







Bahasa
Halaman
Hukum


Feed the Future Ethiopia Growth through Nutrition Activity
Blended Integrated Nutrition Learning Module (BINLM):
Review of training material, training approach, knowledge
and skill retention among participants and related factors
March 2019
2
Contents List of Tables and Figures ....................................................................................................................... 2 Acronym ..................................................................................................................................................... 4 Acknowledgement ................................................................................................................................... 4 Executive Summary ................................................................................................................................. 5 Background and Rationale ..................................................................................................................... 8 Objective .................................................................................................................................................... 9 Methods ...................................................................................................................................................... 9 Result ......................................................................................................................................................... 12
1. Material Review........................................................................................................................... 12 1.1. Introduction Module .......................................................................................................... 12 1.2. Micronutrient Module ........................................................................................................ 13 1.3. Adolescent, Maternal, Infant and Young Child Nutrition ......................................... 14 1.4. Acute Malnutrition Module .............................................................................................. 14 1.5. Nutrition in Communicable, Non-communicable Diseases and Special Health
Conditions ........................................................................................................................................ 16 1.6. Nutrition Program Management .................................................................................... 16
2. Review of Training Approach .................................................................................................. 17 3. Knowledge and skill retention among trained health workers ........................................ 21
3.1. General Characteristics of Respondents ....................................................................... 21 3.2. Introduction Module .......................................................................................................... 22 3.3. Micronutrient Module ........................................................................................................ 23 3.4. AMIYCN Module ................................................................................................................ 24 3.5. Acute Malnutrition Module .............................................................................................. 25 3.6. Nutrition and Communicable Diseases Module.......................................................... 27 3.7. Program management ...................................................................................................... 27
4. Potential personal and institutional factors contributing to training effectiveness and
health workers’ preferences ............................................................................................................ 28
Conclusion .................................................................................................................................................. 31 Recommendations ..................................................................................................................................... 33 Annexes ...................................................................................................................................................... 34
Annex I: Material Review Checklist ......................................................................................................... 34 Annex II: Knowledge and Related Factors Assessment Questionnaire .................................................. 37 Annex III: Skill Assessment Questionnaire .............................................................................................. 48 Annex IV: Observation Guide at Health Facility Level ............................................................................. 51 Annex V: Semi-structured KII Guide........................................................................................................ 55 Annex VI: Frequency tables of aggregated score of study participants for each module and general scores ...................................................................................................................................................... 58
List of Tables and Figures
Table 1: Major findings from Introduction Module review, September 2018 ........................................... 12
Table 2: Major findings from Micronutrient module review, September 2018. ........................................ 13
Table 3: Major findings from the AMIYCN Module review, September 2018 ............................................ 14
Table 4: Major findings from the Acute Malnutrition Module review, September 2018 .......................... 15

3
Table 5: Major findings from Nutrition in Diseases and Special Health Conditions Module review,
September 2018 .......................................................................................................................................... 16
Table 6: Major findings from Nutrition Program Management Module review, September 2018 ........... 17
Table 7: Variations in attendance of knowledge and skill session among surveyed health workers in the
four regions, October 2018 ......................................................................................................................... 18
Table 8: General characteristics of health workers who participated in the study in the four regions,
October 2018 .............................................................................................................................................. 22
Table 9: Proportion of health workers who performed tasks listed in conducting prioritized skill in the
micronutrient module in the four regions, October 2018 .......................................................................... 24
Table 10: Proportion of health workers who performed tasks listed in conducting prioritized skill in the
AMIYCN module in the four regions, October 2018 ................................................................................... 25
Table 11: Proportion of health workers who performed tasks listed in conducting prioritized skill in the
MUAC measurement in the four regions, October 2018 ............................................................................ 26
Table 12: Proportion of health workers who performed expected tasks during preparation of F-75 and F-
100, October 2018 ...................................................................................................................................... 28
Table 13: Proportion of health workers who responded to potential individual attributes that can affect
delivery of BINLM training, October 2018 .................................................................................................. 29
Table 14: Proportion of health centers with key inputs for quality delivery of BINLM and subsequent
knowledge and skill retention, October 2018 ............................................................................................ 30
Table 15: Proportion of health centers with key inputs for quality delivery of BINLM and subsequent
knowledge and skill retention, October 2018 ............................................................................................ 30
Figure 1: Proportion of BINLM trained health workers who responded correctly for undernutrition
related questions in the four regions, October 2018 ................................................................................. 22
Figure 2: Percentage of BINLM trained health workers who responded correctly for selected question
from the micronutrient module in the four regions, October 2018 ........................................................... 23
Figure 3: Percentage of BINLM trained health workers who responded correctly for selected question
from the AMIYCN module in the four regions, October 2018 .................................................................... 24
Figure 4: Percentage of BINLM trained health workers who responded correctly for selected question
from the Acute Malnutrition module in the four regions, October 2018 .................................................. 26
Figure 5: Percentage of BINLM trained health workers who responded correctly for selected question
from the Acute Malnutrition module in the four regions, October 2018 .................................................. 27
Figure 6: Percentage of BINLM trained health workers who responded correctly for selected question
from the Acute Malnutrition module in the four regions, October 2018 .................................................. 28
Figure 7: Percentage of BINLM trained health workers who shared to colleagues, October 2018 ........... 29

4
Acronym
AMIYCN Adolescent, Maternal, infant and Young Child Nutrition
BINLM Blended, integrated Nutrition Learning Module
PHCU Primary Health Care Unit
FMoH Federal Ministry of Health
KII Key Informant Interview
e-based Electronic based
SNNPR Southern Nations nationalities and Peoples Regional State
SURE Sustainable Undernutrition Reduction in Ethiopia
ENGINE Empowering the New Generation to Improve Nutrition and Economic opportunities
NNP National Nutrition Program
NGO Non-governmental Organization
UNICEF United Nations Children’s Fund
WaSH Water, Sanitation and Hygiene
HC Health Center
HW Health Worker
ToT Training of Trainers
RHB Regional Health Bureau
WrHO Woreda Health Office
CD Computer Disc
TVET Technical and Vocational Education and Training
ICT Information and Communication Technology
OTP Outpatient Therapeutic Program
SC Stabilization Center
MUAC Mid-upper Arm Circumference
F-75, F-100 Therapeutic milks for children admitted to health centers as in-patient
Acknowledgement
We are thankful to the Nutrition Case Team of FMoH for its determination to see this task concluded
before the start of BINLM revision and supported it from inception to completion. The support letter
from the Ministry and presence of two members of the case team as supervisors during data collection
facilitated the whole process. Our thanks also goes to the members of the technical working group who
participated in the initial meeting called by the nutrition case team and forwarded valuable feedback on
the study methods and tools. The role of the study coordinators and nutrition experts, who engaged in
final revisions of the study tools, as reviewers of the modules and in data collection on the ground, was
central to the success of this task and they deserve huge appreciation. This assessment would not also
come to fruition without participation and genuine reflections of KII respondents from regional health
bureau, woreda health offices, nutrition partners as well as health workers. Let our heartfelt gratitude
reach them.
We believe this output is a step towards ensuring that those mothers and children who visited our
health centers today, seeking for quality health services yet missed some elements, are to enjoy much
better services when they come back tomorrow.
Growth through Nutrition Activity

5
Executive Summary
Background: The National Nutrition Program (NNP) II of Ethiopia specifically recommends provision
of in-service nutrition trainings to health workers through use of blended integrated nutrition learning
module (BINLM). The blended training approach combines self-paced, e-based knowledge sessions
learning with face-to-face learning focused on practical sessions while ‘integration’ brings multiple
training modules that used to be delivered separately, into one package. The modules include, an
introduction; Micronutrients; Adolescent, Maternal, Infant and Young Child Nutrition; Management of
Acute Malnutrition; Nutrition in Communicable, Non-Communicable Diseases and Special Health
Conditions and Nutrition Program Management.
Since its endorsement in 2015, FMoH, regional health bureaus and partners have applied this
standardized approach to deliver in-service nutrition training to health workers. Growth through
Nutrition is one of the multi-regional nutrition projects that adhere to this standard approach to build
capacity of health workers at PHCUs jointly with health authorities at different levels. Its predecessor
project, ENGINE, has also contributed to the development and finalization of BINLM. In 2017 and early
2018, Growth through Nutrition has provided training to more than 1100 health workers.
Rationale and Objectives: As the BINLM-based training gets rolled out across regions, however,
challenges related to its unique features of being ‘e-based’ and ‘integrated’ started surfacing out from
anecdotal reports of nutrition program implementers and preliminary assessment conducted by
Transform PHC. Hence, in discussion with FMoH that planned to revise the training material in 2019/20,
Growth through Nutrition conducted an operational research with the aim of ensuring effectiveness of
BINLM training. Specific objectives of the assessment included; to review all courses in the module, to
evaluate adherence of trainings conducted so far to the recommended approach, assessing knowledge
and skill retention among health workers trained and to identify potential individual and institutional
factors that contribute to the effectiveness of the training.
Methods: The operational research was a cross-sectional survey that applied mixed qualitative and
quantitative methods. In September and October 2018, Growth through Nutrition discussed on the
methods and tools with FMoH and nutrition partners and started the BINLM material review by
recruiting ten technical experts who worked as BINLM master trainers for the past two years. The
experts applied uniform checklist to review multiple attributes of the training module including its
design, content, user-friendliness and assessment mechanisms. After finalizing the desk review, experts
were deployed to Amhara, Oromiya, SNNPR and Tigray to conduct KII among purposively selected
regional and woreda nutrition focal persons on delivery of BINLM trainings, and to review training
reports. Led by principal investigator and two study coordinators from Save the Children, the reviewers
conducted a quantitative survey to assess knowledge and skill retention among health workers within a
year after taking BINLM training. The survey covered 127 health workers from 51 health centers in the
four regions. Experts also conducted observation of health facilities using a checklist. Data from
qualitative assessment were summarized into frequently appearing themes and quantitative data was
entered into SPSS 20.0, cleaned and analyzed using descriptive statistics.
Findings: Training material review component of the assessment has identified both strengths and areas
of improvement. Most of the courses were reported to have clear learning outcomes, contents aligned
with learning outcomes and proper assessment mechanism. Commonly reported gaps included bulkiness

6
of specific courses, lack of readily downloadable/alternative content materials, outdated epidemiological
content, initiatives and programs; failure to show linkage between knowledge and skill sessions; slow
navigability and freezing presentation slides. Reading speed and pronunciation of the narrator and
relevance of courses such as the Program Management course to nutrition service providers were also
suggested to be re-considered.
Regarding evaluation of adherence to recommended training approaches in trainings conducted so far,
variation in delivery was observed across regions and zones within regions. Reported practices included;
ToTs tended to adhere to recommended duration and self-paced approach, but not most of the cascade
trainings. More than a quarter of skill session participants were not asked for knowledge course
certificates before proceeding to skill sessions. Both knowledge and skill sessions were consecutively
facilitated in a single event. And, skill sessions were in some cases facilitated in venues that did not allow
for adequate practical exercise.
Assessment of individual and institutional factors showed gaps that can contribute to training
effectiveness. Nearly half (49.2%) of the health workers lacked basic computer skills. They could access
computer either sometimes (57%) or not at all (22%). Slightly higher than one in ten of the participants
rated their English proficiency as low and thus could miss some spoken or written language. At health
facility level, a tenth of the health centers where trainees were from lacked electric power and slightly
more (14%) functional computers. Observation findings disclosed absence of stabilization centers in
more than half of the facilities, lack of anthropometric measurement tool – length/height board in 55% of
the HCs, counseling materials and therapeutic foods. Institutional culture as characterized by not
supervising training sessions and limited coaching and mentoring practices in the health system were also
cited to affect retention of basic knowledge and skill elements among the trained.
Finally, analysis of knowledge and skill retention in all components of the training module among trained
health workers trained has brought up findings that demand immediate attention. More than half of the
participants (56%) could not score equal to or above the half mark, 50%, for the entire knowledge
module. Similarly, significant proportion of them failed to perform recommended skill tests/tasks for
major nutrition services such as anthropometric measurement, nutrition counseling and therapeutic milk
preparation.
Recommendations:
When working on BINLM material revision:
Use gaps identified and recommendations from course reviewers as general guidance alongside
applying the review checklist to complement and enrich their outputs
Go beyond reviewing and revising technical content of knowledge session by paying equal attention
to other attributes of the training material including the skill sessions. Use of the review checklist at
the start of the revision process helps for this purpose
While addressing specific technical content of specific courses, technical working groups also need
to equally work on commonly identified areas of improvement including:
o Availing of alternative learning tools
o Reducing the bulk of course material by focusing on practical aspects
o Modulating the speed of the narrator and check for pronunciation related complaints
o Linking knowledge sessions with skill training by alerting participants on areas they should
focus at

7
o Setting minimum quality standards for skill sessions including recommending venue,
minimum duration and expertise/experience of facilitators
o Incorporating tips for sharing knowledge and skills and also including sharing of acquired
competencies as one objective of the training
On training delivery approach:
If health authorities are to apply different approaches pressed by the local context, different
approaches for integrated training need to be pre identified and
o Minimum quality standards should be set for the alternatives to which training
organizers that opted for these alternatives must adhere.
o Training guides (Training facilitation tips) for alternatives such as; computer-based group
sessions, which is one of the alternatives approaches currently mostly practiced, need to
be prepared
Compulsory completion of the entire package also need to be weighed against need-based
specific course training attendance
Training sessions need to be supervised by higher level authorities for fulfilling minimum
standards
Technical report of trainings need to be availed by implementing partners as it helps to audit
quality
To address potential individual and institutional factors that affect effectiveness:
Identify and support trainees that require tutoring to go through knowledge sessions
Provide need-based coaching and mentoring
Design alternative training approach, as recommended above, that lack essential amenities
(electric power, computer access)
On case-by-case basis address key gaps of health centers that lack essential services and
basic equipment/supplies that affect overall health service quality
Addressing the broader context and further investigation:
Continue working to improve quality of pre-service nutrition education
Instill the culture of e-based learning during pre-service education

8
Background and Rationale
The National Nutrition Program (NNP) II of Ethiopia underlines the need for providing competency-based
capacity building to health professionals to operationalize nutrition initiatives of the health sector,
effectively. The program specifically recommends provision of in-service trainings to health workers
through use of blended integrated nutrition learning material (BINLM). The blended training approach
combines self-paced, e-based learning with face-to-face learning while ‘integration’ brings multiple training
modules that used to be delivered separately, into one package.
In Ethiopia, the blended and integrated nutrition learning material was finalized and endorsed by Federal
Ministry of Health (FMoH) in 2015. It comprises of an e- (computer)-based self-learning that takes 10-21
days and a face-to-face skills training of 5 days. The modules include, an introduction; Micronutrients;
Adolescent, Maternal, Infant and Young Child Nutrition; Management of Acute Malnutrition; Nutrition in
Communicable, Non-Communicable Diseases and Special Health Conditions and Nutrition Program
Management.
Currently, most nutrition stakeholders supporting nutrition-related in-service trainings of health workers
in Ethiopia apply the BINLM based approach. Growth through Nutrition is one of the multi-regional
nutrition projects that adhere to this standard approach. A USAID-funded multisectoral nutrition project
(2016-2021) that aims to reduce stunting by supporting multiple sectors to implement their roles in the
NNP. The project, led by Save the Children Ethiopia and run in partnership with international and local
NGOs1, is being implemented in 102 woredas across four regions; Amhara, Oromiya, SNNPR and Tigray.
It primarily targets mothers and children in ‘the first 1000 days’ through supportive agriculture/livelihood,
WASH, SBCC, nutrition-specific and multisectoral nutrition coordination efforts that mainstream gender,
research and learning and strategic coordination with other nutrition related projects. Need-based
capacity building to health workers in project-targeted woredas by using standard training approach is one
of the major activities that it carries out with the health sector.
Growth through Nutrition continued supporting the BINLM training approach by building off the technical
role of its predecessor project (ENGINE, 2011-2016) played to the development and finalization of the
blended learning material. By March 2018, through application of the recommended training approach and
using ToT trained facilitators from the health sector, Growth through Nutrition provided BINLM-based
training to more than 1100 health workers across the four intervention regions.
As the BINLM-based training gets rolled out across regions, however, challenges related to its unique
features of being ‘e-based’ and ‘integrated’ started surfacing out. Electricity coverage and access to
computers including computer skill of potential trainees, which are key elements for completing the
knowledge part of the training, started posing challenges in some areas. This was reported to force training
organizers to shift training approach back to the traditional way of inviting trainees to where they can
access computers together. Secondly, the ‘integrated’ approach that brings separate trainings into one
package was questioned from the point of relevance to some of the trainees and the lack of ‘focus’ that
may diminish effectiveness of the training. Growth through Nutrition thus proposed to conduct
operational research that compiles lessons and challenges in running the training as recommended and
1 International NGOs: Jhpiego, Tufts University, The Manoff Group, Land O’Lakes International Development, PSI
and World Vision, Local NGOs: EOTC-DICAC, EMERDA, FIDO, Mums for Mums, CVDA

9
assesses effectiveness of the training in terms of knowledge and skill retention among participants. As
FMoH plans to revise the BINLM in 2019, findings of this assessment would be an input for the revision.
This assessment was also informed and driven by findings of a qualitative assessment conducted in Oromiya
and SNNPR by TRANSFORM PHC2, a USAID funded health project that mainly assessed effectiveness of
the training approach with regard to feasibility related issues and views of trainees on the training
approach. The study found out that the training approach is regarded as interesting by trainees whereas -
access to computers and electricity, doubts on its effectiveness in building essential skills, contrasting views
on integration of several modules in one package, irregularities in implementing trainings across different
areas were cited as major concerns. The assessment also recommended a quantitative assessment that
looks into effectiveness of the training. Growth through Nutrition, together with FMoH and other
nutrition stakeholders invested on this study to comprehensively dive into the concerns, challenges and,
thus, see how the BINLM-based training is enabling health workers to provide quality nutrition-specific
services.
Objective
General Objective: To ensure effectiveness of the BINLM training in building capacity of health
workers to deliver quality nutrition services
Specific Objectives:
1. To review contents of the training in terms of being fit-for-purpose and target audience
2. Evaluate level of adherence to the recommended approach of applying ‘blended’ and ‘integrated’
training in woredas of varying contexts in the four regions
3. Assess retention of key knowledge and skill competencies among BINLM trained health workers
4. Identify potential individual and institutional factors that can affect effectiveness of BINLM training
Methods
After discussion with FMoH’s Nutrition Case Team in August 2018, Growth through Nutrition proceeded
towards a comprehensive BINLM assessment starting from September 2018.
Study Design: The study applied a cross-sectional mixed approach study design with qualitative and
quantitative components was applied.
Qualitative component consisted of -
Desk review- review of the BINLM training module components and technical reports of BINLM-
based trainings facilitated by government and nutrition partners mainly UNICEF, Growth through
Nutrition, Transform PHC and SURE program
Key informants interview: Regional Health Bureau and woreda health office nutrition focal persons,
training organizers and facilitators
Quantitative survey: Cross-sectional survey among randomly selected BINLM trained health workers
and observation of health centers they work in
2 BINLM effectiveness: Preliminary Assessment: Qualitative assessment findings and proposal for further
investigations/studies. USAID: Transform Primary Health Care

10
Study period: September-October 2018
Study Area: Growth through Nutrition implementation region I.e., all 101 intervention woredas and
health centers where health workers were trained from constituted sampling frame of the study
Study population: For the qualitative assessment, regional and woreda level nutrition focal persons and
training organizers and facilitators from UNICEF, Growth through Nutrition Project regional managers
and Transform PHC relevant staff. For the quantitative survey, those health workers trained via training
sessions that Growth through Nutrition jointly organized with regional health bureaus and woreda health
offices, from June 2017 to March 2018, and health centers where the trainees practice
Sampling Method:
Qualitative: All components of the training module and available training reports were included for the
qualitative review. KIIs included purposively selected respondents from the four regions and all woredas:
RHB and WrHO nutrition focal persons or their delegates, training facilitators/their representative from
BINLM implementing bodies (government/partners). This added up to 29 key informants.
Quantitative: A list of all trainees who completed BINLM course in trainings facilitated by Growth
through Nutrition from June 2017 to March 2018 across all regions was used as a sampling frame. Sample
size was calculated using a single population proportion formula. Assuming a proportion of knowledgeable
participants, trained health workers with an average score of 80% in the e-based knowledge courses as
90%, the standard formula was applied.
n = Z2
p(1-p) = (1.96)²0.90(1-0.90) => 136
w2 (0.05)²
Where Z = Z value, which is 1.96, P = the proportion of trained health workers for passing score
have >80% to 100%, w= the margin of error, N = sample population and n = sample size
Finite population correction formula = n/ (1+n/N) = 136/1+136/1108 => 121
Non-response rate of 5% was assumed resulting in final sample size of 127. Samples were distributed
across regions based on number of trained health workers and considering resources, 10 woredas were
selected purposefully, targeting those woredas where larger number of trained health workers could be
reached at a time. All HCs where study participants worked in were included in the survey.
Study Tools:
Desk review: A checklist to review the e-based BINLM course was adopted from an evaluation checklist
prepared for a related e-based course.3 The tool was commented upon by the technical working group
led by FMoH’s nutrition team at the start of the assessment. (Annex I)
KII Guide: A semi-structured interview guide was developed with sections on respondents background,
training related experience and views. (Annex V)
Quantitative survey questionnaires: This included individual questionnaire and facility-based
observation checklist. The individual questionnaire had three major components: a section on general
socio-demographic characteristics, personal and training related factors; a second part on knowledge
3 University of New Hampshire: Course Review Checklist
file:///C:/Users/L.Berhanu/Downloads/UNH_Course_Review_Checklist%20(1).pdf

11
questions extracted from the BINLM manual (mostly in line with practice questions presented in the
module) and a third section with observation checklist that assesses practice level of selected skill sets
among sampled respondents. (Annex II and III) The facility-based observation checklist had sections that
assessed availability of electricity, computers, and services (in-patient management for acute
malnutrition/SC and outpatient management/OTP) and key nutrition commodities. (Annex IV)
Data Collection: Nutrition Advisor of Growth through Nutrition was principal investigator and two
experienced study coordinators from Save the Children, Ethiopia Office managed the whole assessment
process. Ten experienced BINLM ToT trainers including two experts from FMoH nutrition team were
recruited by Save the Children. They participated in finalization of data collection tools, conducted KIIs
at regional and woreda levels and reviewed training reports. Each module was independently reviewed
by two experts. Two observers per participant assessed skill.
Data Quality Management, Data Entry and Analysis: Selection of nutrition experts for material
review and skill assessment was merit-based and three days orientation and material finalization session
was done involving all assessment team. Supervisors, one per each region, provided on-site support to
data collectors by checking data for completeness and consistency on daily basis. At field level, study
participants were given adequate time to complete the self-administered knowledge questions. Data
were initially entered into EPI 3.5.3 Software Package. Data analysis was done using SPSS 20.
Ethical Consideration: FMoH issued support letter that outlined the purpose of the study. Individual
informed consent was taken from all qualitative and quantitative study participants. Health workers with
identified skill gaps were coached on correct procedure after the skill-sets tests were finalized.
Limitations of the Assessment: For the quantitative component, woredas included in the survey were
purposively selected considering operational constraints. While random selection of trained professionals
from the sampling frame could allow acceptable generalizability, likely inclusion of less remote sites in the
study might allow assuming findings from assessed health facilities are relatively better estimates. Experts’
review of the training module, two per course, while it provides a reasonable evaluation of the course
along multiple attributes, it is not expected to be technically exhaustive. The actual module revision will
benefit more from similar exercise by technical experts who participate in the revision. For the qualitative
assessment, absence of appropriate respondents in some cases and training reports might have affected
quality of output. Finally, measurement of knowledge and skill retention among health workers trained in
the past is not the best method to measure training effectiveness. However, given the BINLM approach is
currently the standard for in-service capacity building on nutrition, study outcomes can be taken as proxy
indicators for BINLM effectiveness.

12
Result
This chapter is structured into four sections that respond for each study objective by applying mixed
methods. The Material Review section presents findings from the exercise where each module was
reviewed on multiple attributes by two BINLM master trainers. The Review of Training Approach section
looks into adherence to recommended training approach as reported by key informants in the four
regions, documented in reviewed written reports and reported by trained health workers. The
Knowledge and Skill among trained health workers presents quantitative findings from the knowledge and
skill survey of trained health workers. ‘Potential personal and institutional factors contributing to training
effectiveness and participants’ preference’ presents findings from the health workers survey and
observation of the health facilities and sets the context in which BINLM training takes place.
1. Material Review
Two reviewers applied a uniform checklist per each six module to evaluate content, design, user-
friendliness and presentation of the learning materials. They used the version of the training modules
that FMoH and TRANSFORM PHC revised in 2018. Findings are presented for each module as follows.
1.1. Introduction Module
Reviewers appreciated the level of information given in the general course overview. The technology
used (e-based learning) was, by principle, deemed appropriate to transfer introductory knowledge on
nutrition and for the learning objectives set in the module. Besides, learning outcomes were rated as
clear, concise and measureable. Content of the module is also well aligned with expected outcomes.
Assessment and feedback components are also in a good shape and need no or minimal revision.
Table 1: Major findings from Introduction Module review, September 2018
Reviewed Attribute Gaps
Course overview
Lacks information on -
Minimum and maximum days to cover knowledge and skill
part of the whole course
Facilitation skills to transfer knowledge and skills by
facilitators/among trained,
What is expected from training organizers and trainees at
different levels
How to install the module
Prerequisites- minimum level of computer and language skill,
materials for practice where required
How knowledge sessions link with knowledge
Course technology
and tools
Lack of access to computers among trainees
Trainees need to have computer skills
Takes time to browse through material- sometimes fails to
resume to the next page or go back
Lack alternative tools: easily downloadable/printable version
(as PPT,DOC,PDF) for use as reference or refreshment
purpose

13
Reviewed Attribute Gaps
Design and layout
There are some unreadable texts in the slides.
Few slides in need of being more eye caching
Content
Pronunciation of the narrator might be difficult those with
lower English proficiency
Epidemiological data need to be updated using latest global
and local figures
Volume/bulk of content need to be checked from
introductory session perspective
Session goes beyond comprehensive introduction and delves
deeper into nutrition education and counseling.
Make sessions more local and focus on easily doable points
Some contents lack source documents
Course summarizes key facts of the session before ending
Assessment and
Feedback
No need for revision on methods (content to be reviewed
with overall introductory part revision
1.2. Micronutrient Module
Reviewers acknowledged the general information given on purpose, structure and tasks, who developed
the course and citation of key references in the overview section. They believed that technology applied
to transfer knowledge related to the module is appropriate, learning outcomes are clear and
measureable, written from participant’s perspective. Content is mostly directly related to objectives and
exercises for practice are aligned with specific course objectives. Table xx summarizes major concerns
raised by the reviewers.
Table 2: Major findings from Micronutrient module review, September 2018.
Reviewed Attribute Gaps
Course overview Lacks information on time required for completion of the
session and how the course links with practical/skill sessions
Course technology
and tools
Session requires computer skill & competencies, availability
of computer, access to electric power
No printable materials- solely dependent on e-learning
(computer based)
Design and layout Font size of content is, mostly, very small & slides cannot be
easily zoomed
It is not easily to navigate or proceed from one page to the
next. Trying to do so sometimes results in re-opening of the
whole module.
Hyperlinked information cannot be easily opened and viewed
Content All sessions are very vast and take longer to complete
Some of the content more appropriate to program managers
than HWs
Not updated data (Epidemiology of Vit A, goiter from 2005)
Some of the language not easily understandable (fast reading)
Sources not cited for some of the references

14
Reviewed Attribute Gaps
Focuses more on facts and less likely to drive trainees to
action
Assessment and
Feedback
Fails to provide certificate, and in some cases prefer
computers with appropriate applications to do so.
1.3. Adolescent, Maternal, Infant and Young Child Nutrition
Reviewers noted that the course overview captures purpose, structure of the course and tasks due. The
technology used is also believed to be appropriate to transfer knowledge in AMIYCN and help trainees
meet set competencies. The course presents learning outcomes clearly and content is directly related to
learning outcomes. The volume of the material is believed to be manageable within the assumed
workload of target trainees. Module consists of practical exercises and provides additional and relevant
material for further reading. In general, reviewers reported that this section is improved compared to
the earlier version that they have used to provide training.
Table 3: Major findings from the AMIYCN Module review, September 2018
Reviewed Attribute Gaps
Course overview Information on how to access different sections not available
Lacks information on how knowledge session links with
practical/skill sessions
Course technology
and tools
Technology appropriate to transfer AMIYCN related
knowledge, however,
Better if a word or PDF document was prepared as
alternative for easy access
Good to put instruction on how to access different sections
easily
Design and layout
Font size (e.g. conceptual framework and other diagrams) is
small. Notes & menu section less visible
Content
Update figures based on latest epidemiological data
Areas like counseling(GALIDRAA) need more detail
Adolescent nutrition needs to be presented in a practical
way
Preparation of CF recipes (particularly, for12-24months)
lacking
No demonstration on how to prepare varieties of CF
recipes such as shiro, firfir from locally available food items
besides porridge
Sections on the introduction module on counseling can best
fit here
Assessment and
Feedback Requires establishing effective mechanism not to
systematically cheat exams
1.4. Acute Malnutrition Module
The need for slight revision across multiple attributes is emphasized here. Reviewers appreciated
presence of clear and measureable learning outcomes and direct relation of content with learning

15
objectives. The volume and depth of content is deemed appropriate for the primary targets though they
are not clearly defined. Case scenarios and case stories are clearly presented and relevant for local
context, which allowed content to focus on applicable knowledge rather than simple facts. Content also
provides further reading materials and summarizes key points in the sessions before proceeding to
assessment part. The skill sessions have appropriate objectives and content well aligned with the
knowledge component.
Table 4: Major findings from the Acute Malnutrition Module review, September 2018
Reviewed Attribute Gaps
Course
overview
Lacks information on
Minimum hours/time period recommended to complete knowledge
session
Who the module is primarily targeting
How to easily resume the course from where one has stopped,
What trainees are expected to prepare to attend training
effectively, and
how to access additional references
Course
technology and
tools
Unreadable contents on some slides-
Charts, scenarios on Daily care and patient monitoring session not
readable
Contents can’t be zoomed
Session stops/freezes repeatedly at some slides
Power point not printable- limits better access to trainees without
computers and constant access to electric power
Also consider other alternatives such as making material accessible
via smart phone
Design and
layout
Difficult to scroll up and down e.g. the patho-physiology content
and contents can’t be zoomed,
Not easy to proceed to next sections after completing quizzes
Sessions on pathophysiology of malnutrition, multi charts for in-
patient monitoring cannot be fully read and easily zoomed
Content
Pronunciation of words might be difficult to lower level health
workers
Some slides do not have notes
Recommends Cotrimoxazole to treat pneumonia that WHO
currently disagree with, recommend referral of cases when there is
no physician/skilled senior staff in case of danger sign,
Update with the new way of preparing F-75 & F-100
Repetition of similar scenarios in daily care and patient monitoring
session
Less emphasis on use of recording and reporting formats and
documented patient monitoring as a whole
Assessment
and Feedback
Some parts of the questions are not accessible e.g. multi chart
(Monitoring patient and ward session)
Daily care session and Monitoring sessions do not allow review of
responses
Wrong answers for quizzes in daily care session
16
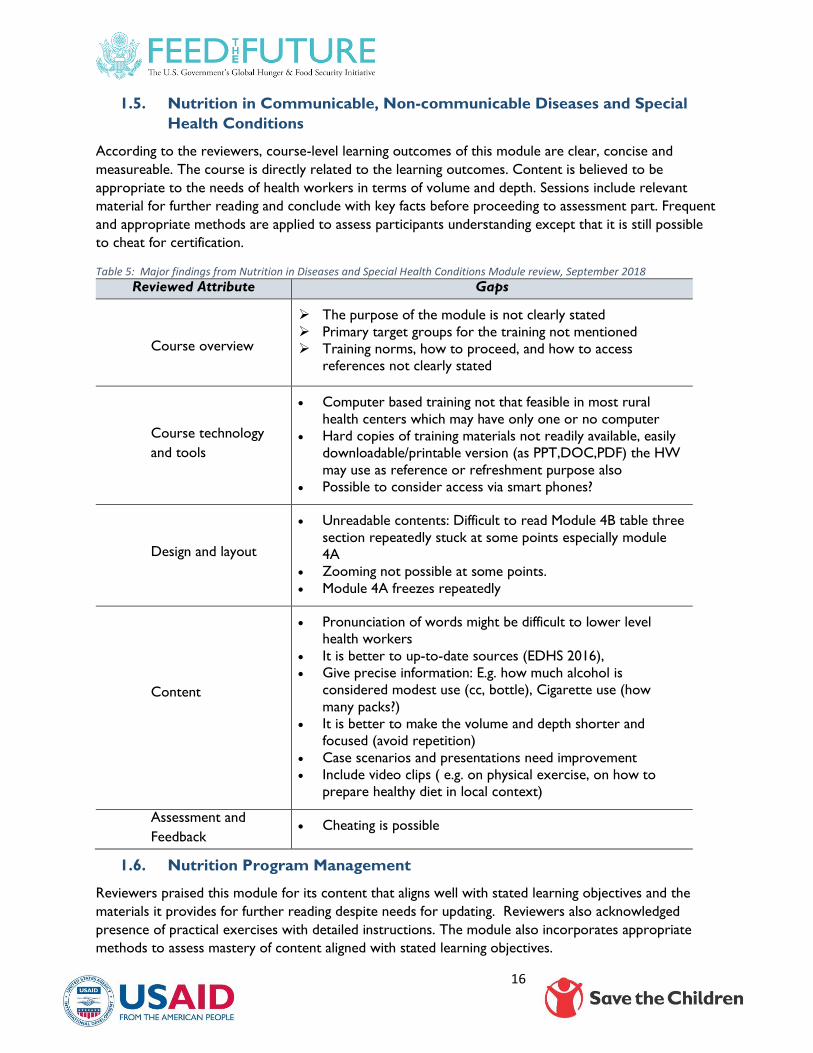
1.5. Nutrition in Communicable, Non-communicable Diseases and Special
Health Conditions
According to the reviewers, course-level learning outcomes of this module are clear, concise and
measureable. The course is directly related to the learning outcomes. Content is believed to be
appropriate to the needs of health workers in terms of volume and depth. Sessions include relevant
material for further reading and conclude with key facts before proceeding to assessment part. Frequent
and appropriate methods are applied to assess participants understanding except that it is still possible
to cheat for certification.
Table 5: Major findings from Nutrition in Diseases and Special Health Conditions Module review, September 2018
Reviewed Attribute Gaps
Course overview
The purpose of the module is not clearly stated
Primary target groups for the training not mentioned
Training norms, how to proceed, and how to access
references not clearly stated
Course technology
and tools
Computer based training not that feasible in most rural
health centers which may have only one or no computer
Hard copies of training materials not readily available, easily
downloadable/printable version (as PPT,DOC,PDF) the HW
may use as reference or refreshment purpose also
Possible to consider access via smart phones?
Design and layout
Unreadable contents: Difficult to read Module 4B table three
section repeatedly stuck at some points especially module
4A
Zooming not possible at some points.
Module 4A freezes repeatedly
Content
Pronunciation of words might be difficult to lower level
health workers
It is better to up-to-date sources (EDHS 2016),
Give precise information: E.g. how much alcohol is
considered modest use (cc, bottle), Cigarette use (how
many packs?)
It is better to make the volume and depth shorter and
focused (avoid repetition)
Case scenarios and presentations need improvement
Include video clips ( e.g. on physical exercise, on how to
prepare healthy diet in local context)
Assessment and
Feedback Cheating is possible
1.6. Nutrition Program Management
Reviewers praised this module for its content that aligns well with stated learning objectives and the
materials it provides for further reading despite needs for updating. Reviewers also acknowledged
presence of practical exercises with detailed instructions. The module also incorporates appropriate
methods to assess mastery of content aligned with stated learning objectives.

17
Table 6: Major findings from Nutrition Program Management Module review, September 2018
Reviewed Attribute Gaps
Course overview
No overview on Nutrition Program Management and its
contents.
No Information on to whom this module is primary
targeted
Course technology
and tools
Check appropriateness against,
Trainees’ lack of basic computer skills
Access to computer
Access to power/ electricity at rural HCs.
Consider alternatives such as hard copy and mobile
application
Design and layout
Guideline part not navigable
Hyperlinks not accessible (NNCB,NNCC)
Missing audio records(Components of Supply management)
Nutrition Supply Management Assessment (Questions not
reviewed, and Finish button freezes)
Content
Narration may not understood by trainees for their lack of
language competency
Updated NNP II (2016-2020) not availed
Health Workers at Facility level may not be primary targets
for the program management module
Better if focus on major duties of the front line service
provider (HW).
Content more befitting to the duties of nutrition program
manager
Assessment and
Feedback
Short answer Questions cannot be reviewed at least against
a strongly suggested response/ ( e.g. Principle to lubricate
the Mechanism of Coordination)
2. Review of Training Approach
This section presents findings health workers responses for quantitative and qualitative questions on the
way training sessions were conducted, responses of KIIs who organized/supervised trainings as well as
from review of accessible training reports of regional health bureaus and nutrition partners.
All four regions provided BINLM-based trainings in the past two years. According to the survey among
health workers, irrespective of the region they are from, apparent variation was observed in the way
participants attended the trainings. As shown in Table 7, a fifth (22%) of the participants attended all
knowledge modules together and a quarter of the participants (27.6%) did have certificates only for
some of the modules or none.
Average duration for attending self-paced knowledge sessions was 14 days (range of two days to three
months) whereas a third of the trainees (33.6%) reported of attending skill sessions for three or less
days. Slightly more than a quarter (27%) of the respondents felt cases were not adequate for practical
session whereas majority of them (86.6%) rated skill of facilitators either as good or very good.

18
Table 7: Variations in attendance of knowledge and skill session among surveyed health workers in the four regions, October 2018
Variable Response Frequency Percent
Took part in knowledge orientation
session (n=125)
116 92.8
Attended knowledge sessions
Alone and where convenient 55 43.3
With a colleague 38 30
All together where computer is
available
28 22
Other 6 4.7
Certified for knowledge session
Yes for all, verified 76 59.8
Yes for all but not verified 14 11.0
Yes, for some 17 13.4
No 18 14.2
Duration of Skill training in Days
One 11 8.8
Two 21 16.8
Three 10 8.0
Four to Five 83 66.41
Location of skill training
Training center/Hotel with
attachment at health facility
67 53.1
Hospital 5 3.9
Health Center 39 30.1
Other 15 11.9
Perceived adequacy of cases to practice
at skill sessions
90 72
Perceived skill of facilitators of the skill
sessions
Very good 54 42.9
Good 55 43.7
Not good 17 13.5
As there was significant variation in mode of training delivery across regions, KII findings are presented
separately for the four regions.
Oromiya: Six KII respondents who responded to the survey reported that trainings were provided by
government, in collaboration with UNICEF, Growth through Nutrition, Transform PHCU and SURE
Program. Three rounds of trainings are provided in the region in the past two years at regional level
claimed that there was no variation during this period. Orientation of two days was provided for the
knowledge part and 30 days were given for self-learning. Skill training was provided for five days.
Respondents reported that self-learning method in BINLM is a good for adult learning and time saving.
The training material consists of rich reference materials. All respondents claimed that the skill part of
the training relatively went well. Study participants did clinical attachments at hospital and health posts.
They also believed that the training was effective in equipping HWs with the appropriate knowledge and
skill though they feel that the knowledge part requires revision in mode of delivery and content.
However, they also noted challenges that particularly affected the knowledge part of the training such as
lack of personal computers and computers at health facilities. Time constraint of health workers also
affected timely completion of courses. One respondent noted that provision of knowledge and skill

19
components separately by itself time taking. Failure of some modules to provide certificate, presence of
duplicated questions and presence of some questions without response were also reported.
KII participants also pointed the need to reduce the volume of some modules and updating resources.
Other suggestions included, providing knowledge and skill phases in one, making hard copies of the
training resources accessible, increasing access through other alternatives such as smart phones,
translating training material into local languages and improving the security issues for some modules.
Follow-up after trainings was also recommended. (However, it is not clear (They were not probed on
whether they have been using the revised version of the training material or not.). Training reports were
not available for review.
Health workers who responded to the question on general feedback on the training frequently
mentioned the need to reduce volume of the modules, increasing training duration, providing the
trainings in the traditional manner, improving the format of the presentations, particularly font size and
making the language simple and clear. They also recommended availing hard copies of the training
materials and allowing specific modules to be taken by specific trainees.
SNNPR: Seven KII respondent reported that BINLM-based trainings were provided in the past two
years mainly by FMoH in collaboration with UNICEF, Growth through Nutrition, Transform PHC and
regional health bureau and zonal health department.
They claimed that there was variation in the way that ToT and cascade trainings were provided. The
CD-based Knowledge part orientation and skill sessions were provided separately during the ToT
whereas in most of the cascade trainings the two sessions were mostly delivered consecutively.
Trainings also varied in the number of days allocated for knowledge and skill sessions. In general, the
ToTs were often adhered to the standard but not the cascade trainings.
None of the KII respondents thought the training was effective in meeting its objectives. They claimed
that most of the trainees did not understand the knowledge component fully, much attention is not
given to the quality of the training, the training is bulky to finish in the given period and health facilities
were not well equipped to practice skill from the trainings. Lack of computer access at health facility and
woreda, limited HWs language and computer skills were noted to affect effectiveness of the knowledge
component. Lack of equipment for skill session such as length board and materials for food preparation.
Participants suggested that training can be improved by conducting proper need and capacity assessment
before providing trainings including addressing challenges of access to computers and HWs capacity,
preparing hard copies of the training materials and if possible increasing access by adapting material to
smart phone application, translating into local language and reducing the size of the training materials.
Improving follow up activities and mentoring after trainings were also recommended.
A training report from a project showed that training was provided according to the recommended
approach with two days orientation on knowledge component and skill session was provided to those
who came with certificates. Challenges faced include lack of computers and power interruptions.
Training facilitators agreed with woreda health offices to use computers at health facilities, where
available, to address this challenge.
Amhara: Seven respondents participated in the KIIs. According to them, FMoH and RHBs, UNICEF,
SCI/Growth through Nutrition, SURE project and TRANSFORM PHC provided BINLM trainings.
Nonetheless, interviewees reported that there was variation in the way the trainings are provided. The
orientation on knowledge sessions lasted for 1-2 days and self-learning from two weeks to one-month.

20
Skill sessions also lasted for three to five days. In other cases, both knowledge and skill sessions were
provided combined. There were also cases where participants did not take part in skill sessions at health
facilities, as trainings were limited to training rooms. Some reported being trained for skills without
being certified on the knowledge modules. In one case, knowledge sessions were provided without CDs
or in a TVET, ICT room, which brought all trainees together.
Despite all such variations, participants believed that trainees could still acquire knowledge and refresh
their pre-service knowledge from the trainings. Most of them are however skeptical about the quality of
the skill sessions and do not believe BINLM alone will not equip health workers with skills to manage
nutritional problems such as acute malnutrition cases.
Challenges faced during trainings include access to computers and lack of computer skills by the
trainees. Difficulties in opening some of the modules and certifying trainees were also reported (did not
specific whether they faced this challenge while using the revised version). Some participants did not
complete the knowledge sessions when they join for the skill part and the skill sessions were affected by
time shortage that left some sessions uncovered. The case of participants being certified without
completing the module were also reported.
As factors that affect the quality of the trainings, respondents mentioned participation in skill sessions
without completion of knowledge sessions, focus on getting certified without reading among trainees,
lack of computers and computer skills, lack of electric power in as nearly 40% of the health centers in
rural areas and lack constant power supply. Quality of skill sessions were also affected by sessions being
limited to classroom demonstrations, caseload for facility level practice being dependent on where the
sessions take place and facilitation of trainings by limited number of, usually two, facilitators. Not all
participants were also asked for knowledge session certificates to proceed to skill trainings.
On the way forward, respondents suggested the need to review the duration given for the training,
supervising the trainings closely and providing comprehensive exam before proceeding to skills session.
To improve knowledge sessions, providing adequate inputs including computers, CDs, earphones were
suggested. Follow up during and after trainings were believed to be vital to maintain in-training quality
and subsequent application of knowledge and skills. Arrangement of skill session also should factor in
days where there will be adequate number of cases for practice. Participants also suggested extra days
for skill sessions. Most of the participants also underscored the need to provide training for more health
workers and as a gap filler.
According to a training report availed from Growth through Nutrition, a two-day orientation on
knowledge sessions and 15 days CD-based self-learning was followed by skill training. The report
claimed that training was conducted according to BINLM recommendations and no major challenges
were faced.
Health workers responding to qualitative feedback on trainings they participated in suggested the need
to increase duration of training and allocating sufficient period, updating particularly the AM module,
making the sessions under this module simple and clear and assigning facilitators with better knowledge
and skill. They recommended reducing the bulk of the material, availing hard copies, separating trainees
based on need and providing knowledge and skill sessions consecutively as the time gap between the
two sessions creates memory lapse.
Tigray: Eight KII respondents participated in the survey and according to them regional health bureau
together with UNICEF, Save the Children/ Growth through Nutrition and Transform Primary Health
Care facilitated BINLM-based trainings over the past two years.

21
All of them mentioned that trainings were provided using the traditional approach where knowledge and
skill components were delivered consecutively. Duration of the training also varied from five to ten days.
Most of the trainings did not have the skills sessions being limited to providing knowledge sessions in a
classroom. In the cascade training, knowledge sessions were mainly delivered in groups at ICT centers.
Respondents acknowledged the presentation of nutrition in a comprehensive manner in the BINLM.
They appreciated attributes including its role in making HWs assess their computer skills and being
familiar with self-learning. Other positive traits included preparation of the training material with
abundant reference materials, practical exercises, and delivery of knowledge session that will not be
affected by facilitators’ variations.
Most respondents, however, reflected negative attitude when it comes to effectiveness of the trainings.
The major reason forwarded was delivery of the training that is not in line with the intended delivery
approach. This has made the training liable to group based training, which may not be helpful for
individual capacity building. Other factors believed to affect effectiveness included language barrier, lack
of commitment and responsibility by training organizers particularly for the skill part, facilitators’
competence, particularly experience on the area that they are assigned on, provision of the whole
course to all types of health workers and lack of equipment and supplies.
Challenges faced include lack of computers and computer skills by trainees, irregularity in power supply,
language barrier and limited time for knowledge sessions. Material related challenges including corrupted
CDs, readability of training materials, sessions that freeze were some practical problems they faced to
attending the e-based course.
Respondents highlighted that focus should be given to the effectiveness of the training. They believe this
can be done by organizing trainings based on profession of health workers, reducing the volume of the
training material, making the material friendlier and the format readable, assigning well-experienced skill
session facilitators. If possible, translating material into local language and preparing hard copies were
also recommended.
Technical training reports were shared from projects but not from RHBs or woreda health offices.
Challenges highlighted in the reports include inability to finalize knowledge sessions of all modules in
four days (as the whole training was delivered consecutively within eight days), language capacity of
trainees, limited computer skills and computer access, repeated power interruptions and participation of
some health workers in courses less relevant to their routine work. Limited capacity of skill session
facilitators was also noted in the Transform PHC report. Training organizers tried to address these
challenges via intensive support during training period.
3. Knowledge and skill retention among trained health workers
3.1. General Characteristics of Respondents
From 51 health centers, 127 health workers participated in the study with slight majority being female
(56%). Half of them were Diploma holders (51%) and the majority clinical Nurses by profession (47.2%).
The majority of the trained (61.9%) were working in maternal and child health units during the time of
the survey. Participants had an average of five years of professional experience and have stayed for
nearly three years at the health facility they were working at the time of the assessment.

22
Table 8: General characteristics of health workers who participated in the study in the four regions, October 2018
Variable Category Frequency Percent
Sex Male 56 44.1
Female 71 55.9
Mean age 27.5 Years
Education level
Diploma holder 65 51.2
B.Sc. Degree 57 44.9
MD/Master’s Degree 3 2.4
Other 2 1.6
Profession
Clinical Nurse 60 47.2
Health Officer 31 24.4
Midwife 28 22.0
Physician 4 3.1
Other 4 3.1
Current department
Under five Clinic 39 30.9
Immunization 8 6.3
ANC/PNC/FP 31 24.6
Others(eg, OPD,TB etc) 48 38.1
Mean year of
professional
experience
5 Years
Mean duration of
stay at the health
facility
2.9 Years
3.2. Introduction Module
This module mainly explained the concept of nutrition, malnutrition and level incidence and prevalence
of major nutritional problems at global and local levels. Out of eight questions, responses to those
related to the definition of stunting, its prevalence, and understanding on immediate and underlying
causes of malnutrition are presented in the figure below. In general, 40-60% of the participants failed to
respond correctly to questions related to these variables.
Figure 1: Proportion of BINLM trained health workers who responded correctly for undernutrition related questions in the four regions, October 2018
On remaining questions related to nutrition education and counseling, which the introduction module
addresses in relative detail, more than two thirds (70% of the respondents identified assessing nutrition
51%
60%
44%40%
Correct definition of stunting Stunting the most prevalentform in Ethiopia
Identified disease asimmediate cause of
malnutrition
Identified HH food insecurityas immediate cause

23
problem of clients as the first step to conduct nutrition education. Around 60% of the respondents also
identified nutrition counseling as a process that helps to assess, analyze and plan solutions for nutrition
related problems. Majority rejected the option of attempting to convince a client is a component of
GALIDRAA approach. (For frequency table for responses on these variables, see Annex xx).
In general, nearly four fifth (79%) of the participants responded correctly four or more out of the eight
questions (≥ 50%) in the introductory module. (See scores in Annex VI.)
3.3. Micronutrient Module
Out of 126 health workers who responded to all questions for this module, the role of zinc as a
micronutrient that decreases incidence and duration of diarrhea, consequences of iron deficiency on
maternal and newborn health and pregnant women as the most vulnerable group for iron deficiency
anemia were responded correctly by more than 85% of the participants. The least proportion of
participants came for timing for deworming during pregnancy and the role of delayed cord clamping in
improving iron status during early infancy, 25% and 11% respectively. Frequencies worth further
reflection are highlighted in red in the figure below.
Figure 2: Percentage of BINLM trained health workers who responded correctly for selected question from the micronutrient module in the four regions, October 2018
Nearly two-thirds (78%) of the participants scored a passing mark, more than 50%, for this module. (See
detail aggregate score in Annex VI).
87
32
92
87
25
67
43
54
71
11
0 10 20 30 40 50 60 70 80 90 100
Iron deficiency- consequence
Vitamin A Role
Zinc in diarrhea management
Group that requres more iron
Deworming starts from the first trimester
Right advice on IFA side effect
Continued IFA postnatally IFA supplementation
Folic acid deficiency
Care for Iodized salt
Delayed cord clamping improves iron status during early…

24
Regarding demonstration of skill in Vitamin A delivery for 6-23 months old infants and children, at least
two-thirds of the participants performed expected tasks for all evaluated tasks. (Table 9)
Table 9: Proportion of health workers who performed tasks listed in conducting prioritized skill in the micronutrient module in the four regions, October 2018
Task Percent
Greet mother 75.6
Asked for age of child 89.0
Asked if child received in the last one month 69.3
Selected appropriate dose 83.5
Cut nipple at the middle 85.0
Asked care taker to hold the child firmly 74.8
Checked if the child is comfortable after swallowing drops 63.8
Discarded capsule into bag and wipe hands clean 67.7
Recorded on tally sheet 68.5
3.4. AMIYCN Module
Twelve questions were presented to assess knowledge retention under this module. The question
related to the need for increased breastfeeding for a sick infant was responded by the highest majority
(84%). Questions on weight gain during pregnancy, nutrient requirements during pregnancy and lactation
as well as the recommended mix for complementary food (porridge) preparation were responded by
less than a third of the participants.
Figure 3: Percentage of BINLM trained health workers who responded correctly for selected question from the AMIYCN module in the four regions, October 2018
Slightly more than half (54.3%) of the participants scored ≥ 50% on this module. (See Annex VI for
aggregate scores.)
42
31
73
33
52
47
47
32
48
84
46
65
0 10 20 30 40 50 60 70 80 90
Disease as Immediate cause of maternal malnutrition
Nutrient requirement of PLW
Care and nutrition during P&L
Weight gain during pregnancy
Intervention for adolescents
Proper positioning during breast feeding
Complementary food for 12-24 month child
Mix recommended for child's porridge
Benefit of adequate nutrient during Pregnancy
Infant feeding during sickness
Feeding low-birth weight babies
Community involvement for nutrition

25
Skill of participants was assessed on application of the GALIDRAA approach in counseling for optimal
maternal infant and young child feeding. As shown in Table 10, relatively higher proportion of the
respondents (>60%) identified the most important problem. However, around a third of the health
workers were evaluated to be poor listeners. Majority failed to use of counseling cards and in more than
a quarter of the cases there was no discussion on whether recommended practices were do-able, and in
letting mothers repeat agreed upon recommendations. More than a third of the health workers also
failed to appoint the mother for the next meeting.
Table 10: Proportion of health workers who performed tasks listed in conducting prioritized skill in the AMIYCN module in the four regions, October 2018
Task
Rating
Not Done Good Not Good
Greet the mother 9.4 55.1 35.4
Asked key questions for a child 12.6 52.8 27.6
Asked key questions for P/L mother 11.8 47.2 22.8
Listened attentively 13.4 54.3 32.3
Identified difficulty and prioritized the most important problem 26.0 61.4 11.8
Used counseling cards properly 61.4 31.5 7.1
Discussed simple doable actions based on identified and
prioritized problems 23.6 67.7 8.7
Discuss optimal breastfeeding/complementary feeding options
appropriate to the age of the child 19.7 62.2 15.7
Discussed if suggestions are easy or not to practice 29.9 55.9 11.8
Help the mother/care giver to agree and to try one of the options, and
asks them to repeat the agreed-upon actions. 26.8 59.8 11.8
Appointed the mother 36.2 44.1 17.3
3.5. Acute Malnutrition Module
Participants responded for ten questions under this module starting with definition of wasting and
focusing on acute malnutrition case classification and case management. Except for a question, where
they correctly classified a case as normal and selected the right mode of management, less than half of
the participants failed to choose the correct answer for the remaining nine questions. Cumulative
scores showed that less than half (44.9%) of the respondents scored greater than 50% for this module.
(See annex VI for detail)

26
Figure 4: Percentage of BINLM trained health workers who responded correctly for selected question from the Acute Malnutrition module in the four regions, October 2018
For assessing skill in acute malnutrition identification and case management, anthropometric
measurement and preparation of F-75 and F-100 feeds were selected. Observation of health workers in
demonstration of skills showed that procedures are not often followed as recommended. MUAC
measurement showed that gaps are observed mostly in identifying the mid-point (performed correctly
by <50%).
Table 11: Proportion of health workers who performed tasks listed in conducting prioritized skill in the MUAC measurement in the four regions, October 2018
Activity Performed (%)
Located tip of shoulder 55.9
Located tip of elbow 52.0
Placed tape at tip of shoulder 51.2
Pulled tape past tip of bent elbow 44.9
Marked mid-point 46.5
Wrapped the tape on the arm across the marked point 71.7
Corrected tape tension 70.9
Corrected tape position for arm circumference 63.0
Measured MUAC to the last completed 0.1 cm and record it
immediately. 60.6
Regarding skill assessment, as shown in table 11, less than 40% of the respondents performed key tasks
expected in preparation of F-75 and F-100 feeds for acute malnutrition cases managed under Phase 1
and Transition phases.
26
40
28
61
49
39
44
38
23
14
0 10 20 30 40 50 60 70
Definition of wasting
OTP case definition
Inpatient-case classification
Normal case management
OTP case classification
Under 6 months SAM classification
SAM management
Misdiagnosis as Commonest cause of death
Mangement of common complications
Under six months SAM case management

27
Table 12: Proportion of health workers who performed expected tasks during preparation of F-75 and F-100, October 2018
Task Performed (%)
Summarized total ml of milk to be prepared for both Phase 1 and transition 40.9
Calculated the number of red scoops and amount of water accurately 37.8
Washed hands 37.8
Measured the amount of water for each phase 41.7
Put the right number of red scoops for each phase 37
Used whisk and prepared the milk 40.9
Measured the right amount and (to) offer to the children 38.6
3.6. Nutrition and Communicable Diseases Module
Seven questions were forwarded to test knowledge for this module. White refined flour as a risk factor
for increased total blood cholesterol was identified by the least proportion of participants (29%),
whereas the majority responded correctly for no need of administering insulin in management of Type 2
diabetes. Nearly half (49%) of the respondents scored above 50% under this module. (See Annex VI for
detail.)
Figure 5: Percentage of BINLM trained health workers who responded correctly for selected question from the Acute Malnutrition module in the four regions, October 2018
3.7. Program management
Six questions on concepts of nutrition-specific and –sensitive interventions, multisectoral coordination
and crosscutting issues such as communication and supply related issues were focused at under this
module. As shown in Figure 6, majority of the respondents (60%) failed to identify the concept behind
nutrition-specific intervention. A quarter of the study participants (25%) scored above 50% for this
module.
38
51 50
65
79
49
29
Correct aboutHIV/TB andmalnutriton
Not CriticalNutrition
Practice forPLHIV
Dietarymanagement of
diarrhea
BMI basedclassification
Type 2 diabetesmanagement
Directcontributer to
chronic diseasein developing
countries
White refinedflour as a risk
factor

28
Figure 6: Percentage of BINLM trained health workers who responded correctly for selected question from the Acute Malnutrition module in the four regions, October 2018
Finally, aggregated score of each study participant showed that 45% of the participants scored above
50% for all six modules. (See Annex VI for aggregate scores)
4. Potential personal and institutional factors contributing to training
effectiveness and health workers’ preferences
Knowledge and skill retention among respondents is likely to be affected by different factors including
exposure to nutrition related trainings. Responding to the question whether they have participated in
modular trainings similar to the one in BINLM, more than a fifth (23%) replied positively. Acute
malnutrition management and Adolescent malnutrition were the topics on which most of the
participants were trained.
Table 12: Proportion of health workers who performed expected tasks during preparation of F-75 and F-100, October 2018
Item Response Percent
Participated in separate modular trainings 29 23.2
Type of training
Acute Malnutrition 11 8.7
AMIYCN 9 7.1
Micronutrient 4 3.1
SBCC 4 3.1
Specific to BINLM training, as a computer-based training to transfer knowledge, it is expected to be
affected by trainees access to computer, computer skill and being a self-teaching one with less chance
for translation a good command of English language. As presented in Table xx, nearly half of the study
participants self-reported of lacking basic skills in use of common computer applications such as word,
excel and internet. Around a fifth of them (22%) can access computers all the time whereas one in ten
founds it hard to understand written and spoken English.
31
48
33
2630
13
Nutrition-specificintervention
defintion
Concept ofnutriton-specific
and -sensitive
Types of nutritioncommunication
Multisectoralcoordination
concept
Supplymanagement
NNP strategicobjective to address
underlying causes

29
Table 13: Proportion of health workers who responded to potential individual attributes that can affect delivery of BINLM training, October 2018
Training Inputs Category Frequency Percent
Computer skill
No expertise in using either MS word, excel,
internet
62 49.2%
Basic skill in using either MS word, excel,
internet
53 42%
Proficient in using either MS word, excel,
internet
12 9.5%
Computer Access
Yes, always 28 22.0%
Yes, sometimes 72 56.7%
Not at all 27 21.3%
Perceived English
Language Skill
Very good (Can fully understand written and
spoken English and is quite OK to be trained
with English)
25 19.8%
Good (understand most of written and spoken
English and does not mind to be trained with
English)
86 68%
Not bad (Finds it somehow hard to fully
understand written and spoken English)
14 11.1%
Not good (Finds it hard to understand written
and spoken English and prefer to be trained
with another language)
1 0.01%
Sharing of knowledge and skills garnered from
trainings also helps in better retention of trained
individuals in addition to extending the reach of key
competencies to other staff not taking part in
formal in-service trainings. The assessment showed
that training materials and acquired knowledge in a
form of on-the-job training was shared by nearly
60% of the study participants.
Figure 7: Percentage of BINLM trained health workers who shared learning to colleagues, October 2018
Other potential factor that affects quality delivery of BINLM training and retention of knowledge and
skill among study participants is the institutional environment they work in. Slightly more than a tenth of
the health centers do not have access to uninterrupted electric power and functional computer.
Therapeutic foods are the least available supplies mainly due to limited presence of stabilization centers,
in less than half of the health centers (47%), followed by lack of nutrition counseling materials in nearly
half (50%-60%) of the health centers.
58.9
59.3
28.1
0.0 20.0 40.0 60.0 80.0
Share training materials tountrained
Provided on-the job K&Straining
Did not get the chance toshare

30
Table 14: Proportion of health centers with key inputs for quality delivery of BINLM and subsequent knowledge and skill retention, October 2018
Available at Health Center Percent
Electric power 88.2
Computer 86.3
Stabilization center 47.1
Weight scale 100
Child MUAC 90.0
Separate room for SC 48.0
RUTF where OTP service provided 76.0
Length/height board 78.0
F75 45.1
F100 43.1
Nutrition counseling card 57.1
Growth monitoring Chart 54.2
Family Health Guide 57.8
Finally, when it comes to preference of trained health workers on ‘computer-based’ and ‘integrated’
nature of the training, around two-thirds (64%) preferred computer-based courses to classroom based
ones and integrated courses (60%) compared to separate modules.
Table 15: Proportion of health centers with key inputs for quality delivery of BINLM and subsequent knowledge and skill retention, October 2018
Item Category Percent
Computer based course vs. class-room based course
Strongly prefer 42 34.1
Prefer 37 30.1
Both are the same 2 1.6
Prefer class-room based course 23 18.7
Strongly prefer class-room based course 19 15.4
Integrated vs. separate courses
Strongly prefer integrated 47 37.3
Prefer integrated course 28 22.2
Both are the same 3 2.3
Prefer modular course 35 27.8
Strongly prefer modular course 13 10.3

31
Conclusion
Application of BINLM, a combination of e-based knowledge sessions and face-to-face skill training, is a
relatively new approach to capacity building efforts of health workers in Ethiopia. BINLM brings core
topics of nutrition under a single package and thereby contributes towards building health workers’
capacity towards FMoH’s ‘Comprehensive and Integrated Nutrition Services’ delivery approach.
Moreover, it avoids long absence of health workers from their duty station as computer-based and self-
paced study covers much part of the training. In contexts where high staff turnover and staff rotation
prevails, all-rounded basic knowledge and skill on nutrition services among all health workers may
guarantee uninterrupted services delivery at PHCUs. However, the benefits of any training approach can
be realized if only the training is effective in improving knowledge and skills of the trainees.
In general, this study has shown that knowledge and skill competencies directly related to the training
outcomes are low among the trained. More than half of the study participants did not achieve passing
mark for the entire knowledge module and significant proportion failed to perform key skill sets as
recommended. These quantitative findings are in line with another in-depth interview findings of a
qualitative assessment where key informants doubted effectiveness of BINLM. Although the method
applied in this study does not allow attributing positive or negative results directly to the BINLM
trainings, the BINLM approach being the current widely implemented in-service capacity building on
nutrition, study outcomes can be taken as proxy indicators for its effectiveness.
Effectiveness of a training is a factor of adequacy and quality of the training material, its mode of delivery,
and participants’ and institutional factors that are prerequisites for effective participation or practicing of
acquired knowledge and skill. The need for BINLM revision to upgrade quality of the training is already
acknowledged by FMoH. Together with Transform PHC, the material was revised mainly towards
making the module less vulnerable to certifying trainees who did not navigate through a given course
and pass the exams. The ministry has then planned for BINLM content revision in 2019/20.
The training material review of this study identified strengths and gaps to serve as input for the intended
revision. Most of the courses in the module have clear learning outcomes, course content aligned with
these outcomes, and proper assessment and feedback mechanism. On the contrary, commonly shared
gaps include bulkiness of specific courses, lack of readily downloadable/printable alternative content,
failure to show linkage between knowledge and skill sessions, outdated epidemiological data/programs/
strategies and policies, and speed and pronunciation of the narrator. Relevance of courses such as
‘Nutrition Program Management’ to all trainees was also questioned. Reviewers suggested the need to
inform actual revision by further comprehensive look into design, content, user friendliness of the
material by course-specific technical experts, using the checklist applied in this study.
Besides having the appropriate training material, mode of training delivery is another factor that
contributes to effectiveness. Review of the trainings conducted in the past one year by government,
often with UNICEF’s support; Growth through Nutrition and Transform PHC showed considerable
variation among regions, zones and woredas. Trainings mostly organized by government health
bureaus/offices did not adhere to recommended duration and delivery mechanisms. Self-paced feature of
the training was often replaced by group knowledge sessions. ToT trainings tended to adhere to the
standard but not cascade trainings. At times, study participants were not asked for certificates of
knowledge courses before they join skill sessions; both knowledge and skill sessions were delivered in a

32
single training event, and skill sessions were facilitated in locations that did not allow for acceptable level
of practical exercise. There was also no standard for number, mix and minimum experience of
facilitators required for the skill sessions. In general, there was lack of direction for alternative
approaches to BINLM, so that widely practiced trainings could meet minimum quality standards.
BINLM rapidly evolved as a sole approach for nutrition focused in-service capacity building of health
workers on nutrition, in Ethiopia. This relied on assumptions of expanded coverage of electric power,
better access to computers among rural health workers, better health workers’ exposure to basic
computer skills and good level of English language proficiency. However, this assessment showed that
majority of the study participants did not have access to computer; more than half did not have basic
computer skills; and, a tenth of the trainees and material reviewers pointed out language limitations even
recommending local language translation. These findings, as a whole, indicate the need for close support
some trainees may need during the knowledge sessions, if they are to attain desired outcomes.
At institutional level, a tenth of visited health centers lacked electric power and slightly higher
proportion did not have functional computers. Such situations, often likely to affect remote health
centers, call for reflecting on the effect of uniform approaches on equitable access to quality trainings.
Observation findings of health centers that revealed gaps in available service packages and/or key
supplies is expected to lead towards knowledge and skill depreciation among the trained.
Similarly, institutional culture that promotes continuous knowledge and skill building among health
workers and complements one-off training sessions was reported to be mostly absent. Training sessions
were not supervised and followed by mentoring. Trained health workers could fortify acquired
competence by sharing it to their peers and downwards to their supervisees (mainly HEWs). However,
the assessment showed substantial proportion of the trained did not report of knowledge and skill
sharing. Lack of such practices is likely to affect knowledge and skill retention.
At a broader level, the average years of experience of the study participants, 5 years, reminds one that,
at least, around half of the health workers joined the health sector in an era where better attention
started to be given to nutrition education. They might have attended their studies through a decade
where Essential Nutrition Actions and management of acute malnutrition were incorporated into pre-
service nutrition curricula of health cadres. They are also more likely to be members of the computer-
friendly generation. Hence, failure of majority to score pass mark on core knowledge and skill
parameters might call for in-depth look at the quality of pre-service nutrition education and students
exposure to contemporary technology that can advance technical knowledge and skills.
Going forward, since application of BINLM is a pioneer for in-service health workers training in Ethiopia
and is likely to be adopted by other health programs; it is advised to focus more on how to build on the
good start that exists. Study participants have also reported higher level of preference to this type of
training. Hence, improving BINLM-based trainings requires sustaining what is going well and
systematically addressing gaps that affect quality at the different layers of the system, identifying
alternative modes of training delivery where the recommended approach is shown to be less practical,
and setting standards for identified alternatives approaches. Most importantly, it demands going beyond
mere updating of material content when carrying out the BINLM revision.

33
Recommendations
When working on BINLM material revision:
Use gaps identified and recommendations from course reviewers as general guidance alongside
applying the review checklist to complement and enrich their outputs
Go beyond reviewing and revising technical content of knowledge session by paying equal attention
to other attributes of the training material including the skill sessions. Use of the review checklist at
the start of the revision process helps for this purpose
While addressing specific technical content of specific courses, technical working groups also need
to equally work on commonly identified areas of improvement including:
o Availing of alternative learning tools
o Reducing the bulk of course material by focusing on practical aspects
o Moderating the speed of the narrator and check for pronunciation related complaints
o Linking knowledge sessions with skill training by alerting participants on areas they should
focus at
o Setting minimum quality standards for skill sessions including recommending venue,
minimum duration and expertise/experience of facilitators
o Incorporating tips for sharing knowledge and skills and also including sharing of acquired
competencies as one objective of the training
On training delivery approach:
If health authorities are to apply different approaches pressed by the local context, different
approaches for integrated training need to be pre identified and
o Minimum quality standards should be set for the alternatives to which training
organizers that opted for these alternatives must adhere.
o Training guides (Training facilitation tips) for alternatives such as; computer-based group
sessions, which is one of the alternatives approaches currently mostly practiced, need to
be prepared
Compulsory completion of the entire package also need to be weighed against need-based
specific course training attendance
Training sessions need to be supervised by higher level authorities for fulfilling minimum
standards
Technical report of trainings need to be availed by implementing partners as it helps to audit
quality
To address potential individual and institutional factors that affect effectiveness:
Identify and support trainees that require tutoring to go through knowledge sessions
Provide need-based coaching and mentoring
Design alternative training approach, as recommended above, that lack essential amenities
(electric power, computer access)
On case-by-case basis address key gaps of health centers that lack essential services and
basic equipment/supplies that affect overall health service quality
Addressing the broader context and further investigation:
Continue working to improve quality of pre-service nutrition education
Instill the culture of e-based learning during pre-service education

34
Annexes
Annex I: Material Review Checklist Course evaluated: _________________________
Blended and Integrated Nutrition Learning Module (BINLM) Review Checklist to
Be Completed by Selected Experts
SECTION I: Respondent’s Identification and Course Related Information
S.N Question Response
1 Name of the evaluator
2 Sex
3 Profession
4 Current Position and Organization
5 BINLM related experience
1. Material content developer
2. ToT trainer (Master trainer)
3. ToT trained nutrition expert
4. Material designer
5. Other (specify)_________________
|___|
6 Period of evaluation ______to ___________(Month and Date)
7 Course evaluated
1. Introduction
2. Micronutrient
3. Adolescent, Maternal, Infant and Young Child
Nutrition
4. Acute Malnutrition
5. Nutrition and Communicable Diseases, Nutrition and
Non communicable diseases, Nutrition and Special
Health Conditions
6. Program Management
(DIRECTION: A single checklist is applied
for a specific Course in the Module)
|___|
SECTION II: Content and Design Review
DIRECTION: Dear Respondent, please give score to each parameter under the 2nd column with
the scores of 0, 1 and 2 or N/A as described under the 3rd column. Write all specific points you
noted for revision in the 4th column. PLEASE refer to the Skill Manual of the course for Q#24.
S.N
Review Components and Questions
Does not need revision=0
Needs minor revision=1
Needs major revision= 2
Not applicable= N/A
Remark:
I. COURSE OVERVIEW and GENERAL INFOMRATION

35
S.N
Review Components and Questions
Does not need revision=0
Needs minor revision=1
Needs major revision= 2
Not applicable= N/A
Remark:
1 An overview is provided for the Course which includes
purpose, structure, navigation and what major tasks are
due.
|___|
2 Information on who developed the Course and to whom
the courses are primarily targeted is provided.
|___|
3 Information on prerequisites, if any required, and key
references including on how to access them is stated.
|___|
II. COURSE TECHNOLOGY AND TOOLS
4 The technology used in the Course is appropriate for the
learning objectives and competencies expected.
|___|
5 The technology used to provide the Course can be easily
accessed by training targets.
|___|
6 The technology applied for the Course is appropriate to
the computer skill of the majority of the trainees.
|___|
7 The Course and specific sessions can be easily accessed,
do not ‘stuck’, frequently’ and allow back and forth
navigation.
|___|
8 Alternative tool (e.g. easily downloadable/printable
version) is suggested if primarily recommended
tool/approach does not work.
|___|
III. DESIGN and LAYOUT
9 A logical, consistent, and uncluttered layout is developed |___|
10 There is enough contrast between text and background
for the content to be easily viewed.
|___|
11 The title of the Course links to content and resources
working order.
|___|
12 The Course is easy to navigate: consistent color scheme
and icon layout, related content organized together.
|___|
13 Contents in the Course have visible slides, fonts are
readable and can be zoomed to improve visibility.
|___|
IV. CONTENT
14 The Course-level learning outcomes are clear, concise
and measurable, written from the participant's
perspective and appropriate for the level of the module.
|___|
15 Content is directly related to the learning
outcomes/objectives for the training.
|___|
16 Content is written and narrated in an understandable
language.
|___|

36
S.N
Review Components and Questions
Does not need revision=0
Needs minor revision=1
Needs major revision= 2
Not applicable= N/A
Remark:
17 Content is up-to-date, scientifically correct, locally
appropriate and logically coherent.
|___|
18 Content is appropriate to the needs of the primary
target /health worker/ in terms of volume and depth.
|___|
19 Volume and depth of the module considers the workload
of the primary target for the training.
|___|
20 Case scenarios, case stories and related examples
provided in the content are clear and relevant for the
local context.
|___|
21 Content drives trainees towards immediate application
of knowledge and behavior rather than focusing on facts.
|___|
22 Content provides additional and relevant material for
further reading.
|___|
23 Course summarizes/ concludes key facts of the session
before ending/ proceeding to the assessment part.
|___|
24 Skill sessions in the skill module for the Course, have
appropriate objectives and content aligned with the
knowledge component of the course.
|___|
V. ASSESSMENT and FEEDBACK
25 The module includes frequent and appropriate methods
to assess participants’ mastery of content.
|___|
26 Criteria for the assessment of a graded quizzes are
clearly articulated (instructions, examples given).
|___|
27 Participants have opportunities to review their
performance and assess their own learning throughout
the module (pre-tests, automated self-tests, etc.).
|___|
28 The assessments are structured to align with their stated
learning objectives.
|___|
29 Assessment questions have clear and specific answers.
|___|
30 Assessment and completion of the course is fairly
protected from cheating.
|___|
SECTION III: General Feedback on the Evaluated Course and the Whole Module
31. General feedback on the Evaluated Course or the Whole Module:
THANK YOU FOR YOUR SIGNIFICANT CONTRIBUTION!
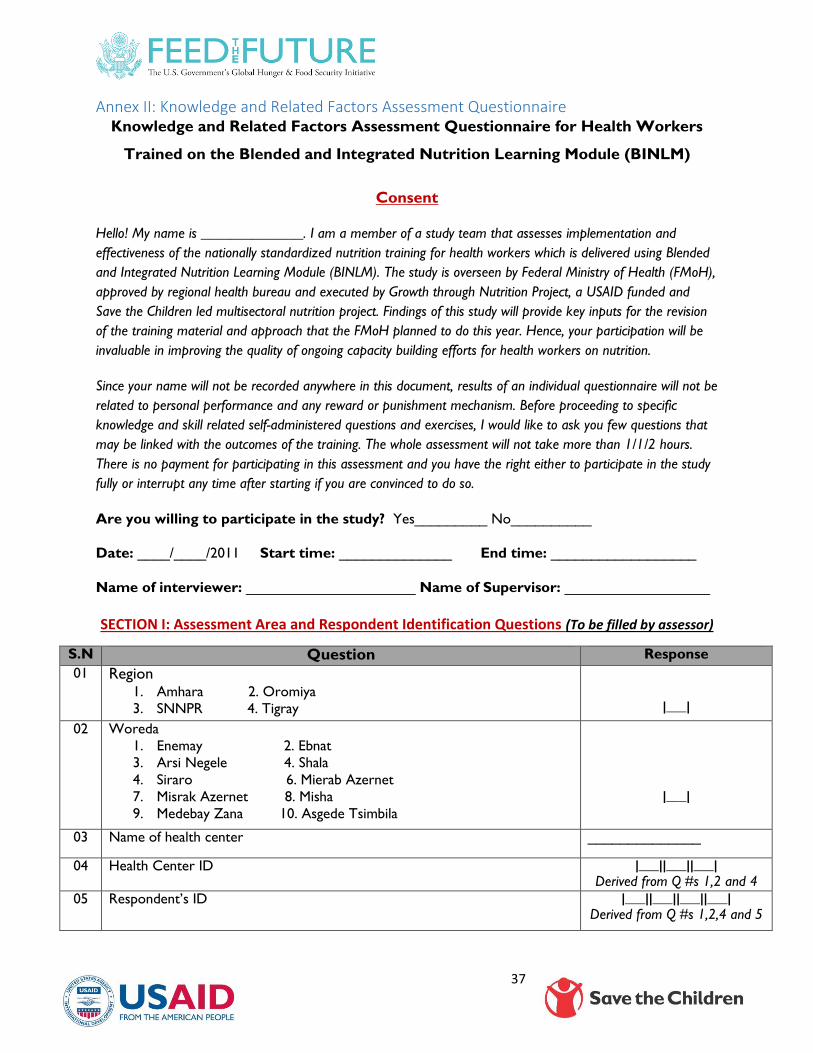
37
Annex II: Knowledge and Related Factors Assessment Questionnaire Knowledge and Related Factors Assessment Questionnaire for Health Workers
Trained on the Blended and Integrated Nutrition Learning Module (BINLM)
Consent
Hello! My name is ______________. I am a member of a study team that assesses implementation and
effectiveness of the nationally standardized nutrition training for health workers which is delivered using Blended
and Integrated Nutrition Learning Module (BINLM). The study is overseen by Federal Ministry of Health (FMoH),
approved by regional health bureau and executed by Growth through Nutrition Project, a USAID funded and
Save the Children led multisectoral nutrition project. Findings of this study will provide key inputs for the revision
of the training material and approach that the FMoH planned to do this year. Hence, your participation will be
invaluable in improving the quality of ongoing capacity building efforts for health workers on nutrition.
Since your name will not be recorded anywhere in this document, results of an individual questionnaire will not be
related to personal performance and any reward or punishment mechanism. Before proceeding to specific
knowledge and skill related self-administered questions and exercises, I would like to ask you few questions that
may be linked with the outcomes of the training. The whole assessment will not take more than 1/1/2 hours.
There is no payment for participating in this assessment and you have the right either to participate in the study
fully or interrupt any time after starting if you are convinced to do so.
Are you willing to participate in the study? Yes_________ No__________
Date: ____/____/2011 Start time: ______________ End time: __________________
Name of interviewer: _____________________ Name of Supervisor: __________________
SECTION I: Assessment Area and Respondent Identification Questions (To be filled by assessor)
S.N Question Response
01 Region 1. Amhara 2. Oromiya
3. SNNPR 4. Tigray
|___|
02 Woreda
1. Enemay 2. Ebnat
3. Arsi Negele 4. Shala
4. Siraro 6. Mierab Azernet
7. Misrak Azernet 8. Misha
9. Medebay Zana 10. Asgede Tsimbila
|___|
03 Name of health center ______________
04 Health Center ID |___||___||___| Derived from Q #s 1,2 and 4
05 Respondent’s ID
|___||___||___||___|
Derived from Q #s 1,2,4 and 5

38
SECTION II: Socio-demographic and Selected Characteristics of Respondents
DIRECTION: Please WRITE the choice in the given space in the right column.
S.N Question Response
1 Sex
1. Female 2. Male
|___|
2 Age _____________
3 Highest attained level of education
1. Diploma 3. MD/M.Sc./MPH
2. B.Sc. 4. Other _______
|___|
_____________
4 Profession
1. Clinical Nurse
2. Health Officer
3. Midwife
4. Physician
5. Other (Specify)________________
|___|
______________
5 Current department you work in the health center:
1. Under-five clinic 3. ANC/PNC/FP
2. Immunization 4. Other
|___|
________________
6 Year of service __________________
7 Duration of stay in this health facility in completed months __________________
8 How do you rate your computer skills?
1. No expertise in using either MS word, excel, internet
2. Basic skill in using either MS word, excel, internet
3. Proficient in using either MS word, excel, internet
4. Other (level and type of skill, if any)
|___|
__________________
9 Do you have your own computer (desktop/laptop/tablet)?
1. Yes 2. No
|___|
10 Can you have access to computer at your work place or elsewhere when you
need it?
1. Yes, always 2. Yes, sometimes 3. Not at all
|___|

39
S.N Question Response
11 How do you rate your English language skill and language preference?
1. Very good (Can fully understand written and spoken English and is
quite OK to be trained with English)
2. Good (understand most of written and spoken English and does not
mind to be trained with English)
3. Not bad (Finds it somehow hard to fully understand written and
spoken English)
4. Not good (Finds it hard to understand written and spoken English and
prefer to be trained with another language)
|___|
SECTION III: Nutrition and BINLM-based Training Related Questions
S.N Questions Response
12 Did you participate in any training that focuses separately on any the following
technical areas in the past 1 year? (PAST one year refers to the period from Meskerem
2010-Meskerem 2011) 1. Yes 2. No
|___|
13 If Yes, to Q 12 what was the training on? READ all choices for respondent and
write choices for each. If ‘No’ to all SKIP to Q 15.
1. Acute malnutrition management 1. Yes 2. No
2. Adolescent, Maternal, Infant and Young Child Nutrition (A/MIYCN)
1. Yes 2. No
3. Micronutrient 1. Yes 2. No
4. Behavior change communication (S/BCC) on nutrition 1. Yes 2. No
5. Other
1. |___| 2. |___|
3. |___| 4. |___|
5. ____________
14 If any is chosen for Q 11, please specify Month(s) of training within 2010/11EC. Month _____ Year _________
Month _____ Year _________
15 Did you take the Orientation (introduction and start-up of first modules) at
the beginning of BINLM knowledge part of the training?
1. Yes 2. No
__________________
16 How long did you take to complete the KNOWLEDGE part of the training? __________________ (WRITE
in number of days) 17 How did you take the KNOWLEDGE part of the training?
1. Alone and where I found it convenient
2. With a colleague (s) where we found it convenient
3. All trainees together where computers are available
4. Other
|___|
__________________
18 Were you certified for the KNOWLEDGE part before starting the skill part?
1. Yes, for all modules and showed the certificates
2. Yes, for all modules but no certificate shown
3. Yes, for some of the modules
4. Not at all
|___|

40
S.N Questions Response
19
For how many days did you take the SKILL part of the training?
|___|
20 Where did you take the SKILL part of the training?
1. Training center/Hotel with attachment to health facility
2. Health center 3. Hospital 4. Other/Specify
|___|
__________________
21 When you take the SKILL part of the training, did you feel there were enough
cases to practice relevant skills?
1. Yes 2. No
|___|
22 How do you rate the skill of the trainers for the SKILL part of the training?
1. Very good 2. Good 3. Not bad 4. Bad
|___|
23
How do you compare the computer-based (e-learning) course with classroom-
based knowledge course?
1. I strongly prefer computer based course
2. I prefer computer based course
3. Both are the same
4. I prefer class-room based course
5. I strongly prefer class-room based knowledge course
|___|
24 How do you compare the integrated (all modules in one) course with separate
modules training?
1. I strongly prefer all-modules integrated course
2. I prefer all modules integrated course
3. Both separate and integrated module courses are the same for me.
4. I prefer trainings delivered separately for specific modules.
5. I strongly prefer separate course than integrated ones.
|___|
25 Did you shift/change your position in the health center (from one unit to
another) after you completed the training?
1. Yes 2. No
|___|
26
If Yes, from which Unit to which unit? If No, SKIP to Q#27.
__________________
27 If Yes, is the health workers that is working in your place trained on BINLM?
1. Yes 2. No
|___|
28 Is there a colleague working with you in the department/unit you are currently
working in?
1. Yes 2. No
|___|
29 If Yes, is s/he trained on BINLM?
1. Yes 2. No
|___|
30 After you completed the training, did you get the chance to
1. Share the training materials to untrained staff 1. Yes, 2. No
2. Give on-the job knowledge and skill training to the staff 1. Yes 2. No
3. Did not get the chance to share 1. Yes 2. No
1. |___|
2. |___|
3. |___|

41
SECTION IV: BINLM-based Knowledge Assessment Questions: PLEASE note that this is a SELF-
ADMINISTERED tool.
DIRECTION: Please WRITE your choice in the space provided in the right column.
S.N Questions per module Response
1. Introduction
1.1 Which one of the following is TRUE about types/indicators of malnutrition?
1. Shortness of a child with respect to its age refers to wasting and shows acute
malnutrition.
2. Wasting refers to rapid loss of weight with respect to child’s age and indicates chronic
malnutrition.
3. Shortness of child with respect to its age refers to stunting and shows chronic
malnutrition.
4. Below standard weight to age for child and shows chronic malnutrition.
|___|
1.2 Currently, which type of nutritional index has the highest level in Ethiopia?
1. Wasting
2. Stunting
3. Overweight
4. Underweight
|___|
1.3 Which of the following is an immediate cause of malnutrition?
1. Household food insecurity
2. Disease
3. Inadequate care
4. Unhealthy household environment
|___|
1.4 Choose the primary process in nutrition education among the following.
1. Selecting education delivery method
2. Assessing problems related with nutrition
3. Selecting follow-up method
4. Preparing nutrition education material
|___|
1.5 Which one of the following is a key element of counseling?
1. Building trust
2. Speaking too quickly
3. Forming working alliance
4. Telling the client what to do
|___|
1.6 One of the following is NOT a component of GALIDRAA counseling approach.
1. Greeting the client
2. Attempting/trying to convince the client
3. Listening to the client
4. Discussing options with the client
|___|
1.7 Which of the following is a COMMON ERROR in counseling?
1. Maintaining eye contact with the client.
2. Sitting in the same level with the client.
3. Finishing sentences of the client.
4. Avoiding physical barriers during counseling.
|___|

42
S.N Questions per module Response
1.8 Which one of the following is TRUE about counseling?
1. It is a one-way communication system.
2. It is the same with nutrition education.
3. It happens when a more knowledgeable person tells a less knowledgeable person what
to do.
4. It helps to assess, analyze and plan solutions for nutrition related problems.
|___|
2. Micronutrient
2.1 Maternal mortality, low birth weight, preterm babies and anemia are highly related to:
1. Zinc deficiency
2. Iron deficiency
3. Vitamin A deficiency
4. Iodine deficiency
|___|
2.2 Which one of the following is TRUE about Vitamin A?
1. Plant source foods are the best source of Vitamin A for human body.
2. Mature breastmilk is the best source of Vit A compared to colostrum.
3. It plays role in immunity, reproduction and fetal development.
4. Dose and frequency of Vit. A supplementation is not affected by age of the child.
5. % of children 0-59 months supplemented with Vit A is an indicator of Vitamin A
supplementation/VAS.
|___|
2.3 Which of the following is TRUE about zinc?
1. Fruits and vegetables are the richest sources of zinc.
2. Currently there is a guideline for zinc supplementation to all children in Ethiopia.
3. Zinc deficiency results in impaired growth and development.
4. In Ethiopia, percentage of children supplemented with zinc helps monitor Zinc
supplementation coverage.
|___|
2.4 Provision of which micronutrient helps to decrease the incidence and duration of diarrhea?
1. Vitamin A
2. Iron
3. Zinc
4. Iodine
|___|
2.5 Which nutritionally vulnerable group requires the highest level of iron intake?
1. Adolescent boys
2. Adolescent girls
3. Pregnant women
4. Lactating women
|___|
2.6 Which of the following is TRUE regarding prevention and control iron deficiency anemia?
1. Deworming of pregnant women starting from the first trimester is recommended.
2. Intermittent IFA supplementation for menstruating women is recommended where
anemia among Women of Reproductive Age (WRA) p is </20%.
3. Delayed cord clamping improves iron status of infant for up to six months.
4. Promoting exclusive breastfeeding does not help as breastmilk has low iron content.
|___|
2.7 For a mother complaining of nausea and vomiting while taking iron supplements, you advise;
1. Drink less fluid
2. Take supplement with meal
3. Start with higher dose and decrease gradually
4. Stop taking supplement if you see dark stool
|___|

43
S.N Questions per module Response
2.8 The National Iron Folic Acid (IFA) supplementation protocol of Ethiopia recommends,
1. To start iron supplementation during the second trimester of pregnancy
2. To discontinue taking IFA if a mother gave birth after taking iron for 90 days
3. To continue taking IFA postnatally if she gave birth before taking for 6 months
4. To take two doses together for a forgotten dose
|___|
2.9 Which of the following is TRUE regarding folic acid?
1. The highest daily requirement of folate occurs during adolescence.
2. Its deficiency results in neural tube defect, low birthweight and cardiovascular disease.
3. Iron and folate supplements are often given separately.
4. Folic acid supplementation is advised to start late during pregnancy.
|___|
2.10 Iodized salt,
1. Should be washed before use
2. Should be added at the start of cooking
3. Is not affected by direct exposure to moisture
4. Is affected by exposure to heat and sunlight
|___|
3. Adolescent Maternal, Infant and Young Child Nutrition
3.1 Which of the following is TRUE regarding nutrient requirement during pregnancy and lactation?
1. Pregnancy requires around 500 additional Kcal each day.
2. Pregnant woman should gain approximately 20 Kg during pregnancy.
3. Lactating women need additional 285 Kcal per day for the first six months.
4. Pregnancy requires less additional kcal per day than lactation.
|___|
3.2 Which of the following is an immediate cause of maternal malnutrition?
1. Ignorance
2. Uneven distribution of available food
3. Infectious disease
4. Insufficient food supply
|___|
3.3 Which of the following is TRUE regarding nutrition during pregnancy and lactation?
1. Exemption from any work is required during lactation and pregnancy.
2. Avoiding animal source food is advised to prevent big baby.
3. Iron folate supplement should not be provided during lactation if mother took 60
tablets during pregnancy.
4. Two extra meals are recommended during lactation and one extra meal during
pregnancy.
|___|
3.4 Regarding weight gain during pregnancy, which one of the following is TRUE?
1. Pre-pregnancy weight is important to estimate the amount of weight a pregnant woman
need to gain during pregnancy.
2. BMI for women can be calculated by dividing weight in Kg per height in cm
3. A normal healthy pregnant women gain at least 2Kg per month
4. Pregnant woman should gain approximately 20 Kg during pregnancy.
|___|
3.5 Which of the following intervention is NOT important for adolescents?
1. Health facility and school linkage
2. Healthy diet
3. Iron folate supplementation
4. Vitamin A supplementation
|___|

44
S.N Questions per module Response
3.6 Which of the following phrases do NOT relate to proper positioning of baby during breast
feeding?
1. The mother’s hand must support the whole body of the baby at the back
2. Baby and mother should touch abdomen to abdomen
3. Baby’s head should be turned to the breast
4. Baby should be facing the breast
|___|
3.7 For a child of 12 up to 24 months of age, how much complementary food should be given per
day?
1. 2 full coffee cups and one-time snack
2. 3 full coffee cups and one-time snack
3. 4 full coffee cups and 1 to 2 snacks
4. 1 full coffee cup and 3 snacks
|___|
3.8 Which of the following example of mixture is recommended in preparing flour for a child’s
porridge?
1. Barley, red teff and wheat
2. Lentils, pea, chick pea and beans
3. Barley, teff, wheat and corn
4. Barely, chick pea and wheat
|___|
3.9 One of the following is NOT among the benefits of adequate nutrient intake during pregnancy.
1. Prevents intrauterine growth restriction
2. Ensures energy storage for lactation
3. Ensures normal presentation of the fetus
4. Decreases the risk of complications during pregnancy and delivery
|___|
3.10 Which of the following sentences relates to proper feeding recommendation during sickness for
children less than six months of age?
1. Breastfeeding should be increased
2. Any form of medication is possible
3. Fluid intake should be increased
4. Fluid intake should be decreased
|___|
3.11 Which of the following is TRUE regarding feeding of low birth weight (LBW) babies?
1. Give formula milk
2. Cup feed breastmilk if needed
3. LBW babies do not need to be followed while feeding
4. LBWs require less fluid and energy
|___|
3.12 Which of the following is NOT true about community involvement for nutrition?
1. Community leaders can be change agents to make behavior change towards IYCN.
2. Implementing IYCN program by consulting the community is a good strategy.
3. Community mobilization fosters collaboration between community and health facilities.
4. Discussion on optimal IYCF practices does not relate to fathers.
|___|
4. Acute Malnutrition
4.1 Wasting is defined as:
1. Weight for height <-2 Z score
2. Weight for age <-2 Z score
3. Weight for height -2 Z score to -2 Z score
4. Weight for age <-3 Z score
|___|

45
S.N Questions per module Response
4.2 Which case of child malnutrition can be managed in OTP?
1. WFL/H <70% or MUAC<11 cm with medical complication and good appetite test
2. Edema of both feet (+, ++) without medical complication and good appetite
3. WFL/H ≥70% to <80% or ≥-3Z to -2Z score
4. WFL/H <70% or MUAC<11 cm without medical complication and fails appetite test
|___|
4.3 Which case of child malnutrition should be managed as in-patient?
1. WFL/H <70% or MUAC<11 cm without medical complication and fails appetite test
2. Edema of both feet (+, ++) and no medical complication and passes appetite test
3. WFL/H>/70% to <80% or ≥-3Z to -2Z score
4. WFL/H <70% or MUAC<11 cm without medical complication and passes appetite test
|___|
4.4 If WFL/H ≥ 80% or ≥-2Z, MUAC ≥12cm and no edema of both feet, a health worker should
1. Refer the case to supplementary feeding
2. Congratulate and counsel the mother on IYCF
3. Manage the case in OTP
4. Admit the case for in-patient management
|___|
4.5 Mulu is an 18-month-old girl with W/H <70% and has edema (+) of both feet. She has no other
medical complication and has good appetite. What is the appropriate classification and
management for Mulu? 1. Moderate Acute Malnutrition, refer to supplementary feeding program and start with
RUTF.
2. Complicated Severe Acute Malnutrition, admit for in-patient management and start with
F75.
3. Uncomplicated Severe Acute Malnutrition, manage in OTP and start with RUTF.
4. Complicated Severe Acute Malnutrition, admit for in-patient management and start with
F100
|___|
4.6 Abebe is a 4 months old infant. Upon examination, the nurse found out that he is clinically
stable without apparent medical condition except that his weight for height is below -3 Z score.
What is the appropriate classification and mode of management for Abebe?
1. Moderate acute malnutrition: refer to supplementary feeding program
2. No acute malnutrition: no need for treatment
3. Uncomplicated severe acute malnutrition: treat as outpatient
4. Complicated Severe Acute Malnutrition: treat as inpatient
|___|
4.7 Which of the following is NOT TRUE about management of severely malnourished children?
1. All severely malnourished children should be given antibiotics as most have hidden
bacterial infection.
2. Feeding should start slowly as the systems of the body slows down with severe
malnutrition.
3. Iron should not be given early in treatment as there is less iron stored in severely
malnourished child.
4. Sodium should be provided via ORS but not potassium.
|___|
4.8 Misdiagnosis and mistreatment of which of the following is the COMMONEST cause of death in
a child with SAM?
1. Hypoglycemia
2. Hypothermia
3. Dehydration
4. Abdominal distension
|___|

46
S.N Questions per module Response
4.9 Which of the following is NOT correct about management of medical complication in a child
with SAM?
1. For alert child with hypoglycemia 50ml of 10% glucose can be given orally or via NG
tube
2. Kangaroo mother technique helps to actively re-warm a child with hypothermia
3. 5ml/kg/30 min of Resomal is given for 12 hours for a conscious and dehydrated child.
4. If no medical complication is present oral amoxicillin is preferable.
|___|
4.10 Which of the following applies for management of severe malnutrition in children>6 months of
age?
1. F75 is used in transition phase management.
2. F100 is used during phase 1 management.
3. Ready to use therapeutic food (RUTF) is introduced during the transition phase.
4. Iron can be given at the start of treatment.
|___|
5. Nutrition and communicable Diseases, Non, communicable Diseases and Nutrition in Special
Health Conditions
5.1 One of the following is CORRECT about HIV, TB and nutrition.
1. All HIV infected individuals are not at risk of weight loss and malnutrition.
2. Active TB decreases energy requirement of the body.
3. HIV infected individuals need high amount of proteins and vitamins.
4. Malnutrition increases mother to child transmission of HIV in pregnant women.
|___|
5.2 Which one of the following is NOT Critical Nutrition Practices for PLHIV?
1. Doing regular physical exercise
2. Regular nutritional assessment
3. Using herbal medications to treat HIV related symptoms
4. Eating variety of foods
|___|
5.3 Which of the following is NOT a means of dietary management of diarrhea?
1. Eating foods rich in soluble fiber (bananas, peas and lentils)
2. Drinking lots of fluids
3. Consuming too much sweet drinks
4. Consuming easily digestible rice, bread, potato
|___|
5.4 What is the classification of an adult with a BMI of less than 16?
1. Normal
2. Mild malnutrition
3. Severe malnutrition
4. Moderate malnutrition
|___|
5.5 In the management of Type 2 diabetes mellitus, one of the following is NOT required.
1. Physical exercise
2. Nutrition therapy
3. Insulin administration
4. Multidisciplinary approach
|___|
5.6 Which has a direct effect in the development of chronic diseases in developing countries?
1. Economic growth and technology transfer
2. Changing life styles and dietary practices
3. Persistence of food insecurity
4. Transformation from agrarian to industrial society
|___|

47
S.N Questions per module Response
5.7 Which one of these grain products need to be limited or avoided not to increase one’s total
blood cholesterol?
1. Whole wheat flour
2. High fiber cereal
3. White refined flour
4. Whole grain pasta
|___|
6. Program Management
6.1 A term that refers to interventions that directly address the immediate causes of malnutrition:
1. Nutrition-sensitive interventions
2. Food security
3. Nutrition-specific interventions
4. Family planning
|___|
6.2 Which of the following shows a CORRECT match between specific intervention and category?
1. Treatment of severe acute malnutrition: Nutrition-sensitive intervention
2. Optimal breastfeeding: Nutrition-specific intervention
3. Women empowerment: Nutrition-specific intervention
4. Social protection: Nutrition-specific intervention
|___|
6.3 Which one shows a CORRECT match for the different types of nutrition communication?
1. Advocacy: helps to change knowledge, attitude and practice of specific audience
2. Social mobilization: increases resources and political or social commitment
3. Social mobilization: best used when people are generally unaware of an issue
4. BCC: promotes wider participation, collective action and ownership
|___|
6.4 Which of the following is wrong about coordination?
1. Coordination is exchanging information and altering activities for mutual benefit and
to achieve a common purpose.
2. Multisectoral coordination means all sectors merge their plans and resources and
works together for a common objective.
3. Coordination, collaboration, cooperation differ in their scope of working together.
4. Multi-sector coordination increases program impact and lowers program costs.
|___|
6.5 Which one of the following is FALSE about supply management?
1. Quantification is a process that estimates the total quantities and costs of products
that will be used during a specific time period
2. Forecasting is estimating quantity and cost required of each product to meet
demand for the forecast period
3. Supply planning is a type of supply quantification that answers the question how
much to procure, when to receive and with what quantities.
4. During storage of supplies, supplies should be rotated on ‘first expiry, last out’ basis.
|___|
6.6 Which of the following strategic objective of the NNP addresses the underlying causes of
malnutrition?
1. Improve the nutritional status of women and adolescents
2. Improve the nutritional status of infants, young children and children under 5
3. Improved the delivery of nutrition services of communicable and non-
communicable diseases
4. Strengthen implementation of nutrition sensitive intervention across sectors
5. Improve multisectoral coordination and capacity to ensure NNP implementation
|___|

48
SECTION V: General Feedback on the whole BINLM-based Course
1. General suggestion to improve the BINLM-based training
Annex III: Skill Assessment Questionnaire Skill Assessment Checklist for Health Workers Trained on the Blended and
Integrated Nutrition Learning Material (BINLM)
I. Vitamin A Administration
Step Task/Activity:
Did the Health worker,
Yes=1
No=0
1 Greet the caregiver and introduce his/herself? |___|
2 Ask for the age of the child? |___|
3 Ask the caretaker if the child has received vitamin A capsule in the last one month. If the
answer is YES, confirmed that and did not administer Vitamin A?
|___|
4
Select appropriate dose based on child’s age, if the answer to STEP 3 is ‘NO’?
100,000 IU to child 6-11 months
200,000 IU to child 12-59 months
|___|
5 Cut the nipple of the capsule at the middle (NOT at the tip or bottom) with scissors and
immediately squeeze the drops of liquid into the child’s mouth?
|___|
6 Ask the caretaker to hold the child firmly, make sure the child is calm, give the appropriate dose
of vitamin A to the child?
|___|
7 Check if the child is comfortable after swallowing the drops? |___|
8 Put all capsules that have been used into a plastic bags and, Wipe your hands to clean off oil? |___|
9 Record the dose on the tally sheet. |___|

49
II. Maternal and IYCF Counseling Skill
DIRECTION: Please ask the BINLM trained health worker to apply the procedures for
counseling on a real client at the visited health center. And rate performance as ‘Very Good=2’,
‘Good=1’ or ‘Not Done=0’. The client should be either a mother/caregiver with a child of
under two years of age or a pregnant/lactating women.
Step
Task/Activity: Did the Health worker,
Very Good=2
Good=1
Not Done= 0
1 Greet the mother/care giver of the child or the pregnant/lactating woman? |___|
2 Ask the mother/care giver/Pregnant/lactating women
2.1 For a child: Ask for age of the child, breastfeeding status, if the child has started
food or not, If ‘Yes’ what type of foods, If ‘No’, why not? Frequency of feeding?
general health condition? Foods available at home or locally accessible)
|___|
2.2 For a pregnant/lactating women: Ask for gestational age, ANC follow-up (If
pregnant); Frequency of maternal feeding, variety/types of food , IFA intake and
adherence, Foods available at home or locally accessible)
|___|
3 Listen attentively to what the parents said |___|
4
Identify difficulties & prioritize the most important one to work on based on
mother’s/caregivers
|___|
5 Discuss feeding options & Recommend simple doable actions.
5.1 Use counseling cards properly |___|
5.2 Discuss simple doable actions based on identified and prioritized problems (did
not mention all the recommended behaviors)
|___|
5.3 Discuss optimal breastfeeding/complementary feeding options appropriate to the
age of the child
|___|
5.4 Discussed if suggestions are easy or not to practice
|___|
5.5 Help the mother/care giver to agree and to try one of the options, and asks them
to repeat the agreed-upon actions.
|___|
6 Appoint mother/care giver for next visit |___|
III. Anthropometric measurement: Taking weight of children
Steps Task/activity: Did the Health worker, Yes=1
No=0
1 Remove the child's clothes, but keep the child warm with a blanket or cloth while carrying
to the scale.
|___|
2 Put a cloth in the scale pan to prevent chilling the child. |___|

50
3 Adjust the scale to zero with the cloth in the pan. (If using a scale with a sling or pants or
basin, adjust the scale to zero with that in place.)
|___|
4 Place the naked child gently in the pan (or in the sling or pants). |___|
5 Wait for the child to settle and the weight to stabilize. |___|
6 Measure weight to the nearest 100gm or as precisely as possible. Record immediately on
multi-chart.
|___|
7 Wrap the child immediately to re-warm. |___|
8 Make sure the weighing scale is calibrated to zero before each measurement is taken. |___|
9 Record the weight to the nearest 100 grams. |___|

51
Annex IV: Observation Guide at Health Facility Level Observation Guide on Blended and Integrated Nutrition Learning Module
(BINLM)-based Training
Name of Observer: _____________________
SECTION I: Assessment Area Identification Questions
S.N Question Response
01 Region 2. Amhara 2. Oromiya
5. SNNPR 4. Tigray
|___|
02 Woreda (Write N/A if respondent is at regional/zonal level)
2. Enemay 2. Ebnat
4. Arsi Negele 4. Shala
6. Siraro 6. Mierab Azernet
8. Misrak Azernet 8. Misha
10. Medebay Zana 10. Asgede Tsimbila
|___|
03 Name of Health Center
04 Health center ID |___||___||___
|
05 Health center provides OTP service 1. Yes 2. No
|___|
06 The health center has Stabilization Center 1. Yes 2. No
|___|
SECTION II: Observation Checklist by component
S.N Question Yes=1
No=0
1. General
1 Electric power available 24/7 |___|
2 Computers available at the HC 1=Yes 2=No |___|
3 If yes, how many? |___|
II. Key measurement tools and supplies
2.1 Weighing scale |___|
2.2 Length/Height board |___|
2.3 MUAC tape |___|
2.4 Zinc + Oral Rehydration Salt |___|
2.5 Iron/Folic acid |___|
2.6 Amoxicillin |___|
2.7 Albendazole/Mebendazole Tablets |___|
2.8 Vitamin A |___|

52
S.N Question Yes=1
No=0
2.9 If OTP service is provided, RUTF available |___|
2.10 OTP cards, registration book |___|
If SC service is provided
2.11 Separate SC room |___|
2.12 F-75 |___|
2.13 F-100 |___|
2.14 SC utensils ( cup, measuring jar e. t .c) |___|
2.15 SC cards, Registration book, reference charts |___|
III. Counseling related Job Aids
3.1 Counseling card on MIYCN available at under 5 clinic, ANC/PNC room |___|
3.2 Growth monitoring charts (both for boys and girls) |___|
3.3 Family Health Guide available
IV. Record Keeping, Data Compilation and Reporting:
Direction: Take a sample of 2 cards from each quarter in 2010 EC and two monthly reports where
SC service is available. Mark as ‘Yes’ if half of the sampled satisfies the stated criteria and ‘No’ if not. Filling out individual follow up chart (Multi-chart and OTP Card)
4.1 Identification part is completed fully
4.2 Anthropometry part is completed fully
4.3 History part is completed fully
4.4 Physical examination part is completed fully
4.5 The classification is indicated clearly
4.6 Routine medication part filled fully
Filling out registration book
4.7 Date recorded accurately
4.8 Anthropometric measurements completed for admission date
4.9 Date of discharge recorded appropriately
4.10 Outcome recorded accurately
Completing monthly reporting format
4.11 Identification of the facility recorded accurately
4.12 Total at the beginning of this month matches with total at the end of last month
4.13 Admission information filled our correctly
4.14 Discharge information filled our correctly
4.15 Total at the end of the month is calculated accurately
4.16 Average length of stay is accurately calculated from the registration book

53
DIRECTION: The health worker will take either length or height depending on the age and
measure of the child (length between 85 to 110 cm). But not both skill tests.
IV. Anthropometric measurement: Taking LENGTH of children Steps Task/activity: Did the Health worker, Yes=1
No=0
1 Place the measuring board flat, preferably on a stable, level table |___|
2 Ensure cloths do not get in the way of measurement |___|
3 Let one person stand or kneel behind the head board and |___|
3.1 Position the child lying on his back on the measuring board, supporting the
head and placing it against the headboard.
|___|
3.2 Position the crown of the head against the headboard, compressing the hair |___|
3.3 Hold the head with two hands and tilt upwards until the eyes look straight up,
and the line of sight is perpendicular to the measuring board.
|___|
3.4 Check that the child lies straight along the center line of the measuring board
and does not change position.
|___|
4 Let himself/the other person stand alongside the measuring board and: |___|
4.1 Support the child's trunk as the child is positioned on the board. |___|
4.2 Place one hand on the shins or knees and press gently but firmly. |___|
4.2 Straighten the knees as much as possible without harming the child. |___|
4.3 With the other hand, place the foot piece firmly against the feet. The soles of
the feet should be flat on the foot piece, toes pointing up.
|___|
5 Measure length to the last completed 0.1 cm and record immediately on the Multi-
chart.
|___|
V. Anthropometric measurement: Taking HEIGHT of children Steps Task/activity: Did the Health worker, Yes=1
No=0
1 Place the stadiometer (height board) on a level floor. |___|
2 Remove the child’s socks and shoes for accurate measurement. Also remove hair
ornaments and undo braids IF they interfere with measurement.
|___|
3 Let one person kneel or crouch near the child’s feet and: |___|

54
Steps Task/activity: Did the Health worker, Yes=1
No=0
3.1 Help the child stand with back of the head, shoulder blades, buttocks, calves
and heels touching the vertical board.
|___|
3.2 Hold the child’s knees and ankles to keep the legs straight and feet flat. Prevent
children from standing on their toes.
|___|
4 Let himself/the other person bend to level of the child’s face and: |___|
4.1 Position the head so that the child is looking straight ahead (line of sight is
parallel to the base of the board).
|___|
4.2 Place thumb and forefinger over the child’s chin to help keep the head in an
upright position
|___|
4.3 With the other hand, pull down the head board to rest firmly on top of the
head and compress hair.
|___|
5 Measure the height to the last completed 0.1 cm and record it immediately on the Multi
chart.
|___|
VI. Anthropometric Measurement: Taking MUAC of Children Step Task/Activity:
Did the Health worker,
Yes=1
No=0
1 Locate tip of shoulder |___|
2 Locate tip of elbow |___|
3 Place tape at tip of shoulder
|___|
4
Pull tape past tip of bent elbow
|___|
5 Mark mid-point |___|
6 Wrap the tape on the arm across the marked point |___|
7 Correct tape tension |___|
8 Correct tape position for arm circumference |___|
9 Measure MUAC to the last completed 0.1 cm and record it immediately. |___|

55
VII. Preparation of F100 and F75 Feeds
DIRECTION: Please provide the following case to the health worker, check the
calculated Total ml/day with the last column and use the checklist in the last table to
follow actual preparation.
Name Age in month Weight in Kg Phase Type of
Milk
Number
of feed
Total
ml/day
Asnake 14 months 6.2 1 F 75 6 840ml
Lema 12 months 5.7 Transition F 100 6 720ml
Step Task/Activity: Did the health worker, Yes=1
No=0
1 Summarize total ml of milk to be prepared for both Phase 1 and transition |___|
2 Calculate the number of red scoops and amount of water accurately |___|
3 Wash hands |___|
4 Measure the amount of water for each phase |___|
5 Put the right number of red scoops for each phase |___|
6 Use whisk and prepare the milk |___|
7 Measure the right amount and offer to the children |___|
Annex V: Semi-structured KII Guide
Semi-structured Key Informant Interview and Key Data Capturing Guide on
Blended and Integrated Nutrition Learning Module (BINLM)-based Training
Consent
Hello! My name is ______________. I am a member of a study team that assesses implementation and
effectiveness of the nationally standardized nutrition training for health workers which is delivered using Blended
and Integrated Nutrition Learning Module (BINLM). The study is overseen by Federal Ministry of Health,
approved by regional health bureau and executed by Growth through Nutrition Project, a USAID funded and
Save the Children led multisectoral nutrition project. Findings of this study will provide key inputs for the revision
of the training material and approach that the FMoH planned to do this year. Hence, your participation will be
invaluable in improving the quality of ongoing capacity building efforts for health workers on nutrition.

56
I will ask for your name here only to clarify on any information I might have missed or misunderstood from you
later; otherwise it will not be reported anywhere in the findings. To retain the most out of our communication, the
interview will be audio-recorded. I may ask for to see some relevant documentation for further desk review and
verification purpose and collect copies, if allowed. The interview takes around 40 minutes and it can be stopped
whenever you wish.
Are you willing to participate in the study? Yes_________ No__________
Date: ____/____/2011 Start time: ______________ End time: __________________
Name of interviewer: _____________________
SECTION I: Assessment Area and Respondent Identification Questions
S.N Question Response
01 Region 3. Amhara 2. Oromiya
7. SNNPR 4. Tigray
|___|
02 Woreda (Write N/A if respondent is at regional/zonal level)
3. Enemay 2. Ebnat
5. Arsi Negele 4. Shala
8. Siraro 6. Mierab Azernet
9. Misrak Azernet 8. Misha
11. Medebay Zana 10. Asgede Tsimbila
|___|
03 Respondent’s profession
04 Respondent’s organization and position
05 Duration of stay in the position (In months)
06 Took part in BINLM training or orientation in the past 2 years? (Meskerem
2008-Meskerem 2011/till now) as
1. Organizer 2. Trainer 3. Participant 4. None 5. Other (Specify)
|___|
SECTION II: BINLM-based Training Related Experience and Views
1. Was BINLM based training conducted in your region in the past two years?
2. If yes, which body supported the training/s? (Government itself or partner/Specify)
3. In what way were the ‘Knowledge’ and ‘Skill’ components of the training provided?

57
4. Was there any variation in the way the trainings were provided across time (in the Past 2 Years)
or was it similar?
5. If there were variations, can you tell me WHY and WHAT kind of variation was there?
6. Which part of the training often goes well? The Knowledge or the Skill part?
7. Which part of the training often faced a challenge, if any? Can you tell me WHAT the challenges
were? WHAT did you do to address these challenge?
8. What do you think are the major strengths/advantages of BINLM based training?
9. Do you think BINLM is effective in equipping HWs with the appropriate knowledge and skill? If
‘Yes’, WHY? If ‘No’, WHY?
10. What do you think are/can be major factors that affect quality of BINLM-based training? WHY?

58
11. Would you please tell me key areas of improvement that can make the BINLM training more
effective? (PROBE for clarity whenever required.)
12. Would it be possible to see a sample of the training reports?
THANK the Key Informant here as you have finished qualitative questions here and you
can stop audio recording.
13. Would you please provide me data on the following areas that are related to BINLM training
and its effectiveness? (Data can be available other units such as Plan and Program).
S.N Question Response
1 # of HC in the region/zone/woreda
2 # of HCs with regular electricity supply
3 # of HC with computer facility accessible by staff
4 # of HWs trained on BINLM in the past 2 years4 (if not available take for the past 1
year)
5 Any plan to train HWs on BINLM this year? (Yes/No)
6 If Yes to Q5, # of HWs planned to be trained
5 # of HWs trained on other specific nutrition trainings in the past two years1
1. CMAM
2. AMIYCN
3. Others
Annex VI: Frequency tables of aggregated score of study participants for each module
and general scores Scores for the introductory module
Scores for the micronutrient module –Knowledge section
4 Document for the time period available but SPECIFY time period in the remark column.
# of correct responses Frequency Valid Percent Cumulative Percent
1 5 4.0 4.0
2 11 8.7 12.7
3 10 7.9 20.6
4 31 24.6 45.2
5 25 19.8 65.1
6 22 17.5 82.5
7 13 10.3 92.9
8 9 7.1 100.0
# of correct responses Frequency Valid Percent Cumulative Percent
0 1 .8 .8
2 4 3.1 3.9
3 11 8.7 12.6

59
Aggregate scores for the AMIYCN module
# of correct responses Frequency Valid Percent Cumulative Percent
0 2 1.6 1.6
1 2 1.6 3.1
2 4 3.1 6.3
3 13 10.2 16.5
4 14 11.0 27.6
5 23 18.1 45.7
6 16 12.6 58.3
7 16 12.6 70.9
8 18 14.2 85.0
9 10 7.9 92.9
10 2 1.6 94.5
11 4 3.1 97.6
12 3 2.4 100.0
Aggregate score for Acute Malnutrition Module
# of correct responses Frequency Valid Percent Cumulative Percent
0 1 .8 .8
1 12 9.4 10.2
2 20 15.7 26.0
3 23 18.1 44.1
4 14 11.0 55.1
5 18 14.2 69.3
6 16 12.6 81.9
7 13 10.2 92.1
8 6 4.7 96.9
9 4 3.1 100.0
4 12 9.4 22.0
5 18 14.2 36.2
6 30 23.6 59.8
7 23 18.1 78.0
8 21 16.5 94.5
9 5 3.9 98.4
10 2 1.6 100.0

60
Aggregate scores for Nutrition in communicable and non-communicable diseases module
Aggregate score for nutrition program management
# of correct responses Frequency Valid Percent Cumulative Percent
0 18 14.2 14.2
1 48 37.8 52.0
2 29 22.8 74.8
3 25 19.7 94.5
4 4 3.1 97.6
5 3 2.4 100.0
Aggregated score for all six modules
Score Valid Percent Score Valid Percent Score Valid Percent
12 .8 24 9.5 35 1.6
13 2.4 25 4.8 36 1.6
14 4.0 26 4.0 37 .8
15 2.4 27 3.2 38 .8
17 1.6 28 6.3 39 .8
18 4.8 29 2.4 40 .8
19 2.4 30 6.3 43 2.4
# of correct responses Frequency Valid Percent Cumulative Percent
0 3 2.4 2.4
1 9 7.1 9.4
2 24 18.9 28.3
3 29 22.8 51.2
4 27 21.3 72.4
5 14 11.0 83.5
6 15 11.8 95.3
7 6 4.7 100.0
Copyright © 2022 FDOKUMEN

