



![RLRT-PPT Template_ Tanning_V3[1] (Read-Only)](https://static.fdokumen.com/doc/165x107/63169137c72bc2f2dd0521e6/rlrt-ppt-template-tanningv31-read-only.jpg)
![Hank Howie Biz & Mktg From Console to[2].ppt (Read-Only)](https://static.fdokumen.com/doc/165x107/63191b740255356abc081fd8/hank-howie-biz-mktg-from-console-to2ppt-read-only.jpg)

Bahasa
Halaman
Hukum

![Page 1: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/1.jpg)
Division of Clinical Laboratory Division of Clinical Laboratory Devices Devices ---- an updatean update
![Page 2: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/2.jpg)
DCLD Summary
uPeople uWorkloaduPerformanceuImplementation of Least Burdensome
ProgramuStrategic Plan
![Page 3: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/3.jpg)
PeoplePeople
uNew Deputy Commissioner – Dr. CrawforduSeasoned Chief Counsel – Dan TroyuNew Associate Director Science - Norris
AldersonuSeasoned Center Director – Dr. FeigaluNew Center Organization – Linda Kahan
and Lillian Gill
![Page 4: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/4.jpg)
PeoplePeople
u60 FTEsuNew Genetics HiresuNo Growth
![Page 5: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/5.jpg)
PeoplePeople ---- ProgramsPrograms
uPremarket ReviewuCLIA categorizationuPharmacogenomics working groupuBioterrorism initiativesuTPLC initiative
![Page 6: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/6.jpg)
510(k) Program
uHeart of workloadu650 submissionsuReview times average 65 days (target 90)
![Page 7: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/7.jpg)
Decreasing Workload
uReplacement reagent policyuASR policyuClarification in modification policyuBusiness environment
![Page 8: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/8.jpg)
PMA Program
uVariable workloaduApproved approximately 6uMeeting all review targets
![Page 9: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/9.jpg)
Protocol Review (pre IDE) Program
uCurrently projected at 90/yearuHigh octane stuffu60 day reviewsuMultiple interactions
![Page 10: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/10.jpg)
CLIA Review Program
uActive – more than 2000 determinations/year
uRemains program in evolution
![Page 11: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/11.jpg)
FDAMAFDAMA
u Improved market accessuLeast burdensome pathwaysuPremarket to postmarket balanceu Increased interaction with industry
![Page 12: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/12.jpg)
Least BurdensomeLeast Burdensome
uAppropriate questionsuAppropriate thresholdsuNon-academic pursuits
![Page 13: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/13.jpg)
Least BurdensomeLeast Burdensome
uMatter of lawuMatter of policyuMatter of spirit
![Page 14: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/14.jpg)
Least BurdensomeLeast Burdensome
uTwo Guidance DocumentuSystems Approach – ensure appropriate
process applied to use of regulatory toolsuReview Guidance
![Page 15: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/15.jpg)
Least BurdensomeLeast Burdensome
uReview changes are profounduParallel genetics initiativeuShift to data summariesuShift to more focused labeling reviewuShift to use of clinical literatureuShift to postmarket analysis
![Page 16: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/16.jpg)
Strategic Plan -- Goals
uMission relateduTotal Product Life CycleuKnowledge Management
![Page 17: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/17.jpg)
Total Product Life CycleTotal Product Life Cycle
uCradle to graveuSeamless oversight
![Page 18: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/18.jpg)
Intellectual AppealIntellectual Appeal
uPremarket review limitationuOutdated lawuSnapshot approachu Impact of scale-upu Impact of wide-use
![Page 19: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/19.jpg)
Intellectual AppealIntellectual Appeal
uPostmarket review strengthsuQuality system regulationsuRequire quality assessmentuRequire process controlsuRequire corrective actionsuUnrealized potential
![Page 20: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/20.jpg)
Intellectual AppealIntellectual Appeal
uNeed for harmonizationu IVD directive u ISO labeling initiativeuGrowing regulatory program in Canada
![Page 21: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/21.jpg)
TPLC IVD Pilot
u Ideal targetuStereotyped review issuesuCadre of like minded scientistsuEngaged communities interested in
partnering
![Page 22: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/22.jpg)
Goals
u Increased transparencyuExpedited technology transferuProvide support and improvements
application of ASRsu Improve surveillance and use of
surveillance
![Page 23: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/23.jpg)
Core MissionCore Mission
uPromote public healthuApply good scienceuEvolving programuRelevant, focused, safe and effective
![Page 24: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/24.jpg)
CLIACSept. 11, 2002
![Page 25: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/25.jpg)
Testing of Public Health SignificanceNumbers of Laboratories:
• 4,414 Level A “capable” for Bioterrorism • 1,959 Mycobacteriology (TB)• 2,516 HIV Antibody• 5,074 Syphilis serology• 824 Blood lead
![Page 26: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/26.jpg)
Private
Labs
• Funding
• Consensus Standards
• Technology Transfer
• Training
50
State
PHL
Current Paradigm• The current network of laboratories that perform
tests of public health significance is a loose association of public health (state, county and city), hospital, and independent laboratories throughout
the country.
Inconsistent
Collaboration
![Page 27: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/27.jpg)
Program Support
50
State Systems of
Public/Private Coordination
Technical Capacity
• LRN / BT
•Pulsenet
•ELC / EIP
• TB - HIV - STD
• Blood lead
• Biomonitoring
•LIP
•NEDSS
•HAN
System Capacity
![Page 28: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/28.jpg)
Role of Laboratories“Provide information for decision making”
Private LabsPrivate Labs•• Diagnostic testingDiagnostic testing
•• Medical managementMedical management
•• Mission = Mission = Individual healthIndividual health
Public LabsPublic Labs•• Some diagnostic testingSome diagnostic testing
•• Reference testingReference testing
•• Surveillance and monitoringSurveillance and monitoring
•• Mission = Mission = Public healthPublic health
![Page 29: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/29.jpg)
Role of Laboratories“Provide information for decision making”
Private LabsPrivate Labs•• Diagnostic testingDiagnostic testing
•• Some reference testingSome reference testing
•• Medical managementMedical management
•• Focus = Focus = Individual healthIndividual health
Public LabsPublic Labs•• Some diagnostic testingSome diagnostic testing
•• Reference testingReference testing
•• Surveillance and monitoringSurveillance and monitoring
•• Focus = Focus = Public healthPublic health
Identify Public Health Threats
Interdependent Network
![Page 30: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/30.jpg)
Statement of Problem• GAO Report (February ’99)
“Emerging Infectious Diseases”– The nation's public health surveillance of infectious diseases
critically needs improvement with Federal leadership
• GWU Report – (January, 1999)“Reporting by Out-of-State Laboratories”– Under-reporting is due to: out-of-state testing, lack of
experienced personnel, and cost-shifting under capitation
• Lewin Group Report (October 1997)“Public Health Laboratories & Health System Change”
– There has been a lack of proactive leadership from the public sector. The entire system should be carefully reviewed.
![Page 31: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/31.jpg)
Barriers To Overcome
SustainabilitySustainability
Geographic separation
Resource limitations
Mission differences
Transport difficulties
Non-culture methods
Out-of-state laboratories
Communication disparities
![Page 32: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/32.jpg)
![Page 33: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/33.jpg)
NLS Consultants Group
• ASM• ACLA• ASCP• APHL• AAB
• CDC- NCID• CDC- BPRP• CSTE• ASTHO• CAP
The Consultants Group has met several times and will be expanded to include additional interests
![Page 34: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/34.jpg)
NLS demonstration projectsMichigan Bureau of Laboratories
Frances Pouch Downes, DrPHJohn Dyke, PhD
Minnesota Public Health LaboratoryNorman Crouch, Ph.D.Paula Snippes
Nebraska Public Health LaboratoryStephen Hinrichs, M.D. Tony Sambol
University of Washington Jon Counts, DrPH
![Page 35: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/35.jpg)
Demonstration Project Focal Areas
PARTNERSHIPSPARTNERSHIPS ASSESSMENTASSESSMENT
STANDARDSSTANDARDSTRAININGTRAINING
![Page 36: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/36.jpg)
Assessment of AST Laboratory Practice
• Majority of labs do not have current NCCLS tables
• Poor understanding of tables• Inconsistent testing for drug resistance in
Streptococcus pneumoniae• Priority training needs were identified• Interventions
• CDC staff involvement• Teleconference • Train-the-Trainer
![Page 37: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/37.jpg)
Minnesota
ML SMINNESOTA
LABORATORY SYSTEMA PUBLIC AND PRIVATE COLLABORATION
Norman Crouch, Ph.D.Laboratory Director
Paula Snippes, MT (ASCP)Laboratory Program Advisor
![Page 38: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/38.jpg)
MLS Laboratory Alerts
First Alert! September 11, 2001
• Encouraged heightened suspicion• Listed 4 “priority threat agents”• Provided agent characteristics• Listed phone number to call
MinnesotaCommunications
![Page 39: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/39.jpg)
MinnesotaPromotional Poster
![Page 40: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/40.jpg)
MinnesotaChallenge Set
1. Bacillus megaterium
2. Streptococcus pneumoniae
3. E. coli O157:H7
![Page 41: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/41.jpg)
NEBRASKANetworking of the NNetworking of the N--LRS Hub Labs to LRS Hub Labs to
Regional “Spoke” LabsRegional “Spoke” Labs
NPHL
Blue: N-LRS Hub Labs Green: N-LRS “Spoke” Labs
![Page 42: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/42.jpg)
MICHIGANCourier System
![Page 43: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/43.jpg)
Public Health Preparedness
Cooperative Agreement Award Guidance for FY 2002 Supplemental Funds for Public Health Preparedness and Response for Bioterrorism
Ensure Nation is Prepared forBioterrorismOther Infectious Disease OutbreaksOther Public Health Threats and Emergencies
![Page 44: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/44.jpg)
Focus Area C: Laboratory Capacity
Biologic Agents
![Page 45: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/45.jpg)
Critical BenchmarkLaboratory Capacity Biologic Agents
• #10: Develop a plan to improve working relationships and communication between Level A (clinical) laboratories and Level B/C laboratories, (i.e. Laboratory Response Network laboratories) as well as other public health officials.
![Page 46: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/46.jpg)
Identify All Clinical Labs
LA County
NYC
DC
BegunDone PlannedNot Addressed
![Page 47: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/47.jpg)
Searchable Laboratory Database
LA County
NYC
DC
BegunDone PlannedNot Addressed
![Page 48: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/48.jpg)
Enlist Clinical Laboratory Participation
LA County
NYC
DC
BegunDone PlannedNot Addressed
![Page 49: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/49.jpg)
Convene Laboratory Forum or“Advisory” Committees
LA County
NYC
DC
BegunDone PlannedNot Addressed
![Page 50: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/50.jpg)
Best Practices: Assessment
BSL-3 module (23)
Proficiency Testing (14)
Surge capacity (8)
Advisory committee (6)
Simulation exercises (5)
Safety Assessment (4)
MA
NYC
RICT
NJDEMD
LA County
Chicago
![Page 51: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/51.jpg)
Best Practices: Communication
Collaborations with First Responders-EMS, FBI, HazMat, etc (31)
Triage procedures (12)
Database of Level A labs (10)
24/7 Human contact (8)
Blast email/fax (7)
Directory of directors and supervisors (1)
Emergency plan for government (1)
LA County
MA
NYC
RICT
NJDEMD
![Page 52: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/52.jpg)
Best Practices: Training
Collaborations with Level A labs (12)
Training for shipping, handling, and packing instructions for specimen (5)
Collaborations with other states (1)
MACT
![Page 53: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/53.jpg)
Chain of custody (16)
Protocols for receiving, processing, evidence storage, disposal (14)
Security (9)
Specimen transport systems/courier (3)
MARI
NJDE
LA County
Best Practices: Specimen Transportation
![Page 54: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/54.jpg)
Laboratory Integration Program Activities
• Convene the NLS Consultants Group
• Maintain the National Laboratory Database of laboratories and their testing services and assist with development of state databases
• Convene regular national conference calls between CDC, the LPC’s & SLTC’s
• With APHL, through the Leadership Institute, provide leadership training
![Page 55: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/55.jpg)
Leadership for Public Health Laboratories
![Page 56: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/56.jpg)
Laboratory Integration Program Activities
• Support dissemination of state’s model activities
• Provide advice on the creation and maintenance of PT programs
• Provide consultation on laboratory management and administration
• With APHL and other stakeholders, create performance standards for PH laboratories
![Page 57: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/57.jpg)
Expected Outcomes
• Formalized relationships between clinical and public health laboratories
• Coordination of activities• Development of Intra- and Inter-state
Collaborations• Improved PH surveillance and response
![Page 58: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/58.jpg)
What are the next steps?
• Promote successful state models • Develop connectivity and standardization
for state-based assessments• Foster the support of national
organizations for state systems• Support a leadership role for state public
health laboratories
![Page 59: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/59.jpg)
9/11/02
Summary of International Conference on Proficiency
Testing for Medical Laboratories February 24-26, 2002
D. Joe Boone, Ph.D.September 11, 2002
![Page 60: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/60.jpg)
9/11/02
Objectives
• Explore Advances in EQA• Create Opportunities for Sharing
and Partnerships• Promote Role of EQA in Global
Health
![Page 61: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/61.jpg)
9/11/02
Conference Participants
• Attendance - 202• Attendees - 54 Countries• Posters - 22 Countries
![Page 62: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/62.jpg)
9/11/02
Conference Outcomes
• Developed Global Inventory of EQA Programs http://www.phppo.cdc.gov/mlp/eqa.asp– Currently 151 EQA Programs in the Inventory – Information on 106 Programs in Printable List
• Created Web-site for Conference Presentations • Proceedings Published in
Accreditation and Quality Assurance,September 2002 by Springer-Verlaghttp://link.springer-ny.com
![Page 63: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/63.jpg)
9/11/02
Conference Outcomes
Defined Seven Post-Conference Workgroups • Coordination – ISO, EQALM, CLIA, etc. • Information – Programs and Meetings• Matchmaking – Country Partners• Advocacy – Brochure • Logistics – Trade, Transportation Barriers • Developmental – New Tests/Technology• Information Technology – EQA Specific
![Page 64: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/64.jpg)
9/11/02
Vision
• Better communication – PT Inventory, Future Meetings, Publications, Internet
• Better collaboration – Resources, Mentors • Better global health – Quality Testing• Ongoing collaboration – Coalition
![Page 65: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/65.jpg)
9/11/02
ProfessionalOrganizat ions
AccreditorsPrivate Sector
W H O
P TProviders
USAID
StandardSett ingGroups
RegionalPrograms
CDC
WorldBank
Global Partnership Global Partnership Quality AssuranceQuality Assurance
![Page 66: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/66.jpg)
9/11/02 Supporting EQA Programs Worldwide
![Page 67: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/67.jpg)
9/11/02
![Page 68: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/68.jpg)
Joe Boone, Ph.D.9/11/02
![Page 69: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/69.jpg)
Conference Information
• Location - J.W. Marriott HotelLenox Rd, Atlanta, Georgia
• Dates - April 13-15, 2003• Starting Time – Noon, April 13• Maximum Attendance - 400
![Page 70: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/70.jpg)
Why?
• Healthcare System Changes Affect Health Laboratory Services – Access, Cost, Quality and Patient Safety
• Significant Role of Health Laboratory Services in the Healthcare System
• Improvement in Health Laboratory Service Depends on Better Collaboration and Coordination within the Healthcare System
![Page 71: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/71.jpg)
Conference Goals
• Develop Framework for National Report on the Quality of Laboratory Services
• Develop Criteria for Quality Indicators for Laboratory Services
• Develop a Process for Ongoing Data Collection and Analysis – Quality Institute
![Page 72: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/72.jpg)
• Keynotes - Dr. Lucian Leape - Dr. Brent James
• Perspectives: Healthcare Providers, Policy Makers, Laboratory Professionals, Accrediting and Standard Setting Groups, Diagnostics Industry, Patient Advocates, Hospital Administrators, Payers/Insurers
• Experiences • Workgroups
Program
![Page 73: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/73.jpg)
• Perspectives in the Healthcare System 1) Patient Experiences 2) Providers of Care3) Organizations that Provide Care4) Environment of Care
• Reactor Panel
Program
![Page 74: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/74.jpg)
• Perspectives: – Introduction and Overview
1) Patient ExperiencesPatient Example
2) Providers of CareAnesthesiology ExamplePharmacy Example
Program
![Page 75: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/75.jpg)
• Perspectives: 3) Organizations the Support Care
Hospital/HMO Example4) Environment of Care
Government’s RolePayer/Purchaser’s Role
Program
![Page 76: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/76.jpg)
• Experiences: Introduction and Overview1) Four Presentations2) Reactor Panel
Program
![Page 77: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/77.jpg)
• Workgroups: Introduction and Overview1) Creating National Report2) Criteria for Quality Indicators3) Creating a Quality Institute
Program
![Page 78: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/78.jpg)
• Better Collaboration and Coordination between Health Laboratories and other parts of the Healthcare System
• Disseminated National Report Highlighting Successes and Identifying Needs of Health Laboratories
• Measures for Quality in Health Laboratory Services:Safety, Timeliness, Effectiveness, Efficiency, and Patient-centeredness
• Ongoing Process to Collect and Analyze Data related to the Quality of Nation’s Health Laboratory Services
Long- and Short-Term Conference Outcomes?
![Page 79: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/79.jpg)
![Page 80: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/80.jpg)
September 10, 2002
The Honorable Claude Allen Deputy Secretary U.S. Department of Health and Human Services 200 Independence Avenue, SW Washington, DC 20201 Dear Mr. Allen: The undersigned organizations are writing to you with a concern over the possible waiver of regulations for rapid HIV (Human Immunodeficiency Virus) tests. We believe that a test as critical as HIV screening must be conducted in a controlled and monitored environment, and conducted by trained personnel. Additionally, there is fear that rapid HIV tests, once waived, may be used in hospital and clinical settings. In these settings, there is great potential for immediate pharmacological treatment, due to false test results. The accuracy of rapid HIV tests must be improved prior to the use of these tests in a clinical setting. The rapid HIV antibody screening test has a lower specificity and sensitivity than Enzyme Linked Immunoabsorbent Assay (ELISA) tests. For example, a specificity of 98% might sound good for a rapid HIV test. Unfortunately, if this test is used by members of a population with a low prevalence of HIV infection, such as normal healthy blood donors, most of the people who get a positive test result are getting a wrong test result. We understand the desire for patient accessible HIV testing. However, due to the inaccuracy of rapid HIV tests and the implications for both patient and public safety, we respectfully ask that any recommendation for waiver of these tests be denied. If you have questions or need additional information, please contact any of the organizations below, or call Rachel Judas at (202) 347-4450. Thank you for your attention to this important public health matter.
Sincerely,
American Association of Bioanalysts American Society for Clinical Laboratory Science
American Medical Association American Society for Clinical Pathology
![Page 81: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/81.jpg)
Update onRapid HIV Tests
Elliot P. Cowan, Ph.D.Senior Regulatory Scientist
Office of Blood Research and ReviewCenter for Biologics Evaluation and Research
Food and Drug Administration
CLIACSeptember 10, 2002
![Page 82: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/82.jpg)
Purpose of This Presentation
To inform CLIAC of progress made toward the approval of new rapid HIV tests since the last meeting
![Page 83: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/83.jpg)
Discussion of Submission Status
uFDA is prohibited from releasing any information related to submissions, as this is considered proprietary
uLimited to discussion of public information only, or information authorized for release by the applicant
![Page 84: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/84.jpg)
Public Information Related to Rapid HIV Test Submissions
uOn May 1, 2002, MedMira Incorporated announced, “the completion of a site inspection of the Company's facilities in Halifax by the U.S. Food and Drug Administration in connection with MedMira's application for Pre-Market Approval of its RevealTM Rapid HIV Test.”(http://www.medmira.ca/press_releases_f.htm)
u In addition, MedMira has given FDA permission to disclose that they received an approvable letter for their PMA on May 24, 2002
![Page 85: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/85.jpg)
u On May 13, 2002, OraSure Technologies, Inc, announced, "it has received notification from the U.S. Food and Drug Administration (‘FDA’) that the OraQuick® Rapid HIV-1 Antibody Test is approvable…Final approval is subject to the Company submitting product labeling and resolving specific validation and design control issues identified during FDA’s recent pre-approval inspection of the Company’s manufacturing facilities…”(http://www.orasure.com/news/default.asp?art_id=185)
Public Information Related to Rapid HIV Test Submissions, cont.
![Page 86: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/86.jpg)
Toby Merlin, M.D., Chairperson Clinical Laboratory Improvement Advisory Committee
5400 Gibson Boulevard, S.E. Albuquerque, New Mexico 87108
(505) 262-7949:[email protected]
September 12, 2002 The Honorable Tommy G. Thompson Secretary Department of Health and Human Services 200 Independence Avenue, S.W. Washington, DC 20220 Dear Secretary Thompson: I am writing on behalf of the Clinical Laboratory Improvement Advisory Committee (CLIAC) to express the Committee’s deep concern that rapid tests for human immunodeficiency virus (HIV) infection are being promoted for a waiver under the Clinical Laboratory Improvement Amendments of 1988 (CLIA) without presentation and review of data demonstrating that the CLIA waiver criteria are met. Data must be evaluated before an appropriate decision regarding waiver can be made.
As you know, CLIAC was chartered in February, 1992 to provide you and the Assistant Secretary of Health with scientific and technical advice and guidance relative to quality laboratory testing. CLIAC has, at several of its meetings, discussed in-depth the criteria used to obtain waiver under CLIA and the process for waiver review. CLIAC has also reviewed the potential public health benefits and risks of a waiver of a rapid HIV test. On September 11-12, 2002, CLIAC again considered this issue. After careful review and thoughtful discussion, the Committee’s voting members unanimously requested that I share with you our concerns in this matter. We believe that consideration of rapid HIV tests for waiver under CLIA requires a review of objective data for the following reasons:
• The results of HIV tests are of enormous consequence to the persons being tested. • Erroneous HIV test results – both false positives and false negatives – pose a
substantial risk to the persons being tested and their partners. • Even the simplest HIV testing device requires oversight, training of personnel,
quality control, proficiency testing, and quality assurance to provide accurate results.
• Waiver under CLIA provides no mechanism to assure proper oversight, personnel training, quality control, proficiency testing, and quality assurance.
• Studies performed by the Centers for Disease Control and Prevention, the Centers for Medicare & Medicaid Services and the Office of the Inspector General have shown that CLIA-waived tests are often incorrectly performed.
• Incorrectly performed waived tests have resulted in harm to patients.
![Page 87: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/87.jpg)
Page 2 - The Honorable Tommy G. Thompson We agree that HIV testing should be made broadly and rapidly available, and we believe this can be accomplished without waiver under CLIA. Mechanisms exist within CLIA to permit rapid HIV tests to be performed in mobile and non-traditional settings with a minimum of burden, while assuring appropriate oversight, quality control, and quality assurance. Although we support broad dissemination of rapid HIV testing as soon as these tests are approved for market, we urge you to require careful review of objective evidence of test performance by waived testing personnel in waived settings before these tests are considered for waiver under CLIA. We welcome the opportunity to work with you and other interested parties in this matter and thank you for your consideration.
Sincerely yours,
Toby L. Merlin, M.D. Chairperson Clinical Laboratory Improvement Advisory Committee
cc: Joseph O’Neill, M.D. Director, Office of National AIDS Policy The White House Washington, DC 20502 Claude Allen, J.D. Deputy Secretary Department of Health and Human Services Louis W. Sullivan, M.D. Co-Chair, Secretary’s Advisory Council on HIV/AIDS Department of Health and Human Services Thomas Coburn, M.D. Co-Chair, Secretary’s Advisory Council on HIV/AIDS Department of Health and Human Services
![Page 88: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/88.jpg)
CLIA Update
Judith A. YostDirector, Division of Laboratories
![Page 89: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/89.jpg)
Status• Waived Lab Survey Project• 2001 Lab Registry • New & Improved CLIA Website • Rapid HIV CLIA Categorization• DOD Lab Program Re-Approval & MOU• Secretary’s Regulatory Reform Initiative• Final QC Regulation Clearance• DAB/ALJ Hearing Master Index• Criteria for Test Waiver Final Regulation
![Page 90: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/90.jpg)
CLIA Statistics Jan. 2002
Total Laboratories Enrolled 174, 504-Certificate of Compliance 21,809(13%)-Certificate of Waiver 93,129(55%)-Certificate of PPM 37,755(22%)-Certificate of Accreditation 16,312(10%)
Exempt State Labs 5499-New York (Except POL’s) 2747-Washington 2752
![Page 91: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/91.jpg)
CLIA Authority
• CMS has delegated authority for all CLIA regulations.
• CMS is working with Tri-Agencies to coordinate program policies & priorities.
• Regular Tri-Agency meetings are being convened.
• Progress has been made, communication enhanced & mutual priorities determined.
![Page 92: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/92.jpg)
Waived Lab Project• Studies by CMS & others indicated 50% of
waived labs have quality problems.– Not following mfgrs.’ instructions; not doing QC.
• Followup data of problem labs reflects compliance is maintained 75% of time using education.
• CMS compiling “Clearinghouse” of existing educational programs for CLIA Website.
• CMS initiated surveys of 2% of waived labs annually for 3 years in all states Apr. 15, 2002.– Comprehensive information collection including
”outcomes”.
![Page 93: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/93.jpg)
Waived Lab Project Cont’d.
• CMS working with manufacturers to enhance clarity of instructions.
• CMS, FDA & manufacturers on NCCLS workgroup to develop international labeling standards.
• Tri-Agencies working on final rule for waived criteria.
• CMS will evaluate survey findings annually & at 3 yrs. to determine appropriate oversight of waived labs.
![Page 94: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/94.jpg)
2001 Lab Registry
• Can be found on CLIA web site.• Lists 221 labs with sanctions completed.
– 196 individual labs; some listed twice.• Reflects more labs than previously(207);
includes repeat offenders.• Incorporates labs from exempt states, OIG
& accrediting organizations in eight categories.
![Page 95: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/95.jpg)
Successes
• Hearing Decisions Web Index• CLIA Website Transition • Department of Defense (DOD) MOU
![Page 96: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/96.jpg)
Hearing Decision Master Index
• Decision, Synopsis, Summary Points.• Basis for Sanctions.• Arguments by both sides of case.• Excerpts from the ruling & referenced cases.• Complete actual hearing decision, applicable
regulatory references.• Updated annually.• CLIA Web site:
www.cms.hhs.gov/clia/hearinggroup.asp.• CLIA has never lost a case!!
![Page 97: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/97.jpg)
www.cms.hhs.gov/clia/
• News• Special Alerts• How to Apply• Program
Description/Projects
• Regulations & Federal Register Documents
• Test Categorizations• Fee Schedule • State Agency Contacts• CMS Regional Office
Contacts
![Page 98: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/98.jpg)
www.cms.hhs.gov/clia/ (Cont)
• Approved Accrediting Organizations
• Exempt States• State Lab Licensure
Programs• PT Providers• Certification Boards
• FAQs• Statistics • Hearing Decisions• Lab Registries• Medicaid CLIA
Releases• OIG Reports
![Page 99: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/99.jpg)
DOD Re-Approval
• Secretary DHHS & Secretary DOD MOU for approval of DOD lab oversight program.– AFIP works with DOD on standards.– Extended for 5 years.
• Most DOD labs accredited by CAP.• DOD regulations are equivalent to CLIA.• DOD labs may have unusual circumstances.
![Page 100: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/100.jpg)
To Be Announced
• Secretary’s Regulatory Reform Initiative• Rapid HIV Test Categorization Status• Final QC Regulation• Waived Test Criteria Final Regulation
![Page 101: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/101.jpg)
Regulatory Reform InitiativeDraft Recommendations (1)
• Simplify/clarify regulations.• Provide information to POLs about training
opportunities.• Update website/ possible link to NLTN.• Develop & disseminate basic laboratory practices
document.• Offer technical assistance in interpreting reg
requirements.• Modify the AQAS as an educational tool.
![Page 102: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/102.jpg)
Regulatory Reform InitiativeDraft Recommendations (2)
• Increase the number of POL reps on CLIAC. • Conduct training at industry meetings.• Design educational brochure for POLs.• Solicit feedback at Open Forums.• Place education clearinghouse on CLIA website.• Promote self assessment tools for laboratories.
![Page 103: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/103.jpg)
Final QC Regulation• Finalizes QC, PTM & QA—due end 2002.
– Most standards unchanged.
• Closes phase-ins that expire 12/31/2002.– Ph.D lab dir.; mod. comp. QC; FDA role.
• Reflects new technology; responds to comments.• Incorporates basic Quality Systems concepts &
CLIAC recommendations.– Follows lab workflow/prevents errors.
• Streamlines, simplifies & adds QC flexibility.• Has 90 day effective date to educate & implement.
– Guidance will be forthcoming.
![Page 104: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/104.jpg)
Waived Test Criteria Regulation• Revised criteria published by FDA in draft
guidance to be withdrawn.• FDA now using ’95 proposed rule used by CDC
for waiver reviews.• Final rule including comments under development
by Tri-Agencies.• Issue 1: Movement to waive rapid HIV test.
– Pre & post analytical considerations.– PACHA meeting conclusions.
• Issue 2: QC for waived tests—recommended or required when no failsafe is present.
![Page 105: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/105.jpg)
THE END!!
THANK YOU!!Questions???
![Page 106: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/106.jpg)
Coordinating Council on the Coordinating Council on the Clinical Laboratory Workforce Clinical Laboratory Workforce
(CCCLW)(CCCLW)
Summit Meeting Report to CLIACSeptember 11, 2002
![Page 107: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/107.jpg)
OverviewOverview
lMeeting held on April 2, 2002 in Chicagol Hosted by ASCLSl Previously known as the Summit on
Laboratory Workforce Shortagel New name proposed: Coordinating Council
on Clinical Laboratory Workforce (CCCLW)
![Page 108: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/108.jpg)
Strategic Plan UpdateStrategic Plan UpdateReview of Current StatusReview of Current Status
l Data Collection – ASCPl Recruitment – ASCLSlMarketing – CLMAl Financing Education - NAACLS
![Page 109: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/109.jpg)
Data CollectionData Collection
lWage and Vacancy SurveylMedical Technologist Prospective Study (in
9th year)l Annual Survey of Programs (from Program
Directors)l Job task/Practice Analysis for MT, MLT,
and PBT in progress
![Page 110: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/110.jpg)
RecruitmentRecruitment
l Career brochure and CD video to promote laboratory careers
l Career Toolboxl Career video for PBS (possible joint venture
with Johnson and Johnson)
![Page 111: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/111.jpg)
Marketing and FinancingMarketing and Financing
l Not much progress on Field Guide for laboratory managers on addressing workforce shortage
l Discussion on available scholarships for clinical laboratory students
![Page 112: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/112.jpg)
Other OpportunitiesOther Opportunities
l Professional licensure - ASCLSl National Preparedness for Bioterrorism –
FDA Office of Science and Technologyl Loan Forgiveness – ASCP (HR 1948)l Logo/Identity – ASCLSl Career Ladders – ASCLS
![Page 113: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/113.jpg)
Workgroup Summary for Workgroup Summary for Strategic PlanStrategic PlanData CollectionData Collection
l Enhance ASCP Wage and Vacancy survey questions to fill gaps (i.e. hiring trends, expand database of targeted individuals)
l Terminology – have glossary of definitions of categories for better correlation of answers
l Error rates – obtain tangible datal Licensure – do labs in licensed states perform
better on PT than those without licensure
![Page 114: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/114.jpg)
Workgroup SummaryWorkgroup SummaryRecruitmentRecruitment
l Organize available materials; pool resourcesl Develop consistent message for material
packets along with dissemination planl Use career ladder/licensure information as
positive recruitment tools
![Page 115: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/115.jpg)
Workgroup SummaryWorkgroup SummaryMarketingMarketing
l Joint CLMA/Educator’s Forum – schedule another? Proposed timeframe of March 2003
l Career pathways – how to form partnership with hospital HR departments
l Implementation strategy for Field Guidel Improve recognition of problem – invite
AHA, AMA, HRSA to CCCLW meetings
![Page 116: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/116.jpg)
Workgroup SummaryWorkgroup SummaryFinancing EducationFinancing Education
l Expand base for soliciting scholarship funding (schools/universities, state societies)
l Establish CCCLW website for informationl Develop list of “local” resourcesl Identify “free” training (i.e. military)l Potential industry support of programs
![Page 117: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/117.jpg)
SummarySummary
l Joint support of subsequent meetings (estimated ~ $250 each)
l Steering committee to set agenda and organize meetings (initial committee includes ASCP, ASCLS, CLMA, NAACLS)
l Keeping information flowing in between face-to-face meetings
l Distribute list of meeting participants and e-mail addresses
l Revise Strategic Plan; disseminate to all organizations
![Page 118: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/118.jpg)
Coordinating Council on the Coordinating Council on the Clinical Laboratory WorkforceClinical Laboratory Workforce
![Page 119: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/119.jpg)
CCCLW ACTIVITYCCCLW ACTIVITYUpdate Since April 2002Update Since April 2002
Report to CLIACSeptember 2002
Brenta G. Davis, Ed.D
![Page 120: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/120.jpg)
Status of Manpower ShortageStatus of Manpower Shortage
l Still exists because of lack of applicants to educational programs.
– We are producing about half the number of graduates we need each year
– Programs that are open are only 77% full (July 2002)
![Page 121: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/121.jpg)
Status of Shortage Cont.Status of Shortage Cont.
l Signs of hope
– About half of programs report a modest increase in applicant pools and enrollments
– Overall, median salaries in US have increased approximately 19% since 2000
– Health care careers seem more attractive in current economic climate
![Page 122: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/122.jpg)
CCCLW Since April 2002CCCLW Since April 2002
l Recognition of CCCLW as focal point of information and action– AMA Health Professions e-letter article and web site item
– Inclusion on program of G-2 Lab Institute in October
– J&J/Ortho-Clinical Diagnostics(OCD) contact
![Page 123: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/123.jpg)
CCCLW since April, contCCCLW since April, cont
l J&J/OCD proposed project
– Special web site and targeted brochures for high school and college students
–Turnkey Media Kit•Primary implementation by PR professionals to media outlets throughout the US
– OCD will meet with CCCLW in fall before final decision to proceed
![Page 124: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/124.jpg)
HOW CLIAC HELPSHOW CLIAC HELPS
l Continued concern about the shortage signals its significance to healthcare community and government
l Continued participation in CCCLW
l Participation in other meetings and informational sessions about workforce issues
![Page 125: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/125.jpg)
![Page 126: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/126.jpg)
![Page 127: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/127.jpg)
![Page 128: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/128.jpg)
![Page 129: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/129.jpg)
![Page 130: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/130.jpg)
![Page 131: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/131.jpg)
![Page 132: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/132.jpg)
![Page 133: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/133.jpg)
![Page 134: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/134.jpg)
![Page 135: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/135.jpg)
![Page 136: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/136.jpg)
![Page 137: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/137.jpg)
![Page 138: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/138.jpg)
![Page 139: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/139.jpg)
![Page 140: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/140.jpg)
![Page 141: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/141.jpg)
![Page 142: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/142.jpg)
![Page 143: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/143.jpg)
![Page 144: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/144.jpg)
![Page 145: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/145.jpg)
![Page 146: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/146.jpg)
![Page 147: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/147.jpg)
![Page 148: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/148.jpg)
![Page 149: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/149.jpg)
![Page 150: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/150.jpg)
![Page 151: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/151.jpg)
![Page 152: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/152.jpg)
![Page 153: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/153.jpg)
![Page 154: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/154.jpg)
![Page 155: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/155.jpg)
Sentinel Event Data andSentinel Event Data andStaffing EffectivenessStaffing Effectiveness
Joint Commission on Accreditation of Joint Commission on Accreditation of Healthcare OrganizationsHealthcare Organizations
Joanne Born, Executive DirectorJoanne Born, Executive DirectorLaboratory ProgramLaboratory Program
![Page 156: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/156.jpg)
OverviewOverview
nn JCAHO accredits more than 17,000 healthcare JCAHO accredits more than 17,000 healthcare organizations in the US and overseasorganizations in the US and overseas
nn 2500 laboratory organizations (4500) CLIA 2500 laboratory organizations (4500) CLIA certificatescertificates
nn Mission is to promote patient safety and Mission is to promote patient safety and performance improvement through accreditation performance improvement through accreditation surveysurvey
nn Survey of compliance with professionally derived Survey of compliance with professionally derived standardsstandards
![Page 157: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/157.jpg)
Sentinel Events and JCAHOSentinel Events and JCAHO
nn Any unexpected occurrence involving death Any unexpected occurrence involving death or serious physical or psychological injury, or serious physical or psychological injury, or the risk thereofor the risk thereof
nn Thorough and credible root cause analysis, Thorough and credible root cause analysis, risk reduction strategiesrisk reduction strategies
nn Leadership expectations standardsLeadership expectations standards--basedbasednn Voluntary selfVoluntary self--reportingreportingnn DatabaseDatabase
![Page 158: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/158.jpg)
Sentinel Event CategoriesSentinel Event Categories
Suicide, 17.1%Suicide, 17.1%Operative/postoperative complications, 12.2%Operative/postoperative complications, 12.2%Medication Error, 11.5%Medication Error, 11.5%WrongWrong--site surgery, 11.2%site surgery, 11.2%Delay in treatment, 5.3%Delay in treatment, 5.3%Transfusion error, 2.6%Transfusion error, 2.6%EquipmentEquipment--related, 1.6%related, 1.6%12 other categories12 other categories
![Page 159: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/159.jpg)
SettingsSettings
nn 82% in hospitals (general, psychiatric)82% in hospitals (general, psychiatric)nn 3.6% in emergency department3.6% in emergency departmentnn 0.3% in clinical laboratory0.3% in clinical laboratorynn Remainder, varied settingsRemainder, varied settings
![Page 160: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/160.jpg)
Categories of Root CausesCategories of Root Causes
nn Communication, 63% of all eventsCommunication, 63% of all eventsnn Orientation/training, 58%Orientation/training, 58%nn Availability of information, 20%Availability of information, 20%nn Staffing levels, 18%Staffing levels, 18%nn Competency/credentialing, 12%Competency/credentialing, 12%nn Procedural compliance, 12%Procedural compliance, 12%nn OthersOthers
![Page 161: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/161.jpg)
Orientation/Training, identified Orientation/Training, identified as root cause…as root cause…
nn 62% of inpatient suicides62% of inpatient suicidesnn 80% of op/post80% of op/post--op eventsop eventsnn 60% of medication errors (number one)60% of medication errors (number one)nn 38% wrong site surgery38% wrong site surgerynn 28% delays in treatment28% delays in treatmentnn 75% transfusion events75% transfusion events
![Page 162: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/162.jpg)
Staffing Levels, as root cause…Staffing Levels, as root cause…
nn 42% of op/post42% of op/post--op eventsop eventsnn 18% of medication errors18% of medication errorsnn 25% of delays in treatment25% of delays in treatmentnn 25% of transfusion events25% of transfusion events
![Page 163: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/163.jpg)
Competency/Credentialing…Competency/Credentialing…
nn 24% of op/post24% of op/post--op eventsop eventsnn 21% of medication errors21% of medication errorsnn 28% of delays in treatment28% of delays in treatment
![Page 164: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/164.jpg)
Lab Compliance IssuesLab Compliance Issues
nn Staff competency (includes point of care)Staff competency (includes point of care)nn Proficiency testing performance, corrective Proficiency testing performance, corrective
action, regulated action, regulated analytesanalytesnn Quality control performance Hematology Quality control performance Hematology
and Chemistry, remedial action, reviewand Chemistry, remedial action, reviewnn Waived testing quality control (nonWaived testing quality control (non--lab) and lab) and
staff training (incl. Manufacturer’s staff training (incl. Manufacturer’s instructions)instructions)
nn Training of staff monitoring transfusionsTraining of staff monitoring transfusions
![Page 165: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/165.jpg)
JCAHO and Staffing JCAHO and Staffing EffectivenessEffectiveness
nn Shortage of qualified professional personnelShortage of qualified professional personnelnn Identified linkages between staffing Identified linkages between staffing
effectiveness and patient safetyeffectiveness and patient safetynn LegislationLegislationnn Develop approach for ALL types of Develop approach for ALL types of
organizationsorganizationsnn Link to clinical/service outcomesLink to clinical/service outcomesnn Engage field in developmentEngage field in development
![Page 166: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/166.jpg)
Staffing Effectiveness:Staffing Effectiveness:
““The number, competency, and skill mix of The number, competency, and skill mix of staff as related to the provision of needed staff as related to the provision of needed services.services.
![Page 167: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/167.jpg)
Development…Development…
nn National panel of over 100 experts, 2000National panel of over 100 experts, 2000nn Representatives from various settings and Representatives from various settings and
disciplines (20% providing direct care)disciplines (20% providing direct care)nn Analyzed staffing models and sensitivity of Analyzed staffing models and sensitivity of
screening indicatorsscreening indicators
![Page 168: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/168.jpg)
ApproachApproach
nn Multiple indicators in combination (human Multiple indicators in combination (human resource indicator and service indicator)resource indicator and service indicator)
nn Indicators as screening tool for staffing issuesIndicators as screening tool for staffing issuesnn Allows flexibilityAllows flexibilitynn Requires analysis of variation from expectedRequires analysis of variation from expectednn Expects response if indicatedExpects response if indicatednn No prescribed staffing levelsNo prescribed staffing levels
![Page 169: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/169.jpg)
Under ConsiderationUnder Consideration
Service IndicatorsService Indicatorsnn Patient complaintsPatient complaintsnn TATTATnn Delayed testsDelayed testsnn Repeat testsRepeat testsnn MisMis--ID of specimensID of specimensnn Left without being seenLeft without being seennn Increase in STAT orders Increase in STAT orders
(outside of rounds)(outside of rounds)
HR IndicatorsHR Indicatorsnn Staff turnoverStaff turnovernn Staff injuryStaff injurynn OvertimeOvertimenn Education hoursEducation hoursnn Vacancy rateVacancy ratenn Sick timeSick timenn Satisfaction of staffSatisfaction of staffnn Understaffed according to Understaffed according to
planplannn Agency useAgency use
![Page 170: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/170.jpg)
Questions?…Questions?…
![Page 171: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/171.jpg)
Legislative Solutions to the
Laboratory Workforce Shortage
By Robin E. StomblerVice President, Government AffairsAmerican Society for Clinical Pathology
![Page 172: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/172.jpg)
Two Approaches
![Page 173: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/173.jpg)
Laboratory Budget Issues
n CPI Updaten Copayments & Competitive Biddingn Specimen Collection Feen Physician Payment Updaten Regulatory Reform
![Page 174: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/174.jpg)
Focus on Education
n Allied Health Project Grants- Title VII, Public Health Service Act- Attract professionals to field and
underserved communities- Proven success
![Page 175: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/175.jpg)
Allied Health Project Grants
n “Such sums”n $9.49 million - FY 2002n $0 – FY 2003 ???
![Page 176: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/176.jpg)
The Shortage
n ASCP Board of Registry & MORPACEWage and Vacancy Survey March 2001
n General Accounting Office Nov 2001In wake of the decline of medical technology education program enrollees, GAO noted that the overall supply of workers may be affected in coming years. "While little is known about recent trends in the utilization of laboratory services, demand is expected to rise as the U.S. population ages," the agency contended.
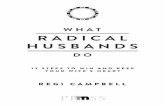
![Page 177: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/177.jpg)
0% 5% 10% 15% 20% 25%
Vacancy Rate
Histologic Technologist
Cytotechnologist
Medical Technologist
Medical LaboratoryTechnician
Vacancy Rate Percentages For Medical Laboratory Professions
1996
1998
2000
Source: 1996, 1998, 2000 Wage and Vacancy Survey. From ASCP Board of Registry, Chicago, IL, and Morpace International, Detroit, MI.
![Page 178: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/178.jpg)
Accredited Medical Laboratory Technology Programs
0
50
100
150
200
250
300
350
400
450
1990 1995 1999
Med
ical
Tec
hn
olo
gis
t P
rog
ram
s
0
5
10
15
20
25
30
35
40
His
tolo
gic
Tec
hn
icia
n P
rog
ram
s
MT Programs HT Programs
![Page 179: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/179.jpg)
Additional Concerns
![Page 180: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/180.jpg)
n Fall 2000 – ASCP Proposal- Focus on Laboratory Personnel Needs- No new programs- Education
Seeking Solutions
![Page 181: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/181.jpg)
Medical Laboratory Personnel Shortage Act of 2001
n Reps. John Shimkus, Jesse Jackson, Jr., Michael Bilirakis, Sherrod Brown
n HR 1948n Over 40 bipartisan cosponsorsn Focus on laboratory personnel
![Page 182: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/182.jpg)
HR 1948
n National Health Service Corpsn Allied Health Project Grantsn Breast and Cervical Cancern Public Health Improvement Actn NHLBI
![Page 183: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/183.jpg)
HR 1948 - Action
n Thousands of letters, phone calls, emailsn Joint letters to Congressn Testimonies & statementsn Hundreds of visits
![Page 184: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/184.jpg)
HR 1948 - Accomplishments
n “Laboratory techs are on par with nurses" n Congressional recognitionn Appropriations increase/recognitionn Public Health Security and Bioterrorism
Preparedness and Response Act
![Page 185: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/185.jpg)
Bioterrorism Law
The Secretary may make awards of grants and cooperative agreements to appropriate public and nonprofit private health or educational entities, including health professions schools and programs as defined in section 799B, for the purpose of providing low-interest loans, partial scholarships, partial fellowships, revolving loan funds, or other cost-sharing forms of assistance for the education and training of individuals in any category of health professions for which there is a shortage that the Secretary determines should be alleviated in order to prepare for or respond effectively to bioterrorism and other public health emergencies.
![Page 186: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/186.jpg)
A State Approach
n California SB 1809n MLTs able to practicen Governor signed!
![Page 187: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/187.jpg)
For CLIAC Consideration
n HHS Strategic Plan
n Importance of Education Funding
n Patient Safety
![Page 188: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/188.jpg)
American Society for Clinical Pathology1225 New York Avenue, NW
Suite 250Washington, DC 20005
(202) 347-4450www.ascp.org
![Page 189: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/189.jpg)
1
Clinical Laboratory WorkersCLIAC Meeting, September 12, 2002
Atul GroverChief Medical Officer
National Center for Health Workforce Information and AnalysisBureau of Health Professions
Health Resources and Services Administration
![Page 190: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/190.jpg)
2
Functions
l Develop the health professions workforce through research, analysis, and planning
l Improve distribution and diversity of health professionals to rural/urban underserved areas
l Improve the quality of health professions practice and education
l Focus on key 21st century health professions issues (geriatrics, genetics, diversity/distribution)
Bureau of Health ProfessionsMission and Functions
Mission: To increase health care access by assuring a health professions workforce that meets the needs of the public.
![Page 191: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/191.jpg)
3
Assuring an Adequate Health Care Workforce Requires:
Workforce Planning and
Analyses-----------------------à To Train the Right People
High Quality Education----à The Right Skills
Equitable Distribution-----à The Right places
![Page 192: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/192.jpg)
4
National Center for Health Workforce Information and Analysis
• Mission: Collect, analyze, and disseminate health workforce information and facilitate national, State, and local workforce planning efforts.
– Collect health professions-related data
– Assist State and local workforce planning efforts
– Conduct issues-related analyses
– Conduct evaluations of health professions training programs
– Develop tools and conduct research on the health workforce
![Page 193: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/193.jpg)
5
More Than 1 in 10 Americans Works in Health Care or is a Health Professional
141,558,183130,748,01610,810,167Total
128,817,103126,649,6852,167,418Other work settings
12,741,0804,098,3318,642,749Health service setting
TotalOther Workers
Health Professionals
2.9%4,098,498Other workers in health service settings
10.5%14,908,498US health workforce
100.0%141,558,183US civilian labor force
1.5%2,167,418Health professionals working in other settings
6.1%8,642,749Health professionals working in health service settings
4.1 million other
workers
8.6 million health
professions
2.2 million health
professions
Health professions Occupations
Health service settings
Bureau of Labor Statistics, 2001Figures shown are the average of 12 months’ data(October 2000 – September 2001)
![Page 194: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/194.jpg)
6
National Center for Health Workforce Analysis
Recent Products
4State Health Workforce Profiles
4Pharmacist Shortage Study
4GME Primer
4Comprehensive Health Workforce Profiles Pilot Project: 10 States
![Page 195: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/195.jpg)
7
National Center for Health Workforce Analysis
4State Health Workforce Profiles 2nd Edition
4Health Workforce: Trends, Issues, and Supply and Demand Projections
4Supply, Demand, and Shortages of RNs
4Comprehensive Health Workforce ProfilesPilot Project: 8 Additional States
4Activities
![Page 196: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/196.jpg)
8
National Center for Health Workforce Analysis
4Supply and Demand for Nursing Aides and Home Health Care Aides
4Scope of Practice Laws and Effect on Access
4State GME Financing and Health Workforce Goals
4The Impact of Changing Demographics on Requirements for Health Care Providers
4Activities
![Page 197: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/197.jpg)
9
National Center for Health Workforce Analysis
ØUniversity of California/San Francisco (UCSF) (http://futurehealth.ucsf.edu/cchws.html)
ØState University of NY Albany (SUNY/Albany) (http://chws.albany.edu)
ØUniversity of Illinois Chicago (UIC) (http://www.uic.edu/sph/ichws)
ØUniversity of Washington Seattle (UW) (http://www.fammed.washington.edu/CHWS/index.html)
ØUniversity of Texas Health Sciences Center at San Antonio (Coming Soon!)
Regional Centers for Health Workforce Studies
![Page 198: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/198.jpg)
10
National Conference of State Legislatures
Comprehensive Health Workforce Profiles Pilot Project: 18 States
In 2002 = CO, ME, MO, MN, NM, NY, OH, TN
![Page 199: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/199.jpg)
11
Demand for Health Professionals Will Grow at Twice the Rate of All Occupations Between
2000-2010
Source: Dept. of Labor, Bureau of Labor Statistics, Occupational Employment Statistics
2000 2010 Percent
(000's) (000's) Change
Total U.S Employment 145,594 167,754 15%
Total Health Occupations 10,984 14,186 29%
Physicians 598 705 18%
Dentists 152 161 6%
Pharmacists 217 270 24%
Registered Nurses 2,194 2,755 26%
Mental and Behavioral Health Occupations 518 657 27%
Therapists 479 639 33%
Public and Environmental Health 241 302 25%
Health Technicians and Technologists 2,459 3,090 26%
Health Service Occupations 3,197 4,264 33%
![Page 200: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/200.jpg)
12
The Growth in the Number of Elderly Citizens Will Increase Requirements for Health Care
Providers
The Number of Elderly Citizens is Growing Steadilyin the United States
0
10
20
30
40
50
60
70
80
90
1960
1970
1980
1990
2000
2010
2020
2030
2040
2050
Millions
Population 65 thru 84 Population 85 and older
![Page 201: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/201.jpg)
13
National Center (SUNY Albany)The Health Workforce: Trends, Issues, and
Supply and Demand Projections
1.9
2
2.1
2.2
2.3
2.4
2.5
2.6
2.7
2000 2005 2010 2015 2020
Millions
FTE RN Requirements
FTE RN Supply
Source: Projections by Division of Nursing, BHPr, HRSA, HHS, 1996
Projections and Requirements of FTE RNs
![Page 202: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/202.jpg)
14
Pharmacists per 100,000 Population: 1970-2000
0
10
20
30
40
50
60
70
80
1970 1975 1980 1985 1990 1995 2000
RPhs/100,000population
Pharmacists--Shortage?
Source: Bureau of the Census
![Page 203: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/203.jpg)
15
Pharmacist Shortage—Rx Growth Rate
0
2
4
6
8
10
91 92 93 94 95 96 97 98 99 00
Perc
ent
Pharmacists Prescriptions
Source: IMS, 2000 (No. of prescriptions), HRSA/BHPr Pharmacist Supply Model (pharmacists)
![Page 204: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/204.jpg)
16
Health Care Worker Shortages• Registered nurses
• Direct care workers
• Clinical lab technologists and technicians
• Radiology techs
• Pharmacists
• Dentists
• Information system specialists
• Medical coders
![Page 205: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/205.jpg)
17
Clinical Laboratory Workers• Generally, clinical laboratory technologists
hold a bachelor’s degree with a major in medical technology or in a life science
• Clinical laboratory technicians generally hold an associate’s degree or certificate
• Employment for both categories expected to grow
Source: Bureau of Labor Statistics, Occupational Outlook Handbook
![Page 206: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/206.jpg)
18
Clinical Lab Worker Job Growth
• Lab technologists and technicians held 295,000 jobs in 2000
• Half working in hospitals, remainder in labs, offices, physician clinics (some in blood banks, research and testing)
• Employment expected to grow 15% through 2010 (equal to other occupations)
Source: BLS
![Page 207: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/207.jpg)
19
Job Growth Factors• Technological advances: Dual effects
– Additional diagnostic tests developed to increase demand
– R&D simplifying routine testing, allowing for movement out of the laboratory setting
• Aging population with increased needs
• Need to replace workers who retire, transition to other fields
Source: BLS
![Page 208: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/208.jpg)
20
Tasks of Medical Technologists
• Collect and prepare specimens• Perform routine & specialized lab tests• Recognize QC, instrument, data problems• Train other lab personnel• Communicate results to technical/lay people• Participate in continuing education• Recognize normal and abnormal values• Correlate abnormal values with disease
status
Survey data from certified MT (ASCP) Lab Medicine, 31(7), July 2000
![Page 209: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/209.jpg)
21
Training: Medical Technologists (MT)
Hospital 46%
University45%
Medical Center6%
Other3%
Baccalaureate Degree in MT or Biological Sciences with Training
Lab Medicine 2001. 32(11): pp 655-660
![Page 210: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/210.jpg)
22
Demographics: Medical Technologists
• 76% Female
• 97% Baccalaureate degrees (3% Grad/other)
• 58% Urban, 24% Suburban, 18% Rural
• 46% Married
Survey data from certified MT (ASCP) Lab Medicine, 31(7), July 2000
![Page 211: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/211.jpg)
23
Demographics: Medical Technologists
Survey data from certified MT (ASCP) Lab Medicine, 31(7), July 2000
Black/AA13%
White69%
Latino8%
Asian9%
Other1%
![Page 212: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/212.jpg)
24
Medical Technologists: Specialization
• Clinical chemistry technologists
• Microbiology technologists
• Blood bank (immunohematology) technologists
• Immunology technologists
• Cytotechnologists
• Molecular biology technologists
Source: BLS
![Page 213: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/213.jpg)
25
Training: Specialists in Blood Banking (SBB)
Hospital 30%
University20%
Blood Center40%
Medical Center10%
Baccalaureate Degree in Health Sciences, One Year Training Program
Lab Medicine 2001. 32(11): pp 655-660
![Page 214: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/214.jpg)
26
Training: Cytotechnologists (CT)
Hospital 25%
Comm College2%
University25%
Medical Center39%
Other9%
Baccalaureate Degree and Completion of Accredited CT Program
Lab Medicine 2001. 32(11): pp 655-660
![Page 215: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/215.jpg)
27
Medical and Clinical Laboratory Technicians
• Perform less complex tests than technologists
• May prepare specimens and operate automated analyzers
• May also specialize– Histology technicians– Phlebotomists
Source: BLS
![Page 216: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/216.jpg)
28
Training: Medical Laboratory Technicians (MLT)
Hospital 1%
Comm College70%
University11%
Medical Center1%
Other17%
Associate Degree, Completion of Accredited CLT/MLT or Certificate Program
Lab Medicine 2001. 32(11): pp 655-660
![Page 217: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/217.jpg)
29
Training: Histologic Technician (HT)
Hospital 31%
Comm College37%
University16%
Medical Center16%
Baccalaureate Degree, Completion of Accredited HLT Program
Lab Medicine 2001. 32(11): pp 655-660
![Page 218: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/218.jpg)
30
Total Number of US Medical Laboratory Technologists and Technicians
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998
Source: BLS
![Page 219: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/219.jpg)
31
Accreditation• National Accrediting Agency for Clinical
Laboratory Sciences (NAACLS) – Medical/clinical technologists, technicians,
histologic technologists/technicians, pathologists assistants
– Programs in phlebotomy, cytogenetic technology, molecular biology, clinical assisting
• Commission on Accreditation of Allied Health Education Programs (CAAHEP)
• Accrediting Bureau of Health Education Schools (ABHES)
![Page 220: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/220.jpg)
32
Licensure• Licensure requirements vary by state
• Certification is voluntary, though required by many employers– American Society of Clinical Pathologists
Board of Registry – American Medical Technologists– National Credentialing Agency for Laboratory
Personnel– Board of Registry of the American Association
of Bioanalysts
![Page 221: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/221.jpg)
33
ASCP Certification--- Technicians and Technologists
Medical Technologists
Medical Laboratory Technicians
1980 6,340 2,865
1985 5,085 2,447
1990 2,849 1,647
1995 3,217 2,120
1996 3,051 2,263
1997 2,760 2,001
1998 2,476 1,766
1999 2,216 1,395What Has Happened to All the Techs ? Pennell C. Painter, Ph.D . http://www.ivdtrials.com/TechStaff.htm
![Page 222: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/222.jpg)
34What Has Happened to All the Techs ? Pennell C. Painter, Ph.D . http://www.ivdtrials.com/TechStaff.htm
![Page 223: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/223.jpg)
35
Medical Laboratory Technician and Techologist
Training Program Declines.
Source: AMA, Health Professions Career and Education Directory
Health Professions Education Programs: 1985-2000
Change1985 1990 1995 2000 1985-2000
Medical Laboratory Technologists 584 420 357 255 -56.3%Medical Laboratory Technicians 281 256 260 242 -13.9%
Total 865 676 617 497 -42.5%
![Page 224: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/224.jpg)
36
Number of Graduates Declining
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
1995 1996 1997 1998 1999 2000
Clinical LaboratoryTechs.
RadiologicTechnologist
Cytotechonologist
Year
Nu
mb
er o
fG
radu
ates
Source: AMA, Health Professions Career and Education Directory (various eds.)
Occupation % Change-29%
-14%
-30%
![Page 225: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/225.jpg)
37
Total Enrollment in NAACLS and CAAHEP Accredited Programs
0
500
1,000
1,500
2,000
2,500
3,000
3,500
1997 1998 1999 2000
CT HT MLT MT SBB
ASCP BOR Survey, 2001
![Page 226: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/226.jpg)
38
Vacancy rates—a good measure of shortages
• In 2000, the vacancy rates for these disciplines exceed the average unemployment rate—typically about 5%--by two- to four-fold.
• Conversely, very high employment for new grads– Cytotechnologists 98%– Histologic Technicians 96%– Medical Laboratory Technicians 96%– Medical Technologists 96%– Specialists in Blood Banking 100%
Sources: National Society for Histotechnology, Lab Medicine 2001: 32(11) pp 655-660
![Page 227: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/227.jpg)
39
0
5
10
15
20
25
1994 2000
Perc
ent
Histo. Technicians HistotechnologistCytotechnologist PhlebotomizesMedical Technologists
Vacancy Rates for Select Laboratory Personnel: 1994-2000
Source: Lab Medicine 2001: 32(3) pp 124-138
![Page 228: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/228.jpg)
40
Washington State—Example of Shortages
54%
52%
53%
63%
100%
75%
82%
100%
31%
42%
55%
77%
79%
96%
92%
88%
42%
46%
54%
71%
84%
87%
88%
91%
0% 25% 50% 75% 100%
Medical LaboratoryTechnicians
Medical Technologists
Medical Records Coders
Radiographers/RadiologyTechnologists
Radiation TherapyTechnologists
Licensed Pharmacists
Ultrasound Technologists
Nuclear MedicineTechnologists
% of Hospitals Reporting
overallurbanrural
* Of hospitals employing the position
Percent of Hospitals Reporting Difficulty Recruiting Personnel for Select Occupations
![Page 229: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/229.jpg)
41
Medical Technologists and Medical Laboratory Technicians
Median Annual Salaries, 2000[1]Medical
TechnologistsMedical
LaboratoryTechnicians
All Settings $40,518 $27,539
Office and Clinics of Medical Doctors
$38,854 $27,186
Hospitals $40,851 $28,870
Medical and Dental Laboratories
$39,790 $25,251
[1] Occupational Employment Statistics, Bureau of Labor Statistics.
![Page 230: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/230.jpg)
42
Mean Annual Salaries, Medical and Clinical Lab Technologists (2000)
$0$10,000$20,000$30,000$40,000$50,000$60,000
NYC
Syrac
use LA
SanF
ran.
Chicag
oMiam
i
Tampa
Dallas
Housto
n
Louis
ville
BLS Data
![Page 231: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/231.jpg)
43
Salary data can help identify a shortage.
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
1983 '84 '85 '86 '87 '88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 '00
Clinical Lab. Workers Radiologic technicians
Pharmacists Physical therapists
Median Annual Earnings of Select Health Occupations: 1983-2000
Source: Bureau of Labor Statistics, Current Population Survey
![Page 232: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/232.jpg)
44
Factors Affecting Labor MarketBLS predicts need for 120,000 new technicians
and technologists between 2000-2010
Supply factors include• Retirement of a large number of clinical
laboratory technicians
• Individuals choosing more lucrative technical careers over clinical laboratory sciences
• Like nursing, which is also heavily a women dominated field, women now have more career opportunities and can choose better paying jobs
![Page 233: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/233.jpg)
45
Increased Demand for Laboratorians
• Volume of tests expected to increase with population growth and the aging of population
• Technological advances and new tests
• Need to replace transitioning workers
![Page 234: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/234.jpg)
46
Laboratorian Shortages: Reported Factors
• Salary levels
• Few opportunities for advancement
• Stressful working conditions
• Lack of visibility on the health care team
• Lack of a professional image
• Risk of infectious diseases
• Increased legal liabilities
![Page 235: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/235.jpg)
47
Barriers to Addressing Lab Worker Shortages
• Diversity of professions and professional training, including training sites
• Lack of data on all laboratorians
• Difficulty in predicting technological changes
• Unknown usage of alternate workers (and ability to substitute)
![Page 236: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/236.jpg)
48
![Page 237: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/237.jpg)
49
Clinical Laboratory Sciences Personnel Shortage Study
• Employment of clinical lab workers estimated at 295,000 in 2000
• Vacancies reported from 10% to 22%
• Employment projected to grow to 348,000 by 2010• Study to assess supply, demand, and shortages of
– Clinical Laboratory Scientists & Medical Laboratory Technologists
– Histotechnologists– Histologic Technicians– Cytotechnologists– Pathologist Assistants
2003
![Page 238: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/238.jpg)
50
Key Questions to be Addressed
• How many lab workers will be needed, and where?
• How many will be formally trained?
• How many will come from alternate career paths/training?
• How are responsibilities affected by education/training?
![Page 239: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/239.jpg)
51
Key Questions to be Addressed• Where will supply fall short of demand?
• What are key factors influencing supply/demand now and in the future?
• What is the impact of a clinical lab worker shortage on the health care system?
• What are the recommendations of the clinical lab worker professions to address workforce?
![Page 240: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/240.jpg)
Report To CLIACon SACGT
Patricia Charache, M.D.September, 12, 2002
![Page 241: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/241.jpg)
SACGT ReportSeptember 12, 2002
The Charter for SACGT expired in August.
• DHHS has decided not to renew the charter of SACGT
![Page 242: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/242.jpg)
Format of This Presentation • Summarize the premise and outputs of
SACGT in areas in which its activities relate to issues that impact directly on quality of patient care laboratory practices.
• (The body of SACGT’s activities involved areas not in CLIAC’s purview.)
![Page 243: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/243.jpg)
Background Premise• Over 800 genetic tests now exist, (577 in CLIA
approved labs, 368 in research labs). Most target rare genetic disorders; others are being developed.
• These tests have multiple uses, e.g. newborn screening, carrier screening, predictive testing, disease diagnosis or prognosis, pharmacogenetics.
• Some, especially predictive tests, raise sensitive medical, social, ethical, and legal issues.
![Page 244: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/244.jpg)
SACGT Charter• Advise the Secretary on all aspects of the
development and use of genetic tests. Includes– safe and effective incorporation of genetic
technologies into health care– assessing the effectiveness of existing and
future measures for oversight of genetic tests, and
– identifying research needs related to the Committee’s purview.
![Page 245: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/245.jpg)
Accomplishments• Recommendations By SACGT (7/00)
There is a need:– To improve the oversight of genetic tests– For Federal legislation to prevent
discrimination in insurance and employment– Study the effect of gene patents and licensure– Study further the issue of informed consent
of third parties in human research subjects.
![Page 246: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/246.jpg)
Recommendations Pertaining to Adequacy of Oversight of Genetic Tests
(Continued)
• The FDA should regulate laboratory developed genetic tests (“home brews”), using an innovative, flexible approach
• CLIA should be augmented to incorporate specific provisions for genetic testing laboratories
• Private-public collaborations are needed to ensure continued analysis of post market data
![Page 247: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/247.jpg)
Definitions: (PC痴)• Analytical Validity: Primarily concerned with
ability to accurately measure a given analyte.• Clinical validity: Ability to separate clinical
disease from no disease or risk of disease through measuring that analyte.
• Clinical utility: Clinical validity plus full knowledge of test , including gene penetrance, etc.significance in populations to be tested.
![Page 248: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/248.jpg)
Ongoing SACGT Considerations:Oversight
Who is responsibleActivity IRB CLIA FDA
Research (development) X
Research, (validatedanalytically, clinically)limited patient reports X X
Wide use patient reports, +/- X Xfully validated, +/-continued research
![Page 249: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/249.jpg)
Ongoing SACGT Activities:Work Groups and Task Forces
• Pursued recommendation issues • Established work groups for additional
issues related to other aspects of testing– Education – IRB/Consent– Rare Diseases– Access– Data collection, clinical utility information
![Page 250: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/250.jpg)
Education Work Group• Assess the adequacy of current efforts to
advance genetics education of health professionals
• Year-long data gathering and fact finding; educational summit in Baltimore, May, 2002.
Issues: For appropriate pre- and post-analytical aspects of testing, educated users are required. Laboratory Directors, IRB’s, clinicians, others need knowledge base.
![Page 251: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/251.jpg)
Consent/IRB Work Group• A brochure was developed to explain genetic
testing and informed consent to the public• White paper was under development on
principles of informed consent, defining levels of consent, and consent recommendations for various types of genetic tests
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Laboratory Issues: Who decides level of consent What is the laboratory痴 role in assuring patient consent?
![Page 252: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/252.jpg)
Rare Disease Testing Work Group • Definition of a rare genetic disease• Developmental and practice incentives• Special access issues• Quality assurance and validation assistance for
research laboratories testing for rare diseases. --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Issues: Limited test sites, mainly research labs , home brew tests if limited industrial interest, no proficiency tests, patent issues
![Page 253: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/253.jpg)
Access Work Group Discussions• Reimbursement for:
– Test cost– Genetic education and counseling– Other professional services– Non-reimbursed laboratory costs
• Health care disparities • Gene patents and licensing:
– Value for industrial interest in development– Issue for access and quality assurance
![Page 254: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/254.jpg)
Data Work GroupGoal: To improve knowledge of the disease and
the clinical validity and utility of a test• Needs: Improved post market data collection, access to
data, resources for data organization, and analysis. Both clinical and laboratory data are required
• Survey of HHS activities to advance knowledge of clinical validity and utility (translational research)
---------------------------------------------------------------Lab Issues: Who is to provide the data and how?
Privacy? Cost? Definitions of a test, etc.
![Page 255: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/255.jpg)
Additional Concerns Supportive of CLIAC’s Reports
• Waived tests (of major concern as they apply to genetic testing because of pre- and post analytical considerations)
• CMS study of laboratories performing waived tests
![Page 256: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/256.jpg)
SummarySACGT recommendations and considerations:• Oversight functions, including FDA review of
tests, template approach and enhanced CLIA• Additional subject matter covered by work
groups and task forces: Education, IRB/Consent, Rare Diseases, Access, Data Work Group
• Other issues: Patent issues; (Waived tests, CMS findings of Waived testing laboratories)
![Page 257: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/257.jpg)
Outstanding Issues • Classification of laboratory oversight
responsibilities, clarifying when CLIA applies to research facilities
• Provision of education/guidance documents for IRB’s, and/or research laboratories interested in patient care
• Oversight of laboratory developed tests: CMS and deemed status organization feasible assessment instruments for analytical and clinical validation (not full clinical utility).
![Page 258: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/258.jpg)
Outstanding Issues • Informed consent issues, (check off box on lab
requests?)• Reimbursement for laboratory expenses associated
with clinical user discussions.• Education of Laboratory Directors and Technical
Supervisors specific to genetic testing• Consideration of result implications in test
categorization decisions, e.g. waived vs. other .
![Page 259: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/259.jpg)
Molecular genetic test orders
Kathy LaBeau, Network Director Pacific Northwest Laboratory Medicine Sentinel Monitoring Network
Presentation to CLIAC – September 12, 2002
![Page 260: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/260.jpg)
Genetic testing in Washington and the Pacific Northwest
n Snapshot of testing in 2001/2002n What tests are being ordered?n Where are tests being performed?n How is the genetic testing laboratory
chosen?
![Page 261: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/261.jpg)
Washington State database
n WA Medical Test Site (MTS) Programn CLIA-exempt state programn More detail about genetic tests than CLIA
database n Molecularn Biochemicaln Cytogeneticn Maternal serum AFP
![Page 262: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/262.jpg)
Genetic testing in Washingtonn 13 of 716 moderate/high
complexity labs (1.8%) perform genetic testingn 12/13 molecular n 6/13 cytogeneticn 2/13 biochemical
![Page 263: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/263.jpg)
Genetic testing in Washington
n 6 research labs n Providing results for patient care
n 4 hospitals (university & children’s)n 2 independent labs (1 hospital-based)n 1 State public health lab (newborn
screening)n 85% are accredited by private organization
n CAP, AABB, ASHI
![Page 264: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/264.jpg)
Genetic testing in Washington
n 11 of 716 moderate/high complexity labs (1.5%) perform maternal serum AFP
n Genetic testing accounts for 0.4% of total volume of testing in Washington’s moderate/high complexity labs
n 0.37% of which is newborn screening
![Page 265: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/265.jpg)
Data from Pacific NW network
n Lab Medicine Sentinel Monitoring Network n Voluntary participation by 600+ laboratories
n Waived, PPMP, moderate, high complexityn POL, hospital, independent labsn Alaska, Idaho, Oregon, Washington
n Questionnaire sent to 330 moderate & high complexity labs in January 2002
n 204 respondents - Genetic testing orders
![Page 266: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/266.jpg)
Questionnaire respondents
464950WA (%)
322222OR (%)
161919ID (%)
699AK (%)
All labs in Pacific NWN = 1539
All network participantsN = 330
Questionnaire respondentsN = 204
![Page 267: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/267.jpg)
Questionnaire respondents
303332Accredited(%)
73/17/1059/31/1059/31/9 POL/Hosp/IL(%)
68/3256/4454/46Urban/Rural(%)
All labs in Pacific NWN = 1539
All network participantsN = 330
Questionnaire respondentsN = 204
![Page 268: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/268.jpg)
Network questionnaire results
n 53% of respondents handled orders for molecular genetic tests in previous 3 months (October - December 2001)n 66% of hospitalsn 58% of independent (reference) labsn 46% of physician office labs
![Page 269: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/269.jpg)
What tests are most commonly ordered?
n 1) Factor V Leiden Thrombophilia
n 2) Fragile X Syndromen 3) Hemochromatosisn 4) Cystic Fibrosisn 5) Hemoglobin S
n 6) BCR/ABL Translocation
n 7) BRCA-1 or BRCA-2n 8) Huntington Diseasen 9) Prader-Willi Syndromen 10) Y Chromosome
Detection
![Page 270: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/270.jpg)
On-site testing
n 2% of the network respondents performed molecular genetic testing on-siten 3 independent, 1 hospital n All urbann All accredited
![Page 271: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/271.jpg)
Send-out testing
n 62% sent orders to their reference lab, who in turn decided where the test would be performed
n 7% sent orders directly to the genetic testing lab
n 31% did some combination of these
![Page 272: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/272.jpg)
How is the genetic testing laboratory chosen?
n Of 95 responses:n 39 % Information from reference lab (37%) or
Internet resource about reference labs (2%)n 39 % Information from health care provider
n Genetic counselor (12%)n Patient’s provider (12%)n Medical geneticist (10%)n Neurologist, oncologist, pathologist, etc (5%)
n 8 % Do not known 4 % Mandated by managed care contract agreement
![Page 273: Gutman 0902.ppt [Read-Only] - CDC](https://reader039.fdokumen.com/reader039/viewer/2023050401/63384eb09a134d8bc704bcc0/html5/page/273.jpg)
Where does testing go?
n 52% stays within the Pacific NW regionn 48% is sent out of the region
n 15% to large national reference labsn Quest/Nichols Institute - California n Lab Corp - North Carolina
n 33% to other genetic testing labs
Copyright © 2022 FDOKUMEN

