






Bahasa
Halaman
Hukum


A
OoDsaSSMttRoidfCht©
K
I
ftisitrds
0d
Physiotherapy 97 (2011) 47–54
Impact of using the ICF framework as an assessment tool for students inpaediatric physiotherapy: a preliminary study
Jennifer Jelsma, Des Scott ∗Department of Health and Rehabilitation Sciences, Faculty of Health Sciences, University of Cape Town, Observatory 7925, Cape Town, South Africa
bstract
bjective To determine if clinical assessment of children with neurological conditions by physiotherapy students was improved through thevert use of the International Classification of Functioning, Disability and Health (ICF).esign and participants A retrospective, pragmatic audit of practice using written patient assessments completed by third-year physiotherapy
tudents. Assessments completed by third-year students in 2008 were compared with assessments completed by third-year students in 2009. Thessessment format used in 2008 was very loosely based on the ICF model, while the 2009 assessments made rigorous use of the ICF approach.etting Two schools for children with special needs to which physiotherapy students from the Department of Health and Rehabilitationciences, Faculty of Health Sciences, Division of Physiotherapy, University of Cape Town are sent for clinical exposure.ethod A score sheet was drawn up to evaluate specific criteria in each assessment, using a five-point marking scheme. The mark sheet was
ested for reliability. All assessments were evaluated independently using the score sheet by two external physiotherapists who were blindo the purpose of the exercise.esults There was a significant difference between the scores obtained on the score sheet for the 2008 group and the 2009 group. The 2009 groupbtained a median score of 60, compared with a median score of 50 for the 2008 group (median difference between groups 9.2, 95% confidencenterval 4.2 to 14.1). The overall impression mark given to the 2009 group was also higher than that given to the 2008 group, with a medianifference between the groups of 5.9 (95% confidence interval 3.2 to 12.7). It would appear that the 2009 students, using the ICF frameworkor assessing patients, were able to include more function-related information in their assessments, resulting in a more holistic assessment.
onclusion Teaching students to use the ICF framework when assessing paediatric patients encourages clinical reasoning and an improvedolistic approach to identifying the patient’s problems in context. This, in turn, enables the student to plan a more appropriate interventionreatment, to the patient’s benefit.2010 Chartered Society of Physiotherapy. Published by Elsevier Ltd. All rights reserved.
kio[
kast
eywords: ICF; Physiotherapy; Education; Clinical assessment
ntroduction
The training of health professionals is complex as dif-erent cognitive and handling skills need to be taught andhen applied in a clinical context. This clinical reason-ng is one of the most difficult skills that a physiotherapytudent has to learn [1], and there are several theories regard-ng the methods utilised by physiotherapists [2]. In theraining of physiotherapy students, various different clinical
easoning strategies are used. These include hypothetico-eductive reasoning [3], which arises from a cognitivecience perspective and focuses on the accessibility of stored∗ Corresponding author. Tel.: +27 21 4066401; fax: +27 21 4066323.E-mail address: [email protected] (D. Scott).
pitpbp
031-9406/$ – see front matter © 2010 Chartered Society of Physiotherapy. Publisoi:10.1016/j.physio.2010.09.004
nowledge in the student’s memory; and narrative reason-ng, which is used to understand the patient’s experiencesf their disability and their needs, as explained by them3].
In order to meet the needs of a patient, the student needs tonow what the needs of the patient are, analyse these needsnd the problems that are causing them, choose and applyuitable techniques, and assess whether or not the interven-ion has been effective [4]. Several models of the clinicalrocess have been developed, but the most common models a cyclical model in which assessment leads to appropriate
reatment which then leads to changes in the condition of theatient [5]. These changes need to be assessed and the cycleegins once more. An example of this ‘rehab cycle’ has beenresented by various authors [6,7].hed by Elsevier Ltd. All rights reserved.

4 ysiothe
tbhgoiatr
dowTdaioadphioa
fu[iaaitapos[
oatioactuscacap
wigpcei
atuascTrO
ameepctlTic[‘stAvoac
R
ctrwdwpcea
8 J. Jelsma, D. Scott / Ph
The problem lies in the amount of information that needso be gathered. Some of it is not important and some ends upeing essential. The inexperienced clinician needs to learnow to gather all relevant data, but not to waste time byathering information that has no bearing on the planningf the patient’s management [8]. This is particularly difficultn paediatrics in which the health condition, impairments andctivity limitations are mediated by the developmental stagehat the child is undergoing and the associated alteration inelevant environmental factors [9].
A useful framework to manage the information gaineduring patient assessment is the International Classificationf Functioning, Disability and Health (ICF) [10]. The ICFas published in 2001 by the World Health Organization.he purpose of the ICF is to ‘provide a unified and stan-ard language and framework for the description of healthnd health-related states’. It defines health in terms of var-ous health-related domains. These domains include areasf physiological function and anatomical structures, as wells actions, tasks and involvement in social situations. Theomains are described from bodily, individual and societalerspectives within a given context [10]. The ICF definesealth in terms of health domains of well-being (e.g. walk-ng, self-care abilities, communication) and other domainsf well-being (e.g. ability to learn, participation in socialctivities) [10].
The ICF can be used to describe all aspects of a patient’sunctioning, disability and health. This information can besed to ensure a holistic approach to managing the patient4]. The ICF is divided into two main categories: function-ng and disability, and contextual factors. Under functioningnd disability, there are body functions and structure, whichre organised according to body system and include changesn the physiological and anatomical structures. Also inhis category are activities and participation, both fromn individual and societal perspective. These are inter-reted by capacity and performance. The second categoryf the ICF classification includes environmental and per-onal factors. These can either facilitate or hinder functioning10].
As the education of physiotherapists is increasingly basedn the biopsychosocial approach to disability and man-gement of health conditions, the ICF model can providehe conceptual linkages between management of disabil-ty (activity limitations and participation restrictions) andther basic, cognitive sciences taught in the curriculum asnatomical sciences (impairments), clinical sciences (healthonditions), psychology (personal factors) and environmen-al sciences (socio-economic factors) [4]. Similarly, it can besed in conjunction with the rehab cycle as a clinical rea-oning tool to guide students in bridging the gap betweenognitive knowledge and interaction in the clinical setting,
s the ICF approach is an interaction between the healthondition and contextual factors [3], and to plan holistic man-gement [7]. The advantage of teaching students to assessatients using the ICF approach is that it provides the studentaocA
rapy 97 (2011) 47–54
ith a conceptual framework which guides their question-ng of a patient, assists them in organising the informationained from both subjective and objective assessments, andrompts them to integrate the information into the variousomponents of the ICF [4]. In this way, clinical reasoning isnhanced to provide a full and complete picture of the patientn his/her own context [3].
This approach is also useful in generating outcome-basedssessments which focus the student’s treatment interven-ions on improving function [11]. Palisano presented a veryseful application of the ICF to the multidisciplinary man-gement and treatment planning of children [12]. The processuggested entails the identification of all problems that thehild experiences under the different components of the ICF.he next step is to use the ICF framework to map out the inter-
elationships and causal chains between these components.n this basis, treatment can be planned and monitored.Similar challenges in educating physiotherapy students
re highlighted in an article which investigates the align-ent of a South African physiotherapy curriculum and the
xpectations of the healthcare system [13]. Two main themesmerged: relating physiotherapy theory to practice, and inter-ersonal relationships around different cultural practices andaring. The author suggests that encouraging students to usehe ICF approach might assist in overcoming these chal-enges as it is a valuable tool in linking theory to practice.he ICF also has 11 ethical provisions which can be divided
nto three main categories: respect and confidentiality, clini-al use of ICF information and social use of ICF information14]. Under social use, ICF information can be used todevelop social policy and political change to enhance andupport the participation of individuals’ [14] as is neededo meet the healthcare expectations of post-apartheid Southfrica. The ICF encourages users to determine an indi-idual’s interpersonal, organisational and societal spheresf living [14]. With this understanding, people with a dis-bility can be rehabilitated back into their own societalulture.
esearch setting and description of intervention
In the third year of study, physiotherapy students attendlinical practice at sites which include special schools. Thehird-year students whose assessments were evaluated for thisesearch were at two different primary schools for childrenith special needs. One school caters specifically for chil-ren with cerebral palsy, and the other school is for childrenith congenital abnormalities, muscular dystrophy and otherhysical conditions. The students are supervised by the samelinical educator who spends one morning per week withach group of students. The students are required to assessnd treat the children assigned to them, and to write up a full
ssessment including treatment planning and functional goalsf intervention. This written assessment is handed in to thelinical educator each week for marking and further input.t the end of each clinical block, the student is awarded a
ysiothe
ca
vfppftacoisifstnihwppi
stIifitddaaiBtlcswdfiIaf
pa
aopu
M
TpcwaTft
I
sdimttwstOiaiit5iswaea1y(Ttsl0
P
aat
J. Jelsma, D. Scott / Ph
linical mark based on his/her performance on the block andclinical examination.
Prior to 2008, the Division of Physiotherapy at the Uni-ersity of Cape Town subscribed rather loosely to the ICFramework as an underlying philosophical approach to under-in the assessment and intervention planning of paediatricatients. These students were given lectures on the ICFramework and an assignment in their second year in whichhey were required to apply the ICF analysis of disabilitynd functioning to a paper patient, a case of a child witherebral palsy. The article by Palisano [12] on applicationf the ICF to the collaborative model of decision makingn children with movement disorders was referenced. Thetudents from this cohort, who were in the paediatric clin-cs in 2008, were not actively encouraged to use the ICFramework, and objective assessment of function was nottrongly linked to participation limitations. The emphasis ofhe assessments was mainly on impairments, with little oro focus on participation. The child’s input was also min-mal and mainly focused on activities of daily living andome environment. A functional problem list was drawn up,ith underlying reasons (impairments) being given for eachroblem. No actual links were made between the functionalroblems and any other aspect of the assessment, except formpairments.
In 2008, lectures were given on the ICF to the newecond-year students, but the approach to assessment in theheoretical lectures was structured along the lines of theCF model. Students were given case studies and asked todentify which aspects of the child described could be classi-ed under each ICF component. They were then required
o analyse the causal and association links between theomains. The following year, in 2009, this group of stu-ents was required to overtly include the ICF frameworks a basis for assessing and decision making in the clinic,nd the clinical educator reinforced the use of the modeln clinical tutorials. The assessment form (see Appendix) was restructured to include sections on health condi-
ion, body functions and structures, activities, participationimitations, and environmental and personal factors. Oncelinical data had been gathered under these components, thetudents were required to insert each problem into the frame-ork and analyse inter-relationships and causal chains byrawing arrows between related components. At this point,nal priority problem setting and goal setting was done.n order to achieve this, the students had to make use ofll the information gained about the child’s disability andunctioning.
The aim of this study was to compare the quality and com-rehensiveness of the written assessments submitted beforend after introduction of the new assessment format.
The expected outcome was that the students using the ICF
pproach to assessment would have a more holistic picturef the child’s participation limitations, and would be able tolan a more appropriate intervention plan than the studentssing the previous form of assessment.pttt
rapy 97 (2011) 47–54 49
ethods
A retrospective, pragmatic audit of practice was instituted.he sample consisted of the written assessments of third-yearhysiotherapy students produced during their paediatric clini-al rotation in 2008 and 2009. In December 2008, the studentsho had been in the paediatric placements that year were
sked to submit their assessments for review (2008 cohort).he assessments of the 2009 student cohort were collected
rom January to June 2009 during the students’ last week athe clinical placement.
nstrumentation
A form was developed to score the quality and scope of thetudents’ assessments and to gather basic information aboutiagnosis of the children. The information included in thenitial rating form reflected the learning outcomes of assess-
ent for the paediatric clinical block, and included gradinghe quality of the information that the student presented inheir assessment (see Appendix A). The emphasis was not onhether the ICF had been applied, but rather on whether the
tudent had approached the assessment holistically and iden-ified the full range of problems that the children experienced.ne of the investigators was the clinical educator and was
n contact with all the children assessed, and therefore wasware of the problems experienced by them. Once the list oftems had been compiled, a five-point marking scheme (1 = nonformation, 2 = some information, 3 = adequate informa-ion but lacks detail, 4 = complete and detailed information,= outstanding) was applied. In addition to scoring individual
tems, the assessors were required to give an overall impres-ion percentage of the assessment. The 23 assessments usedere shuffled to achieve a random order before being evalu-
ted. The researchers filled out three of the forms together tostablish the scoring criteria. Subsequently, to ensure the reli-bility of application of criteria for mark allocation, a further0 forms were assessed separately and the results were anal-sed using a two-way random model. Intra-class correlationICC) for absolute agreement for single measures was used.he correlation of the component items was also assessed. As
wo items in the initial criteria (identification of appropriatehort- and long-term goals, problem list prioritisation) hadow correlation, these were excluded; the overall ICC was.93 (95% confidence interval 0.76 to 0.98; P < 0.001).
rocedure
All patient names, student names, dates of assessmentsnd feedback comments were removed from the assessmentsnd recorded elsewhere. The assessments were then given towo independent assessors, both of whom were physiothera-
ists with postgraduate degrees who had been involved in theeaching of undergraduate students and who were experts inhe field of paediatrics. They were asked to use the score sheeto grade the assessments, and to award an overall impression
5 ysiotherapy 97 (2011) 47–54
paw
D
wttss2apMSaiwiloatdt
R
radpgdga
(d(ttct
bTsam
t
Table 1Conditions treated.
Year 2008 2009 Both groups
Hemiplegic cerebral palsy 2 2 4Quadriplegic cerebral palsy 3 0 3Diplegic cerebral palsy 1 2 3Spina bifida 2 1 3Muscular dystrophy 3 3 6Triplegic cerebral palsy 1 1 2Paraplegia 0 2 2
Total 12 11 23
20092008Year
30
40
50
60
70
80
90
Tot
al %
Median 25%-75% Min-Max
Fm
wpb(smf9
D
uhealth states, rehabilitation and outcome evaluation’ [7]. Thisaudit has demonstrated the utility of the ICF framework, inthat physiotherapy students who overtly used the framework
Table 2Comparison of the clinical performance marks of the two student groups,excluding marks obtained on the paediatric block.
Cohort Valid n Median % Minimum % Maximum %
2008 12 69 61 73
0 J. Jelsma, D. Scott / Ph
ercentage mark. They were blinded to the students’ groupsnd were not informed of the purpose of the study. The ICFas not mentioned at any stage.
ata analysis
The data sets were small and non-parametric statisticsere used throughout. Descriptive statistics were used
o describe the frequencies. Chi-squared test was used toest if the two groups had had equal exposure to the twochools, because each student would only have attended onechool. As there was a concern that only the more competent008 students might have submitted their assessments, theverage clinical marks were compared, which includedlacements other than the paediatric placement, using theann–Whitney U-test. To test for internal validity, the
pearman’s correlation coefficient between the externalssessors’ score based on the score sheet and their overallmpression was calculated. In addition, Cronbach’s alphaas used to determine how well the set of items included
n the questionnaire measured a single unidimensionalatent construct, which was hypothesised to be qualityf assessment. A high Cronbach’s alpha would allow forddition of the scores on the different items as they measurehe same construct. The Mann–Whitney U-test was used toetermine if there was a difference in the rank ordering of theotal score and the impression mark awarded to each student.
esults
Of the 2008 cohort, 12 students (out of a possible 23)esponded and submitted a total of 16 assessments. Onessessment per student was chosen at random. The other stu-ents in that cohort had not kept their assessments from therevious year, limiting the number. As the assessments wereathered after one semester from the 2009 cohort, only 15 stu-ents had attended these schools, and 11 assessments wereathered. For administrative reasons, assessments were notvailable for the remaining four students.
There was no difference in the proportion of each cohortapproximately 50%) attending the two different clinical sitesuring the paediatric placement between 2008 and 2009χ2 = 0.381, df = 1, P = 0.537). The conditions which werereated by the students are listed in Table 1. In general, the dis-ribution was similar, although the 2008 group treated morehildren with quadriplegic cerebral palsy and the 2009 groupreated more children with paraplegia.
There was no difference in the rank ordering of the clinicallock performance of the two groups of students (Table 2).he characteristics of the students in the two years wereimilar regarding block performance, which takes clinical
dministration, application to work, communication, patientanagement and clinical competencies into account.There was a significant difference between the cohorts inhe scores obtained on the score sheet (U = 18.50, P = 0.006),
2
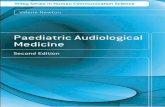
ig. 1. Overall scores given by the two assessors using the score sheet:edian and quartiles of the mean (2008 n = 11, 2009 n = 12).
ith a median score of 50.5 for the 2008 students com-ared with 58 for the 2009 students (median differenceetween groups 9.2, 95% confidence interval 4.2 to 14.1)Figs. 1 and 2). Similarly, the difference in the overall impres-ion marks was significant (U = 27.50, P = 0.032), with aedian score of 58 for the 2008 students compared with 62.5
or the 2009 students (median difference between groups 5.9,5% confidence interval 3.2 to 12.7).
iscussion
Within the clinical context, the ICF was ‘intended forse in needs assessment, matching interventions to specific
009 11 67 62 79
Rank sum 2008 Rank sum 2009 U Z
153 123 57 −0.55

J. Jelsma, D. Scott / Physiothe
20092008Year
40
45
50
55
60
65
70
75
80
85
90
Impr
essi
on %
Median 25%-75% Min-Max
Fo
tdabtirglcpittwtaaastta
alads2
mchdswom
mmdh
otbat
C
afilaaprcbtttc
A
t
EU
C
F
A
N
YDI••••••••• Treatment plan/intervention: addresses all aspects of child’s functional needs
ig. 2. Impression scores given by the two assessors: median and quartilesf the mean (2008 n = 11, 2009 n = 12).
o gather information, analyse and plan interventions pro-uced assessments of a higher quality than students who onlypplied the ICF concepts loosely. The second cohort wereetter able to recognise the relationships that exist betweenhe different components of the ICF and, in particular, thenteraction between activity limitations and participationestrictions as a result of the patient’s social situation, as sug-ested by Homa and Peterson [4]. Encouraging students toink theory to practice by communicating their thought pro-esses while assessing and planning the management of eachatient promotes clinical reasoning. Using clinical reason-ng to determine how to make these daily activities easierhrough therapy, how to change the environment to facilitatehe child’s performance, and being aware of personal factorshich might impede or enhance this performance improved
he students’ management of the patients. In addition tochieving higher scores on the score sheet, the 2009 cohortlso performed better than the 2008 cohort in terms of over-ll impression. This implies that use of the ICF did not resultimply in the inclusion of more relevant ICF data regardinghe child’s participation in age-appropriate activities, but thathe assessments were more comprehensive overall and betterble to identify the extent of the children’s problems.
This study was a pragmatic, retrospective audit of practice,nd cannot be regarded as having proved a definitive causalink between the change in approach to clinical assessmentnd the quality of student assessments. In addition, such aesign lends itself to bias in several ways. However, all theources of bias described below would have favoured the008 cohort but, in fact, the 2009 cohort performed better.
Not all the 2008 students complied with the request to sub-it their assessments, which might have resulted in the more
onscientious students complying and their assessments mayave been of a higher standard. However, as there was noifference in the clinical marks (over several assessments,
ettings and clinical educators) between the two cohorts, itould appear that the two groups were equivalent in termsf their clinical abilities. In addition, the inclusion of assess-ents from the second semester of study in the 2008 cohort•TIO
rapy 97 (2011) 47–54 51
ight have biased the results as the students would have hadore exposure to clinical work in this group. However, this
id not seem to influence the results, as the 2009 cohort whoad only completed their first semester performed better.
The impact of didactic teaching in the absence of overt usef the ICF in the clinic was minimal. The need to strengthenhe links between theory and clinical practice is clear and haseen identified by other authors [1]. Clinical reasoning onlyppears to occur once the student has applied the frameworko assessment in a real situation.
onclusion
The ICF is a useful framework within which students canssess paediatric patients. With rigorous application of thisormat, students were able to assess the children holistically,dentifying the extent of functional problems and activityimitations in the related setting. The ICF framework encour-ged the students to form links between activity limitationsnd participation restrictions, and to analyse the children’sroblems against a full contextual background, taking envi-onment and personal factors into account, thus enhancinglinical reasoning. Once this has been achieved, students areetter able to plan appropriate and holistic treatment interven-ions. This will ultimately improve the quality of students’reatment interventions for children. Based on the results ofhis audit, the ICF appears to be useful as a framework forlinical assessment and treatment planning.
cknowledgements
The contribution of Pam Versfeld and Mariette Burger tohe study as external assessors is gratefully acknowledged.
thical approval: Medical Research Ethics Committee of theniversity of Cape Town (Ref. No. 294/2009).
onflict of interest: None declared.
unding: No funding received.
ppendix A. Data collection form
umber of assessment
ear of assessmentiagnosis of child (demographic data from student assessment)
tems scored out of fiveMedical historySubjective assessment: interaction with family and friendsSubjective assessment: living environmentObjective examination: impairments, body structure and body functionObjective examination: functioningProblem list: addresses all relevant aspects of child’s functioningProblem list: analysis of problemComparable signs to monitor improvement
Holistic approach to interventionotal %mpression %verall mark for all clinical blocks, excluding this paediatric block

5
A
1NDAD
FBDSSMVX
2
b
2 J. Jelsma, D. Scott / Physiotherapy 97 (2011) 47–54
ppendix B. Physiotherapy assessment form outline for paediatrics 2009
ICF Framework
. Demographic detailsame: Assessed by:ate of birth: Date of assessment:ge:iagnosis:
rom folder:irth history:evelopmental history:ubsequent medical history:urgical history – date and typeedication – type and what it is forital signs – if appropriate-Ray findings – if appropriate
. Subjective assessment
a. Impairments• Mental function• Sight, hearing• Speech• Feeding• Pain, sensory loss• Respiratory and/or cardiac function• Continence• Skin condition
. Activity limitations
Health condition(disorder)
Body function &structure
Activities Participation
Environmental factors
Personal factors
••••
Learning and applying knowledge, as appropriate for ageCommunicationSelf-care: dressing, bathing, brushing teeth, toiletingPhysical activity/mobility (an indication of highest level of activity and duration or distance)

ysiotherapy 97 (2011) 47–54 53
c
istsicipation in family outings
d
ople sleeping per room; pace to move around in
G
H
I s?O
3
a
the child is capable of
able to achieve in his what function is difficult functions are missing for
th static and dynamic
b
4
R fill in diagram, making t
5
Dg the following table
Indicator
Objective measure
nt sessions. Give target
J. Jelsma, D. Scott / Ph
. Participation• Domestic life (how does he spend his day?)• School life (what activities does he participate in at school?)• Interpersonal relationships with family, friends, staff, therap• Community and social life regarding leisure time, sport, part
. Environment• Appliances used• Transport to and from school• Accessibility in home (type of house; no. of rooms; no. of pe
available amenities such as water, electricity, indoor toilet, shouse with aids and type of outdoor surface areas)
• Support of community and family involvement• Services (disability and child support grant)
eneral observation
ow did child get to physiotherapy department?
s child in a buggy or wheelchair or walking, with or without appliancebserve child undressing and comment
. Objective assessment
. Activity
• Observe and describe posture in the highest functional levelachieving
• Observe and describe all the functional activities the child ishighest functional level. Analyse what the child is doing and or can only be achieved with facilitation. Be aware of which his age
• Assess balance, if appropriate, in highest functional level, bo• Describe transitioning in and out of highest functional level
. Impairments
• Respiratory• Muscle tone• Sensory loss• Range of movement• Muscle strength
. Identification and analysis of problems
eview ICF framework above before analysing problems. Draw andhe appropriate connections with arrows
. Problem list
ocument functional problemsPrioritise the most important problems and analyse completely, usin
Functional Missing Underlying Interventionproblems components reasonsUsually Usually Usually Treatment plan activity or activity linkedparticipation could berestrictions
and/or personal
6. Short-term aims
Must be functional aim (likely to be achieved in the next few treatmetimes)
environmental
impairment,
7. Long-term aim
Think of one function you would like to improve in 6 months time
8. Soap notes

5 ysiothe
R
[
[
[
[
4 J. Jelsma, D. Scott / Ph
eferences
[1] Shoemaker MJ, Riemersma L, Perkins R. Use of high fidelity humansimulation to teach physical therapist decision-making skills for theintensive care setting. Cardiopulm Phys Ther J 2009;20:13–8.
[2] Doody C, McAteer M. Clinical reasoning of expert and novicephysiotherapists in an outpatient orthopaedic setting. Physiotherapy2002;88:258–68.
[3] Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen GM. Clini-cal reasoning strategies in physical therapy. Med Educ 2004;84:312–29.
[4] Homa D, Peterson D. Using the international classification of func-tioning, disability and health (ICF) in teaching rehabilitation clientassessment. Rehabil Educ 2005;19:119–28.
[5] Smith M, Higgs J, Ellis E. Characteristics and processes of physiother-apy clinical decision making: a study of acute care cardiorespiratory
physiotherapy. Physiother Res Int 2008;13:209–22.[6] Steiner WA, Ryser L, Huber E, Uebelhart D, Aeschlimann A, StuckiG. Use of the ICF model as a clinical problem-solving tool inphysical therapy and rehabilitation medicine. Phys Ther 2002;82:1098–107.
[
Available online at www.s
rapy 97 (2011) 47–54
[7] Stucki G, Ewert T, Cieza A. Value and application of the ICF in reha-bilitation medicine. Disabil Rehabil 2002;24:932–8.
[8] Sackett DL, Haynes RB, Tugwell P. Clinical epidemiology. Boston:Little, Brown and Company; 1985.
[9] Peterson D, Kosciulek J. Introduction to the special issue of Rehabilita-tion Education: the international classification of functioning, disabilityand health (ICF). Rehabil Educ 2005;19:75–80.
10] World Health Organization. International classification of functioning,disability and health. Geneva: WHO; 2001.
11] Peterson B, Rosenthal DA. The international classification of function-ing, disability and health (ICF): a primer for rehabilitation educators.Rehabil Educ 2005;19:81–94.
12] Palisano RJ. A collaborative model of service delivery for children withmovement disorders: a framework for evidence-based decision making.Phys Ther 2006;86:1295–305.
13] Ramklass S. An investigation into the alignment of a South African
physiotherapy curriculum and the expectations of the healthcare sys-tem. Physiotherapy 2009;95:215–22.14] Peterson D, Threats T. Ethical and clinical implications of the inter-national classification of functioning, disability and health (ICF) inrehabilitation education. Rehabil Educ 2005;19:129–37.
ciencedirect.com
Top Related
Copyright © 2022 FDOKUMEN

