 4.1: Age of respondents in 10 year increments
4.2.2 Number of children
Participants were asked how many children they had. As seen in Figure 4.2, 40.8% (n=62) had
one child; 39.5% (n=60) had two children; 15.1% (n=23) had three children; 4% (n=6) had four
children; and 0.66% (n=1) had five or more children.
Figure 4.2: Number of children
32.2% (n=49)
44.1% (n=67)
23.7% (n=36)
0
10
20
30
40
50
60
70
80
18-29 years 30-39 years 40-45 years
Nu
mb
er o
f p
arti
ciap
nts
(n)
Age of respondent
40.8% (n=62)
39.5% (n=60)
15.1% (n=23)
4% (n=6) 0.6%
(n=1) 0
10
20
30
40
50
60
70
1 Child 2 Children 3 Children 4 Children 5 Children ormore
Nu
mb
er o
f P
aric
ipan
ts (
n)
Number of children
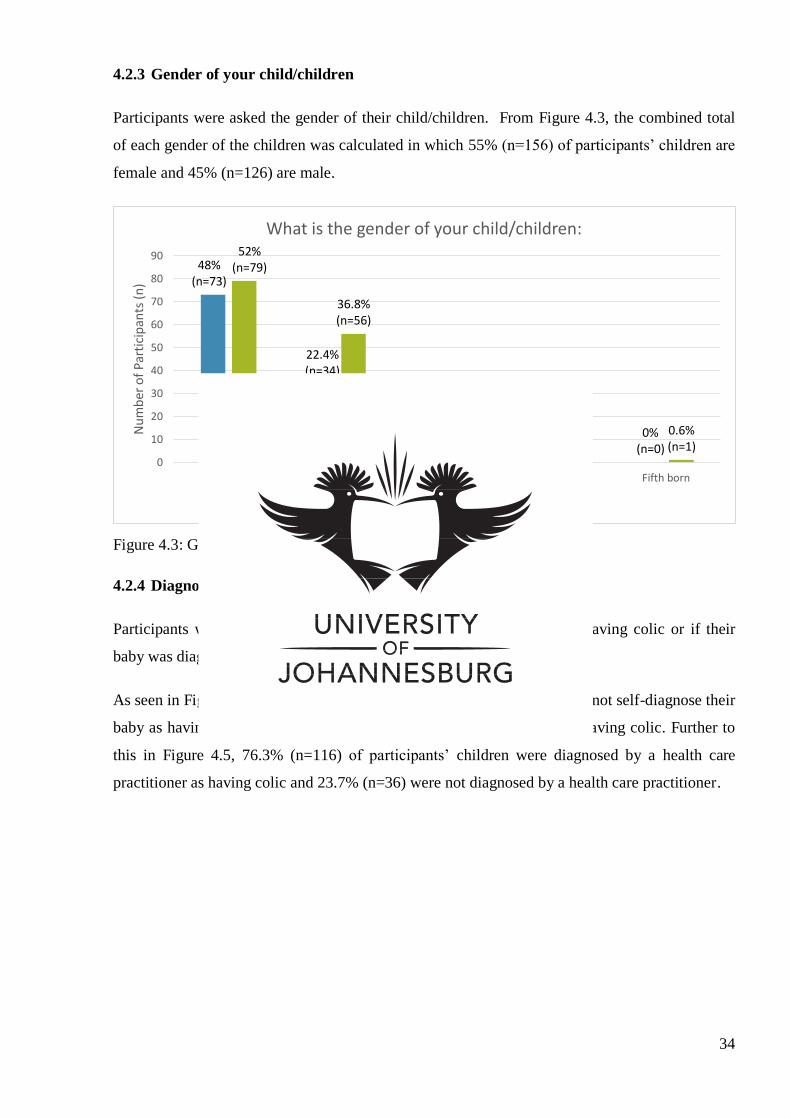
34
4.2.3 Gender of your child/children
Participants were asked the gender of their child/children. From Figure 4.3, the combined total
of each gender of the children was calculated in which 55% (n=156) of participants’ children are
female and 45% (n=126) are male.
Figure 4.3: Gender of child
4.2.4 Diagnosis of colic
Participants were asked whether they had self-diagnosed their baby as having colic or if their
baby was diagnosed by a healthcare practitioner as having colic.
As seen in Figure 4.4, 56.6% (n=86) of participants indicated that they did not self-diagnose their
baby as having colic; whilst 43.4% (n=66) self-diagnosed their baby as having colic. Further to
this in Figure 4.5, 76.3% (n=116) of participants’ children were diagnosed by a health care
practitioner as having colic and 23.7% (n=36) were not diagnosed by a health care practitioner.
48% (n=73)
22.4% (n=34)
10% (n=15)
2.6% (n=4)
0% (n=0)
52% (n=79)
36.8% (n=56)
10.5% (n=16)
2.6% (n=4)
0.6% (n=1)
0
10
20
30
40
50
60
70
80
90
First born Second born Third born Fourth born Fifth born
Nu
mb
er o
f P
arti
cip
ants
(n
)
What is the gender of your child/children:
Male Female
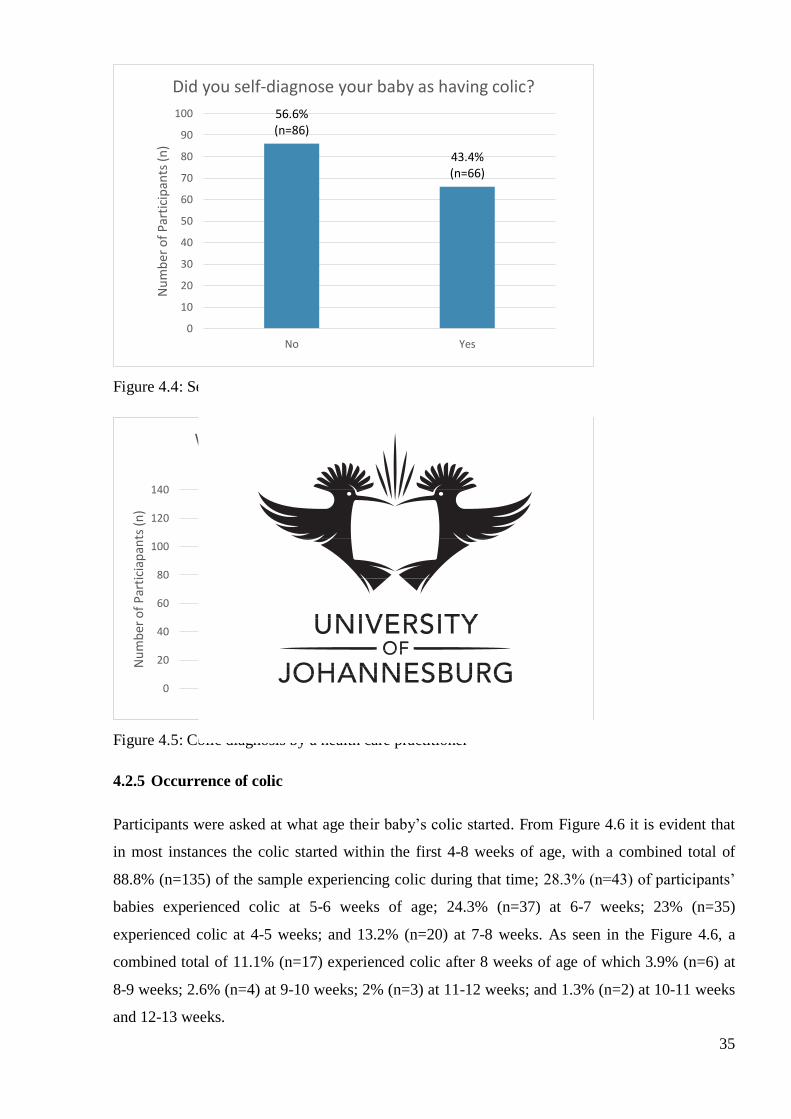
35
Figure 4.4: Self-diagnosis of colic
Figure 4.5: Colic diagnosis by a health care practitioner
4.2.5 Occurrence of colic
Participants were asked at what age their baby’s colic started. From Figure 4.6 it is evident that
in most instances the colic started within the first 4-8 weeks of age, with a combined total of
88.8% (n=135) of the sample experiencing colic during that time; 28.3% (n=43) of participants’
babies experienced colic at 5-6 weeks of age; 24.3% (n=37) at 6-7 weeks; 23% (n=35)
experienced colic at 4-5 weeks; and 13.2% (n=20) at 7-8 weeks. As seen in the Figure 4.6, a
combined total of 11.1% (n=17) experienced colic after 8 weeks of age of which 3.9% (n=6) at
8-9 weeks; 2.6% (n=4) at 9-10 weeks; 2% (n=3) at 11-12 weeks; and 1.3% (n=2) at 10-11 weeks
and 12-13 weeks.
56.6% (n=86)
43.4% (n=66)
0
10
20
30
40
50
60
70
80
90
100
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Did you self-diagnose your baby as having colic?
23.7% (n=36)
76.3% (n=116)
0
20
40
60
80
100
120
140
No Yes
Nu
mb
er o
f P
arti
ciap
ants
(n
)
Was your baby diagnosed by a health care practitioner as having colic?
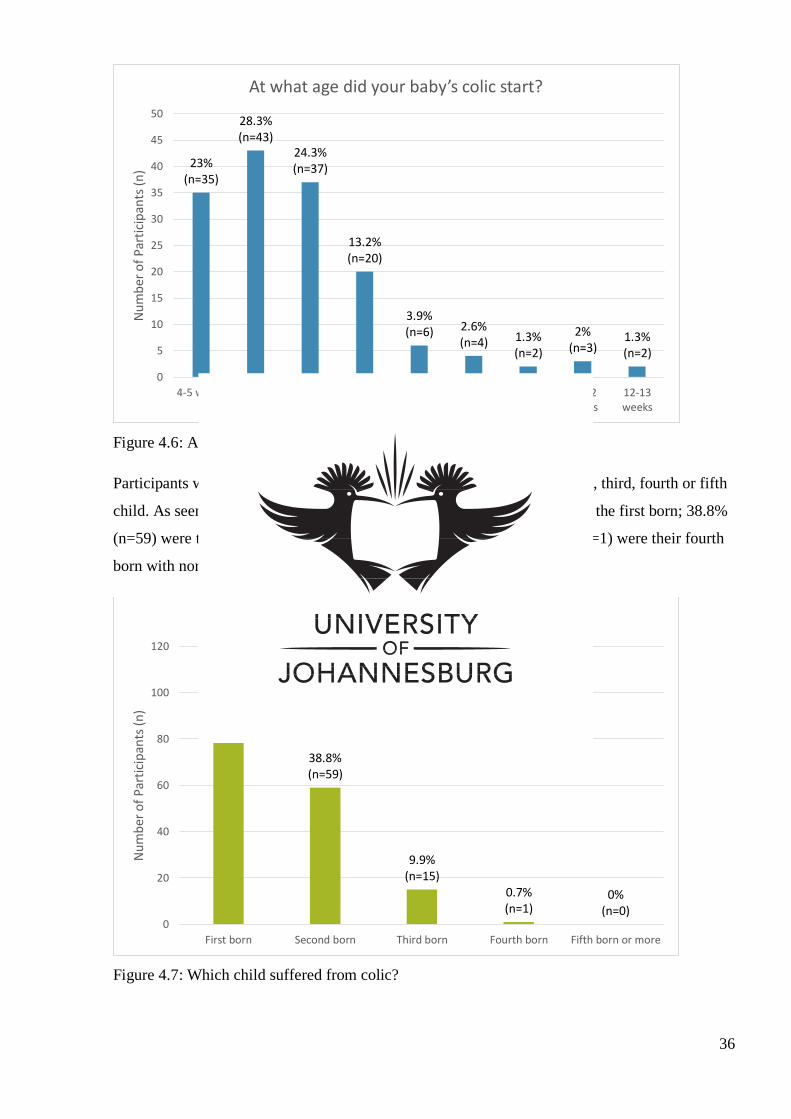
36
Figure 4.6: Age the colic started
Participants were asked whether their suffering baby was their first, second, third, fourth or fifth
child. As seen in Figure 4.7, 68.4 % (n=104) of the suffering children were the first born; 38.8%
(n=59) were their second born; 9.9% (n=15) were their third born; 0.7% (n=1) were their fourth
born with none of the suffering children being their fifth born or more.
Figure 4.7: Which child suffered from colic?
23% (n=35)
28.3% (n=43)
24.3% (n=37)
13.2% (n=20)
3.9% (n=6) 2.6%
(n=4) 1.3% (n=2)
2% (n=3)
1.3% (n=2)
0
5
10
15
20
25
30
35
40
45
50
4-5 weeks 5-6 weeks 6-7 weeks 7-8 weeks 8-9 weeks 9-10weeks
10-11weeks
11-12weeks
12-13weeks
Nu
mb
er o
f P
arti
cip
ants
(n
)
At what age did your baby’s colic start?
68.4% (n=104)
38.8% (n=59)
9.9% (n=15)
0.7% (n=1)
0% (n=0)
0
20
40
60
80
100
120
First born Second born Third born Fourth born Fifth born or more
Nu
mb
er o
f P
arti
cip
ants
(n
)
Is/were your suffering child/children your:
37
Participants were then asked how many of their children experienced colic, 82.2% (n=125) of
participants indicated that only one of their children experienced colic; 15.1% (n=23) indicated
that two of their children experienced colic; and 2.6% (n=4) of participants indicated that three
of their children experienced colic. Please refer to Appendix J for bar graph J.1.
4.2.6 Antenatal class attendance
Participants were asked whether they attended an ante-natal class. If the participants had
attended an ante-natal class, the participants were then asked whether they had learned enough in
the class to care for their new-born in the post-natal stages.
As seen in Figure 4.8, 53% (n=81) of participants responded that they had attended an ante-natal
class; whilst 47% (n=71) of participants had not attended an ante-natal class.
Figure 4.8: Antenatal class attendance
Of the 81 participants that had responded yes to having attended an ante-natal class: 67.9%
(n=55) of participants felt that the ante-natal classes taught them enough to care for their new-
borns in the post-natal stage; whilst 32.1% (n=26) did not feel that the ante-natal class prepared
them sufficiently. Please refer to Appendix J, bar graph J.2. Participants who did not feel
sufficiently prepared were asked to state what would have better prepared them. A few
participants reported that they needed more information on what colic was and how to handle a
child with colic as well as methods on soothing the child. Additional responses may be found in
Appendix K.
47% (n=71)
53% (n=81)
66
68
70
72
74
76
78
80
82
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Did you attend an antenatal class?
38
4.3 Behaviours
4.3.1 Crying
Participants were asked, on average, how many times in a single day their babies experienced
colic and how long the bout of colic would last for.
As seen in Figure 4.9, 32.2% (n=49) of babies experienced colic twice a day; 27.6% (n=42) three
times a day; 22.4% (n=34) once a day; 9.2% (n=14) four times a day; 7.2% (n=11) five times a
day; and 1.3% (n=2) more than five times a day. Two participants responded with different
answers: one saying that the child experienced colic the whole time and that it only subsided
after bath time and up until 12am; the second participant said that her child experienced colic
every 2 hours, which was after every feed.
Figure 4.9: Incidence of colic in a day
Further to this, Figure 4.10 shows that 31.6% (n=48) of babies experienced colic for 11-20
minutes at a time; 26.3% (n=40) for 21-30 minutes; 24.3% (n=37) of babies experienced colic
for 10 minutes or less; 8.6% (n=13) for 31-45 minutes; 5.3% (n=8) experienced colic for more
than one hour; and 3.9% (n=6) for 46-60 minutes.
0% (n=0)
22.4% (n=34)
32.2% (n=49)
27.6% (n=42)
9.2% (n=14) 7.2%
(n=11)
1.3% (n=2)
0
10
20
30
40
50
60
None Once Twice Three times Four times Five times More thanfive times
Nu
mb
er o
f P
arti
cip
ants
(n
)
On average, how many times does/did your baby experience colic in a day?
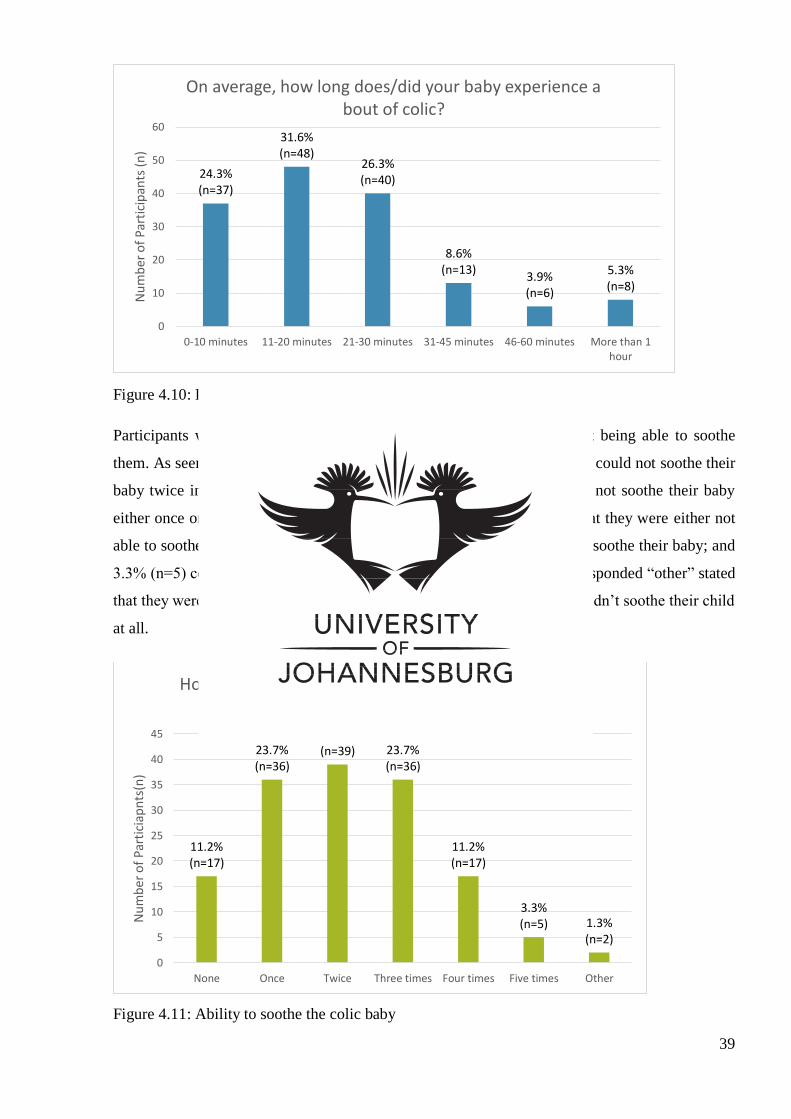
39
Figure 4.10: Duration of colic episode
Participants were asked how many times a day their baby cried without being able to soothe
them. As seen in Figure 4.11, 25.7% (n=39) of participants stated that they could not soothe their
baby twice in a day; 23.7% (n=36) of participants stated that they could not soothe their baby
either once or three times in the day; 11.2% (n=17) of participants felt that they were either not
able to soothe their baby four times a day or that they were always able to soothe their baby; and
3.3% (n=5) couldn’t soothe their baby five times. Two participants who responded “other” stated
that they weren’t able to soothe their child countless times or that they couldn’t soothe their child
at all.
Figure 4.11: Ability to soothe the colic baby
24.3% (n=37)
31.6% (n=48)
26.3% (n=40)
8.6% (n=13)
3.9% (n=6)
5.3% (n=8)
0
10
20
30
40
50
60
0-10 minutes 11-20 minutes 21-30 minutes 31-45 minutes 46-60 minutes More than 1hour
Nu
mb
er o
f P
arti
cip
ants
(n
)
On average, how long does/did your baby experience a bout of colic?
11.2% (n=17)
23.7% (n=36)
25.7% (n=39) 23.7%
(n=36)
11.2% (n=17)
3.3% (n=5) 1.3%
(n=2)
0
5
10
15
20
25
30
35
40
45
None Once Twice Three times Four times Five times Other
Nu
mb
er o
f P
arti
ciap
nts
(n)
How many times does/did your baby cry without you being able to soothe him/her in a day?
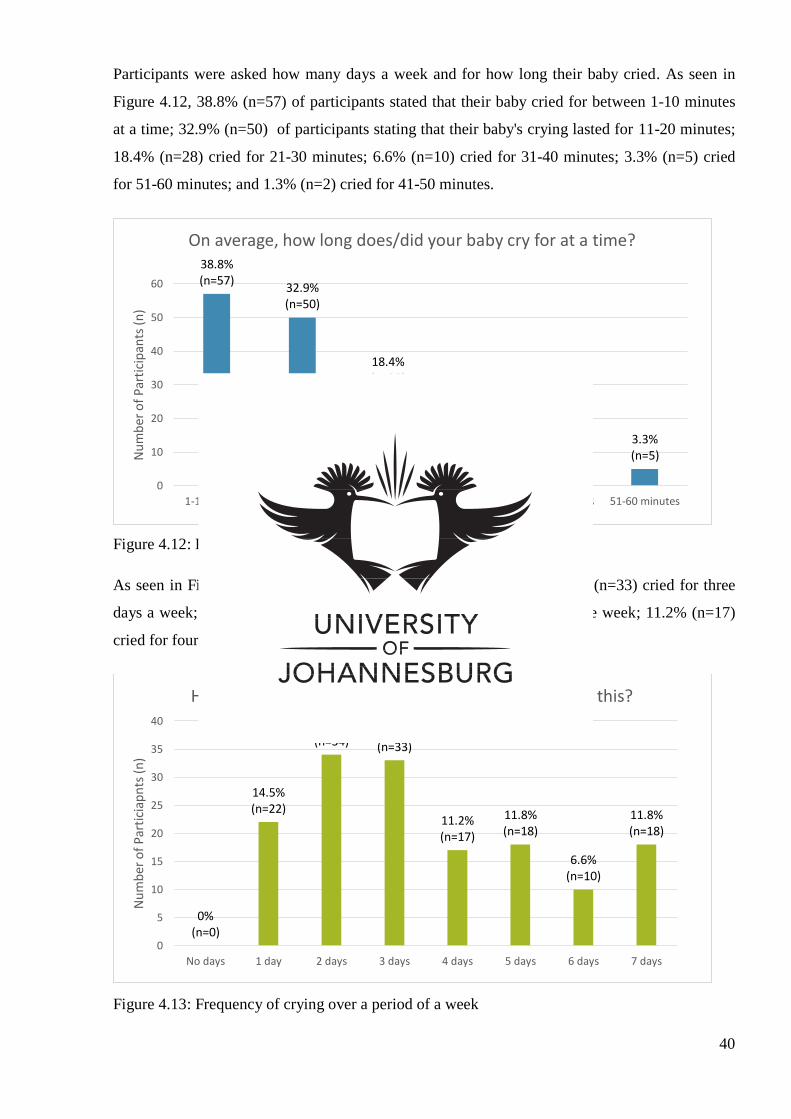
40
Participants were asked how many days a week and for how long their baby cried. As seen in
Figure 4.12, 38.8% (n=57) of participants stated that their baby cried for between 1-10 minutes
at a time; 32.9% (n=50) of participants stating that their baby's crying lasted for 11-20 minutes;
18.4% (n=28) cried for 21-30 minutes; 6.6% (n=10) cried for 31-40 minutes; 3.3% (n=5) cried
for 51-60 minutes; and 1.3% (n=2) cried for 41-50 minutes.
Figure 4.12: Duration of crying at any given time
As seen in Figure 4.13, 22.4% (n=34) cried for two days a week; 21.7% (n=33) cried for three
days a week; 11.8% (n=18) cried for five days a week or every day of the week; 11.2% (n=17)
cried for four days a week; and 6.6% (n=10) cried for six days a week.
Figure 4.13: Frequency of crying over a period of a week
38.8% (n=57)
32.9% (n=50)
18.4% (n=28)
6.6% (n=10)
1.3% (n=2)
3.3% (n=5)
0
10
20
30
40
50
60
1-10 minutes 11-20 minutes 21-30 minutes 31-40 minutes 41-50 minutes 51-60 minutes
Nu
mb
er o
f P
arti
cip
ants
(n
)
On average, how long does/did your baby cry for at a time?
0% (n=0)
14.5% (n=22)
22.4% (n=34)
21.7% (n=33)
11.2% (n=17)
11.8% (n=18)
6.6% (n=10)
11.8% (n=18)
0
5
10
15
20
25
30
35
40
No days 1 day 2 days 3 days 4 days 5 days 6 days 7 days
Nu
mb
er o
f P
arti
ciap
nts
(n
)
How many days in a week does/did your baby cry like this?
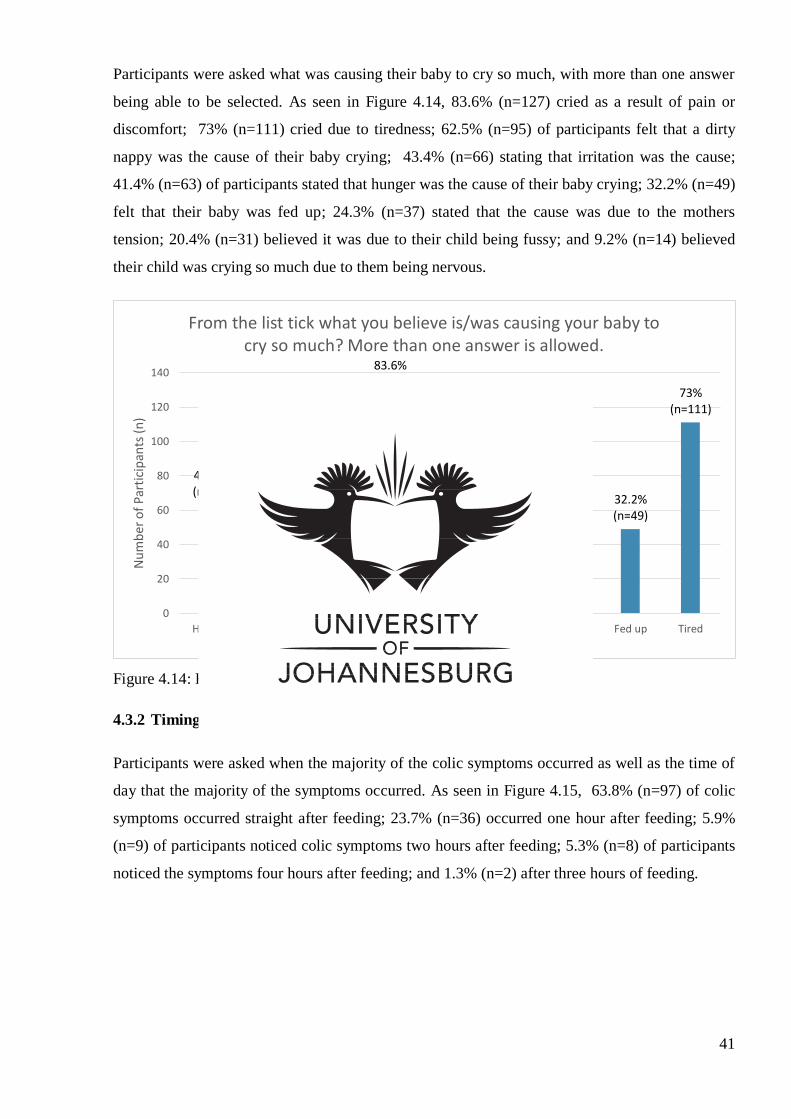
41
Participants were asked what was causing their baby to cry so much, with more than one answer
being able to be selected. As seen in Figure 4.14, 83.6% (n=127) cried as a result of pain or
discomfort; 73% (n=111) cried due to tiredness; 62.5% (n=95) of participants felt that a dirty
nappy was the cause of their baby crying; 43.4% (n=66) stating that irritation was the cause;
41.4% (n=63) of participants stated that hunger was the cause of their baby crying; 32.2% (n=49)
felt that their baby was fed up; 24.3% (n=37) stated that the cause was due to the mothers
tension; 20.4% (n=31) believed it was due to their child being fussy; and 9.2% (n=14) believed
their child was crying so much due to them being nervous.
Figure 4.14: Believed reasons for excessive crying
4.3.2 Timing of colic symptoms
Participants were asked when the majority of the colic symptoms occurred as well as the time of
day that the majority of the symptoms occurred. As seen in Figure 4.15, 63.8% (n=97) of colic
symptoms occurred straight after feeding; 23.7% (n=36) occurred one hour after feeding; 5.9%
(n=9) of participants noticed colic symptoms two hours after feeding; 5.3% (n=8) of participants
noticed the symptoms four hours after feeding; and 1.3% (n=2) after three hours of feeding.
41.4% (n=63)
62.5% (n=95)
24.3% (n=37)
83.6% (n=127)
20.4% (n=31)
43.4% (n=66)
9.2% (n=14)
32.2% (n=49)
73% (n=111)
0
20
40
60
80
100
120
140
Hunger Dirty nappy Yourtension
Pain ordiscomfort
Fussy Irritated Nervous Fed up Tired
Nu
mb
er o
f P
arti
cip
ants
(n
)
From the list tick what you believe is/was causing your baby to cry so much? More than one answer is allowed.
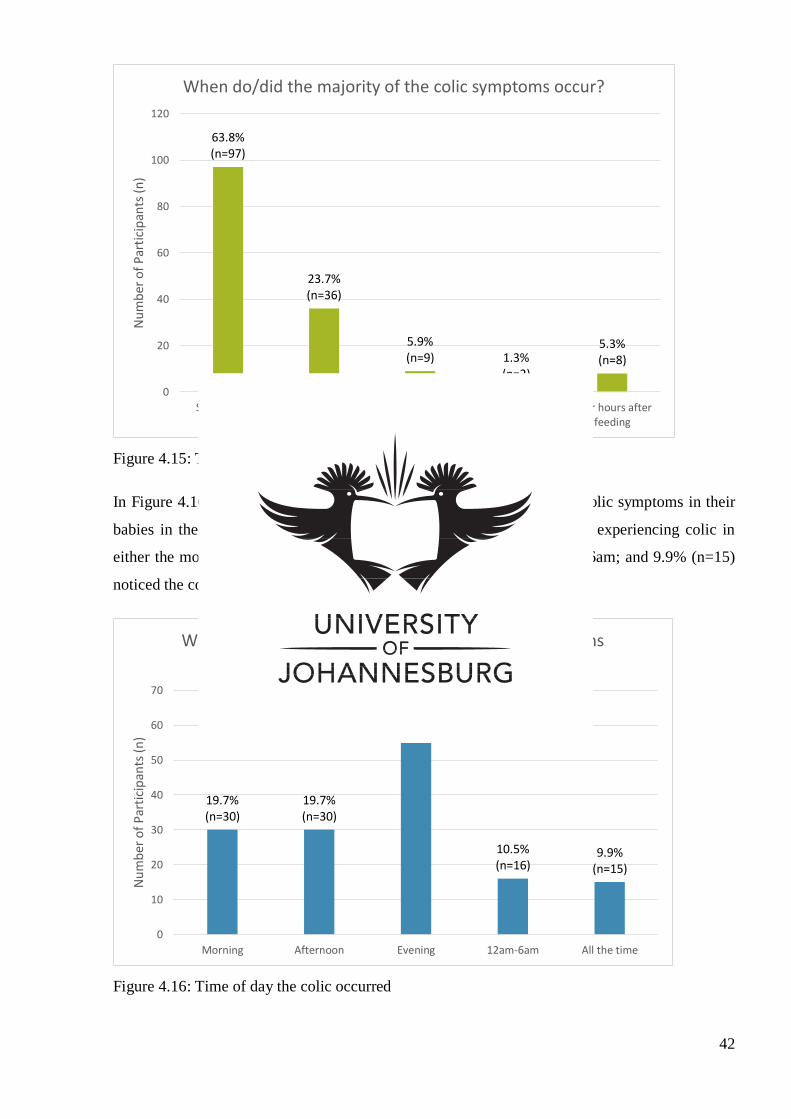
42
Figure 4.15: Timing of colic symptoms in relation to feeding
In Figure 4.16 it can be seen that: 40.1% (n=61) of participants noticed colic symptoms in their
babies in the evening; 19.7% (n=30) of participants noticed their babies experiencing colic in
either the morning or afternoon; 10.5% (n=16) noticed it between 12am-6am; and 9.9% (n=15)
noticed the colic symptoms all the time.
Figure 4.16: Time of day the colic occurred
63.8% (n=97)
23.7% (n=36)
5.9% (n=9) 1.3%
(n=2)
5.3% (n=8)
0
20
40
60
80
100
120
Straight afterfeeding
One hour afterfeeding
Two hours afterfeeding
Three hours afterfeeding
Four hours afterfeeding
Nu
mb
er o
f P
arti
cip
ants
(n
)
When do/did the majority of the colic symptoms occur?
19.7% (n=30)
19.7% (n=30)
40.1% (n=61)
10.5% (n=16)
9.9% (n=15)
0
10
20
30
40
50
60
70
Morning Afternoon Evening 12am-6am All the time
Nu
mb
er o
f P
arti
cip
ants
(n
)
What time of day do/did majority of the colic symptoms occur?
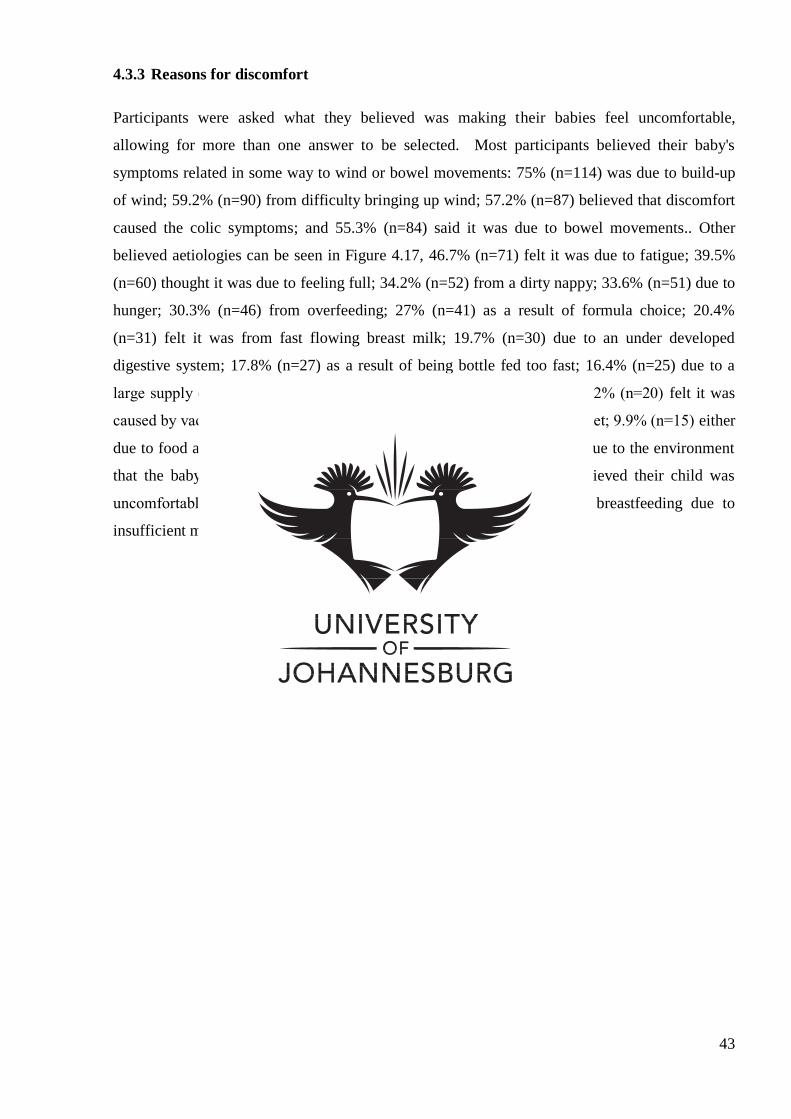
43
4.3.3 Reasons for discomfort
Participants were asked what they believed was making their babies feel uncomfortable,
allowing for more than one answer to be selected. Most participants believed their baby's
symptoms related in some way to wind or bowel movements: 75% (n=114) was due to build-up
of wind; 59.2% (n=90) from difficulty bringing up wind; 57.2% (n=87) believed that discomfort
caused the colic symptoms; and 55.3% (n=84) said it was due to bowel movements.. Other
believed aetiologies can be seen in Figure 4.17, 46.7% (n=71) felt it was due to fatigue; 39.5%
(n=60) thought it was due to feeling full; 34.2% (n=52) from a dirty nappy; 33.6% (n=51) due to
hunger; 30.3% (n=46) from overfeeding; 27% (n=41) as a result of formula choice; 20.4%
(n=31) felt it was from fast flowing breast milk; 19.7% (n=30) due to an under developed
digestive system; 17.8% (n=27) as a result of being bottle fed too fast; 16.4% (n=25) due to a
large supply of breast milk; 13.8% (n=21) from the mother’s tension; 13.2% (n=20) felt it was
caused by vaccinations; 12.5% (n=19) due to the food from the mother’s diet; 9.9% (n=15) either
due to food allergies or a growth spurt; and 9.2% (n=14) felt that it was due to the environment
that the baby was in. Three participants stated that the reason they believed their child was
uncomfortable was due to genetics, “bad digestive system”, frequent breastfeeding due to
insufficient milk supply and that their baby was premature.
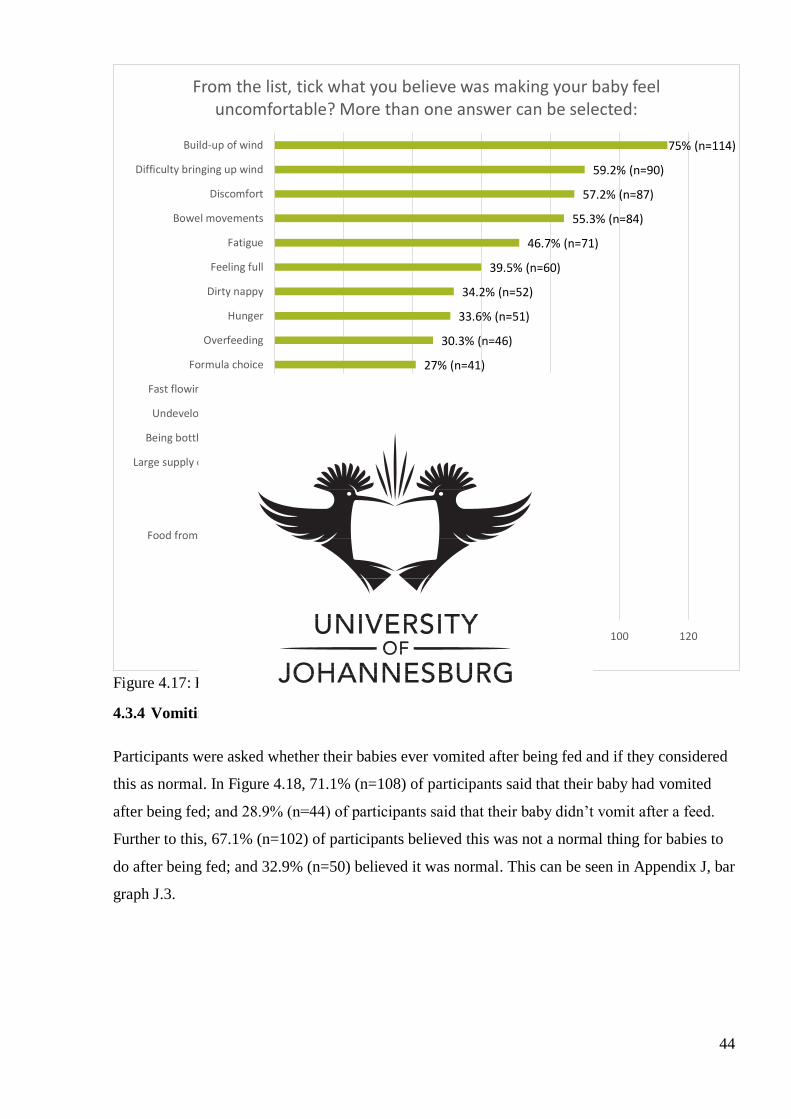
44
Figure 4.17: Reasons for discomfort
4.3.4 Vomiting
Participants were asked whether their babies ever vomited after being fed and if they considered
this as normal. In Figure 4.18, 71.1% (n=108) of participants said that their baby had vomited
after being fed; and 28.9% (n=44) of participants said that their baby didn’t vomit after a feed.
Further to this, 67.1% (n=102) of participants believed this was not a normal thing for babies to
do after being fed; and 32.9% (n=50) believed it was normal. This can be seen in Appendix J, bar
graph J.3.
9.2% (n=14)
9.9% (n=15)
9.9% (n=15)
12.5% (n=19)
13.2% (n=20)
13.8%(n=21)
16.4% (n=25)
17.8% (n=27)
19.7% (n=30)
20.4% (n=31)
27% (n=41)
30.3% (n=46)
33.6% (n=51)
34.2% (n=52)
39.5% (n=60)
46.7% (n=71)
55.3% (n=84)
57.2% (n=87)
59.2% (n=90)
75% (n=114)
0 20 40 60 80 100 120
Environment
Growth spurt
Food allergy
Food from mothers diet
Vaccinations
Your tension
Large supply of breast milk
Being bottle fed too fast
Undeveloped digestive…
Fast flowing breast milk
Formula choice
Overfeeding
Hunger
Dirty nappy
Feeling full
Fatigue
Bowel movements
Discomfort
Difficulty bringing up wind
Build-up of wind
Number of Participants (n)
From the list, tick what you believe was making your baby feel uncomfortable? More than one answer can be selected:
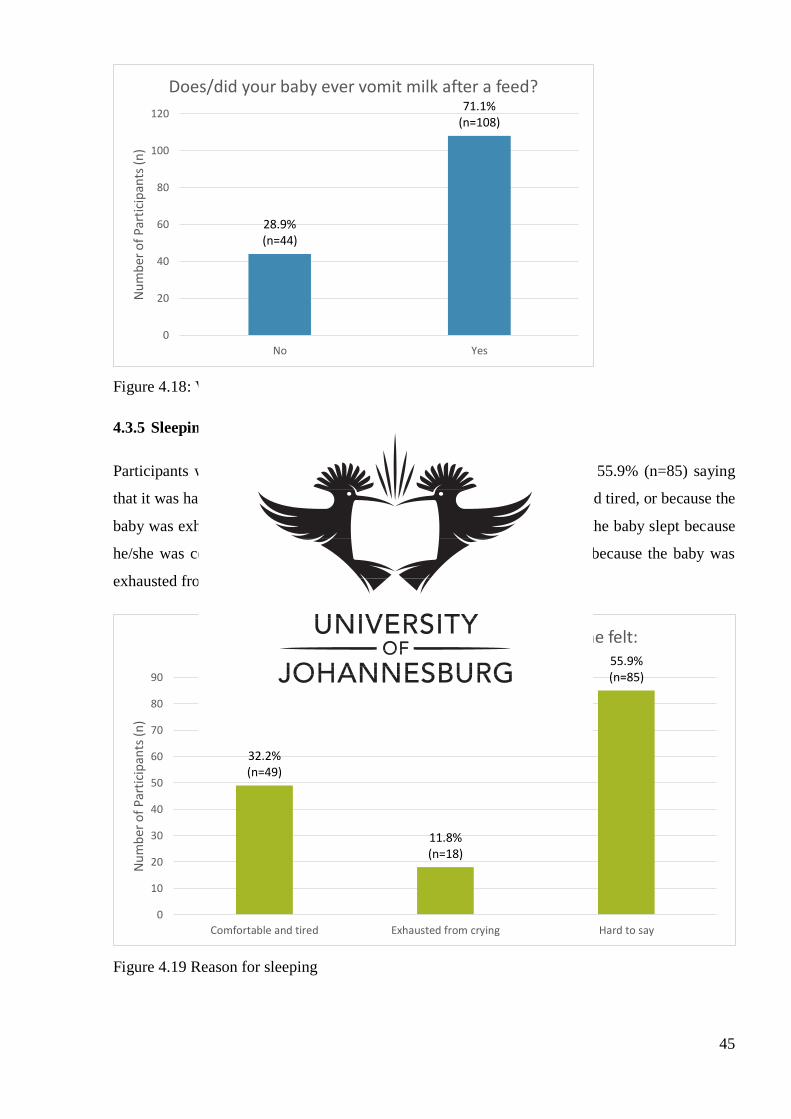
45
Figure 4.18: Vomiting milk after a feed
4.3.5 Sleeping
Participants were asked what caused their baby to sleep. In Figure 4.19, 55.9% (n=85) saying
that it was hard to say whether it was because the baby was comfortable and tired, or because the
baby was exhausted from crying; 32.2% (n=49) stated that they believed the baby slept because
he/she was comfortable and tired; and 11.8% (n=18) stating that it was because the baby was
exhausted from crying.
Figure 4.19 Reason for sleeping
28.9% (n=44)
71.1% (n=108)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Does/did your baby ever vomit milk after a feed?
32.2% (n=49)
11.8% (n=18)
55.9% (n=85)
0
10
20
30
40
50
60
70
80
90
Comfortable and tired Exhausted from crying Hard to say
Nu
mb
er o
f P
arti
cip
ants
(n
)
Do you feel your baby sleeps mostly because he/she felt:
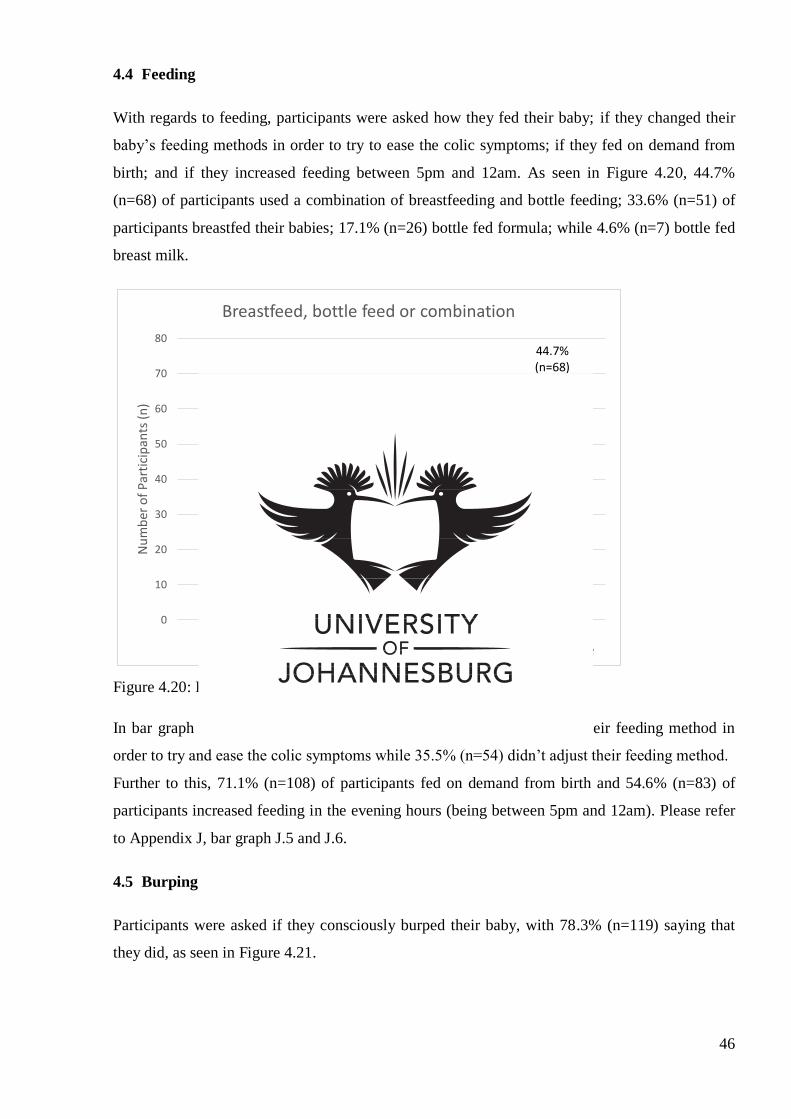
46
4.4 Feeding
With regards to feeding, participants were asked how they fed their baby; if they changed their
baby’s feeding methods in order to try to ease the colic symptoms; if they fed on demand from
birth; and if they increased feeding between 5pm and 12am. As seen in Figure 4.20, 44.7%
(n=68) of participants used a combination of breastfeeding and bottle feeding; 33.6% (n=51) of
participants breastfed their babies; 17.1% (n=26) bottle fed formula; while 4.6% (n=7) bottle fed
breast milk.
Figure 4.20: Feeding methods
In bar graph J.4 in Appendix J, 64.5% (n=98) of participants changed their feeding method in
order to try and ease the colic symptoms while 35.5% (n=54) didn’t adjust their feeding method.
Further to this, 71.1% (n=108) of participants fed on demand from birth and 54.6% (n=83) of
participants increased feeding in the evening hours (being between 5pm and 12am). Please refer
to Appendix J, bar graph J.5 and J.6.
4.5 Burping
Participants were asked if they consciously burped their baby, with 78.3% (n=119) saying that
they did, as seen in Figure 4.21.
36.6% (n=51)
4.6% (n=7)
17.1% (n=26)
44.7% (n=68)
0
10
20
30
40
50
60
70
80
Breastfeed Bottle feed breastmilk
Bottle feed formula Combination ofbreast and bottle
Nu
mb
er o
f P
arti
cip
ants
(n
)
Breastfeed, bottle feed or combination
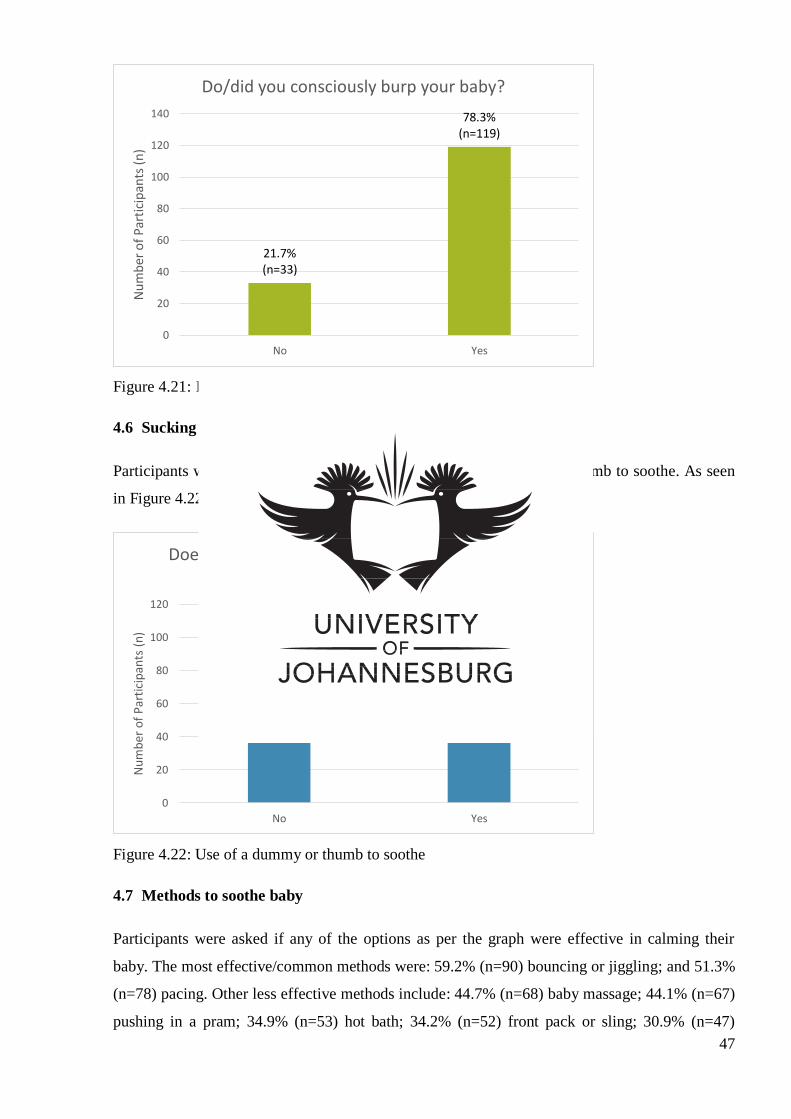
47
Figure 4.21: Burping
4.6 Sucking for comfort
Participants were asked if their baby used a dummy or sucked his/her thumb to soothe. As seen
in Figure 4.22, 71.1% (n=108) stated that this was the case.
Figure 4.22: Use of a dummy or thumb to soothe
4.7 Methods to soothe baby
Participants were asked if any of the options as per the graph were effective in calming their
baby. The most effective/common methods were: 59.2% (n=90) bouncing or jiggling; and 51.3%
(n=78) pacing. Other less effective methods include: 44.7% (n=68) baby massage; 44.1% (n=67)
pushing in a pram; 34.9% (n=53) hot bath; 34.2% (n=52) front pack or sling; 30.9% (n=47)
21.7% (n=33)
78.3% (n=119)
0
20
40
60
80
100
120
140
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Do/did you consciously burp your baby?
28.9% (n=44)
71.1% (n=108)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Does/did your baby use a dummy or suck his/her thumb to soothe?
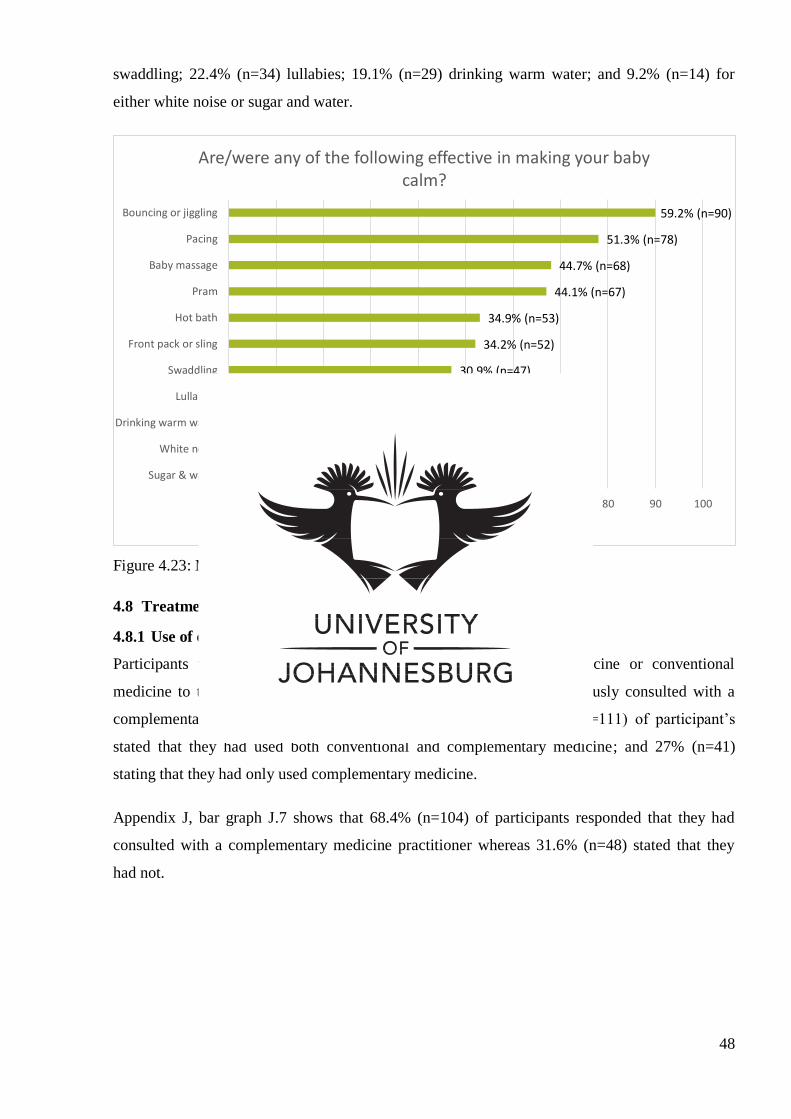
48
swaddling; 22.4% (n=34) lullabies; 19.1% (n=29) drinking warm water; and 9.2% (n=14) for
either white noise or sugar and water.
Figure 4.23: Methods to soothe baby
4.8 Treatment
4.8.1 Use of complementary medicine
Participants were asked whether they had used complementary medicine or conventional
medicine to treat their baby's colic; and whether or not they had previously consulted with a
complementary medicine practitioner. As seen in Figure 4.24, 73% (n=111) of participant’s
stated that they had used both conventional and complementary medicine; and 27% (n=41)
stating that they had only used complementary medicine.
Appendix J, bar graph J.7 shows that 68.4% (n=104) of participants responded that they had
consulted with a complementary medicine practitioner whereas 31.6% (n=48) stated that they
had not.
9.2% (n=14)
9.2% (n=14)
19.1% (n=29)
22.4% (n=34)
30.9% (n=47)
34.2% (n=52)
34.9% (n=53)
44.1% (n=67)
44.7% (n=68)
51.3% (n=78)
59.2% (n=90)
0 10 20 30 40 50 60 70 80 90 100
Sugar & water
White noise
Drinking warm water
Lullabies
Swaddling
Front pack or sling
Hot bath
Pram
Baby massage
Pacing
Bouncing or jiggling
Number of Participants (n)
Are/were any of the following effective in making your baby calm?
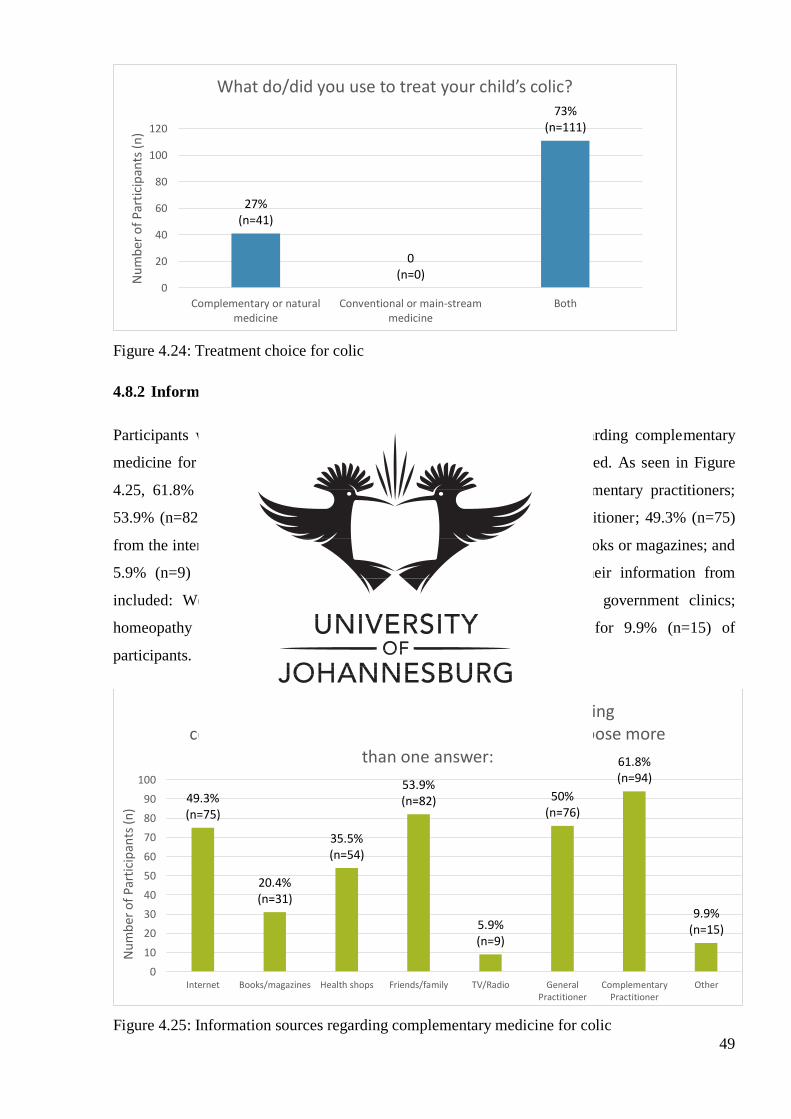
49
Figure 4.24: Treatment choice for colic
4.8.2 Information about complementary medicine
Participants were asked where they had received their information regarding complementary
medicine for colic from, allowing for more than one answer to be selected. As seen in Figure
4.25, 61.8% (n=94) of participants got their information from complementary practitioners;
53.9% (n=82) from friends and family; 50% (n=76) from a general practitioner; 49.3% (n=75)
from the internet; 35.5% (n=54) from health shops; 20.4% (n=31) from books or magazines; and
5.9% (n=9) from the television. Other places that participants got their information from
included: Weleda pharmacy group staff; chiropractors; clinic sisters; government clinics;
homeopathy course; midwives and sangomas, which all accounted for 9.9% (n=15) of
participants.
Figure 4.25: Information sources regarding complementary medicine for colic
27% (n=41)
0 (n=0)
73% (n=111)
0
20
40
60
80
100
120
Complementary or naturalmedicine
Conventional or main-streammedicine
Both
Nu
mb
er o
f P
arti
cip
ants
(n
)
What do/did you use to treat your child’s colic?
49.3% (n=75)
20.4% (n=31)
35.5% (n=54)
53.9% (n=82)
5.9% (n=9)
50% (n=76)
61.8% (n=94)
9.9% (n=15)
0
10
20
30
40
50
60
70
80
90
100
Internet Books/magazines Health shops Friends/family TV/Radio GeneralPractitioner
ComplementaryPractitioner
Other
Nu
mb
er o
f P
arti
cip
ants
(n
)
Where do/did you get your information regarding complementary medicine for colic from? You may choose more
than one answer:
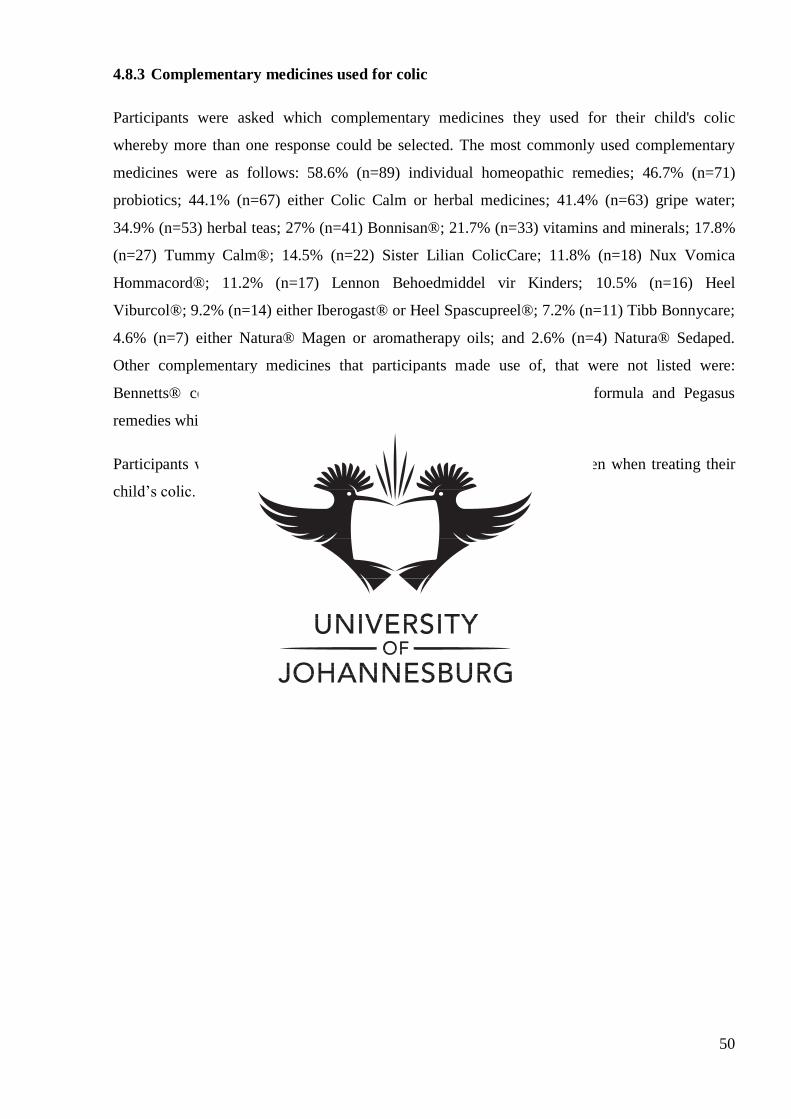
50
4.8.3 Complementary medicines used for colic
Participants were asked which complementary medicines they used for their child's colic
whereby more than one response could be selected. The most commonly used complementary
medicines were as follows: 58.6% (n=89) individual homeopathic remedies; 46.7% (n=71)
probiotics; 44.1% (n=67) either Colic Calm or herbal medicines; 41.4% (n=63) gripe water;
34.9% (n=53) herbal teas; 27% (n=41) Bonnisan®; 21.7% (n=33) vitamins and minerals; 17.8%
(n=27) Tummy Calm®; 14.5% (n=22) Sister Lilian ColicCare; 11.8% (n=18) Nux Vomica
Hommacord®; 11.2% (n=17) Lennon Behoedmiddel vir Kinders; 10.5% (n=16) Heel
Viburcol®; 9.2% (n=14) either Iberogast® or Heel Spascupreel®; 7.2% (n=11) Tibb Bonnycare;
4.6% (n=7) either Natura® Magen or aromatherapy oils; and 2.6% (n=4) Natura® Sedaped.
Other complementary medicines that participants made use of, that were not listed were:
Bennetts® colic mixture; Hylands colic tablets; Infacol and Neocate formula and Pegasus
remedies which all accounted for 5.2% (n=8) participants.
Participants were asked reasons why complementary medicine was chosen when treating their
child’s colic. These responses can be found in Appendix L.
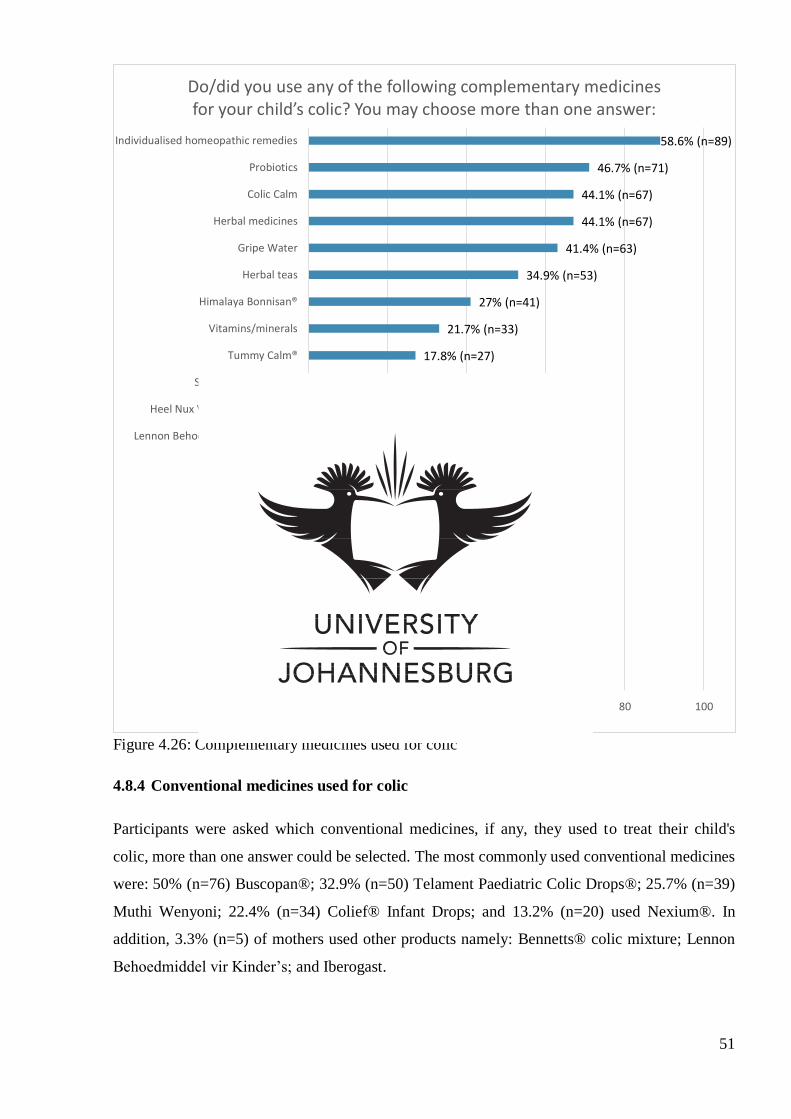
51
Figure 4.26: Complementary medicines used for colic
4.8.4 Conventional medicines used for colic
Participants were asked which conventional medicines, if any, they used to treat their child's
colic, more than one answer could be selected. The most commonly used conventional medicines
were: 50% (n=76) Buscopan®; 32.9% (n=50) Telament Paediatric Colic Drops®; 25.7% (n=39)
Muthi Wenyoni; 22.4% (n=34) Colief® Infant Drops; and 13.2% (n=20) used Nexium®. In
addition, 3.3% (n=5) of mothers used other products namely: Bennetts® colic mixture; Lennon
Behoedmiddel vir Kinder’s; and Iberogast.
0 %(n=0)
2.6% (n=4)
4.6% (n=7)
4.6% (n=7)
5.2% (n=8)
7.2% (n=11)
9.2 % (n=14)
9.2% (n=14)
10.5% (n=16)
11.2% (n=17)
11.8% (n=18)
14.5% (n=22)
17.8% (n=27)
21.7% (n=33)
27% (n=41)
34.9% (n=53)
41.4% (n=63)
44.1% (n=67)
44.1% (n=67)
46.7% (n=71)
58.6% (n=89)
0 20 40 60 80 100
None
Natura® Sedaped
Aromatherapy oils
Natura® Magen
Other
Tibb Bonnycare
Heel Spascupreel®
Iberogast®
Heel Viburcol®
Lennon Behoedmiddel vir Kinders
Heel Nux Vomica Homaccord®
Sister Lilian ColicCare
Tummy Calm®
Vitamins/minerals
Himalaya Bonnisan®
Herbal teas
Gripe Water
Herbal medicines
Colic Calm
Probiotics
Individualised homeopathic remedies
Number of Participants (n)
Do/did you use any of the following complementary medicines for your child’s colic? You may choose more than one answer:
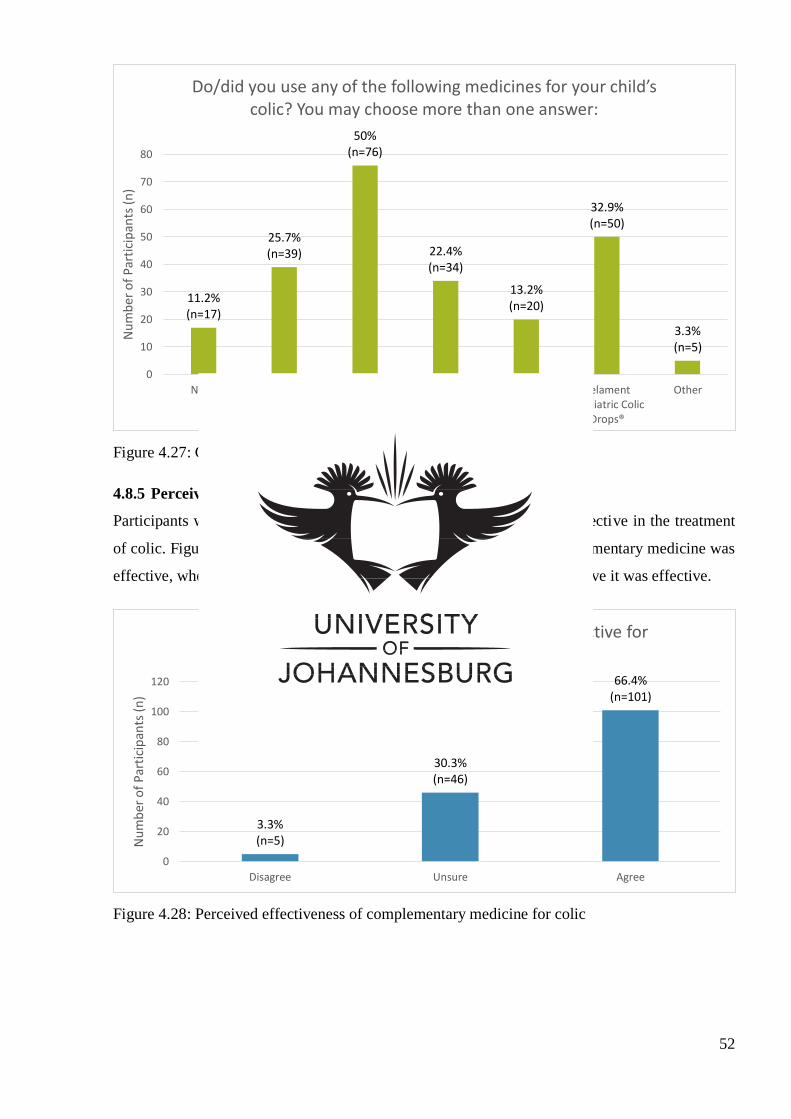
52
Figure 4.27: Conventional medication used to treat colic
4.8.5 Perceived effectiveness of complementary medicine for colic
Participants were asked if they felt that complementary medicine was effective in the treatment
of colic. Figure 4.28 shows 66.4% (n=101) of participants felt that complementary medicine was
effective, whereas 30.3% (n=46) were unsure and 3.3% (n=5) did not believe it was effective.
Figure 4.28: Perceived effectiveness of complementary medicine for colic
11.2% (n=17)
25.7% (n=39)
50% (n=76)
22.4% (n=34)
13.2% (n=20)
32.9% (n=50)
3.3% (n=5)
0
10
20
30
40
50
60
70
80
None Muthi Wenyoni Buscopan® Colief® Infantdrops
Nexium® TelamentPaediatric Colic
Drops®
Other
Nu
mb
er o
f P
arti
cip
ants
(n
)
Do/did you use any of the following medicines for your child’s colic? You may choose more than one answer:
3.3% (n=5)
30.3% (n=46)
66.4% (n=101)
0
20
40
60
80
100
120
Disagree Unsure Agree
Nu
mb
er o
f P
arti
cip
ants
(n
)
In your experience is complementary medicine effective for colic:
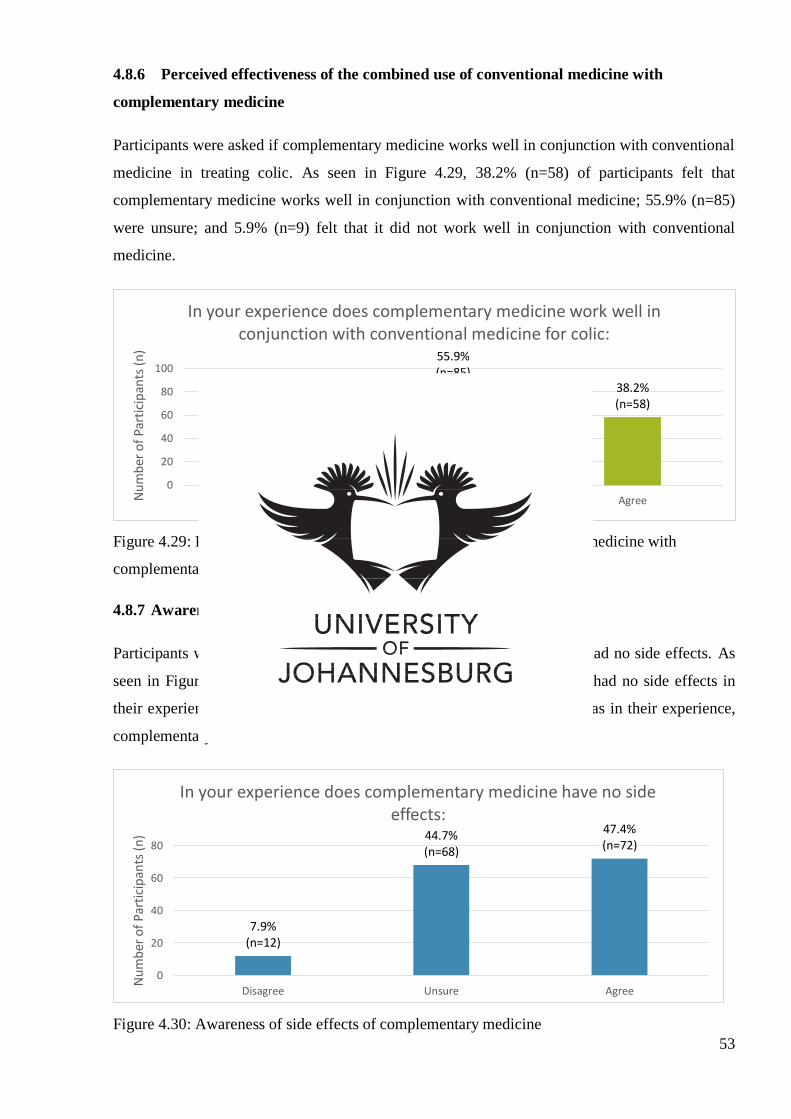
53
4.8.6 Perceived effectiveness of the combined use of conventional medicine with
complementary medicine
Participants were asked if complementary medicine works well in conjunction with conventional
medicine in treating colic. As seen in Figure 4.29, 38.2% (n=58) of participants felt that
complementary medicine works well in conjunction with conventional medicine; 55.9% (n=85)
were unsure; and 5.9% (n=9) felt that it did not work well in conjunction with conventional
medicine.
Figure 4.29: Perceived effectiveness of the combined use of conventional medicine with
complementary medicine
4.8.7 Awareness of side effects of complementary medicine
Participants were asked if, in their experience, complementary medicine had no side effects. As
seen in Figure 4.30, 47.4% (n=72) agreed that complementary medicine had no side effects in
their experience; 44.7% (n=68) were unsure; and 7.9% (n=12) disagreed as in their experience,
complementary medicine had side effects.
Figure 4.30: Awareness of side effects of complementary medicine
5.9% (n=9)
55.9% (n=85)
38.2% (n=58)
0
20
40
60
80
100
Disagree Unsure AgreeNu
mb
er o
f P
arti
cip
ants
(n
)
In your experience does complementary medicine work well in conjunction with conventional medicine for colic:
7.9% (n=12)
44.7% (n=68)
47.4% (n=72)
0
20
40
60
80
Disagree Unsure Agree
Nu
mb
er o
f P
arti
cip
ants
(n
)
In your experience does complementary medicine have no side effects:
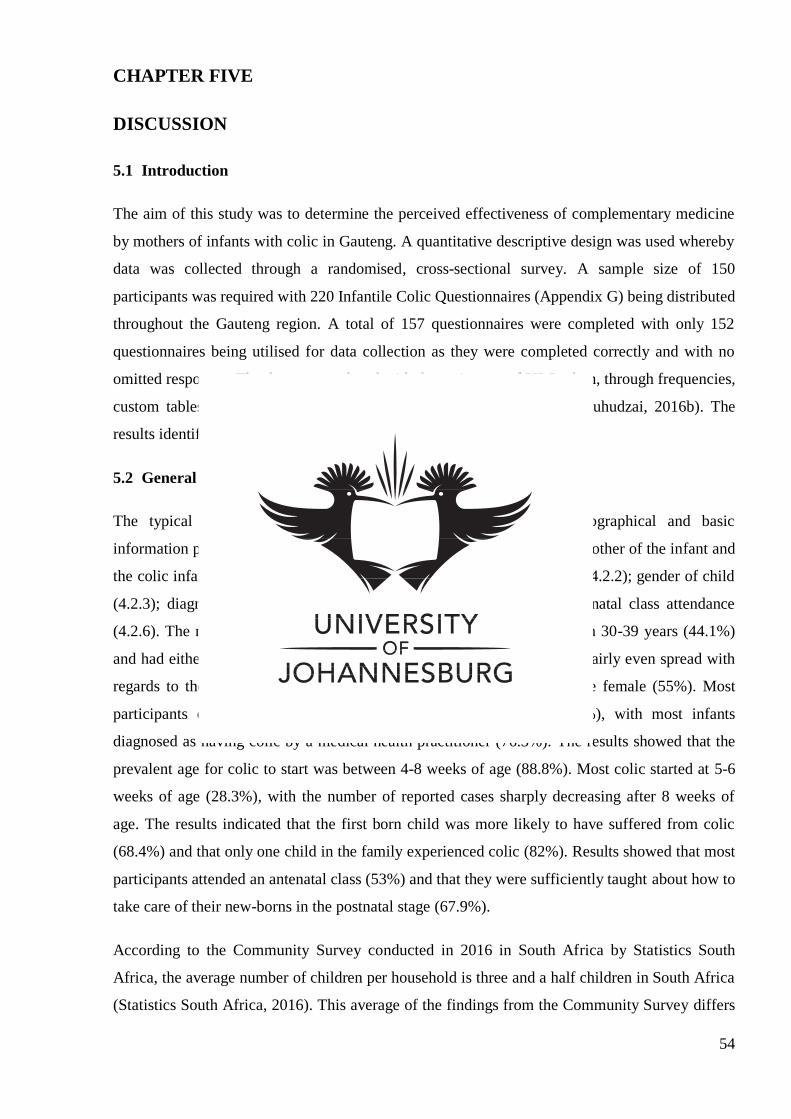
54
CHAPTER FIVE
DISCUSSION
5.1 Introduction
The aim of this study was to determine the perceived effectiveness of complementary medicine
by mothers of infants with colic in Gauteng. A quantitative descriptive design was used whereby
data was collected through a randomised, cross-sectional survey. A sample size of 150
participants was required with 220 Infantile Colic Questionnaires (Appendix G) being distributed
throughout the Gauteng region. A total of 157 questionnaires were completed with only 152
questionnaires being utilised for data collection as they were completed correctly and with no
omitted responses. The data was analysed with the assistance of UJ Statkon, through frequencies,
custom tables, multiple response analysis and open ended responses (Kuhudzai, 2016b). The
results identified the following areas of statistical significance.
5.2 General information
The typical occurrence of infantile colic was determined by demographical and basic
information provided by participants. Data obtained referenced both the mother of the infant and
the colic infant, this included: age of mother (4.2.1); number of children (4.2.2); gender of child
(4.2.3); diagnosis of colic (4.2.4); occurrence of colic (4.2.5); and antenatal class attendance
(4.2.6). The results indicated that majority of mothers were aged between 30-39 years (44.1%)
and had either one (40.8%) or two (39.5%) children. Results indicated a fairly even spread with
regards to the gender of the child however, majority of the infants were female (55%). Most
participants did not self-diagnosis their child as having colic (56.6%), with most infants
diagnosed as having colic by a medical health practitioner (76.3%). The results showed that the
prevalent age for colic to start was between 4-8 weeks of age (88.8%). Most colic started at 5-6
weeks of age (28.3%), with the number of reported cases sharply decreasing after 8 weeks of
age. The results indicated that the first born child was more likely to have suffered from colic
(68.4%) and that only one child in the family experienced colic (82%). Results showed that most
participants attended an antenatal class (53%) and that they were sufficiently taught about how to
take care of their new-borns in the postnatal stage (67.9%).
According to the Community Survey conducted in 2016 in South Africa by Statistics South
Africa, the average number of children per household is three and a half children in South Africa
(Statistics South Africa, 2016). This average of the findings from the Community Survey differs
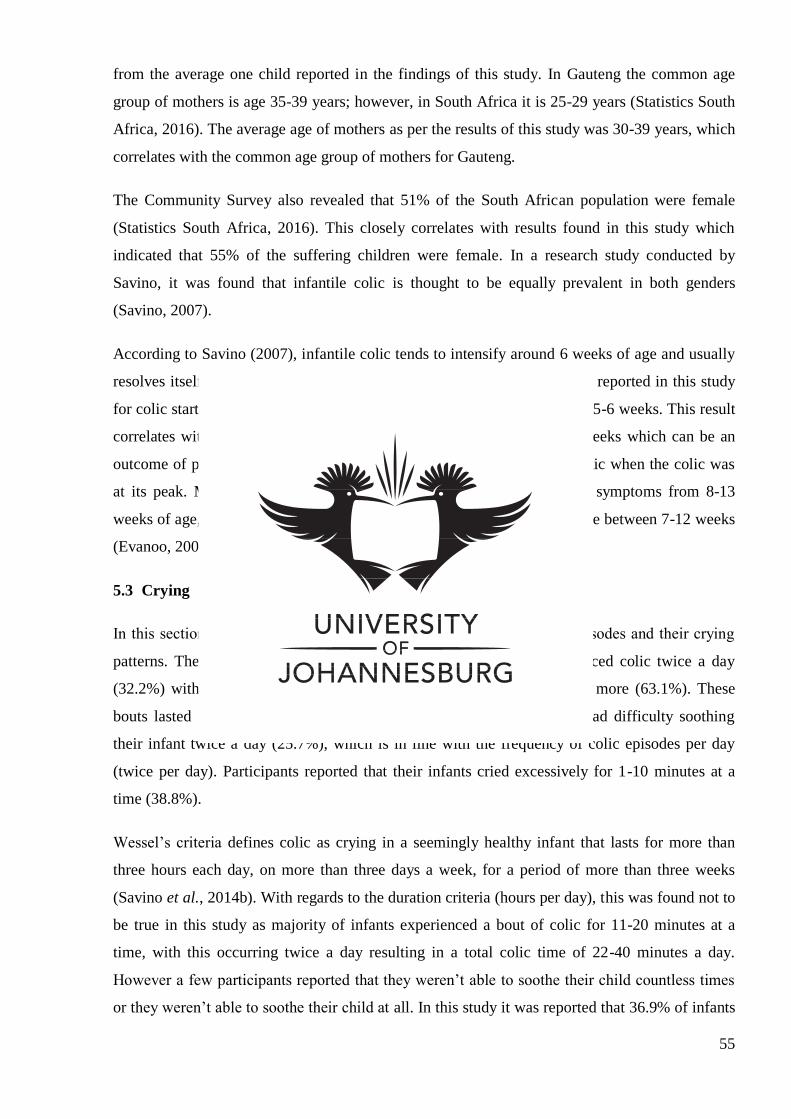
55
from the average one child reported in the findings of this study. In Gauteng the common age
group of mothers is age 35-39 years; however, in South Africa it is 25-29 years (Statistics South
Africa, 2016). The average age of mothers as per the results of this study was 30-39 years, which
correlates with the common age group of mothers for Gauteng.
The Community Survey also revealed that 51% of the South African population were female
(Statistics South Africa, 2016). This closely correlates with results found in this study which
indicated that 55% of the suffering children were female. In a research study conducted by
Savino, it was found that infantile colic is thought to be equally prevalent in both genders
(Savino, 2007).
According to Savino (2007), infantile colic tends to intensify around 6 weeks of age and usually
resolves itself at 12 weeks of age (Savino, 2007). The most prevalent age reported in this study
for colic starting, was around 4-8 weeks with the most common age being 5-6 weeks. This result
correlates with another research study that shows colic intensifies at 6 weeks which can be an
outcome of parents only became fully aware that their child may have colic when the colic was
at its peak. Most participants in this study noted a decline in the colic symptoms from 8-13
weeks of age, in line with other reported trends where colic tends to decline between 7-12 weeks
(Evanoo, 2007).
5.3 Crying
In this section (4.3.1) participants were asked about the infant’s colic episodes and their crying
patterns. The majority of participants reported that their infant experienced colic twice a day
(32.2%) with a combined total of bouts occurring three days a week or more (63.1%). These
bouts lasted 11-20 minutes at a time (31.6%). Participants stated they had difficulty soothing
their infant twice a day (25.7%), which is in line with the frequency of colic episodes per day
(twice per day). Participants reported that their infants cried excessively for 1-10 minutes at a
time (38.8%).
Wessel’s criteria defines colic as crying in a seemingly healthy infant that lasts for more than
three hours each day, on more than three days a week, for a period of more than three weeks
(Savino et al., 2014b). With regards to the duration criteria (hours per day), this was found not to
be true in this study as majority of infants experienced a bout of colic for 11-20 minutes at a
time, with this occurring twice a day resulting in a total colic time of 22-40 minutes a day.
However a few participants reported that they weren’t able to soothe their child countless times
or they weren’t able to soothe their child at all. In this study it was reported that 36.9% of infants
56
experienced colic one to two days a week however, 63.1% of participants experienced colic three
or more times a week. The results from this study therefore, correlate to the Wessel’s criteria of
three times a week.
In this study, the most common reasons stated for excessive crying in the infant were: pain or
discomfort (83.6%); being tired (73%); and a dirty nappy (62.5%); while the least reported
reasons were: the mothers’ tension (24.3%); the infant being fussy (20.4%); and the infant being
nervous (9.2%).
The above results correlates with a study conducted in New Zealand on colic and reflux, where it
was found that majority of respondents (78.6%) reported that the apparent reason for the infants
excessive crying was due to general discomfort and fatigue (Hodge & Murphy, 2014).
The most common causes for crying as reported by Halpern & Coelho (2016) was as a result of
either colic, infections, gastrointestinal causes, trauma, behavioural disorders, drug reactions,
violence or abuse, haematological causes or cardiovascular causes. Colic is reported to affect 20-
30% of infants which manifests itself in excessive crying (Halpern & Coelho, 2016).
5.4 Timing of colic symptoms
In this section, participants were asked when most of the colic symptoms occurred as well as the
time of the day that they occurred (4.3.2). The majority of participants noted colic symptoms
occurred straight after feeding (63.8%) and that colic most often occurred in the evening
(40.1%).
According to Savino (2007), colic and crying episodes tend to occur more frequently in the late
afternoon and evening. This is a characteristic symptom that differentiates colic from other
severe conditions. Many parents increase the frequency of feeding in the evenings. The findings
from this study are therefore consistent with the findings of Savino (2007). When considering the
size of the infant’s stomach and the time it takes for the food to be digested, it is likely some
infants are being over fed. Overfeeding is known to produce colic and reflux symptoms (Hodge
& Murphy, 2014).
5.5 Reasons for discomfort
Participants were asked what they believed was making their infant uncomfortable (4.3.3). The
most common reasons were: build-up of wind (75%); difficulty bringing up wind (59.2%); and
57
discomfort (57.2%); while the least common reasons were: food from the mother’s diet (12.5%);
either food allergy or growth spurt (9.9%); and the environment (9.2%).
In a study by Hodge and Murphy (2014), it was found that majority of parents believed that the
discomfort in their colic child was due to symptoms associated with wind. This included wind
build-up and difficulty bringing up wind. The results of Hodge and Murphy’s (2014) study are
therefore consistent with the findings compiled in this study.
5.6 Vomiting
Participants were asked if their infant vomited and if they felt this was a normal thing for their
baby to do (4.3.4). It was reported that 71.1% of participants noted that their baby did vomit after
being fed and that this was not a normal thing for their baby to do (67.1%).
According to Hegar, Dewanti, Kadim, Alatas, Firmansyah, and Vandenplas (2009), most infants
vomit after a feed and many parents find this distressing. Small amounts of vomit or spit up after
a feed is considered normal and often occurs in the first three months of life. Vomit or spit up
peaks at 4 months of age but resolves by 12 months. Vomiting after a feed should only be a
concern if the infant doesn’t gain weight or is uncomfortable.
5.7 Sleeping
Participants were asked what resulted in their infants sleeping (4.3.5). Majority of participants
(55.9%) stated that it was difficult to determine the factor that induced sleep and they weren’t
sure if it was due to the infant being comfortable and tired, or exhausted from crying.
Findings from a study conducted in New Zealand on colic and reflux suggested that majority of
parents (60%) believed that their infants were sleeping due to exhaustion from crying compared
to 9% of parents who believed it was due to the infant being comfortable and tired (Hodge &
Murphy, 2014).
5.8 Feeding and burping
In this section, participants were asked about their feeding methods; if they changed their infants
feeding method; if they fed their infant on demand from birth; and if they increased their feeding
in the evening (4.4). Participants were also asked if they consciously burped their babies (4.5).
Most participants used a combination of breastfeeding and bottle feeding (44.7%) and the
feeding method was changed by 65.4% of participants in order to try and ease the colic
symptoms.
58
Rosen (2007) found that solely breastfeeding infants will not necessarily prevent the occurrence
of colic despite the fact that breastfeeding is the best source of nutrition for infants. Certain foods
either ingested by breastfeeding mothers or by formula fed infants can cause irritability or
fussiness in infants. This may be due to food allergies in the infant and avoidance of these
allergy foods may prevent colic or assist the colic symptoms. In a randomised trial by Critch
(2011), allergenic foods such as cow’s milk, soy, wheat, eggs, peanuts, tree nuts and fish were
eliminated from the breastfeeding mother’s diet to try and ease the infant’s colic. A total of 161
infants who are solely breastfed and experienced excessive irritability and extended periods of
crying were randomly selected for a one week trial. Of these participants, 90 were put on a low
allergen maternal diet, while the other 54 were put in a control group where no dietary changes
were made. There was a significant improvement in the crying time in 74% of the low allergen
breastfed infants compared to the control group which showed only a 34% improvement. This
indicates that colic symptoms can be eased by altering or eliminating allergenic foods from the
maternal diet. Colic symptoms in infants who are partially or fully formula fed cow’s milk or soy
formulas tend to aggravate if they are atopic infants. Introduction of hydrolysed formulas have
shown to reduce colic symptoms in infants who had excessive irritability (Savino, 2007).
In this study it was reported that 71.1% of participants fed their infant on demand from birth and
they increased feeding hours in the evening between 5:00pm-12:00am (54.6%).
In a survey conducted on colic and reflux by Hodge and Murphy (2014), it was found that 70%
of mothers increase their feeding intervals in the evening hours with some mothers almost
continuously feeding their infants throughout the night, supporting the findings in this study that
majority of participants increased their feeding hours in the evening.
Majority of participants (78.3%) in this study consciously burped their infant.
In a randomised controlled study conducted on the efficacy of burping in lowering colic and
regurgitation episodes in healthy term babies, a total of 71 participants were recruited for period
of 3 months. The study concluded that in 95% of cases, burping did not significantly lower the
occurrence of colic. However, due to the small sample size, research should be conducted to
further validate this result (Kaur, Bharti & Saini, 2014).
5.9 Methods to soothe
In this section participants, were asked if their infants used a dummy (pacifier) and/or their
thumb to self soothe (4.6) as well as what methods were effective in soothing their baby (4.7).
The majority of participants reported that their baby used a dummy and/or their thumb (71.1%)
59
to self soothe. The most effective methods of soothing reported by participants were: bouncing
or jiggling (59.2%); pacing (51.3%); and baby massage (44.7%), with the least effective being:
drinking warm water (19.1%); white noise (9.2%); and drinking sugar water (9.2%).
A recent study conducted by Hodge and Murphy (2014) revealed that the most common methods
to soothe a crying infant were pacing with the child, bouncing the baby, swaddling the baby and
carrying the baby in a sling. The majority of participants made use of a dummy or allowed their
infant to suck their thumb in an attempt for the child to self soothe.
These results correlate with the results found in this study that common methods to soothe an
infant are bouncing and making use of a dummy or thumb sucking.
5.10 Treatments
The use of both complementary medicine and conventional medicine (4.8.1) was seen in 73% of
participants, while complementary medicine alone was only used by 27% of participants to treat
their infant’s colic.
There is no widely accepted conventional treatment for colic and many parents feel dissatisfied
with conventional health care, resulting in those parents seeking out complementary medicine
treatments (Savino & Tarasco, 2010). In a systematic review on randomised clinical trials on
nutritional supplements and other complementary medicines for infantile colic, it was found that
there was significant evidence on the effectiveness of fennel extract, mixed herbal teas and sugar
solutions for infantile colic. Of the 15 included randomised clinical trials, 11 trials showed
significant results in favour of complementary medicine. However, flaws did exist in these
clinical trials. Despite the favourable outcome of complementary medicine for infantile colic, the
flaws in the trials resulted in inadequate conclusions regarding the use of complementary
medicine for infantile colic. Recommendations for further research on complementary medicine
for colic are suggested due to the prevalence of colic and the difficulty in treating the condition
(Perry et al., 2011).
5.11 Consultation with a complementary medicine practitioner
In this section 4.8.2, it is observed that the majority of participants (68.4%) had consulted with a
complementary medicine practitioner. This could be directly related to the fact that three
complementary/natural pharmacies were utilised for data collection compared to the one
conventional/main-stream pharmacy. This resulted in a high probability of the participants
having been referred to a natural pharmacy by a complementary medicine practitioner.
60
Of the 152 participants, 31.6% of participants had not consulted with a complementary medicine
practitioner. This could be due to participants being unfamiliar with the term complementary
medicine practitioner and therefore not fully understanding which health practitioners are
classified as complementary medicine practitioners. The recent influx of complementary
medicines into the South African market has allowed the medicines to be purchased in numerous
shops. The majority of the medicines are currently unscheduled, allowing for them to be
purchased over-the-counter without a practitioner prescription resulting in an increase in self-
medication (Gqaleni et al., 2016).
According to Savino and Tarasco (2010), no widely accepted conventional treatment is available
for colic, resulting in many parents turning to complementary medicine. Homeopathic
medications are commonly used for infantile colic due to its low risk for adverse reactions,
causing parents to consider it a safe treatment for their infants (Rosen, 2007).
5.12 Sources of complementary information
Participants gained their information regarding complementary medicine for colic (4.8.2) mainly
from complementary practitioners (61.8%), friends and family (53.9%), general practitioner
(50%) and the internet (49.3%). The reason numerous participants received information from a
complementary practitioner and a general practitioner could be correlated to the fact that 68.4%
of participants had consulted with a complementary medicine practitioner for their infant’s colic
and that 73% of participants had used both conventional and complementary medicine for the
colic. Furthermore, one of the most common reasons for parents taking their infants to a
paediatric healthcare practitioner is due to infantile colic (Rosen, 2007).
Shapiro (2007) states that in today’s technological era, the use of the internet to access
information about colic is likely, as 3.2 billion people worldwide and 52.4% of Gauteng’s
population have access to the internet. It is common for people to research medical or health
related issues on the internet with the majority of people searching on behalf of a family member
or friend. However, not only do people use the internet for health information but they also use it
as a support group.
5.13 Complementary medicine
Participants were asked to state which complementary products they had used for their infants
colic (4.8.3). The following products were utilised by majority of participants: individualised
homeopathic remedies (58.6%); probiotics (46.7%); either Colic Calm or herbal medicines
(44.1%); and gripe water (41.4%). The high use of individualised homeopathic remedies could
61
correlate to the fact that 68.4% of participants had consulted with a complementary medicine
practitioner.
According to Savino and Tarasco (2010), parents have been choosing homeopathic remedies to
relieve colic symptoms due to their non-toxic nature and very low concentrations of active
ingredients. Individualised homeopathic remedies, prescribed by homeopaths, take into account
all aspects of the infant and the disease picture thus, providing you with a holistic individualised
treatment (Vermeulen, 2011). Colic Calm is also a homeopathic preparation indicated to relieve
abdominal discomfort, flatulence and gastro-oesophageal reflux (Colic Calm, 2013). Due to most
participants having consulted with a complementary medicine practitioner, it could be assumed
that due to the high use of individualised homeopathic remedies that majority of participants
were consulting with a homeopath. Infantile colic accounts for the most visits to a paediatric
practitioner as well as for the use of complementary medicine in infants. Colic is generally the
first crises in a new families life and therefore opting for an integrative approach, where the mind
and body are take into account, is important (Rosen, 2007).
The use of probiotics and herbal remedies has been found to reduce the median crying time in
infants with colic. Probiotics are effective at reducing crying time in infants (Bailey et al., 2013).
In a recent study by Chau et al. (2015), it was found that the probiotic Lactobacillus reuteri was
more effective than placebo in reducing the crying and fussing time in infants with colic. Savino
and Tarassco (2010) found that breastfed infants who received a herbal formula containing
Matricariae recrutita, Foeniculum vulgare and Melissa officinalis, had a reduction in their colic
symptoms within one week of use.
Gripe water is a widely known product for colic. Gripe water formulas are not standardised and
according to the Natural Medicines Comprehensive Database, five different formulas are listed
for gripe water (Rosen, 2007). The herbs found in gripe water are effective antispasmodics and
analgesics however there are no well conducted clinical trials to support the use of gripe water
(Whittaker, 2010).
In this study participants were also asked to provide reasons why they chose to treat their infant’s
colic with complementary medicine. Most participants stated that it was recommended to them
by a health care practitioner; friends or family; that it has no side effects; and is perceived as
safer and less harmful for their child (Appendix L), which is in line with Savino and Tarasco
(2010).
62
Complementary medicine is popular due to its lower incidence of adverse effects when
compared to pharmaceutical treatments. There has been an increase in patients selecting
complementary medicine over conventional medicine due to this fact. Herbal products are
viewed as natural products and patients assume that it is far safer and less likely to have side
effects; however this may not always be the case (Gqaleni et al., 2016). This is due to the lack of
standardisation of the dosage of herbal formulas and the possible content of sugar and alcohol in
the formulas available. Parents are advised to use herbal products with care or only through
prescription by a registered practitioner (Savino & Tarasco, 2010).
5.14 Conventional medicine
The most commonly used conventional medicines (4.8.4) reported were: Buscopan® (50%);
Telament Paediatric Colic Drops® (32.9%); Muthi Wenyoni (25.7%); and Colief® Infant Drops
(22.4%).
Simethicone (Telament Paediatric Colic Drops®), lactase (Colief® Infant Drops) and hyoscine
butylbromide (Buscopan®) are commonly recommended over-the-counter medications, in South
Africa, for infantile colic. Pharmacists are advised to counsel customers that if the over-the-
counter colic preparation provides no relief for the colic after a few days, that the product should
be discontinued and they should consult with a doctor (Whittaker, 2010).
Simethicone aims to reduce gas production however, in several randomised controlled trials,
simethicone was found to be as effective as placebo (Bailey et al., 2013). Lactase is an effective
form of treatment if colic is due to transient lactose intolerance. However, if the colic is not due
to lactose intolerance, lactase is not an effective form of treatment (Savino, 2007). A study
conducted on the efficacy of hyoscine butylbromide found it to be an effective form of treatment
for abdominal pain and cramping and that hyoscine butylbromide is safe and well tolerated
(Lacy, Wang, Bhowal, & Schaefer, 2013). No clinical studies have been conducted on the
efficacy of Muthi Wenyoni. It is suggested that the possible perceived effectiveness of Muthi
Wenyoni is due to the alcohol content which may induce sleep and relaxation in the infant
(Bland et al., 2014). The unconvincing efficacy of the conventional medicine products may be
due to the potential side effects and unknown mode of action (Halpern & Coelho, 2016).
A study conducted on the use of complementary and alternative medicine in a general paediatric
clinic found that 47% of participants made use of both conventional and complementary
medications (Jean & Cyr, 2007). An additional study was conducted on the use of
complementary medicine by children and the impact it has on parent-doctor communication and
63
general practitioner-complementary medicine practitioner communication. Results indicated that
parents expect integrative care from both their practitioners and want to be able to freely discuss
the use of both treatment modalities with both practitioners (Ben-Arye, Traube, Schachter,
Haimi, Levy, Schiff et al., 2010).
5.15 Statements regarding complementary medicine
Participants were asked their opinions on statements regarding complementary medicine. More
than half the participants (66.4%) agreed that complementary medicine is an effective form of
treatment for infantile colic; this opinion is supported by Rosen, Bukutu, Le, Shamseer and
Vohra (2007) whereby complementary therapies have shown to be beneficial in infantile colic.
Participants stated that they were uncertain if complementary medicine works well in
conjunction with conventional medicine for infantile colic (55.9%), this opinion is supported by
Ben-Arye et al., (2010) as more clinical studies are needed on the integration of complementary
and conventional medicine. Most participants (47.4%) agreed with the statement that
complementary medicine had no side effects however; 44.7% of participants were uncertain
about the statement. The opinion that most participants felt that complementary medicine had no
side effects is supported by Gqaleni et al., (2016) as the increase in the use of complementary
medicine can be associated with its low frequency of adverse effects.
5.16 Limitations and assumptions
There were a few factors that could have negatively affected the study and yielded an
unfavourable outcome by influencing the validity of the study.
Numerous participants were unfamiliar with the term “complementary medicine” and which
over-the-counter products fell into the complementary medicine category. It was also evident
that some participants were unable to differentiate between complementary medicine and
conventional medicine. This resulted in some participants selecting conflicting answers or stating
that they made use of other over-the-counter conventional medications for colic that were in fact
complementary products (e.g.: Iberogast), and vice versa. The lack of understanding of the terms
could have affected the answering of the questions and thus the outcome of the study.
A few participants (27%) made use of both complementary medicine and conventional medicine
simultaneously while treating their infant’s colic rendering it difficult to isolate the efficacy of
complementary medicine. This also relates back to the misunderstanding of the two terms,
“complementary medicine” and “conventional medicine”, in which participants were uncertain
64
that they were using two different modalities to treat their infant’s colic (Wieland, Manheimer, &
Berman, 2011). It was assumed that the positive effects were due to complementary medicine.
Added to this, sometimes the distinction between a complementary medicine product and
conventional medicine product is vague (Wieland et al., 2011). For example a product such as
gripe water contains both conventional and herbal ingredients; including dill seed oil, and
sodium bicarbonate. The same is true for the Bennetts® colic formula that contains
diphenhydramine and Atropa belladonna (Kilian, 2011). Therefore further patient education and
knowledge sharing is required to correctly differentiate the two treatment modalities. It is vital
that health care practitioners are able to educated and inform their patients about the difference
(Wieland et al., 2011).
Participants who had more than one child with colic were conflicted when answering questions
where the answer differed for each child. This resulted in a few questions having multiple
answers and resulted in data capturing conflicts or the questionnaire having to be excluded from
the study all together. Potentially valuable information regarding colic and complementary
medicine could have been omitted due to this.
It was assumed that all participants had an infant that suffered from colic and that they had
utilised complementary medicine as a form of treatment. Patients are often reluctant to admit to a
health care provider that they are using both forms of treatment, complementary medicine and
conventional medicine (Gqaleni, et al., 2016). Due to the fact that the research conducted is on
complementary medicine, participants could have felt uncomfortable to reveal their use of
conventional medications. This however, was assumed not to be a possibility, and that all
participants completed the questionnaire truthfully, honestly and without bias.
The participant’s demographic information such as race and financial status was not asked in the
questionnaire so as to not isolate a social group as potentially having infants that appeared to cry
more than other social groups. Socio-economic aspects have been noted to influence the
manifestation of, and increased the chance of seeking medical assistance for infantile colic. Such
aspects or factors include level/standard of education of participants, economic situation and
employment type (Yalçın, Örün, Mutlu, Madendağ, Sinici, Dursun et al., 2010). Research
conducted on the socio-economic groupings within South Africa (more specifically Gauteng
with respect to this research) may be valuable when accessing the prevalence of colic within
each socio-economic group. This combined with information on the lifestyle of the participants
(e.g. diet, smoking, alcohol, drugs/medication) would provide valuable information (Yalçın et
al., 2010).
65
CHAPTER SIX
CONCLUSIONS AND RECOMMENDATIONS
6.1 Conclusions
Infantile colic is a common concern for parents whose children suffer from the condition,
resulting in many parents consulting a health care practitioner. This study found colic to be the
most prevalent around 5-6 weeks of age and that it tends to ease between 8-13 weeks of age.
Infants experienced prolonged and continual bouts of crying and discomfort however, most
infants did not satisfy Wessel’s criteria, “the rule of three”. The aim of this study was to
determine the perceived effectiveness of complementary medicine by mothers of infants with
colic in Gauteng, by means of an Infantile Colic Questionnaire (Appendix G). A quantitative
descriptive design was used whereby data was collected through a randomised, cross-sectional
survey. Recruitment of participants occurred through advertisements (Appendix C) and word-of-
mouth. The Infantile Colic Questionnaires (Appendix G) were distributed at various baby and
health clinics; health shops; nursery schools; and health and beauty businesses in the Gauteng
region. A total of 152 surveys were completed and analysed through frequencies, custom tables,
multiple responses and open ended responses.
Analysis of the results indicated that most participants made use of both complementary
medicine and conventional medicine for their infant’s colic. However it was evident that most
participants aren’t familiar with the term “complementary medicine” and were therefore
confused as to which products are classified as complementary medicine. For some products the
distinction is vague as the products contain both complementary and conventional medicine,
which further contributed to the misunderstanding of the terms. This appears to be a common
trend amongst other studies on complementary medicine, indicating a need for further education
and research conduction (Wieland et al., 2011).
The most commonly used complementary products for infantile colic were individualised
homeopathic remedies, probiotics and over-the-counter herbal medicines. These results are
consistent with other studies conducted on integrative treatment approaches for infantile colic
(Rosen, 2007). The use of these complementary products correlates to the result that most
participants had consulted with a complementary medicine practitioner. Results showed that
complementary medicine practitioners, family and friends and general practitioners were the
main sources of information for parents. Complementary medicine was chosen as a modality for
treatment due to it being perceived as safe, less harmful and with fewer or no side effects.
66
The most commonly used over-the-counter conventional medications were products containing:
hyoscine butylbromide, lactase and simethicone. This finding is consistent with other studies on
commonly recommended products by pharmacists for infants (Whittaker, 2010).
As a result of parents concern with infantile colic, the frequency of consultations with healthcare
practitioners increased as well as the use of complementary medicine (Rosen, 2007). Results
from the research conducted on the perceived effectiveness of complementary medicine by
mothers of infants with colic in Gauteng, indicated that participants perceived complementary
medicine as an effective form of treatment for infantile colic. However, there is uncertainty
whether it works well in conjunction with conventional medicine.
The outcome of this research study indicated that further education is needed on complementary
medicine due to the misunderstanding of terms, complementary medicine and conventional
medicine. Complementary medicine is perceived to be an effective form of treatment for
infantile colic; however, further research and larger scale studies should be conducted to validate
this result.
6.2 Recommendations
This study or future studies, may offer potential improvement or refinement by incorporating the
following recommendations:
The number of participants in the study may be increased. A sample group larger than 152
participants should be utilised to allow for further validation of these results and to allow for a
representation of a wider population.
Conducting a similar study in other regions of the country will yield a more comprehensive
perspective of the use of complementary medicine for colic in South Africa.
Providing definitions, synonyms and examples of complementary medicine and conventional
medicine on the questionnaire so that participants may have a better understanding of the
terms. This will allow participants to feel more comfortable in answering the questions as
they will have a better understanding of the terms and it will also not subject them to feeling
uncomfortable for asking for an explanation of the term. This will also indirectly result in
more of the population becoming educated on complementary medicine.
The inclusion criteria for the study should only include participants who have only used
complementary medicine as a singular form of treatment for colic. The outcome of the
67
confusion between the terms, complementary medicine and conventional medicine, made
isolating the effects of only the complementary medicine difficult.
The inclusion criteria should be more in line with Wessel’s criteria for colic, so that the
timing, duration and frequency of the colic will be able to be fully determined. This will allow
for a better understanding of the severity of the colic and if complementary medicine is
effective in more severe colic cases.
The data collection tool should take into consideration participants who have had more than
one infant suffering from colic. Participants should be required to fill in a questionnaire
pertaining to each colicky infant or the questionnaire should be designed in such a way that
permits participants to answer the questions for multiple suffering children. If not, the
participant should be requested to answer the questionnaire based on the most recent suffering
infant.
A more intensive pilot study should be conducted to determine the reliability of the
questionnaire as questions 16 and 27 in the Infantile Colic Questionnaire were very similar.
Both questions enquired about the reasons for the baby feeling uncomfortable and the reasons
for the baby crying so much. The question could either be combined or the repetition deleted.
Include the demographical and socioeconomic information of the participants in the
questionnaire in order to obtain further valuable information about the access to
complementary medicine.
68
REFERENCES
Adcock Ingram (2004a). Telament® Paediatric Colic Drops (Leaflet). Johannesburg: Adcock
Ingram Limited.
Adcock Ingram (2004b). Telament® Paediatric Gripe Water (Leaflet). Johannesburg: Adcock
Ingram Limited.
AHPCSA (2015). Welcome to The Allied Health Professions Council of South Africa. Available
from: http://ahpcsa.co.za/ (Last accessed 7th
June 2017).
The American Association of Naturopathic Practitioners (2016). Natural medicine. Available
from: http://www.naturopathic.org/content.asp?contentid=59 (Last accessed 2nd
March 2017).
Anderson, L.A. (2014). Nexium®. Available from: https://www.drugs.com/pro/nexium-
capsules.html (Last accessed 7th
June 2016).
Aroma SA (2016). About Aromatherapy - Aroma South Africa. Available from:
http://aromasa.org.za/about-aromatherapy/ (Last accessed: 1st March 2017).
AstraZeneca (2015). Nexium® 2.5mg Sachets (Granules) (Leaflet). Johannesburg. AstraZeneca
Pharmaceuticals (Pty) Ltd.
Bailey, S., D’Auria, J. & Haushalter, J. (2013). Information on Infantile Colic on the World
Wide Web. Journal of Pediatric Health Care, 27(6), pp. 443-450. Available from: http://0-
www.sciencedirect.com.ujlink.uj.ac.za/science/article/pii/S0891524512000806 (Last accessed
9th
June 2017).
Bayer (2015). Iberogast® (Leaflet). Sydney: Bayer Australia Ltd.
Ben-Arye, E., Traube, Z., Schachter, L., Haimi, M., Levy, M., Schiff, E. et al. (2010). Integrative
Pediatric Care: Parents' Attitudes Toward Communication of Physicians and CAM Practitioners.
Peadiatrics, 127(1), pp. 84-95. Available from:
http://pediatrics.aappublications.org/content/pediatrics/early/2010/12/27/peds.2010-1286.full.pdf
(Last accessed 7th
June 2017).
69
Bland, R., Rollins, N., Broeck, J. & Coovadia, H. (2014). The use of non-prescribed medication
in the first 3 months of life in rural South Africa. Tropical Medicine and International Health,
9(1), pp. 118-124.
Boehringer Ingelheim (2013). Buscopan® (Leaflet). Johannesburg: Ingelheim Pharmaceuticals
(Pty) Ltd.
Çetinkaya, B. & Başbakkal, Z. (2012). The effectiveness of aromatherapy massage using
lavender oil as a treatment for infantile colic. International Journal of Nursing Practice, 18(2),
pp. 164-169. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22435980 (Last accessed
16th
May 2017).
Chau, K., Lau, E., Greenberg, S., Jacobson, S., Yazdani-Brojeni, P., Verma, N. et al. (2015).
Probiotics for Infantile Colic: A Randomized, Double-Blind, Placebo-Controlled Trial
Investigating Lactobacillus reuteri DSM 17938. The Journal of Pediatrics. 166(1), pp. 74-78.
Available from:
http://0-www.sciencedirect.com.ujlink.uj.ac.za/science/article/pii/S0022347614008488
(Last accessed 6th
June 2017).
Chopra, D. (2017). What is Ayurveda. Available from: http://www.chopra.com/articles/what-is-
ayurveda#sm.001mmzt4v13xjfa3zft1gek77w5k0 (Last accessed: 2nd
March 2017).
Colic Calm (2013). Frequently Asked Questions. Available from: http://www.coliccalm.co.za/
(Last accessed 10th
July 2016).
Colief (2011). What are Colief Infant Drops? Available from: https://www.colief.com/2014-11-
15-10-41-49 (Last accessed 10th
July 2016).
Critch, J. (2011). Infantile colic: Is there a role for dietary interventions? Paediatrics and Child
Health. 16(1), pp. 47-49. Available from: https://academic.oup.com/pch/article/16/1/47/2639470
(Last accessed 7th
June 2017).
De Schepper, L. (2008). Hahnemann revisited: A Textbook of Classical Homeopathy for the
Professional. 4th edition. India: B Jain Publishers Pvt, pp. 26-47.
70
Embrey, M. (2013). MDS-3: Managing Access to Medicines and Health Technologies. 1st
edition. Arlingtion, VA: Kumarian Press, pp. 74-90.
Eshelman, D. (2013). Baby Exercise for Relief from Baby Constipation - Stellar Caterpillar.
Available from: http://stellarcaterpillar.com/2013/02/07/baby-exercises-for-relief-from-
constipation/ (Last accessed 6th
June 2017).
Evanoo, G. (2007). Infant Crying: A Clinical Conundrum. Journal of Pediatric Health Care,
21(5), pp. 333-338.
Freedman, S., Al-Harthy, N. & Thull-Freedman, J. (2009). The Crying Infant: Diagnostic
Testing and Frequency of Serious Underlying Disease. Pediatrics, 123(3), pp. 841-848.
Available from:
https://pdfs.semanticscholar.org/37b2/fae3d6658f8421363180711d89f1fb76fcb3.pdf
(Last accessed 20th
July 2017).
Gelfand, A. (2016). Infant Colic. Seminars in Pediatric Neurology, 23(1), pp. 79-82. Available
from: http://www.sempedneurjnl.com/article/S1071-9091(15)00062-5/fulltext (Last accessed 6th
February 2017).
Gqaleni, N., Moodley, I., Kruger, H., Ntuli, A. & McLeod, H. (2016). Traditional and
Complementary Medicine. Available from: http://www.hst.org.za/uploads/files/chap12_07.pdf
(Last accessed 31st July 2016).
Halpern, R. & Coelho, R. (2016). Excessive crying in infants. Jornal de Pediatria, 92(3), pp. 40-
45. Available from
http://0-www.sciencedirect.com.ujlink.uj.ac.za/science/article/pii/S0021755716000462
(Last accessed 24th
November 2016).
Heel Inc. (2014a). Nux Vomica Homaccord® (Leaflet). Montreal: Heel Canada Inc.
Heel Inc. (2014b). Spascupreel® Tablets (Leaflet). Montreal: Heel Canada Inc.
Heel Inc. (2014c). Viburcol® Suppositories (Leaflet). Montreal: Heel Canada Inc.
71
Hegar, B., Dewanti, N., Kadim, M., Alatas, S., Firmansyah, A. & Vandenplas, Y. (2009).
Natural evolution of regurgitation in healthy infants. Acta Paediatrica, 98(7), pp. 1189-1193.
Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1651-2227.2009.01306.x/full (Last
accessed 7th
July 2017).
Herman, M. & Le, A. (2007). The Crying Infant. Emergency Medicine Clinics of North America,
25(4), pp. 1137-1159. Available from:
http://www.sciencedirect.com/science/article/pii/S0733862707000788?via%3Dihub
(Last accessed 20th
July 2017).
Himalaya (2016). Bonnisan. Available from:
http://www.himalayawellness.com/products/pharmaceuticals/bonnisan.htm (Last accessed 10th
July 2016).
Hodge, S. & Murphy, P. (2014). Crying Newborns: The Colic and Reflux Situation in New
Zealand as depicted by an Online Questionnaire. International Journal of Nursing and
Midwifery. 6 (8), pp. 97-107.
Jana, S. & Shekhawat, G.S. (2010). Anethum graveolens: An Indian traditional medicinal herb
and spice. Pharmacognosy Reviews, 4(8), pp. 179-184. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249919/ (Last accessed 10th
September 2016).
Jean, D. & Cyr, C. (2007). Use of Complementary and Alternative Medicine in a General
Pediatric Clinic. Pediatrics, 120(1), pp. 138-141. Available from:
http://pediatrics.aappublications.org/content/120/1/e138 (Last accessed 7th
June 2017).
Jellin, J.M. (2015). Natural Medicines Comprehensive Database: Yarrow; Dill; Anise; Fennel;
Lavender; German Chamomile. Natural Medicines – Professional. Nativa Pharmaceuticals.
Kaur, R., Bharti, B. & Saini, S. (2014). A randomized controlled trial of burping for the
prevention of colic and regurgitation in healthy infants. Child: Care, Health and Development,
41(1), pp. 52-56.
Kayne, L.R. & Kayne, S.B. (2007). Homeopathic prescribing. London: Pharmaceutical Press.
pp. 5-7, 11-18.
72
Kheir, A. (2012). Infantile colic, facts and fiction. Italian Journal of Pediatrics, 38(1), p. 34.
Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3411470/ (Last accessed 30th
October 2016).
Kilian, F. (2011). Infant Colic. Frontshop Pharmacy Magazine. Available from:
https://www.frontshop.co.za/infant-colic-2/ (Last accessed 7th
June 2017).
Kirjavainen, J., Jahnukainen, T., Huhtala, V., Lehtonen, L., Kirjavainen, T., Korvenranta, H. et
al.(2007). The balance of the autonomic nervous system is normal in colicky infants. Acta
Paediatrica, 90(3), pp. 250-254. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/11332162 (Last accessed 9th
January 2017).
Kuhudzai, A. (2016a). Statkon. Personal conversation on 26th
July 2016. [email protected], 20
Chiselhurst Avenue Kingsway Campus, (011) 559 4407.
Kuhudzai, A. ([email protected]). (13th
December 2016b). Emailing: Custom Tables,
Frequencies & Open Ended Responses, Infantile Colic Data File, Other Open Ended Responses.
Email to Di Gaspero, N. ([email protected]).
Kumral, A., Tuzun, F., Yesilirmak, D., Duman, N. & Ozkan, H. (2009). Circadian genes:
Mystery underlying the physiopathology of infantile colic. Medical Hypotheses, 72(1), pp. 103-
104. Available from: http://www.medical-hypotheses.com/article/S0306-9877(08)00396-
4/fulltext (Last accessed 14th
June 2017).
Lacy, B., Wang, F., Bhowal, S. & Schaefer, E. (2013). On-demand hyoscine butylbromide for
the treatment of self-reported functional cramping abdominal pain. Scandinavian Journal of
Gastroenterology, 48(8), pp. 926-935. Available from:
http://www.tandfonline.com/doi/abs/10.3109/00365521.2013.804117 (Last accessed 7th
June
2017).
Lennon (2000). Behoedmiddel Vir Kinders (Suspension) (Leaflet). Port Elizabeth: Pharmacare
Limited.
Loo, M. (2008). Integrative medicine for children. United States: Elsevier Health Sciences.
73
Marek, H. (2011). Understanding Colic. Available from: http://www.lulu.com/shop/hillary-
marek/understanding-colic/ebook/product-17387313.html?ppn=1 (Last accessed: 31st July 2016).
MCC (2016). About the MCC - Overview. Available from: http://www.mccza.com/About (Last
accessed 1st July 2016).
Muller-Krampe, B., Gottwald, R. & Weiser, M. (2007). Treatment of Acute Feverish Infections
with a Modern Homeopathic Medication. Biologische Medzin, 31(2), pp. 79-85.
Muller-Krampe, B., Oberbaum, M., Dipl-Math, P. & Weiser, M. (2007). Effects of Spascupreel
versus hyoscine butylbromide for gastrointestinal cramps in children. Pediatrics International,
49(3), pp. 328-334.
Murphy, P. (2015). RE: Colic Questionnaire – Reliability and Validity. Email to Di Gaspero, N.
[email protected]. Email date 2nd
August 2015
National Cancer Institute (2016). NCI Dictionary of Cancer Terms. Available from:
https://www.cancer.gov/publications/dictionaries/cancer-terms?cdrid=449752 (Last accessed 31st
May 2017).
Natura (2016a). Digestion - Magen. Available from: http://www.natura.co.za/B_PD_Magen.asp
(Last accessed 10th
July 2016).
Natura (2016b). Mom & Baby - Sedaped. Available from:
http://www.natura.co.za/B_PMomB_Sedaped.asp (Last accessed 10th
July 2016).
Ottillinger, B., Storr, M., Malfertheiner, P. & Allescher, H. (2012). STW 5 (Iberogast®) a safe
and effective standard in the treatment of functional gastrointestinal disorders. Wiener
Medizinische Wochenschrift, 163(3-4), pp. 65-72. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3580135/ (Last accessed 23rd
July 2017).
74
Perry, R., Hunt, K. & Ernst, E. (2011). Nutritional Supplements and Other Complementary
Medicines for Infantile Colic: A Systematic Review. The American Academy of Pediatrics,
127(4), pp. 720-733. Available from:
http://pediatrics.aappublications.org/content/127/4/720.long (Last accessed 15th November
2016).
Pestana-Caldeira, J.N. (2010). The Efficacy of Magen on Infantile Colic. Johannesburg:
University of Johannesburg. Master’s Dissertation, unpublished. University of Johannesburg, pp.
iii, 2, 23.
Porter, R.S. & Kaplan, J.L. (Editors) (2011). The Merck Manual of Diagnosis and Therapy. 19th
edition. United States of America: Merck Sharp & Dohme Corp, pp. 2735-2749.
Radhakrishna, R.B. (2007). Tips for Developing and Testing Questionnaires/Instruments.
Available from: http://www.joe.org/joe/2007february/tt2.php (Last accessed 20th
July 2016).
Renee, A. (2014). Colic Symptoms Explained. Available from:
http://www.webmd.com/parenting/baby/colic-symptoms (Last accessed 31st July 2016).
Resmed (2016). Intungwa Umuthi Wenyoni. Available from: http://resmed.co.za/product?id=52
(Last accessed 10th
July 2016).
Roberts, M. (2012). My 100 Favourite Herbs. South Africa: Struik Nature. pp. 27, 91, 118.
Rosen, L.D. (2007). "The Gripe": An Integrative Approach to Infant Colic. Pediatrics. 3 (4), pp.
417-422.
Rosen, L.D., Bukutu, C., Le, C., Shamseer, L. & Vohra, S. (2007). Complementary, Holistic, and
Integrative Medicine: Colic. Pediatrics in Review, 28(10), pp. 381-385. Available from:
http://www.nccpeds.com/ContinuityModules-
Fall/Fall%20Continuity%20Source%20Materials/Colic-CAM.pdf (Last accessed 7th
June 2017).
Saeidnia, S., Gohari, A.R., Mokhber-Dezfuli, N. & Kiuchi, F. (2011). A review on
phytochemistry and medicinal properties of the genus Achillea. DARU Journal of
Pharmaceutical Sciences. 19 (3), pp. 173-186.
75
Savino, F. (2007). Focus on infantile colic. Acta Paediatrica, 96(9), pp. 1259-1264. Available
from: http://onlinelibrary.wiley.com/wol1/doi/10.1111/j.1651-2227.2007.00428.x/full
(Last accessed 10th
March 2016).
Savino, F., Ceratto, S., De Marco, A. & Cordero di Montezemolo, L. (2014a). Looking for new
treatments of Infantile Colic. Italian Journal of Pediatrics, 40(1), p. 53. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4050441/ (Last accessed 14th
June 2016).
Savino, F. & Tarasco, V. (2010). New treatments for infant colic. Current Opinion in Pediatrics,
22(6), pp. 791-797. Available from:
http://media.mycme.com/documents/45/savino_tarasco_2010_11186.pdf (Last accessed 23rd
August 2016).
Savino, F., Tarasco, V., Sorrenti, M., Lingua, C., Moja, L., Gordon, M. et al. (2014b). Dietary
modifications for infantile colic. Cochrane Database of Systematic Reviews. Available from:
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011029/full (Last accessed 14th
June
2017).
School of Homeopathy (2012). What is Homeopathy: Natural health care. Available from:
http://www.homeopathyschool.com/why-study-with-us/what-is-homeopathy/ (Last accessed: 1st
March 2017).
Shapiro, J. (2007). Patients Turn to the Internet for Health Information. NPR.org. Available
from: http://www.npr.org/templates/story/story.php?storyId=15166387 (Last accessed 24th
May
2017).
Sister Lilian Remedies (2016). Care Range - ColicCare. Available from:
https://www.sisterlilianremedies.co.za/shop/care-range/sister-lilian-coliccare/
(Last accessed 10th
July 2016).
South African Association of Herbal Practitioners (SAAHP) (2011). Phytotherapy. Available
from: http://herbalpractitionerssa.co.za/about/phytotherapy/ (Last accessed: 2nd
March 2017).
76
The South African Society of Integrative Medicine (SASIM) (2015). Integrative medicine South
Africa. Available from: http://www.integrativemedicine.co.za/unani-tibb-medicine.html (Last
accessed: 2nd
March 2017).
Snyman, W. (2014). A Survey to Determine Attitudes and Perceptions of Complementary and
Alternative Medicine users in Johannesburg Health Shops. Johannesburg: University of
Johannesburg. Master’s Dissertation, unpublished. University of Johannesburg. pp. 11-19, 27-39.
Statistics South Africa (2016). Community Survey 2016 - Statistical Release P0301. Pretoria:
Statistics South Africa, pp. 1-23.
Stiverson, J., Williams, T., Chen, J., Adams, S., Hustead, D., Price, P. et al. (2014). Prebiotic
Oligosaccharides: Comparative Evaluation Using In Vitro Cultures of Infants' Fecal
Microbiomes. Applied and Environmental Microbiology, 80(23), pp. 7388-7397.
Tibb (2016). Concepts in Tibb. Available from: http://tibb.co.za/concepts_tibb.html (Last
accessed: 2nd
March 2017).
Tibb Health Sciences (2011). Infant Care - Bonnycare. Available from:
http://tibbherbals.com/bonnycare.html (Last accessed 10th
July 2016).
Tummy Calm (2014). Tummy Calm Gas Relief Drops. Available from: http://tummycalm.com/
(Last accessed 10th
July 2016).
van den Nieuwboer, M., Claassen, E., Morelli, L., Guarner, F. & Brummer, R. (2014). Probiotic
and synbiotic safety in infants under two years of age. Beneficial Microbes, 5(1), pp. 45-60.
Available from: https://www.ncbi.nlm.nih.gov/pubmed/24463207 (Last accessed 23rd
July
2017).
Vermeulen, A. (2004). The Treatment of Infant Colic using the Homoeopathic similimum.
Johannesburg: University of Johannesburg. Master’s Dissertation, unpublished. University of
Johannesburg. pp. iii, iv, 1.
Vermeulen, F. (2011). Concordant reference complete classic materia medica, Belgium: B. Jain
Archibel S.P.R.L, pp. 553, 554, 558, 1357
77
Walker, W.A., Goulet, O. & Mieli-Vergani, G. (2004). Pediatric gastrointestinal disease set:
Pathophysiology, diagnosis, management. Edited by W. Allan Walker. 4th edition. USA: PMPH
USA Ltd.
Whittaker, C. (2010). Over-the-counter medicines for infants (0-6 months). SA Pharmaceutical
Journal, pp. 22-26.
WHO (1999). WHO monographs on selected medicinal plants. Vol. 1. Geneva: World Health
Organization, p. 92.
WHO (2007). WHO monographs on selected medicinal plants. Vol. 3. Geneva: World Health
Organization, pp. 38, 49, 145,225.
WHO (2009). WHO monographs on selected medicinal plants. Vol. 4. Geneva: World Health
Organization, p. 188.
WHO (2016). Traditional Medicine: Definitions. Available from:
http://www.who.int/medicines/areas/traditional/definitions/en/ (Last accessed 1st July 2016).
Wieland, S., Manheimer, E. & Berman, B. (2011). Development and classification of an
operational definition of complementary and alternative medicine for the Cochrane
Collaboration. Alternative therapies in health and medicine, 17(2), pp. 50-59. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/21717826 (Last accessed 6th June 2017).
Wilson Van Voorhis, C.R. & Morgan, B.L. (2007). Understanding Power and Rules of Thumb
for Determining Sample Sizes. Tutorials in Quantitative Methods for Psychology. 3 (2), pp. 43-
50.
Woodwards (2017). Gripe Water (Leaflet). United Kingdom: Reckitt Benckiser Healthcare (UK)
Ltd.
Wyllie, R., Hyams, J.S. & Kay, M. (2015). Pediatric gastrointestinal and liver disease.
Philadelphia, PA, United States: Elsevier Science Publishing Co.
78
Yalçın, S., Örün, E., Mutlu, B., Madendağ, Y., Sinici, İ., Dursun, A. et al. (2010). Why are they
having infant colic? A nested case-control study. Paediatric and Perinatal Epidemiology, 24(6),
pp. 584-596. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-
3016.2010.01150.x/abstract (Last accessed 19th
October 2016).
79
APPENDIX A
HIGHER DEGREES APPROVAL LETTER
80
APPENDIX B
ETHICS COMMITTEE APPROVAL LETTER
81
APPENDIX C
ADVERTISEMENT
If so, you may be able to participate in a research survey that is looking at the perceived
effectiveness of complementary medicine in the treatment of Infantile Colic.
Moms between the ages of 18-45 years are invited to participate in the research study.
The research study is being conducted by the Department of Homeopathy at the University of
Johannesburg.
Ethical Clearance Number: REC-01-126-2016
If you are interested, please contact:
Natalie on 083 227 7110

82
APPENDIX D
PERMISSION LETTERS
83
84
85
86
87
88
89
90
91
92

93
APPENDIX E
INFORMATION LEAFLET
DEPARTMENT OF HOMOEOPATHY
RESEARCH STUDY INFORMATION SHEET
10th October 2016
Good Day
My name is Natalie Christina Di Gaspero and I WOULD LIKE TO INVITE YOU TO
PARTICIPATE in a research study on The Perceived Effectiveness of Complementary
Medicine by Mothers of Infants with Colic in Gauteng.
Before you decide on whether to participate, I would like to explain to you why the research is
being done and what it will involve for you. I will go through the information sheet with you
and answer any questions you have. This should take about 10-20 minutes. The study is part of
a research project being completed as a requirement for a Masters Degree in Homoeopathy
through the University of Johannesburg.
THE PURPOSE OF THIS STUDY is to determine the perceived effectiveness of
complementary medicine by mothers of infants with colic in Gauteng in order to develop an
approach for the treatment of colic.
Below, I have compiled a set of questions and answers that I believe will assist you in
understanding the relevant details of participation in this research study. Please read through
these. If you have any further questions I will be happy to answer them for you.
DO I HAVE TO TAKE PART? No, you don’t have to. It is up to you to decide to participate
in the study. I will describe the study and go through this information sheet. If you agree to take
part, I will then ask you to sign a consent form.
94
WHAT EXACTLY WILL I BE EXPECTED TO DO IF I AGREE TO PARTICIPATE?
You will be asked to complete a short survey about your child’s colic and the survey should take
approximately 10 minutes to complete. The survey is completed on a voluntary basis and should
you wish to participate, you will need to sign a consent form. No identifying information will be
requested from you and you will remain anonymous throughout the study. To ensure your
privacy, the survey will be completed in a private area. Participation is voluntary and you are
free to withdraw from the study for whatever reason and without consequence, up until the point
that the survey is placed in a lockable box. Once you have completed the survey it will be placed
into a sealable envelope and placed into a lockable box. All completed surveys will be treated as
strictly confidential and only the researcher, supervisor and statistician will have access to the
information.
WHAT WILL HAPPEN IF I WANT TO WITHDRAW FROM THE STUDY? If you
decide to participate, you are free to withdraw your consent without giving a reason and without
any consequences, up until the point that the completed survey is placed in the lockable box. If
you wish to withdraw your consent, you must inform me as soon as possible.
IF I CHOOSE TO PARTICIPATE, WILL THERE BE ANY EXPENSES FOR ME, OR
PAYMENT DUE TO ME: There will be no expense to you should you decide to participate in
the study. You will not be paid to participate in this study.
RISKS INVOLVED IN PARTICIPATION: There are no anticipated risks for participating in
this study.
BENEFITS INVOLVED IN PARTICIPATION: By participating in this study you are able to
assist in providing more information on colic and the use of complementary medicines for colic
in infants.
WILL MY TAKING PART IN THIS STUDY BE ANONYMOUS? Yes. Anonymous means
that your personal details will not be recorded anywhere by me. As a result, it will not be
possible for me or anyone else to identify your responses once these have been submitted.
WHAT WILL HAPPEN TO THE RESULTS OF THE RESEARCH STUDY? The results
will be written into a research report that will be assessed. In some cases, results may also be
published in a scientific journal. In either case, you will not be identifiable in any documents,
95
reports or publications. You will be given access to the study results if you would like to see
them, by contacting me.
WHO IS ORGANISING AND FUNDING THE STUDY? The study is being organised by
me, under the guidance of my research supervisor at the Department of Homoeopathy in the
University of Johannesburg. The study is being funded by the University of Johannesburg
Masters Supervisor Linked Research Bursary.
WHO HAS REVIEWED AND APPROVED THIS STUDY? Before this study was allowed
to start, it was reviewed in order to protect your interests. This review was done first by the
Department of Homoeopathy, and then secondly by the Faculty of Health Sciences Research
Ethics Committee at the University of Johannesburg. In both cases, the study was approved.
Ethics Clearance number: REC-126-2016
Higher Degrees Clearance number: HDC-01-46-2016
WHAT IF THERE IS A PROBLEM? If you have any concerns or complaints about this
research study, its procedures or risks and benefits, you should ask me. You should contact me at
any time if you feel you have any concerns about being a part of this study. My contact details
are:
Natalie Di Gaspero
083 227 7110
You may also contact my research supervisor:
Dr Radmila Razlog
011 559-6233
Or you may contact my research co-supervisor:
Dr Patel
011 559-6780
96
If you feel that any questions or complaints regarding your participation in this study have not
been dealt with adequately, you may contact the Chairperson of the Faculty of Health Sciences
Research Ethics Committee at the University of Johannesburg:
Prof Marie Poggenpoel
011 559-6686
FURTHER INFORMATION AND CONTACT DETAILS: Should you wish to have more
specific information about this research project information, have any questions, concerns or
complaints about this research study, its procedures, risks and benefits, you should communicate
with me using any of the contact details given above.
Researcher:
Natalie Di Gaspero
97
APPENDIX F
CONSENT FORM
DEPARTMENT OF HOMOEOPATHY
RESEARCH CONSENT FORM
The Perceived Effectiveness of Complementary Medicine by Mothers of Children with Infantile Colic in
Gauteng
Please initial each box below:
I confirm that I have read and understand the information sheet dated Click here to enter the
date, as is appears on the information sheet. for the above study. I have had the opportunity to consider
the information, ask questions and have had these answered satisfactorily.
I understand that my participation is voluntary and that I am free to withdraw from this study
at any time without giving any reason and without any consequences to me.
I agree to take part in the above study.
________________________________ ________________
Signature of Participant Date
_______________________ _________________________________ ________________
Name of Researcher Signature of Researcher Date
98
APPENDIX G
Infantile Colic Questionnaire
Philippa Murphy©
The purpose of this questionnaire is to collect data about your child’s colic.
Please answer the following questions below as accurately as you can.
Mark your desired answer with an X or provide a description on the line where required.
Your answers will remain anonymous.
Inclusion Criteria
1. Your age:
18-29 years 1
30-39 years 2
40-45 years 3
2. How many children do you have?
1 Child 1
2 Children 2
3 Children 3
4 Children 4
5 Children or more 5
3. Does/did your baby/babies suffer from symptoms of colic?
No 0
Yes 1
Instructions
99
General
4. What is the gender of your child/children:
N/A Male Female
4.1 First born 0 1 2
4.2 Second born 0 1 2
4.3 Third born 0 1 2
4.4 Fourth born 0 1 2
4.5 Fifth born 0 1 2
5. Did you self-diagnose your baby as having colic?
No 0
Yes 1
6. Was your baby diagnosed by a health care practitioner as having colic?
No 0
Yes 1
7. At what age did your baby’s colic start?
4-5 weeks 1
5-6 weeks 2
6-7 weeks 3
7-8 weeks 4
8-9 weeks 5
9-10 weeks 6
10-11 weeks 7
11-12 weeks 8
12-13 weeks 9
13-14 weeks 10
14-15 weeks 11
15-16 weeks 12
100
8. Is/were your suffering child/children your:
No Yes
8.1 First born 0 1
8.2 Second born 0 1
8.3 Third born 0 1
8.4 Fourth born 0 1
8.5 Fifth born or more 0 1
9. How many of your children suffered from colic?
1 Child 1
2 Children 2
3 Children 3
4 Children 4
5 Children or more 5
10. Did you attend an antenatal class?
No 0
Yes 1
11. If so, do you feel you learnt enough in the class to care for your new-born in the post-natal
stages?
No 0
Yes 1
Not Applicable (N/A) 2
If not, what learning do you feel would have better prepared you?
101
12. On average, how many times does/did your baby experience colic in a day?
None 1
Once 2
Twice 3
Three times 4
Four times 5
Five times 6
More than five times 7
If more, please specify:
13. On average, how long does/did your baby experience a bout of colic?
0-10 minutes 1
11-20 minutes 2
21-30 minutes 3
31-45 minutes 4
46-60 minutes 5
More than 1 hour 6
14. When do/did the majority of the colic symptoms occur?
Straight after feeding 1
One hour after feeding 2
Two hours after feeding 3
Three hours after feeding 4
Four hours after feeding 5
15. What time of day do/did majority of the colic symptoms occur?
Morning 1
Afternoon 2
Evening 3
12am-6am 4
Behaviours
102
All the time 5
16. From the list, tick what you believe was making your baby feel uncomfortable? More than
one answer can be selected:
No Yes
16.1 Hunger 0 1
16.2 Feeling full 0 1
16.3 Bowel movements 0 1
16.4 Build-up of wind 0 1
16.5 Difficulty bringing up wind 0 1
16.5 Dirty nappy 0 1
16.6 Growth spurt 0 1
16.7 Formula choice 0 1
16.8 Your tension 0 1
16.9 Overfeeding 0 1
16.10 Environment 0 1
16.11 Large supply of breast milk 0 1
16.12 Fast flowing breast milk 0 1
16.13 Being bottle fed too fast 0 1
16.14 Food from mothers diet 0 1
16.15 Undeveloped digestive system 0 1
16.16 Food allergy 0 1
16.17 Vaccinations 0 1
16.18 Discomfort 0 1
16.19 Fatigue 0 1
If other, please specify:
17. Does/did your baby ever vomit milk after a feed?
No 0
Yes 1
103
18. Do/did you feel that vomiting after feeding is a normal thing for your baby to do?
No 0
Yes 1
Feeding
19. Do/did you:
Breastfeed 1
Bottle feed breast milk 2
Bottle feed formula 3
Combination of breast and bottle 4
20. Did you change your baby’s feeding method to try and ease the colic symptoms?
No 0
Yes 1
21. Have/did you fed/feed on demand from birth?
No 0
Yes 1
22. Does/did your feeding increase in the evening hours (from around 5pm to 12am)?
No 0
Yes 1
Burping
23. Do/did you consciously burp your baby?
No 0
Yes 1
104
Behaviours
24. How many times does/did your baby cry without you being able to sooth him/her in a day?
None 1
Once 2
Twice 3
Three times 4
Four times 5
Five times 6
Other 7
If more, please specify:
25. On average, how long does/did your baby cry for at a time?
1-10 minutes 1
11-20 minutes 2
21-30 minutes 3
31-40 minutes 4
41-50 minutes 5
51-60 minutes 6
26. How many days in a week does/did your baby cry like this?
No days 1
1 day 2
2 days 3
3 days 4
4 days 5
5 days 6
6 days 7
7 days 8
105
27. From the list tick what you believe is/was causing your baby to cry so much? More than one
answer is allowed.
No Yes
27.1 Hunger 0 1
27.2 Dirty nappy 0 1
27.3 Your tension 0 1
27.4 Pain or discomfort 0 1
27.5 Fussy 0 1
27.6 Irritated 0 1
27.7 Nervous 0 1
27.8 Fed up 0 1
27.9 Tired 0 1
28. Do you feel your baby sleeps mostly because he/she felt:
Comfortable and tired 1
Exhausted from crying 2
Hard to say 3
Sucking for comfort
29. Does/did your baby use a dummy or suck his/her thumb to soothe?
No 0
Yes 1
106
Miscellaneous
30. Are/were any of the following effective in making your baby calm?
No Yes
30.1 Drinking warm water 0 1
30.2 Hot bath 0 1
30.3 Baby massage 0 1
30.4 Sugar and water 0 1
30.5 Swaddling 0 1
30.6 Front pack or sling 0 1
30.7 Pram 0 1
30.8 Pacing 0 1
30.9 Bouncing or jiggling 0 1
30.10 Lullabies 0 1
30.11 White noise 0 1
Treatment
31. Do you use complementary medicine?
No 0
Yes 1
32. What do/did you use to treat your child’s colic?
Complementary or natural
medicine 1
Conventional or main-stream
medicine 2
Both 3
107
33. Have you consulted with a complementary medicine practitioner for your child’s colic
before?
No 0
Yes 1
34. Where do/did you get your information regarding complementary medicine for colic from?
You may choose more than one answer:
If other, please specify:
35. Do/did you use any of the following complementary medicines for your child’s colic? You
may choose more than one answer:
No Yes
35.1 None 0 1
35.2 Individualised homeopathic
remedies 0 1
35.3 Herbal medicines 0 1
35.4 Herbal teas 0 1
35.5 Probiotics 0 1
35.6 Vitamins/minerals 0 1
35.7 Aromatherapy oils 0 1
35.8 Colic Calm 0 1
No Yes
34.1 Internet 0 1
34.2 Books/magazines 0 1
34.3 Health shops 0 1
34.4 Friends/family 0 1
34.5 TV/Radio 0 1
34.6 General Practitioner 0 1
34.7 Complementary Practitioner 0 1
34.8 Other 0 1
108
35.9 Gripe Water 0 1
35.10 Heel Nux Vomica Homaccord® 0 1
35.11 Heel Spascupreel® 0 1
35.12 Heel Viburcol® 0 1
35.13 Himalaya Bonnisan® 0 1
35.14 Iberogast® 0 1
35.15 Lennon Behoedmiddel vir
Kinders 0 1
35.16 Natura® Magen 0 1
35.17 Natura® Sedaped 0 1
35.18 Sister Lilian ColicCare 0 1
35.19 Tibb Bonnycare 0 1
35.20 Tummy Calm® 0 1
35.21 Other 0 1
If other, please specify:
36. Why do/did you choose complementary medicine as a treatment for your child’s colic?
37. Do/did you use any of the following medicines for your child’s colic? You may choose more
than one answer:
No Yes
37.1 None 0 1
37.2 Muthi Wenyoni 0 1
37.3 Buscopan® 0 1
37.4 Colief® Infant drops 0 1
37.5 Nexium® 0 1
37.6 Telament Paediatric Colic
Drops® 0 1
37.7 Other 0 1
109
If other, please specify:
38. In your experience is complementary medicine effective for colic:
Disagree 1
Unsure 2
Agree 3
39. In your experience does complementary medicine work well in conjunction with
conventional medicine (Western medicine) for colic:
Disagree 1
Unsure 2
Agree 3
40. In your experience does complementary medicine have no side effects:
Disagree 1
Unsure 2
Agree 3
Thank you for completing the questionnaire.
110
APPENDIX H
RESEARCH PROCEDURE
Research Procedure
Hand participant an envelope, clipboard (if needed) and a pen.
Inside the envelope is an information leaflet, consent form and
questionnaire.
Participant needs to read the information leaflet and then should they wish
to participate, they need to sign the consent form, allowing the researcher
permission to use their responses for data collection.
Participant then needs to complete the questionnaire by marking each
answer with an X or description where required.
Once completed, the consent form and questionnaire needs to be put into the
envelope.
Envelope must be sealed and a completed sticker to be stuck across the
envelope seal.
Participant may keep the information leaflet.
Place completed envelope in lockable box.
Participant can withdraw from participating in the research but only before
the envelope is sealed and placed in the lockable box.
The research is now complete, thank you.
Any questions, contact Natalie on 083 227 7110.
Thank you so much for your assistance.
111
APPENDIX I
LETTER OF PERMISSION FOR QUESTIONNAIRE
BabyCues
PO Box 35081
Shirley
Christchurch 8640
NEW ZEALAND
2nd
August 2015
To Whom It May Concern
I, Philippa Murphy, the author of the questionnaire, Infantile Colic and Reflux, utilised in New
Zealand in 2012, give permission for Natalie Di Gaspero my questionnaire for her study, which
aims to determine the perceived effectiveness of complementary medicine by mothers of
children with infantile colic in Gauteng.
Kind Regards
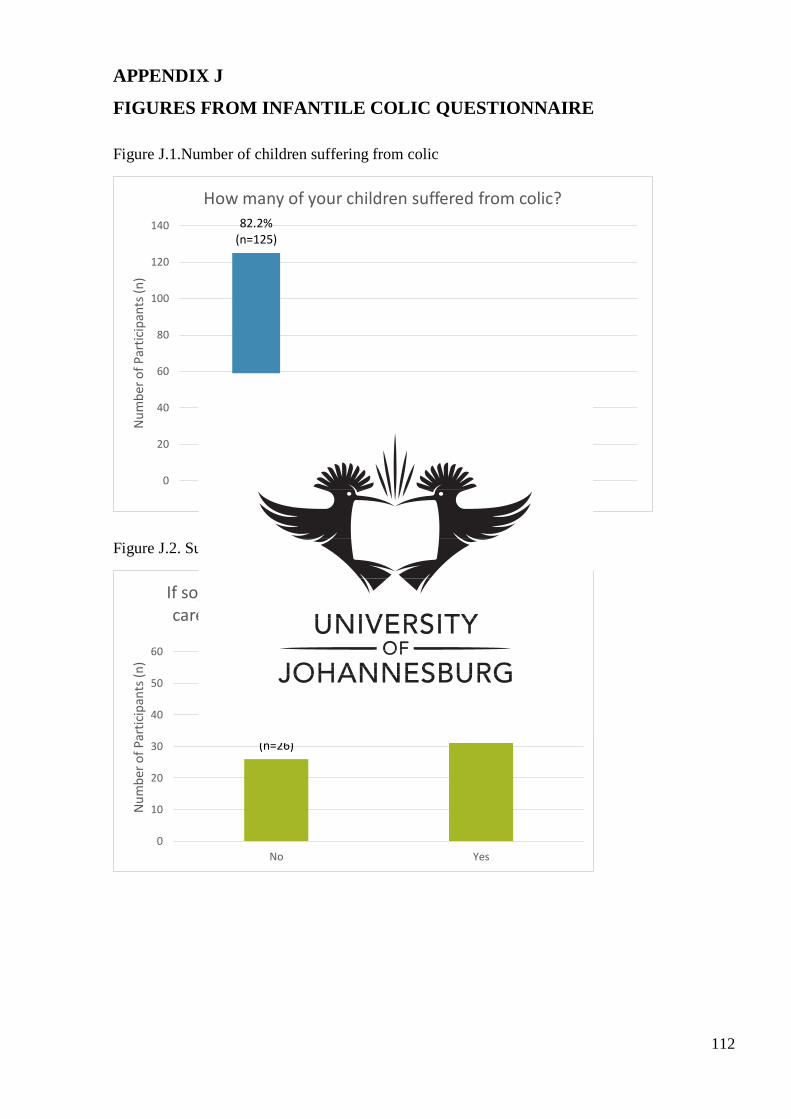
112
APPENDIX J
FIGURES FROM INFANTILE COLIC QUESTIONNAIRE
Figure J.1.Number of children suffering from colic
Figure J.2. Sufficiency of the ante-natal class.
82.2% (n=125)
15.1% (n=23)
2.6% (n=4)
0
20
40
60
80
100
120
140
1 Child 2 Children 3 Children
Nu
mb
er o
f P
arti
cip
ants
(n
)
How many of your children suffered from colic?
32.1% (n=26)
67.9% (n=55)
0
10
20
30
40
50
60
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
If so, do you feel you learnt enough in the class to care for your new-born in the post-natal stages?
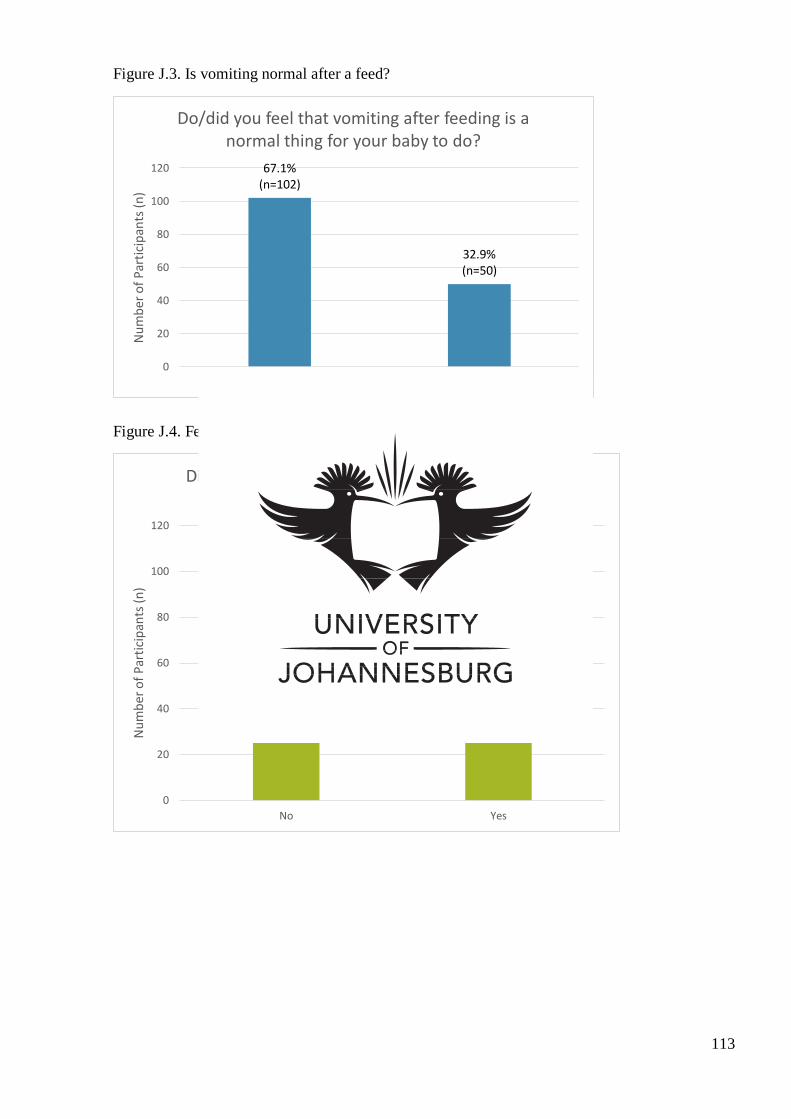
113
Figure J.3. Is vomiting normal after a feed?
Figure J.4. Feeding method changes
67.1% (n=102)
32.9% (n=50)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
) Do/did you feel that vomiting after feeding is a
normal thing for your baby to do?
35.5% (n=54)
64.5% (n=98)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Did you change your baby’s feeding method to try and ease the colic symptoms?
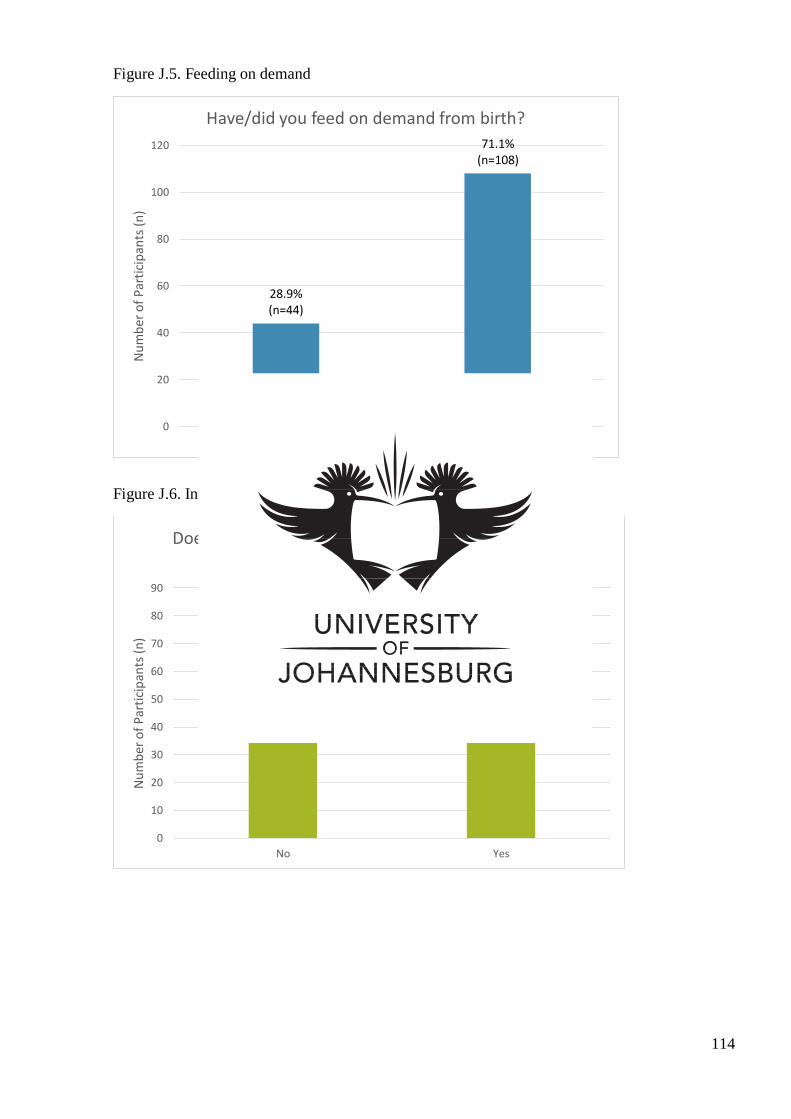
114
Figure J.5. Feeding on demand
Figure J.6. Increase in feeding hours between 5pm and 12am
28.9% (n=44)
71.1% (n=108)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
) Have/did you feed on demand from birth?
45.4% (n=69)
54.6% (n=83)
0
10
20
30
40
50
60
70
80
90
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
)
Does/did your feeding increase in the evening hours (from around 5pm to 12am)?
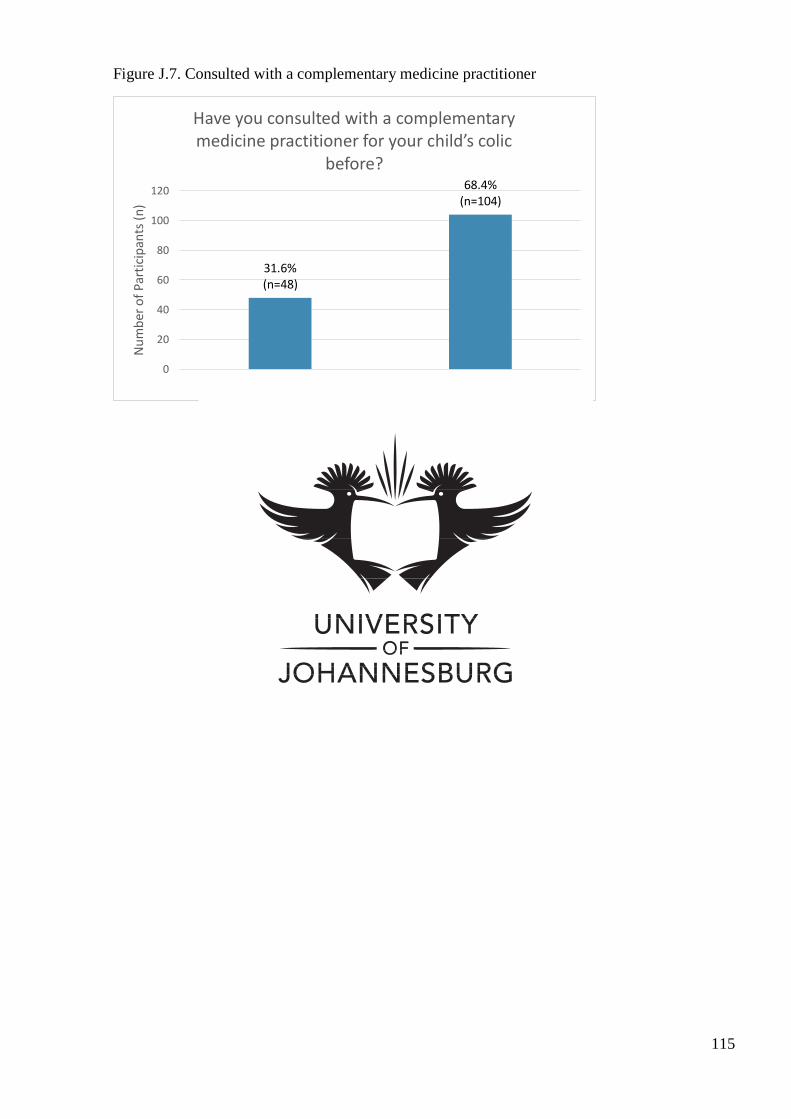
115
Figure J.7. Consulted with a complementary medicine practitioner
31.6% (n=48)
68.4% (n=104)
0
20
40
60
80
100
120
No Yes
Nu
mb
er o
f P
arti
cip
ants
(n
) Have you consulted with a complementary medicine practitioner for your child’s colic
before?
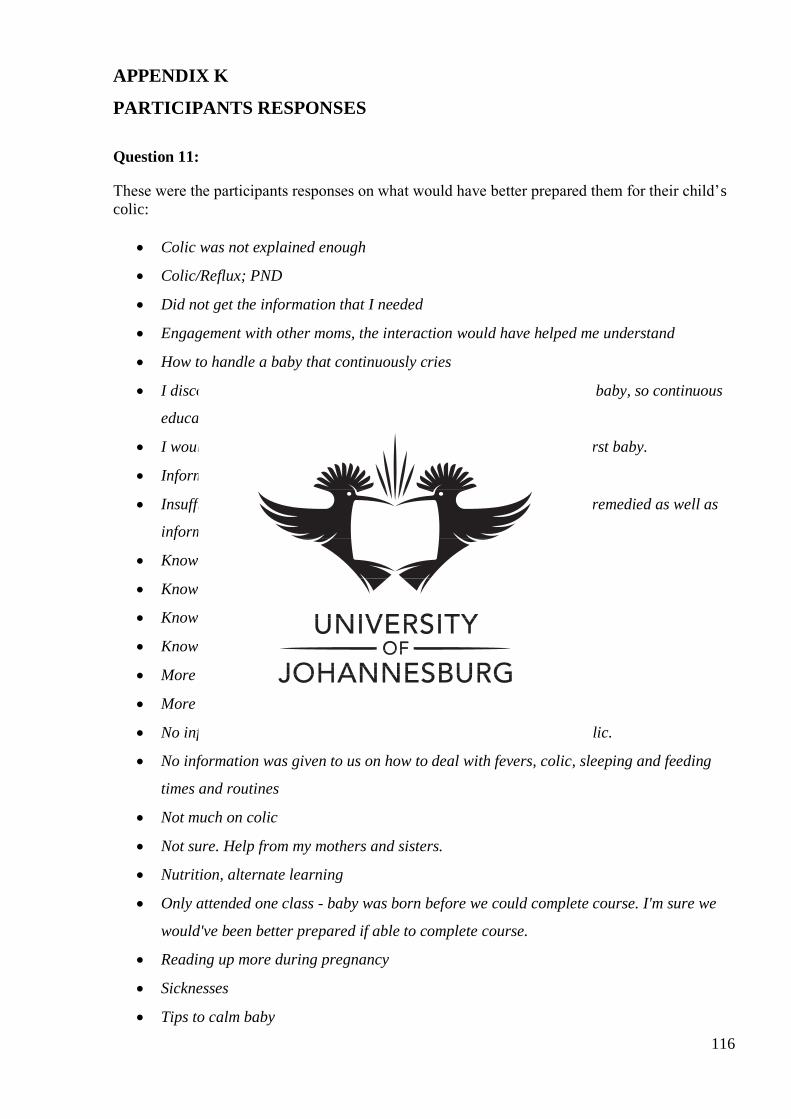
116
APPENDIX K
PARTICIPANTS RESPONSES
Question 11:
These were the participants responses on what would have better prepared them for their child’s
colic:
Colic was not explained enough
Colic/Reflux; PND
Did not get the information that I needed
Engagement with other moms, the interaction would have helped me understand
How to handle a baby that continuously cries
I discovered some situations as I went along with taking care of the baby, so continuous
education is necessary with regular visits to the health practitioner.
I would have been better prepared if I was told how to deliver my first baby.
Information about it
Insufficient information on colic was an issue that could have been remedied as well as
information on how to wind children.
Knowing the symptoms and experience
Knowing what was wrong while baby cries
Knowledge about colic and what to do
Knowledge on natural medicine would have helped
More information on how to wind and soothe child.
More should be emphasised on complementary colic medication
No information on how to wind/burp child. More information on colic.
No information was given to us on how to deal with fevers, colic, sleeping and feeding
times and routines
Not much on colic
Not sure. Help from my mothers and sisters.
Nutrition, alternate learning
Only attended one class - baby was born before we could complete course. I'm sure we
would've been better prepared if able to complete course.
Reading up more during pregnancy
Sicknesses
Tips to calm baby
117
To be taught about it at the clinic before you get a baby, like while still pregnant
To be taught how to handle a child with colic symptoms/calm the body down when crying
What food to avoid to help avoid colic
What to do when the child is not consolable
What to expect when having your baby
Winding techniques! This was hardly covered. Chiropractor has helped in this.
118
APPENDIX L
PARTICIPANTS RESPONSES
Question 36:
These were the following responses from participants as to why they chose to use
complementary medicine as a form of treatment for their child’s colic:
Advice by friends(21) to stick to natural medicines, advice from my sisters/mother(2),
recommended by family (16), it was passed on from Grandparents, from word of mouth
(2)
Health shop recommendation.(3)
Recommendation by a doctor/homeopath (16),
Alternative
Because it was recommended as good for colic
Because it’s safe and it can be used for the whole family (2).
Believe in homeopathic remedies over conventional medicine in general
Conventional medicines didn’t seem to be working effectively (2)
Effective, safer and less side effects, don't like using too many chemicals with my baby
Felt it would be the best. I did not want general medicine that would sedate my baby.
I believe in Homeopathy. It works very well for me and my child.
I have grown up using it
I have used homeopathic medicine myself with great results.
I believe that complementary medicine is a much healthier option for the baby
I didn’t like the idea of giving baby anything besides breast milk so preferred to give
complementary medicine (because natural)
It had no side effects, safer, less harmful (11)
Less side effects & non-toxic , baby responded much better to complementary rather than
conventional
Safer for my child, puts mine and the babies mind at ease
I fully agree with it and don’t want harming, Western medicine for my child
I prefer the gentler approach and Telament made my daughter sick.
Western medicine is too harsh on a child
Did not like conventional (2)
A mother will try anything, I actually tried everything that could work (5)
119
Crying baby gives stress to the mother and worrying about your child is one thing that
makes a mother to try what’s best for the child
Did not know what else to use (2), would have used Chiropractor if had known
I only chose the medicine first because I thought it will help and it did not help much
I will try anything that will help(2)
It was cheaper (2) and worked well
It works well(3)
No specific reason(2)
The problem was not serious and generally a warm bath and lullaby was enough
To calm my baby down and to take out the winds
To find out if it will soothe my babies colic problem
Top Related
Copyright © 2022 FDOKUMEN

