Working Together to Build a Respectful Workplace: Transforming OR Culture
12
Working Together to Build a Respectful Workplace: Transforming OR Culture JUDY COSTELLO, MScN, RN, CCN(C); CATHY CLARKE, MA; GILLIAN GRAVELY, BScN, RN, CPN(C); DINA D’AGOSTINO-ROSE, MA, RN; ROSE PUOPOLO, MN, RN, CPN(C) ABSTRACT Respect is important in the creation of a positive perioperative work environment and effective OR teams. Low scores for respect in the OR on an employee opinion survey and responses on a more customized survey that examined issues associated with respect prompted leaders at the University Health Network to undertake a multiyear organizational strategy to address respect and quality of worklife initia- tives. An interprofessional quality of worklife task force convened to create an action plan to address the outcomes of the surveys. The work of the task force included developing and implementing a code of conduct team charter for the OR, empow- ering leaders to better manage conflict through education and coaching, creating a collaborative, consistent approach to conflict resolution, and designing an education strategy for staff members to enhance communication and conflict resolution. Re- sults of recent employee opinion surveys have reflected positive outcomes. Efforts to sustain the effects of the project include quarterly recognition awards and ongoing education focused on wellness and communication skills. AORN J 93 (January 2011) 115-126. © AORN, Inc, 2011. doi: 10.1016/j.aorn.2010.05.030 Key words: workplace respect, perioperative work environments, quality of worklife, OR culture. O perating rooms are high-intensity, often high-stress environments where team members must work together to provide patient-centered care. Managing the demands of the daily schedule; integrating emergency surger- ies; balancing budgets and ensuring revenue streams; and dealing with staffing shortages and the varied personalities of physicians, nurses, and support staff can be daunting tasks. The influence of hierarchical and unbalanced power relation- ships also can add stress to an already challenging work environment. As a result, a variety of be- haviors are exhibited in the OR, including inter- personal conflict, bullying, verbal abuse, horizon- tal violence, and harassment. 1-4 Professional organizations have called on hos- pitals to establish code of conduct policies and educational interventions to enable staff members to manage and report disruptive behaviors. 5 Em- ployers have been challenged to create healthy work environments that focus on improving staff members’ well-being, patient outcomes, and doi: 10.1016/j.aorn.2010.05.030 © AORN, Inc, 2011 January 2011 Vol 93 No 1 ● AORN Journal 115
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Working Together to Build a Respectful Workplace: Transforming OR Culture

PN(C);
Working Together to Build aRespectful Workplace:Transforming OR CultureJUDY COSTELLO, MScN, RN, CCN(C); CATHY CLARKE, MA; GILLIAN GRAVELY, BScN, RN, C
DINA D’AGOSTINO-ROSE, MA, RN; ROSE PUOPOLO, MN, RN, CPN(C)vironmentee opinionassociateddertake alife initia-e an actione included, empow-creating aeducationution. Re-. Efforts tod ongoingary 2011)
y of
ABSTRACT
Respect is important in the creation of a positive perioperative work enand effective OR teams. Low scores for respect in the OR on an employsurvey and responses on a more customized survey that examined issueswith respect prompted leaders at the University Health Network to unmultiyear organizational strategy to address respect and quality of worktives. An interprofessional quality of worklife task force convened to creatplan to address the outcomes of the surveys. The work of the task forcdeveloping and implementing a code of conduct team charter for the ORering leaders to better manage conflict through education and coaching,collaborative, consistent approach to conflict resolution, and designing anstrategy for staff members to enhance communication and conflict resolsults of recent employee opinion surveys have reflected positive outcomessustain the effects of the project include quarterly recognition awards aneducation focused on wellness and communication skills. AORN J 93 (Janu115-126. © AORN, Inc, 2011. doi: 10.1016/j.aorn.2010.05.030
Key words: workplace respect, perioperative work environments, qualitworklife, OR culture.
nsity
ere t
r to p
eman
ency
evenu
rtage
, nurs
he in
relat
iety of be-
ding inter-
se, horizon-
lled on hos-
licies and
aff members
viors.5 Em-
te healthy
roving staff
Operating rooms are high-inte
high-stress environments wh
members must work togethe
patient-centered care. Managing the d
the daily schedule; integrating emerg
ies; balancing budgets and ensuring r
streams; and dealing with staffing sho
the varied personalities of physicians
support staff can be daunting tasks. T
of hierarchical and unbalanced power
ships also can add stress to an already cha
doi: 10.1016/j.aorn.2010.05.030
© AORN, Inc, 2011
, often
eam
rovide
ds of
surger-
e
s and
es, and
fluence
ion-
work environment. As a result, a var
haviors are exhibited in the OR, inclu
personal conflict, bullying, verbal abu
tal violence, and harassment.1-4
Professional organizations have ca
pitals to establish code of conduct po
educational interventions to enable st
to manage and report disruptive beha
ployers have been challenged to crea
work environments that focus on imp
llenging members’ well-being, patient outcomes, and
January 2011 Vol 93 No 1 ● AORN Journal 115

heale empber
envirt carethe
mploic hememstemarespe
N) iter loted w767(TGHd Pritheseurgicmberrocedcludevasc
he fooskels twoncolothe thons,
departmentbers, and 40sion, anes-
s). Statisticspercentage ofotal proce-imes) are
surveysine surveyon surveyres regard-overall wasH ORs, thes) and 49%ecause ofthe PMH
ort was notof 10 re-
port).gy requiredir depart-
gers presentedrs. Some ex-ons of theles and up-n the lowison with theanagers,
izational
Averageprocedure
time
4.0 hours
2.1 hours
1.8 hours
January 2011 Vol 93 No 1 COSTELLO ET AL
performance at the organizational andsystem level.6 Organizations often usopinion surveys to measure staff memtion and perceptions about key workissues, including the quality of patienspect, communication, teamwork, andenvironment. In 2003, the results of eopinion surveys in a multisite academscience center indicated the need forof the organization to take a more syapproach to exploring the concept ofthe OR.
OUR HOSPITALSThe University Health Network (UHtertiary-quaternary health science cenToronto, Ontario, Canada, and affiliaUniversity of Toronto. The UHN hasthree sites: Toronto General HospitalToronto Western Hospital (TWH), anMargaret Hospital (PMH). Together,sites have 31 ORs with 15 different ssions and departments where staff meform approximately 23,000 surgical pannually. At TGH, areas of service incal oncology, cardiovascular surgery,surgery, and multiorgan transplant. TTWH is on neurosurgery and musculhealth and arthritis, whereas PMH hafocused on low-complexity surgical ocedures. The number of OR staff forhospitals totals 200 nurses, 120 surge
TABLE 1. University Health Netw
Site Hours of opera
Toronto GeneralHospital
24 hours 7 days perweek
Toronto WesternHospital
24 hours 7 days perweek
Princess MargaretHospital
10-hour days, 4 dayweek
116 AORN Journal
th careloyee
satisfac-onment, re-
learningyeealthbersticct in
s acated inith thebeds at),
ncessthree
al divi-s per-uressurgi-
ularcus atetal
ORsgy pro-ree
57 an-
esthesiologists, 95 central processingstaff members, 50 support staff memallied health staff members (eg, perfuthesia assistants, respiratory therapistfor each site (ie, hours of operation,inpatient and outpatient procedures, tdures performed, average procedure tdescribed in Table 1.
THE SURVEYSThe UHN conducts employee opinionevery two to three years using an onlweb site. In the 2003 employee opiniresults, the percentage of positive scoing the issue of respect for the UHN72%; however, for the TGH and TWscores were 51% (n � 37 respondent(n � 48 respondents), respectively. Bthe small number of staff members inORs, an employee opinion survey repavailable for this site (ie, a minimumspondents is required to produce a re
The organizational follow-up stratemanagers to take action related to thement’s or unit’s results. The OR manaand discussed results with staff membeamples of actions taken included revisiOR booking policy and staffing schedudates to staff member orientation. Givescores for respect in the OR in comparoverall organization scores, the OR mdirectors, and human resources organ
R Statistics
Inpatientprocedures
Day surgeryprocedures
Total proceduresper year
89.0% 11.0% 8,647
40.8% 59.2% 11,815
54.7% 45.3% 1,660
ork O
tion
s per

p toovideResp
n titlian, nff mea parsome
pect
reatindisreOR
in whd to p
havioto re
our p
supp
there
entlyR?
eived248
/anesrs (1%). Dculturs ands at edisresiodicaemb
theyd tha
ith disre-s that 20% toisrespect
cy and atitable use ofrding to pol-bumped” foreet the defi-
f the com-dicated thatnted, how-lready stress-
f examples ofnd language,nd inappro-
overruns, notisuse ofs and rude-rs of theom seniord staff mem-
agreed thatddressed andoth formally
on.s, and hu-ment team
surveys andt all staffre of theking to re-rtunity toere taken.s for thenal issues,ore quickly
y were beingemployee
ble. Thed to respect75% from
TRANSFORMING OPERATING ROOM CULTURE www.aornjournal.org
development staff members teamed ua short, eight-item tool that would prdeeper understanding of the problem.dents were asked to select the positioapplied to them in the OR (ie, physicallied health professional, support staFive questions focused on how oftensituation was experienced (ie, never,often):
� Have you been treated with disresmember of the OR surgical team?
� Have you witnessed a colleague tmember of the surgical team with
� Have you treated a member of thecal team with disrespect?
� Do you think there are situationsdisrespectful behavior is warranteappropriate patient care?
� Do you think that disrespectful beto be addressed and actions taken
In addition, participants were asked:
� Which choice best characterizes yin the OR?� I am a member of a team that
each other.� Members of the OR team are
port me.� What would help you to be consist
ful with everyone working in the O
In 2005, all OR staff members receight-item respect survey. There weredents: 101 nurses (41%), 87 surgeonsogists (35%), 44 support staff membeand 16 allied health staff members (6the differences in site structures andsults were similar across all three siteplines. More than 60% of respondentindicated they had been treated withtimes and indicated that they had pernessed disrespect among other staff mpercent of respondents indicated thatwitnessed disrespect, and 7% indicate
were often treated with disrespect. Respondevelopaon-
e thaturse,mber).ticulartimes,
by a
g aspect?surgi-
ichrovide
r needsctify it?
osition
orts
to sup-
respect-
therespon-thesiol-8%),espite
es, re-disci-
ach sitepect atlly wit-
ers. Tenoftent they
also admitted having treated others wspect at times (30%). Of interest, wa35% of staff members believed that dwas warranted in a crisis or emergentimes when practices to facilitate equOR resources were not followed accoicy (eg, when scheduled cases were “nonelective procedures that did not mnition for emergency cases). Many oments expressed by staff members indisrespectful behavior is never warraever, because it only aggravates an aful situation.
Respondents provided a number odisrespect, including rude behaviors aunprofessional conduct (eg, gossip), apriate use of OR resources (eg, timefollowing policies and procedures, mequipment). Disrespectful interactionness occurred at times among membesame professional group as well as frstaff members toward less experiencebers and trainees. Staff members alldisrespectful behavior needed to be athat managers needed to take action band informally to improve the situati
Operating room managers, directorman resources organizational developmembers analyzed the results of thedeveloped presentations to ensure thamembers heard the results, were awacommitments that managers were maspond to the results, and had an oppogive feedback before the next steps wThis work happened at different paceORs surveyed because of organizatiowith the manager at TWH moving mwith improvement strategies.
As the results of the respect survecirculated to staff members, the 2006opinion survey results became availapercentage of positive scores in regarat the UHN overall had increased to
dents 72%. For the TGH and TWH ORs, the positive
AORN Journal 117

s) anhe reed sigscore. Of n, the tarkedt struthe
or wobers
2005sultsity imrgicalitiatiAs T
ng thars aon p
Tn Printo
ntinga fo
proje
iatedof ca3 anfocuse dithe O
ders anclud
s important
am’s use of
rs. The re-
process is-
outcomes for
ed the fol-
d workflow:
cy,
finish time
surgeon,
cedure dura-
,
of the
ion survey
ts (eg, affected
ent safety inentire OR
ite)survey on
survey
onsmation Projectand peopleg valueidmultipleent flow and
elopment and
f the team
ability of the
n strategy
January 2011 Vol 93 No 1 COSTELLO ET AL
scores were 47% (n � 35 respondent(n � 82 respondents), respectively. Trate and scores for TWH had increascantly since 2003, whereas the TGHresponse rates had decreased slightlythat at both the TWH and TGH sitesframe between 2003 and 2006 was mreorganization of the OR managemenhiring of new leaders; and a focus onresponsibilities, and accountabilities fture and behavior. At TGH, staff memmoved into new ORs in 2003.
While concurrently reviewing theand 2006 employee opinion survey reship personnel launched a major qualment transformational initiative in suvices. It was important that respect inalign with the transformation project.illustrates, the journey toward changiculture occurred over a number of yecluded several initiatives that focusedand processes.
OR TRANSFORMATION PROJECThe purpose of the OR Transformatiowas to transform the ORs at the UHNperforming clinical areas by implemetainable process redesign strategies inand outcome driven framework. Thecluded five key areas:
1. OR day redesign,2. workflow,3. human resources analysis,4. supply and technology, and5. quality of worklife.
Each area had a working group assocEssentially, we focused on processes(items 1, 2, and 4) and people (itemsWe identified the quality of worklifefoundational element in the project. Winitially include a focus on respect inTransformation Project, but UHN leacated to have the subject of respect i
this major OR initiative.118 AORN Journal
d 86%sponsenifi-s andote wasimeby the
ctures;roles,rk cul-also
respect, leader-prove-ser-
vesable 2
e ORnd in-eople
ojecthighersus-
cusedct in-
with it.red 5).
as ad notRdvo-
ed in
Our focus on processes of care wa
to determine how the perioperative te
resources affects culture and behavio
spect survey highlighted a number of
sues that required attention. The key
the processes of care redesign includ
lowing changes for OR day design an
� an update of the OR booking poli
� creation of procedure booking and
reports categorized by service and
� implementation of an average pro
tion report by service and surgeon
TABLE 2. Time Frame and ScopeOR Transformation Project
Timeframe Initiatives
2003-2004 � Review of employee opinresults
� Response to critical evenbehavioral incident that acommunication and patithe OR; retirement of theleadership team at one s
2005-2006 � Dissemination of focusedrespect
� Analysis of survey results� Recommendations from
results� Staff member presentati
2006-2008 � Start of the OR Transfor� Evaluation of processes
2007-2008 � LEAN initiatives, includinstream mapping and rapimprovement events (ie,projects to enhance patiimprove efficiency)
� Educational strategy devimplementation
2008-present � Celebration and launch ocharter
� Evaluation of the sustainproject
� Evolution of the project� Launch of the recognitio
� development of a cancellation policy, and

ue toere c
uresituatiity, an
groupcreatansfo
resoe for
sitesstaffi
struklife
usinct surey foes idterprmemhum
ctedon p
nt eld ethcondn keyn the
urvey resultsct survey,dentifiedelationships,rtant compo-
membersegardinge literaturets that pro-to high lev-
ployee en-ffectivenessl teams,ition, weforce ex-
am membersute and de-
their
loped recom-nior leadersrecommen-ask forceor changingr leadersequested thatplan. We
next stepsrk focused
arter for the
nagers tocess fornsibilities.n process.
ding a
TRANSFORMING OPERATING ROOM CULTURE www.aornjournal.org
� development of a cancellation quewhen patients whose procedures wcelled finally underwent surgery.
Introducing standard operating procedthese potentially conflict-generating sprovided structure, transparency, claraccountability.
A human resources managementquality of worklife task force werethe people component of the OR Trtion Project. Members of the humanmanagement group were responsibling roles and responsibilities acrossdating role descriptions, reviewingcation, and standardizing leadershipacross the sites. The quality of worforce members were responsible foremployee opinion survey and resperesults and any other information thcreate a plan for addressing the issufied. Committee membership was insional and included direct care staffmanagers, directors, physicians, andresources staff members. We condutailed literature review with a focuscentered care, MagnetTM environmeteamwork, leadership, education, anaddition, direct care staff membersshort “pulse” survey that focused ofying or dissatisfying components i
TABLE 3. OR Transformation: QuOrganizational Commitment
Key recommenda
� Define respectful OR behavior based onNetwork code of conduct.
� Empower and hold members of the OR laccountable for managing conflicts effecculture of respect.
� Create and follow clear guidelines for resconsequences for repeat offenders.
� Provide education in advanced communand diffusing hostility.
trackan-
foronsd
and aed forrma-urcesreview-, up-ng allo-cturestaskg theveyund toenti-ofes-bers,an
a de-atient-ements,ics. Inucted a
satis-current
OR environment. In reviewing all s(ie, employee opinion survey, respepulse survey), task force members ihierarchies and differential power rparticularly with surgeons, as imponents to address to ensure that staffwere confident about speaking up rpatient-centered care and safety. Threview emphasized that environmenmote a culture of respect are linkedels of staff member satisfaction, emgagement and retention, improved eand productivity of interprofessionaand improved patient safety. In addnoted that members of today’s workpect an environment in which all teare respected, are enabled to contribvelop fully, and are recognized forcontributions.7-10
The task force members then devemendations and presented them to seto gain support for the plan. The keydations from the quality of worklife tand its organizational commitments fculture are outlined in Table 3. Seniosupported the recommendations and rtask force members develop an actiondeveloped a framework to guide the(Figure 1). The task force’s framewoon four key commitments:
of Worklife Committee Recommendations and
Commitments
iversity Health � Create a code of conduct team chOR.
hip teamnd creating a
� Provide a coaching course for mateach a collaborative resolution proconflict and define roles and respo
conflicts and ensure � Commit to a collaborative resolutio
, conflict resolution, � Educate staff members about builrespectful workplace.
ality
tions
the Un
eaderstively a
olving
ication
AORN Journal 119

OR tecode
s to band
procnflic
for stnicati
develr (FiOR
n theg othee andhe emexpeche les straram
designed toin manag-
al ap-est-basedways toe course
y, and con-
ve resolutionN code of
ing a step-sonal con-laborative
ember andisputes. Forirect caressional staffded an all-ce Full ofurse wasle undermanagement
tools and
f work
January 2011 Vol 93 No 1 COSTELLO ET AL
� developing and implementing ancharter that aligned with the UHNconduct,
� empowering managers and leadermanage conflict through educationcoaching,
� creating a collaborative resolutionensure a consistent approach to cotion, and
� designing an educational strategymembers to enhance their commuconflict resolution competencies.
The quality of worklife task forcethe perioperative services team chartethat defines respectful behavior in thesets standards for all team members iof communication, teamwork, treatinrespect, and being part of a supportivsive workplace. The team charter is tment of how OR team members arelive out the UHN code of conduct. Tship development component of thiincluded a full-day educational prog
Figure 1. Respect survey and quality o
conflict coaching for perioperative servic
120 AORN Journal
amof
etter
ess tot resolu-
affon and
opedgure 2)andareasrs withinclu-bodi-
ted toader-tegyon
agers and leaders. The program wasaddress the leaders’ accountabilitiesing conflict, an analysis of individuproaches to resolving conflict, interconflict resolution approaches, andcoach others to resolve conflicts. Thincluded a self-assessment, role plaflict coaching simulation.
We then developed the collaboratiprocess. This process supports the UHconduct and team charter by establishby-step process for resolving interperflicts respectfully (Figure 3). The colresolution process also defines team mleader responsibilities for resolving dthe final component of the strategy, dstaff member education, all interprofemembers (excluding physicians) attenday course titled “Making a WorkplaRespect.” The overall focus of the coabout communicating effectively whipressure. Staff members learned self-in the moment and three conversation
life task force commitments.
e man- approaches for constructively resolving conflict

g actiaff mas, “
to figuunde
orklificatio
munto meent. Ting au,” wl staf
with physi-urvey resultse surgical
rgery, thestaff mem-
zational de-on or depart-issues,
tabilities for
al celebra-ny initiativessformationworklife task
.
rioper
TRANSFORMING OPERATING ROOM CULTURE www.aornjournal.org
(ie, speaking up respectfully, listeningaining perspective). For example, stwere taught to use key phrases, suchsorry you are upset by this, let’s trywhat to do” and “It’s hard for me towhen you are shouting at me.”
Last but not least, the quality of wforce members developed a communegy to ensure that their work was comto all staff members in the ORs andof the organization’s senior managemcommunication strategy, titled “Buildplace Full of Respect Starts With Yomeant to be a personal message to al
University H
As members of the perioperati
• supportive,
• reliable,
• hard working,
• cooperative, and
• patient-centered in our ca
Communication: We will
• communicate in an open,
• be active listeners.
• clarify what we see and h
• take responsibility for ho
• discuss concerns directly
• use the collaborative reso
• use respectful humor in o
Teamwork: We will
• understand our own and o
care.
• offer and accept help to p
• solve problems in new an
Respect for others: We will
• avoid gossip and making
• embrace diversity and res
• recognize and value our t
thank you), by introducin
Supportive and inclusive work
• follow standards, policies
• trust that each other’s inte
• support a safe work envir
• discuss observations of p
• share what we know to p
• hold ourselves and others
Figure 2. University Health Network pe
bers to engage them in the required chang
vely,embersI amre out
rstand
e taskn strat-icatedmbersheWork-
asf mem-
cess. The strategy for communicationcians included a presentation of the sand organizational commitments to thexecutive committee. The chief of susite OR administrative director, and aber from the human resources organivelopment group attended each divisiment physician meeting to review thesurvey results, next steps, and accounall staff members and physicians.
In the fall of 2008, we held a formtion to highlight the results of the mathat had emanated from the OR TranProject. The efforts of the quality of
etwork Perioperative Services Team Charter
ices department we aspire to be:
, positive, respectful, and professional manner.
ommunicate, both verbally and nonverbally.
nstructive and private manner with other persons as soon as possible
rocess or other resources if a conflict or issue cannot be resolved.
interactions.
roles in the department to maximize teamwork and enhance patient
and foster teamwork and our own professional development.
e ways to improve our effectiveness.
comments about others.
ch team member’s culture, values, beliefs, and uniqueness.
mbers by using courteous terms to address each other (eg, please,
lves, and by addressing people by name.
e will
sses, and protocols to support all aspects of patient care.
make decisions that are inclusive and patient-centered.
t.
ly unsafe practices with our team members.
a positive teaching and learning environment.
table for following the team charter.
ative services team charter.
ealth N
ve serv
re.
honest
ear.
w we c
in a co
lution p
ur daily
thers’
romote
d activ
hurtful
pect ea
eam me
g ourse
place: W
, proce
nt is to
onmen
otential
romote
accoun
e pro- force were highlighted. Team members, including
AORN Journal 121

rs, anexamchartmema bointroHN
ices teounta, theonstrcomm
ath, changeresources
rocess isr monitoringrs, and hu-ed key met-tainabilityRespect”
ess.
January 2011 Vol 93 No 1 COSTELLO ET AL
RNs, central processing staff membethesia assistant, and a surgeon, gavethat illustrated the effect of the teamplementation on their work. All staffwho attended the celebration receivedthat outlined the respect initiative, anletter from the chief of surgery, the Uconduct, the UHN perioperative servcharter, team member and leader acca definition of inappropriate behaviorcollaborative resolution process, the cconflict resolution approach, tips and
Figure 3. Collaborative resolution proc
tion tools to manage stress in the moment
122 AORN Journal
anes-pleser im-bersokletductorycode ofam
bilities,
uctiveunica-
reframe the situation, take a deep brethe scene), and a list of other helpfulavailable to them in the organization.
OUTCOMES MONITORINGAND SUSTAINABILITYOne of the key steps in any change pensuring that metrics are identified fooutcomes. The OR managers, directoman resources staff members identifirics for monitoring the effect and susof the “Building a Workplace Full of
(eg, strategy. Turnover rates and results from the

reas ihangm 20
anged50%
stainrganimbedSharimake
ion. TH an
ctively. Atthe em-
, recognition/mitment,ork, and re-87 respon-
cores is amitment ofing the cul-ss changeswell as im-site, the highthe 2006
inion survey
TRANSFORMING OPERATING ROOM CULTURE www.aornjournal.org
employee opinion surveys were the afied for monitoring outcomes of the cing the course of the initiative (ie, fro2009), staff turnover rates were unchTWH at 6% and reduced at TGH byfrom 8% to 4%).
We evaluate the effectiveness and suof the project by conducting ongoing oemployee opinion surveys, which are eorganizational improvement strategies.results of the employee opinion surveyresults transparent within the organizatemployee opinion survey results for TG
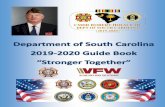
Data source: employee opinion sur
Respondents: n = 35 in 2006; n = 8
Positive score based on response o
Teamwork
Commitment
Work practice
Recognition/
compensation
Physical/
environmental
safety
Communication
Respect
0% 10%
TGH OR 2006
Figure 4. Toronto General Hospital (TG
results.denti-es. Dur-05 tofor
(ie,
abilityzationalded inng thes thehe 2009d TWH
can be found in Figures 4 and 5, respethe TGH site, scores on all elements ofployee opinion surveys, work practicescompensation, communication, comphysical/environmental safety, teamwspect, increased more than 40% (n �
dents). We believe that this shift in sresult of the respect strategy, the comthe new OR leadership team to changture, and implementation of the procein the OR Transformation Project, asproved response rates. For the TWHemployee opinion survey scores from
ducted in 2006 and 2009
9
ery good/excellent or moderately agree/strongly agree
Subscale Score (%)
76%
74%
42%
77%
80%
53%
81%
76%
55%
71%
69%
41%
80%
79%
55%
66%
59%
30%
79%
74%
53%
30% 40% 50% 60% 70% 80% 90% 100%
TGH OR 2009 UHN 2009
iversity Health Network (UHN) 2009 OR employee op
veys con
7 in 200
f good/v
20%
H)/Un
AORN Journal 123

t receelebraand os is a
ome
ect sin alllet to
ation,mem
ect’s
on Awards.o honor anthe six cru-rter by being
members
pinion survey
January 2011 Vol 93 No 1 COSTELLO ET AL
survey were sustained. After the mossults were made available, we held cthat acknowledged the collaborationachieved. Celebrating such milestoneportant component of sustaining the mof change in the ORs.
The sustainability plan for the respincluded posting of the team charterareas, distribution of the respect bookperioperative staff members at orientall-day “respect” course for new staffAnother key component of the proj
Data source: employee opinion sur
Respondents: n = 82 in 2006; n = 1
Positive score based on response o
Teamwork
Commitment
Work practice
Recognition/
compensation
Physical/
environmental
safety
Communication
Respect
0% 10%
TWH OR 2006
Figure 5. Toronto Western Hospital (TWresults.
sustainability was the creation of a recogn
124 AORN Journal
nt re-tionsutcomesn im-ntum
trategyclinicalalland anbers.
strategy, the Team Charter RecognitiWe designed the recognition award tindividual or team that demonstratescial qualities outlined in the team cha
� supportive,� reliable,� respectful,� hard working,� cooperative, and� patient centered.
We held a contest during which staff
ducted in 2006 and 2009
09
ery good/excellent or moderately agree/strongly agree
Subscale Score (%)
76%
88%
85%
77%
86%
89%
81%
87%
88%
71%
78%
86%
80%
89%
92%
66%
82%
78%
79%
84%
85%
30% 40% 50% 60% 70% 80% 90% 100%
TWH OR 2009 UHN 2009
niversity Health Network (UHN) 2009 OR employee o
veys con
06 in 20
f good/v
20%
H)/U
ition were asked to submit slogans or catchy phrases

ived a“Respwho snd re
emenwilly sta
tion”heir cbodifor o
sed sticatioife in
ensuoingcommopmempor
EARf respthe O
t inclt of af initiuccesor chwellrespet wasnt ind ou
“Youworltheir
how tticalect wd woat alrs in
ensure at-bers andes from theg the exper-nior manag-t and imple-y. Finally,membersr their be-
s the interestnd outcomesfor copies ofhough wee accompa-
t the qualityof staffr outcomes.
ents inres can lead
al culturerecruitmentfety. It isagers imple-to improve
gers and staffand processlture and theoting re-stainable
human re-table for andnt, leading
sly monitor-
of theer, Silver
owledge theor, MD, chief
TRANSFORMING OPERATING ROOM CULTURE www.aornjournal.org
for the recognition strategy. We receber of slogans and chose the winnerMotion.” We gave the staff memberted the winning slogan a gift basket ation in the UHN News for the achievplan to give the awards quarterly andwinner from nominations submitted bbers. We designed a “Respect in Mobe awarded to winners to recognize tment to the team charter and all it em
This work has served as a catalyststaff member engagement and increamember education regarding communoverall wellness and quality of workltives. Finally, the OR leadership teamannual education days include an ongon wellness initiatives and advancedtion skills to ensure continuous develstaff member competencies in these iareas.
REFLECTIONS AND LESSONS LThe journey to enhance the culture otransform the perioperative culture inthe UHN was a multiyear project thadata collection, analysis, developmenplans, implementation of a number oand creation of sustainability plans. Stors included having a strong vision fand persistence and perseverance, assuring that all communications werenature and that the concept of respecunderpinning of any unit or departmeThe words of Mahatma Gandhi guidedeavors and commitment to change,be the change you wish to see in theWe asked staff members to reflect onbehavior and take accountability forand treat other team members. Of critance to the sustainability of the projfocus on the importance of respect anculture by staff members and leadersThe chief of surgery and senior leade
surgical program were strong champions fnum-ect inubmit-cogni-
t. Wedraw aff mem-pin toommit-es.ngoingaffn and
itia-res thatfocusunica-
nt oftant
NEDect andRs at
udedctionatives,s fac-angeas en-ctful inthe
itiative.r en-must
d.”11
ownhey actimpor-as therkplace
l levels.the
these initiatives. Their support helpedtendance at workshops for staff memleaders. The involvement of colleaguhuman resources department, includintise of organizational development seers, was important in the developmenmentation of a comprehensive strategall interprofessional leaders and staffhad to hold each other accountable fohaviors and actions.
Of note throughout the process waof other departments in the strategy aachieved. There were many requeststhe perioperative respect booklet. Altprovided these booklets with pride, wnied the booklets with the advice thaof worklife strategy and engagementmembers is critical to produce simila
SUMMARYThe ORs are high-intensity environmwhich competing demands and pressuto disruptive behaviors. Organizationand respect are key for staff memberand retention as well as for patient saimperative that an organization’s manment, monitor, and sustain initiativesrespect and workplace culture. Manamembers must understand the peopleelements that affect organizational cukey roles these elements play in promspect in the workplace. To achieve suresults, OR managers, directors, andsource staff members must be accouncommitted to staff member engagemethe process of change, and continuouing its outcomes.
Editor’s note: Magnet is a trademarkAmerican Nurses Credentialing CentSpring, MD.
Acknowledgement: The authors acknsupport and leadership of Bryce Tayl
or all of surgery and program medical director of the
AORN Journal 125

ervicntariodent o, andwork,he me
sment;13(2):vent v48-150tility?es EatA: HP
raw Criopera
n Nursng in nww.a
ericand Aug
e guidursesrage/2ed Aug
dershido I
0-22.ace. M
a heal223.AORN
. http_you_wAugus
nalysis05;81(
onnas
. NurscommersingCare
nts/Revised%20-%20Dec%
0.lationship in2005;15(3):
re change on:407-415.
), is theeneral, Toronto,
o declareds posing aublication
of organi-niversityanada. Msat could be
flict of in-le.
), is aospital OR
, Universityanada. Ms
that couldonflict ofticle.
the clinicaltis Program,Health Net-
D’Agostino-could bect of interest
a patientital, Univer-, Canada.n that couldnflict of in-
January 2011 Vol 93 No 1 COSTELLO ET AL
Surgical Programs and Critical Care SUniversity Health Network, Toronto, Oada, and Scott McIntaggart, vice presigrated Surgical Services, Critical Careplantation at the University Health NetToronto, Ontario, Canada, and thank tof the quality of worklife task force.
References1. Gilmour D, Hamlin L. Bullying and haras
erative settings. Br J Perioper Nurs. 20042. Buback D. Assertiveness training to pre
abuse in the OR. AORN J. 2004;79(1):13. Bartholomew K. What is horizontal hos
ing Nurse-to-Nurse Hostility: Why NursYoung and Each Other. Marblehead, M2006:3-22.
4. Bigony L, Lipke TG, Lundberg A, McGG, Rogers A. Lateral violence in the peting. AORN J. 2009;9(4):688-696.
5. AORN supports the Center for Americafor an end to lateral violence and bullyiwork environments. AORN, Inc. http://wNews/March2008News/CENTERForAmCallsForAnEndToLateralViole/. Accesse2010.
6. Healthy work environments best practicprofessionalism in nursing. Registered Ntion of Ontario. http://www.rnao.org/Sto2303_BPG_Professionalism.pdf. Access2010.
7. Shewchuck M. Pearls of wisdom for leaLooking in the mirror and asking, “Hownow?” Can Oper Room J. 2004;22(4):2
8. Sutton R. Building the civilized workplQ. 2007;2(May):47-55.
9. Parsons ML, Newcomb M. Developingworkplace. AORN J. 2007;85(6):1222-1
10. Hamlin L. The OR and a “just culture.”90(4):495-498.
11. Mahatma Gandhi quotes. Thinkexist.comthinkexist.com/quotation/be_the_changesee_in_the_world/148490.html. Accessed2010.
ResourcesForsythe L. Using an organizational culture a
sign interventions for change. AORN J. 201302.
Girard N. Dealing with perioperative prima dORs. AORN J. 2005;82(2):187-189.
O’Brien-Pallas L, Hiroz J, Cook A, Mildon BPhysician Relationships: Solutions and Refor Change. Comprehensive Report for Nuiat and Ministry of Health and Long-Term
Unit. Toronto, Canada: Nursing Health Services126 AORN Journal
es at the, Can-f Inte-Trans-
mbers
in periop-79-85.erbal.In: End-Their
ro, Inc;
, Pagactive set-
es callursing
orn.org/Nursesust 24,
elines:Associa-8/ust 24,
p skills.like me
cKinsey
thy OR
J. 2009;
://ant_to_
t 27,
to de-6):1290-
in your
e-ndations
Secretar-Research
Unit; 2005. http://www.nhsru.com/docume20FINAL%20Nurse-physician%20Report%2013%2005.pdf. Accessed August 24, 201
Reynolds A, Timmons S. The doctor-nurse rethe operating theatre. Br J Perioper Nurs.110-115.
Shermont H, Krepcio D. The impact of cultunurse retention. J Nurs Admin. 2006;36(9)
Judy Costello, MScN, RN, CCN(Cdirector surgical services, Toronto GHospital, University Health NetworkOntario, Canada. Ms Costello has naffiliation that could be perceived apotential conflict of interest in the pof this article.
Cathy Clarke, MA, is the managerzation and employee development, UHealth Network, Toronto, Ontario, CClarke has no declared affiliation thperceived as posing a potential conterest in the publication of this artic
Gillian Gravely, BScN, RN, CPN(Cnurse manager at Toronto General Hand Princess Margaret Hospital ORHealth Network, Toronto, Ontario, CGravely has no declared affiliationbe perceived as posing a potential cinterest in the publication of this ar
Dina D’Agostino-Rose, MA, RN, isdirector, Surgical Services and ArthriToronto Western Hospital, Universitywork, Toronto, Ontario, Canada. MsRose has no declared affiliation thatperceived as posing a potential confliin the publication of this article.
Rose Puopolo, MN, RN, CPN(C), iscare manager, Toronto Western Hospsity Health Network, Toronto, OntarioMs Puopolo has no declared affiliatiobe perceived as posing a potential co
Researchterest in the publication of this article.