






Bahasa
Halaman
Hukum

Histological Analysis of the Ankylos Peri-implant Soft Tissues in a Dog Model
Henri Tenenbaum, DDS, PhD,* Jean-François Schaaf, DDS,** and Frédéric J. G. Cuisinier, DDS, PhD***
Osteointegration is a recognizedmeans of anchoring implants inbone. However, few studies
have investigated the relationship be-tween the implant/abutment deviceand the soft tissues. Supracrestal tis-sues around implants seem to be sim-ilar to gingiva around teeth in manyways.1 This tissue has a dense, collag-enous lamina propria and is coveredwith stratified squamous, attached oralepithelium. The apical part of the gin-gival sulcus is lined by a junctionalepithelium of typical tooth morphol-ogy. In the connective tissue, the col-lagen fibers originate from the bonecrest, adjacent teeth, and epithelial pa-pillae and they converge on the im-plant to form circular fibers around theimplant. It is clear that there is noinsertion of fibers on the implant sur-face as it is in the cementum of atooth. However, it may be important tonotice if the majority of fibers are ori-ented perpendicular or parallel to theimplant surface, especially regardingthe resistance of the tissues to externalaggression. Resistance to probing isgreater around teeth than around im-plants, so probing depths are signifi-cantly deeper around implants.2 Histo-logically, the probe tip (which is about0.5 mm in diameter) is coronal to theapical extension of the junctional epi-thelium around teeth, whereas aroundimplants the probe tip is always apical to
the junctional epithelium and close tothe bone crest.2 This may be related tothe orientation of the collagen fibers be-cause the major connective tissue fibersare parallel to the long axis of the im-plant. The importance of the soft tissue–implant interface is enhanced by thepresence of a microgap between the im-plant and the abutment. This microgaprepresents a potential contamination sitefor plaque and bacteria.3 In nonsub-merged implants, the microgap can bekept away from the gingival tissues.4
However, in the case of submerged im-plants, the microgap is positioned justover the bone crest, in front of collagenfibers mostly oriented parallel to theabutment surface, so that it provides anopportunity for bacterial infection.
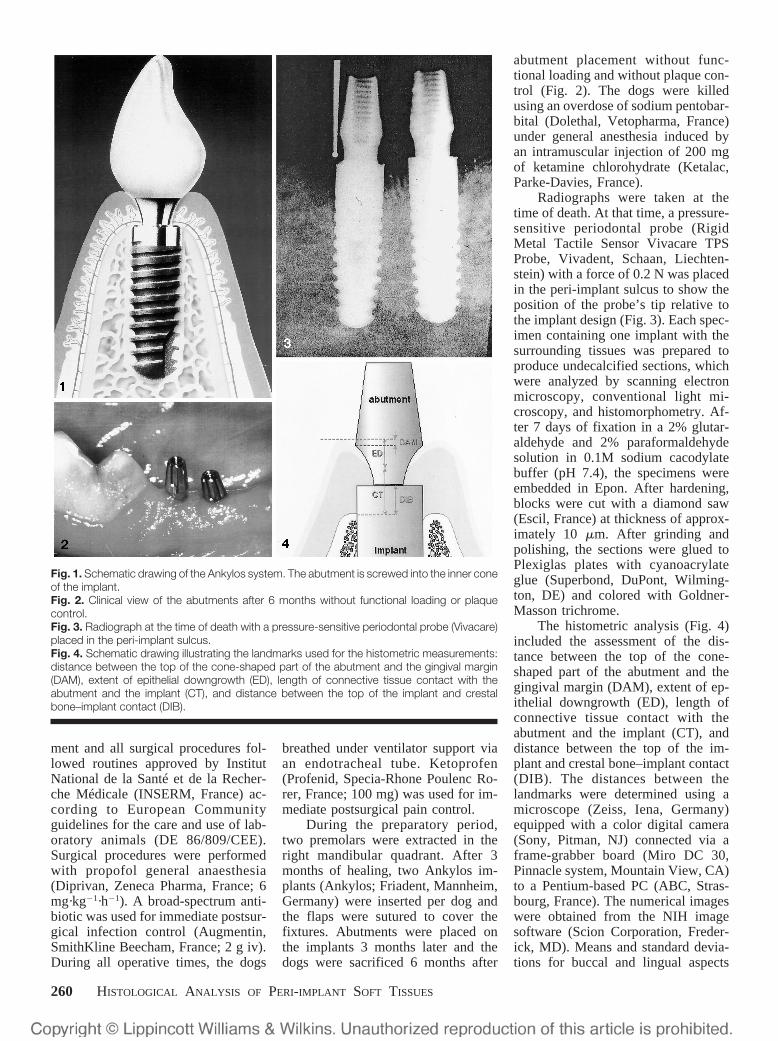
Accordingly, two-phase implantsystems require new approaches tofulfil the requirements of being gap-free and bacteria resistant if the con-nection point between the implant andthe abutment is to be positioned sub-gingivally. In the Ankylos system, theabutment is screwed into the innercone of the implant element and themicrogap is small (1 �m) (Fig. 1). Theaim of this study was to examine theperi-implant soft tissues around theAnkylos implant in a dog model.
MATERIALS AND METHODS
Six adult (age 9 � 2 years) femaleLabrador dogs were included in thestudy. Animal selection and manage-
*Professor and Head, Department of Periodontology, DentalSchool of the Louis Pasteur University of Strasbourg and UnitéInstitut National de la Santé et de la Recherché Médicale (IN-SERM) U 424, Strasbourg, France.**Postdoctoral Researcher, Unité INSERM U 424, Strasbourg,France.***Associate Professor and Head, Department of Biomaterials,Dental School of the Louis Pasteur University of Strasbourg andUnité INSERM U 424, Strasbourg, France.
ISSN 1056-6163/03/01203-259$3.00Implant DentistryVolume 12 • Number 3Copyright © 2003 by Lippincott Williams & Wilkins, Inc.
DOI: 10.1097/01.ID.0000075720.78252.54
Purpose: The importance of thesoft tissue–implant interface is en-hanced by the presence of a micro-gap between the implant and theabutment, which represents a con-tamination site for bacteria. The aimof this study was to investigate theinterface between the Ankylos gap-free implant system and the sur-rounding soft tissues in a dog model.Materials and Methods: Six Labra-dor dogs were included in the studyand two Ankylos implants were in-serted per dog. The dogs were killed6 months after abutment placementwithout functional loading and with-out plaque control. The implantswere analysed histologically byscanning electron microscopy, lightmicroscopy, and histomorphometry.Results: Some sections exhibitedhistologic signs of a mild inflamma-tion. The connective tissue betweenthe most apical epithelial cells of the
junctional epithelium and the alveo-lar crest was characterized by colla-gen fibers running from the perios-teum and the alveolar crest towardthe oral epithelium and, in front ofthe cone-shaped abutment, by a nar-row zone of extracellular matrixwith a few collagen fibers. Conclu-sion: Compared with results ob-tained in other studies using differ-ent types of implant (Astra,Bränemark, ITI), the Ankylos im-plant showed a higher length and alarger width of connective tissuecontact as well as a shorter epithe-lial downgrowth. The absence of amicrogap in the Ankylos systemcould explain the histologic mild in-flammation in the connective tissue.(Implant Dent 2003;12:259–265)Key Words: junctional epithelium,connective tissues, histomorphom-etry, microgap
IMPLANT DENTISTRY / VOLUME 12, NUMBER 3 2003 259
ment and all surgical procedures fol-lowed routines approved by InstitutNational de la Santé et de la Recher-che Médicale (INSERM, France) ac-cording to European Communityguidelines for the care and use of lab-oratory animals (DE 86/809/CEE).Surgical procedures were performedwith propofol general anaesthesia(Diprivan, Zeneca Pharma, France; 6mg·kg�1·h�1). A broad-spectrum anti-biotic was used for immediate postsur-gical infection control (Augmentin,SmithKline Beecham, France; 2 g iv).During all operative times, the dogs
breathed under ventilator support viaan endotracheal tube. Ketoprofen(Profenid, Specia-Rhone Poulenc Ro-rer, France; 100 mg) was used for im-mediate postsurgical pain control.
During the preparatory period,two premolars were extracted in theright mandibular quadrant. After 3months of healing, two Ankylos im-plants (Ankylos; Friadent, Mannheim,Germany) were inserted per dog andthe flaps were sutured to cover thefixtures. Abutments were placed onthe implants 3 months later and thedogs were sacrificed 6 months after
abutment placement without func-tional loading and without plaque con-trol (Fig. 2). The dogs were killedusing an overdose of sodium pentobar-bital (Dolethal, Vetopharma, France)under general anesthesia induced byan intramuscular injection of 200 mgof ketamine chlorohydrate (Ketalac,Parke-Davies, France).
Radiographs were taken at thetime of death. At that time, a pressure-sensitive periodontal probe (RigidMetal Tactile Sensor Vivacare TPSProbe, Vivadent, Schaan, Liechten-stein) with a force of 0.2 N was placedin the peri-implant sulcus to show theposition of the probe’s tip relative tothe implant design (Fig. 3). Each spec-imen containing one implant with thesurrounding tissues was prepared toproduce undecalcified sections, whichwere analyzed by scanning electronmicroscopy, conventional light mi-croscopy, and histomorphometry. Af-ter 7 days of fixation in a 2% glutar-aldehyde and 2% paraformaldehydesolution in 0.1M sodium cacodylatebuffer (pH 7.4), the specimens wereembedded in Epon. After hardening,blocks were cut with a diamond saw(Escil, France) at thickness of approx-imately 10 �m. After grinding andpolishing, the sections were glued toPlexiglas plates with cyanoacrylateglue (Superbond, DuPont, Wilming-ton, DE) and colored with Goldner-Masson trichrome.
The histometric analysis (Fig. 4)included the assessment of the dis-tance between the top of the cone-shaped part of the abutment and thegingival margin (DAM), extent of ep-ithelial downgrowth (ED), length ofconnective tissue contact with theabutment and the implant (CT), anddistance between the top of the im-plant and crestal bone–implant contact(DIB). The distances between thelandmarks were determined using amicroscope (Zeiss, Iena, Germany)equipped with a color digital camera(Sony, Pitman, NJ) connected via aframe-grabber board (Miro DC 30,Pinnacle system, Mountain View, CA)to a Pentium-based PC (ABC, Stras-bourg, France). The numerical imageswere obtained from the NIH imagesoftware (Scion Corporation, Freder-ick, MD). Means and standard devia-tions for buccal and lingual aspects
Fig. 1. Schematic drawing of the Ankylos system. The abutment is screwed into the inner coneof the implant.Fig. 2. Clinical view of the abutments after 6 months without functional loading or plaquecontrol.Fig. 3. Radiograph at the time of death with a pressure-sensitive periodontal probe (Vivacare)placed in the peri-implant sulcus.Fig. 4. Schematic drawing illustrating the landmarks used for the histometric measurements:distance between the top of the cone-shaped part of the abutment and the gingival margin(DAM), extent of epithelial downgrowth (ED), length of connective tissue contact with theabutment and the implant (CT), and distance between the top of the implant and crestalbone–implant contact (DIB).
260 HISTOLOGICAL ANALYSIS OF PERI-IMPLANT SOFT TISSUES

were calculated for each dog that com-pleted the study.
RESULTS
After the surgical procedure,complication-free healing of the softtissues was observed for all implants.After healing, all implants were firmlyanchored in the jaws. None of the ra-diographs showed signs of a continu-ous peri-implant radiolucency. All 12implants achieved osseointegrationdemonstrating direct bone contact.The peri-implant oral mucosa revealed
a keratinized epithelium consisting ofnumerous layers of epithelial cellsforming rete pegs. The peri-implantsulcus was lined with nonkeratinizedepithelial cells (Fig. 5). The most api-cal epithelial cells of the junctionalepithelium were always locatedclearly above the alveolar crest so thatthe implant and abutment surface be-tween the most apical epithelial cellsand the alveolar bone crest showed adirect connective tissue contact (Fig.6). This connective tissue was charac-terized by collagen fibers running indifferent directions. Vertical fibers ranfrom the periosteum and the alveolarcrest toward the oral epithelium,whereas perpendicular fibers that di-rectly contacted the implant and abut-ment surface were observed in a fewsections (Fig. 7). A narrow zone of ex-tracellular matrix with a few collagenfibers characterized the connective tis-sue close to the implant and abutmentsurface, especially in front of the cone-shaped abutment. Some sections exhib-ited histologic signs of a mild inflamma-tion with transmigrating polymorpho-nuclear leukocytes and lymphocytes inthe sulcular epithelium.
Histometric Observations
The results of the histometric mea-surements are reported in Table 1. Thedistances between the top of the cone-shaped part of the abutment and the gin-gival margin were similar on the buccaland lingual aspects. The mean DAMwas 0.68 � 0.94 mm on buccal sidesand 0.46 � 0.41 mm on lingual sides.
The mean extent of ED was longer onbuccal sides (1.31 � 0.63 mm) com-pared with the lingual sides (0.84 �0.53 mm). In contrast, the mean CT wasshorter on buccal sides (2.01 � 1.17mm) than on lingual sides (3.62 � 0.67mm). The mean DIB was shorter onbuccal sides (1.17 � 0.95 mm) than onlingual sides (2.14 � 0.28 mm).
DISCUSSION
The shape of the peri-implant mu-cosa found in our study (ie, a belly-shaped anatomy on the buccal sidecompared with the lingual mucosa,which tapers off coronally to a knife-edge shape) is consistent with that re-ported in other dog studies.5–7 In thisstudy, the vertical dimension of theperi-implant mucosa (distance be-tween the gingival margin to the firstbone–implant contact � DAM � ED� CT) seemed to be 4.00 mm on thebuccal side and 4.92 mm on the lin-gual aspect. Various results werefound in other studies.5–8 Using a non-submerged approach with differenttypes of implants, Buser et al5 ob-served values between 2.39 and 2.70
Fig. 5. Scanning electron microscope images of the Ankylos implant. a, Overview of atransverse section through implant, bone, and soft tissues. b, Enlarged view of the softtissue–implant interface. Notice the dark aspect of oral and peri-implant epithelium.
Fig. 6. Light microscope view showing atransverse section through the abutment, im-plant, and soft tissues. AB, abutment; E, ep-ithelium; CF, connective fibers; A, artifactspace between connective fibers andabutment.
Fig. 7. Light microscope view showing theconnective tissue–abutment interface. AB,abutment; CF, circular fibers; PF, perpendic-ular fibers; A, artifact space between collagenfibers and the abutment. The space betweenthe abutment and the connective tissue wasdue to specimen preparation.
IMPLANT DENTISTRY / VOLUME 12, NUMBER 3 2003 261

mm on the buccal side and between1.58 and 2.00 mm on the lingual side.Comparing submerged and nonsub-merged ITI implants, Weber et al6
measured the vertical dimension of theperi-implant mucosa and found 2.49mm and 2.53 mm, respectively.
In a study using Bränemark fix-tures, Berglundh and Lindhe7 noticedthat the distance between the outersurface of the oral epithelium (gingi-val margin) and the bone crest was onaverage 3.65 mm. They did not mea-sure the bone saucerization that wasfound to vary from 0.08 to 0.39 mm inthe Buser et al5 study. The results ofBerglundh and Lindhe7 seems to beconsistent with a previous study byEricsson and Lindhe2 in which thesame distance between the gingivalmargin and the bone crest was an av-erage 3.3 mm using Bränemark fix-tures. In a comparative study usingthree types of implants (Astra, Bräne-mark, and ITI) placed using a nonsub-merged approach,8 the distance fromthe gingival margin to the marginallevel of bone-to-implant contact was3.10, 3.15, and 3.03 mm, respectively,even without any plaque control pro-tocol during a 5-month period.
The difference between our re-sults and those of previous studiesseems to be related mainly to a higherlength of connective tissue contactwith the abutment and the implant,because the epithelial downgrowth isshorter. The 1.31 mm of epithelialdowngrowth found on the buccal sideis less than that found in the Ericssonand Lindhe2 study (1.7 mm), whereasthe length of connective tissue contactfound in this study (ie, more than 2.0mm) exceeds that measured by Erics-son and Lindhe2 (1.6 mm). Previousstudies5,6 demonstrated that the extentof epithelial downgrowth was signifi-cantly more apical adjacent to sub-merged implants compared with non-submerged implants, and that the
height of connective tissue contactwas greater in nonsubmerged im-plants. In contrast, Abrahamsson et al9
demonstrated that the extent of epithe-lial downgrowth was about 2 mm longin both the submerged and nonsub-merged implants, matching the lengthof epithelium lining in the submergedgroup of Weber et al6 The Ankylosimplant, which used a submerged ap-proach, revealed a shorter epithelialdowngrowth than that observed withother nonsubmerged implants.
In previous studies,10 –12 plaqueformation on titanium implants re-sulted in the establishment of inflam-matory lesions in the adjacent mucosa.Nevertheless, the infiltrated tissue oc-cupied a small portion of the connec-tive tissue lateral to the junctional ep-ithelium. Ericsson et al13 reported thatthe distance between the mucosal mar-gin and the apical border of the infil-trated connective tissue following 9months of plaque accumulation in La-brador dogs was 0.84 mm; the samedistance was 1.6 mm after 5 months ofplaque accumulation in beagle dogs.9
Our histologic findings of a mild in-flammation in the connective tissueunderneath the sulcular and junctionalepithelium are probably more inagreement with those of Ericsson etal13 in the same Labrador dogs. If thedifference in the infiltrated connectivetissue extension was due to the ani-mals used in the study (Labrador ver-sus beagle dogs), this would have tobe confirmed in other experiments. Itis interesting to note that Isidor14
showed (in monkeys) a dense inflam-matory infiltrate in the supracrestalperi-implant mucosa after 18 monthsof plaque accumulation enhanced bycotton cords twisted around the abut-ments. Another explanation of the his-tologic mild inflammation in the con-nective tissue could be the absence ofa microgap in the Ankylos system.
Weber et al6 showed a slight ery-
thema around several two-stage im-plants despite an oral hygiene regi-men, and speculated that theconsequent presence of a microgap be-tween implant and transmucosal abut-ment could have contributed to the find-ing. Quirynen and Van Steenberghe3
confirmed the possibility of microbialleakage through the transmucosal abut-ment and the microgap between implantand abutment, particularly when the gapexceeded 30 �m. In the Ankylos sys-tem, especially the implant–abutmentconnection, the connective tissue iswider and longer and the microgap isvirtually absent, which could help pro-tect against microbial invasion.
CONCLUSIONS
The soft tissue–implant interfaceis the key to the long-term success ofan implant. The significance of thatinterface is enhanced by the fact thatthe presence of a microgap betweenthe implant and the abutment repre-sents a contamination site for bacteria.In the Ankylos system, the absence ofthe microgap, combined with a largerwidth and a higher length of connec-tive tissue, could be more protectiveagainst microbial leakage and soft tis-sue inflammation.
Disclosure
The authors claim to have no fi-nancial interest in any company orproduct mentioned in this article.
REFERENCES
1. Cochran D. Implant therapy I. AnnPeriodontol. 1996;1:707–790.
2. Ericsson I, Lindhe J. Probing depthat implants and teeth. An experimentalstudy in the dog. J Clin Periodontol. 1993;20:623–627.
3. Quirynen M, Van Steenberghe D.Bacterial colonization of the internal part oftwo stage implants. An in vivo study. ClinOral Implants Res. 1993;4:158–161.
4. Buser D, Weber HP, Lang NP. Tissueintegration of non-submerged implants. ClinOral Implants Res. 1990;1:33–40.
5. Buser D, Weber JP, Donath K, et al.Soft tissue reactions to non-submergedunloaded titanium implants in beagle dogs.J Periodontol. 1992;63:226–236.
6. Weber JP, Buser D, Donath K, et al.Comparison of healed tissues adjacent tosubmerged and non-submerged unloadedtitanium dental implants. A histometricstudy in beagle dogs. Clin Oral ImplantsRes. 1996;7:11–19.
Table 1. Detailed Results of the Histometric Measurements
Measurement(mm) DAM ED CT DIB
buccal 0.68 (0.94) 1.31 (0.63) 2.01 (1.17) 1.17 (0.95)lingual 0.46 (0.41) 0.84 (0.53) 3.62 (0.67) 2.14 (0.28)
Data are mean (SD).
DAM, distance between the top of the cone-shaped part of the abutment and the gingival margin; ED, extent of epithelial downgrowth;CT, length of connective tissue contact with the abutment and the implant; DIB, distance between the top of the implant and crestalbone implant contact.
262 HISTOLOGICAL ANALYSIS OF PERI-IMPLANT SOFT TISSUES

7. Berglundh T, Lindhe J. Dimension ofthe peri-implant mucosa. Biological widthrevisited. J Clin Periodontol. 1996;23:971–973.
8. Abrahamsson I, Berglundh T,Lindhe J. Soft tissue response to plaqueformation at different implant systems. Acomparative study in the dog. Clin Oral Im-plants Res. 1998;9:73–79.
9. Abrahamsson I, Berglundh T, MoonIS, et al. Peri-implant tissues at submergedand non-submerged titanium implants.J Clin Periodontol. 1999;26:600–607.
10. Berglundh T, Lindhe J, MarinelloCP, et al. Soft tissue reactions to de novo
plaque formation at implants and teeth.Clin Oral Implants Res. 1992;3:1–8.
11. Ericsson I, Berglundh T, MarinelloCP, et al. Long-standing plaque and gingi-vitis at implants and teeth in the dog. ClinOral Implants Res. 1992;3:99–103.
12. Abrahamsson I, Berglundh T,Wennström J, et al. The peri-implant hardand soft tissues at different implant sys-tems. A comparative study in the dog ClinOral Implants Res. 1996;7:212–219.
13. Ericsson I, Person LG, BerglundhT, et al. Different types of inflammatory re-actions in peri-implant soft tissues. J ClinPeriodontol. 1995;22:255–261.
14. Isidor F. Clinical probing and radio-graphic assessments in relation to the histo-logic bone level at oral implants in monkeys.Clin Oral Implants Res. 1997;8:255–264.
Reprint requests and correspondence to:Henri Tenenbaum, DDS, PhDDepartment of Periodontology, Dental Faculty1 Place de l’Hôpital67000 Strasbourg, FrancePhone: (33) 3 90 24 38 68Fax: (33) 3 90 24 39 00E-Mail : [email protected]
Abstract Translations [German, Spanish, Portuguese, Japanese]
AUTOR(EN): Henri Tenenbaum, DDS,PhD*, Jean-François Schaaf, DDS**, FrédéricJ.G. Cuisinier, DDS, PhD*** *Professor undLeiter, Abteilung für Parodontologie, zahn-medizinische Fakultät der Louis Pasteur Uni-versität Straßburg und Unité INSERM U 424,Straßburg, Frankreich. **Mitglied des Fors-chungsteams, absolvierter Doktorand, UnitéINSERM U 424, Straßburg, Frankreich.***A.O. Professor und Leiter, Abteilung fürBiomaterialien, zahnmedizinische Fakultätder Louis Pasteur Universität Straßburg undUnité INSERM U 424, Straßburg, Frankreich.Schriftwerkehr:Henri Tenenbaum, DDS, PhD,Abteilung für Parodontologie (Dept of Peri-odontology), zahnmedizinische Fakultät (Den-tal Faculty), place de l’Hôpital, 67000 Stras-bourg, France. Telefon: (33) 3 90 24 38 68,Fax: (33) 3 90 24 39 00. eMail: [email protected]
An Hunden durchgeführte Versuchsreihe zur histologischen Untersuchung derAnkylos-Implantate umlagernden Weichgewebsteile
ZUSAMMENFASSUNG: Zielsetzung: Zunehmend wird bei Implantierungsbehandlun-gen das Augenmerk auf die Berührungsfläche zwischen dem das Implantat umlagerndenWeichegewebe und dem Implantat selbst gerichtet, da man inzwischen um die Existenzvon Minimalspalten zwischen Implantat und Stützzahn weiß, die eine ideale Brutstätte zurBakterienbildung darstellen. Die vorliegende Studie zielte darauf ab, diese Berührungs-fläche bei Verwendung des Ankylos Implantierungssystems, das sich durch absolutenSchluss zwischen Implantat und Stützzahn ohne Spaltenbildung auszeichnet, anhand eineran Hunden durchgeführten Versuchsreihe zu untersuchen. Materialien und Methoden:Jedem der sechs zur Studie herangezogenen Labrador-Hunden wurden je zwei AnkylosImplantate eingepflanzt. Sechs Monate nach Stützzahnsetzung erfolgte die Einschläferungder Tiere. Es wurde weder eine funktionelle Belastung des Implantats noch eine unter-suchende Kontrolle hinsichtlich Plaque-Bildung durchgeführt. Die histologische Unter-suchung der Implantate wurde mittels Rasterelektronenmikroskop, Lichtmikroskop sowiedurch histomorphologische Messungen vorgenommen. Ergebnisse: Manche der unter-suchten Bereiche wiesen eine geringfügige Entzündungsneigung auf. Das Verbundgewebezwischen den äußersten Epithelzellen des verbindenden Epithels und dem Alveolärkammwurde von kollagenen Fasern durchzogen, die sich vom Periosteum und dem Alve-olärkamm zum Epithel der Mundschleimhaut erstreckten. Das Gewebe war außerdem imvorderen Bereich des konusförmigen Stützzahns von einem schmalen Streifen extrazel-lulären Muttergewebes mit einigen durchlaufenden Kollagenfasern geprägt.Schlussfolgerung: Im direkten Vergleich zu den in anderen Studien unter Verwendungverschiedener Implantatsysteme (Astra, Bränemark, ITI) erzielten Ergebnissen wies dasAnkylos System eine größere Kontaktlänge und -breite des verbindenden Gewebes sowieein kürzeres Epitheltiefenwachstum auf. Die im verbindenden Gewebe der Berührungs-fläche bei histologischer Untersuchung entdeckte geringfügige Entzündung erklärt sichvoraussichtlich durch das Fehlen des Minimalspalts zwischen Implantat und Stützzahndurch Einsatz eines Implantats der Ankylos Serie.
SCHLÜSSELWÖRTER: Verbindungsepithel, verbindende Gewebsteile, histomorpholo-gische Messungen, Minimalspalt
Análisis histológico de los tejidos suaves periimplantes Ankylos® en un modelo enperros.
IMPLANT DENTISTRY / VOLUME 12, NUMBER 3 2003 263

AUTOR(ES): Henri Tenenbaum, DDS, PhD*,Jean-Francois Schaaf, DDS**, Frédéric J.G.Cuisinier, DDS, PhD***. *Profesor y Jefe,Departamento de Periodontología, Facultadde Odontología de la Universidad de Estras-burgo Luis Pasteur y Unité INSERM U 424,Estrasburgo, Francia. **Investigador post-doctoral, Unité INSERM U 424, Estrasburgo,Francia. ***Profesor Asociado y Jefe, Depar-tamento de Biomateriales, Facultad de Odon-tología de la Universidad de Estrasburgo LuisPasteur y Unité INSERM U 424, Estrasburgo,Francia. Correspondencia a: Henri Tenen-baum, DDS, PhD, Dept. of Periodontology,Dental Faculty L Place de l’Hôpital, 67000Strasbourg, Francia. Teléfono: (33) 3 90 2438 68, Fax: (33) 3 24 39 00. Correo elec-trónico: [email protected]
ABSTRACTO: PROPÓSITO: La importancia de la interfaz de tejido suave-implante esmejorada por la presencia de un microespacio entre el implante y el pilar que representaun lugar de contaminación con bacteria. El propósito de este estudio fue investigar lainterfaz entre el Ankylos, un sistema de implante sin espacio, y los tejidos suaves que lorodean en un modelo en perros. MATERIALES Y MÉTODOS: Seis perros labradores seincluyeron en el estudio y se insertaron 2 implantes Ankylos por perro. Los perros fueronsacrificados 6 meses después de la colocación del pilar sin carga funcional y sin controldel sarro. Los implantes fueron analizados histológicamente con un microscopio debarrido electrónico, microcopio de luz y histomorfometría. RESULTADOS: Algunassecciones exhibieron señales histológicas de una suave inflamación. El tejido conectivoentre las células epiteliales más apical del epitelio de la unión y la cresta alveolar secaracterizó por fibras de colágeno que corrían desde el periostio y la cresta alveolar haciael epitelio oral y, al frente del pilar con forma de cono, en una zona delgada de una matrizextracelular con algunas fibras de colágeno. CONCLUSIÓN: Comparados con los re-sultados obtenidos en otros estudios usando distintos tipos de implantes (Astra, Brane-mark, ITI), el Ankylos demostró una longitud más alta y un ancho más grande de contactocon el tejido conectivo así como un crecimiento epitelial más corto. La ausencia delmicroespacio en el sistema Ankylos podría explicar la suave inflamación histológica en eltejido conectivo.
PALABRAS CLAVES: epitelio de la unión, tejidos conectivos, histomorfometría,microespacio
Análise histológica dos tecidos moles em um peri-implante Ankylos em um cachorrocomo modelo.
AUTOR(ES): Henri Tenenbaum,DDS,PhD*,Jean-François Schaaf, DDS**, Frédèric J.G-.Cuisinier, DDS, PhD*** . * Professor e Chefedo Departamento de Periodontia, Faculdadede Odontologia da Universidade Louis Pas-teur de Strasbourg e Unité INSERM U 424,Strasburgo, França. ** Pesquisador de Pós-Doutoramento, Unité INSERM 424, Stras-burgo, França. *** Professor Associado eChefe do Departamento de Bio-Materiais,Faculdade de Odontologia da UniversidadeLouis Pasteur de Strasbourg e Unité INSERMU 424, Strasburgo, França. Correspondênciapara: Henri Tenenbaum, DDS, PhD, Dept ofPeriodontology, Dental Faculty 1 place del’Hôpital, 67000 Strasbroug, France. Tele-fone: (33) 3 90 24 38 68, Fax (33) 3 90 24 3900 E-mail:[email protected]
SUMÁRIO: PROPÓSITO: a importância da interface do implante de tecido mole éincrementada pela presença de uma micro abertura entre o implante e o suporte o querepresenta um local de contaminação para bactérias. O objetivo deste estudo foi investigara interface entre o Ankylos, um sistema de implante sem abertura, e os tecidos molescircundantes em um cachorro como modelo. MATERIAIS E MÉTODOS: 6 cães raçaLabrador forma incluídos no estudo e 2 implantes Ankylos foram insertados por cachorro.Os cães foram sacrificados 6 meses depois da colocação do suporte sem a carga funcionale sem controle de placa. Os implantes foram analisados histológicamente utilizando-se ummicroscópio de elétrons, um microscópio leve e histomorfometria. RESULTADOS:alguma seções exibiram sinais histológicos de uma inflamação leve. O tecido conjuntivoentre as células epiteliais mais apicais do epitélio de conexão e a crista alveolar foicaracterizado por fibras de colágeno crescidas desde o perósteo e a crista alveolar emdireção ao epitélio oral e, em frente do suporte em forma de cone, por uma zona estreitade matriz extracelular com algumas poucas fibras de colágeno. CONCLUSÃO: com-parado aos resultados obtidos em outros estudos usando diferentes tipos de implante(Astra, Bränemark, ITI) o Ankylos mostrou um comprimento e largura maiores de contatode tecido conjuntivo bem como um encolhimento menor epitelial. A ausência de umamicro abertura no sistema Ankylos poderia explicar a leve inflamação histológica dotecido conjuntivo.
PALAVRAS CHAVE: epitélio de conexão, tecidos conjuntivos, histomorfometria, microabertura
264 HISTOLOGICAL ANALYSIS OF PERI-IMPLANT SOFT TISSUES
IMPLANT DENTISTRY / VOLUME 12, NUMBER 3 2003 265
Copyright © 2022 FDOKUMEN

