





Bahasa
Halaman
Hukum

IMPROVING DPT-HepB +Hib 3rd DOSE COVERAGE AT MUNGULA HEALTH
CENTRE IV-ADJUMANI DISTRICT
BY
AMBAYO WILLIAM- BMLS (IHSU); Dip. MLT (JINJA)AMANDU KADARA ZAIDA- Dip. Nursing (LACOR); Dip.OCO, (JINJA)
MEDIUM-TERM FELLOWS (HEALTH SERVICE IMPROVEMENT)
MENTORS
DR. VIOLET GWOKYALYA – MakSPH-CDC FELLOWSHIP PROGRAM
Dr. AMBAKU MICHEAL- MUNGULA HEALTH CENTRE
FEBUARY, 2015
M A K E R E R E U N I V E R S I T Y
SCHOOL OF PUBLIC HEALTH (MakSPH-CDC FELLOWSHIP PROGRAM)
ii
TABLE OF CONTENTS
TABLE OF CONTENTS.................................................................................................................. ii
DECLARATION .............................................................................................................................. iv
ACKNOWLEDGEMENT ................................................................................................................ v
LIST OF ACRONYMS/ABBREVIATIONS ................................................................................. vi
EXECUTIVE SUMMARY............................................................................................................. vii
1:0 INTRODUCTION AND ORGANIZATIONAL BACKGROUND........................................ 2
1:1 INTRODUCTION....................................................................................................................... 2
1:2 ORGANIZATIONAL BACKGROUND................................................................................... 2
1:3 DPT-Hep B + Hib 3 IMMUNIZATION.................................................................................... 2
2:0 REASONS FOR IMPROVEMENT .......................................................................................... 5
2:1 PROBLEM IDENTIFICATION AND PRIORITIZATION .................................................. 5
2:2 FORMATION OF CONTINUOUS QUALITY IMPROVEMENT TEAM.......................... 6
3:0 CURRENT SITUATION ........................................................................................................... 7
3:1 DPT-Hep B + Hib 3 IMMUNIZATION SITUATION ............................................................ 7
3:2 PROBLEM STATEMENT & JUSTIFICATION.................................................................... 8
3:3 CONTINUOUS QUALITY IMPROVEMENT TARGET...................................................... 8
3.4 PROJECT OBJECTIVES .......................................................................................................... 9
3:4:1 SPECIFIC OBJECTIVES ...................................................................................................... 9
4:0 PROBLEM ANALYSIS ........................................................................................................... 10
4:1 ROOT CAUSE ANALYSIS OF THE PROBLEM................................................................ 10
5:1 IMPLEMENTATION OF COUNTER MEASURES............................................................ 12
6:0 PR OJECT RESULTS ........................................................................................................ 13
6:3 OTHER IMPROVEMENT OUTCOMES.............................................................................. 14
iii
6:3:1 ALLOCATION OF SENIOR STAFF FOR YCC DEPARTMENT................................. 14
6:3:2 HEALTH SERVICE MONITORING................................................................................. 15
6:3:3 HEALTH FACILITY - COMMUNITY PARTNERSHIP ................................................ 15
6:3:4 A CASE SCENARIO............................................................................................................. 15
7:0 LESSONS LEARNED AND CHALLENGES........................................................................ 16
7:1 LESSON LEARNED ................................................................................................................ 16
7:2 CHALLENGES......................................................................................................................... 16
8:0 CONCLUSIONS, RECOMMENDATIONS AND NEXT STEPS........................................ 17
8:1 CONCLUSIONS ....................................................................................................................... 17
8:2 RECOMMENDATIONS.......................................................................................................... 17
8.3 NEXT STEPS............................................................................................................................. 18
8.3.1 DISSEMINATION PLAN ..................................................................................................... 18
8.3.2 SCALE UP PLAN................................................................................................................... 18
REFERENCES ................................................................................................................................ 19
APPENDICES.................................................................................................................................. 20
APPENDIX 1: CQI ORIENTATION AND PROBLEM IDENTIFICATION MEETING .... 20
iv
DECLARATION
I, AMBAYO WILLIAM and KADARA AMANDU ZAIDA do hereby declare that this end-of-
project report entitled, Improving DPT-Hep B + Hib 3 Coverage at Mungula HCIV, Adjumani
District has been prepared and submitted in fulfillment of the requirements of the Medium-term
Fellowship Program at Makerere University School of Public Health and has not been submitted for
any academic or non-academic qualifications.
Signed ………………………………… Date…………………………………..
Mr. AMBAYO WILLIAM (Medium-term Fellow 2014)
Signed ………………………………… Date…………………………………….
Mrs. KADARA ZAIDA AMANDU (Medium- term Fellow 2014)
Signed ………………………………… Date…………………………………..
Dr. AMBAKU MICHEAL (Institution Supervisor/Mentor)
Signed ………………………………… Date…………………………………..
Dr. VIOLET GWOKYALYA (Academic Supervisor/Mentor)
All the fellows actively participated in the activities related with the implementation of the Quality
Improvement Project and Mungula HC IV.

v
ACKNOWLEDGEMENT
We are grateful to a number of people who guided us in the design and eventual implementation of
the project. Our sincere thanks go to institutional mentor who provided us with the technical
support but also created an enabling environment for us to attend the course. We are also indebted
to our academic mentor for all the advice throughout the design and implementation of the project.
Lastly, we are thankful to our families for the moral and spiritual support.
vi
LIST OF ACRONYMS/ABBREVIATIONS
DPT-Hep B + Hib Diphtheria, Pertusis, Tetanus –Hepatitis B + Heamophilusinfluezaetype b
EPI Expanded Program for Immunization
GAVI Global Alliance for Vaccine Initiative
HCIV Health Centre Level Four
MoH Ministry of Health
WHO World Health Organisation
YCC Young Child’s Clinic
VHT Village Health Team
vii
EXECUTIVE SUMMARY
The series of immunizations known as DPT-Hep B + Hibcan prevent diphtheria, pertusis
(whooping cough) and tetanus, hepatitis B and Heamophilusinfluezae type B but these diseases still
kill 600,000 children and afflict millions of others every year in developing countries
WHO/UNICEF, 2012.To be fully protected, children must receive three doses of the vaccine,
administered at the ages of six (6) weeks, ten (10) weeksand fourteen (14) weeks. Completing the
immunization schedule helps a child to get adequate protection from all the immunisable diseases
such as polio, measles, whooping cough, diphtheria, pertusis and tetanus. In Uganda, Immunization
remains a key priority of the Minimum Health Care Package by the health sector. Despite efforts to
accelerate immunization coverage in general and DPT-Hep B + Hib 3in particular, about 22%
districts in Uganda were below the national target of 90% in the July to September quarter of
2013/2014 financial year. Almost all the districts in the West Nile region except Arua performed
poorly with regard to this target. Against this background, the mid-term fellows at Mungulu HC IV
identified lowDPT-Hep B + Hib 3coverage as a priority problem to address.
With support from the fellowship program, a QI project was designed aiming atincreasingthe
percentage coverage of DPT-Hep B + Hib 3immunization completion at Mungula HCIV from 68.6
% to 95% by end of November 2014. In the five months of the project implementation, impressive
results have been achieved as follows; July 79%, August 114%, September 112%, October 116%
and November 125%. The capacity of the YCC clinic was also improved through the allocation of
senior nurses and a community partnership for mobilization was also established. Finally, a
performance monitoring review that was established has resulted into improved performance as it
provides an opportunity for staff to assess performance and lay strategies for improvement.
The biggest lesson learnt from this project is that community partnerships are very important in the
success of immunization campaigns. Consequently, it is recommended that other health workers
should get opportunities to train in CQI.
2
1:0 INTRODUCTION AND ORGANIZATIONAL BACKGROUND
1:1 INTRODUCTION
The series of immunizations known as DPT-Hep B + Hib can prevent diphtheria, pertusis
(whooping cough) and tetanus, Hepatitis B and Heamophilus influezae type b infections but these
diseases still kill 600,000 children and afflict millions of others every year in developing countries
WHO/UNICEF, 2012. To be fully protected, children must receive three doses of the vaccine,
administered at the ages of six (6) weeks, ten (10) weeksand fourteen (14) weeks; completing the
immunization schedule helps a child to get adequate protection from all the immunisable diseases
such as polio, measles, whooping cough, diphtheria, pertusis and tetanus. The percentage of
children receiving the final dose (DPT-Hep B + Hib 3) is therefore a revealing and vital gauge of
how well countries are providing immunization coverage for their children.
In Uganda, Immunization remains a key priority of the Minimum Health Care Package of the health
sector. Over the past years, implementation of the expanded program for immunization
revitalization and strategic plans has accelerated government efforts to achieve better health for the
children and women of Uganda, thereby contributing to the enhancement of the quality of life and
productivity.
1:2 ORGANIZATIONAL BACKGROUND
Mungula HCIV, is a government health facility located in Itirikwa Sub County about 23kms south
of Adjumani town, it serves a catchment population of 12,227 persons. The health facility provides
diverse health care services within various departments including Outpatient department,
laboratory, general ward, maternity, ANC, immunization (YCC), operating theatre etc
1:3 DPT-Hep B + Hib 3 IMMUNIZATION
Diphtheria is a disease caused by a germ called ‘Corynebacterium diphtheriae’. The germ produces
toxins that harm or destroy human body tissues and organs. One type of the disease affects the
pharynx and other parts of the throat. Another type, commoner in the tropics, causes ulcers on the
skin. The disease affects people of all ages, but mostly un-immunized children.The most effective
way of preventing diphtheria is to maintain a high level of immunization in the community.

3
InUganda, Diphtheria toxoid is given together with Pertussis, Tetanus, Hepatitis B and
Heamophilus influenzae type B vaccines (DPT-Hep B + Hib).
Pertussis, or whooping cough is a disease of the respiratory tract caused by a germ called Bordetella
pertussis, which lives in the mouth, nose and throat. Many children with pertussis have coughing
spells lasting four to eightweeks. The disease is most dangerous in children aged under 1 year
especially those who are un-immunized, this bacterial infection spreads from an infected person
(droplets) through sneezing. The disease is extremely contagious, especially where people live in
crowded conditions and nutrition is poor. Infants and children under five years are the people most
likely to be infected. They may also develop life-threatening complications like bacterial
pneumonia and die from the disease. The most effective way to prevent pertussis is to immunize all
children under 1 year.
Tetanus affects people of all ages. The disease is particularly common and serious in newborn
babies where it is called Neonatal tetanus. Neonatal tetanus kills between 500,000 and 1 million
babies every year worldwide (WHO). Almost all neonates who get the disease die. Neonatal tetanus
is particularly common in rural areas where most deliveries are at home without adequate sterile
procedures. In Uganda, neonatal tetanus remains a serious problem in districts with poor
immunization coverage and unclean practices associated with childbirth. If untreated, tetanus is a
very serious disease at any age, almost every person contracting tetanus dies. All children should be
immunized against tetanus because antibodies transferred from the mother before birth last for only
a few months. Infection occurs when contaminated objects puncture or cut the skin and umbilical
cord. It can also occur during unclean delivery practices. the most important way to achieve
prevention is to immunize women of childbearing age 5 doses of TT vaccine and to ensure clean
delivery practices Children receive protection from tetanus by receiving 3 doses of DPT- HepB
+Hib vaccine.
Hepatitis B is a disease caused by the hepatitis B virus and it affects the liver. Adults who get
hepatitis B usually recover.However most infants infected at birth become chronic carriers i.e. they
continue to carry the virus for many yearsand can spread the infection to others.In the year 2000,
there were an estimated 5.7 million cases of acute hepatitis B and more than 521,000 deaths from
hepatitis B related diseases worldwide. It is estimated that there are about 350 million carriers of
4
hepatitis B virus worldwide. In Uganda, it is estimated that 1.4 million people are infected with
hepatitis B (National Hepatitis B Sero survey 2005). This ranks Uganda among countries with high
endemicity. It is recommended that all infants receive three doses of hepatitis B vaccine during the
first year of life. In Uganda Hepatitis B vaccine is given in combination with Diphtheria, Pertussis,
Tetanus and Heamophilus influenzae type b vaccines as DPT-Hep B + Hib vaccine.
Haemophilus influenzae type b (Hib) is the commonest form of Haemophilus influenzae. Hib is a
leading cause of bacterial meningitis and is also responsible for about 2.7 million cases of
pneumonia in developing countries. According to WHO, 5% to 10% cases of Hib meningitis are at
risk of dying. This comes as a result of seeking health care late, improper treatment or use of
inappropriate drugs.
Low DPT-Hep B + Hib 3completion is one of the bottlenecks in attainmentof quality immunization
services in resource limited settings. Although there is a 90% increase in immunization coverage in
every district of Uganda, most districts are slow when it comes to the utilization of these services.
About 78% of districts are above the national target for DPT-Hep B + Hib 3 coverage of 90% for
the quarter (July- September) 2 013/2014;only 22% of the districts are below 90% DPT-Hep B +
Hib 3coverage for the targeted infants in that quarter(UNEPI, 2014).Accordingly all the districts in
Westnile region (Adjumani, Moyo, Yumbe, Maracha, Koboko and Nebbi) scored poorly except
Arua on the utilization of the immunizations services despite the fact that the access to these
services was good in the July-September quarter.
5
2:0 REASONS FOR IMPROVEMENTMungula HCIV is public/government health facility that is mandated to provide and implement
ministry of health activities. One of the key services in the primary health care package expected to
be provided at all health centers is immunization. The goal of improving immunization coverage is
to improve quality of life through protective vaccination of children against all the immunisable
diseases; polio, measles tetanus, diphtheria, whooping cough, pneumonia hepatitis b in corners of
the country.
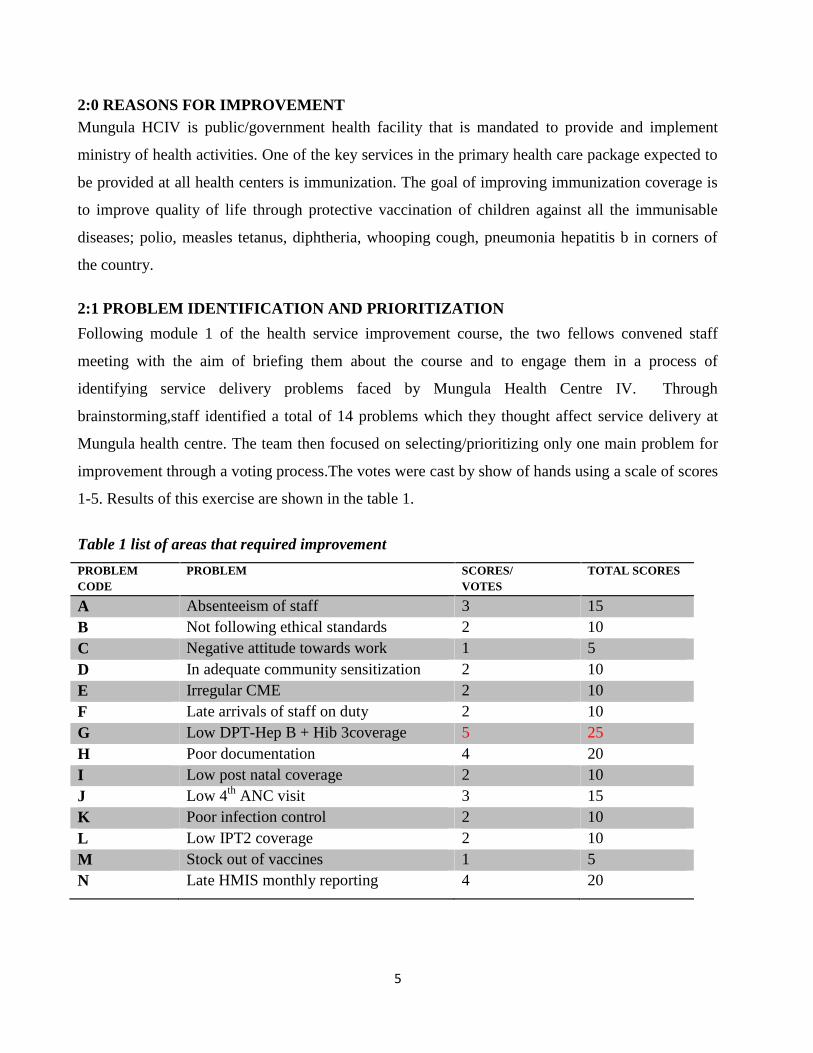
2:1 PROBLEM IDENTIFICATION AND PRIORITIZATION
Following module 1 of the health service improvement course, the two fellows convened staff
meeting with the aim of briefing them about the course and to engage them in a process of
identifying service delivery problems faced by Mungula Health Centre IV. Through
brainstorming,staff identified a total of 14 problems which they thought affect service delivery at
Mungula health centre. The team then focused on selecting/prioritizing only one main problem for
improvement through a voting process.The votes were cast by show of hands using a scale of scores
1-5. Results of this exercise are shown in the table 1.
Table 1 list of areas that required improvement
PROBLEMCODE
PROBLEM SCORES/VOTES
TOTAL SCORES
A Absenteeism of staff 3 15B Not following ethical standards 2 10C Negative attitude towards work 1 5D In adequate community sensitization 2 10E Irregular CME 2 10F Late arrivals of staff on duty 2 10G Low DPT-Hep B + Hib 3coverage 5 25H Poor documentation 4 20I Low post natal coverage 2 10J Low 4th ANC visit 3 15K Poor infection control 2 10L Low IPT2 coverage 2 10M Stock out of vaccines 1 5N Late HMIS monthly reporting 4 20
6
From the results above low DPT-Hep B + Hib 3coverage emerged as the most pressing problem
which the staff selected as the facility project. Officers present during this meeting are listed in
Appendix 1
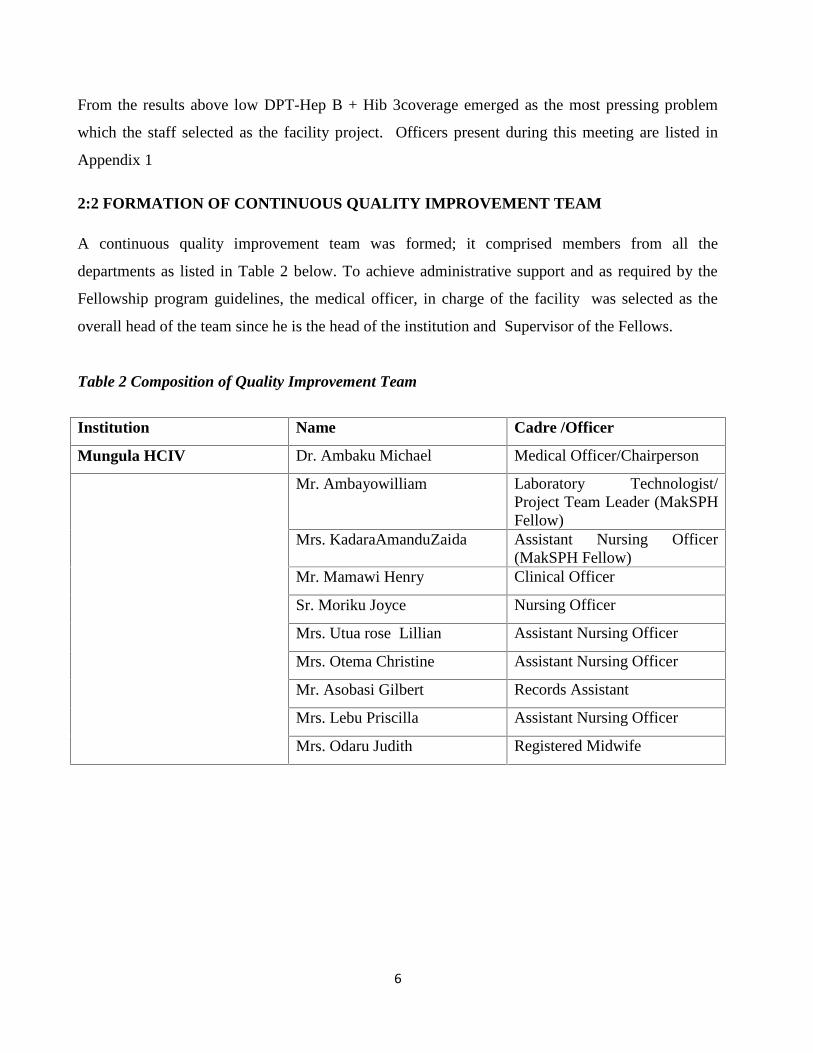
2:2 FORMATION OF CONTINUOUS QUALITY IMPROVEMENT TEAM
A continuous quality improvement team was formed; it comprised members from all the
departments as listed in Table 2 below. To achieve administrative support and as required by the
Fellowship program guidelines, the medical officer, in charge of the facility was selected as the
overall head of the team since he is the head of the institution and Supervisor of the Fellows.
Table 2 Composition of Quality Improvement Team
Institution Name Cadre /Officer
Mungula HCIV Dr. Ambaku Michael Medical Officer/Chairperson
Mr. Ambayowilliam Laboratory Technologist/Project Team Leader (MakSPHFellow)
Mrs. KadaraAmanduZaida Assistant Nursing Officer(MakSPH Fellow)
Mr. Mamawi Henry Clinical Officer
Sr. Moriku Joyce Nursing Officer
Mrs. Utua rose Lillian Assistant Nursing Officer
Mrs. Otema Christine Assistant Nursing Officer
Mr. Asobasi Gilbert Records Assistant
Mrs. Lebu Priscilla Assistant Nursing Officer
Mrs. Odaru Judith Registered Midwife
7
3:0 CURRENT SITUATION
3:1 DPT-Hep B + Hib 3 IMMUNIZATION SITUATIONMungula HCIV is equipped with essential tools required to provide immunization services. The
ministry of health is responsible for supply of all vaccines in the facility and maintenance of cold
chain equipment such as refrigerators through UNEPI program. The health facility also receives
funding to cater for immunization outreaches on quarterly basis. Immunization services at Mungula
HC IV are provided in the young child clinic (YCC) routinely as mothers bring their children for
first time vaccination or return visits (static Mode). In addition, the facility conducts outreaches in
the community once a week as provided for in the facility work plan and when resources permit.
During outreaches, prior notifications are given to village health teams to inform community
members on the planned health facility visits for immunization activity.
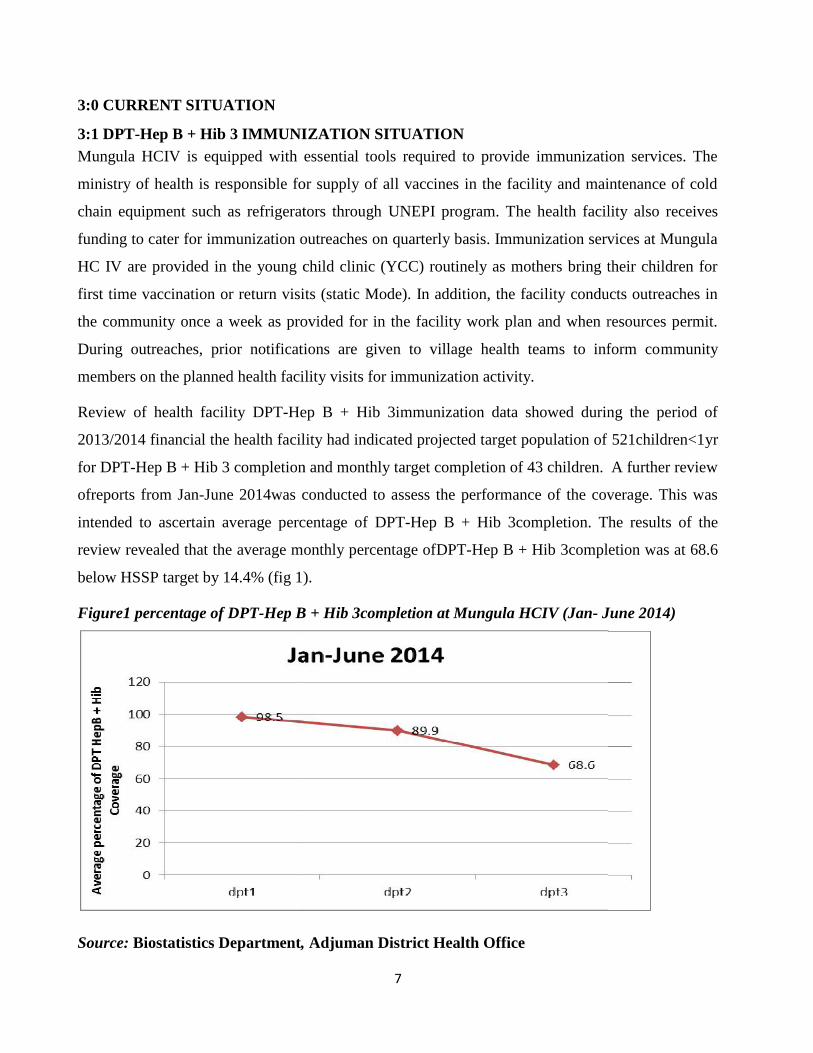
Review of health facility DPT-Hep B + Hib 3immunization data showed during the period of
2013/2014 financial the health facility had indicated projected target population of 521children<1yr
for DPT-Hep B + Hib 3 completion and monthly target completion of 43 children. A further review
ofreports from Jan-June 2014was conducted to assess the performance of the coverage. This was
intended to ascertain average percentage of DPT-Hep B + Hib 3completion. The results of the
review revealed that the average monthly percentage ofDPT-Hep B + Hib 3completion was at 68.6
below HSSP target by 14.4% (fig 1).
Figure1 percentage of DPT-Hep B + Hib 3completion at Mungula HCIV (Jan- June 2014)
Source: Biostatistics Department, Adjuman District Health Office
7
3:0 CURRENT SITUATION
3:1 DPT-Hep B + Hib 3 IMMUNIZATION SITUATIONMungula HCIV is equipped with essential tools required to provide immunization services. The
ministry of health is responsible for supply of all vaccines in the facility and maintenance of cold
chain equipment such as refrigerators through UNEPI program. The health facility also receives
funding to cater for immunization outreaches on quarterly basis. Immunization services at Mungula
HC IV are provided in the young child clinic (YCC) routinely as mothers bring their children for
first time vaccination or return visits (static Mode). In addition, the facility conducts outreaches in
the community once a week as provided for in the facility work plan and when resources permit.
During outreaches, prior notifications are given to village health teams to inform community
members on the planned health facility visits for immunization activity.
Review of health facility DPT-Hep B + Hib 3immunization data showed during the period of
2013/2014 financial the health facility had indicated projected target population of 521children<1yr
for DPT-Hep B + Hib 3 completion and monthly target completion of 43 children. A further review
ofreports from Jan-June 2014was conducted to assess the performance of the coverage. This was
intended to ascertain average percentage of DPT-Hep B + Hib 3completion. The results of the
review revealed that the average monthly percentage ofDPT-Hep B + Hib 3completion was at 68.6
below HSSP target by 14.4% (fig 1).
Figure1 percentage of DPT-Hep B + Hib 3completion at Mungula HCIV (Jan- June 2014)
Source: Biostatistics Department, Adjuman District Health Office
7
3:0 CURRENT SITUATION
3:1 DPT-Hep B + Hib 3 IMMUNIZATION SITUATIONMungula HCIV is equipped with essential tools required to provide immunization services. The
ministry of health is responsible for supply of all vaccines in the facility and maintenance of cold
chain equipment such as refrigerators through UNEPI program. The health facility also receives
funding to cater for immunization outreaches on quarterly basis. Immunization services at Mungula
HC IV are provided in the young child clinic (YCC) routinely as mothers bring their children for
first time vaccination or return visits (static Mode). In addition, the facility conducts outreaches in
the community once a week as provided for in the facility work plan and when resources permit.
During outreaches, prior notifications are given to village health teams to inform community
members on the planned health facility visits for immunization activity.
Review of health facility DPT-Hep B + Hib 3immunization data showed during the period of
2013/2014 financial the health facility had indicated projected target population of 521children<1yr
for DPT-Hep B + Hib 3 completion and monthly target completion of 43 children. A further review
ofreports from Jan-June 2014was conducted to assess the performance of the coverage. This was
intended to ascertain average percentage of DPT-Hep B + Hib 3completion. The results of the
review revealed that the average monthly percentage ofDPT-Hep B + Hib 3completion was at 68.6
below HSSP target by 14.4% (fig 1).
Figure1 percentage of DPT-Hep B + Hib 3completion at Mungula HCIV (Jan- June 2014)
Source: Biostatistics Department, Adjuman District Health Office
8
3:2 PROBLEM STATEMENT & JUSTIFICATION
The M.O.H and W.H.O guidelines recommends that all children <1 yr complete their vaccination
against all the immunisable killer diseases for adequate/complete protection. However, the target
population of DPT-Hep B + Hib 3completion among children <1 yr for 2013/2014 (n=521) at
Mungula HCIVwasn’t achievedthus the facility recorded below coverage during the period of Jan-
May compared to HSSIP target of 83% indicating a gap of 14.4%; this has been attributed to
inadequate community awareness on the benefits of immunization coupled with circulation of
rumors and misconceptions about immunization, lack of follow up of DPT-Hep B + Hib 3dropouts
from the community and poor delivery of immunization to clients/mother by health
workers.Although there is immunization activities taking place both static and outreach, DPT-Hep
B + Hib3 coverage continues to perform below national target. Therefore, if this trend is not
addressed it could result into sudden outbreak of immunisable diseases leading to secondary effects
detrimental to the quality of life, It is against this background, the quality improvement project at
Mungula HC IV targeted to sensitize village health teams (VHTs) on EPI in 100% of villages by
November 2014, reaching every child in homestead and conducting health facility review meetings
to check immunization progress and improve on the information delivery to clients on benefits of
completing DPT-Hep B + Hib 3rd dose vaccination.
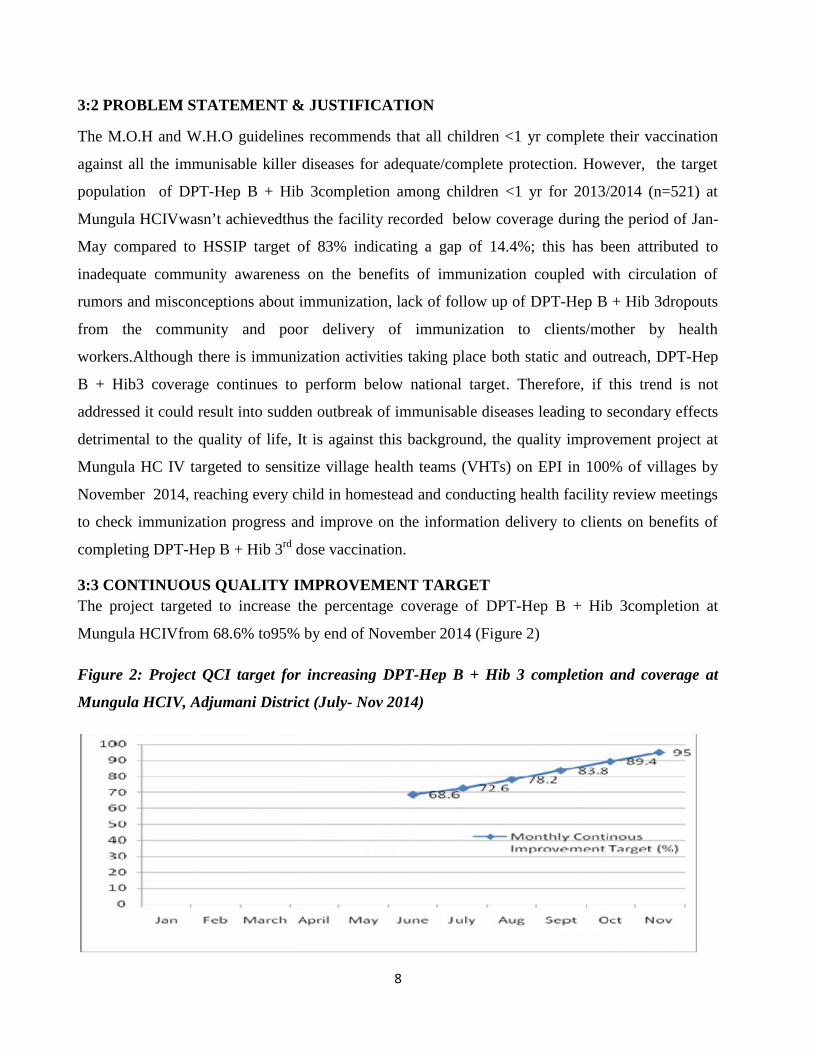
3:3 CONTINUOUS QUALITY IMPROVEMENT TARGETThe project targeted to increase the percentage coverage of DPT-Hep B + Hib 3completion at
Mungula HCIVfrom 68.6% to95% by end of November 2014 (Figure 2)
Figure 2: Project QCI target for increasing DPT-Hep B + Hib 3 completion and coverage at
Mungula HCIV, Adjumani District (July- Nov 2014)
8
3:2 PROBLEM STATEMENT & JUSTIFICATION
The M.O.H and W.H.O guidelines recommends that all children <1 yr complete their vaccination
against all the immunisable killer diseases for adequate/complete protection. However, the target
population of DPT-Hep B + Hib 3completion among children <1 yr for 2013/2014 (n=521) at
Mungula HCIVwasn’t achievedthus the facility recorded below coverage during the period of Jan-
May compared to HSSIP target of 83% indicating a gap of 14.4%; this has been attributed to
inadequate community awareness on the benefits of immunization coupled with circulation of
rumors and misconceptions about immunization, lack of follow up of DPT-Hep B + Hib 3dropouts
from the community and poor delivery of immunization to clients/mother by health
workers.Although there is immunization activities taking place both static and outreach, DPT-Hep
B + Hib3 coverage continues to perform below national target. Therefore, if this trend is not
addressed it could result into sudden outbreak of immunisable diseases leading to secondary effects
detrimental to the quality of life, It is against this background, the quality improvement project at
Mungula HC IV targeted to sensitize village health teams (VHTs) on EPI in 100% of villages by
November 2014, reaching every child in homestead and conducting health facility review meetings
to check immunization progress and improve on the information delivery to clients on benefits of
completing DPT-Hep B + Hib 3rd dose vaccination.
3:3 CONTINUOUS QUALITY IMPROVEMENT TARGETThe project targeted to increase the percentage coverage of DPT-Hep B + Hib 3completion at
Mungula HCIVfrom 68.6% to95% by end of November 2014 (Figure 2)
Figure 2: Project QCI target for increasing DPT-Hep B + Hib 3 completion and coverage at
Mungula HCIV, Adjumani District (July- Nov 2014)
8
3:2 PROBLEM STATEMENT & JUSTIFICATION
The M.O.H and W.H.O guidelines recommends that all children <1 yr complete their vaccination
against all the immunisable killer diseases for adequate/complete protection. However, the target
population of DPT-Hep B + Hib 3completion among children <1 yr for 2013/2014 (n=521) at
Mungula HCIVwasn’t achievedthus the facility recorded below coverage during the period of Jan-
May compared to HSSIP target of 83% indicating a gap of 14.4%; this has been attributed to
inadequate community awareness on the benefits of immunization coupled with circulation of
rumors and misconceptions about immunization, lack of follow up of DPT-Hep B + Hib 3dropouts
from the community and poor delivery of immunization to clients/mother by health
workers.Although there is immunization activities taking place both static and outreach, DPT-Hep
B + Hib3 coverage continues to perform below national target. Therefore, if this trend is not
addressed it could result into sudden outbreak of immunisable diseases leading to secondary effects
detrimental to the quality of life, It is against this background, the quality improvement project at
Mungula HC IV targeted to sensitize village health teams (VHTs) on EPI in 100% of villages by
November 2014, reaching every child in homestead and conducting health facility review meetings
to check immunization progress and improve on the information delivery to clients on benefits of
completing DPT-Hep B + Hib 3rd dose vaccination.
3:3 CONTINUOUS QUALITY IMPROVEMENT TARGETThe project targeted to increase the percentage coverage of DPT-Hep B + Hib 3completion at
Mungula HCIVfrom 68.6% to95% by end of November 2014 (Figure 2)
Figure 2: Project QCI target for increasing DPT-Hep B + Hib 3 completion and coverage at
Mungula HCIV, Adjumani District (July- Nov 2014)
9
3.4 PROJECT OBJECTIVES
To improve DPT-Hep B + Hib 3coverage from the current average of 68.6 % to 95 % in order to
improve health services delivery in Mungula health center IV from July –November 2014
3:4:1 SPECIFIC OBJECTIVES
1. Sensitization of community stake holders and village health teams
2. Establish monitoring and defaulter follow up mechanism
3. Create linkage between VHT registers (HMIS 097) and child register (HMIS 073) for
tracking purposes
4. Supplement on immunization community outreaches
10
4:0 PROBLEM ANALYSIS
4:1 ROOT CAUSE ANALYSIS OF THE PROBLEM
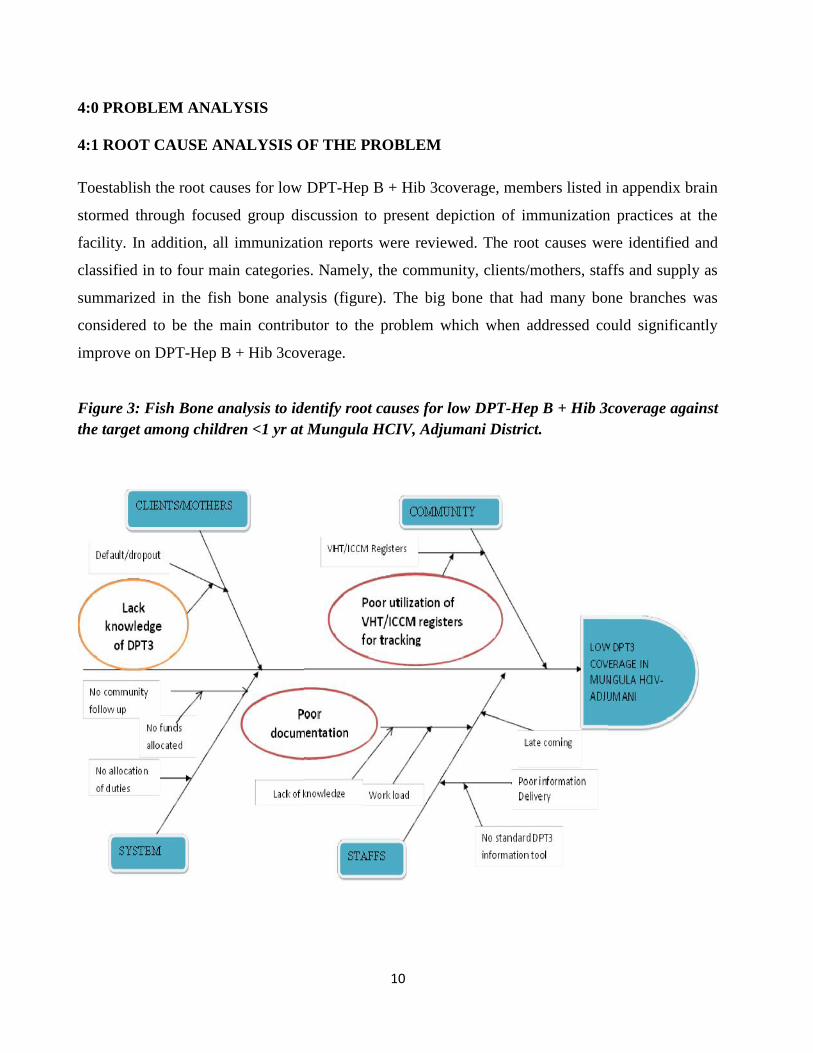
Toestablish the root causes for low DPT-Hep B + Hib 3coverage, members listed in appendix brain
stormed through focused group discussion to present depiction of immunization practices at the
facility. In addition, all immunization reports were reviewed. The root causes were identified and
classified in to four main categories. Namely, the community, clients/mothers, staffs and supply as
summarized in the fish bone analysis (figure). The big bone that had many bone branches was
considered to be the main contributor to the problem which when addressed could significantly
improve on DPT-Hep B + Hib 3coverage.
Figure 3: Fish Bone analysis to identify root causes for low DPT-Hep B + Hib 3coverage againstthe target among children <1 yr at Mungula HCIV, Adjumani District.
10
4:0 PROBLEM ANALYSIS
4:1 ROOT CAUSE ANALYSIS OF THE PROBLEM
Toestablish the root causes for low DPT-Hep B + Hib 3coverage, members listed in appendix brain
stormed through focused group discussion to present depiction of immunization practices at the
facility. In addition, all immunization reports were reviewed. The root causes were identified and
classified in to four main categories. Namely, the community, clients/mothers, staffs and supply as
summarized in the fish bone analysis (figure). The big bone that had many bone branches was
considered to be the main contributor to the problem which when addressed could significantly
improve on DPT-Hep B + Hib 3coverage.
Figure 3: Fish Bone analysis to identify root causes for low DPT-Hep B + Hib 3coverage againstthe target among children <1 yr at Mungula HCIV, Adjumani District.
10
4:0 PROBLEM ANALYSIS
4:1 ROOT CAUSE ANALYSIS OF THE PROBLEM
Toestablish the root causes for low DPT-Hep B + Hib 3coverage, members listed in appendix brain
stormed through focused group discussion to present depiction of immunization practices at the
facility. In addition, all immunization reports were reviewed. The root causes were identified and
classified in to four main categories. Namely, the community, clients/mothers, staffs and supply as
summarized in the fish bone analysis (figure). The big bone that had many bone branches was
considered to be the main contributor to the problem which when addressed could significantly
improve on DPT-Hep B + Hib 3coverage.
Figure 3: Fish Bone analysis to identify root causes for low DPT-Hep B + Hib 3coverage againstthe target among children <1 yr at Mungula HCIV, Adjumani District.
11
Figure: 4 MakSPH Fellows Facilitating a Quality Improvement Meeting at Mungula HCIV,
Adjumani District
Figure 5: Officers attending a quality improvement meeting convened by MakSPH fellows at the
health facility below
12
5:0 PRACTICAL COUNTER MEASURES
5:1 IMPLEMENTATION OF COUNTER MEASURES
ProblemStatement
Identified Root Causes Counter Measures Implemented
Low DPT-Hep B +Hib 3Coverage
Poor documentation becausestaff don’t update childhealth register aftercommunity outreachimmunization
Updated child health registers
Developed standard operatingprocedure for outreach immunizations
Conducted on job mentorship oncompleteness of immunization reports
No community defaulterfollow ups because of poortracking mechanism
With support of the project funds,staffs and VHTs followed outdefaulters in the community
Activated utilization of village childregister for children <1 yr as adefaulter monitoring mechanism
Poor information delivery forclients to examineimmunization benefitsbecause of limited IECmaterials to guide staffsduring Health Education.
With support from other UNHCRImplementing partners such as ACFand CONCERN WORLDWIDEprovided enough IEC materials
Poor duty allocation becausethere is overwhelming workat YCC
With health facility Administrativesupport, 2 staffs were allocated tomanage the work at YCC
Communication gap withcommunity leaders/stakeholders
Conducted immunizationregularsensitization meetings with VHTs,Local councils (LCs), Religiousleaders
Availed community immunizationoutreach programs to VHTs beforeanticipated outreach date.
13
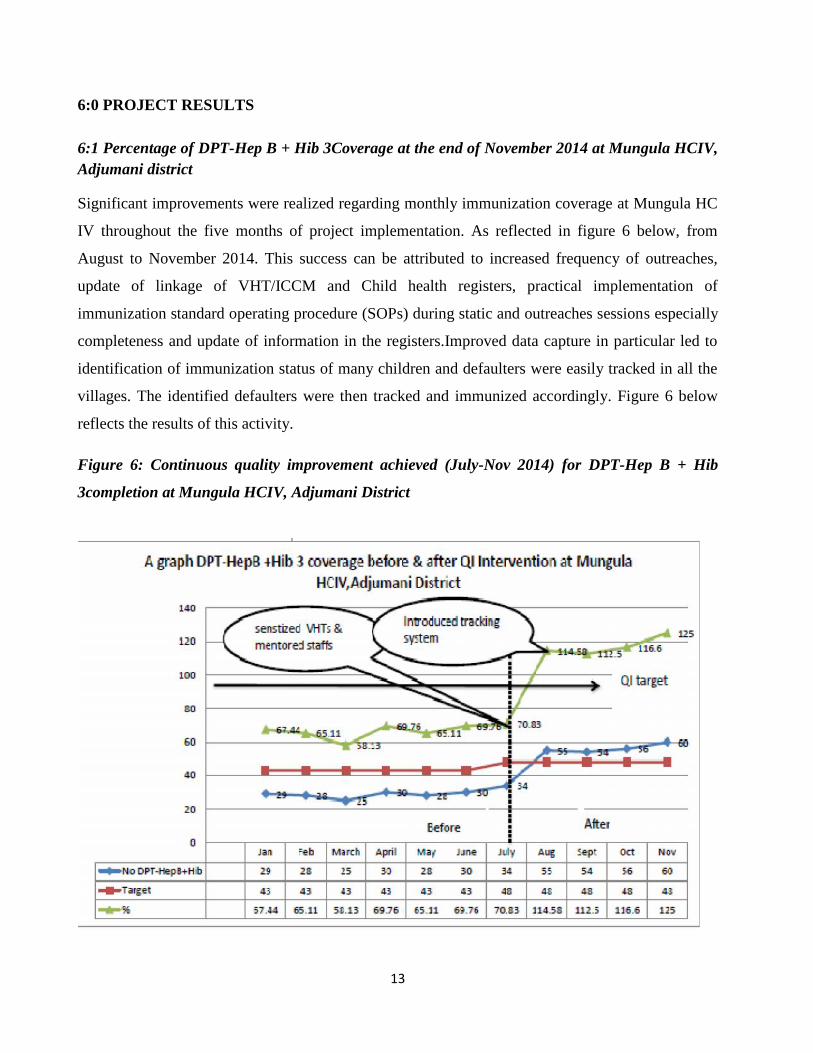
6:0 PROJECT RESULTS
6:1 Percentage of DPT-Hep B + Hib 3Coverage at the end of November 2014 at Mungula HCIV,Adjumani district
Significant improvements were realized regarding monthly immunization coverage at Mungula HC
IV throughout the five months of project implementation. As reflected in figure 6 below, from
August to November 2014. This success can be attributed to increased frequency of outreaches,
update of linkage of VHT/ICCM and Child health registers, practical implementation of
immunization standard operating procedure (SOPs) during static and outreaches sessions especially
completeness and update of information in the registers.Improved data capture in particular led to
identification of immunization status of many children and defaulters were easily tracked in all the
villages. The identified defaulters were then tracked and immunized accordingly. Figure 6 below
reflects the results of this activity.
Figure 6: Continuous quality improvement achieved (July-Nov 2014) for DPT-Hep B + Hib
3completion at Mungula HCIV, Adjumani District
14
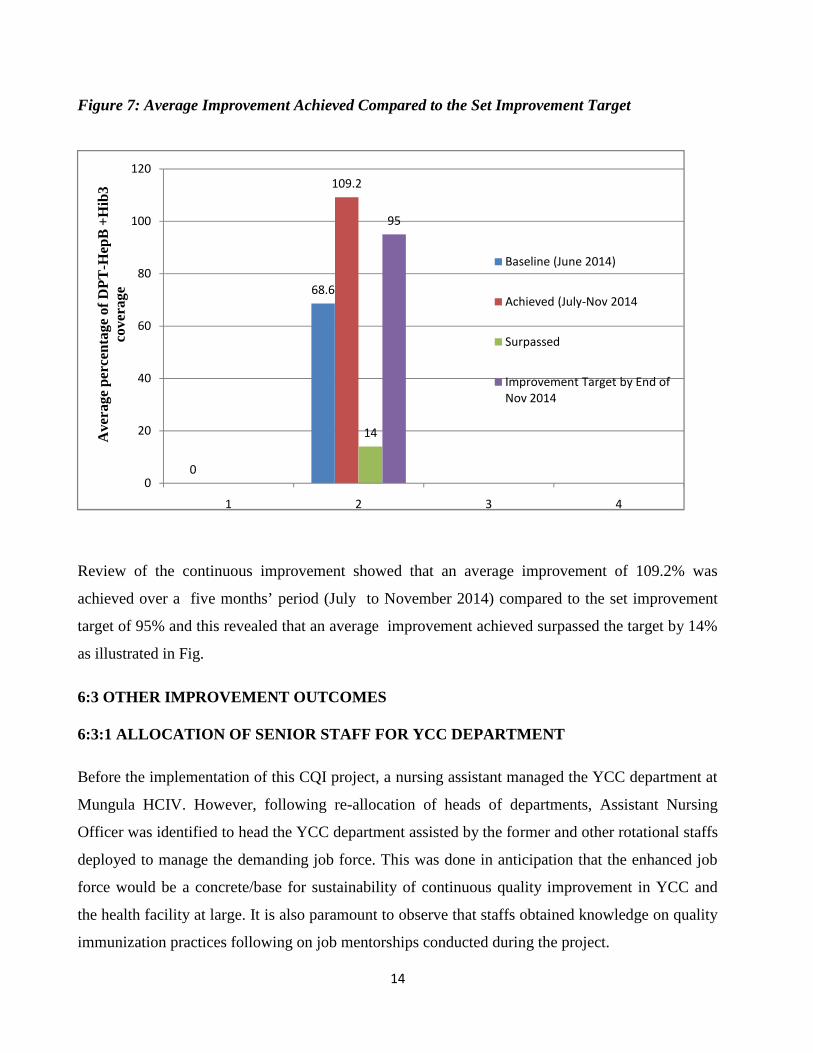
Figure 7: Average Improvement Achieved Compared to the Set Improvement Target
Review of the continuous improvement showed that an average improvement of 109.2% was
achieved over a five months’ period (July to November 2014) compared to the set improvement
target of 95% and this revealed that an average improvement achieved surpassed the target by 14%
as illustrated in Fig.
6:3 OTHER IMPROVEMENT OUTCOMES
6:3:1 ALLOCATION OF SENIOR STAFF FOR YCC DEPARTMENT
Before the implementation of this CQI project, a nursing assistant managed the YCC department at
Mungula HCIV. However, following re-allocation of heads of departments, Assistant Nursing
Officer was identified to head the YCC department assisted by the former and other rotational staffs
deployed to manage the demanding job force. This was done in anticipation that the enhanced job
force would be a concrete/base for sustainability of continuous quality improvement in YCC and
the health facility at large. It is also paramount to observe that staffs obtained knowledge on quality
immunization practices following on job mentorships conducted during the project.
0
68.6
109.2
14
95
0
20
40
60
80
100
120
1 2 3 4
Ave
rage
per
cent
age
of D
PT
-Hep
B +
Hib
3co
vera
ge
Baseline (June 2014)
Achieved (July-Nov 2014
Surpassed
Improvement Target by End ofNov 2014
15
6:3:2 HEALTH SERVICE MONITORING
Prior to the implementation of the CQI project, there was no health facility based performance
monitoring and action plan reviews at Mungula HCIV. Though, there is still inconsistency when it
comes to bi- weekly performance review and action plan meetings, the project implemented this
activity with hope of easily identifying and addressing root causes of problems of low health
services performance against the set targets. It must also be noted that during the implementation of
activities strategies were continuously changed according to bi-weekly reports on immunization
challenges, achievement and action plans.
6:3:3 HEALTH FACILITY - COMMUNITY PARTNERSHIP
Previously, there was poor partnership with the community. During the implementation of these
CQI project activities through sensitization of VHTs/stake holders namely Local Councils and
religious leaders on child immunization a very strong partnership was formed that led to easy
identification of children who were not fully immunized through strengthening utilization and
update of village child registers. Such children were able to complete their immunizations to stay
protected against immunisable killer diseases.
6:3:4 A CASE SCENARIO
At some point in the project partnership improved, complete immunization was attained. A case of
one religious leader who identified a mother with male child of 2 months delivered from home and
never brought for immunization for fear of being criticized. This prompted the health facility to
recognize negative community perception of inappropriate language used by health workers.
16
7:0 LESSONS LEARNED AND CHALLENGES
7:1 LESSON LEARNED
One of main lessons learnt was that community leaders/stakeholders and village health
teams play a fundamental role in realization of increased immunization coverage,
continuous quality improvement provision of basic services in the health care systems. This
was because all became active and motivated towards seeing the health facility attains
widerimmunization coverage as result during the project, wider coverage was reached that
surpasses the projected improvement target by 14.2% from July-November 2014.Such a
support enabled health workers to save time for other duties.
Completeness and update of information in registers at health facility and in the villages
eases tracking and monitoring immunization status of every child <1yr.
7:2 CHALLENGES
Throughout the implementation of the CQI project, there were challenges experienced as reflected
below;
1. It was observed that mobilization of general staff became difficult thus communicating
information to the every staff was difficult especially on outreach practices and performance
progress. This is mainly because management takes long to convey staff meetings.
Consequently not all staffswere involved in continuous quality improvement activities as
required by CQI principles.
2. Challenges related to migration in the community were also observed during follow up of
defaulters, this was noted mainly among refugee camps.
3. During the implementation of this project, some substantial CQI team members showed less
commitment towards the project. This was because most of members in the team were naïve
on CQI principles and health services delivery performance indicators.
17
8:0 CONCLUSIONS, RECOMMENDATIONS AND NEXT STEPS
8:1 CONCLUSIONS
In a period of 5 months (July to Nov 2014) of implementing counter measures for this CQI project,
the average percentage of DPT-Hep B + Hib 3coverage at Mungula HCIV increased from average
68.6% in June 2014 to 109.2% by end of November 2014. Although the 95% target was surpassed,
the average 109.2% improvement achieved within this period demonstrated that regular
immunization outreaches, defaulter follow up, strengthened utilization and update of master village
child register for easy identification of defaulters and establishment every child’s immunization
status in every house hold.
8:2 RECOMMENDATIONS
To standardize and uphold the improvement achieved, the following recommendations are
proposed:
To improve every staff involvement in CQI activities, it is recommended that the health
facility management should address some managerial gaps such lack of routine and
consistent mobilization of general meetings, performance review meetings. Through this
approach, team work can be enhanced.
To sustain quality improvement projects, there should be managerial will to formulate a
very strong CQI team members based on performance and personnel’s commitment not by
seniority or administrative hierarchy.
To expand and reach a bigger multiplier result on acquaintance and skills of CQI concepts,
it is recommended that in prospect Fellowship projects, MakSPH-CDC considers providing
an abridged training to the other team members who work with the main stream Fellow.
This will enable the permanence long after the Fellow stir on.
18
8.3 NEXT STEPS
8.3.1 DISSEMINATION PLAN
The next step in thoughtfulness is to publicize in February 2015 the achievements, deliverable and
outputs attained in this CQI project to MakSPH-CDC that sponsored and synchronized this Program
implementation.
8.3.2 SCALE UP PLAN
Besides Itirikwa sub-county, Mungula HCIV in particular, there some health facilities with low
DPT-Hep B + Hib 3coverage noted in sub-counties of Arinyapi Sub-County (Arinyapi HCIII),
Ukosijoni Sub-County (Ukosijoni HCIII), Pacara Sub-County (Pacara HCIII), and Ofua Sub-
County (Ofua HCIII). As a plan hence, a similar CQI project focusing on improving immunization
coverage will be proposed for implementation at these sub-counties and health center IIIs.
8.3.3 SATELITE TRACKING, MONITORING AND FOLLOW UP OF CHILDREN
It was observed that as common practice, children born at Mungula HCIV coming outside the
facility’s population catchment area were not registered in the health center child register after the
first immunization. Instead they were referred to continue from the nearest health facility of their
origin. Therefore, it is important that Mungula HCIV, the facilities of referral and village leaders
conduct a joint tracking, monitoring and follow up to ensure such children are not lost but rather
complete their immunization. In the future plans, it is planned that monthly systematic inter-facility
data review will be instituted and adhered to by service providers as an path to improve quality of
service delivery.

19
REFERENCES
1. Uganda National Expanded ProgrammeOn Immunization Multiyear Plan 2010 – 2014
2. Immunization Practice In Uganda, A Manual For Operation Level Health Workers, 2nd
Edition ,August-2007
3. WHO/UNICEF Immunization Summary Data, 2012, 2nd Edition 2014
4. http://www.newvision.co.ug/news/650408-uganda-s-immunisation-coverage-improves.html
20
APPENDICES
APPENDIX 1: STAFF ATTENDANCE LIST OF THE CQI ORIENTATION ANDPROBLEM IDENTIFICATION MEETING
Top Related
Copyright © 2022 FDOKUMEN

