






Bahasa
Halaman
Hukum


J
R
IA
JS
a
ARRAA
KEASR
1
terputdrsmap
h1
ARTICLE IN PRESSG ModelSAMS-1126; No. of Pages 7
Journal of Science and Medicine in Sport xxx (2015) xxx–xxx
Contents lists available at ScienceDirect
Journal of Science and Medicine in Sport
journa l h om epage: www.elsev ier .com/ locate / j sams
eview
nfluence of exercise training mode on arterial diameter: systematic review and meta-analysis
ane M. Black ∗, Eric J. Stöhr, Rob Shave, Joseph I. Esformeschool of Sport, Cardiff Metropolitan University, United Kingdom
r t i c l e i n f o
rticle history:eceived 22 October 2014eceived in revised form 3 December 2014ccepted 17 December 2014vailable online xxx
eywords:xercise adaptationrterytructureemodelling
a b s t r a c t
Objectives: To examine whether differences in arterial diameter exist between athletes participating inendurance, resistance or mixed exercise training.Design: A systematic review with meta-analysis.Methods: Random effects meta-analyses of the weighted mean difference in aortic, carotid, brachial andfemoral arterial diameters, height and body mass were conducted on data from 16 peer-reviewed studiesindexed on PubMed, MEDLINE, SCOPUS and Sport Discus. Effect sizes were calculated as the standardiseddifference in means (ı), and used to compare endurance (n = 163), resistance (n = 192), and mixed trainedathletes (n = 360), with controls (n = 440).Results: Compared to controls, endurance athletes displayed the greatest difference in diameter in thebrachial artery (ı = 1.84, 95% CI: 0.59, 3.09, p < 0.01), whereas for mixed athletes, the greatest differencein diameter occurred in the femoral artery (ı = 3.65, 95% CI: 2.21, 5.10, p < 0.01), despite there being nodifferences in height or body mass between these groups. Resistance athletes had a significantly greaterbody mass (p = 0.047) and aortic diameter (ı = 1.81, 95% CI: 1.58, 2.05, p < 0.01) than controls, howeverdifferences in other vessels could not be determined through meta-analysis due to insufficient data.
Conclusions: Our results provide evidence for localised arterial differences, which occur more extensivelyin peripheral vessels (brachial and femoral). Chronically, vascular remodelling may occur as a result ofthe specific haemodynamic conditions within each vessel, which likely differs depending on the modeof exercise. In the future, empirical research is needed to understand the effect of resistance training onchronic vascular remodelling, as this is not well documented.© 2014 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserved.
. Introduction
Chronic vascular remodelling, including changes in arterial wallhickness,1 diameter2 and wall-to-lumen ratio,3 in response toxercise training has been widely debated. Whilst the majority ofesearch supports differences in arterial diameter in athletes com-ared to sedentary or recreationally active controls,1–9 it remainsnclear whether the mode of exercise training (endurance, resis-ance or mixed) plays a role in these differences. This may beue, in part, to the examination of different arteries and the wideange of sports studied. Previously, both blood flow and sheartress patterns have been shown to vary depending on exercise
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
odality,10 and chronic vascular remodelling has been suggesteds a mechanism to reduce exercise-specific shear stress.7 Structuralroperties, such as the distribution of collagen and elastin, differs
∗ Corresponding author.E-mail address: [email protected] (J.M. Black).
ttp://dx.doi.org/10.1016/j.jsams.2014.12.007440-2440/© 2014 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserve
significantly between central and peripheral arteries11 such thatarteries located distally to the heart are stiffer than those locatedmore proximal.12 Therefore it is conceivable that arterial remod-elling in response to chronic exercise training may differ in eachvascular bed; occurring more extensively in peripheral arteries andspecifically in response to the blood flow and shear stress patternsto which each vessel is exposed during exercise.
The current disparity in results makes it difficult to ascertainwhether arterial remodelling occurs regionally in response to aspecific type of exercise stimulus or whether remodelling occursconsistently in all vascular beds. Longitudinal studies that haveexamined arterial diameter following a period of resistance exer-cise training have reported increases in brachial,3,6 carotid andfemoral13 diameter, yet others report no change.3,14 Studies ofendurance athletes have also reported larger carotid and femoral
se training mode on arterial diameter: A systematic review ands.2014.12.007
diameters compared to controls,2,15 and conflict exists in relationto brachial3,16,17 and aortic diameters.2,15 Assimilating all avail-able data, and grouping current studies according to the mode ofexercise, would yield the large sample sizes needed to draw high
d.

ARTICLE IN PRESSG ModelJSAMS-1126; No. of Pages 7
2 J.M. Black et al. / Journal of Science and Medicine in Sport xxx (2015) xxx–xxx
proc
pirafta
2
bcaoetmeris
tptatfeV
Fig. 1. Flow diagram illustrating the literature search
owered statistical conclusions about the existence of differencesn arterial diameter between athletes engaged with endurance,esistance and mixed training. A meta-analysis of such data wouldlso help in evaluating the current state of research, providinguture direction for empirical studies and determining whetherhe mode of exercise training is a potential moderator of arterialdaptation.
. Methods
A literature search for peer-reviewed publications publishedefore June 2013, and examining the arterial adaptations to exer-ise training was conducted using the PubMed, MEDLINE, SCOPUSnd Sport Discus databases. The keywords and phrases used in thenline search were aortic root, artery, arterial, athletes, diameter,xercise, structure, training, and vascular remodelling. In addition tohe online search, reference lists from recently published experi-
ental studies, review papers and meta-analyses were manuallyxamined to locate any other relevant studies not identified as aesult of the online search. If articles were unavailable, or presentednsufficient data, authors were contacted by email and asked toupply relevant information.
To be included in the current meta-analysis, studies had to meethe following criteria: (1) be written in the English-language; (2)resent data for absolute arterial diameter; (3) include male par-icipants only, to prevent any influence of the menstrual cycles a potential confounding variable18; (4) have a mean age of
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
he study cohort between 18 and 40 years to avoid age as a co-actor; (5) recruit homogenous groups of athletes involved in eitherndurance (exercise comprised of a high dynamic component, >70%˙ O2max), resistance (exercise comprised of a high static component,
ess and disposition of articles screened for inclusion.
>50% maximum voluntary contraction), or mixed training (exercisecomprised of both a high dynamic component, >70% V̇O2max and ahigh static component, >50% maximum voluntary contraction) aspreviously defined by Mitchell et al.19; (6) include an age-matcheduntrained control group in the original study, and (7) participantsto have no history of illness or current cardiovascular disease in thestudy groups. Review papers and experimental cohorts of athletesbelonging to different sporting classifications were excluded. Twolongitudinal studies13,14 were excluded from the meta-analysisto prevent incorrect assessments of the variance of the summaryeffect being produced by including a repetitive sample.
One investigator (JB) performed database searches and cross ref-erencing, subsequently removing duplicate studies and screeningabstracts for appropriateness. The search process highlighted 146potential studies which could have been included in the meta-analysis. Based on abstract screening, 84 studies were excluded forfailing to conform to the inclusion criteria. The remaining 62 studieswere independently assessed by two reviewers (JB, JE), with dis-crepancies resolved by consensus. If any studies presented closelyrelated data, the paper published first was selected for inclusionin the meta-analysis. In four cases, data were reported graphicallyand after contacting the authors, raw data were obtained fromone of these four studies20 resulting in exclusion of the remainingthree.5,21,22 The search and filtration processes are illustrated inFig. 1.
A total of 16 studies were entered into the final meta-analysisfor arterial diameter,1,20,23–36 resulting in an overall sample of
se training mode on arterial diameter: A systematic review ands.2014.12.007
1155 men (see Table 1). Participants were categorised into one offour groups, depending on the mode of exercise training under-taken (endurance, resistance, mixed and control). For all 16 studiesincluded in the meta-analysis, the control group were described

Please cite
this
article in
press
as: B
lack JM
, et
al. In
flu
ence
of exercise
trainin
g m
ode
on arterial
diam
eter: A
systematic
review an
dm
eta-analysis.
J Sci
Med
Sport (2015),
http
://dx.d
oi.org/10.1016/j.jsams.2014.12.007
AR
TIC
LE
IN P
RE
SS
G M
odelJSA
MS-1126;
N
o. of
Pages 7
J.M.
Black et
al. /
Journal of
Science and
Medicine
in Sport
xxx (2015)
xxx–xxx
3
Table 1Forest plot of the studies included in the meta-analyses of arterial diameter, grouped by exercise mode and by vessel.
ET, endurance trained (squares); MT, mixed trained (triangles); RT, resistance trained (circles); results of published studies are shown in White; meta-analysis results are shown in black.
IN PRESSG ModelJ
4 nd Medicine in Sport xxx (2015) xxx–xxx
ecwlarnvst
mafmw2
difpawsseactadtmb
mu0ncayv
3
fA8etaasd(mmewire
ARTICLESAMS-1126; No. of Pages 7
J.M. Black et al. / Journal of Science a
ither as sedentary or recreationally active however none of theontrols were participating in more than 3 h of physical activity pereek. Data were subdivided further by anatomical location of four
arge arteries (carotid, brachial, femoral, and aorta), provided thatt least two studies were available for each artery, as previouslyecommended.37 Other parameters, such as intima-media thick-ess, flow-mediated dilation and wall to lumen ratio, and otheressels, including popliteal, subclavian and tibial arteries were con-idered at initial screening but too few papers reported these datao undertake a meaningful analysis.
Data related to the mode of training (endurance, resistance andixed) and the artery under investigation (aorta, brachial, carotid
nd femoral) were coded discretely for each study. Continuous dataor arterial diameter, height and body mass were recorded as group
ean ± SD for each study and transferred into a spreadsheet alongith sample sizes for both the trained and control groups (Excel
010, Microsoft Corporation, Redmond, WA).A random effects meta-analysis model was applied to pooled
iameter data for all athletes. Relative weights, calculated as thenverse of the overall study error, were assigned to the mean changeor each study on the basis of sample size and between partici-ants’ standard error such that studies with a larger sample sizend smaller standard error were assigned more weight than studiesith a smaller sample size and larger standard error. A Q test and I2
tatistic were employed to assess study-to-study heterogeneity. Atatistically significant Q test (p < 0.05) and an I2 statistic >50% werexplored further by subgroup analysis based on mode of trainingnd arterial vessel. Meta-regression for each vessel (aorta, brachial,arotid and femoral) within each exercise group (endurance, resis-ance and mixed) would have allowed for assessment of body sizes a potential covariate of arterial diameter; however, insufficientata prevented meaningful application of this technique. Therefore,o address the issue of body size, a random effects meta-analysis
odel was used to identify any differences in height or body massetween athletes and controls.
Effect sizes were calculated as the standardised difference ineans (ı) and differences between subgroups were examined
sing the 95% CI of each summary mean difference, with alpha set at.05. The presence of publication bias was investigated using a fun-el plot of standard error and standardised difference in means, inonjunction with Egger’s regression intercept test, which provided
quantitative assessment of publication bias.38 All statistical anal-ses were carried out with Comprehensive Meta-analysis softwareersion 2.0 (Biostat, Englewood, NJ).
. Results
Egger’s regression test did not achieve statistical significanceor diameter (p = 0.55), suggesting no presence of publication bias.
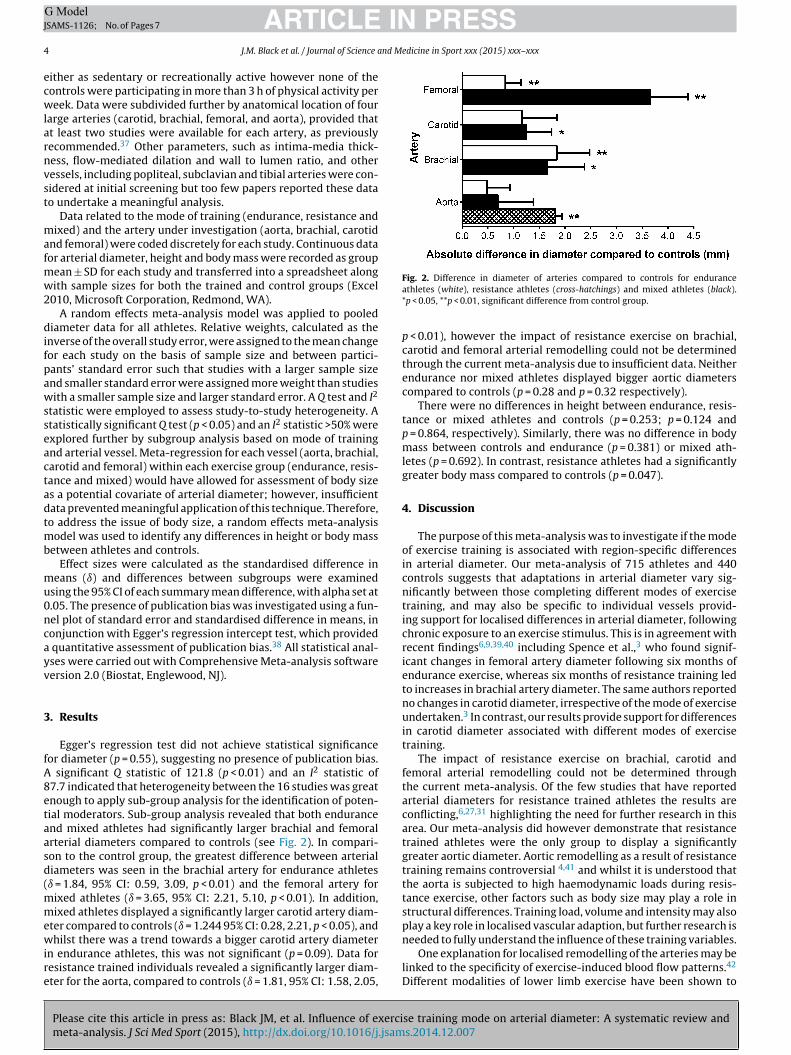
significant Q statistic of 121.8 (p < 0.01) and an I2 statistic of7.7 indicated that heterogeneity between the 16 studies was greatnough to apply sub-group analysis for the identification of poten-ial moderators. Sub-group analysis revealed that both endurancend mixed athletes had significantly larger brachial and femoralrterial diameters compared to controls (see Fig. 2). In compari-on to the control group, the greatest difference between arterialiameters was seen in the brachial artery for endurance athletesı = 1.84, 95% CI: 0.59, 3.09, p < 0.01) and the femoral artery for
ixed athletes (ı = 3.65, 95% CI: 2.21, 5.10, p < 0.01). In addition,ixed athletes displayed a significantly larger carotid artery diam-
ter compared to controls (ı = 1.244 95% CI: 0.28, 2.21, p < 0.05), and
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
hilst there was a trend towards a bigger carotid artery diametern endurance athletes, this was not significant (p = 0.09). Data foresistance trained individuals revealed a significantly larger diam-ter for the aorta, compared to controls (ı = 1.81, 95% CI: 1.58, 2.05,
Fig. 2. Difference in diameter of arteries compared to controls for enduranceathletes (white), resistance athletes (cross-hatchings) and mixed athletes (black).*p < 0.05, **p < 0.01, significant difference from control group.
p < 0.01), however the impact of resistance exercise on brachial,carotid and femoral arterial remodelling could not be determinedthrough the current meta-analysis due to insufficient data. Neitherendurance nor mixed athletes displayed bigger aortic diameterscompared to controls (p = 0.28 and p = 0.32 respectively).
There were no differences in height between endurance, resis-tance or mixed athletes and controls (p = 0.253; p = 0.124 andp = 0.864, respectively). Similarly, there was no difference in bodymass between controls and endurance (p = 0.381) or mixed ath-letes (p = 0.692). In contrast, resistance athletes had a significantlygreater body mass compared to controls (p = 0.047).
4. Discussion
The purpose of this meta-analysis was to investigate if the modeof exercise training is associated with region-specific differencesin arterial diameter. Our meta-analysis of 715 athletes and 440controls suggests that adaptations in arterial diameter vary sig-nificantly between those completing different modes of exercisetraining, and may also be specific to individual vessels provid-ing support for localised differences in arterial diameter, followingchronic exposure to an exercise stimulus. This is in agreement withrecent findings6,9,39,40 including Spence et al.,3 who found signif-icant changes in femoral artery diameter following six months ofendurance exercise, whereas six months of resistance training ledto increases in brachial artery diameter. The same authors reportedno changes in carotid diameter, irrespective of the mode of exerciseundertaken.3 In contrast, our results provide support for differencesin carotid diameter associated with different modes of exercisetraining.
The impact of resistance exercise on brachial, carotid andfemoral arterial remodelling could not be determined throughthe current meta-analysis. Of the few studies that have reportedarterial diameters for resistance trained athletes the results areconflicting,6,27,31 highlighting the need for further research in thisarea. Our meta-analysis did however demonstrate that resistancetrained athletes were the only group to display a significantlygreater aortic diameter. Aortic remodelling as a result of resistancetraining remains controversial 4,41 and whilst it is understood thatthe aorta is subjected to high haemodynamic loads during resis-tance exercise, other factors such as body size may play a role instructural differences. Training load, volume and intensity may alsoplay a key role in localised vascular adaption, but further research is
se training mode on arterial diameter: A systematic review ands.2014.12.007
needed to fully understand the influence of these training variables.One explanation for localised remodelling of the arteries may be
linked to the specificity of exercise-induced blood flow patterns.42
Different modalities of lower limb exercise have been shown to

ING ModelJ
nd M
csswictwair
dtgcmvaifdebbiabitiba
blecrtDaosovtblsnimtap
otddbvldw
ARTICLESAMS-1126; No. of Pages 7
J.M. Black et al. / Journal of Science a
ause variation in brachial artery blood flow responses and sheartress patterns.10 Additionally, during the cardiac cycle blood pres-ure (BP) fluctuates rapidly and produces stretch on the arterialall, which is augmented during exercise.43 Resistance exercise
ncreases shear stress, and is associated with intermittent postontraction increases in blood flow, under a high BP,44 comparedo a continuous increase in blood flow under relatively low BPith endurance exercise.45 These differences in BP patterns may
ffect the stretch produced on the arterial wall resulting in changesn arterial diameter which are specific to the exercise stimuluseceived.
It could also be speculated that localised changes in arterialiameter are augmented by the presence of ischaemic muscle con-ractions, which are believed to occur during continuous forceeneration above 40% MVC.7 Ischaemic contractions cause largehanges in retrograde blood flow with the concomitant develop-ent of muscle tension, and in antegrade flow as the redirected
olume of blood is released during the subsequent muscle relax-tion phase.46 Greater changes in flow pulsatility associated withschaemic muscle contractions may act as a more powerful stimulusor increasing shear stress and the associated release of endothelial-erived nitric oxide,47 causing bigger changes in arterial size. Thusxercise that produces ischaemia in specific vascular beds maye expected to stimulate greater vascular adaptation in thoseeds when compared to the vessels with less ischaemia. Whilst
schaemic muscle contractions occur naturally during force gener-tion at 40% MVC, recently the use of tourniquet cuffs to restrictlood flow during resistance exercise has been used to promote
ncreases in muscle strength and size at much lower intensitieshan conventional strength training.48,49 This may have importantmplications in a clinical or rehabilitation setting, particularly aslood flow restricted resistance exercise at low intensities provides
stimulus sufficient to cause changes in arterial diameter.50
A recent study concluded that significant relationships existetween brachial arterial diameter and measures of whole body,
ean mass and regional mass but not fat mass or height.51 If differ-nces in body size and composition or changes in anthropometricharacteristics occur simultaneously with modifications in arte-ial diameter, allometric scaling techniques have been suggestedo ensure data are comparable within and between populations.51
espite there being insufficient data for successful and meaningfulpplication of meta-regression to assess the influence of body sizen each artery for each mode of exercise training in the presenttudy, we were able to use meta-analysis to identify the presencef any differences in body size between the groups. Height did notary significantly between athletes and controls, which suggestshat, in support of previous research,51 there is no relationshipetween arterial diameter and height. In contrast, resistance ath-
etes did display a significantly larger body mass than controls, andubsequently the larger absolute aortic diameters reported mayot exist if the data were normalised using appropriate scaling
ndices.52 There were no differences in body mass in endurance orixed athletes compared to controls. However, our results did illus-
rate significantly larger brachial and femoral diameters in thesethletes, suggesting that differences in arterial structure are inde-endent of body size.
The relationship between structural and functional adaptationf the artery would suggest that our findings may have implica-ions for some measures of arterial function, such as flow-mediatedilation (FMD), for which the principal determinant is baselineiameter.53 Recent research has illustrated an inverse relationshipetween arterial diameter and FMD.39 Indeed, up to 64% of the
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
ariability in FMD values can be explained by variability in base-ine diameter.54 This meta-analysis has shown variations in arterialiameter depending on the mode of exercise, but insufficient dataere available to investigate the effect of these structural changes
PRESSedicine in Sport xxx (2015) xxx–xxx 5
on FMD. Additionally, it is not known how changes in arterial diam-eter associated with different modes of exercise training mightaffect BP, blood flow or arterial stiffness. Changes in arterial diam-eter appear to improve the efficiency of blood flow but maintainblood flow velocity and shear stress acting on the vessel.5 Reduc-tions in resting BP of 3–4 mmHg have been reported as a result ofchronic exercise,45,55,56 irrespective of the mode, although it is notclear whether these reductions are related to changes in arterialdiameter. Similarly, disparity in previous findings makes it diffi-cult to ascertain whether changes in diameter and arterial stiffnessare interrelated.14,57 A greater understanding of the relationshipbetween changes in diameter, blood pressure, blood flow and arte-rial stiffness, and the interaction with different modes of exercisetraining may help to identify underlying mechanisms responsiblefor arterial remodelling.
Regular exercise has previously been shown to reduce both pri-mary and secondary vascular events.58 The beneficial effects ofexercise on traditional cardiovascular risk factors are thought toaccount for approximately half of the risk reduction associated withexercise and suggestions have been made that direct effects of exer-cise on the vessel wall may account for some of the remainingrisk factor gap.59 Exercise training in older subjects has shownremodelling of conduit arteries, leading to decreased wall thick-ness, and increased lumen diameters, with consequent decreasein wall-to-lumen ratio.59 The results of this meta-analysis providesupport for increased lumen diameters in athletes who have under-taken endurance, resistance or mixed exercise training, and thesedifferences appear to be vessel dependent. It is well known thatperipheral arteries are subject to wall thickening, plaque formationand atherosclerosis.43 Our findings suggest that these peripheralarteries are likely to be the most responsive to exercise training,with the largest femoral vessels observed in athletes engaged inmixed training and the largest brachial vessels in endurance ath-letes. It is possible therefore, that different modes of training couldbe prescribed for different stages of vascular disease, however fur-ther work is required.
This systematic review was limited by the small number of avail-able studies which met our inclusion criteria. Previous studies haveexamined participants with a wide variation in age, however dueto the known influence of age on arterial structure we chose to onlyexamine athletes aged 18–40 years. We therefore acknowledge thatour findings can only be applied to this younger population. Simi-larly, due to a lack of reporting or differentiation in previous studies,we have not examined the potential confounding influence of BPor sex on arterial diameter in athletes. Future studies should reportdata for males and females separately to ensure that the effect ofsex can be assessed, particularly for female athletes where there iscurrently a lack of available data. The search and filtration processwas unblended and limited to English-language studies, which mayintroduce selection bias. It should also be noted that the capacityof Egger’s regression test to detect bias is limited in meta-analysesbased on a low number of small trials; therefore, the results shouldbe interpreted with caution. Similarly not all of the sixteen studiesincluded in the meta-analysis reported on the reliability of theirdata, making it difficult to determine the quality of diameter mea-surements. We acknowledge that different methods of diameterassessment exist, ranging from single point calliper measures toadvanced automated edge detection software and this variabilityin practice may have influenced our findings. Future studies shouldemploy the most valid techniques60 and report the reliability oftheir measurements.
Whilst athletes were grouped using a classification of sports,19 it
se training mode on arterial diameter: A systematic review ands.2014.12.007
is unlikely that training occurs exclusively using the mode of exer-cise in which they compete. However, without detailed informationabout training programmes, it is difficult to establish conclusivelythat the differences presented are related solely to the training

ING ModelJ
6 nd M
mdons
ctcpifrc
5
aao(cEt
A
bo
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
ARTICLESAMS-1126; No. of Pages 7
J.M. Black et al. / Journal of Science a
odality. Therefore, we recommend that future studies provideetails about the level of experience, training intensity and volumef their participants. Finally the use of appropriate scaling tech-iques should be adopted, to remove the possible influence of bodyize and composition.
Research is still needed to systematically document arterialhanges in response to specific training stimuli, especially resis-ance training. The use of appropriate scaling indices should beonsidered when interpreting vascular data and making com-arisons within and between different populations. Finally the
nteraction between cardiac and vascular adaptation is a key areaor future research and may help to identify the mechanismsesponsible for the structural arterial changes associated with exer-ise.
. Conclusion
Our analysis supports that differences in arterial diameterre related to the specific mode of exercise training. Addition-lly localised differences in arterial diameter exist for each modef exercise, which appear to be greater in peripheral vesselsbrachial and femoral). This may be associated with the spe-ific haemodynamic conditions within each vessel during exercise.mpirical research investigating arterial remodelling in responseo resistance exercise is lacking and requires further investigation.
cknowledgements
There is no funding, financial support or technical assistance toe declared in relation to this study and the authors have no conflictf interest to report.
eferences
1. Abergel E, Linhart A, Chatellier G et al. Vascular and cardiac remodeling in worldclass professional cyclists. Am Heart J 1998; 136(5):818–823.
2. Huonker M, Schmid A, Schmidt-Trucksass A et al. Size and blood flow of centraland peripheral arteries in highly trained able-bodied and disabled athletes. JAppl Physiol 2003; 95(2):685–691.
3. Spence AL, Carter HH, Naylor LH et al. A prospective randomized longitudinalstudy involving 6 months of endurance or resistance exercise. Conduit arteryadaptation in humans. J Physiol 2013; 591(5):1265–1275.
4. Iskandar A, Thompson PD. A meta-analysis of aortic root size in elite athletes.Circulation 2013; 127(7):791–798.
5. Miyachi M, Iemitsu M, Okutsu M et al. Effects of endurance training on the sizeand blood flow of the arterial conductance vessels in humans. Acta Physiol Scand1998; 163(1):13–16.
6. Rakobowchuk M, McGowan CL, de Groot PC et al. Endothelial function of younghealthy males following whole body resistance training. J Appl Physiol 2005;98(6):2185–2190.
7. Zoeller RF, Angelopoulos TJ, Thompson BC et al. Vascular remodeling in responseto 12 wk of upper arm unilateral resistance training. Med Sci Sports Exerc 2009;41(11):2003–2008.
8. Welsch M, Blalock P, Credeur D et al. Comparison of brachial artery vasore-activity in elite power athletes and age-matched controls. PLOS ONE 2013;8(1):e54718.
9. Dinenno FA, Tanaka H, Monahan KD et al. Regular endurance exercise inducesexpansive arterial remodelling in the trained limbs of healthy men. J Physiol2001; 534(1):287–295.
0. Thijssen DH, Dawson EA, Black MA et al. Brachial artery blood flow responsesto different modalities of lower limb exercise. Med Sci Sports Exerc 2009;41(5):1072–1079.
1. Fischer G, Llaurado J. Collagen and elastin content in canine arteries selectedfrom functionally different vascular beds. Circ Res 1966; 19(2):394–399.
2. McVeigh G, Bank A, Cohn J. Arterial compliance, Chapter 85, in CardiovascularMedicine, 2nd ed. Philadelphia, Churchill Livingstone, 2000.
3. Stebbings G, Morse C, McMahon G et al. Resting arterial diameter and blood flowchanges with resistance training and detraining in healthy young individuals. JAthl Train 2013; 48(2):209–219.
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
4. Miyachi M, Kawano H, Sugawara J et al. Unfavourable effects of resistance train-ing on central arterial compliance. A randomized intervention study. Circulation2004; 110:2858–2863.
5. Zeppilli P, Vannicelli R, Santini C et al. Echocardiographic size of conductancevessels in athletes and sedentary people. Int J Sports Med 1995; 16(1):38–44.
4
4
PRESSedicine in Sport xxx (2015) xxx–xxx
6. Tinken T, Thijssen D, Black M et al. Time course of change in vasodilator func-tion and capacity in response to exercise training in humans. J Physiol 2008;586(20):5003–5012.
7. Libonati J. Aerobic run training improves brachial artery flow-mediated dilation.J Strength Cond Res 2007; 21(4):1291–1295.
8. Williams MR, Westerman RA, Kingwell BA et al. Variations in endothelial func-tion and arterial compliance during the menstrual cycle. J Clin Endocrinol Metab2001; 86(11):5389–5395.
9. Mitchell JH, Haskell W, Snell P et al. Task Force 8: classification of sports. J AmColl Cardiol 2005; 45(8):1364–1367.
0. Rognmo O, Bjornstad TH, Kahrs C et al. Endothelial function in highly endurance-trained men: effects of acute exercise. J Strength Cond Res 2008; 22(2):535–542.
1. Moreau KL, Silver AE, Dinenno FA et al. Habitual aerobic exercise is associatedwith smaller femoral artery intima-media thickness with age in healthy menand women. Eur J Cardiovasc Prev Rehabil 2006; 13(5):805–811.
2. Tanaka H, Seals DR, Monahan KD et al. Regular aerobic exercise and the age-related increase in carotid artery intima-media thickness in healthy men. J ApplPhysiol 2002; 92(4):1458–1464.
3. Babaee Bigi MA, Aslani A. Aortic root size and prevalence of aortic regurgitationin elite strength trained athletes. Am J Cardiol 2007; 100(3):528–530.
4. Carlsson L, Lind B, Laaksonen MS et al. Enhanced systolic myocardial functionin elite endurance athletes during combined arm-and-leg exercise. Eur J ApplPhysiol 2011; 111(6):905–913.
5. Dzudie A, Menanga A, Hamadou B et al. Ultrasonographic study of left ventricularfunction at rest in a group of highly trained black African handball players. EurJ Echocardiogr 2007; 8(2):122–127.
6. Florescu M, Stoicescu C, Magda S et al. Supranormal cardiac function in ath-letes related to better arterial and endothelial function. Echocardiography 2010;27(6):659–667.
7. Karagounis P, Maridaki M, Papaharalampous X et al. Exercise-induced arterialadaptations in elite judo athletes. J Sports Sci Med 2009; 8:428–434.
8. Kool MJ, Struijker-Boudier HA, Wijnen JA et al. Effects of diurnal variabilityand exercise training on properties of large arteries. J Hypertens Suppl 1992;10(6):S49–S52.
9. Naylor LH, O’Driscoll G, Fitzsimons M et al. Effects of training resumption onconduit arterial diameter in elite rowers. Med Sci Sports Exerc 2006; 38(1):86–92.
0. Rowley NJ, Dawson EA, Birk GK et al. Exercise and arterial adaptation inhumans: uncoupling localized and systemic effects. J Appl Physiol 2011;110(5):1190–1195.
1. Schmidt-Trucksass A, Schmid A, Dorr B et al. The relationship of left ventri-cular to femoral artery structure in male athletes. Med Sci Sports Exerc 2003;35(2):214–219.
2. Spataro A, Pelliccia A, Caselli G et al. Echocardiographic standards in top-classathletes: a morphological study. J Sports Cardiol 1985; 2:17–27.
3. Walther G, Nottin S, Karpoff L et al. Flow-mediated dilation and exercise-inducedhyperaemia in highly trained athletes: comparison of the upper and lower limbvasculature. Acta Physiol (Oxf) 2008; 193(2):139–150.
4. Weiling W, Borghols E, Hollander A et al. Echocardiographic dimensionsand maximal oxygen uptake in oarsmen during training. Br Heart J 1981;46(2):190–195.
5. Wijnen JA, Kuipers H, Kool MJ et al. Vessel wall properties of large arteries intrained and sedentary subjects. Basic Res Cardiol 1991; 86(Suppl 1):25–29.
6. Wimer G, Baldi J. Limb-specific training affects exercise hyperemia but not sym-pathetic vasoconstriction. Eur J Appl Physiol 2012; 112:3819–3828.
7. Valentine J. How many studies do you need? A primer on statistical power formeta-analysis. J Educ Behav Stat 2010; 35(2):215–247.
8. Egger M, Davey Smith G, Schneider M et al. Bias in meta-analysis detected by asimple, graphical test. Br Med J 1997; 315(7109):629–634.
9. Green DJ, Rowley N, Spence A et al. Why isn’t flow-mediated dilation enhancedin athletes? Med Sci Sports Exerc 2013; 45(1):75–82.
0. Rowley NJ, Dawson EA, Hopman MT et al. Conduit diameter and wall remodellingin elite athletes and spinal cord injury. Med Sci Sports Exerc 2012; 44(5):844–849.
1. D’Andrea A, Cocchia R, Riegler L et al. Aortic root dimensions in elite athletes.Am J Cardiol 2010; 105:1629–1634.
2. Green DJ, Bilsborough W, Naylor LH et al. Comparison of forearm blood flowresponses to incremental handgrip and cycle ergometer exercise: relative con-tribution of nitric oxide. J Physiol 2005; 562(2):617–628.
3. Thijssen D, Cable T, Green D. Impact of exercise training on arterial wall thicknessin humans. Clin Sci (Lond) 2012; 122(7):311–322.
4. Gotshall R, Gootman J, Byrnes W et al. Noninvasive characterization of theblood pressure response to the double-leg press exercise. J Exerc Physiol 1999;2(4):1–6.
5. Smith D, Fernhall B. Advanced Cardiovascular Exercise Physiology, Illinois, HumanKinetics, 2011.
6. Gonzales JU, Thompson BC, Thistlethwaite JR et al. Role of retrograde flow in theshear stimulus associated with exercise blood flow. Clin Physiol Funct Imaging2008; 28(5):318–325.
7. Green DJ, Maiorana A, O’Driscoll G et al. Effect of exercise training onendothelium-derived nitric oxide function in humans. J Physiol 2004; 561(1):1–25.
se training mode on arterial diameter: A systematic review ands.2014.12.007
8. Wernbom M, Augustsson J, Raastad T. Ischemic strength training: a low-load alternative to heavy resistance exercise? Scand J Med Sci Sports 2008;4(18):1–416.
9. Laurentino G, Ugrinowitsch C, Aihara A et al. Effects of strength training andvascular occlusion. Int J Sports Med 2008; 29(8):664–667.

ING ModelJ
nd M
5
5
5
5
5
5
5
5
5
ARTICLESAMS-1126; No. of Pages 7
J.M. Black et al. / Journal of Science a
0. Hunt J, Walton L, Ferguson R. Brachial artery modifications to blood flow-restricted handgrip training and detraining. J Appl Physiol 2012; 112(6):956–961.
1. Hopkins N, Green D, Tinken T et al. Does conduit artery diameter vary accordingto the anthropometric characteristics of children or men? Am J Physiol Heart CircPhysiol 2009; 297(6):H2182–H2187.
2. Utomi V, Oxborough D, Whyte GP et al. Systematic review and meta-analysis oftraining mode, imaging modality and body size influences on the morphologyand function of the male athlete’s heart. Heart 2013; 99(23):1727–1733.
Please cite this article in press as: Black JM, et al. Influence of exercimeta-analysis. J Sci Med Sport (2015), http://dx.doi.org/10.1016/j.jsam
3. Celermajer DS, Sorensen KE, Gooch VM et al. Non-invasive detection of endothe-lial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992;340(8828):1111–1115.
4. Atkinson G, Batterham AM. Allometric scaling of diameter change in the originalflow-mediated dilation protocol. Atherosclerosis 2013; 226(2):425–427.
5
6
PRESSedicine in Sport xxx (2015) xxx–xxx 7
5. Fagard R. Exercise is good for your blood pressure: effects of endurance trainingand resistance training. Clin Exp Pharmacol Physiol 2006; 33(9):853–856.
6. Kelley G, Kelley K. Progressive resistance exercise and resting blood pressure. Ameta-analysis of randomized controlled trials. Hypertension 2000; 35:838–843.
7. Sugawara J, Hayashi K, Yokoi T et al. Age-associated elongation of the ascendingaorta in adults. J Am Coll Cardiol Img 2008; 1(6):739–748.
8. Thijssen D, Maiorana A, O’Driscoll G et al. Impact of inactivity and exercise onthe vasculature in humans. Eur J Appl Physiol 2010; 108(5):845–875.
se training mode on arterial diameter: A systematic review ands.2014.12.007
9. Green D, Spence A, Halliwell J et al. Exercise and vascular adaptation in asymp-tomatic humans. Exp Physiol 2010; 96(2):57–70.
0. Woodman R, Playford D, Watts F et al. Improved analysis of brachial arteryultrasound using a novel edge-detection software system. J Appl Physiol 2001;91(2):929–937.
Top Related
Copyright © 2022 FDOKUMEN

