







Bahasa
Halaman
Hukum


DECEPTION IN F A C I A L EXPRESSIONS OF PAIN:
STRATEGIES TO IMPROVE DETECTION
by
M A R I L Y N LOUISE HILL
B.A. (Honours), Queen's University, 1989
M . S c , Memorial University of Newfoundland, 1992
A THESIS SUBMITTED IN PARTIAL F U L F I L L M E N T OF
THE REQUIREMENTS FOR THE DEGREE OF
DOCTOR OF PHILOSOPHY
in
THE F A C U L T Y OF G R A D U A T E STUDIES
Department of Psychology
We accept this thesis as conforming
to the required standard
THE UNIVERSITY OF BRITISH C O L U M B I A
AUGUST 1996
© Marilyn Louise Hi l l , 1996

In presenting this thesis in partial fulfilment of the requirements for an advanced
degree at the University of British Columbia, I agree that the Library shall make it
freely available for reference and study. I further agree that permission for extensive
copying of this thesis for scholarly purposes may be granted by the head of my
department or by his or her representatives. It is understood that copying or
publication of this thesis for financial gain shall not be allowed without my written
permission.
Department
The University of British Columbia Vancouver, Canada
DE-6 (2/88)

Abstract
Research suggests that clinicians assign greater weight to nonverbal expression than to
patients' self-report when judging the location and severity of their pain. However, it has also
been found that pain patients are fairly successful at altering their facial expressions of pain, as
their deceptive and genuine pain expressions show few differences in the frequency and intensity
of pain-related facial actions. The general aim of the present research was to improve the
detection of deceptive pain expressions using both an empirical and a clinical approach. The first
study had an empirical focus to pain identification, and provided a more detailed description of
genuine and deceptive pain expressions by using a more comprehensive range of facial coding
procedures than previous research. A review of research on facial expressions, pain research and
deception suggested that facial analyses of genuine and deceptive pain expressions could be
expanded to include new variables such as temporal patterns and contiguity of facial actions, as
well as an increased focus on facial cues thought to be indicative of lying. Low back patients
(n=40) were videotaped at rest and while undergoing a painful straight leg raise under three sets
of instructions: 1) to genuinely express any pain they felt, 2) pretend that it didn't hurt, 3) to fake
pain without moving their legs. FACS coding was used to describe and quantify their facial
activity and the neutral, genuine pain, masked pain and faked pain expressions were compared on
the number, type, intensity, temporal qualities , and contiguity in time of individual facial
actions, as well as the incidence of facial actions thought to be indicative of deception. Findings
confirmed the difficulty of discriminating the various facial expressions, but indicated that the
faked pain expressions show a greater number of pain-related and non pain-related actions,
remain at peak intensity longer, and last for a longer period of time than do genuine pain
i i

expressions. The difference between masked pain and neutral expressions were more subtle,
with masked pain expressions exhibiting a greater frequency of mouth opening and residual
movement of the eyebrows.
The second study was more clinical in nature and was designed to see i f specific training
could improve the detection skills of naive judges by increasing their knowledge and awareness
of possible cues to deception. University students (60 male, 60 female) were randomly assigned
to one of four experimental groups: l)control, 2) corrective feedback, 3) deception training, and
4) deception training plus feedback. Each subject was shown the videotaped data of the pain
patients in all four conditions (neutral expressions, genuine, masked and faked pain expressions).
For each videoclip, the subjects rated the intensity and unpleasantness of the pain experienced by
the patient, decided which category each of the four videoclips represented, and described which
cues they used to make their decision. There were significant individual differences in accuracy,
with accuracy being unrelated to past pain experience, empathy, or the number or type of facial
cues used. There was, however, a significant sex difference in judgement accuracy, with females
being more accurate than males. Results also showed that immediate corrective feedback led to
significant improvements in subjects' detection accuracy, while there was no support for the use
of an information-based training program.
ii i

Table of Contents
Pag
Abstract : i i
Table of Contents iv
List of tables ix
Acknowledgement xi
Introduction 1
Literature Review ; 4
Describing genuine and deceptive pain expressions 4
Facial expressions of pain 5
Factors contributing to the discrepancies in pain expression research 5
Type and severity of pain 5
Methodological differences 7
Situational variables 8
Validity and utility of the pain expression 8
Discriminating genuine versus deceptive pain expressions 11
Genuine pain..... 11
Faked pain 12
Masked pain 12
Individual difference variables 14
Summary J. 15
Deception theory and research '. 16
Types of deception 16
Theoretical basis for differences between genuine and deceptive expressions 17
Cues to deception 18
Concealing a genuine expression 18
Falsifying an expression 18
Temporal qualities of facial expressions 19
Temporal contiguity of pain expressions 19
Patterns of facial expression 20
iv

Blinking 21
Asymmetry 22
Describing and quantifying facial expressions 25
Increasing the comprehensiveness of FACS coding 25
Detecting pain through facial expression 26
Judging genuine pain using facial expression 27
Detecting genuine versus deceptive pain 28
Detecting deception in others 30
Individual differences in detection accuracy 32
Possible individual difference variables 32
Cue utilization 32
Decision-making confidence 33
Sex differences 34
Empathy 35
Summary 36
Training to improve lie detection 36
Prospects for deception training specific to pain .....37
Summary 40
Study one: A comprehensive description of genuine and deceptive pain expressions ....41
Hypotheses 42
Study two: Effectiveness of training strategies to improve the discrimination
of genuine and deceptive pain expressions 43
Hypotheses 43
Study one: Analysis of genuine, faked and masked pain expressions 44
Method 44
Subjects 44
Videotape equipment 44
Coding videotape 44
Measures 45
Personal data sheet 45
Descriptor differential scales 45
v

Procedure 45
Videotaping protocol 46
Quantification of facial activity 47
Results 49
Description of patient population 49
Reliability coding 49
Preliminary analyses 50
Frequency 50
Intensity 54
Apex duration 57
Onset duration 58
Facial action duration 58
Asymmetry and pulsating apexes 63
Temporal contiguity of facial actions 63
Study two: training to detect deception 65
Method 65
Subjects 65
Materials 65
Video equipment 65
Videotape 65
Training manual 66
Measures 66
Personal information sheet 66
Interpersonal Reactivity Index 67
Procedure 67
Training conditions 67
Judgement task 68
Results 69
Judgements of pain 69
Sex 69
Training group 69
vi

Pain condition 73
Perceived judgement accuracy 74
Decision-making process variables 74
Number of cues used 74
Type of cues used 77
Individual difference variables 85
Pain experience 85
Empathy 86
Comparison of successful and unsuccessful judges 87
Discussion 88
Describing genuine and deceptive pain expressions 88
Genuine pain expressions 88
Faked pain expressions 90
Masked pain expressions 92
Individual differences in facial expressions of pain 93
Temporal qualities of deceptive versus genuine pain expressions 94
Incidence of deception cues in deceptive vs genuine pain expressions 95
Summary 95
Detecting genuine and deceptive pain displays 96
Judgements of intensity and unpleasantness 97
Discrimination of genuine and deceptive pain expressions 99
The effects of training on facial expression judgements 101
Individual differences in judgement accuracy 104
Sex differences 105
Pain experience and empathy 106
Comparison of successful and unsuccessful judges 107
Summary 107
Future directions 108
Limits to generalizability 109
vii

References I l l
Appendices
Appendix A : FACS action units 118
Appendix B: Research identifying pain-related AU ' s 119
Appendix C: Study one questionnaire package 121
Appendix D: Consent form for pain patients 124
Appendix E: Physiotherapy protocol 125
Appendix F: Descriptor differential scales 126
Appendix G: Training manual 128
Appendix H: Questionnaire package 142
Appendix I: Videotape description and rating forms 147
Appendix J: Frequency of facial cue use per subject 151
Appendix K : Categorization of facial cues 156
Appendix L: Type and frequency of subjects' pain experiences 158
Appendix M : Correlation matrix 159
viii
List of Tables
Table Page
1 Results of M A N O V A and Followup A N O V A ' s Examining
Frequency of Facial Actions Across Pain Conditions 51
2 Mean Facial Action Frequency Across Pain Conditions 52
3 Results of M A N O V A and Followup A N O V A ' s Examining
Intensity of Facial Actions Across Pain Conditions 55
4 Mean Facial Action Intensity Across Pain Condition 56
5 Results of M A N O V A and Followup A N O V A ' s Examining
Apex Duration of Facial Actions Across Pain Conditions 59
6 Mean Facial Action Apex Duration Across Pain Condition 60
7 Results of M A N O V A and Followup A N O V A ' s Examining
the Duration of Facial Actions Across Pain Conditions 61
8 Mean Facial Action Duration Across Pain Condition 62
9 Results of M A N O V A on the Effects of Sex, Training and
Pain Condition on Judgements of Pain 70 10 Mean Accuracy and Decision-Making Confidence Across
Training Group and Pain Condition 71
11 Mean Ratings of Pain Intensity and Unpleasantness Across
Training group and Pain Condition 72
ix

Results of M A N O V A on the Effects of Sex, Training and Pain
Condition on Number of Cues Used
Mean Number of Facial Cues Detected Across Training
Groups and Pain Condition
Results of M A N O V A on the Effects of Training Group
on Individual Cue Use
Results of M A N O V A on the Effects of Pain Condition
on Individual Cue Use
Mean Individual Cue Use Across Pain Condition
Results of M A N O V A on the Effects of Training Group
on the Use of Cue Type
Mean Cue Type Use Across Training Group
x

Acknowledgement
I would like to take this opportunity to thank the many individuals who were involved with this
project in some capacity over the years. First, a sincere thanks to my research supervisor, Dr.
Ken Craig, for both his creative input and his impressive editorial skills. His financial
contributions must also be acknowledged, as he supported my dissertation research with funds
provided by his SSHRC grant,as well as providing me with R A funding in times of dire financial
need. Within the research lab itself, many individuals provided research assistanceship,
including Neda Dadmand, Terri Wilmon, and Debbie Sandbrand. Jyotika Reddy deserves a
special mention for her capable handling of the data collection with only minimal long-distance
supervision. I am also indebted to Bruce McMurtry and Christine Lilley for many things,
including the support and humour they provided in response to both graduate school and real-life
crises. In addition, I will never be able to thank them enough for their willingness to complete
the very tedious and time consuming FACS coding required for this project. A last heartfelt
thank-you to my family, for being so supportive and involved, and for not asking (at least not too
often) why this degree was taking so long. Finally, I would like to dedicate the final product to
my grandfather, Percy Hi l l , for his interest in my work and for his overwhelming pride in my
ambition.
xi

1
INTRODUCTION
Pain is a private experience with complex sensory, affective and evaluative qualities. To
properly assess pain and provide effective management, information is needed regarding these
often subtle complexities of experience. Access to these subjective events can only be achieved
through inference from verbal descriptions, nonverbal behaviours, and situational information.
Although sensitivity to such information, using contemporary measures, can lead to relatively
accurate judgements about another's internal pain state (Turk & Melzack, 1993), the ability to
engage in voluntary control of verbal and nonverbal pain expressions may diminish the observer's
ability to make accurate inferences. It is the purposeful and intentional misrepresentation of the
nature of the pain experience that constitutes the focus of these investigations.
The capacity for deception has become an important issue in clinical settings because some
patients report pain and disability levels inconsistent with their degree of physical injury. It could
be that the patient exaggerates or fakes pain due to perceived personal benefit, e.g., influencing
pending litigation or compensation claims. Alternatively, s/he may minimize the report of pain
experience due to fear of adverse consequences, e.g., prescription of addictive pain medications.
Based on these examples, and many other possibilities, it is clear that the possibility of deception
needs to be considered during the assessment of clinical pain. It is equally clear that discrepancies
between physical pathology and behavioural evidence of pain do not justify decisions about
deception. To begin with, current diagnostic systems for identifying physical pathology can be
quite limited. In addition, research has shown that there is a fairly tenuous relationship between
organic damage and reports of pain (Turk & Melzack, 1993).
Where does one begin to look for cues to deception in the range of information currently
available? When assessing pain in a clinical population, the clinician may have access to verbal
information, including standardized questionnaires, and interviews, and nonverbal information,
such as pain behaviours (e.g. limping, guarding movements) and facial expression (Keefe &
Block, 1982; Keefe, Brantley, Manuel & Crisson, 1985). Ekman and Friesen (1969,1974) have
shown that observers often assume that nonverbal behaviour is less amenable to deception, which
is consistent with the finding that observers assign greater importance to people's nonverbal
2
behaviour when it is discordant with their verbal self-reports of emotion (Craig & Prkachin, 1980;
1983; DePaulo, Rosenthal, Eisenstat, Rogers & Finkelstein, 1978; Jacox, 1980). Research
specific to pain supports this finding; naive judges provided with both verbal report and facial
activity, considered facial expressions to be the more salient source of information on which to
base their judgements (Poole & Craig, 1992). Clinicians also assign greater weight to nonverbal
expression than to patient self-reports when judging the location and severity of pain experienced
(Johnson, 1977). Nonverbal cues, including posture, body movements, vocalizations and facial
expression, are clearly crucial sources of information about the nature of an individual's pain
experience. Compared to other nonverbal cues, facial expression is a rich source of information
because of its plasticity and dynamic range (Craig, 1992).
It has been suggested that another advantage of facial expression as a measure of pain is
that it is less subject to conscious deception than are verbalizations (Craig & Prkachin, 1980;
1983). However, it is equally clear that facial expressions of pain cannot be considered to be
simply innate or reflexive responses. Affect and cognition significantly moderate the experience
of pain (Turk, Meichenbaum & Genest, 1983), and research has shown only a modest relationship
between the severity of painful stimulation and the individual's behavioural response (Craig,
1986). Research has also found that individuals can inhibit their facial displays of pain when
under observation (Kleck et a l , 1976). It appears that complete confidence in the genuineness of
facial expressions as an immediate source of information about subjective experience is premature.
Facial expressions therefore, do not represent a direct measure of pain intensity, and are amenable
to manipulation.
Nevertheless, useful information in facial expressions is available to the clinician and other
observers when assessing the credibility of self-report. Recent studies using intensive analyses of
facial activity have found that deceptive and genuine pain expressions differ in the frequency and
intensity of certain facial actions, although relatively few differences have been found and the
differences that exist are quite subtle (Craig, Hyde & Patrick, 1991; Hadjistavropoulos & Craig,
1994). When naive undergraduate observers were asked to judge whether these expressions were
genuine or deceptive, accuracy was extremely poor (Poole & Craig, 1992), although use of a

3
forced choice design indicated judges were better than chance and sources of error could be
identified (Hadjistavropoulos, Craig, Hadjistavropoulos & Poole, 1996). This research suggests
that pain patients can be fairly successful in their attempts to alter their facial expressions of pain.
The general aim of the present research was to improve the detection of deceptive pain
expressions using both an empirical and a clinical approach. The first study had an empirical
focus to pain identification, and provided a more detailed description of genuine and deceptive
pain expressions by using a more comprehensive range of facial coding procedures than previous
research. A review of research on facial expression, pain research, and deception suggested that
the facial analyses of genuine and deceptive pain expressions could be expanded to include new
variables such as the temporal patterns and contiguity of specific units in facial expressions, as
well as the occurrence of facial cues thought to be indicative of lying.
The second study was more clinical in nature and was designed to see if specific training
could improve the detection skills of naive judges by increasing their knowledge and awareness of
possible facial cues to deception. The training programe was based on previous research on facial
expression, pain, and deception, and attempted to increase the breadth and acuity of judges'
decision making procedures. Subjects receiving each of three different training strategies were
compared to one another and to a control group of naive observers in their accuracy of detection
of deception.

4
LITERATURE REVIEW
Describing Genuine and Deceptive Pain Expressions
The face has long been believed to represent a source of information about an individual's
conscious and unconscious experience. Aristotle, for example, noted that characteristic facial
expressions accompanied the experience of many emotions (Russell, 1994). Since the rise of
psychological science, research on the facial expression of emotion has flourished, and several
conflicting theories describing the precise role of facial expression in emotion have appeared
(Buck, 1984; Fridlund, 1991; Izard, 1990; Tomkins, 1962). Similar controversies appeared
regarding the role of facial expression and emotion in the experience of pain (Craig, 1994).
Research investigating the inference of pain and emotion through facial expression shares similar
challenges of assessing subjective experience. The study of pain offers an advantage, however, in
that the instigating event for these subjective experiences can often be more clearly identified.
It has been difficult to empirically validate facial expression theories because of the
problematic description and measurement of facial actions which are complex and fleeting. The
research literature contains a long history of measurement schemes, including category checklists
of facial behaviour, verbal descriptions of facial gestalts, photographs of movement within specific
facial areas, and electromyographic measurement (Ekman & Friesen, 1978a). The present study
used one of the best-known systems: Ekman & Friesen's (1978a, 1978b) Facial Action Coding
System (FACS).
The FACS method provides a comprehensive, objective analysis of all possible facial
actions which can be distinguished reliably by observers. An anatomically based system, FACS
provides a fine-grained description of 44 visible facial Action Units (AU's) resulting from
activation of individual or units of facial muscles. Each of the AU's represents a discrete,
minimally distinguishable action of a facial muscle or combination of facial muscles (See Appendix
A). As a result of this detailed focus, FACS provides a comprehensive descriptive approach to
facial activity independent of inference regarding the underlying emotions or meanings of the
facial expression. FACS coding provides a means for investigating a broad range of psychological
states, and lends itself to the present study of pain assessment.

5
Facial Expressions of Pain
While the many pain expression studies using FACS have not agreed on the precise
constellation of facial actions constituting the "prototypical" pain response, there have been many
consistent findings. In general, only a small subset of the 44 possible AUs has been found to be
responsive during pain. People experiencing pain have been found to exhibit primarily a lowered
brow, raised cheeks, tightened eye lids, a raised upper lip or opened mouth, and closed eyes (Craig
et al., 1991; Prkachin & Mercer, 1989). Specifically, all but one study in the area (Galin & Thorn,
1993) have identified brow lowering and tightening of the eyelids as a response to pain. In addition,
the majority of studies identified cheek raising, eyes closed or blinking, upper lip raise, parting of
the lips, or jaw dropping as pain-related AU"s. In contrast, horizontal or vertical stretching of the
lips, a wrinkled nose, deepening of the nasolabial fold and drooping eyelids were identified in only a
few studies. A breakdown of the particular facial actions identified in each study can be found in
Appendix B. Craig (1992) noted that variations between studies regarding such factors as the type
of pain experienced, the severity of discomfort, methodological differences, and situational and
individual difference variables could account for at least some of the discrepancies in A U s described
above.
Factors Contributing to the Discrepancies in Pain Expression Research
Type and Severity of Pain. Differences between studies on facial expressions associated
with pain could be due to the pain stimulus used. For example, experimentally induced pain studies
often expose university students to novel pain stimuli such as the cold pressor test (Craig & Patrick,
1985) , pressure algometry (Prkachin & Mercer, 1989), or electric shock (Patrick, Craig & Prkachin,
1986) . Subjects in these studies may have little prior experience with the specific type of pain
stimulus. In contrast, clinical pain studies often use patients suffering from varying types of acute
and chronic pain such as low back pain (Hadjistavropoulos & Craig, 1994), shoulder pain (Prkachin
& Mercer, 1989; Prkachin, Solomon, Hwang & Mercer, 1995), cancer pain (Wilkie, 1995), and
temporomandibular disorder pain (LeResche & Dworkin, 1988). The pain stimulus in this case is
often an exacerbation of the acute or chronic pain instigated by medical procedures. For the pain
patient population then, there may have been a fairly lengthy experience with clinical pain and,

6
perhaps more importantly, the pain stimulus itself is likely to have been familiar. As a result, the
clinical pain stimulus probably elicits sensory, cognitive and affective responses that are distinctly
different from responses to the novel, acute pain induced during experimental pain studies. While
there has been some consistency across studies, the variability in findings dictates careful delineation
of the parameters of pain-inducing stimuli, as these differences may be reflected in the facial
expression of pain exhibited by experimental and clinical subjects.
Prkachin and Mercer (1989) have provided evidence for the differential influence of pain-
inducing stimuli on pain experience with their comparison of clinical and experimental pain using
healthy volunteer and patient populations. In the clinical population, some facial expressions were
related to patient ratings of the intensity and unpleasantness of the clinical pain stimulus, yet no
relationship was found between facial expression and similar ratings of experimental pain in either
the clinical or experimental subjects (Prkachin & Mercer, 1989). These results contrast with those
of Patrick et al. (1986) who reported a modest correlation between the magnitude of facial activity
and the intensity of the pain stimulus during induced pain in healthy volunteers. Prkachin and
Mercer (1989) also showed that while the facial expressions induced by experimental pain and
clinical pain shared the features of brow lowering and eye closing, the clinical pain expression
contained a greater variety of facial movements. These differences between clinical and
experimental pain expressions may be a reflection of a less complex reaction to the experimental
pain stimulus, due to a lack of previous experience and thus, a different meaning attributed to the
pain experience
Pain expressions of patients may vary in response to various types of clinical pain.
LeResche (1982) examined individuals undergoing severe acute rather than chronic pain and found
such facial actions as horizontal and vertical lip stretches and nasolabial fold deepening were
extremely common, although they occur only rarely in studies of chronic pain patients. It is
noteworthy that both vertical and horizontal lip stretches have been established as part of the
prototypical fear expression. This suggests that the acute pain stimuli in LeResche's photographs
might reasonably have elicited fear as well as pain. Likewise, experimental studies of pain
expressions may differ depending on the qualities of the pain stimulus used. Patrick et al. (1986)

7
found relatively few facial actions were exhibited in response to an acute electric shock, whereas
Craig and Patrick's (1985) cold pressor pain study found a wide assortment of AU's.
Methodological differences. Some of the differences in pain expressions may be due to
specific methodological differences among studies. A comparison of Galin and Thorn's (1993)
results with those of Craig and Patrick (1985) shows that both studies found a greater incidence of
lip part during the pain condition than during baseline, but Galin and Thorn (1993) did not find the
increased incidence of several other AU's found by Craig and Patrick (1985). These discrepant
results may have resulted simply from the time segment chosen for FACS coding. Whereas Craig
and Patrick (1985) measured facial activity during the first 10 seconds of cold pressor exposure (as
well as 40 - 50 seconds after onset, 10 seconds prior to the highest pain rating, and the final 10
seconds of cold pressor exposure), Galin and Thorn (1993) measured only during the final 20
seconds of cold-pressor pain. They assumed that there would be an increase in facial activity with
increasing cold pressor exposure, and that there was a need to eliminate any non-pain expressions
concomitant with pain expression such as a startle response or orienting behaviour. Craig and
Patrick's (1985) findings indicate that facial activity seems most salient at the onset of exposure, a
finding which fits with current pain theories.
Pain theories focus on the interplay between sensory, cognitive and emotional dimensions of
the painful experience. Rather than considering the complex reactions immediately following pain
onset as a confound of the precise measurement of pain, this time period should be considered a
fuller, richer display of the many factors which comprise the experience of pain: methodology which
ignores this interval is missing important information about pain. By examining this initial period,
Craig and Patrick (1985) found AU's most often seen in a surprise or startle expression occurring
most frequently immediately following onset of the pain stimulus. It is clear that the available
research on facial expressions of pain should be evaluated with respect to how particular coding
methodologies were used. Unfortunately, FACS coding is such a well-documented and commonly
used method of facial coding that past studies have often simply stated that FACS coding has been
used, without specifically describing the way that FACS coding has been implemented.

8
Finally, since by definition pain is a complex experience comprised of sensory, cognitive and
emotional components, the role and relative contributions of these factors may change radically
over the course of the pain stimulation. For example, following the initial pain stimulus, factors
such as the individual's past experience with the pain, coping responses and habituation to the pain
stimulus may lead to marked changes in both the experience and the expression of pain over time.
Research on the timing and pattern of responses to pain in relation to facial expression is clearly
needed.
Situational variables. Some of the variation between findings on pain expression may be due
to situational factors. For example, research has shown that exposure to social models with higher
tolerance to pain will diminish subjects' nonverbal displays of pain (Prkachin et al., 1983; Prkachin
& Craig, 1985). The presence of facial actions which are not pain-related may also be a result of
the social situation in which the pain stimulus occurred; it has been suggested that pulling of the lip
corners plus cheek raising may be an indication of embarrassed smiling (Ekman & Friesen, 1982;
LeResche, Ehrlick & Dworkin, 1990). At least three studies reported these individual actions
during facial responses to pain, most likely as a result of being watched or videotaped. (Craig et al.,
1991; Craig & Patrick, 1985; Swalm & Craig, 1991). In addition, LeResche, Ehrlich & Dworkin
(1990) have shown an increase in masking smiles versus genuine smiles during experimental pain
but not during clinical pain.
Validity and utility of the pain expression
Despite the inconsistencies and complications found in the research reviewed above, the
concept of a "prototypical" facial expression of pain seems to be both valid and clinically useful,
although what one is likely to observe is a variation in a basic core set of actions along with a
limited range of other actions, an expression that perhaps is better characterized as "fuzzy" than
invariant. Research using both experimental and clinical pain have isolated a parsimonious set of
core facial actions which follow a pairiful stimulus. Evidence suggests that this "core" facial
expression is consistently found in adults experiencing both acute pain and exacerbations of chronic
pain. Prkachin (1992b) has also demonstrated this basic facial expression across four different types
of experimentally induced pain: electric shock, cold, pressure and ischemia. These results suggest

9
that the "core" pain-related facial actions are common to many different pain states. This led
Prkachin (1992b) to suggest that for time-limited experimental and clinical pain stimuli, the
assessment of pain via facial expression could be limited to brow lowering, lid tightening / cheek
raising, nose wrinkling / lip raising and eye closing, as they provide the bulk of pain-related
information. However, there may be other facial actions which are unique to certain pain
modalities, arguing for some degree of stimulus specificity. For example, increased bunking rates
have been found following pain onset in some studies; the pain stimulus in each case had an abrupt
onset, adding a startle component to the pain experience. In addition, clinical pain that is chronic or
of higher intensity than that possible during experimental studies may be associated with other facial
actions.
In terms of its clinical utility, the magnitude of facial activity has been found to increase with
the intensity of noxious stimulation (Prkachin et al., 1983) and to correlate with self reports of pain
severity (Patrick et al., 1986; Prkachin & Mercer, 1989) and unpleasantness (LeResche & Dworkin,
1988; Prkachin & Mercer, 1989). This information on pain magnitude seems to be discriminable by
naive observers. Prkachin (1992a) found that the ability to discriminate a painless and a painful
stimuli through facial expression improved reliably and directly with the intensity of the pain stimuli,
suggesting that facial expressions of pain can communicate quantitatively graded pain information.
Despite these findings, the relationship between intensity of noxious events and facial.expression is
not a direct one. For example, in Prkachin's (1992a) study, females responding to a lower pain
intensity than males exhibited more intense facial expressions of pain. Prkachin and Mercer (1989)
have proposed that brow lowering and narrowing of the eyes, signals the probability that the
stimulus intensity has passed some personal threshold of pain. An increase in intensity of these
actions and/or the addition of the other specific facial actions commonly associated with pain would
be recruited as the discomfort approaches and surpasses tolerance levels, providing a mechanism by
which intensity could be coded in the face. Finally, research has shown a relationship between the
intensity and/or duration of some facial actions (brow lowering, cheek raising, lip corner pull and
mouth opening) and self-reports of pain associated disability (Prkachin & Mercer, 1989).

10
Using facial expression as a clinical assessment measure may also provide information that is
not available through other channels. Based on the findings that facial expressions of pain are only
moderately correlated with verbal pain measures, pain threshold and pain tolerance levels, several
researchers have concluded that pain expression carries unique information about the pain
experience (LeResche & Dworkin, 1988; Patrick et al., 1986; Prkachin, 1992b; Prkachin & Mercer,
1989).
The facial expressions described above also seem to be relatively specific to pain; research
has not found a relationship between self-report measures of anxiety and depression and the facial
expression of pain (LeResche & Dworkin, 1988), despite consistent findings of a correlation
between anxiety, depression and verbal pain reports (Craig, 1994). In addition, it has been found
that the pain face can be differentiated from several other negative subjective states, such as disgust,
fear, anger and sadness (LeResche, 1982). The facial expression seems to tap fairly specific aspects
of the pain experience, without confounding with other types of psychological distress. However, it
also shares some common elements with other prototypic facial expressions (Ekman & Ffiesen,
1978a), such as brow lowering during fear, sadness and anger, or mouth opening during fear,
disgust and anger, or eyelid tightening during anger. Eye closing or cheek raising do not occur in
any of these prototypes, with the exception of one variant of sadness.
There are two features which discriminate between the constellation of facial actions during
the facial expression of pain and that of other negative emotions. First, there are several AU's
which occur during these other emotions which are not found during pain. For example, fear is
characterized by inner brow raise, outer brow raise, and upper eyelid raise in addition to the brow
lowering and mouth opening; these actions do not occur during pain. Facial actions unique to other
emotions include: 1) inner brow raise, nasolabial deepening and lip corner depression (sadness), 2)
nose wrinkle, lip corner depression, lower lip depressions, and chin raise (disgust), 3) upper lid
raise, upper lip raise, lip funnel, lip tightening, lip press and chin raise (anger) (Ekman & Frieseh,
1978a). Second, although the pain expression shares some common elements with the facial
expressions of other negative states, the pain face represents a unique pattern of facial actions which
is as distinct as any of those previously described for fear, anger, disgust and sadness.

11
Discriminating Genuine versus Deceptive Pain Expressions
It is important to note that the term "genuine" is not meant to represent a "pure" response to
a painful stimulus; situational determinants are assumed to influence any pain response. This is a
particularly important distinction in light of Fridlund's (1991) view that facial expression reflects
contextual demands rather than a direct representation of conscious experience. Genuine pain
expressions are defined here as those which are spontaneous or without apparent intention to
manipulate the observer; any individual differences are a result of biological variation, situational
factors and socialization (familial and cultural). In contrast, during deceptive pain, there is a
deliberate choice to mislead another person. With respect to pain patients, deceptive pain can take
two forms, exaggeration / faking or masking / suppression. In some cases, clinicians and others
become concerned that patients are exaggerating or faking their pain for financial, social or other
benefits. Perhaps less often, but also of considerable importance, are concerns that patients are
trying to conceal their pain. Masking pain may be motivated by issues such as fear of injections,
addiction or side effects due to pain medications (Lander, 1990), fear of unemployment (Kotarba,
1983), or social/interpersonal factors (Craig, Prkachin & Grunau, 1992).
Three studies to date have examined the voluntary control of facial activity during
experimental pain (Galin & Thorn, 1993) and clinical pain (Craig et al., 1991; Hadjistavropoulos &
Craig, 1994). In two of the studies, subjects were videotaped during a neutral "at rest" condition,
and while exhibiting genuine pain in response to a painful stimulus. In addition, they were asked to
mask their pain while undergoing a painful stimulus, and to fake pain without a pain stimulus.
Hadjistavropoulos and Craig (1994) varied the methodology slightly by asking the subjects to
exaggerate their pain rather than faking a nonexistent pain experience. Trained coders then
completed FACS analyses of the baseline, genuine, suppressed and faked (or exaggerated)
expressions of pain to determine if the baseline and the three types of pain expression could be
distinguished based on the frequency of individual facial action units.
Genuine Pain
In both of the studies involving clinical pain, patients suffering from chronic low back pain
performed a specific physiotherapy exercise (straight leg raising) designed to provoke pain by

12
exacerbating their condition (Craig et al., 1991; Hadjistavropoulos & Craig, 1994). The genuine
facial expressions of pain exhibited in these two studies were consistent with past research and
involved an increased frequency of the following actions: brow lowering, cheek raising, tightening
of the eyelids, raising of the upper lip, parting of the lips and eyes closing. In addition,
Hadjistavropoulos and Craig (1994) extended their FACS analyses to include intensity, and found
that compared to baseline measures, genuine facial expressions also showed a greater intensity of
orbit tightening (cheek raising and eye lid tightening), levator contraction (upper lip raise and nose
wrinkle), and mouth opening. The results of Galin and Thorn's (1993) study were distinctly
different from the two studies outlined above and past research on genuine pain; subjects' genuine
pain expressions differed from the baseline facial expression only in the frequency of Hp corner pull,
likely reflecting the substantial differences in their research methodology.
Faked Pain
When asked to fake their pain, subjects in all three studies exhibited the same facial actions
as in the genuine pain condition. However, the faked pain expression can be described as a
stronger, more "prototypical" or caricatured expression of pain, as all three studies found that brow
lowering and cheek raising occurred more often during the faked than during the genuine pain
display. In addition, the following facial actions were found to occur more frequently during the
faked condition in some studies: closing of the eyes (Craig et al., 1991; Hadjistavropoulos & Craig,
1994), lip corner pull (Craig et al., 1991; Hadjistavropoulos & Craig, 1994), lip stretch
(Hadjistavropoulos & Craig, 1994), and lip tightening (Galin & Thorn, 1993). Evidence was also
found to suggest that faked facial expressions showed a reduced frequency of blinking (Craig et al.,
1991). Hadjistavropoulos and Craig's (1994) analysis of facial action intensity also found that faked
expressions of pain were characterized by an increased intensity of inner and outer brow raising,
brow lowering, eyes narrowing, lip stretch, eyes closing, upper lip raising and nose wrinkling.
Masked Pain
When asked to suppress their pain, people were remarkably successful. FACS analyses
indicated that the only facial activity which distinguished masked pain from the baseline facial
expression was a reduced rate of blinking (Craig et al., 1991). A closer look at the data suggests
13
that some residual activity remained on the face while the patients were trying to mask pain; masked
facial expressions did not differ from either baseline on FACS analysis or the genuine pain
expression (which did differ significantly from baseline) on the frequency of the following actions:
brow lowering, lids tightening (Craig et al, 1991; Hadjistavropoulos & Craig, 1994), mouth
opening, upper lip raise, nose wrinkling (Hadjistavropoulos & Craig, 1994), and lip corner pull
(Galin & Thorn, 1993). Additional support for the presence of residual facial activity during
masked pain is provided by Poole and Craig's (1992) finding that untrained subjects had little
difficulty identifying pain in the faces of patients masking the display, albeit at levels 50% lower
than the amount of pain attributed to the genuine pain expression.
In essence, the research suggests that certain patterns of facial activity are associated with
attempts to exert voluntary control over the facial activity associated with pain. However, the study
by Galin and Thorn (1993) produced results which were extremely different from those of Craig et
al. (1991) and Hadjistavropoulos and Craig (1994), particularly with respect to their lack of
consensus with the large body of work on genuine pain expressions. There are, however, several
methodological issues which might account for Galin and Thorn's discrepant results, including
differences in pain stimuli, the timing of facial expression measurement, and procedural differences
in FACS coding. While these were noted above, a more detailed analysis follows in order to
highlight improvements in methodology for the present study.
Galin and Thorn (1993) used experimental pain as their pain stimulus rather than the
exacerbation of clinical pain used in the other two studies. This simple difference may account for
many of the differences they found since research has already shown that clinical pain is associated
with a greater variety of facial movements than experimental pain (Prkachin & Mercer, 1989).
However, experimental and clinical pain have been shown to share the key features of brow
lowering and eye closing, and even these features were not replicated in the Galin and Thorn (1993)
study. It seems then, that the nature of the pain stimulus alone is not enough to explain their
findings.
The timing of videotaped segments used for FACS analysis in the various studies may also
have led to some of the discrepancies. Craig et al. (1991) and Hadjistavropoulos and Craig (1994)

14
used a 4 to 6 second interval immediately before and after the instant of maximum facial activity
during the genuine and the faked condition, and the final 4 to 6 seconds of the masked condition. In
contrast, Galin arid Thorn (1993) FACS analysed the final 20 seconds of the genuine, faked and
masked cold-pressor procedures; the time periods immediately following the pain stimuli were not
coded. Their choice of segments was based on the assumption that there would be an increase in
facial activity with increasing cold-pressor exposure and that one's immediate reaction to the onset
of a painful stimulus might reflect startle responses or orienting behaviours. However, the work of
Craig and Patrick (1985) has shown that the facial actions decrease in frequency after the first 10
seconds of exposure to experimental pain. Therefore, Galin and Thorn may have missed
considerable information about the genuine pain state and reaction. It also seems likely that there
may be many cues to genuine versus deceptive pain expressions which might appear within the first
few seconds of exposure to the pain stimulus. For example, the immediate impact of a painful event
may be difficult to control, and subjects asked to mask their pain response may allow elements of a
pain expression to "leak" through initially, until they gain control of their expression. Likewise,
genuine, masked and faked pain expressions may differ in the speed of onset.
Finally, slight differences in FACS coding procedures may have resulted in some of the
studies' discrepancies. For example, Craig et al. (1991) found a decreased frequency of blinking in
the deceptive pain conditions, while Galin and Thorn (1993) combined eyes closed and blink into
one facial action variable, and therefore could not investigate the incidence of blinking in isolation.
Individual Difference Variables. Research has shown that there are large individual
differences in the facial actions observed in response to genuine pain. For example, only 45% of
the subjects in one study exhibited one or both of the most common facial actions, brow lowering
and closing of the eyes. Some of these variations have been related to personal dispositions, with
some people being generally impassive, and others very reactive (Craig, 1992). Experimental
studies have shown that subjects with a low pain tolerance exhibited more expressive genuine pain
displays, suggesting that personal pain thresholds also influence nonverbal pain reactions (Galin &
Thorn, 1993). Prkachin and Mercer (1989) found that patients whose pain problem had a greater
psychological and physical impact showed greater facial activity in response to pain. Finally, pain

15
interventions and coping strategies have substantial effects on self-reports of pain, and may have a
similar impact on facial expression, although this is an untested proposition.
Similar variables are thought to influence the ability to display deceptive pain expressions.
One such personality variable, role playing ability, influenced the appearance of genuine and
deceptive pain displays, such that the intensity of faked pain expressions increased with role-
playing ability but was unrelated to the discriminability of the spontaneous and faked pain
expressions (Prkachin, 1992a). Similarly, subjects scoring higher on Pilowsky's general
hypochondriasis factor of the Illness Behaviour Questionnaire displayed genuine and faked pain
expressions which were less intense and harder to discriminate (Prkachin, 1992a). The single
study which related pain symptomatology to deception ability discovered that subjects who rated
the pain experienced as low intensity were better at masking their pain (Galin & Thorn, 1993). It
seems reasonable to suggest that many of the variables found to influence genuine pain
expressions would also influence the ability to present deceptive pain expressions.
Summary
Research on the voluntary control of pain expressions has confirmed that subjects are able to
pose deceptive pain faces and that several FACS-coded differences in facial actions distinguish
between the genuine, faked, masked and no pain displays. The genuine facial expressions of pain
exhibited in the two studies of clinical pain were found to be consistent with past research, involving
an increased frequency and/or intensity of brow lowering, cheek raising, tightening of the eyelids,
raising of the upper lip, wrinkling of the nose, parting of the lips, and closing of the eyes. The faked
pain expression might be described as a stronger, more "prototypical" or "caricatured" expression of
the genuine pain response, as all of the components of the genuine pain expression have been
observed to occur more frequently and/or more intensely during the faked condition. In addition,
several studies have noted the presence of several non-pain related actions which distinguish faked
from genuine pain displays (Craig et al., 1991; Prkachin, 1992a; Hadjistavropoulos & Craig, 1994).
Unlike the faked pain expression, the masked pain expression did not have any uniquely
distinguishing features and is perhaps best described as a mid-point between the neutral baseline
and the genuine pain expression. This may represent residual facial activity which "leaks out" when
16
attempting to neutralize a genuine facial display, a phenomenon described by Ekman and Friesen as
a "microexpression" (Ekman & Friesen, 1969). It is noteworthy that Craig et al. (1991) found both
types of deceptive pain displays to show decreased rates of blinking, a facial action which the
authors postulated to be an indicator of deceptive displays due to the increase in cognitive activity
resulting from instructions to fake or mask pain.
These differences are extremely subtle, and would likely be quite difficult for observers to
distinguish. There are, however, many other qualities of facial expressions which might conceivably
discriminate posed from non-posed reactions. For example, the temporal qualities of a facial display
may differ; a genuine facial display may have a shorter latency to onset, a quicker time from onset to
peak intensity, and a shorter duration than a deceptive display. A review of the deception literature
points to temporal qualities and other facial cues to deception which may be relevant to pain
displays.
Deception Theory and Research
According to Ekman (1985), there are few human relationships that do not involve deceit,
or at least the possibility of it. Many of these lies are harmless; for example, a "little white lie"
meant to protect someone's feelings. Most of us are aware of the commonplace nature of small
lies and many people would not want to expose or uncover the truth behind such messages. In
contrast, there are many situations in which lying can be legally, financially, and personally
harmful. In these situations, uncovering the truth behind the lies becomes extremely important.
The term "lie detection" probably brings to mind criminal activity, political intrigue and the FBI
rather than health care. In fact, Ekman's research on deception was originally developed for
health care uses; specifically, identifying patients who denied suicidal intentions. The cost of
deception in health care settings is high, with "concealers" not receiving the treatment they need
and "fakers" getting treatment and tying up unnecessary medical time, money and resources.
Types of Deception
Deception takes many forms arid occurs in many different situations. In general, deception
implies that an actor tries to induce a false belief in, or judgement by, a perceiver. As such,
deception includes such diverse concepts as practical jokes, criminal fraud, forgery, scams, and

17
white lies. While all of these behaviours share a common goal of deceiving an individual, they
may differ from one another in the complexity, degree and duration of the deception, as well as the
scope and severity of the intended consequences. As yet, research in the area of deception has not
determined how the various types of deception differ in verbal and nonverbal expression.
However, Ekman (1985) has outlined the nonverbal clues that may be present during the two main
types of lying: concealment and falsification. In addition, we have general information on the
nonverbal behaviour of people who have been asked to lie about their feelings and emotions, or
about their reactions to certain situations. Research on emotion has also provided evidence for the
difference between genuine and faked facial expressions of emotion (Caccioppo & Petty, 1981;
Ekman, Hager & Friesen, 1981; Ekman & Friesen, 1982).
Theoretical Basis for Differences Between Genuine and Deceptive Facial Expressions
Results from various research areas suggest that genuine and faked facial expressions of
emotion may be discriminable (Caccioppo & Petty, 1981; Ekman et al., 1981; Ekman & Friesen,
1982). Neurological research has suggested that there may be separate neural systems responsible
for voluntary and involuntary facial movements (Rinn, 1984). The pyramidal system, which
descends from cortical areas, seems to play a role in voluntary movements, as lesions in that area
lead to deficits in the ability to produce certain facial actions on demand, while the individual
retains the ability to exhibit the same expression spontaneously. Involuntary facial movements
tend to depend more on the subcortical, extrapyramidal system. Lesions in this area may result in
deficits in spontaneous facial expressions of emotion, while leaving unaffected the ability to
deliberately produce these movements (Rinn, 1984). These observations may have implications
for the detection of deception in facial expression. While it is unclear whether these two systems
operate in isolation with, for example, the cortical system only functioning during voluntary facial
expression, there is the possibility that cortical mechanisms play a more dominant role in
deliberate facial expressions than does the subcortical system. If one assumes that there is separate
neural control for genuine and deliberate facial expressions, it is possible that there are identifiable
differences in the topography of genuine and deliberate facial expressions.

18
Cues to Deception
Concealing a Genuine Expression. Deceptive facial expressions may be produced by
masking a felt emotion with a deliberately posed neutral facial expression. In order to detect the
true pain state, one would have to detect a hypothetical underlying genuine facial expression.
There are several methods by which a genuine facial expression could be "covered up". First, a
genuine facial expression may be disguised by tightening antagonistic muscles in the face to
"hold in" the real expression. Alternatively, one could attempt to inhibit any muscle action
completely, in order to maintain a neutral facial expression. It has been suggested that either
approach may provide clues for deception as the attempt to control muscles may make the face
appear stiff, unnatural or controlled. In addition, muscle control is difficult to achieve without
some form of leakage of the concealed information (Ekman & Friesen, 1969). This mainly
occurs because the face has such a short latency before transmission, with a microexpression of
the genuine feeling likely to emerge before there is time to neutralize or mask it properly. These
microexpressions, which are so brief as to be barely perceptible, may then be followed by
simulated neutral or antithetical expressions (Ekman, 1985).
Falsifying an Expression. A genuine facial expression may also be replaced by another
contradictory expression, such as a smile falsified to hide sadness. If one is trying to disguise a
negative emotion, it may be very difficult to neutralize the face completely. By posing a positive
expression, such as a smile, the deceiver is not only concealing the true emotion but is conveying
false information that their emotional state is positive. When this occurs, the posed smile may
differ from a genuine smile in some small way, such as the absence of the raised cheeks that give
the little crows feet at the edges of the eyes (Ekman & Friesen, 1982; Ekman, Friesen &
O'Sullivan, 1988). However, such subtle cues would be very difficult for the untrained observer
to pick up. Another cue to deception in this case could be a display consisting of an unnatural
number or type of facial actions. Hager and Ekman (1985) found that a deliberately produced
startle expression contained more facial actions not prototypical of a startle response than during
a genuine startle response. Some of these "extra" facial actions may simply arise because we are
not consciously aware of what a genuine facial expression looks like on our own face. As well,

19
people's feelings about engaging in deception may provide additional cues. For example, some
people feel shame or a fear of being caught when lying that may be observed on the face.
Temporal Qualities of Facial Expressions. Ekman and Friesen (1982) suggested that the
apex, or the duration of peak intensity, of faked expressions will be longer than during a genuine
expression. Indirect evidence for differences in duration between faked and genuine expressions
was provided by these authors. The majority (86%) of smiles categorized as "felt" or genuine
smiles were found to last between 2/3 of a second and 4 seconds in length, while only 36% of
faked smiles fell within this duration range. In addition, they may differ in the peak intensity
reached, the timing of apex onset, or in the timing of the initial facial action onset or offset. For
example, faked expressions may appear too soon or they may have a delayed onset. Ekman and
Friesen (1982) suggest that faked expressions will have a shorter onset time so that the expression
will appear more abruptly than genuine expressions, and that the offset will either be abrupt or
irregular. Empirical support for such claims has yet to be gathered.
Many of these assumptions about the timing of deceptive versus genuine facial expressions
have been developed through general observation or through anecdotal evidence. Rarely have the
temporal qualities of facial expressions in general been investigated; this limitation is particularly
true for research on pain expressions. This dissertation will compare genuine pain expressions
and two types of deceptive pain expressions (faked pain and masked pain) with respect to their
temporal qualities: overall duration, onset duration, offset duration, and apex duration.
Temporal Contiguity of Pain Expressions. By definition, a genuine facial expression
consists of a group of individual facial actions which appear together on the face, in a pattern that
is associated with some underlying emotional state. As such, temporal contiguity of the
component individual facial actions is an important feature of genuine facial expressions (Ekman,
1978a). Evidence for the importance of temporal contiguity on judgements of others' facial
expressions has been provided indirectly in pain research. Lee and Craig (1991) had actors
portray several pain expressions, manipulating both the number of pain-related AU's and the
temporal overlap or non-overlap of the apex intensities of these AU's, Pain ratings by naive
observers were found to increase with the number of AU's, but only if temporal overlap of the
20 AU's occurred. Obviously, temporal contiguity serves a very clear communicative function.
Theory also suggests that deceptive facial expressions may not have the same degree of
temporal contiguity: although they may contain the same component facial actions, the
actions may appear serially rather than all at once.
Studies have not yet investigated the degree of temporal contiguity present in genuine
pain expressions; however, the relationship among individual facial actions has been
investigated. Patrick et al. (1986) and Craig and Patrick (1985) found that pain-related AU's
have small, but significant, intercorrelations, ranging from .11 to .33 and .14 to .65
respectively, which suggests that there is substantial independence among them. It is
important to note that relatively small intercorrelations among component facial actions
found in adult pain expressions to date does not argue against temporal contiguity of genuine
pain expressions. Based on the previous review of pain studies, it seems reasonable to
assume that these small intercorrelations, as well as some of the differences in facial actions
found across pain studies, may have been due to the time segment that was coded. The
various facial actions involved in pain reactions may have different temporal qualities. To
date, most research has computed correlations among the component facial actions during the
entire time segment selected for study in a particular project, a span of time ranging between
4 and 20 seconds. However, since AU's can occur very briefly, in the millisecond range,
research which specifically investigates individual facial actions for contiguous temporal
occurrence is required. The present study used cluster analysis procedures to compare
genuine pain, faked pain and masked pain expressions with respect to the intercorrelations
among pain-related AU's which occured within specified time intervals.
Patterns of Facial Expression. The final temporal quality of facial expressions
investigated in the present study involves a description of the number and type of facial
expression "patterns" exhibited. That is, depending on the nature of the pain stimulus, the
individual's reaction may include expressions of pain, fear, startle, anger or sadness . Rather
than limiting facial analyses to individual facial action units, or analysis of the temporal
contiguity of a single facial expression, one may look for the presence of multiple emotional
expressions within the observation period. LeResche and Dworkin's (1988) research found
that pain patients often exhibited one expression of negative affect in addition to their pain
21
expression. This second emotional expression was most often contempt, although sadness,
disgust, anger and fear were also noted. Likewise, deceptive facial expressions may be composed
of an unlikely mix of emotions, as the faked pain face may cover an underlying positive emotion,
embarrassment, discomfort or fear of being discovered. Although both pain and deceptive pain
are thought to be comprised of a mix of emotions, there may be a difference in the number or type
of facial action "patterns" observed.
Rather than looking at the presence of individual facial actions which are not associated
with pain, it might be useful to look at the temporal contiguity of any "extra" facial actions which
appear with faked pain in order to determine i f they form any meaningful emotional expression
constellations. With the addition of the temporal analyses mentioned above, FACS analysis of
individual facial actions can be grouped into clusters of facial actions occurring together in time.
These clusters can be compared to A U combinations which have been identified for the basic
emotions outlined by Ekman and Friesen (1978a). The present research will be the first to
attempt a comparison of genuine and deceptive pain responses using cluster analyses and
classification of patterns of facial expression.
Blinking. Blinking rates are also thought to change when deception occurs. While some
researchers speculate that blinking will increase because of general emotional arousal (Ekman,
1985) or due to a startle response (Prkachin, 1992), others believe that conscious efforts to control
emotions will lead to an unconscious decrease in blinking. Research has shown that people blink
less often when they are engaged in vigorous cognitive activities (Holland & Tarlow, 1972;
1975). However, looking at the incidence of blinking in deceptive pain states is complicated by
the confusion regarding blinking within the genuine pain literature. Studies focusing on changes
in blinking rates during pain have produced evidence to suggest that blinking rates increase
following pain (Craig & Patrick, 1985; Patrick et al., 1986) and decrease following pain (Craig et
al., 1991; Prkachin, 1992b; Prkachin & Mercer, 1989). Prkachin (1992b) noted that increases in
blinking rates during pain tend to occur only when the pain stimulus has an abrupt onset,
therefore producing a startle response. Thus, it seems that decreased blinking may be a
particularly salient cue to deception when the faked pain has a sudden onset, such as with active

22
manipulation of an injured limb. Research by Craig et al. (1991) provided evidence that faked and
masked pain were characterized by decreased blinking rates, when compared to both a neutral
face and to a genuine pain condition with an insidious onset. Decreased blinking, then, might be a
cue to pain deception regardless of the pain stimuli involved. The present research will attempt to
replicate these results.
Asymmetry. Past research has suggested that the incidence of asymmetrical facial activity
might differentiate genuine and deceptive facial displays (Ekman, 1981; Hager & Ekman,1985).
Some studies have suggested that right hemispheric specialization should occur since the right
hemisphere, has an important function in emotional processes, and facial expressions are an
integral part of emotion (Ley & Bryden, 1981). Others assume that asymmetry results from right
hemisphere specialization for cognitive, nonverbal processes, such as the recognition of faces
(Benton, 1980; Heller & Levy, 1981). Both views would suggest that asymmetry should consist
of stronger facial action on the left side of the face during spontaneous or genuine emotional
states.
Other theorists have suggested that the lateralization of facial asymmetry will depend on
the emotion being expressed; right hemispheric specialization would occur only for negative
emotions, while left hemispheric specialization would occur for positive emotions (Schwartz,
Ahern & Brown, 1979; Reuter-Lorenz & Davidson, 1981; Sackeim & Gur, 1978). Based on this
theory, positive emotions would show more activity on the right side of the face, and negative
emotions would be stronger on the left side of the face.
Ekman (1980) suggested that asymmetry would be more prevalent in deliberate, requested
facial actions (e.g. nonemotional) than during facial movements related to emotion. Ekman et al.
(1981) found that children asked to imitate facial actions showed stronger facial movement on the
left side of the face. Compared to faked smiles, genuine smiles were found to be more
symmetrical than those performed on request, and "genuine" asymmetries were not lateralized.
However, spontaneous negative emotions weren't elicited, and as asymmetries occur more
frequently during spontaneous negative emotions than during positive emotions, a comparison of
spontaneous and deliberate negative emotions is needed (Ekman et al., 1981).

23
A second study by Hager and Ekman (1985) compared facial asymmetry during deliberate
facial movements, spontaneous movements and startle expressions. Genuine facial expressions of
enjoyment and startle were elicited from subjects, after which they were required to simulate
emotional expressions, the startle response and individual facial actions. Results showed that
there were no asymmetry differences between the genuine and simulated startle responses.
However, spontaneous smiles were significantly more symmetrical than were the simulated ones.
Further, the finding that simulated enjoyment expressions were intermediate in asymmetry
between spontaneous happy expressions and deliberate smile action units suggests that the degree
of asymmetry is a function of the degree to which movements are emotional versus deliberate
(Hager & Ekman, 1985). There was no evidence for hemispheric specialization for emotion. In
fact, two of the deliberate facial actions, AU9 (nose wrinkle) and AU15( lip corner depress), most
often associated with negative emotions such as disgust and sadness, were stronger on the right
side of the face, while AU12 (smile), a positive facial action, was lateralized more strongly on the
left side of the face. These results suggest that facial asymmetry occurs during the directed
control of actions, rather than as a function of emotion per se (Hager & Ekman, 1985).
Ekman and Friesen (1979) suggest that lateralization of facial control may depend on the
type of control, inhibition or faking, which was occurring. Ekman et al. (1981) extended this
hypothesis by suggesting that the right hemisphere might be specialized for inhibiting or
modulating emotional expression, which fits with the findings that smiling, which is often feigned
or repressed, shows left laterality. Further research is still needed to determine if the actions
showing left laterality are controlled more often, or in a different manner than right lateralized
actions (Hager & Ekman, 1985). A further argument for the need to consider facial actions
individually is that the various facial actions may have different neural innervations (such as the
brow versus the lower face) (Rinn, 1984) and/or the underlying muscles may serve different
functions, such as talking versus emotional expressions, all of which may lead to asymmetry which
differs in intensity or lateralization (Hager & Ekman, 1985).
The asymmetry research has several implications for the present study. First, it seems that
asymmetry may occur more frequently during deliberate facial displays. If so, we should see an

24
increased frequency of asymmetry in both the faked expressions of pain and masked pain
expressions in comparison to a genuine pain response. Past research has not included a masked
condition, however, and therefore the assumption that asymmetries will occur during this
particular type of facial control is speculative. Asymmetries during a masked condition may
appear in different facial actions than during a faked condition, may differ in temporal qualities
arid may appear on the same or on the opposite side of the face. It is clear that the cues to
deception may be very different depending on the type of facial control being attempted.
In summary, based on a review of the deception literature, several cues to deception may
be useful in improving our description of deceptive facial expressions of pain. First, faking pain
may be exhibited in the face as a mix of emotional expressions. For instance, faked pain hiay be
exhibited as a pain face overlying the true emotional state, while masked pain may be either
covered by a positive emotional expression, or by a stiff, unnatural neutral face, with "leakage" of
the pain expression. Second, faking may occur with the presence of certain emotional expressions
or signals which are incongruous or seem out of context, such as shame, guilt, or smiles. Such
cues may be difficult to pick up, as pain itself is a complex experience which may include or be
influenced by many emotions (Craig, 1994). There is a possibility, however, that certain
emotional expressions may appear more often in deceptive versus genuine pain displays. Third,
there may be certain cues seen in the face which are associated with deception, such as blushing,
sweating, blinking, or asymmetrical actions. Fourth, faked pain expressions may consist of an
exaggerated display, with all of the facial action components of genuine pain being displayed with
greater intensity. Fifth, certain regions of the face may be crucial in the identification of deceptive
pain displays. Research has shown that there may be less differentiated control of the musculature
in the upper face than of the lower face, which may explain the finding of "leaked action" around
the eyes in masked pain displays. Finally, research has suggested that faked facial expressions
may differ with respect to temporal qualities. They may have a delayed onset, a longer duration,
or the individual facial actions may appear serially, rather than in a "constellation" typical of
genuine facial expressions.

25
Describing and Quantifying Facial Expressions
In order to compare genuine and deceptive pain expressions based on the predictions
above, there needs to be a detailed analysis of the numerous facial cues which occur during each
condition. The Facial Action Coding System (FACS) developed by Ekman and Friesen (1978a,
1978b) provides a comprehensive, objective analysis of all of the facial actions which are
distinguished reliably by observers. Although the FACS system itself is well established and
requires highly trained coders to adhere to strict rules regarding the type and degree of facial
action required to reach minimal requirements for coding, the system may be implemented in
several ways. Coders may simply note the presence of any facial action unit which meets the
minimum coding requirements during the coding interval, providing a measure of the frequency of
each individual AU. While this is the most economical approach in terms of time and effort, it
does not provide important information on either the intensity or the duration of the AU's. In
addition, it has been hypothesized that the temporal qualities of facial actions may differentiate
between genuine and deceptive expressions, and this information is not derived using the
foregoing simple FACS approach. In order to tap this information, the basic FACS coding
approach was modified.
Increasing the comprehensiveness of FACS coding
To isolate information on the timing, intensity and duration of facial actions, coding can
take one of two forms. The coding interval may be divided into several smaller segments, with
coders rating the presence or absence of each A U and their intensity during each segment.
Although this approach allows for the collection of detailed information on the changes in
intensity of facial actions over time, it provides only a crude estimate of the timing of facial
activity. A further disadvantage of this approach is that it is extremely labour-intensive to code
the intensity of each facial action repeatedly during a single coding interval.
Another option is to directly code the times of onset and offset of each occurrence of an
individual facial action unit, as well as coding the intensity and duration of the apex. In addition
to providing information on the presence or absence of specific AU's, these coding components

26
provide several parameters of facial activity descriptive of the "pattern" of facial activation: 1)
response latency (the time from event onset to the time of facial action onset), 2) speed of onset
(the time from facial action onset to the start of the apex), 3) maximum intensity (intensity at the
apex), 4) duration of the apex, 5) response duration (the time from facial action onset to the time
of facial action offset) and 6) the speed of offset (the time from the end of the apex to facial action
offset).
There are several advantages to this approach. It provides a wealth of information on the
timing of facial actions and will allow for detailed analyses of temporal patterns during genuine
and deceptive facial expressions. Further, it provides a means of investigating the patterns of
overlap and timing among individual AU's. Albeit time consuming and rarely used by others for
this reason, it is the most comprehensive approach. The one pain study which investigated some
of these parameters suggests that apex intensity, onset times and offset times can be identified
very reliably by trained FACS coders (LeResche & Dworkin, 1988) The present study is the first
to analyse genuine and deceptive pain expressions using the comprehensive FACS coding system.
Detecting Pain Through Facial Expression
Health care practitioners are often concerned with ascertaining the degree of pain
experienced by their patients, as are family and friends of those suffering from acute or chronic pain.
Due to the complex, subjective nature of pain, this can be a very difficult judgement to make. While
people may take into account the many sources of information available to them when making
decisions about others' experiences of pain, it has been shown that both naive judges and clinicians
assign greater weight to nonverbals than to verbal self-report when judging pain (Poole & Craig,
1992). This is most likely due to the commonly held assumption that nonverbal behaviour is less
amenable to deception (Ekman & Friesen, 1969, 1974). Craig and Prkachin (1984) argue that
nonverbal expression may be less subject to response bias because people appear to monitor it less
rigorously than the contents of their verbal report. Based on these arguments, it is clear that it is
important to know how accurately people can judge the pain experience of another through facial
expression. It is also of interest to determine what types of information observers use when making
27
such judgements, and how successfully they can distinguish genuine from deceptive expressions of
pain.
Judging genuine pain using facial expression
Most people believe that they can distinguish a facial expression of pain and recent research
generally supports this belief. It has been shown that people can discriminate facial expressions of
pain from various emotional states, and are able to identify the individual's degree of suffering based
on facial information (Boucher, 1969; Prkachin & Craig, 1985; von Baeyer, Johnson & McMillan,
1984). Research shows that observers attribute higher pain levels to facial expressions in response
to high intensity shocks than to those expressions following low and medium shock intensities
(Patrick et al., 1986; Prkachin & Craig, 1985; Prkachin et al., 1983). This suggests that expressions
do transmit information on pain intensity which is detectable by naive observers.
Patrick etal. (1986) also provided evidence that observers used specific facial cues to judge
pain levels. In their study, pain-related facial actions accounted for 74% of the variance in observer
judgements of pain, an impressively strong relationship when one considers the degree of individual
differences found in expressive pain behaviour. Brow lowering and eye blinking accounted for the
the largest proportion of variance, followed by upper lip raise and cheek raise.
A further finding of the Patrick et al. (1986) study suggests that observers using facial
expression as the basis of pain judgements are tapping different aspects of the pain reaction than is
provided by self-report alone. Subjects who underwent the pain stimuli were in the presence of
either a pain-tolerant model or a pain-intolerant model throughout the procedure. Results showed
that subjects who were exposed to a pain-tolerant model accepted more intense shocks than other
subjects, without increasing their levels of self-reported discomfort. That is, compared to control
subjects and those receiving shocks in the presence of an intolerant pain model, these subjects' self-
reports were inconsistent with the actual shock intensities they received. Despite these subjects'
lower self-reports of pain, observers rated the pain experience of these subjects higher than the
other subject groups, a result which was more consistent with the actual intensity level of the
noxious stimuli administered, than with the subjects' self-reports of pain. This suggests that the
social modeling manipulation exerted an effect oh the self-report measure of pain but did not affect

28
the nonverbal pain display, hence reflecting different aspects of the pain experience. In contrast,
results of a second study found that exposure to a tolerant model led to differences in the magnitude
of facial activity (Prkachin et al., 1983). These results suggest that while self-report is probably
more plastic and responsive to context, situational variables may also have an impact upon
nonverbal expression.
Detecting genuine versus deceptive pain
Two studies that examined the differences between genuine and deceptive pain displays
(Craig et al., 1991; Hadjistavropoulos & Craig, 1994) used the videotaped data in subsequent
studies to investigate observer pain judgements based on these facial expressions
(Hadjistavropoulos et al., 1996; Poole & Craig, 1992). Poole & Craig (1992) had untrained judges
rate the severity of pain being experienced by the patients in the Craig et al. (1991) videoclips. In
this study, the judges were fooled by the patients' attempts to fake their pain experience and
consistently attributed more pain to the faked pain faces than to the genuine and masked pain faces.
Similarly, judges consistently rated masked pain faces to be lower in pain intensity than genuine pain
faces. However, the judges were not completely fooled by the suppressed pain face, as they rated
the suppressed pain face to fall approximately halfway between the genuine and baseline facial
expressions on the pain severity scale. Hence, the judges were able to discern some pain, an
impressive feat considering that the only facial action which statistically discriminated the
suppressed pain condition from the baseline expression was a decreased incidence of blinking.
These results suggest that the judges could identify the residual pain activity which remained on the
face during the masked pain condition.
From the Poole and Craig (1992) study, we can conclude that when untrained observers are
asked to rate the amount of pain experienced by the patient, based on his/her facial expression, their
responses seem to correspond to the magnitude of pain-related facial activity that has been isolated
through FACS coding, regardless of whether that activity level was genuine or deceptive. Both the
empirical analysis and the judgement task determined that facial activity was greatest in the faked
pain condition, followed by the genuine pain condition, the masked pain condition and the neutral
baseline.
29
An additional focus of the Poole and Craig (1992) study was to determine the effect of
priming on the observers' judgements of pain. One half of the observers were told that they were
seeing baseline, genuine, faked and masked pain expressions, the remaining observers were told
simply that they were seeing pain and no pain conditions. Results showed that making the
observers aware of the possibility of deception did not increase their ability to estimate the actual
pain experienced. Instead, priming was found to reduce the observers' willingness to attribute pain
to the patients' facial expressions. So, although observers who were primed attributed less pain to
the faked faces, they also showed a reduced tendency to attribute pain during other conditions.
This finding fits with past research showing that increasing the base rate expectation of deception
has little effect on the success with which deception is detected (Faust, Hart, Guilmette & Arkes,
1988):
Hadjistavropoulos et al. (1996) asked naive observers to rate the pain experience of the
patients in the Hadjistavropoulos and Craig (1994) videoclips. In addition to being asked to rate
the severity and unpleasantness of the pain experienced in each videoclip, subjects were asked to
determine if the videoclip represented a neutral, genuine pain, masked pain or exaggerated pain
expression using a forced choice format. Unlike the Poole and Craig (1992) study, these subjects
rated the intensity and unpleasantness of the genuine, masked and exaggerated pain to be equal,
and significantly greater than the neutral expression. Similar to Poole and Craig's (1992) priming
effect, the knowledge that patients were performing the same movement in all three conditions
and were exhibiting deceptive displays tempered the trend to assign pain intensity ratings which
correspond to the magnitude of pain-related facial activity.
When asked to categorize the various pain expressions, subjects were 53% accurate in
their discrimination of the spontaneous and deliberate facial displays, which is significantly greater
than the 25% accuracy expected by chance. Unfortunately, the use of a forced choice format in
itself would lead to inflated judgement accuracy, and thus does not provide clearcut evidence
about naive judges' ability to categorize spontaneous and deliberate facial expressions. Unlike
past research, Hadjistavropoulos et al. (1996) found very little variation in judges' ability to

30
identify the various expressions, which suggests that the use of a forced choice design may also
obscure individual differences in detection ability.
In general, research has shown that observers perform poorly when asked to discriminate
among genuine and deceptive pain displays. Since deception can have serious consequences in
certain situations, it is important and useful to determine if observers' detection accuracy could be
improved. In order to answer this question, research is needed to determine: (1) the
characteristics that differentiate which deceptive facial expressions are easier or harder to detect,
(2) the facial cues and detection strategies used by successful "lie detectors" versus unsuccessful
ones and (3) whether various training strategies could improve detection abilities. As research of
this type has not been done using pain patients and judgements of pain expressions, a review of
"lie detection" studies in the deception literature provides a starting point for an investigation of
variables related to detection abilities.
Detecting Deception in Others
Research in the area of deception has shown that, in general, people are quite poor at "lie
detection", defined here as judgements based on another's behaviour, as opposed to being based
on psychophysiological data. A review of the available research has determined that the average
accuracy of subjects in these studies has rarely exceeded 60%, which is barely above chance levels
when the base rate is 50% (Ekman & O'Sullivan, 1991). However, Ekman and O'Sullivan (1991)
determined that these accuracy levels might have been improved, as subjects in lie detection
studies were often college students who might not have had any reason to learn how to detect
deception. Ekman and O'Sullivan (1991) assumed that people in occupations which require the
detection of deception would show greater accuracy than the standard college student population.
Surprisingly, three earlier studies, which set out to investigate this assumption, did not show any
improvements in accuracy when using police officers, customs officials and federal law
enforcement officers (Kraut & Poe, 1980; DePaulo & Pfeifer, 1986; Kohnken, 1987). However,
one important design flaw present in all three studies was posited to account for the lack of
accuracy by "professional lie catchers". There was no evidence in two of the studies that the
videotaped behaviour differed between the tmthful and deceptive messages. In the third study,

31
the materials did differ between truthful and deceptive communications, but the authors did not
relate the detectability of the patients' deceptive messages to the degree of observably "different"
behaviour (DePaulo & Pfeifer,1986). It was concluded that the general lack of accuracy and the
lack of advantage for professionals found in past studies was due to a lack of information in the
videotaped deceptive behaviours (Ekman & O'Sullivan, 1991).
Ekman and O'Sullivan (1991) improved upon studies in the area of lie detection by using
videotaped samples of behaviour which were shown to differentiate between truthful and lying
messages. Measures of facial activity using FACS showed that people displayed more masking
smiles when they lied and more enjoyment smiles when they told the truth. These two types of
smiles are discriminate because facial activity in deceptive smiles is restricted to the mouth
region, while felt smiles also involve activity in the eye region. There was also a vocal cue to
deception; when subjects lied, there was an increase in fundamental pitch. The combined use of
facial and vocal cues correctly classified 86% of the subjects in terms of the tmthfulness of their
messages (Ekman, O'Sullivan, Friesen & Scherer, 1991). Ekman and O'Sullivan (1991) selected
subjects from several professional groups expected to have some experience in lie detection: the
U.S. Secret Service, Central Intelligence Agency, Federal Bureau of Investigation, National
Security Agency, Drug Enforcement Agency, police, judges, and psychiatrists. In addition,
college students and other adults assumed to be inexperienced in lie detection were tested.
Results of the study showed that most of the subject groups had average accuracy scores
ranging from 53-58% . In contrast, the Secret Service agents, the only group to score
significantly above chance (50%) levels, had an average accuracy score of 64%. Splitting the
individuals within each group into low (0 to 30%), medium (40 to 60%) and high scorers (70 to
100%) further highlights the differences between the groups. None of the Secret Service agents
scored below chance levels, while all of the remaining groups had members who performed worse
than chance. In addition, 53% of the Secret Service agents scored above 70% accuracy and 29%
were above 80% accuracy. The next best group, the psychiatrists, had Only 12% of their subjects
reach 80% accuracy.

32
Ekman and O'Sullivan have provided evidence to suggest that some people are better at
detecting deception than others, a result which suggests that there is some skill or "trick" to lie
detection that many observers do not possess. However, the state of current research in the lie
detection area leaves several questions unanswered, many of which may also apply to the question
of how one might best detect deceptive pain expressions. To begin, although Ekman and
O'Sullivan's (1991) study suggests that there are substantial individual differences in lie detection
ability, there has been relatively little work done to determine what makes these people perform
above average levels. An additional question of interest is whether individuals can be trained to
become better lie detectors. The following sections address both of these questions in turn,
looking at evidence first within the lie detection literature, and then within pain research.
Individual differences in detection accuracy
Individual differences in lie detection accuracy has been yet another relatively unexplored
area in the deception literature. Past studies have focused on group averages when investigating
lie detection accuracy, and have concluded that people can detect deception at only slightly better
than chance levels. While people as a whole might be poor at detecting deception, there are
individuals who are relatively good at it. Ekman and O'Sullivan (1991) found a large range in
detection abilities, with accuracy levels ranging from highly successful (greater than 80%
accuracy) to performance below chance levels. Although pain research has not investigated the
possibility of individual differences in detection abilities, it seems reasonable to assume that some
people may be be better than others in their ability to detect deceptive pain expressions. Variables
which might influence the ability to detect genuine pain include: the cues used by the detector,
past experience with pain patients, and interpersonal sensitivity skills in general.
Possible Individual Difference Variables
Cue Utilization. Ekman and O'Sullivan (1991) made the first attempt to isolate the
differences in decision-making which differentiate good and bad lie detectors. All subjects in their
study were asked to describe the behavioural cues they used to detect deception both before
participating in the study and again on two occasions during the judgement process. No
relationship was found between accuracy and cues reported prior to beginning the study.

33
However, the accurate and inaccurate groups were found to use different cues when actually
describing how they made their judgements about two individual cases. Those who were good at
detecting deception listed more varied behaviours and emphasized nonverbal behaviours more
than verbal behaviours. In addition, the ability to recognize microexpressions was correlated with
detection accuracy. These results, based on one type of deception (the concealment of strong
negative emotions), suggest that successful "lie catchers" use different information than do
unsuccessful lie detectors, despite their lack of awareness of these cues at pretest.
As stated previously, pain research has not looked specifically at individual differences in
detection accuracy. We do not know if individuals who are relatively good at detecting deceptive
differ in their method of "lie detection" from those who perform worse than chance. Preliminary
research has asked judges to rank the relative importance of various facial and body elements to
their pain ratings and have found that movements of the eyes, eyebrows, eyelids and the mouth
were the most important sources of information (Prkachin et al., 1983). Further information is
needed on the specific cues judges use when judging the veracity of others' pain.
Situational cues are also important determinants of pain judgements. Research has shown
that observers attribute greater pain to facial expressions when told that the patient is
hypersensitive to pain than when under the impression that the patient had received an analgesic
(Prkachin & Craig, 1985). This study show that situational information which is independent of
the pain expression and the actual pain experience of the patient, can bias pain judgements. Based
on this research, we may assume that there are various situational constraints which might
influence observers' judgements of pain, such as information that compensation is pending, that
the self-report of pain is incongruent with the degree of observable tissue damage, etc.
Decision-Making Confidence. There is little evidence for a relationship between subjects'
confidence about their detection ability and actual detection accuracy. Some studies found that
subjects' confidence in their abilities was not correlated to their subsequent performance (DePaulo
& Pfeifer, 1986; Kohnken, 1987). However, this research has simply correlated overall accuracy
with the subjects' retrospective rating of their general performance. As subjects presumably
predict some "deceivers" better than others, relating overall accuracy and confidence measures

34
makes little sense; research needs to look at the relationship between subject's accuracy on
individual cases with their rated confidence in each decision.
Sex Differences. Differences in ability to detect deception related to sex have not been
consistently found. However, these results should be interpreted with caution, as the majority of
studies have looked solely at overall accuracy of detection. In order to investigate sex
differences thoroughly, one should not only look for sex differences in accuracy, but should also
use an individual differences approach to compare the number of highly accurate individuals
belonging to each sex, as well as overall group effects. Also, sex differences may show up in the
process of detection rather than in the overall accuracy.
Hurd and Noller (1988) have done the most thorough investigation of sex differences in
deception decoding. They investigated not only sex differences in accuracy but also looked at
process variables, such as awareness of the possibility of deception, confidence, cue utilization
and response time. In this study, females were found to use more cues, to have a longer latency
to response time, and to be judged as less confident by raters who coded their decision making
process. The finding that females were more likely to mention the use of cues contradicts Buck's
(1984) research which concludes that females use a perception-based decoding strategy versus
males who use an analytic cognitively based decoding strategy. It would seem from Hurd and
Noller (1988) that men use an intuitive coding strategy more often, resulting in quicker, more
confident decisions based less on cues. In contrast, females used a slower, more cue-based
process, which may suggest an analytic approach. The alternative explanation for these sex
differences is, of course, that males simply are not reporting their use of cues. Accuracy scores
were completely unrelated to any of the process variables measured in this study. However,
accuracy scores in general were very low and this lack of variability alone could explain the low
correlations.
Although past research on the ability to detect deceptive facial expressions of pain has not
found sex differences, the present study provided a more thorough investigation of sex
differences. Males and females were compared for overall accuracy, number and type of cues
used, effectiveness of feedback and/or training, and decision-making confidence.

35
Empathy. While research in the area of deception has not investigated the relationship
between empathy and the ability to detect deception, there are several reasons to suggest that
individuals high in empathy may be better "lie detectors". Currently held definitions of empathy
stress not only an emotional identification with others but also an increased social acuity
(Chlopan, McCain, Carbonell & Hagen, 1985). That is, empathy seems to be composed of both
emotional arousability and a more accurate person perception. Intuitively, it seems likely that
person perception would be related to accuracy in judging others, while the emotional arousability
component might be more highly related to the probability of actual helping behaviour.
Past attempts to relate empathy to actual skills, such as judgements of others or helping
behaviour, have been complicated by the lack of consensus across studies on the precise definition
of empathy. Researchers' conceptualizations vary widely, with disagreements on whether
empathy is an active or passive ability and a cognitive or emotional ability (Chlopan et al., 1985).
Empathy has been regarded as both an involuntary vicarious experience of emotion (Clark, 1980;
Mehrabian & Epstein, 1972) and as an active construction of another's mental state (Hogan,
1969). In general, the majority of research has been based on two different definitions of empathy
and their corresponding measurements, The Questionnaire Measure of Emotional Empathy
(Mehrabian & Epstein, 1972) and Hogan's Empathy Scale (EM) respectively (Hogan, 1969).
It is likely that empathy is a much more complicated process than even a combination of
the cognitive or affective approaches. One aspect of empathy, perspective-taking, can be divided
into three distinct categories: perceptual (to predict the visual perspective of another), social-
cognitive (the identification of another's thoughts, intentions, motivations or behaviour), and
affective (the inference of another's feelings, reactions or concerns). Although these components
of empathy are conceptually different, they are probably interrelated and very likely tap
overlapping processes (Moore, 1990). In order to clarify the relationship between empathy and
behaviour, the complex processes involved in an empathic response must be made more explicit.
Davis (1980) has developed a multidimensional measure of empathy, The Interpersonal
Reactivity Index (IRI), which focuses on four separate subscales: Perspective-Taking, Fantasy,
Empathic Concern and Personal Distress. Two of the IRI scales are relevant to the judgement

36
task in the proposed study. Perspective-Taking (PT), the tendency to adopt the psychological
point of view of others, has been found to correlate highly with the "cognitive" Hogan measure
(Davis, 1983) and with accuracy in person perception (Bernstein & Davis, 1982). The Empathic
Concern (EC) scale, a measure of other oriented feelings of sympathy and concern, has been
found to correlate highly with the "emotional" Mehrabian and Epstein measure and with
emotional reactions and helping behaviours towards someone in distress (Davis, 1983). Scores
on the Empathic Concern Scale were not found to correlate with accuracy of person perception
(Bernstein & Davis, 1982). For the current study, it is predicted that the PT scale will be
correlated with individuals' ability to detect deception, while the E C scale will not show such a
relationship.
Summary
The "lie detection" literature suggests that individuals are not highly skilled at
discriminating between genuine and deceptive messages, although there are indications that some
people may be more successful "lie detectors" than others. Several variables have been postulated
to be associated with these variations in detection ability, including cue utilization, decision
making confidence, sex differences and empathy. This study examines the relationship between
these variables and the ability to detect deceptive pain expressions.
Training to Improve Lie Detection
Several studies on lie detection have shown that naive observers are very poor at detecting
deception; however, it is possible that observers can be trained to improve their detection abilities.
There have been many debates about the feasibility of such training (Kohnken, 1987; Zuckerman,
Koestner & Colella, 1985). Evidence against the utility of training to improve "lie detection"
includes the surprising finding that law enforcement groups and psychologists are no better at
detecting deception than college students (Ekman & O'Sullivan, 1991). In addition, the few
studies that have tried to improve detection through the use of training programs have failed
(Kohnken, 1987; Zuckerman, Koestner & Alton, 1984).
Despite the lack of empirical support, there are several reasons to assume that training is
still a viable approach to improve lie detection accuracy. Lie detection studies published to date

37
show that "training" thus far has meant the provision of corrective feedback to observers. The
assumption behind the use of corrective feedback is that subjects who are made aware of their
errors will look for alternative strategies to improve their performance. In general, corrective
feedback has not been found to improve lie detection, resulting in the conclusion that subjects
simply do not see, or do not use, the facial cues which distinguish deceptive and truthful
communications.
In addition, although naive observers have performed no better than chance at lie
detection, Ekman and O'Sullivan (1991) have provided evidence to suggest that some individuals
perform considerably better than chance, suggesting that the task is possible if a certain approach
is used. Further support is provided by the findings of one study which showed that experienced
Facial Affect Scoring Technique (FAST) trained coders were able to correctly classify the honest
and deceptive behaviour of almost all of the subjects (Ekman & Friesen, 1974). This suggests
that observers may be trained to pick up the cues which distinguish truthful from deceptive facial
behaviour. Although it is not practical to train observers to FACS standards due to the hours of
training required, it would be interesting to determine if short-term training programs based on
FACS coding analyses of deception would improve detection accuracy.
Prospects for Deception Training Specific to Pain
A preliminary investigation of the relative merits of corrective feedback versus
information-based training to improve discrimination between genuine and deceptive pain displays
has recently been provided (Galin & Thorn, 1993). The authors investigated the effects of two
deception training approaches on judges' accuracies in identifying genuine cold-pressor induced
pain, masked pain, posed pain or no pain. Subjects in the feedback group were given corrective
feedback on the first half of their judgements. The training group subjects were given a short
description of the FACS facial action units which had been found to discriminate between the pain
conditions in the stimulus clips. They were then shown photographs portraying these
characteristics and were taught how to reproduce these movements on their own faces. Finally,
subjects in this group were given feedback on the first 10% of the judgements they made.

38
During the pretrial task, the subjects in the four groups did not differ in their detection
accuracy and were significantly poorer at identifying genuine pain than the masked, posed and no
pain conditions. This pattern of detection accuracy held for control subjects on trial two, as did
their overall accuracy levels. However, the feedback group were more accurate in identifying the
posed pain condition than the other three pain conditions. In contrast, the training group showed
a different pattern, with the no pain and posed pain conditions identified more often than the
masked and genuine pain conditions. The identification of genuine pain was below chance levels
for all but the feedback group, with the overall accuracy levels for the remaining pain conditions
ranging from 31.5% accuracy for the training group's identification of the masked condition to
55.4% accuracy for the feedback group's identification of the posed condition.
Analyzing overall levels of accuracy for each of the pain conditions yielded surprising
results. In general, subjects in the feedback group were the most accurate in detecting the
genuine and posed pain conditions, while the control group was most accurate at detecting the
masked pain condition. The no-pain condition was detected most often by the control and
training groups. It is noteworthy that the training group was superior to the control condition
only on the posed pain segments.
Several design flaws might have influenced the results of Galin and Thorn's (1993) study.
To begin with, the length of the pretraining task was very long (120 judgements), likely leading to
fatigue effects. More importantly, the type of feedback used did not allow for the most effective
test of its effectiveness as a training strategy. The feedback used in the study was delayed,
providing subjects with the correct categorization for the facial expressions only after all 120 had
been completed. Feedback might be more effective if it were given immediately after each
decision-making process, at which time subjects would be more aware of the strategy they used to
classify each facial expression, and immediate feedback would help to identify the most and least
effective strategies. The feedback only and training plus feedback conditions did not utilize the
same feedback procedures, therefore not providing a true comparison of the possibility of additive
effects. The feedback only group received feedback on all 120 segments, while those in the
training plus feedback condition only received feedback on the first 20 segments. In addition to

39
being provided with feedback on fewer judgements, as the segments were in random order, we do
not know if subjects in this group were given equal amounts of feedback for all four types of
facial expression.
Additional methodological concerns are specific to the training condition used by Galin
and Thorn (1993). First, training alone was not used as a condition, making it difficult to
determine if any of the improvements shown by the training group were in fact due to training, or
due to the limited feedback training they received. Second, the information contained in the
FAGS based training program was sketchy at best, as it was based solely on the FACS analysis of
the stimulus tapes. Unfortunately, contrary to past research^ FACS analysis in this study isolated
few differences among genuine and deceptive pain expressions. The largest number of facial cues
differed between genuine and posed pain; therefore the training package would have contained the
most information about this particular pain condition. In fact, the training group were successful
at discriminating only these two conditions. Since the pattern of AU's identified using FACS
coding did not clearly distinguish among the remaining three pain conditions, subjects would not
have been presented with enough information to allow further discrimination. Despite the
authors' conclusions to the contrary, these results clearly provide support for training.
Finally, the individual differences that exist in pain expressions are an important factor to
take into consideration when designing a training program for the detection of deception in such
patients. Galin and Thorn's (1993) training package was based on the AU's which were found to
discriminate between the various pain conditions. They found very few differences in facial
activity between the groups; their training program did not seem to mention individual differences.
No mention was made of the fact that all people do not show the "prototypical" pain face, nor
that deceptive pain expressions do not look the same for all people. Training judges to look
specifically for the prototypes of pain may be detrimental to performance.
Of course, it is difficult to devise a deception training program when we have no clear idea
about what makes an effective perceiver. We know that FACS coding appears to provide some
cues judges could use to facilitate the discrimination between genuine and deceptive expressions,
but FACS training is hardly a practical and cost-effective detection strategy. However, we do

40
have some general knowledge regarding the elements of facial activity which occur frequently
during deception. In addition, training subjects to detect faked pain should include information on
the typical pain face, as well as the facial elements which may change during masked or faked
conditions.
Summary
This review suggests that attempting to train individuals in the detection of deceptive pain
might be a worthwhile endeavor. Based on the reliance of corrective feedback as a "training
program" in the past, it would be reasonable to compare the efficacy of feedback with that of an
information-based training program. Galin and Thorn (1993) attempted to do this, and found that
both training and corrective feedback led to very limited improvements in detecting deceptive
pain. Unfortunately, they did not provide a clear test of the accuracy of training versus feedback
due to the content of their training session, the manner in which feedback was provided, and
methodological difficulties. Improvements that could be made upon their work include: (1)
providing more information in the training session, including information on the genuine, masked
and no pain conditions based on all past research findings, an emphasis on individual differences in
pain displays, a focus on the facial expressions thought to be related to deception in general, and
consideration of temporal cues; (2) providing feedback following each judgement, in order to
highlight the errors being made and to allow the opportunity to improve their decision-making
process; and (3) accurately assessing the possibility of additive effects when training and feedback
are combined by having a third training group which receives the full training package as well as
the complete feedback procedure.

41
Study One: A comprehensive description of genuine and deceptive facial expressions of pain
The general purpose of the first study is to extend the description of genuine and
deceptive facial expressions of pain by investigating the possibility that the deceptive pain states
differ in the frequency with which deception cues occur. The study will use a clinical population
of low back pain patients who are undergoing physiotherapy for their injuries. Patients suffering
from low back pain were chosen as the focus of this study due to the high prevalence rates and
social impact of the condition. Back pain is one of the most frequently reported types of pain in
the general population, with lifetime estimates in the North American population of 80%, and a
yearly incidence of 4% (Crook, Rideout & Brown, 1984; Mayer et al., 1986). Low back pain
may also be the most expensive condition in North America, with extremely high costs associated
with medical and surgical care, injury litigation, worker's compensation, long term disability
insurance, social security payments and lost work time (Mayer et al., 1986). In addition,
diagnoses of low back pain are notoriously difficult, involving a large subjective component, poor
correlation between degeneration and symptomatology, and a lack of objective physical findings
(Mayer et al., 1986). Based on these facts, it is understandable that both physicians and insurance
companies might be more aware of the possibility of deception in this population, as well as being
highly invested in conducting an accurate assessment of clients' pain experiences.
The pain stimulus will involve an exacerbation of chronic low back pain, using a standard
range of motion exercise performed during physiotherapy assessments. While capable of
instigating sharp, intense pain, range of motion exercises have negligible risk of harming the
patients. These patients will be videotaped while being asked to perform these exercises
repeatedly under instructions to genuinely express their pain, mask their pain, exaggerate their
pain and fake their pain following established protocols (e.g. Hadjistavropoulos & Craig, 1994).
The facial expressions observed within these conditions will be compared on the following
measures: 1) the number, type, and intensity of individual facial actions; 2) the temporal qualities
of the individual facial actions, such as the time of onset, duration, duration of peak intensity, and
speed of onset and offset; 3) the contiguity in time, or the cohesiveness of the facial actions
making up the facial expression; 4) the number and type of facial expessions or constellations

42
exhibited; and 5) the incidence of actions thought to be indicative of deception, such as blinking,
smiling and asymmetry of facial actions.
The specific hypotheses of the study are:
1. The faked expression will appear as a stronger version of the genuine pain face. It will
consist of a significantly larger number of pain-related facial actions than will the genuine pain
expression, and these facial actions will be displayed more intensely in the faked pain expression.
2. The faked expression will have a significantly higher incidence of facial actions not
typically associated with genuine pain.
3. The masked pain expression will be indistinguishable from the baseline neutral
expression except for low intensity activity in the region of the eye orbit.
4. The masked and faked pain conditions will show decreased frequency of blinking, and
an increase in asymmetry.
5. Genuine pain expressions will have a shorter period of peak intensity, and will be of
shorter overall duration than the faked pain expression. However, the speed of onset (i.e., the
time to peak intensity) and the speed of offset (time from peak intensity offset to facial action
offset) may be longer in the genuine expression.
6. There will be greater cohesiveness, or temporal contiguity, of the pain-related facial
actions making up the genuine pain expression than those in the faked pain condition.
7. Faked pain expressions will be composed of either more "constellations" of facial
actions representing multiple emotional expressions or of a different mix of emotional expressions.

43
Study Two: Effectiveness of Training Strategies to Improve the Discrimination
of Genuine and Deceptive Pain Expressions
The purpose of this study is twofold: (1) to determine if there are individual differences in
the ability to detect deceptive pain displays and (2) to determine if people's ability to detect faked or
masked pain can be improved through the use of various training strategies. The following study
will be the first to investigate individual differences in the judgement of deception in pain patients,
by comparing successful and unsuccessful judges on such variables as the number and type of cues
used, their decision-making confidence, and empathy scores. As an attempt to assess the feasibility
of training to improve detection accuracies, the present study will fill a gap in the literature by
utilizing a training program based on the results of recent research in the areas of pain and
deception.
The specific hypotheses of the study are as follows:
1. There will be individual differences in the ability to discriminate genuine and deceptive
pain expressions. That is, the percent of patients' facial expressions which can be correctly
classified into neutral* genuine, faked and masked pain will differ across subjects, ranging from
accuracy levels well below chance to better than chance accuracy.
2. Detection ability will be related to the subjects' score on the Perspective-taking subscale
of the Interpersonal Reactivity Index, but will not be related to scores on the other three subscales.
3. Detection ability will be correlated with the subjects' degree of past experience with pain.
4. Detection ability will also be related to several aspects of the judges' decision-making
process. Specifically, successful "detectors" will report that they use more facial cues, and will
utilize different judgement cues.
5. Detection accuracy will be correlated with decision-making confidence for each rating.
6. Accuracy levels will differ between training groups. Subjects given training plus
corrective feedback will perform best, followed by the training group, the feedback only group and
controls. Similar changes in the number and type of cues used, and decision making confidence are
expected to occur. Due to the proposed individual differences in detection accuracy, there will be
considerable overlap in the range of accuracies across the training groups.

44
Study 1: Analysis of Genuine, Faked, and Masked Pain Expressions
Method
Subjects
The 40 subjects who provided the facial expression data in this study were patients
undergoing treatment for low back pain at either the Point Grey Physiotherapy Clinic in Vancouver,
B.C. or the Lansdowne Physiotherapy Clinic in Richmond, B.C. To be included in the study, the
patients were required to: (a) be experiencing low back pain at the time of the assessment, and (b)
to have sufficient command of the English language to complete the questionnaire packages and to
follow study instructions. Subjects were not excluded because of pending litigation, compensation
claims or medication use. All patients were paid $10 for their participation.
Videotape Equipment
Subjects were videotaped on Sony Ffi-8 metal-P NTSC 120 tapes using a Sony Hi-8 CCD-
TR81 NTSC video camera. The video data was then be transfered to 1/2 inch video cassettes (Fuji
HQ T-120) and dubbed with a digital time display (minutes, seconds, 60ths of a second) using an
R C A video time/date generator, model TC-1440-B. The time display allowed coders to identify the
time segments to be coded without listening to the audio portion of the tape, which identified the
instruction set. The video data was edited into the final form required for coding, using two
Panasonic PC14A51R 14"" Colour T V Monitors, two Panasonic A G 1970 S-VHS Editing VCR's
and a Future Video EC-1000 Pro M K 11 editing board. A Videomics TM-1 Title Maker was used
to label each segment with an A, B, C or D in order of presentation.
The viewing system used for coding the facial expression data was a 20" Sharp MTS Stereo
Monitor hooked up to a Panasonic AG-6300 video cassette recorder. A remote control equipped
with a shuttle allowed coders to view the segments in frame by frame slow motion and stop frame
playback when necessary.
Coding Videotape
In order to ensure that coders' ratings were not influenced by the patients' behaviour
between events, these sections of the tape were edited out, leaving 5 seconds of blank tape between

45
each coding segment. The 160 segments were coded in random order, with the coder blind to the
neutral, genuine or deceptive conditions.
Measures
Each patient completed a questionnaire package consisting of a personal data sheet and the
Descriptor Differential Scales (See Appendix C).
Personal Data Sheet. The personal data sheet asked simple questions about the patient's
sex, age, occupation, marital status and employment status. In addition, questions were asked
about the intensity, location, and duration of their pain condition, as well as about the frequency and
type of medication used for pain.
Descriptor Differential Scales (DPS). The patients were asked to rate the unpleasantness
and intensity of the pain sensations they experienced on an average day using the DDS (Gracely,
Dubner & McGrath, 1979). The scale provides 13 descriptive adjectives on two scales, ranging
from "not painful" to extremely painful", and "not unpleasant" to "extremely unpleasant",
respectively. These descriptors are reliable measures of the pain experience and have been ratio-
scaled using cross-modality matching procedures to provide numerical equivalents for the verbal
descriptors (Gracely, Dubner & McGrath, 1982).
Procedure
Potential subjects were informed of the study by the physiotherapist when they called to
make appointments for treatment sessions. If a patient indicated interest on the phone, they were
approached by the investigators upon their arrival for their scheduled session. The investigators
followed a standard protocol for both recruitment and study procedures. The investigators
approached patients by introducing themselves and stating their affiliation with the Psychology
Department at the University of British Columbia. They then proceeded to describe the purpose of
the study and the procedures which would be involved.
The patients were told that the study had two aims: 1) to see if factors such as nonverbal
pain expressions and physical attractiveness have an effect on other's judgements of the patient's
pain intensity and overall health and 2) to see how closely these judgements compare to the patient's
actual pain and health status. The patients were told that they would be asked to complete a

46
number of questionnaires on their pain experience and coping strategies. They were also informed
that they would be asked to perform certain movements during their normal physiotherapy session
which might cause discomfort and that these movements would be repeated following different
instructions and their facial expressions would be videotaped. Permission to obtain additional
information from their physiotherapy charts was also obtained.
If the patients were still willing to participate at this point, they were given a consent form to
read which reiterated the information given by the investigator (see Appendix D). Patients were
told that the information was for research purposes only, and that their participation would remain
confidential and anonymous. They were also be advised that only their videotaped session would be
viewed by university students and health professionals. Finally, all patients were informed that their
participation was voluntary and that they could withdraw from the study at any time. Patients were
then required to sign the consent form before proceeding with the study.
Patients were given the questionnaire package to complete while they were in the
physiotherapy examination room, awaiting the start of their physiotherapy session. During this
time, the investigator set up the video equipment and adjusted the height and focus of the
equipment based on the height of the patient. When the patient had completed the package, the
physiotherapist was called in and the second portion of the study began. At this point, the
physiotherapist was given his script and the presentation order for the range of motion procedures.
Videotaping protocol. Each patient was videotaped during a standard range of motion
assessment conducted by their physiotherapist. Patients were videotaped in one of the clinic's
examination rooms, while lying on their backs on the examining table, with head and shoulders
propped up slightly with a head rest. The video camera was mounted on a tripod positioned at the
foot of the examining table, and was focused on the head and shoulders of the patients.
To begin the session, patients were videotaped during a neutral "at rest" condition, in both a
sitting up and lying down position. Once baseline recording was completed, the range of motion
exercise was introduced. During this test, the physiotherapist asked patients to straighten their legs
and raise them 10 inches off the examination table, a movement which low back pain patients report
to be very painful. A series of instructions were provided in varying orders. Patients performed the

47
leg raise two times, with instructions to: 1) genuinely express any pain that they felt, and 2) pretend
that it didn't hurt. In a third set of instructions, the patients were asked to give a faked expression,
by pretending that they were in a lot of pain without actually moving their legs (see Appendix E).
The three pain conditions or sets of instructions were counterbalanced for each patient to reduce
order effects, as past research has shown that subjects who fake pain first exhibit more intense faked
and genuine facial expressions (Prkachin, 1992a). The patient's facial expressions were videotaped
for 10 seconds following the initiation of each movement / expression condition. Following
completion of the range of motion procedures, the patients completed another set of Descriptive
Differential Scales to rate the unpleasantness and intensity of the most severe pain they experienced
during the leg-lifting exercises (see Appendix F).
Quantification of Facial Activity. Each patient's five videotaped segments were coded by a
trained FACS coder to describe and quantify their facial activity. For each of the 44 FACS action
units (AU's), the following parameters were measured during the 10 second interval: the time of
A U onset, the time of A U offset, the maximum intensity or "apex" of the A U , and the duration of
the apex. The apex of an A U is defined as "the period during which the movement was held at the
highest intensity it reached". In accordance with past research, certain AU's which involve the same
muscle action were combined to produce new AU's which would allow for more meaningful
intensity and temporal coding: AU1 (inner brow raise) and AU2 (outer brow raise) produced the
variable "brow raise", A U 6 (cheek raise) and A U 7 (lid tighten) produced the variable "orbit
tightening", A U 9 (nose wrinkle) and 10 (upper lip raise) produced the variable "levator
contraction" and A U 25 (lips apart), 26 (jaw drop) and 27 (mouth stretch) produced the variable
"mouth opening" (Hadjistavropolous & Craig, 1994; Prkachin, 1992a).
Intensity for each A U was rated oh a standardized 5-point rating scale, ranging from "trace"
to "maximum". Three AU's which do not lend themselves to intensity coding (AU 11, nasolabial
deepening; A U 38, nostril dilation; AU45, blinking) were coded simply for time of onset and time of
offset, while the mouth opening variable was coded on a 3 point scale, with a score of 1 for A U 25,
a 2 for AU26 and a 3 for A U 27 (Ekman & Friesen, 1983; Prkachin, 1992a). Finally, coders noted
the occurence of any asymmetry in individual facial actions.

48
FACS coding was performed by two trained coders who had completed FACS training and
reached the certified proficiency level (Ekman & Friesen, 1978). A third trained FACS coder
completed reliability coding for 20% of the videotaped segments, including reliability estimates for
the frequency, intensity and temporal parameters for each AU. To avoid inflated reliability
estimates, agreements were not be counted for the nonoccurence of AU's, as nonoccurence of AU's
tends to be far more frequent. For a more conservative measure of reliability, percent agreement
was calculated as the proportion of agreements on the presence of AU's relative to the total number
of AU's scored using the following formula:
Percent Agreement = (# of AU's on which coder 1 and coder 2 agreed) X 2 # of AU's scored by coder 1 + # of AU's scored by coder 2
Agreements were scored only if both coders agreed that an A U occured within a 0.2 second
time frame. The proper method for scoring the reliability for A U onset and offset is less well
established. Based on past work, it was likely that acceptable reliability would be attained using
agreements within 0.10 seconds, however, due to the relative lack of information on temporal
coding, reliability was calculated a second time for both onset and offset, using the percent
agreement within 0.50 seconds. The reliability of intensity judgements was calculated using Pearson
correlation coefficients comparing the intensity scoring of both coders for each agreed upon AU.

49
Results
Description of Patient Population
Subjects were 23 males and 17 females, ranging from 19 to 75 years of age, with an
average age of 32.6 years (s.d = 10.89). 60.0% of the subjects were single, 20.0% were married,
2.86% widowed, 8.57% living common-law and 2.86% were separated. 31.43 % of subjects
experienced constant pain, while 65.71% experienced their pain intermittently. Subjects had
experienced pain for an average of 3.01 years, with 74.29% of subjects suffering from low back
pain, 40.0% from upper back pain, 31.4% from neck pain, 11.4% from shoulder pain, 11.4% from
leg pain, 5.7% from hip pain, and 2.9% each from chest pain, TMJ, pelvis pain, headaches, and
sciatica. When asked about pain onset, 42.9% did not respond or could not identify the
precipitant, 22.9% of subjects were injured on the job, 22.9% in a car accident, and 5.7% each in
a fall or while walking. 42.9% of patients used prescription or non-prescription drugs on a daily
basis to cope with their pain.
Reliability Coding
The reliability of FACS coding was analyzed for the frequency, intensity and temporal
parameters of each AU. The FACS coders showed 82.5% agreement for the occurrence of
individual AU's, which is slightly higher than reliability's reported by Ekman and Friesen (1978a).
The reliability of intensity ratings of agreed upon AU's, measured using a pearson correlation, was
.85. Both the frequency and intensity reliabilities were determined to be acceptable. Given the
infrequent use of temporal coding, and thus a lack of information regarding acceptable reliability,
the percent agreement between coders was calculated for varying degrees of temporal overlap. The
reliability of coding on the temporal parameters varied widely. The coding of A U onset was highly
reliable, with 95.2% agreement, calculated when AU's coincided within 0.1 second. The remaining
temporal parameters (onset duration, apex duration, response duration) which involve more subtle
distinctions of intensity and/or two temporal estimations, were not reliably coded within 0.1
seconds, with percent agreements of 62.7%, 52.0% and 54.7% respectively. Widening the degree
of temporal overlap to within 0.2 seconds resulted in acceptable reliability estimates of 70.7% for
both onset duration and overall response duration, however, apex duration was coded with only

50
66.7% agreement at this level of overlap. Using the upper limit of temporal overlap proposed for
the temporal coding (0.5 seconds), all temporal indices fell well within acceptable ranges for
reliability (onset duration (82.7%), apex duration (80.0%), response duration (84.0%)). Given that
duration estimates involve two temporal estimations, and that apex duration involves subtle
distinctions in intensity compared to coding the presence or absence of an A U , it was determined
that widening the range of temporal overlap was reasonable, and that acceptable levels of reliability
had been reached for all FACS variables.
Preliminary Analyses
One FACS variable, offset duration, was omitted from analysis. Offset duration was not
codeable in several instances, due to the continuation of AU's beyond the end of the recorded
segment. The amount of missing data for the remaining FACS variables was negligible.
Initial analyses of the FACS data established that 15 facial actions (AU's) were observed in
more than 5% of the coded segments. These were retained for the analyses of facial activity: inner
and outer brow raise (AU1 & 2), lowered brow (AU4), orbit tightening (AU6 & 7), levator
contraction (AU9 & 10), lip corner pull (AU12), dimpler (AU14), chin raise (AU17), tongue show
(AU19), lip press (AU24), lip part, jaw drop, mouth stretch (AU25/26/27), nostril dilate (AU38),
eye slit (AU42), squint (AU44), eyes closed (AU43) and blink (AU45).
Frequency
A mixed-model M A N O V A was carried out to determine if the frequency of individual facial
actions differed across pain conditions. It was predicted that: (1) the faked pain expressions would
have a greater incidence of both pain-related and noh-pain-related facial actions than the genuine
pain expression, (2) genuine pain expressions would have a greater frequency of pain-related facial
actions than either the neutral or masked pain expressions, (3) the masked pain expression would
have a greater frequency of movements in the eye area, but would be otherwise indistinguishable
from the neutral expression, and (4) that the masked and faked pain conditions would show
significantly less blinking than neutral and genuine pain conditions. The results of the analysis are
presented in Table 1, while mean frequency scores across pain conditions are presented in Table 2.

Table 1
Results of M A N O V A and Followup ANOVA's Examining Frequency of Facial Actions Across
Pain Conditions
Df F E<
Multivariate Main Effect 45,315 2.18 .001
Univariate F-tests
Brow Raise (AU 1/AU 2) 3,117 6.22 .001
Brow Lowering (AU4) 3, 117 16.85 .001
Orbit Tightening (AU6 / AU7) 3, 117 7.82 .001
Levator Contraction (AU9 / AU10) 3, 117 5.05 .003
Lip Corner Pull (AU12) 3, 117 1.89 .136
Dimpler (AU14) 3, 117 1.95 .125
Chin Raise (AU17) 3, 117 1.66 .180
Tongue Show (AU19) 3, 117 1.72 .168
Lip Press (AU24) 3, 117 1.05 .373
Opened Mouth (AU25/26/27) 3, 117 6.52 .001
Nostril Flare (AU38) 3, 117 0.75 .525
Eye Slit (AU42) 3, 117 2.16 .096
Eyes Closed (AU43) 3, 117 7.37 .001
Eye Squint (AU44) 3,117 3.33 .022
Blinking (AU45) 3, 117 3.20 .026
Note: Bonferroni adjustments suggest a significance level of .003

52
Table 2
Mean Facial Action Frequency Across Pain Conditions
(AU) Facial Action Neutral Genuine Masked Faked (AU) Facial Action
M SD M SD M SD M SD
Brow Raise 0.12 0 56 0.20 0.56 0.10 0 44 0 75a,b,c 1 32
Brow Lowering 0.00 0 00 0.50a 0.99 0.10 0 38 1 20a>b>c 1 38
Orbit Tightening 0.00 0 00 0.22 0.53 0.20 0 46 0 55a-c 0 75
Levator Contraction 0.00 0 00 0.25 0.63 0.08 0 35 0 35a>c 0 66
Lip Corner Pull 0.05 0 22 0.20 0.46 0.20 0 46 0 25 0 44
Dimpler 0.00 0 00 0.12 0.33 0.08 0 27 0 15 0 43
Chin Raise 0.02 0 16 0.22 0.58 0.20 0 56 0 12 0 40
Tongue Show 0.00 0 00 0.12 0.40 0.10 0 30 0 05 0 22
Lip Press 0.02 0 16 0.12 0.33 0.12 0 40 0 10 0 30
Open Mouth 0.18 0 45 0.70a 0.85 0.62a 0 87 0 90a,b,c 0 98
Nostril Dilate 0.00 0 00 0.08 0.27 0.10 0 50 0 10 0 38
Eye Slit 0.00 0 00 0.08 0.27 0.02 0 16 0 15 0 48
Closed Eyes 0.00 0 00 0.25 0.54 0.05 0 32 0 42a>c 0 75
Eye Squint 0.00 0 00 0.10 0.38 0.00 0 00 0 20 0 56
Blinking 2.50 2 70 3.95 3.44 2.60 2 35 3 28 3 43
a Mean is significantly greater than neutral mean (p<05)
b Mean is significantly greater than genuine mean (p<05)
c Mean is significantly greater than masked mean (p<05)

53
Multivariate analyses showed that the overall frequency of facial actions differed
significantly across pain conditions. Univariate F-tests examining the frequency of individual facial
actions across pain conditions provided partial support for the study hypotheses. The incidence of
one usually non pain-related facial action (brow raise) was found to vary across pain condition,
while the remaining non pain-related facial action (eye slit, eye squint, lip corner pull, dimpler, chin
raise, tongue show, lip press and nostril flare) occurred equally frequently in all conditions. Tukey's
post hoc analyses for A U s yielding significant univariate ANOVA's showed that brow raise
occurred more often in faked pain than in genuine pain expressions (p < .05), masked pain
expressions (p < .01) or neutral expressions (p < .01). Genuine pain expressions, in comparison,
showed as many brow raises as masked pain and neutral expressions. The incidence of blinking,
predicted to be an indicator of deception, did not vary across pain condition.
Five pain-related facial actions (actions observed in past pain research) also differed across
pain condition (brow lowering, opened mouth, orbit tightening, levator contraction, and closed
eyes). Tukey's post hoc analyses provided comparisons of individual facial actions between pain
expressions. Brow lowering occurred more often in faked pain expressions than in either the
genuine pain, masked pain or neutral expressions (p < .01). The genuine pain expression did not
differ from the masked pain expression in the frequency of brow lowering, but exhibited a greater
frequency of brow lowering than the neutral expression. Masked pain and neutral expressions did
not differ with respect to the frequency of brow lowering. An opened mouth was also seen more
frequently in faked pain expressions than in either the genuine pain, masked pain, or neutral
expressions (p < .01). Genuine and masked pain expressions did not differ in the frequency of
mouth opening, but both exhibited a greater frequency of mouth opening than the neutral
expression (p < .01). Orbit tightening, levator contraction and eye closure movements all occured
more frequently in the faked pain expressions than in either the masked pain (p < .05) or neutral
expressions (p < .01), but occured as frequently in the genuine pain expressions. There was
however, no significant difference between the genuine, masked and neutral expressions in any of
these three facial actions.

54
Results of the frequency analyses provided some support for the study's hypotheses.
Compared to the genuine pain expression, the faked pain expressions showed a greater incidence of
one non pain-related facial actions (brow raise), as well as a greater frequency of two pain-related
facial actions (brow lowering, open mouth). Contrary to expectation, there was no difference in the
incidence of pain-related facial actions between the genuine and masked pain expressions, although
the frequency of brow lowering did not differentiate masked and neutral expressions, whereas
genuine expressions were assicated with a greater incidence than neutral expressions. Genuine pain
expressions differed from the neutral expression only in the frequency of two pain-related facial
actions: showing more brow lowering and mouth opening. As expected, the masked pain
expression and the neutral expression were almost indistinguishable, differing only in the frequency
of mouth opening.
Although patients' pain expressions were comprised of facial actions that have been
associated with the experience of pain, there was substantial variation in the facial expressions
exhibited. For example, only 30% of patients exhibited brow lowering in response to genuine pain,
while 45% of patients responded with mouth opening. In comparison, there appeared to be less
variation in the display of faked pain expressions, with 62.5% of patients exhibiting brow lowering,
and 55% of patients showing mouth opening.
Intensity
A mixed-model M A N O V A was carried out to determine if the intensity of individual facial
actions differed across pain conditions. Significant multivariate main effects indicated that the
overall intensity of facial actions differed significantly across pain condition (See Table 3).
Univariate F-tests examining individual facial actions showed that the intensity of one non pain-
related facial action (brow raise) differed across condition. Tukey's post hoc analyses indicated that
the intensity brow raise movements was greater in the faked pain condition than either the genuine,
masked or neutral expressions (p < .01). The intensity of brow raise movements observed in the
genuine pain, masked pain and neutral expressions did not differ. The intensity of the remaining non
pain-related facial actions (eye slit, eye squint, lip corner pull, dimpler, chin raise, tongue show, and
lip press) did not vary across pain condition. Mean intensity scores are presented in Table 4.

55
Table 3
Results of M A N O V A and Followup ANO V A's Examining Intensity of Facial Actions Across Pain
Conditions
Df F E <
Multivariate Main Effect 39, 312 2.35 .001
Univariate F-tests
Brow Raise (AU 1/AU2) 3, 114 7.33 .001
Brow Lowering (AU4) 3, 114 22.70 .001
Orbit Tightening (AU6 / AU7) 3, 114 6.26 :001
Levator Contraction (AU9 / AU10) 3, 114 8.10 .001
Lip Corner Pull (AU12) 3, 114 2.17 .095
Dimpler (AU14) 3, 114 1.85 .141
Chin Raise (AU17) 3, 114 1.83 .145
Tongue Show (AU19) 3, 114 2.52 .061
Lip Press (AU24) 3, 114 1.53 .211
Opened Mouth (AU25/26/27) 3, 114 4.41 .006
Eye Slit (AU42) 3, 114 1.42 .240
Eyes Closed (AU43) 3, 114 4.52 .005
Eye Squint (AU44) 3,114 3.81 .012
Note: Bonferroni adjustments suggest a significance level of .003.

56
Table 4
Mean Facial Action Intensity Across Pain Conditions
(AU) Facial Action Neutral Genuine Masked Faked
M SD M SD M SD M SD
Brow Raise 0.08 0 35 0 13 0 57 0 05 0 32 0 80a>b>c 1.5
Brow Lowering 0.00 0 00 0 85a 1 60 0 13 0 57 2 36a,b,c 2.33
Orbit Tightening 0.00 0 00 0 54 1 37 0 44 1 11 1 15a>c 1.71
Levator Contraction 0.00 0 00 0 62a 1 39 0 13 0 57 0 95a,c 1.64
Lip Corner Pull 0.15 0 67 0 38 0 99 0 62 1 40 0 80 1.59
Dimpler 0.00 0 00 0 38 1 04 0 33 1 06 0 41 1.12
Chin Raise 0.3 0 16 0 46 1 12 0 44 1 10 0 28 0.97
Tongue Show 0.00 0 00 0 26 0 78 0 36 1 09 0 05 0.32
Lip Press 0.03 0 16 0 33 0 93 0 28 0 89 0 23 0.71
Open Mouth 0.23 0 58 0 69 0 86 0 74 0 91 0 80 0.83
Eye Slit 0.00 0 00 0 20 0 92 0 10 0 64 0 36 1.18
Closed Eyes 0.00 0 00 0 18 0 82 0 00 0 00 0 62 1.48
Eye Squint 0.00 0 o o 0 33 1 18 0 00 0 00 0 62 1.52
a Mean is significantly greater than neutral mean
b Mean is significantly greater than genuine mean
c Mean is significantly greater than masked mean

57
The intensity analyses of the pain-related AU's yielded more complex results, with three of
the pain-related facial actions varying across condition (brow lowering, orbit tightening and levator
contraction) and the remaining facial actions (opened mouth, and closed eyes) maintaining a
consistent intensity across condition. The intensity of brow lowering was greater in the faked pain
expressions than in either the genuine pain, masked pain or neutral expressions (p < .01). The
intensity of brow lowering in the genuine pain expressions was equivalent to that in the masked pain
expressions, but greater than that seen in neutral expressions (p < .05), while the masked pain and
neutral expressions did not differ. Orbit tightening intensity was found to be greater during faked
pain than during a masked pain (p < .05) or neutral expression (p < .01), with no significant
differences in intensity between the masked pain and neutral expressions. The intensity of orbit
tightening movements in genuine pain expressions did not differ from either the faked pain
expressions or the masked pain and neutral expressions. The intensity of levator contraction
movements were also higher in the faked condition than in either the neutral or the masked pain
expression (p < .01), with no differences in intensity between the masked pain and neutral
expressions. Faked pain and genuine pain expressions were equal in the intensity of these
movements however, as were genuine pain and masked pain expressions. Genuine pain
expressions, however, exhibited a greater intensity of levator contraction than did the neutral
expressions.
Results of the intensity analyses provided some support for the study's hypotheses.
Compared to the genuine pain expression, faked pain showed a greater intensity of one non pain-
related facial actions (brow raise), as well as a more intense display of several pain-related facial
actions (brow lowering, orbit tightening and levator contraction), In terms of facial action intensity,
the distinction between genuine pain, masked pain and neutral expressions was very subtle.
Genuine pain expressions exhibited a greater intensity of brow lowering and levator contraction
than seen in the neutral expressions, while the remaining facial actions (pain-related and non pain-
related) did not differ among these three conditions.
Apex Duration. The average duration of peak intensity for each individual A U was
compared across pain conditions using a mixedTinodel M A N O V A . Multivariate analyses showed
58
that apex duration differed significantly across pain conditions (See Table 5). Univariate F tests
examining the duration of peak intensity for individual facial actions provided partial support for the
study hypotheses. The apex duration for all of the non pain-related facial actions (brow raise, eye
slit, eye squint, lip corner pull, dimpler, chin raise, tongue show, and lip press) was found to be
consistent across pain conditions. Mean apex duration scores are presented in Table 6.
Significant differences in apex duration across pain condition were found in three pain-
related facial actions: brow lowering, orbit tightening, and eye closure. Tukey's post-hoc analyses
showed that the apex duration brow lowering intensity was significantly longer in the faked pain
condition (p< 01) than in the genuine, masked and neutral facial expressions, which were
equivalent. The apex duration of orbit tightening and eye closure were equivalent in the faked and
genuine condition, with the apex in faked pain faces being of longer duration then either the masked
or neutral expression (p < .01). Apex durations in the genuine pain expression did not differ from
either the masked pain or neutral expressions. The apex duration of the remaining pain-related facial
actions (opened mouth, and levator contraction) did not vary across pain condition.
Onset Duration. To determine the onset duration, the average time lag between the initial
onset of a facial action and peak intensity was calculated across all AU's, and was compared across
pain condition using a mixed-model ANOVA. A significant difference in overall onset duration was
found (F (3,37) = 15.02, p < .001). Tukey's post hoc analyses did not support study hypotheses,
showing that genuine and faked pain displays were equivalent in the time from facial expression
onset to peak intensity. Neutral facial expressions showed a longer onset duration (X = 1.44 sec,
s.d = 0.38, p < .01) than either the faked (X = 0.89 sec, s.d. = 0.61) or genuine pain expressions (X
= 0.93 sec, s.d. = 0.49). The onset duration of masked pain expressions were equivalent to both the
neutral and genuine pain expressions, but were of significantly longer onset duration than the faked
pain expressions (X = 1.24, s.d = 0.70, p < .05).
Facial Action Duration. A mixed-model M A N O V A was used to test the hypothesis that
faked facial actions would last significantly longer than genuine facial actions. Multivariate
analyses showed that the overall response duration of facial actions varied across pain condition
(See Tables 7 & 8). Univariate F-tests examining the duration of individual AU's showed that the

59
Table 5
Results of M A N O V A and Followup ANOVA's Examining Apex Duration of Facial Actions
Across Pain Conditions
Df F E<
Multivariate Main Effect 42, 318 2.35 .001
Univariate F-tests
Brow Raise (AU 1/AU2) 3, 117 0.79 .499
Brow Lowering (AU4) 3, 117 13.60 .001
Orbit Tightening (AU6 / AU7) 3, 117 4.66 .004
Levator Contraction (AU9 / AU10) 3, 117 1.88 .136
Lip Corner Pull (AU12) 3, 117 0.99 .398
Dimpler (AU14) 3, 117 2.07 .108
Chin Raise (AU17) 3, 117 0.18 .909
Tongue Show (AU19) 3, 117 0.99 .402
Lip Press (AU24) 3, 117 0.35 .792
Opened Mouth (AU25/26/27) 3, 117 1.76 .159
Eye Slit (AU42) 3, 117 2.27 .084
Eyes Closed (AU43) 3, 117 5.26 .002
Eye Squint (AU44) 3, 117 2.44 .068
Note: Bonferroni adjustments suggest a significance level of .004.

60
Table 6
Mean Facial Action Apex Duration Across Pain Conditions
(AU) Facial Action Neutral Genuine Masked Faked (AU) Facial Action
M (sec) SD M(sec) SD M (sec) SD M (sec) SD
Brow Raise 0 09 0.53 0.05 0 22 0.03 0.21 0.14 0 36
Brow Lowering 0 00 0.00 0.05 0 18 0.01 0.02 0.24a>b>c 0 37
Orbit Tightening 0 00 0.00 0.07 0 31 0.04 0.16 0.23a>c 0 50
Levator Contraction 0 83 0.00 0.82 0 13 0.83 0.04 0.82 0 13
Lip Corner Pull 0 06 0.27 0.07 0 21 0.17 0.61 0.22 0 73
Dimpler 0 00 0.00 0.02 0 07 0.02 0.06 0.10 0 39
Chin Raise 0 04 0.23 0.04 0 17 0.02 0.07 0.05 0 31
Tongue Show 0 00 0.00 0.00 0 01 0.00 0.01 0.00 0 01
Lip Press 0 06 0.40 0.11 0 59 0.05 0.21 0.03 0 10
Open Mouth 0 13 0.54 0.37 0 74 0.32 0.74 0.48 0 82
Eye Slit 0 00 0.00 0.00 0 01 0.00 0.00 0.20 0 82
Closed Eyes 0 00 0.00 0.07 0 22 0.00 0.00 0.18a>c 0 44
Eye Squint 0 00 0.00 0.01 0 03 0.00 0.00 0.12 0 48
a Mean is significantly greater than neutral mean
b Mean is significantly greater than genuine mean
c Mean is significantly greater than masked mean

61
Table 7
Results of M A N O V A and Followup ANOVA's Examining the Duration of Facial Actions Across
Pain Conditions
Df F
Multivariate Main Effect 42, 318 2.26 .001
Univariate F-tests >
Brow Raise (AU 1/AU 2) 3, 117 2.02 .115
Brow Lowering (AU4) 3, 117 20.07 .001
Orbit Tightening (AU6 / AU7) 3, 117 8.80 .001
Levator Contraction (AU9 / AU10) 3, 117 4.64 .004
Lip Corner Pull (AU 12) 3, 117 1.86 .140
Dimpler (AU14) 3, 117 2.19 .093
Chin Raise (AU17) 3, 117 0.27 .848
Tongue Show (AU19) 3, 117 1.16 .326
Lip Press (AU24) 3, 117 0.35 .785
Opened Mouth (AU25/26/27) 3, 117 2.82 .042 •
Nostril Flare (AU38) 3, 117 0.82 .484
Eye Slit (AU42) 3, 117 2.57 .058
Eyes Closed (AU43) 3, 117 7.75 .001
Eye Squint (AU44) 3, 117 4.61 .004
Note: Bonferroni adjustments suggest a significance level of .004

62
Table 8
Mean Facial Action Duration Across Pain Conditions
(AU) Facial Action Neutral Genuine Masked Faked
M(sec) SD M(sec) SD M(sec) SD M(sec) SD
Brow Raise 0 09 0 53 0 10 0.36 0 08 0 38 0.30 0 58
Brow Lowering 0 00 0 00 0 13 0.28 0 01 0 04 0.46a>b>c 0 56
Orbit Tightening 0 00 0 00 0 16 0.48 0 06 0 18 0.55a>b>c 0 98
Levator Contraction 0 41 0 00 0 57 0.53 0 44 0 11 0.68a>c 0 63
Lip Corner Pull 0 11 0 41 0 14 0.38 0 36 1 02 0.45 1 15
Dimpler 0 00 0 00 0 12 0.38 0 04 0 12 0.16 0 56
Chin Raise 0 04 0 23 0 06 0.18 0 04 0 12 0.09 0 50
Tongue Show 0 00 0 00 0 02 0.08 0 03 0 10 0.01 0 07
Lip Press 0 06 0 40 0 15 0.62 0 19 0 83 0.11 0 38
Open Mouth 0 16 0 56 0 48 0.81 0 45 0 92 0.66 0 98
Eye Slit 0 00 0 00 0 01 0.03 0 00 0 02 0.22 0 83
Closed Eyes 0 00 0 00 0 13 0.31 0 02 0 12 0.47a,b,c 0 97
Eye Squint 0 00 0 00 0 03 0.15 0 00 0 00 0.30a>b>c 0 84
a Mean is significantly greater than neutral mean
b Mean is significantly greater than genuine mean
c Mean is significantly greater than masked mean

63
changes in A U duration were limited to four pain-related facial actions (brow lowering, orbit
tightening, levator contraction, and eye closure) and one non pain-related facial action (eye squint).
Tukey's post hoc analyses determined that the duration of brow lowering (p < .01), orbit tightening
(p < .01), and eye squint (p < .05) were significantly longer in the faked pain expressions than in the
genuine pain, masked pain and neutral expressions, with no differences in duration between the
other three facial expressions. The duration of eye closure showed a similar pattern, being longer in
the faked pain expression than in either the genuine pain expression (p < .05), masked pain (p < .01)
or neutral expressions (p < .01), with no differences between the final three expressions. The
duration of levator contraction was also longer in the faked pain expression than in either the
masked (p < .05) or neutral (p < .01) expressions, however, the faked and genuine pain expressions
were of equal duration.
Asymmetry & Pulsating Apexes. A mixed-model M A N O V A determined that the overall
frequency of asymmetrical facial actions and pulsating apexes varied across pain conditions
(F = 2.58, p < .03). Univariate F tests and post-hoc analyses showed that study hypotheses were
not supported: genuine and faked pain expressions exhibited similar frequencies of both
asymmetrical facial actions and pulsating apices. However, faked facial actions showed asymmetry
and pulsating apices significantly (p < .01) more frequently than either the masked pain or neutral
expressions, while there were no significant differences between the genuine pain, masked pain and
neutral expressions.
Temporal Contiguity of Facial Actions. The current study proposed to use cluster analysis
techniques to determine if there would be greater temporal contiguity of pain-related facial actions
in genuine versus faked pain expressions, as well as investigating the idea that faked pain
expressions would contain either a greater number of facial action "constellations" or a different mix
of facial actions in the isolated clusters. Unfortunately, established procedures for performing
cluster analysis on FACS data (Friesen, 1982) utilize both facial action onset and offset, and facial
action offset was not analyzed in the current study due to missing data. A second difficulty
involved the large variation in facial actions exhibited by the subjects, which resulted in temporal
variables being coded as "missing data" when a facial action was not exhibited by a subject. Cluster

64
analysis procedures are not appropriate for small sample sizes, and do not tolerate large amounts of
missing data, therefore missing data was replaced by group means. This allowed for a generalized
investigation of temporal patterns using agglomerative (within group) average linkage cluster
analysis, with pearson correlations as the similarity grouping measure.
The time of onset for the most frequently occuring AU's were analysed separately for the
genuine and faked pain expressions. As replacing large amounts of missing data with group means
makes a detailed investigation of temporal contiguity questionable, clusters were simply examined
to determine if onset time of pain-related AU's were similar. Results showed that for genuine pain
expressions, a four cluster solution produced two clusters containing pain-related and non pain-
related facial actions, and two clusters containing only non pain-related facial actions. The first
"pain" cluster contained orbit tightening, levator contraction, and eyes closed, as well as blinking
and eyebrow raise. The second "pain" cluster contained brow lowering and mouth opening, as well
as squinting and lip corner pull. The first "no pain" cluster included eye slit, nostril dilate, lip press
and chin raise, while the second was comprosed of dimpler and tongue show movements. Results
suggest that the facial actions identified by past research as "pain-related" appeared fairly closely
together in time during genuine pain expressions. In comparison, a four cluster solution for faked
pain expressions showed pain-related facial actions spread across all four clusters. In addition,
brow lowering and mouth opening, which appeared together and were the most frequent facial
response to genuine pain, did not occur within the same cluster. Faked pain expressions then,
seemed to be comprised of pain-related facial actions which did not appear closely together in time.

65
Study 2: Training to detect deception
Methods
Subjects
Judges were 120 undergraduate students (60 male, 60 female) attending the University of
British Columbia, who were either given course credit or were paid $10 for their participation. To
be included in the study, subjects were required to have a sufficient command of the English
language to complete the questionnaire packages. The subjects ranged from 17 to 43 years of age,
with a mean age of 21.7 years (s.d. = 4.6).
Materials
Video Equipment. The video data collected in Study 1 was edited into stimulus tapes using
a Panasonic editing system comprised of two Panasonic PC14A51R 14"" Colour T V Monitors, two
Panasonic A G 1970 S-VHS Editing VCR's and a Future Video EC-1000 Pro M K 11 editing board.
A Videomics TM-1 Title Maker was used to label each segment with an A, B, C or D in order of
presentation.
The judges' viewing system consisted of a 20" Sharp MTS Stereo Monitor hooked up to a
Panasonic AG-6300 videocassette recorder equipped with a shuttle board which allowed the
subjects to pause, stop, rewind and review the tape in frame by frame slow motion.
Videotape. The stimulus tape for the study contained the video data of 30 of the subjects
from study one. The remaining subjects were excluded due to imperfect data: six patients because
they were inclined on the bed during their neutral videoclip instead of lying down flat and four
because at least one of their four videoclips was less than 10 seconds in length. To construct the
stimulus tape, the video clips of the 30 patients were rearranged with editing equipment in
randomized order, with the limiting condition that successive clips alternated between male and
female patients. As it was determined that there was insufficient time available for subjects to make
the full set of 30 judgements and there was a risk of fatigue effects, each subject only viewed the
videotaped data for 20 of the subjects on the stimulus tape. Subjects were then assigned a
particular patient's videoclip as their first to rate. They then watched the next 20 subjects on the
tape. Subject's starting points were assigned in counterbalanced order to eliminate any order

66
effects, and so that each of the 30 patients' data was viewed by the same number of subjects. The
stimulus tape was dubbed so that 2 copies of the 30 patients' clips were on the same tape, which
allowed the experimenter to begin the judgement task with any of the 30 patients. Subjects
beginning on the latter part of the first set of 30 continued with the beginning clips of the second set
of 30.
The four video clips for each patient (baseline, genuine, faked and masked) were presented
at once, with the order of presentation being the counterbalanced order in which the segments were
filmed. The videotape consisted of 120 segments, each of which were approximately 10 seconds in
length. Each clip was followed by 5 seconds of blank tape to allow the judges time to pause the
tape, rate the intensity of the patient's pain experience and to decide which category the expression
represented.
Training Manual. The training manual provided a written description of the typical facial
expression of pain, as well as current information on the facial cues which may differentiate genuine,
faked and masked pain expressions. Subjects were provided with information on the changes in
frequency and intensity of facial expressions found in past studies. The postulated temporal factors
being investigated in study one were also described as possible cues to deception. In addition, they
were provided with a description of the facial cues thought to be indicative of deceit in general,
including asymmetry^ timing and contiguity of facial expressions and multiple emotion expressions.
This information constituted the best of our knowledge to date about the cues which might enable
us to detect deceit in pain patients. Where possible, photographs or drawings of the various facial
expressions were included in the manual. After reading the training manual, subjects completed a
14-item training test, as a measure of their retention of the material (See Appendix G).
Measures
Each patient was asked to complete a questionnaire package containing, a personal
information sheet, the Interpersonal Reactivity Index and the consent form (See Appendix H).
Personal Information Sheet. Each subject was asked to fill out a personal information sheet
containing questions regarding their age, sex, ethnic background and previous experience with pain,
or relationship with others experiencing pain.

67
Interpersonal Reactivity Index (IRD. Subjects' responsivity / empathy to others was be
measured using the IRI, a 28-item self-report measure. The IRI consists of four 7-item subscales,
each tapping a separate aspect of the global concept of empathy: Perspective-Taking (PT), Fantasy
(FT), Empathic Concern (EC) and Personal Distress (PD).
Procedure
Upon the subject's arrival, the experimenter described the purpose of the study and the
procedures involved. The subjects were told that the aims of the study were: (1) to determine how
skilled people are at judging when someone is in pain through their facial expression, and (2) to
determine what qualities makes someone a good judge of others' pain experiences. They were also
told that they would be asked to complete a questionnaire on their own pain experience and another
which asks questions about their personality. Subjects were assured that their participation would
remain confidential and anonymous. In addition, they were informed that their participation was
completely voluntary and that they would be able to withdraw from the study at any time. If
subjects were still willing to participate, they were given a consent form to read which reiterated the
information provided by the experimenter. Subjects were required to sign the form before
proceeding with the study. At this point, subjects were brought into the viewing room and were
asked to complete the questionnaire package. When the package was completed, all subjects were
given a verbal description of the videotape they were about to see and instructions on the judgement
task, the rating materials and the use of the shuttle board.
Training Conditions. Subjects were randomly assigned to one of four experimental
groups: (1) control, (2) feedback, (3) deception training, and (4) deception training plus feedback.
The subjects in the control group viewed the videotape and made their judgements without any
further information on how to make their decisions, nor did they receive any feedback on their
performance. The feedback groups were given corrective feedback on the type of facial
expression depicted in each segment after each patient's four clips had been viewed and
categorized. That is, they were informed of their performance and the correct categorizations
following the judgement tasks for each patient. This information was provided in written format,
to ensure that differences in performance among the groups were not a result of the

68
experimenter's presence during the judgement task. The deception training groups were required
to read the training manual and complete the training test before beginning the judgement task.
Finally, the deception training plus feedback were given feedback on their performance for each
patient as well as being given the training manual to read beforehand.
Judgement Task Procedure. Each subject was shown the videotape data of 20 patients, with
all patients' data being viewed by an equal number of subjects in each training group. Subjects were
allowed to view all four clips for each patient before making their judgements. In addition, the four
clips could be viewed again if the subject felt they require a second viewing in order to come to a
decision. For each videoclip, the subjects rated the intensity and unpleasantness of the pain
experienced by the patient. Ratings were made using the DDS, which provides 13 pain adjectives
on two scales, ranging from "not painful" to "extremely painful", and "not unpleasant" to "extremely
unpleasant", respectively, and which have been ratio-scaled using cross-modality procedures to
provide numerical equivalents (Gracely et al., 1978; Gracely et al., 1979; Gracely et al., 1982). The
subjects were also asked to decide which category each of the four videoclips represented: baseline,
genuine pain, faked pain or masked pain. It is important to note that this was not a forced choice
design, in that subjects were not informed that all four categories were represented for each patient.
Following their categorization of the four clips, the subjects were asked to describe which cues they
used to make their decision. Using this format, each subject was required to make two judgements
about the facial expressions: 1) to estimate the degree of intensity and unpleasantness of pain
experienced by the patient and 2) to make a decision about the category of each facial expression.
Judgements for each patient were made before proceeding to the next (See Appendix I).

69
Results
Judgements of Pain
The overall accuracy of study participants ranged from 18.3% to 63.3%, with the mean
judgement accuracy of students being 32.9% (S.D. = 7.5). A mixed-model M A N O V A was
conducted in order to determine if pain judgements differed across sex, training group or pain
condition. Analyses were performed for judgement accuracy, decision-making confidence, and
ratings of pain unpleasantness and intensity. The results of the analyses are presented in Table 9.
Mean accuracy scores and decision-making confidence are presented in Table 10, and mean
ratings of pain intensity and unpleasantness are presented in Table 11.
Sex. Multivariate analyses showed that pain judgements differed significantly across sex.
Univariate F-tests suggest that females overall judgement accuracy was significantly higher than
males. A comparison of means shows that females classified 35.6% of pain expressions
accurately, as compared to 30.2% accuracy for males, both of which are significantly above
chance levels (t = 10.29, p< .01; t = 7.94, p < .01). There was no sex difference for decision
making confidence, nor did males and females differ in the degree of unpleasantness or intensity
they ascribed to various pain expressions.
Training Group. Multivariate and univariate F-tests suggest that both judgement
accuracy and decision-making confidence were influenced by the training group of the judges.
Planned comparisons showed that subjects in the feedback and feedback plus deception training
groups were equally accurate, correctly classifying 34.4% and 37.1% of pain expressions
respectively (p < .086), both of which are significantly above chance levels (t = 6.33, p< .01; t =
8.49, p < .01). Subjects in the control and deception training only groups were significantly less
accurate in their judgements, correctly classifying 30.4% (p< .001, p<.001) and 29.7% (p< .008,
p<.001) of expressions, both of which are significantly above chance levels (t = 4.88, p< .01; t =
4.76, p < .01). With respect to decision-making confidence, subjects in the control group were
significantly more confident (70.4%) in their decision-making than were the groups receiving
feedback (63.9%; p<.005) or feedback plus deception training (58.8%; p<.002). The deception
training subjects, with 67.6% decision-making confidence, did not differ significantly from
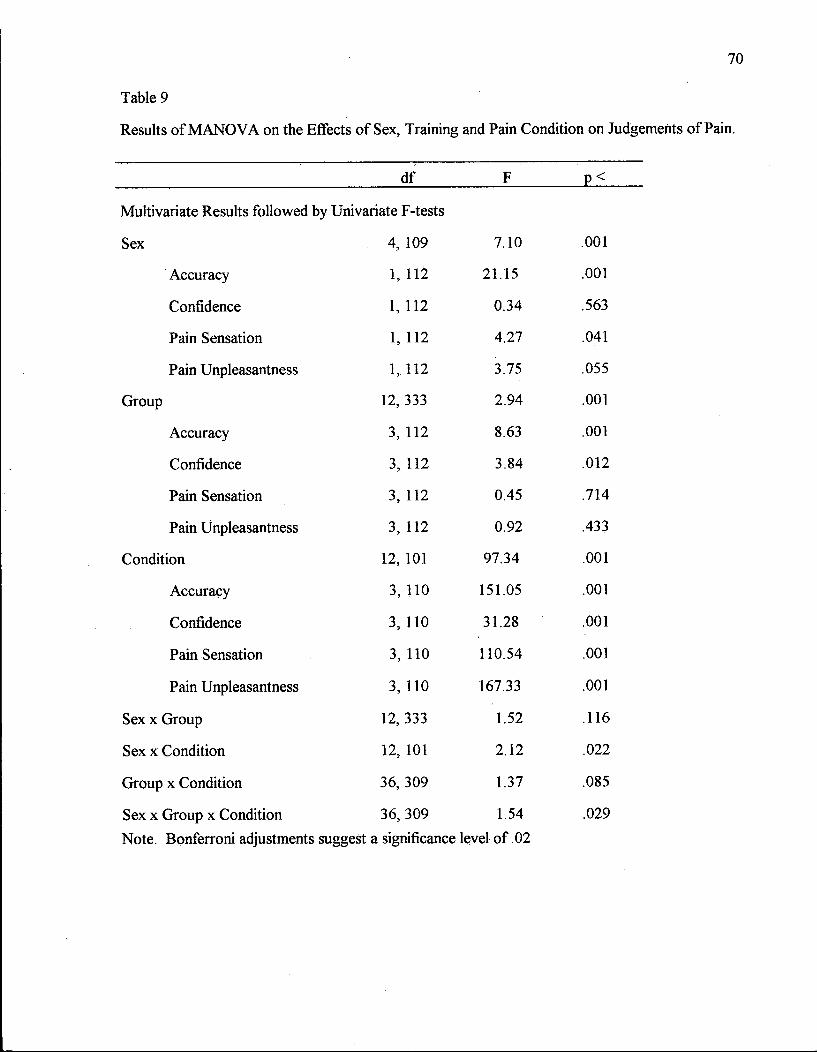
70
Table 9
Results of M A N O V A on the Effects of Sex, Training and Pain Condition on Judgements of Pain.
df F p<
Multivariate Results followed by Univariate F-tests
Sex 4, 109 7.10 .001
Accuracy 1, 112 21.15 .001
Confidence 1, 112 0.34 .563
Pain Sensation 1, 112 4.27 .041
Pain Unpleasantness 1, 112 3.75 .055
Group 12,333 2.94 .001
Accuracy 3, 112 8.63 .001
Confidence 3, 112 3.84 .012
Pain Sensation 3, 112 0.45 .714
Pain Unpleasantness 3, 112 0.92 .433
Condition 12, 101 97.34 .001
Accuracy 3, 110 151.05 .001
Confidence 3, 110 31.28 .001
Pain Sensation 3, 110 110.54 .001
Pain Unpleasantness 3, 110 167.33 .001
Sex x Group 12, 333 1.52 .116
Sex x Condition 12, 101 2.12 .022
Group x Condition 36, 309 1.37 .085
Sex x Group x Condition 36, 309 1.54 .029
Note. Bonferroni adjustments suggest a significance level of .02

71
Table 10
Mean Accuracy and Decision-Making Confidence Across Training Group and Pain Condition
Accuracy Confidence
M SD M SD
Training Group
Control 30.44 6.11 70.36 13.29
Neutral 49.11 9.14 72.13 17.10
Genuine 24.89 8.92 70.47 10.99
Faked 25.00 10.24 71.00 12.62
Masked 22.78 8.93 67.82 14.30
Feedback 34.25 8.00 63.92 13.32
Neutral 47.33 11.02 66.58 13.82
Genuine 28.33 10.39 62.88 14.59
Faked 31.67 11.51 65.15 12.73
Masked 29.67 9.36 61.06 14.56
Training 29.72 5.47 67.63 12.02
Neutral 46.89 8.92 69.75 13.07
Genuine 23.67 11.08 66.73 11.94
Faked 27.33 8.99 69.39 12.32
Masked 21.00 9.02 64.66 12.47
Feedback / Training 37.14 7.82 58.75 16.99
Neutral 48.33 8.20 60.94 17.35
Genuine 31.22 11.86 57.80 17.87
Faked 34.22 10.47 61.20 16.82
Masked 34.78 12.46 55.07 17.55

72
Table 11
Mean Ratings of Pain Intensity and Unpleasantness Across Training Group and Pain Condition
Pain Intensity Pain Unpleasantness
M SD M SD
Training Group
Control 7.41 3.70 3.46 0.97
Neutral 1.78 1.67 1.79 1.52
Genuine 11.58 6.18 4.41 0.79
Faked 9.12 5.89 3.77 1.08
Masked 7.16 3.84 3.86 1.29
Feedback 8.16 5.61 3.75 1.18
Neutral 2.38 2.80 1.93 1.65
Genuine 11.79 8.19 4.72 1.27
Faked 8.32 4.39 3.96 1.56
Masked 10.13 10.04 4.38 1.21
Training 7.96 4.27 3.51 0.92
Neutral 2.25 2.19 1.74 1.23
Genuine 10.94 5.65 4.40 1.01
Faked 10.56 6.54 3.89 1.21
Masked 8.09 5.23 4.00 1.24
Feedback / Training 8.81 5.63 3.80 0.83
Neutral 2.56 2.07 1.96 0.94
Genuine 12.86 9.15 4.62 1.23
Faked 9.39 7.10 4.05 1.48
Masked 10.44 6.26 4.55 1.15

73
either the control (p < .454) or feedback groups (p < .308), although they were significantly more
confident than subjects in the feedback plus training group (p<02) (see Table 10). Univariate F-
tests determined that subjects in the various training groups did not differ in the degree of
unpleasantness or intensity they ascribed to various pain expressions.
In order to determine if subjects in the training conditions read, understood and retained
the information presented, they were given a training test prior to beginning the judgement task.
Subjects scores on the training tests ranged from 7 to 14, out of a total of 14 points, with an
average score of 11.0 (s.d. = 2.1). Further analyses were conducted to determine if judgement
accuracy was influenced by the subjects' training test scores. Pearson correlations showed that
subjects' scores on the training test were not correlated with judgement accuracy (r = .0826).
Finally, there was no correlation between training test scores and subjects' confidence in their
decision-making ability (r = -.0592). Given the relatively high test scores, it is obvious that the
majority of training group subjects understood and remembered the material presented, however,
the information provided did not improve the subject's judgement accuracy.
Pain Condition. Multivariate analyses showed that pain judgements varied significantly
across neutral, genuine, faked and masked pain conditions. Univariate F-tests determined that
judgement accuracy, decision-making confidence, and ratings of pain unpleasantness and intensity
experienced by the patient all differed significantly across pain condition. Tukey's post-hoc
analyses indicated that judges were more accurate at determining a neutral expression (X - 47.9,
s.d. = 9.3) than a faked (X = 29.6, s.d. - 10.8), genuine (X = 27.03, s.d. - 10.9) or masked (X
- 27.06, s.d. = 11.4) pain expression (p < .01), while the detection accuracy for faked, genuine
and masked pain expressions did not differ.
Decision-making confidence was also found to vary with pain condition. Tukey's post hoc
analyses indicated that judges were more confident in their ability to detect neutral (X = 67.35,
s.d. = 15.83) and faked pain (X = 66.69, s.d. = 14.10) expressions than they were for their
judgements of genuine pain (X = 64.47, s.d. = 14.70) and masked pain (X = 62.15, s.d. = 15.40)
expressions (p< .01). Judges were also significantly more confident in their identification of
genuine pain expressions than of masked pain expressions.
74
Judge's estimates of both pain intensity and unpleasantness differed depending on pain
condition. Tukey's post hoc analyses showed that genuine pain faces were rated as exhibiting pain
that was both more intense and unpleasant than either faked, masked or neutral pain expressions.
An approximate comparison of the average intensity and unpleasantness scores to the Gracely
descriptor terms indicates that genuine pain expressions were rated as "moderate" in intensity and
"unpleasant". Both the masked and faked pain expressions were thought to be experiencing more
intense and unpleasant pain than the neutral expression, while faked and masked pain expressions
were rated to be equal in perceived pain intensity and unpleasantness. The approximate Gracely
equivalents for the faked and masked expressions were "moderate" intensity and "slightly
annoying", while neutral expressions were rated to be of "very weak" intensity and "slightly
unpleasant".
Perceived Judgement Accuracy
Upon completion of their judgement task, subjects were asked to rate their overall
accuracy in identifying the four types of facial expression. Subjects identified an accuracy level of
70.67% for neutral facial expressions, 56.75% for genuine pain expressions, 59.34% for faked
pain expressions, and 54.78% accuracy for masked pain expressions.
Decision-Making Process Variables
Number of Cues Used. In an attempt to explain the influence of sex differences, training
group and pain condition on judgement accuracy, analyses were conducted to determine if pain
judgements differed in terms of the number or type of cues used to reach each decision. A mixed-
model A N O V A was carried out to determine if the number of cues identified by each subject
varied across sex, training group and pain condition. The results of the analysis are presented in
Table 12, while the mean cue use scores are presented in Table 13.
Results of the analysis showed that, despite their greater accuracy, females identified the
same number of cues as males when making their judgements. Similarly, although overall
accuracy differed across training groups, training condition did not significantly influence the
average number of cues used in judging facial expressions. Predictably, the number of facial cues
identified by the subjects differed significantly depending on the pain condition being judged.

75
Table 12
Results of M A N O V A on the Effects of Sex, Training and Pain Condition on Number of Cues
Used.
df F P<
Sex 1, 112 116 .284
Group 3, 112 0.41 .743
Condition 3, 110 113.54 .001
Sex x Group 3, 112 0.14 .936
Sex x Condition 3, 110 1.10 .354 i
Group x Condition 9, 336 1.82 .063
Sex x Group x Condition 9,336 1.05 .397

76
Table 13
Mean Number of Facial Cues Detected Across Treatment Groups and Pain Condition
Pain Condition
Treatment Groups Neutral Genuine Masked Faked Treatment Groups
M SD M SD M SD M SD
Control Group 1.12 0.35 1.48 0.35 1.44 0.29 1.45 0.36
Feedback 1.09 0.19 1.29 0.29 1.30 0.24 1.30 0.22
Training 1.07 0.27 1.47 0.32 1.34 0.34 1.45 0.33
Training and Feedback 1.00 0.33 1.44 0.38 1.39 0.33 1.47 0.32

77
Tukey's post hoc analyses showed that subjects identified a greater number of cues for genuine
and faked pain expressions than for either masked pain or neutral expressions (p < .01). Subjects
also identified significantly more facial cues in the masked pain condition than in the neutral
expressions (p < .01).
Type of Cues Used. Subjects identified a total of 299 different facial cues that were used
to make their judgements. The number of times each of these cues was used across all
judgements was calculated for each subject, with the frequency of individual cues ranging from
.01 to 10.18 occurrences per subject (See Appendix J). Two types of analyses were conducted oh
facial cue use: 1) by using the cues individually as identified by the subjects, and 2) by grouping
similar cues into cue use categories.
Of the 299 facial cues identified by the subjects, 15 facial cues were identified in greater
than 3% of the pain expressions (faked, genuine, masked) and were retained in two separate
MANOVAs to investigate the change in frequency across training group, sex and pain condition
(See Table 14). The interaction effects of training group, gender and pain condition on cue use
were not investigated, as separate analyses yielded more power. Multivariate analyses showed
that the use of individual facial cues differed significantly across training group (F = 2.54, p <
.001), and across pain condition (F = 16.85, p < .001), but did not vary with the judges' gender (F
- 1.19, p < .287). Univariate analyses determined that the following facial actions were identified
more or less frequently depending on the training group: lowered eyebrows, closed eyes,
exaggerated facial movements, and eye squinting (See Table 14). Tukey's post-hoc analyses
indicated that lowered eyebrows were identified more frequently by subjects in the training group
than in the training plus feedback group (p < .05), with both the training (p < .01) and training
plus feedback (p < .05) groups using this cue more frequently than either the control or feedback
groups. Eye closure and eye squinting were also identified more frequently by the training group
than either the control Or feedback groups (p < .01), while the training plus feedback group used
these cues a moderate amount, with no difference in frequency between either the training group
or the control and feedback groups. Exaggerated facial movements were identified more
frequently by the training plus feedback group than either the control or feedback groups (p <
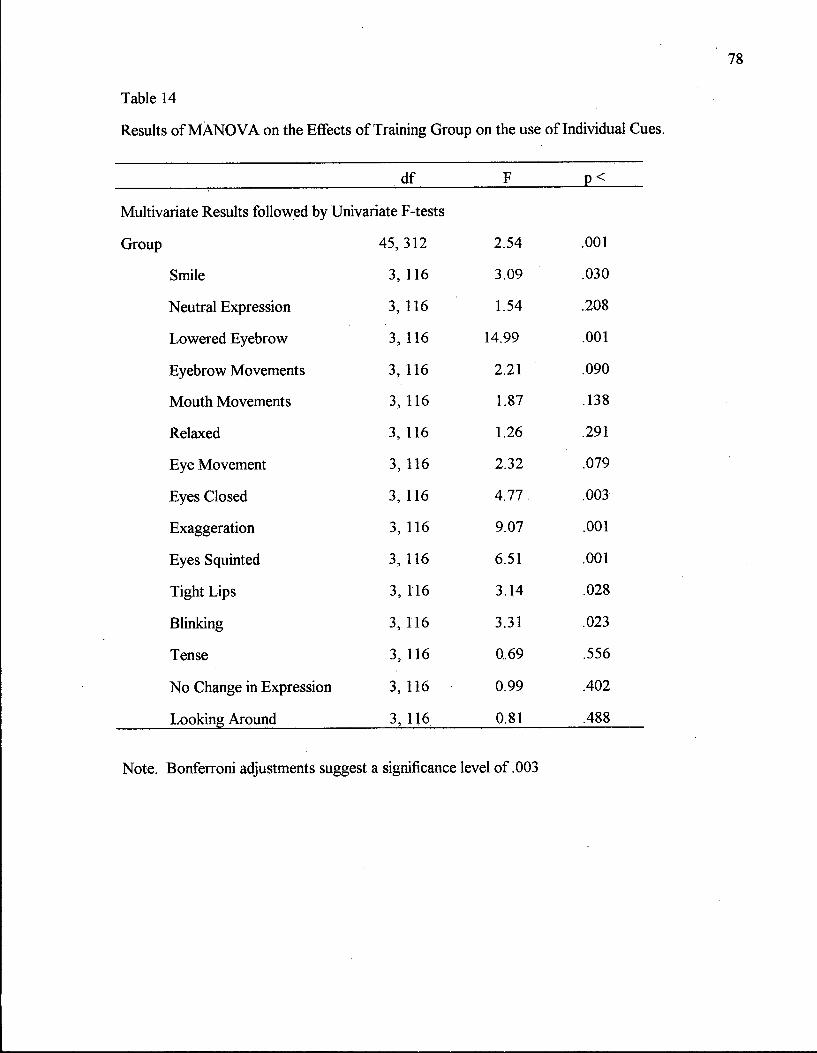
Table 14
Results of M A N O V A on the Effects of Training Group on the use of Individual Cues.
_df F p_<
Multivariate Results followed by Univariate F-tests
45,312 2.54 .001
Smile 3, 116 3.09 .030
Neutral Expression 3,116 1.54 .208
Lowered Eyebrow 3, 116 14.99 .001
Eyebrow Movements 3, 116 2.21 .090
Mouth Movements 3, 116 1.87 .138
Relaxed 3, 116 1.26 .291
Eye Movement 3, 116 2.32 .079
Eyes Closed 3, 116 4.77 .003
Exaggeration 3, 116 9.07 .001
Eyes Squinted 3, 116 6.51 .001
Tight Lips 3, 116 3.14 .028
Blinking 3, 116 3.31 .023
Tense 3, 116 0.69 .556
No Change in Expression 3,116 0.99 .402
Looking Around 3, 116 0.81 .488
Note. Bonferroni adjustments suggest a significance level of .003

79
.01), while the training group identified exaggeration with a frequency that fell between the
training plus feedback group and the control and feedback groups. Finally, the frequency of
smiling, lack of facial movement, eyebrow movements, mouth movements, eye movements,
relaxed features, tight lips, muscle tension, looking around, blinking and "no change in facial
expression" did not differ across training group.
Multivariate analyses determined that the use of facial cues varied across pain conditions,
while univariate analyses indicated that all 15 facial cues differed in frequency across the four pain
conditions (see Tables 15 and 16). Tukey's post hoc analyses indicated that subjects identified
"neutral", "relaxed" and "no change in expression" as cues when judging neutral facial expressions
more frequently than the masked, genuine or faked pain expressions (p < .01). In contrast, mouth
movements, closed eyes and eye movements were identified as facial cues more often when
judging masked, faked and genuine pain expressions than for neutral facial expressions (p < .01).
Lowered eyebrows and exaggerated facial actions were identified most often while observing
faked pain expressions, followed by genuine and masked pain expressions. These cues were
identified equally as frequently in masked pain and neutral expressions, but were identified more
frequently in genuine pain than in neutral expressions (p < .01). Eyebrow movement in general
was identified most frequently during faked pain expressions, followed by genuine pain, with the
least frequency in masked pain and neutral expressions (p < .01). Eye squint was also identified
most frequently in faked pain expressions, followed by genuine pain and masked pain expressions,
with the least frequent cue use during neutral expressions. Blinking was identified with equal
frequency in faked pain, genuine pain and neutral expressions, and was identified less frequently
during masked pain conditions (p < .05). Smiling was observed most frequently during the two
deceptive conditions, faked pain and masked pain, and with less frequency during the genuine pain
and neutral expressions. Tension and looking around were identified most frequently when
observing actual pain experiences (genuine, masked), and less frequently in faked pain and neutral
expressions (p < .01). Finally, tight lips were identified more frequently during genuine pain than
during faked pain (p < .05), with the frequency of tight lips identified during masked pain differing
neither from genuine or faked pain expressions. Tight lips were observed less frequently during

Table 15
Results of M A N O V A on the Effects of Pain Condition on the use of Individual Cues.
df F p_<
Multivariate Results followed by Univariate F-tests
Pain Condition 45, 1035 2.54 .001
Smile 3, 357 67.53 .001
Neutral Expression 3, 357 134.62 .001
Lowered Eyebrow 3, 357 21.29 .001
Eyebrow Movements 3, 357 31.70 .001
Mouth Movements 3, 357 18.88 .001
Relaxed 3, 357 38.85 .001
Eye Movement 3, 357 11.61 .001
Eyes Closed 3,357 23.74 .001
Exaggeration 3, 357 46.48 .001
Eyes Squinted 3, 357 25.80 .001
Tight Lips 3,357 13.01 .001
Blinking 3,357 5.62 .001
Tense 3, 357 8.80 .001
No Change in Expression 3,357 16.07 .001
Looking Around 3, 357 16.24 .001
Note. Bonferroni adjustments suggest a significance level of .003

81
Table 16
Mean Individual Cue Use Across Pain Condition
Facial Action (AU) Neutral Genuine Faked Masked
M SD M SD M SD . M SD
Smile 0.24 0.52 0.54 0.85 1.75 1.75 1.76 1.51
Neutral Face 6.43 5.41 1.20 1.41 1.22 1.34 1.48 1.67
Lowered Eyebrows 0.15 0.40 0.53 1.20 0.94 1.69 0.26 0.76
Eyebrow Movement 0.13 0.37 0.67 1.13 1.15 1.67 0.30 0.76
Mouth Movement 0.11 0.48 0.83 1.59 0.83 1.69 0.68 1.32
Relaxed 2.40 3.75 0.57 1.16 0.4? 1.08 0.69 1.44
Eye Movement 1.17 2.69 2.11 3.17 1.93 2.76 2.25 2.81
Eyes Closed 0.16 0.57 0.89 1.39 0.93 1.45 0.68 1.05
Exaggerated 0.05 0.22 0.43 0.76 1.50 2.05 0.20 0.46
Eye Squint 0.09 0.32 0.57 1.19 1.02 1.69 0.38 0.83
Tight Lips 0.13 0.43 0.66 1.34 0.38 0.79 0.59 1.17
Blinking 0.70 1.21 0.74 1.21 0.82 1.31 0.38 0.75
Tense 0.37 1.01 0.82 1.73 0.40 0.85 0.77 1.78
No Change in Face 1.18 2.98 0.27 0.77 0.31 0.85 0.29 1.09
Looking Around 0.23 0.53 0.68 1.20 0.30 0.73 0.92 1.62
3 Mean is significantly greater than control group
b Mean is significantly greater then feedback group
c Mean is significantly greater than training group
d Mean is significantly greater than training / feedback group

82
neutral expressions than during either genuine (p < .01), masked (p < .01) or faked pain
expressions (p < .05).
In order to provide a more comprehensive analysis of subject's judgement cues, the 299
facial cues identified by the judges were grouped according to muscle group or conceptual
similarity . For example, the facial cue group labeled "eyebrows" consisted of the following cues:
lowered eyebrows, eyebrow movements, eyebrow twitch, pinched eyebrows, and raised
eyebrows. Similarly, the category labeled "timing" included the following cues: short and long
duration, sudden movements, delayed onset, slow movements, early onset and actions which are
not simultaneous. Facial actions which were identified fewer than five times were deleted from
the analyses, as were several miscellaneous facial cues. Additional cues of interest, such as those
involving asymmetry and leakage were also deleted due to infrequency. The final categorization
scheme is outlined in Appendix K.
Grouping judgement cues yielded fifteen facial cue categories: eyes, eyebrows,
cheeks/nose, mouth, smile, repressed facial actions, breathing pattern, incongruent facial actions,
pain expression, blinking, timing of facial actions, exaggeration, tension, sudden movements and
relaxed muscles. As above, the judgement cue categories were used in two separate MANOVAs
investigating the frequency of identification across training group and gender. Similar to the
results for individual judgement cues, multivariate analyses isolated a significant difference in
judgement cue use across training groups, but not across gender (See Tables 17 and 18).
Univariate analyses determined that the use of the following judgement cue categories differed
across training group: eyebrow movements, cheek/nose movements, breathing patterns, and
timing of facial movements.
Post hoc analyses indicated that the training and training plus feedback groups identified
eyebrow movements more frequently then either the control or feedback groups (p < .01).
Movement of the cheeks or nose were identified most frequently by subjects in the training group,
with the remaining groups showing an equal frequency. Breathing patterns were identified more
frequently by the control (p < .01) and feedback groups (p < .05) than by subjects in the training
group. Subjects who received training.and feedback identified breathing patterns with moderate

Table 17
Results of M A N O V A on the Effects of Training Group on the use of Cue Type.
df F p<
Multivariate Results followed by Univariate F-tests
45, 312 2.84 .001
Eye Movements 3, 116 0.39 .757
Eyebrow Movements 3, 116 13.08 .001
Nose / Cheek Movements 3, 116 11.08 .001
Mouth Movements 3, 116 0.84 .475
Smiles 3, 116 2.76 .045
Repressed Expressions 3, 116 1.97 .122
Breathing Patterns 3, 116 5.36 .002
Incongruent Facial Actions 3, 116 4.14 .008
Pain Expressions 3, 116 0.31 .818
Timing 3, 116 6.50 .001
Blinking 3, 116 3.73 .013
Exaggerated Movements 3, 116 3.83 .012
Tension 3, 116 1.36 .259
Sudden Movements 3, 116 0.85 .471
Relaxed 3, 116 0.74 .528
Note. Bonferroni adjustments suggest a significance level of .003

84
Table 18
Mean Cue Type Use Across Training Group
Facial Action (AU) Control Feedback Training Train/Feed Facial Action (AU)
M SD M SD M SD M SD
Eyes 19.80 10.11 22.43 13.78 22.57 9.74 22.00 10.92
Eyebrows 3.40 3.47 2.60 2.58 8.70a>b 6.44 8.67a>b 6.29
Nasolabial 0.60 1.19 0.83 1.78 447a,b,d 4.42 1.93 3.13
Mouth 15.57 10.12 15.20 10.92 18.13 8.62 14.60 7:15
Smile 6.73 4.55 4.93 3.04 4.80 3.60 4.23 2.84
Repressed Actions 4.77 4.77 4.70 5.17 7.27 6.20 7.60 7.81
Breathing Patterns 8.97c 6.19 8.37C 9.56 3.13 4.73 4.77 5.03
Incongruent 1.00 1.36 0.37 0.93 2.00b 3.01 1.00 1.20
Pain Expression 3.30 4.91 3.33 5.59 2.60 3.49 2.50 3.00
Timing of Actions 0.97 1.43 0.73 1.62 2.90b 3.13 3.83^b 5.23
Blinking 4.20 3.63 3.67 3.68 5.67 4.92 7.23b 5.64
Exaggerated 4.70 3.92 4.00 4.01 6.37 5.24 7.70b 5.31
Tense 7.77 7.65 7.87 9.21 11.77 10.12 9.60 8.09
Sudden Movements 2.17 3.60 1.43 191 1.13 1.78 1.77 2.86
Relaxed 6.60 7.90 4.13 5.30 6.47 9.21 5.20 6.58
a Mean is significantly greater than control group
b Mean is significantly greater then feedback group
c Mean is significantly greater than training group
d Mean is significantly greater than training / feedback group

85
frequency, and did not differ significantly from the other three groups. The timing of facial
actions was identified as a judgement cue more frequently by the training plus feedback group
than by either the control or feedback groups (p < .01). Subjects in the training group identified
timing more frequently than the feedback group (p < .05), while not differing from either the
training plus feedback or control groups.
Individual Difference Variables
Pain Experience. In order to determine if subject's degree of experience with pain
influenced their ability to judge pain in others, subjects were asked about the their own incidence
of acute, recurrent and chronic pain, as well as about the pain experiences of their immediate
family. Results showed that 73.3% of subjects reported having experienced acute pain, with
subjects citing surgery, a broken bone, sports injuries and wisdom teeth as the most common
causes. Recurrent pain was experienced by 40.8% of subjects, with the most frequent causes
being headaches, stomach aches, ulcers, back pain and cramps. Chronic pain was the least
frequent pain experience, endorsed by only 19.2% of subjects. Chronic pain was most often due
to chronic back pain, sports injuries, broken bones and torn ligaments. With respect to their
family member's pain experiences, 65.8% of subjects stated that someone in their family had
experienced an acute pain episode, with surgery, broken bones and gallstones cited as the most
common causes. Recurrent pain had been observed in the families of 48.3% of subjects, most
often due to headaches and ulcers. Chronic pain was again the least commonly reported pain
experience, reported by 39.2% of subjects. Family members with chronic pain most often
suffered from chronic back pain. (See Appendix L).
An investigation of sex differences determined that females and males reported a similar
amount of experience with pain (selves and family) (t=l .67, p<098). Separating out the various
types of pain however, showed that fewer females (65.0%) than males (81.7%) reported having
an incident of acute pain (x 2 = 3.74, p< .05), while more females (53.3%) than males (28.3%)
reported experiencing recurrent pain {y} = 8.24, p< .004). The incidence of chronic pain was
comparable in females and males (21.7%) (x2 = 0.32, p<58), p< .04) With respect to their
family members' pain experiences, more females (56.7%) than males (40.0%) had observed a

86
family member suffering from recurrent pain {y} = 4.09, p< .04), while females and males
observed similar frequencies of acute (68.3%; 63.3%) and chronic pain ( 46.7%; 31.7%) within
their families.
A measure of overall pain experience was created by adding the number of pain
experiences endorsed by subjects, and correlation analyses were conducted to determine if overall
pain experience was related to subject's judgement accuracy, decision-making confidence or
ratings of pain intensity and unpleasantness. Results showed that general pain experience was not
significantly correlated with any aspect of the subjects' facial expression judgements. Performing
separate analyses for males and females yielded similar results (See Appendix M).
Empathy. Analyses were conducted to determine if there was a relationship between
subject scores on a multidimensional empathy measure and various aspects of facial expression
judgements: judgement accuracy, decision-making confidence, and ratings of pain unpleasantness
and intensity. It was predicted that the Perspective-taking subscale of the Interpersonal Reactivity
Index would correlate significantly with an individual's ability to detect deception, while the total
IRI score and other sub scale scores (Empathic Concern, Personal Distress and Fantasy) would
not be related to judgement accuracy. Results showed that the total empathy score and the
various subscales were not significantly correlated with either subjects' judgement accuracy,
decision-making confidence or ratings of unpleasantness and intensity (p > .05) (Appendix N).
In order to determine if there were sex difference with respect to the relationship between
empathy and facial expression judgements, correlation analyses were conducted separately for
male and female subjects. Results of the correlation analyses for female subjects paralleled the
overall analyses; neither the overall empathy scores nor the various subscale scores were
significantly correlated with judgement accuracy, decision-making confidence, or ratings of pain
intensity or unpleasantness. Correlation analyses for the male subjects, however, yielded a
different pattern of results. Total scores on the IRI, representing a general empathy score, were
found to be positively correlated with subjects' ratings of the unpleasantness of pain in the patients
facial expressions (p < .05). In addition, scores on the personal distress subscale were found to be
negatively correlated with subject's decision-making confidence (p < .05) and positively correlated
87
with the ratings of pain unpleasantness (p < .01). In general, males who described themselves as
more empathic rated other's pain experience as more unpleasant, however, their level of empathy
was unrelated to their judgement accuracy, decision-making confidence or their ratings of the
intensity of pain experienced. In addition, males who tend to experience feelings of anxiety and
unease in their own interpersonal interactions also rated other's pain experience as more
unpleasant. Interestingly, they also tended to have less confidence in their own ability to judge
other's facial expressions. The degree of personal distress experienced, however, was not related
to judgement accuracy or to ratings of pain intensity.
Comparison of Successful and Unsuccessful Judges
Further explanation for the individual differences in judgement accuracy was sought by
exploring the decision-making process of the most successful judges, those scoring 45% accuracy
or above. The comparison group for these analyses was comprised of eleven subjects whose
judgement accuracy was 32.5%, which is the median accuracy score, and is approximately equal
to the mean for all subjects (32.9%). The distributions of sexes were skewed in both groups;
Eight of the top nine judges were females, as were nine of the eleven subjects with average
judgement accuracies. The judgement variables chosen for the analysis included the total number
of cues used per decision, and the seven categories of facial expression cues whose use was found
to differ among training groups: eyebrow movements, cheek and nose movements, breathing
patterns, incongruent facial actions, blinking, timing of facial actions and exaggerated facial
actions. Results of the between subjects M A N O V A suggested that the groups did not differ
significantly with respect to these aspects of the decision-making process ( F = 1.36, p < .306).

88
Discussion
Describing Genuine and Deceptive Pain Expressions
The general purpose of the first study was to provide a comprehensive description of
genuine and deceptive pain expressions, including the frequencies and qualitative features of specific
facial actions, and relationships among them. This study was the first attempt to analyze genuine
and deceptive pain expressions using a more comprehensive version of the FACS coding system
which incorporates temporal coding. Results provided support for the position that the empirical
description of genuine and deceptive pain expressions could be enhanced by an investigation of the
temporal qualities of facial expressions.
Confirming past studies, genuine and deceptive pain expressions were found to differ in the
type, frequency, and intensity of facial actions. Deceptive and genuine pain expressions also
differed with respect to several temporal parameters, and there was support for the hypothesis that
temporal contiguity among facial action components would differ between genuine and deceptive
pain expressions. In contrast, results did not support the idea that facial cues thought to be
indicative of lying would be seen with increased frequency in deceptive facial expressions.
Frequency and Intensity of Pain-Related Facial Actions
Genuine Pain Expressions. Past research has identified several facial actions which are
consistently exhibited during genuine facial expressions of pain. These have included an increased
frequency of brow lowering, cheek raising, tightening of the eyelids, raising of the upper lip, parting
of the lips and eye closure (Craig et al., 1991; Prkachin & Mercer, 1989). In the present study,
genuine pain expressions exhibited a greater frequency of brow lowering and parting of the lips than
the neutral expression. However, cheek raising / eyelid tightening, nose wrinkle / upper lip raising,
and eye closure were exhibited with equal frequency in genuine pain and neutral expressions.
Previous research has also demonstrated that several pain-related facial actibns were exhibited at a
higher intensity in genuine pain expressions than in neutral expressions. Hadjistavropoulos and
Craig (1994), for example, identified cheek raising / eyelid tightening, nose wrinkle / upper lip raise
and mouth opening as more intense in genuine pain expressions. The current study also isolated
89
differences in the intensity of pain-related facial actions, with genuine pain showing an increased
intensity of brow lowering and nose wrinkle / upper lip raise.
Genuine facial expressions in the present study, then, were characterized by an increased
frequency and intensity of several pain-related facial actions identified in past research; however, the
facial displays did not include the full range of predicted facial actions. One explanation for the
reduced range of facial actions differentiating genuine and neutral conditions is that some of the
pain-related facial actions may also have been present in the neutral condition, possibly in
anticipation of the upcoming painful event. Facial expressions appear to change systematically
during painful events, with movements in the brow and eye area first evident, followed successively
by other facial actions (Prkachin & Mercer, 1989). The current finding that the neutral condition
did not differ in the frequency or intensity of pain-related movements in cheek raise / eyelid
tightening or eye closure, along with the finding that genuine facial displays consisted of a more
intense movement in the region of the nose and lips, suggests that neutral expressions may have
exhibited some anticipatory pain-related facial activity. Examination of the mean frequencies of
facial actions across conditions contradicts this interpretation, as neutral facial expressions did not
exhibit any pain-related facial actions other than mouth opening.
Another explanation for the reduced range of facial actions could be that the patients in the
current study did not find the range of motion procedures to be extremely painful. An approximate
comparison of the average intensity and unpleasantness scores to the Gracely descriptor terms
indicates that the range of motion exercises produced pain rated as "barely strong" in intensity and
"slightly distressing" in unpleasantness. Nevertheless, the fact that patients found the pain stimulus
only moderately painful does not account for the reduced range of facial actions during genuine
pain, as patients in the Hadjistavropoulos and Craig (1994) study reported the stimulus to be of
similar intensity, these patients, in comparison, exhibited a much fuller pain display. It is
interesting to note, however, that the patients in the two studies did differ when rating the intensity
and unpleasantness of their daily pain. Patients in the current study described their chronic pain to
be "barely strong" in intensity and "very unpleasant". In comparison, patients in the

90
Hadjistavropoulos and Craig (1994) study rated their daily pain as "strong" and "slightly
intolerable".
It is possible that a patient's past pain experience might influence his/her facial displays of
pain. Past research provides some support for this explanation. Patients whose pain problems have
had a greater psychological and physical impact on their lives have been shown to exhibit a greater
intensity and duration of pain-related facial actions in response to a painful stimulus (Prkachin &
Mercer, 1989). Although an increased intensity and unpleasantness of pain does not suggest
increased pain-related disability, there are reasons to believe that there may be similar effects on
facial expressions of pain. It seems reasonable to assume that patients who experience more intense
pain on a daily basis would approach the range of motion procedure with greater trepidation, for
fear of exacerbating their pain. Experiencing anxiety about pain has the effect of directing attention
to the pain experience, which in turn leads to stronger pain responses (Arntz, Dreesen &
Merckelbach, 1991). Research has also shown that the increased muscle tension caused by anxiety
can exacerbate musculoskeletal disorders, leading to increased pain nociception (Keefe & Gil,
1986). Similarly, experiencing pain as more unpleasant, may lead to increased negative affect in
response to future pain, which will, in turn, intensify the unpleasant affect and help to perpetuate the
pain (Eich, Rachman & Lopatka, 1990).
Faked Pain Expressions. Faked pain expressions in the present study were comprised of
many facial actions which have been identified as part of the "prototypical" genuine pain display. In
accordance with past research, some of these pain-related facial actions were exhibited with a
greater frequency or intensity than in the genuine pain expression. Two pain-related facial actions,
brow lowering and opened mouth, were seen with greater frequency in the faked pain expression
compared to the genuine pain expressions. Brow lowering was also exhibited at a higher intensity
in the faked pain expressions versus the genuine pain expressions. The remaining pain-related facial
actions were seen with equal frequency and intensity in the genuine and deceptive pain expressions.
Patients in the Hadjistavropoulos and Craig (1994) study produced faked pain expressions which
were more exaggerated than those found in the current study, with several other pain-related facial
actions appearing with greater frequency and intensity. Again, it is possible that a more negative or

91
intense history of pain could exaggerate one's deceptive pain display, due to differences in the
meaning and interpretation of pain.
The instruction to fake a pain display also led to an increased frequency of facial actions
which are not associated with genuine pain. Results showed that faked pain expressions exhibited
an increased frequency and intensity of one non pain-related facial action, brow raise. The
frequency and intensity of the remaining non pain-related facial actions investigated did not vary
across pain condition. These findings provided some support for the hypothesis that faked
expression may contain some "extra" facial actions that are not typical of a genuine facial
expression. These non pain-related facial actions may arise because the poser is not consciously
aware of what a genuine expression looks like on his/her face. It may also be a result of a person's
state or emotions while engaging in deception; for example, there may be individual facial actions
present which are usually associated with surprise or embarrassment. It is interesting to note that
the "extra" facial actions observed in this study, inner / outer brow raise, is a facial action typically
associated with the experience of fear or a startle response. If subjects were faking a pain
expression in response to an acute pain stimulus with rapid onset, one might expect elements of a
surprise or "startle" expression; however, when faking a response to a familiar pain stimulus which
causes an exacerbation of a chronic pain condition, "surprise" would not be an appropriate
response. This suggests that people may base their deceptive pain displays on reactions to acute
pain, which people have typically experienced and observed more frequently.
In general, patients were fairly good at fabricating a pain display, in that faked pain
expressions were, on the whole, appropriately comprised of pain-related facial actions. Based on
the amount of experience most people have with pain and pain behaviours, through their personal
experiences and observations of others, it is not surprising that pain expressions can be readily
assumed. The attempt to fake pain expressions was not wholly successful, however, as a number of
pain-related facial actions were seen more frequently and at a greater intensity than during the
genuine expression. This suggests that, even when asked to recreate a reaction to a very familiar
pain stimulus (physiotherapy exercises), people seem to have a difficult time reconstructing the pain

92
experience. It would be reasonable to assume, then, that people with less frequent and less recent
pain experience would have greater difficulties dissimulating pain.
Masked Pain Expressions. When asked to mask their pain expression during a painful leg
lift, patients were very successful at minimizing their pain display, as differences between the
masked pain and neutral expression were very subtle. Unlike the faked pain expression, the
masking form of deception did not result in any uniquely distinguishing facial features. Masked pain
expressions might best be described as being a midpoint between the genuine pain and neutral
expressions. When masking pain, patients exhibited a greater frequency of mouth opening than
during a neutral expression. In addition to mouth opening, there appears to be residual brow
lowering, as the frequency and intensity of this facial action in masked expressions did not differ
significantly either from the genuine or neutral expressions, while the latter two were significantly
different. This picture of masked pain expressions as a midpoint between genuine pain and neutral
expressions may represent the residual facial activity which "leaks out" when attempting to
neutralize a genuine pain display. This also suggests that there are subtle facial cues available which
would allow the sensitive observer to question a patient's reported lack of pain.
It was hypothesized that any differences in the masked and neutral conditions would consist
of activity in the eye region, which is thought to be more difficult to control. Although the presence
of residual brow lowering provides some evidence for "leakage" in the eye region, it is interesting to
note that the most significant difference between the masked and neutral conditions was increased
mouth movements. When making judgements of another's emotional state based on his/her facial
expressions, observers tend to attach more importance to movements in the area of the eyes and
upper face (Lee & Craig, 1991). When deceiving others, there may be a similar awareness that
greater effort should be expended to control movements around the eyes.
The theory that pain expressions change systematically during painful events may provide a
second explanation for the differences between the masked and neutral expressions. Prkachin and
Mercer (1989) suggest that brow lowering and eye closing will be the first facial actions to appear
in response to pain, followed by mid-face actions such as upper lip raise and nose wrinkling. The
final facial actions to appear would be mouth opening, followed by a horizontal stretching of the lips

93
during extreme pain. The increased frequency of mouth opening during masked pain suggests that
deceivers might exert a reasonable amount of control over their facial actions immediately, with a
gradual lessening of control as the urgency of the pain response decreases.
Individual Differences in the Facial Expression of Pain.
Past research has shown that there are large individual differences in the facial actions
observed in response to genuine pain. For example, only 45% of the subjects in one study
exhibited one Or both of the most common facial actions, brow lowering and closing of the eyes.
In the current study, the facial actions found to discriminate between genuine pain and neutral
facial expressions (brow lowering arid mouth opening) were exhibited by only 30% and 45% of
patients respectively. Some of the variations in pain expression have been related to personal
dispositions, with some people being generally impassive, and others very reactive (Craig, 1992).
Experimental studies have shown that subjects with a low pain tolerance exhibited more
expressive genuine pain displays, suggesting that personal pain thresholds also influence nonverbal
pain reactions (Galin & Thorn, 1993). Prkachin and Mercer (1989) found that patients whose
pain problem had a greater psychological and physical impact showed greater facial activity in
response to pain. Finally, pain interventions and coping strategies have substantial effects on self-
reports of pain, and may have a similar impact on facial expression, although this remains an
untested proposition.
Similar variables are thought to influence the ability to display deceptive pain expressions.
One such personality variable, role-playing ability, influenced the appearance of genuine and
deceptive pain displays, such that the intensity of faked pain expressions increased with role-
playing ability but was unrelated to the discriminability of the spontaneous and faked pain
expressions (Prkachin, 1992a). Similarly, subjects scoring higher on Pilowsky's general
hypochondriasis factor of the Illness Behaviour Questionnaire displayed genuine and faked pain
expressions which were less intense and harder to discriminate (Prkachin, 1992a). The single
study which related pain symptomatology to deception ability discovered that subjects who rated
the pain experienced as low intensity were better at masking their pain (Galin & Thorn, 1993). It

94
seems reasonable to suggest that many of the variables found to influence genuine pain
expressions would also influence the ability to present deceptive pain expressions.
Temporal Qualities of Deceptive Versus Genuine Pain Expressions
Another study hypothesis was that deceptive pain expressions would differ from genuine
pain displays in temporal qualities. Ekman and Friesen (1982) suggested that faked facial
expressions might have a shorter onset time, a longer period of peak intensity and a longer overall
response duration. Results of the present study partially support these findings. Faked pain
expressions were found to have an onset time, the length of time from facial action onset to peak
intensity, similar to that of genuine pain expressions. The findings on apex duration were more
complicated. Brow lowering had a longer peak intensity in the faked condition; however, there
were no differences in apex duration for the remaining pain-related facial actions. Finally, the
overall response duration of two pain-related facial actions in the faked pain expression (brow
lowering, mouth opening) was significantly longer than that of the genuine pain expressions. These
analyses suggest that, when expressions are faked, there is a tendency to exaggerate not only the
number and intensity of pain-related facial actions but also the length of peak intensity and the
overall length of the facial expression. An investigation of the temporal qualities of the second type
of deceptive pain display, masked pain expressions, further reinforces the subtlety of differences
among genuine pain and masked pain expressions. None of the temporal variables were found to
differentiate between the three expressions.
Another temporal quality of facial expressions which was of interest in the present study was
temporal contiguity, or the closeness with which facial actions appear together on the face.
Unfortunately, the available data did not allow for the full use of established clustering procedures
for facial expressions. Preliminary analyses, in which the non-occurrence of a facial actions was
coded with the group mean, yielded cluster analyses which must be interpreted with caution.
Results provided some support for study hypotheses, however, as pain-related facial actions
appeared together in two of four clusters based on onset times. In comparison, cluster analysis of
faked pain expressions yielded a four factor solution in which pain-related facial actions were
scattered throughout all four clusters. It seems then, that when asked to fake pain, people tend to

95
exhibit the component facial actions in more of a sequential manner than during genuine pain when
pain-related facial actions appear more closely together on the face. Again, it appears that the
temporal "errors" made when faking pain may arise because the poser is not consciously aware of
the timing of genuine pain expressions, and how facial actions appear on his/her face.
Incidence of Deception Cues in Deceptive versus Genuine Pain Expressions
The final analysis investigated the incidence of facial cues thought to be indicative of
deception: blinking, facial asymmetry and pulsating apexes. Researchers have suggested that
blinking rates will change during deception, either increasing due to an increase in general emotional
arousal (Ekman, 1985), or decreasing due to conscious efforts to control one's emotions. The
present study did not support either of these hypotheses, as blinking rates did not differ across pain
conditions. However, the issue of blinking as an indicator of deception in pain expressions is
complicated by the confusion regarding the incidence of blinking during genuine pain, as past
research has suggested both that blinking rates increase (Craig & Patrick, 1985; Patrick et al, 1986)
and decrease following pain (Craig et al, 1991; Prkachin, 1992b; Prkachin & Mercer, 1989).
Visual inspection of blinking frequency showed almost identical rates of blinking in neutral, genuine
pain, faked pain and masked pain expressions. It might be hypothesized that the unnatural
experimental situation, particularly the prospect of being videotaped, led to an increase in general
arousal which affected blinking rates across all pain conditions. Two other hypothesized deception
cues, facial action asymmetry and pulsating apexes, did not differentiate among neutral, genuine
pain, faked pain and masked pain expressions. Cues thought to be indicative of deception, then, did
not provide additional information to improve the detectability of deceptive and genuine pains
expressions.
Summary
The present study confirmed the hypothesis that increasing the comprehensiveness of FACS
coding to include temporal parameters of facial expressions would provide cues to improve our
description and discrimination of deceptive pain expressions from genuine pain expressions. This
investigation was the first to provide evidence that the facial actions presented during deliberately
dissimulated pain expressions show significantly different temporal patterns than do genuine pain

96
expressions. Patients were fairly good at fabricating a pain display, in that faked pain expressions
were appropriately comprised of pain-related facial actions. The attempt to fake pain expressions
was not wholly successful, however, as a number of pain-related facial actions were seen more
frequently and at a greater intensity than during the genuine expression. Faked pain expressions
were also found to remain at peak intensity longer, and last for a longer period of time. In addition,
pain-related facial actions did not seem to appear as closely together in time as did those exhibited
in a genuine pain expression. Faked pain expressions were also found to have a greater incidence of
facial actions unrelated to pain; in this case exhibiting brow raising, a movement often associated
with fear.
The differences between genuine pain expressions, masked pain expressions and neutral
expressions were much more subtle. Masked pain expressions might best be described as being a
midpoint between the genuine pain and neutral expressions, consisting of a greater frequency of
mouth opening than during a neutral expression, as well as some residual brow lowering. This may
represent facial activity which "leaks out" when attempting to neutralize a genuine pain display.
The results suggest that it would be very difficult to discriminate neutral and masked pain
expressions; however, there are subtle facial cues available which would allow the sensitive
observer to question a patient's reported lack of pain.
It is obvious that the temporal qualities of facial expressions provide information both when
patients are projecting pain they don't feel, and when they are attempting to mask a genuine pain
experience. Further research is needed to determine the level of discrimination among the pain
conditions that these additional cues will provide. The aim of the second study was to determine if
observers' judgement skills could be improved by increasing their knowledge and awareness of the
various cues to deception elicited in the present study.
Detecting Genuine and Deceptive Pain Displays
The purpose of the second study was twofold: (1) to determine if there are individual
differences in the ability to detect deceptive pain displays and (2) to determine if people's ability to
detect faked or masked pain can be improved through the use of various training strategies. The
present study was the first to investigate individual differences in the judgement of deception in

97
pain patients, by comparing successful and unsuccessful judges on variables postulated to
influence the decision-making process. Results indicated that there were significant individual
differences in judgement accuracy, ranging from accuracy levels well below chance to a 63%
accuracy level, when the base rate was 25%. However, none of the decision-making variables
explained the differences between good "lie detectors" and average judges.
The training program used in the current study was based on the various cues to deception
elicited in the first study, and attempted to increase the breadth and acuity of judges' decision
making procedures. Subjects receiving training, corrective feedback or training plus feedback
were compared to one another and to a control group of naive observers on their ratings of the
intensity and unpleasantness of pain experienced by the patient, as well as accuracy of detecting
deception. Results indicated that providing corrective feedback led to significant improvements in
detection accuracy across all types of pain expressions. In contrast, an information-based training
program was ineffective, as the average judgement accuracy of this group was no better than that
of control subjects.
Judgements of Intensity and Unpleasantness
In previous research, judges were largely fooled by patients' attempts to fake their pain,
and consistently attributed more pain to the faked pain faces than to the genuine and masked pain
faces (Poole & Craig, 1992). In the present study, judges attributed more pain to the genuine
pain expressions than they did to the faked pain expressions, despite the fact that the faked pain
expressions were shown to be comprised of an equal, if not greater frequency and intensity of
pain-related facial actions in study one. Using the DDS descriptor terms closest to the mean
ratings observed, subjects rated genuine pain to be "moderate" in intensity and "unpleasant", while
faked pain displays were describes as "moderate" and only "slightly annoying". Obviously,
subjects were not fooled by the faked pain display, in that they did not equate a stronger pain
display with either increased intensity or unpleasantness. Subjects rated the faked pain
expressions to be equal in pain intensity and unpleasantness to the masked pain expressions. It
would seem that while the judges did not believe the exaggerated pain displays, neither were they
comfortable stating that the patient was experiencing no pain.

98
Similar to the judges in the Poole and Craig (1992) study, judges in the current study rated
the pain intensity and unpleasantness of masked pain expressions to be greater than the neutral
facial expressions, but less than that of the genuine pain expressions. The descriptor term
equivalents for their ratings were "moderate" intensity and "slightly annoying" for the masked pain
expressions, while neutral expressions were rated to be of "very weak" intensity and only "slightly
unpleasant". These results suggest that subjects were able to discern some pain in the masked
pain expressions, an impressive distinction given the relative scarcity of facial actions which
differentiated the three expressions in the FACS analysis.
For the neutral, masked pain and genuine pain expressions, subjects' ratings of pain
intensity and unpleasantness roughly corresponded to the frequency and number of pain related
facial actions isolated through FACS coding of the facial expressions. While rating the faked pain
display, however, they did not equate a stronger pain display with either increased pain intensity
or unpleasantness. One way to clarify the way in which subjects' judgements of genuine pain and
faked pain differed would be to determine which cues helped them to make their decisions
regarding pain intensity and unpleasantness. Further analyses could look at the FACS coding of
patients' genuine and deceptive pain expressions in order to determine which cues or combination
of cues best predicted subjects' pain ratings.
Compared to the judges in the Poole and Craig (1992) study, therefore, subjects were less
likely to be fooled by patients' attempts to fake their pain experience. The increased accuracy of
pain judgements in the current study may be explained by the explicit focus on detecting
deception. The awareness of deception alone should not account for the increased accuracy in
ratings of faked pain. Past research has shown that "priming" a subject to expect deception does
not increase his/her accuracy, but instead leads to a decreased willingness to attribute pain to both
genuine and deceptive pain expressions (Poole & Craig, 1992). Nonetheless, the improved
accuracy cannot be attributed to detection training, as there were no differences in judgements of
pain intensity or unpleasantness between the control group and any of the training groups.
Finally, different study methodologies might account for the difference in results between the two
studies. For example, it is possible that being asked to identify the facial cues they used to make
99
their judgements might have influenced the decision-making process Of subjects in the current
study.
Discrimination of Genuine and Deceptive Pain Expressions
When asked to categorize observed facial expressions as neutral, genuine pain, faked pain
or masked pain, judges' average judgement accuracy was 32.9%, with their accuracy for neutral
expressions being significantly higher than that for any of the three pain expressions. In fact, the
categorization of neutral facial expressions was the only expression identified at higher than
chance levels. This may, in part, be explained by subjects' tendency to overuse the neutral
expression category. Judges were not informed that all four expressions were presented for each
patient, and they identified expressions as neutral more frequently than other categories. Subjects'
tendency to use the neutral category excessively suggests that the patients' facial expressions often
did not provide much information with which to make a decision. Past research, which has
established that people have a general tendency to underestimate patients' reports of pain (Lander,
1990), may also help to explain an increased likelihood of rating a facial expression as neutral.
It is interesting to note that subjects' perceived judgement accuracy mirrored their actual
judgement accuracy. Judges felt that they were most accurate at identifying neutral expressions,
with the three pain expressions identified much less accurately. Although the relative detection
accuracies of the various facial expression types was correct, their perceived accuracy was twice
that of their actual judgement accuracy for all four facial expression categories.
Past research has shown little evidence for a relationship between subjects' overall
confidence in their detection ability and their actual overall detection accuracy (DePaulo &
Pfeiffer, 1986; Kohnken, 1987). Based on the assumption that subjects would presumably predict
some "deceivers" better than others, the present study looked at subjects' decision-making
confidence for each individual case. Results showed that judges were most confident in their
ability to detect neutral and faked pain expressions, followed by judgements of genuine pain, with
decisions about masked pain expressions being the least confident. Overall, subjects were overly
confident in their judgement ability, suggesting that they did not fully appreciate the difficulty of
the judgement task.

100
It is interesting to note that although subjects' perceived accuracy ratings suggest that they
were aware that their judgement of faked expressions was less accurate then that of neutral
expressions, on an individual case basis, they were equally confident in neutral and faked
expressions. This divergence between decision-making confidence and judgement accuracy
across pain conditions may be explained by the clarity of decision-making strategies subjects use
for each pain condition. Similar to the current study, subjects in Hadjistavropoulos et al's (1996)
study reported greater overall decision-making confidence for neutral and faked pain expressions
compared to genuine and masked pain expressions. An investigation of the facial cues which
were present on the patients' faces when subjects rated expressions as neutral, genuine, masked or
faked pain allowed investigators to describe the decision-making strategies used for each
condition. Judges were found to have well defined strategies for making decisions of faked pain
or neutral expressions, while they had less well defined methods of identifying the genuine and
masked pain conditions. It is iniportant to note, however, that the Hadjistavropoulos et al (1996)
results describe cues which were present on the face when certain judgements were made;
therefore, it does not necessarily identify the cues actually used by the judges, nor did it answer
the question of whether judges would be able to articulate their decision-making strategies.
In the current study, judges were asked to describe the facial cues they used to make each
judgement, providing the first in-depth investigation of subjects' actual decision-making process.
Results indicated that subjects identified a greater number of facial cues in the faked and genuine
facial expressions than in either the masked or neutral expressions. Although the first study
determined that faked pain expressions were comprised of a greater frequency and intensity of
facial actions than genuine pain, subjects in the current study reported using the same number of
facial cues to identify faked and genuine pain expressions. Study methodology may account for
this result, as subjects were asked to list the cues they used in their judgements rather than being
asked to list all cues available on the face. Subjects also identified more facial cues in the masked
pain expression than in the neutral expression, which suggests that observers could perceive the
very subtle facial cues which differentiated the masked pain and neutral facial expressions in the
first study. In general, comparing these results to the FACS description of patients' pain

101 expressions suggests that subjects were fairly perceptive in identifying and reporting the
quantitative increase in facial expressions corresponding to neutral, masked, genuine and
faked pain expressions.
A comparison of the facial cues subjects identified with the various pain
expressions and the facial actions which actually comprise the various expressions
provides some information on the efficiency of subjects' decision-making process. For
example, in the first study, brow lowering was found to occur more frequently in genuine
and masked pain expressions than in neutral expressions, with faked pain expressions
showing the greatest frequency of brow lowering. The subjects' use of brow lowering as
a facial cue in judging facial expressions shows a similar pattern. Brow lowering was
identified as a facial cue most frequently when subjects rated a facial expression as faked,
followed by genuine and masked pain expressions, with brow lowering being identified
as a cue less frequently in the neutral expression than in the genuine pain expression. The
use of brow raise, a non pain-related facial action also showed a pattern similar to that
seen in the actual facial expressions. Subjects use of cues which were empirically shown
not to differentiate among pain conditions was less accurate. Eye closure was correctly
used with equal frequency when judging the various pain conditions, however, other
facial actions, such as eye squint and tight lips were identified with progressively greater
frequency in neutral, masked, genuine and faked pain expressions. In general then, it
seems that in many cases, subjects may have made their judgements based on the number
of facial actions they perceived.
The Effects of Training on Facial Expression Judgements
Results of the second study provided partial support for the position that
deception training would improve detection of the various types of facial expressions. As
opposed to studies in the general deception field (Kohnken, 1987; Zuckerman et al.,
1985), providing corrective feedback led to significant improvements in detection
accuracy. Subjects in the feedback group showed a significantly greater judgement
accuracy than either control group or training group subjects, and the advantage of
feedback appeared to be maintained across all types of pain expressions, unlike the
102
Galin and Thorn (1993) study, where feedback subjects were more accurate than control subjects
only when identifying faked and genuine pain expressions.
Changes in the feedback procedure may account for the increased utility of feedback as a
training strategy. As opposed to studies in the deception and pain fields (Galin & Thorn, 1993;
Kohnken, 1987; Zuckerman et al., 1985), the current study used immediate rather than delayed
feedback; therefore the information was more salient to the judgement task and allowed subjects
to improve their detection technique on a case by case basis. In addition, when provided with
feedback, subjects were not simply informed whether or not their judgements were correct.
Instead, they were told precisely which type of face was being depicted in each video clip.
Therefore, subjects in the current study were provided with more information than typical of past
feedback paradigms. As a result, subjects were given an opportunity to compare the faces
associated with the different pain categories. Results would suggest that subjects were then
successful at abstracting unique cues associated with the different pain conditions. These results
suggest that immediate feedback is more effective than the delayed feedback used in past studies,
and suggests that with detailed information, judges can be made aware of the decision-making
cues which have or have not been effective for them in their judgement task and can benefit from
this information.
In contrast, results of the present study did not provide support for an information-based
training program, as the average judgement accuracy of this group was no better than that of
control subjects. There was also no support for the possibility of additive effects of providing
both training and corrective feedback, as the feedback only group performed equally well. Thus,
a training program providing detailed information about the cues that would facilitate the
discrimination between the categories of facial expressions was not effective in the absence of
opportunities to carefully inspect the faces and deliberate upon the usefulness of the various cues
available. As well, the training program did not enhance the successful discriminations that could
be made on the strength of feedback alone. It is likely that the feedback condition was sufficiently
instructive that the information provided by the training program could add little to that which
103
could be learned through inspecting instances of the various expressions and receiving corrective
feedback.
Several aspects of the decision-making process were investigated in an attempt to explain
the relative superiority of subjects in the feedback groups. For example, it was hypothesized that
more effective judges would report the use of both a greater number of facial cues and different
types of facial cues in making their decisions. However, despite their greater accuracy, subjects in
the feedback group believed they used the same number of facial cues as subjects in any of the
other training groups. A comparison of the training groups' reported cue use shows that the
feedback group did not identify any unique facial cues not used by the remaining groups. In
particular, the types of cues reported by subjects in the feedback group did not differ significantly
from those reported by the control group, which suggests that the cues reported by the feedback
subjects were also those used intuitively by naive judges. As the judgement accuracies of the two
groups were significantly different, subjects' reported cue use does not explain the relative
superiority of the feedback group. It is possible that feedback subjects may not have been able to
perceive and/or articulate their decision-making strategies. It is also possible that although the
two groups used similar facial cues, these cues either assumed a different meaning for the
feedback group, or were used more effectively. In order to answer these questions, subjects'
judgements and their reported cue use would have to be directly compared to the facial cues
available in the patients' various expressions.
The poor performance of subjects in the training groups was not due to their inability to
learn and retain the material presented in the training package, as scores on a training test were
fairly high. In addition, an examination of the types of cues reported by the training groups
suggests that they actively used the information presented in the training manual. For example,
subjects in the training groups reported the greatest use of pain-related facial cues, such as brow
lowering, eye closure, eye squinting, nose / cheek movements. Other cues to deception
presented in the training manual were also identified more frequently by the training groups, such
as exaggerated facial actions, and the timing of facial actions. It is also interesting to note that the
feedback and control groups used only one type of detection cue, breathing patterns, more

104
frequently than the groups which received training. Breathing patterns, a detection cue not
included in the training package, and therefore disregarded by subjects in the training groups,
could then be considered to be used intuitively.
Compared to the feedback group, the treatment group reported an increased frequency of
the following facial cues: eyebrow movements, nose / cheek movements, incongruent facial
actions, temporal cues, and lowered eyebrows. Compared to the feedback group, the treatment
plus feedback group reported using an increased frequency of the following facial cues: eyebrow
movements, temporal cues, blinking, exaggerated movements, eye squint, and lowered eyebrows.
The training group differed from the training plus feedback only in an increased use of nose/cheek
movements and lowered eyebrows. It appears that, when given the chance to deliberate upon the
usefulness of cues presented in the training program, subjects in the training plus feedback group
decreased their reported use of nose/cheek movements and lowered eyebrows. It is interesting to
note that nose/cheek and lowered eyebrow movements helped to differentiate faked pain
expressions from genuine, masked and neutral expressions in study one, while lowered eyebrows
helped to differentiate genuine pain expressions from neutral expressions. Perhaps it was difficult
to perceive the difference in frequency of these variables among faked, genuine and masked pain
expressions.
Individual Differences in Judgement Accuracy
Despite the discouragingly low level of judgement accuracy observed in the current study,
it would be misleading to conclude that subjects were unable to discriminate genuine and
deceptive pain displays, as there were substantial individual differences in judgement accuracy.
Judgement accuracy ranged from a dismal 18% to 63%; which is an impressive four standard
deviations above the mean. There was a fair amount of variation in subjects' ability to identify the
various expressions, with 22 subjects scoring a standard deviation below the mean, and 16 scoring
higher than one standard deviation above the mean. The finding of substantial individual
differences in detection accuracy corroborates findings in the general deception literature (Ekman
& O'Sullivan, 1991), but is in opposition to the lack of variation in the recent Hadjistavropoulos et
al (1996) study. This discrepancy could easily be an artifact of the forced choice design used in
105
the latter study. Several variables were investigated in order to explain the variation in accuracy
scores found in the current study.
Sex Differences. Unlike past research (Poole & Craig, 1992), the current study found
significant sex differences in the ability to detect deceptive facial expressions of pain, with female
judges having a significantly higher overall accuracy level than males across all facial expression
types. It is difficult to explain the observed sex difference in judgement accuracy, however, as
there were no gender differences in the other facial expression judgements. For example, males'
and females' ratings of the pain intensity and unpleasantness exhibited in patients' facial expression
were similar across all four types of facial expression, therefore, gender differences in accuracy
were not due to differences in the ability to perceive a quantitative degree of "distress" in facial
expressions. It is also interesting to note that there were no gender differences in subjects'
subjective ratings of their own performance. Despite females' greater judgement accuracy, males
and females did not differ with respect to their confidence in their categorization of facial
expressions, nor did their perception of their overall accuracy differ.
The observed sex differences in judgement accuracy were also unrelated to any of the
decision-making process variables included in the study. For example, the lack of interaction
effects between sex and training group indicates that there were no gender differences in the
ability to benefit from the various training approaches. With respect to the use of facial cues, the
Hurd and Noller (1988) study suggested that females use a slower, cue-based decision-making
approach, while males used a quicker, intuitive approach and reported fewer cues, results which
contradict Buck's (1984) theory. In the present study, males and females reported using the same
number of cues during their judgement process. There was also no significant difference in the
type of facial cues identified by males and females. The current study then, provides no support
for the idea that men and women differ in their use of an intuitive versus cue-based decision
making approach. Nevertheless, men and women did differ in their detection ability. It is
possible, therefore, that while there were no gender differences in the perception of facial cues,
males and females might differ in their interpretation of facial movements.

106
Popular stereotypes portray women as being more sensitive, more understanding, and
more aware of others' feelings (Hall & Briton, 1993). Research has isolated gender differences in
the area of emotional expression which support stereotypes of nonverbal behaviour. Survey data
has shown that women are believed to use more expressive and involved nonverbal behaviours
than men, and to be more skilled at both sending and receiving nonverbal messages (Briton &
Hall, 1995). Observational studies have generally confirmed people's perceptions of gender
differences in nonverbal behaviour. Women were found to be more alert to nonverbal behaviour
in general (Hall, 1984), and were better able to decode nonverbal cues of emotion (Hall, 1978;
Hall, 1984; Costanzo & Archer, 1989). The process by which females become better encoders
and decoders of nonverbal behaviour is unclear; however, it is thought that gender role
socialization plays an important role. In Western cultures, girls and women are encouraged to be
emotionally expressive, while boys are often taught to suppress their emotions. As a result, men
may learn that the nonverbal communication of emotion is relatively unimportant, while for
women nonverbal behaviours may merit a greater focus of attention (Briton & Hall, 1995).
Pain Experience & Empathy. It was hypothesized that subjects who had more personal
experience with various types of pain, or who had observed pain more often in others might be
more accurate in their judgements of deceptive and genuine pain. Results did not support this
hypothesis, nor was there any relationship between pain experience and subjects' ratings of pain
intensity and unpleasantness.
It was also thought that individuals high in empathy might be better "lie detectors", as the
concept of empathy suggests not only an emotional identification with others, but also an
increased social acuity. A multidimensional measure of empathy, the IRI, which includes a person
perception type subscale was used to correlate various aspects of empathy with judgements of
pain. Results of the correlation analyses for female subjects paralleled the overall analyses; neither
the overall empathy scores nor the various subscale scores were significantly correlated with
judgement accuracy, decision-making confidence, or ratings of pain intensity or unpleasantness.
Correlation analyses for the male subjects, however, yielded a different pattern of results. In
general, males who described themselves as more empathic rated others' pain experience as more

107
unpleasant; however, their level of empathy had no effect on their judgement accuracy, decision
making confidence or their ratings of the intensity of pain experienced. In addition, males who
tend to experience feelings of anxiety and unease in their own interpersonal interactions also rated
others' pain experience as more unpleasant. Interestingly, they also tended to have less confidence
in their own ability to judge others' facial expressions. The degree of personal distress
experienced, however, was not related to judgement accuracy or to ratings of pain intensity.
Comparison of Successful and Unsuccessful Judges. Further explanation for the individual
differences in judgement accuracy was sought by comparing the decision-making process of the
most successful judges, those scoring 45% accuracy or above, and those subjects whose
judgement accuracy was at the mean/median for all subjects (32.5%). The distribution of sexes
were skewed in both groups; Eight of the top nine judges were females, as were nine of the
\ eleven subjects with average judgement accuracy's. The decision-making process for these two
groups did not differ either in the number or type of facial cues reported.
Summary
In the current study, subjects' ratings of pain intensity and unpleasantness roughly
corresponded to the frequency and number of pain-related facial actions isolated through FACS
coding of the facial expressions. While rating the faked pain display, however, they did not
equate a stronger pain display with either increased pain intensity or unpleasantness. Unlike the
subjects in Poole and Craig's (1992) study, then, subjects in the current study were not fooled by
the faked pain display. However, when asked to categorize facial expressions as neutral, genuine
pain, faked pain or masked pain, the judges' accuracy levels were disappointingly low, averaging
only 32.9% when the base rate would have been 25%. However, it would be misleading to
conclude that subjects were unable to discriminate among genuine and deceptive pain displays, as
there were significant differences in judgement accuracy, ranging from 18.0 to 63.0%.
Several variables were analyzed in an attempt to explain the wide variation in judgement
accuracy, however, accuracy was unrelated to either the number or type of reported facial cues
used, the subjects previous pain experience or their empathy scores on the IRI. Females'

108
judgement accuracy was significantly higher than males' accuracy, but again, there were no sex
differences in any of the decision-making process variables measured.
Results of the study provided partial support for the position that training would improve
detection of the various types of facial expressions. Providing immediate, rather than the delayed
feedback used in past research, led to significant improvements in subjects' detection accuracy. It
would appear that, when given the opportunity to compare the faces associated with the different
pain categories, subjects became aware of the decision-making cues which have or have not been
effective for them and can benefit from this information. In comparison, there was no support for
an information-based training program. Once again, the number and type of facial cues used in
the decision-making process of teh feedback group did not differ from that of the control group,
suggesting that while feedback subjects used only the cues used intuitively by naive judges, they
may have assumed a different meaning or simply have been used more effectively.
Future Directions
In general, future research needs to further explore individual differences in: a) people's
ability to deceive others through facial expression, and b) people's ability to detect deception. The
first study increased the comprehensiveness of the current description of genuine and deceptive
pain displays by incorporating temporal parameters, as well as an analysis of the frequency and
intensity of pain-related and non pain-related facial actions. The study did not analyze the
difference in these parameters between patients who were good deceivers and those who were
bad deceivers, nor did it investigate pain history variables as a possible predictor of deception
ability. It would be interesting to know what makes a patient more accurate at posing a pain
display, and therefore more difficult to detect. Do they experience less pain-related worry and
emotionality? Do their strategies for coping with pain differ? For example, if someone tends to
cope with pain by ignoring it, are they better able to mask their pain expressions? If someone
tends to exhibit considerable pain behaviour in an attempt to communicate their distress, will their
faked pain expressions be more exaggerated? It would also be interesting to look at faked pain
expressions which were successful to see how closely the FACS coding approximates genuine
pain expressions on the various parameters: frequency, intensity and temporally.

109
With respect to the ability to detect deception, further research is needed to investigate the
decision-making strategies which differentiate successful versus unsuccesful detectors. Reported
cue use did not provide any information which would help explain the superiority of females'
judgement accuracy or that of the feedback group. It seems likely that while they report using the
same facial cues, they may be using them in a more effective manner. A comparison of empirical
prediction using FACS coding, and the clinical prediction of judges might allow us to determine
whether judges were using the available facial cues efficiently.
Finally, the present study indicated that the use of deception training in the form of
corrective feedback can improve subjects' detection accuracy. The improvement in accuracy was
fairly small, and might not be considered clinically significant, but must be evaluated in light of the
short duration of training. It would be of clinical interest to determine if greater exposure to
genuine and deceptive facial expressions using a corrective feedback approach would lead to
further gains in judgement accuracy.
In general, the current study determined that there is information in facial expressions
which may be useful to observers when assessing the credibility of pain experiences, and that one
can improve the detection skills of naive judges by increasing their awareness of available facial
cues. However, this research did not provide an explanation for the significant individual
differences in either people's ability to pose deceptive facial expressions and their ability to detect
deception. These questions are of considerable clinical interest and importance, and point to a
potentially productive area of research.
Limits to Generalizability
Past research has shown that clinicians use nonverbal information to form clinical
judgements during pain assessments. The current study helped to clarify the decision-making
process that judges use when assessing pain experience through facial expression, and provided
support for the position that training would improve the detection of deception. When given the
opportunity to compare genuine and deceptive pain expressions, subjects became aware of the
decision-making cues which have or have not been effective for them and were able to benefit
1 1 0
from this information. However, several factors impede the generalizability of these results to a
clinical setting.
First, judgement accuracy in the current study was generally low, suggesting that one
cannot confidently make decisions regarding the veracity of pain reports based solely on facial
expression. In addition, the significant individual differences in pain expressions suggest that
training judges to use consistent "rules" for detecting deception through facial expression would
not be appropriate
Second, the information on genuine and deceptive facial expressions obtained in this study
was collected in a clinical setting, but were subject to artificial conditions, such as videotaping,
which may have influenced the patients' pain presentations. Similarly, the judgement task used in
the current study focused solely on facial expression, and differed significantly from the judgement
task of a clinician. Clinicians have many sources of information available to them when
conducting pain assessments, including medical records, self-report and nonverbal cues. As a
result, deception cues based on facial expressions would be weighed against the remaining
available information. The purpose of the current study was to determine how one could improve
a judge's use of one type of deception cue available. Additional research is needed to determine
the process by which judges combine information from the various modalities during clinical
decision-making. Furthermore, the need to construct validated protocols for enhancing the
accuracy of detection precludes the direct application of these findings to clinical settings at this
time.

I l l
References
Arntz, A., Dreessen, L. & Merckelbach, H. (1991). Attention, not anxiety, influences pain. Behaviour Research and Therapy. 29. 41-50.
Benton, A.L. (1980). The neuropsychology of facial recognition. American Psychologist. 35. 176-186.
Bernstein, W.M. & Davis, M.H. (1982). Perspective-taking, self-consciousness and accuracy in person perception. Basic and Applied Social Psychology. 3. 1-19.
Boucher, J.D. (1969). Facial displays of fear, sadness and pain. Perceptual and Motor Skills. 28. 239-242
Briton, N.J. & Hall, J.A. (1995). Beliefs about female and male nonverbal communication. Sex Roles. 32. 79-90.
Buck, R. (1984). The communication of emotion. New York: Guildford Press.
Cacioppo, J.T. & Petty, R.E. (1981). Lateral asymmetry in the expression of cognition and emotion. Journal of Experimental Psychology: Human Perception and Performance. 7. 333-341.
Chlopan, B E , McCain, M L . , Carbonell, J L . & Hagen, R.L. (1985). Empathy: Review of available measures. Journal of Personality and Social Psychology. 48. 635-653.
Clark, K.B. (1980). Empathy: A neglected topic in psychological research. American Psychologist. 35. 187-190.
Costanzo, M . & Archer, D. (1989). Interpreting the expressive behaviour of others: The Interpersonal Perception Task (IPT). Journal of Nonverbal Behaviour. 13. 225-245.
Craig, K.D. (1986). Social modeling influences: Pain in context. In R.A. Sternbach (Ed.), The psychology of pain. New York: Raven Press.
Craig, K.D. (1992). The facial expression of pain: Better than a thousand words? American Pain Society Journal. 1. 153-162.
Craig, K.D. (1994). Emotional aspects of pain. In P.D. Wall & R. Melzack (Eds.) Textbook of pain. 3rd edition. Edinburgh: Churchill-Livingstone.
Craig, K.D., Hyde, S. & Patrick, C.J. (1991). Genuine, supressed, and faked facial behaviour during exacerbation of chronic low back pain. Pain, 46, 161-172.
Craig, K.D. & Patrick, C.J. (1985). Facial expression during induced pain. Journal of Personality and Social Psychology. 48. 1080-1091.

112
Craig, K D . & Prkachin, K . M . (1980). Social influences on public and private components of pain. In I.G. Sarason and C. Spielberger (Eds.), Stress and anxiety. ("Vol. 7). New York: Hemisphere.
Craig, K.D. & Prkachin, K . M . (1983). Nonverbal measures of pain. In R. Melzack (Ed.), Pain measurement and assessment. New York: Raven Press.
Craig, K.D., Prkachin, K . M . & Grunau, R.V.E. (1992). The facial expression of pain. In D.C. Turk & R. Melzack (Eds.). Handbook of pain assessment. New York. Guilford Press.
Crook, J., Rideout, E . & Brown, G. (1984). The prevalence of pain complaints in a general pain population. Pain. 18.299-314.
Davis, M . (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology. 10. 85.
Davis, M.H. (1983). Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of Personality and Social Psychology, 44. 113-126.
DePaulo, B M . & Pfeifer, R.L. (1986). On the job experience and skill at detecting deception. Journal of Applied Social Psychology. 16. 249-267.
DePaulo, B.M. , Rosenthal, R., Eisenstat, R.A., Rogers, P.C. & Finkelstein, S. (1978). Decoding discrepant nonverbal cues. Journal of Personality and Social Psychology. 36. 313-323.
Eich, E . , Rachman, S. & Lopatka, C. (1990). Affect, pain and autobiographical memory. Journal of Abnormal Psychology. 99. 174-178.
Ekman, P. (1980). Facial asymmetry. Science. 209. 833-834.
Ekman, P. (1985). Telling lies: Clues to deceit in the marketplace, marriage and politics. New York: Norton.
Ekman, P. & Friesen, W. V. (1969). Nonverbal leakage and clues to deception. Psychiatry. 32. 88-105.
Ekman, P. & Friesen, W.V. (1974). Detecting deception from the body or face. Journal of Personality and Social Psychology. 29. 288-298.
Ekman, P. & Friesen, W.V. (1978a). Investigator's guide to the Facial Action Coding System. Palo Alto, CA: Consulting Psychologists Press.
Ekman, P. & Friesen, W.V. (1978b). Manual for the Facial Action Coding System. Palo Alto, CA: Consulting Psychologists Press.

113
Ekman, P & Friesen, W.V. (1982). Felt, false and miserable smiles. Journal of Nonverbal Behavior. 6. 238-249.
Ekman, P. & Friesen, W.V. (1983). EMFACS: Coders instructions. Unpublished manuscript, University of California, Human Interaction Laboratory, San Francisco, CA.
Ekman, P., Friesen, W. V., & O'Sullivan, M . (1988). Smiles when lying. Journal of Personality and Social Psychology, 54, 414-420.
Ekman, P., Friesen, W.V., O'Sullivan, M . & Scherer, K. (1991). Invited article: Face, voice and body in detecting deceit. Journal of Nonverbal Behavior. 15. 125-135.
Ekman, P., Hager, J.C. & Friesen, W.V. (1981). The symmetry of emotional and deliberate facial actions. Psychophysiology. 18. 101-106.
Ekman, P., & O'Sullivan, M . (1991). Who can catch a liar? American Psychologist, 46. 913-920.
Faust, D., Hart, K.J., Guilmette, T.J. & Arkes, H R . (1988). Neuropsychologists' capacity to detect adolescent malingerers. Professional Psychology: Research & Practice. 19. 508-515.
Fridlund, A.J. (1991). Evolution and facial action in reflex, social motive, and paralanguage. Biological Psychology. 32. 3-100.
Friesen, W.V. (1982). Program for integrating FACS scoring ('CLUSTER''). Unpublished manuscript, University of California, San Francisco, CA.
Galin, K.E . & Thorn, B.E. (1993). Unmasking pain: Detection of deception in facial expressions. Journal of Social and Clinical Psychology. 12. 182-197.
Gracely, R., Dubner, R. & McGrath, P. (1979). Narcotic analgesia: Fentanyl reduces the intensity but not the unpleasantness of painful pulp sensations. Science. 203, 1261-1263.
Gracely, R., McGrath, P. & Dubner, R. (1978a). Ratio scales of sensory and affective verbal pain descriptors. Pain. 5. 5-18.
Gracely, R., McGrath, P. & Dubner, R. (1978b). Validity and sensitivity of ratio scales of sensory and affective verbal pain descriptors: Manipulation of affect by diazepam. Pain. 5, 19-29.
Hadjistavropoulos, H.D. & Craig, K.D. (1994). Acute and chronic low back pain: Cognitive, affective and behavioral dimensions. Journal of Consulting and Clinical Psychology. 62. 341-349.
Hadjistavropoulos, H.D., Craig, K.D., Hadjistavropoulos, T. & Poole, G.D. (1996). Subjective judgments of deception in pain expression: Accuracy and errors. Pain. 65. 247-254.

114
Hager, J.C. & Ekman, P. (1985). The asymmetry of facial actions is inconsistent with models of hemispheric specialization. Psychophysiology, 22. 307-318.
Hall, J.A. (1978). Gender effects in decoding nonverbal cues. Psychological Bulletin. 85, 845-857.
Hall, J.A. (1984). Nonverbal sex differences: Communication accuracy and expressive style. Baltimore, MD: John's Hopkins University Press.
Hall, J.A. & Briton, N.J. (1993). Gender, nonverbal behavior and expectations. In P.D. Blanck (Ed) Interpersonal expectations: Theory, research and applications.
Heller, W. & Levy, J. (1981). Perception and expression of emotion in right-handers and lefthanders. Neuropsychologia. 19, 263-272.
Hogan, R. (1969). Development of an empathy scale. Journal of Consulting and Clinical Psychology. 33. 307-316.
Holland, M.K. & Tarlow, G. (1972). Blinking and mental load. Psychological Reports. 323. 119-127.
Holland, M.K. & Tarlow, G. (1975). Blinking and thinking. Perceptual and Motor Skills. 41. 403-406.
Hurd, K., & Noller, P. (1988). Decoding deception: A look at the process. Journal of Nonverbal Behavior. 12. 217-233.
Izard, C.E. (1990). Facial expression and the regulation of emotions. Journal of Personality and Social Psychology. 58. 487-498.
Jacox, A.K. (1980). The assessment of pain. In L. Smith, H. Merskey & S. Grass (Eds.). Pain, meaning and management. New York: Spectrum.
Johnson, M . (1977). Assessment of clinical pain. In A.K. Jakox (Ed.). Pain: A sourcebook for nurses and other health professionals. Boston: Little, Brown.
Keefe, F.J. & Block, A.R. (1982). Development of an observation method for assessing pain behavior in chronic low back pain patients. Behavior Therapy. 13. 363-375.
Keefe, F.J., Brantley, A., Manuel, G. & Crisson, J.E. (1985). Behavioral assessment of head and neck cancer pain. Pain. 23, 327-336.
Keefe, F.J. & Gil, K . M . (1986). Behavioral concepts in the analysis of chronic pain syndromes. Journal of Consulting and Clinical Psychology. 54. 776-783.
Kleck, R.E., Vaughan, R.C., Cartwright-Smith, J., Vaughan, K.B., Colby, C.Z. & Lanzetta, J.T. (1976). Effects of being observed on expressive, subjective, and physiological

115
responses to painful stimuli. Journal of Personality and Social Psychology, 34, 1211-1218.
Kohnken, G. (1987). Training police officers to detect deceptive eyewitness statements: Does it work? Social Behaviour. 2, 1-17.
Kotarba, J.A. (1983). Chronic pain: Its social dimensions. Beverly Hills: Sage.
Kraut, R.E. & Poe, D. (1980). On the line: The deception judgements of customs inspectors and laymen. Journal of Personality and Social Psychology. 39, 784-798.
Lander, J. (1990). Clinical judgements in pain management. Pain, 42, 15-22.
Lee, D.S. & Craig, K.D. (1991). Facial action determinants of observer pain judgements: Complexity and configuration. Unpublished manuscript, University of British Columbia, Vancouver.
LeResche, L. (1982). Facial expression in pain: A study of candid photographs. Journal of Nonverbal Behaviour. 7. 46-56.
LeResche, L. & Dworkin, S.F. (1988). Facial expression of pain and emotions in chronic T M D patients, Pain. 35. 71-78.
LeResche, L. , Ehrlick, K.J. & Dworkin, S. (1990). Facial expressions of pain and masking smiles: Is "Grin and Bear it" a pain behavior? Pain. Suppl. 5. S286.
Ley, R.G. & Bryden, M.F. (1981). Consciousness, emotion, and the right hemisphere. In R. Stevens & G. Underwood (Eds.) Aspects of consciousness: Structural issues. New York: Academic Press.
Mayer, T.G. , Gatchel, R.J., Kishino, N., Keeley, J., Mayer, H , Capra, P. & Mooney, V. 1986). A prospective short-term study of low back pain patients utilizing novel objective functional measurement. Pain. 25. 53-68.
Mehrabian, A. & Epstein, N. (1972). A measure of emotional empathy. Journal of Personality, 40,525-543.
Moore, B.S. (1990). The origins and development of empathy. Motivation and Emotion. 14, 75-80.
Patrick, C.J., Craig, K.D. & Prkachin, K M . (1986). Observer judgements of acute pain: Facial action determinants. Journal of Personality and Social Psychology, 50, 1291-1298.
Poole, G. D., & Craig, K. D. (1992). Judgements of Genuine, Suppressed, and Faked Facial Expressions of Pain. Journal of Personality and Social Psychology, 63, 797-805.
Prkachin, K . M . (1992a). Dissociating spontaneous and deliberate expressions of pain: Signal detection analyses. Pain. 51. 57-65.

116
Prkachin, K . M . (1992b). The consistency of facial expressions of pain: A comparison across modalities. Pain. 51. 297-306.
Prkachin, K . M . & Craig, K.D. (1985). Influencing non-verbal expressions of pain: Signal detection analysis. Pain. 21. 399-409.
Prkachin, K . M . , Currie, N.A. & Craig, K.D. (1983). Judging nonverbal expressions of pain. Canadian Journal of Behavioural Science. 15. 43-73.
Prkachin, K . M . , Solomon, P.S., Hwang, T. & Mercer, S.R. (1995). Does experience affect judgements of pain behaviour? Evidence from relatives of pain patients and health-care providers. Manuscript submitted for publication.
Prkachin, K . M . & Mercer, S.R. (1989). Pain expression in patients with shoulder pathology: Validity, properties and relationship to sickness impact. Pain. 39. 257-265.
Reuter-Lorenz, P. & Davidson, R J . (1981). Differential contributions of the two cerebral hemispheres to the perception of happy and sad faces. Neuropsychologia, 19. 609-613.
Rinn, W E . (1984). The neuropsyhology of facial expression: A review of the neurological and psychological mechanisms for producing facial expression. Psychological Bulletin. 95. 52-77.
Russell, J.A. (1994). Is there universal recognition of emotion from facial expression? A review of the cross-cultural studies. Psychological Bulletin. 115, 102-141.
Sackeim, H.A. & Gur, R.C. (1978). Lateral asymmetry in intensity of emotional expression. Neuropsychologia. 16. 473-481.
Schwartz, G.E., Ahern, G.L. & Brown, S. (1979). Lateralized facial muscle response to positive and negative emotional stimuli. Psychophysiology, 16, 561-571.
Swalm, D. & Craig, K.D. (1991). Differential impact of placebo on verbal and nonverbal measures of pain in men and women. Unpublished manuscript, University of British Columbia, Vancouver.
Tomkins, S.S. (1962). Affect, imagery, consciousness (Vol. 1). The positive affects. New York: Springer.
Turk, D C , Meichenbaum, D.H. & Genest, M . (1983). Pain and behavioural medicine: Theory, research and clinical guide. New< York : Guilford.
Turk, D C . & Melzack, R. (1993). The measurement of pain and the assessment of people experiencing pain. In D.C. Turk & R. Melzack (Eds.) Handbook of pain assessment. New York: Guilford Press.

117
von Baeyer, C.L., Johnson, M.E. & McMillan, M.J. (1984). Consequences of nonverbal expressions of pain: Patient distress and observer concern. Social Sciences & Medicine. 19, 1319-1324.
Wilkie, D.J. (1995). Facial expressions of pain in lung cancer. Analgesia. 1. 91-99.
Zuckerman, M . , Koestner, R., & Alton, A. O. (1984). Learning to Detect Deception. Journal of Personality and Social Psychology. 46. 519-528.
Zuckerman, M . , Koestner, R., & Colella, M . J. (1985). Learning to communicate deception from three communication channels. Journal of Nonverbal Behavior. 9. 188-194.

Appendix A
Description of FACS Action Units
AU# Action AU# Action
1 inner brow raise 34 puff
2 outer brow raise 35 cheek suck
4 brow lower 36 tongue bulge
5 upper lid raise 37 lip wipe
6 cheek raise 38 nostril dilate
7 lids tight 39 nostril compress
8 lips toward 41 lids droop
9 nose wrinkle 42 slit
10 upper lip raise 43 closed
11 nasolabial deepen 44 squint
12 lip corner pull 45 blink
13 cheek puff 46 wink
14 dimpler
15 lip corner depress
16 lower lip depress
17 chin raise
18 , lip pucker
19 tongue show
20 lip stretch
21 neck tighten
22 lip funnel
23 lip tight
24 lip press
25 lips part
26 jaw drop
27 mouth stretch
28 lip suck
29 jaw thrust
30 jaw to sideways
31 jaw clench
32 bite
33 blow

119
Appendix B
Research Identifiying Pain-Related Action Units
Facial Action Units Studies Identifying as Pain related facial actions
brow lowering Craig & Patrick, 1985
Craig, Hyde & Patrick, 1991
Hadjistavropoulos & Craig, 1994
LeResche, 1982
LeResche & Dworkin, 1988
LeResche, Ehrlick & Dworkin, 1990
Patrick, Craig & Prkachin, 1986
Prkachin, 1992b
Prkachin, Currie & Craig, 1983
Prkachin & Mercer, 1989
Swalm& Craig, 1991
tightened eyelids same as above
raised cheeks Craig & Patrick, 1985
Craig, Hyde & Patrick, 1991
Hadjistavropoulos & Craig, 1994
LeResche, 1982;
Le Resche & Dworkin, 1988
LeResche, Ehrlick & Dworkin, 1990
Patrick, Craig & Prkachin, 1986
Prkachin, Currie & Craig, 1983
eyes closed / blinking Craig & Patrick, 1985
LeResche, 1982
LeResche & Dworkin, 1988
LeResche, Ehrlick & Dworkin, 1990
Patrick, Craig & Prkachin, 1986
Prkachin, Currie & Craig, 1983
Prkachin & Mercer, 1989
Swalm& Craig, 1991

120
upper lip raised Craig & Patrick, 1985
Craig, Hyde & Patrick, 1991
Hadjistavropoulos & Craig, 1994
LeResche & Dworkin, 1988
LeResche, Ehflick & Dworkin, 1990
Patrick, Craig & Prkachin, 1986
Prkachin 1992b
lips parted Craig & Patrick, 1985
Craig, Hyde & Patrick, 1991
Galin & Thorn, 1993
Hadjistavropoulos & Craig, 1994
LeResche, 1982
LeResche & Dworkin, 1988
Prkachin & Mercer, 1989
Swalm & Craig, 1991
jaw drop Craig & Patrick, 1985
Hadjistavropoulos & Craig, 1994
LeResche, 1982
LeResche & Dworkin, 1988
LeResche & Dworkin, 1988
Prkachin & Mercer, 1989
horizontal lip stretch Galin & Thorn, 1993
LeResche, 1982
LeResche & Dworkin, 1988
LeResche, Ehrlick & Dworkin, 1990
Prkachin & Mercer, 1989
lip corner pull Craig & Patrick, 1985
Prkachin & Mercer, 1989
Swalm & Craig, 1991
vertical lip stretch Craig & Patrick, 1985
Hadjistavropoulos & Craig, 1994
LeResche, 1982
Prkachin & Mercer, 1989
nose wrinkled Hadjistavropoulos & Craig, 1994
LeResche & Dworkin, 1988
Prkachin & Mercer, 1989
deepened nasolabial fold LeResche, 1982

121
Appendix C
Study One Questionnaires
Personal Data
Sex: Male Female Age:
Marital Status: Profession:
Number of persons Living in Your Home:
Are you presently employed? Yes_ No
If yes: fulltime parttime
In which job?
If no: when did you stop work?
Did you stop because of pain?
How has your pain been diagnosed?
Where is your pain located?
Do you have other pains?
When did your pain begin? Year Occasion
When did you first seek professional help?
How many hospitalizations or surgical procedures have you had since then?
What kind of medication do you take for pain: Daily
Occasionally
What kind of medication do you take for other problems?
Do you smoke? How much per day?
Do you drink alcohol? How much per day?
Is your pain: Constant? Intermittent?

Descriptor Differential Scales
(Gracely, 1980)
Please circle one word or word-pair on the scale below to describe:
the pain you experience on an average day.
Pain Sensation
A. Extremely Intense
B. Very Intense
C. Intense
D. Strong
E. Slightly Intense
F. Barely Strong
G. Moderate
H. Mild
I. Very Mild
J. Weak
K. Very Weak
L. Faint
M . No Sensation of Pain

123
Descriptor Differential Scales
(Gracely, 1980)
Please circle one word or word-pair on the scale below to describe:
the pain you experience on an average day.
Unpleasantness
A. Very Intolerable
B. Intolerable
C. Very Distressing
D. Slightly Intolerable
E. Very Annoying
F. Distressing
G. Very Unpleasant
H. Slightly Distressing
I. Annoying
J. Unpleasant
K. Slightly Annoying
L. Slightly Unpleasant
M . No Discomfort

124
Appendix D
Consent Form for Pain Patients Appearance-based stereotypes of professionals: Biased or valid?
Investigators: Dr. Thomas Hadjistavropoulos (822-9231) and Dr. Ken Craig (822-3948) Department of Psychology, University of British Columbia
Health professionals' judgements about patients are based in part on facial cues. Factors such as nonverbal pain expressions and patient physical attractiveness have been found to affect professionals' impressions of health and pain intensity. We are interested in determining whether or not such impressions carry any validity. For our study we are requesting your permission to videotape a short segment of the physiotherapy session you are about to undergo. During this segment of the physiotherapy session we will be asking you to carry out certain movements under different instructions. These movements are not harmful but may lead you to experience some discomfort. In order to assess your reactions to the procedures, the videotapes will be coded and viewed by independent observers. Several observers (10-15) will rate the physical attractiveness of your face (all ratings are strictly confidential). The physical attractiveness ratings will be used to determine the extent to which they are related to health professionals' judgements. You will aslo be requested to fill out several brief questionnaires related to the discomfort you may experience during these movements and more generally on a day-to-day basis. We are also interested in understanding how back pain affects your life and how you have come to cope with the discomfort you may be experiencing. Therefore, we will be asking you to fill out some questionnaires concerning your pain experience and your coping strategies. All your responses will be kept strictly confidential.
Photographs of yourself and/or a short video may be shown to health professionals (including individuals training to become health professionals) who will be asked to estimate different dimensions of your pain experience including coping strategies, pain intensity, anxiety, likelihood that you are receiving compensation etc. The health professionals will have no access to your responses and their responses to your videotape will remain strictly confidential. Our goal is to determine how well, on average, the professionals' appearance-based judgements correspond to reality. In a related health experiment, health professionals and college students may eb shown your video, along with those of other patients. They will also be shown a brief summary of information that will be collected from you through an interview and some questionnaires. The professionals and the college students will be asked to match each image with the corresponding description. We will compare their ability to do this correctly. We would also like to point out that we may wish to use the information collected from you for the purposes of additional research. We will not do so however, without writing you first and requesting your written consent. If you have any questions about this study, feel free to ask the experimenter or to contact the investigators. You have the right to refuse participation in this research and even if you agree to participate, you have the right to withdraw at any time. Refusal to participate in this research will in no way affect your treatment.
I agree to participate in this study and give permission for the Point Grey Physiotherapy Clinic to release medical information solely for the purposes of this investigation and subject to the condition that this information is kept in confidence. I am aware that I can stop participation at any time wihtout penalty. I further acknowledge the receipt of a copy of this consent form. Signature Date

Appendix E
Physiotherapy Protocol
125
Neutral Sitting Up & Neutral Lying Down:
"Please maintain a neutral facial expression while looking at the camera. Neck
straight, lips closed, and facial muscles relaxed."
The following four sets of instructions should be presented in random order:
A. Genuine
"Lift both your legs up tp about here (10 - 12 inches) and hold it for 10 seconds. Please
genuinely express the pain or discomfort you are feeling."
B. Exaggerated
"This time I will ask you to lift both your legs up to about here (10 - 12 inches) for
about 10 seconds, but I would like you to pretend that it hurts more than it really does."
C. Masked
"Please lift both your legs up to about here (10 -12 inches) for about 10 seconds, but I'd
like you to pretend that it doesn't bother you at all, no matter how much it does."
D. Faked
"I'm not going to ask you to make any movement this time, but I'd like you to pretend that
you're experienceing pain. Let me know by your facial expression. Begin now."

Appendix F
Descriptor Differential Scales
(Gracely, 1980)
Please circle one word or word-pair on the scale below to describe:
the most severe pain you experienced in response to the leg raises you just completed.
Pain Sensation
A. Extremely Intense
B. Very Intense
C. Intense
D. Strong
E. Slightly Intense
F. Barely Strong
G. Moderate
H. Mild
I. Very Mild
J. Weak
K. Very Weak
L. Faint
M . No Sensation of Pain
127
Descriptor Differential Scales
(Gracely, 1980)
Please circle one word or word-pair on the scale below to describe:
the most severe pain you experienced in response to the leg raises you just completed.
Unpleasantness
A. Very Intolerable
B. Intolerable
C. Very Distressing
D. Slightly Intolerable
E . Very Annoying
F. Distressing
G. Very Unpleasant
F£. Slightly Distressing
I. Annoying
J. Unpleasant
K. Slightly Annoying
L. Slightly Unpleasant
M . No Discomfort

Appendix G
128
Training Manual
It is very important to know how much pain a patient is feeling in order to provide a correct
diagnosis and effective pain control. Unfortunately, physicians cannot always rely on patients to
provide accurate information about their pain experience. Patients can either minimize or
exaggerate their pain levels, and both misrepresentations have medical, social and financial
consequences.
When do patients suffering from severe pain minimize their pain experience?
• the patient may believe that one should be strong and "endure" pain rather than giving in to it
• the patient may be afraid of becoming addicted to pain medications
• the patient may be afraid of needles used for morphine injections
• the patient worries that pain medications will make them "fuzzy headed" or unable to
function
Consequences:
• quality of life goes down
• pain disrupts sleep, decreases appetite and drains patients energy resources
• patients take longer to recover because they don't have the energy required to heal
• pain is a symptom of illness and misreporting it can hamper proper diagnosis
• ties up hospital resources due to longer hospital stays etc.
When do pain patients exaggerate their pain experience?
• the patient may feel he/she is not receiving adequate medication for the pain
• the patient may feel that his/her condition is not being taken seriously enough by medical
staff
• the patient may be undergoing an evaluation for Worker's Compensation, insurance or
litigation purposes
(in all cases, exaggeration may be an attempt to emphasize the seriousness of their condition)
• the patient may be attempting Worker's Compensation or insurance fraud
Consequences:
• increases in unnecesary health care costs
. • tying up limited medical resources (personnel, diagnostic equipment, hospital beds)
• increased insurance premiums
• increased suspicion towards, and possible mistreatment of,- valid pain patients
• unnecessary treatment, including overmedication, increased risk of dependence and addiction
129
T H E PROBLEM:
• medical professionals need to improve their ability to detect deception in pain patients
• there needs to be a focus on pain information other than patient self-report.
• how do we distinguish between patients who are suppressing or exaggerating their pain
and patients who are quite insensitive or highly sensitive to pain?
A POSSIBLE SOLUTION:
• training medical professionals to improve their pain judgement skills with pain patients
• increasing their focus on, and their ability to detect, cues to deception in facial expressions
EVIDENCE AGAINST THIS APPROACH:
• Most people are very poor at detecting deception from a person's facial expression
• accuracy doesn't improve even when people are told to expect deception
• "lie detection" is difficult because there isn't a facial cue highly specific to lying
• lying must be inferred from very subtle cues, such as inconsistent or inappropriate facial
movements.
EVIDENCE FOR THIS APPROACH:
• there is a facial expression associated with genuine pain
• genuine pain expressions do differ slightly from faked pain and masked pain expressions
• research suggests that observers don't pay attention to the facial cues which differentiate
among genuine, faked and masked pain expressions
• with intensive training, people can see very subtle movements of the facial muscles
PURPOSE OF THIS STUDY:
• to see if we can improve people's ability to detect faked or masked pain by:
- providing information on the typical genuine facial expression of pain
- providing information on the facial cues which may occur when someone is lying.
Genuine Pain Expressions
The most common facial actions seen during genuine pain are:
• a lowered brow
• tightened eye lids
• raised cheeks
• eyes narrowed, closed or blinking
This drawing of a genuine pain face shows you what these facial actions look like.
lowered brow
tightened eye lids
eyes closed
raised cheeks
NOTE:* These actions are often very brief (a second, or even a fraction of a second long)
• You might not see all of these facial ations when a person is in genuine pain
• There are substantial individual differences in how people respond
The following pictures will show each of the most common facial actions
131
Most Common Pain-Related Facial Actions
Lowered Brow - Subtle Movement Lowered Brow - Stronger Movement
Tightened Eyelids - Subtle Movement Tightened Eyelids - Intense Movement

132
Raised Cheeks - Subtle Movement Raised Cheeks - Intense Movement
Eyes Narrowed Eyes Closed

133
IMPORTANT:
• these facial actions are common in people experiencing pain BUT everyone's "pain face"
looks different.
• several other facial actions have been frequently seen during people's reactions to pain.
Other facial actions seen during genuine pain are:
• a raised upper lip
• an opened mouth
• a mouth stretched wide open, either horizontally or vertically
• a wrinkled nose
• a deepened nasolabial fold
This drawing of a genuine pain face shows you what these facial actions look like:
wrinkled nose
deepened nasolabial fold
raised upper lip
an opened mouth
Neutral Expression Genuine Pain Expression
IMPORTANT:
• a pain face may include only one or two of these facial actions
• these facial actions may be very subtle (e.g. not very intense)
• these actions are often very brief ( a second, or even a fraction of a second long)
• there are substantial individual differences in people's responses to pain, therfore some
people may display facial actions other than those described here.
NOTE: The following pictures show each of these facial actions individually.

Other Common Pain-Related Facial Actions
Raised Upper Lip - Subtle Movement Raised Upper Lip - Intense Movement
Lips Parted Jaw Drop

135
Vertical Lip Stretch
Horizontal Lip Stretch - Subtle Movement Horizontal Lip Stretch - Intense Movement
Wrinkled Nose - Subtle Movement
136
Wrinkled Nose - Intense Movement
Deepened Nasolabial Fold

137
Faked Pain FACTS:
• people are very good at faking a pain expression
• people asked to fake their pain exhibit the same facial actions as genuine pain patients
• observers have considerable difficulty distinguishing between genuine and faked pain
expressions
• BUT there are a few differences between faked and genuine pain expressions.
DIFFERENCES B E T W E E N F A K E D AND GENUINE PAIN EXPRESSIONS:
• the individual facial actions are usually more intense when faked than when genuine
Note: it is difficult to discriminate between a faked expression and a severe genuine pain
expression as pain severity is communicated through increasingly intense facial
expressions.
• genuine pain expressions are usually only made up of a few pain-related facial actions BUT
faked pain expression usually contain several pain-related facial actions
THEREFORE:
• faked pain faces are often stronger or more exaggerated than genuine pain expressions
• faked pain faces are often more "prototypical" or "perfect" than a genuine pain expression
E X A M P L E :
GENUINE PAIN F A K E D PAIN
• brow lowered • brow lowered
• eyes shut
• raised upper lip
• eyes squeezed shut
• raised upper lip
• deepened nasolabial fold
• lips slightly opened
Note: increased intensity of all facial actions in the faked pain face

Masked Pain.
138
FACTS:
• people are not as successful at masking their genuine pain expressions
• very little of the genuine pain expression remains on their faces BUT observers seem to pick
it up
• subtle facial cues of pain often "leak out" despite the patients efforts to conceal them.
• forehead and brow muscles are difficult to control, so "leakage" may occur most around
the eyes
DIFFERENCES B E T W E E N M A S K E D PAIN EXPRESSIONS AND A N E U T R A L F A C E :
• slightly raised cheeks
• slightly narrowed eyes
• a neutral face that is held unnaturally still
• a neutral face which looks unusually tense, like they are trying to "hold in" a facial
expression
• reduced frequency of blinking
• a very brief "flash" of a pain expression, followed by a prolonged neutral face.
E X A M P L E :
N E U T R A L M A S K E D PAIN
residual activity around the eyes

Cues to General Deception
139
HOW TO F A K E A FACIAL EXPRESSION:
• cover your genuine emotion / expression with the desired facial expression
Cues: • look for an underlying expression or a mix of expressions
• look for small facial actions which are incompatible with the faked emotion
HOW TO HIDE OR M A S K A GENUINE EXPRESSION
• cover the genuine expression with a different facial expression (e.g. a smile)
Cues: • look for incompatible facial actions (e.g. sad eyes with a smile)
• look for signs of an underlying expression (e.g. 1 or 2 pain-related facial actions)
• face seems unnatural
• hide a genuine expression by tightening antagonistic muscles in the face to "hold it in"
Cues: • muscle tightening may make the face appear stiff, unnatural or
controlled.
• "leakage" of the genuine pain expression, a brief "micro-expression"
which is very brief (as short as 1/4 of a second)
OTHER GENERAL CUES TO DECEPTION:
Emotions: • shame or fear of being caught lying
• signs of guilt, such as blushing, blanching or facial sweating.
Timing: • faked expressions seem to last longer than genuine ones
• during faked expressions, individual facial actions actions may appear serially
versus all at once
• faked expressions may have a delayed onset.
Blinking: • changes in blinking rates are also thought to occur during deception.
• blinking may increase because of increased emotion OR conscious efforts to
control emotions will lead to an unconscious decrease in blinking.

140
Asymmetry: • faked expressions sometimes appear lopsided of asymmetrical
• muscle action may be stronger on one side of tfie face than the other.
EXAMPLES:
- in each example, there is asymmetry
- muscle movement on the right is stronger
IMPORTANT:
• the signs of deception described above have not been completely proven through research.
• taken individually, they are not necessarily a sure sign that someone is lying.
• these are not the only signs of deception - there may be others we are unaware of.
• none of these "signs" have been looked for in pain patients.
141
Training Test
1. When people are told that there may be deception occuring, their deception T F
accuracy increases considerably.
2. It should be fairly simple to train lie detectors because there are facial cues
highly specific to lying. T F
3. One of the most common facial actions during genuine pain is tightened
eyelids T F
4. One of the most common facial actions during genuine pain is a wrinkled
nose. T F
5. One of the most common facial actions during genuine pain is an opened
mouth. T F
6. One of the most common facial actions during genuine pain is a lowered
brow. T F
7. Facial reactions to pain are usually pretty intense when compared to other
emotional expressions like sadness, which are pretty brief and subtle. T F
8. Pain expressions always include more than one facial action. T F
9. People aren't very good at faking a pain expression. T F
10. Genuine pain expressions are usually stronger than faked pain expressions. T F
11. When compared to genuine pain expressions, faked pian expressions look
more like a "perfect" pain reaction. T F
12. People are very good at masking their genuine pain expressions. T F
13. When someone is trying to hide their pain, facial activity is most likely to "leak out" in the area around the eyes. T F
14. Faked expressions last longer than genuine ones. T F

142
Appendix H
Study Two Questionnaire Package
Judgement Study Consent Form
June 29, 1992.
Dear Students
We are conducting a study on the facial expression of pain, and the ability of observers to
distinguish between genuine, faked, and masked pain. Our objective is to improve the ability of
health care professionals to make appropriate decisions about diagnosis and treatment.
This study asks you to view videotapes of low back pain patients undergoing a physical
examination which involves painful movements. During these examinations, patients were given
certain instructions regarding their facial expressions. You would view a series of different
patients' reactions and provide brief ratings of how much discomfort, if any, they were
experiencing.
This study will require 60 to 90 minutes of your time. Your participation in this study will remain
completely confidential; any information you provide will be identified by a numbered code and
will be accessible only to researchers involved in this study. We hope that you will be able to
participate and aid us in our research. However, please feel free to decline now or at any time
during the course of this study. If you do wish to participate, you will receive course participation
credit. A copy of this consent form will be provided to you for your own records.
For further information, please contact:
Marilyn Hill, M S c , U.B.C. 822-5280
Ken Craig, Ph.D., Psychologist, Professor, U.B.C. 822-3948
Thank-you in advance for your assistance.
I CONSENT
I DO NOT CONSENT
SIGNATURE

PERSONAL D A T A
Age_
Sex: Male Female
Marital Status:
What country were you born in?
If you were not born in Canada, when did you move here?
What country were your parents born in?
Mother?
Father?
What language do you use at home?
What is your ethnic descent? (e.g. Taiwanese, German / Irish etc.) ?

PERSONAL PAIN EXPERIENCE
144
Have you ever experienced:
1. acute pain, (e.g. an injury or surgery)? Yes No
If yes: -what was the cause of the pain?
-on a scale from 0 (no pain) to 10 (severe pain) how intense was the pain?
- how long did the acute pain last?
2. a recurrent painful condition (e.g. migraine headaches, ulcers)? Yes No
If yes: - what was the cause of the pain? .
- on a scale from 0 (no pain) to 10 (severe pain) how intense was the pain?
- how long have you suffered from recurrent pain?
3. chronic pain (e.g. chronic low back pain)? Yes No
If yes: - what was the cause of the pain? . .
- on a scale from 0 (no pain) to 10 (severe pain) how intense was the pain?
- how long have you suffered from chronic pain?
FAMILY HISTORY OF PAIN
Has anyone in your immediate family ever experienced:
1. acute pain, (e.g. an injury or surgery)? Yes No
If yes: -which family member (s)?
-what was the cause of the pain?
-on a scale from 0 (no pain) to 10 (severe pain) how intense was the pain?
- how long did the acute pain last?
2. a recurrent painful condition (e.g. migraine headaches, ulcers)? Yes No
If yes: -which family member (s)?
- what was the cause of the pain?
- on a scale from 0 (no pain) to 10 (severe pain) how intense was the pain?
- how long have they suffered from recurrent pain?
3. chronic pain (e.g. chronic low back pain)? Yes No
If yes: -which family member (s)?
- what is the cause of the pain?
- on a scale from 0 (no pain) to 10 (severe pain) how intense is the pain?
- how long have they suffered from chronic pain?

145
Interpersonal Reactivity Index
1. I daydream and fantasize, with some regularity, about things that 0 1 2 3 4 might happen to me.
2. 1 often have tender, concerned feelings for people less fortunate 0 1 2 3 4 than me.
3. I sometimes find it difficult to see things from the "other guy's" 0 1 2 3 4 point of view.
4. Sometimes I don't feel very sorry for other people when they are 0 1 2 3 4 having problems.
5. I really get involved with the feelings of the characters in a novel. 0 1 2 3 4
6. In emergency situations, I feel apprehensive and ill-at-ease. 0 1 2 3 4
7. I am usually objective when when I watch a movie or play, and I 0 1 2 3 4 don't often get completely caught up in it.
8. I try to look at everybody's side of a disagreement before I make 0 1 2 3 4 a decision.
9. When I see someone being taken advantage of, I feel kind of 0 1 2 3 4 protective towards them.
10. I sometimes feel helpless when I am in the middle of a very 0 1 2 3 4 emotional situation. .
11. I sometimes try to understand my friends better by imagining how 0 1 2 3 4 things look from their perspective.
12. Becoming extremely involved in a good book or movie is 0 1 2 3 4 somewhat rare for me.
13. When I see someone get hurt, I tend to remain calm. 0 1 2 3 4
14. Other people's misfortunes do not usually disturb me a great deal. 0 1 2 3 4
15. If I'm sure I'm right about something, I don't waste much time 0 1 2 3 4 listening to other people's arguments.
16. After seeing a play or movie, I have felt as though I were one of 0 1 2 3 4 the characters.
17. Being in a tense emotional situation scares me. 0 1 2 3 4

146
18. When I see someone being treated unfairly, I sometimes don't 0 1 2 3 4 feel very much pity for them.
19. I am usually pretty effective in dealing with emergencies. 0 1 2 3 4
20. I am often quite touched by things that I see happen. 0 1 2 3 4
21. I believe that there are two sides to every question and try to look at 0 1 2 3 4 them both.
22. I would describe myself as a pretty soft-hearted person. 0 1 2 3 4
23. When watching a good movie, I can very easily put myself in the 0 1 2 3 4 place of a leading character.
24. I tend to lose control during emergencies. 0 1 2 3 4
25. When I'm upset at someone, I usually try to "put myself in his 0 1 2 3 4 shoes" for a while.
26. When I am reading an interesting story or novel, I imagine how I 0 1 2 3 4 would feel if the events in the story were happening to me.
27. When I see someone who badly needs help in an emergency, I 0 1 2 3 4 go to pieces.
28. Before criticizing somebody, I try to imagine how I would feel if I 0 1 2 3 4 were in their place.

Appendix I
147
Description of Videotapes & Rating Forms
Description of Videotapes
The videotapes you are about to watch are of patients with back pain who are undergoing a a
routine physical examination by their physiotherapist. During this examination, patients were
asked to raise their legs 10 inches off the examination table while keeping them straight. Patients
with low back pain experience this movement as painful.
Patients performed the leg raise twice. During one of these movements they were asked to
genuinely express any pain that they felt. During the other movement, they were asked to pretend
that it didn't hurt. They were also asked to give a faked expression, by pretending that they were
in a lot of pain while not actually moving their legs. The patients' facial expressions were
videotaped in each of these conditions.
For each patient on the videotape you will see 4 kinds of faces: a neutral face videotaped before
the examination began, a genuine pain expression, a faked pain expression, and a masked pain
expression. These 4 clips will not be in any particular order. After each clip, you will be asked to
estimate the pain experienced based on the facial expression you see. You will also be asked to
decide which category the facial expression represents: a neutral expression, a genuine pain face, a
faked pain expression or a masked pain expression. You will also be asked how confident you are
about your decisions and how you came to your decision.

Description of Videotapes (Feedback Group)
148
The videotapes you are about to watch are of patients with back pain who are undergoing a a
routine physical examination by their physiotherapist. During this examination, patients were
asked to raise their legs 10 inches off the examination table while keeping them straight. Patients
with low back pain experience this movement as painful.
Patients performed the leg raise twice. During one of these movements they were asked to
genuinely express any pain that they felt. During the other movement, they were asked to pretend
that it didn't hurt. They were also asked to give a faked expression, by pretending that they were
in a lot of pain while not actually moving their legs. The patients' facial expressions were
videotaped in each of these conditions.
For each patient on the videotape you will see 4 kinds of faces: a neutral face videotaped before
the examination began, a genuine pain expression, a faked pain expression, and a masked pain
expression. These 4 clips will not be in any particular order. After each clip, you will be asked to
estimate the pain experienced based on the facial expression you see. You will also be asked to
decide which category the facial expression represents: a neutral expression, a genuine pain face, a
faked pain expression or a masked pain expression. You will also be asked how confident you are
about your decisions and how you came to your decision. You will be given feedback on the
accuracy of your pain judgements. Once you have completed all of your ratings on a patient, you
check your accuracy by reading the appropriate feedback card. It will tell you which category
each of the 4 facial expressions represents.
When you begin your pain judgement task, you will be given a stack of feedback cards labelled on
one side with the patients ED# (which will match the ones on the tv screen). The other side of the
card contains the correct categorizations of the facial expressions. You may only turn the cards
over one at a time and O N L Y when you have already completed the ratings on that patient. DO
NOT change your ratings once you have seen the feedback card. If you accidentally see a card
before you have rated a patient, please make a note of it so that we can discard the rating you
made on that patient.
This is how you complete your judgement task:
1. Watch the video clip for your first patient.
2. Pause the tape;
3. Make your judgements (pain intensity, categorize the expressions, rate your accuracy)
4. Check your accuracy
5. Continue on to the next subject.

z o oo
. re 3 CO P 5" 3
= 3
§ re*
8
< m re x •3 „
3 ^ re 3
re* 3 8
00 re 3 co P S' 3 00 o EL re
2; oo oo c O C - K g _0Q OQ T3
3 3 3 S-S»T3 3
2 sr o . S0Q
>_<o
3 re s;-
J Q 0"° 3
3 1 co 5 £2 3
O Q
( J Q O Q _ 3" 3 -^
•<<5f 2 O O P re re S2 • l »-t 3 re" re*
3 £
/ p 3 : 2 5
c r re*
re o n cr
T 3
n
a 3
'3 re*
K*
2* "T*
o B 2 re re e? ?? *"^ ""i _<•
* cr g« § re*
re
< m
re X
= 1 3 5* 3 re
oo re 3 CO P o' 3 00 o EL re
2s2 2 2 "
o 3 C
3
oo a O Q - a
'gre, >"_2< 3 _ re
o"2 _ re
3
>EJ0Q C 3 <-* S
— re On Co
EE Cr re S3, O Q O Q ^
3 O 5*
O Q
re 3
OQ
cr 3 *
*<*<9 W I—I CO 3 3 Ef r - * r - * r~. o o 8 re re S2. 3 3 = 2 2 re" re"
n <"
P re"
G 3
'O re* P CO
3 O CO CO 00 O re"
149
Q. re o n •5" >
2 ; T I < < : < : _ _ D O O O o o _ <cn
oo re 3 co P 5' 3
re O 3 0Q
— o _
? = % re
0Q <3£ re
3 5* 3 CO re
3
3 ^ 55 »—1
re 3 re*
3 co re
• _ * r ^ ^ ~ „ a ; r - c n o n w >
00 re 3 co SS-o" 3 00 o BL re
*Zc_c_G> O •-• ~ 3 3 _ 0 Q 0Q >_) 5
3 3 3 =* 3
to SJ-£2 O Q
2 < 0
O Q -3 s. 3* 5
0Q D*SL 5 co' 5 co
3 O Q
00 00 < 00 O Q ^
i3 3* 3"
3 < 5 "
g » J»
re 3 . 2" 2 re* re
co _
2«5 3 5*
E?
p' M*
re _ _ Co * re £2.
^ 3 0Q
re 3 J _ re*
o. re o
n o
3 re CO CO 00 O re.
T3 B 5' oo re 3 co 5' 3 00 o &L re
2r^*^r„o**f lwonw>
£5 £2 < =r < re 5? re
-•-=•03 g o re*
" 0
5' G 3 re* P co
3 re CO CO 00 o p re*
o. re
• o Q •5' 03
T3 CO
n s

w >
Video
Clip
Type ( E
xpr (N
/G
acial ion IM
)
o
*! o _
| o _
# | © _ * 1
Confidence in D
ecision
<=> 1 # 1
u < 1
© 1 # 1
<=> | ~ # 1
L/l 1
© 1 * 1
Confidence in D
ecision
§ i 5$ -
1 1UU%
1 100%
§!
Cues U
sed U
sed

15
Appendix J
Frequency of Facial Cue Use per Subject
Facial Cue Mean SD Facial Cue Mean SD
smile 4.29 3.45 large expression changes 0.08 0.33
neutral / no reaction 10.18 8.34 long duration 0.89 1.88
frown 1.32 3.63 decreased movements 0.01 0.09
repressed expression 0.48 1.14 drawn eyes 0.03 0.37
lowered eyebrows 1.87 3.42 exaggerated movements 2.20 2.64
eye narrows 0.57 1.26 rapid eye movements 0.32 0.73
eyebrow movements 2.'22 3.12 too much expression 0.34 0.90
mouth movements 2.52 4.56 head movements 1.78 2.39
eyebrow twitch 0.28' 0.64 looked fresh 0.01 0.09
relaxed eyes 0.15 0.66' eyes squinting / tightened 2.12 3.48
chewing (gum) 0.14 0.35 tight jaw 0.33 1.10
eyes move upward 0.90 1.61 rapid tongue movements 0.01 0.09
steady breathing pattern 1.62 4.08 rapid breathing 0.70 1.45
eyelid movement 0.30 0.98 shakiness 0.70 1.53
relaxed 4.09 6.45 too much movement 0.48 0.99
smile with pain expression 0.24 0.53 tight hps 1.82 3.17
no emotion 0.09 0.43 too much effort / energy 0.03 0.29
eyes moved 7.47" lti09 grimace 0.92 3.19
throat moved 0.19 0.96 tighdy closed eyes 0.34 1.27
hps moved 1.28. 2.54 change in eyes 0.01 0.09
eyebrows pinched 0.77 1.74 gritting teeth 0.15 0.57
corner mouth twitch 0.08 0.31 tight neck muscles 0.45 1.32
hps curled 0.06 0.47 no change in eyes 1.08 1.91
watery eyes 0.18 0.71 too much cheek movement 0.01 0.09
eyes widened 0.28 0.66 swallowed 0.80 1.17
eyelids hooded 0.01 0.09 sudden movements 0.17 0.75
eyes open 0.15 0.53 exaggerated blinking 0.20 0.56
laugh 0.38 1.01 blinking 2.7.3 3.43
fast blinking 0.69 1.05 eyelid tightening 0.36 1.25
lips drawn 0.13 0.90 too quick to respond 0.01 0:09
short duration 0.60 1.87 deep breathing 1.79 2.75
eyes closed 2.86 3.86 too much neck movement 0.04 0.20

152
Facial Cue Mean SD
tense 2.37 4.75
looking into camera 0.35 1.16 asymmetry 0.86 1.47
cheek movement 0.32 1.12 licking lips 0.21 0.63
sad face 0.18 0.67
nose movement 0.13 0.58
forehead movement 0.08 0.29
no blinking 0.43 1.24
nostril movement 0.47 1.09
tongue movement 0.11 0.38 fake smile 0.32 0.82
symmetry 0.08 0.57
exaggerated nose move 0.01 0.09
sad eyes 0.11 0.46
nose wrinkle 0.23 0.88
no change in expression 2.01 5.17
abrupt head movement 0.09 0.41
raised head 0.04 0.27
raised eyebrows 0.69 1.61 sudden expression change 0.14 0.47
eye bulge 0.06 0,55 sour look 0.01 0.09
raised upper lip 0.49 2.16
sudden jump / jolt 0.93 2.14
stiff face / controlled face 1.36 2.72
lip shiver / wobble 0.11 0.36 biting lips 0.52 1.09
open mouth 1.65 2.36
strange movements 0.15 0.44
silly / comical 0.06 0.27
fake / forced / unnatural 1.38 1.83
eyes in pain 0.17 0.51
stronger movements 0.04 0.20 missing data 369.5 25.47
Facial Cue Mean SD
chin 0.10 0.42
hps closed 0.33 0.97
no pain expression 0.59 2.37
body movement 1.50 2.82
real discomfort 0.62 1.41
no discomfort 0.23 0.73 fake cheeks 0.01 0.09
raised cheeks 0.75 1.94
fast eye shut 0.04 0.46 normal expression 1.02 3.26
unpleasant / cool / irritated 0.27 0.79 very slight movement 0.07 0.28
nervous / worried 0.72 1.50
widened mouth 0.20 0.72
slight pain expression 0.22 1.11 repressed pain expression 0.38 0.93
perfect expression 0.14 0.87
rubbing shoulder 0.12 0.32
fidgety 0.14 0.55
contradictory expressions 0.18 1.03
fleeting expression' 0.01 0.09
"leakage @ eyes 0.06 0.35
timing off 0.03 0.27
tried not to shout 0.01 0.09
looked down 0.22 0.97
too little movement 0.24 0:74
too painful 0.09 0.48
looked relieved 0.16 0.47
jaw movement 0.13 0.48
intense look 0.30 0.91
red face 0.04 0.24
face movements 1.31 7.78
glazed eyes 0.05 0.25
lips pursed 0.32 0.99
no smile 0.03 0.26

153
Facial Cue Mean SD Facial Cue Mean SD
no body movement 0.63 2.33 wince 0.01 0.09
vocalization 0.21 0.63 muscle tension 0.76 2.08
holding breath 0.80 1.99 fake muscle tension 0.03 0.37
wrinkled face 0.04 0.24 head tilted 0.04 0.30
looks sedated 0.09 0.34 "pain, what pain?" 0.01 0.09
nasolabial fold 0.08 0.36 eyelid relaxation 0.13 0.63
happy 0.07 0.28 tense then relaxed 0.15 0.60
weird look in eyes 0.04 0.30 satisfied expression 0.01 0.09
alert eyes / inquisitive 0.05 0.25 controlled breathing 0.13 0.59
strange.expression 0.03 0.20 posture 0.01 0.09
no head movement 0.07 0.34 not distracted by pain 0.06 0.55
trying to hide 0.11 0.31 distracted by pain 0.07 0.36
involuntary movement 0.08 0.65 eyes unfocused 0,03 0.20
serious expression 0.16 0.47 no change in breathing 0.06 0.42
stoic expression 0.05 0.46 twisted facial expression 0.08 0.44
waiting 0.03 0.16 no pain in eyes 0.04 0.30
fear 0.07 0.31 relaxed squint 0.01 0.09
dry mouth 0.02 0.18 no eye squint 0.02 0.13
repressed smile 0.05 0.22 eyes fade 0.01 0.09
conspiratory smile 0.01 0.09 smirk 0.05 0.25
surprise 0.07 0.36 eyes straining 0.03 0.16
pouting 0r04 -0:38 looking at Dr. 0.05 0.39
concentration 0.35 1.32 animated 0.02 0.13
hands 0.02 0.18 horizontal mouth move 0.09 0.43
shoulders 0.01 0.09 abrupt expression 0.03 0.27
face harmony 0,03 0.37 relaxed / normal breathing 0.69 1.69
pain face leakage 0.04 0.24 lopsided mouth 0.01 0.09
looks hurried 0.03 0.20 no mouth movement 0.06 0.33
leakage 0.04 0.30 yawn 0.01 0.09
unnatural gazing 0.03 0.27 boredom 0.16 0.73
distant 0.03 0.29 sudden intake of breath 0.21 0.62
pain face 0.24 0.66 delayed onset 0.19 0.60
pleasant face 0.06 0.40 about to cry 0.03 0.18
looking around 2.05 3.10 prep for pain 0.02 0.18
inconsistant 0.20 0.74 not neutral 0.02 0.18

1
Facial Cue Mean SD
lip stretch 0.03 0.16
shifty/furtive eyes 0.60 1.99
loose facial actions 0.01 0.09
eye twitch 0.34 0.87
no pain in mouth 0.01 0.09
hp twitch 0.30 1.04
hp twist 0.04 0.38
looks weak 0.01 0.09
smile to hide 0.03 0.16
tired eyes 0.03 0.16
shudder 0.02 0.18
trying to remain calm 0.20 0.72
fast movements 0.27 0.81
no grimace 0.03 0.29
arms crossed 0.01 0.09
amused 0.02 0.13
unpleasant / strange smile 0.03 0.22
less swallowing . 0.01 0.09
change in expression 0.01 0.09
smile disappears 0.05 0.41
expecting pain 0.03 0.16
no relief 0.01 0.09
wobbly chin 0.01 0.09
irregular breathing 0.31 0.91
forced smile 0.17 0.63
nervous smile 0.02 0.13
quick glance 0.01 0.09
vertical hp movement 0.01 0.09
partial expression 0.01 0.09
full reaction 0.06 0.64
more reaction 0.01 0.09
simultaneous facial actions 0.03 0.29
few abnormal actions 0.01 0.09
genuine eyes 0.02 0.13
genuine pain 0.04 0.33
Facial Cue Mean SD
looks guilty 0.03 0.22
not exaggerated 0.05 0.25
mean eyes 0.02 0.13
upper lip raise 0.03 0.20
slow movements 0.07 0.32
not shaking 0.01 0.09
showing teeth 0.03 0.27
no intensity 0.07 0.31
not worried 0.03 0.16
repeated pain expressions 0.02 0.13
repeated movements 0.06 0.24
decreased blinking 0.07 0.31
no leakage 0.02 0.13
expectant face 0.01 0.09
slight body movement 0.02 0.18
breathing through mouth 0.02 0.13
breathing through nose 0.01 0.09
barely breathing 0.03 0.16
one eye open, one closed 0.01 0.09
extreme pain to neutral 0.03 0.16
slow eye movement 0.03 0.22
extreme eye lowering 0.04 0.46
hp lowered 0.02 0.18
mouth wrenched 0.01 0.09
collected strength 0.01 0.09
diverted attention 0.03 0.18
not constant 0.04 0.24
no jolt or jerk 0.03 0.29
not simultaneous actions 0.13 1.05
unclear 0.01 0.09
no eyebrow movements 0.05 0.2-2
pain in mouth 0.01 0.09
relaxed mouth 0.13 0.79
relaxed cheeks 0.06 0.42
cheek twitch 0.03 0.20

Facial Cue Mean SD
fake eye movement 0 03 0 16
early onset 0 05 0 31
no tension 0 10 0 70
sigh 0 02 0 13
puzzled 0 01 0 09
chewing interrupted 0 01 0 09
normal blinking 0 15 0 75
drooled 0 03 0 20
very slight smile 0 03 0 20
sad 0 01 0 09
resistant 0 01 0 09
laughing eyes 0 01 0 09
fake mouth 0 01 0 09
cough 0 01 0 09
consistant 0 03 0 20
more realistic 0 01 0 09
decreased intensity 0 02 0 18
swooned 0 01 0 09
decreased tension 0 01 0 09
not neutral 0 01 0 09
relaxed jaw 0 01 0 09
couldn't hold expression 0 01 0 09
eyes crossed 0 01 0 09
abrupt end of expression 0 01 0 09
too consistant 0 01 0 09
forehead tension 0 02 0 18
constant expression 0 01 0 09

156
Eye Movements
eye narrows
eyes moved
eyes closed
staring
eye bulge
weird look in eyes
furtive eyes
Appendix K
Categorization of Facial Cues
relaxed eyes
watery eyes
eyes squinted
eyelid tightening
eyes in pain
alert eyes
eye twitch
eyes rolling
eyes widened
eyes squeezed shut
looking into camera
glazed eyes
looking around
eyelid movements
eyes open
rapid eye movements
sad eyes
leakage around eyes
eyes relaxed
Eyebrow Movements
lowered eyebrows eyebrow twitch
raised eyebrows
eyebrows pinched eyebrow movements
Cheek / Nose Movements
cheek movement raised cheeks
nostril movement nose wrinkle
relaxed cheeks nose movement
Mouth Movements
smile
lips curled
licking lips
open mouth
lip twitch
frown
lips drawn
raised upper lip
lips closed
lip twist
mouth movement
tight lips
lip wobble
widened mouth
relaxed mouth
lips moved
corner mouth twitch
biting lips
lips pursed
horizontal mouth movement
Smile
repressed smile
smirk
fake smile
smile disappears
smile
forced smile
smile with pain expression
"Held In" Facial Actions
staring no blinking
hiding emotions repressed smile
trying to remain neutral
fixed expression repressed expression
stiff / controlled face repressed pain expression
Breathing Patterns
steady breathing rapid breathing deep breathing holding breath
157
controlled breathing relaxed breathing irregular breathing sudden intake of breath
Incongruent Facial Actions
inconsistant smile with paincontradictory actions too many expressions
actions not simultaneous
Pain Expression
grimace real discomfort
pain face twisted face
perfect pain expression
too painful slight pain expression
repressed pain expression
smile with pain expression
Blinking Patterns
fast blinking
no blinking
strange blinking
decreased blinking
staring blinking
Timing
short duration
slow movements
long duration
early onset
sudden movements delayed onset
not simultaneous
Exaggeration
silly
fake
too much movement
fake smile
intense look
too painful too many expressions
strange movements exaggerated movements
Tense / Tight
tight lips tight jaw eye squint eyebrows pinched
eyes squeezed shut gritting teeth tight neck muscles tense
muscle tension tense then relaxed
Sudden Movements
sudden jolt / twitch sudden movements early onset sudden change in expressio
nfast movement involuntary movement
Relaxed
looks relieved looks sedated relaxed eyelid relaxation
relaxed breathing relaxed mouth relaxed cheeks no tension
relaxed eyes

Appendix L
Type and frequency of Subjects' Pain Experiences
Self Family
Cause Acute Recurent Chronic Acute Recurrent Chrc
surgery 7.5 0 0 13.3 0 0.8
sports injury 5.8 0.8 3.3 1.7 1.7
eating disorder 0 0 0 0.8 0 0.8
knee pain 2.5 2.5 0.8 0 0.8 0.8
bacterial infection 1.7 0 0 0.8 0 0
compressed nerve 0 0.8 0 0 0 0.8
ruptured spleen 0.8 0 0 0 0.8 0
headaches 0.8 11.7 0 0.8 20.8 0.8
broken bone 7.5 0 1.7 13.3 0.8 1.7
Osgood schlater's 0 0 0.8 0 0.8 0
back pain 5.0 3.3 6.7 3.3 2.5 18.3
cut 3.3 0 0 1.7 0 0
burn 1.7 0 0 1.7 0 0
blood clot 0 0 0 0.8 0 0
neck pain 0 0 0 0 0 0.8
torn ligaments 2.5 0.8 1.7 0 0 0.8
cataracts 0 0 0 1.7 0 0
ulcer 0 4.2 0 0 5.8 0
cramps 0 3.3 0 0 1.7 0
wisdom teeth 5.8 0 0 0.8 0 0
sore throat 0 0.8 0 P 0 0
gallstone 0 0 0 4.2 0 0
dehydration 0.8 0 0 0 0 0
work injury 0 0 0 0.8 0 0.8
car accident 4.2 0 0.8 3.3 0 2.5
head injury 2.5 0 0 0.8 0 0
leg injury 0 0 0 0.8 0.8 0.8
hemerroids 0.8 0 0 0 0 0
dislocation 0.8 0 0 2.5 0 0
stomachaches 0 5.8 0 0 2.5 0.8
stress 0 1.7 0 0 1.7 0.8
unknown 0.8 0.8 0.8 0 0 0.8

PMS 0 0.8 0.8 0 0 0
allergies 0.8 0 0 0 0 0
appendicitis 0 0 0 1.7 0 0
cut leg with saw 0 0 0 0.8 0 0
worm }n stomach 0 0 0 0 0.8 0
arthritis 0 0 0 0.8 1.7 1.7
rash 0.8 0 0 0.8 0 0
sprain 4.2 0 0 0 0 0
throat infection 0 0 0 0 0.8 0
poor posture 0 0 0.8 0 0 0
a fall 5.0 0 0 0.8 0 0
ingrown toenail 0 0 0.8 0 0 0
gallbladder 0 0 0 0.8 0 0
seizure 0.8 0 0 0 0 0
heart attack 0 0 0 1.7 0.8 0
a growth 0 0 0 0.8 0 0
toothache 0.8 0.8 0 0.8 0 0
poor nutrition 0 0 0 0 0.8 0
gout 0.8 0 0 0 0.8 0
labor 1.7 0 0 0.8 0 0
cancer 0 0 0 1.7 0.8 0
liver 0 0 0 0 0.8 0
water in legs 0 0 0 0 0 0.8
kidney stones 0 0 0 0 0.8 0
lack of sleep 0 0.8 0 0 0 0
too busy 0 0 0 0 0.8 1.7
foot pain 0.8 0 0 0 0 0.8
inflamed ganglion 0.8 0 0 0 0 0
exercise 0 0.8 0.8 0 0 0
finger injury 1.7 0 0 0 0 0
dysmennorhea 0 0.8 0 0 0 0
gum pain 0 0 0 0.8 0 0
ovarian cysts 0 0 0.8 0 0 0

Appendix M
Correlation Matrix: Empathy and Experience with Judgement Variables
160
IRI score Perspectiv Concern
e
Distress Fantasy Experience
Pain Judgements
Accuracy -.02 -.06 -.01 -.04 .04 .08
Confidence -.08 .02 .01 -.17 -.10 -.10
Unpleasantness .16 .05 .15 .17 .12 -.04
Intensity .10 .14 .00 .07 .08 .16
Experience .15 .22* .03 7.01 .20* 1.00
Females
Accuracy -:12 -.16 -.08 .04 -.11 .01
Confidence .02 .10 .06 -.04 -.06 -.11
Unpleasantness .06 -.03 .19 -.05 .07 -.02
Intensity .07 .18 -.06 .16 -.07 .09
Experience .19 ,23 .14 -.02 .18 1.00
Males
Accuracy -.05 -.05 -.05 -.11 04 .05
Confidence -.17 -.07 -.05 -.27* -.16 -.12
Unpleasantness .29* .16 .18 .34** .25 -.01
Intensity .08 .06 .02 -.03 .22 .24
Experience .08 .17 -.10 .00 .17 1.00
* significance less than .05 ** significance less than .01 (two tailed)
IRI score = Interpersonal Reactivity Index Distress = Personal Distress IRI subscale
Perspective = Perspective-taking IRI subscale Fantasy = Fantasy IRI subscale
Concern = Empathic Concern IRI subscale Experience = Sum of pain experiences
Top Related
Copyright © 2022 FDOKUMEN

