







Bahasa
Halaman
Hukum

Journal of the Renin-Angiotensin-Aldosterone System 1 –10© The Author(s) 2015Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1470320315600086jra.sagepub.com
Creative Commons CC-BY-NC: This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 3.0 License (http://www.creativecommons.org/licenses/by-nc/3.0/) which permits non-commercial use, reproduction and
distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access page (https://us.sagepub.com/en-us/nam/open-access-at-sage).
Introduction
Hypertension is a major risk factor for cardiovascular and cerebrovascular diseases and mortality,1–4 affecting approximately 1 billion individuals worldwide.5 It is esti-mated that this number will escalate to more than 1.56 bil-lion by the year 2025,6 putting a tremendous burden on our health care systems.6–9 Hypertension is also a complex dis-ease influenced by an interaction between environmental and genetic factors.10 Regarding these environmental fac-tors, lifestyle changes, including physical activity, play a primordial role in the prevention and treatment of high blood pressure (BP).11,12 There is substantial evidence sup-porting the beneficial effect of aerobic endurance training on resting and ambulatory BP (ABP).13–18 In addition, it has also been demonstrated that one single bout of endur-ance exercise may cause a transient reduction in BP for
prolonged periods of time.11,19–23 This phenomenon has been called postexercise hypotension (PEH)11,21,22 and may vary in magnitude and duration depending on the exercise characteristics.16,24,25 However, it is also widely
ACE polymorphisms and the acute response of blood pressure to a walk in medicated hypertensive patients
Karla F Goessler1,2, Véronique A Cornelissen2, Edilamar M de Oliveira3, Glória de F Mota3 and Marcos D Polito1
AbstractHypothesis/Introduction: Polymorphisms of the angiotensin converting enzyme (ACE) gene can interfere with exercise-induced acute blood pressure (BP) reduction. This cross-over study investigated the acute effect of a single walk on BP and tested whether polymorphisms of the ACE gene might explain the variation in BP responses.Materials and methods: Thirty-four healthy medicated individuals were randomized to one control and one walking session at 60–75% of heart rate reserve. Subjects left the laboratory wearing an ambulatory BP monitor until waking the next morning.Results: Overall, systolic BP was somewhat lower following the walking session (p=.06), which could be attributed to a consistently lower systolic BP for 5 h after exercise (p-interaction<.04) compared with control rest. Similarly, II/ID individuals had a lower systolic BP (p-interaction=.02) and diastolic BP (p-interaction<.01) for 5 h after walking compared with control rest. Among DD individuals, a single walk did not induce a reduction in BP (p-interaction>.05).Conclusions: Our results showed that postexercise hypotension can occur after a walk at moderate intensity in carriers of the I allele; we were not able to demonstrate this in DD individuals. Our results suggest that genetic variation in the ACE gene might affect the BP response to exercise, although more research is needed to confirm these findings.
KeywordsAmbulatory blood pressure monitoring, postexercise hypotension, genetic polymorphisms, renin-angiotensin-aldosterone system, aerobic exercise.
Date received: 23 March 2014; accepted: 20 June 2015
1 Research Group of Cardiovascular Response and Exercise, State University of Londrina, Brazil
2 Research Group of Cardiovascular Rehabilitation, Department of Rehabilitation Sciences, KU Leuven, Belgium
3School of Physical Education and Sport, University of São Paulo, Brazil
Corresponding author:Karla F Goessler, State University of Londrina, Department of Physical Education, Rodovia Celso Garcia Cid, PR445 Km 380, zipcode: 86051-990, Londrina-PR, Brazil. Email: [email protected]
600086 JRA0010.1177/1470320315600086Journal of the Renin-Angiotensin-Aldosterone SystemGoessler et al.research-article2015
Original Article
by guest on August 22, 2015jra.sagepub.comDownloaded from

2 Journal of the Renin-Angiotensin-Aldosterone System
known that not all individuals respond in the same way to such an acute bout of exercise or to exercise training, which might partly be explained by genetic variations.26 The HEalth, RIsk factors, exercise Training And Genetics (HERITAGE) family study concluded that genetic factors explain up to 17% of the training-induced reduction in sys-tolic BP (SBP).27
The renin-angiotensin-aldosterone system (RAAS) is an important BP-regulating mechanism, with angiotensin II (Ang II) being an important and powerful vasoconstric-tor, increasing renal sodium and fluid reabsorption by aldosterone release, and consequently resulting in an increase in BP.10 Given its role in BP regulation, it is rea-sonable to assume that genetic variations in the RAAS influence BP and its response to exercise. Indeed, earlier studies already demonstrated that individuals with the deletion polymorphism (DD) of the angiotensin convert-ing enzyme (ACE) gene have higher circulating ACE lev-els compared with individuals with the insertion polymorphism (II),28–30 resulting in a higher BP and an increased risk for hypertension in DD homozygotes.31–34 Less is known about the role of the RAAS system and its polymorphisms in BP reduction following a single exer-cise session. It is generally accepted that in most subjects, PEH is due to a persistent drop in vascular resistance, which is not completely offset by increases in cardiac out-put.35 Although the mechanisms of the vasodilatation underlying this PEH largely remain to be elucidated, changes in the sympathetic nervous system and nitric oxide (NO) have all been implicated,35–38 with studies demonstrating an association between RAAS and these mechanisms.39,40 Similarly, ACE polymorphisms have also been shown to be related to NO release postexercise, with carriers of the I allele presenting greater NO bioavailabil-ity after a single bout of aerobic exercise compared with DD individuals, and consequently larger PEH.40 Finally, exercise also triggers an increase in release of Ang (1–7) as well as ACE2, which are vasodilators, leading to greater NO production and resulting in a reduction in BP.36 To the best of our knowledge, only a few studies have directly investigated the effects of ACE polymorphisms on post-aerobic exercise hypotension.19,26,40,41 Blanchard et al.26 observed a lower SBP in DD individuals compared with individuals with an I allele after light-intensity exercise (40% VO2max) but not following moderate intensity exer-cise (60% VO2max). On the other hand, Santana et al.40 showed a significantly larger decrease in SBP over the course of 1 h after a maximal incremental cycle test and a single bout of exercise at 90% of anaerobic threshold in II/ID individuals compared with DD.
Nevertheless, participants in these studies were unmed-icated healthy patients, or had been treated with medica-tion but undergone a washout period before enrollment in the study. However, today, 58.9% of the population are treated with BP-lowering medication.42 Therefore, it
would be of interest to see whether exercise still has some adjunctive effect in reducing BP in patients already treated with medication. Therefore, given the current limited and inconsistent results, we aimed in the present study (1) to investigate the acute effect of one single walking session at moderate intensity on PEH and (2) to test whether poly-morphisms of the ACE gene contribute to the variation in PEH response in medicated patients.
Methods
Subjects
Potential participants were recruited by means of announcements in journals and magazines and on the internet. After being screened and signing the informed consent, 34 individuals (Table 1) performed one control session and one exercise session. The inclusion criteria were: healthy men or women without known cardiovascu-lar or pulmonary disease, age ⩾40 years, non-smokers, clinically diagnosed with hypertension according to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure5 and having been treated for at least 3 months with antihypertensive medication acting on RAAS. The study was approved by the Research Ethics Committee of the State University of Londrina - Brazil (232/2013).
Study design
This study was performed as a randomized controlled cross-over trial. During the screening visit, patients received information about the study and filled in a ques-tionnaire about their habitual physical activity behavior, medication and medical history. In addition, anthropomet-rics (height and weight) and resting BP were assessed, and volunteers completed a maximal graded exercise test on a treadmill (T170, h/p/cosmos, Traunstein, Germany) until volitional exhaustion using an individualized ramp proto-col.43 The criteria for test interruption followed the recom-mendations of the American Heart Association.44 The oxygen uptake was evaluated continuously by a breath by breath analysis of expired gases (QuarKCPET, Cosmed, Rome, Italy), and a polar heart rate (HR) monitor (FS1, Polar, Kempele, Finland) was used to assess the HR. Peak oxygen consumption (VO2 peak) was defined as the mean oxygen uptake of the final 30 s of the exercise test. The maximal duration of the test was between 7 and 12 min. This test was used to define the target HR for the exercise session and to evaluate the current physical fitness of the participants.
Following this visit and having signed the informed consent, participants returned to the laboratory twice, dur-ing which they completed the control and the exercise
by guest on August 22, 2015jra.sagepub.comDownloaded from
Goessler et al. 3
session. The randomization order was determined by a computer program (http://www.random.org/). All tests were performed in the morning (9:00–12:00) at the same time of day for each individual patient to control for diur-nal variation in BP and to avoid any influence of time of medication intake. All measurements were performed by the same investigator (KG).
Exercise and control intervention
Each session started with a 10 min seated rest period, after which BP and HR were measured by means of an auto-matic device (Omron HEM 742 INT, Comfort, Japan). This pre-intervention BP was measured three times with a 5 min interval between measurements. Following pre-intervention measurements, each volunteer performed one of the two sessions in random order: a control session of seated rest and one walking session of 55 min, including a warming up and cooling down of 5 min each and 45 min of walking at 60–75% of HR reserve. During the supervised walking session, training intensity was controlled by a HR monitor (FT1, Polar, Kempele, Finland).
Ambulatory blood pressure monitoring
After the exercise and control sessions, individuals left the laboratory wearing an ABP device (Meditech, ABPM04, Budapest, Hungary) on the left arm until waking the next
morning. The ABP monitor was programmed to measure BP every 30 min, and the first BP reading was assessed 30 min following the sessions. Patients were instructed to proceed with their normal daily activities and were asked to fill in an activity diary. Daytime ABP was defined as the average of all BPs recorded between 06:00 and 22:00; nighttime BP was defined as the mean BP of all values between 22:00 and 06:00. All ABP readings were manu-ally checked and invalid measurements were excluded. A reading was considered invalid if it differed by more than 40 mmHg from the previous and the next reading and this could not be explained by a change in physical activity. We subsequently manually calculated hourly averages on the edited data.
Blood sampling and ACE genotyping
Blood samples (5 ml) were collected from the brachial artery during the screening visit and prepared by an inde-pendent biochemical laboratory (The Novaes Center for Clinical Analysis), after which they were stored at −80ºC. Genotyping was performed by the polymerase chain reac-tion (PCR) method45 at the Laboratory of Biomechanical and Molecular Biology (University of São Paulo). DNA was extracted from whole blood and the ACE gene (II/ID and DD) was determined by means of a two-primer system (I/D: forward: 5ʹ CTGGAGACCACTTCCCATCCTTTCT 3ʹ and reverse: 5ʹ GATGTGGCCATCACATTCGTCAGAT 3ʹ;
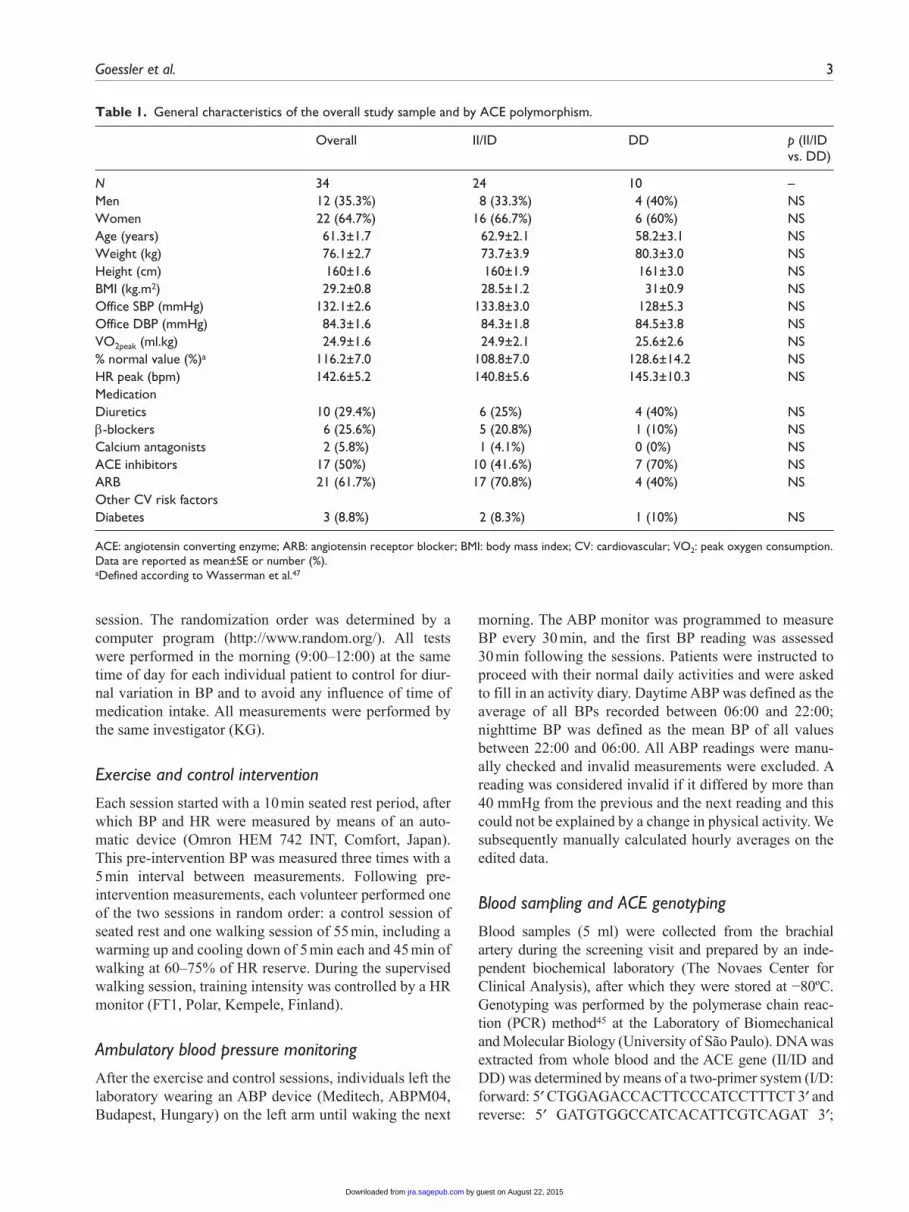
Table 1. General characteristics of the overall study sample and by ACE polymorphism.
Overall II/ID DD p (II/ID vs. DD)
N 34 24 10 –Men 12 (35.3%) 8 (33.3%) 4 (40%) NSWomen 22 (64.7%) 16 (66.7%) 6 (60%) NSAge (years) 61.3±1.7 62.9±2.1 58.2±3.1 NSWeight (kg) 76.1±2.7 73.7±3.9 80.3±3.0 NSHeight (cm) 160±1.6 160±1.9 161±3.0 NSBMI (kg.m2) 29.2±0.8 28.5±1.2 31±0.9 NSOffice SBP (mmHg) 132.1±2.6 133.8±3.0 128±5.3 NSOffice DBP (mmHg) 84.3±1.6 84.3±1.8 84.5±3.8 NSVO2peak (ml.kg) 24.9±1.6 24.9±2.1 25.6±2.6 NS% normal value (%)a 116.2±7.0 108.8±7.0 128.6±14.2 NSHR peak (bpm) 142.6±5.2 140.8±5.6 145.3±10.3 NSMedication Diuretics 10 (29.4%) 6 (25%) 4 (40%) NSβ-blockers 6 (25.6%) 5 (20.8%) 1 (10%) NSCalcium antagonists 2 (5.8%) 1 (4.1%) 0 (0%) NSACE inhibitors 17 (50%) 10 (41.6%) 7 (70%) NSARB 21 (61.7%) 17 (70.8%) 4 (40%) NSOther CV risk factors Diabetes 3 (8.8%) 2 (8.3%) 1 (10%) NS
ACE: angiotensin converting enzyme; ARB: angiotensin receptor blocker; BMI: body mass index; CV: cardiovascular; VO2: peak oxygen consumption.Data are reported as mean±SE or number (%).aDefined according to Wasserman et al.47
by guest on August 22, 2015jra.sagepub.comDownloaded from
4 Journal of the Renin-Angiotensin-Aldosterone System
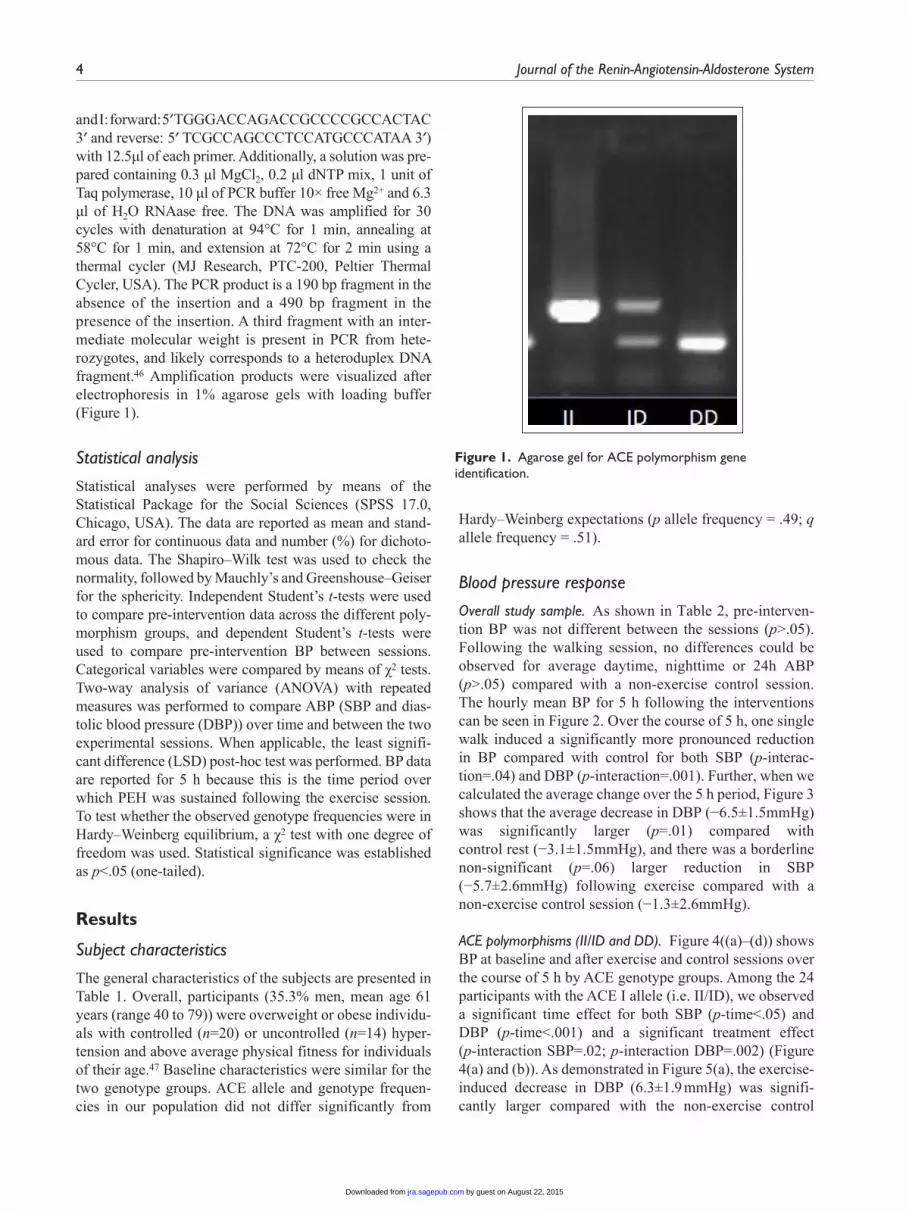
and I: forward: 5ʹ TGGGACCAGACCGCCCCGCCACTAC 3ʹ and reverse: 5ʹ TCGCCAGCCCTCCATGCCCATAA 3ʹ) with 12.5µl of each primer. Additionally, a solution was pre-pared containing 0.3 µl MgCl2, 0.2 µl dNTP mix, 1 unit of Taq polymerase, 10 µl of PCR buffer 10× free Mg2+ and 6.3 µl of H2O RNAase free. The DNA was amplified for 30 cycles with denaturation at 94°C for 1 min, annealing at 58°C for 1 min, and extension at 72°C for 2 min using a thermal cycler (MJ Research, PTC-200, Peltier Thermal Cycler, USA). The PCR product is a 190 bp fragment in the absence of the insertion and a 490 bp fragment in the presence of the insertion. A third fragment with an inter-mediate molecular weight is present in PCR from hete-rozygotes, and likely corresponds to a heteroduplex DNA fragment.46 Amplification products were visualized after electrophoresis in 1% agarose gels with loading buffer (Figure 1).
Statistical analysis
Statistical analyses were performed by means of the Statistical Package for the Social Sciences (SPSS 17.0, Chicago, USA). The data are reported as mean and stand-ard error for continuous data and number (%) for dichoto-mous data. The Shapiro–Wilk test was used to check the normality, followed by Mauchly’s and Greenshouse–Geiser for the sphericity. Independent Student’s t-tests were used to compare pre-intervention data across the different poly-morphism groups, and dependent Student’s t-tests were used to compare pre-intervention BP between sessions. Categorical variables were compared by means of χ2 tests. Two-way analysis of variance (ANOVA) with repeated measures was performed to compare ABP (SBP and dias-tolic blood pressure (DBP)) over time and between the two experimental sessions. When applicable, the least signifi-cant difference (LSD) post-hoc test was performed. BP data are reported for 5 h because this is the time period over which PEH was sustained following the exercise session. To test whether the observed genotype frequencies were in Hardy–Weinberg equilibrium, a χ2 test with one degree of freedom was used. Statistical significance was established as p<.05 (one-tailed).
Results
Subject characteristics
The general characteristics of the subjects are presented in Table 1. Overall, participants (35.3% men, mean age 61 years (range 40 to 79)) were overweight or obese individu-als with controlled (n=20) or uncontrolled (n=14) hyper-tension and above average physical fitness for individuals of their age.47 Baseline characteristics were similar for the two genotype groups. ACE allele and genotype frequen-cies in our population did not differ significantly from
Hardy–Weinberg expectations (p allele frequency = .49; q allele frequency = .51).
Blood pressure response
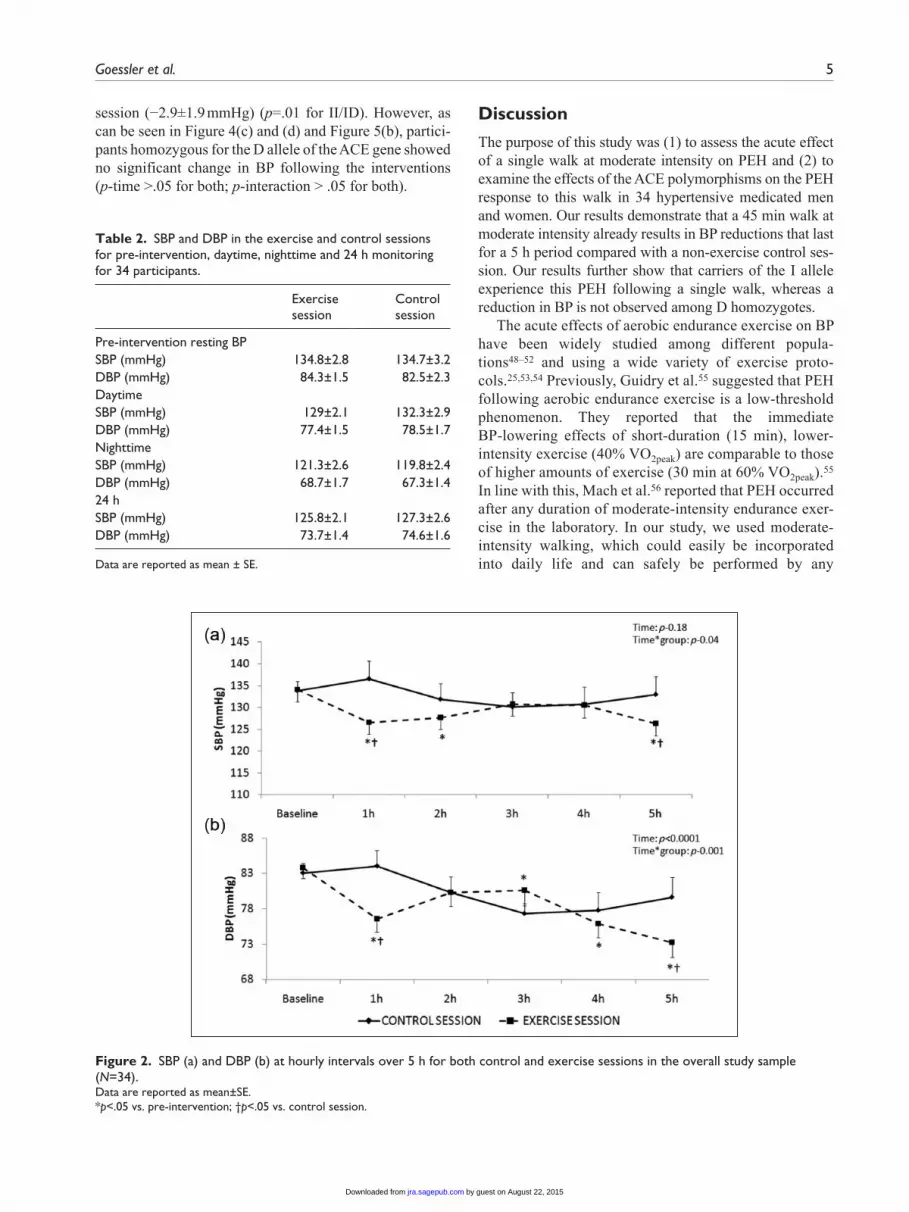
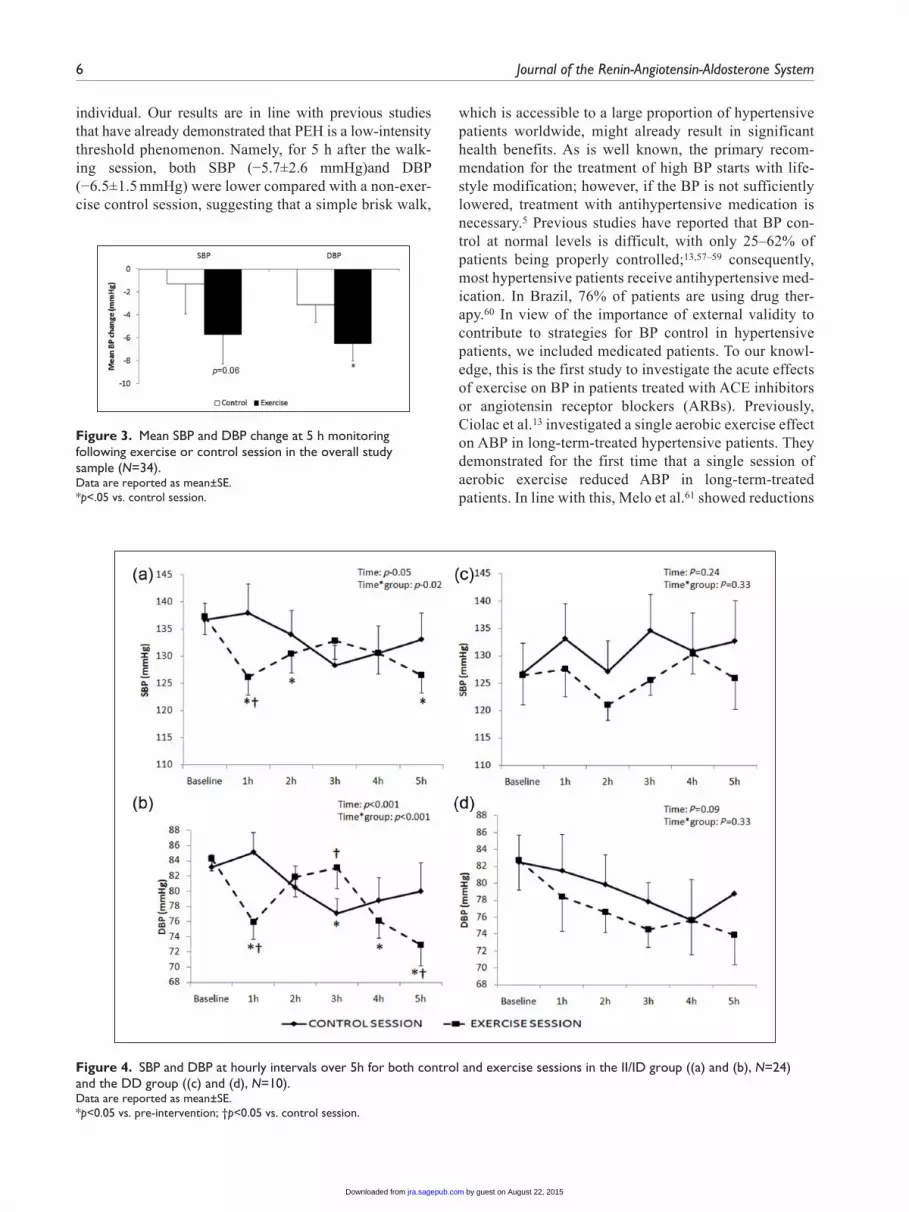
Overall study sample. As shown in Table 2, pre-interven-tion BP was not different between the sessions (p>.05). Following the walking session, no differences could be observed for average daytime, nighttime or 24h ABP (p>.05) compared with a non-exercise control session. The hourly mean BP for 5 h following the interventions can be seen in Figure 2. Over the course of 5 h, one single walk induced a significantly more pronounced reduction in BP compared with control for both SBP (p-interac-tion=.04) and DBP (p-interaction=.001). Further, when we calculated the average change over the 5 h period, Figure 3 shows that the average decrease in DBP (−6.5±1.5mmHg) was significantly larger (p=.01) compared with control rest (−3.1±1.5mmHg), and there was a borderline non-significant (p=.06) larger reduction in SBP (−5.7±2.6mmHg) following exercise compared with a non-exercise control session (−1.3±2.6mmHg).
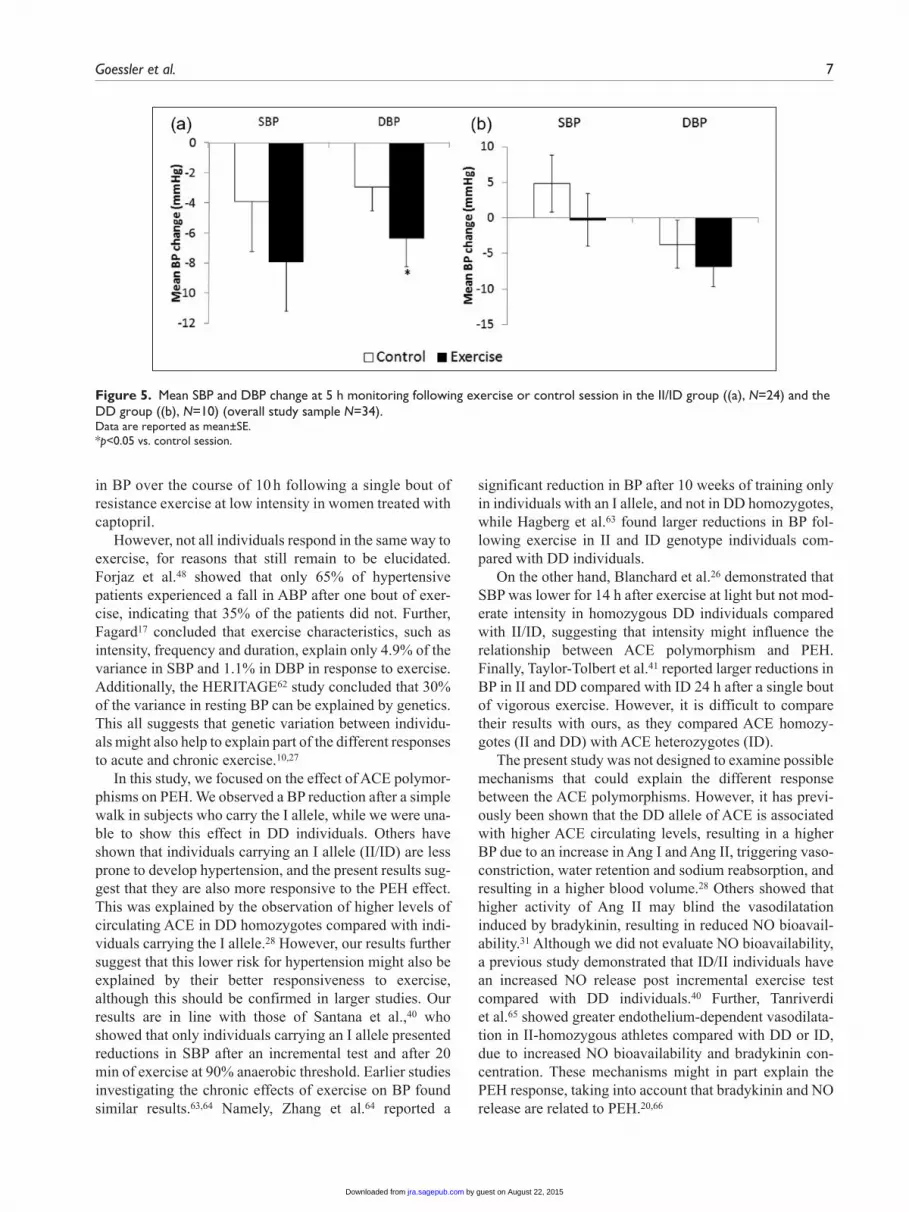
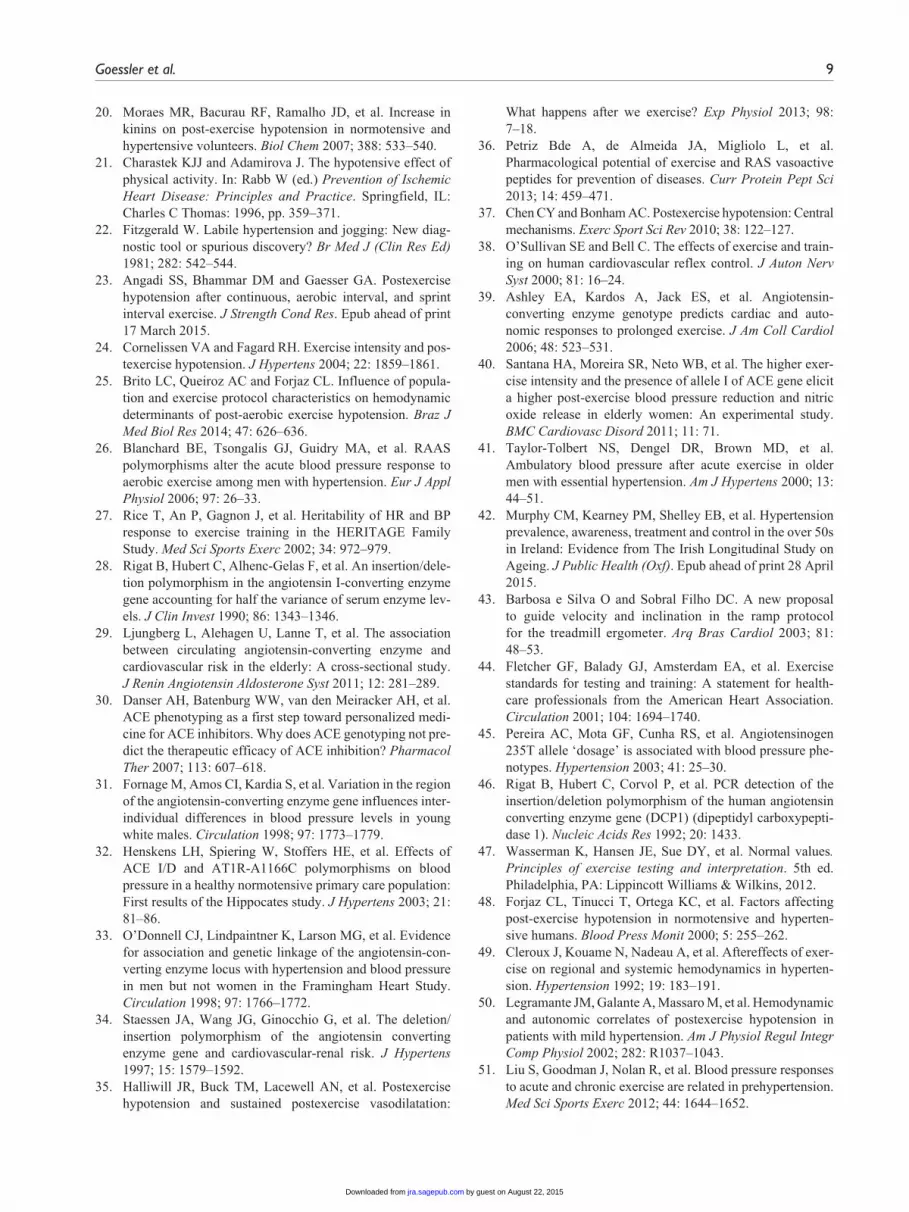
ACE polymorphisms (II/ID and DD). Figure 4((a)–(d)) shows BP at baseline and after exercise and control sessions over the course of 5 h by ACE genotype groups. Among the 24 participants with the ACE I allele (i.e. II/ID), we observed a significant time effect for both SBP (p-time<.05) and DBP (p-time<.001) and a significant treatment effect (p-interaction SBP=.02; p-interaction DBP=.002) (Figure 4(a) and (b)). As demonstrated in Figure 5(a), the exercise-induced decrease in DBP (6.3±1.9 mmHg) was signifi-cantly larger compared with the non-exercise control
Figure 1. Agarose gel for ACE polymorphism gene identification.
by guest on August 22, 2015jra.sagepub.comDownloaded from
Goessler et al. 5
session (−2.9±1.9 mmHg) (p=.01 for II/ID). However, as can be seen in Figure 4(c) and (d) and Figure 5(b), partici-pants homozygous for the D allele of the ACE gene showed no significant change in BP following the interventions (p-time >.05 for both; p-interaction > .05 for both).
Discussion
The purpose of this study was (1) to assess the acute effect of a single walk at moderate intensity on PEH and (2) to examine the effects of the ACE polymorphisms on the PEH response to this walk in 34 hypertensive medicated men and women. Our results demonstrate that a 45 min walk at moderate intensity already results in BP reductions that last for a 5 h period compared with a non-exercise control ses-sion. Our results further show that carriers of the I allele experience this PEH following a single walk, whereas a reduction in BP is not observed among D homozygotes.
The acute effects of aerobic endurance exercise on BP have been widely studied among different popula-tions48–52 and using a wide variety of exercise proto-cols.25,53,54 Previously, Guidry et al.55 suggested that PEH following aerobic endurance exercise is a low-threshold phenomenon. They reported that the immediate BP-lowering effects of short-duration (15 min), lower-intensity exercise (40% VO2peak) are comparable to those of higher amounts of exercise (30 min at 60% VO2peak).55 In line with this, Mach et al.56 reported that PEH occurred after any duration of moderate-intensity endurance exer-cise in the laboratory. In our study, we used moderate-intensity walking, which could easily be incorporated into daily life and can safely be performed by any
Table 2. SBP and DBP in the exercise and control sessions for pre-intervention, daytime, nighttime and 24 h monitoring for 34 participants.
Exercise session
Control session
Pre-intervention resting BP SBP (mmHg) 134.8±2.8 134.7±3.2DBP (mmHg) 84.3±1.5 82.5±2.3Daytime SBP (mmHg) 129±2.1 132.3±2.9DBP (mmHg) 77.4±1.5 78.5±1.7Nighttime SBP (mmHg) 121.3±2.6 119.8±2.4DBP (mmHg) 68.7±1.7 67.3±1.424 h SBP (mmHg) 125.8±2.1 127.3±2.6DBP (mmHg) 73.7±1.4 74.6±1.6
Data are reported as mean ± SE.
Figure 2. SBP (a) and DBP (b) at hourly intervals over 5 h for both control and exercise sessions in the overall study sample (N=34).Data are reported as mean±SE.*p<.05 vs. pre-intervention; †p<.05 vs. control session.
by guest on August 22, 2015jra.sagepub.comDownloaded from
6 Journal of the Renin-Angiotensin-Aldosterone System
individual. Our results are in line with previous studies that have already demonstrated that PEH is a low-intensity threshold phenomenon. Namely, for 5 h after the walk-ing session, both SBP (−5.7±2.6 mmHg)and DBP (−6.5±1.5 mmHg) were lower compared with a non-exer-cise control session, suggesting that a simple brisk walk,
which is accessible to a large proportion of hypertensive patients worldwide, might already result in significant health benefits. As is well known, the primary recom-mendation for the treatment of high BP starts with life-style modification; however, if the BP is not sufficiently lowered, treatment with antihypertensive medication is necessary.5 Previous studies have reported that BP con-trol at normal levels is difficult, with only 25–62% of patients being properly controlled;13,57–59 consequently, most hypertensive patients receive antihypertensive med-ication. In Brazil, 76% of patients are using drug ther-apy.60 In view of the importance of external validity to contribute to strategies for BP control in hypertensive patients, we included medicated patients. To our knowl-edge, this is the first study to investigate the acute effects of exercise on BP in patients treated with ACE inhibitors or angiotensin receptor blockers (ARBs). Previously, Ciolac et al.13 investigated a single aerobic exercise effect on ABP in long-term-treated hypertensive patients. They demonstrated for the first time that a single session of aerobic exercise reduced ABP in long-term-treated patients. In line with this, Melo et al.61 showed reductions
Figure 3. Mean SBP and DBP change at 5 h monitoring following exercise or control session in the overall study sample (N=34).Data are reported as mean±SE.*p<.05 vs. control session.
Figure 4. SBP and DBP at hourly intervals over 5h for both control and exercise sessions in the II/ID group ((a) and (b), N=24) and the DD group ((c) and (d), N=10).Data are reported as mean±SE.*p<0.05 vs. pre-intervention; †p<0.05 vs. control session.
by guest on August 22, 2015jra.sagepub.comDownloaded from
Goessler et al. 7
in BP over the course of 10 h following a single bout of resistance exercise at low intensity in women treated with captopril.
However, not all individuals respond in the same way to exercise, for reasons that still remain to be elucidated. Forjaz et al.48 showed that only 65% of hypertensive patients experienced a fall in ABP after one bout of exer-cise, indicating that 35% of the patients did not. Further, Fagard17 concluded that exercise characteristics, such as intensity, frequency and duration, explain only 4.9% of the variance in SBP and 1.1% in DBP in response to exercise. Additionally, the HERITAGE62 study concluded that 30% of the variance in resting BP can be explained by genetics. This all suggests that genetic variation between individu-als might also help to explain part of the different responses to acute and chronic exercise.10,27
In this study, we focused on the effect of ACE polymor-phisms on PEH. We observed a BP reduction after a simple walk in subjects who carry the I allele, while we were una-ble to show this effect in DD individuals. Others have shown that individuals carrying an I allele (II/ID) are less prone to develop hypertension, and the present results sug-gest that they are also more responsive to the PEH effect. This was explained by the observation of higher levels of circulating ACE in DD homozygotes compared with indi-viduals carrying the I allele.28 However, our results further suggest that this lower risk for hypertension might also be explained by their better responsiveness to exercise, although this should be confirmed in larger studies. Our results are in line with those of Santana et al.,40 who showed that only individuals carrying an I allele presented reductions in SBP after an incremental test and after 20 min of exercise at 90% anaerobic threshold. Earlier studies investigating the chronic effects of exercise on BP found similar results.63,64 Namely, Zhang et al.64 reported a
significant reduction in BP after 10 weeks of training only in individuals with an I allele, and not in DD homozygotes, while Hagberg et al.63 found larger reductions in BP fol-lowing exercise in II and ID genotype individuals com-pared with DD individuals.
On the other hand, Blanchard et al.26 demonstrated that SBP was lower for 14 h after exercise at light but not mod-erate intensity in homozygous DD individuals compared with II/ID, suggesting that intensity might influence the relationship between ACE polymorphism and PEH. Finally, Taylor-Tolbert et al.41 reported larger reductions in BP in II and DD compared with ID 24 h after a single bout of vigorous exercise. However, it is difficult to compare their results with ours, as they compared ACE homozy-gotes (II and DD) with ACE heterozygotes (ID).
The present study was not designed to examine possible mechanisms that could explain the different response between the ACE polymorphisms. However, it has previ-ously been shown that the DD allele of ACE is associated with higher ACE circulating levels, resulting in a higher BP due to an increase in Ang I and Ang II, triggering vaso-constriction, water retention and sodium reabsorption, and resulting in a higher blood volume.28 Others showed that higher activity of Ang II may blind the vasodilatation induced by bradykinin, resulting in reduced NO bioavail-ability.31 Although we did not evaluate NO bioavailability, a previous study demonstrated that ID/II individuals have an increased NO release post incremental exercise test compared with DD individuals.40 Further, Tanriverdi et al.65 showed greater endothelium-dependent vasodilata-tion in II-homozygous athletes compared with DD or ID, due to increased NO bioavailability and bradykinin con-centration. These mechanisms might in part explain the PEH response, taking into account that bradykinin and NO release are related to PEH.20,66
Figure 5. Mean SBP and DBP change at 5 h monitoring following exercise or control session in the II/ID group ((a), N=24) and the DD group ((b), N=10) (overall study sample N=34).Data are reported as mean±SE.*p<0.05 vs. control session.
by guest on August 22, 2015jra.sagepub.comDownloaded from

8 Journal of the Renin-Angiotensin-Aldosterone System
The present study has some limitations. We only evaluated insertion/deletion polymorphisms of the ACE gene, and did not include other polymorphisms or parameters of the RAAS, such as plasma renin levels, ACE plasma levels, angiotensin levels and angiotensinogen. Based on a previous review by Pescatello et al.,67 we calculated that we would need a sample size of 33 patients to detect an absolute net difference of 4.7 mmHg, assuming a standard deviation of 8.5 mmHg with a statistical power of 0.8 and alpha of 0.05. Although the num-ber of participants in the DD group corresponds to the overall representation of this group in the general population, this lower number of participants might have resulted in a lack of power to detect changes in BP following exercise. Consequently, we lacked the power to perform a three-way ANOVA in which we could have included the polymorphism groups as a covariate. Therefore, we suggest that the results of this study should be interpreted as hypothesis generating, and further studies are needed to confirm our findings.
Conclusions
In hypertensive subjects receiving medications for the RAAS, a single walk at moderate intensity promotes a reduction in BP compared with a rest session. Overall, a single walk at moderate intensity promoted somewhat larger reductions in BP compared with a control rest ses-sion. Further, our results suggest that this PEH might be influenced by genetic factors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KFG is supported as a doctoral fellow by the Brazilian Agency for Support and Evaluation of Graduate Education - CAPES founda-tion (process 2446/14-6); VAC is supported as a postdoctoral research fellow by the Research Foundation Flanders (FWO); MDP is supported by the Brazilian Council for the Scientific and Technological Development (CNPq, process 303566/2013-2).
References
1. Wang D, Zhou Y, Guo Y, et al. Arterial pre-hypertension and hypertension in intracranial versus extracranial cerebro-vascular stenosis. Eur J Neurol 2015; 22: 533–539.
2. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2224–2260.
3. Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360: 1903–1913.
4. Lawes CM, Vander Hoorn S and Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet 2008; 371: 1513–1518.
5. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206–1252.
6. Chockalingam A, Campbell NR and Fodor JG. Worldwide epidemic of hypertension. Can J Cardiol 2006; 22: 553–555.
7. 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens 2013; 31: 1925–1938.
8. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: Analysis of worldwide data. Lancet 2005; 365: 217–223.
9. Wolf-Maier K, Cooper RS, Banegas JR, et al. Hypertension prevalence and blood pressure levels in 6 European coun-tries, Canada, and the United States. JAMA 2003; 289: 2363–2369.
10. Rankinen T, Gagnon J, Perusse L, et al. AGT M235T and ACE ID polymorphisms and exercise blood pressure in the HERITAGE Family Study. Am J Physiol Heart Circ Physiol 2000; 279: H368–374.
11. Pescatello LS, Franklin BA, Fagard R, et al. American College of Sports Medicine position stand. Exercise and hypertension. Med Sci Sports Exerc 2004; 36: 533–553.
12. Vanhees L, Geladas N, Hansen D, et al. Importance of char-acteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: Recommendations from the EACPR. Part II. Eur J Prev Cardiol 2012; 19: 1005–1033.
13. Ciolac EG, Guimaraes GV, D’Avila VM, et al. Acute aero-bic exercise reduces 24-h ambulatory blood pressure lev-els in long-term-treated hypertensive patients. Clinics (Sao Paulo) 2008; 63: 753–758.
14. Cornelissen VA, Buys R and Smart NA. Endurance exer-cise beneficially affects ambulatory blood pressure: A sys-tematic review and meta-analysis. J Hypertens 2013; 31: 639–648.
15. Cornelissen VA and Fagard RH. Effects of endurance train-ing on blood pressure, blood pressure-regulating mecha-nisms, and cardiovascular risk factors. Hypertension 2005; 46: 667–675.
16. Cornelissen VA and Smart NA. Exercise training for blood pressure: A systematic review and meta-analysis. J Am Heart Assoc 2013; 2: e004473.
17. Fagard RH. Exercise characteristics and the blood pres-sure response to dynamic physical training. Med Sci Sports Exerc 2001; 33: S484–492; discussion S493–494.
18. Kelley GA and Sharpe Kelley K. Aerobic exercise and rest-ing blood pressure in older adults: A meta-analytic review of randomized controlled trials. J Gerontol A Biol Sci Med Sci 2001; 56: M298–303.
19. Pescatello LS, Turner D, Rodriguez N, et al. Dietary cal-cium intake and renin angiotensin system polymorphisms alter the blood pressure response to aerobic exercise: A ran-domized control design. Nutr Metab (Lond) 2007; 4: 1.
by guest on August 22, 2015jra.sagepub.comDownloaded from
Goessler et al. 9
20. Moraes MR, Bacurau RF, Ramalho JD, et al. Increase in kinins on post-exercise hypotension in normotensive and hypertensive volunteers. Biol Chem 2007; 388: 533–540.
21. Charastek KJJ and Adamirova J. The hypotensive effect of physical activity. In: Rabb W (ed.) Prevention of Ischemic Heart Disease: Principles and Practice. Springfield, IL: Charles C Thomas: 1996, pp. 359–371.
22. Fitzgerald W. Labile hypertension and jogging: New diag-nostic tool or spurious discovery? Br Med J (Clin Res Ed) 1981; 282: 542–544.
23. Angadi SS, Bhammar DM and Gaesser GA. Postexercise hypotension after continuous, aerobic interval, and sprint interval exercise. J Strength Cond Res. Epub ahead of print 17 March 2015.
24. Cornelissen VA and Fagard RH. Exercise intensity and pos-texercise hypotension. J Hypertens 2004; 22: 1859–1861.
25. Brito LC, Queiroz AC and Forjaz CL. Influence of popula-tion and exercise protocol characteristics on hemodynamic determinants of post-aerobic exercise hypotension. Braz J Med Biol Res 2014; 47: 626–636.
26. Blanchard BE, Tsongalis GJ, Guidry MA, et al. RAAS polymorphisms alter the acute blood pressure response to aerobic exercise among men with hypertension. Eur J Appl Physiol 2006; 97: 26–33.
27. Rice T, An P, Gagnon J, et al. Heritability of HR and BP response to exercise training in the HERITAGE Family Study. Med Sci Sports Exerc 2002; 34: 972–979.
28. Rigat B, Hubert C, Alhenc-Gelas F, et al. An insertion/dele-tion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme lev-els. J Clin Invest 1990; 86: 1343–1346.
29. Ljungberg L, Alehagen U, Lanne T, et al. The association between circulating angiotensin-converting enzyme and cardiovascular risk in the elderly: A cross-sectional study. J Renin Angiotensin Aldosterone Syst 2011; 12: 281–289.
30. Danser AH, Batenburg WW, van den Meiracker AH, et al. ACE phenotyping as a first step toward personalized medi-cine for ACE inhibitors. Why does ACE genotyping not pre-dict the therapeutic efficacy of ACE inhibition? Pharmacol Ther 2007; 113: 607–618.
31. Fornage M, Amos CI, Kardia S, et al. Variation in the region of the angiotensin-converting enzyme gene influences inter-individual differences in blood pressure levels in young white males. Circulation 1998; 97: 1773–1779.
32. Henskens LH, Spiering W, Stoffers HE, et al. Effects of ACE I/D and AT1R-A1166C polymorphisms on blood pressure in a healthy normotensive primary care population: First results of the Hippocates study. J Hypertens 2003; 21: 81–86.
33. O’Donnell CJ, Lindpaintner K, Larson MG, et al. Evidence for association and genetic linkage of the angiotensin-con-verting enzyme locus with hypertension and blood pressure in men but not women in the Framingham Heart Study. Circulation 1998; 97: 1766–1772.
34. Staessen JA, Wang JG, Ginocchio G, et al. The deletion/insertion polymorphism of the angiotensin converting enzyme gene and cardiovascular-renal risk. J Hypertens 1997; 15: 1579–1592.
35. Halliwill JR, Buck TM, Lacewell AN, et al. Postexercise hypotension and sustained postexercise vasodilatation:
What happens after we exercise? Exp Physiol 2013; 98: 7–18.
36. Petriz Bde A, de Almeida JA, Migliolo L, et al. Pharmacological potential of exercise and RAS vasoactive peptides for prevention of diseases. Curr Protein Pept Sci 2013; 14: 459–471.
37. Chen CY and Bonham AC. Postexercise hypotension: Central mechanisms. Exerc Sport Sci Rev 2010; 38: 122–127.
38. O’Sullivan SE and Bell C. The effects of exercise and train-ing on human cardiovascular reflex control. J Auton Nerv Syst 2000; 81: 16–24.
39. Ashley EA, Kardos A, Jack ES, et al. Angiotensin-converting enzyme genotype predicts cardiac and auto-nomic responses to prolonged exercise. J Am Coll Cardiol 2006; 48: 523–531.
40. Santana HA, Moreira SR, Neto WB, et al. The higher exer-cise intensity and the presence of allele I of ACE gene elicit a higher post-exercise blood pressure reduction and nitric oxide release in elderly women: An experimental study. BMC Cardiovasc Disord 2011; 11: 71.
41. Taylor-Tolbert NS, Dengel DR, Brown MD, et al. Ambulatory blood pressure after acute exercise in older men with essential hypertension. Am J Hypertens 2000; 13: 44–51.
42. Murphy CM, Kearney PM, Shelley EB, et al. Hypertension prevalence, awareness, treatment and control in the over 50s in Ireland: Evidence from The Irish Longitudinal Study on Ageing. J Public Health (Oxf). Epub ahead of print 28 April 2015.
43. Barbosa e Silva O and Sobral Filho DC. A new proposal to guide velocity and inclination in the ramp protocol for the treadmill ergometer. Arq Bras Cardiol 2003; 81: 48–53.
44. Fletcher GF, Balady GJ, Amsterdam EA, et al. Exercise standards for testing and training: A statement for health-care professionals from the American Heart Association. Circulation 2001; 104: 1694–1740.
45. Pereira AC, Mota GF, Cunha RS, et al. Angiotensinogen 235T allele ‘dosage’ is associated with blood pressure phe-notypes. Hypertension 2003; 41: 25–30.
46. Rigat B, Hubert C, Corvol P, et al. PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP1) (dipeptidyl carboxypepti-dase 1). Nucleic Acids Res 1992; 20: 1433.
47. Wasserman K, Hansen JE, Sue DY, et al. Normal values. Principles of exercise testing and interpretation. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2012.
48. Forjaz CL, Tinucci T, Ortega KC, et al. Factors affecting post-exercise hypotension in normotensive and hyperten-sive humans. Blood Press Monit 2000; 5: 255–262.
49. Cleroux J, Kouame N, Nadeau A, et al. Aftereffects of exer-cise on regional and systemic hemodynamics in hyperten-sion. Hypertension 1992; 19: 183–191.
50. Legramante JM, Galante A, Massaro M, et al. Hemodynamic and autonomic correlates of postexercise hypotension in patients with mild hypertension. Am J Physiol Regul Integr Comp Physiol 2002; 282: R1037–1043.
51. Liu S, Goodman J, Nolan R, et al. Blood pressure responses to acute and chronic exercise are related in prehypertension. Med Sci Sports Exerc 2012; 44: 1644–1652.
by guest on August 22, 2015jra.sagepub.comDownloaded from
10 Journal of the Renin-Angiotensin-Aldosterone System
52. Raine NM, Cable NT, George KP, et al. The influence of recovery posture on post-exercise hypotension in normoten-sive men. Med Sci Sports Exerc 2001; 33: 404–412.
53. Gomes Anunciacao P and Doederlein Polito M. A review on post-exercise hypotension in hypertensive individuals. Arq Bras Cardiol 2011; 96: e100–109.
54. MacDonald JR. Potential causes, mechanisms, and implica-tions of post exercise hypotension. J Hum Hypertens 2002; 16: 225–236.
55. Guidry MA, Blanchard BE, Thompson PD, et al. The influence of short and long duration on the blood pressure response to an acute bout of dynamic exercise. Am Heart J 2006; 151: 1322 e5–12.
56. Mach C, Foster C, Brice G, et al. Effect of exercise duration on postexercise hypotension. J Cardiopulm Rehabil 2005; 25: 366–369.
57. Zanchetti A and Waeber B. Hypertension: Which aspects of hypertension should we impact on and how? J Hypertens Suppl 2006; 24: S2–5.
58. Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hyper-tensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: The VALUE randomised trial. Lancet 2004; 363: 2022–2031.
59. Niiranen TJ, Kantola IM, Vesalainen R, et al. A comparison of home measurement and ambulatory monitoring of blood pressure in the adjustment of antihypertensive treatment. Am J Hypertens 2006; 19: 468–474.
60. Akashi D, Issa FK, Pereira AC, et al. [Antihypertensive treatment. Prescription and cost of drugs. Survey in a tertiary
care hospital] [in Portuguese]. Arq Bras Cardiol 1998; 71: 55–57.
61. Melo CM, Alencar Filho AC, Tinucci T, et al. Postexercise hypotension induced by low-intensity resistance exercise in hypertensive women receiving captopril. Blood Press Monit 2006; 11: 183–189.
62. Rice T, Rankinen T, Chagnon YC, et al. Genomewide link-age scan of resting blood pressure: HERITAGE Family Study. Health, Risk Factors, Exercise Training, and Genetics. Hypertension 2002; 39: 1037–1043.
63. Hagberg JM, Ferrell RE, Dengel DR, et al. Exercise train-ing-induced blood pressure and plasma lipid improvements in hypertensives may be genotype dependent. Hypertension 1999; 34: 18–23.
64. Zhang B, Sakai T, Miura S, et al. Association of angiotensin-converting-enzyme gene polymorphism with the depressor response to mild exercise therapy in patients with mild to mod-erate essential hypertension. Clin Genet 2002; 62: 328–333.
65. Tanriverdi H, Evrengul H, Tanriverdi S, et al. Improved endothelium dependent vasodilation in endurance athletes and its relation with ACE I/D polymorphism. Circ J 2005; 69: 1105–1110.
66. Santana HA, Moreira SR, Asano RY, et al. Exercise inten-sity modulates nitric oxide and blood pressure responses in hypertensive older women. Aging Clin Exp Res 2013; 25: 43–48.
67. Pescatello LS and Kulikowich JM. The aftereffects of dynamic exercise on ambulatory blood pressure. Med Sci Sports Exerc 2001; 33: 1855–1861.
by guest on August 22, 2015jra.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN

