







Bahasa
Halaman
Hukum


Barriers to Communication: Improving Cultural Awareness withLatino Patients
A program proposal submitted to the faculty ofSan Francisco State Universityin partial fulfillment of the
requirements forthe degree
Master of Sciencein
Nursing
byMarcos Taquechel, RN
i
San Francisco, CA
December 2010
CETIFICATE OF APPROVAL
I certify that I have read Barriers to communication: improving cultural awareness with Latino patients by Marcos Taquechel, and that in my opinion, this meets the criteria for approving the field study submitted for partial fulfillment of the requirements for the degree: Master’s of Science in Nursing at San Francisco State University
ii
ii
_________________________________________
Dr. Pamela Baj , DNSc, RN, FAANProfessor of Nursing
_________________________________________
Dr. Harvey “Skip” Davis, RN, PhDAssociate Professor
BARRIERS TO COMMUNICATION: IMPROVING CULTURAL COMMUNICATION AWARENESS WITH LATINO PATIENTS
Marcos TaquechelSan Francisco State University
2010Abstract
Latinos are the fastest growing ethnic population in the United
States. The steady increase in this population segment poses
special communication problems between health care professionals
and Latino patients. Although many health care professionals are
aware of the cultural barriers Latinos encounter, some still lack
cultural competency. The implementation of online courses offered
to health care professionals can help bridge the cultural gap by
introducing an insider’s view on how Latinos perceive and react
iii
iii
to health care in the United States. The purpose of this field
study is to introduce new teaching methodology through employing
latest cultural research. New technology and the online format
may improve the level of cultural competency of health care
professionals treating Latino patients in the clinical setting.
The theoretical framework for this field study was based on the
theory of culture care diversity and universality by Madelaine Leininger’s
which incorporate broad humanist dimensions about people in their
cultural life context, and focuses on identifying values,
beliefs, life-ways, and symbolic referents related to culture
care phenomena. This concept was then applied to web-learning
design using videos and narration with pictures illustrating real
clinical scenarios. An evaluation component is planned to
determine outcome for this field study. Further research is
recommended based on the literature review to evaluate effective
teaching methodology and relevant development of cultural
competency programs.
Dr. Pamela Baj , DNSc, RN, FAAN Date
iv
iv
Professor of Nursing TABLE OF CONTENTS
Chapter One: Introduction .................................... 1Description of this program proposal.................3Purpose of the study.................................5Significance of the study............................7Objectives...........................................8Assumptions..........................................9Summary.............................................10
Chapter Two: Review of literature ............................ 12Cultural Competency in Nursing......................14Racial and Ethnic Discrimination in Health Care.....30Race and Ethnicity and Satisfaction with Health Care34Theoretical Framework...............................36
Chapter Three: ....................................Implementation 40
Introduction........................................40Evidence............................................42Program objectives..................................45Population, Setting, and Stakeholders...............47Implementation of plan..............................49Resource allocation and costs.......................52............................................................................................................Summary.............................................53
Chapter Four: Evaluation.......................................56Introduction........................................56Stakeholders........................................57Evaluation design...................................58Gathering Credible Evidence.........................60Justifying Conclusions..............................61Ensuring use and Sharing Lessons Learned............62Time Frame for Evaluation...........................63
v
v
Summary.............................................64Chapter Five: Conclusion.......................................65
Introduction........................................65Implications........................................65Limitations of the field study......................66Recommendations.....................................67Summary.............................................69
References ..................................................70Appendices ..................................................81
vi
vi
vii
vii
Chapter 1
Introduction
The United States (U.S.) is the sum of many ethnic groups
adding different languages and cultures to form a tapestry rich
in diversity. However, cultural diversity brings challenges to
health care professionals who need to expedite specific
instructions and make assessments with limited time availability.
As a minority group, Latinos are the fastest growing ethnic
population in the U.S. (Shaya & Gbarayor, 2006). Latinos
encounter difficulty obtaining health care due to low
socioeconomic status, language and cultural barriers as they have
difficulties understanding the American mainstream health care
system (Ku & Flores, 2005). Lack of access and lack of insurance
add to this problem, compromising Latino patient satisfaction in
hospitals and clinics (Shi & Stevens, 2005). Health care
providers (HCP) must be able to meet these challenges in order to
offer health and pharmaceutical needs for the fast emerging
Latino population.
1
The United States Census Bureau (USCB) projects that the
overall U.S. population will increase by 50%, from 263 million in
1995 to 394 million in 2050. The Hispanic population is on the
rise and represents the largest minority in the U. S. and will
comprise almost 25% of the U.S. inhabitants by 2050. Of all
nurses in the U. S., 82.3% are White Non-Hispanic and only 6.5%
speak Spanish (Board of Registered Nurses, 2008). Based on this
projected population data, it is safe to estimate that at some
point in their careers, most nurses will take care of Latino
patients, and their families especially in heavy Latino populated
areas such as California and the Southwest of the United States
(Rivers & Patino, 2006).
With limited amounts of time, non Spanish speaking nurses
and physicians rely on official translators over the phone or
family members to aid communication with their Latino patients.
According to new ratings, limited English proficient (LEP)
patients perceive quality care to be associated with HCP and
don’t think having an interpreter is a substitute for Cultural
Competency (CC) (Ngo-Metzger et al., 2007). Thousands of patients
may be facing cultural barriers every day because of their lack
2
of communication skills in another language or may be assisted by
inexperienced translators who might distort important medical
health conditions and interpretations (Ku & Flores, 2005). In
order to become culturally proficient, nurses will need to
acquire CC on their own or have their agencies provide means for
them to acquire it. The lack of CC and language skills have been
found to compromise patient care resulting in more medical
errors, lack of compliancy, longer hospital stays, and lower
patient satisfaction (Ngo-Metzger et al., 2007). Implementation
of CC could also help Latinos in treating chronic diseases. A
study focusing on Latino adults with chronic diseases found that
deficits in communication can lead to chronic diseases as health
care providers fail to catch illnesses which can progress to
chronic conditions (Bachman, Tobias, Master, Scovron, & Tierney,
2008).
Obesity is a major cause of morbidity and disability (Wee et
al., 2005). Obesity is the second-leading cause of preventable
death in the United States. A significant percentage of Americans
have weight problems: estimates show that 64% are overweight and
30% obese (Wee et al., 2005). The estimated annual cost of
3
treating obesity related illnesses in the U.S. reached $ 147
billion in 2009 (Dentzer, 2010). Fifty one percent of Mexican-
American women 40–59 years of age were obese compared with about
39% of non-Hispanic white women of the same age (Centers for
Disease Control, 2007). Demographic factors influence projections
of future health care costs given that current increases in
obesity disproportionately affect women, Hispanics and Blacks
(Wee et al., 2005). Obesity leads to diabetes type II, which can
cause complications such as heart disease, hyperglycemic crises,
end-stage renal disease, lower extremity conditions and visual
impairment (Wee et al., 2005).
Hispanic/Latino Americans are at a particularly high risk
for type II diabetes and its complications. The Latino population
has an 11.7% rate of type II diabetes to 4.8% of non-Latino; this
represents a diabetes risk increase of 100%. Despite the diabetes
predominance, diabetes-related healthcare services such as annual
dilated eye examinations, glycosylated hemoglobin tests, self-
monitoring blood glucose meters, doctor visits for diabetes, foot
examinations, and attendance at diabetes self-management classes
are all lower for Latinos than among non-Latino whites (Centers
4
for Disease Control, 2007). Latinos also have higher rates for
major diabetes risk factors due to being overweight and being
physically inactive (Escamilla & Putnik, 2007). These are a few
examples of disease that affect Latinos and are of importance to
this project.
Development and implementation of CC courses in hospital and
clinics are a good approach to raise cultural competency levels
among health care professionals. The curriculum for such teaching
programs should focus on evidence-based health disparities among
Latino populations. It should provide culturally competent care
education and exposure to health cultural traits in Latin
countries. Health care providers who engage in CC learning should
increase cultural awareness and cultural sensitivity thereby
increasing efficiency communicating, teaching and preventing
diabetes and obesity in low English proficient (LEP) patients
(Shaya & Gbarayor, 2006).
Description of the program
This field study is primarily dedicated to the evaluation of
cultural competency programs and the investigation of the current
5
status of Latinos and their cultural barriers to health care.
This study and its final objective will have 3 phases of
development. The first is a literature search of evidence base
studies regarding Latinos and health care. This first part is
intended to familiarize the target population with Latino
culture, habits, common health conditions and how Latinos
perceive the health care world. The second part will focus on
several aspects of clinical care and the identification of useful
cultural elements which promote better communication between
Latino patient and HCP. A web-site will be created containing
cases, common words, and scenarios encountered in clinics and
hospitals. Health care workers can use this web-site as a guide
and begin to practice their cultural competency skills. The third
and final part of the program will focus on the implementation
and use of this web-site in several educational applications.
A web site as a distribution vehicle is preferable for its
ease of access and user interactive potential. Also the Internet
and its widespread availability is an affordable and efficient
way to deliver information, offering almost unlimited
possibilities of content delivery. Videos, text, sound and
6
interactive animation can be conveniently accessed from personal
or agency computers or from hand held devices. The Internet is
also rapidly becoming the most trusted information vehicle where
the HCP obtain medical related information (Hesse et al., 2005).
Web based media can also be useful for data collection, test
taking, data input management, and it can be connected virtually
anywhere. This web site is designed to help promote better
communication as well as the identification of specific cultural
communications patterns related to Latino and health care. At the
end of the course, an optional questionnaire or test will be
administered to participating HCP who are supposed to achieve at
≥ 80% correct answers.
The target population for this field study will be mostly
non-Latino HCP working in hospitals and clinics in Northern
California who are often in charge of Latino patients. According
to the United States Census Bureau, Latinos in California account
for 37% of the population (U.S. Census Bureau, 2008). HCP mostly
likely to benefit from this CC program are nurses who have
limited or no experience with the Latino population or have moved
7
from areas of the country where the Latino patient population is
small.
One agency in Northern California has been chosen for its
large Latino population and also because it hosted similar CC
programs in the past. This project will be implemented as part of
the training program for new nurse graduates or as part of the
ongoing staff training. Other forms of implementation will take
place as the program is inserted and authorized by nursing
agencies which want to enable CC programs or use it as continuing
education credits for nurses’ license renewal.
Purpose to the study
The purpose of this field study is to improve satisfaction
among Latino patient population seeking health care service in
the United States by the creation of tools to that will promote
cultural understanding related to health care issues among HCP.
The expectations are that incremental improvements in HCP ability
to communicate with a culturally diverse group will generate
better patient satisfaction and safer nursing. Ultimately the
study seeks to promote a mutual cultural understanding between
Latino patient population and HCP producing verifiable benefits
8
in areas such as patient assessments, discharge instruction,
regular scheduled visits and medication instructions compliance
and understanding.
One immediate goal of this project is to first identify and
study the problem areas Latinos face when they seek health care,
and also the possible obstacles HCP face when treating Latino
patients. The research in these areas aim at understanding the
wide-range of perspectives, beliefs, values, and behaviors
concerning health and well being, Latinos bring with them to the
health care environment (Betancourt & Maina, 2007). These include
variations in identification of symptoms, thresholds for seeking
care and understanding of management strategies; also preferences
for being diagnosed or not and the choice for therapeutic
procedures and preventive measures and medication compliance (Ku
& Flores, 2005). A teaching methodology will then be created
utilizing the available research to be further incorporated into
teaching units assessed by a web site and also printed material.
A main goal of this project is the creation of a web site
incorporating the current research as well the teaching
9
methodology with the purpose of providing a comprehensive web
based education in CC regarding Latino culture. The creation and
implementation of a web site seek to accomplish current and
comprehensive learning as health disparities could be minimized
by several factors including the proper training of HCP to better
navigate cultural diverse patient populations (Kripalani, Jones,
Katz & Genao, 2006). In addition to the web site, another goal is
the creation of a booklet which will work as a companion book to
the web based learning course program.
The web site creation and availability offers only a
potential for learning but without correct implementation,
learning efficacy could be jeopardized by the lack of usage and
low penetration of target audience. Another goal of this project
is the implementation of the proposed web site as a training tool
to be used in hospitals by HCP and the establishment of this same
web program as part of nursing license renewal credit hours. This
goal translates into implementation efforts to bring this CC
course into health care institutions such as hospital and clinics
who are interested in starting CC education or already have CC
curricula in their establishments. This goal has also the
10
objective of utilizing the existent infra-structure of
established organizations to help bring this web site to its full
potential.
Significance of the study
The U.S. Hispanic population is growing at a rate four times
faster than the general population (U.S. Census Bureau, 2008).
Hispanics have surpassed African Americans as the largest
minority group in the United States (U.S. Census Bureau, 2008).
The U.S. Census Bureau, 2008 also estimates that 13.8% or 41
million people in the U.S. will be of Hispanic/Latino descent by
the year 2010, growing to 16% or 51 million individuals by 2020.
This jump in population presents an exceptional challenge to
primary care providers who must communicate and provide care to a
patient population whose primary language and cultural background
is often not that of the caregivers. As the Latino population
grows, so grows the susceptibility for widespread health problems
associated with this increasing population segment. The increase
of cultural awareness among HCP could potentially address socio-
11
cultural disparities, increasing patient satisfaction and
improving health among all patients.
The adult Latino population reporting having diabetes is
more than 6% compared to 5.3% for the rest of the non Latino
population (Campos, 2007). In a study addressing cultural
barriers to successful use of insulin in Hispanics with type II,
diabetes was found to be metabolically more severe in Latinos
leading to more complications such as neuropathy, diabetic
retinopathy, peripheral vascular disease, and end stage renal
disease (Campos, 2007). Adding to this problem, Latinos have high
risk factors such as physical inactivity, obesity in woman and
high blood pressure. For most Latinos diabetes is considered a
high co morbidity factor (Lorig, Ritter & Jacquez, 2005). Since
diabetes is associated with education and patient provider
interaction, it is imperative that communication is safe and
effective (Campos, 2007).
Latino health problems have origins that can be traced back
to childhood years growing up in the United States. Because
Latinos are much more likely to be uninsured than non-Latinos and
82% of uninsured Latinos constitute families, children are the
12
most at risk group within the Latino community to suffer lack of
health care (Passel, 2009). Children make up more than 42% of
U.S. - born Latinos with no health coverage bringing serious
implications for Latino age development compromising healthy
development leading to possible illnesses in adulthood (Passel,
2009). Lack of insurance also aggravates economic troubles in the
Latino community. More than half of the adult illegal immigrants,
or 59%, had no health insurance during 2007, and had to withdraw
money from savings to pay for health care (Passel, 2009).
Economic hardship can also be a contributor to poor health care
as families scramble to make ends meet and cut corners utilizing
low quality foods and further delaying treatment of health
conditions. Another study demonstrate that a third of the
children of unauthorized immigrants and a fifth of adult
unauthorized immigrants live in poverty (Passel, 2009). The
economic disadvantages experienced by Latinos can further burden
the health care system in general as uninsured Latinos rush to
the emergency rooms seeking treatment for conditions which could
have been prevented with regular health care services (Okie,
2007). Attempts to address CC competency issues are significant
13
because they can help disenfranchised populations, facilitating
access and utilization of health care system.
Objectives of the study
(1) To increase cultural awareness of Latino health habits
among HCP. This will be measured by the ability health
care professionals have when identifying significant
symbols related to health and treatment important to
Latinos. They should be able to identify at least 80% of
listed important elements in post test questionnaires.
(2) The provision and completion of CC web based course by
HCP should increase patient satisfaction, medication
compliance, and decrease recidivism in the Latino patient
population in hospitals. Latino patients should be able
to interact with HCP demonstrating better understanding
of discharge instructions and seek regular treatments.
(3) To provide a web based resource center to HCP involving
aspects of Latino culture as it relates to health care.
Items should include but not be limited to, language
14
resources such as medical terminology in Spanish,
specific instructions on how to address Latinos with
limited English ability, Latino disease data base, Latino
disease risk, and an assortment of cultural material for
Latin studies. The effectiveness of this web resource
should be measured by the number of visits registered in
the site data base list. Is expected that this site will
have more than 100 visits a day, and online courses be
completed by at least five HCP per month.
Assumptions
The majority of research papers gathered for this project
indicated the existence of health disparities created by language
and communication barriers between the Latino patient community
and the HCP community. Addressing the causes of these disparities
in order to increase patient satisfaction among Latino patients
is a major assumption of this project. The existence of these
communication barriers is expected provided the groups being
studied are from different cultures. Another assumption is that
educational programs will also help to enhance HCP efficiency in
general by becoming more skilled in understanding and treating
15
other cultures, other than their own. Studies have shown that HCP
must be aware and willing to participate in the integration of
the Latino community by becoming knowledgeable of their culture
and customs (Betancourt et al., 2005). Other assumptions of this
study are that HCP will first develop a general interest in Latin
culture after embracing this CC course. This initial interest
will than provide the desire to become genuinely culturally
competent by absorbing and observing the Latino patient
population up close in the clinical setting as HCP have more
tools such as better cultural vocabulary. We can also estimate
that Latino patients should benefit from a favorable environment
where they feel more comfortable. This project assumes that
patients who feel more comfortable with their HCP will disclose
more information crucial to correct assessment and diagnosis as
trust in their HCP has a special and distinct meaning among
Latinos.
Summary
Bridging the cultural gap between Latino patients and HCP is
very important for safety and patient satisfaction (Ku & Flores,
2005). This program seeks to utilize the latest research in CC
16
and bring it to an online course creating an appealing learning
experience to HCP. With the projected increase in the Latino
population in the U.S. and the steady Latinos migration to the
U.S., acculturation tools which can be updated with current
information will be needed more frequently making the online
distribution a plus. Health disparities could be minimized by the
implementation of cultural education including the proper
training of health care professionals (HCP) to better navigate
cultural diverse patient populations (Kripalani, Jones, Katz &
Genao, 2006).
The creation of a CC tool can also promote patient
satisfaction by improving the level of trust Latinos have for
their HCP as they perceive being understood and their cultural
identity more respected. Finally, some immigrants reach the
United States borders unprepared and unexpectedly due to problems
they cannot control and do not have the luxury of a proper
acculturation such as prior English education. CC is important
because it promotes a cushion aiding cultural refugees who are in
need of health care and don’t know how to navigate the health
care system proficiently.
17

18
Chapter 2
Literature Review
To source available literature regarding communication
barriers in health care with the Latino population in the United
States (U.S.), a search was conducted using the following
electronic data bases: Cumulative Index to Nursing and Allied
Health Literature (CINAHL), PubMed, Journal of Nursing Education,
Google Scholar, and SpringerLink for articles published between
2005 and 2010. Search terms used to find relevant material in
these databases were “Latinos, health care, cultural barriers,
patient satisfaction, and Cultural Competency.” An initial search
was conducted using top hierarchy engines such as Google Scholar
and Elton B Stephens Company (EBSCO) information services which
returned a wealth of results. Each database individually yielded
different results. From all searches, 126 items were chosen; from
this first selection 66 were eliminated leaving 60. Of these, 39
were qualitative studies with varying degrees of quantitative
data supporting the research question, and 21 were mostly
quantitative and tended to be centered on specific areas of
health care such as heart attack and stroke awareness among U.S.
19
Hispanics. The criteria for choosing the most relevant research
article were, “uniqueness, data relevancy, size of study, and
reliability of sources.” Two meta-analysis studies were chosen
for review. To support the theoretical framework of this study,
two studies using Madeleine Leininger’s educational theories were
selected. Finally, 10 items were chosen for this literature
review based on their degree of relevancy, and how closely it
mirrored this field study.
Other methods used to obtain literature were contacting
authors through e-mail. Dr Chevannes, an author from the United
Kingdom was contacted in regards to relevant articles similar to
his educational paper, Issues in Educating Health Professionals to Meet Diverse
Needs of Patients and Other Service Users from Ethnic Minority Groups (Chevannes,
2001).
Other relevant literature was obtained throughout contacts
made with professionals working with the Latino community in the
Bay Area. Contacts and interviews with nonprofit organizations,
as well as clinics and hospitals serving Latinos produced
additional relevant literature. The book, Nursing an Hispanic Patient
(Homestead Schools, Inc, 2004), became a vital resource for this
20
study because it is part of a full credited course offered by a
school located in Torrance, California. The objective of this
course is to teach nurses how to work with Latino patients. It
contains a wealth of information about Latino culture, health
care and items relevant to better understand Latino patients and
their cultural identity and useful for this field study.
The articles reviewed here are organized into three
different headings: the first heading Cultural Competency in Nursing
contain seven articles regarding cultural and linguistic
competency, among these, Current Approaches to Integrating Elements of
Cultural Competence in Nursing Education (Lipson & Desantis, 2007) is a
report review, The Evidence Base for Cultural and Linguistic Competency on
Health Care (Goode, Dunne, & Bronheim, 2006) is a longitudinal
meta-analysis. Remaining under this heading, Effects of Limited English
Proficiency and Physician Language on Health Care Comprehension (Wilson, Chen,
Grumbach, Wang, & Fernandez, 2005) and Listening to Patients: Culture and
Linguistic Barriers to Health Care Access (Barr & Wanat, 2005) are articles
relevant to cultural and linguistic barriers effects on Latino
minority population. Caring for the Underserved (Cox et al., 2006),
Community-Based Strategies to Improve the Health of Mexican American Men
21
(Sobralske, 2006), and Teaching Methods and an Outcome Tool for Measuring
Cultural Sensitivity in Undergraduate Nursing Students (Hughes, & Hood, 2007)
are relevant studies in teaching strategies for CC affecting
Latinos. The second heading, Racial and Ethnic Discrimination in Health Care
include, Perceived Discrimination and Self-Reported Quality of Care Among Latinos
in the United States (Perez, Sribney, Rodríguez, 2009), and Racial/Ethnic
Discrimination in Health Care: Impact on Perceived Quality of Care,( Sorkin,
Metzger & Alba, 2010). The third heading: Race and Ethnicity and
Satisfaction with Health Care includes: Race/Ethnicity, Socioeconomic Status, and
Satisfaction with Health Care (Haviland, Morales, Dial & Pincus, 2005),
and focus on patient satisfaction in the Latino community.
Cultural Competency in Nursing
Providing optimal health care to a growing numbers of
Hispanic Latinos offers a unique challenge for the health care
provider who has minimal foreign language skill and understanding
of Latino culture (Araiza, Ignacia & Kelley, 2005). The bulk of
reviewed articles for this field study focus on language
comprehension, cultural competence in health care, and cultural
teaching methodology designed to aid health care professionals
(HCP) in the care of Latino patients.
22
In the language comprehension study, Effects of Limited English
Proficiency and Physician Language on Health Care Comprehension Wilson, Chen,
Grumbach, Wang, and Fernandez (2005), hypothesized that patients
with limited English proficiency (LEP) might be affected by poor
health care treatments due to deficiencies in comprehension of
medical instructions. The goal was to investigate language
barriers with a linguistically diverse population-base sample and
evaluate the extent to which limited English proficiency impairs
medical comprehension. Another important goal of this study was
to evaluate levels of medical understanding by LEP patients when
treated by language concordant physicians versus language
discordant physicians. The variables investigated were a group of
LEP patients speaking 11 different languages, and English
proficient patients.
A state wide telephone survey of 1,200 Californians speaking
11 different languages was conducted. This survey contained four
items relative to medical comprehension. These included
understanding of medical situations, confusion about medication
use, trouble understanding labels, and bad reactions to
medications. Respondents were also asked if their physician spoke
23
their native language. A Likert-type scale method was used as
sampling and respondents were separated in two categories, one
group consisted of LEP persons and the other group was made of
English proficient individuals. Odds ratios and x2 analysis were
used to compare responses between LEP and English-proficient
respondents. Logistic regression models were used to isolate the
effect of language proficiency from that of age, sex, education,
insurance, income, years in the United States, ethnicity, and
having a regular source of care.
The researchers found that LEP respondents were
significantly more likely than their English proficient
counterparts to show problems understanding medical instructions.
Elderly, female, less educated, low income, uninsured and
resident in the United States for a short period of time
consisted of 49% of the 1,200 respondents. 57% of LEP, either
with language concordant or discordant physicians, reported
problems understanding medical instructions. Fewer English-
proficient respondents reported problems understanding medical
instructions and for these respondents, physician language had no
significant effect on comprehension.
24
This study included the large sample size including
respondents of 11 different languages, and the author’s choice of
U.S. Census type questions included in the questionnaire. This
study also uses statistical analysis and significance detailed by
many useful graphics displaying Pearson correlations
distinguishing groups and comparing all parameters. One
weaknesses of this study is to be confined to the state of
California limiting respondents sample and therefore may not
represent all LEP populations. Other limitations are that only
respondents who chose to answer questions in their own language
were selected, weakening results by excluding LEP population.
The relevancy of this study for this field study is based on
the findings regarding language comprehension and interpretation,
a core concern in the creation of CC programs such as the one in
this field study. This study is one of the first multilingual
studies which is population based and focus on the impact of
English proficiency and HCP comprehension. Data from the study is
useful for this field study because it validates the creation of
CC curricula aiding language concordance nursing staff; it also
25
substantiates and verifies the extent to which Latino patients
are affected by lacking culturally concordant health care.
The Evidence Base for Cultural and Linguistic Competency in Health Care
(2006), Goode, Dunne, and Bronheim conducted an 11 year
longitudinal review and analysis of evidence based studies which
impact cultural and linguistic competencies in health and mental
health, its outcomes and cost benefit for the overall healthcare
system. This study isolates and compares two variables. The first
concerns the increased satisfaction among patients and providers,
and well being of patients as a direct result of cultural and
linguistic competence; the second pertains to the cost and
benefits to the health care system.
To identify the evidence and gaps in research for cultural
and linguistic competence, two approaches were used. First a
structured research on Medline from January 1995 to March 2006
was conducted to identify primary research articles for review on
health outcomes and well-being. Second an investigative search of
several databases was performed to identify cost and benefit to
the system. Primary sources, selected reviews, technical reports,
and conceptual papers were chosen given their importance in
26
establishing a business case for cultural and linguistic
competence in relation to cost.
Articles reviewed in this study can be grouped into two
categories: the level of service delivery and organizational
policy level. Design methodology for reviewed articles was
presented in six bar graph charts and parameters were: (a) no
control, (b) no intervention control, (c) usual care control, (d)
usual care, (e) CC model, and (f) not CC model. The second part
of this analytic process looked for the evidence and a gap in
systems costs. To verify this, the authors created a table of
estimated costs for LEP services and compared the cost and
benefits.
This study major finding are a large volume of evidence
supporting linguistic competence as a critical component of
quality and effectiveness in relation to health outcomes for
minorities, and a majority of studies recognizing cultural and
linguistic competence as fundamental aspects of quality in health
care. This study accomplishes a substantial review and
classification of important studies in the subject and offers
significant analysis investigating the hypothesis that cultural
27
and linguistic competency are critical components of quality and
effective care in relation to health outcomes and well-being.
The study also hypothesizes that cultural and linguistic
competence results in decreased system costs is inconclusive and
makes further recommendations for a more robust research agenda
on cultural and linguistic competence in health care. The
findings of this study also conclude that cultural linguistics is
in its developmental stages.
The characteristics of this study lies in a large, extensive
and encompassing investigation that lasted 11 years contained in
a 46 page document. The first structured approached research
utilized a Medline search methodology yielding 365 studies that
addressed cultural and linguistic competence and health outcomes
but only 25 primary research studies met the criteria for final
review. The study also offers cost and benefits analysis
methodology of CC in health care.
The weaknesses of the study lie in the absence of a clear
final conclusion and the narrow scope of the current studies.
Studies do not consistently present conceptual framework, logic
model or definition for what constitutes CC. None of the
28
literature on system costs or business case described
methodological approach referencing patient, community, or key
stakeholder involvement. Other difficulties pointed out by the
authors are the complexity of methodology gathering data among
race and ethnicity which are viewed as being the same but cannot
be analyzed by the same principles.
This field study directly benefits from this extensive study
by helping it to develop a conceptual model of cultural and
linguistic competence for patients, their families, and
communities. This study enumerates a list of linguistic
competence policies which supports and mirrors this field study
purposes. The concept of a “cultural broker” emphasized here
promotes the education of HCP with the ability to tread two
cultures and facilitate understanding. Useful recommendations
includes: English proficiency issues, multilingual
telecommunication technologies, translations, cultural brokers,
teaching materials, and ethnic media languages other than
English.
In another qualitative study, Current Approaches to Integrating
Elements of Cultural Competence in Nursing Education the authors Lipson &
29
Desantis (2006), focus on existing CC programs by initially
describing, in brief, the two longest running CC programs in the
U.S. and then comparing landmark CC curricula. Five methods of CC
are described and analyzed in this study: specialty focus, required
courses, models, immersion experiences, and distance learning or simulation.
This study evaluates the efficacy of each method and compares
reports from institutions using those methods in their CC
courses. The study also focuses on factors that facilitate or
inhibit their intended results.
Lipson and Desantis (2006) demonstrate the type and models
of curricular format used in these institutions followed by a
detailed presentation of how they are implemented. The Purnell
Model for Cultural Competence, Giger and Davidhizar Transcultural
Assessment Model, and The Campinha-Bacote Process of Cultural
Competence are examined in detail by observation of results from
several types of data collection: from telephone calls and face
to face interview, e-mail correspondence and the participation of
active researchers in the field. The authors also provide a
comprehensive examination in their review and evaluate factors
which have positively or negatively affected these programs,
30
including community involvement, long distance learning and
simulation.
The authors found several outcome determinants related to
teaching cultural competence in schools of nursing. These factors
were evaluation, facilitators, and inhibitors. The study gathered evidence
provided from schools and teachers on the difficulty of
evaluation of efficacy of these cultural programs examined. The
facilitating and inhibiting factors were found to be associated
with the institutions and their support, as well as funding and
patient nurse relationships. These variables were then used to
correlate an institutions’ capacity to launch successful CC
curricula.
This qualitative study offers a complex and careful analysis
of each program producing clear distinctions among the different
courses. Parameters for evaluations of these programs included,
(a) increased student self awareness, cultural preconceptions,
beliefs, values and behavior affecting care, (b) enhanced ability
to deal with environmental and socio cultural factors affecting
the client (c) learning ability of students when negotiating
mutually satisfactory interventions with clients. Comparisons
31
were also made between immersion type courses where a student
participates in the community, with distance learning courses,
and where students learn from simulations. Even though this is
not an extensive study, its strength is being a unique and
somewhat rare study on existing CC methods and their results. Of
all articles in this literature review this was the only one
examining course evaluation and analysis on individual basis. The
courses are described and analysis of its methodology is made.
The utilization of graphics and a rich list of references, and an
extensive critique highlight the failures and successes of the
courses.
Lacking in this study are specific information about how
each program was conducted and implemented which could alter
final results and objectives; even though this is a qualitative
study, it could have been instrumental and useful to have
additional data in regards to how each program was implemented.
There is also a lack of definable target population. It is
difficult to determine the socio-demographics of nursing students
that participated in the cultural courses.
32
This article is of importance to this field study because it
helps to determine outcomes for each different choice of program
available, helping the creation and right implementation of CC
curricula which is the intention of this field study. The
methodology of each study brought forth in this study such:
“immersion experiences, distance learning, specialty focus,
models, and required focus”, demonstrate the options available in
some of these CC methods. The information contained in this study
is essential for the creation of new CC programs for HCP.
In the study Caring for the Underserved (Cox et al., 2006)
focusing on minorities and health care, a comparison is made
between two health care curricula formats designed specifically
to address the need of underserved communities. One format was
faculty-led; the other was web-based. The main purpose of this
study was the creation of curricula and its methods aimed at
improving the health of underserved communities such as Latino
immigrants, uninsured, socially isolated, substance addicted,
poorly educated and LEP. Evaluation of each curriculum, faculty-
led or web-based was performed by the comparison between changes
33
in attitude of students and their display of competence and
ability to translate content into behavior at the clinical
setting.
The settings for this study were six pediatric clerkship
rotations between 2003 and 2004 academic years, with the
participation of 100 third year medical students lead by a
coordinator into the existing six week pediatric clerkship study.
Students were assigned instructions either by the established
faculty-led or web-based methodology. Students were required to
complete the assigned course without having any other task of
caring for patients in order to isolate the curriculum providing
more accuracy. Results were than evaluated on basis of
understanding and displaying care for the underserved population
at hand.
A survey with a total possible score of 18 points was given
to all students participating in the three groups; the survey
consisted of eight 1 point multiple choice questions, one 5-point
question, and five 1 point questions about resources. Attitudinal
assessment and clinical skills were the main criteria of
evaluation. Attitudinal assessment, consisted of 26 items with
34
responses ranging from 1 (strongly disagree) to 4 (strongly agree) on a
4-point Likert scale. Several methods of evaluation were created
for this study: Curriculum Development, Core Curriculum Elements, “I CARE”
Screening Tool, and Independent Clinical Project (ICP).
The findings suggested that both faculty-led curricula and
web-based learning are equally effective in improving learning
relevant to care of underserved population. Differences in
attitude and knowledge between web-based and faculty-led groups
were not significant. Compared to the established curricula, both
web-based and faculty lead demonstrated improvement, (p < .001)
for knowledge and (p < .05) for caring for the underserved. The
authors found that the web-based format could be as good and
effective as traditional face to face instruction for promoting
the caring of the underserved. Several reasons led to that
conclusion: among them, the attractiveness of the web-based
system in general; less demand on the instructor without
compromising learning; two hours less instructional time on
average was required and less traveling needed to get to classes.
The strengths of this study are the presence of screening
development of a tool for analysis of two different curricula by
35
medical students; one group with knowledge of underserved patient
and the other without knowledge creating an impact mechanism for
evaluation producing more clear result evidence. The allotted
time of one year and a program spanning at six hospital site
locations also offers a larger sample leading to more expected
accuracy in the results. Other strengths are the use of graphics
and charts to display analysis of covariance (ANCOVA), standard
deviation, and Fishers exact test assessment the program offered
in its charts.
The limitations in this study can be attributed to a small
number of subjects and sample population along with being in a
pediatric clinic which limits the study to that specific group
population and a certain age group. There were problems with
instructions of the “I CARE” tool were some of the students were
unable to recognize undeserved families or felt uncomfortable
inquiring about underserved issues. This might have impacted the
results of the established curriculum group which had a deficit
with I CARE use. Also the long term gains in this study are not
demonstrated since the study focused on evaluating students
36
short-term learning outcomes it cannot predict how gains would
translate into subsequent clinical practices.
The importance of this study is that it explores the use of
Web based learning potentials, which is the main objective of
this field study for a future for CC teaching curricula.
Examination of Web-based mechanisms must be well researched
before resources are used in its creation. This study could also
be instrumental in the writing of a future proposal and support
for web-learning development of CC curricula.
C. Sobralske (2006) in the investigative study, Community-
Based Strategies to Improve the Health of Mexican American Men seeks to
understand how much, and by what means cultural barriers and
values prevent Mexican American men from seeking health care in
the United States. This study looks at culture, masculinity and
acculturation factors affecting health in Mexican males.
Sobralske also highlights community-based programs strategies
aimed at improving the likelihood Mexican men will seek health
care. The participant groups were: (a) well informed and
accessible, (b) willing to participate in the interviews, (c)
were stable residents, (d) identify themselves as similar to
37
other Mexican American men in their community. This group was
than divided into two. One was able to provide or point out
health care-seeking behaviors of the primary group, and the other
did not. Participant observation was the investigative method for
this study seeking to understand the behavior, values, and
customs of a group of people. The difference between the primary
group and the secondary was that the secondary group contributes
to insights about health care seeking behaviors of the first
group. The primary group was not responsible for this action.
This technique was created mainly to confirm data gathered from
the first group and create cross reference data for evaluation by
the researcher. A total of 36 men were chosen for the study, and
eight were chosen as the primary group. Their average age was
47.5 years old.
The variables investigated were (a) level of acculturation,
(b) level of education, (c) age, (d) religious affiliation, (e)
occupation, (f) birthplace of participants and their parents, (g)
amount of time in the United States if born in Mexico, (h)
general living environment, kind of foods eaten, and clothes
worn. Level of acculturation verification was based on existing
38
acculturation rating scales which are well established in
research with Mexican Americans such as the Park model (Lanza,
Armbrister, Flórez & Aguirre, 2006). Analysis progressed from
lower to higher levels of abstraction, from collection of raw
data to identifying usual patterns to formulating major cultural
themes.
The major relevant findings for this field study are clearly
identified. How Mexican American males view health care and how
the influence of Latino masculinity influences their decision
when seeking health care are well tested and analyzed in several
paragraphs and demonstrated with graphics. The authors found that
Latino men do not seek health care until chronic diseases have
progressed far enough to produce bothersome symptoms. Delayed
decisions regarding of health treatment can be life threatening
and can shorten a man’s life. The inability of the Latino patient
to speak English well has been identified as a significant
barrier to health care assessment. Latinos can greatly benefit
from having “health brokers” to help navigate the allopathic
health care system and to assure greater adherence to recommended
health treatments (Sobralske, 2006).
39
The methodology of this study lies in the in-depth nature
and detail of the investigation of subjects and their families.
Subjects were interviewed in their place of choice to avoid
exterior influencing. Another unique quality of this study was
the participant observation method where the men were observed in
their community. Researchers were immersed in the community and
participated in community activities with friends, family and co-
workers leading to understanding of masculine identity. From
observing these interactions researchers were able to identify
emerging patterns blocking men’s health care activities.
This study has a limited number of participants, a non
specified time frame, and the confining of subjects to a small
geographical area northwest of the U.S. The exclusion of other
areas in the U.S. could create inconsistent results due to small
samples. Other problems are the lack of allopathic health care
system as a point of entry; instead it uses the folk healer
approach or the lay person in the community. This may be more
effective as a starting point in the investigation but does not
measure well how Latinos react in the traditional allopathic
health care system.
40
This study is significant for this field study because the
understanding of how Latinos think and react to health care is
fundamental for the creation of educational programs for training
nurses in CC, the intent of this field study. The data gathered
in this study becomes vitally important for the understanding of
cultural sensitivities of Latino families, in particular Latino
men, when seeking health care and can be directly applied to
instruction relevant to Latino man.
In the study, Listening to Patients: Cultural and Linguistic Barriers to
Health Care Access, Barr & Wanat (2005) attempt to identify barriers
to health care access encountered by cultural and linguistic
characteristics of ethnic low-income minorities. The study then
proceeds to investigate why some health care organizations (HCO)
have a tendency to impede access and others to facilitate access.
The study focuses on African American, Latino, Native American,
and Pacific Islander patients; for the purposes of this field
study, the focus of this review will be on Latino patients.
Increasing health care access has more implications than simply
having money to pay for care. Access also requires no
discrimination based on race or ethnicity and that services be
41
provided in a manner that is culturally and linguistically
appropriate (Barr & Wanat, 2005). Based on this assumption, the
study investigate minority patient’s perceptions on general
issues of culture and linguistic access to care such as: (a)
physicians, (b) non-physician staff, (c) HCO’s physical
environments, (d) different types of services provided by
physicians, and (e) different types of services provided by non-
physician staff.
The patient population selected for this research was
composed of low-income African American, Latino, Native
American/American Indian, and Pacific Islander community members
of the San Francisco Bay Area. A focus group format was used to
elicit information that assessed study participants through
various stages of their health care encounters. Forty one adults
were recruited to participate in an ethnically homogeneous focus
group composed of the four target groups. Patients were than
invited to participate in the focus groups responding to ads
posted in several HCO’s. Each participant was offered a small
cash stipend for their participation. With the Spanish speaking
segment the focus group was conducted in Spanish. The questions
42
directed at study participants focus on the specifics of what
might be said and done by HCO physicians and staff at different
stages of the patient-HCO encounters. Each focus group session
was videotaped, with an additional audiotape which was played
back to allow additional information and corrections to be made.
The methodology of this study utilizes focus groups as an
investigative tool. The presence of standard qualitative data
analysis procedures and the mapping of respondents’ experiences
and perceptions relating to characteristics of patient to HCO
encounters impeding or increasing its occurrence are also an
important component of the study. Two project team members
independently coded and analyzed samples of interview transcripts
for more reliability.
Even though it is believed the insights and perspectives
contained in this study suggest certain policy directions making
health care more accessible to minorities. This study has no
control design which could compromise reliable evaluation. Other
problems were that focus groups were not large enough to form a
representative sample. Finally since the participants of this
study obtained their health care from a variety of community-
43
based sources, the study cannot determine the extent to which
characteristics of the individual HCO affects participants.
The findings of this study reflect discrimination as being a
pervasive theme in the Latino community with their encounters
with HCO staff. These findings include discrimination on non-
Latinos against Latinos, discrimination by Latino staff who “feel
superior” to Latino patient, and discrimination by other minority
staff against Latino patients that don’t “look minority” (Barr &
Wanat, 2005). Major language barriers to accessing health care
were reported, including unavailable Spanish speaking staff and
incompetent translators. Latino participants also expressed
intolerance towards patients with limited English proficiency.
There are several important aspects in this study that are
relevant to this field study. It substantiates the need for
closer collaboration between health care organizations and ethnic
minority patients. Minority patients are more concerned with
communication problems with non-physician staff rather than
physician-patient relationship; another finding that low-income,
minority patients express preferences for unhurried, humanistic
health-care. These findings are important data which can be
44
instrumental in the designing of a curriculum focusing on nursing
education; it also aid in targeting a population for training.
Hughes & Hood (2007), in their educational related study,
Teaching Methods and an Outcome Tool for Measuring Cultural Sensitivity in
Undergraduate Nursing Students, illustrates one school of
multicultural curriculum for baccalaureate nursing students and a
tool to gauge changes in behavior called: Cross-Cultural
Interaction Scores (CIS) scale. The design of this study is
centered on the administration of transcultural learning courses
to baccalaureate nursing students. Two types of courses were
given. In level 1 course, students learned to deliver basic
nursing care to clients with alterations in health. Cultural
awareness was emphasized as important in all aspects of care.
Students performed cultural assessments and identified several
nursing diagnoses that may easily be misidentified because of a
nurse’s lack of knowledge related to client cultural practices.
In level 2 courses, the greatest amount of transcultural nursing
content is presented to the students. Curriculum involved caring
for adults, children, families, and clients with mental health
needs. Prior to beginning the cultural content in the second
45
course, a CIS evaluation is applied as a pretest to measure
attitudes and behaviors students have at this point. The tool
consists of 20 items and assesses behavior and attitude using a
five-point Likert-type scale.
The investigation of variables was performed using the CIS
tool. Tests were given to five different groups who participated
in the transcultural curricula; students were given a pretest and
a posttest before and after the administration of the course.
Variables were divided into four major themes for competency
analysis and the tool was subjected to factor analysis using
Principal Components Analysis. The four factors account for 51.9%
of the variance of the scores for the concept of cross-cultural
interaction. Factor 1 theme centered on sharing across cultures
with appreciation for individual perceptions and was 24.4% of
variance. Factor 2 major theme focused on acting with cultural
awareness and sensitivity and had a 13.1% of variance. Factor 3
theme was collaborating with persons from different cultures with
fairness and openness and was 8.1% of variance. Finally, Factor 4
major theme was the embracing of cultural diversity without
losing personal culture and had 6.0% of variance.
46
This study finds that though nurses have been taught to be
holistic according to previous studies, culturally relevant
nursing practice is almost nonexistent in many nursing schools.
In order for students to develop cultural competence, specific
knowledge and behaviors must be acquired in order to change
previously held attitudes, values, feelings, and beliefs about
persons from cultural backgrounds different from their own.
This study test students in a clinical setting before and
after the course has been administered and the CIS tool indicates
how well they make culturally sensitive choices which might
indicate reliability by direct comparison. Comparisons were made
between these two groups which clearly demonstrated an
improvement in cultural sensitivity. Higher scores indicate an
increased tendency to make culturally sensitive choices,
Cronbach’s alphas for the CIS range from .73 to .84. Significant
Cronbach’s alpha increases in student CIS scores were detected
after students engaged in the learning activities. Quantitative
measurements were high, but student comments about clinical
experience provided the depth and embodiment of cultural
sensitivity.
47
This study has several limitations. Important variables are
not included in the report such as age group, duration of courses
and number of participants. Other problems are that no population
target is presented. Minority patients who were the subjects of
this study are not clearly specified, and no information is given
about the type of clinical setting in which evaluations took
place. Even though the study points out an increase in cultural
sensitivity after the course implementation, reliability would be
more well-defined by a larger sample size and sample population
description data.
The finding of this study is of great relevancy for the
creation of CC curriculum, which is the objective of this field
study. This study mirror the final proposal of this field study
in several ways and its models for curriculum evaluation are
useful for CC programs. The three interrelated principles used in
this study, knowledge, development and use, mirror the objectives
of this field study’s end product. The nursing programs evaluated
in this study engage the idea of holism and adopt Leininger’s
cultural theory which is also the objective of this field study.
Racial and Ethnic Discrimination in Health Care
48
The notion that disparities in health care are attributed to
racism or genetics still persists even though the problem is
known to be complex, involving socioeconomic status and cultural
and environmental factors (Shaya & Gbarayor, 2006). There is need
for more study to evaluate what are the specific causes and
reasons attributed to health care disparities within the Latino
population. Disparities may act in insidious ways permeating
health care and affecting quality of care. Therefore it is
essential to investigate the current status of discrimination
perception within the Latino population and health care for the
creation of programs aiming at improving patient satisfaction.
Despite the existence of several studies measuring the
effects of racial and ethnic discrimination, this subject remains
a relatively understudied area among the Latino population.
Perez, Sribney, and Rodriguez, (2009) in their study, Perceived
Discrimination and Self-Reported Quality of Care Among Latinos in the United States
examines the relationship of perceived discrimination and self-
reported quality of health care and health provider-patient
communication. In this study the authors examined the association
between perceived discrimination in two measures of quality of
49
care: patient reporting’s of quality of care and quality of
health care provider-patient communication.
Variables investigated in this study were the (a) Detroit
Area Study (DAS) consisting of a six-point item: sex, age,
foreign born, language of interview, education, and self reported
health status; and (b) a doctor or medical staff discrimination
measure from the Commonwealth Fund Health Quality Survey
consisting of three yes or no items: age, education, and
household income. This study examines the extent racial
differences in socio-economic status, social class and acute and
chronic indicators of perceived discrimination. Two outcomes were
researched. A five-point self-reported quality of health care
received in the past year, scored as 1 (excellent), 2 (very good), 3
(good), 4 ( fair), and 5 (poor). The second outcome measure was a
scale with five-point item from the Interpersonal Processes of
Care Survey short form, reflecting the quality of communication
between health care professionals and the study participants.
Participants were part of a stratified, random digit dialing
telephone survey (The Pew Hispanic Center/Robert Wood Johnson
Foundation Latino Health Survey) of (N=3,899) adult Latinos aged
50
≥ 18 years which made the methodology of the study strong.
Initial telephone interviews (Wave 1) were conducted in summer
2007 and had a response rate of 39.5%. Participants were again
called in the spring of 2008 for a second interview (Wave 2),
focusing on medical care received and chronic disorders. Subjects
for this study are the (N=1,067) persons who completed the (Wave
2) interview. These methods produced a statistically
representative sample in the contiguous United States.
Major findings indicated only 19% of all persons reported
any discrimination from doctors or medical staff. Discrimination
was significantly associated with age (P=.02). Younger population
(18-29 years) were 22% more likely to report discrimination than
persons of ≥ 65 years. Persons of poor health reported 39% more
health care staff discrimination. On the discrimination scales,
younger persons reported more discrimination and U.S. born
Latinos reported more discrimination than foreign-born (0.32 SD
versus -0.23 SD).
The limitations of this study lies in the fact that a cross-
sectional study cannot make a good argument on the specific
causes of the problem. The DAS mean scale is relatively low,
51
discriminatory experiences are occurring only a few times a year.
The follow up of (Wave 2) was also limited due to financial
constraints; there was a short time window to complete the call
back. Issues pertaining discrimination were not well defined
whether they were medical or non-medical. When paired together
they were not so collinear and didn’t appear to create models as
presented in the study.
This paper is important to this field study because it
perceives discrimination and its association with quality of care
measures among U.S. - born Latinos. Discrimination knowledge is
an important variable and indispensible knowledge in the creation
of a teaching program intended to address cultural deficiencies
among health care professionals. It is important to know specific
details on how a minority population feels discriminated against
so the same discriminatory factors can be avoided in the
conception of CC programs.
In this study, Racial/Ethnic Discrimination in Health Care: Impact on
Perceived Quality of Care Sorkin, Metzger, and Alba, (2009) evaluate
whether the perception of poor health care is involved with
discrimination perceptions by minorities, and its associations
52
with socio-demographics, access to care, and patient satisfaction
across racial and ethnic groups. The methods for this study
included a survey of the California Health Interview Survey
(CHIS), which is a telephone survey of the state of California
civilian non-institutionalized population and interviews randomly
selected adults in more than 40,000 households. The CHIS include
California’s major racial and ethnic groups.
Five languages were used in this survey: English, Spanish,
Chinese, Vietnamese, and Korean. Adjustments for non-response
households without telephones were made and the sample of the
analyses was restricted to adults, 18 years or older who rated
the quality of their health care in the last 12 months
(N=36,831). An 11-point Likert scale (0 = worst health care
possible, 10 = best health care possible) was used and the
primary independent variables were race, ethnicity and feeling
discriminated against in health care because of race and/or
ethnicity. Other variables used were health status, insurance
status, education level, English proficiency, chronic health
conditions and country of birth.
53
To determine how respondents felt about how discrimination
affected their health care, an extensive analysis was performed
with the Statistical Software for Analysis of Complex Survey
(SUDAAN). This is a statistical software package that specializes
in providing efficient and accurate analysis of data from complex
studies. The analysis design had four distinct phases: (a)
generation of descriptive statistics, (b) multivariable logistic
regression models to determine impact of race, (c) models were
than built in a sequential manner: race/ethnicity, discrimination
and other social variables, and (d) stratified analysis to test
four separate regression models to determine the relationship
between experience of discrimination in health care and ratings
of quality of care for each group adjusting for socio-demographic
variables and indicators of access and satisfaction.
The large sample population consisting of more than 40,000
households in the state of California which are a significant
number if compared with other similar studies and are strength in
the study. The response rate was 60%. The CHIS data was also
weighted to account for the complex sample design and to adjust
54
for non-response households. The study also uses a wide range of
discriminating variables that were used in the assessment.
The authors of this study found that respondents from all
ethnic minority backgrounds were more likely to report
discrimination and have an unfavorable view of their health care
system. Health care in the United States is not evenly
distributed and it negatively affects racial and ethnic
minorities. Ethnic minorities are more likely to have a lower
quality of health care but the mediators of such reports are not
known. The study also finds that among Latinos one of the most
important variables of perceived satisfaction has a close
relationship with perceived quality suggesting that Latinos are
more satisfied with their health care when a linguistic and
culturally sensitive environment is provided.
The limitation in this cross sectional study design is that
it precludes causal inferences between racial and ethnic
discrimination in health care. Reports can be skewed as the group
that is sensitive to discrimination is more likely to report
problems with their health care. Due to this model, authors
55
cannot determine if the reported quality differences were due to
actual care received or patient’s expectations.
This article is important for this field study because it
highlights the significance of racial discrimination and its
possible detrimental effects in communication affecting health
care among minorities such as Latino populations. In order to
create curricula for cultural competence, there must be a good
understanding of how Latinos view health care. This study
emphasizes special communication needs that can generate more
patient satisfaction among the Latino population.
Race and Ethnicity and Satisfaction with Health Care
In the study, Race / Ethnicity, Socioeconomic Status, and Satisfaction with
Health Care, the authors Aviland, Morales, Dial, and Pincus (2005)
evaluated the effects of race, ethnicity and socioeconomic status
on consumer health satisfaction levels. This study also seeks to
understand the findings which are consistent with continuing
health care disparities among ethnic and minority populations and
make recommendations for ways to improve the quality of care
among minority groups. The authors compare four global and three
56
composite ratings and their level of satisfaction among ethnic
minorities versus white and non-ethnic populations.
The study used dependant and independent variables using
questions regarding satisfaction with health plan and
satisfaction with medical care. The independent variables were
race, ethnicity and poverty status. There were also Case-Mix
(adjustment) variables. These included age, gender, perceived
health status, presence of medical problems in the family, health
plan type, Medicaid coverage, living in a rural area, and
education. The first two global questions focused on satisfaction
with health plan and satisfaction with medical care, a seven-
point Likert scale was used (1 = completely dissatisfied, 7 = completely
satisfied). The second set of two questions concerned whether one
would recommend their health care plan to family and friends and
intentions about switching to another plan, rated on four-point
scale (1 = definitely not, 4 = definitely yes). Data from surveyed
respondents with the analytic sample were compared with case-mix
variables. Multi-item composite measures were analyzed using a
Cronbach’s α. Linear regression was used to assess differences in
global and composite ratings by race ethnicity and poverty,
57
controlling for age, gender, perceived health status, family
medical problems, health plan type, Medicaid coverage, living in
a rural area, and education.
The study utilizes a large sample of surveying participants,
250,000 U.S. households mailed across 48 contiguous states,
obtaining a total of 152, 208 respondents. Also the utilization
of complex and sophisticated analytical designs such as,
multiple-Item composite questions, case-mix (adjustment)
variables, and regression gives this study strength by covering a
wide range of diversity and cultural variations and responses
from wide range ethnic groups in different areas of the country.
A significant number of charts with respondent’s analytical
samples are compared and cross measured and available in the
study.
One limitation of this study includes a survey that was
administered in English only. Since satisfaction ratings are
generally lower in non-English speaking groups, the exclusion of
non-English speaking individuals may have shown unreliable
results indicating a higher patient satisfaction. One factor to
take into consideration is that it only covers subjective
58
experiences with coverage and care and it does not evaluate
technical quality of care.
The major findings indicate a lower satisfaction rate among
non-English speakers or limited English speaking ability. This
study recommends the engagement of strategies for CC among health
care providers to increase minorities’ satisfaction with health
care. The recommendations made by this study are addresses the
main focus of this field study and are of significance for the
designing and implementation of CC curricula by understanding the
current level of satisfaction.
This study is significant to this field study because it
addresses minority satisfaction with health care and examines its
causes. This finding supports this field study hypothesis that
Latino patients with low English ability have lower satisfaction
with health care. The main findings of the study further support
this field study objective by making recommendations and
demonstrating how critical is the understanding of minority
patient satisfaction in the creation of cultural programs aiming
at improving patient satisfaction.
Theoretical Framework
59
In the field study: Culture Care: Diversity and Universality, theories
were derived from the disciplines of anthropology and nursing by
Madeleine Leininger (2002) and it was first written in 1960.
Leininger’s theory is based on the belief that a patient
population of a diverse cultural background can guide health care
professionals to provide care that is relevant to their cultural
beliefs. This theory is directed towards nurses’ ability to
develop their own core personal views of other cultures (Hughes &
Hood, 2007). This theory assumes that cultural specific care can
only be meaningful when nurses develop an inner understanding of
culturally diverse patients and their needs; it also assumes that
beyond inner core learning, knowledge of cultural care should be
learned from outside sources as well. The central thesis of this
theory is that care is the most powerful construct and the
central phenomena of nursing. If the meaning of culture care can
be fully understood, then the health care and well being of
individuals can be better addressed by culturally sensitive
nursing care.
Leininger maintains that cultural care can be learned
inductively or deductively. Nurses should obtain grounded
60
knowledge from Emic (insider) and Etic (outsider) sources. An
Emic source establishes that knowledge should be obtained from
the people or the culture because it makes information more
accurate. Etic refers to knowledge that comes from the outside
such as formal instruction, books and studies. Leininger’s theory
can be viewed as one of the most holistic because it uses diverse
learning methods and a wide spectrum of cultural understanding by
using two approaches to learning. Leininger focuses on the
concept of care based on the principle that people and their
perception of care are the most important element.
Leininger maintains there are four distinct reasons
culturally based care should be studied. Care appears to be
critically to human growth, development, and survival of the
human species to provide cultural congruent care according the
patients cultural needs. Care knowledge can be used to promote
healing and well being in clients to face death or to ensure the
survival of cultures through time to understand systematically
the broad and holistic cultural perspective to discover
expression and meaning of care, health, illness, and well being
as nursing knowledge. Hughes, and Hood (2007) in the study:
61
Teaching Methods and an Outcome Tool for Measuring Cultural Sensitivity in
Undergraduate Nursing Students, applied Leininger’s cultural theories
in the creation of curricula aimed at improving cultural
competencies among baccalaureate nursing students. Their study
has emphasized that when culturally competent care is understood
and practiced, nursing education, research, consultation,
teaching, and clinical practice is improved. The idea of their
study is also founded on Leininger’s statistics, indicating that
fewer than 15% of nursing graduates have taken transcultural
courses and fewer have received instruction on how to work on a
transcultural clinical setting (Hughes & Hoods, 2007). The
authors had a goal to decrease stereotypes and demonstrate the
importance of having a culturally sensitive background in
professional practice. The authors used Leininger’s theory to
develop a multicultural curriculum so students could function
effectively within American culture and also minority ethnic
cultures.
This field study mirrors Hughes and Hood’s (2007) study in
several aspects. Leininger’s cultural theories will be used with
the intent of helping students formulate a valid comparative
62

generalization based on cultural theories that have been
previously tested with success. Before courses can be planned or
designed it is necessary to ensure a conceptual framework with
the commitment to cultural care. Leininger’s cultural theory has
been accepted as one of the most adopted frameworks for nursing
cultural projects for over 20 years (Hughes & Hood, 2007). The
Culture Care theory model is also significant to this field study
because it defines fundamental principles for CC education. Its
assumptions serve as blueprints for the creation of an
educational tool. Its major assumptions are building blocks for
educational modalities of learning. Tomey and Alligood (2001)
found these assumptions to be: care is considered the central
essence of nursing; cultural care is the broadest holistic means
to know, explain, interpret, and predict nursing care phenomena
and to guide nursing care practice. Cultural care values, beliefs
are influenced by world view, language, religion, economic, and
environmental factors. Nurses must learn by using their inner
knowledge as well as research study material
Bacote and Bacote (2009) found that only when individuals
recognize their own assumptions of others who are different from
63
them and become conscious of their own personal bias and
prejudices, are then able to obtain cultural awareness. Bacote
and Bacote (2009), point out that it is not our skills in
observing details of cultural traits that makes us culturally
competent, but rather our self-awareness and respectful attitude
toward another culture’s point of view. Leininger’s theory
maintains social structure, worldviews, and cultural beliefs from
health, wellness, and illness that are closely linked and cannot
be viewed in a fragmentary way.
Shaya and Gbarayor (2006) suggest that in order to meet the
demands of a rapidly growing multi-ethnic population, training
for cultural competence courses must be created with curricula
focusing on evidence-based health disparities among racial and
ethnic minorities. Students should be culturally aware and
culturally sensitive. Another study by Chevannes (2002)
demonstrates the need to integrate cultural competence into the
foundations of educational competencies for health care
professionals. Subjects who participated aimed at assessing what
health professionals knew about care for multiethnic patient
groups. Another area of assessment was to measure student’s
64
perception of training needs in their area of work. It was found
also that 65% of participants confirmed that no attention was
given to their initial education of health care needs of
minorities; instead participants initiated self learning to
improve knowledge and understanding. Chevannes study validates
the need for implementation of methodology such as Leininger’s
theory as a guideline for communication improvements for minority
groups.
Chapter 3
Implementation
Introduction
Cultural competence in health care is important for
successful treatment outcomes as diagnosis, assessment and
discharge instructions are significantly associated with
65
communication exchanges between patients and health care
providers (HCP) (Cohen, Rivara, Marcuse, McPhillips & Davis,
2005). Language barriers, lack of health insurance, stereotyping
and prejudice are some of the variables contributing to health
disparities in the Latino patient population (Shaya & Gbarayor,
2006). Comprehension deficits between Latino patients and HCP are
also associated with low English proficiency, cultural
interpretation of medical-related events, and to some degree a
lack of cultural sensitivity by untrained HCP. Therefore,
facilitating cultural competency (CC) among HCP is important
because it increases patient satisfaction and diminishes
recidivism and medication errors (Cohen et al., 2005). The
establishment of cultural competency curricula and the provision
of instruments to increase cultural competency among HCP can also
help decrease the cultural gap between Latinos and HCP, and thus
contribute to an overall increase in positive health care
outcomes. Cultural competence in health can be described as the
ability of systems and health care professionals to provide high
quality care to patients with diverse values, beliefs and
behaviors, including the implementation of differential delivery
66
of care to meet patients’ social, cultural and linguistic needs
(Betancourt, Green & Carrillo, 2002).
Cultural competency tools can be better implemented and
accepted if some assumptions about today’s medical environment
are clarified. First, consider the assumption that CC education
does not justify its costs, and therefore should not be a
priority. A wealth of research shows how language barriers
obstruct access to health care, compromising quality of care,
increasing the risk of adverse health outcomes among LEP
patients, costing taxpayers billions of dollars in
hospitalization and litigation fees due to medical errors and
misdiagnosis (Ku & Flores, 2005; Cohen, et al. & Nailon, 2005).
Misdiagnosis and medical errors may be caused by lack of
effective communication between patients and HCP from different
cultures as many studies have shown. Medication errors are among
the most common hospital errors, accounting for 3% to 28% of all
hospitalizations due to inappropriate drug administration (Ronda
& Eduardo, 2005).The extra medical cost of treating drug-related
injuries occurring in hospitals alone is between $1.56 billion
and $5.6 billion dollars (Ronda & Eduardo, 2005). CC can be one
67
of many step measures helping address this problem at a low cost.
Education prevention would cost far less than hospitalization and
liability costs related to injuries caused by medical errors (Ku
& Flores, 2005). The Office of Management and Budget Costs (OMB)
reported that it would cost the nation $268 million dollars a
year to provide interpretation services in hospitals, outpatient
physicians, emergency, and dental visits (Ku & Flores, 2005).
Web-based learning (WBL) methodology, the objective of this field
study, would cost less than the translation services
implementation as budgeted by the OMB (Sitzmann, Kraiger, Stewart
& Wisher, 2006).
This field study proposes the implementation of CC
curricula, utilizing the creation of an electronic resource tool
for the improvement of care among the Latino population in the
clinical setting. Curricula for this program will utilize a web-
based format and will function as an electronic resource binder
and a CC on-line course available to nurses from any Internet
abled device.
68
Evidence
As evidenced by one study, a cultural deficit exists between
the nurses lacking proper CC education and Latino patients
(Nerenz, 2005). Due to cultural upbringing, Latinos have
developed a unique health literacy and perception relative to
medicine and medication treatments which differs from mainstream
American values. According to a study by Campos (2007), these
cultural traits are not always visible as Latino patients have a
tendency not to confront HCP on how they feel because their
cultural values require that they show “respecto” (respect) to
HCP. The implementation of this field study WBL project seeks to
address this and other similar discrepancies by making HCP more
aware of cultural differences. With increased awareness, HCP will
be able to better interact with Latino patients by being more
careful, omitting certain assumptions, and emphasizing and
inquiring about important issues.
Health insurers such as BlueCross BlueShield of Florida
(BCBSF) and Kaiser Permanente (KP) have implemented successful CC
programs (Tervalon, 2009; BlueCross BlueShield of Florida, 2007).
BCBSF’s “Cultural Competence and Diversity Imperative” program,
69
designed to aid workers, reflects the changing composition of
Florida’s state population, now numbering 20% Latino and African-
American. The BCBSF (2007) program works with all staff levels to
develop a five-year strategy plan identifying actions and
initiatives to move BCBSF from recognizing cultural issues to
fully understanding them. Kaiser Permanente is a leader in CC
initiatives, and has created a wide range of measures to fully
address specific ethnic populations, from educational guidelines
in cultural competence to in-depth programs such as “Centers of
Excellence in Cultural Competence” (Betancourt et al., 2005).
The Federal Government is also stepping up the CC
implementation in various ways. The Health Resources and Services
Administration (HRSA), along with the Institute for Health Care
Improvement (IHI) which are branches of the federal government,
have developed the “Health Disparity Collaboratives” (HDC), which
address racial and ethnic disparities in community health centers
(Landon et al., 2010). Intervention centers which have adopted
HDC have consistently improved services and outcomes for patients
with asthma and diabetes. Intervention centers have had
significant results in measures of prevention and screening,
70
including a 21% increase in foot examinations for patients with
diabetes, 14% increase in the use of anti-inflammatory
medication, and a 16% increased in the assessment of blood sugar
levels (Landon et al., 2010).
The delivery method chosen for this educational project is
based on evidence supporting the use of new technologies such as
video and computer learning designs and WBL (Balslev, Grave,
Muijtjens, & Scherpbier, 2005; Cherrett, Wills, Price, Maynard, &
Dror, 2009; Sánchez, 2010). Eight out of ten case studies on
average indicate positive gains when students use WBL over
traditional learning. They also indicated that is WBL is not by
nature superior to traditional learning processes, but depend on
its implementation methods and tools that are appropriate for the
teaching objectives. Problems with WBL appear to be associated
with the use of technology without a well defined purpose (Cook,
2007). Disadvantages of WBL also include social isolation, poor
instructional design, and lack of personal interaction. Other
studies have shown that one of the largest sources of
dissatisfaction with WBL is the lack interaction with the
instructor and other participants (Curran et al., 2005). An in-
71
depth analysis of WBL tools and processes are beyond the scope of
this project; instead we will discuss the tools selected for this
project and briefly discuss their benefits and rationale.
The WBL format was chosen for this project for several
reasons. In a survey of organizations conducted by the American
Society of Training and Development, the percentage of companies
using WBL technology to deliver training increased from 8% in
1999 to 27% in 2004 (Chou & Liu, 2005). WBL is becoming a
favorite training option in the industry, including corporations,
government and higher education. There are several reasons for
this increase; its unlimited distribution points, lower costs,
and is easily delivered via computer using the Internet. Another
WBL advantage is that websites can be easily updated with rich
media content such as text, audio and video, allowing student
interaction and data storage and management (Sitzmann et al.,
2006).
This WBL project will use a construct design which is based
on the Person-Centered Learning (PCL) method developed by the American
psychologist Carl Rogers (Derntl & Motschnig-Pitrik, 2005). The
PCL hypothesis is that if students are given the freedom to
72
explore areas based on their personal interests and encouraged to
seek solutions based on their personal values, they will reach
higher academic results and be more self confident. PCL is also
known as PCeL or Person Centered Electronic Learning or “e-learning”
(Derntl & Motschnig-Pitrik, 2005). Implementation of models such
as PCeL in a computer educational environment can take advantage
of several media tools available today. The tools at the core of
this proposed learning program are patient case simulation (PCS)
and educational and interactive video.
Some studies have demonstrated the efficacy of video in
training and education (Balslev et al., 2005; Cherrett et al.,
2009; Sánchez et al., 2010). In one study evaluating the
learning performance of Black and Hispanic male patients on
increasing syphilis education prevention, 206 males were studied
and the intervention group scored 24 percent higher than control
groups (p<.001) (Sánchez et al., 2010). Results of comparisons
made between the effects of video learning and paper based
learning resulted in higher data exploration, theory building and
theory evaluation suggesting that the cognitive process were
stimulated by video screenings. Findings are congruent with other
73
studies pointing to an increased capacity of memory storage due
to visual and auditory information (Balslev, 2005). Video can
also be a powerful and rich medium in e-learning. Information can
be presented in an attractive and consistent manner achieving
better learning results (Zhang, Zhou, Briggs & Nunamaker, 2005).
To potentiate the effectiveness of video learning,
interactivity will be added in order to promote engagement and
involvement from students. In one study, 75% of subjects
‘strongly agreed’ that interactive video had enhanced their
learning experiences (Cherrett, 2009).
Program Objectives
The goals of this field study are overarching. The immediate
goals however are objectives concerning improved efficiency and
safety in caring for Latinos in the clinical setting by providing
critical cultural information. After taken the web based learning
program, HCP should demonstrate an increase in awareness in the
following areas:
Improved communication with Latino patients. HCP should demonstrate
an increase in their ability to interview a Latino patient
74
effectively; understanding of Latino cultural background; an
increase in the ability to give health instructions to
Latino patients. HCP should also demonstrate a good
understanding of the patient’s conceptualizations and
preferences. HCP should be able to identify at least 80% of
interview and communication strategies techniques provided
in the CC course.
Ability to successful make recommendations. HCP should demonstrate
improvements in their rate of success for recommendations of
treatments. HCP should be able to gain patients involvement
in regards to their treatment. HCP should demonstrate
understanding on how to implement cultural relevant
approaches leading to successful health treatments and
outcomes.
Ability to negotiate with Latino patients. HCP should demonstrate
increasing understanding of patient’s perceptions and to
negotiate the provider’s perspective to the patients’
perspective so that treatment plans can be successfully
implemented. HCP should be able to create partnerships with
patients by using all skills learned in the CC course.
75
The overarching goals of this project are harder to be
evaluated. They concern long term gains to be achieved with the
implementation of this CC project over an extended period of
time. HCP who engage in this type of CC curricula should improve
in the following areas:
Cultural awareness. HCP should demonstrate an increase in
deliberate cognitive process in which sensitivity, values,
beliefs and life ways become incorporated in practice as HCP
successful strategizes treatment for clients from other
cultures.
Improvements in cultural skills. This is defined as the ability to
collect relevant cultural data regarding the client’s health
histories and presenting problems as well as accurately
performing cultural and physical assessments.
Cultural desire. HCP should begin to develop self motivation to
become culturally competent and a desire to engage in the
process of CC. A genuine self motivated desire to become
76
culturally competent is beneficial because it leads to
further knowledge and sustainability.
Population, Setting, and Stakeholders
The target population includes HCP working in hospitals in
Northern California where there is a large Latino population.
According to the U.S. Census Bureau, Latinos in California
account for 37% of the population (U.S. Census Bureau, 2008). HCP
most likely to benefit from this CC program are nurses and
doctors who have limited or no experience with Latino populations
or have moved from areas of the country where Latino patient
population is small.
The Board of Registered Nurses (BRN) in a 2008 survey
indicated that white non-Hispanic nurses in the Bay Area comprise
63% of the work force, yet fewer than 7% speak Spanish. The
assumption is that the lack of Spanish comprehension signifies a
lack of Latino culture familiarity and understanding, making this
sample group an ideal target for this CC literacy project, even
though it is possible that some nurses might be Latino cultural
savvy without knowing how to speak Spanish.
77
Several stakeholders with links and involvement in this
project and its target population are identified. Three
institutions have been reviewed and were found to hold similar
and close values associated with this CC project, as well as
Latino community improvement issues; both are potential financial
contributors and supporters. The California Healthcare
Foundation, with its program Innovations for the underserved, is a
philanthropic public foundation with educational, leadership, and
health programs involving the Hispanic community of Northern
California. The Health Trust, a charitable foundation supporting
healthy living, healthy aging, and healthy Latino community in
Silicon Valley offers grants ranging from $15,000 to $75,000.
This organization has supported similar educational projects
aimed at the improvement of health conditions of Latinos. Health
Trust’s mission supports health projects to facilitate health
care services for the underserved by promoting education and
cultural understanding among HCP and the community it serves.
Another potential source of funding is The Baxter International
Foundation which in 2008 has made contributions totaling more
than $4 million, including $2.82 million earmarked for the
78
improvement of quality and accessibility of healthcare among the
disadvantaged and undeserved communities, as well as training HCP
to address health needs and several other projects involving
cultural deficiencies of the underserved.
Kaiser Permanente (KP) is another important partner.
According to the Permanente Journal, KP has been a leader in
culturally competent care to a diverse patient population for the
past 29 years (Tervalon, 2009). Under the direction of its
National Diversity Council, the organization is a leader in
advancing culturally competent care. Among several others, KP has
established “Centers of Excellence,” a project which supports
innovative clinical models responding to the needs of minority
populations by providing language-specific primary care in
Spanish and Chinese as well as interpreter services. KP was also
ranked No. one among the 10 companies for Latinos in 2009 by
Diversity inc., as determined by a statistical analysis of
responses to a 200 question survey (Frankel, 2010). This CC
project will be piloted by Kaiser Health Center and its personnel
in collaboration with staff exclusively associated with the
project.
79
Other possible stakeholders are existing schools of
continuing education for nurses such as The American Nurses
Credentialing Center (ANCC), a subsidiary of the American Nurses
Association (ANA). The ANCC provides continuing education courses
promoting safe, positive work environments through the Magnet
Recognition Program and the Pathway to Excellence programs; they also
accredit providers of continuing nursing education. This CC
course can be considered for approval in their process of
Accreditation of Continuing Nursing Education Providers, a voluntary process
wherein ANCC reviews and accredits providers of continuing
nursing education credits. The criteria for approval includes
planning, needs assessment, purpose and objectives,
implementation, activity evaluation, and outcomes evaluation.
Implementation of Plan
One strategy for successful implementation and positive
outcomes of this project is to increase nurses’ interest by
promoting a “genuine desire” to be culturally competent (Bacote &
Bacote, 2009). Genuine desire can be defined as motivation
inherited in the HCP to want to engage in the process of cultural
competency. Madelaine Leininger’s theory of culture care diversity and
80
universality was chosen with this task in mind. Leininger’s theory
incorporates broad humanist dimensions about people in their
cultural life context, focuses on identifying values, beliefs,
life-ways, and symbolic referents related to culture care
phenomena (appendix D). Leininger’s theory promotes one’s own
discovery of cultural concepts and the use of cultural congruent
care that is appropriate to families and individuals (Leininger,
2002).
The creation of this project will involve different phases
and processes: (a) content research to fulfill the objectives of
a full web-based CC course focusing on Latino culture relating to
health care. The bulk of the research will rely on the wealth of
research available which has been delineated in Chapter Two.
Additional information is being gathered through professional
clinics and organizations which serve Latino populations in the
Bay Area; (b) the design of a web-based course using researched
cultural content. This will require the hiring of professionals
with specific expertise to ensure course quality and academic and
didactic consistency and flow; (c) the assembling of this
material into a web-based medium will require the hiring of a
81
professional webmaster to implement the latest technologies for
quality experience; (e) additional help will be needed to enhance
the web experience adding audio and video. San Francisco State
University Broadcast department students will be contacted to
produce these items; and (f) the final web-based learning course
will be implemented using two different approaches.
The method of distribution for this CC course will function
in two areas but target the same population group. The first area
of distribution will be the inclusion of the course into an
annual competencies program or in-house education requirement in
hospitals. The hospital is the setting where distribution and
advertising takes place. Hospitals may also want to incorporate
this CC course in their new graduate programs. Flyers will be
created containing information on course content and collaborator
scheduling instructions (appendix G). The course will be hosted
on a private server and available through the Internet. Staff
Clinical Nurse Specialists (CNS) will be invited to take part
promoting the course in their regular educational updates and
lectures, and visiting staff from other member hospitals will be
encouraged to examine and comment on the program.
82
The second distribution method is broad-based and intends to
make the course available to a larger population of nurses. The
main target population will be any nurse with Internet access
seeking to engage in a CC program for accreditation of continuing
education credits or simple cultural skills improvement. It will
require State of California Accreditation of Continuing Nursing Education
Providers approval for its addition into the web-based program for
continuing education and license renewal credit hours.
The web-based learning method for this project will utilize
video, text, narration, graphics, resources, interactive
presentations and lessons (appendix C 1-3). The web-site will
provide two main services: the first is to serve as a real time
resource binder for HCP working with Latinos. These resources are
designed to be assessed as needed by HCP at work. The main
features will include a medical Spanish dictionary and a resource
page entitled “e-manual for the Hispanic patient care”. Some of
the help resources will be available for download to hand held
devices. The e-manual will provide an alphabetical listing of
health care scenarios and conditions with relevancy to Latinos
83
and their care. Strategies for quick referencing will be also
available in this page.
The second main function will provide six interactive
modules with videos and interactive media (appendix C 3). The
video modules will be: Pre-Test, Hispanic Culture, Know your Latino patient,
Latino health beliefs and practices, Patient Cases and Post Test (appendix F). The
first three modules following the pre-test are videos intended to
develop some cultural understanding of Hispanic culture; typical
expected behaviors from Latino patients and what health
conditions Latinos are at risk. The module called Patient Cases
contains interactive media where students will be given a virtual
patient to interact with. Patient cases will be converted to e-
learning experiences. The virtual patients in this module will
emulate common scenarios and difficult communication situations
encounter by nurses (appendix C-3). A picture of the patient will
appear along with text explaining the patients’ condition. A set
of questions and answers will be given as choices for students to
use. Depending on questions and answers students select, a
progress display levels at the bottom of the page will indicate
84
positive or negative outcome (appendix C-3). At any time students
will be able to assess rationales concerning the effectiveness of
their choices. Students will be able to create an account and
take the modules at their own pace. The site will also have the
ability to test and keep student scores. Students will need to
score ≥70% in order to pass to following module.
Resource allocation and costs
Most major expenses will be allocated for website
construction and hosting, the hiring of professionals for content
research and web-based course development, and associated costs
for developing and producing ancillary materials consisting of
brochures or booklets that will serve as companion pieces for the
web-based learning modules. Donation of materials and volunteer
work have been considered (appendix A).
Grant-awarding foundations have been chosen as primary
sources of funding for this project and institutions which match
this project’s criteria were searched. These institutions are:
85
(1) The Health Trust of Silicon Valley, (2) The Baxter
International Foundation, (3) and The California Healthcare
Foundation. Details about these foundations can be found under
the stakeholders heading.
The project’s implementation costs are divided into three
areas: technology, research content and course assembling.
Technology costs are associated with the technical construction
of a website; these costs include (a) hiring a webmaster for site
architecture and development; (b) hosting server costs; and (c)
maintenance and technical support. Web construction costs are
estimated to be between $6,000 and $7,000 until site is fully
functional. Research and content creation involves hiring
professional researchers and consultants experienced in Latino
cultural issues. Another professional will be hired to further
develop the content into a web-based learning format producing a
high quality experience in web-based learning. Research costs are
estimated to be between $2,500 to $3,000 dollars. Finally the
implementation of the program, in concert with the participating
institutions, will require the hiring of promotional experts and
86
professional organizer and event planners with estimated costs
between $1,000 to $2,000 dollars.
The non-profit customer-based Web developer “NGO web
solutions” is providing templates of a temporary website which
will serve as a project pilot for grant-writing proposals. The
future creation of the site will follow after funds have been
made available. Video segments for content creation are being
provided in kind by students from San Francisco State
University’s (SFSU) Broadcast and Electronic Communication Arts
department. Support for site implementation and promotion is also
being provided in kind by volunteers from SFSU’s César E. Chávez
Institute.
Summary
Research reviewed for this project has consistently pointed
to the need of effective communication between Latino patients
and HCP for achieving better health outcomes. Latinos are
significantly at risk due to deficiencies in language
comprehension, lack of insurance and stereotyping by HCP who may
be unaware of cultural diversity. It’s widely assumed that the
implementation of cultural competency courses can help bridge the
87
cultural gap between HCP and Latino patient population. Small
investments in CC can produce significant savings in hospital
litigations, fees due to medical errors and misdiagnosis which
can be caused by ineffective communication between HCP and low
English proficiency patients. This field study proposes the
implementation of CC courses and the creation of an electronic
resource tool for the improvement of care among the Latino
population in the clinical setting.
Latinos when migrating to the United States bring with them
a unique health literacy and cultural perception which are
different than the American main stream. These traits are not
always visible and have a tendency to be ignored by untrained
HCP. A culturally trained health care staff can also produce
positive changes in areas beyond the immediate clinical setting
promoting less racial discrimination and less stereotype
formation. Some well established health organizations have been
using successful CC programs for over five years. The Federal
Government has also stepped up efforts to create CC programs
which have improved patient satisfaction among ethnic diverse
88
communities aiding in treatment of diabetes, increased access of
blood sugar levels and medication compliance.
This field study has objectives that are immediate and
overarching. The immediate objectives centers on improved
efficiency and safety in caring for Latinos in the clinical
setting. Improvements on listening to the patient, explaining,
acknowledging, recommending and negotiating should be observed
among HCP who take the CC course. The overarching objectives
should be an increase in cultural awareness, cultural skills and
a display of self initiative to become culturally competent which
is coined “cultural desire”. The target population of this
project consists of HCP providers from health establishments who
participate in this cultural competency program in Northern
California. This HCP target population are likely to have little
training and lack of experience treating Latino patient
populations.
There are several stake holders with links to this project.
The institutions involved hold values that are similar to this
project’s goals. The contributors and supporters are foundations,
corporations and trusts with which hold interest in minorities
89
and health care projects. Partners are also the health
institutions such as hospitals and clinics who will host this
project adding or incorporating it to their ongoing cultural
competency relevant to Latinos.
One strategy for implementing this project has utilization
of Madelaine Leininger’s theory of culture care diversity and universality. The
creation and implementation of this project will involve three
phases: research, web-site creation and the project’s
implementation into educational programs of stakeholder’s
institution. Major expenses incurred in this project are the
website construction, the hiring of professionals for content
research and web-based course development, and brochures or
booklets production.
90
Chapter 4
Evaluation
The evaluation of this program has ties with stakeholders
who sponsor cultural competency or cultural education programs
such as the one in this field study. The efficacy of this
educational tool will require stakeholders’ engagement,
91
evaluation, testing and revisions. The focus of this evaluation
will be the program goals previously explained in chapter 3. The
evaluation tools selected for this field study can also measure
the overarching goals and long term use of the project; however
it will require an entire new evaluation process due to the
complexities associated with overarching goal evaluations. The
subjects Included in the evaluation are all participants in the
project.
This program will utilize two evaluation tools: The Centers
for Disease Control Framework for Program Evaluation (CDCFPE) (Centers for
Disease Control and Prevention 2010), a complex evaluating system
consisting of 6 steps; and the Inventory for Assessing the Process of
Cultural Competence among Healthcare Professionals-Revised (IAPCC-R)
(Appendix E). The IAPCC-R method was chosen specifically because
it was created exclusively for the evaluation of cultural
competency programs among HCP and graduate students in the allied
health fields. It is important to point out that the IAPCC-R is a
questionnaire based structure which assesses 25 items measuring
five cultural constructs using a 4-point likert scale (appendix
E).
92
The CDCFPE is the main structure for this evaluation. It is
a complex method providing a robust structure organized into six
steps: engagement of stakeholders, description of program, design
evaluation, evidence, justification of conclusions, and ensuring
share and learning. Following is a detailed description of the 6
steps. The description of the program which is the step 2 of the
CDCFPE program was fully covered in chapter 3 and will not be
included in the following steps description.
Step 1: Engaging StakeholdersCultural competency projects such as the one proposed by
this field study requires partnerships. Partners bring with them
a set of value systems they want to see reflected in the project
they sponsor; therefore stakeholders must be engaged in the
inquiry and evaluation process to ensure that their perspectives
are understood. Findings will have a tendency to be disregarded
if evaluation fails to address stakeholders’ objectives thus
making the role of engagement, a crucial one. Three main critical
areas of stakeholders’ relationships with the evaluating process
must be identified: program’s operations, target population, and
users.
93
The program’s operations for this project are all groups
involved in the funding, donations or any other benefit made to
the project. The groups most involved in this project are: The
California Healthcare Foundation, The Health Trust, and The
Baxter International Foundation which are this project’s main
financial backers. Even though these organizations are vital,
they are not necessarily the ones responsible for handling the
actual physical production and execution. Other subgroups such as
individuals’ contributors or volunteers are involved and a
distinction must be made between evaluations of organizations as
entities and personal evaluations of individuals. Personal
evaluations should have different criteria from corporate
evaluations as a whole.
The target population is also considered a stakeholder and a
participant in the evaluation process. All the individuals,
communities, workplaces, advocacy groups, professional
associations and anyone who is directly or indirectly affected by
this program should also be identified and included in the
evaluation process. Another target population is the staff nurses
and doctors and other health care staff who will be taking this
94
CC course. Other groups are the Latino patients who are directly
affected by changes in behavior and education among HCP. These
groups are important because their approval or disapproval or
criticism can affect the input and influence evaluation results.
The inclusion of proponents or opponents to this project can
strengthen the evaluation credibility.
Finally the entire body of participants must be identified
and a representative or a specific person in charge for each
subgroup chosen so changes are reflected for each area of the
project and in control of stakeholders objectives. This action
will take place early in the project and each representative will
be required to maintain constant and frequent interaction with
all groups and subgroups involved in workings of the project.
Sharing information through meetings and briefings with the all
the groups will ascertain equilibrium and help to avoid conflicts
of interest and over emphasis from a single individual or
stakeholder over the entire project.
Step 3: Focusing the Evaluation Design
The focus of the evaluation design begins with the
understanding that some designs may not meet the needs of
95
stakeholders. Design options must be evaluated so that the best
format meets the informational needs of all stakeholders.
Therefore the focus of the evaluation must address the core
values of stakeholders or the issues stakeholders are most
concerned. While meeting these criteria, the design must also
meet the demands of time and resource limitations. An evaluation
procedure must also be established before collection begins;
changing procedures when evaluation is in progress might be
impossible and a thorough plan must be created before evaluation
begins. Among the items to be considered in the evaluation are:
purpose, users, uses, questions, methods, and agreements.
The purpose as a consideration for this evaluation design is
to assess the effects and gain insight. To investigate effect
changes we will look at the relationship between this CC program
agenda and improvements in Latino patient care resulting in
improved satisfaction. Even though patient satisfaction is part
of the overarching goal of this program, its evaluation is beyond
the scope of this field study. The effect assessment focus on
measurements of changes in behaviors among the target population
and HCP associated with the administration of this program.
96
Effect evaluation will also determine the direct and indirect
action or effectiveness of the program. Parameters also will be
established to determine if program produces similar of better
results than other compatible CC programs.
The users and uses parameters will be established in
accordance with the program scope including age group, target
population and stakeholders’ core ideologies. The users are the
individuals who will receive evaluation. In the case of this
field study, the users are the HCP participating in the program.
The uses refer to the specific useful objectives the evaluation
data will create: to gain insight, assess needs, identify
barriers for future program changes, assess effect, and affect
participants.
The questions parameter defines boundaries for the
evaluation, pointing to what the focus of the CC program will be.
The formatting of questions encourages stakeholders to expose
what they believe or desire from the program goals as a whole.
The question development may also produce and expose differences
between stakeholders and their expectation. At the heart of this
evaluation design are the issues of greatest concern for the
97
stakeholders, and only the options which best address their needs
are considered priority.
The method for evaluation is based on scientific research
and evidence based practice. The evaluating methods should be
designed so it provides information that meets the stakeholders’
informational needs. The methods should also match the
informational needs of the primary users, uses, and the set of
evaluating questions. The choice of design should be carefully
selected as it has implications for what will count as evidence
and validity. The methodological decision also has implications
on how the program will operate and how the program participants
will be involved; what data collection instruments will be used;
what are the appropriate methods of analysis, and
interpretations. Methods may need to be revised or modified
during the implementation process.
The agreements clarify and summarize the roles and
responsibilities among those in charge of the evaluating plan
execution. The agreement also provides guidelines for the
implementation plan and what and how resources will be allocated
such as money, personnel, time and information. Agreement plays a
98
significant role in this field study where ethical and cultural
issues are at the core of the project. Agreement is also provides
guidelines for administrative matters.
Step 4: Gathering Credible Evidence
Another important function of the evaluation is to produce a
complete picture of the program in all its relevant details so
that the information is credible and useful for primary users
which are the objective of step four of the CDC evaluation
framework (CDC, 2010). This information should be represented by
the evidence of these evaluations and should be trusted by the
stakeholders as reliable and relevant. This evidence is produced
by the type of questions being asked and what are the motives
behind them (CDC, 2010). Before the program begins there will be
meetings with stakeholders and their participation in the general
process of choosing parameters, program indicators, expected
outcomes and general core concepts. Among the relevant aspects
needing evaluation are increased HCP perception of cultural
issues relative to Latino patient population; and understanding
of cultural perceptions in Latino patient population relative to
health care and an overall increased ability to communicate with
99
Latinos. Other parameters which are important to stakeholders
will be discussed or added to the evaluation program. Multiple
sources of data evaluation and gathering procedures will be used
to ensure improved data credibility. Another important provision
is that special training provided to the staff who will conduct
educational and evaluating sessions such as administration of the
pretest and posttest (appendix F).
Evaluation will be performed by analysis of quantitative and
qualitative data. The data will be collected by managers and CNS
staff involved in the project. The data will originate from
answers to tests and questionnaires administered to participants.
Qualitative data will be evaluated by trained staff and all final
data will be entered into a computer running dedicated analysis
software. Prior to the test administration there will be a
consultation with statisticians and data analysis specialists to
determine the ideal psychometric method to start data gathering.
The evaluation of overarching objectives of this study will be
planned as an additional longitudinal project which could take up
to 5 years to implement.
Step 5: Justifying Conclusions
100
The evaluation of conclusions is the fifth step of the CDC
framework. The justification for the conclusions is tied to
previously agreed parameters by the stakeholders, therefore they
must agree with an evaluation criterion before data is gathered
and evaluation process begins (CDC, 2010). The parameters for
conclusion justification in step 5 of this framework are:
standards, analysis and synthesis, interpretation, judgment, and recommendations
(CDC, 2010). The standards for this evaluation will also reflect
the values of the stakeholders which provide the basis for
judging the program performance. These values are centered in
promoting cultural awareness in health care and are the basis for
considering the program successful or unsuccessful. The analysis
and synthesis requires that each isolated finding be analyzed
independently to insure that a larger picture is formed and is
accurate. In the case of this field study items such as the
degree in which students have dedicated to the program and the
level of communication they have achieved with patients are some
of the parameters of independent analysis. One of the principal
assumptions of this study’s evaluation is that participants who
score higher in their posttest have improved their cultural
101
competency levels in regards to treating Latino patients. The
merit, worth, or significance and changes needed for improvement
of the program are contained in the judgment and recommendation
parameters of step five. These parameters will be evaluated by
panels and voting sessions among the stakeholders. Comparison of
this program with others should be easily obtained since there
are a great number of CC programs in existence and their
respective evaluation results can make this evaluation more
reliable.
Step 6: Ensuring Use and Sharing Lessons Learned
Steps six of CDC’s framework addresses usage parameters and
follow up procedures. Specific efforts are needed to ensure that
evaluating processes are used and disseminated correctly. All HCP
participating in this CC will be encouraged to continue studies
leading to a better understanding of cross cultural backgrounds
emphasizing learning and expanding foreign vocabulary. Health
institutions such as clinics and hospitals will be informed of
results and evaluation processes with the objective of promoting
interest in CC programs. The overall reduction in communication
problems can lower the rate of incorrect assessments and
102
diagnosis among Latino patients’ resulting in decreased length of
stay, and hospital cost (Cohen et al., 2005). The findings will
be used to assist the expansion of similar programs in other
hospital and clinics.
Additional methods
The Inventory for assessing the process of cultural competence among health
professionals (IAPCC) will be used as part of the assessment for
cultural competency improvements and consist of a four-point
Likert scale and five sub-scales and it was revised in 2003 (Tan
et al., 2007). IAPCC scores indicate on which level a
professional is operating: cultural proficiency, cultural competence, cultural
awareness, or cultural incompetence. It consists of a 25 item
methodology assessing five constructs: desire, awareness,
knowledge, skill, and encounters (appendix E). The key pivotal
construct “cultural desire” is defined as the “motivation of HCP
to “want” to engage in the process of becoming culturally
competent (Musolino, et al., 2009). Details of IAPCC-R®.
Questionnaires using a 4 point likert scale will also be used to
103
evaluate the good performance of the course and its overall
functionality as well as its efficiency and how students feel
about the methodology used and technology innovation such as
interactive video.
Time frame for evaluation
To effectively evaluate the efficacy of this program will
require a longitudinal study. It is estimated that at least 5
years longitudinal study will be needed to evaluate the full
impact of this CC project. In order to conduct a longitudinal
evaluation is also suggested the creation of 3 distinct phases.
Phase 1 of the project is called the pilot phase where the
project would be implemented on a trial basis. In this phase only
minimal or essential elements would be used seeking low cost and
easy implementation. This first step is designed to obtain
feedback and to chart directions of the upcoming phases. Phase 2
begins after the implementation and evaluation of phase 1 has
been completed. Evaluation of phase 1 would significantly help
the implementation of phase 2 by working as an experimental
showcase, convincing stakeholders of the viability and allowing
them to have a snap shot of the project. On phase 2 the
104
established design outlined in this paper would be fully
implemented. Some changes might be added conforming to previous
experience learned on phase 1. At the end of 4 years, phase 3
would be implemented and it will signify the culmination,
refinement and inclusion of new technologies creating a well
established CC course beyond the original plan. The inclusion of
data from the evaluation of phase 1 and 2 would be included as
improvements in the final phase 3.
The long term evaluation can be performed after phase 3 is
operational. Phase 3 if successful would cement and consolidate a
long term budget relationship with the stakeholders ensuring
monitoring and frequent evaluations and the creation of audits.
It is suggested that at the end of each phase, an evaluation is
performed and its results analysis and presented to stakeholders.
Evaluation design for phase 3 will be created at a future date
when changes are well absorbed.
SummaryEvaluation is an important part of this cultural competency
program because it produces measurable and identifiable strengths
and gains, but also finds the weaknesses, limitations and makes
105
recommendations. Evaluation can also be instrumental in creating
parameters for change and improvements for the program and other
programs with similar goals. Another crucial role of evaluation
is to produce a mechanism in which stakeholders can have
participation and input in the programs they are funding and also
satisfy their desire to see if the program is in par with their
goals and objectives. Evaluation also serves to demonstrate the
program cost effectiveness after input and output are measured
and analyzed. Evaluation can also measure any improvement or
degree of involvement with staff conducting the program. Finally,
evaluation can function as a guarantee of program credibility
relative to its proposed goals and objectives.
Chapter 5
Conclusion
Introduction
The implications, limitations, and recommendations of this
field study are examined in this chapter. The implications of
this study affecting nurses, doctors and other health care
providers will be evaluated; the global impact of CC in the
106
health care environment will also be evaluated. This CC program
also presents limitations that will be discussed as well as the
limitation encountered during the creation of this field study.
Included are also the recommendations for further research needed
for updating and changes for upcoming versions of this CC program
which focuses on the improvement of communication between Latino
patients and HCP in the United States.
Implications
This field study intends to impact the nursing profession,
and specifically nurses working among large Latino patient
populations. By increasing awareness of Latino culture, nurses
may play a role in the improvement of well-being among the Latino
patients with positive repercussions to the Latino community.
Patient education is an important part of the nursing profession,
and the improvements made in the communication skills involving
diverse populations fits within the nurse scope of practice.
Other important interactions demanding communication is patient
assessment requiring correct interpretation of cultural
perceptions. Improvements in communication among HCP in a
cultural diverse environment can improve the quality of care and
107
patient satisfaction.
This field study has also implications for nurse educators
and hospital staff such as social workers responsible for
discharging patients and arranging community placement after
patient discharge. This is particularly true for the CNS who
identifies nursing related problems in the hospital and seeks
solutions by providing educational agenda. Promoting
participation and integration to this CC program in hospitals
will require the CNS to be knowledgeable of Latino population
related problems. She will need to educate others of the
necessity of being culturally savvy in the health care
environment in order to promote successful adhesion to the
program. In addition, the CNS will need to organize and
coordinate other members of the health care team to facilitate
the flow of the studies and manage the access to this CC program.
This field study has also global and encompassing
implications for the health care system as a whole. Cultural
competency can make Latino patients more confident and welcomed
in the health care system, this positive integration can
increasing the number of visitations and help prevent illnesses
108
from progressing or worsening, lowering health care costs on a
long term basis. Better communications with M.D.’s can also lead
to successful detection of disease in the early stages. The
implications for the Latino community are the improvement of
quality of life. The preservation of life and the well being of
the Latino community are proposed in this field study and mirrors
a global health care concern aimed at the improvement of life in
all communities; this program enables HCP to concentrate efforts
aimed at diminishing the cultural gap between Latino patients and
HCP providers in the United States to achieve well being.
Limitations of the field study
To make future improvements to this field study is necessary
to understand its limitations. Even though there is a wealth of
cultural competency studies available through several electronic
databases, the relevancy and accuracy of this study would gain
from having been conducted as a thesis. This field study did not
have the available funding and human resources to conduct its own
investigative research. It would have been preferred if data were
generated from specific Latino populations and the target
population concerning this study for more result accuracy and
109
relevancy.
Another limitation was the time allotted to the completion
of the project. This cultural competency course is expected to be
completed within one year. This is a limited time frame and not
sufficient time to investigate the effectiveness of the methods
used and the desired effects on the specific target populations.
Additional time would have ensured a longitudinal evaluation thus
generating more descriptive evaluating data. Important
information from these studies could have been: rates of re-
visitation from Latino patients prior and after the course
implementation, health outcome directly related to services after
program implementation, and hospital savings directly correlated
with Latino population segments. Lastly, with more time available
this program could have benefited from the input of professional
educators associated with similar cultural competency programs.
This was not possible due to the resource constraints encountered
in this study. Live input from educators or industry
professionals could have also clarified some flaws fond in the
project by determining if assumptions made for the project were
actually worthwhile to implement or if they offered any
110
significant results based on previous experiences from these
educational professionals.
Recommendations
The implementation of this cultural competency web program
to other hospitals and health institutions in addition to the
ones proposed in this study is one recommendation from the author
of this project. Hospital educational staff responsible for
implementing and documenting this CC programs could be
instrumental in contacting other health institutions and
facilitating the expansion of similar programs if evaluation
results are positive. Other independent educational institutions
could become potential centers for distribution for CC courses.
After development and refinement, this course could be packaged
and distributed to interested parties such as health educational
centers interested in providing cultural curricula. Consequently,
these centers could potentially produce entrepreneurial ventures
or marketing of cultural educational products or become
consultants to other institutions.
Another recommendation is the expansion of this CC program
to other areas of cultural integration and learning. Extensions
111
could be created to address areas such as: how to navigate the
health care in the United States. This could serve as a tool to
Latinos with poor comprehension of how health care issues are
addressed in the United States. This recommendation includes more
research to identify who are the Latinos at risk and what
populations suffer from these specific health care utilization
and navigation deficits.
Research in this area will need to be directed at the
assessment of current understanding on how Latinos perceive
health care, and what are the geographic areas where Latinos have
the most deficit when seeking health care in the United States.
More research is needed to evaluate if the largest problem areas
are in the regions of heavy migration or the remote areas where
few Latinos live. The assumption is that the unprivileged and
underserved areas with the most Latino population are the problem
areas but much research is needed to investigate high and low
population areas. This CC system can be more effective as the
roots of cultural deficit are uncovered.
It is also recommended that findings and results be
published and made available to institutions which could
112
potentially benefit from cultural competency program such as
this. Even though much research and studies can be found in the
cultural competency area, the large variety can be confusing and
not necessarily address the educational needs of certain groups.
A need to find cultural competency measurement tool is necessary.
Further research in the classification and validity of different
cultural competency courses is advised. Other research is also
necessary in the areas of diagnosis of Latino patients with the
creation of study cases and the area of mental health. Lastly the
creation of a national Latino health utilization database is
recommended for better access to information and uniformity,
facilitating the improvement of CC programs such as this.
Summary
This field study offers an educational option to the lack of
cultural awareness common in some health care settings where
Latino populations exist. This cultural competency program was
created to serve nurses, doctors and any HCP in seeding cultural
competency with Latinos. The program increases awareness of
differences in the Latino patient and provides comprehensive set
of solutions for discharge teaching, communication, assessment
113
and health instructions by utilizing evidence base research. The
objective is to create better communication and the elimination
of treatment and diagnosis errors creating more patient
satisfaction and safety for the Latino community in the United
States.
References
114
American Nurses Association. (2010). American nurses credentialing center:
Accreditation of continuing nursing education providers. Retrieved from:
http://www.nursecredentialing.org/ContinuingEducation/Accred
itation.aspx
and underserved/v021/21.1.sanchez.html
Anderson, L.M., Scrimshaw, S.C., Fullilove, M.T., Fielding, J.E.,
Normand, J. (2003). Culturally competent healthcare systems
a systematic review. American Journal of Preventive Medicine, 24(3),
0749-3797. doi: 10.1016/S0749-3797(02)00657-8
Araiza, R., Klopf, M., & Kelley, F. (2005). Forces of change.
Nurse practitioner education and second language learning:
Using the Internet as a tool. Clinical Excellence for Nurse
Practitioners, 9(1), 41-47.
Bachman, S.S., Tobias, C., Master, R.J., Scavron, J., & Tierney,
K. (2008) A managed care model for Latino adults with
chronic illness and disability. Journal of Disability Policy Studies,
18(4), 197-204. doi: 10.1177/1044207307311304
Bacote, A.C., Bacote, J.C. (2009). Extending a model of cultural
competence in health care delivery to the field of health
115
care law. Journal of Nursing Law, 13(2), 36-44. doi: 10.1891/1073-
7472.13.2.36
Balslev, T., Grave, W.S., Muijtjens, A.M.M., Scherpbier, A.J.J.A.
(2005). Comparison of text and video cases in a postgraduate
problem-based learning format. Medical Education, 39, 1086-1092.
doi: 10.111/j.1365-2929.2005.02314.x
Barr, D.A., & Wanat, S.F., (2005). Listening to patients:
Cultural and linguistic barriers to health care access.
Stanford University Sociology Department, 37(3), 199-204. Retrieved
from http://www.stfm.org/fmhub/fm2005/March/Donald199.pdf
Betancourt, J.R., & Maina, A., (2007). Barriers to eliminating
disparities in clinical practice. In Betencourt, J.R., &
Maina, A., Eliminating Healthcare Disparities in America (pp. 83-97).
Retrieved from
http://www.springerlink.com/content/kj3373785tml138p/
Betancourt, J.R., Green, A.R., Carrillo, J.M., & Park, E.R.
(2005). Cultural competence and health care disparities: Key
perspectives and trends. Health Affairs, 24(2), 499-505. doi:
10.1377/hlthaff.24.2.499
116
Betancourt, J.R., Green, A.R., Carrillo, J.M., Park, (2002).
Cultural competence and health care: Emerging frameworks and practical
approaches (Research Report No. 576). Retrieved from The
Commonwealth Fund website:
http://www.commonwealthfund.org/usr_doc/betancourt_culturalc
ompetence_576.pdf
BlueCross BlueShield of Florida. (2007). Many cultures one goal your
health. Retrieved from BCBSF website:
http://www.bcbsfl.com/DocumentLibrary/AboutOurCompany/Divers
ityReport.pdf
California Board of Registered Nursing. (2008) Survey of RNs:
Data by Ethinicity. Available at:
http://www.rn.ca.gov/forms/xcelsius_ethnicity_export.shtml.
Accessed March 1, 2010
Campos, C. (2007). Addressing cultural barriers to the successful
use of insulin in Hispanics with type 2 diabetes. Southern
Medical Association, 100(8), 812-820. Retrieve from: http://0-
web.ebscohost.com.opac.sfsu.edu/
Cengage, G. (2002). Acculturation. In L. Breslow (Ed.),
Encyclopedia of public health (May 2006 ed.). Retrieved from
117
http://www.enotes.com/public-health-encyclopedia/acculturati
on
Centers for Disease Control and Prevention, Diabetes Public
Health Resource. National diabetes fact sheet: General information
and national estimates on diabetes in the United States
(2007). Retrieved from
http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf
Centers for Disease Control and Prevention, Framework for Program
Evaluation, Framework for Program Evaluation in Public Health.
MMWR (2010);48(No. RR-11). Retrieved from:
http://www.cdc.gov/eval/framework.htm
Centers for Disease Control and Prevention, Healthy Youth. Health
risks and disparities experienced by Hispanic youth. General information
and national estimates on Hispanic youth (2010). Retrieved
from:
http://www.cdc.gov/HealthyYouth/disparities/hispanic/hispani
c_disparities.htm
Centers for Disease Control and Prevention, Office of Minority
Health & Health Disparities. (2010). Eliminating racial and ethnic
118
health disparities. Retrieved from
http://pewhispanic.org/files/reports/107.pdf
Cheng, E.C., Chen, A., Cunningham, W. (2007). Primary language
and receipt of recommended health care among Hispanics in
the United States. Society of General Medicine, 22 (2). 283-8.doi:
10.1007/s11606-007-0346-6
Cherrett, T., Wills, G., Price, J., Maynard, S., Dror, I.E.
(2009). Making training more cognitively effective: Making
videos interactive. British Journal of Educational Technology, 40(6),
1124-1134. doi: 10.1111/j.1467-8535.2009.00985.x
Chevannes, M., (2001). Issues in education health professionals
to meet the diverse needs of patients and other service
users from ethnic minority groups. Journal of Advanced Nursing,
39(3), 290-298.
Chou, S., Liu, C. (2005). Learning effectiveness in a web-based
virtual learning environment: A learner control perspective.
Journal of Computer Assisted Learning, 21, 65-76. Retrieved from:
http://www3.interscience.wiley.com/cgi-bin/home
119
Christina C Wee, Russell S Phillips, Anna T R Legedza, Roger B
Davis, & et al. (2005). Health Care Expenditures Associated
With Overweight and Obesity Among US Adults: Importance of
Age and Race. American Journal of Public Health, 95(1), 159-65.
Retrieved June 23, 2010, from ABI/INFORM Global. (Document
ID: 777724131).
Coffman, M., Shobe, M., Dmochowski, J., & Fox, S. (2007). Health
care access and utilization among Latino immigrants. Hispanic
Health Care International, 5(2), 73-80. Retrieved from CINAHL Plus
with Full Text database.
Cohen, A.L., Rivara, F., Marcuse, E.K., McPhillips, H., Davis, R.
(2005). Are language barriers associated with serious
medical events in hospitalized pediatric patients? Journal of
the American Academy of Pediatrics, 166,575-579. doi:
10.1542/peds.2005-0521
Cook, D.A., Dupras, D.M., Thompson, W.G., Pankratz, V.S. (2005)
Web-based learning in residents’ continuity clinics: A
randomized, controlled trial. Academic Medicine, 80(1), 90-97.
Retrieved from:
120
http://journals.lww.com/academicmedicine/Abstract/2005/01000
/Web_Based_Learning_in_Residents__Continuity.22.aspx
Cox, E.D, Koscik, R.L., Olson, C.A., Behrmann, A.T., Hambrecht,
M.A., McIntosh, G.C., & Kokotailo, P.K., (2006). Carring for
the underserved blending service learning and a web-based
curriculum. American Journal of Preventive Medicine, 31(4), 342-349.
doi: 10.1016/j.amepre.2006.06.024
Curran, V., Lockyer, J., Kirby, F., Sargeant, J., Fleet, L., &
Wright, D. (2005). The Nature of the Interaction Between
Participants and Facilitators in Online Asynchronous
Continuing Medical Education Learning Environments. Teaching
& Learning in Medicine, 17(3), 240-246.
doi:10.1207/s15328015tlm1703_7.
Dentzer, S. (2010). The child abuse we inflict through child
obesity. Health Affairs. Advance online publication.
doi:10.1377/hlthaff.2010.0152
Derntl, M.; Hummel, K.A.; , "Modeling context-aware e-learning
scenarios," Pervasive Computing and Communications Workshops, 2005.
PerCom 2005 Workshops. Third IEEE International Conference
121
on , vol., no., pp. 337- 342, 8-12 March 2005
doi: 10.1109/PERCOMW.2005.60
Escamilla, R.P., & Putnik, P. (2007). The role of acculturation
in nutrition lifestyle and incidence of type II diabetes
among Latinos. Journal of Nutrition, 137(4), 860-870.
ethnic. Medical-Glossary.com. Retrieved May 19, 2010, from
Medical-Glossary.com website: http://www.medical-
glossary.com/definition/ethnic.html
Frankel, B. (2010, April). The DiversityInc top 10 companies for
latinos. DiversityInc, Retrieved from
http://www.diversityinc.com/article/7452/The-DiversityInc-
Top-10-Companies-for-Latinos/Freeman J: Towards a definition
of holism. Br J Gen Pract
Glenn, F. (2006). Language barriers to health care in the United
States. The New England Journal of Medicine. 355(3). www.NEJM.org
Goode, T.D., Dunne, M.C., & Bronheim, S.M. (2006). The evidence base
for cultural and linguistic competency in health care (Commonwealth Fund
Pub No. 962). Retrieved from The Commonwealth Fund website:
http://www.commonwealthfund.org/ Content/Publications/Fund-
122
Reports/2006/Oct/The-Evidence-Base-for-Cultural-and-
Linguistic-Competency-in-Health-Care.aspx
Gulas, Charles J. (2005). Establishing the reliability of using
the Inventory for Assessing the process of cultural
competence among healthcare professionals with physical
therapy students. Ph.D. dissertation, Saint Louis
University, United States -- Missouri. Retrieved May 15,
2010, from Dissertations & Theses: The Humanities and Social
Sciences Collection.(Publication No. AAT 3185062).
Haviland, M.G., Morales, L.S., Dial, T.S., & Pincus, H.A. (2005).
Race/Ethnicity, socioeconomic status, and satisfaction with
health care. American Journal of Medical Quality, 20, 195-203. doi:
10.1177/1062860605275754
Helms, J.E., Henze, K.T., Sass, T.L., Mifsud, V.A. (2006).
Treating Cronbach’s alpha reliability coefficients as data
in counseling research. The Counsiling Psychologist.34(5), 630-660.
doi: 10.1177/0011000006288308
Hesse, B.W., Nelson, D.E., Kreps, G.L., Croyle, R.T., Arora,
N.K., Rimer, B.K., & Viswanath, K., (2005). The impact of
123
the internet and its implications for health care providers:
Findings from the first health information national trends
survey. Archive of Internal Medicine. 165(22), 2618-2624
Homestead Schools, Inc. (2004). In Homestead Schools, Inc. (Ed.),
Nursing an Hispanic Patient. Torrance, CA: Homestead Schools, Inc.
Hughes, K.H., & Hood, L.J., (2007). Teaching methods and an
outcome tool for measuring cultural sensitivity in
undergraduate nursing students. Journal of Trascultural Nursing, 18,
57-62. doi: 10.1177/1043659606294196
Hunt, L.M., Voogd, K.B., (2005). Clinica myths of the cultural
“other”: Implications for Latino patient care. Academic
Medicine, 80(10), 918-924. Retrieve from:
http://journals.lww.com/academicmedicine/Fulltext/2007/06000
/Measures_of_Cultural_Competence__Examining_Hidden.5.aspx
Kaiser Permanente, News Center, Press Releases. (2006). Kaiser
Permanente health video targets Latinos (publication: August 31,
2006). Retrieved from
http://xnet.kp.org/newscenter/pressreleases/nat/2006/083106e
scogelasalud.html
124

Kripalani, S., Jones, J.B., Katz, M., & Genao, I. (2006). A
prescription of cultural competency in medical education.
Journal of General Internal Medicine, 21(10), 1116-1120. doi:
10.1111/j.1525-1497.2006.00557.x
Ku, L., & Flores, G. (2005). Pay now or pay later: Providing
interpreter services in health care. Health Affairs,24(2), 435-
444. doi: 10.1377/hlthaff.24.2.435
Landon, B.E., Hicks, L.S., O’Malley, A.J., Lieu, T.A., Keegan,
T., McNeil, B.J., Gaudagnoli, E. (2007). Improving the
management of chronic disease at community health centers.
New England Journal of Medicine, 356(9), 921-934. Retrieved from
http://www.nejm.org
Lanza, A.F., Armbrister, A.N., Flórez, K.R., & Aguirre, A.N.,
(2006). Towards a theory-driven model of acculturation in
public health research. American Journal of Public Health, 96, 1342-
1346. doi: 10.2105/AJPH.2005.064980
Latinos. U.S. Census Bureau. Retrieved May 19, 2010, from U.S.
Census Bureau website:
http://quickfacts.census.gov/qfd/meta/long_68188.htm
125
Leininger, M. (2002). Culture care theory: A major contribution
to advance transcultural nursing knowledge and practices.
Journal of Transcultural nursing, 13(3), 189-192. doi:
10.1177/1045602013003005
Lipson, J.G., & Desantis, L.A. (2007). Current approaches to
integrating elements of cultural competence in nursing
education. Journal of Transcultural Nursing, 18, 10-20. doi:
10.1177/1043659606295498
Lorig, R.K., Ritter, P.L., Jacquez, A. (2005). Outcomes of border
health Spanish/English chronic disease self-management
programs. The Diabetes Educator, 31(401). 401-409. doi:
10.1177/0145721705276574
McDermott, R., O'Dell, C. (2001). Overcoming cultural barriers to
sharing. Journal of knowledge management, 5(1), 76-85. Retrieved
from http://mapule276883.pbworks.com/f/Overcoming%20cultural
%20barriers.pdf
Musolino, G.M., Babitz, M., Burkhalter, S.T., Harris, R., Ward,
R.S., Cantarini, S.C. (2009). Mutual respect in healthcare:
Assessing cultural competence for the university of Utah
126
interdisciplinary health sciences. Journal of Allied Health, 38, e54-
e62. Retrieved from http://www.ingentaconnect.com/
Nailon, R.E. (2006). Nurses’ concerns and practices with using
interpreters in the care of Latino patients in the emergency
department. Journal of Transcultural Nursing, 17, 119-128. doi:
10.1177/1043659605285414
National Center for Cultural Competence (2010). Conceptual
frameworks. Retrieved May 19, 2010 from the NCCC website:
http://nccc.georgetown.edu/foundations/frameworks.html
Nerenz, D. (2005). Health care organizations’ use of
race/ethnicity data to address quality disparities. Health
Affairs, 24(2), 409-416. Doi: 10.1377/hlthaff.24.2.409
Ngo-Metzger, Q., Sorkin, H., Phillips, S., Greenfield, S.,
Massagli, P., Clarridge, B., & Kaplan, H. (2007). Providing
high-quality care for limited English proficient patients:
The importance of language concordance and interpreter use.
Society of General Internal Medicine, 22(2),324-303. doi:
10.1007/s11606-007-0340-z
Okie, S. (2007). Immigrants and health care at the intersection
of two broken systems. The New England Journal of Medicine, 357(6).
127
Retrieved from:
http://0-content.nejm.org.opac.sfsu.edu/cgi/content/full/357
/6/525
Passel, J.S. & D’Vera Cohn. (2009). A portrait of unauthorized immigrants
in the United States (Report April 14, 2009). Retrieved from: Pew
Research Center Publications website:
http://pewresearch.org/pubs/1190/portrait-unauthorized-
immigrants-states
Perez, D., Sribney, W.M., & Rodríguez, M.A., (2009). Perceived
discrimination and self-reported quality of care among
Latinos in the United States. Society of General Internal Medicine, 24,
548-54. doi: 10.1007/s11606-009-1097-3
Pérez-Escamila, R., & Putnik, P. (2007). The role acculturation
in nutrition, lifestyle, and incidence of type 2 diabetes
among Latinos. The Journal of Nutritition, 137,860-870.
Quintana, J.M., Gonzalez, N., Bilbao, A., Aizpuru, F., Escobar,
A., Esteban, C., ... Thompson, A. (2006). Predictors of
128
patient satisfaction with hospital health care. BMC Health
Services Research. 6(102). doi: 10.1186/1472-6963-6-102
Rivers, P.A., & Patino, F.G. (2006). Barriers to health care
access for Latino immigrants in the USA. International Journal of
Social Economics, 33(3), 207-220. doi: 10.1108/03068290610646234
Robert Wood Johnson Foundation, Quality/Equality.
(2010). Glossary of health care quality terms. Retrieved
from: http://www.rwjf.org/qualityequality/glossary.
jsp
Ronda, H., Eduardo, O. (2005). Medication errors: Why they
happen, and how they can be prevented. American Journal of
Nursing, 105(3), 14-24. Retrieved from http://www.ovidsp.com
Sánchez, J.P., Kaltwassar, S., McClellan, M., Burton, W.B.,
Blank, A., Calderon, Y. (2010). Educational video tool to
increase syphilis knowledge among Black and Hispanic males
patients. Journal of Health Care for the Poor and Undeserved, 21, 371-385.
Retrieved from:
129
http://0-muse.jhu.edu.opac.sfsu.edu/journals/journal_of_heal
th_care_for_the_poor_
Shaya, F.T., & Gbarayor, C.M., (2006). The case for cultural
competence in health professions education. American Journal of
Pharmaceutical Education, 70(6), 1-6. Retrieved from
http://www.ncbi.nlm.nih.gov/PubMed/
Shi, L., & Stevens, D. (2005). Vulnerability and unmet health
care needs: The influence of multiple risk factors. Journal of
Internal Medicine, 20(2), 148-154. doi: 10.1111/j.1525-
1497.2005.40136.x
Sitzmann, T., Kraiger, K., Stewart, D., Wisher, R. (2005). The
comparative effectiveness of web-based and classroom
instruction: A meta-analysis. Personnel Psychology 3(59), 623-
664. Retrieved from http://www.ebscohost.com
Sobralske, M.C. (2006). Community-based strategies to improve the
health of Mexican American men. International Journal of Men’s Health,
5(2), 153-171.
Sorkin, D.H., & Metzger, Q., Alba, I. (2010). Racial/Ethnic
discrimination in health care: Impact on perceived quality
130
of care. Journal of Internal Medicine. Advance online publication.
doi: 10.1007/s11606-010-1257-5
Tan, Z., Beagan, B., Loppie, C., MacLeod, A., Frank, B. (2007).
Measures of cultural competence: Examining hidden
assumptions. Academic Medicine, 86(6), 548-557. Retrieved from:
http://www3.interscience.wiley.com/cgi-bin/home
Tervalon, M. (2009, winter). At a decade: Centers of excellence
in culturally competent care. The Permanente Journal, 13(1).
Retrieved from:
http://xnet.kp.org/permanentejournal/winter09/culturalcompet
ence.html
Tomey, A.M., & Alligood, M.R. (2001). Culture care: Diversity and
universality theory. In Y. Alexopoulos (Eds.), Nursing
Theorists and Their Work (pp. 501-526). St. Louis, Missouri:
Mosby.
U.S. Census Bureau. (2008). Annual estimates of the resident population by
sex, race, and Hispanic origin for the United States. ( April 1, 2000 to
July 1, 2008) Retrieved from:
http://www.census.gov/popest/national/asrh/NC-EST2008-
srh.html
131
Wilson, E., Chen, A., Grumbach, K., Wang, F., & Fernandez, A.
(2005). Effects of limited english proficiency and physician
language on health care comprehension. Journal of Internal
Medicine, 20,800-806. doi: 10.111/j.1525-1497.2005.0174.x
Zhang, D., Zhou, L., Briggs, R., Nunamaker, J.F. (2005).
Instructional video in e-learning: Assessing the impact of
interactive video on learning effectiveness. Information &
Management, 43, 15-27. doi: 10.1016/j.im.2005.01.004
132

Appendix A
Budget
133
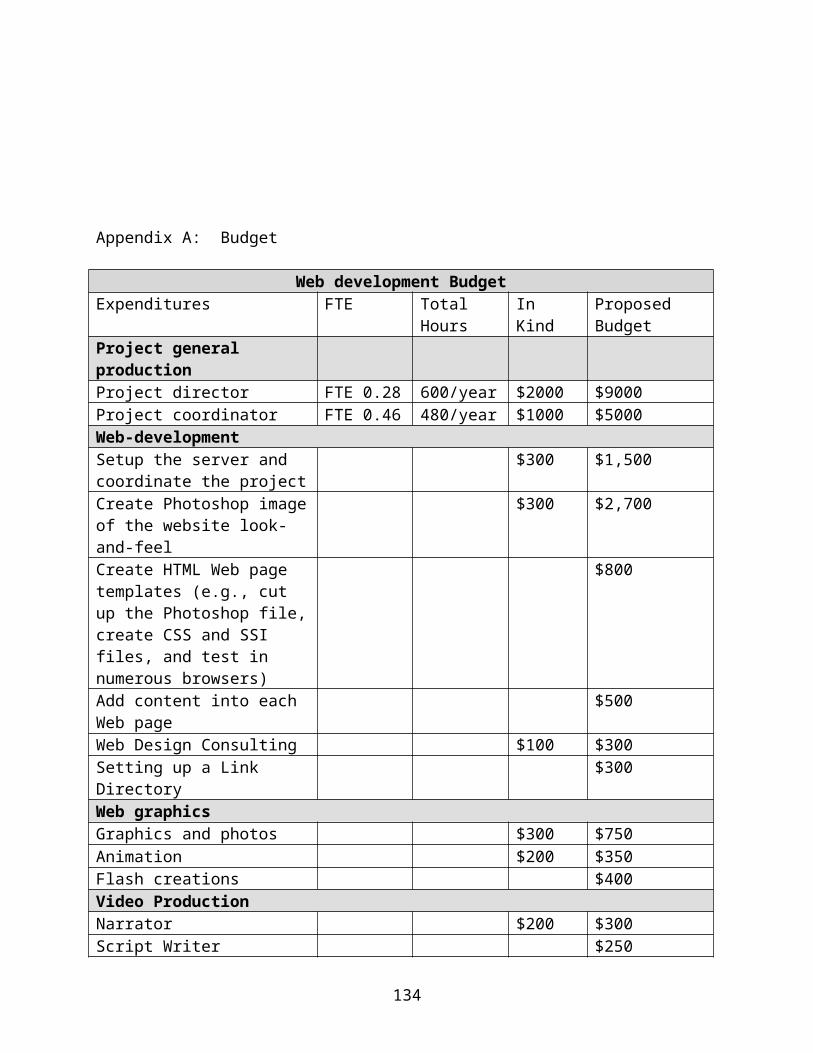
Appendix A: Budget
Web development BudgetExpenditures FTE Total
HoursIn Kind
Proposed Budget
Project general productionProject director FTE 0.28 600/year $2000 $9000Project coordinator FTE 0.46 480/year $1000 $5000Web-developmentSetup the server and coordinate the project
$300 $1,500
Create Photoshop imageof the website look-and-feel
$300 $2,700
Create HTML Web page templates (e.g., cut up the Photoshop file,create CSS and SSI files, and test in numerous browsers)
$800
Add content into each Web page
$500
Web Design Consulting $100 $300Setting up a Link Directory
$300
Web graphicsGraphics and photos $300 $750Animation $200 $350Flash creations $400Video ProductionNarrator $200 $300Script Writer $250
134
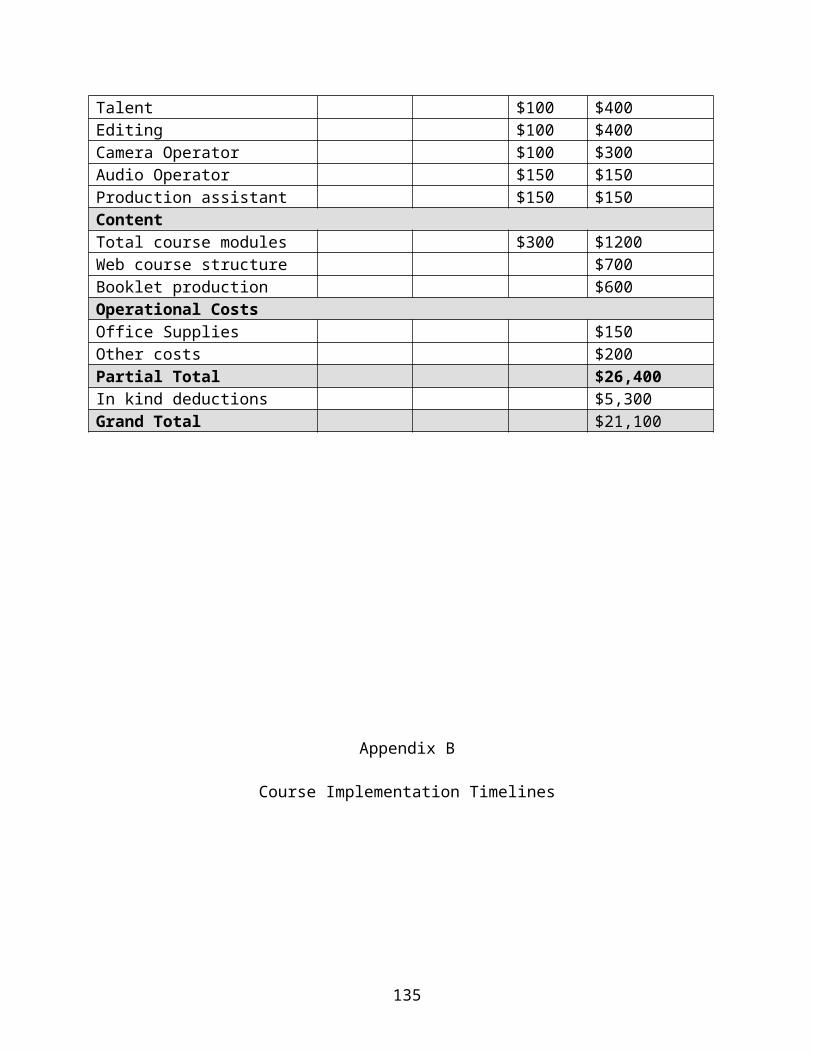
Talent $100 $400Editing $100 $400Camera Operator $100 $300Audio Operator $150 $150Production assistant $150 $150Content Total course modules $300 $1200Web course structure $700Booklet production $600Operational CostsOffice Supplies $150Other costs $200Partial Total $26,400In kind deductions $5,300Grand Total $21,100
Appendix B
Course Implementation Timelines
135

136
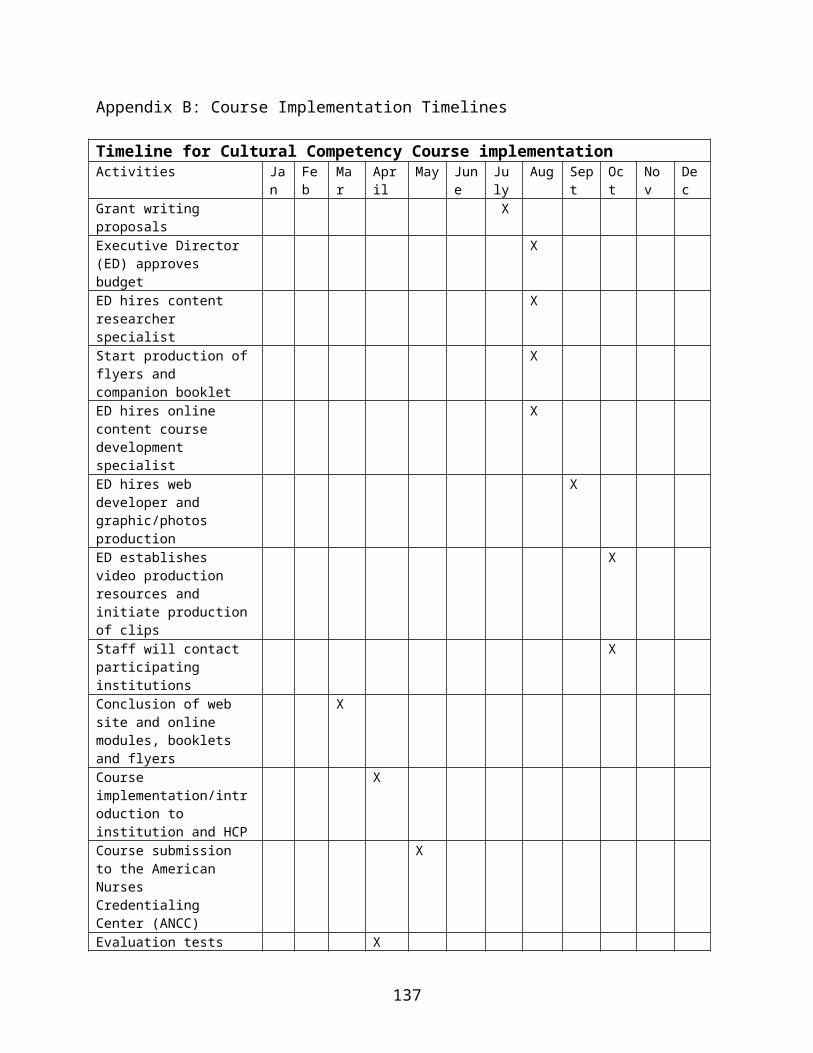
Appendix B: Course Implementation Timelines
Timeline for Cultural Competency Course implementationActivities Ja
nFeb
Mar
April
May June
July
Aug Sept
Oct
Nov
Dec
Grant writing proposals
X
Executive Director (ED) approves budget
X
ED hires content researcher specialist
X
Start production offlyers and companion booklet
X
ED hires online content course development specialist
X
ED hires web developer and graphic/photos production
X
ED establishes video production resources and initiate productionof clips
X
Staff will contact participating institutions
X
Conclusion of web site and online modules, booklets and flyers
X
Course implementation/introduction to institution and HCP
X
Course submission to the American Nurses Credentialing Center (ANCC)
X
Evaluation tests X
137
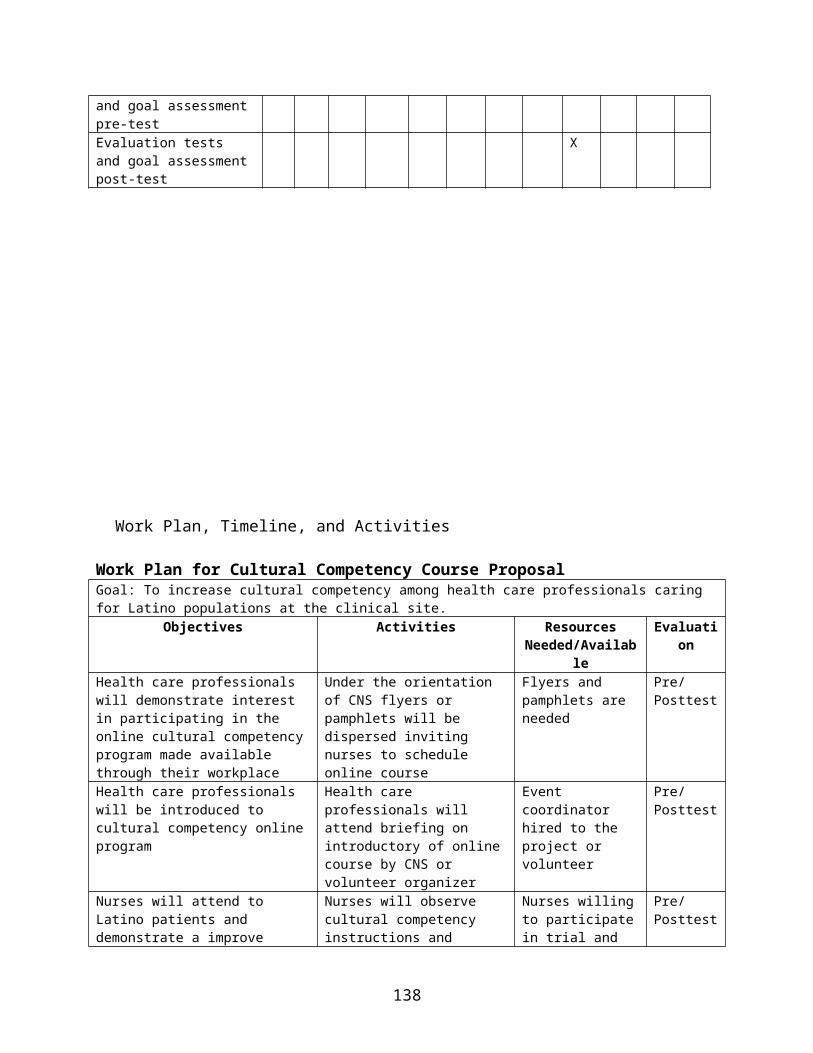
and goal assessmentpre-testEvaluation tests and goal assessmentpost-test
X
Work Plan, Timeline, and Activities
Work Plan for Cultural Competency Course ProposalGoal: To increase cultural competency among health care professionals caring for Latino populations at the clinical site.
Objectives Activities ResourcesNeeded/Availab
le
Evaluation
Health care professionals will demonstrate interest in participating in the online cultural competencyprogram made available through their workplace
Under the orientation of CNS flyers or pamphlets will be dispersed inviting nurses to schedule online course
Flyers and pamphlets are needed
Pre/Posttest
Health care professionals will be introduced to cultural competency onlineprogram
Health care professionals will attend briefing on introductory of onlinecourse by CNS or volunteer organizer
Event coordinator hired to the project or volunteer
Pre/Posttest
Nurses will attend to Latino patients and demonstrate a improve
Nurses will observe cultural competency instructions and
Nurses willingto participatein trial and
Pre/Posttest
138
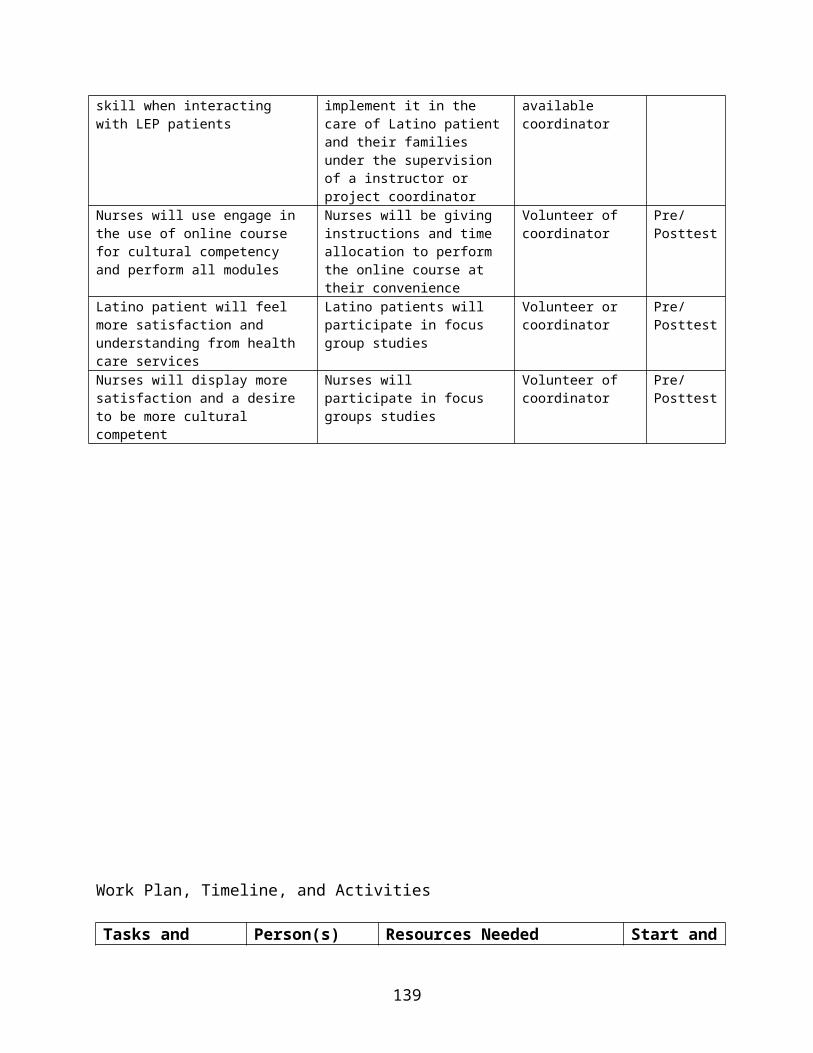
skill when interacting with LEP patients
implement it in the care of Latino patientand their families under the supervision of a instructor or project coordinator
available coordinator
Nurses will use engage in the use of online course for cultural competency and perform all modules
Nurses will be giving instructions and time allocation to perform the online course at their convenience
Volunteer of coordinator
Pre/Posttest
Latino patient will feel more satisfaction and understanding from health care services
Latino patients will participate in focus group studies
Volunteer or coordinator
Pre/Posttest
Nurses will display more satisfaction and a desire to be more cultural competent
Nurses will participate in focus groups studies
Volunteer of coordinator
Pre/Posttest
Work Plan, Timeline, and Activities
Tasks and Person(s) Resources Needed Start and
139
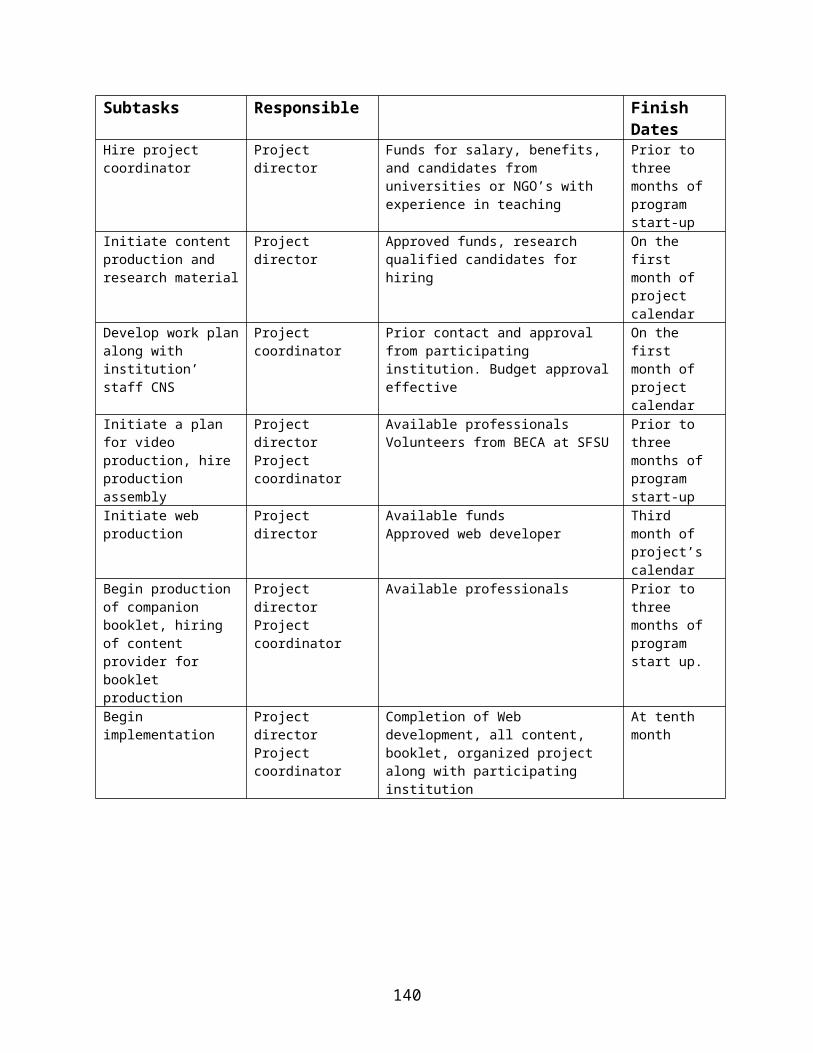
Subtasks Responsible Finish Dates
Hire project coordinator
Project director
Funds for salary, benefits, and candidates from universities or NGO’s with experience in teaching
Prior to three months of program start-up
Initiate content production and research material
Project director
Approved funds, research qualified candidates for hiring
On the first month of project calendar
Develop work planalong with institution’ staff CNS
Project coordinator
Prior contact and approval from participating institution. Budget approvaleffective
On the first month of project calendar
Initiate a plan for video production, hire production assembly
Project directorProject coordinator
Available professionalsVolunteers from BECA at SFSU
Prior to three months of program start-up
Initiate web production
Project director
Available fundsApproved web developer
Third month of project’s calendar
Begin production of companion booklet, hiring of content provider for booklet production
Project directorProject coordinator
Available professionals Prior to three months of program start up.
Begin implementation
Project directorProject coordinator
Completion of Web development, all content, booklet, organized project along with participating institution
At tenth month
140
Appendix C 1-3
Web-site sample diagrams
141

Appendix C-1: Web-site sample diagram
142
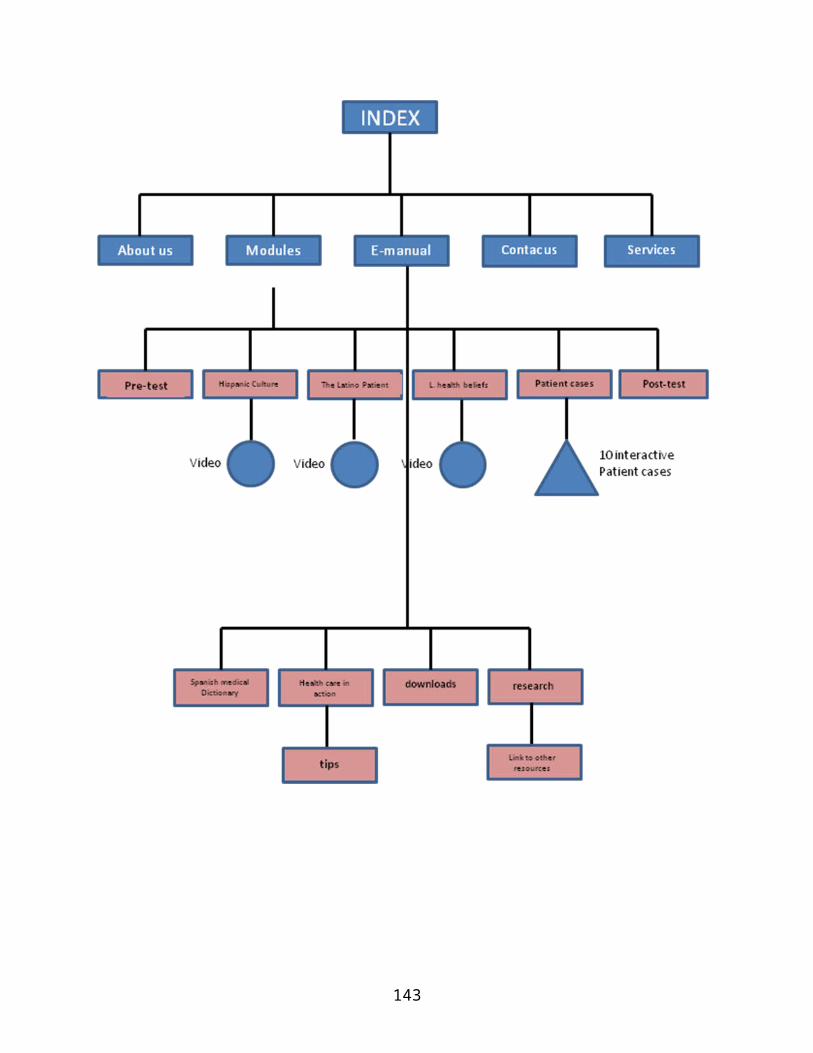
143
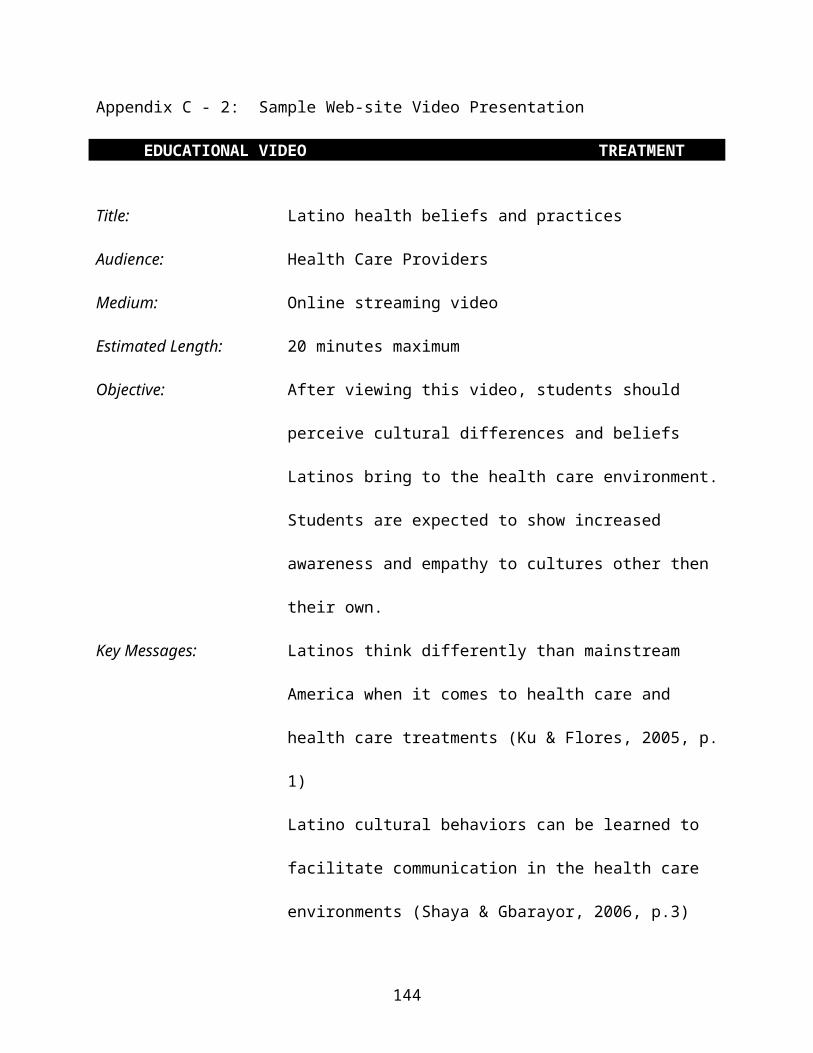
Appendix C - 2: Sample Web-site Video Presentation JCM
EDUCATIONAL VIDEO TREATMENT 352: Corporate Video Sample Treatment
Title: Latino health beliefs and practices
Audience: Health Care Providers
Medium: Online streaming video
Estimated Length: 20 minutes maximum
Objective: After viewing this video, students should
perceive cultural differences and beliefs
Latinos bring to the health care environment.
Students are expected to show increased
awareness and empathy to cultures other then
their own.
Key Messages: Latinos think differently than mainstream
America when it comes to health care and
health care treatments (Ku & Flores, 2005, p.
1)
Latino cultural behaviors can be learned to
facilitate communication in the health care
environments (Shaya & Gbarayor, 2006, p.3)
144
Learning to recognize and understand these
cultural differences can enhance HCP ability
to deal with Latinos (Betancourt & Maina,
2007, p.5).
The following is a description of Latino health beliefs and practices video
presentation. The percentages (given in parentheses) indicate the
amount of emphasis each section will have.
1. Introduction (10 percent)
This is the attention grabber and it should let the viewer know
what this video is all about. The piece opens with a long shot of
an undisclosed hospital. Cut to a shot of the admission desk, we
see emergencies coming through the door on a busy day. (dramatic
music) People are waiting at the lounge and some patients are
feeling ill or frustrated. A Latino family brings their daughter
with bruises to the head. Cut to flash back style shots of how
this accident took place as the Latino family hurriedly describes
the accident of their child who is badly bruised and bloody. The
parents repeat constantly in broken English “hit herself…hit
145
herself” with a heavy Spanish accent. The poor cultural
proficiency of HCP led them to understand the child was abused by
some family member as they assume that the parents were trying to
say that someone hit herself.
Following we see a sequence of shots which let the audience know
the parents are signing the custody of their two children.
Presenter on camera (American Latino): “If Lucia received
inappropriate care owing to the doctor’s misinterpretation , she
would not be alone”…narrator explains how this is a common
problem in emergency rooms and hospitals where misinterpretation
of cases takes place every day and wrong diagnosis can occur.
Graphics and shots of similar cases are presented displaying how
wrong diagnosis can result in serious injuries and deaths,
leading to millions of dollars in lawsuits. “A similar case
happened with a 12 year old boy in a Boston emergency room”…As
the narrator tell the story; photos of the new case are
introduced. “Problems such as this can be greatly diminished if
cultural competency is achieved among HCP (Glenn, 2006).
Presenter enters addressing the audience, graphic remain in
background. Music fades out. “In order to understand the Latino
146
patients we first must know to some degree, who are the Latinos?”
cut to a graphic with words: UNDERSTANDING THE LATINO PATIENT.
2. Understanding the Latino patient (15 percent)
Voice over: “Where do they come from? What is their culture like?
How do they think about their health? (Campos, 2007, p. 42)
Language can become an obvious barrier, challenge, and a point of
identity when working with Latino patients that it can sometimes
obscure other critical more subtle aspects of cross cultural
understanding”. Narration introduces the importance of being
culturally aware and how it can be an asset to health care
professionals (Fernandez, 2005, p. 14). (pictures and shots of
Latinos in their country of origin, Latinos in the United States,
Hispanic culturally related items). Cut to a sequence of small
interviews and statements edited in fast pace by several Latino
community members such as a University professor, street ice
cream vendor, doctor and a house wife. Ice cream vendor on
camera: “We’re a touching people. If you’re more than a handshake
distance from your customer or patient you’re too far” (Homestead
Schools, Inc, 2004, P. 13). In another shot the Latino doctor
147
says that in the early 80’s the American Diabetic Association had
nothing in the Latino diet and it was hard to make a plan for
Latinos but now things are changing (Campos, 2007, p. 7).
Statements should represent widely accepted views of Latinos have
about their cultural group. Narrator: “Let’s talk more in detail
about some common characteristics.
3. Common characteristics (20 percent)
The following is an introduction and brief explanation of
characteristic traits known and studied by cultural competency
educational courses. These items are: personalismo, confianza, respecto,
family structures, communication and social interaction, simapatia and time
orientation (appendix G, P. 104; Homestead Schools, Inc, 2004, P.
13). The following segment goes in detail over each of these
traits. Narrator will explain these items in the following order
or combine them when necessary. Using the same treatment adopted
throughout the video, this segment will combine on on-camera
narrator, voice over and a combination of pictures and graphics
providing a rich visual content aimed at maintaining interest
from the audience. Re-enactment scenes displaying interactions
148
concerning the items being explained will be shown at this point.
At the end of this segment the Narrator will introduce the next
section. Voice over: “But how does that apply to health care?
What are the key health concepts, Latinos bring to hospitals and
clinics when they seek help? (Ngo-Metzger et al., 2007, p.
2)...music up
4. Concepts of health for Latinos and related concerns among Latino patients (25 percent)
Music slows down, goes under. “Next we will talk about how
Latinos generally view health and illness (the hot and cold
principle), how do they view treatments (the concepts of the four
body humors) and some of the strategies that can use to better
communicate with the Latino patient (Homestead Schools, Inc,
2004, P. 13; appendix G, P. 104). More graphics and voice over
than footage are displayed in this segment. At the end of this
segment there will be a listing of related concerns and what are
the potential problems and health conditions HCP should be paying
attention in regards to Latino patients (Homestead Schools, Inc,
2004, P. 13). Voice over: “After learning health care concerns of
Latinos how do we promote health and prevent illnesses among
149
Latinos” segue into next segment (Kripalani, Jones, Katz & Genao,
2006, p. 6; Homestead Schools, Inc, 2004, P. 13).
5. Promotion and prevention (25 percent)
Music slows down, under, voice over. “In this segment we will
learn how to better promote health among Latinos by understanding
the importance and relevancy of family, traditional healing
methods, their views of western medicine and religious beliefs”
(Homestead Schools, Inc, 2004, P. 13) . Cut to a shot of a Latina
talking to a nurse. The narrator will explore why Latinos have a
difficulties using preventative medicine. Some of the common
statements Latinos use suggesting health is the result of luck or
fate and how to better approach these statements positively. Next
the video will explore how Latinos rely on family and friends and
its effects on treatment. Finally this segment will end with a
brief description of common botanical remedies used by Latinos
and what to look for in patients (Homestead Schools, Inc, 2004,
P. 13).
6. Conclusion (5 percent)
150
Music segue. Dissolve back to shot of narrator/presenter. He
addresses the camera: The conclusion is brief and specific.
Narrator on camera reiterates material just covered. Some
suggestions for better communications with Latinos, and some
bullet point graphics. Music up and video ends.
Appendix C - 3: Sample Web-site interactive video page
151
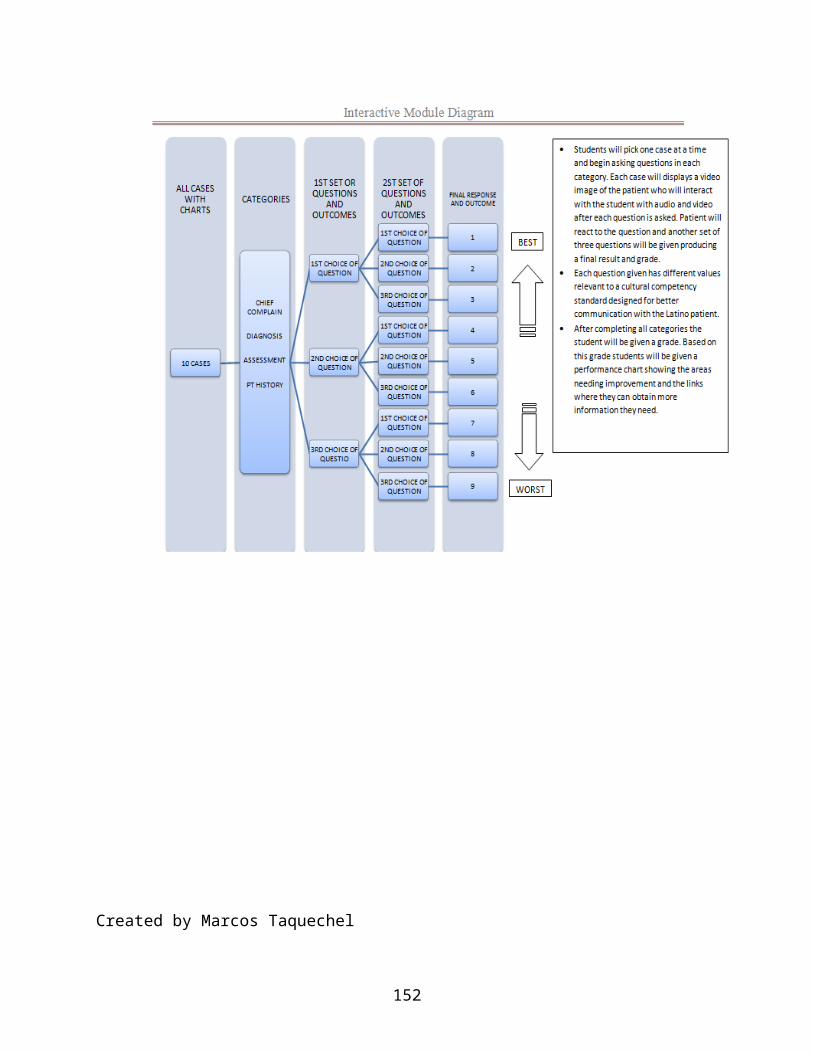
Created by Marcos Taquechel
152

Appendix D:
Communication model diagram
153
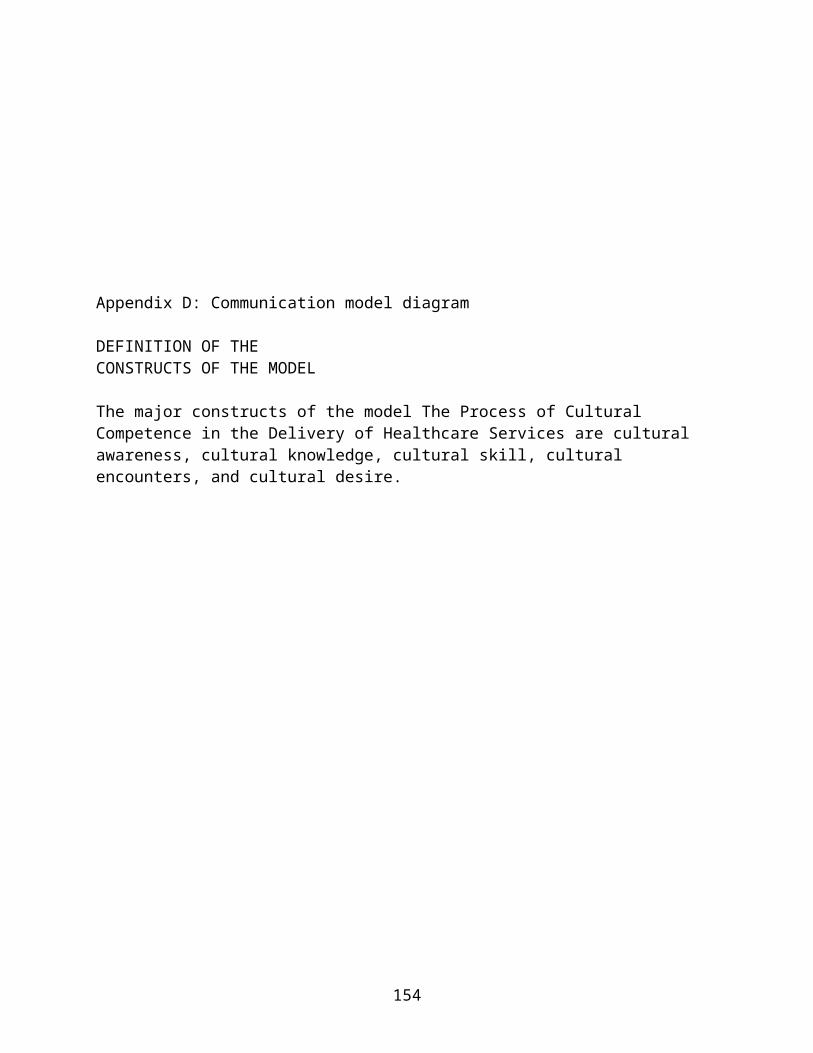
Appendix D: Communication model diagram
DEFINITION OF THECONSTRUCTS OF THE MODEL
The major constructs of the model The Process of CulturalCompetence in the Delivery of Healthcare Services are culturalawareness, cultural knowledge, cultural skill, culturalencounters, and cultural desire.
154
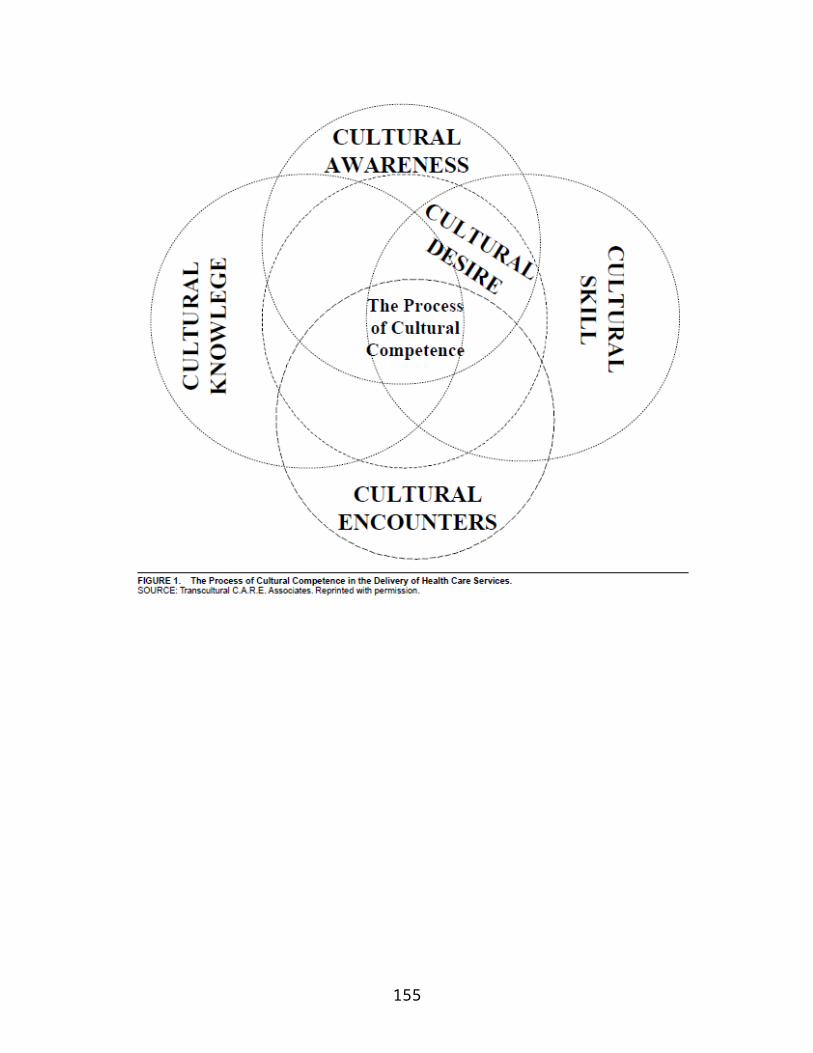
155

Appendix E:
Evaluation Methods
Appendix E: Evaluation Methods
156
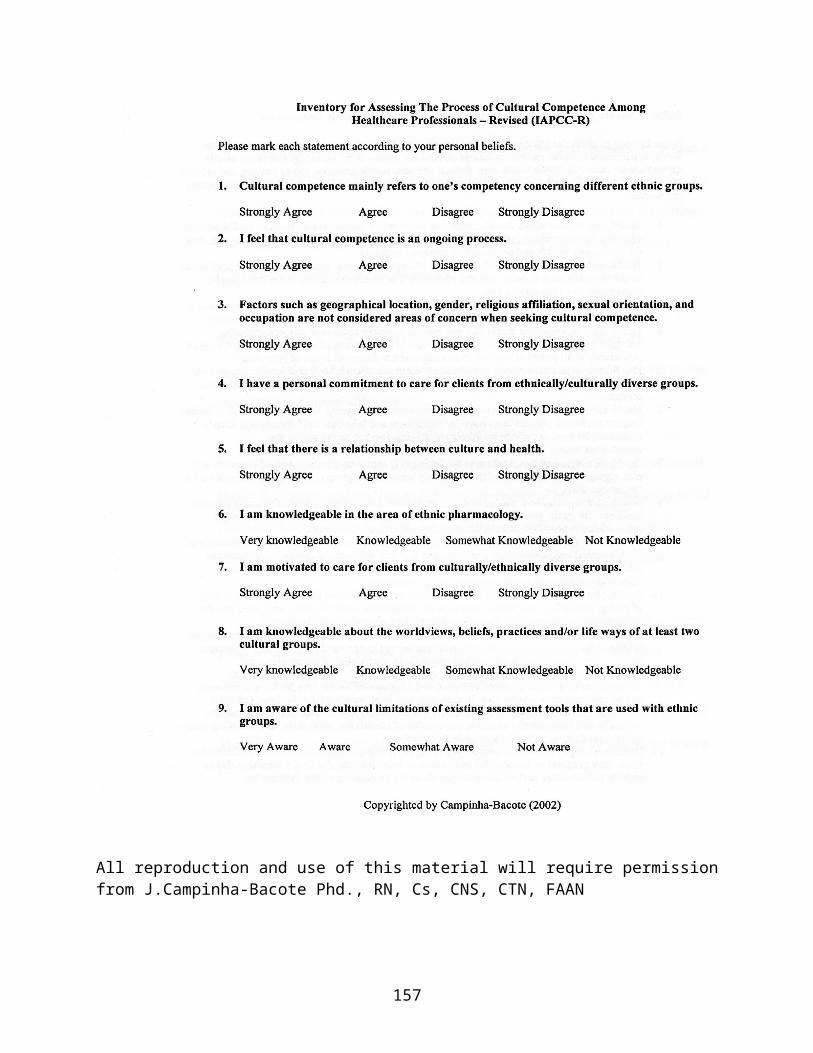
All reproduction and use of this material will require permissionfrom J.Campinha-Bacote Phd., RN, Cs, CNS, CTN, FAAN
157
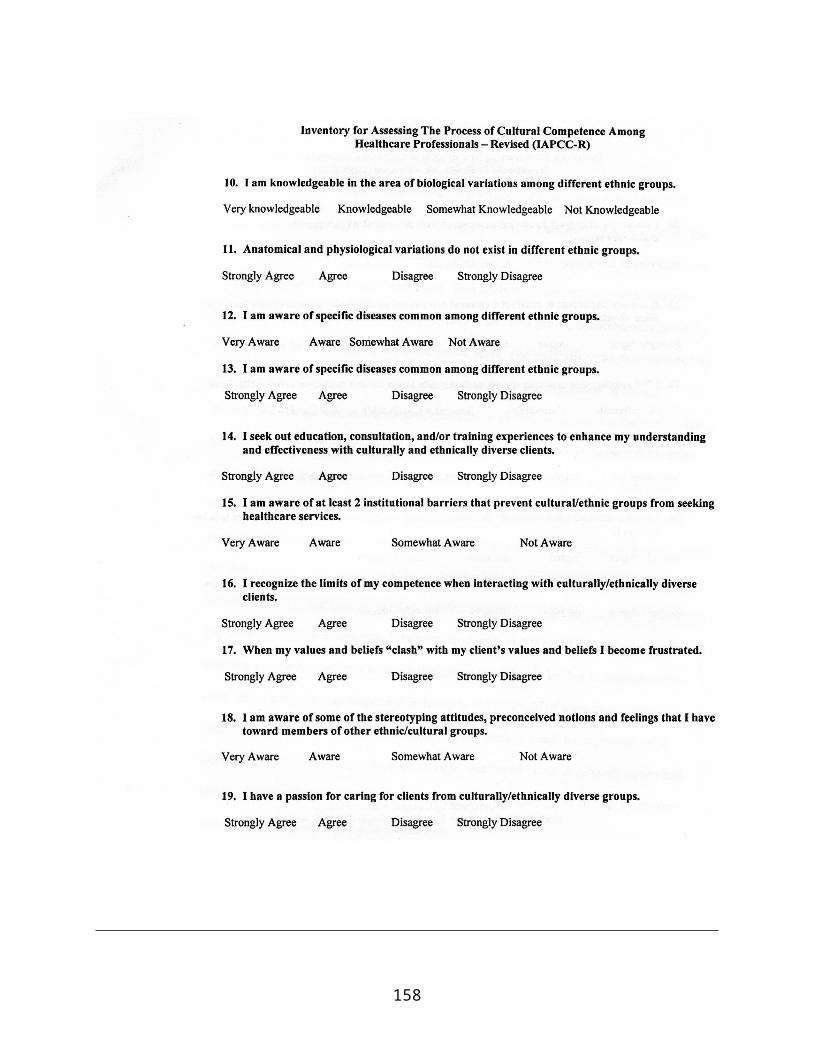
158
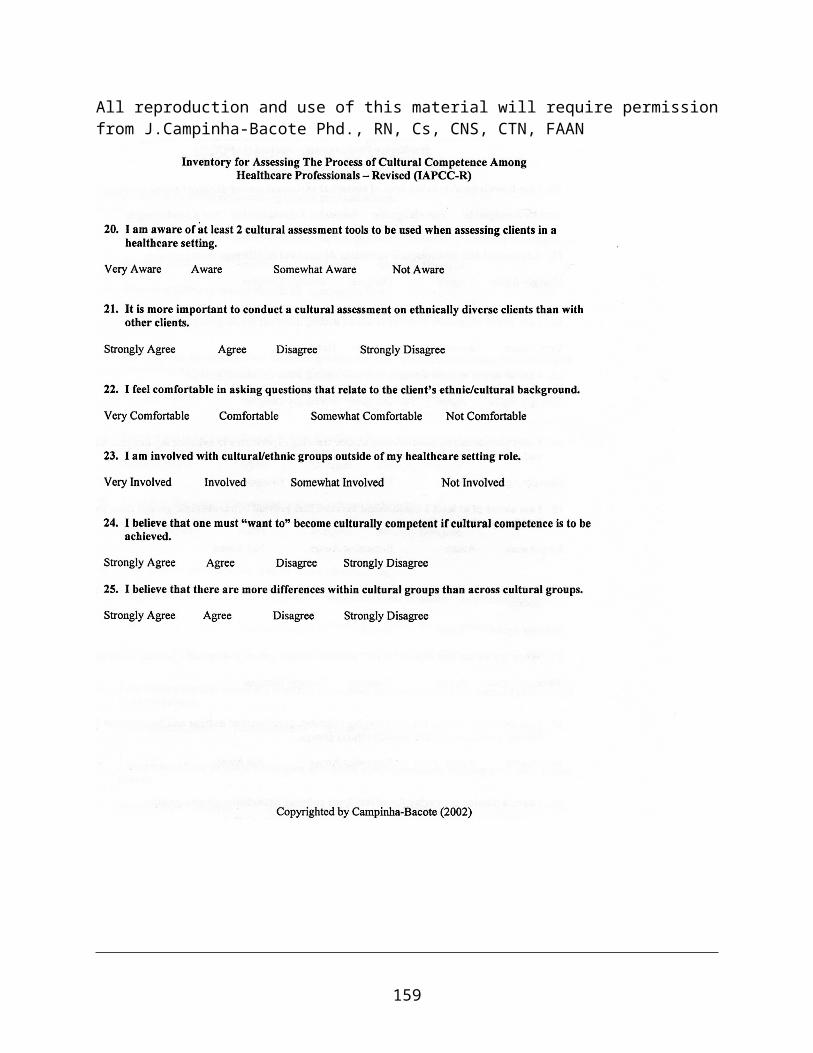
All reproduction and use of this material will require permissionfrom J.Campinha-Bacote Phd., RN, Cs, CNS, CTN, FAAN
159
All reproduction and use of this material will require permissionfrom J.Campinha-Bacote Phd., RN, Cs, CNS, CTN, FAAN
Appendix F:
Pre Test and Post test
160
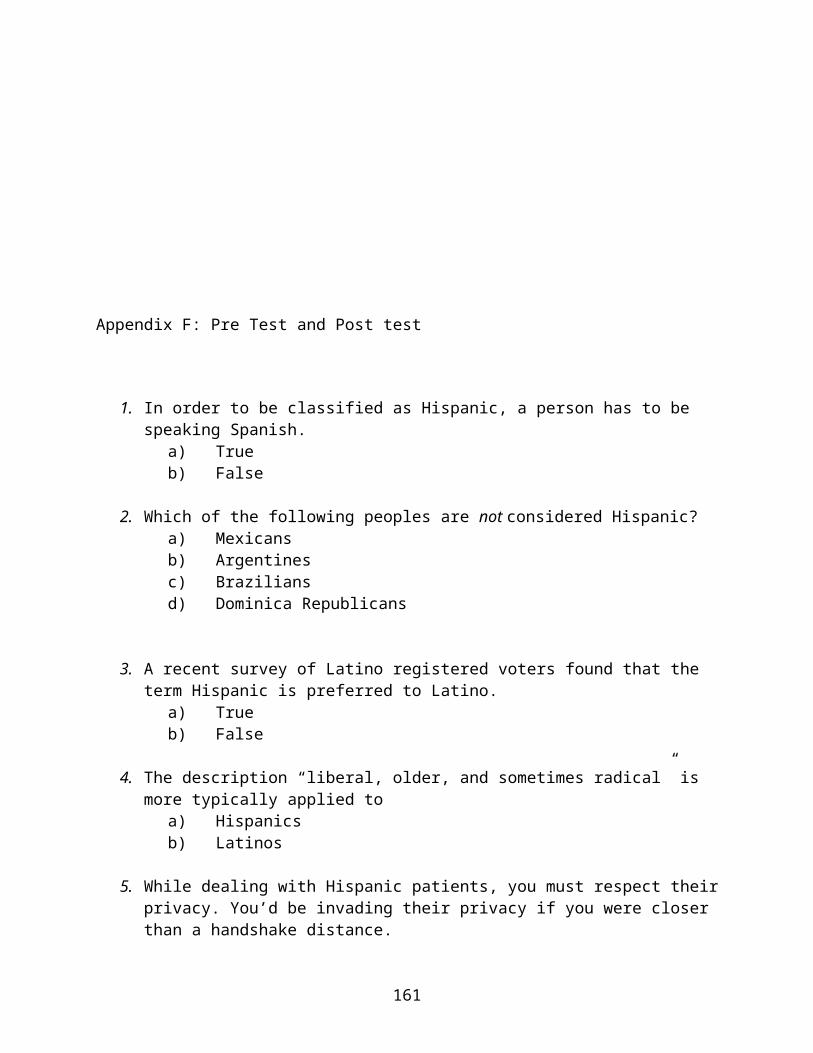
Appendix F: Pre Test and Post test
1. In order to be classified as Hispanic, a person has to be speaking Spanish.
a) Trueb) False
2. Which of the following peoples are not considered Hispanic?a) Mexicansb) Argentinesc) Braziliansd) Dominica Republicans
3. A recent survey of Latino registered voters found that the term Hispanic is preferred to Latino.
a) Trueb) False
4. The description “liberal, older, and sometimes radical” is more typically applied to
a) Hispanicsb) Latinos
5. While dealing with Hispanic patients, you must respect theirprivacy. You’d be invading their privacy if you were closer than a handshake distance.
161
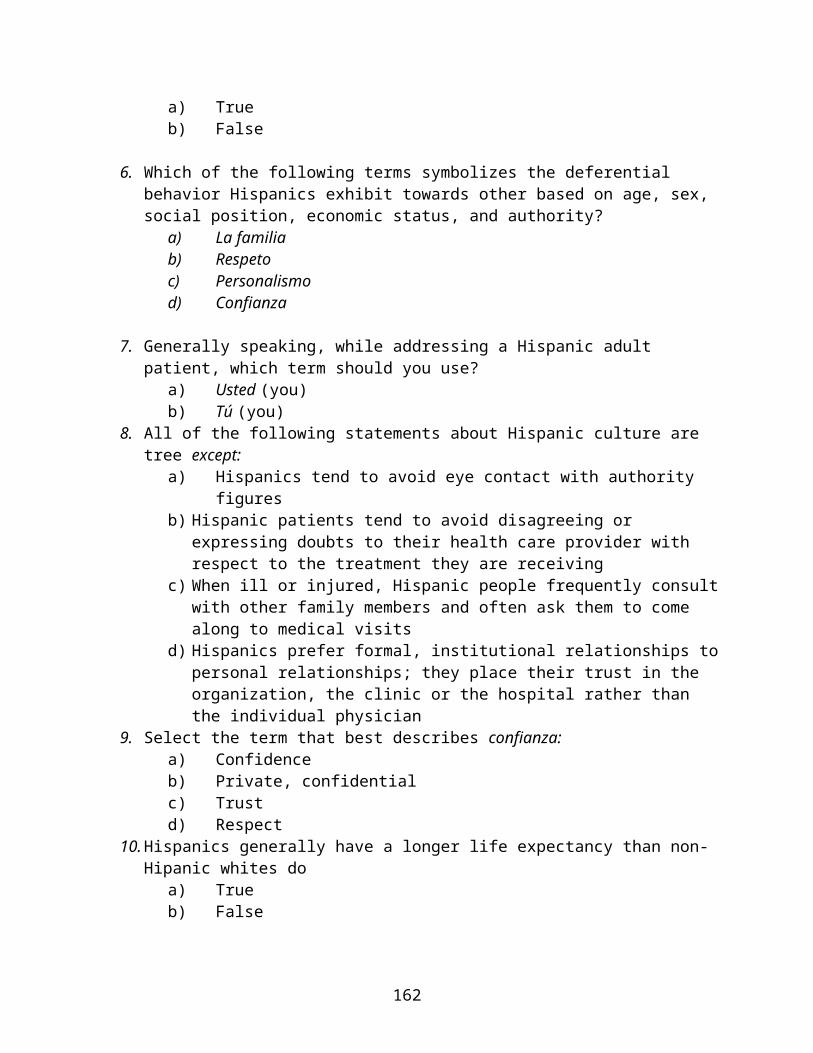
a) Trueb) False
6. Which of the following terms symbolizes the deferential behavior Hispanics exhibit towards other based on age, sex, social position, economic status, and authority?
a) La familiab) Respetoc) Personalismod) Confianza
7. Generally speaking, while addressing a Hispanic adult patient, which term should you use?
a) Usted (you)b) Tú (you)
8. All of the following statements about Hispanic culture are tree except:
a) Hispanics tend to avoid eye contact with authority figures
b) Hispanic patients tend to avoid disagreeing or expressing doubts to their health care provider with respect to the treatment they are receiving
c) When ill or injured, Hispanic people frequently consultwith other family members and often ask them to come along to medical visits
d) Hispanics prefer formal, institutional relationships topersonal relationships; they place their trust in the organization, the clinic or the hospital rather than the individual physician
9. Select the term that best describes confianza:a) Confidenceb) Private, confidentialc) Trustd) Respect
10.Hispanics generally have a longer life expectancy than non-Hipanic whites do
a) Trueb) False
162
11.Identify the leading cause of death for Hispanics of all agegroups
a) Accidentsb) Cancerc) Homicided) Heart disease
12.Select the true statement belowa) Hispanic adults have the lowest rates of smokingb) Hispanic teenagers have the highest rates of smoking
among all their peersc) Both of the aboved) None of the above
13.Which of the following groups has the lowest rate of breast-feeding their infants?
a) Hispanic womenb) Non-Hispanic white womanc) Non-Hispanic black woman
14.Which group tops the list in terms of unhealthy weight?a) Non-Hispanic whitesb) Mexican Americansc) Non-Hispanic blacks
15.A lifestyle issue facing the Hispanic community is excessivealcohol use. Data indicate that rates of alcohol use_________with acculturation among all U.S. Hispanic groups
a) Increaseb) Decrease
All reproduction and use of this material will require permissionfrom Nursing a Hispanic Patient, Homestead schools©
163

Appendix G:
Introductory Brochure
With permission of Homestead Schools, Inc. (2004).
164
165
Top Related
Copyright © 2022 FDOKUMEN

