Utilization and outcomes of mental health services among patients in drug treatment
46
Utilization and Outcomes of Mental Health Services among Patients in Drug Treatment Yih-Ing Hser, Ph.D., Christine Grella, Ph.D., Elizabeth Evans, M.A., & Yu-Chuang Huang, Dr. P.H. UCLA Integrated Substance Abuse Programs Neuropsychiatric Institute University of California, Los Angeles December 2004 Correspondence: Yih-Ing Hser, Ph.D., UCLA Integrated Substance Abuse Programs, 1640 S. Sepulveda Blvd., Suite 200, Los Angeles, CA 90025. Phone: (310) 445-0874, ext. 264; E-mail: [email protected] Acknowledgment: The study was supported in part by the California Department of Alcohol and Drug Programs (ADP; Contract No. 98-00245). Dr. Hser is also supported by an Independent Scientist Award from the National Institute on Drug Abuse (NIDA K02DA00139). The content of this publication does not necessarily reflect the views or policies of the funding agencies. The authors thank the publication support provided by staff at the UCLA Integrated Substance Abuse Programs. Hser, Y.-I., Grella, C., Evans, E., & Huang, Y.-U. (2006). Utilization and outcomes of mental health services among patients in drug treatment. Journal of Addictive Diseases, 25 (1): 73-85. PMID: 16597575. document.doc10/16/20227:33 PM 1
Transcript of Utilization and outcomes of mental health services among patients in drug treatment

Utilization and Outcomes of Mental Health Services among Patients
in Drug Treatment
Yih-Ing Hser, Ph.D., Christine Grella, Ph.D., Elizabeth Evans, M.A., & Yu-Chuang Huang, Dr. P.H.
UCLA Integrated Substance Abuse ProgramsNeuropsychiatric Institute
University of California, Los Angeles
December 2004Correspondence: Yih-Ing Hser, Ph.D., UCLA Integrated Substance Abuse Programs, 1640 S. Sepulveda Blvd., Suite 200, Los Angeles, CA 90025. Phone: (310) 445-0874, ext. 264; E-mail: [email protected]
Acknowledgment: The study was supported in part by the California Department of Alcohol and Drug Programs (ADP; ContractNo. 98-00245). Dr. Hser is also supported by an Independent Scientist Award from the National Institute on Drug Abuse (NIDA K02DA00139). The content of this publication does not necessarily reflect the views or policies of the funding agencies. The authors thank the publication support provided by staff at the UCLA Integrated Substance Abuse Programs.
Hser, Y.-I., Grella, C., Evans, E., & Huang, Y.-U. (2006). Utilization and outcomes of mental health services among patientsin drug treatment. Journal of Addictive Diseases, 25 (1): 73-85. PMID: 16597575.
document.doc10/16/20227:33 PM1
AbstractThis study examined utilization of mental health services and
treatment outcomes among 1,091 patients with mental health
problems recruited from 39 treatment programs in 13 California
counties. We compared three groups: one that received dual
treatment from drug and mental health programs (N = 294), one
that received mental health services only within drug treatment
programs (N = 578), and one that received no mental health
services (N = 219). Individuals who received dual treatment had
more severe substance use and mental health problems, followed in
severity by those who received mental health services within drug
treatment, and those who received no services. All groups
significantly reduced their psychiatric severity at the follow-
up, although there were no group differences in treatment
retention and drug use outcomes. These findings suggest that
individuals with mental health problems can be successfully
treated within drug treatment programs and/or in conjunction with
mental health providers.
document.doc10/16/20227:33 PM2
Introduction
In the past 20 years, service providers have increasingly
recognized that individuals entering into substance abuse
treatment programs frequently have co-occurring mental disorders.
National epidemiological studies have demonstrated that
individuals with co-occurring disorders have higher utilization
rates for both mental health and substance abuse treatment.1-4
Moreover, the presence of a mental disorder has been shown to
affect the severity and course of co-occurring substance
dependence, such that both disorders interact and typically
require simultaneous treatment.5-8 Individuals with co-occurring
disorders have higher levels of psychological distress and poorer
psychosocial functioning, as compared with individuals with
substance dependence only, and hence may need more intensive
treatment and comprehensive services in order to benefit from
treatment.9-11 Further, there is evidence that substance abusers
with co-occurring mental disorders generally have shorter stays
in substance abuse treatment and poorer posttreatment outcomes,
as compared to individuals without co-occurring mental
disorders.12-17 As a result, there has been an increased
document.doc10/16/20227:33 PM3
understanding of the need to provide simultaneous and coordinated
mental health and substance abuse treatment for individuals who
have co-occurring disorders.
Yet individuals who have co-occurring disorders face
numerous obstacles when seeking treatment for either or both
disorders.18-19 These obstacles stem from continuing
administrative and financial policies that undergird the
separation of substance abuse and mental health treatment into
two separate service systems.20 For example, exclusionary
criteria for admission to either type of program often restrict
treatment to individuals with one type of “primary” disorder.21
Publicly funded mental health programs are mandated to provide
treatment only to those individuals who meet the threshold of a
“severe and disabling” disorder, which excludes many others who
have mental health problems of lesser severity, but need
treatment nonetheless. Similarly, historically, individuals who
were taking psychotropic medications for psychiatric disorders
were commonly excluded from substance abuse treatment agencies
that adhered to a strict definition of “abstinence.” Although
there is evidence that such attitudes are changing, treatment
document.doc10/16/20227:33 PM4

providers in the two systems still adhere to divergent
perceptions regarding appropriate treatment approaches for this
population, particularly regarding the issue of abstinence.22
Consequently, individuals with co-occurring disorders are often
referred back and forth across the two treatment systems or fail
to receive treatment for either disorder altogether.23-24
Nevertheless, progress has been made in recent years in the
development of clinical protocols for diagnosis and assessment,
motivational interventions, and relapse prevention for patients
with co-occurring disorders.25-30 Some substance abuse treatment
programs now “specialize” in providing treatment specifically for
this population and have adopted a “dual diagnosis” orientation
to treatment.31-33 Yet many, if not most, substance abuse
treatment programs are still not equipped to provide services to
this population. Data from the annual national survey of
substance abuse treatment programs conducted by the government
show that about half provide on-site services for individuals
with co-occurring disorders ,34 which is consistent with regional
35 and state-level surveys.36 Lacking the capacity to provide
mental health services on-site, many substance abuse programs
document.doc10/16/20227:33 PM5
refer these patients for mental health services off-site,
although coordination of service delivery across treatment
systems presents additional obstacles to patient care.37-39
At present, most studies that examine the outcomes of
treatment for patients who have co-occurring disorders focus on
those who receive treatment within one system or the other. To
date, no studies have directly examined patient characteristics
and treatment outcomes associated with different patterns of
service delivery – either receipt of mental health services on-
site within substance abuse programs or receipt of mental health
services from a separate provider, in addition to substance abuse
treatment.
The present study takes advantage of data collected in the
California Treatment Outcome Project (CalTOP) as part of a pilot
implementation of an ongoing outcome monitoring system tracking
treatment of alcohol and drug abuse in California. CalTOP
included existing drug treatment programs in diverse communities
and collected assessment data from a large sample of patients in
these programs. Services provided by these programs were
obtained by a program survey. Services received by patients were
document.doc10/16/20227:33 PM6

collected by a phone interview at 3-months following treatment
admission. Additionally, records were obtained from the
California Mental Health Department for individuals who received
publicly funded mental health services during the treatment and
follow-up period. Thus, we were able to categorize the sample
into three analytic groups: those receiving dual treatment from
both drug treatment and mental health programs, those receiving
mental health services from drug treatment programs only, and
those not receiving mental health services from either source.
By comparing the three analytic groups, we address the following
key research questions: (1) What were the patient
characteristics related to receiving dual treatment, receiving
mental health services only in the drug treatment programs, and
not receiving services from either source? (2) What types of
treatment services were provided to these patients in these two
types of settings? And (3) What were the treatment outcomes for
the three groups defined by type of service delivery?
Methods
Study Design
document.doc10/16/20227:33 PM7

The source of the data examined in this study was CalTOP, a
multisite and multicounty prospective treatment outcome study.40
As part of the national Treatment Outcomes and Performance Pilot
Studies Enhancement (TOPPSII) funded by the Center for Substance
Abuse Treatment, CalTOP began data collection in April 2000 from
all adult patients consecutively admitted to 43 programs in 13
counties in California. Criteria for selecting the participating
counties and providers included demographic breadth and adequate
flow of the patient population, automation readiness, familiarity
with assessment tools, geographic scope, and commitment to
CalTOP. The participating programs represent all major
modalities currently available in California (25 outpatient drug-
free, 11 residential, 4 methadone maintenance, and 3 multiple
modality). The counties represented in the study (Alameda, El
Dorado, Kern, Lassen, Orange, Riverside, Sacramento, San Benito,
San Diego, San Francisco, San Joaquin, San Luis Obispo, and San
Mateo) cover wide geographic locations (e.g., northern, central,
and southern regions) and include both urban and rural areas.
As part of the evaluation of CalTOP, the first 3,314 adult
admissions in 2001 and 2002 were targeted for the 3-month follow-
document.doc10/16/20227:33 PM8
up. Excluding the ineligible (5 deceased, 110 incarcerated, 17
deported or unable to answer the questions), 2,850 of the 3,182
eligible completed the interview (a 90% completion rate). For
the 9-month follow-up, in order to achieve the target of 2,700
completed interviews, the first 3,715 patients were targeted,
which included an additional 400 patients not targeted for the 3-
month interview. (The 2,700 subjects were determined by (1) a
statistical consideration to achieve adequate power for outcome
analyses, and (2) the logistic consideration for accomplishing
the task within the contract period.) Excluding the ineligible
(29 deceased, 182 incarcerated, 7 deported), 2,730 of the 3,497
eligible completed the interview (a 78% completion rate).
Because the present study focuses on the nature of mental
health service delivery, we include in the study sample only
those subjects who reported at least some mental health or
psychological problem at treatment intake (N = 1,091); excluded
were those who had no evidence of mental health problems as
revealed by a score of 0 on the Addiction Severity Index (ASI; n
= 977), or who did not have 3-month or 9-month follow-up
interviews.
document.doc10/16/20227:33 PM9
Participants
As noted above, the present study includes 1,091 patients
who reported mental health or psychological problems at intake
(i.e., ASI psychiatric severity > 0) and who completed the intake
assessment and the 3-month and 9-month follow-up interviews. We
categorized the sample into three groups based on the type of
mental health services received: (1) Dual-Treatment Group, who
received services from both drug and mental health programs (N =
294, 27% of the sample), (2) Drug-Treatment Group, who received
services only from drug treatment (N = 578, 53% of the sample),
and (3) No-Service Group, who received no mental health services
(N = 219, 20% of the sample).
The overall study sample was 57.1% female, 58.9% White,
17.6% Black, 17.8% Hispanic, and 5.9% other ethnic groups. The
mean age at treatment admission was 34.9 + 9.8 years. Table 1
presents demographic and background characteristics of the three
groups and total study sample.
____________________
Insert Table 1 about here
____________________
document.doc10/16/20227:33 PM10
Among patients in the Dual-Treatment Group, the leading
diagnosis (based on administrative records) was affective
psychoses (28.9%), followed by depressive disorder (18.4%), other
psychoses (8.4), adjustment reaction (8.5%), and schizophrenic
disorder (6.5%). For the most part, mental health services were
provided in outpatient (90%) and day services (8%), although a
small percentage (less than 2%) were provided within hospital or
other inpatient treatment.
Treatment Programs
Questionnaires completed by the program directors provided
the description of treatment characteristics of the participating
CalTOP facilities. The “typical” treatment facility had been in
operation for more than 15 years, was part of a larger
organization, and had an average daily census of 112 patients (a
median of 50). All were primarily drug treatment programs, as
opposed to alcohol-only treatment programs, and most had a
mixture of funding from both public and private sources.
Most programs offered intake assessment and both individual
and group alcohol and drug counseling. In terms of mental health
services, almost all programs provided biopsychosocial assessment
document.doc10/16/20227:33 PM11
and referral and 25.6% conducted psychiatric or psychological
evaluation. More than half offered individual counseling (51.3%)
and group counseling (41.0%) specifically for mental health
issues. About 25.6% prescribed and/or monitored psychotropic
medications on-site.
Patient Intake Assessment and Follow-up
Patients were assessed at intake, discharge, 3-month follow-
up, and 9-month follow-up. Treatment staff at participating
programs completed an in-person assessment with all entering
adult patients as part of the normal admission process.
Treatment staff also completed an exit assessment. Follow-up
interviews were conducted by UCLA-trained interviewers over the
phone at 3 months and 9 months after treatment admission. Each
interview lasted approximately 30 minutes. Patients were paid
$10 for the 3-month interview and $15 for the 9-month interview.
Data Sources, Instruments, and Measures
Data sources included patient self-report at multiple
assessment points as well as official records for mental health
services utilization, arrests, and drug treatment participation.
document.doc10/16/20227:33 PM12
Mental Health Services Data
Mental health services provided by the mental health
programs to CalTOP patients were obtained by searching the Client
and Service Information (CSI) database maintained by the
Department of Mental Health (DMH). The database includes all
Medi-Cal and state-funded mental health services, including 24-
hour, day services, and outpatient programs, and excluding state
hospitals. The Mental Health Client Service Information system
is an event database. Each service received is registered as a
record. Therefore, one client can have multiple records if more
than one service is received. The data linkage process linked
7,589 records to the 294 of the subjects during the follow-up
period (approximately 9 months) since treatment admission.40
Arrest Records
Arrest records for CalTOP clients were obtained from the
California Department of Justice (DOJ), which maintains the
Criminal Identification and Information (CII) database in the
Automated Criminal History System for all California criminal
justice records.
CalTOP Data System
document.doc10/16/20227:33 PM13
Addiction Severity Index (ASI). The ASI 41-42 is a structured interview
that assesses problem severity in seven areas: alcohol use, drug
use, employment, family and social relationships, legal,
psychological, and medical status. A composite score can be
computed for each of the scales to indicate severity in that area;
the range of scores is 0 to 1 with higher scores indicating
greater severity. Also presented are selected individual items in
the psychiatric problem domain. Using a median split (.367) of
the ASI psychiatric severity score at intake, we calculated the
percentage of high severity versus low severity in each of the
three groups. The ASI was administered at treatment admission and
9 months post-admission. One major outcome measure is the
difference in ASI composite scores from baseline to the 9-month
follow-up.
Other intake measures. Additional derived measures at intake
included multiple drug use (use of three or more drugs), heavy
alcohol use (primary alcohol use and daily alcohol use in the
previous 30 days), criminally active (currently on
probation/parole, awaiting trial or case pending, or having been
arrested or incarcerated in the previous 30 days), and on public
document.doc10/16/20227:33 PM14
assistance (receiving food stamps, Medi-Cal, etc.). All these
derived problem indicators were dichotomous variables.
Treatment Services Review (TSR). The TSR 43 was used to collect
information on services provided to patients during treatment.
The TSR recorded the number of professional services (e.g., doctor
appointments, medications) and discussion sessions (e.g., group or
individual counseling or education sessions, Alcoholic
Anonymous/Narcotics Anonymous meetings) that the patient received
in the previous 3 months in each of the seven problem areas of the
ASI. We reported mental health services received (either on-site
in the program or off-site through referrals) collected using the
TSR. This instrument was administered during the 3-month follow-
up interview.
Treatment retention was based on treatment records reported to
the California Alcohol and Drug Data System (CADDS), which is the
state database tracking all admission and discharge episodes
within publicly funded and/or licensed programs. Retention was
defined as the number of days between CalTOP program admission
and discharge. For those without discharge records, we
calculated their length of stay from admission to the last date
document.doc10/16/20227:33 PM15
of program participation or the date of the 9-month interview.
Patients were classified as having sufficient retention if they
stayed in treatment for 90 days or longer, or if they completed
treatment as stipulated by the program. These retention
thresholds have been demonstrated to be predictive of positive
outcomes in previous treatment outcome research.44-45
Drug treatment success. Individuals are considered to be
successful if they reported no use of alcohol or drugs and had an
independent living arrangement in the community (i.e., not in a
controlled environment such as prison, jail, or hospital) in the
30 days prior to the 9-month follow-up interview.
Analytic approach
We conducted ANOVA to examine the main effects of mental
health service utilization patterns as represented by the three
analytic groups. Pair-wise post-hoc comparisons were conducted
to identify which group differences were significant if the main
group effect was significant. Changes in ASI psychiatric
severity scores for the three groups were tested using repeated
measures of ANOVA with Group, Time, and Group and Time
Interaction as the independent variables. To control for Type I
document.doc10/16/20227:33 PM16

error due to multiple tests, we set the significance level at p <
.01 to be conservative.
Results
Pre-treatment Characteristics
Background. As shown in Table 1, the three analytic groups
did not differ in age at drug treatment admission and legal
status. However, the highest percentage of females was in the
Dual-Treatment Group, followed by the Drug-Treatment Group and
the No-Service Group. The No Service Group had more African
Americans and Latinos and fewer Whites than the Dual-Treatment
Group. Individuals receiving no services were also the most
likely to be employed and the least likely to be on public
assistance, while individuals in the Dual Treatment Group were
least likely to be employed and most likely to be on public
assistance.
Drug use, treatment, and criminal history. Patterns of drug use,
treatment participation, and criminal involvement at intake are
presented in Table 2. In general, the Dual Treatment Group had
the most severe use of alcohol and drugs, followed by the Drug
Treatment Group and the No Service Group, as reflected by higher
document.doc10/16/20227:33 PM17
rates of using heroin and cocaine, younger ages at initiation
(e.g., alcohol), and more years of use (alcohol), although the
significant differences were mostly between the Dual Treatment
and No Services groups. There were no significant differences
among groups in the rates of multiple drug use, injection drug
use, or type of primary drug use. Individuals in the Dual
Treatment Group had the highest mean number of prior alcohol or
drug treatment episodes, followed by the Drug Treatment Group,
and the No Service Group. Not surprisingly, relative to the
other two groups, more individuals in the No Service Group were
treated in outpatient drug-free programs and less in residential
programs.
____________________
Insert Table 2 about here
____________________
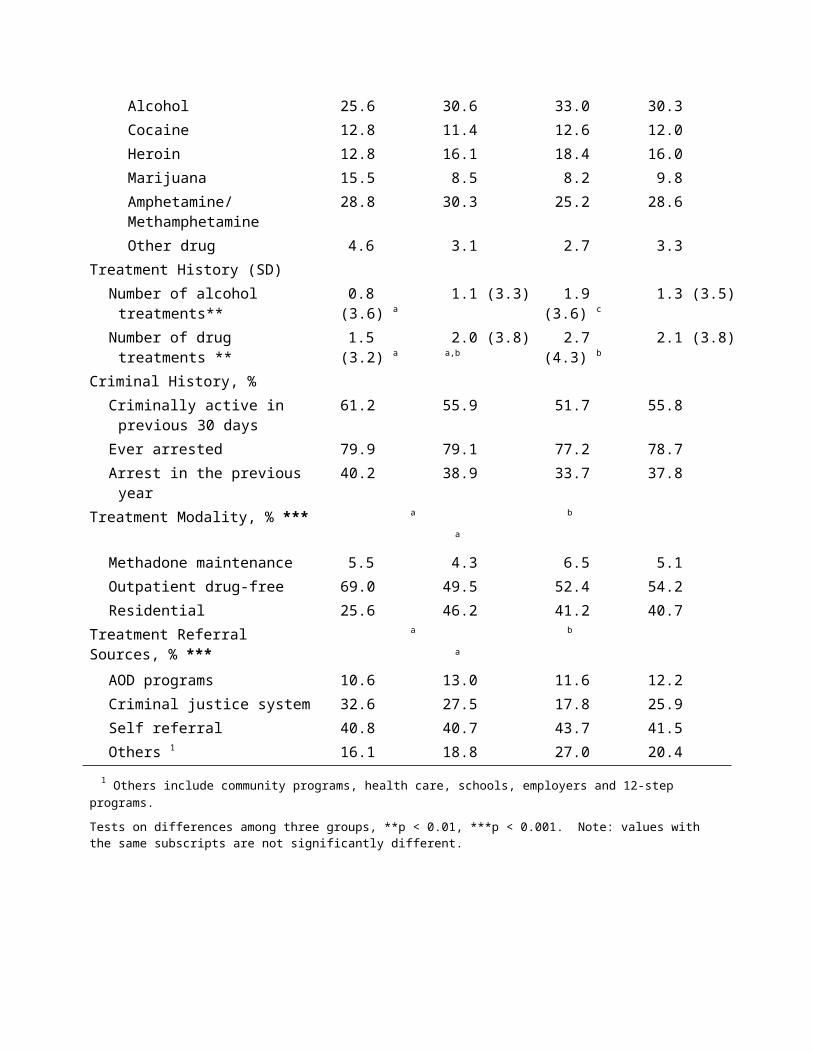
There were no significant differences among groups in regard
to criminal history; however, the No Service Group had the
highest rate of referral to treatment through the criminal
justice system, followed by the Drug –Treatment Group and Dual
Treatment Group. A greater proportion of the Dual Treatment
document.doc10/16/20227:33 PM18
Group was referred by “other” providers, which can include mental
health or other types of health care providers and community
programs.
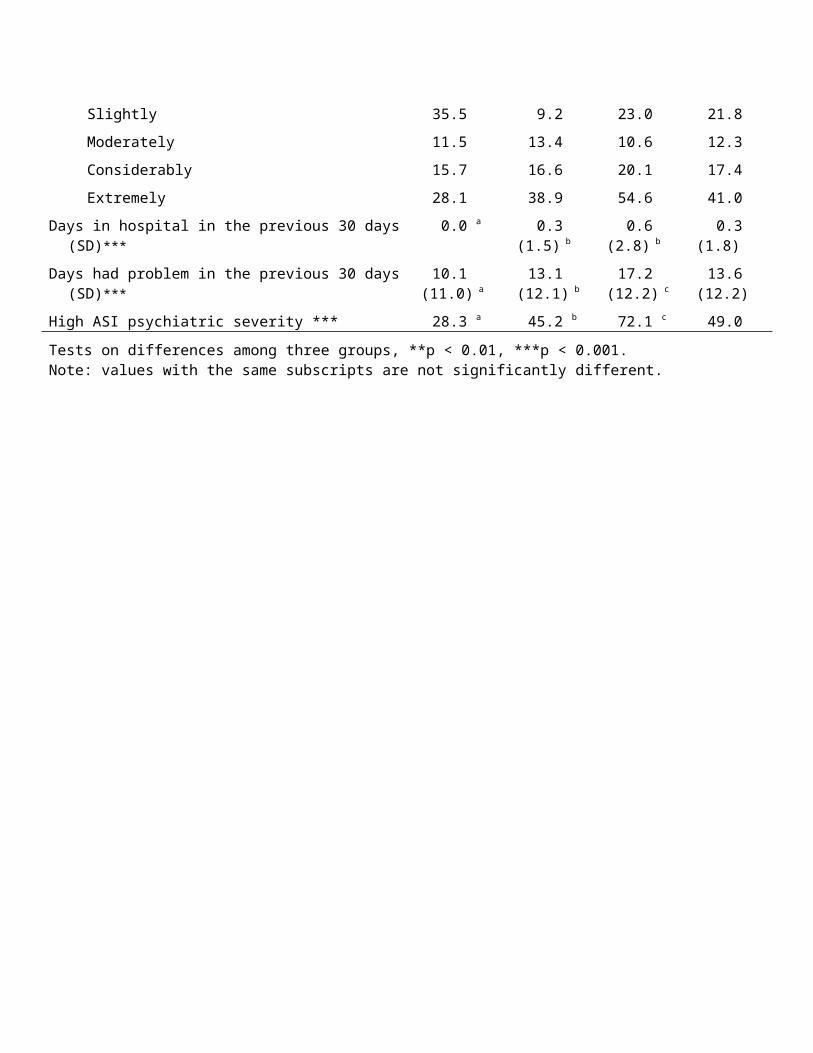
Psychiatric problems. The three groups differed significantly in
their lifetime utilization of mental health services, their
psychiatric symptoms, and perceived need for mental health
treatment at intake into the CalTOP treatment episode (Table 3).
The Dual Treatment Group consistently reported the highest rates
of prior mental health treatment, use of prescription medications
for mental health problems, current psychiatric symptoms, days
hospitalized in the previous 30, and days with psychiatric
problems in the previous 30, followed by the Drug Treatment Group
and the No Service Group. This group also reported being more
troubled by their mental health problems and as having a greater
need for mental health treatment. Consistent with these other
indicators, nearly three quarters of the Dual Treatment Group had
a “high” level of psychiatric severity (based on the median of
the intake sample), compared with fewer than half of the Drug
Treatment Group and less than one third of the No Services Group.
____________________
document.doc10/16/20227:33 PM19

Insert Table 3 about here
____________________
Mental Health Treatment Services, Drug Treatment Retention, and
Self-Help Participation
document.doc10/16/20227:33 PM20

Table 4 presents the mental health services received during
the 3 months following treatment admission (for the Dual
Treatment Group and Drug Treatment Group) based on the TSR
collected at the 3-month follow-up interview. In these analyses,
we included the ASI psychiatric score as covariate in order to
control for the psychiatric severity at intake. A greater
proportion of individuals in the Dual Treatment Group than the
Drug Treatment Group reported receiving mental health tests,
hospitalization, and medication for psychiatric problems. In
contrast, a greater proportion of individuals in the Drug
Treatment Group than the Dual Treatment Group received mental
health services in forms of relaxation training and interpersonal
skills. There were no significant differences between groups
regarding receipt of behavioral modification (about one third of
both groups) or having “significant” discussions with a service
provider (e.g., with a mental health specialist, counselor, or
social worker in an individual or group session) related to one’s
psychological problems (about three quarters of both groups).
_____________________
Insert Table 4 about here
document.doc10/16/20227:33 PM21
_____________________
As shown in table 5, about 54% of the No Service Group
stayed in treatment for at least 90 days or completed treatment
(which in some programs was less than 90 days duration), as did
62% of the Drug Treatment Group, and 59% of the Dual Treatment
Group. Between 59% to 67% in each of the three groups attended
self-help groups in the month prior to the 9-month follow-up. No
group differences were found in either drug treatment retention
or self-help group participation.
_____________________
Insert Table 5 about here
_____________________
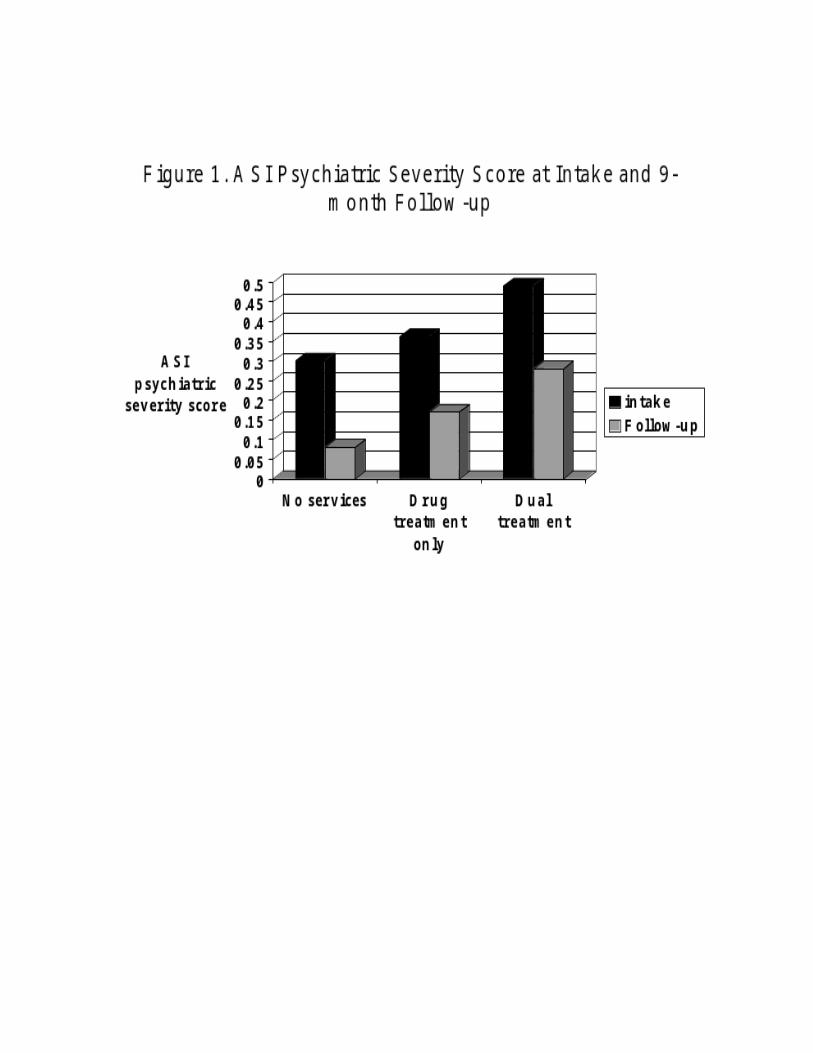
Posttreatment Outcomes
Changes in the ASI psychiatric composite scores from
baseline to follow-up most succinctly summarize changes in mental
health problems after treatment. Repeated measures of ANOVA
showed significant time and group effects (p < .0001) but not
their interaction. As illustrated in Figure 1, significant
reductions in psychiatric severity were observed for all three
document.doc10/16/20227:33 PM22

groups. Controlling for pretreatment differences, the Dual
Treatment Group continued to show the highest level of
psychiatric severity, followed by the Drug Treatment Group and
the No Service Group.
_____________________
Insert Figure 1 about here
_____________________
In terms of overall drug treatment success defined as no use
of alcohol or drugs and having a stable living in the community,
45% of the Dual Treatment Group and 51% to 52% of the other two
groups were considered as successful at 9 months following
treatment admission; again, no significant group difference was
found (Table 5). Combining across the three groups, there were
significant correlations between psychiatric severity and alcohol
use (.25, p < .001, at intake, .32, p < .001, at follow-up), and
drug use (.21, p < .001, at intake, .27, p < .001, at follow-up).
Discussion
This study is one of the first to examine the types of
mental health services utilization among patients in drug
treatment and the relationship of these service patterns to
document.doc10/16/20227:33 PM23
posttreatment outcomes. Moreover, the study has the advantage of
a relatively large number of patients, multiple types of
programs, and the linkage of self-report data with information
from administrative data systems. The study demonstrated that
more than a quarter of those expressing some level of mental
health problems at admission into drug treatment also received
services from mental health programs (i.e., the Dual Treatment
Group), one-fifth received no services, and the remainder
received some type of mental health services within the context
of drug treatment only. The group receiving dual treatment
demonstrated the most severe profile of mental health problems,
both over the lifetime and at treatment intake. Individuals who
received dual treatment were more likely to be women (70%), to be
White (66%), and to rely on public assistance, and were less
likely to be employed at the time of intake. They also displayed
more severe drug use and were more likely to have a history of
prior drug treatment. This group was also more likely to use
more intensive mental health services (e.g., hospitalization,
medications).
document.doc10/16/20227:33 PM24
In contrast, one-fifth of the sample did not receive any
mental health services (i.e., No Service Group) even though their
intake assessment indicated mental health problems. Relative to
the other two groups, the No Service Group had the lowest
percentage of female and individuals on public assistance, and
the highest percentages of African American and Latino/Hispanics
and individuals employed. Although the group’s mean ASI
psychiatric scores were lower than the other two groups, about
28% of this group had scores higher than the median (.366) of the
overall sample. It is unclear why this group did not receive
services addressing their mental health issues.
About half of the sample who reported mental health problems
at drug treatment intake received mental health services within
the drug treatment programs (Drug Treatment Group), and this
group’s outcomes often fell between the Dual Treatment Group and
No Service Group, particularly in terms of psychiatric severity
and service utilization, with some aspects (e.g., drug use) more
similar to the Dual Treatment Group, and other aspects (e.g.,
demographics, prior alcohol or drug treatment) more similar to
the No Service Group.
document.doc10/16/20227:33 PM25
The three groups did not differ much in their stay in drug
treatment or later participation in self-help groups. Their
overall drug treatment success rates were also similar, ranging
from 45% to 52%. Although all three groups showed significant
improvement in level of psychiatric severity, the Dual Treatment
Group continued to have the highest severity and the No Service
Group the lowest, following the same order observed at intake.
The study suggests that individuals who access services from
mental health programs, rather than solely through drug
treatment, have more severe types of mental health problems that
require extended care or more intensive interventions. More than
35% of these dually treated individuals had affective or other
psychoses. Unfortunately, psychiatric diagnoses (which were
obtained from mental health records) were not available in the
other two groups to make further comparisons across diagnostic
categories. Other research has shown that patients with co-
occurring disorders, in either substance abuse or mental health
programs, differ in regard to types of mental disorders.21
However, the Dual Treatment Group reported the highest level of
mental health problem severity and service utilization.
document.doc10/16/20227:33 PM26
Additionally, severity levels of alcohol and drug use increase
with psychiatric severity as evidenced by the significant
correlations between psychiatric severity and alcohol and drug
use at both intake and follow-up.
It is not clear why close to a quarter of those reporting
mental health problems at treatment admission did not receive any
services related to mental health issues. Service utilization
can be a function of access as well as compliance by the
patients. That is, some patients may fail to receive services
because they are treated in drug treatment programs that fail to
properly screen and assess for mental health disorders or that
lack the capability to either provide these services on-site or
to refer patients to off-site providers. Alternatively, the
failure to receive mental health services may reflect a patient’s
lack of interest or willingness to address these issues, or may
even reflect their inability to recall or to accurately report
having received these services.
It is important to note some cautions and limitations of the
present study. The counties and treatment programs participating
in CalTOP were not randomly selected. Observed patterns may not
document.doc10/16/20227:33 PM27
be generalizable to other programs that do not provide similar
services to their patients. Some of the measures relied on data
derived from patient self-report; however, the instruments (e.g.,
ASI, TSR) and procedures used in this study are those most widely
used in the substance abuse treatment field and have been
validated in studies with similar populations. Additionally, the
study has been strengthened by including data sources obtained
from official records such as mental health and criminal justice
involvement.
Few studies are available to assess mental health service
utilization and treatment outcomes in community-based treatment
programs. The present study provides evidence that individuals
with mental health problems are found within mainstream
community-based drug treatment programs and that fully half of
them receive mental health services within the context of their
substance abuse treatment, while another quarter receives
treatment simultaneously from a separate mental health provider.
Future studies should assess the extent to which treatment across
substance abuse and mental health providers is coordinated and
document.doc10/16/20227:33 PM28
identify ways to improve service delivery to dually diagnosed
individuals.
document.doc10/16/20227:33 PM29
References
1. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M,
Eshleman S, Wittchen H, Kendler KS. Lifetime and 12-month
prevalence of DSM-III-R psychiatric disorders in the
United States: Results from the National Comorbidity
Study. Arch Gen Psychiatry. 1994; 51(1):8-19.
2. Kessler RC, Nelson CB, McGonagle KA, Edlund MJ, Frank RG,
Leaf PJ. The epidemiology of co-occurring addictive and
mental disorders: Implications for prevention and service
utilization. Am J Orthopsychiatry. 1996; 66:17-31.
3. Regier D, Narrow W, Rae D, Mandersheid R, Locke B, Goodwin
F. The de facto U.S. Mental and addictive disorders
service system. Arch Gen Psychiatry. 1993; 50:85-94.
4. Wu LT, Ringwalt CL, Williams CE. Use of substance abuse
treatment services by persons with mental health and
substance use problems. Psychiatr Serv. 2003; 54(3):363-69.
5. Bartels SJ, Drake RE, Wallach MA. Long-term course of
substance use disorders among patients with severe mental
illness. Psychiatr Serv. 1995; 46(3):248-51.
6. Drake RE, Mueser KT, Clark RE, Wallach MA. The course,
document.doc10/16/20227:33 PM30
treatment, and outcome of substance disorder in persons
with severe mental illness. Am J Orthopsychiatry. 1996;
66(1): 42-51.
7. Hasin D, Liu X, Nunes E, McCloud S, Samet S, Endicott J.
Effects of major depression on remission and relapse of
substance dependence. Arch Gen Psychiatry. 2002;
59(4):375-80.
8. Minkoff K. Best practices: Developing standards of care
for individuals with co- occurring psychiatric and
substance use disorders. Psychiatr Serv. 2001a; 52:597-99.
9. McLellan AT, Luborsky L, Woody G , O'Brien, CP, Druley KA.
Predicting response to alcohol and drug abuse treatments.
Role of psychiatric severity. Arch Gen Psychiatry. 1983;
40(6):620-25.
10. McLellan AT, Alterman AI, Metzger DS, Grissom GR, Woody
GE, Luborsky L, O'Brien CP. Similarity of outcome
predictors across opiate, cocaine, and alcohol treatments:
Role of treatment services. J Consult Clin Psychol.
1994;62(6):1141-58.
11. Schmitz JM, Stotts AL, Averill PM, Rothfleisch JM,
document.doc10/16/20227:33 PM31
Bailley SE, Sayre SL, Grabowski J. Cocaine dependence with
and without comorbid depression: A comparison of patient
characteristics. Drug Alcohol Depend. 2000; 60(2000):189-
98.
12. Brown RA, Monti PM, Myers MG, Martin RA, Rivinus T,
Dubreuil ME, Rohsenow DJ. Depression among cocaine abusers
in treatment: Relation to cocaine and alcohol use and
treatment outcome. Am J Psychiatry. 1998; 155(2):220-5.
13. Carroll KM, Power ME, Bryant K, Rounsaville BJ. One-
year follow-up status of treatment-seeking cocaine
abusers: Psychopathology and dependence severity as
predictors of outcome. J Nerv Ment Dis. 1993; 181(2):71-9.
14. Compton WM, Cottler LB, Jacobs JL, Ben-Abdallah A,
Spitznagel ED. The role of psychiatric disorders in
predicting drug dependence treatment outcomes. Am J
Psychiatry. 2003; 160(5): 890-5.
15. Rounsaville BJ, Kosten TR, Weissman MM, Kleber HD.
Prognostic significance of psychopathology in treated
opiate addicts: A 2.5-year follow-up study. Arch Gen
Psychiatry. 1986; 43(8):739-45.
document.doc10/16/20227:33 PM32
16. Rounsaville BJ, Dolinsky ZS, Babor TF, Meyer RE.
Psychopathology as a predictor of treatment outcome in
alcoholics. Arch Gen Psychiatry. 1987; 44(6):505-13.
17. Weisner C, Matzger H, Kaskutas LA. How important is
treatment? One-year outcomes of treated and untreated
alcohol-dependent individuals. Addiction. 2003; 98:901-11.
18. Brown VB, Ridgely MS, Pepper B, Levine IS, Ryglewicz H.
The dual crisis: Mental illness and substance abuse. Am
Psychol. 1989; 44:565-9.
19. Zweben JE. Severely and persistently mentally ill
substance abusers: Clinical and policy issues. J
Psychoactive Drugs. 2000; 32: 383-389.
20. Osher FC, Drake RE. Reversing a history of unmet needs:
Approaches to care for persons with co-occurring addictive
and mental disorders. Am J Orthopsychiatry. 1996; 66(1):4-
11.
21. Primm AB, Gomez MB, Tzolova-Iontchev I, Perry W, Vu HT,
Crum RM. Mental health versus substance abuse treatment
programs for dually diagnosed patients. J Subst Abuse
Treat. 2000; 19(3): 285-90.
document.doc10/16/20227:33 PM33
22. Grella CE. Contrasting the views of substance misuse
and mental health treatment providers on treating the
dually diagnosed. Subst Use Misuse. 2003; 38(10):1433-
1446.
23. Drake RE, Mueser KT. Psychosocial approaches to dual
diagnosis. Schizophr Bull. 2000; 26(1):105-18.
24. Watkins KE, Burnam A, Kung F, Paddock SA. A national
survey of care for persons with co-occurring mental and
substance use disorders. Psychiatr Serv. 2001; 52(8):
1062-68.
25. Barrowclough C, Haddock G, Tarrier N, Lewis SW, Moring
J, O'Brien R, Schofield N, McGovern J. Randomized
controlled trial of motivational interviewing, cognitive
behavior therapy, and family intervention for patients
with comorbid schizophrenia and substance use disorders.
Am J Psychiatry. 2001; 158(10):1706-13.
26. Carey KB. Substance use reduction in the context of
outpatient psychiatric treatment: A collaborative,
motivational, harm reduction approach. Community Ment
Health J. 1996; 32(3): 291-306.
document.doc10/16/20227:33 PM34
27. Drake RE, Mercer-McFadden C, Mueser KT, McHugo GJ, Bond
GR. Review of integrated mental health and substance abuse
treatment for patients with dual disorders. Schizophr
Bull. 1998; 24(4):589-608.
28. Drake RE, Essock SM, Shaner A, Carey KB, Minkoff K,
Kola L, Lynde D, Osher FC, Clark RE, Rickards L.
Implementing dual diagnosis services for clients with
severe mental illness. Psychiatr Serv. 2001; 52(4):469-76.
29. Roberts LJ, Shaner A, Eckman TA. Overcoming addictions:
Skills training for people with schizophrenia. New York:
W. W. Norton, 1999.
30. Ziedonis DM, Trudeau K. Motivation to quit using
substances among individuals with schizophrenia:
Implications for a motivation-based treatment model.
Schizophr Bull. 1997; 23(2):229-38.
31. Grella CE, Gilmore J. Improving service delivery to the
dually diagnosed in Los Angeles County. J Subst Abuse
Treat. 2002; 23:115-22.
32. Moos RH, Finney JW, Federman EB, Suchinsky R. Specialty
mental health care improves patients' outcomes: Findings
document.doc10/16/20227:33 PM35
from a nationwide program to monitor the quality of care
for patients with substance use disorders. J Stud Alcohol.
2000; 61(5):704-13.
33. Sacks S. Co-occurring mental and substance use
disorders: Promising approaches and research issues. Subst
Use Misuse. 2000; 35(12-14):2061-93.
34. Substance Abuse and Mental Health Services
Administration, Office of Applied Studies. The DASIS
report: Facilities offering special programs for dually
diagnosed clients. Rockville, MD: U.S. Department of
Health and Human Services, 2002.
35. Grella CE, Hser YI. A county survey of mental health
services in drug treatment programs. Psychiatr Serv. 1997;
48(7):950-52.
36. Young N, Grella CE. Mental health and substance abuse
treatment services for dually-diagnosed clients: Results of
a state-wide survey of county administrators. J Ment Health
Adm. 1998; 25(1):83-92.
37. Drake RE, Wallach MA. Dual diagnosis: 15 years of
progress. Psychiatr Serv. 2000; 51(9):1126-1129.
document.doc10/16/20227:33 PM36
38. Grella CE, Gil-Rivas V, Cooper L. Perceptions of mental
health and substance abuse program administrators and
staff on service delivery to persons with co-occurring
substance abuse and mental disorders. J Behav Health Serv
Res. 2004; 31(1):38-49.
39. Jerrell JM, Wilson JL, Hiller DC. Issues and outcomes
in integrated treatment programs for dual disorders. J
Behav Health Serv Res. 2000; 27:303-13.
40. Hser Y-I, Evans E, Teruya C, Hardy M, Urada D, Huang Y,
Picazo R, Shen H, Hsieh J, Anglin MD. Final report: The
California Treatment Outcome Project. California State
Department of Alcohol and Drug Programs. Los Angeles, CA:
UCLA Integrated Substance Abuse Programs, 2002.
41. McLellan AT, Luborsky L, Woody GE, O'Brien CP. An
improved diagnostic evaluation instrument for substance
abuse patients. The Addiction Severity Index. J Nerv Ment
Dis. 1980; 168:26-33.
42. McLellan AT, Kushner H, Metzger D, Peters R, Smith I,
Grissom G, Pettinati H, Argeriou M. The fifth edition of
the Addiction Severity Index. J Subst Abuse Treat. 1992;
document.doc10/16/20227:33 PM37
9:199-213.
43. McLellan AT, Alterman AI, Cacciola J, Metzger D,
O'Brien CP. A new measure of substance abuse treatment.
Initial studies of the treatment services review. J Nerv
Ment Dis. 1992; 18:101-10.
44. De Leon G. Retention in drug-free therapeutic
communities. In: Pickens RW, Leukefeld CG, Schuster CR,
eds. Improving drug abuse treatment (NIDA Research
Monograph 106, DHHS Pub. No. ADM 91-1754; Rockville, MD:
National Institute on Drug Abuse, 1991.
45. Simpson DD, Joe GW, Fletcher BW, Hubbard RL, Anglin MD.
A national evaluation of treatment outcomes for cocaine
dependence Arch Gen Psychiatry. 1999; 56:507-14.
document.doc10/16/20227:33 PM38
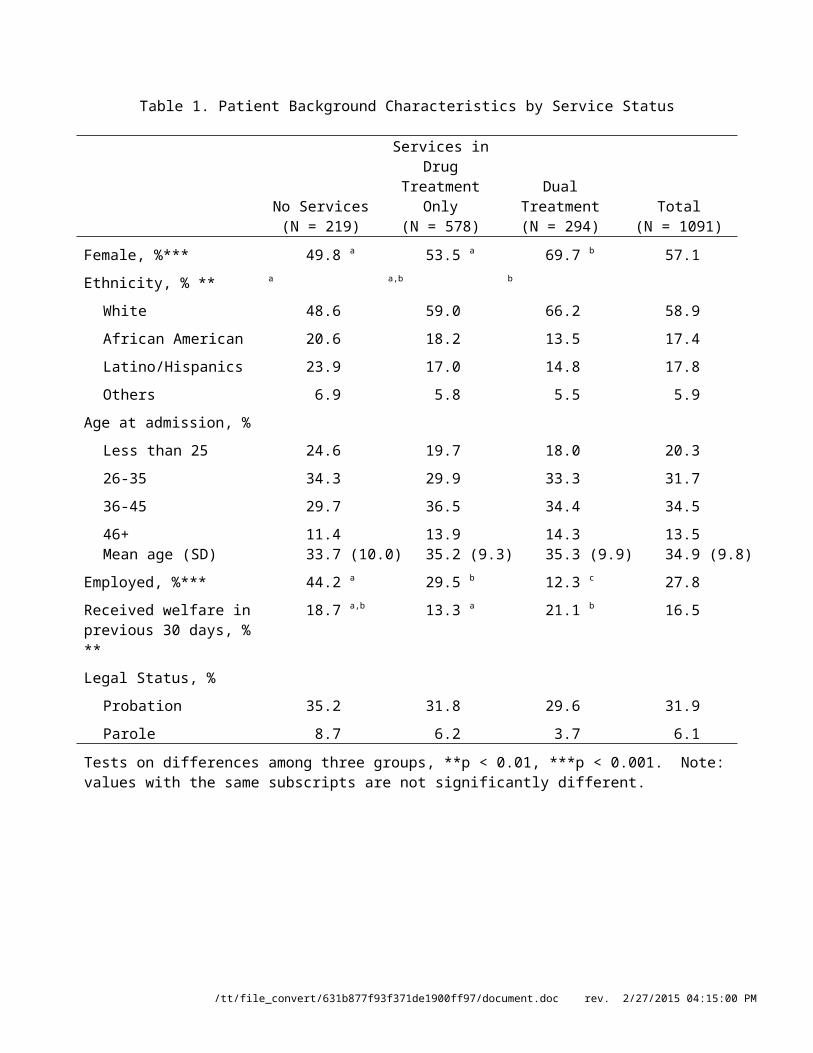
Table 1. Patient Background Characteristics by Service Status
No Services(N = 219)
Services inDrug
TreatmentOnly
(N = 578)
DualTreatment(N = 294)
Total(N = 1091)
Female, %*** 49.8 a 53.5 a 69.7 b 57.1Ethnicity, % **
a
a,b
b
White 48.6 59.0 66.2 58.9African American 20.6 18.2 13.5 17.4Latino/Hispanics 23.9 17.0 14.8 17.8Others 6.9 5.8 5.5 5.9
Age at admission, %Less than 25 24.6 19.7 18.0 20.326-35 34.3 29.9 33.3 31.736-45 29.7 36.5 34.4 34.546+ 11.4 13.9 14.3 13.5Mean age (SD) 33.7 (10.0) 35.2 (9.3) 35.3 (9.9) 34.9 (9.8)
Employed, %*** 44.2 a 29.5 b 12.3 c 27.8Received welfare inprevious 30 days, %**
18.7 a,b 13.3 a 21.1 b 16.5
Legal Status, %Probation 35.2 31.8 29.6 31.9Parole 8.7 6.2 3.7 6.1
Tests on differences among three groups, **p < 0.01, ***p < 0.001. Note:values with the same subscripts are not significantly different.
/tt/file_convert/631b877f93f371de1900ff97/document.doc rev. 2/27/2015 04:15:00 PM
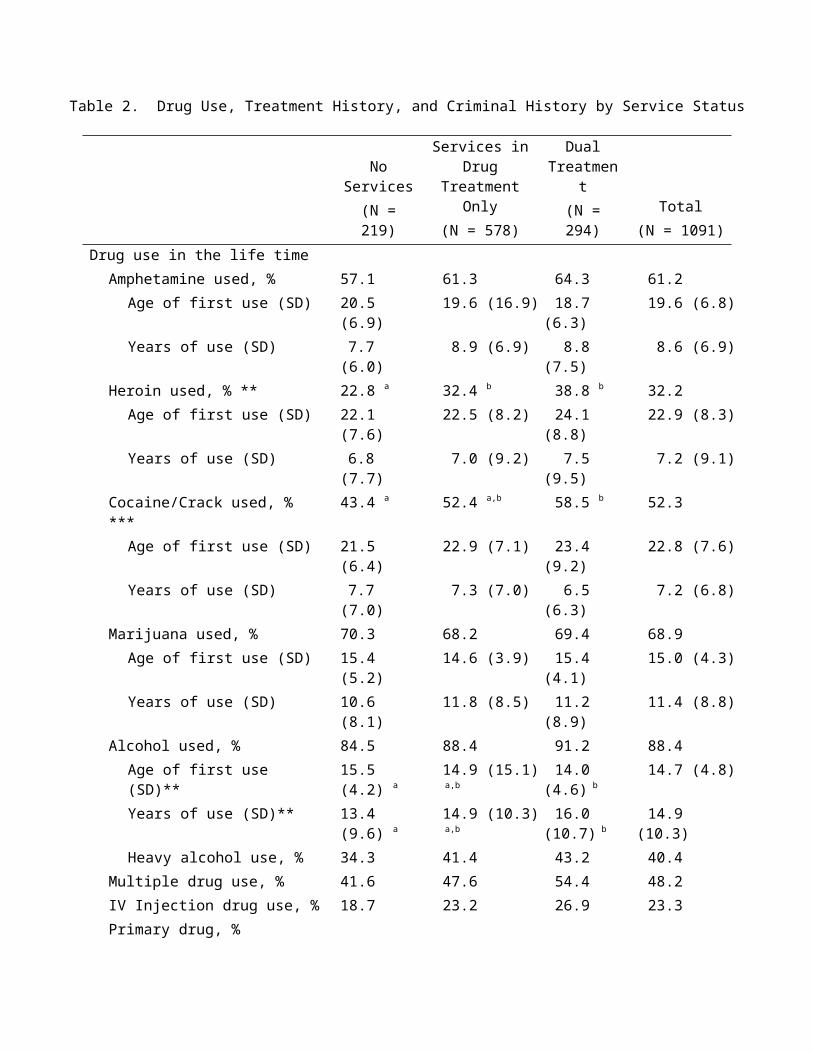
Table 2. Drug Use, Treatment History, and Criminal History by Service Status
NoServices(N =219)
Services inDrug
TreatmentOnly
(N = 578)
DualTreatmen
t(N =294)
Total(N = 1091)
Drug use in the life timeAmphetamine used, % 57.1 61.3 64.3 61.2
Age of first use (SD) 20.5 (6.9)
19.6 (16.9) 18.7 (6.3)
19.6 (6.8)
Years of use (SD) 7.7 (6.0)
8.9 (6.9) 8.8 (7.5)
8.6 (6.9)
Heroin used, % ** 22.8 a 32.4 b 38.8 b 32.2Age of first use (SD) 22.1
(7.6)22.5 (8.2) 24.1
(8.8)22.9 (8.3)
Years of use (SD) 6.8 (7.7)
7.0 (9.2) 7.5 (9.5)
7.2 (9.1)
Cocaine/Crack used, % ***
43.4 a 52.4 a,b 58.5 b 52.3
Age of first use (SD) 21.5 (6.4)
22.9 (7.1) 23.4 (9.2)
22.8 (7.6)
Years of use (SD) 7.7 (7.0)
7.3 (7.0) 6.5 (6.3)
7.2 (6.8)
Marijuana used, % 70.3 68.2 69.4 68.9Age of first use (SD) 15.4
(5.2)14.6 (3.9) 15.4
(4.1)15.0 (4.3)
Years of use (SD) 10.6 (8.1)
11.8 (8.5) 11.2 (8.9)
11.4 (8.8)
Alcohol used, % 84.5 88.4 91.2 88.4Age of first use (SD)**
15.5 (4.2) a
14.9 (15.1)a,b
14.0 (4.6) b
14.7 (4.8)
Years of use (SD)** 13.4 (9.6) a
14.9 (10.3)a,b
16.0 (10.7) b
14.9 (10.3)
Heavy alcohol use, % 34.3 41.4 43.2 40.4Multiple drug use, % 41.6 47.6 54.4 48.2IV Injection drug use, % 18.7 23.2 26.9 23.3Primary drug, %
Alcohol 25.6 30.6 33.0 30.3Cocaine 12.8 11.4 12.6 12.0Heroin 12.8 16.1 18.4 16.0Marijuana 15.5 8.5 8.2 9.8Amphetamine/Methamphetamine
28.8 30.3 25.2 28.6
Other drug 4.6 3.1 2.7 3.3Treatment History (SD)
Number of alcohol treatments**
0.8 (3.6) a
1.1 (3.3) 1.9 (3.6) c
1.3 (3.5)
Number of drug treatments **
1.5 (3.2) a
2.0 (3.8) a,b
2.7 (4.3) b
2.1 (3.8)
Criminal History, %Criminally active in previous 30 days
61.2 55.9 51.7 55.8
Ever arrested 79.9 79.1 77.2 78.7Arrest in the previous year
40.2 38.9 33.7 37.8
Treatment Modality, % *** a a
b
Methadone maintenance 5.5 4.3 6.5 5.1Outpatient drug-free 69.0 49.5 52.4 54.2Residential 25.6 46.2 41.2 40.7
Treatment Referral Sources, % ***
a a
b
AOD programs 10.6 13.0 11.6 12.2Criminal justice system 32.6 27.5 17.8 25.9Self referral 40.8 40.7 43.7 41.5Others 1 16.1 18.8 27.0 20.4
1 Others include community programs, health care, schools, employers and 12-step programs.Tests on differences among three groups, **p < 0.01, ***p < 0.001. Note: values with the same subscripts are not significantly different.
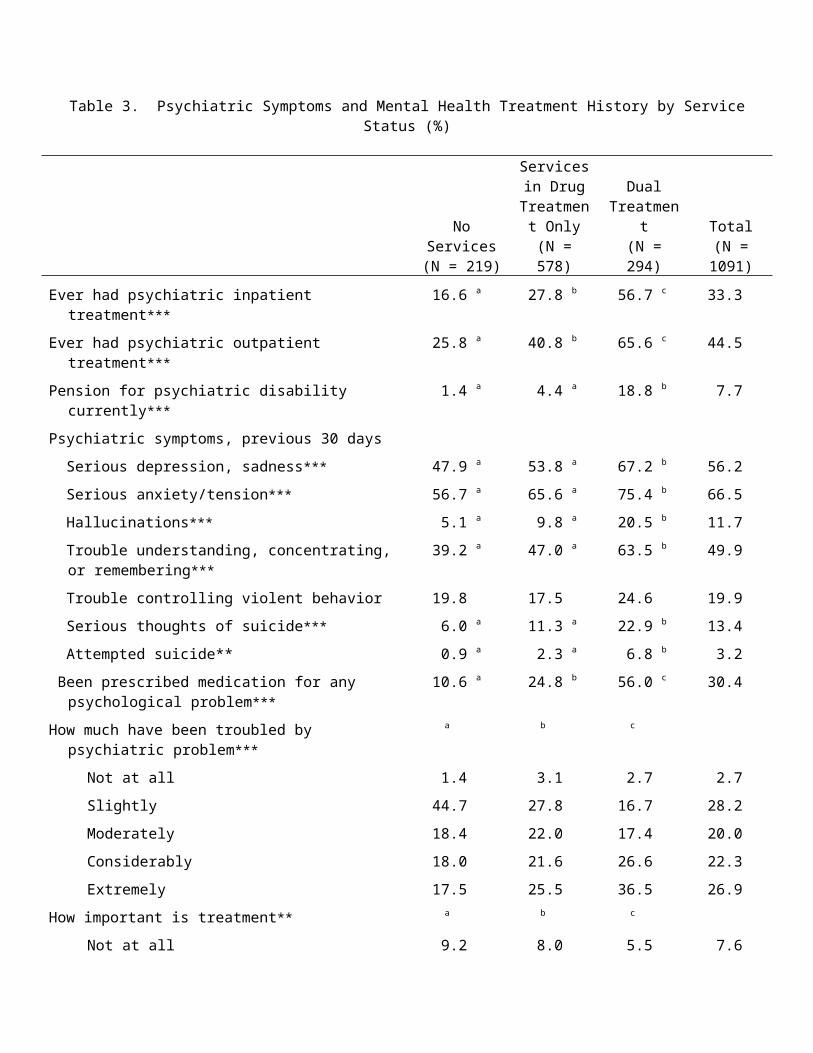
Table 3. Psychiatric Symptoms and Mental Health Treatment History by ServiceStatus (%)
NoServices(N = 219)
Servicesin DrugTreatment Only(N =578)
DualTreatmen
t(N =294)
Total(N =1091)
Ever had psychiatric inpatient treatment***
16.6 a 27.8 b 56.7 c 33.3
Ever had psychiatric outpatient treatment***
25.8 a 40.8 b 65.6 c 44.5
Pension for psychiatric disability currently***
1.4 a 4.4 a 18.8 b 7.7
Psychiatric symptoms, previous 30 days Serious depression, sadness*** 47.9 a 53.8 a 67.2 b 56.2 Serious anxiety/tension*** 56.7 a 65.6 a 75.4 b 66.5 Hallucinations*** 5.1 a 9.8 a 20.5 b 11.7 Trouble understanding, concentrating,
or remembering*** 39.2 a 47.0 a 63.5 b 49.9
Trouble controlling violent behavior 19.8 17.5 24.6 19.9 Serious thoughts of suicide*** 6.0 a 11.3 a 22.9 b 13.4 Attempted suicide** 0.9 a 2.3 a 6.8 b 3.2 Been prescribed medication for any
psychological problem***10.6 a 24.8 b 56.0 c 30.4
How much have been troubled by psychiatric problem***
a
b
c
Not at all 1.4 3.1 2.7 2.7Slightly 44.7 27.8 16.7 28.2Moderately 18.4 22.0 17.4 20.0Considerably 18.0 21.6 26.6 22.3Extremely 17.5 25.5 36.5 26.9
How important is treatment**
a
b
c
Not at all 9.2 8.0 5.5 7.6
Slightly 35.5 9.2 23.0 21.8Moderately 11.5 13.4 10.6 12.3Considerably 15.7 16.6 20.1 17.4Extremely 28.1 38.9 54.6 41.0
Days in hospital in the previous 30 days(SD)***
0.0 a 0.3 (1.5) b
0.6 (2.8) b
0.3 (1.8)
Days had problem in the previous 30 days(SD)***
10.1 (11.0) a
13.1 (12.1) b
17.2 (12.2) c
13.6 (12.2)
High ASI psychiatric severity *** 28.3 a 45.2 b 72.1 c 49.0Tests on differences among three groups, **p < 0.01, ***p < 0.001. Note: values with the same subscripts are not significantly different.
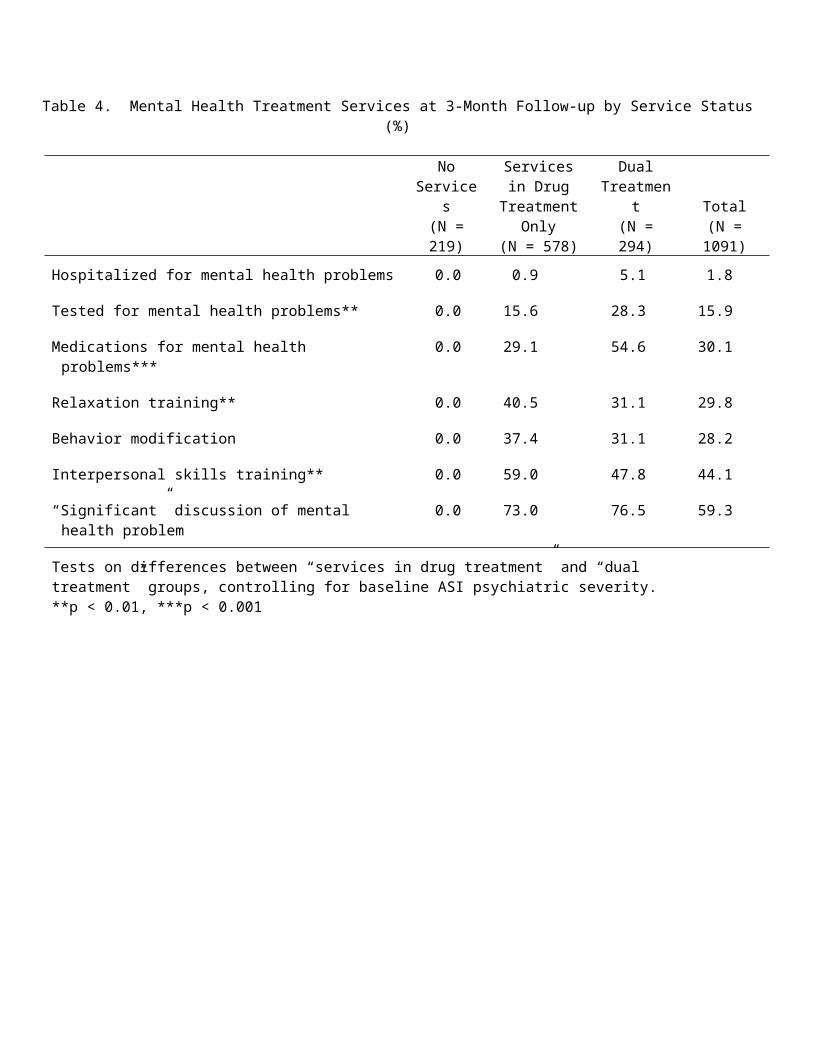
Table 4. Mental Health Treatment Services at 3-Month Follow-up by Service Status(%)
NoService
s(N =219)
Servicesin Drug
TreatmentOnly
(N = 578)
DualTreatmen
t(N =294)
Total(N =1091)
Hospitalized for mental health problems 0.0 0.9 5.1 1.8
Tested for mental health problems** 0.0 15.6 28.3 15.9
Medications for mental health problems***
0.0 29.1 54.6 30.1
Relaxation training** 0.0 40.5 31.1 29.8
Behavior modification 0.0 37.4 31.1 28.2
Interpersonal skills training** 0.0 59.0 47.8 44.1
“Significant” discussion of mental health problem
0.0 73.0 76.5 59.3
Tests on differences between “services in drug treatment” and “dual treatment” groups, controlling for baseline ASI psychiatric severity. **p < 0.01, ***p < 0.001
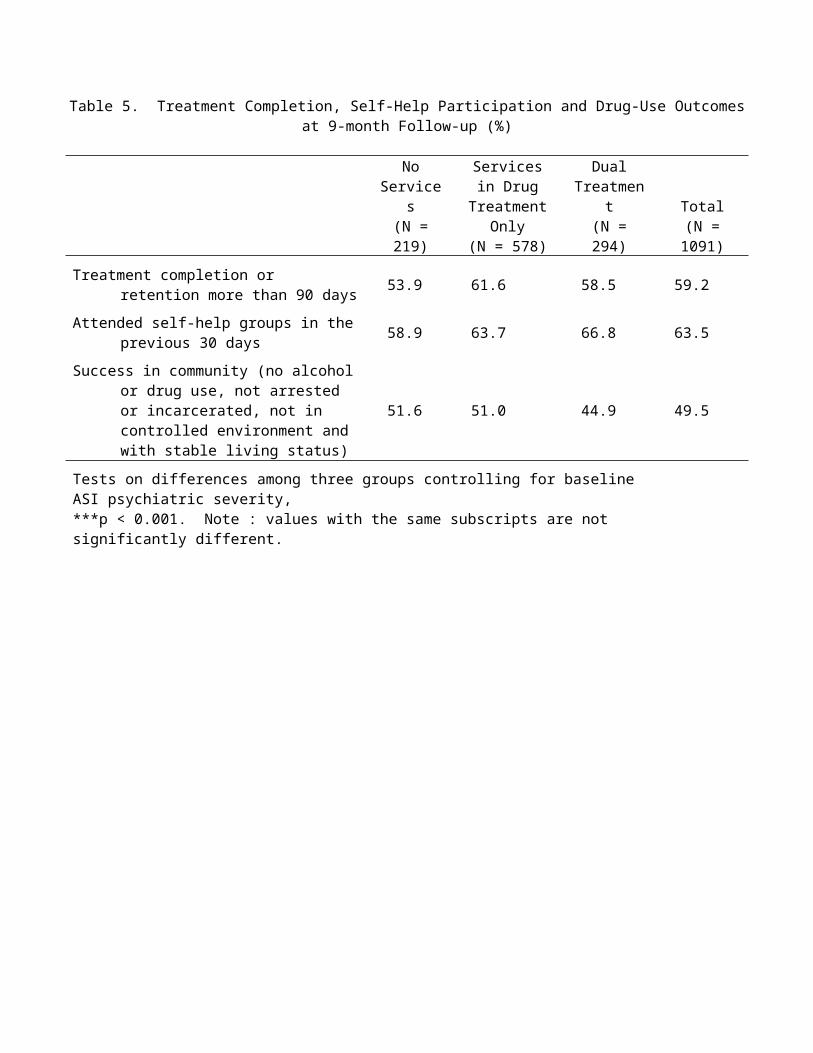
Table 5. Treatment Completion, Self-Help Participation and Drug-Use Outcomesat 9-month Follow-up (%)
NoService
s(N =219)
Servicesin Drug
TreatmentOnly
(N = 578)
DualTreatmen
t(N =294)
Total(N =1091)
Treatment completion or retention more than 90 days 53.9 61.6 58.5 59.2
Attended self-help groups in theprevious 30 days 58.9 63.7 66.8 63.5
Success in community (no alcoholor drug use, not arrested or incarcerated, not in controlled environment and with stable living status)
51.6 51.0 44.9 49.5
Tests on differences among three groups controlling for baseline ASI psychiatric severity, ***p < 0.001. Note : values with the same subscripts are not significantly different.