




Bahasa
Halaman
Hukum


Index
Note: Page numbers of article titles are in boldface type.
A
Abdomen, interventional ultrasonography in. See
Interventional ultrasonography.
Abdominal aortic aneurysms, aortic endografting for,
372–373
complications of, 369–370
CT of, 373
Ehlers-Danlos syndrome and, 370
risk factors for, 368
ultrasonography of, 365–373
anatomy and histology in, 365–366
as screening tool, 370
false aneurysms, 370–371
flow characteristics in, 366
for aortic dissection, 371–372
inflammatory aneurysms, 371
limitations of, 370
mycotic aneurysms, 371
technique for, 366–368
Abdominal ectopic pregnancy, ultrasonography
of, 333
Abdominal injuries, emergency ultrasonography
of, 421
Abdominal surgery, during pregnancy,
ultrasonography in, 323
Abortion, spontaneous, and first-trimester bleeding,
301–303, 306
ultrasonography of, 322
Abruption, placental, ultrasonography of, 319
Abscesses, abdominal, interventional ultrasonogra-
phy for. See Interventional ultrasonography.
intratesticular, ultrasonography of, 353–354
liver, diagnosis of, 268–270
lung, interventional ultrasonography for, 462
tubo-ovarian, ultrasonography of, 338–339
Abscess-pleural symphysis, lung abscesses and, 462
Acalculous cholecystitis, acute, ultrasonography
of, 260
Acute painful scrotum, ultrasonography of, 349–363
anatomy in, 349–350
for appendageal torsion, 356–357for cellulitis, 353
for epididymo-orchitis, 351–353for Fournier’s gangrene, 351
for idiopathic varicocele, 357–358
for inguinal hernia, 360–361
for intratesticular abscess, 353–354
for intratesticular arteriovenous
malformation, 359
for intratesticular varicocele, 358–359
for primary orchitis, 353
for secondary varicocele, 358
for testicular torsion, 354–356
for testicular trauma, 359–360
for testicular tumor, 361
technique for, 350–351
Adenomas, hepatic, ultrasonography of, 271–273
Adnexal masses, ultrasonography of, 329–348
corpus luteal cysts, 329–331
cystadenocarcinoma, 342
cystic teratomas, 341
diverticulitis, 344
ectopic pregnancy, 331–334
abdominal, 333
adnexal ring sign in, 332
cervical, 333
double decidual sac sign in, 332
b-human chorionic gonadotropin in, 334
interstitial, 333
intradecidual sign in, 331–332
management of, 333–334
endometriomas, 339–340
epiploic appendages, 345
follicular cysts, 329
leiomyomata, 340–341luteoma of pregnancy, 338
ovarian hyperstimulation syndrome, 334–336
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/S0033-8389(04)00032-6
Radiol Clin N Am 42 (2004) 479–486

ovarian neoplasms, 341
ovarian torsion, 336–338
pelvic inflammatory disease and tubo-ovarian
abscess, 338–339
perforated appendicitis, 343–344
serous and mucinous cystadenomas, 341–342
theca lutein cysts, 334
Adnexal ring sign, in ectopic pregnancy, 332
Amniotic sac, ultrasonography of, 301
Androgens, and priapism, 430–431
Aneurysms, ultrasonography of, abdominal aortic.
See Abdominal aortic aneurysms.
iliac artery, 377–379
peripheral artery, 379
popliteal, 379
splanchnic artery, 377
splenic artery, 377
in pregnancy, 325
Ankle-brachial index, in arterial injuries, 383–384
Antipsychotic drugs, and priapism, 430
Aortic dissection, ultrasonography of, 371–372
Aortic endografting, for abdominal aortic aneurysms,
372–373
Appendageal torsion, scrotal, ultrasonography of,
356–357
Appendicitis, acute, in infants and children, 452–454
ultrasonography of, 453–454
perforated, ultrasonography of, 343–344
Arterial embolization, for acute limb ischemia,
392–394
for priapism, 436–437
Arterial injuries, ankle-brachial index in, 383–384
pathologic validation of, 383
ultrasonography of, 383–396
acute limb ischemia, 392–394
arteriovenous fistulas, 388–389
craniocervical dissections, 389–391
diabetic foot, 394
hematomas, 386–388
pseudoaneurysms, 384–386
stroke and carotid artery stenosis, 391–392
upper limb ischemia, 394–395
Arteriovenous fistulas, renal, ultrasonography of,
406–407
ultrasonography of, 388–389
Arteriovenous malformations, and first-trimester
bleeding, 309–311
intratesticular, ultrasonography of, 359
B
Barium enema examination, of intussusception, in
infants and children, 449–450
Bell-clapper deformity, scrotal, ultrasonography
of, 354
Biliary duct dilatation, diagnosis of, 264–266
Biliary obstruction, diagnosis of, 266
Biopsy, renal, complications of, 406–407, 410
Bleeding, first-trimester. See First-trimester bleeding.
Bowel strangulation, inguinal hernias and, 360–361
Budd-Chiari syndrome, ultrasonography of, 275
C
Calf veins, ultrasonography of, for thromboembolic
disease, 287–288
Carotid artery dissection, ultrasonography of,
389–390
Carotid artery stenosis, and stroke, ultrasonography
of, 391–392
Cellulitis, scrotal, ultrasonography of, 353
Cervical ectopic pregnancy, ultrasonography of, 333
Chest, interventional ultrasonography in. See
Interventional ultrasonography.
Chest injuries, emergency ultrasonography of,
421–424
Chest tube insertion, ultrasonography in, 459–462
Chlorpromazine, and priapism, 430
Cholecystitis, ultrasonography of, acute, 257
acute acalculous, 260
complicated, 260–261
emphysematous, 263–264
gangrenous, 261–262
Cholecystostomy, percutaneous, ultrasonography in,
463–465
Choriocarcinoma, and first-trimester bleeding, 309
Chronic intestinal ischemia, ultrasonography of,
373–377
Cirrhotic native liver, ultrasonography of. See Liver.
Cocaine, and priapism, 430
Compression ultrasonography, of thromboembolic
disease, 281, 283, 286, 287, 291, 294
Computed tomography, in trauma patients, versus
ultrasonography, 420
Index / Radiol Clin N Am 42 (2004) 479–486480

of abdominal aortic aneurysms, 373
of acute hepatic vein thrombosis, 275
of diverticulitis, 344
of intra-abdominal abscesses, 465–466
Corpus luteal cysts, ultrasonography of, 329–331
Craniocervical dissections, ultrasonography of,
389–391
Crown-rump length, of embryo, 301, 305
Cystadenocarcinoma, ultrasonography of, 342
Cystadenomas, ultrasonography of, 341–342
Cystic teratomas, ultrasonography of, 341
Cysts, corpus luteal, ultrasonography of, 329–331
follicular, ultrasonography of, 329
theca lutein, ultrasonography of, 334
Cytotec, and spontaneous abortion, 322
D
Deep venous thrombosis, ultrasonography of,
286–294
Diabetic foot, ultrasonography of, 394
D-dimer test, for thromboembolic disease, 284, 286
Diverticulitis, CT of, 344
ultrasonography of, 344
Double decidual sac sign, in ectopic pregnancy, 332
in transvaginal ultrasonography, 299
E
Echinococcal abscesses, interventional
ultrasonography for, 470
Ectopic pregnancy, ultrasonography of. See Adnexal
masses.
Edema, re-expansion pulmonary, thoracentesis
and, 459
Ehlers-Danlos syndrome, and abdominal aortic
aneurysms, 370
Embolization, arterial, for acute limb ischemia,
392–394
for priapism, 436–437
transcatheter, for priapism, 437–438
Embryo, ultrasonography of, 300–301, 305
Emphysematous cholecystitis, ultrasonography of,
263–264
Empyema, chest tubes for, 460–462
versus lung abscesses, 462
Endoluminal repair, of abdominal aortic aneurysms,
372–373
Endometriomas, ultrasonography of, 339–340
Endometrium, sonographic anatomy of, 297
Endovaginal ultrasonography, of ectopic
pregnancy, 331
Epididymo-orchitis, ultrasonography of, 351–353
Epiploic appendages, ultrasonography of, 345
F
Fatty infiltration of liver, and liver enlargement, 270
Fatty liver of pregnancy, and liver enlargement,
270–271
Fibroids, uterine, ultrasonography of, 322–323
First-trimester bleeding. See also Pregnancy.
ultrasonography of, 297–314
anatomy in, 297–298
for absent intrauterine gestational sac,
303–304
for arteriovenous malformations, 309–311
for choriocarcinoma, 309
for gestational sac with embryo, 305
for gestational trophoblastic disease, 306–309
for hydatidiform mole, 307–309
for intrauterine growth restriction, 305
for retained products of conception, 306
for spontaneous abortion, 301–303
for subchorionic hematoma, 305–306
for trophoblastic tumors, 309
technique for, 298
versus normal ultrasonography, 298–301
amniotic sac in, 301
embryo in, 300–301
gestational sac in, 298–300
yolk sac in, 300
yolk sac criteria for, 304–305
Fistulas, abdominal, interventional ultrasonography
for, 468, 470
arteriovenous, renal, ultrasonography of,
406–407
ultrasonography of, 388–389
Focal hemorrhagic lesions, hepatic, diagnosis of,
271–274
Focused abdominal sonography for trauma
technique. See Trauma patients, emergency
ultrasonography in.
Index / Radiol Clin N Am 42 (2004) 479–486 481

Follicular cysts, ultrasonography of, 329
Foot, diabetic, ultrasonography of, 394
Fournier’s gangrene, ultrasonography of, 351
Fungal abscesses, interventional ultrasonography
for, 470
G
Gallbladder disease, in pregnancy, ultrasonography
of, 324
Gallbladder perforation, ultrasonography of,
262–263
Gallbladder wall thickening, ultrasonography of, 260
Gallstones, ultrasonography of, 257–260
Gangrene, Fournier’s, ultrasonography of, 351
Gangrenous cholecystitis, ultrasonography of,
261–262
Gestational sac, ultrasonography of, 298–300,
303–305
Gestational trophoblastic disease, and first-trimester
bleeding, 306–309
H
HELLP syndrome, ultrasonography of, 316–317
Hematoceles, ultrasonography of, 359
Hematomas, infected, interventional ultrasonography
for, 470
scrotal, ultrasonography of, 359–360
subchorionic, and first-trimester bleeding,
305–306
ultrasonography of, 386–388
Hemorrhage, postpartum, ultrasonography of, 321
thoracentesis and, 459
Hemorrhagic lesions, hepatic, diagnosis of, 271–274
Hepatic abscesses, interventional ultrasonography
for, 466–467
Hepatic artery stenosis, ultrasonography of, 398, 399
Hepatic artery thrombosis, ultrasonography of,
275–276, 398
Hepatic vein thrombosis, ultrasonography of, 275
Hepatic veins, ultrasonography of, 399–400
Hepatitis, diagnosis of, 266–268
Hepatobiliary ultrasonography, 257–278
Murphy’s sign in, 257
of acute acalculous cholecystitis, 260
of acute cholecystitis, 257
of acute right upper quadrant pain, 276
of biliary duct dilatation, 264–266
of biliary obstruction, 266
of complicated cholecystitis, 260–261
of emphysematous cholecystitis, 263–264
of focal hemorrhagic lesions, 271–274
of gallbladder perforation, 262–263
of gallbladder wall thickening and pericholecystic
fluid, 260
of gallstones, 257–260
of gangrenous cholecystitis, 261–262
of hepatic artery stenosis, 398, 399
of hepatic artery thrombosis, 275–276, 398
of hepatic vascular abnormalities, 274–276
of hepatic vein thrombosis, 275
of hepatitis, 266–268
of liver abscesses, 268–270
of noninfectious liver enlargement, 270–271
of portal vein thrombosis, 274–275, 399,
401–402, 405
Hepatocellular carcinoma, ultrasonography of,
273–274
Hepatofugal flow, ultrasonography of, 402
Hernias, inguinal, ultrasonography of, 360–361
b-Human chorionic gonadotropin, in ectopic
pregnancy, 334
in molar pregnancy, 308–309
in ovarian hyperstimulation syndrome, 334
in pregnancy, 299–300
Hydatidiform mole, and first-trimester bleeding,
307–309
Hydronephrosis, in pregnancy, ultrasonography
of, 325
Hydrosalpinx, ultrasonography of, 339
Hypertension, in pregnancy, ultrasonography of,
316–317
portal, ultrasonography of, 402
Hypertrophic pyloric stenosis, in infants and children,
445–449
clinical features of, 445
incidence of, 445
management of, 448–449
I
Iliac artery aneurysms, ultrasonography of, 377–379
Inferior vena cava, ultrasonography of, 399–400
Inflammatory aneurysms, ultrasonography of, 371
Index / Radiol Clin N Am 42 (2004) 479–486482

Inguinal hernias, ultrasonography of, 360–361
Interstitial ectopic pregnancy, ultrasonography
of, 333
Interventional ultrasonography, 457–478
abdominal, 463–474
for echinococcal abscesses, 470for fistulas, 468, 470
for fungal abscesses, 470for hepatic abscesses, 466–467
for infected hematomas, 470for pelvic abscesses, 470, 472–474
for renal and perinephric abscesses, 467for splenic abscesses, 468
in intra-abdominal abscess drainage, 465–466in paracentesis, 463
in percutaneous cholecystostomy, 463–465in percutaneous nephrostomy, 467–468
of chest, 457–462
for lung abscesses, 462
in chest tube insertion, 459–462
in thoracentesis, 457–459
Intestinal ischemia, chronic, ultrasonography of,
373–377
Intracavernosal arteries, laceration of, and
priapism, 431
Intracorporeal injection therapy, and priapism, 430
Intradecidual sign, in ectopic pregnancy, 331–332
in transvaginal ultrasonography, 299
Intratesticular abscesses, ultrasonography of,
353–354
Intratesticular arteriovenous malformations,
ultrasonography of, 359
Intratesticular varicoceles, ultrasonography of,
358–359
Intrauterine growth restriction, ultrasonography
of, 305
Intussusception, in infants and children, 449–452
barium enema examination for, 449–450
diagnosis of, 449–450
management of, 452
plain films of, 449
J
Jugular vein, ultrasonography of, for thromboembolic
disease, 289–290
K
Kidneys, ultrasonography of, 405–412
after transplantation, 405–409
allograft dysfunction, 408–409
arteriovenous fistulas, 406–407
pseudoaneurysms, 406
renal artery stenosis, 407
renal vein thrombosis, 408
anatomy and appearance in, 405
during transplantation, 407
native kidney, 409–412
for biopsy complications, 410
for pyelonephritis, 410
for renal artery stenosis, 411–412
for renal trauma, 411
for renal vein thrombosis, 411
for urinary obstruction, 410
L
Leiomyomata, ultrasonography of, 340–341
Limb ischemia, ultrasonography of, 392–395
Liver, ultrasonography of, 397–405
after transplantation, 398–400
hepatic artery stenosis, 398, 399
hepatic artery thrombosis, 398
hepatic veins and inferior vena cava,
399–400
portal vein thrombosis, 399
pseudoaneurysms, 400
anatomy and appearance in, 397–398
native cirrhotic liver, 400–404
after transjugular intrahepatic
portosystemic shunt, 400–404
for portal hypertension, 402
for portal vein aneurysmal ectasia, 404
for portal vein thrombosis, 401–402
noncirrhotic native liver, 404–405
Liver abscesses, diagnosis of, 268–270
interventional ultrasonography for, 466–467
Liver enlargement, noninfectious, diagnosis of,
270–272
Lower extremities, thromboembolic disease in,
ultrasonography of, 286–288, 291, 293–294
Lung abscesses, interventional ultrasonography
for, 462
Luteoma of pregnancy, ultrasonography of, 338
Index / Radiol Clin N Am 42 (2004) 479–486 483

M
Magnetic resonance imaging, of acute hepatic vein
thrombosis, 275
Mesenteric vasculature, ultrasonography of, 373–377
Metastatic disease, and liver enlargement, 270
Methotrexate, for ectopic pregnancy, 333–334
Mifepristone, and spontaneous abortion, 322
Molar pregnancy, and first-trimester bleeding,
307–309
Mucinous cystadenomas, ultrasonography of,
341–342
Murphy’s sign, in hepatobiliary ultrasonography, 257
Mycotic aneurysms, ultrasonography of, 371
Myometrium, sonographic anatomy of, 297
N
Nephrostomy, percutaneous, interventional
ultrasonography in, 467–468
Neurologic disease, and priapism, 431
O
Orchitis, ultrasonography of, 353
Ovarian hyperstimulation syndrome, ultrasonography
of, 334–336
Ovarian neoplasms, ultrasonography of, 341
Ovarian torsion, ultrasonography of, 336–338
Ovaries, sonographic anatomy of, 297
Ovulation induction therapy, and ovarian
hyperstimulation syndrome, 335
P
Paracentesis, ultrasonography in, 463
Parapneumonic effusions, chest tubes for, 459–460
Pelvic abscesses, interventional ultrasonography for,
470, 472–474
Pelvic inflammatory disease, ultrasonography of,
338–339
Pelvic pain, adnexal masses and. See
Adnexal masses.
Pelvic thrombophlebitis, in pregnancy,
ultrasonography of, 324
Percutaneous cholecystostomy, ultrasonography in,
463–465
Percutaneous nephrostomy, interventional
ultrasonography in, 467–468
Pericholecystic fluid, ultrasonography of, 260
Perinephric abscesses, interventional ultrasonography
for, 467
Peripheral artery aneurysms, ultrasonography of, 379
Placentation, abnormal, ultrasonography of, 317–319
Plain films, in trauma patients, versus
ultrasonography, 422–424
of intussusception, in infants and children, 449
Pleural effusions, chest tubes for, 459–462
emergency ultrasonography of, 421
Pleuritic pain, thoracentesis and, 459
Pneumothorax, emergency ultrasonography of,
421–423
thoracentesis and, 458–459
Popliteal aneurysms, ultrasonography of, 379
Popliteal vein, ultrasonography of, for
thromboembolic disease, 287
Portal hypertension, ultrasonography of, 402
Portal vein aneurysmal ectasia, ultrasonography
of, 404
Portal vein thrombosis, ultrasonography of,
274–275, 399, 401–402, 405
Pregnancy. See also First-trimester bleeding.
ectopic, ultrasonography of. See Adnexal masses.
molar, and first-trimester bleeding, 307–309
ultrasonography in, 315–327
during abdominal surgery and trauma, 323
for abnormal placentation, 317–318
for acute renal disorders, 324–325
for gallbladder disease, 324
for pelvic thrombophlebitis, 324
for placenta previa, 318–319
for placental abruption, 319
for postpartum hemorrhage, 321
for pregnancy-induced hypertension, 316–317
for retained products of conception, 321–322
for splenic artery aneurysms, 325
for spontaneous abortion, 322
for uterine fibroids, 322–323
for uterine rupture, 317
for vasa previa, 320–321
for venous thromboembolism, 323–324
technique for, 315–316
Index / Radiol Clin N Am 42 (2004) 479–486484

Priapism, 427–443
arterial embolization for, 436–437
definition of, 427–428
diagnosis of, 434–436
epidemiology of, 428, 430
etiology of, 430–431
management of, 438–439
complications of, 439–440
pathophysiology of, 431–434
sickle cell anemia and, 430, 433, 439
transcatheter embolization for, 437–438
ultrasonography of, 436, 438
anatomy in, 428
technique for, 428
Pseudoaneurysms, hepatic, ultrasonography of, 400
renal, ultrasonography of, 406
ultrasonography of, 384–386
Pulmonary edema, re-expansion, thoracentesis
and, 459
Pulmonary embolism, ultrasonography of, 294
Pyelonephritis, ultrasonography of, 410
Pyogenic liver abscesses, interventional
ultrasonography for, 466–467
R
Raynaud’s phenomenon, ultrasonography of,
394–395
Renal abscesses, interventional ultrasonography
for, 467
Renal artery stenosis, ultrasonography of, 407,
411–412
Renal disorders, in pregnancy, ultrasonography of,
324–325
Renal trauma, ultrasonography of, 411
Renal vein thrombosis, ultrasonography of, 408, 411
Retained products of conception, and first-trimester
bleeding, 306
ultrasonography of, 321–322
RU 486, and spontaneous abortion, 322
S
Scrotum, acute painful. See Acute painful scrotum.
Seldinger technique, for percutaneous
cholecystostomy, 464
Serous cystadenomas, ultrasonography of, 341–342
Shunts, for priapism, 439
Sickle cell anemia, and priapism, 430, 433, 439
Solid organ injuries, emergency ultrasonography of,
420–421
Splanchnic artery aneurysms, ultrasonography
of, 377
Splenic abscesses, interventional ultrasonography
for, 468
Splenic artery aneurysms, ultrasonography of, 377
in pregnancy, 325
Spontaneous abortion, and first-trimester bleeding,
301–303, 306
ultrasonography of, 322
Stroke, carotid artery stenosis and, ultrasonography
of, 391–392
Subchorionic hematomas, and first-trimester
bleeding, 305–306
T
Testicular torsion, ultrasonography of, 354–356
Testicular trauma, ultrasonography of, 359–360
Testicular tumors, ultrasonography of, 361
Theca lutein cysts, ultrasonography of, 334
Thioridazine, and priapism, 430
Thoracentesis, ultrasonography in, 457–459
Thrombin injection, for pseudoaneurysms, 386
Thromboembolic disease, clinical evaluation of,
283–284
clinical features of, 279–281
D-dimer test for, 284, 286
ultrasonography of, 279–296
adjuncts to, 291
deep venous thrombosis, 286–294
in lower extremities, 286–288, 293–294
in pregnancy, 323–324
in upper extremities, 288–290, 294
pitfalls of, 291
pulmonary embolism, 294
Thrombophlebitis, pelvic, in pregnancy,
ultrasonography of, 324
Transabdominal ultrasonography, technique for, 298
Transcatheter embolization, for priapism, 437–438
Transhepatic approach, to percutaneous
cholecystostomy, 464
Index / Radiol Clin N Am 42 (2004) 479–486 485

Transjugular intrahepatic portosystemic shunt,
ultrasonography after, 400–404
Transplantation, kidney, ultrasonography after.
See Kidneys.
liver, ultrasonography after. See Liver.
Transvaginal approach, to pelvic abscess drainage,
472–474
Transvaginal ultrasonography, of embryo, 300–301
of gestational sac, 298–300
of molar pregnancy, 308–309
of yolk sac, 300
technique for, 298
Trauma, during pregnancy, ultrasonography of, 323
renal, ultrasonography of, 411
testicular, ultrasonography of, 359–360
Trauma patients, emergency ultrasonography in,
417–425
for chest injuries, 421–424
for solid organ injuries, 420–421
free fluid in, 417–418
free fluid scoring systems in, 419–420
pitfalls in, 418–419
sensitivity of, 420
versus CT, 420
versus plain films, 422–424
Trazodone, and priapism, 430
Trophoblastic tumors, and first-trimester
bleeding, 309
Tubo-ovarian abscesses, ultrasonography of,
338–339
U
Ultrasonography, endovaginal, of ectopic
pregnancy, 331
hepatobiliary. See Hepatobiliary ultrasonography.
in trauma patients. See Trauma patients.
interventional. See Interventional ultrasonography.
of abdominal aortic aneurysms. See Abdominal
aortic aneurysms.
of adnexal masses. See Adnexal masses.
of arterial injuries. See Arterial injuries.
of first-trimester bleeding. See
First-trimester bleeding.
of hypertrophic pyloric stenosis, in infants and
children. See Hypertrophic pyloric stenosis.
of intussusception, in infants and children.
See Intussusception.
of kidneys. See Kidneys.
of liver. See Liver.
of mesenteric vasculature, 373–377
of pregnancy-related emergencies. See Pregnancy.
of priapism, 428, 436, 438
of thromboembolic disease. See
Thromboembolic disease.
transvaginal. See Transvaginal ultrasonography.
Upper extremities, thromboembolic disease in,
ultrasonography of, 288–290, 294
Urinary obstruction, ultrasonography of, 410
Urolithiasis, in pregnancy, ultrasonography of, 325
Uterine fibroids, ultrasonography of, 322–323
Uterine rupture, in pregnancy, ultrasonography
of, 317
Uterus, sonographic anatomy of, 297
V
Varicoceles, ultrasonography of. See Acute
painful scrotum.
Vasa previa, in pregnancy, ultrasonography of,
320–321
Vasovagal reactions, thoracentesis and, 459
Venous thromboembolism, in pregnancy,
ultrasonography of, 323–324
Y
Yolk sac, ultrasonography of, 300, 304–305
Index / Radiol Clin N Am 42 (2004) 479–486486

FORTHCOMING ISSUES
May 2004
Cardiac ImagingMartin Lipton, MD, andLawrence Boxt, MD, Guest Editors
July 2004
Breast ImagingCarl D’Orsi, MD, Guest Editor
September 2004
PET Imaging IAbass Alavi, MD, Guest Editor
RECENT ISSUES
January 2004
Arthritis ImagingBarbara N. Weissman, MD, Guest Editor
November 2003
Imaging of the Acute AbdomenEmil J. Balthazar, MD, Guest Editor
September 2003
Advances in Renal ImagingPhilip J. Kenney, MD, Guest Editor
THE CLINICS ARE NOW AVAILABLE ONLINE!
Access your subscription at:http://www.TheClinics.com

Radiol Clin N Am 42 (2004) xi
Preface
Emergency ultrasound
Vikram Dogra, MD
Guest Editor
Ultrasonography has undergone many technologic tient care. Most of the articles describe sonography
changes resulting in its present state-of-the-art equip-
ment that is capable of high-resolution real-time
gray-scale imaging and tissue harmonics, including
color and power Doppler. These advances in ultra-
sound technology have resulted in improved work-up
of patients undergoing evaluation in emergency de-
partments because it is the first imaging performed on
almost all patients presenting to an emergency facil-
ity. This easily available imaging modality remains
the primary workhorse in diagnostic radiology not
only in day-to-day practice but also in emergency
situations. There has been a need for the Radiologic
Clinics of North America to dedicate an issue solely
to the practice of emergency ultrasound and I am
honored to be the guest editor of this issue. Great care
has been given to the selection of topics for this issue,
and pertinent findings have been summarized in the
form of tables for easy reference in most of the
articles where problem-solving algorithms are also
included. Relevant topics have been included that
are helpful to all clinicians involved in emergency pa-
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.004
techniques and pertinent sonographic anatomy to help
those who are new to the field of ultrasonography.
This issue on emergency ultrasound provides the
reader with up-to-date information on what is new,
exciting, and relevant in the practice of ultrasonog-
raphy as it pertains to acutely ill patients.
I wish to express my thanks to Joseph Molter for
preparing the illustrations, to Bonnie Hami, MA, for
her editorial assistance, and to Adrienne Jones for her
secretarial assistance. In addition, my sincere thanks
go to Barton Dudlick at Elsevier Science for his
administrative and editorial assistance.
Vikram Dogra, MD
Division of Ultrasound
Department of Radiology
Case Western Reserve University
University Hospitals
11100 Euclid Avenue
Cleveland, OH 44106, USA
E-mail address: [email protected]
s reserved.

Radiol Clin N Am 42 (2004) 257–278
Hepatobiliary imaging and its pitfalls
Deborah J. Rubens, MD
Departments of Radiology and Surgery, University of Rochester Medical Center, 601 Elmwood Avenue,
Rochester, NY 14642-8648, USA
Diagnosis of acute cholecystitis Sonographic Murphy’s sign
Acute cholecystitis is the result of obstruction of
the gallbladder and accompanying inflammation of
the gallbladder wall with associated infection and
sometimes necrosis. Ninety percent to 95% of cases
of acute cholecystitis are caused by obstruction by
gallstones in either the gallbladder neck or the cystic
duct [1]. Acute cholecystitis occurs in only approxi-
mately 20% of patients who have gallstones [2]. This
means that many patients with gallstones have no
symptoms, and their right upper quadrant pain may
be caused by a different etiology [3]. Of patients who
present with right upper quadrant pain, only 20% to
35% have acute cholecystitis [1,2]. As the definition
of ‘‘right upper quadrant pain’’ becomes less specific,
especially lacking an accompanying elevated white
blood cell count and fever, the percentage of patients
who actually have acute cholecystitis given the his-
tory of right upper quadrant pain diminishes further.
Specific criteria for the diagnosis of acute cholecys-
titis are important, because many patients have gall-
stones but may not have acute cholecystitis. The
primary diagnostic criterion is a positive sonographic
Murphy’s sign in the presence of gallstones. Second-
ary signs of acute cholecystitis include gallbladder
wall thickening more than 3 mm, a distended or
hydropic gallbladder (loss of the normal tapered neck
and development of an elliptical or rounded shape),
and pericholecystic fluid.
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.004
E-mail address: [email protected]
The sonographic Murphy’s sign is defined as
specific reproducible point tenderness over the gall-
bladder as the transducer applies pressure. In a classic
article by Dr. Phillip Ralls [4], which included only
patients with right upper quadrant pain, fever, and an
elevated white blood cell count, a sonographic Mur-
phy’s sign was 87% specific for the diagnosis of
acute cholecystitis. When a positive sonographic
Murphy’s sign is used in conjunction with the pres-
ence of gallstones, it has a positive predictive value of
92% for diagnosing acute cholecystitis. Persons in
whom a sonographic Murphy’s sign may be absent
include persons who are medicated; therefore, careful
attention to a patient’s clinical status is important.
Denervated gallbladders in patients who have diabe-
tes or gangrenous cholecystitis may result in the loss
of a sonographic Murphy’s sign.
Gallstone diagnosis and pitfalls
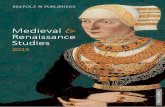
Gallstones are diagnosed by the presence of
gravity-dependent, mobile intraluminal echoes within
the gallbladder, which cast a posterior shadow
(Fig. 1). Although ultrasound (US) has a high accu-
racy ( > 95%) for the diagnosis of gallstones, some
stones may be missed [3]. False-negative results
occur because of stones that are too small to cast a
shadow (usually smaller than 1 mm), soft stones that
lack strong echoes [1], and gallstones that are im-
pacted in the gallbladder neck or in the cystic duct
and may not be as readily visible (see Fig. 1) [5]. If
the gallbladder is focally tender but no gallstones are
appreciated, the patient should be examined from
s reserved.

Fig. 1. Gallstones. (A, left) Gallstone in the gallbladder neck (arrow) casts no significant shadow and is nearly invisible. Gas in
the duodenum (arrowhead) obscures the fundus and casts a strong sharp shadow (asterisk). (Right) With patient in sitting
position, stone (arrow) moves out of the neck and casts a clear shadow (asterisk). Adjacent duodenum (arrowheads) is separate
from the gallbladder but still casts a strong shadow, equivalent to the gallstone. (B, left) Multiple gallstones (arrowheads), some
of which cast shadows (arrows) and some of which do not. (Right) Normal caliber common duct (6 mm at the porta) with stones
(arrows) in same patient. Choledocholithiasis may be difficult to detect, especially in the distal duct, if the stones do not shadow
or are not outlined by the distal fluid. (C, left) Longitudinal US shows a normal gallbladder. (Right) Harmonic imaging reveals
multiple small stones (arrows).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278258
multiple positions, including prone position or up-
right position, to help stretch out the gallbladder
[3,6]. Decubitus or intercostal scanning also may
help visualize the neck, which may not be as easily
apparent from a subcostal supine approach.
Resolution of small stones in the gallbladder can
be improved with use of harmonic imaging [7,8]. This
approach uses the higher frequency of the returning
sound beam for better resolution and decreases the
scattering from superficial structures in the abdominal
wall and in the adjacent liver. Harmonic imaging
improves the echoes cast by stones and strengthens
their posterior shadows. This improved resolution
may permit visualization of stones not seen with
conventional gray scale US (see Fig. 1).
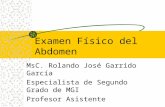
Fig. 2. Pseudo gallbladders. (A) Transverse image in the right upper
containing debris (asterisk). Note that the ‘‘gallbladder’’ does not ex
(B, left) CT image of the same area as in A shows a fluid-containin
aorta (A). This was a hematoma.(Right) The true gallbladder (GB) is
fluid- and debris-containing structure believed to represent an abnor
(Right) The true gallbladder (arrows) is compressed and displaced
pancreatic pseudocyst (P) displacing the gallbladder (arrows).
Echogenicity of stones may be decreased in soft
pigment stones. These stones are commonly associ-
ated with recurrent pyogenic cholangiohepatitis and
are more often seen in the bile ducts than in the
gallbladder. They look more like soft-tissue masses
than stones and may or may not cast acoustic shad-
ows. They may be misinterpreted as sludge or debris
and give a false-negative diagnosis for gallstones.
False-positive results may arise from side lobe
artifacts, which give rise to echoes that seem to arise
within the gallbladder lumen but are actually gener-
ated from the wall or outside the wall [1]. Similarly,
partial volume artifacts from gas in the adjacent bowel
may mimic stones with strong echoes and posterior
shadowing (see Fig. 1A). A calcium bile salt precipi-
quadrant with structure identified as the gallbladder (arrows)
tend anteriorly and that the aorta (A) is immediately adjacent.
g structure (arrows) with similar attenuation to blood in the
lateral to the aorta and extends anteriorly. (C, left) Distended
mal gallbladder in this patient with right upper quadrant pain.
by the adjacent mass, a pancreatic pseudocyst. (D) CT of the

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 259

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278260
tate may form with the use of Ceftriaxone and mimic
gallstones on sonographic examination. These precip-
itates resolve after the patient ends therapy.
Other fluid-containing structures may mimic the
gallbladder, especially if the gallbladder is out of its
normal position or is small and contracted. These
structures include the duodenum, gastric antrum or
colon, hematomas, pancreatic pseudocysts (Fig. 2), or
even dilated vascular collaterals. Mistaking these
structures for the gallbladder may result in missed
pathology in the true gallbladder or a false-positive
diagnosis of gallbladder disease (ie, obstructed gall-
bladder or acalculous cholecystitis).
Gallbladder wall thickening and pericholecystic
fluid
Gallbladder wall thickening is defined as a wall
diameter more than 3 mm and is present in 50% of
patients with acute cholecystitis (Fig. 3) [1]. The
gallbladder wall may be thickened because of hepatic
congestion or edema from liver disease, right heart
failure, or generalized edema from hypoproteinemia,
which is often associated with renal disease or hepatic
dysfunction [3]. A thickened gallbladder wall also
can occur in association with adjacent inflammatory
conditions, including hepatitis, peptic ulcer disease
(Fig. 4), pancreatitis, perihepatitis (Fitz-Hugh-Curtis
syndrome), and pyelonephritis (Fig. 5).
A thickened, striated gallbladder wall consists of
alternating hyper- and hypoechoic layers. When seen
in the setting of acute cholecystitis, it is strongly
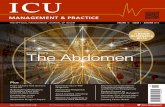
Fig. 3. Acute cholecystitis. This patient presented with right
upper quadrant pain and a positive sonographic Murphy’s
sign. Longitudinal US shows stones (arrows) and diffuse
gallbladder wall thickening (cursors) that measures 5 mm.
associated with complications such as gangrenous
cholecystitis [9]. A striated wall also is nonspecific,
however, and may be seen in all the other causes of
wall thickening, including hepatitis (Fig. 6) [10].
Similarly, pericholecystic fluid is a nonspecific
finding; it may occur because of ascites or localized
inflammation from other causes, such as peptic ulcer
disease (see Fig. 4) [2]. Teefey et al [10] described
two specific patterns of pericholecystic fluid. Type I,
a thin, anechoic, crescent-shaped collection adjacent
to the gallbladder wall, is nonspecific (see Fig. 4B).
Type II, a round or irregular shaped collection with
thick walls, septations, or internal debris, is associated
with gallbladder perforation and abscess formation
(Fig. 7) [10]
Acute acalculous cholecystitis
This is an acute inflammation of the gallbladder
that occurs in up to 14% of patients with acute
cholecystitis [11]. It is most frequently seen in post-
trauma and postsurgical patients and other hospital-
ized patients and occurs because of conditions that
lead to ischemia, hypotension, or sepsis [12]. These
critically ill patients are often medicated with nar-
cotics, are on ventilators, and receive hyperalimenta-
tion, which contributes to biliary stasis and functional
cystic duct obstruction [2,12]. Gallbladder gangrene
is associated in 40% to 60% of cases, with increased
risk of perforation [2]. Mortality ranges from 6% to
44% but can be reduced by early diagnosis and
therapy [12]. In the series by Cornwall et al [12],
only 50% had a sonographic Murphy’s sign. This is
a difficult clinical and ultrasonic diagnosis, because
gallstones are absent and the sonographic Murphy’s
sign may be limited because of other illnesses
and medication. The diagnosis is made by gallblad-
der tenderness (if present) and is associated with
gallbladder distension, intraluminal debris, and gall-
bladder wall thickening that is not caused by other
etiologies, such as hypoalbuminemia, congestive
heart failure, or hepatic congestion (Fig. 8). Because
gallbladder wall thickening is nonspecific, CT can be
used to visualize pericholecystic inflammation to
improve diagnostic specificity [2,13].
Complicated cholecystitis
Complications of acute cholecystitis include gan-
grenous cholecystitis, emphysematous cholecystitis,

Fig. 4. Peptic ulcer perforation and thick gallbladder wall. (A) Patient with right upper quadrant pain, fever, and elevated white
blood cell count. US shows focal gallbladder wall thickening (7-mm cursors) and gallstones (asterisks) and could be interpreted
as cholecystitis. The free air with reverberation shadows (arrows) that leads to the correct diagnosis could be overlooked easily.
(B) Transverse US shows wall thickening (cursors) and simple pericholecystic fluid (arrow). (C) CT image shows peri-
cholecystic fluid (arrows), free air (arrowheads), and extraluminal accumulated air (paired arrowheads) in perforated duo-
denal ulcer.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 261
and gallbladder perforation. These complications oc-
cur in up to 20% of patients [3]. Complications of
acute cholecystitis are important to detect because they
are associated with increased morbidity (10%) and
mortality (15%) [14] and require emergency surgery
[2]. There is also approximately a 30% conversion
for laparoscopic cholecystectomy to an open proce-
dure in the setting of complicated cholecystitis [14].
Gangrenous cholecystitis
Gangrenous cholecystitis is defined histologically
as coagulative necrosis of the mucosa or the entire
wall associated with acute or chronic inflammation
[10]. It occurs in up to 20% of patients with acute
cholecystitis and has an increased risk of perforation
[3]. Unfortunately, US is relatively nonspecific for the

Fig. 5. Pyelonephritis with gallbladder wall thickening. (A) Gallbladder wall shows marked 1.3 cm thickening (cursors) and
hypoechoic fluid within the wall. (B) Transverse US of the lower pole of the right kidney shows a 3-cm echogenic mass
(arrows). (C) CT through the right lower pole shows the characteristic round, heterogeneous decreased attenuation area of
pyelonephritis (arrows).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278262
diagnosis of gangrenous cholecystitis because a sono-
graphic Murphy’s sign is absent in two thirds of
patients [15]. A relatively specific finding is intra-
luminal membranes caused by a fibrous exudate or
necrosis and sloughing of the gallbladder mucosa
(Fig. 9). This finding is present, however, in only
5% of patients [10].
Gallbladder perforation
Gallbladder perforation occurs in 5% to 10% of
patients with acute cholecystitis, most often in asso-
ciation with gangrenous cholecystitis [3]. The fundus
is the most common site for perforation because it has
the least blood supply. Acute perforation with free
intraperitoneal bile results in peritonitis and is rare.
More commonly, subacute perforation occurs, which
results in pericholecystic abscess formation [2].
These abscesses may occur in or adjacent to the
gallbladder wall in the gallbladder fossa, within the
liver, or along the free margin of the gallbladder
within the peritoneal cavity [10]. They are character-
ized by complex fluid collections with inflammatory
changes in the adjacent fat on US or CT [2]. Patients
with peritoneal or liver abscesses require immediate
surgery and drainage, respectively, whereas abscesses

Fig. 6. Hepatitis, with striated gallbladder wall thickening.
Longitudinal US of contracted gallbladder with a thickened
striated wall (arrows) with alternating echogenic and hypo-
echoic layers. This patient had right upper quadrant pain,
fever, abnormal liver function tests, and a negative sono-
graphicMurphy’s sign. She tested positive for hepatitis B and
clinically had acute alcoholic hepatitis. The striated wall is
not specific for gallbladder disease.
Fig. 7. Complicated cholecystitis with gallbladder perforation. (A
irregularly marginated pericholecystic intrahepatic fluid (arrows)
surgery and was found to have acute cholecystitis with an adjacent
shows a pericholecystic collection (arrow) that contains debris. Th
contained within the gallbladder wall (double arrow). (C) CT
inflammatory edema in the adjacent fat (arrowheads).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 263
in the gallbladder wall and fossa may respond to
conservative management [16].
Pericholecystic fluid adjacent to the gallbladder
wall may mimic perforation. Upon careful inspection,
however, the wall is intact and the fluid anechoic (see
Fig. 4B). Fluid that appears within the walls been
noted to precede perforation in one case [17]; how-
ever, no specific US features predict which gallblad-
ders will perforate.
Emphysematous cholecystitis
This is a rare complication of acute cholecystitis
(less than 1% of all complicated cases) and is
associated with gas-forming bacteria in the gallblad-
der lumen or in the gallbladder wall. As many as 40%
of patients with emphysematous cholecystitis have
diabetes [2]. The clinical course is rapidly progres-
sive, with 75% incidence of gallbladder gangrene and
20% incidence of perforation [18]. Emphysematous
cholecystitis can be recognized by the antidependent
gas echoes within the lumen (Fig. 10). Intramural gas
may be more difficult to identify because it may
mimic the calcified wall of a porcelain gallbladder.
The type of shadowing (‘‘clean’’ versus ‘‘dirty’’) does
not differentiate between calcium and air. The loca-
tion of the echoes does. If the presence of gas is
) Longitudinal US of the gallbladder (GB) with adjacent
. This patient presented with sepsis 2 weeks after prostate
liver abscess. (B) Longitudinal US of gallbladder with stones
e collection abuts the free wall of the gallbladder and is not
shows an enhancing rim around the fluid (arrows) and

Fig. 7 (continued).
Fig. 9. Gallbladder gangrene/mucosal sloughing. Longitu-
dinal US of patient with acute cholecystitis secondary to
stone (arrow) impacted in the gallbladder neck. Note the
intraluminal membranes (arrowheads), which are associ-
ated with gallbladder gangrene.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278264
uncertain, either CT or plain film radiography can be
used to differentiate between gas and calcification.
Biliary ducts
Dilated biliary ducts in the acute patient represent
a relative emergency because sepsis in association
with dilated ducts requires rapid decompression.
Biliary duct dilatation may be the result of multiple
causes, including stones, tumor, stricture, or adjacent
Fig. 8. Acalculous cholecystitis. Longitudinal US of a debris-
filled (asterisk) gallbladder with a thick, striated wall (ar-
rows). No stones are visualized. At surgery, this was acute
acalculous cholecystitis.
extrinsic masses with biliary duct compression and
obstruction. The diagnosis is made by evaluation of
intra- and extrahepatic ducts, because one or both
may be dilated, depending on the level of obstruction.
Ultrasound diagnosis of duct dilatation
The extrahepatic common duct is measured from
outer wall to outer wall at the level of the crossing of
the right hepatic artery. The diameter at this level
should not exceed 6 mm [1]. The diameter of the
common duct is slightly greater distally as it ap-
proaches the pancreas, sometimes as much as 1 to
2 mm. There is still debate in literature as to whether
the bile duct dilates with age or after cholecystectomy
[1]. Most laboratories consider a duct smaller than
6 mm normal and a duct 8 mm or larger abnormal
[1,19]. Clinically, if a patient has dilated ducts but no
accompanying symptoms—elevated bilirubin, pain,
sepsis, or elevated liver enzymes, including alkaline
phosphatase—the dilated ducts are unlikely to be
clinically relevant. Similar to the presence of gall-
stones, when assessing the ducts for biliary disease,
the clinical scenario is of prime importance. Intra-
hepatic biliary ducts are normal if they are 2 mm or
smaller in the porta or no more than 40% of the
diameter of the accompanying portal vein [1]. With
the advent of newer equipment, however, it is possi-
ble to see intrahepatic biliary ducts in normal patients,
especially with the use of harmonic imaging, which
diminishes scatter. Clinical correlation is important,
because many young and slender patients may show
normal ducts with high-frequency transducers
(Fig. 11A). In general, intrahepatic biliary duct dila-

Fig. 10. Emphysematous cholecystitis. (A) Transverse supine view of the gallbladder reveals nondependent echoes anteriorly
(arrowheads), which cast a dense posterior shadow. (B) When viewed longitudinally from the flank, the dependent echogenic
gallstones (arrows) can be seen. Note that the shadow cast by the gas in (A) is denser and sharper than that from the stones (B).
The bowel gas does not necessarily cast a ‘‘dirty’’ or reverberant echo-filled shadow. Thus, the shadow cannot distinguish gas
from the stones.
Fig. 11. Normal ducts. (A) Normal intrahepatic ducts (cursors) in a post-cholecystectomy patient. Multicolored vessel in the
center of the color box is the hepatic artery (HA), and dark red adjacent vessel is the portal vein (PV). (B,C) Patient with
abdominal pain, nausea, and jaundice, 1 month after cholecystectomy. Note multiple anechoic irregularly branching tubes with
confluence in the porta hepatis. Color Doppler image (C) confirms that some are avascular and represent ducts (arrowheads), and
the portal veins (red), hepatic veins(blue) and hepatic arteries (HA) are correctly identified. The inferior vena cava (IVC) and
hepatic vein (HV) as shown can be recognized by its anatomic position.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 265

Fig. 11 (continued).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278266
tation can be diagnosed by irregular angular branch-
ing, a central stellate configuration, and acoustic
enhancement posteriorly to the ducts (Fig. 11B) [1].
The use of color and power Doppler may be valuable
to demonstrate that the dilated structures are ducts
and that the normal portal veins and hepatic arteries
course adjacent to them (Fig. 11C). Biliary duct
necrosis is a critical complication that occurs after
liver transplant. In this situation, the ducts may not be
filled with bile but may be filled with pus or necrotic
debris. They also may appear echogenic and irregular
and enlarged without any fluid component (Fig. 12).
If the diagnosis of biliary disease is in question on
US, CT scan or transhepatic cholangiography may be
helpful in posttransplant patients.
Diagnosis of biliary obstruction
Assuming a patient has a dilated duct (6 mm or
larger) associated with clinical signs of obstruction
(including elevated bilirubin or elevated alkaline
phosphatase), how well does US identify the level
and cause of obstruction?
With good technique, the level of obstruction can
be defined in up to 92% of patients and the cause in
up to 71% [1]. Important technical factors include
positioning the patient in the erect right posterior
oblique or right lateral decubitus position to minimize
overlying bowel gas from the antrum or the duode-
num and using transverse scans to follow the duct
accurately [1]. Additional technical improvements
sometimes can be achieved by having the patient
drink water to displace gas or by using large a
footprint curvilinear transducer to compress bowel
and bowel gas away from the distal duct. Ninety
percent of obstruction occurs in the distal duct be-
cause of common duct stones, pancreatic carcinoma,
or pancreatitis [1]. Obstruction also may occur at the
level of the porta hepatis, usually because of tumor
(cholangiocarcinoma) or adenopathy. Sclerosing
cholangitis gives rise to segmentally dilated ducts,
often only in one portion of the liver (Fig. 13). These
patients may develop infection and present with
sepsis. Other causes of obstruction between the
pancreas and the porta hepatis include masses of
the colon or duodenum (Fig. 14), primary biliary
malignancy, or adenopathy.
Pitfalls include patients who have obstruction
without dilatation, which can occur in ascending
cholangitis, intermittent obstruction from stones, or
sclerosing cholangitis. As many as one third of
common bile duct calculi are found in nondilated bile
ducts (see Fig. 1B) [1]. In this group of patients, US is
relatively insensitive to make the diagnosis. MR
cholangiopancreatography (MRCP) and endoscopic
retrograde cholangiopancreatography (ERCP) should
be considered the alternative diagnostic modalities,
especially for stone disease.
Acute hepatic disease processes
Multiple abnormalities of the liver may present
with right upper quadrant pain. Some of these situa-
tions involve medical emergencies, including lesions
that are hemorrhagic or patients who have infection
and sepsis. Space-occupying disorders that stress the
liver capsule also may present with right upper
quadrant pain. These disorders range from acute fatty
infiltration to hepatitis to diffuse metastatic disease.
The important clinical features to determine are
whether the patient has infection or sepsis and if
the pain is localized to the liver or is more diffuse
(peritoneal signs). Anatomically the hepatic processes
can be divided into diffuse disease, focal disease, and
diseases that involve the vasculature.
Hepatitis
Hepatitis is a viral infection of the liver. The most
common acute presentation is from hepatitis A,
which is spread via oral ingestion with a 99%
recovery rate [20]. Patients present acutely with
jaundice, fever, and hepatomegaly. Sonographically,

Fig. 12. Biliary duct necrosis. (A) Transverse US of a liver transplant patient who presented with sepsis. Amorphous echogenic
debris (arrows) is seen on gray scale. (B) Two months later, the process has progressed. The echogenic areas (arrows) are more
confluent and linear and cast acoustic shadows, which obscure the adjacent parenchyma. (C) Color Doppler image shows
echogenic debris in a ductal distribution (arrows) and a low resistive index (less then 0.5) in the hepatic artery, which signifies
hepatic arterial stenosis or thrombosis. (D) The extensive biliary duct necrosis (arrows) and the resulting liver abscess
(arrowheads) are documented by CT. The abscess was obscured on the US because of shadowing from the ducts.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 267
most often the liver parenchyma is normal [20,21].
Rarely, the liver may have diffusely decreased echo-
genicity with relatively increased echogenicity of the
portal triads—the ‘‘starry-sky’’ appearance [21]. The
overall echogenicity of the liver is decreased relative
to the adjacent kidney (Fig. 15). Confirmation should
be obtained by checking the echogenicity of the
spleen relative to the left kidney to confirm that there
is no medical renal disease [20]. More commonly,
hepatitis has associated gallbladder findings, includ-
ing gallbladder wall thickening (see Fig. 6) and
sometimes a contracted gallbladder [20,21]. When

Fig. 13. Sclerosing cholangitis. Patient presented with sepsis and abdominal pain. (A) Longitudinal US of the right lobe is
normal, with a common duct (cursors) measuring 2 mm. (B) Longitudinal US of the left lobe shows multiple markedly enlarged
ducts (arrows). (C) CT shows the asymmetrically enlarged ducts (arrows) with enhancing walls, which indicates inflammation.
Emergent biliary drainage was performed, which alleviated the patient’s symptoms.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278268
the patient recovers from hepatitis, the gallbladder
wall and distention return to normal. Other viral
infections that involve the liver, such as mononucleo-
sis, may cause a similar pattern, with liver swelling,
tenderness, and gallbladder wall thickening (Fig. 16).
Liver abscess
The most common liver abscesses are pyogenic,
caused by bacteria. Patients most often present with
right upper quadrant pain, fever, and malaise. The
cause may be biliary (ascending cholangitis or from
the adjacent gallbladder), portal venous (from diver-
ticulosis or Crohn’s disease), or arterial. Fifty percent
of liver abscesses do not have a clear source [20]. The
appearance of liver abscesses varies. Microabscesses,
lesions smaller than 2 cm, may be widely scattered in
the liver or may cluster in a single focus. Pyogenic
abscess cavities probably begin as a small cluster of
microabscesses, which coalesce into a larger drainable
collection [22]. Sonographically, abscess margins are
often indistinct; which make abscesses less conspicu-
ous than on contrasted CT scans. This is particularly
true in small clustered microabscesses (Fig. 17A, B).
Predominately abscesses are hypoechoic (see Fig. 7A)
but also may be isoechoic, solid appearing, or even
hyperechoic if they contain gas and debris (Fig. 17C).
Fifty percent or less have enhanced through transmis-
sion. Because of this variable appearance, the differ-
ential diagnosis is large and includes tumor, simple
cyst with hemorrhage, hematoma, or other forms of
infection, including amebic abscess or ecchinococcal
infection. The absence of flow centrally helps to

Fig. 14. Duodenal mass with biliary, pancreatic, and bowel obstruction. Patient presented to the emergency department with
nausea and rising bilirubin. (A) Transverse US of the pancreas shows a 1.8-cm common duct (CD) and a dilated pancreatic duct
(arrowheads). (B) Longitudinal US shows a distended gallbladder with a soft-tissue mass (arrows) behind it. (C) On transverse
imaging, the mass (arrows) obstructs the duodenum (Duod), which has a fluid-filled proximal lumen. GB, gallbladder. (D) CT
confirms the circumferential duodenal tumor (arrows). Note distended gallbladder (GB) and common duct (CD).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 269
confirm that these are not solid tumors; however,
necrotic neoplasm remains in the differential diagno-
sis. The most helpful feature is a clinical scenario that
includes signs of infection. Abscesses are frequently
multiple, and US may be limited near the dome or
underneath the ribs for identifying the extent of
abscess involvement. In this case, contrast-enhanced
CT is often helpful in detecting the total abscess
burden and may identify the cause, especially if the
abscess arises from the bowel. After liver transplant,
patients are particularly prone to abscesses, especially
if biliary necrosis is present because of hepatic arterial

Fig. 15. Acute hepatitis. Transverse image shows a hypo-
echoic liver relative to the kidney (K) and bright portal triads
(arrowheads), the ‘‘Starry Sky’’ appearance. Although strik-
ing, this appearance is rare. Most often the hepatic echo-
genicity is normal.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278270
thrombosis. If a transplant patient presents with a
hepatic abscess, the patency of the hepatic arteries
should be assessed (see Fig. 12).
Noninfectious diffuse enlargement of the liver
Patients with diffuse metastatic disease may pres-
ent with right upper quadrant pain, sometimes with
fever and jaundice. When patients are questioned
closely, their symptoms are usually not as acute as
Fig. 16. Mononucleosis. (A) Initial longitudinal US in a patient 18
vomiting. The gallbladder is thick walled (arrows) and contains deb
(B) One week later the galbladder wall (arrows) has returned to nor
for mononucleosis.
that of cholecystitis or hepatitis. On imaging, meta-
static disease may be of any type from cystic metas-
tases of carcinoid to echogenic metastases from colon
carcinoma or any other primary lesion. The liver is
enlarged and tender to palpation, usually because of
stretching of the liver capsule (Fig. 18A). Another
disease process that causes rapid hepatic enlargement
is acute fatty infiltration of the liver, which may be
diffuse and homogenous fatty infiltration (Fig. 18B)
of the liver or segmental fatty infiltration with areas
of focal sparing. The liver may enlarge rapidly and
give rise to the clinical symptoms of right upper
quadrant tenderness. Vessels are not distorted, how-
ever, and if there are areas of focal fatty infiltration,
they should have a geographic margin. If metastatic
disease is in the differential diagnosis, a sulfur colloid
nuclear medicine scan can be performed, which
should produce normal results in the setting of fatty
infiltration. An MR imaging scan with and without
fat suppression also defines the cause of the US
abnormalities. Acute fatty liver of pregnancy is a
relatively rare but serious complication that occurs in
the third trimester and peripartum. Two-thirds of
patients have associated pre-eclampsia or the hemo-
lysis, elevated liver enzymes and low platelets
(HELLP) syndrome [23]. Patients present with vari-
ous symptoms, most commonly nausea, vomiting,
abdominal pain, fever, and jaundice [23,24]. Symp-
toms commonly mimic hepatitis. Laboratory ab-
normalities include elevated liver enzymes and
coagulopathy (prolonged prothrombin time [PTT]).
Disseminated intravascular coagulation occurs in up
to 50% [23]. US and CT may have high false-
weeks pregnant with right upper quadrant pain, nausea, and
ris. A diagnosis of acute acalculous cholecystitis was offered.
mal and the sludge is diminishing. The patient tested positive

Fig. 17. Liver abscesses. (A) Transverse US of nearly invisible microabscesses (cursors) within the liver. There are no specific
US features to identify this as an abscess. The area is slightly heterogeneous and lacks a normal vessel pattern. (B) CT of the left
lobe contains a typical rosette pattern diagnostic of clustered small abscesses with enhancing rims (arrows). A right lobe abscess
(arrow) could not be seen by US. (C) Mixed abscesses and gas. Longitudinal US of a patient with multifocal abscesses. The
fluid-containing abscess (A) anteriorly contains gas (arrow) with a reverberant echo posteriorly. The isoechoic abscess more
posteriorly (arrowheads) with central gas is more difficult to detect. (D) CT scan shows both abscesses. The more central abscess
(arrowheads) is much more extensive on CT than on US.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 271
negative rates (as high as 80%), and the diagnosis
largely depends on clinical features and biopsy, if
necessary [23,24].
Focal lesions with hemorrhage
Any focal hepatic lesion can potentially bleed,
which leads to acute right upper quadrant pain with
subsequent presentation of the patient for emergency
US. Even innocuous lesions, such as benign liver
cysts, occasionally can hemorrhage with resultant
symptoms. Hemangiomas, the most common benign
tumors of the liver, are mostly small and asympto-
matic and discovered incidentally. Lesions larger than
5 or 6 cm occasionally may present with either
hemorrhage or thrombosis [20]. Hepatic adenoma, a
benign tumor associated with estrogen or anabolic

Fig. 18. Diffuse liver enlargement. (A) Carcinoid metastases. Longitudinal US of a patient with acute right upper quadrant pain to
‘‘rule out (R/O) cholecystitis.’’ The gallbladder is normal; however, the liver was enlarged at 21 cm and riddled with cystic thick-
walled metastases (arrows) from a carcinoid primary. (B) Acute fatty infiltration. Longitudinal US in a patient with acute right
upper quadrant pain and abnormal liver function tests. The liver is enlarged at 18.4 cm with diffusely increased echogenicity, loss
of the normal vascular pattern, and increased attenuation, which causes poor delineation of the diaphragm posteriorly (arrows).
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278272
steroid therapy, does have a predisposition for bleed-
ing [25]. The rate of intratumoral or intra-abdominal
hemorrhage with adenomas is reported as high
50% to 65% [26]. Contrary to focal nodular hyper-
plasia and hemangioma, which are usually managed
conservatively, except if the patient has significant
symptoms, adenomas are usually resected, especially
Fig. 19. Hemorrhagic adenoma. (A) Transverse US in a patient
contraceptive pills shows a mixed echogenicity mass (arrows) wi
(arrowhead). The through transmission indicates fluid. (B) CT sh
enhanced, whereas the remaining hemorrhage did not.
if larger than 5 cm. On US, hepatic adenomas have a
variable appearance that ranges from hypoechoic
masses to mixed heterogeneous masses, which cor-
respond pathologically with intratumoral hemorrhage
and necrosis [25]. Masses also may be isoechoic to
the liver with a hypoechoic rim or even hyperechoic
if they contain fat. The mixed echogenic pattern is
with acute right upper quadrant pain who is taking oral
th through transmission (asterisk) displacing the gallbladder
ows a heterogenous mass (arrows). The tumor portion (A)

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 273
most likely to correspond to hemorrhagic necrosis;
however, it cannot be distinguished from other tu-
mors that can hemorrhage (Fig. 19) [25].
After adenoma, the other hepatic tumor likely to
present with hemorrhage is hepatocellular carcinoma.
Similar to adenomas, the US appearance of these
Fig. 20. Hepatocellular carcinoma with hemorrhage. (A) Trans
hypoechoic fluid (F) and an echogenic region that has a straight-line
(H). (B) Color Doppler image from the liver shows an area with hig
of 0.49) flow, which indicates tumor shunt flow. (C, D) CT confirm
image (D) shows the acute clot (H) bordering the lateral liver mar
Fig. 19A. F, fluid.
lesions varies greatly and ranges from echogenic to
hypoechoic or mixed [21]. Tumors even may be
diffuse and infiltrative and relatively invisible by
US. A clue to the presence of an underlying malig-
nancy is increased hepatic arterial flow in the lesion
compared with the remaining normal liver (Fig. 20).
verse US shows a heterogeneous liver echogenicity with
margin (arrows) with the more superficial hypoechoic tissue
h velocity (1.6 m/second) and low resistance (resistive index
s enhancing tumor at the dome (arrows), and a more caudal
gin (arrows). This accounted for the straight margin seen in

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278274
Most patients with hepatocellular carcinomas also
have predisposing risk factors, including cirrhosis or
hepatitis B or C.
The important feature to remember about acute
hemorrhage is that it may mimic the adjacent liver
parenchyma. Color Doppler imaging is useful for
showing vessels in a normal liver or in the tumor,
whereas the hemorrhage has no vascularity within the
hematoma. Straight lines and geographic margins are
also a clue to the presence of hemorrhage (Fig. 20).
Usually this indicates a subcapsular component with
compression of the adjacent liver capsule. Because
US can have difficulty differentiating between the
acute blood and the adjacent liver, CT scan is often
used to map the extent of the process and differentiate
hepatic tissue from blood and tumor.
Abnormalities of hepatic vasculature
Pathologic processes that involve the hepatic
vasculature may result in acute symptoms and emer-
gent presentations of the patient for US examination.
The liver has three vascular systems: the hepatic
arterial and portal venous for incoming blood and
the hepatic venous for outgoing blood.
Acute portal vein thrombosis
Acute portal venous thrombosis has multiple
causes, including septic thrombophlebitis [27], as-
sociated pancreatitis, and hypercoagulable states,
Fig. 21. Portal vein thrombosis. (A) Longitudinal US in a patient
portal vein (arrows) is distended and hypoechoic with no flow on c
portal vein (arrow), which fails to enhance. Thrombus also involv
including stem cell transplantation [28]. Septic throm-
bophlebitis has a mortality rate as high as 50% [27].
The most common cause is diverticulitis, with inflam-
matory bowel disease, bowel perforation, and suppu-
rative pelvic and pancreatitis infections as potential
sources. Most patients present with sepsis, fever,
chills, and upper abdominal pain because the primary
bowel source is often asymptomatic [27].
Patients without sepsis and acute portal vein
thrombosis present with nonspecific right upper
quadrant or epigastric pain. Some patients also have
abnormal liver function tests without hyperbilirubi-
nemia [29]. On US, the portal vein is dilated and may
be completely anechoic, but it is more often filled
with low-level echoes and shows no flow on color or
power Doppler (Fig. 21). The main portal vein is seen
on 97% of upper abdominal US [30]. Failure to
visualize a patent main portal vein on gray scale
and Doppler US should indicate portal vein throm-
bosis. False-positive results may occur in patients
with slow flow caused by portal hypertension. In
these cases, maximum Doppler sensitivity should be
achieved with low wall filter and lower Doppler
angles and lower Doppler frequencies to improve
penetration at depth. Spectral Doppler always should
be used to confirm absent flow on color or power
Doppler images [29]. If flow remains absent but no
thrombosis can be visualized, contrast-enhanced US,
CT, or MR imaging could be used to confirm the
presence of thrombosis [31]. In the subacute to
chronic phase, older thrombosis becomes hyper-
echoic and recanalizes, or the patient forms collater-
als. These smaller multiple portal channels are called
cavernous transformation of the portal vein. On
with right upper quadrant pain on oral contraceptives. The
olor Doppler. (B) Contrasted CT scan shows low-attenuation
es the splenic vein (paired arrows).

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 275
spectral Doppler they have the typical monophasic
spectral waveform of the portal system.
Acute hepatic venous thrombosis
Acute hepatic venous thrombosis is otherwise
known as Budd-Chiari syndrome. This rare entity
results from venous obstruction usually caused by
thrombosis of the hepatic veins, although proximal
suprahepatic webs or obstruction of the inferior vena
cava (IVC) also can cause it [30,31]. Etiologic factors
include hypercoagulable states, including pregnancy,
birth control pill use, and post–bone marrow trans-
plant status, and other malignancies, including hepa-
toma, which may directly invade the veins [30].
Patients present with abdominal pain, ascites, and liver
enlargement. US findings include abnormal flow in
one or more hepatic veins [32]. Flow may be absent or
completely monophasic on spectral Doppler, which
indicates loss of cardiac pulsatility because of inter-
ruption between the vein and the heart. Reversed or ‘‘to
and fro’’ flow also may be seen in these excluded
segments if they form collaterals with the portal veins
or the IVC [30,33]. Nonvisualization of the veins on
color or power Doppler is nonspecific because they
may be compressed in the setting of cirrhosis [32].
Portal venous flow is present, although it may be
biphasic or reversed in fairly severe cases [30]. Ob-
struction of the suprahepatic IVC also can be docu-
mented by US, visualization of the thrombus, or absent
flow in the obstructed segment. The inferior IVC and
iliacs may be patent but should have a monophasic
spectral Doppler waveform and lack the normal re-
Fig. 22. Hepatic artery thrombosis with infarction postpartum. A
failure 3 days postpartum. (A) US shows a diffusely disorgan
(arrowheads). Echogenic lines (arrows) represent gas. (B) CT scan s
ducts (arrows).
sponse to a Valsalva’s maneuver [30]. Findings may
be confirmed with either CT or MR imaging. CT in
acute cases shows global ascites and liver enlargement
with decreased attenuation in the affected areas before
contrast and heterogeneous patchy enhancement after
contrast with rim enhancement of the hepatic veins
[34]. MR imaging may show heterogeneous enhance-
ment of the hepatic parenchyma with edema and
relative caudate sparing because the caudate drains di-
rectly into the IVC and does not go through the hepa-
tic veins [35]. Severe involvement of the veins may
lead to liver failure, which requires transplantation.
Hepatic artery thrombosis
Hepatic arterial thrombosis is a major contributor
to acute hepatic dysfunction in patients after liver
transplant. In particular, the biliary ducts depend on
adequate hepatic arterial perfusion for oxygenation.
Hepatic arterial thrombosis or stenosis occurs in up to
13% of patients after liver transplant and is a major
cause of graft failure [36]. Clinically, hepatic arterial
thrombosis is suspected when liver function studies
deteriorate, fever of unknown origin occurs, or the
biliary tract is involved, with either a delayed biliary
leak secondary to ischemia or development of liver
abscesses [37]. Without treatment, mortality rate may
be as high as 70%. Graft salvage may be achieved by
arterial revision, or retransplantation may be required
[38]. The diagnosis could be made by Doppler US in
as many as 10% of patients who are clinically
asymptomatic by using aggressive US screening in
the early postoperative period (days 1–3) [37]. US
liver transplant patient presented with acute pain and liver
ized liver pattern with no discernable vessels anteriorly
hows the large infarct (arrowheads) and the gas in the biliary

Fig. 23. Hemorrhagic adrenal adenoma. Patient presented with fever and acute right upper quadrant pain. Clinically the attending
surgeon was convinced she had acute cholecystitis. (Left) Longitudinal US shows mass (M) posterior to retroperitoneal reflection
(arrows) and separate from kidney (K). The gallbladder was normal. (Right) Transverse CT shows non-enhancing adrenal mass
(M) caused by hemorrhage of an adrenal adenoma.
D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278276
diagnosis consists of color Doppler and spectral
Doppler examination. Absent hepatic arteries indicate
thrombosis, although vessels may be small and diffi-
cult to visualize in the immediate postoperative
patient. This may be a situation in which US contrast
is useful. If flow is visualized in the vessels, a
resistive index is obtained (peak systolic velocity =
end diastolic velocity divided by systolic velocity). A
resistive index of less than 0.5 or acceleration from
beginning of systolic to systolic peak of more than
0.08 seconds yields 73% to 81% sensitivity for
hepatic thrombosis or stenosis [39,40]. Additional
diagnostic criteria include a resistive index of 1 in
the extrahepatic artery with no flow visualized in the
intrahepatic arteries [37]. Confirmation of US find-
ings is usually performed angiographically. Prompt
revascularization or retransplantation is desirable be-
cause asymptomatic patients may achieve up to an
80% graft salvage rate versus 43% on symptomatic
patients [37]. Massive acute hepatic arterial throm-
bosis may result in liver infarction (Fig. 22).
Acute right upper quadrant pain, outside the
hepatobiliary system
The differential diagnosis for patients with right
upper quadrant pain is extensive and includes pneu-
monia, appendicitis, peritoneal tumor, primary bowel
disease, pancreatitis, and peritonitis caused by either
bowel or pelvic pathology, such as hemorrhagic
adnexal masses. Retroperitoneal processes, such as
renal infarction, renal obstruction, and renal or adre-
nal hemorrhage (Fig. 23), also can present occasion-
ally with right upper quadrant pain, which mimics
acute cholecystitis.
Summary
In summary, US is the initial imaging modality for
the evaluation of acute right upper quadrant pain. It
permits accurate diagnosis of acute cholecystitis and
successfully identifies multiple other causes of patient
symptomatology. Some of these processes lie outside
the hepatobiliary system and include renal infection
and obstruction, pancreatitis and its sequelae, duode-
nal or colonic perforation or mass lesions, peritoneal
tumor spread, adrenal hemorrhage, and even remote
problems, such as pneumonia. The limitations on US
include incomplete imaging of the liver, most often at
the dome or beneath ribs on the surface, and incom-
plete visualization of lesion boundaries, particularly
with some infections and tumors. For these clinical
scenarios, contrast-enhanced CT is complementary to
US and should be encouraged. In the biliary tree, US
has limitations in situations in which the ducts are not
dilated and sometimes with imaging the extrahepatic
ducts, especially distally. For these patients, CT or
MR imaging (MRCP) is especially useful. If one
keeps the clinical scenario in mind and always images
a patient where he or she hurts, US is a powerful and
effective diagnostic method for evaluating acute right
upper quadrant pain.

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278 277
References
[1] Laing FC. The gallbladder and bile ducts. In: Rumack
CM, Wilson SR, Charboneau JW, editors. 2nd edition.
Diagnostic ultrasound, volume 1. St. Louis: Mosby-
Year Book; 1998. p. 175–223.
[2] Gore RM, Yaghmai V, Newmark GM, Berlin JW,
Miller FH. Imaging benign and malignant disease of
the gallbladder. RCNA 2002;40(6):1307–23.
[3] Coopersberg PL, et al. Imaging of the gallbladder. Ra-
diology 1987;163:605–13.
[4] Ralls PW, Colletti PM, Lapin SA, et al. Real-time
sonography in suspected acute cholecystitis. Radiology
1985;155:767–71.
[5] Laing FC, Jeffrey Jr RB. Choledocholithiasis and cys-
tic duct obstruction: difficult ultrasonographic diagno-
sis. Radiology 1983;146:475–9.
[6] Hough DM, Glazebrook KN, Paulson ER, et al. Value
of prone positioning in the ultrasonographic diagnosis
of gallstones: prospective study. J Ultrasound Med
2000;19:633–8.
[7] Choudry S, Gorman B, Charboneau JW, et al. Com-
parison of tissue harmonic imaging with conventional
us in abdominal disease. Radiographics 2000;20:
1127–35.
[8] Hong HS, Han JK, Kim TK, et al. Ultrasonic evalua-
tion of the gallbladder. J Ultrasound Med 2001;20:
35–41.
[9] Teefey SA, Baron RL, Bigler SA. Sonography of the
gallbladder: significance of striated (layered) thicken-
ing of the gallbladder wall. AJR Am J Roentgenol
1991;156:945–7.
[10] Teefey SA, Baron RL, Radke HM, et al. Gangrenous
cholecystitis: new observations on sonography. J Ul-
trasound Med 1991;10:603–6.
[11] Kalliafas S, Ziegler DW, Flancbaum L, et al. Acute
acalculous cholecystitis: incidence, risk factors, diag-
nosis, and outcome. Am Surg 1998;64(5):471–5.
[12] Cornwell EE, Rodriguez A, Mirvis SE, et al. Acute
acalculous cholecystitis in critically injured patients.
Ann Surg 1989;219(1):52–5.
[13] Blankenberg F, Wirth R, Jeffrey RB, et al. Computed
tomography as an adjunct to ultrasound in the diagnosis
of acute acalculous cholecystitis. Gastrointest Radiol
1991;196:149–53.
[14] Habib FA, Kolachalam RB, Khilnani R, et al. Role
of laparoscopic cholecystectomy in the management
of gangrenous cholecystitis. Am J Surg 2001;181:
71–5.
[15] Simeone JF, Brink JA, Mueller PR, et al. The sono-
graphic diagnosis of acute gangrenous cholecystitis:
importance of the Murphy sign. AJR Am J Roentgenol
1989;152:289–90.
[16] Takada T, Yasuda H, Uchiyama K, et al. Pericholecys-
tic abscess: classification of us findings to determine
the proper therapy. Radiology 1989;172:693–7.
[17] Forsberg L, Andersson R, Hederstrom E, et al. Ultra-
sonography and gallbladder perforation in acute cho-
lecystitis. Radiology 1988;29(2):203–5.
[18] Bloom RA, Libson E, Lebensart PD, et al. The ultra-
sound spectrum of emphysematous cholecystitis. J Clin
Ultrasound 1989;17(4):251–6.
[19] Ralls PW, Jeffrey RB, Kane RA, Robbin M. Ultra-
sonography. Gastroenterol Clin North Am 2002;31:
801–25.
[20] Withers CE, Wilson SR. The liver. In: Rumack CM,
Wilson SR, Charboneau JW, editors. 2nd edition. Di-
agnostic ultrasound, volume 1. St. Louis: Mosby-Year
Book; 1998. p. 87–154.
[21] Tchelepi H, Ralls PW, Radin R, et al. Sonography
of diffuse liver disease. J Ultrasound Med 2002;21:
1023–32.
[22] Ralls PW. Inflammatory disease of the liver. Clin Liver
Dis 2002;6(1):203–25.
[23] Usta IM, Barton JR, Amon EA, et al. Obstetrics: acute
fatty liver of pregnancy. An experience in the diagnosis
and management of fourteen cases. Am J Obstet Gyne-
col 1994;171(5):1342–7.
[24] Castro MA, Fassett MJ, Reynolds TB, et al. Reversible
peripartum liver failure: a new perspective on the di-
agnosis, treatment, and cause of acute fatty liver preg-
nancy, based on 28 consecutive cases. Am J Obstet
Gynecol 1999;181(2):389–95.
[25] Hung CH, Changchien CS, Lu SN, et al. Sonographic
features of hepatic adenomas with pathologic correla-
tion. Abdom Imaging 2001;26(5):500–6.
[26] Terkivatan T, de Witt J, de Man RA, et al. Indications
and long-term outcome of treatment for benign hepatic
tumors: a critical appraisal. Arch Surg 2001;136(9):
1033–8.
[27] Balthazar EJ, Gollapudi P. Septic thrombophlebitis of
the mesenteric and portal veins: CT imaging. J Comput
Assist Tomogr 2000;24(5):755–60.
[28] Grigg A, Gibson R, Bardy P, et al. Acute portal vein
thrombosis after autologous stem cell transplantation.
Bone Marrow Transplant 1996;18:949–53.
[29] Sheen CL, Lampareli H, Milne A, et al. Clinical fea-
tures, diagnosis and outcome of acute portal vein throm-
bosis. QJM 2000;93(8):531–4.
[30] Zwiebel WJ. Sonographic diagnosis of hepatic vascu-
lar disorders. Semin Ultrasound CT MR 1995;16(1):
34–8.
[31] Grant EG, Schiller VL, Millener P, et al. Color Doppler
imaging of the hepatic vasculature. AJR AM J Roent-
genol 1992;159(5):943–50.
[32] Millener P, Grant EG, Rose S, et al. Color Doppler
imaging findings in patients with Budd-Chiari syn-
drome: correlation with venographic findings. AJR
Am J Roentgenol 1993;161(2):307–12.
[33] Ralls PW, Johnson MB, Radin DR, et al. Budd-Chiari
syndrome: detection with color Doppler sonography.
AJR Am J Roentgenol 1992;159(1):113–6.
[34] Didier M, Vasile V, Menu Y, et al. Budd-Chiari syn-
drome: dynamic CT. Radiology 1987;165(2):409–13.
[35] Noone TC, Semekla RC, Woosley JT, et al. Case re-
port: US and MR findings in acute Budd-Chiari syn-
drome with histopathologic correlation. J Comput
Assist Tomogr 1996;29(5):819–22.

D.J. Rubens / Radiol Clin N Am 42 (2004) 257–278278
[36] Degaetano AM, Cotroneo AR, Maresca G, et al. Color
Doppler sonography in the diagnosis and monitoring
of arterial complications after liver transplantation.
J Clin Ultrasound 2000;28(8):373–80.
[37] Garcia-Criado A, Gilarbert R, Nicolau C, et al. Early
detection of hepatic artery thrombosis after liver trans-
plantation by Doppler ultrasonography: prognostic
implications. J Ultrasound Med 2001;20(1):51–8.
[38] Sakamoto Y, Harihara Y, Nakatsuka T, et al. Rescue
of liver grafts from hepatic artery occlusion in living-
related liver transplantation. Br J Surg 1999;86(7):
886–9.
[39] Dodd GD, Memel DS, Zajko AB, et al. Hepatic artery
stenosis and thrombosis in transplant recipients: Dopp-
ler diagnosis with resistive index and systolic accelera-
tion time. Radiology 1994;192:657–61.
[40] Platt JF, Yutzy GG, Bude RO, et al. Use of Doppler
sonography for revealing hepatic artery stenosis in
liver transplant recipients. AJR 1997;168(2):473–6.

Radiol Clin N Am 42 (2004) 279–296
Venous protocols, techniques, and interpretations of the
upper and lower extremities
James D. Fraser, MDa,*, David R. Anderson, MDb
aDepartment of Diagnostic Radiology, Dalhousie University, Queen Elizabeth II Health Sciences Centre, 3rd Floor,
Victoria Building, 1278 Tower Road, Halifax, Nova Scotia, Canada B3H 2Y9bDivision of Hematology, Department of Medicine, Dalhousie University, Queen Elizabeth II Health Sciences Centre,
Victoria General Site, 4th Floor, Bethune Building, 1278 Tower Road, Halifax, Nova Scotia, Canada B3H 2Y9
Deep venous thrombosis (DVT) and pulmonary Clinical presentations
embolism (PE), collectively known as venous throm-
boembolism, are common problems and are frequent-
ly in the differential diagnosis of patients presenting
to the emergency department and in the acute care
setting. In the United States, the annual combined in-
cidence of DVT and PE is at least 70 per 100,000 in-
dividuals [1,2]. Clinical signs and symptoms of both
of these entities are nonspecific and it is important
to perform objective testing to confirm the diagnosis
and initiate appropriate therapy. This approach leads
to a demand for emergent diagnostic studies. Com-
pression ultrasonography (CUS) is the diagnostic pro-
cedure of choice for the assessment of patients with
suspected DVT. It has been shown to be highly sen-
sitive and specific for the diagnosis of DVT, particu-
larly in the lower extremities in symptomatic patients.
Bilateral leg CUS combined with assessment of the
clinical pretest probability and D-dimer testing has
also been shown safely to reduce the need for pul-
monary angiography in patients with suspected PE.
This article reviews the clinical indications, diag-
nostic techniques, and interpretation of CUS for the
assessment of DVT in the upper and lower extrem-
ities and evaluates the role of CUS in the assessment
of patients with suspected PE.
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.001
* Corresponding author.
E-mail address: [email protected] (J.D. Fraser).
Patients who eventually require assessment for
potential venous thromboembolic disease may pres-
ent with symptoms suggestive of DVT of the upper or
lower extremity, PE, or both. Most commonly, DVT
begins in the veins of the calf and moves proximally
with time. Patients who present with acute calf-
popliteal vein thrombosis experience pain and swell-
ing in the calf of one leg, which is exacerbated with
ambulation and improved with rest. There may be
associated warmth, redness, and tenderness in the calf
area [3]. Over time, these symptoms tend to become
more severe and may progress proximally to the
popliteal fossa and into the medial thigh area. On
average, these patients’ symptoms persist for about
7 days before presenting for medical assessment
[4,5]. Less than 20% of patients who are confirmed
to have lower-extremity DVT have thrombi isolated
to the calf veins.
In approximately 10% of patients with lower-
extremity DVT, the thrombus is isolated in the
iliofemoral region (Fig. 1) [6]. These patients initially
present with symptoms of pain in the buttock or
groin region, which over time extend to the medial
thigh and cause swelling and dusky discoloration of
the proximal leg. Superficial veins in the groin and
proximal thigh become prominent because of venous
engorgement [7]. Iliofemoral disease is a common
presentation of DVT during pregnancy with over
90% occurring on the left side usually caused by
extrinsic compression of the left iliac vein. Iliofe-
s reserved.

Fig. 1. Iliofemoral DVT. A 35-year-old pregnant woman with isolated iliofemoral DVT, who presented with left buttock pain.
(A) Longitudinal image with color flow Doppler shows a small amount of spontaneous venous flow around the thrombus (T).
(B) A transverse image of the iliac with compression was obtained with the maximum compressed anteroposterior diameter
measured. Normal compressibility of the (C) superficial femoral vein and (D) popliteal veins (arrowheads), which are free of
thrombus. Arrowheads in (A) and (B) delineate the left iliac vein. The arrows in (C) and (D) designate the accompanying artery.
The asterisk in (C) denotes the deep femoral artery branch. Note the superficial position of the vein relative to the artery in the
popliteal fossa.
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296280

Fig. 1 (continued).
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 281
moral DVT is associated with pelvic masses, recent
pelvic surgery, oral contraceptive use, and the anti-
phospholipid antibody syndrome.
In contrast, patients presenting with upper-extrem-
ity DVT (Fig. 2) usually have thrombosis initiating in
the proximal veins (subclavian and brachiocephalic).
Pain and swelling of the proximal arm and superficial
vein distention in the upper chest and proximal arm
are commonly seen. Functional impairment also may
be present. Upper-extremity DVT most commonly
occurs in patients with malignancy and incidence is
much higher when they have indwelling central ve-
nous catheters. It occasionally occurs in otherwise
healthy individuals or following strenuous upper-
extremity exercise, such as weight lifting [8].
Patients with acute PE may present with dyspnea,
pleuritic chest pain, dizziness, and loss of conscious-
ness with or without symptoms of DVT. Tachypnea,
tachycardia, and hypotension may be noted on phys-
ical examination. The range of presentation of PE is
great, from minimal chest symptoms to life-threaten-
ing shock.
The role of ultrasound in the evaluation of
thromboembolic disease
Because of the nonspecific nature of the presen-
tation of venous thromboembolic disease, clinical
assessment is certainly not sufficient to make a
diagnosis. Given the possible serious consequences
of a misdiagnosis, objective testing for DVT and PE
is crucial.
In the lower extremities, CUS is the method of
choice to evaluate patients with symptoms suspected
to be DVT. The sensitivity and specificity exceeds
97% for the diagnosis of DVT involving the proximal
leg veins. Accuracy studies using CUS for evaluation
of the calf veins have been relatively few and have
demonstrated much greater variation. The range of
sensitivities varies between 11% and 100%, whereas
the specificity ranges between 90% and 100% [9–12].
A meta-analysis of methodologically high-quality
studies reported the sensitivity of CUS for the diag-
nosis of DVT isolated to the calf to be 73% [11]. The
rate of technically inadequate studies has been re-
ported to be much higher than those for the evaluation
of proximal DVT (ie, in the range of 20%–40%)
[12,13].
In contrast to patients with suspected DVT of the
lower extremities, the validity of ultrasound for the
evaluation of upper-extremity DVT is less well estab-
lished. In a recent systematic review of the sensitivity
and specificity of ultrasonography in the diagnosis of
upper-extremity DVT, Mustafa et al [14] found only
six original prospective studies, only one of which
met their predefined criteria for adequately determin-
ing sensitivity and specificity and included a total of
58 patients [8]. The sensitivity of duplex ultrasound
from this review ranged from 56% to 100% with a
specificity ranging from 94% to 100%. None of
these studies evaluated the safety of withholding
anticoagulation therapy in a patient with a negative
result on ultrasound evaluation who did not undergo
further testing and concluded that the safety of this
approach is uncertain [14]. More recently in a pro-
spective study published in 2002 comparing color
Doppler with contrast venography in 126 patients,
Baarslag et al [15] reported a sensitivity and speci-
ficity of 82%. He also noted that incompressibility of
the vein during ultrasound correlated well with
thrombus, whereas only 50% of isolated flow-related
abnormalities proved to be thrombus-related. He
concluded that patients with isolated flow abnormal-

Fig. 2. Upper-extremity DVT. Cancer patient who developed a painful swollen right arm secondary to extensive DVT of the
upper extremity. (A) Longitudinal color flow image of the internal jugular vein with spontaneous flow above the thrombus.
(B) Thrombus (arrow) can be seen within the distal jugular vein (arrowheads). (C) Clot is seen (arrowheads) extending down to
the confluence with the subclavian vein (arrows). (D) Color flow Doppler demonstrates complete occlusion of the subclavian
vein (arrowheads). The presence of clot in the axillary (arrowhead) vein (E) and basilic vein (arrowhead) (F) is confirmed
because of the inability to compress the vein in the transverse plane. The arrows denote the associated arteries.
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296282
ities on duplex color ultrasound should have contrast
venography performed for further evaluation.
The optimal strategy to diagnose PE remains
controversial. Spiral CT and ventilation-perfusion
scanning are used routinely for the evaluation of
patients with suspected PE, but neither test is partic-
ularly sensitive. Ultrasonography may be added to
diagnostic algorithms for suspected PE to increase
the sensitivity of noninvasive testing because most
PEs are believed to originate in the veins of the legs.
Patients with nondiagnostic pulmonary investigation
may be confirmed to have venous thromboembolism
by leg ultrasonography and thereby avoid the need
for angiography [16]. A definitive diagnosis or ex-
clusion of PE may not be possible at the initial
presentation using noninvasive testing. Most cases
of DVT (approximately 90%) start in the calf and
rarely cause clinically important PE unless they

Fig. 2 (continued).
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 283
extend into the proximal deep venous system. Eighty
percent of clots isolated to the calf are asympto-
matic; however, if left untreated approximately 25%
extend to involve the proximal veins. This usually
occurs within the first week or so after presentation.
Seventy-five percent of patients diagnosed with PE
have DVT, two thirds of which are located in the
proximal veins (Fig. 3). Up to one-quarter of patients
with symptomatic PE have clinical evidence of DVT
[17]. Given this information, various algorithms have
been developed that incorporate the use of CUS in the
work-up of patients with suspected PE (Fig. 4).
Clinical assessment and the use of D-dimer
Clinical assessment
Although the clinical presentation of DVT is
nonspecific and clinical assessment alone is unreli-
able, recent studies have shown that with explicit
clinical criteria, patients can be categorized accurately
into high, moderate, or low pretest probability groups
based solely on a clinical evaluation [18]. These
criteria combine the signs and risk factors for DVT
and take into consideration the likelihood of an

Fig. 2 (continued).
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296284
alternate diagnosis as the cause for the patient’s
presentation. A simple, nine-point clinical criteria
scoring system has been developed to determine the
pretest probability for DVT (Table 1) [19]. Using
such criteria, patients with a high pretest probability
have a greater than 75% prevalence of DVT con-
firmed by objective testing. Patients in whom the
diagnosis of DVT cannot be excluded on clinical
grounds but who have a low pretest probability have
less than a 5% prevalence of DVT. The use of this
clinical categorization tool has proved to be a valu-
able adjunct to noninvasive testing for the evaluation
of patients with suspected DVT and PE [16,20,21].
D-dimer
Several serologic markers of thrombosis have
been investigated for their predictive value in the
diagnosis of DVT. The test that has emerged as the
most useful is the D-dimer test. D-dimer represents a
breakdown product of the cross-linked fibrin clot.
Several D-dimer assays have been validated to be
sensitive but nonspecific markers of DVT and PE,
indicating that a positive test has a low predictive
value but a negative test has a reported negative
predictive value of more than 97% [16,22–29].
Combinations of clinical assessment and D-dimer

Fig. 3. Lower-extremity DVT with PE. Patient presenting with shortness of breath and chest pain who underwent chest CT as
per PE protocol. (A) It revealed bilateral pulmonary emboli (arrowheads). CUS of the legs confirmed DVT involving the
popliteal and superficial femoral veins (arrowheads) to the mid thigh (B,C) with normal venous flow and no clot present within
the superficial femoral veins (arrowheads) above the mid thigh (D). Arrows in (B) and (C) designate the accompanying arteries.
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 285

Fig. 3 (continued).
Table 1
Clinical evaluation table for predicting pretest probability of
deep vein thrombosis
Clinical characteristics Score
Active cancer (treatment ongoing, within
previous 6 mo or palliative)
1
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296286
results have been shown safely to reduce or eliminate
the need for noninvasive testing in certain patient
groups [30,31]. For example, patients with a low
suspicion of DVT or PE but in whom a diagnosis
cannot be excluded on clinical assessment alone may
safely avoid the need for radiographic imaging on the
basis of a negative D-dimer study (see Figs. 4–6). D-
dimer is less useful for excluding venous throm-
boembolism in hospital patients, particularly those
having had major surgery or trauma in whom the test
is highly likely to be positive [32].
A variety of D-dimer assays have been validated
for diagnostic testing for venous thromboembolism.
The accuracy parameters of these assays (sensitivity,
specificity) vary and physicians need to be aware of
these and of the validated laboratory cut-off points
for defining a positive and negative test.
Non-diagnostic Ventilation Perfusion (VQ)/Computerized axial Tomography (CT) Scan
Bilateral Compression Ultrasound (CUS)
Pretest Probability (PTP) + D-dimer (DD)
Low PTPor - DD
Mod/High PTPand + DD
PE excluded Pulmonary angiogram or 1 wk CUS
Treat for PE
+
+ -
Fig. 4. Algorithm for investigation of patients with sus-
pected PE. CUS, compression ultrasound; DD, D-dimer; PE,
pulmonary embolism; PTP, pretest probability.
Ultrasound technique for the evaluation of deep
venous thrombosis of the extremities
Lower extremities
The venous anatomy of the lower extremity is
shown in Fig. 7. CUS of the deep venous system of
the lower extremities is performed with the patient
in the supine position ideally with the head elevated
Paralysis, paresis, or recent plaster
immobilization of the lower extremities
1
Recently bedridden > 3 d or major surgery
within 12 wk requiring general or regional
anesthesia
1
Localized tenderness along the distribution
of the deep venous system
1
Entire leg swollen 1
Calf swelling 3 cm larger than asymptomatic
side (measured 10 cm below tibial tuberosity)
1
Pitting edema confined to the symptomatic leg 1
Collateral superficial veins (nonvaricose) 1
Alternative diagnosis at least as likely as deep
vein thrombosis
�2
A score of 3 or higher indicates a high probability of deep
vein thrombosis; 1 or 2, a moderate probability: and 0 or
lower, a low probability. In patients with symptoms in both
legs, the more symptomatic leg is used.

Clinically Suspected DVT
Pretest Probability (PTP)
Low
D-dimer (DD) Compression Ultrasound (CUS)
DD/PTP
DVT Excluded
Low PTPor - DD
Mod/High PTPand + DD
Venogram Treat for DVT
- +
+ -
-
+
Moderate/High
Fig. 6. Algorithm for suspected DVT in the upper extremity.
CUS, compression ultrasound; DD, D-dimer; DVT, deep
vein thrombosis; PTP, pretest probability.
Clinically Suspected Deep Vein Thrombosis (DVT)
Pretest Probability (PTP)
Low
D-dimer (DD) Compression Ultrasound (CUS)
DD/PTP
DVT Excluded
Low PTPor - DD
Mod/High PTPand + DD
1 wk CUS Treat for DVT
-
+
+
+-
-
Moderate/High
Fig. 5. Algorithm for clinically suspected DVT. CUS,
compression ultrasound; DD, D-dimer; DVT, deep vein
thrombosis; PTP, pretest probability.
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 287
20 to 30 degrees to promote venous pooling and
distention of the veins. A linear transducer with a
frequency in the 5- to 10-MHz range is used, ideally
with duplex and color Doppler capability, although
these are not required but can be helpful in localizing
the vessels and characterizing their flow. The leg is
rotated externally and flexed slightly at the knee. The
transducer is placed transversely in the groin area to
identify the common femoral vein just medial to the
common femoral artery. Gentle pressure is applied to
the vessels with the transducer and in the absence of
DVT, the lumen of the vein should collapse with
complete apposition of the anterior and posterior walls
(see Fig. 1C, D). In the presence of DVT, the lumen
does not collapse completely even with enough pres-
sure to occlude the adjacent artery (Fig. 8). This
compression is performed at 1-cm intervals moving
down the leg following the common femoral vein,
superficial femoral vein, and popliteal vein until it
divides into the three calf branches at the popliteal
trifurcation. Compression of the veins within the
muscular adductor (Hunter’s) canal is often difficult
and visualization limited because of the depth of the
vein. This can usually be overcome by placing one
hand underneath the medial aspect of the distal thigh
and compressing the vein between the fingers and the
transducer. This not only aids in compressing the
vein but also brings the vein closer to the transducer
head, allowing better visualization.
Scanning along the axis of the vein is often ad-
vantageous for following the course of the vein and
for assessing flow (see Figs. 2A, 3D). It is important,
however, to confirm compressibility in the transverse
plane; compression in the longitudinal plane is unre-
liable because the transducer may slide off the vessel,
possibly resulting in a false-negative interpretation.
In a mobile patient, the popliteal vein is assessed
most easily with the patient in the lateral decubitus or
prone position with the knee passively flexed to
approximately 10 to 15 degrees to avoid collapse of
the vein. Very often the patient is not able to move
from the supine position but the popliteal vein can
usually be assessed adequately by lifting the affected
leg with a hand sufficiently under the distal thigh to
place the transducer behind the knee. The popliteal
vein is superficial to the popliteal artery (see Fig. 1D)
in the popliteal fossa and can be compressed easily by
the extended knee. It is important to keep the knee
slightly flexed while interrogating the popliteal vein.
There remains controversy over the value of
performing CUS of the calf veins if the more proximal
veins are normal. Approximately 10% to 20% of
patients with symptomatic DVT have thrombus iso-
lated to the calf veins of, which 20% to 30% eventu-
ally extend into the proximal venous system [33,34].
The positive predictive value of CUS for detecting
DVT in the calf is significantly lower than it is for
proximal DVT, and there are a relatively large number
of cases in which the studies are considered non-
diagnostic or inadequate. Reported rates of nondiag-
nostic studies vary in the literature from 9.3% to
82.7%. Gottlieb et al [35] had a nondiagnostic rate
of 41% for the evaluation of calf veins. The same
study found no significant difference in adverse out-
comes in patients undergoing a protocol in which the
deep calf veins were routinely evaluated or a protocol
in which the calf was evaluated only if physical signs
or symptoms were present.

Inferior vena cava
Common iliac vein
External iliac vein
Common femoral vein
Superficial femoralvein
Great saphenous vein(superficial)
Poplitealvein
Anteriortibial vein
PeronealveinSmallSaphenous(superficial)
Posteriortibial vein
Poplitealvein
Peronealvein
Anterior tibialvein
Fig. 7. Diagrammatic representation of the veins of the lower extremity.
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296288
The authors have previously described the tech-
nique for the evaluation of the calf veins [1]; however,
their present protocols for the evaluation of patients
with suspected thromboembolic disease do not in-
clude evaluation of the calf and the technique is not
discussed in this article. It should be stressed, how-
ever, that when assessing the proximal venous system,
one should ensure that the examination includes the
distal popliteal vein all the way down to its trifurca-
tion point to have the highest possible sensitivity for
DVT. In addition, if there is focal tenderness or
swelling within the calf region, it is useful to scan
this area to evaluate for nonvenous focal pathology,
such as a hematoma, which might explain the pa-
tient’s symptoms.
Upper extremities
The venous anatomy of the upper extremity is
shown in (Fig. 9). The technique for evaluating the
upper extremities for DVT is similar to that for the
lower extremities; however, compression of the deep
venous system is more limited particularly in the area
where the subclavian vein passes beneath the clavi-
cle. Because of this limitation, technical modifications
are required, such as the use of adjunctive procedures

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 289
and the findings of Doppler and color flow Doppler
analysis (see Fig. 2). Once again, a linear transducer
with a frequency in the 5- to 10-MHz range with
Doppler or color flow Doppler is preferable. With the
patient in the supine position, the head is tilted slightly
away from the side of interrogation. It is often easiest
to begin by evaluating the internal jugular vein,
following this down to the confluence with the sub-
clavian vein (see Fig. 2C), which is located under the
proximal third of the clavicle, and is best visualized
by placing the transducer longitudinally along the
Fig. 8. Extensive lower-extremity DVT involving the iliac vein.
involving the popliteal vein (A) and extending up to involve the supe
(C) (arrowheads), all of which are not compressible despite sufficie
course of the vessel just below the clavicle and
angling it slightly cephalad. The vein can be differen-
tiated from the adjacent artery by its generally larger
size, lack of internal pulsations, and its vascular flow
pattern as assessed by Doppler. Attempts to compress
the vein with the transducer in the transverse plain
often fail because of the presence of the clavicle. At-
tempts should then be made to compress the vein with
the transducer along the length of the vessel. If
compression is not possible, one must evaluate with
spectral or color flow Doppler to determine if the lack
Patient with painful swollen left leg with extensive DVT
rficial femoral veins (not shown), CFV (B), and the iliac vein
nt pressure to partially compress the adjacent artery (arrows).

Fig. 8 (continued).
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296290
of compressibility is caused by thrombus or by over-
lying structures preventing adequate force to be trans-
mitted to the vein. The subclavian vein is followed
distally to the axillary, cephalic, brachial, and basilic
veins, which are assessed with transverse compression
similar to the evaluation of the lower-extremity veins
(see Fig. 2E, F). Assessment of the axillary, brachial,
and basilic veins is performed using an axillary ap-
proach by raising the arm. High in the axilla, the vein is
superficial to the artery [36]. In such areas as the sub-
clavian where the vein may not be accessible to com-
Internal jugular veinExternal jugular vein
Subclavian vein
Axillary vein
Cephalic vein
Brachial vein
Basalic vein
Median cubital vein
Fig. 9. Diagrammatic representation of the veins of the upper lim
superior vena cava.
pression and color Doppler is used for assessment of
patency, it is important to pay close attention to the
color flow gain settings to avoid oversaturation,
which may obscure small intraluminal clots or areas
of incomplete thrombosis [37]. Similar to assessment
of the leg, if thrombosis is discovered it is important to
document the full extent of the disease including
evaluation of the contralateral neck and proximal
arm because this information may be important for
subsequent evaluation for progression or recurrence of
disease or for the effectiveness of treatment.
BCP veinSVC
b and thoracic inlet. BCP vein, brachiocephalic vein; SVC,

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 291
Diagnostic criteria for the diagnosis of deep
venous thrombosis of the extremity
In the absence of DVT, the vein being evaluated
should collapse and the walls of the vein should
be completely apposed with less pressure than re-
quired to occlude the adjacent artery. The inability
completely to compress the vein lumen is the prin-
cipal criterion for the diagnosis of DVT [6,7,38–40].
Other adjunctive findings are often observed in the
presence of DVT but have much poorer sensitivi-
ties and specificities. These include distention of
the involved vein in acute DVT and the absence of
or reduced spontaneous blood flow on Doppler
evaluation (see Fig. 8). In patients with incomp-
lete obstruction, there is usually loss of the normal
phasic respiratory venous flow pattern, often giving
a reduced continuous flow pattern (monophasic
flow), which is minimally affected by the Valsalva’s
maneuver or attempts to augment flow, such as
gently squeezing the calf. The monophasic pattern
indicates some degree of obstruction to venous flow
returning to the right side of the heart and should
increase one’s suspicion for the presence of DVT.
This pattern can also be seen, however, in the ab-
sence of thrombosis when sufficient external com-
pression on the deep venous system exists. The
appearance of the vein alone is unreliable because
acute thrombus is often anechoic mimicking a patent
vein and internal echoes are not infrequently seen
within a patent vein lumen in the presence of slow-
flowing blood.
The ultrasound appearance of DVT changes over
time with the clot retracting and becoming more
echogenic. The vein wall in the area of previous
thrombus may become thickened, echogenic, and
resistant to compression [41]. Over a 12- to 24-month
period, only about 50% of patients have complete
resolution of thrombus and normal compressibility of
the proximal leg veins [41–43]. Although the ultra-
sound appearance in patients with previous DVT may
be suggestive of chronic disease, it is usually difficult
to rule out acute or chronic disease unless the patient
has a posttreatment baseline study available for com-
parison. In the latter setting, unequivocal evidence of
thrombosis in a venous segment previously demon-
strated to be free of disease or increase in compressed
venous diameter greater than 4 mm from a baseline
study may be considered diagnostic of recurrent DVT
in the appropriate clinical setting.
Compression ultrasound occasionally diagnoses
an alternative cause for pain and swelling of the
lower extremity in the absence of DVT, such as a
ruptured Baker’s cyst or a calf hematoma (Fig. 10).
Adjunctive procedures, pitfalls, and limitations
There are a number of procedures that may be
helpful when examining a patient whose deep venous
system is difficult to localize. Placing the patient in a
position that promotes venous pooling in the extrem-
ity of interest distends the veins, making them easier
to localize and assess. Similarly, having the patient
perform a Valsalva’s maneuver also results in venous
distention [7]. When duplex or color flow Doppler is
available, it can be used to localize the venous system
based on its flow characteristics. The presence of
spontaneous flow, normal respiratory phasic flow
variation, and flow augmentation with manual com-
pression of the limb suggests patency. It is, however,
important to remember that spontaneous flow and
flow augmentation can occur in the presence of
incomplete thrombosis (see Fig. 1A), adequate collat-
eralization, and in patients with duplication of the
deep venous system. Augmentation may even force
blood around an area of complete thrombosis and
should probably be used only to aid in the localization
of venous segments that are difficult to visualize.
Patients in whom adequate compression studies of
the proximal deep venous system may be difficult to
perform include obese patients, patients with tense
swollen extremities, burn patients, and patients with
recent surgery in the area of interest. These limitations
seldom preclude evaluation of the areas where DVT
most commonly occurs (ie, the common femoral and
popliteal veins).
Pitfalls occasionally encountered include missing
a thrombosed vein segment when a nonthrombosed
duplicated vein segment is present (Fig. 11) and
occasionally mistaking a large collateral for a patent
venous segment when thrombosis is present in the
underlying vein. The latter can usually be avoided by
confirming the normal course of the vein in relation-
ship to the adjacent artery.
Suggested protocols
Diagnosis of acute deep venous thrombosis of the
lower extremities
To maximize patient safety and the efficiency of
resources, clinicians should be encouraged to follow
validated nomograms that encompass consideration
of clinical probability, D-dimer testing, and venous
ultrasound imaging. The algorithm outlined in Fig. 5
has been demonstrated to be safe for patients with
low pretest probability for DVT because only less
than 1% of these patients, if left untreated, develop

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296292

Fig. 11. Duplicated superficial femoral and popliteal veins. Patient with symptomatic DVT who has duplication of the poplit-
eal veins (A) and the superficial femoral veins (B) of the leg. Noncompressible clot is seen within the more superficial of the two
deep veins at both levels (2), with the deeper vein (1) demonstrating normal compressibility (A,B). Duplication of the artery
within the popliteal fossa is appreciated only on the color Doppler images with a more superficial artery (A) and a deeper
J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 293
objective evidence of DVT or PE in follow-up over
a 3-month period.
The ultrasound examination in this algorithm is
restricted to the proximal venous system. Pretest
probability should be judged either by experienced
clinicians or by using a validated clinical model.
D-dimer testing should be done using a validated as-
say for the diagnosis of venous thromboembolism.
Fig. 10. Calf hematoma. Patient who presented to the emergency
DVT. The deep venous system (arrowheads) within the common
with normal compressibility. A hematoma was discovered (arrow
muscles (C), explaining the patient’s calf pain and tenderness.
Using this approach, most patients can have a diag-
nosis of DVT confirmed or excluded on initial
testing. Recognizing that a small proportion of
patients may have DVT isolated to the calf veins, it
is advisable that these higher-risk patients as defined
by moderate or high pretest probability and positive
D-dimer should have the ultrasound repeated ap-
proximately 1 week following their initial evaluation.
department with a painful swollen calf area suspicious for
femoral (A) and popliteal regions (B) demonstrates patency
s) between the heads of the gastrocnemius and the soleus

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296294
This is to detect patients whose calf DVT may have
extended to the proximal venous system, which has
thereby increased the risk of PE.
Diagnosis of deep venous thrombosis of the upper
extremities
Unfortunately, validated diagnostic algorithms
are not available for patients presenting with DVT
of the upper extremity. There also are no models to
assist clinicians in determining pretest probability.
Fig. 6 contains an algorithm based on one of the
principles of DVT investigation of the lower extrem-
ities with the recognition that CUS is less sensitive in
the evaluation of the upper extremities. This algo-
rithm is based on the opinion and clinical experience
of the authors. It is their opinion that venography
should be performed in patients in whom the clin-
ical suspicion of upper extremity DVT is moderate or
high, D-dimer is positive, and the ultrasound is neg-
ative. As a second option, a repeat ultrasound may
be performed 1 week later; however, the safety of
this approach has not been demonstrated in con-
trolled trials.
Diagnosis of pulmonary embolism
Ultrasonography is particularly valuable in the
investigation of patients in whom PE is not conclu-
sively confirmed or refuted by other radiographic
imaging techniques. Patients with high-probability
ventilation-perfusion lung scans or positive spiral
CT may be treated for PE. Those with normal venti-
lation-perfusion scans may be considered to have PE
excluded. For patients with abnormal ventilation-per-
fusion scans that are not high probability or with
normal spiral CT scans, however, a significant pro-
portion may have underlying PE. It is recommended
that these patients undergo bilateral ultrasound imag-
ing of the proximal venous system of the lower ex-
tremities. Those with positive studies may be treated
for venous thromboembolism. Those patients with
negative ultrasound investigations have a much lower
likelihood of having PE responsible for their symp-
toms. Clinical trials have demonstrated that patients
with suspected PEs who have the combination of
negative spiral CT and bilateral CUS may safely have
the diagnosis of PE excluded [44–46]. Patients with
non–high-probability ventilation-perfusion scans
with normal spiral CT may have the diagnosis of
PE excluded if clinical pretest probability is low or the
D-dimer is negative. Other patients should be consid-
ered for 1-week follow-up CUS or pulmonary angi-
ography, particularly if the clinical pretest probability
is high.
Other considerations
Frequently, patients with suspected venous throm-
boembolism present at inopportune times when im-
mediate access to diagnostic testing may not be
available. With the advent of low-molecular-weight
heparin, diagnostic testing can be scheduled safely
within 24 hours of presentation. Such patients may
receive a single dose of subcutaneous low-molecular-
weight heparin designed to treat DVT or PE while
awaiting diagnostic testing [16,30]. The only restric-
tion to this regimen is that patients are at increased risk
of major bleeding.
References
[1] Fraser JD, Anderson DR. Deep venous thrombosis:
recent advances and optimal investigation with US.
Radiology 1999;211:9–24.
[2] Anderson DR, Wells PS. Improvements in the diagnos-
tic approach for patients with suspected deep vein
thrombosis for pulmonary embolism. Thromb Haemost
1999;82:878–86.
[3] Cogo A, Lensing AWA, Prandoni P, Hirsh J. Dis-
tribution of venous thrombosis in patients with symp-
tomatic deep vein thrombosis: implications for
simplifying the diagnostic process with compression
ultrasound. Arch Intern Med 1993;153:2777–80.
[4] Birdwell BG, Raskob GE, Whitsett TL, et al. The clini-
cal validity of normal compression ultrasonography
in outpatients suspected of having deep venous throm-
bosis. Ann Intern Med 1998;128:1–7.
[5] DeBaleu ME, Ochner A. Phlegmasia cerulea dolens
associated with thrombophlebitis: case reports and re-
view of the literature. Surgery 1966;59:997–1007.
[6] Cronan JJ. Venous thromboembolic disease: the role
of US. Radiology 1993;186:619–30.
[7] Cogo A, Lensing AWA, Wells P, Prandoni P, Buller
HR. Noninvasive objective tests for the diagnosis of
clinically suspected deep-vein thrombosis. Haemo-
stasis 1995;25:27–39.
[8] Prandoni P, Polistena P, Bernardi E, et al. Upper-
extremity deep vein thrombosis: risk factors, diagnosis
and complications. Arch Intern Med 1997;157:57–62.
[9] Simons GR, Skibo LK, Polak JF. Utility of leg ultra-
sonography in suspected symptomatic isolated calf
deep venous thrombosis. Am J Med 1995;99:43–7.
[10] Atri M, Herba MJ, Reinhold C, et al. Accuracy of
sonography in the evaluation of calf deep vein throm-
bosis in both postoperative surveillance and symptom-
atic patients. AJR Am J Roentgenol 1996;166:1361–7.
[11] Kearon C, Julian JA, Newman TE, Ginsberg JS.

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296 295
Noninvasive diagnosis of deep venous thrombosis:
McMaster diagnostic imaging practice guidelines
initiative. Ann Intern Med 1998;128:663–77.
[12] Rose SC, Zwiebel WJ, Nelson BD, et al. Symptomatic
lower extremity deep venous thrombosis: accuracy,
limitations, and role of color duplex flow imaging in
diagnosis. Radiology 1990;175:639–44.
[13] Noren A, Ottosson E, Rosfors S. Is it safe to withhold
anticoagulation based on a single negative color duplex
examination in patients with suspected deep venous
thrombosis? A prospective 3-month follow-up study.
Angiology 2002;53:521–7.
[14] Mustafa BO, Rathbun SW, Whitsett TL, Raskob GE.
Sensitivity and specificity of ultrasonography in the
diagnosis of upper extremity deep vein thrombosis: a
systematic review. Arch Intern Med 2002;162:401–4.
[15] Baarslag H-J, van Beek EJR, Koopman MWM, Reek-
ers JA. Prospective study of color duplex ultrasonog-
raphy compared with contrast venography in patients
suspected of having deep venous thrombosis of the
upper extremities. Ann Intern Med 2002;136:865–72.
[16] Wells PS, Anderson DR, Rodger M, Stiell I, Dreyer J,
Barnes D, et al. Excluding pulmonary embolism at
the bedside without diagnostic imaging: management
of patients with suspected pulmonary embolism pre-
senting to the emergency department using a simple
clinical model and D-dimer. Ann Intern Med 2001;
135:98–107.
[17] Kearon C. Natural history of venous thromboembo-
lism. Circulation 2003;107:I22–30.
[18] Wells PS, Hirsh J, Anderson DR, et al. Accuracy of
clinical assessment of deep-vein thrombosis. Lancet
1995;345:1326–30.
[19] Anderson DR, Wells PS, Stiell I, MacLeod B, Simms
M, Gray L, et al. Use of a clinical diagnosis model to
safely avoid the need for urgent radiological investiga-
tion. Arch Intern Med 1999;159:477–82.
[20] Wells PS, Anderson DR, Bormanis J, et al. Value
of assessment of pretest probability of deep-vein
thrombosis in clinical management. Lancet 1997;350:
1795–8.
[21] Kearon C. Diagnosis of pulmonary embolism. CMAJ
2003;168:183–94.
[22] Wells PS, Anderson DR, Rodger M, Forgie M, Kearon
C, Kovacs G, et al. Evaluation of D-dimer in the diag-
nosis of suspected deep-vein thrombosis. N Engl J Med
2003;349:1227–35.
[23] Bounameaux H, Cirafici IP, de Moerloose P, et al.
Measurement of D-dimer in plasma as diagnostic aid
in suspected pulmonary embolism. Lancet 1991;337:
196–200.
[24] Turkstra F, van Beek JR, ten Cate JW, Buller HR. Re-
liable rapid blood test for the exclusion of venous
thromboembolism in symptomatic outpatients. Thromb
Haemost 1996;76:9–11.
[25] Bounameaux H, Schneider PA, Reber G, Moerloose P,
Krahenbuhl B. Measurement of plasma D-dimer for
diagnosis of deep venous thrombosis. Am J Clin Pathol
1989;91:82–5.
[26] Boneu B, Bes G, Pelzer H, Sie P, Boccalon H. D-Di-
mers, thrombin antithrombin III complexes and pro-
thrombin fragment 1 + 2: diagnostic value in
clinically suspected deep vein thrombosis. Thromb
Haemost 1991;65:28–32.
[27] Heaton DC, Billings JD, Hickton CM. Assessment of
D-dimer assays for the diagnosis of deep vein throm-
bosis. J Lab Clin Med 1987;110:588–91.
[28] Wells PS, Brill-Edwards P, Stevens P, et al. A novel and
rapid whole-blood assay for D-dimer in patients with
clinically suspected deep vein thrombosis. Circulation
1995;91:2184–7.
[29] Wells PS, Anderson DR, Bormanis J, Guy F, Mitchell
M, Lewandowski B. Simpli-RED D-dimer can reduce
the diagnostic tests in suspected deep vein thrombosis.
Lancet 1998;351:1405–6.
[30] Anderson DR, Kovacs MJ, Kovacs G, Stiell I, Mitchell
M, Khoury V, et al. Combined use of clinical assess-
ment and D-dimer to improve the management of
patients presenting to the emergency department with
suspected deep vein thrombosis (The EDITED Study).
Journal of Thrombosis and Haemostasis 2003;1:1–7.
[31] Anderson DR, Wells PS, Stiell I, MacLeod B, Simms
M, Gray L, et al. Management of patients with sus-
pected deep vein thrombosis in the emergency depart-
ment: combining use of a clinical diagnosis model
with D-dimer testing. J Emerg Med 2000;19:225–30.
[32] Schutgens REG, Esseboom EU, Haas FJLM, Nieuwen-
huis HK, Biesma DH. Usefulness of a semiquantitative
D-dimer test for the exclusion of deep venous throm-
bosis in outpatients. Am J Med 2002;112:617–21.
[33] Kakkar VV, Howe CT, Flanc C, Clarke MB. Natural
history of postoperative deep-vein thrombosis. Lancet
1969;2:230–2.
[34] Lagerstedt CI, Olsson CG, Fagher BO, Oqvist BW,
Albrechtsson U. Need for long-term anticoagulant
treatment in symptomatic calf-vein thrombosis. Lancet
1985;2:515–8.
[35] Gottlieb RH, Voci SL, Syed L, Shyu C, Fultz PJ,
Rubens DJ, et al. Randomized prospective study com-
paring routine versus selective use of sonography of
the complete calf in patients with suspected deep ve-
nous thrombosis. AJR Am J Roentgenol 2003;180:
241–5.
[36] Talbot SR. B-mode evaluation of peripheral veins.
Semin Ultrasound CT MR 1988;9:295–319.
[37] Machi J, Sigel B, Roberts AB, Kahn MB. Oversatura-
tion of color may obscure small intraluminal partial
occlusions in color Doppler imaging. J Ultrasound
Med 1994;13:735–41.
[38] Lensing AW, Prandoni P, Brandjes D, et al. Detection
of deep-vein thrombosis by real-time B-mode ultraso-
nography. N Engl J Med 1989;320:342–5.
[39] Raghavendra BN, Rosen RJ, Lam S, Riles T, Horii
SC. Deep venous thrombosis: detection by high-reso-
lution real-time ultrasonography. Radiology 1984;152:
789–93.
[40] Raghavendra BN, Horii SC, Hilton S, Sabramanyam
BR, Rosen RJ, Lam S. Deep venous thrombosis: detec-

J.D. Fraser, D.R. Anderson / Radiol Clin N Am 42 (2004) 279–296296
tion by probe compression of veins. J Ultrasound Med
1986;5:89–95.
[41] Cronan JJ, Leen V. Recurrent deep venous thrombosis:
limitations of US. Radiology 1989;170:739–42.
[42] Prandoni P, Lensing AWA, Cattelan AM, Cogo A,
Cuppini S, Ruol A. Outcome of abnormal compression
ultrasonography after acute deep venous thrombosis
(DVT) and its implications for diagnosis of recurrent
DVT [abstract]. Thromb Haemost 1991;66:1175.
[43] Killewich LA, Bedford GR, Beach KW, Strandness
DE. Spontaneous lysis of deep venous thrombi: rate
and outcome. J Vasc Surg 1989;9:89–97.
[44] Kearon C. Excluding pulmonary embolism with helical
(spiral) computed tomography: evidence is catching
up with enthusiasm. CMAJ 2003;168:1430–1.
[45] Musset D, Parent F, Meyer G, Maitre S, Girard P,
Leroyer C, et al. Diagnostic strategy for patients with
suspected pulmonary embolism: a prospective multi-
centre outcome study. Lancet 2002;360:1914–20.
[46] van Strijen MJ, de Monye W, Schiereck J, Kieft GJ,
Prins MH, Huisman MV, et al. Single-detector helical
computed tomography as the primary diagnostic test in
suspected pulmonary embolism: a multicenter clinical
management study of 510 patients. Ann Intern Med
2003;138:307–14.

Radiol Clin N Am 42 (2004) 297–314
Sonographic evaluation of first-trimester bleeding
Raj Mohan Paspulati, MD*, Shweta Bhatt, DMRD, DMRE, Sherif Nour, MD
Department of Radiology, University Hospitals of Cleveland, Case Western Reserve University, 11100 Euclid Avenue,
Cleveland, OH 44106, USA
Vaginal bleeding in the first trimester of preg- and external cervical os. The internal os is the
nancy is a common presentation in emergency care
facilities. About 25% of all gestations present with
vaginal spotting or frank bleeding in the first few
weeks of pregnancy; half of these progress into
miscarriage or abortion [1]. The acuity of these
symptoms may vary from occasional spotting to se-
vere hemorrhage, associated with cramping and ab-
dominal pain. The bleeding often is self-limited and
is most likely caused by implantation of the concep-
tus into the endometrium. The important causes of
first-trimester bleeding are spontaneous abortion, ec-
topic pregnancy, and gestational trophoblastic dis-
ease. The clinical assessment of pregnancy outcome
is unreliable and ultrasound (US) evaluation com-
bined with quantitative beta human chorionic gonado-
tropin (b-hCG) is an established diagnostic tool in
these patients. This article reviews the role of ultra-
sonography in the evaluation of patients presenting
with first-trimester bleeding.
Sonographic anatomy
The uterus is a pear-shaped, muscular organ that
varies greatly in size and shape depending on age and
prior pregnancies. The normal postpuberty uterus in
an adult measures approximately 7.5 to 8 cm in
length, 4 to 5 cm in width, and about 2 cm in an-
teroposterior dimension. The normal cervix is 3.5 to
4 cm in length. The cervix is comprised of internal
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.005
* Corresponding author.
E-mail address: [email protected] (R.M. Paspulati).
junction of the uterine cavity and the cervical canal
and the external os is the junction of the cervical
canal and the vagina. Transvaginal US (TVUS) of the
normal myometrium reveals three distinct layers.
Arcuate vessels separate the thin outer layer from
the thick middle layer, and both layers are homoge-
neous with the outer layer more hypoechoic relative
to the middle layer [2]. The inner layer consists of a
thin hypoechoic halo that surrounds the endometrium
and corresponds to the junctional zone seen on MR
imaging. The endometrial thickness measurements
are optimally made on sagittal (long-axis) images of
the uterus; this measurement should be performed
on the thickest portion of the endometrium excluding
the hypoechoic inner myometrium (Fig. 1). The en-
dometrial thickness should be reported as the ‘‘dou-
ble thickness’’ measurement [3]. If endometrial fluid
is present, its diameter should be omitted; in such
cases the endometrial thickness should be reported
as the sum of the measurements obtained from the
anterior and posterior endometrial walls. An endo-
metrial thickness of 4 to 14 mm is normal in an adult
premenopausal woman. Endometrial thickness and
appearance vary with the phase of the menstrual
cycle [4].
The position of the ovaries is variable but they are
usually found in the posterior fold of the broad
ligament, posterior and distal to the fallopian tubes.
On sonography the ovaries can be localized anterior
to the internal iliac vessels. The postpubertal ovary
measures approximately 3 cm in length, 2 cm in
width, and 1 cm in anteroposterior dimension. The
upper limit for normal ovarian volume is highest in
young adult women measuring approximately 9.8 to
14 mL and declines with increasing age [5]. Normal
s reserved.

Fig. 1. Sagittal TVUS of the uterus demonstrates a normal
endometrial lining (arrowheads).
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314298
fallopian tubes cannot be visualized with current US
imaging equipment
Table 1
First-trimester scanning milestones
Parameter Transabdominal US Transvaginal US
Gestational sac — Present at 5 wk
(5 mm)
Yolk sac Always present
if GS > 20 mm
Always present
when GS > 10 mm
Cardiac activity GS > 2.5 cm GS > 18 mm
Abbreviations: GS, gestational sac; US, ultrasound.
Scanning technique
Ultrasound evaluation of the female pelvis is
conducted with a real-time scanner, preferably using
a sector or curvilinear transducer. The scanner is
adjusted to operate at the highest clinically appropri-
ate frequency, realizing that there is a trade-off
between the resolution and beam penetration.
Transabdominal pelvic US is performed with a
full bladder using transducer frequencies of 3.5 MHz
and above. Adequate distention of the bladder dis-
places the bowel from the field of view. Transab-
dominal US gives an initial overview of the uterus,
adnexa, and any intra-abdominal free fluid. TVUS is
performed with the patient’s bladder being empty,
using a transducer frequency of 5 to 7.5 MHz. TVUS
gives detailed information about the uterus and the
adnexa. Higher-frequency transvaginal probes can be
positioned closer to the pelvic organs resulting in
improved spatial resolution and diagnostic accuracy.
Currently available transducers of 10 MHz and above
can identify the finer details of intrauterine gestation
and have greatly contributed to the early diagnosis of
abnormal gestation and to the management of first-
trimester bleeding. Color flow Doppler and pulsed
Doppler may be added to the examination, as indi-
cated by the gray-scale US findings. It is important to
bear in mind that the energy output of Doppler US is
substantially higher than that used for imaging and it
may have potentially harmful effects on the concep-
tus [6]. Because of this risk, caution has been
expressed over the routine use of Doppler US in
early pregnancy evaluation. While performing Dopp-
ler US in early pregnancy, the concept of ‘‘as low as
reasonably achievable’’ is important [7] and the
advantages of the Doppler US should outweigh the
potentially harmful effects on the conceptus.
Normal first-trimester sonography
Scanning in the first trimester may be performed
either transabdominally or transvaginally. TVUS is
preferred and is the community standard. The first-
trimester milestones are given in Tables 1 and 2.
A gestational sac can be identified with TVUS at
5 weeks of gestational age, when it measures 5 mm.
The yolk sac should always be seen by TVUS when
a gestational sac measures greater than 10 mm and
by transabdominal US when the mean sac diameter
is greater than 20 mm [8,9]. An embryo with car-
diac activity should be seen transvaginally when the
gestational sac measures greater than 18 mm, and
transabdominally when the gestational sac measures
2.5 cm. These discriminatory criteria should be used
as guidelines. If the findings of the US examination
are equivocal and the examination is technically
difficult, a follow-up examination should be obtained.
Gestational sac
The blastocyst implants into the endometrium by
approximately 23 days of menstrual age [10]. It mea-
sures 0.1 mm and is too small to be visualized on
TVUS. Demonstration of peritrophoblastic flow by
transvaginal color flow Doppler at this focal decidual
thickening has improved the diagnostic sensitivity of
intrauterine pregnancy (IUP) from 90% with TVUS
alone to 99% using transvaginal color flow Dopp-
ler [11,12]. The peritrophoblastic flow has a charac-
teristic high-velocity and low-impedance flow caused
by shunting of blood from the spiral arteries into the
intervillous spaces. According to Emerson et al [11],
the peak systolic velocity of peritrophoblastic flow
in a normal IUP ranges from 8 to 30 cm/second, be-
fore the visualization of the gestational sac. Yeh et al

Table 2
Land marks of normal first-trimester pregnancy
Gestational age Embryologic change Sonographic appearance
23 d Blastocyst implantation Blastocyst measures 0.1 mm and is too small to visualize
3.5–4 wk Decidual changes at
implantation site
Focal echogenic decidual thickening at implantation site
4–4.5 wk Trophoblastic tissue High-velocity and low-impedance trophoblastic flow at the implantation site
on TVCFD
4.5–5 wk Exocoelomic cavity of
the blastocyst
Gestational sac (a sonographic term) is always seen when it measures > 5 mm
and the serum b-hCG is between 1000 and 2000 mIU/mL (IRP)
5–5.5 wk Secondary yolk sac Yolk sac is seen as a thin-walled cystic structure within the gestational sac and
should always be seen when the GS is > 10 mm; it is the first sign of a true
gestational sac before the visualization of embryo
5–6 wk Embryo Seen as a focal echogenic area adjacent to the yolk sac; should always be seen
when the GS is > 18 mm
5–6 wk Embryonic cardiac
activity
Embryonic cardiac activity should always be seen when the embryo is > 5 mm;
normal heart rate ranges from 100–115 beats/min between 5–6 wk of gestation
Abbreviations: CG, human chorionic goradotropin; GS, gestational sac; IRP, international reference preparation; TVCFD,
transvaginal color flow Doppler.
Fig. 2. Coronal TVUS of the uterus shows a gestational sac
with hyperechoic margins (arrow) and endometrial cavity
(curved arrow).
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 299
[13] described a focal, eccentric, anechoic area in the
endometrium caused by the embedded blastocyst as
the ‘‘intradecidual sign.’’ They described this sign as
early as 3.5 weeks of menstrual age on transabdomi-
nal US and reported a sensitivity rate of 92%, a
specificity rate of 100%, and an accuracy rate of
93%. Laing et al [14] used TVUS to demonstrate this
sign and found that the overall sensitivity, specificity,
and accuracy for the intradecidual sign were only
48%, 66%, and 45%, respectively. With currently
available high-frequency transvaginal probes, a ges-
tational sac as small as 2 to 3 mm can be demon-
strated at 4 weeks of gestational age [15–17]. On
TVUS, the gestational sac is seen as a well-defined
fluid-filled cavity with a surrounding hyperechoic
rim, embedded eccentrically in the endometrial lining
of the fundus or midbody of the uterus (Fig. 2). The
sonographic term ‘‘gestational sac’’ represents the
exocoelomic cavity of the blastocyst and the sur-
rounding echogenic rim is caused by the developing
chorionic villi and decidual tissue. The echogenic rim
should have a minimum thickness of 2 mm and its
echogenicity should exceed that of myometrium [1].
The double decidual sac sign of intrauterine
gestation was first described in 1982 [18]. The double
decidual sac sign consists of two concentric echo-
genic rings encasing a central anechoic focus that im-
press on the endometrial stripe. The inner echogenic
rim represents the decidua capsularis and chorion
laeve, whereas the outer echogenic rim represents
the decidua parietalis; these echogenic rims are sepa-
rated by a thin rim of fluid in the endometrial cavity
(Fig. 3). This is a useful sign of IUP between 4 and
6 weeks of gestation. The crown-rump length (CRL)
of the embryo is a more accurate indicator of gesta-
tional age than the mean gestational sac diameter. The
mean gestational sac diameter should be recorded,
however, when an embryo is not identified.
Because hCG production and gestational sac
growth are related to trophoblastic function, there is
excellent correlation of the serum hCG level, sac size,
and the stage of pregnancy [19]. Kadar et al [20] first
introduced the concept of a discriminatory level of
the b subunit of hCG. The range of the serum b-hCGlevel at which an intrauterine gestational sac is
visualized is the discriminatory zone. Although the
discriminatory range of b-hCG varies from one labo-
ratory to another, the widely accepted range is from

Fig. 3. Double decidual sac sign. (A) Coronal TVUS of the uterus reveals an intrauterine gestational sac (straight arrow),
decidua capsularis (curved arrow), decidua parietalis (arrowhead), and effaced endometrial cavity (asterisks). (B) Corresponding
line diagram.
Fig. 4. TVUS of the uterus demonstrates a yolk sac (thin
arrow) outside the amniotic membrane (arrowhead), which
has not yet fused with the chorion (curved arrow). Embryo
(thick arrow) is seen within the amniotic sac.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314300
1000 to 2000 mIU/mL international reference prepa-
ration (IRP) for TVUS and 2400 to 3600 mIU/mL
(IRP) for transabdominal US [10]. In normal preg-
nancy serum b-hCG should double or increase by at
least 66% in 48 hours.
Yolk sac
The first structure to be seen within the gestational
sac is the secondary yolk sac, which is a reliable
indicator of a true IUP with a positive predictive
value of 100%. The primary yolk sac is not seen by
US because it shrinks at 4 weeks menstrual age and
gradually disappears with the formation of the sec-
ondary yolk sac [21]. The secondary yolk sac is first
seen on TVUS as a thin-walled cystic structure by the
fifth gestational week and is virtually always seen by
5.5 weeks gestational age (Fig. 4) [22]. The yolk sac
is round, measures less than 6 mm, and should be
visualized by TVUS when a gestational sac measures
more than 10 mm [10]. The yolk sac is involved in
nutritive, metabolic, hemopoietic, and secretive func-
tions during early embryonic development and or-
ganogenesis [23,24]. Abnormalities in its size and
appearance are predictors of abnormal gestation [25].
Embryo
The embryo should always be visualized by
TVUS when the gestational sac measures greater than
18 mm, and transabdominally when the gestational
sac measures 2.5 cm (Fig. 5). With the currently
available high-frequency transvaginal transducers,
the embryonic disk is initially seen as a focal echo-
genic area of 1- to 2-mm thickness adjacent to the
yolk sac between 5 and 6 weeks of gestational age
[26–29]. Embryonic cardiac activity should always
be seen when an embryo measures greater than 5 mm.
Occasionally the heartbeat may be seen adjacent to
the yolk sac even before the embryo is clearly visible.

Fig. 5. TVUS of the uterus shows a normal embryo and
separate amniotic membrane (arrow) in close relation to the
embryo. This should not be mistaken for nuchal translucency.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 301
Levi et al [3] suggested a 4-mm CRL cutoff because
their study demonstrated cardiac activity in all em-
bryos with a CRL of 4 mm [30]. Other studies
demonstrated 5 mm as the discriminatory CRL for
detecting cardiac activity [31,32]. Although visual-
ization of a living embryo does not ensure a viable
pregnancy, the abortion rate decreases for living em-
bryos as the gestational age increases, with a 0.5%
demise rate for living embryos between 6 and 10 mm
[33]. If the length of the embryo is less than 5 mm,
follow-up US should be performed until the expected
CRL exceeds the discriminatory value. Most of the
studies reported a heart rate of 100 to 115 beats per
minute between 5 and 6 weeks [34–36]. By 9 weeks
of gestational age, the mean heart rate increases to
about 140 beats per minute. The cardiac activity
should be documented by M-mode.
Amniotic sac
The amniotic sac is formed in the fourth week
of gestation between the ectoderm layer and the adja-
cent trophoblast. Before 6.5 weeks the amniotic
membrane is so close to the embryo that the amniotic
cavity around the embryo is not easily seen. The di-
ameter of the amniotic cavity is nearly equal to the
CRL. Between 5 and 7 weeks of gestational age the
embryo is located between the amniotic and yolk
sacs. On US, this amniotic sac–embryo–yolk sac
complex appears as two small sacs and is called the
double bleb sign [9]. The embryo and the inner
amnion grow at a faster rate than the outer chorionic
cavity with eventual fusion of the amniotic and
chorionic membranes by 16 weeks of gestation
[37]. Separation of the amniotic and chorionic mem-
branes before 14 weeks of gestation is considered
normal (see Figs. 4 and 5).
Spontaneous abortion
Spontaneous abortion is defined as pregnancy
terminating before the 20th completed week of ges-
tation. Approximately 80% of spontaneous abortions
occur in the first trimester. The causes of spontaneous
abortions fall into two categories: genetic and envi-
ronmental (maternal) as listed next:
Genetic or fetal causes
Trisomy
Polyploidy or aneuploidy
Translocations
Environmental or maternal causes
Uterine
Congenital uterine anomalies
Leiomyoma
Intrauterine adhesions or synechiae (Asherman’s
syndrome)
Endocrine
Progesterone deficiency (luteal phase defect)
Hypothyroidism
Diabetes mellitus (poorly controlled)
Luteinizing hormone hypersecretion
Immunologic
Autoimmunity: antiphospholipid syndrome, sys-
temic lupus erythematosus
Infections
Toxoplasma gondii, Listeria monocytogenes,
Chlamydia trachomatis, Ureaplasma urea-
lyticum, Mycoplasma hominis, herpes simplex,
Treponema pallidum, Borrelia burgdorferi,
Neisseria gonorrhoeae
Genetic abnormalities are the most common cause
of spontaneous abortions accounting for almost 50%
to 60% of cases. Autosomal trisomy is the most
frequently identified chromosomal abnormality re-
sulting in first-trimester abortions. The incidence of
abortions secondary to chromosomal abnormalities
markedly increases after the maternal age of 35 years.
The environmental or maternal causes account for
a small percentage of spontaneous abortions. These in-
clude infection; anatomic defects (maternal mullerian
defects); endocrine factors (failure of corpus luteum);
immunologic factors (antiphospholipid antibody syn-
drome); and maternal systemic disease (diabetes mel-
litus, hypothyroidism). The algorithmic approach to
first-trimester bleeding is summarized in Fig. 6.

First Trimester Ultrasound
MSD > 18MM
ED
YS present
F/U re: sacgrowth andembryo
1
MSD < 10MM
ED
MSD > 10MM
YS absent
MSD < 18MM
Embryo not visualized
A
F/Ure: growth andcardiac activity
1
EDF/U2wksre: growthand cardiacactivity
1
F/U2
? F/U18 wks
1
HR N HR AbN
MSD-CRL> 5MM
MSD-CRL< 5MM
YS normal YS abnormal
YS present YS absent
CRL > 5MM CRL < 5MM
Cardiac activitypresent
CRL > 5MM CRL < 5MM
Cardiac activityabsent
Embryo visualizedB
Fig. 6. (A, B) Proposed algorithms for evaluating women with first trimester bleeding. ED, embryonal demise; F/U, follow-up;
HR ABN, heart rate abnormal; HR N, heart rate normal; YS, yolk sac. (From McGahan J, Goldberg B. Diagnostic ultrasound:
a logical approach. Philadelphia: Lippincott, Williams & Wilkins; 1998; p. 142–3; with permission.)
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314302
The most common morphologic finding in early
spontaneous abortions is an abnormality of devel-
opment of the zygote, embryo, early fetus, or the
placenta. Spontaneous abortion is clinically classified
into threatened, inevitable, missed, incomplete, and
complete abortions (Table 3).
Ultrasound findings in abortion
The US findings depend on the developmental
stage of the pregnancy at which the patient presents
with symptoms. Familiarity with normal sonographic
landmarks of first-trimester pregnancy is essential

Table 3
Classification of spontaneous abortion
Types Clinical features US findings
Threatened abortion Vaginal bleeding before 20 wk gestation
without cervical dilatation
Depending on the stage of pregnancy, US may show an
empty uterus, intrauterine gestational sac with or without
an embryo
Incomplete abortion Vaginal bleeding with partial expulsion
of products of conception before 20 wk
gestation and cervical dilatation
Thick, irregular endometrial lining caused by residual
trophoblastic tissue and fluid
Missed abortion Embryonic demise before 20 wk of
gestation without expulsion of products
of conception; may or may not have
vaginal bleeding
Embryo without cardiac activity; small size of the embryo
for the gestational age (see Fig. 10)
Complete abortion Vaginal bleeding and expulsion of all
products of conception before 20 wk
gestation
Empty uterus
Inevitable abortion Vaginal bleeding before 20 wk gestation
with cervical dilatation
Variable depending on the degree of bleeding and expulsion
of the products of conception
Abbreviations: US, ultrasound.
Table 4
TVUS features of pregnancy failure
Ultrasound findings Comments
Absence of IUGS with serum
b-hCG above the
discriminatory level
(1000 mIU/mL)
Ectopic pregnancy
has to be excluded
IUGS > 10 mm without
a yolk sac
Follow-up with serum
b-hCG and TVUS
IUGS of >18 mm without
an embryo
Anembryonic pregnancy
Embryo of 5 mm and above
without cardiac activity
Embryonic demise
Embryo with bradycardia
(< 100 beats/min)
Poor prognosis and
needs close follow-up
with TVUS
Subchorionic hematoma Correlation of pregnancy
outcome with the size
of hematoma is not well
established and needs
TVUS follow-up
Abbreviations: hCG, human chorionic gonadotropin; IUGS,
intrauterine gestational sac; TVUS, transvaginal ultrasound.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 303
to diagnose a failing pregnancy. TVUS features of
failing pregnancy are summarized in Table 4. The
sonographic findings are to be correlated with serum
b-hCG and menstrual age. In the pre-embryonic stage,
the pregnancy outcome depends on the presence of
the gestational sac and yolk sac and their morpho-
logic features.
Absent intrauterine gestational sac
Failure to demonstrate intrauterine gestational sac
by TVUS may be secondary to early IUP (b-hCG <
1000 mIU/mL) or secondary to ectopic pregnancy.
When the serum b-hCG is more than 1000 mIU/mL
(IRP) and there is no IUP, an ectopic pregnancy
[19,20] must be excluded by careful evaluation of
the adnexa. If there is no identifiable ectopic gesta-
tional sac, adnexal mass, or a large amount of adnexal
fluid in the cul-de-sac, follow-up with b-hCG and
TVUS is necessary until a definite diagnosis is made.
When the endometrial lining is thick with echoes in
the endometrial cavity and no intrauterine gestational
sacs, an incomplete abortion with retained products
of conception must be distinguished from decidual
reaction of ectopic gestation. Transvaginal color flow
Doppler of the endometrial contents is useful in dif-
ferentiating trophoblastic tissue from blood clots and
pseudogestational sac. Sparse flow on color Doppler
with low peak systolic velocities (< 6 cm/second) and
low to absent end diastolic flow suggests decidual re-
action of an ectopic pregnancy (Fig. 7) [38,39]. With
early IUP (< 5 weeks) multiple flashes of color with a
peak systolic velocity of greater than 8 cm/second
and high diastolic component caused by trophoblastic
arterial flow are noted [40].
Intrauterine gestational sac without an embryo
A common and difficult problem arises when the
gestational sac in the uterus lacks an embryo or yolk
sac [41–43]. This can be caused by early normal IUP,

Fig. 7. Decidual reaction. (A) Sagittal TVUS shows thick echogenic endometrial lining without a gestational sac (arrowheads).
This sonographic appearance can be seen in molar pregnancy; correlation with beta hCG is very important. (B) Sagittal TVUS
with color Doppler did not demonstrate trophoblastic flow, confirming it to be decidual reaction (arrowheads). Patient’s beta
hCG was 650 IU. On follow-up, the patient was shown to have a normal intrauterine pregnancy.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314304
anembryonic gestation, or a pseudogestational sac of
ectopic pregnancy. Anembryonic gestation is a form
of failed pregnancy defined as a gestational sac in
which the embryo failed to develop (Fig. 8A). A
mean gestational sac diameter greater than 18 mm
(TVUS) without a visualized embryo is unequivocal
evidence of a failed, anembryonic pregnancy [44].
This also is referred to as an ‘‘empty amnion’’ sign
(Fig. 8B) because of its sonographic appearance of a
large well-defined amniotic sac without an embryo
[45]. The growth rate of an anembryonic gestational
sac is slower than that of a normal gestational sac,
which increases by 1.13 mm/day. An abnormal ges-
tational sac can be identified confidently when the
rate of increase of the mean sac diameter is less than
Fig. 8. Anembryonic pregnancy. (A) TVUS of uterus shows a large (
‘‘empty amnion sign’’ of anembryonic gestation (arrow).
0.6 mm/d on follow-up US [46]. Other minor crite-
ria of an abnormal gestational sac include distorted
sac shape and weakly echogenic or irregular chorio-
decidual reaction (Fig. 9). The presence of gestational
sac in the lower uterine segment or cervix is usually
seen in patients with abortion in progress (Fig. 10),
but can also be seen secondary to low implantation.
Demonstration of trophoblastic vascular flow on
color Doppler is useful in differentiating low implan-
tation from abortion.
Yolk sac criteria of an abnormal gestation
The absence of a yolk sac when the mean sac
diameter of the gestational sac is more than 10 mm is
> 18 mm) gestational sac (arrow) without an embryo. (B) An

Fig. 9. Abnormal shape of the gestational sac. A 30-year-old
woman with 5 week’s of amenorrhea presents with vaginal
spotting. A TVUS of the uterus shows an intrauterine gest-
ational sac of abnormal shape and lobulated contour. On fol-
low-up patient had a spontaneous complete abortion.
Fig. 10. Abortion in progress. ATVUS of the uterus shows a
low-lying gestational sac (arrow). Mixed hyperechoic and
hypoechoic contents in the endometrial cavity of the fundus
(arrowheads) represent decidual reaction and hemorrhage.
The patient had a complete spontaneous abortion a few
hours after the scan.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 305
indicative of an abnormal gestation and is associated
with spontaneous abortion [47–49]. A failing or
failed pregnancy is also suggested when the yolk
sac is abnormal in size and shape. Large (> 6 mm)
irregular and calcified yolk sacs have been found to
correlate with early pregnancy failure [50–52]. A
large yolk sac is considered to be caused by an
alteration of the metabolic functions of the yolk sac
membrane with accumulation of secretions following
embryonic death [53]. The association of a large yolk
sac with aneuploidy has also been reported [50].
Although abnormal large yolk sac size is reported
to be associated with subsequent pregnancy failure,
another study with yolk sac diameter greater than the
95th percentile for gestational age reported normal
pregnancy outcomes [54]. Because of this controver-
sial issue, any patient with a large yolk sac should
have a follow-up US because there is increased risk
of spontaneous abortion. Apart from size, irregular,
echogenic, calcified, or double yolk sacs (vitelline
duct cyst) also are associated with early pregnancy
failure [55,56].
Gestational sac with an embryo
Although visualization of a living embryo does
not ensure a viable pregnancy, the abortion rate
decreases for living embryos as the gestational age
increases, with a 0.5% demise rate for living embryos
between 6 and 10 mm [29]. Because cardiac activity
may not be demonstrated [57] in early normal em-
bryos (CRL < 4 mm), follow-up US and correlation
with the serum b-hCG level is useful in determining
the viability of the gestation. The most convincing
evidence that a pregnancy has failed is to document
absence of cardiac activity when CRL length is
greater than 5 mm. In a missed abortion, the embryo
may be small for the gestational age with a discrep-
ancy between the mean sac diameter and the CRL
(Fig. 11). Embryonic bradycardia is a poor prognos-
ticator of pregnancy viability and requires follow-up
[58]. Embryonic bradycardia is defined as a heart rate
of less than 100 beats per minute before 6.2 weeks
gestational age and less than 120 beats per minute
between 6.3 and 7 weeks [59].
Intrauterine growth restriction
First-trimester growth restriction is a sign of a
failing pregnancy. Growth restriction is detected by
comparing the mean sac diameter with the CRL or
by serial follow-up of these growth parameters. The
average gestational sac diameters should be at least
5 mm larger than the CRL. A difference in size be-
tween mean sac diameter and CRL of less than 5 mm
caries a high risk of subsequent embryonic demise
[60]. When there is sac size and CRL discrepancy, a
follow-up US examination is recommended because
these fetuses have higher incidence of low birth
weight and premature delivery [61,62].
Subchorionic hematoma
Up to 20% of women with a threatened abortion
have a subchorionic hematoma [44]. Perigestational

Fig. 11. Missed abortion. A 35-year-old woman with
10 weeks of amenorrhea presents with intermittent vaginal
bleeding. TVUS shows a relatively small-sized embryo (ar-
row) compared with the gestational sac. No cardiac activity
was demonstrated on pulsed Doppler.
Fig. 12. Subchorionic hemorrhage. TVUS shows a gesta-
tional sac (curved arrow), chorion (straight thick arrow),
and a subchorionic hemorrhage (straight thin arrow).
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314306
hemorrhage from chorionic frondosum is the most
common source of vaginal bleeding in the first
trimester of pregnancy. Subchorionic hemorrhage is
secondary to abruption of the edge of the chorion
frondosum–decidua basalis complex or may be
caused by marginal sinus rupture [63,64]. Although
the hemorrhage usually abuts or elevates the edge of
the chorion frondosum–decidua basalis complex, the
bulk of the hemorrhage is usually situated between
the decidua capsularis, chorion laeve, and the decidua
vera. Acute hemorrhage may be hyperechoic or
isoechoic relative to the chorion, and it becomes
isoechoic with the chorionic fluid in 1 to 2 weeks
(Fig. 12). Several studies have correlated the preg-
nancy outcome in these patients with the size of the
subchorionic hematoma, gestational age, and the
maternal age. One of the largest studies [65] showed
that the rate of pregnancy loss increases with hema-
toma size, advancing maternal age, and earlier gesta-
tional age. In this study, the size of the hematoma was
graded according to the percentage of the chorionic
sac circumference elevated by the hematoma. It was
graded as small when it involved less than one third
of the chorionic sac circumference, moderate when it
involved one-third to one-half of the chorionic sac
circumference, and large when two-thirds or greater
of the chorionic sac circumference was involved.
There was little difference in the rates of spontaneous
abortion between pregnancies with small- and mod-
erate-size hematomas (7.7% and 9.2%, respectively),
but the rate doubled with large hematomas (18.8%).
The spontaneous abortion rate was also twice as
high in women 35 years of age or older compared
with that in younger women (13.8% versus 7.3%, re-
spectively), and was 2.3 times higher in women who
presented with vaginal bleeding at 8 weeks gesta-
tional age or less compared with that in women who
presented with bleeding at more than 8 weeks gesta-
tional age (13.7% versus 5.9%, respectively). Some
investigators have calculated the volume of a sub-
chorionic hematoma as a percentage of the gesta-
tional sac volume. When the volume of a hematoma
is less than 40% of the gestational sac volume, the
pregnancy outcome is favorable [64,66].
Retained products of conception
Retained products of conception typically consist
of retained placental tissue. An echogenic mass in the
uterine cavity is the most suggestive US finding. A
heterogeneous mass or collection in the central cavity
may represent a blood clot, or some combination of
retained placenta, necrotic debris, and clot (Fig. 13).
Color Doppler may help to differentiate vascularized
trophoblastic tissue from nonvascularized blood clots.
A normal-appearing endometrial stripe or punctate
echogenic foci not associated with a discrete mass
makes retained products of conception unlikely.
Gestational trophoblastic disease
Gestational trophoblastic disease is a spectrum of
pregnancy-related trophoblastic proliferative abnor-
malities that can present with first-trimester bleeding.

Fig. 13. Retained products of conception with variable appearance. Sagittal (A) and coronal (B) TVUS in two different patients
with persistent vaginal bleeding after spontaneous abortion show retained products of conception with increased echogenicity
(arrowheads) in (A) and heterogeneous appearance in (B). This appearance is secondary to necrosis and blood clots. (C) Increased
vascularity on color flow Doppler evaluation in a patient with retained products of conception.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 307
Classification of gestational trophoblastic disease is
as follows:
Hydatidiform mole
Complete mole
Partial mole
Gestational trophoblastic tumors
Choriocarcinoma
Invasive mole
Placental site trophoblastic tumor
Hydatidiform mole (molar pregnancy)
Molar pregnancy is a noninvasive process charac-
terized by varying degrees of trophoblastic prolif-
eration and edema of villous stroma. Its incidence is
1 in every 1000 to 2000 pregnancies [67] and is
estimated to be as high as 1 in 41 in patients with
miscarriages [68]. Hydatidiform mole constitutes
80% of the cases of gestational trophoblastic disease
with relatively high frequency of molar pregnancy at
the beginning and end of the childbearing period.
Mole recurrence is seen in about 1% to 2% of cases
[69]. The absence or presence of fetus or embryonic
elements is used to classify a molar pregnancy into
complete or partial moles. Complete molar pregnan-
cies are most often 46 XX, with the chromosomes
completely of paternal origin and are referred to as
‘‘androgenesis.’’ The karyotype in partial mole is usu-
ally triploid (69 XXY) or even tetraploid (92 XXXY)
with one maternal and two paternal haploid compo-

R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314308
nents. The fetus in partial mole is usually nonviable
and exhibits features of triploidy, which include
multiple congenital anomalies and growth restriction
[70]. Histologically, the molar tissue has prominent
villi with central acellular space corresponding to the
macroscopic appearance of vesicles. In partial mole
these changes are focal and less advanced.
The clinical presentation of molar pregnancy,
listed below, has changed appreciably over the last
decades because of early diagnosis with TVUS and
quantitative b-hCG estimation.
� Uterine bleeding, which may vary from spotting
to profuse hemorrhage� Uterine enlargement out of proportion to the
duration of pregnancy in 50% of cases� Absence of fetal parts or fetal heart sounds
despite an enlarged uterus� Pregnancy-induced hypertension before
24 weeks gestation� Hyperemesis� Thyrotoxicosis, which is usually subclinical� History of passage of grape-like vesicles trans-
vaginally
Uterine bleeding is the most common presentation
and it may vary from spotting to profuse bleeding.
Occasionally patients may pass grape-like vesicles
transvaginally. Clinically the uterine fundal height is
more than is expected for the gestational period. Di-
Fig. 14. Complete hydatidiform mole. (A) Transabdominal sonogr
defined anechoic cystic areas (arrows) corresponding to the vesic
(B) Corresponding T1-weighted postgadolinium image of the uteru
multiple well-defined hypointense lesions that are not enhancing a
agnosis is made by markedly elevated serum b-hCGlevels expected for the stage of gestation and by the
characteristic sonographic appearance.
Sonographic features of molar pregnancy
Molar changes can be detected from 8 weeks of
pregnancy by US. The uterine cavity is filled with
multiple sonolucent areas of varying size and shape.
This has been described as a ‘‘snow storm’’ appear-
ance with low-frequency transabdominal scanning.
With high-frequency transvaginal transducers, nu-
merous discrete, anechoic (cystic) spaces are visual-
ized corresponding to the hydropic villi (Fig. 14).
These cystic spaces range from 1 to 30 mm in size
and increase in size with gestational age. Large sono-
lucent areas or maternal lakes resulting from the stasis
of maternal blood are seen between the vesicles. In
partial mole, an intrauterine embryo is noted along
with molar changes [71,72]. Because the trophoblas-
tic changes develop at a slower rate in partial mole,
it may present as enlarged placenta without macro-
scopic vesicular changes [73]. Women with a high
b-hCG level for the gestational age without sono-
graphic molar changes should have follow-up US to
exclude partial mole. In missed abortion, impaired
trophoblastic vascularity leads to hydropic degenera-
tion of villi and can resemble a partial hydatidiform
mole on US. The serum b-hCG is not elevated, how-
ever, and may be normal or at a lower level than for
am of the uterus shows a complex mass with multiple well-
les of hydatidiform mole. There was no associated embryo.
s demonstrates intrauterine complex mass (arrowheads) with
nd represent vesicles of hydatidiform mole (arrow).

R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 309
the expected gestational age. Rarely, a viable fetus
may be associated with complete molar pregnancy
[74] and is caused by the coexistence of a true mole
and a normal fetus in dizygotic twin gestation. Dem-
onstration of the typical trophoblastic flow is useful
in differentiating the trophoblastic tissue of molar
pregnancy from intrauterine blood clots in a patient
with abortion. Theca-leutin ovarian cysts are seen in
up to 25% to 60% of cases because of hyperstimu-
lation of the ovaries by chorionic gonadotrophin
secreted by the trophoblastic tissue [75]. In this con-
dition, the ovaries are enlarged with multiple cysts
having a soap bubble or spoke-wheel appearance.
Treatment of hydatidiform mole consists of im-
mediate evacuation of the mole and subsequent fol-
low-up with serial measurement of serum b-hCG for
detection of persistent trophoblastic proliferation
or malignant change. TVUS is useful in monitor-
ing patients following evacuation and chemotherapy
[76–79]. If the b-hCG levels plateau or continue to
rise, persistent trophoblastic tissue is diagnosed. Fol-
lowing evacuation of a hydatidiform mole, 18% to
29% with complete hydatidiform mole and 1% to
11% with partial mole develop a persistent tropho-
blastic tumor [80–83]. TVUS reveals nodules of
residual echogenic trophoblastic tissue and central
hypoechoic blood spaces. Doppler interrogation
reveals typical low-resistance and high-peak systolic
velocity vascular flow of trophoblastic tissue.
Gestational trophoblastic tumors
Gestational trophoblastic tumor refers to chorio-
carcinoma, invasive mole, and placental site tropho-
blastic tumor. It may follow a normal or a molar
pregnancy, abortion, or ectopic pregnancy. Diagnosis
is made primarily by persistent elevation of the serum
b-hCG. Fifty percent of these tumors arise following
hydatidiform mole, 25% following abortion, and 25%
following normal or ectopic pregnancy [84].
Choriocarcinoma
Choriocarcinoma is a malignant form of tropho-
blastic tumor that invades uterine myometrium and
blood vessels resulting in distant metastasis. The ab-
sence of villous pattern is characteristic of chorio-
carcinoma, in contrast to hydatidiform mole and
invasive mole. The most common sites of metastases
are the lungs (over 75%) and the vagina (50%). Other
sites of metastases include the vulva, liver, kidneys,
brain, ovaries, and bowel [85]. The US appearance
is indistinguishable from a complete mole, except
in cases with myometrial and parametrial extension.
TVUS reveals a heterogeneous intrauterine mass with
or without myometrial invasion. Doppler interroga-
tion reveals typical trophoblastic flow and differen-
tiates trophoblastic tissue from areas of hemorrhage
and necrosis. Ovarian theca-leutin cysts are identified
in more than a third of such cases. Cross-sectional
imaging with CT and MR imaging is more accurate in
demonstrating invasion of the myometrium and para-
metrium. Radiologic evaluation for distant metastases
is mandatory in all cases of choriocarcinoma.
Invasive mole
This is defined as excessive trophoblastic over-
growth with invasion of the myometrium and oc-
casional extension to the peritoneum or adjacent
parametrium. Unlike choriocarcinoma there are no
distant metastases. Invasive mole presents clinically
as heavy vaginal bleeding after the evacuation of the
molar pregnancy with persistent elevation of serum
b-hCG. On TVUS it appears as focal areas of in-
creased echogenicity within the myometrium [86].
Doppler color flow mapping of this area can evaluate
the extent of this lesion and its subsequent response
to chemotherapy (Fig. 15) [87–89].
Placental site trophoblastic tumor
This is a very rare trophoblastic tumor, which arises
from the placental implantation site following either a
normal term pregnancy or abortion. These patients
present with either abnormal bleeding or amenorrhea
and might be presumed to be pregnant. Moreover, the
b-hCG levels are not as high as in other forms of
gestational trophoblastic disease [90,91]. They may
invade the myometrium and in 15% to 20% cases
behave in a malignant fashion with distant metastases.
US features are indistinguishable from those of other
gestational trophoblastic tumors [92,93].
Arteriovenous malformation of the uterus
It is important to consider arteriovenous malfor-
mations in the differential diagnosis of first-trimester
bleeding because of their sonographic resemblance
to retained products of conception and gestational
trophoblastic disease. Vascular malformations of the
uterus are rare and potentially life-threatening le-
sions. They can be congenital or acquired following
uterine trauma (surgery or curettage); use of intra-
uterine contraceptive devices; endometrial or cervi-
cal carcinoma; and previous treatment of gestational
trophoblastic tumors [94]. Congenital arteriovenous
malformations have multiple arteriovenous commu-
nications and may extend through the myometrium
into the parametrium. Acquired lesions are arterio-

Fig. 15. Invasive mole. (A) TVUS showing molar tissue invading the myometrial wall (arrowheads) of the fundus and
endometrial cavity (arrow). (B) Color flow Doppler evaluation shows vascularity of the invaded myometrium. Endometrial
cavity is shown by arrow. (C) Corresponding T2-weighted, sagittal image of the uterus demonstrates hyperintense myometrium
(arrow) representing invasive molar tissue. Uninvolved endometrial lining is shown (arrowheads).
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314310
venous fistulas between a single artery and a vein.
Vascular malformations persist following treatment
in 10% to 15% of patients with gestational trophoblas-
tic tumors. Gray-scale US shows multiple anechoic
spaces with mosaic pattern of color signals within the
cystic spaces on color Doppler US. Spectral analysis
of the vessels shows high-velocity blood flow with a
low resistive index [95,96], indistinguishable from a
gestational trophoblastic disease (Fig. 16). These
vessels can be distinguished from gestational tropho-
blastic disease because the serum b-hCG is normal.
Uterine arteriovenous malformations are one of the
common causes of spontaneous abortions. Contrast-
enhanced CT, MR imaging, and angiography are other
imaging modalities used to diagnose uterine arterio-
venous malformations. The diagnosis of uterine arte-
riovenous malformations as the cause of vaginal
bleeding is crucial because treatment is entirely dif-
ferent from that for retained products of conception or
gestational trophoblastic disease, which can mimic
arteriovenous malformations. The treatment of arte-
riovenous malformations is by embolization if the

Fig. 16. Uterine arteriovenous malformation in a 35-year-old woman with history of spontaneous abortion presenting with
vaginal bleeding. She was referred to exclude retained products of conception. (A) TVUS shows complex endometrial mass
(arrowheads) with anechoic spaces (arrow). (B) Corresponding color flow Doppler demonstrates the mosaic pattern of flow
within the mass (arrowheads). Arrow points to endometrial cavity. Pulsed Doppler (C) shows arterialized venous flow,
diagnostic of arteriovenous malformation.
R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 311
patient desires fertility and by hysterectomy if fertility
is not an issue.
Summary
Vaginal bleeding is a leading cause of presentation
for emergency care during the first trimester of the
pregnancy. Clinical assessment of the pregnancy
outcome at this stage is less reliable. US examination
is crucial in establishing IUP and early pregnancy
failure and to exclude other causes of bleeding, such
as ectopic pregnancy and molar pregnancy. Diagnosis
of a normal IUP at this stage not only assists the
physician in an expectant management, but also gives
a psychologic boost to the patient. With recent ad-
vances in US technology and the availability of high-
frequency transvaginal transducers, reliable diagnosis
of early pregnancy failure can be made even before
the embryo is visible.
Acknowledgment
The authors thank Bonnie Hami, MA, Department
of Radiology, University Hospitals of Cleveland,
Ohio, for her editorial assistance in the preparation of
this article.
References
[1] Nyberg DA, Laing FC, Filly RA. Threatened abortion:
sonographic distribution of normal and abnormal ges-
tation sacs. Radiology 1986;158:397–400.

R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314312
[2] Laing FC, Brown DL, DiSalvo DN. Gynecologic ul-
trasound. Radiol Clin North Am 2001;39:523–40.
[3] Goldstein RB, Bree RL, Benson CB, Benacerraf BR,
Bloss JD, Carlos R, et al. Evaluation of the woman
with postmenopausal bleeding: Society of Radiologists
in Ultrasound-Sponsored Consensus Conference state-
ment. J Ultrasound Med 2001;20:1025–36.
[4] Forrest TS, Elyaderani MK, Mulenberg MI, et al. Cy-
clic endometrial changes: US assessment with histo-
logic correlation. Radiology 1988;167:233–7.
[5] Tamarkin S, Dogra V. Benign and malignant adnexal
lesions. In: Dogra V, Rubens D, editors. Ultrasound se-
crets. Philadelphia: Hanley & Belfus; 2004. p. 97–104.
[6] Kremkeu FW. Performance and safety. In: Kremkau
FW, editor. Diagnostic ultrasound: principles and in-
struments. 4th edition. Philadelphia: WB Saunders;
1993. p. 286.
[7] Implementation of the principle of as low as reasonably
achievable (ALARA) for medical and dental personnel.
NRCP report 107. Bethesda, MD: National Council
on Radiation Protection and Measurements; 1990.
[8] Nyberg DA, Hill LM. Normal early intrauterine preg-
nancy: sonographic development and HCG correlation.
In: Patterson AS, editor. Transvaginal ultrasound. St.
Louis: Mosby; 1992. p. 64–85.
[9] Yeh HC, Rabinowitz JG. Amniotic sac development:
ultrasound features of early pregnancy: The bouble
bleb sign. Radiology 1988;166:97–103.
[10] Moore KL. Formation of the bilaminar embryo: the
second week. In: Keith L, editor. The developing hu-
man: clinically oriented embryology. 5th edition. Phila-
delphia: WB Saunders; 1988. p. 38.
[11] Emerson DS, Cartier MS, Altieri LA, et al. Diagnostic
efficacy of endovaginal color flow imaging in an ec-
topic pregnancy scanning program. Radiology 1992;
183:413–20.
[12] Dillon EH, Feyock AL, Taylor KJ. Pseudogestational
sacs: Doppler US differentiation from normal or abnor-
mal intrauterine pregnancies. Radiology 1990;176:
359–64.
[13] Yeh HC, Goodman JD, Carr L, Rabinowitz JG. Intra-
decidual sign: a US criterion of early intrauterine preg-
nancy. Radiology 1986;161:463–7.
[14] Laing FC, Brown DL, Price JF, et al. Intradecidual
sign: Is it effective in diagnosis of an early intrauterine
pregnancy? Radiology 1997;204:655–60.
[15] Trimor-Tritsch IE, Farine D, RosenMG. A close look at
early embryonic development with the high frequency
transvaginal transducer. Am J Obstet Gynecol 1988;
159:676–81.
[16] Rosavic IK, Torjusen GO, Gibbons WE. Conceptual
age and ultrasound measurements of gestational sac
and crown-rump length in vitro fertilization pregnan-
cies. Fertil Steril 1988;49:1012–7.
[17] de crespigny LC, Cooper D, Mckenna M. Early detec-
tion of intrauterine pregnancy with ultrasound. J Ultra-
sound Med 1988;7:7–10.
[18] Bradley WG, Fiske CE, Filly RA. The double sac sign
of early intrauterine pregnancy: use in exclusion of
ectopic pregnancy. Radiology 1982;143:223–6.
[19] Nyberg DA, Filly RA, Duarte DL, et al. Abnormal
pregnancy: early diagnosis by US and serum chori-
onic gonadotropin levels. Radiology 1986;158:393–6.
[20] Kadar N, Devore G, Romero R. Discriminatory hCG
zone: its use in the sonographic evaluation for ectopic
pregnancy. Obstet Gynecol 1981;58:156.
[21] Moore KL. Formation of bilaminar embryo. In: Won-
siewicz M, editor. The developing embryo. 4th edition.
Philadelphia: WB Saunders; 1988. p. 38–49.
[22] Levi CS, Lyons EA, Lindsay DJ. Early diagnosis of
non viable pregnancy with transvaginal US. Radiology
1988;167:383–5.
[23] Moore KL. The placenta and fetal membrane. In:
Moore KL, editor. The developing human embryo:
clinically oriented embryology. 4th edition. Philadel-
phia: WB Saunders; 1988. p. 121.
[24] Gitlin D, Pericelli A. Synthesis of serum albumin, pre-
albumin, alpha 1-antitrypsin and transferin by the hu-
man yolk sac. Nature 1970;228:995.
[25] Jauniaux E, Jurkovic D, Henreity Y, et al. Development
of the secondary human yolk sac: correlation of sono-
graphic and anatomical features. Hum Reprod 1991;6:
1160–6.
[26] Yeh HC, Rabinowitz JG. Letter. J Ultrasound Med
1995;14:97–9.
[27] Goldstein SR, Wolfson R. Transvaginal ultrasono-
graphic measurement of early embryonic size as a
means of assessing gestational age. J Ultrasound Med
1994;13:27–31.
[28] Daya S. Accuracy of gestational age estimation by
means of the fetal crown-rump length measurement.
Am J Obstet Gynecol 1993;168:903–8.
[29] Wisser J, Dirschedl P, Krone S. Estimation of gesta-
tional age by transvaginal sonographic measurement of
the greatest embryonic length in dated human embryos.
Ultrasound Obstet Gynecol 1994;4:457–62.
[30] Levi CS, Lyons EA, Zheng XH, et al. Transvaginal US:
demonstration of cardiac activity in embryos of less
than 5.0 mm in crown rump length. Radiology 1990;
176:71–4.
[31] Brown DL, Emerson DS, Fleker RF, et al. Diagnosis of
early embryonic demise by transvaginal sonography.
J Ultrasound Med 1990;9:631–6.
[32] Pennell RG, Needleman L, Pajak T, et al. Prospective
comparison of vaginal and abdominal sonography in
normal early pregnancy. J Ultrasound Med 1991;10:
63–7.
[33] Goldstein SR. Embryonic death in early pregnancy: a
new look at the first trimester. Obstet Gynecol 1994;
84:294–7.
[34] Hertzberg BS, Mahony BS, Bowie JD. First trimester
fetal cardiac activity: sonographic documentation of a
progressive early rise in heart rate. J Ultrasound Med
1988;7:573–5.
[35] Achiron R, Tadmor O, Machiac S. Heart rate as a
predictor of first-trimester spontaneous abortion after

R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314 313
ultrasound proven viability. Obstet Gynecol 1991;78:
330–3.
[36] May DA, Sturtevant NV. Embryonal heart rate as a
predictor of pregnancy out come: a prospective analy-
sis. J Ultrasound 1991;10:591–3.
[37] Fleischer AC, James AE, Dawes WJ, Paige M, Rob-
inson HP. Sonographic depiction of pregnancy during
embryonic development. In: Sanders RC, James AE,
editors. The principles and practice of ultrasonography
in obstetrics and gynaecology. 3rd edition. Norwalk
(CT): Appleton-Century- Crofts; 1985. p. 61–74.
[38] Jaffe R, Dorgan A, Abramowicz JS. Color Doppler
imaging of the uteroplacental circulation in the first
trimester: value in predicting pregnancy failure or com-
plication. AJR Am J Roentgenol 1995;164:1255–8.
[39] Emerson DS, Cartier MS, Altieri LA, et al. Diagnostic
efficacy of transvaginal color Doppler flow imaging in
an ectopic pregnancy program. Radiology 1992;183:
413–20.
[40] Parvey HR, Dubinsky TJ, Johnston DA, Maklad NF.
The chorionic rim and low-impedance intrauterine ar-
terial flow in the diagnosis of early intrauterine preg-
nancy: evaluation of efficacy. AJR Am J Roentgenol
1996;167:1479–85.
[41] Robinson HP. The diagnosis of early pregnancy failure
by sonar. Br J Obstet Gynaecol 1975;82:849–57.
[42] Donald I, Mosley P, Barnett E. The diagnosis of the
blighted ovum by sonar. Br J Obstet Gynaecol 1972;
79:304–10.
[43] Jouppila P, Hesva T. Study of blighted ovum by ultra-
sonic and histopathology methods. Obstet Gynecol
1980;55:574–8.
[44] Nyberg DA, Laing FC. Threatened abortion and abnor-
mal first trimester intrauterine pregnancy. In: Patterson
AS, editor. Transvaginal ultrasound. St Louis: Mosby;
1992. p. 85–103.
[45] McKenna KM, Feldstein VA, Goldstein RB, Filly RA.
The ‘‘empty amnion’’: a sign of early pregnancy fail-
ure. J Ultrasound Med 1995;14:117–21.
[46] Bromley B, Harlow BL, et al. Small sac size in the first
trimester: a predictor of poor fetal out come. Radiology
1991;178:375–7.
[47] Levi CS, Lyons EA, Lindsay DJ. Early diagnosis of
non viable pregnancy with endovaginal US. Radiology
1988;167:383.
[48] Crooij MJ, Westhuis J, Schoemaker J, et al. Ultraso-
nographic measurement of the yolk sac. Br J Obstet
Gynecol 1982;89:931–4.
[49] Green JJ, Hobbins JC. Abdominal ultrasound exami-
nation of the first-trimester fetus. Am J Obstet Gynecol
1988;159:165–75.
[50] Lindsay DJ, Lovett IS, Lyons EA, et al. Yolk sac di-
ameter and shape at endovaginal US: predictors of
pregnancy outcome in the first trimester. Radiology
1992;183:115–8.
[51] Stampone C, Nicotra M, Muttinelli C, et al. Trans-
vaginal sonography of the yolk sac in normal and ab-
normal pregnancy. J Clin Ultrasound 1996;24:3–9.
[52] Dugoff L, Persutte WH, Schultz L, Hobbins JC. Prog-
nostic significance of the large yolk sac. Am J Obstet
Gynaecol 1998;178:S165.
[53] Ferrazi E, Brambati B, Lauzani A, et al. The yolk sac
in early pregnancy failure. Am J Obstet Gynaecol
1988;158:137.
[54] Stampone C, Nicotra M, Muttinelli C, Cosmi EV.
Transvaginal sonography of the yolk sac in normal
and abnormal pregnancy. J Clin Ultrasound 1996;24:
3–9.
[55] Harris RD, Vincent LM, Askin FB. Yolk sac calcifica-
tion: a sonographic finding associated with intrauterine
embryonic demise in the first trimester. Radiology
1988;166:109–10.
[56] Barzilai M, Lyons EA, Levi CS, Lindsay DJ. Vitelline
duct cyst or double yolk sac. J Ultrasound Med 1989;8:
523–6.
[57] Brown DL, Emerson DS, Felker RE, et al. Diagnosis
of early embryonic demise by endovaginal sonogra-
phy. J Ultrasound Med 1990;9:631–6.
[58] Benson CB, Doubilet PM. Slow embryonic heart rate
in early first trimester: indicator of poor pregnancy out
come. Radiology 1994;192:343–4.
[59] Doubilet PM, Benson CB. Embryonic heart rate in the
early first trimester: What rate is normal? J Ultrasound
Med 1995;14:431–4.
[60] Bromley B, Harlow BL, Laboda LA, et al. Small sac
size in the first trimester: a predictor of poor fetal out
come. Radiology 1991;178:375–7.
[61] Dickey RP, Gasser RF. Ultrasound evidence for vari-
ability in the size and development of normal human
embryos before the tenth post insemination week after
assisted reproductive technologies. Hum Reprod 1993;
8:331–7.
[62] Smith GS, Smith MF, McNay MB, Flemming JEE.
First trimester growth and the risk of low birth weight.
N Engl J Med 1998;339:1817–22.
[63] Nyberg DA, Cyr DR, Mack LA, et al. Sonographic
spectrum of placental abruption. AJR Am J Roent-
genol 1987;148:161.
[64] Sauerbrei EE, Pham DH. Placental abruption and sub
chorionic haemorrhage in the first half of pregnancy:
US appearance and clinical out come. Radiology 1986;
160:109–12.
[65] Bennett GL, Bromley B, Lieberman E, Benacerraf BR.
Subchorionic hemorrhage in first trimester pregnan-
cies: prediction of pregnancy outcome with sonogra-
phy. Radiology 1996;200:803–6.
[66] Stabile I, Campbell S, Grudzinskas JG. Threatened
miscarriage and intrauterine hematomas: sonographic
and biochemical studies. J Ultrasound Med 1989;
8:289.
[67] Contran RS, Kumar V, Robbins SL. Female genital
tract. In: Contran RS, Kumar V, Robbins SL, editors.
Robbins pathologic basis of disease. 4th edition. Phila-
delphia: WB Saunders; 1989. p. 1174–8.
[68] Jeffers MD, O’Dwyer P, Curran B, et al. Partial hyda-
tidiform mole: a common but under diagnosed condi-
tion. Int J Gynecol Pathol 1993;12:315.
[69] Miller DS, Ballon SC, Teng NNH. Gestational tropho-

R.M. Paspulati et al / Radiol Clin N Am 42 (2004) 297–314314
blastic diseases. In: Broody SA, Veland K, editors. En-
docrine disorders in pregnancy. Norwalk (CT): Apple-
ton & Lange; 1989. p. 451.
[70] Lawler SD, Fisher RA, Dent J. A prospective genetic
study of complete and partial hydatidiform moles. Am
J Obstet Gynecol 1991;164:1270–7.
[71] Szulman AE, Surti U. The syndromes of hydatidiform
mole: I. Cytogenetic and morphologic correlations.
Am J Obstet Gynecol 1978;131:665.
[72] Szulman AE, Surti U. The syndromes of hydatidiform
mole: II. Morphologic evolution of the complete and
partial mole. Am J Obstet Gynecol 1978;132:22.
[73] Fine C, Bundy AL, Berkowitz RS, et al. Sonographic
diagnosis of partial hydatidiform mole. Obstet Gynecol
1989;73:414.
[74] Steller MA, Genest DR, Bernstein MR, et al. Natural
history of twin pregnancy with complete hydatidi-
form mole and coexisting fetus. Obstet Gynecol 1994;
83:35.
[75] Green CL, Angtuaco TL, Shah HR, Parmley TH. Ges-
tational trophoblastic disease: a spectrum of radiologic
diagnosis. Radiographics 1996;16:1371–84.
[76] Tepper R, Shulman A, Altaras M, et al. The role of
color Doppler flow in the management of nonmetat-
static gestational trophoblastic disease. Gynecol Obstet
Invest 1994;38:14.
[77] Mayman R, Schneider D, Schulman A, et al. Serial
color Doppler flow of uterine vasculature combined
with serum beta-hCG measurements for improved
monitoring of patients with gestational trophoblastic
disease. Gynecol Obstet Invest 1996;42:201.
[78] Zanetta G, Lissoni A, Colombo M, et al. Detection of
abnormal intrauterine vascularization by color Doppler
imaging: a possible additional aid for the follow up of
patients with gestational trophoblastic tumors. Ultra-
sound Obstet Gynecol 1996;7:32.
[79] Long MG, Boultbee JE, Begent RH, et al. Preliminary
Doppler studies on the uterine artery and myometrium
in trophoblastic tumors requiring chemotherapy. Br J
Obstet Gynaecol 1990;97:686.
[80] Jauniaux E, Gulbis B, Hyett J, et al. Biochemical analy-
sis of mesenchymal fluid in early pregnancy. Am J Ob-
stet Gynecol 1998;178:765.
[81] Berkowitz RS, Goldstein DP. Chorionic tumors. N Engl
J Med 1996;335:1740.
[82] Bagshave KD, Lawler SD, Paradinas FJ, et al. Gesta-
tional trophoblastic tumors following initial diagnosis
of partial hydatidiform mole. Lancet 1990;335:1074.
[83] Chen RJ, Huang SC, Chow SN, et al. Persistent gesta-
tional trophoblastic tumour with partial hydatidiform
mole as the antecedent pregnancy. Br J Obstet Gynaecol
1994;101:330.
[84] Cunningham FG, MacDonald PC, Grant NF, Leveno
KJ, Gilstrap LC. Diseases and abnormalities of
the placenta. In: Licht J, editor. Williams obstetrics.
19th edition. Norwalk (CT): Appleton & Lange; 1993.
p. 748–59.
[85] Fine C, Bundy AL, Berkowitz RS, et al. Sonographic
diagnosis of partial hydatidiform mole. Obstet Gynecol
1989;73:414.
[86] Aoki S, Hata T, Hata K, et al. Doppler color flow
mapping of an invasive mole. Gynecol Obstet Invest
1989;27:52.
[87] Desai RK,DesbergAL.Diagnosis of gestational tropho-
blastic disease: value of endovaginal color flow Dopp-
ler sonography. AJR Am J Roentgenol 1991;157:787.
[88] Chau MT, Chan FY, Pun TC, et al. Perforation of the
uterus by an invasive mole using color Doppler ultra-
sound: case report. Ultrasound Obstet Gynecol 1993;
3:51.
[89] Bagshawe KD. Choriocarcinoma: a model for tumour
markers. Acta Oncol 1992;31:99–106.
[90] Mazur MT, Kurman RJ. Gestational trophoblastic dis-
ease and related lesions. In: Kurman RJ, editor. Blaus-
tein’s pathology of the female genital tract. New York:
Springer Verlag; 1994. p. 1049–92.
[91] Caspi B, Elchalal U, Dgani R, Ben-Hur H, Rozenman
D, Nissim F. Invasive mole and placental site tropho-
blastic tumor: two entities of gestational trophoblastic
disease with a common ultrasonographic appearance.
J Ultrasound Med 1991;10:517–9.
[92] Abulafia O, Sherer DM, Fultz PJ, Sternberg LB, An-
gel C. Unusual endovaginal ultrasonography and
magnetic resonance imaging of placental site tropho-
blastic tumor. Am J Obstet Gynecol 1993;170:750–2.
[93] Newlands ES, Barghawe KD, Begent HJ, Rustin GJS,
Holden L, Dent J. Developments in chemotherapy for
medium and high risk patients with gestational tropho-
blastic tumors. Br J Obstet Gynaecol 1986;93:63–9.
[94] Abu Musa A, Hata T, Hata K, Kitao M. Pelvic arterio-
venous malformation diagnosed by color flow Doppler
imaging. AJR Am J Roentgenol 1989;152:1311–2.
[95] Sugiyama T. Diagnosis of uterine arterivenous malfor-
mation by color and pulsed Doppler ultrasonography.
Ultrasound Obstet Gynecol 1996;8:359–60.
[96] Pelage JP, Soyer P, Repiquet D, et al. Secondary post
partum hemorrhage: treatment with selective arterial
embolization. Radiology 1999;212:385–9.

Radiol Clin N Am 42 (2004) 315–327
The role of ultrasound in pregnancy-related emergencies
Noam Lazebnik, MD*, Roee S. Lazebnik, PhD
Department of Obstetrics and Gynecology, MacDonald Women’s Hospital, University Hospitals of Cleveland,
Case Western Reserve University School of Medicine, 11100 Euclid Avenue, Cleveland, OH 44106, USA
Although most births are uneventful, about 15% Ultrasound examinations in emergency situations
of all birthing women experience potentially life-
threatening complications, and at least 1% to 2%
require major surgery. Although some complications
can be prevented, and some predicted preemptively,
most of the severe complications cannot be antici-
pated. To reduce mortality, a key component of ma-
ternal health care is the ability to diagnose, confirm,
and treat women whose medical status is unstable
in the antenatal, delivery, and postpartum periods.
Sonography is the imaging modality of choice for
diagnosing maternal-related abnormalities both dur-
ing and following pregnancy and delivery. Pelvic
ultrasound has long been the mainstay for evaluation
of the female pelvis. It is widely used during preg-
nancy in countries where antenatal care is available.
Most pregnant women are referred for ultrasound
study to confirm gestational age and to rule out fetal
malformations, abnormal placentation, and uterine
and cervical abnormalities. At University Hospitals
of Cleveland, Case Western Reserve University, a
tertiary care medical facility, more than 12,000 ob-
stetric ultrasound studies are performed yearly. About
13% of the total studies are performed in an emer-
gency obstetric setup. This article describes the
emergency conditions during pregnancy and the
immediate postpartum period that might lead to a
life-threatening situation for the pregnant patient or
her fetus, and the spectrum of imaging findings
associated with these conditions.
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.006
* Corresponding author.
E-mail address: [email protected] (N. Lazebnik).
are ordered to obtain specific, limited information
when it is necessary or impossible to perform a
complete fetal, placental, or pelvic organ survey.
Limited examinations in antepartum and intrapartum
emergency settings may include identification of
fetal number, fetal presentation, presence or absence
of fetal cardiac activity, localization of the placenta,
assessment of amniotic fluid volume, and a biophysi-
cal profile. The relevant clinical information can be
obtained by performing transabdominal study, trans-
vaginal study, or combination of the two modalities.
Occasionally, additional ultrasound studies are needed
in cases of medical or surgical complications of the
pregnant patient. Examples of such disorders include
renal and gastrointestinal abnormalities and maternal
vascular abnormalities.
Sonographic technique
Modern ultrasound devices have variable-focus
depths that allow the examiner to study structures
in the near or far field as needed without changing
transducers. A 2- to 5-MHz and 4- to 9-MHz trans-
ducer for transabdominal and transvaginal study,
respectively, is very well suited. For a pelvic sono-
gram, performed transabdominally, the patient’s uri-
nary bladder should be distended. A full bladder
usually is unnecessary. The more advanced the preg-
nancy, the lesser the need for a full bladder. When-
ever cervical and lower uterine segment or pelvic
organs images are needed, endovaginal scanning is
superior to transabdominal scanning. Improved visu-
alization may be achieved using the vaginal ap-
proach, because the transducer is brought closer to
s reserved.

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327316
the area being examined. It can be very helpful in
studying the lower uterine segment and its relation
to the placenta, evaluating the uterus, or measuring a
cyst in an ovary in the early stage of pregnancy. The
sonologist performing the study decides whether
one or a combination of approaches is best for the
particular case.
There are no known contraindications to abdomi-
nal ultrasound study. Transvaginal studies are not
recommended in case of premature rupture of the
membranes. The use of this modality is controversial
in cases of placenta previa, as discussed later. Careful
judgment should always be applied in choosing to
perform a transvaginal study because it might be
contraindicated for maternal or fetal reasons. Further-
more, regardless of the indication for the study, one
should always perform a transabdominal evaluation
before considering vaginal scanning. The added
views obtained by combining the two scanning
modalities might be of significant help in establish-
ing a correct diagnosis.
It is highly advisable to follow a strict routine
when one performs ultrasound study for an obstetric
emergency. The first priority in a true obstetric
emergency is to document a live in utero gestation,
with a stable and normal heartbeat. Once this has
been achieved one should document that there is no
suspicion for a significant volume of free fluid or
blood clots inside the gestational sac, the abdominal
cavity, or the posterior cul-de-sac. The bladder and
uterus should appear normal and intact, and no
adnexal mass should be present.
Second- and third-trimester obstetric emergencies
Pregnancy-induced hypertension
Pregnancy-induced hypertension complicates 6%
to 8% of pregnancies in the United States and ac-
counts for 15% of maternal deaths. It ranks second
only to embolic events as a cause of maternal mor-
tality. It also is an important cause of perinatal mor-
bidity and mortality. In pregnant women, two distinct
hypertensive disorders are common: chronic hyper-
tension and pregnancy-induced hypertension. Women
with chronic underlying hypertension are at risk for
pregnancy-induced hypertension, a multiorgan patho-
logic state with various subsets. One of the more
severe forms of hypertensive disorder during preg-
nancy is HELLP syndrome.
The HELLP syndrome in a pregnant woman is
characterized by hemolytic anemia, elevated liver
enzymes, and a low platelet count. Progressive nau-
sea and vomiting, upper right quadrant abdominal
pain, and headache are usually the most common
symptoms. During the physical examination, the
physician notes impressive abdominal tenderness,
especially in the right upper quadrant. The liver
may be enlarged and liver function tests are abnor-
mally elevated with evidence of hemolysis on a
peripheral blood smear and the red blood cell and
platelet counts may be low. When the disease is not
treated early, up to 25% of affected women develop
serious complications. Without treatment, approxi-
mately 1.1% to 3.5% of patients die from HELLP
syndrome, usually because of liver rupture or other
related maternal complications [1]. The pathophysio-
logic process of this condition begins with arteriolar
vasospasm, which causes endothelial damage and
fibrin deposition in the vessel lumen. This leads to
the following events: (1) platelet deposition on the
fibrin aggregates, reducing the number of circulat-
ing platelets (unlike disseminated intravascular co-
agulation, coagulation factors are not involved);
(2) erythrocyte destruction by the fibrin aggregates
(a microangiopathic hemolytic anemia), leading to
abnormal cells in the peripheral smear (burr cells and
schistocytes), an elevated indirect bilirubin level, and
anemia; and (3) hepatocyte destruction caused by
hepatic microemboli [2]. HELLP syndrome occurs
in approximately 10% of pregnant women with
preeclampsia or eclampsia. Preeclampsia may be mild
or severe. Severe cases with high blood pressure and
protein in the urine can progress to seizures (eclamp-
sia). Severe cases are life-threatening to both the
mother and fetus. Many women have a high blood
pressure and are diagnosed with preeclampsia before
they develop the HELLP syndrome. In some cases,
however, HELLP symptoms are the first warning of
preeclampsia and the condition is misdiagnosed as
hepatitis, gallbladder disease, idiopathic thrombocy-
topenic purpura, hemolytic uremic syndrome, or
thrombotic thrombocytopenic purpura.
The fatality rate among neonates born to mothers
with HELLP syndrome varies, depending on such
factors as birth weight. The main treatment is delivery
of the baby as soon as possible, because liver func-
tion in the mother rapidly deteriorates with this con-
dition, a harmful state for both the mother and fetus.
Sonographic findings
Unlike the traditional role of sonography during
pregnancy where the fetus, placenta, or the pelvic
organs are the targets of the study, sonography plays a
different role in HELLP syndrome; it can exclude
biliary tract disease and identify altered hepatic
and renal echo textures. Possible findings include

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 317
patchy areas of increased echogenicity in the liver,
diffusely increased renal echo texture and size, peri-
renal fluid, and hepatic subcapsular hematoma [3,4].
Uterine rupture
One of the major causes of maternal and perinatal
mortalities is rupture of the uterus. This obstetric
hazard is also associated with short-term maternal
morbidities, such as vesicovaginal fistula, rectovagi-
nal fistula, bladder rupture, foot drop, psychologic
trauma, and anemia [5]. In the long-term, because of
the surgical intervention, the woman may become
infertile as a result of indicated hysterectomy.
Uterine rupture is defined as separation that
requires operative intervention or is symptomatic. It
involves the full thickness of the uterine wall. Uterine
rupture may occur spontaneously but is more com-
monly associated with history of uterine surgery,
such as dilation and curretage, classical cesarean or
low transverse cesarean section, and myomectomy.
Induction of labor using low- and high-dose regi-
mens of prostaglandin E2 or with misoprostol might
also result in uterine rupture. Prolonged deceleration
(alone or proceeded by either severe late or variable
decelerations) is the most reliable clinical finding
occurring in 100% of cases when total fetal extrusion
occurred [6]. The incidence of uterine rupture is
0.05% of all pregnancies [7], occurring between 1 in
140 and 1 in 300 of women with a pre-existing scar
[8]. The risk of uterine rupture increases with the
number of caesarean sections [9]. The perinatal mor-
tality is 10 times that of the maternal mortality [7].
Leung et al [6] evaluated 78 cases of uterine rupture
in a large tertiary care medical center and reported
significant neonatal morbidity when 18 minutes or
more elapsed between the onset of prolonged decel-
eration and birth. When the prolonged deceleration
was preceded by severe late or variable decelera-
tions, fetal asphyxia occurred as early as 10 minutes
from the onset of prolonged deceleration.
Sonographic findings
The sonographic findings of uterine rupture dur-
ing pregnancy include extrauterine blood collection,
fetal parts outside the uterine cavity, intra-amniotic
hemorrhage, and focal bulging of membranes through
the site of dehiscence [10]. In a recently published
study the authors raised numerous questions regard-
ing the significance of cesarean scar defects and the
ability of transvaginal ultrasound to predict the risk
of uterine rupture in women choosing trial labor after
cesarean section [11]. Transvaginal ultrasound dem-
onstrated a cesarean scar as an echogenic line through
the myometrium near the level of the internal os, and
a cesarean scar defect was present when there was
an anechoic area (fluid) within the scar. Women who
had prolonged labor before cesarean section were
more likely to show a cesarean scar defect, and so
were women who had multiple cesarean deliveries.
The researcher reported that real-time transvaginal
ultrasound was 87% sensitive and 100% specific
for detecting cesarean scars [11].
Abnormal placentation
Abnormal placentation in the form of placenta
accreta, percreta, or increta is a rare but potentially
life-threatening complication of pregnancy that is
an increasingly frequent cause of maternal morbidity
and mortality. The term refers to any placental im-
plantation resulting in abnormal adherence to the
uterine wall. Life-threatening hemorrhage can occur
at delivery because of failure of placental separation
from the uterine wall and occurs in about 40% of
cases. It is associated with significant maternal mor-
bidity and in rare cases maternal mortality [12].
Pathologically it occurs when the decidua basalis is
partially or totally absent in conjunction with an
imperfect development of Nitabuch’s membrane, a
fibrinoid layer that separates the decidua basalis
from the placental villi [13]. The placental villi are
in direct contact with the myometrium without in-
tervening endometrial decidua. Clark et al [14] dem-
onstrated the effect of previous cesarean section
deliveries on the incidence of placenta accreta. They
showed that the risk of placenta previa increases
proportionately with the number of previous cesarean
section deliveries (0.26% in an unscarred uterus, and
up to 10% in women with four or more previous
cesarean sections). Surgical intervention in the form
of total abdominal hysterectomy is often indicated
because of life-threatening hemorrhage at delivery,
secondary to failure of placental separation from
the uterine wall.
Sonographic findings
Placenta accreta can be diagnosed using gray-
scale and color Doppler sonography. Gray-scale
findings include loss of the normally visible retropla-
cental hypoechoic rim corresponding to the decidua
basalis and dilated venous vessels [12]. Progressive
thinning of the retroplacental hypoechoic zone on
serial examinations is an important clue (Fig. 1).
Multiple placental lakes that may represent dilated
vessels extending from the placenta through the myo-
metrium form the so-called ‘‘Swiss cheese’’ appear-

Fig. 1. Placenta accreta. Longitudinal color Doppler image
of placenta demonstrates thinning of the retroplacental
hypoechoic zone (arrowheads). Color flow Doppler ultra-
sound highlights areas of increased turbulent flow that
extend from the placenta into the surrounding uterine wall
and cervix (arrows).
N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327318
ance of the placenta [15]. Depending on the location
of the implantation, the condition is referred to as
‘‘placenta accreta,’’ ‘‘placenta increta,’’ or ‘‘placenta
percreta.’’ If the placental villi extend beyond the
confines of the endometrium and attach to the super-
ficial aspect of the myometrium, the term ‘‘placenta
accreta’’ is used. Placenta increta refers to a situation
in which the villi invade the myometrium, whereas
the term ‘‘placenta percreta’’ is used if the villi ad-
vance into the serosa or parametria. Although this
classification scheme is widely accepted, most pub-
lished literature discusses these abnormalities collec-
tively as placenta accreta [16]. Doppler ultrasound
highlights areas of increased turbulent flow that
may extend from the placenta into the surrounding
uterine wall and cervix (see Fig. 1). Lerner et al [17]
reported a sensitivity of 100% and a specificity of
94% for the prenatal detection of placenta accreta
using color Doppler.
This technique also allows turbulent flow to be
visualized in cases of placenta percreta where placen-
tal vessels extend beyond the uterine serosa and may
involve other pelvic organs, such as the bladder.
Chou et al [18] have described the following findings
associated with placenta accreta: dilated vascular
channels with diffuse lacunar flow, irregular vascular
lakes with focal lacunar flow, hypervascularity linking
the placenta to the bladder, dilated vascular channels
with pulsatile venous flow over cervix, and poor
vascularity at sites of loss of hypoechoic zone.
Placenta previa
Placenta previa occurs in approximately 1 in
200 to 250 pregnancies and is associated with po-
tentially serious consequences from hemorrhage,
abruption of the placenta, or emergency cesarean
delivery. Abruption of the placenta occurs 14 times
more frequently in pregnancies with placenta previa
than in normal pregnancies, and cesarean delivery
occurs four times more frequently because of the
potentially serious consequences of persistent pla-
centa previa at delivery. There are three types of
placenta previa: (1) marginal previa where the edge
of the placenta is less than 2 cm from the opening
of the cervix, (2) partial placenta previa where the
placenta partly covers the cervical opening, and
(3) total previa where the placenta completely covers
the cervical os (Fig. 2A).
Marginal placenta previa is also known as ‘‘low-
lying’’ placenta. The natural history of marginal
placenta previa was studied by Rizos et al [19].
Placental localization by diagnostic ultrasound was
performed at 16 to 18 weeks’ gestation in 1098 pa-
tients before amniocentesis for genetic indications.
Marginal placenta previa was diagnosed in 58 pa-
tients, 47 of whom went on to delivery uncompli-
cated by placenta previa. There were five patients
with placenta previa at delivery, four of whom had
third-trimester bleeding. One patient was diagnosed
as having a normal placental implantation at mid-
trimester but placenta previa was demonstrated at
delivery. The incidence of placenta previa at 16 to
18 weeks’ was 5.3% and fell to 0.58% at delivery,
indicating a 90% conversion rate. This conversion
occurs secondary to rapid growth of lower uterine
segment in the third trimester resulting in superior
migration of placenta relative to the internal cervical
os. Most cases of asymptomatic low-lying placenta
convert to normal location of the placenta before
delivery. The authors concluded that these patients
should be observed with serial ultrasound studies at
6- to 8-week intervals until delivery or unequivocal
conversion. They also recommended no restriction
in activity unless the placenta previa persists beyond
30 weeks or becomes clinically manifest [19].
Traditionally, transabdominal study is used to
document sagittal midline images of the lower uter-
ine segment and cervix, preferably with a full bladder
to document the presence of placental tissue extend-

Fig. 2. Placenta previa. (A) Transvaginal sonographic view at 10 weeks gestation reveals the placenta completely covering the
internal cervical os. (B) Transabdominal view of the same case at 34 weeks gestation. The placenta covers the entire internal
cervical os. The retroplacental hypoechoic zone is invisible in the lower uterine segment adjacent to the cervix also suggesting
placenta accrete (arrows).
N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 319
ing down to the region of the cervix (Fig. 2B). Be-
cause of concerns regarding the use of transvaginal
study in patients with vaginal bleeding, possibly as a
result of placenta previa, translabial (transperineal)
study has been suggested as an alternative to trans-
abdominal study [20].
Farine et al [21] compared the accuracy of the
diagnosis of placenta previa using transvaginal so-
nography with that of the traditional transabdominal
sonography. They concluded that transvaginal sonog-
raphy was superior to transabdominal sonography in
diagnosing placenta previa and invariably correct in
ruling it out. Timor-Tritsch and Yunis [22] confirmed
the safety of transvaginal sonography in patients
suspected of placenta previa. They concluded that
the angle between the cervix and vaginal probe is
sufficient to prevent the probe from inadvertently
slipping into the cervix and initiating or further
aggravating vaginal bleeding.
Placental abruption
Third-trimester placental abruption complicates
less than 1% of pregnancies but is associated with
increased risk of preterm delivery and fetal death
when it does occur [23]. The clinical diagnosis is
usually based on bleeding, abdominal pain, and con-
tractions, but sonography is often performed to visu-
alize the extent of subchorionic or retroplacental
hematoma (Fig. 3). The diagnostic sensitivity for
abruption has not improved despite significant
improvements in ultrasound technology. Only one of
every nine sonograms obtained to rule out placental
abruption revealed evidence of a subchorionic or
retroplacental hematoma [23]. Ultrasound study
performed specifically to document placental abrup-
tion is usually unremarkable and is positive in only
25% of cases of placental abruption that are con-
firmed at delivery [24]. These researchers noted that
there were no significant differences in clinical char-
acteristics between women with positive or negative
sonographic findings. They concluded that sonogra-
phy is not sensitive for detecting abruption, but
when a clot is visualized on sonography, the positive
predictive value for abruption at delivery is high.
They also noted that the shorter the scan-to-delivery
interval, the greater the positive predictive value.
When delivery occurred within 2 weeks of a positive
sonographic finding, the diagnosis of placental abrup-
tion was confirmed in 100% of cases. Given that
sonography is not a sensitive tool to diagnose pla-
cental abruption, sound clinical judgment suggests
that even if the placenta appears grossly normal, a
diagnosis of abruption should be considered when
vaginal bleeding, abdominal pain, and uterine hyper-
tonicity are present.

Fig. 3. Placental abruption. (A) Retroplacental blood clot (arrows). (B) Large blood clot resulting from placental abruption
occupying most of the fundal region of the uterus. Hyperechoic and hypoechoic irregular areas are seen within the clot (arrows).
segment (arrows).
N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327320
Vasa previa
Despite dramatic improvements in diagnosis of
maternal, fetal, and placental abnormalities vasa
previa remains a true diagnostic challenge and con-
tinues to be a fatal condition for the fetus. For many
years even following the introduction of ultrasound
technology the diagnosis was made only after the
membranes were ruptured and fetal exsanguina-
tion occurred.
Vasa previa is a condition in which vessels run
through the membranes below the presenting part,
running over, or in close proximity to, the internal
cervical os, unsupported by placenta or cord (Fig. 4)
[25]. Spontaneous or artificial rupture of the mem-
branes in labor often leads to fetal exsanguination,
with mortality approaching 100%. With a high index
(C) A second blood clot is seen in the anterior lower uterine
of suspicion, however, vasa previa can be diagnosed
prenatally using ultrasound and color Doppler, allow-
ing for elective delivery by cesarean section before
membrane rupture with almost universal fetal sur-
vival [25]. Fung and Lau [26], Oyelese et al [27], and
Lee et al [28] showed that a good outcome in vasa
previa depended entirely on antenatal diagnosis
of the condition by ultrasound. Screening all patients
for vasa previa is time consuming and unnecessary
because of low incidence. Documentation of placen-
tal cord insertion, however, should be part of any
detailed obstetric sonographic examination. Recently
Fung and Lau [26] and Oyelese et al [27] indepen-
dently concluded that a low-lying placenta in the
second trimester was the most important risk factor
for vasa previa at term, whether or not the placenta
subsequently remained low-lying at term. Other risk

Fig. 4. Vasa previa. The placenta is posterior in location
with marginal previa. The vessels (red and blue) commu-
nicate with an accessory placental lobe implanted on the left
anterior lower uterine segment. Arrow points to the cervix.
Fig. 5. Retained products of conception. An echogenic area
(calipers) representing placental tissue, debris, and blood is
present in the endometrial cavity following manual removal
of the placenta. Patient underwent dilation and curettage for
continued uterine bleeding. The arrows point to retained
products of conception still present subsequent to the
dilation and curettage.
N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 321
factors for vasa previa include multiple pregnancies,
pregnancies resulting from in vitro fertilization, and
those with succenturiate lobe and bilobed placen-
tae [25]. In all such pregnancies it is prudent to
examine the region overlying the internal cervical
os for evidence of vessels running over it.
Postpartum hemorrhage
Obstetric delivery has been associated with the
potential for acute, massive blood loss to a degree
unparalleled by other surgical procedures. Data from
the Maternal Mortality Collaborative in 1988 indicate
that hemorrhage was responsible for 11% of direct
maternal deaths occurring in 1980 through 1985 [29].
No other condition in obstetrics, except perhaps
shoulder dystocia, requires such rapid recognition
and skillful response by the clinician to prevent
loss of life.
Sonographic findings
The sonographic findings of retained placental
tissue are often nonspecific because blood clots and
retained products feature considerable overlap in
sonographic appearance. In the first and early second
trimester on transabdominal or transvaginal views
of the endometrial cavity, thickened hyperechoic
endometrial stripe greater than 5 mm, gestational
sac (with or without a nonliving embryo), and round
to ovoid fluid sac are suggestive of retained prod-
ucts. If the endometrial stripe is less than 5 mm,
especially if it is less than 2 mm, retained blood in
the endometrial cavity is more likely than retained
products of conception.
Hertzberg and Bowie [30] reviewed the ultra-
sound images of 53 postpartum patients referred for
possible retained products of conception and corre-
lated specific ultrasound patterns with clinical and
pathologic follow-up. The most common finding in
patients with retained placental tissue was an echo-
genic mass in the uterine cavity, seen in 9 of
11 patients with pathologically proved retained pla-
cental tissue. In the remaining two patients with
pathologically confirmed retained placenta, a hetero-
geneous mass was seen in the uterine cavity some-
time during the course of serial sonography. Retained
placental tissue was found unlikely when ultrasound
demonstrated a normal uterine stripe endometrial
fluid, or hyperechoic foci in the uterine cavity with-
out an associated mass. The latter finding often was
associated with recent uterine instrumentation. The
sonographic appearance of retained placental tissue
was shown to be variable, but detection of an echo-
genic mass in the uterus strongly supported the
diagnosis. The authors concluded that solid echogenic
masses in the lumen or uterine wall are the most
specific findings for a retained placenta, whereas
heterogeneous mass could be caused by retained pla-
centa or from blood clots or infected or necrotic ma-
terial in the absence of placental tissue [30]. The

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327322
authors suggested that sonographic evaluation for
retained products of conception is best performed
before uterine instrumentation to avoid confusion
with iatrogenically introduced air. An example of
retained products following term vaginal delivery is
illustrated in Fig. 5.
Di Salvo [10] noted anecdotally that low-resist-
ance Doppler signals in these masses also can be
predictive. When using Doppler sonography in this
setting, however, it is important not to confuse low-
resistance arterial signals that arise within the myo-
metrium, which represent the placental implantation
site, with similarly appearing Doppler signals arising
from tissue within the endometrial cavity, which
represent retained products [10].
Retained products of conception
A spontaneous abortion is the loss of a fetus dur-
ing pregnancy because of natural causes. The term
‘‘miscarriage’’ is the spontaneous termination of a
pregnancy before fetal development has reached
20 weeks. The term ‘‘spontaneous abortion’’ refers
to these naturally occurring events, not elective or
therapeutic abortion procedures. More specific terms
include missed abortion (a pregnancy demise where
nothing is expelled); incomplete abortion (not all of
the products of conception are expelled); complete
abortion (all of the products of conception are ex-
pelled); threatened abortion (symptoms indicate a
miscarriage is possible); inevitable abortion (the
symptoms cannot be stopped and a miscarriage will
happen); and infected abortion. Any one of these
conditions might be associated with some degree of
vaginal bleeding. The bleeding in incomplete abor-
tion in which parts of the fetus or placental material
are retained within the uterus might be associated
with significant blood loss, however, and mandate
surgical intervention in the form of uterine curettage
to remove the remaining material from the uterus [31].
In the last decade with the introduction of mife-
pristone (RU 486) and oral or vaginal misoprostol to
induce abortion in the first trimester, vaginal bleeding
secondary to retained products of conception became
more common [32]. Studies clearly establish miso-
prostol as an effective agent to ‘‘empty’’ the pregnant
uterus in the first trimester [33]. Chia and Ogbo [32]
showed medical evacuation of missed abortion with
misoprostol to be an effective, safe, and cost-effective
alternative to surgical evacuation of the uterus, and
particularly suited for women not desiring hospital
admission or a surgical procedure under general
anesthesia [32]. Misoprostol is a synthetic prostaglan-
din E1 analogue. It was developed and marketed for
prevention of peptic ulcer disease caused by prosta-
glandin synthetase inhibitors, but with its potent
uterotonic and cervical ripening activity has found
applications in the management of gynecologic and
obstetric problems. In the United States it has been
marketed as Cytotec, in 100- and 200-mg tablets. Simi-
lar effectiveness has been shown when it is given
for a ‘‘failed’’ pregnancy or missed abortion [34,35].
Potential hypertonus as a result of drug accumu-
lation has been associated with uterine rupture in the
second or third trimester, and retained products of
conception with significant bleeding [36]. Transvagi-
nal sonography is a useful supplement to the clinical
assessment in women who experience a spontaneous
first-trimester abortion. Its use results in reduction
of unnecessary general anesthesia and uterine curet-
tage. Wong et al [37] showed that a first-trimester
vaginal ultrasound study has a sensitivity and speci-
ficity of 100% and 80%, respectively, using a bilayer
endometrial thickness of 8 mm or less. The ultra-
sound findings suggesting retained products of con-
ception are a thickened endometrium of greater than
8 mm; complex hyperechogenic (blood and tissue
debris) and hypoechogenic fluid material inside the
endometrial cavity; a gestational saclike structure; or
a space-occupying collection.
Uterine fibroids
Fibroid tumors are benign growths that develop
in the muscular wall of the uterus. Although fibroids
do not always cause symptoms, their size and loca-
tion could lead to complications during pregnancy for
some women including recurrent miscarriage, infer-
tility, premature labor, fetal malpresentations, and
complications of labor [38]. Lev-Toaff et al [39]
reported their ultrasound findings of uterine fibroids
during pregnancy. Fibroid size changes were ana-
lyzed on the basis of trimesters. In the second tri-
mester, smaller fibroids increased in size, whereas
larger fibroids decreased in size. In the third trimester,
a decrease in size was documented regardless of
initial size.
The most common patterns of echotexture were
hypoechoic, heterogeneous, and echogenic rim. The
development of a heterogeneous pattern or anechoic-
cystic spaces on a follow-up study was accompa-
nied by severe abdominal pain. The development
of these patterns apparently indicates significant
degeneration of the fibroid (Fig. 6). Fibroids located
in the lower uterine segment were accompanied by
a higher frequency of cesarean section and retained
placenta. Fibroids located in the uterine corpus were

Fig. 6. Color flow Doppler of uterus demonstrates a poste-
rior lower uterine segment degenerating fibroid. The
heterogeneous pattern with anechoic-cystic spaces suggests
degeneration process within the fibroid. A ‘‘feeding’’ ves-
sel can be seen between the myometrium and the fi-
broid (arrow).
Fig. 7. Gray-scale ultrasound longitudinal view shows a
posterior lower uterine segment fibroid undergoing degen-
eration. The patient experienced premature uterine con-
tractions starting at 29 weeks and delivered prematurely at
31 weeks by cesarean section secondary to lower uterine
segment obstruction from the fibroid. Arrowhead points to
the internal cervical os and calipers depict the whole length
of the cervix.
N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 323
more frequently associated with early abortions.
Multiple fibroids were accompanied by a higher
frequency of malpresentation and premature con-
tractions compared with cases with one or two
fibroids (Fig. 7) [39].
Abdominal surgery and trauma during pregnancy
Emergency surgery is indicated during pregnancy
for the management of trauma, malignancy, or acute
medical illness. Women in the childbearing years
are among the population at greatest risk for trauma.
Trauma occurs in 5% to 10% of pregnancies and is
responsible for 36 maternal deaths per 100,000
pregnancies, which is considerably higher than preg-
nancy-related mortality [40]. Penetrating abdominal
injury from gunshot and knife wounds or associated
with motor vehicle accidents results in 5% maternal
mortality. A much higher perinatal death rate in the
range of 41% to 71% is reported [41]. Fetal death
can be the result of maternal instability, placental
abruption, direct fetal injury and hemorrhage, or as a
consequence of premature delivery. The fetal status
must be assessed carefully for evidence of develop-
ing compromise. Monitoring fetal heart rate is an
important aspect of these procedures, and is techni-
cally feasible after the 16th week for nonabdominal
surgery. The surgeon and obstetrician alike must be
aware that fetal heart rate monitoring helps guide the
management of maternal cardiorespiratory parame-
ters, and is useful even if it does not influence a
decision to deliver the fetus [42]. Anesthetic drugs
create loss of heart rate variability, presumably by
anesthetizing the brainstem center that modulates
intrinsic cardiac automaticity. In addition, vasoactive
agents cross the placenta and produce predictable
changes to fetal heart rate and further influence the
interpretation of the fetal tracing, rendering fetal
heart rate monitoring through the use of standard
external Doppler probes useless. In many similar
challenging cases, the use of real-time ultrasound
and color Doppler adds valuable data to assess the
fetal status. Intermittent abdominal real-time ultra-
sound assessment of the fetus and placenta can be
used for abdominal procedures that do not permit
the use of standard external Doppler probes by
covering the ultrasound transducer with a sterile
sleeve. Abrupt changes in heart rate, baseline rates
outside the acceptable range of 120 to 160 beats per
minutes, and abnormal Doppler readings of the fetus
or the placental vasculature should prompt the
anesthesiologist to look for obvious causes of ute-
roplacental insufficiency.
Maternal nonobstetric emergencies during
pregnancy
Venous thromboembolism
Venous thromboembolism occurs infrequently
during pregnancy. It is a leading cause of illness
and death during pregnancy and the puerperium and

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327324
remains a diagnostic and therapeutic challenge [43].
In the general population the incidence of pregnancy-
associated venous thromboembolism has been esti-
mated to vary from 1 in 1000 to 1 in 2000 deliveries
[43]. The risk of venous thromboembolism is five
times higher in a pregnant woman than in a nonpreg-
nant woman of similar age. Postpartum venous
thromboembolism is more common than antepartum
venous thromboembolism [43]. Women with congen-
ital thrombophilic abnormalities, such as mutations
within factor II or V of the coagulation factors,
mutations leading to deficiency of protein S, or
protein Cor persistent presence of antiphospholipid
antibodies have an increased risk of venous throm-
boembolism during pregnancy and the puerperium. In
individuals with well-defined hereditary thrombosis
risk factors, such as the factor V:R506Q mutation, the
factor II:G20210A mutation, antithrombin deficiency,
or protein C deficiency, a relative risk of pregnancy-
associated venous thromboembolism between 3.4 and
15.2 has been found [43]. Women with previous
venous thromboembolism have an approximately
3.5-fold increased risk of recurrent venous thrombo-
embolism during pregnancy compared with nonpreg-
nant periods [43].
Pelvic thrombophlebitis
Pelvic thrombophlebitis is considered to be a rare
disorder of the puerperium with an incidence of
0.05% to 0.18% [44]. The ovarian veins are the most
frequently involved veins in puerperal pelvic venous
thrombosis. The clinical manifestations of the condi-
tion range from asymptomatic or dull abdominal pain
to sepsis, pulmonary embolism, and even death.
Unremitting fever and lower-quadrant or flank pain
usually occurs within the first 1 to 2 days after
delivery [45]. An abdominal mass is palpable in
about half of the patients, which may lead to the
suspicion of acute appendicitis. Torsion of the ovar-
ian pedicle, broad ligament hematoma, and pelvic
abscess may also occur. This condition is usually
managed conservatively, with intravenous heparin
and antibiotics, and rarely surgically. Imaging mo-
dalities used in the diagnosis include sonography, CT,
and MR imaging [44].
Gallbladder disease
Gallbladder disease is four times as common in
women as in men, and pregnancy seems to contribute
to the development of gallstones [46]. The symptoms
of gallbladder disease during pregnancy do not differ
from those reported for the nonpregnant population
and include steady, severe pain in the upper abdomen
that increases rapidly and lasts from 30 minutes to
several hours, pain in the back between the shoulder
blades, pain under the right shoulder, nausea or
vomiting, abdominal bloating, recurring intolerance
of fatty foods, belching, and indigestion. Ultrasound
scans are highly sensitive to the detection of gall-
stones. Sonographic findings with biliary disease
include gallstones, sludge, wall thickening, the sono-
graphic Murphy’s sign, biliary dilatation, and ductal
stones [47]. In a study done in Dublin, Ireland, real-
time ultrasound scanning was used to examine the
pelvic area and the upper part of the abdomen in a
prospective study of 512 healthy, pregnant women to
determine the prevalence of gallstones [47]. Twenty-
three women (4.5%) had gallstones. Fourteen
(60.9%) of the pregnant women were unaware of
the presence of gallstones. Ultrasound technique was
shown as the modality of choice to diagnose gall-
bladder disease in the parous and nonparous state
including acute gallbladder disease [46]
Acute renal disorders
Acute renal failure has become a rare complica-
tion of pregnancy [48]. This is the result of the
significant decline of septic abortion and its related
complications; the improvement of prenatal care; the
prevention of volume contraction, which is mainly
caused by uterine hemorrhage; early diagnosis; and
the treatment of other classic maternal complications,
such as preeclampsia and acute pyelonephritis [48].
The incidence of bilateral renal cortical necrosis has
also been declining during the last decade. Acute
fatty liver, a potentially fatal disease, often is com-
plicated by acute renal failure [48].
Ultrasound often is the first imaging technique
to be used in patients with renal failure, hematuria,
or proteinuria. Gray-scale ultrasound evaluation,
color flow Doppler, and resistive indices provide
adequate renal evaluation. In the initial clinical stages
of renal parenchymal diseases, the kidneys may
present normal ultrasound appearance and normal
resistive indices values. Different renal parenchymal
diseases may reveal similar appearance on ultrasound
and Doppler ultrasound evaluation [48]. Percutane-
ous renal biopsy is often necessary to reach definite
diagnosis. Renal vasculitides and tubular-interstitial
nephropathies are identified more frequently by
gray-scale ultrasound and Doppler ultrasound than
glomerular nephropathies, because glomerular com-
ponent accounts only for 8% of the renal paren-
chyma, whereas the highest percentage is occupied
by vascular and tubulointerstitial component [48].

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 325
Follow-up of acute renal failure, during and after
medical treatment, is the most useful field of use of
gray-scale ultrasound and Doppler ultrasound techni-
ques, because a progressive lowering of resistive
indices is correlated to a progressive recovery of
renal function [48].
Hydronephrosis in pregnancy occurs in more than
80% of pregnancies and begins as early as 11 to
15 weeks [49]. The dilatation of the ureters in the
early months of pregnancy is probably caused by
atony of the neuromuscular apparatus, but what un-
derlies this is not clear. The cause of the later dilata-
tion of the abdominal segment of the right ureter
and renal pelvis is a somewhat controversial sub-
ject. It is believed to be caused by pressure on the
right ureter at the pelvic brim by the natural inclina-
tion to the right of the enlarged uterus, whereas the
left ureter is protected by the rectosigmoid.
Urolithiasis during pregnancy is a difficult clinical
problem in which carefully selected radiologic stud-
ies play an essential role. It has been shown that
sonography, particularly Doppler sonography, plays
a major role in the diagnosis of urolithiasis in preg-
nancy [49]. Studies evaluating the intrarenal resistive
index in asymptomatic pregnant patients have shown
that both right and left kidneys have similar resistive
indices, and there is no change in resistive indices
during pregnancy [50]. In the absence of underlying
renal disease, however, a difference of greater than
0.1 in resistive indices should prompt further sono-
graphic confirmation of mechanical ureteral obstruc-
tion. This includes unilateral absence of a distal
ureteral jet or direct visualization of a stone either
at the ureterovesical or ureteropelvic junction [10].
Unilateral absence of a ureteral jet with the patient
supine should always be confirmed by re-evaluation
with the patient in the contralateral decubitus posi-
tion, because the cause of the absent jet may merely
be compression of the ureter by the uterus rather than
an obstructing calculus [51].
Splenic artery aneurysm
Splenic artery aneurysm occurs predominantly in
women and most of the aneurysms are asymptomatic
until rupture [52]. Over half of those that rupture
occur during pregnancy or in women who have had
children. Rupture during pregnancy is associated
with a very high maternal and fetal mortality rate
[52]. Although this condition is uncommon, good
maternal-fetal outcome can only be achieved by early
diagnosis and prompt treatment. Ordinarily, in sus-
pected unruptured splenic artery aneurysm the gold
standard for diagnosis is arteriography [53]. Ultraso-
nography and pulsed Doppler, however, are prefera-
ble in pregnancy [54]. Gray-scale sonography might
fail to detect the unruptured splenic artery aneurysm
if marked calcification of the aneurysmal wall is
present [54]. Pulsed Doppler sonography has been
used to document turbulent pulsatile flow along the
aneurysmal wall. When patients with ruptured splenic
artery aneurysm present with acute abdominal pain,
an emergency ultrasound scan may reveal free fluid
in the upper abdomen and the diagnosis is subse-
quently confirmed at laparotomy [54].
Summary
Most complications of pregnancy allow time for
transfer to specialized obstetric ultrasound units, but
many women present to the emergency room or the
labor and delivery unit with signs and symptoms
suggesting genuine acute medical emergencies,
where successful outcome depends on prompt diag-
nosis of the disorder and rapid appropriate medical
management. The use of ultrasound technology in
obstetric emergencies is well established. Ultrasonog-
raphy plays a major role in such cases as the most
important tool clinicians are using to identify the
correct etiology and diagnosis, whereas in other cases
it helps limit the differential diagnosis. One of the
goals of any advanced training program in obstetrics
and gynecology and radiology is to allow the skilled
physician to perform the proper ultrasound study in
case of an obstetric emergency to facilitate the proper
diagnosis, enabling the medical team to provide the
best possible care.
References
[1] Weinstein L. Syndrome of hemolysis, elevated liver
enzymes and low platelet count: a consequence of
hypertension in pregnancy. Am J Obstet Gynecol
1982;142:159–67.
[2] Sibai BM, Taslimi MM, El-Nazer A, et al. Maternal-
perinatal outcome associated with the syndrome of
hemolysis, elevated liver enzymes and low platelets
in severe preeclampsia-eclampsia. Am J Obstet Gyne-
col 1986;155:501–9.
[3] Benacerraf BR, Frigoletto Jr FD, Martini CA. Sono-
graphic findings in severe pre-eclampsia twenty-four
hours prior to clinical signs. Am J Obstet Gynecol
1985;152:684–5.
[4] Kronthol AJ, Fishman EK, Kuhlman JE, et al. Hepa-
tic infarction in preeclampsia. Radiology 1990;177:
726–8.

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327326
[5] Chauhan SP, Martin Jr JN, Henrichs CE, et al. Mater-
nal and perinatal complications with uterine rupture
in 142,075 patients who attempted vaginal birth after
cesarean delivery: a review of the literature. Am J
Obstet Gynecol 2003;189:408–17.
[6] Leung AS, Leung EK, Paul RH. Uterine rupture after
previous cesarean delivery: maternal and fetal conse-
quences. Am J Obstet Gynecol 1993;169:945–50.
[7] Lynch JC. Uterine rupture and scar dehiscence: a
five year survey. Anaesth Intensive Care 1996;24:
699–704.
[8] CESDI 5th Annual Report. Maternal and Child Health
Research Consortium; 1998.
[9] Caughey AB. Rate of uterine rupture during a trial of
labor in women with one or two prior caesarian sec-
tions. Am J Obstet Gynecol 1999;181:872–6.
[10] Di Salvo DN. Sonographic imaging of maternal com-
plications of pregnancy. J Ultrasound Med 2003;22:
69–89.
[11] Armstrong V, Hansen WF, Van Voorhis BJ, et al. De-
tection of cesarean scars by transvaginal ultrasound.
Obstet Gynecol 2003;101:61–5.
[12] Breen JL, Neubecker R, Gregori CA, et al. Placenta
accreta, increta, and percreta: a survey of 40 cases.
Obstet Gynecol 1997;49:43–7.
[13] Benirschke K, Kaufmann P. Pathology of the hu-
man placenta. 2nd edition. New York: Springer-Ver-
lag; 1990.
[14] Clark SL, Koonings PP, Phelan JP. Placenta previa/
accreta and prior cesarean section. Obstet Gynecol
1985;66:89–92.
[15] Hoffman-Tretin JC, Koenigsberg M, Rabin A, et al.
Placenta accreta: additional sonographic observations.
J Ultrasound Med 1992;11:29–34.
[16] Avva R, Shah HR, Angtuaco T. US case of the day.
Radiographics 1999;19:1089–92.
[17] Lerner JP, Deane S, Timor-Tritsch IE. Characterization
of placenta accreta using transvaginal sonography and
color Doppler imaging. Ultrasound Obstet Gynecol
1995;5:198–201.
[18] Chou MM, Ho ES, Lee YH. Prenatal diagnosis of
placenta previa accreta by transabdominal color Dopp-
ler ultrasound. Ultrasound Obstet Gynecol 2000;15:
282–5.
[19] Rizos N, Doran TA, Miskin M, et al. Natural history of
placenta previa ascertained by diagnostic ultrasound.
Am J Obstet Gynecol 1979;133:287–91.
[20] Hertzberg BS, Bowie JD, Carroll BA, et al. Diagnosis
of placenta previa during the third trimester: role
of transperineal sonography. AJR Am J Roentgenol
1992;159:83–7.
[21] Farine D, Peisner DB, Timor-Tritsch IE. Placenta pre-
via: is the traditional diagnostic approach satisfactory?
J Clin Ultrasound 1990;18:328–30.
[22] Timor-Tritsch IE, Yunis RA. Confirming the safety
of transvaginal sonography in patients suspected of
placenta previa. Obstet Gynecol 1993;81:742–4.
[23] Combs CA, Nyberg DA, Mack LA, Smith JR, Bene-
detti TJ. Expectant management after sonographic
diagnosis of placental abruption. Am J Perinatol
1992;9:170–4.
[24] Glantz C, Purnell L. Clinical utility of sonography in
the diagnosis and treatment of placental abruption.
J Ultrasound Med 2002;21:837–40.
[25] Oyelese KO, Turner M, Lees CC, et al. Vasa previa:
an avoidable obstetric tragedy. Obstet Gynecol Surv
1999;54:138–45.
[26] Fung TY, Lau TK. Poor perinatal outcome associated
with vasa previa: is it preventable? A report of three
cases and review of the literature. Ultrasound Obstet
Gynecol 1998;12:430–3.
[27] Oyelese KO, Schwarzler P, Coates S, et al. A strategy
for reducing the mortality rate from vasa previa using
transvaginal sonography with color Doppler. Ultra-
sound Obstet Gynecol 1998;12:434–8.
[28] Lee W, Kirk JS, Comstock CH, et al. Vasa previa:
prenatal detection by three-dimensional ultrasonogra-
phy. Ultrasound Obstet Gynecol 2000;16:384–7.
[29] Rochat RW, Koonin LM, Atrash HK, et al. Maternal
mortality in the United States: report from the Mater-
nal Mortality Collaborative. Obstet Gynecol 1988;
72:91–7.
[30] Hertzberg BS, Bowie JD. Ultrasound of the postpartum
uterus: prediction of retained placental tissue. J Ultra-
sound Med 1991;10:451–6.
[31] Jurkovic D. Modern management of miscarriage: is
there a place for non-surgical treatment? Ultrasound
Obstet Gynecol 1998;11:161–3.
[32] Chia KV, Ogbo VI. Medical termination of missed
abortion. J Obstet Gynaecol 2002;22:184–6.
[33] Carbonell JL, Varela L, Velazco A, et al. The use of
misoprostol for abortion at < 9 weeks’ gestation. Eur
J Contracept Reprod Health Care 1997;2:181–5.
[34] Chipcase J, James D. Randomised trial of expectant
versus surgical management of spontaneous miscar-
riage. BJOG 1997;104:840–1.
[35] Creinin MD, Moyer R, Guido R. Misoprostol for
medical evacuation of early pregnancy failure. Obstet
Gynecol 1997;89:768–72.
[36] Faundes A, Santos LC, Carvalho M, et al. Postabortion
complications after interruption of pregnancy with
misoprostol. Adv Contracept 1996;12:1–9.
[37] Wong SF, Lam MH, Ho LC. Transvaginal sonogra-
phy in the detection of retained products of concep-
tion after first-trimester spontaneous abortion. J Clin
Ultrasound 2002;7:428–32.
[38] Benson CB, Chow JS, Chang-Lee W, et al. Outcome of
pregnancies in women with uterine leiomyomas
identified by sonography in the first trimester. J Clin
Ultrasound 2001;29:261–4.
[39] Lev-Toaff AS, Coleman BG, Arger PH, et al. Leiomyo-
mas in pregnancy: sonographic study. Radiology 1987;
164:375–80.
[40] Pearlman MA, Tintinalli JE, Lorenz RP. A prospective
controlled study of outcome after trauma during preg-
nancy. Am J Obstet Gynecol 1990;162:1502–7.

N. Lazebnik, R.S. Lazebnik / Radiol Clin N Am 42 (2004) 315–327 327
[41] Crosby WM, Costiloe JP. Safety of lapbelt restraint
for pregnant victims of automobile collisions. N Engl
J Med 1971;284:632–6.
[42] Liu PL, Warren TM, et al. Fetal monitoring in parturi-
ents undergoing surgery unrelated to pregnancy. Can
Anaesth Soc J 1985;32:525–32.
[43] Pabinger I, Grafenhofer H. Thrombosis during preg-
nancy: risk factors, diagnosis and treatment. Patho-
physiol Haemost Thromb 2002;32:322–4.
[44] Zuckerman J, Levine D, McMicholas MMJ, et al. Im-
aging of pelvic postpartum complications. AJR Am J
Roentgenol 1997;168:663–8.
[45] Dunnihoo DR, Gallaspy JW, Wise RB, Otterson WN.
Postpartum ovarian vein thrombophlebitis: a review.
Obstet Gynecol Surv 1991;46:415–27.
[46] Hossain GA, Islam SM, Mahmood S, et al. Gall stone
in pregnancy. Mymensingh Med J 2003;12:112–6.
[47] Basso L, McCollum PT, Darling MR, et al. A study of
cholelithiasis during pregnancy and its relationship
with age, parity, menarche, breast-feeding, dysmen-
orrhea, oral contraception and a maternal history of
cholelithiasis. Surg Gynecol Obstet 1992;175:41–6.
[48] Quaia E, Bertolotto M. Renal parenchymal diseases:
is characterization feasible with ultrasound? Eur Radiol
2002;12:2006–20.
[49] Boridy IC, Maklad N, Sandler CM. Suspected uro-
lithiasis in pregnant women: imaging algorithm and
literature review. AJR Am J Roentgenol 1996;167:
869–75.
[50] Nazarian GK, Platt JF, Rubin JM, et al. Renal duplex
Doppler sonography in asymptomatic women during
pregnancy. J Ultrasound Med 1993;12:441–4.
[51] Wachsberg RH. Unilateral absence of ureteral jets
in the third trimester of pregnancy: pitfall in color
Doppler US diagnosis of urinary obstruction. Radi-
ology 1998;209:279–81.
[52] Selo-Ojeme DO, Welch CC. Spontaneous rupture of
splenic artery aneurysm in pregnancy. Eur J Obstet
Gynecol Reprod Biol 2003;109:124–7.
[53] Wagner WH, Allins AD, Treiman RL, et al. Ruptured
visceral artery aneurysms. Ann Vasc Surg 1997;11:
342–7.
[54] Lang W, Strobel D, Beinder E, et al. Surgery of a
splenic aneurysm during pregnancy. Eur J Obstet
Gynecol 2002;102:215–6.

Radiol Clin N Am 42 (2004) 329–348
Adnexal mass with pelvic pain
Emily M. Webb, MD, Gretchen E. Green, MD, Leslie M. Scoutt, MD*
Department of Diagnostic Radiology, Yale University School of Medicine, 333 Cedar Street, New Haven, CT 06520, USA
The routine use of ultrasound (US) in the evalua- and unnecessary surgery can be avoided, to the
tion of pregnant patients has resulted in more fre-
quent detection of adnexal masses, which occur in
approximately 2% of pregnancies. This estimation in-
cludes masses with a wide variety of appearances
and etiologies that range from asymptomatic ovarian
cysts to surgical emergencies, including ovarian tor-
sion, ectopic pregnancy, and tubo-ovarian abscess [1].
Although many adnexal masses are detected inciden-
tally, this article focuses on the evaluation of preg-
nant women who present with an adnexal mass in
the setting of acute pelvic pain. Clinical diagnosis in
pregnancy is a challenge because the differential di-
agnosis for an adnexal mass that presents with pelvic
pain is broad and includes pregnancy-related and
unrelated causes. The clinical presentation and natu-
ral history of abdominal and pelvic disease may be
altered in pregnancy. US is an ideal tool for evaluating
a pregnant patient. It is excellent in defining pelvic
anatomy and pathology without the risks of ionizing
radiation inherent to many imaging techniques.
Pregnancy-related disease
Several disease processes, either specific to preg-
nancy or with an increased incidence in pregnant
patients, can cause acute pelvic pain and an associ-
ated adnexal mass. These disease processes vary
from benign, often asymptomatic entities to diseases
that require emergent treatment. Differentiation is
critical so that appropriate treatment can be provided
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.006
* Corresponding author.
E-mail address: [email protected]
(L.M. Scoutt).
benefit of mother and fetus.
Follicular cysts and corpus luteal cysts
Most adnexal masses identified during pregnancy
are non-neoplastic, physiologic cysts, including cor-
pus luteal cysts and follicular cysts. These cysts can
be seen in early pregnancy but usually involute by
midterm [1]. Follicular cysts vary in size from 3 to
8 cm in diameter. They result from failure in ovu-
lation, most likely secondary to changes in the re-
lease of pituitary gonadotropins. The fluid contained
within the immature follicle is not completely re-
absorbed, which produces an enlarged follicular cyst
[2]. On US examination, a follicular cyst should ap-
pear as a thin-walled, anechoic, round, or oval struc-
ture that demonstrates increased through transmission
(Fig. 1). After ovulation has occurred from a mature
follicle, the granulosa cells, which line the follicle,
become luteinized. Blood accumulates in the central
cavity during vascularization and then resorbs to form
the corpus luteum [2]. The corpus luteum is described
as a cyst when it reaches more than 2.5 to 3 cm [2].
Corpus luteal cysts are typically thin-walled, uni-
locular cysts that can range in diameter from approxi-
mately 3 to 11 cm [2]. The corpus luteum can have
a wide range of appearances on US in the first tri-
mester of pregnancy, however. The most common ap-
pearance is that of a round, thin-walled hypoechoic
structure that demonstrates diffuse, homogenous, low-
level echoes (Fig. 2) [3]. Other reported gray scale
appearances in order of decreasing frequency include
a cyst with a thick wall and anechoic center (Fig. 3), a
cyst that contains scattered internal echoes, or a thin-
walled simple cyst that is similar in appearance to
a follicular cyst [3]. In most cases, color Doppler
s reserved.

Fig. 1. Simple ovarian or follicular cysts. These two ovarian
cysts are completely anechoic, with thin, nearly impercep-
tible walls (arrow), and they demonstrate increased through
transmission (arrowheads).
Fig. 3. Atypical corpus luteal cyst. This exophytic cyst has
an anechoic center with a thick, relatively hypoechoic wall
(arrow) with a thin rim of vascularity. Although it may be
difficult to differentiate such a structure from an ectopic
pregnancy, in general the wall of an ectopic pregnancy is
more echogenic and usually not so thick.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348330
evaluation of the corpus luteum demonstrates a cir-
cumferential ‘‘ring of fire’’ of vascularity with a low
resistance waveform pattern. In a study by Durfee
and Frates [3], 92% of corpus luteal cysts demon-
strated this pattern of blood flow with a mean resist-
ance index of 0.49 and mean peak systolic velocity of
17 cm/second.
Acute pelvic pain in pregnancy is commonly
caused by hemorrhage into a follicular or corpus
luteal cyst. Cyst rupture or leakage also may cause
severe pelvic pain and hemorrhage, sometimes re-
quiring laparoscopy or laparotomy [2,4]. The US
appearance of hemorrhagic ovarian cysts varies be-
cause the US characteristics of hemorrhage change
over time [4–7]. Initially a hemorrhagic cyst dem-
onstrates a diffuse, homogeneous pattern of low-
Fig. 2. Corpus luteal cyst. This exophytic corpus luteal cyst
contains low-level internal echoes. The cyst wall is mark-
edly vascular on color Doppler evaluation, which dem-
onstrates ring of fire (arrows).
level echoes. The wall may be vascular but should
be thin and regular. In a study by Baltarowich et al
[6], most hemorrhagic cysts (92%) demonstrated
increased through transmission. Over time as the clot
forms, a lace-like, reticular pattern of internal echoes
develops because of the presence of fine fibrous
Fig. 4. Hemorrhagic cyst. Note lace-like or spider web
pattern of internal echoes. The cyst wall is smooth and
regular. Increased through transmission is present. Doppler
interrogation reveals no evidence of internal blood flow,
and the appearance changes over time as the blood clot
continues to resorb.

Fig. 5. Hemorrhagic cyst. Clot within a hemorrhagic cyst
often adheres to the cyst wall and is lenticular in shape
(arrow). Doppler examination does not demonstrate internal
vascularity within adherent clot but may do so in a neo-
plastic mural nodule. Despite the absence of vascularity on
this color Doppler image, follow-up imaging in 6 weeks is
recommended to ensure that the clot continues to resolve.
Occasionally Doppler interrogation does not demonstrate
vascularity in tumor nodules because of low velocity, low
volume flow, or sampling error.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 331
septae (‘‘fish net’’) (Fig. 4). The clot may appear as
an echogenic mass either mobile or adherent to the
cyst wall but without evidence of vascularity. Typi-
cally, the clot retracts over time and adheres to the
cyst wall in a lenticular shape (Fig. 5). Lysis of red
blood cells may result in layering fluid or debris.
Follow-up examination at a 6- to 8-week interval
should demonstrate that a hemorrhagic cyst changes
in appearance and decreases in size [7]. In patients
with rupture or leakage of fluid from the corpus luteal
cyst, the cyst may have an angular or crenated
appearance, and free fluid that contains low-level
echoes or frank clots may be observed in the cul-
de-sac or surrounding the ovary [2,7].
Box 1. Conditions that predispose toectopic pregnancy
� Prior pelvic inflammatory disease� Presence of an intrauterine device� Treatment of infertility� Tubal surgery� Previous ectopic pregnancy� Diethylstillbestrol exposure
Ectopic pregnancy
The incidence of ectopic pregnancy has increased
over the past three decades, and it recently reached a
plateau at a reported rate of 19.7 per 1000 pregnan-
cies [8]. Ectopic pregnancy remains the leading cause
of maternal death in the first trimester and the second
leading cause of maternal mortality overall [8]. Im-
proved treatments for infertility and pelvic inflam-
matory disease and an increase in the size of the
patient population at risk for ectopic pregnancy in
large part account for the increased incidence. Other
risk factors include presence of an intrauterine device,
exposure to diethylstilbestrol, adhesions from prior
surgery, and previous ectopic pregnancy (Box 1).
The reported increased incidence of ectopic preg-
nancy is also likely in part accounted for by an
‘‘apparent’’ increase because of early US evaluation
of symptomatic pregnant patients. Endovaginal US
almost certainly documents some early ectopic preg-
nancies that otherwise would have resolved without
coming to medical attention. Endovaginal US, com-
bined with quantitative b-human chorionic gonado-
tropin (b-HCG) analysis, is an excellent tool for
identifying ectopic pregnancy and differentiating
from other causes of adnexal mass in the pregnant
patient with pelvic pain. The first goal of endovaginal
US in the patient suspected of harboring an ectopic
pregnancy is to assess for an intrauterine pregnancy
because ectopic pregnancy can be reasonably ex-
cluded when an intrauterine pregnancy is identified
[9]. Only rarely does an ectopic pregnancy occur
synchronously with an intrauterine gestation. Hetero-
topic pregnancy is estimated to occur in only 1 in
2600 to 1 in 30,000 pregnancies in the general
population [10], but it likely occurs in up to 1 in
100 in patients with multiple risk factors who are
undergoing infertility treatment [11].
An intrauterine gestational sac should be seen
on endovaginal US when the b-HCG is more than
2000 mIU/mL (approximately 4–6 weeks’ gestation).
The earliest positive sign of an intrauterine pregnancy
is the intradecidual sign, which is defined as a fluid
collection with an echogenic rim located eccentrically
within either the anterior or posterior layer of the
endometrium adjacent to the echogenic line that
represents the endometrium [12,13]. The intradecid-
ual sign should be visible at 4.5 weeks’ gestation, but
it can be confused with a pseudosac or decidual cyst.
A study reported by Laing et al [12] demonstrated a
low enough sensitivity and specificity to warrant a
recommendation to document the development of
a yolk sac or fetal pole on follow-up examination to

Fig. 7. Ectopic pregnancy. Note echogenic tubal ring
(arrow) medial to the right ovary (cursors). Amorphous
hypoechoic material between ovary and ectopic pregnancy
likely represents hemorrhage.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348332
confirm an intrauterine pregnancy. The double decid-
ual sac sign is formed when the gestational sac is
surrounded, at least in part, by two echogenic
layers—decidual capsulans (inner) and decidual parie-
talis (outer)—and is separated by the hypoechoic
endometrial cavity [9]. It should be seen when the
mean sac diameter is more than 10 mm. Because
endovaginal US (when using a high-frequency trans-
ducer) typically demonstrates a yolk sac with an
intrauterine pregnancy by the time the mean sac
diameter (MSD) is more than 8 mm, the double
decidual sign is of limited use in the evaluation of
patients with suspected ectopic pregnancy. The pres-
ence of trophoblastic flow (high velocity, low imped-
ance) around an endometrial fluid collection further
supports the diagnosis of an intrauterine pregnancy,
although pulsed Doppler should be used with caution
because of concerns regarding heat deposition in the
developing fetus.
A pseudosac, an intrauterine fluid collection
formed in response to hormonal influences on the
endometrium as the result of the presence of an
ectopic pregnancy, can be distinguished from an
intrauterine pregnancy by its central location in the
endometrial cavity, oval shape, poorly defined mar-
gins, absence of decidual reaction, single decidual
layer, and absence of trophoblastic flow.
Ectopic pregnancy most commonly (95%) occurs
in the ampullary or isthmic portions of the fallopian
tube. An ectopic pregnancy can be diagnosed with
confidence when an adnexal mass that contains a
yolk sac or viable embryo is identified (Fig. 6) [14].
In the absence of a visualized yolk sac or fetal pole,
the so-called echogenic adnexal (or tubal) ring sign
Fig. 6. Ectopic pregnancy. A yolk sac (arrow) and fetal pole
(arrowhead) are present within this echogenic tubal ring
(curved arrow) located in the cul de sac. U, uterus. Note that
the wall or ring of this ectopic pregnancy is much more
echogenic than the wall of the corpus luteal cyst in Fig. 3.
is the next most specific US finding for ectopic
pregnancy (Fig. 7) [15]. Adnexal rings are usually
located between the ovary and uterus. In 14% to 33%
of cases, the adnexal ring is contralateral to the cor-
pus luteum [16]. The echogenic adnexal ring typi-
cally has a relatively anechoic center and vascular
wall (sometimes only focally). It may be difficult to
differentiate the tubal ring of an ectopic pregnancy
from an exophytic corpus luteal cyst. An anechoic
structure with an echogenic, vascular rim truly lo-
cated within the ovary is statistically much more
likely to be a corpus luteal cyst, because true intra-
ovarian ectopic pregnancies are rare.
Frates et al [17] reported that the wall of the
adnexal ring is more echogenic compared with the
ovarian stroma in 88% of ectopic pregnancies, where-
as the wall of the corpus luteal cyst was usually
relatively hypoechoic. Corpus luteal cysts and ectopic
pregnancy demonstrate low-resistance arterial flow
on Doppler examination [18]. Color Doppler is
helpful primarily for increasing conspicuity. Differ-
entiation between an ectopic pregnancy and an
exophtic corpus luteal cyst can be aided by gently
tapping on the ovary with the transducer. Independent
movement of the ovary indicates an extraovarian
location of the adnexal ring, which confirms ectopic
pregnancy. A hemorrhagic ovarian cyst occasionally
can produce an adnexal ring sign, and when associ-
ated with significant hemoperitoneum, it may mimic
ectopic pregnancy [19].
Evaluation of the cul-de-sac and Morrison’s pouch
is important to detect echogenic fluid that could
represent blood (Fig. 8) [20]. Transabdominal US is
particularly helpful for evaluation of these areas and
visualization of the patient’s point of maximal ten-
derness if not imaged on endovaginal US. Blood need

Fig. 8. Hemoperitoneum from a ruptured ectopic pregnancy.
Note echogenic free fluid (arrow) outlining loops of bowel.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 333
neither be echogenic nor the consequence of tubal
rupture, however; hemoperitoneum may be anechoic
(albeit rarely) and can occur secondary to leakage
from the fimbriated end of the fallopian tube or even
from a ruptured hemorrhagic corpus luteal cyst.
Endovaginal US has replaced culdocentesis as the
method of choice for detecting hemoperitoneum
[21]. Brown and Doubilet [14] reported that demon-
stration on US of an extrauterine gestational sac that
contains a yolk sac or embryo or a tubal ring has high
specificity rate (99.5%–100%) and high positive
predictive value (97.8%–100%) for the diagnosis
of ectopic pregnancy. Sensitivity rate was, however,
found to be low (20.1%–64.6%). When the most non-
specific finding that suggests ectopic pregnancy—
the presence of any adnexal mass other than a simple
cyst—was used as the sole diagnostic criterion, sen-
sitivity rate was improved (84.4%) with only slightly
diminished specificity rate (98.9%) and positive pre-
dictive value (96.3%) [14]. The sonographer should
remember that in up to 26% of ectopic pregnancies,
no intrauterine pregnancy or adnexal abnormality
may be detectable by endovaginal sonography [22].
Clinical correlation and close follow-up are of para-
mount importance.
Although the terms are occasionally used inter-
changeably, the term ‘‘cornual pregnancy’’ should be
reserved for an intrauterine pregnancy implanted in
one horn of a bicornuate or septate uterus, whereas an
interstitial ectopic pregnancy (approximately 2%–4%
of all ectopic pregnancies) occurs in the interstitial
(or intramyometrial) portion of the fallopian tube. An
interstitial ectopic pregnancy typically develops much
longer before becoming symptomatic, and it often
presents late in the first trimester or early in the
second trimester. A ruptured interstitial pregnancy
poses a significantly increased risk of severe, life-
threatening hemorrhage. On US examination, the sac
is eccentrically located within the uterine wall, and
the surrounding myometrium is thinned (<5 mm) or
even absent laterally. The ‘‘interstitial line sign’’
describes an echogenic line that reflects the two
opposing layers of endometrium seen adjacent to
the gestational sac but not surrounding it. This sign
has been reported to be 80% sensitive and 99%
specific for diagnosing interstitial ectopic pregnancy,
compared with 40% sensitive and 62% specific for
eccentric location or 40% sensitive and 74% specific
for myometrial thinning [23]. Even more convinc-
ing is visualization of myometrial tissue interposed
between the gestational sac and echogenic line (en-
dometrial cavity). It may be difficult to distinguish
interstitial and cornual pregnancies. Braxton Hicks
contractions or fibroids occasionally can cause a nor-
mal intrauterine pregnancy to be eccentrically placed.
If there is doubt about the diagnosis, follow-up may
be helpful.
Cervical pregnancies are rare but are important
to diagnose accurately because routine dilation and
curettage may cause life-threatening hemorrhage.
Cervical ectopic pregnancies may be difficult to
differentiate from pregnancies implanted in the lower
uterine segment or miscarriages. An hourglass ap-
pearance of the uterus, a gestational sac seen within
the cervical canal or in an eccentric location, invasion
of the cervical stroma or the presence of trophoblastic
flow, and visualization between the external and
internal cervical os may be helpful in differentiating
a cervical pregnancy from an impending miscarriage,
although trophoblastic flow occasionally can be noted
during miscarriage.
Abdominal pregnancy, defined as an ectopic preg-
nancy located in the peritoneal cavity, occurs in 1 in
10,000 pregnancies. It is a medical emergency be-
cause of high associated maternal and fetal morbidity
and mortality. Surgery is indicated as soon as the
diagnosis is made. In rare cases of undetected ad-
vanced abdominal pregnancy with fetal demise, litho-
pedion formation (fetal calcification) can occur.
This is usually found incidentally and can appear
on US as a large echogenic mass.
Treatment for ectopic pregnancy increasingly in-
cludes medical and even expectant management,
in addition to laparoscopic surgery. Close interval
follow-up with endovaginal US, monitoring serial
b-HCG levels, and reassessment of the patient’s clini-
cal stability are crucial elements of expectant therapy
[24]. Methotrexate is a folic acid antagonist that in-
hibits the synthesis of purines and pyrimidines, which

Box 3. Medical contraindications tomethotrexate therapy
� Abnormal liver function tests (LFTs)(elevated transaminases)
� Immunodeficiency� Any type of blood dyscrasia� Leukocyte count of <2000� Platelet count of >100,000� Peptic ulcer disease� Active pulmonary disease� Renal disease� Known sensitivity to methotrexate
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348334
prevents DNA synthesis and cell multiplication. It
acts primarily on the rapidly dividing trophoblastic
cells of the embryo [87]. Although exact eligibility
criteria continue to change with increasing experience
and vary somewhat among institutions, medical man-
agement with methotrexate is most effective when an
ectopic pregnancy is small (<3–4 cm), b-HCG is
low (<15,000–20,000 IU/mL International Reference
Preparation [IRP]), and cardiac activity is absent.
Medical management of ectopic pregnancy may,
however, be attempted despite one or more of these
criteria not being met. These patients have a higher
incidence of failure of treatment and may require
multiple doses of methotrexate [88]. Absolute
contraindications to medical therapy include pain,
hemodynamic instability, or evidence of large hemo-
peritoneum. Eligibility criteria and absolute contra-
indications of methotrexate treatment are further
discussed in Boxes 2 and 3 [87,88].
In the 2 to 4 weeks after methotrexate adminis-
tration, an ectopic pregnancy can demonstrate persist-
ent vascularity and can increase in size secondary to
infarction and hemorrhage. These findings are nor-
mal, and, in an asymptomatic patient, do not represent
failure of treatment. To avoid confusion, sonographic
follow-up is sometimes avoided during this time as
long as the patient remains asymptomatic. If a patient
develops pain, US follow-up is necessary to evaluate
for signs of tubal rupture, such as a dramatic increase
in the size of the ectopic pregnancy or large hemoperi-
toneum. Pain can develop during the normal course
of methotrexate therapy, 4 to 5 days after adminis-
tration, because of the infarction of trophoblastic
tissue. The development of pain does not necessarily
indicate failure of treatment or tubal rupture. Pain
secondary to trophoblastic tissue infarction should
resolve within 12 to 24 hours. Baseline b-HCG levels
are recorded before methotrexate administration. The
b-HCG begins to fall gradually after 4 days. If there is
Box 2. Eligibility criteria for methotrexatetherapy
� Hemodynamically stable� Absence of large hemoperitoneum� Absence of pain� Ectopic size <3.5–4 cm� C-HCG levels with peak values>15,000–20,000 mIU/mL (IRP)
� F Cardiac activity in gestational sac� Absence of any contraindications
more than a 15% fall in b-HCG from the baseline, a
second injection of methotrexate is not required [88].
Theca lutein cysts
Theca lutein cysts are caused by elevated levels
of chorionic gonadotropin and are seen in patients
with hydatidiform mole or choriocarcinoma and in
the setting of exogenous chorionic gonadotropin ad-
ministration for treatment of infertility [2]. The cysts
are lined by theca cells, which may or may not be
luteinized [2]. Cysts are usually multiple and bilateral
and typically range in diameter from 3 to 20 cm [25].
Symptoms are usually mild, including pelvic fullness
and dull pelvic pain. Acute pain can occur in the
setting of cyst rupture or hemorrhage [2]. The cysts
resolve spontaneously after treatment of gestational
trophoblastic disease or cessation of fertility therapy.
Theca lutein cysts may persist for long periods,
however, despite relatively low levels of b-HCG[25]. US examination demonstrates multiple simple
cysts in both ovaries (Fig. 9).
Ovarian hyperstimulation syndrome
Ovarian hyperstimulation syndrome (OHSS) is a
potentially dangerous iatrogenic complication of
pharmacologic ovulation induction for the treatment
of infertility [26]. It occurs in the setting of abnor-
mally high levels of b-HCG and less frequently has
been reported in spontaneous singleton and multi-
ple pregnancies, sex hormone–producing tumors,
and choriocarcinoma [26–28]. Although the precise
pathophysiology remains unknown, b-HCG seems to
trigger an increase in vascular permeability that

Fig. 9. Theca lutein cysts. Note multiple simple bilateral
ovarian cysts in this patient with a hydatidiform mole.
A pocket of free fluid is present between the two ova-
ries (arrow).
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 335
results in ovarian enlargement, cyst formation, and
third spacing of fluid. The renin-angiotensin system,
vascular endothelial growth factor, and cytokines are
believed to be chemical mediators in this process
[29,30]. Whelan and Vlahos [31] emphasize risk
stratification as the key to preventing OHSS or
minimizing its severity. Generally accepted risk fac-
tors include young age, presence of theca lutein
cysts, and elevated estradiol levels. Known polycys-
tic ovarian syndrome or the presence of multiple pe-
ripheral ovarian follicles (the ‘‘necklace sign’’) on US
in a patient with a clinical presentation that suggests
polycystic ovarian syndrome is also a risk factor for
OHSS [32].
Women who undergo ovulation induction ther-
apy whose ovaries contain several small or interme-
diate-sized follicles are at greater risk for developing
OHSS than women with large (>15 mm) follicles,
especially when seen in conjunction with high levels
of estradiol (>3000 pg/mL) [33]. Higher baseline
ovarian volume of more than 10 mL also has been
shown by Danninger et al [34] to predict subsequent
development of OHSS and may become a more
important predictor with the widespread availability
of US units capable of providing three-dimensional
images with highly accurate, reproducible measure-
ments of ovarian volume. A patient at higher risk for
OHSS may require more intensive monitoring (in-
cluding US) or undergo an alternative pharmacologic
ovulation induction technique. It is estimated that
mild OHSS may occur in as many as 65% of women
who undergo ovulation induction. The incidence of
clinically important (moderate to severe) OHSS
ranges from 1% to 10% of exogenously induced
ovulation cycles, but only a small percentage of these
cases are severe (0.5% to 5%) [35,36].
OHSS is more severe in patients who become
pregnant after ovulation induction. The spectrum of
clinical presentation ranges from nausea, vomiting,
and abdominal pain to massive ascites, acute respi-
ratory distress syndrome, and hypotension, classified
according to severity by Golan et al [30]. Pain may be
caused by rupture of or hemorrhage into the enlarged
cysts or ovarian torsion. Approximately 20% of
patients who receive gonadotropin therapy develop
mild to moderate ovarian enlargement [37]. Ovarian
diameter more than 5 cm is a criterion for diagnosis
of mild OHSS, although the ovaries are frequently
more than 10 cm in diameter. US is the most exact
method of detecting ovarian enlargement. It is also
preferable to bimanual examination because of the
risk of ovarian rupture [30]. On US, multiple large,
thin-walled cysts are identified. Pulsed Doppler may
demonstrate increased intra-ovarian arterial diastolic
flow or nonphasic venous flow, which indicates de-
creased venous return [38]. Acute pain may be caused
by hemorrhage into a cyst, cyst rupture, or ovarian
torsion. Debris or low-level echoes within the cysts
may be seen when hemorrhage occurs. Cyst rupture
can result in an irregularly shaped cyst with adjacent
free fluid or fluid in the cul-de-sac (Fig. 10).
Because ovarian enlargement predisposes to ovar-
ian torsion, documentation of ovarian blood flow is
important in patients who present with acute pain (see
next section). In severe cases of OHSS, US can be
used to detect and monitor complications. US exami-
nation may demonstrate ascites or pleural fluid,
criteria used in determining whether hospitalization
is necessary [31]. Oliguria may prompt a request for
renal US evaluation, although in the setting of OHSS
this is usually secondary to impaired venous return
from the kidneys secondary to extrinsic compression
by ascites. Patients with OHSS are at increased risk
of thromboembolism caused by hemoconcentration
and may benefit further from US examination for
various complications, such as deep venous throm-
bosis. Thoracic complications, such as pulmonary em-
bolism (1.9%), acute respiratory distress syndrome
(2.4%), infection (3.8%), atelectasis (20%), and pleu-
ral effusion (29%; usually right-sided), may occur
[39]. Unilateral pleural effusion has been reported
as an isolated finding in OHSS [40,41]. A large pleu-
ral effusion often predicts hemodynamic instability.
Treatment is supportive: hemodynamics, hemato-
crit, electrolytes, liver and kidney function (includ-
ing urine output), and coagulation parameters are
monitored. Some authors have advocated an out-
patient treatment approach, facilitated in part by

Fig. 10. Ovarian hyperstimulation syndrome. (A) Note marked enlargement of the right ovary within calipers. Numerous cysts
are seen, several of which contain internal echoes. There is a small amount of free fluid adjacent to the enlarged ovary. (B) Pulse
Doppler interrogation reveals high-velocity systolic and diastolic flow, which excludes the diagnosis of ovarian torsion. The
patient’s pain is likely caused by hemorrhage into these cysts or rupture of these hemorrhagic cysts.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348336
US-guided follicular aspiration [42]. Navot et al [32]
reported US-guided paracentesis as the treatment of
choice when medical therapy is insufficient; alter-
natives include transvaginal aspiration of ascites or
follicular cysts. OHSS typically resolves in 7 to
10 days unless pregnancy ensues, in which case
recovery is more prolonged.
Ovarian torsion
Ovarian or adnexal (ovary and fallopian tube)
torsion is a surgical emergency that requires prompt
diagnosis and treatment. There is increased risk
during pregnancy, and ovarian torsion occurs in ap-
proximately 1 in 1800 pregnancies [1,43]. Approxi-
mately 25% of adnexal torsions occur in pregnant
patients [1]. Adnexal torsion most commonly occurs
between 6 and 14 weeks’ gestation and in the
immediate puerperium [1,44]. Ovarian torsion is the
result of partial or complete rotation of the ovarian
pedicle on its axis, which results initially in impaired
lymphatic and venous drainage and eventual loss of
arterial perfusion [43,45]. It occurs more commonly
on the right side [44]. Torsion can be difficult to
diagnose clinically because the presenting symptoms,
including pain, nausea, and vomiting, are nonspecific
and similar to many causes of acute abdomen [43,45].

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 337
Because ovarian enlargement of more than 6 cm
predisposes to ovarian torsion [46,47], women who
undergo ovulation induction have the highest inci-
dence because of the development of numerous theca
lutein cysts, which can massively enlarge the ova-
ries [2,30]. Mashiach et al [47] reported that tor-
sion was more common in women with OHSS
who subsequently became pregnant, compared with
women with OHSS alone. Enlargement of the ovary
secondary to a corpus luteal cyst or incidental benign
ovarian neoplasm, most commonly a mature mature
cystic teratomas or cystademoma, also can predispose
to ovarian torsion [44]. Ovarian torsion rarely occurs
in the presence of ovarian carcinoma or endometri-
osis because of fixation of the ovaries to adjacent
structures by adhesions.
The US appearance of ovarian torsion varies de-
pending on the degree of ischemia and infarction
and the time course [44]. The ovary is typically
enlarged. Numerous small follicles are often seen at
the periphery of the ovary [43,45,48]. The central
ovarian stroma becomes heterogeneous with areas of
increased echogenicity, which represent hemorrhage,
and more hypoechoic areas, which represent edema
Fig. 11. Ovarian torsion. (A) The ovary is enlarged with several sm
stroma is heterogeneous, with echogenic areas representing hemor
detected with color Doppler. (B) Because pulse Doppler is more sen
with pulse Doppler should be performed. No flow could be demo
(Fig. 11A) [44]. With frank infarction, cystic, clotted
areas may be observed. Free fluid within the pelvis
or adjacent to the ovary also can be seen [44,50].
Although the range of gray scale features varies, the
ovary rarely has a completely normal appearance.
Classically, Doppler interrogation demonstrates ab-
sence of arterial flow (Fig. 11B). It is important,
however, to remember that early in the process there
may be obstruction of lymphatic and venous flow with
preservation of arterial perfusion [49–51]. Occasion-
ally only diastolic or venous flow is lost early on.
Because the ovary has dual arterial supply, in
early torsion only one may be occluded [51]. In a
patient who presents with acute pain and an ovary
that demonstrates real-time findings consistent with
ovarian torsion, the diagnosis should be suggested
even in the presence of documented arterial blood
flow (Fig. 12) [48–51]. When color Doppler imaging
and pulsed Doppler sampling do not demonstrate
arterial flow within the ovarian parenchyma, the
diagnosis is more easily made. All Doppler parame-
ters must be set carefully to maximize detection of
slow flow to avoid a false-positive diagnosis caused
by technical factors. Sampling error also may cause
all peripherally located cysts (arrows). The central ovarian
rhage and hypoechoic areas representing edema. No flow is
sitive to low-velocity, low-volume flow, meticulous sampling
nstrated in this case.

Fig. 12. Early ovarian torsion. Note classic gray scale
features of torsion: ovarian enlargement, central amorphous,
heterogeneous stroma, and small peripheral cysts. Pulse
Doppler interrogation revealed some arterial flow in this
woman, who presented less than 2 hours after the acute
onset of severe pelvic pain.
Box 4. Sonographic findings of ovariantorsion
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348338
false-positive diagnoses. Fleischer et al [52] reported
that the preservation of parenchymal venous flow
is a useful indicator of ovarian viability. The twisted
vascular pedicle also can be seen on color Doppler
sonography. Demonstration of flow within the
twisted vascular pedicle may be a useful marker of
ovarian viability (Box 4).
Adnexal torsion that is diagnosed before tissue
infarction is managed with laparoscopic ‘‘detorsion’’
surgery followed by progesterone replacement if
the corpus luteum is removed. If tissue infarction
and necrosis have occurred, then laparotomy with
salpingo-oophorectomy is usually required to pre-
vent peritonitis.
Gray scale findings
Ovarian enlargementPeripherally located folliclesHeterogeneous central ovarian stroma
� Internal hemorrhage (echogenic)� Internal edema (hypoechoic)
Cystic necrosis of the ovaryFree fluidF Underlying precipitating mass
Range of color/pulsed Doppler findings
NormalLoss of venous flowLoss of diastolic flowAbsence of flowTwisted vascular pedicle
Luteoma of pregnancy
Luteoma of pregnancy is a rare entity, with fewer
than 200 cases reported in the literature [53]. Luteo-
mas consist of non-neoplastic tumor-like masses of
lutein cells and are often multifocal and bilateral
[2,53]. The luteoma range up to 20 cm in diameter,
but most are in the 5- to 10-cm range [2]. Luteomas
are usually clinically occult, only coming to attention
when visualized during cesarean section or postpar-
tum tubal ligation [2]. Occasionally, luteomas can
have androgenic effects that result in fetal hirsutism
and virilization. As is the case with any large adnexal
mass, however, luteomas may precipitate ovarian
torsion that results in acute pelvic pain. Although
their morphologic appearance can be ominous and
suggest malignancy, biopsy is adequate for diagnosis,
and masses spontaneously resolve several months
after delivery [53]. The diagnosis should be enter-
tained to avoid unnecessary oophorectomy. In case
reports, the lesions have been described on US as
solid ovarian masses. Cystic components may be
present secondary to necrosis [53].
Disease unrelated to pregnancy
Diagnoses such as ectopic pregnancy and ovarian
torsion are likely to be at the top of the differential
list in a pregnant patient who presents with acute
pelvic pain and an adnexal mass. There are, however,
many gynecologic and nongynecologic causes of
acute pelvic pain and pelvic mass that are unrelated
to pregnancy and may still occur in this population.
Pelvic inflammatory disease and tubo-ovarian
abscess
Pelvic inflammatory disease (PID) is most com-
monly caused by sexually transmitted infection by
Chlamydia species or Neisseria gonorrhea. Uterine
instrumentation and the placement of intrauterine
contraceptive devices also are risk factors [44]. Less
frequently, PID may be caused by direct extension

Fig. 14. Tubovarian abscess. Note complex fluid collection
engulfing right ovary (arrow).
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 339
of infection from appendicular or diverticular ab-
scesses, and in these instances disease tends to be
unilateral [44,46]. Fortunately, acute PID is a rare
entity in the pregnant patient. The cause of PID in
pregnancy is uncertain, but recurrence of old in-
flammatory disease is considered the most common
cause [54]. PID is typically an ascending infection
that begins as a cervicitis, progresses to endometritis,
and ultimately involves fallopian tubes or ovaries
(tubo-ovarian complex). Only approximately 5% of
patients with PID progress to abscess formation.
PID can be difficult to diagnosis secondary to vague
or confusing symptoms. It should be suspected in
the setting of fever, pelvic discomfort, and purulent
vaginal discharge. Many patients do not demonstrate
these classic symptoms, however, and US imaging
often plays a crucial role in diagnosis and patient
management [4].
Pelvic US is frequently normal in the early stages
of PID [44,46]. As disease worsens or becomes
more chronic, several appearances can be identified
on US imaging. US may reveal dilatation of one or
both fallopian tubes. Hydrosalpinx is characterized
by its tubular shape or folded configuration [55]. A
well-defined echogenic wall and linear echoes that
protrude into the anechoic tubal lumen are also
characteristic [55]. Hydrosalpinx can be differentiated
from fluid-filled bowel loops by the absence of
peristalsis [55]. Dilated fallopian tubes also may
contain diffuse, low-level echoes that represent debris
or hemorrhage (Fig. 13) or appear as a complex cys-
tic adnexal mass that demonstrates multiple fluid
levels and septations [4,44]. Once the disease has
progressed to abscess formation (Fig. 14), a complex
adnexal mass is observed on US examination. The
ovary may not be identifiable separate from the
mass but actually may be engulfed by the infection,
Fig. 13. Pyosalpinx. Note layering debris or pus (curved
arrow) in the dilated fallopian tube.
although relative sparing of the ovary has been re-
ported. The ovary is sometimes enlarged with indis-
tinct margins secondary to peri-ovarian inflammation,
termed the tubo-ovarian complex [4].
Pressure from the transducer often causes pain
during the examination, and the pelvic organs may
appear fixed to the surrounding tissues. The serosal
contour of the uterus may be indistinct because of
surrounding inflammatory exudate. Pus may be seen
within the cul-de-sac or around the liver with an
appearance of free fluid–containing low-level echoes
[4,44,46]. A US that demonstrates findings that sug-
gest PID (ie, a thick-walled, fluid-filled tubular ad-
nexal mass with or without free intrapelvic fluid) has
been reported to have a sensitivity rate of 85% and a
specificity rate of 100% for the diagnosis [56]. Any
complex multilocular adnexal mass in an appropriate
clinical setting can represent PID, however. Hydro-
salpinx is not always present. Abscess drainage or
conservative surgical procedures with antibiotic
therapy are often recommended in managing PID
complicated by tubo-ovarian abscess during preg-
nancy. There is no true consensus on management
in this population, however [54].
Endometrioma
Endometriosis is a common cause of abdominal
pain. In younger women, endometriosis is defined
as the presence of functional endometrial tissue out-
side of the uterus [43]. The classic triad of clinical
symptoms includes pelvic pain, dysmenorrhea, and
infertility [43,57]. Endometriosis has an estimated
prevalence of 1% in reproductive age women [57];
however, the incidence of endometriosis in women
with infertility is closer to 40% [43]. Overall, endo-

Fig. 15. Endometrioma. The cystic lesion medial to the right
ovary contains diffuse low-level echoes (arrow) and demon-
strates increased through transmission. The wall is thin
and regular.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348340
metriomas account for approximately 4% of adnexal
masses diagnosed during pregnancy [1]. Endometrio-
mas can have a diverse range of appearances on US,
from anechoic cysts to complex cystic masses that
contain multiple septations to heterogeneous echo-
genicity. Classically endometriomas appear on US as
thin-walled unilocular cystic masses that contain
diffuse, low-level echoes (Fig. 15) [43,57–59]. Patel
et al [59] reported that hyperechoic wall foci and
multilocularity, in the absence of malignant features,
highly suggest endometrioma. Layering or anechoic
foci within a background of homogeneous low-level
echoes also have been described. Margins may be
indistinct and angulated secondary to associated
adhesions. The appearance on US may be similar to
Fig. 16. Acute hemorrhagic infarction of a fibroid in a patient
(A) Sagittal US image of the uterus (U) reveals an echogenic subs
fluid. (B) Follow-up CT scan demonstrates lack of enhancement
hemorrhagic infarction.
that of a hemorrhagic cyst [60]. The pattern of in-
ternal echoes within a hemorrhagic cyst is more
often lace-like, however, as opposed to the homoge-
neous hypoechoic internal echoes characteristic of
endometrioma, and hemorrhagic cysts more often
present with acute pain [43].
Endometriomas are more frequently multiple,
and their appearance is more stable over time when
compared with hemorrhagic cysts. Hemorrhagic cysts
and endometriomas may have vascular walls on color
Doppler interrogation [61]. An increased likelihood
of mural vascularity in endometriomas has been re-
ported in patients with acute pelvic pain and may
serve as a relative marker of disease activity, although
this is somewhat controversial [62]. Endometriomas
can be bizarre looking and cannot always be distin-
guished readily from malignancy. The presence of
irregular walls or vascular nodularity should raise
concern, because clear cell or endometroid carcino-
mas rarely may develop within endometriomas (<1%).
MR imaging may be useful to document the presence
of hemorrhage within an ovarian mass when US
examination is equivocal.
Leiomyomata
Leiomyomata are the most common benign uter-
ine neoplasms and are composed of smooth muscle
cells with varying amounts of fibrous connective
tissue and collagen. Leiomyomata are most com-
monly diagnosed in premenopausal women, with an
incidence of 20% to 30% in women over the age
of 30 [43]. Some studies have indicated that careful
who presented with acute pelvic pain 4 days postpartum.
erosal fibroid (arrow) with a small amount of adjacent free
of the uterine mass (arrow), which is consistent with acute

Fig. 17. Pedunculated leiomyoma. Note large left leiomyoma
connected to the uterus by a thin pedicle (arrowhead).
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 341
pathologic evaluation can demonstrate leiomyomas
in up to 80% of women of reproductive age [1].
Uterine leiomyomata are diagnosed in 0.3% to 4% of
pregnancies, usually because a pedunculated subse-
rosal leiomyoma simulates an ovarian neoplasm
[1,45]. Pedunculated leiomyomata may undergo tor-
sion and necrosis, which results in acute pelvic pain
[45]. Fibroids are hormonally dependent and can
rapidly increase in size during pregnancy, which
results in hemorrhagic infarction, which may cause
acute, severe pelvic pain (Fig. 16). Leiomyomata
have variable appearance on US. They most fre-
quently appear as round, homogeneous solid, well-
circumscribed masses that are usually hypoechoic or
isoehoic to the myometrium and more rarely rela-
tively echogenic. Areas of decreased echogenicity
secondary to degeneration and necrosis may be seen,
especially in lesions larger than 5 cm. Distal acoustic
shadowing, often in a striated pattern, is commonly
noted. Calcification is most common in older women
[63]. It may be difficult to identify the site of myo-
metrial attachment of a pedunculated leiomyoma on
gray scale imaging. Both ovaries should be identifi-
able separate from the mass, however (Fig. 17), and
color Doppler imaging may help to identify a vascu-
lar pedicle. When sonographic evaluation of an
adnexal lesion is indeterminate in differentiating a
pedunculated leiomyoma from a solid ovarian neo-
plasm, MR imaging can be useful in further charac-
terization [64].
Fig. 18. Mature cystic teratoma of the ovary. Note large
echogenic mass on the left (arrowheads).
Benign and malignant neoplasms
Ovarian neoplasms are most often asymptomatic
unless they precipitate ovarian torsion, although such
lesions may present with vague abdominal or pelvic
pain and urinary frequency. Most ovarian neoplasms
detected during pregnancy are benign. The most
common of these are mature cystic teratomas and
cystadenomas [1]. Mature cystic teratomas are benign
neoplasms that usually contain tissue derived from
all three germ cell layers [2,43]. Occurring most
commonly in the active reproductive years [43],
dermoids account for 40% to 50% of benign ovarian
neoplasms and are bilateral in 10% to 15% of cases
[43]. Malignant transformation is rare (<2% of
cases) and is most common in older women [47].
Dermoids are usually asymptomatic unless torsion
or rupture occurs [43]. US appearance of mature
cystic teratomas ranges from that of a solid homo-
geneously echogenic mass with posterior attenuation
(Fig. 18) to a completely anechoic structure that
mimics an ovarian cyst.
Several US features, however, have been described
as specific to mature cystic teratomas. A predomi-
nately cystic mass with an echogenic mural nodule
is a characteristic appearance. The mural nodule, or
dermoid plug, may contain hair, teeth, or fat [65]. If
calcium is present, distal acoustic shadowing is ob-
served. [43,66]. Linear echogenic foci that represent
hair fibers, an echogenic hair ball floating at a fluid-
fluid interface (Fig. 19), and fat-fluid levels are also
specific features [43,67,68]. A study by Patel et al
[66] found that the positive predictive value was
100% when an ovarian mass had two or more US
features considered specific for mature cystic terato-
mas. In this study, the sensitivity of US for detection
of dermoids was reported as 85% [66]. Diffusely
echogenic mature cystic teratomas can escape detec-
tion by US because they appear similar to bowel [43].
When a palpable adnexal mass can be diagnosed
confidently as a mature cystic teratoma, surgery can
be delayed safely until after delivery. If US is non-
diagnostic but suspicious, CT or MR imaging may

Fig. 19. Mature cystic teratoma of the ovary. Note echogenic
hairball ‘‘floating’’ (arrow) at the fat/fluid interface. The
liquid fatty layer contains low-level echoes. Becuase the fat
is lighter than the serous fluid, the more echogenic layer is
more anterior in this supine patient.
Fig. 20. Serous cystadenoma. Note thin, regular septations
(arrow) in this cystic adnexal mass.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348342
document the presence of fat within dermoids, thereby
confirming the diagnosis.
Serous and mucinous cystadenomas are benign
neoplasms that most commonly occur in reproductive
age women [43]. They can be difficult to differentiate
sonographically from malignant cystadenocarci-
nomas because of the wide spectrum of appearances
on US. Serous cystadenomas typically are large,
unilocular, thin-walled cystic lesions that may demon-
strate thin septations or papillary projections (Fig. 20).
They are bilateral in 20% of cases [43]. Mucinous
cystadenomas are typically larger, measure up to
30 cm, and may contain internal low-level echoes
secondary to mucin content. Septations are common.
Papillary projections are less common and the mass
usually unilateral [43]. Malignant neoplasms com-
prise approximately 3% of adnexal masses diagnosed
in pregnancy [1]. The most common malignant neo-
plasms that come to attention during pregnancy in-
clude germ cell tumors, low-grade ovarian cancers,
and invasive epithelial ovarian cancers. Most women
diagnosed with ovarian cancer during pregnancy
present with stage 1 disease [1].
In many cases the US appearance of complex
cystic adnexal masses is indeterminate and the differ-
ential diagnosis of cystadenoma or cystadenocarci-
noma must be considered. The presence of thick
vascular septations (>3 mm), mural nodularity, papil-
lary processes, thick, irregular walls, solid areas,
invasion or fixation of adjacent structures, and asso-
ciated findings, such as ascites or serosal implants,
increase the likelihood of malignancy (Figs. 21, 22)
[68,69]. The likelihood of malignancy also increases
with age, elevation of serum CA-125 level, and
positive family history [70]. It is not possible to dif-
ferentiate benign solid lesions (eg, fibromas or theco-
mas) from malignant germ cell or stromal tumors [69].
The presence of a purely solid tumor indicates a
higher probability of metastatic carcinoma than pri-
mary ovarian cancer (Fig. 23) [71]. Numerous authors
have reported that ovarian malignancies tend to have
increased peak systolic flow (peak systolic velocity
>35 cm/second) and low resistance perfusion (resis-
tive index <0.4 or perfusion index <1) [68,70,72,73].
There is significant overlap in the distribution
of peak systolic velocity, resistive index, and perfu-
sion index values between benign and malignant
lesions, however, and no discriminatory value is
accepted [68,70,72,73]. Lack of detectable flow by
means of color Doppler US does not exclude ovarian
malignancy [72]. The management of an ovarian
mass during pregnancy is controversial. Surgery in
the first trimester is associated with pregnancy loss,
and surgery in the third trimester can result in
premature labor [1]. Although US is excellent at
detecting adnexal masses, it is not always accurate
in differentiating benign from malignant lesions.
Although the previously described morphologic char-
acteristics and internal vascularity with high peak
systolic velocity and low resistive index suggest
malignancy, these features are nonspecific, with a
positive predictive value of approximately 50% [73].
The real value of US lies in the high negative
predictive value (nearly 99%) of US features con-
sidered to be benign [73]. In a pregnant patient with a
palpable adnexal mass and US features diagnostic of
a benign entity, such as a serous or hemorrhagic cyst,
dermoid or pedunculated fibroid, surgery may be
postponed safely until after delivery or avoided

Fig. 21. Stage 1 serous cystadenocarcinoma. This 28-year-old patient presented at 12 weeks’ gestation with a palpable right
adnexal mass. (A) US reveals mural irregularity (arrow), which represents small papillary projections. (B) These papillary
projections (arrow) are seen on corresponding MR image. Gravid uterus (U) is anterior.
E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 343
altogether. Masses with multiple malignant features
require prompt surgery. Masses that appear more
benign are often followed by serial examinations
until the second trimester, which is the optimal time
for surgery in terms of maternal and fetal safety. In
equivocal cases, MR imaging may be useful in
further characterizing an adnexal mass.
Perforated appendicitis
Appendicitis is the most common cause of non-
gynecologic acute pelvic pain in women and the most
common diagnosis that requires emergent surgical
intervention during pregnancy [4,74]. The inci-
Fig. 22. Serous cystadenocarcinoma. Note large complex
adnexal mass on color Doppler with a vascular solid com-
ponent (arrow).
dence of gestational appendicitis has been reported
as 0.05% to 0.14% [45,74]. Although the incidence
of acute appendicitis is not increased in pregnancy,
appendiceal rupture occurs two to three times more
frequently and occurs in up to 25% of cases, second-
ary to delay in diagnosis and surgery [1,45]. Patients
with appendicitis typically present with fever, leuko-
cytosis, nausea, vomiting, and peri-umbilical pain,
which gradually moves to the right lower quadrant.
These symptoms may be altered, muted, or absent in
pregnancy, however, which contributes to delays in
Fig. 23. Krukenberg tumor (metastasis from gastric carci-
noma). This 27-year-old woman presented at 32 weeks’
gestation with acute abdominal pain, bilateral solid ovarian
masses, and ascites (only one mass is shown here). Although
the differential diagnosis would include benign lesions, such
as fibroma and fibrothecoma, the pronounced vascularity
and ascites are worrisome for malignancy.

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348344
diagnosis and the increased incidence of perforation
and associated morbidity and mortality in this popu-
lation [1,45,74–76].
In pregnancy, the most common presenting symp-
tom is right-sided abdominal pain, regardless of the
gestational age [76]. The position of the appendix is
elevated above McBurney’s point after the first tri-
mester, however, and pain may be more localized to
the right upper quadrant than the right lower quad-
rant and is often confused with cholecystitis [45].
Although CT is the imaging modality of choice in
evaluating patients with suspected appendicitis, it is
to be avoided in pregnant patients because of the
risks of ionizing radiation to the fetus. US examina-
tion is often the first-line imaging modality in this
patient population. US is a specific, although rela-
tively insensitive, test for the diagnosis of acute
appendicitis. Prospective studies have reported US
specificity rates of 86% to 100% and sensitivity rates
as high as 75% to 90% in patients with clinically
suspected appendicitis [4]. In most clinical practices,
however, the appendix is infrequently visualized,
which limits the sensitivity and negative predictive
value of the examination. In one study, on-call
residents were only able to detect the appendix by
US in 13% of cases in which appendicitis was
clinically suspected [77]. Sensitivity for detection
of appendicitis was 50% on US compared with
100% on CT [77].
Fig. 24. Acute appendicitis. Transverse view demonstrates a
thick-walled (arrow), noncompressible appendix with a
surrounding fluid collection (F).
The examination is performed with a linear array
transducer. The cecum and psoas muscle can be used
as landmarks to help localize the appendix. Graded
compression is used to displace overlying bowel at
the point of maximum tenderness [4,78]. An abnor-
mal appendix appears as a blind-ending, aperistaltic
loop of bowel that does not compress [4,79]. Trans-
versely, the loop should be more than 6 mm in
diameter (outer wall to outer wall) (Fig. 24) [4,
80–82]. This measurement criterion provides high
sensitivity but limited specificity, because the normal
appendix has been reported to have a diameter of up
to 13 mm secondary to intraluminal contents [81,82].
The combined wall thickness should not exceed 6 mm
in a normal appendix [4,82]. Increased vascularity
may be noted on Doppler interrogation. In some
cases, a shadowing appendicolith is seen [4]. The
surrounding area also should be evaluated carefully to
exclude loculated periappendiceal fluid or gas, which
suggests abscess formation [4,78]. Recent reports
suggest that MR imaging may be beneficial in eval-
uating patients for suspected appendicitis when US is
nondiagnostic [83,84]. Appendicitis in pregnancy
requires prompt surgery. Maternal mortality from
appendicitis has diminished to approximately 0.1%
but still exceeds 4% when perforation occurs [1].
Fetal mortality is less than 2% but is more than 30%
in the case of perforation [1].
Diverticulitis
Diverticulitis is uncommon in pregnant women.
Patients present with lower quadrant (usually left)
pain, fever, and leukocytosis [4]. Whereas CT is the
gold standard in evaluation of suspected diverticu-
litis, US is a preferred modality in the pregnant
patient, and a small body of literature has indicated
that US can be used to make this diagnosis accu-
rately. Pradel et al [85] reported that CT and US
had an accuracy rate of 84% in diagnosing diverticu-
litis. US and CT findings were not statistically
significantly different in terms of sensitivity rates
(85% and 91%, respectively) and specificity rates
(84% and 77%, respectively) [85]. Although trans-
abdominal US scanning seems less sensitive in iden-
tifying diverticular abscess compared with CT,
endovaginal US scanning is just as sensitive if the
area is within reach of the vaginal probe [4]. US
may identify an abnormal loop of bowel in the re-
gion of the patient’s pain with an irregular lumen
and outpouchings beyond the bowel wall. The co-
lonic wall may appear thickened but less concentri-
cally so than in primary colitis. An adjacent walled

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 345
off fluid collection or extraluminal shadowing air
suggests perforation and abscess formation [4]. These
results are operator dependent; however, US should
not be overlooked as a viable alternative imaging
modality for diagnosing diverticulitis in the preg-
nant patient.
Epiploic appendigitis
Epiploic appendigitis is an uncommon entity. It
is caused by torsion or ischemic infarction of one of
the epiploic appendages of the colon, which incites a
subsequent inflammatory reaction [4,86]. Epiploic
appendages are rudimentary in children and reach
their full size in adulthood. Most of them measure
2 to 5 cm in length and are 1 to 2 cm thick [4,86]. The
largest appendages are found in the descending colon
and cecum, which are the most common locations
for torsion to occur [86]. Epiploic appendages are
enlarged in obese patients, which increases their risk
for torsion [86]. Patients most commonly present
with acute or subacute left lower quadrant pain and
leukocytosis. When cecal epiploic appendages are
involved, the clinical picture may mimic appendicitis.
Fever is usually absent [4,86]. Normal epiploic appen-
dages are not visible on US unless the colon is
surrounded by extraluminal fluid. In epiploic ap-
pendigitis, US demonstrates an ovoid, hyperechoic,
solid, noncompressible mass at the point of maxi-
mum tenderness. The mass is often surrounded by a
thin hypoechoic rim, believed to represent thicken-
ing of the serosa of the appendage and the adjacent
parietal peritoneum [4,86]. The lesions are typically
located between the anterior abdominal wall and the
colon, from which they arise. The mass often adheres
to the adjacent peritoneum, which can be observed
on real-time sonography during inspiration and expi-
ration [86]. Color Doppler signal is typically absent
within the echogenic mass. Minimal blood flow is
sometimes identified immediately external to the
hypoechoic rim, however. This lack of vascularity is
in contrast to the prominent color flow that is seen
in secondary inflammation of the epiploic append-
ages in persons with diverticulitis [86].
Summary
In a pregnant woman who presents with acute
pelvic pain and an adnexal mass, pregnancy-related
etiologies, such as ectopic pregnancy or ovarian tor-
sion, are typically the first diagnoses to be consid-
ered. Many other causes of pelvic pain associated
with an adnexal mass can occur in pregnant patients,
however. Some causes are benign and others require
urgent management and treatment. Clinical presenta-
tion and physical examination can be misleading
in pregnancy. The location of pain may be atypical
for the pathologic entity, the pain may be muted, and
in the case of infection, fever and leukocytosis can
be absent. US examination is a safe and effective
method for evaluating these patients. Sonographic
characterization of adnexal masses may make a de-
finitive diagnosis or focus the differential, which al-
lows for prompt and appropriate treatment of patients.
References
[1] Cappell MS, Friedel D. Abdominal pain during preg-
nancy. Gastroenterol Clin North Am 2003;32(1):1–58.
[2] Purcell K, Wheeler JE. Benign disorders of the ova-
ries and oviducts. In: DeCerney A, Nathan L, editors.
Current obstetric and gynecologic diagnosis and treat-
ment. New York: McGraw-Hill; 2003.
[3] Durfee SM, Frates MC. Sonographic spectrum of the
corpus luteum in early pregnancy: gray-scale, color,
and pulsed Doppler appearance. J Clin Ultrasound
1999;27(2):55–9.
[4] Bau A, Atri M. Acute female pelvic pain: ultrasound
evaluation. Semin Ultrasound CT MR 2000;21(1):
79–93.
[5] Jain KA. Sonographic spectrum of hemorrhagic
ovarian cysts. J Ultrasound Med 2002;21(8):879–86.
[6] Baltarowich OH, Kurtz AB, Pasto ME, Rifkin MD,
Needleman L, Goldberg BB. The spectrum of sono-
graphic findings in hemorrhagic ovarian cysts. AJR
Am J Roentgenol 1987;148(5):901–5.
[7] Okai T, Kobayashi K, Ryo E, Kagawa H, Kozuma S,
Taketani Y. Transvaginal sonographic appearance of
hemorrhagic functional ovarian cysts and their spon-
taneous regression. Int J Gynaecol Obstet 1994;44(1):
47–52.
[8] Centers for Disease Control. Current trends in ectopic
pregnancy: United States, 1990–92. MMWR Morb
Mortal Wkly Rep 1995;44:46–8.
[9] Mahony BS, Filly RA, Nyberg DA, Callen PW. Sono-
graphic evaluation of ectopic pregnancy. J Ultrasound
Med 1985;4(5):221–8.
[10] Bright DA, Gaupp FB. Heterotopic pregnancy: a re-
evaluation. J Am Board Fam Pract 1990;3(2):125–8.
[11] Tal J, Haddad S, Gordon N, Timor-Tritsch I. Hetero-
topic pregnancy after ovulation induction and assisted
reproductive technologies: a literature review from
1971 to 1993. Fertil Steril 1996;66(1):1–12.
[12] Laing FC, Brown DL, Price JF, Teeger S, Wong ML.
Intradecidual sign: is it effective in diagnosis of an
early intrauterine pregnancy? Radiology 1997;204(3):
655–60.
[13] Yeh HC, Goodman JD, Carr L, Rabinowitz JG. Intra-

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348346
decidual sign: a US criterion of early intrauterine preg-
nancy. Radiology 1986;161(2):463–7.
[14] Brown DL, Doubilet PM. Transvaginal sonography for
diagnosing ectopic pregnancy: positivity criteria and
performance characteristics. J Ultrasound Med 1994;
13(4):259–66.
[15] Levine D. Ectopic pregnancy. In: Callen P, editor. Ul-
trasonography in obstetrics and gynecology. 4th edi-
tion. Philadelphia: WB Saunders; 2000. p. 924.
[16] Pellerito JS, Taylor KJ, Quedens-Case C, Hammers
LW, Scoutt LM, Ramos IM, et al. Ectopic pregnancy:
evaluation with endovaginal color flow imaging.
Radiology 1992;183(2):407–11.
[17] Frates MC, Visweswaran A, Laing FC. Comparison
of tubal ring and corpus luteum echogenicities: a use-
ful differentiating characteristic. J Ultrasound Med
2001;20(1):27–31.
[18] Taylor KJ, et al. Ectopic pregnancy: duplex Doppler
evaluation. Radiology 1989;173(1):93–7.
[19] Hertzberg BS, Kliewer MA, Bowie JD. Adnexal ring
sign and hemoperitoneum caused by hemorrhagic
ovarian cyst: pitfall in the sonographic diagnosis
of ectopic pregnancy. AJR Am J Roentgenol 1999;
173(5):1301–2.
[20] Dart R, McLean SA, Dart L. Isolated fluid in the cul-
de-sac: how well does it predict ectopic pregnancy?
Am J Emerg Med 2002;20(1):1–4.
[21] Chen PC, Sickler GK, Dubinsky TJ, Maklad N, Jacobi
RL, Weaver JE. Sonographic detection of echogenic
fluid and correlation with culdocentesis in the evalua-
tion of ectopic pregnancy. AJR Am J Roentgenol
1998;170(5):1299–302.
[22] Russell SA, Filly RA, Damato N. Sonographic diag-
nosis of ectopic pregnancy with endovaginal probes:
what really has changed? J Ultrasound Med 1993;
12(3):145–51.
[23] Ackerman TE, Levi CS, Dashefsky SM, Holt SC,
Lindsay DJ. Interstitial line: sonographic finding in
interstitial (cornual) ectopic pregnancy. Radiology
1993;189(1):83–7.
[24] Atri M, et al. Expectant treatment of ectopic pregnan-
cies: clinical and sonographic predictors. AJR Am J
Roentgenol 2001;176(1):123–7.
[25] Montz FJ, Schlaerth JB, Morrow CP. The natural his-
tory of theca lutein cysts. Obstet Gynecol 1988;72(2):
247–51.
[26] Al-Shawaf T, Grudzinskas JG. Prevention and treat-
ment of ovarian hyperstimulation syndrome. Best
Pract Res Clin Obstet Gynaecol 2003;17(2):249–61.
[27] Abu-Louz SK, Ahmed AA, Swan RW. Spontaneous
ovarian hyperstimulation syndrome with pregnancy.
Am J Obstet Gynecol 1997;177(2):476–7.
[28] Shimon I. Ovarian hyperstimulation without elevated
serum estradiol associated with pure follicle-stimulat-
ing hormone-secreting pituitary adenoma. J Clin Endo-
crinol Metab 2001;86(8):3635–40.
[29] Rutkowski A, Dubinsky I. Ovarian hyperstimulation
syndrome: imperatives for the emergency physician.
J Emerg Med 1999;17(4):669–72.
[30] Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z,
Caspi E. Ovarian hyperstimulation syndrome: an up-
date review. Obstet Gynecol Surv 1989;44(6):430–40.
[31] Whelan III JG, Vlahos NF. The ovarian hyperstimula-
tion syndrome. Fertil Steril 2000;73(5):883–96.
[32] Navot D, Bergh PA, Laufer N. Ovarian hyperstimula-
tion syndrome in novel reproductive technologies:
prevention and treatment. Fertil Steril 1992;58(2):
249–61.
[33] Blankstein J, et al. Ovarian hyperstimulation syn-
drome: prediction by number and size of preovulatory
ovarian follicles. Fertil Steril 1987;47(4):597–602.
[34] Danninger B, Brunner M, Obruca A, Feichtinger W.
Prediction of ovarian hyperstimulation syndrome by
ultrasound volumetric assessment [corrected] of base-
line ovarian volume prior to stimulation. Hum Reprod
1996;11(8):1597–9.
[35] Delvigne A, Rozenberg S. Epidemiology and preven-
tion of ovarian hyperstimulation syndrome (OHSS):
a review. Hum Reprod Update 2002;8(6):559–77.
[36] Brinsden PR, Wada I, Tan SL, Balen A, Jacobs HS.
Diagnosis, prevention and management of ovarian
hyperstimulation syndrome. Br J Obstet Gynaecol
1995;102(10):767–72.
[37] Kim HH, Fox JH. The fallopian tube and ectopic preg-
nancy. In: Ryan KJ, Berkowitz RS, Barbieri RL,
Dunaif A, editors. Kistner’s gynecology and women’s
health. St. Louis: Mosby; 1999. p. 338.
[38] Tekay A, Martikainen H, Jouppila P. Doppler parame-
ters of the ovarian and uterine blood circulation in
ovarian hyperstimulation syndrome. Ultrasound Obstet
Gynecol 1995;6:50–3.
[39] Abramov Y, Elchalal U, Schenker JG. Pulmonary mani-
festations of severe ovarian hyperstimulation syn-
drome: a multicenter study. Fertil Steril 1999;71(4):
645–51.
[40] Roden S, Juvin K, Homasson JP, Israel-Biet D. An
uncommon etiology of isolated pleural effusion: the
ovarian hyperstimulation syndrome. Chest 2000;
118(1):256–8.
[41] Gregory WT, Patton PE. Isolated pleural effusion in
severe ovarian hyperstimulation: a case report. Am J
Obstet Gynecol 1999;180(6 Pt 1):1468–71.
[42] Fakih H, Bello S. Ovarian cyst aspiration: a therapeutic
approach to ovarian hyperstimulation syndrome. Fertil
Steril 1992;58(4):829–32.
[43] Salem S. The uterus and adnexa. In: Rumack CM,
Wilson SR, Charboneau JW, editors. Diagnostic ultra-
sound. 2nd edition. St. Louis: Mosby; 1998. p. 550.
[44] Holschneider CH. Surgical diseases and disorders in
pregnancy. In: DeCerney A, Nathan L, editors. Current
obstetric and gynecologic diagnosis and treatment.
New York: McGraw-Hill; 2003.
[45] Kaakaji Y, Nghiem HV, Nodell C, Winter TC. Sonog-
raphy of obstetric and gynecologic emergencies, Part 2.
Gynecologic emergencies. AJR Am J Roentgenol
2000;174(3):651.
[46] Gorkemli H, Camus M, Clasen K. Adnexal torsion
after gonadotrophin ovulation induction for IVF or

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348 347
ICSI and its conservative treatment. Arch Gynecol
Obstet 2002;267(1):4–6.
[47] Mashiach S, Bider D, Moran O, Goldenberg M, Ben-
Rafael Z. Adnexal torsion of hyperstimulated ovaries
in pregnancies after gonadotropin therapy. Arch Gyne-
col Obstet 2002;267(1):4–6.
[48] Hurh PJ, Meyer JS, Shaaban A. Ultrasound of a torsed
ovary: characteristic gray-scale appearance despite
normal arterial and venous flow on Doppler. Pediatr
Radiol 2002;32(8):586–8.
[49] Albayram F, Hamper UM. Ovarian and adnexal tor-
sion: spectrum of sonographic findings with patho-
logic correlation. J Ultrasound Med 2001;20(10):
1083–9.
[50] Stark JE, Siegel MJ. Ovarian torsion in prepubertal and
pubertal girls: sonographic findings. AJR Am J Roent-
genol 1994;163(6):1479–82.
[51] Rosado Jr WM, Trambert MA, Gosink BB, Pretorius
DH. Adnexal torsion: diagnosis by using Doppler
sonography. AJR Am J Roentgenol 1992;159(6):
1251–3.
[52] Fleischer AC, Stein SM, Cullinan JA, Warner MA.
Color Doppler sonography of adnexal torsion. J Ultra-
sound Med 1995;14(7):523–8.
[53] Choi JR, Levine D, Finberg H. Luteoma of pregnancy:
sonographic findings in two cases. J Ultrasound Med
2000;19(12):877–81.
[54] Yalcin OT, Tanir HM, Eskalen M. Unruptured pelvic
abscesses in pregnancy: report of two cases. Gynecol
Obstet Invest 2002;53(2):133–4.
[55] Tessler FN, Perrella RR, Fleischer AC, Grant EG.
Endovaginal sonographic diagnosis of dilated fallopian
tubes. AJR Am J Roentgenol 1989;153(3):523–5.
[56] Cacciatore B, Leminen A, Ingman-Friberg S, Ylostalo
P, Paavonen J. Transvaginal sonographic findings in
ambulatory patients with suspected pelvic inflamma-
tory disease. Obstet Gynecol 1992;80(6):912–6.
[57] Wiseman DA, Greene CA, Pierson RA. Infertility.
In: Rumack CM, Wilson SR, Charboneau JW, editors.
Diagnostic ultrasound, volume 2. 2nd edition. St.
Louis: Mosby; 1998. p. 1420.
[58] Kupfer MC, Schwimer SR, Lebovic J. Transvaginal
sonographic appearance of endometriomata: spectrum
of findings. J Ultrasound Med 1992;11(4):129–33.
[59] Patel MD, Feldstein VA, Chen DC, Lipson SD, Filly
RA. Endometriomas: diagnostic performance of US.
Radiology 1999;210(3):739–45.
[60] Athey PA, Diment DD. The spectrum of sonographic
findings in endometriomas. J Ultrasound Med 1989;
8(9):487–91.
[61] Pascual MA, Tresserra F, Lopez-Marin L, Ubeda A,
Grases PJ, Dexeus S. Role of color Doppler ultraso-
nography in the diagnosis of endometriotic cyst. J
Ultrasound Med 2000;19(10):695–9.
[62] Alcazar JL. Transvaginal colour Doppler in patients
with ovarian endometriomas and pelvic pain. Hum
Reprod 2001;16(12):2672–5.
[63] Baltarowich OH, Kurtz AB, Pennell RG, Needleman
L, Vilaro MM, Goldberg BB. Pitfalls in the sono-
graphic diagnosis of uterine fibroids. AJR Am J
Roentgenol 1988;151(4):725–8.
[64] Weinreb JC, Barkoff ND, Megibow A, Demopoulos R.
The value of MR imaging in distinguishing leiomyo-
mas from other solid pelvic masses when sonography
is indeterminate. AJR Am J Roentgenol 1990;154(2):
295–9.
[65] Quinn SF, Erickson S, Black WC. Cystic ovarian tera-
tomas: the sonographic appearance of the dermoid
plug. Radiology 1985;155(2):477–8.
[66] Patel MD, Feldstein VA, Lipson SD, Chen DC, Filly
RA. Cystic teratomas of the ovary: diagnostic value
of sonography. AJR Am J Roentgenol 1998;171(4):
1061–5.
[67] Bronshtein M, Yoffe N, Brandes JM, Blumenfeld Z.
Hair as a sonographic marker of ovarian teratomas:
improved identification using transvaginal sonography
and simulation model. J Clin Ultrasound 1991;19(6):
351–5.
[68] Jain KA. Prospective evaluation of adnexal masses
with endovaginal gray-scale and duplex and color
Doppler US: correlation with pathologic findings.
Radiology 1994;191(1):63–7.
[69] Brown DL, et al. Benign and malignant ovarian
masses: selection of the most discriminating gray-scale
and Doppler sonographic features. Radiology 1998;
208(1):103–10.
[70] Van Nagell Jr JR, Ueland FR. Ultrasound evaluation
of pelvic masses: predictors of malignancy for the
general gynecologist. Curr Opin Obstet Gynecol 1999;
11(1):45–9.
[71] Alcazar JL, Galan MJ, Ceamanos C, Garcia-Manero
M. Transvaginal gray scale and color Doppler sono-
graphy in primary ovarian cancer and metastatic
tumors to the ovary. J Ultrasound Med 2003;22(3):
243–7.
[72] Brown DL, et al. Ovarian masses: can benign and
malignant lesions be differentiated with color and
pulsed Doppler US? Radiology 1994;190(2):333–6.
[73] Stein SM. Differentiation of benign and malignant
adnexal masses: relative value of gray-scale, color
Doppler, and spectral Doppler sonography. AJR Am
J Roentgenol 1995;164(2):381–6.
[74] Tracey M, Fletcher HS. Appendicitis in pregnancy.
Am Surg 2000;66(6):555–60.
[75] Tamir IL, Bongard FS, Klein SR. Acute appendicitis
in the pregnant patient. Am J Surg 1990;160(6):571–5;
discussion 575–6.
[76] Mourad J, Elliott JP, Erickson L, Lisboa L. Appendi-
citis in pregnancy: new information that contradicts
long-held clinical beliefs. Am J Obstet Gynecol 2000;
182(5):1027–9.
[77] Kan JH, Fines BP, Funaki B. Conventional and hydro-
colonic US of the appendix with CT correlation per-
formed by on-call radiology residents. Acad Radiol
2001;8(12):1208–14.
[78] Abu-Yousef MM, Phillips ME, Franken Jr EA, Al-Jurf

E.M. Webb et al / Radiol Clin N Am 42 (2004) 329–348348
AS, Smith WL. Sonography of acute appendicitis:
a critical review. Crit Rev Diagn Imaging 1989;29(4):
381–408.
[79] Jeffrey Jr RB, Laing FC, Lewis FR. Acute appendici-
tis: high-resolution real-time US findings. Radiology
1987;163(1):11–4.
[80] Jeffrey Jr RB, Laing FC, Townsend RR. Acute appen-
dicitis: sonographic criteria based on 250 cases. Radi-
ology 1988;167(2):327–9.
[81] Simonovsky V. Sonographic detection of normal and
abnormal appendix. Clin Radiol 1999;54(8):533–9.
[82] Rettenbacher T, et al. Outer diameter of the vermiform
appendix as a sign of acute appendicitis: evaluation
at US. Radiology 2001;218(3):757–62.
[83] Incesu L, Coskun A, Selcuk MB, Akan H, Sozubir S,
Bernay F. Acute appendicitis: MR imaging and sono-
graphic correlation. AJR Am J Roentgenol 1997;
168(3):669–74.
[84] Hormann M, et al. MR imaging in children with
nonperforated acute appendicitis: value of unenhanced
MR imaging in sonographically selected cases. AJR
Am J Roentgenol 1998;171(2):467–70.
[85] Pradel JA, Adell JF, Taourel P, Djafari M, Monnin-
Delhom E, Bruel JM. Acute colonic diverticulitis:
prospective comparative evaluation with US and CT.
Radiology 1997;205(2):503–12.
[86] Hollerweger A, Macheiner P, Rettenbacher T, Gritz-
mann N. Primary epiploic appendigitis: sonographic
findings with CT correlation. J Clin Ultrasound 2002;
30:481–95.
[87] Ander DS, Ward KR. Medical management of ectopic
pregnancy– the role of methotrexate. J Emerg Med
1997;15(2):177–82.
[88] Barnhart K, Esposito M, Coutifaris C. An update on
the medical treatment of ectopic pregnancy. Obstet
Gynecol Clin North Am 2000;27(3):653–67.

Radiol Clin N Am 42 (2004) 349–363
Acute painful scrotum
Vikram Dogra, MD*, Shweta Bhatt, DMRD, DMRE
Department of Radiology, Case Western Reserve University, University Hospitals, 11100 Euclid Avenue,
Cleveland, OH 44106, USA
High-frequency transducer sonography using across the testis in the craniocaudal direction. If
gray scale along with pulsed and color Doppler is
the imaging modality of choice for evaluating pa-
tients who present with acute scrotal pain. Disease
processes such as testicular torsion, epididymo-orchi-
tis, and intratesticular tumors have the common
symptom of pain at presentation, and sonographic
evaluation helps in differentiating patients who re-
quire surgical from patients for whom conservative
management is sufficient. Sonography with a high-
frequency transducer helps to characterize better the
testicular flow and, in many instances, suggests more
specific diagnoses. This article is organized on the
basis of the pathophysiology of the disease process
with emphasis on color Doppler when applicable.
This article is intended to familiarize the reader with
new technology and provide new insights into the
sonographic diagnosis of painful scrotum.
Imaging anatomy
A normal adult testis has medium-level echoes
and measures 5�3�2 cm [1]. The tunica albuginea is
the fibrous sheath that covers the testicle. The tunica
albuginea is covered by the tunica vaginalis. Septae
extend from the tunica albuginea into the testicle and
divide the testes into lobules (Fig. 1). The posterior
surface of the tunica albuginea is reflected into the
interior of the gland, which forms the incomplete
septum known as the mediastinum of the testis. Sono-
graphically, the mediastinum of the testis is an echo-
genic band (Fig. 2) of variable thickness that extends
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.002
* Corresponding author.
E-mail address: [email protected] (V. Dogra).
imaged at an angle, it may resemble a testicular tumor.
Each lobule is composed of many seminiferous tu-
bules that open via tubuli recti into dilated spaces
called the rete testes within the mediastinum. The
normal rete testis can be identified at high-frequency
ultrasound (US) in 18% of patients as a hypoechoic
area with a striated configuration adjacent to the
mediastinum testis [1]. These in turn communicate
via efferent ductules with the epididymal head. The
epididymis is composed of a head, body, and tail,
the ducts of which continue as the vas deferens in
the spermatic cord. The epididymis is seen as a 5- to
12-mm pyramidal structure lying atop the superior
pole of the testes. The head of the epididymis is usu-
ally isoechoic to the testis, and its echotexture may be
coarser than that of the testicle [2,3]. High-frequency
transducer sonography permits visualization of the
body of epididymis, which measures 2 to 4 mm.
The right and left testicular arteries—branches of
the abdominal aorta—provide the vascular supply to
the testis. A transmediastinal artery branch of the
testicular artery occurs in approximately one half of
normal testes (Fig. 3) [4]. It courses through the
mediastinum to supply the capsular arteries and is
usually accompanied by a large vein. The deferential
artery, a branch of the superior vesicle artery, and the
cremasteric artery, a branch of the inferior epigastric
artery, supply the epididymis, vas deferens, and
peritesticular tissue [5]. Branches of the pudendal ar-
tery supply the scrotal wall [6]. Venous drainage is
via the pampiniform plexus.
Four testicular appendages have been described:
the appendix testis, the appendix epididymis, the vas
aberrans, and the paradidymis. They are remnants of
embryologic ducts [7]. The appendix testis and the
appendix epididymis are usually seen on scrotal so-
s reserved.

Fig. 1. Diagrammatic transverse representation of the anatomy of the testis illustrates the relationships of the tunica albuginea
to the mediastinum testis and the mediastinum testis to the rete testis. (Courtesy of Vikram Dogra, MD.)
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363350
nography. The appendix testis is attached to the upper
pole of the testis in the groove between the testis and
the epididymis (Fig. 4A). The appendix epididymis,
another appendage (Fig. 4B), is attached to the head
of the epididymis and is encountered unilaterally in
34% and bilaterally in 12% of postmortem series.
Presence of minimal fluid facilitates their visualiza-
tion on sonography.
Scanning technique
Scrotal sonography is performed with the patient
lying in a supine position and the scrotum supported
by a towel placed between the thighs. Optimal results
Fig. 2. Longitudinal view of a normal testis demonstrates
the mediastinum testis (arrow) as an echogenic band.
are obtained with 7- to 14-MHz high-frequency
linear-array transducers.
The testes are studied in two planes (ie, along the
long and transverse axes). The size and echogenicity
of each testicle and the epididymis are compared with
those on the opposite side. In patients being evaluated
for an acute scrotum, the asymptomatic side should
be scanned initially to set the gray scale and color
Doppler gains to allow comparison with the affected
side. Color Doppler and pulsed Doppler are opti-
mized to display low-flow velocities, and blood flow
in the testis and surrounding scrotal structures is
documented, including the spectral Doppler recording
of the intratesticular arterial flow in both testes.
Transverse images with portions of each testis on
the same image should be recorded in gray scale and
color Doppler. Power Doppler also may be used to
Fig. 3. Transverse oblique view of the testis demonstrates the
transmediastinal artery as a linear hypo-echoic band (arrow).

Fig. 4. (A) Appendix testis (arrow) directly attached to the testis (T). Presence of fluid (asterisk) facilitates its visualization.
(B) The appendix of the epididymis (cystic appearance) (arrow) is seen attached to the head of the epididymis (E).
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 351
visualize intratesticular flow in patients with an acute
scrotum. Additional techniques, such as the Valsal-
va’s maneuver or upright positioning, can be used as
needed for venous evaluation.
Inflammatory causes
Fournier’s gangrene
Fournier’s gangrene constitutes a urologic emer-
gency that demands early recognition because of its
high mortality rate, which is reportedly as great as
75% [8]. The diagnosis of Fournier’s gangrene is
based primarily on clinical examination rather than
on imaging studies. When clinical findings are am-
biguous, however, diagnostic imaging is useful [1].
Fournier’s gangrene is a synergistic polymicrobial
necrotizing fasciitis of the perineum or perirectal or
genital area that predominantly affects the scrotum in
men and frequently extends to involve the lower
abdominal wall. Predisposing conditions include di-
abetes mellitus, alcoholism, advanced age, and im-
munodeficiency syndrome [9]. Fournier’s gangrene
is characterized by obliterative endarteritis, which re-
sults in a cutaneous and subcutaneous vascular necro-
sis. The most common pathogens isolated in patients
with this syndrome are Klebsiella, Proteus, Strepto-
coccus, Staphylococcus, Peptostreptococcus, Esche-
richia coli, and Clostridium perfringens [8,10,11]. It
was first described in 1883 as an idiopathic condition
of the scrotum. The disease currently differs from
the original description in that it includes women and
is known to be secondary to a defined source of in-
fection in 95% of the cases.
Conventional radiography, CT, and sonography
can aid in determining the location and cause of gas
in the scrotum. Crepitus (gas in the tissue) has been
reported in 18% to 62% of cases and can be detected
by US, CT, and conventional radiography. Subcuta-
neous gas within the scrotal wall is the sonographic
hallmark of Fournier’s gangrene [12]. Sonographi-
cally, the gas appears as numerous discrete hyper-
echoic foci with reverberation artifacts (Fig. 5A, B)
[12,13]. Other sonographic findings include scrotal
wall thickening while the echotexture of the testis
and epididymis remains normal. Inguinoscrotal her-
nia can present with gas on sonographic examination
and can be differentiated from Fournier’s gangrene
by the presence of gas within the protruding bowel
lumen and away from the scrotal wall [1].
Epididymo-orchitis
Acute epididymo-orchitis or epididymitis is the
most common cause of acute scrotum in adolescent
boys and adults. Sexually transmitted Chlamydia
trachomatis and Neisseria gonorrhea are common
pathogens in men younger than 35 years. In prepu-
bertal boys and men over 35 years of age, the dis-

Fig. 5. (A) Surgically confirmed case of Fournier gangrene. Longitudinal US of the testis (T) shows sparing of the testis. Both
sonograms show air (arrowhead) parallel to the transducer face with reverberation artifact (arrow). (B) Axial CT in another
patient with proven Fournier gangrene, which shows subcutaneous air (arrowhead) dissecting the fascial planes.
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363352
ease is most frequently caused by E coli and Proteus
mirabilis [14]. Prehn [15] described the clinical dif-
ferentiation of scrotal pain associated with epididy-
mitis and acute torsion. Pain associated with acute
epididymo-orchitis is usually relieved when the tes-
ticles are elevated over the symphysis pubis; how-
ever, the scrotal pain associated with testicular torsion
is not lessened with this maneuver (Prehn’s sign).
Other causes, such as sarcoidosis, brucellosis, tuber-
culosis, cryptococcus, and mumps, also may cause
epididymitis and orchitis. Drugs, such as amiodarone,
also may cause epididymitis (chemical epididymitis)
[16]. Complications of acute epididymitis include
chronic pain, infarction, abscess, gangrene, infertility,
atrophy, and pyocele.
Epididymitis first affects the tail of the epididymis
and then spreads to involve the body and head of the
Fig. 6. Clinically proven epididymo-orchitis. Transverse
US of the testis (T) shows a markedly enlarged epididymis
(arrows) with variable echotexture.
epididymis. Orchitis develops in 20% to 40% of cases
of epididymo-orchitis by direct spread of infection.
On gray scale, the epididymis is enlarged and
usually appears hypoechoic or hyperechoic (second-
ary to hemorrhage) (Fig. 6) [17]. Other signs of in-
flammation, such as reactive hydrocele or pyocele
with scrotal wall thickening, are present in most cases.
Diffuse testicular involvement is confirmed by testicu-
lar enlargement and an inhomogeneous testicular
echotexture. Gray scale sonographic findings are non-
specific, but acute epididymo-orchitis is the most
common disorder with this combination of findings.
In one study that involved 20 cases of epididymo-
orchitis, 11 of 20 cases had enlarged and heteroge-
neous appearance of the epididymis or testis [18].
In orchitis there is edema of the testis contained within
an unyielding tunica albuginea, which results in var-
ious scales of reflectivity, seen as heterogeneity on
sonography [16,19]. This variable reflectivity may be
seen as a diffuse process or focal involvement, the
latter manifested as multiple hypoechoic lesions
within the testicular parenchyma. It is difficult to
differentiate focal areas of heterogeneity from neo-
plastic lesions. A heterogeneous echo pattern does not
always signify orchitis.
The increased blood flow to the epididymis and
testis on color Doppler examination is a well-estab-
lished criterion for the diagnosis of epididymo-orchi-
tis (Fig. 7) [20]. Normally, epididymal arterial flow is
of a low-resistance, high-flow state. With the US
machines currently in use, blood flow can be seen in
a normal epididymis on color Doppler sonography. In
one study it was seen in 100% of the cases [21]. The
mere presence of color flow in epididymis is not
equivalent to epididymitis; therefore, it is important
to compare the vascularity in both epididymii.

Fig. 7. Clinically proven epididymo-orchitis. Color Dopp-
ler of the testis (T) shows marked hyperemia of the epi-
didymis (arrow).
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 353
Increase of vascularity in acute epididymitis is
secondary to the increased number and concentration
of identifiable vessels with hyperemia, which results
in a high-flow/low-resistance pattern [22–24]. Analy-
sis of the spectral waveform also can provide use-
ful information, because inflammation of epididymis
and testis is associated with decreased vascular resist-
ance to that seen in normal individuals. In the testes
of a normal healthy volunteer, the resistive index (RI)
is rarely less than 0.5, but more than half the patients
with epididymo-orchitis have an RI of less than 0.5
(Fig. 8) [22,24,25]. In normal testes, intratesticular
venous flow is difficult to detect. Easy detectability
and increased venous flow in the testes greatly
suggest orchitis. The absence of venous flow in the
presence of arterial signal in orchitis is abnormal
and suggests venous occlusion, which may be sec-
ondary to impending infarction or underlying coagu-
lopathic disorder. Reversal of the spectral Doppler
diastolic plateau in acute epididymo-orchitis suggests
venous infarction. In all cases of testicular inhomo-
geneity diagnosed as epididymo-orchitis, if there is
no demonstrable improvement with antibiotic treat-
ment, the diagnosis should be reconsidered. Tumor
markers, a hypercoagulation profile, or repeat US
may reveal a different diagnosis, such as testicular
tumor or thrombosis.
Fig. 8. Duplex Doppler evaluation of the testis demonstrates
an RI of 0.44 and increased vascularity of the testis in a
patient with epididymo-orchitis.
Primary orchitis
Mumps is the commonest cause of orchitis without
accompanying epididymitis and is bilateral in 14% to
35% of cases [1]. Sonographically, the testes appear
enlarged with decreased echogenicity. In one study of
mumps-related epididymo-orchitis, 9 of 11 cases were
unilateral, and all 11 cases had an enlarged testis and
increased testicular vascularity. Testicular echogeni-
city was uniformly decreased in all 11 cases [26].
Hyperemia and heterogeneity isolated to the testis can
be seen in cases of orchitis, tumor, infarction, and
especially transient torsion of the testis. Because
intratesticular venous flow is difficult to detect in
normal testes, increased and easily detected venous
flow in the testes greatly suggests orchitis [20].
Cellulitis
Scrotal wall cellulitis is common in patients who
are obese or immunocompromised or have diabetes.
The sonographic signs are an increase in scrotal wall
thickness and the presence of hypoechoic areas with
increased blood flow shown on color Doppler. Scrotal
wall cellulitis may lead to scrotal abscess. Such ab-
scesses are usually well loculated, with irregular
walls and low-level internal echoes [1].
Intratesticular abscess
This condition is usually secondary to epididymo-
orchitis, but other causes include mumps, trauma, and
testicular infarction (Fig. 9). The sonographic features
include shaggy irregular walls, an intratesticular lo-

Fig. 9. Surgically confirmed testicular abscess. Transverse
US of the testis (T) shows fluid-debris level (arrow) con-
sistent with intratesticular abscess that developed secondary
to epididymo-orchitis.
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363354
cation, low-level internal echoes, and occasional
hypervascular margins [27].
Fig. 10. Diagram represents abnormal (Bell-Clapper defor-
mity) and normal insertion of the tunica vaginalis. (From
Dogra V, Ledwidge ME, Winter III TC, et al. Bell-Clap-
per deformity. AJR Am J Roentgenol 2003;180:1176–7;
with permission.)
Vascular
Testicular torsion
Testicular torsion and epididymo-orchitis com-
monly present with pain. The main role of US is to
differentiate acute testicular torsion, which is a sur-
gical emergency, from epididymo-orchitis. Clinical
differentiation of these conditions is difficult, with
a nearly 50% false-positive rate for diagnoses of
testicular torsion based solely on clinical findings,
which often results in unnecessary surgical explora-
tion [28]. Hunter described the first case of testicular
torsion [15]. Torsion of the spermatic cord occurs
most commonly from 12 to 18 years of age but can
occur at any age. The chance of torsion of the testis or
its appendage developing by age 25 is approximately
1 in 160 [29], with 2% of testicular torsions being
bilateral [30].
Patients with acute torsion present after a sudden
onset of pain followed by nausea, vomiting, and a
low-grade fever. Physical examination reveals a swol-
len, tender, and inflamed hemiscrotum. The cremas-
teric reflex is usually absent [31], and the pain cannot
be relieved by elevation of the scrotum [15].
Testicular torsion causes venous engorgement that
results in edema, hemorrhage, and subsequent arterial
compromise, which results in testicular ischemia. The
extent of testicular ischemia depends on the degree of
torsion, which ranges from 180� to 720� or more.
Experimental studies indicate that 720� torsion is
required to occlude the testicular artery [32]. When
torsion is 180� or less, diminished flow is seen. The
testicular salvage rate depends on the degree of tor-
sion and the duration of ischemia. A nearly 100%
salvage rate exists within the first 6 hours after the
onset of symptoms, a 70% rate in 6 to 12 hours, and a
20% rate in 12 to 24 hours [33].
Intravaginal torsion occurs within the tunica va-
ginalis. In patients with ‘‘Bell-Clapper deformity’’
(Fig. 10), tunica vaginalis completely encircles the
epididymis, distal spermatic cord, and the testis
rather than attaches to the posterolateral aspect of the
testis [1,34]. This leaves the testis free to swing and
rotate within the tunica vaginalis, much like a clapper
inside a bell. Bell-Clapper deformity is bilateral in
80% of patients.
Testicular perfusion can be evaluated by color
Doppler, power Doppler, or spectral Doppler sonog-
raphy. Color Doppler sonography can demonstrate
intratesticular flow reliably [17,24,35]. Power Dopp-
ler sonography uses the integrated power of the
Doppler signal to depict the presence of blood flow.
Higher power gains are more likely with power
Doppler sonography than with standard color Dopp-
ler sonography, which results in increased sensitivity
for detecting blood flow. Power Doppler sonography
is valuable in scrotal sonography because of its
increased sensitivity to low-flow states and its inde-
pendence from the Doppler angle correction [36,37].
Pulsed Doppler sonography is a useful method to
identify flow in the testis using the time-velocity
spectrum to quantify blood flow [38]. The spectral
waveform of the intratesticular arteries characteristi-
cally has a low-resistance pattern [35], with a mean
RI of 0.62 (range, 0.48–0.75) [17]. This is not true for
testicular volumes less than 4 cm3, however, which

Fig. 11. Surgically confirmed testicular torsion. (A) Color Doppler US of the testis (T) demonstrates the absence of intrates-
ticular blood flow with peripheral hyperemia (arrows). (B) Involvement of the epididymis in testicular torsion. There is no blood
flow within the testis (T) or epididymis (E). Peripheral hyperemia is seen (arrow).
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 355
are often found in prepubertal boys, in whom dia-
stolic arterial flow may not be detectable [39].
The role of color Doppler and power Doppler
sonography in the diagnosis of acute testicular torsion
is well established [24,40]. Using the presence or ab-
sence of identifiable intratesticular flow as the only
criterion for detecting testicular torsion, color Dopp-
ler was 86% sensitive, 100% specific, and 97% ac-
curate in the diagnosis of torsion and ischemia in
painful scrotum (Fig. 11A, B) [23]. The high degree
of accuracy is attributable to the improved depiction
of power Doppler sonography over color Doppler
sonography in normal prepubertal and postpubertal
testes [41]. Sonographic findings vary with the dura-
tion and degree of rotation of the spermatic cord.
Fig. 12. Surgically confirmed testicular torsion. Gray scale US o
appearance. (B) Epididymal involvement in testicular torsion in a
hypoechoic. There was no blood flow in the testis or epididymis o
Gray scale images are nonspecific for detecting
testicular torsion [22] and often appear normal if the
torsion has just occurred. Testicular swelling and
decreased echogenicity are the most commonly en-
countered findings 4 to 6 hours after the onset of
torsion. Twenty-four hours after the onset, the testis
has a heterogeneous echotexture secondary to vascu-
lar congestion, hemorrhage, and infarction, which is
referred to as late or missed torsion. An enlarged and
hypoechoic epididymal head may be visible because
the deferential artery that supplies the epididymis is
often involved in the torsion (Fig. 12A, B). In the
setting of testicular torsion, normal testicular echo-
genicity is a strong predictor of the testicular viability
[42]. Gray scale findings of testicular torsion are sum-
f the testis (A) shows an enlarged testis with a hypoechoic
nother patient. The epididymis (E) is enlarged and appears
n color Doppler examination (not shown).

Table 1
Gray scale findings of testicular torsion
Testicular torsion Gray scale patterns
Acute torsion with
viable testis
Normal
Acute torsion
with infarction
Hypoechoic pattern that may be
total or partial in case of a
partial infarct
Acute torsion with
hemorrhagic infarction
Hyperechoic and heterogeneous
echo patterns
Chronic torsion Hypoechoic with small testis
Box 1. Testicular torsion: color flowDoppler patterns
1. Absent arterial and venous flow2. Increased RI on affected side (dimin-
ished or reversed diastolic flow)3. Decreased flow velocity difficult to
measure because of small vessels/angle correction but may be subjec-tively inferred by relative difficulty infinding small, low-amplitude flow onsymptomatic side
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363356
marized in (Table 1). Other indicators include the pres-
ence of scrotal wall thickening and reactive hydrocele.
Because gray scale findings are often normal in the
early phases of torsion, the Doppler component of the
examination is essential. The absence of testicular
flow on color and power Doppler sonography is con-
sidered diagnostic of ischemia provided that the US
scanner is optimized to detect slow flow, is limited to
the use of a small color-sampling box, and is adjusted
for the lowest repetition frequency and the lowest
possible threshold setting [43]. The threshold should
be set just above the detection of color noise. The
absence of color flow Doppler on US examination is
not synonymous with testicular torsion, because other
conditions, such as testicular polyarteritis nodosa,
can mimic torsion [44]. The color flow Doppler and
spectral Doppler waveform findings in testicular tor-
sion are summarized in Box 1.
Torsion may be complete, incomplete, or transient.
Cases that show partial or transient torsion present a
diagnostic challenge. The ability of color Doppler
imaging to diagnose incomplete torsion accurately
remains undetermined. The role of spectral Doppler
analysis is not well established for diagnosing partial
torsion, but the findings may be useful (Fig. 13A, B)
[45]. No studies are available to validate the role of
spectral Doppler in partial torsion; however, sporadic
case reports exist to suggest its usefulness [46,47].
Asymmetry in the testicular RIs with decreased dia-
stolic flow or diastolic flow reversal may be seen. The
presence of a color or power Doppler signal in a
patient with the clinical presentation of torsion does
not exclude torsion [47].
Extravaginal testicular torsion occurs exclusively
in newborns. Torsion occurs outside the tunica vagi-
nalis when the testis and gubernaculums are not fixed
and are free to rotate [48]. The affected neonate
presents with swelling, discoloration of the scrotum
on the affected side, and a firm painless mass in the
scrotum [49,50]. The testis is typically infarcted and
necrotic at birth. Sonographic findings include an
enlarged, heterogeneous testis, ipsilateral hydrocele,
skin thickening, and no color flow Doppler signal
in the testis or the spermatic cord [51]. In children,
power Doppler US is more sensitive than color Dopp-
ler US for detection of intratesticular blood flow. In
one study, power Doppler US demonstrated intra-
testicular blood flow in 66 (97%) testes, whereas
color Doppler US demonstrated intratesticular blood
flow in 60 (88%) testes. Combined techniques de-
picted blood flow in all 68 (100%) testes [52].
Appendiceal torsion
The normal appendix testis appears as an ovoid
structure 5 mm in length in the groove between the
testis and the epididymis. The appendix testis is iso-
echoic to the testis and occasionally may be cystic.
The appendix epididymis is of the same approximate
dimensions as the appendix testis but is more often
pedunculated [53]. These appendages may become
twisted. Torsion of either appendage produces pain
similar to that experienced with testicular torsion, but
the onset is more gradual. The classic finding on
physical examination is a small, firm nodule that is
palpable on the superior aspect of the testis and
exhibits a bluish discoloration through the overlying
skin; this is called the ‘‘blue dot’’ sign [54]. The cre-
masteric reflex still can be elicited, although it is usu-
ally absent in testicular torsion. Approximately 91%
to 95% of twisted testicular appendices involve the
appendix testis and occur most often in boys aged 7 to
14 years.
Sonographic evaluation of torsion of the append-
ages of the testes usually reveals a circular mass with
variable echogenicity adjacent to the testis or epididy-
mis (Fig. 14) [55,56]. Reactive hydrocele and skin
thickening are common in these cases. Increased
peripheral flow may be seen around the torsed testicu-

Fig. 13. Surgically confirmed partial torsion. (A) The left testis shows normal intratesticular arterial spectral waveform. (B) In
the same patient, the right testis demonstrates diastolic flow below the baseline, which indicates loss of tissue perfusion. This
waveform pattern is abnormal and suggests partial testicular torsion. (From Dogra VS, Sessions A, Mevorach A, et al. Reversal
of diastolic plateau in partial testicular torsion. J Clin Ultrasound 2001;29:105–8; with permission.)
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 357
lar appendage on color Doppler US [14,23,24]. These
cases are managed conservatively with attention given
to pain management. The pain usually resolves in 2 to
3 days with atrophy of the appendix that may calcify.
The role of sonographic examination in torsion of the
testicular appendages is to exclude testicular torsion
and acute epididymo-orchitis.
Varicocele
Idiopathic varicocele
Venous drainage of the scrotum is via the pam-
piniform plexus of draining veins; it is formed around
the upper half of the epididymis in a variable fashion
and continues as the testicular vein through the deep
inguinal ring. The right testicular vein empties into
Fig. 14. Clinically proven case of appendiceal torsion. Lon-
gitudinal view of the testis (T) shows a predominantly
hypoechoic area (arrow) adjacent to the epididymis (E).
the inferior vena cava and the left testicular vein
into the left renal vein. Abnormal dilatation of the
veins of the pampiniform plexus results in varicocele,
which is usually caused by incompetent valves in the
internal spermatic vein. This results in impaired
drainage of blood into the spermatic cord veins when
the patient assumes an upright position or during a
Valsalva’s maneuver. Varicoceles have been noted in
approximately 15% of the general population and in
up to 40% of men with infertility [57]. Patients with
idiopathic varicoceles usually present between the
ages of 15 and 25 years. The veins of the pampini-
form plexus normally range from 0.5 to 1.5 mm in
diameter, with the main draining vein as large as
2 mm in diameter. Varicoceles are more common
on the left side for the following reasons: (1) the left
testicular vein is longer, (2) the left testicular vein
enters the left renal vein at a right angle, (3) in some
men, the left testicular artery arches over the left renal
vein, thereby compressing it, (4) the descending
colon distended with feces may compress the left
testicular vein [58], and (5) a ‘‘nutcracker’’ effect of
compression of the left renal vein may occur be-
tween the superior mesenteric artery and the abdomi-
nal aorta [59].
Varicocele is a clinical diagnosis, and palpation
reveals a scrotal mass that may feel like a bag of
worms with or without a palpable thrill. In one study,
all patients with palpable varicoceles had a spermatic
vein diameter of 5 to 6 mm [60]. The clinical gra-
dation of varicoceles is given in Table 2.
Sonography should be performed in supine and
upright positions. The sonographic appearance of

Table 2
Grade I Not visible but palpable on
Valsalva’s maneuver.
Grade II Less visible but palpable
without Valsalva’s maneuver
Grade III Always visually identifiable
and palpable without
Valsalva’s maneuver.
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363358
varicocele consists of multiple, serpigenous, tubular
structures of varying sizes larger than 2 mm in diam-
eter, which are usually best visualized superior or
lateral to the testis. When large, they can extend
posterior and inferior to the testis. Occasionally, low-
level internal echoes can be detected in these dilated
veins secondary to slow flow. Color flow and duplex
Doppler sonography optimized for low-flow velocities
confirms the venous flow pattern with phasic variation
and retrograde filling with Valsalva’s maneuver. The
sensitivity and specificity rates of varicocele detec-
tion approach 100% with color Doppler sonography.
The relationship between nonpalpable (subclini-
cal) varicocele and infertility remains controversial.
After treatment, however, these patients’ partners
have a 40% pregnancy rate [61]. Approximately one
third of men who undergo evaluation for infertility
present with varicocele; however, not all patients with
infertility have a palpable varicocele. In a study of
1372 infertile men, varicocele was found in 29% by
sonography; however, only 60% had a palpable vari-
cocele [62]. Diagnosis of subclinical varicocele is
important because treatment improves sperm quality
in as much as 53% of these cases.
Fig. 15. Intratesticular varicocele. (A) Longitudinal view of the
within the testis. (B) Corresponding spectral Doppler waveform d
va’s maneuver.
Secondary varicoceles
Secondary varicoceles result from increased
pressure on the spermatic vein produced by disease
processes, such as hydronephrosis, cirrhosis, or ab-
dominal neoplasm. Neoplasm is the most likely
cause of nondecompressible varicocele in men over
40 years of age. It is classically from a left renal
malignancy invading the renal vein [3]. Nondecom-
pressible varicoceles on the left or right should
prompt evaluation of the retroperitoneum to exclude
retroperitoneal masses and thrombus or tumor exten-
sion to the left renal vein. An abdominal mass always
should be suspected when an older man presents with
a new varicocele.
Intratesticular varicocele
An intratesticular varicocele can occur in associa-
tion with an extratesticular varicocele, but intrates-
ticular varicoceles are more commonly found alone
[63]. Clinical implications and the pathogenesis of
the newly defined condition, intratesticular varico-
cele, are not yet well established. Patients with intra-
testicular varicocele may have pain related to passive
congestion of the testis, which eventually stretches
the tunica albuginea. The sonographic findings of
intratesticular varicocele are similar to those of pam-
piniform plexus varicocele [58].
Sonographic features include multiple anechoic,
serpigenous, tubular structures of varying sizes within
the testis. Color flow and duplex Doppler sonography
demonstrate the venous flow pattern with a charac-
teristic venous spectral wave form, which increases
testis (T) shows tortuous anechoic, tubular areas (arrow)
emonstrates characteristic venous flow with positive Valsal-

V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 359
with Valsalva’s maneuver (Fig. 15A, B) [58]. The
main differential considerations are cyst, hematoma,
epidermoid cyst (echogenic rim), and tubular ectasia.
Use of color flow and duplex Doppler affords easy
differentiation. In every longstanding case of varico-
cele that presents with pain, this entity should be
considered and sought [58].
Fig. 17. Surgically confirmed testicular fracture secondary
Intratesticular arteriovenous malformation
Intratesticular arteriovenous malformation is a
rare, benign entity. Its pathogenesis may be congeni-
tal or posttraumatic. The characteristic arterialized
venous spectral waveform is universal to all arterio-
venous malformations [64], and the main differential
consideration is intratesticular hemangioma [65].
to trauma. Color Doppler US of the testis demonstrates alinear hypoechoic area (arrow) that runs obliquely across the
testis and represents the testicular fracture line.
Testicular traumaTesticular trauma typically results from athletic
injury, a motor vehicle accident, a direct blow, straddle
injury, or penetrating gunshot trauma. Blunt trauma
accounts for approximately 85% of these cases, and
penetrating trauma comprises the remaining 15%. A
direct blow to the testis with impingement against the
symphysis pubis or ischial ramus is the most common
mechanism of injury from blunt trauma. Approxi-
mately 50 kg of pressure is necessary to rupture the
tunica albuginea during blunt trauma. Testicular rup-
ture is a surgical emergency, and more than 80% of
Fig. 16. Surgically confirmed tunica albuginea rupture. In
this case of testicular trauma, color Doppler US shows a
contour abnormality (arrow) that represents extruded tes-
ticular contents through the ruptured tunica albuginea. The
asterisk represents accompanying hematocele.
ruptured testes can be saved if surgery is performed
within 72 hours after injury [66,67].
Trauma can result in contusion, hematoma, frac-
ture, or rupture of the testis [1]. Scrotal US with color
flow Doppler is helpful in determining the nature and
extent of the injury. The scrotal sonography has 100%
sensitivity for testicular injuries and 80% specificity
for tunica albuginea fractures [68]. Approximately
20% of patients who seek medical attention after
testicular trauma have testicular rupture [69]. Sono-
graphic findings in testicular rupture include inter-
ruption of the tunica albuginea, contour abnormality
(Fig. 16), a heterogeneous testis with irregular, poorly
defined borders, scrotal wall thickening, and a large
hematocele [70,71]. Color and power Doppler sonog-
raphy are helpful because either can detect disruption
of the normal capsular blood flow of the tunica
vasculosa. Heterogeneous intratesticular lesions are
caused by hemorrhage or infarction. Direct visual-
ization of a fracture line is rare and is seen only in
17% of cases (Fig. 17) [71]. Sonographic findings in
testicular trauma are summarized in Box 2.
Hematocele is a blood collection within the tu-
nica vaginalis. On sonography, acute hematoceles
are echogenic, whereas older hematoceles appear as
fluid collections with low-level echogenicity, fluid-
fluid levels, or septations. Hematoceles may be
caused by extratesticular or intratesticular bleeding,
although there is no definite US evidence of testicular
rupture. The presence of associated hyperechoic or
hypoechoic changes in the testicular parenchyma
suggests testicular rupture.

Box 2. Sonographic findings in testiculartrauma
1. Contour abnormality of the testis2. Disruption of the tunica albuginea
(evidenced by interruption of tunicavasculosa)
3. Direct visualization of a fracture line4. Presence of hematocele5. Intra- or extratesticular hematoma6. Heterogeneous appearance of the
testis7. Hyperemia of the epididymis
Note that any of the above mentionedfindings may be seen in isolation or inany combination.
V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363360
Hematomas can involve the testis, epididymis, or
scrotal wall. Their sonographic appearance varies
with time. Acute hematomas appear hyperechoic
and subsequently become complex with cystic com-
ponents. Hematoma appears avascular on color
Doppler sonography [14,40]. Color Doppler sonog-
raphy in posttrauma patients may reveal focal or
diffuse hyperemia of epididymis, which is called
traumatic epididymitis [72].
Patients with intratesticular hematomas fare
poorly without exploration, and 40% of the hema-
tomas result in testicular infection or necrosis, which
often requires orchiectomy. Scrotal exploration is
warranted if there is compelling evidence of testicular
fracture or rupture on scrotal sonography or physical
examination. The presence of a large hematocele is
another indication for exploration. Small hematoceles,
epididymal hematomas, or contusions of the testis
generally pose little risk to the patient and do not
require surgical exploration [73]. In posttrauma
patients with sonographic testicular abnormality, if
surgical exploration is not immediate, their progress
should be followed to demonstrate sonographic reso-
lution of the lesion, because 10% to 15% of testicular
tumors first present after an episode of scrotal trauma
[6]. Complications of testicular trauma include testic-
ular atrophy, infection, infarction, and infertility.
Fig. 18. Surgically confirmed case of inguinal hernia. Gray
scale US of the testis (T) shows the presence of air (arrow-
head) in a loop of bowel away from the skin surface with
reverberation artifact (arrow). (Compare with Fig. 5A.)
Miscellaneous conditions
Inguinal hernia
A hernia may present acutely as a nonpainful
mass or as a painful swelling with incarcerated bowel.
Hernias occur because of persistent patency of the
process vaginalis with protrusion of the peritoneal
contents, such as omentum or bowel, through it into
the tunica vaginalis [32].
US is helpful for patients with equivocal physical
findings and patients who present with acute inguino-
scrotal swelling. Herniation of the abdominal or
pelvic contents in the groin region may be divided
into two main categories: inguinal and femoral. In-
guinal hernias are the most common and can be sub-
divided into direct and indirect types. Direct inguinal
hernias travel through the Hassalbach’s triangle, a
weakness in the anterior abdominal wall. The borders
of this triangle are formed by the lateral border of
the rectus sheath medially, the inferior epigastric
artery laterally, and the inguinal ligament inferiorly
[74]. Indirect hernias travel lateral to the inferior
epigastric artery and through the inguinal canal; they
constitute 80% of all hernias. A femoral hernia occurs
within the femoral canal that lies medial to the femo-
ral vein. Because of the narrowness of the femoral
ring (the opening that forms the neck of a femoral her-
nia), it is more likely than an inguinal hernia to be-
come incarcerated [75]. Femoral hernia is common in
women, with the right side more frequently affected.

V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 361
Sonographic appearance depends on the hernial
sac contents. Most commonly it contains bowel; the
next most common content is omentum. Other rare
contents include Meckel’s diverticulum and urinary
bladder. Gray scale findings are a fluid- or air-filled
loop of bowel in the scrotum (Fig. 18). Finding real-
time peristalsis indicates the presence of bowel. Oc-
casionally, because contraction of the dartos also can
mimic peristalsis on real-time sonography; the exam-
iner should be aware of this possibility to avoid
misdiagnosis [1]. If the omentum has herniated, areas
of high echogenicity are present, which correspond to
omental fat.
Bowel strangulation is more common with indi-
rect than direct inguinal hernia. An akinetic dilated
loop of bowel observed sonographically in the hernial
sac is reported to have high sensitivity (90%) and
specificity (93%) rates for the recognition of bowel
strangulation [76]. Hyperemia of the scrotal soft tis-
sue and bowel wall suggests strangulation [17].
Patients with Richter’s hernia, a strangulated hernia
in which only a portion of the circumference of the
bowel is obstructed [77], usually present with gastro-
enteritis. Such cases can present a diagnostic chal-
lenge because of the hernia’s small size and the
eccentric bowel wall involvement with limited lumi-
nal compromise. This hernia commonly occurs at a
femoral site. It is important to recognize this condi-
tion because preoperative delays in diagnosis and
high postoperative morbidity are common compared
with other types of strangulated hernias [78].
Testicular tumors
Testicular tumors sometimes can present with
acute pain. This presentation is usually secondary
to epididymo-orchitis or hemorrhage within the tu-
mor. Ten percent of testicular tumors are brought to
attention secondary to epididymo-orchitis [1]. Semi-
noma is the most common tumor to masquerade
as acute orchitis. It is presumed to infiltrate and
obstruct the seminiferous tubules, and it results in
orchitis [1]. Leukemia and lymphoma can have a
similar presentation.
Gray scale findings of intratesticular tumors are
nonspecific and usually hypoechoic in appearance.
Hyperemia also can be seen in testicular tumors.
Acute epididymo-orchitis and intratesticular tumors
larger than 1.5 cm may have increased blood flow on
color Doppler examination. Hypervascularity seen
with tumors is sonographically indistinguishable
from inflammatory hypervascularity [2]. There are
no reliable sonographic criteria to distinguish malig-
nant from focal benign intratesticular lesions, such as
infarction, hemorrhage, infection, or non–germ-cell
tumor [79]. The presence of epididymal involvement
strongly suggests a nonneoplastic process.
All patients with a heterogeneous echo pattern of
testis should be followed to demonstrate their sono-
graphic resolution so that tumors with epididymo-
orchitis presentation are not missed.
Summary
The ability of US to diagnose the pathogenesis of
the acute scrotum is unsurpassed by any other imaging
modality. It is the first imaging performed in patients
with acute scrotum. Knowledge of the normal and
pathologic sonographic appearance of the scrotum and
proper sonographic technique is essential for accurate
diagnosis of acute scrotum. High-frequency trans-
ducer sonography combined with color flow Doppler
sonography provides the information essential to
reach a specific diagnosis in patients with testicular
torsion, epididymo-orchitis, and testicular trauma.
Acknowledgments
The authors would like to acknowledge Bonnie
Hami, MA, for her assistance in the preparation of the
manuscript and Joseph Molter for his assistance in
preparation of photographs.
References
[1] Dogra VS, Gottlieb RH, Oka M, Rubens DJ. Sonog-
raphy of the scrotum. Radiology 2003;227:18–36.
[2] Bree RL, Hoang DT. Scrotal ultrasound. Radiol Clin
North Am 1996;34:1183–205.
[3] Dambro TJ, Stewart RR, Barbara CA. The scrotum.
In: Rumack CM, Wilson SR, Charboneau JW, editors.
Diagnostic ultrasound. 2nd edition. St. Louis: Mosby;
1998. p. 791–821.
[4] Middleton WD, Bell MW. Analysis of intratesticular
arterial anatomy with emphasis on transmediastinal ar-
teries. Radiology 1993;189:157–60.
[5] Siegel BA, editor. Diagnostic ultrasonography test and
syllabus (second series). Reston (VA): American Col-
lege of Radiology; 1994. p. 148–9.
[6] Tumeh SS, Benson CB, Richie JP. Acute diseases of
the scrotum. Semin Ultrasound CT MR 1991;12:
115–30.
[7] Trainer TD. Testis and the excretory duct system. In:
Sternberg S, editor. Histology for pathologists. New
York: Raven Press; 1992. p. 744–6.
[8] Vick R, Carson III CC. Fournier’s disease. Urol Clin
North Am 1999;26:841–9.

V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363362
[9] Elem B, Ranjan P. Impact of immunodeficiency virus
(HIV) on Fournier’s gangrene: observations in Zambia.
Ann R Coll Surg Engl 1995;77:283–6.
[10] Kane CJ, Nash P, McAninch JW. Ultrasonographic
appearance of necrotizing gangrene: aid in early diag-
nosis. Urology 1996;48:142–4.
[11] Benizri E, Fabiani P, Migliori G, et al. Gangrene of
the perineum. Urology 1996;47:935–9.
[12] Dogra VS, Smeltzer JS, Poblette J. Sonographic diag-
nosis of Fournier’s gangrene. J Clin Ultrasound 1994;
22:571–2.
[13] Rajan DK, Scharer KA. Radiology of Fournier’s gan-
grene. AJR Am J Roentgenol 1998;170:163–8.
[14] Luker GD, Siegel MJ. Color Doppler sonography of
the scrotum in children. AJR Am J Roentgenol 1994;
163:649–55.
[15] Noske HD, Kraus SW, Altinkilic BM, Weidner W.
Historical milestones regarding torsion of the scrotal
organs. J Urol 1998;159:13–6.
[16] Cook JL, Dewbury K. The changes seen on high-reso-
lution ultrasound in orchitis. Clin Radiol 2000;55:
13–8.
[17] Siegel MJ. The acute scrotum. Radiol Clin North Am
1997;35:959–76.
[18] Farriol VG, Comella XP, Agromayor EG, Creixams
XS, Martinez De La Torre IB. Gray-scale and power
Doppler sonographic appearances of acute inflamma-
tory diseases of the scrotum. J Clin Ultrasound 2000;
28:67–72.
[19] Dewbury KC. Scrotal ultrasonography: an update.
BJU Int 2000;86(Suppl 1):143–52.
[20] Horstman WG, Middleton WD, Melson GL. Scrotal
inflammatory disease: color Doppler US findings.
Radiology 1991;179:55–9.
[21] Keener TS, Winter TC, Nghiem HV, Schmiedl UP.
Normal adult epididymis: evaluation with color Dopp-
ler US. Radiology 1997;202:712–4.
[22] Horstman WG. Scrotal imaging. Urol Clin North Am
1997;24:653–71.
[23] Burks DD, Markey BJ, Burkhard TK, Balsara ZN,
Haluszka MM, Canning DA. Suspected testicular tor-
sion and ischemia: evaluation with color Doppler so-
nography. Radiology 1990;175:815–21.
[24] Lerner RM, Mevorach RA, Hulbert WC, Rabinowitz
R. Color Doppler US in the evaluation of acute scrotal
disease. Radiology 1990;176:355–8.
[25] Jee WH, Choe BY, Byun JY, Shinn KS, Hwang TK.
Resistive index of the intrascrotal artery in scrotal in-
flammatory disease. Acta Radiol 1997;38:1026–30.
[26] Basekim CC, Kizilkaya E, Pekkafali Z, Baykal KV,
Karsli AF. Mumps epididymo-orchitis: sonography
and color Doppler sonographic findings. Abdom Im-
aging 2000;25:322–5.
[27] Dogra VS, Gottlieb RH, Rubens DJ, Liao L. Benign
intratesticular cystic lesions: US features. Radio-
graphics 2001;21(Spec No):S273–81.
[28] Dubinsky TJ, Chen P, Maklad N. Color-flow and
power Doppler imaging of the testes. World J Urol
1998;16:35–40.
[29] Williamson RC. Torsion of the testis and allied con-
ditions. Br J Surg 1976;63:465–76.
[30] Washowich L. Synchronous bilateral testicular torsion
in an adult. J Ultrasound Med 2001;20:933–5.
[31] Rabinowitz R. The importance of the cremasteric
reflex in acute scrotal swelling in children. J Urol
1984;132:89–90.
[32] Herbener TE. Ultrasound in the assessment of the
acute scrotum. J Clin Ultrasound 1996;24:405–21.
[33] Patriquin HB, Yazbeck S, Trinh B, et al. Testicular
torsion in infants and children: diagnosis with Doppler
sonography. Radiology 1993;188:781–5.
[34] Dogra V, Ledwidge ME, Winter III TC, Lee Jr FT.
Bell-Clapper deformity. AJR Am J Roentgenol
2003;180:1176–7.
[35] Middleton WD, Thorne DA, Melson GL. Color Dopp-
ler ultrasound of the normal testis. AJR Am J Roent-
genol 1989;152:293–7.
[36] Hamper UM, DeJong MR, Caskey CI, Sheth S. Power
Doppler imaging: clinical experience and correlation
with color Doppler US and other imaging modalities.
Radiographics 1997;17:499–513.
[37] Rubin JM, Bude RO, Carson PL, Bree RL, Adler RS.
Power Doppler US: a potentially useful alternative to
mean frequency-based color Doppler US. Radiology
1994;190:853–6.
[38] Scoutt LM, Zawin ML, Taylor KJ, Doppler US. Part II.
Clinical applications. Radiology 1990;174:309–19.
[39] Paltiel HJ, Rupich RC, Babcock DS. Maturational
changes in arterial impedance of the normal testis in
boys: Doppler sonographic study. AJR Am J Roent-
genol 1994;163:1189–93.
[40] Horstman WG, Middleton WD, Melson GL, Siegel
BA. Color Doppler US of the scrotum. Radiographics
1991;11:941–57.
[41] Luker GD, Siegel MJ. Scrotal US in pediatric patients:
comparison of power and standard color Doppler US.
Radiology 1996;198:381–5.
[42] Middleton WD, Middleton MA, Dierks M, Keetch D,
Dierks S. Sonographic prediction of viability in testic-
ular torsion: preliminary observations. J Ultrasound
Med 1997;16:23–7.
[43] Wilbert DM, Schaerfe CW, Stern WD, Strohmaier
WL, Bichler KH. Evaluation of the acute scrotum by
color-coded Doppler ultrasonography. J Urol 1993;
149:1475–7.
[44] Dotan ZA, Laufer M, Heldenberg E, Langevitz P,
Fridman E, Duvdevan M, et al. Isolated testicular
polyarteritis nodosa mimicking testicular neoplasm:
long-term follow up. Urology 2003;62(2):352.
[45] Fitzgerald SW, Erickson S, DeWire DM, et al. Color
Doppler sonography in the evaluation of the adult
acute scrotum. J Ultrasound Med 1992;11:543–8.
[46] Sanelli PC, Burke BJ, Lee L. Color and spectral Dopp-
ler sonography of partial torsion of the spermatic cord.
AJR Am J Roentgenol 1999;172:49–51.
[47] Dogra VS, Sessions A, Mevorach A, Rubens DJ.
Reversal of diastolic plateau in partial testicular tor-
sion. J Clin Ultrasound 2001;29:105–8.

V. Dogra, S. Bhatt / Radiol Clin N Am 42 (2004) 349–363 363
[48] Backhouse K. Embryology of testicular descent and
maldescent. Urol Clin North Am 1982;9:315–25.
[49] Zerin J, DiPietro M, Grignon A, Shea D. Testicular
infarction in the newborn: ultrasound findings. Pediatr
Radiol 1990;20:329–30.
[50] Hawtrey CE. Assessment of acute scrotal symptoms
and findings: a clinician’s dilemma. Urol Clin North
Am 1998;25:715–23.
[51] Brown SM, Casillas VJ, Montalvo BM, Albores-Saa-
vedra J. Intrauterine spermatic cord torsion in the
newborn: sonographic and pathologic correlation. Ra-
diology 1990;177:755–7.
[52] Barth RA, Shortliffe LD. Normal pediatric testis:
comparison of power Doppler and color Doppler US
in the detection of blood flow. Radiology 1997;204:
389–93.
[53] Hricak H, Filly RA. Sonography of the scrotum. Invest
Radiol 1983;18:112–21.
[54] Skoglund RW, McRoberts JW, Ragde H. Torsion of
testicular appendages: presentation of 43 new cases
and a collective review. J Urol 1970;104:598–600.
[55] Strauss S, Faingold R, Manor H. Torsion of the tes-
ticular appendages: sonographic appearance. J Ultra-
sound Med 1997;16:189–92.
[56] Hesser U, Rosenborg M, Gierup J, Karpe B, Nystrom
A, Hedenborg L. Gray-scale sonography in torsion
of the testicular appendages. Pediatr Radiol 1993;23:
529–32.
[57] Kim ED, Lipshultz LI. Role of ultrasound in the as-
sessment of male infertility. J Clin Ultrasound 1996;24:
437–53.
[58] Mehta AL, Dogra VS. Intratesticular varicocele. J Clin
Ultrasound 1998;26:49–51.
[59] Woodward PJ, Schwab CM, Sesterhenn IA. Extrates-
ticular scrotal masses: radiologic-pathologic correla-
tion. Radiographics 2003;23:215–40.
[60] Metin A, Bulut O, Temizkan M. Relationship between
the left spermatic vein diameter measured by ultra-
sound and palpated varicocele and Doppler ultrasound
findings. Int Urol Nephrol 1991;23:65–8.
[61] Gonda Jr RL, Karo JJ, Forte RA, O’Donnell KT.
Diagnosis of subclinical varicocele in infertility. AJR
Am J Roentgenol 1987;148:71–5.
[62] Pierik FH, Dohle GR, van Muiswinkel JM, Vreeburg
JT, Weber RF. Is routine scrotal ultrasound advanta-
geous in infertile men? J Urol 1999;162:1618–20.
[63] Das KM, Prasad K, Szmigielski W, Noorani N. Intra-
testicular varicocele: evaluation using conventional
and Doppler sonography. AJR Am J Roentgenol
1999;173:1079–83.
[64] Konus OL, Ilgit ET, Yucel C, Ozbek E, Onal B. Scrotal
arteriovenous malformation and its preoperative embo-
lization. Eur Radiol 1999;9(3):425–7.
[65] Kutlu R, Alkan A, Soylu A, Sigirci A, Dusak A. Intra-
testicular arteriovenous malformation: color Doppler
sonographic findings. J Ultrasound Med 2003;22:
295–8.
[66] Bhandary P, Abbitt PL, Watson L. Ultrasound diagno-
sis of traumatic testicular rupture. J Clin Ultrasound
1992;20:346–8.
[67] Cass AS, Luxenberg M. Testicular injuries. Urology
1991;37:528–30.
[68] Sasso F, Gulino G, Di Pinto A, Alcine E. Correlation
between ultrasonography imaging and surgical find-
ings in scrotal trauma. Arch Ital Urol Androl 1995;
67(2):159–62.
[69] Lewis CA, Michell MJ. The use of real-time ultra-
sound in the management of scrotal trauma. Br J Ra-
diol 1991;64:792–5.
[70] Siegel MJ. Male pelvis. In: Siegel MJ, editor. Pediatric
sonography. 2nd edition. New York: Raven Press;
1995. p. 479–512.
[71] Jeffrey RB, Laing FC, Hricak H, McAninch JW.
Sonography of testicular trauma. AJR Am J Roent-
genol 1983;141:993–5.
[72] Gordon LM, Stein SM, Ralls PW. Traumatic epididy-
mitis: evaluation with color Doppler sonography.
AJR Am J Roentgenol 1996;166:1323–5.
[73] Haas CA, Brown SL, Spirnak JP. Penile fracture and
testicular rupture. World J Urol 1999;17:101–6.
[74] Subramanyam BR, Balthazar EJ, Raghavendra BN,
Horii SC, Hilton S. Sonographic diagnosis of scrotal
hernia. AJR Am J Roentgenol 1982;139:535–8.
[75] Shadbolt CL, Heinze SBJ, Dietrich RB. Imaging of
groin masses: inguinal anatomy and pathologic condi-
tions revisited. Radiographics 2001;21:S261–71.
[76] Ogata M, Imai S, Hosotani R, Aoyama H, Hayashi M,
Ishikawa T. Abdominal ultrasonography for the diag-
nosis of strangulation in small bowel obstruction. Br J
Surg 1994;81:421–4.
[77] Middlebrook MR, Eftekhari F. Sonographic findings in
Richter’s hernia. Gastrointest Radiol 1992;17:229–30.
[78] Kadirov S, Sayfan J, Friedman S, Orda R. Richter’s
hernia: a surgical pitfall. J Am Coll Surg 1996;182:
60–2.
[79] Lentini JF, Benson CB, Richie JP. Sonographic fea-
tures of focal orchitis. J Ultrasound Med 1989;8:
361–5.

Radiol Clin N Am 42 (2004) 365–381
Ultrasound evaluation of abdominal aortic and iliac
aneurysms and mesenteric ischemia
Kathryn Hermsen, MD*, Wui K. Chong, MB, FRCR
Department of Radiology, CB #7510, University of North Carolina, 101 Manning Drive, Chapel Hill, NC 27599, USA
Ultrasound (US) has been used routinely since of an endothelial lining, a connective tissue layer, and
the mid 1980s to evaluate the abdominal aorta. Color
Doppler imaging allows characterization of flow pat-
terns [1]. It is the preferred method for diagnosis and
surveillance of abdominal aortic aneurysms (AAAs)
because of its accuracy, ease of use, and cost effec-
tiveness [1,2]. US has been used to characterize aor-
tic diseases, such as mycotic aneurysm, posttraumatic
pseudoaneurysm, dissection, and detection of mural
thrombus and AAA rupture [3,4]. Other applications
of sonography include characterization of iliac arterial
disease and postoperative evaluation of endovascular
AAA repair. US plays a role in noninvasive diagnosis
of mesenteric vascular occlusive disease in patients
with suspected chronic intestinal ischemia.
Anatomy and histology
The aorta enters the abdomen at the aortic hiatus
at the T12 level. It descends anterior to the lumbar
vertebrae immediately left of midline and tapers dis-
tally [5]. The normal luminal diameter of the in-
frarenal abdominal aorta varies according to age and
gender. In young patients without vascular disease, it
measures 2.3 cm in men and 1.9 cm in women [6].
It increases in size with age. In one study, average
luminal diameter in men without aneurysm with a
mean age 70.4 years was 2.8 cm [2].
The aorta is an elastic artery composed of three
layers: the tunica intima, tunica media, and tunica ad-
ventitia. The aortic intima is thick and is composed
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.003
* Corresponding author.
E-mail address: [email protected] (K. Hermsen).
an internal elastic membrane. The endothelium con-
sists of squamous cells oriented parallel to the direc-
tion of blood flow and connected by tight junctions.
The tunica media is composed of smooth muscle
and connective tissue. The tunica adventitia of the
aorta is thin and consists of connective tissue fibers,
fibroblasts, and macrophages. It also contains the in-
nervation of the aorta and its blood supply (vasa va-
sorum) [7].
The aorta bifurcates to form the common iliac ar-
teries near the level of the umbilicus (approximately
L4). The common iliac arteries proceed anterolaterally
in association with the common iliac veins and bifur-
cate into the internal and external iliac arteries [5].
Major branches of the abdominal aorta routinely
visualized by US include the celiac axis, superior
mesenteric artery (SMA), and renal arteries. The ce-
liac axis is the first major division of the abdominal
aorta. It generally gives rise to the left gastric, hepatic,
and splenic arteries, although anatomic variants are
frequent [3]. The left gastric artery is seldom visual-
ized by US [8]. The SMA arises anterior to the L1
vertebra and posterior to the body of the pancreas [9].
It travels with the superior mesenteric vein anterior to
the duodenum and inferiorly to divide within the
mesentery 5 to 6 cm from its origin. The normal
inferior mesenteric artery is infrequently visualized by
US. In disease states it may hypertrophy and become
visible [8]. The renal arteries arise from the lateral
wall of the aorta within 1.5 cm of the SMA [3].
Supernumerary renal arteries are frequent [3].
Branches of the aorta and the iliac arteries are
classified as muscular arteries. When compared with
the elastic arteries, such as the aorta, their intima
are thinner and have less subendothelial connective
s reserved.

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381366
tissue. Likewise, the tunica media contains less elas-
tic material. The tunica adventitia is thicker and has
greater collagen content [7].
Flow characteristics
As characterized by color Doppler, the aorta is
a high-resistance vessel. Velocity climbs rapidly in
early systole and falls rapidly in early diastole [3].
The proximal aorta demonstrates biphasic waveforms
with reversal of flow in early diastole. The distal aorta
demonstrates triphasic waveforms (small component
of forward flow in late diastole). Normal blood flow
is laminar (Fig. 1) [1].
The celiac axis demonstrates high-resistance flow
at its origin with rapid systolic upstroke and rapid de-
cline (Fig. 2). Hepatic and splenic arteries are low-
resistance vessels with substantial forward flow
throughout diastole [3].
The SMA is a high-resistance vessel in the fasting
state. In the fasting patient, flow is triphasic, with
rapid systolic upstroke and reversal of flow in early
diastole. In the postprandial state, spectral Doppler
waveform of the SMA changes to a low-resistance,
high-flow pattern secondary to decrease in splanchnic
vascular resistance. Peak systolic velocity (PSV)
increases and forward flow is seen throughout dias-
tole (Fig. 3) [8]. Moneta et al [10] described the
effects of meal content on mesenteric vascular resist-
ance. Test subjects were imaged after ingesting vary-
ing amounts of fat, proteins, and carbohydrates.
Control meals consisted of water or mannitol. In the
Fig. 1. (A) Normal aorta with normal triphasic waveform. Note rapid
flow characteristic of a high resistance vessel. (B) Normal aortic t
SMA, PSV, end diastolic velocity (EDV), and mean
velocity increased with all except water. The great-
est changes were demonstrated in end diastolic flow
[10]. The neurohumoral mechanisms behind this
response are incompletely understood. Hormones re-
leased in the presence of fat, carbohydrates, and pro-
teins, including cholecystekinin, vasoactive intestinal
peptide, gastrin, secretin, and kinins, are released into
the bowel wall and act as vasodilators. Decreased
oxygen concentration that results from increased con-
sumption associated with active transport of nutrients
may act as a vasodilatory stimulus [11]. Postpran-
dial changes in vascular resistance are considerably
less pronounced in the celiac axis (CA), which indi-
cates that this is a low-resistance circuit regardless of
feeding [8]. In the study by Moneta et al, minimal
changes were observed in the CA with feeding [10].
Imaging techniques
The primary limitations in imaging the abdominal
aorta are patient body habitus and the presence of
bowel gas. Thinner patients are more easily imaged.
No bowel preparations have proved effective in lim-
iting the effect of interposed bowel gas. In imaging of
the abdominal aorta, patients are usually scanned after
an 8- to 10-hour fast. The presence of barium within
the bowel attenuates US transmission, and imaging
should be postponed after gastrointestinal procedures.
The patient is initially scanned in the supine position
using linear 4-, 3.5-, or 2.5-MHz transducers; curved
5- or 3.5-MHz transducers are also used, depending
systolic peak followed by rapid decline and brief reversal of
ransverse diameter measurement.

Fig. 2. Normal celiac axis origin and bifurcation. The left
gastric artery is seldom seen.
Fig. 4. (A, B) Importance of obtaining measurement per-
pendicular to plane of vessel. Oblique measurements may
overestimate lumen diameter.
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 367
on patient body habitus [1]. The aorta is imaged in
sagittal and transverse planes at its proximal, mid, and
distal portions. In the presence of a tortuous aorta, it is
important to obtain measurements perpendicular to
the long axis of the vessel. Oblique measurements
Fig. 3. (A) Fasting SMA. Note rapid systolic upstroke and
low diastolic flow. (B) Postprandial SMA. Note increased
diastolic forward flow.
may overestimate the lumen diameter (Fig. 4) [12].
The anteroposterior and transverse diameters are mea-
sured from outer wall to outer wall. The common iliac
arteries are imaged at the level of the bifurcation in
anteroposterior and transverse diameter. In the upper
abdomen, a good acoustic window is often found in
the midline between the rectus abdominus muscles.
The lateral aspect of the rectus muscles also may
provide a good window, especially for visualizing
the iliac vessels [3]. A left lateral decubitus or oblique
approach is often helpful in patients with excessive
bowel gas and for visualizing the mid and lower ab-
dominal aorta. Use of slow graded compression with
the transducer may displace bowel loops. Color
Doppler may aid in identifying the aorta [1]. Flow
characteristics (laminar versus turbulent) and mea-
surements, including PSV and EDV, are documented.
Flow within the renal arteries is demonstrated, and
each kidney is observed in long axis.
The aorta is visualized similarly after endovascu-
lar stenting using 2.5- and 3.75-MHz curved trans-
ducers. Duplex and color flow Doppler analysis is
obtained at the level superior to the stent, at its
proximal attachment, including right and left iliac
attachments. Flow within the SMA and renal arteries
is documented. The maximum transverse diameters
of the graft lumen and aneurysm sac are measured in
the anteroposterior and transverse planes. The clot
within the aneurysm sac is observed with color
Doppler in the transverse and longitudinal planes to
evaluate for leak around the stent or flow within the
sac. Detectable flow is considered an indication of
leak [13]. Another indicator of graft compromise is
enlargement of the aneurysm sac or failure of the
aneurysm sac to regress. Multiple types of endoleaks
have been described. In 1997, White first described
endoleaks (Box 1) [14,15].
Cursory evaluation of the mesenteric arterial vas-
culature is undertaken in routine imaging of the

Box 1. White classification ofendoleaks[15]
Type I: Direct communication betweenthe graft and aneurysm sac via anineffective seal at the graft ends orattachment sites.
Type II: Retrograde flow through lum-bar arterials, the inferior mesentericartery (IMA), or accessory renal ar-teries feeds into the aneurysm sac.
Type III: Seen in modular, multisegmen-tal grafts. Leak occurs through defi-ciency in graft fabric and may be aresult of altered hemodynamics sec-ondary to aneurysm sac shrinkage.
Type IV: On contrast, CT appears as ablush of contrast outside the graftfrom contrast diffusion through thenaturally porous graft fabric orthrough small defects in the fabricat the site of sutures or struts. Mayrequire angiography to distinguishfrom Type III graft.
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381368
abdominal aorta. More detailed examination to assess
for mesenteric occlusive disease faces several techni-
cal challenges. Bowel gas, respiratory motion, and
vessel depth confound identification of the mesen-
teric vessels [8]. Various methods have been used to
reduce interference by gas, including cathartic bowel
preparation the night before, oral simethicone 15 min-
utes before examination, liquid diet the evening be-
fore followed by 8- to 12-hour fast, and fasting alone
[16,17].
The CA is scanned from its origin to its bifurca-
tion. The SMA is examined from its origin and
followed 5 to 6 cm distally. In the fasting state, the
normal SMAwaveform is triphasic. Should a biphasic
waveform be observed, the sonographer searches for a
replaced hepatic artery. This anatomic variant occurs
in approximately 20% of the population. It arises from
the lateral SMA and travels cephalad and right to
supply the liver. The presence of a replaced hepatic
artery results in biphasic SMA flow [16,17]. The
position of the CA and SMA in the upper abdomen
often requires high Doppler angles of insonation.
Unfortunately, this introduces error in determining
flow velocities, which usually results in falsely ele-
vated values [8]. Care must be taken to maintain a
Doppler angle of 60� or less while obtaining velocity
measurements [8,18–20].
Abdominal aortic pathology
Aneurysm
An aneurysm is an abnormal expansion of a vessel.
Aneurysms are classified as false or true. True aneu-
rysms include all three layers of the vessel wall. Mul-
tiple configurations of true aneurysms are described.
Most AAAs are true aneurysms and are fusiform; 97%
are infrarenal. Only 2% to 7% extend to the juxtarenal
or suprarenal aorta [21]. Aneurysms that occur proxi-
mal to the renal arteries are more likely to be mycotic
or posttraumatic. AAA is a common condition, with
a prevalence of 1% to 4% in people aged 50 or older
[1]. Most of these aneurysms are idiopathic. The
strongest association with AAA is atherosclerotic
disease. Other risk factors for development of AAAs
include male gender, smoking, chronic obstructive
pulmonary disease, age, and family history. Most pa-
tients with AAA are asymptomatic. Some patients
may present with abdominal or lower extremity pain
[3]. The most common physical examination finding
is a pulsatile abdominal mass. The physical examina-
tion, however, has poor predictive value in the detec-
tion of AAA [22].
Sonography is the primary imaging study for
detection of aortic aneurysms. The accuracy of US
in the diagnosis of AAA approaches 100% [3,27]. The
typical US appearance of AAA is of a dilated vessel
with an irregular lumen. Ulceration or cystic changes
may be seen as focal hypoechoic regions within
the vessel wall [3]. Echogenic mural thrombus is
present in most large lesions and may be circumfer-
ential or eccentric (Figs. 5, 6). Juxtarenal AAAs may
appear to involve the renal arteries at US because
of apparent overlap of the aneurysm wall with the
renal ostia. Careful evaluation of the course of the
renal arteries and aorta in multiple planes may clarify
the relationship of the aneurysm to the renal arteries.
Multidetector CT with coronal reconstruction or aor-
tography is usually required to evaluate renal artery
involvement in juxtarenal aneurysms, however [1].
Flow within AAAs may be laminar or turbulent.
Turbulent flow is associated with formation of mural
thrombus (Fig. 7). It has been proposed that thrombus
imparts tensile strength to the aneurysm wall by
absorbing forces generated by flow. Mower used
computer-generated models of AAA that ranged in
size from 2 to 4 cm to study the effects of thrombus
size and composition on wall stress [23]. In this

Fig. 5. (A) Transverse view of AAA with mural thrombus
(arrow). (B) Color Doppler demonstrates turbulent flow
within lumen outlining thrombus.
Fig. 6. Pitfalls in measuring AAA. (A) This echogenic line
(solid arrow) is easily mistaken for the aortic wall. It ac-
tually represents the surface of the thrombus that lines the
wall of a large AAA. Open arrow demarcates the true aortic
wall. (B) On the transverse view, the large mural thrombus is
better seen. (Open arrows mark the true vessel wall.)
Fig. 7. Turbulent flow within AAA. Note the hypoechoic
thrombus (arrow).
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 369
study, the larger the mural thrombus, the greater the re-
duction in wall stress. Organized mural thrombi im-
parted greater tensile strength than more pliant ones.
The authors speculated that the tendency of eccen-
tric mural thrombi to collect along the ventral wall
may explain the rarity of ventral rupture [23]. The
presence of mural thrombus also may help to restore
laminar flow.
The most catastrophic complication of abdominal
aortic aneurysm is rupture. Rupture carries a high
mortality rate. Fifty percent of patients do not reach
the hospital alive. The overall mortality rate is 80% to
94% [1]. Signs and symptoms associated with rupture
include severe abdominal and back pain, nausea and
vomiting, and hypotension [1]. Aneurysm size and
rate of enlargement are the most important factors in
predicting potential rupture. In a 15-year study,
Brown et al [24] followed 476 patients with AAA
larger than 5 cm who were deemed unfit surgical
candidates. The risk of rupture in male patients with
AAA of 5 to 5.9 cm was 1% per year; in male patients
with AAA 6 cm or larger, the risk was 14.1%. Gender
differences also were noted in this study. Women with
aneurysms of similar size were at fourfold higher risk
for rupture [24]. Aneurysms are generally expected to
enlarge 2 to 4 mm per year. Aneurysms that enlarge by
5.5 to 6 mm per year are regarded as high risk for
rupture [12]. Sharp et al [25] identified 32 patients
with aneurysms less than 5.5 cm per year that had
enlarged 5 mm or more in the past 6 months. Over a
period of 50 patient years, none ruptured. Thus,
the risk of rupture was calculated to be 0 to 6 per
100 patient years [25]. CT is the imaging modality of
choice in the setting of rupture because it is not subject
to technical factors, such as interposed bowel gas, and
grants a greater perspective on the extent of bleeding

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381370
[3]. The US appearance of rupture is that of a large,
usually hypoechoic retroperitoneal fluid collection.
Other complications of AAA include embolization
of mural thrombus, occlusion of the renal and splanch-
nic arteries, obstructive uropathy (usually on the left),
and arteriovenous fistula (usually with the inferior
vena cava [IVC], or left renal vein) (Fig. 8) [2,3]. A
less common complication is duodenal obstruction,
which results from compression of the duodenum
(SMA syndrome) between an enlarging AAA and
the SMA [26].
US is ideal for monitoring AAAs because it is
inexpensive, does not require the use of contrast
material or radiation, and is highly accurate. CT is
often used in AAA evaluation, but it faces some
technical limitations. Because the aneurysmal aorta is
frequently ectatic, slices obtained in the axial plane
only may be obtained with a degree of obliquity,
which potentially overestimates the size of the aneu-
rysm. Because changes in measurements of only a
few millimeters may influence management greatly,
potential effects of measurement variability be-
tween CT and US are an important consideration.
Fig. 8. Left ureteral obstruction by AAA. (A) Distal AAA.
Lumen diameter is normal proximally and expands distally.
(B) Mild left hydronephrosis secondary to compression
by AAA.
Wanhainen et al [2] evaluated differences in observer
measurements between CT and US in 475 patients.
Thirty-three were found to have AAAs (defined as
diameter larger than 3 cm). In patients with normal
aortas (<3 cm), US overestimated the diameter by
2.8 mm in anteroposterior diameter and 3.8 in trans-
verse diameter. The difference in aneurysmal aortas
was greater, with a variability of 8 mm or less in
anteroposterior and 10.6 mm in transverse measure-
ments. The authors found the variability in transverse
measurements to be unacceptably high and preferred
using anteroposterior diameters in assessing aneurysm
size [2]. There is no true ‘‘gold standard’’ modality in
the measurement of AAA. Lanne et al [12] reported
greater reliability for US using an automated echo
tracking device for measurement of the aortic lumen.
Frequent indications for aortic US are the finding
of a pulsatile abdominal mass on physical exami-
nation and evaluation of an AAA incidentally dis-
covered on a CT performed for another purpose.
Unfortunately, however, many AAAs are not discov-
ered until rupture. Given the dismal prognosis of
rupture and the relatively low mortality rate for repair
(2%–5%), is screening for AAA in high-risk patients
a viable option? Lee et al [27] examined the cost
effectiveness of conducting a ‘‘quick screen’’ (ie, ab-
breviated US) evaluation of the abdominal aorta in at-
risk populations. The examination was limited to less
than 5 minutes and was performed at reduced cost.
The sensitivities and specificities for the quick screen
and standard duplex US were 100%. The emphasis
was on screening patients with known risk factors,
such as male gender, smoking, hypertension, hyper-
lipidemia, other peripheral vascular disease, and coro-
nary artery disease. They found screening in at-risk
populations to be cost effective and recommend
screening in men over age 60 [27].
Although most AAAs are idiopathic, certain con-
nective tissue disorders carry an increased risk of
AAA. Ehler-Danlos syndrome is a group of disorders
associated with abnormal collagen synthesis. Type IV
Ehler-Danlos syndrome is associated with vascular
abnormalities, including aneurysms of the elastic ar-
teries and their major branches. Catastrophic com-
plications have been reported with angiography in
patients with Type IV Ehlers-Danlos syndrome, and it
is generally avoided [28].
Pseudo or false aneurysms are generally the result
of a defect in the intima through which blood flows.
Blood escapes through a defect in the arterial wall
and is contained by the surrounding soft tissue. Blood
flows into the aneurysm during systole and out during
diastole, which produces a characteristic appearance
on color Doppler imaging that has been likened to the

Fig. 9. Classic color Doppler ‘‘Yin-Yang’’ appearance of
pseudoaneurysm. Blood enters the false aneurysm (red),
strikes the back wall, and reverses direction (blue).
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 371
Yin-Yang sign (Fig. 9). False aneurysms caused
by penetrating trauma show ‘‘to and fro’’ flow in the
neck, with blood leaving the artery during systole and
re-entering during diastole. Aortic pseudoaneurysms
are most frequently posttraumatic or mycotic [3,28].
Mycotic aneurysms refer to aneurysms of any type
that have become infected. They are more frequent in
patients younger than 50 years, unlike idiopathic
AAAs, which are more frequent in patients over age
60. Two broad categories of mycotic aneurysms have
been described: those that form secondary to aortic
wall factors (atherosclerosis or stents) and those that
are seeded from a distant source. The second group is
divided according to source of infection: intravascular
(frequently in the form a septic emboli) and extravas-
cular (usually formed by contiguous spread from a
nearby infected site). The most frequent causative
organisms are staphylococci and salmonella. An im-
portant feature of mycotic aneurysms is their tendency
to enlarge rapidly and their propensity for rupture
[4,29]. Few specific US findings are reported. Naga-
numa et al [4] described the presence of gas echoes in
the wall of a mycotic aneurysm with sonography.
Inflammatory aneurysms are a relatively uncom-
mon type of true aneurysm that constitutes approxi-
mately 4% of AAA. They are characterized by fibrotic
thickening of the adventitia and chronic inflammatory
changes [30]. They most frequently occur in the iliacs,
followed by the aorta. On sonography, the aneurysm
wall is thickened with surrounding hypoechoic fi-
brotic tissue. US and CT have proved the most useful
modalities in diagnosing inflammatory aneurysms
[31]. Inflammatory AAAs may be seen in the setting
of retroperitoneal fibrosis. In this setting, the fibrotic
tissue may extend laterally into the retroperitoneum,
and the ureters may become obstructed [32]. Inflam-
matory aneurysms carry a higher rate of morbidity and
mortality than idiopathic AAAs and are more likely to
present with pain in the absence of rupture [30].
Erythrocyte sedimentation rate is usually elevated.
Pennell et al [33] described a triad of chronic abdom-
inal pain, weight loss, and elevated erythrocyte sedi-
mentation rate in a patient with AAA as highly
suggesting inflammatory AAA.
Dissection
Aortic dissection occurs when a defect in the
aortic wall allows the entry of blood, which separates
the intima from the media [34]. Two lumens are
created: a false lumen, which consists of blood within
the vessel wall, and the true vessel lumen. Although
the vessel does enlarge, dilatation is considerably less
pronounced than with true aneurysms. Most often,
dissection occurs along a segment of varying length
and ends with re-entry of the blood column into the
true lumen via a second intimal defect. This serves to
decompress the hematoma and delay rupture [35].
Isolated abdominal aortic dissection is exceedingly
rare in the absence of blunt abdominal trauma [36].
Most aortic dissections originate in the thoracic aorta,
usually the ascending aorta. Several classifications
exist; the most commonly used are the DeBakey and
Stanford classifications. Two thirds of dissections
involve the ascending aorta, usually within a few
centimeters of the aortic valve. In DeBakey types 1
and 3, the dissection plane may extend into the
abdominal aorta [37].
The pathogenesis behind dissection remains con-
troversial. Dissection in the absence of a clear intimal
tear has been documented, which suggests that dis-
section occurs through a defect in the media created
by intramural hemorrhage. The importance of abnor-
malities of the media has been a topic of interest in
the pathogenesis of dissection. Increased incidence of
dissection in patients with Turner’s, Ehlers-Danlos, or
Marfan syndrome, all of which have underlying ab-
normalities of the media, suggests that a primary
defect of the media underlies dissection. To date, no
specific histologic abnormalities have been demon-
strated [38]. Sonesson et al [39] used US to show that

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381372
patients with Marfan syndrome had abnormal com-
pliance of the aorta. Most dissections occur in pa-
tients without connective tissue disorders, however.
In these cases, by far the strongest association with
dissection is the presence of hypertension [37].
CT and MR imaging are the imaging modalities of
choice in dissection that involves the abdominal
aorta. Dissection may be an incidental finding in
US evaluation of the aorta, however. The intimal flap
created between the true and false lumen is best
visualized with US in the transverse plane [38]. The
flap moves with arterial pulsation if flow through the
false lumen is preserved. (This may not be seen if
the flap is thickened.) Doppler waveforms in both lu-
mens may appear bizarre, with spectral broadening
and reversed flow. Velocity tends to be slower in the
false lumen (Fig. 10).
A true AAA with organizing thrombus may look
like a dissection on sonography. The outer layer of
thrombus can appear echogenic and be mistaken for
an intimal flap, whereas deeper thrombus appears
anechoic and can mimic the false lumen [40]. Color
Doppler increases the specificity of US in evaluating
dissection. Flow in the false lumen may be too slow
for detection with Doppler. Thrombosis within the
false lumen frequently occurs and is a significant
Fig. 10. (A, B) Abdominal aortic dissection with intimal
pitfall in the use of US for characterization of dis-
section. Nguyen [41] described a case of ‘‘pseudo-
dissection’’ in which an intimal flap with flow on
either side was described with sonography. This was
shown on CT to be an AAA with mural thrombus.
The perception of flow within the ‘‘false lumen’’ was
attributed to mirror image artifact caused by a calci-
fied thrombus surface layer or incorrect color flow
assignment in the anechoic portion of the throm-
bus [41].
US is not the primary imaging modality for aortic
dissection because most dissections involve the tho-
racic aorta.
Ultrasound and aortic endografting
In the early 1990s, Parodi [42] first reported the
endoluminal repair of abdominal aortic aneurysm.
Given the relatively high operative morbidity and
mortality rates associated with open repair (3% –
10% mortality and 15%–40% perioperative morbid-
ity) [43], AAA repair using stent grafts offers a less
invasive alternative to open repair, with reduced
morbidity and mortality rates. The most frequent com-
plication of endografting is the development of leak-
flap (arrow). (C) Turbulent flow within dissection.

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 373
age into the aneurysm sac excluded by the graft. This
may occur via direct communication with the graft
lumen at its attachment site or back flow from
collateral arteries communicating with the aneurysm
sac. Leaks are frequent, with cited incidences as high
as 40% [13]. Lifelong monitoring is required. Al-
though the gold standard for postoperative monitor-
ing is CT, US has been used with varying success. It
offers several potential advantages, including avoid-
ance of potentially nephrotoxic contrast agents and
radiation exposure [3,44,45]. Initial studies that
compared CT and US demonstrated promising results
for US. In 1998, Kronzon et al [43] studied 17 pa-
tients after stent repair of AAA with color Doppler
imaging (CDI) and CT. US was successful in dem-
onstrating flow within the excluded aneurysm lumen
using color Doppler and in measuring aneurysm size
(Figs. 11, 12).
Sato et al [44] reported a sensitivity rate of 97%,
specificity rate of 74%, and accuracy rate of 82% for
US in detecting endoleak. With the advent of im-
proved helical scanning techniques, including thinner
collimation and delayed imaging, Golzarian et al [45]
demonstrated improved reliability of CT compared
with US. US detected clinically significant leaks
within the stent graft and iliac limbs; however, it
frequently missed small perigraft leaks. Using CT as
the standard for evaluating US performance, US
detected endoleak with a sensitivity rate of 77% and
specificity rate of 90% [45]. After this, Pages et al [13]
demonstrated a poorer sensitivity and specificity in
endoleak detection of 48% and 93%, respectively.
Although CDI did detect some endoleaks not detected
on CT, the use of delayed postcontrast CT imaging
could detect these leaks. CDI performed better in
monitoring aneurysm size, with a sensitivity rate of
88% and specificity rate of 76% in demonstrating no
change in AAA size. As with unrepaired AAA, US
Fig. 11. (A) Longitudinal image of AAA shows stent (arrow) an
Doppler demonstrates flow within the graft lumen and hypoechoic
and CT demonstrated some discrepancy in measure-
ments. If a preoperative US is available as a baseline,
however, US can be effective in monitoring aneurysm
size [13]. Some authors suggest using both CTand US
when following endografts [13,45].
In a recent study, Greenfield et al [46] found that
US was more accurate than CT for characterizing
endoleaks. In a study of seven endoleaks classified as
type II by CT, US demonstrated two of these to be
type I leaks. Type I leaks generally require immediate
repair, whereas type II are often managed conserva-
tively because they tend to resolve without treatment.
These findings dramatically altered care. US findings
in proximal limb type I leaks were high velocity flow
at the site of the proximal attachment. Distal limb
attachment site leaks demonstrated flow in the sac
opposite the direction of that in the lumen. IMA flow
was antegrade in type I leaks. Type II leaks were
characterized by slower flow within the aneurysm sac
and retrograde flow in the IMA. These finding sug-
gest an adjunct role for US in characterizing endo-
leaks detected by CT [46].
Mesenteric vascular ultrasound
Chronic intestinal ischemia
Chronic intestinal ischemia (CII) is caused by
inadequate blood supply to meet the metabolic de-
mands of the enteric tract after feeding. In the post-
prandial state, intestinal motility increases, as does
oxygen demand from active transport of nutrients.
Clinically, this presents as postprandial pain.
The clinical diagnosis is one of exclusion. It is a
relatively rare entity with no pathognomonic find-
ings. CII occurs most commonly in elderly women
(75%) [8,20]. Patients typically present with colicky
d wall of aneurysm (thick arrow). (B) Application of color
clot (arrow) in the excluded aneurysm sac.

Fig. 12. Type 2 endoleak. (A, B) Color Doppler demonstrates flow outside the graft lumen (arrow). (C) CT correlate: blush of
contrast outside the limbs of the stent (arrow).
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381374
postprandial epigastric pain, occasionally with radia-
tion to the back. Symptoms begin 15 to 30 minutes
after eating and persist 1 to 3 hours. Patients associate
feeding with pain and frequently develop ‘‘food
phobia,’’ with anorexia and marked weight loss.
Changes in bowel habits are also frequent [16]. The
abdominal examination is usually nonspecific, with
no localizing or peritoneal signs. An abdominal bruit
is often present, but this finding is too nonspecific to
make the diagnosis of CII to make the diagnosis of
CII. Laboratory data are neither sensitive nor specific.
Malabsorption of various nutrients has been de-
scribed in the setting of CII. Villous atrophy and
epithelial flattening has been shown in biopsy series.
These findings are unreliable and nonspecific, how-
ever [8,16,20,47].
Atherosclerotic narrowing at the origin of the mes-
enteric vessels is the most common factor that pre-
disposes to CII. Other processes, such as vasculitis,
extrinsic or intrinsic compression, and drug reactions,
also may produce symptoms (Box 2). Although CII
is relatively rare, atherosclerotic narrowing of the
mesenteric vasculature is common. In one autopsy
series, 6% to 10% of patients had stenosis of 50% or
more. High-grade CA stenosis is also frequently well
tolerated. In high-grade CA stenosis or occlusion, the

Box 2. Associations with chronicintestinal ischemia
Atherosclerotic diseaseInflammatory vasculitis
RadiationPolyarteritis nodosa (PAN)
Connective tissue disease
1. Berger’s2. Systemic lupus erythematosus
(SLE)3. Rheumatoid arthritis (RA)
Extrinsic compression
1. Neurofibromatosis2. Median arcuate ligament
syndrome
Drug reactions
Cocaine
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 375
gastro- and pancreaticoduodenal arteries form an
important collateral pathway. In SMA stenosis or
occlusion, flow may be reconstituted via the hepatic
artery and pancreaticoduodenal arteries. In high-
grade stenosis or occlusion of the SMA and CA,
the IMA may form sufficient collaterals via the
middle colic artery and pancreaticoduodenals (the
arch of Riolan) to supply the foregut. IMA stenosis
is most frequently asymptomatic [8]. Because the
splanchnic vessels are able to form extensive collat-
eral pathways, significant stenosis or occlusion of
two of the three mesenteric vessels is generally
required to produce symptomatic ischemia, although
high-grade stenosis of the SMA alone may produce
symptoms. Collateralization also makes prediction of
CII difficult. The presence of two-vessel disease or
complete SMA occlusion does not imply the presence
of CII in the absence of symptoms [8].
The diagnosis of CII frequently is delayed because
of its tendency to mimic more common disorders,
such as symptomatic gallstones, cholecystitis, pancre-
atic cancer, and peptic ulcer disease. The average time
from onset of symptoms to diagnosis is 18 months
[16]. Traditionally, CII has been diagnosed via an-
giography. There is reluctance to perform angio-
grams for nonspecific clinical findings because of
its invasiveness, cost, and potential complications in
elderly patients. Noninvasive screening tests in
symptomatic patients are needed to evaluate the mes-
enteric vasculature.
The successful application of Doppler sonography
for diagnosis of mesenteric ischemia was first de-
scribed by Jager in 1984 [47]. High PSVs were found
at the origins of the SMA and celiac arteries. PSV in
the SMA was more than 300 cm/second. Spectral
broadening and monophasic waveforms with loss of
reversed diastolic flow also were noted [47].
In a subsequent validation study, Moneta [19]
sought to establish specific US criteria for high-grade
SMA and CA stenosis. One hundred patients under-
went mesenteric duplex scanning followed by arteri-
ography. In this study, a PSV of 275 cm/second or
more predicted 70% stenosis, with a sensitivity rate of
92% and specificity rate of 96%. In CA stenosis, a
PSVof 200 cm/second or more predicted stenosis with
87% sensitivity rate and 80% specificity rate (Fig. 13).
Although elevations in EDVwere observed in stenotic
vessels, use of EDV did not improve the sensitivity or
specificity of results. In a different study, Moneta [18]
found that the ratios of PSV to EDV were not pre-
dictive. These studies addressed one important tech-
nical factor in acquiring PSV data. In patients with
peripheral atherosclerotic disease but no mesenteric
occlusive disease, PSVs were elevated over control
subjects. This result suggests that tortuousity of the
mesenteric vessels in patients with atherosclerosis
may limit the sonographer’s ability to maintain Dopp-
ler angles less than 60� [18]. This inability could resultin falsely elevated PSVs.
Bowersox [20] found that EDV and PSV were
elevated in confirmed SMA stenosis . The study
accepted 50% or more stenosis as being significant.
In normal control subjects, SMA flow was triphasic
with a normal PSV of 134 (F 18) cm/second and
EDV of 24 (F 4) cm/second. (except in replaced
hepatic artery, in which flow was biphasic). PSVs
increased with increasing SMA stenosis. PSV of 300
cm/second diagnosed 50% or more stenosis with a
sensitivity rate of 63% and specificity rate of 100%.
Unlike Moneta, however, Bowersox [20] found that
EDV was more sensitive and specific than PSV. An
EDV of more than 45 cm/second was found to be
100% sensitive and 92% specific in detecting severe
stenosis. Significant CA values could not be estab-
lished in this study. One proposed reason is that col-
laterals through the gastroduodenal arcade can restore
CA flow in the presence of severe stenosis [20].
Two more recent publications favor the use of
EDVs in predicting significant stenosis. Perko et al
[44] evaluated 39 patients with suspected intestinal

Fig. 13. Celiac stenosis. (A) Color Doppler with narrowing at the celiac origin and turbulent flow. (B) Doppler spectrum with
elevated PSV (>300 cm/second) and spectral broadening. (C) Angiogram demonstrates narrowing of the CA (arrow) and SMA.
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381376
ischemia using Moneta’s criteria in addition to the
following other parameters: EDV, early diastolic ve-
locity (EaDV), and PDV. A control group of hyper-
thyroid patients was included in this study. They
found that the Moneta criteria (PSV >275 cm/second)
were 90% accurate for stenoses more than 50%. Ac-
curacy improved dramatically, however, when EDV,
EaDV, and PDV were considered. EDVof more than
50cm/second, EaDV of more than 50cm/second, and
PDV of more than 70 cm/second predicted signifi-
cant stenosis with a sensitivity and specificity rate of
100%. PSV in the CA also was examined according
to Moneta’s criteria. An accuracy rate of 94% was
demonstrated using a PSV of more than 200 cm/sec-
ond to predict more than 50% stenosis. As with SMA
disease, evaluation of EDV, EaDV, and PDV pre-
dicted significant CA stenosis with 100% sensitivity
and specificity. In this study, two false-positive results
were noted using PSV as a criteria, one in a hyper-
thyroid patient and the other in a hypertensive patient
with extensive atherosclerotic calcification. Elevated
PSVs occurred in the thyrotoxic group, likely related
to increased stroke volume. EDVand EaDV were un-
affected. High output states may elevate PSV artifi-
cially [48].
Zwolack et al [17] found similar results to the
Perko study. In a retrospective study of 243 patients
with suspected mesenteric ischemia, an EDVof more

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 377
than 45 cm/second predicted more than 50% stenosis
with an accuracy rate of 91% (sensitivity 90%, speci-
ficity 91%). Their results for using PSV to predict
SMA stenosis were similar to the Bowersox study,
with a low sensitivity rate (60%) but high specificity
rate (100%) for PSVs of more than 300 cm/second.
Similar to the Perko study, a PSVof more than 200 cm/
second and an EDVof more than 55 cm/sec predicted
CA stenosis with good accuracy, although EDV
demonstrated the greatest accuracy (95% for EDV
versus 93% for PSV). This study also demonstrated
high-grade CA stenosis or occlusion in 100% of
patients with reversed hepatic flow. Because the CA
is frequently difficult to visualize, this finding may be
particularly helpful in inferring CA stenosis [17].
Several factors may account for disagreement
regarding the accuracy in PSV in SMA stenosis.
Zwolack et al [17] described several potential explan-
ations for the discrepancies in results. First, in the
Moneta study [18], 88% of subjects were men. In the
Zwolack study, 70% percent were women. Gender
differences in flow characteristics in the mesenteric
vasculature may be present, although to date these
have not been explored fully. Second, aliasing is more
frequent at PSVs more than 200 cm/second and vary
according to the type of equipment used. This occur-
rence may account for the low sensitivity encountered
using the Moneta criteria for SMA stenosis of 300 cm/
second, whereas PSVs of 200 cm/second predicted
CA stenosis in both studies [17]. Another potential
pitfall in the use of PSV, as described by Moneta et al
[19], is the difficulty encountered in acquiring veloc-
ities at the level of stenosis. Stenoses usually arise at
the origin of the vessel. Distal to this, the PSV is
expected to fall. The reduced sensitivity in PSV
described in some studies may be the result of
sampling of the SMA distal to the stenosis.
The studies described have used different percent
stenoses as significant values. The Moneta criteria
use 70% as a critical value, whereas the remaining
studies use 50%. Using different percentages to
define significant stenoses did not significantly alter
the findings between the studies. In the study by
Zwolack et al [17], the diagnosis of CII was sus-
pected in all patients. Approximately half were found
to have occlusive disease; symptoms in the remaining
patients were attributed to other causes. In the CII
group, most had stenoses of 70% or more at arteri-
ography. In the group without CII, most had stenosis
less than 50%. This finding created a bimodal distri-
bution of vascular lesions. Only 12% of patients fell
between these two groups. This result suggests that
either value is acceptable and may explain the accu-
racy the Perko group demonstrated using the Moneta
criteria of PSV 275 cm/second to predict lesions of
50% or more [17].
In conclusion, duplex US scanning of the mesen-
teric vasculature has been demonstrated to be an
effective screening test in patients with suspected
CII. An adequate examination of the splanchnic ves-
sels can be achieved in only 60% of the general
population. The remaining 40% are limited by body
habitus and interposed bowel gas. Patients with CII
tend to be thinner than the general population and
are easier to scan. Although controversy still exists in
the literature as to the sensitivity and specificity of
using PSV to predict SMA stenosis, PSV is a reliable
parameter for diagnosing CA stenosis. Reversal of
hepatic flow also has been shown to predict CA oc-
clusion [17,19]. EDV reliably predicted significant
SMA and CA stenosis in several studies. In clinical
practice, the US finding of normal vasculature or
subcritical stenoses in patients with abdominal pain
and weight loss can exclude CII. Most patients
with positive duplex US proceed to CT or conven-
tional angiography. Mesenteric US may be a valuable
screening tool.
Splanchnic artery aneurysms
Historically, splenic artery aneurysms have been
the most common visceral artery aneurysms. In recent
years, hepatic artery aneurysms have surpassed splen-
ic aneurysms in incidence with increasing use of
percutaneous biliary procedures [49]. Posttraumatic
pseudoaneurysms in the splanchnic vasculature, most
commonly the hepatic artery, have been reported after
trauma in children (Fig. 14). Blunt trauma is most
frequently implicated, although it has been described
in penetrating trauma. Embolization is the treatment
of choice, although spontaneous thrombosis has been
reported [50,51]. Splenic artery aneurysms are asso-
ciated with acute pancreatitis. They occur in 10% of
elderly patients [52]. In women of childbearing age,
more than half of ruptured splenic artery aneurysms
are related to pregnancy, and survival is uncommon
[53]. Hepatic and splenic artery aneurysms appear as
cystic structures in communication with the parent
artery, which demonstrates arterial flow within the
cystic portion on color Doppler (Fig. 15).
Iliac artery aneurysm
Seventy-five percent of iliac artery aneurysms
(IAAs) occur in association with AAA either as a

Fig. 14. Traumatic hepatic artery aneurysm. (A) Cystic central area surrounded by thrombus (arrow). (B) Color Doppler
shows turbulent flow within cystic portion of aneurysm.
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381378
direct extension of AAA or coincident with AAA
[54,55]. The common iliac artery is the most com-
monly involved (99%), followed by the internal then
external iliac [54]. According to standards created by
the Subcommittee on Reporting Standards for Arterial
Aneurysms, Ad Hoc Committee on Reporting Stan-
dards, Society for Vascular Surgery and the North
American Chapter of the International Society for
Cardiovascular surgery, IAA is defined by a lumi-
nal diameter that exceeds 1.5 cm [55]. They may be
Fig. 15. Splenic artery aneurysm. (A) Cystic structure communicate
ler shows turbulent flow.
fusiform, saccular, or bilobed. Atherosclerotic disease
is the most common predisposing factor [54,55].
Pseudoaneurysms are less frequent and may be asso-
ciated with trauma (accidental or iatrogenic), preg-
nancy, infection, or collagen vascular disease (Fig. 16)
[54]. Several hypotheses have been proposed to
explain the association with pregnancy, including
trauma and instrumentation associated with delivery,
infection, and increased vascular demand associated
with pregnancy [56].
s with vessel lumen. Note disordered flow. (B) Color Dopp-

Fig. 16. Right internal iliac artery with surrounding hypo-
echoic fluid collection represents hematoma after stent pro-
cedure (arrow).
K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 379
IAAs are frequently asymptomatic but may cause
pelvic, flank, or groin pain [54,55]. Ureteral obstruc-
tion may complicate IAA because of the close prox-
imity to the genitourinary tract. Sciatic and femoral
root compression may result in symptoms. Arteriove-
nous fistula with resulting lower extremity ischemia is
a less frequent manifestation [54,56,57]. Santilli et al
[55] found that rate of expansion depended on aneu-
rysm size. Common IAAs smaller than 3 cm expand-
ed approximately 1 mm per year; IAAs larger than
3 cm expanded 2.6 mm per year. In that study,
approximately 50% of the patient population with
IAA was symptomatic. All symptomatic patients had
aneurysms larger than 4 cm. The risk of rupture
increased with increasing aneurysm size. For common
IAAs, the risk of rupture for aneurysms smaller than
5 cm in diameter was 0%; for aneurysms larger than
5 cm, it was 33% [55]. Richardson and Greenfield
[58] found that internal IAAs tended to be larger at
detection and carried a 33% incidence of rupture.
Santilli et al [55] found that B-mode US and CT
had similar accuracy in measuring iliac aneurysms.
US is most effective in diagnosing IAA when it is
large enough to cause a palpable mass. Under these
circumstances, IAAs are more likely to displace bowel
loops, which aids visualization. Gentle graded com-
pression is also helpful in displacing bowel loops [54].
Color Doppler shows a characteristic swirling pattern
along with intraluminal thrombus, if present [54].
Santilli et al [55] recommended annual screening
with B-mode US of IAAs smaller than 3 cm and
biannually for those larger than 3 cm. Repair is
frequently undertaken in association with AAA repair.
Elective IAA repair is indicated in symptomatic IAA
and IAA larger than 4 cm. More urgent repair is
performed in IAA larger than 5 cm given their higher
risk of rupture [55].
IAAs, although uncommon, carry a risk of rupture
with high associated mortality. As in AAA, US is a
modality well suited to surveillance of IAA. Because
75% of IAAs occur in association with AAA [55], the
routing screening for AAA as proposed by Lee [27]
could potentially unmask most IAAs.
Other peripheral arterial aneurysms
The most common lower extremity aneurysms are
popliteal, which comprise 80% of all peripheral
arterial aneurysms. They tend to be bilateral (50%).
Patients often present with acute limb ischemia sec-
ondary to embolization or thrombosis. This carries
a poor prognosis, with 15% requiring amputation
[59]. Forty percent of patients with popliteal aneu-
rysms have coincident AAA [56]. In a prospective
study of patients with AAA, Diwan et al [60] found
popliteal or femoral artery aneurysms in 51 of 313
patients. The association of femoral and popliteal
aneurysms with AAA suggests a common pathogen-
esis. Jacob et al [61] found reduced vascular smooth
muscle, increased inflammatory infiltrate, and in-
creased expression of signaling molecules involved
in cell death in surgical specimens obtained from
AAA, iliac, popliteal, femoral, and carotid artery
repairs. US is the imaging modality of choice in
diagnosing popliteal aneurysm. In a series of 21
patients, MacGowan et al [62] found that sonography
was superior to angiography in detecting surgically
confirmed popliteal aneurysm. Popliteal aneurysm is
diagnosed by focal dilatation of more than 20% of the
vessel diameter. As with AAA, popliteal aneurysm
can be followed sonographically. Popliteal aneurysm
larger than 2 cm generally require surgical interven-
tion regardless of the presence or absence of symp-
toms although much controversy regarding this still
exists [63,64].
Summary
The role of US in imaging of the abdominal
vasculature has broadened over recent years. Long

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381380
considered the modality of choice in the detection of
AAA, its use has expanded to diagnosing and moni-
toring IAAs and PAAs, screening for mesenteric
ischemia, and posttreatment monitoring of endovas-
cular stents.
References
[1] Bluth E, LoCascio L. Ultrasound evaluation of the
abdominal aorta. Echocardiography 1996;13(2):
197–206.
[2] Wanhainen A, Bergqvist D, Bjorck M. Measuring the
abdominal aorta with ultrasonography and computed
tomography: difference and variability. Eur J Vasc
Endovasc Surg 2002;24(5):428–34.
[3] Downey D. The retroperitoneum and great vessels. In:
Rumack CM, Wilson SR, Charboneau JW, editors.
Diagnostic ultrasound. St. Louis: Mosby-Year Book;
1998. p. 453–86.
[4] Naganuma H, Ishida H, Konno K, Sato M, Ishida J,
Watanabe S. Mycotic abdominal aneurysm: report of a
case with emphasis on the presence of gas echoes.
Abdom Imaging 2001;26(4):420–2.
[5] Hollinshead WH. The abdomen. In: Hollinshead WH,
editor. Textbook of anatomy. New York: Harper and
Row; 1967. p. 662–3.
[6] Pedersen OM, Aslaksen A, Vik-Mo H. Ultrasound
measurement of the luminal diameter of the abdominal
aorta and iliac arteries in patients without vascular
disease. J Vasc Surg 1993;17(3):596–601.
[7] Ross MH, Romrell LJ, Kaye GI. Cardiovascular sys-
tem. In: Histology: a text and atlas. Baltimore: Wil-
liams and Wilkins; 1995. p. 304–9.
[8] Moneta G. Diagnosis of chronic intestinal ischemia.
Semin Vasc Surg 1990;3(3):176–85.
[9] Nebesar RA, Kornblith PL, Pollard JJ, Michels N. Ana-
tomic considerations in celiac and superior mesenteric
arteries: a correlation of angiograms and dissections.
Boston: Little, Brown and Company; 1969. p. 26.
[10] Moneta GL, Taylor DC, Helton WS, Mulholland MW,
Strandness DE. Duplex ultrasound measurement of
post prandial intestinal blood flow: effect of meal com-
position. Gastroentereology 1988;95(5):1294–301.
[11] Guyton AC, Hall JE. General principles of gastroin-
testinal function: motility, nervous control, and blood
circulation. In: Textbook of medical physiology. Phila-
delphia: WB Saunders; 1996. p. 800–1.
[12] Lanne T, Sandgren T, Mangell P, Sonesson B, Hansen
F. Improved reliability of ultrasonic surveillance of
abdominal aortic aneurysms. Eur J Vasc Endovasc
Surg 1997;13(2):149–53.
[13] Pages S, Favre JP, Cerisier A, Pyneeandee S, Boissier
C, Veyret C. Comparison of color Duplex ultrasound
and computed tomography scan for surveillance af-
ter aortic endografting. Ann Vasc Surg 2001;15(2):
155–62.
[14] White GH, Yu W, May J, Chaufour X, Stephen MS.
Endoleak as a complication of endoluminal grafting of
abdominal aortic aneurysms: classification, incidence,
diagnosis, and management. J Endovasc Surg 1997;
4(2):152–68.
[15] Pacanowski JP, Dieter RS, Stevens SL, Freeman MB,
Goldman MH. Endoleak: the Achilles heel of endovas-
cular abdominal aneurysm exclusion: a case report.
Wis Med J 2002;101(7):57–63.
[16] Harward T, Smith S, Seeger J. Detection of celiac axis
and SMA occlusive disease with use of abdominal
duplex scanning. J Vasc Surg 1993;17(4):738–45.
[17] Zwolak R, Fillinger M, Walsh D, LaBombard F,
Musson A, Darling C. Mesenteric and celiac duplex
scanning: a validation study. J Vasc Surg 1998;27(6):
1078–87; discussion 1088.
[18] Moneta G, Yeager R, Dalman R, Antonovic R, Hall L,
Porter J. Duplex ultrasound criteria for diagnosis of
splanchnic artery stenosis or occlusion. J Vasc Surg
1991;14(4):511–8; discussion 518–20.
[19] Moneta G, Lee R, Yeager R, Taylor L, Porter J. Mes-
enteric duplex scanning: a blinded prospective study.
J Vasc Surg 1993;17(1):79–84; discussion 85–6.
[20] Bowersox J, Zwolak R, Walsh D, Schneider J, Musson
A, LaBombard E, et al. Duplex ultrasonography in
the diagnosis of celiac and mesenteric artery occlusive
disease. J Vasc Surg 1991;14(6):780–6; discussion
786–8.
[21] Durham J, Kaufman J. Imaging of acquired thoracic
and abdominal aortic disease. In: Strandness DE, Van
Breda A, editors. Vascular diseases: surgical and inter-
ventional therapy. New York: Churchill-Livingstone;
1994. p. 240–72.
[22] Beede S, Ballard D, James E, et al. Positive predictive
value in clinical suspicion of abdominal aortic aneu-
rysms. J Gen Intern Med 1990;150:549–51.
[23] Mower W, Quinones J, Gambhir S. Effect of intra-
luminal thrombus on abdominal aortic aneurysm wall
stress. J Vasc Surg 1997;26(4):602–8.
[24] Brown PM, Zelt DT, Sobolev B. The risk of rupture in
untreated aneurysms: the impact of size, gender, and
expansion rate. J Vasc Surg 2003;37(2):280–4.
[25] Sharp MA, Collin J. A myth exposed: fast growth in
diameter does not justify precocious abdominal aortic
aneurysm repair. Eur J Vasc Endovasc Surg 2003;
25(5):408–11.
[26] Sostek M, Fine SN, Harris TL. Duodenal obstruction
by abdominal aortic aneurysm. Am J Med 1993;94(2):
220–1.
[27] Lee TY, Korn P, Heller J, Kilaru S, Beaver F, Bush HL.
The cost-effectiveness of a ‘‘quick-screen’’ program for
abdominal aortic aneurysms. Surgery 2002;132(2):
399–407.
[28] Griffith JF, Yang WT, Lam WWM, Metreweli C. Un-
common features of abdominal aorto-iliac disease. Br
J Radiol 1997;70:536–42.
[29] Rogoff SM, Lipchik EO. Aneurysms of the abdominal
aorta. In: Abrams HL, Cook PH, editors. Angiography.
Boston: Little, Brown and Company; 1971. p. 761.
[30] Fiorani P, Bondanini S, Faraglia V, Spartera C, Spe-

K. Hermsen, W.K. Chong / Radiol Clin N Am 42 (2004) 365–381 381
ziale F, Taurina M, et al. Clinical and therapeutical
evaluation of inflammatory aneurysms of the abdomi-
nal aorta. Int Angiol 1986;5(1):49–53.
[31] Bartels C, Wedekind G, Claeys L, Beyer D, Horsch S.
Significance of radiologic diagnosis for detection and
staging of inflammatory abdominal aortic aneurysm.
Cardiovasc Surg 1995:3(6);665–70.
[32] Moosa HH, Peitzman AB, Steed DL, Julian TB, Jarrett
F, Webster MW. Inflammatory aneurysms of the ab-
dominal aorta. Arch Surg 1989:124;673–5.
[33] Pennell RC, Hollier LH, Lie JT, Bernatz PE, Joyce JW,
Pairolero PC. Inflammatory abdominal aortic aneu-
rysms: a thirty year review. J Vasc Surg 1985;2(6):
859–69.
[34] Dowd SB, Wilson BG, Hall JD, Steves A, Benson T.
Review of techniques used to image aortic dissection.
Radiol Technol 1996;67(3):223–30.
[35] Zwiebel WJ. Aorta, iliac arteries, and inferior vena
cava. In: Introduction of vascular ultrasonography.
Philadelpha: WB Saunders; 2000. p. 411–2.
[36] Ferko A, Krajina A, Jon B, Lesko M, Voboril Z, Zizka
J. Dissection of the infrarenal aorta treated by stent
graft placement. Eur Radiol 1998;8(2):298–300.
[37] Lindsay J. Aortic dissection. In: Diseases of the aorta.
Malvern (PA): Lea and Febiger; 1994. p. 127–41.
[38] Zaccardi M. Aneurysmal disease. In: Strandness DE,
editor. Duplex scanning in vascular disorders. Philadel-
phia: Lippincott Williams and Wilkins; 2002. p. 335.
[39] Sonesson B, Hansen F, Lanne T. Abnormal mechanical
properties of the aorta in Marfan’s syndrome. Eur J
Vasc Surg 1994;8(5):595–601.
[40] King PS, Cooperberg PL, Madigan SM. The anechoic
crescent in abdominal aortic aneurysms. not as sign of
dissection. AJR Am J Roentgenol 1986;146(2):345–8.
[41] Nguyen BD, Ulrike MH. False positive dissection
of abdominal aortic aneurysm by color Doppler du-
plex ultrasonogrophy. J Ultrasound Med 1995;14(6):
467–9.
[42] Parodi JC. Endovascular repair of abdominal aortic
aneurysms and other arterial lesions. J Vasc Surg 1995;
21:549–57.
[43] Kronzon I, Tunick PA, Rosen R, Riles T. Ultrasound
evaluation of endovascular repair of abdominal aor-
tic aneurysms. J Am Soc Echocardiogr 1998;11(4):
377–80.
[44] Sato DT, Goff CD, Gregory RT, Robinson KD, Carter
KA, Herts BR, et al. Endoleak after aortic stent graft
repair: diagnosis by color duplex ultrasound scan ver-
sus computed tomography scan. J Vasc Surg 1998;
28(4):657–63.
[45] Golzarian J, Murgo S, Dussaussois L, Guyot S, Said
KA, Wautrecht JC, et al. Evaluation of abdominal aor-
tic aneurysm after endoluminal treatment: comparison
of color Doppler sonography with biphasic helical CT.
AJR Am J Roentgenol 2002;178:623–8.
[46] Greenfield AL, Halpern EJ, Bonn J, Wechsler RJ,
Kahn MB. Application of duplex US for characteriza-
tion of endoleaks in abdominal aortic stent-grafts: re-
port of five cases. Radiology 2002;225(3):845–51.
[47] Jager KA, Fortner GS, Thiele BL, Strandness DE.
Noninvasive diagnosis of intestinal angina. J Clin Ul-
trasound 1984;12(9):588–91.
[48] Perko M, Just S, Schroeder T. Importance of diastolic
velocities in the detection of celiac and mesenteric
artery disease by duplex ultrasound. J Vasc Surg
1997;2:288–93.
[49] Messina LM, Shanley CJ. Visceral artery aneurysms.
Surg Clin North Am 1997;77(2):425–42.
[50] Soudack M, Epelman M, Gaitini D. Spontaneous
thrombosis of hepatic posttraumatic pseudoaneurysms:
sonographic and computed tomographic features.
J Ultrasound Med 2003;22(1):99–103.
[51] Sidhu MK, Shaw DW, Daly CP, Waldhausen JH, Cold-
well D. Post-traumatic hepatic pseudoaneurysms in
children. Pediatr Radiol 1999;29(1):46–52.
[52] Babb RR. Aneurysm of the splenic artery. Arch Surg
1976;111(8):924–5.
[53] Barrett JM, Van Hooydonk JE, Boehm FH. Pregnancy-
related rupture of arterial aneurysms. Obstet Gynecol
Surv 1982;37(9):557–66.
[54] Zuckerman DA, Yucel EK. Iliac artery aneurysms:
radiographic evaluation. Clin Imaging 1993;17(3):
213–21.
[55] Santilli SM, Wernsing SE, Lee ES. Expansion rates
and outcomes for iliac artery aneurysms. J Vasc Surg
2000;31(1 Pt 1):114–21.
[56] Hashimoto BE, Kenny K, Kramer D. Duplex and color
Doppler appearance of isolated internal iliac aneu-
rysms. J Ultrasound Med 1992;11(1):45–7.
[57] Nachbur BH, Inderbitzi RG, Bar W. Isolated iliac
aneurysms. Eur J Vasc Surg 1991;5(4):375–81.
[58] Richardson JW, Greenfield LJ. Natural history and
management of iliac aneurysms. J Vasc Surg 1988;
8(2):165–71.
[59] Thompson MM, Bell PRF. Arterial aneurysms. BMJ
2000;320:1193–6.
[60] Diwan A, Sarkar R, Stanley JC, Zelenock GB, Wake-
field TW. Incidence of femoral and popliteal artery
aneurysms in patients with abdominal aortic aneu-
rysms. J Vasc Surg 2000;31(5):863–9.
[61] Jacob T, Ascher E, Hingorani A, Gunduz Y, Kallakuri
S. Initial steps in the unifying theory of pathogenesis of
artery aneurysms. J Surg Res 2001;101(1):37–43.
[62] MacGowan SW, Saif MF, O’Neill G, Fitzsimons P,
Bouchier-Hayes D. Ultrasound examination in the di-
agnosis of popliteal artery aneurysms. Br J Surg 1985;
72(7):528–9.
[63] Schellack J, Smith III RB, Perdue GD. Nonoperative
management of selected popliteal aneurysms. Arch
Surg 1987;122:372–5.
[64] Shortell CK, DeWeese JA, Ouriel K, Green RM. Pop-
liteal artery aneurysms: a 25-year surgical experience.
J Vasc Surg 1991;14(6):771–6.

Radiol Clin N Am 42 (2004) 383–396
Arterial injuries: a sonographic approach
Brian D. Davison, MDa,*, Joseph F. Polak, MD, MPHb
aDepartment of Radiology, Harvard Medical School, Brigham and Women’s Hospital, 75 Francis Street, Boston, MA 02115, USAbDepartment of Radiology, Tufts Medical School, New England Medical Center, Box 299, 750 Washington Street, Boston,
MA 02111, USA
Acute arterial emergencies can arise from direct setting of proximity injuries or where a mechanism of
traumatic injury to the artery or be spontaneous. In the
case of spontaneous injuries, the likelihood of a spe-
cific arterial event increases in the presence of certain
risk factors or medical conditions. For example, the
incidence of acute arterial occlusions is increased in
the presence of popliteal artery aneurysms or atrial
fibrillation. This article emphasizes the various pre-
sentations of arterial emergencies. These include acute
arterial occlusions; excessive bleeding; and hematoma
formation caused by penetrating arterial wall injuries,
pseudoaneurysms, and arteriovenous fistulas. The
broad category of arterial occlusions includes trau-
matic lacerations, embolizations, and arterial dissec-
tions. The caliber of the artery can also, on occasion,
be significantly narrowed because of spasm. This of-
ten exacerbates the clinical impact of the injury.
Modern ultrasound equipment is a rapid and con-
venient imaging approach in many of these clinical
scenarios. In combination with MR angiography and
CT angiography, these noninvasive tests can diagnose
the presence of most arterial injuries, and be used to
measure their impact. Conventional angiography is
reserved for problem solving or directed therapy.
Validation studies: pathologic validation
In the emergency setting color Doppler imaging
and duplex ultrasound have shown use in the evalua-
tion of potential vascular injuries, especially in the
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.007
* Corresponding author.
E-mail address: [email protected]
(B.D. Davison).
injury is not in accordance with other physical find-
ings. Since the late 1980s studies have been conducted
to screen patients with vascular injuries that need
possible surgical management. Ultrasound can be up
to 95% to 100% sensitive for diagnosing vascular
injuries in the hands of highly qualified personnel
with a high index of suspicion [1]. This high diag-
nostic accuracy has actually been validated with
animal studies. Panetta et al [2] created different types
of arterial injuries in the femoral and carotid arteries of
dogs. These injuries including intimal flaps, crush
injuries, and lacerations, and were compared with
control limbs. The studies were performed by a
sonographer blinded to the type and location of the
injury. Results were correlated against operative ob-
servation and pathologic study of the injured artery
1 month after the injury. The sensitivity and specific-
ity of ultrasound were 96.5% and 86.4%, respectively,
with an accuracy of 95%. The ultrasound findings
correlated well with the histopathologic examination.
All arteries subjected to crush injury in these studies
showed abnormal duplex findings with measurable
changes in the arterial wall thickness. The site of the
crush injury showed intramural hemorrhage or mural
thrombus at the site of injury. Most intimal flaps had
healed at the time of pathologic examination, 1 month
after the injury. Overall, the findings of Doppler
ultrasound suggested that it has clinical use in the
evaluation of acute arterial trauma.
Nonimaging Doppler techniques
The ankle-brachial index is a quick comparison of
blood pressure readings. Doppler is used instead of a
stethoscope. Systolic pressures are obtained in both
s reserved.

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396384
brachial arteries. Pressures are obtained in the poste-
rior tibial artery, or the dorsalis pedis in both legs. By
dividing the highest left and right ankle values by the
highest brachial value an ankle-brachial index is
calculated. Someone with no disease should have a
ratio of greater than 0.96. For evaluation of periph-
eral vascular disease a value of 0.81 to 0.95 suggests
mild disease, 0.51 to 0.80 suggests moderate disease,
0.31 to 0.50 suggests moderate to severe disease, and
0.30 or below suggests severe disease. Simple mea-
surement of the ankle-brachial index can be used to
screen for lower-extremity arterial injuries. This adds
value to the clinical finding of depressed pulses or
pulses that change strength, waxing and waning over
a few minutes. More direct comparisons of pressure
in one limb with the other can also be done. Johansen
et al [3] used the Doppler arterial-pressure index to
compare the systolic arterial pressure in the injured
extremity to the arterial pressure in the uninvolved
side. A ratio of 0.9 or less was indicative of major
arterial injury with a sensitivity and specificity of
95% and 90%, respectively. The negative predictive
value was high. Most physicians, however, consider
a negative arterial-pressure index as a poor indica-
tor of potentially unstable injuries, such as arterial
dissections, disruptions, and pseudoaneurysms. These
findings were confirmed in a study by Lynch and Jo-
hansen [4] where the arterial-pressure index calculated
in 100 consecutive injured limbs in 93 trauma vic-
tims. All of these patients subsequently had angiog-
raphy. An arterial-pressure index of less than 0.9 had
a sensitivity of 80% and specificity of 97% for the
presence of arterial disruption.
Overall, the sensitivity of the pressure index for
detecting injuries requiring intervention ranges from
44% to 95%, depending on clinical circumstances and
extent of the injury. Angiography remains the gold
standard for the evaluation of traumatic arterial inju-
ries. There are several disadvantages include cost,
time delay, and a 0.6% major complication rate.
Vascular injuries requiring intervention are present
on only 1% to 1.5% of angiograms in patients missing
true signs of vascular injury. Impaired renal function
and the amount of iodinated contrast already given
should be weighed before an angiographic procedure.
Pseudoaneurysm
Pseudoaneurysm or false aneurysm is defined by
the loss of integrity of the three layers of the arterial
wall. This results in a contained rupture of the blood
vessel. The most common origin of pseudoaneurysms
is traumatic, secondary to a penetrating injury. Of
these, iatrogenic compromise of the arterial wall
following medical interventions is most common.
Diagnostic and interventional arterial catheterizations
are the most common sources of iatrogenic pseudo-
aneurysms. Other common sources are postsurgical,
typically at the site of an arterial anastomosis or
following an arterial repair.
Pseudoaneurysms following femoral artery cathe-
terization have a reported incidence of 7% to 8% [5].
The likelihood of an iatrogenic pseudoaneurysm fol-
lowing arterial catheterization increases with the size
of the catheter, the length of the procedure, and the
concurrent use of anticoagulants. Additional factors
include poor puncture [6] and compression techniques
[5]. Antegrade punctures and use of compression
devices increase the likelihood of pseudoaneurysm
formation. Other factors include poor coagulation
factors caused by liver failure and thrombocytopenia,
and other patient factors, such as obesity, hyperten-
sion, and stresses to the catheter entry site [5,7].
The patient who presents acutely to the emergency
room typically has suspicious physical signs, such as
swelling in the injured region, a pulsatile mass, or the
presence of a thrill. This occurs in the case of
postcatheterization pseudoaneurysm 1 to 10 days
after the actual catheterization. Ecchymotic skin
changes are often present starting 1 to 2 days post-
injury. If the mass of the pseudoaneurysm presses
sufficiently on the native arteries, then blood flow can
be decreased despite intact or even increased pulses.
A bruit may be heard on auscultation.
Gray-scale ultrasound analysis reveals anechoic
or hypoechoic areas resembling fluid collections
(Fig. 1A). These are located adjacent to or can abut
the arterial wall. Color Doppler ultrasound, however,
is most useful in identifying the nature of the lesion.
Classically, the description of the blood flow pattern
as seen on color Doppler ultrasound has been de-
scribed as the yin and yang sign (Fig. 1B). These
signals are caused by swirling motion of blood within
the pseudoaneurysm cavity. The inflow jet of blood is
directed along one wall causing a positive frequency
shift (red color), and the outflow is along the opposite
wall causing a negative frequency shift (blue color).
The presence of a communicating channel or neck
between the artery and the collection is needed,
however, to confirm the diagnosis. Blood flow in this
communicating channel has a very typical pattern.
Inflow of blood causes the pseudoaneurysm collection
to expand during systole. Sampling of the Doppler
waveform in the neck of the pseudoaneurysm shows a
positive inflow into the channel. During diastole,
blood flows out of the collection into the artery. This
is caused by the release of elastic energy stored by the

Fig. 1. (A) Color Doppler image in a patient with a knife wound shows a superficial hematoma (arrow) and a collection
containing flow signals. (B) The presence of a pseudoaneurysm is confirmed by the alternating to-and-fro signals at the neck
of the pseudoaneurysm.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 385
soft tissues surrounding the pseudoaneurysm cavity.
Blood flow is directed out of the collection into the
artery. This biphasic to-and-fro blood flow pattern
with pandiastolic reversal of flow is characteristic of
a pseudoaneurysm.
Once diagnosed, gray-scale ultrasound can be
used to estimate the size of the neck of the pseudo-
aneurysm. Smaller diameter and long necks are more
suitable for percutaneous interventions than pseudo-
aneurysms with short (less than 1 cm) and wide necks
(larger than 2–3 cm), and location must be consid-
ered. The natural history is varied. Most pseudo-
aneurysms spontaneously thrombose [8]. Over time
pseudoaneurysms can mature and a fibrous capsule
may form. The dreaded complication of a pseudo-
aneurysm is continued expansion and bleeding into
the thigh or retrograde bleeding into the pelvis. With
rapid enough expansion, the dissecting blood can
cause a compartment syndrome, compromise blood
flow to the distal limb, and lead to ischemia and
irreversible tissue loss. Many pseudoaneurysms at
presentation contain varying degrees of clotted blood.
Pseudoaneurysms can have multiple separate com-
partments or collections connected by thin tracts or
canals. Expanding pseudoaneurysms can cause limb
ischemia through compression. The thrombus form-
ing within them theoretically can escape and cause
distal emboli [9].
Pseudoaneurysms involving surgical sites, most
often the anastomosis of bypass grafts, typically have
very wide necks. They tend to be large and have well-
formed capsules. They often contain mural thrombus.
Pseudoaneurysms caused by gunshot wounds or
penetrating knife wounds should be considered as
potentially being infected. This type of pseudoaneu-
rysm seldom resolves spontaneously, and often re-
quires direct surgical intervention.
Historically, treatment of pseudoaneurysms has
been by open surgical repair, but evolution in endo-
vascular devices has allowed multiple options for
treating these lesions. Ultrasonography should be
used to assess the neck of the pseudoaneurysm. If it
is wide or in a position not directly accessible for
compression, other therapies should be considered.
Ultrasound-guided manual compression of the pseu-
doaneurysm has been used for over 15 to 20 years as
a treatment for pseudoaneurysms. The procedure
allows natural thrombosis of the pseudoaneurysm
cavity. Using gray-scale imaging as a guide, force
can be applied directly to the skin overlying the neck.
With enough pressure, blood flow stops and the con-
tents of the pseudoaneurysm thrombose. Success rates
are reported in the range of 51% to 73% [10–13].
The procedure is noninvasive, but can be time con-
suming and painful for both the patient and operator.
Unfortunately, this technique may require several

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396386
attempts before complete obliteration of the pseudo-
aneurysm. Patients treated with anticoagulants can be
refractory to this form of therapy. The recurrence rate
of pseudoaneurysms after ultrasound-guided com-
pression may be as high as 20% [5].
Direct thrombin injection using a sterile technique
and real-time Doppler ultrasound guidance into a
pseudoaneurysm causes thrombosis of the pseudo-
aneurysmwithin seconds. The procedure usually takes
less than 15 minutes. This procedure is safe and can be
performed on outpatients. A 20-gauge can be used and
the tip should be directed away from the neck.
Percutaneous thrombin injection for the treatment of
pseudoaneurysm has been described in the subclavian,
brachial, radial, and tibial arteries and carotid and
temporal arteries [14–16]. The proximity to these key
arteries requires that the operator have great technical
skills to prevent excess injection of thrombin and
thrombosis of the native artery. Success rates for
thrombin injection vary between 93% and 100% in
the literature [12,14–19]. Patients on antiplatelet
therapy or heparin can have thrombin injection with-
out decreasing success rates [14,19].
Pseudoaneurysms that have very short and wide
necks or that are located posterior to the artery are at
higher risk for failure or complications than those
with long necks and located near the skin. Compli-
cations include inadvertent direct injection of throm-
bin into the artery, or subsequent emboli emission
through a large neck. Sensitivity or allergy to throm-
bin has been reported [20]. The long-term effects of
bovine thrombin injection are not known.
Percutaneous transcatheter embolization and other
endovascular techniques, such as exclusion of the
pseudoaneurysm with covered stent placement, are
Fig. 2. (A) Transverse scan of the right groin in a patient with acut
dial to the vein. (B) The CT of the pelvis shows a right pubic ram
successful but invasive. Covered wall grafts have
been percutaneously placed to treat internal carotid
artery aneurysms [21]. In a small series, 16-month
follow-up did not show evidence of occlusion or
stenosis or reperfusion to the pseudoaneurysm. In-
dications included penetrating trauma and compli-
cations of percutaneous interventions [5,7,22].
Temporary balloon occlusion has been tried and can
be successful in properly selected patients. Repair of
large neck aneurysm with balloon occlusion and
thrombin injection has not been shown to be an
acceptably safe procedure.
In the event that the previously described proce-
dures fail or rupture is threatened by the rapid
expansion of the pseudoaneurysm, surgery should
be performed. Other surgical indications include
infection, distal ischemia, an embolic event, or ex-
tensive tissue damage. There is significant morbidity
associated with emergently performed surgery [12].
Hematoma
A hematoma is the natural outcome of a vascular
disruption. This can occur spontaneously in smaller
arteries especially in the setting of anticoagulation
[2,23,24]. The hematoma can be the result of blunt or
penetrating trauma or represent a thrombosed pseu-
doaneurysm (Figs. 2–4). The hematoma may remain
restricted to the surrounding soft tissue especially if it
occurs in a muscle, or it can tract through fascial
planes when caused by a larger arterial disruption.
Hematomas commonly occur in the retroperitoneum
[23,25], the rectus sheath [26], and in the extremities
around joints associated with muscle tears [24].
e pain following a fall shows an avascular mass (arrow) me-
us fracture (arrow) and the hematoma lying superior to it.

Fig. 3. (A) Arteriogram of the upper limb shows an intact duplicated brachial artery (arrows) and a distal humeral fracture.
(B) The corresponding color Doppler image shows a hematoma (within calipers) and no evidence of a pseudoaneurysm.
A, duplicated brachial artery.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 387
Physical finding include swelling in the injured
region, which is most often nonpulsatile, and silent on
auscultation. Ecchymotic skin changes are almost al-
ways present. If causing compression and narrowing,
hematomas can present with diminished blood flow
and pulses to the affected limb. If bleeding is severe
and within a fascial compartment, then a compartment
syndrome can ensue, causing severe pain, markedly
diminished pulses, pallor, and paresthesias. Hemato-
mas should be delineated with a marking pen on the
skin and measured carefully on ultrasound to rule out a
rapidly evolving hematoma. Although not a common
site of arterial puncture, a high brachial puncture used
for catheterization is difficult to compress following
catheter removal. This can result in an extensive
hematoma. Extension into the axilla is of great con-
cern because the resulting hematoma can compress
and injure the brachial plexus [27,28]. The common
femoral artery remains the preferred site for arterial
access for catheterization procedures. Hematomas
here usually result in local groin swelling adjacent to
the puncture site. Rarely, they can expand to pelvis,
leg, or retroperitoneum. Vigorously compressed to
break apart, the hematoma ultimately decreases pa-
tient discomfort. Careful fluoroscopic checking of the
anatomic landmark of the femoral head ensures proper
needle placement, and is paramount in minimizing the
risk of postprocedure hematoma.
Gray-scale ultrasound analysis shows variable
findings dependent on the time interval since the
original hemorrhage and possibly intermittent nature
of bleeding episodes. In the acute period (hours)
hematoma may present as solid or mixed echogenic
structures because of mixing of liquid with clotting
blood [11,26]. It can be well or ill defined, and should
be imaged carefully to document its extent, location,
and dimensions. The size seen on ultrasound should
be compared with the physical effect on the extrem-
ity. Hematomas can often dissect in a diffuse fashion
and not form a well-circumscribed mass. A baseline

Fig. 4. (A) Color flow Doppler image shows a large hematoma in a patient following penetrating trauma. (B) Doppler signals
confirm the presence of an additional arteriovenous fistula.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396388
measurement of size should be done because this can
help document possible rebleeding and expansion of
the hematoma. Over the course of days the clotted
blood breaks down to fluid in areas, giving a complex
cystic and solid appearance. At this point, without
proper history, the collection can be misdiagnosed an
abscess cavity or perhaps a pseudoaneurysm. Cystic,
necrotic, or hemorrhagic neoplasms may also have
similar imaging findings, and should be excluded
with follow-up. As discussed previously, however,
color flow Doppler is most useful in identifying and
differentiating these lesions from pseudoaneurysms
(see Fig. 1). Over weeks liquefactive necrosis of the
entire hematoma usually occurs [11,26]. Ultrasound
at this point shows all fluid signals, but a hematocrit
level may be seen within. A 2- to 3-month follow-up
scan is recommended to assess for decreasing size or
resolution to differentiate the hematoma from a mass.
Secondary infections are relatively rare. Their
likelihood increases if there is a persistent foreign
body in the case of penetrating trauma. Other exam-
ples where foreign material remains in the soft tissues
include after the use of closure devices used to seal
the needle access site following catheterization, or
post–synthetic graft placement.
Arteriovenous fistulas
Arteriovenous fistulas represent a direct connec-
tion between a vein and an artery. Like hematomas
and pseudoaneurysms, arteriovenous fistulas can be
spontaneous, but are often the result of penetrating
trauma. Arteriovenous fistulas are often asympto-
matic, but when significant can cause rapid shunting
with return of oxygenated blood to the right heart.
Rarely, they can contribute to high-output cardiac
failure [29]. They can also shunt away blood from the
extremity and cause symptoms of distal ischemia.
Arteriovenous fistulas are often caused by
low-arterial punctures, large-diameter catheters, anti-
coagulant use, and they are associated with pseudo-
aneurysms [2,30–32]. The femoral artery and vein
are parallel and side-by-side in the region of the
groin. Variant anatomy or punctures in the lower thigh
(where the femoral vein travels behind superficial
femoral and profunda arteries) are risk factors for
the formation of iatrogenic arteriovenous fistulas. Iat-
rogenic arteriovenous fistulas are not uncommon
elsewhere in the body, and not infrequently seen as
a consequence of a biopsy, such as in the kidney.
Physical examination can reveal little to no swelling
or ecchymosis, but a palpable thrill is often present.
Patients may present with pain but are most often
asymptomatic, but have a bruit on local auscultation.
Gray-scale ultrasound imaging is not helpful in
the evaluation of arteriovenous fistulas unless the
arteriovenous fistula is chronic and the high flow
state has caused dilatation of the vein and artery.
Color Doppler imaging and pulsed wave Doppler are
usually diagnostic. Tissue vibrations caused by tur-
bulent flow are the most notable color Doppler
finding (see Fig. 4). Also, the track between artery
and vein can sometimes be directly visualized. The
Doppler waveform in the feeding artery shows a low
resistance pattern with increased diastolic flow. The

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 389
jet of arterial flow entering the vein can cause a
marked flow disturbance and chaotic waveform or in
more severe case an arterial waveform is present.
Compression repair is usually not successful for
closing arteriovenous fistulas. Small arteriovenous
fistulas can spontaneously remit [8]. Percutaneous
placement of a covered stent or surgical repair is
often indicated.
Craniocervical dissections
There are two types of dissections likely to affect
the carotid and vertebral arteries. The first is a
primary dissection of the artery, sometimes associated
with a vague history of trauma or rapid movement of
the head. This is seen more often in young patents
less than 50 years of age. Secondary dissections occur
as an extension of a ‘‘type A’’ dissection of the aortic
arch into the origins of the brachycephalic, carotid,
and subclavian arteries. This is typically seen in older
patients or patients with a weakness of the media in
the aortic wall, typically with cystic medial necrosis.
Primary dissections
Although any of the arteries in the neck may be
affected, primary dissections of the internal carotid
Fig. 5. (A) Spectral Doppler waveform demonstrates a high resis
25-year-old patient. (B) The corresponding arteriogram shows abru
of an internal carotid artery dissection.
artery are the most common. Internal carotid artery
dissections typically occur in the proximal internal
carotid artery, just beyond the carotid bulb. Primary
dissections of the intracranial portion of the internal
carotid artery can occur but they are much less
common than the classic primary dissection of the
internal carotid artery (Fig. 5). Dissections of the
vertebral arteries are also seen but a careful investi-
gation is rarely done because symptoms, if present,
tend to be minimal. Patients with an internal carotid
artery dissection have nonspecific presenting symp-
toms, such as a sensory or motor deficit. The classic
presentation is that of a headache. The dissection
often happens in a previously healthy individual and
develops either spontaneously or following various
degrees of trauma. As medical imaging equipment
has evolved, better visualization of this area is pos-
sible. This fact coupled with more awareness has
made this diagnosis less difficult.
A dissection is the disruption of the media or
second layer of the artery. Once the dissection starts,
the intima along with a portion of the media is lifted
from the artery wall. Collagen is exposed to blood
and this usually starts a clotting cascade. The pathol-
ogy of the primary dissection of the internal carotid
artery is one of an intramural blood clot. If the size
and volume of the blood clot is large enough, the
artery occludes. If the size of the clot is intermediate,
tance and low amplitude in the internal carotid artery of a
pt termination of the internal carotid artery (arrow) at the site

Fig. 6. This patient was found to have an acute traumatic
intimal tear of the internal carotid artery on the carotid
arteriogram (not shown). The internal carotid artery color
Doppler image demonstrates evidence of a periarterial soft
tissue mass consistent with a hematoma (arrow). The inti-
mal tear seen in arteriogram could not be seen on color
flow Doppler.
Fig. 7. Gray-scale ultrasound image shows the leading edge
of an aortic dissection extending from the arch into the
common carotid artery. The leading edge of the dissection
has re-entered the lumen of the artery.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396390
then the lesion causes a stenosis or even occlusion of
the proximal internal carotid artery (see Fig. 5). If
relatively small, the patient can present with acute
symptoms and no neurologic deficit because the
lesion does not compromise blood flow in the internal
carotid artery. This can occur in spontaneous and
posttraumatic dissections (Fig. 6). The latter scenario
is typical of up to 40% of patients with primary
internal carotid artery dissections. Physical examina-
tion can reveal motor weakness or a sensory deficit.
Rarely, the patient can present clinically with cranial
nerve palsy, such as Horner’s syndrome [33–35].
A double lumen with a separating intimal flap can
be seen on gray-scale imaging in cases of primary
internal carotid artery dissections, but is less common
than an intramural hematoma. Typically, the dissec-
tion consists of an intramural hematoma or thrombus
that is hypoechoic and hard to perceive. The Doppler
findings are variable. In the absence of a significant
obstruction, the signals can be normal. A more
significant dissection with large intramural hematoma
shows direct evidence of a stenosis with a zone of
elevated blood flow velocities. Very severe dissec-
tions can occlude or subtotally occlude the internal
carotid artery. Doppler ultrasound is quite specific for
the detection of significant vessel obstruction when
the Doppler waveform is altered and shows a high-
resistance pattern (see Fig. 5). This pattern, however,
is the least common of the patterns seen in patients
with proved dissections. Internal carotid artery dis-
sections may or may not cause symptoms depending
on the integrity of the circle of Willis. Atherosclerotic
disease may be present in the adjacent arterial seg-
ment. Spectrum analysis may demonstrate two sepa-
rate frequency curves when the dissected lumen is
still open. Doppler ultrasound has been used to
monitor and follow patients with internal carotid
artery dissection.
Secondary dissections
These dissections extend into the neck arteries
from a primary dissection arising from the ascending
aorta (Fig. 7). The patients present with the symptoms
of acute chest pain, radiating to the back. Because
these ‘‘type A’’ dissections are, a priori, triaged to
surgical intervention, it is very likely that the aorta
will be repaired. The extension of the dissection into
the neck arteries is rarely symptomatic, probably be-
cause the dissecting lumen re-enters the lumen at varia-
ble locations in the common or, less often, the internal
carotid arteries. Neurologic symptoms are rare.
Gray-scale imaging shows the typical luminal
flap. Doppler waveforms are altered. If there is a site
of re-entry, forward blood flow is mainly seen. If one
of the lumens (the false lumen) does not re-enter the

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 391
carotid lumen, then an alternating systolic-diastolic
waveform is seen in that lumen.
Stroke and carotid artery stenosis
The patient who presents with a stroke (or sig-
nificant transient ischemic attack) likely has an arte-
rial embolus in the intracranial circulation or primary
disease of the intracranial branches. Other and more
common sources of stroke include emboli from the
heart and from the aorta. In the aggregate, most
Fig. 8. (A) Color Doppler image shows an abrupt termination of
the proximal internal carotid artery. This corresponds to an embol
sound image shows the filling defect. (C) The spectral Doppler w
presence of the obstructing embolus.
patients with strokes have nonsignificant lesions in
the carotid arteries. If a significant lesion is detected,
then the focus shifts to this lesion. It is then consid-
ered to be a ‘‘culprit’’ lesion. Significance is defined
in one of three ways. A 50% or greater narrowing of
the internal carotid artery is considered a hemo-
dynamic significant stenosis. In asymptomatic pa-
tients, a 60% or greater narrowing of the lumen
diameter of the internal carotid artery is considered
significant. In symptomatic patients, the definition
varies. The North American Symptomatic Carotid
Endarterectomy Trial (NASCET) study showed that
color Doppler signals before an echogenic filling defect in
us in a 35-year-old patient. (B) Transverse gray-scale ultra-
aveform shows a high resistance pattern consistent with the

Fig. 9. Triphasic spectral Doppler waveform. The systolic
peak is marked (arrowhead) followed by an area of flow
reversal (short arrow). This is followed by a small area of
antegrade flow (long arrow).
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396392
a 70% diameter stenosis was a threshold above which
there was a high-risk for a permanent stroke in the
next few months or years [36]. A second NASCET
report indicated that a 50% or greater stenosis should
be considered to be significant [37]. Rarely, an acute
embolus can occlude the carotid artery proper; the
source of the embolus is then the heart or even the
aortic arch (Fig. 8).
Physical examination shows diminished pulses
only for the most severe stenoses. Presence of a carotid
bruit can be heard on auscultation. A carotid bruit
is, however, an unreliable sign of significant stenosis.
Gray-scale imaging can show the fibrofatty
changes (hypoechoic) of carotid artery plaque. The
most common finding, however, is the presence of a
heterogeneous plaque with mixed dense and hypo-
echoic elements. Calcium deposits cause acoustic
shadowing. Pulsed wave Doppler is the most impor-
tant ultrasound approach to evaluating the degree of
carotid stenosis. The degree of carotid stenosis is
graded by the blood flow velocity elevation caused at
the site of stenotic narrowing. The peak systolic and
end-diastolic velocity is correlated to the degree of
internal carotid artery stenosis. The ratio of the inter-
nal carotid artery to common carotid artery peak
systolic velocities is considered a sturdy diagnostic
criterion that accounts for changes in blood flow ve-
locities caused by altered (either lowered or increased)
cardiac output. When a stenosis in the internal carotid
arteries lumen is reduced by 50%, a noticeable change
in blood flow velocity can be measured. This corre-
sponds to a 50% diameter stenosis. When flow values
approach and exceed 230 cm/second, then the pres-
ence of a 70% or greater stenosis is very likely. Rarely,
a critical stenosis is so severe as to decrease blood
flow volume and blood flow velocity to the point that
the Doppler signal is no longer detectable. This
remains a limitation of Doppler ultrasound: mistaking
a subtotal occlusion to be a total occlusion is still a
diagnostic limitation of ultrasound imaging. Patients
with a subtotal occlusion could still benefit from an
intervention, whereas there is no lasting benefit to
opening a previously occluded internal carotid artery.
In the setting of recurrent transient ischemic at-
tacks in a patient with an ipsilateral high-grade carotid
lesion, carotid endarterectomy should be considered.
Currently, appropriate therapy in an acute setting is
not necessarily surgical endarterectomy. Percutaneous
stenting of the carotid is a viable option in the
emergent setting, especially if the patient is evolving
toward a major stroke. There is increasing controversy
as to how and when to treat the culprit lesion in the
neck, especially if an acute revascularization of the
intracranial arteries is being attempted. In this context,
a fully percutaneous approach with stenting of the
carotid and lysis of the embolus offers a reasonable
therapeutic option.
Acute limb ischemia: arterial embolization
The normal appearance of an extremity artery is
triphasic (Fig. 9). Pulse Doppler waveform shows an
initial narrow antegrade systolic peak, followed by an
early diastolic retrograde peak or notch. Finally, a
variable antegrade diastolic peak is seen. Under the
arterial envelope a clear area is seen. Extremity arte-
rial waveforms convert to a lower resistance pattern
during exercise, with a broadened spectral peak, and
pandiastolic antegrade flow.
Acute limb ischemia is usually caused by a sudden
arterial obstruction. There are two main causes: acute
thrombosis of an existing arterial lesion; and embo-
lism from the heart or from a more central arterial
lesion, such as an aneurysm or an ulcerated plaque.
Emboli usually lodge at major branch points in the
arteries. Symptom onset is rapid. Depending on the
physiologic impact of the occlusion, the patient may
have severe claudication, rest pain, or sensory loss.
Emergent intervention by surgical embolectomy,
surgical bypass, or percutaneous thrombolysis is re-
quired to save the limb from necrosis of the muscles.
In severe cases, amputation may be needed because
further myonecrosis causes release of myoglobin and
can trigger further metabolic pathways that lead to
organ failure and finally death. The impact of the
arterial occlusion depends on the extent of arterial
disease and the presence of arterial collaterals. For
example, acute occlusion of an artery in a young,
relatively healthy patient can be devastating, because
there are almost no collateral branches to feed the
more distal leg arteries. A patent with claudication
and slowly progressing arterial disease likely has

Fig. 10. (A) This patient with acute onset of calf pain had evidence of a Baker cyst (within calipers) on ultrasound examina-
tion. (B) Imaging lower in the calf shows a hypoechoic mass extending along the fascia. This is consistent with an acute dis-
secting Baker cyst.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 393
well-developed collateral branches. An acute occlu-
sion in this patient may only cause an abrupt increase
in the severity of claudication.
Gray-scale imaging from the groin to the calf
arteries is relatively easy, as is the upper arm. Diffi-
culty can be experienced, especially in diabetic pa-
tients, when calcium deposits in the arterial walls
impair ultrasound beam penetration. Sometimes an
alternative diagnosis for acute pain can be made with
gray-scale imaging (Fig. 10). Long-standing occlu-
sion can result in contraction of the artery to a small
scarred cord that runs parallel to the deep vein. New
thrombus in the vessel lumen can appear hyper-
Fig. 11. (A) Transverse color flow Doppler image shows low-amp
spectral Doppler waveform shows low-amplitude signals in the art
echoic, especially if it originates from the heart.
Thrombus is most often anechoic with echogenicity
similar to that of blood. Dilation of the artery proxi-
mal to an occlusion is rarely seen.
Acute occlusions are most likely diagnosed by
combining color flow Doppler with pulsed wave
Doppler waveform analysis. Absence of flow or
low amplitude signal in the affected vessel is diag-
nostic of occlusion (Fig. 11), whereas high-grade
stenosis is associated with increased blood flow
velocities. Care should be taken to reduce the pulse
repetition frequency and to scan in orthogonal planes
to assess for the presence of very slow blood flow.
litude signals in the brachial artery. (B) The corresponding
ery just proximal to an acute embolus to the brachial artery.

Fig. 12. (A) Spectral Doppler waveform from the superficial femoral artery shows a reversing component to blood flow during
diastole. This is caused by high peripheral resistance from a distal (calf) compartment syndrome following trauma. (B) The
contralateral normal superficial femoral artery spectral Doppler waveform is shown for comparison.
B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396394
This helps distinguish an occlusion from a stenosis.
In transverse plane, tortuous small collaterals may be
seen in both cases. One should look for reconstitution
of the occluded vessel, distal to the occlusion.
Extensive thrombosis extending over long seg-
ments is more difficult to treat using endovascular
approaches than shorter occlusions. Thrombolysis
can be used alone or in combination with a surgical
bypass operation. Surgical thrombectomy alone or in
combination with surgical bypass operations is a very
common therapeutic option. Uncommonly, a compart-
ment syndrome can occur where tissue pressures in
the compartment exceed systolic pressure (Fig. 12).
Diabetic foot
Vascular disease in the diabetic patient is usually
insidious in its presentation and slowly progressive.
Close control of the diabetic status and medical
examination of known diabetics is the best way to
avoid an emergency. Careful routine clinical exami-
nation and self-inspection of the diabetic foot on a
regular basis is the most effective preventive mea-
sure. Peripheral neuropathy is a risk factor associated
with poor outcome. Loss of sensory feedback adds to
the effects of arterial obstruction because symptoms
are ignored and the extent of tissue loss can increase
without the patient noticing. The prevalence of lower-
extremity occlusive arterial disease in diabetics is four
times more prevalent than in nondiabetics of a similar
age [38]. Calcification of the arterial wall is generally
widespread, and the larger vessels of the pelvis are
less affected than the small vessels of the calf and foot.
Falsely elevated pressures that are measured with
external pressure cuffs, typically greater than 30 mm
Hg above the brachial pressure, suggest the presence
of noncompliant arteries. Of the run-off vessels, the
dorsalis pedis artery is often spared [39]. The calcifi-
cation of the peripheral vasculature generally affects
the more distal vessels to a lesser degree. Distal pedal
pulses can be intact and the vessels remain compress-
ible. This allows pressures measured at the toe to be
used as an alternative noninvasive approach to assess
lower-extremity arterial disease. A toe-to-brachial
index of greater than 0.6 is considered normal. A
vascular work-up including transcutaneous oxygen
measurement [40], the ankle-brachial index, and the
absolute toe systolic pressure [41] is appropriate. In
the acute setting, where lower-extremity ischemia is
strongly suspected, arteriography or MR imaging
should be performed to confirm or rule out ischemia.
Ischemia of the upper limbs
Acute ischemia in the upper extremity can be
caused by other etiologies than arterial embolization
from central arteries, heart, and aorta. An accurate
diagnosis can sometimes be difficult in the presence of
an underlying vascular disease. The most noticeable
signs and symptoms are changes in color and sensa-
tion in the hand caused by Raynaud’s phenomenon.
This can be seen in as much as a fifth of the

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396 395
population, and is four times more likely to occur in
women. The disorder affects the smallest blood ves-
sels in the hand with exposure to stress, vibration, or
cold triggering arterial-arteriole contraction and vaso-
spasm. This contraction results in blanching or bluing
of the skin of the digits from diminished blood supply.
There is marked rubor and paresthesias as hyperemia
results on rewarming.
Raynaud’s phenomenon is a manifestation of many
diseases, most often collagen vascular processes,
whereas primary or idiopathic Raynaud’s phenome-
non is called Raynaud’s disease. The etiology of these
changes is thought to be multifactorial and variable.
Noninvasive vascular testing is occasionally used
to evaluate patients with Raynaud’s disease and
includes digital pulse volume recordings and mea-
surement of digital systolic blood pressure and digital
blood flow. Stress testing for cold sensitivity should
be considered. Past medical history is most important
diagnosing the etiology of Raynaud’s. Laboratory
testing for antinuclear antibody, cryoglobulins, rheu-
matoid factor, sedimentation rate, and others may
suggest a specific secondary cause of Raynaud’s
phenomenon. Atherosclerosis, thromboembolism,
acrocyanosis, reflex sympathetic dystrophy, throm-
boangiitis obliterans, and hypothenar hammer syn-
drome are in the differential diagnosis. These entities
may all result in macrothrombus or microthrombus in
the circulatory system and can all present acutely.
Noninvasive diagnosis is limited in the acute,
limb-threatening situation. Arteriography and possi-
bly MR angiography are more useful for confirming
the diagnosis on morphologic basis. Doppler ultra-
sound is useful when it confirms patency of the large
conduit arteries to the hand. It can also be used to
confirm the presence of arterial aneurysms as are seen
in cases of hypothenar hammer syndrome.
References
[1] Bynoe RP, Miles WS, Bell RM, Greenwold DR,
Sessions G, Haynes JL, et al. Noninvasive diagnosis
of vascular trauma by duplex ultrasonography. J Vasc
Surg 1991;14:346–52.
[2] Panetta TF, Sales CM, Marin ML, Schwartz ML, Jones
AM, Berdejo GL, et al. Natural history, duplex charac-
teristics, and histopathologic correlation of arterial in-
juries in a canine model. J Vasc Surg 1992;16:867–74;
discussion 874–6.
[3] JohansenK, LynchK, PaunM,CopassM.Non-invasive
vascular tests reliably exclude occult arterial trauma in
injured extremities. J Trauma 1991;31:515–9; discus-
sion 519–22.
[4] Lynch K, Johansen K. Can Doppler pressure measure-
ment replace ‘‘exclusion’’ arteriography in the diagno-
sis of occult extremity arterial trauma? Ann Surg 1991;
214:737–41.
[5] Katzenschlager R, Ugurluoglu A, Ahmadi A, Huls-
mann M, Koppensteiner R, Larch E, et al. Incidence
of pseudoaneurysm after diagnostic and therapeutic an-
giography. Radiology 1995;195:463–6.
[6] Rapoport S, SnidermanKW,Morse SS, ProtoMH, Ross
GR. Pseudoaneurysm: a complication of faulty tech-
nique in femoral arterial puncture. Radiology 1985;
154:529–30.
[7] Forster T, Kardos A, Kiss E, Varga A, Gaal T, Csanady
M. Diagnosis of femoral pseudoaneurysm and factors
contributing to its incidence after heart catheterization.
Orv Hetil 1991;132:2897–9.
[8] Toursarkissian B, Allen BT, Petrinec D, Thompson
RW, Rubin BG, Reilly JM, et al. Spontaneous closure
of selected iatrogenic pseudoaneurysms and arterio-
venous fistulae. J Vasc Surg 1997;25:803–8; discus-
sion 808–9.
[9] Perry MO. Complications of missed arterial injuries.
J Vasc Surg 1993;17:399–407.
[10] Morgan R, Belli A. Current treatment methods for post-
catheterization pseudoaneurysms. J Vasc Interv Radiol
2003;14:697–710.
[11] Paulson EK, Sheafor DH, Kliewer MA, Nelson RC,
Eisenberg LB, Sebastian MW, et al. Treatment of iat-
rogenic femoral arterial pseudoaneurysms: comparison
of US-guided thrombin injection with compression re-
pair. Radiology 2000;215:403–8.
[12] Taylor BS, Rhee RY, Muluk S, Trachtenberg J, Walters
D, Steed DL, et al. Thrombin injection versus compres-
sion of femoral artery pseudoaneurysms. J Vasc Surg
1999;30:1052–9.
[13] Trertola SO, Savader SJ, Prescott CA, Osterman Jr
FA. US-guided pseudoaneurysm repair with a com-
pression device. Radiology 1993;189:285–6.
[14] Kang SS, Labropolous N, Mansour MA, Michelini M,
Filliung D, Baubly MP, et al. Expanded indications
for ultrasound-guided thrombin injection of pseudo-
aneurysms. J Vasc Surg 2000;31:289–98.
[15] Partap VA, Cassoff J, Glikstein R. US-guided percuta-
neous thrombin injection: a new method of repair of
superficial temporal artery pseudoaneurysm. J Vasc
Interv Radiol 2000;11:461–3.
[16] Sheiman RG, Brophy DP, Perry LJ, Akbari C. Throm-
bin injection for the repair of brachial artery pseudo-
aneurysms. AJR Am J Roentgenol 1999;173:1029–30.
[17] Kang SS, Labropolous N, Mansour MA, Baker WH.
Percutaneous ultrasound guided thrombin injection:
a new method for treating postcatheterization femo-
ral pseudoaneurysms [comment]. J Vasc Surg 1998;
27:1032–8.
[18] Liau CS, Ho FM, Chen MF, Lee YT. Treatment of
iatrogenic femoral artery pseudoaneurysm with percu-
taneous thrombin injection [comment]. J Vasc Surg
1997;26:18–23.
[19] Brophy DP, Sheiman RG, Amatulle P, Akbari CM.
Iatrogenic femoral pseudoaneurysms: thrombin injec-

B.D. Davison, J.F. Polak / Radiol Clin N Am 42 (2004) 383–396396
tion after failed US-guided compression. Radiology
2000;214:278–82.
[20] Sheldon PJ, Oglevie SB, Kaplan LA. Prolonged gen-
eralized urticarial reaction after percutaneous thrombin
injection for treatment of a femoral artery pseudoaneu-
rysm. J Vasc Interv Radiol 2000;11:759–61.
[21] Kubaska S, Greenberg R, Clair D, Barber G, Srivastava
S, Green R, et al. Internal carotid artery pseudoaneu-
rysms: treatment with the wall graft enoprosthesis.
J Endovasc Ther 2003;10:182–9.
[22] Hood DB, Mattos MA, Douglas MG, Barkmeier LD,
Hodgson KJ, Ramsey DE, et al. Determinants of suc-
cess of color-flow duplex-guided compression repair of
femoral pseudoaneurysms. Surgery 1996;120:585–8;
discussion 588–90.
[23] Sharp KW, Spees EK, Selby LR, Zachary JB, Ernst
CB. Diagnosis and management of retroperitoneal he-
matomas after femoral vein cannulation for hemodi-
alysis. Surgery 1984;95(1):90–5.
[24] Bianchi S, Martinoli C, Abdelwahab IF, Derchi LE,
Damiani S. Sonographic evaluation of tears of the gas-
trocnemius medial head (tennis leg). J Ultrasound Med
1998;17:157–62.
[25] Tomlinson MA, Beese R, Banwell M, Loosemore T,
Buckenham TM, Dormandy JA. Sequential retroperito-
neal venous hemorrhage and embolism of an angio-seal
puncture closure device complicating iliac artery angio-
plasty. J Endovasc Surg 1999;6:264–9.
[26] Fukuda T, Sakamoto I, Kohzaki S, Uetani M, Mori M,
Fujimoto T, et al. Spontaneous rectus sheath hemato-
mas: clinical and radiological features. Abdom Imaging
1996;21:58–61.
[27] Elesber AA, Kent PD, Jennings CA. Compressive neu-
ropathy of the brachial plexus and long thoracic nerve:
a rare complication of heparin anticoagulation. Chest
2001;120:309–11.
[28] Klein SR, Bongard FS, White RA. Neurovascular inju-
ries of the thoracic outlet and axilla. Am J Surg 1988;
156:115–8.
[29] Abreo G, Lenihan DJ, Nguyen P, Runge MS. High-
output heart failure resulting from a remote traumatic
aorto-caval fistula: diagnosis by echocardiography.
Clin Cardiol 2000;23:304–6.
[30] Cwikiel W, Midia M, Williams D. Non-traumatic vas-
cular emergencies: imaging and intervention in acute
arterial conditions. Eur Radiol 2002;12:2619–26.
[31] Knudson MM, Lewis FR, Atkinson K, Neuhaus A.
The role of duplex ultrasound arterial imaging in
patients with penetrating extremity trauma. Arch Surg
1993;128:1033–7; discussion 1037–8.
[32] Pellerito JS. Current approach to peripheral arterial so-
nography. Radiol Clin North Am 2001;39:553–67.
[33] Patel S, Ilsen PF. Acquired Horner’s syndrome: clinical
review. Optometry 2003;74:245–56.
[34] Aanonsen NO, Kerty E, Nyberg-Hansen R, Nakstad P.
Spontaneous dissection of the internal carotid artery.
Tidsskr Nor Laegeforen 1991;111:330–2.
[35] Anzola GP, Gualandi GF, Orlandini A, Scipione V.
Lower cranial nerve palsy produced by internal carotid
artery dilatation: report of two cases. Ital J Neurol Sci
1987;8:375–9.
[36] North American Symptomatic Carotid Endarterectomy
Trial Collaborators. Beneficial effect of carotid endar-
terectomy in symptomatic patients with high-grade
carotid stenosis. N Engl J Med 1991;325:445–53.
[37] Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson
GG, Haynes RB, et al. Benefit of carotid endarterec-
tomy in patients with symptomatic moderate or severe
stenosis. North American Symptomatic Carotid Endar-
terectomy Trial Collaborators. N Engl J Med 1998;
339:1415–25.
[38] Kannel WB, McGee DL. Diabetes and glucose toler-
ance as risk factors for cardiovascular disease: the Fra-
mingham study. Diabetes Care 1979;2:120–6.
[39] LoGerfo FW, Coffman JD. Current concepts: vascu-
lar and microvascular disease of the foot in diabetes.
Implications for foot care. N Engl J Med 1984;311:
1615–9.
[40] Bacharach JM, Rooke TW, Osmundson PJ, Gloviczki
P. Predictive value of transcutaneous oxygen pressure
and amputation success by use of supine and elevation
measurements. J Vasc Surg 1992;15:558–63.
[41] Apelqvist J, Castenfors J, Larsson J, Stenstrom A,
Agardh CD. Prognostic value of systolic ankle and
toe blood pressure levels in outcome of diabetic foot
ulcer. Diabetes Care 1989;12:373–8.

Radiol Clin N Am 42 (2004) 397–415
Emergency Doppler evaluation of the liver and kidneys
Michelle M. McNamara, MD*, Mark E. Lockhart, MD, MPH,Michelle L. Robbin, MD
Abdominal Imaging Section, Department of Radiology, University of Alabama at Birmingham, 619 19th Street South, JTN 353,
Birmingham, AL 35249-6830, USA
Vascular complications of hepatic and renal trans- orly. The left intersegmental fissure separates the left
plants are potentially catastrophic. They may result
in loss of the allograft with significant morbidity for
the recipient. Doppler evaluation of renal and he-
patic transplants may provide data that are essential
for preserving allograft function. Timely recogni-
tion of these problems improves the likelihood that
intervention to correct vascular abnormalities will
be successful.
Emergent applications of Doppler in the native
liver and kidneys are more limited. Sonographic
evaluation of patients with cirrhosis, with or without a
transjugular intrahepatic portosystemic shunt (TIPS),
may elucidate a cause for acute clinical decompen-
sation. Ultrasound is a readily available means of
assessing patients with acute renal dysfunction. Im-
portantly, ultrasound can be used to determine if
active hemorrhage is present at liver or renal biopsy
sites in the postbiopsy patient with a decreasing he-
matocrit level.
Hepatic ultrasound
Anatomy and appearance
The liver is divided into lobes and segments by
three fissures. The main lobar fissure divides the right
and left lobes. The boundaries of this fissure are the
middle hepatic vein superiorly, the gallbladder neck
in the midportion, and the inferior vena cava inferi-
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.001
* Corresponding author.
E-mail address: [email protected]
(M.M. McNamara).
lobe into the lateral and medial segments. The ana-
tomic boundaries of this fissure are the left hepatic
vein superiorly and the falciform ligament inferiorly.
The ascending portion of the left portal vein is at the
midportion of this fissure. The right intersegmental
fissure separates the right lobe into anterior and
posterior segments. The right hepatic vein defines
this fissure superiorly.
The main portal vein divides into right and left
branches in the liver hilum. The left portal vein
courses horizontally (horizontal segment) and then
changes to a more vertical orientation in the left
intersegmental fissure, termed the ‘‘ascending por-
tion,’’ or umbilical segment of the left portal vein.
The right portal vein divides into anterior and poste-
rior divisions. The anterior and posterior divisions
of the right portal vein course centrally in the ante-
rior and posterior right hepatic lobe segments, respec-
tively, and are equidistant from the middle and right
hepatic veins.
The hepatic veins, surrounded by liver paren-
chyma, drain into the inferior vena cava. They are
in open communication with the right heart. Cardiac
physiology and hepatic parenchymal compliance in-
fluence the hepatic vein waveform. The normal
hepatic vein waveform is phasic, similar to the in-
ferior vena cava (Fig. 1A). Two large antegrade
waves reflect atrial diastole and ventricular systole.
A small reversal in flow is seen between the larger
antegrade waves at atrial systole.
The main portal vein provides 70% to 80% of
hepatic blood flow. Normal portal venous waveforms
reflect minimal undulations from respiratory and
cardiac activity, because they are normally isolated
from the central venous system (Fig. 1B). The hepatic
s reserved.

Fig. 1. Spectral Doppler of normal hepatic waveforms. (A) Right hepatic vein shows triphasic flow. (B) Portal vein waveform
demonstrates monophasic flow. (C) Hepatic artery with sharp systolic upstroke.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415398
artery, which provides 20% to 30% of hepatic blood
flow, originates from the celiac trunk. The common
hepatic artery (Fig. 1C) becomes the proper hepatic
artery after it gives rise to the gastroduodenal artery.
The proper hepatic artery bifurcates into the right and
left hepatic arteries. Variations in hepatic anatomy are
common, however, and may not be sonographically
apparent [1].
Transplant liver
Clinical
Hepatic artery thrombosis is the most common
vascular complication of orthotopic liver transplant,
and it occurs in 3% to 10% of all recipients [2,3]. The
incidence is at the higher end of the spectrum in
pediatric recipients, and it occurs in up to 12% of
transplant recipients [3,4]. If this complication oc-
curs, it is most often seen in the first 2 weeks after
transplant [4]. Clinical manifestations include biliary
dysfunction and sepsis [4]. Hepatic artery anasto-
motic stenosis usually precedes thrombosis [5]. He-
patic artery stenosis and thrombosis can be detected
with Doppler ultrasound.
Early arterial occlusion is associated with liver
failure and may require retransplantation. Alterna-
tively, if significant hepatic artery stenosis can be
detected before life-threatening ischemia occurs, an-
gioplasty or surgical revascularization may salvage
the liver transplant [4–6]. Doppler spectral analysis
is an effective tool for evaluating a patient for hepatic
artery thrombosis or stenosis, and it has sensitiv-
ity and specificity rates of 97% and 64%, respec-
tively [6].
Other vascular complications include portal vein,
hepatic vein, and inferior vena cava (IVC) stenosis
and thrombosis, and pseudoaneurysm formation at the
arterial anastomosis [7]. The narrowing that results
from nonocclusive thrombus cannot always be differ-
entiated sonographically from stenosis secondary to
other causes [6]. These less frequent complications

Fig. 1 (continued).
Fig. 2. Immediate post – liver transplant hepatic artery
Doppler. Color and spectral Doppler documents antegrade
flow with RI of 1. In the perioperative period, a high re-
sistance waveform does not necessarily indicate a patho-
logic condition.
M.M. McNamara et al / Radiol Cl
may develop independently or concomitantly. Prompt
diagnosis and treatment of vascular complications are
crucial to graft and patient survival [8].
Sonographic technique
For most adult patients, a 3.5-MHz or lower
frequency transducer is preferred, especially in the
immediate posttransplant period, when available
sonographic imaging windows may be limited. Lower
frequency transducers facilitate adequate tissue pene-
tration without compromising resolution for Doppler
evaluation. Optimum Doppler angle is less than 60�.Low wall filter settings increase sensitivity for detec-
tion of low flow [9]. Direct gray scale inspection of
the vessels is performed, as is color and spectral
Doppler analysis of the main, right, and left hepatic
arteries, the main, right, and left hepatic veins, the
main, right, and left portal veins, IVC, and splenic
vein. Patency, flow direction, velocities, resistive
indices (RIs), and waveforms are assessed. Anasto-
motic sites are interrogated for narrowing [7].
Sonographic criteria
Hepatic artery stenosis
Hepatic artery stenosis is suspected if RIs are less
than 0.5 [5] or if there is a focal peak systolic velocity
(PSV) more than 200 to 300 cm/second [2]. Other
indicators of significant hepatic arterial narrowing
include a systolic acceleration time (end diastole to
first systolic peak) more than 0.08 seconds [5]. In the
first 48 hours after transplant, RIs may be low or high
(Fig. 2) [10]. Essentially, the presence of an arterial
signal in the immediate postoperative period is satis-
factory, as long as a focal gradient is not found [6]. In
the authors’ experience, a PSV ratio at the anastomo-
sis of more than approximately 3:1 correlates with a
hemodynamically significant stenosis. A low resis-
tance arterial waveform may be seen downstream
from the stenosis (Fig. 3).
Portal vein thrombus
The portal vein is evaluated for presence or ab-
sence of flow, nonocclusive filling defects, and flow
direction. In the authors’ experience, a PSV gradient
equal to or more than approximately 3:1 at the anas-
tomosis is consistent with a hemodynamically signifi-
cant stenosis, a finding rarely encountered.
Hepatic veins and inferior vena cava
Flow direction and pulsatility are evaluated in the
hepatic veins with spectral Doppler. Monophasic
flow in the hepatic veins after transplant is a rela-
in N Am 42 (2004) 397–415 399

Fig. 3. Hepatic artery stenosis in a transplant liver. Color and
spectral Doppler of the right hepatic artery (Doppler gate)
shows abnormal waveform with RI of 0.37. RIs in the left
and main hepatic arteries (not shown) were 0.32 and 0.44,
respectively. Angiography documented 80% stenosis at the
hepatic artery surgical anastomosis.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415400
tively common finding. Although it is not always
clinically significant, monophasic flow in the hepatic
veins can be a result of outflow stenosis or obstruc-
tion at the cranial IVC anastomosis. In the authors’
experience, a distended IVC with a peak systolic ratio
of more than approximately 3:1 can be seen in cases
with IVC anastomotic stenosis (Fig. 4A–C). An IVC
venogram with measurement of pressures across the
stenosis can be a useful confirmation of clinically
significant abnormality. Hepatic vein thrombosis is
uncommonly seen on Doppler (Fig. 5).
Pseudoaneurysm
Pseudoaneurysms appear as a simple or complex
hypoechoic lesion on grayscale ultrasound. Unless a
pseudoaneurysm is completely thrombosed, typical
‘‘to-and-fro’’ color and spectral Doppler findings
should be elicited (Fig. 6) [9].
Cirrhotic native liver
Clinical
Cirrhosis is a diffuse process characterized by
fibrosis and alteration of normal liver architecture.
Pathologic mechanisms include cell death, fibrosis,
and regeneration, which result in the formation of
nodules. In the micronodular type of cirrhosis, nod-
ules measure less than 1 cm, whereas in the macro-
nodular type, nodules of varying size may measure up
to 5 cm. Alcoholism and viral hepatitis are common
causes. Other causes include biliary cirrhosis, scle-
rosing cholangitis, Wilson’s disease, and hemochro-
matosis. Cirrhosis is a common cause of intrahepatic
portal hypertension, with resultant ascites, portosys-
temic collateral formation, and gastrointestinal bleed-
ing. Doppler ultrasound is a useful noninvasive
means of assessing the status of a TIPS and portal
vein flow in patients with cirrhosis who present with
acute decompensation [11]. Depending on criteria
selected to define abnormal, Doppler ultrasound
sensitivity rate for detection of TIPS malfunction
ranges from 92% to 94% [12], with a specificity rate
of 72% to 100% [12].
Sonographic technique
Comprehensive evaluation of the hepatic vessels
includes acquiring angle-corrected color and spectral
Doppler to determine flow direction, pulsatility, PSV,
and patency. As with transplant liver Doppler evalua-
tion, a lower frequency transducer may facilitate
penetration [13]. Low pulse repetition frequency
settings increase color Doppler sensitivity but may
result in aliasing, which can mimic flow reversal
[11,14]. Direction of flow should be confirmed by
modifying pulse repetition settings or with spectral
Doppler [14]. High wall filter settings should be
avoided because they may decrease the ability to
detect low velocity flow [2].
The main, right, and left portal veins, middle left
and right hepatic veins, hepatic artery, splenic vein,
and IVC are evaluated with gray scale followed by
assessment with color and spectral Doppler. Varices
are sought in the coronary, periumbilical, peripancre-
atic, and splenic regions, typically the most fruitful
locations for sonographic variceal detection. Vessels
are sampled proximal to (upstream) and at any abnor-
mality. Parenchymal abnormalities are imaged in
transverse and longitudinal planes. Doppler interro-
gation of any thrombus seen is performed to aid in
determining if it is bland or tumor thrombus, particu-
larly in the presence of a liver mass. Tumor thrombus
may demonstrate flow on color or spectral Doppler.
Sonographic evaluation of TIPS is complex. Ve-
locities in as much of the shunt as is acoustically
visible should be evaluated. A complete assessment

Fig. 4. IVC stenosis after liver transplant. (A) Narrowing is visually apparent on gray scale images (arrows). (B) Spectral Doppler
demonstrates PSV of 24 cm/second 2 cm caudal to the infrahepatic anastomosis. (C) PSV at the anastomosis is 115 cm/second,
which results in a PSV ratio of 115/24, or 4.8. IVC venogram (not shown) showed stenosis without significant pressure gradient
at this level.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 401
may require changes in patient position during the
examination—including the left lateral decubitus and
prone positions—to get the best angle and shunt
visualization. Main portal vein velocity and flow
direction should be assessed. Values for the hepatic
venous end within the stent, mid-shunt and portal
venous end within the stent, and highest and lowest
intrashunt velocities (if at a different location) are
recorded [2,13,15]. Flow direction and PSV in the
intrahepatic right and left portal veins and in the right,
middle, and left hepatic veins are also evaluated [2].
Stent diameter is measured.
Sonographic criteria
Portal vein thrombosis
The presence of occlusive low-level echoes, or a
nonocclusive filling defect, may be observed at gray
scale imaging. Color Doppler may be useful in
finding hypoechoic thrombus not apparent on gray
scale imaging (Fig. 7). Normal portal vein caliber
ranges from 9 to 13 mm [16]. A small vessel in the
region of the portal vein is suspicious for prior
portal vein thrombus, with subsequent vein sclero-
sis or collateral formation. Cavernous transformation,

Fig. 5. Hepatic vein thrombosis after liver transplant. Color
Doppler shows a hypoechoic linear structure (arrows) in the
region of the right hepatic vein without Doppler flow.
Fig. 7. Cirrhotic liver with nonocclusive portal vein throm-
bus. Color Doppler demonstrates linear hypoechoic throm-
bus (asterisks) within the portal vein (arrows). Spectral
Doppler (not shown) also documented vessel patency.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415402
which represents multiple small periportal venous
collaterals, suggests chronic portal vein thrombosis.
Portal hypertension
Portal venous hypertension may manifest sono-
graphically as slow antegrade, stagnant, or hepatofu-
gal flow in the main portal vein, intrahepatic branches
only, or extrahepatic collaterals only [11]. The portal
vein may be enlarged and measure more than 1.3 cm,
a sensitive but not specific sign of portal venous
Fig. 6. A 6.2-cm hepatic artery pseudoaneurysm at the ar-
terial anastomosis. Liver transplant was performed at an
outside institution. Color and spectral Doppler show typical
biphasic ‘‘to and fro’’ pattern.
hypertension [17]. Bi-directional flow may precede
reversal of flow [11].
Although cirrhosis is the most common cause of
hepatofugal flow, there are exceptions. Large porto-
systemic collaterals may persist after transplantation
and result in reversed flow in the absence of recurrent
portal hypertension. Liver function and portal vein
patency may be compromised as a result. Hepatofu-
gal flow in one or more intrahepatic portal veins may
occur with a focal arterioportal shunt from a biopsy or
tumor and is not specific for portal hypertension [11].
Transjugular intrahepatic portosystemic shunt
malfunction
TIPS is an effective and widely used means of
treating symptomatic portal hypertension. Timely
identification of TIPS malfunction increases the
probability of successful shunt revision with a conse-
quent decrease in recurrence of complications of portal
hypertension. Sensitivity and specificity rates for de-
tection of TIPS dysfunction range from 92% to 94%
and 72% to 100%, respectively, depending on the
number of abnormal criteria present [12,18]. Clinical
manifestations of TIPS dysfunction may include as-
cites recurrence, variceal bleeding, and splenomegaly.
A wide range of velocities is seen in patent shunts
[13,15], which necessitates determination of baseline
velocities in individual patients for long-term follow-
up [13]. Integration of data from several parameters is
needed to suggest TIPS malfunction. If multiple
abnormalities are identified, the likelihood of TIPS
dysfunction increases [12,18,19]. Stenosis most com-
monly involves the draining hepatic vein.

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 403
Direct signs of TIPS malfunction include lack of
flow with color and spectral Doppler, consistent with
shunt occlusion. Stenosis is suggested by a velocity
within the shunt that is less than 90 cm/second or
exceeds 189 cm/second. Velocity gradient across the
shunt also correlates with stenosis. Similar sensitivity
and specificity for detection of stenosis has been
shown when either 50 cm/second or 100 cm/second
is selected as the upper limit of normal for velocity
Fig. 8. Stenotic TIPS. (A) Main portal vein velocity is abnormally
gradient within the TIPS. Velocity at the hepatic vein side is 135
(not shown) were 60 and 50 cm/second, respectively. (C) The steno
is 206 cm/second.
gradient [12,20]. Normal main portal vein velocity
when a TIPS is present is approximately 43 cm/
second. Velocities in the main portal vein less than
30 to 33 cm/second correlate with TIPS malfunction
(Fig. 8A–C) [12,18,20].
Comparison with prior studies is helpful for
evaluating for TIPS malfunction. Decrease in main
portal vein velocity of 20% from baseline or peak
shunt velocity decrease of more than 40 cm/second
low, 28 cm/second. (B) Spectral Doppler shows a velocity
cm/second. Velocities mid-shunt and at the portal vein side
sis is located in the draining hepatic vein, where the velocity

Table 1
Indicators of transjugular intrahepatic portosystemic shunt stenosis [12]
Criteria Diagnostic threshold Sensitivity/specificity
Main portal vein velocity Less than 30 cm/sec Sensitivity 82%, specificity 77%
Decrease of 20% from baseline Sensitivity 78%, specificity 75%
Velocity within the TIPS <90 or >189 cm/sec Sensitivity 84%, specificity 70%
Decrease of >40 cm/sec or increase of
>60 cm/sec from baseline
Sensitivity 71%, specificity 88%
Gradient across the TIPS More than 100 cm/sec Sensitivity 56%, specificity 78%
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415404
or increase more than 60 cm/second correlates with
stenosis [12]. A change from retrograde to antegrade
flow in a portal vein not drained by the TIPS and
reappearance of varices or patent periumbilical col-
lateral strongly suggests shunt malfunction [13] but
may be a relatively late sign (Table 1).
Main portal vein velocity after TIPS placement
may be influenced by the size of the stent. Higher
flow velocities may be observed with 12-mm versus
10-mm shunts. A higher main portal vein velocity
threshold for shunt malfunction may be necessary;
however, significant differences in maximum and
minimum intrashunt velocities are not likely [19].
Portal vein aneurysmal ectasia
Aneurysmal ectasia of the portal vein is uncom-
monly seen and may be congenital or secondary to
portal venous hypertension or vessel wall weakening
related to inflammatory processes, such as acute
pancreatitis. There is considerable variation in the
size of the portal vein. The measurement at which
dilatation is called aneurysmal is somewhat arbitrary.
Aneurysmal ectasia is present if there is significant
focal portal vein diameter enlargement compared
with the rest of the vessel, especially if a saccular
or fusiform appearance is identified [21,22]. It gen-
erally appears as a cystic structure. Turbulent or ‘‘to
and fro’’ flow is identified with Doppler interrogation
[23], unless the vein is thrombosed.
Fig. 9. Postbiopsy hemorrhage. Color Doppler of native
liver after biopsy shows active hemorrhage demonstrated
by a jet from the biopsy tract to the liver surface (arrow).
Noncirrhotic native liver
Clinical
Applications of urgent Doppler ultrasound in
patients without cirrhosis include evaluation for
post– liver biopsy complications, sequela of inflam-
matory processes, and determination of the cause of
acutely elevated liver function tests. An acute drop in
hematocrit or unusual pain after biopsy may warrant
sonographic evaluation for active hemorrhage or
pseudoaneurysm. Portal vein thrombus and pseudo-
aneurysm are rare, usually sequelae to inflammatory
processes such as pancreatitis or septicemia. Portal
vein thrombus also may be seen with hypercoagula-
ble states and malignancy.
Sonographic technique
Comprehensive sonographic evaluation is similar
to evaluation of the cirrhotic native liver. All anechoic
structures are evaluated for flow. If the evaluation is
for a postbiopsy complication, evidence of active
hemorrhage also is sought.
Sonographic criteria
Postbiopsy complications
Active hemorrhage may be observed as a jet on
color Doppler (Fig. 9) and demonstrate an arterial
spectral waveform. Additional findings consistent
with hemorrhage include the presence of hematoma
or fluid adjacent to the liver or in the pelvis. A non-

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 405
thrombosed pseudoaneurysm demonstrates the typi-
cal ‘‘to and fro’’ color and spectral pattern.
Portal vein thrombosis
Evaluation is the same as for a cirrhotic liver.
Portal vein thrombosis is rare in the native noncir-
rhotic liver and may not be detected on a routine
abdominal ultrasound. The authors have found that a
brief look at the main portal vein with gray scale and
color Doppler on routine abdominal ultrasound ex-
amination occasionally has been useful in detecting
clinically unsuspected portal vein thrombus.
Renal ultrasound
Anatomy and appearance
The kidney has several distinct anatomic features
that may be differentiated by ultrasound. The renal
cortex and medullary pyramids are similar in echo-
texture in the normal kidney. Each pyramid and sur-
rounding cortex converges into a renal papilla and
collecting system infundibulum. In echogenic kid-
neys, the pyramids of the renal medullary region are
hypoechoic to the renal cortex. Each of these struc-
tures may be distinguished easily from the echogenic
fat of the central sinus. The anechoic renal calyces
course into the renal pelvis and proximal ureter, struc-
tures that may be visualized if distended with urine.
Normal cortical thickness averages 10 mm, but
differentiation of medulla and cortex may be difficult.
Instead, the combined thickness of the capsule to the
renal sinus may be better depicted and normally mea-
sures approximately 15 to 16 mm [24]. The length of
kidneys varies with patient height, but their median
length is 11 cm; most kidneys measure 9.8 to 12.3 cm
long and are symmetric in length [24].
A single renal artery arises from each side of the
abdominal aorta caudal to the superior mesenteric
artery to supply each kidney. In up to 30% of
kidneys, however, accessory renal arteries may be
present [25]. Accessory arteries may arise near the
main renal artery, distal aorta, or common iliac
arteries. The main renal artery bifurcates or trifurcates
into branches that supply the dorsal and ventral
portions of the kidney. Segmental renal arteries
course within the renal parenchyma near the pyra-
mids. Multiple renal vein branches join to form the
main renal veins, which drain directly into the inferior
vena cava.
The normal spectral waveform in the native renal
artery is a rapid systolic upstroke with a small early
systolic peak followed by smooth tapering to the end
diastolic velocity. Flow should be laminar without
aliasing. In the normal kidney, diastolic flow should
be present in the artery, and the upper limit of RI
has been described as 0.7 in adults [26,27]. Flow in
the main renal vein should have normal mild respi-
ratory phasicity.
Transplant kidney
Clinical
Ultrasound is the best initial imaging modality in
the renal transplant patient with elevated creatinine
level. Using ultrasound as the initial screening test
avoids the use of radiation, increased cost, and the
potential nephrotoxic effects of iodinated contrast
associated with CT. Common allograft abnormalities
include hydronephrosis with ureteral obstruction,
renovascular disease, acute tubular necrosis, and
rejection. Peritransplant seromas or lymphoceles
may cause hydronephrosis or compress the renal
vessels. Rarely, a mass from posttransplant lympho-
proliferative disorder may cause renal artery stenosis
or hydronephrosis [28]. Many of these etiologies
overlap in their clinical symptomatology, and the
underlying problem must be diagnosed accurately to
guide therapy.
Doppler ultrasound can document patency of a
transplant renal artery and vein and may aid in the
detection of renal artery stenosis or an arteriovenous
fistula. Decreased or absent perfusion in the post-
operative allograft is rare but requires immediate
intervention [29]. Gray scale ultrasound is sensitive
and specific for hydronephrosis, which is caused by
obstruction in up to 8% of transplanted kidneys [30].
Ultrasound may evaluate delayed function of the
kidney or a sudden functional decline after good
initial results.
Sonographic technique
Sonographic characteristics of the renal transplant
are similar to native kidneys with a few significant
differences. Renal transplants are most commonly
placed within the right or left pelvis. The superficial
location may allow easier visualization of the trans-
plant vessels and anastomoses compared with the
vessels of the native kidneys. A higher frequency
transducer—3.5 mHz or higher (usually a curved
transducer, which allows good visualization of the
near and far portions of the kidney)—is used. The
entire course of the renal artery and vein should be

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415406
visualized, with special attention paid to the anasto-
moses, usually at the external iliac artery and vein.
Rarely, a transplant may be placed in the midabdo-
men with anastomoses to visceral vessels. The kidney
is often best visualized from an anterolateral approach
with displacement of any overlying bowel loops with
gentle graded compression by the ultrasound trans-
ducer. Adynamic ileus in the perioperative period
may hinder the sonographic examination, however.
Once the allograft is localized, the renal vessels
can be traced to the areas of anastomosis. Angle-
corrected flow evaluation should maintain an angle
less than 60� from the sonographic beam. An initial
scan with power or color Doppler to demonstrate
areas of decreased flow is useful. Regional decreased
flow may be the only suggestion of a segmental
stenosis or infarction. Subsequently, a representative
segmental renal artery waveform in the upper pole,
midportion, and lower pole is evaluated with spectral
Doppler, and an RI is calculated. The detection of an
abnormal acceleration time or absence of the early
systolic peak may suggest transplant renal artery
stenosis [31].
Color Doppler is used to identify turbulent vessel
flow by the depiction of aliasing. Spectral Doppler is
obtained in the areas of aliasing to evaluate for
potential stenosis. PSV measurements are obtained
at and approximately 2 cm proximal to the area of
aliasing or visual narrowing, which allows the calcu-
lation of a PSV ratio. The main renal artery anasto-
mosis is specifically evaluated with color and spectral
Fig. 10. Postrenal biopsy hemorrhage. (A) Color Doppler of kidne
capsule (arrow) into a perinephric hematoma. Renal parenchym
demonstrates arterial waveform.
Doppler at each examination, because it is a relatively
common site of abnormality. If a stenosis at the renal
artery anastomosis is suspected, a PSV is obtained in
the proximal iliac artery approximately 2 cm from the
anastomosis, which allows for the calculation of a
renal artery anastomosis to proximal iliac artery PSV
ratio. The main renal vein is also evaluated with color
and spectral Doppler, which usually demonstrates a
normal antegrade venous waveform.
Sonographic criteria
Postbiopsy complications
Interrogating the transplant kidney after instru-
mentation or biopsy is important to assess for com-
plications that could result in loss of life or loss of the
allograft. Color Doppler can detect active extravasa-
tion (Fig. 10A, B) of blood from the margin of the
kidney at the point of biopsy. The biopsy tract is often
visible, and active hemorrhage presents as a jet of
color that projects from this region into the perineph-
ric fat.
Pseudoaneurysm is a documented complication of
renal biopsy [32]. In a kidney with history of instru-
mentation, any anechoic structure should be evalu-
ated with Doppler to exclude a vascular structure
[33]. Flow that fills a cavity that does not conform to
the renal vessels confirms a pseudoaneurysm. Spec-
tral Doppler may detect the ‘‘to and fro’’ waveform
that diagnoses pseudoaneurysm in other sites.
y after biopsy shows jet of active extravasation through the
al denoted by asterisk. (B) Spectral Doppler of the jet

Fig. 11. Postbiopsy 0.6-cm arteriovenous fistula (cursors)
in a transplant kidney. Spectral Doppler (not shown) dem-
onstrated bidirectional flow in the renal parenchyma de-
noted by asterisks. Also, a needle track pseudoaneurysm is
seen (arrows).
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 407
Arteriovenous fistula is a common complication
of renal biopsy (Fig. 11), and it is detected on follow-
up imaging in 10% to 15% of biopsies [34,35]. It is
important to find a fistula if present, because it can
cause a significant steal from normal parenchyma,
which causes transplant dysfunction. A fistula may be
suspected based on low resistance main renal artery
flow in the absence of a vascularized collection.
There may be aliasing of signal on color Doppler
[35]. On color Doppler, tissue reverberation may
cause color artifact in the renal parenchyma [35,36].
High volume of flow may be present on spectral
Doppler in the renal artery and vein [37]. Close to the
arteriovenous fistula (AVF), the draining vein typi-
cally has an arterialized waveform [35,38].
Intraoperative renal ultrasound
Although intraoperatively the surgeon may note
by visual inspection that kidney perfusion is failing,
the cause of the abnormal perfusion may not be clear.
The sonologist can be helpful to the surgeon during a
difficult surgical procedure by documenting renal
flow characteristics. Doppler ultrasound can docu-
ment patency of the main renal artery and main renal
vein. It can detect an arterial dissection and may be
able to differentiate it from renal artery thrombosis.
Intraoperative Doppler may assist the surgeon in
differentiating an inflow problem with low renal
artery resistance downstream in the segmental arter-
ies, from an inflow, or intrinsic transplant abnormality
with high-resistance arterial waveforms.
Transplant vascular compromise
Severe vascular complications can result in rapid
loss of the transplant allograft. In this setting, emer-
gent Doppler may identify the cause of the dysfunc-
tion and allow intervention in a timely manner. In one
series, emergent ultrasound and intervention in pa-
tients decreased loss of the organ from 4.7% to
1.05%. In that series, the most common cause of
severe perfusional failure of the transplant was renal
artery stenosis [29], which may occur in as many as
8% to 16% of renal transplant allografts [39,40].
In the authors’ experience, there is an increased
incidence of transplant renal artery stenosis in living
related donor allografts compared with cadaveric
kidneys. This is likely because of different surgical
techniques in the cadaveric renal transplant versus
living related donor. In the cadaveric transplant, a
patch of the aorta is taken around the main renal artery
aorta takeoff. The anastomosis in the cadaveric trans-
plant is actually a larger anastomosis than just that of
the main renal artery, from the aortic patch to the iliac
artery, with resultant decrease in technical complica-
tions. Taking an aortic patch would not be desirable in
the living related transplant. The main renal artery
anastomosis with the iliac artery is generally a much
smaller diameter anastomosis, with increased poten-
tial for technical problems that cause stenosis.
Critical vascular compromise of a transplant kid-
ney may be demonstrated with abnormal color Dopp-
ler perfusion. In the setting of rapid allograft failure,
reduced or absent flow in the kidney and main renal
artery suggests renal artery thrombosis [29]. This is a
rare occurrence but may have severe impact on the
allograft. Occasionally, only segmental arteries are
thrombosed. In these cases, segmental infarctions
may be detected on color Doppler [41]. Power
Doppler may increase confidence for detection of
perfusional defects associated with areas of allograft
infarction, however [42]. Renal artery stenosis also
may cause allograft dysfunction.
In transplant renal artery stenosis, high PSVs of
more than 200 cm/second have been described at the
site of a significant renal artery stenosis (Fig. 12A)
[43]. The accuracy is improved if a PSVof more than
350 cm/second criterion is used in combination with
acceleration time and evaluation for dampened intra-
renal waveforms [31]. Measurement of a tardus-par-
vus waveform (slow systolic acceleration with low
peak flow velocity) of poststenotic flow in the allo-
graft also may suggest main renal artery stenosis

Fig. 12. Renal artery stenosis in a transplant kidney. Spectral Doppler shows an elevated velocity of 469 cm/second at the
arterial anastomosis (A) and parvus-tardus waveform (B) in an intrarenal segmental artery.
Fig. 13. Spectral Doppler shows reversal of diastolic flow in
the main renal artery. The renal vein was not definitely iden-
tified (not shown). At surgery, a large peritransplant hema-
toma was evacuated, which restored flow in the renal vein.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415408
(Fig. 12B) [31,44]. Iliac artery stenosis proximal to
the transplant artery may affect a renal transplant
adversely in much the same way as renal artery
stenosis [45,46].
Renal vein thrombosis is rare, but it may cause
allograft loss if the diagnosis remains unrecognized.
Diastolic reversal of flow (Fig. 13) or absent flow in
the main renal artery has been documented in renal
transplant allografts with renal vein thrombosis
[43,47,48]. Both findings are nonspecific and may
occur with severe rejection [49], acute tubular necro-
sis, or acute interstitial nephritis [47]. Recognition of
the arterial waveform abnormality is useful to prompt
directed main renal vein evaluation for thrombus,
however. The normal main renal vein flow should
be antegrade with minimal variability, unlike the
rapid pulsatile waveforms of the renal artery.
Posttransplant allograft dysfunction
In a functioning, normal renal transplant, an RI of
0.5 to 0.7 has been generally reported [29]. Elevation
of the RI in a transplant has been described as an
indicator of allograft dysfunction (Fig. 14A) [50–52],
but it is not specific in determining the cause of the
allograft failure [52,53]. Elevated RIs may be associ-
ated with hydronephrosis (Fig. 14B). More worrisome
is a change in RIs over time without a morphologic
cause, such as hydronephrosis [54]. Interval increases
in RI are also nonspecific, however, and may be
caused by acute rejection, chronic rejection, acute

Fig. 14. Elevated RIs in two separate renal allografts. Spectral Doppler demonstrates increased RIs in segmental arterial
branches. (A) The RI of 0.91 was secondary to acute rejection 3 days after transplant, documented by Tc 99m MAG 3 study and
clinical findings. (B) The cause of the RI of 1 was severe hydronephrosis.
M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 409
tubular necrosis, or cyclosporine toxicity. The RI in a
transplant kidney may be elevated in the perioperative
period because of acute tubular necrosis [55].
Native kidney
Clinical
Sonography is commonly used in the evaluation
of abnormal renal function or evidence of urinary
pathology. In the emergency setting, ultrasound is
often the first imaging test to evaluate acute renal
failure, flank pain, hematuria, or a postbiopsy drop in
hematocrit because it is rapid and inexpensive and
does not use ionizing radiation or potentially neph-
rotoxic contrast agents. Ultrasound may help differ-
entiate between various causes of renal dysfunction
that may be clinically similar in physical examination
and laboratory tests.
For most chronic renal pathologic conditions, gray
scale ultrasound is adequate to differentiate medical
renal disease from hydronephrosis or renovascular
abnormality. Renal vascular abnormality and hydro-
nephrosis must be discerned from medical renal
disease, because the therapies differ. Renal artery
stenosis may be suggested by hypertension and renal
atrophy on gray scale images. Renal artery occlusion
may occur secondary to embolus or thrombus and
may affect the main renal artery or branches. Renal
vein thrombosis is another cause of renal failure.
Renal vein thrombosis may occur acutely and is
usually secondary to an underlying abnormality of
the kidney, abnormal hydration, or coagulation status.
The cause may be suggested in the presence of the
nonspecific finding of an enlarged kidney [56].
There are several situations in which the use of
Doppler ultrasound is more controversial. Doppler
ultrasound is not considered adequate for exclusion of
acute renal trauma [57]. Although gray scale ultra-
sound may grade the severity of hydronephrosis
caused by acute obstruction by a renal stone, Doppler
assessment of RIs in this clinical setting is no longer
generally performed. If hydronephrosis is detected
and there is clinical concern for ureteral calculus, a
noncontrast CT for urinary calculi is obtained.

Fig. 15. Pyelonephritis in a native kidney. Interval delay
transverse image using ultrasound contrast with agent detec-
tion imaging shows focal area of decreased perfusion (arrow)
in the mid-kidney. Ps, psoas; SP, spleen.
iol Clin N Am 42 (2004) 397–415
Sonographic technique
Sonographic settings and imaging technique for
evaluation of the kidneys must be optimized individ-
ually because the patient and scanning situation are
often suboptimal in the emergent setting. Flow de-
tection by color Doppler should be maximized with-
out introducing too much color artifact in the adjacent
tissues. The gain should be increased until artifact
occurs and then slightly reduced below the level
where artifacts are noted. Spectral Doppler should
use a gate that overlies most of the vessel diameter
and is angled with the direction of flow.
If evaluating for renal artery stenosis, complete
color and spectral Doppler of renal artery always
should be attempted. Any areas of turbulent flow or
aliasing on color Doppler should be evaluated closely
with gray scale and spectral Doppler for stenosis. The
arterial waveform of the aorta at the level of the renal
arteries should be obtained if renal artery stenosis is
suspected. If there is a focal site of injury, such as in a
renal biopsy, the biopsy site should be investigated
carefully with gray scale for adjacent hematoma and
Doppler for active hemorrhage. In this setting, any
intrarenal anechoic structure should be checked with
Doppler for the possibility of pseudoaneurysm.
Sonographic findings
Postbiopsy complications
Immediately after renal biopsy, color Doppler is
useful for evaluating active bleeding from the site
of biopsy. The authors generally wait approximately
2 minutes after the biopsy before looking for sig-
nificant bleeding, however, because brief bleeding
is common with the large 14- to 16-gauge biopsy
needles used. Hemorrhage and urinoma are the most
common complications after renal biopsy [32]. Ac-
tive hemorrhage is detected as a fountain of color
that originates from the edge of the renal parenchyma
on color Doppler. The scale and filters must be ad-
justed to optimize for detection of flow. Typically
there is no sonographic evidence of arteriovenous
fistula in the immediate postprocedural setting. Arte-
riovenous fistulas and pseudoaneurysms from renal
biopsies occasionally can be seen on subsequent ul-
trasound evaluations, however.
Severe acute urinary obstruction
Severe acute urinary obstruction may be associ-
ated with Doppler abnormalities. The RI may be ele-
vated in a severely hydronephrotic kidney [58–60].
Comparison of RIs with the contralateral normal
kidney also may be helpful [26]. The usefulness of
M.M. McNamara et al / Rad410
RI criteria is limited because of the lack of sensitivity
of Doppler for partial obstruction or moderate hydro-
nephrosis [61]. In pregnant patients with clinical
concern for ureteral obstruction and additional con-
cern about exposure to ionizing radiation, an RI more
than 0.7 or more than the contralateral kidney may be
accurate and useful for detecting obstruction [62].
Current clinical practice includes evaluating most
patients with suspected renal colic with noncontrast
CT rather than ultrasound.
Pyelonephritis
Pyelonephritis is a common clinical diagnosis in
the emergent setting that is often referred to a
radiologist for imaging. The differentiation between
pyelonephritis and cystitis may be difficult in a
patient with leukocytes in the urine. Ultrasound
may be requested to evaluate for renal abscess or
perinephric abscess. Color and power Doppler have
been documented to show focal peripheral areas of
decreased perfusion in an infected kidney [63]. Al-
though not approved in the United States for clinical
use within the urinary system, microbubble contrast
agents may demonstrate focal areas of infarction
associated with pyelonephritis with good detail and
may obviate the need for CT (Fig. 15) [64].

iol Clin N Am 42 (2004) 397–415 411
Renal vein thrombosis
Renal vein thrombosis is associated with dehy-
dration, hypercoagulability, renal disease, tumor, sur-
gery, extension of existing venous thrombus, and
trauma [65]. Color or power Doppler may detect ab-
sent renal vein flow or thrombus as a filling defect
within the detected flow [66,67] or demonstrate ab-
sent or slow flow. It is important to realize that
venous collaterals develop quickly after native renal
vein thrombosis, in contradistinction to the renal
transplant. It is important to evaluate the entire
renal vein—and not just the renal vein at the hi-
lum—if this diagnosis is a clinical consideration.
Monophasic venous flow is also abnormal and may
indicate collateral flow or incomplete thrombosis
[65]. Absent diastolic flow may be noted in the native
renal artery. Absent or reversed diastolic flow is
neither sensitive nor specific for renal vein thrombo-
sis in the native kidney, however [68].
Renal trauma
Gray scale ultrasound may detect a renal lacera-
tion or contusion in the emergency setting; however,
there is little use of color or spectral Doppler evalua-
tion of the kidneys in the setting of acute abdominal
trauma. The ability of ultrasound to visualize a renal
M.M. McNamara et al / Rad
Fig. 16. Renal artery stenosis in a native kidney. (A) Spectral Do
with a PSV of 57 cm/second. (B) Elevated PSV of 610 cm/second
which resulted in a renal artery to aorta PSV ratio of 10.7.
injury is low [57]. Although demonstration of active
hemorrhage may direct a surgeon to the appropriate
area of the body, absence of visualization does not
exclude a significant renal injury. Patients with active
extravasation of urine or blood are often treated with
conservative management [69] or angiographically
directed embolization.
Renal artery stenosis
Many sonographic criteria are reported for the
evaluation of renal artery stenosis in the native
kidneys with variable degrees of success [70]. The
most widely accepted criteria are based on direct
visualization of the main renal artery with elevated
PSV of more than 180 to 200 cm/second [70–72].
Stenosis may be detected as a focal area of turbulence
or an area aliasing on color Doppler, confirmed by
spectral Doppler [67,73]. Other direct criteria include
a ratio of the PSV within the renal artery divided by
the PSV of the aorta of at least 3.5:1 (Fig. 16A, B)
[74–76].
Several indirect criteria also have been suggested
and are sometimes reported in conjunction with direct
criteria to increase detection of renal artery stenosis.
The loss of the normal early systolic peak was the
most sensitive of the indirect criteria in one series
ppler demonstrates normal aorta (Doppler gate) waveform
is detected in the proximal main renal artery (Doppler gate),

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415412
[77]. Other criteria include the tardus-parvus wave-
form in the segmental renal arteries [67,78]. Delayed
acceleration time of the systolic upstroke has been
useful in some studies [79]. A difference in the RI
between the kidneys may suggest renal artery stenosis
[80]. A low RI can be seen downstream from an area
of focal narrowing in renal artery stenosis [81,82].
Poor detection of stenosis of accessory renal
arteries has been a limitation of ultrasound. In one
sonographic study of renal artery stenosis, nearly half
of the false-negative results were caused by stenosis
of an accessory renal artery [82]. A recent article
suggested that significant stenosis isolated to an
accessory renal artery occurs in only 1.5% of patients
with clinically significant renal artery stenosis [83].
Another important consideration in the assessment of
renal artery stenosis deals with the potential to correct
hypertension by angioplasty or surgery. In patients
with renal artery stenosis and RI more than 0.8, there
may be little improvement in a patient’s hypertension,
kidney survival, or renal function after repair of the
focal stenosis [84].
Renal artery occlusion is less common than renal
vein thrombosis, but it is also devastating to the
kidney. No flow is documented in the renal artery if
complete occlusion is present. Partial arterial throm-
bosis may be more difficult to detect, however, and
careful insonation of the entirety of the renal artery is
necessary. Segmental arterial occlusion is sonograph-
ically indistinguishable from decreased perfusion
secondary to pyelonephritis, which presents as a
focal area of decreased or absent flow on color or
power Doppler.
Summary
Doppler ultrasound is useful in the emergent
evaluation of the liver and kidney transplant patient.
Arterial stenosis, pseudoaneurysm, and venous throm-
bosis are treatable causes of allograft failure that can
be detected easily with color and spectral Doppler.
Doppler has a limited but important role in the
emergent evaluation of the native liver and kidneys,
usually involving prior biopsy or instrumentation.
Acknowledgments
The authors would like to thank Trish Thurman
for her assistance in manuscript preparation and
Anthony Zagar for photographic assistance.
References
[1] Martinez-Noguera A, Montserrat E, Torrubia S, Vil-
lalba J. Doppler in hepatic cirrhosis and chronic hepa-
titis. Semin Ultrasound CT MR 2002;23(1):19–36.
[2] Withers CE, Wilson SR. The liver. In: Rumack CM,
Wilson SR, Charboneau JW, editors. Diagnostic ultra-
sound. 2nd edition. St. Louis: Mosby Year Book; 1998.
p. 87–154.
[3] Cook GJR, Crofton ME. Hepatic artery thrombosis and
infarction: evolution of the ultrasound appearances
in liver transplant recipients. Br J Radiol 1997;70:
248–51.
[4] Nishida S, Kato T, Levi D, et al. Effect of protocol
Doppler ultrasonography and urgent revascularization
on early hepatic artery thrombosis after pediatric liver
transplantation. Arch Surg 2002;137:1279–83.
[5] Rode A, Ducerf C, Adham M, et al. Influence of sys-
tematic echo Doppler arterial survey on hepatic artery
thrombosis after liver transplantation in adults. Transpl
Int 1998;11(Suppl 1):S292–5.
[6] Dodd III GD, Memel DS, Zajko AB, Baron RL, Santa-
guida LA. Hepatic artery stenosis and thrombosis in
transplant recipients: Doppler diagnosis with resistive
index and systolic acceleration time. Radiology 1994;
192(3):657–61.
[7] Hamper UM. Doppler sonography in the evaluation of
liver transplants: advances in sonography. Presented at
the SRU 12th Annual Meeting. San Francisco, October
26, 2002.
[8] Kok T, Slooff MJH, Thijn CJP, et al. Routine Doppler
ultrasound for the detection of clinically unsuspected
vascular complications in the early postoperative phase
after orthotopic liver transplantation. Transpl Int 1998;
11:272–6.
[9] Grant EG, Schiller VL, Millener P, et al. Color Doppler
imaging of the hepatic vasculature. AJR Am J Roent-
genol 1992;159:943–50.
[10] Garcia-Criado A, Gilabert R, Salmeron JM, et al. Sig-
nificance of and contributing factors for a high resistive
index on Doppler sonography of the hepatic artery
immediately after surgery: prognostic implications for
liver transplant recipients. AJR Am J Roentgenol 2003;
181:831–8.
[11] Wachsberg RH, Bahramipour P, Sofocleous CT, Bar-
one A. Hepatofugal flow in the portal venous system:
pathophysiology, imaging findings, and diagnostic pit-
falls. RadioGraphics 2002;22(1):123–60.
[12] Kanterman RY, Darcy MD, Middleton WD, et al.
Doppler sonography findings associated with trans-
jugular intrahepatic portosystemic shunt malfunction.
AJR Am J Roentgenol 1997;164:467–72.
[13] Foshager MC, Ferral H, Finlay DE, Castaneda-Zuniga
WR, Letourneau JG. Color Doppler sonography of
transjugular intrahepatic portosystemic shunts (TIPS).
AJR Am J Roentgenol 1994;163:105–11.
[14] Ralls PW. Color Doppler sonography of the hepatic
artery and portal venous system. AJR Am J Roent-
genol 1990;155:517–25.

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 413
[15] Bodner G, Peer S, Fries D, Dessl A, Jaschke W. Color
and pulsed Doppler ultrasound findings in normally
functioning transjugular intrahepatic portosystemic
shunts. Eur J Ultrasound 2000;12:131–6.
[16] Weinreb J, Kumari S, Phillips G, Pochaczevsky R.
Portal vein measurements by real-time sonography.
AJR Am J Roentgenol 1982;139(3):497–9.
[17] Zwiebel WJ. Sonographic diagnosis of hepatic vascu-
lar disorders. Semin Ultrasound CT MR 1995;16(1):
34–48.
[18] Zizka J, Elias P, Krajina A, et al. Value of Doppler
sonography in revealing transjugular intrahepatic
portosystemic shunt malfunction: a 5-year experience
in 216 patients. AJR Am J Roentgenol 2000;175:
141–8.
[19] Lin EC, Middleton WD, Darcy MD, Teefey SA. He-
modynamics revealed by Doppler sonography in
patients who have undergone creation of transjugu-
lar intrahepatic portosystemic shunts: comparison of
10- and 12-mm metallic stents. AJR Am J Roentgenol
1999;172:1245–8.
[20] Middleton WD, Teefey SA, Darcy MD. Doppler evalu-
ation of transjugular intrahepatic portosystemic shunts.
Ultrasound Q 2003;19(2):56–70.
[21] Gallego C, Velasco M, Marcuello P, Tejedor D, De
Campo L, Friera A. Congenital and acquired anomalies
of the portal venous system. Radiographics 2002;22(1):
141–59.
[22] Atasoy KC, Fitoz S, Akyar G, Aytac� S, Erden I. Aneur-
ysms of the portal venous system Gray-scale and color
Doppler ultrasonographic findings with CT and MRI
correlation. Clin Imaging 1998;22(6):414–7.
[23] Tanaka S, Kitamura T, Fujita M, et al. Intrahepatic
venous and portal venous aneurysms examined by
color Doppler flow imaging. J Clin Ultrasound 1992;
20(2):89–98.
[24] Emamian SA, Nielsen MB, Pedersen JF, Ytte L. Kid-
ney dimensions at sonography: correlation with age,
sex, and habitus in 665 adult volunteers. AJR Am J
Roentgenol 1993;160:83–6.
[25] Cochran ST, Krasny RM, Danovitch GM, et al. Helical
CT angiography for examination of living renal donors.
AJR Am J Roentgenol 1997;168:1569–73.
[26] Platt JF, Rubin JM, Ellis JH. Distinction between ob-
structive and nonobstructive pyelocaliectasis with du-
plex Doppler sonography. AJR Am J Roentgenol 1989;
153:997–1000.
[27] Platt JF. Duplex Doppler evaluation of native kidney
dysfunction: obstruction and nonobstructive disease.
AJR Am J Roentgenol 1992;158:1035–42.
[28] Lopez-Ben R, Smith JK, Kew II CE, Kenney PJ, Julian
BA, Robbin ML. Focal posttransplantation lymphopro-
liferative disorder at the renal allograft hilum. AJR Am
J Roentgenol 2000;175:1417–22.
[29] Urbancic A, Buturovic-Panikvar J. Emergency intra-
and perioperative Doppler after kidney transplantation:
a guide for immediate surgical intervention. Transplant
Proc 2001;33:3320–1.
[30] Straiton JA, McMillan A, Morley P. Ultrasound in
suspected obstruction complicating renal transplanta-
tion. Br J Radiol 1989;62(741):803–6.
[31] Gottlieb RH, Lieberman JL, Pabico RC, Waldman DL.
Diagnosis of renal artery stenosis in transplanted
kidneys: value of Doppler waveform analysis of the
intrarenal arteries. AJR Am J Roentgenol 1995;165:
1441–6.
[32] Hubsch PJ, Mostbeck G, Barton PB. Evaluation of
arteriovenous fistulas and pseudoaneurysms in renal
allografts following percutaneous needle biopsy:
color-coded Doppler sonography versus duplex Dopp-
ler sonography. J Ultrasound Med 1991;9:95–100.
[33] Tobben PJ, Zajko AB, Sumkin JH, et al. Pseudoaneu-
rysms complicating organ transplantation: roles of CT:
duplex sonography, and angiography. Radiology 1988;
169:65–70.
[34] Merkus JWS, Zeebregts CJAM, Hoitsma AJ, van
Asten WNJC, Koene RAP, Skotnicki SH. High inci-
dence of arteriovenous fistula after biopsy of kidney
allografts. Br J Surg 1993;80(3):310–2.
[35] Middleton WD, Picus Daniel D, Marx MV, Melson
GL. Color Doppler sonography of hemodialysis vas-
cular access: comparison with angiography. Am J
Radiol 1989;152:633–9.
[36] Renowden SA, Blethyn J, Cochlin DL. Duplex and
colour flow sonography in the diagnosis of post-biopsy
arteriovenous fistulae in the transplant kidney. Clin
Radiol 1992;45:233–7.
[37] Middleton MA, Middleton WD, Wiele K. Sonography
case of the day: postbiopsy renal transplant arteriove-
nous fistula. AJR Am J Roentgenol 1989;152:1323–4.
[38] Dodd III GD, Tubin ME, Shah A, Zajko AB. Imaging
of vascular complications associated with renal trans-
plants. AJR Am J Roentgenol 1991;157:449–59.
[39] Taylor KJW, Morse SS, Rigsby CM, Bia M, Schiff M.
Vascular complications in renal allografts: detection
with duplex Doppler US. Radiology 1987;162(1):
31–8.
[40] Faenza A, Spolaore R, Poggioli G, Selleri S, Roversi
R, Gozzetti G. Renal artery stenosis after renal trans-
plantation. Kidney Int 1983;23(Suppl 14):S54–9.
[41] Helenon O, Melki P, Correas JM, Boyer JC, Moreau
JF. Renovascular disease: Doppler ultrasound. Semin
Ultrasound CT MR 1997;18(2):136–46.
[42] Turetschek K, Nasel C, Wunderbaldinger P, Diem K,
Hittmair K, Mostbeck GH. Power Doppler versus color
Doppler imaging in renal allograft evaluation. J Ultra-
sound Med 1996;15:517–22.
[43] Pozniak MA, Dodd III GD, Kelcz F. Ultrasonographic
evaluation of renal transplantation. Radiol Clin N Am
1992;30(5):1053–66.
[44] Handa N, Fukunaga R, Uehara A, et al. Echo-Doppler
velocimeter in the diagnosis of hypertensive patients:
the renal artery Doppler technique. Ultrasound Med
Biol 1986;12(12):945–52.
[45] Voiculescu A, Hollenbeck M, Plum J, et al. Iliac artery
stenosis proximal to a kidney transplant: clinical find-
ings, duplex-sonographic criteria, treatment, and out-
come. Transplantation 2003;76(2):332–9.

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415414
[46] Nghiem DD, Ercolani L, Corry RJ. Stenosis of the
iliac artery: an unusual cause of hypertension in the re-
nal transplant recipient. Transplant Proc 1983;15(4):
2161–3.
[47] Kaveggia LP, Perella RR, Grant EG, Tessler FN, Ro-
senthal JT, Danovitch GM. Duplex Doppler sonogra-
phy in renal allografts: the significance of reversed
flow in diastole. AJR Am J Roentgenol 1990;155:
295–8.
[48] Baxter GM, Morley P, Dall B. Acute renal vein throm-
bosis in renal allografts: new Doppler ultrasonic find-
ings. Clin Radiol 1991;43:125–7.
[49] Reuther G, Wanjura D, Bauer H. Acute renal vein
thrombosis in renal allografts: detection with duplex
Doppler US. Radiology 1989;170:557–8.
[50] Rifkin MD, Needleman L, Pasto ME, et al. Evaluation
of renal transplant rejection by duplex Doppler exami-
nation: value of the resistive index. AJR Am J Roent-
genol 1987;148:759–62.
[51] Rigsby CM, Taylor KJW, Weltin G, et al. Renal allo-
grafts in acute rejection: evaluation using duplex so-
nography. Radiology 1986;158:375–8.
[52] Genkins SM, Sanfilippo FP, Carroll BA. Duplex Dopp-
ler sonography of renal transplants: lack of sensitivity
and specificity in establishing pathologic diagnosis.
AJR Am J Roentgenol 1989;152:535–9.
[53] Perrella RR, Duerinckx AJ, Tessler FN, et al. Evalua-
tion of renal transplant dysfunction by duplex Doppler
sonography: a prospective study and review of the
literature. Am J Kidney Dis 1990;15(6):544–50.
[54] Hollenbeck M, Hilbert N, Meusel F, Grabensee B. In-
creasing sensitivity and specificity of Doppler sono-
graphic detection of renal transplant rejection with
serial investigation technique. Clin Invest 1994;72:
609–15.
[55] Harris DCH, Antico V, Allen R, et al. Doppler assess-
ment in renal transplantation. Transplant Proc 1989;
21(1):1895–6.
[56] Braun B. Ultrasonic demonstration of renal vein
thrombosis. Radiology 1981;138:157–8.
[57] McGahan JP, Richards JR, Jones CD, Gerscovich EO.
Use of ultrasonography in the patient with acute renal
trauma. J Ultrasound Med 1999;18:207–13.
[58] Platt JF, Rubin JM, Ellis JH. Acute renal obstruction:
evaluation with intrarenal duplex Doppler and conven-
tional US. Radiology 1993;186(3):685–8.
[59] Rodgers PM, Bates JA, Irving HC. Intrarenal Doppler
ultrasound studies in normal and acutely obstructed
kidneys. Br J Radiol 1992;65(771):207–12.
[60] Gottlieb RH, Luhmann IV K, Oates RP. Duplex ultra-
sound evaluation of normal native kidneys and native
kidneys with urinary tract obstruction. J Ultrasound
Med 1989;8:609–11.
[61] Chen JH, Pu YS, Liu SP, Chiu TY. Renal hemodynam-
ics in patients with obstructive uropathy evaluated by
duplex Doppler sonography. J Urol 1993;150:18–21.
[62] Shokeir AA, Mahran MR, Abdulmaaboud M. Renal
colic in pregnant women: role of renal resistive index.
Urology 2000;55(3):344–7.
[63] Dacher JN, Pfister C, Monroc M, Eurin D, Dosseur PL.
Power Doppler sonographic pattern of acute pyelone-
phritis in children: comparison with CT. AJR Am J
Roentgenol 1996;166:1451–5.
[64] Robbin ML, Lockhart ME, Barr RG. Renal imaging
with US contrast: current status. Radiol Clin N Am
2003;41(5):963–78.
[65] Mulligan SA, Koslin DB, Berland LL. Duplex evalua-
tion of native renal vessels and renal allografts. Semin
Ultrasound CT MR 1992;13(1):40–52.
[66] Platt JF, Ellis JH, Rubin JM. Intrarenal arterial Doppler
sonography in the detection of renal vein thrombosis of
the native kidney. AJR Am J Roentgenol 1994;162:
1367–70.
[67] Helenon O, el Rody F, Correas JM, et al. Color Dopp-
ler US of renovascular disease in native kidneys.
RadioGraphics 1995;15(4):833–54.
[68] Platt JF. Doppler ultrasound of the kidney. Semin Ul-
trasound CT MR 1997;18(1):22–32.
[69] Husmann DA, Gilling PJ, Perry MO, Morris JS, Boone
TB. Major renal lacerations with a devitalized fragment
following blunt abdominal trauma: a comparison be-
tween nonoperative (expectant) versus surgical man-
agement. J Urol 1993;150:1774–7.
[70] Stavros AT, Harshfield D. Renal Doppler, renal artery
stenosis, and renovascular hypertension: direct and in-
direct duplex sonographic abnormalities in patients
with renal artery stenosis. Ultrasound Q 1994;4:
217–63.
[71] House MK, Dowling RJ, King P, Gibson RN. Using
Doppler sonography to reveal renal artery stenosis: an
evaluation of optimal imaging parameters. AJR Am J
Roentgenol 1999;173:761–5.
[72] Pellerito J.S. Renal artery stenosis: advances in sonog-
raphy. Society of Radiologists in Ultrasound, 12th An-
nual Meeting and Postgraduate Educational Course,
San Francisco, October 25–27, 2002.
[73] Dubbins PA. Renal artery stenosis: duplex Doppler
evaluation. Br J Radiol 1986;59:225–9.
[74] Kohler TR, Zierler RE, Martin RL, et al. Noninvasive
diagnosis of renal artery stenosis by ultrasonic duplex
scanning. J Vasc Surg 1986;4(5):450–6.
[75] Taylor DC, Kettler MD, Moneta GL, et al. Duplex ul-
trasound scanning in the diagnosis of renal artery ste-
nosis: a prospective evaluation. J Vasc Surg 1988;7(2):
363–9.
[76] Strandness Jr DE. Duplex scanning in diagnosis of re-
novascular hypertension. Surg Clin N Am 1990;70(1):
109–17.
[77] Stavros T, Harshfield D. Renal Doppler, renal artery
stenosis, and renovascular hypertension: direct and in-
direct duplex sonographic abnormalities in patients
with renal artery stenosis. Ultrasound Q 1994;12(4):
217–63.
[78] Downey DB. The retroperitoneum and great vessels.
In: Rumack CM, Wilson SR, Charboneau JW, editors.
Diagnostic ultrasound. 2nd edition. St. Louis: Mosby
Year Book; 1998. p. 453–86.
[79] Handa N, Fukunaga R, Uehara A, et al. Efficacy of

M.M. McNamara et al / Radiol Clin N Am 42 (2004) 397–415 415
echo-Doppler examination for the evaluation of reno-
vascular disease. UltrasoundMedBiol 1988;14(1):1–5.
[80] Schwerk WB, Testrepo IK, Stellwaag M, Klose KJ,
Schade-Brittinger C. Renal artery stenosis: grading
with image-directed Doppler US evaluation of renal
resistive index. Radiology 1994;190(3):785–90.
[81] Bude RO, Rubin JM, Platt JF, Fechner KP, Adler RS.
Pulsus tardus: its cause and potential limitations in
detection of arterial stenosis. Radiology 1994;190(3):
779–84.
[82] Kliewer MA, Tupler RH, Carroll BA, et al. Renal ar-
tery stenosis: analysis of Doppler waveform parame-
ters and tardus-parvus pattern. Radiology 1993;189(3):
779–87.
[83] Bude RO, Forauer AR, Caoili EM, Nghiem HV. Is it
necessary to study accessory arteries when screening
the renal arteries for renovascular hypertension. Radi-
ology 2003;226(2):411–6.
[84] Radermacher J, Chavan A, Bleck J, et al. Use of Dopp-
ler ultrasonography to predict the outcome of therapy
for renal-artery stenosis. N Engl J Med 2001;344(6):
410–7.

Radiol Clin N Am 42 (2004) 417–425
Emergency ultrasound in trauma patients
John P. McGahan, MDa,*, John Richards, MDb, Maria Luisa C. Fogata, MDa
aDivision of Diagnostic Radiology, University of California, Davis, School of Medicine, 4860 Y Street, Suite 3100,
Sacramento, CA 95817, USAbDivision of Emergency Medicine, University of California, Davis, School of Medicine, 2315 Stockton Boulevard,
PSSB 2100, Sacramento, CA 95817, USA
Although ultrasound (US) was first described in documented that sonographic sensitivity for the de-
the detection of blunt traumatic splenic injuries more
than 30 years ago [1], it was never widely advocated
until approximately 10 years ago [2–4]. There are
probably two reasons for the initial limited use of
sonography in blunt traumatized patients. The first is
that the use of CT evolved at approximately the
same time and was shown to be highly sensitive for
evaluation of blunt abdominal trauma [5]. CT not
only detected free fluid but also directly demonstrated
the organ injury. Sonography also was used initially
to detect specific organ injury rather than the free
fluid associated with the injury. There were limita-
tions in the ability and sensitivity of sonography in
directly demonstrating the injured organ. It was not
until the 1990s that the focused abdominal sonogra-
phy for trauma (FAST) was developed for the main
objective of detecting free fluid in patients with blunt
abdominal trauma [2–4].
Sonographic examination
The initial focus of sonographic examination was
a single view of the hepatorenal fossa (Morison’s
pouch) [2]. It was soon realized that a more compre-
hensive examination of the abdomen improved de-
tection of free fluid, however [4]. This included
examinations of both upper quadrants, the paracolic
gutters, and pelvis. In 1997, McGahan et al [4]
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2003.12.005
* Corresponding author.
E-mail address: [email protected]
(J.P. McGahan).
tection of free fluid could be improved by having a
full bladder. Often in traumatized patients a Foley
catheter is placed and the bladder is decompressed,
which eliminates the acoustic window in the pelvis
needed to detect small or moderate amounts of free
fluid. More recently, in an article by Hahn et al [6],
patients with proven intra-abdominal injuries after
blunt abdominal trauma were evaluated and it was
demonstrated that the finding of free fluid with
sonography was important. Seventy-eight percent of
patients with free fluid on sonography required lapa-
rotomy, whereas only 27% without free fluid needed
laparotomy. They also showed that examination of
Morison’s pouch had the highest detection rate of
free fluid in these patients (66%), whereas free fluid
was detected 56% of the time in the upper quadrants,
48% of the time in the paracolic gutters, and 36% of
the time in the pelvis. Examination of all areas was
important, however, because 3 of the 604 patients
with intra-abdominal injuries had free fluid only in
paracolic gutters [6]. At our institution we always
include an examination of the heart for pericardial
fluid as a part of the FAST scan. US is also useful in
examinations of the chest for pneumothorax or pleu-
ral effusion, which are discussed later in this article.
Sonographic findings
Free fluid
Free fluid typically appears as a hypoechoic
region within the peritoneal cavity or pelvis and is
usually linear or triangular in shape (Fig. 1). The
s reserved.

Fig. 1. Patterns of free fluid. (A) Real-time US examination of the right upper quadrant demonstrates small triangular-shaped
hypoechoic region (arrow) that corresponds to free fluid. (B) Real-time US of the right upper quadrant demonstrates larger
hypoechoic region, with acute angles (arrow), noted just inferior to the liver and the right kidney that corresponds to free fluid.
(C) In the same patient as B, linear hypoechoic region in the hepatorenal fossa (Morison’s pouch) corresponds to free
fluid (arrow).
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425418
shape of the fluid depends on its compression by the
surrounding structures. For instance, in Morison’s
pouch, the fluid between the kidney and liver usually
has a linear shape (see Fig. 1). Fluid that surrounds
bowel often appears triangular. Fluid often accumu-
lates at the site of injury but then flows throughout
the abdomen and into the pelvis. At the site of in-
jury, the blood may appear echogenic as it forms a
clot adjacent to the injured organ (Figs. 2, 3). There
maybe several pitfalls in recognition of free fluid
within the abdomen (Box 1).
Pitfalls
Patients with pre-existing ascites or iatrogenic
free fluid (eg, dialysis patients) may have false-
positive sonogram results. It is impossible in these
patients to know if the free fluid is caused by pre-
existing ascites, traumatic injury, or a combination of
the two. In women of childbearing age, a small
amount of ‘‘physiologic’’ free fluid may be noted in
the pelvis. It is important to recognize that although
this free fluid is most likely pre-existing and probably
physiologic, it may be secondary to an injury. In
this situation, searching for free fluid in other sites
is important.
Loops of fluid-filled bowel should not be con-
fused with free intraperitoneal fluid. Bowel loops
can be distinguished from free fluid because they
are round and have peristalsis. This should cause little
confusion. In almost all recent studies of the use
of sonography for detection of free fluid in patients
with blunt abdominal trauma, the specificity of so-
nography is high [4]. In some cases sonography may
detect small amounts of free fluid that are not vi-
sualized with CT [4].
Sonographic sensitivity in detecting injuries in
patients with blunt abdominal trauma may be de-
creased for several reasons. The sensitivity of sonog-
raphy for detection of free fluid in the pelvis may be
decreased if a full bladder is not used. With the
bladder decompressed after placement of a Foley
catheter, free fluid in the dependant portion of the
pelvis can be missed. Another potential pitfall of US
detection of free fluid is that hematomas may appear
echogenic. With severe injury, clotted blood at the

Fig. 2. Echogenic clot/liver laceration. (A) Real-time US examination of the right upper quadrant of the abdomen shows right
kidney (RTK) and echogenic clot anterior to the liver (RT LOBE). (B) Real-time examination of the liver demonstrates fairly well
marginated echogenic region in the liver (arrows) that corresponds to liver laceration.
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425 419
site of the injury may be echogenic and should not be
overlooked (see Figs. 2, 3). Finally, there is often no
free fluid associated with contained injuries of solid
organs, such as the liver, spleen, or kidney. In the
article by Hahn et al [6], in several patients no free
fluid was detected, yet 27% of these patients required
laparotomy. This may be the greatest pitfall of the
FAST scan and is discussed later in this article.
Finally, sonography is limited and unable to show
some types of injuries, including spinal and pelvic
fractures, bowel and mesentery injuries, pancreatic
injuries, vascular injuries, diaphragmatic ruptures,
and adrenal injuries [4].
Fig. 3. Subcapsular hematoma of the spleen. Longitudinal
real-time US of the spleen demonstrates well-demarcated,
slightly hyperechoic region along the anterior aspect of the
spleen (arrow) that corresponds to subcapsular hematoma.
(From McGahan JP, Wang L, Richards JR. From the RSNA
refresher courses: focused abdominal US for trauma. Ra-
diographics 2001;21(Spec No):S191–9; with permission.)
Free fluid scoring systems
Scoring systems have been developed to help
stratify patients into groups who may or may not
require laparotomy. Others have stratified patients
based on either the amount of free fluid in one
location or the number of locations in which free
fluid was detected. For instance, Sirlin et al [7,8]
described a scoring system based on the location of
the fluid. For each anatomic region in which fluid
was detected, one point was given. The percentage of
patients with a score of 0 who had intra-abdominal
injury or required surgical intervention (based on this
scoring system) was 1.4% and 0.4%, respectively.
For the score of 1, the rate of intra-abdominal injury
was 59%, and the rate of surgical intervention was
13%. The rate of intra-abdominal injury increased to
85% and rate of surgical intervention was 36%, for
a score of 2. For a score of 3, the percentage of pa-
Box 1. Pitfalls in examination of theabdomen for free fluid
� Pre-existing fluid (ascites)� Iatrogenic free fluid as in dialysis ordirect peritoneal lavage
� Pelvic fluid (female)� Loops of fluid filled bowel� Incomplete or empty bladder� Echogenic clot� Contained injury

Fig. 4. Splenic laceration. US examination of the left up-
per quadrant demonstrates poorly marginated spleen with
mixed echo pattern (arrows), which corresponds to severe
splenic laceration.
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425420
tients with intra-abdominal injury remained static at
83%, but rate of surgical intervention was 63%. The
higher the score, the higher the injury rate and the
greater the need for laparotomy. Others have advo-
cated scoring systems based on the number of free
fluid sites or the vertical height of free fluid [9,10]. A
common theme would be the more the amount of
free fluid, the greater the likelihood of injury or the
need for surgical intervention.
Sensitivity of sonography
The sensitivity of sonography depends on what is
used as the ‘‘gold’’ standard to which US is com-
pared. When sonographic results are compared with
clinical outcome, the sensitivity rates of sonography
are high, usually more than 95% [11–13]. McGahan
et al [4] calculated a sensitivity rate of only 63%
when sonography was compared with CT or laparot-
omy and not using clinical observation as a gold
standard. The probable reason for this discrepancy
in sensitivities is that McGahan et al [4] showed that
several minor lacerations of the liver or spleen were
detected on CT but not detected by FAST. These
patients did not require surgical intervention, and all
improved clinically. If clinical improvement had
been used as the ‘‘gold’’ standard, these patients
would have been deemed as having true negative
results. When using CT as the ‘‘gold’’ standard,
however, they were deemed as having false-negative
results. This is the main reason for discrepancies in
the sensitivities of FAST scan.
Numerous other studies have been published on
the topic of the sensitivity of FAST. For instance, in
744 pediatric patients with blunt abdominal trauma,
Richards et al [14] demonstrated a sonographic sen-
sitivity rate of 68% for detecting free fluid or solid
organ injuries. In a large review of 3264 patients, this
same study group showed that sonography had a sen-
sitivity rate of 67% in detection of intra-abdominal
injury [15]. Other results from recent literature vary.
Miller et al [16] reported a sensitivity rate of 42%
for the FAST scan when compared with CT. Polletti
et al [17] demonstrated a sensitivity rate of 93% for
sonography, however. Other studies have shown that
sonography may miss injuries that may require sur-
gery. Dolich et al [18] reported on 43 patients with
false-negative sonography results, 10 of whom (33%)
required surgery. Shanmuganathan et al [19] studied
the use of sonography in more than 11,000 patients
with blunt abdominal trauma: 467 patients had intra-
abdominal injury, 310 (66%) of whom had free fluid
detected by sonography. This detection rate is simi-
lar to past studies. In this larger study by Shanmuga-
nathan et al, 157 patients (34%) with intra-abdominal
injury had no free fluid, and 26 of these patients
required surgery or further intervention. Sonography
can be used to triage patients, but one must remember
that it may miss significant injuries that require
further intervention. CT should be used for patients
with a negative sonography result in whom there is a
suggestion of intra-abdominal injury [20,21].
Solid organ injury
After the initial studies on the use of sonography
in detecting organ injuries in the 1970s [1], more
recent studies focused on the detection of free fluid
[11–13]. A few recent studies have demonstrated the
ability of sonography to detect parenchymal organ
abnormalities directly. Rothhin et al [12] reported a
sensitivity rate of 41.4% for the direct detection of
solid organ injuries by sonography. McGahan et al [4]
also reported a sensitivity rate of 41% detection in
solid organ injuries. More recently, Polletti et al [17]
showed a sensitivity rate of 41% for direct demon-
stration of organ injury. Stengel et al [22] showed
that a 7.5-MHz linear ray probe detected solid or-
gan injuries much more readily than a 3.5-MHz
convex probe.
Sonographic appearance of solid organ injuries
Much of the work on sonographic classification
and appearance of solid organ injuries has been
performed by McGahan et al [23,24] and Richards
et al [25,26]. When identified, acute solid organ
injuries are often echogenic on sonography. A diffuse
heterogeneous echogenic pattern is the predominant

J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425 421
pattern identified with splenic injuries (Fig. 4). A dis-
crete hyperechoic or diffuse hyperechoic pattern is
seen with hepatic injuries (see Fig. 2). Renal injuries
are echogenic, with a disorganized appearance that
occurs with severe renal lacerations (Fig. 5).
More recently, contrast-enhanced abdominal US
has been used in the evaluation of solid organ inju-
ries in trauma patients (Fig. 6). For instance, Marte-
gani et al [27] presented the preliminary evaluation
of micro-bubble–enhanced US of abdominal organs
in blunt and penetrating trauma. They evaluated
14 patients with abdominal trauma who were scanned
with unenhanced US and contrast-enhanced sonogra-
phy. These authors use SonoVue (Bracco/ ALTANA
Pharm, Konstanz, Germany), a phospholipid coated
micro-bubble, at the dose of 1.2 to 2.4 mL scanned
with a low mechanical index. The liver, spleen, and
kidneys were studied over a 3- to 5-minute interval.
They demonstrated that on the unenhanced scan, no
lesions were confidently visualized. Excellent en-
hancement of the parenchymal organs was obtained
in all cases using contrast-enhanced sonography,
however. They detected injuries in the liver in 5 pa-
tients, the spleen in 5 patients, and the kidney in
4 patients. In 7 patients there was confirmation with
CT, and there was good correlation between contrast-
enhanced sonography and contrast-enhanced CT in
terms of the position and size of the abnormality.
The authors believed that the contrast-enhanced so-
nography might expedite management of trauma
patients [27].
The chest
Sonography has been shown to detect pleural
effusions [28]. In traumatized patients, sonography
Fig. 5. Renal laceration. (A) Longitudinal scan of the right uppe
without reniform shape, which corresponds to severe renal lacer
performed immediately after the US examination. (B) Real-time
an echogenic region inferior to the kidney in the right paracolic g
can be used to diagnose pneumothorax or free fluid
within the thorax. More recently, sonography also
has been shown to be helpful in diagnosing peri-
cardial effusions [29,30] in traumatized patients. The
main reason for diagnosing pericardial effusions is to
prevent patients from having a traumatically induced
pericardial tamponade. We incorporate the subcostal
view of the heart as a portion of the FAST scan in all
patients with blunt abdominal trauma. This is helpful
in diagnosing pericardial effusions (Fig. 7). It must
be emphasized that inexperienced examiners often
have problems diagnosing pericardial effusions. For
instance, Blavias et al [30] set up a study with
emergency medicine residents and fellows trained in
sonography. They had trouble discerning the epicar-
dial fat, which appeared hypoechoic on US, from a
true pericardial effusion. Sonography had a sensitiv-
ity rate of 73% and a specificity rate of only 44%
in this study [30]. With more experienced examiners,
sonography may be useful in detecting moderate
pericardial effusions.
More recently, sonography also has been proved
to be useful in diagnosing pneumothorax [31,32]. The
parietal pleura adheres to the inner muscle of the tho-
rax, whereas the visceral pleura adheres to the lung.
During inspiration and expiration the visceral pleura
‘‘slides’’ back and forth adjacent to the parietal
pleura. The bright echogenic line of the visceral
pleura, which adheres to the lung as it moves and
slides during normal inspiration and expiration, may
be observed on real-time sonography and is a normal
finding (Fig. 8). Absence of the sliding lung is a
direct sign of pneumothorax (Fig. 9). Remembering
that the free air within the thorax rises to the most
nondependent portion of the thoracic cavity, the US
probe is placed in this area to check for pneumotho-
r quadrant of the abdomen demonstrates ill-defined region
ation (shattered kidney) (arrows). Right nephrectomy was
US examination of the right paracolic gutter demonstrates
utter that corresponds to hematoma (arrow).

Fig. 6. Contrast-enhanced US of splenic laceration. (A) Noncontrast US of the spleen appears normal. (B) Contrast-enhanced US
with SonoVue demonstrates a large, wedge-shaped defect in the central portion of the spleen. (C) Correlative CT demonstrates
splenic laceration. (Courtesy of Thomas Albrecht, MD, FRCR, Berlin, Germany.)
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425422
rax. Either a curved array probe or, better yet, a linear
array probe may be used to detect pneumothorax. The
US probe is placed in the intercostal space. The
normal ‘‘to and fro’’ motion of the visceral pleura
against the parietal pleura is observed in a normal
Fig. 7. Pericardial effusion. Subcostal real-time US of the
heart demonstrates anechoic region (long arrow) anterior
to the heart, which corresponds to pericardial effusion.
patient. The normal motion of the visceral pleura
against the parietal pleura is absent with pneumotho-
rax, however. In a normal patient, a ‘‘reverberation
artifact’’ usually is noted posterior to the parietal
visceral pleura interface in a normal patient (see
Fig. 8). This is observed as lines that are equally
spaced from one another and gradually decrease in
echogenicity. This is the reverberation of the US
beam as it strikes the interface between the parietal
and visceral pleura and the air in the lung and is
reflected back to the transducer. This reverberation
produces multiple equally spaced echoes. The rever-
beration artifact is not identified when there is a
pneumothorax. A pneumothorax may produce acous-
tic shadowing. Absence or decrease of the reverber-
ation artifact also may occur in a normal patient if
the gain settings are set too low.
An article by Rowan et al [33] compared the
accuracy of sonography with that of the supine
chest radiograph in detecting traumatic pneumotho-
rax, with CT serving as the reference or ‘‘gold’’
standard. They studied 27 patients who sustained

Fig. 8. Normal lung. (A) Real-time US examination using linear array probe demonstrates the appearance of the normal lung on
US. Note that the first echogenic line (open arrow) corresponds to the interface between the parietal and the visceral pleura.
Parallel equally spaced lines of decreasing echogenicity are observed posterior to this, which corresponds to reverberation
artifacts (arrows). (B) Drawing of reverberation artifact. The US probe is placed on the skin surface (S). R refers to the interface
between the parietal and visceral pleura. Lines labeled as numbers 1 and 2, which are of decreasing echogenicity posterior to this,
correspond to reverberation artifacts caused by the US beam ‘‘reverberating’’ or ‘‘bouncing’’ between the pleura and transducer.
(C) Similar pattern is seen with sector scan of the lung in another patient.
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425 423
blunt thoracic trauma and had US. The radiographic
and US findings were compared with CT findings.
Eleven of 27 patients had pneumothoraces as seen
with CT. All of the pneumothoraces were detected
by sonography, for a sensitivity rate of 100%. The
specificity rate of sonography was 94%, and 1 of
16 patients had a false-positive diagnosis of pneu-
mothorax. Supine chest radiography had a sensitivity
rate of only 36% (4 of 11 patients), with a specificity
rate of 100%. In their study, US was more sensitive

Fig. 9. Small pneumothorax. Real-time US examination of
thorax in this patient with a small pneumothorax demon-
strates the echogenic line that corresponds to the parietal
and visceral pleura, which is noted to the left side of image.
Note more distal reverberation artifacts. To the right side
of the image there is loss of this pattern because of a
small pneumothorax.
J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425424
than chest radiography in the detection of trauma-
tic pneumothoraces.
Summary
US will be used more frequently in the future for
the evaluation of traumatized patients. Previously,
the main focus of the sonographic examination was
for the detection of free fluid. Unstable patients with
free fluid often can be triaged to the operation room
without further imaging tests. In patients who are
more stable or in whom US results are negative, CT
is required. Based on recent studies, sonography has
a sensitivity rate of approximately 40% in direct
detection of solid organ injuries. In the future, how-
ever, with the use of contrast-enhanced agents, so-
nography may more reliably detect solid organ
injuries. Within the chest, US has been shown to be
helpful in detecting pleural effusions and may be
useful in detecting pericardial effusions. US has been
shown to be sensitive in detecting pneumothoraces in
traumatized patients.
References
[1] Kristensen JK, Buemann B, Kuehl E. Ultrasonic scan-
ning in the diagnosis of splenic haematomas. Acta
Chir Scand 1971;137:653–7.
[2] Jehle D, Guarino J, Karamanoukian H. Emergency
department ultrasound in the evaluation of blunt ab-
dominal trauma. Am J Emerg Med 1993;11:342–6.
[3] Kimura A, Otsuka T. Emergency center ultrasonogra-
phy in the evaluation of hemoperitoneum: a prospec-
tive study. J Trauma 1991;31:20–3.
[4] McGahan JP, Rose J, Coates TL, Wisner DH, New-
berry P. Use of ultrasonography in the patient with
acute abdominal trauma. J Ultrasound Med 1997;16:
653–62.
[5] Federle MP, Griffiths B, Minagl H, Jeffrey Jr RB.
Splenic trauma: evaluation with CT. Radiology 1987;
162:69–71.
[6] Hahn DD, Offerman SR, Homes JF. Clinical impor-
tance of intraperitoneal fluid in patients with blunt
intra-abdominal injury. Am J Emerg Med 2002;20:
595–600.
[7] Sirlin CB, Casola G, Brown MA, Patel N, Bendavid
EJ, Hoyt DB. Patterns of fluid accumulation on screen-
ing ultrasonography for blunt abdominal trauma:
comparison with site of injury. J Ultrasound Med
2001;20:351–7.
[8] Sirlin CB, Casola G, Brown MA, Patel N, Bendavid
EJ, Hoyt DB. Quantification of fluid on screening
ultrasonography for blunt abdominal trauma: a simple
scoring system to predict severity of injury. J Ultra-
sound Med 2001;20:359–64.
[9] Huang MS, Liu M, Wu JK, Shih HC, Ko TJ, Lee
CH. Ultrasonography for the evaluation of hemoperi-
toneum during resuscitation: a simple scoring system.
J Trauma 1994;36:173–7.
[10] McKenney KL, McKenney MG, Nunez DB, et al.
Interpreting the trauma ultrasound: observations in
62 positive cases. Emerg Radiol 1996;3:113–7.
[11] McKenney MG, Martin L, Lentz K, Lopez C, Sleeman
D, Aristide G, et al. 1,000 consecutive ultrasounds for
blunt abdominal trauma. J Trauma 1996;40:607–10.
[12] Rothlin MA, Naf R, Amgwerd M, Candinas D, Frick
T, Trentz O. Ultrasound in blunt abdominal and tho-
racic trauma. J Trauma 1993;34:488–95.
[13] Rozycki GS, Ochsner MG, Jaffin JH, Champion HR.
Prospective evaluation of surgeons’ use of ultrasound
in the evaluation of trauma patients. J Trauma 1993;
34:516–26.
[14] Richards JR, Knopf NA, Wang L, McGahan JP. Blunt
abdominal trauma in children: evaluation with emer-
gency US. Radiology 2002;222:749–54.
[15] Richards JR, Schleper NH, Woo BD, Bohnen PA,
McGahan JP. Sonographic assessment of blunt ab-

J.P. McGahan et al / Radiol Clin N Am 42 (2004) 417–425 425
dominal trauma: a 4-year prospective study. J Clin
Ultrasound 2002;30:59–67.
[16] Miller MT, Pasquale MD, Bromberg WJ, Wasser TE,
Cox J. Not so fast. J Trauma 2003;54:52–9.
[17] Polletti PA, Kinkel K, Vermeulen B, Irmay F, Unger
PF, Terrier F. Blunt abdominal trauma: should US
be used to detect both free fluid and organ injuries?
Radiology 2003;227:95–103.
[18] Dolich MO, McKenney MG, Varela JE, Compton RP,
McKenney KL, Cohn SM. 2,576 ultrasounds for blunt
abdominal trauma. J Trauma 2001;50:108–12.
[19] Shanmuganathan K, Mirvis SE, Sherbourne CD, Chiu
WC, Rodriguez A. Hemoperitoneum as the sole indi-
cator of abdominal visceral injuries: a potential limita-
tion of screening abdominal US for trauma. Radiology
1999;212:423–30.
[20] McGahan JP, Richards J, Gillen M. The focused ab-
dominal sonography for trauma scan: pearls and pit-
falls. J Ultrasound Med 2002;21:789–800.
[21] McGahan JP, Richards JR. Blunt abdominal trauma:
the role of emergent sonography and a review of the
literature. AJR Am J Roentgenol 1999;172:897–903.
[22] Stengel D, Bauwens K, Sehouli J, Nantke J, Ekkern-
kamp A. Discriminatory power of 3.5 MHz convex and
7.5 MHz linear ultrasound probes for the imaging of
traumatic splenic lesions: a feasibility study. J Trauma
2001;51:37–43.
[23] McGahan JP, Richards JR, Jones CD, Gerscovich EO.
Use of ultrasonography in the patient with acute renal
trauma. J Ultrasound Med 1999;18:207–13.
[24] McGahan JP, Wang L, Richards JR. From the RSNA
refresher courses: focused abdominal US for trauma.
Radiographics 2001;21(Spec No):S191–9.
[25] Richards JR, McGahan JP, Jones CD, Zhan S, Gersco-
vich E. Ultrasound detection of blunt splenic injury.
Injury 2001;32:95–103.
[26] Richards JR, McGahan JP, Pali MJ, Bohnen PA. Sono-
graphic detection of blunt hepatic trauma: hemoperito-
neum and parenchymal patterns of injury. J Trauma
1999;47:1092–7.
[27] Martegani A, Cosgrove DO, Del Favero C, Aiani L,
Harvey CJ. Contrast enhanced abdominal ultrasound
in trauma using SonoVue. Radiology 2002;225(P):358.
[28] Ma OJ, Mateer JR. Trauma ultrasound examination
versus chest radiography in the detection of hemo-
thorax. Ann Emerg Med 1997;29:312–6.
[29] Aaland MO, Bryan III FC, Sherman R. Two-di-
mensional echocardiogram in hemodynamically stable
victims of penetrating precordial trauma. Am Surg
1994;60:412–5.
[30] Blaivas M, DeBehnke D, Phelan MB. Potential errors
in the diagnosis of pericardial effusion on trauma ul-
trasound for penetrating injuries. Acad Emerg Med
2000;7:1261–6.
[31] Dulchavsky SA, Schwarz KL, Kirkpatrick AW, et al.
Prospective evaluation of thoracic ultrasound in the
detection of pneumothorax. J Trauma 2001;50:201–5.
[32] Sargsyan AE, Hamilton DR, Nicolaou S, et al. Ultra-
sound evaluation of the magnitude of pneumothorax:
a new concept. Am Surg 2001;67:232–6.
[33] Rowan KR, Kirkpatrick AW, Liu D, Forkheim KE,
Mayo JR, Nicolaou S. Traumatic pneumothorax detec-
tion with thoracic US: correlation with chest radiogra-
phy and CT. Initial experience. Radiology 2002;225:
210–4.

Radiol Clin N Am 42 (2004) 427–443
Priapism
Hossein Sadeghi-Nejad, MDa,b,*, Vikram Dogra, MDc, Allen D. Seftel, MDd,Mamdouh A. Mohamed, MDd,e
aDivision of Urology, University of Medicine and Dentistry of New Jersey, Medical School, 185 South Orange Avenue,
MSB G536, Newark, NJ 07103-2714, USAbCenter for Human Sexuality and Male Reproductive Medicine, Hackensack University Medical Center, 20 Prospect Avenue,
#711, Hackensack, NJ 07601, USAcDivision of Ultrasound, Department of Radiology, Case Western Reserve University, University Hospitals, 11100 Euclid Avenue,
Cleveland, OH 44106, USAdDepartment of Urology, Case Western Reserve University, University Hospitals of Cleveland,
Cleveland Veterans Affairs Medical Center, 11100 Euclid Avenue, Cleveland, OH 44106–5046, USAeDepartment of Urology, El-Mina University Hospital, El-Mina, Egypt
Priapism is a relatively uncommon medical con- Definition
dition that is defined as a pathologic prolonged en-
gorgement or erection of the penis or clitoris that is
unrelated to sexual arousal. Recent advances in the
study of erectile physiology and the pathophysiology
of erectile dysfunction have resulted in better under-
standing of the processes leading to various subtypes
of priapism and the factors implicated in its resolu-
tion or recurrence. Despite these advances, there is a
paucity of randomized studies and basic science
investigations pertaining to priapism. The recently
published American Urological Association (AUA)
Guideline on the management of priapism sheds
further light on the management of this potentially
emergent condition, but the guideline ‘‘does not es-
tablish a fixed set of rules or define the legal standard
of care for the treatment of priapism’’ [1].
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.008
* Corresponding author. Division of Urology, Univer-
sity of Medicine and Dentistry of New Jersey, Medical
School, 185 South Orange Avenue, MSB G536, Newark,
NJ 07103-2714.
E-mail addresses: [email protected],
www.hsadeghi.com (H. Sadeghi-Nejad).
The term ‘‘priapism’’ is derived from Priapus, a
minor god of fertility, luck, and the deity of gardens
and fields in Greek mythology [2]. A famous painting
in the entrance to the House of Vettii in Pompeii
depicts Priapus with a disproportionately large phal-
lus, leaning against a pillar and weighing his massive
penis. Conditions related to the prolonged engorge-
ment of the penis were associated with Priapus in
the Greek language and were later assimilated into
Latin and modern languages [2]. In the early twenti-
eth century, Hinman [3] classified priapism as either
mechanical or nervous in etiology and suggested
corporal vein thrombosis as the cause of mechanical
priapism. The condition is more common in men and
typically involves the paired corpora cavernosa, al-
though rare exceptions with involvement of the
corpus spongiosum and sparing of the cavernosal
spaces have been reported [4].
Priapism is broadly classified as low-flow (ische-
mic) or high-flow (arterial and nonischemic). Low-
flow priapism and the associated severe decrease in
venous drainage from the corpora cavernosa is a
potential medical emergency and may lead to irre-
versible ischemic tissue changes. High-flow priapism
is less commonly encountered and involves unregu-
s reserved.

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443428
lated inflow that is typically secondary to some form
of arterial trauma. One of the earliest reports of
arterial priapism was published in 1960 following a
case of traumatic coitus that was surgically managed
by ligation of the internal pudendal artery [5]. Unlike
the ischemic subtype, arterial priapism is not consid-
ered an emergency: the patient does not have pain
and spontaneous resolution is the likely outcome in
more than half the cases. Hauri et al [6] elaborated on
the different management approaches to arterial ver-
sus veno-occlusive priapism and was one of the first
to suggest that the prognosis of the latter is far less
favorable than arterial priapism. Nonetheless, the
long-term outcome of nonischemic priapism has not
been thoroughly investigated and it is clear that
completely normal erectile function after these epi-
sodes cannot be guaranteed in all cases. Stuttering
priapism refers to a condition of recurrent, intermit-
tent, painful erections. These episodes are more
common in patients with various hemoglobinopa-
thies. Stuttering priapism is especially troublesome
for both the affected patient, facing repeated painful
episodes and potential emergency room visits, and
the physician challenged to arrive at a practical and
efficacious management plan for the patient. Malig-
nant priapism is a rare clinical entity that is caused
by metastasis of solid tumors to the penis.
Sonographic anatomy of the penis
The penis is composed of two dorsal corpora
cavernosa and one ventral corpus spongiosum. The
two corpora cavernosa are enclosed in a fibrous
sheath, the tunica albuginea, which partially covers
the corpus spongiosum. The tunica albuginea is com-
posed of elastic fibers that form an irregular, latticed
network on which collagen fibers rest. The septum
between the two corpora cavernosa is complete proxi-
mally and is incomplete in its distal two thirds. The
corpora cavernosa join beneath the pubis (penile
hilum) to form the major portion of the body of the
penis. The corpora cavernosa are composed of si-
nusoidal spaces lined by smooth muscles (erectile
tissue) and endothelium. The glans penis is formed
by the expansion of the corpus spongiosum.
The corpus spongiosum is traversed throughout
its length by the anterior urethra, which begins at the
perineal membrane. The corpus spongiosum provides
support to the urethra and helps with the expulsion
of semen from the urethra. Buck’s fascia surrounds
both cavernosal bodies dorsally and splits to sur-
round the spongiosum ventrally (Fig. 1).
The penile blood vessels arise from the internal
pudendal artery. The common penile artery continues
in the Alcock’s canal above the perineal membrane
and terminates in three branches to supply the erectile
bodies. The bulbourethral artery supplies the urethra,
spongiosum, and the glans. The cavernosal artery
enters the corpora cavernosa on the superomedial
surface of the penis. The cavernosal artery travels in
the center of each corporal body and gives off straight
and helicine arteries. Helicine arteries form a bridge
between the cavernosal artery and the lacunar spaces
in the corpora cavernosa [7]. It is the cavernosal artery
and its branches that dilate and bring extra blood to the
erectile tissue during penile erection. The dorsal artery
of the penis passes between the crus penis and the
pubis to reach the dorsal surface of the corporal
bodies. The dorsal artery mainly supplies blood to
the glans and runs between the dorsal vein and the
dorsal penile nerve. The venous blood is returned by
the venous plexus beneath the tunica albuginea. The
emissary veins perforate the tunica albuginea, and
the blood is drained by the venae circumflexae into
the deep dorsal veins.
Sonographic technique
A penile sonographic examination is performed
with the patient supine with the penis lying on the
anterior abdominal wall or supported with towels
between the thighs. High frequency (7.5–12 MHz)
linear array ultrasound transducers provide high-reso-
lution images of the penis [7]. Copious amounts of
acoustic gel should be used on the surface of the
penis to optimize visualization and avoid excessive
compression by the transducer.
Transverse images of the penis are recorded start-
ing at the level of the glans and moving down to the
base of the penis. The two corpora cavernosa are iden-
tified as two adjacent circular hypoechoic structures.
The tunica albuginea is identified as a hyperechoic
linear structure covering the corpora. The cavernosal
artery is visualized on the medial portion of each
corpora cavernosa. The corpus spongiosum is often
compressed and is difficult to visualize from the ven-
tral aspect (see Fig. 1). Longitudinal evaluation of the
corporal bodies should also be obtained and recorded.
During the transverse and longitudinal scanning, close
attention should be given to any plaques, calcific foci,
or arteriovenous fistulas. In the case of veno-occlu-
sive priapism, the sonographer should be extremely
gentle while performing the sonographic examination
because this is an exceedingly painful condition.

Dorsal Artery
CavernosalArtery
CorpusCavernosum
Corpus Spongiosum
Dorsal Veins
Tunica Albuginea
Buck's Fascia
Urethra
A
Internal Pudendal Artery
Dorsal Artery
Cavernosal Artery
Helicine Arteries
Bulbar ArterySpongiosal Artery
C
Fig. 1. (A) Diagrammatic representation of penile anatomy in cross-section. (B) Corresponding gray-scale ultrasound image.
(C) Diagrammatic representation of penile anatomy in longitudinal view. (From Fitzgerald SW, Erickson SJ, Foley WD, et al.
Color Doppler sonography in the evaluation of erectile dysfunction. Radiographics 1992;12(1):3–17; with permission.)
H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 429

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443430
The presence of the cavernosal artery in each
corpora cavernosa along with a spectral Doppler
waveform of each should be obtained and recorded.
Color Doppler images in both transverse and longi-
tudinal views should also be obtained.
Epidemiology and etiology
Eland et al [8] have evaluated the incidence of
priapism in the general population. These investiga-
tors conducted a population-based retrospective co-
hort study using a longitudinal observational database
from the patient records of a group of general practi-
tioners in The Netherlands. They found an overall
incidence rate of 1.5 per 100,000 person-years. The
incidence rate in men 40 years old and older was
2.9 per 100,000 person-years. The authors acknowl-
edged that not all patients with priapism seek medical
care and the reported data may be an underestimation
of the actual rate in the general population. The
incidence of priapism in special at-risk subpopula-
tions is much higher. At-risk populations include men
with cocaine drug use, advanced pelvic or hemato-
logic malignancy, and those on antipsychotic medi-
cations [9–12]. Pohl et al [13] evaluated various
etiologies for priapism in a study of 230 single case
reports in the literature: idiopathic causes comprised
one-third of the cases, whereas 21% were attributed
to alcohol abuse or medications, 12% to perineal
trauma, and 11% to sickle cell anemia (SCA) [13].
For individuals on intracorporal injection ther-
apy for erectile dysfunction, the incidence range of
priapism episodes is from 1% for those on prostaglan-
din E1 and as high as 17% for patients who receive
intracorporeal injections of papaverine [14]. The most
likely cause of prolonged erection as a result of
intracavernous injection therapy is overdosage. Proper
injection technique and gradual upward titration of the
dose by the patient helps decrease this adverse event.
Priapism associated with sickle cell disease is
classically described as ischemic, although rare ex-
ceptions of high-flow priapism in association with
sickle cell disease have been reported. The pathophys-
iology of high-flow priapism in patients with sickle
cell disease is not known [15]. Fowler et al [16]
evaluated the incidence and prevalence of priapism
in sickle cell conditions. The authors reported fre-
quent self-limited priapistic episodes, mostly occur-
ring during sleep, which last less than 3 hours.
Priapism associated with SCA was unusual before
puberty and in keeping with the previously reported
6% prevalence of priapism in children with SCA
[16,17]. No correlations are observed between the
average number of priapism episodes per year and
the duration of a typical episode. A similar study from
Jamaica documented a 42% prevalence of priapism in
SCA patients [18]. Priapism was significantly associ-
ated with low hemoglobin F levels and high platelet
counts and over one fourth of those who had suffered
priapism had some degree of impotence. A more
recent survey of patients with homozygous SCA
(hemoglobin SS) and sickle cell b(0) thalassemia
(hemoglobin S-b[0]) between 5 and 20 years of age
found an 89% actuarial probability of experiencing
priapism by 20 years of age. The mean duration of an
episode in this study was 125 minutes. Episodes
typically occurred around 4:00 AM, and 75% of the
patients surveyed had at least one episode starting
during sleep or on awakening from sleep [19].
Drug-induced priapism has been reported with a
variety of medications, most commonly related to
the antihypertensive drugs guanethidine, prazosin,
and hydralazine and psychotropic medications [20].
Antipsychotics are associated with a small, but defi-
nite risk of priapism and the most commonly cited
agents are trazodone (Desyrel), thioridazine, and
chlorpromazine [21]. Abber et al [22] investigated
the mechanism of drug-induced priapism in dogs by
intravenous and intracorporeal injection of the anti-
psychotic agent chlorpromazine and the antidepres-
sant trazodone. The authors demonstrated that both
drugs induced erection in a manner similar to that of
intracorporeal injection of papaverine and showed
venous restriction and slight increases in internal
pudendal arterial flow at the beginning of tumescence.
The authors stated that the a-adrenergic antagonist
properties of chlorpromazine and trazodone probably
cause priapism by local action. Psychotropic-induced
priapism is almost always associated with low-flow
pathology and is currently believed to be caused by
the a1-adrenergic antagonism of these medications.
Chlorpromazine and thioridazine are conventional
antipsychotics with the greatest a1-adrenergic affin-
ity and have been most frequently reported to be
associated with priapism [9]. The exact pathophysiol-
ogy has not been elucidated, but is likely multifacto-
rial and may be related to the ratio of a-adrenergicblockade to anticholinergic activity. Risperidone,
olanzapine, and clozapine are the atypical antipsy-
chotics that have been reported to cause priapism on
rare occasions [9].
It has been reported that trazodone and cocaine
may have synergistic effects in promoting priapism
and their combination may pose an additional risk of
priapism. Clinicians should be aware of the possible
additive risk of priapism in this patient population,

Box 1. Etiology (AFUD classification)
� Drug induced� Hematologic� Sickle cell disease and other hemo-globinopathies
� Thrombophilia states (protein C andother thrombophilias, lupus)
� Hyperviscosity states (hyperleukocy-tosis, polycythemia)
� Idiopathic� Central nervous system mediated� Other
H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 431
because trazodone is commonly used as a hypnotic
and is often chosen for polysubstance abusers because
of its low abuse potential [23]. Cocaine-induced
priapism has been reported in association with topical
application to enhance sexual performance, and intra-
nasal and intracavernous injections [24–26]. Priapism
has also been reported in association with the recrea-
tional drug ecstasy [27].
Androgens have been implicated as an important
etiologic factor with reports of priapism in hypogo-
nadal men receiving gonadotropin-releasing hormone
or high-dose testosterone, testosterone-induced pria-
pism in adolescents with SCA, and priapism after
androstenedione intake for athletic performance en-
hancement [28–31].
Examples of neurologic etiologic factors include
priapism in patients with degenerative stenosis of
the lumbar canal, where symptoms may be fully re-
lieved by surgical decompression, and priapism
secondary to cauda equina syndrome (following de-
generative stenosis of the lumbar canal and lumbar
arachnoiditis), herniated disk, or blockage of the
central inhibitory influences as seen during general
or regional anesthesia.
Noteworthy reports of systemic illnesses impli-
cated as etiologic factors include reports of priapism
occurring in widespread amyloidosis [32]. Other un-
common etiologies include glucose phosphate isom-
erase deficiency (third most commonly occurring
erythroenzymopathy), which can cause priapism
through increased rigidity of red blood cell membrane
and resultant increased blood viscosity, cell sludging
in the corpora, and increased acidity; Fabry’s disease
(glycosphingolipid lipidosis) presenting with a com-
bination of renal insufficiency and priapism; high
concentration (ie, 20% rather than 10%) fat emulsion
in total parenteral nutrition; and paradoxical throm-
boembolic events in heparin- or warfarin-induced
priapism [33–37]. Possible etiologies for increased
thromboembolic events in total parenteral nutrition–
induced priapism include increased blood coagulabil-
ity and fat emboli and direct cellular effects by high fat
content. Increased platelet function assessed by the
levels of antiheparin platelet factor 4 and b-thrombo-
globulin has been documented in priapism following
20% fat emulsion total parenteral nutrition [35].
The mechanism of malignant priapism has not
been definitively elucidated, but may be caused by
extensive organ replacement by carcinoma, venous
obstruction by the tumor, or continual stimulus to the
erectile afferent or efferent neural pathways [38].
Tumor infiltration is most frequently from the bladder
and prostate (32% and 28%, respectively) followed by
kidney (17%), gastrointestinal tract (8%), and rarely
from testis, lung, liver, bone, and sarcomas as the
primary source [39]. It has been reported that 20% to
53% of cases of penile metastasis from other primary
tumors initially present with priapism [40].
When Witt et al [41] published their paper on
traumatic laceration of intracavernosal arteries and
the pathophysiology of nonischemic high-flow pria-
pism in 1990, only five additional cases of priapism
with similar features to the reported case were cited.
Although more attention has been focused on this
subtype of priapism and numerous related papers have
been published since the early 1990s, there is general
agreement that arterial priapism is far less common
than the ischemic variant. It is estimated that the
condition is rare enough that few urologists treat more
than two cases in their lifetime [42]. Nonetheless,
because the presentation of arterial priapism is pain-
less and far less distressful to the patient, it is entirely
possible that many more cases of arterial priapism
are unreported. Nonischemic priapism has been de-
scribed in a variety of conditions causing perineal
trauma including bicycling and other straddle injuries
[43–47]. The resultant injury to the arterial system
and formation of an arteriolacunar fistula is most often
implicated as the causative factor in nonischemic
high-flow priapism. The venous outflow system is
typically unaffected in these conditions and the blood
in the corpora remains well oxygenated. The condi-
tion may also be iatrogenic following deep dorsal
vein arterialization for vasculogenic impotence [48].
This etiology is exceedingly unlikely to be reported in
the future, however, because deep dorsal vein arteri-
alization is rarely performed anymore. The most
common etiology for high-flow priapism in children
is traumatic arterial laceration, but cases associated

Box 2. Etiologic factors in priapism
Low-flow states (veno-occlusive orischemic type)
� Hemoglobinopathies and sickle celldisease
� Thrombophilia states (lupus,protein C)
� Warfarin or heparin induced� Fabry’s disease� Dialysis� Total parenteral nutrition (high fatcontent)
� Vasculitis� Hematologic malignancies� Pelvic or lower genitourinary tract(bladder and prostate) cancer andmetastatic (ie, renal) malignancies
� Psychotropics and antidepressants(chlorpromazine, trazodone,risperidol)
� Antihypertensives (guanethidine,hydralazine, prazosin)
� Erectogenic agents (intracavernosalvasoactives; sildenafil; intraurethralprostaglandin E1)
� Spinal cord stenosis� Amyloidosis� Glucose phosphate isomerasedeficiency
� Alcohol� Androgens or testosterone
High-flow states (arterial or nonischemictype)
� Penile or perineal trauma� Straddle injury� Cavernosal artery injury� Arteriosinusoidal fistula� Cocaine� Metastatic malignancy� Fabry’s disease� Iatrogenic (following deep dorsal veinarterialization)
H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443432
with inherited metabolic disorders (ie, Fabry’s dis-
ease) or hematologic diseases, such as SCA, also have
been described [49–51].
Box 1 is a classification of priapism by etiology
as agreed on by the American Foundation for Uro-
logic Disease (AFUD) Thought Leader Panel on Pria-
pism [43,52]. A more detailed list of etiologic factors
based on low-flow versus high-flow subtypes of
priapism is shown in Box 2.
Pathophysiology
In broad terms, priapism may be regarded as an
imbalance between arterial inflow and outflow. Bur-
nett [53] has recently reviewed the pathophysiology
of priapism and suggested derangements in the di-
verse systems of regulatory control in erectile func-
tion. These dysregulatory functions include possible
overactivity of the veno-occlusive mechanism, arte-
rial inflow, or neurogenic processes that can affect
inflow or outflow. Conversely, the problem may be
secondary to malfunction of the normal contractile
activities of cavernosal smooth muscle cells.
Low flow
Ischemic or veno-occlusive priapism is a medical
emergency and the most common form of priapism.
It is characterized by a painful, rigid erection; absent
cavernosal blood flow; and severely acidotic corpora
(Fig. 2). The spectrum of clinical symptoms and signs
is analogous to those found in other compartment
syndromes and mandates immediate decompression
to minimize the chances of long-term sequelae. The
combination of venous outflow obstruction, high-
pressure chambers, and poor-to-absent inflow can
lead to trabecular interstitial edema and ultrastruc-
tural changes in trabecular smooth muscle cells and
functional transformation to fibroblast-like cells. In
priapism lasting more than 24 hours, severe cellular
damage and widespread necrosis may occur [54].
Destruction of the endothelial lining, formation of
blood clots within the corpora, and widespread trans-
formation of the smooth muscle cells to fibroblast-like
cells or necrosis occurs in cases lasting beyond
48 hours and eventually results in irreversible erectile
dysfunction [54]. Lack of these changes in priapism
lasting less than 12 hours emphasizes the importance
of patient education and early intervention.
In an animal model, anoxia has been shown to
eliminate spontaneous and drug-induced contractile
activity, suggesting a likely explanation for the failure
of penile injection of a-adrenergic agonists to reverse
prolonged ischemic priapism when the penis is in its
maximal rigid state [55]. The failure of detumescence
seen in low-flow priapism may be secondary to failed
a-adrenergic neurotransmission, endothelin deficit, or

Fig. 2. Low-flow priapism in a patient with sickle cell
disease. Longitudinal sonogram of the corpora cavernosa
demonstrates high-resistance flow in the cavernosal artery
suggestive of priapism. Cavernosal arterial flow is usually
absent in patients with low-flow priapism; however, high-
resistance flow may be observed.
H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 433
inactivation of intracellular cofactors of smooth mus-
cle contraction caused by hypoxia or hypercarbia [55].
Recurrent episodes of veno-occlusive priapism,
occurring anywhere from a few times monthly to
recurrent daily episodes, are quite disabling and often
have an idiopathic etiology. Levine et al [56] evalu-
ated six patients with recurrent veno-occlusive pria-
pism and ruled out mechanical occlusion of corporeal
venous drainage by demonstrating elevated flows to
maintain intracavernosal pressures following smooth
muscle contraction and markedly decreased flow rates
following smooth muscle relaxation. The authors
proposed that a functional alteration of the adrenergic
or endothelial-mediated mechanisms that control pe-
nile tumescence and maintain penile flaccidity may
develop secondary to the initial ischemic episode and
reported that the use of oral phenylpropanolamine
reduced the frequency and duration of the recurrences,
and markedly reduced the need for adrenergic self-
injection. Treatment of the recurrent episodes with
intracavernous self-injection of phenylephrine re-
sulted in successful detumescence in that series and
the authors’ experience with similar cases. The pa-
tients must be instructed on the proper and early
use of phenylephrine self-injections. Most recently,
Lin et al [57] have postulated that the mechanism
of stuttering priapism in patients with sickle cell
hemoglobinopathies may involve abnormally low
expression of phosphodiesterase type 5 secondary to
hypoxia. In the human corpus cavernosum, phos-
phodiesterase type 5 is responsible for degradation
of cGMP and phosphodiesterase type 5 inhibitors,
such as sildenafil and vardenafil, have become the
mainstay of oral pharmacotherapy in the treatment of
erectile dysfunction.
Seftel et al [58] have reported on two cases of
veno-occlusive priapism refractory to conventional
therapy that later converted to high-flow priapism.
The authors suggested that the high-flow state ob-
served after treatment of veno-occlusive priapism may
represent a variant of nonischemic priapism or, alter-
natively, may be the pathophysiology of recurrent
idiopathic priapism.
Neurologic control of the efferent erectile pathway
is by the pelvic nerves that are joined by the pregan-
glionic parasympathetic nerves. The pelvic nerves
join the pelvic plexus that gives rise to the cavernous
nerve of the penis. Normally, penile stimulation
causes reflexogenic erections that are primarily con-
trolled by the sacral parasympathetic nerves originat-
ing from the S2-4 segment located at the T11-L1
vertebral levels. The afferent limb of the erection
response is mediated by the dorsal penile nerve
(a branch of the pudendal nerve), which transmits
sensory impulses to the spinal cord. The role of the
sympathetic nervous system in penile erection is not
entirely clear, but its activation is generally associated
with contraction of corpus cavernosal smooth muscle
and penile detumescence. The neuropathophysiology
of priapism in patients with lumbar stenosis has not
been fully elucidated, but it is postulated that it may
be caused by parasympathetic efferent hyperactivity
in the S2-4 cauda equina nerve roots within the
narrowed thecal sac. The parasympathetic hyperactiv-
ity may be secondary to increased intrathecal pressure
at the stenotic level and altered circulation within the
cauda equina during walking [59].
Sickle cell hemoglobinopathy results from the
inheritance of one or two genes coding for an abnor-
mal S hemoglobin and manifests in 0.15% of black
Americans in the form of sickle cell disease (homo-
zygous for hemoglobin S) and in 8% as sickle cell trait
(heterozygous for hemoglobin S). Inheritance of a
combination of a hemoglobin S gene and a second
gene coding for abnormal hemoglobin (ie, B + thal-
assemia or C hemoglobin) is possible and, as in the
homozygous type, may result in ischemic complica-

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443434
tions [16]. The pathophysiology of SCA-induced
priapism is thought to result from decreased oxygen
tension and pH developing in stagnant blood within
the corporal sinusoids, which in turn leads to a cycle
of erythrocyte sickling and sludging followed by even
more hypoxemia and acidosis [60]. Although most
cases are of the low-flow ischemic type, high-flow
priapism may be observed in patients with sickle cell
hemoglobinopathy in rare instances [15].
High flow
Nonischemic or arterial priapism is a less common
form of priapism that presents clinically as a painless
erection that typically follows some type of penile or
perineal trauma leading to unregulated arterial inflow
into the sinusoidal space. Unlike the veno-occlusive
variant, high-flow priapism is not an emergency: the
outflow mechanism is intact and the cavernosal milieu
is not anoxic. The penis is often not maximally rigid
in these cases, but intercourse may be possible. Other
clinical observations include delayed onset of pria-
pism after perineal trauma and a state of constant
suboptimal rigidity that may become more rigid with
arousal [61]. Diagnosis is typically based on the
aforementioned clinical history and physical exami-
nation, and demonstration of arterial blood on aspi-
rated cavernosal blood gas studies. A number of
recent studies have pointed to cycling trauma as the
cause of both transient neurogenic impotence and
vasculogenic pathologies in the form of arterial pria-
pism or permanent erectile dysfunction [43,46,62].
Spycher and Hauri [54] have shown that at the level of
trabecular smooth muscle cells, the ultrastructural
changes and fibroblast-like cellular transformation
seen in low-flow states do not occur with arteriogenic
priapism, even when the latter has been present for
prolonged (as late as 5 months) periods. A mechanism
for the pathophysiology of high-flow priapism is
described by Goldstein’s group in Boston: unlike a
traditional arteriovenous fistula, the condition is de-
scribed as an arterial-lacunar fistula where the helicine
arteries are bypassed and the blood passes directly into
the lacunar spaces. In turn, the high flow in the lacunar
space creates shear stress in adjacent areas, leading
to increased nitric oxide release, activation of the
cGMP pathway, and smooth muscle relaxation and
trabecular dilatation [61]. The authors also postulate
that the delay in onset of high-flow priapism may be
secondary to a delay in the complete necrosis of the
arterial wall after the initial penile or perineal trauma.
Alternatively, the delay may be secondary to clot
formation at the site of injury followed by the normal
lytic pathways, which follow in a few days.
Diagnosis
Physicians caring for patients with priapism should
remember at all times the significant anxiety and fear
experienced by most patients with this condition and
make a genuine effort to alleviate their apprehension.
A thorough history and physical examination are
prerequisites to diagnostic accuracy. The sexual and
medical history should especially focus on medica-
tions, trauma, and predisposing comorbidities. Pres-
ence or absence of pain is a fairly reliable predictor of
low-flow versus high-flow priapism, respectively. The
latter diagnosis is further suggested by a history
of penile or perineal trauma. Absence of pain in arte-
rial priapism frequently results in less patient anxiety
and discomfort as compared with veno-occlusive
priapism. Consequently, those with arterial priapism
may present days or even weeks after the original
injury. The fundamental aim of the initial phase of
assessment is to distinguish arterial from ischemic
priapism. The AFUD panel recommendations for the
management of priapism are illustrated in Fig. 3 and
follow a step-care model that has been modified and
refined over the years [43,52,63].
Physical examination of the penis is critical and
typically reveals firm corpora cavernosa and a soft
glans, indicating sparing of the corpus spongiosum in
low-flow priapism. Findings in high-flow states usu-
ally reveal a partial to full erection and sparing of the
corpus spongiosum in most cases (as in low-flow
states). General diagnostic tests include urine toxicol-
ogy screening for psychoactive drugs and metabolites
of cocaine [10,43]. These tests are particularly helpful
if the diagnosis is unclear. The AFUD panel has
additionally suggested reticulocyte count (if indi-
cated); urinalysis (if indicated); complete blood count;
platelets, and differential white blood cell count; and
urologic consultation. The reticulocyte count is often
elevated in men with SCA. The most important
warning with regard to hematologic testing is to
remember that hemoglobinopathies are not restricted
to African American men and other groups, especially
those of Mediterranean descent, may be affected
(ie, thalassemia or sickle-thalassemia). The sickledex
test and examination of the peripheral smear are less
time consuming than hemoglobin electrophoresis and
may be more appropriate for the emergency room
setting. These recommendations are similarly empha-
sized in the more recent AUA guideline on pria-
pism [1].
Urologic management of priapism includes his-
tory and physical (including penile) examination, and
assessment of corporal blood flow status (corporal
aspirate and visual inspection by color and consist-

Fig. 3. Step-care treatment model for the management of priapism recommended by the AFUD thought leader panel. CA,
cavernosal artery; CBC, complete blood count; DDU, duplex Doppler ultrasonography; HB, hemoglobin; NB, nerve block; PE,
physical examination; PSA, prostate-specific antigen; UA, urinalysis; VS, vital signs. (Data from references [43] and [52].)
H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 435
ency or corporal blood gas including pH, PO2, and
PCO2, or penile duplex Doppler ultrasound) [43].
Low-flow priapism is suggested by finding low
oxygen, high carbon dioxide, and low pH in the
blood gas analysis of the aspirate. When a high-flow
state is suspected based on the bright red appearance
or blood gas analysis of the corporal aspirate, duplex
Doppler sonography may identify a dilated caver-
nosal artery or pseudocapsule formation at the site of
arterial sinusoidal fistula. These findings are helpful
if superselective arterial embolization is performed
[64]. The AUA Guideline states that the use of penile
arteriography for the identification of the site of a
cavernous artery fistula may be warranted in some
cases, but that arteriography has been largely replaced
by color duplex sonography and the former is only

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443436
used as part of an embolization procedure [1]. Fur-
thermore, penile aspiration has mainly a diagnostic
role in the management of arterial priapism (not
therapeutic). Although the data reviewed by the
AUA guideline panel did not reveal any instances
of arterial priapism resolution after aspiration or
irrigation, two separate case reports in the literature
have documented the rare resolution of arterial pria-
pism after aspiration or irrigation in cases of adult
and pediatric posttraumatic priapism [65,66].
Patients presenting with refractory low-flow
priapism who later convert to a high-flow state
represent a less common cohort of priapism patients.
Because the management of the low-flow and high-
flow states is radically different, sonography should
be considered if conventional corporal irrigation and
intracavernosal sympathomimetics (ie, phenyleph-
rine) fail to resolve the initial veno-occlusive pria-
pism [58]. When a hemoglobinopathy is suspected,
hemoglobin electrophoresis may be performed. The
AFUD panel has also recommended testing for pros-
tate-specific antigen when indicated.
Role of radiology in the diagnosis and treatment of
priapism
Most of the reports on the use of sonographic
imaging in the diagnostic and therapeutic algorithms
of priapism are focused on the high-flow variant,
although sonography may be used instead of blood
gas sampling to differentiate ischemic (low-flow
priapism) from high-flow priapism. Color duplex
Doppler sonography has replaced arteriography as
the imaging modality of choice for the diagnosis of
priapism. Penile color duplex Doppler sonography is
noninvasive, does not expose the patient to ionizing
radiation, and can reveal important information re-
garding the location of arterial injury in high-flow
priapism. Most published studies on the subject indi-
cate that in experienced hands, differentiation of the
increased color flow on the affected side from the
normal flow on the contralateral side is not problem-
atic. Two important papers from Goldstein’s group
at Boston University have shown color Doppler
ultrasound to be as sensitive as angiography for the
diagnosis of high-flow priapism [61,67]. More spe-
cifically, penile duplex Doppler sonography had a
sensitivity of 100% and a specificity of 73% with a
predictive value of 81% for a positive test and 100%
for a negative test [67]. Mabjeesh et al [68] have
reported therapeutic use of color duplex Doppler
ultrasound in one patient in whom sonography was
used to localize the fistula and subsequently apply
external compression to achieve permanent fistula
occlusion and resolution of priapism.
In a posttraumatic case of priapism with an arterial
tear, gray-scale ultrasound reveals an irregular hypo-
echoic region secondary to tissue injury or distended
lacunar spaces in the corpus cavernosum. This irregu-
lar area appears with well-circumscribed margins
analogous to a capsule formation if the injury has
been long-standing [69]. The arteries exhibit normal
or increased flows within the cavernosal arteries and
an irregular flow from the artery to the cavernosal
body at the site of injury. Arterial signs may be seen
in the pseudoaneurysm and, unlike veno-occlusive
priapism, increased venous flow may be observed in
high-flow priapism [42]. The arterial lacunar fistula
seen in high-flow priapism essentially bypasses the
helicine arteries and appears as a characteristic color
blush extending into the cavernosal tissue on color
duplex sonography. It is reported that 90% of fistulas
in adults appear as unilateral, whereas at least 50% of
arterial priapism in children is associated with bilat-
eral or multiple arterial lacerations [42,51]. Bertolotto
et al [69] recommend increasing the color Doppler
velocity scale for better detection of the cavernosal
artery tear region as a focal area with very high flow.
Because aspiration is only used for diagnostic pur-
poses in cases of arterial priapism, if the history is
suggestive of high-flow pathology and color duplex
sonography is conclusive, the patient may be spared
the discomfort of needle aspiration. Kang et al [70]
warn about the potential difficulty of accurate lesion
localization caused by pubic bone sonic attenuation
when the injury is in the region of the proximal
cavernosal artery or the distal common penile artery.
They further reiterate the importance of accurate
sonographic localization in cases where embolization
may be anticipated because internal iliac artery or
internal pudendal artery cannulization is easier from
the contralateral femoral artery.
The use of selective arterial embolization for the
management of arterial priapism is somewhat contro-
versial. The embolization of an arteriolacunar fistula
in nonischemic priapism with an autologous clot was
first reported by Wear et al [71] in 1977. Numerous
reports in the literature have since documented use
of this approach in high-flow priapism with variable
success [72–82]. The recently published AUA guide-
line recommends that the initial management of
nonischemic priapism should be observation [1]. This
approach is based on the finding that expectant
management results in spontaneous resolution in
62% of the reported cases (with erectile dysfunction
in one third of cases) reviewed by the AUA Guideline

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 437
panel. Many investigators have shown complete reso-
lution of posttraumatic high-flow priapism without
any invasive measures and the historical trend on the
management of high-flow priapism gradually seems
to be moving from surgery to embolization to expect-
ant management [1,67,83]. Selective arterial emboli-
zation with autologous clot and absorbable gels are
recommended for ‘‘patients who request treatment’’
[1]. The AUA guideline further states that any dis-
cussion of invasive treatment modalities including
Fig. 4. A 40-year-old man with cocaine-induced priapism. He
examination. After failure of urologic treatment, he was referre
angiography (A, B) demonstrates the internal pudendal artery (strai
the dorsal artery of the penis (arrowhead). (C) Complete occlusio
absorbable gelatin sponge using coaxial microcatheter. Arrow ind
(Courtesy of A. Blum, MD, and P. Kang, MD, Cleveland, OH.)
surgery or embolization must be preceded by a thor-
ough discussion of the various aspects of expectant
management and the chances of spontaneous reso-
lution. It should be noted that autologous clot is
reported to be unstable by some investigators and is
not widely used [80].
Superselective transcatheter embolization (Fig. 4)
has been performed to occlude the source of arterial
inflow with potential preservation of potency in up to
80% of patients in one recent report [84]. In rare
was confirmed to have low-flow priapism on ultrasound
d to radiology for embolization of the penile artery. The
ght arrow), the artery to the scrotal wall (curved arrow), and
n of the penile artery (arrowhead) after embolization with
icates the artery to the scrotal wall. B, bladder; P, priapism.

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443438
instances, this treatment has been associated with
perineal abscess formation [85]. When embolization
is used, serial penile duplex studies should be per-
formed in follow-up to ‘‘assure complete resolution of
the arterial lacunar fistula and ultimate restoration
of normal cavernosal blood flow’’ [67]. Based on
the AUA Guideline recommendations and earlier
work by the Boston University group, a course of
watchful waiting with regular follow-up examinations
should be discussed with the patient as a reasonable
(if not preferred) alternative to maximize the chances
of preserving potency and avoiding nonessential in-
tervention in high-flow priapism [67]. When avail-
able, arterial embolization of arteriocavernous fistulas
has been advocated by Volkmer et al [51] as the first
line of therapy in prepubertal boys with traumatic
high-flow priapism when hematologic or metabolic
causes have been eliminated [51]. The authors report
26-month mean follow-up in three cases of high-flow
priapism diagnosed by color Doppler ultrasound that
presented 4 to 7 days after the injury. After diagnosis
of the fistula location by angiography (branches of the
internal pudendal artery in two and the bulbourethral
artery in one patient), gelatin sponge (bulbourethral
artery) or microcoil (internal pudendal artery) were
used to occlude the fistula and achieve detumescence
with preservation of erectile function in all three cases
[51]. Traditionally, when embolization is performed, a
unilateral approach has been recommended to avoid
the dreaded complications of penile gangrene, gluteal
ischemia, or erectile dysfunction [61,86]. Langenhuij-
sen et al [80], however, have described highly selec-
tive embolization of bilateral cavernous arteries in a
case where unilateral embolization was unsuccessful.
The authors advocate the use of the highly selective
technique (cannulization of the cavernosal arteries) to
minimize the risk of distal embolization of embolic
material and use of resorbable materials (gelatin
sponge) to allow for later recanalization and potential
preservation of potency. The disadvantage of the
absorbable materials is that they are not radiopaque
and accurate placement can only be accomplished by
frequent control arteriography during the procedure
[80,87,88]. Callewaert et al [89] were the first to
report superselective embolization in children using
microcoils. Again, the advantage of the microcoils is
that they allow precise placement into the branch
supplying the fistula and may be performed bilaterally
and yet maintain adequate penile blood flow to
potentially preserve erectile function. Volkmer et al
[42] advocate a combined interventional approach
with intraoperative penile color Doppler ultrasound
while performing arterial embolization to minimize
iodinated contrast use and radiation exposure. This
approach allows precise angiographic catheter place-
ment and is especially useful for reducing radiation
exposure in children because of the higher likelihood
of multiple arterial lacerations.
For patients requesting treatment in areas with no
access to tertiary care centers and angiographic ex-
pertise, a trial of cavernosal aspiration and corporal
irrigation with a-adrenergic agents may be tried early
in the course of priapism and has been associated
with a positive outcome (resolution of priapism and
ability to achieve normal erections with follow-up) in
at least one case report [66].
Treatment
The duration of the veno-occlusive period in pri-
apism has a significant impact on the potential for
recovery of spontaneous erections. Conservative mea-
sures and a trial of medical therapy should always be
attempted before surgical therapy. Immediate reduc-
tion of intracorporeal pressure in low-flow states is
of paramount importance. Treatment options are fur-
ther separated based on the etiology. For patients with
non–sickle cell priapism, initial comfort measures
include local penile or systemic anesthesia in the form
of dorsal nerve block, circumferential penile block,
subcutaneous local penile shaft block, and oral con-
scious sedation for the pediatric patient [43]. The
initial diagnostic penile aspiration is also used as a
therapeutic measure and, except where contraindi-
cated, should be combined with intracavernosal instil-
lation of a sympathomimetic agent (ie, phenylephrine
injection after aspiration) to induce detumescence.
This combination addresses the two important goals
of therapy in low-flow states: decreased inflow
(phenylephrine), and increased outflow and reduced
pressures (aspiration). Transient increases in systemic
blood pressure are possible and monitoring of vital
signs is indicated when using sympathomimetic
agents. Because of its potent and selective a1-adre-
nergic stimulatory properties and lack of b1-stimula-
tory effect, which could cause arrhythmias and angina
in susceptible patients, phenylephrine is a preferred
agent for achieving detumescence by intracavernosal
injection and has been extensively reviewed by Lee
et al [90]. These authors also have prepared a useful
chart for preparation of dilutions of a-adrenergicagonists for intermittent injection or irrigation. Fail-
ing this approach, the next step in the process is
irrigation with saline with or without pharmacologic
agent except when contraindicated. The authors have
successfully used a closed system for corporeal aspi-
ration and irrigation as described by Futral and Witt

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 439
[91] that has the advantages of reduced risk of body
fluid exposure and corporeal contamination and the
capacity for extended irrigation without repeated
corporeal puncture.
The authors agree with observations by Pautler
and Brock [64] indicating that most cases of veno-
occlusive priapism treated without excessive delay
(< 12 hours) respond to a-agonist therapy and that
failure of resolution after 20 minutes of injection
(0.1 mL/minute of a 500–1000 mg/mL phenylephrine
solution for a total infused dose of 1 mg) calls for
alternative strategies for management because these
patients are unlikely to respond. The AFUD panel
highly recommended first-line treatments (aspiration
and irrigation) for low-flow priapism of more than
4-hours duration before undertaking more invasive
surgical shunts and further suggested that these ther-
apies have not shown a benefit in preserving potency
when priapism has persisted beyond 72 hours [43].
Failure of resolution after conservative measures as
described moves the step-care process to the surgical
level. A number of different surgical shunts for
diversion of blood away from the corpus cavernosum
have been described. The consensus among authori-
ties is that, in general, distal corporospongiosal shunts
should be undertaken before proximal shunts; how-
ever, there is no consensus regarding the choice of
percutaneous versus open surgical shunts. The
authors prefer to start with a transglandular Winter
shunt (corporoglandular) using a biopty gun biopsy
device to create multiple channels between the corpus
spongiosum and the corpora cavernosa [92]. If this
technique is not successful, a larger communication
between the corpora cavernosa and the corpus spon-
giosum may be created by a modified Al-Ghorab
shunt in which the distal tunica albuginea of the
corpora cavernosa is removed through a transglan-
dular incision. Proximal shunts have been described
by a number of authors and are recommended if these
shunts fail and absent cavernosal artery flow is
assessed by Doppler sonography [43,93]. A few
authors have advocated early use of penile prostheses
in cases of refractory or recurrent priapism associated
with corporal fibrosis and erectile dysfunction [94].
The AFUD panel recommendations for manage-
ment of priapism in patients with SCA include intra-
venous hydration and parenteral narcotic analgesia
while preparing for aspiration and irrigation, supple-
mental oxygen, and exchange transfusion [43]. Initial
efforts are directed at relief of pain and anxiety, and
hydration with hypotonic fluids at 1.5 times mainte-
nance. Powars and Johnson [95] state that in the static,
hypoxic, and acidotic corporal environment, it is
unlikely that red cells can reach the area of involve-
ment and question the use of red cell transfusion.
Furthermore, they emphasize that blood volume and
viscosity must be monitored closely in patients un-
dergoing exchange transfusion or rapid single-unit
transfusion, because there is an increased risk of
cerebrovascular accident, coma, and intracranial
hemorrhage. Low-flow infarctive priapism is uncom-
mon. Nonetheless, adolescent patients are more likely
to develop this condition compared with younger
children who are more likely to respond to hydration,
rest, analgesia, and warmth [95]. Failing conservative
measures as described, the rest of the management
algorithm for SCA patients with low-flow priapism is
very similar to that described for non-SCA priapism.
Stuttering or recurrent painful priapism episodes in
this population have been managed successfully with
instruction on sympathomimetic self-injection and
gonadotropin-releasing hormone analogue injection
in refractory cases [96,97]. This experience has been
corroborated by the authors. Rutchik et al [98] have
reported on a single case of refractory veno-occlusive
priapism (failure of response to intracavernosal
a-adrenergic injection or irrigation and recurrence
after an Al Ghorab surgical shunt) that responded to
intracavernosal injection of 15-mg tissue plasminogen
activator [98]. The authors resorted to this therapy
because of severe penile congestion and risk of penile
necrosis with further shunting. It must be emphasized,
however, that experience with this approach is very
limited. A novel approach for treatment of priapism
was suggested by deHoll et al [99] who described the
use of methylene blue, a guanylate cyclase inhibitor,
in 11 patients with priapism and reported immediate
detumescence in 67%. A possible explanation for the
success of this therapy is blockage of cyclic GMP-
induced muscle relaxation following the initial aspi-
ration attempts. Recently, successful treatment of
recurrent idiopathic priapism with oral baclofen has
been reported in two patients [100]. The treatment
options for high-flow arteriogenic priapism mainly
consist of conservative measures aimed at preserva-
tion of sexual function. Mechanical measures include
external compression with occlusion of arterial inflow
and topical application of ice. If these approaches fail,
surgical, pharmacologic, or radiologic approaches
may be used. Surgical and pharmacologic interven-
tions have not had great success in resolution of high-
flow priapism and restoration of potency [67]. A
detailed discussion of embolization therapy was pre-
sented in the previous section. There are very limited
data on the safety and efficacy of surgical procedures
for management of high-flow priapism and surgery
was recommended as the ‘‘option of last resort’’ by the
AUA Guideline panel [1].

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443440
Complications
Early complications typically result from injection
of a-adrenergic agents and include headaches, palpi-
tation, hypertension, and cardiac arrhythmias. Vital
signs should bemonitored during this phase of therapy.
Additional adverse events include urethral injury and
urethrocutaneous or urethrocavernosal fistula from
aggressive needle decompression, bleeding, and infec-
tion [101]. Rare cases of gangrene of the penis after
corporospongiosal shunt have been reported [102].
Complications in high-flow states are usually second-
ary to the angiographic embolization used in the
therapeutic stage of management. Use of angiography
for diagnostic purposes is seldom necessary. Color
duplex Doppler ultrasound evaluation and a thorough
history and physical examination readily delineate the
diagnosis in nearly all cases. Late complications are
usually the sequelae of ischemic damage to cavernosal
tissue and commonly manifest as corporal fibrosis and
erectile dysfunction. Early decompression of the penis
in the low-flow state is the most important preventive
measure against these adverse events.
Summary
Priapism is a relatively uncommon condition that
may present as a medical emergency associated with
significant pain and anxiety in the veno-occlusive or
low-flow variant. Pharmacologic advances and, spe-
cifically, the availability of intracavernosal a-agonisttherapy have dramatically improved the prospects
of resolution for patients with low-flow priapism
presenting within the first few hours of the acute
episode. High-flow priapism is not considered an
emergency and treatment measures are typically con-
servative aimed at preservation of potency. Urolo-
gists, radiologists, and other health care personnel
caring for the patient with priapism must be familiar
with various etiologic factors implicated in low-flow
and high-flow priapism to formulate a logical step-
care approach. Differentiation of the low-flow from
the high-flow state is perhaps the most critical initial
diagnostic challenge that determines the sequence of
further interventions including surgical shunts in low-
flow priapism refractory to medical therapy.
References
[1] Montague DK, Jarow J, Broderick GA, et al. Ameri-
can Urological Association guideline on the manage-
ment of priapism. J Urol 2003;170:1318–24.
[2] Papadopoulos I, Kelami A. Priapus and priapism:
from mythology to medicine. Urology 1988;32:385.
[3] Hinman F. Priapism: report of cases in a clinical study
of the literature with reference to its pathogenesis
and surgical treatments. Ann Surg 1914;60:689.
[4] Taylor WN. Priapism of the corpus spongiosum
and glans penis. J Urol 1980;123:961.
[5] Burt FS, Scott WW. A new concept in the manage-
ment of priapism. J Urol 1960;83:60.
[6] Hauri D, Spycher M, Bruhlmann W. Erection and
priapism: a new physiopathological concept. Urol
Int 1983;38:138.
[7] Dogra V, Bhatt S. Erectile dysfunction and priapism.
In: Dogra V, Rubens D, editors. Ultrasound secrets.
1st edition. Philadelphia: Hanley & Belfus; 2004.
p. 420–4.
[8] Eland IA, van der Lei J, Stricker BH, et al. Incidence
of priapism in the general population. Urology 2001;
57:970.
[9] Compton MT, Miller AH. Priapism associated with
conventional and atypical antipsychotic medications:
a review. J Clin Psychiatry 2001;62:362.
[10] Altman AL, Seftel AD, Brown SL, et al. Cocaine
associated priapism. J Urol 1999;161:1817.
[11] Steinhardt GF, Steinhardt E. Priapism in children with
leukemia. Urology 1981;18:604.
[12] Suri R, Goldman JM, Catovsky D, et al. Priapism
complicating chronic granulocytic leukemia. Am J
Hematol 1980;9:295.
[13] Pohl J, Pott B, Kleinhans G. Priapism: a three-phase
concept of management according to aetiology and
prognosis. Br J Urol 1986;58:113.
[14] Linet OI, Ogrinc FG. Efficacy and safety of intra-
cavernosal alprostadil in men with erectile dysfunc-
tion. The Alprostadil Study Group. N Engl J Med
1996;334:873.
[15] Ramos CE, Park JS, Ritchey ML, et al. High flow
priapism associated with sickle cell disease. J Urol
1995;153:1619.
[16] Fowler Jr JE, Koshy M, Strub M, et al. Priapism
associated with the sickle cell hemoglobinopathies:
prevalence, natural history and sequelae. J Urol 1991;
145:65.
[17] Tarry WF, Duckett Jr JW, Snyder III HM. Urological
complications of sickle cell disease in a pediatric
population. J Urol 1987;138:592.
[18] Emond AM, Holman R, Hayes RJ, et al. Priapism and
impotence in homozygous sickle cell disease. Arch
Intern Med 1980;140:1434.
[19] Mantadakis E, Cavender JD, Rogers ZR, et al. Preva-
lence of priapism in children and adolescents with
sickle cell anemia. J Pediatr Hematol Oncol 1999;
21:518.
[20] Rubin SO. Priapism as a probable sequel to medica-
tion. Scand J Urol Nephrol 1968;2:81.
[21] Ankem MK, Ferlise VJ, Han KR, et al. Risperi-
done-induced priapism. Scand J Urol Nephrol 2002;
36:91.
[22] Abber JC, Lue TF, Luo JA, et al. Priapism induced by

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 441
chlorpromazine and trazodone: mechanism of action.
J Urol 1987;137:1039.
[23] Myrick H, Markowitz JS, Henderson S. Priapism fol-
lowing trazodone overdose with cocaine use. Ann
Clin Psychiatry 1998;10:81.
[24] Fiorelli RL, Manfrey SJ, Belkoff LH, et al. Priapism
associated with intranasal cocaine abuse. J Urol 1990;
143:584.
[25] Mireku-Boateng AO, Tasie B. Priapism associated
with intracavernosal injection of cocaine. Urol Int
2001;67:109.
[26] Rodriguez-Blaquez HM, Cardona PE, Rivera-Herrera
JL. Priapism associated with the use of topical co-
caine. J Urol 1990;143:358.
[27] Dubin NN, Razack AH. Priapism: ecstasy related?
Urology 2000;56:1057.
[28] Kachhi PN, Henderson SO. Priapism after andro-
stenedione intake for athletic performance enhance-
ment. Ann Emerg Med 2000;35:391.
[29] Slayton W, Kedar A, Schatz D. Testosterone induced
priapism in two adolescents with sickle cell disease.
J Pediatr Endocrinol Metab 1995;8:199.
[30] Whalen RK, Whitcomb RW, Crowley Jr WF, et al.
Priapism in hypogonadal men receiving gonadotropin
releasing hormone. J Urol 1991;145:1051.
[31] Zargooshi J. Priapism as a complication of high dose
testosterone therapy in a man with hypogonadism.
J Urol 2000;163:907.
[32] Lapan DI, Graham AR, Bangert JL, et al. Amyloi-
dosis presenting as priapism. Urology 1980;15:167.
[33] Bschleipfer TH, Hauck EW, Diemer TH, et al. Hepa-
rin-induced priapism. Int J Impot Res 2001;13:357.
[34] Goulding FJ. Priapism caused by glucose phosphate
isomerase deficiency. J Urol 1976;116:819.
[35] Hebuterne X, Frere AM, Bayle J, et al. Priapism in a
patient treated with total parenteral nutrition. JPEN J
Parenter Enteral Nutr 1992;16:171.
[36] Wilson SK, Klionsky BL, Rhamy RK. A new etiol-
ogy of priapism: Fabry’s disease. J Urol 1973;109:646.
[37] Zimbelman J, Lefkowitz J, Schaeffer C, et al. Un-
usual complications of warfarin therapy: skin necrosis
and priapism. J Pediatr 2000;137:266.
[38] Wilson F, Staff WG. Malignant priapism: an unex-
pected response to local anaesthetic infiltration of
the dorsal nerves of the penis. Br J Surg 1982;69:469.
[39] Krco MJ, Jacobs SC, Lawson RK. Priapism due to
solid malignancy. Urology 1984;23:264.
[40] Chan PT, Begin LR, Arnold D, et al. Priapism sec-
ondary to penile metastasis: a report of two cases
and a review of the literature. J Surg Oncol 1998;
68:51.
[41] Witt MA, Goldstein I, Saenz de Tejada I, et al.
Traumatic laceration of intracavernosal arteries: the
pathophysiology of nonischemic, high flow, arterial
priapism. J Urol 1990;143:129.
[42] Volkmer BG, Nesslauer T, Kuefer R, et al. High-flow
priapism: a combined interventional approach with
angiography and colour Doppler. Ultrasound Med
Biol 2002;28:165.
[43] Berger R, Billups K, Brock G, et al. Report of the
American Foundation for Urologic Disease (AFUD)
Thought Leader Panel for evaluation and treatment
of priapism. Int J Impot Res 2001;13(Suppl 5):S39.
[44] Alvarez Gonzalez E, Pamplona M, Rodriguez A, et al.
High flow priapism after blunt perineal trauma: reso-
lution with bucrylate embolization. J Urol 1994;
151:426.
[45] Dewan PA, Lorenz C, Davies RP. Posttraumatic pria-
pism in a 7-year-old boy. Eur Urol 1994;25:85.
[46] Golash A, Gray R, Ruttley MS, et al. Traumatic pria-
pism: an unusual cycling injury. Br J Sports Med
2000;34:310.
[47] Touge H,Watanabe T, Fujinaga T, et al. Post-traumatic
high flow priapism: a case report. Int J Urol 1999;
6:623.
[48] Wolf Jr JS, Lue TF. High-flow priapism and glans
hypervascularization following deep dorsal vein arte-
rialization for vasculogenic impotence. Urol Int 1992;
49:227.
[49] Dewan PA, Tan HL, Auldist AW, et al. Priapism in
childhood. Br J Urol 1989;64:541.
[50] Miller ST, Rao SP, Dunn EK, et al. Priapism in chil-
dren with sickle cell disease. J Urol 1995;154:844.
[51] Volkmer BG, Nesslauer T, Kraemer SC, et al. Prepu-
bertal high flow priapism: incidence, diagnosis and
treatment. J Urol 2001;166:1018.
[52] Sadeghi-Nejad H, Seftel AD. The etiology, diagnosis,
and treatment of priapism: review of the American
Foundation for Urologic Disease Consensus Panel
Report. Curr Urol Rep 2002;3:492.
[53] Burnett AL. Pathophysiology of priapism: dysregula-
tory erection physiology thesis. J Urol 2003;170:26.
[54] Spycher MA, Hauri D. The ultrastructure of the erec-
tile tissue in priapism. J Urol 1986;135:142.
[55] Broderick GA, Gordon D, Hypolite J, et al. Anoxia
and corporal smooth muscle dysfunction: a model for
ischemic priapism. J Urol 1994;151:259.
[56] Levine JF, Saenz de Tejada I, Payton TR, et al. Recur-
rent prolonged erections and priapism as a sequela
of priapism: pathophysiology and management. J Urol
1991;145:764.
[57] Lin G, Xin ZC, Lue TF, et al. Up and down-regulation
of phosphodiesterase-5 as related to tachyphylaxis
and priapism. J Urol 2003;170:S15.
[58] Seftel AD, Haas CA, Brown SL, et al. High flow pria-
pism complicating veno-occlusive priapism: patho-
physiology of recurrent idiopathic priapism? J Urol
1998;159:1300.
[59] Baba H, Furusawa N, Tanaka Y, et al. Intermittent
priapism associated with lumbar spinal stenosis. Int
Orthop 1994;18:150.
[60] Siegel JF, Rich MA, Brock WA. Association of sickle
cell disease, priapism, exchange transfusion and neu-
rological events: ASPEN syndrome. J Urol 1993;
150:1480.
[61] Bastuba MD, Saenz de Tejada I, Dinlenc CZ, et al.
Arterial priapism: diagnosis, treatment and long-term
follow-up. J Urol 1994;151:1231.

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443442
[62] Desai KGJ. Hazards of long distance cycling. BMJ
1989;298:1072.
[63] Lue TF, Hellstrom WJ, McAninch JW, et al. Pria-
pism: a refined approach to diagnosis and treatment.
J Urol 1986;136:104.
[64] Pautler SE, Brock GB. Priapism: from Priapus to the
present time. Urol Clin North Am 2001;28:391.
[65] Koga S, Shiraishi K, Saito Y. Post-traumatic priapism
treated with metaraminol bitartrate: case report.
J Trauma 1990;30:1591.
[66] Rudick DH. Successful treatment of arterial priapism
with alpha-agonist irrigation: a rural experience.
J Urol 2002;167:2132.
[67] Hakim LS, Kulaksizoglu H, Mulligan R, et al. Evolv-
ing concepts in the diagnosis and treatment of arterial
high flow priapism. J Urol 1996;155:541.
[68] Mabjeesh NJ, Shemesh D, Abramowitz HB. Post-
traumatic high flow priapism: successful manage-
ment using duplex guided compression. J Urol
1999;161:215.
[69] Bertolotto M, Quaia E, Mucelli FP, et al. Color Dopp-
ler imaging of posttraumatic priapism before and
after selective embolization. Radiographics 2003;
23:495.
[70] Kang BC, Lee DY, Byun JY, et al. Post-traumatic
arterial priapism: colour Doppler examination and
superselective arterial embolization. Clin Radiol
1998;53:830.
[71] Wear Jr JB, Crummy AB, Munson BO. A new ap-
proach to the treatment of priapism. J Urol 1977;
117:252.
[72] Belgrano E, Puppo P, Quattrini S, et al. Percutaneous
temporary embolization of the internal pudendal ar-
teries in idiopathic priapism: 2 additional cases. J Urol
1984;131:756.
[73] Carmignani G, Belgrano E, Puppo P, et al. Idiopathic
priapism successfully treated by unilateral emboliza-
tion of internal pudendal artery. J Urol 1980;124:553.
[74] Cohen GS, Braunstein L, Ball DS, et al. Selective
arterial embolization of idiopathic priapism. Cardio-
vasc Intervent Radiol 1996;19:47.
[75] Fratezi AC, Martins VM, Pereira Porta RM, et al.
Endovascular therapy for priapism secondary to peri-
neal trauma. J Trauma 2001;50:581.
[76] Gorich J, Ermis C, Kramer SC, et al. Interven-
tional treatment of traumatic priapism. J Endovasc
Ther 2002;9:614.
[77] Gujral S, MacDonagh RP, Cavanagh PM. Bilateral
superselective arterial microcoil embolisation in de-
layed post-traumatic high flow priapism. Postgrad
Med J 2001;77:193.
[78] Kawakami M, Minagawa T, Inoue H, et al. Successful
treatment of arterial priapism with radiologic selective
transcatheter embolization of the internal pudendal
artery. Urology 2003;61:645.
[79] Kress O, Heidenreich A, Klose KJ, et al. Superselec-
tive embolization with coils in high-flow priapism.
Cardiovasc Intervent Radiol 2002;25:326.
[80] Langenhuijsen JF, Reisman Y, Reekers JA, et al.
Highly selective embolization of bilateral cavernous
arteries for post-traumatic penile arterial priapism.
Int J Impot Res 2001;13:354.
[81] Ravi R, Baijal SS, Roy S. Embolotherapy of pria-
pism. Arch Esp Urol 1992;45:587.
[82] Webber RJ, Thirsk I, Moffat LE, et al. Selective ar-
terial embolization in the treatment of arterial pria-
pism. J R Coll Surg Edinb 1998;43:61.
[83] Arango O, Castro R, Dominguez J, et al. Complete
resolution of post-traumatic high-flow priapism with
conservative treatment. Int J Impot Res 1999;11:115.
[84] Ciampalini S, Savoca G, Buttazzi L, et al. High-flow
priapism: treatment and long-term follow-up. Urology
2002;59:110.
[85] Sandock DS, Seftel AD, Herbener TE, et al. Perineal
abscess after embolization for high-flow priapism.
Urology 1996;48:308.
[86] Steers WD, Selby Jr JB. Use of methylene blue and
selective embolization of the pudendal artery for high
flow priapism refractory to medical and surgical treat-
ments. J Urol 1991;146:1361.
[87] Colombo F, Lovaria A, Saccheri S, et al. Arterial
embolization in the treatment of post-traumatic pria-
pism. Ann Urol 1999;33:210.
[88] Kerlan Jr RK, Gordon RL, LaBerge JM, et al. Super-
selective microcoil embolization in the management
of high-flow priapism. J Vasc Interv Radiol 1998;
9:85.
[89] Callewaert P, Stockx L, Bogaert G, et al. Post-trau-
matic high-flow priapism in a 6-year-old boy: man-
agement by percutaneous placement of bilateral
vascular coils. Urology 1998;52:134.
[90] Lee M, Cannon B, Sharifi R. Chart for preparation
of dilutions of alpha-adrenergic agonists for intracav-
ernous use in treatment of priapism. J Urol 1995;
153:1182.
[91] Futral AA, Witt MA. A closed system for corporeal
irrigation in the treatment of refractory priapism.
Urology 1995;46:403.
[92] Winter CC. Priapism cured by creation of fistulas
between glans penis and corpora cavernosa. Trans
Am Assoc Genitourin Surg 1977;69:31.
[93] Sacher EC, Sayegh E, Frensilli F, et al. Cavernospon-
giosum shunt in the treatment of priapism. J Urol
1972;108:97.
[94] Sundaram CP, Fernandes ET, Ercole C, et al. Man-
agement of refractory priapism with penile prosthe-
ses. Br J Urol 1997;79:659.
[95] Powars DR, Johnson CS. Priapism. Hematol Oncol
Clin North Am 1996;10:1363.
[96] Levine LA, Guss SP. Gonadotropin-releasing hor-
mone analogues in the treatment of sickle cell
anemia-associated priapism. J Urol 1993;150:475.
[97] Steinberg J, Eyre RC. Management of recurrent pria-
pism with epinephrine self-injection and gonado-
tropin-releasing hormone analogue. J Urol 1995;
153:152.

H. Sadeghi-Nejad et al / Radiol Clin N Am 42 (2004) 427–443 443
[98] Rutchik S, Sorbera T, Rayford RW, et al. Successful
treatment of recalcitrant priapism using intercorporeal
injection of tissue plasminogen activator. J Urol
2001;166:628.
[99] deHoll JD, Shin PA, Angle JF, et al. Alternative
approaches to the management of priapism. Int J
Impot Res 1998;10:11.
[100] Rourke KF, Fischler AH, Jordan GH. Treatment of
recurrent idiopathic priapism with oral baclofen.
J Urol 2002;168:2552; discussion 2552.
[101] De Stefani S, Savoca G, Ciampalini S, et al. Urethro-
cutaneous fistula as a severe complication of treat-
ment for priapism. BJU Int 2001;88:642.
[102] Fortuno RF, Carrillo R. Gangrene of the penis follow-
ing cavernospongiosum shunt in a case of priapism.
J Urol 1972;108:752.

Radiol Clin N Am 42 (2004) 445–456
Ultrasound evaluation of acute abdominal emergencies in
infants and children
Pauravi Vasavada, MD
Department of Pediatric Radiology, University Hospitals of Cleveland, 11100 Euclid Avenue, Cleveland, OH 44106, USA
Ultrasonography is an essential component in the position. Close to 7% of children with HPS have pa-
evaluation of acute abdominal pain and vomiting in
children. Radiation exposure is a prime consideration
in the pediatric population. Ultrasonography, unlike
CT or fluoroscopy, allows the radiologist to acquire
diagnostic information without the use of ionizing
radiation. Ultrasound (US) can be performed in any
imaging plane, which is advantageous when evaluat-
ing such structures as the pylorus and appendix,
which may not be fixed in their orientation. Small
children with abdominal pain often are not able to lie
down quietly for a CT or MR image without the
use of sedation. US, however, is able to obtain diag-
nostic images in nonsedated children. It is also cost
effective, being far less expensive than CT or MR
imaging. Real-time ultrasonography can be per-
formed in the radiology department or at bedside in
the emergency department [1,2].
Hypertrophic pyloric stenosis
Hypertrophic pyloric stenosis (HPS) is the most
common surgical disorder producing emesis in in-
fancy [1,3]. The incidence of HPS is approximately
2 to 5 per 1000 births per year and it varies with the
geographic area. HPS is less common in India, and
among black and Asian population, with a frequency
that is one third to one fifth compared with that in the
white population [3]. Boys are four times more likely
to be affected than girls, with the incidence signifi-
cantly higher in first-born boys [2–4]. Although it’s
etiology remains unknown, there is a familial predis-
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.003
E-mail address: [email protected]
rents with the same condition [2,4].
Hypertrophic pyloric stenosis is characterized by
a defect in contractility or relaxation of the circular
muscle of the pylorus that results in hypertrophy of
the pyloric circular muscle and narrowing of the
pyloric channel [3,4]. This leads to stomach dilation
and gastric outlet obstruction of variable severity.
Pyloric stenosis should be suspected in neonates 3 to
6 weeks old with postprandial nonbilious vomiting.
Symptoms, however, can be present in the first week
of life or as late as 5 months of age. The patient
classically presents with nonbilious vomiting that is
projectile secondary to the pressures generated by the
hypertrophied gastric muscles [5]. Persistent vomiting
results in large losses of gastric secretions. Because
only gastric secretions are lost, prolonged vomiting
leads to hypokalemic, hypochloremic metabolic alka-
losis. If uncorrected the condition can lead to malnu-
trition, weight loss, dehydration, and death. More
recent evidence suggests, however, that more than
90% of infants with HPS present without any meta-
bolic disorders. This lower incidence has been linked
to proper diagnosis before protracted vomiting is
allowed to occur, and it has been suggested that easy
access to ultrasonography may be contributing to
earlier diagnosis [6]. Nonbilious vomiting can present
in several other conditions including gastroesophageal
reflux disease and pylorospasm [4].
The clinical diagnosis of HPS has traditionally
been made by palpation of an olive-shaped mass in
the epigastrium representing the hypertrophic pyloric
muscle. Palpation of a tumor-like mass in the right
upper quadrant by an experienced examiner is usually
considered specific and diagnostic without further
testing [3,4,7]. In those infants in whom a mass is
s reserved.

Fig. 1. Fluoroscopic image from an upper gastrointestinal
study in a patient with HPS. The double track sign (arrows)
is formed by contrast material coming through the mucosal
interstices of the canal.
P. Vasavada / Radiol Clin N Am 42 (2004) 445–456446
not palpated unequivocally, an imaging examination
is required. The diagnosis of HPS can be established
by imaging upper gastrointestinal tract with the help
of a radiographic contrast, such as barium, or by
sonography. An upper gastrointestinal tract reveals a
beak or a ‘‘string‘‘ sign because of the narrow open-
ing of the pylorus or the double tract sign (Fig. 1) [2].
In patients with pyloric stenosis the muscle is hyper-
trophied and the intervening mucosa is crowded and
Fig. 2. (A,B) Sonograms in a patient with a normal pylorus. Longitu
muscle. The pyloric channel is not elongated measuring 1.1 cm, a
thickened and protrudes into the distended portion
of the antrum resulting in the nipple sign. The upper
gastrointestinal tract provides indirect information
about the status of the pyloric channel based on the
morphology of the canal lumen as outlined by contrast
material. Secondary to this fact, failure of relaxation
of the pyloric channel, known as ‘‘pylorospasm,’’ may
be confused with pyloric stenosis. Upper gastro-
intestinal tract can be time consuming, because the ra-
diologist has to wait for contrast to pass through the
high-grade obstruction. Fluoroscopy time and radia-
tion exposure may be prolonged. Upper gastrointes-
tinal tract sensitivity rate has been reported to be
approximately 95% but error rate as high as 11%
has also been reported [3,7].
Sonography has become the modality of choice
for the diagnosis of HPS. Sonography is documented
to be a highly sensitive (90%–96%) and specific
modality for the diagnosis of HPS [4]. US avoids
radiation and allows direct visualization of the py-
loric muscle as opposed to the upper gastrointestinal
tract where the morphology of the muscle is inferred
by the thinness and length of the barium through the
area [1–3]. The sonographic examination is typically
performed with a 5- to 7.5-MHz linear array trans-
ducer. A transducer up to 10 MHz can be used
adjusted to the size of the infant and the depth of
the pylorus [3,4]. The patient is placed in the right
posterior oblique position, which allows fluid in the
stomach to distend the antrum and pyloric region.
dinal views demonstrate normal measurement of the pyloric
nd the muscle wall is not thickened measuring 2.6 mm.

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456 447
Because the stomach in infants with pyloric stenosis is
normally distended it is usually not necessary to
introduce more fluid. If the antrum does not contain
adequate fluid, a glucose solution or water can be
given orally or through a nasogastric tube [3,4,7].
Occasionally, the stomach may become so distended
and displace the duodenal cap caudally and medially
rendering the pylorus difficult to visualize. In these
cases, if the patient is placed in the supine or left pos-
terior oblique (LPO) position, the pylorus is able to
rise anteriorly for more optimal evaluation.
Fig. 3. Hypertrophic pyloric stenosis. (A,B) Longitudinal sonogr
measuring 5.8 mm. The pyloric channel is elongated measurin
hypoechoic muscle surrounding the echogenic mucosa.
The pylorus is viewed in longitudinal and trans-
verse planes. The examination begins by placing the
transducer in the transverse plane, beginning at the
gastroesophageal junction and following the contour
of the stomach to its antrum. The duodenal cap is
recognized by its arrowhead shape. By positively
identifying the gastric antrum and the duodenal cap,
the interposed pyloric channel can be imaged [7]. A
negative study hinges on the diagnosis of a normal
pyloric ring and a distensible pyloric portion of the
stomach (Fig. 2) [3,7].
aphic views demonstrate the hypertrophied pyloric muscle
g 23 mm. (C) Cross-sectional view shows the thickened

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456448
On longitudinal views the muscle has a uniformly
hypoechoic appearance. In the short axis view, the
hypertrophic pyloric muscle has a target or bull’s eye
appearance reflecting the thickened hypoechoic mus-
cle surrounding the echogenic mucosa. The sono-
graphic hallmark of HPS is the thickened pyloric
muscle (Fig. 3). The numeric value for the diagnostic
muscle thickness has varied greatly. The exact recom-
mended measurement includes a range of numbers
with a broad range of sensitivities and specifications
[8]. Controversy persists regarding the significance
of muscle thickness between 3 and 4 mm. Some au-
thors consider 3 mm as diagnostic, whereas others
believe that this diagnosis cannot be made reliably
until a muscle thickness of 3.5 to 4 mm has been
attained [3,8]. The length of the hypertrophic canal is
variable and may range from as little as 14 mm to
more than 20 mm. Despite this variability in numbers
in the literature, a patient with HPS has an examina-
tion and overall morphology of the pylorus that is
characteristic of pyloric stenosis. The muscle thick-
ness is at least 3 mm or more during the examination
and the intervening lumen is filled with crowded or
redundant mucosa through the center of the canal.
Additionally, gastric peristaltic activity fails to distend
the preduodenal portion of the stomach [3].
In patients without HPS the muscle does not
measure more than 3 mm at any given time. Thick-
Fig. 4. (A, B) Sonographic images of the pylorus after the infant
within the antrum passing through a normal pylorus (P, arrow) int
ening of the pyloric channel may be a transient
phenomenon because of peristaltic activity or pylo-
rospasm. During a normal examination, one can
document the pyloric canal changing from a rigid
linear morphology to a relaxed canal that permits
pockets of fluid within the lumen. If the stomach is
empty and the antrum is collapsed a small amount of
fluid may be fed to the infant to document a normal
fluid-filled antrum (Fig. 4). Patients in whom the
pyloric canal relaxes to a normal morphology do not
have pyloric stenosis. Patients in whom the muscle is
2 to 3 mm thick during the examination and does not
relax warrant monitoring and follow-up examination.
Because the cause and evolution of HPS are unknown,
it is uncertain whether a young infant in whom the
canal fails to relax completely will go on to develop
HPS requiring surgery or whether the changes will be
arrested and resolve with sequelae [3].
Potential causes of errors in the diagnosis of
HPS are overdistention of the stomach, which may
lead to displacement of the pylorus posteriorly
making identification and measurement of the py-
loric thickness more difficult. Additionally, off-
midline or tangential images can lead to erroneous
diagnosis of a thickened muscle [3,4].
The treatment of HPS is pyloromyotomy in which
the hypertrophic muscle is split longitudinally. A
study by Yoshizawa et al [9] showed that although
was given a small amount of fluid. Both images show fluid
o the duodenum (D, arrow).

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456 449
the pyloric muscle thickness remains abnormal after
surgery, by 5 months the dimensions gradually return
to less than or equal to normal values.
Fig. 5. Intussusception. Plain radiograph demonstrates a
round soft tissue density mass (arrows) in the right upper
quadrant protruding into the gas-filled transverse colon.
Intussusception
Intussusception is one of the most common causes
of acute abdomen in infancy. The condition occurs
when a segment of intestine (the intussusceptum) pro-
lapses into a more caudal segment of intestine (the
intussuscipiens). This condition usually occurs in chil-
dren between 5 months to 2 years of age. In this age
group most intussusceptions are idiopathic with no
pathologic lead point demonstrated. More than 90%
of intussusceptions are believed to be secondary to
enlarged lymphoid follicles in the terminal ileum.
Intussusception is more common in boys and the
condition is rare in children younger than 3 months.
The peak incidence is between 5 and 9 months of age.
Lead points are noted in children younger than
3 months of age or greater than 2 years of age. Lead
points include such entities as Meckel’s diverticulum,
duplication cysts, intestinal polyps, lymphoma, and
intramural hematomas [4]. Transient intussusception
is seen in patients with celiac disease (sprue).
Most intussusceptions involve the ileocolic region
(75%), where the ileum becomes telescoped into the
colon. This is followed in decreasing frequency by
ileoileocolic, ileoileal, and colocolic intussusceptions.
The classic clinical triad of acute abdominal pain
(colic), currant jelly stools or hematochezia, and a
palpable abdominal mass is present in less than 50%
of children with intussusception [10,11]. Up to 20%
of patients may be pain free at presentation. Addi-
tionally, in some instances lethargy or convulsion is
the predominant sign or symptom. This situation
results in consideration of a neurologic disorder rather
than intussusception. Given the uncertainty of achiev-
ing an accurate clinical diagnosis, imaging is required
in most cases to achieve an early and quick diagnosis
to reduce morbidity and mortality. Delay may be life-
threatening because of the development of bowel
necrosis and its complications [12].
Much controversy exists in the literature related to
the diagnosis and management of intussusception.
Realistically speaking children with intussusception
can be managed successfully in a number of different
ways. It is best to use diagnostic tools that are as
benign as possible, however, to avoid potential harm
to these children and to lessen the discomfort to the
children who are not shown to have intussusception.
Conventional radiography and the contrast enema
examination have been the principal methods used for
the diagnosis and treatment of intussusception.
Radiographs of the abdomen are useful and can
suggest the diagnosis by showing a mass usually
located in the right upper quadrant effacing the
adjacent hepatic contour (Fig. 5). Other signs include
reduced air in the small intestine, gasless abdomen, or
obstruction of the small intestine [13–15]. Identifi-
cation of a cecum filled with gas or feces in the
normal location is the finding that allows exclusion
of intussusception with most confidence [10,13]. In
the presence of intussusception, plain radiography
allows exclusion of bowel perforation, a major com-
plication of intussusception. The accuracy of plain
radiography in diagnosis on exclusion of intussuscep-
tion ranges from 40% to 90% [13,16,17].
Barium enema examination has been the standard
of reference for the diagnosis of intussusception for
many years. At many institutions liquid enema or air
enema examination is the principal diagnostic tool.

Fig. 6. Meniscus sign. Image from barium enema reduction
shows the rounded apex of the intussusception protruding
into the column of contrast material.
Fig. 7. Intestinal intussusception. Transverse sonographic
image demonstrates a soft tissue mass in the right upper
quadrant adjacent to the gallbladder (GB).
P. Vasavada / Radiol Clin N Am 42 (2004) 445–456450
The classic signs of intussusception at enema exami-
nation are the meniscus sign and the coiled spring
sign. The meniscus sign is produced by the rounded
apex of the intussusception (the intussusceptum) pro-
truding into the column of contrast material (Fig. 6).
The coiled spring sign is produced when the edema-
tous mucosal folds of the returning limb of the in-
tussusception are outlined by contrast material in the
lumen of the colon. The enema examination, however,
can be a very unpleasant experience for both the
parent and child and is also associated with radiation.
The role of sonography in the diagnosis of intus-
susception is well established with a sensitivity of
98% to 100% and a specificity of 88% to 100% [18].
It has been suggested that sonography should be the
initial imaging modality and that the enema exami-
nation should only be performed for therapeutic
reasons [11,18,19]. Sonography not only aids in the
diagnosis of intussusception but it also allows the
identification of patients who are candidates for
therapeutic reduction. Sonography may also detect
other abnormalities that are overlooked by the enema
examination [4]. In addition, there is a high level of
patient comfort and safety with US.
A technique of graded compression is used for
the sonographic evaluation of suspected intussuscep-
tion. Because deep penetration of the US beam is not
necessary in small children, a linear high-resolution
transducer, 5 to 10 MHz, can be used to improve the
definition of the image. The abdomen and the pelvis
should be scanned in both longitudinal and transverse
planes [1]. The intussusception mass is a large struc-
ture, usually greater than 5 cm. Most intussusception
occurs in the subhepatic region often displacing adja-
cent bowel loops (Fig. 7). Even inexperienced opera-
tors can readily identify the intussusception on
sonography. An intussusception is a complex struc-
ture. The intussuscipiens (the receiving loop) contains
the folded intussusceptum (the donor loop), which has
two components: the entering limb and the returning
limb. The attached mesentery is dragged between the
entering and returning limbs. Sonographically, the
intussusception may demonstrate an outer hypoechoic
region surrounding an echogenic center, referred to as
a ‘‘target’’ or ‘‘doughnut’’ appearance (Fig. 8) [20].
The hypoechoic outer ring seen on axial scans is
formed by the everted returning limb, which is the
thickest component of the intussusception and the thin
intussuscipiens. The echogenic center of intussuscep-
tion contains the central or entering limb, which is of
normal thickness and is eccentrically surrounded by
hyperechoic mesentery [20]. Another pattern of imag-
ing that has been described is that of multiple con-

Fig. 8. Target appearance. Transverse sonographic view de-
monstrates the intussusception. The hypoechoic outer layer
represents the intussuscipiens and the central echogenic layer
represents the intussusceptum (arrow).
P. Vasavada / Radiol Clin N Am 42 (2004) 445–456 451
centric rings. Within the bowel wall the mucosa and
submucosa are echogenic, whereas the muscularis
layer is hypoechoic. Multiple hypoechoic and hyper-
echoic layers are identified when there is little bowel
edema present. This represents the mucosa, submu-
cosa, and muscularis layers of the intussusceptum and
intussuscipiens. With increasing degrees of bowel
edema, the hyperechoic mucosal and submucosal
echoes are obliterated in the intussusceptum resulting
in fewer layers. On long axis scans the hypoechoic
layers on each side of the echogenic center may result
in a reniform or pseudokidney appearance (Fig. 9).
Fig. 9. Long-axis sonographic view shows an elongated
appearance resulting in a pseudokidney appearance (arrow).
The pseudokidney sign is seen if the intussusception
is curved or imaged obliquely [1].
Although the target and pseudokidney signs are
the most common ultrasonographic signs used, they
are not pathognomic because they have also been
seen in normal or pathologic intestinal loops. Differ-
ential consideration for the US findings includes
other causes of bowel wall thickening, such as
neoplasm, edema, and hematomas. An inexperienced
operator may mistake stool or psoas muscle for
an intussusception.
In addition to diagnosing the intussusception US
has other advantages. US may detect the presence
of a lead point, which is present in approximately 5%
of intussusception. Various sonographic findings
have been reported to be predictive of success of hy-
drostatic reduction. A study by Koumanidou et al [18]
shows that the sonographic presence of enlarged
mesenteric lymph node in the intussusception is a
prediction of hydrostatic irreducibility. Small amounts
of free peritoneal fluid are seen in up to 50% of cases.
The presence of trapped peritoneal fluid within an
intussusception correlates significantly with ischemia
and irreducibility, however, because it reflects vascu-
lar compromise of the everted limb.
Fig. 10. Use of Doppler ultrasound to evaluate intussuscep-
tion. Doppler ultrasound shows blood flow within the
intussusception, suggesting its reducibility.

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456452
Additionally, the absence of flow within the intus-
susception on color Doppler sonography correlates
with a decreased success of reduction and a higher
likelihood of bowel ischemia [21–23], and presence
of color flow within the intussusception correlates
with higher success rate of its reduction (Fig. 10).
There are many different techniques used to reduce
intussusception described in the literature. Water-sol-
uble contrast material, barium, air enema guided by
fluoroscopy, and physiologic saline solution com-
bined with US have all been used [24,25]. The use
of sonography to guide hydrostatic reduction has
been predominately performed in the eastern hemi-
sphere and is increasingly being used in Europe. The
reduction rate is high (76%–95%), with only 1
perforation in 825 cases reported [25,26]. The proce-
dure may be performed with water, saline solution, or
Hartmann solution. The instilled fluid is followed as it
courses through the large bowel until the intussuscep-
tion is no longer visualized and the terminal ileum and
distal small bowel are filled with fluid or air. There has
been little experience with US-guided air enema
therapy. Because air prevents the passage of the US
beam, it may be difficult to visualize the ileocecal
valve; therefore, small residual ileoileal intussuscep-
tion can be observed. Additionally, it is difficult to de-
tect perforation resulting in pneumoperitoneum [24].
Sonography has been shown to be highly success-
ful in the diagnoses and reduction of intussusception.
The appropriate use of US in children with suspected
intussusception obviates the necessity for diagnostic
enema, and the use of enema should be limited to
therapeutic purposes [27].
Acute appendicitis
Acute appendicitis is one of the major causes of
hospitalization in children and it is the most common
condition requiring emergency abdominal surgery in
the pediatric population. The condition typically
develops in older children and young adults with the
diagnosis being rare under the age of 2. Clinical signs
and symptoms associated with acute appendicitis
include crampy, periumbilical, or right lower quad-
rant pain; nausea; vomiting; point tenderness in the
right lower quadrant; rebound tenderness; and leuko-
cytosis with a left shift [28]. When the history and
clinical findings are classic, the diagnosis of acute
appendicitis is often straightforward [29]. Not only do
one-third of children with acute appendicitis have
atypical findings, however, but also the presenting
signs and symptoms of many nonsurgical conditions
may mimic those of acute appendicitis. Most children
with acute abdominal pain have self-limited non-
surgical disease. Upper respiratory tract infections,
pharyngitis, viral syndrome, gastroenteritis, and con-
stipation are the most common associated conditions
noted in these children. The actual prevalence of acute
appendicitis in children presenting in the outpatient
setting with acute abdominal pain ranges from 1% to
4% [28,30].
The delayed diagnosis of acute appendicitis can
carry serious consequences. Perforation, abscess for-
mation, peritonitis, wound infection, sepsis, infertil-
ity, adhesions, bowel obstruction, and death have
been reported. Morbidity and mortality in acute
appendicitis are related almost entirely to appendiceal
perforation. The prevalence of appendiceal perfora-
tion in various pediatric series has ranged from 23% to
73%, with the perforation rate even higher in young
children [28,31–33]. Up to half of children with
perforated appendicitis may experience a complica-
tion, with nearly all deaths associated with perforated
appendix [28]. For fear of missing the diagnosis and
allowing the development of perforation, peritonitis,
and sepsis, a low index of suspicion and early opera-
tive intervention have been recommended. As a result,
negative laboratory rates as high as 20% have been
reported with rates of 10% to 15% widely accepted
[29,34,35]. Unnecessary appendectomy carries po-
tentially major risks and substantial costs, however,
prompting many to advocate increased efforts to avoid
unnecessary appendectomy [36]. The goal of imaging
in a child with suspected appendicitis should be to
identify the presence of disease in patients with
equivocal clinical findings. Used correctly, imaging
should reduce the negative laparotomy and perfora-
tion rates and reduce the intensity and cost of care.
The ideal diagnostic test should be fast, noninvasive,
highly accurate, and readily available [37]. The pri-
mary imaging technique over the past decade for
evaluating children with suspected appendicitis has
been graded-compression US because it is widely
available, noninvasive, and does not involve radiation
[28,38–40].
The reported diagnostic accuracy of US in the
diagnosis of acute appendicitis has varied greatly. The
sensitivity of US has ranged from 44% to 94% and
the specificity has ranged from 47% to 95% [28]. The
clinical use of US lies primarily in the subgroup of
children in whom the clinical findings are equivocal.
Not only can it establish the diagnosis of appendicitis
but also it can identify other abdominal and pelvic
conditions, especially gynecologic, that present as
right lower quadrant pain [28,41].
The graded-compression technique of US is per-
formed with a high-resolution, linear-array transducer

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456 453
of 5 to 10 MHz. Graded-compression sonography
primarily consists of anterior forced compression to
reduce the distance between the pathologic process
and the transducer and to displace or compress bowel
structures to eliminate gas artifacts. Reducing the
abdominal cavity by compression enables clear visu-
alization of the retroperitoneal structures [42]. Ante-
rior compression is considered adequate when the
iliac vessels and psoas muscles are visualized because
the appendix is anterior to these structures.
Scanning is performed in both longitudinal and
transverse planes. The examination begins with the
identification of the cecum and the terminal ileum.
The ascending colon is a nonperistaltic structure
containing gas and fluid. The terminal ileum is com-
pressible easily and displays active peristalsis. The
cecal tip where the appendix arises is approximately
1 to 2 cm below the terminal ileum. The examination
can be expedited by asking the patient to point to the
area of maximal tenderness. This can also aid in
locating a retrocecal appendix [28].
In early nonperforated appendicitis, an inner
echogenic lining representing submucosa can be
identified. The inflamed, nonperforated appendix ap-
pears as a fluid-filled, noncompressible, blind-ending
Fig. 11. Acute appendicitis. Longitudinal (A) and transverse (B) u
calipers), which is enlarged.
tubular structure on longitudinal US image. The
maximal appendiceal diameter from outside wall to
outside wall is greater than 6 mm in an inflamed
appendix. A noncompressible enlarged appendix
measuring greater than 6 mm in maximal diameter
is the only US sign that is specific for appendicitis
(Fig. 11). Other findings of appendicitis include an
appendicolith, which appears as an echogenic focus
with acoustic shadowing; pericecal or periappendi-
ceal fluid; and enlarged mesenteric lymph nodes. On
transverse imaging a target appearance is delineated.
This is characterized by a fluid-filled appendiceal
lumen, which is surrounded by the echogenic mucosa
and submucosa and hypoechoic muscularis layer.
The US features of perforation include loss of the
echogenic submucosal layer and presence of a locu-
lated periappendiceal or pelvic fluid collection or
abscess (Fig. 12) [43,44]. The appendix is visible
in 50% to 70% of patients with perforated appendi-
citis [44].
The use of color Doppler has also been described
in the evaluation of appendicitis. Color Doppler US
of nonperforated appendicitis demonstrates periph-
eral wall hyperemia reflecting inflammatory hyper-
perfusion. Color flow may be absent in gangrenous
ltrasound images show an inflamed appendix (between the

Fig. 12. Right lower quadrant abscess. Two-year-old girl
presented with abdominal pain. A complex mass in the right
lower quadrant consistent with an appendiceal abscess was
demonstrated on ultrasound.
P. Vasavada / Radiol Clin N Am 42 (2004) 445–456454
appendicitis or early inflammation [45]. Color Dopp-
ler findings of appendiceal perforation include hyper-
emia in the periappendiceal soft tissue or within a
well-defined abscess [46]. Color Doppler US does not
increase the sensitivity of the examination but it does
make interpretation of the gray-scale US findings
easier and can increase observer confidence in the
diagnosis of acute appendicitis.
Most false-negative diagnosis results from failure
to visualize the appendix. This may be secondary to
operator dependency, inability to compress the right
lower quadrant adequately, a retrocecal position of
the appendix, or appendiceal perforation [37,42]. In
patients with obesity the high-frequency transducer
may fail to reach the necessary depth, which makes
accurate diagnosis difficult because of decreased spa-
tial resolution. Another pitfall is early inflammation
limited to the appendiceal tip, which can be missed
if only the proximal appendix is imaged [47,48].
False-positive diagnosis has also been reported.
The normal appendix, which may be visible in 10%
to 50% of children and adolescents, may be mistaken
for appendicitis. The normal appendix measures 6 mm
or less, is compressible, and lacks adjacent inflamma-
tory changes. Periappendiceal changes may also be
secondary to causes other than appendicitis, such as
Crohn’s disease or pelvic inflammatory disease. The
use of US in patients with acute appendicitis is a
subject of controversy in the literature [42]. Many
studies have been performed to evaluate the use of
US in the ultimate outcome of children with suspected
appendicitis. Some studies have suggested that the
use of US has not improved outcome in children with
suspected appendicitis. A study by Roosevelt and
Reynolds [49] showed no significant differences in
the perforation rate or cost of care in children who
underwent US compared with those who did not. A
study by Lessin et al [29], however, suggests that the
early and selective US in clinically equivocal cases
could rapidly allow an accurate diagnosis, without the
need for prolonged observation or hospitalization.
There are several other tests that have been used to
facilitate the diagnosis of acute appendicitis but the
advantage of ultrasonography is its low cost, lack of
radiation exposure, easy availability, and noninvasive
nature [38].
Summary
Ultrasound is extremely beneficial in the evalua-
tion of acute pediatric abdominal disease, such
as HPS, intussusception, and acute appendicitis. As
techniques and equipment improve, its role in the eval-
uation of infants and children continues to increase.
References
[1] Mendelson KL. Emergency abdominal ultrasound
in children: current concepts. Med Health 1999;82:
198–201.
[2] Hudson PA, Promes SB. Abdominal ultrasonography.
Emerg Med Clin North Am 1997;15:826–48.
[3] Hernanz-Schulman M. Infantile hypertrophic pyloric
stenosis. Radiology 2003;227:319–31.
[4] Sivit CJ, Siegel MJ. Gastrointestinal tract. Pediatric
Sonography 2002;3:337–83.
[5] Haider N, Spicer R, Grier D. Ultrasound diagnosis of
infantile hypertrophic pyloric stenosis: determinants
of pyloric length and the effect of prematurity. Clin
Radiol 2002;57(2):136–9.
[6] Papadakis K, Chen EA, Luks FI, Lessin MS, Wessel-
hoeft Jr CW, DeLuca FG. The changing presentation
of pyloric stenosis. Am J Emerg Med 1999;17:67–9.
[7] Hernanz-Schulman M, Sells LL, Ambrosino MM,
Heller RM, Stein SM, Neblett III WW. Hypertrophic
pyloric stenosis in the infant without a palpable olive:
accuracy of sonographic diagnosis. Radiology 1994;
193:771–6.
[8] Lowe LH, Banks WJ, Shyr Y. Pyloric ratio: efficacy

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456 455
in the diagnosis of hypertrophic pyloric stenosis. J Ul-
trasound Med 1999;18:773–7.
[9] Yoshizawa J, Eto T, Higashimoto Y, Saitou T, Maie M.
Ultrasonographic features of normalization of the py-
lorus after pyloromyotomy for hypertrophic pyloric
stenosis. J Pediatr Surg 2001;36:582–6.
[10] del-Pozo G, Albillos JC, Tejedor D, Calero R, Rasero
M, de-la-Calle U. Intussusception in children: current
concepts in diagnosis and enema reduction. Radio-
graphics 1999;19:299–319.
[11] Shanbhogue RL, Hussain SM, Meradji M, Robben
SG, Vernooij JE, Molenaar JC. Ultrasonography is ac-
curate enough for the diagnosis of intussusception.
J Pediatr Surg 1994;29:324–8.
[12] Kim MC, Strouse PJ, Peh WC. Clinics in diagnostic
imaging (80). Ileocolic intussusception. Singapore
Med J 2002;43:645–8.
[13] Sargent MA, Babyn P, Alton DJ. Plain abdominal ra-
diography in suspected intussusception: a reassess-
ment. Pediatr Radiol 1994;24:17–20.
[14] Bisset III GS, Kirks DR. Intussusception in infants
and children: diagnosis and therapy. Radiology 1988;
168:141–3.
[15] Ratcliffe JF, Fong S, Cheong I, O’Connell P. Plain film
diagnoses of intussusception: prevalence of the target
sign. AJR Am J Roentgenol 1992;158:619–21.
[16] Eklof O, Hartelius H. Reliability of the abdominal plain
film diagnosis in pediatric patients with suspected in-
tussusception. Pediatr Radiol 1980;9:199–206.
[17] Meradji M, Hussain SM, Robben SG, Hop WC. Plain
film diagnosis in intussusception. Br J Radiol 1994;67:
147–9.
[18] Koumanidou C, Vakaki M, Pitsoulakis G, Kakavakis
K, Mirilas P. Sonographic detection of lymph nodes
in the intussusception of infants and young children:
clinical evaluation and hydrostatic reduction. AJR Am
J Roentgenol 2002;178:445–50.
[19] Verschelden P, Filiatrault D, Garel L, Grignon A,
Perreault G, Boisvert J. Intussusception in children:
reliability of US in diagnosis–a prospective study. Ra-
diology 1992;184:741–4.
[20] del Pozo G, Albillos JC, Tejedor D. Intussusception:
US findings with pathologic correlation-the crescent-
in-doughnut sign. Radiology 1996;199:688–92.
[21] Lim HK, Bae SH, Lee KH, Seo GS, Yoon GS. As-
sessment of reducibility of ileocolic intussusception
in children: usefulness of color Doppler sonography.
Radiology 1994;191:781–5.
[22] Lam AH, Firman K. Value of sonography including
color Doppler in the diagnosis and management of
long standing intussusception. Pediatr Radiol 1992;
22:112–4.
[23] Lagalla R, Caruso G, Novara V, Derchi LE, Cardinale
AE. Color Doppler ultrasonography in pediatric intus-
susception. J Ultrasound Med 1994;13:171–4.
[24] Rubi I, Vera R, Rubi SC, Torres EE, Luna A, Arcos J,
et al. Air reduction of intussusception. Eur J Pediatr
Surg 2002;12:387–90.
[25] Riebel TW, Nasir R, Weber K. US-guided hydrostatic
reduction of intussusception in children. Radiology
1993;188:513–6.
[26] Rohrschneider WK, Troger J. Hydrostatic reduction
of intussusception under US guidance. Pediatr Radiol
1995;25:530–4.
[27] Henrikson S, Blane CE, Koujok K, Strouse PJ, Di-
Pietro MA, Goodsitt MM. The effect of screening
sonography on the positive rate of enemas for intus-
susception. Pediatr Radiol 2003;33:190–3.
[28] Sivit CJ, Siegel MJ, Applegate KE, Newman KD.
When appendicitis is suspected in children. Radio-
graphics 2001;21:247–62.
[29] Lessin MS, Chan M, Catallozzi M, Gilchrist MF,
Richards C, Manera L. Selective use of ultrasonogra-
phy for acute appendicitis in children. Am J Surg 1999;
177:193–6.
[30] Scholer SJ, Pituch K, Orr DP, Dittus RS. Clinical out-
comes of children with acute abdominal pain. Pedi-
atrics 1996;98:680–5.
[31] Gamal R, Moore TC. Appendicitis in children aged
13 years and younger. Am J Surg 1990;159:589–92.
[32] Adolph VR, Fallerman KW. Appendicitis in children
in the managed care era. J Pediatr Surg 1996;31:
164–9.
[33] Rao PM, Rhea JT, Rattmer DW, et al. Introduction
of appendiceal CT: impact on negative appendectomy
and appendiceal perforation rates. Ann Surg 1999;
229:344–9.
[34] Bell MJ, Bower RJ, Ternberg JL. Appendectomy in
childhood: analysis of 105 negative exploration. Am
J Surg 1982;144:335–7.
[35] Puylaert JB. Acute appendicitis: ultrasound evalua-
tion using graded compression. Radiology 1986;158:
355–60.
[36] Bendeck SE, Nino-Murcia M, Berry GJ, Jeffrey Jr RB.
Imaging for suspected appendicitis: negative appen-
dectomy and perforation rates. Radiology 2002;225:
131–6.
[37] Sivit CJ, Applegate KE, Stallion A, Dudgeon DL,
Salvator A, Schluchter M. Imaging evaluation of sus-
pected appendicitis in a pediatric population: effective-
ness of sonography versus CT . AJR Am J Roentgenol
2000;175:977–80.
[38] Pena BM, Taylor GA, Fishman SJ, Mandl KD. Cost
and effectiveness of ultrasonography and limited com-
puted tomography for diagnosing appendicitis in
children. Pediatrics 2000;106:672–6.
[39] Pena BM, Taylor GA. Radiologists’ confidence in
interpretation of sonography and CT in suspected pe-
diatric appendicitis. AJR Am J Roentgenol 2000;175:
71–4.
[40] Sivit CJ, Newman KD, Boenning DA, Nussbaum-
Blask AR, Bulas DI, Bond SJ. Appendicitis: useful-
ness of US in diagnosis in a pediatric population.
Radiology 1992;185:549–52.
[41] Even-Bendahan G, Lazar I, Erez I, Gullemacker M,
Verner M, Konen O. Role of imaging in the diagnosis
of acute appendicitis in children. Clin Pediatr (Phila)
2003;42:23–7.

P. Vasavada / Radiol Clin N Am 42 (2004) 445–456456
[42] Lee JH, Jeong YK, Hwang JC, Ham SY, Yang SO.
Graded compression sonography with adjuvant use
of a posterior manual compression technique in the
sonographic diagnosis of acute appendicitis. AJR Am
J Roentgenol 2002;178:863–8.
[43] Quillin SP, Siegel MJ, Coffin CM. Acute appendicitis
in children: value of sonography in detecting perfora-
tion. AJR Am J Roentgenol 1991;159:1265–8.
[44] Borushok KF, Jeffrey RB, Laing FC, Townsend RR.
Sonographic diagnosis of perforation in patients with
acute appendicitis. AJR Am J Roentgenol 1990;154:
275–8.
[45] Quillin SP, Siegel MJ. Appendicitis: efficacy of color
Doppler sonography. Radiology 1994;191:557–60.
[46] Quillin SP, Siegel MJ. Diagnosis of appendiceal ab-
scess in children with acute appendicitis: value of color
Doppler sonography. AJR Am J Roentgenol 1995;164:
1251–4.
[47] Lim HK, Lee WJ, Lee SJ, Namgung S, Lim JH. Focal
appendicitis confined to the tip: diagnosis at US. Ra-
diology 1996;200:799–801.
[48] Sivit CJ. Diagnosis of acute appendicitis in children:
spectrum of sonographic findings. AJR Am J Roent-
genol 1993;161:147–52.
[49] Roosevelt GE, Reynolds SL. Does the use of ultraso-
nography improve the outcome of children with appen-
dicitis? Acad Emerg Med 1998;5:1071–5.

Radiol Clin N Am 42 (2004) 457–478
Emergent ultrasound interventions
Dean A. Nakamoto, MD*, John R. Haaga, MD
Department of Radiology, Case Western Reserve University, 11100 Euclid Avenue, Cleveland, OH 44106, USA
Interventional radiologists are frequently asked to effusion. Ultrasound evaluation before the procedure
perform emergent diagnostic and therapeutic proce-
dures. The choice of image guidance depends on
user preference; availability of CT, ultrasound, and
MR imaging; and the ability of the modality to
visualize the target. Ultrasound is the most preferred
modality and has many advantages including real-time
imaging of the needle tip during the procedure; multi-
planar imaging capabilities; its relatively low cost; and
the equipment is mobile, so procedures can be per-
formed at the bedside of critically ill patients in the
intensive care unit. Ultrasound-guided interventions
have become very common in many institutions [1,2].
Emergent procedures frequently performed with ultra-
sound guidance include thoracentesis, paracentesis,
percutaneous nephrostomy, and percutaneous chole-
cystostomy. The role of ultrasound guidance has also
expanded to include abscess drainage, particularly in
the pelvis, and chest tube placement. This article
discusses various emergent interventions performed
with ultrasound imaging guidance.
Ultrasound-guided chest interventions
Thoracentesis
Ultrasound-guided thoracentesis is usually per-
formed easily because most pleural fluid collections
are accessible using percutaneous methods. In the
septic patient, a diagnostic thoracentesis is usually
performed to evaluate for empyema. Other indications
include evaluation for chylous, bloody, or malignant
0033-8389/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/j.rcl.2004.01.002
* Corresponding author.
E-mail address: [email protected]
(D.A. Nakamoto).
confirms the presence of fluid and distinguishes
pleural fluid from atelectasis, mass, or elevated dia-
phragm. Typically, the patient is seated upright. Pleu-
ral fluid is generally anechoic, although debris or
septations may be present. The diaphragm must be
identified, and the underlying liver or spleen. A 3- to
4-MHz sector or vector probe is usually sufficient to
survey the hemithorax quickly.
Technique
Most diagnostic and therapeutic thoracenteses are
performed with ultrasound guidance. Typically, the
patient is seated upright with his or her back to the
interventionalist. To perform the procedure safely,
there should be at least one rib interspace of fluid
above and below the puncture site. If there is less
fluid, the procedure may be deferred depending on the
clinical urgency and the ability of the patient to
cooperate. Very small pleural fluid collections can
be aspirated safely, however, if the patient can coop-
erate with breath-holding. Patients who cannot sit
upright are placed either supine or in a lateral decu-
bitus position. In either of the latter two positions,
there must be a larger amount of fluid to attempt
thoracentesis. Because ultrasound can be performed
portably, ultrasound-guided thoracenteses can be per-
formed in an ICU, even on mechanically ventilated
patients [3]. If visualization is difficult because of
patient body habitus, air in the pleural fluid, or the
patient’s inability to be positioned adequately, CT
guidance may be helpful.
Initial scanning should be performed with a sector,
vector, or curvilinear probe. This is to document the
amount of fluid and quickly to find the largest pocket
of fluid. At this time, it is important to verify the
location of the diaphragm. Scanning can then be
performed with a linear probe of 6 MHz. This enables
s reserved.

Fig. 1. Aberrant intercostal artery. This sagittal color Doppler
scan performed with a 6-MHz linear probe demonstrates an
aberrant, tortuous course of the intercostal artery (arrow).
Here the artery is situated close to the midpoint of the rib
interspace. In this location, the artery is more susceptible to
injury from a needle.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478458
accurate localization of the rib interspace, particularly
in obese patients. The location of the intercostal artery
(Fig. 1) also is verified at this time. Although the
artery is usually directly adjacent to the inferior aspect
of the rib, it can be located more inferiorly and in the
rib interspace. If the patient has a malignancy, pleural-
based metastases can also be visualized at this time
and avoided (Fig. 2). It is important to be able to
recognize hypoechoic, consolidated lung and not
mistake it for pleural fluid. Sometimes consolidated
Fig. 2. Pleural-based metastases. This patient with metastatic lung c
based mass was noted (cursors); a different location was used.
lung may mimic complex fluid (Fig. 3) and color
Doppler may be helpful to verify the presence of
pulmonary vessels in consolidated lung. Following
sterile preparation of the skin, local anesthesia should
be administered from the skin surface to the pleural
surface. Although one could use ultrasound to visual-
ize needle insertion directly, typically a site is marked
on the skin surface and the needle is advanced until
fluid is obtained.
A variety of needles and catheters are available for
thoracenteses. The simplest method is to use an 18- or
20-gauge angiocatheter. The angiocatheter with punc-
ture needle is advanced into the pleural space until
fluid is aspirated, and then the angiocatheter is ad-
vanced into the pleural space over the puncture
needle. Single-step 6F trocar-based catheters (Skater,
Medical Device Technologies, Gainesville, Florida)
are also available, particularly if the procedure is
both diagnostic and therapeutic. These are used in a
similar fashion.
After a thoracentesis, the authors obtain a chest
radiograph in posteroanterior view to evaluate for
pneumothorax. The chance of pneumothorax is small
and generally ranges from 2.5% to 7.5% [4–7],
although rates up to 13.9% have been reported [8].
Symptoms caused by pneumothorax include shortness
of breath and shoulder pain on the affected side. Some
investigators do not advocate routine postprocedure
chest radiograph for the asymptomatic patient, be-
cause of the low complication rate [4,9,10]; however,
because sizable pneumothoraces may be asymptom-
atic, the authors routinely obtain a chest radiograph.
The mechanisms of postthoracentesis pneumothorax
ancer was referred for therapeutic thoracentesis. The pleural-

Fig. 3. Consolidated lung mimicking complex pleural fluid. This patient was referred for possible thoracenteses. Longitudinal
vector scan of the left hemithorax demonstrates complex-appearing mixed solid and cystic foci in the hemithorax (arrowheads)
consistent with consolidation of the lung.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 459
include (1) inadvertent introduction of air into the
pleural space, usually by leaving the needle or catheter
open to the air after the tip is in the pleural space;
(2) puncture of the lung; and (3) rupture of the vis-
ceral pleura because of a decrease in pleural pressure
[4,11]. If the pneumothorax is large, is symptomatic,
or increases with time, the patient may require a chest
tube placement.
Other significant complications of thoracentesis
include pain, vasovagal reaction, bleeding, and re-
expansion pulmonary edema. Pleuritic pain may be
caused by the rubbing of the visceral and parietal
pleural surfaces after the fluid has been removed. Pain
during the procedure may also be caused by the
inability of the patient’s collapsed lung to re-expand
as the fluid is removed. This may be an indication to
stop the procedure [4,7].
Vasovagal reactions may occur during any inter-
ventional procedure. The patient may become tran-
siently bradycardic, hypotensive, and may then lose
consciousness. Predisposing factors include volume
depletion. A quick physical examination of these pa-
tients shows bradycardia, diaphoresis, dilated pupils,
and hypotension. These vasovagal reactions are usu-
ally minor and temporary. Placing the patient in the
Trendelenburg position to improve venous return to
the heart usually resolves the problem. If the patient
improves within a few minutes, no other action is
needed. If significant, the patient may require atro-
pine. Typical atropine doses are as follows: adult—
1 mg intravenously; children—0.02 mg/kg to 0.60 mg
(maximum) intravenously. The treatment interval is
every 3 to 5 minutes to a total of 3 mg for adults or
2 mg for children. If the atropine does not improve the
situation, then urgent consultation with the resuscita-
tion team is appropriate.
Re-expansion pulmonary edema is an uncommon
complication of uncertain etiology. It may be asymp-
tomatic; however, it can cause various degrees of
hypoxia and can even be life-threatening [12,13]. It
presents as unilateral pulmonary edema, which may
progress to bilateral edema [4,12]. Re-expansion pul-
monary edema is believed to be more likely if a large
volume (ie, greater than 1 L) of pleural fluid is as-
pirated at one time. Some investigators have removed
up to 2 L at one time, however, without adverse con-
sequences [4,7].
Bleeding is an uncommon complication. The risk
is higher in patients with coagulopathies. It also may
occur with inadvertent laceration of the intercostal
artery [14]. The authors typically check platelets,
prothrombin time and partial thromboplastin time,
and International Normalized Ratio (INR) before
any procedure and adjust accordingly. They prefer
platelet counts over 50,000, and the prothrombin time
to be within 2 seconds of normal, or INR less than
1.5. Fine-needle aspirations may be performed out-
side of these ranges. Every case, however, should be
individually tailored.
Ultrasound-guided chest tube insertion
Pleural effusions can occur in a variety of settings,
including pneumonia (parapneumonic effusion); ma-
lignancy; bleeding; and fluid overload. The pleural
fluid can be classified as transudative or exudative,
depending on the laboratory analysis as described
in Box 1. Parapneumonic effusions are generally

Box 1. Light’s criteria for diagnosis ofexudative effusions
� Pleural fluid protein to serum proteinratio > 0.5
� Pleural fluid to serum L-lactatedehydrogenase ratio > 0.6
� Pleural L-lactate dehydrogenase con-centration more than two thirds ofthe normal upper limit for serumL-lactate dehydrogenase
*satisfying any one of these criteriasuggests exudative natureData from reference [16].
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478460
divided into complicated and uncomplicated effu-
sions. The uncomplicated effusions are transudative
effusions and small free-flowing exudative effusions.
These effusions can resolve spontaneously with anti-
biotic treatment.
The complicated effusions are exudative effusions
that do not respond to medical treatment and require
drainage. Empyema, hemothorax, and malignant effu-
sions are all complicated effusions. Indications for
drainage of pleural fluid are given in Box 2.
Regarding parapneumonic effusions, there are
three stages in the evolution of empyema [15,16].
The first stage is a free-flowing exudative effusion.
The second stage is the fibrinopurulent stage during
which the cellularity and protein content of the effu-
sion increase. Fibrin is deposited on the visceral and
parietal surfaces. The third stage is the organization
stage; fibroblasts and capillaries grow into exudates
and form a pleural peel. If untreated, this stage can
result in lung entrapment and subsequent fluid drain-
age into the chest wall or into the lung. Empyema
requires emergent drainage to control sepsis. The first
two stages should be drained by closed-tube drainage,
Box 2. Indications for drainage of pleuralfluid
� A very large pleural effusion causingcardiorespiratory embarrassment
� Grossly purulent or hemorrhagicpleural fluid
� Positive Gram stain� pH > 7.2� Glucose < 40 mg/dL� L-lactate dehydrogenase > 1000 U/L
either radiologic or surgical. The third stage usually
requires surgical decortication, although there are
some data suggesting that the pleural peels may re-
solve with closed-tube drainage [17].
Anechoic pleural collections or collections with
fine linear septations on ultrasound respond best to
catheter drainage, whereas those with a complex
honeycomb pattern usually fail catheter drainage and
require decortication. Patients showing parietal pleu-
ral thickness greater than 5 mm are unlikely to re-
spond to catheter drainage.
Indications for chest tubes and technique
The primary indication for chest tube placement is
to drain an empyema and prevent progression to the
organized stage. This can be accomplished with
surgical drainage or closed-tube drainage. Closed-
tube drainage can be performed with blind insertion
of a large-bore (22–34F catheter) chest tube placed by
a surgeon or with image-guided chest tube placement
using CT or ultrasound. Typically, smaller-bore, 8 to
14F catheters are used with the image-guided meth-
ods. The smaller tubes placed by imaging methods are
usually better tolerated by the patients than the larger,
surgically placed tubes. Therapeutic options for in-
fected pleural collections are summarized in Box 3.
Large pleural fluid collections are amenable to
single-step trocar catheters. The patient can be posi-
tioned either upright or in a lateral decubitus position
with the affected side up. As with a thoracentesis,
initial scanning should confirm the location of the
diaphragm and the overall size of the effusion. Once a
site is marked and the skin is sterilely prepared,
adequate local anesthesia should be used from the
skin surface to the pleural surface. A small incision
should be made with a scalpel, and the tract should be
dilated with a small hemostat. An initial aspiration
can be performed with a 19-gauge sheath needle with
a disposable 5F tetra-fluoro-ethylene (TFE) catheter
(Yueh centesis disposable catheter needle, Cook,
Box 3. Therapeutic options for infectedpleural collections
� Antibiotics� Tube thoracotomy� Intrapleural fibrinolytics (urokinase)� Thoracoscopy with lysisof adhesions
� Decortication� Open surgical drainage

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 461
Bloomington, Indiana) to determine the viscosity of
the fluid. A trocar–based, self-retaining catheter can
then be inserted blindly or under ultrasound visuali-
zation, depending on the size of the effusion. If the
effusion is thin, a single-step, 6 to 8F catheter (Skater,
Medical Technologies, Gainesville, Florida) can be
placed. Although 10F and larger catheters are avail-
Fig. 4. Complex left pleural effusion in heart transplant patien
demonstrates a large loculated left pleural effusion, which inve
illustrating the procedure. Under ultrasound guidance, a 19-gauge d
the effusion at the level of the midaxillary line. The needle is with
7.5-mm J 0.035-inch angiographic guidewire is placed. (C) The tra
self-retaining nephrostomy-type tube is placed. Arrows point to ne
able on single-step trocars, the authors have found
that these larger catheters can be difficult to insert in a
single-step procedure. If a 10F or larger catheter is
needed, the Seldinger technique can make catheter
insertion easier (Fig. 4). A standard 0.035-inch
angiographic guidewire can be placed through the
5F Yueh catheter and the tract can then be dilated.
t, left chest tube placement. (A) Longitudinal vector scan
rts the left hemidiaphragm. (B) Schematic representation
isposable sheath needle (Yueh centesis needle) is placed into
drawn, a small amount of fluid is aspirated, and a standard
ct is sequentially dilated to 10F catheter, and a 10F catheter
phrostomy tube.

Box 4. Indications for external drainage oflung abscess
� Persistent sepsis after 5 to 7 days ofantibiotic therapy
� Abscesses 4 cm or more in diameterthat are under tension
� Abscesses 4 cm or more in diameterthat are enlarging
� Failure to wean from a ventilatorbecause of a large abscess
Box 5. Relative contraindications forexternal drainage of lung abscess
� Noncompliant patient� Lack of an abscess-pleuralsymphysis
� Coagulopathy
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478462
CT is the preferred method for smaller effusions or
effusions close to vital structures, such as the heart or
major vessels. When placing the chest tube, a lateral
approach is preferred rather than a direct posterior
approach, if possible. The ideal site for catheter
placement is usually at the level of the midaxillary
line; the authors try to avoid a direct posterior
approach so that the patient does not lay on the tube.
Once the tube is placed, some of the fluid should
be withdrawn to confirm the location of the tube.
Direct visualization with ultrasound should also doc-
ument the location. The tube should be secured to the
skin and placed to a water-seal pleural drainage
system (Pleur-Evac, Deknatel, Fall River, Massachu-
setts) with suction at �20 cm H2O. Patients are
monitored daily to ensure proper tube functioning
and to record the amount of drained fluid. Once the
fluid becomes serous, the tube output has decreased to
20 mL or less per 24 hours, and the patient has
defervesced, the tube may be removed. A CT scan
should be performed before tube removal to ensure
that there are no undrained collections. Additional
drainage tubes may be placed for any separate collec-
tions not being drained.
Many empyemas are loculated, which can make
chest tube drainage difficult. Fibrinolytic agents, such
as streptokinase and urokinase, have been used suc-
cessfully to lyse septations [18–20]. Because uro-
kinase is not always available, the authors have been
using streptokinase, 125,000 IU every 12 hours for up
to 2 days.
Success rates range from 70% to 94%, with a
cumulative success rate of approximately 85% in
various radiologic studies [19–27]. Not all empyema
are amenable to percutaneous drainage. Patients who
develop a pleural peel or who have persistent fevers
and elevated white blood cell counts despite adequate
drainage and appropriate antibiotics may require sur-
gical drainage and decortication. Surgical treatment
for such patients should not be delayed. Complica-
tions from chest tube insertion include sepsis, inap-
propriate pathway of chest tube, bleeding, and injury
to adjacent organs.
Lung abscesses
Most lung abscesses are caused by oropharyngeal
aspiration of bacteria as can occur with alcoholic
stupor, general anesthesia, seizures, or cerebral vas-
cular accidents [28,29]. Other causes include malig-
nancy, septic emboli, foreign bodies, and lung cysts
[28,29]. It is important to distinguish between lung
abscess and empyema because empyema requires
external drainage, whereas most lung abscesses re-
solve with medical management [30]. The distinction
between lung abscess and empyema is best made with
contrast-enhanced CT. A lung abscess appears round
and if it contacts the pleural surface, it forms an acute
angle with the pleura. Empyema is more biconvex in
shape and forms obtuse angles with the pleura. The
wall of an abscess may have thick and irregular en-
hancement, whereas the enhancing pleura with empy-
ema has a smooth curvilinear appearance (ie, the split
pleura sign) [31].
Indications for external drainage of lung abscess
[32] are summarized in Box 4.
Relative contraindications for external drainage of
lung abscess are given in Box 5.
The abscess-pleural symphysis occurs when a lung
abscess is continuous with the pleura. It is important to
have a needle traverse the abscess-pleural symphy-
sis to decrease the chances of complications, such as
leak of abscess fluid into the pleural space and bron-
chopleural fistula. Catheter drainage is usually per-
formed by CT; however, ultrasound can be used in
selected cases. If the abscess-pleural symphysis is
small, CT is the modality of choice because it is easier
to place the needle accurately under CT guidance.
Because lung abscesses may have fine strands of
residual normal parenchyma, which can bleed, one
should not be too aggressive with catheter insertions or
guidewire manipulations [32].

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 463
Ultrasound-guided abdominal interventions
Paracentesis
Ultrasound-guided paracentesis is a commonly
performed procedure. Typically, the procedure is per-
formed emergently in a septic patient as a diagnostic
procedure to evaluate for spontaneous bacterial peri-
tonitis [33] or for hemoperitoneum in the setting of
trauma [34]. More commonly, this procedure is per-
formed urgently as a therapeutic measure for symp-
tomatic relief of tense ascites.
Initial scanning is performed with a sector or cur-
vilinear probe to find the largest pocket. Attention is
then made to the abdominal wall to ensure that there
are no vessels at the site of subsequent needle punc-
ture, such as the epigastric artery or collateral vessels
in a patient with cirrhosis. In patients with malignan-
cy, one should ensure that there are no peritoneal
metastases at the needle insertion site. This can be
performed with a linear transducer, usually of 6 MHz
or greater. The preferred site for large-volume para-
centesis is chosen in the dependent position, such as
right or left lower quadrants. The site of puncture is
chosen usually lateral to the rectus muscle to avoid the
accidental puncture of the inferior epigastric artery.
The inferior epigastric artery normally travels at the
junction of the medial two thirds and lateral one third
of the rectus or approximately 5 cm laterally from the
midline (Fig. 5). After standard sterile skin prepara-
tion, 1% lidocaine is injected into the abdominal wall
for local anesthesia. The authors anesthetize all the
Fig. 5. Paracentesis, epigastric artery. (A) Color Doppler transvers
transducer was used to localize the location of the inferior epiga
location along the lateral aspect of the rectus abdominis muscle. (B
the epigastric arteries (arrowheads).
way to the parietal peritoneum. Then they perform the
aspiration with a standard 18-gauge angiocatheter. If
the patient is obese, the authors use a 15- or 20-cm-
long, 19-gauge sheath needle (Yueh centesis dispos-
able catheter needle; Cook, Bloomington, Indiana).
For smaller collections or collections adjacent to ma-
jor vessels or to the spleen, the authors use direct
ultrasound guidance with either the freehand tech-
nique or the needle guide.
Large-volume paracentesis provides rapid resolu-
tion of symptoms with minimal complications and is
well tolerated by most patients. Complications from
paracentesis have rarely been reported, and include
inferior epigastric artery pseudoaneurysm [35], hem-
orrhage after large-volume paracentesis [36–38],
bowel perforation [38], hypotension [39], and a frag-
ment of the catheter left in the abdominal wall or
peritoneum [38]. Postparacentesis circulatory dys-
function has been reported and is characterized by
hyponatremia, azotemia, and an increase in plasma
renin activity. Postparacentesis circulatory dysfunc-
tion is associated with an increased mortality and may
be prevented by administration of albumin intrave-
nously (6 to 8 g/L of ascites removed) along with large
volume parasynthesis (LVP).
Percutaneous cholecystostomy
Acute cholecystitis in high-risk patients in the
ICU is difficult to manage. In critically ill, oftentimes
septic patients with possible acalculous or gangrenous
cholecystitis, percutaneous cholecystostomy may be
e image of the anterior abdominal wall with a 6-MHz linear
stric artery (arrow) before paracentesis. This is the typical
) CT scan on a different patient demonstrates the location of

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478464
both diagnostic and therapeutic. These patients are not
suitable candidates for surgery. Percutaneous chole-
cystostomy is used as a diagnostic and therapeutic
procedure in these critically ill and difficult to manage
patients [26,40–43]. In unstable patients with calcu-
lous cholecystitis, percutaneous cholecystostomy per-
mits stabilization so that cholecystectomy can be
performed electively.
Indications
Percutaneous cholecystostomy may be performed
in critically ill septic patients to exclude acute cho-
lecystitis, because of the difficulties of establishing
the diagnosis of acute cholecystitis in these patients
[26,44,45]. The findings on the various diagnostic
tests can be nonspecific. A sonographically normal
gallbladder virtually excludes cholecystitis in an ICU
patient, and a positive sonographic Murphy’s sign
may be the most specific finding of acute cholecystitis
in these patients [46]. Other findings, such as sludge,
distention, pericholecystic fluid, wall thickening, and
striations, are nonspecific in this setting [46,47]. The
presence of gallstones, distention, and pericholecystic
fluid, however, have been described as findings that
may predict a more favorable response to percutane-
ous cholecystostomy [41,47]
Technique
Two access routes are used. The transhepatic route
approaches from the right midaxillary line and aims
for the ‘‘bare’’ area of the gallbladder. This route is
preferred by most investigators and theoretically
reduces the risk of bile peritonitis [26,41,42,48]. The
transperitoneal approach is from the anterior abdomen
and is aimed at the gallbladder fundus [41,49–51].
Because of the risks of bile peritonitis and inadvertent
perforation of the colon, the transperitoneal approach
is probably best reserved for patients with very dis-
tended gallbladder in which the gallbladder fundus
abuts the anterior abdominal wall. This approach is
also useful in patients with coagulopathy or underly-
ing liver disease [41,43,49–51]. The transhepatic
route for percutaneous cholecystostomy does not al-
ways result in a puncture of the ‘‘bare area’’ of the
gallbladder and the ‘‘free’’ peritoneal surface of the
gallbladder may still be punctured [52]. Some inves-
tigators have also used simple aspiration of the gall-
bladder contents without placement of a drainage tube
[45,53]. The authors typically use the transhepatic
approach and ultrasound guidance. Sometimes CT
guidance may be necessary, however, particularly
for a liver in a high subcostal location. Typically, a
small 6F single-step trocar catheter (Skater, Medical
Device Technologies, Gainesville, Florida) is used. If
the trocar-based catheter buckles against the liver or
gallbladder wall, the Seldinger technique can be used
(Fig. 6). The acutely inflamed gallbladder wall can be
friable and catheter and wire manipulations should not
be too aggressive. If the Seldinger technique is used,
the authors use a 5F catheter on a 19-gauge needle
(Yueh centesis disposable catheter needle, Cook,
Bloomington, Indiana) to puncture the gallbladder
lumen. They then use a standard 0.035-inch guide-
wire; carefully dilate the tract to 8F catheter; and then
place an 8F catheter, self-retaining nephrostomy tube.
The authors recommend not using a super-stiff guide-
wire, such as an Amplatz, because it may perforate the
gallbladder wall. If the transperitoneal approach is
used, a small 8F catheter or less, single-step trocar
catheter is recommended. The gallbladder lumen
should be punctured with a sharp jab, and the gall-
bladder should be emptied once the catheter is within
[49]. The Seldinger technique is not favored with this
technique, because there is a theoretical risk of bile
leakage into the peritoneum.
Once the self-retaining tube is within the gallblad-
der, it is recommended that it remain there for at least
2 to 3 weeks to allow formation of a mature tract along
the catheter; otherwise, there may be bile leakage once
the catheter is removed [42,48]. It also is recom-
mended that a cholangiogram be performed before
catheter removal to ensure patency of the cystic duct
and common bile duct [26,48,54]. Some investigators
also advise imaging the tract at the time of tube
removal [26,43,44], although other investigators dis-
agree [41,49] even if the transperitoneal approach is
used [49].
Complication rates generally range from 5% to
13.8% [41,43,45,49,51,55]. Complications include
bleeding, bile leakage, catheter dislodgement, and
vasovagal events. Bile leakage has been reported with
both the transhepatic and transperitoneal approaches.
Technical success rates (ie, adequate placement of a
drain in the gallbladder) are high (ie, as great as 97%–
100%) [26,41–43,45,47–49,56]. Overall patient re-
sponse is lower, however, because of the relatively
low threshold of clinicians to request the procedure
and the nonspecificity of the diagnostic tests; no
clinical response to the procedure can be found in up
to 42% of the patients [26,42]. Placement of a chole-
cystostomy tube is still helpful in these circumstances,
however, because it does reassure the clinicians that
cholecystitis is not a cause of a patient’s sepsis.
Some investigators have used simple gallbladder
aspiration in patients with suspected acute cholecys-
titis [45,53]. Simple percutaneous gallbladder aspira-
tion does seem to be beneficial in patients with acute
cholecystitis and comorbid conditions. Chopra’s et al

Fig. 6. Ultrasound-guided percutaneous cholecystostomy in a patient status-post recent myocardial infarction. (A) Longitudinal
vector scan demonstrates distended gallbladder with sludge and a thick wall. Initial attempts with a 6F catheter one-step trocar-
based catheter were not successful, because of the thickened gallbladder wall. The catheter buckled on the trocar. The Seldinger
technique was used. A 19-gauge disposable sheath needle (Yueh centesis needle) was used to enter the gallbladder lumen. A
standard 0.035-inch angiographic guidewire was placed, the tract was carefully dilated to 8F catheter, and a self-retaining 8F
catheter nephrostomy-type tube (arrowhead) was placed. (B) Schematic representation of the procedure described in Fig. 6A.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 465
[45] patient population, although at high surgical risk,
consisted of noncritically ill patients. As stated in their
article, they excluded patients who had had prolonged
admission to the ICU.
Intra-abdominal abscess drainage
Image-guided percutaneous abscess drainage is a
well-established technique, which has become the
primary method of treatment for many patients with
intra-abdominal abscess [18,57–60]. In many hospi-
tals in the United States, CT is the imaging modality of
choice to detect abscesses. Once detected, an abscess
can be drained using either CT or ultrasound guidance
depending on which modality best delineates the
abscess and its surrounding structures. In general,
CT is used for abscesses inaccessible to ultrasound,
such as abscesses in deep locations adjacent to vital

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478466
structures (eg, major vessels or those adjacent to
bone), which may block the ultrasound beam. These
abscesses include pancreatic, interloop, and deep
retroperitoneal abscesses. Abscesses in more superfi-
cial locations of the peritoneum or visceral organs are
usually amenable to ultrasound guidance. Ultrasound
has many advantages, including its lower cost, its
ability to be performed portably at the patient’s bed-
side, and its multiplanar imaging capabilities.
Indications
In general, intraperitoneal abscesses adjacent to the
abdominal wall and abscesses in the periphery of
visceral organs, such as the liver or kidney, are
amenable to ultrasound-guided aspiration and drain-
age. The authors always avoid traversing uninvolved
spaces or organs, such as the liver or bowel, when
performing any interventional procedure. The excep-
tions are traversing the stomach for pancreatic proce-
dures and traversing the rectum or vagina for pelvic
abscess drainages. Other investigators have reported
success without significant complications from tra-
versing uninvolved spaces or organs while performing
interventional procedures [61–63]. If a loop of bowel
is inadvertently traversed with a catheter, the catheter
should be left in place for 2 to 3 weeks so a tract can
form. After this period the catheter can usually be
removed safely without spillage of bowel contents
into the peritoneum [64,65]. This assumes that the
underlying bowel is otherwise normal and that there is
no distal bowel obstruction. Relative contraindica-
tions common to all percutaneous procedures include
coagulopathy, the patient’s inability to cooperate, and
lack of safe access to the abscess.
Technique
Simple, uncomplicated abscess drainage is de-
scribed next.Management of more complex abscesses,
such as infected hematomas, abscesses associated
with fistulae, and fungal abscesses, is also discussed.
Pelvic abscesses, particularly those caused by gyne-
cologic sources, are discussed separately.
Preprocedure imaging is best performed with CT
because the size of the fluid collection, its location,
and extent can be well-delineated. The authors typi-
cally review the patient’s CT before the procedure and
if possible have a copy of the CT in the ultrasound
suite when performing the procedure. The CT pro-
vides an excellent roadmap to help plan the needle
trajectory. The authors frequently use a commercially
available needle guide, although for superficial ab-
scesses they use the freehand technique. For most
abscesses, the Seldinger technique is favored unless
the abscess is very large and superficial.
After obtaining informed consent, the fluid is
localized and the needle trajectory planned. The site
for needle insertion is marked, and the skin is prepared
and draped in a sterile manner. The ultrasound probe
is then covered with a sterile cover, and the needle
guide is attached unless the procedure is performed
freehand. A skin wheal is raised with local 1% lido-
caine, and a skin nick is made with a scalpel. Using a
19-gauge sheath needle (Yueh centesis disposable
catheter needle; Cook, Bloomington, Indiana), the
projected needle tract is anesthetized to the fluid
collection. The fluid collection is then punctured with
the 19-gauge sheath needle, the 5F disposable sheath
catheter is advanced over the needle, the sharp needle
is then removed, and the fluid is aspirated through the
5F disposable catheter sheath. If the fluid is purulent, a
standard 0.035-inch angiographic guidewire can be
advanced into the abscess. After confirming the loca-
tion of the guidewire, the tract can be dilated and an
appropriate-sized, self-retaining nephrostomy tube
can be placed. For thin pus, 8 to 10F catheters are
usually sufficient. Catheters up to 14F can be used for
more viscous pus. The tube position should then be
verified so that additional purulent fluid can be
aspirated. The catheter is then secured to the skin
either with sutures or adhesive fixation devices
(Percu-Stay Percutaneous Catheter Fastener, Derma
Sciences, Princeton, New Jersey).
Routine catheter care is then performed. The
authors place catheters to gravity drainage. Daily tube
rounds are made to evaluate the drainage progress.
Once the fluid becomes serous, the tube output has
decreased to less than 20 mL per 24 hours, the patient
has defervesced, and the white blood cell count is
normal, the tube may be removed. The authors typi-
cally repeat a CT scan before tube removal to ensure
that there are no residual fluid collections.
Liver abscess
Pyogenic liver abscesses located in the periphery
are amenable to ultrasound aspiration and drainage.
Those located more centrally are better approached
with CT guidance. Typically, a cuff of normal paren-
chyma should be included within the needle trajec-
tory to prevent spillage of the abscess contents into
the peritoneum (Fig. 7). The pleural space, loops
of bowel, and large intrahepatic vessels should be
avoided. Multilocular abscesses may be drained;
however, close follow-up and additional catheters
may be necessary [62]. The cure rate for liver abscess

Fig. 7. Ultrasound-guided liver abscess drainage in a septic patient whose previous catheter was inadvertently pulled out. (A) CT
scan demonstrates residual abscess in the dome of the right lobe of the liver (arrows). (B) Transverse ultrasound of the liver
demonstrates the 8F pigtail catheter (arrowhead) placed by the Seldinger technique into the abscess by a subphrenic approach.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 467
is about 80% to 90%. Causes of failures of percuta-
neous drainage of liver abscess are given in Box 6.
Renal and perinephric abscess
Renal and perirenal abscesses may be drained
using ultrasound guidance; however, such abscesses
are usually better detected and delineated by CT [66].
This is particularly important for abscesses in the
pararenal space because they can extend from the
pelvis to the diaphragm. A posterolateral approach is
preferred because it avoids the erector spinal muscles,
colon, liver, and spleen.
Percutaneous nephrostomy
The main emergent indication for percutaneous
nephrostomy is pyohydronephrosis, which can occur
in native or a transplant kidney. Other urgent indica-
tions include a rapidly rising creatinine level or recent
endourologic complication. Indications of percutane-
ous nephrostomy are summarized in Box 7. Ultra-
sound is an excellent method to guide the initial
needle placement for percutaneous nephrostomy.
These procedures are typically performed in the
angiography suite using a portable ultrasound unit.
Although the entire procedure can be performed
with fluoroscopic guidance only, ultrasound is very

Box 6. Causes of failures of percutaneousdrainage of liver abscess
Preprocedure
Unable to access the abscess safelyImproper pathway to abscessInability to place the catheter appropri-
ately within the abscess
Postprocedure
Premature withdrawal of catheterDislodged catheterCatheter kinked or occludedHigh-output fistula to gastrointesti-
nal tractFungal abscessInfected necrotic tumorViscous pus or multiple septations,
resistant to fibrinolytic therapySepsis or death
Box 7. Indications for percutaneousnephrostomy
1. Relief of urinary obstructionImprove renal functionEvacuate pyonephrosisAssess recoverable renal function in
chronic obstruction2. Diversion of urine in case of urinary
leakageTraumatic or iatrogenic urinary
tract injuryInflammatory or malignant
urinary fistula3. Provide access for urinary
manipulationPerform dynamic flow-pressure
studies (Whitaker test)BiopsyStone therapyBenign stricture dilatationUreteral stent placementForeign body retrievalNephroscopic surgery
(eg, endopyelotomy)Administration of antifungal agents
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478468
useful for obtaining initial access to the renal collect-
ing system [20,67], particularly in cases where the
hydronephrosis is mild, or for renal transplants where
the renal axis can vary. For a native kidney, the
authors target a posterior calyx using a posterolateral
approach to avoid most of the erector spinus muscles.
For transplant kidneys, the authors target an anterior
calyx. Typically, they use a 20-gauge Chiba needle for
initial access, followed by instillation of contrast and a
small amount of air (3–5 mL) to confirm the needle
position (Fig. 8). The air rises to the nondependent
calices. If the needle position is satisfactory, the tract
can be dilated with a micropuncture set through the
20-gauge Chiba needle. If there is a better site to
access the collecting system, a second needle can then
be placed under fluoroscopic guidance using either a
20-gauge Chiba needle or 19-gauge sheath needle
(Yueh centesis needle). The tract is dilated using the
Seldinger technique, and an 8 to 14F catheter self-
retaining nephrostomy tube can be placed.
Splenic abscess
Splenic abscess if untreated have a mortality rate
of 80% to 100% and mortality rate of 14% to 30%
with surgical drainage. Experience with percutaneous
drainage is limited [59,68–70]. Although no major
complications were reported in these series [59,70],
their numbers were small. Green [68] described suc-
cessful percutaneous drainage in only one of four
patients. Lucey et al [67] successfully drained five
of six splenic abscesses; the one failure required a
splenectomy. The authors believe that splenic abscess
drainage should only be performed in rare circum-
stances and should generally be reserved for select
patients. Close consultation with the surgical service
is recommended so that an emergent splenectomy can
be performed if needed. If percutaneous drainage of a
splenic abscess is to be attempted, the abscess ideally
should be peripheral so that the least amount of nor-
mal splenic parenchyma is traversed. Thanos et al
[69], however, have performed drainages in two pa-
tients where the needle and catheter traversed 2.3 cm
of normal splenic parenchyma.
Fistulae
Uncomplicated abscesses have gradually decreas-
ing output following percutaneous drainage. In those
abscesses with persistently elevated output (ie, greater
than 100 mL per 24 hours) more than 3 to 4 days after

Fig. 8. Ultrasound-guided percutaneous nephrostomy in a renal transplant with pyohydronephrosis caused by ureteral calculus.
(A) Initial ultrasound demonstrates complex-appearing urine within the hydronephrotic transplant, which is consistent with
pyohydronephrosis. The indwelling stent is noted (arrows). (B) Longitudinal ultrasound of the dilated distal transplant ureter
demonstrates an obstructing calculus in the cursors. Note the ‘‘twinkle’’ artifact from the calculus with the color Doppler.
(C) Longitudinal image during placement of a nephrostomy tube (arrowhead). (D) Schematic representation of the kidney and
positioning of the catheter.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 469

Fig. 8 (continued ).
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478470
initial catheter placement, especially drainage consist-
ing of bilious or enteric material, a gastrointestinal
fistula is likely [71,72]. At this point a sinogram con-
firms the communication to the gastrointestinal tract.
The cause of the fistula should then be determined so
that appropriate treatment may be initiated. Fistulae
caused by distal obstruction, neoplastic involvement,
or ongoing infection must have these underlying
conditions corrected or the abscess does not heal.
Low-output fistulae (ie, less than 320 mL per day)
usually close spontaneously without additional thera-
py [18]. High-output fistulae may require additional
treatment, including suction on the abscess catheter,
and bowel rest often with nasogastric tube placement.
Hyperalimentation may be necessary, and surgical
intervention may be required [18].
Infected hematomas
Most infected hematomas do not drain with simple
catheter placement because of their extensive amount
of fibrin and the protective effects of fibrin on bacteria
[18]. For patients with a suspected infected hema-
toma, the authors perform an initial aspiration. If
the fluid is bloody but not grossly infected, they only
take a sample for laboratory analysis and do not place
a catheter for the fear of secondary infection. If
the fluid is grossly purulent or if the cultures subse-
quently come back positive for infection, a drainage
catheter is placed. Sometimes local instillation of fi-
brinolytic agents, such as streptokinase, 125,000 IU
twice a day-for 2 days, may improve drainage from
such hematomas.
Fungal abscess
Fungal abscesses are difficult to treat with percu-
taneous drainage and may require surgical drainage
and debridement [18,73]. This is probably caused by
the extensive tissue invasion, necrosis, and mycotic
plaque formation in the wall of the cavity [18].
Echinococcal abscess
A number of investigators have described success-
ful treatment of hydatid cysts using percutaneous
aspiration and drainage [74–79]. The technique is
similar to routine abscess aspiration and drainage.
Various catheter irrigants are used, such as hyperto-
nic saline [74,79], scolicidal agent [75], or alcohol
[76,77,79]. Anaphylaxis is a potential complication,
which can be severe or even fatal [78]. Many of the
patients were given prophylaxis with albendazole.
Some investigators perform single-step aspiration
[74,77], whereas others aspirate the smaller cysts
and leave catheters in larger (> 6 cm) cysts [75,78,79].
Pelvic abscesses
Image-guided percutaneous drainage (Fig. 9) is
commonly performed for pelvic abscesses. Typically,
pelvic abscesses arise from gastrointestinal sources,
such as diverticulitis, ruptured appendicitis, and
Crohn’s disease, and from postoperative fluid collec-
tions. In female patients, pelvic abscesses may also
arise from gynecologic sources, such as tubo-ovarian
abscess from pelvic inflammatory disease. Such pel-
vic abscesses are traditionally treated with medical
therapy and if drainage of abscess is required many
investigators prefer image-guided interventional tech-
niques [80–87]. Pelvic abscesses in a female second-
ary to gynecologic causes are a special category and
usually have acute presentation.
Imaging-guided pelvic abscess drainage offers
several advantages to traditional surgical drainage.
The imaging-directed methods are less invasive and
do not require general anesthesia. The indications for
surgical drainage include ruptured tubo-ovarian ab-
scess, when diagnosis is uncertain; pelvic abscess
secondary to appendicitis or ruptured viscus [88];
and failed percutaneous drainage. The imaging-guid-
ed methods include transabdominal, transgluteal,
transrectal, and transvaginal approaches. The trans-
perineal approach has also been described [89]. In
general, the transabdominal approach is preferred,

Fig. 9. Ultrasound-guided pelvic abscess drainage, transabdominal, in a postsurgical patient. (A) Initial CT scan demonstrates
abscesses in the right and left lower quadrants of the pelvis (arrows). (B) Under ultrasound guidance the abscess in the right
lower quadrant was localized and punctured with a 19-gauge sheath needle. After confirming pus, a standard 0.035-inch
angiographic guidewire (Rosen) was advanced into the abscess. The tract was dilated to 10F catheter, and a self-retaining 10F
catheter nephrostomy tube (arrowhead) was placed. (C) The left lower quadrant abscess was then localized. Initial attempts were
made with a 12F one-step catheter; however, the patient complained of too much discomfort. This abscess was also punctured
with a 19-gauge sheath needle. After confirming pus, the tract was dilated and a 12F catheter nephrostomy tube was placed
(arrowhead). (D) Schematic representation of the procedure.
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 471

Fig. 9 (continued ).
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478472
using CT or ultrasound, because it is very well-
tolerated by patients. Pelvic abscesses may not be
accessible using the transabdominal approach, how-
ever, because of the presence of intervening loops of
bowel, urinary bladder, major blood vessels, or the
uterus. The transgluteal approach has several disad-
vantages, including patient discomfort, injury to the
sciatic nerve, and an increased chance of catheter
kinking and subsequent malfunction [84,90]. Al-
though initially underused, some investigators have
recently been successful using the transgluteal ap-
proach [90–93]. The transrectal [94–97] and trans-
vaginal approaches are well established [60,80–
84,88,98]. The transrectal approach can be guided
using CT [94], ultrasound [95–97,99], or ultrasound
combined with fluoroscopy [100]. The transvaginal
approach is usually guided with ultrasound.
Most patients with tubo-ovarian abscesses respond
to intravenous antibiotic therapy. As expected, the
response to antibiotics is inversely related to the size
of the abscess [82]. In unruptured tubo-ovarian ab-
scesses not responding to antibiotics, image-guided
drainage is indicated. The decision to proceed with
drainage is usually made in conjunction with the
gynecologic service. The authors prefer the trans-
abdominal approach, if possible, followed by the
transrectal approach with CT guidance, and finally
the transvaginal approach with ultrasound. Female
patients tolerate transrectal catheter placement better
as compared with transvaginal placement [99]. The
authors use the transgluteal approach only when
necessary (ie, a deep pelvic abscess in a patient with
underlying rectal mucosal disease or in premenarchal
or sexually inactive females). The transperineal ap-
proach provides an additional option for deep pelvic
abscess drainage and may be a viable alternative for
patients who have undergone abdominoperineal re-
section [89].
Technique
The transvaginal approach is best performed with
ultrasound guidance (Fig. 10). First, the abscess
should be localized by endovaginal ultrasound. The
abscess should be directly adjacent to the vaginal
vault with no intervening structures. The ultrasound
probe then is removed and the perineum and vagina
are prepared with a standard povidone-iodine solu-
tion. A vaginal speculum is then inserted and the
vaginal vault is prepared using sponges soaked in io-
dine-iodine solution. The speculum is then removed.
Despite the iodine-iodine preparation, the vagina is
still semi-sterile. If the patient is not already receiving
intravenous antibiotics, she should be given an appro-
priate antibiotic before beginning the procedure. Be-
cause it can be difficult to hold the ultrasound probe
while doing the various catheter manipulations, the
procedure generally requires two people.
The endovaginal ultrasound probe is then fitted
with a modified guide to allow catheter insertion. The
commercially available needle guides typically do not
allow placement of trocar-based catheters. Various
methods can be used [80,88], although the authors
prefer using the plastic sheath that comes with the
catheter, as described by O’Neill et al [79]. The
endovaginal probe is initially placed in a sterile probe
cover with coupling gel. A modified guide then is
made from the plastic catheter protector. The plastic
protector is cut so that approximately 5 cm of the
catheter protrudes beyond the end of the guide; a slit is
then made along the length of the guide, which
facilitates subsequent removal of the guide from the
catheter. This modified guide is then attached to the
sterilely prepared endovaginal probe with sterile rub-
ber bands along the groove intended for the metal
probe guide. The 6 to 8F trocar-based catheter (Skater,
Medical Device Technologies, Gainesville, Florida) is
then placed into the modified guide and a second
sterile probe cover is placed over the catheter and
guide. The catheter punctures the outer sterile probe
cover before puncturing the vaginal wall. One can
attempt to use local lidocaine at the vaginal wall but
this can be difficult because there are no landmarks to
ensure that the same area is traversed with the catheter.
Before placing a catheter, an initial aspiration should
be performed using an 18- to 20-gauge needle to
document infection. Initial scanning should be done
to place the abscess centrally within the scan plane
and to visualize where the catheter enters the abscess.
The tip of the trocar-based catheter should indent the

Fig. 10. Ultrasound-guided transvaginal pelvic abscess drainage. (A) Photograph shows the trocar catheter advanced through the
guide and projecting approximately 5 cm past the end of the probe (arrow). Note that the guide (plastic sheath) needs to be cut to
a length such that it allows at least 5 cm of catheter advancement so that the catheter can be advanced through the vaginal vault.
(B) Photograph shows the catheter has been fed off and the pigtail has been formed. The inner needle has been removed, but the
outer metal cannula stiffener is left in the straight portion of the catheter to stiffen it and ease the peeling away of the guide from
the catheter. (C) CT scan shows a complex right adnexal fluid collection (straight arrow). An incidentally noted right-sided
fundal fibroid is noted (curved arrow). (D) Transvaginal ultrasound scan shows trocar-catheter assembly (arrow) in the right
adnexal collection along the guide. (From O’Neill MJ, Rafferty EA, Lee SI, et al. Transvaginal interventional procedures:
aspiration, biopsy, and catheter drainage. Radiographics 2001;21:657–72; with permission.)
D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 473
wall of the abscess during light palpation. Assuming
there are no intervening structures and the trajectory is
appropriate, the abscess wall is punctured using a
sharp thrust of 1 to 2 cm. This is the most difficult part
of the procedure. It is helpful to apply enough pressure
with the endovaginal ultrasound probe so that the
vaginal wall is taut before being punctured with the
trocar. The sharp needle of the trocar is removed and a
diagnostic aspiration is performed. Once pus is aspi-
rated, the catheter is advanced over the metal stiffener
of the trocar until the self-retaining loop is formed and
locked. The endovaginal probe is then removed care-
fully and the rubber bands and outer sterile cover
gradually are cut. The modified guide is then removed
from the catheter. This is easier to perform if the metal
stiffener is placed partially within the catheter. The
stiffener is then removed and more pus is aspirated.
Because of difficulties in penetrating the vaginal wall,
the authors have found that 10F or smaller catheters
are easier to insert.
Although the single-step trocar-based catheter is in
general easier to perform, the authors find the Sel-
dinger technique useful for inserting larger catheters
into abscesses with thick pus [84,101,102]. For expe-
rienced operators, ultrasound alone can be used.
Alternatively, a combination of ultrasound and fluo-
roscopy can be performed. With the Seldinger tech-
nique, the abscess is punctured with a 19-gauge sheath

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478474
needle with a disposable 5F TFE catheter (Yueh
centesis disposable catheter needle; Cook, Blooming-
ton, Inidana). After aspirating pus to confirm its
location, the 19-gauge needle is removed, leaving
the 5F catheter in the abscess, and a standard 0.035-
inch angiographic guidewire is advanced into the
abscess. The 5F TFE catheter is then removed and a
standard 5F pigtail catheter is placed over the guide-
wire and coiled into the abscess. Placement should be
confirmed with ultrasound. The disposable 5F TFE
catheter is not long enough to allow a guidewire to
coil within the abscess. The 0.035-inch guidewire is
removed, and a 0.035-inch Amplatz wire (Amplatz
Super Stiff, Boston Scientific, Medi-Tech, Miami,
Florida) is advanced into the 5F pigtail catheter. The
5F pigtail catheter is then removed, the tract can be
dilated up to 14F catheter, and an appropriate size of
self-retaining nephrostomy-type tube can be placed. If
the abscess is large enough, an Amplatz wire can be
introduced initially; however, this must be done care-
fully to avoid perforating the wall of the abscess with
the super-stiff wire. The stiffness of the Amplatz wire
(Amplatz Super Stiff, Boston Scientific, Medi-Tech,
Miami, Florida) allows the tract to be dilated despite
the distance between the operator’s hands and the
point of wire insertion in the vaginal wall. Less stiff
guidewires may kink. All of the dilatations can be
performed through the modified guide on the endo-
vaginal probe.
Some investigators perform simple needle aspi-
ration of an abscess without catheter placement
[81,103–106]. Although large, multiloculated collec-
tions can be treated this way, this method may be most
useful for small, unilocular collections. Nelson et al
[80] found no correlation between the size of an
abscess and the success rates for simple aspiration.
The advantages of this method are that it is safe, easier
to perform than catheter drainage, and there is no
problem with catheter misplacement or dislodging.
The disadvantages include multiple punctures for
multiloculated abscesses, an extended period of anti-
biotic coverage to control residual infection, and re-
peat aspiration for recurrent abscess [81,88]. For this
method, a standard needle guide attached to an endo-
vaginal probe can be used with an 18- to 20-gauge
needle. The needle must be at least 18 to 20 cm long to
fit through the needle guide. Contraindications in-
clude diffuse multifocal abscesses or abscess with
peritonitis, abscesses associated with fistulas, foreign
bodies, or abscesses caused by pancreatitis.
After the catheter is placed in the abscess and
locked in position, the authors tape the catheter to the
patient’s leg. Routine catheter care is then used. The
catheters are left to gravity drainage. The authors do
not routinely flush the catheters unless they are using
fibrinolytic agents, such as streptokinase.
Success rates for transvaginal drainage range from
78% to 100% [60,81,82,84,98,106]. Similar success
rates are noted for the other methods (ie, transabdomi-
nal, transrectal, and transgluteal) of pelvic abscess
drainage, ranging from 94% to 100% [83,91,94,96].
Complications from transvaginal drainage are infre-
quent and include bleeding, infection, underlying
organ damage, and vaginal fistula formation. Catheter
dislodgement may occur following any drainage pro-
cedure; however, this did not adversely affect patient
outcome in three of four patients in the study of Ryan
et al [94].
Summary
The interventionist can perform many emergent
procedures with ultrasound guidance, because of its
real-time, multiplanar imaging capability and porta-
bility. With the use of color Doppler, additional im-
portant information, such as aberrant vessels, can be
ascertained to help plan needle trajectory. Ultrasound
is also useful for nonemergent procedures, such as
biopsies. All interventionists are encouraged to be
facile with the use of ultrasound.
Acknowledgment
The authors thank Elena DuPont of the radiology
department at University Hospitals of Cleveland for
the line drawings and Joe Molter for assisting in the
preparation of images.
References
[1] Dodd III GD, Esola CC, Memel DS, et al. Sonogra-
phy: the undiscovered jewel of interventional radiol-
ogy. Radiographics 1996;16:1271–81.
[2] Sheafor DH, Paulson EK, Simmons CM, et al. Ab-
dominal percutaneous interventional procedures: com-
parison of CT and US guidance. Radiology 1998;
207:705–10.
[3] Lichentstein D, Hulot JS, Rabiller A, Tostivint I. Fea-
sibility and safety of ultrasound-aided thoracentesis in
mechanically ventilated patients. Intensive Care Med
1999;25:955–8.
[4] Jones PW, Moyers JP, Rogers J, Rodriquez R, et al.
Ultrasound-guided thoracentesis: is it a safer method?
Chest 2003;123:418–23.
[5] Raptopoulos V, Davis L, Lee G, Umali C, et al. Fac-
tors affecting the development of pneumothorax as-

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 475
sociated with thoracentesis. AJR Am J Roentgenol
1991;156:917–20.
[6] Alemen C, Alegre J, Armadans L, Andreu J, Falco V,
et al. The value of chest roentgenography in the diag-
nosis of pneumothorax after thoracentesis. Am J Med
1999;107:340–3.
[7] Boland GW, Lee MJ, Silverman S, Mueller PR. Inter-
ventional radiology of the pleural space. Clin Radiol
1995;50:205–14.
[8] Peterson W, Zimmerman R. Limited utility of
chest radiograph after thoracentesis. Chest 2000;4:
1038–42.
[9] Doyle JJ, Hnatiuk O, Torrington K, Slade A, Howard
R. Necessity of routine test roentgenography after
photosynthesis. Ann Intern Med 1996;124:816–20.
[10] Capizzi SA, Prakash U. Chest roentgenography after
outpatient thoracentesis. Mayo Clin Proc 1998;73:
948–50.
[11] Gervais DA, Petersein A, Lee M, Hahn P, et al. US-
guided thoracentesis: requirement for postprocedure
chest radiography in patients with receive mechani-
cal ventilation versus patients who breathe spontane-
ously. Radiology 1997;204:503–6.
[12] Mahfood S, Hix W, Aaron B, Blaes P, et al. Re-
expansion pulmonary edema. Ann Thorac Surg 1988;
45:340–5.
[13] Gascoigne A, Appleton A, Taylor R, Batchelor A,
Cook S. Catastrophic circulatory collapse following
re-expansion pulmonary oedema. Resuscitation 1996;
31:265–9.
[14] Carney M, Ravin CE. Intercostal artery laceration
during thoracentesis: increased risk in elderly pa-
tients. Chest 1979;75(4):520–2.
[15] Sahn SA. Management of complicated parapneu-
monic effusions. Am Rev Respir Dis 1993;148:
813–7.
[16] Light RW. Parapneumonic effusions and empyema.
Clin Chest Med 1985;6:55–62.
[17] Neff CC, vanSonnenberg E, Lawson D, Patton A. CT
follow-up of empyemas: pleural peels resolve after
percutaneous catheter drainage. Radiology 1990;176:
195–7.
[18] Haaga JR. Image-guided micro procedures. In: Haaga
JR, Lanzieri CF, Gilkeson RC, editors. CT and MR
imaging of the whole body. 4th edition. St. Louis:
Mosby; 2003. p. 2123–257.
[19] Moulton JS, Moore PT, Mencini RA. Treatment of
loculated pleural effusions with transcatheter intra-
cavitary urokinase. AJR Am J Roentgenol 1989;153:
941–5.
[20] Lee KS, Im J, Kim YH, Hwang SH, Bae WK, Lee
BH. Treatment of thoracic multiloculated empyemas
with intracavitary urokinase: a prospective study. Ra-
diology 1991;179:771–5.
[21] Silverman SG, Mueller PR, Saini S, Hahn PF,
Simeone JF, et al. Thoracic empyema: management
with image-guided catheter drainage. Radiology
1988;169:5–9.
[22] Hunnan GR, Flower CD. Radiologically-guided per-
cutaneous catheter drainage of empyemas. Clin Radiol
1988;39:121–6.
[23] Merriam MA, Cronan JJ, Dorfman GS, Lambiase
RE, Haas RA. Radiographically guided percutaneous
catheter drainage of pleural fluid collections. AJR
Am J Roentgenol 1988;151:1113–6.
[24] Westcott JL. Percutaneous catheter drainage of pleural
effusion and empyema. AJR Am J Roentgenol 1985;
144:1189–93.
[25] vanSonneberg E, Mueller PR, Ferrucci Jr JT. Percuta-
neous drainage of 250 abdominal abscesses and fluid
collections. Pt I. Results, failures, and complications.
Radiology 1984;151:337–41.
[26] Lee MJ, Saini S, Brink J, Hahn P, et al. Treatment of
critically ill patients with sepsis of unknown cause:
value of percutaneous cholecystostomy. AJR Am J
Roentgenol 1991;156:1163–6.
[27] Moulton JS, Benkert RE, Weisiger KH, Chambers
JA. Treatment of complicated pleural fluid collec-
tions with image-guided drainage and intracavitary
urokinase. Chest 1995;108:1252–9.
[28] Moore AV, Zuger JH, Kelley MJ. Lung abscess: an
interventional radiology perspective. Semin Interv
Radiol 1991;1:36–43.
[29] Bartlett JG. Anaerobic bacterial infections of the lung.
Chest 1987;91:901–9.
[30] Weissberg D. Percutaneous drainage of lung abscess.
J Thorac Cardiovasc Surg 1984;87:308–12.
[31] Stark DD, Federle MP, Goodman PC, Polrasky AE,
Webb WR. Differentiating lung abscess and empy-
ema: radiography and computed tomography. AJR
Am J Roentgenol 1983;141:163–7.
[32] Rice TW, Ginsberg RJ, Todd TR. Tube drainage of
lung abscesses. Ann Thorac Surg 1987;44:356–9.
[33] Guarner C, Runyon BA. Spontaneous bacterial peri-
tonitis: pathogenesis, diagnosis, and management.
Gastroenterologist 1995;3(4):311–28.
[34] Goletti O, Ghiselli G, Lippolis PV, Chiarugi M, Brac-
cini G, Macaluso C, et al. The role of ultrasonography
in blunt abdominal trauma: results in 250 consecutive
cases. J Trauma 1994;36:178–81.
[35] Lam EY, McLafferty RB, Taylor Jr LM, Moneta
GL, et al. Inferior epigastric artery pseudoaneurysm:
a complication of paracentesis. J Vasc Surg 1998;28:
566–9.
[36] Webster ST, Brown KL, Lucey MR, Nostrant TT.
Hemorrhagic complications of large volume ab-
dominal paracentesis. Am J Gastroenterol 1996;91:
366–8.
[37] Arnold C, Haag K, Blum HE, et al. Acute hemo-
peritoneum after large-volume paracentesis. Gastro-
enterology 1997;113:978–82.
[38] Mallory A, Schaefer JW. Complications of diagnostic
paracentesis in patients with liver disease. JAMA
1978;239:628–30.
[39] Ross GJ, Kessler HB, Clair MR, Gatenby RA, et al.
Sonographically guided paracentesis for palliation of
symptomatic malignant ascites. AJR Am J Roent-
genol 1989;153:1309–11.

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478476
[40] Boland G, Slater G, Lu D, Eisenberg P, et al. Preva-
lence and significance of gallbladder abnormalities
seen on sonography in intensive care unit patients.
AJR Am J Roentgenol 2000;174:973–7.
[41] Boland GW, Lee MJ, Leung J, et al. Percutaneous
cholecystostomy in critically ill patients: early re-
sponse and final outcome in 82 patients. AJR Am J
Roentgenol 1994;163:339–42.
[42] vanSonnenberg E, D’Agostino H, Sanchez R, Casola
G. Percutaneous abscess drainage. Radiology 1992;
184:27–9.
[43] vanOverhagen H, Meyers H, Tilanus HW, Jeekel J,
Lemeris JS. Percutaneous cholecystectomy for pa-
tients with acute cholecystitis and an increased surgi-
cal risk. Cardiovasc Intervent Radiol 1996;19:72–6.
[44] Chopra S, Dodd G, Mumbower A, Chintapalli K, et al.
Treatment of acute cholecystitis in non-critically ill
patients at high surgical risk: comparison of clinical
outcomes after gallbladder aspiration and after per-
cutaneous cholecystostomy. AJR Am J Roentgenol
2001;176:1025–31.
[45] England RE, McDermott VG, Smith TP, Suhocki PV,
Payne CS, Newman GE. Percutaneous cholecys-
tostomy: who responds? AJR Am J Roentgenol 1997;
168:1247–51.
[46] Browning PD, McGahan JP, Gersovich EO. Percuta-
neous cholecystostomy for suspected acute cholecys-
titis in the hospitalized patient. J Vasc Interv Radiol
1993;4:531–8.
[47] Boggi U, Di Candio G, Campetelli A, et al. Percu-
taneous cholecystostomy for acute cholecystitis in criti-
cally ill patients. Hepatogastroenterology 1999;46:
121–5.
[48] Garber SJ, Mathleson J, Cooperberg P, MacFarlane
J. Percutaneous cholecystostomy: safety of the trans-
peritoneal route. J Vasc Interv Radiol 1994;5:295–8.
[49] Hatzidakis AA, Prassopoulos P, Petinarakis I, et al.
Acute cholecystitis in high-risk patients: percuta-
neous cholecystostomy vs conservative treatment.
Eur Radiol 2002;12:1778–84.
[50] Teplick SK, Brandon JC, Wolferth CC, Amron G,
Gambescia R, Zitomer N. Percutaneous interventional
gallbladder procedures: personal experience and liter-
ature review. Gastrointest Radiol 1990;15:133–6.
[51] Nemcek Jr AA, Bernstein JE, Vogelzang RL. Percu-
taneous cholecystostomy: does transhepatic puncture
preclude a transperitoneal catheter route? J Vasc
Interv Radiol 1991;2:543–7.
[52] Verbanck JJ, Demol JW, Ghillebert GL, Rutgeerts
LJ, Surmont IP. Ultrasound-guided puncture of the
gallbladder for acute cholecystitis. Lancet 1993;341:
1132–3.
[53] D’Agostino H, vanSonnenberg E, Sanchez R, Gooda-
cre B, Casola G. Imaging of the percutaneous chole-
cystostomy tract: observations and utility. Radiology
1991;181:675–8.
[54] Teplick SK. Diagnostic and therapeutic interventional
gallbladder procedures. AJR Am J Roentgenol 1989;
152:913–6.
[55] Patel M, Miedema BW, James MA, Marshall JB.
Percutaneous cholecystostomy is an effective treat-
ment for high-risk patient: with acute cholecystitis.
Am Surg 2000;66:33–7.
[56] vanSonnenberg E, Wittich GR, Goodacre BW, Casola
G. Percutaneous abscess drainage: update. World J
Surg 2001;25:362–9.
[57] Nakamoto DA, Haaga JR. Percutaneous drainage of
postoperative intra-abdominal abscesses and collec-
tions. In: Cope C, editor. Current techniques in in-
terventional radiology. 2nd edition. Philadelphia:
Current Medicine; 1995. p. 111–23.
[58] Lambiase RE, Deyoe L, Cronan JJ, et al. Percuta-
neous drainage of 335 consecutive abscesses: results
of primary drainage with 1-year follow-up. Radiology
1992;184:167–79.
[59] VanSonnenberg E, D’Agostino HB, Casola G,
Goodacre BW, et al. US-guided transvaginal drain-
age of pelvic abscesses and fluid collections. Radiol-
ogy 1991;181:53–6.
[60] McNicholas MM, Mueller PR, Lee MJ, Echeverri J,
et al. Percutaneous drainage of subphrenic fluid col-
lections that occur after splenectomy: efficacy and
safety of transpleural versus extrapleural approach.
AJR Am J Roentgenol 1995;165:355–9.
[61] Shankar S, van Sonneberg E, Silverman SG, Tuncali
K. Interventional radiology procedures in the liver:
biopsy, drainage, and ablation. Clin Liver Dis 2002;
6:91–118.
[62] Brandt KR, Charboneau JW, Stephens DH, et al. CT-
and US-guided biopsy of the pancreas. Radiology
1993;187:99–104.
[63] Boland GW, Lee MJ, Mueller PR, Dawson SL, et al.
Gallstones in critically ill patients with acute calculus
cholecystitis treated by percutaneous cholecystos-
tomy: nonsurgical therapeutic options. AJR Am J
Roentgenol 1994;162:1101–3.
[64] Mueller PR, Ferrucci Jr JT, Butch RJ, Simeone JR,
et al. Inadvertent percutaneous catheter gastroenteros-
tomy during abscess drainage: significance and man-
agement. AJR Am J Roentgenol 1985;145:387–91.
[65] Papanicolaou N, Pfister RC. Acute renal infections.
Radiol Clin North Am 1996;34:965–95.
[66] Farrell TA, Hicks ME. A review of radiologically
guided percutaneous nephrostomies in 303 patients.
J Vasc Interv Radiol 1997;8:769–74.
[67] Lucey BC, Boland GW, Maher MM, Hahn PF,
et al. Percutaneous nonvascular splenic intervention:
a 10-year review. AJR Am J Roentgenol 2002;179:
1591–6.
[68] Green BT. Splenic abscess: report of six cases and
review of the literature. Am Surg 2001;67:80–5.
[69] Thanos L, Dailiana T, Papaioannou G, et al. Percuta-
neous CT-guided drainage of splenic abscess. AJR
Am J Roentgenol 2002;179:629–32.
[70] Schuster MR, Crummy AB, Wojtowycz MM, et al.
Abdominal abscesses associated with enteric fistulas:
percutaneous management. J Vasc Interv Radiol 1992;
3:359–63.

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478 477
[71] Gazelle GS, Mueller PR. Abdominal abscess: imag-
ing and intervention. Radiol Clin North Am 1994;32:
913–32.
[72] Casola G, vanSonneberg E, Neff CC, et al. Abscesses
in Crohn’s disease: percutaneous drainage. Radiology
1987;163:19–22.
[73] Khuroo MS, Zargar SA, Mahajan R. Echinococcus
granulosus cysts in the liver: management with per-
cutaneous drainage. Radiology 1991;180:141–5.
[74] Bret PM, Fond A, Bretagnolle M, Valette PJ, et al.
Percutaneous aspiration and drainage of hydatid cysts
in the liver. Radiology 1988;168:617–20.
[75] Sayek I, Onat D. Diagnosis and treatment of uncom-
plicated hydatid cyst of the liver. World J Surg 2001;
25:21–7.
[76] Filice C, Pirola F, Brunetti E, et al. A new therapeutic
approach for hydatid liver cysts: aspiration and alco-
hol injection under sonographic guidance. Gastroen-
terology 1990;98:1366–8.
[77] Men S, Hekimoglu B. Percutaneous treatment of he-
patic hydatid cysts: an alternative to surgery. AJR Am
J Roentgenol 1999;172:83–9.
[78] Ustunsoz B, Akhan O, Kamiloglu MA, Somuncu I,
Ugurel MS, Cetiner S. Percutaneous treatment of hy-
datid cysts of the liver: long-term results. AJR Am J
Roentgenol 1999;172:91–6.
[79] O’Neill MJ, Rafferty EA, Lee SI, et al. Transvaginal
interventional procedures: aspiration, biopsy, and
catheter drainage. Radiographics 2001;21:657–72.
[80] Nelson AL, Sinow RM, Renslo R, et al. Endovaginal
ultrasonographically guided transvaginal drainage for
treatment of pelvic abscesses. Am J Obstet Gynecol
1995;172:1926–32.
[81] Perez-Medina T, Huertas MA, Bajo JM. Early ultra-
sound-guided transvaginal drainage of tubo-ovarian
abscesses: a randomized study. Ultrasound Obstet
Gynecol 1996;7:435–8.
[82] Casola G, vanSonnenberg E, D’Agostino HB, Harker
CP. Percutaneous drainage of tubo-ovarian abscesses.
Radiology 1992;182:399–402.
[83] Feld R, Eschelman DJ, Sagerman JE, et al. Treatment
of pelvic abscesses and other fluid collections: effi-
cacy of transvaginal sonographically guided aspira-
tion and drainage. AJR Am J Roentgenol 1994;163:
1141–5.
[84] Kuligowska E, Keller E, Ferrucci JT. Treatment of
pelvic abscesses: value of one-step sonographically
guided transrectal needle aspiration and lavage. AJR
Am J Roentgenol 1995;164:201–6.
[85] Nosher JL, Winchman HK, Needell GS. Transvaginal
pelvic abscess drainage with US guidance. Radiology
1987;165:872–3.
[86] Parsons AK. Regarding the best approach to the
pyosalpinx. Ultrasound Obstet Gynecol 1996;7:
398–400.
[87] Varghese JC, O’Neill MJ, Gervais DA, et al. Trans-
vaginal catheter drainage of tubo-ovarian abscess
using the trocar method: technique and literature re-
view. AJR Am J Roentgenol 2001;177:139–44.
[88] Sperling DC, Needleman L, Eschelman DJ, Hovse-
pian DM, et al. Deep pelvic abscesses: transperineal
US-guided drainage. Radiology 1998;208:111–5.
[89] Harisinghani MG, Dervais DA, Hahn PF, et al. CT-
guided transgluteal drainage of deep pelvic abscesses:
indications, technique, procedure-related complica-
tions, and clinical outcome. Radiographics 2002;22:
1353–67.
[90] Gervais DA, Hahn PF, O’Neill MJ, Mueller PR. CT-
guided transgluteal drainage of deep pelvic abscesses
in children: selective use as an alternative to trans-
rectal drainage. AJR Am J Roentgenol 2000;175:
1393–6.
[91] Harisinghani MG, Gervais DA, Hahn PF, et al. Trans-
gluteal approach for percutaneous drainage of deep
pelvic abscesses: 154 cases. Radiology 2003;228:
701–5.
[92] Butch RJ, Mueller PR, Ferrucci Jr JT, et al. Drainage
of pelvic abscesses through the greater sciatic fora-
men. Radiology 1986;158:487–91.
[93] Gazelle GS, Haaga JR, Stellato TA, et al. Pelvic ab-
scesses: CT-guided transrectal drainage. Radiology
1991;181:49–51.
[94] Ryan RS, McGrath PR, Haslam PJ, Varghese JC, Lee
MJ. Ultrasound-guided endocavitary drainage of pel-
vic abscesses: technique, results and complications.
Clin Radiol 2003;58:75–9.
[95] Alexander AA, Eschelman DJ, Nazarian LN, et al.
Transrectal sonographically guided drainage of deep
pelvic abscesses. AJR Am J Roentgenol 1994;162:
1227–30.
[96] Nosher JL, Needell GS, Amorosa JK, Krasna IH.
Transrectal pelvic abscess drainage with sono-
graphic guidance. AJR Am J Roentgenol 1986;146:
1047–8.
[97] McGahan JP, Brown B, Jones CD, Stein M. Pelvic
abscesses: transvaginal US-guided drainage with the
trocar method. Radiology 1996;200(2):579–81.
[98] Hovsepian DM. Transrectal and transvaginal abscess
drainage. J Vasc Interv Radiol 1997;8:501–15.
[99] Kastan DJ, Nelsen KM, Shetty PC, Burke MW, et al.
Combined transrectal sonographic and fluoroscopic
guidance for deep pelvic abscess drainage. J Ultra-
sound Med 1996;15:235–9.
[100] Abbitt PL, Goldwag S, Urbanski S. Endovaginal so-
nography for guidance in draining pelvic fluid collec-
tions. AJR Am J Roentgenol 1990;154:849–50.
[101] VanDerKolk HL. Small, deep pelvic abscesses: defi-
nition and drainage guided with an endovaginal probe.
Radiology 1991;181:283–4.
[102] Kuligowska E, Keller E, Ferrucci JT. Treatment of
pelvic abscesses: value of one-step sonographically
guided transrectal needle aspiration and lavage. AJR
Am J Roentgenol 1995;164:201–6.
[103] Aboulghar MA, Mansour RT, Serour GI. Ultra-
sonographically guided transvaginal aspiration of
tubo-ovarian abscesses and pyosalpinges: an optional
treatment for acute pelvic inflammatory disease. Am
J Obstet Gynecol 1995;172:1501–3.

D.A. Nakamoto, J.R. Haaga / Radiol Clin N Am 42 (2004) 457–478478
[104] Caspi B, Zalel Y, Or Y, Bar Dayan Y, et al. Sono-
graphically guided aspiration: an alternative therapy
for tubo-ovarian abscess. Ultrasound Obstet Gynecol
1996;7:439–42.
[105] Corsi PJ, Johnson SC, Gonik B, Hendrick SL, et al.
Transvaginal ultrasound-guided aspiration of pel-
vic abscesses. Infect Dis Obstet Gynecol 1999;7:
216–21.
[106] Wroblicka JT, Kuligowska E. One-step needle as-
piration and lavage for the treatment of abdominal
and pelvic abscesses. AJR Am J Roentgenol 1998;
170:1197–203.
Copyright © 2022 FDOKUMEN

