







Bahasa
Halaman
Hukum


METHODOLOGICAL AND ETHICAL ISSUES IN THE STUDY OF MATERNAL SMOKING AND
ADVERSE PREGNANCY OUTCOMES
Matthew Roy Wong
A thesis submitted in conformity with the requirements for the degree of Master of Science
Graduate Department of Pharmaceutical Sciences University of Toronto
O Copyright by Matthew Roy Wong 2000

National Library 1+1 ,,na, Biôiiitheque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services services bibliographiques 395 Wellington Strwt 395. IW Wdlingtm OctawaON K I A M -ON KlAOIJ4 canada Canade
The author has granted a non- exclusive licence ailowing the National Libmy of Canada to reproduce, loan, distribute or seii copies of this thesis in microforni, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantiai extracts fiom it may be printed or otherwise reproduced without the author's permission.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfiche/^ de reproduction sur papier ou sur format électronique.
L'auteur conserve la propriété du droit d'auteur qui protège cette thèse. Ni la thése ni des extraits substantiels de celle-ci ne doivent être imprimés ou autrement reproduits sans son autorisation.

METHODOLOGICAL, AND ETHICAL ISSUES LN
THE STUDY OF MATERNAL SMOKING AND
ADVERSE PREGNANCY OUTCOMES
Master of Science 2000
Matthew Roy Wong
Graduate Department of Pharmaceutical Sciences, University of Toronto
ABSTRACT:
In Canada an estimated 20 to 30 percent of women smoke during pregnancy. The study
of maternal smoking in adverse pregnancy outcornes presents complex methodological and
ethical issues, iiicluding potential reporting bias and maternal guilt.
Matemal reports of smoking before and afier an incident of fetal distress were compared.
Ethical issues surrounding matemal guilt and informed consent were articulated. The impact of
methodological and ethical issues was assessed in a feasibility study exarnining matemal
smoking as a risk factor in neonatal hypoxic-ischemic encephalopathy (HIE).
Among women who had events of fetal distress, a significant decrease in their report of
smoking occurred. Mothers who smoked during pregnancy with an adverse outcome may be at
risk for psychological damage fiom exposure to the research hypothesis. Methcdological and
ethical issues significantly affected the feasibility study, and preliminary data suggests a high
level of smoking may be occumng amongst mothers o f infants with HIE.
ACKNOWLEDGEMENTS
First and forernost, 1 wish to thank my supervisor Dr. Gideon Koren for his ongoing support and
direction for this work. He has taught me that research must be practical, and should be
conducted with an entrepreneurial spirit. 1 would especially like to express my appreciation for
the support of Dr. Andrew James who has been an integral part of my devetopment both
personally and professionaily. 1 am also particularly indebted to Drs. Shinya Ito, Reina
Bendayan, Ingeborg Radde and Christine Harrison for their guidance and instruction. 1 would
also like to thank, Dr. Max Perlman and Ms. Julia Klein at The Hospital for Sick Children for
their assistance and insights into this research. Finally, 1 am indebted to my farnily for their
invaluable encouragement, suggestions and providence.
iii

TABLE OF CONTENTS
1 INTRODUCTION 1.1 Matemal Smoking as a Risk Factor in Adverse Pregnancy Outcomes
1.1.1 The Problem of Bias in Matemal Self-Report of Smoking 1.1.2 Ethical Considerations in the Study of Maternal Smoking in Adverse
Pregnanc y Out comes 1.1.3 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
1.2 Purpose of Objectives of The Study 1.2.1 Reporting Bias 1 -2.2 Ethical Considerations 1.2.3 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
1.3 Research Hypothesis and Rationale for Hypotheses 1 -3.1 Reporting Bias 1.3.2 Ethical Considerations 1.3.3 Maternal Smoking and Neonatal Hypoxic-lschemic Encephalopathy
2 METHODS 2.1 Reporting Bias Methodology 2.2 Ethical Considerations Methodology 2.3 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
Methodology 2.3.1 Retrospective Studies 2.3.2 Prospective Studies
3 R E S a T S 3.1 Reporting Bias Results 3.2 Ethical Considerations Results
3.2.1 Ethical Concems 3.2.2 Outcome of REB/IRB Review 3 -2.3 Final Solution
3.3 -Matemal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy Results 3.3.1 Retrospective Data 3.3.2 Prospective Data
3.3.2.1 Clinical Data and Hair Cotinine Analysis Results 3.3.2.2 Assessment of Feasibility
4 DISCUSSION 4.1 Reporting Bias 4.2 Ethical Considerations 4.3 Matemal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
4.3.1 Retrospective Data 4.3 -2 Prospective Data
4.4 Summary of Findings 4.5 Recommendations for Future Studies
Page 1 1 4 5
5 REFERENCES
6 APPENDICES

Table 1
Table 2
Table 3
Table 4
Table 5
Table 6
Table 7
Table 8
Table 9
Table 10
Table 11
Table 12
Table 13
Table 14
Table 15
LIST OF TABLES Page
Causes of Fetal Asphyxia 8
Sarnat and Sarnat Staging of Hypoxic-Ischemic Encephalopatby (HIE)
Additional Information Provided by Mothers Reporting "Fetal Distress"
Materna1 Characteristics at Clinic 31
Follow-up Characteristics 32
Materna1 Self-Report of Smoking 34
Changes in Self-Report of Materna1 Smoking 35
Self-Reported Cigarette Consumption in Mothers of 43 Infants with HIE at the Hospital for Sick Children (1985-92) vs. All Live Births at the Ottawa Civic Hospital (1989-90)
Materna1 Characteristics of Infants with HIE Presenting 45 at the Hospital for Sick Children (Nov. 1998-July 1999)
Delivery Factors of Infants with HIE Presenting at the Hospital for Sick Children (Nov. 19984uly 1999)
Neonatal Characteristics of Infants witb HIE Presenting at the 48 Hospital for Sick Children (Nov. 1998- July 1999)
Smoking Status for Mothers of Infants with Neonatal HIE 50 Presenting at the Hospital for Sick Children (Nov. 1998JuIy 1999)
Maternal Characteristics Categorized by Smoking Status in Infants with Neonatal HIE Presenting at the Hospital for Sick Children (Nov. 1998-July 1999)
Delivery Factors of Infants with HIE Categorued by Maternal Smoking Status Presenting a t the Hospital for Sick Children (Nov. 1998-July 1999)
Neonatal Characteristics of Infants with HIE Presenting at the Hospital for Sick Children (Nov. 1998duly 1999) Categorized by Maternal Smoking

LIST OF APPENDICIES
Appendix 1 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy (HIE)
Study: Clinical Data Collection Form
Appendix 2 Maternal Smoking and Neonatal Hypoxic-lschemic Encephalopathy (ME)
Study: Actual Hair Cotinine Values €rom Neonates with HIE (The Hospital
for Sick Children November 1998 - July 1999)
Appendix 3 Manuscript: "Proposed Non-Consensual Research to Avoid Potential
Iatrogenic Parental Guilt: An Example in Hypoxic-ischemic Encephalopathy
(HIE)" M Wong, BSc, C Hanison, PhD, A Moore, MD, G Koren, MD
Appendix 4 Manuscript: CLBias in Maternal Reports Of Smoking During Pregnancy
Associated With Fetal Distress" M Wong, BSc, G Koren, MD
Appendix5 Abstract from The Toronto Fetal Centre Newsletter Number 14/15:
"Proposed Non-Consensual Research to Avoid Potential Iatrogenic Parental
GuiIt: An Example in Hypoxic-ischemic Encephalopathy (HIE)"
Appendix 6 Abstract from Oral Presentation at the Canadian Bioethics Society meeting
October 1998 (Delta Chelsea Inn, Toronto, Ontario, Canada): "Proposed
Nonconsensual Research: An Example in Hypoiric-Ischemic
Encephalopathyn

1 INTRODUCTION
1.1 Maternal Smoking as a Risk Factor in Adverse Pregnancy Outcomes
Despite overwhelming evidence underlining the possible harms to the fetus, in Canada it
is estimated that approximately 20 to 30 percent of women continue to smoke during pregnancy
( B r e ~ a n , 1997). Increasing results indicate that smoking during pregnancy is associated with a
dose-dependent decrease in birth weight, an increased risk for spontaneous abortions, as well as
a higher likelihood of placental abruption and higher perinatal mortality rates (Brennan, 1997;
Cnattingius and Nordstrom, 1996; Koren, 1995). Maternal smoking has also been associated
with sudden infant death syndrome (SDS) (MacDoman MF et al., 1997; Golding, 1997; Oyen
et al., 1997).
Yet aithough these women continue to smoke during their pregnancies, the vast majority
of them experience a significant amount of guilt and self-blame because of their addiction and
largely express a desire to quit, but for a number of reasons feel incapable of doing so (Sherman,
Sanders and Tnnh, 1998; Cuskey and Wathey, 1982; Finnegan, 1980). In addition to the self-
imposed negative thoughts associated with this behaviour, society also contributes significantly
to this state of mind. Smoking is looked upon unfavorably by society and this serves to label and
stigmatize these women (Welte and Russell, 1993).
The societal exclusion and negative feelings caused by smoking during pregnancy can
lead to a significant problem in clinical research that relies on matemal report. Because of the
feelings of guilt and shame that some wornen rnay experience, they may not be tnithfbl when
answering questions relating to their smoking status, and may misrepresent the nurnber of
cigarettes which they smoke each day. With regards to smoking status, this may introduce a
severe bias in determining the proportion of women in a given cohort who smoked during
pregnancy. When asked, women who did in fact smoke during pregnancy may simply Say that
they did not. Further to this, if we assume that women who smoked during pregnancy correctly

2
identim that they did smoke, what if they misrepresent the amount that they smoked? If for
example they do not accurately report the number of cigarettes they smoked per day, if a dose-
response relationship exists, the effect rnay not be seen. Additionally, if such a bias existed in
previous research, those results rnay have in fact overstated the significance of what were
thought to be low levels of smoking but were in fact due to maternal underreporting.
Given that this bias rnay occur in mothers with uneventful pregnancy outcornes, how
much more powerful a sense of guilt and social disapproval might there be in light of an adverse
pregnancy outcome? And how much more an inclination to underreport behaviour which a
mother rnay attribute to causing her infant's condition? Fetal distress for example is a serious
perinatal condition associated with perinatal rnortaIity, and is well recognized by most women.
If a mother who srnoked during pregnancy were to have an infant who experienced fetal distress
during delivery, her report of smoking rnay potentially becorne highly unreliable.
In light of the fact that this source of bias rnay exist in maternal reports, we then turn to
the question of biological markers. Both neonatal meconium (a baby's first bowel movement)
(Ostrea, 1994) and neonatal hair (Eliopolous et al., 1994) have been identified as sensitive,
specific and non-invasive markers of fetal exposure to cigarette smoke. In addition to showing
positivity or negativity regarding smoking status, these rnarkers are also able to give ana
approximation of the extent to which smoking occurred. This being the case, biological markers
would most likely provide a more reliable indication of self-reported smoking status and some
estimate as to the quantity of smoking that took place.
Seeking to obtain a biological marker, we then tum to the question of obtaining this
sample. Would women be willing to consent to this research? In the context of an uneventful
pregnancy, some women might feel hesitant to consent. And again, what of the question about
seeking consent for this biological sample in the context of an adverse pregnancy outcome?

3
One such adverse pregnancy outcome exists in neonatal hypoxic-ischemic
encephalopathy (HIE). In this condition, a decrease in oxygen to the fetal brain during delivery
results in neurological sequelae, and in extreme cases c m potentially cause permanent brain
damage (Ekertet al., 1997; Thornberg et al., 1995; Sarnat and Sarnat, 1976). In addition to a
number o f other factors, because of the baseline decrease in oxygen supply to the fehis that
occurs during smoking (Schardein, 1993; Longo, 1977), there is concern that smoking could
potentially contribute to the etiology of neonatal HIE.
In light of this potentially devastating outcome, an important question presents itself
which can affect Our research methodology. First, if we were to examine the role of matemal
smoking during pregnancy in neonatal HIE and wished to use a biological marker, what impact
could simply posing the research question to the subject have? We have already stressed that an
underlying feeling of guilt and shame exists in a smoking mother. Hypothetically, what effect
would suggesting that her smoking was related to this outcome have? Although there is a
working hypothesis, nonetheless it is still unproven. The suggestion, however, that smoking
may have played some role in her baby's condition may cause considerable psychological
damage. In spite of this potential for h m , the importance of the research also needs to be
considered. If smoking was associated with the condition, it might be one of the few etiologic
factors that could be avoided in the development of neonatal HIE. Our ultimate ethical question
then becomes a question of whether it is possible to conduct this research without putting these
women at risk.
In summary, the study of matemal smoking as a risk factor in adverse pregnancy
outcomes presents two main problems. First, ethical issues that exist in these circumstances
need to be considered not only for their own sake (as this in of itself is a field of research) but
also in Iight of how these issues affect study methodology; narnely, in the case of neonatal HIE,
how methodology should be constructed in order to avoid potential psychologicai damage to the

4
research subject. Secondly, methodological issues need to be addressed regarding the validity of
rnaternal report in the context of an adverse pregnancy outcome and also regarding the feasibility
of investigating maternal smoking as a risk factor in a condition such as neonatal HIE. This
second question of feasibility is an important one in that the ethical issues may shape a
methodology such that it inay, although ethically sound, prove to be untenable for practical or
technical reasons.
These methodological and ethical issues in the study of matemal smoking and adverse
pregnancy outcomes are the focus of this thesis.
1 1 The Problem of Bias in Materna1 Self-Report of Smoking
Studies examining the potential adverse effects on the fetus of certain rnaternal
exposures, such as smoking during pregnancy, comrnonly rely on maternal self-reports. In the
event of a negative result, researchers will ofien cite undeneporting as a potential source of bias
(Jedrychowski et al., 1998). The problern of undeneporting of cigarette smoking during
pregnancy can have a profound effect on the results of such studies. n ie magnitude of this
problem can be appreciated when one compares matemal reports to a biological rnarker. Three
studies comparing biochemical markers of smoking, such as serum or urine cotinine levels, with
matemal report of smoking found that between 5 and 15 percent of wornen who identified
themselves as nonsmokers in fact had cotinine levels that were consistent with active smoking
(Klebanoff et al., 1998; Murray et al., 1993; Walsh et al., 1996). However, the use of biological
markers is not always feasible for a number of reasons including reluctance of patients to give
consent, which in of itself can introduce a severe bias, and particularly in the case of
retrospective studies where one has only a patient record to examine. Moreover, the existing
studies (Klebanoff et al., 1998; Murray et al., 1993; Walsh et al., 1996), while identiGing a
reporting bias of smoking dichotomously (i-e., yes or no smoking), were not designed to address
a bias in the amount of cigarettes reported.

5
At least two reasons for underreporting have been suggested. Firstly, because of the
diminishing social acceptance of smoking during pregnancy, expectant mothers rnay provide
false reports of their smoking which they believe will be more acceptable to the researcher and
to the public at large (Welte and Russell, 1993). Secondly, in the instance of an adverse event
during the pregnancy or delivery, it is possible that women may underreport a behaviour which
in their own minds rnay have been associated with these adverse events. This, however, has
never previously been demonstrated empirically.
1.12 Ethical Considerations in the Study of iMaternai Smoking in Adverse Pregnancy
Ou tcomes
The study of maternal behaviour and its effect upon fetal well-being is an extremely
complex task. Beyond the scientific or technical obstacles that rnay present themselves, there
are a multitude of psychosocial and ethical dimensions that rnay be difficult and, perhaps in
some cases, impossible to completely overcome.
In situations where a child was born with a condition resulting in permanent disability,
mothers often expenenced tremendous feelings of guilt even in situations where their behaviour
during pregnancy could not have had an impact upon the infant's outcome (Affleck et al., 1982).
Given that this occurs, it is Iikely that conducting research into a maternal behaviour such as
smoking during pregnancy in circumstances of an adverse pregnancy outcome rnay ampli@ any
underlying feelings of guilt that exist as the fact that there is a hypothesis put forward by the
researcher rnay point a finger of blarne towards the mother. This could potentially inflict serious
psychological damage upon the subject. The very act of obtaining an infonned consent could
initiate thoughts of self-blame that rnight not be warranted nor even be scientifically valid as at
that point in time it would be a reaction to an idea that was only a hypothesis and not a proven
fact.
6
The loss of a baby during childbirth is a devastating event associated with feelings of
extreme grief, disappointment, helplessness, and self-blame. Perhaps even more tragic and
ernotionally complex is an event during childbirth that may result in the chiId having a life-long
disability. One such outcorne can occur in babies who develop a perinatal condition known as
hypoxic-ischemic encephalopathy (HIE). Our group wished to investigate the hypothesis that
maternal smoking is a risk factor for HIE, using a combination of maternal obstetncal history
and biological waste products as markers of smoking. At the onset of developing Our
hypothesis, several ethical concems arose regarding Our study population. These included the
potential psychological harm to parents who might infer from the study that they were
responsibie for their child's condition, ambiguity regarding the moral status of biological waste
such as meconium (a baby's first bowel movement), and the apparently absolute requirements of
The Hospital for Sick Children's Research Ethics Committee to obtain informed consent.
Given the potentially fragile nature of the study population and the possibility of causing
psychological damage, the question of conducting non-invasive, observational, nonconsensual
research needed to be considered in order to protect the subject from the theoretical hami that
could be caused by being exposed to the research question.
1.1.3 Materna1 Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
Neonatal Hypoxic-Ischemic Encephalopathy is a potentially devastating perinatal
complication affecting between 3 and 5 in every 1000 live births (Roberton, 1992). In this
condition, a decrease in the oxygen supply to the fetal brain occurs dunng the delivery process.
Although the pathogenesis of HIE is not h l ly understood, a number of causes related to either
decreased oxygenation of the maternal-fetal unit or restricted uteroplacental perfusion have been
identified (Perlman and Kirpalani, 1992), summarized in Table 1.
The severity of the hypoxic-ischemic insult to the central nervous system can ofien be
differentiated clinically, and infants are described as having mild, moderate, or severe HIE

7
(Stage 1, 2, and 3, respectively) according to clinical criteria (Sarnat and Sarnat, 1976) as
illustrated in Table 2. In the more severe forms, these infants may die or develop severe cerebral
palsy and/or cognitive deficits of varying degree (Cnattingius and Nordstrom, 1996; Ekert et al.,
1997; Thornberg et al., 1995).
Matemal smoking has been associated with a wide range of perinatal complications,
including increased rates of miscarriage, stillbirth, intrauterine growth restriction, prematurity,
and the Sudden Infant Death Syndrome (MacDorman et al., 1997; Golding, 1997; Oyen et al.,
1997). Tobacco smoke emits over one thousand different chemicals, some of which have been
shown to cause fetal toxicity. Dwing smoking, circulating levels of carbon monoxide (CO) may
cause as much as 20% of materna1 and fetal bemoglobin (Hb) to be converted into carboxy-Hb
which does not carry oxygen (Schardein, 1993). Because fetal Hb has a much higher affinity for
CO than adult Hb, carboxy-Hb levels tend to be higher, and are sustained for longer periods in
the fetus than in the mother (Longo, 1977). It is this binding to CO which results in decreased
oxygen carrying capacity in the blood for the mother and the fetus. In addition, CO also binds to
intracellular cytochrome enzymes, thus its effect on intracellular respiration is much greater than
those predicted by circulating CO levels (Longo, 1977).
Nicotine is a potent neurotoxin, shown in animal studies to affect the fetus morphologically and
developmentaHy (Schardein, 1993). As well, it acts as a vasoconstrictor, causing decreased
uteroplacental perfùsion (Schardein, 1993). In addition, inhibition of prostacydin activity has
been demonstrated in the umbilical cords of heavy smokers (Ahlsten et al., 1990). Prostacyclin-
dependent vasodilation is an important part of maintaining uteroplacental perfusion and, hence,
inhibition may cause reduced fetal blood supply. Gross anatomical differences in umbilical
cords between heavy smokers have also been observed. The presentation of an increased
number of blood vessels above the standard three in the umbilical cord has been documented in
heavy smokers (Gupta et al., 1993), which the authors believed to be consistent with chronic

8
hypoxia. It is also felt that with this abnorrnal profile, the vascular system may be less resilient
to compression or other insults during delivery.
Recently, it has also been shown that long term exposure to cigarette smoke has the
ability to cause an increase in the expression of CD18 integrin cell-surface molecules on
neutrophils, thereby facilitating their adhesion to other ce11 surfaces particularly during
extravasation (Ryder et al., 1998). Inhibition of CD18 adhesion molecules using monoclonal
antibodies has been shown to decrease ischemia-reperfusion injury in primates (Wim et al.,
1 998). Taken together, these observations suggest that exposure to cigarette smoke may cause
an upregulation of CD 18 molecu~es on neutrophils and may thereby potentiate hypoxic-ischemic
damage.
To date, despite great concerns regarding the adverse fetal effects of materna1 smoking,
no study has addressed the potential risks of tobacco smoke for causation of HIE. Because HIE
is characterized by fetal brain hypoxia, the current research sought to investigate feasibility of
conducting a study that addressed the hypothesis that materna1 smoking is a risk factor for HIE.
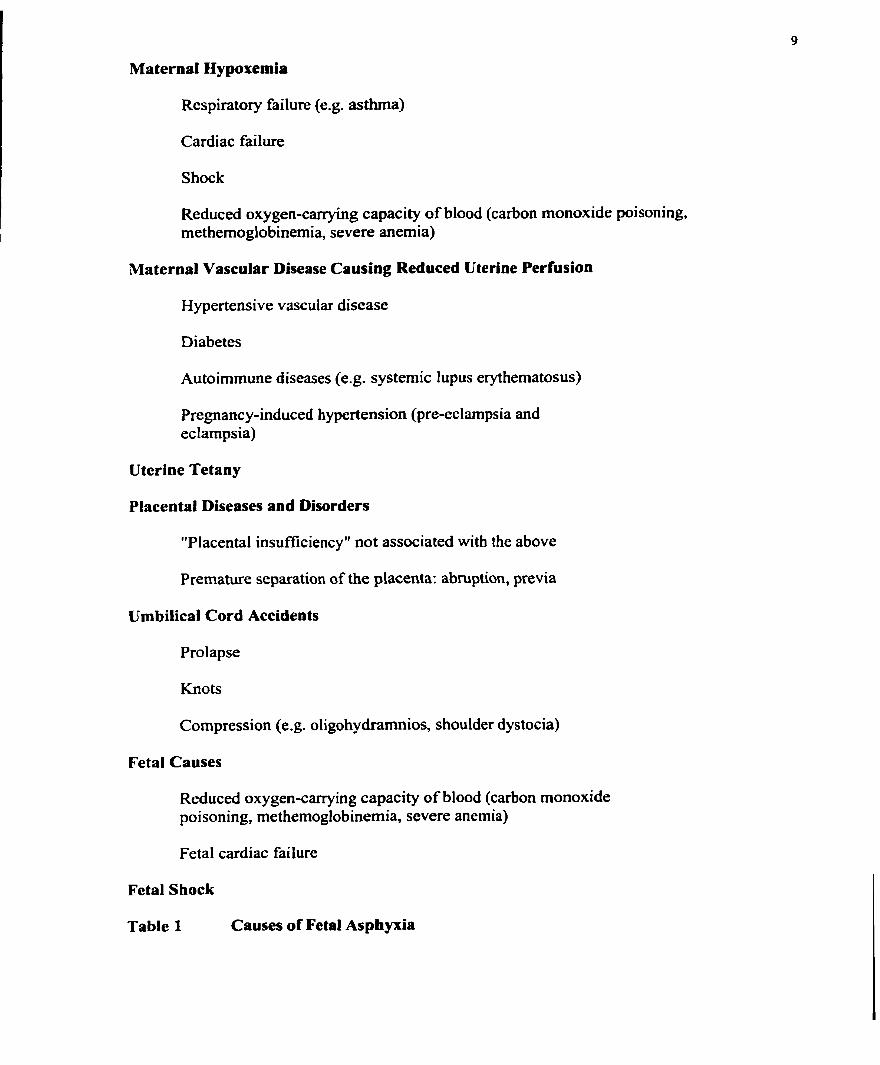
Maternal Hypoxemia
Respiratory failure (e.g. asthma)
Cardiac failure
Shock
Reduced oxygen-caiTying capacity of blood (carbon monoxide poisoning, rnethemoglobinemia, severe anemia)
Maternal Vascular Disease Causing Reduced Uterine Perfusion
Hypertensive vascular disease
Diabetes
Autoimmune diseases (e.g. systemic lupus erythematosus)
Pregnancy-induced hypertension @re-eclampsia and eclampsia)
Uterine Tetany
Placental Diseases and Disorders
"Placenta1 insufficiency" not associated with the above
Premature separation of the placenta: abruption, previa
Umbilical Cord Accidents
Prolapse
ff io ts
Compression (e.g. oligohydramnios, shoulder dystocia)
Fetal Causes
Reduced oxygen-canying capacity of blood (carbon monoxide poisoning, methemoglobinemia, severe anemia)
Fetal cardiac failure
Fetal Shock
Table 1 Causes of Fetal Asphyxia

Classification Cliaical Signs
Stage 1 (Mild) Hyperalertness
Hyperexcitabili ty
Stage 2 (Moderate) Lethargy
Hypotonia
Suppressed primitive reflexes
Stage 3 (Severe) Stupor
Flaccidity
Absent primitive reflexes
Table 2 Sarnat and Sarnat Staging of Hypoxic-lschemic Encephalopathy (HIE)

11
1.2 Purpose and Objectives of The Study
The purpose of this study was threefold. First, to determine if bias exists in the maternai
reporting of smoking in the context of an adverse pregnancy outcome, using fetal distress as an
example. Second, to explore the ethical issues that exist in circumstances of an adverse
pregnancy outcome which need to be considered and how these issues affect study methodology;
namely in the case of neonatal HIE, and how study methodology should be constmcted in order
to avoid potential psychological damage to the research subject. Third, to determine the
feasibility of investigating matemal smoking as a risk factor in the perinatal condition of HIE in
light of the ethical and methodological issues presented by the first and second purposes above.
To this end, the following three objectives were pursued.
1.2.1 Reporting Bias
The objective of this component of the present study was to investigate whether there is
bias in maternal reporting of the arnount of cigarette consumption when fetal distress is
diagnosed. Fetal distress is described as a cluster of clinical situations, including oxygen
deprivation (e.g. presence of meconium, low Apgar score), heart rate abnormality, or
biochemical disturbances (e-g. fetal acidemia) (Hill, 1979; Parer and Livingston, 1990; Mead,
1996). Fetal distress presented at birth often requires medical intervention and admission to a
neonatal intensive care unit; these infants may suffer long tenn sequelae (Gilstrap et al., 1989).
Although fetal distress is lacking an accurate clinical definition, most mothers are aware of its
significance and wiIl recall its occurrence. This research exarnined whether bias would occur in
matemal report of smoking if a woman had an event of fetal distress during delivery.
1.2.2 Ethical Considerations
The object of this component was to illustrate the ethical considerations involved in
determining a study methodology for the research of maternal smoking as a risk factor in
neonatal HIE. In particular, this component sought to investigate three areas. First, to describe

12
the nature of matemal guilt resulting from an adverse pregnancy outcorne surrounding the
question of a maternal behaviour such as smoking. Second, to delineate the requirements of
informed consent from an institutionaVregulatory perspective (venus a philosophical
perspective). Third, to determine the requirements for noninvasive, nonconsensual research in
light of the concems put forth in the previous two components. These areas were then to be
looked at in light of the Hospital for Sick Children's Research Ethics Cornmittee review decision
and incorporated with the cornmittee's requirements to form an ethically coherent study
rnethodology which took al1 ethical factors into account.
1.2.3 Materna1 Smoking and Neonatal Hypoxic-Ischemic Encephalopathy
The objectives of this part of the research were: One, to determine the ethical,
methodological, and practical feasibility of studying the incidence and degree of maternal
smoking during pregnancy as a risk factor for neonatal HIE at the Hospital for Sick Children.
Two, to validate the hypothesis for the study with retrospective and prospective data.
As there were a number of ethical concerns raised in the development of the research
protocol, the objective of this component was to evaluate the proposed methodology in the
process of obtaining consent from research subjects and to establish if the ethical guidelines
derived from the research outlined in Section 1.2.2 were feasible from an ethical perspective. In
essence, this component sought to address the question of whether the proposed solution by the
Hospital for Sick Children's ethics committee to the ethical problems was in fact entirely ethical,
and to make observations on any difficulties in the implementation of the solution.
Along with ethical feasibility, a critical appraisal of the methodological feasibility was
another objective. The methodology utilized in this feasibility study was to be scrutinized with
the idea of this methodology being used in the context of a larger definitive study of matemal
smoking and HIE.

13
An assessrnent of the practical feasibility of this research was also to be explored. This
was to include several elements including characterizing the study population with regard to
geographical concerns (for the purposes of matching in fiiture studies), logistical concems (how
to contact parents in order to obtain consent, etc.), and data collection concerns (quality of
information in charts, difficulty [not related to consent] in obtaining biological samples, etc.). In
addition, the rate of presentation (number of admissions in a given time) at the Hospital for Sick
Children's NICU for infants with HIE was to be assessed (to estimate how quickly data could be
collected from this institution) as well as the declination rate of subjects and establishing their
reasons for declining to participate.
Finally, the validity of our hypothesis was to be tested through an investigation of
existing data through retrospective analysis and prospective data collection. Retrospective data
at the Hospital for Sick Children NlCU between 1985 and 1992 were to be examined for
evidence of materna1 smoking, and to compare the prevalence or amount of smoking in mothers
of infants with HIE with a population-based historical control group. Prospective data were to
be collected from mother-infant pairs presenting at the Hospital for Sick Children's NICU with a
neonatal diagnosis of HIE in order to analyze both the prevalence and amount of cigarette
consumption during pregnancy through the use of a biological marker. These data were then to
be compared to population-based historical data for cornparison of the prevalence of smoking,
and the actual levels from infants of active smokers as indicated by the biological marker were to
be cornpared with historical data from infants who did not suffer from HIE.

14
1.3 Research Hypotheses and Rationale for Hypotheses
Although the hypotheses for scme of the cornponents of my research are dependent on
the results from previous components, the hypotheses below are stated independently for the
sake of clarity. Any assumptions are stated explicitly.
1.3.1 ReportingBias
The hypothesis was that women who smoke during pregnancy and have events of fetal
distress during delivery will decrease their report of smoking during pregnancy reported at the
time of follow-up when compared to their initial "reat time" report. That is, it was hypothesized
that the number of cigarettes consumed per day reported during pregnancy would decrease
postnatally due to the event of fetal distress.
It is well accepted that smoking during pregnancy puts the fetus at increased health risks.
Studies have clearly illustrated the nsk for decreased birthweight and an increased incidence of
perinatal mortality and deIivery complications, such as fetal distress (DiFranza and Lew, 1995;
Walsh, 1994). These nsks are oAen explained by health professionals to women who smoke
during their pregnancy, and these women are ofien cited as being aware of these risks pnor to
receiving counseling for smoking cessation (Haslam et al., 1997).
The rationale for the hypothesis is that, because of the additional social stigrna that rnay
be caused by admission of smoking during pregnancy in Iight of an adverse outcome potentially
due to smoking, a mother rnay actively decrease her report of smoking which she believes will
be more acceptable to the researcher and to the public at large (Welte and Russell, 1993).
1.3.2 Ethical Considerations
There were three hypotheses in this component of the research.
The first hypothesis was that women who have an adverse pregnancy outcome would
experience significant underlying feelings of guilt and would engage in self blame. The
rationale was based on two examples of anecdotal evidence. First, dunng pregnancy women

15
express great concems regarding their behaviour, particularly regarding exposures to cigarette
smoke. This is seen frequently in calls to the MotheRisk program at the Hospital for Sick
Children which answers questions regarding exposures during pregnancy and their effects on the
fetus. Second, in instances of an adverse pregnancy outcome requiring admission of the infant to
the Hospital for Sick Children's NICU, physicians often report that women ask numerous
questions regarding the potential causative role of their behaviour in the pregnancy outcome and
show a great degree of anxiety around this topic. Accordingly, it was hypothesized that this
group would be psychologically vulnerable and that, in investigating maternal smoking as a risk
factor for HIE, the posing of the research question might unjustifiably increase the feelings of
guitt and self-blame that preexisted and could result in psychological damage.
The second hypothesis was that, assuming the first hypothesis to be true, informed
consent might not be required in this unique research situation according to exceptions stated in
institutional regulations and requirements. The rationale being that since the research initially
proposed was non-invasive and to be completely anonymous, it could be hypothesized that
institutional guidelines would allow for a nonconsensual methodology to be adopted.
In light of the assumption in the first hypothesis that the potential existed for causing
considerable psychological damage to research subjects by highlighting the issue of smoking
during pregnancy, and assuming fiom Our second hypothesis that institutional policy would
allow exceptions for nonconsensual research, the ultimate hypothesis was that nonconsensual
research methods needed to be considered to avoid this serious potential harm.
1.3.3 Materna1 Smoking and Neooatal Hypoxic-lschemic Encephalopathy
The working hypothesis was that maternal smoking increases the risk for HIE by
decreasing fetal oxygenation. Both through diminishing oxygen transport by hemoglobin as well
as intracellular cytochrorne enzyme binding (Shardein, 1993; Longo, 1977), maternal smoking
increases the risk of decreasing fetal oxygenation, and therefore may increase the nsk for HIE.

16
This may be especially crucial if CO-factors such as placental abruption, insuficiency or previa
coexist. In addition, cigarette smoke may potentiate hypoxic-ischemic damage by increasing
neutrophil adhesion during ischemic-reperfusion injury (Ryder et al., 1998; W i n et al., 1998).
When this occurs in the brain, increased neutrophil adhesion in the cerebral vasculature creates
an excess of neutrophil aggregation in a damaged vesse1 which resû-icts normal blood flow
downstrearn. This deprives more distant tissues of oxygen and hence may exacerbate cerebral
injury.
A biological marker was to be used to identifL smokers and to quanti@ intrauterine
exposure to tobacco smoke.
Cotinine, the major metabolite of nicotine, has a longer elimination half life than nicotine
and is the most widely used rnarker of exposure to tobacco smoke (Koren, 1995). Matemal
serum concentrations of cotinine have been s h o w to reflect accurately the number of cigarettes
smoked by the mother, when the time of the last cigarette smoked is known. However, direct
measurement of fetal exposure to cotinine will allow a more accurate estimate of the intrauterine
burden of constituents of tobacco smoke (Eliopolous et ai., 1994). Umbilical cord levels of
cotinine rnay be spunously low if the mother has not smoked for 2-3 days before or during
delivery. On the other hand, cotinine is trapped in meconium (Ostrea et al., 1994) and hair
(El iopolous et al., 1 994) throughout the second half of pregnancy, and their measurement allows
long-term, cumulative estimates of fetal exposure.
Therefore, in addition to allowing us to determine positivity or negativity of smoking
status, measurement of cotinine allows for an estimation of the amount of cigarette smoking that
had occurred during the latter part of pregnancy. In this way, the prevalence and amount of
smoking can be compared to historical data.
Our specific hypotheses therefore were as follows. First, that in the retrospective study
an increase in either prevalence or amount o f cigarette smoking in active smokers as indicated by

17
materna1 report in the Hospital for Sick Children's patient charts for cases of infants with HIE
between 1985 and 1992 would be seen when compared to population-based historical data fiom
approximately the same time period. Second, that in a prospective study, infants with H E at the
Hospital for Sick Children would have a higher prevalence of smoking compared to the
population-based historical data of approxirnately the same time period, or that the actual
cotinine Ievels seen in active smokers would be higher than historical data fiom infants whose
mother smoked during pregnancy and who did not have HIE.

18
2 METHODS --
2.1 Reporting Bias Methodolow
The original data on smoking status were collected prospectively fiom pregnant patients
who were seen between 1988 and 1997 in clinic by a physician through The MotheRisk Program
(The Hospital For Sick Children, Toronto, Ontario, Canada) - a counseling service for women
with medicinal, chemical, illicit drug or other exposures in pregnancy. During the clinic visit,
maternal characteristics including age, gravidity, parity, and previous spontaneous or therapeutic
abortions were collected as were details of any underlying medical condition and previous
pregnancy outcornes. Detailed reports of the patient's exposures during the pregnancy were
made ascertaining the time of exposure, dose and frequency of use, where applicable. These
included the exposures that the patient had corne to ch i c for specifically, as well as other
exposures including cigarettes, alcohol and illicit drugs.
Afier collection of al1 data, the concept of a baseline nsk that exists in every pregnancy
for a woman to have a child with a major birth defect even in the absence of any teratogenic
exposure was explained to the patients. Patients were then informed of the potential risk to the
fetus (if any) of such fetal exposures by way of critical evaluation of the current medical
literature. Documentation of the counseling along with the specific literature references is then
forwarded to the physician caring for the woman and also to the patient directly if requested.
As a part of this research program, patients seen in clinic are followed up with a
telephone interview one to two years after their clinic visit to confirm exposure details and to
inquire about pregnancy outcome.
For the present study, patients were selected based on three cnteria: 1) Live birth with
completion of the follow-up interview, 2) documented delivery details, and 3) documented
details of maternal smoking bebaviour in both clinic and follow-up files. Exclusion was based
on documentation in the tiles of intentional decrease or cessation of smoking, or where details of

19
smoking were not complete for either clinic or follow-up information (e.g. 16 cigarettes per day
at c h i c vs. response of only 4'yes" at follow-up). During follow-up interviews, patients were
asked if there was an event of "Fetal Distress" during delivery and the interviewer then gave
examples summarized in Table 1. The mother's response to this question was documented and
any narrative coxnments made by the mother about the delivery were detailed. Patients were
categorized into one of two groups based on their report of "Fetal Distress" or "Uneventful
delivery".
These two groups were then compared with regards to materna1 characteristics at clinic,
number and nature of exposures (teratogenic, unknown, nonteratogenic), use of alcohol or illicit
drugs, presence of matemal illness, and incidents of fetal distress in a previous delivery.
Neonatal characteristics at follow-up including gestational age, birthweight and presence of
major malformations as well as the time between clinic visit and follow-up were also compared.
Cornparisons between the two groups were done using the Student's t-test, Mann-Whitney Rank
Sum Test or Chi-square, as appropriate.
The primary endpoint of interest was the difference in the reported daily number of
cigarettes in the first trimester between the first interview ("real time") and the second (post
partum) interview. The raw number of cigarettes smoked per day as reported at clinic, at follow-
up and the difference between the two values (follow-up value minus clinic value) were
compared between women reporting "Fetal Distress" venus "Uneventful Delivery" using the
Mann-Whitney Rank Sum Test. The numerical difference in number of cigarettes per day
reported in the second compared to the first interview was then categonzed as having increased
(positive value), remained the same (zero value), or decreased (negative value) and these were
then compared using Chi-squared.

20
2.2 Etbical Considerations Methodology
In order to determine the ethical factors involved in developing a methodology for the
"Matemal Smoking and Neonatal HIE" study, a literature review was conducted exarnining the
areas of materna1 guilt surrounding an adverse pregnancy outcome, informed consent, and the
specific requirements for conducting ethically acceptable nonconsensual research.
A MEDLINE search was conducted to locate articles relating to matemal guilt resulting
fiom an adverse pregnancy outcome using the keywords and textwords "guilt, pregnancy,
outcome, infant, newborn, mother/psychology, emotions, attitude". Relevant articles were then
selected and sumrnarized.
For the components of infonned consent and requirements for nonconsensual research,
the American Department of Health and Human Services Code of Federal Regulations for
conducting Human Research (DHHS, 1983), and the Medical Research Council of Canada's
Guidelines on Research Involving Human Subjects (MRC, 1987) were used to identiQ relevant
ethical considerations surrounding informed consent and allowable exceptions to this doctrine in
the context of nonconsensual research. Although there was a considerable body of literature on
the theoretical rationale for the doctrine of informed consent, these documents represented the
most recent statements publicly available at that time and were considered to be authoritative as
they were federat guidelines.
These elements were then articulated in a chronological account of the application to the
Hospi ta1 for Sick Children's Research Ethics Commi ttee (alternatively known as a Research
Ethics Board (REB) or Institutional Review Board (IRB)) for the "Materna1 Smoking and
Neonatal H I E study in the following order:
1) Ethical Concerns
2) Outcome of REB/IRB Review

2 1
3) Final Solution
The ethical concerns resulting fiom the literature review were stated first as a surnmary of the
ethical arguments put forth to the Research Ethics Cornmittee. Second, the outcorne of the
cornmittee's review was detailed as the committee's reaction to the proposai highlights
alternative perspectives on the ethical situation at hand. This is of course largely important as
the committee's response gives suggestions to the researcher as to how the methods should be
changed. Lastly, the final solution to the ethical problem in light of the committee's response
was documented as this illustrated the methodological changes that were made as a result, and
also presented the reaction of the investigators to the cornmittee's initial response.

22
2.3 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephalopathy Methodology
2.3.1 Maternal Smoking and Neonatal Hypoxic-Ischemic Encephaiopathy:
Retrospective Studies
Retrospective analysis of HIE cases was done by reviewing the original data which
supplied information for The Hospital for Sick Children's NlCU computerized database on
outcornes of infants presenting with neonatal HIE (maintained by Dr. Max Perlman). This
database consists of al1 cases of infants with HIE seen at The Hospital for Sick Children NICU
between 1985 and 1992, including details of clinical care and conesponding outcorne. As
information on matemal exposure to cigarette snioke during pregnancy was not included in the
computerized database, the original data collection forms were retrieved and analyzed.
Al1 information relating to materna1 exposure to cigarette srnoke during pregnancy was
documented exactly as it appeared in the original records with regards to positivity (where "yes"
or "no" was indicated) and the number of cigarettes smoked per day where available. The data
were tabulated and categorized where possible in order to be compared with population based
historical matemal smoking data from the Ottawa Civic Hospital during the years 1989 and 1990
(Perkins, Belcher and Livesey, 1997), in order to infer differences in either prevalence or amount
of smoking among pregnant mothers. These particular historical data were used for three
reasons. First, the data was based on a population sample of al1 pregnant women who were seen
at the Ottawa Civic Hospital between July 1989 and May 1990. Second, the geographical area
from which the sample originated was in close proximity to the Hospital for Sick Children and in
fact these two service areas see some degree of overlap for cases of neonatal HIE. Third, this
data was collected in the middle of the time period in which the data in the Hospital for Sick
Children's NICU database was collected. This is particularly important as smoking prevalence
amongst pregnant women has been s h o w to change over time (Britton, 1998; Stewart et al.,
1995).

23
The Chi-square test was then used to test for a significant difference in the proportion of
smokers in each group, and to test for a significant difference in the distribution of the amount of
smoking in each group.
2.3.2 Maternai Smoking and Neonatal Hypoxic-Ischemic Encephalopathy:
Prospective Studies
The study group consisted of al1 term (237 weeks gestational age) infants with a
diagnosis of HIE who presented to the Hospital for Sick Children's Neonatal Intensive Care Unit
over a 9-month period between November 1998 and July 1999. Inclusion was based on a
diagnosis of HIE as determined by the guidelines set forth by the American College of
Obstetricians and Gynecologists (Poland and Freeman, 1992). In order for this diagnosis to be
made, one or more of the following must be present:
1) 5-minute Apgar score 13, metabolic acidosis (serum bicarbonate 4 2 mrnoVL in the
first hour of Iife), or delayed onset of spontaneous respirations beyond 5 minutes.
2) Mechanical ventilation at birth.
3) Evidence of encephaIopathy including clinical seizures, altered state of
consciousness, atypical neuroimaging, or electroencepalographic findings.
4) Evidence of multisystem involvement (i.e., encephalopathy and at least one other
organ system, including abnormal renal function (urine output c l ml/kg/hour for 2 24
hours after birth and a rising serum creatinine after birth), electrocardiographic
evidence of myocardial ischemia, hypotension, coagulopathy (clinical bleeding with
abnormal results of clotting studies consistent with disseminated intravascular
coagulation or hepatic coagulopathy), bone marrow depression (platelet count
400,000 per cu.mm), elevated liver transaminase leveis (AST >200 IU, ALT HO0
IV , pulmonary hypertension (a PO, difference >20 torr between pre- and postductal

24
sites, or evidence of right-to-left shunting through the ductus arteriosis or foramen
ovale on echocardiography).
Exclusion of infants fiom the study was based on the presence of either of the following
criteria:
1) A diagnosis of HIE due to an insult that occurred prior to the delivery
process (e-g., intracranial hemorrhage)
2) A gestational age (37 weeks
The severity of HIE was established by the cnteria described by Sarnat and Sarnat
(Sarnat and Sarnat, 1976) in Table 2.
Afier obtaining consent from the subjects, a one-page data sheet (see Appendix 1) was
completed where a chart analysis was done to collect the relevant obstetrical details fiom patient
records. In addition, a limited number of questions were asked to ascertain parental
socioeconomic status and to clarify any data that were missing or unclear in the charts.
Socioeconomic status was determined using the Hollingshead Four Factor Index of Social Status
(Hollingshead, 1975). Materna1 and paternal characteristics including education and
employment, and factors affecting matemal health, reproductive history, previous pregnancy
outcornes, delivery factors, abnormalities of the placenta or umbilical cord, and neonatal heaIth
were documented. An identification number was assigned for each data form in order to link
clinical data with laboratory results.
A sample of hair was taken fiom the neonate using scissors and methods described by
EIiopolous (Eliopolous et al., 1994), and a meconium sample was obtained using the methods of
Ostrea (Ostrea et al., 1994). According to these established methods, hair samples were stored at
room temperature until the time of analysis in individual envelopes with an identification
number corresponding to that of the data fom. As only one meconium sample was available, it

25
was stored at -70°C and was not analyzed. Ailet the linking of the clinical data to the biological
sample, al1 identiSing personal information for each subject was removed
Cotinine concentrations in neonatal hair were measured by radioimmunoassay (RIA)
(EliopoIous et al., 1994). Hair samples were first washed with a miId detergent, rinsed with
distilled water, and dried in a warm (37°C) oven ovemight. The following day, each neonatal
hair sarnple was cut into small segments and thoroughly mixed in order to determine the average
content of cotinine in the hair sample. Two to five milligrams of each hair sample were weighed
on an analytical balance (Mettler AE 100) and placed in a glass container with 1 rnL of 0.6 N
sodium hydroxide in order to digest the hair samples. The glass vials were sealed with parafilm
to prevent evaporation of the solutions. The samples were agitated overnight at 50°C to allow
for digestion. The following day, the samples were neutralized with 50 to 70 pL of concentrated
hydrochloric acid, and 100 pL aliquots of the neutral solutions were used to measure cotinine
concentrations by M A as originally described by Langone (Langone et al., 1973). The results
were expressed in nanogram of cotinine per milligram of neonatal hair.
The RIA materials required for determination of cotinine were purchased from the
Department of Biochemistry, Brandeis University, Massachusetts. The procedures used in this
study involved adding fixed amounts of tritiated cotinine to each sample, followed by incubation
for one hour at 37°C with the respective rabbit antiserum. A sufficient amount of antibody was
used in these assays to bind 40% to 95% of the total radioactive ligand. After allowing the
reaction to reach equihbrium, a goat anti-rabbit gamma globulin was added to each sample to
separate the antibody-bound cotinine from the free analyte. After overnight storage at 4"C, the
antibody-bound fiactions were precipitated from solution by centrifugation at 1000 x g for 45
minutes. The temperature of the centrifuge (Beckman TJ-6) was also set at 4°C.

26
The amount of radioactivity in the precipitate was expressed as the average counts per
minute (CPM) with a counting time of two minutes per sample using a Beckman LS 5000 CE
scintillation counter.
The concentration of cotinine in each sample was determined by cornparison to a
standard curve. The standard curve was prepared at the same time and in the same manner as the
samples in order to account for day-to-day variability and decay of the isotope. Standards were
prepared by diluting stock of 500 pL of cotinine in isogel TRIS HCl (trimethamine
hydrochloride) buffer. Cotinine standards of 0.25, 0.5, 1, 2, 5, 10, and 25 ng/mL were used for
quantification. The total binding of antibody by radiolabeled antigen was represented by a zero
standard which did not contain any quantity of unlabeled cotinine. In addition, an antibody
blank which did not contain the unlabeled antigen or the rabbit antiserum was used to determine
nonspecific binding (i-e. possible binding of the radiolabeled antigen to test tube contents and
components other than the antibody). The counts per minute value of the antibody blank was
then subtracted fiom al1 values obtained for standards and samples to correct for nonspecific
binding.
To produce the standard curve, the log standard concentration of cotinine was plotted on
the abscissa against the respective logit per cent radioactivity on the ordinate. This type of plot
gives a straight line rather than a curve simpliQing calculation. The line of best fit was
determined by least square regression analysis using the Stat View SE+ graphicsM statistics
software (Abacus Concepts, Inc., 1988) on an Apple Macintosh cornputer. The unknown
concentrations of analyte in the samples were extrapolated from the regression equation.
Al1 standards and samples were run in duplicate and positive and negative controls were
run with each batch of samples assayed.

27
When 2 mg of hair was used, the lowest sensitivity of the assay was 0.1 ng cotinine per
mg hair. In this assay, 3-hydroxycotinine, a metabolite of cotinine, exhibited less than 10%
cross-reactivity.
Recovery of analytes was established by adding known amounts of cotinine to a negative
hair sample afier it had been digested in solution. An aliquot of the same hair sample had been
tested prior to spiking and confirmed to be negative for cotinine. AIiquots (100 uL) of the
spiked solution were analyzed and the recovery of each analyte was calculated. A recovery
value of 92% for cotinine had been calculated in six previous experiments (Eliopolous et al.,
1994).
For the purposes of this study, a neonatal hair cotinine value 5 2.6 ng cotinine per mg of
hair was defined as indicating that the mother was a nonsmoker or a passive smoker as jn
previous work by Elipolous and her colleagues illustrated that amongst nonsmokers and passive
smokers the range of neonatal cotinine was between 0.04 ng cotininelmg hair (the limit of
detection) and 2.54 ng cotinine/mg hair (Eliopolous et al., 1996). Accordingly, any value greater
than 2.6 ng cotinine/mg hair was defined as being positive for active smoking.
After this determination of smoking status, the clinicai characteristics were summarized
both collectively disregarding smoking status and comparatively by categorizing smokers and
nonsmokers into two groups. Where appropriate, student's t-test and Fischer's exact test were
used to test for statistically significant differences between these groups.
The resulting data were then compared with population-based historical data collected in
the Ottawa-Carleton region during 1992 (Stewart et al., 1995) using the Fischer's exact test to
determine if a significant difference existed in the HIE infants with respect to the proportion of
mothers smoking during pregnancy. As with the retrospective studies, these historical data were
chosen due to their being based on a population sarnple, originating from a similar geographical

28
area and being sarnpled at a tirne as close as possible to the time when the prospective data were
being collected.
The actual cotinine levels in the hair of infants whose mothers were identified as active
smokers were then compared with previous data (Eliopolous et al., 1996) for infants who did not
suffer fiom HIE. As these previous data were not population-based, no statistical tests were
performed.
Feasibility was also assessed in several ways.
First, the ethical feasibility of this study was characterized by documenting ethical issues
that arose during the course of conducting the research in light of the guidelines set forth by the
Hospital for Sick Children's Research Ethics Cornmittee and by reevaluating the stance of the
ethics cornmittee in light of these ethical issues which presented themselves.
Second, methodological feasibility was assessed through documenting any dificulties
that arose through the use of the proposed methods and cntically appraising the methodology
and comrnenting on its suitability in light of these difficulties.
Lastly, the practical feasibility of examining the role of materna1 smoking as a risk factor
for neonatal HIE was explored through documenting and highlighting problerns that arose in
terms of geographical concems, logistical concerns such as contacting parents for consent, and
data collection concerns such as the collection of chart information and the problems in
obtaining biological samples. The rate of presentation was also detennined based on averaging
the number of cases which arriveci at the Hospital for Sick Children's NICU between November
1998 and July 1999.

29
3 RESULTS
3.1 Reporting Bias Results
In total, 132 cases were collected which met the inclusion criteria. However, in 7 cases the
patients had expressly mentioned that they had quit, and in 2 cases had mentioned that they had
been successful in decreasing their smoking. In 2 cases the data were not sufficiently quantified
to be analyzed and in one case the patient told the interviewer that she had "memory problerns".
Afier these exclusions, there were 120 eligible cases. Of these 120 women, 95 reported an
uneventful delivery and 25 reported an event which foltowed the definition of "Fetal Distress".
These women provided details of the events in narratives which are summarized in Table 3.
Materna1 charactenstics at clinic between women who had an uneventful delivery and those
who had "Fetal Distress" were not significantly different (Table 4). There were no significant
differences in matemal age, gravidity, parity, spontaneous or therapeutic abortions. The number
of exposures to agents with teratogenic or nonteratogenic effects did not differ. Use of illicit
dmgs or aicohoi during pregnancy also did not differ between the two groups. The two groups
did not significantly differ with regards to the proportion of women who had a chronic illness in
general or a psychiatrie illness in particular. Finally, there were no significant differences in the
number of women who had an event of "FetaI Distress" during a previous pregnancy.
Other than the selection critena of "Fetal Distress", pregnancy outcome characteristics at
follow-up also did not differ significantly between the two groups as shown in Table 5. There
was no difference between the two groups in the number of infants bom with major
malformations, nor were there any differences in gestational age at birth or birth weight. in
addition, there was no significant difference in the number of months that had elapsed between
clinic visit and follow-up among the two groups.

Comment No. of Occurrencesa
Emergency Caesarian Section Performed
Baby's Heart Rate Was Low 5
Cord Around Neck 4
Baby's Heart Rate Elevated 3
Induced Labor 3
Baby Admitted to NICU 2
No Additional Commentsm 2
Decreased Oxygen to Fetus 1
Presence of Meconium 1
Baby Aspirated Meconium 1
"Baby Was Blue" 1
Baby Received Oxygen 1
*-2 women did not elaborate on the circumstances of Fetal Distress a-Not mutually exclusive
Table 3 Additional Information Provided by Mothers Reporting "Fetal Distress"

Uneventful Delivery
n=95
Materna1 Age' 29.1 k4.9
Gravidityb 2 [l-71
TA^ O [O-21
No. Exposures for C h i c b 1 [l-71
( No. Exposures Teratogenicb 1 O [O-11
I No. Exposures Unknownb
No. Exposures Nonteratogenicb
1 Use of Illicit Drugs b
Use of Alcohol 37 (38.9%)
1 Maternal Illness 1 72 (75m8%) Psychiatric Illness 27 (28.4%)
1
I Prev. "Fetal Distress" l O (0%) - - --
a - Values expressed as mean + S.D. b - Values expressed as median with range I - Student's t-test 2 - Mann-Whitney Rank Sum Test 3 - Chi-squared
Table 4 Materna1 Characteristics at C h i c Visit

l Major Malformations
( Gestational Age ( ~ k ) ~ 1 40 [35-421 1 40 [3442] 1 0.502
P value Uneventful Delivery ' b6Fetal Distress" n=9S
Time to Follow-up OS)^ 1 16[7-35-51 1 20[236.5] 1 0.3 l2
n=ZS
Birth Weight (g)'
a - Values expressed as mean I S.D. b - Values expressed as median with range 1 - Student's t-test 2 - Mann-Whitney Rank Sum Test 3 - Chi-squared
Table 5 FoUow-up C haracteristics
327 1k546 3250k565 0.86'

33
Details of materna1 self-report of smoking are shown in Table 6. There was no
significant difference between the two groups in the number of cigarettes smoked per day dunng
pregnancy as reported at c h i c . There was also no significant difference @=0.32) in the
proportion of mothers who at follow-up declared themselves to be non-srnokers (decreased to
zero cigarettes). There was, however, a statistically significant difference between the two
groups in the change in reporting of cigarette consumption during pregnancy in c h i c versus at
follow-up afler pregnancy. That is, mothers who experienced Fetal Distress in their babies
reported significantly !ess smoking during pregnancy at follow-up than during their initial c h i c
visit. This difference was categonzed and compared as shown in Table 7. The two groups were
significantly different in terms of the change in the report of number of cigarettes per day at
follow-up with respect to whether it had increased, remained unchanged or decreased. These
resuits indicate that mothers who had events of fetal distress during delivery were significantly
more likely to decrease their subsequent report of smoking during pregnancy cornpared to
mothers who had uneventhl deliveries, who did not change their reports.

Uneventful Delivery n=93
No. Cig/d reported at Follow-up'
No. Cig/d reported at Clinic'
Difference in No. Cig/d reported at Follow-up vs. Clinics
10 [O-401
Values expressed as median with range Mann-Whitney Rank Sum Test
Tab Materna1 Self-Report of Smoking

Change in No. Cig/d Reported at Follow-up vs. Clinic
Uneven tful Delivery n=95
Increased
Table 7 Changes in Self-Report of Materna1 Smoking
"Fetal Distress" n=25
Same
Decreased
P value
24 (25.3%)
34 (35.8%)
37 (38.9%)
5 (20%)
3 (12%)
17 (68%)
0.02'

3.2 Ethical Consideratioos Results
3.2.1 Ethical Concerns
At the onset of developing the hypothesis, several ethical concems arose regarding the
study population. These included the potential psychological harm to parents who might infer
from the study that they were responsible for their child's condition, ambiguity regarding the
moral status of biological waste such as meconiurn, and the apparently absolute requirements of
the Research Ethics Board / Institutional Review Board (REBARB) of the Hospital for Sick
ChiIdren to obtain infonned consent.
Whereas previously it was believed that women who smoked during pregnancy were less
aware than nonsmokers of the specific risks to the fetus (Butters and Howie, 19901, from the
results of several studies it now appears that women who smoke during pregnancy are becoming
increasingly aware of at least some of the risks that this behaviour poses to the fetus (Buist and
Yu, 1987; Haslarn, Draper and Goyder, 1997; Lelong et al., 1995). In one prenatal survey study
(Buist and Yu, 1987), it was demonstrated that both smoking and non-smoking expectant
mothers during pregnancy are generally aware of the known potential risk of low birth weight as
a result of smoking during pregnancy. Additionally, in this particular study, the investigators
used open-ended questionnaires which allowed women to suggest any risks that they thought
might exist while smoking during pregnancy. Amongst their responses, although more senous
possible outcomes such as increased mortality were suggested, very few women in fact felt that
these were a possibility. Therefore, we assumed that women who smoke during pregnancy may
not envision a potential nsk for a condition such as HIE which if moderate or severe may result
in a number of severe adverse outcomes including cerebral palsy, cognitive deficits or death
(Shaywitz and Fletcher, 1993).

37
In a study examining maternai reaction to the birth of an infant who suffered fiom a long-
term disability (of genetic or perinatal cause), three types o f causal attributions have been
documented (not mutually exclusive)(Affleck et al., 1982):
The behaviour of others (e-g. obstetrician - 22%)
Materna1 behaviour (self-blame) - 26%
No behavioral causes (e.g. chance, Act of God, "fate") - 57%
Although the final category does not directly attribute the outcome to a particular person,
the author states that it may lead to self-blarne as some mothers developed the idea that
somehow they "deserved it". This category is also believed to be associated with depression and
low self-esteem both of which have been linked with smoking populations (Fidler et al., 1992;
Fergusson et al., 1996; Hurst et al., 1997). In cases where a child is born with a long-tenn
disability, mothers will undoubtedly look for some reason for this outcome; even in cases where
there was an obvious genetic cause for the outcome, mothers still felt some degree of
responsibility and had begun to examine their own behaviour in order to look for some cause.
In light of this potentially vulnerable study group, we felt that seeking consent would
represent a risk for psychological harm as exposure to the hypothesis itself might provide a
mechanism for developing self-blame. Sirnply stating that there was a possibility of a mother
being responsible for this outcome might convert ail of the smokers to the seif-blame category.
In addition, any underlying anxiety of the non-smoking mothers might be exacerbated by
thoughts of exposure to second hand smoke, which has also been shown to have an effect on the
fetus (Koren, 1996). One may argue that since our hypothesis is pure speculation, that it has no
potential for h m ; however, just the fact that the research is being undertaken may suggest to
the mother the likely validity of the hypothesis.
Given the importance of this project and the nature of the study population, we began to
consider carrying out this research without consent. As we sought to obtain a biological marker

38
of maternal smoking, we felt that using the discarded waste meconiurn (a baby's first bowel
movement) would be appropriate as it is non-invasive, can be collected unobtrusively, and is an
excellent indicator of maternal smoking status (Ostrea et al., 1994). We could then link this
information with relevant obstetrical information from a baby's chart. AAer linking, al1
identifiing characteristics would be removed maintaining anonymity for both the babies and
their parents.
As stated by the American Department of Health and Human Services (DHHS)
conditions under which research can be conducted without consent must conforrn to the
following guidelines (DHHS, 1983):
1) Procedure(s) involve minimal risk
2) No violation of nghtslwelfare of subject
3) Could not be carried out otherwise
4) When appropriate, subjects be informed after participating
(Section 46.1
As our proposed research involved no risk to the subject, condition 1
16d)
. was met. The
interpretation of the criteria set out under conditions 2 and 3, however, was not as clear. Under
condition 2, Our research could be interpreted as a violation of the subject's right to privacy. As
we would be examining the baby's waste, it could be regarded in a similar light to police
searches through garbage being considered an illegal invasion of privacy as the baby's waste
would provide insight into the prenatal activities of the baby's mother. However, the study of
biological waste products, in the past, has been seen as not requiring consent (Medical Research
Council of Canada, 1987). We would also be examining the baby's and the mother's medical
information, both from the baby's chart. Historically, conducting retrospective "chart studies"
without consent had been common practice, although this practice has been looked upon less
favorably in recent years (Emson, 1994). Although there was room for debate, we felt that as we

39
had proposed to eliminate any identiQing characteristics, thereby retaining anonymity, that
violation of privacy would be minimal and hence this would sat ise condition 2. We viewed
Condition 3 as being satisfied in that we felt that we would not be able to carry out the research
obtaining consent as it could put some mothers at risk for psychological harrn. Again, with
regards to Condition 4 we would seek to avoid causing harm to the subjects, and hence we would
likely not be informing subjects aAer participating.
Upon reviewing the cnteria set out in the DHHS, we felt that we had fulfilled al1 of the 3
essential criteria required for permission to conduct nonconsensuaI research. We subsequently
made our request to Our REBARB in the Spring of 1998 to do our research without consent,
presenting the above arguments. Because we felt that seeking consent would represent an
unjustifiable nsk to the subject, we considered a nonconsensual methodology to be the most
ethically reasonable.
3.2.2 Outcome of REB/IRB Revîew
Our request to conduct this research without consent was subsequently denied and
several suggestions were made by the REBIIRB:
First, we were required to inform parents and obtain consent for this study. At the time
of our submission, the Medical Research Council of Canada (MRC) was in the process of
releasing its "Tri-Council Policy Statement on Code of Ethical Conduct for Research Involving
Humans". In Article 1.1 the Code States that al1 research must be consensual and that subjects
must be given the opportunity to make an informed choice in accordance with the principle of
autonomy (MRC, 1998). In light of the Code, The R E B W felt that it was of utmost
importance to obtain consent in showing respect for persons. As well, in the interests of
planning fhture pregnancies the REB/IRB felt that parents should be informed of the
hypothetical link between smoking and HIE.

40
Second, we were required to present to the parents a list of potential causes of HIE and
to include smoking in that list, thereby diMusing the unconfirmed association with smoking.
Hence, the posing of the study question was to be such that it appeared that we were in fact in
search of new risk factors, or clarification of the roles of known nsk factors. The REB/IRB felt
that because our study would at best be only able to show an association between materna1
smoking and HIE that this listing of potential risk factors would be suitable. This is to Say that
our study would not be able to show that matemal smoking was a cause of HIE, but rather that it
is one of several factors which together or in combination with other unknown reasons could
potentially cause HIE. Hence, this study would not in fact be able to show that a mother had a
causative role in this outcorne.
Finally, it wos also requested that counseling be available to any mothers who were
experiencing any fonns of self-blarne and that the results of this study be provided to families
with personalized comments where appropriate. At this point, the REB/IRB assigned a member
to Our case in order to handle any further issues which did not require a full cornmittee review.
3.2.3 Final Solution
In accordance with the decision of the REB/IRB, we complied with their requests. As
hlly infonned consent would be sought, we expressed Our desire to obtain more biological
samples and to obtain detailed obstetrical information which would enhance the quality of the
study and make Our results more valid. The REB/IRB approved our request at which point we
proceeded to compose a parent information and consent form requesting permission to obtain
these samples and information. The consent form included smoking as a risk factor in a large
list of possible risk factors. This first version of Our information form was then approved by Our
REBARB.
Afier REB/IRB approval, we then proceeded to inform staff rnembers in the Neonatal
Intensive Care Unit (MCU) as to the particulars of our study. Several staff members, however,

4 1
had concems regarding the information form. They cited that physicians do everything in their
power to try and reassure parents of these babies with HIE that there is no evidence that they
were in no way at fault, and they felt that such an information form was contrary to this notion,
The physicians felt that al1 references to smoking should be removed fkom the fonn and that the
information should be presented in a more general fashion in order to convey the idea that we
were searching for new risk factors with no suggestion that we had a working hypothesis and
that this was in fact more of a "fishing expedition" than anything else. Accordingly, a second
finalized version which did not have smoking Iisted as a risk factor, but included a reference to
decreased oxygen as a risk, was submitted to the assigned member of the REBnRB and was
approved.

42
3.3 Materaal Smoking and Neooatal Hypoxîc-Ischemic Encephalopathy Results
3.3.1 Retrospective Data
A total of 300 infants with HIE presented to the Hospital for Sick Children's NICU
between 1985 and 1992. Hence during this time period, the rate of presentation of infants with
HIE to this institution was approximately 3 per month. For the purposes of the aforementioned
outcome study reported by Ekert et al. (Ekert et al. 1997), 133 infants were excluded as their HIE
was considered to be mild or where there was evidence of head trauma or a gross physical insult
unrelated to asphyxia. Hence, a total of 167 cases were reviewed and were utikw! for the
current research.
Of the 167 cases, 7 1 had documentation of smoking status. Among these 7 1 cases, 13
(18%) mothers reported smoking during pregnancy. In the research reported by Perkins et al., in
a population sample of al1 pregnant women who delivered their babies at the Ottawa Civic
Hospital between the months of July 1989 and May 1990, 734 (23%) out of 3220 identified
themselves as active smokers (Perkins et al., 1997). After comparing these proportions with the
Chi-squared test using Yates correction, it was found that the proportions of smokers in each
group were not significantly different w . 4 5 ) .
Of the 13 mothers who reported smoking in the HIE group, their reported quantity of
smoking ranged fiom 2 cigarettes per day up to 60 cigarettes per day. The distribution of this
data is s h o w along with the distribution found at the Ottawa Civic Hospital in Table 8. Chi-
square testing showed a statistically significant difference @<0.001) in the distribution of
smoking suggesting that in this limited sample, mothers of infants with HIE smoked
significantly more cigarettes per day compared to the population of pregnant mothers seen at the
Ottawa Civic Hospital.

Self-Reported
Cigarettes/Day
Ottawa Civic Hospital
1989-90
(n=734)
Hospital for Sick Children
HIE Cases 1985-92
(n=13)
a-C hi-square test
Table 8 Self-Reported Cigarette Consumption in Mothers of Infants with HIE at the
Hospital for Sick Children (1985-92) vs. All Live Births at the Ottawa Civic
Hospital (1989-90)

3.3.2 Prospective Data
3.3.2.1 Clinical Data and Hair Cotinine Analysis Results
A total of 12 term infants presented to the Hospital for Sick Children NICU with a
diagnosis of hypoxic-ischemic encephalopathy (HIE) between November 1998 and July 1999.
In total the parents of 11 cases agreed to participate and were enrolled in the study. The parents
of one infant refused to participate in the study specifically indicating that they were doing so
under legal counsel as a Lawsuit against the delivering obstetrician was being pursued.
A summary of the matemal characteristics for the 11 infants is s h o w in Table 9.
Matemal age ranged fiorn 22 to 43 years of age, with an average of age of 33. The Hollingshead
Scores for the parents of these infants were consistent with a low to mid-level socioeconomic
status (Socioeconornic status of IV or V). For 5 of the 1 1 mothers, this was their first pregnancy.
Of the remaining 6 mothers, two had at least one child, and the remaining 4 mothers had
between I and 3 spontaneous abortions in previous pregnancies. Arnongst these 1 1 mothers, 5
had ongoing medical concems during their pregnancy and 1 had a pregnancy induced medical
condition. Of these 6 cases, 4 were identified as potential causes of fetal asphyxia as per Table
1, namely, two cases of diabetes, one case of asthrna, and one case of pregnancy induced
hypertension. One woman also experienced polyhydramnios during her pregnancy.

No. of Occurrenccs @=il)
Maternal Age (yrs.)
Gravidity
Parity
Spontaneous Abortion
None
One
Three
Maternal Health Problem
Essential Diabetes
Asthma
Infertility Requinng Treatment
Hepatitis B Carrier
Abnormal Prenatal Conditions
Pregnancy-Induced Hypertension
Pol y hydramnios
a-mean value + standard deviation
b-rnedian value with range in brackets
Table 9 Materna1 Characteristics of Infants with HIE Preseoting at the Hospital for
Sick Children (Nov. 1998-July 1999)

46
Deliveiy factors for the case infants are displayed in Table 10. In 5 cases, delivery was
induced and in 6 cases assistance during delivery was required (forceps or vacuum). In 3 cases
emergency caesarian section was required due to abnormalities of fetal heart beats, and 1 case
presented as a breech birth. One case of placenta previa, one case of an umbilical ho t , 3 cases
of nuchal cord (cord wrapped around the baby's neck) and one case of cord prolapse were seen
and are identified as risks for asphyxia as per Table 1. In a11 but one case there was evidence of
fetal cardiac abnormalities during delivery. Of the 11 infants, 8 had meconium staining during
delivery and in 4 cases there was evidence of meconium aspiration.
Characteristics of the 1 1 neonates are shown in Table 1 1. These infants had an average
gestational age of approximately 39 weeks, with 4 cases greater than 40 weeks gestation. The
infants had an average birthweight of approximately 3.4 kg and there were 6 females, and 5
males. Apgar scores for these infants were low with a 1 minute average score of 1.5, and 5
minute average score of 5 . The severity of HIE in these infants was primarily moderate as one,
eight and two infants had Stage 1,2 and 3 HIE, respectively.

No. of Occurrences (n=ll)
Precipitous Delivery
Forceps Used
Rotation
Extraction
Vacuum Used
Emergency Caesarian Section
Breech Birth
Placental Factors
Previa
Cord Factors
Urnbilical Cord Knot
Nuchal Cord
Proiapsed Cord
Fetal Cardiovascular Factors
Bradycardia
Decelerations
Loss of Variability
Meconium Aspiration
Meconium Staining
Table 10 Delivery Factors of Infants with HIE Presenting nt the Hospital for Sick
Children (Nov. 1998-July 1999)

No. of Occurrences @=il)
Gestational Age (wk)
No. Postmature (>40 wk)
Gender
Male
Female
Birthweight (g)
Apgar Scores
1 Minute
5 Minute
HIE Severity
Stage 1
Stage 2
Stage 3
a-mean value + standard deviation
b-median value with range in brackets
Table 11 Neonatal Characteristics of Infants with HIE Presenting at the Hospital for
Sick Children (Nov, 1998-July 1999)

49
The results of neonatal hair cotinine analysis are summarized in Table 12 (actual cotinine
values for each case are available in Appendix 2). Eight of the 11 mothers were categorized as
nonsmokers based on their infants hair cotinine value ( a . 6 ng/mg hair), and 3 mothers were
categorized as active smokers based on their infants hair cotinine value (>2.6 ng/mg hair) as per
previous findings (Eliopolous et al., 1996).
Based on the results in Table 12, infants were then categorized by matemal smoking and
compared by category.
Materna1 characteristics of smokers and nonsmokers are shown in Table 13. There were
no statistically significant differences between the two groups including differences in matemal
age, gravidity or parity. Amongst al1 active smokers, this was the first pregnancy, and none of
these women had any underlying health problems (one woman had pregnancy-induced
hypertension).
Delivery factors of smokers and nonsmokers are summarized in Table 14. There were no
statisticaily significant differences between the two groups. Although not statistically
significant, it is noteworthy that a higher proportion of infants in the materna1 smoking group
required assistance in delivery, showed signs of fetal heart monitoring abnormalities and had
incidents of meconiurn aspiration than the infants of nonsmokers.

Number of Cases
Table 12 Smoking Status for Mothers of Infants with Neonatal HIE Presenting at the
Hospital for Sick Children (Nov. 1998-July 1999)
-
Range (ng cotinine/
mg neonatal hair)
Nonsmoker / Passive Smoker
Active Smoker
8 (73%)
3 (27%)
0.05-0.98
15.05-45.5

1 Maternal Age (yrs.)
Parity
1 Spontaneous Abortion
1 Three
Maternal Health Problem
Essential Diabetes
1 Infertility Requiring Treatment
1 Pregnancy Induced Hypertension
1 Hepatitis B Carrier
Abnormal Prenatal Conditions
a-mean value f; standard deviation b-median value with range in brackets
Non-Smoker/ f assive Smoker
(n=8)
Table 13 Materna1 Characteristics Categorized by Smoking Status in Infants with
Neonatal HIE Presenting at the Hospital for Sick Children (Nov. 1998-July
1999)
Active Smoker (n=3)
O [O-21 0 [O-O]

Non-Smokerl Passive Smoker
(n=8)
Forceps ~ s e d I
1 , Precipitous Delivery
Rotation I O (0%)
4 (50%)
Extraction I 2 (25%)
Vacuum Used O (0%)
Emergency Caesarian Section
Placental Factors I
2 (25%)
Breech Birth
Previa I 1 (12.5%)
1 (12.5%)
Cord Factors
--
Nuchal Cord I 1 (12.5%)
Umbilicai Cord h o t
Prolapsed Cord 1 (12.5%)
1 (12.5%)
Fetal Cardiovascular Factors I Bradycardia
LOSS of Variability ( 3 (37.5%)
5 (62.5%)
Decelerations 3 (37.5%)
-
' Active Smoker I (n=3)
Meconium Aspiration
Meconium Staining -- - - - - - -- - - -
Table 14 Delivery Factors of Infants with HIE Categorized by Materna1 Smoking
Status Presenting at the Hospital for Sick Childrea (Nov. 1998-July 1999)
2 (25%)
6 (75%)

53
Neonatal characteristics categorized by matemal smoking are shown in Table 15. There
were no statistically significant differences between the groups. The birthweight for infants in
the group of active srnokers was lower and almost reached statistical significance (p=0.07).
Although not statistically significant, a difference was seen in the two groups in the proportion
of infants who were born afier 40 weeks gestation as there were 4 cases (50%) in the nonsrnoker
group and none in the smoking group. Further to this, although amongst nonsmokers there was
some degree of difference in the severity of HIE, al1 infants of rnothers who smoked were of the
moderatdy severe category of HLE (Stage 2).
In this cohort, 3 of 11 (27%) mothers smoked, assumedly, throughout their pregnancy.
This proportion was found not to be statisticaIIy significant @=0.73) compared to the
population-based data fiom the Ottawa-Carleton region in 1992 where the investigators found
that amongst 7940 women, 1485 (18.7%) continued to smoke throughout pregnancy (Stewart et
al., 1995)
Amongst active smokers, cotinine values ranged fiom approximately 15 up to 45 ng/mg
hair. Based on the data reported by Eliopolous and her colleagues, this would be consistent with
a minimum leveI of 40 cigarettes or approximately 2 packs per day (Eliopolous et al., 1996). In
the previous data neonatal hair fiom 36 active smokers was measured and cotinine values above
19 ng/mg hair were not seen and hence estirnates of the nurnber of cigarette per day consumption
of the two remaining mothers could not be calculated.

Non-Smokerl Passive Smoker
(n=8)
1 Female 1 5 (62.5%) 1 1 (33.3%)
Active Smoker (II=~)
Gestational Age (wk)
No. Postmature
Gender
1 Birthweight (g) 1 3514k376" 1 30325249'
39.5k2.3"
4 (50%)
1 Stage 1 ( 1 (12.5%) I o (0%)
38.7k2.3"
O (0%)
Apgar Scores
1 Minute
5 Minute
a-mean value I standard deviation b-median value with range in brackets c-data unavailable
1.5 [l-61b
5 [l-71
I
Stage 2
Stage 3
Table 15 Neonatal Characteristics of Infants with HIE Presenting at the Hospital for
Sick Children (Nov. 1998-July 1999) Categorized by Materna1 Smoking
C -
C -
5 (62.5%)
2 (25%)
3 (100%)
O (0%)

3.3.2.2 Assessrnent of Feasibility
Ethical Feasibility
During the course of this research several ethical issues were brought to light by the
researcher and the staff of the Hospital for Sick Children's NICU. First, as docurnented in
Section 3.2.3 several staff physicians expressed concem about the idea of smoking as a potential
risk entering into the minds of the mothers of infants with HIE. There was ongoing concern
dunng the course of the research as to how this topic would be addressed if the researcher was
asked by parents about the exact nature of the research and what the working hypothesis was.
Second, as the nursing staff was closely involved in contacting parents and reminding them of
the study during the tirne when parents were reading over the consent form (which usually took
place over one to hvo days), there was concem on behalf of the nursing staff about the exact
scientific nature of the study. Third, there was ongoing concem on behalf of the researcher
about the possibility of parents persisting in questioning the nature of the research and the exact
rationaIe behind it.
Taken together, the above ethical concems posed serious concerns as to the requirements
of the ethics cornmittee as the research environment seerned to leave parents open to the
potential psychological harms illustrated in Section 3.2.1 as there was an ongoing possibility of
being exposed to the research hypothesis.
Met hodological Feasibility
The methods utilized in the research examining materna1 smoking as a risk factor for
neonatal HIE worked efficiently when elements of practical feasibility were not a concem (i.e.,
excellent methods can oniy work well when one can successfûlly contact subjects and obtain
consent). The only limitation noted was that neonata1 meconium proved difficult if not
impossible to obtain. in many instances as seen in Section 3.3.2.1, meconium was passed in
utero and hence was not obtainable. In addition, due to the severity of the asphyxia1 insult, many

56
infants had multiple organ damage which ofien resulted in the inability to pass their first bowel
movement for several days. Neonatal hair by contrat was easy to obtain and no parents
objected to the taking of the sample. As well, discarded neonatal hair was occasionally available
if an infant required a medical intervention requiring shaving of the head.
Practical Feasibility
Several practical concerns arose during the course of the research.
Geographical issues could pose a theoretical problem in that because the Hospital for
Sick Children admits infants boni throughout central and northern Ontario. Hence, if
geographically matched controls were needed, it could potentially be very difficult to obtain
them.
Logistical concerns also emerged as contacting parents proved to be difficult for at least
two reasons. First, as mothers had ofien undergone caesarian section they Frequently remained
at the refemng hospitai during recovery for a number of days while the infant was attended to at
the Hospital for Sick Children. Second, parents frequently did not have any fixed pattern of
visiting hours at the hospital and their location was otten unknown which rendered contacting
them in order to obtain consent dificult.
Data collection concems aside from the methodological concems sunounding meconium
did not occur. Patient charts were adequate for obtaining the necessary clinical information, and
determining socioeconomic status through parental report was not difficult.
A total of 12 term infants with HIE presented to the Hospital for Sick Children over the
course of 9 months between November 1998 and July 1999. This presentation rate of less than 2
per month could prove to be a serious impediment for future studies. Staff physicians felt that
this rate was considerably less than in previous years and may have been due to ongoing
cutbacks resulting in limited bed space.

5 7
4 DISCUSSION
4.1 Reporting Bias
The problem of underreporting in epidemiological research poses a threat to the validity
of a study. Our results suggest that in studies of adverse outcomes during pregnancy, mothers
tend to underreport their smoking which they may feel had in some way contributed to the event.
Because the two groups were similar in many matemal charactenstics and outcome
measures, it is highly probable that it is the adverse pregnancy outcome that led to the reporting
bias. Moreover, women who had uneventfui pregnancy outcome did not change their reported
number of cigarettes (median change=O), indicating that because of the chronic and stable nature
of smoking, there is no problem of recall per se (Feldman et al., 1989).
The major limitation in a i s study was sample size. Because of the limited sarnpfe size,
the statistical power to show a tme difference between groups was low. Gravidity and parity for
example were higher in the group of women who had uneventhl deliveries but were not
statistically different fiom the cases of women who had events of fetal distress. It is possible
that women who had uneventhl pregnancies had previous pregnancies in which they smoked
and had no adverse outcomes that they may have become more socially confident in their ability
to admit to their smoking behaviour during pregnancy. Use of alcohol is another factor that did
not reach statistical significance. Its reported value was in fact higher in women who had events
of fetal distress. If in fact there was a link between alcohol use and fetal distress, this also would
not be seen because of limited sample size.
It is noteworthy that the event of fetal distress may in fact have caused women to have a
better recall of their smoking during pregnancy. In a study looking at bottled water consumption
during pregnancy and pregnancy outcome, it was concluded that women who had spontaneous
abortions in fact had a significantly better recall of their water intake when compared to women

5 8
with normal outcomes (Neutra e t al., 1992). Hence, it is not an issue of recall per se, but rather
of recall bias.
The results of our study reinforce the need to obtain biological markers of exposures
during pregnancy as we have demonstrated that in instances of adverse outcomes, materna1 self-
report may be unreliable. However, while biological markers such as blood, urine or hair
cotinine can help distinguish smoken from nonsmokers, they may not be adequate for the
detection of changes in pregnancy consumption, as nicotine undergoes pharmacokinetic changes
during pregnancy (Seaton and Vessell, 1993). These changes can result in altered nicotine
clearance making dose estimates by extrapolation unreliable.

59
4.2 Et hical Considerations
In this unique ethical situation, there is perhaps no one answer that would satisQ al1
individuals involved. Clinical and research ethics is the process of striking a balance between
what provides appropriate protection to human subjects and what best fiirthers medical research
and patients' wellbeing. While seeking to obtain consent shows respect for the study participant
and a desire to enter into a "contract" of mutual exploration we also realize that in some
situations, as proposed by our REB/TRB, that partial disclosure, or deception, is permissible if it
is "not Iikely to be harmfbl in and of itself and that sufficient information will be disclosed to
give subjects a fair opportunity to decide whether they want to participate in the research."
(Levine, 1988)
In this situation, however, tbere are two consciences at risk. First, there is the individual
who is involved in obtaining the consent. This penon is asked to approach a potential subject
knowing that he/she is required to interact with these particularly vulnerable subjects attempting
to obtain their consent and inform them and at the same time insulate them fiom knowledge
which could potentially be harmfùl. In this context, it can be interpreted as the obtaining of an
invalid consent as we are not in fact disclosing our true purpose. These conflicting obligations
may cause moral distress in the person seeking the consent, confemng a sense of dishonesty and
deceit. Secondly, there is the subject of the research. It is generally held that within the
allowance of incomplete disclosure, "investigators should always give truthfûl answers to
questions" (Levine, 1988). This being the case, there is still a possibility within this framework
that parents could be "exposed" to our potentially damaging hypothesis by virtue of the fact that
if they demand to know exactly what we are looking for then we are obliged to be tmthfùl in our
response.
The notion of protecting the subjects fiom potential psychological h m in this instance
hinges upon the hope that subjects are in fact ignorant of or uninterested in the fact that we are

60
indeed only investigating one hypottiesis. Hence, although the final solution of the R E B m
combined with the suggestions of the NICU staff seems to be the most reasonable, it still leaves
individuals at risk for psychological h m . In this situation, it is diffiçult to see how the goal of
protecting hurnan subjects would best be achieved.
This portion of the research highlights the way in which ethical considerations shape
study methodology at the onset of the research initially during the proposa1 stage, in the
secondary phase of the response to the concerns of the research ethics comrnittee and through to
the point of the final phase at the point of initiating the research.

4.3 Materna1 Smoking and Neonatal Hypoxic-Ischemic EncephaIopathy
4.3.1 Retrospective Data
The retrospective data in this research suggest that women who had infants with HIE
smoked significantly more cigarettes per day when compared to a population based historical
control within the sarne time period. This suggests that a dose-response relationship may be
occumng such that high levels of maternal smoking are associated with an increased risk for
infants developing neonatal HIE dunng delivery. This strengthens the overall hypothesis
governing the present research. The overall difference in prevalence of smoking between the
hvo groups, however, was not statistically significant. If in fact this is sbown to be true in a
larger sample size, it suggests that maternai smoking in general may not be a risk for neonatal
HIE, but that a certain threshold exists in dosage after which point there is an increased risk for
this condition.
This component of the research had three main limitations. First, the small sample size
of infants with known materna1 smoking status provided low statistical power and hence if a true
difference existed between groups, this could not have been seen. Second, out of 167 cases, only
71 (43%) had documentation of smoking status. As smoking was not considered in the
retrospective study conducted by Ekert and his colleagues on infant outcome (Ekert et al., 1997),
the availability of data on smoking was sporadic. Because of this fact, it is impossible to know if
the data used for the retrospective study of maternal smoking as a risk factor for HIE are tmly
representative of that infant population. If for example the question was not asked because
parents seemed particularly distraught, and the reason for this psychological state was partially
due to guilt because of smoking during pregnancy, this would introduce a severe bias in the
results. Third, as this research relied on maternal report and did not utilize a biological marker,
it is subject to al1 of the shortcomings illustrated by the current research into reporting bias due
to an adverse pregnancy outcome. Although the results suggest that a higher amount of smoking

62
was occwring, it is possible that an even higher amount was actually taking place and this fact
would be lost due to underreporting.
During the time when the retrospective data were originally collected, there was a higher
rate of infants presenting to the Hospital for Sick Children's NICU than there is currently
(approximately 3 per month between 1985 and 1992 versus less than 2 per month in 1998/99).
At this time, the hospital saw a wider range of HIE cases than is seen currently. For example,
during those years it was quite cornmon for an infant with Stage 1 or mild HIE to be referred to
the Hospital for Sick Children. In recent years, mild cases of HIE are rarely adrnitted as these
infants can often be cared for adequately at the refen-ing hospital. The effect of this selective
presentation of more severe cases of HIE to the hospital in recent years is that cases with more
severe etiologies will arrive at the hospital. Accordingly, cases where there is an obvious,
physically traumatic cause of HIE make up the majority of cases seen in the Hospital for Sick
Children's NICU. As a result, the more subtle cases where there is no obvious cause are lost to
the Hospital for Sick Children as they remain at the referring hospital. This makes previous data
that much more robust, but has senous implications for the qualityhreadth of data that can be
collected fkom the Hospital for Sick Children's NICU.
4.3.2 Prospective Data
The results of this prospective component of the research further support the
retrospective data and serve to reinforce the working hypothesis. Through the prospective
research, it was determined that three women were active smokers dunng their pregnancy.
Arnongst these women, cotinine values ranged from approximately 15 up to 45 ng/mg hair.
Based on the data reported by Eliopolous and her colleagues, this would be consistent with a
minimum level of 40 cigarettes or approximately 2 packs per day (Eliopolous et al., 1996). In
fact, these three cases represent a level of smoking that was only seen in the top 1% of the data
based on the Ottawa Civic Hospital population (Perkins et al., 1997). This high level supports

63
the hypothesis that a nsk for developing neonatal HIE is associated with an elevated level of
maternal smoking.
The clinical findings in this prospective research also veri@ the likelihood of a high level
of smoking. The birthweight of the three infants bom to women who smoked actively dunng
pregnancy was lower than that of infants bom to nonsmokers and almost reached statistical
significance (p=0.07), although there was no difference in gestational age. This finding of
decreased birthweight has been s h o w in numerous stcdies to be associated with maternal
smoking (MacDorrnan et al., 1997; Golding, 1997; Oyen et al., 1997; Koren, 1995).
The prospective component of the research did show a significant difference in
proportion of smokers amongst mothers of infants with HIE when compared to historical data
from the Ottawa-Carleton region (Stewart et al., 1995). This result was not surprising given the
sample size; however, this finding brings to light an interesting finding in the study. During the
study period, a total of 12 eligible infants with HIE were seen at the Hospital for Sick Children.
Eleven of these cases were enrolled into the study; however, there was one refusa1 on the
grounds that they had been instructed by their lawyer not to participate. If in fact the parents in
this case refùsed participation because the mother had actively smoked during her pregnancy,
which could potentially weaken a legal case alleging negligence on behalf of the attending
obstetrician, this would be a source of a powerful bias. During the course of the study, the
parents of two infants who had enrolled in the study had asked the researcher confidentially
about what was required for an investigation of obstetrician cornpetence for the purposes of a
potential lawsuit. Given that this occurs, there is a concem that this potential knowledge of
smoking behaviour through a methodology that is not completely anonymous may be a serious
disincentive for parents to participate in future studies.
The results of the prospective research also suggest some interesting roles for maternal
smoking in the etiology of HIE. In the cornparison of delivery factors between nonsmokers and

64
smokers, it was noted, that although not significantly different, a higher proportion of women,
who actively smoked during pregnancy, required assistance during delivery and showed more
abnormalities of fetal heart monitoring. If there was an underlying problem of decreased
oxygenation of the feus at the start of the delivery due to smoking, then this could in
combination with other factors which although may restrict oxygen supply or blood flow but are
normally not suffrcient to cause a severe degree of hypoxia, could potentially result in fetal heart
rate abnormalities due to hypoxia (Perlman and Kirpalani, 1992; Hill, 1979). These events
usually prompt the obstetrician to move for a prompt extraction of the fetus which necessitates
the use of assistance such as forceps and vacuum. In two of three cases of active smokers, these
events unfolded, albeit without the knowledge of the potential role of smoking in the etiology of'
HIE. If this supposition about smoking is true, this may establish smoking as a risk factor in that
it potentiates the risk of other events which normally would prove innocuous.
However, the role of smoking may be more serious than this. In one case of neonatal
HIE in this cohort, there were no obvious risk factors identified. This young woman had no
underlying health problems, and no history of reproductive problems. By definition, the infant
was a tenn infant and was normal in every regard other than the diagnosis of HIE. However, this
particular infant showed al1 of the documented signs of fetal heart rate abnormalities consistent
with fetal hypoxia. In addition, this infant gave the highest level of hair cotinine at
approximately 45 ng/mg hair. If we were to assume a linear relationship in the arnount of
smoking and the amount present in neonatal hair, it is possible that this woman was smoking 4
packs of cigarettes per day, or was in an environment which together with her own smoking
resulted in that level of exposure. In this particular case, it is possible that there was an as yet
undocumented risk factor at work in the etiology of HIE. It is of greater concern that because of
this level of smoking, the oxygen supply was so greatly reduced to the fetus that it was not able
to endure the process of an otherwise normal delivery.
65
The main limitation to this component of the research, as with other components, was
sample size. Possibly due to this small sample, no difference in smoking prevalence was seen.
In addition, it was not possible to effectively compare clinical factors between smokers and
nonsmokers because of the limited numbers.
One of the strengths of this research is that a bioIogica1 marker was used to determine
smoking status and an estimation of the actual level of smoking that occurred. This method
allowed the research to minimize the problems inherent in relying on maternal report of smoking
which was demonstrated in the current research, and is a potential limitation in the retrospective
study of maternal smoking as a nsk for neonatal HIE.
In addition to seeking to strengthen the working hypothesis of the research, this purpose
of this study was to determine the feasibility of doing research into the role of matemal smoking
in neonatal HIE at the Hospital for Sick Children. While conducting the research, several
concems arose considering the ethical feasibility of investigating this problem using the
proposed rnethods. The primary concem is the problem of potential psychological damage due
to a vulnerable subject being exposed to the research hypothesis. This is a novel concept in
bioethics as the need to seek an informed consent has become paramount and there has been no
prior consideration in the literature as to the risks of seeking consent in such a context as this
one.
Two problems remain regarding the ethical feasibility of this study. First, there is an
ongoing concem that due to either persistent questioning on behalf of parents, or lack of
discretion on behalf of staff or the individual obtaining consent, or for other reasons, that there is
still a potentiaI for vulnerable subjects to be exposed to the research hypothesis and therefore the
possibility of psychological damage still exists. As was illustrated in Section 4.2, this is an
exceedingly dificuit situation as it has become imperative to obtain an infonned consent (MRC,
1998). As a non-invasive, anonymous nonconsensual methodology was not considered to be
66
ethically acceptable, in subsequent designs it may be necessary to h e the research question as
a more generalized research problem which does not make the "background" hypothesis of
smoking as a risk factor known to anyone other than the pnmary investigîtor and others
performing data analysis. In this way, not even the individual obtaining consent would be aware
as to what the tnie objective was and hence the potential for psychological damage could
theoretically be reduced to a minimum. Yet by the same token, this practice is inherently
dishonest and poses a serious problem in that the "background" hypothesis is of great
importance to explore and drives the need to conduct the study. The second problem that
became evident is the question of the ethical status of the investigator or the individual obtaining
consent if they know the hypothesis. If ethics seeks to provide a solution where no one comrnits
a wrongfùl act, then it will likely be impossible to attain this goal given the current methodology
and circumstance. This affects feasibility in that if there is to be another person obtaining
consent, for example an investigator at a different site in a multicentre study, then if this person
is to be made aware of the "background" hypothesis they must be willing to engage in the same
deceptive behaviow as the primary investigator. It is quite possible that other persons, and their
institutions, will not be willing to do this.
The methodology utifized in this research proved to be efficient. Data collection using
the developed fonn (Appendix 1) was straightforward and required a minimum arnount of time
to complete once consent was obtained. A physician who was fmiliar with a particular case
could likely complete the clinical details in 5 minutes. Determination of socioeconomic status
was easily done with the Hollingshead index (Hollingshead, 1975). Using this index, marital
status, and the highest levels of education and employment are al1 that need be obtained from
each parent. As mentioned in Section 3.3.2.1, meconium was difficult to obtain for a number of
reasons. In planning future studies, due to the diffculties noted and also the problems in storing
and shipping the matenal it should not be included as a biological sample, but rather neonatal

67
hair should exclusively be used. Ln addition to being a sensitive and specific biological marker,
neonatal hair is conveniently obtained, easily stored in an envelope at room temperature and is
easily shipped.
The practical issues of geographic distribution, logistics, and presentation rate have
important implications for future research. In a subsequent study design, the methodology
shouId seek to address the issue of matching index cases with geographically similar controls.
This present research at first sought to enroll infants fiom the Hospital for Sick Children's NICU
as controls which would address this problem. This, however, proved to be difiicult as the
majority of infants without HIE were premature andor often had severe congenital defects
which would have made approaching parents for consent extraordinarily difficult. In light of
this, future studies will need to address this concem. Logistical problems arose due to
difficulties in contacting parents. This could be addressed by a different methodology that
utilized hospitals where the NICU is located on site with the rnatemity ward. In this way,
parents would be physically accessible to researchers much more easily. Finally, there is a large
concem regarding presentation rate. Between November 1998 and July 1999, a total of 12
eligible infants with HIE were seen at the Hospital for Sick Children. This resulted in a rate of
presentation of less than 2 per month, which was lower than what would have been predicted by
previous data. In order for further studies to be conducted expediently, other centres will need to
be included in order to collect data at an appropriate speed.

68
4.4 Surnmary of Findings
This research addresses the larger question of how to conduct research examining the
role of materna1 smoking in adverse pregnancy outcornes, both fiom a methodological and
ethical standpoint.
The results from the first part of this research highlight the fact that maternal report of
smoking dwing pregnancy may be unreliable, particularly in the context of an adverse
pregnancy outcome. It was demonstrated that in situations of fetal distress during detivery,
mothers may reduce their report of smoking that occuned during pregnancy. This bias can
severely affect the results of a study seeking to delineate the role of matemal smoking in this
outcome. Our study has hvo major advantages over previous attempts to characterize this
reporting bias: This was a prospectiveiy collected cohort, and at the time of the initial interview,
women were very open about their smoking habits as they were eager to receive accurate
estimates of their risk. Secondly, we could assess not just smoking status, but also changes in
the number of reported cigarettes.
From these results, it was inferred that maternal report will not be adequate to address the
study question. This prompted a consideration of the use of a biological marker such as cotinine
trapped in neonatal meconium. The question then becarne that of how to obtain this marker,
which led to the questions of informed consent, institutional policy, and the prospect of doing
noninvasive, nonconsensual research. This was proposed in order to avoid psychological h a m
to the research subject that could result from the indirect accusation that her behaviour played a
role in the adverse outcome of her infant.
In the process of submitting the proposa1 for this research to the Hospital for Sick
Children's research ethics cornmittee, it was required that a partially informed consent be
obtained and that the study proceed seeking to obtain neonatal meconium and neonatal hair.
From the course of arguments put forth to support Our initial hypothesis and in light of the ethics

69
comrnittee's decision, it was demonstrated that indeed there were indeed possible risks to the
subject in the form of induced maternal guilt by the nature of the research hypothesis. It was
also illustrated that this potential risk exists in the study methodology proposed by the ethics
cornmittee.
The pilot research into the role of maternal smoking and neonatal HIE provided data,
both retrospectively and prospectively, that support Our hypothesis that maternal smoking may
confer an increased risk for the development of neonatal HIE during delivery. Although having
several limitations, the retrospective data suggest that a significantly higher amount of smoking
had occurred amongst mothers of infants with HIE compared to a general population of women
who had also smoked during pregnancy. Prospectively, there was also an initial signal that this
supposition may indeed be true as evidenced by very high levels of neonatal hair cotinine
amongst mothers who smoked and had infants with HIE.
In addition, this pilot research also highlighted several issues of feasibility in the research
on materna1 smoking and neonatal HIE.
Regarding methodology and study design, frorn a purely technical perspective it was
suggested that a study collecting clinical data and neonatal hair samples would be relatively easy
and effective. Appropriate controls would need to be obtained and issues of contacting parents
quickly to consent needs to be addressed, perhaps in centres where the NICU and maternity
wards are located close to each other. When the presentation rate at the Hospital for Sick
Children is considered, it would be imperative for this study to adopt a multicentre design to
collect data at an appropriate speed.
When we examine the ethical considerations involved in this potential multicentre design
however, two issues come to bear. First, although there currently exists a form of insulative
deception in the obtaining of a partially informed consent in the study, this still leaves a
possibility of subjects learning of the Eue hypothesis and hence the potential for psychological

70
damage remains. Second, the requirement of the site investigator to be involved in some degree
of deception may dissuade potential site investigators, or their institutions fiom collaborating in
this study. Because of these concerns, the presentation of the study may have to be done in such
a way as to keep site investigators uninformed so as to avoid any accidental leaks of the
hypothesis that could potentially cause damage. It may in fact be necessary to address the study
as a "fishing expedition" as the ethics cornmittee had suggested.
From these results, it has been demonstrated that there are numerous methodological and
ethical issues in the study of maternal smoking and adverse pregnancy outcomes. This research
shows not only that these aspects are substantial, but that they interact in the research process.
Methodology has an impact on ethics in that methods may potentially be subject to ethical
scmtiny. This issue is well known to researchers, yet in this unique context the method of
obtaining an informed consent itself poses an ethical concern not from the principle of
autonomy, but rather fiom that of "doing no ham". This results in the formation of ethical
judgments regarding the methodology, and hence the methodology is shaped by the ethics in
order to meets its demands. In the study of maternal smoking and adverse pregnancy outcomes,
this delicate interplay between methodology and ethics is of great importance.

7 1
4.5 Recommendations for Future Studies
Areas of need for hture investigation are extensions of the related areas of study
presented in this thesis.
Further studies in the area of underreporting should be undertaken in order to determine
if there is some predictive value that can be elucidated. If one cari determine a consistent pattern
of underreporting or detenninants leading to underreporting, this would be important
information in an attempt to improve the understanding of the matemal fetal toxicology of
tobacco smoke or other addictive substances.
Bioethics is a rapidly expanding field, yet the topic of adverse pregnancy outcomes and
the surrounding ethical questions of investigating matemal behaviour as a risk factor in these
outcomes has been poorly studied. Future research into the specific topic of materna1 guilt
resolution in light of scientific evidence and hypotheses should be explored. Knowledge on the
nature of how mothers weigh scientific evidence or hypotheses in their development of self-
blame would allow better formulation of methods and consent forms that would be sensitive to
these issues. Although perhaps dificult to realize, criticisms of the institutional policies used in
determining ethical solutions should be undertaken. In Canada, the Medical Research Council
now requires informed consent as a blanket policy (MRC, 1998). Perhaps this policy should be
reviewed in order to allow exceptions that represent minor infkingements such as those
exceptions delineated in the United States (Levine, 1988).
It has been suggested that a multicentre study will be necessary in order to more clearly
establish the role of materna1 smoking in neonatal HIE. This is clearly a future research
direction as a larger sample size is most certainly required.

If matemal smoking proves to be associated with HIE, a full scale study will need to be
designed based on these results to adâress the following questions:
1) Dose-response characteristics: How much fetal exposure is associated with how
much risk? Also, is there a correlation between materna1 smoking and the clinical
severity of the encephalopathy?
2) Confounders: Large sample sizes will be needed to control for potential confounders.
3) The relative validity of different biological markers (e.g. where hair and meconium
are readily obtainable).
HIE is a devastating pennatal complication, ofien leading to serious lifelong morbidity. If an
association exists between HIE and smoking, this may be one of very few etiologies of HIE
which can be prevented.
Finally, studies examining the interplay between methodology and ethics should be
undertaken. If it is possible to delineate underlying principles that existed in the modification of
proposed methodologies because of ethical considerations, perhaps it would be possible to
incorporate those principles into the methodology earlier, such that it might enable the
production of more ethically sound protocols. It is hoped that this research would serve not only
to expedite the study development and review process, but also to raise the awareness of
researchers to the ethical requirements involved in research design.

73
5 REFERENCES
Affleck G, Allen D, McGrade BJ, McQueeney M. Matemal causal attributions at hospital
discharge of high-risk infants. Arnerican Journal of Mental Deficiency. l982;86(6):575-
Ahlsten G, Ewald U, Tuvemo T. Prostacyclin-like activity in umbilical arteries is dose-
dependently reduced by matemal smoking and related to nicotine levels. Biology of the
Neonate. l99O;S8(5):27 1-8.
Breman, BG. Smoking in Pregnancy. Journal of the Society of Obstetncs and G y n e c o k of
Canada. 1997; 1 9: 1405- 10.
Bitton GA. A review of women and tobacco: have we corne such a long way? Journal of
Obstetric, Gyriecologic, & Neonatal Nursing. 1998;27(3):24 1-9.
Buist A, Yu D. Smoking and pregnancy: awareness, attitudes and habit changes. Healrh
Bulletin. l987;45(4): 179-84.
Butters L, Howie CA. Awareness among pregnant women of the effect on the fetus of
comrnonly used dnigs. Midwifery. 1990;6(3): 146-54.
Cnattingius S, Nordstdm M-L. Matemal smoking and feto-infant mortality: Biological
pathways and public health significance. Acta Paediatrica. 1996;85(12): 1400-2.
Cuskey WR, Wathey B. Female addiction. Lexington Books, Lexington, MA, 1982.
Department of Health and Human Services. Title 45 Code of Federal Regulations 46. March 8,
1983.
DiFranza JR, Lew RA. Effect of materna1 cigarette smoking on pregnancy complications and
sudden infant death syndrome. Journal of Famiiy Practice. 1995;40(4):385-94.
Ekert P, Perlman M, Steinlin M, Hao Y. Predicting the outcome of postasphyxial hypoxic-
ischemic encephalopathy within 4 hours of birth. Journal of Pediatrics. 1997; 1 3 1 :6 13-
7.

Eliopoulos C, Klein J, Chitayat D, Greenwald M, Koren G. Nicotine and cotinine in materna1
and neonatal hair as marken of gestational smoking. CZinical & lnvesrigarive Medicine.
1996; 19(4):23 1-42.
Eliopoulos C, Klein J, Phan MK, Knie B, Greenwald M, Chitayat D, Koren G. Hair
concentrations of nicotine and cotinine in women and their newbom infants. Journal of
the American Medical Association. 1994;27 1 (8):62 1 -3.
Emson HE. Minimal breaches of confidentiality in health care research: a Canadian perspective.
Journal of Medicai Efhics. l994;20(3): 1 65-8.
Feldman Y, Koren G, Mattice K, Shear H, Pellegrini E, MacLeod SM. Determinants of recall
and recall bias in studying dmg and chemical exposure in pregnancy. Teratology.
1989;40(1):37-45.
Fergusson DM, Lynskey MT, Horwood LJ. Comorbidity between depressive disorders and
nicotine dependence in a cohort of 16-year-olds. Archives of General Psychiatry.
1996;53(11): 1043-7.
Fidler W, Michel1 L, Raab G, Charlton A. Smoking: a special need? British Journal of
Addiction. 1992;87(11): 1583-9 1.
Fimegan, L.P. Dmg dependence in Pregnancy. Crown House Publishing, London, 1980.
Gilstrap LC 3d, Leveno KI, Burris J, Williams ML, Little BB. Diagnosis of birth asphyxia on
the basis of fetal pH, Apgar score, and newbom cerebral dysfunction. Am J Obstet
GynecoZ. 1989; 16 1 :825-830.
Golding J. Sudden infant death syndrome and parental smoking--a literature review. Paediatric
& PerinafaZ Epiderniology. 1997; 1 1(1):67-77.
Gupta 1, Hillier VF, Edwards JM. Multiple vascular profiles in the umbilical cord; an indication
of materna1 smoking habits and intrautenne distress. Placenta. 14(1): 1 17-23, 1993.

75
Haslam C, Draper ES, Goyder E. The pregnant smoker: a preliminary investigation of the social
and psychological influences. Journal of Public Health Medicine 1997; 1 g(2): 187-92.
Hill A, Volpe JJ. Perinatal asphyxia: clinical aspects. Clinics in Perinaiology. 1989; l6(2):435-
57.
Hill LM. Diagnosis and management of fetal distress. Mayo Clinic Proceedings
1979;54(12):784-93.
Hollingshead AB. Four factor index of social status. Dept. of Sociology, Yale University, New
Haven, CT, 1975.
Hurst DF, Boswell DL, Boogaard SE, Watson MW. The relationship of self-esteem to the
health-related behaviors of the patients of a primary care clinic. Archives of Family
Medicine. 1 997;6( 1):67-70.
Jedrychowski W, Whyatt RM, Cooper TB, Flak E, Perera FP. Exposure misclassification error
in studies on prenatal effects of tobacco smoking in pregnancy and the birth weight of
children. Journal of Exposure Analysis & Environmetrtal Epiderniology. 1998;8(3):347-
57.
Klebanoff MA, Levine RJ, Clemens JD, Dersirnonian R, Wilkins DG. Serum cotinine
concentration and self-reported smoking during pregnancy. American Jounial of
EpidenlioZow. 1998; 148(3):259-62.
Koren G. Fetal toxicology of environmental tobacco smoke. Cuwent Opinion in Pediarrics.
1995;7(2): 128-3 1 .
Koren G. The fetus as a passive smoker. Canadian Family Physician. l996;42: 130 1-3.
Langone IJ, Gjika HB, Van Vunakis H. Nicotine and its metabolites. Radioimmunoassays for
nicotine and cotinine. Biochemistry. 1973; 12(24):5025-30.

76
Lelong N, Kaminski M, Chwalow J, Bean K, Subtil D. Attitudes and behavior of pregnant
women and health professionals towards alcohol and tobacco consumption. Patient
Education & Counseling. 1 995;25(1):39-49.
Levine, Ri. Ethics and Regulation of Clinical Research. Yale University Press, New Haven,
1988.
Longo L. The biological effects of carbon monoxide on the pregnant woman, fetus, and and
newbom infant. A m e e n Journal of Obstetrics & Gynecol~gy~ 1 977; l29( 1 ):69- 1 03.
MacDorrnan MF, Cnattingius S, Hoffian HJ, Kramer MS, Haglund B. Sudden infant death
syndrome and smoking in the United States and Sweden. Arnerican Journal of
Epidemiology. 1997;146(3):249-57.
Mead M. The diagnosis of foetal distress: a challenge to midwives. Journal of Advanced
Nursing. l996;23(5):975-83.
Medical Research Council of Canada (MRC). Tri-Council Policy Statement Document: Code of
Ethical Conduct for Research Involving Humans. Ottawa, 1998.
Medical Research Council of Canada (MRC): Guidelines on research involving human subjects.
MRC, Ottawa, 1987.
Murray RP, C o ~ e t t JE, Lauger GG, Voelker HT. Error in smoking measwes: effects of
intervention on relations of cotinine and carbon monoxide to self-reported smoking. The
Lung Health Study Research Group. American Journal of Public Hedth.
1 W3;83(9): 125 1-7.
Neutra RR, Swan SH, Hertz-Picciotto 1, Windham GC, Wrensch M, Shaw GM, Fenster L, Deane
M. Potential sources of bias and confounding in environmental epidemiologic studies of
pregnancy outcomes. Epidemiologv. 1 992;3(2): 1 34-42.

77
Ostrea EM Jr, Knapp DK, Romero A, Montes M, Ostrea AR. Meconiurn analysis to assess fetal
exposure to nicotine by active and passive materna1 smoking. Journal of Pediatrics.
1 994; l24(3):47 1-6.
Oyen N, HagIund B, Skjaerven R, irgens LM. Materna1 smoking, birthweight and gestational
age in sudden infant death syndrome (SIDS) babies and their surviving siblings.
Paediatric & Perinatal Epiderniology. 1 997; 1 1 Suppl 1 : 84-95.
Parer JT, Livingston EG. What is fetal distress? American Journal of Ubstetrics and
Gynecolobgy. 1 990; l62(6): 142 1-5.
Perkins S, Belcher JM, Livesey JF. A Canadian Tertiary Care Centre Study of Matemal and
Umbilical Cord Cotinine Levels as Markers of Smoking During Pregnancy: Relationship
to Neonatal Effects. Canadian Journal of Public Health. 1997; 88(4):232-7.
Perlman M, Kirpalani H. Residents Handbook of Neonatology. Mosby Year Book, Toronto,
1992.
Poland RL, Freeman RK, eds. Guidelines for pennatal care. 3" ed. Elk Grove Village, IL:
American Academy of Pediatrics; 1992.
Ryder MI, Fujitaki R, Lebus S, Mahboub M, Faia B, Muhaimin D, Hamada M, Hyun W.
Alterations of neutrophil L-selection and CD18 expression by tobacco smoke:
implications for periodontal diseases. Journal of Periodontal Research. 1998;33(6):359-
68.
Sarnat H, Samat M. Neonatal encephalopathy following fetal distress. A clinical and
electroencephalographic study. Archives of Neurology. 1 976;3 3 : 696-705.
Schardein, JL. Chemically induced birth defects, 2"* Ed. Dekker, New York, 1993.
Seaton MJ, Vesell ES. Variables affecting nicotine metabolism. Pharmacology & Therapeutics.
l993;60(3):46 1-500.

78
Shaywitz BA, Fletcher JM. Newological, cognitive, and behavioral sequelae of hypoxic-
ischemic encephalopathy. Seminars in Perinato20gy~ 1993; 17(5):3 57-66.
Sherman BR, Sanders LM, Trinh C, eds. Addiction and Pregnancy. Praeger Publishers,
Westport, CT, 1998.
Stewart PJ, Potter J, Dulberg C, Niday P, Nirnrod C, Tawagi G. Change in smoking prevalence
arnong pregnant women 1982-93. Canadian Journal of Public Health. 1995;86(1):37-
41.
Roberton NRC. Textbook of neonatology, 2nd ed. New York: Churchill Livingstone, 1992.
Thomberg E, Thiringer K, Odeback A, Milsom 1. Birth asphyxia: incidence, clinical course and
outcome in a Swedish population. Acta Paediatrica. 1995;84(8):927-32.
Walsh RA, Redman S, Adamson L. The accuracy of self-report of smoking status in pregnant
women. Addictive Behaviors. 1996;2 1 (5):675-9.
Walsh RA. Effects of materna1 smoking on adverse pregnancy outcornes: examination of the
criteria of causation. Human Biology. 1994;66(6): 1059-92.
Welte JW, Russell M. Influence of socially desirable responding in a study of stress and
substance abuse. Alcoholism, CZinical & E-rperimental Research. 1993; 17(4):758-6 1.
Winn R, Vedder N, Ramamoorthy C, Sharar S, Harlan J. Endothdial and leukocyte adhesion
molecules in inflammation and disease. Blood Coagulation & Fibrinolysis. 1998;9
Suppl2:S 17-23, 1998.

79
6 APPENDICES
Appendix 1
HIE STUDY fORY MatemaUPaternal Characteristics and SES MATERNAL AG€ G e - SA - TA - GESTATIONAL AGE wks MARITAL STATUS- MOTHER'S: EDUCATION
OCCUPATION FATHER'S: EDUCATION
OCCUPATION COMMENTSIOTHER Matemal Disease ANXIETY P HYPOTENSION O PIH O ESS HTN P GESTDIABETES P An/ DECREASE O AFV INCREASE O SEV M D TRIM APH P THYROXINE TREAT O COMMENTSfOTHER Maternal CV Factors HY POXlA P CARDIACCOND O PULMONARYCOND O COMMENTSIOTHER Reproductive History INFERTlLlTY RX O PREV STILLBIRTHS Q NEONATAL DEATHS O COMMENTSIOTHER Previous Neonatal Mortality SEIZURES O INTRACRANIAL HEMORRHAGE P FRACTURED SKULL O HIE O SlBLlNG HEALTH PROBLEMS O COMMENTSIOTHER Maternal Infections RUBELLA O CMV 0 HERPES O GBS O COMMENTSIOTHER Delivery Factors HOME BIRTH O ABN UTERINECONT O PROM Q C-SECTION P HEADTRAUMA Q PRECP. DELIV Q UTERlNERUPTURE O VACUUM O If yes, RURAL? P If yes, CAST SB O BREECH O BLOOD LOSS Ci
FORCEPS (Rotation) O FORCEPS (Extraction) O IUGR SYM Q IUGR ASYM P SGA O CEPHALOHEMATOMA P COMMENTSIOTHER Placental Factors ANTPLACENTA P PL PRNlA O ABRUPTION O PLANOMALY Q COMMENTS/OTHER Cord Factors UMBlLlCAL KNOT P PROLAPSED CORD O NUCHAL CORD O
If yes, SGA Q CORD HEMATOMA O COMMENTS/OTHER Neonatal Characteristics s u - BIRTH WEIGHT g / kg / lb APGARs 1 min 5 min CO TWlN SIB P MECASP P MEC STAlN O PPHN O COMMENTS/OTHER Fetal CV Factors FETAL BRADY O DECELS O LOSS OF VARlABlLlTY O COMMENTSIOTHER Neonatal Infections NEC O PNEUMONIA O MENlNGlTlS O COMMENTSIOTHER SequenceIAdditional Comment8

Actual Hair Cotinine Values from Neonates with HIE (The Hospital for Sick Children November 1998 - July 1999)
Sample Cotinine (nglmg hair)

Appendix 3
Proposed Non-Consensual Research to Avoid Potential Iatrogenic Parental Guilt: An Example in Hypoxic-ischemic Encephalopathy (HIE)
Matthew Wong, BSc, Christine Hamson, PhD, Aideen Moore, MD, Gideon Koren, MD
The Division of Clinical Pharmacology/Toxicology (MW,GK), The Department of Bioethics (CH), The Division of Neonatology (AM) and The MotheRisk Program (GK), The Hospital for Sick Children, Toronto. The Faculty of Pharmacy (MW,GK), The Department of Pharrnacology (GK), The Faculty of Medicine (AM,GK), The Institute of Medical Science (CH,GK), The University of Toronto Joint Centre for Bioethics (CH), The Department of Pediatrics (CH,AM,GK), and the CIBC Wood Gundy Children's Miracle Foundation Chair in Child Health Research (GK), University of Toronto.
Dr. Aideen Moore was the Chair of the Hospital for Sick Children's Research Ethics Cornmittee during the time of subrnitting the proposa1 described in the text.
Supported in part by the Medical Research Council of Canada, and the Seed Grant Program, The Hospital for Sick Children.
Address for Correspondence:
Gideon Koren, MD, ABMT, FRCPC The Division of Clinical Pharmacology and Toxicology The Hospital for Sick Children 555 University Ave. Toronto, ON M5G 1 X8 Canada Tek (416) 813-578 1 Fax: (416) 8 13-7562

Abstract
The loss of a baby during childbirth is a devastating event associated with
feelings of extreme grief, disappointment, helplessness, and seIf-blame. Perhaps even
more tragic and emotionally complex is an event during childbirth that may result in the
child having a life-long disability. One such outcome occurs in babies who develop a
perinatal condition known as hypoxic-ischemic encephalopathy or HIE. In HIE, the
oxygen supply to the fetus is decreased during delivery resulting in temporary or
permanent brain damage. Although many obstetrical risk factors have been identified, a
Iarge number of cases present no obvious cause. Our research is to investigate the
hypothesis that maternal smoking is a risk factor for HIE.
In light of this psychologically vulnerable study group, we sought to do an
anonymous study using discarded meconiurn (a baby's first bowel movernent) as an
indicator of maternal smoking status. As smoking has not been established in this role,
we felt that it would be unethical to suggest to a mother of a baby with this serious
condition that she might be in some way responsible for this tragedy. However, given
the importance of this project, we consequently requested that our REBARB allow us to
cany out this research without consent as it would be anonymous and completely non-
invasive. Our request was subsequently denied and we were required to inform parents
of the study. This article documents the ethical framework which prompted our request,
an account of the REBARB response, and the final solution to this dilemma.

Background
The loss of a baby dun ng childbirth is a devastating event associated with
feelings of extreme grief, disappointment, helplessness, and self-blarne. Perhaps even
more tragic and emotionally complex is an event during childbirth that may result in the
child having a life-long disability. One such outcome can occur in babies who develop a
pennatal condition known as Hypoxic-Ischemic Encephalopathy (HIE). In this
condition, the oxygen supply to the fetus is decreased during delivery potentially
resulting in significant brain damage. The etiology of this condition is not fully
understood, and although many obstetncal risk factors have been identified, a Iarge
proportion of these cases present no obvious cause (1). Because of the potential for a
baseline decrease in oxygenation and vascular changes that can occur during smoking
(2,3), Our group wished to investigate the hypothesis that materna1 smoking is a risk
factor for HIE, using a combination of matemal obstetncal history and biological
markers of smoking.
Ethical Concerns
At the onset of developing our hypothesis, several ethical concerns arose
regarding our study population. These included the potential psychological harm to
parents who might infer from the study that they were responsible for their child's
condition, ambiguity regarding the moral status of biological waste such as meconium,
and the apparently absolute requirements of Our Research Ethics Board / institutional
Review Board (REBARB) to obtain informed consent.
Whereas previously it was believed that women who smoked during pregnancy
were less aware than nonsmokers of the specific risks to the fetus (4), from the results of

several studies it now appears that women who smoke during pregnancy are becoming
increasingly aware of at least some of the risks that this behaviow poses to the fetus (5-
7). In one prenatal s w e y study (9, it was demcjnstrated that both smoking and non-
smoking expectant mothers during pregnancy are generally aware of the known potential
risk of low birth weight as a result of smoking during pregnancy. Additionally, in this
particular study, the investigators used open-ended questionnaires which allowed women
to suggest any risks that they thought rnight exist while smoking during pregnancy.
Amongst their responses, although more serious possible outcomes such as increased
mortality were suggested, very few women in fact felt that tbese were a possibility.
Therefore, we assumed that women who smoke dunng pregnancy may not envision a
potential risk for a condition such as HIE which if moderate or severe may result in a
number of severe adverse outcomes including cerebral palsy, cognitive deficits or death
In a study examining materna1 reaction to the birth of an infant who suffered fiom
a long- tenn disabiiity (of genetic or perinatal cause), three types of causal attributions
have been documented (not mutually exclusive)(9):
The behaviour of others (e.g. obstetrician - 22%) Matemal behaviour (self-blarne) - 26% No behavioral causes (e.g. chance, Act of God, "fate") - 57%
AIthough the final category does not directly attribute the outcorne to a particular person,
the author states that it may lead to self-blame as some mothers developed the idea that
somehow they "deserved it". This category is also believed to be associated with
depression and low self-esteem both of which have been associated with smoking
populations (10-12). In cases where a child is boni with a long-tenn disability, mothers

will undoubtedly look for some reason for tbis outcome; even in cases where there was
an obvious genetic cause for the outcome, mothers still felt some degree of responsibility
and had begun to examine their own behaviour in order to look for some cause.
In light of this potentially vulnerable study group, we felt that seeking consent
would represent a nsk for psychological h m as exposure to the hypothesis itself rnight
provide a mechanism for developing self-blame. Simply stating that there was a
possibility of a mother being responsible for this outcorne might convert al1 of the
smokers to the self-blame category. In addition, any underlying anxiety of the non-
smoking mothers might be exacerbated by thoiights of exposure to second hand smoke,
which has also been shown to have an effect on the fetus (13). One may argue that since
Our hypothesis is purely speculation that it has no potential for h m , however just the
fact that the research is being undertaken may suggest to the mother the likely validity of
the hypothesis.
Given the importance of this project and the nature of the study population, we
began to consider carrying out this research without consent. As we sought to obtain a
biological marker of materna1 smoking, we felt that using the discarded waste meconium
(a baby's first bowel movement) would be appropriate as it is non-invasive, can be
coIlected unobtrusively, and is an excellent indicator of matemal smoking status (14).
We could then link this information with relevant obstetrical information from a baby's
chart. After linking, al1 identiQing characteristics would be removed maintaining
anonyrnity for both the babies and their parents.

As stated in the American Department of Health and Human Services (DHHS),
conditions under which research can be conducted without consent must conform to the
following guidelines (1 5):
1) Procedure(s) involve minimal risk 2) No violation of rightdwelfare of subject 3) Could not be carried out otherwise 4) When appropriate, subjects be informed afier participating
DHHS, Section 46.1 16d
As our proposed research involved no risk to the subject, condition I was met. The
interpretation of the criteria set out under conditions 2 and 3 however was not as clear.
Under condition 2, our research could be interpreted as a violation of the subject's right
to privacy. As we would be examining the baby's waste, it could be regarded in a similar
light to police searches through garbage being considered an illegal invasion of privacy
as the baby's waste would provide insight into the prenatal activities of the baby's
mother. However, the study of biological waste products, in the past, has been seen as
not requiring consent (16). We would also be examining the baby's and the mother's
medical information, both fiom the baby's chart. Historically, conducting retrospective
"chart studies" without consent had been common practice, although this practice has
been looked upon less favorably in recent years (17). Although there was room for
debate, we felt that as we had proposed to eliminate any identifying characteristics
thereby retaining anonymity, that violation of privacy would be minimal and hence this
would satisfi condition 2. We viewed Condition 3 as being satisfied in that we felt that
we wouId not be able to carry out the research obtaining consent as it could put some
mothers at risk for psychological harm. Again, with regards tu Condition 4 we would

seek to avoid causing h m to the subjects, and hence we would likely not be informing
subjects after participating.
Upon reviewing the criteria set out in the DHHS, we felt that we had fùlfilled al1
of the 3 essential critena required for permission to conduct nonconsensual research. We
subsequently made our request to our REB/IRB in the Spring of 1998 to do Our research
without consent, presenting the above arguments. Because we felt that seeking consent
would represent an unjustifiable risk to the subject, we considered a nonconsensual
methodology to be the most ethically reasonable.
Outcome of REBflRB Review
Our request to conduct this research without consent was subsequently denied and
several suggestions were made by the R E B W :
First, we were required to inform parents and obtain consent for this study. At the
time of our submission, the Medical Research Council of Canada (MRC) was in the
process of releasing its "Tri-Council Policy Statement on Code of Ethical Conduct for
Research Involving Humans". In Article 1.1 the Code states that al1 research rnust be
consensual and that subjects rnust be given the opportunity to make an informed choice
in accordance with the principle of autonomy (18). In Iight of the Code, The REB/IRB
felt that it was of utrnost importance to obtain consent in showing respect for persons. As
weI1, in the interests of planning future pregnancies the REBARB felt that parents should
be informed of the hypothetical link between smoking and HIE.
Second, we were required to present to the parents a list of potential causes of
HIE and to include smoking in that list, thereby diffising the yet unconfinned
association with smoking. Hence, the posing of the study question was to be such that it

appeared that we were in fact in search of new risk factors, or clarification of the roles of
h o w n nsk factors. The REB/IRB felt that because our study would at best be only able
to show an association between materna1 smoking and HIE that this listing of potential
risk factors would be suitable. This is to Say that Our study would not be able to show
that matemal smoking was a cause of HIE, but rather that it is one of several factors
which together or in combination with other unknown reasons could potentially cause
HIE. Hence, this study would not in fact be able to show that a mother had a causative
role in this outcorne.
Finally, it was also requested that counseling be available to any mothers who
were experiencing any forms of self-blame and that the results of this study be provided
to families with personalized comrnents where appropriate.
At this point, the REB/IRB assigned a member to our case in order to handle any
fiirther issues which did not require a full cornmittee review.
Final Solution
In accordance with the decision of the REBARB, we complied with their requests.
As fully informed consent would be sought, we expressed Our desire to obtain more
biological samples and to obtain detailed obstetricai information which would enhance
the quality of the study and make our results more valid. The REB/IRB approved Our
request at which point we proceeded to compuse a parent information and consent form
requesting permission to obtain these samples and information. The consent form
included smoking as a risk factor in a large list of possible risk factors. This first version
of our information f o m was then approved by our REBflRB.

After REB/IRB approval, we then proceeded to inform staff members in the
Neonatal Intensive Care Unit (NICU) as to the particulars of Our study. Several staff
members however had concerns regarding the information fonn. They cited that
physicians do everything in their power to try and reassure parents of these babies with
HIE that there is no evidence that they were in no way at fault, and they felt that such an
information form was contrary to this notion. The physicians felt that al1 references to
smoking should be rernoved fiom the form and that the information should be presented
in a more general fashion in order to convey the idea that we were searching for new risk
factors with no suggestion that we had a working hypothesis and that this was in fact
more of a "fishing expedition" than anything else. Accordingly, a second finalized
version which did not have smoking listed as a risk factor, but included a reference to
decreased oxygen as a risk, was submitted to the assigned member of the REB/IRB and
was approved.
Discussion
In this unique ethical situation, there is perhaps no one answer that would satisQ
ail individuals involved. Clinical and research ethics is the process of stnking a balance
between what provides appropriate protection to human subjects and what best furthers
medical research. While seeking to obtain consent shows respect for the study
participant and a desire to enter into a "contract" of mutual exploration we also realize
that in some situations, as proposed by Our REBARB, that partial disclosure, or
deception, is permissible if it is "not likely to be harmful in and of itself and that
sufficient information will be disclosed to give subjects a fair opportunity to decide
whether they want to participate in the research." (19)

In this situation however, there are two consciences at risk. First, there is the
individual who is involved in obtaining the consent. This person is asked to approach a
potential subject knowing that he/she is required to interact with these particularly
vulnerable subjects attempting to obbin their consent and inform them and at the same
tirne insulate them from knowiedge which could potentially be harrnful. In this context,
it can be interpreted as the obtaining of an invalid consent as we are not in fact disclosing
Our tnie purpose. These conflicting obligations may cause moral distress in the person
seeking the consent, confemng a sense of dishonesty and deceit. Secondly, there is the
subject of the researcb. It is generally held that within the allowance of incomplete
disclosure, "investigators should always give tnithful answers to questions" (19). This
being the case, there is still a possibility within this fiamework that parents could be
"exposed" to our potentially damaging hypothesis by virtue of the fact that if they
demand to know exactly what we are looking for then we are obliged to be tmthfûl in Our
response.
The notion of protecting the subjects from potential psychological harm in this
instance hinges upon the hope that subjects are in fact ignorant of or uninterested in the
fact that we are indeed only investigating one hypothesis. Hence, although the final
solution of the REB/IRB combined with the suggestions of the NICU staff seems to be
the most reasonable, it still leaves individuals at risk for psychologicaI ham. In this
situation, it is diffkult to see how the protection of human subjects, would best be served.

References
Hill A, Volpe JJ. Perinatal asphyxia: clinical aspects. Clinics in Perinatology. l6(2):435-57, 1989. Cnattingius S, Nordstrôm M-L. Materna1 smoking and feto-infant mortality: Biological pathways and public health significance. Acta Paediatrica 8S(lS): 1400-2, 1996 Dec. Gupta 1, Hillier VF. Edwards JM. Multiple vascular profiles in the umbilical cord; an indication of materna1 smoking habits and intrautenne distress. Placenta. 14(1): 1 17-23, 1993 Jan-Feb. Butters L, Howie CA. Awareness arnong pregnant women of the effect on the fetus of commonly used drugs. Midwifery. 6(3): 146-54, 1990. Buist A, Yu D. Smoking and pregnancy: awareness, attitudes and habit changes. Fiealth Bu1 letin. 45(4): 1 79-84, 1987. Haslam C, Draper ES, Goyder E. The pregnant smoker: a preliminary investigation of the social and psychological influences. Journal of Public Health Medicine. I9(2): 1 87-92, 1997. Lelong N, et al. Attitudes and behavior of pregnant women and health professionals towards alcohol and tobacco consurnption. Patient Education & Counseling. 25(1):39-49, 1995. Shaywitz BA, Fletcher JM. Neurological, cognitive, and behavioral sequelae of hypoxic-ischemic encephalopathy. Seminars in Perinatology. 17(5)357-66, 1993. Affïeck G, Allen D, McGrade BJ, McQueeney M. Matemal causal attributions at hospital discharge of high-risk infants. Amencan Journal of Mental Deficiency. 86(6):575-80, 1982. Fidler W, Michel1 L, Raab G, Charlton A. Smoking: a special need? British Journal of Addiction. 87(11): 1583-9 1, 1992. Fergusson DM, Lynskey MT, Horwood LJ. Comorbidity between depressive disorders and nicotine dependence in a cohort of 16-year-olds. Archives of General Psychiatry. 53(11): 1043-7, 1996. Hurst DF, Boswell DL, Boogaard SE, Watson MW. The relationship of self- esteem to the health-related behaviors of the patients of a primary care clinic. Archives of Family Medicine. 6( 1):67-70, 1997. Koren G. The fetus as a passive smoker. Canadian Family Physician. 42: 1301- 3, 1996. Ostrea EM Jr, et al. Meconium analysis to assess fetal exposure to nicotine by active and passive matemal smoking. Journal of Pediatrics. l24(3):47 1-6, 1994. Department of Health and Human Services. Title 45 Code of Federal Regdations 46. Mach 8, 1983. Medical Research Council of Canada: Guidelines on research involving human subjects. MRC, Ottawa, 1987. Emson HE. Minimal breaches of confidentiality in health care research: a Canadian perspective. Journal of Medical Ethics. 20(3): 165-8, 1994.

18. Medical Research Council of Canada (MRC). Tri-Council Policy Statement Document: Code of Ethical Conduct for Research Involving Humans. Ottawa, 1998.
19. Levine, W. Ethics and Regulation of Clinical Research. Yale University Press, New Haven, 1988.

Appendix 4
Title:
Bias in Maternal Reports Of Smoking During Pregnancy Associated With Fetal Distress
Running Title:
Bias in Maternal Reports of Smoking
Matthew Wong, BSc, Gideon Koren, MD
The Faculty of Pharmacy, University of Toronto (MW,GK) and The Division of Clinical Phannacology/Toxicology, The Hospital for Sick Children, Toronto (MW,GK), The MotheRisk Program and The Division of Clinical Pharmacology/Toxicology, The Hospital for Sick Children, Toronto, The Departments of Pediatrics, Pharmacology, and Medicine, University of Toronto and the CIBC Wood Gundy Children's Miracle Foundation Chair in Child Health Research, University of Toronto (GK).
Supported in part by the Medical Research Council of Canada, and the Seed Grant Program, The Hospital for Sick Children.
Address for Correspondence and Reprints:
Gideon Koren, MD, FACMT, FRCPC The Division of Clinical Pharrnacology and Toxicology The Hospital for Sick Children 555 University Ave. Toronto, ON M5G 1x8 Canada Tel: (416)813-5781 Fax: (4 16) 8 13-7562

Abstract
BACKGROUND: Studies examining the adverse effects of smoking during pregnancy
comrnonly use matemal reports. We hypothesized that if an adverse event occured during
pregnancy, women rnay underreport smoking. This study looked for bias in matemal report of
smoking if fetal distress occurs.
METHODS: Data was collected prospectively fkom patients attending The MotheRisk Program
who smoked during pregnancy. Categorized by delivery outcome, matemal and neonatal
charactenstics, and the raw number of cigarettes smoked per day during pregnancy reported at
cIinic, at follow-up, and the difference between the two values were compared.
RESULTS: 95 wornen had uneventfiil deliveries and 25 had fetd distress. Women who
reported fetal distress decreased their report of smoking after delivery compared to their original
report during pregnancy, whereas wornen with an uneventhl labour did not @=0.04).
CONCLUSIONS: Our results suggest that if an adverse pregnancy outcome occurs, mothers
rnay tend to underreport their cigarette consumption.
Keywords: Bias (Epidemiology). Fetal distress. Pregnancy. Pregnancy outcome. Prospective
studies. Smoking.

Introduction
Studies exarnining the potential adverse effects on the fetus of certain maternal exposures
such as smoking during pregnancy cornmonly rely on matemal self-reports. In the event of a
negative result, researchers will often cite underreporting as a potential source of bias.(l) The
problem of underreporting of cigarette smoking during pregnancy c m have a profound effect on
the results of such studies. The magnitude of this problem c m be appreciated when one
compares maternal reports to a biological marker. Three studies comparing biochernical markers
of smoking, such as s e m or wine cotinine levels, with maternal report of smoking found that
between 5 and 15 percent of women who identified themselves as nonsrnokers in fact had
cotinine levels that were consistent with active smoking.(2-4) However, biological markers are
not always feasible for a number of reasons including reluctance of patients to give consent,
which in of itself can introduce a severe bias, and particularly in the case of retrospective studies
where one has only a patient record to examine. Moreover, the existing studies (24) , while
identifying a reporting bias of smoking dichotomously (i.e. yes or no smoking), were not
designed to address a bias in the amount of cigarettes reported.
At least two reasons for underreporting have been suggested. Firstly, because of the
dirninishing social acceptance of smoking during pregnancy, expectant mothers may provide
false reports of their smoking which they believe will be more acceptable to the researcher and
to the public at large.(5) Secondly, in the instance of an adverse event during the pregnancy or
delivery, it is possible that women may underreport a behaviour which in their own minds may
have been associated with these adverse events. This however has never previously been
demonstrated empirically.
It is well accepted that smoking during pregnancy puts the fetus at increased health risks.
Studies have clearly illustrated the risk for decreased birthweight and an increased incidence of
perinatal rnortality and delivery complications.(6,7) These risks are often explained to %orner?
who smoke during their pregnancy by health prokssionals, and these women are often cited as
being aware of these risks pnor to receiving counseling for smoking cessation.(g)
The objective of the present study was to investigate whether there is bias in maternal
reporting of the amount of cigarette consumption if fetal distress is diagnosed. Fetal distress is
described as a cluster of clinical situations, including oxygen deprivation (e-g. presence of
meconium, low Apgar score), heart rate abnorrnality or biochemical disturbances (e.g. fetal
acidemia).(9-11) Fetal distress presented at birth, often requires medical interventions,
admission to a neonatal intensive care unit and these infants may suffer long term sequelae.(l2)
Although fetal distress is lacking an accurate clinical definition, most mothers are aware of it and
report it.
Methods
The original data on smoking status were collected prospectively fkom pregnant patients
who were seen between 1988 and 1997 in clinic by a physician through The MotheRisk Program
(The Hospital For Sick Children, Toronto, Ontario, Canada) - a counseling service for women
with medicinal, chemical, illicit h g or other exposures in pregnancy. Dunng the clinic visit,
maternal characteristics including age, gravidity, parity, and previous spontaneous or therapeutic
abortions were collected as were details of any underlying medical condition and previous
pregnancy outcornes. Detailed reports of the patient's exposures during the pregnancy were
made ascertaining the time of exposure, dose and frequency of use, where applicable. These

included the exposures that the patient had corne to clinic for specifically, as well as other
exposwes including cigarettes, alcohol and illicit dmgs.
After collection of al1 data, patients were explained the concept of a baseline risk that
exists in every pregnancy for a woman to have a child with a major birth defect even in the
absence of any teratogenic exposure. Patients were then infomed of the potential risk (if any) of
their exposures to the fetus by way of critical evaluation of the current medical literature.
Documentation of the counseling along with the specific literature references is then forwarded
to the physician caring for the woman and also to the patient directly if requested.
As a part of our research program, patients seen in c h i c are followed up with a
telephone interview one to two years afier their clinic visit to confirm exposure details and to
inquire about pregnancy outcorne.
For the present study, patients were selected based on three criteria: 1) Live birth with
completion of the follow-up interview, 2) docurnented delivery details, and 3) documented
details of materna1 smoking behaviour in both c h i c and follow-up files. Exclusion was based
on documentation in the files of intentional decrease or cessation of smoking, or where details of
smoking were not complete for either clinic or follow-up information (e.g. 16 cigarettes per day
at c h i c vs. response of only "yes" at follow-up). During follow-up interviews, patients were
asked if there was an event of "Fetal Distress" during delivery and the interviewer then gave
examples surnrnarized in Table 1. The mother's response to this question was docurnented and
any narrative comrnents made by the mother about the delivery were detailed. Patients were
categorized into one of two groups based on their report of "Fetal Distress" or "Uneventful
de 1 ivery".
These two groups were then compared with regards to materna1 characteristics at chic ,
number and nature of exposures (teratogenic, unknown, nonteratogenic), use of alcohol or illicit
dmgs, presence of matemal illness, and incidents of fetal distress in a previous delivery.
Neonatal charactenstics at follow-up including gestational age, birthweight and presence of
major malformations as well as the time between clinic visit and follow-up were also compared.
Cornparisons between the two groups were done using the Student's t-test, Mann-Whitney Rank
Sum Test or Chi-square as appropriate.
The primary endpoint of interest was the difference in the reported daily number of
cigarettes in the first trimester between the first interview ("real time") versus the second (post
partum) interview. The raw number of cigarettes smoked per day as reported at clinic, at follow-
up and the difference between the two values (follow-up value minus clinic value) were
compared between women reporting "Fetal Distress" versus "Uneventfiil Delivery" using the
Mann-Whitney Rank Sum Test. The numerical difference in number of cigarettes per day
reported in the second versus the first interviews was then categorized as having increased
(positive value), rernained the same (zero value), or decreased (negative value) and these were
then compared using Chi-squared.
Results
In total, 132 cases were collected which met the inclusion criteria. However, in 7 cases
the patients had expressly mentioned that they had quit, and in 2 cases had mentioned that they
had been successfiil in decreasing their smoking. In 2 cases the data were not sufficiently
quantified to be analyzed and in one case the patient told the interviewer that she had "memory
problems". Afier these exclusions, there were 120 eligible cases. Of these 120 women, 95
reported an uneventhl delivery and 25 reported an event which followed the definition of "Fetal

Distress". These women provided details of the events in narratives which are summarized in
Table 1.
Matemal charactenstics at c h i c between women who had an uneventfùl delivery and
those who had "FetaI Distress" were not significantly different (Table 2). There were no
significant differences in matemal age, gravidity, parity, spontaneous or therapeutic abortions.
The number of exposures to agents with teratogenic or nonteratogenic effects did not differ. Use
of illicit drugs or alcohol during pregnancy also did not differ between the two groups. The two
groups did not significantly differ with regards to the proportion of women who had a chronic
ilIness in general or a psychiatric illness in particular. Finally, there were no significant
differences in the nurnber of women who had an event of "Fetal Distress" during a previous
pregnancy.
Other than the selection criteria of "Fetal Distress", pregnancy outcome characteristics at
follow-up also did not differ significantly between the two groups as shown in Table 3. There
was no difference between the two groups in the number of infants bom with major
malformations, nor were there any differences in gestational age at birth, or birth weight. In
addition, there was no significant difference in the number of months that had elapsed between
clinic visit and follow-up among the two groups.
Details of materna1 self-report of smoking are shown in Table 4. There was no
significant difference in the number of cigarettes smoked per day during pregnancy as reported
at c h i c between the two groups. There was also no significant difference (p4.32) in the
proportion of mothers who at follow-up declared themselves to be non-srnokers (decreased to
zero cigarettes). There was however a statistically significant difference between the two groups
in the change in reporting of cigarette consumption dunng pregnancy in clinic versus at follow-

up after pregnancy. That is, mothers who experienced Fetal Disîress in their babies reported
significantly less smoking during pregnancy at follow-up han during their initial clinic visit.
This difference was categorized and compared as shown in Table 5. The two groups were
significantly different in ternis of the change in the report of number of cigarettes per day at
follow-up with respect to whether it had increased, remained unchanged or decreased. These
results indicate that mothers who had events of fetal distress during delivery were significantly
more likely to decrease their subsequent report of smoking during pregnancy compared to
mothers who had uneventful deliveries, who did not change their reports.
Discussion
The probIem of underreporting in epidemiological research poses a threat to the validity
of a study. Our results suggest that in studies of adverse outcomes during pregnancy, mothers
tend to underreport their smoking which they rnay feel had in some way contributed to the event.
Because the two groups were similar in a large number of materna1 characteristics and
outcome measures, it is highly probable that it is the adverse pregnancy outcome that led to the
reporting bias. Moreover, women who had uneventhl pregnancy outcome did not change their
reported number of cigarettes (median change*), indicating that because of the chronic and
stable nature of smoking, there is no problem of recall per se.( f 3)
Moreover, it is noteworthy that the event of fetal distress may in fact have caused women
to have a better recall of their smoking during pregnancy. In a study looking at bottled water
consumption during pregnancy and pregnancy outcome, it was concluded that wornen who had
spontaneous abortions in fact had a significantly better recall of their water intake when
compared to women with normal outcomes.(l4) Hence, it is not an issue of recall per se, but
rather of recall bias.

The results of our study reinforce the need to obtain biological marken of exposures
during pregnancy as we have demonstrated that in instances of adverse outcomes, matemal self-
report may be unreliable. However, while biological markers such as blood, urine or hair
cotinine can help distinguish smokers from nonsmokers, they may not be adequate for the
detection of changes in pregnancy consurnption, as nicotine undergoes phamacokinetic changes
during pregnancy.( 1 5)
Our study has two major advantages over previous attempts to charactenze this reporting
bias: This was a prospectively collected cohort, and at the time of the initial interview, women
were very open about their smoking habits as they were eager to receive accurate estimates of
their nsk. Secondly, we could assess not just smoking status, but also changes in the number of
reported cigarettes.
Further studies in the area of underreporting should be undertaken in order to determine
if there is some predictive value that can be elucidated. If one can determine a consistent pattern
of underreporting or determinants leading to underreporting, this would be important
information in an attempt to improve the understanding of the materna1 fetal toxicology of
tobacco smoke.

References
Jedrychowski W, et al. Exposure misclassification error in studies on prenatal effects of
tobacco smoking in pregnancy and the birth weight of children. Journal of Exposure
Analysis d Environmental Epidernioiogp 1998;8(3):347-57.
Klebanoff MA., et al. S e m cotinine concentration and self-reported smoking during
pregnancy. American Journal of Epidemio(ogy 1998; 148(3):259-62.
Murray RP, Comett JE, Lauger GG, Voelker HT. Error in smoking measures: effects of
intervention on relations of cotinine and carbon monoxide to self-reported smoking. The
Lung Health Study Research Group. American Journal of Public Heaith
1993;83(9): 125 1-7.
Walsh RA, Redman S, Adamson L. The accuracy of self-report of smoking status in
pregnant women. Addictive Behaviors l996;2 1 (5):675-9.
Welte JW, Russell M. Influence of socially desirable responding in a study of stress and
substance abuse. Alcoholism, Chtical & Experimental Research 1993; 17(4):758-6 1.
DiFrama JR, Lew RA. Effect of matemal cigarette smoking on pregnancy complications
and sudden infant death syndrome. Journal of Famiij Practice 1995;40(4):385-91.
Walsh R A . Effects of matemal smoking on adverse pregnancy outcornes: examination of
the criteria of causation. Human Biology 1994;66(6): 1059-92.
Haslam C, Draper ES, Goyder E. The pregnant smoker: a prelirninary investigation of
the social and psychological influences. Journal of Public Health Medicine
1997; l9(2): 1 87-92.
Hi1 1 LM. Diagnosis and management of fetal distress. Mayo Clinic Proceedings
l979;54(12):784-93.

10. Parer JT, Livingston EG. What is fetal distress? Am J Obstet Gynecof
lWO;l62(6): 1421-5.
1 1. Mead M. The diagnosis of foetal distress: a challenge to midwives. Journal ofAdvanced
Nursing I996;23@):97$-83.
12. Gilstrap L, et aI. Diagnosis of birth asphyxia on the basis of fetal pH, Apgar score, and
newbom cerebral dysfunction. Am J Obstet Gynecol 1989; 16 1 :825-830.
13. Feldman, Y et al. Determinants of recall and recall bias in studying dnig and chemical
exposure in pregnancy. Teratology l989;4O( 1 ):37-45.
14. Neutra RR, et al. Potential sources of bias and confounding in environmental
epidemiologic studies of pregnancy outcornes. Epidemioiogy l992;3(2): 1 34-42.
15. Seaton MJ, Vesell ES. Variables affecting nicotine metabolism. Pharmacology &
Therupeutics 1993;60(3):46 1-500.

Additional Information Provided by Mothers Reporting "Fetal Distress"
Comment No. of Occurrences'
Emergency Caesarian Section Perfonned
Baby's Heart Rate Was Low Cord Around Neck Baby's Heart Rate Elevated Induced Labor Baby Adrnitted to MCU No Additional ~ornments. Decreased Oxygen to Fetus Presence of Meconium Baby Aspirated Meconium "Baby Was Blue" Baby Received Oxygen
*-2 women did not elaborate on the circumstances of Fetal Distress a-Not rnutuaIly exclusive
Table 1

Maternal Characteristics at Clinic
Materna1 Age' Gravidityb Parity b
SAb TA^ No. Exposures for Clinicb No. Exposures Teratogeoicb No. Exposures Unknownb
a - Values expressed as mean I S.D.
No. Exposures Nonteratogenicb Use of Illicit Drugs Use of Alcohol Materna1 IUness Psyc hiatric Iiiness Prev. "Fetal Distressn
b - Values expressed as median with range
P value
0.09' O. 16' O. 12' 0.82' 0.852 0.6 1 *
Uneventful Deliver y
n=95 29.lk4.9
&Fetal Distress" n=25
3 1 .Ok4.9 1 :1-61 O ;O-51 O :O-2:
1 - Student's t-test 2 - Mann-Whitney Rank S m Test 3 - Chi-squared
2 1 O O 1
O 2
O
1 10-71 1 1 (1 1.6%) 37 (38.9%) 72 (75.8%) 27 (28.4%) O (0%)
Table 2
r1-71 :O41 10-6: :0-2: il-71
10-2:. :1-8:
O [O-II O [O-21
10- 11 0.9g2 0.65' O :O-31
1 [O-81 3 (12%) 14 (56%) 18 (72%) 6 (24%) 1 (4%)
0.8 1' 0.773 O. 1g3 0.903 0.8S3 0.473

Foiiow-up Characteristics
a - Values expressed as mean + S.D.
Major Malformations Gestational Age ( ~ k ) ~ Birth Weight (g)' Time to Follow-up (rnoslb
b - Values expressed as median with range 1 - Student's t-test 2 - Mann-Whitney Rank Sum Test 3 - Chi-squared
Table 3
P value
0.863 0.50' 0.86' 0.3 l2
Uneventful Delivery n=95
3 (3.2%) 40 l35-421 327 1+546 16 17-35.51
&Fetal Distress" n=25
O (0%) 40 t34-421 325W565 20 12-36.51

Materna1 Self-Report of Smoking
1 ( Uneventful Delivery
1 Clinic' 1 No. Cig/d reported at
n=93 1 O [O401
Wetal Distress" 1 P value 1
No. Cig/d reported at ~ollow-upb Difference in No. Cig/d reported at FoUow-up vs. Clinic'
10 [O-401
O [-24-+30]
b - Values expressed as median with range 2 - Mann-Whitney Rank Sum Test
Table 4

Changes in Self-Report of Materna1 Smoking
Table 5
Change in No. Cig/d Reported at Follow-up vs. Clinic Increased Same Decreased
Uneventful Delivery n=95
24 (?5.3%) 34 (35.8%) 37 (38.9%)
"Fetal Distress" n=25
5 (20%) . 3 (12%) 17 (68%)
P value
0.02'

--
0 Pdornaki G, a aï. R i s k - b d prenatai screcnll\g for tnsomy 18 using alpha-fetoprokin, unconjugated oatnol and human duorionic gonadotropin. R a u t Diagn 1995;15:7ï3-23.
0 Philiips O, et al. h4aterml saum sanning for ktal Down syndrome in women l a s than 35 yeus of age using aipha fetoprotein, hCG and unconjugated estnol: a prospective 2-year study. Obstet Gynecol 1992;80334.
0 Piggott M, et al. hphentation of an antexutai unmi screning progrunme for Down's syndrome in two districts (Brighton and Eastboume). J Med Screcn 1994;1:4549- Spencer K, et al. Free-&hCG as first-trimester marker for fetal trisomy. Lancet 19!32~1W.
O StapIes AJ, et al. A mitenul serum scriéen for trisomy 18: an extension of matenul senun saeaiing for Down syndrome. Am J Hum Genet 1991,49102133.
0 Tafas T, et al. An automated image anaiysis method for the measurement of neutrophil alkaline phosphatase in the prenatal saeening of Down syndrome. Fetal Diagn 'Iher 1%1129-259. Van Lith J, et al. First-trimester mateml semm immunoreactive inhibin in dvomosomally mm1 and abnorrml prpgruncies. Obstet Cynecol 1994;83:661a64.
0 Wald NJ, et al. Mateml secum scmming for Down's syndrome in earl y pregnancy. Br4 1988,297S83-887.
0 Wald NJ, George L, Smith D, Densem JW, Petterson K. Semm screening for Down syndrome between 8 and 14 weeks of pregnancy. Br J Obstet Gynaecol1996;11)3:407-412.
0 Wald NJ, Kennard A: Prenatal biodiemial xreening for Down's syndrome and neuat tube defects. Curr Opin Obstet Gynecol 1992,4:302-307. Wald Nj, Kennard A, Densem JW, CuckJe HS, Chard T, Butler L Antenatal maternal senun m g for Down's syndrome: resuits of a demonstration pmpct. BMJ 1992,3û5391-394. Watt H, Wald N, Huttly W. The pattern of materna1 senun inhibin-A concentrations in the second trimester of pregnancy. Prenat Diagn 1998;18â46-848. Yankowitz J, Fulton A, W i n R, Grant S, Budelier W. Prospective waluation of prenatal matemal serum screening for trisorny 18. Am J Obstet CynecoL1998;1fs:44645û.
Dr. Rosalinde Snijders
ABSTRACTS FROM THE TORONTO FETAL CENTRE
Prospective Non-Invasive Monitoring Of Pngnancies Complicated By Red Cell Alloimmunüation. iskaros J, Kin dom J, Morrison J, Rodeck C. Ultrnsound O%SM Gynecol lW?;ll:62-7
Our objective was to evaluate the impact of non-invasive assessrnent of fetal anemia and anti-D antibody quantification on the timing and frequency of invasive procedures in pregnanaes complicated by rhesus alloimrnuniza tion
Ninetwn consecutive non-hydropic pregnanaes referred to the fetal mediane center were assigneci a pnor risk category (none/mild, moderate, or severe) and monitored by: (1) serial fetal measurernents of umbilical vein maximal flow velocity (UVV-), liver length and spleen perimeter measurernents; and (2) serial anti-D antibody concentration.
Invasive tests for fetal anernia (amniocentesis or fetal blood sampling) were deferred in the absene of abnormal ultrasound findings and/or rishg antibody levels. In six
@FETAL CENTRE NEWSlEïER cases, serial non-invasive tests were normal with stable antibody levels, and no invasive tests were performed; four infurts were mildly affected, one was unaffeded and one required pastnatai exchange transfusion.
in the remaining 13 affecteci cases, amniocentesis was performed in 9 cases for: elwated UVV- alone (n=3), elevated UVV- and an increased antibody lwel (n=2), or normd UVV- with an increased antibody lwel(>15 IU /mL) and severe prior risk ca tegory (n=4). Six fetuses undemrent fetal blood sampüng (initial hematocrit 9 to 2%), and five of these had an elevated UVV-. Liver length and spleen perimeter meammmmrS were increased in only one anemic khrs (hematocrit 13%). Of 17 infants bom alive, an elwated W- prior to delivery was predictive of the need for exchange transfusion (six of seven cases with an elwated UVV- versus one of ten with a normal UW-- chi- square=5.73, pd.017 with Yates' correction).
These preliminary data suggest that pregnanaes with a mild or no history of fetal anemia may be monitored by a combination of serial antibody quantification and Doppler m o n i t o ~ g of UVV-.
John Kingdom, M B Dept. of Obstetncs & Gynaecology, Mount Sinai Hospital
Pnrrrited at the Canadian Bioethics Society Meetin& Oct. ï9!M
Proposcd Non-Consensual Research to Avoid Potential Iatrogtnic Parental Guilt: An Example in Hypoxic- ischemic Encephalopathy (HIE) Badcground: The loss of a baby d u ~ g childbirth is a dwastating event associated with feelings of extreme grief, disappointment, helpfessness, and self-blame. Perhaps wen more tragic and emotionaliy cornplex is an event during childbirth that may tesult in the child having a lifdong disability. One such outcome occurs in babies who develop a perinatal condition known as hypoxic-ischemic encephalopathy or HIE In HIE, the oxygen supply to the fetus is decreased during delivery resulting in temporary or permanent brain damage. Although many obstetncal rkk factors have been identifieci, approximately 40% of cases present no obvious cause. Because of the baseline decrease in oxygenation and vascular changes that occur during smoking, our group wishes to investigate the hypothesis that maternai smoking is a risk hctor for HIE.
Expectant mothers who smoke are generally aware of at least =me of the risis of smoking during pregnancy induding dmeased birth weight, increased chance of mixamage, and inaeased chance of stillbirth. In addition, some cigarette wamïngs indude statements indicating some potentîaî for other wents. One example is "May cause fetal harm". It is assumeci that these women may not envision a potential N k for a condition such as HIE which if moderate or severe may result in a number of outcornes including cerebral palsy, cognitive defiab or death. In a study exarnining maternal reaction to the birth of an infant who suffered h m a long- terrn disability (of genetic or perinatal cause), üuee types of causal attributions have been documented that were not mutually exclusive (AffIeck 1984):
The behaviour of others (includes obstetrician - 22G%) Materna1 behaviour (self-blame) - 26% No behavioral causes (chance, Act of God, "fate") - 57%
Page 5

Although the hirul a- does not d i d y attriôute the outcome to a particuiar persan, the author states that it may lead to self-blame as some mothers developed the idea tht somehow they "deserveci it'. This category is alsa believed to be associated with depression and low self-esteern both of which have been associatd with smoking populations. In light of this psychologidy vulnerable study p u p , we felt that seeking consent would represent a potential risk for psychologicai hm. Simply stating that there was a possibility of a mother k i n g responsible for this outcome might convert al1 of the smokers to the self-blame category. In addition, any underlying paranoia of the non-smoking mothers might be exacerbateci by thoughts of any exposure to second hand smoke. We therefore sought to do an anonymous study using discardeci meconium (a baby's first bowel rnovement) as an indicator of materna1 smoking status. Given the importance of this project and in light of this fragile population, we consequently requested that ouf Research Ethi- b a r d REB) / Interna1 Rwiew Board (IRE) allow us to carry out this research without consent as it would be anonymous and cornpletely non-invasive.
Our request was subsequently denied and we were required to fully inform parents and obtain consent in this study. ï h e ethics cornmittee felt that in the interests of planning future
0 FETAL CENTRE N E W S L ~ R ' orrnnuries ~ u e n t s should be inforniod of the h l e link &een smdcing uid HIE. In addition, because'mokikïng carmot be pmed h m this study to cause HIE (only a risk factor) Uiey felt that it would not represent an ethical fraud to indude -mlcing as a possible risk factor in a study deigned to examine HIE risk factors in g e n d thereby diffusing the accusation of smoking. It was also requested that counseling be available to any mothem who were experiencing any foms of self-blarne and that the results of this study be provided to families with personalùed comments where appropriate.
in accordance with the decision of the ethics cornmittee, we decidd to comply with th& reqwsts- As fuiiy informeci consent would be sought, the REB/IRB agreed with our desire to obtain complete obstetrical details of these patients and additional biological samples to improve the quality of the study.
Matthew Won& BSc, gduatc studmt, U of T Cideon Koren, MD, Director, Dept. Pharmacology, HSC
Christine Harrison, PhD, Director, Dept. Biocthics, HSC
O CASE MANAGEMENT in THE TORONTO FETAL CENTRE
Antenatal Dirgnorh Of Uhl'r Anomily
Uhl's anomaly of the heart is a rare congenital cardiac malformation characterized by aplasia or hypoplasia of the myocardium of the right ventride, such that the free wall of the right ventride is paper thin. The pathogenesis is undear, but could be explaineci on the basis of 'apoptosis'(cell death) in a developing human heart (1). We report a case of Uhl's anornaly identifid at 24wks gestation.
A 3û-year old primi gravida healthy caucasian woman was re fend at 24 weeks of gestation given the finding of an enlarged fetal heart on a level II obstetrical ultrasound. She had an wiremarkable early pregnancy. The general fetal ultrasound revealed a single fetus with severe hydrops (ascites and pleural effusion). A biparietal diameter consistent with 24-25 weeks of gestation ïhe placenta was normal and the amniotic fluid volume was adequate. There was massive cardiac enlargement such that the heart nearly fUed both the right and leH chest. The right atrium and ventride were severely dilated and Ebstein's anornaly of the tricuspid valve was suspected. There was no obvious extra-cardiac abnorrnality. A genetic amniocentesis was performed that showed a normal 46XY.
Segmental approach to cardiovascular system revealed: A regular heart rate of approximately 140bpm with an atrial rhythm, lwocardia (apex pointing to the left), s ihs solitus, A-V and V-A concordance, marked cardiomegaly with the heart occupying an estimated 90% of the thoaac cavity (Figure l), severely dilated right atrium and nght ventride with normal position of the tricuspid valve but with an extremely thin right ventricular free wall/myocardium, and moderate tricuspid inmffiaency. The right ventricular function was severely depresseci. The right ventricular outflow tract and pulmonary arteries were difficult to visualize. ïhere was compression of the left atrium and ventride which appeared to have nonnal morphology, and there was a normal aortic outflow tract with antegrade flow. Both urnbilical vein and artery flows were normal.
At 28 weeks there was spontaneous intrauterine demise. Autopsy was dedineci. To our knowledge, this is the third reported antenatal diagnosis of Uhl's anornaly (2-3).
The differential diagnosis of Uhl's anornaly indudes anomalies of the tricuspid valve: Ebstein's anomaly, unguarded N orifice, and TV dysplasia. In Ebstein's anomaly the W is abnormal in position with displacement of the leafleb(septa1 and postenor)into the right ventricular sinus and atrialization of the proximal right ventricular chamber. However, in unguarded N, there is no identifiable tricuspid leaflet tissue visualized at the tricuspid valve annulus along the ventricular septum or posterior free wall. Rudimentary leaflets rnay be seen within the RV cavity at poshnortem. In N dysplasia, the N leaflets are thick and hequentiy redundant or hypoplastic and usually fail to coapt properly such that there is significant tricuspid regurgi ta tion.
The prognosis for fetuses diagnosed with any of t h e lesions, particularly with significant tricuspid regurgitation or RV dysfunction is very poor, with as much as a 48% antenatal mortality (due to congestive heart failure/hydrops or dysrhythmias) and 38% mortality in the neonatal period (due to heart hilure, dysrhythmias or lung hypoplasia) based on one

The 10th CBS Conference: Reflections on a Decade of Bioethics/
Le 10e Colloque annuel de la SCB: Réflexions sur une décennie de bioéthique
October 15th to 18th. 1998 Delto Chelsea Inn, Toronto, Ontario/
1 5 - 18 octobre 1 998 Hôtel Delta Chelsea, Toronto, Ontario
Conference hosted by the University of Toronto Joint Centre for Bioethics/ Organisé pa le Centre conjoint de bioéthique de runivenité de Toronto

3 - 1225 1 Austen 5 - 1 145 1 Duchesse
115 111
' McLeod, Carolyn W. 1 16 Octobcr
Moore, Aideen M. , Munden, L. Martina . Nathoo, AbNoor . Nisker, Jeff
, McNally. Mary 1 6 October Morgan, Kathryn Pauly Morin, Benoit
3 - 1545 5 - 1225 3 - 1625 3 - 1 105 3 - 1 105 5 - 1630 3 - 1545 1 - 1505 i - 1505 .a 1 - t 145 1- 1625
-
16 Octobcr 17 October 17 October 16 October
1 7 October 1151 16 October i l 1 5
- - Rossetti James Duchesse Windsor i
Duchesse I
Windsor Newton James Rossetti Churchill Courryud James J ~ C S
4
155 1 03 1 03 150
Robinson. D.
151 143
, Page, Staccy A f 17 October
, Rosenberg, Zahava R. S.
, Parks, Jennifa A
Rock, Melanie 17 October 1110- 1145 Duchesse 1
17 Octobcr
, Sepinwdl Amy Sepinwall, Amy Shah, Nirav Dinesh S hanner, Laura Sheldon, Sally -
17 October , Peter, Elizabeth Pidwysocky, Stephen J. Poole, Gai1 F. Pullnian, Duyl
16 ûctober
Sori, Caroline Storcb, Janet L. Sullivan, William Szebik, Imre
1030 - 1 105
16 October 17 October 16 October 17 October 16 October
17 Octoôer 1 143
Newton
Russell, M.L. 1030- 1100
16 Octobcr 16 ûctober 16 October 17 October
-- --
Windsor Duchesse
Trevor-Deutsch, Burleigh 1 17 October ( 1 150 - 1225
16 0ct0ber 16 October 16 O c t o k
16 October ' ChurchiliBallfoom
1510- 1545 .
1 550 - 1 625 Poster 1550 - 1625 Poster 1 churchill Courtyard .
, Weijcr, Charles
Pos 11 1 155
Duchesse ,
Churchill Ballroom Churchill Cowtyud ,
Austen
1510-1545 1510-1545 1550 - 1625
Poster 1430 - 1505 1030 - 1 105 1510-1545
WilIiams-Jones, Bryn , Williron, Kathieen , Won& Matthcw Wolbnn~ Gregor Yeo, Michael
, Savard, Anne-Marie , Schachter, Debbie
Duchesse Austen Rossetti
16 October
17 October 16 October
1030- 1100 , James Churchi 1 l Courtyard , James Austen
1430 - 1 SOS 16 October 16 October 17 October 1 7 October 16 Octobcr
, Schrecka. Ted 16 October
J
Windsor
Poster Churchill Courtyard . Poster 1 550 - 1625 11 50 - 1225 1 1 50 - 1225
' Churchill Courtyard ,
Newton I
Duchesse Duchesse 1
Top Related
Copyright © 2022 FDOKUMEN

