







Bahasa
Halaman
Hukum


BILIARY CYSTADENOMA AND CYSTADENOCARCINOMA Report of 14 Cases and Reuiew of the Literature
KAMALG. ISHAK, MD, PHD, G. W. WILLIS, MD, S. D. CUMMINS, MD, AND A. A. BULLOCK, MD
The clinical and pathologic features and long-term follow-up of eight patients with biliary cystadenoma and six patients with biliary cystadenocarcinoma are reported and the previous literature is reviewed. All the cystadenomas were in middle-aged women, but the six cystadenocarcinomas occurred in both male (4) and female (2) patients. The majority of the patients with cystadenoma and half of those with cystadenocarcinoma presented with an abdominal mass. Four of the patients whose cystadenoma was excised are alive and well for periods of time ranging from 2 % to 13 years. Two of the patients with cystadenocarcinoma have survived for three years and for three years and eight months, respec- tively, after subtotal hepatic lobectomy. Morphologically the cyst- adenocarcinomas differ from the cystadenomas in that the former have cellular pleomorphism and anaplasia and infiltration of the underlying fribrous stroma; they can invade adjacent viscera and may occasionally metastasize to distant sites. The presence of benign epithelium in most cystadenocarcinomas supports their origin from cystadenoma.
Cancer 38:322-338, 1977.
I L I A R Y C Y S T A D E N O M A S A N D CYST- B adenocarcinomas are rare tumors that arise in the liver or, less frequently, in the extra- hepatic biliary system. The cystadenomas of the liver and bile ducts bear a resemblance to those that arise in the pancreas and, like them may be subclassified into multilocular and papillary va- rieties, the former being the most frequent. The cystadenocarcinomas have thus far been found only in the liver, but these, too, may be multi- locular or papillary. A survey of the literature revealed 38 cases of cystadenoma '*'*'- 13,'8~'8v
and ten cases of
cases reported before the turn of the century were not available for review. These are men- tioned in the reviews of Geist," Jones,27 Lepp- m~ann,~ ' and Sonntag." Most of the previously published cases have been isolated case reports;
20.21.23.24.20.28- 31.33.34,38,38,40- 44.47- 49
cystadenocarcinoma, 2,3,13.15,25.33.37.38,48,50 A few
From the '4rrned Forces Institute of Pathology, Washing- ton, DC; Ochsner Foundation Hospital New Orleans, Loui- siana; Confederate hlemorial hledical Center, Shreveport, Louisiana; and the Willis-Knighton Memorial Hospital and Clinic, Shreveport, Louisiana.
Address for reprints: Kamal G. Ishak, M.D., Ph.D., Divi- sion of Hepatic Pathology, Armed Forces Institute of Pathol- ogy. Washington, DC, 20306.
The opinions or assertions contained herein are the pri- vate views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
Received for publication March 2. 1976.
the largest series of five cases of hepatic cyst- adenomas was reported by Delannoy and La- gache." The opportunity to study eight cases of cystadenoma and six cases of cyst- adenocarcinoma prompted this clini- copathologic study. The present cases are com- pared and contrasted with previously published ones.
CLINICAL FINDINGS Biliary Cystadenoma (Table 1)
All eight tumors occurred in middle-aged Caucasian women whose ages ranged from 34 to 71 years. The majority (six of the eight) pre- sented with a mass in the abdomen. Two patients (Cases 2 and 3 ) also had intermittent abdominal pain, while one patient (Case 7) complained of epigastric discomfort, anorexia, and indigestion. One of the patients (Case 5) had an abdominal mass that at laparotomy was discovered to be a cystadenoma attached by a pedicle to the region of the celiac axis; this tu- mor was excised. The liver showed multiple cys- tic lesions which were not biopsied because of their marked vascularity. The patient died seven years later from myocardial infarction. At ne- cropsy almost the entire liver was replaced by a multiloculated cystadenoma.
O n e of the patients (Case 1 ) with a palpable abdominal mass had scleral icterus (total serum
322
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS lshak et al. 323
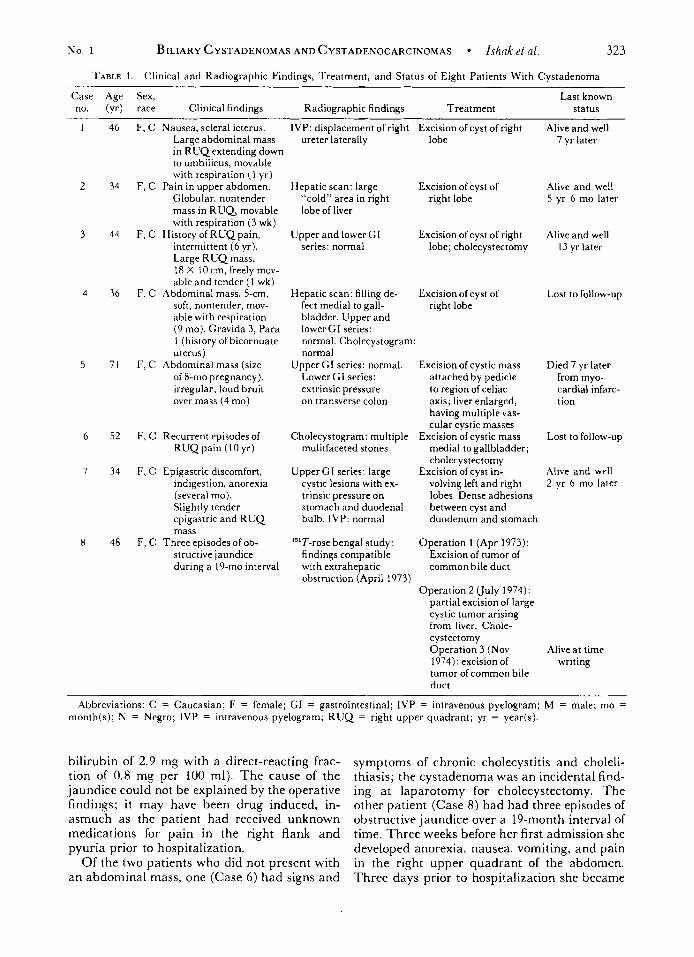
TABLE I . Clinical and Radiographic Findings, Treatment, and Status of Eight Patients With Cystadenoma
Case Age Sex, no. (yr) race Clinical findings Radiographic findings Treatment
Last known status
46
34
44
36
71
52
34
48
F, C Nausea, scleral icterus. Large abdominal mass in R U Q extending down to umbilicus, movable with respiration (1 yr)
F, C Pain in upper abdomen. Globular. nontender mass in R U Q movable with respiration (3 wk)
F, C History of RUQpain , intermittent (6 yr). Large R U Q mass, 18 X I0 cm, freely mov- able and tender (1 wk)
F, C Abdominal mass, 5-cm, soft, nontender, mov- able with respiration (9 mo). Gravida 3, Para 1 (history of bicornuate uterus)
F, C Abdominal mass (size of 8-mo pregnancy), irregular, loud bruit over mass (4 mo)
F, C Recurrent episodes of R U Q pain ( 1 0 yr)
F, C Epigastric discomfort, indigestion, anorexia (several mo). Slightly tender epigastric and RUQ mass
structive jaundice during a 19-mo interval
F, C Three episodes of ob-
IVP: displacement of right ureter laterally
Hepatic scan: large “cold” area in right lobe of liver
Upper and lower GI series: normal
Hepatic scan: filling de- fect medial to gall- bladder. Upper and lower GI series: normal. Cholecystogram: normal
Lower GI series: extrinsic pressure on transverse colon
Upper GI series: normal.
Cholecystogram: multiple mulitfaceted stones
UpperGI series: large cystic lesions with ex- trinsic pressure on stomach and duodenal bulb. IVP: normal
13’T-rose bengal study: findings compatible with extrahepatic obstruction (April 1973)
Excision of cyst of right lobe
Excision of cyst of right lobe
Excision of cyst of right lobe; cholecystectomy
Excision of cyst of right lobe
Excision of cystic mass attached by pedicle to region of celiac axis; liver enlarged, having multiple vas- cular cystic masses
Excision ofcystic mass medial to gallbladder; cholecystectomy
Excision of cyst in- volving left and right lobes. Dense adhesions between cyst and duodenum and stomach
Operation 1 (Apr 1973): Excision of tumor of common bile duct
Operation 2 (July 1974): partial excision of large cystic tumor arising from- liver. Chole- cystectomy Operation 3 (Nov 1974): excision of tumor of common bile duct
Alive and well 7 yr later
Alive and well 5 yr 6 mo later
Alive and well 13 yr later
Lost to follow-up
Died 7 yr later from myo- cardial infarc- tion
Lost to follow-up
Alive and well 2 yr 6 mo later
Alive at time writing
Abbreviations: C = Caucasian; F = female; GI = gastrointestinal; IVP = intravenous pyelogram; M = male; mo = month(s); N = Negro; IVP = intravenous pyelogram; R U Q = right upper quadrant; yr = year(s).
bilirubin of 2.9 mg with a direct-reacting frac- tion of 0.8 mg per 100 ml). The cause of the jaundice could not be explained by the operative findings; i t may have been drug induced, in- asmuch as the patient had received unknown medications for pain in the right flank and pyuria prior to hospitalization.
Of the two patients who did not present with a n abdominal mass, one (Case 6) had signs and
symptoms of chronic cholecystitis and choleli- thiasis; the cystadenoma was an incidental find- ing at laparotomy for cholecystectomy. The other patient (Case 8) had had three episodes of obstructive jaundice over a 19-month interval of time. Three weeks before her first admission she developed anorexia, nausea, vomiting, and pain in the right upper quadrant of the abdomen. Three days prior to hospitalization she became

324 CANCER January 1977 V O l . 39
jaundiced. Her total serum bilirubin value peaked at 23.4 mg/100 ml (of which half was direct reacting), and the highest serum alkaline phosphatase value was 388 units (normal 20 to 48 units). At exploratory laparotomy, a tumor that completely occluded the common bile duct was excised. The patient was readmitted 15 months later because of a second bout of jaun- dice. Re-exploration showed a large cystic tu- mor arising from the liver and extending to the vertebral column. The tumor compressed the common bile duct but was not connected to it. Complete excision was not possible because of adhesions between the tumor and the portal vein and inferior vena cava. The gallbladder, which contained multiple calculi, was removed. The patient was re-admitted for the third time four months later because of recurrence of her jaun- dice. At celiotomy dense adhesions were found at the site of previous surgery. The common bile duct was again found to contain a tumor, which was excised in toto.
A preoperative diagnosis of a cystic tumor arising from the anterior surface of the right lobe of the liver was made in one patient by peri- toneoscopy (Case 4).
Findings from tests of hepatic function were within the normal range in all except for the two patients (Cases 1 and 8) who were clinically jaundiced.
Radiographic studies showed displacement of the transverse colon in one patient (Case 5) and extrinsic pressure on the stomach and duodenal bulb in another (Case 7). There was lateral displacement of the right ureter in one patient (Case 1) . Two patients (Cases 2 and 4) had a filling defect demonstrated by hepatic scanning. The cystadenomas in all patients were surgically excised either by “shelling out’’ by blunt dis- section or by ligation and excision of the pedicle. All patients made an uneventful postoperative recovery. Four of the patients (Cases 1, 2, 3, and 7) are alive and asymptomatic 7, 5 % , 13, and 2 Yi years postoperatively. As noted earlier, the patient with the extrahepatic and hepatic cyst- adenomas (Case 5) died from myocardial in- farction seven years after surgery. No long-term follow-up is available on the remaining patients (Cases 4, 6, and 8).
Biliary Cystadenocarcinoma (Table 2) Four of the patients were male (all Cauca-
sian), while two were female (one Negro and one Caucasian). Their ages ranged from 23 to 75 years. In three of the patients the cyst- adenocarcinoma was an incidental finding at
necropsy (Cases 10 and 11) or at surgery (Case 13). Three patients (Cases 9, 12, and 14) com- plained of upper abdominal fullness or a mass of several months’ duration. One of these patients (Case 9) gave a history of epigastric distress for 19 years and of cramping and dull epigastric pain for six months prior to exploratory lap- arotomy. The abdominal mass in another patient (Case 12) was associated with dis- comfort only when she was lying down, while the third patient (Case 14) was otherwise asymptomatic. Two of the patients (Case 13, third admission, and Case 14) complained of weight loss.
Results of tests of hepatic function in three of the patients with cystadenocarcinoma (Cases 9, 10, and 12) were reported to be within the nor- mal range.
Radiographic studies showed distortion of the stomach by an extrinsic mass in one patient (Case 9) and a double right collecting system and ureter in another (Case 12). Hepatic scans during the second and third admissions of one patient (Case 13) demonstrated a large filling defect.
In two of the patients with cystadeno- carcinoma a subtotal lobectomy was per- formed; both are alive and well with no evidence of recurrence three years and eight months (Case 9) and three years (Case 12) later. One patient (Case 14) had a simple excision of his cystadenocarcinoma. He was readmitted two years and four months later with the diagnosis of duodenal obstruction. At laparotomy the duode- num was invaded and occluded by a mass aris- ing from the liver. The mass had also invaded the hepatic flexure of the colon and the anterior abdominal wall through an adhesion. A biopsy specimen from the paraduodenal mass showed metastatic adenocarcinoma. The patient refused further treatment and was discharged to the care of his family. In one patient (Case 13) the cyst was drained, biopsied, and marsupialized when it was discovered at laparotomy for cho- lecystitis and cholelithiasis. The stoma closed, and the cyst reaccumulated fluid on two sub- sequent occasions, necessitating further surgery. This patient died two years and eight months after her first operation but was not autopsied.
PATHOLOGIC FINDINGS Gross Features (Tables 3 and 4)
The cystadenomas (Table 3) in six of eight cases were located in the right lobe of the liver, and in one (Case 6) the tumor involved both lobes. In
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Ishak el a / . 325
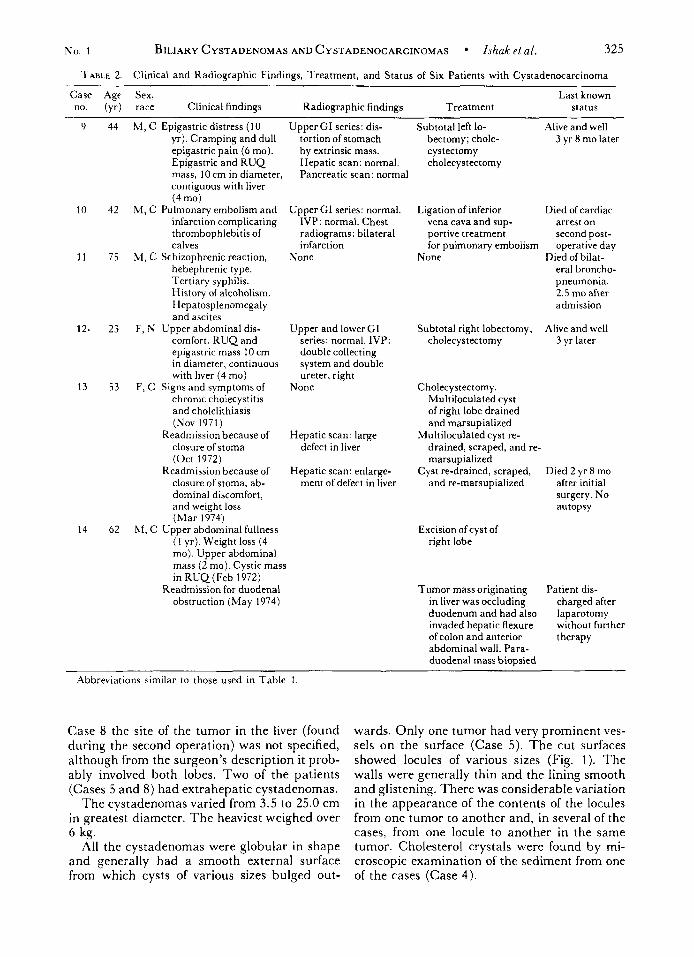
TABLE 2. Clinical and Radiographic Findings, Treatment, and Status of Six Patients with Cystadenocarcinoma
9
10
11
12.
13
14
Case Age Sex, Last known
44 M , C Epigastric distress (10 Upper GI series: dis- Subtotal left lo- Alive and well
no. (yr) raze Clinical findings Radiographic findings Treatment status
yr). Cramping and dull tortion of stomach bectomy; chole- 3 yr 8 mo later . - epigastric pain (6 mo). Epigastric and R U Q mass, 10 cm in diameter, contiguous with liver (4 mo)
by extrinsic mass. Hepatic scan: normal. Pancreatic scan: normal
42 M, C Pulmonary embolism and Upper GI series: normal. infarction complicating IVP: normal. Chest thrombophlebitis of radiograms: bilateral calves infarction
75 M, C Schizophrenic reaction, None hebephrenic type. Tertiary syphilis. History of alcoholism. Hepatosplenomegaly and ascites
comfort. R U Q and epigastric mass 10 cm in diameter, continuous with liver (4 mo)
53 F, C Signs and symptomsof None chronic choiecystitis and cholelithiasis (Nov 1971)
closure of stoma (Oct 1972)
Readmission because of closure of stoma, ab- dominal discomfort, and weight loss (Mar 1974)
hf, C Upper abdominal fullness (1 yr). Weight loss (4 mo). Upper abdominal mass (2 mo). Cystic mass in R U Q (Feb 1972)
Readmission for duodenal obstruction (May 1974)
23 F, N Upper abdominal dis- Upper and lower GI series: normal. IVP: double collecting system and double ureter, right
Readmission because of Hepatic scan: large defect in liver
Hepatic scan: enlarge- ment of defect in liver
62
cystectorny cholecystectomy
Ligation of inferior Died of cardiac vena cava and sup- arrest on portive treatment second post- for pulmonary embolism operative day
era1 broncho- pneumonia. 2.5 mo after admission
Alive and well
None Died of bilat-
Subtotal right lobectomy; cholecystectomy 3 yr later
Cholecystectomy . Multiloculated cyst of right lobe drained and marsupialized
Multiloculated cyst re- drained, scraped, and re- marsupialized
Died 2 yr 8 mo and re-marsupialized after initial
surgery. No autopsy
Cyst re-drained, scraped,
Excision of cyst of right lobe
Tumor mass originating Patient dis- in liver was occluding duodenum and had also laparotomy invaded hepatic flexure without further of colon and anterior therapy abdominal wall. Para- duodenal mass biopsied
charged after
Abbreviations similar to those used in Table 1
Case 8 the site of the tumor in the liver (found during the second operation) was not specified, although from the surgeon’s description it prob- ably involved both lobes. Two of the patients (Cases 5 and 8) had extrahepatic cystadenomas.
The cystadenomas varied from 3.5 to 25.0 cm in greatest diameter. T h e heaviest weighed over 6 kg.
All the cystadenomas were globular in shape and generally had a smooth external surface from which cysts of various sizes bulged out-
wards. Only one tumor had very prominent ves- sels on the surface (Case 5). The cut surfaces showed locules of various sizes (Fig. 1). The walls were generally thin and the lining smooth and glistening. There was considerable variation in the appearance of the contents of the locules from one tumor to another and, in several of the cases, from one locule to another in the same tumor. Cholesterol crystals were found by mi- croscopic examination of the sediment from one of the cases (Case 4) .
326 CANCER January 1977 Vol. 39
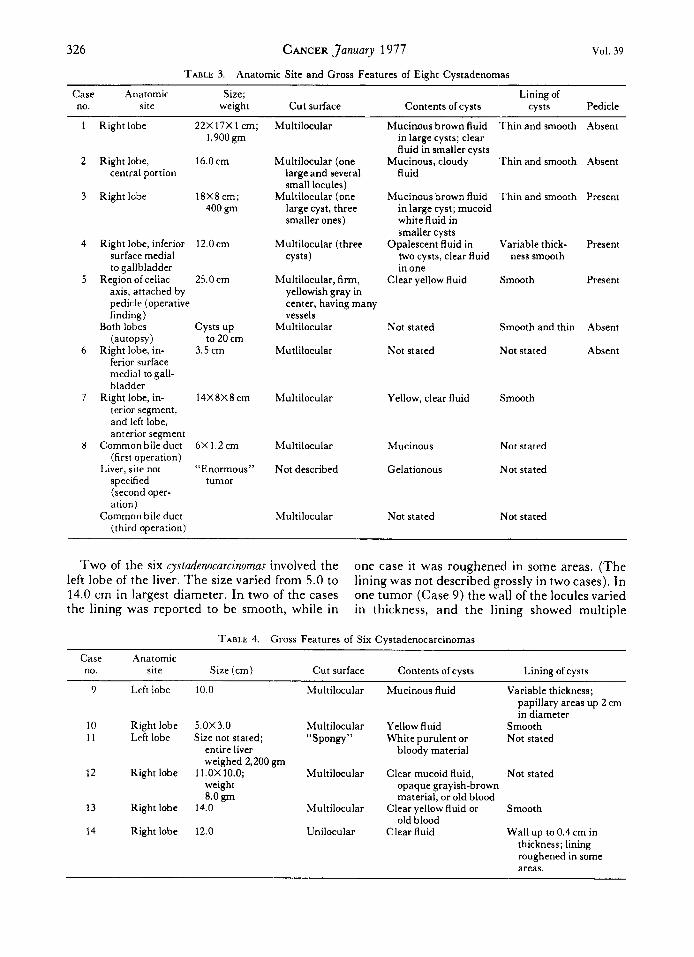
TABLE 3. Anatomic Site and Gross Features of Eight Cystadenomas
Case Anatomic Size; Lining of no. site weight Cut surface Contents of cysts cysts Pedicle
Mucinous brown fluid Thin and smooth Right lobe 22X 17X 1 cm; 1,900gm
Multilocular
Right lobe, 16.0 cm central portion
Right lobe 18X8cm; 400 gm
Right lobe, inferior 12.0cm surface medial to gallbladder
axis, attached by pedicle (operative finding)
(autopsy) to 20 cm
ferior surface medial to gall- bladder
terior segment, and left lobe, anterior segment
Common bile duct (first operation)
Liver, site not “Enormous” specified tumor (second oper- ation)
Common bile duct (third operation)
Region of celiac 25.0 cm
Both lobes cysts up
Right lobe, in- 3.5 cm
Right lobe, in- 14X8X8cm
6X 1.2 cm
Multilocular (one large and several small locules)
Multilocular (one large cyst, three smaller ones)
Multilocular (three cysts)
Multilocular, firm, yellowish gray in center, having many vessels
Multilocular
Mutlilocular
Multilocular
Multilocular
Not described
Multilocular
in large cysts; clear fluid in smaller cysts
fluid Mucinous, cloudy Thin and smooth
Mucinous brown fluid Thin and smooth in large cyst; mucoid white fluid in smaller cysts
two cysts, clear fluid in one
Opalescent fluid in Variable thick- ness smooth
Clear yellow fluid Smooth
Not stated Smooth and thin
Not stated Not stated
Yellow, clear fluid Smooth
Mucinous Not stated
Gelationous Not stated
Not stated Not stated
Absent
Absent
Present
Present
Present
Absent
Absent
Two of the six cystadenocarcinomas involved the left lobe of the liver. The size varied from 5.0 to 14.0 cm in largest diameter. In two of the cases the lining was reported to be smooth, while in
one case it was roughened in some areas. (The lining was not described grossly in two cases). In one tumor (Case 9) the wall of the locules varied in thickness, and the lining showed multiple
TABLE 4. Gross Features of Six Cystadenocarcinomas ~ ~
Case Anatomic no. site Size (cm) Cut surface Contents of cysts Lining of cysts
9 Left lobe 10.0 Multilocular Mucinous fluid Variable thickness; papillary areas up 2 cm in diameter
10 Right lobe 5.0X3.0 Multilocular Yellow fluid Smooth 11 L& lobe Size not stated; “Spongy” White purulent or Not stated
entire liver bloody material weighed 2,200 gm
weight opaque grayish-brown 8.0 gm
12 Right lobe ll.OX10.0; Multilocular Clear mucoid fluid, Not stated
material, or old blood
old blood 13 Right lobe 14.0 Multilocular Clear yellow fluid or Smooth
14 Right lobe 12.0 Unilocular Clear fluid Wall up to 0.4 cm in thickness; lining roughened in some areas.
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Ishak et nl. 327
papillary projections that measured up to 2 cm in diameter. As shown in Table 4, there was considerable variation in the gross appearance of the contents of the locules. One of the excised cystadenocarcinomas (Case 14) had an aberrant duct 4 to 5 mm long that was attached to the cyst and the common hepatic duct but could not be probed.
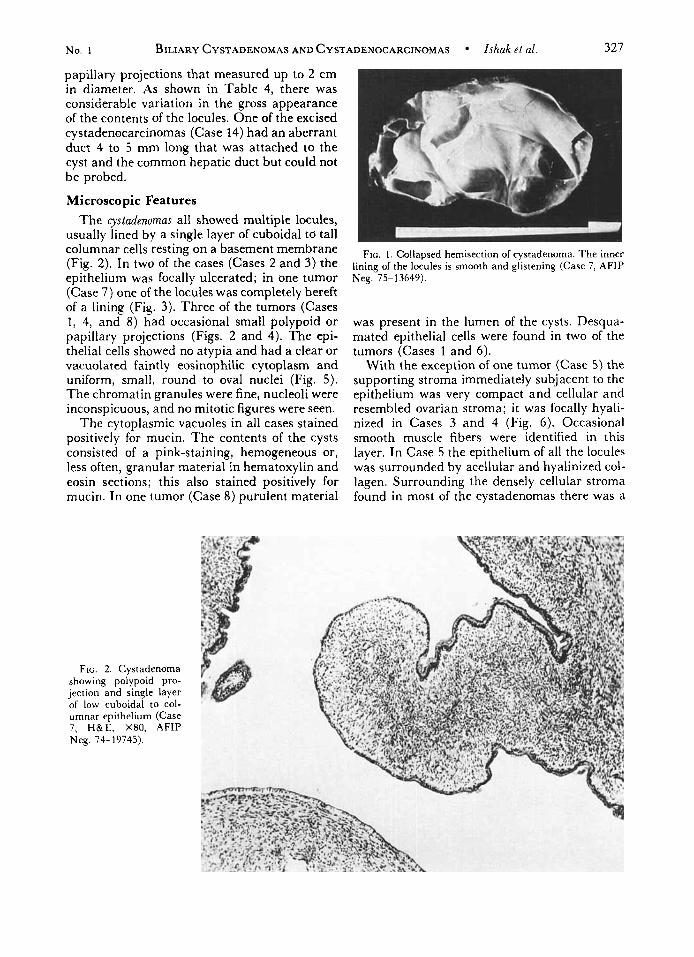
Microscopic Features The cystadenomas all showed multiple locules,
usually lined by a single layer of cuboidal tci tall columnar cells resting on a basement membrane (Fig. 2). In two of the cases (Cases 2 and 3) the epithelium was focally ulcerated; in one tumor (Case 7) one of the locules was completely bereft of a lining (Fig. 3 ) . Three of the tumors (Cases 1, 4, and 8) had occasional small polypoid or papillary projections (Figs. 2 and 4). The epi- thelial cells showed no atypia and had a clear or vacuolated faintly eosinophilic cytoplasm and uniform, small, round to oval nuclei (Fig. 5 ) . The chromatin granules were fine, nucleoli were inconspicuous, and no mitotic figures were seen.
The cytoplasmic vacuoles in all cases stained positively for mucin. The contents of the cysts consisted of a pink-staining, hemogeneous or, less often, granular material in hematoxylin and eosin sections; this also stained positively for mucin. In one tumor (Case 8) purulent material
FIG. 2. Cystadenoma showing polypoid pro- jection and single layer of low cuboidal to col- umnar epithelium (Case 7, H&E, X80, AFIP Neg. 74-19745).
FIG. 1 . Collapsed hemisection of cystadenorna. The inner lining of the locules is smooth and glistening (Case 7, AFIP Neg. 75-13649).
was present in the lumen of the cysts. Desqua- mated epithelial cells were found in two of the tumors (Cases 1 and 6).
With the exception of one tumor (Case 5) the supporting stroma immediately subjacent to the epithelium was very compact and cellular and resembled ovarian stroma; it was focally hyali- nized in Cases 3 and 4 (Fig. 6). Occasional smooth muscle fibers were identified in this layer. In Case 5 the epithelium of all the locules was surrounded by acellular and hyalinized col- lagen. Surrounding the densely cellular stroma found in most of the cystadenomas there was a

328 CANCER January 1977 Vol. 39
FIG. 3. Wall of locule of cystadenoma showing ulceration of epithelium (top). Wall contains nu- merous dark-stained macrophag-e cells as well as a few inflammatory cells (Case 1 , PAS, X180, AFIP Neg. 74- 6758).
loose layer of fibroblasts and collagen. This tis- sue, when it intervened between the cyst and the adjacent liver, contained veins, arteries, lyrn- phatics, and nerve bundles, as well as occasional small and medium-sized bile ducts; the latter
were often surrounded by a thick ring of colla- gen. In the locules with ulceration the base of the ulcers consisted of granulation tissue, and free rnucin could be demonstrated in its inter- stices.
FIG. 4. Locule of cyst- adenoma showing mul- tiple small papillary pro- jections into the lumen (Case 3, H&E, X70, AFIP Neg. 74-7052).
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Ishak et al. 329
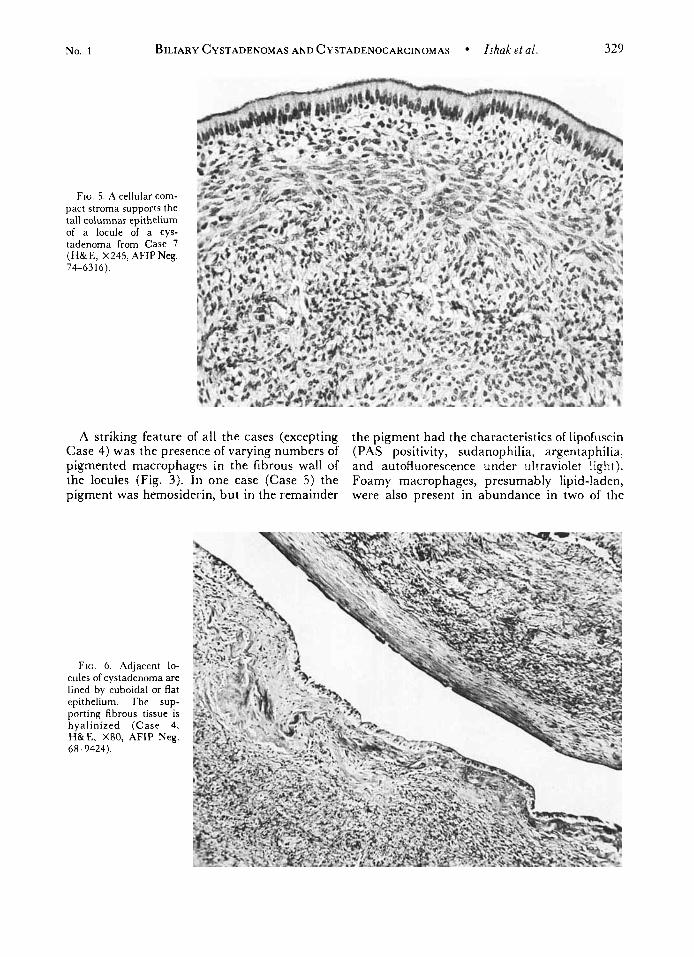
FIG. 5. A cellular com- pact stroma supports the tall columnar epithelium of a locule of a cys- tadenoma from Case 7 (H& E, X245, AFIP Neg. 74-63 16).
A striking feature of all the cases (excepting the pigment had the characteristics of lipofuscin Case 4) was the presence of varying numbers of (PAS positivity, sudanophilia, argentaphilia, pigmented macrophages in the fibrous wall of and autofluorescence under ultraviolet light). the locules (Fig. 3). In one case (Case 5) the Foamy macrophages, presumably lipid-laden, pigment was hemosiderin, but in the remainder were also present in abundance in two of the
FIG. 6. .4djacent lo- cules of cystadenoma are lined by cuboidal or flat epithelium. The sup- porting fibrous tissue is hyalinized (Case 4, H&E, X80, AFIP Neg. 68-9424).
330 CANCER January 1977 Vol. 39
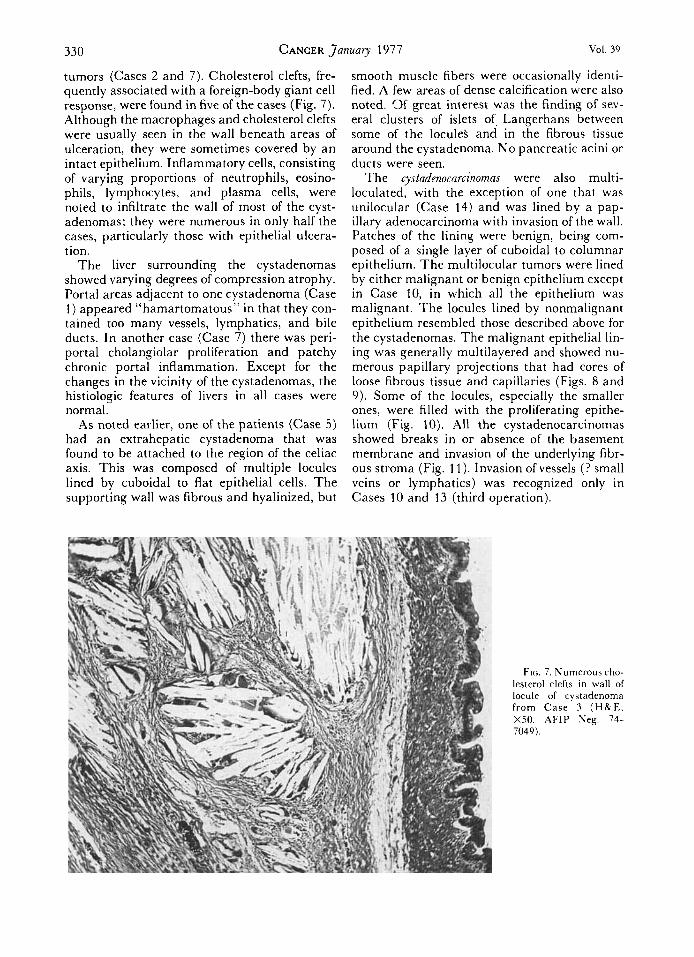
tumors (Cases 2 and 7). Cholesterol clefts, fre- quently associated with a foreign-body giant cell response, were found in five of the cases (Fig. 7). Although the macrophages and cholesterol clefts were usually seen in the wall beneath areas of ulceration, they were sometimes covered by a n intact epithelium. Inflammatory cells, consisting of varying proportions of neutrophils, eosino- phils, lymphocytes, and plasma cells, were noted to infiltrate the wall of most of the cyst- adenomas; they were numerous in only half the cases, particularly those with epithelial ulcera- tion.
The liver surrounding the cystadenomas showed varying degrees of compression atrophy. Portal areas adjacent to one cystadenoma (Case 1) appeared “hamartomatous” in that they con- tained too many vessels, lymphatics, and bile ducts. In another case (Case 7) there was peri- portal cholangiolar proliferation and patchy chronic portal inflammation. Except for the changes in the vicinity of the cystadenomas, the histiologic features of livers in all cases were normal.
As noted earlier, one of the patients (Case 5) had an extrahepatic cystadenoma that was found to be attached to the region of the celiac axis. This was composed of multiple locules lined by cuboidal to flat epithelial cells. The supporting wall was fibrous and hyalinized, but
smooth muscle fibers were occasionally identi- fied. A few areas of dense calcification were also noted. 3 f great interest was the finding of sev- eral clusters of islets of. Langerhans between some of the IoculeS and in the fibrous tissue around the cystadenoma. N o pancreatic acini or ducts were seen.
The cystadenocarcinomas were also multi- loculated, with the exception of one that was unilocular (Case 14) and was lined by a pap- illary adenocarcinoma with invasion of the wall. Patches of the lining were benign, being com- posed of a single layer of cuboidal to columnar epithelium. T h e multilocular tumors were lined by either malignant or benign epithelium except in Case 10, in which all the epithelium was malignant. The locules lined by nonmalignant epithelium resembled those described above for the cystadenomas. The malignant epithelial lin- ing was generally multilayered and showed nu- merous papillary projections that had cores of loose fibrous tissue and capillaries (Figs. 8 and 9). Some of the locules, especially the smaller ones, were filled with the proliferating epithe- lium (Fig. 10). All the cystadenocarcinomas showed breaks in or absence of the basement membrane and invasion of the underlying fibr- ous stroma (Fig. 11) . Invasion of vessels (? small veins or lymphatics) was recognized only in Cases 10 and 13 (third operation).
FIG. 7. Numerous cho- lesterol clefts in wall of locule of cystadenorna from C a s e 3 (HBrE. XSO, AFIP Neg. 74- 7049).
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS lshak et al. 331
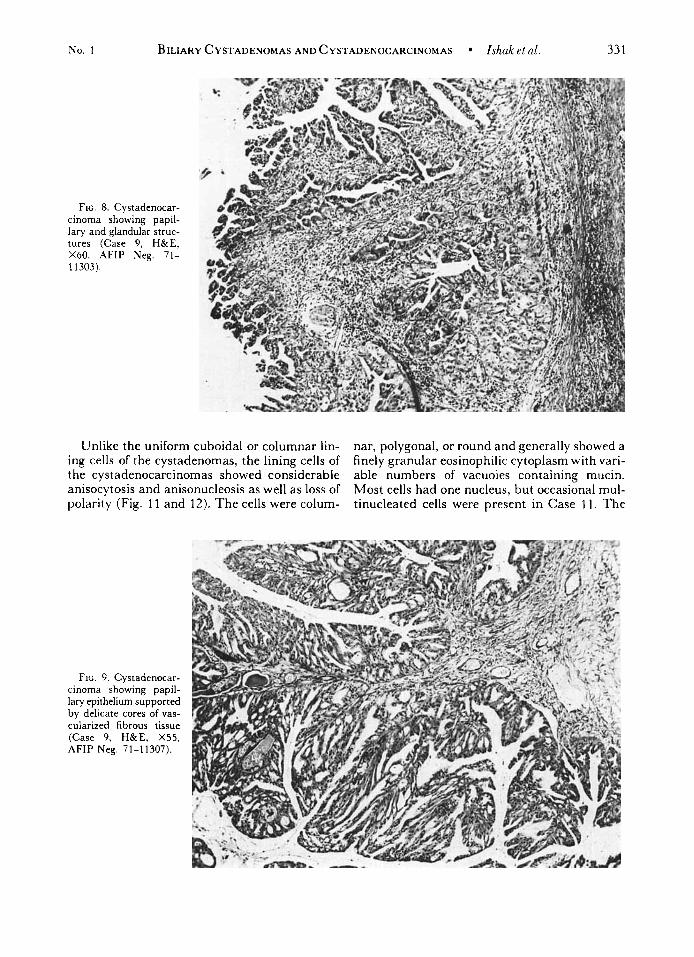
FIG. 8. Cystadenocar- cinoma showing papil- lary and glandular struc- tures (Case 9, H&E, X60, AFIP Neg. 71- 1 1303).
Unlike the uniform cuboidal or columnar lin- ing cells of the cystadenomas, the lining cells of the cystadenocarcinomas showed considerable anisocytosis and anisonucleosis as well as loss of polarity (Fig. l l and 12). The cells were colum-
nar, polygonal, or round and generally showed a finely granular eosinophilic cytoplasm with vari- able numbers of vacuoles containing mucin. Most cells had one nucleus, but occasional mul- tinucleated cells were present in Case 11. The
FIG. 9. Cystadenocar- cinoma showing papil- lary epithelium supported by delicate cores of vas- cularized fibrous tissue (Case 9, H&E, X55, AFIP Neg. 71-11307).
332 CANCER January 1977 V O l . 39
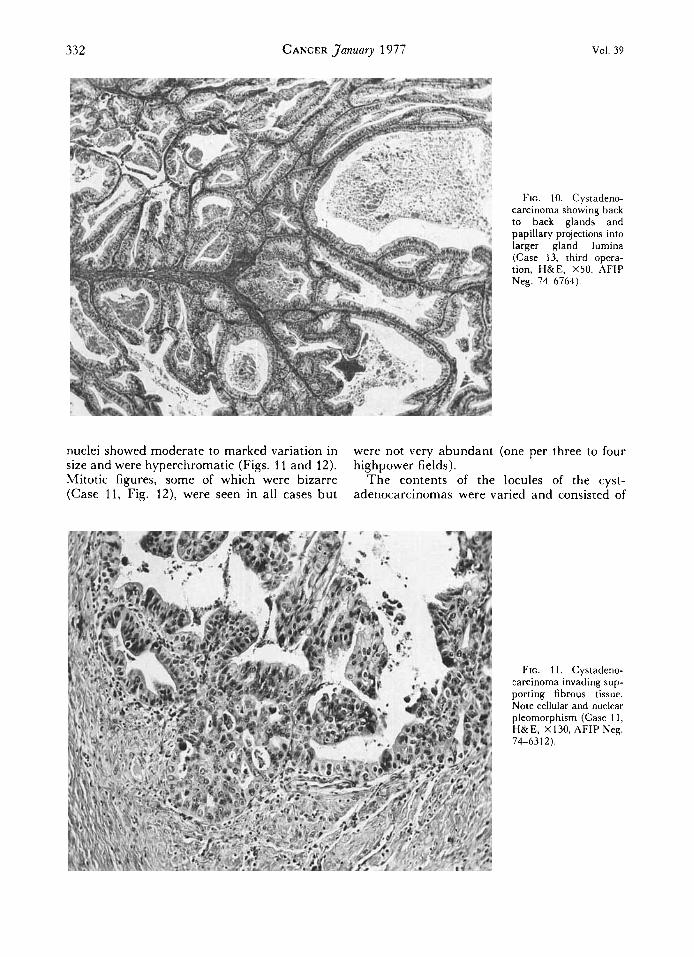
FIG. 10. Cystadeno- carcinoma showing back to back glands and papillary projections into larger gland lumina (Case 13, third opera- tion, H&E, X50, AFIP Neg. 74-6764).
nuclei showed moderate to marked variation in were not very abundant (one per three to four size and were hyperchromatic (Figs. 11 and 12). highpower fields). Mitotic figures, some of which were bizarre The contents of the locules of the cyst- (Case 11, Fig. 12), were seen in all cases but adenocarcinomas were varied and consisted of
FIG. 11. Cystadeno- carcinoma invading sup- porting fibrous tissue. Note cellular and nuclear pleomorphism (Case 11 , H&E, X130, AFIP Neg. 74-631 2).
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Zshak et al. 333
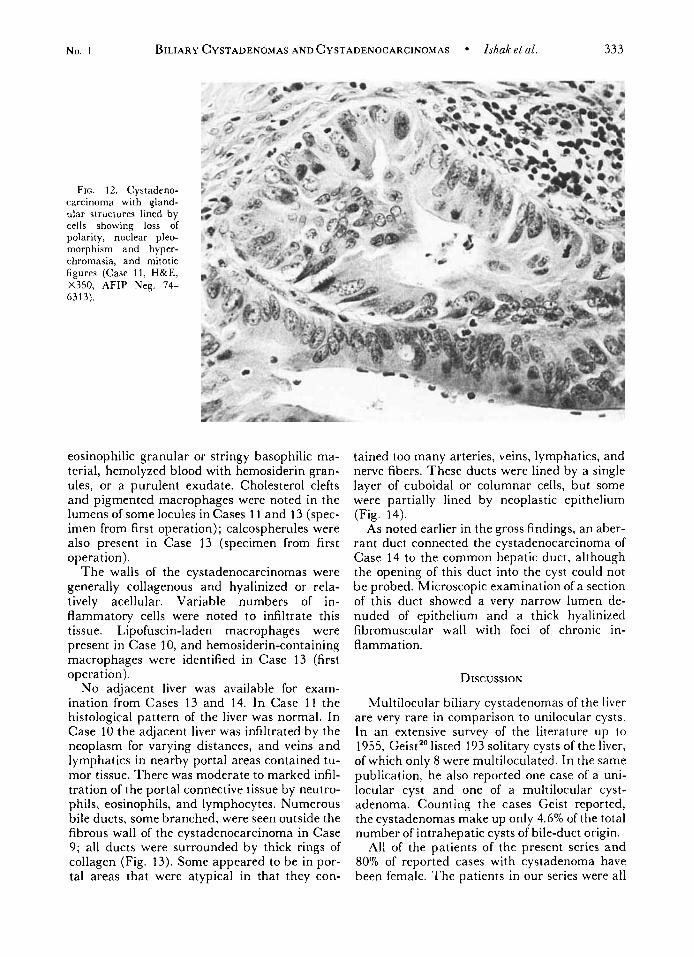
FIG. 12. Cystadeno- carcinoma with gland- ular structures lined by cells showing loss of polarity, nuclear pleo- morphism and hyper- chromasia, and mitotic figures (Case 11, H&E, X350, AFIP Neg. 74- 631 3) .
eosinophilic granular or stringy basophilic ma- terial, hemolyzed blood with hemosiderin gran- ules, or a purulent exudate. Cholesterol clefts and pigmented macrophages were noted in the lumens of some locules in Cases 1 1 and 13 (spec- imen from first operation); calcospherules were also present in Case 13 (specimen from first operat ion).
The walls of the cystadenocarcinomas were generally collagenous and hyalinized or rela- tively acellular. Variable numbers of in- flammatory cells were noted to infiltrate this tissue. Lipofuscin-laden macrophages were present in Case 10, and hemosiderin-containing macrophages were identified in Case 13 (first operation).
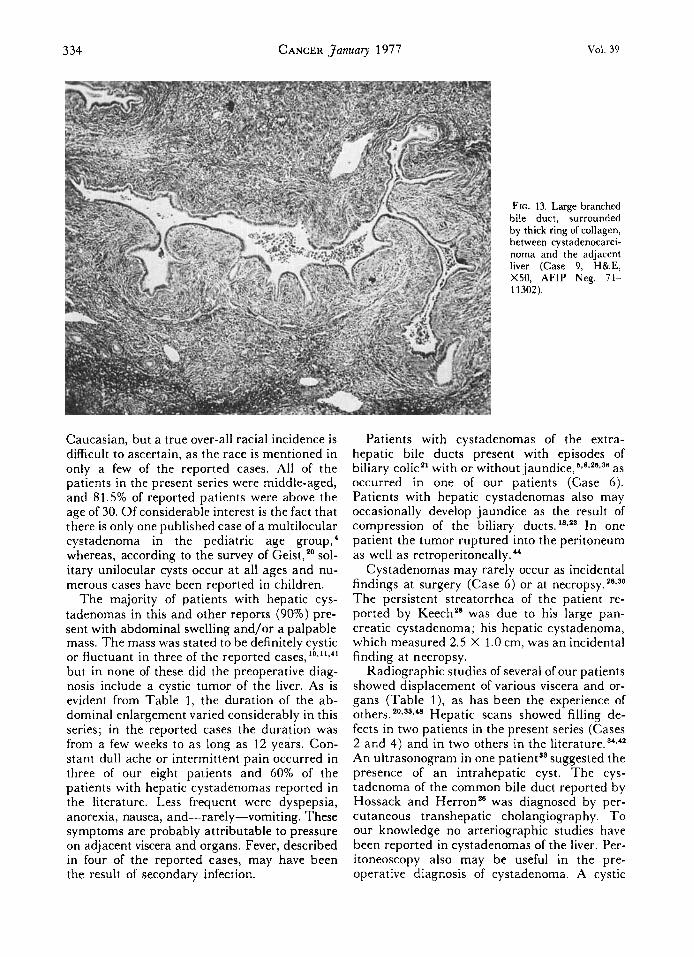
No adjacent liver was available for exam- ination from Cases 13 and 14. In Case 11 the histological pattern of the liver was normal. In Case 10 the adjacent liver was infiltrated by the neoplasm for varying distances, and veins and lymphatics in nearby portal areas contained tu- mor tissue. There was moderate to marked infil- tration of the portal connective tissue by neutro- phils, eosinophils, and lymphocytes. Numerous bile ducts, some branched, were seen outside the fibrous wall of the cystadenocarcinoma in Case 9; all ducts were surrounded by thick rings of collagen (Fig. 13). Some appeared to be in por- tal areas that were atypical in that they con-
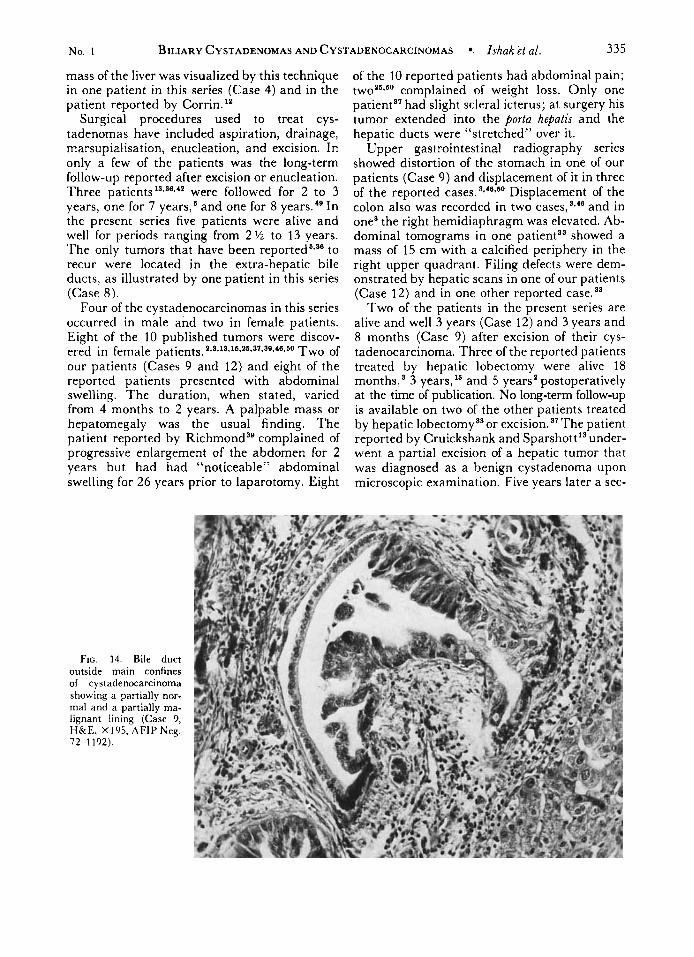
tained too many arteries, veins, lymphatics, and nerve fibers. These ducts were lined by a single layer of cuboidal or columnar cells, but some were partially lined by neoplastic epithelium (Fig. 14).
As noted earlier in the gross findings, an aber- rant duct connected the cystadenocarcinoma of Case 14 to the common hepatic duct, although the opening of this duct into the cyst could not be probed. Microscopic examination of a section of this duct showed a very narrow lumen de- nuded of epithelium and a thick hyalinized fibromuscular wall with foci of chronic in- flammation.
DISCUSSION
Multilocular biliary cystadenomas of the liver are very rare in comparison to unilocular cysts. In an extensive survey of the literature up to 1955, Geist" listed 193 solitary cysts of the liver, of which only 8 were multiloculated. In the same publication, he also reported one case of a uni- locular cyst and one of a multilocular cyst- adenoma. Counting the cases Geist reported, the cystadenomas make up only 4.6% of the total number of intrahepatic cysts of bile-duct origin.
All of the patients of the present series and 80% of reported cases with cystadenoma have been female. The patients in our series were all
334 CANCER January 1977 Vol. 39
Caucasian, but a true over-all racial incidence is difficult to ascertain, as the race is mentioned in only a few of the reported cases. All of the patients in the present series were middle-aged, and 81.5% of reported patients were above the age of 30. Of considerable interest is the fact that there is only one published case of a multilocular cystadenoma in the pediatric age group,' whereas, according to the survey of Geist," sol- itary unilocular cysts occur at all ages and nu- merous cases have been reported in children.
The majority of patients with hepatic cys- tadenomas in this and other reports (90%) pre- sent with abdominal swelling and/or a palpable mass. The mass was stated to be definitely cystic or fluctuant in three of the reported cases,10*11,41 but in none of these did the preoperative diag- nosis include a cystic tumor of the liver. As is evident from Table 1, the duration of the ab- dominal enlargement varied considerably in this series; in the reported cases the duration was from a few weeks to as long as 12 years. Con- stant dull ache or intermittent pain occurred in three of our eight patients and 60% of the patients with hepatic cystadenomas reported in the literature. Less frequent were dyspepsia, anorexia, nausea, and-rarely-vomiting. These symptoms are probably attributable to pressure on adjacent viscera and organs. Fever, described in four of the reported cases, may have been the result of secondary infection.
FIG. 13. Large branched bile duct, surrounded by thick ring of collagen, between cystadenocarci- noma and the adjacent liver (Case 9, H&E, X50, AFIP Neg. 71- 1 1302).
Patients with cystadenomas of the extra- hepatic bile ducts present with episodes of biliary colicz1 with or without jaundice,6,8.2"-3a as occurred in one of our patients (Case 6 ) . Patients with hepatic cystadenomas also may occasionally develop jaundice as the result of compression of the biliary ducts. 18*28 In one patient the tumor ruptured into the peritoneum as well as re t r~peri toneal ly .~~
Cystadenomas may rarely occur as incidental findings at surgery (Case 6) or at n e c r o p ~ y . ~ ~ ~ ~ ~ The persistent streatorrhea of the patient re- ported by Keech2* was due to his large pan- creatic cystadenoma; his hepatic cystadenoma, which measured 2.5 X 1.0 cm, was an incidental finding at necropsy.
Radiographic studies of several of our patients showed displacement of various viscera and or- gans (Table l ) , as has been the experience of others. 2 0 ~ 3 3 ~ 4 8 Hepatic scans showed filling de- fects in two patients in the present series (Cases 2 and 4) and in two others in the l i terat~re .~ '*~* An ultrasonogram in one patient" suggested the presence of an intrahepatic cyst. The cys- tadenoma of the common bile duct reported by Hossack and Herron2' was diagnosed by per- cutaneous transhepatic cholangiography. To our knowledge no arteriographic studies have been reported in cystadenomas of the liver. Per- itoneoscopy also may be useful in the pre- operative diagnosis of cystadenoma. A cystic
No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Ishak et al. 335
mass of the liver was visualized by this technique in one patient in this series (Case 4) and in the patient reported by Corrin.”
Surgical procedures used to treat cys- tadenomas have included aspiration, drainage, marsupialisation, enucleation, and excision. In only a few of the patients was the long-term follow-up reported after excision or enucleation. Three patients 13~36942 were followed for 2 to 3 years, one for 7 years,’ and one for 8 years.“ In the present series five patients were alive and well for periods ranging from 2 % to 13 years. The only tumors that have been reported6v3‘ to recur were located in the extra-hepatic bile ducts, as illustrated by one patient in this series (Case 8).
Four of the cystadenocarcinomas in this series occurred in male and two in female patients. Eight of the 10 published tumors were discov-
our patients (Cases 9 and 12) and eight of the reported patients presented with abdominal swelling. The duration, when stated, varied from 4 months to 2 years. A palpable mass or hepatomegaly was the usual finding. The patient reported by Richmond’’ complained of progressive enlargement of the abdomen for 2 years but had had “noticeable” abdominal swelling for 26 years prior to laparotomy. Eight
ered in female patients. 2,9.18,16,26.31,38,46.60 T wo of
FIG. 14. Bile duct outside main confines of cystadenocarcinoma showing a partially nor- mal and a partially ma- lignant lining (Case 9, H&E, X195, A F l P Neg. 72-1 192).
of the 10 reported patients had abdominal pain; twoZs-bo complained of weight loss. Only one patienta’ had slight scleral icterus; at surgery his tumor extended into the porta hepatis and the hepatic ducts were “stretched” over it.
Upper gastrointestinal radiography series showed distortion of the stomach in one of our patients (Case 9) and displacement of it in three of the reported cases. 3*46360 Displacement of the colon also was recorded in two cases,S*‘’ and in one* the right hemidiaphragm was elevated. Ab- dominal tomograms in one patient” showed a mass of 15 cm with a calcified periphery in the right upper quadrant. Filing defects were dem- onstrated by hepatic scans in one of our patients (Case 12) and in one other reported case.”
Two of the patients in the present series are alive and well 3 years (Case 12) and 3 years and 8 months (Case 9) after excision of their cys- tadenocarcinoma. Three of the reported patients treated by hepatic lobectomy were alive 18 months,s 3 years,“ and 5 years’ postoperatively at the time of publication. No long-term follow-up is available on two of the other patients treated by hepatic lobectomya3 or excision. “The patient reported by Cruickshank and Sparshott l3 under- went a partial excision of a hepatic tumor that was diagnosed as a benign cystadenoma upon microscopic examination. Five years later a sec-
336 CANCER January 1977 Vol. 39
ond laparotomy was performed, at which time the tumor was drained and biopsied; the speci- men was interpreted as malignant and possibly "sarcomatous." The patient died 10 days later. At necropsy there was a large multilocular cystic mass in the left lobe that had a solid part that had invaded the stomach and duodenum and metastasized to a lymph node in the porta he- patis. The solid component was histologically malignant and composed of spindle cells but could not be characterized any further. T h e re- maining four reported patients with cys- tadenocarcinomas died from a few weeks to 15 months after seeking medical attention. '6*a9-48.50
Surgical excision was carried out in two of these patients. "4' Of the three patients who were autopsied, '5*3g*60 two had extra hepatic met as t atic growths. Thompson and Wolff's'' patient, who underwent hepatic lobectomy was reexplored 6 months later for excision of a metastatic lesion in his omentum; he died 5 ?h months later but was not autopsied.
While the cystadenocarcinomas are capable of spreading beyond the confines of the liver and metastasizing to distant sites, the long survival of some of the patients in this series and in some of the reported patients suggest that this tumor has a better prognosis than intrahepatic cho- langiocarcinoma. According to Edmondson,'' the average survival of patients with the latter type of tumor is 6 months from the onset.
The majority of hepatic cystadenomas in the present series were found in the right lobe. In the published cases in which the site was speci- fied, 50% were in the right lobe, 29.2% were in the left lobe, and 16.6% involved both lobes of the liver. One tumor was located in the caudate lobe. 33
One patient in the present series (Case 8) had a cystadenoma that involved the common bile ddct (and later recurred) as well as a hepatic cystadenoma. A similar case was reported by Short et al.;" their patient had a cystadenoma in the left lobe as well as one in the common he- patic duct. Another patient in our series (Case 5) had an extrahepatic cystadenoma that con- tained pancreatic islet cell tissue and may have arisen in heterotopic pancreatic tissue; this patient also had a huge hepatic cystadenoma. One patient had both pancreatic and hepatic cystadenomas. Several other cystadenomas arising in the extrahepatic biliary tract have been reported.6*8*Se T h e cystadenoma in Ger- ber's patient" was found in an intrahepatic bile duct that communicated with the left hepatic duct and a large unilocular retention cyst lo- cated in the right lobe.
As in the present series, most of the reported cystadenomas were multiloculated. Two uni- locular cystadenomas with papillary or polypoid areas have, however, been reported. 1'931 There was considerable variability in the appearance of the liquid contents of the locules in the pres- ent series and in published cases. The majority of the reported tumors have been quite large, their maximum diameters frequently exceeding 10 cm. Two of the largest tumors contained 10 and 11 liters, respectively, of f l ~ i d . ~ ' . ~ '
The locules of cystadenoma are lined by biliary-type epithelium (with polypoid or pap- illary projections) that is supported by a dense cellular fibrous stroma in which smooth muscle fibers may be identified. This layer is in turn surrounded by a looser and less cellular layer of collagen that contains the arteries and veins (presumably supplying blood and draining it from the tumor), as well as nerve fibers and bile ducts. A connection between a large in- trahepatic bile duct and a cystadenoma has not to our knowledge been demonstrated, except for Gerber's case," in which the tumor had arisen in an intrahepatic duct. Such connections are, however, suggested by bile staining of the con- t e n t ~ , ~ ' * ~ * by the finding of a large bile duct at one extremity of a cy~tadenoma,~ ' by the identi- fication of an aberrant duct connecting the cys- tadenoma to the common hepatic duct (Case 14), or by the discovery of a transected bile duct in the defect left in the liver after surgical ex- cision of the cystadenoma. '@
A striking feature of the majority of cys- tadenomas we have studied is the presence of macrophages with phagocytosed lipofuscin, which is presumed to be a reaction to degenera- tion and inflammation in the cyst wall. The cholesterol in the wall is probably absorbed from the contents of the cyst through areas of epithelial ulceration. Cholesterol crystals were identified in the contents of the cystadenoma from one of our patients (Case 4) and from two of the reported
The cystadenocarcinomas in the present study were all multilocular except for one tumor (Case 14). Of the 10 published cases, 6 were multilocular and 3 unilocular. (No description is given of the case reported by Adson and Jones).' T w o of t h e published unilocular cys- t a d e n o c a r c i n ~ m a s ' ~ ~ ' ~ and one in the present series (Case 14) had a shaggy or roughened lining; a fourth tumorm had two gray-white fleshy areas that were microscopically malig- nant. Of the multilocular tumors, three13.33.50 also had solid areas. I t is significant that four of the six reported tumors whose contents were

No. 1 BILIARY CYSTADENOMAS AND CYSTADENOCARCINOMAS Ishak et al. 337
described contained blood-stained, frankly he- morrhagic, or chocolate-colored material. In the present series two of the tumors contained bloody material in some of the locules. In con- trast, only 2 of 16 reported cystadenomas con- tained blood-stained fluid.
With the exception of one tumor (Case lo), all of the cystadenocarcinomas in the present study showed both benign and malignant com- ponents. In addition to the microscopic features characteristic of malignant neoplastic epithe- lium, we wish to stress the occurrence of breaks in the basement membrane and invasion of the underlying stroma. Intestinal metaplasia, with both goblet and argentaffin cells, was present in the cystadenocarcinoma reported by More. 37 Of special interest in the present series was Case 10, in which abnormal “hamartomatous” bile ducts surrounded the main tumor, some being lined by both benign and malignant epithelium.
In the present series, the demonstration of benign epithelium in the majority of the cys- tadenocarcinomas makes it highly probable that they arose in previously benign cystadenomas. Transformation of a benign to a malignant tu- mor has been definitely documented in only one case. l3 The fate of patients reported in the liter- ature whose cystadenomas were only drained or marsupialized is unknown, since long-term fol- low-up information is not available. Inasmuch as the latent period for malignant transforma- tion is unknown, prompt excision of the cys- tadenoma would seem to be advisable.
The cause of cystadenoma of the liver and extrahepatic bile ducts remains unknown. The various theories of origin of hepatic cysts have been discussed at length by several au- thors. 14.20,27*36 The oft-quoted theory of Mos- chow it^^^ that nonparasitic cysts of the liver have their origin in aberrant bile ducts was in refer- ence to polycystic disease of the liver and/or kidney. Dardik et al.,“ who reported a solitary cyst of the liver lined by ciliated epithelium, raised the possibility of an analogous origin for
certain respiratory and enteric malformations from the pleuripotential embryonic foregut.
In support of a congenital origin is the finding of an aberrant duct in a reported cystadenoma3’ and in one of the cystadenocarcinomas in the present series (Case 14) and the occurrence of a cystadenoma within an intrahepatic duct that may have been anomalous.’ Clearly abnormal “hamartomatous” bile ducts were interposed between a cystadenoma in the present series (Case 10) and the adjacent liver. The portal areas in the same case and in one of the cys- tadenomas (Case 1 ) also had an abnormal “hamartomatous” structure. I t is also of interest that 2 of the 14 patients in the present series had developmental anomalies. One of the patients with a cystadenoma was known to have a bicor- nuate uterus (Case 4), while one of the patients with a cystadenocarcinoma had a double col- lecting system and double ureter on the right (Case 12).
If the cystadenomas are of developmental ori- gin, then their late presentation must be as- cribed to very slow growth and/or accumulation of fluid, but, as noted earlier, symptoms related to the tumors of some of the reported patients were of many years’ duration. There is little evidence to support an acquired origin of cys- tadenoma, but note should be made of the ex- perimental production of benign and malignant cysts in the liver of rats fed on a diet containing afl at oxi n. ”
As mentioned earlier, we believe that the cys- tadenocarcinomas arise by malignant transfor- mation of the epithelium of a cystadenoma. In this context it is worth noting that adenocarci- nomas may also arise in congenital abnor- malities of the intrahepatic and extrahepatic bile ducts, such as choledochal cysts, Caroli’s dis- ease, congenital hepatic fibrosis, and polycystic disease, a subject that has recently been re- viewed by Gallagher et al.” A squamous cell carcinoma arising in a solitary bile duct cyst has also been reported.”
REFERENCES
1. Ackman, F. D., and Rhea, L. J.: Non-parasitic cysts of the liver. Their clinical and pathological aspects. E r . 1. Surg. 18:648-654, 1931.
2. Adson, M . A,, and Jones, R. R : Hepatic lobsctorny. Arch. Surg. 92:631-635, 1965.
3. Ameriks, J., Appleman, H., and Frey, C.: Malignant nonparasitic cyst of the liver. Case report. Ann. Surg. l76:7 13-717, 1972.
4. Alexander, R. C.: Solitary nonparasitic cysts of the liver. Edinburgh Med. 3. 32:61-68, 1925.
5. Barber, K . W . , J r , , ReMine, W. H . , Harrison, E C, , Jr.? and Priestley, J. T.: Benign neoplasms of extrahepatic bile ducts, including papilla of Vater. Arch. Surg. 81 :479-484, 1960.
6. Bevan, A. D.: Multilocular cystadenorna of the liver. Surg. Clm. North Am. 3:887-892, 191 9.
7. Bisgaard-Frantzen, C. F.: Et Tilfaelde af en rnansho- vedstor, ikke parasitaer, solitaer, multiloculaer Levercyste. .,Vord. M e d . 16:3542-3543, 1942.
8. Bishop, E. S.: An undescribed innocent (?) growth of
338 CANCER January 1977 Vol. 39
the gallbladder. Lancet 2:72-78, 1901. 9. Bland-Sutton, J . : Solitary nonparasitic cysts of the
liver. Br. Med.,3. 2:1167-1168, 1905. 10. Burch, J. C., and Jones, H. E.: Large nonparasitic
cyst of the liver simulating an ovarian cyst. Am. 3. Obstet. Gynecol. 63:441-444, 1952.
11. Clagett, 0. T., and Hawkins, W. J . : Cystic disease of the liver. Report of a case. A n n . Surg. 123:lll-118, 1946.
12. Corrin, B . : Cystadenoma of the liver. 3. Pathol. Bacte- rzol. 84:441-443, 1962.
13. Cruickshank, A. H., and Sparshott, S. M . : Malig- nancy in natural and experimental hepatic cysts. Experi- ments with aflatoxin in rats and the malignant transforma- tion of cysts in human livers. 3. Pathol. 104:185-190, 1971.
14. Dardik, H., Glotzer, P., and Silver, C.: Congenital hepatic cyst causing jaundice. Report of a case and analogies with respiratory malformations. Ann . Surg. 159:585-592, 1964.
15. Dean, D. L., and Bauer, H . hl.: Primary cystic carci- noma of the liver. Am. 3. Surg. 117:416-320, 1969.
16. Delannoy,. E., and Lagache, G. : Adenomes biliares kystiques a propos de 5 observations personnelles. Arch. M a / . Appar. Dzg. 36:452-456, 1947.
17. Edmondson, H. A , : Tumors of the Liver and In- trahepatic Bile Ducts. Atlas of Tumor Pathology, Sect. VII, Fascicle 25. Washington, DC, Armed Forces Institute of Pathology, 1958.
18. Evans, A. : Cystic adenoma of the bile ducts. BY. 3. Surg. 9:155-156, 1921.
19. Gallagher, P. J. , Millis, R. R., and Mitchinson, M. J.: Congenital dilatation of the intrahepatic bile ducts with cholangiocarcinoma, 3. Clin. Pathol. 25:804-808, 1972.
20. Geist, D. C.: Solitary nonparasitic cyst of the liver. Arch. Surg. 71:867-880, 1955.
21. Gerber, A , : Retention cyst of the liver due to a bile duct polyp. Ann. Surg. 140:906-910, 1954.
22. Greenwood, N., and Orr, W. McN.: Primary squamous-cell carcinoma arising in a solitary non-parasitic cyst of the liver. ,7. Pathol. 107:145-148, 1972.
23. Grieg, D. M.: A case of adenoma of the bile ducts. Edinburgh Med. J . 27:145-148, 1921.
24. Harrington, W. W. : Solitary nonparasitic cyst of the liver. Surg. Clin. North Am. 6:1191-1193, 1926.
25. Hodel, C. : Primares Cystadenocarcinom der Leber. zentralbl. Allg. Pathol. 109:62-66, 1966.
26. Hossack, K. F., and Herron, J. J.: Benign tumours of the common bile duct. Report of a case and review of the literature. A u s ~ N . 2. J . Surg. 42:22-26, 1972.
27. Jones, J. F. X. : Removal of a retention cyst from the liver. Ann. Surg. 77:68-89, 1923.
28. Keech, M. K.: Cystadenomata of the pancreas and intrahepatic bile ducts. Gastroenterolog~~ 19:568-574, 1951.
29. Keen, W. W.: O n resection of the liver, especially for
hepatic tumors. Boston M e d . Surg. 3. 126:405-409, 1892. 30. Kelemen, A , : Ein aus den Gallengzngen hervorge-
hendes Cystadenoma papilliferm hepatis. Frankfurl zentralbl. Pathol. 33:423-427, 1956.
31. Lasnier, E. P., and Rodriguez Estevan, C. M.: Dos casos de cistadenoma biliar. Ann. Fac. Med. Montevideo 14: 142- 160, 1929.
32. Lepprnann, F. : Ueber die echten Cysten der Leber. Deutsch. z, Chzr. 54:446-467, 1900.
33. March, J. L., Dahms, B . , and Longmire, W. P. Cys- tadenoma and cystadenocarcinoma of the biliary sys- tem.Arch. Surg. 109:41-43, 1974.
34. Merchant, F. J.: Multiloculated cystadenoma of the liver. Il l . Med. 3.1 144:129-139, 1973.
35. Moschowitz, E.: Non-parasitic cysts (congenital) of the liver, with a study of aberrant bile ducts. Am. J . Med. Scz. 131:674-699, 1906.
36. Moore, S. W., and McElwee, R. S.: Benign tumor of the biliary tract. JAMA 150:999-1002, 1952.
37. More, J. R. S. : Cystadenocarcinoma of the liver. 3. Clzn. Pathol. 19:470-474, 1966.
38. QuPnu, M. J . : Un gros kyste non parasitaire du foie. Mim. Acad. Chzr. 62:1425-1426, 1936.
39. Richmond, H. G. : Carcinoma arising in congenital cysts of the liver. 3. Pathol. Bacteriol. 72:681-683, 1956.
40. Sandberg, I . : Zur Kasuistik solitarer, nicht-para- sitlrer Leberzysten. Acta Chir. Scand. 70:555-562, 1933.
41. Shattuck, F. C.: Adenocystoma of the liver. Boston Med. Surg. 3. 142:427-428, 1900.
42. Short, W. S., Nedwich, A. , Levy, H . A,, and Howard, J. M. : Biliary cystadenoma. Report of a case and review of the 1iterature.Arch. Surg. 102:78-80, 1971.
43. Skaliczki, J., Fiizesi, K., and Altorjay, I : Operativ entferntes Gallengangszystadenom. zentralbl. Allg. Pathol.
44. Snedecor, P. A. : Bile duct cystadenoma of the liver. A m . Surg. 33:581-583, 1967.
45. Sonntag, E. : Beitrag zur Frage den solitlren, nicht parasitzren Lebercysten.Beitr. 2. klin. Chir. 86:227-377, 1913.
46. Thompson, J. E., and Wolff, M.: Intra-hepatic cys- tadenoma of bile duct origin, with malignant alteration. Report of a case, treated with total left hepatic lobectomy. Mzlzt. hfed. 130:218-224, 1965.
47. Tuffier, M.: Kyste non parasitaire du foie (angiome biliare). Bull. Mem. Soc. Chir. Paris 38:1252-1261, 1912.
48. Warren, K. W., and Pararo, L. L.: Solitary non- parasitic cysts of the liver. Lahey Clzn. Found. Bull. 8:162-169, 1953.
49. Williams, B. : Cystadenoma of the liver. P m . Roy. Soc. Med. 54:157-158, 1961.
50. Willis, K. A : Carcinoma arising in congenital cysts of the liver. 3. Pathol. Backmd. 50:492-495, 1943.
11:131-135, 1968.
Top Related
Copyright © 2022 FDOKUMEN

