Using Formative Research to Develop a Worksite Health Promotion Program for African American Women
19
Using Formative Research to Develop a Worksite Health Promotion Program for African American Women Christie Zunker, MA, CHES Tiffany L. Cox, MPH Brooks C. Wingo, MSW Bern’Nadette Knight, MSPH Wendy K. Jefferson, BS Jamy D. Ard, MD ABSTRACT. Objectives: To describe the development of a cultur- ally appropriate worksite health promotion program (WHPP) de- signed to promote increased physical activity and improved nutrition in a high risk group of African American women. Methods: The program was based on EatRight, which is a lifestyle- oriented weight control program that focuses on food volume, rather than calories. Formative research included four nominal group tech- nique (NGT) sessions conducted with 14 African American women from the selected worksite to gather input on job factors that affected their weight and daily life factors that affected their amount of phys- ical activity. Their responses were used to adapt existing EatRight materials to target areas of special need for this unique group. Christie Zunker, Tiffany L. Cox, Brooks C. Wingo, Bern’Nadette Knight, Wendy K. Jefferson, and Jamy D. Ard are affiliated with University of Alabama at Birmingham, Department of Nutrition Sciences, Division of Clinical Nutrition and Dietetics, 445 Webb Building, 1675 University Boulevard, Birmingham, AL 35294- 3360. Address correspondence to: Christie Zunker at the above address (E-mail: cbz9@ uab.edu). Women & Health, Vol. 48(2) 2008 Available online at http://www.haworthpress.com © 2008 by The Haworth Press. All rights reserved. doi: 10.1080/03630240802313514 189
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Using Formative Research to Develop a Worksite Health Promotion Program for African American Women

Using Formative Research to Developa Worksite Health Promotion Program
for African American Women
Christie Zunker, MA, CHES
Tiffany L. Cox, MPHBrooks C. Wingo, MSW
Bern’Nadette Knight, MSPHWendy K. Jefferson, BS
Jamy D. Ard, MD
ABSTRACT. Objectives: To describe the development of a cultur-ally appropriate worksite health promotion program (WHPP) de-signed to promote increased physical activity and improved nutritionin a high risk group of African American women.
Methods: The program was based on EatRight, which is a lifestyle-oriented weight control program that focuses on food volume, ratherthan calories. Formative research included four nominal group tech-nique (NGT) sessions conducted with 14 African American womenfrom the selected worksite to gather input on job factors that affectedtheir weight and daily life factors that affected their amount of phys-ical activity. Their responses were used to adapt existing EatRightmaterials to target areas of special need for this unique group.
Christie Zunker, Tiffany L. Cox, Brooks C. Wingo, Bern’Nadette Knight, WendyK. Jefferson, and Jamy D. Ard are affiliated with University of Alabama atBirmingham, Department of Nutrition Sciences, Division of Clinical Nutrition andDietetics, 445 Webb Building, 1675 University Boulevard, Birmingham, AL 35294-3360.
Address correspondence to: Christie Zunker at the above address (E-mail: [email protected]).
Women & Health, Vol. 48(2) 2008Available online at http://www.haworthpress.com
© 2008 by The Haworth Press. All rights reserved.doi: 10.1080/03630240802313514 189

190 WOMEN & HEALTH
Results: Themes emerged from the NGT sessions that indicatedstress at work and an environment of unhealthy eating, in addition tosocial eating and lack of social support for healthy eating added tounhealthy eating patterns at work. In response to physical activity, theprimary themes included lack of time to exercise, stress of multiplefamily roles and responsibilities, and perceived physical barriers tophysical activity.
Discussion: Based on the NGT themes, EatRight materials wereadapted and additional topics (e.g., increasing social support, over-coming limitations, and time management) were included to developa WHPP that addressed issues that the participants identified asrelevant for their work and home lives. Conducting the NGT sessionsand EatRight classes in the work environment, we were able toprovide a convenient, familiar environment which fostered socialsupport among participants. We believe that a culturally appropriatemodification of EatRight holds great promise in addressing healthdisparities seen among African American women by offering educa-tion on lifestyle changes that will decrease weight through nutritionand physical activity.
KEYWORDS. Worksite health, African American, women, nutri-tion, physical activity
Physical inactivity and poor nutrition are major public health prob-lems thatincrease the risk of chronic disease morbidity and mor-tality, particularly among African American women and lower so-cioeconomic status (SES) groups (USDHHS, 1996; Wilcox et al.,2000). Most chronic disease and mortality is preventable by modifyinglifestyle-related behaviors (Mokdad et al., 2005). Promoting healthierlifestyles, including increased physical activity and improved nutri-tion, through health education in the workplace may be a convenient,feasible option. Worksites have the potential to reach a large numberof employees, including many who may not otherwise participate inhealthy behaviors (Glasgow, McCaul, & Fisher, 1993). Furthermore,because a larger proportion of African American women compared towomen of other racial groups currently make up the workforce, theworksite setting may be an especially convenient means to capture thetarget audience. Recent employment status annual averages reportedby the U.S. Department of Labor (2004) indicated that a larger pro-

Zunker et al. 191
portion of African American women aged 16 years and older wereemployed compared with white, Asian, or Hispanic women.
Worksite health promotion programs (WHPPs) may produce ben-efits for employees and employers, including reduced sick leave andhealth plan costs (Chapman, 2003; Griffin-Blake & DeJoy, 2006).For example, a systematic review indicated WHPPs that incorporateenvironmental modifications (e.g., promoting stair usage) can havewide-ranging effects on health behaviors, including influencing dietaryintake (Engbers et al., 2005). Comprehensive worksite programs thatinclude both nutrition and physical activity components (e.g., dietaryeducation, group physical activity, behavioral skill training) have beenrecommended by the Task Force on Community Preventive Services(Katz et al., 2005). In addition, a review by Marcus et al. (2006)reported that methodologically strong workplace interventions usingindividually tailored, theory-based materials often produce favorableoutcomes (e.g., increased physical activity) among employees, butmay not be generalized to less motivated employees or continue forthe long term.
It is unclear whether WHPP participation is affected by behav-ioral risk characteristics (i.e., actual behaviors) because many studiesto date have had limited external validity, typically only includinghighly motivated volunteers who were already physically active, iden-tified as low risk, or white men (Marshall, 2004). For example, aWHPP offering on-site wellness and fitness programs found that moreemployees with fewer behavioral risk factors, such as inadequateamounts of physical activity and excessive caloric intake, partici-pated than employees at high risk (Lewis, Huebner, & Yarborough,1996). However, other researchers have reported that healthy employ-ees do not consistently participate more than nonhealthy employeesand suggest changing the work environment to encourage employeeinvolvement (Grosch et al., 1998). The feasibility and effectivenessof these programs in different work environments and other pop-ulations, such as African American women, remains a significantquestion.
Multi-component WHPPs that include physical activity and nu-trition education are most effective when built on components thatrelate specifically to the population of interest (Malpede et al., 2007).Equally as important as knowing which interventions work to improvehealth, is understanding why they work and how to deliver themsuccessfully. Formative research guides the initial development ofthe program and allows researchers to shape the program strategies,including identifying key decision points and determining the neces-

192 WOMEN & HEALTH
sary information to make the decisions (Weinreich, 1999). In addition,formative research can be used to develop culturally and regionallyappropriate programs (Gittelsohn et al., 2006).
An example of a successful lifestyle weight management programthat could be tailored to a specific population is the EatRight Program.The authors’ past work with African American groups in the areasuggest that this program could be successful in changing physicalactivity and diet behaviors of African American women. The EatRightProgram is based on the concept of “time-calorie displacement,” whichemphasizes the ingestion of large quantities of high-bulk, low-energy-density foods (primarily vegetables, fruits, high-fiber grains, and ce-reals) and moderation in high-energy-density foods (meats, cheeses,sugars, and fats; see Greene et al., 2006). The program also uses basicprinciples of behavior modification related to dietary and physicalactivity habits to promote a calorie deficit and achieve moderateweight loss goals.
Leisure time physical activity is often low in African Americanwomen and may be even more so in those African American womenwho work and have multiple roles outside of the home (Crespo et al.,1999; USDHHS, 1996). Preliminary work suggested that this mightbe especially true for the employees of the current worksite: a Com-munity Action Agency that provided social and child developmentservices to low-income citizens in the community. This article de-scribes the iterative process and its findings used to formulate aculturally appropriate WHPP designed to promote increased physi-cal activity and improved nutrition in a high risk group of AfricanAmerican women. The target group of the current project was mostlymiddle-aged, overweight or obese African American women with ahigh disease risk and low to middle socioeconomic status. To ourknowledge, no one has conducted a WHPP with this unique group.The theoretical models underlying intervention development were pri-marily social cognitive theory and the social ecology model, be-cause numerous factors influence health behaviors, including self-efficacy beliefs with the social environment, community norms, andpolicy level factors (Bandura, 2004; McLeroy et al., 1988). Thisstudy is unique for a number of reasons, including implementationof a comprehensive behavioral nutrition and physical activity pro-gram (which might lead to weight loss) in working, high risk, obeseAfrican American women within the context of their work environ-ment. The main objective addressed by this project was to describethe formative research process of culturally modifying existing WHPPmaterials.

Zunker et al. 193
METHODS
Participant Recruitment
The current worksite included a headquarters that supports a staffof over 400 employees at 40 sites throughout the county with three di-visions: administrative support, child development services, and com-munity services. The study was announced to all employees of thecurrent worksite with paycheck mailers and via flyers distributed atheadquarters and posted at worksites. The worksite chosen for thecurrent study provided a variety of federal, state, and local programsto improve quality of life among low-income individuals. Informedconsent was written and signed by all participants. This study wasreviewed and approved by the University of Alabama at BirminghamInstitutional Review Board to ensure the protection of human subjects.
The only eligibility criterion was that the participant had to be acurrent employee of the worksite. This stipulation was a conditionof the agency’s agreement to participate in the research study. There-fore, all employees were notified of the opportunity to participatein the worksite program using bulletins posted throughout the work-site, announcements placed in paycheck stubs, and announcementsplaced in the intra-agency newsletter. A total of 39 employees wererecruited for the program, including 14 individuals who took part inthe formative assessment. Ten participants did not continue throughthe control period because of subsequent job conflicts .n D 5/; lackof interest/reason not known .n D 4/; or health issues .n D 1/:Thus, 29 participants began the intervention, which included 60- to90-minute group sessions led by a registered dietician. Participantsattended weekly sessions provided either after typical working hoursor during the workday and received modified EatRight materials. Inaddition, one 60-minute weekly group fitness class led by certifiedfitness instructors was offered onsite.
Control Period
Participants who inquired about enrolling in the study completeda baseline assessment within the first month of the study. Followingthe baseline assessment, participants received a usual care interven-tion that consisted of one counseling session during a health fairat their worksite. The counseling session included written materialon approaches for adopting a healthy lifestyle to improve health

194 WOMEN & HEALTH
conditions such as overweight/obesity, hypertension, and diabetes.Participants also received two newsletters during the control period.The newsletters included one healthy recipe idea and a brief articleon a behavioral approach to improve their lifestyle. Within one monthof the completion of the control period, a series of repeat assessmentmeasurements were obtained, and participants began the program.
Formative Assessment
The control period was also used as a time to complete a for-mative assessment and gather data upon which to base the culturalmodification of the standard EatRight materials. The formative as-sessment included data collection from a pilot intervention (i.e., a6-week version of the intervention program) with a small group ofemployees who were recruited by word of mouth from the sameagency and information distilled from a series of group meetings usingthe Nominal Group Technique (NGT). Data from the pilot interven-tion influenced modification of the intervention materials and guidedquestion development for the NGTs. The NGT format is useful foreliciting and systematically organizing perceptions among participantsby gathering equally weighted responses that offer valid representationof group views (Elliott & Shewchuk, 2002).
Because our intervention was to be delivered at the worksite, itappeared to be an opportune time to deal with the impact of a highdemand job environment and its role in affecting eating behaviors.In addition, some of the agency worksite locations provide food forclients and employees. As a result of being an agency of primarilyAfrican American female employees, it was also considered importantto address the cultural attitudes and beliefs that were prevalent withinthe agency regarding dietary habits, body image/appearance, wellness,and physical activity. We purposely chose the term “physical activity”rather than “exercise” because we wanted to include any form ofbodily movement that expended energy, and many women perceivethe different meanings between the two terms (Kline, Lackland, &Wheeler, 1992). Based on these objectives, we wanted to identifycore values of the participants and gather responses to the followingtwo questions: “What factors about your job affect your weight?”and “What factors in your daily life affect your amount of physicalactivity?” Each question was directed to two groups of participants,resulting in a total of four NGT groups. Women who attended the firstand second NGT sessions answered question one, and women who

Zunker et al. 195
participated in the third and fourth NGT sessions answered questiontwo. A total of 14 participants were involved in deriving the themes.
Procedures
The first step of the NGT process was for the facilitator to posea specific question to the group. Each participant also received ahandout with the question printed on it. Therefore, each of the groupsreceived one of the aforementioned questions. After the question wasposed, participants were asked to work independently for five minutesand write down as many words or short phrases that reflected theirindividual perceptions in response to the question.
The second step involved sharing written responses with the groupin a round-robin fashion. Each participant was asked to list one ideaat a time. They were encouraged to make their responses brief andremain neutral (i.e., refrain from giving positive or negative feedback)to help avoid influencing participants. An assistant numerically listedeach response verbatim on a flipchart, which was visual to eachparticipant throughout the group.
The third step provided a time for clarification to ensure that all re-sponses were understood by all members of the group. Again, partici-pants were discouraged from sharing evaluative comments or opinions.
During the fourth step, participants were asked to look over theresponses generated by the group carefully and choose three that werethe most important to them in response to the question. Each partici-pant wrote her top three responses on note cards. Finally, during thefifth step, participants were asked to rank order those three responsesin order of importance to them (3 D most important and 1 D leastimportant). Finally, research assistants gathered the note cards fromthe participants and thanked them for their effort.
Data Analysis
When all NGT meetings had been conducted, the investigativeteam employed a formal distillation process to identify the commonthemes that were generated across the different meetings. This processinvolved examining the three top-ranked responses from each partic-ipant and grouping through consensus those responses that appearedto be substantively similar into themes. The themes and supportingstatements were then used to direct the modification of the standardEatRight material.

196 WOMEN & HEALTH
Cultural Modification of WHPP Basedon EatRight Material
The modification of the EatRight material followed the approachof Ard and colleagues (2003; 2005). Information gathered from theNGT groups was used to develop intervention methods based onunderstanding more about the cultural experiences of the participants,including their life experiences (e.g., financial strain, caregiving re-sponsibilities, work stressors), and how these experiences and perspec-tives might affect adoption of dietary and physical activity goals. Theprimary goal of the research team was to decrease inherent bias in theintervention, where bias represents the ethnocentric viewpoint of theexisting material, which may be a different perspective than that of thetarget audience. The research team used the themes and supportingstatements to identify differences systematically and potential conflictsbetween the standard intervention and core values of the study par-ticipants. The differences and conflicts were resolved by integratingnew material or removing existing material as necessary, resulting inthe addition of new topic areas, practical examples, and interventionprinciples that were congruent with core values, thereby decreasingbias. For example, the research team identified a need for developingskills to effectively handle and prioritize multiple tasks in a smallamount of time and added a new topic area for time management.
RESULTS
Characteristics of the Study Sample
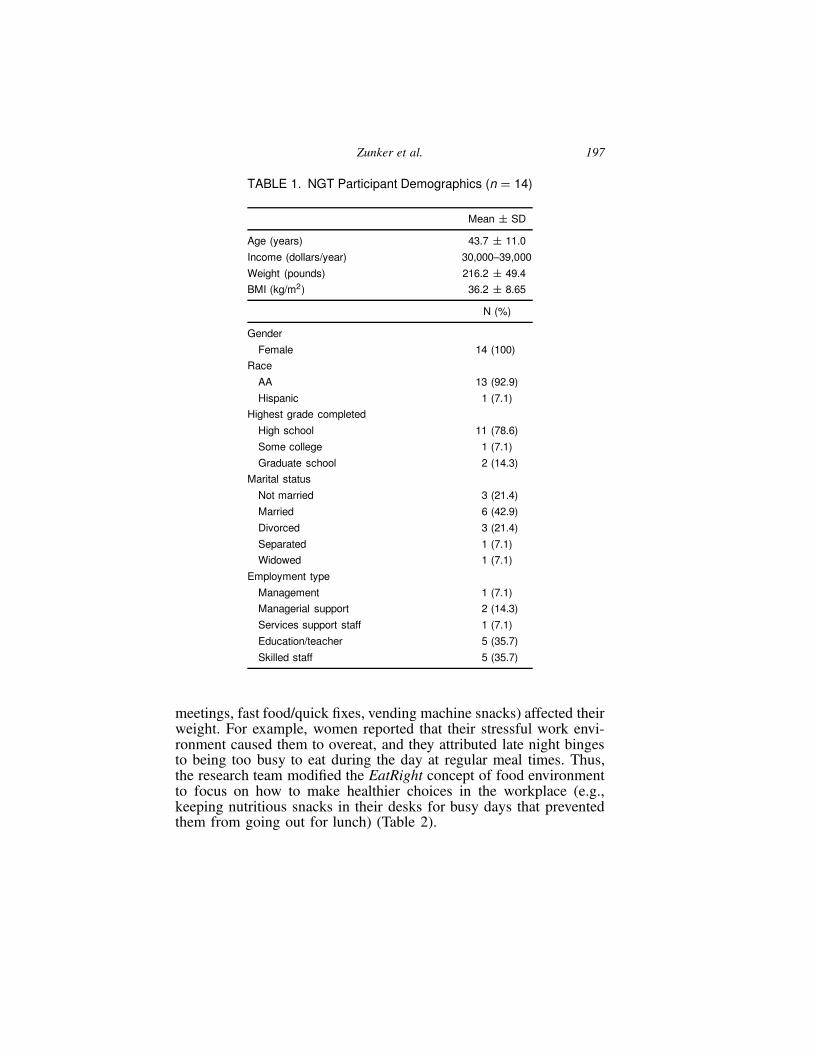
Fourteen women with a mean age of 44 years old participated inthe NGT sessions. Their mean weight was 216.2 (˙49.4) poundsand body-mass-index (BMI) was 36.2 kg/m2. All of the women hada high school education or more, 93% were African American, and43% were married (Table 1).
Nutrition
For the first question, “What factors about your job affect yourweight?” many women reported that job-related stress (e.g., multipleresponsibilities, constant interruptions, uncooperative and judgmen-tal co-workers) and unhealthy food choices (e.g., unhealthy food at
Zunker et al. 197
TABLE 1. NGT Participant Demographics (n D 14)
Mean ˙ SD
Age (years) 43.7 ˙ 11.0
Income (dollars/year) 30,000–39,000
Weight (pounds) 216.2 ˙ 49.4
BMI (kg/m2) 36.2 ˙ 8.65
N (%)
Gender
Female 14 (100)
Race
AA 13 (92.9)
Hispanic 1 (7.1)
Highest grade completed
High school 11 (78.6)
Some college 1 (7.1)
Graduate school 2 (14.3)
Marital status
Not married 3 (21.4)
Married 6 (42.9)
Divorced 3 (21.4)
Separated 1 (7.1)
Widowed 1 (7.1)
Employment type
Management 1 (7.1)
Managerial support 2 (14.3)
Services support staff 1 (7.1)
Education/teacher 5 (35.7)
Skilled staff 5 (35.7)
meetings, fast food/quick fixes, vending machine snacks) affected theirweight. For example, women reported that their stressful work envi-ronment caused them to overeat, and they attributed late night bingesto being too busy to eat during the day at regular meal times. Thus,the research team modified the EatRight concept of food environmentto focus on how to make healthier choices in the workplace (e.g.,keeping nutritious snacks in their desks for busy days that preventedthem from going out for lunch) (Table 2).

198 WOMEN & HEALTH
TABLE 2. Development of Appropriate Intervention Topics: What FactorsAbout Your Job Affect Your Weight?
NGT Theme EatRight Concept Adapted EatRight Program Topic
High stress level at work:
—Too many things to do
—Urgent phone calls
—Interruptions
—Poor morale
—Judged by others
—Unexpected, last minutetasks
—Co-workers take credit foryour work
—Clients miss appointments
Emotional eating Discovering how to deal with job demands andexploring alternatives to eating high-energydense food in reaction to stress, includingdeep breathing, yoga poses, and relaxationtechniques
Unhealthy food environment:
(Within Workplace)
—Generous portions fromkitchen at work
—High calorie snacks (e.g.,donuts) at every meeting
—Work emergencies causemissed meals
—Unhealthy vending machinesnacks
—Food is a status symbol
(Outside of Workplace)
—Fast food for lunch isconvenient
—Most of the places near workare fast food restaurants
Food environment Learning about portion size, keeping healthysnacks in your desk, and making healthy fastfood choices
Lack of social support forhealthy behaviors:
—Negative commentsregarding weight loss
—Judgmental beliefs andattitudes
Not addressed inprevious materials
Learning how to politely decline ‘‘foodpushers,’’ deal with others’ perceptions, andincrease self-efficacy with self-monitoring andmeal planning, posted signs to prompt stairuse
Social eating behaviors
—Unhealthy foods sanctionedby employer
—Co-workers bring sweets toshare
—Social norms
Not addressed inprevious materials
Encourage reciprocal determinism andobservational learning (healthy interactions toinfluence each other) by reinforcing personsbringing healthy lunch to class

Zunker et al. 199
During the third step of the NGT process, the facilitator askedparticipants to clarify some of their responses to provide a betterunderstanding of their perspective. For example, a participant initiallyreported “stress” in response to the question. When asked for clar-ification she responded that, “stress makes me want to eat chickenwings and fries at work.” In that same NGT, a woman stated that shewas “judged for what I eat” and further explained that her lunch wasoften the topic of the day: if she ate a salad her co-workers teased herthat she was trying to be skinny, and if she ate McDonald’s she wasgoing to get fat. In addition, she reported that older female co-workerscriticized her body shape when she lost weight.
Employees at this worksite also described food as an expression ofstatus and a facilitator of social life, which the authors hypothesizedas a norm in the African American community because the act ofsharing food with others has been observed as socially reinforcing.For example, any gathering—business related or social—was usuallycatered with “unhealthy” foods. After these gatherings, the remainingfood was given to the favored employees as an expression of approvalor endearment toward that individual, further perpetuating overeatingand an overall unhealthy nutrition environment at their worksite.
Physical Activity
For the second question, “What factors in your daily life affectyour amount of physical activity?” many women reported that timeconstraints (e.g., working long hours, working two jobs, watching toomuch TV) and other demands (e.g., outside activities, caretaking) tookpriority over physical activity. For example, a woman reported thatshe tried waking up earlier to exercise, but was unable to maintainthis regimen because she was tired after a long day at work and stillneeded to help her child with homework, cook dinner, and tend toother domestic responsibilities (e.g., laundry, cleaning, caring for anelderly parent). Another woman reported that she was tired from “theweight [she was] carrying.” Others clarified the idea of being tired bystating that they felt “burnout” from dealing with client problems andclarified by reporting that it “affects you when you listen to othersproblems.”
Several participants reported a fear of “extreme” exercise and thattheir bodies were not prepared physically. In addition, women reporteda concern over physical appearance during exercise (e.g., “not wantingto see myself in the workout gear”; “see others in biking shorts”). The

200 WOMEN & HEALTH
TABLE 3. Development of Appropriate Intervention Topics: What Factors inYour Daily Life Affect Your Amount of Physical Activity?
NGT Theme EatRight Concept Adapted EatRight Program Topic
Time management:
—No time to exercise
—Watching too much TV
—Constantly on the phone
—Sleeping late
—Too tired
—Working longer hours
—Many other activities (e.g.,band, choir, church meetings)
Not addressed inprevious materials
Practical examples of managing time,including best time of day to exercise basedon personality, identifying enjoyable activities,fitting in small amounts of physical activity, andfinding places to walk near worksite
Physical activity is not a priority:
—Other things come up
—Go directly home after workinstead of exercising
—Always finding time to carefor others, not for self
—Not motivated enough
Not addressed inprevious materials
Discussing the benefits of physical activity,discovering alternatives to going to the gym,making time for self, and motivationalstrategies (e.g., workout partner)
Perceived limitations andphysical limitations:
—Fear of ‘‘extreme’’ exercise
—Not enough sleep
—Carrying excess weight
—Physical appearance
—Not prepared
—Medical issues
—Lack of ability
Not addressed inprevious materials
Increase knowledge of appropriate physicalactivity for ability level, learn how to modifyexercises, proper attire (e.g., supportivefootwear), change perception of acceptableappearance during physical activity
Multiple roles:
—Mother
—Caretaker
—Various demands at workand in social life
Not addressed inprevious materials
Teach self-care and assertiveness training
research team addressed these concerns by adding EatRight lessonson how to safely begin an exercise program, emphasized enjoyable ac-tivities, and encouraged women to wear clothes they felt comfortablewearing when they participated in physical activity (Table 3).
A few women reported that their medical conditions (e.g., degen-erative arthritis, spinal stenosis, foot surgeries, hernia, medications)limited their physical activity, but only two persons ranked this themeas important. In addition, the theme of overeating (e.g., “too much

Zunker et al. 201
junk food”; “too full—don’t feel like doing anything”) and lack oftime was reported during both groups.
The NGT themes that emerged were mapped to relevant areas of theexisting EatRight material to determine if the concept was addressed,the adequacy of coverage, and the cultural appropriateness (i.e., howmuch bias was presented by the approach used in the current material)(Tables 2 and 3). In many areas, such as time management or lackof social support, these issues were not addressed in the EatRightmaterial because of general assumptions regarding the typical clientseeking weight loss services. The assumption was that these indi-viduals would make time available for the recommended behaviors,giving them priority over other activities, and that these individualswould have a supportive environment to help promote the adoption ofhealthy behaviors. However, our formative assessments with AfricanAmerican women challenged many of these assumptions. As a re-sult, we specifically addressed skills for prioritizing time and healthactivities and skills to build self-efficacy and intrinsic motivation forrecommended behavior changes.
DISCUSSION
The primary goal of this article was to describe the developmentof a culturally appropriate WHPP for a group of African Ameri-can women. Formative research guided the research team to partnerwith worksite leadership and engage potential participants prior toimplementing the program. We also addressed potential recruitmentand participation barriers (e.g., transportation, time, cultural differ-ences) by conducting the activities at a convenient time and location(Escobar-Chaves et al., 2002). In addition, we provided tokens ofappreciation (e.g., $20 for completing the NGT session), emphasizedthat their input was essential to accomplish the task, and explainedthat the study was sponsored by a legitimate authority (i.e., the uni-versity and a grant from the Minority Health Research Center), tobuild trust, which is important for African American recruitment andparticipation. These foundational steps assisted with stakeholder buy–in, as well as program development and modification of EatRightmaterials. The EatRight Program materials in their original formatused commonly taught behavioral skills (e.g., self-monitoring, goalsetting, problem solving), combined with nutrition education on a lowenergy dense dietary pattern to assist patients in losing weight. Whilegenerally successful, the program lacked specification for the cultural

202 WOMEN & HEALTH
needs of this target audience. The formative assessment allowed theresearch team to reframe the key behavioral concepts and nutritionalgoals and target the specific needs of the African American womenin their particular work environment.
Formative assessment, especially primary research with the targetaudience, has the benefit of guiding program developers to tailormessages that fit the specific needs of the target group (Weinreich,1999; Klesges et al., 2005; Kumanyika et al., 2003; Zapka et al.,2007). More specifically, qualitative research methods helped us torecognize their issues and gain a deeper overall understanding fromthe target audience’s point of view by placing their responses in thecontext of African American women and weight loss. Often formativeassessment in the area of lifestyle behavior modification has serveda wide variety of needs, from identifying potential logistic concernsto being a key process for community based participatory research(Klesges et al., 2005; Kumanyika et al., 2003; Zapka et al., 2007).While these practical concerns are critical to the success of anyintervention, equally important is the perspective of the interventionand how it is framed relative to the experience of the target audi-ence. Using this approach to deal with cultural appropriateness alsoprovides investigators and other research personnel with a complexview of the interrelationship between personal, social, and contextualelements, that otherwise would not be considered in the context ofthe intervention (Kumanyika et al., 2003).
An additional justification for tailoring the weight loss interventionfor African American women was their disproportionate prevalenceof overweight and obesity. Approximately 50% of African Ameri-can women are overweight or obese compared to 30% of Caucasianwomen (Flegal et al., 2002; Mokdad et al., 2000). Moreover, in the2004 Behavioral Risk Factor Surveillance Survey (BRFSS) 34% ofAfrican American women reported no leisure-time physical activity inthe past month, compared with 22% of Caucasian women (BRFSS,2005). These findings suggest a need for alternative approaches toaddress the sociocultural beliefs and attitudes that affect weight trendsas they relate to African American women. For example, in a quali-tative study women were asked how their race affected their weight,and African American women frequently reported that their weightwas adversely influenced by unhealthy food preparation, poor foodchoices, lack of exercise, and overeating due to stress, while Caucasianwomen reported sociocultural pressure to achieve an ideal body imagebased on mainstream standards of beauty and desires for thinness thatwere reinforced by friends and family (Malpede et al., 2007). In a

Zunker et al. 203
qualitative study by Wilbur et al. (2002), African American womenreported a number of barriers to physical activity, including a lack ofrole models (i.e., they did not personally know any physically activewomen), lack of social support (i.e., feel out of place and anticipatedcriticism from neighbors; fear of teasing if exercising in public sincethey were not physically fit), and cultural influences (i.e., exercise ispart of a Caucasian woman’s culture; Wilbur et al., 2002). Similarlyin the present study, NGT participants reported that they did not wantto see themselves in exercise outfits and may have been discouragedby seeing smaller/fit women in body conscious workout clothing (e.g.,“biking shorts”).
The current study used the NGT to create a safe environment forparticipants to express their opinions and perceptions that were criticalto adaptation of the EatRight materials. Small groups of womenopenly discussed their job-related concerns surrounding factors af-fecting their weight and physical activity, including the lack of long-term wellness programs to meet the needs of most employees. Theyreported that past programs excluded many employees from partici-pating because the wellness activities were only available after workhours. Furthermore, many women expressed their concerns over deal-ing with stress at work and managing their time efficiently. Severalwomen typically responded to work-related stress by overeating, mak-ing poor food choices, and avoiding physical activity. This stressresponse was generally supported by other co-workers and the work-place culture. For example, it was the social norm to go out for lunchat a nearby fast food restaurant that had few healthy menu options orto take the elevator at work, even though the worksite building wasonly two floors. Time management was often reported as a perceivedchallenge due to the multiple demands many experienced as a resultof a challenging job, busy social and civic life, and family respon-sibilities. However, this perceived barrier may not accurately reflectactual time commitments (Heesch & Masse, 2004). The expressionof these sensitive and critical perceptions was facilitated by the NGTprocess, allowing precise identification of salient program targets.
Limitations
The employees that participated in the formative research mayhave been non-representative of the rest of the worksite, reflectingpotential participation bias. In addition, their replies may have notbeen representative of those other groups of employees, reflecting

204 WOMEN & HEALTH
potential selection bias, thus reducing the generalizability of findings.Furthermore, the potential for social desirability bias (e.g., participantsmight have told us what they think we wanted to hear) was possible.Cost effectiveness of the program was not examined. Additional stud-ies with women from a variety of different age groups, geographicareas, economic backgrounds, and educational levels would providea greater sense of generalizability.
Implications
As healthcare costs related to obesity continue to rise, businesseswill incur greater financial burdens trying to provide adequate health-care coverage for employees (Chapman, 2003). This burden will begreater for small businesses and organizations. To preclude this, manyorganizations have begun adopting policies that encourage the creationof WHPPs.
Worksite wellness plans have become increasingly attractive aslong-term solutions for controlling healthcare costs and fostering anorm of health of behaviors within the workplace (Carpenter, 2003).Providing traction for healthy behaviors to become the norm within aworkplace can be the primary challenge for initiating WHPPs. Suc-cessful interventions need to address individual, social environmental,and cultural factors to change unhealthy behaviors (McLeroy et al.,1988). For example, African American and Caucasian women maydiffer in seeking professional assistance for weight loss and reportdifferent reasons for weight control behaviors (Malpede et al., 2007).Developing policy level interventions may reach more employees andprovide greater sustainability than enforcing individual changes. Forexample, allowing employees to dress casual or wear jeans one daya week instead of normal business attire has been show to increasephysical activity levels by 8% (Anders, 2007).
Based on the results of our formative assessment, it is clear thatthe workplace culture related to health and wellness is influenced bythe sociocultural perspective of those that make up the workforce.Therefore, interventions need to be successful at challenging individ-ual as well as organizational cultural norms, particularly in the caseof African Americans. Incorporating employee input in the type andformat of activities offered allows the program to be more salient andcost effective rather than simply offering a wide array of services.The results given here provide practical applications for developing aculturally tailored WHPP for a group of African American women.

Zunker et al. 205
Future intervention studies should consider the unique personal, so-cial, cultural, environmental, and policy factors when designing theirprogram.
REFERENCES
Anders, M. (2007). New research identifies the fitness benefits of wearing casualclothing to work. American Council on Exercise. Retrieved 04/23/07, from www.acefitness.org/getfit/casualclothesstudy.cfm
Ard, J. D., Carter-Edwards, L., & Svetkey, L. P. (2003). A new model for develop-ing and executing culturally appropriate behavior modification clinical trials forAfrican Americans. Ethnicity & Disease, 13, 279–285.
Ard, J. D., Durant, R. W., Edwards, L. C., & Svetkey, L. P. (2005). Perceptions ofAfrican-American culture and implications for clinical trial design. Ethnicity &Disease, 15, 292–299.
Bandura, A. (2004). Health promotion by social cognitive means. Health Education
& Behavior, 31(2), 143–164.Behavioral Risk Factor Surveillance System. (2005). Trends in leisure-time physical-
inactivity by age, sex, and race/ethnicity—United States, 1994–2004. Morbidityand Mortality Weekly Report, 54(39), 991–994.
Carpenter, D. (2003). Why small business is sick over health care costs. Hospital
Health Network, 77, 38–42, 44, 46.Chapman, L. (2003). Meta-evaluation of worksite health promotion economic return
studies. Art of Health Promotion, 6(6), 1–10.Crespo, C., Ainsworth, B., Keteyian, S., Heath, G., & Smit, E. (1999). Prevalence of
physical inactivity and its relation to social class in U.S. adults: Results from theThird National Health and Nutrition Examination Survey, 1988–1994. Medicine
and Science in Sport and Exercise, 31, 1821–1827.Elliott, T. R., & Shewchuk, R. M. (2002). Using the nominal group technique
to identify the problems experienced by persons living with severe physicaldisabilities. Journal of Clinical Psychology in Medical Settings, 9(2), 65–76.
Engbers, L. H., van Poppel, M. N. M., Chin A Paw, M. J. M., & van Mechelen,W. (2005). Worksite health promotion programs with environmental changes: Asystematic review. American Journal of Preventive Medicine, 29(1), 61–70.
Escobar-Chaves, S. L., Tortolero, S. R., Masse, L. C., Watson, K. B., & Fulton, J.E. (2002). Recruiting and retaining minority women: Findings from the Womenon the Move Study. Ethnicity & Disease, 12, 242–251.
Flegal, K. M., Carroll, M. D., Ogden, C. L., & Johnson, C. L. (2002). Prevalence andtrends in obesity among US adults. Journal of the American Medical Association,288, 1723–1727.
Gittelsohn, J., Steckler, A., Johnson, C. C., Pratt, C., Grieser, M., Pickrel, J., et al.(2006). Formative research in school and community-based health programsand studies: “State of the Art” and the TAAG Approach. Health Education &Behavior, 33(1), 25–39.
206 WOMEN & HEALTH
Glasgow, R. E., McCaul, K. D., & Fisher, K. J. (1993). Participation in worksitehealth promotion: A critique of the literature and recommendations for futurepractice. Health Education Quarterly, 20(3), 391–408.
Greene, L. F., Malpede, C. Z., Henson, C. S., Hubbert, K. A., Heimburger, D. C.,& Ard, J. D. (2006). Weight maintenance 2 years after participation in a weightloss program promoting low-energy density foods. Obesity, 14(10), 1795–1801.
Griffin-Blake, C. S., & DeJoy, D. M. (2006). Evaluation of social-cognitive versusstage-matched, self-help physical activity interventions at the workplace. Ameri-can Journal of Health Promotion, 20(3), 200–209.
Grosch, J. W., Alterman, T., Petersen, M. R., & Murphy, L. R. (1998). Worksitehealth promotion programs in the U.S.: Factors associated with availability andparticipation. American Journal of Health Promotion, 13(1), 36–45.
Heesch, K. C., Mâsse, L. C., (2004). Lack of time for physical activity: perceptionor reality for African American and Hispanic women? Women & Health, 39(3),45–62.
Katz, D. L., O’Conell, M., Yeh, M., Nawaz, H., Nijike, V., Anderson, L. M., Cory,S., & Dietz, W. (2005). Public health strategies for preventing and controllingoverweight and obesity in school worksite settings: A report on recommendationsof the Task Force on Community Preventive Services. Morbidity and Mortality
Weekly Report, 54(RR10), 1–12.Klesges, L. M., Estabrooks, P. A., Dzewaltowski, D. A., Bull, S. S., & Glasgow, R. E.
(2005). Beginning with the application in mind: Designing and planning healthbehavior change interventions to enhance dissemination. Annals of Behavioral
Medicine, 29(Suppl), S66–S75.Kumanyika, S. K., Story, M., Beech, B. M., Sherwood, N. E., Baranowski, J. C.,
Powell, T. M., Cullen, K. W., & Owen, A. S. (2003). Collaborative planning forformative assessment and cultural appropriateness in the Girls health EnrichmentMulti-site Studies (GEMS): A retrospection. Ethnicity & Disease, 13(1 Suppl 1),S15–S29.
Lewis, R. J., Huebner, W. W., & Yarborough, C. M., 3rd. (1996). Characteristics ofparticipants and nonparticipants in worksite health promotion. American Journal
of Health Promotion, 11(2), 99–106.Malpede, C. Z., Greene, F. L., Fitzpatrick, S. L., Jefferson, W. K., Shewchuk, R.
M., Baskin, M. L., & Ard, J. D. (2007). Racial influences associated with weightrelated beliefs in African American and Caucasian Women. Ethnicity & Disease,17, 1–5.
Marcus, B. H., Williams, D. M., Dubbert, P. M., Sallis, J. F., King, A. C., Yancey,A. K., et al. (2006). Physical activity intervention studies: What we know andwhat we need to know. Circulation, 114, 2739–2752.
Marshall, A. L. (2004). Challenges and opportunities for promoting physical activityin the workplace. Journal of Sports Science and Medicine, 7(1 Suppl), 60–66.
McLeroy, K., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspectiveon health promotion programs. Health Education Quarterly, 15, 379–397.
Mokdad, A. H., Serdula, M. K., Dietz, W. H., Bowman, B. A., Marks, J. S., &Kaplan, J. P. (2000). The continuing epidemic of obesity. Journal of the American
Medical Association, 284, 1650–1651.

Zunker et al. 207
Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2005). Correction:Actual causes of death in the United States, 2000. Journal of the American
Medical Association, 293(3), 293–294.U.S. Department of Health and Human Services. (1996). Physical activity and health.
A report of the Surgeon General. Atlanta, GA: U.S. Department of Health andHuman Services, Centers for Disease Control and Prevention, National Centerfor Chronic Disease Control and Prevention.
US Department of Labor: Bureau of Labor Statistics. (2004). Employment status byrace, age, sex, and Hispanic or Latino ethnicity, 2004 annual averages. Retrieved3/7/2007, from http://www.bls.gov/cps/wlf-table3-2005.pdf
Weinreich, N. K. (1999). Hands-on Social Marketing: A Step-by-Step Guide. Thou-sand Oaks, CA: Sage Publications, Inc.
Wilbur, J., Chandler, P., Dancy, B., Choi, J., & Plonczynski, D. (2002). Environ-mental, policy, and cultural factors related to physical activity in urban AfricanAmerican women. Women & Health, 36(2), 17–28.
Wilcox, S., Castro, C., King, A. C., Housemann, R., & Brownson, R. C. (2000).Determinants of leisure time physical activity in rural compared with urban olderand ethnically diverse women in the United States. Journal of Epidemiology andCommunity Health, 54, 667–672.
Zapka, J., Lemon, S. C., Estabrook, B. B., & Jolicoeur, D. G. (2007). Keeping aStep Ahead: Formative phase of a workplace intervention trial to prevent obesity.Obesity, 15(Suppl 1), 27S–36S.