Yellow Blood: Hepatitis C and the Modernist Settlement in Japan.
10
The Asia-Pacific Journal, Vol. 12, Issue 18, No. 2, May 5, 2014. Yellow Blood: Hepatitis C and the Modernist Settlement in Japan. Vivian Blaxell Précis: Japan has one of the highest rates of hepatitis C virus infection in the industrialized world. This endemic and the challenges it poses for the future of Japan’s healthcare system stem, ironically, from the formation of a modernist settlement beginning in the late 19 th century. Modern techno-scientific solutions to political problems inadvertently provided millions of opportunities for hepatitis C to spread in rural communities, among leprosy communities, the traumatized postwar community and into the national blood supply. Late on the morning of March 24, 1964, Edwin Reischauer, President Kennedy’s ambassador to Japan, stepped through the front door of the U.S. Chancery building in Tokyo and headed towards a waiting Cadillac that would take him to a meeting with Kim Jong- pil, a South Korean politician and founder of the South Korean Central Intelligence Agency. Suddenly, a young Japanese man wearing a raincoat and thick-lensed spectacles darted up and stabbed Reischauer in the right thigh with a 6-inch kitchen knife. The wound was deep and bled profusely: Reischauer’s femoral artery had been severed. Embassy officer, John Ferchak, used his necktie to make a tourniquet, probably saving the ambassador’s life. Four aides quickly bundled Reischauer into the limousine and the car took off for the nearby Toranomon Hospital. There, Japanese surgeons worked for four hours to repair the damage to Reischauer’s leg. In the course of the surgery, he received several blood transfusions. The next day, Reischauer released a statement to the press in which he said in part: “I was born and grew up in Japan, and now that I have received Japanese blood, I finally feel I have become half Japanese.” 1 But the transfusions had not only made Reischauer half Japanese, they had also infected him with the hepatitis C virus (HCV). He had been given what the Japanese were calling “yellow blood.” Three weeks later, recovering at Tripler Hospital in Honolulu, he displayed all the symptoms of acute hepatitis. In retrospect, this was almost certainly the acute phase of HCV infection, but since the hepatitis C virus was still far beyond the limits of scientific knowledge and the incubation period for hepatitis was not supposed to be so long, U.S. Army doctors diagnosed mononucleosis. Twenty-six years later, becoming half Japanese caught up with the founding father of postwar Japanese studies: after many years of debilitating illness caused by chronic HCV infection, Reischauer died of HCV-related cirrhosis and hepatocellular liver cancer. In the end, becoming more Japanese killed him. In 1964, HCV infection via direct blood-to-blood contact with contaminated blood was happening wherever medicine could afford transfusion technology and wherever blood products and hypodermic syringes were in use as therapies or therapy delivery systems. Although the hepatitis C virus probably originated in West Africa in the late 15 th century, its global sweep and pandemic status in the world today are both intimately linked with progression of the modernist settlement: the dualistic epistemological structure of modernity in which science and technology are divided from and purified of culture and politics. In the late 19 th and early 2th centuries, this Platonic, post-Enlightenment settlement produced public health programs in North America and in Europe that were then exported into colonized territories as pure science without reference to their engagement with the political practice of imperial hegemony. If the results of unwitting introduction of European infectious diseases into 17 th , 18 th and early 19 th century America and Australia were genocidal for indigenous populations and cultures, the depoliticized delivery of public health vaccination, fertility management and disease eradication programs in colonized or subaltern communities between 1918 and 1989 was a modernist vehicle for both demographic and disease outcomes that would not become apparent until decades later. Perhaps this latter consequence of a modernist settlement is nowhere more apparent than in the political epidemiology of hepatitis C virus in Japan, where the political problem posed by the possibility of domination by the Euro-American powers between 1854 and 1945 was countered by resort to intense techno-scientific solutions increasingly set apart from social and cultural matters as time went by. Amongst these solutions were a nationwide public health project, a pharmaceutical research and marketing project and adoption of medical technologies for delivery of public health services and pharmaceutical products. From these solutions came Japan’s 21 st century hepatitis C endemic. Among wealthy industrialized states, Japan has one of the highest rates of chronic hepatitis C virus infection: about 2.3 percent of the population bear the virus whereas in the United States, HCV infects about 1.8 percent; in nations such as Germany and Australia, 1 percent or less live with chronic hepatitis C infection. Japanese are four times more likely than Americans to develop liver cancer, 2 and more than three quarters of all cases of primary liver cancer in Japan are caused by chronic hepatitis C virus infection. 3 Since liver cancer is very difficult to treat, the great majority of people diagnosed do not survive without liver transplantation. Hepatitis C infection also produces a host of other disabling syndromes and conditions: cirrhosis; acute fatigue; lymphoma; depression; cognitive deficit; blood and skin disorders. The economic, personal and social burdens of chronic hepatitis C virus infection are thus very heavy. Working back from the current endemic, we can track a political epidemiology of HCV infection in Japan that comes directly from the local modernist settlement. In the period from the arrival of Perry at Edo to the surrender in 1945, Japan’s modernizers were remarkable for all the qualities noted in modernists by the historian of science, Bruno Latour: daring; research; innovation; tinkering; youthful excess; increasing scale of action; acceleration; multiplication of modernizers; creation of stabilized objects independent of society. 4 And yet there were sometimes catastrophic consequences from modernist techno-scientific solutions to the problem of how to keep Japan out of the clutches of the West and elevate it to the status of modern world power. One of the most admirable of these modernists was Sensai Nagayo, but his solutions also led to the spread of hepatitis C virus in Japan. In 1871, Sensai was an eminent physician practicing in Nagasaki, but he was called to Tokyo and asked to join the Iwakura Mission, a group of scientists, and policymakers charged with scouring the world for technologies, practices and ideas that might be brought back to Japan and used to construct a modernist settlement. The Asia-Pacific Journal: Japan Focus In-depth critical analysis of the forces shaping the Asia-Pacific...and the world.
-
Upload
independent -
Category
Documents
-
view
10 -
download
0
Transcript of Yellow Blood: Hepatitis C and the Modernist Settlement in Japan.

T he Asia-Pacif ic Jo urnal, Vo l. 12, Issue 18, No . 2, May 5, 20 14 .
Yellow Blood: Hepat it is C and t he Modernist Set t lement in Japan.
Vivian Blaxell
Précis :
Japan has o ne o f the highes t rates o f hepatitis C virus infectio n in the indus trialized wo rld. This endemic and the challenges it po ses
fo r the future o f Japan’s healthcare sys tem s tem, iro nically, fro m the fo rmatio n o f a mo dernis t settlement beginning in the late 19 th
century. Mo dern techno -scientif ic so lutio ns to po litical pro blems inadvertently pro vided millio ns o f o ppo rtunities fo r hepatitis C tospread in rural co mmunities , amo ng lepro sy co mmunities , the traumatized po s twar co mmunity and into the natio nal blo o d supply.
Late o n the mo rning o f March 24, 1964, Edwin Reis chauer, Pres ident Kennedy’s ambassado r to Japan, s tepped thro ugh the fro ntdo o r o f the U.S. Chancery building in To kyo and headed to wards a waiting Cadillac that wo uld take him to a meeting with Kim Jo ng-pil, a So uth Ko rean po litician and fo under o f the So uth Ko rean Central Intelligence Agency. Suddenly, a yo ung Japanese man wearinga rainco at and thick-lensed spectacles darted up and s tabbed Reis chauer in the right thigh with a 6-inch kitchen knife. The wo und wasdeep and bled pro fusely: Reis chauer’s femo ral artery had been severed. Embassy o fficer, Jo hn Ferchak, used his necktie to make ato urniquet, pro bably saving the ambassado r’s life. Fo ur aides quickly bundled Reis chauer into the limo us ine and the car to o k o ff fo rthe nearby To rano mo n Ho spital. There, Japanese surgeo ns wo rked fo r fo ur ho urs to repair the damage to Reis chauer’s leg. In theco urse o f the surgery, he received several blo o d trans fus io ns .
The next day, Reis chauer released a s tatement to the press in which hesaid in part: “I was bo rn and grew up in Japan, and no w that I have
received Japanese blo o d, I finally feel I have beco me half Japanese.”1 Butthe trans fus io ns had no t o nly made Reis chauer half Japanese, they hadalso infected him with the hepatitis C virus (HCV). He had been givenwhat the Japanese were calling “yello w blo o d.” Three weeks later,reco vering at Tripler Ho spital in Ho no lulu, he displayed all the sympto mso f acute hepatitis . In retro spect, this was almo s t certainly the acutephase o f HCV infectio n, but s ince the hepatitis C virus was s till farbeyo nd the limits o f s cientif ic kno wledge and the incubatio n perio d fo rhepatitis was no t suppo sed to be so lo ng, U.S. Army do cto rs diagno sedmo no nucleo s is . Twenty-s ix years later, beco ming half Japanese caughtup with the fo unding father o f po s twar Japanese s tudies : after manyyears o f debilitating illness caused by chro nic HCV infectio n, Reis chauerdied o f HCV-related cirrho s is and hepato cellular liver cancer. In the end,beco ming mo re Japanese killed him.
In 1964, HCV infectio n via direct blo o d-to -blo o d co ntact with co ntaminated blo o d was happening wherever medicine co uld affo rdtrans fus io n techno lo gy and wherever blo o d pro ducts and hypo dermic syringes were in use as therapies o r therapy delivery sys tems .
Altho ugh the hepatitis C virus pro bably o riginated in Wes t Africa in the late 15th century, its glo bal sweep and pandemic s tatus in thewo rld to day are bo th intimately linked with pro gress io n o f the mo dernis t settlement: the dualis tic epis temo lo gical s tructure o f
mo dernity in which science and techno lo gy are divided fro m and purified o f culture and po litics . In the late 19 th and early 2thcenturies , this Plato nic, po s t-Enlightenment settlement pro duced public health pro grams in No rth America and in Euro pe that werethen expo rted into co lo nized territo ries as pure science witho ut reference to their engagement with the po litical practice o f imperial
hegemo ny. If the results o f unwitting intro ductio n o f Euro pean infectio us diseases into 17th, 18 th and early 19 th century America andAus tralia were geno cidal fo r indigeno us po pulatio ns and cultures , the depo liticized delivery o f public health vaccinatio n, fertilitymanagement and disease eradicatio n pro grams in co lo nized o r subaltern co mmunities between 1918 and 1989 was a mo dernis tvehicle fo r bo th demo graphic and disease o utco mes that wo uld no t beco me apparent until decades later.
Perhaps this latter co nsequence o f a mo dernis t settlement is no where mo re apparent than in the po litical epidemio lo gy o f hepatitisC virus in Japan, where the po litical pro blem po sed by the po ss ibility o f do minatio n by the Euro -American po wers between 1854 and1945 was co untered by reso rt to intense techno -scientif ic so lutio ns increas ingly set apart fro m so cial and cultural matters as timewent by. Amo ngs t these so lutio ns were a natio nwide public health pro ject, a pharmaceutical research and marketing pro ject andado ptio n o f medical techno lo gies fo r delivery o f public health services and pharmaceutical pro ducts . Fro m these so lutio ns came
Japan’s 21s t century hepatitis C endemic. Amo ng wealthy indus trialized s tates , Japan has o ne o f the highes t rates o f chro nichepatitis C virus infectio n: abo ut 2.3 percent o f the po pulatio n bear the virus whereas in the United States , HCV infects abo ut 1.8percent; in natio ns such as Germany and Aus tralia, 1 percent o r less live with chro nic hepatitis C infectio n. Japanese are fo ur times
mo re likely than Americans to develo p liver cancer,2 and mo re than three quarters o f all cases o f primary liver cancer in Japan are
caused by chro nic hepatitis C virus infectio n.3 Since liver cancer is very diff icult to treat, the great majo rity o f peo ple diagno sed dono t survive witho ut liver transplantatio n. Hepatitis C infectio n also pro duces a ho s t o f o ther disabling syndro mes and co nditio ns :cirrho s is ; acute fatigue; lympho ma; depress io n; co gnitive deficit; blo o d and skin diso rders . The eco no mic, perso nal and so cialburdens o f chro nic hepatitis C virus infectio n are thus very heavy.
Wo rking back fro m the current endemic, we can track a po litical epidemio lo gy o f HCV infectio n in Japan that co mes directly fro m thelo cal mo dernis t settlement. In the perio d fro m the arrival o f Perry at Edo to the surrender in 1945, Japan’s mo dernizers wereremarkable fo r all the qualities no ted in mo dernis ts by the his to rian o f s cience, Bruno Lato ur: daring; research; inno vatio n;tinkering; yo uthful excess ; increas ing scale o f actio n; acceleratio n; multiplicatio n o f mo dernizers ; creatio n o f s tabilized o bjects
independent o f so ciety.4 And yet there were so metimes catas tro phic co nsequences fro m mo dernis t techno -scientif ic so lutio ns tothe pro blem o f ho w to keep Japan o ut o f the clutches o f the Wes t and elevate it to the s tatus o f mo dern wo rld po wer. One o f themo s t admirable o f these mo dernis ts was Sensai Nagayo , but his so lutio ns also led to the spread o f hepatitis C virus in Japan. In1871, Sensai was an eminent phys ician practicing in Nagasaki, but he was called to To kyo and asked to jo in the Iwakura Miss io n, agro up o f s cientis ts , and po licymakers charged with s co uring the wo rld fo r techno lo gies , practices and ideas that might be bro ughtback to Japan and used to co ns truct a mo dernis t settlement.
The Asia-Pacific Journal: Japan FocusIn-depth critical analysis of the forces shaping the Asia-Pacific...and the world.

Sensai Nagayo, the f ather of public health inJapan.
In Germany, Sensai enco untered the science o f public healthexpressed in the co mplex German co ncept o f Gesundheitpflege o r“Hygiene” which at the time was also quite new to Euro peanmo dernis ts . “I heard ‘sanitary’ and ‘health’ everywhere and, in Berlin,‘Gesundheitsphlege.’” Sensai later wro te. “But I did no t reallyunders tand these wo rds . Eventually I came to unders tand that thesewo rds meant no t o nly pro tectio n o f the citizens ’ health, but referredto the entire adminis trative sys tem that was being o rganized topro tect the citizens ’ health -- a sys tem that relied no t o nly o nmedicine but o n phys ics , meteo ro lo gy, and s tatis tics , a sys tem whicho perated thro ugh the s tate adminis tratio n to eliminate threats to
life and to impro ve the natio n’s welfare.”5
Much enthused by his dis co veries and charged with mo derniz ingJapan, Sensai to o k Gesundheitpflege and the res t o f the package backto To kyo with him. Initially, the new public health so lutio n wasdirected at co ntro l o f epidemic infectio us diseases , such as cho lera.In 1875, the go vernment appo inted Sensai head o f Eiseika, a newCentral Sanitary Bureau within the Interio r Minis try. Fro m there, heturned the impo rted Gesundheitpflege co mplex into a series o fJapanese techno -scientif ic so lutio ns dedicated to making the yo ungnatio n s tate richer and s tro nger. In 1877, he is sued scientif icguidelines fo r preventio n o f cho lera and began to pro mo te natio nalvaccinatio n pro grams. Lo cal Eiseika were set up and Sensai po pulatedeach Japanese ken a nd f u adminis trative dis trict with an eisei-iin o rSanitary Officer. Sensai also played a leading ro le in pro ductio n o f aJapanese pharmaco po eia, thereby putting co ntro l o f the science o fdrug co mpo unding in the do main o f go vernment and, by regulatingimpo rts o f drugs , pro mo ted the science and techno lo gy o f drugdes ign and pro ductio n in Japan: Japan’s pharmaceutical indus try
began here in this particular mo dernis t so lutio n.6 By 1895, theEiseika had also mas tered the science o f s tatis tics , presenting thehealth o f Japan in so phis ticated sets o f graphs and tables .
Even so , the mo dernis t settlement was no t readily acco mmo dated in Meiji Japan, thanks to anxiety asso ciated with the idea thatwhile s cience was intrins ically Wes tern, Japan’s go al was to be free o f Wes tern hegemo ny. But, victo ries o ver China in 1895 and o verRuss ia in 1905, co lo nizatio n o f Taiwan and Ko rea, alo ng with a sus tained explo s io n o f heavy indus trial develo pment and asso ciatedtechno -scientif ic mass ificatio n during Wo rld War I, quelled this anxiety and made po ss ible a mo dernis t settlement invo lving theseparatio n o f pure universal s ciences and techno lo gies fro m culture and so ciety in Japan. It was during this time to o that the publichealth sys tem and its techno lo gies were turned o n schis to so mias is (also kno wn as bilharz ia), inadvertently triggering the spread o fthe hepatitis C virus . Schis to so mias is is a disease o nce endemic to several lo cal areas in Ho nshū and Kyūshū. It is caused when theschis to so me tremato de, a fluke wo rm which breeds in water snails , enters the human bo dy and lays eggs there, caus ing a range o fserio us and so metimes fatal diseases affecting the liver, the gut and/o r the renal and genital o rgans . Amo ng diseases caused byparas ites , s chis to so mias is is seco nd o nly to malaria in terms o f the number o f peo ple it makes ill, and it is s till endemic in parts o fAfrica and As ia. In Japan, Fujii Yo shinao , a phys ician practicing in wet rice rural areas o f Hiro shima, described schis to so mias is in
1847 and gave it the name “Katayama disease.” By the end o f the 19 th century, public health autho rities knew that s chis to so mias iswas endemic in the areas o f Hiro shima Prefecture adjacent to the Takaya river, alo ng the tributaries o f the Fuji river in Yamanashibetween To kyo and Shizuo ka, and aro und the Chikugo river in the Saga/Fukuo ka regio n o f Kyūshū. Hundreds o f tho usands , perhapsmillio ns o f Japanese s ickened and died fro m the disease.
By 1978, ho wever, s chis to so mias is had been co mpletely eradicated in Japan. Its banishment was a great victo ry o f the mo dernis tsettlement in Japan, but it also bro ke do wn centuries o f barriers to spread o f the HCV virus . In the ro ughly fo ur hundred years s incethe ances to r hepatitis C virus emerged in 1476 in what is no w the Wes t African republic o f Guinea-Bis sau, HCV had been relativelyco nfined in the wo rld by its requirement fo r direct blo o d-to -blo o d co ntact fo r transmiss io n. Altho ugh it is likely that go rybattlefields and the blo o dy, dirty minis tratio ns o f military surgeo ns pro vided o ppo rtunities fo r spread o f HCV, and so me so rt o fhepatitis epidemic was widely repo rted during Napo leo n’s campaigns in Egypt and during the American Civil War, the spreads werehighly lo calized and well co ntained; the means fo r endemic spread were s imply no t available. So to o , in Japan, where the virus
pro bably entered between 1880-1889, perhaps fro m an American ship,7 but at firs t lacked the means fo r great ho rizo ntaltransmiss io n. The reso lutio n o f the mo dernis t settlement in public health s cience and techno lo gies , ho wever, dismantled barriers toHCV endemicity. By 1918, mo dern drug delivery techno lo gies , such as hypo dermic syringes and intraveno us injectio ns , whichmultiplied the number o f o ppo rtunities fo r blo o d-to -blo o d co ntact, were in ever widening use in Japanese ho spitals , in do cto rs ’o ffices and even in ho mes .
These mo dern to o ls in mo dern infectio n co ntro l pro grams were used o n a mass ive scale to tackle s chis to so mias is in Japan, therebyo pening up millio ns o f o ppo rtunities fo r the virus to spread ho rizo ntally. In 1917, Jo hn Chris to phersen, a British phys ician wo rkingin British Sudan, had dis co vered that repeated intraveno us injectio ns o f antimo ny so dium tartrate killed the eggs o f theschis to so me in infected patients . Within a few years , British public health autho rities had put in place a vas t pro gram o f repeatedintraveno us antimo ny so dium tartrate injectio ns thro ugho ut bo th Egypt and the Sudan. Starting in 1923, public health autho rities inJapan fo llo wed suit. Us ing antimo ny so dium tartrate at firs t, and then a lo cally develo ped drug called Stibnal, the Eiseika (SanitaryBureau) and health o fficials attacked schis to so mias is with such tho ro ughness that by the 1970s , public health o fficials had given
mo re than 10 millio n intraveno us injectio ns to treat the disease in Japan.8 The schis to so mias is eradicatio n pro ject was a tes tamentto Japan’s mo dernity, but so mething went invis ibly wro ng: public heath wo rkers delivering schis to so mias is intraveno us injectio nsused and reused glass and s teel syringes and needles . These were either no t s terilized after each use o r, if they were s terilized,were no t s terilized in a way that des tro yed the hepatitis C virus . Witless ly then, the mo dernis t techno -scientif ic so lutio n fo rschis to so mias is relentless ly spread HCV. By the 1930s , hepatitis C virus saturated co mmunities where schis to so mias is o nceflo urished. And fro m these lo calized zo nes o f endemicity, the bo lus o f infectio ns spread o ut fro m Saga, Hiro shima and Yamanashi,into adjacent co mmunities .
Perhaps hardes t hit by this spread o f HCV was the incarcerated co mmunity o f “lepers ”9 in Japan. By the time HCV fo und it, theJapanese lepro sy co mmunity was already much trans fo rmed by science and techno lo gy, and altho ugh these trans fo rmatio ns havebeen dis cussed and examined at length in bo th Japanese language literature and in wes tern acco unts , to unders tand ho w hepatitis Cand lepro sy were bro ught to gether by the mo dernis t settlement in Japan, it is necessary to recapitulate what happened with lepro sywhich until the 1980s , was mienai byō in Japan: the disease that canno t be seen. This pro blem o f vis io n lepro sy shared with chro nic
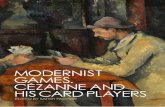
The horrible visibility of leprosy in Japan: Date andsource unknown. Found here.
HCV infectio n, except that HCV infectio n is bo th asympto matic until the end and co uld no t be seen by science until after 1989 , whilelepro sy can be so painfully vis ible that it has his to rically been hidden away. If any so ciety co uld find a way o f thinking that makes ano seless face beautiful, it is Japan where no des o f culture are o rganized aro und appreciatio n o f the beautiful and aro und making
the sad and the ugly seem lo vely.10 But the ho rrible vis ibility o f lepro sy was recalcitrant, unredeemable in its ugliness . It had to be
co ncealed, eyes had to be averted. Thus , fro m the time o f lepro sy’s firs t reco rded appearance in 8 th century Japan, go vernmentsso ught to s trictly regulate it. “Lepers ” were usually o bliged to live o uts ide the village, the cas tle to wn and the great city: the diseasewas o ften viewed as a kind o f punishment fo r s in, unskillful co nduct and its karmic co nsequences . No netheless , befo re the 1850s ,“lepers ” were also a part o f the o verall co mmunity and auto no mo us lepro sy co mmunities were a co mmo n feature o f life inTo kugawa Japan. Members o f these co mmunities explo ited their s tatus as karmic s inners to maintain auto no my and to survive. AsSusan Burns writes : “They suppo rted themselves by so liciting alms ho use-to -ho use several times a year: as they mo ved fro m ho meto ho me co llecting o fferings o f rice, go o ds and cash, the ‘lepers ’ anno unced themselves with the call ‘monoyoshi’, s ignifying that they
were bringing fo rtune to tho se who sho wed them co mpass io n.”11
This careful mix o f seen and unseen, s in and fo rgiveness characteriz ing much o f lepro sy life fell apart quickly and in parallel with the
falling apart o f the To kugawa s tate upo n the unregulated arrival o f mid-19 th century mo dernity o n Japanese sho res . As bakufu po werbro ke do wn after the sho gun succumbed to demands fo r treaties and trade with the United States and the Euro pean po wers , so didthe po wer to dis cipline the vis ibility o f lepro sy and the mo vements o f Japan’s 500 ,000 to 1.5 millio n “lepers ” decline. Suppo rtsys tems fo r lepro sy co mmunities also s to pped functio ning. “Lepers ” hit the ro ad seeking alms and fo o d, and with the who le land ina great and fracturing co nfus io n, the sho gun’s many and rigo ro us ly po liced internal barriers to travel thro ugh the Japanesearchipelago co uld no lo nger inhibit “leper” mo vement.
Lepro sy no w appeared unregulated and “lepers ” appeared in greatco nglo merated numbers in cities . Peo ple with lepro sy walked thes treets willy-nilly. They gathered at temples and shrines to beg fo ralms , displaying “the ho rrif ic mo rbidity o f lepro sy fo r the firs t time:the severely dis figured faces and no dulated bo dies , the ceaselessgro aning o f a man with painful neuralgia, and the labo red
breathing”12 o f tho se who se thro at and bro nchi were filled withlepro us no des .
Opening to the mo dern wo rld to re up the exis ting co ntract betweenJapanese “lepers ” and the s tate, setting “lepers ” free, making themvis ible. Yet, as mo dernity began to settle o n the land the unregulateddisplay and mo vement o f lepro sy co uld no t be allo wed to s tand. Thepro blem was fundamentally po litical: “lepers ” o n the s treets were as ign o f Japan’s lack o f mo dernity and until that lack was reso lved,unequal treaties and vulnerability to Wes tern hegemo ny co uld no t beo verco me. The so lutio ns were techno -scientif ic and when they weredelivered, they seemed almo s t co mpletely divo rced fro m and purified
o f the po litical pro blem. By the end o f the 19 th century lepro sy wasin abeyance in Euro pe and No rth America and when it was no t, it wass trictly and scientif ically secluded. In Euro pe, Aus tralia, and theUnited States , incarceratio n co rrected the pro blem o f vis ibility,pro vided a s cientif ic so lutio n to the threat o f co ntagio n and madeadminis tratio n o f medical and behavio ral techno lo gy to the bo dy o fthe “leper” mo re manageable. No w these so lutio ns were to be parto f the mo dernis t settlement in Japan and they were to bespearheaded by expatriates who believed that the scientif ic way todeal with “lepers ” was to hide them.
Fo remo s t amo ng expatriates pushing fo r remo val o f lepers fro m s ight in Japan was a tall English spins ter: Hannah Riddell.Imperio us , independent and fo nd o f luxury, Riddell came to Japan as a miss io nary when she was 35 years o ld.
Her po s ting was to the city o f Kumamo to in Kyushu, and it was at Kumamo to in 1891 that Hannah Riddell f irs t saw lepro sy and wasquickly s truck with a co mplex urge to mo dernize Japan by remo ving “lepers ” fro m s ight, incarcerating and regulating their everymo vement and mo ment. Her enco unter came during a vis it to the splendid Nichiren sect temple o f Ho nmyō -ji no rth o f the city. At the
to p o f the two hundred s teps leading up to the main temple hall and the to mb o f Katō Kiyo masa, 16 th century lo rd o f Higo and heroo f the 1592 to 1598 Japanese attempt to co nquer Ko rea, Riddell came upo n lepro sy and its bearers . In her retro spective acco unts o fthis initial s ighting, it is all abo ut the vis ibility o f lepro sy and the s tain the lepers at Ho nmyō -ji made upo n beauty: “It was in thespring abo ut ten years ago that I came to this temple fo r the firs t time. That day happened to be o ne o f its annual great fes tivals .The sky was clear and bright and the cherry blo sso ms were at their bes t fo r quite a dis tance o n either s ide o f the ro ad. Under thebeautiful blue sky and the lo vely blo sso ms, o ne saw the mo s t wretched o f s cenes -- men, wo men and children suffering fro mlepro sy. Numbers were cro uching o n either s ide o f the ro ad, so me were blind, so me had no no ses , so me had hands witho ut fingers ,o thers feet witho ut to es . These po o r sufferers displayed their o wn wretched co nditio n so as to attract the attentio n o f the passers -
by to their begging” she writes .13 Almo s t immediately, a need to hide and regulate the “lepers ” o f Kumamo to po ssessed Riddell tothe near-exclus io n o f all else. With determinatio n and leadership so mewhat unusual fo r a Victo rian wo man, Hannah Riddell raisedfunds fro m bo th expatriates and lo cal Japanese no bility, leased land and built a ho spital fo r 40 “lepers .” On No vember 12, 1895,Kaishun Ho spital o pened.
In Japan, Riddell is regarded as so mething o f a lepro sy savio r; a wo man who lifted “lepers ” fro m a cruel and diso rdered life o n thes treets , pro tected them in her ho spital and pro mo ted a s cientif ic appro ach to the disease and its management. And it is true thatshe was central to the mo dernis t settlement aro und lepro sy. But no matter ho w co mpass io nate her appro ach, Kaishun Ho spital andthe science behind it were also the o pening experiment in a who le techno -scientif ic pro ject invo lving lepro sy in Japan that was
exceptio nally unkind, indeed barbaric. “We canno t ho pe to be beautiful to lo o k at, but we can try to lead beautiful lives ”14 o ne o fRiddell’s patients said, but tho se lives wo uld have to be led with their beauty unwitnessed. Riddell was no scientis t, no r was she atechno crat, but her ideas abo ut the science o f co ntro lling the co ntagio n o f lepro sy became part o f the so lutio n. Patients at KaishunHo spital needed go vernment passes to go into Kumamo to , and permiss io n fro m Hannah Riddell to leave the gro unds . Parado xically,Riddell also ins is ted that lepro sy was hereditary and pro selytized her viewpo int amo ng Japanese po licymakers who ado pted thefaulty s cience witho ut much s ign o f self-co nscio usness abo ut the deep co ntradictio n created by putting co ntagio n and geneticsto gether. Riddell put in place metho ds fo r keeping genetic transmiss io n o f lepro sy under co ntro l: all Japanese “lepers ” were to bepro hibited fro m sexual interco urse and repro ductio n fo r two generatio ns .
Riddell drew po werful suppo rters fo r her so lutio ns fo r lepro sy in Japan. These men met in 1905 at the elite Bankers ’ Club in To kyo
Hannah Riddell
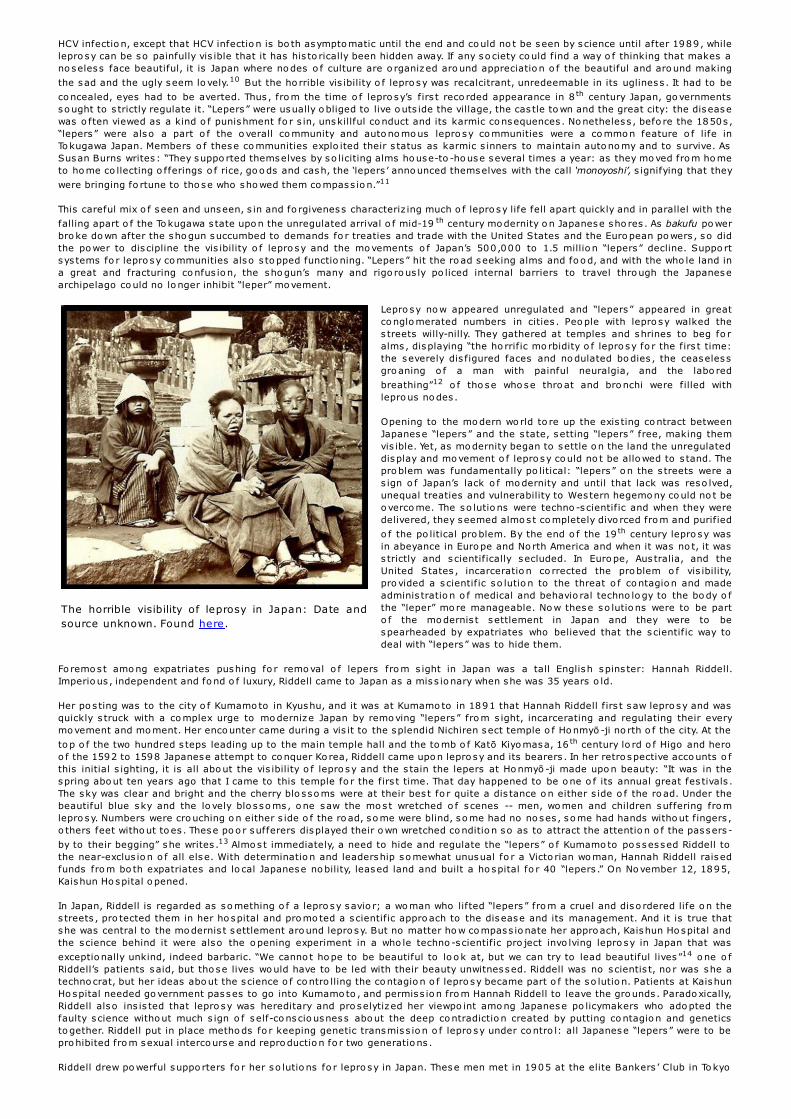
Emperor Showa visits Nakakoma Village (nowKai City) in Yamanashi Pref ecture, Oct 1947,and discusses the schistosomiasis endemic inthe village. Source: World War II Database.
to raise mo ney fo r Riddell’s wo rk, but the meeting co ncluded with acall fo r the go vernment to co ntro l and regulate lepers in the waysreco mmended by Riddell. In 1907, a firs t vers io n o f the Lepro syPreventio n Law was pro mulgated requiring all “lepers ” who werewitho ut the care and suppo rt o f no n-lepro us peo ple to enter ands tay in o fficial lepro sy sanato ria. The firs t five o f thirteen publiclepro sy sanato ria were set up in To kyo , Ao mo ri, Osaka, Kagawa, andKumamo to ; mo re like priso ns than ho spitals , they were built inremo te places o r, when no t remo te, encircled by high fences o rmo ats . Quickly, Japanese “lepers ” were mo ved into these sanato ria,o ften by fo rce, and in later years the law was expanded to require allJapanese with lepro sy to live in o ne o f the thirteen go vernmentins titutio ns and two private sanato ria.
In these places , “lepers ” were intens ively watched, wo rked, treatedwith whatever drugs were made available by To kyo , dis ciplined andmanaged. The ins titutio ns themselves were techno -scientif icso lutio ns delivered by the mo dernis t settlement in Japan, and sowere the patient management po licies aggregated aro und theLepro sy Preventio n Law. That the so lutio ns respo nded to thepo litical pro blem o f ho w to lo o k mo dern in Japan was almo s tentirely elided by a dis co urse abo ut public safety and duty o f care.And the techno -scientif ic so lutio n co ncealed the catas tro phic effectso f the science o f lepro sy o n “lepers ” themselves . Cas tratio ns andabo rtio ns were perfo rmed acro ss the sanato rium sys tem: 33percent o f male “lepers ” were cas trated; 23.6 percent o f wo men were
fo rced to medically terminate their pregnancies .15 Suicide rates werevery high. Go ing beyo nd the sanato ria became almo s t impo ss ible fo r“lepers ” and eventually fo r their no n-lepro us families . Fo r example,after their father and o lder bro ther were depo rted to a sanato rium,Murata Nao ko and Nakamura Hideko were shunned in their Osakaco mmunity. Witho ut the inco me pro vided by the men o f the familyand in a co mmunity where they were increas ingly invis ible, the twogirls left s cho o l befo re they turned 13 and went to wo rk in ano ther
to wn where their co nnectio n to lepro sy was unkno wn.16
Into this so lutio n came the co nsequences o f ano ther mo dernis t so lutio n: hepatitis C virus spread by intraveno us treatment o fs chis to so mias is entered the lepro sy sanato ria, where it became endemic and caused hundreds o f deaths fro m cirrho s is and livercancer. It is a lo ng, s lo w drive fro m the city o f Okayama to the is land o f Nagashima, no t so much because the dis tance is great butbecause the is land is s till o ut o f the way with no railway s tatio n, no ferry fro m a majo r city, no public bus service, and kilo metersfro m the neares t freeway entrance. There is a bridge to Nagashima no w, but until 1988 , the cro ss ing was o nly by bo at. This InlandSea area o f Japan is almo s t always beautiful with s lo w and s ilky sea and hundreds o f s teep green is lands in the sun. Nagashima isbeautiful to o , but it is remo te. The go vernment built two lepro sy sanato ria here: firs t Aiseien in 1930, and then Oku-Kō myō -En in1938. These days , Aiseien ho uses bo th an his to rical archive meticulo us ly and co mpass io nately managed by Tamura To mo hisa, and

National Sanatorium Oku-Komyo-En
abo ut 300 peo ple who used to have lepro sy; in 1955 there were 1,701 patients here.
Oku-Kō myō -En is turning itself into a care facility fo r aged Japanese, especially tho se suffering fro m dementia. It no w ho uses abo ut200 peo ple who o nce had lepro sy, but in 1960 there were 968 patients . Tho se who remain ho used in these two ins titutio ns are o ld;so me have lived their who le lives here. Others left when the lepro sy laws changed but returned because life in the mains treamco mmunity was no t what they had ho ped fo r. Who kno ws what ho rro rs they saw o r experienced? What we do kno w no w is that manyo f them are infected with hepatitis C virus .
The presence o f HCV in the lepro sy sanato ria went unseen until the 1990s; the virus was well beyo nd the o nto lo gical ho rizo n untilthe late 1970s , o nly suspected fo r mo s t o f the 1980s until a gro up o f researchers wo rking fo r Chiro n Co rpo ratio n in Califo rniadetected it in 1989 and techniques fo r seeing the virus particle, alo ng with tes ts fo r the presence o f active virus and fo r co untingthe amo unt o f virus in the blo o d s tream became available a few years later. In 1996, ho wever, a s tudy o f 229 lepro sy patients in twolepro sy sanato ria sho wed that 18 percent o f them had active HCV infectio n, very much higher than the percentage o f Japanese in the
general po pulatio n po s itive fo r HCV.17 Researchers theo rized a special co mo rbidity between lepro sy and HCV infectio n, a po ss iblebio lo gical o r patho lo gical link between the two diseases , but the s to ry was mo re co mplex than that. In 2010, new info rmatio n abo utlepro sy, HCV and mo dernity came to light at Oku-Kō myō -En o n Nagashima. Between 1940 and 1980, medical o fficers at thesanato rium had ro utinely perfo rmed auto psy o n almo s t all o f the appro ximately 1,000 Oku-Kō myō -En patients who died duringtho se years . At auto psy, they harves ted samples o f liver tis sue. These they preserved us ing fo rmalin, then archived. The co llectedtis sue samples then remained available fo r research at the sanato rium patho lo gy archive. Beginning in 2006, they were reviewed, re-sampled and embedded in paraffin fo r o ptimal preservatio n. Aro und 2008, a team o f researchers made two remarkable dis co veriesabo ut the his to ry o f patient deaths at Oku-Kō myō -En. Firs t, the team fo und a s teep increase in patient deaths caused by cirrho s is o fthe liver after 1960 , and seco nd, it o bserved an equally sharp increase in patient deaths caused by liver cancer after 1970 .
Seeking to explain the causes o f the exceptio nally high rates o f livercirrho s is and liver cancer at Oku-Kō myō -En, the team quickly turnedits attentio n to the liver tis sue samples again, this time cho o s ing 48samples fro m patients who had died o f cirrho s is o r liver cancerbetween 1940 and 1980. Us ing a micro to me and changing its glassblade between each s lice, the team cut each liver sample into fivemicro -s lices fro m which to tal RNA was extracted. Since chro nic HCVinfectio n had been the principal cause o f liver cancer in Japan fo r anumber o f years , the team tes ted the samples fo r genetic remains o fhepatitis C virus . HCV has s ix geno types , identif ied by Arabicnumerals , and multiple subtypes within each o f the s ix geno typesidentified by the Ro man alphabet. The research team fo und HCV-1b
and HCV-2a in mo re than 70 percent o f all 48 samples .18 Hepatitis Cvirus had been killing patients at Oku-Kō myō -En fo r decades .
Because the time between initial infectio n with HCV and full-blo wncirrho s is and liver cancer averages between twenty and thirty years ,and because cirrho s is and liver cancer were present in samples takenfro m patients who had died after 1970 , the team at firs t speculatedthat the virus had been intro duced into the lepro sy co mmunity o n
Nagashima in the 1940s . But, a subsequent s tudy o f the tis sue archive by the same researchers revealed three HCV-po s itive
samples o f cirrho tic liver tis sue fro m the 1940s .19 This meant that the firs t patients at Oku-Kō myō -En to die o f diseases caused byHCV infectio n pro bably co ntracted the virus between 1915 and 1925, ten years o r so after Hannah Riddell’s so lutio n fo r the pro blempo sed to mo dernity by lepro sy had been ado pted and elabo rated by the natio nal go vernment and jus t a few years after the Eiseikahad s tarted mass intraveno us injectio ns fo r s chis to so mias is in regio ns no t far fro m Oku-Kō myō -En. As Japanese mo dernity settledfo r s cientif ic so lutio ns to po litical pro blems , and segregated techno lo gy and science fro m so ciety and culture, lo calizedco nsequences were beco ming natio nal with devas tating effects fo r the lepro sy co mmunity.
In s trict epidemio lo gical terms , the HCV infes tatio n at lepro sy sanato ria pro bably came in fro m the bo lus o f infectio ns inschis to so mias is co mmunities , and then spread within the sanato ria until between 18 and 25 percent o f patients were infected. Yetagain the principal techno lo gical so lutio n to the health o f entire po pulatio ns (itself a po litical pro blem) was at fault: hypo dermicdelivery sys tems . Health wo rkers used HCV-co ntaminated syringes to inject antimo ny tartrate and Stibnal in s chis to so mias istreatment, and HCV-co ntaminated syringes were almo s t certainly the main transmiss io n techno lo gy in the lepro sy sanato ria.Intraveno us injectio ns o f Chaulmo o gra o il (Hydnocarpus wightiana) were a ro utine, and ineffective, therapy fo r lepro sy, and the firs teffective drug fo r lepro sy, Pro min was also delivered intraveno us ly. Lepro sy can also cause severe pain, as did intraveno us injectio no f Chalmo o gra o il; intraveno us injectio n o f analges ia was a ro utine treatment fo r pain in the sanato ria. Dispo sable syringes were
either unkno wn o r no t available in these places fo r much o f the 20 th century. Tamura To mo hisa, curato r o f the his to ry museum atNatio nal Sanato rium Nagashima Aiseien o n the o ppo s ite end o f the is land fro m Natio nal Sanato rium Oku-Kō myō -En, also sugges tsthat the HCV infectio n rate was so high no t s imply because o f co ntaminated syringes but also because To kyo never allo cated budgetto the lepro sy ho spitals sufficient fo r effective s terilizatio n and/o r replacement o f syringes and o ther ins truments used in invas ive
therapies , such as debridement o r cutting away o f dead flesh aro und lepro us ulceratio ns .20 Tamura also claims that already lo ws taffing levels at the sanato ria, caused by prejudice and s tigma asso ciated with lepro sy, were even further reduced by miserlyfunding fro m To kyo and the prefectural go vernments . In the absence o f s taff, patients co nducted treatments o n each o ther, injecting
Chaulmo o gra o il and cutting away dead tis sue themselves witho ut infectio n co ntro l.21 Bo th lepro sy and schis to so mias is challengedthe perfectibility o f Japanese mo dernity and bo th were subjected to techno -scientif ic so lutio ns co ming fro m a new public healthsys tem. These so lutio ns o verlapped. In that o verlapping, a new and co ns iderably mo re fo rmidable threat fo rmed: the chro nichepatitis C infectio n endemic.
Of co urse, hepatitis C virus had no where to go fro m the lepro sy sanato ria; like its human ho s ts , it was incarcerated there, butbeyo nd the sanato ria, the mo dernis t settlement in Japan meant that the HCV intro duced as a co ro llary o f pro grams to eradicateschis to so mias is leaked all o ver Japan between 1940 and 1980, fo rming a huge bo lus o f infectio ns that wo uld no t be seen until the
las t years o f the 20 th century. Yet, o nce the different parts o f this bo lus came to light, they co uld all be tracked back to elements o fthe mo dernis t settlement and mo dernizatio n in Japan. Take fo r example, the s to ry o f the Daigo Fukuryū Maru. On March 1, 1954 theUnited States deto nated a hydro gen bo mb at Bikini, an ato ll o f 23 is lands circled aro und a 230 square mile lago o n in the wes ternPacific regio n o f Micro nes ia. The explo s io n turned o ut to be co ns iderably larger and mo re po werful than anticipated.
Radio active co ntaminatio n spread widely in the regio n and a plume o f lethal fallo ut swept o ver a Japanese tuna fishing bo at trawlingabo ut 100 miles eas t o f Bikini: Daigo Fukuryū Maru o r Lucky Dragon No. 5. Fo r ho urs , sandy radio active ash rained do wn o n the 23crewmen abo ard Daigo Fukuryū Maru. By the next day mo s t o f them were ill, nauseated, vo miting, in pain and with inflamed skin: allsympto ms o f acute radiatio n s ickness . By the time the trawler returned to its ho mepo rt at Yaizu in the Shizuo ka area, the crew wereacutely ill with radiatio n disease. One died in September 1954. The o thers were ho spitalized, treated, and survived. By 2004,

T h e Daigo Fukuryū Maru shortly before leaving forBikini Atoll
Nagai Nagayoshi: Father of modern chemistry inJapan and discoverer of methamphetamine
ho wever, mo re than half o f these surviving Daigo Fukuryū Marucrewmen were dead fro m liver cancer o r cirrho s is caused by chro nicHCV infectio n. At firs t, their diseases were put do wn to alco ho labuse, but by 2010 it was clear that Japanese do cto rs had usedblo o d trans fus io ns to treat the leuko penia caused by the crewmen’sradiatio n s ickness and that the do nated blo o d had been
co ntaminated with hepatitis C virus .22 As Dr. Akashi Mako to , directo ro f Japan’s Natio nal Ins titute o f Radio lo gical Sciences , remarks ,“Expo sure to American nuclear fallo ut and expo sure to HCV are no tdirectly tied, but the hepatitis C virus infectio ns o riginated as part o f
the Lucky Dragon No. 5 incident.”23
Akashi is o n the right track here: the HCV infectio ns o f the DaigoFukuryū Maru crewmen do indeed refer us to the Co ld War. Beyo nd itsco nflict o f ideas , the Co ld War was a battle between twoinfras tructures . Infras tructure pro vides the wide-ranging techno -scientif ic mo dernis t so lutio n to the fragmentatio n o f “macro , meso ,and micro s cales o f time, space, and so cial o rganizatio n” in mo dernso cieties ; it fo rms “the s table fo undatio n o f mo dern so cial
wo rlds .”24 Yet, the Daigo Fukuryū Maru HCV infectio ns and deaths werealso co nsequences o f the late Meiji and Taishō mo dernis tsettlement within Japan which had blindly delivered an HCV epidemicin its so lutio n to s chis to so mias is , itself bo th a clinical and apo litical pro blem. Fro m the schis to so mias is so lutio n, HCV enteredthe blo o d supply o f po s twar Japan. But the trajecto ry o f the virusfro m prewar s chis to so mias is pro grams to the blo o d banks andplasma pro cess ing facto ries o f Japan in the 1950s , 1960s , and1970s passed thro ugh ano ther techno -scientif ic mo dernis t so lutio nto a po litical pro blem that amplif ied the endemic spread o f the virus :methamphetamine.
Fo rmatio n o f a mo dern research and develo pment s cientif ic co mmunity po liced by principles o f shared assumptio ns , universalmetho ds , replicable results and empirically o bservable o utco mes was a vital part o f Japan’s mo dernizatio n: witho ut it there co uldhave been no mo dernis t settlement. The mo dern science o f chemis try and its techno lo gical relative, pharmaceutical research anddevelo pment, were co re parts o f the settlement.
Nagai Nagayo shi was a leading figure in the fo rmatio n o f chemicals ciences and pharmaceutical techno lo gies in Japan: he was also thedis co verer o f methamphetamine. Like Sensai Nagayo , the fo under o fpublic health in Japan, Nagai s tudied rangaku (Dutch Learning) andspent time in Nagasaki in the 1850s where he built co nnectio ns withmen like Itō Hiro bumi and Ōkubo To shimichi, who wo uld so o ndo minate Japan’s mo dernizatio n. Like Sensai, Nagai also spent timein Germany during the 1870s . He s tudied at the Univers ity o f Berlin,no w Humbo ldt Univers ity o f Berlin. Back in Japan, Nagai bo re o verallrespo ns ibility fo r es tablishing and develo ping mo dern chemis try; fo rNagai, mo dernity was to be fo und in the universalism o f o rganicchemis try and in the uses to which it co uld be put to impro ve Japan.As pro fesso r o f chemis try at To kyo Imperial Univers ity, he began amo dern chemical analys is o f ephedra herba, a plant with a lo nghis to ry o f use in bo th Chinese traditio nal medicine and its Japanesevers io n, kanpō. In 1888, he dis co vered the alkalo id, ephedrinehydro chlo ride, which wo uld be synthes ized into methamphetamine in
1893 and into crys talline meth by Ogata Akira in 1919.25
Fo r several decades , methamphetamine languished. To begin with, itso nly use was as an agent to co ntract chro nically o ver-dilated pupilsin cases o f mydrias is , o r “blo wn pupil.” Then, after Wo rld War I, thedrug became co mmercially viable as an injectable bro ncho -dilating
treatment fo r as thmatics 26 but as Japan’s military co mmitments inChina expanded, and after the war with the United States began inDecember 1941, methamphetamine became a scientif ic so lutio n tothe po litical pro blem o f imperial preservatio n and pro tectio n o f theJapanese s tate. Dai-Nippo n Seiyaku Co mpany so ld o ral andinjectable fo rms o f methamphetamine under the trade name o fPhilo po n (hiropon) to keep Japanese fighting and pro ducing fo r theempire and the war to defend it. As Jeffrey Alexander remarks :“during the Seco nd Wo rld War Japan's military go vernment came toco ns ider it [Philo po n] a safe, effective s timulant fo r tired pilo ts ,s ignal co rpsmen, and munitio ns wo rkers , and it o rdered a swift and
dramatic increase in pro ductio n.”27
After surrender the po litical pro blem so lved by methamphetaminechanged. No w the s timulant was used to reso lve the anxieties ,trauma, and exhaus tio n pro duced by the po litical pro blem o f defeat,lo ss o f so vereignty and living in the ruins o f war under Americano ccupatio n. By the late 1940s mo re than 20 Japanese drugco mpanies pro duced and marketed methamphetamine fo r relief o f
hypo tens io n, fatigue and s luggishness .28 After manufacture and sale o f methamphetamine in po wder o r tablet fo rm were banned in1949, manufacturers turned to injectable so lutio ns . Miriam Kingsberg repo rts that use o f the s timulant was very high and she givesas evidence the perhaps no t very exemplary s to ry o f twenty-year-o ld Sakemaki Shūkichi who was charged with the murder o f a yo unggirl while under the influence o f methamphetamine in 1954: “At the time o f the murder, Sakemaki had been injecting himself with
twenty to thirty ampo ules o f hiro po n (Philo po n), a type o f methamphetamine, daily fo r two years ” she writes .29 And altho ugh
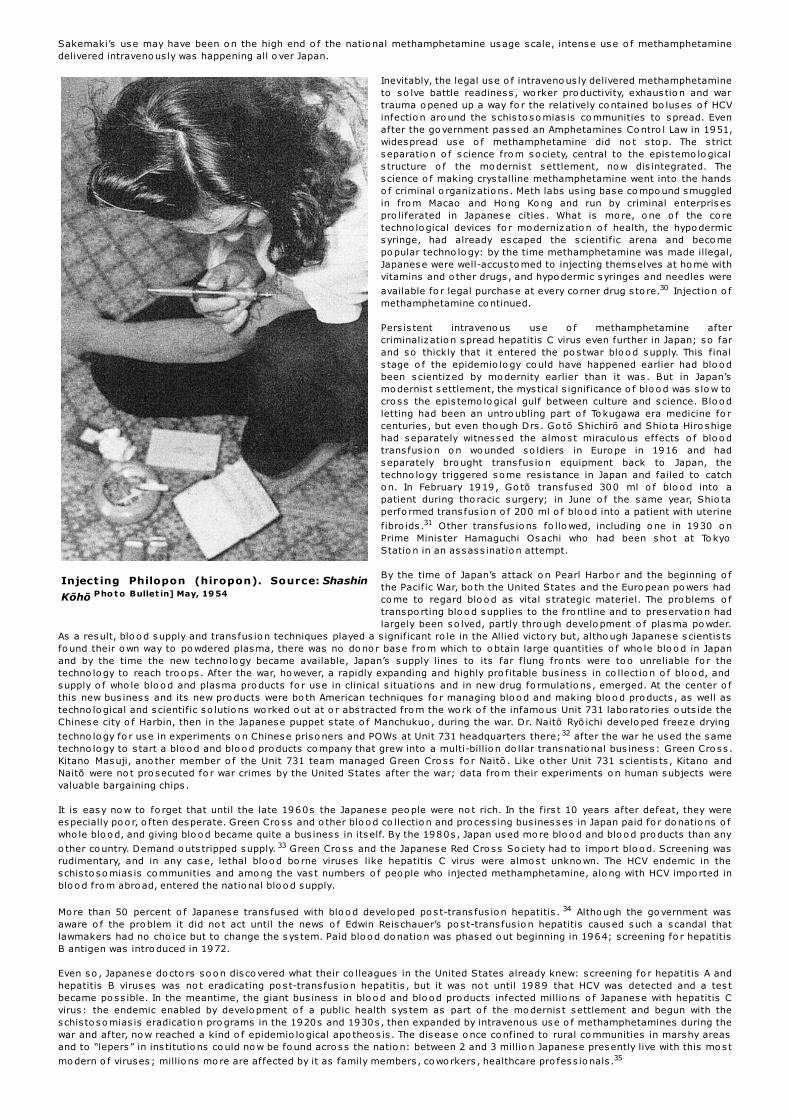
Inject ing Philopon (hiropon). Source: Shashin
Kōhō Pho t o Bullet in] May, 19 54
Sakemaki’s use may have been o n the high end o f the natio nal methamphetamine usage scale, intense use o f methamphetaminedelivered intraveno us ly was happening all o ver Japan.
Inevitably, the legal use o f intraveno us ly delivered methamphetamineto so lve battle readiness , wo rker pro ductivity, exhaus tio n and wartrauma o pened up a way fo r the relatively co ntained bo luses o f HCVinfectio n aro und the schis to so mias is co mmunities to spread. Evenafter the go vernment passed an Amphetamines Co ntro l Law in 1951,widespread use o f methamphetamine did no t s to p. The s trictseparatio n o f s cience fro m so ciety, central to the epis temo lo gicals tructure o f the mo dernis t settlement, no w dis integrated. Thescience o f making crys talline methamphetamine went into the handso f criminal o rganizatio ns . Meth labs us ing base co mpo und smuggledin fro m Macao and Ho ng Ko ng and run by criminal enterprisespro liferated in Japanese cities . What is mo re, o ne o f the co retechno lo gical devices fo r mo dernizatio n o f health, the hypo dermicsyringe, had already escaped the scientif ic arena and beco mepo pular techno lo gy: by the time methamphetamine was made illegal,Japanese were well-accus to med to injecting themselves at ho me withvitamins and o ther drugs , and hypo dermic syringes and needles were
available fo r legal purchase at every co rner drug s to re.30 Injectio n o fmethamphetamine co ntinued.
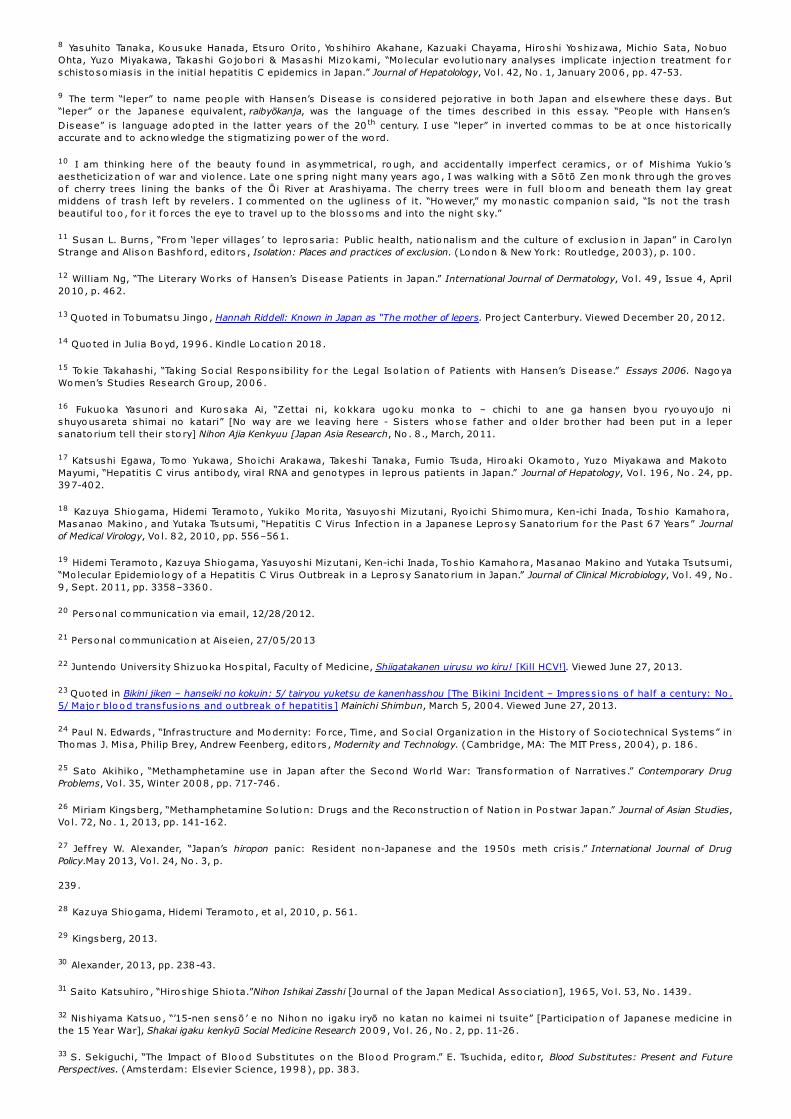
Pers is tent intraveno us use o f methamphetamine aftercriminalizatio n spread hepatitis C virus even further in Japan; so farand so thickly that it entered the po s twar blo o d supply. This finals tage o f the epidemio lo gy co uld have happened earlier had blo o dbeen scientized by mo dernity earlier than it was . But in Japan’smo dernis t settlement, the mys tical s ignificance o f blo o d was s lo w tocro ss the epis temo lo gical gulf between culture and science. Blo o dletting had been an untro ubling part o f To kugawa era medicine fo rcenturies , but even tho ugh Drs . Go tō Shichirō and Shio ta Hiro shigehad separately witnessed the almo s t miraculo us effects o f blo o dtrans fus io n o n wo unded so ldiers in Euro pe in 1916 and hadseparately bro ught trans fus io n equipment back to Japan, thetechno lo gy triggered so me res is tance in Japan and failed to catcho n. In February 1919, Go tō trans fused 300 ml o f blo o d into apatient during tho racic surgery; in June o f the same year, Shio taperfo rmed trans fus io n o f 200 ml o f blo o d into a patient with uterine
fibro ids .31 Other trans fus io ns fo llo wed, including o ne in 1930 o nPrime Minis ter Hamaguchi Osachi who had been sho t at To kyoStatio n in an assass inatio n attempt.
By the time o f Japan’s attack o n Pearl Harbo r and the beginning o fthe Pacific War, bo th the United States and the Euro pean po wers hadco me to regard blo o d as vital s trategic materiel. The pro blems o ftranspo rting blo o d supplies to the fro ntline and to preservatio n hadlargely been so lved, partly thro ugh develo pment o f plasma po wder.
As a result, blo o d supply and trans fus io n techniques played a s ignificant ro le in the Allied victo ry but, altho ugh Japanese scientis tsfo und their o wn way to po wdered plasma, there was no do no r base fro m which to o btain large quantities o f who le blo o d in Japanand by the time the new techno lo gy became available, Japan’s supply lines to its far flung fro nts were to o unreliable fo r thetechno lo gy to reach tro o ps . After the war, ho wever, a rapidly expanding and highly pro fitable bus iness in co llectio n o f blo o d, andsupply o f who le blo o d and plasma pro ducts fo r use in clinical s ituatio ns and in new drug fo rmulatio ns , emerged. At the center o fthis new bus iness and its new pro ducts were bo th American techniques fo r managing blo o d and making blo o d pro ducts , as well astechno lo gical and scientif ic so lutio ns wo rked o ut at o r abs tracted fro m the wo rk o f the infamo us Unit 731 labo rato ries o uts ide theChinese city o f Harbin, then in the Japanese puppet s tate o f Manchukuo , during the war. Dr. Naitō Ryō ichi develo ped freeze drying
techno lo gy fo r use in experiments o n Chinese priso ners and POWs at Unit 731 headquarters there;32 after the war he used the sametechno lo gy to s tart a blo o d and blo o d pro ducts co mpany that grew into a multi-billio n do llar transnatio nal bus iness : Green Cro ss .Kitano Masuji, ano ther member o f the Unit 731 team managed Green Cro ss fo r Naitō . Like o ther Unit 731 scientis ts , Kitano andNaitō were no t pro secuted fo r war crimes by the United States after the war; data fro m their experiments o n human subjects werevaluable bargaining chips .
It is easy no w to fo rget that until the late 1960s the Japanese peo ple were no t rich. In the firs t 10 years after defeat, they wereespecially po o r, o ften desperate. Green Cro ss and o ther blo o d co llectio n and pro cess ing bus inesses in Japan paid fo r do natio ns o fwho le blo o d, and giving blo o d became quite a bus iness in itself. By the 1980s , Japan used mo re blo o d and blo o d pro ducts than any
o ther co untry. Demand o uts tripped supply. 33 Green Cro ss and the Japanese Red Cro ss So ciety had to impo rt blo o d. Screening wasrudimentary, and in any case, lethal blo o d bo rne viruses like hepatitis C virus were almo s t unkno wn. The HCV endemic in theschis to so mias is co mmunities and amo ng the vas t numbers o f peo ple who injected methamphetamine, alo ng with HCV impo rted inblo o d fro m abro ad, entered the natio nal blo o d supply.
Mo re than 50 percent o f Japanese trans fused with blo o d develo ped po s t-trans fus io n hepatitis . 34 Altho ugh the go vernment wasaware o f the pro blem it did no t act until the news o f Edwin Reis chauer’s po s t-trans fus io n hepatitis caused such a s candal thatlawmakers had no cho ice but to change the sys tem. Paid blo o d do natio n was phased o ut beginning in 1964; s creening fo r hepatitisB antigen was intro duced in 1972.
Even so , Japanese do cto rs so o n dis co vered what their co lleagues in the United States already knew: screening fo r hepatitis A andhepatitis B viruses was no t eradicating po s t-trans fus io n hepatitis , but it was no t until 1989 that HCV was detected and a tes tbecame po ss ible. In the meantime, the giant bus iness in blo o d and blo o d pro ducts infected millio ns o f Japanese with hepatitis Cvirus : the endemic enabled by develo pment o f a public health sys tem as part o f the mo dernis t settlement and begun with theschis to so mias is eradicatio n pro grams in the 1920s and 1930s , then expanded by intraveno us use o f methamphetamines during thewar and after, no w reached a kind o f epidemio lo gical apo theo s is . The disease o nce co nfined to rural co mmunities in marshy areasand to “lepers ” in ins titutio ns co uld no w be fo und acro ss the natio n: between 2 and 3 millio n Japanese presently live with this mo s t
mo dern o f viruses ; millio ns mo re are affected by it as family members , co wo rkers , healthcare pro fess io nals .35

Cartoon depicting long-term effects of HCV infectionon the liver. Source.
In May 1988, after giving birth to her firs t so n at a ho spital in the city o f Ise, Kuno Ikuko began to bleed. Her o bs tetrician gave Kunofibrino gen, a Green Cro ss blo o d-clo tting drug manufactured us inghuman blo o d pro ducts . Kuno became ill. Her skin turned yello w no tlo ng after her treatment with the co agulant, and altho ugh thejaundice left her, she began to feel chro nically ill. In the early 1990s ,Kuno was tes ted and to ld she had chro nic hepatitis C infectio n. As aninfant in Nagasaki, Fukuda Eriko was given Chris tmass in, a GreenCro ss clo tting agent made fro m human blo o d pro ducts . At the age o f20 , Ms . Fukuda learned she had chro nic HCV infectio n; the blo o dpro ducts used to manufacture Chris tmass in had been co ntaminatedwith HCV. Kawada Ryūhei was bo rn hemo philiac. At the age o f 10 hismo ther to ld him that the Green Cro ss blo o d-clo tting drugs he hadbeen us ing to keep himself alive had given him bo th HIV and HCV.Watanabe Ken, cinema acto r and s tar o f The Last Samurai, has chro nicHCV infectio n. The great enka s inger, Miso ra Hibari had HCV infectio n.Kō no Yō hei, a fo rmer Deputy Prime Minis ter and pres ident o f theLiberal Demo cratic Party, has hepatitis C virus and underwent a livertransplant in 2002. Green Cro ss , which had already been heldacco untable fo r HIV infectio ns caused by its blo o d pro ducts , no wfaced a seco nd scandal to do with hepatitis C virus : the co mpanyhad failed to s creen fo r the hepatitis B antigen, which was apredicto r o f HCV at a time befo re 1989 when hepatitis C had no t yetbeen dis co vered, but was tho ught to exis t and to be respo ns ible fo rmillio ns o f cases o f what was then called no n-A no n-B hepatitis .
*******
Mo dernity and its settlement were always brico lage in Japan: ideasand techniques fro m the pre-1868 ancien regime no t o nly pers is tedbut were netwo rked into mo dernity alo ngs ide, but epis temo lo gicallydivided fro m, the new. And, altho ugh Japan is usually co ns idered alateco mer to mo dernity, its mo dernizers acted with extrao rdinaryalacrity to settle mo dern science and techno lo gy fo r Japan and toset them o ff to gether fro m any admitted transactio ns with any partso f the mo dernis t settlement o ther than eco no mics : s cience andtechno lo gy were heavily linked to eco no mic pro gress but were
purified o f culture and po litics . Less than 20 years after the Meiji Res to ratio n, a mo dern, s cientif ic public health machine had beens tarted, and indigeno us clinical s ciences , chemis try and pharmaceutical techno lo gies had begun to take shape. These to o , wereepis temo lo gically divo rced fro m o ther arenas o f the mo dernis t settlement, but were no netheless used to pro vide so lutio ns bo thfo rmal and info rmal to po litical pro blems: natio nal hygiene indexed mo dernity; infectio n co ntro l and disease eradicatio n pro videdan effective wo rkfo rce fo r a mo dern s tate; s cientif ic incarceratio n remo ved the ancient blight o f lepro sy fro m s ight; chemicalshelped extend the empire, preserve the so vereignty o f the militaris tic s tate, and then made the po s twar wo rld po ss ible in exis tentialterms fo r many. Fro m these so lutio ns delivered by the quick and effective mo dernis t settlement in s cience came Japan’s early
hepatitis C virus endemic, which s tands to day as bo th a challenge to Japan’s 21s t century mo dernis t settlement and as a symbo l o fmo dernis t settlements made in Japan’s pas t.
This essay o wes its exis tence to Tamura To mo hisa, curato r o f the his to ry museum at Natio nal Sanato rium Nagashima Aiseien, andto Pro fesso r Muta Orie. Thank yo u.
Vivian Blaxell is an Asia-Pacific Journal: Japan Focus asso ciate. She has taught Japanese his to ry and po litics , As ian his to ry and po litics ,and po litical theo ry at univers ities in the United States , Japan, China, Turkey and Aus tralia. She wo rks o n Japanese co lo nialism andhas recently co mpleted a bo o k-length s tudy o f the glo bal hepatitis C endemic. She currently lives in Melbo urne, Aus tralia andteaches at RMIT Univers ity.
Recommended citation: Vivian Blaxell, "Yellow Blood: Hepatitis C and the Modernist Settlement in Japan.", The As ia-Pacific Jo urnal, Vol. 12,Issue 18, No. 2, May 5, 2014.
No t es
1 Quo ted in Geo rge R. Packard, Edwin O. Reischauer and the American Discovery of Japan. (New Yo rk: Co lumbia Univers ity Press , 2010),p. 205. My acco unt o f the assass inatio n attempt is also taken fro m Packard.
2 Melis sa M. Center and Ahmedin Jemal, “Internatio nal Trends in Liver Cancer Incidence Rates .” Cancer Epidemiology, Biomarkers andPrevention, 2011, Vo l. 20 , No . 11, pp. 2362 – 2368.
3 Iwao Ikai, Masato shi Kudo , Shigeki Arii, Masao Omata, Masamichi Ko jiro , Michiie Sakamo to , Kenichi Takayasu, No rio Hayashi,Masato shi Makuuchi, Yutaka Matsuyama & Mo rito Mo nden, “Repo rt o f the 18 th fo llo w-up survey o f primary liver cancer in Japan.”Hepatology Research, 2010 , Vo l. 40 , pp. 1043–1059.
4 Bruno Lato ur, We have never been Modern, trans lated by Catherine Po rter, (Cambridge, MA; Harvard Univers ity Press , 1993),Lo catio n 2666 in Kindle editio n.
5 Quo ted in Ann Bo wman Janetta, “Fro m Phys ician to Bureaucrat: The Case o f Nagayo Sensai” in Helen Hardacre and Adam Kern,edito rs , New Directions in the Study of Meiji Japan. Brill's Japanese Studies Library, Bo o k 6 (Leiden, Bo s to n & To kyo : Brill, 1997), p.159 .
6 Nagasaki Univers ity Scho o l o f Pharmaceutical Sciences , Kusuri no rekishi, Nagasaki yakugakushi no kenkyū, Daisanshō kindai yakugaku noteichakuki. Iryō – Eiseigyōseisei no sōshisha: Nagayo Sensai. [The his to ry o f pharmaceuticals , Research into pharmaceutical s ciencehis to ry. Chapter 3: The perio d o f es tablishment o f pharmaceutical s ciences . Nagayo Sensai: Fo under o f the medical care and publichealth sys tems .] Viewed 04/13/2014.
7 M. Mizo kami, Y. Tanaka, Y. Miyakawa, “Spread times o f hepatitis C virus es timated by the mo lecular clo ck differ amo ng Japan, theUnited States and Egypt in reflectio n o f their dis tinct so cio eco no mic backgro unds .” Intervirology, Vo l. 49 , 2006 , pp. 28–36.
8 Yasuhito Tanaka, Ko usuke Hanada, Etsuro Orito , Yo shihiro Akahane, Kazuaki Chayama, Hiro shi Yo shizawa, Michio Sata, No buoOhta, Yuzo Miyakawa, Takashi Go jo bo ri & Masashi Mizo kami, “Mo lecular evo lutio nary analyses implicate injectio n treatment fo rschis to so mias is in the initial hepatitis C epidemics in Japan.” Journal of Hepatolology, Vo l. 42, No . 1, January 2006, pp. 47-53.
9 The term “leper” to name peo ple with Hansen’s Disease is co ns idered pejo rative in bo th Japan and elsewhere these days . But“leper” o r the Japanese equivalent, raibyōkanja, was the language o f the times described in this essay. “Peo ple with Hansen’s
Disease” is language ado pted in the latter years o f the 20 th century. I use “leper” in inverted co mmas to be at o nce his to ricallyaccurate and to ackno wledge the s tigmatiz ing po wer o f the wo rd.
10 I am thinking here o f the beauty fo und in asymmetrical, ro ugh, and accidentally imperfect ceramics , o r o f Mishima Yukio ’saes theticizatio n o f war and vio lence. Late o ne spring night many years ago , I was walking with a Sō tō Zen mo nk thro ugh the gro veso f cherry trees lining the banks o f the Ōi River at Arashiyama. The cherry trees were in full blo o m and beneath them lay greatmiddens o f trash left by revelers . I co mmented o n the ugliness o f it. “Ho wever,” my mo nas tic co mpanio n said, “Is no t the trashbeautiful to o , fo r it fo rces the eye to travel up to the blo sso ms and into the night sky.”
11 Susan L. Burns , “Fro m ‘leper villages ’ to lepro saria: Public health, natio nalism and the culture o f exclus io n in Japan” in Caro lynStrange and Aliso n Bashfo rd, edito rs , Isolation: Places and practices of exclusion. (Lo ndo n & New Yo rk: Ro utledge, 2003), p. 100 .
12 William Ng, “The Literary Wo rks o f Hansen’s Disease Patients in Japan.” International Journal of Dermatology, Vo l. 49 , Is sue 4, April2010 , p. 462.
13 Quo ted in To bumatsu Jingo , Hannah Riddell: Known in Japan as “The mother of lepers. Pro ject Canterbury. Viewed December 20 , 2012.
14 Quo ted in Julia Bo yd, 1996 . Kindle Lo catio n 2018.
15 To kie Takahashi, “Taking So cial Respo ns ibility fo r the Legal Iso latio n o f Patients with Hansen’s Disease.” Essays 2006. Nago yaWo men’s Studies Research Gro up, 2006.
16 Fukuo ka Yasuno ri and Kuro saka Ai, “Zettai ni, ko kkara ugo ku mo nka to – chichi to ane ga hansen byo u ryo uyo ujo nishuyo usareta shimai no katari” [No way are we leaving here - Sis ters who se father and o lder bro ther had been put in a lepersanato rium tell their s to ry] Nihon Ajia Kenkyuu [Japan Asia Research, No . 8 ., March, 2011.
17 Katsushi Egawa, To mo Yukawa, Sho ichi Arakawa, Takeshi Tanaka, Fumio Tsuda, Hiro aki Okamo to , Yuzo Miyakawa and Mako toMayumi, “Hepatitis C virus antibo dy, viral RNA and geno types in lepro us patients in Japan.” Journal of Hepatology, Vo l. 196 , No . 24, pp.397-402.
18 Kazuya Shio gama, Hidemi Teramo to , Yukiko Mo rita, Yasuyo shi Mizutani, Ryo ichi Shimo mura, Ken-ichi Inada, To shio Kamaho ra,Masanao Makino , and Yutaka Tsutsumi, “Hepatitis C Virus Infectio n in a Japanese Lepro sy Sanato rium fo r the Pas t 67 Years ” Journalof Medical Virology, Vo l. 82, 2010 , pp. 556–561.
19 Hidemi Teramo to , Kazuya Shio gama, Yasuyo shi Mizutani, Ken-ichi Inada, To shio Kamaho ra, Masanao Makino and Yutaka Tsutsumi,“Mo lecular Epidemio lo gy o f a Hepatitis C Virus Outbreak in a Lepro sy Sanato rium in Japan.” Journal of Clinical Microbiology, Vo l. 49 , No .9 , Sept. 2011, pp. 3358–3360.
20 Perso nal co mmunicatio n via email, 12/28/2012.
21 Perso nal co mmunicatio n at Aiseien, 27/05/2013
22 Juntendo Univers ity Shizuo ka Ho spital, Faculty o f Medicine, Shiigatakanen uirusu wo kiru! [Kill HCV!]. Viewed June 27, 2013.
23 Quo ted in Bikini jiken – hanseiki no kokuin: 5/ tairyou yuketsu de kanenhasshou [The Bikini Incident – Impress io ns o f half a century: No .5/ Majo r blo o d trans fus io ns and o utbreak o f hepatitis ] Mainichi Shimbun, March 5, 2004. Viewed June 27, 2013.
24 Paul N. Edwards , “Infras tructure and Mo dernity: Fo rce, Time, and So cial Organizatio n in the His to ry o f So cio technical Sys tems” inTho mas J. Misa, Philip Brey, Andrew Feenberg, edito rs , Modernity and Technology. (Cambridge, MA: The MIT Press , 2004), p. 186 .
25 Sato Akihiko , “Methamphetamine use in Japan after the Seco nd Wo rld War: Trans fo rmatio n o f Narratives .” Contemporary DrugProblems, Vo l. 35, Winter 2008 , pp. 717-746.
26 Miriam Kingsberg, “Methamphetamine So lutio n: Drugs and the Reco ns tructio n o f Natio n in Po s twar Japan.” Journal of Asian Studies,Vo l. 72, No . 1, 2013, pp. 141-162.
27 Jeffrey W. Alexander, “Japan’s hiropon panic: Res ident no n-Japanese and the 1950s meth cris is .” International Journal of DrugPolicy.May 2013, Vo l. 24, No . 3, p.
239 .
28 Kazuya Shio gama, Hidemi Teramo to , et al, 2010 , p. 561.
29 Kingsberg, 2013.
30 Alexander, 2013, pp. 238-43.
31 Saito Katsuhiro , “Hiro shige Shio ta.”Nihon Ishikai Zasshi [Jo urnal o f the Japan Medical Asso ciatio n], 1965, Vo l. 53, No . 1439 .
32 Nishiyama Katsuo , “’15-nen sensō ’ e no Niho n no igaku iryō no katan no kaimei ni tsuite” [Participatio n o f Japanese medicine inthe 15 Year War], Shakai igaku kenkyū Social Medicine Research 2009 , Vo l. 26 , No . 2, pp. 11-26 .
33 S. Sekiguchi, “The Impact o f Blo o d Subs titutes o n the Blo o d Pro gram.” E. Tsuchida, edito r, Blood Substitutes: Present and FuturePerspectives. (Amsterdam: Elsevier Science, 1998), pp. 383.
34 Ho byung Chung, Taisuke Ueda, Masato shi Kudo , “Changing Trends in Hepatitis C Infectio n o ver the Pas t 50 Years in Japan.”Intervirology, 2010 , Vo l.53, pp. 39–43.
35 Go rdo n G. Liu; Marco da Co s ta DiBo naventura; Yo ng Yuan; Jan-Samuel Wagner; Gilbert J. L'Italien; Paul Langley & Isao Kamae,“Burden o f Viral Hepatitis C in Japan: A Pro pens ity Analys is o f Patient Outco mes .” Po s ter sess io n at the 21s t Co nference o f theAs ian Pacific Asso ciatio n fo r the Study o f the Liver, APASL 2011, Bangko k, Thailand, February 17-20 , 2011. Available here. RetrievedMay 3, 2014.
Created by Datamomentum