United States and Mexico
243
United States and Mexico High Level Contact Group Proceedings of the Third Bi-National Drug Demand Reduction Conference co-sponsored by the U.S. Office of National Drug Control Policy and Mexico National Council on Addictions May 31 - June 2, 2000 Phoenix, Arizona
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of United States and Mexico
United States and MexicoHigh Level Contact Group
Proceedingsof the
Third Bi-NationalDrug Demand Reduction Conference
co-sponsored bythe U.S. Office of National Drug Control Policy
and Mexico National Council on Addictions
May 31 - June 2, 2000Phoenix, Arizona
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 1 Foreword
FOREWORD
For the third time in as many years, Mexican and American officials and experts gathered at a bi-national conference to collaborate in reducing drug use in both countries. The understanding,goodwill, cooperation and work products generated during and in preparation for theseconferences demonstrate what can result when suspicion and blame are set aside for thecommon good. With each successive conference, bi-national relationships and tools werecreated that can continue to effectively serve the people of the United States and Mexicothroughout the normal periodic changes in leadership that take place in both countries.
While Mexico and the United States have worked together on drug issues for many years, ourcollaboration took dramatic steps forward under the leadership of Presidents Zedillo and Clinton,prompted in part by the greater economic interdependency fostered during their administrationsby the creation and implementation of the North American Free Trade Agreement. In March1996 the U.S.-Mexico High Level Contact Group for Drug Control (HLCG) was created. In May1997 at the Mexico City Summit, the two presidents signed a 16-point Alliance against Drugsdesigned to strengthen our nations’ joint commitment to reducing drug use. Then in February1998 the two countries produced a Bi-National Drug Strategy that committed both nations tospecific measures in the fight against illegal drugs. Both documents reinforce our commitment toreduce the availability of drugs through aggressive interdiction, tough law enforcement andsound judicial processes, but their first priority is together meeting the challenge of eliminatingthe demand for drugs in both countries.
One of the demand reduction measures in the Bi-National Drug Strategy was to convene a bi-national conference on demand reduction. The first conference, held in El Paso, Texas, USA, inMarch 1998, was exploratory in nature. Over 250 researchers, practitioners, and treatment andprevention experts in both countries gathered to share their expertise, exchange ideas, andstrengthen our shared ability to reduce drug use. From the conference came the beginnings of aframework for joint efforts in demand reduction. Working groups generated explicit strategies ineight areas including research cooperation and the exchange of technical information, publicawareness, community participation, youth, special populations, the workplace, HIV/AIDS, andviolence and drug-related problems.
Between the first and second conferences, the bi-national demand reduction working groupformed by the HLCG developed Performance Measures of Effectiveness (PMEs) to implement thestrategies conceived at the first conference. The group identified 108 target actions, 22 of whichwere bi-national in nature. Before the second conference, 19 of those bi-national target actionswere accomplished.
Over 300 people attended the second Bi-National Conference on Demand Reduction June 1999 inTijuana, Baja California, Mexico. The PMEs developed between conferences to implement thefirst year’s workgroup strategies were reviewed, adjusted, and supplemented by the secondyear’s workgroups (reduced to five from eight: research, treatment, prevention, publicawareness, and the workplace). Participants were encouraged and excited by all that had beenaccomplished between conferences and were anxious to build on that momentum.
In addition to plenary sessions and work groups, this second conference featured pre-conferenceprofessional development workshops and guided tours to Tijuana research and treatment andprevention centers. Also, special sessions were held for representatives of non-governmentalorganizations (NGOs) involved in prevention and treatment and for youth participants. Among

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 2 Foreword
other actions, the youth agreed to work toward the creation of a Bi-National Youth OrganizationCoalition for the Prevention and Control of Addictions.
The third Bi-National Demand Reduction Conference, which is described in these proceedings,met in Phoenix, Arizona, USA, in May 2000. Building on the accomplishments of the prior twoconferences, this conference’s objectives were:
• To identify future needs within drug control policy and ways the U.S. and Mexico can workdomestically and bi-nationally, benefiting from one another’s ideas and experiences;
• To bring together key policy makers, researchers, community members, and others fromboth countries to encourage networking, information sharing, and long-term relationships;
• To develop a bi-national research agenda;
• To expand bi-national youth-oriented substance abuse treatment and prevention efforts;
• To expand bi-national linkages and exchange of technical expertise in the field of substanceabuse treatment, especially within the criminal justice system.
The 2000 conference brought together 426 participants for 2 ½ days of meetings. It waspreceded by a research symposium and by three concurrent sessions for non-researchers:Advancements in Prevention Interventions; Advancements in Treatment Interventions; andInitiating and Evaluating Public Awareness Campaigns. Throughout the conference, workshopswere organized along three tracks: Prevention, Treatment, and a new emphasis: Linking thePublic Health and Public Safety Systems. While these were going on, youth participantsconvened the first annual meeting of the Bi-National Youth Organization Coalition for thePrevention and Control of Addictions that had been organized the year before. A fourth bi-national conference is scheduled for September 2001 in Mexico.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings i Table of Contents
TABLE OF CONTENTS
WELCOME LETTERS .......................................................... 1
CONFERENCE OVERVIEW.................................................. 9
PLENARY SESSIONS ........................................................13
Opening Plenary Remarks ...............................................15
Daniel Schecter, Deputy Director for Demand Reduction (Acting), Office of NationalDrug Control Policy, United States
Sofia Magaly CamorlingaYouth representative, Mexico
Barry R. McCaffrey, Director, Office of National Drug Control Policy, Executive Office ofthe President, United States
Jeffrey Davidow, Ambassador of the United States to Mexico
Nelba Chavez, Ph.D., Administrator, Substance Abuse and Mental Health ServicesAdministration, Department of Health and Human Services, United States
Jorge Madrazo Cuellar, Attorney General, Mexico
José Antonio González Fernández, Secretary of Health, Mexico
Challenges and Opportunities in DrugDemand Reduction ..........................................................28
Moderator: John W. Wilson, Acting Administrator, Office of Juvenile Justice andDelinquency Prevention, Department of Justice, United States
Providing Effective TreatmentH. Westley Clark, M.D., J.D., M.P.H., CAS, FASAM, Director, Center for SubstanceAbuse Treatment, Department of Health and Human Services, United States
What We Have Learned From ResearchTimothy Condon, Ph.D., Associate Director, National Institute on Drug Abuse,Department of Health and Human Services, United States

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings ii Table of Contents
Preventing Drug Abuse Among Our YouthHaydée Rosovsky, Technical Secretary, National Council on Addictions (CONADIC),Ministry of Health, Mexico
Drug Free Workplaces: A Critical Prevention ComponentMary Bernstein, Office of Drug and Alcohol Policy and Compliance, Department ofTransportation, United States
Drug Free Workplaces: A Critical Prevention ComponentAgustín Vélez, General Director, Trusteeship for the Institute for Street Kids andAddiction (FINCA), Mexico
Bridging the Public Health and Public Safety SystemsMelody Heaps, President and Founder, Illinois Treatment Assessment Screening Center(TASC), Inc., United States
Rafael Velasco Fernández, President, Center in Studies on Alcohol and Alcoholism(CESAAL), Mexico
Mobilizing Parents for Prevention ...................................58
Jesús Cabrera Solís, Director, Centers for Youth Integration, (CIJ) Mexico
L.A. Jose Luis Perez Bautista, President, National Association of Parents, Mexico
Henry Lozano, President, Californians for Drug Free Youth, United States
Program Evaluation .................................................................................. 62
Moderator: José Vila del Castillo, Representative for Mexico and Central America,United Nations International Drug Control Program (PNUFID)
Evaluation of Prevention ProgramsAbraham Wandersman, Ph.D., University of South Carolina, United States
Evaluation of Treatment ProgramsD. Dwayne Simpson, Ph.D., Texas Christian University, United StatesJesús Cabrera Solís, Director, Centers for Youth Integration (CIJ), Mexico
Evaluation of Prison-Based Therapeutic Communities – Current Status and FutureStepsGeorge De Leon, Ph.D., Center for Therapeutic Community Research, United States

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings iii Table of Contents
Focus on Youth ...............................................................66
Moderator: Ruth Sanchez-Way, Ph.D., Acting Director, Center for Substance AbusePrevention, Department of Health and Human Services, United States
Report From the YouthMaria Christina Diaz Jimenez, Carlos Alejandro Espinoza Dominguez, MexicoCarla Perez, Ricardo Hernandez, United States
Adolescent TreatmentJorge Sánchez Mejorada, Researcher, Veracruzana University, Mexico
Prevention for High-Risk YouthSusan Kunz, Director, U.S.-Mexico Border Center for the Application of PreventionTechnologies, United States
Addressing the Needs of Youth in Criminal Justice/ Substance Abuse-Public HealthProgramsEugenia Ortega, Superintendent, Karl Holton Youth Correctional Drug and AlcoholTreatment Facility, California Youth Authority, United States
Closing Remarks ...........................................................82
Daniel Schecter, Deputy Director for Demand Reduction (Acting), Office of NationalDrug Control Policy, United States
PREVENTION...................................................................83
Pre-Conference SessionsSuccessful Intervention Programs...................................85
Moderator: Ruth Sanchez-Way, Substance Abuse and Mental Health ServicesAdministration, Department of Health and Human Services, United States
FAMILIES AND COMMUNITIES
Hablemos En ConfianzaMark Weber, Luisa Pollard, Substance Abuse and Mental Health ServicesAdministration, Department of Health and Human Services, United States
Supporting and Financing Prevention Projects Focused on YouthJesus Garcia, Director, Mexican Institute for Youth
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings iv Table of Contents
CHILD DEVELOPMENT PROGRAMS: A SCHOOL AND FAMILY MODELBuilding MeAimee Graves, CODAC Behavioral Health Services, Tucson, Arizona, United StatesRaul Zapata, Centers for Youth Integration (CIJ), Mexico
Drug Prevention in the WorkplaceBernie McCann, Office of National Drug Control Policy, United StatesJuan Roman Uriarte Galvan, Secretary of Communications and Transportation,Mexico
Drugs and Violence: Overview of Border Crime Prevention Program in Baja,California and San Diego
Developing a Culture of LawfulnessEdward Brand, Superintendent of Sweetwater Union School District, Chula Vista,California, United StatesRosalia Salinas, Director of Curricula, Sweetwater Union School District, Chula Vista,California, United StatesCarlos Franco, Director of Curricula, Baja School District, MexicoLuciana Ramos, Mexican Institute of Psychiatry, Mexico
PreventionTraining Sessions .........................................................101
COMPREHENSIVE SCHOOL-BASED PROGRAMS INVOLVING THE FAMILYIntroduction to Programs on Schools and FamiliesCarmen Mille, National Council on Addictions (CONADIC), Ministry of Health,Mexico
“Construye tu Vida sin Adicciones” (Build your Life without Addictions) Program inSchoolsCarmen Mille, Maria Teresa Sanchez Fragoso, Fernando Bilbao, Norma Merena,Council on Addictions (CONADIC), Ministry of Health, Mexico
Bi-national Implementation of “Construye tu Vida sin Adicciones” ProgramDr. Ignacio Benedicto Reyes, Baja, California, Mexico
EFFECTIVE COMMUNITY MOBILIZATION APPROACHES: DRUG FREECOMMUNITIESDrug-Free Communities Support Program: Community Mobilization in the BorderStates to Reduce Substance AbuseMary Ann Solberg, Co-Chair, Advisory Commission on Drug-Free Communities,United StatesHarry Montoya, Hands Across Cultures Inc., Espanola, New Mexico, United StatesLuz Arriola, West Texas Council Alcoholism and Drug Abuse, El Paso, Texas, UnitedStatesLorenzo Merritt, Project HEAVY, Los Angeles, California, United States
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings v Table of Contents
National Projects in CommunitiesLuis Navarro, Chimalli System for the Integral Development of the Family (DIF),Mexico
BUILDING EFFECTIVE PARTNERSHIPS FOR DRUG PREVENTION IN THEWORKPLACERobert Stephenson, Acting Director, Division of Workplace Programs, SubstanceAbuse and Mental Health Services Administration, Center for Substance AbusePrevention, Department of Health and Human Services, United States
Building Partnerships for Drug Prevention in the WorkplaceElizabeth Edwards, Gabriela Garcia, Arizonans for a Drug-Free Workplace, UnitedStates
Model Program on Alcohol and Drug Use Prevention for Workers and Their FamiliesAgustin Vélez, General Director, Trusteeship for the Institute for Street Kids andAddictions (FINCA), Mexico
PREVENTION ACROSS THE LIFE CYCLEIntroductory Remarks: Ruth Sanchez-Way, Substance Abuse and Mental HealthServices Administration, Department of Health and Human Services, United States
Prevention in Early ChildhoodRosa Bonifaz, Carmen Mille, National Council on Addictions (CONADIC), Ministry ofHealth, Mexico
US Efforts - Prevention in Early ChildhoodEileen O’Brien, Casey Family Program, Substance Abuse and Mental Health ServicesAdministration, Department of Health and Human Services, United States
INTRODUCTION TO YOUNG ADULTHOOD AND ELDERLY SEGMENTSPREVENTION IN YOUNG ADULTHOODHigher Education ProgramsJohn Clapp, San Diego State University, United States
Prevention Education for Parents in the WorkplaceBernie McCann, Office of National Drug Control Policy, United States
Prevention of Substance Abuse in Older AdultsKristen Barry, University of Michigan, United States
DRUG AND VIOLENCE PREVENTIONModerator: William Modzeleski, Director, Safe Schools Program, Department ofEducation, United States
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings vi Table of Contents
PRESENTATIONS ON SAFE-SCHOOLS - HEALTHY STUDENTS INITIATIVEAnn Clark, Houston Independent School District, Houston, Texas, United StatesPhilmer Bluehouse, Pinon Unified School District #4, Pinon, Arizona, United StatesForrest Van Camp, Leon County School District, Tallahassee, Florida, United StatesMartha Fletcher, Leon County School District, Tallahassee, Florida, United States
Latin American Institute for Family StudiesMarisa Oceguera, Latin American Institute for Family Studies, Mexico
TREATMENT ..................................................................123
TreatmentPre-Conference Sessions ..............................................125
Moderator: Arturo Ongay Pérez, National Council on Addictions (CONADIC),Ministry of Health, Mexico
COMPREHENSIVE TREATMENT PLANSComprehensive Treatment Approaches for WomenRobin Hoskins, Women’s Treatment Network
THERAPEUTIC COMMUNITIESStandards for Prison-Based Therapeutic CommunitiesGeorge DeLeon, Center for Therapeutic Community Research, United States
Treatment Program for Heroin UseMaría Elena Ramos, Programa Compañeros, A.C., Mexico
RECOVERY PROGRAMS: FAITH-BASED MODELSChristianity InterventionsRoberto Bital Pineda, Alcance Victoria, Mexico
RECOVERY PROGRAMS: SOCIAL MODELSEVAC and PREHAB of Arizona: Successful Multi-Systemic Approaches within aCommunity ContextTom Hutchinson, Prehab of Arizona, United States
HIV Prevention, Addictions and Social Reintegration of Street KidsMartín Pérez, El Caracol, Mexico
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings vii Table of Contents
TreatmentTraining Sessions .........................................................136
New Developments in Oversight and Treatment of Opiate Addiction: Pharmacologyand Behavioral TherapiesMark W. Parrino, M.P.A., President, American Methadone Treatment Association,United StatesAndrea G. Barthwell, M.D., President, Encounter Medical Group, United StatesVíctor Manuel Guisa, Centers for Youth Integration (CIJ), Mexico
Program AccreditationStephen Shearer, health care consultant, United StatesNora Gallegos, National Council on Addictions (CONADIC), Ministry of Health,Mexico
Innovations in the Treatment of Stimulant Use DisordersJeanne Obert, Executive Director, Matrix Center, Los Angeles, California, United StatesVíctor Manuel Guisa, Centers for Youth Integration (CIJ), Mexico
PUBLIC AWARENESS CAMPAIGNS..................................159
Initiating and Evaluating Public Awareness CampaignsPre-Conference Sessions ...............................................161
IntroductionJennifer Bishop, Office of National Drug Control Policy, United States
Crafting Effective Messages for Behavioral ChangesAmelie G. Ramirez, Dr. P.H., Associate Professor, Department of Medicine, BaylorCollege of Medicine, United StatesAntonieta Martin, Ph.D., Researcher, John Hopkins University, United States
Developing and Implementing Community AwarenessIsabel Gomez-Bassols, Ph.D., Radio Unica Network, United StatesMario Bejos, Liber Addictus, Mexico
Evaluating Media CampaignsTerry Zobeck, Ph.D., Office of National Drug Control Policy, United StatesJaime Quintanilla, Centers for Youth Integration (CIJ), Mexico
Building Private Public Partnership for Social MarketingBeverly Schwartz, Senior Vice President, Fleishman Hillard InternationalCommunications, United StatesEduardo Chacón Vizcaino, Azteca Foundation, Mexico

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings viii Table of Contents
PUBLIC HEALTH AND PUBLIC SAFETY ............................165
Linking Public Health and Public SafetyTraining Sessions .........................................................167
ModeratorsSteve Wing, Substance Abuse and Mental Health Services Administration, Departmentof Health and Human Services, United StatesOscar Fuentes, Attorney General’s Special Office for Crimes against Health (FEADS/PGR), Mexico
IntroductionAllen Ault, National Institute of Corrections, Department of Justice, United States
Special Populations: Adolescents and Dually-Diagnosed AdolescentsWilfred Rios Sánchez, Attorney General’s Special Office for Crimes against Health(FEADS/PGR), MexicoDuane McBride, Andrews University, Berrien Springs, Michigan, United StatesRichard Dembo, University of South Florida, United StatesMario Alva Rodriguez, National Institute of Sciences of Penal Investigations(INACIPE), Mexico
Dually-DiagnosedDavid M. Wertheimer, M.S.W., King County Dept. of Community and Human ServicesMario Alva Rodriguez, National Institute of Sciences of Penal Investigations(INACIPE), Mexico
Engagement, Retention, and Relapse PreventionEngagement into Treatment and RetentionTom McLellan, University of Pennsylvania, United StatesRelapse Prevention and Recovery SupportD. Dwayne Simpson, Texas Christian University, United States
A System-Based ApproachDiversion and Community Corrections: Pre-trial Diversion and Drug CourtsPre-Trial DiversionBarbara Zugor, Executive Director, Treatment Assessment Screening Center (TASC)Arizona, United States
Drug CourtsTim Murray, Bureau of Justice Assistance, Department of Justice, United States
Incarceration: Adult and Juvenile Populations.AdultsAllen Ault, National Institute of Corrections, Department of Justice, United States
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings ix Table of Contents
Parole and Community CorrectionsDave Gaspar, Arizona Department of Juvenile Corrections, United StatesAdolescentsJennifer Mankey, Project Director, Denver Juvenile Justice Integrated TreatmentNetwork, United StatesHiram Suárez Villa, Office of Secretary of the Government, Mexico
NATIONAL INSTITUTE ON DRUG ABUSE (NIDA)PRE-CONFERENCE SESSION...........................................181
National Institute on Drug Abuse Research SymposiumSummary ......................................................................183
OTHER CONFERENCE INFORMATION..............................185
Acknowledgements .......................................................187
Exhibitors .....................................................................193
Speakers from the United States ...................................195
Speakers from Mexico ...................................................203
Attendees from the United States..................................205
Attendees from Mexico..................................................219
National Institute on Drug AbuseResearch Symposium Participants .................................227

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 1 Welcome Letters
WELCOME LETTERS
THE WHITE HOUSE
WASHINGTON
May 26, 2000
Warm greetings to everyone gathered in Phoenix to participate in the third U.S.-MexicoBi-National Drug Demand Reduction Conference. This conference culminates another year ofeffective partnership between our two nations in the struggle to combat illegal drugs.
Since President Zedillo and I signed the Declaration of Alliance Against Drugs in 1997,the United States and Mexico have closely cooperated to achieve a comprehensive, balancedapproach to reducing the demand for and supply of illegal drugs. In the area of law enforcement,we have seen the arrest of some major traffickers and cooperated with mutual respect onimportant cases. We have improved interdiction and cracked down on money laundering. Wehave also worked together to reduce demand for illegal drugs in both countries.
I am confident that this third Bi-National Drug Demand Reduction Conference will buildon the achievements of your earlier gatherings. I applaud each participant for your commitmentto protecting a new generation of youth on both sides of the border from destructive drug use. Aswe stand at the dawn of a new century, we must reaffirm our obligation to ensure a safer,healthier future for all our citizens.
Best wishes for a successful conference.

Vienna International CenterP.O. Box 500, A-1400, Vienna, Austria
Telephone: +43-1- 26060-0 Telefax +43-1-26060-5866E-Mail: [email protected]
THE EXECUTIVE DIRECTOR
Message to the Third U.S./Mexico Bi-NationalDrug Demand Reduction Conference
Phoenix, Arizona, 31 May - 2 June 2000
As you know, the work of the United Nations International Drug Control Programme is guided byagreements reached by the international community in inter-governmental bodies. In March thisyear, the Commission on Narcotic Drugs continued to devote special attention to drug demandreduction, particularly regarding follow-up to the Action Plan for the Implementation of theDeclaration on the Guiding Principles of Drug Demand Reduction.
During the debate the Commission identified four substantive priority areas for U7NDCP’sactivities:
Firstly, drug abuse among children and youth and the globalization of youth culture and associatedpatterns of drug abuse, with special attention to young people’s involvement and participation inthe design and implementation of drug prevention programmes.
Secondly, the growing problem of ATS abuse, and the need to develop effective responses in thisarea. The abuse of ATS increased dramatically throughout the 1 990s and diffused to regionswhere it was previously unknown. There is a need to identify and develop culturally appropriateapproaches to prevention and treatment.
Thirdly, the health consequences of drug abuse and particularly drug injection, such as HIVinfection, hepatitis C and other communicable diseases, as well as overdoses. In many countries,and in developing countries in particular, the increase in heroin abuse has been accompanied bythe introduction of drug injecting. Furthermore, the number of countries reporting HIV infectionamong drug injectors is increasing.
Fourthly, cutting across all the three above-mentioned areas, the need for improved data collçctionto provide a sound knowledge base for the development of effective responses, and in particularthe important role UNDCP should play in supporting the development of capacity for datacollection and analysis in countries where this is absent or deficient.
Concentrating on these four priority areas in drug demand reduction constitutes plenty of work forus all in the coming year. I wish you fruitful deliberations and a successful conference.
Pino Arlacchi
ODCCPUNUnited Nations Office
for Drug Controland Crime Prevention
EXECUTIVE OFFICE OF THE PRESIDENT OFFICE OF NATIONAL DRUG CONTROL POLICY
Washington, D.C. 20503
May 31, 2000
Dear colleague:
The Office of National Drug Control Policy welcomes participants in the ThirdU.S.-Mexico Bi-National Drug Demand Reduction Conference. This conference marks animportant milestone in the evolving cooperation between our two countries in reducingthe demand for illegal drugs.
The United States and Mexico are two dynamic societies whose present andfutures are intertwined. We share a 1,800-mile border, the world’s busiest. We are majortrading partners. We share a common culture, with the U.S. now possessing the world’sfifth largest Hispanic population. Although we share much that is positive, we also face acommon threat to the health and safety of our citizens: the use of illegal drugs. That iswhy our presidents signed, in May 1997, the Declaration of the U.S.-Mexico AllianceAgainst Drugs, outlining 16 principles under which cooperation would be carried out.Reducing drug demand was the first of these principles, and this conference — the thirdsuch conference — is a fundamental vehicle for advancing collaborative efforts.
Like those that preceded it, this is a working conference. It brings together experts,scholars, program administrators and practitioners from the U.S. and Mexico to exchangeinformation, highlight effective approaches, and work together on issues that require across-border solution. Our cooperation is already showing tangible results. Communityanti-drug coalitions on both sides of the border are working together as never, before.Researchers are developing a common framework for future studies. Regionalconferences have been held on drug and violence prevention approaches. A specialwebsite has been developed to facilitate binational information exchange. And ourcountries are mounting unprecedented drug prevention media campaigns in cooperation,not in isolation.
Our partnership must continue and be strengthened in the years ahead if we are tosucceed in reducing the devastating impact of drug abuse on our societies. We lookforward to working with each of you on this long-term approach to ensuring a healthier,safer future for our. children and our families.
Best wishes,
THE SECRETARY OF EDUCATIONWASHINGTON, D.C. 20202
THIRD U.S./MEXICO BI-NATIONALDEMAND REDUCTION CONFERENCE
Phoenix, ArizonaMay31 —June 2, 2000
I wish to extend my warmest greetings to all of you who are participating in the Third U.S./Mexico Bi-National Demand Reduction Conference.
This conference provides an important opportunity for our countries to share informationabout promising and effective strategies to prevent drug use and violence. The Department ofEducation is engaged in a number of new initiatives to ensure that our children have access tosafe, disciplined, and drug-free schools.
One approach the Department of Education is taking is to collaborate with other Federalagencies on initiatives that support comprehensive, multidisciplinary drug and violenceprevention strategies involving the whole community. An example is the Safe Schools/HealthyStudents Initiative, a joint effort of the U.S. Departments of Education, Health and HumanServices, and Justice that awards grants to school districts to implement comprehensive,community-wide strategies for safe, drug-free learning environments and healthy childhooddevelopment. The initiative draws on the best practices of the education, justice, social service,and mental health systems to help children avoid drug use and violent behavior.
We look forward to sharing information about our current initiatives and learning aboutsimilar prevention initiatives in Mexico. We are committed to our continuing partnership inthis bi-national effort. Best wishes for a successful and productive conference.
Our mission is to ensure equal access to education and to promote educational excellence throughout the Nation.
THE SECRETARY OF TRANSPORTATIONWASHINGTON, D.C. 20590
May 16, 2000
Dear Colleague,
I am pleased once again to have the opportunity to extend my greetings to the participants in thethird Bi-National Drug Demand Reduction Conference, this year in Phoenix, Arizona.
Safety is President Clinton and Vice President Gore’s highest transportation priority and theNorth Star by which the Department of Transportation is guided and willing to be judged. Safetyis a partnership in commitment. Each of us -- government, industry, and private citizens alike --
must take personal responsibility for reducing crashes on our highways and ensuring that thosewho are entrusted with the safety of our public are drug and alcohol free.
The bi-national meetings focus on developing and expanding the partnership between our twocountries in the vital interest of reducing the demand for drugs. This vision continues within eachof you this year. Nowhere is it more important to send a signal to the public that we arecommitted to reducing drug and alcohol usage than in our workplaces. Together we shouldexpect nothing less than workplaces that are completely drug and alcohol-free, making for evensafer workplaces for our employees, their families, and the traveling public.
Transportation is more than concrete, asphalt, and steel, it is about people and providing them thesecurity of being able to enjoy safe travel. Together we can make this happen and this conferencewill go a long way to ensuring that the people of our countries working collaboratively canreduce the demand for drugs. I applaud all of your efforts in achieving our mutual goals.
Sincerely,
DEPARTMENT OF HEALTH & HUMAN SERVICES Substance Abuse and MentalHealth Services Administration
Center for Mental Health ServicesCenter for Substance AbusePrevention
Center for Substance AbuseTreatmentRockville MD 20857
May 26 2000
Dear Colleagues:
Welcome to the third annual High Level Contact Group U.S.-Mexico Demand ReductionConference — the first in this new millennium. This key meeting — “Strengthening the Bi-NationalPartnership in the New Century” — will give still further concrete structure and form to theblueprints for action that we have crafted together in past meetings.
There is no better time for us to get down to the work of training and education, sharing what“works” in prevention, in treatment, and in linking public health and public safety. The issues onwhich we will work transcend nationality, transcend politics and ideology. They are at the veryheart of our purpose: reducing substance abuse for our people today, and eliminating it for thosewho will come tomorrow.
This meeting most assuredly will set the tone and direction for the new century of collaborationsand individual demand reduction efforts within and across our borders. The commitment,dedication and, above all, collaboration of the leaders in substance abuse prevention and treatmentat this key meeting can and, I am certain, will serve as the springboard to meaningful and targetedsubstance abuse-related programs for both the Mexican and American people.
It has been said that “progress occurs when courageous, skillful leaders seize the opportunity tochange things for the better.” Let us work together to live up to those words. We have alreadyseized the opportunity; let us now demonstrate once again, that capacity to change things for thebetter not just for our nations, but for all the Americas.
Sincerely yours,
Office of the Administrator—Office of Applied Studies—Office of Communications—Office of Equal Employment Opportunity & Civil Rights—Office of Managed Care—Office of Minority Health—Office of Policy & Program Coordination—Office of Program Services
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 9 Overview
CONFERENCE OVERVIEW

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 10 Overview
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 11 Overview
CONFERENCE OVERVIEW
The Third Bi-national Drug Demand Reduction Conference in Phoenix featured sharing of innovations andbest practices in the area of substance abuse prevention and treatment, training for Mexican officials onadvances in heroin and amphetamine treatment, and expert presentations on ways to better integratethe public health and public safety systems.
Concurrent pre-conference sessions were held on advances in prevention and treatment, and in initiatingand evaluating public awareness campaigns. Both Mexican and US programs were featured, such asSAMHSA’s media campaign, Hablemos En Confianza, as well as Mexico’s prevention program, ConstruyeTu Vida Sin Addiciones. Officials from Baja, California, Mexico and San Diego jointly presented aninnovative school curriculum to prevent drug-related border crime. Treatment professionals discussedfaith-based and social models of recovery, and participants shared best practices in crafting andevaluating public awareness campaigns and heard from experts in social marketing.
The conference featured several plenary sessions covering a range of topics and was divided into threetracks: Prevention, Treatment, and Linking Public Health and Public Safety. Plenary sessions includedopening remarks, challenges and opportunities in drug demand reduction, mobilizing parents, youth, andprogram evaluation ― for prevention, treatment, and public health-public safety programs.
The prevention track featured prevention experts from both Mexico and the US on topics such as familystrengthening and community mobilization, while the treatment track consisted of two training sessions― one on opiate treatment, and a shorter training on amphetamine treatment. The track on linkingpublic health and public safety featured presentations on the dually-diagnosed, relapse prevention,recovery, diversion and community corrections, and drug courts.
ORGANIZATION OF THIS BOOK
These Proceedings are organized thematically rather than chronologically. All plenary sessions across thethree days are presented first. Then materials are grouped for each track: prevention, treatment, publicmedia campaigns, and public health-public safety. Each grouping contains speech transcripts, papersprovided by the speaker, or slides presented at the conference. Those materials are followed by the NIDApre-conference session overview. The final components are lists of attendees.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 12 Overview

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 13 Plenary Sessions
PLENARY SESSIONS

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 14 Plenary Sessions
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 15 Plenary Sessions
PLENARY SESSIONSOpening Remarks
Daniel SchecterDeputy Director for DemandReduction (Acting)Office of National Drug ControlPolicyUnited StatesGood Morning. Welcome to the third Bi-NationalU.S.- Mexico Drug Demand ReductionConference.
Many of you will remember two years ago whenwe held the first bi-national conference in ElPaso, Texas. This kind of gathering had neverbeen done before. There were no examples inhistory of twocontiguous nationsconvening theirexperts together tojointly hold aconversation on howto cooperativelyreduce the use ofillegal drugs.Well, thatconference was atremendous success.In fact, those of you who were there wouldremember that on the final day of theconference, on a Friday afternoon, in the finalmoments of the final plenary session, the roomwas packed; nobody had left. I think thatspeaks to the interest and the commitment onboth sides of the border to find commonsolutions to common problems.
A second conference was hosted by Mexico lastyear in Tijuana, again, a highly successfulconference. Now, here we are; a third U.S.-Mexico conference which we hope will be themost successful of all. And it will be followed, Iam sure, by a fourth, a fifth, and a sixth. Thereason I am so confident of this is because ofthe many relationships that have been formed,collegial relationships among experts from bothcountries, working together outside of theseconferences throughout the year in many, many
different settings. You will be hearing aboutthose collaborations over the next two days.
Although this is the official opening of theconference many of us have already beenmeeting for two days. On Tuesday, we had avery successful day-long meeting of bi-nationalresearchers, hosted by the National Institute onDrug Abuse. Yesterday, we held pre-conferencesessions on prevention, treatment and oncommunicating anti-drug messages.
Before we get to our distinguished panel ofspeakers, I would like to call upon a very specialyoung lady to say a few words to us. Her nameis Sofia Magaly Camorlinga; she is twenty yearsold, from the State of Colima, and attends theUniversity of Colima, majoring in PublicAdministration. She was a participant in ourfirst youth forum last year in Tijuana and we arecontinuing that youth forum here. As a result ofthis conversation, Sofia and others in Mexicoformed a national youth coalition organizationfor the prevention of addictions ? yet anothertangible example of the benefits of thiscollaboration.
Sofia Magaly CamorlingaYouth RepresentativeMexicoGood Morning. First of all I would like to thankeveryone for the opportunity provided us, aspart of the youngpeople of theworld, to come toa forum such asthis to expressourselves. I wouldlike to convey amessage that wascollectively draftedby youthorganizations herepresent as well asthose who have been working in theircommunities. I’m going to be reading themessage in order not to omit any details.
We are here speaking the different views of thecoalition of youth organizations for the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 16 Plenary Sessions
prevention of addiction and critical conditionsassociated with it. This is from the organization,the neighborhood, the rock band, the dancegroup, the football team or just the boys andgirls out in the field; in the cities, in the schools,on the corner of the street; those of us whoundertake different actions to prevent the useand dependence on psychoactive drugs andsubstances. This coalition is comprised of youngpeople of different ages, ways of thinking,identities, political affiliations and even withdifferent beliefs, religious beliefs and sexualpreferences. We have interests as diverse asthe cultural economic and political conditionsthat we find in Chiapas or Quintana Roo, inMexico City or Morelos, in Tijuana or CiudadJuarez.
In spite of our differences, which we assumewith joy in order to enrich each other, we havebeen working together, so that in our own smallway we might transcend our local livingconditions. We are a hundred and twenty youthorganizations working throughout almost all ofthe states of Mexico. We are most willing totake action and we have the desire to achievemuch in our coalition.
Today our youth, both in the United States andMexico, are here to talk about our concerns andproposals for continuing the work. We want toshare this with government agencies and non-government organizations that are alsoconcerned about the conditions of youth in orderto jointly build public policies that will take intoaccount our contributions.
We know that the phenomenon of production,trafficking, distribution and consumption ofdrugs is increasingly complex and growing inboth countries. This is related to poverty,violence, insecurity, delinquency and socialexclusion. It is not merely a legal issue or anational security issue. The consequences ofdrug use concerns youth, the family, the priest,teachers, police, community leaders andofficials. With their support we strive to put inplace the promotion of prevention programs thataddress these issues and the critical relatedconsequences. We feel that is very important topromote the distinct efforts and models thattake place at the local level in youthorganizations that are based on the prevailing
local conditions. We know that this can takeplace at different levels, but we hope thatefforts will be undertaken jointly so thatgovernments, institutions, youth organizationand young people can go forward together.
We presented our desires at the second bi-national conference in Tijuana and you havebeen working for us and with us. We want youto continue working with us. It is our proposalthat we continue working collectively with theyoung people of both Mexico and the UnitedStates. We want to build this coalition further.What we have done thus far has been hardwork and we have run into certain obstacles, butwe realize that we have progressed to the pointwhere our efforts can transcend any border.
After our participation in the second bi-nationalconference where 50 young people attended inorder to build a coalition, we in Mexico decidedto invite other youth organizations so that theycould join our fight. We met at a national campthat was held in the State of Morelos, and wealso had two regional meetings, one in CiudadJuarez, Chihuahua and the other in TuxtlaGutierrez, Chiapas. In December we held ourfirst national meeting in Mexico City with 120organizations participating.
There we decided on an action plan for thisyear. A communication structure was alsocreated so that we could all keep in touch withthe work that each organization is doing. Itwould take a very long time for me to tell youwhat every organization has done, but on thesecond floor of this hotel, we have a display thatshows the work being done by eachorganization.
We youth agree that the drug demand reductionwork requires political, social and economicsupport in order to reduce drug use. And wemust not forget the commitment of the last bi-national conference to create a fund that willsupport the projects of youth organizations.
For a long time young people have beenconsidered as passive role players in thephenomenon of drug use and abuse. And nowwe enthusiastically see that the governments ofboth of our countries, Mexico and the UnitedStates, are again demonstrating that they’re

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 17 Plenary Sessions
quite open to us by inviting us and supportingour participation in this event.
Together with the experts and those responsiblefor programs, we are capable of collaborating inthis program as well as many others that impactour young people. The message ofirresponsibility or lack of social awareness thathas for many years been the weight upon theshoulders of our youth, is now being reversedthrough the dynamics and creativity of ouryoung people.
Together with government organizations, socialorganizations, as well as with the help ofresearchers and others, we wish to no longer bepart of the problem. We want to become anessential component for its solution. We knowthat our contribution will add up and that thisthird bi-national conference will end withcommitments and agreements that theassociations will undertake and live up to.
We invite you to join forces with us and tocommit to working together with us so that wecan reduce the demand for drugs in ourcountries. Thank you.
Barry R. McCaffreyDirectorOffice of National Drug ControlPolicyExecutive Office of the PresidentUnited States
Thank you for thatintroduction. Youknow, each yearthere’s one part ofthe introduction thatbecomes more andmore important forme to hear— theyoungest four-starGeneral. I cling toit, and I thank youDan for includingthat. Let me, if Imay, very briefly make some remarks.
To begin, I want to tell you our corporate senseof pride, satisfaction and optimism for the futureto see all of you here. The most senior,engaged, and experienced officials in both ofthese huge democracies are here, charged withthe important responsibility of the reduction ofdrug abuse in our societies. We have enormousexpectations that what we are doing here ismore of a process than a snapshot in time. Wehave committed ourselves to partnership on thisvery essential issue of reduction in drugconsumption.
I really thank all of you for the gift of your mostprecious personal asset, your time, to come herefrom all over these two great nations. Let mealso thank the Mexican delegation leadership.Quite specifically, we’ve become not onlypartners, but also friends. We had a breakfastamong thirty of us this morning; it’s an unusualrelationship. We have some very strongpartnerships in the international community, butI would suggest that there is almost nothing likethe growing sense of very continuous contactbetween our two governments at the mostsenior levels.
I thank Attorney General Jorge Madrazo for hisown leadership, for his integrity, for his couragein facing one of the most violent, corruptinginternational criminal threats history has everseen. It’s unfortunate Mariano Herrán could notbe here, but he has his representatives here.We thank them for their commitment toresponding to President Zedillo’s instructions tosee this as a most significant threat facingMexico.
We also welcome the Minister of Health ofMexico, José Antonio González Fernández; wethank him for the tremendous experience hebrings to this public policy position. He is agreat partner in the last months of ouradministrations.
Haydée Rosovsky, who as you know, is the headof CONADIC, and Dr. Roberto Tapia Conyer—we thank them for their continuing support.The heavy lifting of this relationship is reallydone by those two in many ways.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 18 Plenary Sessions
And congratulations to Jesús Cabrera Solís, theDirector of the Juvenile Integration Institute, ontheir 30th anniversary for all they do.
And to the many other Mexican partners wehave come to know, we thank you for the abilityto work with you for three days here in Phoenix.
In the U.S. delegation, there are too many hereto identify specifically, but, Ambassador JeffDavidow, our U.S. Ambassador to Mexico, thankyou for your presence here, underscoring that inthe world of diplomacy we understand that the21st Century has very different concerns thanthe 19th Century. And so his own involvementand indeed that of Secretary Madeline Albrighthas been crucial to try and build a new sense ofmultinational partnership.
The most important person in our governmentin the drug issue is Dr. Nelba Chavez. She’shere, fortunately, with both Dr. Westley Clark,who is in charge of our Center for SubstanceAbuse Treatment, as well as Dr. Ruth Sanchez-Way, who monitors our Substance AbusePrevention programs, and I thank the two ofthem. They’re making spectacular progress inour own internal domestic challenges.John Wilson, the Acting Director of the Office ofJuvenile Justice and Delinquency Prevention inthe Department of Justice, is here. You shouldmake sure you get to know him. They’ve beena very important part in our U.S. effort ofbringing together these two worlds of thecriminal justice system and the chronic offender,without which, there can be no progress indealing with the chronic addict, so we thank himfor being here.
There are many other people. Mr. Dan Schecteris my principal permanent civilian official incharge of Demand Reduction. We thank him forhis leadership. He will be here in the next threeU.S.-Mexico Demand Reduction conferences.
I notice we have Art Dean, right over here,retired general officer, one of the reasons helooks so good. We thank you, Art, for yourleadership with Community Anti-Drug Coalitionsof America (CADCA). He started with 4,000community anti-drug coalitions around America;we’re now up to 5,000.
We’re also working on funding some newinnovative approaches, and both Henry Lozanoand Mary Ann Solberg are here from ourAdvisory Commission on Drug-FreeCommunities. I thank you for your leadership.They’re really involved in helping us establishwhat have been to date more than 200 newfunded community coalitions. They’ve hadmodest amounts of money, a hundred thousanddollars or less, to let communities begin to pulltogether the leadership that counts in thiscountry.
We often say that our nation doesn’t have anational drug problem; it has a series ofcommunity drug epidemics. So you can’tpossibly hope to confront these issues unlessdata is collected locally. Organizations are local— parents coalitions, the health community, theeducators, the local law enforcement — that’sreally what CADCA is doing, as well as thethousands of anti-drug coalitions.
I hope Sunna Rasch is here. Last night it was agreat treat and a privilege for many of us to seeThe Periwinkle Theatre production “HalfwayThere.” This group of young people puts onwhat is probably the best acted and the mostcreative anti-drug play that I’ve seen. They aretrying to communicate with young people thenotion of the terrible destructive potential ofdrug abuse in their lives. We thank them fortheir involvement.
Let me also, if I may, pay note to two lettersthat we are very proud to have. The first isfrom my own President Bill Clinton. He hasprovided his greetings to this assembly andtakes note of the enormous personalcooperation between these two Presidents overthe last five-plus years. You know, I am a non-political officer of government by law and Ihelped change the law to make it that way. But,I personally have to articulate my own gratitudeand respect for these two Presidents to stepbeyond domestic politics and to keep us on trackworking this common solution. We thank bothof them.
We also have a letter from the United NationsDrug Control Program Secretary, Mr. PinoArlacchi. I hope all of you know about his workand of him personally. They’re based in Vienna,

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 19 Plenary Sessions
of course, and just last week I was very proudto lead a delegation to New York, to the UnitedNations, and to spend some time, first with ourSecretary General Kofi Annan and also with PinoArlacchi. We talked about how we will continueto stress multi-national cooperation.
Now, at every one of these conferences, onething I can always count on is Mexican civility.And so, with your permission let me read a fewwords in Spanish. Creo que es importante subrayarel éxito que se está logrando con la estrategianacional para el control de drogas en los EstadosUnidos. En los últimos 20 años, por ejemplo, elconsumo general en los Estados Unidos representauna reducción del 50 por ciento, mientras que elconsumo de cocaína representa una reducción del 70por ciento. En los últimos dos años nuestros jovenesnorte-americanos han empezado a rechazar lasdrogas. Hemos lanzado una campaña de prevenciónhistorica. No se puede dudar nuestra determinaciónpara reducir la demanda. It’s a miracle what threeyears of West Point Spanish thirty years ago canproduce.
With your permission, a few continuingcomments in English. Some of them perhapsunderscore the general idea that the older I get,the more that I believe the most importantthings in life are obvious and need to be stated.One of those is that the U.S. and Mexico haveno option but to cooperate. We are sitting inthe same lifeboat. There is almost no frontierbetween these two nations. 350 million peoplea year cross that two thousand mile border. Inmost places, the border is barely marked. Thisis not North Korea next to another nation.These two nations have huge common cultural,economic, and political interests. We also havea history of ignorance and animosity toward oneanother on an official level, but not on apersonal level. Because when you look at theimpact of these two societies on one another infood, in art, in music, in religion, in cooperation,there has always been a tremendous sense ofpeople-to-people cooperation and warmth over200-plus years. But now, fortunately, whatwe’ve begun to do is to understand that onlythrough the success of the three of us, Canada,the United States and Mexico, will ourgrandchildren’s futures be preserved.
And so, I would just underscore, it would besimply remiss for officials in these two nations to
not also recognize that an issue of suchtremendous consequence to our societies suchas drug abuse also deserves to have a responsewhich is crafted in respectful, cooperativepartnership. That’s why we’re here. Becausewe are serving our own self interests byextending a hand of dialogue, friendship, andpartnership across that border. I think it’s aneasy message to make, given the fact that oursenior leadership, the Presidents and their seniorofficials, have publicly continued to say that.
Now the second observation is that bi-nationaldrug cooperation is really key to either societyhoping to confront the issue. I do not believe itis possible for the United States standing alone,nor Bolivia, nor Thailand, nor other nationswhich are fundamentally threatened by thisissue, to confront the problem withoutmechanisms of cooperation. This extends evento the most obvious and arguably bestorchestrated part of international cooperationwhich is law enforcement. The law enforcementpeople do pretty well, almost naturally. Our twoAttorneys General, thank God, have telephonesthat go to each other’s direct linecommunications. So, in accordance with theirown laws, the police, the intelligence, there is acontinuing dialogue. How could we addressdrugs without money laundering, precursorchemical control, guns going from the UnitedStates into Mexico, the kind of system problemsof crime that we address? It’s a requirement,we would argue, to have a sense of cooperation.Clearly, that cooperation also extends into the21st century. The most important aspect, Iwould argue, the most important institutions,are the legislative bodies. How can wecooperate on money laundering issues if therearen’t 21st century laws that allow multiplesystems in the hemisphere to share evidence, todo extradition, to have wire-tapping authority,where a Mexican wire tap can be used in a SanDiego trial and vice versa? So I would justargue again, that any of us who hope tosuccessfully confront the issue have tounderstand that we no longer live in a world ofnational concerns; we’re in a global community.
The third point I would underscore is thedynamic nature of drug abuse. We talked ofthis at breakfast. Ambassador Davidow askedthe question, “Now wait a minute, I understand

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 20 Plenary Sessions
the past, I hear your programs. What is thefuture? Where is this drug problem moving?”Many of us are still holding old stereotypes ofthe problem, both in the national communityand the international community. There’s adanger that we will continue to work on pastproblems. This is a dynamic situation. It hastaken me years to get U.S. officials to stopsaying in their public speeches that the UnitedStates consumes half the drugs in the world.It’s a curious kind of statement. It’s not onlycompletely wrong, but it produces an impact inwhich policy won’t address the problems that weface.
Drug data is the worst aspect of this issue; it’stoo soft. If we were dealing with internationaleconomic questions, if we’re dealing withhighway construction problems, you never argueabout facts. You find out what the facts are,you argue about conclusions.
But in the drug issue we have difficulty withdata; addressing this is another aspect of ourcooperation. I think that’s very encouraging thatMexico and Argentina and other nations are nowgetting in front of the problem in collecting data.I would clearly suggest, straight out, that whenI talk to the international community I say theUnited States has a huge drug consumptionproblem, around 6% of the population in thepast month used drugs. In 1979, it was 14% ofthe population; in 2007, it will be below 3% ofthe population. It’ll be the lowest recorded inmodern American history. That’s where we’regoing.
Meanwhile, Mexico is fortunate to be in asituation where the culture, the family, theCatholicism all combined to make your nationresistant to adolescent drug use. But times arechanging. All of us are being immersed in thesame modern communications and change infamily values, change in how women relate tothe work force. We are converging in manyways, which is largely good.
And the worldwide plague, the nature of thedrug threat is changing. It’s not just heroin; theworld is submerged in heroin. The increase inproduction in the last ten years is unbelievable.In Afghanistan, now the number one producerof heroin on the face of the earth, it’s the only
aspect of that society that works. In Myanmar,we have huge rates of production of heroin.And then we come to Mexico. Fortunately, ithas reduced heroin production. Thanks to theMexican armed forces’ courage, integrity anddedication, it has gone down by 25%. And yetthe United States, we believe, consumes 3% ofthe world’s heroin, so almost the entireconsumption in the U.S. can come fromColombia and Mexico. It’s a global problem.What we really fear and what many of us arelooking at is that ten years from now—when mydaughter who is an intensive care unit nurse ishere as the U.S. Drug Policy Director— she willnot be talking about cocaine as the number oneaddiction problem. But instead she will talkabout methamphetamines, MDMA, ecstasy, andGHB and PCP, chemically manufacturedpsychoactive substances.
We need to understand this is a global problem.Mexico has a tremendous opportunity to ensurethat what happened to the United States in the1970’s will not occur in Mexico. Demandreduction must be central to our partnership.It’s great fun to work with Secretary RosarioGreen, Minister Cervantes, and Attorney GeneralMadrazo. We all have vital national federalresponsibilities and we’ll do them. But at the endof the day, the people who count are those whowork with youth, and those who deal with thetreatment of the chronically addicted. In manycases, these are either private non-profitorganizations, or they deal with organizationsthat don’t necessarily have governmentalstanding. We need to find ways for thesegroups to talk to each other, in particular alongthat border region. I think that is, of course, thecentral purpose of what we are doing here inthe next two plus days.
Finally, let me point to the future. You knownone of us are quite sure how the two politicalprocesses will work out in these twodemocracies. But clearly, by next year at thistime, we’ll have two very new political sets ofleaders in place, and what we are making a verystrong argument for is that regardless who hasthe honor of temporarily serving as officials inthese two democratic governments, they mustcontinue cooperation on the drug issue. Andwe’re going to make that argument verystrongly. We think we have heavily imbued in

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 21 Plenary Sessions
the permanent bureaucracy a commitment toscientific, medical educational cooperation indrug treatment communities in the comingyears. I hope that’s the case. I believe,probably in August, you’ll see us have anothermeeting of our High Level Contact Group, andby then the Mexican election will be over, andthe U.S. system will be in the final weeks of ourelection. It’ll be a good statement, I wouldhope, that on both sides of the border we seethe problems as continuing and the requirementto cooperate as continuing.
Again, if you will, let me just share the sense ofpride all of us at the head table, the ministers ofgovernment from both nations, feel in beingprivileged to provide a forum in which theserious professionals in this room can buildconcrete cooperation.
Thank you for who you are, and what you standfor, and God bless you in your work. Thankyou.
Jeffrey DavidowUnited States Ambassador toMexico
Good Morning. Last week I was in Washington,at the meeting of the Bi-National commission ofthe United States and Mexico. And at thatmeeting, 16 sub-commissions, led by membersof the cabinets ofboth countries,dealt with problemsrelating to healthand education inthe whole range oftopics that uniteand sometimesdivide our twocountries. Whatbecame apparent tome at that meeting,and I think we willsee again at the meeting that will be takingplace just one week from today in Washingtonbetween President Zedillo and Clinton, is thatthere are various components that have to be inplace to deal with problems. They are, it seems
to me, procedures, systems mechanisms andpeople with dedication and vision.The fact that this is the third meeting of thisgroup is immensely important. It means that itis now a tradition and it will continue. It willcontinue because it’s a good idea and it’sproductive. And the people who will be runningthe government of Mexico next year and thepeople who will be running the government ofthe United States next year will understand that.It will recognize that this mechanism mustcontinue to give you, the experts, the dedicatedpeople, the opportunity to come together atleast once a year and hopefully more to dealwith this important problem.
But mechanisms, procedures, systems don’tmean anything without dedicated people. Youknow, President Kennedy had a favorite story,which I’m going to repeat to you because it’sone of my favorite stories. It’s about a very oldman, even older than me, a man in his 90’s ?very wealthy, with a great estate. And one dayhe called his gardener, and he said to hisgardener, “Tomorrow, I want you to go to town,to the little pueblo, to the garden place, thenursery and buy some seedlings ? seedlings ofoak trees. And I want you to plant them overthere.”
And of course the gardener said, “Of course sir,I will. I will do that. I will go and buy theseedlings, but let me ask you a question. Theseoak trees will take 20 or 30 or 40 years to grow,and uh, with all due respect, I don’t think you’llbe here to see them, because you’re already 90years old. “
And the old man thought for a minute and hesaid, “ you’re absolutely right. I don’t want youto go to town tomorrow to buy those little oaktrees. I want you to go this afternoon.”
And this is what I mean about people. Becausewhat is necessary and what that old man had, isdedication and vision. So governments can helpput together the mechanisms, mechanisms suchas this meeting. But without the dedication andvision of you people, the mechanisms meannothing.
And I am very honored to have been invited tocome and meet you. I am very honored and

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 22 Plenary Sessions
very encouraged to see the work that you’redoing, and I wish you every success.
Thank you.
Nelba Chavez, Ph.D.Administrator, Substance Abuseand Mental Health ServicesAdministrationU.S. Department of Health andHuman Services
Thank you for that gracious introduction. Onceagain, I am honored to be here.
And once again, Ibring greetings fromDonna Shalala,Secretary of the U.S.Department ofHealth and HumanServices, whosesupport for programsto address drugabuse has beenunwavering duringher service to the Nation.
President John F. Kennedy said, “when peoplecome together for a common cause, good thingsstart to happen.” Well, since our countries cametogether to develop and implement the U.S.-Mexico Binational Drug Strategy, we have beenable to speak about drug demand reduction as acommon cause.
Over the past years together, we’ve translatedthe theory and reality of drug abuse into alanguage we all understand. It’s the languageof family and home, the language of law andsafe community, the language of forthrightnational leadership.
And that shared language has allowed us tocreate new knowledge, goals, and strategies toaddress drug abuse within our countries andacross our borders.
Our shared language has been heard and readin our agreements to work together, ourtenacity to get over the ticking spots of
disagreement and dissent, and our sharedcommitment to do what is right for the people ofboth the Unites States and Mexico.
And as a result, those “good things” thatPresident Kennedy spoke about, indeed, havestarted to happen.
We have moved from words to action. Thewords contained in Alliance Point 1, to “reducedemand through information, education andrehabilitation” have been actualized in acomprehensive set of performance measures ofeffectiveness for demand reduction – PMEs.
The PMEs capture successes in research, publiceducation and the advance of effectiveprevention and treatment programs. And fromthe framework of the PMEs have comerecommendations - recommendations that arethe very soul of our work together – thecollective wisdom of our insights, ideas andmutual respect.
Those recommendations affirm, above all, thatsubstance abuse demand is a public healthproblem – a problem not dissimilar from insect-borne diseases or natural disasters such asearthquakes and floods. After all, when adisaster strikes, nations come together in sharedpurpose – to be of aid to suffering people,suffering nations.
So, too, it is with substance abuse demand. We– the United States and Mexico – come togetherto be of aid to suffering people – from childrento elders – caught in the web of substanceabuse.
More concretely, those recommendations spaneverything from research cooperation andtechnical information exchange to communityparticipation, from public information andawareness to workplaces and education. Andthat’s the public health model in action; that’sthe Bi-lateral Commission in action.
Now it is time to move these recommendationsinto our communities, as we promote anunderlying base of self-worth, safety, andeconomic security for all.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 23 Plenary Sessions
We know the message must be unified; weknow the message must be ongoing; we knowthe message must come from schoolroom andpulpit, from the circle of family to thecamaraderie of the workplace.
To take that step ? as other steps we havetaken together ? we need sharedunderstandings, harmonized data, andawareness of what works for people at homewhere they live.
And today we’re sharing just that knowledge.What you have found works; what we havefound works - in treatment, in prevention; inschools, in the workplace, in communities; foradults, for youth; and across the health, andjustice, and safety systems.
When we close this meeting, we’ll all have morethan take-away messages. We’ll take-awayknowledge that we can apply at home.
We will have the measuring sticks to tell if we’redoing a good job of it. And we will have theopportunity for continued collaborations ? atthe level of nations and at the level of programs.
I’m reminded of a story from Eastern Europebefore the turn of the last century. Right afteryoung couples married in the village church, theold women of the village would hustle them outof the town and into a forest.
There, the couple was handed a bocksaw –that’s the kind log cutters use, with two handlesand a blade in-between. The old womenpointed to a good-sized tree and demanded thatthe new couple cut it down.
So, the couple is struggling to cut down thedesignated tree in the woods and they’resurrounded by a group of village elders.
When the tree finally falls, the old women gointo a huddle. Based on what they have seen,they will make a prediction on how long thismarriage will likely last.
How do they make their judgment? Not onwhether the couple exchanged loving looks andhugs and kisses. No. Rather, based on howwell they worked together at a common task.
And what does this tale tell us? What does itsuggest for our future together? Well, fromwhat I’ve seen, we’ve met the test.
And, as I mentioned earlier, it’s been said thatgood things start to happen when people cometogether in a common cause.
But, we’ve got to admit, these are challengingtimes. At the start of this new century, it’s atime of transition in so very many ways.
Someone once said that the best way to predictthe future is to create it. And with thisconference, most certainly we’re sharing thetools to help create a safer, drug-freeenvironment for the people of both Mexico andthe United States.
Thank you.
Jorge Madrazo CuellarAttorney GeneralMexico
Very distinguished Secretary of Health, JoseAntonio Gonzalez Fernandez; my dear friendGeneral McCaffrey; dear friends from the UnitedStates and Mexico.
I would like to thankfor the invitation toparticipate in thisThird Bi-NationalConference onDemand Reduction,whose main topic isthe strengthening ofthe bi-nationalrelationship in thefight against drugsin the new century.
The relationship between the United States andMexico on the subject of drugs is one of themost ample and varied in the world. The firstattempt made by our countries to develop ajoint outlook regarding the issue began in May1997 with the presentation by Presidents Zedilloand Clinton of the report entitled "U.S.-Mexico

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 24 Plenary Sessions
Bi-National Drug Threat Assessment", a jointstudy and diagnosis which gives acomprehensive outlook on the jointphenomenon of drug abuse, drug trafficking,and related crimes.
The U.S.-Mexico Bi-National Drug ThreatAssessment comprises an acknowledgement ofthe challenge posed by drugs for the majority ofmodern people and societies, independently ofwhat their level of development might be andhow this issue has been recognized in mostinternational forums, such as the United Nationsand the Organization of American States. Theassessment established that the fight againstdrugs has to be approached from acomprehensive standpoint. In other words,measures to control drug supply will only bearfruit if we simultaneously set up the necessarymeasures that will control demand. Itestablished the commitment made by bothcountries in order to comprehensively fightagainst the problem of drugs and posited thatmeasures to control drug supply will onlysucceed if we simultaneously set up thenecessary measures to control the demand ofdrugs.
In view of the commitment made by bothcountries to comprehensively combat theproblems of drugs, May 1997, Presidents Zedilloand Clinton signed the Declaration ofMexico/United States Alliance Against Drugs,agreeing to establish a bi-national drug strategyfor cooperation. The bi-national drug strategysigned in February 1998 to complement thenational strategies of both countries hascontributed to direct our efforts towards thereduction of illicit drug demand. Thestrengthening of our cooperation in the differentareas affected by the drug phenomenon hasreached the highest priority in the agenda ofboth countries. Bilateral efforts towards demandreduction are evident. This conferenceprecisely, is an example and reflection of theway in which international cooperation withregards to this subject must operate.
Because of all of this and with the holding of thisthird bilateral conference, our two countriesreiterate their commitment to continuestrengthening their collaboration and
cooperation in the fight against drug abuse inboth countries, especially today when the newcentury is beginning. As the internationalcommunity acknowledged during theextraordinary meeting of the United NationsGeneral Assembly, held in order to face theworld problem of drugs, drugs destroy lives aswell as communities and impact all sectors ofsociety. Above all, the abuse of drugs has animpact upon the freedom and development ofyouth that are, undoubtedly, the most valuableasset of humanity.
There is no doubt that the problem of illicit druguse and abuse means a complex challenge forthose of us who are responsible for fightingagainst this scourge. The last National AddictionSurvey that was done in 1998 has allowed theMexican government to analyze what the trendsof consumption have been, as compared withsimilar studies that were done in 1988 and1993. Drug use rates in Mexico are still ratherlow when compared to those of other countries.Nevertheless, there have been increases in usetrends that are cause for concern, particularly inurban centers and the northern region of ourcountry. Marijuana continues to be one of themain drugs used by different population groups.Inhalable solvents tend to be reduced, but theconsumption of cocaine, which is a drug thattraditionally had been used by reducedpopulation groups, has now become popularamong the young people and lower incomegroups. The use of heroin, although low at thenational level, has also gone up in the northerncities of Mexico. Methamphetamine use is notyet a problem that affects a large sector of ourpopulation; however, among some youngpeople its use is now a reason for concern.
As I pointed out in the Meeting of HemisphereLeaders on Drug Policy that was held inWashington, from November 3 to 5, 1999, sinceillicit drugs are one of our most sensitivechallenges, policies at the national level,regional level, and global level must be basedupon humanist principles that will inspire us toface the challenge. In this regard, a humanistpolicy concerning illicit drug use is nothing elsebut the expression of a general state policy thathas its foundation on a social consensus directedtowards that specific challenge. A humanistpolicy against this phenomenon must have as its

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 25 Plenary Sessions
base, the conviction of there having to be a pactbetween government and society, acollaboration among the different levels ofgovernment and population, a pact expressedthrough concrete actions within the family, inthe school, through the media, and in ournational as well as international society.
Therefore, the Mexican government has decidedto enter into a social pact that will destroyideological type barriers and allow us to makeprogress in the fight against drug abuse. In thisregard, the General Attorney's Office hasundertaken enormous efforts to create anetwork with the different civilian organizationsand agencies. We have also set up coordinatingmechanisms with the different agencies of thefederal and local governments, such as theMinistry of Health, the Ministry of PublicEducation, and the General Attorney's Office ofMexico City.
Among the most relevant activities within thisframework of collaboration has been thepresentation of talks regarding crime preventionand drug use and abuse, addressed to thosepopulation groups considered to be at high risk.That is, talks addressed to our young peopleand children. We also have tried to see to itthat parents, teachers, social workers, lawenforcement and public security officials, etc,assume the commitment of communicatingpreventive messages in their homes, school,work centers and communities with the purposeof presenting a common front against addictionsand crime.
Since a humanist policy must be based upon theacknowledgment and defense of human dignity,we have proposed to care for drug users andnot to treat them as delinquents. Because ofthis, together with the Ministry of Health and theGeneral Attorney's Office of Mexico City, wehave set up a Unit for Assistance for Drug Users.The objective of this unit is to channel thoseindividuals with addiction problems who havebeen detained and put before the Federal PublicProsecutor, towards rehabilitation and treatmentcenters.
Our efforts must also have a policy basis formass media to convey to the population theconsequences of illicit drugs. In this regard, our
Institution has had the support of outstandingpersonalities in the world of arts, sports and alsoof the very diverse media that have their ownmessages and policies to communicate to largenumbers of our population.
Ladies and gentlemen, drug use and abuse is aproblem that presents us with severe challengesat the beginning of this century. We cannotconsider the possibility of doing away with thesupply of drugs if we do not do away with thedemand. It is among the children and youngpeople that we must gear our efforts. Wecannot allow for their future to beovershadowed by the possibility of theirbecoming dependent upon drugs. We cannothope to have a better stage of development forour people if we allow for the cancer of drugaddiction and violence that goes hand in handwith it, to contaminate our youth and ourchildren. We must share our experiences onceagain. We must keep these forums open as oneof the main paths for us to exchange ideas,projects, and programs regarding how toprevent the use of drugs, as well as thetreatment for drug users in order to protect thehuman dignity and health of our youth.
I would like to comment that one of the greatestsatisfactions I have had in this joint fight thatwe have taken up between Mexico and UnitedStates has been the friendship and affection ofGeneral McCaffrey. The Mexican delegation hasbeen able to share and learn so much from thisvaluable citizen of the United States, thisextraordinary fighter against drugs, who hasparticipated perhaps, in one of the greatest warsthat humanity has ever fought towards the endof last century and the beginning of this century.General McCaffrey, I would like to say that as apublic servant of the Mexican government andas an individual, it has been a great honor andan enormous privilege to have worked with you.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 26 Plenary Sessions
José Antonio GonzálezFernándezSecretary of HealthMexico
It's almost afternoon, so I think that I must say,"Good afternoon."After these veryweightycontributions, so fullof content, sopurposeful andconcise, I would liketo say that whenyou have to speakafter so many otherswho are sointelligent, you areat a disadvantage,but maybe also at an advantage. The maindisadvantage is that everything has been said,and it has been said very well. One runs intothe problem of what to say in order not torepeat concepts, to not overtire people. Themain advantage on the other hand is if one isvery brief, people will say he was the one whospoke the best. I don't intend for you to saythat I was the one that spoke the best, but I dohope to be the briefest because everything hasbeen said.
Thank you very much on behalf of the Mexicangovernment and President Zedillo, who sent youa most cordial greeting through me. I would liketo show President Clinton our gratitude for hisletter, his comments, and his solidarity with thismeeting. I want to thank also the hostauthorities, headed by General McCaffrey,Donna Shalala, Nelba, Daniel, Jeffrey, all of you.I thank you for having welcomed us to this thirdconference.
With respect to what General McCaffrey saidabout how times change, it is a pleasure for meto see how in fact times have changed ? attimes for the better, but unfortunately in certainthings, for the worst. I had the privilege ofworking in this great country as part of theMexican government some years ago. In 1987 Icame here entrusted by the Attorney General toopen a new office in our embassy in the United
States. I was to open what has become areality today, not only in the United States, butalso around other parts of the world. It's aliaison office between the Attorney General ofMexico and our own embassy in each of thecountries in which we have an embassyincluding the United States, to analyze the issueof drug trafficking and drugs. I had theprivilege of not only working in this greatcountry as a representative of my owngovernment, but in working with an equallycommitted and honorable person, a strict fighteras is Attorney General Jorge Madrazo today,who at that time was our Attorney GeneralSergio Ramirez, a great man that we all loveand acknowledge.
In 1987 there was a great deal of talk aboutdrug traffic. In 1987 there was an exchange ofmany different adjectives between our twocountries. We sort of blamed each other. Wesaid we produce because you consume; if youdidn't consume, we wouldn't produce but todayI find it very encouraging that these types ofcomments are not being put before the table.Times have changed and we all understand thatonly together can we hope to fight these typesof problems. It is a pleasure for me to realizethat not only do we stress, as we did then, theproblem of drug traffic, but that today throughthe political will of our two Presidents, PresidentClinton and President Zedillo, it has beenpossible to hold special meetings intended toreduce demand in our two countries. It's reallya source of pleasure that times have changed inthat direction. It is also excellent that thepractices in both countries have changed ? notonly towards joining our efforts in fighting drugtraffic and reducing drug demand. But it isexcellent that today we can talk about thissubject in an organized way, that coordinatesefforts at an institutional level. For this I thankthe great efforts and tenacity of public officialsin our two governments and I am very gratefulto General McCaffrey, Nelba, Daniel and toJeffrey for what they have said. And with all ofthe role players at various levels present at thismeeting, we have not only those that canimplement government policies. We also havethose who, because of their personal conviction,because of their political vocation, because oftheir social concern, because of their love forthe families in our two countries, have engaged

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 27 Plenary Sessions
in this daily fight in an unpretentious manner.They have done this for the benefit of ourcountries, the families, and the people of ourtwo countries in order to avoid further drug use.
Fourteen years ago when I worked in the UnitedStates, I never would have imagined that in ameeting like this we would have youngsterspresent. It is a pleasure to know that a girlfrom my country, such as Sofia, has come hereto speak. She speaks not because she hasmade use of drugs, not because she is a part ofa rehabilitation program, but because she is sosold on the value of our youth: the youngpeople of Mexico and other young people whowish to put forth their efforts on both sides ofour border in order to avoid the use of drugsamong them. And it is also wonderful thatthroughout these years we have been able towitness how people of non-governmentorganizations, from families, and from privateenterprise have formed groups at the regional,state, or local level. And people from differentlevels of society, no matter what their economicincome or condition might be, have all comehere to try to find new methods to bettercoordinate improved and newer strategies sothat those strategies, actions and shared pointsof view can bear better fruits. This is the goodnews of the time that has elapsed.
The bad news is also there. One item is thatafter so many years of dealing with the subject,in our own country as well as in the UnitedStates, it's a pity that an increase in drug usehas taken place in my country in these last fewyears. Certainly, as Attorney General Madrazohas said, we don't have usage levels as high asprevailing levels in other countries, but in 1987we practically had no use of drugs in Mexico.Back then, the Attorney General at the timeinsisted that we had to clearly understand thatthe drug traffic and drug use phenomenonwould lead to a situation where in the future wewould all be consumers and producers.
General McCaffrey has been so kind in hiscomments and in conversations with him, andI'm very grateful to him. This morning at thebreakfast sponsored by the Border HealthFoundation whose members we had thepleasure of meeting, we were saying that todaythe United States is a great producer of drugs;
back then it was not. And the good news is thatin the United States they have reduced drugconsumption and use. It's excellent that theyhave been able to invest more in new and betterprograms, all of this the result of the efforts,tenaciousness, imagination, greater resources,and of course people at the governmental leveland at the level of society who are greatlycommitted. I am referring here especially to theSecretary of Health, President Clinton, Nelba,and General McCaffrey. All their efforts havehelped to truly reduce drug abuse, which hasbeen so high.
But in Mexico, as the Attorney General said inthe figures and numbers that he has given us,drug use has been on the rise in recent years.The trend is a rising one, not a downward one.That is the bad news resulting from these lastfew years. If we don't undertake all theseefforts to clearly understand the phenomenontaking place in Mexico and to clearly understandthe situation along the border and that of theUnited States; if we don't take advantage of thispotential and resources which are so unique(and our dear friend Jeffrey Davidow said thisvery clearly); if we do not take advantage of thisexcellent relationship, this great joint effortbeing undertaken by these two magnificentcountries and people, I really don't see clearlyhow we might achieve successful results andoutcomes.
I am altogether convinced that with the will andwith the effort that we have witnessed here, wewill truly be able to do things that will haveresults. For the United States these efforts areresulting in reduced consumption and use. Alsoin Mexico, the use will drop, and in the years tocome we will make this social scourge only amemory.
Another piece of bad news I am sorry toacknowledge is something I didn't know beforetoday ? that when we have meetings such asthis we come to agreements and commitmentsand sometimes our side doesn't live up to them.It's a pity that Sofia has said that last year itwas agreed that we would work with them, withour youth, and that we would have to create afund to help our youth with the communitywork. I offer that this month of June, you willhave that fund and that we will be working with

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 28 Plenary Sessions
youth. As to the future, if we are convinced, ifwe have the will, then the future winds blowingwill be most favorable. We certainly have sixmonths to work jointly under this administrationheaded by President Zedillo and which has doneso much in favor of health in Mexico. We haveonly a few months left of witnessing what thisgovernment does, where such distinguishedUnited States citizens have worked such asNelba, General McCaffrey, Daniel and manyothers. But what really matters is that thisconviction prevails in our people and in ourgovernment so that we can continue movingahead at the highest level possible. It'simportant that we share information and that wework together.
I am most pleased then to be able to announcethat President Zedillo together with the AttorneyGeneral, who has done such excellent work inhis position, will announce an extensive programand strategy, not only to fight drug traffic butalso in developing programs to reduce thedemand for drugs. And I'm very pleased thatJorge Madrazo and I are here together today.In any case, the President of Mexico willannounce a program through an officialstandard that will compile the differentstandpoints and views in a way similar to thattaken up in the United States. President Zedillowill announce a creation of a higher level officeentrusted with fighting drugs. I think truly theremust be a commitment to assign greaterresources, not greater bureaucracy, a greateramount of will and greater resources so thatpractices will be taken up that will truly convinceand encourage our society, so that whatever thegovernment does will truly permeate thedifferent levels of our community.
The United States has already done this. Theyhave created this special office. GeneralMcCaffrey has presided over it, and we hope todo the same in order to have greaterpossibilities in our fight against the traffic andthe reduction of demand. So Mexico will alsohave a high commissioner that will doeverything possible to reduce drug demand inthe forthcoming months. This is the reason Ishare Jorge's vision. Together we can do agreat deal in these few months and together wewill be able to do much more in coming years.
Finally, I would like to say, that on behalf of theMexican delegation where we have youngpeople, men and women, working daily invarious organizations to reduce drug demand;the director of Social Security Institute MariaLuis Fuentes; Attorney General Jose Madrazo,myself and many other people with us fromMexico, that it's a privilege for us today to leavea testimonial. We would like to present toGeneral McCaffrey this parchment to remind himof the acknowledgment expressed by thePresident of Mexico for his great talent andgreat vision in the fight against drug traffic andreduction of drug demand in the United States.Thank you very much.
Challenges andOpportunities in DrugDemand Reduction
John W. Wilson
Acting Administrator,Office of Juvenile Justice andDelinquency PreventionDepartment of JusticeUnited States
I want to thank the planning committee forasking me to speak briefly this morning and toserve as moderator for this plenary session. I’mhonored to be here today on behalf of the U.S.Department of Justice, Attorney General JanetReno, and the Office of Juvenile Justice andDelinquency Prevention. I’m here, along withMark Morgan from our Anti-drug Program Unit,and I’m excited to have the opportunity tointroduce the plenary session on the subject,“Challenges and Opportunities in Drug DemandReduction.” Fortunately, we’ve been hearingsome encouraging news about youth attitudestowards drug use lately. Forty percent of teensin a recent survey responded that they stronglyagree that really cool teens do not use drugs.And along with changes in attitude, we’re seeing

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 29 Plenary Sessions
positive changes in behavior. Youth drug usehas been generally decreasing since the mid-1990’s and in 1999 the level of drug use amongAmerican adolescents held steady from theprevious year. We hope that this is a pause andthat the downward trend will continue into thenew millennium.
Yet, even with these gains in the battle againstyouth substance abuse, many challenges lieahead. For even as youth substance abuse wasdeclining in 1998, more than half of Americanhigh school seniors said they used an illicit drug,at least once. And even more admitted toconsuming alcohol. Moreover, it is estimatedthat 3000 youth, those under the age of 18,started smoking every single day in 1997. Wealso know that youth who have used or solddrugs are more likely to engage in otherdelinquent behaviors. Think about this. Youthwho have used marijuana are much more likelyto have sold marijuana – about four times morelikely, three times more likely to have carried agun, and seven times more likely to have beenin a gang. This all happens at some point duringadolescence. That is why it is so important forus to focus on prevention and early interventionof substance abuse. I’m talking aboutintervention at the first sign of trouble. Time andagain, our experiences and research have shownthat the most effective and successful approachto juvenile crime is prevention, including youthdevelopment programs that target at-risk youth,and early intervention programs for youthengaged in high-risk behaviors including druguse.
Our communities pay a high price when weallow even one youth to leave high school for alife of crime and drug abuse: a bill that isestimated to cost over $1.7 million per lostyouth. Based on decades of research in thefields of criminal and juvenile justice, publichealth and youth development, our office, theOffice of Juvenile Justice and DelinquencyPrevention, has developed a comprehensivesystem-wide approach to delinquencyprevention, early intervention and improvementof the juvenile justice system’s response tojuvenile offenders. Our comprehensive strategyfor serious violent and chronic juvenile offendersis a framework that is built on strengtheningfamilies and communities so that they can better
provide guidance and support for their childrenin developing capable, mature and responsibleyouth.
Another key component of the comprehensivestrategy is multi-disciplinary coordination. Tosucceed, we must have the support of keyleaders and the involvement of a strong networkof community based programs and servicespublic and private ? system and non-system,state and local ? collaborating on prevention,intervention, supervision and the provision ofeffective services. We have committed to suchcollaboration at the Federal level with initiativeslike the Drug Free Communities SupportProgram. Together, OJJDP, the Office ofNational Drug Control Policy, and the SubstanceAbuse and Mental Health ServiceAdministration’s Center for Substance AbusePrevention, with private partners such as CADCAare helping coalitions across this country tobring communities together, we support drugprevention programs by providing funding,resources and tools needed to support at-riskyouth, provide services to drug-involved youth,and make neighborhoods safe and drug free forfamilies. And this program has received strongfinancial support. The U.S. Congressappropriated an additional $30 million in fiscalyear 2000, the program’s third year, to ensurethat no child, family or community is left behindin the prevention of substance abuse. Justwithin the border states of Arizona, California,New Mexico and Texas there are currently 43operational Drug-Free Community supportprograms. And if you don’t have one in yourcommunity, or if you’re a visitor from Mexico, Isuggest that you go and see these programs atwork and work to put a coalition together inyour community.
We know that if we can reduce substance abuseamong our children, we will be laying thefoundation that gives them a better opportunityto become drug free and productive adults. Bycoordinating these efforts across agencies anddisciplines and through collaboration betweenjuvenile justice system officials, schools, lawenforcement, child and family services, andcommunity based organizations, we can succeedin creating a community wide network of carefor our children. We have a special challengeand a unique opportunity to reach out further

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 30 Plenary Sessions
and establish a strong collaborative effortbetween the United States and Mexico. Forminglocal, state, Federal and global partnerships, andusing a system-wide approach, a comprehensivestrategic approach, that incorporates the latestresearch into prevention and treatmentprogramming, we can successfully reducesubstance abuse by reducing drug demand.
I think the global nature of the problem hasbeen illustrated recently by a number of articlesand stories that I’ve read about in papers aboutthe use of the Internet for drug sales. We havechildren now who are going on the Internet andbuying drugs for delivery to their homes. Thinkof the implications of that and the need for all ofus to work together nationally andnternationally to address this issue. One of thethings that we pride ourselves on in our office isproviding information resources. We have at theback table here, a sample of publications fromour office. And they include publications abouthow youth can be a bit more involved inreducing crime and delinquency and drugprevention. We work closely with a nationalyouth network to help youth to become involvedas part of the solution. And I applaud you forhaving the youth representation here at thisconference because that’s critical to our success.These publications deal with issues of gangs,guns and drugs. They’re all inter-relatedproblems. You can’t look at one without lookingat the others. And they cover issues includingresearch, evaluation, programs, effectiveprograms that you can adopt in yourcommunity. How to involve youth, families inthe communities, in comprehensive efforts onhow to involve the juvenile justice system as aplayer in these efforts.
In this plenary, our speakers will present someof the components of system wide services thatspan the continuum of prevention andtreatment. This plenary challenges theopportunities in drug demand reduction. It wasdesigned to stimulate continuing discussion andthought on the roles of prevention, treatmentand multi-sector, multi-strategy collaborativeefforts and what role they can play in achievingdemand reduction on the U.S.-Mexico border. Ithank you for your attention. We have sevenspeakers, so we’re going to be moving veryquickly. Our first speaker is H. Westley Clark. Dr.
Clark is the Director of the Center for SubstanceAbuse Treatment in the Department of Healthand Human Services. He leads the nation’s effortto provide effective and accessible treatment toall Americans with addictive disorders. Dr.Clark’s areas of expertise include substanceabuse treatment, methadone maintenance, painmanagement, dual diagnosis, psycho-pharmacology, anger management, and medicaland legal issues. Ladies and gentlemen, it is mypleasure to introduce Dr. Clark.
H. Westley Clark, M.D., J.D.,M.P.H., CAS, FASAM, DirectorCenter for Substance AbuseTreatmentDepartment of Health and HumanServicesUnites States
Estoy muy contento de estar aqui nuevamentecon ustedes. I am very pleased to join youagain to continue the dialogue between the U.S.and Mexico on Drug Demand Reduction. I havebeen asked to focus my comments on providingeffective treatment.
For the Center for Substance Abuse Treatmentknown as CSAT, effective treatment meansscientifically based, culturally relevant treatmentthat can be replicated in different settings andadjusted for use among various ethnic groups. Iwould also like to note that effective treatmentimproves the lives of individuals and familiesaffected by alcohol and drug abuse and reducesthe health and social costs to our communitiesand the nation.
To collect scientific base data, CSAT conductedthe National Treatment Improvement EvaluationStudy, known as NTIES from 1992-1997. Thiswas the largest sample ever studied, with one ofthe longest client follow-up periods in thesubstance abuse treatment field.
This study found that the average economicbenefit to society was over three times theaverage cost of a client treatment episode. Theaverage cost of a treatment episode was
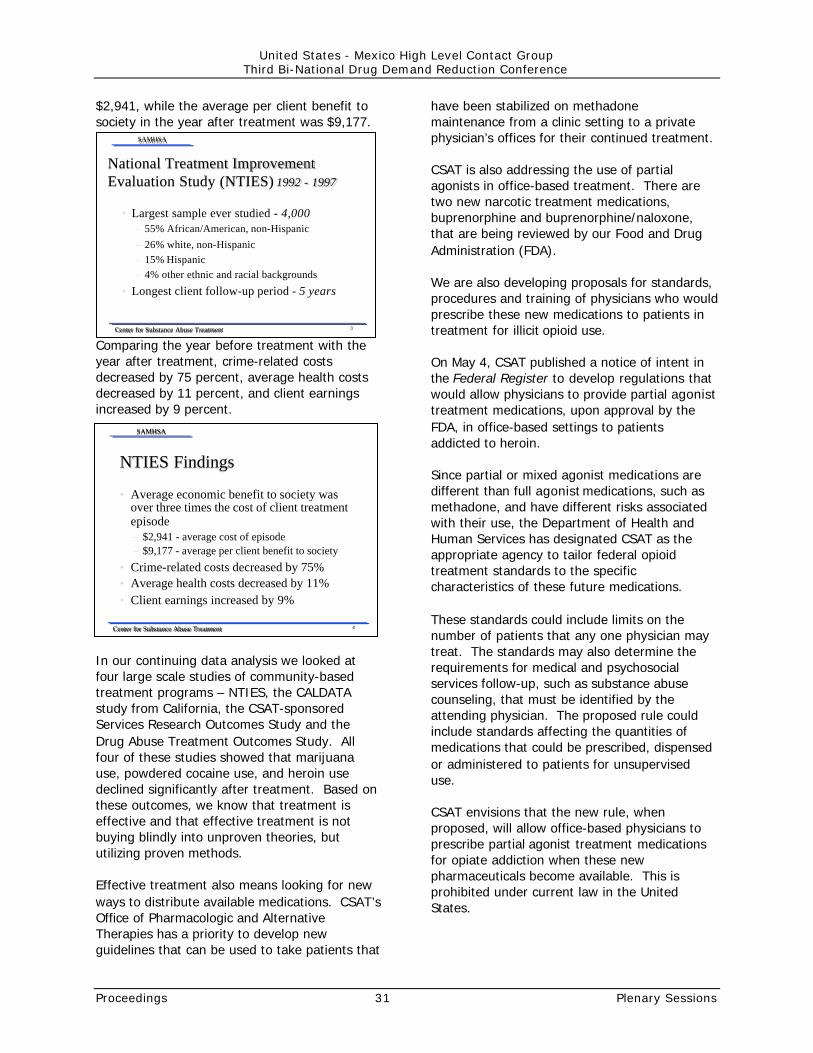
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 31 Plenary Sessions
$2,941, while the average per client benefit tosociety in the year after treatment was $9,177.
Comparing the year before treatment with theyear after treatment, crime-related costsdecreased by 75 percent, average health costsdecreased by 11 percent, and client earningsincreased by 9 percent.
In our continuing data analysis we looked atfour large scale studies of community-basedtreatment programs – NTIES, the CALDATAstudy from California, the CSAT-sponsoredServices Research Outcomes Study and theDrug Abuse Treatment Outcomes Study. Allfour of these studies showed that marijuanause, powdered cocaine use, and heroin usedeclined significantly after treatment. Based onthese outcomes, we know that treatment iseffective and that effective treatment is notbuying blindly into unproven theories, bututilizing proven methods.
Effective treatment also means looking for newways to distribute available medications. CSAT’sOffice of Pharmacologic and AlternativeTherapies has a priority to develop newguidelines that can be used to take patients that
have been stabilized on methadonemaintenance from a clinic setting to a privatephysician’s offices for their continued treatment.
CSAT is also addressing the use of partialagonists in office-based treatment. There aretwo new narcotic treatment medications,buprenorphine and buprenorphine/naloxone,that are being reviewed by our Food and DrugAdministration (FDA).
We are also developing proposals for standards,procedures and training of physicians who wouldprescribe these new medications to patients intreatment for illicit opioid use.
On May 4, CSAT published a notice of intent inthe Federal Register to develop regulations thatwould allow physicians to provide partial agonisttreatment medications, upon approval by theFDA, in office-based settings to patientsaddicted to heroin.
Since partial or mixed agonist medications aredifferent than full agonist medications, such asmethadone, and have different risks associatedwith their use, the Department of Health andHuman Services has designated CSAT as theappropriate agency to tailor federal opioidtreatment standards to the specificcharacteristics of these future medications.
These standards could include limits on thenumber of patients that any one physician maytreat. The standards may also determine therequirements for medical and psychosocialservices follow-up, such as substance abusecounseling, that must be identified by theattending physician. The proposed rule couldinclude standards affecting the quantities ofmedications that could be prescribed, dispensedor administered to patients for unsuperviseduse.
CSAT envisions that the new rule, whenproposed, will allow office-based physicians toprescribe partial agonist treatment medicationsfor opiate addiction when these newpharmaceuticals become available. This isprohibited under current law in the UnitedStates.
Center for Substance Abuse TreatmentCenter for Substance Abuse Treatment
SAMHSASAMHSA
3
National Treatment ImprovementNational Treatment ImprovementEvaluation Study (NTIES) Evaluation Study (NTIES) 1992 - 19971992 - 1997
• Largest sample ever studied - 4,000– 55% African/American, non-Hispanic– 26% white, non-Hispanic– 15% Hispanic– 4% other ethnic and racial backgrounds
• Longest client follow-up period - 5 years
Center for Substance Abuse TreatmentCenter for Substance Abuse Treatment
SAMHSASAMHSA
4
NTIES FindingsNTIES Findings
• Average economic benefit to society wasover three times the cost of client treatmentepisode– $2,941 - average cost of episode– $9,177 - average per client benefit to society
• Crime-related costs decreased by 75%• Average health costs decreased by 11%• Client earnings increased by 9%

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 32 Plenary Sessions
To deal with the problem of methamphetamine,the fastest growing drug problem here inArizona, and a major problem in many otherstates in the southwest, northwest and midwest,CSAT is sponsoring a study to determine themost effective and cost-effective methods oftreating methamphetamine addiction.
The CSAT program is designed to test a 16week psychosocial intervention approachdeveloped by the MATRIX Center in Los Angelesand existing treatment models at seventreatment sites in California, Hawaii andMontana. An eighth site, the UCLA Drug AbuseResearch Center in Los Angeles, will coordinatethe research and analyze the cross-site data.This is a three year program to determine whatmethods can be successfully used to treat thoseaddicted to this very dangerous substance thatis particularly appealing to women, since it doesaffect weight loss.
The study has been designed to see if resultscan be replicated in different user populationssuch as Latino women, pregnant women andwomen with children, and Asian Pacific Islandersor Native Americans, or in the gay community inLos Angeles.
The study is looking at adolescent and adultwhite males, Hispanic males, and white women.The site in Hawaii is looking at effectivetreatment of younger, less-educated userswhose parents are using marijuana or cocaine.
Specifically, the principles of drug addictiontreatment include common-sense approachestowards service delivery. Effective substanceabuse treatment programs have:
• tailored treatment approaches, treatmentsettings and services to each individual’sparticular problems and needs
• availability to treatment services at the timethat the individual needs help (which meansclients will not have to be placed on awaiting list to receive services)
• the program options address the fullspectrum of the individual’s needs including:medical, psychological, social, vocationaland legal problems
• the individual’s treatment plans allows forflexibility in the course of treatment andrecovery and addresses appropriatetreatment approaches based on age,gender, ethnic and cultural needs
• degree to which individuals in the programare allowed to remain in treatment for anacceptable length of time based on theclient’s needs
• degree to which individuals in treatment areoffered individual or group counseling andother behavioral therapies as part of theirtreatment protocol
• degree to which programs offer or haveaccess to pharmacologic alternative optionsas part of the treatment services
• degree to which programs offer or haveaccess to psychological, psychiatric ormental health services for individualsdemonstrating a coexisting mental disorders
• degree to which individuals in recovery aremonitored once the leave formal treatmentand degree to which individuals have theoption to participate in long term treatmentand to join self-help groups once they leavetreatment
• degree to which individuals are providedwith counseling to help them avoid high-riskbehavior and degree to which treatmentprogram provides assessments forHIV/AIDS, Hepatitis B and C, tuberculosis,and other infectious diseases.
Center for Substance Abuse TreatmentCenter for Substance Abuse Treatment
SAMHSASAMHSA
5
Improving Current DeliveryImproving Current DeliverySystemsSystems
• Physician office-based treatment formethadone, buprenorphine and naloxone
• Pharmacy distribution of methadone

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 33 Plenary Sessions
Beyond these factors, what is important tounderscore is the undeniable fact thatdetoxification should not be confused withtreatment. Medical detoxification is meant toovercome acute symptoms of withdrawal. It isnot designed to deal with the underlyingproblems that lead to drug use or to motivatethe patient to work toward long-termabstinence.
Another critical factor is that injection drug useis highly associated with medical problems thatinclude HIV/AIDS, hepatitis, sexually transmitteddiseases, and other medical consequences ofdrug use and unprotected sex.
Just last month, CSAT released a new TreatmentImprovement Protocol, “Substance AbuseTreatment for Persons With HIV/AIDS” – or TIP#37. This new TIP volume provides the latestinformation on what is known about theintersection or interrelatedness of HIV/AIDS andsubstance abuse.
The TIP includes chapters on demographictrends, identifies the information that isimportant for conducting medical assessments,identifies ways to determine mental healthneeds, and discusses issues that might come upfor substance abuse counselors, includingdealing with their own prejudices when treatingHIV/AIDS-positive clients.
The TIP also offers information on how tointegrate other necessary services for thesepatients including the use of case managementtechniques, ways of managing pain, ethical andprivacy issues and funding and policyconsiderations in the delivery of services.
CSAT is working to develop comprehensivetreatment models that programs can replicate toprovide the highest quality of substance abusetreatment available anywhere. This should bethe strongest component of every demandreduction effort. Given the complexities anddifferent variables that influence society as aresult of substance abuse among its population,we need to continue our call for increased levelsof funding for substance abuse treatmentprograms.
My last point is perhaps the most telling point.In the U.S. we are spending an inordinateamount of the Federal tax resources to coverthe costs associated with drug related crimes.These crimes include the use or trafficking ofillegal substances, domestic violence incidentsrelated to substance use, and a cyclical patternto recidivism related to substance use.
CSAT is working diligently with other sectors ofthe Federal government ? the Department ofJustice, Department of Labor, Department ofEducation, Department of Housing and UrbanDevelopment, Department of Transportation –and with states and local governments to try tobetter coordinate substance abuse treatmentprograms at all levels.
Increasingly, these systems realize that we mustwork together to create continuum of care forindividuals that have a substance abuseproblem. The continuum of care means thatonce we have an individual that wants help, heor she will not be turned away from learning anew skill to sustain their recovery and to offerthem an opportunity to earn a decent living.
He or she will not be turned away from finding adecent place to live. He or she will be providedwith the necessary information and parentalskills development so they can attempt to keeptheir families intact and prevent them fromlosing custody of their children.
Center for Substance Abuse TreatmentCenter for Substance Abuse Treatment
SAMHSASAMHSA
10
Critical FactorsCritical Factors
• Detoxification alone IS NOT treatment• Injection drug use is highly associated with
HIV/AIDS, hepatitis, sexually transmitteddisease and other medical consequences ofdrug use and unprotected sex

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 34 Plenary Sessions
He or she will be given the necessary medicalattention to deal with their diabetes, theirHIV/AIDS and any other medical condition thatcan adversely impact the road to recovery.
And, most importantly, he or she will haveaccess to on-going counseling to prevent anirreversible relapse episode from clouding theroad to recovery.
At CSAT, our mission is to determine how wecan best support the coordination of substanceabuse treatment services and to help facilitatethe development and implementation of aintegrated service delivery systems.
Both of our countries need the commitment ofour governments, the health insurance sector,the private sector, the foundations and thededicated throngs of substance abuse serviceproviders and practitioners to work together tocontinue to minimize the adverse effects ofsubstance abuse within our borders.
Together, we will all make a difference as westrive for productive societies unburdened bythe current weight of addictive behavior.
Timothy P. Condon, Ph.D.Associate DirectorNational Institute on Drug AbuseDepartment of Health and HumanServicesUnited States
There are many reasons people take drugs.One is to feel good. And that’s often the peoplewho are sensation seeking and want to feelbetter. Those are people who are taking drugsto help to get through the day. They may bedepressed, have anxiety disorder. They may, infact, be victims of socio-economic problems.
They may be victims of family abuse, spousalabuse, or parental abuse. They take drugs tojust get through the day. And in many casesthey are self-medicated. But the bottom line is,people take drugs because they like what drugsdo to their brain.
And here’s your neuro-science lesson. I am aneuro-scientist and I couldn’t leave you todaywithout a little bit of the neuro-science of whatwe’ve learned in the last five or ten years. Andthis is, and if I had my pointer, I could show youthat this is the reward pathway for the brain, orthe pleasure centers in the brain if you will.
What drugs and abuse do is, they hijack this.You can see here, alcohol, cocaine, heroin, allwork in the various areas of the rewardpathway, and they work at the level of theneuron or the brain cell itself.
This is one of the terminals of the brain cell.They work on many neuro-transmitter systems,seretonin, norepinephrine, gabba. But they allseem to work. There’s some commonality there.And they all work on the dopamine system. Andwhat happens here is that a nerve impulsecomes down into the neuron and it causes therelease of the dopamine. It crosses that spacethere and binds to those dopamine receptorsand stimulates that next cell. You like that. Andin fact, if a lot of dopamine comes down andstimulates that, you get a very euphoric feeling.But Mother Nature, in her wisdom, decidedthere needed to be a mechanism to turn thissystem off because this is the normal way youexperience pleasure. So, there is in fact, as yousee here in the red, mechanisms that reallyscoops up or transports back the dopamine backinto that cell.
That’s where drugs of abuse like cocaine work.They block the reuptake of that dopamine.
Center for Substance Abuse TreatmentCenter for Substance Abuse Treatment
SAMHSASAMHSA
13
Collaborative Support SystemsCollaborative Support SystemsProvide Continuum of CareProvide Continuum of Care
• Helping those who want help to learn newskills and opportunity to earn a decent living
• Availability of decent housing• Parental skill development, keep families
together• Necessary medical attention• Access to on-going counseling to prevent
relapse

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 35 Plenary Sessions
If you measure the amount of dopamine in thatspace with drugs of abuse as you can see here,cocaine, methamphetamine, nicotine, THC, theyall cause a dramatic release of dopamine intothat space. You love that release. That’s part ofwhat causes this euphoric feeling or this highassociated with drugs of abuse.
But this doesn’t happen in the long-term. Infact, long-term changes occur in the brain afteryou stimulate this system over and over again.
So, we know that prolonged drug use changesthe brain in long-lasting and fundamental ways.And it’s as if there’s a switch in the brain thatflips. Something changes. And we don’t havevery much research at this point about whatthat transition is, from somebody who goes fromvoluntary drug use to addiction. They’redifferent states. There is something thathappens in the brain and we don’t actually knowall about it. That’s one of the areas of researchfor the future.
But here’s an example of that change. Thoselong-lasting and fundamental changes thatoccur in the brain. As Dr. Clark pointed out,methamphetamine is a very big problem inmany countries, many communities around theUnited States.
This is the front of the brain. The top is the frontof the brain. The back of the brain, the left andthe right. The area there is the striadum. Andwhat that is showing you is that dopaminetransporter or that scooper molecule, and thefirst one is a control. The second one is amethamphetamine addict three years after hislast methamphetamine. Three years. There’s adramatic reduction in the amount of thatmolecule that’s in this individual’s brain, in hisstriadum.
Methadone addict. Same thing. Three yearsafter his last drug. And the last panel is forcomparison, is a Parkinson’s Disease patientwho has a dramatic deficit in the dopaminesystem in his brain.
People often ask me what that means. And thisis very new data that just came out. Again, topis normal controls. The bottom is individualsand there are about 13 people in this study.
Individuals who are chronic methamphetamineabusers. And you can see on the bottom adramatic reduction in the amount of dopamine.This is actually dopamine transporter inmethamphetamine abusers as it was in the lastslide. But what does that mean? Well, theytested the meth abusers compared to thecontrols and this is the first time there havebeen data on the functionality changesassociated with those long-term changes in thebrain. They found two simple things: motortasks and memory tasks. It took longer for themto walk from here to there for themethamphetamine addicts. And their memorywas not as good in terms of a word recall. So,they’ve got cognitive problems and they’ve gotsome motor problems associated with that long-term change in the brain.
So, as they say then, addiction results fromlong-term effects of drugs on the brain. And thebrains of addicts are different from the brains ofnon-addicts. And those differences are really theessential element of addiction. So addiction isfundamentally a brain disease, but it’s not just abrain disease. That would be a little bit easierfor the scientists to discover how to fix that. It’sin fact, the quintessential bio-behavioraldisorder. What I mean by that is in fact that thebiology, the behavior and the social context allbecome intertwined in this disease. And if, infact, you go to make some progress in treatingpeople with addiction, you need to attend to allof those things. It’s as if the challenge fortreatment is to flip the switch back in the brainby behavioral therapy, counseling, medications,job placement, a number of different thingsfrom biology, behavior and social context. Themost effective treatments will, in fact, attend toall of these. And we have a number of things inour clinical toolbox that can help us do thosethings. These are just some therapy manualsthat the Institute published last year. One oncognitive behavioral approaches and one oncommunity reinforcement. You can order thoseat the NIDA exhibit. And there’s also, of course,a number of medications, as Dr. Clark said.Methadone, nicotine replacement, are comingon line in the coming year and we hopebuprenorphine.
Dr. Clark did a really eloquent andcomprehensive job of listing a lot of the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 36 Plenary Sessions
principles of effective treatment that wepublished in the NIDA Principles of DrugAddiction Treatment last year.
So, as I said, the most effective treatmentstrategies will in fact attend to all those things.Treatment, pharmacology, or counseling arevery important but they’re not the only thingsthat have to be part of the comprehensivesuccessful and effective treatment program.There needs to be childcare services andvocational services as well as a whole host ofother things.
And as we have a variety of effective treatmentoptions in the toolbox, we need to do better. Infact this is just a list to show you what’s in thepipeline for the future. We have a whole host ofbehavioral therapies that are in various stages ofresearch that we hope will be available in theclinic and in the community in the not-too-distant future. So too do we have a host ofmedications as anti-cocaine agents that are invarious stages of development. This is all part ofNIDA’s Future Treatment initiative to movetreatment from the lab into the community, intoreal life settings for new treatment componentsas well as improvement of existing treatmentcomponents.
One of the ways we’re doing that is we’velaunched the clinical trial network; the NationalDrug Abuse Clinical Trial Network will testeffectiveness in real life settings, behavioral andmedication treatment. We envision there will benodes of research, regional research trainingcenters, partnered with community treatmentprograms. Five to ten community treatmentprograms that will test various therapies –behavioral, pharmacological, in various real lifesettings with diverse populations, as Dr. Clarksaid. And in fact, we’ve established the first sixof these through NIDA grandiosity. So, weenvision this to be a national program in thenext few years. We’ve made the first six awards.We’re going to make another six awards thiscoming year. And in the following year we hopeto make an additional five or six. So, with anational clinical trial network, not only to testtherapies in real life settings and to get themincorporated into the community treatmentprograms, but also to use it as a vehicle todisseminate other areas of research, whether it
be neuro-science or genetics. Science isavailable to replace ideology at the local andcommunity level as well as the national level.Thank you.
Slide presentation follows.

Challenges and Opportunities inDrug Demand Reduction:
What We Have Learned FromResearch
Timothy P. Condon, Ph.D.Associate Director,National Institute on Drug Abuse6001 Executive BoulevardRoom 5263 MSC 9591Bethesda, Maryland 20852(301) 443-6480 (301) 443-9127 Fax
U.S. - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Phoenix, ArizonaJune 1, 2000
Advances in ScienceHave Revolutionized Our
Fundamental Views of Drug Abuse and Addiction
Drug Abuse is a Preventable BehaviorDrug Addiction is a Treatable Disease
Partnership for a Drug Free America
Why Do People Take DrugsIn The First Place?
www.drugabuse.gov
�� ineffective parentingineffective parenting�� chaotic home environmentchaotic home environment�� lack of mutual attachments/nurturinglack of mutual attachments/nurturing�� inappropriate behavior in the classroominappropriate behavior in the classroom�� failure in school performancefailure in school performance�� poor social coping skillspoor social coping skills�� affiliations with deviant peersaffiliations with deviant peers�� perceptions of approval of drug-usingperceptions of approval of drug-using
behaviors in the school, peer, and communitybehaviors in the school, peer, and communityenvironmentsenvironments
Prevention Programs Should . . . .Prevention Programs Should . . . .Reduce Risk FactorsReduce Risk Factors
www.drugabuse.gov
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 37 Plenary Sessions
Prevention Programs Should . . . .Prevention Programs Should . . . .
�� strong family bondsstrong family bonds�� parental monitoringparental monitoring�� parental involvementparental involvement�� success in school performancesuccess in school performance�� prosocialprosocial institutions (e.g. such as institutions (e.g. such as
family, school, and religiousfamily, school, and religiousorganizations)organizations)
�� conventional norms about drug useconventional norms about drug use
Enhance Protective FactorsEnhance Protective Factors
www.drugabuse.gov
. . . and be Culturally Sensitive. . . and be Culturally Sensitive
PreventionPrevention Programs Should . . . .Programs Should . . . .
Target all Forms of Drug UseTarget all Forms of Drug Use
www.drugabuse.gov
�� Resist drugsResist drugs
�� Strengthen personalStrengthen personalcommitments against drug usecommitments against drug use
�� Increase social competencyIncrease social competency
�� Reinforce attitudes against drugReinforce attitudes against druguseuse
Prevention Programs Should . . . .Prevention Programs Should . . . .
Include Interactive Skills-BasedInclude Interactive Skills-BasedTrainingTraining
www.drugabuse.gov
�� Provides greater impact thanProvides greater impact thanparent-only or child-onlyparent-only or child-onlyprogramsprograms
�� Include at each stage ofInclude at each stage ofdevelopmentdevelopment
�� Involve effective parenting skillsInvolve effective parenting skills
Prevention Programs Should be . . . .Prevention Programs Should be . . . .
Family-FocusedFamily-Focused
www.drugabuse.gov
Prevention Programs Should . . . .Prevention Programs Should . . . .
Involve Communities and SchoolsInvolve Communities and Schools
�� Media campaigns and policyMedia campaigns and policychangeschanges
�� Strengthen norms against drug useStrengthen norms against drug use
�� Address specific nature of localAddress specific nature of localdrug problemdrug problem
www.drugabuse.gov
People Take Drugs To:People Take Drugs To:
Feel good (sensation seeking)Feel good (sensation seeking)
Feel better (self-medication)Feel better (self-medication)
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 38 Plenary Sessions

A Major Reason People Takea Drug is They Like What
it Does to Their Brains
Prolonged Drug Use Changes
The Brain In Fundamental and
Long-Lasting Ways
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 39 Plenary Sessions

Methamphetamine Neurotoxicity Dopamine Transporters in Methamphetamine AbusersDopamine Transporters in Methamphetamine Abusers
Methamphetamine abusers have significant reductions in dopamineMethamphetamine abusers have significant reductions in dopaminetransporters.transporters.
Normal ControlNormal Control
Methamphetamine AbuserMethamphetamine Abuser p < 0.0002p < 0.0002
Dop
amin
e Tr
ansp
orte
rs(B
max
/Kd)
NormalControls
MethAbusers
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
BNL - UCLA - SUNYBNL - UCLA - SUNYNIDA - ONDCP - DOENIDA - ONDCP - DOE
What We Have Learned FromResearch
Timothy P. CondonAssociate DirectorNational Institute on Drug Abuse6001 Executive BoulevardRoom 5263 MSC 9591Bethesda, Maryland 20852(301) 443-6480
Dopamine Transporters inDopamine Transporters in Methamphetamine Methamphetamine Abusers Abusers
BNL/UCLA/SUNYBNL/UCLA/SUNYNIDA, ONDCP, DOENIDA, ONDCP, DOE
Motor TaskMotor TaskLoss of dopamine transporters Loss of dopamine transporters in the in the methmeth abusers may result abusers may result in slowing of motor reactionsin slowing of motor reactions..
Memory TaskMemory TaskLoss of dopamine transporters Loss of dopamine transporters in the in the methmeth abusers may result abusers may result in memory impairment.in memory impairment.
7 8 9 10 11 12 131.01.21.41.61.82.0
Time Gait(seconds)
468101214161.01.21.41.61.82.0
Delayed Recall(words remembered)
Dop
amin
e Tr
ansp
orte
rBm
ax/K
d
Addiction Results from
Long-Term Effects of Drugs
on the Brain
Addiction Results from
Long-Term Effects of Drugs
on the Brain
The Brains of AddictsAre Different From
the Brains of Non-Addicts
…And Those DifferencesAre An Essential Element
of Addiction
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 40 Plenary Sessions

Dopamine Transporters inDopamine Transporters in Methamphetamine Methamphetamine Abusers Abusers
BNL/UCLA/SUNYBNL/UCLA/SUNYNIDA, ONDCP, DOENIDA, ONDCP, DOE
Motor TaskMotor TaskLoss of dopamine transporters Loss of dopamine transporters in the in the methmeth abusers may result abusers may result in slowing of motor reactionsin slowing of motor reactions..
Memory TaskMemory TaskLoss of dopamine transporters Loss of dopamine transporters in the in the methmeth abusers may result abusers may result in memory impairment.in memory impairment.
7 8 9 10 11 12 131.01.21.41.61.82.0
Time Gait(seconds)
468101214161.01.21.41.61.82.0
Delayed Recall(words remembered)
Dop
amin
e Tr
ansp
orte
rBm
ax/K
d
Addiction Results from
Long-Term Effects of Drugs
on the Brain
Addiction Results from
Long-Term Effects of Drugs
on the Brain
Addiction is, Fundamentally,
a Brain Disease
Addiction is, Fundamentally,
a Brain Disease
Addiction is Not
Just a Brain Disease
Addiction is Not
Just a Brain Disease
Addiction is theQuintessential
Biobehavioral Disorder
Drug Use Addiction TreatmentNormal
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 41 Plenary Sessions
The Most Effective TreatmentStrategies Will Attend to All
Aspects of Addiction:
•Biology
•Behavior
•Social Context
We Have A Variety OfEffective Treatment Options
In The Clinical Toolbox
NIDA THERAPY MANUALS Medications for Drug AddictionMedications for Drug Addiction
�� MethadoneMethadone
�� LAAMLAAM
�� NaltrexoneNaltrexone
�� Nicotine ReplacementNicotine Replacement
•• patchespatches•• gumgum•• buproprionbuproprion
www.drugabuse.gov
www.drugabuse.gov
The Most Effective TreatmentStrategies Will Attend to All
Aspects of Addiction:
• Biology
• Behavior
• Social Context
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 42 Plenary Sessions

Components of ComprehensiveComponents of ComprehensiveDrug Addiction TreatmentDrug Addiction Treatment
www.drugabuse.gov
We Have A Variety OfEffective Treatment Options
In The Clinical Toolbox
…But We Need To AndCan Do Better
Clinical Trials Network
• Infrastructure based on NIH model• Test effectiveness in real-life settings• Behavioral and medications treatment• Diverse populations• Partnership with community treatment
programs
National Drug Abuse Treatment Clinical Trials Network Node
National Drug Abuse Treatment Clinical Trials Network Node
CTP -- Community-Based Treatment Program RRTC -- Regional Research and Training Center
CTPCTP
CTP
CTP
CTPCTP
CTP
CTP
CTP
RRTCRRTC
CTP
National Drug Abuse Treatment Clinical Trials Network
National Drug Abuse Treatment Clinical Trials Network
We’ve Come A Long Way in Replacing
IDEOLOGY
We’ve Come A Long Way in Replacing
IDEOLOGY withwith
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 43 Plenary Sessions

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 44 Plenary Sessions
Haydée RosovskyTechnical SecretaryNational Council on AddictionsMinistry of HealthMexico
I am very happy and I am very proud toparticipate in this plenary session together withoutstanding professionals in this field. I’m goingto make some remarks that have to do with thechallenges we have to face whenever we doprevention that is targeted to the youth. I’mreferring to drug use prevention among youth.First of all, I would like to say that prevention isthe best possible strategy for our programs. Thisis where we would like to invest all of ourresources and we would like to have abundantresources for this purpose. Unfortunately,prevention at present in Mexico has to go hand-in-hand with various important treatmentactions because we already have an importantproportion of the population who started to usedrugs a few years ago and that are nowpresenting problems that require therapy.
From the standpoint of the youth, what I’vebeen able to observe and what my colleagues atNational Institute of Psychiatry have read ininternational literature is that the most, let’s say,universal, recommendation is that preventionshould start as early as possible. Preventiveprograms that expect to achieve a veryimportant impact when targeted to youngstersafter puberty or in middle school or in highschool do not seem to be as effective asprograms that begin from the time the childbegins to develop. What’s the reason for this?Well, the concept of prevention that seems to bethe most successful one is the one dealing notonly with substance abuse but also with anenvironment that promotes positive behaviorsand lifestyles that are created from the earliestchildhood. In these models, the use of drugsmakes us feel better and as we heard a momentago from the presentation of our NIDAcolleague, there is a search for relieving pain orlooking for pleasure. All of these behaviorswould not necessarily be sought when there areother sources of satisfaction in individual’s lives.
Another important element of this education forlife, as we call it, is a proper management ofemotions: growing up in environments wherefreedom goes hand-in-hand with responsibility,and one in which individuals learn to grow upfeeling self-assured and having a realisticjudgment about their self-esteem.
In certain environments, prevention among theyouth is more successful. And this is, these arethe ones we should focus on. Let me mentionsome of these sites where we should reinforceour actions. And I think this is importantbecause many prevention efforts do not reachtheir target population. Let me give you anexample. Let’s say we want to do a lot ofprevention in the setting of health care, theprimary health care setting for instance. In thecase of the young people, we’re not going to bevery successful because youngsters seldom goto primary health care centers. We see mainlyyoung children, or adults that go forimmunization or for a specific problem. Butteenagers do not represent the most frequentclients of primary health care centers.Therefore, the type of educational andinformation materials that we use are not goingto reach our youngsters. But where are they?They are at schools, and this is something thatis universally recognized. However, I would liketo state that basic science is more universal,because in the end, biologically speaking wehave more commonalties among us humans.Whenever we refer to behaviors and to ourpreventive work, we find many reservationsabout international recommendations.
There are some recommendations, for instance,that stem from the experience of institutions inthe United States like SAMHSA. And theserecommendations cannot necessarily besuccessfully taken to Mexico. We need to do atranslation or an adaptation and take someaspects that are applicable, but exclude othersthat are not. For instance at schools you knowthat unfortunately, in Mexico, the meanschooling level of the education, of thepopulation continues to be quite low. Animportant proportion of our youth, especiallywomen, quit school at a very early age.Fortunately, this situation is changing. We aremaking progress, but we are still very far fromhaving all of our youngsters completing high

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 45 Plenary Sessions
school, or graduating from high school, let alonegiving to all of them the opportunity of going tocollege. This is only available for a minority.Therefore, although the school is a veryimportant setting for prevention, we cannotexpect that the young population that we wantto reach with preventive actions are all going tobe at schools.
It’s precisely the young people who are at riskfor drug use, those who quit school probablybecause of their personal life situations thatmake them be very vulnerable, and exposethem to drug use. Another setting where wewould have to work is the community. You weregiven an example of this today and you will hearabout many more later, those who approach theyounger coalitions or coalitions of the young,many of which are represented here, but also atthe community at the neighborhood level, insmall towns. The young people are moving, arethere, and they are very active. They are notnecessarily at home. They are out in parks, outin the street. They are playing. They are havingfun. Some of them are even working in thestreets. That’s why we should approach themwherever they are. And as I already said, thereare many young people who are part of thelabor force, of the working force. Some workunder very poor conditions that further exposethem to drug use. For example, those working incertain areas of big cities where there isprostitution or where one finds adult centers likenightclubs where one can easily have access todrugs, or sell to your economic need see theneed for working in prostitution or as beggars.There is another group of young people whowork, but they are not necessarily so muchexposed to drug use. They may work insupermarkets and self-service stores and maybethey combine work with school.
Another very important setting is that ofrecreation centers. These are meeting places forthe young people. And here we may includethose who play sports. Young people like bars,discos, going to places to listen to rock bands.And probably in every country and in thedifferent regions of our countries, we may finddifferent habits of the young people in doing thistype of activity. But I think that each one of us,in our own country need to define thesedifferent settings, to determine what our target
population is. In working for the youth, in doingprevention efforts, we think that there arecertain actions that we are trying to undertakein Mexico that may have a very importantimpact. And that they be carried out only underthe condition of having a very good coordinationwith other sectors. It’s a fact that thegovernment alone cannot take care of thisproblem. And the government cannot andshould not take care of this problem alone.
We are becoming more and more aware of theneed to work jointly with equality, without oneof the parties being submissive to another one,and with a different group of youth. Preventiveprograms, as I said, cannot be universal for thereasons that I already mentioned, but there areother reasons, for example, cultural aspects,different values, gender aspects. And there arerisk factors and protective factors that pertain tothe different groups, cultures, regions, eveninside one single country. Yesterday we heardsome experiences about research. And let mesay that this is the reason why research is soimportant for prevention purposes. Preventionneeds to be research-based. Research can guideus as to what’s going on, what’s the status ofthe problem in different population groups sothat prevention and treatment resources can bemore successfully allocated. As I said, we heardyesterday about the construction of the genderidea, and the different perspectives one finds indifferent cultures. We heard about self-esteem,assertiveness, and in two neighbor countries likeMexico and the U.S., something might meansomething totally different. For example, for ayoung Mexican woman, being assertive maysound like being too aggressive or a behaviorthat will make her unaccepted vis-a-vis the boysof her community. So these are aspects that inmy view should be based on research.
I also think that drug use prevention cannot liewithin community and government programs asif it were something separate for resourceutilization purposes. We would like to undertakecomprehensive action. Drug use preventionneeds to be part of many other healthprograms. Why? Because we know thatsubstance use and abuse is an extremelyimportant risk factor. For example, for HIV AIDStransmission, for unwanted pregnancies,accidents, violence and dropping out of school.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 46 Plenary Sessions
All of these are important challenges, but thereare other important challenges we face in ourprevention efforts. We frequently see thatdifferent organizations use different conceptualframeworks for prevention. And often, they arenot only not complementary, they are opposed.And this unfortunately, leads to confusionamong the population, and efforts areneutralized or there is suspicion about what’sbeing done.
We also see quite frequently preventive actionsthat are not permanent enough and that are notconsistent with other actions that areundertaken by a different group. That’s why, inorder to reach our young population, in the caseof mass media campaigns, we need to see thatwhenever they are broadcast, it must be a timewhen the young people can hear them or watchthem. This is something we need to think aboutand we have with us some examples of thework we have been doing. Part of this we havedone for a few years. Other actions are morerecent. And we’re working in the setting offamilies and communities. To do preventionamong the youth, we also need to work withtheir parents, with their religious leaders. This issomething that has to do with the cultures andtraditions of every country. You heard Sofia thismorning telling us about the youth coalition. Wehave great hopes for what is being done. Andthe youth have told us that they are suspiciousabout adults and they don’t trust either adults orgovernments or institutions. At least this is thecase in Mexico. So, we need to take this toaccount and ask the young people of ourcountry to become the most active agents ofprevention. Let’s ask them to be, with ourselvesas facilitators, and give them the tools that theyneed.
The educational setting is very important as wellfor us. We have started to organize studentorganizations against addiction under the modelof building a drug-free life. This is a model thatwe have used with other institutions. We have acrusade with teachers. We know that thepreventive experiences at the school settingshould be part of the school’s educationalprograms. These should not be actions that areisolated or that are done intermittently. Theyshould be part of the material that teachers useand be part of the internal school regulations.
In the work setting it is important to develop adhoc programs that consider the socio-economicstratum of individuals and that facilitate a timelyprovision of preventive treatments. In therecreational setting, one of the things we’redoing now is to work with owners of discos, barsand nightclubs. They want to get together onthis because it’s not good for them to haveaccidents or drug problems in their centers ordiscos. So, we have found a possibility to worktogether with them and we will have thespecifics quite soon.
Finally, actions towards responsible alcoholicdrinking. In Mexico the age at which one candrink is 18 years. This is younger than in theUnited States. We know there are certainindividuals that should not drink because theyare prone to addiction or dependency. But thereare many other individuals who may havedrinking problems. There are very interestingprograms aimed at changing this and promotingresponsible drinking. We also have actions incultural and sports centers. This is based onwhat we have learned from our young people.
Mary BernsteinDirectorOffice of Drug and Alcohol Policyand ComplianceDepartment of TransportationUnited States
Slide presentation follows.
THIRD U.S./MEXICO BI-NATIONALDRUG DEMAND REDUCTION
CONFERENCEPhoenix, AZ
May 31 – June 2, 2000
Drug Free WorkplacesA Critical Prevention Component
Mary BernsteinDepartment of Transportation
Office of Drug and Alcohol Policy and Compliance2
� Drug and alcohol abuse are a majorproblem. Its consequences are felt in allsegments of society, including theworkplace.
� Employers want to provide their employeeswith a safe and healthful work environment.
KEY MESSAGES
3
KEY MESSAGES
� Drug and alcohol abuse impairs lifestyle, workproductivity and shortens life span.
� Drug and alcohol abuse may destroy normalfamily life, cause financial difficulties and maylead to spouse and child abuse.
� Drug and alcohol abuse places an extra burdenon friends, coworkers and associates.
4
KEY MESSAGES
� Companies encourage employees having drugor alcohol abuse problems to seek help beforework performance is affected. Through theEmployee Assistance Program employees canavail themselves of drug and alcohol counselingand rehabilitation.
� Drug testing is an effective intervention toidentify and deter drug users.
5
SUBSTANCE ABUSE INTHE WORKPLACE
What Is It?� Alcohol� Drugs� Prescription Drugs
6
SUBSTANCE ABUSE INTHE WORKPLACE
Why Does Business Care?
� Cost to Industry� Liability� Social Conscience� Legislation (United States)
Proceedings 47 Plenary Sessions
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference

7
DRUG-FREE WORKPLACEINTIATIVES
DRUG-FREE WORKPLACE ACT OF 1988� Shot heard throughout United States Industry
OMNIBUS TRANSPORTATION EMPLOYEETESTING ACT OF 1991
� Required mandatory testing for safety sensitive transportation workers
8
PUZZLE PIECES
Training and Education are used tocreate an environment that stresses “Notolerance.”
�Supervisory Training�Employee Education�Employee & Family Communications�Hosting
9
Policies and Procedures which spell out thecompanies position on alcohol and drug use duringworking hours.
�Use of alcohol�Position on illicit drugs�Position on licit drugs�Procedures to be followed after a violation�Consequences of violation�How employees can seek help
PUZZLE PIECES
10
The Employee Assistance Program is the companies vehicle foremployees and family members to seek help for alcohol and drugproblems. It is a proactive program whose goal is education earlyintervention and follow-up.
�Job Performance Based�Education�Prevention Programs�Supervisory Training�Management Consultation�Intervention�Short Term Problem Resolution�Referral�Follow-up
PUZZLE PIECES
11
Drug and Alcohol Testing is a safety program that hasbecome an important tool in identifying and deterringsubstance abuse in the workplace.
�Pre-employment Testing�Random Testing�For Cause Testing�Post Accident Testing�Return-to–Duty Testing�Follow-up Testing
PUZZLE PIECES
12
IT IS IN BOTH THE EMPLOYERS ANDTHE EMPLOYEE’S BEST INTERESTTO HAVE A DRUG-FREEWORKPLACE.
WHEN THE PUZZLEFITS TOGETHER
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 48 Plenary Sessions

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 49 Plenary Sessions
Agustin VélezGeneral DirectorTrusteeship for the Institute forStreet Kids and AddictionsMexico
Gracias, John. There is no doubt that theworkplace is an important place for preventingthe use of substances irrespective of which theyare. Our research project that is being changedonce again shows that drug use is a preventablebehavior. Prevention of this behavior withoutdoubt, has as a purpose, a goal: that a largernumber of individuals at a given point in time ina society would prefer to promote their interestfor health rather than have a brain disorder. So,the questions we must answer with preventiveactions or activities are not only in children andyoung people or in adults. We must be atschools and the workplace. That is where wemust put in place prevention programs.Intervention is quite broad and leads us tointervene with preventive activities at any timein the life of individuals and at any place wherethey can meet. They can be intervened withprevention.
In recent years, we have made great efforts toguide our interventions towards children andteenagers that find themselves studying andgoing to school through many informationactivities. We tell them about their risks, andstrengthening those factors that protect them.However, at schools where our children attend,there are also adults – both the teachers andthose who have other duties in the field ofeducation. And these adult individuals in thisworkplace called school express their attitudes,and with their words, concepts that would notnecessarily be favorable to avoid the use ofsubstances. Quite the contrary, some howconcepts that can lead people to think thatsubstance use is a behavior that is allowable.And this is in most workplaces, includingschools.
For those of us who are between 20 and 50years of age, this age of life is of our greatestwork productivity. This is also the age wheremore substances of any type are used. Clearly,we can say that a large number of workers atschools where our children attend, are using
some type of substance – alcohol, tobacco andsome other type of substance. School must beseen as a place for intervention to tell all thestudents about the risks involved in using thesesubstances, but to we must also consider it as aworkplace under a care modality that I willmention later. So, this workplace will be apriority place for preventive intervention.
Research is pointing out that at any point intime in life, we must do prevention activities andwe must not consider all substances as risky.They can lead to addiction. We must not neglectactions addressed to avoid the use of alcoholand tobacco as we address the use of otherbasically illegal drugs.
Every year in the world, billions of dollars arelost due to the use of alcohol and of other drugsalso in the workplace. And this is due to the factthat substance use is behind absenteeism,injuries, and low productivity in companies.There are many studies that try to measure thecost. Many of them fall short because cost dueto the loss of days of work and the loss due tocost in injuries does not take into account theimpact within a social network: the use ofalcohol on the rest of the family. Because theydon’t go to work, there’s no income and thereare other repercussions in the family setting. Aprevention program on the use of alcohol andother drugs in the workplace must consider atleast this space where people work together asa simulation of what happens at home or asimulation of what happens in the community.For a long period of time, different types ofpeople are together. Values, traditions,standards and laws regarding the use ofsubstances are at stake every day. This is whythis type of program should consider thecreation of an infrastructure inside the companythat will take into account the owners, seniormanagement, the employees through theirunion organizations, and health and manpoweroffices who are the ones that will carry out apreventive action in the workplace. Of course,it’s necessary to put in place any value with amodel that includes all substances and includesall the ways in which these substances are used.The major components of this type of programmust develop the necessary human resourcesfor this end, must strengthen primary healthcare, and must include the component of the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 50 Plenary Sessions
family and the community within the sameworkplace. A program of this type must be partof a more comprehensive one that ensuresquality in the company and can be reinforcedwith health, safety and well-being policiesincluded in the organization’s documents andmade available to any worker, manager, oranybody who’s in the workplace.
This way, top management and unions mustreach an agreement about the various aspectsand objectives of the type of program. Youbecome committed to the project. If the headsand senior management agree that this is a veryimportant subject, the workers will understandthat senior management is worried for them andthey will have greater interest to follow aprogram. There are two basic strategies in theprograms for workplaces – those programs thataddress the existing problems and those thataddress prevention. For problem-orientedprograms, the strength of the concept is alsotheir greatest weakness. They are focused onthe individual that is already sick and is alreadya problem. Most people feel that this approachis stigmatizing, and makes it difficult to seek oraccept help when it’s needed the most. It’s moreeffective to offer prevention before workershave developed any type of dependence andhave infringed upon the work bylaws repeatedly.The highest losses in the worker’s performancemay not come from addicts that have beenidentified as such, but rather of the rest of theworkers of the organization. The most acuterisks are related to sporadic incidents likedrinking too much, or being under the influenceof alcohol or drugs at the wrong time and thewrong place.
All this affects the mechanisms that individualshave to face in a given situation. The risk, thecritical task now is to go beyond the care ofindividuals in order to face broader social issuesthrough prevention methods that will be part ofthe structure. They must be a part of thecompany. Programs must focus on prevention.The major goal is prevention while lessemphasis is made on treatment andrehabilitation. If we use the metaphor of atraffic light, green is primary prevention and itsconcept would be that those who are free ofdrugs and alcohol. A yellow light tells us aboutthe risk and we must create possibilities to go
back to the green light. A red light is when aworker has very severe health problems due toaddiction. This requires constant treatment.
In a culture that accepts the use of alcohol,primary prevention must be pragmatic ratherthan dogmatic. Instead of intending to avoiddrinking, we should focus people on how to facealcohol and how to do it in their daily life and onspecial occasions. Union leaders and managersare also exposed to the same risks. Thus, theyshould also be part of a comprehensive policy ofany company.
And finally, it’s important to recall that in aworkplace where workers have problems, suchuse of substances also indicates problems in thesocial network, basically within the familysetting. So, the support of the family is afundamental part of a program that begins inthe workplace. Thank you very much.
Melody HeapsPresident and FounderIllinois Treatment AssessmentScreening Center, Inc.United States
Let me just very briefly talk to you about what Ithink are some elemental principles having to dowith this issue. You will have a track that indeedall afternoon and tomorrow will go throughsome of the programs that have attempted tobe the bridge between public health and publicsafety within the United States and with thegovernment of Mexico.
Let me begin by suggesting to you, that as wein the United States have faced an increasingillegal drug usage, and in fact even legal drugusage, we have put the burden of handling thatproblem on the criminal justice system to thepoint where the justice system itself has almostfailed. It is groaning with the weight of havingto process cases in our courts, of incarceratingindividuals. If we take my state of Illinois alone,in 1990 there were maybe 800 individuals whowere incarcerated because of drug offenses. Inthe year 2000, there are almost 11,000individuals. My state is not unique. And indeed,

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 51 Plenary Sessions
we focus on those numbers only of drugoffenses but the other offenses related to druguse which happen to be property crime offenseshave also escalated. So that the whole justicesystem, that which has become a foundation forour democracy is struggling to deal with theissue of substance abuse. And it is therefore,very critical that we begin to look at how we canintervene with the justice system to bring peopleout of that system into community treatment.Particularly because we know that there is anever ending cycle of arrest, addiction,incarceration, release, arrest. And so theopportunity to intervene in that cycle in aconstructive way is very important.
At the last conference, the speaker from thegovernment of Mexico talked about the publicsafety and public health systems as interlockingand that metaphor, I thought, was an excellentmetaphor. And what it brought to mind was howour spaceships have space stations and shuttlesto connect. And they’ve had to connect oftenbetween the Soviet Union and the United Stateswhere we’ve had different technologies. If wecan apply that metaphor to public health andpublic safety, the first principle is to understandthat both systems have not only differenttechnologies, but very, very different cultures.And in order to bridge the gap, in order toconnect those systems, there has to be adocking mechanism. At points along the system,we need something very specific which allows,as the Attorney General of Mexico spoke of thismorning, channeling of individuals whom wedon’t want to continue to prosecute or tocontinue to allow to penetrate further into thejustice system and further criminalize. And so adocking mechanism like a TASC program, or amore recent iteration, the drug court movement,is a mechanism which the United States hasused to move people from the justice system atall phases, from courts to corrections, into thecommunity-based treatment system.
The other thing you must understand is that thejustice system provides a unique opportunity asa catchment area to really go to what is perhapsa hot bed of what I consider a communicabledisease. If we are not intervening and looking atways to treat substance abuse, individualswithin the justice system will move into thecommunity and that disease will spread.
The importance that the justice system can offerthe public health system is sanctions, a way toovercome what we know to be one of thehallmarks of our substance abuse disease model– denial. The importance of sanctions instimulating recovery in an individual can be metand melded with the treatment process in sucha way as to encourage recovery as individualsmove along. I think if we begin, and if, forinstance the government of Mexico is beginningto look at the issue of bridging both systems, itis really critical that we understand that if weare going to put mechanisms in the justicesystem, we had better be ready with treatmentprograms. For instances in our correctionscenters if we get the justice system ready toidentify drug users, we’d better have communitytreatment. There ought to be dedicatedcommunity treatment that is rich in resources.That is obviously culturally sensitive but wemust get ready to handle the vast numbers thatseem to move from justice into treatment.
It is also important and a lesson we’ve learnedin the United States that we need to take astrategic macro approach when we look atforming programs and developing this bridge.That macro approach is not by finding the latesttrick or silver bullet or program that may solveour problem within six months. But we look atthe total justice system. We look at theproblems of usage in a community and wedecide to target areas, cases, individuals, to helpset up a systemic movement from justice intotreatment. It is critical that there be cross-cultural training because, again, we are dealingwith individuals in each system that are used todoing different things, thinking different ways,and using different languages. People in thejustice system think enforcement, thinkpunishment. People in the treatment systemthink rehabilitation. So, I suggest that these arevery, very obvious principles, but GeneralMcCaffrey gave me permission to be obvioustoday. That will help us at least conceptualizeand focus on the need to develop this newbridge or interlocking system. And again, Iwould stress to you the need to specifically lookat designing the function that will help dock, andbring together both the public health and publicsafety systems in both Mexico and The UnitedStates. Thank you.
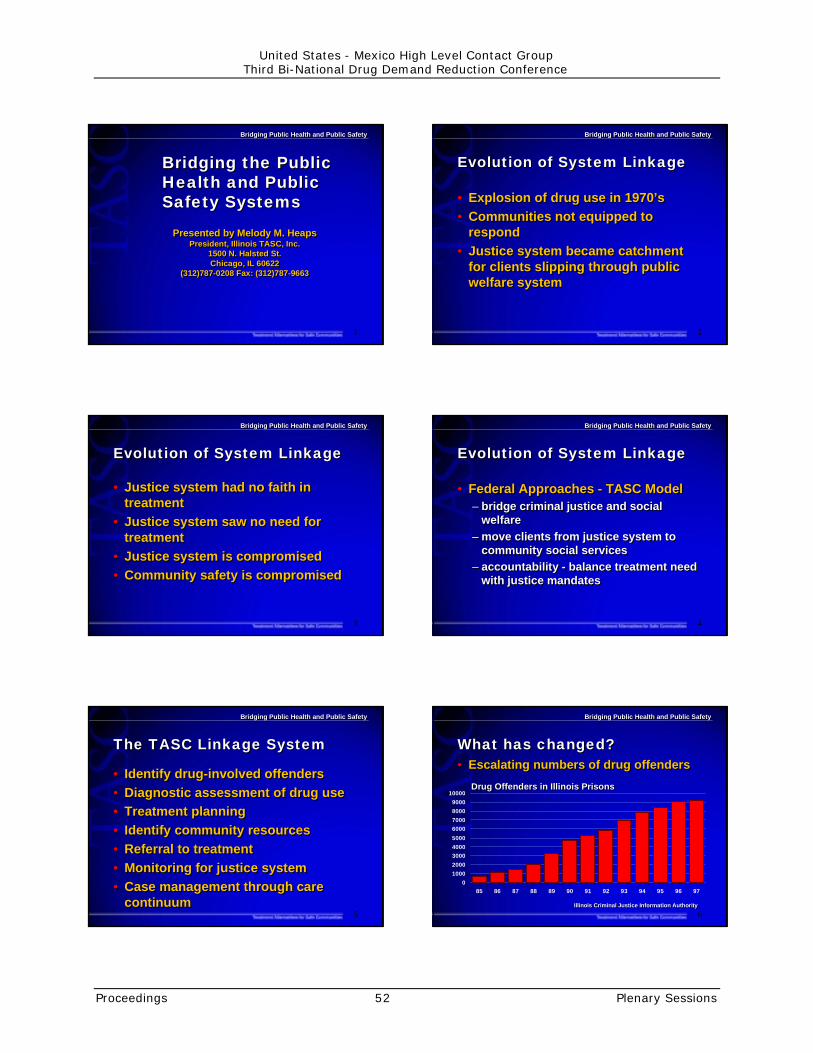
1
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Bridging the PublicHealth and PublicSafety Systems
Bridging the PublicHealth and PublicSafety Systems
Presented by Melody M. HeapsPresident, Illinois TASC, Inc.
1500 N. Halsted St.Chicago, IL 60622
(312)787-0208 Fax: (312)787-9663
Presented by Melody M. HeapsPresident, Illinois TASC, Inc.
1500 N. Halsted St.Chicago, IL 60622
(312)787-0208 Fax: (312)787-9663
2
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Evolution of System LinkageEvolution of System Linkage
•Explosion of drug use in 1970’s•Communities not equipped to
respond•Justice system became catchment
for clients slipping through publicwelfare system
•Explosion of drug use in 1970’s•Communities not equipped to
respond•Justice system became catchment
for clients slipping through publicwelfare system
3
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
•Justice system had no faith intreatment
•Justice system saw no need fortreatment
•Justice system is compromised•Community safety is compromised
•Justice system had no faith intreatment
•Justice system saw no need fortreatment
•Justice system is compromised•Community safety is compromised
Evolution of System LinkageEvolution of System Linkage
4
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Evolution of System LinkageEvolution of System Linkage
•Federal Approaches - TASC Model– bridge criminal justice and social
welfare– move clients from justice system to
community social services– accountability - balance treatment need
with justice mandates
•Federal Approaches - TASC Model– bridge criminal justice and social
welfare– move clients from justice system to
community social services– accountability - balance treatment need
with justice mandates
5
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
The TASC Linkage SystemThe TASC Linkage System
• Identify drug-involved offenders•Diagnostic assessment of drug use•Treatment planning• Identify community resources•Referral to treatment•Monitoring for justice system•Case management through care
continuum
• Identify drug-involved offenders•Diagnostic assessment of drug use•Treatment planning• Identify community resources•Referral to treatment•Monitoring for justice system•Case management through care
continuum6
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What has changed?What has changed?• Escalating numbers of drug offenders• Escalating numbers of drug offenders
0
1000
2000
30004000
5000
60007000
8000
9000
10000
85 86 87 88 89 90 91 92 93 94 95 96 97
Drug Offenders in Illinois PrisonsDrug Offenders in Illinois Prisons
Illinois Criminal Justice Information AuthorityIllinois Criminal Justice Information Authority
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 52 Plenary Sessions

7
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What has changed?What has changed?• Increased drug use among arrestees• Increased drug use among arrestees
70.6
71
70.3
71.5
62.7
64.4
56.8
74.2
MaleFemale
Chicago
Las Vegas
Phoenix
drug of choice - cocaine
drug of choice - cocaine drug of choice - cocaine
drug of choice - cocaine drug of choice - marijuana
Los Angeles
drug of choice - cocaine
drug of choice - cocaine drug of choice - cocaine
From NIJ’s 1998 Arrestee Drug Abuse Monitoring StudyFrom NIJ’s 1998 Arrestee Drug Abuse Monitoring Study8
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Based on estimates from GAO, CASA and the Federal Bureau of PrisonsBased on estimates from GAO, CASA and the Federal Bureau of Prisons
0
100000
200000
300000
400000
500000
600000
700000
800000
900000
1992 1993 1994 1995 1996
Inmates needing TxInmates in Tx
Total State and Federal InmatesTotal State and Federal Inmates
What has changed?What has changed?• Gap between need and availability of treatment• Gap between need and availability of treatment
9
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What has changed?What has changed?
•Client profile– Mix of substance abuse and criminality– Economic & social dysfunction– Mental illness– Compromised/vulnerable health status– Impulsivity & aggression
•Client profile– Mix of substance abuse and criminality– Economic & social dysfunction– Mental illness– Compromised/vulnerable health status– Impulsivity & aggression
10
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What has changed?What has changed?
•Justice system recognizes need forcommunity resources– Federal overcrowding lawsuits
•Justice system more compromised
•Justice system recognizes need forcommunity resources– Federal overcrowding lawsuits
•Justice system more compromised
4700
1130614000
17500
0
5,000
10,000
15,000
20,000
1983 1991 1995 1998
Cook County, Illinois Felony Drug CasesCook County, Illinois Felony Drug Cases
There are now morefelony drug cases inCook County thantotal felony cases inany year before 1988
There are now morefelony drug cases inCook County thantotal felony cases inany year before 1988
11
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What is still needed?What is still needed?
•Federal and local policy that movesfrom program-level response tosystem-level response
•Federal policies that respond to allphases of justice system:– pre-trial– sentencing– corrections– parole
•Federal and local policy that movesfrom program-level response tosystem-level response
•Federal policies that respond to allphases of justice system:– pre-trial– sentencing– corrections– parole
12
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What is still needed?What is still needed?
•Funding that mandates systemlinkage infrastructure
• Increased, dedicated treatment base•Funding for and focus on community
re-entry
•Funding that mandates systemlinkage infrastructure
• Increased, dedicated treatment base•Funding for and focus on community
re-entry
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 53 Plenary Sessions

13
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
What is still needed?What is still needed?
•Funding responsive to clienttreatment issues– culture– gender– co-occurring mental illness– cognitive and behavioral problems
•Funding responsive to clienttreatment issues– culture– gender– co-occurring mental illness– cognitive and behavioral problems
14
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Recommendations:Recommendations:•Macro approach
– addresses drug use impact on justicepopulations
– addresses treatment accessibility
•Target priority justice populations•Develop linkage infrastructure
programs like TASC
•Macro approach– addresses drug use impact on justice
populations– addresses treatment accessibility
•Target priority justice populations•Develop linkage infrastructure
programs like TASC
15
Bridging Public Health and Public SafetyBridging Public Health and Public Safety
Recommendations:Recommendations:
•Develop adequate dedicatedcommunity treatment resource base
•Cross-cultural education for justiceand treatment personnel
•Develop adequate dedicatedcommunity treatment resource base
•Cross-cultural education for justiceand treatment personnel
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 54 Plenary Sessions

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 55 Plenary Sessions
Rafael Velasco FernándezPresident, Center in Studies onAlcohol and Alcoholism, A.C.Mexico
The first thing I want to say is that I feel veryfortunate and surely so do you of having beenhere, listening to people who know what they’retalking about. They are conveying theirexperience and in some point, really update usof things on which we all want to know. If youwill allow me, I would just like to stress on thebasis of my own criteria, which I hope you finduseful, something of what was said here byeach of those who spoke before me. Especiallyas regards those things that have a certainimpact on our own country.
Mr. Wilson gave us a good and bad piece ofnews initially. This has become customarywhenever we speak of drugs. Almost alwayswhen we have piece of good news regardingsome reduction in use and so on, it comes handin hand with something which is not all thatgood. Mr. Wilson was telling us, and this isexcellent, that adolescents in the United Statesand juveniles are consuming less drugs now.Less illegal drug use. This seems to me to beexcellent news and it has already happened inother areas, stages of time. And then it goes upagain. But it seems that the reduction now is asustained one, which is good news. And wehave to begin to ask ourselves whether it isbecause of programs that they have underwayor are providing very good results or whetherthere are other factors involved. Probablythere’s a bit of everything that is responsible,but we would have to research more in depth toknow what is helping to improve things.
The bad news is that more and more youngpeople are initiating the use of alcohol andtobacco. So this leads to other questions. All ofthe fruitful research that is done brings up newquestions. It provides answers to certainquestions, previous questions, but it opens upother questions not yet answered. He also saidsomething that was of great interest to meregarding the youth groups in the United States,along the U.S.-Mexico border. He asked that wehave an exchange so that the groups on ourside, on the Mexican side, can get in touch with
them. Well, probably, the funding of our groups,in spite of what we’ve heard here with ourSecretary of Health giving them the financialsupport, is not very similar to the 30 milliondollars being devoted to such programs in theU.S.
Nevertheless, I believe that establishing linksdoesn’t necessarily mean that they have to lendus some of those 30 million dollars. It meansthat we must work together and do things thatwill really help to improve the programs that wehave along the border. Mr. Wilson has worked agreat deal in the field of drug-relateddelinquency. And it is an excellent thing for meto have had the opportunity of hearing himtoday. Dr. Clark told us about the end product oftreatment as he called it. What happens at theend of these prevention programs and thetreatment of drug addictions and use. Hereminded us of something that we often forget,that the treatment of episodes must be costeffective. And if we don’t do it appropriately, itwill be more costly later on.
Although perhaps not specifically, but Dr. Clarkdid speak in favor of assessments andevaluations. And I’m very pleased because that’sone of the problems that we have in ourMexican programs. We have to work towardsassessment. Not a quantitative type ofassessment or evaluation, not the one that hasto do with how many took the courses, howmany supervisors we have to train. But ratherthe qualitative assessment of what we havedone. Whether the goals of our programs havebeen met, what we expected to do was actuallybeing done. So, a qualitative type of assessmentis fundamental. And it is being done on the U.S.side and it’s producing good results and I’m gladthat he stressed this.
He also announced a study to be done on thebest treatment adapted to specific high-riskgroups. He ended by saying that, this is veryinteresting because it will provide us with furthernews in future that could be useful. What I’msaying is that luckily we are now undergoingmoments during which programs are beingassessed after 20 or more years that they havebeen underway. This discovery which seems tobe a very basic one ? that we have to discoverwhat are the protecting factors and the risk

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 56 Plenary Sessions
factors ? could seem like a truism, somethingvery logical that everybody should be aware of.But if we really don’t know what those riskfactors are and if we don’t identify what theprotective factors are, we cannot really put outvery many protective programs and effectiveones. And here they are undertaking an effort tocontinue to assess programs.
He also said something very interesting. He saiddetoxification is not treatment. At least not thecomprehensive treatment against addictions anddrug use. Nevertheless it is a very importantpart of it. And it must be done.
Fine. I think I should go on to talk about Dr.Condon. His expression that science isinternational is an excellent one, and we allknow it, but we don’t always remember this.Modern imaging and the images that we have ofdrug use and abuse and addictions aresomething which is relatively modern and isincreasing in importance to all of us. But it’s veryimportant that in meetings such as this, andthat’s why I’m saying that we’re fortunate inhaving heard so many points of view, it’s veryimportant that we’re told about basic sciencesand the research that leads to other things, interms of prevention for example. And hisexpression that drug use is preventable, andaddictions are treatable, is something that we allhave to learn. When we first give a conferenceor lecture on subjects such as this, its veryimportant that everybody listening understandthis, especially in the field of health.
Mr. Condon spoke about risk reduction andstrengthening protective factors, and the idea ofintroducing these into the very effectiveprograms. He also said a very basic truth thatwe must all remember: that young people takedrugs in order to feel better and to feel goodabout themselves. This is something we mustnot neglect or forget when we talk to our youngpeople about the problems that they have toface and the reasons why drugs are consumed.He also clearly told to us about activating thepleasure circuit as it has been called lately. Hetalked about the dopamine effects or dopamine-like effects. What happens with certain neuro-transmitters and so on. And I would like to tellour colleagues who are not physicians orbiologists or bio-chemists, but who view this
problem from the field of social psychology,anthropology, and who collaborate with otherspecialists in the field of drug use andprevention, to also read this. They also realizethat in principle, addiction is a relationshipbetween a substance and a living biologicalbeing. It’s fundamental that we know about this,at least as has to do with the general guidelinesof it, the basics of this relationship.
That’s why his statement that addiction is adisease of the brain, seems to me an excellentway of viewing things because in fact the braindoes become ill when it has become used toconsuming these substances. The expression ofthis problem goes beyond the purely biologicalrealm. It has to be something more than just abrain pathology, although basically that is whatit is. Therefore, treatment must becomprehensive, and that’s why I think that if weare talking about a multi-factorial problem, thenthe treatment must be comprehensive. Andinclude all of the factors that have an impact onthe problem when treating.
Haydée Rosovsky stressed the idea of leadingmore healthy lifestyles. She led us from thebasic sciences to the psycho-social sciences. Wealso must take note of. There are other factorsthat we have to research for our youngpopulation, not only those that will lead them todeviations in behavior. She mentions self-esteem and other things. She said that in schooland in the community and in the work place andrecreation centers, we must work towards theself-esteem. And this goes hand in hand withthe idea that is in the minds of many teacherswho view the use of drugs and the appearanceof this use of drugs in the streets. They viewthis, not only as an educational challenge but asa universal failure of education. Many of theseoutstanding teachers have said that we haveforgotten and neglected to shape personalitiesand have devoted more time to providinginformation. It’s a necessary supplement of thebasic sciences of course, this view. And we arereminded to consider cultural diversity. Thatwhich is implemented in one place is not alwaysas successful elsewhere. It is true that there arecertain aspects of basic sciences that are validwithout any borders or obstacles anywhere, butshe marked differences between our youngpeople, their habits and those of other latitudes.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 57 Plenary Sessions
And she almost closed by saying somethingwhich was of great interest to me, which is topoint out that every preventive effort should bebased upon research first and foremost.Research, not only basic research, but alsosocial and other types of research that willprovide support is truly useful for our programs.
Dr. Augustine Velez reminds us that we mustn’tonly ask ourselves about our children andadolescents vis-a-vis drugs, but we should alsowonder about all individuals at all ages,especially in the workplace. This is extremelyimportant and he reminded us not all youngpeople are students. In countries such as ours,much less so. And, on the other hand, adultteachers at school, at the workplace, aresometimes consumers both of legal and illegal,or licit or illicit, drugs. It’s hazardous forteachers to take a mistaken approach to thatproblem at the schools. And that’s one of theissues that we have in our country which is thatof truly and really training our teachersappropriately. This must be said. They are notbeing truly well-trained to face up to thisproblem. Truly in developing countries wedemand a great deal from teachers. If there’s anecological problem, we tell them to talk aboutthe ecology. If there’s a problem in sexualeducation, we introduce sexual education in thecurriculum. If there’s a drug problem, we alsoask them to approach that. And in generalterms, they are not appropriately trained to doit. I’m pleased that this was brought up here.
We were told about the money that is lost.Absenteeism. The drop in productivity. And Iwould yet add something else that wassomewhat expressed, but cannot be measured.The moral suffering of the worker, of his or herfamily and his co-workers. There’s also apolitical issue here at stake, because we have totry and involve entrepreneurs and businessmenmore, as well as the unions. Dr. Velez talkedabout the two strategies: the one that attacksthe already existing problems and the otherpolicy to prevent problems.
Dr. Bernstein told us that in the United Statesmany young people work part-time and also full-time. And that it’s quite fair that we should tryand make sure that their workplace be free of
drugs. We have to sit down and think in Mexicoabout the great differences that still separate usfrom what is being done in the United States. Ithink we still have a long road to cover in termsof knowledge, of training, and of revision of lawsand regulations. This is what I was taught bywhat Mary Bernstein said here about the effortsundertaken in the United States on this issue.Drug users, she told us, get ill more often. Andthis is a cost that we normally don’t take intoaccount. They get ill, not only of the thingsdirectly related to their drug use, but theysimply are generally weaker and can thereforecontract illnesses more frequently. And sincethey generally are less responsible, they havemore accidents, both in the workplace andoutside the workplace.
She also told us about the law. I hadn’t anopportunity to jot it all down, but I doremember that she stressed the aspect oftraining, education, policies of zero tolerance.She said, this is something we really have toponder. And timely care. She also mentionedtesting here which is something we have towork a great deal on in Mexico. I’m not sayingit’s not done. It is done. But the test and thecomparisons of laboratories is a matter that wehave to really study in-depth.
Dr. Melody Heaps stressed the need of linkingthe justice system to the health care system ortreatment system. Here again we in Mexico havea great deal to be done. And what she said wasuseful to me: more than anything we shouldreflect upon the fact that our preventiveprograms should be linked with many otherthings and activities. In Mexico we are still notestablishing those links. So, this meeting, Ithink, leaves behind good experiences andlearning. Each of those that has spoken, hasspoken on the basis of their own excellentpersonal expertise. What they have said mustbe translated to each of our countries so thatthose of us who work in the areas of preventionand treatment can really become enriched withthis knowledge here presented. And I repeat, itwas a pleasure to be here today.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 58 Plenary Sessions
Mobilizing Parents forPrevention
Jesús Cabrera SolísDirectorCenters for Youth Integration (CIJ)Mexico
Today, we have two outstanding people fromour two countries whose contributions willundoubtedly be of great interest to everyonehere today. The first to take the floor shall beMr. Bautista, who is President of the NationalParents Association in my country. He has a BAin business management and specializes inbusiness direction. Prior to being President ofthe National Parents Association, he wasPresident of his State Association for theparents. I briefly would like to tell you howimportant this parents’ association is by first ofall pointing out that in our country we have 19million parents with children in school. There area total of 194,500 committees of parentsthroughout the country, one per school. Therealso are 32 state parents associations, one perstate. And grouped in this national associationare parents whose children are in different typesof schools, such as the special educationchildren, preschool children, grade school,middle school and secondary school children.This association groups together all of theparents with children in private and publicschools.
L.A. Jose Luis Perez BautistaPresidentNational Association of ParentsMexico
Mobilizing parents is a very important goal. Weshould strive in workshops, training sessions,exhibits, conferences, preventative meetings,and at sports events to talk with parents withthe common objective of preventing drug useand addiction. Parent associations have beenimportant sources for sharing information inschools as well as in the home. Parents canattend the school where their children study,
and schools can offer workshops that deal witha great many subjects that benefit therelationships between the home and the school.It is in the schools where subjects of preventionand drug use are delved into and informationcan be brought to all parents. If we considerthat the school, the community and the parentsas well as participating institutions are allworking towards a common end, then we willagree that our joint work toward theseobjectives will produce better and greaterresults than the isolated efforts of only one ofthe parties. Many experiences have shown this.
Experiences that link the school with thecommunity are vital and can be achieved bydevoting an hour per month or every fortnightto holding meetings with parents and childrenand youths. Subjects can be approached in abasic and simple way, for example, entering intoagreements to talk with their family membersabout specific topics of importance to the workof prevention.
It is important to consider that today educationis not to be given in an isolated way. Rather, itoften involves a comprehensive effort by manyinstitutions working together. These institutionscan form a comprehensive development systemwhere the family, the National EducationInstitute for Adults, the Social Security Institute,state workers, Social Services, the Departmentof Health, Youth Integration Centers, GeneralAttorney's Office, and representatives fromMexico City and the country participate togetherconstantly in the area of education. Suchcollaboration allows these agencies andinstitutions to focus their specialized knowledgeof prevention and their experienced preventionstaff to work with teachers in their schools inorder to provide broad knowledge aboutpreventing youth substance use. Also, schoolcurricula contain information regardingdelinquency prevention, lack of safety,preventing drug use and addiction, smoking,and alcoholism. It is important to remember thatmany times these subjects are also important todiscuss with parents.
The right to protect the health of children, ofyoung people and of all Mexican citizens is setforth in our Constitution and its provisions. Tofully comply with this, all institutions and parents

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 59 Plenary Sessions
need to work together. Institutions must offerthose services required for the well-being of thepopulation. And parents in the community atlarge should accept the commitment individuallyand collectively, of developing and implementinga prevention culture, self-care, and safety. Weknow that health, safety and education are ashared responsibility. Parents who haveorganized in our country ratify our commitmentto continue contributing in these areas. Thegovernment of our country must continueforward with firm public health policies, policiesof safety and education that are congruent withthe needs of most Mexicans. Organized parentsin the country and our organization, throughme, have firmly requested that the health andeducation sectors, as well as those institutionsand agencies in charge of law and safetyenforcement, establish closer coordination linksto reinforce the training and education of ouryouth in order to prevent violence anddelinquency. To this end, undoubtedly, the jointresponsibility of everyone is required. In thearea of health and prevention, we and ourchildren require constant orientation campaignsthat will allow our community to reduce the risksand diseases as well as addictions and violencethat they produce.
It is timely to repeat that the National Parents'Association finds it necessary to reinforceguidance programs and information programs inthe areas of drug use, violence and crime, bothfor our parents as well as for our children. Weneed to strengthen the mechanisms that willallow for us to more rigorously inform ourchildren and our youth throughout the schoolsystem, so that we can truly, more efficientlyprevent and alert them regarding the brutal riskthat drugs represent for their own health andthe eventual health of their families. That is whywe must speak to our children objectively andtruthfully with the greatest respect that allfamilies and sectors of the population deserve,but also clearly enough so that all of ourprograms and campaigns will have the impactwe want. We know of no father wishing evil forhis or her children. We know of no teacher thatwishes to shape a poor citizen, but I also knowof no other way of guiding parents and familiesif it is not through the help of everyone thattakes part in the educational process and in ourinstitutions.
The government, headed by President Zedilloand his distinguished wife as well as the parentsof our country have joined efforts. We mustacknowledge that we have a good stretch tocover, but only through the will and organizedwork of institutions and the community, can weforge ahead. Parents will make this effort infavor of our children, for our schools where theygo to receive knowledge, and for Mexico. Thankyou very much.
Henry LozanoPresidentCalifornians for Drug Free YouthUnited States
It’s an honor to be here today. It’s an honor toaddress you. As my esteemed colleagues havealready mentioned, the basic principle of ourdiscussion this afternoon is to think about theimplications of the family. How many of youknow that across this country, and across othercountries, when you mention things likeprevention, and then connect the logicalconnector, in my mind – the family, thatsomehow there’s a bridge that still has to bebuilt to understand the importance, the valueand the implication of families and parentscoming together in communities to address theissue of substance abuse and illicit drugprevention?
How many of you know that there’s still a bridgeout there that has to be crossed? There’s still avast lack of understanding about the value ofcommunity. I’m proud to be part of a numberof institutions and agencies across this countrythat have forged bridges into communities, thathave forged alliances with different agencies,and have gone the extra mile in their efforts toconsider how they might approach bringingtogether agencies, communities, resources, andmost importantly, family. Parents. La familia.The center. The core of every institution withinevery city. You know how we always draw thecase that we have to move to the cities. We’vegot to move to the communities. We’ve got toimpact the legislatures. We’ve got to impact thelocal civil governments and the institutions that

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 60 Plenary Sessions
reside out there. But more at heart, we have toimpact the family.
I compliment the previous speaker in his pointsabout understanding specifically that there isn’ta family anywhere, not one family, that wouldlook upon their children without heart and notwant the best for their child, the best in thatchild’s development, education, welfare, growth,environment, status, and achieving. The onething I do know, that this morning, as thisconference was started, we had a wonderfulcommunicator. A speaker before the dignitaries,a dignitary in her own right. A young lady whoadvanced the charge, a charge about hernation, a charge about her people and a chargeabout the declaration of the value of youngpeople in their incorporated necessity in whatwe call prevention and family dynamics. I wouldsay to you that the reason we continue to callparents and family the hardest domain to reachis because we haven’t understood what they’relistening for. We continue to frighten ourfamilies. The moment we use the word drugs,we have families across this nation and acrossMexico that instantly are perplexed by thedilemma of what it would mean to associatewith a drug prevention organization. Wouldsomebody actually think that my family wasinvolved in that kind of a lifestyle? If I went tohelp and support, would somebody perceive thatwhat I was there for was help? Across thisnation and across Mexico, we have a commonthread, a common theme to involve andincorporate people. One of the campaigns thatI’ve been honored to be involved with was thiscampaign that was under SAMHSA’s directionand The Center for Substance Abuse Prevention(CSAP). Our administrator, Dr. Nelba Chavez,founded this program, moved it across thiscountry with the Association of CollaborativeAgencies, and important individuals in this roomwho advanced it. The project had a primaryfocus. The focus was to deliver to parents, bothEnglish and Spanish, a tool-kit, a digest ofsuggestions and possibilities of programsdialogue forums to encourage communities tostart talking at the family level. And the questionhas always been: what can this do?
Let me give you a quick brief of what this cando. I stand here a proud and honored son oftwo incredible people — two individuals who
gave me my life, who gave me anunderstanding of what it is to work everyday.My father’s side came from Chihuahua, Mexico.My mother’s side are Apache from southwesternNew Mexico. These two people gave me what Iunderstand today to be an honorable son. Theygave me the facility to understand what it is tobe a son of integrity, a son who responded tohis father’s name, a son who respected hismother. Now you smile at that because in thisgathering, that understanding is imperative. Ihad a father who worked seven days a weekand a mother who carried a broom seven days aweek, not to sweep the floor but to crack it onour backs if we didn’t respond the way weshould have while Daddy wasn’t there. Iunderstood at an early age. From the early daysof my upbringing the one thing inside of me, theone thing that held me true to course, the onething that advanced me forward, was theunderstanding that my mother and father caredabout who I was as a child, that my fatherunderstood the value of complimenting me as ason, that my mother understood the value ofalways being my public relations expert.
Every time mother got up and introduced me,she would tell everybody 50% of a non-truth bytelling them how wonderful I was. And shewould tell 50% of the truth. All of those thingsthat I did do. But my mother continued toadvance the prospect that her firstborn son wasa man of honor and integrity like her husbandwas.
Why did my mother do that? Why did mymother continue to advance a son in such aspectacular way? And then subsequently, mybrothers and sisters? Because my motherunderstood that the man she married, EnriqueLozano, was a man of integrity, a man of honor,a man of value. And to inspire that in me, shehad to continue to reinforce in the community’spublic eye, that I was also a man of integrity.And what did that mean in our family? What didthat say about us? What impression did thatgive about us locally? It gave other people theimpression that this firstborn was a man whowas going to carry out his father’s ways.
I want to tell you that that was the mostimportant lesson my family could have evergiven me. All of the curriculum, of the
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 61 Plenary Sessions
institutions, of the programs that wereassembled could never have taught me what mymother and father gave me in my principles oflife. And I’m proud of that. I’m proud of wheremy dad, proud of where my mother’s peoplecome from. On this side of the border I’m proudof who I am. And to understand that pride in meis what I gave to my children. It’s what I hopeto give when I’m a grandfather. I hope to seethat respect come back to me. I’m going to tellyou why. I’m going to tell you that we mustcome to that conclusion as a country.
I’m proud to be of another campaign – TheNational Media Campaign. The Anti-DrugCampaign that is moving across this country tobring a baseline value of understanding andclarity to this nation on how it goes aboutinvesting in its children. In my mind it’s the mostimportant campaign of value that could happenin the United States. I’m proud of theleadership, the director, General BarryMcCaffrey, and the Office of National DrugControl Policy, and the strategy that’s beenimplemented to move a campaign across thisnation, to send this country a message: that ouryoung people are not tomorrow’s future. Pleasehear this. That our young people are nottomorrow’s hope. That our young people are nottomorrow’s future. They are today’s future. Ouryoung people happen to be the pride of today.My mother never said to anybody in public,when this young man finally grows up, then he’llhave some value. When this young man finallygets his degree and five years experience, thenhe’ll be worth something. When this man finallygets to be, well, as tall as my father, when thisyoung man can fill my father’s shoes, or myhusband’s shoes, as my mother would say, andwalk in them in a manly way, then he will be ofvalue. My mother understood intrinsically thatthe value was placed within me coming fromher, from her very words, from her heart. Myfamilia, my family, is a family that’s intact today.A family of brothers and sisters that wait for ourannual reunions, that have a better time whenwe’re together than when we’re not. And it’s allbecause of two people who championed that thecommon thread, the common voice in both ourcountries. We have to speak with confidence,with integrity and dignity to our young people.But not about what they’re doing wrong, butabout what they’re doing right.
We have to move and advance throughout bothof our countries. The honor and respect of thefamily as it is today. The common theme thatboth of our countries understand is that we havesomething of value, imperative value, that existstoday. It’s our young people, working alongsideus. Now. Not tomorrow. Not after they go toschool. Today. It’s moving our young people insuch a primary form that that young womanwho spoke this morning would be the championof every other young voice in both of ourcountries, if they would speak with thededication and honor, knowing that somedaytheir mother and father are going to hear thosesame words, those same suggestions, that anymother or father that would sit right there andlisten to their son.
If it wouldn’t have been that today was the dayand my mother and father were otherwiseengaged, my hope was to have my father andmy mother sitting right there right now. Myhope would have been that with these eyes, Icould have looked at my father and I could havelooked at my mother at this luncheon and Icould have said “Salute” to them. I could havebeen with honor to understand that my peoplegave me a destiny. A proud destiny.
Toolkits. I’m proud of this one. Probablybecause I sit on the steering committee andbecause I get to work with a wonderful group ofpeople. I want you to know that this is awonderful product that would work in Mexico aswell as the United States. And I know theadministrator and the local dignitaries here fromSAMHSA would love to move this to bothcountries. I would love to be invited to advancethis product because it’s a product that has anethic to it. That has a moral support to it.
Another opportunity I’d like to share with you isthat within this nation, there’s a network ofpeople who are working together to advance theissues of alcohol and substance abuse acrossour people’s venues. And there’s a conferencethat’s going to happen. I’m sounding like ahawker now. It’s for the millennium. It’s goingto happen October 18-20 in Albuquerque, NewMexico. That conference will bring together thefinest in research, the finest in researchers, andleadership across this nation to look at our

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 62 Plenary Sessions
issues and to consequently forge together thebridge to the communities, the bridge to theleadership within communities. I would invitethose of you from Mexico who sit here today toknow that we invite you to that conference. Wewould like to forge that bridge with thewonderful work that’s going on. We have beguna bridge to connect to our families. The day istoday. Today is the day to continue to advance.
I would also like to thank our Department ofEducation. I would like to thank Mr. WilliamModzeleski who is here today, because of theschools and the imperative projects that havegone on with our Safe and Drug Free Schoolsand Communities Act, the projects that haveventured across this nation to reach youngpeople. The caretakers who usually become theformal providers for our young people happen tobe those educators across this country who actas surrogate parents in incredible ways. Thetools that are needed are there. The instrumentsthat are needed are there. The collaborationmechanisms for these two countries comingtogether are there. I am proud that there areyoung people here today. Without these youngpeople, without the people right there with us,our wholeness, our young people, young menand young women who are the leadership here,without them, we the fathers and mothers donot have a future.
My closing comment: When I’m a grandfather, itwill be in my honor and dignity to havegrandchildren who want to come and see me.Just like I want to see my mother and father. Itwill be an honor for those little kids to sit in mylap. To sit and look up at grandpa and to say Ilove you. It will be an honor for this grandfatherto tell his grandchildren that, just as my fatherand mother gave me that gift, I love you back.Do you know what? I will never understand thatprivilege unless I create the respect and thetradition of that love and honor within my ownchildren’s lives. Because they will be the onesthat will convey that thought to mygrandchildren. They will be the ones that tell mygrandchildren in their homes that Grandpa’s agood man. Grandma’s a good woman. We needto go see Grandma and Grandpa.
What does this have to do with prevention?Prevention in its heart and soul, is the fabric of
this nation’s mind and the nation’s mind inMexico. It was us remembering that the prizeand the goal that we always had, was to raisechildren of honor, dignity and purpose.
Program Evaluation
José Vila del CastilloModeratorRepresentative for Mexico andCentral AmericaUnited Nations International DrugControl Program (PNUFID)
Thank you very much for inviting me tomoderate this section on program evaluation.I am sure you will agree that we have chosenspeakers who are very highly qualified andhighly respected authorities in the preventionand treatment of drug abuse.
Evaluation of PreventionPrograms
Abraham Wandersman, Ph.D.University of South CarolinaUnited States
Dr. Wandersman’s session described howevaluation can be helpful in achieving substanceabuse prevention, program improvement andprogram outcomes. The session highlighted:
• Empowerment and Evaluation
• Getting to Program Outcomes: A results-based approach to accountability.
Dr. Wandersman pointed out that the goal ofEmpowerment Evaluation is to improve overallprogram success. It provides programdevelopers with tools for assessing the planning,implementation and results of programs. Thus
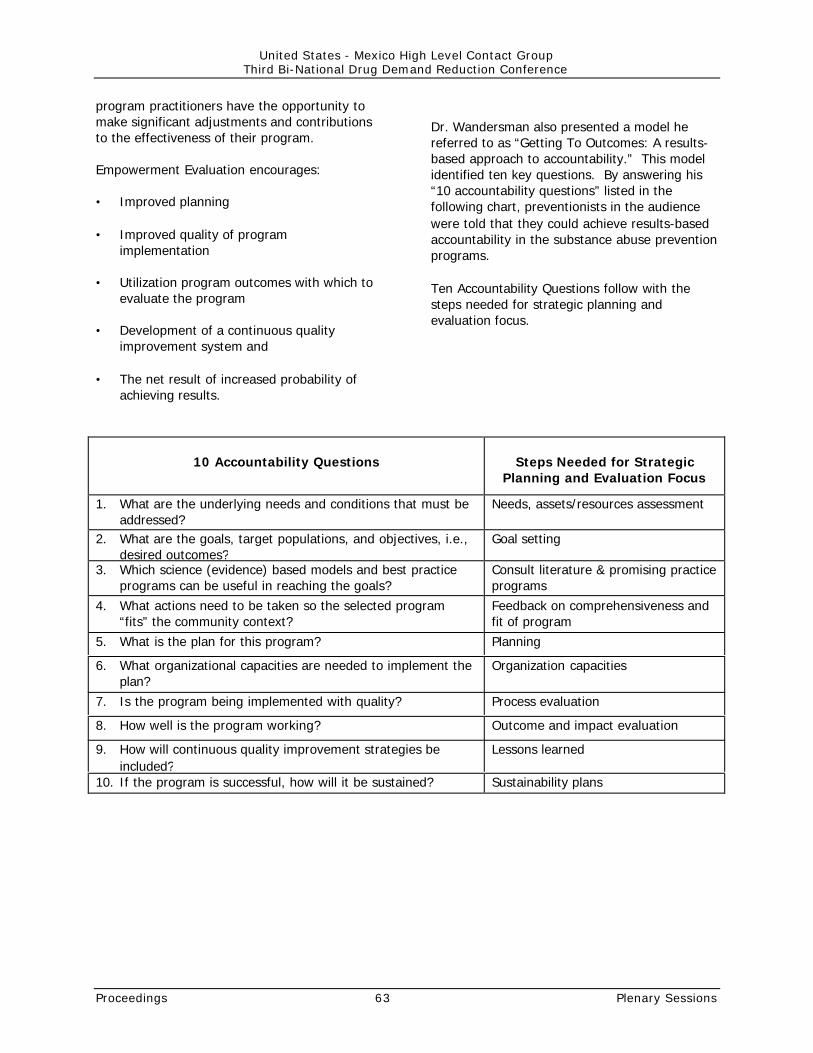
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 63 Plenary Sessions
program practitioners have the opportunity tomake significant adjustments and contributionsto the effectiveness of their program.
Empowerment Evaluation encourages:
• Improved planning
• Improved quality of programimplementation
• Utilization program outcomes with which toevaluate the program
• Development of a continuous qualityimprovement system and
• The net result of increased probability ofachieving results.
Dr. Wandersman also presented a model hereferred to as “Getting To Outcomes: A results-based approach to accountability.” This modelidentified ten key questions. By answering his“10 accountability questions” listed in thefollowing chart, preventionists in the audiencewere told that they could achieve results-basedaccountability in the substance abuse preventionprograms.
Ten Accountability Questions follow with thesteps needed for strategic planning andevaluation focus.
10 Accountability Questions Steps Needed for StrategicPlanning and Evaluation Focus
1. What are the underlying needs and conditions that must beaddressed?
Needs, assets/resources assessment
2. What are the goals, target populations, and objectives, i.e.,desired outcomes?
Goal setting
3. Which science (evidence) based models and best practiceprograms can be useful in reaching the goals?
Consult literature & promising practiceprograms
4. What actions need to be taken so the selected program“fits” the community context?
Feedback on comprehensiveness andfit of program
5. What is the plan for this program? Planning
6. What organizational capacities are needed to implement theplan?
Organization capacities
7. Is the program being implemented with quality? Process evaluation
8. How well is the program working? Outcome and impact evaluation
9. How will continuous quality improvement strategies beincluded?
Lessons learned
10. If the program is successful, how will it be sustained? Sustainability plans
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 64 Plenary Sessions
Evaluation of TreatmentPrograms
D. Dwayne Simpson, Ph.D.Texas Christian UniversityUnited States
Numerous studies based on almost 300 drugabuse treatment programs and 70,000 patientsover the past 30 years have shown thattreatment can be highly effective in reducing oreliminating drug use, criminality and relatedproblems. However, all patients do not have thesame needs and all programs are not equallyeffective, so treatment evaluation research hasexpanded in recent years to focus on how tomaximize treatment effectiveness and efficiency.General findings show that ––
• Problem severity dictates the appropriatetype and intensity of treatment needed.
• Patients with moderate-to-high problemseverity levels usually need at least threemonths of treatment (and for chronic opiateaddiction, this increases to a year or longer)before significant benefits can bedocumented following release. As problemseverity increases, the need for and benefitsof intensive residential care rises. Goodassessments of patient needs and progressare therefore essential.
• Cognitive stages of treatment readiness (ormotivation) influence the chances thatpatients will engage and benefit fromtreatment. Special cognitive-based“induction” strategies for poorly motivatedpatients can be effective antidotes,especially in correctional settings.
• Several distinct, sequential phases oftreatment (e.g., referral, induction,engagement, early recovery and continuingcare) are related to addiction recoveryoutcomes of patients. Establishment oftherapeutic rapport is particularly important.
• Specialized interventions have beendeveloped that can improve each of thesecrucial steps of the therapeutic continuum.
Jesús Cabrera SolísDirectorCenters for Youth IntegrationMexico
Optimizing valuable resources is an overarchingprinciple in selecting effective drug abuse andaddiction treatment. Mr. Cabrera, underscoredthe following points:
Network of Service Providers
At CIJ privileged rights are granted to:
• mixed operating units that offer preventionprograms, community mobilization, andtreatment,
• ambulatory therapeutic service units, whichare promoted in areas of high demand forservices, and
• residential therapeutic units, strategicallylocated across our country for the purposeof providing specialized services to complexcases.
Financial justification
The financial justification is based on thefollowing example:
• At CIJ, residential service is offered through3 month programs; 122 cases are seen, ofwhich 70 cases or 57% go through recoveryand are released.
• The annual operational cost for this type ofservice is approximately U.S. $356,000.
• Through the ambulatory service system, andfor a similar line of cost, effective treatmentcan be offered to 1,284 cases annually, ofwhich 449 or 35% can be treated andreleased.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 65 Plenary Sessions
• At centers with mixed operating units,preventive programs are offered to 70,500persons, services are provided to 512 caseswith addiction problems, of which 130 casesor 25% are treated and released.
Based on these concepts, the 54 operating unitsthat form the institutional network for serviceproviders offer prevention, treatment, andcommunity mobilization programs; 4 unitsprovide ambulatory treatment services; and 3units provide residential services.
Behavioral Training
The institutional training for modality programsis composed of the following:
• Therapists are trained in basic, intermediate,and advanced levels,
• Instructors are trained in individual, family,and group therapy,
• Specialized training is offered to addressspecific modalities, such as cognitivebehavioral therapy for treating personsaddicted to cocaine and are registered andusing ambulatory services, and
• Training in supportive therapy modality,such as acupuncture.
Productivity of networking service provider
• On average, at each therapeutic unit in CIJservices are provided to 300 patients peryear, of which 70 are treated and released;
• If these figures are obtained in the 3000and 9000 treatment centers registered inMexico and in the United States, theprojected result would indicate that 900,000and 2,700,000 persons would be treated fordrug addictions, of which 108,000 and324,000 persons would treated andreleased.
Recommendation: To favor and supportambulatory services over the residential ones inthe design of the networking for serviceproviders and training programs for therapists.
Evaluation of Prison-BasedTherapeutic Communities:Current Status and FutureSteps
George De Leon, Ph.D.Center for Therapeutic CommunityResearchUnited States
Summary of Key Findings:
• Over 80% of admissions to communitybased TC’s have criminal histories.
• TC treatment for CJS clients is effective incommunity based programs in showingreductions in drug use and crime.Improvements are related to length of stay.
• Estimates of the percentage of inmates instate correctional facilities with serioussubstance abuse histories range from 50-80%.
• Modified TC programs in prison and jailsettings are effective in reducing recidivismand relapse to drug use.
• Modified TC programs in prisons plus postrelease aftercare produce the largest andmost consistent reductions in recidivism tocrime and in drug use.
• Aftercare programs which are “continuous”with the prison-based primary treatmentprograms appear to be particularly effective.
• The large majority of inmates withsubstance abuse problems do not electtreatment in prison. Among those who doenter prison TC treatment, most do notvoluntarily elect to continue their treatmentin post release after care settings.
• Individual motivation appears to be a criticalfactor in completing prison-based treatmentas well as post release aftercare.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 66 Plenary Sessions
Conclusion:
Prison-based treatment is highly effective inreducing relapse to drug use and recidivism tocrime when it is followed by aftercare treatmentin the community after release from prison.However, only a minority of substance abusersin prison enter treatment in prison or go on toaftercare.
The implication for treatment, policy andresearch: Based upon the science to date, theimpact, effectiveness and cost effectiveness ofprison-based treatment can be significantlyimproved.
Four specific recommendations are brieflyoutlined.
• Establish continuity of care initiatives:Treatment initiated in prisons must beextended after release from prison.Moreover, aftercare programs should becontinuous with the philosophy andapproach implemented in prison-basedtreatment.
• Enhance Treatment Utilization Initiatives:Strategies are needed to increase theproportion of inmate substance abusers whowill enter and complete prison-basedtreatment and who will continue in postrelease aftercare treatment.
• Implement Quality Assurance And TrainingInitiatives:
Efforts are needed for guiding the conductof prison-based treatment and aftercaretreatment programs. These includestandards for accreditation of treatmentprograms within prisons to assure thefidelity of treatment delivery. Such effortsshould be accompanied by uniform traininginitiatives for criminal justice and treatmentpersonnel.
• Define Research and Evaluation Priorities
Evaluation and research studies shouldaddress the above stated broadrecommendations:
(1) evaluations of the effectiveness ofintegrated vs. non integrated treatmentsystem
(2) research on motivational and otherstrategies to increase treatmentutilization
(3) research on models of training
(4) studies of treatment matching e.g.,clarifying the subgroups of inmatesubstance abusers who require prisontreatment plus aftercare, prisontreatment only or post release treatmentonly.
Focus on Youth
Ruth Sanchez-Way, Ph.D.Acting DirectorCenter for Substance AbusePreventionDepartment of Health and HumanServicesUnited States
The reason why most of us are in the businessof substance abuse prevention and treatment isbecause of our young people. We’re in thisbecause we love our young people. We knowthat they have great potential and that we wantto give them all the opportunities that we’ve hadin life and maybe even more. So, our focus thisafternoon, while it is the closing session, is onyouth, I think that they are really primary in ourconcerns and in our hearts. The youthcomponent of this conference has been meetingthe past two days and they have broken up intofour discussion groups and are going to presentto us their discussion points, their ideas, andtheir recommendations. We have four youthrepresentatives who will present theinformation. And the presenters are: fromMexico, Maria Christina Diaz Jimenez and CarlosEspinoza. From the U.S., we have Carla Perezand Ricardo Hernandez.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 67 Plenary Sessions
Report from the Youth
Maria Christina Diaz JimenezCarlos Alejandro Espinoza DominguezMexico
Carla PerezRicardo HernandezUnited States
Today, fifty youth participants from the U.S. andMexico are here. Their ages vary from 13 to 30years. Youth from different social groups, likestudents, professionals, artists, indigenouspeople and street boys. Youth from across theArizona border and from 32 Mexican states.
Topic ofdiscussion:popular cultureand artisticexpression, sportsand recreation,communication,education andsocial movement,and communitywork.
Recommendations. Establish a pilot youthcoalition between Arizona and Sonora to developactivities and projects. Expand the pilot to anational level coalition.
We would like to establish a pilot youth coalitionbetween Arizona and Sonora as a pilot project.Mexico, as you know, already has a youthcoalition across their country. As a means toexpand into the United States, we would like toestablish a pilot project within the borders ofArizona and Sonora, form connections and forma similar national coalition within the country. Byexpanding the pilot to a national level, we wouldlike to create a bi-national youth coalition whereconnections between all 32 Mexican states, andif possible, all 50 American states, are created.We’d also like to establish a planning committeewith youths, adults, United States and Mexican
officials to gather the opinions of youths forwhom these projects were created, as well asadult feedback. We would like to get theiropinions and suggestions on ways that we canmove around within our government, ourcommunity and non-profit organizations, andU.S.-Mexican officials to make this coalitionhappen. We would be able to establish a bi-national youth camp. This bi-national youthcamp would allow the exchange of ideas toexplore prevention. One way to exchangeaddiction prevention strategies is to createplanning committees. Another way is theexchange of cultural traditions. Among bordertowns within Arizona and Sonora, in religious,social and economic of Mexico and the UnitedStates are very similar. They are inter-dependent because, this is the border. We learnfrom each other, we live with each other, so we
have to learn howto work with eachother.
We want toestablish a bi-national youthcamp, we want toestablish discussiongroups in the fourmain areas thatwere discussedpreviously: sports,recreation, popularculture, artistic
expression, communication, education, socialmovement and community work. By having theexchange of ideas and traditions within theseareas, we have the best of both worlds. Weneed strategies that the United States youthgroups have been using, along with strategiesthat the Mexican youth groups have been using,and that may be implemented bi-nationally. Onething that we, as the American delegation wishto commit to is the free flow of ideas by lettingMexican youth travel within the United Statesfreely, without any reservation, without anyform of denials. We should be able to worktogether to form communities and coalitions andestablish good ideas. As a means of doing this,we would also like American students to go toMexico and to form an exchange of culturaltraditions as well.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 68 Plenary Sessions
The themes that we want to expand on for thebi-national youth camp are, as she said, ManosJóvenes a través de la frontera, United AgainstDrugs; a mixture of English and Spanish;Spanglish as we call it. We are a globalcommunity. We are a community engaged in asociety where nobody is just alone. Nobodystands alone any more. Everybody exchanges,everybody’s connected in one form or another.Within Mexico, the local youth groups haveconnected with each other, linked with eachother, and exchanged ideas with each other.Among themselves, among their governments,among their leaders and adults. That issomething that we, the United States, wish tocommit the United States government to. Wewould like to know if the Mexican governmenthas committed to its youth, will the UnitedStates commit to theirs?
Slide presentation follows.
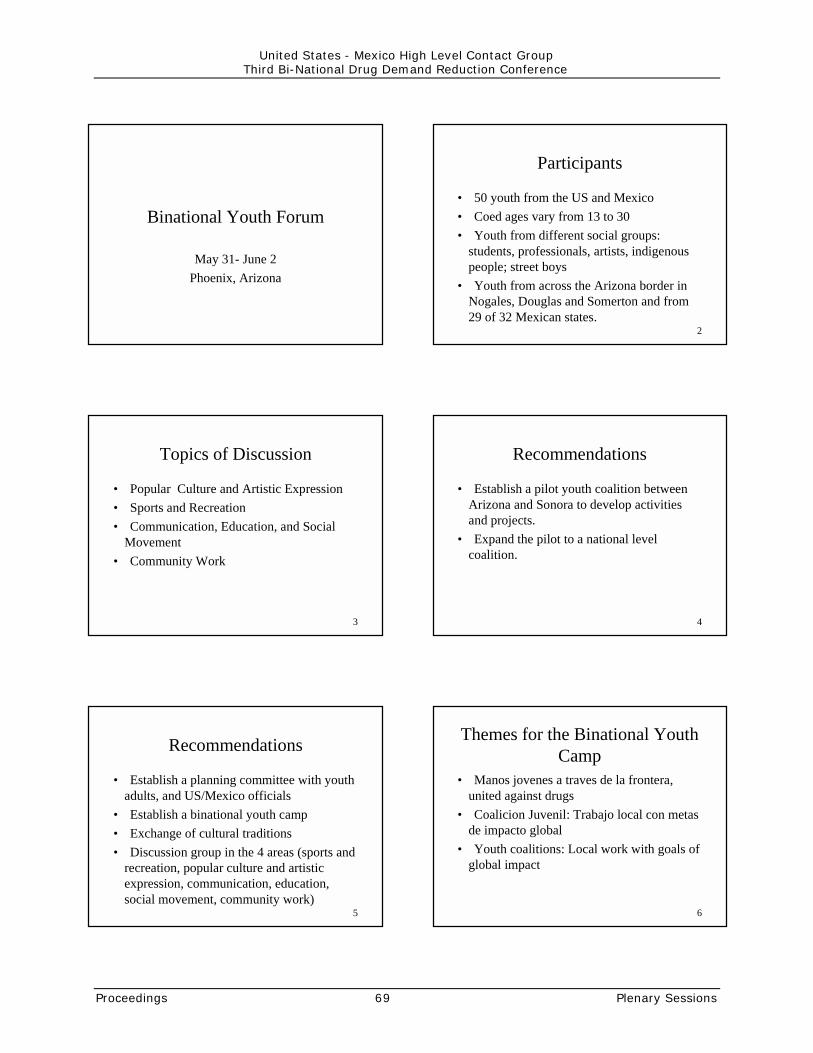
Binational Youth Forum
May 31- June 2Phoenix, Arizona
2
Participants
• 50 youth from the US and Mexico• Coed ages vary from 13 to 30• Youth from different social groups:
students, professionals, artists, indigenouspeople; street boys
• Youth from across the Arizona border inNogales, Douglas and Somerton and from29 of 32 Mexican states.
3
Topics of Discussion
• Popular Culture and Artistic Expression• Sports and Recreation• Communication, Education, and Social
Movement• Community Work
4
Recommendations
• Establish a pilot youth coalition betweenArizona and Sonora to develop activitiesand projects.
• Expand the pilot to a national levelcoalition.
5
Recommendations
• Establish a planning committee with youthadults, and US/Mexico officials
• Establish a binational youth camp• Exchange of cultural traditions• Discussion group in the 4 areas (sports and
recreation, popular culture and artisticexpression, communication, education,social movement, community work)
6
Themes for the Binational YouthCamp
• Manos jovenes a traves de la frontera,united against drugs
• Coalicion Juvenil: Trabajo local con metasde impacto global
• Youth coalitions: Local work with goals ofglobal impact
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 69 Plenary Sessions

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 70 Plenary Sessions
Adolescent TreatmentJorge Sánchez MejoradaResearcherVeracruzana UniversityMexico
I want to welcome you to this closing plenarysession of this bi-national meeting. It is anhonor to be with you this evening, talking toyou, very briefly about the topic which, for me,is a core issue. The participation of the youth, Ithink, is fundamental and I use theirparticipation as a very successful event to saythat from the viewpoint of treatment ofadolescents we will also require theirparticipation. I think this is a core, or a key,participation. I would like to tell you why when Iidentify a specific point. One of the things, andyou youngsters know this very well, you who areworking on a daily basis with the other youngpersons, you who have an impact on theactivities and mindset and lifestyles and fashionsand styles and mores. You who have also animpact on treatment and recovery and have tobe aware of how important your role is.Fortunately, those youngsters who haveaddictions can enter into a recovery programand link to other young persons who canunderstand their problems and move forwardalong this process.
I will briefly share with you a couple ofexperiences, one of them linked with thetestimony of our young persons who have hadan impact upon my professional life. Thishappened about 12 or 13 years ago when I hadthe opportunity to listen to an alcoholic 16 year-old boy. That broke away with many paradigmsbecause I have to confess that for mespecifically, alcoholism was a problem of olderpersons. That was the medical model I had beenworking on. And that addiction as such wasespecially alcohol, it was something which wasnever seen in early ages. The testimony of thisyoung boy really hit me. It moved me. And Ihave to tell you that once in a while I have thepleasure of seeing him again. He’s around 28-29years of age. And he’s been able to take controlof his life and career. The great teaching wasthat I could clearly understand that addiction isa very complex problem. It is a disease if we use
the disease model, which I think is the one tobetter understand addictions. The model can bepresent at any age and much more so now thatat an early age many persons are using drugsthat have a high addictive potential. As you haveheard, the proliferation of the use of cocaine issomething that we more often see amongst veryyoung teenagers or young persons. And this issomething we have to be aware of.
About 10 or 11 years ago, I was invited to go toa treatment center in Minneapolis, Minnesota,called St. Mary’s Chemical Dependence Services.It was quite a novelty to me and highlystimulating. To find a place that had thecharacteristics this center had. The young addictand the adult addict were treated with a broadrange of strategies with a comprehensiveapproach. Different needs were present there,but everything was done with full respect for thedignity of individuals. I thought that to befundamental. And since then, I had this dream,a dream I have tried to make a realitythroughout this year. And I can tell you now,that some steps have been taken in Mexico,although much has yet to be done. And thedream is that any addicted person, youth oradult, can receive professional treatment, withethics, where dignity and an individual’s integrityare respected. So, we have a lot of work to do.Although I have acknowledged that things havebeen done in my country, and that we have thenecessary foundations, it is now time to moveforward at a greater pace.
I would like to share some thoughts specificallywith the young representatives here. Treatingand working with professionals or volunteerpersonnel, young persons, parents, persons inrecovery, what I have been able to realize isthat if you require passion and commitment inmany occupations, in this one much more.When treating, when working in the preventionand treatment of addictions, you’re required tolove your activity. If you believe in healthylifestyles, you have to truly believe so that youcan truly convey the message. Otherwise, ourwords will be empty and will be left hanging outin the air. So, we have to be passionate andfully committed. And, I’m very pleased to seethat there are young persons from Mexico andthe U.S. that are getting involved in all of this,because this had been the missing link. I hope

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 71 Plenary Sessions
you continue moving forward with thisenthusiasm because adults and professionals, bythemselves, won’t be able to cope with the task.It’s evident we need your participation.
I’m going to present to you some ideas herewhich relate to treatment of adolescents. This isa proposal based on literature reviews as well ason direct observations made at treatmentcenters in the U.S. and in other places includingMexico, for example, the ones existing inColombia. Within this field, there’s a lot of workto be done, such as creating different butspecific alternatives of treatment foradolescents. With adolescents’ treatment forproblems of drug dependence and drugaddiction diagnostic difficulties sometimes makeit difficult to differentiate between abuse anddependence. Young persons have to provide usthe guidelines to follow as to the degree ofintervention we should undertake. Going frominterventions which can use tools, the mosttraditional ones, for example, individualpsychotherapy, family psychotherapy, or grouppsychotherapy which is a very good approach tobe used with adolescents. As to the other side,more intensive treatment: outpatient care, homecare, or maybe hospitalizations, with times thatmay vary according to the characteristics ofthose persons affected. The truth is, addictionamongst adolescents as well as within adultsrequires us to resort to strategies that requirehome care. And this is, more or less, what I’ll betalking about in the forthcoming minutes.
This is a specific characteristic in the case ofadolescents and which we have to address.There are different needs, which I wouldcategorize into three groups: those needsrelated to the development stage. Inadolescence, aside from any additional problemsthey may be experiencing, we need to solvespecific issues. Certain things that pertain tothat specific development stage of their life.Some authors call these developmental tasks.You have to answer a set of questions andarrive at a set of conclusions. Throughout thisprocess of growing up and in defining one’s selfin many senses, and getting to know one’s self.And appreciating one’s self and learning aboutour own individual potentials. This is a set ofneeds that have to be undertaken andconsidered within any treatment scheme. Other
needs are linked to the addictive process andrecovery itself. And the third group are thespecific problems like the case of the psychiatricmorbidity or dual diseases or parallel diseases toaddiction.
Here, we have some of the points I hadmentioned that pertain to that developmentalstage. The first one, the personal identityresponding to the question, “Who Am I?”.Fundamentally, who am I? The definition ofsexual orientation, which is also a task to bedone during adolescence. Understanding thedefinition and acceptance of the sexualorientation. The definition of personal values.Moral values. Ethical values. Spiritual values.Religious values. Values relating to daily life.That which is important for each individual. Thatwhich each individual believes in. And evidently,if you live in accordance with all that, there willbe a sense of well-being and be a feeling ofbeing a comprehensive person. Communicatingto others. Getting close to others and living withothers. Vocational choice. The sense ofbelonging. All of us need to belong. But this isfundamental during adolescence. To belong to agroup of peers, that’s very important. You haveto be a member of a peer group. One of thecharacteristics of addiction is that it providesindividuals with a sense of belonging to a groupof peers that identify themselves through theirdifferent behaviors. Well, in addiction recovery,at a certain point in time, you can experiencethat same feeling when the links are establishedin a lifestyle which implies sobriety.
And lastly, to define a life project. Theunderstanding, the vision, that each individualhas as to life in terms of defining one’s selfmission. This is closely linked to values andvocation. And it is also linked to all the otherareas of life. So, these are the things that haveto be considered within any treatment in thelong run when we treat addicted young persons.And we have to walk along as individuals withthese adolescents in trying to identify answersto these questions. The needs which areinherent to recovery, that is to recovery of thosedamages caused by addiction. Starting withdetox, through some drugs, this poses noproblem, but with other drugs it posesproblems, even within the medical and physicalfields, specifically, when we talk about opiates.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 72 Plenary Sessions
It is not common to see withdrawal syndromesamongst adolescents because of the type ofsubstances used – at least in Mexico. However,we are not exempt from having problems andfrom having to address the situation. We haveto confront denial, because you know that partof the characteristic of this addiction is denial.When an individual says, no, I have no problem,nothing is wrong with me; this is denial. And wehave to address the post-acute withdrawalsyndrome with a different characteristic. Themental field, in the emotional arena, and even inthe physical arena. Emergencies, due to the useof drugs such as cocaine, even after some timeafter consumption has been suspended. Wehave to support and foster healthy behaviors.We have to rediscover or restructure cognitivestructures, a new way of thinking, a new way ofvisualizing oneself, and visualizing life in theenvironment, and the individual’s problems.
We also have to look at background information,having to do with badgering or abuse,psychological or physical. And also, we have toconsider HIV and early pregnancy. We have toemphasize sports activity in contexts that willallow socializing to take place. This is somethingvery important that has been somewhat lost.Sport is an element of coming to know eachother and sharing with others in contrast withthe current trends towards this lonely kind ofsport where the only thing being done isheeding one’s body, personal development andself-pride. The recovery of values has to betaken, values that have been somewhat lostalong the way. It enables those people toprovide a meaning to life through thisinteraction and through this range of possibilitiesand of interactions that are developed.
It is also a fact, as it happens within the adultpopulation, that some adolescents, aside fromhaving the drug addiction problem, they haveother psychiatric problems. And we could alsotalk about other medical problems, but herewe’re just referring to the psychiatrists. Andthese are some of the most often-seen problemsamongst adolescents, may they be drug addictsor not. But when we’re at a certain point in timetreating addicted adolescents, we would have toidentify and/or discard the presence of any ofthe aforementioned diseases to be able to treatthese diseases in an efficacious way. So, we
have schizophrenia which is a disease thatusually has its onset during adolescence or earlyadulthood. We also have personality disordersbefore 18 years of age. However, there arecertain traits that could somehow point towardsthis direction and if we see these traits early, wewill then be able to identify specific needs thathave to be considered within treatment. Andalso, it is important to know them in terms ofprognosis. The activity disorders, hyperactivitydisorders that have their onset during earlychildhood, or anxiety disorders or learningproblems or disorders, these are the mostmeaningful ones. This is a broad range ofdisorders that can be associated with drugaddictions. And if they’re not detected andspecifically addressed, then the adolescent willbe at a disadvantage to use the recovery toolsavailable, and to be able make this cognitivechange and behavioral change being proposedto that person.
Now, in trying to respond to all these needs thatI’ve mentioned already, here are someconsiderations which can be used within a broadrange of therapies. First, we have self-help andmutual help and these are main axes, and manytimes they are confused but it’s quite clear herethat self-help is the help that one can renderhim or herself, and mutual help is the helppatients provide each other. By now, you’ll seehow I help myself and how I help you. And this,in turn, does help me. And another alternative inthese therapies is only you can do it, but youcannot do it alone. This emphasizes personalliability but also the need for help, anatmosphere which promotes confidence andself-esteem in the environment of theteenagers. Many of these needs can be coveredand can be found within this atmosphere. It’snot an atmosphere that fosters fear or terror.But, obviously, what you need is discipline. Youneed clearly cut standards and rules. Theserules should be established, especially indysfunctional families, and we try to deal withthem in the centers to make them as functionalas possible. This is difficult and sometimes webecome more dysfunctional than the familiesthat we have diagnosed as such.
Now, on education, recovery and new lifestylesand abilities for being able to play recreationand athletic activities and also occupational
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 73 Plenary Sessions
activities. Service to the community – this isfundamental. And therefore, I restate here theefforts and the participation and involvement ofthese young people that are here today. Toserve is something very important. From manyviewpoints, the one who serves, gives and theone who gives also serves because you feeluseful. So, within the communities, service tothe community itself plays a very important role,and group therapies play a central role. Theyare opportunities for confrontation forknowledge and also feedback.
The involvement of the family is alsofundamental. It’s decisive. We know that inMexico there are places in which the addicts areoften teenagers. The family deposits them as ifthey’re dropping off a package somewhere. So,if we speak of family involvement as beingfundamental and always very important in orderto help in this change process and to make thenecessary changes, this is one way in which thefamily can be part of the solution to theproblem. We have to work intensely with them.This is also a matter of convincing the familythat they must be involved in this fashion.
We’re also dealing with multi-faceted programsbased upon goals or objectives in which thereinsertion which comes later is something thathappens gradually. The social and familyreinsertion. And, obviously, something that hasbeen said in many conferences these last fewdays, is the importance of post-treatment, thatis, follow-up in which the prognosis improvesgreatly if there is post-treatment that also islong-term and continuous. I think this isfundamental.
We also have much to do. In Mexico we knowthis because the profile of the consumers ofdrugs has changed considerably in the last fewyears. Young people begin taking drugs youngerand younger and this is a problem, not just inthe major cities, but rather in manycommunities. I have data in populations where Inever would have imagined that it takes place.
In rural areas they use controlled substancesand alcohol, but at younger and younger ages,10 and 11 years of age, in fact. How can weface this challenge? I think training is the goldenkey. In order to be able to multiply the options
of treatment throughout the country, trainingprofessionals must also train those who havebeen empirically trained, along with volunteerpersonnel who are more than willing to workand may already work in this field. However,many require the necessary training. Therefore,we’d be able to work on models in which thereis intensive inter-disciplinary work taking placewhere the gulf exists between the theories andthe professionals.
And also, there’s work on research. That is,research on the impacts that we’ve seen in theconferences and in the U.S. I think they’re lightyears ahead of us here. But we can learn a lotand we need to do it urgently. It behooves us todo so. We also have to know that in Mexico verygood things are being done, but we don’t havethe necessary elements to say “yes, here’s thedata.” And the data supports this. This can leadto the right path. We need to do it. There’s anurgent need for this. And obviously, we needfunding. We need the funding from differentsources. From governments, Federal, state, fromcivil society. Unfortunately, in Mexico, we do nothave a very altruistic culture in this sense – thatis, with regards to donating money. We have itin other senses, ironically, so we have to knockon these doors and we have to seek out otheroptions. In the case of state or municipalgovernments, I see more and more examples ofsituations in which they donate a house or apiece of land, a property, or they are beingloaned. So, we have to knock on these doors.We have to open them up and therefore, seethe participation of government agencies. Theyare quite useful and obviously the participationof professionals and of volunteer personnelworking together to respond to the problem andto evaluate the measures so that in a few years,we’ll be able to say we’ve done this. And wehave all this data, and we have a series ofstudies which at a given moment will indicatethat we’re on the right path or we have tochange our path. And therefore, be able tocontinue heading towards something we can nolonger delay.
I think the need has been created and theresponse is already within us and around us. Sowe have to start working. Thank you so muchfor your attention.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 74 Plenary Sessions
Prevention for High-RiskYouthSusan KunzDirectorU.S.-Mexico Border Center for theApplication of PreventionTechnologiesUnited States
We have a mechanism that some of you in theroom are also involved in. We have an advisorygroup. This is to keep us honest, to keep usfocused, for you to tell us what you need for usto do as representatives of the bordercommunity that we’re trying to serve. We havea meeting coming up very soon. There arerepresentatives from each border state andseveral Federal agencies and some other localgroups. So, I encourage you to find out who therepresentative is from your area, and use thatperson as a conduit of information. They willreally be guiding the direction of our project. Ifyou don’t contact us, chances are we will notfulfill our mission. These are the people thatcan help you. They can help provide theseresources. They’ve very responsive. They’rereally nice. And they’re very helpful. And,please take advantage of the U.S.-Mexico BorderCAPT, so we can help youth through goodprevention programs. Thank you.
Slide presentation follows.

1
Effective Prevention ProgramsEffective Prevention Programsfor Border Youthfor Border YouthProgramas EfectivosProgramas Efectivos de de
Prevención paraPrevención para la laJuventudJuventud de la de la FronteraFrontera
Susan Kunz, MPHU.S. Mexico Border CAPTBorder Health Foundation
2501 East Elm St.Tucson, AZ 85716
(520) 795-9756 fax [email protected] 2
Basic PremiseBasic Premise
■■ InvolveInvolverepresentative youthrepresentative youth
■■ Reach youth in needReach youth in needPremísa BásicaPremísa Básica
Involucrar a jóvenesrepresentadosAlcanzar las necesidades de losjovenes
3
How do we know whatHow do we know what
is effective?is effective?
¿Cómo sabemos que esefectivo?
4
Science-BasedScience-BasedFrameworkFramework
■■ Población definidaPoblación definida■■ Programa díseñado Programa díseñado en base a en base a las necesidadeslas necesidades
Estructura Estructura Basada en la en la CienciaCiencia
Clear target populationProgram design based on needs
5
Science-BasedScience-BasedFrameworkFramework
■■ Intervenciones relacionadasIntervenciones relacionadas con con loslosresultadosresultados
■■ El El diseño es culturalmente apropiadodiseño es culturalmente apropiado
Estructura Basada en la Ciencia
Interventions tied to outcomesDesign is culturally appropriate
6
Science-BasedScience-BasedFrameworkFramework
■■ Evaluación integradaEvaluación integrada
Estructura Basada en la Ciencia
Integrated evaluation
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 75 Plenary Sessions
7
Basic PrinciplesBasic Principles
■■ Dirigirse Dirigirse a a múltiples áreasmúltiples áreas■■ Utilizar múltiples estrategiasUtilizar múltiples estrategias
Principios Básicos
Address multiple domainsUtilize multiple strategies
8
ResearchResearch PracticePractice
CSAP’s Vision for the FutureCSAP’s Vision for the Future
Improve System Performance & Service Quality
9
What is science-basedWhat is science-basedpractice?practice?
Que es la practica basada en la ciencia?
■■ Model ProgramModel Program■■ Best PracticeBest Practice■■ Promising approachPromising approach
■■ Programa ModeloPrograma Modelo■■ MejoresMejores Practicas Practicas■■ EnfoquesEnfoques
PrometedoresPrometedores
10
CAPTs CAPTs at a Glanceat a Glance
■■ Border CAPT: Tucson,Border CAPT: Tucson,AZ, 520-795-9756AZ, 520-795-9756
■■ Central CAPT: Central CAPT: AnokaAnoka, MN,, MN,800-782-1878800-782-1878
■■ Northeast CAPT: Newton,Northeast CAPT: Newton,MA, 617-969-7100MA, 617-969-7100
■■ Southeast CAPT: Jackson,Southeast CAPT: Jackson,MS, 800-233-7326MS, 800-233-7326
■■ Southwest CAPT: Norman,Southwest CAPT: Norman,Oklahoma, 405-325-1454Oklahoma, 405-325-1454
■■ Western CAPT: Reno, NV,Western CAPT: Reno, NV,888-734-7476888-734-7476
11
U.S.-MexicoU.S.-MexicoBorder RegionBorder Region
12
MissionMission
■■ Increase availability and application ofIncrease availability and application ofscience-based substance abuse preventionscience-based substance abuse preventionknowledge that is responsive to US-Mexicoknowledge that is responsive to US-Mexicoborder dynamicsborder dynamics
Aumentar la disponibilidad y aplicacion del conocimientosobre la prevencion del abuso de sustancias basada en laciencia que responda bien a la dinamica de la fronteraMexico-Estados Unidos
Mision
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 76 Plenary Sessions

13
Border ContextBorder Context
■■ CommunityCommunityconditionsconditions
■■ Drug availabilityDrug availability■■ MigrationMigration■■ TransculturationTransculturation
■■ Las condiciones deLas condiciones dela comunidadla comunidad
■■ La disponibilidad deLa disponibilidad delas drogaslas drogas
■■ La imigracionLa imigracion■■ La transculturizacionLa transculturizacion
CAPT de la Frontera Mexico-Estados Unidos
14
Goals of Border CAPTGoals of Border CAPT
■■ Identify culturally appropriate programsIdentify culturally appropriate programs■■ Help customers apply programsHelp customers apply programs■■ Sustain border prevention effortsSustain border prevention efforts
Identificar programas culturalmente apropriadosAyudar a clientes con aplicacion de programasSostener esfuerzos preventivo fronterizos
Meta del CAPT Fronterizo
15
How?How? Como Como??
■■ Integrate US-Mexican research to adaptIntegrate US-Mexican research to adaptmodels suited to residents of the bordermodels suited to residents of the borderregionregion
Integrar las investigaciones mexicanas y estadounidenses paraadaptar los modelos que sean mas apropiados para losresidentes de la region fronteriza
16
ServicesServices
■■ ElectronicElectronic■■ Technical AssistanceTechnical Assistance■■ Skill BuildingSkill Building
■■ ElectronicosElectronicos■■ Asistencia tecnicaAsistencia tecnica■■ Formacion deFormacion de
habilidadeshabilidades
Servicios
17
Electronic Electronic ElectonicoElectonico
■■ WebsiteWebsite■■ English/SpanishEnglish/Spanish
resourcesresources■■ LinksLinks
Sitio webrecursos en ingles y espanolenlaces
WWW.BorderCAPT.org 18
Technical assistanceTechnical assistance
■■ Expert Network...Expert Network...–– …we want you…we want you
■■ Red de Expertos…Red de Expertos…–– lo(a) queremoslo(a) queremos
Asistencia tecnica
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 77 Plenary Sessions
19
Skill buildingSkill building
■■ Group training…Group training…–– what are yourwhat are your
needs?needs?
■■ Entrenamiento deEntrenamiento degrupo…grupo…–– Cuales son susCuales son sus
necesidades?necesidades?
Formacion de habilidades
20
Adaptation/TranslationAdaptation/Translation
■■ EnglishEnglish■■ InglesIngles
■■ SpanishSpanish■■ EspanolEspanol
Adaptacion/Traduccion
CultureCultureCulturaCultura
21
Research Work GroupResearch Work Group
Grupo de Trabajo de Investigacion
■■ U.S. researchersU.S. researchers■■ InvestigadoresInvestigadores
estadounidensesestadounidenses
Mexican researchersInvestigadores mexicanos
22
Research Work GroupResearch Work Group
Grupo de Trabajo de Investigacion
■■ Review, adapt and recommend bestReview, adapt and recommend bestpractices for border populationspractices for border populations
■■ Revisar, adaptar y recomendar lasRevisar, adaptar y recomendar lasmejores practicas para las mejores practicas para las poblaciónespoblaciónesfronterizasfronterizas
23
Advisory GroupAdvisory Group
■■ Mexico & U.S.Mexico & U.S.■■ State and FederalState and Federal
■■ Mexico y EstadosMexico y EstadosUnidosUnidos
■■ EstatalEstatal y Federal y Federal
Grupo de Asesoria
24
Contact UsContact UsNos puede contactarNos puede contactar en en
nuestra pagínanuestra pagínaelectronicaelectronica
www.bordercapt.org
Courtney Coffey, BHF(520)795-9756
Lorenza Mena, USMBHA(915)833-6450
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 78 Plenary Sessions

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 79 Plenary Sessions
Addressing the Needs ofYouth in Criminal Justice/Substance Abuse-PublicHealth Programs
Eugenia OrtegaSuperintendentKarl Holton Youth CorrectionalDrug and Alcohol TreatmentFacilityCalifornia Youth AuthorityUnited States
Ok, thank you very much. And muchas gracias. Iam very honored to be here. I am veryimpressed with this collaboration. Quite frankly,I wasn’t aware that Mexico and the UnitedStates were making such a conscientious effortto work and address these problems. I wouldlike to also make an observation. Last year Iwas also part of the panel for ONDCP inWashington, DC when they were addressingdrug issues throughout the country. And, ofcourse, I was at the end of the session becauseit dealt with youth. And, today again, we’re atthe end of the session. And, actually it makes ita lot easier to do a presentation to half of acrowd, but I want to challenge both Mr.Schecter and Mr. Cordova, if we continue withthese kinds of conferences, we talk about ouryouth being our primary focus. We talk aboutour youth being the most important reasonwe’re here. We talk about these programs andthe efforts being made so we can address theyouth of not tomorrow – as Henry said – but ofour youth today, and we leave them to the end.So, I challenge you to take an observation ofthat. I would like to see this ballroom full with allour dignitaries here, with all our panel membershere. To listen to what they’re doing. I’m soimpressed, and I just compliment you all.Let me just give you a quick overview of whatthe California Youth Authority is doing. We arean institution, we are a department that houses7,500 juvenile offenders. These juvenileoffenders come to us through the courts. Theyare sentenced by the courts and they end up inthe Youth Authority. We have 11 institutionsstatewide, and four camps, which allow these
young men to establish, develop additionalskills. When these young men come to theYouth Authority, obviously they’re hereinvoluntarily. And I’m going to address that,because as you have heard throughout theconference and the literature clearly speaks to,is that providing substance abuse treatment.whether it’s voluntary or involuntary, has provento have an impact. It has been proven to show achange, even if the person is attending thesedifferent services on an involuntary basis.
Our population in the Youth Authority, is 49%Hispanic. Personally, that saddens me. Twenty-nine percent are African-American, 14% areWhite, 5% Asian, and 2% “other”. The Hispanicpopulation has increased from 33% in 1990 to49% in 1999. That’s quite a change, quite adifference in our population. And right now,we’re looking at different treatment modalities.They’re more culturally related, so that we canintroduce that element to our programs. About,85% of our young men, come to us withsubstance abuse, either drug related offenses ordrug related history. As a result, in 1994, theYouth Authority decided that they needed tolook at an institution and totally dedicate theservices provided to substance abuse treatment.So, in 1994, in Karl Holton, which is located inStockton, California, we housed approximately410 wards. All the wards there addresssubstance abuse.
I’m going to talk a little bit about what we do.First of all, the mission of Karl Holton is toprovide these young men the training, theeducation and the treatment necessary toestablish a substance abuse free lifestyle oncethey go out into the community, once they getout on parole. Karl’s program is from 8 to 12months. The literature clearly speaks to thelonger the stay in treatment the better thesuccess rate. So, we have an established 8month program, but it can go up to 12 months,depending on the particular needs of the youngmen. It’s a transitional program. The literaturealso states that if you provide these servicesupon the end of their stay, while incarcerated,you have a better success rate. In other words,if the young men have a sentence of three tofour years, they will come to Karl approximatelyone year before their release on parole.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 80 Plenary Sessions
Karl has an established therapeutic community.Karl was established in 1966 with that modality.Since then, obviously, many years have goneby. We still have some elements and somecomponents of therapeutic community, butthey’re not as strong as were presented earlierby Dr. De Leon. As a matter of fact, I took hiscard because I want him to give us someadditional training and update our staff in thetherapeutic community. But we still have someof the same concepts and elements that werepresented.
Karl is a three-phase program. When the youngmen arrive, they arrive during an orientationperiod. During the orientation period, they aretaught what we term social thinking skills. It’s acognitive method for these young men to learnhow to deal with their issues, resolve programsand deal with their daily living while at theYouth Authority. Upon completion of theorientation, there is a 12-step Hazelton Programthat’s called Design for Living. It’s a modified12-step program, that is used for correctionalsettings. So, the young men go to school. Inaddition to working towards their high schooldiploma, their GED, they are also working inschool to learn the 12-step program. Once theylearn the concepts, in school, they have to takea test. It’s all cognitive. Then once they go intothe living units, then the youth counselors aresupporting the treatment modality by doingsmall groups, individual counseling with thesame 12-step program.
There’s an aftercare program which providesrelapse prevention and helps the young men getready for parole. They work on establishing,what we call a personal life plan. I’m going toaddress that in a little bit. They’re a number ofthings that our institution does. We do havestatistics, of course. You always have to becareful when quoting statistics because it’s allrelative. Karl’s success rate is: 64% of the youngmen are able to maintain free from incarcerationwithin the first 12 months upon release from theYouth Authority, greater than the YouthAuthority norm at 49%. So, we’re doing a littlebetter than some of the other institutionsbecause of the intensity of our program.
They’re all kinds of components. I’m not evengoing to elaborate any more on the different
services that we provide. What I mainly wantedto focus on in today’s session was on the needsof our juvenile offenders and the needs of theyouth in the criminal justice system. Dr. Sanchezearlier talked about adolescent treatment. Healready elaborated on all the key componentsthat we have that have been recognized asdifferent areas that need attention. So, I’m justgoing to highlight a few of them. Number One:there is a mental health concern. Twenty-fivepercent of the young men sentenced to theYouth Authority, or sentenced to Karl, are duallydiagnosed, which means that they have other,maybe mood disorders, and anxiety disorders.Some of them are schizophrenic and paranoid.Some of them come to us with very extensivehistories of physical abuse or sexual abuse. So,those needs must be addressed, needs that areabove and beyond the substance abuse issuesand concerns.
We talked about some of the other areas thatwere highlighted, such as a sense of self-identity, developing a sense of who they are.Mind you, these young men come to the YouthAuthority at a prime age during theiradolescence. Their sense of seeking their self-identity is no greater or no less than any otheradolescent. When you couple that with havingto deal with incarceration, it exacerbates thesituation. Particularly with self-identity, there’s aconcern of gang involvement. Most of our youngmen have some form of gang affiliation. Wehave extensive programs at Karl that help theseyoung men break away to denounce their gangaffiliation. And we have modeled a couple ofprograms by using some of the 12-stepcomponents and adapting them to gang relatedissues. We’ve looked at using sponsors asmentors. We also have a group calledIndependent Status. These young men meet ona regular basis to look at how they can supporteach other to break away from the gangs. Asyou well know, gang involvement comes with alot of peer pressure, so I think we need toenhance the peer pressure on a positive notejust as well to help them overcome their ganginvolvement, gang affiliation.
Family involvement is so crucial. Unfortunately,that’s probably one of the most difficult areas. Alot of times, and I have to say that particularlymy experience has been in working with the
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 81 Plenary Sessions
Hispanic community, it’s very difficult to involvethe family. I know personally, my parents arevery private, very humble and have the “keep itin your household” mentality. It’s just verydifficult to enlist the family in the treatment, inthe development. So, we’re trying to educatethem by showing them what kind of progress isbeing made by getting the family involved. Andthese young men are returning back to theircommunities, it’s so important that theyunderstand the changes that the young menhave made and accomplished. But that’s verydifficult, I have to admit, very difficult to do.
One of the needs that is crucial upon preparingthese young men is to ensure that their plansfor parole, their plans upon release, are realistic.These young men have made some verypositive changes while incarcerated. But, theystart establishing these very grandiose goals.I’m never going to get involved in gangs. I’mnever going to do this. And some of that maynot be realistic. So, we need to establish andassist these young men in establishing arealistic, what we call a personal life plan. Youcan establish nice, grandiose goals, but theyhave to be coupled with very specific, concreteobjectives. That’s very important. And so wework with these young men. What are theygoing to do about school? What are they goingto do about work? In what areas are they goingto hang out? Are they going to be in the samecommunities, in the same neighborhoods? Whatare they going to do if temptation hits them?What are they going to do if relapse occurs? So,the personal life plan is very, very concrete.
In addressing today’s topic, which spoke to theneeds of the youth, I was reflecting upon ourwork in the Youth Authority, reflecting upon myexperience in working with juveniles. And inessence, it really comes down to the fact thatthese youth have no different needs than youand I. They really don’t. These young men orwomen who are dealing with substance abuse,want to feel important. They want to feel love,and they want to feel cared for. Just like you.Just like me. They want to have this love andthis care demonstrated to them. How many ofus are parents or children or spouses? And, weknow our parents love us. We know our childrenlove us. We know our spouses love us. But wewant to hear it. We want to hear it. I love you.
Honey, you did great today. We need thatpositive reinforcement. The needs of theseyouth that are in criminal justice have the sameneeds in that regard. They want to feelrecognized. They want to feel important. Andthey want to feel part of a bigger good. You andI want to feel accepted by our families, by ourloved ones, by our communities. These youngyouth also want to feel the same. They want tofeel that they are accepted by the biggercommunity, by the bigger good, so, it’s verydifficult. It may appear simplistic, as I present itin that fashion and in someways it is. It’s prettysimple. But I know it’s much more difficult toimplement and to create processes and methodsand treatment programs to help them overcomethis desire that probably they’ve been neglectedby their upbringing, their communities, theirschools. Everybody has turned away from them.
So, it’s really important that we ensure that aswe deal with these youth, that we recognizethat the essence of their needs are very similarto yours and mine. So, I challenge you all. Iempower you all to go back to your work sites,go back to your communities and respond toyour youth, to our youth, that they are acceptedin our community and that we truly care forthem and we’re going to do whatever we can tosalvage this generation to come.
Thank you very much.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 82 Plenary Sessions
Closing Remarks
Daniel SchecterDeputy Director for DemandReduction (Acting)Office of National Drug ControlPolicy, United States
This conference really began four days ago withNIDA’s research conference. On Wednesdaywere the pre-conference sessions, the reception,and the play “Halfway There,” followed by twodays of plenary and breakout sessions, whichwere really like conferences within conferences.So, it’s been a very, very intense four days. Ourheads are filled with information and ideas.
Think about how different the first U.S./Mexicoconference two years ago was from thisconference. In El Paso, Americans andMexicans working on drug abuse problems didn’treally know each other. They weren’t familiarwith what each other was doing. They weren’tfamiliar with the problems in the others’ country.They certainly weren’t working together verymuch. We didn’t have Susan Kunz’s BorderCenter for the Application of PreventionTechnology. None of those things existed. Itwas a very different kind of meeting.
But look at this conference. The wholeatmosphere was different. It was much morecollegial, much more businesslike. We gottogether and talked about ongoing projects,areas in which we were already workingtogether. And we discussed what we were goingto do next together. So, I think we’ve come atremendously long way in two years. And weshould give ourselves a lot of credit for that.
A final thought. We were asked by EugeniaOrtega to focus these conferences on youth. Ithink that’s a wonderful suggestion, the rightsuggestion. A few moments ago, Sofia gave methis shirt with the name of the Mexico youthcoalition on it. When you’re in the drugprevention field, you often come home frommeetings of this sort with at least one T-shirt.But this is a special shirt. In fact, I think
I will put it on the wall in my office, to remindme of the good and important things that comeout of the work that we’re doing together. It’snot just another shirt with a slogan on it. This isa real tangible example of a coalition of Mexicanyouth committed to drug prevention that didn’texist before we began this bi-nationalcooperation in El Paso two years ago. So, I’mgoing to be very proud of having this shirt onmy office wall.
With that thought, let’s bring this conference toa close and let’s give ourselves a great big handfor what we’ve accomplished together.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 83 Prevention
PREVENTION

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 84 Prevention
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 85 Prevention
PREVENTIONPRE-CONFERENCESESSIONSSuccessful InterventionPrograms
Ruth Sanchez-WayModeratorSubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
FAMILIES AND COMMUNITIES
Hablemos En ConfianzaMark Weber and Luisa PollardSubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
Luisa Pollard, of SAMHSA’s Center for SubstanceAbuse Prevention, told participants that the“Hablemos en Confianza” campaign, under theleadership of Dr. Chavez, was launched onSeptember 4, 1999, after careful work with a17-member group representing the largestHispanic groups in the U.S. ? researchers,providers, parents, and kids. Stating that “thisis about communications skills,” Pollard toldparticipants that the family ? in all itsextensions ? was the key focus and tool of thecampaign. Products include various materialsfor 3-6 year olds, and “soap operas” in picturesof three families (Lopez, Ruiz, and Castro) toportray the reality of family-life and the way inwhich prevention messages can be given tochildren by all adult family members. Moreimportant than the well-developed presscomponent, Pollard maintained, was developingthe campaign based on meetings with parentswho asked for practical information about drugs(street names, symptoms of use, etc.) as well asfor prevention messages. Coming soon will beadditional materials for girls ages 9-14, and
materials for their mothers. Pollard said that thekey messages for parents in the campaign were:
• First talk and give clear rules• Then listen/watch/observe• Then speak.
Mark Weber, SAMHSA Associate Administratorfor Communications, noted that it is clear thatdirect translations are not enough; we need tostart with the target group and design materialswith and for them.
Supporting and Financing PreventionProjects Focused on YouthJesus GarciaDirectorMexican Institute for YouthMexico
Mexico Institute for Youth PreventionProgram: Jesus Garcia of Mexico’s Institute forYouth talked about the steps the Institute tookin reaching the broad-based, youth-orientedprevention effort it coordinates today. Initially,school officials had asked the Institute toprovide drug information to youth, which wasn’teffective (as confirmed by a survey of youth).The Institute then developed a lecture series forschools, which they didn’t have time toincorporate into their curricula. So the Instituteturned to youth organizations, where “there wastime to do the lectures.” However, the youthtold the Institute that they had enoughinformation – what they needed was someoneto “tell us how to deal with our families, themedia, and peer pressure. As a result, theInstitute totally revised the prevention program,keeping the information part (primarily for ruralareas), and letting the youth take the lead. TheInstitute brought in health care professionals tohelp the youth develop activities such asfestivals, dramas, youth weeks against smoking,etc. with resources and skills identified by theyouth in their own communities. In 1995,recognizing that the Institute could not reachinto every community that requested this kind ofhelp, it started to identify youth-oriented non-governmental organizations (NGOs), and nowworks with 350 NGOs and individuals to developand support such prevention activitiesthroughout Mexico. The Institute provides small

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 86 Prevention
grants (often matching) to communities andNGOs; the resulting programs are evaluated andtheir results are shared.
CHILD DEVELOPMENT PROGRAMS: ASCHOOL AND FAMILY MODEL
Building MeAimee GravesDirector of Community Based ServicesCODACTucson, ArizonaUnited States
Aimee Graves gave an overview of a highlysuccessful early childhood prevention programfor Hispanic populations in public housing inTucson, Arizona. This five-year programconsisted of a “Building Me” curriculum featuring70 activities to build resiliency, short sessions for3-4 year olds, with transportation, parentingclasses, home visits, support groups, andtreatment services for both mental health andsubstance abuse needs. Parental involvementwas key - and was achieved by a ParentAdvisory Council, and special Family Weekendactivities. The program’s success was due to atrue collaboration of all segments of thecommunity, in-service and cross-training ofstaff, and resource integration. She ended bystating the challenges remaining in conductingsuch a broad-based program - defining roles ofeach player, learning collaboration and valuingindividuals as resources.
Raul ZapataYouth Integration Centers (CIJ)Mexico
Through risk assessments, CIJ identifiedcommunities at risk in Mexico, and found that1.3 million persons received some type ofprevention services. Stating that preventionshould be based in the community so that it cantake root, and that “precarious life conditions”are key risk factors, Garcia noted that CIJ-funded activities target youth ages 10-18. CIJpromotes healthy lifestyles by strengthening
resiliency factors such as assertiveness, stressmanagement, socialization, and commitment toschool. CIJ funds “training of trainers” to helpdifferent communities address their differentneeds. In general, Garcia concluded, suchprevention programs achieved “highly favorable”results, with respondents saying that theinformation was useful and that they were veryinterested in participating in preventionactivities. Difficulties encountered inimplementing such programs were lack of timeand various restrictions. Regarding drug-usingstudents, Garcia noted that teachers hadreported they felt helpless to help such studentswith their obvious anti-social and psychologicalproblems. Garcia concluded that by trainingteachers in prevention, they would see thebenefit to their students in improved academicperformance à increased self-esteem à nomore drug use.
Drug Prevention in the WorkplaceBernie McCannOffice of National Drug Control PolicyUnited States
DRUG-FREE WORKPLACE DATA SUMMARY
Drug Abuse & Workforce Demographics
• According to the most recent HouseholdSurvey in 1998, almost 75% of adults (age18 and up) who reported current illicit druguse (at least once in the past month) areemployed, either full or part-time. Thisnumber represents more than 8.5 millionindividuals. Unpublished Results from the1998 National Household Survey on DrugAbuse, U.S. Department of Health andHuman Services, SAMHSA, Office of AppliedStudies, Rockville, MD, August, 1999.
• The 8.5+ million workers reporting currentillicit drug use represent 6.4% of the 1998adult workforce. Similarly, 7.8% of the adultworkforce reported heavy drinking (5 ormore drinks on 5 or more occasions in thepast month). Preliminary Results from the1998 National Household Survey on DrugAbuse, U.S. Department of Health andHuman Services, SAMHSA, Office of Applied
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 87 Prevention
Studies, Rockville, MD, August, 1999. [Table19, Page 82; Table 24, Page 87]
• Among employed adults, the highest rates ofcurrent drug use and heavy drinking arereported by white, non-Hispanic males, 18-25years old, with less than a high schooleducation. By occupation, significantly higherrates of current drug use and heavy drinkingwere reported by those employed as foodpreparation workers, waiters, waitresses andbartenders (19%), construction workers(14%), other service occupations (13%) andtransportation and material moving workers(10%). Worker Drug Use and WorkplacePolicies and Programs: Results from theNational Household Survey on Drug Abuse[1997], U.S. Department of Health andHuman Services, SAMHSA, Office of AppliedStudies, Rockville, MD, September, 1999.
• A 1999 SAMSHA study reveals workersreporting current drug use were more likelyto have worked for three or moreemployers, to have voluntarily left anemployer in the past year, and skipped oneor more days of work in the past month.Employees in three of four occupationsreporting significantly lower rates of currentdrug use and heavy drinking (protectiveservices; extraction and precisionproductions; electronic equipmentassemblers; and administrative support)were employed in those occupationsidentified with the highest rates of druginformation and policies in the workplace.An Analysis of Worker Drug Use andWorkplace Policies and Programs, 1997. U.S.Department of Health and Human Services,SAMHSA, Office of Applied Studies.Rockville, MD, September 1999.
• About one-half of young adults ages 16-17,work during the year. Those working morethan 20 hours per week are at high risk forsubstance abuse and injury. Protecting Youthat Work: Health, Safety, and Development ofWorking Children and Adolescents in the US.Committee on Health & Safety Implications ofChild Labor, Washington DC: NationalAcademy Press, 1998, [pp. 2-5]. ONDCPDirector Barry McCaffrey, cautioned thatemployers will need to be vigilant regardingthe next generation of workers. There are
signs that youth aged 12 to 17 years usegateway substances ? a predictor of futuresubstance abuse ? at disturbingly high rates.Remarks by Director McCaffrey at theRecovery Month Kick-off, Washington, DCSeptember 8, 1999.
• The number of workers ages 16 - 24 willincrease by more than 3 million between1998 and 2008, making this group the largestit has been in 20 years. U.S. Department ofLabor, Bureau of Labor Statistics, 1998-2008Employment Projections. Nov. 30, 1999.[Table 5 ]
• In 1998, 18.2% of unemployed adults (18and over) reported current drug use asubstantial increase over the 1997 rate of13.8%. 10.8% reported heavy drinking,slightly higher than the 10.1% rate reportedin 1997. Preliminary Results from the 1998National Household Survey on Drug Abuse,U.S. Department of Health and HumanServices, SAMHSA, Office of Applied Studies,Rockville, MD, August, 1999. [Table 19, Page82; Table 24, Page 87]
Alcohol Abuse in the Workforce• Alcohol is the most widely abused drug
among adults, especially among youngadults. According to the 1998 NationalHousehold Survey on Drug Abuse, 85% ofheavy drinkers in the United States areemployed ? about 10 million people. One inthree adults aged 18 to 25 are bingedrinkers (at least 5 drinks at a time). Ratesof binge drinking and heavy drinking(binging at least 5 times a month) areconsistently higher among men than women? 43% of men aged 18 to 25 are bingedrinkers, compared to 21% of women.Preliminary Results from the 1998 NationalHousehold Survey on Drug Abuse, U.S.Department of Health and Human Services,SAMHSA, Office of Applied Studies,Rockville, MD, August, 1999
• Many more employees drink to a lesserdegree. A common misconception amongemployers is that alcoholics are responsiblefor most workplace problems related toalcohol. Casual drinkers, in aggregate,account for far more incidents of

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 88 Prevention
absenteeism, tardiness, and poor quality ofwork than those regarded as alcoholdependent. The Worksite Alcohol Study,National Institutes of Health, NationalInstitute on Alcohol Abuse and Alcoholismand the Robert Wood Johnson Foundation.Rockville, MD, 1998.
• According to the 1998 Harvard School ofPublic Health Corporate Alcohol Study, lightand moderate drinkers cause 60% ofalcohol-related incidents of absenteeism,tardiness and poor quality of work, whiledependent drinkers cause 40%. NewPerspectives for Worksite Alcohol Strategies:Results from a Corporate Drinking Study.Thomas W. Mangione, Jonathan Howlandand Marianne Lee, funded by the RobertWood Johnson Foundation and the NationalInstitute on Alcohol Abuse and Alcoholism,December 1998.
• Alcohol-related job performance problemsare caused not only by on-the-job drinkingbut also by heavy drinking outside of work.Ames and colleagues found a positiverelationship between being "hungover" atwork and feeling sick at work, sleeping onthe job, and having problems with job tasksor co-workers. Among pilots whoseperformance was tested in flight simulators,researchers found evidence of impairment14 hours after pilots reached blood alcoholconcentrations of between 0.10 and 0.12BAC, and significant impairment 8 hoursafter reaching a BAC of 0.10. Drinking atwork, problem drinking, and frequency ofgetting "drunk" in the past 30 days arepositively associated with frequency ofabsenteeism, arriving late or leaving early,doing poor work, doing less work, andarguing with co-workers. Hangover Effectson Aircraft Pilots 14 Hours After AlcoholIngestion: A Preliminary Report. Yesavage,J.A., and Leirer, V.O. American Journal ofPsychiatry 143(12):1546-1550, 1986.;Employee Drinking Practices and WorkPerformance. Mangione, T.W.; Howland, J.;Amick, B.; Cote, J.; Lee, M.; Bell, N.; andLevine, S.Journal of Studies on Alcohol 60(2):261-270, 1999; The Influence of Alcoholand Aging on Radio Communication DuringFlight. Morrow, D.; Leirer, V.; and Yesavage,
J. Aviation, Space, and EnvironmentalMedicine 61(1):12-20, 1990.
• Productivity losses attributed to alcohol wereestimated at $119 billion for 1995. EconomicCosts of Alcohol and Drug Abuse in theUnited States, National Institute on DrugAbuse and National Institute on AlcoholAbuse and Alcoholism, May 1998.Alcoholism accounts for 500 million lostworkdays each year. Treatment is theAnswer: Cost-Effectiveness of Alcoholismand Drug Dependency Treatment. NationalAssociation of Treatment Providers, LagunaHills, CA. March 1991.
• One in 5 workers report being injured,having to cover for a co-worker, or workingharder due to other employees’ drinking.Nearly 1/3 of workers who consider theirjobs to be dangerous report experiencing“secondhand” alcohol effects; ½ ofemployees surveyed supported randomalcohol testing at work; nearly ¾ ofemployees in manufacturing ortransportation supported testing. NewPerspectives for Worksite Alcohol Strategies:Results from a Corporate Drinking Study.Thomas W. Mangione, Jonathan Howlandand Marianne Lee, Robert Wood JohnsonFoundation and National Institute on AlcoholAbuse and Alcoholism, December 1998.
• Many employers (an estimated 20,000nationwide) offer employee assistanceprograms (EAPs) designed to promotehealthy lifestyles for workers. According tothe U.S. Department of Labor, for everydollar invested in an EAP, employers cansave $5-$16. Many companies do not havealcohol policies; those that do may notenforce them effectively. Nearly 60% ofmanagers and supervisors say theircompanies are “tough” on illicit drugs but“soft” on alcohol; 80% say they haveinadequate training in how to addressemployee performance problems. Moremanagers (23%) and supervisors (11%)actually report drinking during the workdayand at company functions than do otheremployees (8%), which may contribute to acorporate culture that encourages drinking.Perspectives for Worksite Alcohol Strategies:
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 89 Prevention
Results from a Corporate Drinking Study.Thomas W. Mangione, Jonathan Howlandand Marianne Lee, funded by the RobertWood Johnson Foundation and the NationalInstitute on Alcohol Abuse and Alcoholism,December 1998.
• In a 1998 Peter Hart poll, employers oftenencounter denial (75%) and anger (42%)when they approach workers about alcoholproblems. However, mandatory referral totreatment and the risk of job loss are strongmotivations for treatment compliance.Coerced Treatment for Substance AbuseProblems Detected Through WorkplaceUrine Surveillance: Is it Effective? EliLewantal et al., Journal of Substance Abuse,8(1): 115-128, 1996.
• A 1996 study by the Pennsylvania VeteransAdministration Center for Studies ofAddiction found employees required to enteralcohol treatment programs tend to performas well in treatment as employees whovoluntarily seek it. Drinking dropped 74%after 6 months of “coerced” treatment and78% after 6 months of “self-referral.” Evenwhen alcohol programs are available, manyemployees do not take advantage of them.Survey Shows Alcohol/Drug Use Has StrongImpact on Workplace. Hazelden Foundation,Center City, MN Oct. 22, 1996.
• Employers can encourage participation byinforming employees about theconfidentiality of programs to help deal withalcohol and other drug problems. Increasedpublic education focused on treatmentsuccesses may encourage more participationin alcohol interventions among bothemployers and employees. The Road toRecovery: A National Study on PublicPerceptions of Alcoholism and Barriers toTreatment. San Francisco, CA: The RecoveryInstitute, 1998.
Drug-free Workplace Programs: Successesand Future Challenges
• Available research demonstrates thatcomprehensive workplace preventionprograms which include: 1) education forworkers and training for supervisors; 2)
equitable, reliable drug testing; and 3)access to assistance and treatment servicescan successfully reduce worker substanceabuse and improve health, safety, andworksite productivity. Workplaces provide anideal opportunity to influence individualbehavior and community norms. Clear andconsistent substance abuse policies anddrug education efforts create an aware andinformed workforce, can significantly reducedrug and alcohol abuse in workplaces, andreach the families of employees and thecommunities where they live. SelectedFindings in Prevention: A Decade of Resultsfrom the Center for Substance AbusePrevention, Department of Health andHuman Services, SAMHSA, Center forSubstance Abuse Prevention, Rockville, MD,1997.
• Since 1986, the Federal government hasmandated a comprehensive drug-freeworkplace program for all Federal workers.Implemented in 120 agencies, this modelprogram covers approximately 1.8 millionemployees. In 1997, the most recentpositive drug test rates available, the rate ofpositive test results for Federal jobapplicants and employees in designatedtesting positions (numbering approximately80,000), was 0.5%; or one-tenth of the 5%positive rate of approximately 4 million testsconducted in 1997 by the largest privatesector workplace testing laboratory in theUS. As the nation’s largest employer, theFederal government continues to provideleadership by example. In June 1999,President Clinton took another historic stepforward to ensuring a drug-free federalworkforce by issuing an Executive Orderdirecting the Federal Employees HealthBenefit Program, the nation’s largest healthinsurance plan, to provide full coverage forsubstance abuse treatment, equal to anyother medical condition, by the year 2001.Annual Survey of Federal Agency Drug FreeWorkplace - 1997, U.S. Department ofHealth and Human Services, SAMHSA,Center for Substance Abuse Prevention,Division of Workplace Programs, Rockville,MD, March 1999; Quest Drug TestingIndex©, Quest Diagnostics, inc., Teterboro,NJ, October 19, 1999
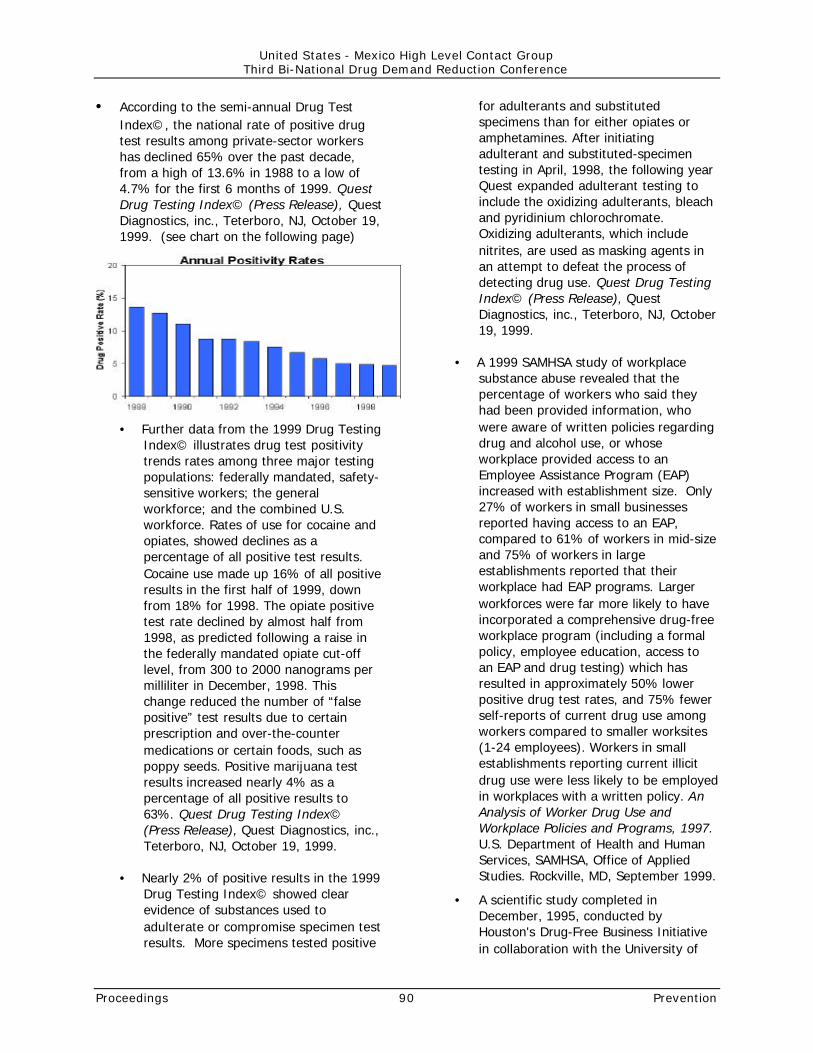
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 90 Prevention
• According to the semi-annual Drug TestIndex©, the national rate of positive drugtest results among private-sector workershas declined 65% over the past decade,from a high of 13.6% in 1988 to a low of4.7% for the first 6 months of 1999. QuestDrug Testing Index© (Press Release), QuestDiagnostics, inc., Teterboro, NJ, October 19,1999. (see chart on the following page)
• Further data from the 1999 Drug TestingIndex© illustrates drug test positivitytrends rates among three major testingpopulations: federally mandated, safety-sensitive workers; the generalworkforce; and the combined U.S.workforce. Rates of use for cocaine andopiates, showed declines as apercentage of all positive test results.Cocaine use made up 16% of all positiveresults in the first half of 1999, downfrom 18% for 1998. The opiate positivetest rate declined by almost half from1998, as predicted following a raise inthe federally mandated opiate cut-offlevel, from 300 to 2000 nanograms permilliliter in December, 1998. Thischange reduced the number of “falsepositive” test results due to certainprescription and over-the-countermedications or certain foods, such aspoppy seeds. Positive marijuana testresults increased nearly 4% as apercentage of all positive results to63%. Quest Drug Testing Index©(Press Release), Quest Diagnostics, inc.,Teterboro, NJ, October 19, 1999.
• Nearly 2% of positive results in the 1999Drug Testing Index© showed clearevidence of substances used toadulterate or compromise specimen testresults. More specimens tested positive
for adulterants and substitutedspecimens than for either opiates oramphetamines. After initiatingadulterant and substituted-specimentesting in April, 1998, the following yearQuest expanded adulterant testing toinclude the oxidizing adulterants, bleachand pyridinium chlorochromate.Oxidizing adulterants, which includenitrites, are used as masking agents inan attempt to defeat the process ofdetecting drug use. Quest Drug TestingIndex© (Press Release), QuestDiagnostics, inc., Teterboro, NJ, October19, 1999.
• A 1999 SAMHSA study of workplacesubstance abuse revealed that thepercentage of workers who said theyhad been provided information, whowere aware of written policies regardingdrug and alcohol use, or whoseworkplace provided access to anEmployee Assistance Program (EAP)increased with establishment size. Only27% of workers in small businessesreported having access to an EAP,compared to 61% of workers in mid-sizeand 75% of workers in largeestablishments reported that theirworkplace had EAP programs. Largerworkforces were far more likely to haveincorporated a comprehensive drug-freeworkplace program (including a formalpolicy, employee education, access toan EAP and drug testing) which hasresulted in approximately 50% lowerpositive drug test rates, and 75% fewerself-reports of current drug use amongworkers compared to smaller worksites(1-24 employees). Workers in smallestablishments reporting current illicitdrug use were less likely to be employedin workplaces with a written policy. AnAnalysis of Worker Drug Use andWorkplace Policies and Programs, 1997.U.S. Department of Health and HumanServices, SAMHSA, Office of AppliedStudies. Rockville, MD, September 1999.
• A scientific study completed inDecember, 1995, conducted byHouston's Drug-Free Business Initiativein collaboration with the University of

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 91 Prevention
Houston, reinforced the belief by manyemployers that drug testing reducesinjuries and workers' compensationclaims in the workplace. The studyfound that companies engaged inrandom drug testing in combination withpre-employment testing reduced theirmean workers' compensation claims per100 employees per year by 63.7% overa 4-year period while the control groupof employers (employers not conductingdrug testing), experienced a 19%increase during that same time period.The study also found that well over halfof the responding employers believedthat the benefits of drug testingoutweighed the cost and just under halffelt that the benefits of an EAPoutweighed the cost. When asked toselect one strategy over the other,40.6% of the respondents stated that itwas more important to conduct drugtesting than have an EAP, while only7.8% thought it was more important tohave an EAP than to test. However,51.6% thought drug testing and EAPswere of equal importance. A Report onEmployer Attitudes and the Impact ofDrug Control Strategies on WorkplaceProductivity Fay, Calvina L., Harlow,Kirk C. , and Durand, Roger. Houston'sDrug-Free Business Initiative and theUniversity of Houston - Clear LakeDecember, 1995.
• In 1990, problems resulting from alcoholand other drugs use cost Americanbusinesses an estimated $81.6 billion inlost productivity due to premature death(37 billion) and illness (44 billion); 86%of these combined costs were attributedto drinking. Substance Abuse andMental Health Statistics Sourcebook,Substance Abuse and Mental HealthServices Administration, U.S.Department of Health and HumanServices. Rockville, MD. 5/95, p.3. In1991, the reported cost of drug abuseto the United States businesscommunity was $75 billion annually.Address delivered to President Bush andthe President's Drug Advisory Council byFrank T. Tasco, Chairman, Marsh &
McLennan Companies. [November 15,1991]
• Workplace safety is the most commonreason employers give for drug testing.In 1997, approximately 25% of workersreported having a drug testing policy intheir workplaces. Of employersimplementing testing, the majority haveadopted urine drug screening as thepreferred methodology. In 1997, pre-employment testing was the mostcommon type of testing reported byworkers (39%), followed by reasonablesuspicion testing (30%), post-accident(29%) and random testing (25%).Current drug users indicate they are farless likely to apply for a job where theyknow that pre-employment or randomdrug testing is used. An Analysis ofWorker Drug Use and Workplace Policiesand Programs, 1997. U.S. Departmentof Health and Human Services,SAMHSA, Office of Applied StudiesRockville, MD, September 1999.
• Results of an extensive U.S. PostalService study indicate that employeeswho tested positive on their pre-employment drug test were 77% morelikely to be discharged within the firstthree years of employment, and wereabsent from work 66% more often thanthose who tested negative. Had the U.S.Postal Service screened out all drugpositive postal service applicants in1987, the authors estimated this wouldhave saved approximately $52 million by1989. An Evaluation of Pre-employmentDrug Testing. Normand, J., Salyards, S.& Maloney, J. Journal of AppliedPsychology. Vol. 75, No. 6, 1990. [pp.629-639]
• According to the American ManagementAssociation’s annual Survey onWorkplace Drug Testing and DrugAbuse Policies, workplace drug testinghas increased by more than 1,200%since 1987. More than 81% ofbusinesses surveyed in 1996 wereconducting some form of applicant oremployee drug testing. Likewise, theperceived effectiveness of drug testing,

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 92 Prevention
as assessed by human resourcesmanagers, has increased from 50% in1987 to 90% in 1996. AMA Survey onWorkplace Drug Testing and DrugAbuse Policies. American ManagementAssociation. New York, NY. 1996.
• Testing for the right reasons has thesupport of most employees and there issome evidence that drug testing helpsprevent illicit drug use. A 1995 Galluppoll of employees found 97% inagreement that workplace drug testingis appropriate under certaincircumstances; 85% believed that urinetesting might deter illicit drug use. TheGallup Organization, Princeton, NJ,October 1995, commissioned by TheInstitute for a Drug-Free Workplace,Washington, DC.
• Referrals to treatment for drug andalcohol abuse and support foremployees to change drug use behaviorare key. Employee Assistance Programs(EAPs) are increasingly being used byemployers to provide a gateway tosubstance abuse treatment, and reflectcost differences related to the quantityand qualities of services, the size andtype of industry and region of theUnited States. (1995 mean cost peremployee $22.19). Cost of EmployeeAssistance Programs: Comparison ofNational Estimates from 1993 and 1995.French, M.T., Zarkin, G.A., Bray, J.W.,Hartwell, T.D., Journal of BehavioralHealth services Research, February1999.
• Employee assistance programs (EAPs)are growing in popularity in all types ofU.S. worksites, according to a 1996study. In 1993, 1/3 of private,nonagricultural worksites with 50 or
more employees had an EAP, asignificant increase over the numbersshown in similar studies in 1988 and1990. Most employers surveyed,especially those with 50 to 99employees, had implemented an EAP inthe 5 years preceding the study.Compared to 1988 results, most of thisgrowth was in external programs: 81%of EAP services in 1993 were providedby external contractors, and 83% at alocation outside the workplace. Largerworksites (more than 1000 workers) andcertain industries (communications,transportation, finance, realty) weremore likely to have an EAP.Demographic findings revealed a greaterlikelihood of an EAP in workplaceswhere employees were unionized andrelatively more educated, and wherethere were relatively low numbers ofvisible minority workers. Geography hadno impact on the existence of aprogram, but program costs did varyregionally, with a median annual costper employee of just under $22 forinternal programs and of $18 forexternal programs. Based on theirsurvey results, the authors concludethat EAPs will continue to grow inimportance, and that health careprofessionals working in the areas ofsubstance abuse and emotional healthwill continue to get numerous referralsof clients who have passed through theEAP process. Consequently, researchinto the costs, characteristics, andresults of EAPs will continue to beimportant. Aiding troubled employees:prevalence, cost, and characteristics ofemployee assistance programs in theUnited States. Hartwell, Tyler D.American Journal of Public Health,86(6): 804-808, 1996
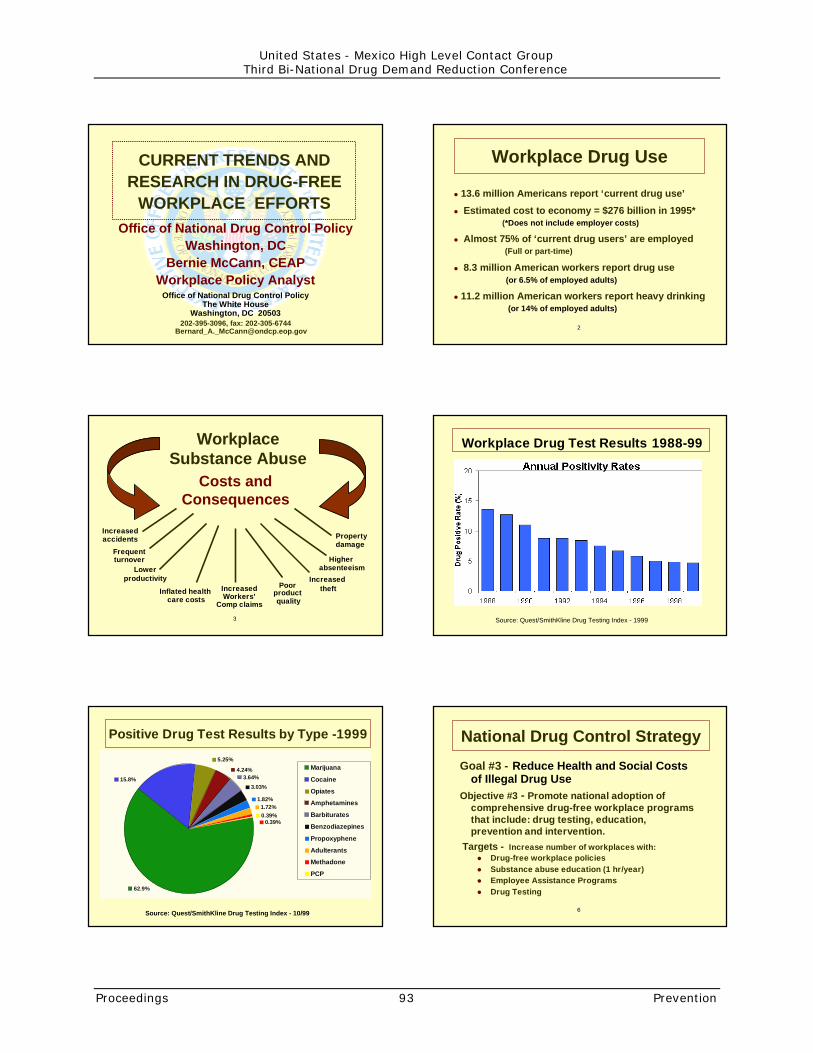
Office of National Drug Control PolicyWashington, DC
Bernie McCann, CEAPWorkplace Policy Analyst
Office of National Drug Control PolicyThe White House
Washington, DC 20503202-395-3096, fax: 202-305-6744
CURRENT TRENDS ANDRESEARCH IN DRUG-FREE
WORKPLACE EFFORTS
!!
Workplace Drug Use
� 13.6 million Americans report ‘current drug use’
� Estimated cost to economy = $276 billion in 1995* (*Does not include employer costs)
� Almost 75% of ‘current drug users’ are employed (Full or part-time)
� 8.3 million American workers report drug use (or 6.5% of employed adults)
� 11.2 million American workers report heavy drinking (or 14% of employed adults)
""
Costs andConsequences
Lowerproductivity
Frequentturnover
Poorproduct quality
Increasedaccidents
WorkplaceSubstance Abuse
Inflated health care costs
IncreasedWorkers’
Comp claims
Increased theft
Property damage
Higher absenteeism
Workplace Drug Test Results 1988-99
Source: Quest/SmithKline Drug Testing Index - 1999
Positive Drug Test Results by Type -1999
0.39%
5.25%
1.72%1.82%
3.03%
3.64%4.24%
0.39%
15.8%
62.9%
Marijuana
Cocaine
Opiates
Amphetamines
Barbiturates
Benzodiazepines
Propoxyphene
Adulterants
Methadone
PCP
Source: Quest/SmithKline Drug Testing Index - 10/99 ##
Goal #3 - Reduce Health and Social Costsof Illegal Drug Use
Objective #3 - Promote national adoption ofcomprehensive drug-free workplace programsthat include: drug testing, education,prevention and intervention.
National Drug Control Strategy
Targets - Increase number of workplaces with:� Drug-free workplace policies� Substance abuse education (1 hr/year)� Employee Assistance Programs� Drug Testing
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 93 Prevention

$$
Role and Objectives ofDrug Prevention
� Deter experimentation and new drug use
� Deter existing users progression into more serious use
� Break intergenerational cycle of substance abuse
� Reduce risk factors and increase protective factors
� Improve knowledge and attitudes
� Reduce drug and alcohol problem behaviors
%%
Workplace Prevention Efforts
➨ The workplace provides an ideal venue andopportunity to influence both individual adultbehavior and community norms.
➨ Clear, consistent workplace substance abuse policies and employee drug education can:
1) create an aware and informed workforce;
2) significantly reduce drug and alcohol abuse problems in the workplace; and
3) reach employees, their families, and into their communities with prevention messages.
&&
Drug-free Workplace ProgramsHistorical Development
� 1940s - Occupational Alcoholism Programs
� 1960s - Employee Assistance Programs
� 1986 - Executive Order 12564� 1988 - Drug-Free Federal Workplace established� Drug-free Workplace Act of 1988
(covers Federal contractors and grantees)
� 1989-94 Transportation (DOT) Regulations(covers safety-sensitive transport employees)
� Drug-free Workplace Act of 1998(provides drug-free workplace assistance to small business)
� National Drug Control Strategy: Workplace'('(
Why would EmployersImplement a DFWP?
� Triggering event� Regulations� Safety of:
� Public� Employees
� Productivity� Cost savings
� Community and/orIndustry norms
� Labor marketinfluences
� Liability exposure� Tax incentives� Health insurance
''''
Components of a Drug-FreeWorkplace Programs
� Policy Statement and Procedures
� Employee Education
� Supervisory Training
� Employee Assistance Program (EAP)
� Drug Testing
'!'!
Workplace Policy Elements
� Rationale (specific to worksite)
� Prohibited behaviors (and substances)
� Employees affected
� Detection of policy violation
� Consequences of prohibited behavior
� Availability of assistance
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 94 Prevention

'"'"
DFW Policy Considerations
� Why implement a DFW policy?� Who or what groups decide?� Who should be covered by policy?� What substances are prohibited?� To test or not to test?� Consequences of policy violations
� Treatment options?� Suspension, termination, etc?� Worker’s comp and unemployment claims?� Return to work procedures?
')')
Employee Education -Learning Objectives
� Clearly communicate policy
� Inform about the dangers of drug use
� Identify signs of drug abuse and effectson job performance and safety
� Describe when, if and how to approachco-workers and/or family members
� Additional resources for help and info
'*'*
Supervisory Training -Learning Objectives
� Identify signs of drug abuse and effects onjob performance and worksite safety
� Clarify supervisors’ role and responsibilityin policy enforcement� Recognize� Document� Intervention� Referral to EAP and/or drug testing� Follow-up job performance monitoring
'#'#
Employee Assistance Programs
� Workplace-based services to assist inproblem identification and resolution
� Confidential service to employees
� Assess, refer to help and follow-up
� Education and training services
� Consultation and training for organization
� Often available to family members
'$'$
To Test or Not to Test?
� Worksite safety - internal� Public Safety - external� Privacy - legal and ethical� Legitimacy of business concern
� Job performance indicators� Off-duty v.s on-duty use� Non-workplace drug convictions
� Risk reduction and liability issues� Business Climate� Organizational culture
'%'%
What Substances are Covered?
� Illicit drugs
� Alcohol
� Prescription drugs� Used with or against medical advise
� Over-the-counter medications
� Non-medical intoxicants
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 95 Prevention

'&'&
To Treat or Not To Treat?
� Zero tolerance or …..?
� Treatment opportunities� Type and number
� Who pays?
� Return to duty restrictions
� Last Chance Agreements
� Expectations from treatment
!(!(
Those who participate in drug treatment: ���� Decrease their drug use
���� Decrease their criminal activity
���� Increase their employment
���� Improve their social functioning
���� Improve their physical health
“Carrying the Message”-about Workers and Treatment
Drug use and criminal activity decrease forvirtually all who enter treatment, with better
results the longer they stay in treatment
!'!'
Easy Access DFW Resources - US
Federally-funded services� Drug-Free Workplace Helpline -
☛ Employers, Labor Unions, Supervisors, & Associations
� National Clearinghouse (NCADI) -
� Department of Labor (Working Partners) -
� Drug Enforcement Administration -☛ Regional Demand Reduction Coordinators
� Department of Transportation -☛ Assists with FAA, FHWA, USCG, FTA, FRA, RSPA regs
� Small Business Administration -☛ 50+ Small Business Development Centers
!!!!
Easy Access DFW Resources, cont.
✔ State Substance Abuse and related WorkforceDevelopment Agencies
✔ Private Sector Resources● Regional and Community groups, i.e., “Drugs don’t
Work” Coalitions, etc.
✔ Professional and Trade Associations -National, State and local, e.g.,� Employee Assistance Professionals Association� National Drug-free Workplace Alliance� Chambers of Commerce� Substance Abuse Professionals Association� Natl. Assn. of State Alcohol & Drug Abuse Directors
!"!"
Opportunities/Challenges
� Creating demand among small employers� Delivering services cost-effectively� Program standards and procedures
� Federal or State issue?� Uniformity and standardization� Employee protections� Enforcement authority
� Certification of professionals and othersdelivering DFW products and services
!)!)
Drug Testing Elements
� Established policy and procedures� Illicit Drugs (or additional substances)
Marijuana, Cocaine, PCP, Opiates, Amphetamines
� Alcohol� Testing Methodology
Screening and Confirmation
� Types of Testing� Consequences of Positive Tests� Due Process and Appeals
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 96 Prevention
!*!*
Types of Workplace Testing
� Pre-employment� Random� Reasonable Suspicion� Post accident/incident� Return-to-duty� Follow-up� Voluntary� Pre-Promotion� Periodic
!#!#
Who Should be Covered?
� Large and/or small businesses?
� All workplaces and all workers?
� Safety-sensitive workers?
� Certain industries?
� Certain professions?
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 97 Prevention

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 98 Prevention
Juan Roman Uriarte GalvanSecretary of Communicationsand TransportationMexicoThe Secretary first noted that the U.S.experience with drug-free workplaceprogramming has been invaluable to Mexico. Heagreed with the list of costs and consequencespresented by the previous speaker, Mr. McCann.He also noted that Mexican labor laws clearlyprohibit alcohol and other drug use in theworkplace by public sector workers.
The main drug prevention activities of theMinistry of Communication and Transportation inthe workplace have been:
• Performing comprehensive occupationalphysicals and medical examinations,including pre-employment and subsequentrandom urine drug testing for drugs ofabuse; and
• Conducting a massive educational campaignto prevent alcohol and drug abuse and thusreduce accidents associated with substanceabuse.
In the post-NAFTA environment, Ministry-sponsored programs have, in effect, adoptedU.S. Department of Transportation guidelines toachieve common protocols necessary to aidcross-border commerce. These activities extendto all modes of transportation: air, land, sea,etc.
Given research revealing that traffic crashes arethe fourth leading cause of death in Mexico(many in which alcohol use is implicated orsuspected) the Transportation Ministry hasundertaken prevention and detection effortswith both public and private sector. To this end,the National Council for Accident Prevention hasbeen established. The National Council providesthe coordinating role for state councils that willadvise and help states to reduce incidents andfatalities. Another agency, CONADIC has beenconducting research regarding transportationaccidents as well as exchanging information withothers and working to implement provenprograms.
In recognition of the key importance oftransportation safety, the Ministry ofTransportation was given the lead in developing
programs in this area, and has recently signed aMemorandum of Understanding with Mexico Cityto cooperate on programs geared to youth andaccident prevention. He also noted that recentlylegislation was passed to regulate toxicologytests and involve more private employers inprevention programs.
One of the Ministry’s priorities is to developcloser working relationships with employers andto increase prevention efforts around holidaytimes, which typically see a rise in accidentsattributable to substance abuse.
As Mr. McCann stated, it is important to realizethat our efforts here and elsewhere have indeedcaused people to become more aware andinterested in making changes to reduceaccidents and other costs of substance abuse. Itis even more important to have the political willto address the plague of substance abuseamong those who are most vulnerable, who inturn endanger the lives of others. An excellentexample would be efforts to increase educationand substance abuse assistance for vehicleoperators.
DRUGS AND VIOLENCE:OVERVIEW OF BORDER CRIMEPREVENTION PROGRAM IN BAJA,CALIFORNIA & SAN DIEGO
Developing a Culture of Lawfulness
Edward BrandSuperintendent of Sweetwater Union SchoolDistrictChula Vista, CaliforniaUnited States
Rosalia SalinasDirector of CurriculaSweetwater Union School DistrictChula Vista, CaliforniaUnited States
Carlos FrancoDirector of CurriculaBaja School DistrictMexico
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 99 Prevention
Luciana RamosMexican Institute of PsychiatryMexico
Dr. Brand, Ms. Salinas, and Sr. Franco spokeabout a middle school curriculum jointlydeveloped by Ms. Salinas, Sr. Franco, and agroup of U.S. and Mexican teachers, to teachstudents about the rule of law and the wayorganized crime can infiltrate a community. Itis based on an approach developed in HongKong and Sicily by the National StrategyInformation Center that focuses on personal andsocial ethical decision making, the rationale forthe rule of law, the temptations of crime andmaterialism, and techniques for resistinginvolvement in criminality and corruption.
The curriculum in Baja and San Diego wasdeveloped as part of a social studies course andis meant to address the problem of drugviolence along the border. According to Dr.Brand, the keys to this program's effectivenessinclude:
• Commitment by senior political leadership inthe communities
• School administrations' support (i.e., countyboards of education)
• Teacher training and assistance, and a goodfit with current social studies curricula.
Ms. Salinas noted the importance of bringing incurriculum experts from both the U.S. andMexico who could develop a course that couldbe integrated into current curricula determining,for example, where such a course could fit intothe schedule and who could teach it. Studentresults from the pilot effort jointly conducted bySweetwater and Baja show the following:
• Increased knowledge about drug-relatedcrime and how to resist it
• Improved interpersonal competency, selfesteem, and problem solving ability
• Improved ability to resist temptation andincreased awareness of life choices andimportance of planning.
She stressed the importance of teacher-to-teacher collaboration and recommended that theprogram be extended to all of SouthernCalifornia.
Sr. Carlos Franco stated that the teachers'common concerns about drug related violencealong the border has really led to thecurriculum’s development and support. Hedescribed the U.S.-Mexican collaboration incurriculum development:
• Agreement to and specification of a pilot(set period of time, evaluation according toobjectives)
• Formed a task force of teachersrepresenting both poor and better-offschools, that developed a curriculum toexplain why society has laws and why theyare important; to show how crime operatescounter to those laws; and to increase thestudents' sense of self-worth andcompetence to support a society of laws.
The teachers are now adding a program onvalues and citizenship training.
He explained that the project has continued fortwo six-month segments and reiterated theresults described by Ms. Salinas, noting the"enormous difference between pilot and non-pilot schools" in terms of student understandingand self esteem. He concluded that the nextstep is to bring the parents into the program.
Dr. Luciana RamosMexican Institute of PsychiatryMexico
Dr. Ramos spoke on drugs and violence fromthe perspective of a researcher on family anddomestic violence. She noted that in Mexico therole of substance abuse (mainly alcohol) israrely acknowledged in domestic violence cases.She called for a clearer understanding by thepublic and by policy makers of this connection,stating that each could be a risk factor for theother. She then reviewed her research on thisissue, which has revealed the following:

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 100 Prevention
• One in every three women in Mexico haveexperienced some sort of abuse
• Between 30-60% of women in the Americasreport some sort of "gender violence"
• Of the women reporting incidents ofdomestic violence, there was moretranquilizer and marijuana use (but nosignificant difference in alcohol use fromwomen who reported no such incidents).
She described results of a survey conducted intwo Mexico City high schools which revealedsexual abuse against both sexes and increaseduse of cocaine and marijuana by these youngpeople. Dr. Ramos concluded by calling forstudies of young people of both countries.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 101 Prevention
PREVENTION TRAININGSESSIONS
COMPREHENSIVE SCHOOL-BASEDPROGRAMS INVOLVING THE FAMILY
Introduction to Programs on Schools andFamilies
Carmen MilleNational Council on Addictions(CONADIC)Ministry of HealthMexico
“Construye tu Vida sin Adicciones” (Buildyour Life without Addictions” Programin SchoolsCarmen Mille,Maria Teresa Sanchez Fragoso,Fernando Bilbao Norma MerenaCouncil on Addictions (CONADIC)Ministry of HealthMexico
Bi-national Implementation of “Construyetu Vida sin Addiciones”Dr. Ignacio Benedicto ReyesBaja, CaliforniaMexico
In a prevention track session on school andfamily-based programs, CONADIC staff providedan overview of Mexico’s wide-ranging preventioneffort, “Construye Tu Vida Sin Addiciones,”(build your life without addictions) followed by apresentation by Dr. Ignacio Benedicto Reyesabout a cross-border implementation ofConstruye in Baja California in both Mexico andthe U.S.. Construye programs have manyelements including role-plays for young peopleon decision making, community work in whichfacilitators form groups of community preventionworkers, and projects specifically planned byand for young people. Materials include posters,bulletins, flyers, four books and three videos.The biggest problem in getting prevention
programs in schools is that school officials thinkthey have no time for such activities. Presentersnoted, however, that the students find time andeven work on Saturdays on tournaments,parties, fairs, basketball games ? all drug-freeand promoting healthy lifestyles. At this time,process evaluations are being done onConstruye programs, and Carmen Mille ofCONADIC stated that a follow-up study will beconducted that will enable measurement ofprogram impact. Other CONADIC staff notedthe need for improved dissemination systems.
Noting that Baja is a “third culture,” Dr. Reyes,of Baja California, described bi-nationalimplementation of Construye programs there.Baja, Mexico’s activities were coordinated withthose of Imperial, California’s, and thesecommunities jointly chose Construye as theirprevention model. A youth committee and anadult prevention committee were formed, andbi-national training was conducted. Construyewent through its entire process, from theidentification of small groups of students to leadthe effort in particular schools, to theiridentification of activities. In this case, underthe theme “Baja Fighting Drugs Together,” thecommunity held prevention fairs and art shows,and a youth-operated hotline has been started.At this point, Construye is at the communitylevel but some training has begun in theschools. In some schools, Construye lessonshave become part of the curriculum; in others, itis an after school activity. Sometimes teachersinvite parent participation and provide trainingfor both students and parents. Reyesconcluded that all models have to be adapted tothe specific culture, be easily understood, andhave direct relevance to the target population.
EFFECTIVE COMMUNITYMOBILIZATION APPROACHES
Drug-Free Communities Support Program:Community Mobilization in the BorderStates to Reduce Substance AbuseMary Ann Solberg, ModeratorAdvisory Commission on Drug-FreeCommunitiesUnited States

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 102 Prevention
Panel:
Harry MontoyaHands Across Cultures, Inc.Espanola, New MexicoUnited States
Luz ArriolaWest Texas Council on Alcoholism andDrug AbuseEl Paso, TexasUnited States
Lorenzo MerrittProject HEAVY WestLos Angeles, CaliforniaUnited States
Luis NavarroChimalli System for the IntegralDevelopment of the Family (DIF)Mexico
Grantees from the Drug-Free CommunitiesSupport Program (DFCSP) facilitated thistraining session. This program is a collaborativeprogram of ONDCP, OJJDP and SAMHSA/CSAPcreated by the Drug-Free Act of 1997 (PublicLaw 105-20). This act funds communitycoalitions (collaboratives) to reduce substanceabuse among youth, and over time amongadults; and increase collaboration amongFederal, State, local, and private non-profitcommunity based organizations.
The DFCSP projects all serve a diverse bi-national target community on the U.S. side ofthe border.
Harry Montoya, presented cultural relevance,vision and principals of community mobilization.Luz Arriola, WTCADA, provided a step-by-stepguide to plan and form a community coalition tomobilize the community to reduce substanceabuse. Dr. Lorenzo Merritt, PHW, presented thedevelopmental stages of communitymobilization, the challenges and opportunities,and the outcomes of community mobilization.Luis Navarro, Chimalli-DIF, Mexico, presentedthe results of a Mexican research project on
homeless children living in the streets in 100cities in Mexico. Mr. Navarro’s presentationprovided the many risk factors that thesechildren are exposed to, including a higherincidence of substance abuse and substanceabuse related violence.
The main points of this training were:
• Assess the community that you are trying tomobilize in order to establish baseline data.
• Balance inter-cultural issues in communitymobilization process.
• Determine steps and developmental stagesrelating to community mobilization for thetarget community.
• Impact negative social norms by using theproven Community Mobilization trainingmodel.
• Utilize community challenges andopportunities for community mobilization todesign, provide ongoing review ofeffectiveness, and revise, if necessary,evaluation of mobilization efforts.
BUILDING EFFECTIVEPARTNERSHIPS FOR DRUGPREVENTION IN THE WORKPLACE
Robert Stephenson, Acting Director,Division of Workplace ProgramsCenter for Substance Abuse Prevention,Substance Abuse and Mental HealthServices AdministrationUnited States
Building Partnerships for Drug Preventionin the Workplace
Elizabeth Edwards, Gabriela Garcia,Arizonans for a Drug-Free WorkplaceUnited States
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 103 Prevention
Model Program on Alcohol and Drug UsePrevention between Workers and TheirFamilies
Agustin Vélez, Director,Trusteeship for the Institute for Street Kidsand AddictionsMexico
Slide presentations follow.
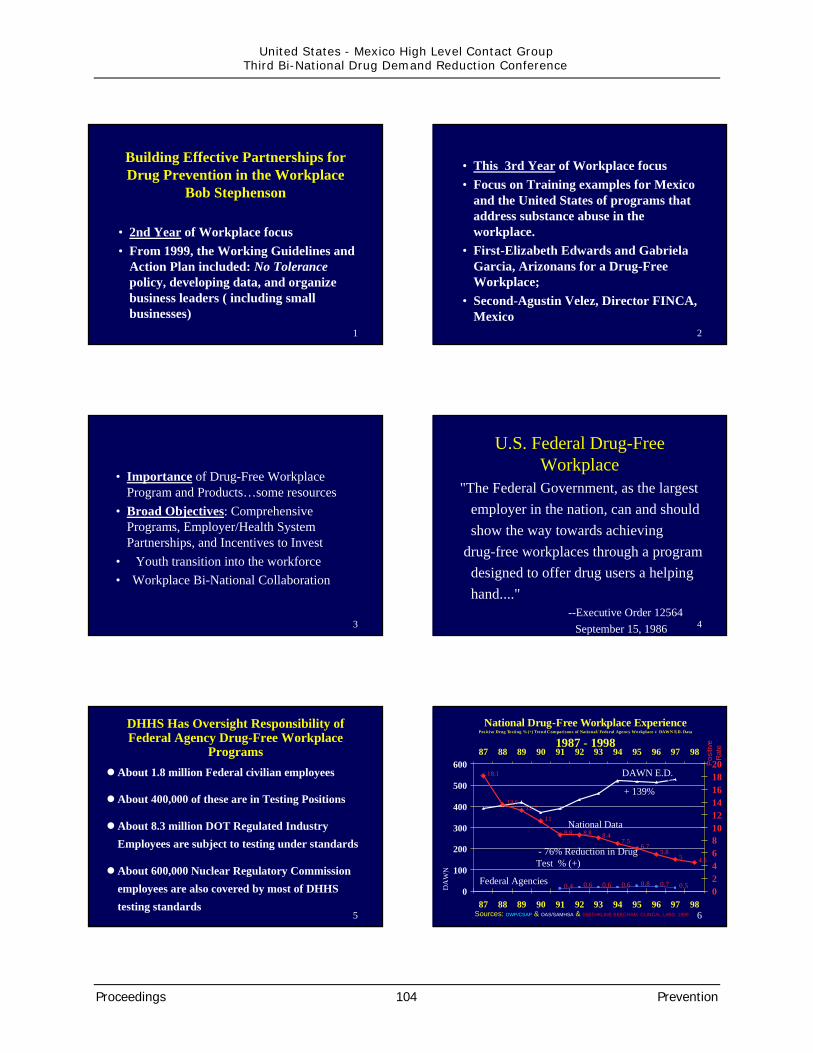
1
•2nd Year of Workplace focus•From 1999, the Working Guidelines and
Action Plan included: No Tolerancepolicy, developing data, and organizebusiness leaders ( including smallbusinesses)
Building Effective Partnerships forDrug Prevention in the Workplace
Bob Stephenson
2
•This 3rd Year of Workplace focus•Focus on Training examples for Mexico
and the United States of programs thataddress substance abuse in theworkplace.
•First-Elizabeth Edwards and GabrielaGarcia, Arizonans for a Drug-FreeWorkplace;
•Second-Agustin Velez, Director FINCA,Mexico
3
•Importance of Drug-Free WorkplaceProgram and Products…some resources
•Broad Objectives: ComprehensivePrograms, Employer/Health SystemPartnerships, and Incentives to Invest
• Youth transition into the workforce• Workplace Bi-National Collaboration
4
U.S. Federal Drug-FreeWorkplace
"The Federal Government, as the largestemployer in the nation, can and shouldshow the way towards achieving
drug-free workplaces through a programdesigned to offer drug users a helpinghand...." --Executive Order 12564 September 15, 1986
5
DHHS Has Oversight Responsibility ofFederal Agency Drug-Free Workplace
Programs� About 1.8 million Federal civilian employees
� About 400,000 of these are in Testing Positions
� About 8.3 million DOT Regulated IndustryEmployees are subject to testing under standards
� About 600,000 Nuclear Regulatory Commissionemployees are also covered by most of DHHStesting standards
6
National Drug-Free Workplace Experience Positive Drug Testing % (+) Trend Comparisons of National/ Federal Agency Workplace v DAWN E.D. Data
1987 - 1998
18.1
13.612.7
11
8.8 8.8 8.47.5
6.75.8
5 4.5
0.4 0.6 0.6 0.6 0.8 0.7 0.50
100
200
300
400
500
60087 88 89 90 91 92 93 94 95 96 97 98
Posi
tive
Rat
e
02468101214161820
87 88 89 90 91 92 93 94 95 96 97 98Sources: DWP/CSAP & OAS/SAMHSA & SMITHKLINE BEECHAM CLINCAL LABS, 1999
DA
WN
E.D
. D
ata
(10 0
0’s)
DAWN E.D.
+139%
National Data
- 76% Reduction in DrugTest % (+)
Federal Agencies
DAWN E.D.
+ 139%
Federal Agencies
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 104 Prevention
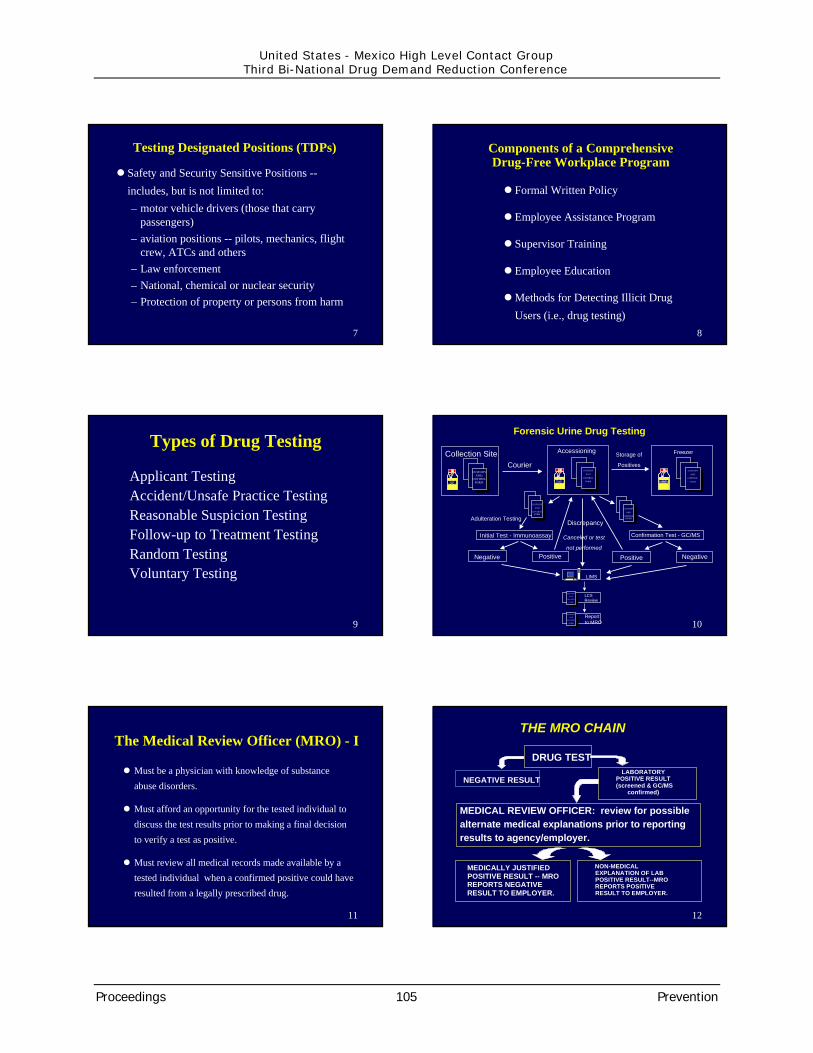
7
Testing Designated Positions (TDPs)
� Safety and Security Sensitive Positions --includes, but is not limited to:– motor vehicle drivers (those that carry
passengers)– aviation positions -- pilots, mechanics, flight
crew, ATCs and others– Law enforcement– National, chemical or nuclear security– Protection of property or persons from harm
8
Components of a ComprehensiveDrug-Free Workplace Program
� Formal Written Policy
� Employee Assistance Program
� Supervisor Training
� Employee Education
� Methods for Detecting Illicit DrugUsers (i.e., drug testing)
9
Types of Drug Testing
Applicant TestingAccident/Unsafe Practice TestingReasonable Suspicion TestingFollow-up to Treatment TestingRandom TestingVoluntary Testing
10
Forensic Urine Drug Testing
Accessioning
CUSTODY
AND
CONTROL
FORM
XXXX
CUSTODY
AND
CONTROLFORM
LIMS
Reportto MRO
LCSReview
CUSTODY
AND
CONTROL
FORM
CUSTODY
AND
CONTROL
FORM
Negative Positive
Initial Test - Immunoassay
Adulteration Testing
Collection Site
CUSTODYAND
CONTROLFORM
XXXX
Courier
Positive Negative
Confirmation Test - GC/MS
Storage of
PositivesCUSTODY
AND
CONTROL
FORM
XXXX
Freezer
CUSTODY
AND
CONTROLFORM
Canceled or test
not performed
Discrepancy
11
The Medical Review Officer (MRO) - I
� Must be a physician with knowledge of substanceabuse disorders.
� Must afford an opportunity for the tested individual todiscuss the test results prior to making a final decisionto verify a test as positive.
� Must review all medical records made available by atested individual when a confirmed positive could haveresulted from a legally prescribed drug.
12
DRUG TEST
NEGATIVE RESULT
MEDICALLY JUSTIFIEDPOSITIVE RESULT -- MROREPORTS NEGATIVERESULT TO EMPLOYER.
NON-MEDICALEXPLANATION OF LABPOSITIVE RESULT--MROREPORTS POSITIVERESULT TO EMPLOYER.
MEDICAL REVIEW OFFICER: review for possiblealternate medical explanations prior to reportingresults to agency/employer.
LABORATORYPOSITIVE RESULT(screened & GC/MS
confirmed)
THE MRO CHAIN
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 105 Prevention

13
OPIATES OTHERTHAN
POSITIVE
MRO ContactsEmployee
Employee DeniesIllegal Drug Use
OPIATES
POSITIVE
MRO PROBES FOREXPLANATION
Review Medical RecordsExamines if Appropriate
Employee AdmitsIllegal Drug use
How MRO Reporting Works - I
Report toEAP/MGT. as
required
14
Report toEAP/Management as Required
Recent prescriptionor treatment
claimed
Conclusion: No urinary confirmation ofabuse; inform employee; take no further
action
Review LabResult; Check QC;Consult with labdirector; retest
specimen
No explanation orother explanation
noted
How MRO Reporting Works- III
NotVerified
Resultsscientificallyinsufficient
No QC/LabProblems
OTHER THANOPIATESPOSITIVE
Verified
15
Non-Testing Activites - 1• DWP administers a drug-free workplace Helpline for
businesses, that receives over 700 inquiries per month, andmay be reached at 1 800-WORKPLACE, or on the Internetat [email protected].
• The“ Workplace Resource Center” is coming to the Internetsoon, and was demonstrated on the evening of May 10, at theSAMHSA Joint Council Meeting. workplace.samhsa.gov
• Workplace Managed Care KDA, exploring the healthcare provisions of private sector employers to identifyeffective and cost efficient models that provide substanceabuse prevention and early identification and interventioncomponents. Nine (9) Three year Cooperative Agreements
16
Non-Testing Activites - 2• Geographic Information System (GIS) applications
for workplace and community substance abuse andviolence reduction. These resources have been usedby SAMHSA in the Congressional Budget Hearingsin 1999 and this year. These GIS resources are beingincorporated into the CSAP Decision Support System(DSS), currently under development, and will also beavailable through the Internet in the next few months.
17CSAP/DWPCSAP/DWP
Number ofSites
9 WMC Grantees Have Numerous Sites Throughout U.S.
18
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 106 Prevention

19 20
21 22
Example: CONGRESSIONAL BLACK CAUCUSHIV/AIDS Outreach Grants Program
(November 10, 1999)
• Assisted CSAP HIV/AIDS Program Office andthe Surgeon General in presenting to theCongressional Black and Hispanic Caucusesthe distribution of funds targeted for theAfrican American Community by analyzing:– Concentration of the Population at Risk, African American
Population and Target Groups (African American Women,Women of Color, Children & Youth)
– Correlated the spread of HIV/AIDS within these community(CDC Data)
– Location of CSAP HIV/AIDS Grants Requested & Approvedwithin CBC Member Districts - HHS-wide data to follow
23 24
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 107 Prevention
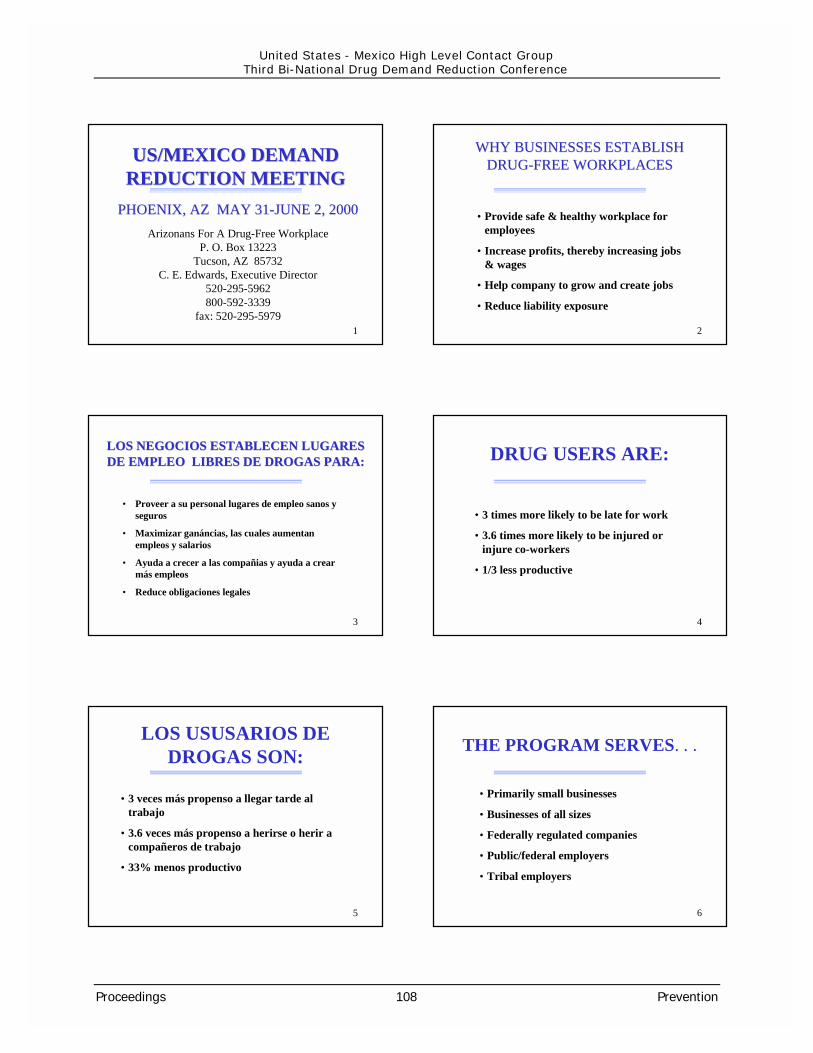
1
US/MEXICO DEMANDUS/MEXICO DEMANDREDUCTION MEETINGREDUCTION MEETING
Arizonans For A Drug-Free WorkplaceP. O. Box 13223
Tucson, AZ 85732C. E. Edwards, Executive Director
520-295-5962800-592-3339
fax: 520-295-5979
PHOENIX, AZ MAY 31-JUNE 2, 2000PHOENIX, AZ MAY 31-JUNE 2, 2000
2
WHY BUSINESSES ESTABLISHWHY BUSINESSES ESTABLISHDRUG-FREE WORKPLACESDRUG-FREE WORKPLACES
•Provide safe & healthy workplace foremployees
•Increase profits, thereby increasing jobs& wages
•Help company to grow and create jobs
•Reduce liability exposure
3
LOS NEGOCIOS ESTABLECEN LUGARESLOS NEGOCIOS ESTABLECEN LUGARESDE EMPLEO LIBRES DE DROGAS PARA:DE EMPLEO LIBRES DE DROGAS PARA:
• Proveer a su personal lugares de empleo sanos yseguros
• Maximizar ganáncias, las cuales aumentanempleos y salarios
• Ayuda a crecer a las compañias y ayuda a crearmás empleos
• Reduce obligaciones legales
4
DRUG USERS ARE:
•3 times more likely to be late for work
•3.6 times more likely to be injured orinjure co-workers
•1/3 less productive
5
LOS USUSARIOS DEDROGAS SON:
•3 veces más propenso a llegar tarde altrabajo
•3.6 veces más propenso a herirse o herir acompañeros de trabajo
•33% menos productivo
6
THE PROGRAM SERVES. . .
•Primarily small businesses
•Businesses of all sizes
•Federally regulated companies
•Public/federal employers
•Tribal employers
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 108 Prevention

7
EL PROGRAMA ASISTE A . .
•Pequeñas industrias
•Industrias de todo tamaño
•Compañias bajo reglamentos del gobierno federal
• Personal público/ federal
• Personal de Naciones Indígenas Norteamericanas
8
ARIZONANS FOR A DRUG-ARIZONANS FOR A DRUG-FREE WORKPLACEFREE WORKPLACE
COMPANIES/ORGANIZATIONSSERVED 1990-2000
Arizona: 4,643
National: 953
9
ARIZONANS FOR A DRUG-ARIZONANS FOR A DRUG-FREE WORKPLACEFREE WORKPLACE
COMPAÑIAS/ ORGANIZACIONESASESORADAS: 1990-2000
En Arizona: 4,643
En la nación: 953
10
ARIZONANS FOR A DRUG-ARIZONANS FOR A DRUG-FREE WORKPLACEFREE WORKPLACE
SERVICES PROVIDED Technical Assistance Training Education Resources
11
ARIZONANS FOR A DRUG-ARIZONANS FOR A DRUG-FREE WORKPLACEFREE WORKPLACE
SERVICIOS BRINDADOS Asistencia técnica Instrucción Educación Recursos
12
HOW BUSINESSES AREREACHED
Business networks & professional organizations Referrals Business conferences Media and direct mail for training programs
Proceedings 109 Prevention
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference

13
COMO SE ATRAEN A LOSCOMO SE ATRAEN A LOSNEGOCIOSNEGOCIOS
Asociaciones de negocios y otras asociacionesprofesionales
Recomendaciones
Conferencias relacionadas con el sector privado
Medios de comunicación y folletos sobre cursosenviados directamente a negocios
14
REACHING RURAL ANDREACHING RURAL ANDSMALL BUSINESSESSMALL BUSINESSES
Increased number of training programs from 8 to 19
5 regions established in Arizona for centers
Arizona zoned for convenient access to training programs
Provide toll-free telephone service and internet site
Provide listing of rural community test collection sites
15
COMO SE ATRAE ACOMO SE ATRAE AREGIONES RURALES YREGIONES RURALES Y
PEQUEÑAS INDUSTRIASPEQUEÑAS INDUSTRIAS
Incrementación de cursos de 8 anuales a 19
5 centros de recursos regionales en Arizona
Cursos impartidos en zonas accessibles pararegiones rurales en Arizona
Acceso a numero telefónico con lada gratuita ypresencia en el internet
Acceso a una lista de localidades para centros decolección de muestras en las regiones rurales
16
HOW THE PROGRAM EXISTSHOW THE PROGRAM EXISTS
•Partnerships with drug demand reductionagencies
•Fees from training programs, products,other materials
•Memberships, donations, sponsorships
•Fund-raising activities
17
COMO EXISTE Y SE SOSTIENE COMO EXISTE Y SE SOSTIENEEL PROGRAMA DE AFDFWEL PROGRAMA DE AFDFW
•Vínculos con agencias de reducción dedemanda
•Honorarios por impartición de cursos,productos, y la venta de otros materiales
•Asociación a AFDFW, donativos,patrocinadores
•Actividades de capturación de fondos
18
BARRIERSBARRIERS ENCOUNTEREDENCOUNTERED
•No funds for advertising to reach ruralbusinesses
•Continual budget shortages
•Demand for services exceeds resourcesand available staff levels
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 110 Prevention
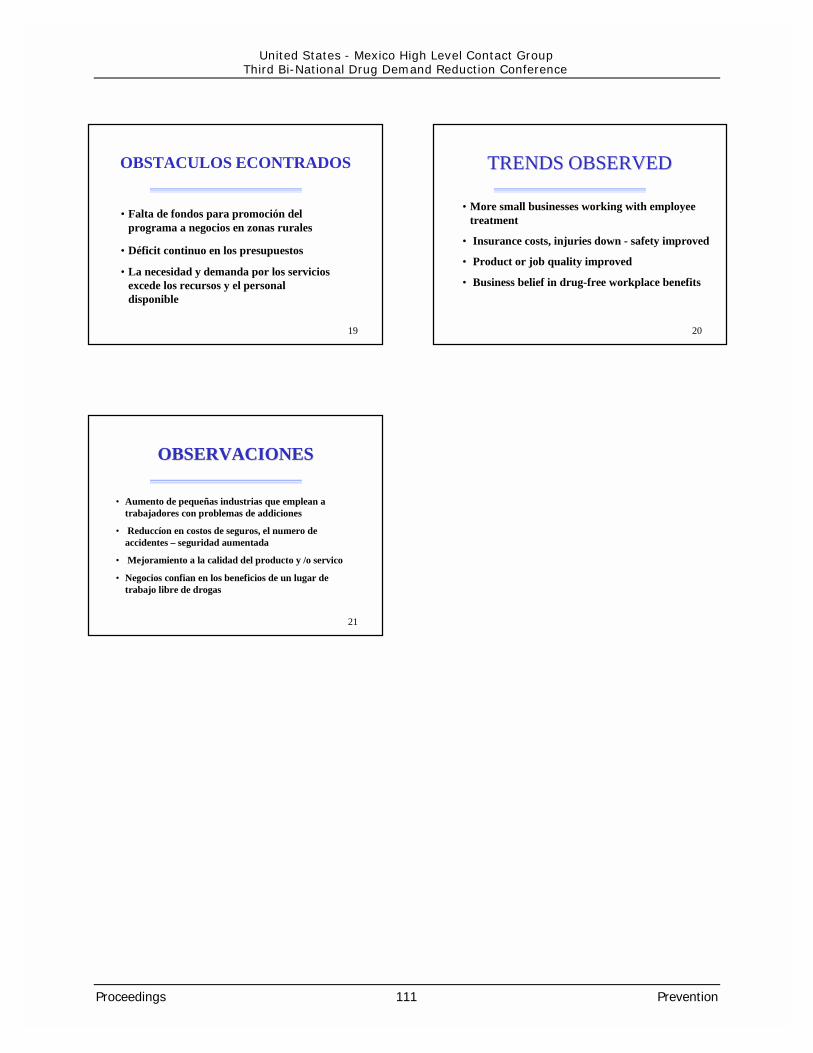
19
OBSTACULOS ECONTRADOS
•Falta de fondos para promoción delprograma a negocios en zonas rurales
•Déficit continuo en los presupuestos
•La necesidad y demanda por los serviciosexcede los recursos y el personaldisponible
20
TRENDSTRENDS OBSERVEDOBSERVED
•More small businesses working with employeetreatment
• Insurance costs, injuries down - safety improved
• Product or job quality improved
• Business belief in drug-free workplace benefits
21
OBSERVACIONESOBSERVACIONES
• Aumento de pequeñas industrias que emplean atrabajadores con problemas de addiciones
• Reduccíon en costos de seguros, el numero deaccidentes – seguridad aumentada
• Mejoramiento a la calidad del producto y /o servico
• Negocios confian en los beneficios de un lugar detrabajo libre de drogas
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 111 Prevention

Programa Modelo de Prevención del AbusoAlcohol y Drogas en Trabajadores y sus Familias
Programa Modelo de Prevención del AbusoAlcohol y Drogas en Trabajadores y sus Familias
RESULTADOS DE INVESTIGACIÓNAdaptaciones al Contexto Mexicano
Dr. Agustín Vélez Barajas
RESULTADOS DE INVESTIGACIÓNRESULTADOS DE INVESTIGACIÓNAdaptaciones al Contexto Mexicano
Dr. Agustín Vélez Barajas
Objetivos de la InvestigaciónObjetivos de la InvestigaciónObjetivos de la Investigación
�Identificar los elementos que favorecen o restringen laprevención de abuso de sustancias en los ámbitos laboraly familiar
�Obtener la información necesaria del proceso yresultados de la instrumentación del programa
�Realizar recomendaciones para la adaptación delprograma a contextos mexicanos
�Realizar la extensión del programa a la familia
FASE I: Evaluación denecesidades
Prioridades�44% Alcohol
� 7% programas de adiccion adrogas
�81% Tienen programas desalud y seguridad
�48% Incluyen un componentede drogas
MetodologíaMetodología
FASE II. Introducción delprograma a las empresas
�Contacto con el departamentode recursos humanos
�Política de recursos humanos
�Asistencia al seminario
�Acuerdo con el marcoconceptual
�Visitas clave del coordinadorinternacional
Desarrollo� Nececidades de información� Normas y valores� Necesidad de asociación de colores
usados� Simbolos y Palabras� Comprensión del texto
Evaluación�Tiempo de exposición�Opinión de expertos, gerentes y médicos�Grupos Focales�Aplicación del cuestionario a través de
entrevistas con los trabajadores
FASE IV. Desarrollo y evaluación demateriales para la intervención
FASE III. Desarrollo de instrumentos ydiagnóstico
� Tabaco, alcohol (AUDIT), otrasdrogas y problemas relacionados
� Lugares para beber
� Razones para beber
� Conocimientos y actitudes acerca delalcohol
� Información sociodemgráfica
� Formas de enfrentamiento y apoyosocial
� Estrés laboral y familiar
MetodologíaMetodología
FASE VI. Evaluación de laIntervención
� Asociación de los colores
� Cambios en creencias y conocimientosacerca de los efectos del alcohol
� Variaciones en la conducta
� Impacto en los problemas relacionadoscon el alcohol
� Percepción de las fuentes de apoyo
� Conocimientos acerca de estrategias deenfrentamiento en la familia
FASE V. Intervención
Sensibilización� Video: política de la empresa, conceptos
básicos de programa, autoevaluación yubicación en zona verde, ámbar o roja
� Carteles: con los colores asociados alalcohol y calidad de la producción
Intervención
� Carteles: “aprenda a contar”
� Folleto: “¿Te estás pasando el alto?”
� Folleto: “Guía para la familia de lostrabajadores”
MetodologíaMetodología CARACTERÍSTICAS GENERALES DE LA MUESTRA DETRABAJADORES DE LA EMPRESA “A”
Distribución de Edad
8% no asistieron a la escuela, 59% 1 - 8 años
Distribución por Turno
7-15 Hrs 15-23 Hrs 23-7Hrs Mixto0
33.3
24.8
18.520.1
5
10
15
20
25
30
35
40
%
0 10 20 30 40 50 %
13
25.5
19.6
14.9
26.1
16-17
18-20
21-23
24-26
27 +
Years
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 112 Prevention
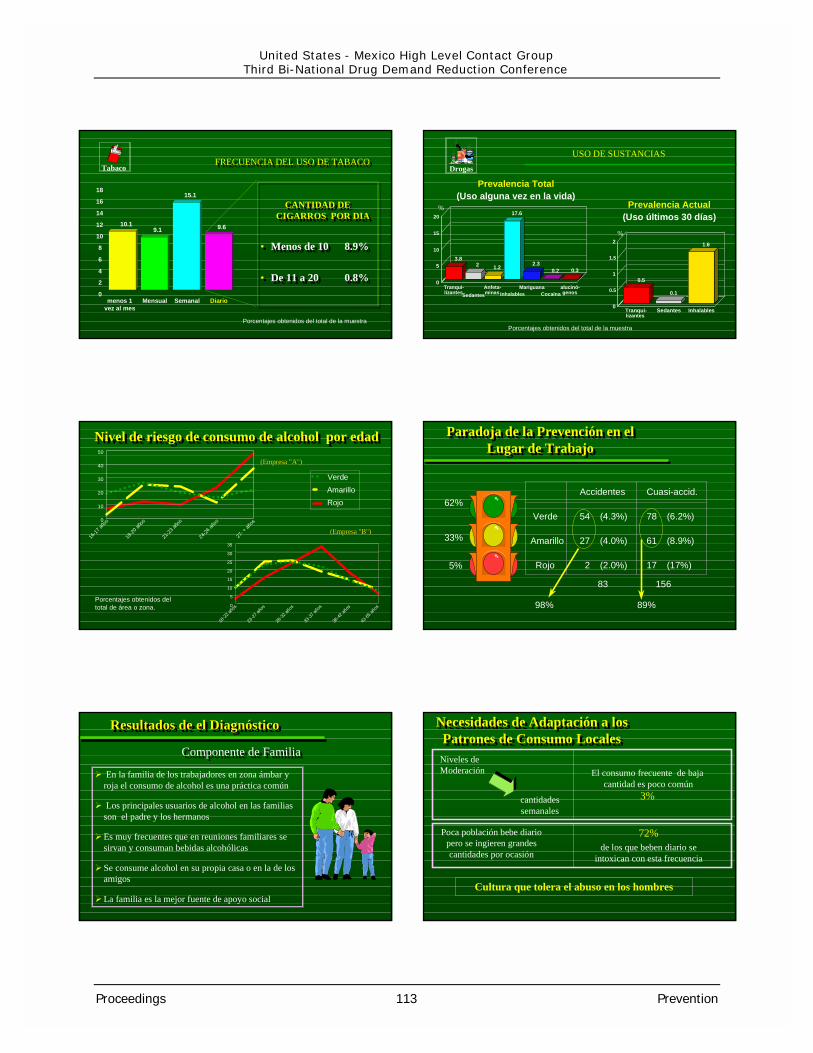
FRECUENCIA DEL USO DE TABACOFRECUENCIA DEL USO DE TABACO
CANTIDAD DECIGARROS POR DIA
• Menos de 10 8.9%
• De 11 a 20 0.8%
CANTIDAD DECIGARROS POR DIA
• Menos de 10 8.9%
• De 11 a 20 0.8%
10.19.1
15.1
9.6
menos 1vez al mes
Mensual Semanal Diario0
2
4
6
8
10
12
14
16
18
Tabaco
Porcentajes obtenidos del total de la muestra
USO DE SUSTANCIASDrogas
Prevalencia Total(Uso alguna vez en la vida)
Prevalencia Actual(Uso últimos 30 días)
Porcentajes obtenidos del total de la muestra
10
15
20
3.82 1.2
17.6
2.30.2 0.3
Tranqui-lizantesSedantes
Anfeta-minas Inhalables
MariguanaCocaína
alucinó-genos
0
5
%
%
0.5
0.1
1.6
Tranqui-lizantes
Sedantes Inhalables0
0.5
1
1.5
2
Nivel de riesgo de consumo de alcohol por edadNivel de riesgo de consumo de alcohol por edad
�
�
�
�
�
�
� �
��
��
�
18-22
años
23-27
años
28-32
años
33-37
años
38-42
años
43-65
años0
5
10
15
20
25
30
35
VerdeAmarilloRojo
Porcentajes obtenidos deltotal de área o zona.
(Empresa "B") (Empresa "B")
�
�
��
�
��
�
��
16-17
años
18-20
años
21-23
años
24-26
años
27- +
años
0
10
20
30
40
50
(Empresa ”A") (Empresa ”A")
62%
33%
5%
Accidentes Cuasi-accid.
Verde 54 (4.3%) 78 (6.2%)
Amarillo 27 (4.0%) 61 (8.9%)
Rojo 2 (2.0%) 17 (17%)
98%
83 156
89%
Paradoja de la Prevención en elLugar de Trabajo
Paradoja de la Prevención en elLugar de Trabajo
Componente de FamiliaComponente de Familia
Resultados de el DiagnósticoResultados de el DiagnósticoResultados de el Diagnóstico
� En la familia de los trabajadores en zona ámbar yroja el consumo de alcohol es una práctica común
� Los principales usuarios de alcohol en las familiasson el padre y los hermanos
�Es muy frecuentes que en reuniones familiares sesirvan y consuman bebidas alcohólicas
�Se consume alcohol en su propia casa o en la de losamigos
�La familia es la mejor fuente de apoyo social
Necesidades de Adaptación a losPatrones de Consumo Locales
Necesidades de Adaptación a losPatrones de Consumo Locales
Niveles deModeración
Poca población bebe diariopero se ingieren grandescantidades por ocasión
El consumo frecuente de bajacantidad es poco común
3%
Cultura que tolera el abuso en los hombres
72%de los que beben diario se
intoxican con esta frecuencia
cantidadessemanales
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 113 Prevention

Consumo ModeradoConsumo Moderado
� 1-2 COPAS POR DÍA
� NO MÁS DE 14 POR SEMANA
� NO MÁS DE 4 POR OCASIÓN
� NO MÁS DE 2 POR HORA.
HOMBRES
MENOS CONSUMO PARA UNA VIDA MEJORMENOS CONSUMO PARA UNA VIDA MEJOR
14 9
Máximo Máximo4 copas por ocasión 3 copas por ocasión
Unidades por semanaUnidades por semana
3 La familia es la principal fuente de apoyo social
3 La cultura es principalmente “colectivista”
3 La mujer es una vía esencial para prevención ytratamiento
¿Por qué la familia debe ser incluida?¿Por qué la familia debe ser incluida?
De esta manera la familia es un ambiente clavepara el desarrollo de políticas sociales
Estrategias por ÁreaEstrategias por Área
Campaña de Sensibilización
CartelesFolletosVideos
Cuente sus Copas
VERDE Manténgase en VERDE
AMARILLO
ROJO
Manual Naranja del Trabajador
Manual de FamiliaEntrenamiento de
Supervisores
Manual de FamiliaReferir a Centros de
tratamiento
Busque Ayuda
CONSEJO ESTRATEGIA
Ejemplos de Carteles de SensibilizaciónEjemplos de Carteles de Sensibilización Ejemplos de Carteles de IntervenciónEjemplos de Carteles de Intervención
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 114 Prevention
Estrategias para la zona naranjaEstrategias para la zona naranja
" Uso responsable de bebidas
alcoholicas: Cómo lograr la
abstinencia o Beber
moderadamente"
Sanchez Craig, M.
MANUAL INSTRUCTIVO
DIRIGIDO A TRABAJADORES
DIRIGIDO AL PERSONAL ENCARGADO DE RECURSOS HUMANOS, TRABAJADORES DE LA SALUD, CAPACITADORES.
"Detección, evaluación y
orientación de personas con problemas de alcohol en el
ambiente laboral"
Romero, M.; Rivera, E.
�Aprenda a sobreponerse a lastentacionesentaciones
��Anote Anote diariamente cuánto bebe
�Evite EmborracharseEmborracharse
�Preparese para situacionespeligrosas
�Desarrolle hábitoshábitos mássaludables
�Aprenda de sus errores, no seno sedesanimedesanime
Como lograr la abstinencia o consumir moderadamenteComo lograr la abstinencia o consumir moderadamente
��DECIDASEDECIDASE A CAMBIAR A CAMBIAR
��EXAMINEEXAMINE SUS HÁBITOS SUS HÁBITOS
��ESTABLEZCAESTABLEZCA SUS SUSLIMITESLIMITES
��MANTENGASEMANTENGASE EN LOS EN LOSLÍMITES.LÍMITES.
�Mida cada copa
�Diluya o rebaje
�Espere una hora para beberotra copa
�Beba Lentamente
�Alterne con bebidas noalcohólicas
�Coma antes y mientras bebe
Paso I. PREGUNTE E INVESTIGUE acerca del consumo de alcoholPaso II. EVALUE los problemas relacionados con el alcoholPaso III. ACONSEJE la acción apropiada a tomar (instrucciones del manual)Paso IV. SIGA el progreso del sujeto
Procedimientos de detección temprana y de intervención breve
"Orientación para las Familias de losTrabajadores"
"Orientación para las Familias de losTrabajadores"
Contenido:
Pedir ayuda
Las manifestaciones más comunes
de tensión
Maneras de enfrentar el problema
Buscar apoyos sociales
¿Qué hacer con los niños ante estas
situaciones?
�Audiovisual�Carteles�Manual para el Orientador "Prevención del
Consumo de Alcohol y Drogas en el Trabajadory sus Familiares".
� Folleto "Orientación para las Familias de losTrabajadores"
�Manual "Uso Responsable de BebidasAlcohólicas. Como Lograr la Abstinencia oBeber Moderado"
Acciones Preventivas que PuedenExtenderse a las Familias
Acciones Preventivas que PuedenExtenderse a las Familias
Efecto de la Intervención en la Frecuencia/Cantidad Consumo de Alcohol
Efecto de la Intervención en la Frecuencia/Cantidad Consumo de Alcohol
Prueba Rápida
Antes Después
X 3.2 2.5S (1.86) 2.1
t = 4.15 p >= 0.0001
Prueba Rápida
Antes Después
X 3.2 2.5S (1.86) 2.1
t = 4.15 p >= 0.0001
COPAS
0
10
20
30
40
50
1 a 2 3 a 4 5 ó más
Antes Después
28
38
29
3742
25
%
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 115 Prevention

� Adaptación de la metáfora y una fácil introducción delconcepto de riesgo asociado a los niveles de consumo dealcohol
� Adaptación del material, lugares y tiempo de exposición
� Bajo impacto en la estrategia de zona verde enconocimientos y creencias
� Cambio satisfactorio en la conducta o al menossensibilización en la asociación del nivel de riesgo con elconsumo de alcohol (76% permanecen en verde o semueven de ámbar a verde)
Evaluación de ResultadosEvaluación de Resultados
� Necesidad hablar de la prevención del uso desubstancias
� Prueba del programa en otros ambientes (con másriesgo en el abuso de substancias, orientación a laproducción comparado con orientación al desarrollohumano)
� Enfatizar las diferencias en los niveles de consumo dealcohol y problemas relacionados en cada empresa
� Precaución en el uso del concepto “moderación”
ConclusionesConclusiones
� El trabajador es un medio para dar información a la familia
� Resaltar la interacción del lugar de trabajo-familia-comunidad
� Altamente recomendable evaluar el uso de alcohol y problemasrelacionados en la familia y la actitud hacia la participación dela familia
� Identificación de caminos más directos para llegar a la familia
� Estrategias para evaluar los cambios en la conducta
� Evaluación continua del impacto
ConclusionesConclusiones
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 116 Prevention

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 117 Prevention
PREVENTION ACROSS THE LIFECYCLE
Ruth Sanchez-WayIntroductory RemarksSubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
Prevention in Early ChildhoodRosa Bonifaz, Carmen MilleNational Council on AddictionsMinistry of HealthMexico
U.S. Efforts – Prevention in EarlyChildhoodEileen O’BrienCasey Family ProgramSubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
Dr. Ruth Sanchez-Way, Acting Director ofSAMHSA's Center for Substance AbusePrevention (CSAP), opened the session byunderscoring the need to view prevention as alife-long process, not just one or twointerventions.
Ms. Mille described Mexico's "Construye Tu Vidasin Addiciones" a comprehensive preventioneffort covering physical, mental, spiritual, social,and cultural aspects of prevention. She notedthat the health promotion aspects of Construyeare based on elements of "care" and a healthyenvironment. Ms. Mille then described thepublic awareness features of the effort,including the use of television, radio (withspecific targets), written guides, and hotlines.
Ms. Rosa Bonifas, also of CONADIC, describedConstruye 's media campaign, which targetsyouth ages 9-14, older adolescents, and adults20+ years of age. Materials for the youthinclude activity guides, self-surveys, anddiscussion guides. For older adolescents, self-
help manuals have been developed, along withself-evaluations. For adults, self-help manualsand facilitator guides have been developed,along with specific guides for parents andteachers.
Ms. Eileen O'Brien, of SAMHSA's CSAP, thendescribed an early childhood prevention programdeveloped by CSAP called Starting Early/StartingSmart (SESS). Describing brain research thatshows early experiences (i.e., positive ornegative interactions) shape neural pathways,she then recounted the various elements of SESSas listed below. In general, she noted that SESSprovides integrated substance abuse and mentalhealth services in early childhood setting, andSESS services may include: case management,pediatric primary care, language development,reading readiness, and family services includingparenting education and support groups. Ms.O'Brien stressed that SESS is based onacknowledging and building family strengths witha direct focus on both substance abuse andmental health, and is implemented throughcollaborations and partnerships.
Pre-natal:
• improving attachment and parenting skillsfor expectant parents
• nutrition support for the future mothers
• general support and encouragement forfuture fathers.
Infants and toddlers:
• health care, child care
• links with Healthy Start, and well-baby care.
Children ages 3-5:
• Access to primary care clinics, child care,pre-school and early reading programs.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 118 Prevention
PREVENTION IN YOUNGADULTHOOD
Higher Education ProgramsJohn ClappResearch DirectorCollege of Health & Human Services,School of Social WorkSan Diego State UniversityUnited States
Dr. John Clapp described a college preventionprogram called CAPP, the Collegiate CommunityAlcohol Prevention Partnership. From 1989-1999, individual colleges in the U.S. conductedprevention programs based on raising awarenessand peer education, with modest success. Now,according to Clapp, colleges are funding"environmental prevention" programs thatinvolve all sectors of a community, fromrecognizing the role of the social environment inpreventing alcohol and other drug abuse bycollege students, to developing preventionprograms that target real needs.
The strategy used to develop these realisticprevention efforts starts with data collection,then goes to strategy identification (e.g., mediaadvocacy, server training, party penaltyprograms), and finally to strategy selection.Clapp stressed the importance of starting withcommunity assessment of problems and needs,in order for communities to identify desiredoutcomes (reduce binge drinking or reducealcohol-related injuries, etc.).
Parent Prevention Education in theWorkplace
Bernie McCannOffice of National Drug Control PolicyUnited States
The National Youth Anti-Drug Media CampaignWorkplace Program Objective is to use theworkplace to communicate Media Campaignmessages and strategies to parents,grandparents and others involved with youth.
The Media Campaign’s workplace component isdesigned in conjunction with National DrugControl Strategy’s Goal Number 1: to educateand enable America’s youth to reject illicit drugsas well as alcohol and tobacco.
Business CaseAmerica’s workplaces offer an efficient, effectiveand, at this time, an underutilized channel toreach parents and guardians with drugprevention information, solutions, and resourcesto help raise drug-free children. And researchdemonstrates there is a need for theseresources in the workplace:
• A recent poll conducted in conjunction withthe Society for Human ResourceManagement (SHRM) showed that mosthuman resource professionals believe anemployee’s concerns over their child’spossible drug use could lead to decreasedmorale and productivity, and a concomitantincrease in turnover, and healthcare costs.The Media Campaign workplace program isdesigned to reduce youth drug use whileassisting with a company’s efforts to findsolutions for critical performance issues.
How the program will workThe Media Campaign will recruit employers towork in partnership to incorporate MediaCampaign messages and in the internalcommunications vehicles employees know andtrust – employee newsletters, company intranetsand e-mail systems, posters, benefit andemployee assistance program kits, workplaceseminars, etc.Media Campaign will accomplish recruitingefforts by:
• A nationwide publicity and promotion effortemphasizing the importance andorganizational benefits of providing youth-focused drug prevention information toemployees who are parents, grandparentsand guardians of teens and tweens.Materials and resources will be easilyadaptable to a company’s existing employeecommunications program.
• Reaching out to business leaders andprofessional, business, labor andgovernment organizations willing to serve as

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 119 Prevention
Media Campaign messengers and asinfluential conduits into employerorganizations.
• Contacting and offering Media Campaigninformation directly to employerorganizations.
What materials will be distributed?Print and electronic media will be made availableto employers for their employees. Print materialswill consist of a collection of items fromnationally recognized drug prevention programs.Each company participating in the workplaceprogram will have the option of orderingmaterials directly from the publisher. Materialswill be available in either print or electronicformats (downloadable files via the World WideWeb). Items include:• Pamphlets, posters, etc., appropriate to the
parent target audience
• Media Campaign-created newsletter articlesfor use in employee magazines, newsletters,human resource benefit kits and employeemailers
• Electronic communications including MediaCampaign-generated e-mails, down-loadablePSAs, screen savers, banner ads for use oncorporate Web pages, and electronic linksfor drug prevention resources available forparents/guardians on the World Wide Web.
Screening and Brief Alcohol Interventionswith Older Adults
Kristen BarrySenior Associate Research ScientistUniversity of MichiganUnited States
The purpose of Dr. Barry’s presentation was toprovide state-of-the-art information andtechniques regarding alcohol screening and briefalcohol interventions targeted to adults age 60and over. Dr. Barry pointed out the fact that agrowing number of people reach later life, andthat the promotion of healthy lifestyles andprimary disease prevention among these olderadults is becoming a critical issue. She
presented information regarding how manyaging adults are seeking costly health care foracute and chronic conditions and how becauseof the increased incidence of health careproblems, elderly adults are more likely to seekhealth care on a regular or semi-regular basisthan are younger adults. In addition, Dr. Barryidentified older adults as being more vulnerableto the effects of alcohol and, this combined withthe increases in co-morbid diseases and theiruse of prescription and over-the-countermedications, may cause them to seek healthcare for a variety of conditions that are notimmediately associated with increased alcoholconsumption.
She stressed the importance of systematicalcohol screening and intervention methods andtools, and said that they can help insure relevantand high quality health care to older adults.Older adults with alcohol problems are a specialand vulnerable population who require elder-specific screening and intervention proceduresfocused on the unique issues associated withdrinking in later life. She stressed the followingimportant points to consider when working withthese older adults, including:
• The prevalence of at-risk drinking incommunity samples of older adults has beenestimated to be between 1-15%, dependingon the group studied.
• Randomized controlled clinical trials indicatethat older adults whose alcohol use exceedsthe National Institute on Alcoholism andAlcohol Abuse (NIAAA) guidelines willsignificantly decrease alcohol use inresponse to brief structured workbook-driven interventions.
• Implementing alcohol screening and briefintervention strategies for older adults inclinical settings will require the developmentof systematized protocols that provide easyservice delivery.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 120 Prevention
DRUG AND VIOLENCE PREVENTIONPRESENTATIONS ON SAFE-SCHOOLS
Healthy Students Initiative
William Modzeleski, ModeratorDirector, Safe and Drug-Free Schools ProgramU.S. Department of EducationUnited States
Presenters: Ann ClarkSupervisor, Safe and Drug-Free SchoolsHouston Independent School DistrictHouston, TexasUnited States
Philmer BluehousePinon Unified School District #4Pinon, ArizonaUnited States
Forrest Van CampLeon County SchoolsTallahassee, FloridaUnited States
Martha FletcherLeon County School DistrictTallahassee, FloridaUnited States
Dra. Marisa OcegueraLatin American Institute for Family StudiesMexico
Overview
The drug and violence prevention session beganwith an introduction by the moderator, followedby presentations on three Safe Schools/HealthyStudents projects in the United States, and apresentation on the Latin American Institute forFamily Studies program in Mexico.
Introduction
Bill Modzeleski opened the session with anoverview of issues and data regarding schoolsafety in the United States. For the most part,U.S. schools are safe. Recent data indicate that43 percent of schools experience no crime, and90 percent experience no serious violent crime.The most common crimes that occur in schoolsare theft and fighting. Serious violent crimesagainst students at school or going to and fromschool have been decreasing since 1992, andremain much lower than the same types ofcrimes committed in communities. With regardto weapon carrying, based on data from 1993-1999, the general trend in weapon carrying onschool grounds has been decreasing.
With regard to the frequently asked question ofhow many homicides there are in schools,according to a study by the Centers for DiseaseControl (CDC) over a two-year period between1992-1994, there were 105 school associatedviolent deaths, of which 85 were homicides.From 1997-1998, there were 58 violent deaths,representing a slight increase from the previousperiod studied. Today, there is a lowerincidence of homicides in schools, but morevictims, due to an increase in multiplehomicides. Much attention is being directed tohomicides; however, not enough attention isgiven to more basic, prevention-related issuessuch as discipline, truancy, and bullying.Prevention of violence needs to start with astrong foundation of clear standards ofbehavior.
How are we addressing the problem of violencein schools? Through the following broadapproaches: 1) improving physical conditions atschools; 2) targeting high-risk youth; 3)implementing drug and violence preventionprograms and 4) increasing security andestablishing strong discipline policies. It isimportant to use comprehensive strategies thatinvolve many partners, including schools, lawenforcement, health services, communityorganizations, families, and many others.
The following recent publications of the U.S.Department of Education and the U.S.Department of Justice can be ordered free of
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 121 Prevention
charge by contacting ED Pubs at 1-800-877-433-7827.
• Safeguarding Our Children: An ActionGuide
• 1999 Annual Report on School Safety
• Early Warning/Timely Response: A Guideto Safe Schools
Safe Schools/Healthy Students Initiative
Houston Independent School District,Houston, Texas
Ann Clark, Safe and Drug-Free SchoolsCoordinator, Houston Independent SchoolDistrict (I.S.D.) presented information onHouston’s Safe Schools/Healthy StudentsInitiative. The purpose of the program is toprovide students, schools, and communities inthe feeder schools to Houston’s secondaryschools with enhanced comprehensiveeducational, mental health, social, lawenforcement, and juvenile justice services thatpromote healthy childhood development andprevent violence, drug and alcohol abuse. TheHouston I.S.D. serves a diverse populationwhich speaks 87 different languages. Theprogram has six goals:
• Establish a safe school environment byreducing the levels of violence, aggression,and substance abuse among children andyouth in the community.
• Improve mental health and increase pro-social behavior through an integrated,coordinated continuum of programs andservices.
• Ensure that children at risk of emotional andbehavioral problems receive appropriateschool and community mental healthpreventive and treatment interventionservices.
• Assist high risk families to build resilience toadversity so that children enter school withthe necessary pro-social and academic skillsto succeed.
• Support educational reform efforts thatincrease academic achievement throughdevelopment of school climate.
• Improve integration and coordination ofservices among Houston I.S.D. and variouscommunity agencies.
Activities for accomplishing these goals includestrategies for increasing parent involvement;improving the availability of after-schoolprograms; providing ongoing training tostudents, parents, and teachers on accessingresources and services; providing mental healthtreatment services for children at risk foremotional and behavioral problems; providingintensive early prevention and therapeuticservices to high-risk families of children ages 0-5; and many other strategies.
Pinon Unified School District, Pinon,Arizona
Philmer Bluehouse, Director of the SafeSchools/Healthy Students Initiative for PinonUnified School District, began his presentationwith the Navajo greeting “Ya’a’te”, which means“I come to you with the universe” and “It isperfect.” As he introduced himself as a full-blooded Navajo of the Many Goats Clan, heexplained that it is critical to teach children whothey are, and that it is Navajo custom tointroduce oneself through one’s clan. One muststart from one’s clan to understand where onefits in. The Many Goats Clan has a “humble” sideand a “warrior” side. We are all designed in thesame way, in that we have a linear side and acultural side, or a peace side and a warrior side.This creates balance.
Pinon School District is very rural, with apopulation of 8,000. Children are bused toschool, leaving their homes at 6:00 a.m. and notreturning until late afternoon. Services arestretched thin, meaning that the communitymust play an important role. The Safe Schools/Healthy Students initiative is looking at astrategy of re-empowering the community todecide what services to provide, and how theservices should be provided, includingeducation, health, and law enforcement. Thereare Federal, State, and Tribal laws that apply.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 122 Prevention
The community must be involved, and all partsof the community must work together.
The goal is to achieve a state of harmony or“hosanosnin.” How can harmony be achieved?How can the process make things better? Howdo we allow the process to heal rather thandestroy? The overall objective is to allow peopleto be involved in making decisions at thecommunity level rather than being acted on byoutside forces, and to encourage traditionalways to flourish. The problems and thesolutions are local.
Leon County School District, Tallahassee,Florida
Forrest Van Camp, Executive Director, LeonCounty School District, provided an overview ofthe Safe Schools/Healthy Students Initiative inLeon County School District.
The initiative places an emphasis on earlychildhood, providing early intervention for at-riskchildren. Five elementary schools are beingtargeted. Objectives are to build studentresiliency and increase access to mental healthand prevention services. Strategies includeincreasing alternative after school programs andrecreational activities for students. Schoolsecurity strategies include increasingsurveillance cameras and radios in schools.
Martha Fletcher, Program Specialist, EarlyChildhood Programs, provided furtherinformation about the Leon County initiative.Leon County is unique in that all funding forearly childhood services is under one umbrella.This blending of funds for early childhoodservices enables more children to be served.Services include programs for teen parents, andmental health programs for young children.Many children are coming to school from chaotichome environments. Mental health interventionservices need to be provided early, rather thanwaiting until children are older. Children need tobe taught how not to become victims. Teachersare being trained through a problem solvingapproach. Leon County has produced a trainingcurriculum for parents and a video entitled“Discipline with Love.” The Safe Schools/Healthy Students initiative will provide an “activeparenting” parent education curriculum.
Latin American Institute for FamilyStudies
Marisa Oceguera presented information on theLatin American Institute for Family Studies andits family therapy services. The focus is onprevention among families. One must considerthe family in various contexts, such as social andeconomic environments, as part of anecosystem. Legislation related to familyviolence in Mexico has been recent. Accordingto a 1999 study, family violence occurs in oneout of three homes in Mexico. In fact, familyviolence is sometimes seen as normal behavior.Another study found that 38.4% of women hadsuffered some type of violence. Family violenceis often associated with alcohol abuse by men.Violence against women is a significant socialproblem. Its impact often extends to children,resulting in behavioral problems and problems atschool. One of the main reasons that girls leavehome is due to sexual abuse. One must havean ecological outlook when considering familyviolence, such as personal history, distribution ofpower within the family, lack of equality, genderroles, stereotypes, and a certain way of lookingat men in relation to women. Many studies onalcoholic men show a close relationship betweenalcohol use and violence. Women with drug andalcohol problems often come from familieswhere there is a lack of care and support. To bea female addict is worse than to be a maleaddict. Women are prey to violence. Accordingto one study, two-thirds of people on controlledsubstances had been subjected to violence.There is a “social silence” on the subject offamily violence. It is hushed up, reinforcing thenegative effects, and creating difficulties inseeking help. The ecosystem approach isrecent. It is an approach that must involve allparts of many complex systems in addressingthe problem.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 123 Treatment
TREATMENT

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 124 Treatment
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 125 Treatment
TREATMENTPRE-CONFERENCESESSIONS
Arturo Ongay PérezModeratorNational Council on Addictions(CONADIC)Ministry of HealthMexico
COMPREHENSIVE TREATMENTPLANSComprehensive Treatment Approaches forWomenRobin HoskinsWomen’s Treatment NetworkPhoenix, ArizonaUnited States
THERAPEUTIC COMMUNITIESStandards for Prison-Based TherapeuticCommunitiesGeorge DeLeonCenter for Therapeutic Research, NationalDevelopment and Research Institute, Inc.United States
Treatment Program for Heroin UseMaría Elena RamosPrograma Compañeros, A.C.Mexico
RECOVERY PROGRAMS: FAITH-BASED MODELSChristianity InterventionsRoberto Bital PinedaAlcance VictoriaMexico
RECOVERY PROGRAMS: SOCIALMODELSEVAC and PREHAB of Arizona:Successful Multi-Systemic ApproachesWithin a Community Context
Tom HutchinsonPrehab of ArizonaUnited States
HIV Prevention, Addictions and SocialReintegration of Street KidsMartín PérezEl CaracolMexico
----------
COMPREHENSIVE TREATMENTPLANSComprehensive Treatment Approaches forWomenRobin HoskinsWomen’s Treatment Network
I want to welcome those of you who are heretoday. We were expecting about 70 peopletoday, so we’re happy that you all are here. Myname is Robin Hoskins and I work here inPhoenix, Arizona for the Adult ProbationDepartment. I am a Director, and I oversee aprogram that supervises female substanceabusers in the criminal justice system. I wasasked to talk about our comprehensivetreatment approach for female offenders. Sowhat I’m going to do is spend a little bit of timetelling you what we do here locally, and myhope is that some of the things that I tell youtoday are things that you can apply to whereyou’re from.
I want to make sure that I have something toshare that’s of value. And so, what you’ll find inmy presentation today is that it’s very simple.When we do our comprehensive treatmentplanning for our women in our program, we usea very, very simple basic concept. What we doat the “Women’s Treatment Network,” which isthe name of the program I oversee in adultprobation, is we treat each individual client asan individual client. And that’s really important.What’s traditionally done in criminal justice isthat our clients are not seen as offenders ordefendants. A lot of times our clients are definedas either just being a substance abuser ormaybe a violent offender. But what we try to do

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 126 Treatment
is to take a look at that client as an individual.In doing that we take a holistic approach in ourtreatment planning. But what’s most importantto tell you in our approach to treatment planningis that it all starts with a comprehensiveassessment. And I don’t really know where youall are from or what your backgrounds are, so ifthis seems very basic and simple, I apologize.I’m not trying to make it too basic or boring foryou. I found in my job in working in ourdepartment is that it’s hard for people to keep itbasic. It’s hard for people to continue to look atour clients as whole people rather than justcriminals.
When we develop our comprehensive treatmentplan for our clients, we focus on seven lifeareas. And those life areas are mental health,family, employment, education, social, medicaland legal. When we develop our treatment planwe assess the need of the client in each of those7 life areas. That’s critical to the success of ourprogram. Also important in what we do, is thatwe put the time and energy at the front end ofour assessment, development of our treatmentplan which is the assessment. What I mean bythat is that we employ Master’s level, certifiedcounselors to do our assessments. Otherprograms will have assessments done by maybeBachelor’s level folks or people that are notcertified in counseling. And we have chosen tospend the time and energy and resources upfront so that we can get a comprehensiveassessment and that will pave the way for abetter treatment plan.
What we also know is not every woman that wesee has needs in every life area. But what we doconsistently is we approach each life area tomake sure that the woman is being addressedas a whole, like I said, as a whole person. Ikeep saying this, but I would imagine that mostof you know what I mean when I talk about thetraditional criminal justice system identifying theclients as just defendants rather than people.
One of the exciting things about what we’redoing in the Women’s Network is, we’re one ofseven programs across the nation that issupported by Washington, DC in our efforts. Andour plan is to take our approach with women ?this comprehensive approach ? and apply it toother populations. For example, we’re in the
process now of developing the same type ofapproach for our juvenile offenders.
What makes our approach unique, and I thinkone of the reasons why I was asked to be heretoday as a resource for you all, is that we havethe same kind of approach, systems deliveryand supervision for our clients whether theycome from jail and they’re pre-sentenced or pre-trial or if they’re coming out of prison on parole.So the whole continuum is covered and we havea consistent approach with these clients. One ofthe main things that we teach our staff whenthey deal with our clients is called a strengths-based approach. This means that we focus onsolutions rather than problems. Our clients, thewomen that we see, are very used to beingunsuccessful and not completing things. Andwhat we do is we focus on their strengths. Weinvolve the client in her treatment planning. Webelieve that the client has the energy withinherself to propel her towards success. It’s notreally our energy, it’s hers. We really focus onthe client and her strengths. We try to mobilizethe client’s attributes so that she can moveforward. And this really gives us the greatestpotential to produce positive outcomes webelieve.
One of the other things that’s important to dowhen you’re trying to develop a comprehensivetreatment plan is that it’s important thateverybody’s on the same page. So what we’vedone here at The Women’s Network, is that wehave a treatment team that includes the client,the probation officer, a case manager, and aclinical director. Any agency in the communitythat’s providing services to that client iswelcome to be a part of the treatment team.And these folks meet every month to discuss theprogress of the client.
By approaching the client in a holistic manner,using a treatment team and sharing thecomprehensive assessment and treatment plan,we’re able to better address the needs of theclient. We save money, we save resources, wesave time. And that’s a key element. I’ve beenin the criminal justice system for a very longtime and my experience has been that it’s a veryfragmented system. Probation usually doesn’tcommunicate well with parole. City governmentsdon’t usually communicate with local or state

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 127 Treatment
governments and it’s very fragmented. And thepeople that are suffering the most from that arethe clients, ultimately.
One of the things I will share with you as someof our outcomes because everyone’s interestedin tangible outcomes. The clients that we seeare probably not very different from the clientsthat you see in your communities. The majorityof the women that we serve choosemethamphetamine as their drug of choice. Andthe second drug of choice is cocaine. And for usthe third drug is alcohol. The majority of ourclients, about 75%, are in their late 30s. And themajority of our clients, again about 75%, havechildren. Also the majority of our clients areunemployed and under-educated. As a result ofour comprehensive approach to taking a look atthe whole person addressing those 7 life areas,I’ll give you some statistics of the women thatwe have in our program.
Eighty percent of our clients are in stablehousing which is key for our clients. When I saystable housing, I mean they’re in a home ontheir own. They’re not relying on family or ahusband or a boyfriend. It’s a stable home thatthey have control of. And that’s a key issue for alot of our clients. Seventy percent of our clientsare employed either part-time or full-time. And62% of our clients are enrolled in education orvocational programs. When we talk aboutdemand reduction, reducing the demand forillegal drugs, what we know we have to do isreduce the barriers that prevent our clients fromsucceeding in their recovery. And some of thosebarriers are housing, childcare, employment,education, health, legal issues ? those life areasthat I talked about – and mental healthproblems. So as the Women’s TreatmentNetwork, what we do is try to break down thosebarriers. I talked about making a commitment atthe assessment level where we hire a qualified,certified counselor to do the assessment.Another thing that we do as part of ourcomprehensive treatment plan is we have fundsset aside that we can spend on housing andchildcare and parenting classes. We pay for rentfor the first couple of months on some of thesehomes for these women until they can get ontheir feet. By doing that, we break down thebarriers, ultimately resulting in demand
reduction. These women are able to take care ofbusiness and they’re not relying on drugs.
You know, you’re going to leave here today andyou probably in a year and one-half or a week,or maybe even six months from now, you won’tremember me. And that’s ok. I don’t take thatpersonally. But I do hope that you remember astatement that I want to read from a client, agraduate. She wrote a statement that I’d justlike to read to you all. Again, this is a tangibleresult. “I’m a Black, 46 year old woman who’shad a problem with drug addiction and self-esteem. As a child, I aspired for great things:being an Olympic track star, being the fastestjump-roper in the world, or a lawyer. But Inever imagined I would be a drug addict. I havea Bachelor’s degree in business and threebeautiful daughters who depend on me foreverything. I’ve overcome many obstacles, butdrug addiction is done on a day-to-day basis.What turned my life around was going to jailand losing custody of my baby. There are somany things that I’ve been blessed with ?where do I begin? I went from living in a shelterafter being released from jail to living in amansion.” She actually owned her first homewhich was a two-bedroom home, but it felt likea mansion after jail. “I found a new career withSt. Mary’s Community Kitchen as a chef trainer,and make money, up to $30,000 a year. I can’tbelieve it. I’m planning on purchasing my ownhome in a year, a larger home, and a decent carfor the first time. I’m on the Board of Advisorsfor the Probation Department. I’m a motivationalspeaker for The Women’s Network, and I’vebeen asked to meet the Drug Czar fromWashington, DC. Some days I question myself.Am I worthy? Do I deserve this? You’re DAMNright I do. I’ve worked hard to achieve thisdream, and I don’t see myself going to a life ofdrugs and crime again with God’s love andgrace. Today I’m successful because I choose tobe.”
It’s these kinds of things that keep me going asfar as developing new programs and changingpolicies and procedures, not only locally butnationally. I hope that your experience here thisweek provides you with some information, someguidance and resources where you can do somethings in your own communities that will make adifference to your clients. My number is in the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 128 Treatment
workbook that was given to you all. And pleasefeel free to call me if you have any questions.
THERAPEUTIC COMMUNITIESStandards for Prison-Based TherapeuticCommunitiesGeorge DeLeonCenter for Therapeutic Research, NationalDevelopment and Research Institute, Inc.United States
Good afternoon. I was asked to speak ontherapeutic communities, in particular, recentdevelopments for therapeutic communities. Wenow have standards in the United States fordelivering therapeutic community programs,both in the general community and particularlyin correctional settings. I don’t know how muchthis audience knows about the therapeuticcommunity approach. That term therapeuticcommunity is used very generally, but theapproach is actually a very specific one. And so,before I talk with you about the standardsthemselves, let me take a few moments andreview with you the basic theoretical approachof the therapeutic community.
As some of you may know, this particulartreatment approach is very well researched.There are some 30 years of research ontherapeutic communities documenting theeffectiveness of this treatment. This treatmenthas been demonstrated to actually serve themost serious of substance abusers: usually anti-social, with many other psychological problemsin addition to their substance abuse. Sotherapeutic communities have been serving themost serious of the addicts over the years. Andthe research has shown, of course, that thetreatment is effective. The basic findings of thatresearch, for those of you that may not beaware of it, is that the longer clients stay inresidential treatment, the greater the likelihoodof their long-term success. The treatmentapproach has been modified and adapted fornumbers of populations including adolescents,mentally ill, chemical abusers, those in homelessshelters, those in mental hospitals, and ofcourse, those in prisons.
The approach that the therapeutic communityhas that governs everything that it does, isstraightforward. This perspective views thedisorder one of the whole person, so substanceabuse essentially is only one component of whathas to change in the treatment.
Secondly, the persons themselves can beunderstood in terms of a variety ofcharacteristics. Many of them may be seen ascharacter disorder features, along with otherpsychological dysfunction like depression,anxiety and low self-esteem.
Recovery of the individual requires a multi-dimensional and a multi-interventional approachto change the individual. The goals of thetherapeutic community are to transformlifestyles and identities. So, the goal is muchbeyond the issue of using drugs.
And finally, the fourth view that constitutes theperspective is that this approach teaches rightliving. The assumption here is that individualscannot sustain their recovery, cannot changetheir lifestyles unless they actually have learnedcertain values to govern them. And so, much ofwhat goes on in the therapeutic communityinvolves teaching those values and teachingindividuals how to live.
That’s the perspective, admittedly very brieflysaid to you, that governs and guides everythingthat is done in a therapeutic community. Thesetreatment programs are generally long-termresidential settings, self-contained, primarilymanaged by recovering people themselves. It’sa self-help approach, a mutual self-helpapproach, with relatively few staff compared tothe number of residents. And that of courseultimately has been shown to be very cost-effective. But, if you actually want to understandthe treatment, the active treatment ingredient inthe therapeutic community, it is the use of thecommunity, which is peers and staff, and all ofthe activities that go on in that community asthe method. So, unlike traditional treatmentapproaches, there is less emphasis on traditionalcounseling, traditional psychotherapy, traditionalpsychiatric approaches, and relatively fewprograms with medication. In the therapeuticcommunity, the primary treatment change agent

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 129 Treatment
is the community itself. And that’s why, over theyears, I have used the term “community asmethod” to indicate what is the primary activetreatment ingredient.
When we actually spell out community asmethod, it can be summarized in four points:the context, which means all of the influences ina contained environment; the people; therelationships; and the daily regimen of activitieswhich is groups, meetings, seminars, recreation,dining, eating together, personal time. All ofthose activities are defined as the context, and itis assumed in the theory that every one of thoseactivities is potentially an intervention forchanging the individual.
So, it is not only whether the individuals go togroups, or whether they attend meetings, butit’s everything that they do. Work, meetings,groups, recreation, informal time together,dining together. Every element of the social lifein the therapeutic community is an interventionto produce change. Every element is used toteach the individual or to train the individual.And the theory says, in order to bring aboutmulti-dimensional change, you have to have amulti-interventional environment. That’s context.
But there is more to community as method. Itsays that the community is not only the contextfor learning and changing, but it also sets theexpectations for individuals’ participation in thatcommunity. This is a very critical feature tounderstand this method. The community itselfestablishes explicit requirements in terms of howthe individual should participate and how muchthey should participate. So, there is a basicdemand characteristic in the community. Notonly is this the place where you can change, butthere is expectation about how you should usethis place to change.
The third assumption in community as method isthat the community is also continually assessing,observing, whether you are in fact participating.So, it is a requirement of the community tocontinually confront, support, provide feedbackto the individual as to whether they areparticipating in the community. And the fourthelement is that the community, peers and staffprovide responses, both positive and negative,concerning whether the individual is
participating. So again, to understandcommunity as method, the community ? all ofits people, its relationships and its daily activities? provide the social learning setting forproducing change in the individual. Thecommunity sets the expectations for how youshould participate. The community will assess,continually observe through challenging you,testing you and exposing you as to whether youare participating and using the community tochange yourself.
And finally, the community will provide theresponses, the affirmations, the supportiveresponses as well as the negative ones and thecorrective responses. Now, while this may seemobvious to you, what needs to be emphasized isthat all of this method essentially describesindividuals living together and carrying out theprocess of recovery. So it’s very unliketraditional treatment.
And now, just a word about how the communityproduces change. What I’ve just described inthe previous slide is what we mean bycommunity as method. And this slide tries tocommunicate briefly to you how communityproduces change. Again, everything that is donein the therapeutic community is addressing abehavior, attitude, value or emotionalmanagement issue in the individual: how theywork, how they relate to people in the diningroom, how they participate in the meeting, howthey participate in groups. All of those activitiesessentially surface individual behavioral,attitudinal, emotional characteristics which canthen be changed. And that’s what we mean byeverything can be an intervention.
In order for change to occur, the individual hasto have some relationship to the community.That’s why I’ve used the words “affiliation,participation and change.” What that means isthat in order for individuals to use thecommunity to change themselves, they have tohave some affiliation with the community, someconnection with the community. So much thatgoes on in the therapeutic community isdesigned to strengthen affiliation. If I amaffiliated with the community, I listen. If I listen,I change.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 130 Treatment
The process of change is a gradual, gradualgradient path of learning that leads tointernalized change. There are really four levelsof internalization, people changing. First, theycan change initially through compliance. I dowhat the community says I have to do because Idon’t want to be thrown out and go to jail or goto the street, or go back home. So one reason Ido what I’m supposed to do is “I’m complying,”with very little internalization. Initially, in thetherapeutic community, the first changes thatwe see in most clients are compliance.
The second stage is conformity. They graduallynow begin to do the behaviors and attitudesthat the community is expecting them to do,based upon their increasing affiliation withothers. They do not want to lose therelationships in the community. It’s still a formof compliance, but it has shifted now torelationships with the community. They don’twant to lose those.
The third stage of learning is one in which theindividuals now are making a commitment, andthe commitment stage of internalization. Theywill make the commitment that they want tofinish the program. These are the first changes,learning and changing in recovery, that areactually related to the experience of theindividual. I keep my room clean, because now Ifeel better about myself and clearer in my head.When I first came into the program I kept myroom clean because I didn’t want them to throwme out. As I stayed on, I kept my room cleanbecause I didn’t want my peers to in some wayto discourage me. The third stage is, I keep myroom clean because when I keep my roomclean, my head is clean. That’s based on myexperience. You’re now entering internalization.
And the last stage of internalization is acommitment to the change process. Theindividuals now learn that for them to continueto change, they have to literally “remain in thechange process even though I may leavetreatment.”
And the fourth point that you see in terms ofhow the process occurs has to do with emphasison motivation and readiness. Most of the changethat comes about in an individual requires acontinuous sustaining of motivation ? I want to
change ? and readiness ? I take action tochange. That must be, those two characteristicsmust be sustained throughout, and much ofwhat goes on in the community is designed tosustain motivation and readiness. And we say, inthe therapeutic community that individuals ofcourse bring about their own recovery but theydo that by using the community to changethemselves. To continually use the community,they have to remain motivated and ready.
Again, the reason why they wanted me to speakabout program standards of therapeuticcommunities is that it is a recent development.And it was a very big step forward in theevolution of this treatment approach. As Imentioned earlier, the treatment approach iswell documented in the research literature. Butuntil recently we did many, many treatmentactivities that would actually call themselvestherapeutic communities because that phrase isa general phrase, therapeutic community. Whatyou have been hearing from me is that it isactually a very, very specific methodology thathas a very sound theory to it and a set ofprescribed practices and a research base. So theneed for standards has been to address theissue of quality assurance, making certain thatprograms that call themselves therapeuticcommunities were in fact treatment programsthat were adhering to the basic theory, methodand model of the therapeutic community. Thisis a great step forward.
Therapeutic communities have been here forabout 40 years. We now have a significant bodyof research, a theoretical framework that is welldescribed in the literature, and now we have aset of standards which will help to prescribe bestpractices. We’re not going to go through thosestandards here, but what I want to make surethat you learn today about these is that thestandards themselves apply to community basedtherapeutic communities as well as specialadapted therapeutic communities such as thosein prison. These were developed for prisons andthey’re very detailed, therefore very educationalfor those of you who want to learn more aboutthe therapeutic community and how actually toimplement properly implement therapeuticcommunity programs.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 131 Treatment
But the other very important feature aboutthese standards is that they are grounded inboth the theory and the research. So I will giveyou some examples of that, just quickly. Theentire theoretical framework of the therapeuticcommunity and what I’ve called the theory ?the program model and various methods whichwe call community as method ? can beorganized into 11 domains. There are some 121item standards across all those domains.
If there’s a therapeutic community in the prison? and there are many of them now in theUnited States ? the field reviewer has a reviewdocument and can spend two or three days inthe prison therapeutic community, and reviewexactly how all of these domains are actuallyfunctioning and whether the program is actuallydelivering the treatment in accordance withthese standards. Let’s look at one or twoexamples of these domains.
For example, there are standards which strictlyreflect the theoretical basis of the therapeuticcommunity. It says in the standards manual thatit’s essential that they have a program groundedin the theory. And then it simply resummarizessome of the key theoretical points. And then itpresent some sample items of exactly how Iwould walk into your program and checkwhether you are meeting this particularstandard. There are more items than thesethree, but this is an example. So that was thetheoretical domain.
Similarly a very critical domain in the standardsis the general clinical principles. I’ll just giveyou one example. It is essential that programparticipants identify with the therapeuticcommunity and feel a sense of belonging inorder to change their patterns of criminality andsubstance use. Remember I mentioned theissues of affiliation. There must be a continuous24 hour atmosphere of constructiveconfrontation and feedback ? 24 hours a day ?to the individuals in the community as a whole,in order to raise personal awareness of theindividual behaviors and attitudes. Now that’sthe principle that governs the standards whichare very explicit items. And then there’s therationale for this principle and then someexamples.
It’s much better that you actually look at thestandards, but what I want to get across to youis the relationship between the basic theory ofthe therapeutic community, the elements thattherefore essentially should flow from thattheory and then the basic assessment methodthrough the standards themselves.
Let’s try one more area. Even on theadministrative level a standard is necessary.Here’s the general principle. It is necessary thatkey administrative and management staffinterface with a particular agency. This happensto be a prison therapeutic community. So that ina prison, the therapeutic community is in theprison and may be provided by an outsideagency for the prison. And this standard saysthat the individual agency, the prison itself andthe treatment provider have to be in a veryclose interface. They have to be closely relatedto the success of the program. And then thereare some standards to essentially assesswhether that relationship between the prisonand the treatment provider exists. I’ll take onemore and then we’ll stop.
It is essential that the entire staff function in amanner consistent with the philosophy and thepractice of the therapeutic community. Let memake a point about this because in my generalintroductory comments I didn’t have the time todetail the roll of staff in a therapeuticcommunity model which is largely a peer, self-help, mutual self-help model. Staff have very,very critical roles in therapeutic communities.Their key role is as a community member. Thatis, they have to role model what the programitself is teaching. But they have other roles. Staffare rational authorities making assessmentsabout individuals in the therapeutic community.But they are not conventional therapists andthey are not conventional counselors althoughcounseling and therapy actually go on all day atall times in the therapeutic community. I callthat informal. There’s much informal counselingand therapy. It may be for two minutes at atime, three minutes at a time. So that thetraditional view of counseling and therapy wherethe client comes in to a counselor’s office for 50minutes or one hour is relatively infrequent in atherapeutic community. Because the primarytreatment agent is the community itself, not theindividual therapist. So that the role of staff,

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 132 Treatment
when they are in a counseling situation, or in atherapeutic situation, are always directing theclient to in fact go back to the community todeal with what they have to deal with. So therole of staff is really as facilitator and guide, notreally as traditional therapists. Even thoughtherapeutic moments go on all the time.
So this notion of the standards is very difficult toget across because traditional professionals,psychologists, social workers, psychiatrists, havetheir own tendencies and want to essentiallycarry out that role as they have learned it. Thetraditional approaches in the therapeuticcommunity are not effective. There has to be achange in the whole staff mindset when theywork in therapeutic communities. That’s been alot of my work over the years to try and teachstaff this model and method ? how to movefrom a primary provider to a primary facilitator.Of course the therapeutic community is not aprovider-consumer model. It is a self-helpmodel. And the role of staff is to facilitate self-help. So the standard becomes very important,particularly as you move into prisons and youmove into mental hospitals. As you use moreand more of the traditional staff, this standardbecomes a very important standard and there isan entire training initiative that essentiallyfollows this standard. How to get staff welltrained in this very powerful self-help model.
There are seven or eight other domains. I’mgoing to not talk about those. You’ll look atthose in the monograph if you’re interested. Butlet me stop and take some questions.
The question was, “How difficult was it to movefrom the general statements, the general levelof the theoretical statements of the therapeuticcommunity to the very specific?” In reality, itwas for many years impossible to do that. Butonce we were able to write a clear theoreticalbasis for the therapeutic community, once wewere able to make that theoretical writing veryclear about what we do and why we do it in thetherapeutic community, then it was much lessdifficult to move from the general statements tothe specific standard items. We needed anexplicit theory to do that. That was the difficultpart ? the years of making that theory explicitand clear. That was the difficult part. This part,beginning to write the specific items for the
standards, this was much easier once we hadthe theory.
Can we consider a little clinic? The answer isyes, we can consider any clinic or any particularenvironment as a therapeutic community if itadheres to the perspective and the method.That’s the important part of your question. AndI’ll answer it, if you allow me, in another way. Ihave developed programs in many settings now,prison settings, shelters for the homeless, in daytreatment settings for methadone clients. Theidea is that once we had a theory and a modeland a method, then you can use it to guide thetransformation of the environment into atherapeutic community. Even if it’s daytreatment, or if you like, outpatient ? even ifthey don’t live there ? you can, in fact,incorporate the essential elements of thetherapeutic community. But you have to havethose essential elements and you have tounderstand the theory behind those essentialelements. So the answer is yes, you can havesmall clinics, schools, shelters, hospital wards,and whole sections of prisons, which we have inthe United States now serving almost 12thousand inmates in therapeutic communities inprisons. So the answer is yes, but it takestraining and you need to know the elements andyou need to know the theory.
EVAC and PREHAB of Arizona:Successful Multi-Systemic ApproachesWithin a Community ContextTom HutchinsonPrehab of ArizonaUnited States
Thank you. I appreciate the opportunity to behere this afternoon. My name is TomHutchinson, and I’m Director of CommunityServices for Prehab of Arizona. A colleague ofmine, Dr. Frank Scarpatti, is sitting to my leftand he works for the organization, East ValleyAddiction Council. These are two separateorganizations. Today, we are going to talk aboutthose two organizations. We are featuring oneprogram that deals mainly with adults and oneprogram that deals mainly with teens.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 133 Treatment
We’re going to talk about general concepts usedin the social model as well as characteristics oftwo successful programs, the one being EastValley Addiction Council, the other being Prehabof Arizona. We want to talk a little bit aboutclient experiences within those programs, andthen we have time for questions and answers.
When Dr. Scarpatti and I were speaking theother day, it was interesting because we foundthings in common that our programs had. Andthe word “caring” came up ? that we havecaring, dedicated and committed staff who workwith our clients. Often these people areforgotten, the people who work directly with ourclients. They show much love to the clients withwhom they are dealing. We also favored smallprogram size, feeling that clients feel cared for.There’s a certain level of intimacy that developsand also it helps with retaining staff membersover time.
Flexibility to meet client needs. We both arefrom Arizona. We’re from the East Valley ofMaricopa County, and there is a variety ofpeople who reside there. So, our programs areboth flexible, in terms of language, in terms oftransportation, in terms of different services thatclients need at various levels. In both of ourprograms there’s integrated treatment thathappens. EVAC features a medical detoxificationand yet there are other elements of treatmentthat are involved – in particular, across acontinuum of care. Our youth programs whichwe will talk more of in a few minutes, are verycomprehensive. Both organizations work with acontinuum. And we have a cooperative,collaborative mindset which we practice in ourcommunity, among organizations. One keyaspect was to protect the length of stay for theclient. Both of our programs are publicly fundedand therefore there is pressure around dollarsand moving people quickly and we felt that it isvery important to protect the length of stay ofthe client in order for the client to be successful.
Our idea of the social model had to do with theidea that substance abuse and addictionsoperate in a context. They are simply notsomething that can be described from abiological or medical point of view or solely froman environmental point of view. They grow outof a person’s environment and also, they have
very serious repercussions across society.Therefore, it’s important that for a person intreatment, a person in recovery, that theprofessionals work with all the client’s socialsystems. We speak mainly of families, but alsoof peer groups, neighborhoods. I would also saythat we need to deal with the various systemsthat the clients find themselves in, whether it bethe public health system in our state, whether itbe the corrections system, whatever kind ofsystem that person is in. Our programs seek tohelp that person understand how to best utilizethe resources available to them. Families arecrucial to success and failure. Peer groups andneighborhoods and communities make atremendous difference in the recovery ofindividuals.
The East Valley Addiction Council is located inMesa, Arizona. It’s located in the south centralpart of the city and it is a gem. It is a very well-kept physical plant. It’s essentially a smallhospital in the neighborhood. Dr. Scarpetti is tobe complimented for the great work he’s donewith building that facility in the last five years. Ithas a budget of about 1.5 million dollars fromvarious sources. Most of that comes from thestate of Arizona, but the East Valley citiessupport the program as well as does The UnitedWay. There is a continuum of care. It is licensedby the Department of Health Services. It isaccredited by the Council on the Accreditation ofRehabilitation Facilities, and 80% of the patientsthat were seen in 1999 ? and there were 4000patients that went through the program ? arehomeless. A good percentage of the remaining20% are low income individuals. So, these arepeople in tremendous need of assistance. EVACprovides some prevention services mainlythrough the schools, provides training for staff,presentations to youth, and various otheractivities in the community. They are veryinvolved with presenting literally hundreds ofdifferent presentations to differentorganizations, to educate those people aboutsubstance abuse.
The core service, SORT, stands for Stabilization,Observation, Referral and Treatment. And whenan individual is referred to the detoxificationcenter, the first day or so is spent in that part ofthe process. Some individuals leave after a dayof treatment. If they are severely affected and

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 134 Treatment
toxified they will go into the medical detox. Theslogan is “detox with dignity,” and the programprides itself on its staff. The medical director is atoxicologist. All the staff members are eitherregistered nurses or trained as emergencymedical technicians. After the detox period theprogram refers them to halfway homes andresidential treatment centers with emphasis onrelapse prevention for these individuals.
When we think of detoxification centers there’ssometimes a problem with the idea that they’rerevolving doors in the sense that we see thesame people, time and time again. The vision ofEVAC is to stop that revolving door. They’vebeen working at it for about 5 years.
In the old model, there would be a crisis andthere would be a crisis team response, includingtransportation and then the individual would endup in the detoxification center and spendanywhere from 0 to 5 days getting various levelsof care. Then they would often be released backto their same circumstances. What EVAC hasdone is included the SORT time, which is anintensive assessment time, as well as astabilization period for the individual, and thenhe or she moves into the detoxification phase.The counselors who are on the staff are knownas transition counselors and they’re moreinterested in transition management than theyare in actual process of giving clients therapy.So, they work with our local healthcareenrollment, social services assessment, familyreconnection, medication management and casemanagement referral. As the person movesthrough the system, they’re given servicesaround relapse prevention. There is an aftercareNaltrexone treatment program that saw about400 people last year. And some individuals aregoing into residential treatment environments.
However, in the state of Arizona, there are notmany residential beds, so most of the people arereferred to some kind of therapeutic community.In the city of Mesa, there were some 80 or sohalfway houses. EVAC studied those and cameup with a list of 12 facilities they felt wereadequate to deal with the individuals that wereplaced there. They audited each site for theproper environment of care for cleanliness, fortraining of staff, for staffing patterns. When itcame right down to it, there were 12 facilities
that met their standards, and many of theindividuals who go into the detox part, go intothe halfway homes. Of those, 75% have notreturned in need of detoxification. So that effortat stopping the revolving door, seems to beworking with a significant number of individualsin our community.
By the way, the most frequently occurringcircumstances that bring people to EVAC aredifficulties with heroin, alcohol, and meth-amphetamine, and various combinations ofthose drugs. The fact that most of the peopleare homeless also leaves them in very physicallyincapacitated, and often, there are 9-1-1 calls,just to assist those people through their detoxphase. These people are suffering a great dealand are given the kinds of comfort at EVAC thatthey need. The model is based on the Americanaddiction medicine treatment model. And allthose standards are applied and monitored bytheir accrediting body.
I appreciate the opportunity to provide twopresentations today.
I am an employee of Prehab of Arizona. We arealso located in Mesa. And we have a budget ofabout $11 million from a wide variety ofsources. We have monies from the court,monies from the Department of Health, from ourlocal Department of Economic Securities, as wellas various grants and foundations. In order tosurvive, we have 2.5 individuals who simplywrite grants and obtain various monies in orderto keep our programs going. We have 13programs. We are private, non-profit, licensedby the state, and we are accredited by the JointCommission on the Accreditation of Health CareOrganizations. We serve children, youth, adultsand families. We have an out-patient counselingservice, with about 1500 open files. We havedomestic violence and family homeless shelters.We have training employment for hard to serveindividuals. We have alternative crisis centers foryouth. Then we have long-term residentialtreatment with the school.
When people come to us, all medical servicesare provided including psychiatric care andpsychological services. We have two doctorsthat we use for psychiatric care as well as apsychologist. The children receive mental health

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 135 Treatment
counseling ? group, individual, and family. Wehave 20 kids, and there are about 20 staff.There are 4 or 5 clinical staff and then othersupport people. Our philosophy is to supportand promote abstinence, and we do that andmonitor individuals on a daily basis. We alsohave support groups using the 12-step modelgenerally speaking with youth: NarcoticsAnonymous. And we also have our own school.So we try and have an integrated program thatinvolves the mental health and t social aspectsof treatment as well as the recovery program.We feel very fortunate that we have been ableto keep the length of stay at a level where wefeel it needs to be.
We also support aftercare. Family involvementstarts early. In fact, in the interview process thefamily is involved. And if the family is unwillingto support the teen who’s in treatment, we willnot accept that teen. There needs to be a levelof support for the treatment process or we willnot accept that individual. We start within 2-4weeks family counseling on an individual familylevel. We do work with extended families. We dowork with Spanish speaking people in particularand have staff that can provide that service.
Also on a weekly basis we have multi-familygroups, most weeks of the year. We have onsitevisitation on a weekly basis on Sundays. And wehave home and neighborhood visits as the youthstart to become ready to return to theirenvironment. If the family is unsupportive andthere are active addictions going on within thefamily setting, we will seek alternativeplacements, whether that be the extendedfamily, other people within that environment, orthrough any other means that we findnecessary.
In terms of the accreditation, we are considereda Level One facility. We are not a locked facility.The elopement rate is quite low because thescreening is pretty rigorous. We screen peopleto make sure that they are willing to do workand to stay in treatment. The elopement rate isnot high. Our environments are more homelikethan they are institutional. We believe increating a healthy milieu for the youth andreally focus on doing that in a thoughtful way.
And of course the idea of having individuals andhaving leaders and having followers who arecommitted to the long-term. Who are willing tostay on a task such as their careers, we feel isvery, very important organizationally andprogrammatically. And it’s important to expressto the community around us that we care aboutand respond to their needs. And in doing so, wegain community support. And that is not only ona formal level through the United Way orthrough the city councils, but also on aninformal level. For example, in Frank’sneighborhood, there is a community garden.And individuals from the neighborhood itselfcome onsite, tend that garden, reap the fruits ofthat effort and feel connected to theirinstitution. So, those kinds of activities we feelare very important to create success, not onlyfor the organization, but for the clients involved.In our youth centers we have celebrations. Wehave graduations from school, graduation fromprograms. We have holiday events, birthdayevents. We bring in service groups to supportthe environment in which they live and try andkeep that environment really appropriate fortheir stays.
We also believe that people need to alwayslearn. That is the staff. We continue toprofessionalize staff. I can speak for ourorganization – it being mainly publically funded,but we make every effort to train staff throughevents like this, or through supporting theireducation, because much of the work is done bydirect care people who maybe are not degreedin some functions. We really promote that andpromote lots of training and education.
Also the need to collaborate and network withother organizations creates strength. It’s not solong ago that people competed with each otherorganizationally, and they competed for thedollars. That atmosphere is changing on theprogram level to a great extent, and that allowsfor more healthy environments overall. In termsof client support, there were times when thedoors were closed to different people who wereinterested. I can speak for our organizationsthat all supportive people who were involvedwith the client are invited to become involvedwith those individuals in the treatment process.We consider it very important within our settingsto do that with immediate families, even families

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 136 Treatment
who are struggling with their own issues andtheir own addictions, and also extended familiesin particular.
I appreciate your time and your attention.
TREATMENT TRAININGSESSIONS
New Developments in Oversight andTreatment of Opiate Addiction:Pharmacology and Behavioral Therapies
Mark W. Parrino, M.P.A.PresidentAmerican Methadone TreatmentAssociationUnited States
Good morning. It’s a pleasure to be here.
Part of my remarks will focus on research andpolicy: Why methadone maintenance treatmentis so widely used in the United States and othercountries. The presentation will also focus oncommunity education – the need to inform thepublic about the value of methadonemaintenance treatment. Some additional issuesof clinical management include pregnancy,treating, and comorbidity, such as HIV infectionand other infectious diseases with people onmethadone maintenance. And in addition, I willcome back after Dr. Barthwell has concluded tofinish some administrative concepts aboutprogram design, how best to operatemethadone maintenance treatment programs,and so that you don’t run into the flaws inMexico the way we did in the United States inthe early part of methadone maintenancetreatment. So, I thank you for your graciousintroduction, for inviting me to speak andhopefully this will help all of you in other partsof the country and in Mexico.
So, with that, I’m the President of the AmericanMethadone Treatment Association, which wasfounded in 1984. The association representsapproximately 650 methadone treatmentprograms in the United States and we’reorganized through statewide methadone
program association chapters. Some of thelargest chapters are from the states ofCalifornia, New York, Illinois and Texas. In fact,in addition to Dr. Barthwell being the Presidentelect of the American Society of AddictionMedicine, she also represents the IllinoisMethadone Provider Association to our Board ofDirectors, which is not atypical of Dr. Barthwell.She represents many different organizations atonce.
The focus here will be three major issueseffecting the future of opiate addition in theUnited States. The first is a change in programoversight in the Federal government from theFood and Drug Administration to the Center forSubstance Abuse Treatment. These are twoFederal agencies in the United States. For thepast 25 years, since 1974, the Food and DrugAdministration has provided Federal oversight tomethadone treatment. This made sense at thebeginning of the major change in methadonetreatment in the early 1970s, but lost itsapplicability over the course of the last 5 years.The plan is to use accreditation standards, whichare outcome oriented standards as a way toevaluate the success of methadone maintenancetreatment, to measure the improvement of thewell-being of the patients who are in treatment.It’s a very serious and major shift in howmethadone maintenance treatment will beevaluated in the United States, and ourassociation has supported such a practice.
The second major issue is having stabilizedmethadone maintained patients who have beenin treatment in methadone programs in theUnited States, have the ability to transfer out ofthe clinics, into private physician office practices.This is called medical maintenance. The ideabehind this is to free up needed places for newpatients to come into methadone maintenancetreatment and to give the successfully stabilizedpatients an opportunity to gain access to adifferent kind of treatment experience oncethey’ve successfully demonstrated stability in thetreatment system.
The third major policy issue is the developmentand use of new medications to treat opioiddependency. Methadone maintenance treatmenthas been the most evaluated, studied and usedtreatment for opiate dependence that we have
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 137 Treatment
in the history of any medicine. No othermedicine has been scrutinized and evaluated socarefully to treat a disease. No other form ofcancer treatment, or any other disease, hasbeen so carefully evaluated. So methadonemaintenance treatment is the most studied care.And according to our Federal agencies and theNational Institute on Drug Abuse and theNational Institute of Alcoholism and AlcoholAbuse, methadone maintenance treatment hasbeen found to be the most effective medicaltreatment available to treat opiate dependence.
Of the new medications, the most current one iscalled buprenorphine. It’s certainly to be foundeffective. The question becomes effective forwhat patient, during what part of the addictioncycle? From our perspective and what we’veknown in reviewing the research, it is probablybest geared to the younger, or more naiveopiate dependent person. The individual whohas not been using opiates for a very longperiod of time. In the United States, if I were togive you a sketch of the most typical opiatedependent person, it would be as follows. Theindividual began using heroin at the age of 17,after using alcohol and some other drugsincluding marijuana. The young person doesn’tcomplete high school in most cases. Rarely getsto college. Generally gets involved with thecriminal justice system. Is arrested. Spendssome time in jail. The individual rarely getstraining for an employable skill. Most times theindividual, as they get into their 20s, because ofusing dirty needles, becomes susceptible tohepatitis C or to HIV infection. The persongenerally enters a methadone treatmentprogram somewhere around the age of 27 to 29years old. As a result, the patient has beenexposed to a lot of other illnesses, to thecriminal justice system and presents theprogram with many challenges in terms ofproviding rehabilitation or in some cases,habilitation. So, keep in mind that treating thisdisease is extremely complex. And all of myremarks should be put in the context that whilemethadone is effective, you need more thanmedication to treat the complexity of opiateaddiction. It is not simple to treat and it willtake some time. It is also important to show atthe outset that while some people will be able tobe free and will not use methadone very long,history shows that the majority of people who
do best in methadone treatment will remain inmethadone treatment for 5 years or for manycases, for the rest of their natural lifetime.
This is not a setback. This is not a problem. Thisis just the treatment they require.
As I said, the Association was founded in 1984.We represent about 650 of the programs in theUnited States. This slide demonstrates from theNational Household Drug Abuse Survey, theincreasing trend of using heroin in the UnitedStates. I know that in Mexico, you’re also havinga very serious problem with people using heroin,including young people. This trend has beenmirrored in other countries. This is not new. Andthe reason is that heroin is becoming moreavailable. It’s more available at purer levels, andit’s less expensive.
Now, understand that when you look from theleft side to the right side of this graph, in 1995,you have 140 thousand brand new heroin usersin the United States. This was for one year. Younotice the increase from 1993 to 1995. I wouldargue that Mexico and other countries arehaving the same problem. To let you know thatthis is not just a problem between the UnitedStates and Mexico, internationally renownedresearchers, Dr. Jerry Stimson and Dr. DonDejoulas, did a worldwide study of the numberof countries using heroin. In 1991, 80 countrieswere reporting heroin use intravenously. In1995, 121 countries were reporting intravenousheroin use. HIV infection follows the pattern. In1991, 50 countries are reporting HIV infection asa result of intravenous heroin use. But by 1995,81 countries are reporting HIV infection as aresult of intravenous drug use.
In Mexico, I don’t know if you’ve seen HIVinfection and AIDS or hepatitis C. And I don’tknow to what degree you see dramaticpercentages. But I can guarantee you, that ifyou do not treat intravenous heroin useeffectively, and if you don’t provide access totreatment, you will see an increase in HIVinfection, of AIDS, of other infectious diseases,hepatitis B, C and Delta, to say nothing of thekind of opportunistic infections that untreatedheroin users get. What this slide does not showis the number of young people using heroin. Ittells you that 140 thousand people in the United

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 138 Treatment
States used heroin for the first time in 1995. Butof this group, 2½ percent of 8th grade studentsused heroin in the United States. This is adramatic difference. It is also striking to notethat in the last nine years, the average age ofthe heroin user was about 22-24 years old. Theaverage age of the heroin user in 1998 droppedto 16½ years old. This may not seem dramaticat first blush, but I can tell you that that drop inthe average age in so short a period of time isalarming. It’s exactly why health officials in theUnited States are trying to increase access totreatment.
What you’re going to be receiving now is theAssociation’s news report from December 1999.In that news report, you will see the breakdownof all the methadone treatment patients andprograms in the United States. It’s in the middleof that booklet and it’s in a purple backgroundand it’s short. Our association conducted thesurvey to demonstrate the number of patients intreatment. This is not an estimate. This is anactual count. So, once again, this gives you abreakdown of where the treatment programsare, what states and what number. According tothe White House Office of National Drug ControlPolicy, the estimate of untreated heroin users isabout 800 thousand. It probably is more, butthe number has increased over the course of thelast several years. So, if I could recommend thatthe Mexican government do anything, myrecommendation is capture good information atthe very beginning. The value of what theUnited States government has done is, it has theNational Institute on Drug Abuse which reallyfunds 85% of the world’s research on drugabuse. The only reason we have such goodinformation about methadone treatment andwhy it works is because of the National Instituteon Drug Abuse. More recently the Center forSubstance Abuse Treatment is a relatively neweragency that’s really been in existence for about10 years or so, and this is a much more criticalagency in terms of treatment and treatmenteffectiveness. In fact, one of the first treatmentapproved protocol statements that CSATdeveloped was on methadone treatment. Andone of the slides that I will show you comesfrom this book.
I would recommend that if you have an interest,please access this document. It took about 18
months to develop and given the quality of thedocument and the material it covers, it isactually remarkable. It is as useful today as itwas 8 years ago when it was first published. So,I really recommend it to you. It’s a basicguidelines of the most effective treatmentpractices.
Now, what we have to do in the United States,when we go to Congress and to statelegislatures, is we have to demonstrate in hardterms what the costs are of dealing with drugabuse. So, here this came from the CaliforniaDrug and Alcohol Treatment Assessment of1994. Dr. Gerstein and his colleagues conductedthe survey. If you look to the right of the chart,in the pie, the cost to society for the impact ofdrug and alcohol abuse in the year beforeentering treatment is $4.4 billion each year. Thisis the cost to society. The reason I show youthis slide first is to demonstrate the reality thatlike it or not, every country has an economicimpact. If the politicians, or governmentagencies wish to ignore it, you’re going to payfor this, one way or another. I will alsodemonstrate how inexpensive treatment iscompared to this kind of number.
The average cost per year for one heroin addictis based on a study in 1991 by Dr. Vincent Doyleand Dr. Don Dejolais. While the slide representsa study of nine years ago, and this is based onNew York State, the average, the relative cost,between the category is pretty much the same.On the left side of the graph, you will notice thatthe cost of untreated heroin is about $45,000per person, per year. And look at how the costis calculated. Security, theft and heroin use.
To incarcerate the person is about $35,000 perinmate per year. For residential treatment,$14,000. For methadone maintenancetreatment, about $4,500 per patient per year. Ifthe society or the government, does not want totreat the patient, you pay $45,000 per year. Ifyou want to treat the patient with methadone,you pay $4,500 to $5,000 per year. Which costsmore? We also have to demonstrate to Congressand state legislatures, the value of methadonemaintenance treatment even compared to otherforms of treatment. So, here, you look at clientswho reduce costs to taxpaying citizens by 50%in the year following treatment. Look all the way

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 139 Treatment
to the right. If patients continue, not end, butcontinue methadone treatment, society gets55% savings for the person staying inmethadone treatment. Look at the bar next to it.The discharged methadone. You notice how thatgoes down to 19.5%, which means if the patientremains in treatment, and the longer the patientremains in treatment, not only is it better for thepatient, but it’s better for the country. It’s betterfor the culture. So, any policy, any directiveabout methadone maintenance treatment shouldalso include the fact that treatment should beopen-ended. What that means is that you leavethe patient in treatment as long as they’re doingwell. You do not create artificial barriers to endtreatment at any particular point in time as longas the patient continues to do well.
This slide shows the strategies for improvingmethadone treatment process and outcome. AsI indicated at the beginning of these remarks,what’s most important is that you follow what’shappening to the patient. The hallmark ofmethadone maintenance treatment is that thepatient improves. That’s its hallmark. That’s itsvalue. You will notice that was in the Journal ofDrug Abuse in 1997, and you probably saw theslide if you were in the morning lecture, becausethis comes from Dr. Dwayne Simpson and hiscolleagues. In the first bar, to the far left of thegraph, the injection frequency drops from 94%in the patient before treatment, to 35% as thepatient is in methadone treatment. The opiateuse, from 100% to 48%. And this is all withinthe first year. If you look at cocaine use, youdon’t see as dramatic a change. You see from43% to 31% because methadone maintenancetreatment is not necessarily going to preventcocaine use. If the patient is at the rightmethadone dosage it will decrease the drugseeking behavior and the use of cocaine, but itwill not eliminate it. Methadone maintenancetreatment at the right dosage level eliminatesthe use of heroin. We know that from research.You will also notice the change in alcohol abuse,from 31% before to 18% during treatment, andcrime or jail decreases dramatically.
One of the true hallmarks of methadonemaintenance treatment is a decrease in crime.You’ll notice this comes from Dr. John Ball’sstudy in 1989, published in 1991. The red barsshow crime in the untreated heroin user before
they enter methadone treatment. The yellowbars show crime during methadone treatment.You notice the dramatic change. Now, thefollowing slides represent a history. Whenmethadone maintenance treatment wasexpanded in the United States, it was in theearly 1970s, during the Nixon Administration.You would not think that the NixonAdministration might expand access tomethadone treatment, but they did so becausecrime would be reduced. It became clear that asthe methadone maintenance patient continuesand as people leave using heroin to get intomethadone treatment, crime decreases sharplyand the reduction continues. This slidedemonstrates it.
This slide is shown to break the myth that theuntreated heroin user is a predatory criminal.Dr. John Ball, who did this study, wanted toknow what kind of crime the untreated heroinuser would commit. Society has the myth thatthe untreated heroin user commits predatorycrime so that people will be hit on the head, willbe held up at gunpoint, or at knifepoint. This isnot true. This study looked at 6 clinics in NewYork, Philadelphia and Baltimore. Go from theleft side to the right side of the graph, and lookat the kind of crime that’s committed. In theNew York City clinics, and Philadelphia andBaltimore, all the way to the left, in the yellowcolor, that’s theft. The blue is drug business.Green is organized crime. And then to the farright is organized crime, but look at violentcrime, all the way to the right. In New Yorkprograms, 1.1% of untreated heroin users wouldcommit violent crime: in Philadelphia, 1.6%; inBaltimore, .7%. The reason I show this slide isto remind you that the untreated heroin usercommits crime to support an illicit addiction.They are not looking to harm people. I’m notforgiving the fact that crime is committed. I’mjust trying to demonstrate the kind of crime thatis committed. These are people who are sick,these are people who have a disease; these arehuman beings who need access to treatment;they are not criminals; they should not be put injail. They should be treated. And as you sawfrom one of the earlier graphs, it’s also lessexpensive.
To bring you back to the 1970’s ? and I showyou this as a piece of history in the United

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 140 Treatment
States ? this slide was developed by Drs. Doyle,Dejolais and Joseph. Between 1971 and 1973,19,900 untreated heroin users enteredmethadone treatment in New York City. This isthe largest single expansion of any methadonesystem in the country. It never happened again.In one city, 20,000 people enter methadonetreatment during a 24 month period. Look atwhat happens in the same period of time:decreases in complaints to the policedepartment for burglary; robbery and grandlarceny decreased by 77,000. So, 20,000 peopleenter methadone treatment, and there are77,000 fewer complaints of burglary in the same24 month period. In terms of drug arrests, yousee 25,000 fewer drug arrests. This means thatfewer police are chasing after untreated heroinusers. This means that courts are not filled withthis kind of case. This means that police are ableto do other kinds of work rather than lock uppeople because they’re buying heroin illegally onthe streets. This saves taxpayers all the moneyyou saw in the first graph. This is part of thecost of untreated addiction and $45,000. This ispart of that cost.
Now, this is also before HIV infection and AIDS.It’s the same period: 1971-1973, New York. Butas those 20,000 entered treatment, you see areduction of contagious serum hepatitis by1,500 cases. The reason methadonemaintenance treatment became much moresupported by public health officials in the UnitedStates is because of HIV infection and AIDS.This is from New York State Department ofHealth, 1996. Compare New York City with therest of the United States, looking at only onereason of transmission for AIDS throughintravenous drug use. In New York City, 45% ofpeople with AIDS get it as a result of untreatedintravenous drug use. If you look throughout theUnited States, 25% of people with AIDS get thatAIDS as a result of untreated intravenous druguse. Treating AIDS is extremely expensive tosay nothing of the human torment that peoplewith AIDS go through. You can prevent this bygetting into methadone treatment, as I willdemonstrate in the subsequent slides.
This was in 1989-1990: HIV seropositivityamong new and established methadonemaintenance treatment patients. For thosepeople who had been newly admitted to
methadone treatment, you had 45% of thepatients entering treatment who were HIVpositive. Compare that to patients who werealready in methadone treatment, who had notbeen exposed to HIV infection. Look at thedifference. It’s 27.2%, a major difference. Thisis another value to methadone treatment. Notonly is it less expensive than untreated, not onlydoes it reduce crime, but it reduces AIDS andHIV infection. If you look at the effect ofmethadone treatment on HIV positivity rates ina different way, you see the value of keeping apatient in treatment. In the first bar to the left,the person who’s not in treatment is 47% HIVpositive. If you’re currently in treatment butwere not infected at the time of enteringtreatment, the percentage drops to 23%. Ifyou’ve been in methadone maintenancetreatment for five years, the percentage dropsto 17%. If you’ve been in treatment withoutneedle use, the percentage of HIV infectiondrops to 12%. And if you’ve been in treatmentfor five years or more without needle use, thepercentage of HIV infection drops to 6%. Onceagain, this demonstrates the value of retentionand treatment as opposed to discharging thepatient. As the patient remains in treatment, youcontinue to see the benefit.
This slide is related to methadone dose. Mostpatients do well with between 80 and 100 mg ofmethadone. It is true that some patients will dowell on lower dosages, but on average, thepatient should be receiving a dosage between80-100 mg per day. Look at the frequency ofheroin use and methadone dose. You will noticethat the percentage of patients usingintravenous heroin decreases steadily as thedose of methadone increases. Ultimately, themost effective dosage range, as you will see, isabove 70 mg. So, for all programs, it’sinstructive to remember this lesson. There are anumber of programs in the United States thathave used 50 and 60 mg for the majority oftheir patients. These patients are not getting theappropriate dosage of methadone. As a result,these patients are using heroin, cocaine,continuing to drink and are using other drugs aswell. The most basic issue for methadone is itseffective pharmacology. Methadone is effectiveat the appropriate dosage level, and willextinguish the use of heroin as this slidedemonstrates.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 141 Treatment
This shows, in another way, as the patiententers and stays in methadone treatment, howthe patient’s use of heroin steadily decreases.This also comes from the John Ball study. And Iwould argue that if the programs in this studyused 80-100 mg of methadone, you would see amuch sharper decline in the number of peopleusing heroin. This slide demonstrates thatbeyond treating heroin, we’re also treating anextremely complex disease. This shows thelifetime and recent prevalence of psychiatricsymptoms among the patients in the John BallStudy. Just look at the first two lines. Theincidents’ prevalence of serious depression andserious anxiety among the people in treatment:48% of the patients have a lifetime prevalenceof serious depression and 51% have a lifetimeprevalence of serious anxiety. So, while you’retreating heroin, you’re also treating otherdiseases as well. And a major component ofmethadone treatment has to be counseling,individual counseling and group counseling,because after the patient is stabilized on a doseof methadone, you must deal with the fact thatso many of the patients have underlyingproblems of mental health. I don’t know if this isthe case also in Mexico, but I would assume thatthe cultures are not that dissimilar. Because thisis also the case in Switzerland, in Italy, inAustralia, in England and in France.
This study that was conducted in the early1990’s, with Dr. Thomas McLellan and hisassociates. Dr. McLellan wanted to study thedifferent levels of methadone maintenancetreatment. How much treatment should you givea patient? And how valuable will it be? What’sthe difference? There were three differentpatient groups in the study. In minimummethadone maintenance, you have a minimumdaily dose of 60 mg per day, but no regularcounseling and no extra service. In the standardmethadone service, which is mostly the kind ofmethadone treatment that’s provided in theUnited States, you have a minimum daily doseof 60 mg plus regular counseling but noadditional service. In the last study group,enhanced methadone treatment, you have thesame dose of 60 mg but regular counseling, on-site medical and psychiatric care, family therapyand employment counseling. Which means thisis a very comprehensive treatment. It’s alsomore expensive. The first group, it’s about
$1,500 per patient per year. The second groupis about $4,500 per patient per year. The thirdgroup is about $7,500 per patient, per year. So,the more treatment is, the more it costs.
Look at the number of patients who actuallyseek additional care when they’re in themethadone program. Remember there are threedifferent study groups. They’re all at the samedosage level, everyone of them. Some peopleimproperly suggest that the patient will notaccess treatment services, even if it’s given tothem. This slide shows that’s not true. If youlook at other drug use, family care andpsychiatric care, when those services areprovided to the patients, the patients will usethe care. This slide demonstrates this.
This slide, from the same study, also shows thedifference in the use of opiates. What’s mostinteresting about this slide however, is thatwhile you see a difference in how the patient isresponding, the top group is showing a veryhigh use of heroin. Fifty to sixty percent of thepatients are using heroin while they’re on theirdose of 60 mg of methadone. In the middlegroup, the standard, they’re using a little lessheroin. But it’s still there. And in the lowergroup, which is the enhanced methadonetreatment in yellow, you have the least amountof heroin being used. Why is this slideinteresting? Because all groups are maintainedon the same dose of 60 mg. So, even thoughopiate addiction is a brain disease, it alsoresponds to behavioral changes, too. If youprovide the patient with adequate counseling,adequate medical care, adequate services torespond to their needs, psychiatric, comordibity,in addition to the other medical problems of HIVinfection and AIDS, what you have are patientsdoing better in the methadone treatmentprograms.
This comes from Dr. Vincent Doyle who is theco-founder of methadone maintenancetreatment with his wife, Dr. Marie Neiswander.And I’m going to read the statement for you.“The problem was one of rehabilitating peoplewith a very complicated mixture of socialproblems on top of a specific medical problem,and that practitioners ought to tailor theirprograms to the kind of problems they weredealing with.” The strength of the early

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 142 Treatment
programs, as designed by Marie Neiswander wastheir sensitivity to individual human problems.What I have demonstrated in the slides is thatyou cannot treat a complicated disease just withsimple solutions like a dose of methadone alone.
This slide comes from Dr. Ball and Ross and hisassociates. They found that the programcharacteristics that were associated with successin methadone treatment are the ones listedhere. If the programs provide comprehensiveservices the patients get better. If the programshave integrated medical, counseling andadministrative services, once again, the patient’shealth will improve. If the patient’s gettingindividualized care where the staff of thetreatment facility responds to the patient, thepatient gets better. If the clinic has adequatedosing policies, the patient will get better. Ifthere is sufficient and stable staff, patients willget better. If there is sufficient staff training, thepatients will get a better quality of care and willultimately improve.
This is the staffing pattern that’s used in theUnited States for most of the treatmentprograms. Nurses comprise 27%, physicians13%, and counselors and social workers makeup the majority. Look at this for a few minutes.It demonstrates the relapse to heroin use at theend of methadone maintenance treatment.Eighty-two percent of people on methadone willrelapse to using heroin within 12 months ofending methadone maintenance treatment.82%. This has been replicated mostly inSwitzerland, in Hong Kong and in Australia. Thisis a geo-political and national and internationalproblem. What you have here is the same thingreplicated in other countries. What thisdemonstrates is as the patient enters andremains in treatment, it’s best to leave them intreatment.
Next, we need to educate the public aboutmethadone. In spite of what I have just shownyou, most people don’t support methadonemaintenance treatment. I understand thatthere’s even a medical society in Mexico –psychiatrists – that don’t support methadonetreatment.
This is not philosophy. This is medicine. This ismedicine treating a disease the way doctors
treat heart disease. Or the way doctors treatdiabetes. So, why is it that we get into a debateabout how to treat heroin users? The reason Isuggest to you is because heroin use is not seenas a disease by most people in the public. Thepeople who use heroin are seen as criminals.They are seen as very strange human beingsthat may not be seen as human at all. It’s seenas a criminal problem, and that people shouldbe locked up, rather than treated. So what ourassociation decided to do, was fund thedevelopment of a brief video tape, which I’mgoing to show to you now. It’s the story ofsuccessful methadone patients and theirfamilies. It only lasts seven minutes, and I knowthat you will have the text of it interpreted butthis is most instructive for you to understand.This is going to be our association’s campaign toeducate the public.
This tells you the narrative story. This is the newkit ? with stripes in it. This is designed for thecommunity, for legislators, for judges. This isdesigned for people who know nothing aboutmethadone maintenance treatment. This kitgoes with this video.
The point of this is to put a human face toheroin addiction. It’s to demonstrate thatmethadone maintenance is a human treatmentand it helps people. The idea is to break downthe barrier that most people have about theperson using heroin, which is pretty similar tothe person who’s using methadone. It’s to breakthrough the stigma. The value of this is toremind people who don’t use drugs and have nounderstanding of methadone, that the peoplethat we’re treating are pretty much just like theyare. This video is from the person’s perspective,not from my perspective as the President of theAssociation, not from the perspective of theresearch scientists who did the graphs. It’s toremind people that we’re all in the same boat,that we’re all dealing with people just likeourselves. Someone who had seen this tape saidto me, why are you making this so emotional?My answer was, because a lot of people don’twant to listen to the science those who take thepoint of view that methadone doesn’t work.
This community education kit, this video is amethod of trying to break through a lot of the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 143 Treatment
cultural barriers. We were told this is the samein many countries – in European countries andthe same thing happened in Germany. InGermany, only until the last five to six years didmethadone treatment expand. At the beginningof the 1990’s, the only way a person usingheroin could get on methadone treatment inGermany was if the person had HIV infection.That was the criteria for admission.
Slides are an effective way to explain tolegislators to policy makers, to people who don’tlike methadone treatment, that this is the storyof methadone treatment in facts. This is notphilosophy. Do I think it works? These slides,this book, ? absolutely. What this does is tellyou our associations, policies and positions ?about everything I’ve talked about: aboutaccreditation, about policies for newmedications. This tells you where ourassociation stands on every major policyinitiative about methadone treatment in theUnited States. The community education booktells you how to educate people in thecommunity. For those of you who operatemethadone treatment programs in Mexico, forthose of you who are in government positions,to try and influence other people, you need touse this kind of community education bookbecause it tells you a great deal aboutmethadone maintenance treatment.
You always will have to educate the public. Itnever ends. I operated a methadone treatmentprogram for 15 years in New York City. I always,every single week, had to educate someoneabout methadone maintenance treatment.Always.
Andrea G. Barthwell, M.D.President, Encounter Medical GroupUnited States
Question and Answer SessionI want to make sure we’re all on equal footingrelative to the biological rationale for methadonetherapy, which then sets out the reason for thechronic care of a patient who needs methadonereplacement therapy in a medical context. We,at this point in the United States have very fewpeople receiving office-based opioid therapy inthe doctor’s office, and there is no established
rate for that. Some physicians who are doing itprovide self-payment option for those patientsreceiving it in that way. And if they are seeingthe patient once a month with the standard costof a medical visit and the patient’s insurance ispicking up the cost of the methadone, it wouldbe expected to average between $40-60 or $80a month. In the least funded publicly fundedclinics, clinics receive anywhere from $38 to upto $80 per week for services, and that would bechronic and lifelong. In those settings wherepatients, or clinics, are subsidized to provide thecare, patients might pay on a sliding fee scaleanywhere between $1 and $50 a week inaddition to what the clinic gets. And clearly, thelarger the clinic, the lower you can get yourcosts. One of the things that artificially inflatesthe cost in the clinic is an arbitrarydetermination of the kinds of services thatpeople receive. So the cost of providing care toindividuals who need less group therapy istransferred over to providing care to thoseindividuals who need more. We have an averagecost that the clinic receives. For some patients ittakes more money to treat, some patients less.
Q. Who is going to continue to pay for clients’methadone treatment?
A. I want to comment that the necessity forthat level of treatment with daily medical visits,daily psychiatric visits and so forth, drops downdramatically as people are restored to morenormal functions. And, we have to consider thatthe treatment in an ideal or perfect world wouldbe phased. And phasing of treatment early onwould provide more intensive support andstructure. But as the person is normalized andcured of the addictive behaviors while onmethadone, the need for those supportiveservices could conceivably drop off. The personcould begin to engage in therapeutic activities ina self-directed way where they’re going to 12-step meetings and they don’t have to have atherapist encouraging or supporting theirparticipation in that. They’re doing that on avoluntary basis, in the same way that long-termrecovered and recovering alcoholics continue togo to their 12-step meetings to support theircontinued growth and change across their life.So, I appreciate your question about who’sgoing to pay for this, and what does it cost long-term, looking at a cost of $40 per week every

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 144 Treatment
week for the rest of your life seems like adifficult proposition. And we really need toencourage the development of other ways ofdelivering the medication when the medicationreplacement therapy is all that’s needed anddeveloping phases to allow for that.
Q: My question to you doctor is, earlier weheard that there’s a rising number ofadolescents using heroin, and in fact it is soimmense of a problem that the average heroinuser now, I believe, is 16 or so? And so thatreally presents a whole different treatment, awhole milieu of different treatment strategiesbecause it seems that up until this point we’vebeen talking about dealing with heroin addicts interms of adults. This really changes a lot. I’d beinterested in any comments that you may havein terms of dealing with adolescent heroinaddicts in the future.
A: The adolescent drug user who is usingheroin is more typically using it within a patternof poly-substance abuse and using it within apattern of emotional behavioral problems thatare not necessarily specifically drug addiction.We know from all of the studies of the onset ofthis disorder, it is more likely to be a primarydisease without greater underlying psycho-pathology if the age of onset is delayed. Whenwe see individuals who start with early druginvolvement, their drug involvement is a part ofa complex of psycho-behavioral problems, and itis more likely to be a symptom of a greaterunderlying problem than when you see onset ofaddiction in an adult. So you cannot talk aboutadolescent drug abuse in the same way that youtalk about adult, or adolescent addiction in thesame way that you talk about adult addiction.The earlier the age of onset, the more likely youare going to find psycho-behavioral problemsunderlying that disorder and that behavior.
Your treatments therefore cannot be as directedat the primary disorder as they are in the adult,and they have to take in to account thedevelopmental stages of the adolescent and beappropriate to that adolescent’s developmentalstage. They also have to take into accountwhether another psycho-behavioral disorderexists along with the addiction, where you’remore likely to be dealing with dual diagnosis orif the addiction is one of the criteria for a
greater psychological disorder. And that’s one ofthe ways in which that psychological disorder isbeing expressed in the adolescent. So, you’renot going to be able to treat it as simply, with abiological intervention, as you are adultaddiction. And again, we’re going to have toencourage treatments directed at the psycho-behavioral disorders for the adolescent and lessfocused on the biological. The adolescent mayneed the biological support if repeatedtreatments fail to turn their behavior around.But the adult is going to be more easilyresponsive to a biological support, areplacement therapy, when placed on a platformof talk therapy. In the adolescent, the platformof talk therapy is going to be critical to haveestablished and you may or may not be able totreat them without the biological therapy.I had a question yesterday about other medicalconditions and the management of this disorderin hospitalized patients, pregnant patients andpatients with pain.
This set of slides was developed by this group ofpeople – Dr. Flowers, from Wisconsin, Dr.Maxwell from Chicago, and Dr. Samosa fromOhio. They came together and developed thisworkshop for the Addiction Technology TransferCenter that’s funded by SAMHSA through CSATwhich exists in the Chicago area. The GreatLakes Addiction Technology Transfer Center.These slides will be available to you onlinethrough the CSAT website by the end of thesummer for individuals who would want to usethem in presentations. We have developed thislecture, and I’m giving you an abbreviatedversion of it, for use in the hospital setting for amedical grand rounds. It can be delivered in lessthan an hour, allowing time for questions andanswers. I’m using it because it illustrates someof those points you discussed yesterday.
We start out by making the point that addictionis a chronic disease of the brain. It’s a primary,chronic disease with genetic, psycho-social, andenvironmental factors that influence itsdevelopment and manifestation. And again,across the life cycle, each of those aspects mayweigh in more than another depending upon theage of initiation and the person’s basic conditionwhen they make their first contact with thechemical. The disease is often progressive and itis fatal. When you look at addiction you don’t

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 145 Treatment
diagnose it by the nature of the drug. It mattersnot what drug is being used, addiction is notdiagnosed by physical dependence alone. Clearlymethadone addresses the physical dependence.I said that because it’s a drug to which theaddict is cross-tolerant, it blocks the withdrawalsyndrome and the withdrawal syndrome is theexternal evidence, that physical dependence hasoccurred. Physical dependence can be definedas one having an experience of adverse physicalconsequences when drug use stops. So it’s acyclical kind of definition. You know it existsbecause when you’re not using, you’re sick. Andwhen you’re sick and you can relieve that byusing again, you know it exists.
It is also not diagnosed by the dosage, howmuch the person is taking, how often they takeit, or how long they’ve been taking it.Individuals have different characteristics to theirdependence. So it’s much broader than whatwas taken, how often, and how much. Addictionis similar to other chronic diseases. It hasfeatures in common with insulin dependentdiabetes mellitus. It has features in commonwith hypertension. It has features in commonwith coronary artery disease. Those featuresinclude that there is both a biology and anenvironmental contribution to its cause. Peoplewho are genetically predisposed to coronaryartery disease can have the chance that geneticpredisposition will become expressed if theygrow up in an impoverished area and eatinferior food that’s high in fat content. Peoplecan have a genetic predisposition to insulin-dependent diabetes mellitus that may never getexpressed if they have grown up in anenvironment where exercise is valued and theyexercise and maintain a very slim figurethroughout their life. So biology andenvironment contribute to the disease.
Chronic diseases often have a poor response tobehavior interventions alone. Have you evertried to treat a diabetic with diet alone and seenhow unsuccessful you are? Chronic disorderstypically require both biological and behavioralinterventions in order to get a more ideamanagement of them. Pharmacologicalmanagement is usually necessary for the controlof high blood pressure. Someone can make adecision that they’re going to eliminate stress,change their diet, workout and do a number of
things. Reduce the salt in their diet to help bringtheir blood pressure within a normal range. Buteven with a strict adherence to a behavioralmanagement program, some individuals will notget their high blood pressure under completecontrol and will have to have that behavioralprogram supplemented with a biologicallydirected program, pharmacological managementin other words.
The chronic course of these diseases ischaracterized by remissions, where the diseasegets worse or it appears to be worse with anaggressive deterioration over time. All of thosethings characterize chronic medical conditionsand characterize addictions, particularly opiateaddiction. But addiction is different from otherchronic diseases because there’s a stigmaattached to it. The behaviors which supportgetting the drugs are criminalized so that thedisease is put in a criminal context. And overtime we have had very limited pharmacologicalinterventions available to us. There is not a lotof incentive for the pharmaceutical industry todevelop treatments for these disorders. Andwhen we have had pharmacological treatmentsdeveloped, there has been a lot ofmisunderstanding and misinterpretation ofthem. For example, methadone.
There are over 900 peer reviewed publicationsover the last 30 years which talk about thesafety and efficacy of methadone. There areonly 237 about the oral hypoglycemic, and thereare only about 426 about a drug for anantidepressant; yet there is generally morepublic acceptance of these other drugs. We lookat the evidence on these other drugs and acceptthat they are an important component thatphysicians can use in the managing high bloodsugar, depression, and other mood disorders.The number of studies which support the safetyand efficacy of them are small and insignificantin comparison to the literature and the dataavailable in high quality, peer reviewed journalsabout methadone. Yet, we find methadone notachieving the same level of acceptability asProzac. Within 6 months of Prozac’s beingreleased for use by physicians of a specializednature, many general practitioners were using itreadily in their personal practices. And patientswere going to their physicians asking for the

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 146 Treatment
drug for a variety of things for which it hadn’tbeen approved, including weight control.
On the other hand, we see no outpouring ofsupport or adoption of this medication,methadone, for a variety of reasons that we’vebeen struggling with over the last two days.Empirical studies have proven that methadone iseffective. More than 900 studies over more than30 years document that methadone is effectivein the treatment of heroin addiction, and theyprove that methadone is extremely safe. Noorgan pathology has ever been associated witheither acute or chronic methadone treatment.There are more deaths annually from the use ofnon-steroidal anti-inflammatory drugs than fromillegal drug use. Yet, when you hear methadonediscussed, you hear a lot of concern aboutmethadone overdose and methadone deaths.And they typically have nothing to do with thefact that the person was on methadone. In fact,methadone has been life-sustaining and life-giving to more people than not.
We do know that methadone is not safe for non-addicts, just as insulin is not safe for non-diabetes. Individuals should not take amedication for which they don’t have a medicaldisorder. There will be some problem with safetyin that instance. Empirical studies have proventhat methadone is life prolonging, and I thinkI’m not going to dwell on this because Markdealt with that. But, you can see that forindividuals in methadone maintenancetreatment, the ratio of observed deaths toexpected, based upon the patient population is8.4. For those who are not in treatment, thedeath rate ratio of observed to expected isseven times that. For those who areinvoluntarily discharged from treatment, it’sabout six times that. It’s surprising to see howmuch of the administrative policy governing thetreatment of narcotics addicts has been basedupon theoretical opinions, political pressures andwishful thinking. And there’s a tremendous bodyof scientific evidence that we have accumulatedover the last 33 years.
Some people are concerned about providingmethadone because they think they’re going tocreate addicts by giving them methadone.Remember, we said yesterday that methadoneworks because the heroin addict is cross-
dependent to it. It therefore maintains theunderlying dependence on heroin but itsuppresses all the other behavioral effects thatan untreated heroin addict would present with.And the incidents of iatric, iatrogenic, meaningphysician-caused opioide addiction is clinicallyinsignificant. We just do not see peoplebecoming heroin addicts because someonetreated their heroin addiction with methadone.We are careful in our review of who needs to goon methadone, as Mark pointed out. Andtypically people have had multiple failures atother forms of treatment before we will initiatemethadone. Methadone treatment is a soundmedical practice. For individuals who areadmitted to the hospital with an untreatedheroin addiction, it can ensure a continuation ofthe medical-surgical stay. Without treatment,the individual will experience withdrawal andleave treatment prematurely. It decreases thephysiological stress on the patient who’spresenting for another medical condition. Itensures that the management, the staff willhave fewer management problems with apatient. If the person is in the hospitalexperiencing heroin withdrawal, they are goingto push the nurses’ buttons regularly andfrequently, trying to get some relief fromwithdrawal. And it increases patient compliancewith prescribed medication regimens during thehospital stay and afterwards because the personisn’t having their life interfered with becausethey need to go get heroin to relievewithdrawal.
We recommend that when patients present tophysicians for medical care, that the physiciancontinue existing methadone maintenance if aperson is in a program. What we find frequently,however, is that when patients get admitted tothe hospital, the admitting physician, who maynot be knowledgeable about methadone, will tryand do us a favor by reducing or eliminatingthat person’s dependence upon methadone. Andthey’ll seize the opportunity of the patient beingin the hospital to reduce or eliminate their dosefor us. And while the person may be able totolerate a reduction in dose while they’re in thehospital and not in that complex environmentwhere they use their heroin, as soon as theyreturn to the street, they’ll resume heroin use.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 147 Treatment
What we try to teach people about individualson methadone, is that when patients present inmedical settings they don’t routinely report aninflated methadone dose. They tell theirhospital-based doctor what they’re getting at theclinic. They don’t increase their dose. Unlessthey’re receiving treatment in a clinic that usesinadequate methadone doses. We advise thephysician to call the clinic to coordinate care andfollow-up. But we also recommend that fortreating physicians, or if you’re going to workwith a patient who’s in your clinic to get themhospitalized, that you advise the admittingphysician to maybe increase their dose by up to20% to cover them during the hospital staybecause, there are additional stressors on ourpatients when they get admitted to the hospital.So, if I have someone on 100 mg, when theypresent to the hospital, if I have a chance towork with the doctor before them going in, I’llask the doctor to cover them with 120 mg whilethey’re there to cover the additional stress. Toallow them to be adequately covered fromwhat’s associated with being in the hospital, thefear, the anxiety, the pain, the personalintrusions that occur when a person ishospitalized.
If a person presents to a medical care withheroin addiction who is not on methadone, werecommend that methadone replacement beinitiated. And our clinics make ourselves readilyavailable to our hospital system to admit thosepatients at discharge. We have found that thereluctance among physicians to treat withmethadone while the patient is in the hospitalcan be reduced or eliminated if the physicianknows that the patient can enter a clinic whenbeing discharged. Otherwise, they feel kind oflike they have been put on the spot by thepatient’s addiction, and they feel helpless interms of managing it long-term. So, we makeourselves available to them.
Methadone in that setting is prescribed not as adefinitive addiction treatment because again, wewant the other services to be provided to theperson, but as an acute replacement to theheroin which is lost to the patient upon beingadmitted to the hospital. Opioide withdrawalsyndrome will not increase the chance ofabstinence after discharge, so by lettingsomebody go through withdrawal in the
hospital, they’re not more likely not to return toheroin once they’ve been discharged. And aperson having a good experience withreplacement therapy while in the hospital mayseek treatment for their heroin addiction afterthey’re discharged. We want people to knowthat there is no medical indication to withdrawmethadone in the hospital setting.
In our country we have some Federalregulations and there is a quote out of theregulation which states, “This section is notintended to impose any limitations on aphysician or authorize hospital staff toadminister or dispense narcotic drugs in ahospital, to maintain or detoxify a person as anincidental adjunct to medical or surgicaltreatment of conditions other than addiction.”While we have a Federal regulation that keepsus from treating addiction with a narcotic drug,except under a methadone program sponsor,that regulation does not keep the physician fromtreating an addiction, as long as the finding ofaddiction is incident to admission to a hospitalfor another reason. So, in order to completetreatment for the primary reason for which theperson’s admitted to the hospital, if you have toprovide methadone under that situation, youcan. There’s nothing in the law that keeps youfrom doing that.
Now, in order to treat this disease, you have torecognize opioide addiction is a disease andhave to understand that patients don’t alwaysvolunteer that they’re heroin dependent or onmethadone. Patients have to be askedspecifically. But they don’t generally give a falsereport of being addicted to heroin if they’re not.So people won’t tell you I’m a heroin addict justto get methadone from you in the hospital. Wehave found no incidents of that. But how youask the patient as to whether they’re an addictor not will certainly influence how they respond.So, if the question sounds like “You don’t usedrugs do you?” You don’t encourage the patientto report it appropriately. You need to say, “Inmy experience, when treating people withhepatitis C, there is a chance that they haveused heroin in the past, or are currently usingheroin. I see this enough in my practice to knowthat this happens, and we’ve developed a wayof helping the person deal with their heroinaddiction while they’re in the hospital for their

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 148 Treatment
hepatitis C. And we use methadone to treat thatwhile you’re in the hospital. So tell me, are youcurrently using heroin, and how much? Are youon a methadone program? Have you ever beenon a methadone program? When you were onmethadone in the past, what was your dose?”So, asking the questions in a way thatcommunicates to the patient that you’reconcerned about them, and that you have somesolutions for the problems that they’re going toface. Some familiarity with those problems,encourages the patient to disclose.
In order to initiate methadone for someonewho’s not on it, you have to assess the degreeof opioide dependence. And I never, everrecommend that you do a narcane challengetest in order to determine how addicted theperson is. What you will do in a narcanechallenge test is precipitate withdrawal in theheroin dependent person and make them verysick, and rupture the therapeutic relationshipyou’re trying to establish. So I encourage you touse the clinical history and understand thatusing $10 worth of heroin is approximatelyequivalent to 10 mg of methadone. You can goup to 30 mg for the initial dose, and add 10 mgevery four hours until the person is comfortable.And at the end of the first 24 hours, add up howmuch you’ve given and you’ve established thedaily dose that will be required.
You want to look for signs and symptoms ofwithdrawal. We’ve talked about them yesterdayand they’re on your handout. And also look forsigns and symptoms of intoxication. If you seesigns and symptoms of withdrawal, the patientneeds more. If you see signs and symptoms ofintoxication, you can stop increasing the dose.And administer the dose that it took to get tothat point the next day.
Understand that if, at a very low dose, you caneliminate the objective signs of withdrawal. At alow dose, you may eliminate subjectivesymptoms of withdrawal. Remember grade 0compared to grade 1 through 4 from yesterday.And you want to exceed both the very low andthe low dose and get them into a therapeuticrange where there are no signs of symptoms ofwithdraw or intoxication, and the patient reportsbeing comfortable. You cannot base where youstop dosing on what you see alone. The patient
has to report being comfortable. If the patientcontinues to report not being comfortable butthey’re exhibiting signs of intoxication, you’llwant to watch them.
Now the pain management. Often you will seepeople who are on a methadone program andthey’ll go into the hospital for surgery and they’llhave post-operative pain. And the doctor willsay well, they’re on methadone. That should betaking care of their pain. So the one take homemessage for you here is that the maintenancedose from a methadone program does notprovide any analgesia. In order to get analgesia,you have to add to the maintenance dose ashort acting opioide. Something that you’regoing to give every 3-6 hours for pain. Now,when the person is on an opioide blockade doseof methadone, it’s going to create a higher doserequirement for the medication that you givethem for pain. So if you were someone that Iwas going to give 100 mg of Demerol to, I’dhave to give you 125 mg in order to bring aboutadequate pain relief. So the rule of thumb is a25% higher dose. If I were going to give youDemerol every 4 hours for pain, I have to give itin shorter intervals, 25% shorter interval, so I’dstart to give it to you every 3 hours. So if astandard dose is 100 mg every four hours forpain, in the individual on methadonemaintenance, I want to give 125 mg every 3hours for pain. A 25% higher dose with a 25%smaller interval. And I also want to review thenursing notes as to the person’s level of comfortfrom pain following the dose and at the end ofthat interval because I might have to shorten iteven more. I might have to increase the dosageeven more. I also want to see whether I’mgetting significant sedation. Because if I’mgetting significant sedation, I might want toback off on the dose or back off on the interval.And lengthen the interval.
Never, ever use the mix antagonist agonist, oran antagonist for pain relief. You will precipitatewithdrawal with mixed agonis antagonist. And apatient controlled analgesia is extremelyappropriate in the population. Since the personhas a greater tolerance for and a greater needfor pain relief, something that they can managethemselves, by pushing the button anddelivering the dose will reduce the managementproblems associated with inadequate relief in

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 149 Treatment
the population. And if your patient controlledanalgesia is turned off at 10 mg every fourhours you want to set it at a 25% higher ceiling,understanding that the patient will require more.
Sometimes physicians and nurse practitionersand other health professionals will see a personwho is addicted and mis-attribute inadequatelytreated pain as addiction. This pseudo addictionis an iatrogenically caused disorder. Physiciansand nurse practitioners who write inadequatepain management regimens bring this diseaseabout. It’s caused by the poor management ofacute pain in addicted and non-addictedpopulations. And it’s characterized by a drug-seeking behavior exhibited on the part of thepatient. The patient is pushing the nursingbutton at shorter and shorter intervals, askingfor more and more pain relief. And it getslabeled as drug-seeking behavior, which it is.They’re seeking adequate medication to relievepain. So it’s medication-seeking behavior thatgets mislabeled as drug-seeking behavior. And itresults in a terrible, terrible misunderstandingbetween the patient and the physician, or thehealthcare provider and the patient. That personmisperceives the patient as an addict and thepatient misperceives their healthcare provider asuncaring. So it needs to be diagnosed where itexists.
Pregnancy: I said yesterday that opioidwithdrawal is not life-threatening to the adult. Itis life-threatening to the fetus. Fetal withdrawalis well-established before the mother becomessymptomatic. Before the mother feelswithdrawal, the fetus is in withdrawal. And thefetus is suffering from withdrawal before themother knows that she’s in withdrawal. Opiatesare extremely benign to fetal tissue when givenin a way that is supportive in a medicalenvironment. There are no known terradigeniceffects of opioide like drugs. Opium, heroin andmethadone are not known to cause birthdefects. We see negative outcomes frompregnancy in the heroin addict because ofrepeated withdrawal for the fetus and becauseof the lifestyle associated with heroin using. Butall of that can be normalized by putting themother on an adequate dose of methadonethroughout her pregnancy. What we see interms of the neo-natal withdrawal once the childhas been delivered has no known direct
relationship to the dose of methadone that themother required to maintain her during thepregnancy. So you may have a mother who’s on10 mg of methadone whose child experiencessome neo-natal withdrawal. You may haveanother on 80 mg whose child does notdemonstrate any visible neo-natal withdrawal.We do not establish the dose for the motherbased upon what we predict the child willexperience. We provide the dose to the motherbased upon what the mother needs in order toachieve the goals of methadone maintenanceduring the pregnancy, which is to eliminate thetarget symptom, heroin use. If we put themother on too low a dose of methadone,thinking we’re doing the child a favor, we willsee continued heroin use on the part of themother, continued fetal withdrawal, continuedrisk of infection, continued premature rupture ofthe membranes, continued early delivery and allof the other complications associated withheroin use during pregnancy.
Multiple dependencies: Methadone does notcover withdrawal from alcohol or sedativehypnotics. So additional treatment will benecessary. If you have a person who isdependent upon heroin and valium and alcoholand cocaine, and you start them on methadone,it will address the heroin addiction, but not theother dependencies. Remember in that settingthat if they stop the valium and the alcohol, itposes a life-threatening withdrawal risk to theadult. You are obligated to treat and address thesedative withdrawal and the alcohol withdrawalwith medication assisted detoxification. It wouldbe recommended in that instance to sequencethe coming off of the alcohol and the sedativehypnotics with a taper of benzyoldiazepines, anda maintenance dose of methadone. If your goalis to detox from all drugs, you don’t havesomeone who is a candidate for methadonemaintenance, for example, you withdraw fromthe benzylodiazepines, and then withdraw fromthe methadone. Otherwise, you withdraw fromthe benzylodiazepines and leave the methadonedose unchanged and initiate psycho-socialtherapies to address the cocaine, alcohol andValium dependence.
Frequently in a methadone program you’ll seeindividuals whose heroin use stops and their useof alcohol or sedatives or cocaine continues, or

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 150 Treatment
they initiate on methadone. Those individualsagain will require psycho-social therapies toaddress their other dependencies. Methadonecannot be held responsible for stopping thoseother dependencies. It is very specificbiologically to the receptors that respond toheroin.
Drug interactions: Certain medications that willbe prescribed by the patient’s physician canlower the methadone level in the blood, creatingfor the patient a crisis of methadone withdrawal.And if it is not anticipated and then addressed,the individual may resume heroin taking to self-medicate the withdrawal they’re experiencing.We recommend that if there is a choice that canbe made for another medication, that thatmedication be selected. Avoid those medicationsthat lower the methadone dose unless they aremedically necessary. And if they are, if there’snot a good alternative medication to use in thepopulation, the fact that the person is going onthese medications be anticipated and thephysician putting this patient on thosemedications coordinate with the methadoneprescriber, to have the methadone doseincreased in response to it, as needed. Thereare also medications that can raise themethadone level, and the patient may complainof sedation after these medications are started.If it is going to be transient, the person mayaccommodate to the increased effective dose.And you may leave them alone. You may wantto reduce it and when they stop taking theseother medications, make sure that you increasetheir methadone level again. But again, youraise or lower the methadone level as needed,based upon both your physical findings and thepatients’ subjective reports of comfort.
If methadone is initiated when the patient is inthe hospital or continued when they’re in thehospital, we recommend that a simple phonecall to the clinic will do when the person’sadmitted to verify the dose and to let the clinicknow that the person won’t be showing up therefor the next few days. And then on the day ofdischarge, call the clinic to let them know whatthe last dose was and when it was administered.If you’ve increased the dose during the hospitalstay from 100 to 120 mg. you’ll want to informthe clinic that the person will probably becomfortable back at 100 but that they should
watch them in the event that their body hasadjusted to the increased dose, depending uponhow long the increased dose was in place. If theperson wasn’t at a clinic at the point where theywere admitted to the hospital, you look for aclinic to transfer them to if the patient hasagreed to that. But if the clinic cannot take thepatient immediately and they’re saying we needthree days to run them through the admissionprocess, in the United States methadone can becontinued up to three days after dischargewhere it is dispensed daily at the hospital. Theycannot be given medication to cover them forthree days. They have to go back to the hospitalevery day for three days.
What are the take home messages? Thataddiction is a brain disease. That over 900studies over 30 years have shown thatmethadone works. Withdrawing someone frommethadone when they go into another medicalsetting is bad medicine. And withdrawingsomeone from methadone when they go to jailis bad medicine. There is no indication towithdraw the person from the medication in thesame way that there is no indication to withdrawsomeone from insulin when they become insulindependent. When you see a stable person onmethadone, there is no indication to withdrawthe methadone. You are doing them no favor.You have to understand that they’re stablebecause they’re on methadone. When you see astable diabetic on insulin, you don’t think todiscontinue the insulin. You’re not doing themany favor and you will precipitate a crisis in theirlife. Likewise, you will precipitate a crisis in theperson’s life who is stable on a dose ofmethadone.
Methadone maintenance is separate from painmanagement. The methadone dose that they’retaking on a daily basis is addressing theaddiction. The pain management has to beaddressed separately. There are no real legalbarriers to the proper care of the heroin addictwithin the medical context. There should be noreal legal barriers to the proper care of heroinaddiction in the prison context. People don’t gofrom needing this medication on one day for itslife-sustaining, life-giving and life-restoringproperties, to not needing it the next day justbecause their life situation changed.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 151 Treatment
Dr. Parrino: With that, there are several piecesof information that both of us have not coveredyet. First, to follow on some of Dr. Barthwell’sremarks. The importance of treating the patientwho’s pregnant and treating the patient properlyis truly important. I’ll give you one examplewhen I was an administrative director of a clinicin New York. It was on a Friday afternoon, atabout 3:00. Our admissions were closed for theday. The clinical supervisor of the facilityapproached me and said, “We have a 41 yearold woman who has just seen the doctor andshe has found that she is six months pregnant.She has just been withdrawn from methadonefrom another methadone treatment program.We believe that it is important to admit herimmediately and try to restore her methadonedose.” Obviously we were concerned about themother and the fetus. We admitted the patient.We tried to increase her dose over the course ofthe weekend, and I called the administrator ofthe clinic that the patient had been maintainedon and inquired why this patient had beenwithdrawn. The answer was, first, they did notknow she was pregnant. Secondly, she was analcoholic and she refused treatment for alcohol.I explained that the patient had been pregnantmore than 6 months, which was determinedthrough medical exam. Unfortunately, within fivedays, the patient had a spontaneous abortionand the child was lost. So, what Dr. Barthwellpresented to you is not only critical, but it’scritical to the child that you don’t see.
Ultimately, everything that we do has been socarefully studied, that we’re giving you thebenefit of these 30 years of research andinformation. In terms of prison facilities, it’sunfortunate that the only prison system in theUnited States that dispenses methadone, isRikers Island in New York City. Our associationhas tried to work to increase access tomethadone treatment in prison systemsthroughout the United States. But, most prisonofficials simply do not want to provide access tomethadone treatment services. Again, the prisonofficials take the position that most of societytakes: that methadone is not really a medicationand that the heroin user is not really sufferingwith a disease, that the heroin users broughtthis disease on themselves. As one warden in aprison said to me, “He created the disease, lethim suffer without it in jail.” So Rikers Island has
demonstrated there is a significant cost savingsfrom giving methadone treatment.
We have found through research that for certainpatients, there is an irreversible change in thebrain structure. In the neuro-chemistry. And forthose people, they are going to need areplacement, pharmaco-therapy as you suggest,for an indefinite period of time, or for the rest oftheir lives. NIDA is still doing research usingsome of the new computer temography studies,and in certain cases you’ll also find that fordifferent people there may be some reversibility.It depends on the individual. It depends on thelength of time the person has used heroin. Itdepends on the individual’s brain chemistry. Dr.Barthwell will talk more about that particularaspect. In terms of other kinds of treatmentintervention, methadone maintenance treatmentis effective. But it’s not necessarily thetreatment of choice for all heroin users. Someheroin users, again depending on length of timein treatment, may not need a pharmaco-therapylike methadone, or even others, likebuprenorphine. Some patients do well with drugfree, in-patient, therapeutic communities. Butwe have found that many of the patients whoare in methadone treatment have tried todiscontinue their use of heroin, whether they’vebeen in residential drug-free treatment orthey’ve been through self-help groups. So, theclear majority of the people on methadonetreatment have tried this already. And have notsucceeded. Ultimately, for most people,methadone is the last treatment choice – notthe first. So, in this regard we have found thatthe replacement pharmaco-therapy is really themost effective for the majority of the peoplebecause of the length of time using, theirhistory, and most of those patients have reallytried using and stopping on their own manytimes over, even in jail, in psychiatric facilitiesand withdrawal wards.
Víctor Manuel GuisaCenters for Youth Integration (CIJ)Mexico
Dr Guisa’s presentation focused in the clinicalresearch for treatment. The psychological,sociological, and environmental factors relatedto drug abuse were emphasized. His
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 152 Treatment
presentation-included discussion of a studyentitled “Imagen del Padre en pacientesadictos,” (English translation: The Father’simage of patients with addictions). Researchprojects that were suggested included:
• Bicultural aspects in migrant populations• The impact of drug abuse on children of
addicts• Drugs and violence• Drug abuse among adolescents and young
adults• Effectiveness of drug treatment• Drug abuse with comorbid conditions• Clinical research in LAAM and Methadone
treatment• Vaccines for cocaine addicts• Epidemiology
In conclusion, Dr Guisa stressed theeffectiveness of treatment of opiate addictionsuch as the use of LAAM and methadone. Heunderscored the need to incorporate methadonetreatment methods at Centers for YouthIntegration.
Program Accreditation
Stephen ShearerHealth Care ConsultantUnited States
The topics of the workshop that Mr. Schearerled included:
• Presenting the benefits of accreditation ofprograms by a recognized accreditationbody
• Describing the program accreditationprocesses of the Joint Commission and CARF
• Discussing the new CSAT guidelines foropioid replacement therapy
• Discussing the concepts in the PatientRights, Assessment and Care standards ofthe Joint Commission
• Question and Answers session
Nora GallegosNational Council on Addictions(CONADIC),Ministry of HealthMexico
Slide presentation follows.
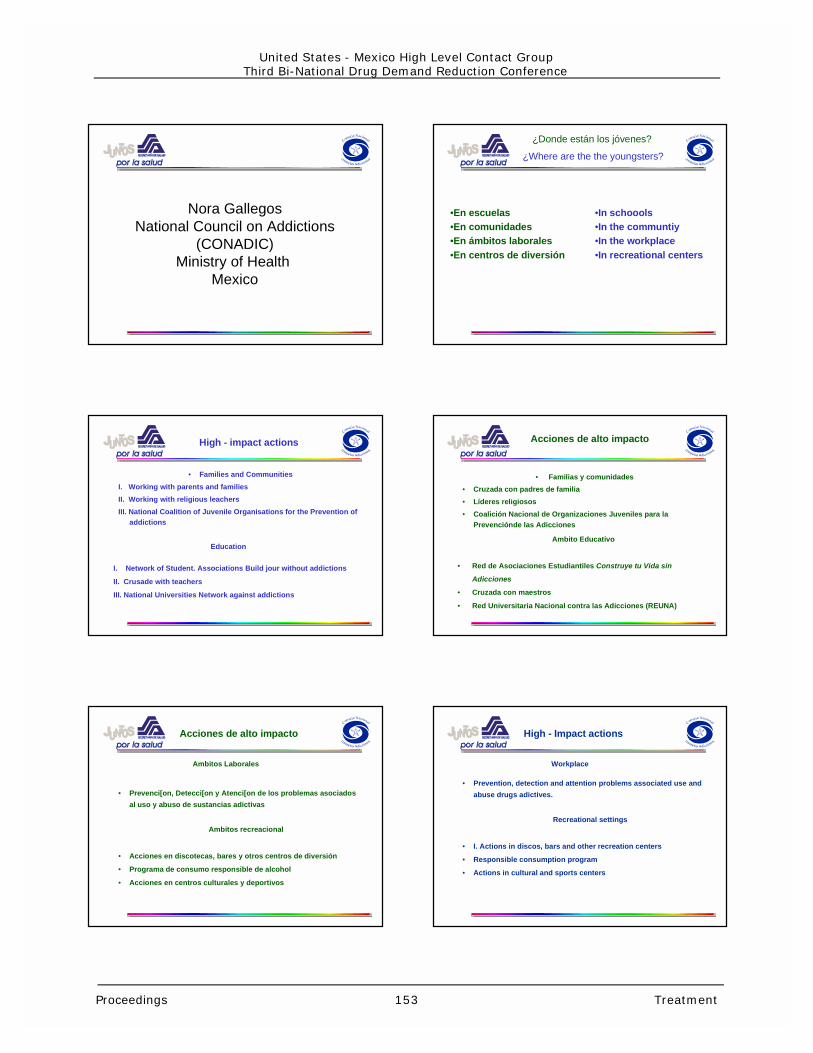
Nora GallegosNational Council on Addictions
(CONADIC)Ministry of Health
Mexico
¿Where are the the youngsters?
•En escuelas•En comunidades•En ámbitos laborales•En centros de diversión
•In schoools•In the communtiy•In the workplace•In recreational centers
¿Donde están los jóvenes?
• Families and Communities
I. Working with parents and families
II. Working with religious leachers
III. National Coalition of Juvenile Organisations for the Prevention ofaddictions
High - impact actions
I. Network of Student. Associations Build jour without addictions
II. Crusade with teachers
III. National Universities Network against addictions
Education
• Familias y comunidades
• Cruzada con padres de familia
• Líderes religiosos
• Coalición Nacional de Organizaciones Juveniles para laPrevenciónde las Adicciones
Acciones de alto impacto
• Red de Asociaciones Estudiantiles Construye tu Vida sin
Adicciones
• Cruzada con maestros
• Red Universitaria Nacional contra las Adicciones (REUNA)
Ambito Educativo
• Prevenci[on, Detecci[on y Atenci[on de los problemas asociados
al uso y abuso de sustancias adictivas
Ambitos recreacional
• Acciones en discotecas, bares y otros centros de diversión
• Programa de consumo responsible de alcohol
• Acciones en centros culturales y deportivos
Ambitos Laborales
Acciones de alto impacto
• Prevention, detection and attention problems associated use and
abuse drugs adictives.
Recreational settings
• I. Actions in discos, bars and other recreation centers
• Responsible consumption program
• Actions in cultural and sports centers
Workplace
High - Impact actions
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 153 Treatment

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 154 Treatment
Innovations in the Treatment of StimulantUse Disorders
Jeanne ObertExecutive DirectorMatrix Institute on AddictionsUniversity of California at Los AngelesUnited States
The cocaine epidemic that began in the UnitedStates in the 1980’s and the present widespreadmethamphetamine problem have presentedtreatment providers with tremendouschallenges. Patients dependent on stimulantshave been particularly unresponsive totraditional psychosocial treatments and noeffective pharmacologic interventions have beendiscovered. The lack of medical necessity forhospitalization during the withdrawal and thetreatment phases argues against inpatienttreatment as an option. The most effectiveinterventions presently available to treatmentproviders working with stimulant abusers are thestructured, outpatient, psychosocialinterventions. This presentation will present anoverview of those models of psychosocialtreatment that have documented efficacy. Oneof the models, the Matrix Model, will bepresented in detail. Participants will be madeaware of specific interventions that have proveneffective for the different stages of recoveryfrom stimulant dependence.
Slide presentation follows.

MATRIX MODELOF
OUTPATIENT CHEMICAL
DEPENDENCY TREATMENT
Matrix Center, Inc.Matrix Institute On Addictions
UCLA Alcoholism and Addiction Medicine Service
Matrix Model ofOutpatient Treatment
Organizing Principles of Matrix Treatment
•Create explicit structure and expectations
•Establish positive, collaborative relationship with patient
•Teach information and cognitive-behavioral concepts
•Positively reinforce positive behavior change
Matrix Model ofOutpatient Treatment
Organizing Principles of Matrix Treatment(cont.)
•Provide corrective feedback when necessary
•Educate family regarding stimulant abuse recovery
•Introduce and encourage self-help participation
•Use urinalysis to monitor drug use
MATRIX TREATMENT MODELDifferent from General Therapy
1. Focus on behavior vs. feelings
2. Visit frequency results in strong transference
3. Transference is encouraged
4. Transference is utilized
5. Goal is stability (vs. comfort)
MATRIX TREATMENT MODELDifferent from General Therapy
6. Focus is abstinence
7. Bottom-line is always continued abstinence
8. Therapist frequently pursues less motivated clients
9. The behavior is more important than the reason behind it
MATRIX TREATMENT MODELDifferent from General Therapy
10. Family system support is encouraged
11. Therapist functions in coach/advocaterole
12. More directive
13. Therapeutic team approach is utilized
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 155 Treatment

MATRIX TREATMENT MODELDifferent from Inpatient Programs
1. Less confrontational
2. Progresses slower
3. Focus is on present
4. “Core issues” not immediately addressed
5. Allegiance is to therapist (vs. group)
MATRIX TREATMENT MODELDifferent from Inpatient Programs
6. Non-judgmental attitude is basis of client-therapist bond
7. Change recommendations based on scientific data
8. Changes incorporated immediately into lifestyle
Outpatient Recovery IssuesStructure - Ways to Create
•Time scheduling•Attending 12-step meetings•Going to treatment•Exercising•Attending school•Going to work•Performing athletic activities•Attending church
Outpatient Recovery IssuesInformation - What
- Substance abuse - Sex and recovery
and the brain - Relapse prevention issues
- Triggers and cravings - Emotional readjustment
- Stages of recovery - Medical effects
- Relationships and recovery - Alcohol/marijuana
Outpatient Recovery IssuesStimulant CravingResponse Sequence
Trigger Thought Craving Use
Phases of Addiction
and
Stages of Recovery
Proceedings 156 Treatment
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
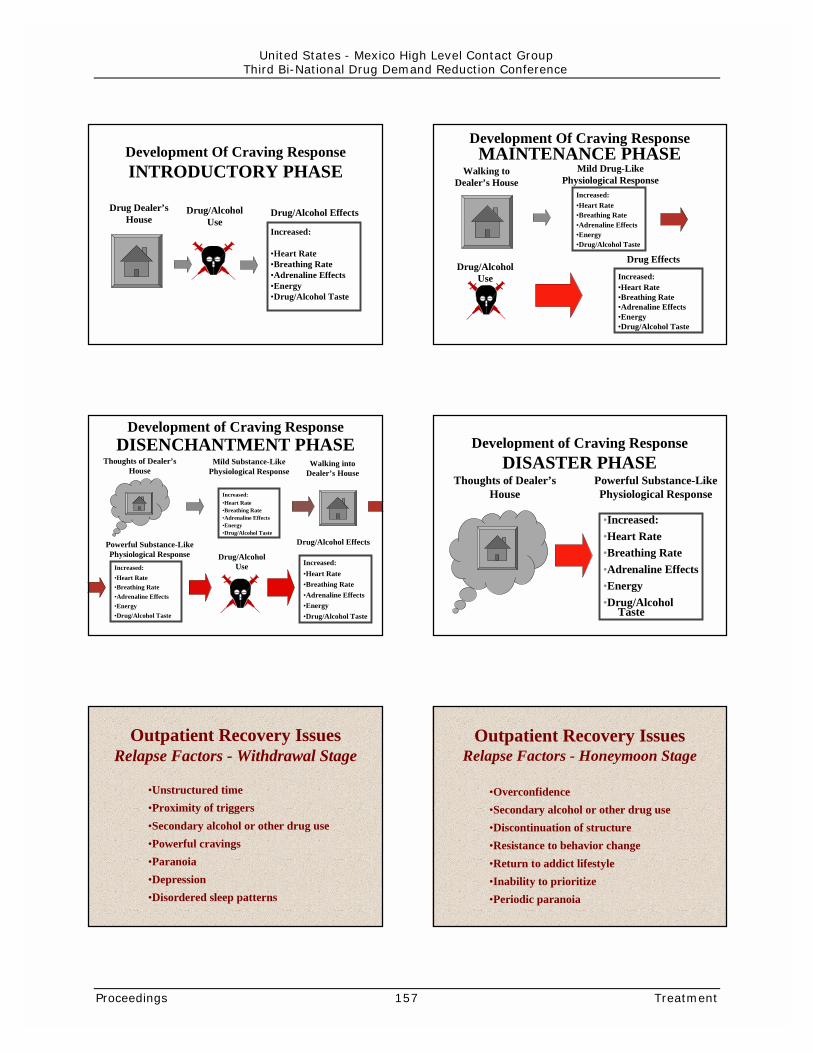
Development Of Craving ResponseINTRODUCTORY PHASE
Drug Dealer’sHouse
Drug/AlcoholUse
Drug/Alcohol Effects
Increased:
•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Development Of Craving ResponseMAINTENANCE PHASE
Increased:•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Mild Drug-LikePhysiological Response
Walking toDealer’s House
Drug/AlcoholUse Increased:
•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Drug Effects
Development of Craving ResponseDISENCHANTMENT PHASE
Increased:•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Powerful Substance-LikePhysiological Response Drug/Alcohol
Use Increased:•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Drug/Alcohol Effects
Increased:•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol Taste
Mild Substance-LikePhysiological Response
Thoughts of Dealer’sHouse
Walking intoDealer’s House
Development of Craving ResponseDISASTER PHASE
Thoughts of Dealer’sHouse
•Increased:•Heart Rate•Breathing Rate•Adrenaline Effects•Energy•Drug/Alcohol
Taste
Powerful Substance-LikePhysiological Response
Outpatient Recovery IssuesRelapse Factors - Withdrawal Stage
•Unstructured time•Proximity of triggers•Secondary alcohol or other drug use•Powerful cravings•Paranoia•Depression•Disordered sleep patterns
Outpatient Recovery IssuesRelapse Factors - Honeymoon Stage
•Overconfidence•Secondary alcohol or other drug use•Discontinuation of structure•Resistance to behavior change•Return to addict lifestyle•Inability to prioritize•Periodic paranoia
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 157 Treatment
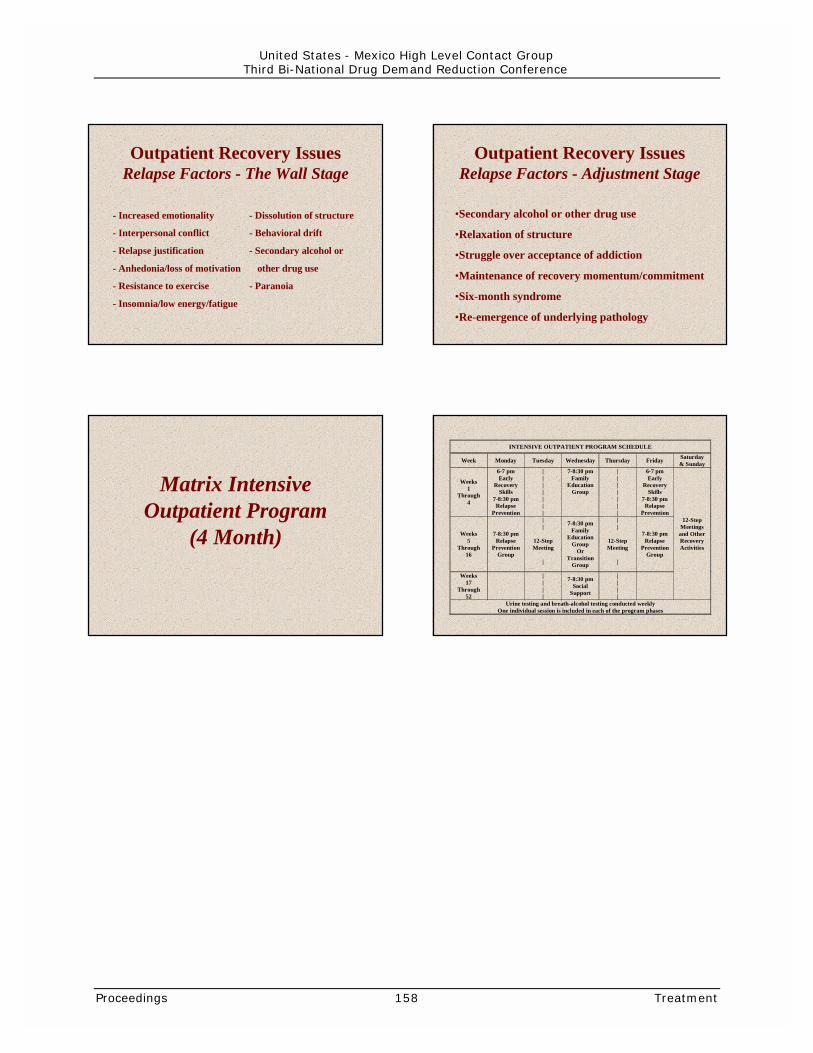
Outpatient Recovery IssuesRelapse Factors - The Wall Stage
- Increased emotionality - Dissolution of structure
- Interpersonal conflict - Behavioral drift
- Relapse justification - Secondary alcohol or
- Anhedonia/loss of motivation other drug use
- Resistance to exercise - Paranoia
- Insomnia/low energy/fatigue
Outpatient Recovery IssuesRelapse Factors - Adjustment Stage
•Secondary alcohol or other drug use
•Relaxation of structure
•Struggle over acceptance of addiction
•Maintenance of recovery momentum/commitment
•Six-month syndrome
•Re-emergence of underlying pathology
Matrix IntensiveOutpatient Program
(4 Month)
INTENSIVE OUTPATIENT PROGRAM SCHEDULE
Week Monday Tuesday Wednesday Thursday Friday Saturday& Sunday
Weeks1
Through4
6-7 pmEarly
RecoverySkills
7-8:30 pmRelapse
Prevention
|||||||
7-8:30 pmFamily
EducationGroup
|||||||
6-7 pmEarly
RecoverySkills
7-8:30 pmRelapse
Prevention
Weeks5
Through16
7-8:30 pmRelapse
PreventionGroup
||
12-StepMeeting
|
7-8:30 pmFamily
EducationGroup
OrTransition
Group
||
12-StepMeeting
|
7-8:30 pmRelapse
PreventionGroup
Weeks17
Through52
||||
7-8:30 pmSocial
Support
||||
12-StepMeetingsand OtherRecoveryActivities
Urine testing and breath-alcohol testing conducted weeklyOne individual session is included in each of the program phases
Proceedings 158 Treatment
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 159 Public Awareness Campaigns
PUBLIC AWARENESSCAMPAIGNS

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 160 Public Awareness Campaigns
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 161 Public Awareness Campaigns
INITIATING ANDEVALUATING PUBLICAWARENESSCAMPAIGNS
Introduction:Jennifer BishopOffice of National Drug Control PolicyUnited States
Crafting Effective Messages forBehavioral ChangesAmelie G. Ramirez, Dr. P.H.Associate ProfessorDepartment of MedicineBaylor College of MedicineUnited StatesTelephone: (210) 348-0255Fax: (210) [email protected]
Dr. Ramirez gave an overview of the ONDCPNational Youth Anti-Drug Media Campaign’sbehavioral change guidelines that are usedfor its outreach to Hispanic communities.
Main points:• Increasing drug use among youth in
the early 1990’s poses a significantpublic health threat that is bestreduced using a Social-Cognitive theoryapproach to offset psychosocialinfluences.
• Acculturated Hispanics in the UnitedStates show higher rates of drug abusecompared to immigrants. Thus, theMedia Campaign is focusing specificallyon reaching first generation teens.
• To reach Hispanic audiences in the US,the Media Campaign will emphasizecultural sensitivity, instill importance oftraditional values, model positivebehavior and increase familialcommunication.
Developing and ImplementingCommunity AwarenessAntonieta Martin, Ph.D.ResearcherJohns Hopkins University
Dr. Martin presented an overview of a youthdrug prevention campaign underway inMexico, that is produce though theassistance from John Hopkins School ofHygiene and Public Health.
Main points:• Campaign focuses on the emotions
associated with drug use, and seeks tofind ways to determine one’s intent touse drugs.
• Behavioral modification based on socialmarketing follows a distinct pathway:
- awareness of preventive message- approval of prevention message- intention to change behavior- practicing the new behavior- advocating new behavior.
• Strategic communication models orinitiatives need to address the cognitive,social and emotional motivations forperforming a drug use behavior.
Developing and ImplementingCommunity AwarenessIsabel Gomez-Bassols, Ph.D.Radio Unica NetworkUnited StatesTelephone: (305) 463-5045Fax: (305) 463-5001
Dr. Bessols hosts a radio program that helpsfamilies deal with drug abuse. Herpresentation shares her experiences usingradio as a prevention medium.
Main points:• To get a drug prevention message out
to the community, you need anattention grabbing mechanism, a radio
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 162 Public Awareness Campaigns
talk show on drug use in the context offamilial effect, has been successful.
• To be successful you must provideresources to empower individuals andfamilies to overcome their drugproblems. This can be facilitatedthrough creating partnerships withorganizations that can provide theinformation, and by using methods thatwill initiate dialogs within families.
• Family development is necessary inprevention and the radio can play a role.
Mario BejosLiber addictusMexico
This session focused on Liber Addictus aMexican magazine designed to discuss theuse of mass media in the prevention of druguse and addiction treatment.
Main points:• Liber Addictus has transformed itself
from a small scientific paper/publicationinto a large publication that addressesthe issue of all addictions.
• The greatest challenge to reducingaddiction and its prevention, is agrowing “toxic culture” which normalizesand promotes drug use and otherdisruptive behaviors. Toxic culturesportray addictive behaviors as cool whilelabels healthy habits as anti-social.
• The media plays an important role inpromulgating addiction as it adds to thecreation of this toxic culture.
Evaluating Media CampaignsTerry Zobeck, Ph.D.Office of National Drug Control PolicyUnited StatesTelephone: (202) 395-5503Fax : (202)395-6729
Dr. Zobeck gave an overview of themethodology currently in use to evaluatethe National Youth Anti-Drug MediaCampaign.
Main Points:• ONDCP is doing an externally contracted
impact evaluation of the campaignwhich will determine the campaign’soverall effectiveness. Additionally theagency has already created internalperformance measures/goals that areused to evaluate the campaign’s efforts.
• The campaign initially collected base linebehavioral data from in school surveys.With time its become increasinglydifficult to conduct survey’s in schooland have since began using householdsurveys which use hour long in personinterviews using youth and parentdyads.
• Continual evaluation during the life ofthe Media Campaign will initiate changein the campaign during its lifetime.
Jaime QuintanillaMexico’s Central Institute of Justice(CIJ)Mexico
Mr. Quintanilla discussed the methodspresently used by (CIJ) to evaluate its massmedia drug prevention initiatives.
Main Points:• A majority of data that was collected
was derived from television advertisingthat featured an 800 number to receiveinformation on treatment and to ordermaterials. Once the CIJ began usingtelevision advertising, call volume to the800 number increased by 500%.Respondents had a number of questionsthat were not directly related totreatment. A Gallup poll was later usedto gauge national attitudes towardsdrugs.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 163 Public Awareness Campaigns
• CIJ established a number of public andprivate partnerships to increase thereach of their messages, especially withchildren.
• The feedback received via the phonelines gave them solid qualitative data bywhich to revise their future efforts.
Building Private Public Partnership forSocial MarketingBeverly SchwartzSenior Vice PresidentFleishman Hillard InternationalCommunicationsUnited States
Ms. Schwartz gave an overview ofFleishman-Hillard’s work with the NationalYouth Anti-Drug Media Campaign todisseminate drug prevention messages inlocal arenas.
Main Points:• Social marketing is voluntary behavior
change for the benefit of society, whichis distinct from consumer productmarketing. It works because it offersbenefits that people want.
• To promote drug prevention messages;you must extend these themes intocommunities by using non-traditionalmethods, and public/privatepartnerships.
• To facilitate these partnerships, youmust know what you want from youpartner, and know what you can do tohelp them. Together you must work towhat resources are available throughthe venture to reach your goal.
The Azteca FoundationEduardo Chacón VizcainoMexico
Described their efforts to use a socialmarketing approach to develop traditional
and non-traditional partnerships to preventdrug use among youth.
Main points:• Campaign messages need to extend into
the community.
• Partnerships are developed around whatthey can do for you and what you cando for them.
• Campaigns need to give their audiencesmore than just information, skills andsupport are necessary. You must tellthem how, not only why.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 164 Public Awareness Campaigns
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 165 Public Health-Public Safety
PUBLIC HEALTH ANDPUBLIC SAFETY

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 166 Public Health-Public Safety
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 167 Public Health-Public Safety
LINKING PUBLIC HEALTHAND PUBLIC SAFETY
ModeratorsSteve WingSenior Advisor for Drug PolicySubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
Oscar Fuentes FierroAttorney General’s Special Office forCrimes against Health (FEADS/PGR)Mexico
IntroductionAllen AultNational Institute of CorrectionsDepartment of JusticeUnited States
Special Populations: AdolescentsWilfred Rios SánchezAttorney General’s Special Office forCrimes against Health (FEADS/PGR)Mexico
Duane McBrideAndrews UniversityUnited States
Richard DemboUniversity of South FloridaUnited States
Mario Alva RodriguezNational Institute of Sciences of PenalInvestigations (INACIPE)Mexico
Special Populations: Dually-DiagnosedDavid M. Wertheimer, M.S.W.King County Department of Community &Human ServicesUnited States
Mark SimpsonLexington Federal PenitentiaryDepartment of JusticeUnited States
Engagement into Treatment and RetentionTom McLellanTreatment Research InstituteUniversity of PennsylvaniaUnited States
Relapse Prevention and Recovery SupportD. Dwayne SimpsonTexas Christian UniversityUnited States
A System-Based ApproachSteve Wing, United StatesOscar Fuentes Fierro, Mexico
Diversion and Community Corrections:Pre-trial Diversion, Drug Courts, and Pre-Trial DiversionBarbara ZugorExecutive DirectorTreatment Assessment Screening Center(TASC)-ArizonaUnited States
Drug CourtsTim MurrayOffice of Justice AssistanceDepartment of JusticeUnited States
Incarceration: Adult PopulationsAllen AultNational Institute of CorrectionsDepartment of JusticeUnited States

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 168 Public Health-Public Safety
Parole and Community CorrectionsDave GasparArizona Department of Juvenile CorrectionsUnited States
Jennifer MankeyDenver Juvenile Justice IntegratedTreatment NetworkUnited States
Hiram Suárez VillaOffice of the Secretary of GovernmentMexico
Lilia Vasquez PortalesOffice of the Attorney General (PGR)Mexico
____________
IntroductionAllen AultNational Institute of CorrectionsDepartment of JusticeUnited States
In the United States, substance abuse leadshundreds of thousands of people into thecriminal justice system each year – many ofthem in need of treatment. This represents aproblem for both the public health and publicsafety systems.
There have been numerous creative responsesto this challenge. An ongoing dialoguesponsored by the U.S. Department of Justice,U.S. Department of Health and Human Services,and the Office of National Drug Control Policyhas focused on how system-wide approachesare needed, including approaches to:
• Prevent entry into the criminal justicesystem for those who can be safely divertedto community social service systems
• Limit penetration into the criminal justicesystem for nonviolent offenders throughcommunity justice interventions
• Intervene with those who must beincarcerated, through treatment andsupervision, both during and afterconfinement.
The ONDCP policy paper Drugs, Alcohol Abuse,and Adult and Juvenile Offenders: Breaking theCycle—Breaking Free of the Cycle: Policy forCommunity and Institutional Interventions toSafeguard Public Safety and Restore PublicHealth outlines the elements of an integratedsystem. Communities employing theseapproaches can reduce recidivism and drug-related crime.
Oscar FuentesAttorney General’s Special Office forCrimes against Health (FEADS/PGR)Mexico
It is a pleasure to participate in this importantconference. In Mexico there are a number ofinstitutions involved with the processing andrehabilitation of persons within the criminaljustice system.
Many speakers from Mexico will address theroles that various government institutions play inreducing drug use and related crime. LiliaVázquez, representing Procuraduría General ofthe Republic (PGR), will address drug treatmentin the criminal justice systems. Addressingsystem-wide challenges will be Wilfred RiosSánchez (FEADS/PGR), Mario Alva Rodriguez(INACIPE), Hiram Suárez (Secretrariat ofGovernment), and Licenciada Vázquez Portales(PGR).
This session examining the linkage betweenpublic health and public safety offers greatopportunity for sharing knowledge and expertisebetween Mexico and the United States. It alsooffers a unique opportunity to build a continuingdialogue on this issue of mutual concern.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 169 Public Health-Public Safety
Special Populations: Adolescents andDually-Diagnosed AdolescentsWilfred Rios SánchezAttorney General’s Special Office forCrimes against Health (FEADS/PGR)Mexico
Mr. Rios discussed the role that the AttorneyGeneral’s Office for Crimes against Health takesin Mexico’s anti-drug prevention campaigns andits efforts to discourage criminal behavior andthe social consequences of drug related crimeand violence.
Drug consumption is given special attention sothat appropriate measures with specific targetscan be applied to attack the supply and thedemand of illicit substances. Information is afundamental mechanism for all social sectorsvulnerable to this phenomenon. Therefore, thediffusion of legal disposition applicable to thecommission for crimes against health is vital, aswell as the diffusion of organic damages broughtby the use and abuse of drugs.
To accomplish these tasks, the Special Office forCrimes against Health is engaged in thefollowing activities:
• Organizing, developing, and implementingconferences, including training the trainercourses for the formation of leaders in drugprevention
• Sponsoring diverse activities include anti-drug messages with special emphasis onschool age youth.
An important concept to understand is thatunder Mexican legislation, addicts are notconsidered delinquents, but rather sick personswho should be treated in a special manner.Cases are reviewed and diagnosed by acompetent authority in the field and inaccordance with the federal penal code system.Diagnosed cases are referred to the appropriatehealth sector for treatment and rehabilitation.
Mexico deems a crime committed against healthto be one where any responsible person isengaged in the production, transportation,
commercialization, and trafficking, including theprovision of drugs as a gift. Sanctions can reachup to 25 years in prison.
In training provided to the community the areasdescribed above are discussed, placing specialemphasis on the effect that trained drugdetecting canines have contributed to thesuccess of anti-drug operations. This tool hasbeen used successfully in preventing drugs frominfiltrating schools.
Special Populations: AdolescentsDuane McBrideAndrews UniversityUnited States
For more than two decades, researchers,clinicians, and juvenile justice programadministrators have been aware of theconsistent relationship between alcohol andother drug (AOD) use and juvenile crime. Poly-drug use in this population is prevalent andmost commonly includes alcohol, marijuana,amphetamines, LSD, and crack.
The consequences of the juvenile drug-crimecycle are severe. AOD use among juveniledelinquents appears to be strongly related toother social and psychological problems,including lowered school performance, poorfamily relationships, arrested social emotionaldevelopment, increased interactions with AOD-using peers, and adult unemployment. AOD usealso appears to be associated with a number ofdelinquent behaviors including recurring,chronic, and violent delinquency that continuesinto adulthood.
The juvenile justice system is a viable point ofentry for a comprehensive collaborative servicedesigned to break the juvenile drug-crime cycle.Very few juvenile justice jurisdictions provideappropriate substance abuse treatment servicesfor youth. In the U.S. treatment for adolescentsubstance offenders has be found to beenavailable in less than 40 percent of the 3,000public and private juvenile detention,correctional, and shelter facilities.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 170 Public Health-Public Safety
The following model program employingresearch-based components can be used toguide improvements within the system.
• Intake. There should be a single point ofentry into the system, an immediatecomprehensive and culturally competentassessment, and a special emphasis onevaluating possible co-occurring mentalillnesses and conditions.
• Cross Systems Case Management. Eachcase should be ensured a continuum of careprovided by coordinating needed servicesfrom various systems.
• Collaborative Systems. In order toprotect the public safety and ensureintegration of relevant community and socialservices, a judge within the Juvenile JusticeSystem should administer the system.Examples of such systems include DrugCourts and Treatment Alternatives to StreetCrime (TASC) programs.
• Treatment Interventions withinGraduated Sanctions. Graduatedsanctions coupled with careful monitoring oftreatment progress can be successful inreducing both drug use and delinquentbehavior.
• Evaluation. The system should have anevaluation system in place that providesongoing feedback to the entire system.
Presentation based on:
McBride, D.C., VanDerWaal, Terry, Y.M.,VanBuren, H. Breaking the Juvenile Drug CrimeCycle. National Institute of Justice ResearchWeb Monograph, www.ncjrs.org/jjsa.htm 1999.
McBride, D.C., Terry, Y.M., & Inciardi, J.A.Alternative Perspectives on the Drug PolicyDebate in The Drug Legalization Debate (secondedition) Sage Publications, Newbury Park,California, (pp:9-54), 1999.
McBride, D.C., Pacula, R.L., VanderWaal, C.V.,Chriqui J. & Terry, Y.M.. Conceptual FrameworkReport to ImpacTeen, April 2000.
Terry, Y.M., VanderWaal, C.J., McBride, D.C., &VanBuren H. Provision of Drug TreatmentServices in the Juvenile Justice System: ASystem Reform. Journal of Behavioral HealthServices and Research, 27 #2: 194-214, May2000.
Richard DemboUniversity of South FloridaUnited States
Over the last few years there has been anincrease in juvenile crime. There is a highcorrelation between juvenile drug use andcrime. In Florida, arrests for drug offenses haveincreased 300% in the last 10 years.Increasingly younger people are entering thecriminal system, bringing with them ever moreserious problems.
Juvenile offenders are in special need of holisticapproaches that address mental health,education, substance use, and otherpsychosocial problems. Communities requiremore effective programs for children andfamilies who have not been able to accessservices.
Much of what we know has been derived fromworking with adults. However, there is agrowing knowledge base about alcohol and drugproblems in youth, and how to handle themmore effectively. Challenges faced by thesystem include:
• Developing consistent evaluation systems toassess the impact of treatment and identifycandidates for early intervention
• Determining the cost effectiveness oftreatment interventions
• Ascertaining approaches for increasing entryinto and retention in treatment programs(especially challenging for an adolescentpopulation)
• Improving community support services toincrease post treatment retention
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 171 Public Health-Public Safety
• Developing integrative systems of care thatfollow clients through their entire timewithin the criminal justice system.
Systems can address these challenges byincorporating interrelated activities into theirefforts by:
• Establishing preliminary screening and triageto identify problem areas that could betargeted during a more in-depthassessment, including the severity andscope of problems
• Involving clients in quality treatmentprograms at the residential and communitylevels
• Developing collaborative systems of care
• Providing aftercare services, including thepost-sanctions period (this is a majorproblem throughout the country, wherelong-term investments in treatment areneeded.)
Model programs have been developed in Floridawhere assessment centers provide centralizedintake facilities for youngsters who are at highrisk. The target population includes juvenileswho: (1) have been taken into custody; (2) aretruant from school; (3) have not been taken intothe justice system, but are at high risk, and (4)have undergone screening process, and arereferred to the program. Assessment centers provide opportunities andchallenges. The centers can gathercomprehensive information on youngsters thathelp inform referrals, court disposition, andprogram placement. (Before centers wereestablished juveniles cases went through thecourt system and youngsters were followed 3weeks later, thereby providing little informationto the court about how best to serve thejuvenile.)
The centers provide an opportunity to employearly intervention and diversion programs.Centers can serve as focal point for coordinatingand evaluating services for families and
individuals. Routine drug testing can be used toidentify new drug use trends in a community.
Assessment centers also face challenges. Forexample, it is important that programs limit theircatchment population so as not to pull inyoungsters not truly in need of treatment (i.e.,minor misdemeanors.) Screening instrumentsshould be as culturally sensitive as possible.Maintaining a strong infrastructure and thesupport of key stakeholders is important forprogram success. And finally, collecting data ontreatment outcomes system-wide is critical forevaluating and creating cost-effective programs.
Mario Alba RodriguezNational Institute of Sciences of PenalInvestigations (INACIPE)Mexico
In Mexico, 75 percent of drug users are betweenthe ages of 12 and 34. Drug use in thispopulation has been on the rise since 1980.Marijuana and inhalers are the drugs of choicewith heroin being the least consumed drug.Drugs are available on the street, schools, bars,and discos. The consequences of addiction arecrimes, accidents, and absenteeism.
Prevention is crucial to combat addiction, witheducation being a priority. Prevention studies inMexico have focused on one of the mostvulnerable populations – males between theages of 10 and 20.
Studies have shown significant tobacco andalcohol in the younger populations, with alcoholbeing the most abused drug. Usage is greaterin tourist and U.S. border areas, which mightindicate that location is a factor in increasedusage. Also, areas close to metropolitan areasare more extensively affected.
Of 6,374 violent deaths analyzed in Mexico City’sCoroner’s Office, over half of the bodies hadexcessive alcohol levels in the blood. Illegalsubstances accounted for a much smalleramount.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 172 Public Health-Public Safety
Special Populations: Dually DiagnosedDavid M. WertheimerKing County Dept. of Community andHuman ServicesUnited States
Dual diagnosis is the co-occurrence of mentalillness and substance use disorders. A widespectrum is possible. Mental health problemscan be a situational crisis or a persistent mentaldisorder. Substance abuse problems can rangefrom use to abuse to dependence.
Persons with co-occurring disorders represent asignificant proportion of the prison and jailpopulations. Sixty-three percent of jaildetainees have a mental illness or a substanceabuse disorder. The rate of serious mentalillness in jails is 3-5 times the rate in thecommunity. Ninety percent of inmates withschizophrenia, major affective disorders, or anti-social personality disorders have co-occurringsubstance abuse problems.
Behaviors that result in incarceration are oftenbyproducts of mental illness and chemicaldependency rather than true sociopathy.Incarceration provides neither a disincentive tocriminal behavior nor a setting for rehabilitation.Rates of recidivism are extremely high.
Integrated treatment (i.e., where a client’smental health and substance abuse disordersare treated simultaneously) provides the mosteffective results. Achieving integration requirescollaboration among the mental health, chemicaldependency, and criminal justice systems – atall entry and exit points in each system.
In a structure with a “No Wrong Door”approach, every entry point into the system isthe “right” door leading to appropriate careregardless of the presenting problem. Majormental health, substance abuse, and criminaljustice linkage points include pre-booking, post-booking, and post-release services.
By focusing on appropriate placement, provisionof quality treatment services, and communitytransition, states and localities can experiencereduced recidivism in this population.
Mark SimpsonLexington Federal PenitentiaryDepartment of JusticeUnited States
Criminal offenders with co-occurring addictivedisorders and psychiatric illnesses pose a specialproblem for the criminal justice system. Ifuntreated, these offenders are often among themost difficult to manage within an institution.Their behaviors are often disruptive to thegeneral inmate population and require increasedstaff supervision. These inmates are at greaterrisk of relapse in substance use and criminalbehavior following their release back to thecommunity. One reason for this is the likelihoodsuch individuals use illicit substances tomedicate their psychiatric symptoms.
In the United States, the criminal justice systemis being increasingly tasked with theresponsibility of providing drug abuse treatmentto its offender population. When done right,drug abuse treatment can effectively reducerelapse in drug use and recidivism in criminalbehavior among offenders following theirrelease back to the community. However, duallydiagnosed criminal offenders often do notrespond as favorably to more traditional formsof substance abuse treatment. There are avariety of reasons for this. Substance abusecounselors often lack the training necessary toassess mental illness. Many programs lack thepsychiatric help needed to treat mental illness.Involvement and retention of dually diagnosedcriminal offenders in treatment are oftendifficult, due to rationalization and blamingothers for their difficulties, distrust of treatmentproviders, and sudden changes in theirpsychiatric symptoms.
In response to the unique challenges posed bydually diagnosed offenders, the U.S. Bureau ofPrisons, Department of Justice created aspecialized drug abuse treatment program in1997 for dually diagnosed male inmates at theFederal Medical Center (FMC) in Lexington,Kentucky. The 16-bed dual–diagnosis programis a 9-month intensive residential program thatoperates within a larger residential program forgeneral population inmates.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 173 Public Health-Public Safety
The experience of the dual diagnosis program atFMC, Lexington has helped to identify criticalelements that significantly impact the success ofsuch treatment initiatives. These elementsinclude:
• accurate assessment of an offender’spsychiatric illness
• skilled drug abuse treatment personnel whoare trained and experienced in working withmentally ill offenders
• long-term and intensive treatment thatintegrates substance abuse treatment andmanagement of psychiatric symptoms
• transitional treatment in the community thatassists dually-diagnosed offenders insuccessfully reintegrating back into society
• the transfer of information betweeninstitution-based treatment staff andcommunity treatment providers to assist inthe offender’s transition back to thecommunity.
Engagement into Treatment and RetentionTom McLellanTreatment Research InstituteUniversity of PennsylvaniaUnited States
Evidence suggests that drug dependence is achronic medical illness with biological,psychological, and social components. Fortreatment to be as effective as possible it shouldaddress these aspects of illness with medication,therapy and counseling, and skill building.
A study looking at treatment for opiate addictionin pregnant women found that addressing theiraddiction in holistic manner with medication,counseling, job and family therapy andpsychiatric care yielded the best outcomes.
Disorders have a genetic, metabolic, andbehavioral influence. The nature of anindividual’s addictive disorder depends on bothinherent tendencies and vulnerabilities in
addition to behavior and environmentalinfluences.
Factors that predict poor outcomes forconditions such as asthma, diabetes, andhypertension treatment are the same as foraddiction, specifically: non-adherence to aphysician’s orders, low socioeconomic status,low family support for change; and psychiatriccomorbidity. Medication adherence and relapserates are similar across these illnesses.
Drug dependence produces significant andlasting changes in brain chemistry and function.Effective medications are available for treatingnicotine, alcohol, and opiate dependence but notstimulant or marijuana dependence. Drugdependence generally has been treated as if itwere an acute illness. However, researchsuggests that long-term care strategies ofmedication management coupled withbehavioral interventions and continuedmonitoring produce lasting benefits. Drugdependence should be insured, treated, andevaluated like other chronic illnesses.
Relapse Prevention and Recovery SupportD. Dwayne SimpsonTexas Christian UniversityUnited States
Numerous studies based on almost 300 drugabuse treatment programs and 70,000 patientsover the past 30 years have shown thattreatment can be highly effective in reducing oreliminating drug use, criminality, and relatedproblems. However, all patients do not have thesame needs and all programs are not equallyeffective, so treatment evaluation research hasbeen expanded in recent years to focusmaximizing treatment effectiveness andefficiency. General findings show that
• Problem severity dictates the appropriatetype and intensity of treatment needed.
• Patients with moderate-to-high problemseverity levels usually need at least 3months of treatment (and for chronic opiateaddiction, this increases to a year or longer)

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 174 Public Health-Public Safety
before significant benefits can bedocumented following release. As problemseverity increases the need for and benefitsof intensive residential care rises. Goodassessments of patient needs and progressare therefore essential.
• Cognitive stages of treatment readiness (ormotivation) influence the chances thatpatients will engage and benefit fromtreatment. Special cognitive-based“induction” strategies for poorly motivatedpatients can be effective antidotes,especially in correctional settings.
• Several distinct, sequential phases oftreatment (e.g., referral, induction,engagement, early recovery, and continuingcare) are related to addiction recoveryoutcomes of patients. Establishment oftherapeutic rapport is particularly important.
• Specialized interventions have beendeveloped that can improve each of thesecrucial steps of the therapeutic continuum.
• Research now being supported by severalfederal agencies emphasizes the need tounderstand and improve the manner inwhich treatment innovations can beeffectively introduced and used in treatmentprograms for community-based andcorrectional populations.
A System-Based ApproachSteve WingSubstance Abuse and Mental HealthServices AdministrationDepartment of Health and Human ServicesUnited States
Working in concert, justice and public healthagencies can establish a continuum ofaccountability and treatment for juvenile andadult offenders with substance use disorders.The criminal and juvenile justice systems shouldoperate in concert with other service systems asa series of opportunities for intervention withoffenders experiencing substance use disorders.Interventions should be carried out in a
systematic manner and at the earliest possibleopportunity.
Improving public safety and public healthrequires systematic interventions to bring aboutlong-term change in the substance abusing andcriminal behaviors of offenders. Treatment mustbe a priority of the justice system andincorporated into the routine practices anddecisions of justice officials. More than simplecoordination is required for the justice system towork effectively with public health serviceproviders, largely because the primary focus ofthe former is public safety, while the latterfocuses primarily on improving the lives ofindividual clients.
Policies and operational procedures must crossorganizational boundaries to make treatmentdecisions a critical element of justice decisions.Nine key elements have been identified to helpcommunities move beyond coordination ofprograms to full collaboration among communityagencies with integrated decisions and services,specifically:
1. Set the stage.Recognize substance abuse as a public healthand public safety problem that requires thecollective efforts of the health and justicecommunities working in an integrated fashion.
2. First things first.Identify areas where collaboration will result inlong-term benefits.
3. Treatment's contribution.Recognize treatment as a key element in crimecontrol. Treatment is not an ancillary service.Rather, treatment is important to the reductionof recidivism and substance seeking and abusingbehaviors.
4. The importance of assessment.Employ assessment protocols that address bothsubstance use and juvenile/criminal justicefactors.
5. Rational placement.Adhere strictly to placement based on anassessment of safety risk and the severity ofsubstance use disorders.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 175 Public Health-Public Safety
6. Individual treatment plans.Employ the assessment to develop an individualtreatment plan for each offender.
7. Rigorous case management.Manage offenders in treatment with testing,supervision, sanctions, and incentives. Adult andjuvenile offenders in treatment must be closelysupervised and their cases tightly managed.
8. Structured accountability.Be fair and predictable in delivering sanctionsand incentives. Offenders respond to situationsthat they believe are fair and just, and tosanctions and incentives that are uniformlyapplied.
9. Follow through.Extend the impact of treatment by providing acontinuum of supervision and support.
Oscar Fuentes FierroAttorney General’s Special Office forCrimes against Health (FEADS/PGR)Mexico
In Mexico, the public health and public safetysystems are linked in several ways. TheGovernment of Mexico has a national programto combat illegal drugs, of which the mainobjective is to combat drugs in its entiredimension including programs in drug demandreduction.
Mexico’s fundamental judiciary framework, theConstitution of Politics, sets forth severalimportant principles. Public safety is embodiedin Article 21 of the basic rule of the Mexicanpenal system, which establishes the authorityand rights of the Public Ministry for prosecutingcriminal acts. Article 73 describes coordinatedactivities that must be established among thefederation, the federal district, municipalities,and States, in matters of public safety. Article73 also establishes the organization, duties,selection, and promotion of members in publicsafety institutions.
Public health is considered a judiciary right ofthe people. The law, however, defines the basisand actions for access to public health servicesthat must be coordinated by the federation andthe States.
Diversion and Community Corrections:Pre-trial Diversion and Drug CourtsPre-Trial DiversionBarbara ZugorExecutive DirectorTreatment Assessment Screening Center(TASC)-ArizonaUnited States
Collaboration between the criminal justice andtreatment systems is essential in assuring thatall available resources are most appropriatelyutilized. Such services should based on athorough evaluation of the needs of theoffender.
System success depends on an objective,comprehensive needs assessment. The initialassessment of substance abuse involvedoffenders should be administered at acentralized location and can take place while theoffender is either in or out of custody. Theassessment process must respect the offender’sconstitutional and statutory rights and followguidelines regarding confidentiality. Acomprehensive treatment plan should becompleted at the earliest possible juncture afterentry into the criminal justice system.
Because no single factor causes substanceabuse disorders, and because the effects ofsubstance abuse extend to multiple areas of aperson’s life, it necessary to evaluate a widerange of individual and environmental factors. Acomprehensive treatment plan should be holisticin nature, covering, key components intreatment plan development also include theparticipation and active input of the offender,the knowledge of the treatment provider, andreferring or supervisory criminal justicepersonnel.

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 176 Public Health-Public Safety
The Women’s Treatment Network wasdeveloped to put these concepts into practice.At the time of the program’s inception there waslittle coordination between criminal justice andthe client service delivery systems for womenentering the system. TASC believed that for theprogram to be successful it must provide earlyintervention to the client on the individual,community, and criminal justice levels.Comprehensive treatment plans should take intoaccount the strengths and needs of theoffender, set realistic goals and objectives, andbe flexible to allow for unplanned orunforeseeable events. Establishing acoordinated service delivery system will helpclients get from treatment to success.
Drug CourtsTim MurrayOffice of Justice AssistanceDepartment of JusticeUnited States
Drug courts in the United States haveexperienced an evolutionary development. Inthe mid-1980’s, many states and local criminaljustice systems were inundated with felony drugcases. Drug courts began in 1989 as anexperiment by the Dade, Florida County FloridaCircuit Court to call upon the authority of asitting judge to devise – and proactively oversee– an intensive, community-based, treatment,rehabilitation, and supervision program for drugdefendants.
The goal of the drug courts was to halt rapidlyincreasing recidivism rates and reduce drugusage. The program is now underway in 48states as well as in the District of Columbia,Puerto Rico, Guam, a number of nativeAmerican tribal courts, and one federal districtcourt.
The appeal of the drug court lies in manysectors: more effective supervision of offendersin the community; more credibility to the lawenforcement function (where arrests of drugoffenders are taken seriously, even by courtsystems overwhelmed by cases); greateraccountability of defendants for complying with
conditions of release and/or probation; greatercoordination and accountability of publicservices provided; and more efficiency for thecourt system by removing a class of cases thatplaces significant resources demands forprocessing on the courts.
Since the program’s inception, close to 100,000drug dependent offenders have drug courtprograms with over 70% either still enrolled orgraduated. Drug court participants reflect allsegments of the community. Approximately66% are parents of minor children.Approximately 15% are veterans. Menparticipate at twice the rate of women althoughthe percent of female participants is rising.Many drug court participants have been usingdrugs for many years and most are poly-drugusers. A large proportion of participants hasnever been exposed to treatment previouslyalthough many have served jail or prison timefor drug-related offenses.
The original goals of drug courts of reducingdrug use and recidivism have largely beenachieved. Challenges however remain.Improving the system to address the repeatoffender remains an area for further work.However, with continued support from federal,state, and local jurisdictions, the advancesachieved under this program can be extendedeven further.
Incarceration: Adult PopulationsAllen AultNational Institute of CorrectionsDepartment of JusticeUnited States
In the United States, 60% of adult malearrestees tested positive for drugs. Eightypercent of men and women behind bars (1.4million) in the United States are seriouslyinvolved with alcohol and other drug use. Itcosts the United States $30 billion per year toincarcerate this population, with an averagelength of stay of 27 months.
Moreover, non-drug users in drug usinghouseholds are 11 times more likely to be killed
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 177 Public Health-Public Safety
compared to those in a drug free household.Drug abuse in a home increases a woman’s riskof being killed 28 times.
Treatment is essential to breaking the cycle ofdrug use and crime. It is important to note thatSanctions without treatment actually increaserecidivism. Inappropriate interventions alsoincrease recidivism.
The length of time in treatment is positivelycorrelated with treatment success. Treatmentassessment and matching inmates to necessaryservices yields better treatment outcomes.Programs that adopt combinations of treatmentcomponents that are suited to individual client’sproblems and needs are more successful than“one size fits all” inflexible programs.
Programs must provide a significant level ofstructure throughout assessment, treatmentplanning, supervision, and swift and certainsanctions. Rewards must be a part of thecorrectional treatment program. A segregatedtreatment unit is found to increase the likelihoodfor success. Segregation provides moretreatment accountability and structure.Transitional services provide significantly betteroutcomes than programs without transitionalservices.
There is a need for better informationdissemination to public and legislative groupsregarding what we know about treatmentprograms that work and how these effortsreduce costs and recidivism. Treatmentoutcomes could improve if there were moreoptions for matching inmates with the necessarytreatment and service needs, including inmateswith co-occurring illnesses. There is also a needfor more evaluation data that is useful tocorrection managers.
Substance abuse treatment coupled with post-release follow-up and support are highlysuccessful in reducing recidivism. Programsrequire both components for success.
Parole and Community CorrectionsDave GasparArizona Department of Juvenile CorrectionsUnited States
The Arizona Department of Juvenile Corrections(ADJC) is the state agency responsible forjuveniles adjudicated delinquent and committedto its jurisdiction by the county juvenile courts.ADJC is accountable to the citizens of Arizonafor the promotion of public safety through themanagement of the state's secure juvenilefacilities and the development and provision of acontinuum of services to juvenile offenders,including rehabilitation, treatment andeducation.
The Department is 10 years old, havingseparated from adult corrections in 1990. It hastwo responsibilities -- the first responsibility is tokeep the public safe and the second is tochange an adolescent’s life. ADJC’s efforts arebased on seven basic values:
• A good future requires a good foundation
• Valuing the safety of youth in our care andthe citizens of Arizona
• Believing that all individuals should have theopportunity to engage in continuousimprovement and learning
• Believing that all people, including the youthin our care, have the right to live productivelives
• Valuing all people regardless of where theyare in their development and who they areas individuals
• Valuing instilling hope in our youth andfamilies
• Valuing data and research-based decisionmaking.
The program begins with a 28-day assessmentperiod. Here, staff conduct a thoroughevaluation, including job skills and interests, andfocus on the key issues to be addressed for the
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 178 Public Health-Public Safety
individual. A number of secure housing facilitiesare available to provide a continuum of carebased on the severity of the problemspresented. Sixteen hours per day are dedicatedto programmed activities with six of those hoursspent in a learning environment. A major goalof the program is to penetrate delinquentthinking and catalyze personal change.
Through this approach of getting young peopleinvolved in education and changing delinquentthinking and behavior, the program gives theprogram participants an opportunity to see newlife paths and hopefully provide a chance at abetter life.
Jennifer MankeyDenver Juvenile Justice IntegratedTreatment NetworkUnited States
The Denver Juvenile Justice IntegratedTreatment Network was founded in 1995. Itspurpose is to bring a variety of juvenileoffender, substance abuse intervention andtreatment as well as other community agenciesto one table to identify ways to assist ininterrupting the cycle of delinquency andsubstance abuse. It is funded by the Center forSubstance Abuse Treatment, U.S. Department ofMental Health and Substance Abuse ServicesAdministration.
Comprised of every state and local juvenilejustice agency with responsibility for Denver'sjuvenile offenders, in addition to a wide varietyof other youth and family serving programs, theNetwork has made significant progress inexpanding access not only to substance abusetreatment but to other needed services in thecommunity for this population. In addition, theNetwork believes that one of the keys to longterm innovation and change within the youthservices community is an investment in currentand future generations of youth workersthrough establishment of a higher educationlink.
Ms. Mankey related the story of a child, David,which illustrated the juvenile justice system's
ability to fail when interventions are not doneearly enough. In his case opportunities forservices were missed, multiple systems andservices were involved but with no single entitywith lead responsibility, and there was no rolefor or engagement of his family.
In addressing the needs of juvenile offenders itis important that collaborative treatmentnetwork be organized to serve their particularneeds. Members of the treatment networkshould include law enforcement (includingparole), state and city agencies, public schools,family members and family advocacy groups,social service agencies, and substance abuseand mental health service agencies andproviders. Members should collectively identifybarriers and options for resolution. Thereshould be cross training for the purpose ofknowledge and skills development. Informationsystems should be integrated and the data usedto evaluate Network efforts.
In Denver this approach has resulted in moreyouth receiving more services and staying intreatment longer. Participants are showing anincreased ability to abstain from alcohol anddrug use, handle life problems, and stay inschool. There is a 23% decrease in theconviction rate one year after release on parole.
The system is also working more collaboratively.There is a more comprehensive intakeassessment conducted, an increase in referralswithin the system, more family involvement,improved case management, and enhancedcommunication and information sharing. Thechanges brought about by the Network have apositive impact on the system, youth,community, and families.
Dr. Hiram Suárez VillaOffice of Secretary of the GovernmentMexico
The Mexican Government agencies that addressprevention and social rehabilitation are
• Prevention and Social Rehabilitation• Prevention and Treatment for Adolescent

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 179 Public Health-Public Safety
• Adolescent Council• Patronage for Employment Social
Rehabilitation• Executive Coordination of Penitentiary
Infrastructure
We will only address two of these organizations,specifically:
• Prevention and Education whichformulates, coordinates, and evaluatessocial programs dealing with prevention andsocial rehabilitation of delinquent adults.
• Prevention and Treatment forAdolescents which runs all programs thataddresses preventing antisocial conductamong adolescents.
The administrative federation to support theseprograms manages five adult federal Institutionsand six for adolescents. Federal prisons foradults in Mexico include Guadalajara, Jalisco,and Matamoros (Tamaulipas), a penal colony inthe Marias Islands, and a Federal Center ofPsychological Rehabilitation.
The adolescent institutions, which arecomplemented with prevention programs fororientating and supporting the adolescent andtheir parents, are:
• The Diagnostic Center for Boys• The Diagnostic and Treatment Center for
Women• The Treatment Center for Men• The Special Needs Center• The Interdisciplinary Center for Walk-in
Treatment
Prevention programs are of utmost importanceand should be a fundamental part of treatmentprograms; this is because it is a sad reality thatdrug usage is high among adults andadolescents during the commission of a crime.The Mexican Government promotes the fight foreradication of this ill that equally affects,institutionalized adolescents and adults throughthe coordination of strategies and programs ofthe various Government’s administrative entities.
In Mexico pharmaco-dependent preventionprograms are a public health issue. Theirimplementation is of public and social interest.The Health Department is in charge ofimplementing these programs which, incoordination with State Governments, promoteand support:
• Prevention and treatment of drugdependency – the rehabilitation of drugdependent users.
• Education on the effects of drugs,psychotropic substances, and othersubstances of probable addiction, as well astheir social consequences.
• Education and instruction of the families andthe community on how to recognize thesymptoms of drug dependency in order toprovide timely prevention and treatment.
The Mexican Government has special interest ininvolving all of the essential health factions withthe penal authorities in charge of theinstitutionalized adult and adolescent populationthrough:
• the design of novel drug preventionprogram within the institution
• the development of lines of communicationwith society as a whole in order to developnew strategies that would reduce anderadicate this terrible epidemic thatthreatens the security and the health of ourcitizens.
Lilia Vasquez PortalesOffice of the Attorney General (PGR)Mexico
Drug usage in Mexico has increased in recentyears due to several factors. A major reason isthe availability of drugs derived from cashtransactions. The usage index has increasedprimarily in urban centers, tourist areas, andnorthern frontier towns. Linking drug usagewith the attorney’s office is difficult in caseswhere the usage of drugs is perceived duringthe commission of a crime and when cases

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 180 Public Health-Public Safety
involving possession of a controlled substanceare transferred to the Public Ministry.
To solve this problem the Mexican institutionsthat comprise the public safety and public healthsystems address the following:
• Substance abuse prevention and crimeprevention.
• Rehabilitation of drug addicts through:
− rehabilitation as an alternative to penalpunishment
− rehabilitation as part of socialreadaptation of the criminal.
The coordination of the public health and publicsafety institutions is addressed in the NationalProgram for Drug Control 1995-2000 (PNCD),which defines the objectives, strategies, andactions to be developed by the MexicanGovernment to confront drug issues. Thenational policy plan has as an objective todevelop complementary programs to reducedrug demand as well as availability. To achievethis goal coordination between twelveGovernment institutions is promoted.
In the area of drug consumption affecting publicsafety, an effort is being made to promote thecoordination between the public health andjustice departments, in order to prevent drugconsumption and to promote rehabilitation ofsubstance abusers, including those whose areon trial or incarcerated. This effort is beingsupported to facilitate the transition of thedelinquent into society.
Important advances have been made insubstance abuse prevention, the rehabilitation ofaddicts, and treatment as part of socialreadaptation. The Public Health Ministry, theState Department, as well as the AttorneyGeneral’s Office have played a fundamental role.There are specific procedures in place thatrequire the coordinated involvement of therespective authorities in concrete cases. Forexample, when a drug addict’s case has beentransferred to the Public Ministry, during theinitial stages of an existing investigation, or
when a penal process is being referred to thecorresponding judicial jurisdiction.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings NIDA Pre-Conference Session181
NATIONAL INSTITUTE ONDRUG ABUSE
(NIDA) PRE-CONFERENCE
SUMMARY

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings NIDA Pre-Conference Session182
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings NIDA Pre-Conference Session183
NATIONAL INSTITUTE ON DRUG ABUSE (NIDA) PRE-CONFERENCE SUMMARY
Developing a Bi-national Research AgendaU.S. – Mexico Cooperation on Drug Abuse Research
Phoenix, ArizonaMay 30, 2000
At a one-day meeting preceding the (Third U.S. – Mexico Bi-national Demand ReductionConference), Mexican and U.S. drug abuse researchers and officials met to discuss therecommendations of the work groups from the two previous bi-national conferences andto identify several potential collaborative research projects. Fifty-six participants fromboth Mexico and the United States came together for a daylong series of presentations,discussions and working group sessions. The meeting was organized by the NationalInstitute on Drug Abuse International Program in cooperation with the U.S. Office ofNational Drug Control Policy.
Welcoming participants, Dr. M. Patricia Needle, International Program Director, NIDAOffice of Science Policy and Communications, opened the meeting and encouragedattendees to network and exchange information regarding research about drug abuse andhealth consequences, as well as to establish future collaborative research initiatives. Sheadded that the comments, suggestions and ideas that emerged from this meeting wouldhelp structure the agenda for the next U.S.-Mexico conference.
Ms. Haydee Rosovsky, Mexican National Council Against Addictions, opened themorning presentations with her discussion of the benefits of exchanging data, instrumentsand information as steps toward building bi-national research cooperation. She alsoreviewed some of the important achievements in research cooperation between Mexicoand the United States over the past three years.
Dr. Richard H. Needle, U.S. Department of Health and Human Services, Office ofHIV/AIDS Policy, presented preliminary results from Rapid Assessment, Response andEvaluation (RARE) projects in three U.S. cities. The RARE methodology will beimplemented in racial and ethnic minority communities around the countrydisproportionately impacted by HIV/AIDS to better understand the changing dynamics ofHIV/AIDS and to implement feasible, science-based best practices to respond to theepidemics of HIV/AIDS and drug abuse in their communities.
Dr. Mary Jeanne Kreek, Rockefeller University, discussed from her extensive experiencein drug abuse science as a basic scientist and clinical researcher the importantcontribution of basic neuroscience for understanding addiction and the translation of thisknowledge into science-based best practices for prevention and treatment of drug abuseand the health consequences of abuse. Dr. Silvia Cruz, Cinvestav, served as a discussant

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings NIDA Pre-Conference Session184
and raised issues of importance for practitioners in implementing programs built onscientific research.
Dr. Judith Brook, Mt. Sinai School of Medicine, described the U.S. National Institutes ofHealth (NIH) grant application process and the advantages of collaboration betweenMexican and U.S. partners, especially NIDA-supported researchers, to secure researchfunding for joint projects. Dr. Brook also provided a list of current topics of specialrelevance in drug abuse research, based on priorities of NIDA and NIDA researchers.
Dr. Luciana Ramos, Mexican Institute of Psychiatry, and Dr. M. Patricia Needlediscussed funding mechanisms available in their respective countries for buildingresearch cooperation between Mexico and the United States. NIDA promotesinternational scientific collaboration in drug abuse through fellowships and grantmechanisms. Other NIH programs were also described.
Research information sessions featured presentations by Mexican and U.S. drug abusescientists, followed by work groups that explored issues on epidemiology and prevention,drug abuse treatment, and basic science. The work group participants developed goalsand objectives for future U.S.-Mexico research collaboration and presented them at theclosing plenary session. These recommendations are listed below.
Recommendations
1. Binational website and/or listserv to facilitate development of researchcooperation.
2. Second research pre-conference in 2001 (or next U.S.-Mexico Bi-nationalDemand Reduction Conference) with scientific presentations that feature bi-national (U.S.-Mexico) research collaborations.
3. Formalize a program of bi-national research cooperation. Topics of importancefor this group include: perception of risk in relation to drug abuse prevalence;program evaluation; HIV prevention interventions for drug abusers;implementation of rapid assessment, response and evaluation on U.S.-Mexicoborder; adolescent drug use, violence and HIV; gender differences, familyinfluences, women, social and cultural factors; patient-treatment matching; andcooperation in the basic science of drug abuse.
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 185 Other Conference Information
OTHER CONFERENCEINFORMATION
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 186 Other Conference Information
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 187 Acknowledgements
ACKNOWLEDGEMENTS
The Office of National Drug Control Policy (ONDCP) acknowledges the cooperation andsupport given by the following organizations and individuals of those sponsoring the event:
In the United States:
The Substance Abuse and Mental Health Services Administration (SAMHSA)The National Institute on Drug Abuse (NIDA)The U.S. Department of Education (ED)The U.S. Department of State, Bureau of International Narcotics and Law Enforcement Affairs
(INL)The U.S. Department of Justice, Drug Enforcement Administration (DEA) and Office of
Juvenile Justice and Delinquency Prevention (OJJDP)The U.S. Department of TransportationThe Arizona National Guard
In Mexico:
The Under-Secretariat for Disease Prevention and Control, Ministry of HealthThe National Council on Addictions (CONADIC), Ministry of HealthThe Directorate of Epidemiology, Ministry of HealthThe Mexican Institute of Psychiatry
The Conference Committee would also like to thank Periwinkle National Theatre and theirExecutive Director Sunna Rasch for their outstanding production of “Halfway There.”
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 188 Acknowledgements
Program Committee for the U. S. and Mexico
In the United States:
Ana AndersPublic Health AnalystOffice for Special PopulationsNational Institutes of HealthNational Institute on Drug Abuse
Gail BeaumontSenior Education Program SpecialistSafe and Drug-Free Schools ProgramUS Department of Education
John CampbellPublic Health AdvisorCenter for Substance Abuse TreatmentSubstance Abuse and Mental Health Services Administration
Javier M. Córdova (Conference Manager)Policy AnalystOffice of Demand ReductionOffice of National Drug Control Policy
Darlind DavisChief, Prevention BranchOffice of Demand ReductionOffice of National Drug Control Policy
Lorinda DanielSpecial Assistant to the AdministratorSubstance Abuse and Mental Health Services Administration
Kenneth EdgellDrug Enforcement and Program ComplianceU.S. Department of Transportation
Dan FletcherSpecial Assistant to the DirectorDivision of State and Community Systems DevelopmentCenter for Substance Abuse PreventionSubstance Abuse and Mental Health Services Administration
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 189 Acknowledgements
Sandra LawsonPolicy AnalystOffice of Demand ReductionOffice of National Drug Control Policy
Winnifred MitchellPublic Health AnalystOffice of Policy and Program CoordinationSubstance Abuse and Mental Health Services Administration
Bernard McCannPolicy AnalystOffice of Demand ReductionOffice of National Drug Control Policy
Mark MorganProgram ManagerOffice of Juvenile Justice and Delinquency Prevention
M. Patricia NeedleDirector, International ProgramOffice of Science Policy and CommunicationNational Institute on Drug Abuse
Barbara RobertsSenior Policy AnalystOffice of Demand ReductionOffice of National Drug Control Policy
Jane SanvillePolicy AnalystOffice of Demand ReductionOffice of national Drug Control Policy
Daniel SchecterDeputy Director for Demand Reduction (Acting)Office of National Drug Control Policy
Barbara WetherellSenior Prevention Programs ManagerDemand Reduction SectionOffice of Congressional and Public AffairsDrug Enforcement Administration

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 190 Acknowledgements
In Mexico:
Mtra. Haydée RosovskySecretaría TécnicaConsejo Nacional contra las Adicciones (CONADIC)
Lic. Nora Gallegos VázquezDirectora de NormatividadCONADIC
Lic. José Castrejón VacioDirector de ProgramasCONADIC
Mtra. Carmen Millé MoyanoDirectora de Capacitación e InformaciónCONADIC
Lic. Alejandro Arroyo DomínguezCoordinador AdministrativoCONADIC
Lic. Juan Nuñez GuadarramaSubdirector de Apoyo a la DescentralizaciónCONADIC
Lic. Patricia Reyes del OlmoSubdirectora de Coordinación SectorialCONADIC
Lic. Rosa Bonifaz PedreroSubdirectora de Documentación y DifusiónCONADIC
Lic. Teresa Sánchez FragosoSubdirectora de CapacitaciónCONADIC
Dr. Arturo OngaySubdirector de Desarrollo TécnicoCONADIC
Lic. Karen Aspuru JuárezJefa del Departamento de NormatividadCONADIC
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 191 Acknowledgements
Sra. Eda González RichmondSecretaria Particular de la C. Secretaría TécnicaCONADIC
Dra. Ma. Elena Medina MoraJefa de la División de Investigaciones Epidemiológicas y SocialesInstituto Mexicano de Psiquiatría (IMP)
Lic. Luis Ignacio Sánchez GómezDirector GeneralInstituto Mexicano de la Juventud (IMJ)

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings 192 Acknowledgements

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants193
EXHIBITORS
Arizona National Guard Demand Reduction California Department of Justice1614 West Roosevelt 4949 Broadway, Room #E-131Phoenix, Arizona 85007 Sacramento, California 95820(602)267-2901 Fax: (602)267-2474 (916)227-3220 Fax: (916)[email protected]
Centros de Integracion Juvenil A.C. Coalicion de Organizaciones Juveniles ParaLa Tlaxcala 208 - Col. Hipodromo Condesa Prevencion de AdiccionesMexico D.F. 06300 2a. Retorno Boulevard Jacarandas(525)286-9597 Fax: (525)286-9597 No. 22, Col. Lomas de [email protected] [email protected]
(527)316-2576 Fax: (527)216-2575
Consejo Nacional Contra Las Adicciones Counterdrug TechnologyAniceto Ortega 1321 1st Piso Col. Del Valle Assessment Center – (CTAC)Mexico D.F. 03100 ONDCPWashington D.C. 20503 750 17th Street, N.W., Suite 731(525)524-5600 Fax: (525)534-9024 Washington [email protected] (202)395-6761 Fax: (202)395-6775
D.A.R.E. Southwest Regional Training Center El Caracol A.C.3110 North 19th Avenue, Suite 290 Rafael Helidoro Valle No. 337Phoenix, Arizona 85015 Col. Lorenzo Boturini(602)223-2544 Fax: (602)279-0853 Mexico, D.F. Distrito Federal 15820
(525)768-1204 Fax: (525)[email protected]
Fiscalia Especializada Para La Atencion de Delitos Contra Fundacion AztecaLa Salud, PGR Vereda No. 80 Col. Jardines delPlaza de la Republica No. 43, 2o. Piso, Col. Tabacalera PedregalDeleg. Cuauhtemoc D.F. 06030 Mexico D.F. [email protected] (015)568-9303 Fax: (015)568-9309
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants194
Instituto Mexicano de La Juventud Narcotics Anonymous World.Serapio Rendon No. 76 Col. San Rafael Services, IncMexico D.F. 06470 19737 Nordhoff Place(525)536-1605 Fax: (525)535-9235 Chatsworth, California 91311
(818)773-9999 Fax: (818)[email protected]
National Institute on Drug Abuse (NIDA) Office of National Drug Control1375 Piccard Drive, Suite 360 Policy (ONDCP)Rockville, Maryland 20850 P.O. Box 6000(240)632-5624 Fax: (240)632-0519 Rockville, Maryland [email protected] (301)519-5520 Fax: (301)519-5212
Operadora Oceanica Internacional, S.A. de C.V. Organizacion Panamericana de LaPorfiro Diaz No. 102 P.H. 01 Col. Nochebuena SaludMexico D.F. 03720 5400 Suncrest C-4(525)615-3001 Fax: (525)611-2207 El Paso Texas 79912oceanica(arroba).spin.com.mx (915)845-5950 Fax: (915)845-4361
Substance Abuse and Mental Health Services U.S. - Mexico Border CenterAdministration(SAMHSA) for the Application of PreventionP.O. Box 2345, Suite 200 TechnologiesRockville, Maryland 20847-2345 2501 East Elm Street(800)729-6686 Fax: (301)468-6433 (520)545-2970 Fax(520)[email protected] [email protected]
U.S. Department of Education United Nations International Drug 400 Maryland Avenue, S.W. Control ProgrammeWashington D.C. 20202-6123 Masarik #29, Col. Chapultepek(202)260-2673 Fax(202)260-7767 [email protected] Mexico D.F. 11570
(525)545-2970 Fax:(525) [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants195
SPEAKERS FROM THE UNITED STATES
Luz Arriola Allen AultProgram Director ChiefWest Texas Council on Alcoholism and Drug Abuse U.S. Department of Justice3210 Dyer Street Washington, D.C. 20534El Paso, Texas 79930 (202)307-3995 Fax: (202)305-2185(915)577-0791 Fax: (915)577-0799 [email protected]@msn.com
Kristen Barry Andrea G. BarthwellUniversity of Michigan President(734)930-5127 Fax: (734)930-5150 Encounter Medical [email protected] 1010 Lake Street, Suite 210
Oak Park, Illinois 60301(708)383-2700 Fax: (708)[email protected]
Mary Bernstein Jennifer BishopDirector, Office of Drug and Alcohol Policy and Office of National Drug Control PolicyCompliance Washington, D.C.U.S. Department of Transportation400 7th Street, S.W., Room 1403Washington, D.C. 20590(202)366-3784 Fax: (202)366-3897
Philmer Bluehouse Edward BrandSafe Schools Director SuperintendentPinon United School District #4 Sweetwater Union DistrictP.O. Box 839 1130 5th AvenuePinon, Arizona 86510 Chula Vista, California 91911(520)725-3450 Fax: (520)725-3278 (619)691-5555 Fax: (619)498-1997
Alejandra Castillo Nelba ChavezOffice of National Drug Control Policy Administrator, SAMSHAThe White House 5600 Fishers Lane, 12-105Washington, D.C. 20503 Rockville, Maryland 20857
(301)443-4795 Fax: (301)[email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants196
John D. Clapp Ann ClarkResearch Director SupervisorCollege of Health & Human Svcs Houston Independent School DistrictSan Diego State University 3830 Richmond AvenueSan Diego, California 92182-4119 Houston, Texas(619)594-6859 Fax: (619)594-5991 (713)892-6690 Fax: (713)[email protected]
H. Westley Clark Timothy P. CondonDirector Associate DirectorSubstance Abuse&Mental Health Svcs. Admin. National Institute on Drug Abuse6001 Executive Boulevard, Room 5263 MSC 9591 U.S. Department of Health & Human SvcsBethesda, Maryland 20852 Rockville, Maryland 20857(301)443-6480 Fax: (301)443-9127 (301)443-5700 Fax: (301)443-8751
Jeffrey Davidow George De LeonAmbassador to Mexico Director
National Development and ResearchInstitutes, Inc.World Trade CenterNew York, New York 10048(212)845-4417 Fax: (212)[email protected]
Richard Dembo Elizabeth EdwardsProfessor Executive DirectorUniversity of South Florida Arizonans for a Drug-Free Workplace4202 East Fowler Avenue P.O. Box 13223Tampa, Florida 22620-8100 Tucson, Arizona 85732-3223(813)931-3345 Fax: (813)933-1146 (520)295-5962 Fax: (520)[email protected] [email protected]
Martha Fletcher Gabriela GarciaProgram Specialist AdministratorLeon County School District Arizonans for a Drug-Free Workplace500 North Appleyard Drive P.O. Box 13223Tallahassee, Florida 32304 Tucson, Arizona 85713(850)487-7598 Fax: (850)487-7614 (520)295-5962 Fax: (520)[email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants197
David Gaspar Isabel Gomez-BassolsArizona Department of Juvenile Corrections Radio Unica NetworkUnited States (305)463-5045 Fax: (305)463-5001
Aimee Graves Melody M. HeapsDirector of Community Based Services PresidentCODAC Behavioral Health Services, Inc. TASC, Inc.Tucson, Arizona 1500 North Halsted Street
Chicago, Illinois 60622(312)787-0208 Fax: (312)[email protected]
Robin Hoskins Tom HutchinsonExecutive Director Prehab of ArizonaWomen's Treatment Network (480)464-9669 Fax: (480)969-1509Phoenix, Arizona(602)506-6456 Fax: (602)506-5381
Susan Kunz Sandra Owens LawsonDirector Office of National Drug Control PolicyU.S. - Mexico Border Center for the Application of Washington DCPrevention Technologies 202)395-6750 Fax: (202)395-67442501 East Elm StreetTucson, Arizona 85716(520)795-9756 Fax: (520)[email protected]
Henry Lozano Jennifer MankeyPresident DirectorCalifornians for Drug Free Youth Denver Juvenile Justice Treatment Network333 West Colfax Avenue, Suite 400 Denver, Colorado 80204
(303)893-6898 Fax: (303)893-6848 [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants198
Antonieta Martin Duane McBrideResearcher Professor and ChairJohn Hopkins University Andrews University
Berrien Springs, Michigan 49104(616)471-3576 Fax: (616)[email protected]
Barry R. McCaffrey Bernard McCannDirector Office of National Drug Control PolicyOffice of National Drug Control Policy Washington D.C.Washington D.C. (202)395-3096 Fax: (202)395-6744
Tom McLellan Lorenzo MerrittTreatment Research Institute Project Heavy West150 South Independence Mall 1600 Sawtelle Boulevard, Suite 300Philadelphia, Pennsylvania 19106-3475 Los Angeles, California 90025(215)399-0980 Fax: (215)399-0987 (310)477-1291 Fax: (310)477-1373
William Modzeleski Harry MontoyaDirector, Safe and Drug Free Schools Program President/CEOU.S. Department of Education Hands Across Cultures, Inc.400 Maryland Avenue, S.W., Room 3E314 P. O. Box 2215Washington, D.C. 20202-6123 Espanola, New Mexico 87532(202)260-3954 Fax: (202)260-7767 (505)747-1889 Fax: (505)[email protected] [email protected]
Tim Murray Eileen O'BrienBureau of Justice Assistance Senior Enterprise DevelopmentDepartment. of Justice Office on Early ChildhoodWashington, DC 5600 Fishers Lane(202)616-8933 Fax: (202)307-0036 Rockville, Maryland 20857
(301)443-7762 Fax: (301)[email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants199
Jeanne Obert Eugenia OrtegaExecutive Director, Matrix Institute on Addictions SuperintendentUniversity of California at Los Angeles California Youth Authority12304 Santa Monica Boulevard, Suite 200 7650 South New Castle RoadLos Angeles, California 90025 Spockton, California 952139002(310)207-4322 Fax: (310)207-6511 (209)944-6331 Fax: (209)[email protected] [email protected]
Mark W. Parrino Luisa Del PollardPresident SAMHSAAmerican Methadone Treatment Association 5600 Fishers Lane217 Broadway, Suite 304 Rockville, Maryland 20857New York, New York 10007 (301)443-6728(212)566-5555 Fax: (212)349-2944 [email protected]@aol.com
Amelie Ramirez Rosalia SalinasAssoc. Professor, Department of Medicine Director, Curriculum Instruction andBaylor College of Medicine Assessment8207 Callaghan Road, Suite 110 6401 Linda Vista RoadSan Antonio, Texas 78230 San Diego, California 92111(210)348-0255 Fax: (210)348-0554 (858)292-3522 Fax: (858)[email protected] [email protected]
Ruth Sanchez-Way Dan SchecterActing Center Director Acting Deputy DirectorSAMHSA Office of National Drug Control Policy5600 Fishers Lane Washington, DC 20503Rockville, Maryland 20857 (202)395-6733 Fax: (202)395-6744(301)443-0365 Fax: (301)443-5447 [email protected]@SAMHSA.gov
Beverly Schwartz Stephen ShearerSenior Vice President ConsultantFleishman Hillard, Inc. Stephen Shearer, Inc.1615 L Street, N.W., #1000 446 Upland RoadWashington, D.C. 20036 Redwood City, California 94062(202)828-8820 Fax: (202)223-8199 (650)599-9007 Fax: (650)599-9008

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants200
D. Dwayne Simpson Mark SimpsonDirector FMC LexingtonTexas Christian University 3301 Leestown RoadTCU Box 298740 Drug-Free Communities Support ProgramFort Worth, Texas 76129 Lexington, Kentucky 40511(817)257-7226 Fax: (817)257-7290 (606)253-8839 Fax: (606)[email protected] [email protected]
Mary Ann Solberg Robert StephensonChair Acting DirectorDrug-Free Communities Support Program SAMHSA/CSAP
Forrest Van Camp Abraham WandersmanExecutive Director, Area 3 University of South CarolinaLeon County Schools Barnwell College2757 West Pensacola Street Columbia, South Carolina 29208Tallahassee, Florida 32304 (803)777-7671 Fax: (803)777-9558(850)487-7525 Fax: (850)[email protected]
Mark Weber David WertheimerDirector Service and Systems IntegrationSAMHSA King County Department of Community5600 Fishers Lane and Human ServicesRockville, Maryland 20857 Seattle, Washington 98104zz(301)443-8956 Fax: (301)443-9050 (206)[email protected] [email protected]
John W. Wilson Steve WingActing Administrator Senior Advisor for Drug PolicyU.S. Department of Justice SAMHSA810 Seventh Street, N.W. 5600 Fishers LaneWashington, D.C. 20531 Rockville, Maryland 20857(202)307-5911 Fax: (202)307-2093 (301)443-0593 Fax: (301)443-7590
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants201
Terry Zobeck Barbara ZugorOffice of National Drug Control Policy Executive DirectorWashington, D.C. 20503 TASC – Arizona(202)395-5503 Fax: (202)395-6729 2234 North 7th Street
Phoenix, Arizona 85006(602)254-7328 Fax: (602)255-0851

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants202
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants203
SPEAKERS FROM MEXICO
Norma Amerena Jose Luis Perez BautistaCONADIC Presidente
Asociación Nacional de Padres deFamilia
Mario Bejos Fernando BilbaoLiber-Addictus CONADIC
Rosa Bonifaz Roberto CantoCONADIC Juventud, Luz y Esperanza
Jose Vila del Castillo José CastrejonRepresentative for Mexico and Central America CONADICDirector de Operacion y ComunicacionUnited Nations International Drug ControlProgramme (UNDCP)
Eduardo Chacon José Antonio Gonzalez FernandezFundacion Azteca Secretary of HealthVereda No. 80 Jardines del Pedrega
Rafael Velasco Fernandez Oscar Fuentes FierroPresident Fiscalia Espcializada Para La deCenter in Studies on Alcohol and Alcoholism Delitos(CESAAL) Contra La Salud, PGR
Carlos FrancoBaja School District
Maria Teresa Sanchez Fragoso Nora GallegosCONADIC CONADIC
Juan Roman Uriarte Galvan Jesus GarciaSecretariat of Communications and Transportation Instituto Mexicano de la Juventud(SCT)
Juan Rebolledo Gout Victor Manuel Guisa Centros de Integracion Juvenil
Jorge Machado Jorge MadrazoFunadacion Azteca Attorney General
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants204
Jorge Sanchez Mejorada Norma MerenaResearcher Council of Addictions CONADICVeracruzana University Mexican Ministry of Health
Carmen Mille Lorenzo MorinCONADIC Secretario de Educacion, BajaCalifornia
Juan Nuñez Marisa OcequeraCONADIC Latin American Institute for Family
Studies
Jose Luis Navarro Padilla Arturo Ongay PerezDIF CONADICMartin Perez Roberton Bital PinedaEl Caracol Mexico
Elizabeth Preciado Ignacio Carrillo PrietoFEADS Ministry of Interior
Jaime Quintanilla Luciano RamosCentros de Integracio Juvenil Mexican Institute of Psychiatry
Maria Elena Ramos Ignacio Benedicto ReyesPrograma Companeros, A.C. Baja California
Mario Alva Rodriguez Haydee RosovskyINACIPE CONADIC
Manuel Carbajal Ruiz Ninfa SadaCESAD Fundación Azteca
Mexico
Wilfred Rios Sanchez Jesus Cabrera SolisFEADS, PGR Center for Youth Integration
Agustin Velez Hiram Juarez VillaGeneral Director SEGOBTrusteeship for the Institute for Street Kids andAddictions (FINCA)
Mr. Raul ZapataYouth Integration Centers
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants205
ATTENDEES FROM THE UNITED STATES
Ms. Ana Anders Dr. Rudy ArredondoNIDA-NIH Texas Tech University-Health Science6001 Executive Boulevard CenterBethesda, Maryland 20892 3601 4th Street(301) 443-0441 Fax: (301) 480-8179 Lubbock, Texas [email protected] (806) 743-2800 Fax: (806) 743-4250
Mr. Luz Arriola Ms. Linda J. AugensteinWTCADA Tucson Unified School District #13210 Dyer Street 2025 E. WinsettEl Paso, Texas 79930 Tucson, Arizona 85719(915) 577-0791 Fax: (915) 577-0799 (520) 617-7174 Fax: (520) [email protected] [email protected]
Dr. Allen Ault Dr. Kristen BarryNational Institute of Corrections University of Michigan320 First Street, NW 400 E. Eisenhower ParkwayWashington, D.C. 20534 Ann Arbor, Michigan 48108(203) 307-3106 Fax: (202) 305-2185 (734) 930-5127 Fax: (734) [email protected] [email protected]
Mr. Carl Battistone Ms. Gail BeaumontLions Clubs International U.S. Department of Education1260 Delfield Drive 400 Maryland Avenue, S.W.Bethel Park, Pennsylvania 15102-2454 Room 3E310(412) 831-0540 Fax: (412) 831-0227 Washington, D.C. [email protected] (202) 260-2673 Fax: (202) 260-7767
Ms. Mary Bernstein Mr. Jeffrey BillingsU.S. Department of Transportation Border Health Initiative400-7th Street, SW, Suite 10403 148 E. 30th Street, Suite Up-SouthWashington, D.C. 20590 National City, California 91950(202) 366-3784 Fax: (202) 366-3897 (619) 791-2610 Fax: (619) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants206
Ms. Jennifer Bishop Mr. John BlackburnOffice of National Drug Control Policy Maricopa County Attorney's OfficeWashington D.C. 301 W. Jefferson
8th FloorPhoenix, Arizona 85003-2151(602) 506-3411 Fax: (602) 506-8102
Mr. Philmer Bluehouse Ms. Kimberley Bonnington KouriPinon Unified School District #4 Greater Detroit Area Health CouncilP.O. Box 839 333 West Fort Street, Suite 1500Pinon, Arizona 86510 Detroit, Michigan 48226(520) 725-3450 Fax: (520) 725-3278 (313) 965-4115 Fax: (313) 965-2031
Ms. Madeline Duran Bosma Ms. Joan BoughtonOracle Board of Education Rotary International65820 E. Rocky Trail Drive 1333 Camino LoradoTucson, Arizona 85739 Lake San Marcos, California 92069(520) 825-5270 Fax: (520) 825-5271 (760) 736-4700 Fax: (760) [email protected] [email protected]
Mr. Michael Branham Mr. John CampbellArizona Criminal Justice Commission HHS3737 North 7th Street Rockwall II, Suite 619Suite 260 5600 Fishers LanePhoenix, Arizona 85014 Rockville, Maryland 20857(602) 728-0752 Fax: (602) 728-0752 (301) 443-9299 Fax: (301) 480-6077
Ms. Linda Carrier Ms. Gail ChadwickGovernor's Community Policy Office Arizona State University3800 North Central Avenue, Suite 1500 641 East Van Buren, Suite B-2Phoenix, Arizona 85012 Phoenix, Arizona 85004(602) 280-1365 Fax: (602) 280-1470 (480) 727-2772 Fax: (480) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants207
Ms. Anna Chisman Ms. Joanne CisnerosCICAD/OAS U.S. DOT/FMCSA1889 F. Street, NW 22690 Cactus AvenueWashington, D.C. 20006 Suite 250(202) 458-6221 Fax: (202) 458-3658 Moreno Valley, California [email protected] (909) 653-2299 Fax: (909) 653-6969
Dr. John D. Clapp Ms. Ann B. ClarkSan Diego State University Houston Independent School District5500 Campanile Drive 3830 Richmond AvenueSan Diego, California 92182 Houston, Texas 77027(619) 594-6359 Fax: (619) 594-5991 (713) 892-6690 Fax: (713) [email protected] [email protected]
Dr. H. Westley Clark Mr. Timothy P. CondonHealth and Human Services National Institute on Drug Abuse5600 Fishers Lane 6001 Executive BlvdRockwall II, Suite 619 Room 5263, MSC 9591Rockville, Maryland 20857 Bethesda, Maryland 20852(301) 443-5700 Fax: (301) 443-8751 (301) 443-6036 Fax: (301) [email protected] [email protected]
Mr. Javier Cordova Mr. Gerardo De CosioONDCP Pan American Health OrganizationWashington D.C. 20503 5400 Suncrest Drive C-4(202) 395-3000 El Paso, Texas [email protected] (915) 845-5950 Fax: (915) 845-4361
Ms. Margaret Cossey Mr. Bill CraneCalifornia Department of Alcohol and Drug Alcohol and Drug ServicesPrograms Health and Human Services Agency1700 K Street, 2nd Floor P.O. Box 85222Sacramento, California 95814-4037 California 92186-5222(916) 324-4468 Fax: (916) 323-0633 (619) 692-5762 Fax: (619) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants208
Ms. Laura Cummings Ms. Lorinda DanielSTCADA SAMHSA1502 Laredo, Suite 2 5600 Fishers LaneLaredo, Texas 28040 Parklawn Building, Room 12-105(800) 487-7752 Fax: (956) 725-0236 Rockville, Maryland
(301) 443-5337 Fax: (301) 442-0284
Major General (Ret.) Arthur T. Dean Mr. George DeLeonCommunity Anti-Drug Coalitions of America Center for Therapeutic Community901 North Pitt, Suite 300 ResearchAlexandria, Virginia 22314 2 World Trade Center(703) 535-8530 Fax: (703) 706-8088 16th [email protected] New York, New York 10048
(212) 845-4417 Fax: (212) [email protected]
Dr. Richard Dembo Mr. Mark F. DemersUniversity of South Florida National Drug Intelligence Center4202 E. Fawler Avenue 319 Washington StreetTampa, Florida 33620 5th Floor(813) 931-3345 Fax: (813) 933-1146 Johnstown, Pennsylvania [email protected] (814) 532-4028 Fax: (814) 532-4690
Mr. Paul J. DeWispelaere Mr. Alejandro DuranPRIDE Youth Programs DEA4684 S. Evergreen 3010 North 2nd StreetNewayso, Michigan 49337 Phoenix, Arizona 85012(800) 668-9277 Fax: (231) 652-2461 (602) 664-5600 [email protected]
Mr. Kenneth Edgell Ms. Elizabeth EdwardsDepartment of Transportation Arizonans for a Drug-Free Workplace400 7th Street, SW P.O. Box 13223Room 9404 Tucson, Arizona 85732Washington, D.C. 20590 (520) 295-5962 Fax: (520) 295-5979(202) 366-3784 Fax: (202) [email protected]

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants209
Mr. A.J. Ernst Ms. Calvina FayATCMHMR Drug Free America Foundation909 W. 45th Street P.O. Box 11298P.O. Box 12668 St. Petersburg, Florida 33733Austin, Texas 78711 (727) 893-2616 Fax: (727) 893-2563(512) 206-4763 Fax: (512) 206-4784 [email protected]@mhmr.staff.tx.us
Mr. Joáo Ferreora-Pinto Mr. Dan FletcherUniversity of Texas, Houston Division of State and Community1100 North Stanton # 110 Systems DevelopmentEl Paso, Texas Center for Substance Abuse Prevention(915) 747-8507 Fax: (915) 747-8512 5515 Security Lanejoá[email protected] Rockville, Maryland 20875
(301) 443-5660 Fax: (301) 443-0526
Ms. Martha Fletcher Ms. Gabriela Garcia-HeadLeon Co. Schools Arizonans for a Drug-Free Workplace500 N. Appleyard Drive P.O. Box 13223Tallahassee, Florida 32304 Tucson, Arizona 85713(850) 922-2099 Fax: (850) 487-7614 (520) 295-5962 Fax: (520) 295-5979
Mr. Jose Gonzalez Ms. Aimee GravesDepartment of Alcohol and Drug Programs CODAC Behavioral Services, Inc.1700 K Street Tucson, ArizonaSacramento, California 95814 (520) 327-4505 Fax: (520) 792-0033(916) 445-0860 Fax: (916) [email protected]
Ms. Melody Heaps Ms. Brenda HendersonTASC, Inc. Governor's Office1500 N. Halsted St. 1700 West WashingtonChicago, Illinois 60622 Phoenix, Arizona 85007(312) 573-8203 Fax: (312) 787-8214 (602) 542-6003 Fax: (602) [email protected] [email protected]

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants210
Mr. Eduardo Hernandez Ms. Sally HolcombCal Partners Coalition Southeastern Arizona Behavioral909 12th Street ServicesSuite 205 382 E. WilcoxSacramento, California 95814 Sierra Vista, Arizona 85635(916) 442-3760 Fax: (916) 447-7052 (520) 459-6377 Fax: (520) [email protected] [email protected]
Mr. Charles E. Holzer Ms. Sheila HoppeUniversity of Texas- Medical Branch Governor's Division of Drug Policy301 University Boulevard 1700 W. WashingtonGalveston, Texas 77555-0189 Room 101(409) 747-8362 Fax: (409) 747-8364 Phoenix, Arizona [email protected] (602) 542-3406 Fax: (602) 542-3643
Ms. Sonja J. Hoppe Mr. Pedro JanerSouthwest Laboratories, Inc. Drug Enforcement Administration2727 W. Baseline Suite #1 1880 Regal RowTempe, Arizona 85283 Dallas, Texas 75235(602) 438-8507 Fax: (602) 438-2737 (972) 574-2111 Fax: (974) [email protected] [email protected]
Mr. Ricardo Jasso Ms. Mary Ann JaurequiLuz Social Services Border Area Mental Health345 E. Toole P.O. Box 1349Suite 101 Silver City, New Mexico 88062Tucson, Arizona 85701 (505) 388-4497 Fax: (505) 534-1150(520) [email protected]
Ms. Susan Jones Mr. Kaare KjosDrugs Don't Work in Arizona San Diego Joint Border Initiative3010 N. 2nd Suite, Suite 301 2838 Granada AvenuePhoenix, Arizona 85012 San Diego, California 92104(602) 248-8453 Fax: (602) 664-5627 (619) 285-1725 Fax: (619) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants211
Mr. Thomas C. Kring Ms. Susan KunzUSDHHS/HRSA Border Health Foundation50 United Nations Plaza Suite #349 2501 East Elm StreetSan Francisco, California 94102 Tucson, Arizona 85716(415) 437-8090 Fax: (415) 437-7664 (520) 795-9756 Fax: (520) [email protected] [email protected]
Ms. Janet Lander Mr. Ronald LardArizona Department of Education D.A.R.E. International1535 West Jefferson 4916 Lincoln AvenuePhoenix, Arizona 85007 Alexandria, Virginia 22362(602) 542-8717 Fax: (602) 542-3818 (703) 750-3321 Fax: (703) 750-7844
dareintrel@
Ms. Cheri Levenson Mr. John LewisArizona Department of Education Alberta Tippecconnic1535 West Jefferson, Mail Bin 6 2214 N. Central AvenuePhoenix, Arizona 85007 Suite 100(602) 542-5045 Fax: (602) 542-5467 Phoenix, Arizona [email protected] (602) 258-4822 Fax: (602) 258-4825
Dr. Don LivingstonCroft Workplace Drug Programs Mr. Henry Lozano4659 S.Lakeshore Drive Californians for Drug-Free Youth, Inc.Suite B P.O. Box 826Tempe, Arizona 85282 Big Bear City, California 92314-0826(480) 496-9116 (909) 584-1170 Fax: (909) 584-4485
Mr. Matthew G. Maggio Ms. Jennifer MankeyNational Drug Intelligence Center Denver Juvenile Justice Network319 Washington Street 333 W.Colfax Ave. .5th Floor #400Johnstown, Pennsylvania 15901 Denver, Colorado 80204(814) 532-4989 Fax: (814) 532-4690 (303) 893-6898 Fax: (303) [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants212
Mr. Ricardo Martinez Mr. Alberto MataSTCADA University of Oklahoma207 Fal St 601 Elm AvenueHeldoronville, Texas 78361 Room 728(361) 527-5132 Fax: (361) 527-4311 Norman, Oklahoma 73019
(405) 325-1756 Fax: (405) [email protected]
Ms. Pastora C. Maytorena Mr. Bernie McCannSan Diego Health Alliance ONDCP234 North Magnolia Avenue Washington, D.C. 20503El Cajon, California 92020 (202) 395-3096 Fax: (202) 395-6744(619) 579-8373 [email protected]
Ms. Lorenza Mena Ms. Adriana MendioleaU.S.-Mexico Border Health Association U.S. Consulate Tijuana5400 Suncrest Drive P.O. Box 439039Suite C5 San Diego, California 92143-9039El Paso, Texas 79912 (6 ) 681-7400 Fax: (6 ) 681-8592(915) 833-6450 Fax: (915) 883-7840 [email protected]@usmbha.org
Mr. Julio Mercado Mr. Lorenzo MerrittDrug Enforcement Administration Project Heavy-West700 Army Navy Drive 1600 Sawtelle BlvdArlington, Virginia 22202 Los Angeles, California 90019(202) 307-7345 Fax: (202) 307-4540 (310) 477-1291 Fax: (310) 477-1373
Mr. Dennis Metrick Mr. John MilesArizona Supreme Court CDC1501 West Washington 1600 Clifton Road, NERoom 410 Mail Stop E-07Phoenix, Arizona 85007 Atlanta, Georgia 30333(602) 542-9453 Fax: (602) 542-9480 (404) 639-8011 Fax: (404) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants213
Ms. Winnifred Mitchell Mr. David MonnetteSAMHSA-HHS Drug Enforcement Administration5600 Fishers Lane 660 N. Mesa Hills, Suite 2000Parklawn Building, Room 12C-105 El Paso, Texas 79912Rockville, Maryland 20857 (915) 832-6000 Fax: (915) 832-6001(301) 443-2324 Fax: (301) [email protected]
Mr. Harry Montoya Mr. Jack G. MoortelHands Across Cultures Paradise Valley School DistrictP.O. Box 2215 15002 North 32nd StreetEspanola, New Mexico 87532 Phoenix, Arizona 85032(505) 747-1889 Fax: (505) 747-1623 (602) 867-5124 Fax: (602) [email protected] [email protected]
Mr. David Morales Mr. Mark MorganTexas Commission on Alcohol and Drug Abuse OJJDP-SEDP.O. Box 80529 810 7th Street, NWAustin, Texas 78708-5233 Room 3307(512) 349-6721 Fax: (512) 837-8624 Washington, D.C. [email protected] (202) 353-9243 Fax: (202) 353-9095
Dr. M. Patricia Needle Dr. Andrew NicholsNIDA Border Health Foundation9000 Rockville Pike 2501 East Elm StreetBuilding 31, Room 1B59 Tucson, Arizona 85716Bethesda, Maryland 20892 (520) 626-7862 Fax: (520) 321-7763(301) 594-1928 Fax: (301) [email protected]
Dr. Eileen O'Brien Ms. Laura O'NeilThe Casey Family Program Sunnyslope Village Alliance5515 Security Lane 8827 N. CentralRockwall II, Suite 950 Phoenix, Arizona 85021Rockville, Maryland 21144 (602) 395-9847 Fax: (602) 749-0618(301) 443-6323 Fax: (301) 443-7878 [email protected]@samhsa.gov

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants214
Ms. Stephania O'Neill Mr. Dee OgleScottsdale Prevention Institute Texas Commission on Alcohol and Drug7428 East Stetson, Suite 215 AbuseScottsdale, Arizona 85251 P.O. Box 80529(480) 994-0004 Fax: (480) 994-3922 Austin, Texas [email protected] (512) 349-6655 Fax: (512) 837-8624
Mr. Eduardo Olivarez Mr. Ranaldo OllieRio Grande Valley Council on AlDA Drug Enforcement Administration3511 West Alberta 1433 West Loop SouthEdinburg, Texas 78539 Suite 600(956) 928-1996 Fax: (956) 928-0004 Houston, Texas [email protected] (713) 693-3354 Fax: (713) 693-3153
Ms. Eugenia Ortega Dr. Luis S. OrtegaCalifornia Youth Authority Arizona Department of Health ServicesP.O. Box 213002 3815 North Black Canyon HighwayStockton, California 95213 Phoenix, Arizona 85015(209) 944-6331 Fax: (209) 465-4164 (602) 230-5880 Fax: (602) [email protected] [email protected]
Ms. Rosa Ortega Mr. Vincent OrtegaCompañeros Southern New Mexico IncDouglas, Arizona P.O. Box 1008 P.O. Box 2285(520) 364-8200 Fax: (520)364-5617 Las Cruces, New Mexico [email protected] (505)882-5101 FaxL (505) 882-2858
Ms. Enid Osborne Ms. Sylvia ParraState of New Mexico Department of Health Tohono O'odham Nation1190 Saint Francis Drive P.O. Box 837Santa Fe, New Mexico 87502 Sells, Arizona 85634(505) 827-1643 (520) [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants215
Mr. Mark W. Parrino Mr. Roger PisaniAmerican Methadone Treatment Association 33 Harding Road217 Broadway, Suite 304 Old Greenwich, Connecticut 6870New York, New York 10007 (203) 698-0433 Fax: (203) 698-0433(212) 566-5555 Fax: (212) 349-2944 [email protected]
Ms. Luisa Pollard Mr. Richard RamirezSAMHSA/CSAP Tohono O'odham NationRockwall II, Room 800 P.O. Box 8375600 Fishers Lane Sells, Arizona 85634Rockville, Maryland 20857 (520) 383-2221(301) [email protected]
Special Agent Ricardo Ramos Ms. Kathy RiceDrug Enforcement Administration Arizona Department of Education8400 NW 53rd Street 1535 West Jefferson, Bin 7Miami, Florida 33166 Phoenix, Arizona 85007(305) 590-4804 Fax: (305) 590-4437 (602) 542-8713 Fax: (602) 542-3818
Mr. Kenneth Rodgers Mr. Ambrose RodriguezFMCSA Department of Mental Health400 7th Street, SW 3333 Wilshire BoulevardWashington, D.C. 20590 Suite 820(202) 316-4016 Los Angeles, California [email protected] (213) 738-2882 Fax: (213) 384-0729
arodriguez @dmh.co.la.ca.us
Mr. Galen E. Rogers Ms. Cecilia RosalesSan Diego Health Alliance Arizona Department of Health234 N. Magnolia 4949 E. Fifth StreetEl Cajon, California 92020 Tucson, Arizona 85716(619) 579-8373 Fax: (619) 579-8155 (520) 795-1531 Fax: (520) 795-1816
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants216
Ms. Lucy Rosario Mr. Jacob L. RuedaJuntos Unidos HRSA- Border HealthP.O. Box 310 3815 No. Black Canyon HighwayNogales, Arizona Phoenix, AZ 85015(520) 761-4412 Fax: (520) 761-4413 (602)230-5949 Fax: (602) [email protected] [email protected]
Mr. Rene T. Salgado Ms. Rosalia SalinasArizona Mexico Border Health Foundation Learning Resources and Educational2501 East Elm Technology DivisionTucson, Arizona 85716 San Diego County Office of Education(520) 795-9756 Fax: (520) 795-1365 6401 Linda Vista [email protected] San Diego, California 92111-7399
(619) 292-3522 Fax: (619) 571-4750
Ms. Dubia Sanchez Ms. Ruth Sanchez-WayPuentes de Amistad CSAPP.O. Box 646 5600 Fishers Lane, Rockwall IISomerton, Arizona 85350 Room 9-30(520) 627-4280 Fax: (520) 627-4277 Rockville, Maryland [email protected] (301)443-0369 Fax: (301)443-0526
Ms. Mary Sandy-Neville Ms. Sylvia J. SapienDrug Enforcement Administration LCDF3010 North Second Street, Suite 301 P.O. Box 3420Phoenix, Arizona 85012 Anthony, New Mexico 88021(602) 664-5630 Fax: (602) 664-5612 (505) 882-7370 Fax: (505) 882-7373
Mr. Daniel Schecter Dr. D. Dwayne SimpsonONDCP Texas Christian UniversityWashington, D.C. 20503 TCU Box 298740(202) 395-6733 Fax: (202) 395-6744 Fort Worth, [email protected] (817) 257-7226 Fax: (817) 257-7290
ibr.tcu.edu
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants217
Mr. Mark Simpson Mr. Shepherd SmithU.S. Bureau of Prisons The Institute for Youth Development3301 Leestown Road P.O. Box 16560Lexington, Kentucky 40511 Washington, D.C. 20041(859) 253-8839 Fax: (859) 253-8839 (703) 471-8750 Fax: (703) [email protected] [email protected]
Ms. Mary Ann Solberg Mr. Harry SteedTroy Community Coalition for the Arizona Elks AssociationPrevention of Drug and Alcohol Abuse 37 South 82nd Way4420 Livernois Mesa, Arizona 85208Troy, Michigan 48098 (480) 984-1219 Fax: (480) 832-9503(248) 823-5088 Fax: (248) 823-5051 [email protected]@moa.net
Mr. Robert Stephenson Ms. Linda SturdivantSAMHSA/CSAP Employee Assistance Professionals5600 Fishers Lane, Rockwall II Room 815 AssociationRockville, Maryland 20857 200 Lothrup Street(301) 443-6780 Fax: (301) 443-3031 Pittsburgh, Pennsylvania 15213
(412) 647-3296 Fax: (412) [email protected]
Ms. Emma Torres Mr. Avelardo ValdezPuentes de Amistad University of Texas at San AntonioP.O. Box 646 1222 N. Main Avenue #650AYuma, Arizona 85350 San Antonio, Texas 78212-5709(520) 627-4280 Fax: (520) 627-4277 (210) 458-2370 Fax: (210) [email protected] [email protected]
Dr. Elizabeth Valdez Mr. Forrest Van CampConcilio Latino de Salud, Inc. Leon Co. Schools546 East Osborn Road, #22 2757 W. Pensacola StreetPhoenix, Arizona 85012 Tallahassee, Florida 32304(602) 285-0970 Fax: (602) 285-0980 (850) 487-7525 Fax: (850) [email protected] [email protected]

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants218
Mr. Luis E. Vazquez Mr. Moises VenegasPuentes de Amistad The Albuquerque Partners143 N. State Avenue 801 Encino Place, NESomerton, Arizona 85350 Suite F21(520) 627-4280 Fax: (520) 627-4277 Albuquerque, New Mexico [email protected] (505) 244-9770 Fax: (505) 244-9771
Mr. Ray Vinsik Mr. Ricky WascherArizona HIDTA Juntos Unidos1750 E. Benson Highway P.O. Box 310Tucson, Arizona 85714 Nogales, Arizona(520) 746-4426 Fax: (520) 746-4405 (520) 761-4412 Fax: (520) [email protected] [email protected]
Mr. Harvey Weiss Major Larry W. WilbanksNational Inhalant Prevention Coalition National Guard Bureau2904 Kerbey Lane Jefferson Plaza 1, Suite 6500Austin, Texas 78703 1411 Jefferson Davis Highway(800) 269-4237 Fax: (512) 477-3932 Arlington, Virginia [email protected] (703) 607-5772 Fax: (703) 601-2733
wilbanksl@

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants219
ATTENDEES FROM MEXICO
Dr. Enrique de Jesus Aceves Arce Lic. Evangelina Aguilar SotoCentros de Integración Juvenil Responsible del Pp y Ca de Sinaloa
Dr. Mario Alva Rodriguez Lic. Norma Amerena CasaoDe la Direccion General Secretaria de Educacion Publica
Dr. Benito Antón Palma Jose Angel Arce GonzalezInstituto Mexicano de Psiquiatría
Jose Arellano Lopez Lic. Alejandro Arroyo DomínguezCasa Juvenil de Villahermosa Consejo Nacional Contra lass Adicciones
Edith Gabriela Arroyo Tinoco Lic. Karen Aspuru JuárezDe Promotores Juveniles de Irapuato Departamento de Normas CONADIC
Dr. Carlos Astorga Othón Dr. Hector E. Ayala VelazquezDirector General de Salud en el Facutad de Psicologia UnamEstado de Baja California
Lic. Adrian Badillo Martinez Arnulfo BanuelosCentros de Integración Juvenil
Dr. Mario Cesar Bejos Lucero Lic. Fernando Beltran AguirreLiber-Adictus Direccion General de Salud Reproductiva
Lic. Ruth Noemí del Pilar Beltrán Ojeda Dr. Fernando de J. Bilbao MarcosComunidad Terapéutica Para Mujeres Universidad Autonoma de Morelos
Lic. Rosa del Carmen Aglae Bonifaz Pedrero Lic. Jaime Luis Brito VazquezCONADIC Cultura Joven
Lic. Jesús Cabrera Solís Dr. Luis Calderón RodríguezCentros de Integración Juvenil Federación Médica de Baja California, A.C
Jose Camarografo Sofia Magaly Camorlinga CamachoDe Programas de Adicciones y Sexualidad
Juan Carlos Camul Cu Dr. P. Roberto Canto AguilarBoys Scouts Juventud "Luz y Esperanza" I.A.P.
Lic. Mónica Cantú de Ainslie C. Veronica Eulalia Caporal PerezFundación Ama la Vida, I. A. P. Casa Dar y Amar Daya
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants220
Dr. Manuel Carbajal Ruiz Ismael Carreto IglesiasClínica Especializada en SolucionarAlcoholismo y Dependencias
Pablo Carrillo Lic. Ignacio Carrillo PrietoDirector General de Prevención yReadaptación Social
Cónsul Salvador Casián Amada CastanonCónsul de México en Phoenix
Dr. Javier Castellanos Countiño Lic. Claudia Angélica Castillo AldanaSubsecretario de Regulación y Tec. de MonterreyFomento Sanitario, SSA
Lic. Jose Castrejon Vacio Dr. Mario Castro RochelCONADIC Responsible del Pp y Ca en Durango
Lic. Sergio Tadeo Cervantes Gallegos Lic. Jesús Cevallos CopelDe Jovenes Oceánica
Eduardo Chacon C. Alma Rosa Colin ColinAnica
Lic. Roberto Cordova Contreras Dr. Francisco Humberto Cordova CorderoServicios de Salud en el Estado de Chihuahua Secretariade Salud en el Estado de Chiapas
Luis Alberto Cordova Gonzales C. Miguel Angel Coria ValdezCIRAD
Lic. Adriana Cortes Jimenez Lic. Maribel Cuellar RamirezFundación Comunitaria Bajio A.C. Radio Neta
Dra. Christine de Agostini Maria de la PazPNUFID
Arturo de la Paz Vega Martin de la Rosa
Dr. Hector de Leo Tovalina Lic. Claudia de Mendieta OrtegaSecretaria de Salud de Veracruz Universidad del Valle de Mexico
Lic. Lino Diaz Barriga Salgado C. Maria Cristina Diaz JimenezCentros de Integración Juvenil Juventud Progresista Chiapaneca

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants221
Lic. David Bruno Diaz Negrete C. yomara Dominguez ContrerasCentros de Integración Juvenil CONALEP
Roberto Duran Lic. Ernesto Enriquez RubioCentros de Integración Juvenil
C. Carlos Alejandro Espinoza Dominguez Lic. Fanny FeldmanInstituto Mexicano de la Juventud Grupo Retorno
Dra. Emilia Figueroa Guillén Luis Manuel FloresClínica Integral de Tratamiento Contralass Adicciones
Lic. Karina Flores Carmelo Carlos FrancoCentros de Integraciòn Juvenil
Lic. Oscar Fuentes Fierro Lic. Laura Elena Gaither JiménezProcuraduria, General de la Republica Responsible del Pp y Ca en Tamaulipas
Lic. Nora Gallegos Vázquez Dr. Jesus GarcíaDirección de Normatividad CONADIC Salud, Equidad y Servicios a Jovenes
Dr. Jose Luis García Aguirre L.P. Erendira García AlcantarCoordinación de Salud Mental Pp y Ca en Michoacan
Lic. Monica García Murrieta C. Roberto García SalgadoOceanica Instituto Mexicano de la Juventud
Lic. Israel Arturo Gomez Daniel Maria Idalia Gomez SilvaDe Atención a la Juventud
Ana Maria Gonzales Medina Acuna GonzalezLic. José Antonio González Fernández Dra. Ma. de Los Angeles GonzálezSecretario de Salud Terapeutica
C. Eda González Richmond Sra. Martha GranadosDirección General CONADIC AMAAR de Chihuahua
Dr. Victor Manuel Guisa Cruz Lic. Maria de Lourdes VelezCentros de Integración Juvenil (CIJ) FIPADIC
Dra. Gladys Guzon Jover Leo HernandezGenesis de Sinaloa
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants222
Victor Miguel Hernandez Sr. Jorge Hernandez VillarealLos Brazos de Dios
Lic. Mariano Herrán Salvatti Miguel Inguanzo BlancoFiscal Especial-PGR
Sr. Jose Israel Jimenez Calvillo Dr. Alvaro Jurado AlonsoPresidencia Municipal de Leon AMAAR de Chihuahua
Dr. Philippe Leff Gelman Marta LohrInstituto Nacional de Psiquiatría Secretariat de Salud de Sonora
Dr. Joaquín López Bárcena Dr. Hèctor López GonzálezDirector General de Servicios Servicios de Salud en TamaulipasMédicos, Unam
Lic. Juan Pablo Lopez Montano Lic. Alejandro Lopez SanchezCIRAD DGPMP
Jorge Machado Lic. Claudia Yanet Machi GermanCausa Joven
Ing. Juan Machin Ramirez Lic. Eduardo Maciel del ValleInstituto Mexicano de la Juventud Club Juventud Siglo XXI
Lic. Jorge Madrazo Cuéllar Dr. Carlos Leonardo Magis RodriguezProcurador General de la República
Raul Marquez Albujar Dr. Hector Marroquin SeguraConasida Servicios de Salud en El Estado San
Luis Potosi
C. Imelda Marrufo Nava Dra. Silvia Cruz Martín del CampoCasa Centro ce Investigación y Estudios
Avanzados Cinvestav
Mtra. Antonieta Martín Gómez Jorge Alejandro Medellin VazquezUniversidad de Johns Hopkins
Lic. Ana Maria Mercadal Martinez Lic. Mauricio Meza BarreraFiscalia Especializada Para la Del Grupo de PacificadoresAtencion de Delitos Contra la Salud
Mtra. Maria Carmen Rosa Millé Moyano Lic. Dina Nohami Molina GomezDirección de Capacitación y Informacion Causa Joven
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants223
Lic. Carlos Oswaldo Morales Buelna Gregorio Moreno ContrerasInstituto Sonorense del Deporte y la Juventud
Lic. María Jesús Muñoz Avila Humberto Munoz GrandeResponsible del Pp y Ca en CampecheLic. Gustavo Ignacio Muñoz Manzo Dr. Armando Muñoz Valenciade Organizaciòn Juvenil Servicios de Salud en el Estado de Mexico
Lic. Fernando Murguia Orozco Lic. Alejandro Narvaez HigueraOceanica Asociacion Dips Por un Consumo Responsible
Dr. Jose Luis Navarro Paredes Lic. Yvette Nuñez BravoPrevencion de Riesgos Sociales en la Infancia Instituto Nacional Para la Educación
de Los Adultos
Lic. Juan Nuñez Guadarrama C. Luis Antonio Obregón ContrerasCONADIC Responsible del Pp yY Ca e en Chihuahua
Lic. Francisco Ojeda Quesney Dr. Arturo Ongay PérezCausa Joven CONADIC
Alfredo Ortega Sanchez Lic. Rosa Maria Ortiz EncinasCentros de Integración Juvenil
C. Ricardo Ortiz Longoria Ernesto Ortiz MaldonadoInstituto Mexicano de la Juventud
Lic. Marisa Oseguera Garcia Lic. Sandra Paola Otalora de GreILEF-CAVIDA Genesis de Sinaloa
Lic. Amir Efren Padilla Espadas Lic. Mario Padilla RamosConsejo Quintanarroense de la Juventud Secretaria de Salud de Sonora
C. Jose Edgar Palma Carrillo Maria Eugenia ParraConsejo Quintanarroense de la Juventud
Lic. Andrea Pastor Padilla Lic. Leonel Penagos FloresCentro de Estudios Superiores Servicios Especiales, PGRMonte Fenix
Jose Luis Perez Bautista Maria Rosalia Perez Garcia
Lic. Juan Martín Pérez García Dr. Jose Luis David Peterson BeltránCentro "El Caracol" Salud Mental en SonoraC. Yazmin Elizabeth Piña Alfaro C. Jose Luis Pino Guerrero
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants224
Opcion Mexico Drogadictos Anonimos
Dr. Jaime Ponce Alcocer Lic. Manuel Ponce BernalEstatal para el Control de Drogas en Queretaro Centros de Integración Juvenil
Lic. Adriana Porter Mejia Psic. Gloria Estela Portillo GarcíaAtencion A la Delincuencia Ciudadana Centros de Integración Juvenil
Lic. Maria Teresa Puebla de Carreño Lic. Gabriela Quiñones CervantesCentros de Integración Juvenil Centros de Integraciòn Juvenil
Lic. Jaime Quintanilla Bendek Lic. Ana Maria Quintanilla EncisoCentros de Integración Juvenil Centros de Integración Juvenil
Lic. Alba Rabling Dr. Miguel Angel Ramirez AlmanzaPNUFID Servicios de Salud de Oxaca
M.C. Martha Ramirez Rambao Oscar RamosClinica Integral de Tratamiento
Lic. Luciana Ramos Lira Mtra. Ma. Elena Ramos RodriguezInstituto Mexicano de Psiquiatría Programa CompañerosGuillermo Rangel Enriquez Reyes
Dr. Ignacio Benedicto Reyes Aguila Lic. Patricia Ines Reyes del OlmoServicios de Salud en Baja California CONADIC
Lic. Claudia Rigalt Gonzalez Lic. Wilfred Rios SanchezUniversidad del Valle de Mexico Procuraduria General de la Republica
Sr. Ruben Rivera Peña Lic. Yasmin Rivera PerezAMAAR de Chihuahua Secretaria de Desarrollo Social
Queretaro
Dr. Manuel Robles Linares Negrete Dra. Rosalía Rodriguez CuevasSecretaria de Salud de Sonora Clinica de Tabaquismo IPN
Sr. Pedro Rodriguez Garcia Sr. Gerardo Rodriguez RiveraEl Caracol El Caracol
Dr. Juan José Roque Segovia Lic. Galia RosembergResponsible del Pp y Ca en el Estado PNUFIDde Nuevo León

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants225
Mtra. Haydée Rosovsky Cesar Rubio GarciaSecretaría de Salud
Sra. Ninfa Sada de Salinas Lic. Epifanio Salido PavlovichDirectora de Fundación Azteca Secretaria de Salud de Sonora
C.P. Alfonso Salinas Corral Lic. Teresa Sanchéz FragosoSecretaria de Comunicaciones y Transporte CONADIC
Dr. José Sánchez Ortega Lic. Mario C. Sánchez TapiaCeca en el Estado de Baja California Presidencia Municipal de Leon, GTO
Dr. Jorge Sánchez-Mejorada Fdez. Dr. Hector Sandoval MartinezUniversidad Veracruzana CETyS
C.P. Irene Sandoval Mejia Dr. Mauro Santiago PedroInstituto Mexicano de la Juventud CONADIC
Dr. Jorge Santibañez Lic. Ma. Cristina Santoscoy GutierrezDirector del Colegio de la Frontera Norte Consejo Estatal Contra las Adicciones
en Jalisco
Lic. Toffie Sasson Hamui Lic. Marta Serafin MorenoCentro Monte Fenix FEADS
C. Engelbert Serna Barraza Dr. Fred SipeDel Secretario General Oceanica
Lic. Sonja Skarstol Dr. Luis Solis RojasOceanica Instituto Nacional ee Psiquiatría
Dr. Ivan Suarez Villa Dr. Roberto Tapia-ConyerSecretaria de Gobernacion Subsecretario de Prevención y
Control de Enfermedades
Lic. Pedro Tonella Trelles C. Andrés Tovilla SaenzPp y Ca en Sonora Narcóticos Anónimos
C. Luz del Carmen Trejo Fernandez de Castro Sra. Socorro Trespalacios GuerreroFundación "Dr. Sergio Berumen" AMAAR de Chihuahua
Sr. Eduardo Trespalacios Lozano Lic. Luis Amador Treviño PeñaAMAAR de Chihuahua Instituto Mexicano de la Juventud
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants226
Dr. Manuel Urbina Fuentes Lic. Juan Ramón Uriarte GalvánSubsecretario de Coordinación Sectorial, SSA Director General de Promoción y
Medicina del Transporte, SCT
Lic. Blas Urquidez Jr. Lic. José Vallejo FloresTransportación Maritima Mexico S.A. de C.V. Fundación Renacimiento
Lic. Lilia Vazquez Portales Aida VelascoPGR Cendro
Dr. Rafael Velasco Fernández Dr. Agustín Vélez BarajasCentro de Estudios Sobre Alcohol y Fideicomiso para los Institutos paraAlcoholismo, A.C. (CESSAL) los Niños de la Calle
Lic. Araceli Vergara Sabbagh Lic. Cesar de Jesus Vergara SabbaghClinica Nazaret Clinica Nazaret
Dr. José Vila del Castillo Cesar ViruegaRepresentante del PNUFID en México
Ing. Roberto Vital Pineda Margarita YbarraCasa de Rehabilitación "Alcance Victoria"
Lic. Joaquin Zamora Ortega Lic. Raul Zapata AguilarDel Proyecto y Educador de Calle Centros de Integración Juvenil
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants227
NIDA PRE-CONFERENCE PARTICIPANTS
Dr. Jaime Ponce Alcocer Mr. Mario AlvaCoordinator Instituto Nacional de Ciencial PenalesEstado de Queretaro Apartado Postal 10830Secretría de GobiernoConse Jo Estatal para el Control de Drogas
Dr. Benito Antón Ms. Esther ArellanoInvestigatador Titular AB@ Prevention Application Management CoordinatorDivisión de Investigaciones Clínicas Center for the Application of Prevention TechnologyInstituto Mexicano de Psiquiatría Arizona Department of Health Services
Division of Behavioral Health
Mr. Hector Ayala Ms. Judith Brook, Ph.D.Coordinador de Enseñanza Profesional ProfessorFacultad de Psicología Department of Community and PreventionUniversidad Nacional Autonoma de Mexico Mount Sinai School of Medicine
Dr. Luis Calderón Dr. Felipe Gonazalez Castro, M.S.W.Director del centro de la Conducta S.C. Department of Psychology
Arizona State University
Patricia Chavez-Anaya Anna ChismanValue Options Investigador Titular Chief of Demand Control
Inter-American Drug Abuse Control CommissionOrganization of American States1889 F Stree NW Washington DC 20006 USAPhone: (202) 458-6119Fax: (202) [email protected]
Dr. Francisco H. Córdova Mr. Javier CórdovaSecretario de Salud Policy AnalystHospital General, María Ignacia gandulfo Prevention BranchEstado de Chiapas, Mexico Office of Demand ReductionPhone: (529) 613-7688 Office of National Drug Control PolicyFax: (529) 613-1309 750 17th St., N.W., St. 612, Washington D.C
20503 USAPhone: (202) 395-6166Fax: (202) [email protected]
Dr. Silvia Cruz Dr. Bruno DiazCINVESTAV, IPN Centros de Integración Juvenil
Calle Vicente Suárez 149Col. Hipódroma CondesaC.P. 06100 Mexico, D.F.Phone: (525) 211-4186Fax: (525) 286-5955investigació[email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants228
Dr. Gerardo DeCosio Mr. Leonel Penagon FloresCoordinator Binacional PGR FEMOSPrograma Binacional Colabrorativo de Diabetes Mexico, D.FFrontera Mexico-Estados UnidosOrganización Pan Americana de la SaludOrganización Mondial de la Salud5400 Suncrest Drive, St. El Paso, TX 79912Phone: (915) 845-5950Fax: (915) [email protected]
Mr. Oscar Fuentes Lic Nora GallegosPGR Directora de NormatividadMexico D.R. Consejo Nacional Contra las Adicciones, SSA
Aniceto Ortega 1321, Piso 5Col. Del Valle03100, Mexico, D.F.Phone: (525) 534-6690Fax: (525) 534-6690ggallegos @supernet.mx
Ms. Elsa Garcia Dr. Victor GuisaChihuahua Director de Tratamiento y Rehabilitación del
Centro de Integración JuvenilCalle Vicente Suárez No. 149Col. Hipó dromo Condesa06100 Mexico D.F.Phone: (525) 534-6690 Tijuana, MexicoFax: (525) [email protected]
Dr. Mary Jeanne Kreek Ms. Susan KuntzThe Laboratory of the Biology of Addictive Diseases DirectorRockefeller University Hospital Border Health Foundation1230 York Avenue 2501 East Elm StreetNew York, NY 10021-6399 USA Tucson, AZ 85716 USAPhone: (202) 327-8247 Phone: (520) 795-9756Fax: (202) 327-8574 Fax: (520) [email protected] [email protected]
Dr. Sandra Owens Lawson, Ph.D. Dr. Phillip LeffSenior Policy Analyst Investigados AsociateWhite House Office of Drug Control Policy División de Investigaciones Clinicas750 17th St. N.W. Washington DC 20503 USA Calzado, Mexico D.F.Phone: (202) 395-6750 [email protected]: (202) [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants229
Dr. Remedios Lozada Dr. Carlos MagisCoordinadora del Programa HIV/SIDA Director de investigaciónEnfermedades de Transmisión Sexual Consejo Nacional para la Prevención y Control delComite Municipal Contra el SIDA SIDA (CONASIDA), SSAAv. ConstituciónEntre call 8 y 9 Calzado de Tlalpan, No. 4585 Piso 2Zona Centro 22000, Baja California Col. Torilello GuerraPhone: (526) 668-3804 C.P. 14050 Mexico D.F.Fax: (526) 685-1338 Phone: (525) 528-1949 / (528)1887
Fax: (525) [email protected]
Mr. Alberto Mata. Jr. Ms. Adriana MendioleaAssociate Professor Border Affairs CoordinatorDivision of Human Relations U.S. Consulate TijuanaUniversity of Oklahoma Office of Public Affairs Tijuana, Mexico601 Elm Ave., Room 728, Norman, OK 73019 USA Phone: (526)-681-7400 ext. 261Phone: (405) 325-1756 Fax: (526)-681-8592Fax: (405) 325-4402 [email protected]@ou.edu
Dr. M. Patricia Needle, Ph. D. Dr. M. Richard H. Needle, Ph. D., M.P.H.Director, International Program Senior Policy Advisor for HIV/AIDS & DrugAbuse National Institute on Drug Abuse U.S. Department of Health and Human ServicesRoom 1B59 Building 31, 9000 Rockville Pk. Room 733-E, 200 Independence Ave, S.W.Bethesda, MD 20892 US Washington DC 20201Phone: (301) 594-1928 Phone: (202) 205-0290Fax: (301) 402-5687 Fax: (202) [email protected] [email protected]
Luis Antonio Obregón Lic. Andrea PastorDirector General DirectoraCoordinador de Atención a las Adicciones y Centro de Estudios Superiores Monte FenixResponsible del Programa de Prevención y Las Flores No 439, Col. San angel InnControl de Adiccciones 01060 Mexico D.F.Niños Heroes 1103-B Phone: (525) 681-3011 ext. 249Col. Centro 31000 Chihuahua, Mexico Fax: (525) 595-3349Phone: (521) 415-3059 [email protected]: (521) 410-7980 / (521)-410-7856
Mr. Juan Paz Dr. Luciana RamosAssociate professor Jefe del Departamento de Investigaciones EspecialesSchool of Social Work Instituto Mexicano de Psiquiatría, SSAArizona State University Calzada Mexico-Xochimilco, No. 1012648 east 6th Street Delegación TlalpanTucson, AZ 85716 USA 14370 Mexico D.F.Phone: (520) 884-5507 Phone: (525) 655-21811 ext. 201Fax: (520) 881-0678 Fax: (525) [email protected] [email protected]
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants230
Ms. Rebecca Ramos Mtra. Haydée RosovskyU.S. – Mexico Border Health Association SecretarÍa TecnicaAsociación Fronteriza Consejo Nacional Contra las Adicciones5400 Suncrest Dr., St. C-a5 Aniceto Ortega 1321 Piso 2El Paso, TX 79912 USA Colonia del BallePhone: (915) 833-6450 03100 Mexico City, MexicoFax (915) 833-7840 Phone: (525) 534-7891 ext. [email protected] Fax: (525) 554-7851
Wilford Rios Sanchez Dr. Jorge SantibañezPGR FEDPS PresidenteInvestigador del Instituto de Investigaciones Colegio de la Frontera Norte, A.C.Psicológicos Blvd. Abelardo L. Rodriguez No. 2925Universidad de Veracruz Zona del RioKm 3.5 de la Carretera Jalap-Las Trancas 22320, Baja California, Tijuana Mexico91100, Jalapa, Veracruz, Mexico Phone: (520) 631-3300Phone: (522) 812-5740 Fax: (520) 631-5266 / (520) 631-3555Fax: (522) 812-8683 [email protected]@infosel.net.mx
Lic Toffie Sasson Dr. Steven Shoptaw, Ph.D.Director Clinico Del Centro Monte Fenix Senior Behavioral ScientistLas Flores No. 439 Friends Research Institute, Inc.Col. San Angel Inn 11075 Santa Monica Blvd., St. 22501060 Mexico, D.F. Las Angeles, CA 90025 USA(525) 681-3011 ext. 249 Phone: (310)479-9330 ext. 239(525) 595-3349 Fax: (310)[email protected] [email protected]
Dr. Luis Solís Mr. Robert L. Stephenson IIJefe del Centro de Ayuda al Alcohólico y Director (Acting)sus Familiares (CAAF) Center for Substance Abuse Prevention/SAMHSAInstituto Mexicana de Psiquiatría Division of Workplace ProgramsCalle Rebública de Venezuela esq. Rodriguez Puebla 5600 Fishers Lane Rockwall II, Room 815Col. Morelos Centro, 06020 Mesico, D.F. Rockville, Maryland USAPhone: (525) 702-7568 Phone: (301) 443-6780Fax (525) 702-7538 Fax: (301) [email protected] [email protected]
Ms. Claire E. Sterk Mr. Avelardo ValdezRollins School of Public Health DirectorEmory University Hispanic Research Center1518 Clifton Road, N.E. Room 516 University of Texas, San AntonioAtlanta, GA 30329-4218 USA 6900 North Loop 1604 WestPhone: (404) 727-9124 San Antonio, TX 78249-0650 USAFax: (404) 727-1369 Phone: (210) [email protected] Fax (210) 458-5155
United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants231
Mr. Fernando Wagner-Echeagaray Mr. Harvey WeissJohns Hopkins University Executive Director624 North Broadway, 8th Floor National Inhalant Prevention CoalitionBaltimore, MD 21209 USA 2904 Kerbey LanePhone: (410) 415-6055 Austin, TX 78703Fax: (410) 955-5155 Phone: (800) [email protected] Fax: (512) 477-3932
Dr. Raúl ZapataDirector de PrevenciónCentros de Integración JuvenilVicente Suárez 149Col. Hipódromo CondesaMexico, D.F.Phone: (525) 286-9230Fax: (525) [email protected]

United States - Mexico High Level Contact GroupThird Bi-National Drug Demand Reduction Conference
Proceedings Participants232