







Bahasa
Halaman
Hukum


Effects of Once-Daily Tadalafil on Treatment Satisfaction,Psychosocial Outcomes, Spontaneous Erections, and Measures ofEndothelial Function in Men With Erectile Dysfunction But Naiveto Phosphodiesterase Type 5 Inhibitors
HARTMUT PORST,* GERALD B. BROCK,{ KRZYSZTOF KULA,{ IGNACIO MONCADA,§ FRANCESCO
MONTORSI,5 BRUCE R. BASSON," KRAIG KINCHEN," AND ANTONIO AVERSA#
From the *Private Practice in Urology and Andrology, Hamburg, Germany; the �Division of Urology, Faculty of
Medicine and Dentistry, University of Western Ontario, London, Ontario, Canada; the `Division of Andrology,
Department of Andrology and Reproductive Endocrinology, Medical University of Lodz, Lodz, Poland; the
§Department of Urology, Hospital La Zarzuela, Madrid, Spain; the 5Department of Urology, Scientific Institute
Hospital, San Raffaele, Milan, Italy; the "Lilly Research Laboratories, Eli Lilly, Indianapolis, Indiana; and the
#Endocrinology Section, Department of Experimental Medicine, University of Rome, La Sapienza, Rome, Italy.
ABSTRACT: Previous studies established the efficacy of once-
daily tadalafil for men with erectile dysfunction. However, no trial has
focused on the effects of such treatment on men without previous
experience using oral phosphodiesterase type 5 inhibitors. Patients
were randomized (2:1) to once-daily tadalafil 5 mg (with possible
down-titration to 2.5 mg; n 5 146) or placebo (n 5 69) for 12 weeks.
Among 215 patients (mean age, 52 years), once-daily tadalafil
treatment resulted in 61.7% of study participants reporting their
ability to achieve and maintain erections as being much better or very
much better (vs 21.7% on placebo; P , .001). Tadalafil significantly
improved treatment satisfaction on the Erectile Dysfunction Inventory
of Treatment Satisfaction (P , .001 vs placebo at end point) and
psychosocial outcomes on the Self-Esteem and Relationship
(SEAR) questionnaire (least squares mean difference in SEAR total
score change from baseline, 11.8 [95% confidence interval, 5.4%–
18.2%; P , .001 vs placebo]). Patients receiving once-daily tadalafil
also experienced a higher proportion of daily self-reported sponta-
neous morning erections at end point (58.7%) compared with
placebo (42.2%; P , .001 for the between-treatment difference in
changes from baseline). However, no significant differences in
parameters of endothelial dysfunction (including biomarkers and
peripheral arterial tonometric measures) or nocturnal erections as
recorded by the nocturnal electrobioimpedance volumetric assess-
ment were observed between treatment groups. Tadalafil was well
tolerated; adverse events included back pain, headache, and
dyspepsia. These findings may contribute to a more comprehensive
understanding of once-daily tadalafil’s effects on phosphodiesterase
type 5 inhibitor–naive men.
Key words: Drug therapy, efficacy, endothelium, erection,
morning, nocturnal, phosphodiesterases, psychosocial assess-
ments, peripheral arterial tonometry, tolerability, treatment outcome.
J Androl 2012;33:1305–1322
The phosphodiesterase type 5 (PDE5) inhibitor
tadalafil can be administered on demand (5–20 mg)
or once daily (2.5–5 mg) to treat erectile dysfunction
(ED). Once-daily treatment largely obviates the need to
plan sexual activity within a narrow therapeutic window
after dosing. A number of recent studies using the
International Index of Erectile Function–Erectile Func-
tion (IIEF-EF) domain (Rosen et al, 1997) as well as the
Sexual Encounter Profile (SEP) questionnaire as out-
comes have supported the efficacy of once-daily tadalafil
(Porst et al, 2006; Rajfer et al, 2007; Donatucci et al, 2008;
Hatzichristou et al, 2008; Seftel et al, 2009, 2011).
Over time, in addition to the IIEF and SEP questions,
measures of the effectiveness of PDE5 inhibitors have
grown to include a number of other patient-reported
outcomes, such as 1) the Self-Esteem and Relationship
(SEAR) questionnaire, which measures male confidence
(subdivided into self-esteem and overall relationship
satisfaction) as well as sexual relationship satisfaction
(Althof et al, 2003; Cappelleri et al, 2004); 2) the Erectile
Dysfunction Inventory of Treatment Satisfaction (ED-
ITS), which assesses ED treatment satisfaction (Althof
et al, 1999); and 3) Global Assessment Questions
(GAQ1 and GAQ2). The wording of, and 7 response
options for, the GAQ questions (from ‘‘very much
Supported by Eli Lilly and Co (Indianapolis, IN), which had a role
in study design, data acquisition and interpretation, and the decision to
publish the findings.
Correspondence to: Dr Hartmut Porst, Private Practice of Urology
and Andrology, Neuer Jungfernstieg 6a, 20354 Hamburg, Germany
(e-mail: [email protected]).
Received for publication August 24, 2011; accepted for publication
June 11, 2012.
DOI: 10.2164/jandrol.111.015289
Journal of Andrology, Vol. 33, No. 6, November/December 2012Copyright E American Society of Andrology
1305

better’’ to ‘‘very much worse’’) were in turn consistent
with the Patient Global Impression of Improvement
(PGI-I) questionnaire previously developed for psycho-pharmacologic research and applied most recently to
enable an overall appraisal of the severity of stress
urinary incontinence and its response to treatment (Guy,
1976; Yalcin and Bump, 2003). Studies across different
cultures have demonstrated that treatment with PDE5
inhibitors enhances erectile function and that these
improvements in turn correlate directly and significantly
with increments in treatment satisfaction and measuresof patient well-being and relationship satisfaction
(Althof et al, 2006a,b; Steidle et al, 2006; Ralph et al,
2007; Seftel et al, 2009). In a recent study, once-daily
tadalafil was associated with significantly (P , .001 vs
placebo) superior improvements in sexual satisfaction,
sexual relationships, confidence, and self-esteem (Seftel
et al, 2009).
Most men with ED enrolled in registration studies foronce-daily tadalafil had previous experience with PDE5
inhibitors, and initial European recommendations for
once-daily tadalafil treatment were for men who had
previously responded to on-demand PDE5 inhibitors. In
the primary manuscript from the current European
randomized, double-blind, placebo-controlled study
(Clinicaltrials.gov identifier NCT00836693), Montorsi
et al (2011) reported that once-daily tadalafil treatmentwas efficacious in, and well tolerated by, PDE5
inhibitor–naive men with ED. Efficacy was assessed
using least squares (LS) mean changes in the IIEF-EF
domain (7.3 for tadalafil 5 mg vs 3.4 for placebo, once
daily), percent of intercourse attempts in which the
patient was able to successfully insert his penis into the
vagina (change in SEP2 score, +23.8% vs +12.2%,
respectively), and percent of attempts lasting longenough for successful intercourse (change in SEP3 score,
+39.5% vs +21.5%, respectively; P , .001 for each
tadalafil-placebo comparison) as coprimary end points.
In the current study, we focus on additional end
points assessed in this study of PDE5-inhibitor–naive
men. Patient-reported outcome measures used in the
present study included the EDITS, SEAR, and GAQ1
and GAQ2 to assess perceived degrees of improvement.
In addition to evaluating these patient-reported out-come measures, this study also explored approaches
aimed at measuring objective end points that might
further inform the understanding of ED and its
treatment. Potential objective end points considered
relevant to ED treatment include assessments of
spontaneous nocturnal erections as well as indices of
endothelial dysfunction. Restoring spontaneous erec-
tions may have beneficial effects on penile hemodynam-ics and overall erectile function by enhancing intracor-
poreal perfusion and oxygenation, and hence combating
the development of hypoxia-induced tissue injury,
including downstream increases in growth factors within
the tunica albuginea (Montorsi et al, 1997, 2004).Devices developed to attempt to measure spontaneous
nocturnal erections include RigiScan (Timm Medical
Technologies Inc, Eden Prairie, Minnesota; Udelson
et al, 1999; Suzuki et al, 2001) and nocturnal electro-
bioimpedance volumetric assessment (NEVA; PJR Inc,
Minnetonka, Minnesota; Knoll and Abrams 1999a,b;
Mizuno et al, 2004).
Cavernous atherosclerotic endothelial dysfunction,with its imbalance of vasodilator (eg, nitric oxide
[NO]) and vasoconstrictor (eg, endothelin-1) factors,
can blunt the penile vascular response to sexual
stimulation necessary for normal erection (Foresta et
al, 2006; Aversa et al, 2007). Because of this intimate
‘‘endothelial-erectile dysfunction’’ connection (Costa
and Virag, 2009), ED is recognized as a sentinel
symptom of atherosclerosis in other vascular beds,including the coronary, cerebral (carotid-artery), and
peripheral (eg, femoral-artery) vasculature (Montorsi
et al, 2003; Gazzaruso et al, 2004, 2006; Caretta et al,
2005; Foresta et al, 2008; Tamler and Bar-Chama,
2008). Promising findings from trials involving partic-
ipants with ED (typically without atherosclerotic
plaque) receiving chronic rather than on-demand
PDE5 inhibitors suggested that therapy can help to‘‘recondition’’ dysfunctional cavernous endothelium,
resume spontaneous erections, and confer sustained
vasoprotective and erectile-rehabilitative effects, even
after treatment discontinuation, through increased NO
levels and/or structural changes in the penile vasculature
(McMahon, 2004; Caretta et al, 2005; Jackson, 2005).
Potential objective measures of cavernous endothelial
function include serum markers, cellular markers, andother physiologic assessments (Tamler and Bar-Chama,
2008). Putative serum markers of endothelial dysfunc-
tion include circulating levels of cellular adhesion
molecules (eg, soluble E-selectin), inflammatory cyto-
kines, the potent vasoconstrictor peptide endothelin-1,
and another inflammatory marker: high-sensitivity C-
reactive protein (hsCRP; Billups et al, 2003; Nawawi
et al, 2003; Giugliano et al, 2004; Bohm and Pernow,2007; Naya et al, 2007b; Ridker, 2007; Tamler and Bar-
Chama, 2008). Putative thromboembolic markers of
endothelial dysfunction include levels of plasminogen
activator inhibitor, tissue-type plasminogen activator
antigen, and von Willebrand factor (Bickel et al, 2002;
Naya et al, 2007a; Tamler and Bar-Chama, 2008).
A physiologic measure of global endothelial function
is the assessment of the reactive hyperemia index (RHI)
by noninvasive peripheral arterial tonometry (Endo-PAT; Itamar Medical Limited, Caesarea, Israel). This
finger plethysmographic device allows detection of
1306 Journal of Andrology N November �December 2012
minute fluxes in digital pulse volumes (pulsatile arterial
volume changes) secondary to microcirculatory endo-
thelial dysfunction (Bonetti et al, 2004; Rubinshtein et al,
2010; Aversa et al, 2011). The aim of the present study
was to investigate treatment satisfaction measures, as
well as other outcomes, such as nocturnal erections and
endothelial function, in patients participating in the
aforementioned clinical study (Montorsi et al, 2011),
whose main outcome comprised evaluations of the IIEF
(Rosen et al, 1997).
Materials and Methods
Study Design
The European multicenter, randomized, double-blind, paral-
lel-group trial was conducted across 22 sites in Germany,
Greece, Italy, Poland, and Spain. Tadalafil doses were based
on currently licensed regimens for once-daily administration in
Europe (European Medicines Agency, 2012). The study was
conducted in accordance with ethical tenets originating in the
Declaration of Helsinki. All study participants provided
written informed consent before participating in any assess-
ment or treatment, and the study protocol and consent
document underwent institutional ethics review.
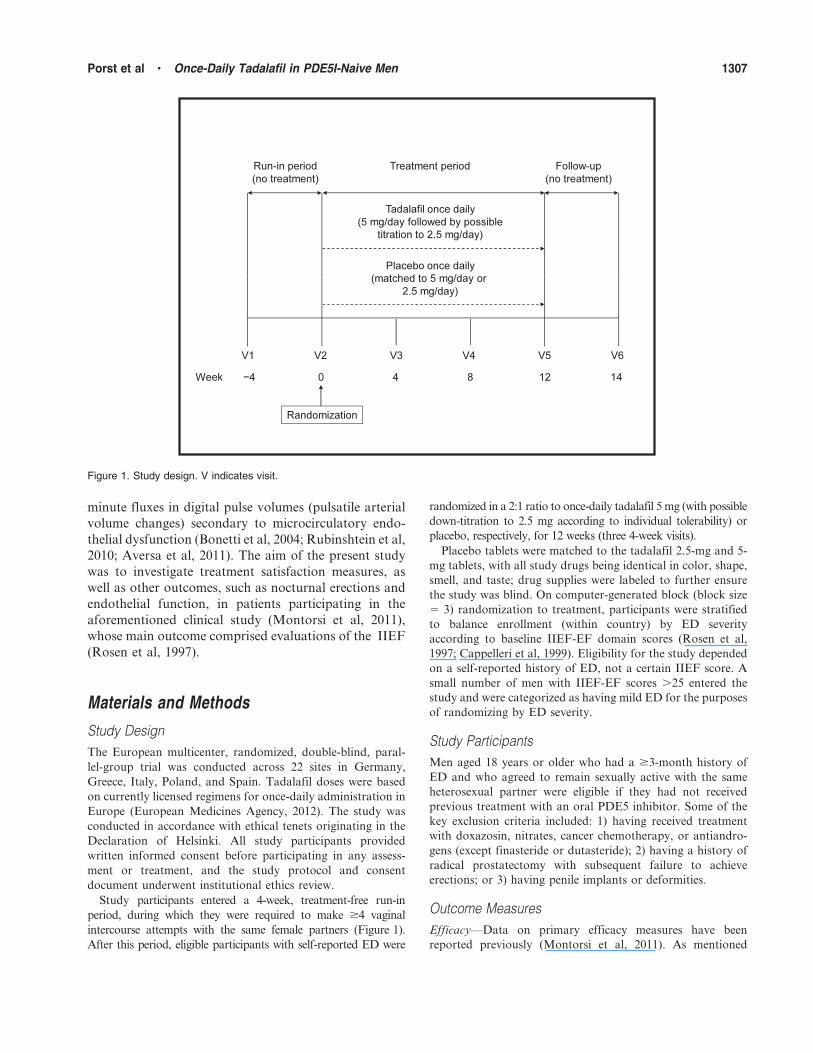
Study participants entered a 4-week, treatment-free run-in
period, during which they were required to make $4 vaginal
intercourse attempts with the same female partners (Figure 1).
After this period, eligible participants with self-reported ED were
randomized in a 2:1 ratio to once-daily tadalafil 5 mg (with possible
down-titration to 2.5 mg according to individual tolerability) or
placebo, respectively, for 12 weeks (three 4-week visits).
Placebo tablets were matched to the tadalafil 2.5-mg and 5-
mg tablets, with all study drugs being identical in color, shape,
smell, and taste; drug supplies were labeled to further ensure
the study was blind. On computer-generated block (block size
5 3) randomization to treatment, participants were stratified
to balance enrollment (within country) by ED severity
according to baseline IIEF-EF domain scores (Rosen et al,
1997; Cappelleri et al, 1999). Eligibility for the study depended
on a self-reported history of ED, not a certain IIEF score. A
small number of men with IIEF-EF scores .25 entered the
study and were categorized as having mild ED for the purposes
of randomizing by ED severity.
Study Participants
Men aged 18 years or older who had a $3-month history of
ED and who agreed to remain sexually active with the same
heterosexual partner were eligible if they had not received
previous treatment with an oral PDE5 inhibitor. Some of the
key exclusion criteria included: 1) having received treatment
with doxazosin, nitrates, cancer chemotherapy, or antiandro-
gens (except finasteride or dutasteride); 2) having a history of
radical prostatectomy with subsequent failure to achieve
erections; or 3) having penile implants or deformities.
Outcome Measures
Efficacy—Data on primary efficacy measures have been
reported previously (Montorsi et al, 2011). As mentioned
Figure 1. Study design. V indicates visit.
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1307

earlier, these outcome variables included mean changes from
baseline to end point on the IIEF-EF, as well as in the per-
patient percentage of successful attempts at vaginal penetra-
tion (SEP2) and of successful attempts at sexual intercourse
(SEP3). Additional patient-reported outcome variables includ-
ed: 1) treatment satisfaction as measured by the EDITS
questionnaire (Althof et al, 1999); 2) psychosocial end points
as measured by the SEAR questionnaire (Althof et al, 2003;
Cappelleri et al, 2004); 3) the number (frequency) of self-
reported daily spontaneous morning erections; and 4) GAQ1
and GAQ2.
Each of the 11 questions on the EDITS was rated from 0
(extremely low) to 4 (extremely high) for treatment satisfaction
(Althof et al, 1999). A summary score ranging from 0 to 100
was obtained by summing the individual scores for all
questions, dividing by the number of questions answered,
and multiplying by 25. The validated SEAR questionnaire was
also completed by each study participant at baseline and the 3-
month final visit (or early discontinuation). This 14-item
questionnaire has two domains assessing sexual relationship
and confidence. Each item was scored from 1 to 5, and scores
were transformed (to 0–100), such that higher scores indicated
more favorable responses. The transformed score was equal to
100 times the actual raw score minus the lowest possible raw
score, divided by the possible range in raw scores.
Study participants also answered GAQ1 and GAQ2 at the
final 3-month visit (or early discontinuation): 1) ‘‘How do you
perceive your ability to achieve and maintain erections now,
compared to before you began taking the study medication?’’
(GAQ1); and 2) ‘‘How do you perceive your sexual life now,
compared to before you began taking the study medication?’’
(GAQ2). Responses were scored using a 7-point scale where a
response of 1 5 very much better, 2 5 much better, 3 5 a little
better, 4 5 no change, 5 5 a little worse, 6 5 much worse, and
7 5 very much worse. As mentioned earlier, questions and
response options were consistent with the validated PGI-I
questionnaire (Yalcin and Bump, 2003). Men completed a
daily diary to indicate whether they experienced morning
erections. For each man, the percent of mornings with waking
erections was calculated.
Nocturnal Electrobioimpedance Volumetric Assessment—
Spontaneous nocturnal erections were measured by nocturnal
electrobioimpedance volumetric assessment (NEVA). To use
NEVA, 2 electrodes are placed on a man’s penis, and 1
electrode is placed on the hip. The underlying operating
principles have been elaborated elsewhere (Levine and Caroll,
1994; Knoll and Abrams, 1999a,b; also see Supplemental Data
available online at http://www.andrologyjournal.org). In brief,
the property of electrobioimpedance changes with minute
variations in blood flow. Consequently, penile volumetric
changes can be calculated from changing measures of
impedance (Salama, 2004). Penile blood volume is computed
from NEVA data, including the cross-sectional area and length
of the penis. Recordings of nocturnal penile blood volume over
2 or 3 consecutive nights impart useful information for
individuals with abnormal erections.
By recording data on the number and duration of
spontaneous nocturnal erectile events and penile volume
changes (ie, erections not induced by sexual stimulation), the
NEVA device was developed to provide objective data on the
integrity of the erectile mechanism. Changes from baseline in
nocturnal penile tumescence (indicated by an increase in
volume, length, and/or area) were assessed by continuously (at
1-second intervals) measuring penile electrobioimpedance.
Consistent with manufacturer guidance, study participants
were instructed (by appropriately trained site personnel) to use
the NEVA device at home on 3 consecutive nights in each 1-
week period before baseline, end point, and 2 weeks after
treatment discontinuation. Studies suggest that 2 or 3 nights
of this type of monitoring are needed to characterize an
individual adequately (Levine and Carroll, 1994). During
this first ‘‘training’’ use of the device (ie, the first of 3 nights),
data on nocturnal tumescence parameters were not recorded
because this session was intended to allow each study par-
ticipant to become acquainted with and accustomed to using
the device.
NEVA data were collected for the 2 nights before the visit
and analyzed for nights on which the device was recorded as
having been worn for .4 hours and #20 hours. If a man had a
NEVA session recorded as .20 hours, the session was not
considered to be valid for analysis. An erectile event was
defined as a nocturnal peak penile volume that exceeded the
baseline value for $15 minutes. Study participants were
advised to avoid sexual activity immediately before testing.
They were also counseled to refrain from consuming coffee,
tea, cola, or alcoholic beverages, or taking sedatives, tranquil-
izers, muscle relaxants, or sleeping pills immediately before
testing. Other precautions included keeping the device away
from liquids (eg, shutting off the device before urinating).
Patients returned their devices to their sites after the period
of monitoring (ie, at randomization, end point, and after a 2-
week treatment-free washout), and the data were downloaded
and managed using the manufacturer’s software. Recorded
data for each erection included the date; start and stop times;
number of erectile events; the minimum and maximum cross-
sectional area, length, blood volume, and duration of each
erectile event; and the percent volume change from baseline.
Peripheral Arterial Tonometry—The EndoPAT2000 device
was used to measure reactive hyperemia (RH–peripheral
arterial tonometry [RH-PAT]) as well as arterial stiffness
(augmentation index [AI]) by PAT at baseline, week 4, end
point, and after a 2-week treatment-free interval. PAT is a
validated, noninvasive method of assessing systemic endothe-
lial function and arterial stiffness based on brachial-artery
occlusion and endothelial-mediated arterial responses at the
distal phalanx of the finger. The AI is a sensitive indicator of
arterial stiffness that: 1) captures the enhancing effects of a
reflected blood pressure pulse wave on central aortic pressure
(ie, augmentation); 2) is associated with target-organ damage;
3) predicts cardiovascular events across diverse populations;
and 4) can be used to discriminate between the vascular effects
of different vasoactive agents (Shimizu and Kario, 2008;
Boutouyrie et al, 2010).
EndoPAT assessments were scheduled to take place between
7 and 11 AM and, when possible, at the same time of day. Study
participants were counseled to fast and refrain from smoking
1308 Journal of Andrology N November �December 2012

from midnight until the time of the assessments. These
evaluations were performed before both blood sampling and
administration of study drug (or concomitant medications) if
possible. Study participants taking calcium channel blockers
were advised to take their previous doses approximately
24 hours before scheduled EndoPAT assessments.
Cellular and Biochemical Markers—Fasting blood samples
were obtained at baseline, end point, and after a 2-week
treatment-free interval to analyze circulating endothelial
progenitor cells (cEPC) and the other biomarkers, including
soluble E-selectin.
Safety—Adverse events were monitored throughout the
study. Treatment-emergent adverse events were defined as
occurring for the first time or worsening upon study treatment.
Statistical Analyses
Sample size was estimated based on an expected between-
treatment difference of 4.7 points (SD 5 8) in the IIEF-EF
domain score, which indicated a sample size of 174 partici-
pants (with a ratio of 2:1 tadalafil-placebo) to provide $95%
power to detect a significant effect between once-daily placebo
and tadalafil at a two-sided a 5 .05. Under the assumption of a
screening failure rate of 20%, 218 participants were needed to
result in the required sample size of 174.
Primary and secondary efficacy analyses were performed on
an intent-to-treat (ITT) basis. The ITT population included all
randomized participants who had $1 baseline and $1
postbaseline observation. Where missing values for the
treatment period were imputed, a last observation carried
forward approach within the treatment period was used.
The primary manuscript (Montorsi et al, 2011) addressed the
primary study hypothesis that once-daily tadalafil, compared
with placebo, would result in statistically significant improve-
ments in erectile function, as measured by the IIEF-EF domain,
SEP2, and SEP3. We also hypothesized that such differences
would be reflected in other measures, including the EDITS,
SEAR, and GAQ questionnaires. Assessments of endothelial
dysfunction were exploratory in nature and did not necessarily
support or contradict the primary analyses of parameters
supporting efficacy on ED as assessed via IIEF questionnaires
or SEP diaries. A priori, one would expect the following findings
in the event that tadalafil improved nocturnal erections and
endothelial function compared with placebo: 1) a decrease in the
PAT measure of arterial stiffness (AI); 2) an increase in the PAT
measure of microvascular endothelial function (RHI-PAT); 3)
reductions in inflammatory (eg, hsCRP, E-selectin) and
thrombotic/antifibrinolytic (t-PA, von Willebrand factor) bio-
markers; and 4) increases in cEPCs (Foresta et al, 2005a,b, 2006,
2009a,b, 2010a,b; Rosano et al, 2005).
Analysis of covariance models were used to evaluate changes
from baseline in the SEAR questionnaire. LS mean (x),
standard error (SE), 2-sided 95% confidence interval, and P
values for differences between placebo and tadalafil 5 mg
derived from an analysis of variance (ANOVA) including
terms for treatment group, country, baseline SEAR score, age
group, ED severity stratum, etiology, testosterone level, and
the RHI at baseline, as well as the baseline-by-treatment group
interaction if significant at P , .01.
The EDITS summary score was analyzed descriptively with
summary statistics, using an ANOVA model with treatment
and country as factors. Mean (6SD) end point EDITS total
scores were compared by baseline treatment assignment; in
those with moderate or severe (vs mild) ED at baseline; and in
those ages 50 to 59 years or $60 years (vs ,50 years) at
baseline. End point GAQ1 and GAQ2 data were analyzed
using the Wilcoxon rank sum test. Mean changes in the IIEF-
EF score, SEP2, and SEP3 were calculated according to levels
of responses to both GAQ1 and GAQ2. Correlations between
and among treatment efficacy, satisfaction, and psychosocial
outcomes were assessed using Spearman’s correlation coeffi-
cients in the ITT population, as were correlations between
numbers of spontaneous morning erections and spontaneous
nocturnal erections. The proportion of participants with IIEF-
EF domain scores ,26 at baseline and $26 (consistent with
‘‘no ED’’ [Cappelleri et al, 1999]) at end point were also
computed by treatment group and compared using Fisher’s
exact test.
NEVA data were analyzed in the ITT population using a
Kruskal-Wallis 1-way ANOVA, with P values generated for
differences in nocturnal erection parameters between the
placebo and tadalafil 5 mg treatment groups at end point.
Endothelial markers were analyzed using a prospectively
defined repeated-measures ANOVA, and correlations with
treatment and ED severity were assessed using Spearman’s
correlation coefficient. RH-PAT results were summarized by
treatment group with descriptive measures.
Post hoc analyses were conducted for 5 selected parameters
(RHI, AI, logarithm of hsCRP, soluble E-selectin, and
numbers of cEPCs) to determine the effects of tadalafil
treatment and other factors on measures of endothelial
function using a more tailored, backward-elimination, stepwise
modeling approach. For each measure, the initial model
included potentially predictive factors such as baseline level of
the measure, smoking, age, race, ED severity, and country.
Terms for treatment, time, and treatment-by-time interaction
were retained in all models, as were any factors with P , .10.
Subsequently, the effect of the number of cardiovascular risk
factors on endothelial function was examined by adding this
term to the model. These risk factors included body mass index
.30 kg/m2; current smoking; and/or a baseline diagnosis of (or
baseline concomitant medications for) hypertension, hyper-
cholesterolemia, diabetes, or coronary artery disease (CAD).
Treatment interactions with baseline response and number of
cardiovascular risk factors were examined where those factors
were found to significantly affect response (P , .10). Mixed-
effect model repeated-measures analyses with baseline mea-
sures as covariates were conducted to assess between-visit
changes in total cEPCs. Post hoc analyses were not adjusted
statistically for multiple comparisons.
Results
Participant Disposition and Baseline Demographics
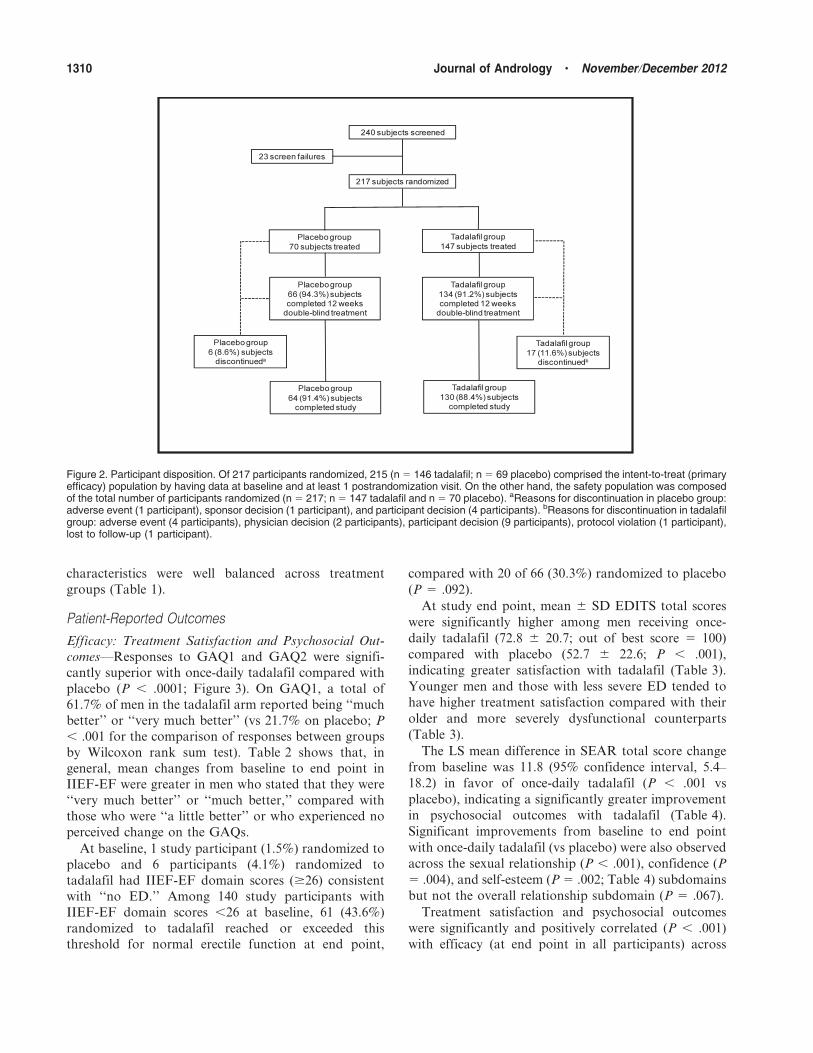
Of 217 participants randomized, 200 (92.2%) completed
the 12-week double-blind treatment (Figure 2). Baseline
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1309
characteristics were well balanced across treatment
groups (Table 1).
Patient-Reported Outcomes
Efficacy: Treatment Satisfaction and Psychosocial Out-
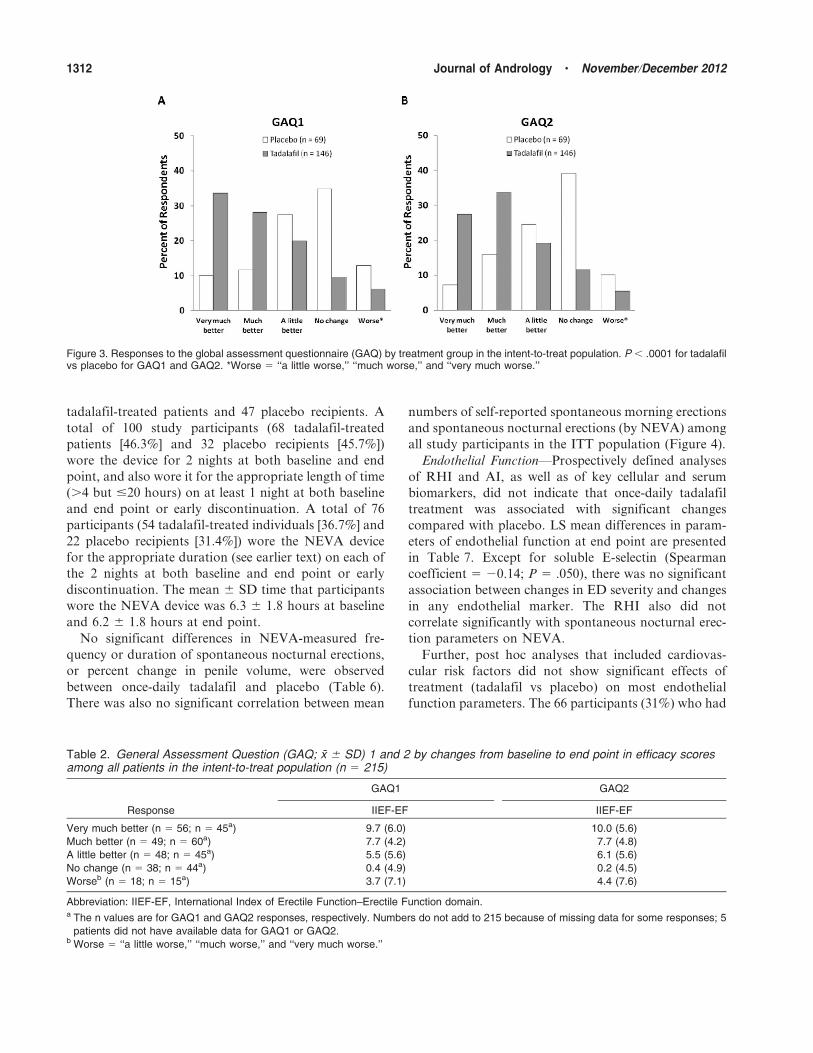
comes—Responses to GAQ1 and GAQ2 were signifi-
cantly superior with once-daily tadalafil compared with
placebo (P , .0001; Figure 3). On GAQ1, a total of
61.7% of men in the tadalafil arm reported being ‘‘much
better’’ or ‘‘very much better’’ (vs 21.7% on placebo; P
, .001 for the comparison of responses between groups
by Wilcoxon rank sum test). Table 2 shows that, in
general, mean changes from baseline to end point in
IIEF-EF were greater in men who stated that they were
‘‘very much better’’ or ‘‘much better,’’ compared with
those who were ‘‘a little better’’ or who experienced no
perceived change on the GAQs.
At baseline, 1 study participant (1.5%) randomized to
placebo and 6 participants (4.1%) randomized to
tadalafil had IIEF-EF domain scores ($26) consistent
with ‘‘no ED.’’ Among 140 study participants with
IIEF-EF domain scores ,26 at baseline, 61 (43.6%)
randomized to tadalafil reached or exceeded this
threshold for normal erectile function at end point,
compared with 20 of 66 (30.3%) randomized to placebo
(P 5 .092).
At study end point, mean 6 SD EDITS total scores
were significantly higher among men receiving once-
daily tadalafil (72.8 6 20.7; out of best score 5 100)
compared with placebo (52.7 6 22.6; P , .001),
indicating greater satisfaction with tadalafil (Table 3).
Younger men and those with less severe ED tended to
have higher treatment satisfaction compared with their
older and more severely dysfunctional counterparts
(Table 3).
The LS mean difference in SEAR total score change
from baseline was 11.8 (95% confidence interval, 5.4–
18.2) in favor of once-daily tadalafil (P , .001 vs
placebo), indicating a significantly greater improvement
in psychosocial outcomes with tadalafil (Table 4).
Significant improvements from baseline to end point
with once-daily tadalafil (vs placebo) were also observed
across the sexual relationship (P , .001), confidence (P
5 .004), and self-esteem (P 5 .002; Table 4) subdomains
but not the overall relationship subdomain (P 5 .067).
Treatment satisfaction and psychosocial outcomes
were significantly and positively correlated (P , .001)
with efficacy (at end point in all participants) across
Figure 2. Participant disposition. Of 217 participants randomized, 215 (n 5 146 tadalafil; n 5 69 placebo) comprised the intent-to-treat (primaryefficacy) population by having data at baseline and at least 1 postrandomization visit. On the other hand, the safety population was composedof the total number of participants randomized (n 5 217; n 5 147 tadalafil and n 5 70 placebo). aReasons for discontinuation in placebo group:adverse event (1 participant), sponsor decision (1 participant), and participant decision (4 participants). bReasons for discontinuation in tadalafilgroup: adverse event (4 participants), physician decision (2 participants), participant decision (9 participants), protocol violation (1 participant),lost to follow-up (1 participant).
1310 Journal of Andrology N November �December 2012

most questionnaires and domains. For each association
between the EDITS or SEAR total score and each
domain of the IIEF (except the SEAR with the
orgasmic-function domain; r 5 0.12; P 5 .090), Pearson
r values ranged from 0.26 to 0.54 and were P , .001 for
correlations (Table 5). Positive correlations between
EDITS and SEAR total scores and SEP questions 3,
4, and 5 were also statistically significant (each P , .001;
Table 5).
Spontaneous Morning Erections—Men receiving once-
daily tadalafil experienced a significantly higher proportion
of self-reported daily spontaneous morning erections at
study end point compared with placebo (58.7% vs 42.2%; P
, .001). The LS mean change in spontaneous morning
erections from baseline to end point in the tadalafil group
was 27.6% (adjusted for treatment group, age, and baseline
score), compared with 11.5% in the placebo group
(adjusted for the mentioned factors; P , .001 between
groups).
Spontaneous Nocturnal Erections—Among 217 men in
the NEVA ITT population, only 138 (63.6%) had
available data at both baseline and end point: 91
Table 1. Baseline patient characteristicsa
Characteristic Placebo (n 5 69) Tadalafil 5 mg (n 5 146)
Age, y, x 6 SD 51.9 6 10.4 52.2 6 10.9
Body mass index, kg/m2, x 6 SD 27.7 6 3.4 27.9 6 4.7
Race, No. (%)
White 69 (100.0) 144 (98.6)
Asian 0 (0) 2 (1.4)
ED etiology, No. (%)b
Psychogenic 9 (13.0) 22 (15.1)
Organic 23 (33.3) 40 (27.4)
Mixed 27 (39.1) 61 (41.8)
Unknown 10 (14.5) 23 (15.8)
ED duration, No. (%)b
3 to ,6 mo 6 (8.7) 10 (6.8)
6 to ,12 mo 14 (20.3) 33 (22.6)
$12 mo 49 (71.0) 103 (70.5)
IIEF-EF domain score, x 6 SD 15.9 6 6.2 15.5 6 6.0
ED severity (categories of IIEF-EF domain scores), No. (%)
Mild (17–30) 31 (44.9) 64 (43.8)
Moderate (11–16) 22 (31.9) 47 (32.2)
Severe (1–10) 16 (23.2) 35 (24.0)
Comorbid cardiovascular risk factors, No. (%)
Hypertension 20 (29.0) 46 (31.5)
Hypercholesterolemia 6 (8.7) 17 (11.6)
Diabetes mellitus 6 (8.7) 19 (13.0)
Coronary artery disease 1 (1.4) 1 (0.7)
Endothelial-function parameters, x 6 SDc
RHI, AU 2.0 6 0.5 1.9 6 0.6
AI, % 8.2 6 14.4 9.3 6 15.7
hsCRP, mg/L 1.8 6 2.3 2.3 6 3.9
No. of cEPCs, cells per milliliter 183.1 6 100.7 169.7 6 124.5
Soluble E-selectin, ng/mL 29.7 6 14.1 27.4 6 13.3
RHI, No. (%) with values AUc,d
,1.67 26 (38.8) 63 (43.8)
1.67–2.07 18 (26.9) 50 (34.7)
.2.07 23 (34.3) 31 (21.5)
Abbreviations: AI, augmentation index; AU, arbitrary units; cEPCs, circulating endothelial progenitor cells; ED, erectile dysfunction; hsCRP,
high-sensitivity C-reactive protein; IIEF-EF, International Index of Erectile Function–Erectile Function domain; RHI, reactive hyperemia index.a Intent-to-treat population (n 5 215): placebo (n 5 69) and tadalafil (n 5 146); 2 participants without follow-up data were excluded from all
outcome analyses except adverse events.b Some percent values do not sum to 100 because of rounding.c The intent-to-treat population with available data for endothelial function parameters included 59–67 participants in the placebo group and
134–145 in the tadalafil group.d One patient (in the tadalafil group) did not have data on this parameter.
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1311
tadalafil-treated patients and 47 placebo recipients. A
total of 100 study participants (68 tadalafil-treated
patients [46.3%] and 32 placebo recipients [45.7%])
wore the device for 2 nights at both baseline and end
point, and also wore it for the appropriate length of time
(.4 but #20 hours) on at least 1 night at both baseline
and end point or early discontinuation. A total of 76
participants (54 tadalafil-treated individuals [36.7%] and
22 placebo recipients [31.4%]) wore the NEVA device
for the appropriate duration (see earlier text) on each of
the 2 nights at both baseline and end point or early
discontinuation. The mean 6 SD time that participants
wore the NEVA device was 6.3 6 1.8 hours at baseline
and 6.2 6 1.8 hours at end point.
No significant differences in NEVA-measured fre-
quency or duration of spontaneous nocturnal erections,
or percent change in penile volume, were observed
between once-daily tadalafil and placebo (Table 6).
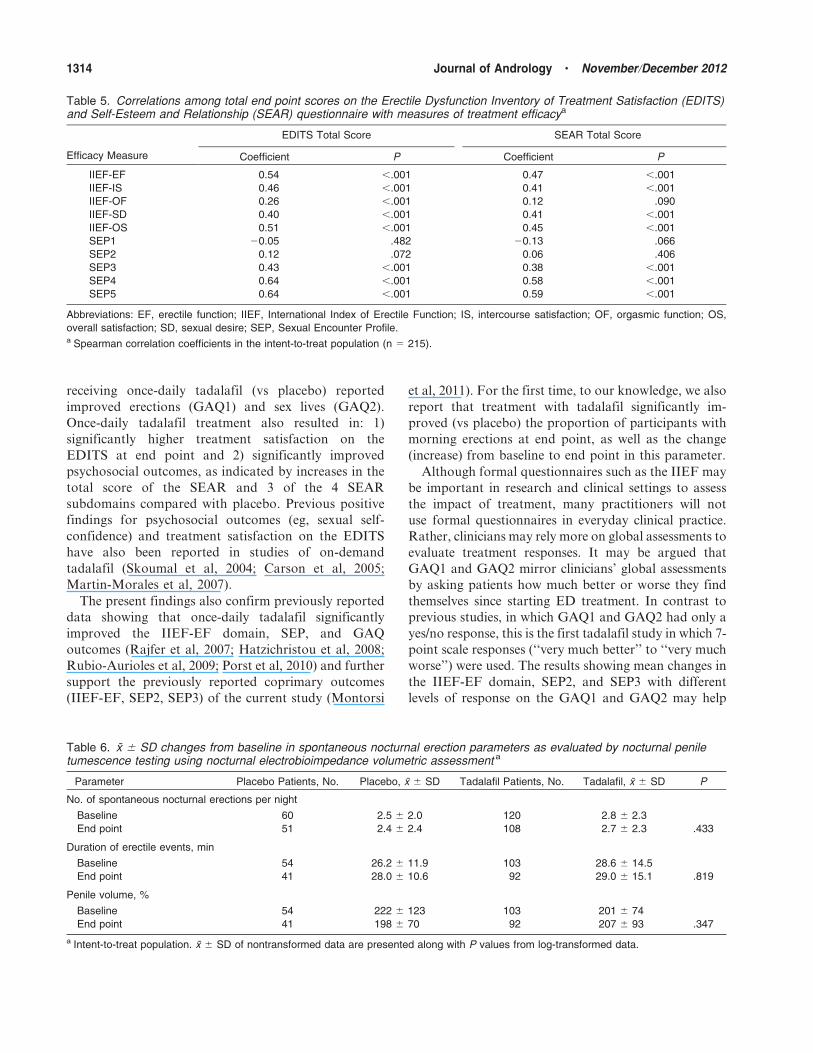
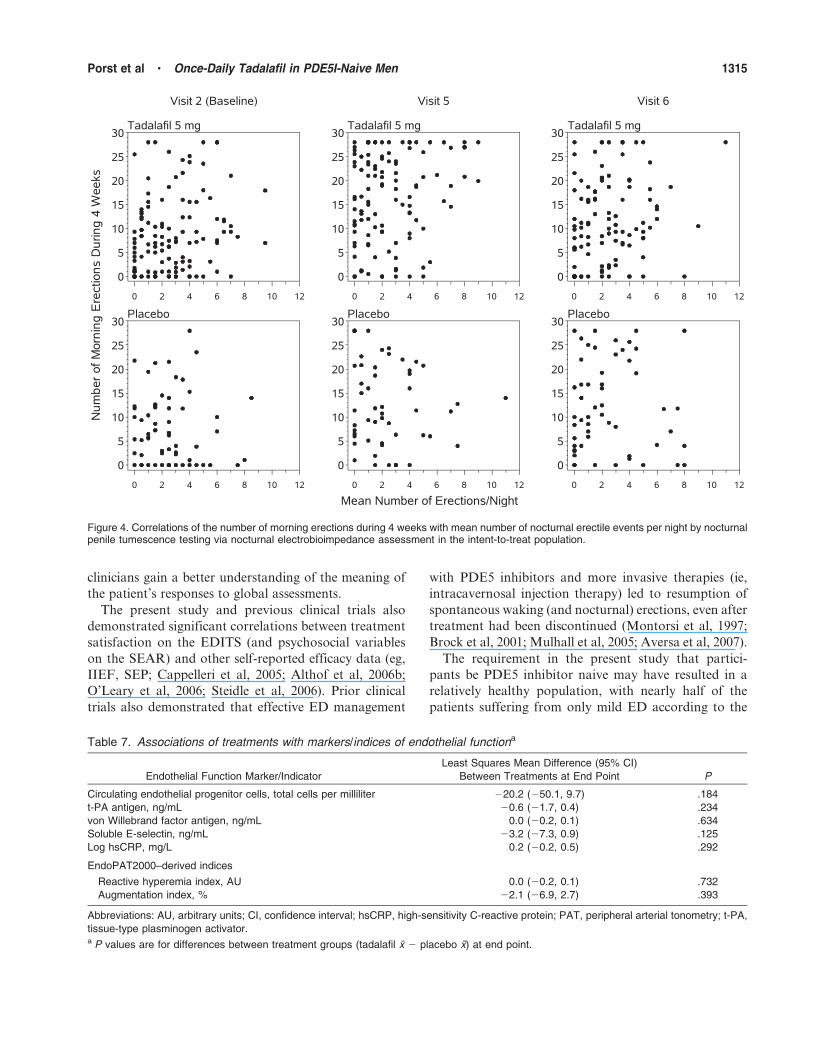
There was also no significant correlation between mean
numbers of self-reported spontaneous morning erections
and spontaneous nocturnal erections (by NEVA) among
all study participants in the ITT population (Figure 4).
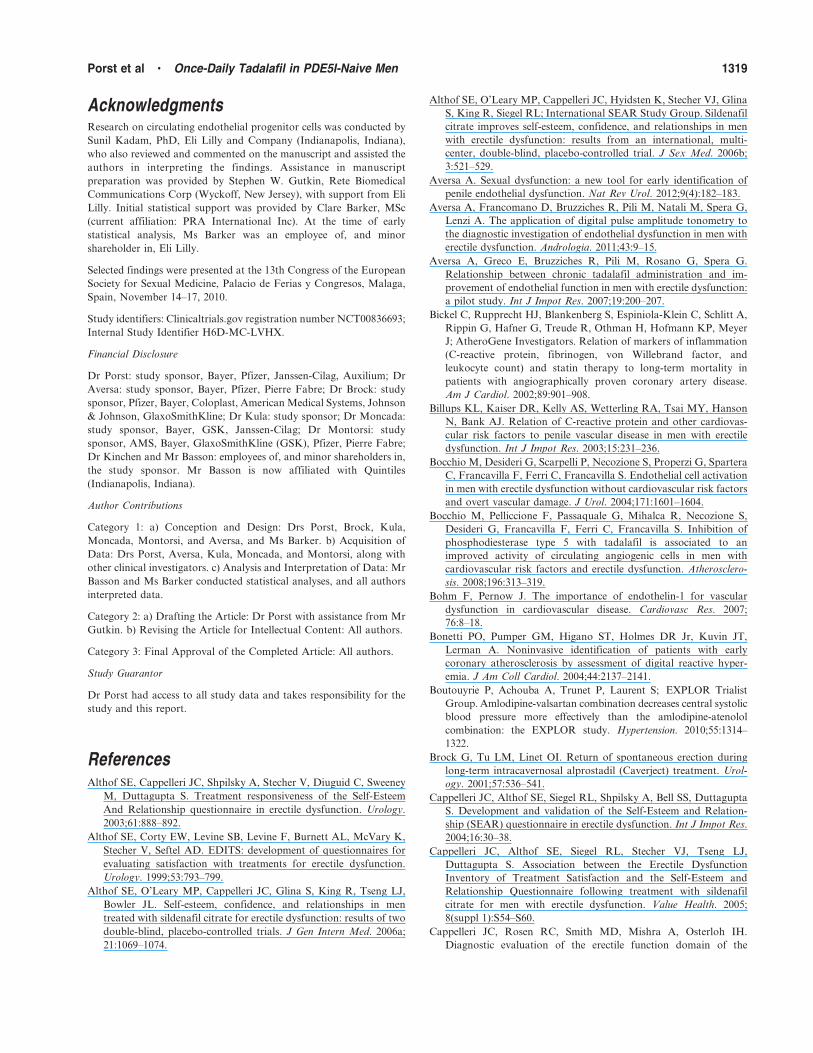
Endothelial Function—Prospectively defined analyses
of RHI and AI, as well as of key cellular and serum
biomarkers, did not indicate that once-daily tadalafil
treatment was associated with significant changes
compared with placebo. LS mean differences in param-
eters of endothelial function at end point are presented
in Table 7. Except for soluble E-selectin (Spearman
coefficient 5 20.14; P 5 .050), there was no significant
association between changes in ED severity and changes
in any endothelial marker. The RHI also did not
correlate significantly with spontaneous nocturnal erec-
tion parameters on NEVA.
Further, post hoc analyses that included cardiovas-
cular risk factors did not show significant effects of
treatment (tadalafil vs placebo) on most endothelial
function parameters. The 66 participants (31%) who had
Figure 3. Responses to the global assessment questionnaire (GAQ) by treatment group in the intent-to-treat population. P , .0001 for tadalafilvs placebo for GAQ1 and GAQ2. *Worse 5 ‘‘a little worse,’’ ‘‘much worse,’’ and ‘‘very much worse.’’
Table 2. General Assessment Question (GAQ; x 6 SD) 1 and 2 by changes from baseline to end point in efficacy scoresamong all patients in the intent-to-treat population (n 5 215)
GAQ1 GAQ2
Response IIEF-EF IIEF-EF
Very much better (n 5 56; n 5 45a) 9.7 (6.0) 10.0 (5.6)
Much better (n 5 49; n 5 60a) 7.7 (4.2) 7.7 (4.8)
A little better (n 5 48; n 5 45a) 5.5 (5.6) 6.1 (5.6)
No change (n 5 38; n 5 44a) 0.4 (4.9) 0.2 (4.5)
Worseb (n 5 18; n 5 15a) 3.7 (7.1) 4.4 (7.6)
Abbreviation: IIEF-EF, International Index of Erectile Function–Erectile Function domain.a The n values are for GAQ1 and GAQ2 responses, respectively. Numbers do not add to 215 because of missing data for some responses; 5
patients did not have available data for GAQ1 or GAQ2.b Worse 5 ‘‘a little worse,’’ ‘‘much worse,’’ and ‘‘very much worse.’’
1312 Journal of Andrology N November �December 2012

at least 2 cardiovascular risk factors also had a
significantly lower mean RHI (ie, greater degree of
endothelial dysfunction) compared with their counter-
parts having fewer risk factors; however, only the
baseline mean RHI value (not tadalafil vs placebo
treatment) was significantly predictive of lower RHI
values (P , .001) on treatment. In models including
cardiovascular risk factors, the baseline AI (P , .001),
age (P , .001), and country (P 5 .043) were
significantly associated with AI values during the study;
a treatment effect of tadalafil (vs placebo) did not reach
statistical significance. Similarly, only the baseline
logarithm of hsCRP was unequivocally significantly
associated with on-treatment levels, and tadalafil did not
exert a significant beneficial effect (vs placebo).
Participants randomized to tadalafil experienced
larger decreases from baseline to end point in raw
numbers of total cEPCs compared with placebo (mean
6 SD changes from baseline, 220.7 6 133.7 cells per
milliliter in the tadalafil group and 212.3 6 115.2 cells
per milliliter in the placebo group). In a post hoc
subgroup analysis, the effects of once-daily tadalafil
on levels of cEPCs were found to depend on each
participant’s number of baseline cardiovascular risk
factors (significant interaction; P 5 .015). In participants
with 2 or more risk factors, tadalafil treatment was
associated with a significant LS mean 6 SE reduction
from baseline to end point of 32.5 6 12.4 cEPCs per
milliliter compared with an increase of 42.6 6 20.3 cEPCs
per milliliter with placebo (P 5 .002). In study partici-
pants with fewer than 2 cardiovascular risk factors, the
between-treatment difference was not significant. Partic-
ipants with hypertension did not have significantly
different changes in cEPCs compared with those without
hypertension, and the presence or absence of hypertension
did not significantly influence the overall treatment effect.
Treatment significantly influenced changes in mean
soluble E-selectin levels, depending on baseline concen-
trations of the marker (significant treatment interaction;
P , .001). Among participants with higher baseline
soluble E-selectin levels (ie, third quartile or .36 ng/
mL), those randomized to tadalafil experienced signif-
icantly greater reductions in soluble E-selectin (23.71 ng/
mL) compared with changes with placebo (+0.06 ng/mL;
P 5 .013). Among study participants with lower
baseline soluble E-selectin levels (ie, first quartile or
,21 ng/mL), however, between-treatment differences
were not statistically significant (P 5 .408).
Safety—Tadalafil was well tolerated in this study. As
previously reported, the leading treatment-emergent
adverse events (each occurring in .2% of tadalafil-
treated participants) included back pain (3.4%) as well as
nasopharyngitis, dyspepsia, headache, and myalgia (each
2.7%; Montorsi et al, 2011). These findings are similar to
previously reported data in other once-daily tadalafil
trials (Porst et al, 2006; Rajfer et al, 2007; Hatzichristou
et al, 2008; Rubio-Aurioles et al, 2009). Less than 3% of
participants in each group discontinued treatment pre-
maturely because of adverse events (Montorsi et al, 2011).
Discussion
In this study of men previously naive to PDE5 inhibitor
therapy, significantly higher proportions of participants
Table 4. Changes in scores on the Self-Esteem and Relationship (SEAR) questionnaire by treatment groupa
SEAR Domain/Subdomain
Change From Baseline, x 6 SELS Mean Treatment Difference (95%
CI) in Change From Baseline PPlacebo (n 5 66) Tadalafil (n 5 141)
Total score 8.3 6 21.1 20.4 6 23.9 11.8 (5.4, 18.2) ,.001
Sexual relationship domain 9.7 6 22.4 23.4 6 25.9 13.1 (6.3, 20.0) ,.001
Confidence domain 6.5 6 24.6 16.5 6 25.6 9.9 (3.3, 16.5) .004
Self-esteem subdomain 9.3 6 30.1 19.2 6 27.9 11.2 (4.2, 18.3) .002
Overall relationship subdomain 0.9 6 30.2 11.0 6 32.5 7.4 (20.5, 15.3) .067
Abbreviations: CI, confidence interval; LS, least squares.a Intent-to-treat population (n 5 215) with data at baseline and end point.
Table 3. End point total scores on the Erectile DysfunctionInventory of Treatment Satisfaction (EDITS) by treatmentgroup, overall and in different groups, by baselinecharacteristicsa
Parameter No. (x 6 SD) P
EDITS
Placebo 67 (52.7 6 22.6) . . .
Tadalafil 142 (72.8 6 20.7) ,.001 vs placebo
ED severity
Mild 94 (71.4 6 21.9) Referent
Moderate 65 (66.2 6 22.9) .106 vs mild
Severe 50 (57.0 6 23.7) ,.001 vs mild
Age, y
,50 87 (72.7 6 20.3) Referent
50–59 60 (62.8 6 23.9) .021 vs ,50 y
$60 62 (60.8 6 24.6) .008 vs ,50 y
Abbreviation: ED, erectile dysfunction.a Intent-to-treat population (n 5 215) with data at end point.
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1313
receiving once-daily tadalafil (vs placebo) reported
improved erections (GAQ1) and sex lives (GAQ2).
Once-daily tadalafil treatment also resulted in: 1)
significantly higher treatment satisfaction on the
EDITS at end point and 2) significantly improved
psychosocial outcomes, as indicated by increases in the
total score of the SEAR and 3 of the 4 SEAR
subdomains compared with placebo. Previous positive
findings for psychosocial outcomes (eg, sexual self-
confidence) and treatment satisfaction on the EDITS
have also been reported in studies of on-demand
tadalafil (Skoumal et al, 2004; Carson et al, 2005;
Martin-Morales et al, 2007).
The present findings also confirm previously reported
data showing that once-daily tadalafil significantly
improved the IIEF-EF domain, SEP, and GAQ
outcomes (Rajfer et al, 2007; Hatzichristou et al, 2008;
Rubio-Aurioles et al, 2009; Porst et al, 2010) and further
support the previously reported coprimary outcomes
(IIEF-EF, SEP2, SEP3) of the current study (Montorsi
et al, 2011). For the first time, to our knowledge, we also
report that treatment with tadalafil significantly im-
proved (vs placebo) the proportion of participants with
morning erections at end point, as well as the change
(increase) from baseline to end point in this parameter.
Although formal questionnaires such as the IIEF may
be important in research and clinical settings to assess
the impact of treatment, many practitioners will not
use formal questionnaires in everyday clinical practice.
Rather, clinicians may rely more on global assessments to
evaluate treatment responses. It may be argued that
GAQ1 and GAQ2 mirror clinicians’ global assessments
by asking patients how much better or worse they find
themselves since starting ED treatment. In contrast to
previous studies, in which GAQ1 and GAQ2 had only a
yes/no response, this is the first tadalafil study in which 7-
point scale responses (‘‘very much better’’ to ‘‘very much
worse’’) were used. The results showing mean changes in
the IIEF-EF domain, SEP2, and SEP3 with different
levels of response on the GAQ1 and GAQ2 may help
Table 6. x 6 SD changes from baseline in spontaneous nocturnal erection parameters as evaluated by nocturnal peniletumescence testing using nocturnal electrobioimpedance volumetric assessment a
Parameter Placebo Patients, No. Placebo, x 6 SD Tadalafil Patients, No. Tadalafil, x 6 SD P
No. of spontaneous nocturnal erections per night
Baseline 60 2.5 6 2.0 120 2.8 6 2.3
End point 51 2.4 6 2.4 108 2.7 6 2.3 .433
Duration of erectile events, min
Baseline 54 26.2 6 11.9 103 28.6 6 14.5
End point 41 28.0 6 10.6 92 29.0 6 15.1 .819
Penile volume, %
Baseline 54 222 6 123 103 201 6 74
End point 41 198 6 70 92 207 6 93 .347
a Intent-to-treat population. x 6 SD of nontransformed data are presented along with P values from log-transformed data.
Table 5. Correlations among total end point scores on the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS)and Self-Esteem and Relationship (SEAR) questionnaire with measures of treatment efficacya
Efficacy Measure
EDITS Total Score SEAR Total Score
Coefficient P Coefficient P
IIEF-EF 0.54 ,.001 0.47 ,.001
IIEF-IS 0.46 ,.001 0.41 ,.001
IIEF-OF 0.26 ,.001 0.12 .090
IIEF-SD 0.40 ,.001 0.41 ,.001
IIEF-OS 0.51 ,.001 0.45 ,.001
SEP1 20.05 .482 20.13 .066
SEP2 0.12 .072 0.06 .406
SEP3 0.43 ,.001 0.38 ,.001
SEP4 0.64 ,.001 0.58 ,.001
SEP5 0.64 ,.001 0.59 ,.001
Abbreviations: EF, erectile function; IIEF, International Index of Erectile Function; IS, intercourse satisfaction; OF, orgasmic function; OS,
overall satisfaction; SD, sexual desire; SEP, Sexual Encounter Profile.a Spearman correlation coefficients in the intent-to-treat population (n 5 215).
1314 Journal of Andrology N November �December 2012
clinicians gain a better understanding of the meaning of
the patient’s responses to global assessments.
The present study and previous clinical trials also
demonstrated significant correlations between treatment
satisfaction on the EDITS (and psychosocial variables
on the SEAR) and other self-reported efficacy data (eg,
IIEF, SEP; Cappelleri et al, 2005; Althof et al, 2006b;
O’Leary et al, 2006; Steidle et al, 2006). Prior clinical
trials also demonstrated that effective ED management
with PDE5 inhibitors and more invasive therapies (ie,
intracavernosal injection therapy) led to resumption of
spontaneous waking (and nocturnal) erections, even after
treatment had been discontinued (Montorsi et al, 1997;
Brock et al, 2001; Mulhall et al, 2005; Aversa et al, 2007).
The requirement in the present study that partici-
pants be PDE5 inhibitor naive may have resulted in a
relatively healthy population, with nearly half of the
patients suffering from only mild ED according to the
Figure 4. Correlations of the number of morning erections during 4 weeks with mean number of nocturnal erectile events per night by nocturnalpenile tumescence testing via nocturnal electrobioimpedance assessment in the intent-to-treat population.
Table 7. Associations of treatments with markers/indices of endothelial functiona
Endothelial Function Marker/Indicator
Least Squares Mean Difference (95% CI)
Between Treatments at End Point P
Circulating endothelial progenitor cells, total cells per milliliter 220.2 (250.1, 9.7) .184
t-PA antigen, ng/mL 20.6 (21.7, 0.4) .234
von Willebrand factor antigen, ng/mL 0.0 (20.2, 0.1) .634
Soluble E-selectin, ng/mL 23.2 (27.3, 0.9) .125
Log hsCRP, mg/L 0.2 (20.2, 0.5) .292
EndoPAT2000–derived indices
Reactive hyperemia index, AU 0.0 (20.2, 0.1) .732
Augmentation index, % 22.1 (26.9, 2.7) .393
Abbreviations: AU, arbitrary units; CI, confidence interval; hsCRP, high-sensitivity C-reactive protein; PAT, peripheral arterial tonometry; t-PA,
tissue-type plasminogen activator.a P values are for differences between treatment groups (tadalafil x 2 placebo x) at end point.
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1315

baseline IIEF-EF. Only 23.7% had severe ED, com-
pared with a range of approximately 24% to 40% in
previous once-daily trials (Porst et al, 2006; Rajfer et al,2007; Rubio-Aurioles et al, 2009). In addition, the mean
age of the present population (52 years) was lower in the
current study compared with previous once-daily
tadalafil trials: approximately 54 years (Rubio-Aurioles
et al, 2009), 56 years (Porst et al, 2006), and 60 years
(Rajfer et al, 2007). Proportions of participants with
vascular risk factors were also near the lower limits of
ranges established in previous studies of once-dailytadalafil that enrolled patients with previous exposure to
PDE5 inhibitors, including hypertension (30.7% vs a range
of 29%–43%), diabetes (11.6% vs a range of 14%–15%),
and hyperlipidemia/hypercholesterolemia (10.7% vs a
range of 10%–22%). Under such conditions, once-daily
tadalafil might not be expected to substantially improve
endothelial function that was not profoundly abnormal
in most patients. The impact of daily tadalafil onendothelial dysfunction might be assessed more appro-
priately in a study specifically focused on men with
defined endothelial dysfunction and documented arter-
iogenic ED.
Once-daily tadalafil did not significantly improve
objective measures of spontaneous nocturnal erections
compared with placebo. However, with regard to the
NEVA data, there was substantial patient attrition,which was largely attributed to operator difficulties (eg,
problems wearing the device throughout the night,
difficulties with batteries). Only 138 of 217 patients
(63.6%) had available data on at least 1 night at baseline
and end point to compute changes in the number of
spontaneous nocturnal erections. Relatively few study
participants successfully wore the device for .4 hours
nightly on consecutive nights, at baseline and end point,as planned. These patient-attrition issues may have
served to minimize any treatment effect with tadalafil
(vs placebo) because of type II (b) statistical error.
The observations of the essentially neutral effects of
tadalafil (vs placebo) on objective measures of endothe-
lial function in the current study are somewhat at odds
with data from previous clinical studies involving
treatment with tadalafil. For example, Rosano et al(2005) studied alternate-day tadalafil (vs placebo) in
men with increased cardiovascular risk and found
improved endothelial function, as measured by flow-
mediated dilatation (FMD) and endothelin-1 levels, in
the tadalafil treatment group.
In another study, treatment with tadalafil 20 mg 3
times per week was associated with improved brachial
artery FMD and increased progenitor cells in men with
ED (Foresta et al, 2006). In general, PDE5 inhibitors arenot effective in improving endothelial function in
healthy individuals (Dishy et al, 2001). This observation
is supported by a study conducted by Bocchio and
colleagues (2008), in which changes in circulating
angiogenic cells and improved brachial artery FMD inmen receiving tadalafil 20 mg every other day (vs
placebo) were associated with the presence of baseline
endothelial dysfunction.
In the current study, we chose a range of putative
cellular markers as exploratory end points in an effort
to better understand the potential impact of tadalafil
once daily on endothelial function. However, there is
no consensus concerning which of these markers shouldbe evaluated in such an analysis. In addition, we do
not yet have reliable population data on normative
values for each of these markers, the sensitivities and
specificities of abnormal levels in detecting endothelial
dysfunction, and the levels of changes in these
parameters that might be clinically meaningful. In a
recent article, for example, Costa and Virag (2009)
observed that, ‘‘To date, many circulating biomarkershave been proposed for the evaluation of endothelial
function; however, none have been considered the ideal
or more specific, and most are unavailable for current
practice.’’ Despite these limitations, we felt that it was
important to contribute our results to this growing area
of scientific investigation.
Given that eligible participants could not have had
previous exposure to PDE5 inhibitors, a ‘‘ceiling’’ effectmay have limited the degree to which once-daily
tadalafil for 12 weeks could further improve objective
measures of endothelial function compared with place-
bo. The fact that our study population involved men
with ED naive to PDE5 inhibitors (and hence with
mainly mild ED) helps to explain why tadalafil did not
result in higher proportions of men with normal IIEF-
EF domain scores at end point: 43.6% compared with30.3% with placebo. In this context, Rosen and
colleagues (2011) demonstrated that minimum clinically
important differences in the IIEF-EF domain are
directly related to baseline ED severity, with patients
having mild ED exhibiting a minimum clinically
important difference of 2; moderate ED, 5; and severe
ED, 7. Hence, given the large proportion of our patient
population with mild ED, it is not entirely surprisingthat tadalafil-associated improvements in normalization
of erectile function according to the IIEF-EF domain
would be modest.
Evidence that patients analyzed in the present study
had mild overall vascular disease and experienced a
ceiling effect with tadalafil included the fact that 122
participants (57.5%) in the ITT population had RHI
data that were considered a priori to be either
inconclusive for endothelial dysfunction (RHI-PATindex $1.67 and #2.07) or normal (.2.07), where a
value of #1.67 has been associated with endothelial
1316 Journal of Andrology N November �December 2012

dysfunction in a population at risk for ischemic heart
disease (Yinon et al, 2006). Although the proportion of
participants with hypertension (30.7%) was not dissim-ilar in our study and previous trials, a smaller
proportion of our patient sample had diabetes: approx-
imately 12% in the total population compared with 14%
to 21% in previous studies of tadalafil once daily and as
needed (Carson et al, 2004; Porst et al, 2006; Rajfer et al,
2007; Donatucci et al, 2008). Corresponding data for
CAD were 0.9% of participants in the present study
compared with 5% to 14% of those in previous tadalafiltrials.
Other baseline data in the current study support the
explanation of a ceiling effect as having limited potential
improvements in endothelial dysfunction with tadalafil
(vs placebo). The mean participant age was 52 years,
approximately 75% of study participants had mild
(44.2% of the total ITT population) or moderate
(32.1%) ED, and 29.3% of the entire study populationhad organic ED.
Most other parameters of endothelial dysfunction
were also not profoundly elevated at baseline. The
baseline RHI-PAT index value in the total ITT
population of the present study was higher than the
previously reported cutoff of #1.67 for endothelial
dysfunction (mean 6 SD, 1.89 6 0.57 in all participants)
and consistent with an inconclusive finding aboutendothelial dysfunction.
On the other hand, it is also possible that the daily
dose of tadalafil evaluated in the present study (5 mg)
was too low to expect consistent beneficial effects on
biomarkers of endothelial dysfunction in a low-risk
population when compared with previous studies
(Foresta et al, 2006, 2009; Aversa et al 2007). In the
future, it might be of interest to compare PAT findings
with results from other forms of testing, including FMDand other, penile hemodynamic and anatomic measures,
such as cavernous artery intima-media thickness (Car-
etta et al, 2009). FMD remains the first-choice
noninvasive method to measure endothelial function
and has the most data relating to CAD risk (Tamler and
Bar-Chama, 2008). Considering that endothelial dys-
function of penile arteries is a different entity from
systemic endothelial dysfunction as detected by othermodalities (ie, veno-occlusive plethysmography and
FMD), the utility of evaluating penile arterial dysfunc-
tion as an early marker of atherosclerotic disease seems
to be more promising than fingertip PAT, especially in
men with ED (Aversa, 2012).
Similarly, the baseline mean 6 SD hsCRP level of
2.12 6 3.44 mg/L (and median of 1.19 mg/L) in the
present study is not consistent with elevated cardiovas-cular risk (Ridker et al, 2008; Genest et al, 2009). In a
randomized, open-label crossover study of 20 individuals
with ED in whom alternate-day tadalafil 20 mg treatment
significantly reduced hsCRP, the baseline value was
considerably higher (x 6 SD, 3.1 6 0.4 mg/L; Aversa etal, 2007).
A 12-week randomized, double-blind, placebo-con-
trolled study of 298 men with comorbid ED and
diabetes showed that once-daily tadalafil 2.5- to 5-mg
treatment did not significantly reduce hsCRP, intercel-
lular adhesion molecule (ICAM-1), or vascular cell
adhesion molecule (VCAM-1), but the baseline values
were within normal limits (Hatzichristou et al, 2008).Two studies involving alternate-day treatment with
tadalafil 20 mg for 4 weeks showed significant reduc-
tions in endothelin-1 on active therapy in study
participants with baseline mean values of 3.3 ng/L in
both studies (Rosano et al, 2005; Aversa et al, 2007).
Our post hoc analyses demonstrated that changes in
levels of the cellular adhesion molecule soluble E-
selectin correlated inversely with ED severity on theIIEF. To our knowledge, this is the first reported
observation of such a relationship. The origins of
circulating adhesion molecules are not entirely clear,
but these cells may derive from shedding or proteolytic
cleavage from endothelial cells, and thus reflect
increased expression of membrane-bound adhesion
molecules (an initiating event in atherogenesis). Men
with ED have increased levels of adhesion molecules,including soluble P-selectin (Bocchio et al, 2004), which
recruits leukocytes to the site of arterial injury, and
hence is intimately involved in the inflammatory
pathway. In the present study, tadalafil treatment
significantly reduced soluble E-selectin levels only in
participants with baseline soluble E-selectin values in the
upper tertile (or above the median; data not shown).
This finding suggests that in such study participants,soluble E-selectin may represent an early marker of
endothelial repair during progression of the atherogenic
process.
The number of EPCs is considered to be an indicator
of the presence of vascular injury as well as an
expression of reparative mechanisms and vascular
protection, including angiogenesis and vasculogenesis
(Rauscher et al, 2003; Foresta et al, 2010a). In previous
studies by Foresta et al (2005a,b, 2006, 2007, 2009a,b,2010a,b), patients with increasing degrees of endothelial
dysfunction exhibited progressive decreases in numbers
of cEPCs. However, age-specific normative values for
cEPCs have yet to be established, and larger studies are
needed to determine the clinical significance of cEPC
numbers in the general population. In a previous study
involving an Asian population, most of whom did not
have cardiovascular risk factors, there was no significantcorrelation between numbers of cEPCs (and surface
marker expression) and blood pressure, cholesterol or
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1317

glucose levels, or a history of smoking (Chen et al,
2010). It is also important to note that not all studies of
EPCs have focused on the same cell types, including
progenitors expressing CD34, CD133, KDR, and/or
VEGFR2. Taken together, these factors may have
contributed to uncertainty in the evaluation of our
results. In this context, Esposito et al (2009) stated that
‘‘. . .there is no clear consensus on which antigenic
profile best identifies progenitor cells with the potential
to repair the endothelium.’’ They concluded that
‘‘literature data evaluating the putative causative role
of EPCs in ED are scanty and discordant.’’
In the current study, there were no statistically
significant differences between tadalafil and placebo
in terms of mean changes in levels of cEPCs. However,
a post hoc analysis showed a reduction in cEPCs with
tadalafil compared with placebo in men with 2 or more
cardiac risk factors. The results of cEPC analyses in the
current study must be interpreted with great caution
given the mentioned discussion on the limitations
introduced by the relatively mild ED population in
this study, the current understanding of how cEPCs
should best be studied in endothelial function, and the
relatively small number of participants in the subgroup
analysis involving those with 2 or more risk factors. It
is possible, for example, that decreases in cEPCs
observed in our study may represent reductions in
ligand-mediated activation of cEPCs, with stabilization
of the cEPC pool and potential long-term beneficial
outcomes, especially in study participants at high
cardiovascular risk. Further, it is plausible that PDE5
inhibitors do not increase cEPCs and other salutary
biomarkers to the same extent as other medications for
vascular diseases; in one small study of patients with
angiographically documented stable CAD, daily treat-
ment with an HMG-CoA reductase inhibitor (statin)
for 4 weeks increased numbers of cEPCs by a factor of
1.5 to 3 (Vasa et al, 2001). Work in one of our
institutions (Aversa, 2012), which included both PAT
and cEPC measures, demonstrated that low-dose once-
daily tadalafil did not affect endothelial function in
men with mild ED.
Potential Study Limitations
As mentioned earlier, the requirement in this study that
eligible participants could have no previous experience
using PDE5 inhibitors may have resulted in our
enrolling a greater proportion of men with less severe
ED and less advanced cavernous endothelial dysfunc-
tion. To reduce the probability of a potential ceiling
effect with tadalafil (vs placebo) because of mild
pathology at baseline, our study could be repeated in
larger and more heterogeneous patient populations
without regard to previous use of or degree of responses
to PDE5 inhibitors; in study participants with more
severe ED and/or more frequent vascular comorbidities
(eg, diabetes); and possibly using more sensitive or
effective objective measures (eg, FMD).
The NEVA device was suboptimally tolerated, and a
relatively small number of participants had data
recorded on consecutive nights at baseline and end
point per the study protocol. At times, patients reported
considerable difficulties in operating the NEVA device.
Taken together, these difficulties likely contributed to
important limitations in the analysis of the NEVA data.
Our choice of NEVA was dictated largely by the fact
that this technology was Conformite Europeenne
(European Conformity) marked, ensuring its overall
safety according to requirements of the European
Union.
The post hoc subgroup analyses were of a mainly
exploratory, hypothesis-generating nature, were subject
to potential biases, and were not adjusted for multiple
comparisons. The present study did not assess potential
diurnal fluctuations in endothelial function (eg, in RHI
[Ohno et al, 2010]) or treatment satisfaction from the
sexual partner’s perspective.
Conclusion
European men with ED who had not previously used
PDE5 inhibitors experienced superior self-reported
treatment satisfaction and improvements in psychoso-
cial function (vs placebo) after receiving once-daily
tadalafil. Data from GAQs (scored for the first time
using a 7-point scale response set in tadalafil studies)
further supported the efficacy of tadalafil in this patient
population. Enhanced treatment satisfaction and psy-
chosocial function were significantly correlated with
improvements in efficacy. Once-daily tadalafil treat-
ment also significantly increased the frequency of self-
reported spontaneous morning erections. No signifi-
cant effects of active treatment on spontaneous
nocturnal erections by NEVA were observed, but a
relatively low proportion of study participants were
able to provide data per protocol. Other objective
measures of endothelial function were not improved by
once-daily tadalafil (vs placebo) in this multicenter
study.
Summary
Once-daily tadalafil significantly improved erectile func-
tion, satisfaction, psychosocial factors, and frequencies of
morning erections, but it did not significantly enhance
objectively measured spontaneous nocturnal erections or
endothelial dysfunction.
1318 Journal of Andrology N November �December 2012
AcknowledgmentsResearch on circulating endothelial progenitor cells was conducted by
Sunil Kadam, PhD, Eli Lilly and Company (Indianapolis, Indiana),
who also reviewed and commented on the manuscript and assisted the
authors in interpreting the findings. Assistance in manuscript
preparation was provided by Stephen W. Gutkin, Rete Biomedical
Communications Corp (Wyckoff, New Jersey), with support from Eli
Lilly. Initial statistical support was provided by Clare Barker, MSc
(current affiliation: PRA International Inc). At the time of early
statistical analysis, Ms Barker was an employee of, and minor
shareholder in, Eli Lilly.
Selected findings were presented at the 13th Congress of the European
Society for Sexual Medicine, Palacio de Ferias y Congresos, Malaga,
Spain, November 14–17, 2010.
Study identifiers: Clinicaltrials.gov registration number NCT00836693;
Internal Study Identifier H6D-MC-LVHX.
Financial Disclosure
Dr Porst: study sponsor, Bayer, Pfizer, Janssen-Cilag, Auxilium; Dr
Aversa: study sponsor, Bayer, Pfizer, Pierre Fabre; Dr Brock: study
sponsor, Pfizer, Bayer, Coloplast, American Medical Systems, Johnson
& Johnson, GlaxoSmithKline; Dr Kula: study sponsor; Dr Moncada:
study sponsor, Bayer, GSK, Janssen-Cilag; Dr Montorsi: study
sponsor, AMS, Bayer, GlaxoSmithKline (GSK), Pfizer, Pierre Fabre;
Dr Kinchen and Mr Basson: employees of, and minor shareholders in,
the study sponsor. Mr Basson is now affiliated with Quintiles
(Indianapolis, Indiana).
Author Contributions
Category 1: a) Conception and Design: Drs Porst, Brock, Kula,
Moncada, Montorsi, and Aversa, and Ms Barker. b) Acquisition of
Data: Drs Porst, Aversa, Kula, Moncada, and Montorsi, along with
other clinical investigators. c) Analysis and Interpretation of Data: Mr
Basson and Ms Barker conducted statistical analyses, and all authors
interpreted data.
Category 2: a) Drafting the Article: Dr Porst with assistance from Mr
Gutkin. b) Revising the Article for Intellectual Content: All authors.
Category 3: Final Approval of the Completed Article: All authors.
Study Guarantor
Dr Porst had access to all study data and takes responsibility for the
study and this report.
ReferencesAlthof SE, Cappelleri JC, Shpilsky A, Stecher V, Diuguid C, Sweeney
M, Duttagupta S. Treatment responsiveness of the Self-Esteem
And Relationship questionnaire in erectile dysfunction. Urology.
2003;61:888–892.
Althof SE, Corty EW, Levine SB, Levine F, Burnett AL, McVary K,
Stecher V, Seftel AD. EDITS: development of questionnaires for
evaluating satisfaction with treatments for erectile dysfunction.
Urology. 1999;53:793–799.
Althof SE, O’Leary MP, Cappelleri JC, Glina S, King R, Tseng LJ,
Bowler JL. Self-esteem, confidence, and relationships in men
treated with sildenafil citrate for erectile dysfunction: results of two
double-blind, placebo-controlled trials. J Gen Intern Med. 2006a;
21:1069–1074.
Althof SE, O’Leary MP, Cappelleri JC, Hyidsten K, Stecher VJ, Glina
S, King R, Siegel RL; International SEAR Study Group. Sildenafil
citrate improves self-esteem, confidence, and relationships in men
with erectile dysfunction: results from an international, multi-
center, double-blind, placebo-controlled trial. J Sex Med. 2006b;
3:521–529.
Aversa A. Sexual dysfunction: a new tool for early identification of
penile endothelial dysfunction. Nat Rev Urol. 2012;9(4):182–183.
Aversa A, Francomano D, Bruzziches R, Pili M, Natali M, Spera G,
Lenzi A. The application of digital pulse amplitude tonometry to
the diagnostic investigation of endothelial dysfunction in men with
erectile dysfunction. Andrologia. 2011;43:9–15.
Aversa A, Greco E, Bruzziches R, Pili M, Rosano G, Spera G.
Relationship between chronic tadalafil administration and im-
provement of endothelial function in men with erectile dysfunction:
a pilot study. Int J Impot Res. 2007;19:200–207.
Bickel C, Rupprecht HJ, Blankenberg S, Espiniola-Klein C, Schlitt A,
Rippin G, Hafner G, Treude R, Othman H, Hofmann KP, Meyer
J; AtheroGene Investigators. Relation of markers of inflammation
(C-reactive protein, fibrinogen, von Willebrand factor, and
leukocyte count) and statin therapy to long-term mortality in
patients with angiographically proven coronary artery disease.
Am J Cardiol. 2002;89:901–908.
Billups KL, Kaiser DR, Kelly AS, Wetterling RA, Tsai MY, Hanson
N, Bank AJ. Relation of C-reactive protein and other cardiovas-
cular risk factors to penile vascular disease in men with erectile
dysfunction. Int J Impot Res. 2003;15:231–236.
Bocchio M, Desideri G, Scarpelli P, Necozione S, Properzi G, Spartera
C, Francavilla F, Ferri C, Francavilla S. Endothelial cell activation
in men with erectile dysfunction without cardiovascular risk factors
and overt vascular damage. J Urol. 2004;171:1601–1604.
Bocchio M, Pelliccione F, Passaquale G, Mihalca R, Necozione S,
Desideri G, Francavilla F, Ferri C, Francavilla S. Inhibition of
phosphodiesterase type 5 with tadalafil is associated to an
improved activity of circulating angiogenic cells in men with
cardiovascular risk factors and erectile dysfunction. Atherosclero-
sis. 2008;196:313–319.
Bohm F, Pernow J. The importance of endothelin-1 for vascular
dysfunction in cardiovascular disease. Cardiovasc Res. 2007;
76:8–18.
Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr, Kuvin JT,
Lerman A. Noninvasive identification of patients with early
coronary atherosclerosis by assessment of digital reactive hyper-
emia. J Am Coll Cardiol. 2004;44:2137–2141.
Boutouyrie P, Achouba A, Trunet P, Laurent S; EXPLOR Trialist
Group. Amlodipine-valsartan combination decreases central systolic
blood pressure more effectively than the amlodipine-atenolol
combination: the EXPLOR study. Hypertension. 2010;55:1314–
1322.
Brock G, Tu LM, Linet OI. Return of spontaneous erection during
long-term intracavernosal alprostadil (Caverject) treatment. Urol-
ogy. 2001;57:536–541.
Cappelleri JC, Althof SE, Siegel RL, Shpilsky A, Bell SS, Duttagupta
S. Development and validation of the Self-Esteem and Relation-
ship (SEAR) questionnaire in erectile dysfunction. Int J Impot Res.
2004;16:30–38.
Cappelleri JC, Althof SE, Siegel RL, Stecher VJ, Tseng LJ,
Duttagupta S. Association between the Erectile Dysfunction
Inventory of Treatment Satisfaction and the Self-Esteem and
Relationship Questionnaire following treatment with sildenafil
citrate for men with erectile dysfunction. Value Health. 2005;
8(suppl 1):S54–S60.
Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH.
Diagnostic evaluation of the erectile function domain of the
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1319
International Index of Erectile Function. Urology. 1999;54:
346–351.
Caretta N, Palego P, Ferlin A, Garolla A, Bettella A, Selice R, Foresta
C. Resumption of spontaneous erections in selected patients
affected by erectile dysfunction and various degrees of carotid
wall alteration: role of tadalafil. Eur Urol. 2005;48:326–331.
Caretta N, Palego P, Schipilliti M, Ferlin A, Di Mamro A, Foresta C.
Cavernous artery intima-media thickness: a new parameter in the
diagnosis of vascular erectile dysfunction. J Sex Med. 2009;
6:1117–1126.
Carson C, Shabsigh R, Segal S, Murphy A, Fredlund P, Kuepfer C.
Efficacy, safety, and treatment satisfaction of tadalafil versus
placebo in patients with erectile dysfunction evaluated at tertiary-
care academic centers. Urology. 2005;65:353–359.
Carson CC, Rajfer J, Eardley I, Carrier S, Denne JS, Walker DJ, Shen
W, Cordell W. The efficacy and safety of tadalafil: an update.
Br J Urol Int. 2004;93:1276–1281.
Chen CH, Cheng BC, Leu S, Chen CH, Tsai TH, Leu S, Chang HW,
Chung SY, Chua S, Yeh KH, Chen YL, Yip HK. Circulating level
of endothelial progenitor cells in healthy Taiwanese. Acta Cardiol
Sing. 2010;26:94–100.
Costa C, Virag R. The endothelial-erectile dysfunction connection: an
essential update. J Sex Med. 2009;6:2390–2404.
Dishy V, Sofowora G, Harris PA, Kandcer M, Zhan F, Wood AJ, Stein
CM. The effect of sildenafil on nitric oxide-mediated vasodilation in
healthy men. Clin Pharmacol Ther. 2001;70:270–279.
Donatucci CF, Wong DG, Giuliano F, Glina S, Dowsett SA, Watts S,
Sorsaburu S. Efficacy and safety of tadalafil once daily:
considerations for the practical application of a daily dosing
option. Curr Med Res Opin. 2008;24:3383–3392.
Esposito K, Ciotola M, Maiorino MI, Giugliano F, Autorino R, De Sio
M, Jannini E, Lenzi A, Giugliano D. Circulating CD34+ KDR+endothelial progenitor cells correlate with erectile function and
endothelial function in overweight men. J Sex Med. 2009;6:107–114.
European Medicines Agency. Cialis summary of product characteristics
2012. Available at http://www.ema.europa.eu/docs/en_GB/document_
library/EPAR_-_Product_Information/human/000436/WC500026318.
pdf. Accessed September 28, 2012.
Foresta C, Caretta N, Lana A, Cabrelle A, Palu G, Ferlin A.
Circulating endothelial progenitor cells in patients with erectile
dysfunction. Int J Impot Res. 2005a;17:288–290.
Foresta C, Caretta N, Lana A, De Toni L, Biagioli A, Vinanzi C,
Ferlin A. Relationship between vascular damage degrees and
endothelial progenitor cells in patients with erectile dysfunction:
effect of vardenafil administration and PDE5 expression in the
bone marrow. Eur Urol. 2007;51:1411–1417.
Foresta C, De Toni L, Biagioli A, Ganz F. Magagna S, Caretta N.
Increased levels of osteocalcin-positive endothelial progenitor cells
in patients affected by erectile dysfunction and cavernous
atherosclerosis. J Sex Med. 2010a;7:751–757.
Foresta C, De Toni L, Garolla A, Ferlin A, Zuccarello D. The PDE5
inhibitor sildenafil increases circulating endothelial progenitor cells
and CXCR4 expression. J Sex Med. 2009a;6:369–372.
Foresta C, De Toni L, Magagna S, Galan A, Garolla A. Phospho-
diesterase-5 inhibitor tadalafil acts on endothelial progenitor cells
by CXCR4 signalling. Curr Drug Deliv. 2010b;7:274–282.
Foresta C, Di Mambro A, Caretta N, De Toni L, Zuccarello D, Ferlin
A. Effect of vardenafil on endothelial progenitor cells in
hypogonadotrophic hypogonadal patients: role of testosterone
treatment. Clin Endocrinol (Oxf). 2009b;71:412–416.
Foresta C, Ferlin A, De Toni L, Lana A, Vinanzi C, Galan A, Caretta
N. Circulating endothelial progenitor cells and endothelial function
after chronic tadalafil treatment in subjects with erectile dysfunc-
tion. Int J Impot Res. 2006;18:484–488.
Foresta C, Lana A, Cabrelle A, Ferigo M, Caretta N, Garolla A, Palu
G, Ferlin A. PDE-5 inhibitor, Vardenafil, increases circulating
progenitor cells in humans. Int J Impot Res. 2005b;17:377–380.
Foresta C, Palego P, Schipilliti M, Selice R, Ferlin A, Caretta N.
Asymmetric development of peripheral atherosclerosis in patients
with erectile dysfunction: an ultrasonographic study. Atherosclero-
sis. 2008;197:889–895.
Gazzaruso C, Giordanetti S, De Amici E, Bertone G, Falcone C,
Geroldi D, Fratino P, Solerte SB, Garzaniti A. Relationship
between erectile dysfunction and silent myocardial ischemia in
apparently uncomplicated type 2 diabetic patients. Circulation.
2004;110:22–26.
Gazzaruso C, Pujia A, Solerte SB, Amici ED, Emanuele E, Falcone C,
Geroldi D, Giustina A, Garzaniti A. Erectile dysfunction and
angiographic extent of coronary artery disease in type II diabetic
patients. Int J Impot Res. 2006;18:311–315.
Genest J, McPherson R, Frohlich J, Anderson T, Campbell N,
Carpentier A, Couture P, Dufour R, Fodor G, Francis GA, Grover
S, Gupta M, Hegele RA, Lau DC, Leiter L, Lewis GF, Lonn E,
Mancini GB, Ng D, Pearson GJ, Sniderman A, Stone JA, Ur E.
2009 Canadian Cardiovascular Society/Canadian guidelines for
the diagnosis and treatment of dyslipidemia and prevention of
cardiovascular disease in the adult - 2009 recommendations.
Can J Cardiol. 2009;25:567–579.
Giugliano F, Esposito K, Di Palo C, Ciotola M, Giugliano G,
Marfella R, D’Armiento M, Giugliano D. Erectile dysfunction
associates with endothelial dysfunction and raised proinflamma-
tory cytokine levels in obese men. J Endocrinol Invest. 2004;
27:665–669.
Guy W. ECDEU Assessment Manual for Psychopharmacology–
Revised. DHEW Publication No. ADM 76-338. Rockville, MD:
National Institute of Mental Health; 1976:218–222.
Hatzichristou D, Gambla M, Rubio-Aurioles E, Buvat J, Brock GB,
Spera G, Rose L, Lording D, Liang S. Efficacy of tadalafil once
daily in men with diabetes mellitus and erectile dysfunction. Diabet
Med. 2008;25:138–146.
Jackson G. Editorial comment on Caretta N et al. Resumption of
spontaneous erections in selected patients affected by erectile
dysfunction and various degrees of carotid wall alteration: role of
tadalafil. Eur Urol. 2005;332.
Knoll LD, Abrams JH. Application of nocturnal electrobioimpedance
volumetric assessment: a feasibility study in men without erectile
dysfunction. J Urol. 1999a;161:1137–1140.
Knoll LD, Abrams JH. Nocturnal electrobioimpedance volumetric
assessment of patients with erectile dysfunction. Urology. 1999b;
53:1200–1204.
Levine LA, Carroll RA. Nocturnal penile tumescence and rigidity in
men without complaints of erectile dysfunction using a new
quantitative analysis software. J Urol. 1994;152:1103–1107.
Martin-Morales A, Haro JM, Beardsworth A, Bertsch J, Kontodimas
S. Therapeutic effectiveness and patient satisfaction after 6 months
of treatment with tadalafil, sildenafil, and vardenafil: results from
the erectile dysfunction observational study (EDOS). Eur Urol.
2007;51:541–550.
McMahon C. Efficacy and safety of daily tadalafil in men with erectile
dysfunction previously unresponsive to on-demand tadalafil. J Sex
Med. 2004;1:292–300.
Mizuno I, Fuse H, Fujiuchi Y, Nakagawa O, Akashi T. Comparative
study between audiovisual sexual stimulation test and nocturnal
penile tumescence test using RigiScan Plus in the evaluation of
erectile dysfunction. Urol Int. 2004;72:221–224.
Montorsi F, Aversa A, Moncada I, Perimenis P, Porst H, Barker C, Shane
MA, Sorsaburu S. A randomized, double-blind, placebo-controlled,
parallel study to assess the efficacy and safety of once-a-day tadalafil in
1320 Journal of Andrology N November �December 2012

men with erectile dysfunction who are naıve to PDE5 inhibitors. J Sex
Med. 2011;8:2617–2624.
Montorsi F, Briganti A, Salonia A, Rigatti P, Burnett AL. Current and
future strategies for preventing and managing erectile dysfunction
following radical prostatectomy. Eur Urol. 2004;45:123–133.
Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi
A, Galli S, Ravagnani PM, Montorsi P. Erectile dysfunction
prevalence, time of onset and association with risk factors in 300
consecutive patients with acute chest pain and angiographically
documented coronary artery disease. Eur Urol. 2003;44:360–364.
Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L, Barbieri
L, Rigatti P, Pizzini G, Miani A. Recovery of spontaneous erectile
function after nerve-sparing radical retropubic prostatectomy
with and without early intracavernous injections of alprostadil:
results of a prospective, randomized trial. J Urol. 1997;158:1408–
1410.
Mulhall J, Land S, Parker M, Waters WB, Flanigan RC. The use of an
erectogenic pharmacotherapy regimen following radical prostatec-
tomy improves recovery of spontaneous erectile function. J Sex
Med. 2005;2:532–540.
Nawawi H, Osman NS, Annuar R, Khalid BA, Yusoff K. Soluble
intercellular adhesion molecule-1 and interleukin-6 levels reflect
endothelial dysfunction in patients with primary hypercholesterol-
aemia treated with atorvastatin. Atherosclerosis. 2003;169:283–291.
Naya M, Tsukamoto T, Inubushi M, Morita K, Katoh C, Furumoto T,
Fujii S, Tsutsui H, Tamaki N. Elevated plasma plasminogen activator
inhibitor type-1 is an independent predictor of coronary microvas-
cular dysfunction in hypertension. Circulation J. 2007a;71:348–
353.
Naya M, Tsukamoto T, Morita K, Katoh C, Furumoto T, Fujii S,
Tamaki N, Tsutsui H. Plasma interleukin-6 and tumor necrosis
factor-alpha can predict coronary endothelial dysfunction in
hypertensive patients. Hypertens Res. 2007b;30:541–548.
Ohno Y, Hashiguchi T, Maenosono R, Yamashita H, Taira Y,
Minowa K, Yamashita Y, Kato Y, Kawahara KI, Maruyama I.
The diagnostic value of endothelial function as a potential sensor of
fatigue in health. Vasc Health Risk Manag. 2010;6:135–144.
O’Leary MP, Althof SE, Cappelleri JC, Crowley A, Sherman N,
Duttagupta S; United States Self-Esteem and Relationship Question-
naire Study Group. Self-esteem, confidence and relationship satisfac-
tion of men with erectile dysfunction treated with sildenafil citrate: a
multicenter, randomized, parallel group, double-blind, placebo con-
trolled study in the United States. J Urol. 2006;175:1058–1062.
Porst H, Giuliano F, Glina S, Ralph D, Casabe AR, Elion-Mboussa
A, Shen W, Whitaker JS. Evaluation of the efficacy and safety of
once-a-day dosing of tadalafil 5mg and 10mg in the treatment of
erectile dysfunction: results of a multicenter, randomized, double-
blind, placebo-controlled trial. Eur Urol. 2006;50:351–359.
Porst H, Glina S, Ralph D, Zeigler H, Wong DG, Woodward B.
Durability of response following cessation of tadalafil taken once
daily as treatment for erectile dysfunction. J Sex Med. 2010;
7:3487–3494.
Rajfer J, Aliotta PJ, Steidle CP, Fitch WP III, Zhao Y, Yu A. Tadalafil
dosed once a day in men with erectile dysfunction: a randomized,
double-blind, placebo-controlled study in the US. Int J Impot Res.
2007;19:95–103.
Ralph D, Eardley I, Kell P, Dean J, Hackett G, Collins O, Edwards D.
Improvement in erectile function on vardenafil treatment correlates
with treatment satisfaction in both patients and their partners.
Br J Urol Int. 2007;100:130–136.
Rauscher FM, Goldschmidt-Clermont PJ, Davis BH, Wang T, Gregg
D, Ramaswami P, Pippen AM, Annex BH, Dong C, Taylor DA.
Aging, progenitor cell exhaustion, and atherosclerosis. Circulation.
2003;108:457–463.
Ridker PM. C-reactive protein and the prediction of cardiovascular
events among those at intermediate risk: moving an inflammatory
hypothesis toward consensus. J Am Coll Cardiol. 2007;49:2129–
2138.
Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr,
Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG,
Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER
Study Group. Rosuvastatin to prevent vascular events in men and
women with elevated C-reactive protein. N Engl J Med. 2008;
359:2195–2207.
Rosano GM, Aversa A, Vitale C, Fabbri A, Fini M, Spera G. Chronic
treatment with tadalafil improves endothelial function in men with
increased cardiovascular risk. Eur Urol. 2005;47:214–220.
Rosen RC, Allen KR, Ni X, Araujo AB. Minimum clinically important
differences in the erectile function domain of the International Index
of Erectile Function Scale. Eur Urol. 2011;60:1010–1016.
Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A.
The international index of erectile function (IIEF): a multidimen-
sional scale for assessment of erectile dysfunction. Urology. 1997;
49:822–830.
Rubinshtein R, Kuvin JT, Soffler M, Lennon RJ, Lavi S, Nelson RE,
Pumper GM, Lerman LO, Lerman A. Assessment of endothelial
function by non-invasive peripheral arterial tonometry predicts late
cardiovascular adverse events. Eur Heart J. 2010;31:1142–1148.
Rubio-Aurioles E, Kim ED, Rosen RC, Porst H, Burns P, Zeigler H,
Wong DG. Impact on erectile function and sexual quality of life of
couples: a double-blind, randomized, placebo-controlled trial of
tadalafil taken once daily. J Sex Med. 2009;6:1314–1323.
Salama N. Nocturnal electrobioimpedance volumetric assessment in
diabetic men with erectile dysfunction before and after tadalafil
intake. Int J Impot Res. 2004;16:441–447.
Seftel A, Goldfischer E, Kim ED, Dula E, Zeigler H, Burns P. Onset of
efficacy of tadalafil once daily in men with erectile dysfunction:
a randomized, double-blind, placebo controlled trial. J Urol.
2011;185:243–248.
Seftel AD, Buvat J, Althof SE, McMurray JG, Zeigler HL, Burns PR,
Wong DG. Improvements in confidence, sexual relationship and
satisfaction measures: results of a randomized trial of tadalafil 5 mg
taken once daily. Int J Impot Res. 2009;21:240–248.
Shimizu M, Kario K. Role of the augmentation index in hypertension.
Ther Adv Cardiovasc Dis. 2008;2:25–35.
Skoumal R, Chen J, Kula K, Breza J, Calomfirescu N, Basson BR,
Kopernicky V. Efficacy and treatment satisfaction with on-demand
tadalafil (Cialis) in men with erectile dysfunction. Eur Urol.
2004;46:362–369.
Steidle CP, Stecher VJ, Pace C, Tseng LJ. Correlation of improved
erectile function and rate of successful intercourse with improved
emotional well-being assessed with the Self-Esteem And Relationship
questionnaire in men treated with sildenafil for erectile dysfunction
and stratified by age. Curr Med Res Opin. 2006;22:939–948.
Suzuki K, Sato Y, Horita H, Adachi H, Kato R, Hisasue S, Itoh N,
Tsukamoto T. The correlation between penile tumescence mea-
sured by the erectometer and penile rigidity by the RigiScan.
Int J Urol. 2001;8:594–598.
Tamler R, Bar-Chama N. Assessment of endothelial function in the
patient with erectile dysfunction: an opportunity for the urologist.
Int J Impot Res. 2008;20:370–377.
Udelson D, Park K, Sadeghi-Nejad H, Salimpour P, Krane RJ,
Goldstein I. Axial penile buckling forces vs. Rigiscan radial rigidity
as a function of intracavernosal pressure: why Rigiscan does not
predict functional erections in individual patients. Int J Impot Res.
1999;11:327–337.
Vasa M, Fichtlscherer S, Adler K, Aicher A, Martin H, Zeiher AM,
Dimmeler S. Increase in circulating progenitor cells by statin
Porst et al N Once-Daily Tadalafil in PDE5I-Naive Men 1321

therapy in patients with stable coronary artery disease. Circulation.
2001;103:2885–2890.
Yalcin I, Bump RC. Validation of two global impression question-
naires for incontinence. Am J Obstet Gynecol. 2003;189:98–101.
Yinon D, Lowenstein L, Suraya S, Beloosesky R, Zmora O, Malhotra
A, Pillar G. Pre-eclampsia is associated with sleep-disordered
breathing and endothelial dysfunction. Eur Respir J. 2006;27:
328–333.
1322 Journal of Andrology N November �December 2012
Top Related
Copyright © 2022 FDOKUMEN

