







Bahasa
Halaman
Hukum


1
NeurologySectionProceduresforEvidence-BasedDocumentDevelopment
I. DefinitionsofEvidenceBasedDocumentsClinicalPracticeGuideline(CPG)Clinicalpracticeguidelinesaregradedrecommendationsonbestpracticeforaspecificconditionbasedonthesystematicreviewandevaluationofthequalityofthescientificliterature.Thesedocumentsaredefinedbyastringentmethodologyandformalprocessfordevelopment.Clinicalpracticeguidelinesarerequiredtobridgethegapbetweenevidenceandrecommendationandaremadeupofbothevidence-basedandexpert-basedinformationtoguideclinicalpracticedecision-making.Althoughvariationcanexist,allmustmeetstandardcriteria.
ClinicalPracticeAppraisals(CPA)/ClinicalGuidanceStatements(CGS)ClinicalpracticeappraisalsorguidancestatementssummarizebestpracticeforanareaofclinicalpracticebasedupontheintegrationofavailableliteraturefromCPGsandexpertopinion.Thesedocumentsaredefinedbyastrongmethodologyincludingananalysisoftheavailableresearchandstructuredprocessfordevelopment.Variationmayexistbutallmustmeetstandardcriteria.
SystematicReview(SR)Asystematicreviewisabalancedsynthesisofevidencerelatedtoadefinedclinicalquestion.Thesystematicreviewappliesanexplicit,reproduciblemethodologyandsystematicsearchoftheliterature.Systematicreviewssearch,appraise,summarize,andidentifygapsinknowledge.UndernocircumstancedoesanSRprovidearecommendationforpractice.Clinicalpracticeguidelinesarerequiredtobridgethegapbetweenevidenceandrecommendation.
ClinicalsummaryClinicalpracticesummariesarereferencedbasedandpeerreviewedsummariesoftheevidence.Thesedocumentsdescribewhatisknownsofarandfocusonclinicalapplicationfollowingastandardformatwhichincludesoverview,classification,screening,examination,diagnosis,prognosis,intervention,medicalmanagement,andcaseexamples.ThesearepublishedonPTNow.
ProceduralsummaryAproceduralsummaryisavariationofaclinicalsummaryfornon-clinicalpopulationcontentsuchassafepatienthandling,electricalstimulation,etc.APTAhasnotformalizedadefinitionforproceduralsummarybeyondthis.TheTaskforceinterpretsthisEBDasastep-by-stepdescription.
Positionstatement/WhitepaperPositionstatementsareintendedtosetforthapositionbasedonclinicalcontentrelatedtothephysicaltherapistsscopeofpractice.Thesedocumentsarereferencedandpeerreviewed.Theyareintendedforaconsumeraudience.
PocketguidePocketguidesareshortsummarystatementsinaportabletool.Apocketguidecouldbederivedfromanyoftheabovedocuments.Whenpocketguidesaredevelopedindependentofanotherdocument,theyareintendedtobebasedonbestavailableevidenceandexpertconsensusandarereferencedandpeerreviewed.
ConsumerdocumentsTheAPTAispresentlytalkingaboutthistypeofdocumentasacompaniontoCPGsorCGSs.

2
II. StructureandPeopleNeededtoDevelopEvidenceBasedDocuments(EBDs)
TheNeurologySectioncompletesthedevelopmentofEBDswiththefollowingstructure:
1. TheDirectorofPracticealongwiththe3-5memberAdvisoryCommitteewilloverseetheprocess.TheFigurebelowillustratestherelationshipoftheDirectorofPracticeandAdvisoryCommitteetotheEBDworkgroups.TheSectionleadershipalongwiththeDirectorofPracticeandAdvisoryCommitteewilldeterminehowmanyworkgroupswillbeinprocessatanyonetime.
Director of Practice/EBP Coordinator
and Advisory Committee
VesUbularHypofuncUonCPGChair
OutcomeMeasuresCPGChair
Workgroup#3Chair(e.g.,LocomoUonin
Stroke)
Workgroup#4Chair
Workgroup#5Chair
Workgroup#6Chair
3
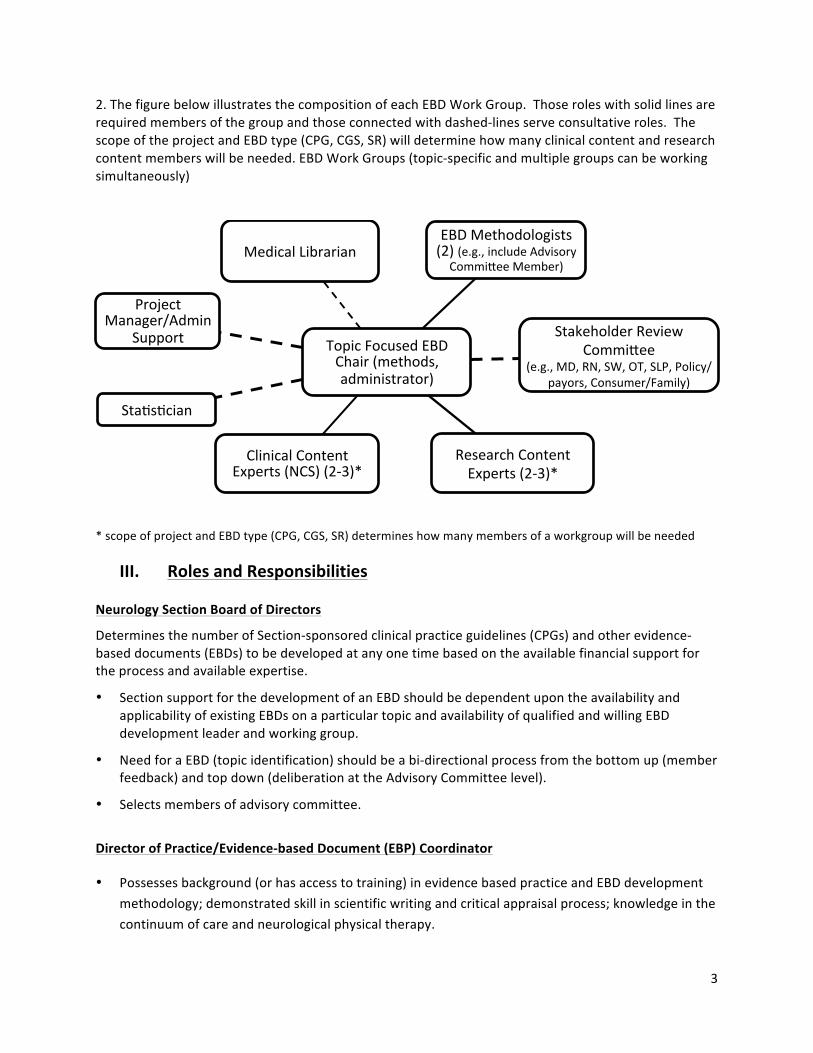
2.ThefigurebelowillustratesthecompositionofeachEBDWorkGroup.Thoseroleswithsolidlinesarerequiredmembersofthegroupandthoseconnectedwithdashed-linesserveconsultativeroles.ThescopeoftheprojectandEBDtype(CPG,CGS,SR)willdeterminehowmanyclinicalcontentandresearchcontentmemberswillbeneeded.EBDWorkGroups(topic-specificandmultiplegroupscanbeworkingsimultaneously)
*scopeofprojectandEBDtype(CPG,CGS,SR)determineshowmanymembersofaworkgroupwillbeneeded
III. RolesandResponsibilitiesNeurologySectionBoardofDirectors
DeterminesthenumberofSection-sponsoredclinicalpracticeguidelines(CPGs)andotherevidence-baseddocuments(EBDs)tobedevelopedatanyonetimebasedontheavailablefinancialsupportfortheprocessandavailableexpertise.
• SectionsupportforthedevelopmentofanEBDshouldbedependentupontheavailabilityandapplicabilityofexistingEBDsonaparticulartopicandavailabilityofqualifiedandwillingEBDdevelopmentleaderandworkinggroup.
• NeedforaEBD(topicidentification)shouldbeabi-directionalprocessfromthebottomup(memberfeedback)andtopdown(deliberationattheAdvisoryCommitteelevel).
• Selectsmembersofadvisorycommittee.
DirectorofPractice/Evidence-basedDocument(EBP)Coordinator
• Possessesbackground(orhasaccesstotraining)inevidencebasedpracticeandEBDdevelopmentmethodology;demonstratedskillinscientificwritingandcriticalappraisalprocess;knowledgeinthecontinuumofcareandneurologicalphysicaltherapy.
TopicFocusedEBDChair(methods,administrator)
MedicalLibrarianEBDMethodologists(2)(e.g.,includeAdvisoryCommi`eeMember)
StakeholderReviewCommi`ee
(e.g.,MD,RN,SW,OT,SLP,Policy/payors,Consumer/Family)
ResearchContentExperts(2-3)*
ClinicalContentExperts(NCS)(2-3)*
StaUsUcian
ProjectManager/Admin
Support

4
• OverseesandmanagesWorkingGroups(WorkingGroupsareheadedbyatopic-focusedEBPChair)andAdvisoryCommitteeactivities.
• ProvidesexpertiseandresourcesonmethodologytoWorkingGroupChairandmembers.• AlongwiththeAdvisoryCommittee,developsaplanfortheupdateofallpublishedEBDsasneeded
(butatleastreviewedevery5years).• AlongwithAdvisorycommittee,maintainsandmanagesallmattersofconflictofinterest.
AdvisoryCommittee
• Consistsof3-5members.DirectorofPractice/EBPCoordinatorandexpertsinknowledgetranslationandEBDdocumentdevelopmentmethodologyandscientificwriting/editing.
• WiththeassistanceofBoardofDirectorsandNeurologySectionMembership,identifies,prioritizes,andrefinestopicstobedeveloped.
• Assistsinperiodically(aswarrantedbychangesinneurologicalphysicaltherapypracticeand/orpoliciesandasstandardsforthedevelopmentofEBDsevolve)conductingneedsassessmentfortopicsidentification.
• OrganizesandplacescalltoSectionmembers,NCS,and/orSIGmembersforvolunteers.WorkswithSIGtoidentifycontentexpertsaspotentialmembersofEBDworkgroups.ScreensCV/resumestodeterminequalificationsasclinicalorresearchexpert.
• RecommendstotheDirectorofPracticeandtheSectionBoDtheappointmentofworkgroupleaders,andworkinggroupmembers.PlacesacalltoSectionmembers,NCS,and/orSIGmembersasappropriate;andscreenCV/resumetodeterminequalificationasclinicalorresearchexperts.
• Assistsworkgroupswithidentifyinganddelineatingthecontentareasoftheirevidencebaseddocuments.
• Assistsworkgroupswithsecuringadditionalexternalreviewers.• AssistsWorkingGrouponscopeofEBDs.• Reviews,editsandapprovesallEBDs(bothoriginalandsubsequentrevisions)submittedbythe
WorkingGroupsattherequestoftheDirectorofPractice/EBPCoordinator.Withrespecttoediting:EditstheCPGsubmissionfromtheworkgroupsothatguidelineshaveaconsistentlabelingsystemthatfollowsbothICFandICDtaxonomiesandareformattedforpublicationineitherJNPTorPTJ.
• WithdirectorofPractice,maintainsandmanagesallmattersofconflictofinterest.• MaintainsalistofpotentialReviewerswithexpertiseinvariouscontentareas.• SubmitsanypublishedCPGtoNationalGuidelinesClearinghouse.
TopicFocusedEBDChairandWorkGroup:
ChairisappointedbyAdvisoryCommittee.
• Mustdeclareconflictofinterestbeforeapprovalofappointment.• Primaryroleismanagerofgroupprocess,aswellas“tiebreaker”duringreviewofabstracts,
researchpapersorotherevidencebaseddocuments.Guidedevelopmentprocess;Facilitatecommunication;Managetasks;Delegateanddirectteamontasks;Conductfirsteditorialreview

5
priortoExternalReviewGroup;Alongwithworkinggroupmembers,identifymembersofexternalreviewgroupanddevelopstimeline.
• Skillsneededincludeefficient,motivated,organized,demonstratedleadershipability,scientificwriting,fluentinuseofInternet,e-mail,andstorageservices(eg,Skydrive,GoogleDocs).PriorexperiencewithEBDsorCPGdevelopmentwouldbebeneficial.
• Familiarwithliteratureandmanagementoftheclinicalconditionorprocedure.• Decides,alongwithworkgroup,onthenatureoftheEBD(eg,CPG,CGS,SR,ClinicalSummary).• CommunicateregularlywithAdvisoryCommittee
WorkGroup(seechart:Recommendapproximately6full-timemembers)
• PotentialmemberscanbeidentifiedbytheChair,AdvisoryCommittee,and/orSectionleadership.• Considerationsasaclinicalexpertincludesexperienceinasetting,yearsofpractice,degreeand
certification,CIexperience,publicationofcasereportsandsimilardocumentsonthetopics,presentationandteachingexperience.Recommend2membershaveclinicalexpertiseintheworkgroup.
• Considerationsasaresearchexpertincludesexperienceinresearchdesignandmethodology,facilityincriticalappraisal,scientificwritinginthecontentarea.Recommend2membershaveresearchexpertiseintheworkgroup.
• Asearchspecialist(medicallibrarian)andstatisticianmayberequiredanditisrecommendedthattheseareadhocandcontractualpositions(budgetedthroughtheAPTAEBDproposalprocessorfundedthroughNeurologySection).
• UnderstandingofEBPandEBDdevelopmentiscriticalforsuccess.• ResponsibilitiesoftheWorkGroupinclude:discloseconflictofinterest,participateinallconference
calls,attendallmeetingswithacommitmenttoteamworkandclearcommunication,readingallrelevantmaterialanddoingallnecessarybackgroundworktofullyparticipate,respondingtoe-mailcommunicationsinatimelyfashion,completingallpersonalassignmentstomeetdeadlines,maintainingconfidentiality.
ThenextpageincludestheConflictofInterestformthateachEBDworkgroupmembershouldcompleteandsubmittotheAdvisoryCommitteefortheirreviewandapproval.

6
CONFLICT OF INTEREST DISCLOSURE FORM
Name: ______________________________________ (Every panelist must complete a separate form)
Guideline name and chapter (if known): __________________________________________________
____________________________________________________________Date: ___________________ The Neurology Section (NS) of the American Physical Therapy Association, and the Evidence-based Documents (EBD) Advisory Committee (AC) of the Practice Committee (PC) strive to produce high-quality, unbiased EBDs. As such the policy requires full disclosure by all guideline authors, editors, and reviewers of all potential conflicts of interest (COI) related to NS activities, real or perceived, including those that are unrelated to the guideline topic. The AC and Director of Practice reviews the disclosures and either recommends approval, approval with management, or disapproval to the NS Board of Directors. It is the AC responsibility to issue the final vote on each candidate. Examples of COIs that clearly disqualify a nominee include employment by a pharmaceutical or device manufacturer, particularly if the drugs or devices manufactured are related to a specific EBD topic. Nominees who serve as consultants or participate on advisory boards should provide as much information as possible in order for the AC and Director of Practice to evaluate the potential COI accordingly. It is not the goal of the AC to preclude all individuals with COIs. Rather, the goal is to ensure full transparency while protecting the integrity of the EBDs, the EBD panelists, and the NS. It is not the role of the AC to serve as a policing body for its EBD panels. However, if the committee or its members discover through other means that non-disclosed COIs exist, then the nomination in question can be revoked.
Annual updates must be submitted to the AC until the date of the final proof of the manuscript. COI forms are stored and archived with the NS Board. DEFINITION: For purposes of the NS and this disclosure form, a COI or competing interest is a financial relationship or other set of circumstances that might affect, or might reasonably be thought by others to affect, an author's judgment, conduct or other work. A COI exists based on the contributor’s circumstances. The contributor’s behavior, subjective beliefs, and outcomes are irrelevant. In other words, the contributor must disclose a COI, even if the circumstances do not actually influence the contributor’s actions or manuscript, and even if the contributor believes that the circumstances cannot or will not affect the contributor’s actions. In parentheses below are some, but not all, examples.
Within the last 3 years and presently (for you and your parents, siblings, spouses, life companion or children):
COI Topic NO Yes (if yes, explain and where applicable provide $ amount Do you have, or are named in, any grants (clinical, educational, research) on EBD topic from any funding body (non-profit, private, corporate)?
Receive royalties or in-kind benefits (travel; accommodations; per diem; meals) from a commercial or professional entity?
Own shares (stock option holder) of a device/equipment or company with ties to EBD topic?
Act as an employee, officer, or director of a device/ equipment or pharmaceutical company? Specify interaction with FDA, financial analysts

7
Serve as a consultant to a device or pharmaceutical company or perform advocacy work related to the EBD topic?
Act as an employee, officer or director of an institution or employer that has a financial relationship with a commercial entity having an interest related to the EBD topic of interest?
Provide money for patient enrollment or other aspect of research related to the EBD topic?
Hold patent rights or pending patent application on EBD topic of interest?
Participate in speaking activities, advisory committee, or other activities related to industry sources, with or without receiving honoraria or in kind benefits (sponsored by a nonprofit university, annual meeting, inservice, symposia; sponsored by a for- profit health company)? Include any participation in CE or related speaking on this EBD topic. If you sit on advisory committees on this EBD topic, include it here.
Make/Made public statements on this EBD?
Provide legal assistance (or expert testimony) on litigation related to EBD topic?
Clinical practice related COI: Do you perform clinical procedures in your clinical practice related to EBD topic of interest? Estimate the percentage of time you treat patients related to EBD topic
Anything else that could be perceived by others to affect your objectivity? Include any published papers (research, educational, perspective, reviews, etc)
ATTESTATION: I attest that my answers are true, that I have disclosed all conflicts of interest in accordance with the conflicts of interest policy and that the disclosed conflicts of interest (if any) will not bias, or in any way impact the integrity of, my work. If I choose to submit this form electronically, I agree that keying in my name and corresponding date at the top of this form indicates my assent to its terms and is equivalent to my signature. SIGNATURE:

8
IV. TOPICIDENTIFICATION• Board,AdvisoryCommittee,and/ormembershipcanproposeatopicforthedevelopmentofan
EBD.
• BoardandAdvisoryCommitteeprioritizetopicstobetransitionedintoanEBD.
• Topicshouldbebasedonclinicianinterest,consumerdemand,prevalenceofthediagnosisinphysicaltherapy,levelsofvariabilityinpractice,abundanceofliteratureorconflictingresultswithintheliterature,theeffectoftheguidelineintermsofcostofrecommendedcare,oritsimportanceforreimbursementandpolicydevelopment(ref:PedsManual-PediatrPhysTher2013;25:257–270).
• Reasonsforsettingtopicpriorities(basedonOxman,Schünemann,andFretheim.Improvingtheuseofresearchevidenceinguidelinedevelopment:2.PrioritysettingHealthResPolicySyst.2006;4:14)
i. Problemsassociatedwithahighburdenofdisability.ii. Noexistingrecommendationsofgoodquality.iii. Astronglikelihoodthatthedevelopedrecommendationswillimprovehealthoutcomes,
reduceinequities,orreduceunnecessarycostsiftheyareimplemented.iv. Implementationisfeasible.
• Considerations(usingICFandPatient/ClientManagementasfoundation)whendiscussingtopicchoicesinclude:usingICFlanguage,followingpatient/clientmanagementprocessordescribingasingularaspect(screening,examination,classification,interventionbyoneormoreactivitiese.g.,walking,secondaryprevention),forasinglesettingoracrossthecontinuumofcare.(seeScope).
V. SCOPE
ThescopeoftheEBDisdependentupontwothings:ThebreadthanddepthoftheEBDandthetypeofEBD.Dependingonthedegreeofdevelopmentofthetopicandquestion(s)thesestepsarecomplementary.
AccordingtoRosenfeldetal.,
“Awell-craftedguidelinehasaclearlydefinedscope.Definingscopewilloccupymostofthefirstconferencecallandmayrequireasecondforcompletion.Inexperiencedguidelinedevelopersattempttocoverallaspectsofacondition,resultinginabroadscopethatwillstalldevelopmentefforts.Thekeytoprogressisarazor-sharpfocusfromthestart,recognizingthatsomeissuesimportanttosomestakeholderswillinevitablybeleftout.Cliniciansmayhavetrouble

9
embracingtheconceptofafocusedguidelinewithrestrictedscopeandalimitednumberofrecommendations.Instead,thedesirewillbetoincludeabroadrangeoftopics,similartowhatappearsinatraditionalreviewarticleorbookchapter.Topicsdeemedimportantbythegroup,butnotaccommodatedintheguidelineactionstatements,maystillbediscussedinthesupportingtextorinanappendix,provideditisclearlyidentifiedasbasedonconsensusorexpertopinion.”(p.S16)

10
Thefollowingfigure(Figure3)providestheprocessfordeterminingtypeofEBD.

11
BreadthandDepthofEBDTodeterminethescopeoftheEBDrequiresthatquestions“WhatexactlyistheEBDintendingtoaccomplish?Whatisitsfocus?”beansweredprecisely.
Thefollowingrecommendationsandconsiderationswillfacilitatedecision-makingintheprocessofdeterminingthescopeoftheEBD:
1. Definetheintendedaudience,targetpatientsorclinicalpresentation,andthetargetconditionorprocedure(itmayincludeassessmentortreatmentorboth)andbeabletopreciselydefinetheconditionorprocedure.
a. TowhomistheEBDdirected?PTs?Allphysicaltherapyprofessionals?Allmedicalprofessionals?Etc.
b. Thetargetpatientorclinicalpresentationcanbedefinedusingdemographics,signs/symptoms,history,diagnostictests.TheWorkingGroupshouldbecleartoidentifywhatpatientsorclinicalpresentationswouldnotbeincludedintheEBD.
c. Theremaybeasingleconditionoralistofmultipleconditions.UsetheICFterminologyandmodelasabasisforthedescriptionofthetarget/healthconditions.
d. Identifythepatients’orconditions’levelwithinthecontinuumofcaretowhichtheEBDisdirected.Thecontinuumincludespracticesettingsfromacutehospitalizationtocommunity–basedprograms.Insomeinstances,therecommendationsaremoreheavilybasedinonesettingandanexplanationrelatedtothebestpracticeareatoimplementtheEBDshouldbeincluded.Furthermore,acuity(hyper-acute,acute,sub-acute,chronic)shouldalsobeaddressedwhenitispertinenttothetopicandassistsindefiningscope.
2. UsethePTmanagementmodelfromtheGuidetoPhysicalTherapistPractice(Exam,Eval,Diagnosis,Prognosis,Intervention)anddelineatehowmuchofthePTmanagementprocesswillbecoveredintheEBD.
3. Prospectivelyidentifyoutcomestoconsider.Outcomescategoriestoconsiderincludehealthstatus,functional,qualityoflife,aswellascost,qualityandutilizationoutcomes.Agreeuponstandardizedoutcomesusingbodystructure/function,activity,and/orparticipationdomainsandprovideMDCandMCIDwhereavailable.Relateinformationonthebenefit/outcometosocietyforimplementingtheEBD.(i.e.costorcost-effectivenessdata,qualityoflifeimprovements)tothestakeholders(boththetargetpatientsandthetargetaudience).
DeterminingtheTypeofEBD
TherearedifferenttypesofEBDs.ThefollowingareEBDsthathavebeendefinedbytheAPTA:
ClinicalPracticeGuideline(CPG)Clinicalpracticeguidelinesaregradedrecommendationsonbestpracticeforaspecificconditionbasedonthesystematicreviewandevaluationofthequalityofthescientificliterature.Thesedocumentsaredefinedbyastringentmethodologyandformalprocessfor

12
development.Clinicalpracticeguidelinesaremadeupofbothevidence-basedandexpert-basedinformationandassuchareintendedtofacilitateinterpretationofresearchevidencetoguideclinicalpracticedecision-making(Fetters&Tilson).Althoughvariationcanexist,allmustmeetstandardcriteria.
ClinicalPracticeAppraisals(CPA)/ClinicalGuidanceStatements(CGS)ClinicalpracticeappraisalsorguidancestatementssummarizebestpracticeforanareaofclinicalpracticebasedupontheintegrationofavailableliteraturefromCPGsandexpertopinion.Thesedocumentsaredefinedbyastrongmethodologyincludingananalysisoftheavailableresearchandstructuredprocessfordevelopment.Variationmayexistbutallmustmeetstandardcriteria.
• DevelopmentofaCGSmaybeprudentwhenmultipleCPGsexistonaparticulartopic.FortheCGS,itsscopeistoappraisetheexistingCPGsandsynthesizetheCPGs’recommendationsintoacoherentsummary.TheappraisalandsynthesismayaddressmuchofthetopicandscopewithouttheneedforanewCPGandalsoprovideanopportunityforagapanalysis.Thus,whereapplicable,PT-specificactionstatementsshouldbedevelopedbasedonasynthesisoflevelsofevidenceandgradesofrecommendationsfromtheexistingCPGs.However,thegapanalysismayalsoprovidedirectivesforarefinementoftheclinicalquestionandscopeforafuturePT-specificCPG.
SystematicReview(SR)Asystematicreviewisabalancedsynthesisofevidencerelatedtoadefinedclinicalquestion.Thesystematicreviewappliesanexplicit,reproduciblemethodologyandsystematicsearchoftheliterature.Systematicreviewssearch,appraise,summarize,andidentifygapsinknowledge.UndernocircumstancedoesanSRprovidearecommendationforpractice.Clinicalpracticeguidelinesarerequiredtobridgethegapbetweenevidenceandrecommendation.
ClinicalsummaryClinicalpracticesummariesarereferencedbasedandpeerreviewedsummariesoftheevidence.Thesedocumentsdescribewhatisknownsofarandfocusonclinicalapplicationfollowingastandardformatwhichincludesoverview,classification,screening,examination,diagnosis,prognosis,intervention,medicalmanagement,andcaseexamples.ThesearepublishedonPTNow.
ProceduralsummaryAproceduralsummaryisavariationofaclinicalsummaryfornon-clinicalpopulationcontentsuchassafepatienthandling,electricalstimulation,etc.APTAhasnotformalizedadefinitionforproceduralsummarybeyondthis.TheTaskforceinterpretsthisEBDasastep-by-stepdescription.
Positionstatement/WhitepaperPositionstatementsareintendedtosetforthapositionbasedonclinicalcontentrelatedtothephysicaltherapistsscopeofpractice.Thesedocumentsarereferencedandpeerreviewed.Theyareintendedforaconsumeraudience.
PocketguidePocketguidesareshortsummarystatementsinaportabletool.Apocketguidecouldbederivedfromanyoftheabovedocuments.Whenpocketguidesaredevelopedindependentofanotherdocument,theyareintendedtobebasedonbestavailableevidenceandexpertconsensusandarereferencedandpeerreviewed.

13
ConsumerdocumentsTheAPTAispresentlytalkingaboutthistypeofdocumentasacompaniontoCPGsorCGSs.
BeforethescopeoftheEBDcanbeformallydefined,thechoiceofEBDmustbeestablished.ThechoiceofEBDisdeterminedbyafirstliteraturesearchtodetermineifCPGsand/orSRsalreadyexistonthetopic.Asearchspecialist(medicallibrarian)maybeneededtoassistwiththesearchprocess.Ataminimum,NationalGuidelinesClearinghouse,GuidelinesInternationalNetwork,andstandardelectronicdatabases(using“guideline”)shouldbesearched.
• CPGrepositoriesinclude:
o http://guidelines.gov/-NationalGuidelinesClearinghouseo http://www.sign.ac.uk/-ScottishCollegiateo http://www.nice.org.uk/-Nat’lInstforHealthandClinicalExcellenceo http://www.pedro.org.au/-PhysiotherapyEvidenceDatabaseo http://www.g-i-n.net/-GuidelinesInternationalNetworko Anydiscipline-specificguidelines(looktoprofessionalorganizationwebsites)
• SystematicReviewsorothersynthesizedevidence?
o http://www.thecochranelibrary.com/view/0/index.htmlo http://srdr.ahrq.gov/-AHRQSystematicReviewDataRepository(New)o http://www.pedro.org.au/-PhysiotherapyEvidenceDatabase(PEDro)o PrimaryReferenceDatabases-(PubMed,CINAHL,etc)
OncetheinitialsearchiscompletedandthetypeofEBDhasbeenestablished,theWorkingGroup,inconsultationwiththeAdvisoryCommittee,definesandagreesuponaspecificscopefortheEBD.
ScopeReferences/Resources
FettersL&TilsonJ.Evidence-basedPhysicalTherapy.FADavis.2012.Kaplanetal.ClinicalPracticeGuideline:PhysicalTherapyManagementofCongenitalMuscularTorticollis:AnEvidence-BasedClinicalPracticeGuidelinefromtheAmericanPhysicalTherapyAssociationSectiononPediatrics.UnderreviewRosenfeldRM,ShiffmanRN,andRobertsonP.Clinicalpracticeguidelinedevelopmentmanual,thirdedition:Aquality-drivenapproachfortranslatingevidenceintoaction.OtolaryngologyHeadNeckSurgery2013148:S1.WoolfS,SchünemannHJ,EcclesMP,GrimshawJMandShekelleP,Developingclinicalpracticeguidelines:typesofevidenceandoutcomes;valuesandeconomics,synthesis,grading,andpresentationandderivingrecommendations.ImplementationScience2012,7:61

14
VI. StatementofIntent
AllCPGsshouldhaveastatementofintentfollowingthescope.BoththeOrthopedicandPediatricSectionshaveusedsimilarphraseologyintheirCPGs.Asarepresentativeexample,thefollowingistakendirectlyfromtheforthcomingPediatricCPGonCongenitalMuscularTorticollis.APTAhasgenerallanguageforstatementofintentwithinCPGsaswell.
“Thisguidelineisintendedforclinicians,familymembers,educators,researchers,policymakersandpayers.Itisnotintendedtobeconstruedortoserveasalegalstandardofcare.Asrehabilitationknowledgeexpands,clinicalguidelinesarepromotedassynthesesofcurrentresearchandprovisionalproposalsofrecommendedactionsunderspecificconditions.Standardsofcarearedeterminedonthebasisofallclinicaldataavailableforanindividualpatient/clientandaresubjecttochangeasknowledgeandtechnologyadvance,patternsofcareevolve,andpatient/familyvaluesareintegrated.ThisCPGisasummaryofpracticerecommendationsthataresupportedwithcurrentpublishedliteraturethathasbeenreviewedbyexpertpractitionersandotherstakeholders.Theseparametersofpracticeshouldbeconsideredguidelinesonly,notmandates.Adherencetothemwillnotensureasuccessfuloutcomeineverypatient,norshouldtheybeconstruedasincludingallpropermethodsofcareorexcludingotheracceptablemethodsofcareaimedatthesameresults.Theultimatedecisionregardingaparticularclinicalprocedureortreatmentplanmustbemadeusingtheclinicaldatapresentedbythepatient/client/family,thediagnosticandtreatmentoptionsavailable,thepatient’svalues,expectationsandpreferences,andtheclinician’sscopeofpracticeandexpertise.TheGDGsuggeststhatsignificantdeparturesfromacceptedguidelinesshouldbedocumentedinpatientrecordsatthetimetherelevantclinicaldecisionsaremade.”

15
VII. CRITICALAPPRAISALOFTHEEVIDENCEandLEVELSOFEVIDENCE
CriticalappraisalrequirestheSECONDLITERATURESEARCHandisusedforthedevelopmentofCPGs,CGSs,andSRs.Oncethescope(s)usingPICOformathasbeenestablished,theWorkgroupperformsasecondliteraturesearch.Theobtaineddocumentswillthenbeappraisedfortheirquality.
Assumptions:
1. the“PICO”questionthatthegroupwantstoaddresshasbeenclearlydefined2. keyconceptualdefinitionsrelevanttotheproposedEBDhavebeenclearlydefined
Steps:
1. Preparation:Cleardelineationofinclusionandexclusioncriteriaforpotentialstudies
Examples:
• agerange,gender,andethnicityofsubjects• samplesize• medicalconditionsallowed• leveloffunction(ICFWHO)oracuitylevelofsubjects• studysetting(community,acutecare,rehabilitation,subacutecare,longtermcareetc)• studyintent(diagnostic,prognostic,efficacyofintervention,epidemiological,instrument
development/clinometric,etc)• studydesign(crosssectional,longitudinal,descriptive,quasi-experimental,experimental)• typeofstatisticalanalysis(relationship,difference,descriptive,predictiveetc.)• language(Englishonly,unlessmedicaltranslatorsareavailabletotheteam)• daterangeforstudies
2. Search:Decisionsaboutwhichdata-basestouseanddevelopmentofkeysearchterms.GuidanceofaMedicalLibrarianisveryhelpfulatthisstep.
• MeshheadingsforPubmed(mostuptodatewithepubs)orMedline• CINAHLtendstocapturemoreofrehabliterature• PEDroforPToutcomestudies/RCTs• Booleanoperators:useofquotations,parentheses,roots*,AND,OR,NOT
(note:goalatthispointistobeasinclusive/broadaspossible)
3. Search:Conductthesearch
• Setupexceldatabasetokeeptrackofeachabstractthatmightpotentiallybeincluded(headings:primaryauthor,co-authors,title,journal,year,citation,othersasdeterminedbyintentofsearch)
• WorkGroupChairisthekeeperofthisfile.Notenumberofduplicatesifmultiplesearchesareundertaken

16
• Recordeverypotentialabstractinthedatabase(decisionsaboutinclusionarethenextstep)• Retrieveandsaveabstractsintolimitedaccesse-storage(GeriEDGEcutandpasted
abstracts,savingfilesbyprimaryauthorlastname,year,andjournalabbreviation;andstoredtheminadropboxfolderaccessibleonlytomembersoftheteam
4. AppraiseAbstracts:Evaluatetheabstractsbasedoninclusionexclusioncriteria
• Definejudgmentcategories:ex:retrieve,exclude,“datamine”(ifarticlereferencesmightyieldadditionalabstracts)
• Establishreliabilityofthereviewprocessbyhavingallreviewteammembersreviewthesamesmallsetofabstractsindependently,thendiscusstheprocessforclarificationandconsensus
• Assignasetnumberofabstracts(alphabetically)toeachteamof(2)reviewers.Eachreviewerevaluatesabstractsindependently.
o Developaformbasedoninclusion/exclusioncriteriathatreviewerscouldusetorecordwhytheymadetheirrecommendationsforeacharticle.
o ProvideExcelfilecutandpastedfromthemasterwiththecitationseachpairwasassignedtouse.Pairscometoconsensusoneachassignedabstract.Ifthisisnotpossible,theWorkGroupChairresolves.
• WorkGroupChairrecordsteamdecisionsonthemasterfile• Retrievearticlesthatmetinclusioncriteria.Savepdfsina“ArticlestobeReviewed”file
(savethembyprimaryauthor,year,journalabbreviation)• Retrievearticlesthatfellinto“datamine”category;reviewreferencestitles,andretrieve
abstractsthatappeartobeinformative;putthesethroughtheabstractreviewprocess
Note:Whenthesecondliteraturesearchresultsinalargenumberofdocuments,theWorkGroupmaywanttoincludeadditionalvolunteersforthecriticalappraisalprocess.TheWorkGroupshouldprovideanorientationandtrainingsession(s)regardingbackgroundtotheprojectandthespecificcriticalappraisalprocess.ReliabilityshouldbeestablishedforeachcriticalappraisaltoolusedwithinthedevelopmentoftheEBD.TheWorkGroupwillneedtoestablishanacceptablelevelofreliability.Werecommenda90%agreementamongappraisers.Consensuscanbeestablishedthroughdiscussion.TheWorkgroupwillberesponsibleforresolvinganyscoringdiscrepancies.
5. Evaluatethearticlesbasedontheappropriatecriticalappraisaltool
• Establishreliabilitybyhavingentirereviewteamindependentlyreviewandrateseveralarticles.Usediscussionofprocessandcometoconsensusonoutcome.Thisshouldbeaccomplishedinoneconferencecall.
• Assignasetofretrievedarticlestoateamof2reviewers.Eachreviewerevaluatesarticlesindependentlythenmustcometoconsensuswithteam.
• Criticalappraisalwhentheevidence-baseddocumentofchoiceiseitherasystematicrevieworaclinicalpracticeguideline.

17
• Appraisingindividualstudies:Therearenumerousevidenceappraisaltools.Center
forEvidencebasedmedicine(CEBM)andScottishIntercollegiateGuidelinesNetwork(SIGN)providetoolsforSRs,RCTs,Cohort,Casecontrol,andDiagnosticstudies.FromCEBM
! http://ktclearinghouse.ca/cebm/teaching/worksheets
FromSIGN! http://www.sign.ac.uk/methodology/checklists.html
CaseSeriesStudies:TheInstituteofHealthEconomicsinAlberta,Canadahasdoneextensiveworkoncriticalappraisalofcaseseriesstudies.Theydevelopedan18-pointappraisaltoolandusea70%cutoffscoreforratinghighqualitystudies.
http://www.ihe.ca/publications/library/2012-publications/development-of-a-quality-appraisal-tool-for-case-series-studies-using-a-modified-delphi-technique/(accessed1/2014)
http://colloquium.cochrane.org/fr/abstracts/development-quality-appraisal-tool-case-series-studies(accessed1/2014)
InterventionStudies:TheAPTAhasdevelopedacriticalappraisaltoolforexperimentalinterventionstudiesandAPTAisencouragingitsuseinallevidence-baseddocumentinitiatives.
MeasurementStudies:Consensus-basedstandardsfortheselectionofhealthmeasurementinstruments(COSMIN)providesatoolspecifictohealthmeasurements.However,thisisaverydensetoolandmayposechallengesfortrainingvolunteerreviewers.
FettersandTilson(2012)withintheirtext,discussandprovideappraisaltoolsacrossthedifferenttypesofstudies:(http://www.fadavis.com/product/physical-therapy-practical-guide-evidence-based-practice-fetters-tilson)
TOOLRECOMMENDATION:TheTaskForcerecommendsthattheAPTACriticalAppraisalToolforExperimentalInterventionStudiesbeusedforallrandomizedcontrolledtrials.WorkgroupsshouldassistAPTAwithvalidationoftheAPTA’sCriticalAppraisalTool.AsSectionsandworkgroupsadoptthistool,thereisalsothepotentialforthedevelopmentofacentralrepositoryofcritically–appraisedinterventionstudies.Atthistime,appraisaltoolsdevelopedbyFetters&Tilson(2012)shouldbeusedforallotherstudies.TheTaskForceevaluatedtheInstituteforHealthEconomics’criticalappraisaltoolforcaseseriesstudiesandfeltitsusewouldbevaluableinsituationswhereatopic/PICOquestion(orsub-question)was

18
answerableonlybyamajorityofcaseseriesevidence.However,appraisalofthistypeofstudywouldresultinaLevelIVlevelofevidence(seeLevelsofEvidencebelow)irrespectiveoftheoutcomeofthecriticalappraisal.
• Appraisingsystematicreviews:Appraisingsystematicreviewswillberequiredwhentheevidence-baseddocumentofchoiceisaclinicalpracticeguideline.
TOOLRECOMMENDATION:TheTaskForcerecommendsusingAMSTARforthecriticalappraisalofsystematicreviews.
http://www.nccmt.ca/registry/view/eng/97.html
• Criticalappraisalwhentheevidence-baseddocumentofchoiceisaclinicalguidancestatement.
• Appraisingclinicalpracticeguidelines:ThebesttoolforappraisingCPGsatthistime
istheAGREEIIdocument.AllCPGsshouldbeappraisedusingAGREEII.Atleast3(preferablyall)membersoftheWorkgroupshouldrevieweachCPGusingAGREEII.TrainingforAGREEIIisavailablehere:
http://www.agreetrust.org/resource-centre/agree-ii/
http://www.agreetrust.org/resource-centre/agree-ii-training-tools/
Iftimeandresourcesarelimited,thenanew,shortversionoftheAGREEII(AGREEII–GRS)documentmaybeconsidered.EachWorkGroupincommunicationwiththeAdvisoryCommitteeshoulddecidewhichversionoftheAGREEIIdocumentshouldbeused.
http://www.agreetrust.org/resource-centre/agree-ii-grs-instrument/
• Inter-raterreliabilityshouldbeestablishedonasampleCPG.ConsensusshouldbeestablishedbyphonecallonallCPGscores.
• Scorecriteriaforeachpaper.Thiswillbeusedtodeterminelevelofevidence(e.g.,LevelIversusLevelII)
6.ScoresfromthecriticalappraisalarelinkedtoLevelsofEvidence.
• TheTaskForcerecommendstheuseoftheCEBMnomenclatureforLevelsofEvidence.TheCEBMnomenclaturehasbeenadaptedbytheOrthopedicsandPediatricsSectionsandispresentlybeingusedbytheVestibularCPGGroup.ThefollowingindicateshowthePediatricCPGonCongenitalMuscularTorticollisintegratedcriticalappraisalscoresintoLevelsof

19
Evidenceusinga>or<50%score.OrthopedicsSectiondidnotprovidecriticalappraisalscoreinformation.
I Evidenceobtainedfromhigh-qualitydiagnosticstudies,prognosticorprospectivestudies,cohortstudiesorrandomizedcontrolledtrials,metaanalysesorsystematicreviews(criticalappraisalscore>50%ofcriteria).
II Evidenceobtainedfromlesser-qualitydiagnosticstudies,prognosticorprospectivestudies,cohortstudiesorrandomizedcontrolledtrials,metaanalysesorsystematicreviews(eg,weakerdiagnosticcriteriaandreferencestandards,improperrandomization,noblinding,<80%follow-up)(criticalappraisalscore<50%ofcriteria).
III Case-controlledstudiesorretrospectivestudiesIV CasestudiesandcaseseriesV Expertopinion
• THRESHOLDRECOMMENDATION:TheTaskForcerecommendsadoptingthe50%thresholdforappraisalsofindividualstudiesonly.o Backgroundonmakingthisrecommendation:
o Presently,therearenumerousandvariableapproachestocriticalappraisalwhichisalsodependentuponthetypeofindividualstudy.Thereisnoestablishedstandardfororconsensusonchoosing50,60,or70%cutofffordelineationofhigherversuslowerlevelofevidence.However,onegroup,theInstituteofHealthEconomicsinAlberta,Canadahasdoneextensiveworkoncriticalappraisalofcaseseriesstudies.Theydevelopedan18-pointappraisaltoolandusea70%cutoffscoreforratinghighqualitycaseseriesstudies.
o TheTaskForcedebatedthisissuequiteextensivelyandcametotheconclusionthat50%wasaprudentthresholdatthistime.Withsomuchvariability,ourintentionistoerroronthesideofinclusionwiththe50%recommendation.However,asthescienceofcriticalappraisalevolves,theAdvisoryCommitteeshouldperiodicallyre-visitthisissue.
• TheTaskForcedoesnotrecommendusingathresholdforappraisalsofCPGs(whentheEBDofchoiceisaCGS)
o AGREEIIprovidesforascaleddomainscore.However,theAGREEIIConsortiumstates“Althoughthedomainscoresareusefulforcomparingguidelinesandwillinformwhetheraguidelineshouldberecommendedforuse,theConsortiumhasnotsetminimumdomainscoresorpatternsofscoresacrossdomainstodifferentiatebetweenhighqualityandpoorqualityguidelines.ThesedecisionsshouldbemadebytheuserandguidedbythecontextinwhichAGREEIIisbeingused.”(p.13ofBrouwersetal).Assuch,theTaskForcedoesnotrecommendaformalthresholdbeestablishedwhenevaluatingCPGsfortheirinclusioninaCGS.MoreappropriatelybasedonthepurposeoftheCPG,aWorkGroupshoulddecidetoincludeonlyhighqualityCPGsandthisshouldbeaccomplishedbyconsensusdiscussionfollowingappraisalusingAGREEII.

20
7. Extractinformationfromthearticlesthatmeetqualitycriteriatoinformthedevelopingevidence-baseddocument.EnterintoanEvidenceTable.ThisstepisdiscussedinthenextsectiononWritingRecommendations.
8.Synthesizeevidenceacrossretrieved/appraisedstudiestocometoconsensusaboutrecommendationforclinicaluse.
• Useofateamdiscussion/consensusbuildingisrecommended• Make“strengthofevidence”determinationforrecommendationforclinicalusebasedon
thecriteria/formatgrouphaspreviouslyagreedupon.
References/Resources
BrouwersM,KhoME,BrowmanGP,CluzeauF,federG,FerversB,HannaS,MakarskiJonbehalfoftheAGREENextStepsConsortium.AGREEII:Advancingguidelinedevelopment,reportingandevaluationinhealthcare.CanMedAssocJ.Dec2010,182:E839-842;doi:10.1503/cmaj.090449FettersL&TilsonJ.EvidenceBasedPhysicalTherapy.FADavisCompany.2012.KaplanSL,CoulterC,FettersL.ClinicalPrracticeGuideline:physicaltherapymanagementofcongenitalmusculartorticollis:anevidence-basedclinicalpracticeguidelinefromtheAmericanPhysicalTherapyAssociationSectiononPediatrics.UnderReview.
MogaC,GuoB,SchopflocherD,HarstallC.DevelopmentofaQualityAppraisalToolforCaseSeriesStudiesUsingaModifiedDelphiTechnique.EdmontonAB:InstituteofHealthEconomics.2012.
SheaBJ,GrimshawJM,WellsGA,BoersM,AnderssonN,HamelC,PorterAC,TugwellP,MoherDandBouterLM.DevelopmentofAMSTAR:ameasurementtooltoassessthemethodologicalqualityofsystematicreviews.BMCMedicalResearchMethodology2007,7:10
SheaBJ,HamelC,WellsGA,BouterLM,KristjanssonE,GrimshawJ,HenryDA,BoersM.AMSTARisareliableandvalidmeasurementtooltoassessthemethodologicalqualityofsystematicreviews.JClinEpidemiol.2009Oct;62(10):1013-20.
WoolfS,SchünemannHJ,EcclesMP,GrimshawJMandShekelleP,Developingclinicalpracticeguidelines:typesofevidenceandoutcomes;valuesandeconomics,synthesis,grading,andpresentationandderivingrecommendations.ImplementationScience2012,7:61.

21
VIII. STRATEGIESFORDATASTORAGE,DATAEXTRACTIONANDSYNTHESISOFFINDINGS
Foranytypeofevidence-baseddocumentbeingdevelopedbyaworkgroup,thenextstep(afterarticleshavebeenretrievedandcriticalappraisaliscompleted)istoextractrelevantinformationfromeacharticle,andbegintheprocessofsynthesis.
DATASTORAGEAmechanismforliteratureanddocumentstorageshouldbeestablished.Workgroupmemberswillbeperformingsearches,appraisals,andsoonbegindraftingtheEBDanditsassociatedsections.Aclear,easilyaccessibledocumentstoragespacewillassurethateachworkgroupmemberhasthetoolsnecessaryforthesetasks.Recommendations/considerationsinclude:
• Establishhowabstracts,articles,andotherdocumentswillbeorganized.Someprogramstoconsiderare:
o Googledocso Mendeleyo Endnoteo Zoteroo DropBoxo Hardcopy
• Considerdifferentcapabilitiesoftheprogram/software:
o Accessibleandconvenienttotheuserso Organizationcapabilities,includingaddinginformationovertimeo Easeofinformationretrievalo Efficientmeansofpreventingduplicateentries;onemainrepositoryo Flexibilityofthesystem,ie.abilitytoattacha.pdfdocumento Costmaybeaconsideration
• Somefeedbackfromprevioususersinclude:
o Googledocs:! Differentversionsofamanuscriptweresaved,anditwaschallengingtokeep
trackofthemostrecent;web-basedo Mendeley:MendeleyReferenceManagerforarticles
! Freeversionhaslowstoragecapacity;$5-10/moextrafor>3peopleandformorethan~150articles
! Haspotentialformultipleprojectswithvariouscollectionsofarticlesforeacho Endnote:
! Costtoastudent=$180! HasInternetcapability-cansynctodesktoporworkcomputer! Softwareexpiresaftersometimeduetonewversions! SomeversionscannotholdPDFs,andsomereportedtroublewithupdatingthe
mostrecentversiono DropBox
! Providedlimitedaccesstothegroup(whenthisisneeded)

22
• Regardlessoforganization/storagesystem,keeptrackofthesearchhistoriestocompileforthe
Methodssectionorafuturerevisionworkgroup
• Namefileswithconsistentformat.Forexample,useof“author’slastname_year_keyword”canmakearticleseasiertofind
• Establishamethodtoprovideworkgroupmemberaccesstofull-textpublications,asappropriate.Allgroupmembersshouldhaveaccesstothedatabaseofallabstracts.Copyrightlawsmaypreventsharingthefullcollectionofarticlestoall.
DATAEXTRACTION
Mostresourcesonevidence-baseddocumentsrecommendthattheteamleader/reviewcoordinator,inconsultationwiththeworkgroup’smethodologistorstatistician,clearlydefinethenecessarypiecesofinformation(datapoints)tobeextractedfromeacharticleinordertoanswertheguidingPICOquestionthatisthefoundationfortheevidence-baseddocument.
Dataextractionformsforevaluationofinterventioneffectiveness,forexample,mightincludeatleastthefollowingpiecesofinformation:
• StudyIDnumber(assignedbyreviewcoordinatorforeacharticle)• Dataextractorinitials• Datedataextractioncompleted• CompleteReferenceasfollows
o PrimaryAuthoro SecondaryAuthorso FullTitleo Journalo Yearo Volume(Issue):pagerange
• Objective—thestudyobjectiveasstatedbytheauthors• Articletype/studydesign:e.g.,metaanalysesorsystematicreviews,diagnosticstudies,prognostic
orprospectivestudies,cohortstudiesorrandomizedcontrolledtrials,case-controlledstudies,retrospectivestudies,casestudiesandcaseseries,orexpertopinion.Note:Thiswillinformdecisionsaboutoflevelsofevidence.
• LevelofEvidence(describedearlier)• CriticalAppraisalToolSummaryScore.• Population—demographicsoftheparticipantsinthestudy• Intervention—descriptionoftheintervention• Control—descriptionofthecontrolgrouporalternativeintervention• Outcomemeasuresused• Typesofanalysesperformed• Resultsoftheintervention• Studylimitations

23
Itisimportanttonotethatthereisnosingletemplatefordataextraction:thecontenttobeextracteddependsonthePICOquestion/sunderlyingtheEBDdevelopmentgroup’sgoalsandpurpose.Oncekey“datapoints”aredefined,theteamleaderandmethodologistmustdecidehowandwhentheinformationtobeextractedwillbedocumentedandstored.Atimelineforcompletionshouldbedeveloped.
DataExtractionOptions
Thereareanumberofoptionstoconsiderincollectingandmanagingthe“data”extractionprocess,eachwithitsownprosandcons:
• “Paperandpencil”orstandardizedformsavailableasWorddocumentsorfunctionalPDFforms.AnexampleofthistypeofdataextractiontoolistheformdevelopedbytheSectiononResearchEDGEgroupandusedbythevariousNeuroEDGEsubgroups;itwasdesignedtogatherinformationonvalidity,reliability,andmeasurementcharacteristicsoffunctionalmeasuresusedtodocumentoutcomesinphysicaltherapycare(http://www.ptresearch.org/article/84/resources/researchers/edge-task-force-evaluation-database-to-guide-effectiveness/edge-rating-forms).
Eachreviewercompletesoneformforeveryarticleonhisorherassignmentlist.Mostresourcesondevelopmentofevidence-baseddocumentsrecommendthattworeviewersindependentlygatherrelevantinformationfromeacharticle,compareresults,andcometoconsensus/agreementthatallkeyinformationhasbeenextracted.Thisstrategyhelpstoreducepotentialbias,aswellasimprovereliabilityduringdatacollection.Followingconsensus,thedocumentcanbeemailedtothereviewcoordinator,whothenperformsordelegatesdataentryintoanexcelfileorotherdatabaseforfurtheranalysis.
• Spreadsheets/DataTables:ToolssuchasMicrosoft’sExcelprogramorGoogleDocsopenaccessonlineprogramscanbedevelopedtomeetthespecificneedsoftheworkgroup.Thedecisionmustbemadeaprioriaboutwhetherreviewersenterdatadirectly,oruse“pencilandpaper”togatherinformationthatasingleassignedperson(e.g.,teamleaderorreviewcoordinator)entersextracteddataintothespreadsheet.Ifthenumberofreviewersisrelativelysmall,enteringdatadirectlymaybemanageable.Ifthenumberofreviewersislarge,theriskofdataentryerrorsincreasessubstantially.Additionally,spreadsheetswithmanycolumnsandrowsofinformationtocompletecanbecumbersomeandconfusing;thiscontributestoriskofdata-entryerrors.
• Databasesoftware:ToolssuchasMicrosoftAccessprogramcanalsobedevelopedtomeetthespecificneedsoftheworkgroup.Bysettingupaseriesofscreensbycontentinformation(e.g.,citationinfo,samplecharacteristics,studydesignandstatisticalanalysis,methodologicalquality,measuresused,interventiondetails,conceptual&operationaldefinitions/outcomemeasuresused,results,etc.asappropriateforthePICOquestion),riskofdataentryerrorsisgreatlyreduced.Thistypeofdatabasealsoallowsmultiplepersonstohaveaccess,andcanbemodifiedasnecessarytomakedatagatheringmoreefficient.ThereisasignificantlearningcurvefornewAccessusershowever;thisoptionwouldworkbestifsomeoneinthegroupwasalreadyfamiliarandfacilewith

24
thesoftwareprogram,oriftherewasfundingtohireanexperttodevelopthemulti-layerinterfaceandtraingroupmembersinitsuse.
• Web-basedSurveys:SurveyMonkeyhttps://www.surveymonkey.comisaweb-basedtoolthatcouldbeusedtodesignadataextractionform.Theteamleader/reviewcoordinatorwouldneedtodesignasurveythatreviewerteamscanrespondtoforeachoftheirassignedarticles.Answerformatcouldbedesignatedasacombinationoffreetextorforcedchoiceoptions.Managementofdatacanbecumbersomeifmanyarticlesaretobeminedforinformation.Surveyresultscanbedownloadedbytheteamleader/reviewcoordinatorintoadatabase,suchasExcel.Thisworksefficientlyonlyifresponseoptionsarewellunderstoodandconsistentacrossthereviewteam.Notethatthereislikelytobeacostforadvancedsurveytools.
• FreeOnlineDatabasesandSoftware:TheCochraneCollaborationhasdatamanagementandanalysissoftware,RevMan(ReviewManager5.3)availablefordownloadforresearchersinvolvedindevelopingsystematicreviews.Itmayalsobeusefulforothertypesofevidence-baseddocumentsaswell.http://tech.cochrane.org/revman.CochranealsohasGRADEprosoftwarethathelpstocreatethesummaryoffindingtablesnecessaryforthesynthesisprocess.http://tech.cochrane.org/revman/gradepro.UsersareabletotailortheirdataformsbasedonthetypeofquestiontheirEBDistryingtoanswer:effectivenessofintervention,diagnostictestaccuracy,methodologyreview,overview,orflexible(prognosis,qualitative,orprototype)review.Oncethetypeofreviewisidentified,thesoftwarehasadefinedsetofinformationtogather.Tables,figuresandappendicescanbedownloadedintoRevMan.TheAPTAisintheprocessofevaluatingacriticalappraisal/datacollectionformforstudiesofphysicaltherapyintervention/outcomestudies.
• FeeforServiceWeb-BasedDatabasesandSoftware:Whentherearemanyarticlesfromwhichdataneedstobeextracted,orwhentherearemultiplepersonsinvolvedinthearticlereviewanddataextractionprocesses,thereareonlineservicesthataredesignedtoassistdatamanagementforcomplexreviews.DistillerSR(http://distillercer.com/products/distillersr-systematic-review-software)isanexampleofonesuchservice
Nomatterwhichstrategyisselectedfordataextraction,theinitialdraftofthe“form”needstobeevaluatedandrevisedsothatitisefficientandeffective.Manydataextractionformsundergoseveraliterationspriortoimplementationinafinalversion.Evaluationoftheformisachievedbyhavingseveralknowledgeablereviewersuseiton“practice”articles,focusingattentiononclarityofinstructions,easeofuse,andidentificationofredundantandmissinginformation.Theiterativefeedbackprovidedbyactualuseisinvaluable,insuringthatthedataneededtosupportsynthesisisavailableinaconsistent,interpretable,andhighqualityformat.
TrainingforDataExtraction
Oncethedataextractionstrategyand“form”arefinalized,theindividualswhowillbeextractingdataneedtobetrainedsothatthereisasconsistency(andthereforelessriskoferror)acrossthereviewteam.Becausethereisgreatvariabilityinhowauthorspresentinformationanddescribemethodsandresultsacrossjournals,effectivedataextractioncanbeverychallengingandtimeintensive.Havingdataextractors“practice”onthesamearticleorsmallsetofarticlesfollowedbydiscussiontoreachconsensusmaybeasolidstrategytodevelopinter-raterreliability.Itisveryhelpfultohavea

25
manual/dictionarythatindividualscanrefertoastheymovefromnovicetoexperienceddataextractors.
Aftertheteamleader/reviewcoordinatorissatisfiedthatthereisconsistencyinprocessandcontentacrossreviewers,pairsofreviewers(ideally)areassignedasetofarticlesfordataextraction.Eachindependentlycompletesdataextractionthencomparesresultswiththeirteammate.Onceconsensusisreached,thefinaldatasetforthatarticleisrecordedinthedataextraction/datamanagementtoolthathasbeenchosen/developedfortheproject.Iftherearemanyarticlesfromwhichdatamustbeextracted(andifdataextractorsareexperienced),analternativeisto“spotcheck”,havingsingledataextractor,withaplanneddualconsensusevaluationonevery15thor20tharticle.
ManagingtheDatabase
Errorsindataentryinacomplexdatabasearelikely,nomatterhowcarefulorexperiencedtheindividual/senteringdataare.ItisimportanttothinkabouttheEBDdatabaseinthesamewayonewouldaresearchdatabase.Dataextractionforms,the“raw”datausedfordevelopmentofEBD,shouldbesavedinane-folderaccessibletotheindividualontheteamdesignatedasthedatabasemanager.Thispersonshouldperiodicallyusesortoptionstoscanforoutofrangeorunusualvaluesinanygivencolumn,referringbacktothe“raw”datatomakecorrections.Oncethedatabasemanagerissatisfiedthatinformationinthedatabaseisaccurate,theteamisreadytomoveintotheprocessofsynthesis.
SortingInformationintheDatabase
Inorderforthegrouptobeabletosynthesizeevidencecontainedinthedatabaseofextracteddata,itisnecessarythatasortingprocessoftheinformationispossible.Inthisway,informationrelevanttospecificcomponentsofthePICOquestioncanbegrouped.Itmaybenecessarytoaddcolumnswithinthedatabasesothatcodingwillallowanefficientsortingprocess.Sortingofthedataprovidesthefoundationfordevelopmentofdata/evidencetablesasthesynthesisprocessbegins.

26
DATASYNTHESIS(MAKINGRECOMMENDATIONS)
Thequalityofanevidence-baseddocumentisdeterminedbythetransparencyandeffectivenessofthesynthesisprocess.JustasintheearlierstagesofEBDdevelopment,riskofbiascanbereducedbyuseofaconsensusbuildingstrategy.Therearenohardandfastrulesaboutthesynthesisprocess.AfterreviewingstrategiesusedbyEBDworkgroupsfromAPTASectionsofOrthopedicsandPediatrics,aswellasmethodologyfromEBDworkgroupsfromotherdisciplines,werecommendthat2-4individuals(dependingonscopeofdocument)beassignedtodraftasynthesisoutline,presenttheiroutlinetothegroup,andthenuseaconsensusorDelphi-typeprocedureforratificationbylargergrouptoensurethatpossibilityofbiasisminimal.AdescriptionoftheDelphimethodcanbefoundat(http://www.healthknowledge.org.uk/public-health-textbook/research-methods/1c-health-care-evaluation-health-care-assessment/use-delphi-methods
Inclinicalpracticeguidelines,inparticular,andotherevidencebaseddocuments,synthesizedinformationleadstoaclinicalrecommendationor“grading”.Oneexampleofaprocesstodeveloprecommendationsisthe“GRADE”process(GradingofRecommendationsAssessment,Development,andEvaluation)(seeGuyattG,etal.JClinicalEpidemiology,2011,64:383-394),developedbyaninternationalcollaborationasatransparentandstructuredmethodforpresentationofsummariesofevidenceanddevelopingrecommendations.GRADEmethodologywasdevelopedtoanswerquestionsconcerningalternativemanagementstrategies,interventions,orhealthpolicies.
StepsintheSynthesisProcess
ThesynthesisprocesshasmultiplestepsthatmustbecarriedoutforeachPICOquestionthathasinformedthesearchforevidence:
• ForallEBDs:o Carefullydetermining/gradingthestrengthoftheevidenceofeachofthearticlestobe
includedintheevidence/datatable.Thiscanbeaccomplishedusingaconsensusprocess,orbyasinglegroupmemberwithexpertiseinresearchmethodology.
o Generationofa“bestestimate”ofeffectsaswellasanindexofuncertainty(e.g.Confidenceintervalsassociatedwiththeestimate).
o ReviewofthedocumentbytheAdvisoryCommitteeandExternalReviewerso Incorporationofrecommendationsforreviewgroupsintothedocument
• ForCPGs:
o Developmentofevidence/datatables(evidenceprofiles)usinginformationinthemasterdatabase(includingqualityratingforeachstudy).SeenextsectiononEvidenceTables.
o Reviewofinformationinthedata/evidencetabletoidentifypotentialrecommendations.
o Decidingaboutthedirection(pro/con)andstrength(strong/weak)oftherecommendation.SeeEvaluating/GradingEvidencebelow.
o Reachingconsensusoneachrecommendationwithintheentireworkgroup.SeeBRIDGEWizsectionbelow.
o Synthesizingrecommendationsintoasingledocument.

27
• ForSRs:
o Developingsummaryoffinding(SOF)table.SOFtablesareashorterdistillationofthelargerevidencetables,focusedonfindingsthatmakekeyinformationmoreaccessibletoreaders.SOFtablesareincludedintheSRdocument,providingasummaryofkeyinformationonwhichasynthesisdecisionorclinicalrecommendationismade.
o Reviewofinformationinthedata/evidencetabletopreparesummaryoffindings.o NorecommendationsaremadeinaSR.
EvidenceTables(DataTables,EvidenceProfiles,SummaryofFindingTables)
EvidencetablesaredevelopedtobeabletoanswerthespecificPICOquestionsposedaswellasscopeofthedocumentbeingdevelopedbytheEBDdevelopmentworkgroup.Theinformationincludedinanevidencetableisselectedfromthecompleteddatabasefollowingdataentry.AworkgroupdevelopingasystematicrevieworCPGaimedatidentifyingwhichoutcomemeasureorcombinationofmeasuresprovidesthebestinformationaboutchangeinfunctionallocomotionforpersonswithstrokemightdesignadatatablethatcouldbeusedforeachoutcomemeasureidentifiedinthesearchandreviewprocess.Aworkgrouplookingspecificallyatbest-practiceinterventionsfordevelopingposturalcontrolnecessaryforindependentsittinginpersonswithquadriplegicandhighparaplegicspinalcordinjurymightchoosetogroupinterventionswithinasingleevidencetable.Agrouplookingatphysicaltherapyforaspecificdiagnosisormovementdysfunctionfromtheviewpointofanepisodeofcare(fromreferraltodischarge)mightorganizetheirdatabythecategoriesoftheAPTA’spatient-clientmanagementmodel
Evidencetablescanbedevelopedeitherinexcelworksheetformat(whichallowssorting)orasaworddocument.Someofthedatacanbecutandpastedfromthemasterdatafile,oncedataextractioniscomplete.Thefirstrowinanevidencetablecontainstheheadingsofinteresttothegroup.Inastudyfocusingoninterventioneffectiveness,forexample,headingsmightinclude:
• PrimaryAuthorName,• Yearofpublication• Class/Levelofevidence• StudyPopulation(n,gender,meanage,dxasappropriate)• Intervention• Outcomemeasures• Strengthofresults.
Eachstudythathasbeenretrieved,criticallyappraisedand“datamined”wouldhaveitsownrowinthetable.Thesummarystatementconsidersthe“evidence”presenteddownthecolumnsoftheevidencetable.UsefulreferencesaboutbuildingevidencetablesincludeAppendix5intheAmericanAcademyofNeurology2011ClinicalPracticeGuidelineProcessManual(St.Paul,MN)p.41,:TheAmericanAcademy

28
ofNeurology;Mlika-Cabanneetal,Sharinghardlabour:developingastandardtemplatefordatasummariesinguidelinedevelopment.BMJQualSaf2011;20:141-145.)
EvaluatingandGradingtheQualityoftheEvidence
TheworkgroupischargedtodeterminethestrengthofeachPICOquestionrecommendation(andtheirrelatedactionstatements)basedonthelevelofevidenceavailableintheliterature.ThegradeassignedtotherecommendationinformsthelanguageofactionstatementsrelatedtoPICOquestion.NotethatrecommendationsofB,C,D,orE(aimedatclinicians),mayalsobeaccompaniedwithanRgrade(aimedatclinicalresearchers).Thekeytodraftingarecommendationstatementisthatitisactionableratherthansimplyastatementoffact.Thefollowingisintendedtoprovidesomeguidanceontheactionverbusagewithrespecttothegradesofrecommendations.
• A-Strongimpliesa“must”or“should”recommendationthatrepresentsbest/optimalclinicalpractice(i.e.,stateoftheart/topofthechart!).Thisrecommendationisclearlyaimedattranslatingtop-notchevidenceintoclinicalpracticetoimprovepatientcare.Thestrengthoftheevidencemightsuggestthatmoreresearchinthisareamaynotaddadditionalunderstandingtowhatisalreadyknown.
Thedecisiontouse“must”vs“should”isbasedonthediscussionandconsensuswithintheGDG.Ausefulreferenceonthisissueis:Lomatanetal.,How“Should”WeWriteGuidelineRecommendations?InterpretationofDeonticTerminologyinClinicalPracticeGuidelines:SurveyoftheHealthServicesCommunity.QualSafHealthCare.2010December;19(6):509–513.doi:10.1136/qshc.2009.032565.
FromLomatanetal:““Must”clearlydefinesthehighestlevelofobligation,butweanticipateonlyrareusageoftheterm…Useof“must”or“mustnot”maybelimitedtosituationswherethereisaclearlegalstandardorwherequalityevidenceindicatesthepotentialforimminentpatientharmifacourseofactionisnotfollowed.“May”isanappropriatechoiceforthelowestlevelofobligation.Wesuggestavoidinganyexpressionusing“consider”…
“Should”isthecommonestdeonticverbfound…andisanappropriatechoicetoconveyanintermediatelevelofobligation.Alternatively,theintermediatelevelcouldbestratifiedinto“should”and“isappropriate.”Overlappingrangesofobligationmaybeacceptableaslongasguidelinedevelopersmakeexplicittheconnectionbetweendeontictermschosenandtheirintendedlevelofobligation.Onestrategywouldbetolinkdeontictermstogradesofrecommendationstrength.Inthisapproach,thenumberofdeontictermsusedwoulddependontheparticulargradingsystemappliedbytheguidelinedevelopers.”p.513
• B-Moderateimpliesa“should”or“isappropriate”recommendationthatsupportsbutmightnotquitefullyrepresentbest/optimalpractice(i.e.,thereissomeroomforimprovement).This

29
recommendationisaimedatchangingclinicalpractice,butalsoidentifieswhere“holes”inexistingevidencemayexistthatneedtobeaddressedbyclinicalresearcherstomovethefieldtowardbest/optimalclinicalpractice.
• C-Weakimpliesan“isappropriate”or“may”recommendationthatrepresentsbetter(butnotquitebest;thereisdefinitelyroomforimprovement)clinicalpractice(i.e.,thereisaclearneedforfurtherresearch).Whileitaimstoimprovepractice,italsochallengesclinicalresearcherstoprovidebetterevidencesuchthatbetterevidencecanbedevelopedsothatthegrademayimproveinfuturerevisionsoftheguideline.
Theuseof“may”whenassociatedwithgradesC,D,andEandIII,IV,andVlevelsofevidencesuggeststhattheGDGbeverycarefultodiscussbenefits/harmsandvaluesintheactionstatementprofile.Higherlevelsofevidenceandstrongergradesofrecommendationsimplyaclearbenefit-harmimpactwhilelowerlevelsofevidenceandlowergradesimplythatthebalancebetweenbenefitsandharmsplaysagreaterroleindecisionmaking.Towardthatend,theclinicianmustespeciallybeabletoweighthebenefits/harmsandpatientvaluesinthesecircumstances.
• D-Theoretical/Foundationalimpliesan“isappropriate”or“may”recommendationthatrepresentsgood(notquitebetter)clinicalpractice(i.e.,thereisgreatneedforfurtherresearch).Itisastrongsignaltoclinicalresearchersthatmoreworkneedstobedoneinevaluatinghowwelltheoreticalmodelsetc.translateintotheclinicalrealm.
• E–ExpertOpinionimpliesan“isappropriate”or“may”recommendationthatrepresentsgood(notquitebetter)clinicalpractice.Thismightbebasedprimarilyonreviewpapers,whitepapers,consensusdocumentsdevelopedbyvariousmethodology(e.g.,Delphi,RAND)andopinionoftheEBDworkgroup.Itcreatesanimperativeforclinicalresearcherstofillthemany“holes”thatwereidentifiedduringtheEBDdevelopment
• R-ResearchcanbeusedindividuallywhenthereisreallynoevidenceavailabletoguidepracticeorincombinationwithB-Egrades(whentheexistingevidenceneedsbolstering).Itgenerateseithera“mustdo”orshoulddo”aimedatclinicalresearchers,ratherthanclinicians.

30
Grade Recommendations QualityofEvidence
A Strong ApreponderanceoflevelIstudies,butleast1levelIstudydirectlyonthetopicsupporttherecommendation.
B Moderate ApreponderanceoflevelIIstudiesbutatleast1levelIIstudydirectlyontopicsupporttherecommendation.
C Weak AsinglelevelIIstudyatlessthan25%criticalappraisalscoreorapreponderanceoflevelIIIandIVstudies,includingstatementsofconsensusbycontentexpertssupporttherecommendation.
D Theoretical/foundational
Apreponderanceofevidencefromanimalorcadaverstudies,fromconceptual/theoreticalmodels/principles,orfrombasicscience/benchresearchsupportsthisconclusion.
E
ExpertOpinion Bestpracticebasedonexpertopinion(reviewpapers,whitepapers,consensusdocumentsdevelopedbyvariousmethodology(e.g.,Delphi,RAND)andtheclinicalexperienceoftheguidelinedevelopmentgroup.
R Research Anabsenceofresearchonthetopic,orconclusionsfromexistingstudiesonthetopicareindisagreement.

31
UseofBridge-WIZforWritingRecommendations
BRIDGE-Wizshouldbeusedforconstructingtherecommendationsandaccompanyingtextandshouldbeagroupactivity(in-personmeetingrecommended)toreducebias.IfWorkingGroupsdecidenottouseBridge-WIZ,theyshouldstillfollowtheformattinglistedbelow:
• Beginwithastatement(ActionStatement1).ActionstatementswillbelocatedonasummarypageatthebeginningoftheEBDandinthebodyofthetext.
• Followactionstatementwithelaboration–whoshoulddowhat,whenandwhere?• Followelaborationsentencewithlevelofevidenceandstrengthofrecommendation.• ExpandedrecommendationsarelocatedintheBodyoftheCPG
Repeattheactionstatementverbatimfromthesummarypage.
Elaborateusingthefollowingactionstatementprofile:
Aggregateevidencequality:Thisisonetotwosentencesofspecificevidencedetail(oddsratios,CIs)orsimplyanindicationoftheoveralllevelofevidencebasedonthedatafromtheevidencetables.
Benefits:Severalsentencesorbulletedremarksdescribingwhatisaccomplishedbyfollowingtheactionstatementand/orwhattheactionstatementoffersthepatient,family,therapistetc.
Risk,Harm,andCost:Listanyrisks,harms,orcostsassociatedwithfollowingtheactionstatement.
Benefit-HarmAssessment:Eachgroupshouldevaluatethisrelationshipandmakeastatement(inmanycases“Preponderanceofbenefit”).Userisk–benefitevidencewhereavailable.
ValueJudgments*:Identifyherewhentheworkinggroupincludesvaluestatements(usingGuidetoPTPractice,CodeofEthics,othervalue-relateddocuments)withinarecommendation.Identifyherewhentheworkinggroupadds,modifies,orotherwisechangesarecommendationbasedonvalueswhentheevidenceisunclearorisaclosecall.Forexample,thissectionmayexplainwhyalessreliablemeasuremaybeadvocatedoveranoverlyexpensive,time-consumingandcostlymeasurewithgreaterreliability.
Intentionalvagueness*:Elaborateonanactionstatementthatiswrittenwithintentionalvagueness.Forexample,examinationofabodystructure’simpairmentmaybestronglyrecommended.However,nospecificmeasurementtoolislisted.Thisisanexampleofknowingunambiguouslywhattodobuttheintentionalvaguenessexistsonhowtodoit.
Roleofpatient/caregiverpreferences*:Identifyif,when,orwherepreferencesand/orroleofcaregiverimpactsdecision-making.

32
Exclusions*:Identifysituationsorcircumstanceswheretheactionstatementshouldnotbeapplied.Clearexceptionswillbeimportantwhenguidelinesareadaptedtomeasureclinicalperformance.
*WrittenafterBRIDGE-Wizgeneratesanactionstatement.
• ThisactionstatementprofileisthenfollowedbyaSupportingEvidenceandClinicalInterpretationsection.Thisincludes1-3paragraphssummarizingtheliteratureandprovidingnecessaryinformationoninterpretationofresults,elementsofarecommendedprocess,redflags,andresearchrecommendations/needs.ThissectionshouldbewrittenbyWorkingGroupmemberswithexpertiseinthetopicarea.
StepsFollowingWritingofRecommendations
Presentdraftrecommendationtorestofthegroupforconsensus
CompletedraftCPGandsubmittoAdvisoryCommitteeforreview.IncorporateACfeedback.
AssessCPGimplementability(seeImplementationSection).
SenddraftCPGtomultidisciplinaryexpertreviewgroup.Actonexternalreviewgroupfeedbackasappropriate.Keepatable/spreadsheetofexternalreviewgroupcommentsandhowtheGDGactedonthesecomments.
SubmittoNeurologySectionthroughtheAdvisoryCommitteetoinitiateacallforpublicreviewbyPTs,MDs,otherhealthprofessionals,patientadvocacygroups,patients/familyasappropriate(esp.ifCPG,orCGS,maynotbenecessaryforothertypesofEBD).
Juryandincorporatepubliccommentsintodocumentasappropriate
Submitdocumenttojournal/publisherforfurtherpeerreview,andrespondstocomments
SubmittoappropriatedatabasesforCPG(egNationalGuidelineClearinghouse).
PublicizepublicationofEBDthroughNeurologySection.
Planforrevisionprocess–seeRevisionPolicy.

33

34
IX. RevisionofEvidence-BasedDocuments
Therevisionprocessisintegraltomaintainclear,updatedrecommendationsorguidelinesbasedonthemostcurrentevidence.TheDirectorofPractice(DoP)andtheAdvisoryCommittee(AC)shouldmaintainapolicyandprocedureformonitoring,reviewing,andupdatinganyEBD.EachEBDshouldbereviewed/revisedatleasteveryfiveyears(ie.someCPGportalspulltheCPGafterthe5yearpublicationdate).
IneachpublishedEBD,threedatesshouldbeclear:
• EBD/CPGpublicationdate• Dateofpertinentsystematicevidencereview• Proposeddateforreview/revisionofthedocumentand/orwhenthedocumentshouldbe
consideredinactiveifanupdateisnotperformed.Forexample,“Thisguidelinewillbeconsideredforreviewin(insertbasedonpresentpublicationdateplus5years),orsoonerifnewevidencebecomesavailable.AnyupdatestotheguidelineintheinterimperiodwillbenotedontheNeurologySectionoftheAPTAwebsite:http://www.neuropt.org/“
Therevisionprocessshouldbeginthreeyearsafterpublicationtoassurecompletionbythefiveyeardeadline.ThefollowingrecommendationswillsupportaseamlesstransitionofworkflowfromtheoriginalEBDworkgrouptotherevisionworkgroup:
• TheinitialEBDworkgroupisresponsibleforregularmonitoringoftheliteratureinordertoassessifnewandsignificantevidenceisavailable,andifupdatingtheEBDshouldoccurpriortoaformalfiveyearreview.Considerationsforrevisingthedocumentpriortothefiveyeartimeframeinclude:
o Newevidenceshowsthatarecommendedinterventioncausespreviouslyunknownsubstantialharm
o Anewexaminationorinterventionisfoundtobesignificantlysuperiortoapreviouslyrecommendedintervention
o Arecommendationcanbeappliedtonewpopulations• TheinitialEBDworkgroupisresponsibleformonitoringtheliteraturefornewandrelevant
publications(uptothreeyearspost-publicationoftheoriginalEBD).Thisincludescompletionofonefinalliteraturesearchtoupdatetheevidenceandcreateabibliographyfortherevisionsgroup.
• Tosupportcontinuity,theinitialEBDworkgroupshouldkeepcleardocumentationandnotes.Forexample,clearrecordsmayincludesearchtermsandstrategies,organizedevidencetables,etc.
• Bythethirdyear,theDoP,ACandLeaderoftheinitialEBDworkgroupidentifyany/allpersonsfromthatgroupthatwillcontinuetoworkontherevisionworkgroup.TheDoPandACconfirmleadershipfortherevisiongroup,andthisgroupmaybegintherevisionprocess.

35
• Therevisionworkgroupshouldworkforafiveyearterm,ormaydefineamoreappropriatetimeframegiventheextentofnewevidencefound.
AsadditionalEBDworkgroupsareformed,orifthevolumeofEBDswarrantsthis,theDoPandACcanopttoaddanadditionalACmemberasRevisionsCoordinator.Thisshouldbeexaminedatleastannuallytomatchresourcesandneedsofnewly-developingorto-be-revisedEBDs.Alternatively,theDoPmayopttoassigntheRevisionsCoordinatorroletoanexistingACmember.Therolesandresponsibilitiesofthispersonwouldbeto:
• KeeptrackofallCPGs/EBDsandwhenrevisionsaredue.
• Contact,onbehalfoftheAC,theoriginalgrouptoidentifypotentialrevisionmembersandreporttotheAC.
• Facilitatehand-offbetweentheoriginalandrevisionCPG/EBDgroups.
TheACwillcontinuetoreviewandeditallsubmittedCPGsirrespectiveoftheirstatus(ie,original;revision).
X. ImplementationofEvidence-BasedRecommendations
OneofthefinalresponsibilitiesoftheEBDWorkgroupistoidentifythepotentialfacilitatorsandbarrierstoimplementingrecommendations.“Implementationreferstothatpartoftheguidelinelifecycleinwhichsystemsareintroducedtoinfluenceclinicians'behaviortowardguidelineadherence”.(GLIA,GuidelineImplementabilityAppraisalv2.0)
ThissectionfocusesspecificallyonCPGs,asonetypeofEBD,astheseinherentlyprovideasetofactionstatements.ForothertypesofEBDs,thatincluderecommendationsoractionstatements(iepositionstatement/whitepaper),itissuggestedthattheEBDworkgroup,atminimum,identifypotentialbarrierstoimplementationandconsiderpotentialstrategiestoenhanceimplementation.
Guidelinedevelopersshouldreflectonthefollowingareaswhenofferingrecommendationsforsupportingguidelineuptake:(modifiedTable3inShekelleetal,originallytakenfromGagliardietal)
• Useofmultipleformatsandchannelsforguidelinedisseminationbasedonpreferencesofthetargetgroupofhealthcarepractitioners.
• Developmentofeducationalresourcesadaptedincontent,andvehicletomeettheneedsofeachtargetgroupofhealthcarepractitioners(andotherstakeholders,asindicated).

36
• Identificationoftheresourceimplicationsofrecommendations,ensuringtheiravailabilitybeforestarting.
• Useofdatacollectiontools(forexample,simpleaudittemplates).
ExamplesofstrategiesthatmaysupportimplementationofaCPGbytheindividual,clinicalprogram,department,orhealthsysteminclude:(KaplanSL,CoulterC,FettersL.Physicaltherapymanagementofcongenitalmusculartorticollis:anevidence-basedclinicalpracticeguideline.PediatricPhysicalTherapy.2013:348-394.)
• KeepacopyoftheCPGinalocationthatiseasytoreference.
• Compareitemsintherecommendedexamination/interventionlisttodeterminewhatshouldbeaddedtoanexaminationorplanofcaretoincreaseadherence.
• Adaptexaminationformstoincludeaplacetodocumenteachoftherecommendedmeasures.
• Adaptformatofdailynotestoincludeaplacetodocumentrecommendedinterventionsintheplanofcare.
• Seektrainingintheuseoftherecommendedstandardizedmeasuresand/orinterventionapproaches.
• BuildrelationshipswithotherhealthprovidersorreferralsourcestoencourageuseofCPG.
• Measureserviceoutcomesofcare(eg,patienteffectacrosstheICFdomains,costs,andcaregiversatisfaction).
Thesestrategiesshouldbeincludedwithinthe“implementation”sectionoftheCPGasawayofguidingindividuals,clinicalprograms,departmentsorhealthsystemsintoimplementingCPG.
AssessingtheImplementabilityofaCPG
TheimplementabilityofaCPGisdefinedas“theeaseandaccuracyoftranslationofguidelineadviceintosystemsthatinfluencecare”.(fromShiffmanRN,DixonJ,BrandtC,EssaihiA,HsiaoA,MichelG,O’ConnellR.TheGuideLineImplementability(GLIA):developmentofaninstrumenttoidentifyobstaclestoguidelineimplementation.BMCMedicalInformaticsandDecisionMaking.2005;5(23)).TheCPGdevelopmentworkgroupcanfacilitateimplementabilityoftheCPGthrough“pre-emptiveidentificationofpotentialbarriersofrecommendationsandwherepossiblesuggestpotentialsolutionstoaddress

37
thembytheguidelineworkgroup.(fromGagliardietal.Howcanweimproveguidelineuse?Aconceptualframeworkofimplementability.ImplementationScience2011,6:26.)
Toaccomplishthis,thegroupshould:
1. Identifybarriersofcurrentpracticeattheprovider,payer,andpatientlevelsthatmayaffectimplementationofaguideline(education/training,requireddosage,paymentlimitations,technologicalresourceneeds)andprovidesuggestionsforimplementation.
a. Examples:structural(significantserviceredesignie.Redesignbusinessmodel),organization(lackoffacility,equipmentorstafforskillmix),individual(lackofknowledge,attitudeandskill)(WhohandbookonGuidelineDevelopment2010)
2. Elucidatenecessarycoordinationofcarewithotherpractitionersandalternativechoicesthatcouldbemadeandwouldrequirereferraltoanotherpractitioner(surgery,medication,etc)
OnetooltoassistinappraisingtheimplementabilityoftheCPGistheGLIA:theGuideLineImplementabilityAppraisalv.2.0.ThistoolshouldbeusedpriortoopeningtheCPGtoexpertpanelreview,publiccommentandpublication.Inthisstep,typically,anexternalpanelcomprisedofpeopleunfamiliarwiththeCPG’scontentanddevelopment,areinvitedtocompletetheGLIA.Eachactionstatementisappraisedacross8dimensionsofguidelineimplementability:
1. Executability(exactlywhattodo)
2. Decidability(preciselyunderwhatconditions(e.g.,age,gender,clinicalfindings,laboratory
results)todosomething)
3. Validity(thedegreetowhichtherecommendationreflectstheintentofthedeveloperandthe
strengthofevidence)
4. Flexibility(thedegreetowhicharecommendationpermitsinterpretationandallowsfor
alternativesinitsexecution)
5. Effectonprocessofcare(thedegreetowhichtherecommendationimpactsupontheusual
workflowinatypicalcaresetting)
6. Measurability(thedegreetowhichtheguidelineidentifiesmarkersorendpointstotrackthe
effectsofimplementationofthisrecommendation)
7. Novelty/innovation(thedegreetowhichtherecommendationproposesbehaviorsconsidered
unconventionalbycliniciansorpatients)
8. Computability(theeasewithwhicharecommendationcanbeoperationalizedinanelectronic
informationsystem)isonlyapplicablewhenanelectronicimplementationisplanned

38
BasedontheGLIAresults,authorsofaCPGmaymodifyitscontentinorderimprovetheeaseinwhichrecommendationsmaybeappliedpriortopublicationorassistadministratorsinidentifyingpotentialproblemsinimplantingaCPGwithintheirorganizations.
AssessingwhetherapublishedCPGhasimpactonphysicaltherapypractice
Ultimately,adoptionandimplementationofCPGrecommendationsoccursthroughtheprocessofknowledgetranslation(Hudonetal).ItisbeyondthescopeoftheCPGworkgrouptoactuallyfacilitateandtomonitorthesuccessoftheknowledgetranslationprocess.BecausetheSectionisencouragingdevelopmentoftheCPGtoenhancephysicaltherapypractice,itmayfalltotheSectiontoundertakeassessmentofbarrierstoimplementationattheleveloftheSection,andtodevelopandimplementstrategiestofacilitateadoptionoftheCPGithassponsored.DevelopmentofaCPGrequiresarigorousinquiryandsynthesisprocessthatresultsin“creation”ofnewknowledge.TheSectiondisseminatesthisnewknowledgeviapublicationinitsjournal,makingitavailableonitswebsite,andpresentationsatCombinedSectionsMeetings.DisseminationalonedoesnotguaranteethattheCPGwillbeadoptedatthehealthcareadministrativeandclinicalpracticelevel.IftheSectionintendsnewlydevelopedCPGstochangeandimprovethepracticeofneurologicalphysicaltherapy,thenitshoulddevelopstrategiestofacilitatetheknowledgetranslationprocess,andtomonitortheimpactofCPGsindailyclinicalpractice.Figure1presentsapotentialmodel,attheleveloftheSection,tofacilitatetheknowledgetranslationprocess,suchthatCPGssupportedanddisseminatedbytheSectionare“living”andeffectivedocuments.(Friedmanetal).

39
Figure1:ConceptualModelfortheknowledgetoactionprocessforimplementationofCPGsinNeurologicalPhysicalTherapyPractice(adaptedfromGrahamID,LoganJ,HarrisonMBetal.Lostinknowledgetranslation:timeforamap?JContinEducHealthProf,2006:26:13-24.)
NewKnowledge:
CPG
(FollowingDissemination)
ID&SELECTPROBLEM
PrioritizebarrierstoCPGimplementationforSoNto
address ADAPTKNOWLEDGE
DetermineSoNMemberneedsforCPGadoption
ADDRESSBARRIERS
Develop“interventions”tofacilitateCPGadoptionthatmeetmemberneeds
IMPLEMENT
DeliverinterventionsdesignedtofacilitateCPG
adoption
MONITOREFFECT
Develop&implementstrategiestosupport
membereffortsforKTpostintervention
EVALUATEOUTCOME
Develop&implementstrategiestodetermineif/howwellCPGhasbeen
adopted
SUSTAINKNOWLEDGEUSE
Recognize/celebratesuccessfuladoption(asmodelforother
settings)
MONITORADOPTION
Develop&implementstrategiestoassesslevelofCPGadoptionbymembersandtheirinstitutions
ONGOINGEVALUATION
Identifynewbarriersand/oradditional
memberneedsreCPG

40
AlthoughtheadoptionofaCPGasa“living”documentcanbeconsideredcyclicalinnature,theSoNcanentertheprocessbyidentifyingwhichofthebarrierstoCPGimplementationidentifiedinthenewCPGcanbebestaddressedattheleveloftheSection.Suchbarriersmightincludealackofknowledgeabout“howto”read/interpretthedocumentamongSoNmembers,lackofunderstandingonthepartofrehabilitationmanagersaboutincorporatingrecommendationsintodailyoperations,ordifficultyinchangingdocumentationsystemstoeffectivelycomplywithrecommendations. Oncesuchbarriersandmemberneedshavebeenidentifiedandprioritized,theSoNwouldbegintoconsiderhowbesttoaddresstheproblem/s.TheSoNmightchoosetoassembleagroupofindividualswithexpertiseinknowledgetranslationormembersoftheEBDAdvisoryBoardtodevelopaseriesof“interventions”toassistmembersintheprocessofadoptingtheCPGintoclinicalpractice.Thismightinclude(asexamples)a)a“howtoread/interpret/applyCPGsasapresentationatmultipleCSMs;b)regionalworkshopsaimedatclinicalmanagersonassessmentofwheretheirpracticesetting“sits”withregardtotheexaminations/evaluations,interventions,andoutcomemeasurementstrategiesrecommendedintheCPG,withanemphasisonhelpingmanagersidentifybarriers/challengesandpotentialsolutionsattheirspecificinstitution;orc)consultationserviceswhereexpertSoNmembers“visit“anorganizationinterestedinadoptingtheCPG.Therearelikelymanyadditionalcreative“interventions”thatcouldbedevelopedtomeetmemberneeds(Friedmanetal).
InordertomonitortheeffectandevaluatetheoutcomesofadoptionofanewCPG,itmaybehelpfulfortheSoNtocreateanetworkofindividuals/agenciesworkingtoimplementtheCPGattheirownsetting.KeepingintouchwithpersonswhohaveattendedSectionsponsored“interventions”wouldprovidepeersupportandnetworkingopportunities,aswellasawaytocollectinformationaboutfacilitators/barrierstochangeacrosssettings(Dulko).SuchpooledinformationwouldassistfutureCPGdevelopmentgroupstobetterunderstandtheprocessofknowledgetranslationandbuildstrategiesforchangeintotheirdocuments,aswellasassisttheCPGrevisionworkgroupbetterunderstandwhatmightneedtobeupdated/changedastheyapproachtherevisionprocess.
TokeepaCPG“alive”overthe5-year-to-revisionpublicationlifetime(i.e.,sustainit’suseintheclinic)theSoNmightchoosetorecognize/celebratesuccessfuladoption(includingbutnotlimitedtothesteps/strategiesusedtoincorporatetheCPGintopractice,changesindocumentation,consequencesintermsofefficiencyandefficacyofcare,andoutcomesintermsofreimbursement)byhighlightingpractices/agenciesthathavemadethetransition.Thismighttaketheformofarticlesinthee-newsletter,presentationsatCSM,orascholarlyarticleinJNPT.SucheffortswouldpotentiallyprovideincentiveaswellasasuccessfulmodelforotherpracticesettingsconsideringadoptionofthenewCPG.OneofthemajorchallengesfacedbygroupswhodevelopanddisseminateCPGsistoreallyunderstandiftheirworkhaseffectivelyimprovedpractice(Countsetal;Brusamentoetal).Bysettingupthe“infrastructure”describedabove,theSoNcreatesforitselfanopportunityto“study”theclinicalimpactofaCPG.Forexample,ayearlysurveysenttothosewhoparticipatedinSoNsponsoredinterventionsaswellastoarandomsampleofmembers(sortedbysettingtowhichtheCPGapplies)wouldprovidedescriptivedataabouttheimpactoftheCPGonpractice.Suchaneffortwouldalsoserveasavehicleforongoingevaluationofmemberneedswithrespecttounderstanding,embracing,andimplementingtheCPG.

41
AdditionalReferences
BrusamentoS,Legido-QuigleyH,PanteliD,etal.AssessingtheeffectivenessofstrategiestoimplementclinicalguidelinesforthemanagementofchronicdiseasesatprimarycarelevelinEUMemberStates:asystematicreview.HealthPolicy.2012Oct;107(2-3):168-183.
CountsJM,AstlesJR,LipmanHB.Assessingphysicianutilizationoflaboratorypracticeguidelines:barriersandopportunitiesforimprovement.ClinBiochem.2013;46(15):1554-60.
DulkoD.Auditandfeedbackasaclinicalpracticeguidelineimplementationstrategy:amodelforacutecarenursepractitioners.WorldviewsEvidBasedNurs.2007;4(4):200-209.
FriedmanL,EngelkingC,WickhamR,HarveyC,ReadM,WhitlockKB.TheEDUCATEStudy:acontinuingeducationexemplarforClinicalPracticeGuidelineImplementation.ClinJOncolNurs.2009;13(2):219-230.doi:10.1188/09.CJON.219-230.
HudonA.GervaisMJ,HuntM.Thecontributionofconceptualframeworkstoknowledgetranslationinphysicaltherapy.PhysTher.2014epubaheadofprinthttp://ptjournal.apta.org/content/early/2014/07/23/ptj.20130483
ShiffmanNR,DixonJ,BrandtC,etal.TheGuideLineImplementabilityAppraisal(GLIA):developmentofaninstrumenttoidentifyobstaclestoguidelineimplementation.BMCMedicalInformatics&DecisionMaking.2005;5(1):23-28.
Top Related
Copyright © 2022 FDOKUMEN

