







Bahasa
Halaman
Hukum


Original article
Factors of morbidity in hemispherectomies:
Surgical technique!pathology
Antonio Nogueira de Almeida*, Raul Marino Jr., Suely Kazuo Marie,
Paulo Henrique Aguiar, Manoel Jacobsen Teixeira
Departamento de Neurologia, Hospital das Clinicas, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, Brazil
Received 15 May 2005; received in revised form 30 July 2005; accepted 1 August 2005
Abstract
Objective: The objective of this paper is to evaluate factors of surgical morbidity from different techniques of hemispherectomy with
emphasis on causative pathology. Patients and methods: Thirty patients underwent hemispherectomy in our institution from 1987 to 2003,
two presented with Sturge–Weber Syndrome (SWS), sixteen with Rasmussen’s Syndrome (RS), eight with established hemispheric lesions
(EHL), and four with cortical development malformations (CDM). Six surgeons operated on three patients using anatomical
hemispherectomies (AH), 11 patients using functional hemispherectomy (FH), and 16 patients employing hemispherotomy (HT). Surgical
technique and causative pathology were studied independently as factors of morbidity in hemispherectomy. Results: Overall mean surgical
time was 11:50G3:20 h and increased proportionately in pathologies with larger hemispheres. Blood transfusion was particularly influenced
by the approach adopted by our team of anesthesiologists, independently of technique or pathology. Pathology was the most important factor
related to hydrocephalus as two out of four patients with CDM needed ventriculoperitoneal shunt whilst none with EHL or SWS. Four
patients undergoing HT and one FH presented residual bridges connecting the hemispheres, three were reoperated and are seizure free. Two
patients with CDM did not improve their seizures worthwhile with surgery and other two (one with RS and other with CDM) were waiting a
second procedure due to incomplete inter-hemispheric disconnection. Five patients presented infection and one died after developing
meningoencephalitis. Conclusion: Hemispherectomies are procedures where pathology and surgical technique interact narrowly. Therefore,
in order to study surgical morbidity or outcome, both pathology and technique have to be analyzed independently.
q 2005 Elsevier B.V. All rights reserved.
Keywords: Hemispherectomy; Hemidecortication; Hemispherotomy; Functional hemispherectomy; Epilepsia; Neurosurgery; Morbidity
1. Introduction
Anatomical hemispherectomy (AH) has been used in
treating seizure since the 1930s. However, it was almost
abandoned in the 1960s after reports of postoperative
fatalities caused by hydrocephalus, hemosiderosis, and
trivial head traumas [1]. Despite serious complications,
patients’ remarkable improvement encouraged surgeons to
0387-7604/$ - see front matter q 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2005.08.005
* Corresponding author. Address: Instituto Neurologico de Sao Paulo,
Rua Maestro Cardim, 808Liberdade, Sao Paulo, SP CEP 01323-001, Brazil.
Tel.: C55 11 9659 2857/3141 9550; fax: C55 11 3141 9556.
E-mail address: [email protected] (A.N. Almeida).
modify the AH in order to lessen its morbidity whilst
preserving efficacy. Efforts to improve the technique gave
rise to several unique procedures, which remain in use to
this day.
Given that all approaches are able to achieve complete
isolation of the damaged hemisphere, sufficient to render the
patient free of seizures [2], the rationale behind choosing a
particular technique should be based on its related
morbidity. Unfortunately, comparing the morbidity of
different techniques drawing from the literature is not
straightforward. Some authors describe blood loss, operat-
ive time, and risk of developing either hydrocephalus or
hemosiderosis, as drawback parameters related specifically
to the technique [3,4]. However, it would be reasonable to
assume that other factors, such as the causative pathology,
Brain & Development 28 (2006) 215–222
www.elsevier.com/locate/braindev

A.N. Almeida et al. / Brain & Development 28 (2006) 215–222216
also bias these parameters. Furthermore, most papers give
an account of a series of cases operated on by the same
individual and as a consequence the experience and ability
of the surgeon in question are bound to have a considerable
influence on results.
In the literature, pathology is already considered the
main determinant for seizure control, where its importance
for intra and postoperative course has been cited but as yet
not fully addressed. The objective of this paper is to evaluate
the surgical morbidity of different techniques of hemi-
spherectomy with emphasis on pathology as a distinct
morbidity factor.
2. Patients and methods
Thirty patients underwent hemispherectomy in our
institution from 1987 to 2003, these being fourteen females
and sixteen males with an average age of 11.5G8.9 years,
ranging from 7 months to 38 years. Pre-operative work up
included a thorough history of the disease, video-EEG with
seizure recordings, neuropsychological evaluation, CT scan,
and MRI. The Wada test was used only when language
lateralization was uncertain. A multidisciplinary group
analyzed the data before a final agreement on surgery was
reached.
In this series, two patients presented with Sturge–Weber
Syndrome (SWS), sixteen with Rasmussen’s Syndrome
(RS), eight with established hemispheric lesions, sequelae
of previous vascular or traumatic event, with or without
porencephalic cyst (EHL), and four with cortical develop-
ment malformations (CDM) (three with hemimegalence-
phaly and one with hemispheric cortical dysplasia).
In order to analyze our data and compare our results to
the literature, hemispherectomy techniques currently in use
were allocated to one of two main groups. Group 1 included
those techniques that completely remove the cortex from the
hemisphere, whilst Group 2 comprised those associated to
partial cortical removal and fiber disconnection. Group 1
presented two sub-divisions based on ventricular integrity
where Group 1A included techniques that involve opening
the lateral ventricles (called anatomical or classical
hemispherectomy) and Group 1B those that kept them
closed (called hemidecortication or hemicorticectomy).
Group 2 was sub-divided into three: functional hemispher-
ectomy (FH), as described by Rasmussen (Group 2A),
techniques that disconnect the hemisphere from a vertical
approach (Group 2B), and techniques disconnecting the
hemisphere from a lateral approach (Group 2C). In the
literature techniques included in the groups 2B and 2C are
frequently known as hemispherotomy. Fig. 1 shows
schematic drawings of techniques included within each
group.
Six surgeons operated on thirty patients. Three patients
underwent anatomical hemispherectomies (Group 1A), 11
patients underwent the functional hemispherectomy (Group
2A) and 16 were operated on employing three different
techniques from the lateral approach group (Group 2C).
Surgical time (from skin incision to skin closure), blood
transfusion, hydrocephalus, postoperative seizures, infec-
tion, and mortality/unexpected-neurological-deficits were
reviewed as parameters of morbidity. At least three samples
of peripheral blood were examined for each patient, one
preoperatively, one within 12 h following surgery, and
another on the third postoperative day.
2.1. Statistical analysis
Mean values and standard deviation were obtained from
all analyzed data. The two groups with different leukocyte
counts were compared using the Mann–Whitney test,
whereas the c2 test was employed to compare groups with
diverse surgical times and diverse volumes of blood
transfusion. Statistical significance was considered present
for P!0.05.
3. Results
3.1. Surgical time
Overall mean surgical time was 11:50G3:20 h, varying
from 6:30 to 19:00 h. Comparing different pathologies,
surgical time increased proportionately with larger hemi-
spheres though figures were not statistically significant.
Hemispherectomies on patients with CDM took on average
13:30 h, while on patients with RS or SWS the time stood at
12:00 h on average, whilst patients with EHL took 11:30 h.
The technique employed did not affect procedure length.
3.2. Blood transfusion
All but one patient in this series received a blood
transfusion during surgery. On average, each patient
received 3.3G1.4 units of packed red blood cells. Despite
transfusion, hemoglobin levels fell 1.0G1.4 g/dl, compar-
ing pre and immediate postoperative values. Hemoglobin
values on immediate postoperative hemogram averaged
12.5G1.5 g/dl. Over the first days after the procedure,
levels of hemoglobin continued to drop, by an average of
2.6G2.0 g/dl, and six patients had a second transfusion,
usually when their hemoglobin levels fell below 10 g/dl.
Hemoglobin reached its lowest values between the second
and the fifth postoperative day. There were no statistical
differences among groups of pathologies, or surgical
techniques in relation to blood transfusion requirement.
Ten patients developed leukocyte counts of over 20,000
cells per mm3 on the blood sample collected within 12 h
after surgery. This group evolved with an average decline in
hemoglobin of 3.8G1.7 g/dl over the proceeding day. In
contrast, patients with leukocyte counts below 20,000 cells
per mm3 presented an average decline of only 2.0G1.7 g/dl
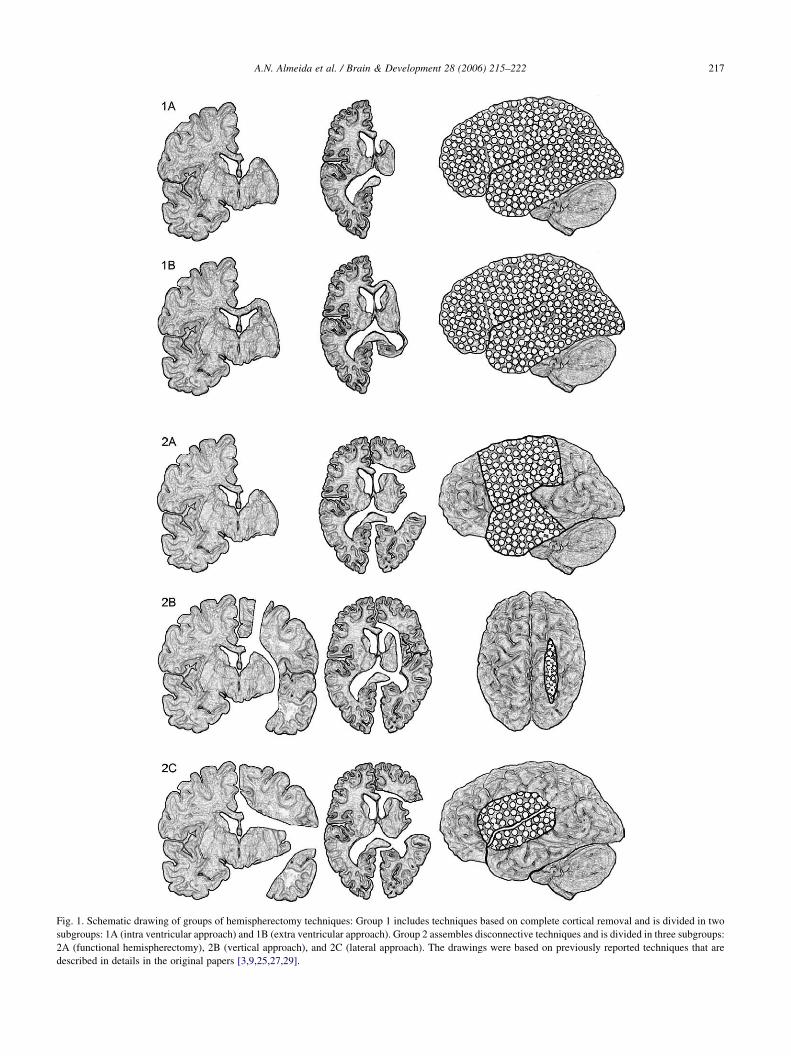
Fig. 1. Schematic drawing of groups of hemispherectomy techniques: Group 1 includes techniques based on complete cortical removal and is divided in two
subgroups: 1A (intra ventricular approach) and 1B (extra ventricular approach). Group 2 assembles disconnective techniques and is divided in three subgroups:
2A (functional hemispherectomy), 2B (vertical approach), and 2C (lateral approach). The drawings were based on previously reported techniques that are
described in details in the original papers [3,9,25,27,29].
A.N. Almeida et al. / Brain & Development 28 (2006) 215–222 217

A.N. Almeida et al. / Brain & Development 28 (2006) 215–222218
in hemoglobin (P!0.01). Variations in early postoperative
leukocyte counts were not linked to causative pathology,
technique, intra-operative blood transfusion, or surgical
length.
Data from each patient regarding surgical time, age,
hemoglobin variation, and the first postoperative white
blood count, separated by pathology and surgical technique
are shown on Tables 1 and 2.
3.3. Hydrocephalus
Three patients developed hydrocephalus three, four, and
six months respectively, after the hemispherectomy, and
underwent ventriculoperitoneal shunts, one with RS and two
with CDM. Two had undergone procedures from Group 2C
and one from Group 1A.
3.3.1. Postoperative Seizures
After surgery, MRI detected a residual bridge in the
corpus callosum connecting the hemispheres in five patients
(four with RS and one with CDM, four had undergone FH,
Table 1
Patient’s data separated by causative pathology
ID Path. Tech. Age Surg. time HB1 H
1 CDM 2C 2.2 17:00 15.8 12
2 CDM 2A 13 12:30 15.2 13
3 CDM 2C 1.7 18:00 14.9 14
4 CDM 1A 0.6 6:30 13.4 14
5 EHL 2C 16 9:00 14.7 12
6 EHL 2C 19 13:00 14.2 12
7 EHL 2C 7 12:00 11.3 13
8 EHL 2C 33 10:30 16.6 11
9 EHL 2C 16 12:30 11.6 10
10 EHL 2C 8 13:30 13.3 10
11 EHL 2C 18 11:30 14.2 12
12 EHL 2C 38 9:30 15.4 14
13 RS 2A 15 11:00 13.9 14
14 RS 2C 11 14:00 12.4 11
15 RS 2C 3 19:30 13.6 12
16 RS 2C 7 15:30 12.2 12
17 RS 2A 8 8:00 12.9 11
18 RS 2A 14 8:50 15 13
19 RS 1A 21 9:00 15.5 14
20 RS 2A 4.5 13:00 12.9 12
21 RS 2A 13.5 14:00 14 13
22 RS 2C 16 15:30 13.5 13
23 RS 2C 7 15:00 12.4 13
24 RS 2A 6.5 13:00 13.5 12
25 RS 2A 5.2 8:30 12.8 13
26 RS 2A 5.5 8:15 12.5 11
27 RS 2A 8 10:30 11.5 10
28 RS 2A 21 8:00 14.5 12
29 SWS 2C 4.5 8:00 13.1 11
30 SWS 1A 0.7 8:00 10 7
Legends: ID (patient’s identification), Pathol. (causative pathology), Tech. (used
surgery in years), Surg. Time (surgical time from skin to skin), HB1 (preoperati
lowest postoperative value), HB1-HB2 (difference between preoperative and imme
and the lowest postoperative hemoglobin), BT (blood transfusion in units of pack
* Patients that receive a second blood transfusion. ** The patient received blood
Group 2A, and one HT, Group 2C). All these patients
developed postoperative seizures and, on closer investi-
gation, scalp EEG disclosed epileptic activity spreading
between the hemispheres. Three patients with RS underwent
a second operation to complete disconnection of the corpus
callosum and became seizure free thereafter. Intense
electrical activity was revealed by electrocorticography
over the insula in one of these patients where the area was
then removed during the operation. The other two patients
with incomplete disconnection are awaiting a second
procedure.
Twenty-one patients received follow-up over one year,
three over less than a year, whilst one deceased, and five
were lost during follow-up. A total of 17, out of 21, were
seizure free or had a 90%, or greater, improvement in their
seizures. Four patients remained with seizures, which
recurred few days after the surgery. Two of these were
awaiting a second procedure, made necessary due to
incomplete disconnection of the corpus callosum (one
with RS and other with CDM) and the remaining two did not
improve significantly with surgery (both had CDM).
B2 HB3 HB1-HB2 HB2-HB3 BT WBC
.1 9.7 3.7 2.4 2 15600
.6 9.6 1.6 4 3 21600
.5 8.6* 0.4 5.9 3.2 30000
.1 10.1 K0.7 4 3.5 14200
.1 11.7 2.6 0.4 3 12620
.8 9.6 1.4 3.2 2 37700
.3 8* K2 5.3 2 26300
.9 10.2 4.7 1.7 0 14370
.4 10.3 1.2 0.1 5 9800
.8 10.2 2.5 0.6 4 17830
.5 12 1.7 0.5 4 11760
10.8 1.4 3.2 1 22780
.7 9.7 K0.8 5 4 12100
.8 11.5 0.6 0.3 4 15200
.7 10.1 0.9 2.6 3 12130
.5 10 K0.3 2.5 4 13200
.9 10 1 1.9 3 10300
9.7 2 3.3 5 13300
8.1* 1.5 5.9 5 23900
.5 10.5 0.4 2 3 22100
.5 10.5 0.5 3 4 15800
.6 8.8* K0.1 4.8 5 22400
.2 9.9 K0.8 3.3 4 23000
.3 11.8 1.2 0.5 3 27600
.9 8.8* K1.1 5.1 2 11600
.9 11.7 0.6 0.2 3,3 16600
.5 10.2 1 0.2 4 12000
.5 7.8* 2 4.7 5 13400
.7 11.5 1.4 0.2 1 13590
.5** 12.1 2.5 0 2,9 14100
surgical technique, specified by groups reported on Fig. 1), Age (age at
ve hemoglobin), HB2 (first postoperative hemoglobin), HB3 (hemoglobin
diate postoperative hemoglobin), HB2-HB3 (difference between immediate
ed red blood cells), and WBC (first postoperative white blood cells count).
transfusion right after his arrival at ICU.

Table 2
Patient’s data separated by surgical technique
ID Tech. Path. Age Surg. time HB1 HB2 HB3 HB1-HB2 HB2-HB3 BT WBC
7 2C EHL 7 12:00 11.3 13.3 8* K2 5.3 2 26300
22 2C RS 16 15:30 13.5 13.6 8.8* K0.1 4.8 5 22400
5 2C EHL 16 9:00 14.7 12.1 11.7 2.6 0.4 3 12620
11 2C EHL 18 11:30 14.2 12.5 12 1.7 0.5 4 11760
14 2C RS 11 14:00 12.4 11.8 11.5 0.6 0.3 4 15200
8 2C EHL 33 10:30 16.6 11.9 10.2 4.7 1.7 0 14370
16 2C RS 7 15:30 12.2 12.5 10 K0.3 2.5 4 13200
23 2C RS 7 15:00 12.4 13.2 9.9 K0.8 3.3 4 23000
29 2C SWS 4.5 8:00 13.1 11.7 11.5 1.4 0.2 1 13590
15 2C RS 3 19:30 13.6 12.7 10.1 0.9 2.6 3 12130
12 2C EHL 38 9:30 15.4 14 10.8 1.4 3.2 1 22780
6 2C EHL 19 13:00 14.2 12.8 9.6 1.4 3.2 2 37700
3 2C CDM 1.7 18:00 14.9 14.5 8.6* 0.4 5.9 3,2 30000
1 2C CDM 2.2 17:00 15.8 12.1 9.7 3.7 2.4 2 15600
10 2C EHL 8 13:30 13.3 10.8 10.2 2.5 0.6 4 17830
9 2C EHL 16 12:30 11.6 10.4 10.3 1.2 0.1 5 9800
17 2A RS 8 8:00 12.9 11.9 10 1 1.9 3 10300
2 2A CDM 13 12:30 15.2 13.6 9.6 1.6 4 3 21600
20 2A RS 4.5 13:00 12.9 12.5 10.5 0.4 2 3 22100
24 2A RS 6.5 13:00 13.5 12.3 11.8 1.2 0.5 3 27600
26 2A RS 5.5 8:15 12.5 11.9 11.7 0.6 0.2 3,3 16600
13 2A RS 15 11:00 13.9 14.7 9.7 K0.8 5 4 12100
21 2A RS 13.5 14:00 14 13.5 10.5 0.5 3 4 15800
25 2A RS 5.2 8:30 12.8 13.9 8.8* K1.1 5.1 2 11600
18 2A RS 14 8:50 15 13 9.7 2 3.3 5 13300
27 2A RS 8 10:30 11.5 10.5 10.2 1 0.2 4 12000
28 2A RS 21 8:00 14.5 12.5 7.8* 2 4.7 5 13400
30 1A SWS 0.7 8:00 10 7.5** 12.1 2.5 0 2,9 14100
4 1A CDM 0.6 6:30 13.4 14.1 10.1 K0.7 4 3,5 14200
19 1A RS 21 9:00 15.5 14 8.1* 1.5 5.9 5 23900
See legend at Table 1.
Table 3
Surgical complications
ID Inc. Disc. VPS CSF fist. Inf.
1 C
3 C C
5 C Osteom.
12 C Mening.*
14 Mening.
15 C Mening.
16 C
17 C18 C
19 C
20 C
26 Skin Inf.
27 Skin Inf.
28 C
ID (patients’ identification as listed on table 1), Inc. Disc. (incomplete
disconnection), VPS (ventriculoperitoneal shunt), CSF fist. (CSF fistulae),
Inf (Infection), Skin inf (skin infection), Mening. (meninigitis), Osteom.
(osteomyelitis). *Patient deceased.
A.N. Almeida et al. / Brain & Development 28 (2006) 215–222 219
3.4. Infection
Seventeen patients presented at least one peak of axillary
temperature S38.5 8C. Ten patients underwent at least one
lumbar puncture to rule out CSF infection. There was no
pathogen growth on CSF but three patients presented
leukocyte counts on CSF of over 1000/mm3 and were
treated for meningitis with broad-spectrum antibiotics. One
of them deceased on the 27 postoperative day. He developed
an incisional fistula and the necropsy revealed meningoen-
cephalitis. Patients without bacterial meningitis averaged
109G136 leukocytes/mm3, 106G69.4 mg/dl of protein,
and 50G13.9 mg/dl of glucose in CSF.
Three other patients developed CSF fistula, two being
incisional and one nasal (two had RS and one EHL). Two
resolved with continuous lumbar drainage and antibiotics.
One developed osteomyelitis requiring bone flap removal,
where dura mater was patched during the procedure. Two
other patients developed skin infection, but were treated
with antibiotics only. Patients’ postoperative complications
are listed on Table 3.
3.5. Mortality/unexpected-neurological-deficits
There was no occurrence of unexpected neurological
deficit aggravation. Two patients with RS and one with
SWS had residual fine motricity in the affected hand before
surgery, which was lost after the procedure. No patient in
this series presented hemosiderosis or late-onset hydro-
cephalus. As mentioned before, one patient deceased after
developing postoperative menigoencephalitis.

A.N. Almeida et al. / Brain & Development 28 (2006) 215–222220
4. Discussion
This series represents a unique combination of several
surgeons performing different hemispherectomy techniques
within the same institution. In such a context, differences
among techniques cannot be attributed to externally
acquired experience as all surgeons were at the same point
in their learning curves. Our results better reflect the reality
in groups having experience in epilepsy surgery but who are
not yet entirely familiar with hemisperectomy. The
parameters of surgical time, blood transfusion, hydrocepha-
lus, postoperative seizures, infection, and mortality/unex-
pected-neurological-deficits were chosen because they are
frequently used to justify development of new surgical
approaches.
Reduction in surgical time has been cited as an advantage
of the techniques from group 2. In our series the surgical
time did not differ appreciably amongst the different
techniques. Nevertheless, surgical procedures on patients
with CDM were approximately 20% longer than those on
patients with EHL, although these differences did not
translate to noticeable morbidities.
Bleeding is still a concern during hemispherectomies,
however, comparing data from different series is not
feasible as authors use different parameters to measure
blood loss. Kestle et al. [5] and Schramm et al. [6] reported
progressive reduction in blood loss or transfusion necessity
when comparing techniques from Group 1B, Group 2A and
Group 2C. Jonas et al. [7], on the other hand, reported
differences in blood loss among pathologies, being higher in
patients with hemimegalencephaly. In our series, 29 patients
received packed red cells intra-operatively. On average, the
amount transfused was higher than in other series but was
not linked to pathology or technique [6,8]. Our increased
blood volume may reflect higher intra-operative bleeding or,
lower tolerance threshold for postoperative anemia adopted
Table 4
Compilation of different series regarding the incidence of subacute hydrocephalu
RS CDM SWD EHL
1A 0/0 15/5 0/0 0/0
0/0 0/0 1/0 15/0
1/1 1/0 1/0 0/0
1/1 16/5 2/0 15/0
1B 27/5 24/10 2/1 4/0
27/5 24/10 2/1 4/0
2A 0/0 12/3 0/0 0/0
10/0 1/0 0/0 0/0
10/0 13/3 0/0 0/0
2B 15/0 20/10 6/0 12/0
15/0 20/10 6/0 12/0
2C 1/0 26/5 0/0 6/0
4/0 10/3 2/0 11/0
1/0 2/0 1/0 16/0
5/0 2/2 1/0 6/0
11/0 40/10 4/0 39/0
Total 64/5 113/38 14/1 70/0
The first figure refers to total of patients reported by the cited series and the seco
by our team of anesthesiologists. Most of our patients left
the operating theater with hemoglobin levels above 12 g/dl
and none presented hemodynamic instability during the
procedure. In the ICU, hemoglobin continued to drop for a
few days and six patients needed a second blood transfusion
when their hemoglobin levels fell below 10 mg/dl. Notably,
postoperative progressive anemia was not associated with
intra-operative blood loss, blood transfusion, technique,
pathology, or patient age. Initially, it was thought to be the
result of bleeding from the subgaleal drain. However, there
was a strong association between hemoglobin reduction and
leukocyte counts of over 20,000/mm3 in the earliest
postoperative hemogram. As fever and hemodynamic
abnormalities are frequent in the postoperative period, it is
reasonable to suppose that this fall in hemoglobin may be
related to some sort of systemic inflammatory response,
however, further studies are needed to clarify this. Thus, the
amount of blood loss during and after the surgery is
attributable to a combination of surgical technique,
pathology and inflammatory factors.
Hydrocephalus is a frequent morbidity following
hemispherectomies and may develop under two different
circumstances: either within months of the procedure, or
years later. Rasmussen believed subacute hydrocephalus
was a defect of CSF absorption secondary to the huge
removal of the subarachnoid space [9]. Late onset
hydrocephalus, for its part, has been attributed to either
superficial cerebral hemosiderosis or low-pressure hydro-
cephalus [10]. In our series however, the most important
factor associated to subacute hydrocephalus was pathology,
whereby 50% of our patients with CDM needed ventricu-
loperitoneal shunt. Compiling series from the literature
whose shunts were reported by surgical technique and
pathology, there is a clear preponderance of subacute
hydrocephalus in patients with CDM (Table 4). Since
patients with CDM have larger hemispheres, the higher
s separated by surgical technique and causative pathology
Total
Di Rocco and Iannelli (2000) [12]
Davies et al. (1993) [27]
Current series
34/6
Vining et al. (1997) [25]
57/16
Carreno et al. (2001) [28]
Current series
23/3
Delalande et al. (2001) [29]
53/10
Shimizu and Maehara (2000) [8]
Devlin et al. (2003) [26]
Schramm et al. (2001) [6]
Current series
94/10
261/44
nd number to total of ventriculoperitoneal shunts inserted.

A.N. Almeida et al. / Brain & Development 28 (2006) 215–222 221
incidence of hydrocephalus may be a consequence of debris
in the surgical cavity, which are more abundant after
operating on a thicker parenchyma. The series of Jonas et al.
[7] reported higher incidence of shunting in all groups of
pathologies although was not included in the table since a
proportion of his patients underwent ventriculoperitoneal
shunt routinely after hemispherectomy [11]. Therefore, it is
not feasible to ascertain the actual rate of hydrocephalus in
their series. Di Rocco and Iannelli [12] found correlation
between subacute hydrocephalus and patient age, yet not
technique. Our results may corroborate these findings to
some extent, as patients with CDM are usually considered
surgical candidates earlier than in other pathologies.
Papers published in the sixties considered superficial
cerebral hemosiderosis (SCH) as an inevitable and fatal
complication of hemispherectomy [13]. Despite the small
number of our patients who underwent anatomical
hemispherectomy (Group 1A), there were no instances of
late onset hydrocephalus or SCH in our series. In 1973,
Rasmussen [14] reported the MNI experiment with follow
up over thirty years, of patients with anatomical and subtotal
hemispherectomy. The author concluded that a small
portion of remnant brain would be sufficient to protect
against SCH. This may account to some extent for the lack
of such problem in the current literature, as more recent
series have used techniques that leave a portion of the brain
in the cavity. Although hydrocephalus and SCH may
manifest several decades after the procedure, it is the
exception, not the rule [15]. The average interval between
surgery and SCH has been described as 8 years [9]. As
Rasmussen’s technique was developed in the seventies, one
could expect several cases of SCH by now if the technique
were not protective against such a condition. On the other
hand, in patients who have undergone AH today (Group
1A), widespread use of CT scan may allow early diagnosis
and treatment for bleeding in the surgical cavity shown to be
effective in preventing the development of SCH [16].
Finally, Cook et al. [17] presented 34 patients who
underwent AH, in which ventriculoperitoneal shunt was
used almost routinely, with at least 14 years of follow up and
none presented SCH. Therefore, although SCH is still
related to AH (group 1A), it may not be considered a
common cause of morbidity today so long as patients
receive proper follow up.
Currently, causative pathology, not surgical technique, is
considered the main factor for postoperative seizure control
[18,19]. However, procedures other than from group 1A
may leave bridges between the hemispheres or epilepto-
genic areas over either the insula or the basal frontal lobe
that perpetuate seizures spreading [20,21]. Incomplete
disconnection occurred in 18.5% of our cases, the same
incidence as reported by Peacock et al., [11] in patients
operated on with functional hemispherectomy (Group 2A).
Shimizu and Maehara [8] reported this in 9% of his patients
using modified peirinsular hemispherotomy, while
Schramm et al., [6] reported none in their series (both
author employed techniques from Group 2C). Finally,
Kossoff et al. [18] reported five patients out of 111
reoperated upon after initial hemidecortication (group 1B)
due to persistent seizures and residual tissue identified on
MRI. Incomplete disconnection may happen using almost
all techniques, although it may be reduced according to
surgeons’ experience. Pathologies with thicker cortical
mantles, such as hemimegalencefalia, may increase the
chances of its occurrence. Therefore, incomplete disconnec-
tion should not be considered a complication but an
expected morbidity, at least, at the beginning of the
surgeon’s learning curve.
Considering operative mortality and major morbidity
together, hemispherectomy is still a risky procedure,
regardless of technique or pathology. Our series presented
a rate of postoperative fever similar to what is reported in
the literature. Temperature elevation after hemispherectomy
is a common phenomenon and has been attributed aseptic
meningitis. On the other hand, we had a high rate of
complications like infection and CSF fistulae. We credited
such drawback to the teaching characteristic of our
institution, where several in-training medical teams con-
tributed to surgeries. One patient deceased in our series due
to meningoencephalitis. Other authors have reported brain
stem lesion, excessive blood loss, brain swelling, general-
ized hypoxia, infection, locked-in syndrome, and shunt
failure as causes of death or permanent sequelae [6–8,
21–25]. The death rate reached up to 5.7% in recent series
and, even in a series without death or permanent sequelae,
life-threatening operative complications occurred in 10% of
cases [26].
5. Conclusions
Hemispherectomies are procedures where pathology and
surgical technique interact narrowly. In order to define
causes of morbidity both factors have to be analyzed
independently. From this standpoint, it is not possible to
infer that a specific technique of hemispherectomy has less
morbidity or better outcome if results are not adjusted for
different causative pathologies.
References
[1] Almeida AN, Marino Jr R. The early years of hemispherectomy.
Pediatr Neurosurg 2005;41:137–40.
[2] Thomas P, Zifkin B, Ghetau G, Delalande O. Persistence of ictal
activity after functional hemispherectomy in Rasmussen syndrome.
Neurology 2003;60:140–2.
[3] Villemure JG, Mascott CR. Peri-insular hemispherotomy: surgical
principles and anatomy. Neurosurgery 1995;37:975–81.
[4] Schramm J, Behrens E, Entzian W. Hemispherical deafferentation: an
alternative to functional hemispherectomy. Neurosurgery 1995;36:
509–16.
[5] Kestle J, Connolly M, Cochrane D. Pediatric peri-insular hemispher-
otomy. Pediatr Neurosurg 2000;32:44–7.

A.N. Almeida et al. / Brain & Development 28 (2006) 215–222222
[6] Schramm J, Kral T, Clusmann H. Transsylvian keyhole functional
hemispherectomy. Neurosurgery 2001;49:891–901.
[7] Jonas R, Nguyen S, Hu B, Asarnow RF, LoPresti C, Curtiss S, et al.
Cerebral hemispherectomy: hospital course, seizure, developmental,
language, and motor outcomes. Neurology 2004;62:1712–21.
[8] Shimizu H, Maehara T. Modification of peri-insular hemispherotomy
and surgical results. Neurosurgery 2000;47:367–73.
[9] Rasmussen T. Hemispherectomy for seizures revisited. Can J Neurol
Sci 1983;10:71–8.
[10] Daniel RT, Lee GY, Halcrow SJ. Low-pressure hydrocephalic state
complicating hemispherectomy: a case report. Epilepsia 2002;43:
563–5.
[11] Peacock WJ, Wehby-Grant MC, Shields WD, Shewmon DA,
Chugani HT, Sankar R, et al. Hemispherectomy for intractable
seizures in children: a report of 58 cases. Childs Nerv Syst 1996;12:
376–84.
[12] Di Rocco C, Iannelli A. Hemimegalencephaly and intractable
epilepsy: complications of hemispherectomy and their correlations
with the surgical technique. A report on 15 cases. Pediatr Neurosurg
2000;33:198–207.
[13] Griffith HB. Cerebral hemispherectomy for infantile hemiplegia in the
light of the late results. Ann R Coll Surg Engl 1967;41(2):183–201.
[14] Rasmussen T. Postoperative superficial hemosiderosis of the brain, its
diagnosis, treatment and prevention. Trans Am Neurol Assoc 1973;
98:133–7.
[15] Kalkanis SN, Blumenfeld H, Sherman JC, Krebs DE, Irizarry MC,
Stephen W, et al. Delayed complications thirty-six years after
hemispherectomy: a case report. Epilepsia 1996;37:758–62.
[16] Falconer MA, Wilson PJE. Complications related to delayed
hemorrhage after hemispherectomy. J Neurosurg 1969;30:413–26.
[17] Cook SW, Nguyen ST, Hu B, Yudovin S, Shields WD, Vinters HV,
et al. Cerebral hemispherectomy in pediatric patients with epilepsy:
comparison of three techniques by pathological substrate in 115
patients. J Neurosurg 2004;100(2 Suppl. Pediatrics):125–41.
[18] Kossoff EH, Vining EP, Pillas DJ, Pyzik PL, Avellino AM,
Carson BS, et al. Hemispherectomy for intractable unihemispheric
epilepsy etiology vs outcome. Neurology 2003;14(61):887–90.
[19] Sugimoto T, Otsubo H, Hwang PA, Hoffman HJ, Jay V, Snead
3rd OC. Outcome of epilepsy surgery in the first three years of life.
Epilepsia 1999;40:560–5.
[20] Mittal S, Farmer JP, Rosenblatt B, Andermann F, Montes JL,
Villemure JG. Intractable epilepsy after a functional hemispher-
ectomy: important lessons from an unusual case. J Neurosurg 2001;
94:510–4.
[21] Comair YG. The transsylvian functional hemispherectomy: patient
selection and results. In: Luders HO, Comair YG, editors. Epilepsy
sugery. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;
2001. p. 699–704.
[22] Behrens E, Schramm J, Zentner J, Konig R. Surgical and neurological
complications in a series of 708 epilepsy surgery procedures.
Neurosurgery 1997;41:1–10.
[23] Villemure JG. Functional hemispherectomy: evolution of technique
and results in 65 cases. In: Luders HO, Comair YG, editors. Epilepsy
surgery. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;
2001. p. 733–9.
[24] Kossoff EH, Vining EP, Pyzik PL, Kriegler S, Min KS, Carson BS,
et al. The postoperative course and management of 106 hemi-
decortications. Pediatr Neurosurg 2002;37:298–303.
[25] Vining EP, Freeman JM, Pillas DJ, Uematsu S, Carson BS, Brandt J,
et al. Why would you remove half a brain? The outcome of 58
children after hemispherectomy—the johns hopkins experience: 1968
to 1996 Pediatrics 1997;100:163–71.
[26] Devlin AM, Cross JH, Harkness W, Chong WK, Harding B, Vargha-
Khadem F, et al. Clinical outcomes of hemispherectomy for epilepsy
in childhood and adolescence. Brain 2003;126:556–66.
[27] Davies KG, Maxwell RE, French LA. Hemispherectomy for
intractable seizures: long-term results in 17 patients followed for up
to 38 years. J Neurosurg 1993;78:733–40.
[28] Carreno M, Wyllie E, Bingaman W, Kotagal P, Comair Y, Ruggieri P.
Seizure outcome after functional hemispherectomy for malformations
of cortical development. Neurology 2001;57:331–3.
[29] Delalande O, Fohlen M, Jalin C, Pinard JM. From hemispherectomy
to hemispherotomy. In: Luders HO, Comair YG, editors. Epilepsy
surgery. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;
2001. p. 741–6.
Copyright © 2022 FDOKUMEN

