







Bahasa
Halaman
Hukum


Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 1

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 2

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 3
Materia Novum: The Journal of Homoeopathy
RNI: #### Print ISSN: ####
Editor –in-Chief
Dr. F. F. Motiwala, MD (Hom)
Dr. Ajay Valke Dr. Sarang RahalkarDr. Dhanashree Kulkarni Dr. Shweta PatilDr. Gayatri Nimbhore Dr. Smitha NairDr. Khuzem Lokhandwala Dr. Subhash YadavDr. Mita Gharte Dr. Vaishali ZodgekarDr. Rita Kundu Dr. Varsha DharneDr. Ruta Patharkar Dr. Sachin BhaleraoDr. Virendra Jain Dr. Vishal Nimbhore
Peer Review Board
Dr. Gangaraju Prasad Dr. Swanand ShuklaDr. Kamlesh Bagmar Dr. Tapas KunduDr. Suhail Sheikh
Editorial Board
VOL. - 2 ISSUE-2 April – June 2018 RS. 40/-

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 4
Materia Novum: The Journal of HomoeopathyOfficial publication of Motiwala Homoeopathic Medical College
The JournalMateria Novum (print ISSN____________ E-ISSN_____________) is a peer reviewed open accessjournal published on behalf of Motiwala Homoeopathic Medical College, Nashik. This journalpublishes articles on the subject of Homoeopathy. The journal is published quarterly in the month ofJanuary, April, July, October.
Information for AuthorsAll manuscript should be submitted online at [email protected] for peer review.
Publisher’s AddressMotiwala Homoeopathic Medical College and Hospital and F. G. Motiwala P. G. Institute ofHomoeopathy and Research centre, Nashik.Motiwala Nagar, Gangapur- Satpur link road, Ashok Nagar, Gangapur, Nasik- 422012.Phone No: 0253-2351693E-mail: [email protected]: www.mhmc.org.in
Printer’s AddressSarvadnya Printer’s , Nashik
Editorial OfficeDr. F. F. MotiwalaMotiwala Homoeopathic Medical College and Hospital andF. G. Motiwala P. G. Institute of Homoeopathy and Research centre, Nashik.Motiwala Nagar, Gangapur- Satpur link road,Via Ashok Nagar, Gangapur, Nasik- 422012.Phone No: 0253-2351693E-mail: [email protected]: www.mhmc.org.in
General Information

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 5
Materia Novum: The Journal of Homoeopathy
Official publication of Motiwala Homoeopathic Medical College
Volume- 2 / Issue 2 / April – June 2018
A Case Report Of Premenstrual Syndrome With Homoeopathic Remedy FolliculinumDr.SnehalSanjivKapadnis. ___________________________________________ 7
Randomized control trial of Magnesium phosphoricum 6X along with homoeopathicsimilimum versus homoeopathic similimum alone in cases of Dysmenorrhoea.Dr. Pratiksha Yadav ________________________________________ 14
The Treatment Of Primary Dysmenorrhea With Homeopathic Remedy-A Case ReportDr. Saba Khan_________________________________________________ 22
A Case Report On InfertilityDr. Swanand Shukla___________________________________________ 27
To Evaluate The Role Of Homoeopathic Medicine In Cases Of Infertility: A Case SeriesDr Gulfisha Mirza__________________________________________________ 30
A case report of Trigeminal NeuralgiaDr Shubhada Borse________________________________________________ 37
Role Of Homoeopathic Medicine in the case of corn, The Case Report.Dr Charushila Gawali. ______________________________________________ 41
Homeopathy In Nocturnal Enuresis:A Case StudyDr Savita Sahani __________________________________________________ 45
CONTENTS

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 6
Dear Friends,
Materia Novum Intends to bridge the gap to its readers the personal experiences that ourauthors gain through their practice, the college OPD as well as the learning through their dayto day discussion and experience.
Articles are the result of actual cases that the authors have come across Homeopathy is aboon and a ray of hope for cases of infertility it is much more cost effective in these caseswhen it comes for comparison with the conventional treatment The articles on Infertility putsHomoeopathy as the primary therapeutic science, Articles on dysmenorrheal problems placesHomoeopathy on upper edge of treatment. The Potential of Homoeopathy in cases ofTrigeminal Neuralgia, Corns are reflected in its case articles
Homoeopathy is Developing and growing as trusted faith of the citizens of Earth is beingstrengthened day by day with its curative powers
The direct collaboration of the Motiwala Homoeopathic Medical College with the apex bodyfor research that is the ‘Central Council for Research in Homoeopathy’. CCRH only goes onto testify the scientific work being done at this institute.
Once again we put before you readers the Materia Novum the endeavor of our Teachers, P.G.Scholars, Students and Supporting Staff.
Dr. F. F. MotiwalaEditor-In-Chief
Email:[email protected]
Editorial

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 7
Snehal Kapadnis (PG Scholar)
AbstractPremenstrual syndrome is a group of symptoms which is physical, psychological and behavioural.The exact cause and etiology is unknown but it seems to related to ovarian function and otherendocrinal factors. The severity of symptoms varies from female to female and it depends onindividuality of the female. Some female may experience such severity that may disturb their dailyactivities and seeking for medication so we want to know the homoeopathic approach inPREMENSTRUAL SYNDROME .A case of premenstrual syndrome of a female treated withhomoeopathy is reported here.This case shows the usefulness of homoeopathic remedy Folliculinum.Key words: Case report, Premenstrual syndrome, ovarian function, Homoeopathy, FolliculinumIntroductionPREMENSTRUAL SYNDROME / TENSION:DEFINITION: There is no universally agreed single definition of premenstrual syndrome. It seems itis a collection of groups of symptoms. The symptoms are physical, psychological and behaviouralwhich appear at the same period in relation to menstrual cycle, usually 8-10 days before the onset ofmenstruation, without any physically detectable cause[1]. The exact cause is not known but it seemsto be related to ovarian function and other endocrinal factors.PATHOPHYSIOLOGY: The exact cause is not known but the following hypotheses are postulateda) Alteration in the level of estrogen and progesterone starting from the midluteal phase .Either thereis altered estrogen: progesterone ratio or diminished progesterone levelb) Neuroendocrine factors- Serotonin: during luteal phase, decreased synthesis of serotonin is observed in women sufferingfrom PMS- Endorphins : the symptom complex of PMS is thought to be due to the withdrawal of endorphinsfrom CNS during the luteal phase- GABA: gamma aminobutyric acid suppresses the anxiety level in the brainc) Psychological and psychosocial factors may be involved to produce behavioural changesd) Others: Variety of factors have been mentioned to explain the symptom complex of PMS. Thesearethyrotrophin releasing hormone, prolactin, renin, prostaglandins, and others. Unfortunately,nothing is conclusive.[3]
Symptoms:[2][3][4]
RELATED TO WATER RETENTION1. Abdominal bloating2. breast tenderness3. swelling of the extremities4. weight gain
NEUROPSYCHIATRIC SYMPTOM1. Irritability 4. Depression
7. Mood swings2. Forgetfulness 5. Restlessness
8. Tearfulness3. Anxiety 6. Anger 9. Confusion
PHYSICAL GENERAL SYMPTOMS1 .Fatigue2 .Tiredness3 .Insomnia4. Increased appetite
A Case Report of Premenstrual Syndrome with Homoeopathic Remedy
Folliculinum

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 8
Management:1. DIET: Avoid: caffeine sugar, salt, fat, honey. Dairy products and white flour,
sometimes aggravates PMS.2. Do’s: Eat more fruits and vegetables, whole grain bread and cereals. Meal high in
carbohydrate and low in fat. Meal rich in vit B6 or Mg. For example meat, fish and wholegrains.
3. LIFE STYLE:Regular exercise, yoga, meditation are helpful. Getting adequate sleep is also an important factor forsuccessful treatment.
4. Homoeopathic medicine: folliculinum [5][6]
Source: Folliculinum is the natural hormone secreted by the ovaries, it is also known as “oestron”.It is a crystalline compound, white, insoluble in water and its first three attenuations are made bytrituration.GENERALITIES:A female remedy affecting primarily the syndrome known as hyperfolliculinia but this syndrome israrely observed in laboratory tests.MIND: Hypersensitive to heat, noise and contact.Congestive headaches either with redness of the face, or the opposite, with pallor but still withsensation of chilliness at the extremities.
- Premenstrual migraines.- Extreme instability with anguish and worse at nightfall.- Alteration of excitability and depression, worse beforeMenses.- Sexual hyper-excitability.- Fixed ideas, of a sexual nature.
Digestive system:-Swallowing of liquids very painful.-Abdominal metearism, worse three or four days before menses.-Liver swollen, soft and hypertrophic.-Feeling of heaviness in the rectum.-Stubborn constipation, sometimes alteration of constipation and diarrhoea.-Nausea, vomiting, pre-menstrual pain in the right hypochondriac.Circulatory system:Tachycardia, palpitations with faintness. Sensation of constriction around the heart with feeling of abar in the pericardial region.Respiratory system:-Need for fresh air takes large breaths of air and sighs deeply.-Coryza with headaches and profuse discharge.Urinary and genital organs:-Vulva pruritus, worse before menses.-Small losses of blood during ovulation. Menses prolonged, blood bright red, with clotting.-Menses painful for 1st few days.-Yellow or brown discharge, sometimes blood- streaked, between menses, especially duringovulation.-Congestive mastitis. Congestion, pre-premenstrual pain.-Breast enormous, swollen cannot bear being constricted or touched.-The pain is ameliorated or disappears with menses.Skin:-Acne on the face, and seborrhoea of the nostrils.-Dry eczema, worse during ovulation before menses.-Worse before menses or during ovulation.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 9
Locomotar system:-Lumbar pains, worse during ovulation, before menses.Modalities:-Aggravation: before menses, during ovulation, from heat, and from resting.-Amelioration: Better after the third day of menses with movement of fresh air.
Case reportA female aged 23 years intern came to the OPD of Motiwala homoeopathic medical college on 15/7/2016with complaints of backache , swollen extrimities , headache throbbing type of pain since 4 to 5 days ,she toldthat this symtoms came before 7 to 8 days prior to the menses.
Mental general before menses: Irritability+++ trifles at menses before, Anxiety & Crying mensesbefore.
I feel sad about the fact that I have never done anything according my wish since childhood, I wasalways forced to do things, I never wanted to become a doctor but still I had to become, all mydesires are suppressed since childhood.
History of presenting complaints: Complaints started since menarche she was taken allopathicmedicines like antispasmodic and painkillers
Menstrual history: Menarche at 14 years of age, LMP: 20/6/2016 , Cycle duration: 4/28 dayscharacter of blood : profuse dark and clotted
Family history: father and mother suffering from renal calculus.
On Examination:
BP : 120/ 70 mm of Hg Pulse : 87 / minWeight : 55 kg
Systemic examinationCVS : S1S2 Normal CNS: Conscious well orientedRS :AeBe clear P/A : Soft and non –tender
Repertorial totality:
1)MIND- Ailments from domination.
2) MIND- Irritability menses before.
3) MIND- Anxiety menses before.
4) MIND- Hood changeable menses before.
5) HEAD- Headache menses before.
6) BACK- Backache menses before.
7) EXTREMITIES- Extremities pain menses before.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 10
REPERTORIALSHEET[8]
PRESCRIPTION: (15/07/2016)
Folliculinum 30/3doses /8 hourly for 1 day,SL 4 pills TDS X 1 Month
DIGNOSTIC TOOL

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 11
SYMPTOMS FOLLOWUP 1(11/8/16)
FOLLOWUP 2(9/9/16)
FOLLOWUP 3(5/10/16)
FOLLOWUP 4(8/11/16)
FOLLOWUP 5(4/12/16 )
FOLLOW UP6(7/1/17)
Backache as it is of lastfollow up
Slightlybetter thanbefore
Reduced 30to 40 %
As it is oflast followup
Slight backache but nostiffness
Mildbackachebeforemenses
Headache as it is of lastfollow up
as it is oflast followup
Reduced 70%
As it is oflast followup
As it is oflast followup
No headachebefore menses
Swollenextremities
Betterslightly
As it is oflast followup
Reduced As it is oflast followup
As it is oflast followup
Swollenextrimitiesincreased
Mood swings Reduced thanbefore
Reducedthan before
Reduced60%
No moodswingsbeforemenses
No moodswingsbeforemenses
No moodswings beforemenses
Irritability Reduced thanbefore
Reducedthan before
Noirritabilitybeforemenses
Mildirritabilitybeforemenses
Noirritabilitybeforemenses
No irritabilitybefore menses
Anxiety No anxietybeforemenses
No anxietybeforemenses
No anxietybeforemenses
No anxietybeforemenses
No anxietybeforemenses
No anxietybefore menses
Menstrual history LMP :24/7/16Cycleduration 4/28Character ofblood :
LMP :25/8/16Cycleduration4/30Character of
LMP :23/9/16Cycleduration5/30Character of
LMP :29/10/16Cycleduration5/30Character of
LMP :23/11/16Cycleduration5/28Character of
LMP : 30/12/16Cycle duration5/30Character ofblood : darkred, normal
Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 12
Normal , Red,offensivenessreduced
blood : darkred, Normalflow , Noodour
blood : darkred, profuseflow , Noodour
blood : darkred, normalflow , Noodour
blood : darkred, profuseflow , Noodour
flow , No odour
Crying , fatigue Newsymptomscame
As it is oflast followup
As it is oflast followup
Fatiguereduced ,crying as itis
Fatiguereduced50%, cryingas it is
Fatigue reduced70 %, cryingreduced 60 %
Medicineprescribed
Folliculinum30 /3 doses /8hrly 1 daySL /4 pillsTDS X 1month
Rubrum /3doses /8hrly for 1daySL /4 pillsTDS X 1month
Cos /3doses /8hrly for 1daySL /4 pillsTDS X 1month
Rubrum /3doses /8hrly for 1daySL /4 pillsTDS X 1month
Folliculinum30 /3 doses/8 hrly for 1daySL /4 pillsTDS X 1month
Cos /3 doses /8hrly for 1 daySL /4 pills TDSX 1 month
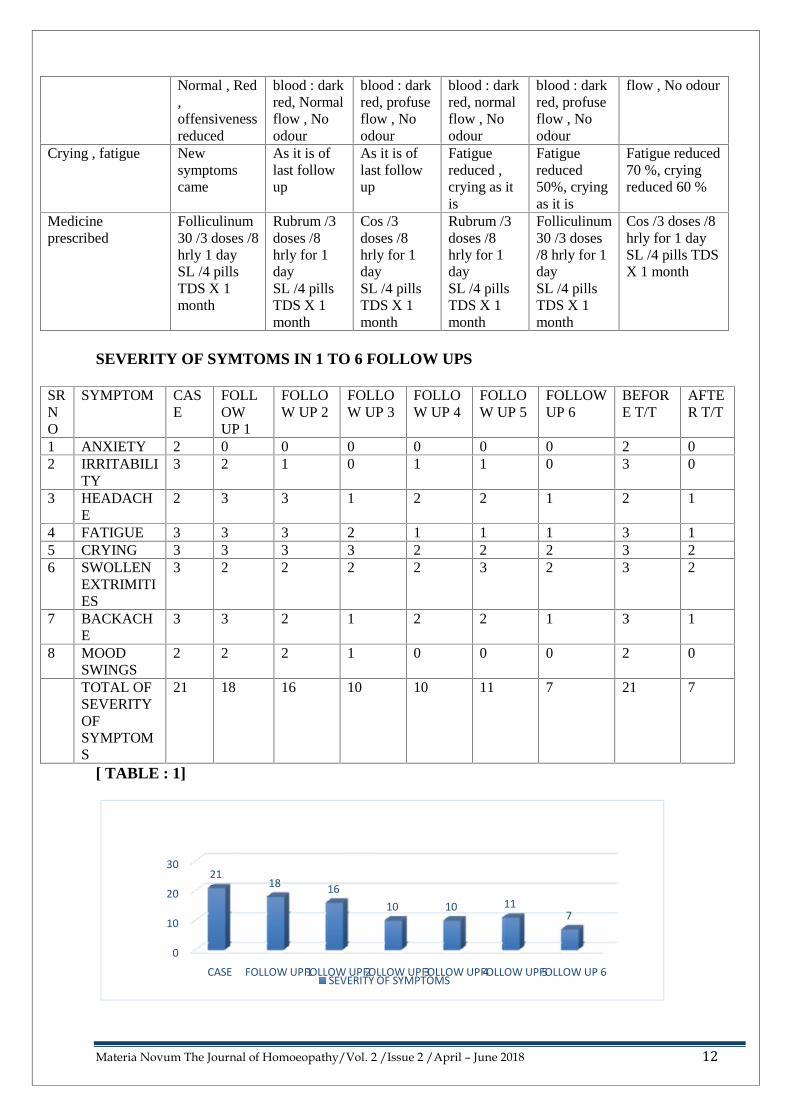
SEVERITY OF SYMTOMS IN 1 TO 6 FOLLOW UPS
SRNO
SYMPTOM CASE
FOLLOWUP 1
FOLLOW UP 2
FOLLOW UP 3
FOLLOW UP 4
FOLLOW UP 5
FOLLOWUP 6
BEFORE T/T
AFTER T/T
1 ANXIETY 2 0 0 0 0 0 0 2 02 IRRITABILI
TY3 2 1 0 1 1 0 3 0
3 HEADACHE
2 3 3 1 2 2 1 2 1
4 FATIGUE 3 3 3 2 1 1 1 3 15 CRYING 3 3 3 3 2 2 2 3 26 SWOLLEN
EXTRIMITIES
3 2 2 2 2 3 2 3 2
7 BACKACHE
3 3 2 1 2 2 1 3 1
8 MOODSWINGS
2 2 2 1 0 0 0 2 0
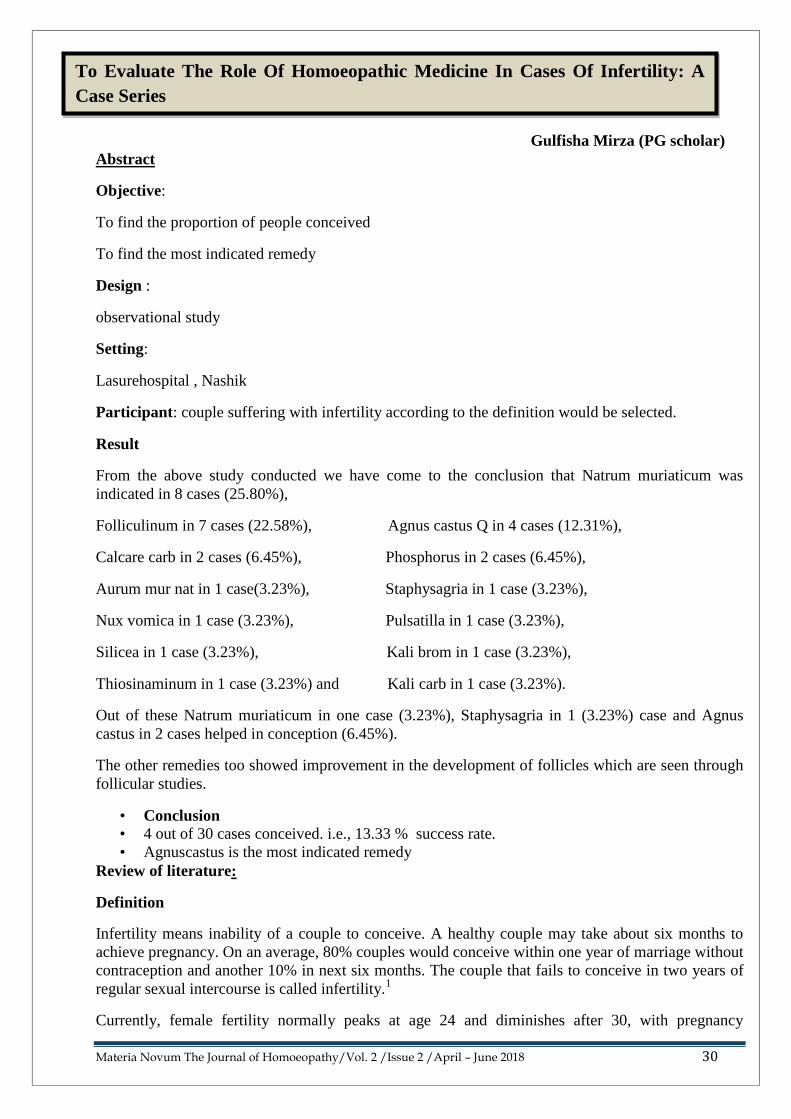
TOTAL OFSEVERITYOFSYMPTOMS
21 18 16 10 10 11 7 21 7
[ TABLE : 1]
0
10
20
30
CASE FOLLOW UP 1FOLLOW UP 2FOLLOW UP 3FOLLOW UP 4FOLLOW UP 5FOLLOW UP 6
2118 16
10 10 117
SEVERITY OF SYMPTOMS

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 13
DISCUSSION –The patient visited the OPD of Motiwala homoeopathic medical college ON 15/7/2016 for thepremenstrual syndrome. She is taking antispasmodic and painkiller for past 2 to 3 yearswithoutdesired results. The case was repertorised with all symptoms and Folliculinum 30C wereprescribed (15/07/2016). In the next follow up (11/8/2016) the severity of symptoms was reduced.Later on, based on the response to these drug the next medicine that is placebo was prescribed. Afterthe fourth follow up the severity of symptoms slightly increased that’s why few doses ofFolliculinum 30 were repeated on 4/12/2016.After giving Folliculinum 30, patientwas much better.Patient started Homoeopathic treatment from Aug 2016 and continued till Jan 2017, during thisperiodthe patient was not taking any allopathic medication for premenstrual syndrome
References:1] Premenstrual syndrome-NHS choices
2]Howkins and Bourne Shaw’s text book of gynaecology.12th edition, Page no. 226
3] Text book of gynaecology by Rashid latif khan.5th edition.
4] D C Duttas textbook of gynecology sixth edition page no 182
5]FOLLICULINUM- A matrimonial remedy to prevent infertility. Indications and results in
treatment of anovulatory female cycle disorders.ByDr.Christina Ari.( article on folliculinum source
internet )
6]Folliculinum: Mist or Miasm?by Melissa Assilem, RSHomhpathy.com/material-
medica/folliculinum-mist-or-miasm ( ARTICLE this paper was presented at society of homoeopaths
seventh international conference at the university of NOTTINGHAM in September 1990
7]Reference www.nhs.uk/conditions/premenstrual-syndrome/pages/symptoms/.aspxdiagnostic tool
for PMS
8]RADAR 10 Homoeopathic software in that Schroyens F, Synthesis 9.0 English repertory.
9]O.A.JulianMateriaMedica of New Homoeopathic Remedies.231
**********************************************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 14
Pratiksha Yadav (PG Scholar)
Abstract
Objectives – To study the effect of magnesium phosphoricum 6X along with homoeopathicsimillimum versus homoeopathic simillimum alone in case of dysmenorrhoea.
Design – Randomized control trial.
Setting – Motiwala Homoeopathic Medical College OPD
Participants – Girls of age 12 to 25 years meeting the Diagnostic Pain Rating Scale fordysmenorrhoea.
Intervention- A total of 45 patients 22 – Homoeopathic simillimum, 23 - Homoeopathicsimilimum along with magnesium phosphoricum 6X, for a period of 6 months.
Outcome measures – Pain Rating Scale, before and after every follow up
Result – - A total of 45 patients 22 – Homoeopathic simillimum, 23 - Homoeopathic similimumalong with magnesium phosphoricum 6X, for a period of 6 months were analysed under modifiedintention to treat. All patient in Magnesium Phosphoricum 6X along homoeopathic simillimumshowed better outcome 86.95% i.e. 20 cases out of 23 cases, cases improved with homoeopathicsimillimum 81.81%, 18 cases out of 22. Cases not improved with magnesium phosphoricum 6Xalong with homoeopathic simillimum 13.04% i.e. 3 cases out of 23, cases not improved withhomoeopathic simillimum 18.18% i.e. 5 out of 22 cases.
Conclusion – Thus Randomized control trial study provides evidence to support the therapeuticeffect of magnesium phosphoricum 6X along with homoeopathic similimum in cases ofdysmenorrhoea in girls with age group of 12 – 25 years.
Keywords – Dysmenorrhoea, Randomized control trial, Magnesium phosphoricum 6X, Pain Ratingscale.
Introduction –
‘PAIN’ be it mental or physical has been constant companion of human being, since a long time.The credit to the increasing mental pain can be given to the ever increasing stress and strain and nowit is a part and parcel of the modern life style.
What we would like to concentrate on the physical pain – this pain could be a manifestation ofvariety of causes. Dysmenorrhoea is the most common gynaecological complaint. It affects half ofall female adolescents today and represents the leading cause of periodic college, school absenteeismamong that population. Many females take antispasmodic and other pain killers which give onlytemporary relief for monthly pain .These medicine are in pharmacological form and gives sideeffects like hyperacidity, giddiness, weakness.
Randomized control trial of Magnesium phosphoricum 6X along withhomoeopathic similimum versus homoeopathic similimum alone in cases ofDysmenorrhoea

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 15
Indicated homeopathic medicines are given in potentized form which gives a mental and physicalcalmness, and relief to the patient.
Signs and symptoms
The main symptom of dysmenorrhoea is pain concentrated in the lower abdomen or pelvis .It is alsocommonly felt in the right or left side of the abdomen. It may radiate to the thighs and lower back.Symptoms often co-occurring with menstrual pain include nausea and vomiting, diarrhoea orconstipation, headache, dizziness, disorientation, hypersensitivity to sound, light, smell and touch,ICD ClassificationSpecialty GynaecologyICD-10 N94.4-N94.6ICD-9-CM 625.3DiseasesDB 10634MedlinePlus 003150eMedicine article/253812Patient UK DysmenorrheaMeSH D004412
Epidemiology
Dysmenorrhea is estimated to affect approximately 25% of women. Reports of dysmenorrhea aregreatest among individuals in their late teens and 20s, with reports usually declining with age. Theprevalence in adolescent females has been reported to be 67.2% by one study and 90% by another.
1) Congestive dysmenorrhoea(secondary, extrinsic or organic )This variety is characterized by premenstrual pain situated either in the back or lowerabdomen, occurring between three and five days or sometimes even longer before the onsetof menstruation. It is always relieved by the menstrual flow. Patient is elderly beyond 30years. The pains always related to pelvic lesions.
Aetiology1) Usually associated with pelvic inflammatory diseases – Salpingo- oophoritis, Parametritis,
Pelvic adhesions.2) Associated with chocolate cysts of ovaries, adenomyomas, endometriosis and acquired
retroversion of uterus.3) Premenstrual congestion or tension syndrome.4) Intra uterine contraceptive devices
Clinical featuresThe pain or discomfort is referred to one or other iliac fossa, usually the left. Usually accompaniedby an alteration in bowel habit mostly constipation, with some flatulent distention of upper colon.The pain is associated with irritability, malaise, headache, feeling of fullness and pain in breasts etc.Other menstrual irregularities like menorrhagia, metrorrhagia & leucorrhoea are frequentlyassociated with the condition.
2) Spasmodic dysmenorrhoea( primary, intrinsic, essential, functional )The majority of cases of dysmenorrhoea fall in to this group. In the true spasmodic variety,the condition does not become established until two or three years after the menarche thoughthere may be a degree of discomfort associated with earlier periods. Probably the most severe

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 16
cases are seen in patients between the age of 19 & 21. It is rare to encounter in women overthe age of 30.
Aetiology1) Cervical obstruction – due to organic stricture of cervix, pinpoint os, narrow cervical canal etc.2) Endocrine factors – dysmenorrhoea is invariably associated with ovulatory cycles. Women on oralcontraceptive pills are rendered anovulatory and thus relieved from pain. Progesteron stimulatesmyometrial contraction of the smooth muscles of the cervix causing narrowing of cervical canal; alsostimulates production of prostaglandin F2alpha which in turn accentuates pain.
MechanismDuring a woman's menstrual cycle, the endometrium thickens in preparation for potential pregnancy.After ovulation, if the ovum is not fertilized and there is no pregnancy, the built-up uterine tissue isnot needed and thus shed. Molecular compounds called prostaglandins are released duringmenstruation, due to the destruction of the endometrial cells, and the resultant release of theircontents. Release of prostaglandins and other inflammatory mediators in the uterus cause the uterusto contract. When the uterine muscles contract, they constrict the blood supply to the tissue of theendometrium, which, in turn, breaks down and dies. These uterine contractions continue as theysqueeze the old, dead endometrial tissue through the cervix and out of the body through the vagina.
DiagnosisThe diagnosis of dysmenorrhea is usually made simply on a medical history of menstrual pain thatinterferes with daily activities. Yet, there are quantification models, called menstrual symptometrics,that can be used to estimate the severity of menstrual pains as well as correlate them with pain inother parts of the body, menstrual bleeding and degree of interference with daily activities.
Menstrual Symptometrics Device :Objective: To validate a menstrual symptometrics device that can quantify menstrual blood loss,dysmenorrhea, and the premenstrual syndrome against traditional methods of collecting data onsymptoms.Design: Validation study.symptometrics device in quantifying and diagnosing menorrhagia, dysmenorrhea, and thepremenstrual syndrome. Most patients preferred the menstrual symptometrics device as a datacollection tool.Conclusion: The menstrual symptometrics device is a rapid and accurate method of quantifyingblood loss,The menstrual symptometrics device displays the following items.Visual analogue scalesScales are displayed that quantify leg pain, back pain, stomach cramps, and the effect of pain ondaily activities. Scales for breast tenderness, headache and bloating, depression, clumsiness, andirritability are also included. All of these scales appear every day throughout the cycle.Research doneA qualitative study on the effect of the homoeopathic similimum in the treatment of primarydysmenorrhoea Christie, Lisa URI: http://hdl.handle.net/10210/4598 Date: 2005
General Management:-1) Hot fomentation during pain.- short management Surya Namaskar [sun salutation]2) Explanation of menstrual process, sex education and reassurance to the patient are important
aspects of management.3) Avoidance of stress and strain, intake of nourishing diet, correction of constipation, mild
physical exercise and adequate rest and proper personal hygiene are necessary adjuvants.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 17
4) When medical treatment fails, dilatation & curettage is advisable in married womenObjective
To study the effect Magnesium phosphoricum 6X versus homoeopathic similimum alone in cases ofDysmenorrhoea.
Material and Methods –
A randomized control trial study was conducted on cases of dysmenorrhoea with age group of 12 to25 years at MHMC OPD, to evaluate the efficacy of Magnesium Phosphoricum 6X withhomoeopathic similimum. Written and informed consent was received from guardians of all girlsenrolled.
Patients and Settngs –
Total study period – 6 months, included 6 months of interventional treatment, which was conductedat MHMC Opd. Girls in age group 12 to 25 years and satisfying the Diagnostic Pain rating scale.Girls suffering from dysmenorrhoea with disturbance in their daily routine activity.were included
Intervention –
Investigators were instructed to make an in depth case taking with the patients as per the guidelineslaid down by DR. Samuel Hahnemann in 6th edition of Organon of medicine. The girls enrolled inthe study were not on any other pharmacological intervention. Kentian Method of evaluation andrepertorization using RADAR software was used to reach the simillimum, however the final decisionwas made after consultation with Materia Medica. The medicines were given from the OPD.
Outcome Measures –
Pain Rating Scale, before and after every follow up, A total of 45 patients 22 – Homoeopathicsimillimum, 23 - Homoeopathic similimum along with magnesium phosphoricum 6X, for a periodof 6 months were analysed under modified intention to treat. All patient in MagnesiumPhosphoricum 6X along homoeopathic simillimum showed better outcome 86.95% i.e. 20 cases outof 23 cases, cases improved with homoeopathic simillimum 81.81%, 18 cases out of 22. Cases notimproved with magnesium phosphoricum 6X along with homoeopathic simillimum 13.04% i.e. 3cases out of 23, cases not improved with homoeopathic simillimum 18.18% i.e. 5 out of 22 cases.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 18
Master chart [mag phos along with homoeopathic similimum ]Srno
Name Age Intensityofsymptombeforestudy
Painintensityscalebeforestudy
Prescription Intensityofsymptomafterstudy
Painintensityscaleafterstudy
Objectivesfulfilled
Result
1 MissM.S
23 Severe,spasmodic
8-10 Nat mur200Mag phos6X
Mild pain 1 – 2 1, 2 Improved
2 MissK.C
14 Severe 7 – 10 Puls 200Mag phos6X
Mild 1 -2 1,2 Improved
3 MissS.N
16 Severe 7 – 10 Ferrum met200Mag phos6X
Mild 1 - 2 1,2 Improved
4 MissM.C
16 Severe 8 – 10 Pul 200Mag phos6X
Mild 1 -2 1,2 Improved
5 MissA.M
15 severe 8 – 10 Pul 200Mag phos6X
Mild 2 - 3 1,2 Improved
6 MissS.O
21 Severe 8 – 10 Puls 200Mag phos6X
Mild 1 – 2 1,2 Improved
7 MissN.R
15 Severe 7 – 10 Nat mur200Mag phos6X
Mild 1 - 2 1,2 Improved
8 MissS.C
21 Severe 8 – 10 Graphitis200Mag phos6X
No pain 0 1 – 2 Improved
9 MissS.S
14 Severe 7 – 8 Nux vomica200 Magphos 200
Severe 7- 8 - NotImproved
10 MissS.S
21 Severe 8 – 9 Nat mur 200Mag phos6X
Moderate 4 -5 1 , 2 Improved
11 MissS.P
22 Severe 7 -8 Nat mur 200Mag phos6X
Mild 3 1,2 Improved
12 MissP.K
18 Severe 8 – 9 Nat mur 200Mag phos6X
Moderate 5 1,2 Improved
13 MissJ.Y
17 Severe 8 – 9 Lyco 200Mag phos6X
Moderate 4 -5 1,2 Improved

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 19
14 MissM.G
14 Severe 7 – 8 Nux vomica200Mag phos6X
Moderate 5 1,2 Improved
15 MissP.K
23 Severe 7 Puls 200Mag phos6X
Moderate 4 -5 1,2 Improved
16 MissS .P
23 Severe 7 -8 Lyco 200Mag phos6X
Mild 3 1,2 Improved
17 MissA.K
23 Severe 9 – 10 Lachesis 200Mag phos
Mild,bearable
3 -4 1,2 Improved
18 MissC.Y
16 Severe 9 – 10 Nat mur 200Mag phos6X
Severe 8 -9 - NotImproved
19 MissO.B
22 Severe 8 – 9 Sepia 200Mag phos6X
Mild 3 – 4 1,2 Improved
20 MissP.B
16 Severe 8 – 9 Puls 200Mag phos6X
Mild 2 – 3 1, 2 Improved
21 MissG. D
16 Severe 9 – 10 Phos 200Mag phos6X
Severe 9 – 10 NotImproved
22 MissR.S
22 Severe 9 – 10 Phos 200Mag phos6X
Mild 2 -3 1,2 Improved
23 MissZ.Q
16 Severe 9 – 10 Lyco 200Mag phos6X
Mild 2 -3 1,2 Improved
Master chart [ Homoeopathic similimum alone ]Srno
Name Age Intensityofsymptombeforestudy
Painintensityscalebeforestudy
Prescription Intensityofsymptomafterstudy
Painintensityscaleafterstudy
Objectivesfulfilled
Result
1 MissN.J
14 Severe 8 – 10 Puls 200 Moderate 5 -6 1,2 Improved
2 MissS.Y
24 Severe 8-10 Nta mur 200 Mild 1 -2 1,2 Improved
3 MissA.P
20 Severe 8 – 10 Lyco 200 Mild 1-2 1,2 Improved
4 MissP.H
20 Severe 7 – 8 Puls 200 Mild 1 -2 1,2 Improved
5 MrsP.D
24 Severe 7 – 10 Lyco 200 Mild 1 -2 1,2 Improved
6 MissP.Y
21 Severe 7– 10 Puls 200 Mild 2 -3 1, 2 Improved
7 Miss 15 Severe 8 – 9 Nat mur 200 Severe 8 – 9 1, 2 Not

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 20
Statistical Analysis – Pain Intensity Scale
0.00%
50.00%
100.00%
15.55%
17.77%
64.44%
2.22%
STATUS AFTER TREATMENT
Medicine PrescribedThe most frequently used remedies for the 45 cases.
U.S improved8 Miss
M.B14 Severe 8 – 9 Phos 200 Mild 3 -4 1,2 Improved
9 MissK.S
15 Severe 8 – 9 Phos 200 Mild 2 -3 1,2 Improved
10 MissS.V
16 Severe 8 – 9 Nat mur 200 Moderate 4 – 5 1,2 Improved
11 MissP.S
13 Severe 7 – 8 Puls 200 Mild 3 1,2 Improved
12 MissA.S
19 Severe 7 – 8 Nat mur 200 Mild 3 – 4 1,2 Improved
13 MissP.K
23 Severe 8 – 9 Nux vomica200
Mild 3 1,2 Improved
14 MissS.M
21 Severe 7 – 8 Lachesis 200 Severe 8 Notimproved
15 MissF.A
23 Severe 9 - 10 Puls 200 Severe 9 - 10 Notimproved
16 MissM.C
14 Severe 8 – 9 Puls 200 Mild 3 -4 1,2 Improved
17 MissR.S
16 Severe 9 – 10 Bryo 200 Moderate 4 -5 1,2 Improved
18 MissR S
21 Severe 8 - 9 sulphur 200 Mild 2-3 1,2 Improved
19 MissS .B
25 Severe 9 - 10 Nat mur 200 Mild 2 -3 1,2 Improved
20 MissS.S
23 Severe 9 – 10 Nat mur 200 Severe 9 – 10 Notimproved
21 MissZ.K
16 Severe 9 – 10 Caust 200 Mild 2 -3 1,2 Notimproved
22 MissK.B
21 Severe 9 – 10 Nat mur 200 Mild 3 -4 1,2 Improved

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 21
13 13
53 3 2 1 1 1 1 1 1
MEDICINES PRESCRIBED
Result
84.44%
15.55%
IMPROVED
NOT IMPROVED
Discussion –
The main results emerged from this study are
(1) There was significant changes in the outcome measures the improvements was found stable overtime of 6 months period with the group of Magnesium Phosphoricum 6X along with homoeopathicsimillimum.
(2) Patients participating in the study were selected by a rigorous diagnostic evaluation followingPain rating scale for DysmenorrhoeaConclusion –This randomized control trial provides evidence to support the therapeutic effect of Magnesiumphosphoricum 6X along with homoeopathic simillimum in cases of dysmenorrhoa with age group og12 to 25 years.
References –1) D.C Dutta – book of Gynaecology pg.-1682) Jeffcoats priciple of gynaecology pg no.- 5323) K.Park- Park’s textbook of preventive and social medicine pg no – 78 - 794) Twelve tissue remedies by Schussler pg no -98 - 1065) Nash materia medica Pg no – 2836) Hering’s guiding symptom pg no – 248 - 2577) kent’s materia medica pg no – pg no – 720 - 7218) Boerick’s matertia medica pg no – 370 – 3719) The Prescriber by J H clarke – pg no – 2 vol pg 370 – 37610) C.S Dawn Textbook of gynaecology contraception and Demography Pg No – 8311) Gynaecology – Rashid latifkhan Pg no – 27912) Shaw’ s Textbook of Gynaecology Pg 277
***************************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 22
Saba Khan (P. G. Scholar)
AbstractPrimary dysmenorrhoea is period pain that cannot be explained by structural gynaecological
pathology. It is highly prevalent in adolescence and starts six to twelve months after painless periodsof menarche. This pain is spasmodic and is often superimposed over background of constant lowerabdominal pain, and may radiate to the back or thigh. Malaise, fatigue, nausea, vomiting, diarrhea, orheadache is often concomitant. Increased production of endometrial prostaglandin has been reportedin suffering women which results in increased uterine tone and stronger and more frequent uterinecontractions that induce the pain [1,&2].In conventional system, analgesics (NSAIDs) are used tomanage primary dysmenorrhoea and if they are ineffective, suppression of ovulation with a low-doseestrogen/progestogen oral contraceptive is tried. However, about 10 percent of affected women donot respond to these measures.[3]
A 20 years old female suffering from severe primary dysmenorrhea.On the basis of totality ofsymptoms and repertorization Sepia 200 was prescribed . Her intensity of symptoms were muchreduced from first cycle till the third month cycle.This case provides documentary evidence aboutthe effectiveness of homoeopathic treatment in severe primary dysmenorrhoea.Keywords: Homoeopathy,Case Report, Primary Dysmenorrhea, Sepia.Introduction -Dysmenorrhea is defined as painful menstruation of sufficient magnitude so as to incapacitate the
day-to-day activities[1].
It is the most common gynecological disorder and one of the most common cause of pelvic pain inwomen. The prevalence rate of dysmenorrheavary widely (16.8% to 81%), and estimates as muchhigh as 90% which have been reported.[2]
Dysmenorrhea can be classified as:1)Primary (spasmodic) dysmenorrhea ;-In primary dysmenorrhea the muscles of uterus squeeze andcontract harder than normal to dislodge the thickened lining that is endometrium. These contractionsmay also reduce the blood flow to the uterus making the pain more worse.[2&3]
The incidence of primary dysmenorrhoea is about 15-20 percent, it is almost alwaysconfined to ovulatory cycle. The pain usually begins when menses start (or just before) and persistsfor the first 1 to 2 days. The pain of primary dysmenorrhoea is described as spasmodic. It issuperimposed over background of constant lower abdominal pain, which may radiate to the back orthigh. The patients may also complain of malaise, fatigue, nausea, vomiting, diarrhea, orheadache[4&5]. Increased production of endometrial prostaglandin, resulting in increased uterine tonestronger.The frequent dysrhythymic uterine contractions, reduced uterine blood flow, and increasedperipheral nerve hypersensitivity induced the pain[6&7]
Published literature indicates that nearly 5 to 15% of women suffering with primarydysmenorrhea, report debility and interference as well as impairment of daily activities[6&7],.
Absenteeism from work and school has been commonly reported (5% to 14% are often absent owingto the severity of symptoms. This absence from school or work due to severity of symptoms oftenlead to poor academic/ or work performance. Feelings of irritability or depression during pain leadsto poor social interaction. Thus, severe primary dysmenorrhoea has physical, psychological, andsocial consequences and this may leads to significant disruption in quality of life.
In conventional system, analgesics (NSAIDs) are used to manage this condition. Analgesicsthat act as prostaglandin synthetase inhibitors are usually started 24 to 48 hour before menses andcontinued for 1 or 2 days after menses begin. Published literature indicates that differentformulations of NSAIDs have similar efficacy and nearly 67% of women achieve pain relief.[6]
However, NSAIDs have known side effects including nausea, vomiting, and/or diarrhoea.Women with a history of gastroduodenal ulcer, gastrointestinal bleeding, or gastroduodenalperforation are advised to avoid pain killersLow-dose estrogen/progestogen oral contraceptives are tried if NSAIDs are found ineffective. OCPs
The Treatment Of Primary Dysmenorrhea With Homeopathic Remedy-ACase Report

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 23
inhibit ovulation and thus cause painless bleeding. There is lack of high quality RCT evidencedemonstrating pain improvement with the use of OCPs over placebo. However, smaller RCTs reportresponse rates as high as 80%. Although combined OCPs may also confer other health benefits sucha reduction in the risk of endometrial and ovarian cancers; several adverse effects such as headache,nausea, abdominal pain, bloating, anxiety, weight gain, and acne have been reported with their use.In rare cases serious health problems, such as venous thrombosis, heart attack, and stroke have alsobeen reported. Women who are already at higher risk of these conditions are generally advised toavoid oral contraceptives.
In all, 10-20% of women with primary dysmenorrhoea do not respond to treatment withNSAIDs or oral contraceptives. In addition, there are known side effects and contraindications tothese treatments. Therefore there is a need to explore effectiveness of alternative methods oftreatment for this condition. This case provides documentary evidence about the effectiveness ofhomoeopathic treatment in severe primary dysmenorrhoea. [7]
Case reportA 20 years female came with the complaints of Primary dysmenorrhea since last 5years. Hersymptoms included lower abdominal pain with nausea and vomiting which starts few hours beforethe menses and last for the next 10-12 hours.Chief complaints-History of Present Illness;-ODP- Lower abdominal pain with nausea and vomiting starts few hours before menses andcontinued for the next 10-12 hours.Cramping and griping Abdominal pain is followed by pain in lower back. .After each episode of vomiting there is generalized weakness.Even from the smell of food her nausea is aggravated and that’s why though she feels hungry sheafraid to eat anything.She also suffered from constipation during every menstrual cycle(2-3days during menses)During each menstrual cycle she is having the same above complaintsThe patient had been prescribed Ipecac, Colocynth, in different potencies before present consultationwithout any relief in her complaints. There was a history of frequent hospital admissions duringmenses with analgesic injections and intravenous infusion of normal saline.MindDuring every menses ,she gets irritated on small things,She do not go out to college or outside the home and spent 2-3 days completely lying on bed due toabdominal pain.Disinterested in talking to everyone, avoids eating or doing any work.Family historyFather- hypertension.Physical generalsThermally- Chilly Appetite- Reduced before and during mensesThirst- Normal Stool- Constipated during mensesUrine- Normal Sleep- Disturbed due to painMenstrual historyMenarche- at the age of 15 yearsCycle/ duration- 28-30 days/ 5-6 daysFlow is normalNumber of pads used/day-2-3 pasds /dayPain- Cramping and griping Abdominal pain is followed by pain in lower back. .
Physical examinationWeight-50Kg BP -110/70mmHg PR- 75/minute. Pallor -face and conjunctiva.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 24
Analysis of symptoms:-Chief complaints Location Sensation Modalities Concomitants Classification of
symptomsLower abdominalpain starts fewhours beforemenses andcontinued for thenext 10-12 hours.
Femalegenitourinary system
Cramping andgriping
>-rest. -low backache during menses-nausea and vomiting startsfew hours before menses andcontinued for the next 10-12hours-Irritability during menses-Disinclination to work DuringMenses- Wants to live alone duringmenses-constipation during menses-sleep disturbed before andduring menses-Appetite reduced before andduring menses
Complete particularsymptoms
Evaluation of Symptoms-Mentals – 1) Irritability during Menses 2) Disinclination to work During Menses
3) Wants to live alone during mensesPhysical Generals-
1) Thermally- Chilly 2) Appetite- Reduced before and during menses3) Stool- Constipated during menses 4) Sleep- Disturbed due to pain
Particulars1) Cramping and griping pain in Lower Abdomen starts few hours before menses and continued forthe next 10-12 hours.2) Dull aching pain in lower back.3) Nausea and vomitting starts few hours before menses and continued for the next 10-12 hoursfollowed by generalized weakness after each episode of vomiting4) Nausea is aggravated even from smell of food
Totality of symptoms-1) Cramping and griping pain in Lower Abdomen starts few hours before menses and continued
for the next 10-12 hours.2) Dull aching pain in lower back.3) Nausea and vomitting starts few hours before menses and continued for
the next 10-12 hours followed by generalized weakness after each episode of vomiting4) Nausea is aggravated evenfrom smell of foodIrritability During Menses5) Disinclination to work During Menses6) Wants to live alone durind menses7) Thermally- Chilly8) Appetite- Reduced before and during menses9) Stool- Constipated during menses10) Sleep- Disturbed due to pain
Repertorial Approach-Used Synthesis Repertory for repertorization
Medicine PrescribedSepia 200,3 doses X 8 hourlySL 4globules TDS for 1 month

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 25
Follow-up-
Date Symptoms Medicine and dose
First month follow up-28/04/2017
The menstrual period started on30th day. There was slight pain atlower abdomen, nausea anddisinclination to eat before start ofmenses that lasted for 3-4hours.Vomiting twice till next morning.She avoided eating anything as shefeared that vomiting mightaggravate.On next day there was no nauseaand vomiting.The patient continued to haveconstipation with feeling ofincomplete evacuation
SL 3doses X 8 hourlycos 4 globules TDS for 1 month
Second month follow up-30/05/2017
The menstrual period started on31st day. There waslower abdominal pain before startof menses that lasted for few hoursonly.There was no vomiting with mildnausea.On next day her appetite wasnormal with no nausea andvomiting.menstrual flow was normal and lastfor 4-5 days.Constipation and other symptomswere better.
SL 3doses X 8 hourlycos 4 globules TDS for 1 month
Third month follow up-30/05/2017
The menstrual period started on30thday. There was milddiscomfortat lower abdomen before start ofmenses that lasted for 2-3 hours.There was nausea but no vomiting.There was no nausea or vomitingnext day.Her appetite was normal.There was no constipation.
SL 3doses X 8 hourlycos 4 globules TDS for 1 month
Discussion Homoeopathic materia medica and repertories were studied to find the “Homoeopathicsimilimum” suitable for this case.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 26
Rubrics taken for repertorization[8,9,10&11]
1. MIND - IRRITABILITY - menses - before2. MIND - IRRITABILITY - menses - during3. MIND - INDIFFERENCE - menses - during4. STOMACH - NAUSEA - menses - before5. STOMACH - NAUSEA - menses - during6. STOMACH - NAUSEA - food - smell of7. STOMACH - VOMITING - menses - before8. STOMACH - VOMITING - menses - during9. ABDOMEN - PAIN - cramping - menses - during10. RECTUM - CONSTIPATION - menses - during11. GENERALS - COLD - agg.12. SLEEP - DISTURBED - menses - during
Repertorial Result[8,9,10&11]
1) Sepia 11/18 2) Nat Mur 10/18 3)puls 10/174)Nux Vom 5)cal 6)Sulph
ConclusionThis case provides documentary evidence about the effectiveness of homoeopathic treatmentIn severe primary dysmenorrhea Homoeopathic medicine prescribed on basis of totality of symptomsand repertorization has positive role in management of severe primarydysmenorrhea.
References
1. Dutta D C. Textbook of Gynecology including contraception. Enlarged and revisedreprint of sixth edition. Jaypee brother’s medical pubishers (P) ltd. New Delhi. Nov 2013.Page 196-202.2)Dysmenorrhoea available on http;.emedicine.medscape.com/article.2538123.Howkins and bourneshaw's Text book of gynaecolody 12th edition4.Text book of gynaecoloy by Rashid Latif Khan 5th edition5.Dysmenorrhoea. Available on http://emedicine.medscape.com/article/253812-overview.6. Dysmenorrhoea. Available on http://emedicine.medscape.com/article/253812-overview7. http://www.merckmanuals.com/professional/gynecology-and-obstetrics/menstrualabnormalities/dysmenorrhea.8. Kent J T. Repertory of the Homoeopathic MateriaMedica. B Jain Publishers Pvt Ltd,9.Allen H C. Allen’s Keynotes Rearranged and Classified with Leading Remedies of theMateria. B. Jain Publishers (P) Ltd, New Delhi, 2002.10.Nash E B. Leaders in Homoeopathic Therapeutics. B. Jain Publishers (P) Ltd, New Delhi,2013.11.RADAR 10 Homeopathic Software
*****************************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 27
Dr.Swanand Shukla
Miss Prachi Rajput , Miss Sana Siddique
Abstract:
Infertility is defined as failure to conceive within one to two years of regular unprotected coitus. 1
Primary infertility denotes those patients who have never conceived. Secondary infertility indicatesprevious pregnancy but failure to conceive subsequently.
80% of couples achieve conception if they so desire, within one year of having regular intercoursewith adequate frequency (4-5 times a week). Another 10 percent will achieve objective by the end ofsecond year. As such 10%remain infertile by end of second year.1
Keywords: infertility, intercourse.
Methodology: A detailed case history was taken and medicine had been selected on the basis oftotality of symptoms. Follow ups were taken on regular intervals.
Case:
A couple came to MHMC OPD on 4/ 11/ 2017 with the complaint of infertility,
Case history was taken in detail separately.
Male:
Presenting complaints:
37 years old male Mr A.P. came with complaint of pain in lumbosacral region a/f overwork, whichaggravated after exertion and was ameliorated by rest and warm fomentation. Since 4-5 months, c/ocough A/F exposure to dust when travelling from one place to another. H/O infertility since 3 years,married 3 years ago (reports S/O = oligospermia).
Generals:
His appetite was good. He has desire for spices and thirst adequately thirsty. Bowel movements arenormal. He had complaint of disturbed sleep as his work schedule was highly disturbed. He haddreams of his work.Mentals:He had aversion to his family members specially his parents who had constant arguments and hencekept himself busy with his work. Hence he is unable to give time to his wife. Mostly he has thoughtsabout his work. He was optimistic that his problem will be solved.Rubrics Selected:MIND – OPTIMISTICMIND - AVERSION - family; to members ofBACK - PAIN - exertion – fromDREAMS - BUSINESSSLEEP – UNREFRESHINGGENERALS - DUST - agg.
A Case Report On Infertility

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 28
GENERALS - FOOD and DRINKS - spices - desireGENERALS - WARM - amel.
Prescription: 4/11/2017- Lycopodium 200/ 3D/ 8 hourly.Phytum 200, 3 doses, 8 hourly for 2 months.Female:Presenting complaints:A 26 year old female Mrs S.P. came with the complaint of inability to conceive in spite of 3 years ofunprotected coition. Had taken treatment but no result obtained She also had c/o headache afterexposure to sunlight.She had h/o delayed menarche.Generals:She had desire for Non veg food with apparently adequate thirst, Had perspiration only on chest andher bowel habits were regular.Her sleep was disturbed. Her menses were regular.LMP: 6/10/17.Mentals:She is introverted person, reserved in nature. She doesn’t express her anger to her in laws as they areelder to her. And is easily irritated at small things but can’t express.Rubrics selected:MIND – RESERVED MIND - AILMENTS FROM - anger - suppressedMIND - IRRITABILITY - trifles, fromFEMALE GENITALIA/SEX - MENSES - delayed in girls, first mensesCHEST - PERSPIRATION SLEEP - DISTURBEDGENERALS - FOOD and DRINKS - meat – desire GENERALS - SUN - exposure to the sun

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 29
Prescription: 4/11/2017- Natrum Mur 200/ 3D/ 8 hourly.Phytum 200 /3 doses / 8 hourly for 2 months.
Follow up:
DATE COMPLAINTS PRESCRIPTION23/ 12/ 2017 (Mr. A.P)Lumbosacral pain reduced, dry cough
after dust exposure reduced, generalities werebetter.
Lycopoium 200/1D /stat.Phytum 200 /tds/ 4 pills for 2months
(Mrs S.P.) LMP 9/12/2017.Anger irritability reduced.No any new complaints after medicine.
Natrum mur 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
3/2/2017 (Mr. A.P)All c/o are better. Lycopoium 200/1D /stat.Phytum 200 /tds/ 4 pills for 2months
(Mrs S.P.) LMP: 9/1/18All c/o are better.
Natrum mur 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
21/3/18 (Mr. A.P) All c/o are better, patient not present,follow up on call.
SL 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
(Mrs S.P.)Patient not present, pregnancy test positive.
SL 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
17/4/2018 (Mr. A.P) All c/o are better SL 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
(Mrs S.P.)USG 10/4/2018Uterus is enlarged and anteverted,Gestational sac seenLMP 13/2/18Foetal pole identified, 10.7mmInternal os closed.
SL 200 /1D/ stat.Phytum 200 /tds/ 4 pills for 2months
Discussion:
Patient was given constitutional on the basis of symptom similarirty along with guidance regardingfertile period and adequate knowledge of menses cycle and advice to healthily increase the frequencyof intercourse in the fertile period, which along with constitutional medicine helped them toconceive.
1. DUTTA D.C Textbook of Gynaceology including contraception, 6th edition, new central bookagency (P) Ltd. London. P 217
******************************************
Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 30
Gulfisha Mirza (PG scholar)Abstract
Objective:
To find the proportion of people conceived
To find the most indicated remedy
Design :
observational study
Setting:
Lasurehospital , Nashik
Participant: couple suffering with infertility according to the definition would be selected.
Result
From the above study conducted we have come to the conclusion that Natrum muriaticum wasindicated in 8 cases (25.80%),
Folliculinum in 7 cases (22.58%), Agnus castus Q in 4 cases (12.31%),
Calcare carb in 2 cases (6.45%), Phosphorus in 2 cases (6.45%),
Aurum mur nat in 1 case(3.23%), Staphysagria in 1 case (3.23%),
Nux vomica in 1 case (3.23%), Pulsatilla in 1 case (3.23%),
Silicea in 1 case (3.23%), Kali brom in 1 case (3.23%),
Thiosinaminum in 1 case (3.23%) and Kali carb in 1 case (3.23%).
Out of these Natrum muriaticum in one case (3.23%), Staphysagria in 1 (3.23%) case and Agnuscastus in 2 cases helped in conception (6.45%).
The other remedies too showed improvement in the development of follicles which are seen throughfollicular studies.
• Conclusion• 4 out of 30 cases conceived. i.e., 13.33 % success rate.• Agnuscastus is the most indicated remedy
Review of literature:
Definition
Infertility means inability of a couple to conceive. A healthy couple may take about six months toachieve pregnancy. On an average, 80% couples would conceive within one year of marriage withoutcontraception and another 10% in next six months. The couple that fails to conceive in two years ofregular sexual intercourse is called infertility.1
Currently, female fertility normally peaks at age 24 and diminishes after 30, with pregnancy
To Evaluate The Role Of Homoeopathic Medicine In Cases Of Infertility: ACase Series

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 31
occurring rarely after age 50. A female is most fertile within 24 hours of ovulation. Male fertilitypeaks usually at age 25 and declines after age 40.
World Health Organization- ICMART glossary
Infertility is a disease of the reproductive system defined by the failure to achieve a clinicalpregnancy after 12 months or more of regular unprotected sexual intercourse2
Epidemiology
Prevalence of infertility varies depending on the definition, i.e. on the time span involved in thefailure to conceive.
Infertility rates have increased by 4% since the 1980s, mostly from problems with fecundity due toan increase in age.
Fertility problems affect one in seven couples in the UK. Most couples (about 84%) who haveregular sexual intercourse (that is, every two to three days) and who do not use contraception getpregnant within a year. About 92 out of 100 couples that are trying to get pregnant do so within twoyears.
Women become less fertile as they get older. For women aged 35, about 94% who have regularunprotected sexual intercourse get pregnant after three years of trying. For women aged 38, however,only about 77%. The effect of age upon men's fertility is less clear.
In people going forward for IVF in the UK, roughly half of fertility problems with a diagnosed causeare due to problems with the man, and about half due to problems with the woman. However, aboutone in five cases of infertility has no clear diagnosed cause.
In Britain, male factor infertility accounts for 25% of infertile couples, while 25% remainunexplained. 50% are female causes with 25% being due to anovulation and 25% tubalproblems/other.
In Sweden, approximately 10% of couples wanting children are infertile.[66] In approximately onethird of these cases the man is the factor, in one third the woman is the factor, and in the remainingthird the infertility is a product of factors on both parts.
Causes
Causes of male infertility may include:
Abnormal sperm production or function due to various problems, such as undescended testicles,genetic defects, health problems including diabetes, prior infections such as mumps, trauma or priorsurgeries on the testicles or inguinal region. Enlarged veins in the testes can increase blood flow andheat, affecting the number and shape of sperm.
Problems with the delivery of sperm due to sexual problems, such as premature ejaculation, semenentering the bladder instead of emerging through the penis during orgasm (retrograde ejaculation),certain genetic diseases, such as cystic fibrosis, structural problems, such as blockage of the part ofthe testicle that contains sperm (epididymis), or damage or injury to the reproductive organs. Menwho have previously undergone a vasectomy and desire a return of fertility will also need to eitherhave the vasectomy reversed (see 'vasectomy reversal' below) or have sperm retrieved through asurgical procedure for use in assisted reproductive techniques.
Overexposure to certain chemicals and toxins, such as pesticides, radiation, tobacco smoke, alcohol,marijuana, and steroids (including testosterone). In addition, frequent exposure to heat, such as in

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 32
saunas or hot tubs, can elevate the testicular temperature, impairing sperm production.
Damage related to cancer and its treatment, including radiation or chemotherapy. Treatment forcancer can impair sperm production, sometimes severely. Removal of one testicle due to cancer alsomay affect male fertility.
Causes of female infertility may include:
Ovulation disorders, which hinder or prevent the ovaries from releasing eggs. Examples includehormonal disorders such as polycystic ovary syndrome, a condition that might relate to your ovariesproducing too much of the male hormone testosterone, and hyperprolactinemia, when you have toomuch prolactin — the hormone that stimulates breast milk production. Other underlying causes mayinclude excessive exercise, eating disorders, injury or tumors.
Uterine or cervical abnormalities, including problems with the opening of the cervix or cervicalmucus, or abnormalities in the shape or cavity of the uterus. Benign tumors in the wall of the uterusthat are common in women (uterine fibroids) may rarely cause infertility by blocking the fallopiantubes. More often, fibroids may distort the uterine cavity interfering with implantation of thefertilized egg.
Fallopian tube damage or blockage, which usually results from inflammation of the fallopian tube(salpingitis). This can result from pelvic inflammatory disease, usually caused by sexuallytransmitted infection, endometriosis or adhesions.
Endometriosis, which occurs when endometrial tissue implants and grows outside of the uterus —often affecting the function of the ovaries, uterus and fallopian tubes.
Primary ovarian insufficiency, also called early menopause, when the ovaries stop working andmenstruation ends before age 40. Although the cause is often unknown, certain conditions areassociated with early menopause, including immune system diseases, radiation or chemotherapytreatment, and smoking.
Pelvic adhesions, bands of scar tissue that bind organs after pelvic infection, appendicitis, orabdominal or pelvic surgery.
Other causes in women include:
Thyroid problems. Disorders of the thyroid gland, either too much thyroid hormone(hyperthyroidism) or too little (hypothyroidism), can interrupt the menstrual cycle or causeinfertility.
Cancer and its treatment. Certain cancers — particularly female reproductive cancers — oftenseverely impair female fertility. Both radiation and chemotherapy may affect a woman's ability toreproduce.
Other conditions. Medical conditions associated with delayed puberty or the absence of menstruation(amenorrhea), such as celiac disease, Cushing's disease, sickle cell disease, kidney disease ordiabetes, can affect a woman's fertility. Also genetic abnormalities can make conception andpregnancy less likely.
Certain medications. Temporary infertility may occur with the use of certain medications. In mostcases, fertility is restored when the medication is stopped.
Many of the risk factors for both male and female infertility are the same. They include:
Age. A woman's fertility gradually declines with age and this decline becomes more pronounced in

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 33
her mid-30s. Infertility in older women may be due to the number and quality of eggs as they age orto health problems that may interfere with fertility. Men over age 40 may be less fertile than youngermen are.
Tobacco use. A couple's chance of achieving a pregnancy is reduced if either partner uses tobacco.Smoking also reduces the possible benefit of fertility treatment. Miscarriages are more frequent inwomen who smoke. Smoking can increase the risk of erectile dysfunction and low sperm count inmen.
Alcohol use. For women, there's no safe level of alcohol use during conception or pregnancy. Avoidalcohol if you're planning to become pregnant because you may not realize you're pregnant for thefirst few weeks. Alcohol use increases the risk of birth defects, and it may also make it more difficultto become pregnant. For men, heavy alcohol use can decrease sperm count and motility.
Being overweight. Among American women, an inactive lifestyle and being overweight mayincrease the risk of infertility. In addition, a man's sperm count and testosterone levels may beaffected if he is overweight.
Being underweight. Women at risk of fertility problems include those with eating disorders, such asanorexia or bulimia, and women who follow a very low calorie or restrictive diet.
Exercise issues. Lack of or not enough exercise contributes to obesity, which increases the risk ofinfertility. Less often, ovulation problems may be associated with frequent strenuous, intenseexercise in women who are not overweight.
Primary and secondary infertility.
Primary infertility is defined as the absence of a live birth for women who desire a child and havebeen in a union for at least five years, during which they have not used any contraceptives.[12] TheWorld Health Organisation also adds that 'women whose pregnancy spontaneously miscarries, orwhose pregnancy results in a still born child, without ever having had a live birth would present withprimarily infertility'.[13]
Secondary infertility is defined as the absence of a live birth for women who desire a child and havebeen in a union for at least five years since their last live birth, during which they did not use anycontraceptives.
Thus the distinguishing feature is whether or not the couple have ever had a pregnancy which led to alive birth.
Effects
A.Psychological impact
The consequences of infertility are manifold and can include societal repercussions and personalsuffering. Advances in assisted reproductive technologies, such as IVF, can offer hope to manycouples where treatment is available, although barriers exist in terms of medical coverage andaffordability. The medicalization of infertility has unwittingly led to a disregard for the emotionalresponses that couples experience, which include distress, loss of control, stigmatization, and adisruption in the developmental trajectory of adulthood.[14]
Infertility may have profound psychological effects. Partners may become more anxious to conceive,increasing sexual dysfunction.[15] Marital discord often develops in infertile couples, especially whenthey are under pressure to make medical decisions. Women trying to conceive often have clinicaldepression rates similar to women who have heart disease or cancer.[16] Even couples undertakingIVF face considerable stress.[17]

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 34
The emotional losses created by infertility include the denial of motherhood as a rite of passage; theloss of one’s anticipated and imagined life; feeling a loss of control over one’s life; doubting one’swomanhood; changed and sometimes lost friendships; and, for many, the loss of one’s religiousenvironment as a support system.[18]
Emotional stress and marital difficulties are greater in couples where the infertility lies with theman.[19]
B.Social impact.
In many cultures, inability to conceive bears a stigma. In closed social groups, a degree of rejection(or a sense of being rejected by the couple) may cause considerable anxiety and disappointment.Some respond by actively avoiding the issue altogether; middle-class men are the most likely torespond in this way.[20]
In an effort to end the shame and secrecy of infertility, Redbook in October 2011 launched a videocampaign, The Truth About Trying, to start an open conversation about infertility, which strikes onein eight women in the United States. In a survey of couples having difficulty conceiving, conductedby the pharmaceutical company Merck, 61 percent of respondents hid their infertility from familyand friends.[21] Nearly half didn't even tell their mothers. The message of those speakingout: It's notalways easy to get pregnant, and there's no shame in that.
There are legal ramifications as well. Infertility has begun to gain more exposure to legal domains.An estimated 4 million workers in the U.S. used the Family and Medical Leave Act (FMLA) in 2004to care for a child, parent or spouse, or because of their own personal illness. Many treatments forinfertility, including diagnostic tests, surgery and therapy for depression, can qualify one for FMLAleave. It has been suggested that infertility be classified as a form of disability.
Materials and methods
Study setting :
Lasure hospital ,Cidco, Nashik
Sample size: 30
Duration of study:
Eight months
Inclusion criteria:
1.Primary infertility in females of reproductive age group.
2.Secondary infertility in females.
3.Bad obstetric history.
4.Males of reproductive age group.
5. Tubal blocks
Exclusion criteria:
1.Married for less than 1year. 2. Azosperm
For females:

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 35
1. Couples with infertility would be selected depending upon the definition, inclusion andexclusion criteria
2. Medicines would be administered in the post menstrual phase3. Follicular studies would be done during which monitoring of follicular growth to be done
with the help of trans vaginal sonography on 10th, 12th and 14th day of menses.If required, follicular studies may be done on 8th, 15th and 16th days as well to keep a watchon the free fluid in pouch og doughlas that indicates rupture of follicules suggestingovulation.The prescriber may repeat the medicines during the follicular studies as per the requirementof the case.
For males:
1. Semen examination would be done.2. Suitable homoeopathic medicine would be administered if needed as per the requirement.
Data collection :Cases of infertility would be selected from lasure hospital ,cidco, nashik.
Observation and result
02468
1012141618
Ovu
latio
n fa
ilure
horm
al im
bala
nce
PCO
Dun
know
ntu
bal b
lock
CAUSES OF INFERTILITY
CAUSES OFINFERTILITY
24
6TYPES OF INFERTILITY
PrimarySecondary
4
26
RESULT OF 30 CASES
CONCEIVED
NOTCONCEIVED

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 36
Result
From the above study conducted we have come to the conclusion that Natrum muriaticum wasindicated in 8 cases (25.80%),
Folliculinum in 7 cases (22.58%), Agnus castus Q in 4 cases (12.31%),Calcare carb in 2 cases (6.45%), Phosphorus in 2 cases (6.45%),Aurum mur nat in 1 case(3.23%), Staphysagria in 1 case (3.23%),Nux vomica in 1 case (3.23%), Pulsatilla in 1 case (3.23%),Silicea in 1 case (3.23%), Kali brom in 1 case (3.23%),Thiosinaminum in 1 case (3.23%) and Kali carb in 1 case (3.23%).
Out of these Natrum muriaticum in one case (3.23%), Staphysagria in 1 (3.23%) case and Agnuscastus in 2 cases helped in conception (6.45%).The other remedies too showed improvement in the development of follicles which are seen throughfollicular studies.
• In this study of 30 cases we observed that 26 cases were of primary infertility and 4 cases ofsecondary infertility.3 cases of primary infertility concieved whereas 1 case of secondaryinfertility concieved.
• 6 cases had an history of ovulation failure ,• 1 case of hormonal imbalance ,• 4 cases of tubal block and• 1 case of PCOD• 18 case with no diagnosable cause.
Conclusion• 4 out of 30 cases conceived. i.e., 13.33 % success rate.• Agnuscastus is the most indicated remedy
Discussion:In this study of 30 cases we observed that 26 cases were of primary infertility and 4 cases ofsecondary infertility.3 cases of primary infertility concieved whereas 1 case of secondaryinfertility concieved.6 cases had an history of ovulation failure ,
1 case of hormonal imbalance ,
4 cases of tubal block and
1 case of PCOD
18 case with no diagnosable cause.
Natrummuriaticum was prescribed for for 8 case out of which 1 concieved.
Folliculinum was prescribed to 7 cases. With folliculinum all 7 cases showed remarkableincrease in follicular size and improvement was seen in ovulation,but none of them concieved. Soour observation is that, folliculinum may be used as intercurrent remedy along with theconstitutional medicine.
Agnuscastus was prescribed to 4 cases out of which 2 cases concieved.Conclusion1) 4 out of 30 cases conceived. i.e., 13.33 % success rate.2) Agnus castus is the most indicated remedy
****************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 37
Shubhada Borse (PG Scholar)
Abstract
Trigeminal neuralgia is characterised by unilateral lancinating severe stabbing recurrent
episodes of facial pain. It most commonly involves the 2nd and 3rd division of the trigeminal nerveterritory.
A case report has been presented below showing the usefulness of calcarea carbonium in thetreatment of trigeminal neuralgia (TN).
Keywords
Trigeminal neuralgia (TN), Homoeopathy, Calc Carb, barrow neurological institute pain intensityscore.
Introduction
Trigeminal neuralgia is a chronic debilitating condition resulting in brief and intense episode offacial pain in the distribution of one or more nerve branches [1]. It is thought to be caused by anirritative lesion involving the trigeminal root zone, in some cases an aberrant loop of artery.Trigeminal neuralgia associated with multiple sclerosis may result from a plaque of demyelination inthe brainstem [2].
The prevalence of TN in the general population is 0.015%. Facial pain has a considerable impact onquality of life. It has been recently shown that TN is the most frequent type of facial pain and thatamong facial pain syndromes the overall incidence of TN has remained constant ranging from12.6/100,000/ years to 27/100,000/ years. The right side is very frequently involved[3]
Unfortunately there is no definitive cure for TN at present. Relapse and reoccurrences may occurwith significant morbidity; however plethors of medical and surgical treatment options do exist toalleviate the patient’s symptoms. [1] In surgery, decompression of vascular loop encroaching on thetrigeminal root is set to have 90% success rate. Otherwise, localised injection of alcohol or phenolinto peripheral branch of the nerve may be effective.
Review of Literature
Trigeminal neuralgia is a chronic debilitating condition resulting in brief and intense episode offacial pain in the distribution of one or more nerve branches [1]. The trigeminal nerve suppliessensation to the skin of the face and anterior half of the hand. It is the second largest of the cranialnerve [4].
TN is relatively common, with an estimated annual incidence of 4-8 per 100,000 individuals. Middleage and elderly person are affected primarily and 60% of cases occur in women. Remission may belong lasting but in most patients, the disorder ultimately recurs. [4]
Idiopathic TN by definition has no causative lesion whereas symptomatic TN has a cause such asvascular compression of the TN root exit zone [2].
Path physiology: Symptoms result from ectopic generation of action potential in pain sensitiveafferent fibers of 5th cranial nerve root just before it enters the lateral surfaces of the pons.[4]
Clinical features: TN is characterised by excruciating paroxysms of pain in the lips, gums, cheek orchin and very rarely in the distribution of the ophthalmic division of the 5th nerve. The pain seldom
A case report of Trigeminal Neuralgia

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 38
lasts more than few a seconds or a minute or two but may be so intense that the patient winces. Theymay occur spontaneously or with movements of affected areas evoked by speaking chewing orsmiling. Another characteristic feature is the presence of trigger zone, typically on face lip or tonguethat provokes attacks, patients may report that tactile stimuli e.g. washing the face, brushing theteeth, or exposure to a draft of air generate excruciating pain [4].
Differential diagnosis:
Pain from migraine or cluster headache must be ruled out as it is stabbing quality of TN. When TNdevelops in a young adult or is bilateral multiple sclerosis is the key consideration [4].
The differential diagnosis also include Trigeminal autonomic cephalgia, which has autonomicaccompaniments that are not associated with TN[5].
Diagnostic criteria for classical trigeminal neuralgia:[6]
- Paroxysmal attacks of pain lasting from a fraction of a second to two minutes that affect oneor more divisions of the trigeminal nerve
- Pain has at least one of the following characteristics- Intense, sharp, superficial, or stabbing precipitated from trigger areas or by trigger factors- Attacks are similar in individual patients- No neurological deficit is clinically evident- Not attributed to another disorder
Case report:
A female patient of 45 years came with complaints of lightning pain on the right side of the faceespecially on the cheek since 12 to 14 days. The patient said that, the pain does not last for more than30-40 seconds and is usually caused on exposure to cold air, cold water and gurgling. The patientwas diagnosed to have trigeminal neuralgia. The totality of the symptoms was formed andrepertorised. And on the basis of totality, calc carb 200 3 doses 8 hourly was prescribed. Accordingto Barrow Neurological institute pain intensity score (table 1) it was 4th grade pain. The patientstarted to show improvement from the first follow up and the condition was completely resolved incouple of follow-up.
Past history: No major illness
Family history: Father-NAD
Mother-NAD Brother-NAD
Physical General: Appetite: Good
Desire: Not specific Aversion: Not specific
Perspiration: Scanty Urine: Normal
Stool: Satisfactory once a day
Sleep: Disturbed sleep. Thinking about complaints when awakens from middle of the sleep
Dreams: Of daily routine Thirst: 2-3 lit/day
Thermal state: Chilly
Mental Generals:

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 39
The patient is worried about the disease. Thinks what if the disease is incurable. The patient is verysad when alone. Constantly thinks about the disease.
Reportorial approach:
MIND-DELUSION-DISEASE-incurable MIND-SADNESS-alone-when
SLEEP-DISTURBED-thoughts; by FACE-PAIN-neuralgia
FACE-PAIN-Cheek-right MOUTH-COLD-taking-agg
GENERALS-COLD-agg
Reportorial imageReportorial outcome: Calcarea carb 200 3 doses 8 hourlyS.L 4 globules TDS for 7 daysDetails of follow up and prescription of medicine are given in table 2Table 1: Barrow neurological institute pain intensity score[7]
Score Pain description
I No pain, No medications
II Occasional pain, No medication required
III Some pain, Adequately controlled with medication
IV Some pain, not adequately controlled with medication
V Severe pain or no pain relief

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 40
Table 2: Follow up:
Follow up 1 Follow up 2 Follow up 3 Follow up 4
Pain intensityduring theepisode of TN
Slightly reduced 3 episode sincelast week
1 episode sincelast week
No episode ofpain
Gradation ofpain
III Grade IV Grade II Grade I Grade
Sadness whenalone
Still the same Still the same Relief , feelshappy
Relief , feelshappy
Disturbed sleep Sound sleep Sound sleep Sound sleep Sound sleep
Discussion and Conclusion:
When medicines don’t work surgery is the only left treatment for trigeminal neuralgia. But withhomoeopathy, a patient can be treated and the possibility of surgery can be avoided completely.
The patient when came, had severe 4th grade pain with sadness when alone and disturbed sleep sincethe complaint had started. The patient was given calc carb 200 3 dose 8 hourly and saclac TDS for 7days. On the 1st follow up the pain had been reduced to 3rd grade and sleep was sound. She wasprescribed saclac TDS for 7 days. On the 2nd followup for which patient was 2 weeks latecomplained of 3 episodes of pain in the last week of the 4th grade. The patient was given calc carb200 3 dose 8 hourly and saclac TDS for 7 days. By the 3rd follow up, pain had been reduced to 2nd
grade and the feeling of alone and sadness had also been reduced. By the 4th followup, there was noepisode of pain and all the other complaints had regressed.
So, it is very clear from the above case that cases of trigeminal neuralgia can be treated and managessuccessfully with homoeopathic medicines.
References:
1) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4368016
2) Brain.R.Walker. Davidson’s principle and practise of medicine,22nd ed.: Churchilllivingstone;2014:p1178
3) http://www.ncbi.nlm.nih.gov/pmc/article/PMC4348120/
4) Kasper.et all. Harrison’s principle of internal medicine vol 2, 19 ed.: McGraw hill education;2015:p2646-2647
5) Goldman Lee et all. Goldman’s Cecil medicine,24th ed.: Elsevier saunder:p 2251
6) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1782012/
7) https://www.cns.org/sites/default/files/clinical_neuro/chapter19_0.pdf
8) Radar 10 Homoeopathic software
********************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 41
Charushila Gawali (PG Scholar)Abstract:
A corn (also termed as clavus) is a thickening of the skin due to intermittent pressure and frictionalforces. These forces result in hyperkeratosis, clinically and histologically. The extensive thickeningof the skin in a corn may result in chronic pain, particularly in the forefoot.
It is not a viral, bacterial or fungal disease. Corn consist of thickened layers of skin that the body hasformed as a barrier to protect the skin and its inner layers from outside pressures. The first signs aregenerally sore, tender areas on the toes which if ignored quickly developed into corns. A majority ofcorns are caused as a result of the footwear a person is wearing. Here we are treating the case ofCorn with the homoeopathic similimum on the basis of totality of symptoms. The case was treatedwith Antimonium Crudum. The Prescriber has given homoeopathic similimum. The remedy wasantimonium crudum.Keywords: Case report, Proliferation, Hyperkeratosis, Hyperplasia, Corn, Antimonium Crudum.Introduction:Corn is a localised hyperkeratosis of the skin. It usually occurs at the side of pressure e.g. on the soleand toes. There is usually a horny induration of the cuticle with a hard centre. Corn may be painfulparticularly where it is rubbed. Corn has a tendency to recur after excision. A corn has deep centralcore which reaches the deeper layer of the dermis.PathophysiologyCorns are the result of mechanical trauma to the skin culminating in hyperplasia of the epidermis.Most commonly, friction and pressure between the bones of the foot and ill-fitting footwear cause anormal physiological response—proliferation of the stratum corneum. One of the primary roles ofthe stratum corneum is to provide a barrier to mechanical injury. Any insult compromising thisbarrier causes homeostatic changes and the release of cytokines into the epidermis, stimulating anincrease in synthesis of the stratum corneum. With corns, external mechanical forces are focused ona localized area of the skin, ultimately leading to impaction of the stratum corneum and theformation of a hard keratin plug that presses painfully into the papillary dermis, which is known as aradix or nucleus. Corns are common worldwide. Any weight-bearing human is susceptible to thedevelopment of corns. Hyperkeratotic lesions of the foot have been reported to affect 20-65% ofpeople aged 65 or older.Anyone can have a clavus, but most individuals acquire the risk factors for clavus formation afterpuberty because of the onset of traumatic footwear use, repetitive motion injuries, and progressivefoot deformities.Clinically, corn can be described in 3 types. The first is a hard corn or heloma durum. It is mostlyfound in interphalangeal joints, top of the toe or the outside of the little toe. The second is a soft corn.It is generally found in interdigital locations and between the 4th &5th toes. The third type is aperiungual, and this type occurs near or on the edge of a nail. We also found in another type of cornthat is seed corn. Seed corns are clusters of tiny corns that can be very tender if they are on a weight-bearing part of a foot. It is tend to occur on the bottom of the foot.
Case report:
A 36 years male, presented with complaints of thorn like stitching pain on sole of foot, feel uneasyand remains irritable due to the pain. The lesion is horny and painful to touch since 5 months, whichwas occurring at the left foot just beneath the 3rdtoe. His pain gets aggravated when he hit his foot onpebble.The patient had complaint of gastric trouble due to over eating followed by constipation andtongue was thick white coated.
Role Of Homoeopathic Medicine in the case of corn, The Case Report.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 42
Past history: No major illness.
Family history:
Father- Hypertension Brother-NAD
Mother- NAD
Physical generals:
Appetite: Good Hunger: Increased.
Desire: sour food. Aversion: Bread
Perspiration: scanty in armpit. Urine: Normal
Stool: constipation due to overeating. Sleep: sound sleep.
Dreams: of daily routine. Thirst: 2-3 lit/day
Thermal state: Can’t tolerate extremes of heat and cold.
Mental generals:
Talkative.He like spiritual things for reading. He is calm and quite.He easily communicate with otherpeople. Helpful in nature. He wants company.
Physical examination:
B.P.-124/80 mm of Hg Pulse -83/min RR- 19/min
Systemic examination:CNS- conscious, oriented CVS-S1 S2 Normal RS- AEBE clearP/A- soft and non- tender.Repertorial totality:
1. MIND- Anger- touched- when.2. EXTRIMITIES- Corn- painful- touched when.3. EXTRIMITIES- Corn – foot – sole- horny.4. EXTRIMITIES- Corns- inflamed.5. GENERALS- Food and drinks- sour food.6. RECTUM- constipation- eating from- overeating.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 43
Figure 1.Selection of remedy: Antimonium Crudum 200 – Single dose.S. L. 4 globules B.D. for 15days.1st Follow up:10/5/2017Pain and inflammation reduced 60%Complaints of constipation relieved and pain reduced 50% (as per patient)Prescription- SL 4 x BD 15 days.
Figure 2.2nd Follow up:30/5/2017The pain and inflammation reduces 60%Complaints of constipation relieved andpain reduced 80% (as per patient)Prescription: Antimonium Crudum 200 single dose S L -4 B.D. for 15 days.

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 44
Figure 3.
3rd follow up:16/6/2017
Complaint of constipation is relieved.
Patient passes stool daily.
The pain and inflammation reduces 80%.
Prescription:S L – 4 B.D. For 15 days.
4th Follow up: 30/6/2017
Corn is completely get cured.
Figure 4.
Discussion
The patient was treated successfully with homoeopathic medicine. Homoeopathic remedy can offergentle and safe relief and reduces the chances of recurrences significantly. In conventional medicinesurgery is choice of such cases. In such a cases homoeopathy is a ‘Ray Of Hope.’
Conclusion
After giving medicine, the size of corn and hardness reduced substantially and patient is notexperiencing any pain. After giving medicine the case was under observation for 3 months and inevery follow up pain and size, hardening has reduced and patient is still under observation.
Reference1.https://emedicine.medscape.com/article/1089807-overview#showall2. Gupta R, Manchanda RK; Textbook of dermatology for homoeopaths. B. Jain Publishers. 2005.3.DAS S; A concise textbook of Surgery. 8th edition. Published by S. Das [page no.151].4.RADAR 9.0 Software synthesis repertory by Schroyens.5.W. Boericke Pocket Manual Of Homoeopathic Materia Medica And Repertory .
******************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 45
Savita Sahani (P.G. Scholar)Abstract:
Enuresis is a common condition. Approximately 5–10% of 7 year-olds regularly wet their beds andthe problem may persist into teenage and adulthood. Boys are more commonly afflicted than girls,and the condition tends to run in families. There are three pathogenetic mechanisms that havesufficient scientific support to be regarded as important, namely, nocturnal polyuria, and nocturnaldepressor over activity and high arousal thresholds. These may all, in turn, be explained by acommon underlying disturbance at the brainstem level.
It is quite evident that there are bedwetting children who produce disproportionately large amountsof urine at night; this polyuria is often explained by a nocturnal lack of the ant diuretic pituitaryhormone vasopressin. It is also known that bedwetting can be provoked in some non-neuroticchildren just by having them drink lots of water before bedtime and that the vasopressin analoguedecompressing makes many budgeters dry—especially the ones with polyuria . There are, however,some important modifications to the hypothesis. First, not all bedwetting children are polyuria;second, some dry children are polyuria (and have nocturnal instead of enuresis); third, the polyuriadoes not explain why the children do not wake up. A Case of nocturnal enuresis shows the usefulnesshomoeopathic medicine. Calc carb, it give symptomatic relief to the patient.(1)
Keyword:
Nocturnal Enuresis, Bed wetting, Enuresis alarm, Homoeopathic medicine.Introduction:
Nocturnal enuresis (bedwetting) is defined by the National Institute for Health and CareExcellence (NICE) guidelines as the involuntary wetting during sleep without any inherentsuggestion of frequency of bedwetting or pathophysiology. It is considered normal up to the age of 5years, and is common up to the age of 10 years.Children with nocturnal enuresis may have excessive nocturnal urine production, poor sleep arousaland/or reduced bladder capacity. Children with nocturnal enuresis may also have daytime urinaryurgency, frequency or incontinence of urine.(2)
Defination:Primary nocturnal enuresis. This is the recurrent involuntary passage of urine during sleep by a
child aged 5 years or older, who has never achieved consistent night-time dryness. This may further besubdivided into:
Primary nocturnal enuresis without daytime symptoms: children who have enuresis only at night.Primary nocturnal enuresis with daytime symptoms: those who also have daytime symptoms, suchas urgency, frequency, or daytime wetting.
Secondary nocturnal enuresis. This is the involuntary passage of urine during sleep by a childwho has previously been dry for at least six months.
Primary enuresis most often represents developmental delay which resolves in time. In secondaryenuresis the patient regresses after a period of continence, which requires the exclusion of underlyingpathology - eg, a urinary infection.
Three aetiological factors are commonly involved:A disorder of sleep arousal. The child is not wakened by the sensation of a full bladder.
Bladder factors. There may be a low nocturnal bladder capacity and/or an overactive bladder.Emptying reflexes are not inhibited during sleep.
Homeopathy In Nocturnal Enuresis:A Case Study
A Homeopathic Perspective on Pre- and Post-surgicalTreatment

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 46
Nocturnal polyuria. Affected children have been found to have low overnight vasopressin levels,and excessive production of dilute urine during the night.(3)
Material and methods:
A case is taken from homeopathic medical college OPD and prescribed on basis of totality ofsymptom.
Case presentation:
A male boy aged 8 yrs, high school student came to the OPD of Homoeopathic Medical College on7/06/2016 With the c/o involuntary urination at mid-night since 5yrs, 5-6 episode in a week withoffensive odour. No sensation while passing urine. aggavation at mid-night .
Past history
-Pneumonia at the age of 5yrs old
Family history
-Mother – Migraine
-Father- Hemorrhoids
Physical general:- Patient is chilly .His appetite is normal. Desire spicy food and salty food.Aversion to vegetable. Thrist small quantity at small interval, Sleep- deep sound. Dreams- notspecific. Stool- unsatisfactory .Urine 2 -3 times in a day and involuntary urination at midnight .
Mental generals:-
He is absent minded, not obedient. He does exactly the opposite of what her mother asks. He like toparticipates in every event in school. He likes to study and he got 1 rank in school .He as fear ofdogs. He wants company. He like to play outside games.
General physical examination:-
Height-3’2”, weight- 23kg, Pulse- 84/min, cyanosis-absent, Pallor- absent, Lymphadenopathy- nill.
Systemic examination
Respiratory system, gastro-intestinal system, locomotor system and nervous system-NAD
Repertorisation:-
MIND – LAZINESS
MIND –OBSTINATE CHILDREN
MIND- COMPANY –DESIRE FOR
MIND –FEAR – DOGS OF –CHILDREN IN
URINE – ODOR-OFFENSIVE
BLADDER-URINATION-INVOLUNTARY- NIGHT

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 47
Nitric acid, Arsenicum Album, Calc carb was the remedies came in front, but Calc carb was the mostsimilimum to the case. Hence it was selected for the case.
Prescription:- CALC CARB 200 stat 1 dose was prescribed.Phytum 30 4 pills TDS for 15days.
Follow up :
SR.NO COMPLAINTS PRESCRIPTION WITH DATE
1) -URINATION AT NIGHT ON ALTERNATEDAYS.-offensive odor reduce by 50%.P/H:-APP:-Good
THRIST :-Small Quantity at short intervalSTOOL:-RegularSLEEP:-SoundWeight-24 kg
27-6-2016
Calc carb 200 1 doseFollowed by 15 days placebo.4 PILLS TDS
2) URINE EPISODE 3 TIME IN A WEEK.- offensive odor reduce by 80%.P/H:-APP:-Good
THRIST :-Small Quantity at short intervalSTOOL:-RegularSLEEP:-Sound
20-7-2016
Followed by 15 days placebo.4 PILLSTDS
3) URINE EPISODE 2 TIME IN A WEEKNO OFFENSIVE ODORP/H:-APP:-GOOD
THRIST :-Small Quantity at short intervalSTOOL:-RegularSLEEP:-Sound
6-8-2016
Calc carb 200 1 dosePlacebo repeated for 15 days.4 PILLS TDS
4) URINE EPISODE 1 TIME IN A WEEKNO OFFENSIVE ODORP/H:-APP:-GOOD
THRIST :-Small Quantity at short intervalSTOOL:-RegularSLEEP:-SoundWEIGHT:-25 KG
25-8-2016
Placebo repeated for 15 days .4 PILLS TDS

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 48
CONCLUSION and DISCUSSION:-
A case of nocturnal enuresis was treated successfully with homoeopathy .patient ‘s quality of lifewas also improved after taking the medicine ,as there is no recurrence of complaint since lastmedicine it can be a permanent gentle cure.
The bed alarm has the most long-lasting success rate and is worthy of consideration if children aretruly distressed by bedwetting. Constitutional cases- 90%.Therapeutic prescription-10%
References:-
1)Nocturnal enuresis: A topic review and Institutional experience John Michael Dibianco, ChadMorley, and Osama Al- Omar;www.pubmed.comBedwetting
2)Betwetting (enuresis);NICE CKS,Caldwell PH ,Deshpande AV ,Von Gontard ;Management ofnocturnal enuresis.
3)Vande Walle J, Ritting ,Bauer S,ET AL;Partical consensus guidelines for the management ofenuresis.
4) Boericke W.Pocket manual of Homoeopathic Materia Medica and repertory. Rep.ed.New delhi:B jain Publishers;1998
5)Lectures on material medica: J T Kent
6)RADAR 9.0 Software synthesis repertory by Schroyens.
*****************************************

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 49

Materia Novum The Journal of Homoeopathy/Vol. 2 /Issue 2 /April – June 2018 50
Top Related
Copyright © 2022 FDOKUMEN

