Usefulness of extra-articular ultrasound applied to systemic ...
Upload
independentCategory
view
0download
0
RESPIRATORY MEDICINE (1998) 92, 1X31-1187
Usefulness of a national registry of alpha-I-antitrypsin deficiency. The Spanish experience
M. MIRAVITLLES”, R. VIDAL*, J. C. BARROS-TIZ~N+, A. BUSTAMANTE*, P. P. EsPAI;JA§, F. CASAS’~, M. T. MART~NEZ~, C. ESCUDERO”” AND R. JARDI++
*Servei de Pneumologia, Hospital Vail d’Hebron, Barcelona ‘Servicio de Neumologia, Hospital Xeral-Cies, Vigo ‘Unidad de Neumologia, Hospital Sierrallana, Torrelavega ‘Servicio de Neumologia, Hospital de Galdakao “Servicio de Neumologia, Hospital de Granada 7Servicio de Neumologia, Hospital 12 de Octubre, Madrid **Servicio de Neumologia, Hospital Central de Asturias, Oviedo “Servei de Bioquimica, Hospital Vall d’Hebron, Barcelona
Severe alpha-1-antitrypsin (AAT) deficiency, phenotype Pi ZZ, is a rare condition with an estimated prevalence of 114500 individuals in Spain. Given this low prevalence, it seems useful to accumulate all the information derived from the care of these patients. In this context, the Spanish Registry of patients with AAT deficiency was founded in 1993; its main objectives were to establish guidelines adapted to our country for the treatment and management of AAT-deficient patients, offer expert support to physicians all over the country treating these patients, and provide technical support on the determination of Pi phenotyping and genotyping of individuals suspected of being AAT-deficient.
From 1993 to January 1998 the number of enrollees increased from 48 to 223, of which 216 were Pi ZZ. Seventy-three per cent were male and only 31.5% were never smokers, mean age was 46 years (SD= 13 years) and mean FEV, 53% predicted (s~=31%). 83% were index cases who, compared with non-index cases, were older (49 i 11 vs. 35 * 13 years, P<O.OOl), more likely to have a smoking history (85% vs. 47%, PcO.01) and displayed more severe impairment in pulmonary function (FEVi%=40% + 19% vs. 96% & 23%, P<O.OOl). Augmentation therapy was administered to 129 patients (58%). Treated patients had more severe impairment in pulmonary function than the untreated (FEV,%=40% & 21% vs. 72% * 32%, P<O.OOl) and were more likely to be index cases (81% vs. 43%, PcO.001).
Characteristics of the patients included are similar to those described for other Registries. The Registry has extended knowledge of the disease throughout the country and has established local guidelines for treatment and follow-up. It may be a valid database for future co-operation in international initiatives.
RESPIR. MED. (1998) 92, 1181-1187
Introduction
Hereditary deficiency of alpha-1-antitrypsin (AAT), the main serum inhibitor of proteolytic enzymes, is associated
Received 24 March 1998 and accepted in revised form 3 June 1998. The Spanish Registry is a workshop of the Brea de Insuficiencia Respiratoria y Trastornos de1 Sueiio (IRTS), Sociedad Espafiola de Neumologia y Cirugia Torgcica (SEPAR). Financial support was obtained from Bayer Q.F., Spain. Correspondence should be addressed to: M. Miravitlles, Rocafort 173-177, 3”-la 08015 Barcelona, Spain.
with increased risk of pulmonary emphysema of early onset, with cigarette smoking being the most important risk factor. Although there are more than 70 biochemical gen- etic variants of AAT, the most important deficient variant is the 2 type. Patients homozygous for the Z allele have only lo-20% of the normal serum concentration of the inhibitor.
AAT deficiency is rare. The deficient Z allele is almost limited to the white population and is almost inexistent among other non-European populations (l-3). Geographi- cal differences are also found in the prevalence of the Z mutation in the form of a north-south gradient. This mutation is more frequent in Scandinavian countries [gene
0954.6111/98/101181+07 $12.00/O 0 1998 W. B. SAUNDERS COMPANY LTD

1182 M. MIRAVITLLES ET AL
frequency 0.023 in Sweden (3) and Denmark (4)], than in Mediterranean countries [O.OlS in Spain (5)]. With these figures, the estimated number of homozygous Pi ZZ (phenotype inhibitor) individuals ranges from l/l600 in Scandinavia to 114500 in Spain.
Owing to the low prevalence of AAT deficiency, there is a need to accumulate information derived from the study of individuals with the disease. In this respect, the Danish Registry was founded in 1978 and in 1994 included more than 500 individuals (6). However, the greatest interest for the registries came with the availability of an augmentation treatment for the disease. It was realized early on that a clinical trial to ascertain the long-term clinical efficacy of such treatment would be unaffordable (7); consequently, some registries appeared as an alternative to a clinical trial (8,9) by comparing the clinical evolution of a great cohort of patients with and without augmentation therapy (10,ll).
The Spanish Registry of patients with AAT deficiency was founded in 1993 (12) but because of the relatively small expected number of individuals to be recruited, the initial purpose of the Registry was not to be an alternative to clinical trials on augmentation therapy. The objectives of the Registry were: (1) to ascertain the frequency and characteristics of AAT deficiency in Spain; (2) to establish guidelines adapted to our country for treatment and man- agement of AAT-deficient patients; (3) to offer expert support to physicians treating these patients all over Spain; (4) to increase interest in this rare disease and attempt to decrease underdiagnosis and delay in recognition of the deficiency; and (5) to offer technical support on the deter- mination of Pi phenotyping and genotyping of individuals suspected of being AAT-deficient.
In this report the experience of the first 5 years of the Registry is described.
Methods
ORGANIZATION OF THE REGISTRY
The Spanish Registry of patients with alpha-1-antitrypsin deficiency (AATD) was founded early in 1993 as a work- shop of the IRTS working group (Insuficiencia Respiratoria y Trastornos de Sueiio) of the SEPAR (Sociedad Espafiola de Neumologia y Cirugia Toracica). Organizational com- ponents of the Registry include two co-ordinators (M.M. and R.V.), a Steering Committee and 62 participating clinical centres, 61 distributed throughout Spain and one in Andorra. A Clinical Co-ordinating Center houses the cen- tral database of the Registry. In this Centre there is also a Central Laboratory (R.J.) which offers support in determin- ing Pi phenotype by isoelectric focusing and genotyping via DNA extraction and amplification; the techniques used have been described extensively in previous works (5,13,14). A list of participants in the Registry is provided in the Appendix.
The Steering Committee provides scientific direction for the Registry and consists of representatives from some of the participating clinical centres and the two co-ordinators.
An annual conference of representatives from the participating clinical centres is held to comment on the situation of the database, characteristics of the patients enrolled and the specific problems derived from the care and treatment of these patients, and the guidelines for treatment and follow-up are updated.
ELIGIBILITY CRITERIA
To be eligible for inclusion in the Registry, an individual must have serum AAT below 35% of normal values (<50 mg dl- ’ or < 11 ,UM) and phenotype Pi ZZ or other severe deficient variants. For patients receiving augmenta- tion therapy, serum AAT levels must have been determined before the first dose, or after therapy has been suspended for 4 weeks. Patients with phenotype Pi SZ are not included in the Registry unless they have serum levels of AAT < 11 ,uM and are administered augmentation therapy on the decision of the corresponding physician.
The Registry collects information at 6-month intervals on demographic data, medical history, pulmonary function measurements which include prebronchodilator and post- bronchodilator FEV, and FVC, and information on the use and frequency of augmentation therapy as well as the possible incidence of adverse side-effects.
Lung function measurements (spirometry) were per- formed in the respective participating clinical centres and reported by the referring physician. All participant centres performed measurements according to European recom- mendations (15). The percentage of the reference values was calculated using Mediterranean population reference values (16). In this report the postbronchodilator FEV, was used in all calculations.
Family study after the diagnosis of an index case was recommended by the Registry, but the Registry itself did not perform the investigation, which depended on the criteria of each participating centre.
DATA MANAGEMENT
Standardized data forms were used to record data at each clinical centre. The forms were mailed to the SEPAR office, from where they were sent to the Co-ordinating Centre. Forms were logged and entered into a microcomputer- based data management system. Exploratory analysis to detect missing or out-of-range values was performed for purging of the database. Characteristics of the patients included in the Registry in January 1998 are described in the present paper.
Statistical analysis was performed using the Statistical Analysis System software (SAS-Institute, Cary, NC, U.S.A.). The Student’s t-test was used for comparisons between means and the chi-square test was used to study the relationship between categoric variables. A difference of PcO.05 was considered significant.
Results
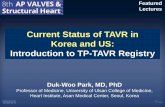
Two hundred and twenty-three individuals had been included in the Registry from 1993, of whom four died

200 -
150 -
100 -
50- r 111 0-
i
1
l/1993 l/1994 l/1995 l/l996 l/l997 l/1998
FIG. 1. Cumulative number of enrollees in the Registry over time.
during follow-up and four received a lung transplant. Pi phenotypes were: 216 Pi ZZ, two Pi SZ, three Pi ZMmalton, two Pi ZMpalermo. The cumulative number of enrollees over time is shown in Fig. 1.
Geographical distribution of the individuals included is uneven with a greater number of individuals belonging to the regions of Northern Spain compared with the centre and the South. Case density in the different autonomous communities of Spain is depicted in Fig. 2. Three commu- nities have not reported any case to the Registry: Murcia, La Rioja and the Balearic Islands.
SPANISH REGISTRY 0~ MT 1183
Demographic, clinical and functional characteristics of enrollees are shown in Table 1. There is a predominance of men (73%) ex-smokers (62.5%) and individuals included because of pulmonary symptoms (83%), while those diagnosed by family screening represent 14%.
Comparison between index cases, i.e. those identified through chest symptoms, and non-index cases is shown in Table 2.
Criteria established by the Registry to initiate augmenta- tion therapy with intravenous AAT (Prolastina@; Bayer Pharmaceutical; West Haven, CT, U.S.A.) are depicted in Table 3. Decisions to treat with augmentation therapy were always left to the discretion of the enrollees’ attending physicians. Frequency and dosage of augmentation therapy recommended by the Registry was 180 mg kg- ’ every 3 weeks. A total of 129 (58%) patients were receiving aug- mentation therapy at the time of enrolment or initiated the treatment the year after enrolment; their characteristics and comparison with those not receiving augmentation therapy are shown in Table 4. Administration frequency of augmen- tation therapy was: weekly four patients (3%), every 2 weeks 16 (12%), every 3 weeks 99 (77%), monthly 3 (2.3%) and not stated seven (54%). Regarding functional impair- ment, 65% (84/129) of patients with FEV,<30% were receiving augmentation therapy, 67% (29143) of those with FEV, between 30% and 49%, 65% (1107) of those with FEV, between 50% and 69%, and 15% (5/34) of those with FEV, 2 70%.
Of the four patients who died, three had an FEV,<30% predicted; two of these died of pulmonary emphysema and the other of acute peritonitis due to diverticulitis. The remaining patient had an FEV, of 60% predicted and died of disseminated stomach cancer.
FIG. 2. Case density of alpha-I-antitrypsin deficient individuals in the different autonomous communitie :s of Spain.

1184 M. MIRAVITLLES ETAL.
TABLE 1. Demographic, clinical and functional characteris- tics of individuals with AAT deficiency at enrolment
n % Mean (SD)
Male gender Age (years) Age at onset (years) Ascertainment*
163 73 46 (13) 39 (10)
Lung disease Family Other
Smoking statust
145 83 25 14
5 3
Never 42 31.5 Ex 83 62.5 Current 8 6
Augmentation therapy 129 58 FEV, (ml) 1726 (1200) FEV, (% predicted) 53 (31)
*Percentages refer to 175 enrollees for whom this information is available. TPercentages refer to 133 enrollees for whom this information is available.
Discussion
Since its foundation in 1993, the Spanish Registry has included a total of 223 patients, of whom four have died and four received a lung transplant up to January 1998. Most of the enrollees are males in the fourth or fifth decade of life with a history of cigarette smoking and pulmonary symptoms and lung function tests consistent with emphysema. More than one half of the enrollees are receiving augmentation therapy, with the patients treated being older, more likely to have smoked and with severe pulmonary function impairment with a mean FEV,
TABLE 3. Criteria for augmentation therapy established by the Spanish Registry of patients with alpha-1-antitrypsin deficiency
1. Evidence of pulmonary emphysema 2. Serum levels of AAT<35% reference values 3. FEV,<70% predicted
Patients with FEV,>SO% should demonstrate a decline in FEV, > 150 ml yr - ’
4. Age > 18 years 5. Non-smokers at least for 1 year 6. No other important co-morbid conditions 7. Ability to attend the corresponding clinical centre
of only 40% predicted. Only 17% of cases have been diagnosed despite not having respiratory symptoms (non- index cases) and the majority were identified through family screening of an index case. This description is similar to that of the NHLBI Registry in the U.S.A. (10) where non-index cases represent 28% of enrollees, but clearly below the Danish Registry where cases diagnosed through family screening constitute almost one half of the enrollees (6).
A recent study in Barcelona observed a gene frequency of the Z allele to be 0.015 (5). If this frequency were valid for the whole country, the expected number of individuals homozygous for Pi ZZ in Spain would be approximately 8400. The number of patients registered is 0.58/100 000, ranging from 0 in three regions or 0.08/100 000 in Valencia to 31100 000 in Cantabria and Asturias, and represents globally 2.6% of the total deficient individuals expected. This percentage lies between that of the NHLBI Registry (10) and other Registries with a longer tradition such as the Danish one, where approximately 28% of the estimated number of patients in the 30-59 year age category are registered (6).
TABLE 2. Comparison between index and non-index cases
Index Non-index n= 145 n=30 P
Men (%) Death (%) Lung transplant (%) Non-smokers (%) Pack-year
(smokers and ex-smokers) Age (years) Augmentation
therapy (%) FEV, (ml) FEV, (%)
Values are mean & SD. *Chi-square test. TStudent’st-test.
78 60 0.21” 3 0 n.s.* 3 0 n.s.*
15 53 cO.Ol* 29* 17 16& 13 10.05?
49& 11 35 zt 13 <o.o01t 78 16 ~o~ool*
1242 =t 699 3358 zt 1252 <O.OOl~ 40* 19 96 rt 23 <o.o01t

SPANISH REGISTRY OF AAT 1185
TABLE 4. Comparison between patients receiving and not receiving augmentation therapy
Treated Untreated n=131 n=92 P
Men (%) 74 Age (%) 48+ 10 Death (“Yo) 2 Lung transplant (%) 3 Index cases (%) 81 Non-smokers (%) 9 FEV, (ml) 1210 + 633 FEV, (%) 40&21
70 0.60” 42f 16 <O.OlT
2 n.s.* 0 n.s.*
43 ~o~ool* 31 co.o01*
2458 zt 1428 <O.OOlt 72 xt 32 <O.OOlT
Values are mean & SD.
*Chi-square test. TStudent’s t-test.
The differences observed in some regions are not likely to be due to differences in gene frequencies (5,17,18) or cigarette smoking habits, but to differences in diagnostic rates due to the existence or not of medical groups inter- ested in the deficiency in different areas. It is well docu- mented that some non-smoking, non-index deficient individuals will never develop significant emphysema and thus will not be detected (6,19,20), but even today many patients with early onset emphysema due to the deficiency are misdiagnosed for many years as having smoking-related disease, until the final diagnosis of the deficiency is (if ever) established. In a national series, mean delay in diagnosis was 10 years (range=3-22 yr) although mean age at diagnosis was only 46 yr and mean FEV, 0.80 1 (21).
The criteria established by the Registry for initiating augmentation therapy are very restrictive. Patients must refrain from smoking for at least 1 year and present pulmonary function impairment consistent with emphy- sema; those with FEV, >50% predicted must show an annual decline of more than 150 ml. The reasons for adopting these restrictive criteria are lack of definitive evidence of the clinical efficacy of the therapy, and lack of information on which patients are going to benefit more from the treatment, together with the fact that the treat- ment is very expensive and of limited availability (22) and its use should be, in our opinion, restricted to patients with well-defined characteristics in the setting of experimental trials or under the supervision of national or international registries. Nevertheless, the decision to treat is left to the corresponding physicians and in our series, at least five patients on augmentation therapy did not fulfil all criteria and, conversely, eight patients who did meet the criteria were not receiving augmentation therapy for different reasons, including the limited availability of the product.
Most of the patients on augmentation therapy were receiving AAT on an every-3-weeks schedule following the recommendations of the Registry. This dosage was adopted because in Spain almost all patients are treated in a hospital-based administration programme, some are still employed, and others depend on their relatives to attend
the hospital. For these reasons, the weekly or even every- 2-weeks schedules are difficult to accept for most patients. The biochemical efficacy of augmentation therapy in terms of obtaining serum AAT levels above those considered protective (80 mg dl - I or 11 pM) and enhanced antineu- trophil elastase activity in both serum and BAL fluid throughout the period between doses has only been proven for the weekly administration (23,24). The efficacy of other administration regimens is under debate; some authors have found good serum AAT levels with a 2 weeks’ interval (25) while others suggest that this interval is too long (26). Hubbard et al. (27) reported that after a single infusion of 250mg kg-’ of AAT, serum levels remained above 80 mg dl- i for approximately 21 days. Considering the pharmacokinetics of the infused AAT, with a rapid decline in serum levels during the first 2 days and a slower phase of elimination proportional to the serum concentration, it seemed more reasonable to reduce the interval between infusions than to increase the total dose. Consequently, the Registry recommended a dose of 180 mg kg - i every 3 weeks, a regimen already reported in another recent study (28).
Two considerations must be made at this point: first, we are only considering biochemical efficacy, and although some promising data exist on the clinical efficacy of the treatment (8,11,21,28-30) definitive evidence is lacking. Furthermore, it is not known to what extent the fact that serum AAT levels are below 80 mg dl - i during the last few days of each cycle of treatment implies a worse outcome of therapy; second, the approach of a standard dose for every patient may be too simple: patients with purulent bronchi- ectasis or frequent infectious exacerbations may need higher doses of AAT to compensate for the higher neu- trophil elastase burden (31). Consequently, a trough serum AAT level of 50 mg dl - ’ may be sufficient for an asymp- tomatic patient (in fact, some Pi ZZ non-smokers do not develop significant emphysema), while a concentration of 120 mg dl - ’ might be insufficient for a patient suffering from recurrent acute infectious exacerbations (3 1,32).
Since the beginning in 1993, the number of enrollees has increased from 48 to 223. They come from almost all the communities in Spain, which demonstrates a more extended awareness of this condition. The Registry has established local guidelines for augmentation therapy and follow-up of patients with the deficiency and has contributed to the rational utilization of a product of limited availability and high cost. Furthermore, the Registry has offered physicians interested in this rare condition the opportunity to meet and work together for better understanding of the disease, and should be a valid platform for co-operation with international initiatives.
References
1. DeCroo S, Kamboh MI, Ferrell RE. Population genet- ics of alpha-1-antitrypsin polymorphism in US whites, US blacks and African blacks. Hum Hered 1991; 41: 215-221.

1186 M. MIRAVITLLES ET AL
2. Yuasa I, Suenaga K, Gotoh Y, Yokoyama N, Okada K. PI (alpha-1-antitrypsin) polymorphism in the Japanese: confirmation of PI*M4 and description of new PI variants. Hum Genet 1984; 67: 209-212.
3. Beckman G, Beckman L, Nordenson I. Alpha-l- antitrypsin phenotypes in Northern Sweden. Hum Hered 1980; 30: 129-135.
4. Thymann M. Distribution of alpha-1-antitrypsin pheno- types in Denmark determined by separator isoelectric focusing in agarose gel. Hum Hered 1986; 36: 19-23.
5. Vidal R, Miravitlles M, Jardi R, et al. Estudio de la frecuencia de 10s diferentes fenotipos de la alfa-l- antitripsina en una poblacion de Barcelona. (A study on the frequency of the different alpha-1-antitrypsin phenotypes in a population from Barcelona, Spain). Med Clin (Bare) 1996; 107: 211-214.
6. Seersholm N, KokJensen A, Dirksen A. Survival of patients with severe alpha-1-antitrypsin deficiency with special reference to nonindex cases. Thorax 1994; 94: 695-698.
7. Anthonisen N (Chair). Design of a clinical trial to test a treatment of the underlying cause of emphysema. Ann NY Acad Sci 1991; 624 (Suppl.): 31-34.
8. Konietzko N. Alpha-1-antitrypsin substitution- treatment or prevention of emphysema. Lung 1990; 168 (Suppl): 5928-598s.
9. The Alpha-1-Antitrypsin Deficiency Registry Study Group. A registry of patients with severe deficiency of alpha-1-antitrypsin. Design and methods. Chest 1994; 106: 1223-1232.
10. McElvaney NG, Stoller JK, Buist AS, et al. Baseline characteristics of enrollees in the National Heart, Lung and Blood Institute Registry of alpha-1-antitrypsin deficiency. Chest 1997; 111: 394403.
11. Seersholm N, Wencker M, Banik N, Viskum K, Dirksen A, Kok-Jensen A, Konietzko N for the Wissenschaftliche Arbeitsgemeinschaft zur Therapie von Lungenerkrankungen (WATL) alpha-l-AT study group. Does alpha-1-antitrypsin augmentation therapy slow the annual decline in FEVl in patients with severe hereditary alpha-1-antitrypsin deficiency? Eur Respiv J 1997; 10: 2260-2263.
12. Vidal R, Miravitlles M y Grupo de Estudio de1 Deficit de Alfalantitripsina. Informe de1 Registro Espanol de Pacientes con Deficit de Alfalantitripsina. Arch Bronconeumol 1995: 31: 299-302.
13. Jardi R, Rodriguez-Frias F, Casas F, et al. Caracter- izacion molecular de dos variantes deficitarias de la alfa-1-antitripsina: PIpalermo y PIlovel. (Molecular characterization of the two deficient variants of alpha- I-antitrypsin: PI Mpalermo and PI Plovel). Med Clin (Bare) 1997; 109: 463466.
14. Jardi R, Rodriguez F, Miravitlles M, et al. Identifica- tion and molecular characterization of the new alpha- 1-antitrypsin deficient allele PI Ybarcelona (Asp256-Val and Pro391 -His). Human Mutation, Mutation in brief# 174 (1998) Online.
15. Quanjer PH. Standardized lung function testing. Report of a Working Party on Standardization of Lung Function Tests. European Community for Coal and
Steel. Bull Eur Physiopathol Respir 1983; 19 (Suppl. 5): l-95.
16. Rota J, Sanchis J, Agusti-Vidal A, et al. Spirometric reference values from a Mediterranean Population. Bull Eur Physiopathol Respir 1986; 22: 217-224.
17. Fagerhol MK, Tenfjord OW. Serum Pi types in some European, American, Asian and African populations. Acta Path Microbial Stand 1968; 72: 601-608.
18. And& Puertas MJ, Arranz Pefia ML. Valoracion de fenotipos de alfalantitripsina en CastillaLeon: estudio en una poblacion de recien nacidos. Rev Clin Esp 1989; 184: 106-108.
19. Silverman EK, Pierce JA, Province MA, Rao DC, Campbell EJ. Variability of pulmonary function in alpha-1-antitrypsin deficiency: clinical correlates. Ann Intern Med 1989; 111: 982-991.
20. Seersholm N, Kok-Jensen A. Clinical features and prognosis of life time non-smokers with severe alpha- 1-antitrypsin deficiency. Thorax 1998; 53: 265-268.
21. Miravitlles M, Vidal R, Torrella M, Bofill JM, Cotrina M, de Gracia J. Evaluation de1 tratamiento sustitutivo de1 enfisema por deficit de alfalantitripsina. (Assessment of alpha- 1 -antitrypsin replacement therapy for emphysema). Arch Bronconeumol 1994; 30: 479484.
22. Horowitz ID. Alpha-1-proteinase inhibitor (human) shortage. Chest 1996; 110: 16241625.
23. Wewers MD, Casolaro MA, Sellers SE, Swayze SC, McPhaul KM, Wittes JT, Crystal RG. Replacement therapy for alpha-1-antitrypsin deficiency associated with emphysema. N Engl JMed 1987; 316: 1.055-1.062.
24. Stone PJ, Morris III TA, Franzblau C, Snider GL. Preliminary evidence that augmentation therapy dimin- ishes degradation of cross-linked elastin in alpha-l- antitrypsin-deficient humans. Respiration 1995; 62: 76-79.
25. Constans J, Carles P, Boneu A, et al. Clinical pharmacokinetics of alpha-1-antitrypsin in homo- zygous PiZ deficient patients. Clin Pharmacokinet 1992; 23: 161-168.
26. Barker AF, Iwata-Morgan I, Oveson L, Roussel R. Pharmacokinetic study of alpha-1-antitrypsin infusion in alpha-1-antitrypsin deficiency. Chest 1997; 112: 607- 613.
27. Hubbard RC, Sellers S, Czerski D, Stephens L, Crystal RG. Biochemical efficacy and safety of monthly aug- mentation therapy for alpha-1-antitrypsin deficiency. J Am Med Assoc 1988; 260: 1.25991.264.
28. Barker AF, Siemsen F, Pasley D, D’Silva R, Buist S. Replacement therapy for hereditary alpha-1-antitrypsin deficiency. A program for long-term administration. Chest 1994; 105: 14061410.
29. Carles P, Constans J, Pujazon MC, Arnaud J, Lauque D, Goudemand M. Bilan a deux ans du traitement substitutif de l’emphyseme PiZZ par l’alpha-l- antitrypsine. Neuf cas. Presse M&d 1990; 19: 514-518.
30. Schwaiblmair M, Volgemeier C, Fruhmann G. Long- term augmentation therapy in twenty patients with severe alpha-1-antitrypsin deficiency. Three-year follow-up. Respiration 1997; 64: 10-15.

SPANISH REGISTRYOF AAT 1187
31. Janus ED, Phillips NT, Carrel1 RW. Smoking, lung function, and alpha-1-antitrypsin deficiency. Lancet 1985; i: 152-154.
32. Wencker M, Denker J, Konietzko N. Serial measure- ments of FEV, over 12 years in a patient with alpha-1-protease inhibitor deficiency: influence of augmentation therapy and infections. Respiration 1994; 61: 195198.
Appendix
Albacete: M. Arevalo, R. Coloma; Alcalh de Henares (Madrid): M. Vazquez; Almeria: A. Martinez; Andorra La Vella: J. Roig; Avilh (Asturias): J. M. Garcia; Badajoz: J. M. Checa; Badalona (Barcelona): E. Fit& J. Izquierdo; Baracaldo (Vizcaya): B. Galdiz; Barcelona: R. Vidal, M. Miravitlles, A. Torres, R. Jardi; CLEceues: A. Sojo; Chdiz: C. Garcia; Cartagena (Murcia): P. Belindres; Ferrol (La ComAa): R. de 10s Reyes; Galdakao (Vizcaya): P. Espaiia; Getafe (Madrid): M. A. Juretschke; Gij& (Asturias): T. Bazus; Girona: M. Rubio; Granada: F. Casas; Guadalajara: J. L. Izquierdo; Hondarribia (San Sebasticin): J. F.
Capellan; Huelva: F. Barragan; La Corufia: C. Montero; Leganb (Madrid): M. Yoldi; Lugo: L. A. Perez; Madrid: L. Maiz, J. Jarefio, F. Villegas, M. J. Chillon, L. Sanchez- Agudo, M. Martinez, B. Ortega, J. Gaudo, J. Lirio, G. Marin, F. Artalejo, M.C. Rodriguez de Guzman, J. M. Carreras; Mhlaga: J. J. Martin, F. Espildora; Orense: A. Rodriguez, A. Gonzalez; Oviedo: J. Palicio, C. Escudero; Pamplona: F. J. Dominguez, J. Boldu; Ponferrada (La Coruria): S. Fernandez; Pontevedra: A. Baloira, A. Pena; Puertollano (Ciudad Real): W. El Jawat; Riafio-Langreo (Asturias): I. Blanco; Sabadell (Barcelona): J. Such; Sala- manca: J. M. Gonzalez; Santander: R. Agiiero; Santiago (La Corufia): R. Arias, L. Valdes; Santa Cruz de Tenerife: I. Garcia; San Sebastih: P. de la Torre; Tarragona: J. Aguilar; Tenerife: Gonzalez Abreu; Teruel: J. A. Domingo; Torrelavega (Santander): A. Bustamante; Tremp (Lleida): J. Alvarez; Trevias (Asturias): J. E. Armengod; Valencia: V. Crescencio, J. France, G. Juan; Valladolid: A. Herrero; Vigo: J. C. Barros-Tizon, J. M. Barreiro, R. Band&, M. Jimenez; Vitoria: J. L. Lobo, M. Perez; Zaragoza: I. Herrero, C. Aguirre.
Copyright © 2022 FDOKUMEN