
Brazil's International Development Cooperation: Old and New Motivations
Upload
khangminh22Category
view
0download
0
1 | P a g e
Understanding Cancer Patients’ Motivations and Experiences in using
Traditional Healers in Ghana, a Constructivist Grounded Theory Approach
By
Isaac Badu Appiah
A thesis submitted for the degree of Doctor of Philosophy
School of Health Science
Faculty of Health and Medical Science
University of Surrey
December 2019
Supervisors: Dr Anne Arber & Dr Afrodita Marcu

2 | P a g e
ACKNOWLEDGEMENTS
My first and foremost thanks and gratitude go to the almighty God for His grace that has
enabled me to complete this journey successfully. I also thank Him for the opportunity to
meet people who have thought me many lessons along the way. I would like to acknowledge
my wife, Esther Appiah and our two sons Janaya and Jayden Appiah. Thank you so much for
your support, love and understanding that you have shown to me over the years. I also want
to acknowledge my late parents, who unfortunately did not live to see me complete this
study. I will miss you both always.
I also want to thank my family, who offered me the emotional and material support in
Ghana. Special thanks to my cousins, Prof. Asabere Ameyaw, Dr Addai Darko and my
brother Rev Ampofo Twumasi.
Many thanks go to my supervisors, Dr Anne Arber and Dr Afrodita Marcu, for their
expertise, patience, empathy and friendship. Thank you for making me feel that you were
always there for my success and encouraging me all the way. Thank you for the
understanding, support and flexibility that you showed me when I lost both my parents in the
last couple of years. I could not have done this without the two of you. I am very grateful. I
want to thank Dr Carin Magnusson, who was part of the supervisory team in the first two
years of the course and has continued to encourage me since leaving the team.
I also want to thank the hospitals and herbal clinics staffs who allowed me access to their
settings and supported me in many ways. A special thanks to the participants who spent their
time to share their views with me.

3 | P a g e
ABSTRACT
Traditional Medicine is embedded in the socio-cultural traditions of most Ghanaian
communities, with about 70-80% of the population using it alone or in parallel with
Conventional Medicine. Some studies have shown that people living with cancer and other
chronic diseases use Traditional Healers more than the ordinary population. However, studies
that have investigated the reason behind such behaviour of people living with cancer are few.
Thus, this study explores and conceptualises people living with cancers’ motivations and
experiences of using Traditional Healers in the Brong-Ahafo region of Ghana. The region is
rich in cultural traditions and has an abundance of Traditional Healers. The methodological
approach for the study was Constructivist Grounded Theory (CGT) in which semi-structured
interviews were conducted in two hospitals and five herbal clinics (n=35). The interviews
backed by a background observation of participants’ interaction with staff at the study sites.
The main categories from the analysis were: “Placing trust in one’s community”, “Finding
solace in the therapeutic hospitality and conviviality”, and “Aiming to avoid upset and
manage emotions”. These categories underpin the theory “Community of Us” which provides
a conceptualised understanding of the subtleties of the trusting and identity relations between
people living with cancer and Traditional Healers. The theory shows how these identities
influence people living with cancer’ help-seeking behaviour for their illnesses and symptoms
and therapeutic interaction. The “Us” exclude Conventional doctors as people living with
cancer did not trust them because they were detached from the local communities’ identities.
Conventional doctors represented “Whiteness” which symbolises colonial power, inequality,
and elitism. The study shows that people living with cancer use of Traditional Healers in
Ghana are more profound than mere socio-economic factors identified in previous studies.

4 | P a g e
DECLARATION
I declare that this thesis is the product of my work. Any ideas, data, text and images form
others were acknowledged and referenced. The thesis has not been submitted partly or in
whole to any other institution for any qualification. I accept that the University has the right
to submit this work to the plagiarism detection service to check the originality. The
University has the right to request an electronic copy or version of this document for any
verification.

5 | P a g e
TABLE OF CONTENTS
ACKNOWLEDGEMENTS ................................................................................................................. 2
ABSTRACT ........................................................................................................................................... 3
DECLARATION ......................................................................................................................................... 4
LIST OF FIGURES ............................................................................................................................ 10
LIST OF TABLES .............................................................................................................................. 11
GLOSSARY OF ABBREVIATIONS ................................................................................................ 12
CHAPTER ONE: BACKGROUND AND INTRODUCTION ....................................................... 13
1.1 Chapter Overview ................................................................................ 13
1.2 Cultural Values, and Conceptualisations of Illness in Ghana ................ 14
1.3 Pluralistic Health Care Approaches in Ghana .................................... 17
1.4 Traditional Medicine and Traditional Healers in Ghana .................... 18
1.4.1 The Profile of Traditional Healers in Ghana ...................................... 22
1.4.2 Apprenticeship and Training of Traditional Healers in Ghana ........... 24
1.5 The Approach of Conventional Medicine ............................................. 27
1.6 Overview of Ghana ................................................................................. 31
1.6.1 Ghana’s Health Service Delivery System .......................................... 32
1.6.2 Access to Conventional Health Services in Ghana ............................ 34
1.6.3 Cancer Incident Statistics in Ghana ................................................... 36
1.7 Pre-Field Reflexivity: Researcher’s Background and Biography ......... 38
1.8 Summary of Chapter One ........................................................................ 40
CHAPTER TWO: LITERATURE REVIEW .................................................................................. 43
2.1. Chapter Overview .................................................................................. 43
2.2 Search Strategy and Critical Appraisal ................................................... 45
2.2.1 Databases and Search Terms ............................................................. 45

6 | P a g e
2.2.2 Inclusion Criteria and Exclusion Criteria .......................................... 46
2.2.3 Critical Appraisal of the Literature .................................................... 49
2. 3 Factors Influencing the Use of Traditional Healers in Ghana ................ 50
2.3.1 Socioeconomic Factors ..................................................................... 50
2.3.2 Sociocultural Factors ........................................................................ 56
2.3.3 Spiritual Belief System ..................................................................... 61
2.3.4. Psychological and Emotional Motivations for Using Traditional
Medicine……………………….. ............................................................... 63
2.4. People Living with cancer’ Silence about Their Use of Various
Traditional Healers ...................................................................................... 66
2.4.1. Prevalence of People Living with cancer’ Use of Traditional Healers
in Ghana…………………. ........................................................................ 67
2.4.2. Different Forms of Traditional Medicine used by People living with
cancer……………….. ...................................................................................... 68
2.4.3 Lack of Doctor-Patient Communication about Traditional Medicine 69
2.5 Cancer Awareness and Help-Seeking for Cancer Symptom .................... 71
2.6 Summary of the chapter and Research Question ..................................... 75
2.7 Research Aims ........................................................................................ 76
2.7.1 Research Questions ........................................................................... 77
2.8 Overview of theoretical literature on trust .............................................. 77
2.9 General Understanding of Trust ............................................................. 78
2.10 Conceptualising Trust as Interconnected Self-Interests ......................... 81
2.11 Trust as Deference to Authority ............................................................ 82
2.12 Trust in Reputational and Good Behaviour Characteristics .................. 84
7 | P a g e
2.13 Endurance of Community Norms and a Generalised Culture of Trust ... 85
2.14 Trust as a System of Language and Communication ............................. 87
2.15 Trust as Familiarity and Habits of Communities ................................... 88
2.16 Summary ............................................................................................... 89
CHAPTER THREE: RESEARCH DESIGN AND METHODOLOGICAL CHOICES ............. 90
3.1 Chapter Overview ................................................................................... 90
3.2 Choosing Interpretivism Approach over Positivism ................................ 90
3.3 The Influence of Constructivism, Social Constructionism and Symbolic
Interactionism on Constructivist Grounded Theory (CGT) ........................... 92
3.4 Choosing Grounded Theory (GT) Methodology ...................................... 95
3.5 Choosing the Constructivist Grounded Theory (CGT) ............................ 99
3.5.1, Brief History of Divisions in Grounded Theory (GT) ...................... 99
3.5.2 Classic Grounded Theory: The Glaserian Approach ....................... 100
3.5.3 Straussian Grounded Theory ........................................................... 101
3.5.4 Constructivist Grounded Theory (CGT) .......................................... 102
3.6 Summary of the Methodological and Philosophical Standpoint in This
Study ........................................................................................................... 104
3.7 Overview of Study Sites and Region ...................................................... 106
3.8 Recruitment and Sampling (Selective to Theoretical Sampling) ............ 107
3.9 Negotiating Access to the Study Sites: Hospitals and Herbal Clinics .... 110
3.10 Data Collection: Interviews ................................................................ 114
3.11 Theoretical Saturation ........................................................................ 117
3.12 Theoretical Sensitivity ......................................................................... 118
3.13 Iteration and Constant Comparison .................................................... 120

8 | P a g e
3.14 Seeking Relevant Ethics Approval in UK and Ghana .......................... 121
3.15 Obtaining Informed Consent (IC) and the Challenges around Cultural
Consent ....................................................................................................... 122
3.16 Observations: The Dynamics of Doctor-Patient versus Herbalist-Patient
Relationships .............................................................................................. 124
3.17 Confidentiality and Sensitivity to Participants and Their Data ........... 129
3.18 Researcher’s Safety and Risk minimisation ......................................... 131
3.19 In-field reflexivity and Emotional Labour ........................................... 131
3.20 Data Analysis ...................................................................................... 134
3.21 Transcribing the Interviews ................................................................ 135
3.22 Open, Focused and Theoretical Coding of the Data............................ 136
3.23 Memo Writing ..................................................................................... 145
3.24 Developing Categories ........................................................................ 146
3.25 Theory Development ........................................................................... 148
3.26 Post field Reflexivity ........................................................................... 149
3.27 Considerations for Rigour and Credibility .......................................... 150
3.28 Summary of Chapter ........................................................................... 154
CHAPTER FOUR: FINDINGS ...................................................................................................... 155
4.1 Chapter Overview ................................................................................. 155
4.2. Power Disparity and Lack of Trust ...................................................... 156
4.3 Placing Trust in One’s Community and Identity ................................... 162
4.3.1 Tradition: Participants shared Ancestral and Cultural Connection with
Traditional Healers .................................................................................. 162
4.3.2 Participants Shared Language with the Traditional Healers ............ 165

9 | P a g e
4.3.3 Perception of Familiarity, Goodwill and Accountability ................. 169
4.3.4 Participants Perceptions of the Traditional Healers Reputable Virtues
……………………………………………………………………………………………174
4.4 Finding Solace in Therapeutic Hospitality and Conviviality ................. 180
4.4.1. Being Reassured by the Friendly and Jovial Manner of the Traditional
Healers …………………………………………………………………………………………….180
4.4.2 Participants perception of Traditional Healers interest in them ....... 182
4.4.3 Being Listen to and Giving Attention .............................................. 186
4.4.4 Feeling Relaxed .............................................................................. 189
4.4.5 Feeling of Lifting the Spirit and Boosting Hope .............................. 191
4.5. Aiming to Avoid Upset and Manage Emotions ..................................... 194
4.5.1 Euphemising: Softening and Placating Participants Situation .......... 194
4.5.2 Concealing: A Non-Disclosure of Participants Illness ..................... 196
4.6 Chapter Summary ................................................................................. 201
4.7 The theory of “Community of Us.” ....................................................... 202
CHAPTER FIVE: DISCUSSION ....................................................................... 204
5.1 Chapter Overview ................................................................................. 204
5.2 Trusting Identities: People Living with cancer’ Relationships and
Motivations for Using Traditional Healers ................................................. 210
5.2.1 Whiteness: Power, Inequality and Lack of Trust ............................. 214
5.2.2 Trust as a Traditional Identity and Shared Sensitivity ..................... 217
5.2.3 Trust as a Shared Language and Identity ......................................... 223
5.2.4 Trust in the Familiar and Habits in Communities ............................ 226

10 | P a g e
5.2.5 Reputational Trust: Reputable Characteristics of the Traditional
Healers …………………………………………………………………………………………230
5.3 Conviviality Interaction and Convivial Therapeutic Landscape ............. 237
5.4 Holistic Support and Quality Human Time ........................................... 242
5.5 Protecting Feelings and Avoiding Distress ........................................... 246
5.5.1 Cultural Telling and Disclosure....................................................... 247
5.5.2 Keeping It to Oneself and Not Washing One’s Clothes in Public .... 253
5.6 Summary of Chapter ............................................................................. 254
CHAPTER SIX: CRITIQUE OF STUDY AND CONTRIBUTION TO KNOWLEDGE ......... 256
6.1 The Study Contributions to Knowledge ................................................. 256
6.2 Strength of the Study ............................................................................. 259
6.3 Limitations and Requirement for Future Research ................................ 260
6.4 Recommendations for practice policy and education ........................... 262
6.4.1 Recommendations for Practice ...................................................... 262
6.4.2 Recommendation for Policy ............................................................ 264
6.4.3 Recommendation for Education ..................................................... 266
6.4.4 Recommendation for Research ....................................................... 268
6.5 Conclusion ......................................................................................... 268
6.6 Dissemination of Findings .................................................................... 270
REFERENCE .......................................................................................................................................... 271
APPENDIXES ........................................................................................................................................ 328
LIST OF FIGURES
Figure 1 Traditional Healers Profile Summary ...................................................................................... 27
Figure 2 Map of Ghana and bordering nations ..................................................................................... 32
11 | P a g e
Figure 3 Ghana Health Delivery Structure ............................................................................................ 34
Figure 4 Summary of chapters to Thesis .............................................................................................. 42
Figure 5 PRISMA Flow Chart ................................................................................................................. 48
Figure 6 Researcher's Multiple Identity .............................................................................................. 113
Figure 7 example of Open line-by-line codes..................................................................................... 140
Figure 8 Sample of analytical core category and subcategory ........................................................... 148
Figure 9 The Developed Substantial Theory ...................................................................................... 202
Figure 10: Participants model of placing Trust in their communities ................................................ 214
LIST OF TABLES
Table 1 Summary of studies on people living with cancer’ use of Traditional Healers ....................... 66
Table 2 Methodological Relevance to Theory Development................................................................ 97
Table 3 Summary of GT Methodologies and the Choice for CGT Approach ....................................... 106
Table 4 Participants demographics (Phase 1 visit).............................................................................. 116
Table 5 Participants demographics (Phase 2 visit).............................................................................. 117

12 | P a g e
GLOSSARY OF ABBREVIATIONS
CASP: Critical Appraisal Skills Programme
CCG: Constructivist Grounded Theory
CP: Conventional Practice or Hospital
HC: Herbal Clinic
GT: Grounded Theory
NHIS: National Health Insurance Scheme
OFN: Observation Field notes
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
SRH: Sunyani Regional Hospital
KHRCIEC: Kintampo Health Research Centre Institutional Ethics Committee

13 | P a g e
CHAPTER ONE: BACKGROUND AND INTRODUCTION
1.1 Chapter Overview
The study aims to explore the experiences of people living with cancer in using Traditional
Healers and why they use them in the Brong- Ahafo region of Ghana. The thesis develops a
new theory of the use of Traditional Healers for patients with cancer. In this first chapter,
there is a discussion of the background social and economic context of Ghana, general
cultural beliefs, practices and values. A demonstration on the elements influencing health-
seeking behaviours and use of Traditional and Conventional Medicine is also present. I also
highlight how existing theories of lay use of Traditional Medicine in Ghana or sub-Saharan
West Africa more broadly provide only a partial explanation for peoples ’behaviour and use
of Traditional Healers.
The chapter considers cultural values and practices and how they influence the
conceptualisation of health and illnesses in Ghana. I also discuss medical pluralism and the
different health care approaches dominant in Ghana. These are primarily the lay networks (
local health beliefs and practices), Traditional Medicine and the Conventional Health
Systems. Additionally, the chapter discusses the concept of Traditional Healers in Ghana,
their profile and the impact of their training within the community to become accepted as
established Traditional Healers. Also, the chapter discusses the Conventional Medical System
and how it conflicts with Traditional Medicine in peoples’ experiences and some of the
common criticism against it. Moreover, this chapter provides a general overview of Ghana,
its health delivery system, access to Conventional Health Services, and cancer incidents and
statistics. Furthermore, the chapter outlines my formative background and how that
influenced my development of personal interest into Traditional Healers and to this research.

14 | P a g e
1.2 Cultural Values, and Conceptualisations of Illness in Ghana
Culture is a set of shared ideas, concepts, practices and their underlying
meanings, and how they are expressed in human behaviours and interactions
(Keesing, Strathern 1998, Tylor 2010). This shared knowledge, concepts and practices
include belief systems, moral frameworks, laws, customs and norms, symbols, art,
language and even habits and behaviours that people acquire or inherit as members of
a society (Helman 2007, Geertz 2017, Tylor 2010, Kleinman 1980). Both culture and
its influence on people or societies’ worldview and way of life is sophisticated and
can be overt or implied (Helman 2007, Geertz 2017), outsider and insider knowledge,
tertiary and deeper, secondary or primary and superficial or profound in layers (Hall.
1989, Hofstede 1991, Helman 2007).
The belief in spirituality, ancestors and supernatural beings are dominant in
most Ghanaian communities (Utley 2016, Darko 2009). Most Ghanaians highly
revere their ancestors and believe the ancestors have established certain moral
traditions and values which strengthens character development, community
interactions and behaviours towards the sick and vulnerable (Utley 2016). These
moral values include community coherence, consideration for others wellbeing in
society and respect for elders and people with traditional statuses such as chiefs,
Traditional Healers and priests (Utley 2016). Ghanaian communities generally
perceive those in traditional positions such as Traditional Healers, traditional kings
and queens, fetish priests and family heads to be in harmony with the ancestors and
have the necessary wisdom and experience. Ghanaians generally consider such elders
to have Traditional Knowledge to offer advice and insight on important issues such as
illnesses and misfortunes (Utley 2016).
15 | P a g e
Ghanaians also inherently believe that the ancestors and other supernatural beings
have the powers to influence or intervene in individual situations, for example, issuing
punishments and rewards to people. Stories of occasions when ancestral spirits have visited
people as sick or weak to test peoples’ behaviours are often told to emphasise the importance
of ethical and moral values. Furthermore, most Ghanaians believe in the importance of
virtues such as kindness, friendliness hospitality, compassion, generosity, faithfulness and
trustworthiness (Utley,2016). Most Ghanaians usually endorse and advocate the idea of
oneness “Yeye Nipa Baako’’, meaning we are one people. The notion of “one people’’ is
pivotal for the collective and reciprocal responsibilities amongst most Ghanaians. What
affects one person affect everyone or the entire community in which almost everyone knows
each other.
In most indigenous Ghanaian communities, people usually knock their neighbours’
door in the morning and the evening to share welfare greetings and to ascertain that the
neighbours’ are feeling well. There is a tradition that we must always help others and greet
them since we do not know when we would need their help. Spiritual and cultural beliefs
influence the understanding and interpretation of health and illnesses, health-seeking
behaviours and preferred treatment methods in most Ghanaian communities (Kleinman 1980,
Helman 2007, Nettleton 2013, Douglas 2003, Landy 1977). These beliefs highlight the
importance of situating, interpreting and discussing health practices in Ghana and other
African countries from the perspective of a broader cultural context (Landy 1977, Helman
2007, Kleinman 1980). Most Ghanaians communities perceive illness as a complex
interaction of physical, psychological, and spiritual factors (Tabi et al. 2006, Kleinman 1980).
Primarily, most Ghanaians consider illness as a misfortune which is sacred (Spiritual),
secular (natural) or both in their origin, which influences the kind of treatment they may seek
(Kleinman 1980, Helman 2007). Most Ghanaians consider illness to be natural if they

16 | P a g e
perceive the disease as part of God's predestined plan (destiny) (Abel, Busia 2005,
Neba 2011). The concept “Oyame’’ (almighty God), permeates in all thoughts of the
Akan tribe (the largest tribe in Ghana) and generally all the tribes in Ghana as a
supreme being who controls life and sustains the universe (Bruce, 2002, Abel, Busia
2005, Neba 2011). Many Ghanaians believe that God assigns a destiny or fate to
every person and that fate eventually take its course or God fulfils that fate at a point
in one's lifetime (Abel, Busia 2005, Hevi 1989, Neba 2011).
Apart from the vertical human relationship with a supreme God in the
Ghanaian belief system is the notion of other lesser supernatural beings such as
ancestral spirits and lesser gods or idols who may cause diseases and misfortunes to
humanity. Such misfortunes may demonstrate their anger and dissatisfaction to certain
behaviours and practices (Abel, Busia 2005, Hevi 1989, Bonsi 1980, Tabi et al. 2006,
Bruce, 2005). In the case of evil spirits and witchcraft, the invocation of illnesses and
misfortunes to a person or entire community may be the result of mere dislike or
doing of evil and not necessarily in response to certain behaviours.
However, culture and spirituality are not the only elements that influence
health-related beliefs, actions and practices in Ghana. Other factors that influence the
populations’ beliefs about health include political, socioeconomics, education, age,
historical and environmental determinants which impinge on the local health care
system (Helman 2007, Kleinman 1980). The health-seeking behaviours and beliefs in
Ghana are very complex, usually influenced by more than one factor and the existence
of different therapeutic approaches.

17 | P a g e
1.3 Pluralistic Health Care Approaches in Ghana
The concept of medical pluralism is seen as using more than one Medical
System or resorting to diverse kinds of therapies even in cases where the various
therapeutic methods have different conceptualisation and explanatory models of
illness (Moshabela et al. 2016, Moshabela et al. 2017, Hsu 2008). In Ghana and most sub-
Saharan African countries, medical pluralism involves ‘shopping and switching’ between
multiple modalities or therapies of care. There are three primary overlapping and
interconnected approaches to health care in Ghana, which are accessible, including lay health
beliefs and practices (lay networks), Traditional Medicine, and the professional health care
system or Conventional Medicine (Helman 2007, Kleinman 1980).
The popular or lay network of health beliefs and practices constitute the most
extensive health care approach in Ghana but challenging to study because of the vast
complexities and lack of any defined or organised structure (Helman 2007, Kleinman 1980).
The activities and the knowledge of the popular or lay health beliefs are informally
interspersed and disseminated amongst ordinary community members (Helman 2007,
Kleinman 1980). The popular sector of health care is described as a matrix containing
several layers of individuals, families, social networks, lay community beliefs, values and
activities (Kleinman 1980).
The popular culture of beliefs, values, local and family definitions of illnesses and
normality influence patients decisions to pursue treatment or not. These elements also affect
what treatment would be sought (Helman, 2007, Kleinman, 1980). Hence, the lay health
network is the starting point of health-seeking or maintenance behaviours for most Ghanaians
before proceeding to interact with both the Traditional and Conventional Medicine.
As part of this interaction, the ill-person may move freely between modalities or use
them simultaneously (Helman, 2007, Kleinman, 1980). The lay network of health practices in

18 | P a g e
Ghana includes self-treatment, pieces of advice and recommendations from society
members such as families, relatives and neighbours. The lay health networks treat
general or specific ailments and allow people to share their experiences of illnesses or
treatments of a condition to support others (de-Graft Aikins, 2005, Aikins et al., 2010,
Gyasi., et al., 2017). For example, older women in Ghana with the experience of
giving birth or having multiple pregnancies are considered able to offer advice on safe
pregnancy and delivery to young women. Also, older men and women in the families
or communities act as health advisors and offer minor treatments to people who
sustain cuts, snake bites, burns, chronic cough and other health issues.
1.4 Traditional Medicine and Traditional Healers in Ghana
An estimated 75% of the global population and between 70% and 80% of the
African population use Traditional Medicine or the services of Traditional Healers
either alone or alongside Conventional Medicine (Oreagba et al. 2011). Furthermore,
people living with cancer and other chronic illnesses have been shown to use
Traditional Medicine or Complementary Alternative Medicine more than the general
population across the globe (Mao et al. 2011, Patterson et al. 2002, Richardson et al.
2000). Many authors pinpoint poverty, lack of available and accessible Conventional
Medicine as the main reasons for the use of Traditional Healers in Ghana (Dove 2008,
Yarney et al. 2013). However, this is not always the case as some people who have
access to Conventional Medicine or have the financial power to afford Conventional
Medicine may continue to use the Traditional Healers services (Chen et al. 2008).
Nonetheless, there is a general understanding that the inadequate and ineffective
provision of Conventional Medicine in Africa, Asia and other developing countries
influence the continuing vivacity of Traditional Medicine (Last, Chavunduka, 2018).

19 | P a g e
Although Traditional Medicine is an active part of most indigenous communities,
their role in modern states is a subject of much debate due to the insufficient evidence for its
safety and efficacy. Equally, there is a lack of a standard definition of Traditional Medicine
and what is included or excluded as Traditional Medicine (Last, Chavunduka, 2018,
Kleinman, 1980, Helman, 2007). A shared definition of Traditional Medicine is contested
across countries and different communities within a country (Kleinman, 1980, Last,
Chavunduka, 2018, Helman, 2007). The heterogeneity, ambiguity and the lack of consensus
on definition and components of Traditional Medicine are indications of divergent views,
assumption and the need to view Traditional Medicine within their specific contexts both
nationally and internationally (Last, Chavunduka, 2018, WHO, 2002).
The World Health Organisation (WHO) is the main body at the forefront in
standardising Traditional Medicine through regulation, safety and gathering of information
on efficacy at the global level and more especially in countries where Traditional Medicine is
popular and widely used. As part of this endeavour, WHO has provided a standard definition
of Traditional Medicine as “the sum total of the knowledge, skills, and practices based on the
theories, beliefs, and experiences indigenous to different cultures, whether explicable or not,
used in the maintenance of health as well as in the prevention, diagnosis, improvement or
treatment of physical and mental illness” (WHO, 2013, page 15), WHO acknowledges that
Traditional Medicine evades a precise definition or description and contains diverse and
sometimes conflicting characteristics and viewpoints (WHO, 2013). The WHO definition is
considered a working definition and not necessarily comprehensive or inclusive of all
contexts (WHO, 2013, WHO, 2002).
Respectively, there is no clarity in the literature about who is responsible for deciding
what is included or excluded as Traditional Medicine. While the WHO broadly provides

20 | P a g e
some information on the components of Traditional Medicine, it leaves the ultimate
responsibility for Traditional Medicine to individual countries and communities (WHO,
2002, Last, Chavunduka, 2018). Traditional Medicine generally includes therapies in
the form of herbs or herbal products, animal parts, minerals and other therapies such
as acupuncture, manual, mental and spiritual therapies or a combination of these to
maintain wellbeing, and to diagnose, prevent and treat illnesses (WHO, 2002).
Although Traditional Medicine has many variations, there seems to be a
consensus that it is opposite to Conventional Medicine, generally part of the cultural
heritage of a nation or community and has evolved as part of their lifestyle (WHO,
2012). Traditional Medicine defers from Conventional Medicine in philosophy,
education, practice and emphasis on current scientific evidence.
In some countries, especially in Europe and America or other developed
countries, Traditional Medicine is often described as Alternative or Complementary
Medicine (WHO, 2002). Herbal Medicine or treatments are the most popular form of
Traditional Medicine and used by 70-80% of the world’s population for therapeutic or
health promotion reasons (WHO, 2012, WHO, 2004). Herbal medicines include herbs
(raw or processed), herbal materials, herbal preparations and finished herbal products
and in some countries may contain additives such as natural organic or inorganic
active ingredients that are not from plants (WHO, 2004).
In General, the concept of Traditional Medicine refers to the use of culturally
embedded health beliefs and practices by indigenous communities for treatment and
therapeutic purposes or general health maintenance (Struthers et al. 2004, Warren et
al. 1995, Berkes 1993, Debas et al. 2006, Zhang 1999, Kincheloe, Steinberg 2008).
Traditional healers are those who are recognised in Ghanaian communities to have the
relevant knowledge and skills entrenched in culture to treat illnesses (Struthers et al.

21 | P a g e
2004, Girardet, Robertson Winn 1994, Reyes-García 2010, Zhang 1999). In Ghana, the
mainstream Traditional Medicine is Traditional Herbal Medicine (Bodeker, Ong 2005,
Shukla, Sinclair 2009), which constitute about 65% of all Traditional Medicines in the
country (Bodeker, Ong 2005).
Traditional Herbal Medicine usually involves the use of medicinal plants or herbs in a
raw or refined form for health purposes (Bodeker, Ong 2005, Girardet, Robertson Winn
1994, Tsey 1997). Hence, Traditional Medicine is sometimes used interchangeably or
synonymously with Traditional Herbal Medicine in the literature. Traditional healing in
Ghana may involve treating the physical and the spiritual components of diseases
simultaneously and perceived to adopt a more holistic approach of restoring the mind, body
and spirit (Nettleton 2013, Kolcaba. 1997, Bierlich 1995, Abel, Busia 2005, Neba 2011).
Also, Traditional Healers regularly involve the family and take their concerns and feelings
into consideration. In this sense, the healing process is the responsibility of patients, their
families and the Traditional Healer (Martin, 1981, Helman 2007, Kleinman 1980).
Moreover, a shared worldview or culture, the warmth of patients’ familiarity to
healers and settings, informality and use of everyday language in consultation give
Traditional Healers an edge over their Conventional counterpart (Helman 2007).
Furthermore, the notion that the Traditional healer is part of the broader socio-cultural
community and will act for the benefits of patients and the total community welfare makes
the Traditional sectors sometimes more attractive to indigenous societies (Helman 2007,
Kleinman 1980).
Specific criticisms and judgments passed on Traditional Healers usually relate to the
conceptual and operational explanations and the lack of parity of evidence with Conventional
Medicine (Darko 2009). However, continuously judging all medicines and treatments by the
scientific objective evidence-based standard inherently underpinning conventional Medicine

22 | P a g e
undermines the sociocultural importance of Traditional Healers in most indigenous
societies (Darko 2009, Helman 2007, Kleinman 1980).
Traditional Healers meet the healthcare and economic needs of some people in
the African and Asian communities who use them or engage in them commercially
for their livelihood (Kleinman 1980, Cunningham 2001, Yeboah 2000, Zhang 1999).
Also, Traditional Medicine serves as a revenue generation to governments (Yeboah
2000, Cunningham 2001), especially in countries like China and India, where they are
better regulated and formalised (Helman 2007). Although the diversity and the lack of
regulation of Traditional Medicine and Traditional Healers make it challenging to
assess the amount of revenue generated from its market activities, available data
suggest an active and substantial fiscal activity with Traditional Medicine. For
example, the revenue output in China in 2012 was US$ 83.1 billion. The annual
expenditure in the Republic of Korea was US$7.4 billion in 2009. In the United
States, the out of pocket spending on natural and medicinal products was US$14.8
billion in 2008 (WHO 2013).
Furthermore, Traditional Herbal Medicine has the potential for future drug
discovery and development through appropriate investment and research (Reyes-
García 2010, Patwardhan, Mashelkar 2009, Bhat 2012, Fabricant, Farnsworth 2001).
These highlight the necessity to preserve Traditional Healers and ensure the
transmission of their depository of knowledge and practices to the younger
generations to prevent extinction (Ohmagari, Berkes 1997, Brundtland 1987).
1.4.1 The Profile of Traditional Healers in Ghana
The family constitutes a primary level depository of individual skills and
traditions of society and equally a mode of training Traditional Healers (Tsey 1997,
Helman 2007). In Ghana, Traditional healing is considered a family asset and

23 | P a g e
reputation (Ryan 1998, Abel, Busia 2005, Osujih 1993, Shukla, Sinclair 2009). Consequently,
the practice is safeguarded and transferred to other family members for perpetuation
(Ndubani, Höjer 1999, Osujih 1993, Tsey 1997). People from a family background of healing
traditions or healers usually inherit or learn the practice of Traditional healing from an
experienced relative or a family member (Tsey 1997, Vandebroek et al. 2004, Shukla,
Sinclair 2009, Abel, Busia 2005, Gessler et al. 1995, Hampshire, Owusu 2012).
Also, some people claimed to have become traditional healers through a divine or
supernatural call and received a revelation from the ancestors or a deity through a dream,
vision, a sign or a direct voice (Hampshire, Owusu 2012, Tsey 1997, Gessler et al. 1995,
Twumasi 2005, Evans-Anfom 1986). Sometimes, the instruction may be conveyed through
the wisdom of the elders who are closely aligned with their ancestors. Usually, those who
become Traditional Healers through this pathway perceive Traditional healing as a higher
“call” which one does not merit and cannot partake without a divine invitation and
authorisation (Tsey 1997, Gessler et al. 1995, Abel, Busia 2005). There are various
experiences, indications or signs of confirmation that an individual has been ‘called’ to the
healing profession by a supernatural power. The individual will usually be possessed by a
spirit which could cause them to exhibit hallucination, hysteria, tremors and ecstatic
behaviours (Lewis 2002, Twumasi 2005, Helman 2007).
In some cases, the “call’’ may be preceded by the potential healer or family
encountering a severe or traumatic emotional encounter (Helman 2007), or a painful
experience or misfortune such as sickness, extreme poverty or family death as a way of
making them sober, but also active and ready for their ‘call’ (Tabuti et al. 2003). These
groups of healers usually claim to have had no choice but to respond to the spirits to avoid
severe repercussions (Gessler et al. 1995, Swantz 1990).
24 | P a g e
Additionally, an individual could come to the Traditional healing profession
through a personal decision (Tsey 1997, Helman 2007). People may develop the
interest to become Traditional Healers during a time they are receiving treatment from
a Traditional Healer or when the Traditional Healer has successfully treated them
(Gessler et al. 1995). Under these circumstances, the request to be trained by an
individual serve as a kind gesticulation to propagate the good work of traditional
healing and give back to the community (Gessler et al. 1995).
1.4.2 Apprenticeship and Training of Traditional Healers in Ghana
In general, regardless of which path or combination of ways people take to
become traditional healers, they must be thought through apprenticeship until they
gain the right medicinal or healing knowledge and cultural skills to practice
(Ohmagari, Berkes 1997, Shukla, Sinclair 2009). Even those children from a family
of healers continue to undergo training until they are old enough and have acquired
enough knowledge to practice independently or take over the family healing tradition
(Ohmagari, Berkes 1997, Zarger, Stepp 2004, Shukla, Sinclair 2009, Tsey 1997, Abel,
Busia 2005, Ndubani, Höjer 1999). Although those who receive divine calling
undergo apprentice training, some claim to have gained insights into medicinal plants
and their purposes through supernatural means (Tsey 1997, Abel, Busia 2005, Evans-
Anfom 1986, Twumasi 2005, Neba 2011). This method of acquiring and transmitting
healing knowledge is contentious on the grounds of subjectivity and verification.
Most Conventional Health Professionals see these groups of healers who have
the divine “calling” as the most difficult to have any meaningful role in the effort to
integrate Herbal Medicine with Conventional Medicine in some recommended
settings (Tsey 1997, Bonsi 1980, Osujih 1993). However, in the context of Ghana
and most African communities, such mode of acquiring healing knowledge is

25 | P a g e
compatible with the inherent worldview of the powers of the ancestors and spirit beings.
The apprenticeship or training of a Traditional Healer in Ghana can be very extensive
and last for many years (Girardet, Robertson Winn 1994, Shukla, Sinclair 2009). The
Traditional Healers’ training could start between 5-7yrs of age and continue until adulthood
(Shukla, Sinclair 2009, Girardet, Robertson Winn 1994, Gessler et al. 1995, Tsey 1997,
Hampshire, Owusu 2012).
Although the training of adult Traditional Healers can take an average of three years
(Abel, Busia 2005), it can also last for about twelve to fourteen years depending on the
learners’ ability (Ohmagari, Berkes 1997, Girardet, Robertson Winn 1994). During the
training period, the apprentice assumes the position of a servant to the trainer and spend most
of their time with him (Tabuti et al. 2003). Usually, the training is an active process of
collaboration between the trainer and trainee (Rogoff 1990) and takes place in an informal
setting in the community, a sacred bush or a forest (Tsey 1997, Zarger, Stepp 2004, Twumasi
2005). The trainer and trainee often travel to the forest together for the trainee to acquire
extensive knowledge in herbs or plants, preparation of treatments and acquisition of practical
skills in harvesting medicinal plants (Tsey 1997, Shukla, Sinclair 2009, Twumasi 2005).
Extensive knowledge in medicinal plants is essential to Traditional Healers in Ghana
and most African countries (Tsey 1997, Shukla, Sinclair 2009, Zarger, Stepp 2004). The
herbal knowledge benefits Traditional Healers and their trainees to avoid the use of
poisonous or harmful plants while at the same time providing a range of plant medicine
option available as a healer (Shukla, Sinclair 2009, Tabuti et al. 2003). For trainees who are
spiritually based, the training involves learning to tune their senses to recognise, understand
and communicate with the spirits (Twumasi 2005).
Fundamentally, the trainer aims to develop the trainee as a ‘whole person’ by
demonstrating and teaching traditional normative values such as discipline, respect, sharing,

26 | P a g e
self-reliance, independence and corporation. It enables the trainee to become a
virtuous member of society, Sendell 1997). Likewise, the trainer tends to be patient to
allow for trial and error and continuous learning and practising by the trainee. Even
when the trainee makes a mistake, the trainer continues to support them if they
continue to show interest and diligence in the endeavour (Ohmagari, Berkes 1997).
The behaviour of the trainer shows the trainees the importance of patience, tolerance
and persistence or resilience in dealing with people, as well as stressful situations. In
Ghana, Traditional Healers are known to have reputation and character, part of which
is due to people’s perception about the nature of their training which strengthens their
understanding and compliance with the socio-cultural traditions and values of their
communities.
Overall, the way an individual becomes a Traditional Healer affects their
practice orientation. Classifying Traditional Healers into spiritual and non-spiritual
practitioners provides a practical and concise working framework to explore the
differences in their worldview. Usually, those who claim to have become Traditional
Healers through spiritual means have explicit spirituality or practices in conjunction
to their herbal or physical treatments of illnesses (Hampshire, Owusu 2012, Tsey
1997, Abel, Busia 2005, Neba 2011). These categories of practitioners offer spiritual
explanations to the causes and treatment of diseases. They are usually required to
consult the spirits for guidance to resolve the perceived spiritual underlie of illnesses
(Ngokwey 1994, Bierlich 1995).
On the other hand, the non-spiritually based practitioners offer a lucid and
physical explanation to illnesses, and their main emphasis is on the use of herbal
medicinal products to treat illnesses (Tsey 1997, Tabuti et al. 2003, Ngokwey 1994,
Bonsi 1980). However, in Ghana, the distinction between the two types of Traditional

27 | P a g e
Healers is a continuum and sometimes blurred with nuances. Although the non-spiritual
practitioners do not overtly make an inference to supernatural powers in their practice, they
inherently recognise the influence of supernatural powers on human endeavours and tend to
look for spiritual explanations, especially for illnesses that come about suddenly or are
difficult to explain or treat. (Tsey 1997, Abel, Busia 2005, Tabi et al. 2006).
Figure 1 Traditional Healers Profile Summary
1.5 The Approach of Conventional Medicine
Conventional Medicine, underpinned by the modern scientific paradigm (Nettleton
2013, Helman 2007, Rose 2001, Kleinman 1980) appears to dominate as the benchmark for
all health discussions. Perhaps, Conventional Medicine is the most organised,

28 | P a g e
professionalised, and well-regulated form of health care or treatment modality across
the globe (Janes 1999, Helman 2007, Kleinman 1980). The Conventional Health Care
System offers a biomedical or scientific explanation for the causes and treatments of
diseases (Hewson 1998, Dick 2010). In principle, Conventional Medicine adheres to
the use of objective evidence and rational patterns of conditions (Wade, Halligan
2004). In the perspective of Conventional Medicine, sicknesses and diseases are
caused by an underlying organ pathology that requires treatment or intervention
targeted to the affected organ (Wade, Halligan 2004).
In Ghana and most countries across the world, Conventional Medicine usually
has statutory ascent and receives funding from the government and external donors
(Helman 2007, Hampshire, Owusu 2012, Nettleton 2013). However, Traditional
Medical Systems in some countries, e.g. Ayurveda in India and Chinese Medicine, are
well established or professionalised to some extent. They also receive some level of
governments’ finance and legal support (Helman 2007, Kleinman 1980).
Most indigenous population criticise Conventional Medicine for alluding to a
single scientific view or conceptualisation of health which segregate the sick body
from the person (Nettleton 2013, Helman 2007). Also, many criticise Conventional
Medicine for its generic approach and lack of consideration to the dynamics of the
sociocultural context and subjective interpretations of causes of illnesses and healing
(Helman 2007, Nettleton 2013, Kleinman 1980, Geertz 2017). The quote below from
Atkinson (2012) summarises the criticisms that many people often argue against
Conventional Medicine :
“It is reductionist in form, seeking explanations of dysfunction in invariant biological
structures and processes; it privileges such explanation at the expense of social, cultural, and
biographical explanations. In its clinical mode, this dominant model of medical reasoning
29 | P a g e
implies: that diseases exist as distinct entities; that those entities are revealed through the
inspection of ‘signs’ and ‘symptoms’ that the individual patient is a more or less passive site
of the disease manifestation; that diseases are to be understood as categorical departures or
deviations from “normality’’ (Atkinson in Lock and Gordon, 2012, page 180).
The quote alludes to the failure of Conventional Medicine to recognise people as
social beings who are dynamically affected by their socio-cultural and historical context and
background and how all these factors interact to affect a person’s biological function and the
concept of illnesses. The quote highlights the importance of a comprehensive approach to the
treatment of illnesses that would encompass all the social, cultural and emotional or
psychological aspects of human life and avoid a body-mind dualism. Nettleton (2013),
identified five fundamental assumptions that underlie Conventional Medicine and how these
assumptions influence the behaviours of its professionals such as doctors, nurses and
pharmacists. These fundamental tenets are body and mind dualism: the notion that the body
and mind can be segregated or treated as different entities instead of focusing holistically on
the entirety of the person. Conventional Medicine also acts as treating a body that requires
repairs, in which case the Conventional Medicine and its professionals' function either as
engineers or mechanics who are qualified enough to mend any dysfunctions or malfunctions
of the body machine. The adoption of a technological imperative or advancement to health to
the extent of downplaying their potential consequences or overplaying their benefits. The
adoption of a reductionist approach or view in which Medicine focuses on explaining
diseases concerning biological, physiological and physical changes and neglecting the
psycho-spiritual and socio-cultural elements impinging on health. Conventional Medicine
also adheres to the doctrine of specific disease causation which assumes that every disease or
illness has a specific identifiable causative organism or explanation.

30 | P a g e
Despite the considerable criticism against Conventional Medicine, it is
essential to acknowledge that Conventional Medical Systems across the globe have
recently evolved and have made improvements in adopting some of the softer skills
which are often associated with Traditional Medicine (King, Hoppe, 2013, Saha, et
al. 2008). Governments across the continents, and regulatory and patients’ advocacy
organisations have implemented several initiatives which have led to improvements in
clinician-patient relationships, patient communications, engagements, empowerment
and involvement in healthcare in recent times (Colombo et al., 2012). The nature of
the relationships between Conventional Medical Practitioners and patients has
dramatically changed, and the once characterised as the experts-lay relationship is
now appropriately described as collaborative or partnership (Nettleton, 2013).
Arguably, there has been massive progress in the education and practice of medical
and other clinical staffs to encompass excellent communications skills, honesty,
openness, respect for patients and their views, confidentiality, autonomy and showing
of interest in other aspects of patients’ lives (King, Hoppe, 2013).
Also, in most countries across the globe, there is a commitment and initiatives
to shift healthcare from institutions to non-institutional environments, encourage
people to take control of their health and involve them in shaping health care policies
and systems (Nettleton, 2013). For example, there has been a considerable
momentum within the UK health service about the patient and public involvement
which has been reflected in various policy initiatives to drive patient empowerment,
participatory approach to care, safety and open culture (Ocloo, Fulop, 2012, Bravo et
al., 2015). Moreover, Conventional Healthcare approaches have now moved from
focusing on only physiological and biological interventions to a more holistic or
comprehensive way of supporting patients psychologically, sociologically and

31 | P a g e
spiritually (Porter, 1997, Kolcaba, R., 1997, Kolcaba, K., 2003). Furthermore, there has been
an increased awareness and integration of ethics in education and practice in medical and
other professions of Conventional Medicine (Terawaki et al., 2014).
1.6 Overview of Ghana
Ghana has an estimated population of about 29 million (WHO: Global Cancer
Observatory 2018), and Capital City is Accra. The country is well administered and a model
of political democracy and economic reform on the African continent (The World Bank 2015,
BBC 2018). Ghana is also one of the most stable countries in the region with a respectable
record of peaceful political elections and transitions. The country also enjoys a stable,
independent judiciary, and secure freedom of speech, press and broadcasting freedom, and
consistently ranking amongst the top in Africa and the globe (The World Bank 2015, BBC
2013, Anku-Tsede 2013). Despite the stability and consistent growth forecast (7.4 for 2019),
the country still has a high poverty rate and inequality of wealth and living standards (The
World Bank 2015). A total of 28.5% of the population live in poverty with a life expectancy
of 61, and percentage literacy of 67.3% (World Bank 2013).
Geographically, Ghana is located on the Gulf of Guinea and the Atlantic Ocean in the
south of the West African sub-region (Sub Saharan Africa) and shares a border with Ivory
Coast (Côte d'Ivoire) to the west, Burkina Faso to the north and Togo to the east (Moellering
et al. 2011, Jackson et al. 2001). The total landmass is nearly the same as that of the United
Kingdom 238.537 kmsq, consisting of different climates and terrains (Moellering et al. 2011,
Utley 2016). The country has three cardinal regions which have different climate, resources
and living activities, namely the northern, southern and coastal (See Figure 2).
The northern part of Ghana is mainly savanna and wildlife, the southern part consists
of mineral resources and fertile agricultural land, and the coast consists of a labyrinth of

32 | P a g e
castles, ports, harbours and beeches (Utley 2016, Moellering et al. 2011). Overall,
Ghana has over fifty languages with English as the national or official language.
Other significant languages include Twi, Fante, Ewe, Ga, Hausa, Nzema and
Dagbani. According to Utely (2016), outsiders sometimes perceive Ghana to be a
monolingual state because most of the population can speak “Twi’’ which is spoken
by the Akan’s’, the largest ethnic group in Ghana, spread across many of the regions.
The Brong -Ahafo region, where the study took place, is dominated by Akan people.
Figure 2 Map of Ghana and bordering nations
1.6.1 Ghana’s Health Service Delivery System
The government of Ghana categorises Ghana’s health system into
conventional and Traditional Medical Systems (Salisu, Prinz 2009, Aseweh Abor et
al. 2008). The government, private companies, individuals and faith-based or non-
governmental organisations operate the Conventional Health System.

33 | P a g e
Administratively, the Ministry of Health is the government department which regulates the
entire health sector through policy planning and formulation, regulation, and coordination of
stakeholders (Salisu, Prinz 2009, Aseweh Abor et al. 2008). The Ministry of Health has three
hierarchies of administrations, which are the Central, Regional, and Metropolitan District
administrations. These administrations are concurrent with operational activities that extend
to the sub-districts and community levels. The Ghana Health Service is responsible for the
implementation of government policies and regulation of public sector health delivery
(Aseweh Abor et al. 2008, Salisu, Prinz 2009, Ghana Health Service 2013).
On the other hand, the Teaching Hospital Board regulates and implement government
policies in the Teaching and Tertiary hospitals (Aseweh Abor et al. 2008, Salisu, Prinz 2009).
The public sector health delivery is through a network of health centres, district hospitals,
regional hospitals, tertiary and teaching hospitals (Govindaraj et al. 1996). Furthermore, the
National Health Insurance Scheme (NHIS) finances the public health sector delivery (Salibu,
Prinz,2009, Gobah, Zhang,2011) and subsidised by central government funding. The
fundamental principle of the NHIS is to provide financial protection for the poor and to
ensure equitable access to primary health care (Salisu, Prinz 2009).
The private health sector consists of faith-based organisations or hospitals, private
medical and dental facilities, private maternity homes or clinics, and private pharmacies (See
Figure 3) (Salisu, Prinz 2009, Aseweh Abor et al. 2008) and provides about 40% of the total
health care services in Ghana, (Abekah-Nkrumah 2006, Olivier et al. 2014). The private
sectors do not receive direct financing from the central government. However, they have
exemptions from some taxation for the services they provide and reimbursed for the cost and
training of health professionals in their facilities. Although the Traditional Medical Sector in
principle is under the authority and administration of the Ministry of Health, in practice, it is

34 | P a g e
less controlled and challenging to do so because they are not formalised and lack an
identifiable professional body and regulations.
Figure 3 Ghana Health Delivery Structure
1.6.2 Access to Conventional Health Services in Ghana
The World Health Organisation (WHO) has called for health systems to move
towards universal coverage and defines universal coverage as the access to adequate
and appropriate health care at affordable prices (McIntyre et al. 2008, Dye et al.
2013). Some health analysts describe accessibility to health as living within 3-5 miles

35 | P a g e
of appropriate health service (Nagelkerk 1994). According to Dye et al. (2013), the eventual
goal of universal health coverage is for people to obtain all the health services they need at
where they are without the risk of financial ruin and impoverishment, now and in future.
Ghana renewed its commitment to ensuring a more extensive and accessible coverage
through the introduction of the NHIS in 2003, which admittedly has achieved some
improvement in reducing out of pocket payment according to some evaluation analysis,
(Okoroh et al. 2018, Dake 2018).
In general, the country’s plan to provide regular and accessible health care for all the
population has been described as patchy by the director of the Ghana Health Service (Salisu,
Prinz 2009). Some studies assessing the impact of the NHIS have concluded that poor
households are less likely to register in the scheme or benefit from it (Sarpong et al. 2010).
Currently, the methods of registration or enrolling into the system appears cumbersome and
bureaucratic, requiring people to travel to the cities or rely on technology to do so, making it
difficult for the rural poor. Also, the NHIS do not cover some treatments and medications,
and this continues to burden the poor in society. Hence, there is the need to evaluate these
obstacles occurring amongst the poor appropriately to ensure that the full benefit of the
scheme is realised by all (Dixon et al. 2011).
In general, underfunding, insufficient workforce and infrastructure, lack of
accessibility due to poor road and transport networks characterises Ghana’s Conventional
Health System (Nagelkerk 1994, Sarpong et al. 2010, Buor 2003). Equally, there is difficulty
in retaining the already insufficient health workforce and in distributing them to deprived
communities (MOH 2000, Asase et al. 2010). In Ghana, the ratio of a Conventional medical
doctor to the population is 1:20,000 while that of a Traditional Healer per population is 1:200
with even more alarming rationing of specialist doctor per population, 1:300,000 (Tabi, Soo
2003). Consequently, Traditional Medicine, which is perceived to be available, accessible
36 | P a g e
and affordable in Ghana and other African communities, is essential in health care
provision to the population (Van den Boom et al. 2004). In other words, many of the
population, especially those in the remote setting, rely on Traditional Healers for their
health care needs. Traditional Healers are readily available in rural communities or
travelled to remote communities where conventional doctors or services cannot reach
or are not willing to go.
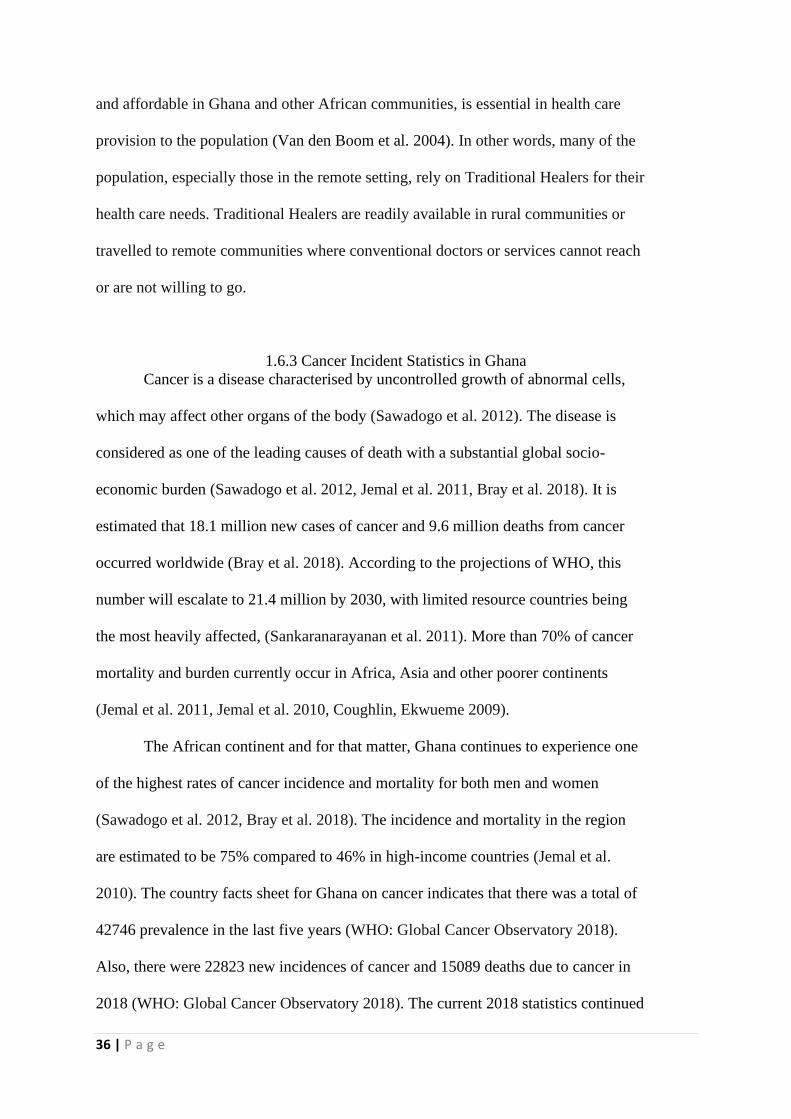
1.6.3 Cancer Incident Statistics in Ghana
Cancer is a disease characterised by uncontrolled growth of abnormal cells,
which may affect other organs of the body (Sawadogo et al. 2012). The disease is
considered as one of the leading causes of death with a substantial global socio-
economic burden (Sawadogo et al. 2012, Jemal et al. 2011, Bray et al. 2018). It is
estimated that 18.1 million new cases of cancer and 9.6 million deaths from cancer
occurred worldwide (Bray et al. 2018). According to the projections of WHO, this
number will escalate to 21.4 million by 2030, with limited resource countries being
the most heavily affected, (Sankaranarayanan et al. 2011). More than 70% of cancer
mortality and burden currently occur in Africa, Asia and other poorer continents
(Jemal et al. 2011, Jemal et al. 2010, Coughlin, Ekwueme 2009).
The African continent and for that matter, Ghana continues to experience one
of the highest rates of cancer incidence and mortality for both men and women
(Sawadogo et al. 2012, Bray et al. 2018). The incidence and mortality in the region
are estimated to be 75% compared to 46% in high-income countries (Jemal et al.
2010). The country facts sheet for Ghana on cancer indicates that there was a total of
42746 prevalence in the last five years (WHO: Global Cancer Observatory 2018).
Also, there were 22823 new incidences of cancer and 15089 deaths due to cancer in
2018 (WHO: Global Cancer Observatory 2018). The current 2018 statistics continued

37 | P a g e
to make the point on the acceleration and effects of cancer on the poor and emerging
economies and low-income countries (Bray et al. 2018).
Ghana like other sub-Saharan African countries continues to find it challenging to
provide an adequate solution to the increasing cancer incidence and burden due to poor
infrastructure, insufficient health workers, lack of diagnostic and screening equipment and
poor access to health care. Admittedly, the benefits of recent advancement in cancer care are
far from being a reality for the higher proportion of the Ghanaian population. Regrettably,
national disease data and statistics precisely for Ghana and most African Countries are
usually not available or accurately reflect the situation on the ground as many people may go
undiagnosed or unaccounted in the statistics (Klufio 2004, Aikins et al. 2010, Jemal, et al.
2011, Wiredu, Armah 2006). The problem is due to the lack of a national register, accurate
capturing, recording and preserving of data at community and institutional facility levels.
Hence the only available data may be confined to few institutions or smaller geographical
settings (Wiredu, Armah 2006, Jemal, et al. 2011).
Although the data from developing countries may be obsolete, limited in coverage,
quality and accuracy, this is mostly the only source of information on some disease profile
made available to the World health organisation (Wiredu, Armah 2006). Moreover, until
recently, cancer, unlike other communicable diseases, had not been given enough attention as
a public health problem in Africa (Wiredu, Armah 2006). Nonetheless, the impact of cancer
continues to challenge the Ghana health system and places an overwhelming burden on the
population that is affected.
38 | P a g e
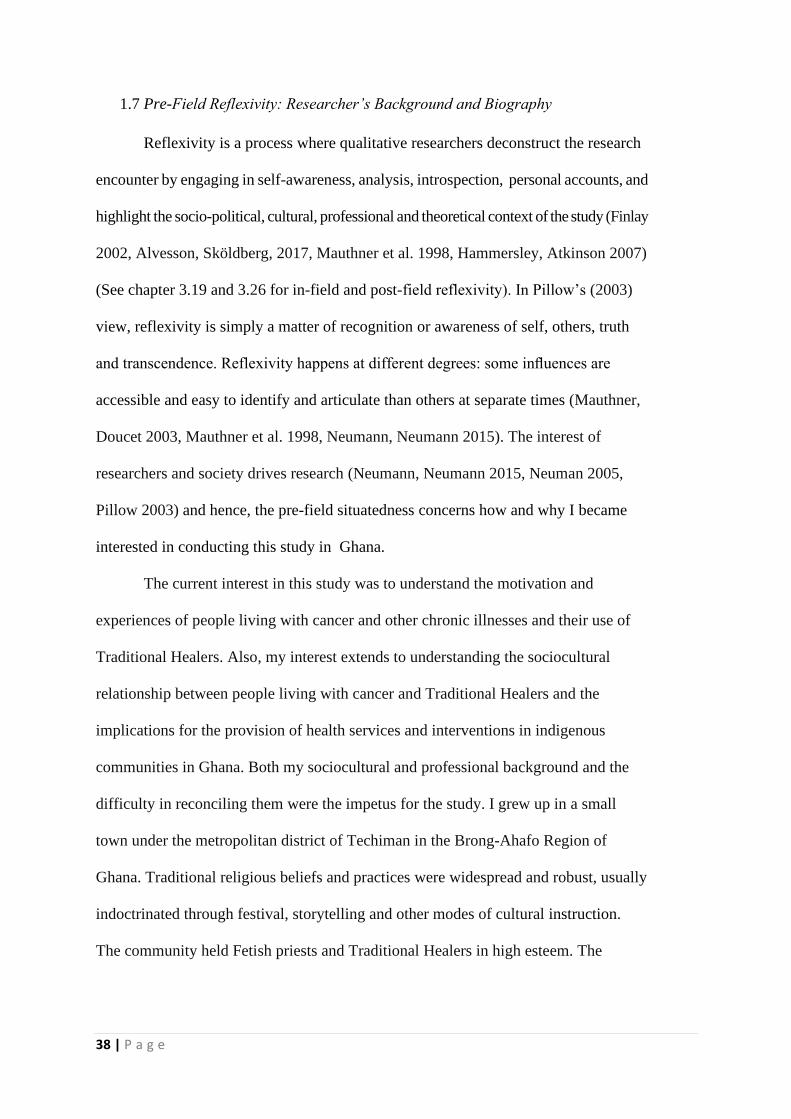
1.7 Pre-Field Reflexivity: Researcher’s Background and Biography
Reflexivity is a process where qualitative researchers deconstruct the research
encounter by engaging in self-awareness, analysis, introspection, personal accounts, and
highlight the socio-political, cultural, professional and theoretical context of the study (Finlay
2002, Alvesson, Sköldberg, 2017, Mauthner et al. 1998, Hammersley, Atkinson 2007)
(See chapter 3.19 and 3.26 for in-field and post-field reflexivity). In Pillow’s (2003)
view, reflexivity is simply a matter of recognition or awareness of self, others, truth
and transcendence. Reflexivity happens at different degrees: some influences are
accessible and easy to identify and articulate than others at separate times (Mauthner,
Doucet 2003, Mauthner et al. 1998, Neumann, Neumann 2015). The interest of
researchers and society drives research (Neumann, Neumann 2015, Neuman 2005,
Pillow 2003) and hence, the pre-field situatedness concerns how and why I became
interested in conducting this study in Ghana.
The current interest in this study was to understand the motivation and
experiences of people living with cancer and other chronic illnesses and their use of
Traditional Healers. Also, my interest extends to understanding the sociocultural
relationship between people living with cancer and Traditional Healers and the
implications for the provision of health services and interventions in indigenous
communities in Ghana. Both my sociocultural and professional background and the
difficulty in reconciling them were the impetus for the study. I grew up in a small
town under the metropolitan district of Techiman in the Brong-Ahafo Region of
Ghana. Traditional religious beliefs and practices were widespread and robust, usually
indoctrinated through festival, storytelling and other modes of cultural instruction.
The community held Fetish priests and Traditional Healers in high esteem. The

39 | P a g e
village forbids members to go and fetch water from the rivers or go to the farm at certain
sacred days and times.
The perception was that the ancestors and the gods would punish those who disobey
or disrespect these rules. The herbalists and the fetish priests acted as health advisers,
performed rituals that could eradicate illness from the village and provided most of the
healthcare needs of the population. The population trusted these practitioners for their
wisdom but also feared them for their possession of supernatural powers to decide matters
and punish people. Although people attended hospitals for emergencies and some illnesses,
they still consulted the herbalist or the priest to discern the spiritual cause of the illness and to
resolve it. Admittedly, the village is now moderate in their cultural beliefs because of the
influx of people from the city. However, it has always had the memories of these experiences
and exposures. I wanted to understand the motivation for the strong relationships between the
community and the Traditional Healers in these settings.
As a professional nurse, I use research or clinical evidence in practice or making
clinical decisions daily and find it difficult to accept some premises of Traditional Healers or
Traditional Medicine such as the supernatural connotations and anecdotal evidence to support
assertions. I usually struggle with the tension between my background (insider) and
professional perspectives (outsider) about Traditional Healers and how to maintain the
appropriate balance (Coffey 1999, Fetterman 2009, O'Reilly 2008). Nonetheless, I remained
open to understanding the practical and deep motivations for users of Traditional Healers.
According to Seale (1999), Allan and Arber (2018), being open about these tensions and
emotions enhance the credibility and integrity of the study. Neumann and Neumann (2015)
were insightful in their suggestion that an individual consists of a fragmented and developing
set of identities. My situation is usually fluid, sometimes accepting some aspects of
Traditional Medicine and rejecting others (Cudmore, Sondermeyer 2007, Allan, Arber 2018).

40 | P a g e
Consciously or unconsciously, these biographies, experiences and identities
entered the field with me and had the potential to influence my thoughts and
decisions. Furthermore, My MSc project laid the foundation by exploring doctors’
views and experiences of Traditional Medicine and the possible integration with
Conventional Medicine as recommended by the World Health Organisation. The
study found that almost all the participant doctors had the experience of using
Traditional Healers or Traditional Medicine in the community or the family when
they were growing up (Badu Appiah 2011). However, most doctors strongly
disagreed with any form of integration between Conventional Medicine and
Traditional Medicine because of Traditional Medicine’s lack of scientific evidence or
medical training for its practitioners (Badu Appiah 2011).
Many of the doctors saw Traditional Healers as a hindrance to better treatment
outcomes by preventing the population from seeking advice early (Badu Appiah
2011). Also, the study found that most of the doctors were resentful towards
Traditional Healers and unsympathetic to patients who use their services (Badu
Appiah 2011). However, the conceptualisation of health and health-seeking
behaviours in indigenous communities is complicated and something that needs more
exploration.
1.8 Summary of Chapter One
The chapter provided an overview of the socio-cultural and economic context of the study
and how health beliefs and practices influence choices regarding pathways to treatment and
care. Also, I discussed the socio-cultural values and health care or health delivery system in
Ghana. These included the general lay health practices, use of Traditional Healer and
Conventional Medicine. Moreover, the chapter considered the profile of the Traditional

41 | P a g e
Healer with regards to the pathways through which they come into Traditional healing, how
they acquire their healing knowledge and their methods of training. Although almost all
Traditional Healers in Ghana tend to seek answers from a supernatural power, some have
more action-oriented to spirituality than others. However, orientation they have depends on
their route or pathway to the Traditional healing profession. The chapter also gives an
overview of the cancer statistics in Ghana, which identifies the rising prevalence of cancer.

42 | P a g e
The literature review is divided into two parts. The first part, which is the general literature review was conducted to establish the gaps in the literature and to help formulate the research question. This part of health beliefs, illness conceptualisation and health seeking behaviours and use of THs/TM in Ghana The second part of the review was a theoretical review that was conducted as per my methodology to place the study findings and theory in the theoretical literature of trust. The Theoretical literature review the importance of true examined the concepts of trust that were relevant to participants motivations and relationships, experiences and re indigenous communities, interaction and relationships with the THs.
In this chapter, I discussed the philosophical and theoretical underpinnings of GT or CGT and justifies why the interpretive-constructive approach is the most suitable for my study. I situate myself in the study through reflexivity and acknowledge my potential biases. I also discuss access negotiation, participants recruitment and data collection and analysis using the method of iterative coding and constant comparison method
The findings chapter discusses and shows evidence of participants motivation and experiences of using THs. I have categorised the findings under three broad headings: Placing trust in one’s community and Identity, Finding solace in Therapeutic Hospitality and Conviviality and Aiming to avoid upset and manage emotions The section shows how trust formed the fundamental premise of participants relationship with THs. Participants trusted the THs because of shared identities and the THs reputation that reflected the shared traditions or cultural values. The section examines participants experience of friendliness and welcoming reception and atmosphere with the THs. Avoidance of upset or the managing of emotion describes how THs behave in a culturally appropriate manner to avoid upsetting participant and managing their emotions. For example, the use of euphemism or indirect language to minimise the impact of their words on participants.
In this chapter, I
discuss and
compare the finding
of the study with
extant theoretical
literature and other
studies. The
discussion was
focused on trust
and how
participants
conceptualised it in
their context and
how that influence
their motivation
and experiences in
using the THs.
The conclusion chapter describes the process of the study and what I learnt in the journey. I also considered the recommendation and implication of the study to health policy and delivery in Ghana. There is also an implication of the study about the training and relationship of doctors in Ghana with the local communities. The need to involve THs in health delivery, as recommended by the World Health Organisation.
Figure 4 Summary of chapters to Thesis

43 | P a g e
CHAPTER TWO: LITERATURE REVIEW
2.1. Chapter Overview
The literature review has two-parts. The first part was the general review that
was done to identify the gaps in the literature and to develop the research questions.
The second part of the literature review was a theoretical review that was performed
as a way of situating the findings and the theory in extant theories about Trust (see section
2.8, for details on a theoretical literature review).
The nature of literature review in Grounded theory methodology has been a matter of
debate since the inception of the methodology by its pioneers (El Hussein et al. 2017,
Charmaz 2014, Gibbs 2015, Ramalho et al. 2015). There is an expectation on researchers
using Grounded theory methodology to minimise their exposure to extant literature and
theories and to limit their influence to ensure that the concepts and categories of their studies
are grounded in data (El Hussein et al. 2017, Gibbs 2015, Charmaz 2014) (See 3.12:
Theoretical Sensitivity). Hence, some authors propose that the literature review in using
Grounded theory methodology should only be conducted after the research or data analysis
(El Hussein et al. 2017, Henwood, Pidgeon 2003). Perhaps, this highlights the debate and
lack of clarity on how the Grounded theory researcher should approach the literature review
and the appropriate time to conduct it.
The Constructivist Grounded theory, the version of the methodology which was used
for this study acknowledges the importance of understanding the discourse around the
research topic and contextualising the research, fulfilling ethics and regulatory requirements
and setting the initial direction of a study (Bryant, Charmaz 2007, Gibbs 2015, Charmaz
2014, Creswell 2012, Ramalho et al. 2015). Equally, research funding bodies require
applicants to demonstrate their knowledge in the field of enquiry through the literature
review, which is discouraged by some versions of the methodology (Ramalho et al. 2015).

44 | P a g e
The Constructivist Grounded theory Methodology approach offers a pragmatic and a
two-stage (pre the study and post the analysis ) approach to the literature review (El
Hussein et al. 2017, Gibbs 2015, Charmaz 2014). This two-stage approach to
literature review was applied to this study.
The first stage of the literature review (the initial or general review) was
conducted to address the initial research interest, identify the gaps in the literature,
and provide a justification for conducting the study (El Hussein et al. 2017, Gibbs
2015, Charmaz 2014). Equally, the initial literature review was essential in
understanding the context of the study and in developing the research questions and
preparing the interview schedule for the study (Gibbs 2015, Charmaz 2014).
Questions around factors influencing the health-seeking behaviours and the use of
Traditional Healers in Ghana and other similar settings were considered in the general
review. Additionally, the general literature review was influenced by questions on
knowledge and barriers to cancer prevention in Ghana. Moreover, the general review
answers the questions on how people who are living with cancer use Traditional
Healers and their motivation for doing so.
The first part of the literature review (general review) begins with an outline
of the search strategy and critical appraisal of the relevant literature. Following this, I
discuss the key factors influencing the use of Traditional Healers or Traditional
Medicine in Ghana. Moreover, the general review considers how people living with
cancer use Traditional Healers more than the ordinary population, the type of
Traditional Medicine that they use, and how they do not seem to talk about it with
their doctors. Furthermore, I discuss cancer awareness and health-seeking for cancer
symptoms in Ghana. Also, I outline the research questions, aims and objectives.
These were based on the synopsis of the knowledge and theory gaps in the literature.

45 | P a g e
I also discuss how my study would help to bridge some of the identified gaps in knowledge.
After this, I present the theoretical literature on trust.
2.2 Search Strategy and Critical Appraisal
The search strategy was developed to identify and appraise the appropriate evidence
and to evaluate them for their values and relevance. Grant and Booth (2009) described the
literature review as a springboard for conceptual innovation and thinking anew through
identifying and engaging with relevant and significant literature on a theme or subject area. It
also includes evaluating their contributions and limitations. The review provides a narrative
on the research through review and analyses of what we know about Traditional Healers and
people living with cancer in Ghana and similar settings. In doing so, the knowledge gaps in
methodology, theory and findings in the literature are identified to influence the research
questions and to make explicit the importance of my study (Grant, Booth 2009). In other
words, the study is justified in seeking to bridge some of these knowledge gaps. I first
describe my search strategy, critical appraisal of existing literature and then evaluate and
discuss their findings.
2.2.1 Databases and Search Terms
A search was conducted using the following databases: MEDLINE, Social Science
Citation Index (Web of Knowledge), CIHNAL, Psych Articles, Psych INFO, PROQUEST
and Psychology and Behavioural Science and Google Scholar to identify scholarly articles on
Traditional Medicine, cancer and health-seeking behaviours. The search was conducted
between June 2013 and 2014 and updated regularly through alerts and re-running of the
search (latest in June 2019). Updating the search helped in capturing the most up to date
knowledge on the subject. There was also a search in relevant journals, books and conference

46 | P a g e
reports at the University of Surrey Library. I also explored the appropriate references
to the literature for their potential inclusion in the review.
The University of Surrey library staff helped to obtain literature that was not
available at the school from the British Library and other external libraries through
the interlibrary request. The searches were conducted using appropriate MESH terms,
subject headings and keywords such as Traditional (Herbal, Indigenous, Folks, and
Alternative Complementary) medicine ( treatment, therapy, care ), (cancer, tumour or
chronic diseases), Ghana (Sub-Saharan Africa, Africa and Asia ) Behaviour (Beliefs,
culture, determinants, motivation, choices, decisions). Boolean operators and
truncators were utilised to capture studies as per eligibility criteria. I uploaded all
papers from the searches into RefWorks and Endnote bibliography software. Using
this software facilitated screening and removing duplicates, keeping track of the
articles and referencing them.
2.2.2 Inclusion Criteria and Exclusion Criteria
The concept of Traditional Healers and Medicine are old, and authors who
wrote on some of the most critical pieces of literature on the subject wrote them long
ago. Hence, I did not intend to limit the years covered in the search, but for practical
purposes, I included published articles spanning the last 20 years in the search.
Empirical research articles with abstract and published in the English language met
the inclusion criteria and vice versa. The included literature also had adults as their
participants, peer-reviewed and had full sources available. I included studies
conducted in a developing or impoverished continent such as Asia and Africa and
excluded those done in Europe and America to ensure relevance or similarity to the
context of my study. Also, some articles were excluded based on the irrelevance of

47 | P a g e
their title and content of the abstract. For this purpose, a PRISMA flow chart was used that
helped to identify what was included and excluded (See Figure 5).

48 | P a g e
Figure 5 PRISMA Flow Chart

49 | P a g e
2.2.3 Critical Appraisal of the Literature
The search results revealed that most of the empirical studies on the use of Traditional
Healers by people living with cancer and their health-seeking behaviours in the indigenous
population were conducted using qualitative methodology. Perhaps, the researchers preferred
qualitative methods because they could explore in more depth lay people's meanings,
motivations, conceptualisations or sociocultural phenomenon. Also, it may allude to the
nature of research in this field, mostly intended to understand peoples’ experiences in using
different health care systems in places of medical pluralism.
Moreover, there may be practical and logistical barriers to conducting extensive
surveys or quantitative studies in rural parts of Ghana or other African countries. Most
studies have focused on the socio-economic factors influencing the use of Traditional Healers
while neglecting the need to understand or conceptualise the experiences of these users and
their cultural, identity and motivations which is the focus of the exploration of my study. I
read, analysed and critically appraised the quality of the literature using the Critical Appraisal
Skills Programme (CASP) (See Appendix 1 for CASP tool) tool for qualitative studies
(Noyes et al. 2015, Joanna Briggs Institute 2015).
In this study, the CASP appraisal tool was found to be very systematic and
appropriate for the type of studies to be appraised and hence used. After assessing the
materials to be included in the review, they were categorised into themes based on the
similarities of their focus and findings (Neill 2000, Joanna Briggs Institute 2015, Noyes et al.
2015). Throughout the review, I referred to the original papers when necessary for
information or content accuracy and representation (Neill 2000; Noyes et al. 2015; Joanna
Briggs Institute 2015).

50 | P a g e
2. 3 Factors Influencing the Use of Traditional Healers in Ghana
I have categorised the factors that influence the use of Traditional Healers in
Ghana and most African countries into socio-economic, socio-cultural and belief
systems. Classifying the elements in this manner reflects the understanding,
conceptualisation and determinants of health behaviours in these settings. However, in
practice, the distinctive categories are blurred with nuances. Multiple factors influence
peoples’ health-seeking behaviours (Langlois-Klassen et al. 2007, Peltzer et al. 2008,
Kwansa 2010) and in Ghana, involves switching between different therapeutic
modalities or using them simultaneously (Tabi et al. 2006, Bazzano et al. 2008,
Awusabo-Asare, Anarfi 1997).
2.3.1 Socioeconomic Factors
Studies have drawn attention to the influence of socio-economic factors on the
health-seeking behaviours in communities that are impoverished. The pieces of
literature highlight factors such as the lack of affordability, availability and
accessibility to Conventional Medicine as the main socio-economic factors
influencing the use of Traditional Healers in these poor resource communities
(Bazzano et al. 2008, Tabi et al. 2006, Aries et al. 2007, Fenny et al. 2015, Dalaba et
al. 2018). Generally, the unavailability or lack of access to Conventional Medicine is
more acute in remote and poor communities in Ghana. Hence, these populations rely
on Traditional Healers who usually reside in their communities (Tabi et al. 2006,
Sarpong et al. 2010, Buor 2003, Tabi, Soo 2003). Other studies have mentioned the
attitude of medical staffs at hospitals and clinics to influence health-seeking
behaviours of patients or the communities they serve (Macha et al. 2012, Agyemang-
Duah et al. 2019, Mwaka et al. 2015).

51 | P a g e
A study by Bazzano et al. (2008) focused on the care-seeking behaviours for the new-
borns in Northern Ghana using both quantitative and qualitative data. The quantitative data
was a birth surveillance data of 2878 children from July 2003 to June 2004. The qualitative
data includes observation (84 hours) and multiple data collection methods including a focus
group of parents, in-depth semi-structured interviews with a key informant (old mothers and
grandmothers), interviews with mothers and expert’s local health providers (n=132). The
study identified financial constraints and remoteness from health facilities to have a
significant influence on the participants’ health decisions. Some parents took their children to
the Traditional Healers because they could not afford the transport and hospital cost (Bazzano
et al. 2008).
The study highlighted the importance of more comprehensive and affordable health
care coverage and improvement in health-seeking behaviours through health education and
removal of financial barriers (Bazzano et al. 2008). Similarly, Aries et al. (2007) study on
fracture treatments after a road traffic accident in Techiman, a city in the Brong-Ahafo
region of Ghana (n=46) identified socio-economic factors to influence the decision to choose
between Traditional Healers and Conventional Medicine. A higher proportion of participants
(n-=29) opted for treatments from the bonesetters. These participants cited the cost of
treatments (Aries et al. 2007) and bonesetters competence or experience in treating bone
fracture (Aries et al. 2007, Solagberu 2005) for using Traditional Healers.
Although most participants in Aries et al. (2007) study were concerned with money,
they attended the hospital immediately after the accident before transferring to the bonesetters
on the basis that the doctors or hospitals had sophisticated diagnostic equipment and the
knowledge to halt emergencies. A study by Sato (2012) on the actions taken for self-reported
episodes of acute and previously diagnosed chronic illnesses supports the notion that doctors
are experts in dealing with emergencies and not so good with chronic diseases. The study

52 | P a g e
found low use of Traditional Healers for acute conditions and higher use of
Traditional Healers for chronic conditions.
However, the cost of treatment was the main reason for most participants in
Aries et al. (2007) study who were admitted as an emergency to the hospital later
requesting to be discharged to the bonesetter and not the issue of competency. In
Amegbor’s (2017) study about the preferences of healthcare therapy in Ghana, most
participants relied on self-care, using both indigenous and biomedical initiatives to
escape the financial burden of Conventional Health Care. Some participants of the
study used home remedies and ordinary herbal products or bought un-prescribed
tablets, ointments and medications from an unqualified chemist or street hawker to
treat themselves (Amegbor 2017). These studies highlight the importance of financial
consideration in health decisions and whether a person would use the Conventional
Medicine or Traditional Healers in Ghana.
Additionally, a study by Macha et al. (2012), explored the manner of health
care financing and the primary beneficiaries of such financing in Ghana, Tanzania and
South Africa. A triangulated data of household surveys, interviews and focus group
were collected in 2008 for the study. The data collected in each country were: Ghana:
2986 households survey interviews (n=14050) and a focus group (n=26), Tanzania:
2234 (n=12200) households survey, interviews and a focus group (n=22) and in South
Africa: 4800 households survey interview (n=22000) and a focus group (n=44). The
study found that the structure and methods of financing Conventional Health Care in
all three countries were similar and favoured the rich or the wealthy. All the three
countries operated with a health insurance system which required initial registration,
regular membership renewal and annual premium payments (Macha et al. 2012).

53 | P a g e
Majority of the rural populations and the poor in all the three countries in the study
faced a financial challenge of paying for the premium, travelling to the cities or registration
centres to register or having the technology and internet access to register (Macha et al.
2012). The general acknowledgement is that arbitrary rolling out and expanding national
health insurance will not necessarily translate to an increased usage of Conventional
Medicine unless it matches with affordable, accessible and functioning facilities or services
(Macha et al. 2012, Kuuire et al. 2016, Fenny et al. 2015, Agyemang-Duah et al. 2019).
The increase in the national health insurance scheme (NHIS) coverage in Ghana has
not adequately addressed the fundamental tenets of the scheme to provide access to adequate
and equitable health services to the entire population, especially the poor and vulnerable
(Kuuire et al. 2016). Studies have highlighted insufficient workforce, poor building
infrastructure, and transport connecting systems as constraints to the rural populations’ ability
to have access to Conventional Medicine (Nagelkerk 1994, Sarpong et al. 2010, Buor 2003).
In most Ghanaian communities, there is a low ratio of Traditional Healers to the
population, and ready availability and unimpeded accessibility to Traditional Healers (Tabi,
Soo 2003). Contrary, there is a high ratio of patients to doctors per population with the
situation even worse regarding the number of specialist doctors per population (Tabi, Soo
2003). The shortage or insufficient doctors are due to the lack of facilities to train more
doctors, government’s inability to provide enough incentives comparable to the developed
countries which have led to brain drain (MOH 2000, Asase et al. 2010).
The impact of such doctors’ shortages is more felt in the remote and rural
communities which are not attractive to doctors. Consequently, the rural populations in
Ghana and most African communities rely on Traditional Healers who are available in their
communities (Van den Boom et al. 2004) or are willing to travel to these communities where
Conventional Health Professionals are not available. Other factors hindering access to

54 | P a g e
Conventional Medicine in Ghana are the lack of proximity to Conventional facilities
and poor road and transportation systems (Tabi et al. 2006, Tabi, Soo 2003, MOH
2000, Dalaba et al. 2018, Fenny et al. 2015). Some authors consider appropriate
healthcare as the one that people need and can access in their immediate communities
(Dye et al. 2013) or at least within three to five miles of where they live (Nagelkerk
1994).
In Ghana, most Conventional Health facilities are established in the cities and
away from rural communities. Equally, most of the linking roads to these facilities
are very rough, has potholes and challenging to use, especially when it rains (Tabi et
al. 2006, MOH 2000). Hence, even those rural populations who manage to get into the
NHIS may be unable to use conventional medical services due to the unfortunate lack
of proximity and transport network (Fenny et al. 2015). On the contrary, the lack of
any requirement for transportation and long-distance travelling make using the
Traditional Healers more attractive and convenient in most Ghanaian indigenous
communities. Furthermore, staff attitudes at Conventional Health facilities influence
the health-seeking behaviour of patients.
In the study by Macha et al. (2012), both the focus group interviews and the
household surveys identified staff attitude to influence health-seeking behaviours. The
study identified negative staff attitudes such as bribery and corruption and asking
participants to pay for drugs and services that should be free to influence patients’
health-seeking decisions. In Ghana, some participants in the more indigent
population did not trust the hospitals and NHIS staffs, and hence, they were unwilling
to register for the NHIS (Macha et al. 2012). Contrary, the same study identified staff
attitudes as positive, such as politeness and excellent interaction in privately own

55 | P a g e
facilities which attracted the rich or those who could afford private care (Macha et al. 2012).
Although the study highlighted functional interactions in the privately own hospitals,
it does not discuss the nature or elements of the interactions. Other studies have documented
in more detail, the influence of staff attitude to the use of health services (Agyemang-Duah et
al. 2019, Mwaka et al. 2015). Both Agyeman-Duah et al. (2019) study (n=35) in Ghana and
Mwaka et al. (2015) (n=24) in Uganda, broadly explored the facilitators and barriers to
biomedical or Conventional Health Care use. Both studies highlighted the importance of staff
attitude to health service use. The study by Mwaka et al. (2015) described negative staff
attitudes such as disrespect, bribery or unofficial payments, and discriminating against the
poor or giving special services to those who have high statuses in society.
On the other hand, Agyeman-Duah et al. (2019) identified positive staff attitudes such
as friendliness, cordiality, approachability and quality of care (quick recovery and
effectiveness of treatment ). It should be noted that 20 participants of Agyeman-Duah et al.
(2019) study were health professionals and may have theoretical knowledge of the influence
of positive behaviours on patients and their health service use. What is not known is how they
demonstrate these in practice. Both studies found the use of English language by hospital
staff and their failure to speak the local dialect and understand the local culture an abhorrent
attitude, a deterrent to Conventional Medicine use and contributed to low patient satisfaction
(Mwaka et al. 2015, Agyemang-Duah et al. 2019)
There is not much clarity on whether the barriers or hindrances to Conventional
Medicine use always drive people to Traditional Healers. However, Mwaka et al.’s. (2015)
clearly stated that patients living with cervical cancer used Traditional Healers mainly
because of language and staff attitude as a barrier to biomedical care. Furthermore, the lack
of practical functionality of most Conventional facilities and staff attitude discouraged the use
of Conventional Medicine (Macha et al. 2012, Agyemang-Duah et al. 2019). Some authors
56 | P a g e
have described incomplete waiver policies and lack of required services at the
institutional levels as a challenge to Ghana’s Conventional Health System (Macha et
al. 2012, Agyemang-Duah et al. 2019).
Agyeman-Duah’s et al. (2019) conducted their study at Ejusu in the Ashanti
Region of Ghana. They discovered that most participants, including NHIS members,
were dissatisfied with the service that they received and described the system as
inoperative. The reason for the study participants dissatisfaction was that the NHIS
did not cover many illnesses, services and drugs (Agyemang-Duah et al. 2019). Some
of the study participants were also concerned about the lack of clarity on what the
scheme covers and, the fact that many of the items covered were in name only and not
available in practice (Agyemang-Duah et al. 2019).
Unfortunately, the study did not mention the specific list of illnesses, drugs
and services that the NHIS covered or did not cover and hence it is not known the
level cover of treatment that people living with cancer were entitled to receive.
Undoubtedly, all the studies above show how multiple socio-economic and health
system factors influence whether people in indigenous communities would choose
Conventional or Traditional Medicine for treatment.
2.3.2 Sociocultural Factors
Culture as a way of life relates to how people of community experience and interact with
others and the wider socio-spiritual or psycho-physical environment (Geertz 2017). At all
stages of human life, socio-cultural processes impinge on health, ill-health and our
perspective and interpretation of them (Nettleton 2013). People’s sociocultural background
and understanding of health influence their preferred method or model of treatment and
whom they identify or recognise as appropriate to provide the treatment (Kleinman 1980,

57 | P a g e
Helman 2007, Nettleton 2013). Equally, culture affects the health decision-making process,
such as which stakeholders are involved and who makes the final decision.
Hence, we should study and discuss treatment-seeking behaviours from a broader
cultural context (Landy 1977, Helman 2007, Kleinman 1980). However, culture should not
serve a broad-gauge or a sole measure of health behaviours because of its lack of
homogeneity and different individual or subgroup behaviours in all communities (Helman
2007, Geertz 2017, Kleinman 1980). Different members of a cultural group may have a
different expectation, understanding and attitude toward the same cultural values and norms
(Koffman 2006) and hence have a varied attitude towards health.
Additionally, there may be multiple distinctions or variation of cultural attributes
within the confines of a specific cultural group or society across the different socio-economic,
professional and religious strata or categories (Helman 2007, Hall, 1989, Leach 1973). These
groups may exhibit different health-seeking behaviours and practices from the rest of the
broader cultural group. Hence, we should always consider culture in the appropriate context
of socioeconomics, politics, history, geography and the influence they may have on the group
of people at a specified period (Kleinman 1980, Helman 2007).
A study by Kakute et al. (2005) considered the barriers of exclusive breastfeeding by
mothers in rural Cameroon, initially using four focus groups discussion (n=40). The
researchers then formulated a survey questionnaire from the focus groups discussions to
recruit breastfeeding mothers from four villages (n=320), 80 from each village (Kakute et al.
2005). Although most of the participants (94.4%) attended the antenatal clinic and received
advice on exclusive breastfeeding, the community’s cultural beliefs influenced their health
behaviours. The study is not clear on the exactness and the quality of advice that the antenatal
clinic staff gave to the women and whether the women understood the information.

58 | P a g e
Many of the participants, two hundred and seventy-one (84.7%) gave solid
food to their infants before the age of six with others doing so at a very early age. All
participants practised mixed feeding and gave additional foods such as chewed
cocoyam, plantain, banana, groundnut and oranges to their babies before they were
six (Kakute et al. 2005). The study identified mixed feeding as an old cultural practice
which the elders or older women enforce in the communities with the intentions of
protecting babies from illnesses. Any attempt by the women to disobey such a
practice could cause a conflict between them and their husbands, mothers-in-law, and
the village elders which could attract curses or misfortunes (Kakute et al. 2005).
Furthermore, all participants had the cultural belief that sexual contact was a
prohibition during breastfeeding as it destroys the milk and can destroy the child. To
eschew such risk, the mother had to feed the child with other foods and then wean
them off the breast milk as soon as possible so that the husband can have sexual
contact with them at the earliest opportunity (Kakute et al. 2005). Most participants
had the notion that breast milk was an incomplete food and could not provide all the
necessary nutritional requirements for the child’s growth. Hence, the mother needs to
give the child solid food to meet the nutritional requirement and equally enjoy the
pride of feeding the child with the families own farm products. More than half
(52.2%) of participants believed that colostrum milk was inadequate and bad for the
baby. Hence, all Fulani women in the study preferred not to commence breastfeeding
immediately but wait until at least after two days. Instead, they preferred to give their
babies cow’s milk and Viindi. Viindi is the water they obtain from washing off
passages of Quran, which they have written with charcoal and believe to be highly
nutritious and offers protection to the child (Kakute et al. 2005).

59 | P a g e
Although the study is critical in highlighting the dynamics of cultural practices in
health behaviours, it does not necessarily say that the participants used the services of
Traditional Healers. However, the participants were breastfeeding women who had no health
issues and hence, it was not necessary for them to see a Traditional Healer. The study
acknowledged that these communities and the practices were controlled and enforced by
Traditional leaders and elders who are in similar positions or provided identical services as
the Traditional Healers.
Other factors such as the influence of family, friends, social networks, education and
occupation influence health behaviours (Aries et al. 2007, Tabi et al. 2006, Moyer et al. 2014,
Ngom et al. 2003, Gyasi et al. 2015, Solagberu 2005). Some participants in Aries et al.
(2007) study were influenced to leave the hospital for treatment at the Traditional Healers per
the family leaders’ experience, advice and the entire families’ perception of the ease to visit.
Also, in a study by Tabi et al. (2006), some participants used Traditional Healers
because of the experiences and persuasions of their parents or family. A study by Moyer et
al. (2014) explored the impact of social factors on the place of delivery or childbirth in
northern Ghana. The study identified power, social hierarchy, and a widespread sense of
shared family or communal responsibility to influence whether a woman delivered in a
Conventional Medical facility or at home. The family head, husband and community
soothsayers all played an essential role in deciding the facility that the women used for
delivery.
The study found that even the women who made their own decisions sometimes
needed the spiritualist and the husband's approval to operationalise this decision (Moyer et al.
2014). A study by Ngom et al. (2003) on gatekeeping and women’s health in the Kassena
Nakanna District in the northern part of Ghana (n=2856), used the terms compound and
husband gatekeepers to describe how hierarchies and cultural practices affect health-seeking

60 | P a g e
behaviours in some communities. The health-seeking behaviour of participants was
affected by their reliance on the compound gatekeepers who provided spiritual and
moral direction and the husbands who provided the legal authority and economic
support (Ngom et al. 2003). The respect for older people, tradition and hierarchy is
fundamental in the Ghanaian culture. Likewise, the hierarchy influences health
decisions, and in most cases, the community elders or stakeholders make the decision
corporately or at least approve the decision.
Education and demands from employers were found by Tabi et al. (2006) to
influence the choice of treatments for some employees. The demand from employers
for the evidence of employees visit the doctors for treatment, and formal education
did not favour the choice of Traditional Medicine. Similarly, Gyasi et al. (2015)
analysis of the predictors of using Traditional Healers in the Ashanti Region of Ghana
found higher use of Traditional Healers amongst market workers or traders than
public sectors workers. Education may have a bearing on the finding as people
working in the public sector in Ghana tend to have formal education or qualification
in contrast to market traders. The findings contradict the findings of Chen et al. (2008)
(n=5046) assessment of the demographics, and socioeconomic statuses of people
living with cancer’ use of Traditional Healers post-diagnosis in China.
The study found that 97% of participants used Traditional Medicine, and they
were associated with higher education, younger age, higher income or socio-economic
status. The disparity between the findings of the two studies suggests that while
Traditional Medicine may be cheaper in Ghana, it may be expensive in China and
more affordable to the affluent. The issue of education and its benefits are usually
contentious within some indigenous populations in Africa. Some see education as
enlightenment to the unhygienic and unscientific superstitious practices of
61 | P a g e
Traditional Healers. Others perceive education as anti-African traditions or cultures which
dissuade people from using Traditional Healers (Tabi et al. 2006).
The study by Awusabo-Asare and Anarfi (1997) did not directly identify non-
spiritual factors in their findings. However, they found that HIV/AIDs patients who believed
in the scientific concept of disease aetiology used Conventional Medicine for treatment.
Some participants also preferred Traditional Healers for the thought that their illnesses may
be a misfortune. Primarily, the scientific theory of disease aetiology offers a non-spiritual
explanation to the cause of a disease (Wade, Halligan 2004, Dick 2010, van der Geest 1997)
and hence encourages people to seek Conventional Medicine.
2.3.3 Spiritual Belief System
A study by Okerefo and Fiaveh (2017) examined how religiosity or spiritual beliefs
influence health-seeking behaviours in Accra, Ghana. The study found an active link between
health-seeking behaviours and religiosity. Participants who believed in spiritual causation
and healing of diseases relied on prayer alone or on both prayer and biomedicine to find
solutions to their illnesses (Okyerefo, Fiaveh 2017). The study also found that participants
who believed in spiritual healing preferred getting away from the routine busy life activities
to a sacred and serene landscape such as the forest where they could wrestle with the mishaps
they had in their life.
Several studies have acknowledged the influence of spiritual beliefs on illness
causation in health-seeking behaviours and choices in Ghana (Tabi et al. 2006, Bazzano et al.
2008, Awusabo-Asare, Anarfi 1997, Kwansa 2010, Adjei et al. 2013, Kpobi et al. 2018,
Farnes et al. 2011). These include diseases such as Asram characterised with ‘green veins’
on a child’s body, excessive crying and growing leaner in Bazzano et al. (2008), epilepsy in
Tabi et al. (2006), Adjei et al. (2013) and Kpobi et al. (2018). Also, HIV/AIDS in Awusabo-

62 | P a g e
Asare and Anarfi (1997) and Kwansa’s (2010) study were seen as the consequence of
a curse or attack from an evil person and hence required treatment from Traditional
Healers. Supernatural beliefs and human vulnerability to spirit and deities are
common in Ghana and underpins most cultural practices. For example, in Farness et
al. (2011) study, pregnant women believed that the pregnancy increased their
vulnerability, exposure and made them a target to spiritual attacks from a jealous
person.
Consequently, they preferred to receive support from the Traditional Healers
who could protect them from evil spirits. A study by Kwansa (2010) acknowledged
the importance of spiritual therapy in Ghana, at least as a coping strategy to find
meaning and hope in life or hereafter. Traditional Healers are perceived to have the
powers to deal with spiritual illnesses and misfortunes or offer the necessary spiritual
protection, guidance and answers under challenging circumstances in conformity with
the indigenous Ghanaian culture (Farnes et al. 2011, Tabi et al. 2006, Awusabo-
Asare, Anarfi 1997, Abel, Busia 2005). Broadly, Ghanaians and Africans, in general,
tend to seek a spiritual explanation to diseases and events because of the inherent
beliefs about God and ancestral spirits (Neba 2011, Castle 1994, Tsey 1997, Abel,
Busia 2005).
Individuals may behave in this manner even for diseases that are viewed to
have no spiritual causation or have a clear medical explanation for their causes
(Musara 1991, Irwin et al. 1991, Lindan et al. 1991). Some people seek spiritual
interpretations due to the shock and uncertainties from suddenly occurring illnesses
and worsening of illnesses and chronicity of health conditions. Others seek
Traditional healing to ascertain answers to why they or their relative may be suffering
from illnesses or misfortunes (Castle 1994, Johnston 2002, Neba 2011).
63 | P a g e
Moreover, people review their health choices and make changes accordingly as
circumstances change. Some participants in both Aries et al. (2007) and Solagberu (2005)
study returned to the hospital when they developed infections or perceived a lack of progress
in their treatment with the Traditional Healers. All these studies have highlighted essential
elements influencing the choice of Traditional Healers in Ghana.
2.3.4. Psychological and Emotional Motivations for Using Traditional Medicine
A study by Yarney et al. (2013) found that participants used Traditional Healers to
improve emotional and physical wellbeing and to manage the perceived toxic and dire
consequences of Conventional treatment. Psychological and emotional support is essential for
people living with cancer throughout their disease trajectory and influences their decision to
use Traditional Healers (Miller et al. 1998, Clegg-Lamptey et al. 2009, Wanchai et al. 2010,
Aziato, Clegg-Lamptey 2015). A study by Clegg-Lamptey et al. (2009), was on people living
with cancer regarding the psychological aspects of breast cancer treatment in Accra-Ghana
(n=89). The study identified specific patient concerns such as fear of destructive
Conventional Medicine treatment (chemotherapy, radiotherapy and mastectomy), depression
and shock of the diagnosis to cause a psychological challenge to people living with cancer.
Several participants in the study had concerns about the lack of psychological support
in Conventional facilities. These included staffs and institutional lack of sympathy and
emotional support, lack of information and communication concerning their treatment, lack
of any available counselling services, and slow or bureaucratic services. Overall, 67% of
participants were dissatisfied with the level of psychological support they received in the
hospitals, and 49.4% ended up with an alternative or non-conventional medical treatment for
their cancer treatment. Although the study did not say whether these patients used alternative
treatments for a psychological reason, it appeared to allude that the lack of psychological
support in the hospitals may have influenced the participants’ choice of Traditional Medicine.

64 | P a g e
The study concluded that people living with breast cancer in Ghana are not
receiving emotional and psychological support and the need for adequate and enough
psychological support for people living with cancer in Ghana. Similarly, the findings
of other studies have supported the severe psychological distress of people who were
living with cancer experienced from the time of diagnosis and throughout their
disease progression. These studies show a complete lack or limited support that
people living with cancer receive for their emotional needs (Wanchai et al. 2010,
Clegg-Lamptey, et al. 2009).
In Ghana, the provision of psychological and emotional support to patients in
Conventional Medicine is limited or lacking with patient care focusing mainly on
physical needs. Most of the population, therefore, use prayers, religious and social
activities and Traditional Healers therapies to address these unmet needs alongside
Conventional Medicine or alone. Although the general perception is that people use
Traditional Healers because of the Traditional Healers acknowledgement and support
for their psychological needs, there is a lack of literature on how Traditional Healers
provide services and support in Ghana. In Wanchai et al. (2010) study, Traditional
Healers were perceived to be holistic practitioners and provided psychological support
through listening, acting humanly, allowing enough time for their patients during the
consultation and therapeutic encounter.
A study by Bignante’s (2015) investigated the culturally specific interaction
between patients and healers in Northern Senegal, (n=160), using interviews, focus
groups interviews and observation. The participants were 100 patients, 20 herbalists
or people selling herbal remedies in the marker and 40 traditional healers. The study
identified elements of psychological and emotional healing or support emanating from
participants relationships with the Traditional Healers to influence their use of the

65 | P a g e
Traditional Healers. To understand the kind of patient-healer relationship that supports
patients emotionally and psychologically, the researcher interacted more intensely with 20
patients and 15 healers who had a high reputation in the communities through extensive
interviews, observation and interactions (Bignante 2015).
Consequently, the researcher was able to provide a clear understanding of the several
elements of the relationship and interaction between participants and the Traditional Healers,
which supported them emotionally and influenced their use of the Traditional Healers. The
study found that the Traditional Healers discussed patients’ problems, fears and things that
were making them unhappy or causing them sadness with the view that these issues affect the
patients' general wellbeing (Bignante 2015). Some participants described how they went to
the Traditional Healers for the opportunity to discuss personal matters such as quarrels with
their friends, issues concerning their partners or spouses, or to deal with feelings of sadness,
depression or grief and impotence and to find peace and emotional wellness (Bignante 2015).
Furthermore, the study discussed that several participants indicated their preference
for the Traditional Healers because of their unique ability to heal with words, keep patients
calm, let patients worries go away and making patients feel protected and at home in their
clinic. Although some of these supports that the Traditional Healers offer may appear social,
they turn to affect or exacerbate the psychological wellbeing of patients and therefore require
health professional attention together with the illnesses and the opportunity for patients to
discuss them. Perhaps, one can understand the complexities of these issues and why
conventional health professional may not want to discuss them or feel they are not equipped
to do so. It appears that in general Traditional Healers are members of their communities and
have the requisite knowledge to interact with patients on a more personal level.

66 | P a g e
2.4. People Living with cancer’ Silence about Their Use of Various Traditional Healers
The use of Traditional Healers by people living with cancer is on the increase in both
the developed and developing world (Verhoef et al. 2005, Paltiel et al. 2001, Boon et
al. 2000, Ernst 1998). Also, studies have reported greater use of Traditional Medicine
by people living with cancer compared to the general population (Mao et al. 2011;
Patterson et al. 2002, Richardson et al. 2000). However, there is a paucity of enough
studies that have investigated the issues of cancer, and Traditional Healers use in
Ghana, which is one of the reasons for this study. Hence, I considered studies that
have looked at other chronic diseases and Traditional Healers for review in this
section. For a coherent structure and discussion, I have included the following themes:
prevalence or percentage of Traditional Medicine use, types of Traditional Medicine
used, and the level of communication between people living with cancer and their
doctors about Traditional Medicine or Traditional Healers.
Table 1 Summary of studies on people living with cancer use of Traditional Healers
Study Number of
participants (n)
Site/source of participants Percentage of
Traditional Medicine
users
Yarney et al.
(2013)
people living with
cancer (n=98)
Korle-Bu Hospital-Ghana 73.5% (herbal,
massage, Chinese
medicine, and
prayers)
Broom et al.
(2010)
People living with
cancer (n=500)
Two Sri-Lankan Hospitals 67.4% (Sinhala,
Ayurveda &
Traditional religious
practices
Gozum et al.
(2003)
people living with
cancer (n=107)
Yakutiye hospital-Turkey 41.1% (herbs)
Brahmi et al.
(2011)
People living with
cancer (n=100)
University Hospital of Fez-
Morocco
46 % (Herbal, Pure
honey, Holy water
from Mecca, special
diets, religious
practices)
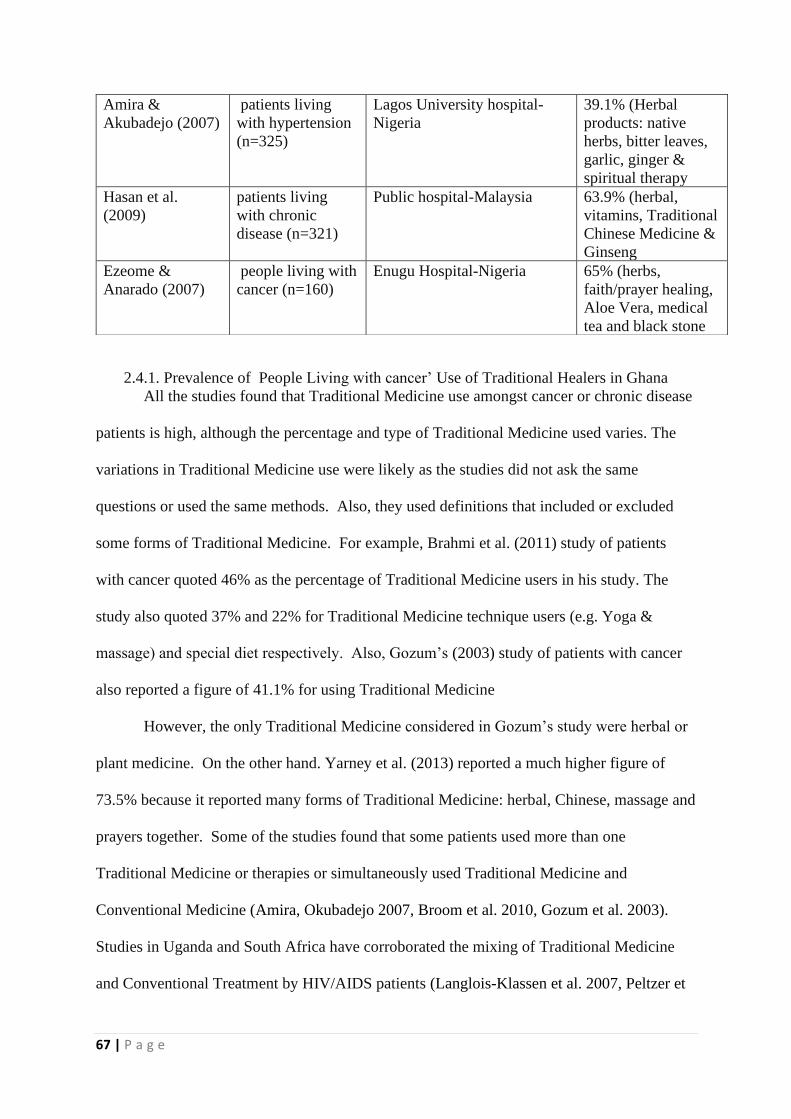
67 | P a g e
2.4.1. Prevalence of People Living with cancer’ Use of Traditional Healers in Ghana
All the studies found that Traditional Medicine use amongst cancer or chronic disease
patients is high, although the percentage and type of Traditional Medicine used varies. The
variations in Traditional Medicine use were likely as the studies did not ask the same
questions or used the same methods. Also, they used definitions that included or excluded
some forms of Traditional Medicine. For example, Brahmi et al. (2011) study of patients
with cancer quoted 46% as the percentage of Traditional Medicine users in his study. The
study also quoted 37% and 22% for Traditional Medicine technique users (e.g. Yoga &
massage) and special diet respectively. Also, Gozum’s (2003) study of patients with cancer
also reported a figure of 41.1% for using Traditional Medicine
However, the only Traditional Medicine considered in Gozum’s study were herbal or
plant medicine. On the other hand. Yarney et al. (2013) reported a much higher figure of
73.5% because it reported many forms of Traditional Medicine: herbal, Chinese, massage and
prayers together. Some of the studies found that some patients used more than one
Traditional Medicine or therapies or simultaneously used Traditional Medicine and
Conventional Medicine (Amira, Okubadejo 2007, Broom et al. 2010, Gozum et al. 2003).
Studies in Uganda and South Africa have corroborated the mixing of Traditional Medicine
and Conventional Treatment by HIV/AIDS patients (Langlois-Klassen et al. 2007, Peltzer et
Amira &
Akubadejo (2007)
patients living
with hypertension
(n=325)
Lagos University hospital-
Nigeria
39.1% (Herbal
products: native
herbs, bitter leaves,
garlic, ginger &
spiritual therapy
Hasan et al.
(2009)
patients living
with chronic
disease (n=321)
Public hospital-Malaysia 63.9% (herbal,
vitamins, Traditional
Chinese Medicine &
Ginseng
Ezeome &
Anarado (2007)
people living with
cancer (n=160)
Enugu Hospital-Nigeria 65% (herbs,
faith/prayer healing,
Aloe Vera, medical
tea and black stone

68 | P a g e
al. 2008). Again, this highlights the complexity of health-seeking behaviour and the
fact that many people use both different treatments simultaneously to achieve
different results.
2.4.2. Different Forms of Traditional Medicine used by People living with cancer
Furthermore, the studies identified a variety of Traditional Medicine that people use in Ghana
and other communities. Broom et al. (2010) study in Sri Lanka found that participants with
cancer used Indian Traditional Medicine such as Ayurveda, Sinhala, and spiritual practices
but the primary medicine used was herbal or plant-based medicine. Herbal medicine was used
by all participants (100%) in Gozum et al. (2003) study, 24% in Brahmi et al. (2011) study,
51.9% in Ezeome and Anarado (2007) study and 26% in Hasan et al. (2009) study. The other
studies asserted that herbal medicine was the most widely used Traditional Medicine but did
not provide any figures to support this assertion. On the other hand, Yarney et al. (2013) (n=
98) reported massage as (66%), herbs (59.2%), vitamins (55.1%) and prayers (42. 9%). The
higher use of massage in this study is not consistent with the view of Herbal medicine as the
mainstream Traditional Medicine in Africa and Asian communities as identified in other
studies (Bodeker, Ong 2005, Burford et al. 2000, Hampshire, Owusu 2012, Shukla, Sinclair
2009).
The study did not offer any explanation for this deviation. However, massage
has been shown to reduce pain, fatigue, stress, anxiety, depression and recommended
in oncology settings (Cassileth, Vickers 2004, Post-White et al. 2003, Myers et al.
2008, Weinrich, Weinrich 1990). Hence, it is possible that massage was offered to
participants as part of their care by oncologists and may explain this aberrancy. The
multiplicity of different items and materials and practices involved in Traditional
Medicine and their variation in different cultures highlight the complexity of
Traditional Medicine.

69 | P a g e
2.4.3 Lack of Doctor-Patient Communication about Traditional Medicine
The World Health Organisation has been embarking on a significant policy initiative
which principally aims to increase research and development of Traditional Medicine,
improve dialogue between Traditional Healers and doctors and utilise Traditional Healers in
the national health systems ( WHO, 2013, Sato,2012). The policy development was in
response to the popularity and increasing use of Traditional Medicine both in the developed
and developing countries in recent times. There is no evidence to suggest that communication
between doctors and their patients about Traditional Medicine will reduce the number of
Traditional Medicine users. However, the assumption or prediction is that open and honest
discussions and conversations between patients and health professional about Traditional
Medicine would ensure safety or avoid drug interaction and provide a better and more
prudent use of Traditional Medicine.
Furthermore, such conversations will dwindle the notion that Traditional Medicine
and its practitioners would and should always remain and function outside the mainstream
Conventional Medical Systems ( Stone, Matthews,1996). Despite this recognition and efforts
to improve communication and safety for Traditional Medicine users, many studies have
highlighted the lack of communication or discussion between patients and their health
professional about Traditional Medicine (Yarner et al. 2013, Gozum et al. 2003, Broom et al.
2010, Brahmi et al. 2011, Ezeome 2007). For instance, 83.3% of Traditional Medicine users
in Yarney’s et al. (2013), 80.5% in Broom’s et al. (2010) study 54.5% in Gozum’s et al.
(2003) study, 55.8% in Ezeome and Anarado (2007) study did not inform their clinician that
they were using Traditional Medicine. Although Brahmi et al. (2011) study made the same
assertion, it did not provide the exact percentage or number of participants who did not tell
their clinicians that they were using Traditional Medicine.
Studies have corroborated the lack of communication about Traditional Medicine
between patients and clinicians (Davis et al. 2012, Langlois-Klassen et al. 2008, Tovey et al.

70 | P a g e
2006). The study by Langlois-Klassen et al. (2008) specifically investigated the level
of communication between HIV/AIDs patients and doctors about Traditional
Medicine in Uganda (n=137). The findings were that 87 % anti-retroviral (n=67) and
84% of none anti-retroviral users (n=70) did not inform their doctors that they were
using Traditional Medicine. Equally, Tovey et al. (2006) study (n=92) found that
62.9% of participants who used Traditional Medicine did not inform their doctors
during encounters. Most patients assumed that the doctor knows it all and will ask
about Traditional Medicine if it was necessary or had an implication on their
biomedical treatment.
Also, some patients were under the impression that doctors are prejudiced to
Traditional Medicine use and hence did not see the reason or the benefits of
discussing or informing them (Davis et al. 2012). Other studies described patients’
ability to judge the doctors perceived lack of interest and apathy to discuss any other
form of treatment and hence such patients felt discouraged to talk about any other
treatment they were using (Langlois-Klassen et al. 2008, Davis et al. 2012, Broom et
al. 2010). However, patients were willing to discuss or talk to their doctors about
Traditional Medicine if the doctors asked them or they perceived that their doctors
were open to the idea and willing to discuss them (Davis et al. 2012, Ezeome,
Anarado 2007, Langlois-Klassen et al. 2008). Perhaps, more studies are needed to
investigate the potential drug interactions between the two treatment modalities
(Langlois-Klassen et al. 2008, Peltzer et al. 2008).
Additionally, it is reported that there should be understanding and acceptance
by health care workers that for socio-cultural and economic reason, some patients will
continue to use other treatment approaches and therefore, health professionals should
encourage discussions about them (Langlois-Klassen et al. 2008, Peltzer et al. 2008).

71 | P a g e
2.5 Cancer Awareness and Help-Seeking for Cancer Symptom
The use of Traditional Medicine by people living with cancer is on the increase in
recent times (Paltiel et al. 2001, Ernst 1998, Boon et al. 2000, Verhoef et al. 2005). However,
several factors hinder the effort to deal with the challenges of cancer in Ghana and most
developing countries (Anderson et al. 2011, Jemal, et al. 2011, Sankaranarayanan et al.
2011). Public awareness, health education, screening, and early detection or diagnosis of
cancer are central to reducing cancer mortality in sub-Saharan Africa (Abotchie, Shokar
2009, Edwin 2010, Mena et al. 2014). For example, increased awareness and uptake of Pap
smear and Human Papillomavirus (HPV) screening schemes help the early detection of
premalignant cell changes for early intervention to avoid the disease progression (Edwin
2010).
However, inadequate infrastructure and equipment, culture and belief systems are
hurdles to the few available preventions and awareness programs in Ghana and other
developing countries (Valsecchi, Steliarova-Foucher 2008, Anderson et al. 2011, Kingham et
al. 2013, Kwok, Sullivan 2006, Williams, Amoateng 2012). Also, a review on optimising
cancer management in Africa has highlighted impediments such as lack of research and
essential data to make informed decisions (Anderson et al. 2011). Ghana, at present does not
have any active screening and education program or policy initiative for preventing or raising
awareness of cancer disease in the population (Abotchie, Shokar 2009, Aikins et al. 2010).
The few and patchy programs aimed at addressing the problem have come from non-
governmental or foreign organisations who have limited capacity and usually focus on a few
rural communities (Mena et al. 2014).
The consequences of the situation are inadequate knowledge and awareness, poor
prognosis, late medical attention and patients’ reliance on Traditional Healers for treatment

72 | P a g e
(O'Brien et al. 2012). Some studies have highlighted the low level of knowledge of
cancer in Ghana and other African communities. First, in Abotchie and Shokar (2009)
cross-sectional study of knowledge, beliefs and acceptability of cervical cancer
screening amongst university students in Ghana (n=140). Second, in Opoku et al.
(2012) study of knowledge, attitudes, beliefs, behaviour and breast cancer screening
practices in Accra and Sunyani-Ghana using both quantitative and qualitative data
collection approaches (n=500). Third, in Mangoma et al. (2006) investigation of the
perception and understanding of women in rural communities on cancer, barriers to
screening and the sources of information on cancer for participants in Zimbabwe
using both quantitative and qualitative data collection tools (n=356). The study by
Opoku et al. (2012) did not provide examples of specific knowledge deficit of
participants. However, Abotchie and Shokar (2009) study specified that 92.1% of
participants did not know there is a relationship between factors such as the Human
Papilloma Virus (HPV) and smoking with cervical cancer. Some participants in both
Mangoma et al. (2006) study and Abotchie and Shokar (2009) study did not know the
signs and symptoms of cervical cancer and the purpose of cervical cancer screening.
However, neither of the studies mentioned the number or percentage of
participants who had this knowledge deficit. Interestingly, participants in Abotchie
and Shokar (2009) understood that indiscriminate sex and multiple sexual partners
could lead to cervical cancer. Mangoma et al. (2006) study further identified other
features of the low level of knowledge, although these appeared to be more of
inadequate knowledge or understanding of the causes of cancer. Women perceived
cancer as dirtiness of the uterus caused by men through the accumulation of sperm
into them or through sexually transmitted diseases (STD) (Mangoma et al. 2006).
Some participants did not see the need for attending cancer screening or discovering

73 | P a g e
their cancer risk or status as they believed that cancer is not curable (William et al. 2014).
Moreover, studies have found transcendent beliefs to influence peoples’ knowledge of
cancer and their attendance of screening intervention. A study by Kwok and Sullivan (2006)
was on the influence of belief systems on cancer screening behaviour of Chinese women in
Australia (n=20). The study observed that some participants’ viewed cancer as part of one’s
destiny supernaturally, and hence, any attempt to alter the process was not necessary.
Moreover, in Opoku et al. (2012) study in Ghana, some participants perceived cancer to have
an esoteric cause, for example, witchcraft. Consequently, some participants in Opoku et al.
(2012) study preferred reliance on God through prayers and Traditional Healers for treatment.
However, participants of Mangoma et al. (2006) study were interested in obtaining
appropriate information about cancer from a health professional if they were available. The
lack of comprehensive health information from qualified persons is a concern in Ghana and
most developing countries (Kingham et al. 2013, Anderson et al. 2011).
A few studies have underlined some of the sources of cancer information in Ghana
and Africa (Opoku et al. 2012, Abotchie, Shokar 2009, Williams 2014, Mangoma et al.
2006). All these studies identified the media (radio, television and newspaper) and traditional
healers (herbalists and spiritualists) as the source of public information on cancer. Mangoma
et al. (2006) study also identified family and friends as sources of information on cancer in
Africa. These sources of information differ from the developed countries where doctors, other
health professionals and reputable organisations and charities provide health information. The
diversity of information outlets in Ghana and the difficulty in verifying them is a challenge to
both patients and the public (Mangoma et al. 2006, Opoku et al. 2012).
However, a good understanding, cooperation and integration between conventional
practitioners and Traditional Healers can be an asset in disseminating health information to
the rural population in Ghana. Doctors in the Conventional Medical System can train and

74 | P a g e
educate Traditional Healers about cancer and work with them to create the needed
awareness and raise the knowledge of cancer in Africa (O’Brien et al. 2012). Many
studies have identified cervical cancer as the most common cancer affecting women
in Ghana (Nkyekyer 2000, Nartey et al. 2016). Although cervical cancer is high in
Ghana, there is still low level of awareness and use of available prevention programs
because of social and psychological barriers in Ghana (William et al. 2014, Abotchie,
Shokar 2009, Williams 2014). All the three studies William et al. (2014) (n=220),
Abotchie and Shokar (2009) (n=140) and Williams (2014) (n=34) were similar in
their focus around exploring their participants' knowledge of cervical cancer
screening and the socio-cultural and psychological barriers or belief about cervical
cancer careening.
These studies (Abotchie, Shokar 2009, William et al. 2014) identified women
fear of being stigmatised as promiscuous to prevent them from attending cervical
screening clinics. In Abotchie and Shokar (2009) study, some women perceived the
procedure to be painful and could lead to the loss of their virginity and give others the
impression that they are promiscuous or without good character. Also, in both
Williams (2014) and William et al. (2014), most participants were concerned that the
procedure of cervical screening and other cancer screening programs would lead to
the invasion of their privacy which was culturally inappropriate, primarily if a male
doctor performed the procedure.
Similarly, women were afraid to ask their husbands for permission to attend
cervical cancer screening for fear that their husbands may react negatively to their
request (Williams 2014, Awusabo-Asare et al. 1993, Abotchie, Shokar 2009). In
William et al. (2014) study, some participants had concerns that they cannot have sex
with their husbands when they get cervical cancer and consequently be divorced and
75 | P a g e
hence, they preferred not to know. The study by Awusabo-Asare et al. (1993) examined the
effect of social values on the vulnerability of women to HIV/AIDS in Ghana and identified
that most marriages or relationships are patriarchal in Ghana. The study concluded that
financial, socio-cultural and sexual emancipation for women was necessary for them to have
access to timely and appropriate treatment to illnesses.
Generically imposing health systems and practices from Europe and America are
unlikely to be useful or benefit some people in Ghana. Cancer awareness and education
programs should involve local stakeholders and focus on developing culturally friendly
programs (Opoku et al. 2012, Abotchie, Shokar 2009). Such a culturally friendly approach by
Government and relevant agencies can help to strengthen public knowledge through
education and increase their uptake of screening programs (Opoku et al. 2012, Abotchie,
Shokar 2009). Although the conclusions and findings of these studies are significant, they did
not focus on understanding peoples’ living with cancer’ motivations and experiences in using
Traditional Healers. Also, no theory currently exists in the literature that conceptualises the
experiences of people living with cancer in using Traditional Healers and their motivations to
do so in Ghana.
2.6 Summary of chapter and Research Question
This chapter shows how the choices of treatment and health-seeking behaviours in
Ghana are affected by different and complex factors such as socio-cultural, socio-economic,
spiritual and psychological. These elements act as barriers to accessing cancer prevention and
education programmes and awareness amongst the population. The review highlights the
importance of designing health programmes and system in Ghana in a manner that takes into
consideration the socio-cultural beliefs of the target populations or communities. Moreover,

76 | P a g e
the literature review shows that people living with cancer use Traditional Healers or
Traditional Medicine more than the rest of the population across the globe.
However, there is a gap in knowledge and understanding of why people living
with cancer are using Traditional Healers or Traditional Medicine and what their
experiences are in the process as most studies have focused on barriers to cancer
prevention and screening programs. Some people living with cancer use of the
Traditional Healers even when they can afford Conventional Medicine or using
Traditional Healers alongside Conventional Medicine suggests a more profound and
complicated reason for people living with cancer use of Traditional Healers than we
currently know. Equally, studies have not focused on investigating and conceptually
understanding the experiences and motivations of people living with cancer in using
Traditional Healers in Ghana and elsewhere. Hence, no theory currently exists to
explain the socio-cultural dynamics between Traditional Healers and people living
with cancer and how such relationships influence people living with cancer decision
to use the Traditional Healers services
2.7 Research Aims
My study proposes to explore the reasons and experiences of people living
with cancer in using Traditional Healers in the Brong-Ahafo region of Ghana. Based
on the gaps in the literature and the purpose of the study, the following are the
research aims and research questions that I intend to answer. The broad aims of my
study are to bridge the identified gaps in the literature. The study intends to offer a
conceptual understanding and explanation of the experiences of people living with
cancer in using Traditional Healers in Ghana. Also, the study explores the dynamics

77 | P a g e
and tenets of the relationship between Traditional Healers and people living with cancer and
how the relationship motivates patients to use Traditional Healers.
Moreover, my study will provide an understanding of the motivations, experiences,
and health-seeking behaviours of people living with cancer and give policymakers some
information in tailoring healthcare and cancer programmes in the rural communities in
Ghana. Furthermore, the study will contribute to the current body of knowledge and act as the
impetus for other students and academics to engage in similar studies in another setting to
create a more understanding of this phenomenon and lead to the possible development of
formal theory in future.
2.7.1 Research Questions
1. What are Ghanaian people living with cancer’ cultural beliefs and motivations for
using Traditional Healers or Traditional Medicine?
2. Why do people living with cancer combine Traditional Medicine with Conventional
Medicine?
3. What sociocultural beliefs and relationships enable the use of Traditional Healers?
4. What are the experiences of using Traditional Healers?
2.8 Overview of Theoretical Literature Review on Trust
The Constructivist Grounded theory methodology requires a final phase literature review
(theoretical review) which is conducted at the end or towards the end of a study to
contextualise the constructed grounded theory or conceptualised ideas concerning established
theoretical concepts or extend theories (current). This review is crucial in situating the study
within and across different disciplines and to compare the constructed grounded theory to
established theories and to highlight the contributions to knowledge (Bryant, Charmaz 2019,
Gibbs 2015, Charmaz 2014)
In this part of the literature review, I provide a theoretical review of the concept of
trust in help-seeking behaviours. I first highlight key definitions of trust, the importance of
78 | P a g e
trust in society, and how trust functions to mitigate the complexities and
vulnerabilities in unforeseen situations. Also, I review trust as an interconnected
concept, comprising deference to authorities and identities (Kramer et al. 1996, Tyler,
DeGoey 1996, Tyler 2001), a reputation (Sztompka 1999, Misztal 2013, Ensminger
2001), encapsulation of self -interest, social coherence and stable systems of
language, and familiarity and habits (Misztal 2019, Misztal 2013, Heckscher 2015,
Sztompka 1999). Trust was found to be essential to my thesis as it was identified in
the literature and eventually formed the foundational identities of both participants
and Traditional Healers regarding help-seeking with symptoms and illness
experiences.
2.9 General Understanding of Trust
Trust is vital for human interaction, relationships, cooperation and smooth
functioning of both indigenous and modern societies (Misztal 2013, Luhmann 2018,
Cook 2001, Hosking 2014, Heckscher 2015, Bok 1979, Hirsch 2005, O'neill 2002).
Whenever trust is misplaced or abused, there is the possibility of destructive
consequences which may be perpetual or take longer to remedy (Hosking 2014;
Hardin 2006; Cook et al. 2005). The actors of trust are a trustor and trustee who
encounter each other in a situation or a relationship involving risk and uncertainty
about the future (PytlikZillig, Kimbrough 2016, Rousseau et al. 1998, Bacharach,
Gambetta 2001, Gambetta 2008). Trust can be conceptualised with regards to the
psychological state of vulnerability because of one’s willingness to place trust in
someone (Mayer et al. 1995, Fink et al. 2010, Rousseau et al. 1998, Möllering 2005).
Others see trust as the trustors' confidence in the trustee to fulfil an expectation
in the future or broadly consider the trustor’s interest in an intended action (Luhmann

79 | P a g e
2018, Misztal 2013). Trust within the healthcare setting conveys patients’ confidence in the
health systems or professionals to function in their best interest or fulfil their expectation
(Hall et al. 2001, Thom et al. 2004, Lord et al. 2012). Patient’s trust is usually in the
behaviours and attributes of health professionals such as their technical and interpersonal or
relational competence, and fiduciary obligations (Thom et al. 2004).
Similarly, Dugan et al. (2001) identified fidelity, confidentiality, honesty and
competence as the main conceptual domain of analysing trust in healthcare. Also, other
definitions of trust focus on the generalised or innate disposition of individuals or people to
do the right thing (Messick, Kramer 2001, Kramer et al. 1996). Some people consider the
work of both the Conventional Health Professional and Traditional Healers as a vocation or a
“calling’’ and hence trust these practitioners because of their innate inclination or
characteristics to do the right thing (Messick, Kramer 2001, Heckscher 2015, Goffman 2017,
Goffman 2010). The different conceptualisations of trust had led to some authors describing
the domain of trust or signals of trustworthiness as a broad spectrum of processes
incorporating various trusting views, linguistic variables and historical and socio-cultural
context (Bacharach, Gambetta 2001, Hampshire et al. 2017, Hosking 2014, PytlikZillig,
Kimbrough 2016, Heimer 1999).
Primarily, trust in someone can explain trust as a feeling, attitude, disposition and
relationship relating to behaviour and actions, or the potential in a dynamic socio-cultural or
relational context (PytlikZillig, Kimbrough 2016, Hosking 2014). Consequently, the varying
signals of trust reflect the different community or sociocultural context and would continue to
vary over time. The complexities, risk and uncertainty in health care decisions can become
overwhelming, especially for illiterate and impoverished indigenous communities who may
have limited access to information or the understanding of it (Northouse, Northouse, 1998,
Berry 2006).

80 | P a g e
In other words, for patients who have low health literacy or unable to
understand and act on medical advice as often in unforeseen situations, trust is
necessary to simplify, reduce complexities and vulnerabilities (Hardin 2006,
Luhmann 2018, Misztal 2013, Cook 2001) and increase the propensity or justification
to act without necessarily eliminating all the risk from the trustee’s behaviour (Misztal
2013, Heimer 1999, Hardin 2006, Dodd 1994). Most of my study participants were
vulnerable by the very nature of their condition and had tremendous anxiety regarding
the outcome or consequences of their illnesses and thus relied on trust in dealing with
these situations.
According to Heimer (1999), traditional communities usually focus on
reducing uncertainty about the intentions and competence of others by focusing on
habits and specific behaviour and values which the community expects every member
to comply. In contrast, modern societies have the unavoidably intense and regular
contact with strangers and hence focus on vulnerability reduction through schemes
such as insurance, contracts, legal certification and accreditation (Heimer 1999)
Although trust is an essential aspect of society, there is a general
acknowledgement that trust carries the risk of uncertainty and disappointment to
trustors as they may not realise their hopes. Some authors describe the risk of
uncertainties and disappointments as the problem of trust regarding the difficulty in
identifying the right people to trust or the correct signals of trustworthiness in others
(Gambetta 2008, Bacharach, Gambetta 2001). Inadequate and deficiencies in
communication and interpretation make it difficult for anyone who engages in trust to
assess or achieve the full motives, potential actions and possible responses of trustees
to changes or contingencies (Coleman 1994, Bacharach, Gambetta 2001, Gambetta
2008). Hence, it is always possible for an opportunist who can learn to mimic the

81 | P a g e
attributes and characteristics of trustworthiness in a society or organisation to achieve their
interest (Bacharach, Gambetta 2001).
In the same manner, people can deceive their trustors by signalling certain behaviours
of someone who has a reputation in order to influence the trustors’ confidence in them
(Bacharach, Gambetta 2001). In such circumstances, it is challenging for the trustor to know
whether the signals exhibited by the trustee are genuine or intended to deceive (Hampshire,
Hamill et al. 2017, Bacharach, Gambetta 2001, Gambetta 2008, Cook 2001). Also, in some
situations, a failure of the trustee to function as deemed appropriate can even leave the trustor
in a worse off situation than before and highlights the inherent risk of believing that another
person would act in our interest or behave appropriately (Faulkner, Simpson 2017).
Moreover, in relationships in which there is a power imbalance, it is difficult to assess
whether the trust is genuine or not as the trustor may not have any opt-out options. Hence, the
trustor may act in a specific manner from fear and unable to hold the trustee accountable for
their actions (Cook et al. 2005, Hardin 2006, Bacharach, Gambetta 2001, Heckscher 2015)
2.10 Conceptualising Trust as Interconnected Self-Interests
Trust is defined as encapsulated or interconnected self-interest in which the trustor
assumes that their interest is interconnected with the trustee’s interest. Hence, the trustor's
actions are influenced based on the conviction that the trustee would look after their interest.
Conceptualising of trust in this manner is relevant in situations in which we believe
that it is in the trustee’s best interest to fulfil our expectation or consider our interest in their
actions (Hardin 2006, Cook 2001). The interconnection of interest may be subtle to the extent
that the trustee may not even be aware that they are fulfilling their interest by considering the
interest of the trustor. The encapsulated interest exists in situations in which the trustor has
82 | P a g e
enough information or have enough knowledge to judge the trustworthiness of the
trustee (Hardin 2006).
Nee and Sanders (2001) proposed that trust in ethnic ties and community
identities are often the de facto position for people when they face uncertainty or
contingent situation of the familiar and unfamiliar. The hypothesis they put forward is
that co-ethnic relationships are incentives for the trustee to fulfil the trust obligations
bestowed on them by the trustor. Typically, people who have a closer sense of identity
are more likely to be interested in being trustworthy than a stranger, as they want to
avoid the intrinsic and informal sanctions of risk in an ongoing relationship. The cost
of betrayal of trust in such relationships would not affect only the trustor but also the
trusted party (Coleman, 1988, Nee, Ingram, 1998).
The criticism of the encapsulated interest trust conceptualisation is that it may
not always indicate a trusting relationship, but instead, a committed relationship in
which one actor can take undue advantage of the other or the situation (Nee, Sanders,
2001). Close community networks, traditions, neighbourhood relationships and
identities influence and strengthen the concept of encapsulated interest relationship
between most indigenous Ghanaian communities in general (Utley 2016, Hardin
2006).
2.11 Trust as Deference to Authority
Peoples’ identification with a group, community or authoritative figure
increases their propensity to trust others in the same group (Tyler, Dawes 1993,
Dawes et al. 1990, Tyler 2001). Tyler (2001) described such trust as social trust,
which develops from socio-cultural bonds, identities or identification within human
institutions and societies. Equally, others see such trust as an in-group dynamic in

83 | P a g e
which members favour or trust their in-group by having the right attitude, behaviour and
perception about them (Kruglanski, Higgins 2007, Brewer 2007, Turner et al. 1979, Tajfel,
Turner 1986, Tajfel 2010). The commitment and deference of trust to a group or a group
authority facilitate the dynamics of groups or social relationships, identity formation and
validation (Tyler, DeGoey 1996, Tyler 2001, Braithwaite, Levi 2003, Adjei 2013).
In indigenous communities, members who have traditional positions, roles and
symbolise any dimension of the ancestral tradition are trusted by the rest of the population to
have moral values. Such trust facilitates voluntary respect and commitment to these members
or authorities and their decisions. Hence, deference trust is usually the attribution to the
motives and intentions of groups or authorities (Tyler, 2001, Heckscher, 2015) to
benevolently act towards the general wellbeing of the trustor in decisions (Tyler 2001,
Heckscher 2015, Abrams, Hogg 2006).
In such situations, the assumed trustworthiness of the motives of authorities or
traditions becomes the crucial factor under consideration and not necessarily evidence of any
concrete outcome. However, there is no suggestion that people arbitrary trust in authorities
and identify with groups. Instead, the authorities must exhibit the right attitude and standards
of their status. There are concerns that deference to socio-cultural group identities or
identification and authorities can create favouritism towards group members while delimiting
outsiders (Kruglanski, Higgins 2007, Brewer 2007, Turner et al. 1979, Tajfel, Turner 1986,
Tajfel 2010).
Another criticism of a deference trust is the notion of apprehension and entrapment
through totally depending and becoming servitudes to those who are considered trustworthy
in the group and ethnic authorities (Nee, Sanders, 2001). Consequently, trust as deference to
authority is not devoid of the potential distrust from the possibility of duplicity by
84 | P a g e
opportunists who may use their positions for unwarranted privileges to take advantage
of vulnerable or ardent members (Nee, Sanders, 2001).
2.12 Trust in Reputational and Good Behaviour Characteristics
Reputational trust depends on the past deeds that people can access through
information, or the trustors’ familiarity and encounter with an organisation, institution
or an individual (Good 2000, Layton 1971, Misztal 2013, Ensminger 2001, Sztompka
1999). Heckscher (2015) described indigenous communities as thick societies which
are tightly knit and in which people closely interact, encounter and know each other.
In such communities, there is the opportunity to access the reputation and
performance of other community members to facilitate the decision to confer trust in
others or not. In contrast, assessing the reputation of people in modern and
sophisticated societies is done through reviews, publicly available collective
knowledge and regulatory bodies (O'neill, 2002, Heckscher, 2015).
In general, people are more likely to believe in the reputation that they can
link to a profession, category or a collective identity than the individual as the former
is more simplified and manageable (Frowe 2005, Bacharach, Gambetta 2001,
Gambetta 2008, Heckscher 2015). Trust in the collective or categories are easy to
manage because of specific standardised reputational characteristics and behaviours
that may define the group (Brewer 2007, Tajfel 2010, Tajfel, Turner 1986).
Respectively, reputational trust can be presented or expressed through appearance and
demeanour of good manners and behaviours which may reveal the identity,
personality, status or professional groups (Giddens 1991, Dasgupta 2008, Bacharach,
Gambetta 2001).

85 | P a g e
In general, Traditional Healers in Ghana learn the values and cultures of behaviour
including the culturally appropriate demeanours such as calmness, patience and resilience in
a stressful and demanding situation which reflect the indigenous socio-cultural and traditional
propriety. However, both collective reputational and appearance trust can be misleading as
individuals can hide behind such a reputation or appearance to act up (Luhmann 2018,
Misztal 2013, Sztompka 1999). Equally, there is always the possibility of mimicry and
pretence of the reputational qualities and characteristics by opportunists or confident
tricksters who have different motives from a group or a community (Dasgupta 2008,
Bacharach, Gambetta 2001, Good 2000, Yeboah 2000, Ensminger 2001).
2.13 Endurance of Community Norms and a Generalised Culture of Trust
Traditional communities assert collective values and trust in their members through
norms of reciprocity, traditions, history and intimately engaging networks (Putnam et al.
1994). The enforcement or binding nature of these elements in indigenous communities and
subscription to a shared moral authority create coherence and order which equally influence
identity trust formation (Sztompka 1999, Heckscher 2015, Kramer et al. 1996, Tyler, Huo
2001, Tyler 2001, Tyler, Blader 2013). The shared ancestral traditions and socio-cultural
morality or values in most Ghanaian communities normatively bound members as the
foundation of their behaviours and identities that can be trusted. Furthermore, in traditional
societies, regular or repeated social order (social stability) is an active ingredient in signalling
trustworthiness (Goffman 2017, Heckscher 2015, Luhmann 2018, Sztompka 1999)
Primarily, the stability of tradition and culture, long-lasting, persistence and
continuity of networks and encounters provide some certainty and reliability for trust.
Generally, tradition and culture act as anchorage of trust or trustworthiness because of their
centrality to the continuity of identity and acting as a springboard for other forms of trust

86 | P a g e
(Giddens 1991, Sztompka 1999, Smith et al. 1982, Hamer 1994). Tradition
encourages trust and trustworthiness through patterning and repeating of practices
(Misztal 2013), reducing irregularities through the summation of distinct values which
facilitate comprehension and continuity of historical experiences (Misztal 2013,
Sztompka 1999, Fentress, Wickham 1992). However, the stability of tradition does
not imply only completely inert societies signal trustworthiness or to say that
communities lose trustworthiness or trust because of a social transition (Giddens
1991, Sztompka 1999).
In contrast, modern societies can undergo changes and development regularly
and at a drastic pace, requiring more than tradition and culture to maintain social
order, stability and reliability (Oneill 2002, Heckscker 2015). Equally, the values for
maintaining trust in modern societies are different from those in traditional
communities and centre on interactive sensibility and civic engagement such as
civility, tolerance, integrity, reasonableness, multiculturalism, inclusiveness and
equality (Misztal 2013, Gambetta, Hamill 2005, Anderson, 2013, Heckscher 2015)
Hence, in modern settings, normative stability and continuity of social order require legally
recognised systems, reputational measurements, a set of private and public institutions,
professional bodies, contracts and plethora of information to ensure cooperation and trust
(Hosking 2014, Putnam et al. 1994, Heckscher 2015, Knight 2001). These institutions have
the power to outlast socio-political transitions and regimes usually. The effective functioning
of the law and these institutions are the pointers and enforcers of an order of stability in
modern societies (Cook 2001, Hardin 2006, Sztompka 1999, O'neill 2002).

87 | P a g e
2.14 Trust as a System of Language and Communication
The Communication Accommodation Theory (CAT) provides a broad framework
which offers an explanation and prediction of the possible alteration we make in creating and
maintaining social distances in community and social interaction using language (Giles, Ogay
2013). According to the CAT, communication, or language is not devoid of a socio-cultural
and historical context in which communities or individuals exist (Garrett 2010, Giles, Ogay
2013). Although personal identities influence communication in individual encounters, there
is the evidence that entirety of both the verbal and nonverbal aspects of even individual
interaction is dominated by sociocultural and community identity of the person (Giles, Ogay
2013).
The theory explains the relational and identity processes in communication and
language interaction (Coupland, Jaworski 1997), including non- verbal communicative
symbols of a socio-cultural group (Giles, Ogay 2013). Similarly, Tracy (2013) described
language as a codified abstract or systematic knowledge that represents something deeper or
substantial than their verbal expression. Equally, language can be used to show the lack of
trust, identification and social distances or divergence with a group or community.
Furthermore, Luhmann (2018) discusses language and communication as a powerful tool
which can be used to regulate identities, statuses, choices and distances in communities and
fundamentally affect interaction and trust. In this sense, language becomes a medium for
creating, maintaining and changing power base into action (Reid, Ng 1999).
Groups and social hegemony turn to be accompanied by linguistic dominance and
style, which, when used continuously, can simplify the power of other groups and lead to
mistrust. Language depoliticises and harmonises power through the deceptive act of covering
up and justifying power through the strategic use of language. While the powerful employ

88 | P a g e
language to maintain and sabotage any act of power or opposition, the powerless
equally use language to gain power or challenge those with higher powers (Reid, Ng
1999). In this sense, there is a power display and dynamics in the anger,
dissatisfaction and resentments that may exist in therapeutic and health care
relationships.
The link between language and power highlights the capacity of language or
linguistics to isolate or include people, raise the social barriers to interaction and
create a sense of exclusion (Giles, Ogay 2013, Garrett 2010, Luhmann 2018, Reid,
Ng 1999). The exclusions, barriers and inequalities created by language can lead to
those who perceive themselves to be victims to frown on the powerful with distrust
and scepticism. People can, therefore, perceive language as common grounds,
leverage or empowerment in their relationships with others and the basis of trust. In
contrast, unfamiliar language can make people feel afraid, dominated and unable to
trust others.
2.15 Trust as Familiarity and Habits of Communities
Furthermore, a key element in estimating the trustworthiness of others is
familiarity (Heckscher 2015, Sztompka 1999, Luhmann 2018, Bacharach, Gambetta
2001) with either the socio-physical environment or relationships and encounters.
People are likely to trust others in the environment that they feel comfortable and
familiar with people whom they have a close association or share relationships. In
effect, familiarity breeds trust (Giddens 1991, Giddens 1990) through the sense of
security, certainty, predictability and positive expectation. Familiarity creates the
opportunity for actors to know each other and to form an opinion about each other.

89 | P a g e
Many Ghanaian trust Traditional Healers and people from their communities because of their
familiarity with them.
Similarly, trust relationships and accountability, blossom in communities which have
relatively persistence interaction, re-encounters and mutual dependence (Luhmann 2018).
From this perspective, some authors conceptualise trust relating to familiarity and trusting in’
’habits’’ as identical (Misztal 2013) Trusting in “habits” is a disposition that offers
predictability, provides security, continuity and strength to face uncertainties and
complexities of social life, particularly in vulnerable and unsettled situations (Misztal, 2013,
Durkheim, 2012, Gulati, 1995, Gilson, 2006, Wuthnow, 2004, Misztal, 2019, Latour, 2013).
Like familiarity, prior knowledge and occurrences build habits which are employed to
alleviate the risk in handling contingencies (Misztal 2019, Misztal 2013). Indigenous
communities usually rely on their past and the shared understanding of the traditional system
and their prior knowledge to trust each other and to distrust the unfamiliar and cumbersome
situations.
2.16 Summary
The chapter provided an overview regarding the importance and conceptualisation of
trust in societies and the therapeutic encounter. It also highlighted the complex facets of risk
and vulnerability, when making health decisions and how trust functions to bridge the gap
and make it easier for people to act and make health decision. The chapter has discussed
some of the theoretical frameworks of trust that are relevant to my study.

90 | P a g e
CHAPTER THREE: RESEARCH DESIGN AND METHODOLOGICAL CHOICES
3.1 Chapter Overview
The chapter primarily is divided into three parts. In keeping with Constructivist
Grounded Theory (CGT), the chosen methodology for this study, I have attended to
reflexivity in these parts (See Chapter 1.7: pre-field reflexivity, 3.19: in-field
reflexivity and 3.26: post-Field reflexivity ). The first part (3.2-3.6), I deal with
methodological concerns. I give an overview of the relevant paradigms associated
with Grounded theory (Interpretivism, Constructivism, Constructionism, Symbolic
Interactionism and Pragmatism) and more specifically, the Constructivist Grounded
theory (CGT) methodology. Also, I give an overview of the selected Grounded theory
methodology over other comparable methodologies that could have been used for the
study (Ethnography and Phenomenology). Additionally, the first part of the chapter
describes the process of choosing Constructivist Grounded theory and the rationale
for choosing it over the Glaserian and Straussian approaches. The second part of the
chapter (3.7-3.19) discusses the study methods, including the critical elements of the
Constructivist Grounded theory method, ethical considerations such as seeking
approval, and how relevant accesses were negotiated and the cultural challenges to
consenting study participants. This part also considers my approaches to recruitment
and data collection (Interviews and Observation). The third part of the chapter (3.20-
3.26) is where I describe the methods of analyses of the data and the development of
categories, leading to theory development.
3.2 Choosing Interpretivism Approach over Positivism
A theoretical or philosophical paradigm serves as the premise that provides a
framework, justification and a guide for academic pursuit and acquisition of

91 | P a g e
knowledge through empirical evidence (Strauss, Corbin 1998, Guba, Lincoln 1994, Kuhn
1970). In social research, a paradigm is seen as interrelated shared worldviews, beliefs and
values that guide research approaches (Schwandt 2001, Crotty 1998). There are diverse types
of paradigms or theoretical assumptions which are a continuum between the positivists and
subjective approaches with positive-objective and the interpretive framework views at their
extremities (Charmaz 2014, Denzin, Lincoln 2011, Orlikowski, Baroudi 1991).
The purpose of my study was to explore participants' subjective interpretation and
construction of the phenomenon through language and interaction. Such interpretation
provides an understanding of participants’ motivations and experiences of using Traditional
Healers in Ghana. An interpretive or qualitative methodology was suitable because it allows
participants with specific and relevant experiences to share their stories (Elster 2015, Willig
2013, Cohen et al., 2011). Similarly, an interpretative methodology allows participants to
express the meanings behind their behaviours and actions (Elster 2015, Willig 2013, Cohen et
al., 2011). Contrary, Positivism which disregards subjective phenomena such as beliefs,
values, and experiences underlying human behaviours would limit my understanding of
participants’ motivations and experiences and the socio-cultural context of the participants’
actions (Gray 2013).
However, some people criticise the qualitative approaches for their lack of objectivity
and generalisability (Creswell, 2017, Denzin, Lincoln, 2011). However, interpretive studies
are not concerned with generalisation or validity but with credibility and transferability and
an in-depth understanding of issues within their social context (Charmaz 2014, Creswell
2012, Yardley 2000, Noble, 2015). Furthermore, the positivist (empiricism), assumes the
existence of an objective, single reality independently of human perception or interaction
which the researcher can discover, measure or characterise (Denzin, Lincoln, 2011,
Thompson, 2000). Thus, the researcher can explain the behaviour of humans through the

92 | P a g e
application of rigorous and systematic procedures of scientific methods of inquiry
(Crotty 1998) of generating and testing hypothesis (Macionis, Gerber 2010, Bowling
2009, Lincoln et al. 2011).
Positivism views the researcher as an independent, neutral or value-free
individual, separate from the influence of social interactions and context of research
(Macionis, Gerber 2010; Bowling 2009; Lincoln 1994). In contrast, the interpretive
paradigm postulates the position of multiple realities and social construction and
subjective interpretation of participants and the researcher (Denzin, Lincoln 2011;
Creswell 2012). My study data and findings are one story or perspective of the reality
that exists. The interpretive paradigm, unlike positivism, acknowledges the centrality
and criticality of a value-laden researcher and their interaction with participants and
the social context (Creswell 2012).
3.3 The Influence of Constructivism, Social Constructionism and Symbolic Interactionism on
Constructivist Grounded Theory (CGT)
The interpretive epistemological paradigms of Constructivism and Social
constructionism influences Constructivist Grounded theory methodology (Creswell
2012). Broadly, the literature uses these epistemological approaches interchangeably
(Denzin, Lincoln 2011, Creswell 2012, Charmaz 2014, Lincoln et al. 2011, Mertens
2014). Constructivism focuses on the individual learning and assumes reality to be an
individual construct, created by an individual’s knowledge and experiences within the
real world (Denzin, Lincoln 2011, Lincoln et al. 2011, Mertens 2014, Guba, Lincoln
1994). Constructivism emphasises on how we develop meaning from what we know
based on individual learning within a social setting (Thomas et al. 2014, Young,
Collin 2004).

93 | P a g e
Ghanaians are familiar with symbolic, cultural and historical strands and attach
meanings and interpretations to them. They also talk about the relevance of their ancestral
history and how Traditional Healers are part of the cultural quintessence of the symbolic
depiction of the ancestral moral framework. Social constructionism focuses on the social
processes, actions and interactions, their historical context, and how they influence
knowledge and meaning construction (Thomas et al. 2014, Young, Collin 2004). The use of
language and Symbolic Interaction help humans to dynamically and flexibly seek knowledge
and adapt to the relevant context. Consequently, a person can develop multiple realities at
separate times and contexts based on social needs and interactions.
The Constructivist Grounded theory methodology, with its emphasis and
underpinning Symbolic Interactions and social context, blurs the boundary between
Constructivism and Constructionism even more (Charmaz 2014). Symbolic Interactionism
and Pragmatism have a tight bond and application with Constructivist Grounded
methodology (Milliken, Schreiber 2012, Lomborg, Kirkevold 2003, Chamberlain-Salaun et
al. 2013). Pragmatism relies on practical consideration of problem-solving and what works
best rather than theoretical concerns (Mounce 2000, Charmaz 2014). Thus, Pragmatism
emphasises the importance of values of theories and beliefs on the effectiveness of their
practical application or usefulness (Mounce 2000, Charmaz 2014). The theoretical
perspective of Symbolic Interactionism with its pragmatic philosophical root views human
beings as active agents. As active agents, they interact with their world to produce multiple
realities and not passive recipients of larger social forces (Charmaz 2014, Corbin, Strauss
2008).
The theory in this study is not a representation of the only reality but a product of the
practical values and meanings that myself and participants gave to situations, experiences and
interactions in the context of the study. Essentially, Pragmatism encourages subjectivity of

94 | P a g e
meaning, human agency, emergent process of actions and interaction to grounded
theory and not structures (Charmaz 2014, Corbin, Strauss 2008). Symbolic
Interactionism adheres to the notion that we construct society, self and reality through
the interpretation of language, interactions and symbols (Charmaz 2014). Also, the
inherent dynamic interpretation of interactions and language means people can change
the meanings they assign to symbols and interactions (Dennis, Smith 2015, Handberg
et al. 2015, Charmaz 2014).
The findings of the study are some perspectives of reality which were a
product or a constructed view of both I and participants experience during interactions
and associated meanings we assigned to language (Charmaz 2014, Handberg et al.
2015, Dennis, Smith 2015, Atkinson et al. 2007). The premise of Symbolic
Interactionism is that human action always occurs in a situation that confronts an
actor and that the actor acts to define or assign meaning to the confronting situation
based on their experience. Therefore, Symbolic Interaction stresses the importance of
the meanings people give to their activities or experiences through the interpretation
of actions, interactions and symbols in contrast to deterministic explanation to human
conduct (Dennis, Smith 2015). The knowledge that this study generates is temporal
and contextual, my interpretation and conceptualisation of the meaning that the
researcher believed participants gave to the situation. Hence, the study intended to
offer a fresh or a new perspective or theory to the phenomenon of using Traditional
Healers rather than offering absolute explanatory categories and outcomes (Dennis,
Smith 2015, Charmaz 2014, Atkinson et al. 2007).

95 | P a g e
3.4 Choosing Grounded Theory (GT) Methodology
I chose Grounded theory methodology, specifically the Constructivist version
because of its suitability to respond to the nature and aims of my study, the research
questions and congruence with my philosophical, ontological and epistemological
assumptions. The phenomenon of my interest shaped the selection of Grounded theory and
the Constructivist approach as the methodological choice. Some authors describe these
choices as a fit or coherence between the researcher and their chosen methodology or method
which makes it easy for the researcher to justify the methodology by enjoying and engaging
with the study (Walsham 2006). Thus, the research aims guided the selection of the
methodological approach (Glaser 2004). I did not just say yes to my biases or indicted any
methodology but instead examined their suitability and possibilities for the nature of the
study and in answering the research questions.
The study followed an inductive and emergent ground-up approach rather than
imposing or handing down any pre-existing theory onto the study (Urquhart 2013, Creswell
2012, Gibbs 2015, Charmaz 2014). Such an approach is consistent which with Grounded
theory or Constructivist Grounded theory approach. Also, the findings from the literature
review indicated the suitability of using a qualitative approach in exploring peoples’
motivations, experiences and interactions. The qualitative methodology had been used in the
past to study peoples’ health-seeking behaviours, and factors influencing health decisions or
choices.
Moreover, Grounded theory (Constructivist Grounded theory) examines and explores
actions, social processes and structures through interaction, and how those interactions
influence events and activities (Corbin, Strauss, 2008, Charmaz 2014). I intended to
understand why most patients with cancer use Traditional Healers in the Brong-Ahafo region
of Ghana and the processes involved in these practices and how they influence health-seeking

96 | P a g e
activities. Grounded theory was suitable in exploring and examining participants’
health-seeking behaviours, motivations, and experiences in using Traditional Healers
in a sociocultural, historical and economic context to provide a broad view of the
phenomenon.
Additionally, Grounded theory (Constructivist Grounded theory) was more
suitable for my study in exploring realities created by individual subjectivities and
inner worlds. These were then raised analytically through data analysis to try and
understand the core dimensions present in these individual realities (Glaser 2002).
The underlying position of my study was that the concept of reality is not sealed or
watertight but continually changing. These changes are due to the influences of
changing groups or individual encounters, social interactions, and dynamic settings or
context. The reality of the study was construction or understanding of meanings and
interpretations that participants assign to the situation or the phenomenon under
investigation.
Furthermore, Grounded theory (Constructivist Grounded theory) was suitable
for my study as the primary purpose was to develop a substantive theory and
conceptual understanding of the participants’ experiences. Thus, the conceptualisation
of participants experiences as it was best fitting to the data or emergent from it, which
is not usually the focus of other qualitative methodologies (See Table 2 in this
chapter: summary of methodological relevance to theory development). Grounded
theory (Constructivist Grounded theory) captures individual participants’ subjective
experiences, motivations and subjectivities of their use of Traditional Healers. The
participants’ accounts are then raised to analytical level through data analysis,
interpretation and provide a theoretical understanding and explanation of the realities
of the phenomenon.

97 | P a g e
Although a qualitative approach like Ethnography and Phenomenology can be
relevant in carrying out the study, I did not find them appropriate. In choosing to use
Grounded theory (Constructivist Grounded theory), I was concerned with the flexibility to
access relevant data from any person or individual with the experience of the topic of interest
(Corbin, Strauss 2014, Lambert et al. 2011). Ethnography focuses on understanding or
describing the cultural meanings of a phenomenon and employs an observational approach
using thick description for data collection. Hence, I did not consider ethnography as the most
appropriate methodology to give me the flexibility and provide a holistic view of the
dynamics of participants experience and motivation, including their socio-cultural and
historical context.
Similarly, Phenomenology is not concerned with conceptualising experiences but
instead looks at the commonalities or essence of an event or phenomena and describes them.
Although phenomenology equally would have enabled me to gain insight into participants’
experiences or their world, the outcome would not be a theory development (Creswell 2012,
Charmaz 2014, Gerrish, Lacey 2010). The table below is a summary of the relevance of
comparative methodology in theory development and how Grounded Theory was selected as
the most suitable.

98 | P a g e
Table 2 Methodological Relevance to Theory Development (Goulding 2005, Starks, Trinidad
2007)
Characteristics Phenomenology Ethnography Grounded Theory
Focus Understanding the essence
of the experience.
Describing and
Interpreting a culture
sharing group
Developing a theory grounded in
the data from the field.
Kind of Problem suited
for the design
Needing to describe the
essence of a lived
phenomenon.
Describing and
Interpreting Shared
patterns of the culture
of a group
Grounding theory in the views of
participants
History or Discipline
Background
Drawing from philosophy,
psychology and Education
Drawing from
Anthropology and
Sociology
Drawing from Sociology
Unit Of analysis Studying several individuals
who have a shared
experience
Studying a group that
shares the same culture
Studying a process, actions or an
interaction involving many
individuals in a context
Study Aim: Developing
Theory to represent
Participants experience
Gain Insight into participant
Worldview. Development of
a theory is not an outcome
Depends on existing
theories to explain a
phenomenon
The primary outcome is towards
theory development. Appropriate
for developing a theory
representative of participants
experiences

99 | P a g e
3.5 Choosing the Constructivist Grounded Theory (CGT)
3.5.1, Brief History of Divisions in Grounded Theory (GT)
The founders of Grounded theory, sociologist Barney Glaser and Anselm Strauss
entered the methodological debate with a successful collaborative seminal work on death and
dying in hospitals and subsequent publication “The Discovery of Grounded Theory:
Strategies for Qualitative Research (Charmaz 2014, Charmaz, Mitchell 2007, Howard-Payne
2016, Glaser, Strauss 2009). The timing of their work and entry to the methodological debate
was critical, especially at a time when qualitative research was losing ground to the positivist
conception of objectivity, generality, and replicability of research and falsification of
competing theories and hypothesis that included quantitative approaches (Charmaz 2014,
Charmaz 2012, Gibbs 2015).
However, Glaser and Strauss refocused qualitative inquiry to an analytic level through
explicit codification and systematic analyses of qualitative data. They encouraged the
development of theories (substantive or theoretical understandings) grounded in data. Soon
after developing Grounded Theory, Strauss and Glaser were contending on their differences
of opinion and position on realism which led to their separation (Howard-Payne 2016).
Strauss went on to work with Juliet Corbin (Strauss, Corbin 1998, Strauss, Corbin 1990,
Strauss, Corbin 2012, Corbin, Strauss 2008). Strauss came from a pragmatic and social
interactionist (interpretive) background and focused on human agency, emergent processes
and subjective understanding to Grounded Theory (Charmaz 2012; Charmaz 2014). In
contrast, Glaser focused on systematic structures, rigorous codification, empiricism and
discovery, a reflection of his quantitative leaning (Charmaz 2012; Charmaz 2014).
Kathy Charmaz, a former student of both Glesser and Strauss at the University of
Chicago (Kenny, Fourie 2015), forged a departure from both Strauss and Glaser. Charmaz
developed a more pragmatic version of Grounded Theory that brought an emphasis on
100 | P a g e
Constructivist and Constructionist approaches into Grounded Theory. These divisions
lead to three main approaches of Grounded theory which are the Constructivist (CGT)
approach, Classic or Glaserian and Straussian approaches. Constructivist Grounded
Theory (CGT) differs from the Straussian and Glaserian approach at the philosophical
and ontological level, use of literature, data analysis and coding practices.
3.5.2 Classic Grounded Theory: The Glaserian Approach
The Glaserian version of Grounded Theory is central and indispensable to data
(Glaser 1992, Glaser 2004, Glaser 2001). Glaser views everything concerning the
phenomenon under investigation as data (all is data) and hence applies loose data
analysis, which will allow the natural emergence of theory from the data. The
researcher assumes the position of an independent or neutral observer who
conceptualises data without taking an interpretive stance, indicating a robust
Positivist-Objectivist leaning (Glaser 2009, Martin, 2006). Glaser alludes to the
possibility of understanding reality from the data without considering the context
(Sosa 1993, Howard-Payne 2016, Charmaz 2014).
Hence, Glaserians treat data as real or objective facts that contain the theory that the
researcher can discover independently of their interaction with participants (Charmaz 2014).
Glaser insists that while employing the coding procedure, the researcher should patiently
“trust that emergence will occur, and it does (Glaser 2007, Glaser 1992, Glaser, Holton
2004). Researchers are to ask a series of questions of concerns to participants in the data and
then look for accounts that resolve the concerns (Glaser 1992, Glaser, Holton 2004). Glaser
developed a system of dealing with the human tendency and inevitability of inadvertently and
unconsciously introducing personal bias or interpretation. Glaser does this by alluding to
careful and rigorous coding procedure, constant comparison, restraint from the literature and
extant theories and collection of a large volume of data from multiple sources (Kenny, Fourie

101 | P a g e
2015, Glaser 1992, Glaser 2004). These premises, he argues, will correct bias and diminish
any personal input or influence of the researcher on the theory and help uncover underlying
patterns of the phenomenon and make data objective (Glaser 2004). However, I rejected the
Glaserian approach because of the over-emphasis on the emergence of the theory and
researcher neutrality.
The limiting of any researcher input is not corresponding to my ontological and
epistemological persuasion about reality and knowledge. Again, the naturalistic approach
supports the use of unstructured interviews and opposes the use of interview schedules in
collecting data (Glaser 2004). Hence, using the Glaserian approach would have denied me the
flexibility and possibility to clarify issues with participants, probe for more responses, and
elaboration and steer the interview to the point of theoretical interest (Charmaz 2014).
Equally, it was not practicable for me not to be exposed to the literature or extant theories
until the end of the study as the university required extensive literature review and
submission of proposal and application for ethical review and the transfer viva.
3.5.3 Straussian Grounded Theory
Although Strauss had some positivist learnings, he acknowledges the relationship
between concepts and Symbolic Interaction and positions Grounded theory as a way of
interrogating data (Strauss, Corbin 1990, Strauss, Corbin 1998). Since these publications, the
position of Strauss and Corbin has shifted towards the pragmatic realism position (Howard-
Payne 2016, Sosa 1993). The pragmatic realism position places reality in settings or contexts
and the possibility of multiple realities and co-construction of data (Howard-Payne 2016,
Strauss, Corbin 2012). To this effect, the revised position of Corbin, a comrade of Strauss,
brings her closer to the Constructivist interpretive theorising perspective (Howard-Payne
2016, Corbin, Strauss 2012, Strauss, Corbin 2018, Corbin et al. 2014, Kenny, Fourie 2015).

102 | P a g e
However, the highly systematic and rigorous coding structures intended to
create (not discover) a meticulous theory closely corresponding to data still espoused
objectivist stands (Strauss, Corbin 1990, Strauss, Corbin 1998). The robust and
systematic procedure mostly follows the same sequential progression as Glaser but
more meticulous and specified (Strauss, Corbin 1990). The Straussian position has
more in common with the Constructivist approach, the version of Grounded Theory
that I used for this study. However, the Straussian approach does not provide enough
subjectivity and flexibility in data analysis and theory development and was not
suitable for my study. Also, I do not allude to the objectivist view of data. Instead, I
see the whole research process as co-constructed.
3.5.4 Constructivist Grounded Theory (CGT)
The choice and interest in Constructivist Grounded Theory methodology were
guided primarily by the research questions and the nature of the study to explore and
understand the experiences and motivation in patients with cancer in using Traditional
Healers in a socio-cultural context. Also, I found the Constructivist Grounded Theory
methodology to be more dynamic and contemporary, offering a systematic but
flexible perspective and approach in responding to the challenges in the field.
Constructivist Grounded Theory emphasises the co-construction of data and open
acknowledgement of subjectivity and open reflexivity, which are corresponding to my
philosophical assumptions. The flexible approach of Constructivist Grounded Theory
also makes it ideal for studying a new terrain and gives the researcher room to work
with what may be available and what participants may be willing to share.
The Constructivist Grounded Theory lays stronger emphasis on co-
construction of knowledge or the shared reality between researchers and research
participants through social interaction (Charmaz, Mitchell 2007, Charmaz 2014,

103 | P a g e
Altheide, Johnson 1994, Guba, Lincoln 1994). The co-constructionist acknowledges that
knowledge and understanding of reality are products of society (Orlikowski, Baroudi 1991).
Apart from considering how participants viewed their experiences and theorise their
interpretation, it was recognised that the resultant theory was co-construction involving
multiple realities. Respectively, Clarke refers to reality as involving different actors in the
research and the impact of the broader environment on the researcher and the researched
(Clarke 2012, Clarke 2005).
Also, the Constructivist approach conceives of the world and reality as a new social
process, an extension of human consciousness, interactions and personal explanations of
experiences and encounters (Burrell, Morgan 2017). Hence, the Constructivist researcher
should broadly seek to understand how, through their participation in social processes and
social practices, members of a social group enact a reality (Orlikowski, Baroudi 1991). Also,
the social group can ascribe meaning to these realities, which then help them to constitute or
formulate a social action (Orlikowski, Baroudi 1991).
Moreover, I chose Constructivist Grounded Theory because it allows for open and
honest acknowledgement of subjectivity and presupposition in my study. The participants'
accounts that I presented were not a generic reflection or representation of the experiences
and motivation of people living with cancer in using Traditional Healers in Ghana. The aim
was to tell the story of participants and to represent their voices instead of generalising their
views. Subjective realities do not merely imprint on individuals. Instead, they develop from
negotiations through interaction with others, and exposures or experiences with languages,
symbols, history, culture and society (Lincoln et al. 2011, Creswell 2012). I relied on the
participants’ narrative of their experiences and subjective views or meanings of the situation.
In the social constructivist approach, individuals attempt to understand their world
through the subjective meanings of experiences directed towards themselves or others

104 | P a g e
(objects or things) (Creswell 2012). Consequently, no conception or model of
research or reality is pristine (Van Maanen 2011). The researchers’ socio-cultural or
economic, exposure and experiences profoundly sway what they see and the meaning
they attach to them (Gilgun 2013, Charmaz 2014, Charmaz 2012). The application of
the Constructivist Grounded theory approach to this study was that the initial
objectives and topic were subject to refinement and amendment as the inquiry
continued.
Although I laid out all the necessary groundwork and framework for the study,
it was not possible to predict all eventualities at any time or phase. Social research is
often unpredictable because of its dependence on many actors’ involvements, e.g.
participants, informants and gatekeepers. In Constructivist Grounded theory, there is
no guarantee that even the initial broad concepts would work in the field. Hence,
researchers should be flexible to work with the tools that participants, stakeholders
and key informants give them in the field (Gibbs 2015, Charmaz 2014, Charmaz
2012).
3.6 Summary of the Methodological and Philosophical Standpoint in This Study
More explicitly, the philosophical or methodological orientation for this study
is based on Constructivism and more specifically the version advocated by Kathy
Charmaz (Gibbs 2015, Charmaz 2014, Charmaz 2012, Charmaz, Mitchell 1996). The
theoretical underpinnings are rooted in the interpretive framework or traditions of
Symbolic Interactionism and pragmatism (Charmaz 2014). My study embraces the
ontological view of multiple contextual realities that actors such as the researcher and
participants constructed through their exposures, experiences and interactions in a
socio-cultural context.

105 | P a g e
Hence, the study did not intend to give a linear view of reality. Instead, my study
reflects the multiple views and interpretation of my participants. I was not a neutral or
independent observer; somewhat, my biography, privileges, culture, or profession influenced
my orientation to this research interpretation and co-construction and analysis of data
(Moustakas 1994). Furthermore, it was impossible to separate my values and research.
Hence, my axiological position is that every study is value-laden, and the onus is on
researchers to openly share them (Moustakas 1994, Creswell 2012, Creswell, Creswell 2017,
Charmaz 2014, Urquhart 2013).
The paradigm that underpins my study makes it clear that qualitative methods of data
collection which minimise the distance between the researcher and the participants and allow
participants to share their experiences in their settings was the best approach. In this study, I
collected and analysed data using an inductive research process to generate a theory on the
experience of people living with cancer in using Herbal Medicine in the Brong-Ahafo region
of Ghana (See this chapter 3.7 overview of study sites)

106 | P a g e
Table 3 Summary of GT Methodologies and the Choice for CGT Approach
Summary of GT methodologies and choosing CGT
Approach Underpinning
Philosophy and
Ontology
Coding
Principles
Position of
researcher Use of literature Selection of
Phenomenon
Uniting
Concepts
Classic or
Glaserian GT
Soft Positivism
The
constant
questioning
of data.
Designed to
discover
GT
Independent,
neutral and
value-free to
the research
process
Should be Avoided
until the end
Does not
commence
with pre-
defined
research
context or
proposal
Memo
Writing
Constant
Comparison
Theoretical
Sampling
Coding and
Theoretical
coding
Nor suitable for
examining
actions and
social processes
Not
suitable.
Against
researcher
input,
subjectivity
and
construction
Not suitable:
Objectivist
orientation.
Not suitable.
Against PhD
research
guidelines, initial
proposal and ethics
committee
Not suitable
Straussian
GT
Post-Positivism:
Influenced by
Symbolic
Interactionism
and Pragmatism
Systematic
procedures
Designed to
create a
Theory
from Data
Findings are
representative
of participants
only.
Appropriate use of
literature at all
stages
The
researcher
chooses a
phenomenon
and setting
Not suitable:
objectivist and
rigid treatment
of data
Not
suitable:
Rigid
analysis and
lack of
flexibility
Not suitable for
the aims of the
study towards
developing a
theory that is
co-constructed.
Suitable: meets
PhD, ethic and
protocol guidelines
and
Suitable for
the current
study and
PhD
research
guidelines
Constructivist
GT
Interpretivism or
Constructivism:
Influenced by
Constructionism,
Symbolic
Interactionism
and Pragmatism
Open-ended
and flexible
approach.
Designed to
construct
GT
Interdependent;
holds that the
findings are co-
constructed
(both
participants
and researchers
views)
Appropriate use of
literature at all
stages. Compile
temporal or Initial
Literature review.
The
researcher
chooses a
phenomenon
and setting.
Suitable for the
kind of question
Suitable:
Flexible
and
innovative
approach
Suitable for co-
construction of
data and
theory.
Suitable: meets
PhD, ethic and
protocol
guidelines.
Suitable for
the current
study and
PhD
research
guidelines
3.7 Overview of Study Sites and Region
The recruitment of study participants took place in two public hospitals and
five herbal clinics in the Brong- Ahafo Region of Ghana. The phenomenon and
interest of the study, methodology and potential for successful recruitment of relevant
patients led to the selection of these sites and the Brong- Ahafo region. I was led to

107 | P a g e
these oncology hospitals based on the possibility of capturing people living with cancer who
had relevant experiences and knowledge of the phenomenon of interest. Also, I had links to
these hospitals that facilitated the negotiation of access to the field.
The region was chosen for the study because of its large rural population, rich cultural
traditions and people who use Traditional Healers (Henry et al., 2013; Addo-Fordjour et
al.,2008). Besides, the region has several herbal clinics or traditional establishments which
treat illnesses (Henry et al., 2013, Addo-Fordjour et al.,2008). Hence, the Brong-Ahafo
region of Ghana provided a safe place of opportunity to conduct this study.
The Brong-Ahafo region is the second-largest region in Ghana with a total landmass
of 39,557 square kilometres and a population of 2,310983 according to the 2010 national
population census (Ghana Tourism Authority 2019). The location of the region is along the
middle belt of Ghana. It shares a local boundary with five other regions, and an international
border with The Republic of Cote D' Ivoire (Ghana Tourism Authority 2019, Government of
Ghana 2015). There are 22 district administration capitals headed by a regional
administration or capital. The farming and fishing are the principal occupations of the
population in the region (Government of Ghana 2015, Ghana Tourism Authority 2019,
Henry et al. 2013).
3.8 Recruitment and Sampling (Selective to Theoretical Sampling)
Participants in this study were male or female people living with cancer from the
Brong-Ahafo region of Ghana. The inclusion criteria considered adult patients (aged 18 years
or older) (Laird 2002), with a current cancer diagnosis who had used or were using
Traditional Healers for their current health condition confirmed by a conventional doctor. I
excluded people living with cancer who were under the age of eighteen or had not used
Traditional Healers (See Table 4 and 5 for details of the participants’ demographics).

108 | P a g e
Participants recruited from the hospitals were asked to confirm their demographics
details as part of the Informed consent process and before starting the interviews.
However, the lack of record-keeping in the Traditional Healers setting made it
impossible to confirm or verify the patients’ details in the herbal clinics.
The study developed interviews schedules or a list of topics that had to be
covered in the semi-structured interviews to allow flexibility and fluidity (Lewis-Beck
et al. 2004, Castillo-Montoya 2016). The interview schedules were developed based
on the literature review, research questions, and the overall phenomenon under
investigation (Lewis-Beck et al. 2004, Castillo-Montoya 2016, Seidman 2012). The
intention of the interview schedules was not to elicit socially correct answers but to
understand participants stories and the meaning they make of it (Castillo-Montoya
2016). Hence, the questions were “open questions’’ that stimulated conversation and
were suitable and relevant to participants understanding based on the local language
and culture without any jargons or prejudice (Brinkmann, Kvale 2015, Patton 2002). I
piloted the interview schedules with five adults from Ghana who live in the UK. The
feedback of their understanding of the questions helped verify that the questions were
able to facilitate a conversation about the topic of interest (Castillo-Montoya 2016,
Brinkmann, Kvale 2015). Using the feedback from the piloting and my supervisors, I
amended and finalised the interview schedule.
Sampling in Constructive Grounded theory (CGT) is a sequential progression
from selective or purposeful sampling to theoretical sampling (Draucker et al. 2007).
Selective sampling in Constructivist Grounded Theory is the initial sampling to
address the initial research question or central idea. It involves establishing criteria
and parameters for samples, situation and settings before starting the fieldwork
(Morse 2010, Bryman 2012, Draucker et al. 2007, Charmaz 2006). The focus is to

109 | P a g e
gather data most relevant to the phenomenon under investigation from people with the
relevant experiences or characteristics (Urquhart 2013, Creswell 2012, Pope, Mays
2008; Thompson,1999). In making the initial sampling decision to recruit people who were
living with cancer and had used or were using Traditional Healers, the Brong -Ahafo Region
and the study sites appeared suitable for my study. It was necessary to visit the recruitment
sites for collection on two separate occasions (Phase 1, 2015 and Phase 2, 2016). At the first
phase of the study, twenty-one participants were interviewed: eleven in the hospitals and ten
in the herbal clinics.
I conducted ten hours of observations: six hours at the hospitals and four at the herbal
clinics. I conducted interviews during the day and then spent the evening and night
transcribing and then analysing the data. The first couple of interviews were conducted in the
hospitals and another couple of interviews in an herbal clinic. The interviews were recorded
on an Olympus digital voice recorder, which has microphones for audio enhancement and
noise reduction, a USB port for charging and uploading data to a computer. The recorder also
had the capability for encrypting files and earpiece for playback at different motion which
facilitated the transcription.
After the analysis and comparison of the first four interviews, there was a
simultaneous data collection at both the hospitals and the herbal clinics based on the evolving
categories (theoretical sampling) such as ‘’boosting spirits, jovial and friendly, cordiality,
informality and as if they know you’’. Theoretical sampling is the collection of data as
directed by the initial data analysis to broaden, elaborate and strengthen emerging categories
(Charmaz 2014; Charmaz, 2012). Hence, both the data analysis and collection co-occur with
the emergent concept and guide the researcher’s decision on what data was needed and where
to get them (Pope, Mays 2008, Draucker et al. 2007, McCann, Clark 2003, Glaser 2009).

110 | P a g e
Using theoretical sampling, I was able to gather pertinent data to elaborate and
develop emerging provisional codes and their theoretical properties. Theoretical sampling is
not very seamless as the literature sometimes portrays it but involves tussling as some puzzles
may not fit together. I made decisions about which of the issues emerging in the data
collection and analysis needed to form the basis of theoretical sampling for further
investigations.
Soon after coming back to the UK and completing the analysis of all the
interviews of the phase one visit, I went back to the field to collect more theoretical
data for saturating the emergent categories and their properties (Bryman 2012,
Creswell 2012, Urquhart 2013). Also, I followed up on saturating properties of my
categories such as tradition, language and familiarity and goodwill. During the second
period of data collection, I extended my data collection to the herbal clinic more
frequently. The herbal clinics provided me with further data about motivations for
using these clinics. The questioning and suggestions from my supervisors rejuvenated
my momentum and thoughts and guided the collection of relevant data to expand
categories and their properties.
3.9 Negotiating Access to the Study Sites: Hospitals and Herbal Clinics
Although I had useful links in making contact and negotiating access to the
hospitals, I anticipated some difficulties and had a sense of trepidation. Through
family and friends, I commenced the negotiation of access using communications and
contacts. The use of support networks and relationships to start access negotiation
before going to the field is recommended in ethnographic research (Hammersley,
Atkinson 2007).
111 | P a g e
Allan & Arber (2018) encourage researchers to take advantage of their social,
professional and cultural links in the field to gain access, establish rapport, gain trust
and information about the communities, institutions and relevant people. My cousin (a
specialist Gynaecologist) and uncle (Consultant medical radiologist) facilitated the access by
discussing with relevant hospital authorities my request to use their facilities for recruitment.
They obtained favourable responses. Moreover, they provided information about the working
patterns of the clinics and sought assurances from staffs’ willingness to support the
recruitment activities.
However, such leads were projections that had to be tested to see whether the host
community would genuinely accept, welcome and provide the necessary support
(Hammersley, Atkinson 2007). When I arrived at the hospitals, I had an introductory meeting
with the medical director, administrators and matron who introduced me to the medical and
nursing team and asked them to support me. However, the negotiation of access was an
ongoing daily activity that required me to continually introduce myself, establish and
maintain rapport and ask for permission and support (Hammersley, Atkinson 2007).
In contrast, the herbal clinics were owned by private individuals and hence making
contact and negotiating access before travelling to Ghana was difficult. I negotiated access to
most of the herbal clinics when I was in Ghana. Three herbalists initially agreed for me to
recruit from their clinics through the assistant of a teacher whom I met during my MSc data
collection in Ghana. However, these herbalists wanted a face to face discussion with me
before they could confirm their participation. In the herbal clinics, I faced the challenge of
staffs’ suspicion as they doubted my identity and intentions. Most of the Traditional Healers
expressed their unhappiness with the doctors’ lack of respect and disdain towards them.
Hence, they were cautious in granting me access to their facilities in case I was a
doctor who wanted to spy on them or expose their practices. Although it was not possible to

112 | P a g e
control these feelings, I needed to remain open, establish rapport and show interest in
both staffs and patients at the clinics (Allan, Arber 2018, O'Reilly 2008, Fetterman
2009). I interacted with the “pharmacists’’ or the staff in charge of the herbs or
medicines. He explained to me some of the components of the medicines and how
they work. Moreover, I adopted the typical cultural greetings, postures, and showed
humility by supporting staffs whenever possible. At the first herbal clinic interview,
the herbalist appeared agitated and concerned that I may be related to doctors or
collecting information to slander his reputation. He kept walking up and down the
corridor and coming to stand behind the entrance of the interview room. I realised the
need to do something profound to break this suspicion and to convey trust.
The only conceivable way of assuring the herbalist that I was not a doctor and
had no ulterior motive was to allow him to listen to part of the interview. However, I
was also aware that allowing the herbalist to listen to some part of the interview
would not be consistent with the ethical principles of confidentiality. Also, doing so
would breach the assurances that I gave to the patient and her confidence in me.
Hence, I asked the patient’s permission to share the interview with the Traditional
Healer. Fortunately, the patient was okay with my request and had no reluctance. The
patient had been coming to the clinic for over a year and knew the herbalist very well.
The patients described how the clinic was a family to her. Hence, she agreed for the
interview to be shared with the herbalist without hesitation.
I invited the herbalist to listen to the recorded interview, and suddenly the
“penny dropped’’. The herbalist listened to the beginning of the interview, which
consisted broadly of the introduction of myself and open demographic questions
about the participant. The herbalist became satisfied in a few minutes and told me he
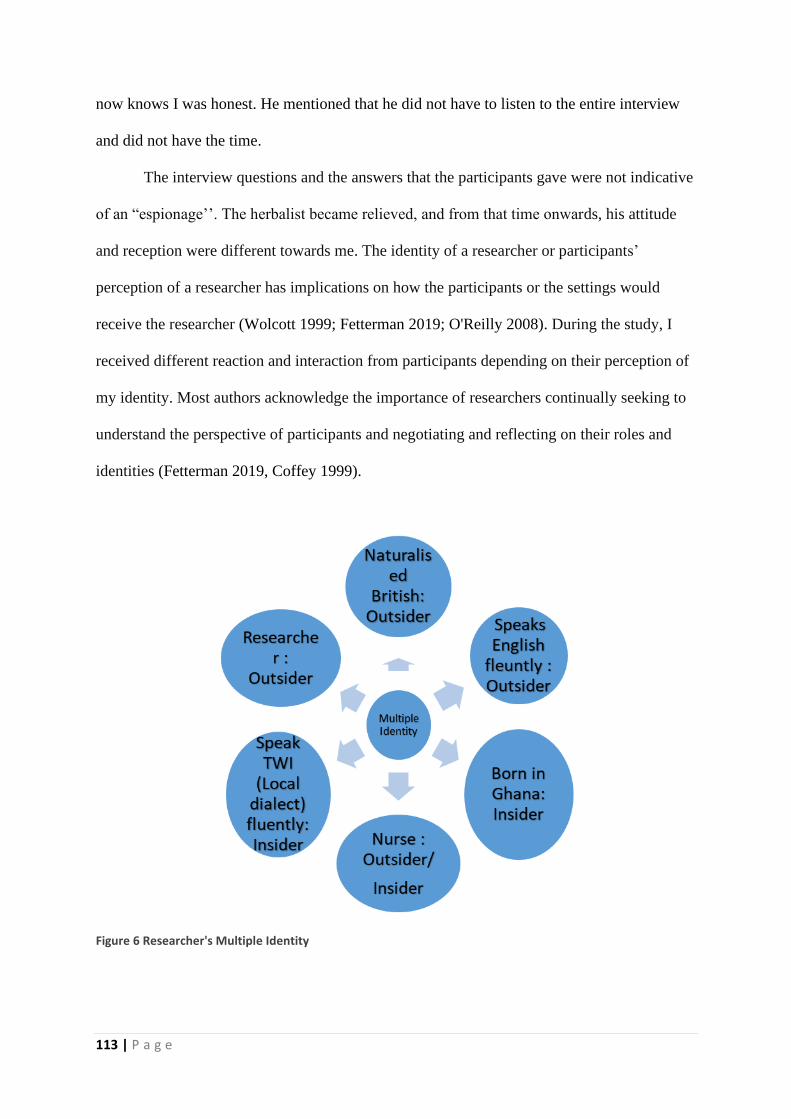
113 | P a g e
now knows I was honest. He mentioned that he did not have to listen to the entire interview
and did not have the time.
The interview questions and the answers that the participants gave were not indicative
of an “espionage’’. The herbalist became relieved, and from that time onwards, his attitude
and reception were different towards me. The identity of a researcher or participants’
perception of a researcher has implications on how the participants or the settings would
receive the researcher (Wolcott 1999; Fetterman 2019; O'Reilly 2008). During the study, I
received different reaction and interaction from participants depending on their perception of
my identity. Most authors acknowledge the importance of researchers continually seeking to
understand the perspective of participants and negotiating and reflecting on their roles and
identities (Fetterman 2019, Coffey 1999).
Figure 6 Researcher's Multiple Identity

114 | P a g e
3.10 Data Collection: Interviews
The primary method of data collection for this study was the use of semi-structured
in-depth interviews (n=35), using an interview schedule. The research interview offers
the opportunity for dialogue through which the researcher listens and facilitates
interaction and then interprets participants' responses to satisfy his or her theoretical
curiosity and understanding (Masson 2002). Interviews were used as the primary
mode of interaction with study participants and their accounts through the perspective
of Symbolic Interaction. The approach gave me an understanding of what the
participants experience meant to them. The approach gave an insight into how
participants juxtaposed their experiences with the Traditional Healers and the
Hospital.
The initial or opening question was a warm-up question that required
participants to tell me about themselves. The initial questions put the participant at
ease and stimulated their interest. I audio recorded the interviews to capture all
participants’ responses and to quickly refer to them for recollection and accuracy
(Kvale 2008). I conducted the interviews in a quiet room and offices where there was
privacy at the sites. However, some participants at the herbal clinics were comfortable
to have the interview under a tree. The interview schedule was useful in covering
specific areas while retaining the sensitivity and flexibility to pick up, probe and
pursue relevant leads and insights (Kvale 2008, Horowitz, Gerson,2002, (Bryman
2012, Masson 2002).
Interviews were ideal in exploring the individual experiences of the
participants and the meanings they attached to these experiences (Horowitz, Gerson
2002, Kvale 2008). The Interviews allowed me to probe participants to share their
stories while at the same time, guiding the dialogue towards a conceptual direction.

115 | P a g e
The use of semi-structured interviews enabled me to listen to the participants' narrations of
their experiences, encounters and construction of the phenomenon under investigation and
was suitable for gathering rich qualitative data for this study (Masson 2002, Kvale 2008).
However, I was cautious not to allow the presuppositions of myself or participants to
force any framework on the entire interview process and outcome (Masson 2002, Charmaz
2014, Howard-Payne 2016, Horowitz, Gerson 2002). I remained focused and alert during the
interviews to ensure salient issues, including what participants said unconsciously were
followed up immediately or during subsequent interviews without free associations (Kvale
2008, Charmaz 2014). I used the approach of probing to explore participants responses in a
more in-depth, clarify any ambiguities, and encouraged participants to talk freely and
spontaneously about their experiences (Bryman 2012, Masson 2002, Bowling 2009, Bryant,
2007, Charmaz 2006).
However, when I had to ask participants to elaborate or clarify their responses, I did it
with ‘open questioning’ to get more details. For example, I asked participants, ‘can you tell
me more about this or that’? Can you explain that in detail? After completing the initial data
analysis, I went back to the field to collect more theoretical data from saturating the emergent
categories and their properties (Bryman 2012; Creswell 2012)

116 | P a g e
Table 4 Participants demographics (Phase 1 visit)
PARTICIP
ANTS
NAME
INTERVIEW
CODE
GEND
ER
A
GE
OCCUPATION NATIVE
TOWN
SETTI
NG
DIAGNOSIS
Abrafi VN870067 Femal
e
29 Traditional
Midwife
Kintampo Hospit
al
Cervical
Ohemaa VN870068 Femal
e
71 Farmer Berekum Herbal Cervical?
Akomea VN870070/71 Femal
e
28 Finance
Institution
Nsoatre Hospit
al
cervical
Assifuah VN870072 Femal
e
68 Businesswoman Intotro so Herbal Cervical?
Serwaa VN870073/74 Femal
e
52 Secretary Bechem Hospit
al
cervical
Kyeremant
eng
VN870075 Male 70 Farmer Berekum Hospit
al
Prostate
Aborampah VN870077 Male 73 Farmer Berekum Hospit
al
Prostate
Kwarteng VN870078 Male 72 Farmer Berekum-
Biadan
Herbal Prostate?
Asantewaa VN870081 Femal
e
77 Farmer Berekum Herbal Breast?
Pinaman VN870083 Femal
e
40 Farmer Bosanko Hospit
al
Vulvar
Buruwa VN870085 Femal
e
30 Hairdresser Drobo Herbal Cervical?
Kwartema VN870090 Femal
e
37 Farmer Sampa Hospit
al
Cervical
Kyeremaa VN870092 Femal
e
32 Sells clothes Kwasiboo
Kurom
Hospit
al
Lung and liver
Kisiwaa VN870101 Femal
e
50 Farmer & Market
woman
Techiman Herbal Cervical
Nkrumah VN870106/07 Male 70 Retired Teacher Techiman Herbal Prostate?
Husain VN870113 Male 56 A sub-Chief Techiman Hospit
al
Lungs and
Liver
Asumadu VN870117 Male 57 Hunter Bore Herbal Ulcer
Kyeremeh VN870120 Male 44 Library Assistant Buoyem Herbal Prostate?
Fremah VN870125 Femal
e
31 Farmer Whediem Hospit
al
cervical
Aboagyewa
a
VN870129 Femal
e
56 Farmer Awurowa Herbal Leg ulcer, Skin
cancer?
Ataa VN870130 Femal
e
43 Farmer Techiman Hospit
al
Breast
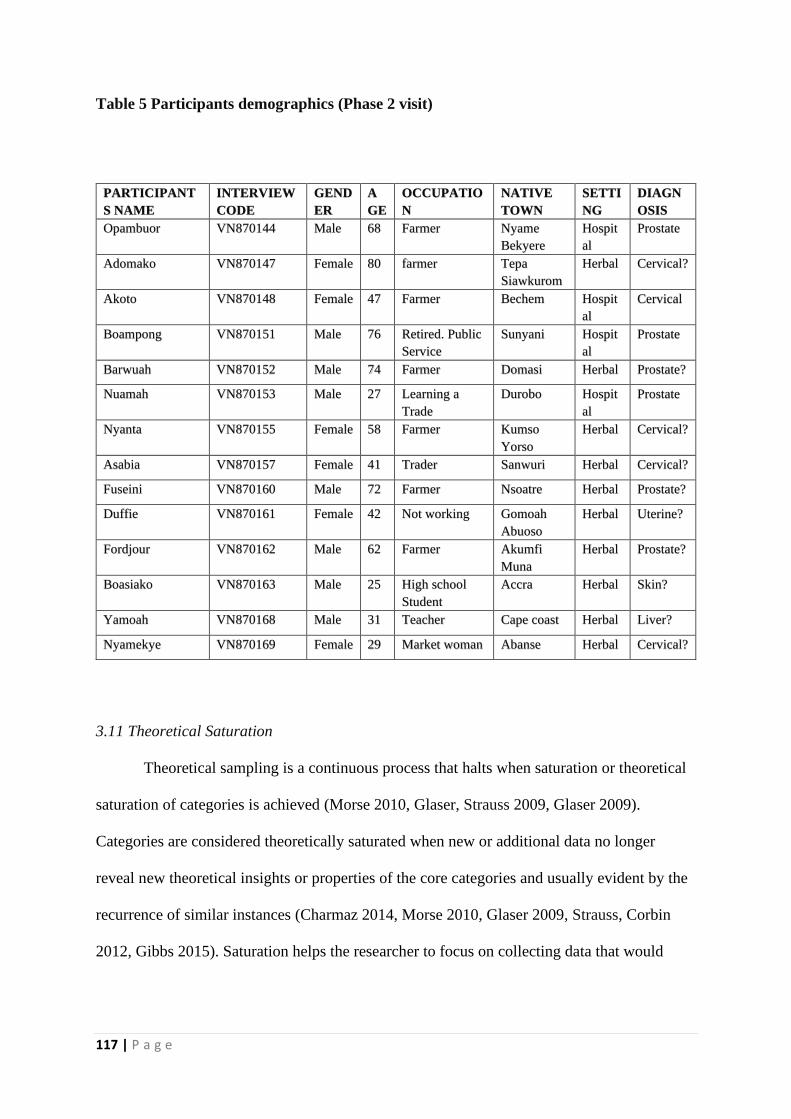
117 | P a g e
Table 5 Participants demographics (Phase 2 visit)
PARTICIPANT
S NAME
INTERVIEW
CODE
GEND
ER
A
GE
OCCUPATIO
N
NATIVE
TOWN
SETTI
NG
DIAGN
OSIS
Opambuor VN870144 Male 68 Farmer Nyame
Bekyere
Hospit
al
Prostate
Adomako VN870147 Female 80 farmer Tepa
Siawkurom
Herbal Cervical?
Akoto VN870148 Female 47 Farmer Bechem Hospit
al
Cervical
Boampong VN870151 Male 76 Retired. Public
Service
Sunyani Hospit
al
Prostate
Barwuah VN870152 Male 74 Farmer Domasi Herbal Prostate?
Nuamah VN870153 Male 27 Learning a
Trade
Durobo Hospit
al
Prostate
Nyanta VN870155 Female 58 Farmer Kumso
Yorso
Herbal Cervical?
Asabia VN870157 Female 41 Trader Sanwuri Herbal Cervical?
Fuseini VN870160 Male 72 Farmer Nsoatre Herbal Prostate?
Duffie VN870161 Female 42 Not working Gomoah
Abuoso
Herbal Uterine?
Fordjour VN870162 Male 62 Farmer Akumfi
Muna
Herbal Prostate?
Boasiako VN870163 Male 25 High school
Student
Accra Herbal Skin?
Yamoah VN870168 Male 31 Teacher Cape coast Herbal Liver?
Nyamekye VN870169 Female 29 Market woman Abanse Herbal Cervical?
3.11 Theoretical Saturation
Theoretical sampling is a continuous process that halts when saturation or theoretical
saturation of categories is achieved (Morse 2010, Glaser, Strauss 2009, Glaser 2009).
Categories are considered theoretically saturated when new or additional data no longer
reveal new theoretical insights or properties of the core categories and usually evident by the
recurrence of similar instances (Charmaz 2014, Morse 2010, Glaser 2009, Strauss, Corbin
2012, Gibbs 2015). Saturation helps the researcher to focus on collecting data that would

118 | P a g e
enhance the theory development or develop the emerging categories rather than
imposing an off the shelf theory on the data.
The number of participants from each setting (hospitals and herbal clinics) in
the end, were guided by saturation and the point by which nothing new was emerging
(Charmaz 2014, Bryman 2012, Guest et al., 2006, Dey 2012). Saturation of all
categories signified the end of the data collection for this study. People question the
practicalities of saturation and its prominence over logistical issues such as time,
money and practical field issues that may influence the completion of a study
(O’reilly, Parker, 2013, Guest et al., 2006, Bryman 2012, Dey 2012, Thorne, 2005).
Moreover, the saturation of a concept or a category is not definitive but a
claim that researchers make when they are satisfied with the explanatory powers of
the newly developed concept (Charmaz, 2014, Gibbs 2015). Admittedly, there were
practical constraints such as not intending to overstay my visa in Ghana or time off
from work. Also, I was aware of the period needed for completing the PhD. However,
there was no decision to leave the field or force saturation because of these external
constraints. Instead, the analysis and data collection continued as usual until
saturation was reached.
3.12 Theoretical Sensitivity
Theoretical sensitivity denotes the ability to generate concepts or categories,
relate them to hypotheses and integrate these hypotheses into emerging theoretical
codes (Glaser 1992, Urquhart 2013). At some point, the researcher must move
beyond the data, define the phenomenon in abstract terms and illustrate their
conceptual relationships (Charmaz 2014). Hence, theoretical sensitivity enables the
researcher to construct analytic codes, leading to abstract concepts that have clear
119 | P a g e
empirical indicators and can be unique from other concepts (Charmaz 2014). Furthermore,
theoretical sensitivity helps researchers to seize unexpected moments of insight in the
interviews and data collection to subsequently guide theoretical sampling and theory
development (Gibbs 2015; Charmaz 2014). My awareness and understanding of a broad
range of related concepts facilitated my thinking about data analysis. However, I did not
impose any concepts on the data as they had to earn their fit and relevance.
My theoretical insights and sensitivity came from academia, reading, profession and
attending conferences and PhD study groups. Also, supervisory and professional discussions
played a part in sharpening my sensitivity to extant concepts and theories. I reviewed the
literature as part of the ethics application and continued to make use of the University of
Surrey’s resources. The notion of having theoretical sensitivity before the study is
contentious on the basis that this might taint and impede the generation of categories from the
data (Glaser 1992).
However, it was unpractical for me to start the study or data analysis on a ‘tabula
rasa’ and sheath myself in pure innocence and substantive ignorance (Henwood, Pidgeon
2003, Charmaz 2012, Charmaz 2014). Instead, I exercised theoretical “agnosticism’’ and
subjected all prior theories and theoretical conjectures to rigorous scrutiny rather than
ignoring or denying them (Henwood, Pidgeon 2003, Gibbs 2015). Thus, I did not impose any
external concept on the study; instead, I pondered and engaged with these concepts and
activities that raised my theoretical sensitivity or acclimatisation with sensitising concepts.
For example, I read about the Comfort theory (Kolcaba, 2003, Kolcaba, 1997, Boudiab,
Kolcaba 2015) and wanted to apply it to my study. However, I dropped it after scrutiny since
it was not fitting to the data. The Comfort theory is the satisfaction of the basic human needs
for relief, ease and transcendence arising from stressful healthcare situation. The Comfort
theory assumes that Human beings have holistic responses to complex stimuli, comfort is a

120 | P a g e
desirable holistic outcome that is germane to the discipline of nursing, and human
beings strive to meet or to have met these basic comfort needs (Kolcaba, 2003,
Kolcaba, 1997, Boudiab, Kolcaba 2015).
3.13 Iteration and Constant Comparison
A unique feature of Grounded theory is that the data analysis and data
collection happen in parallel and not consecutively as with other qualitative methods.
Grounded theory methods commence with inductive data. However, the method
immediately proceeds through iterative strategies of moving back and forth between
the data and analysis using constant comparison (Charmaz 2014, Gibbs 2015). The
constant comparison involves comparing instances of identified categories or
concepts with other instances of data in the same class (Creswell 2012, Urquhart
2013). The use of Constant Comparison method helps to explore variations and draw
analytic distinctions (Hallberg 2006, Charmaz 2014).
The concept of iteration and constant comparison in Grounded theory
safeguards the researcher from adopting participants view uncritically, collecting
randomly partial data and relying on existing theories or concepts (Charmaz 2014).
Repeatedly moving between data collection and data analysis helps to give analytic
structure and direction to the data collection (Coffey 1996, Charmaz 2014). However,
engaging in an iterative process does not necessarily constitute a theory construction
if they do not lead to the explication of abstract concepts (Clarke, Montini 1993,
Charmaz 2014).
Through the iterative, comparative and inductive process, Grounded theory
method encourages persistent interaction between the researcher, the data and the
emerging analysis (Bowen, 2008a, Charmaz 2014, Bowen, 2008b, Draucker et al.
121 | P a g e
2007, Strauss, Corbin 2012). Hence, there is a continuous interplay and simultaneous
proceeding of data collection, analysis and theory development (Bowen, 2008b;
Strauss, Corbin 2012).
3.14 Seeking Relevant Ethics Approval in UK and Ghana
Research Ethics are the principles of moral, rights and legal conducts that inform and
guide research studies (Hardicre 2014, Fathalla, Fathalla 2004). Human research is dynamic
and complex, requiring the excellent co-operation, trust and legally or morally accepted
conventions and expectations between the researcher, potential participants and the setting
(Rubin, Rubin 2011, Silverman 2000). Imperatively, researchers should respect the principle
of self-autonomy or self-determination, non-maleficence, beneficence and justice always
(Murphy, Dingwall 2007, Beauchamp 1982). These principles underpinned the study and
formed a protective mechanism for me and the participants against inadvertent perilous effect
(Long, Johnson 2007, RCN 2011). Ethics committees and institution are necessary to
safeguarding safety and quality assurance in research (Hammersley, Atkinson 2007).
I first submitted the study protocol and relevant documents to the University of Surrey
Ethics Committee for assessment and approval (See Appendix 2-5 for relevant submitted
documents) and received feedback to respond to some concerns. After addressing these
concerns, I received a full approval (See Appendix 6-for approval certificate). Furthermore, I
submitted the study to the Kintampo Health Research Centre Institutional Ethics Committee
(KHRCIEC) (See Appendix 7 for approval certificate). Kintampo is a city in the Brong-
Ahafo region of Ghana where one of the three health research centres of the Ghana health
service is located. The research administrator provided the necessary assistance and guidance
in the process through email and telephone contacts.

122 | P a g e
KHRCIEC after approving the study referred it to the Scientific Review
Committee of the centre to consider its scientific validity. Three independent experts
of the Scientific Review Committee reviewed the study and provided their robust
feedback and suggestions. I addressed their concerns and obtained a full scientific
approval (See Appendix 8 for certificate). Through these reviews, the relevant
authorities assessed the benefits of the study and satisfied themselves that I had
minimised risk from or in the study to potential participants (National Research
Council 2014). Obtaining formal Ethics approval in Ghana was not automatic
permission to operate in the local facilities. The study required another high-level
access, call “clearance’’. Clearance seemed more of a political security pass to the
local institutions and the patients.
The KHRCIEC administrator made me aware of this before I arrived in
Ghana. I submitted a letter requesting for clearance in person to the regional health
administration where the staff asked me to wait to discuss my request with the
regional health director. In Ghana, ones’ profile and wealth or lack of it can open or
block access to high dignitaries. Hence, I felt intimidated that I may not get a
favourable response. Fortunately, the regional director showed interest in the study
and permitted me to recruit from the public hospitals in the region.
3.15 Obtaining Informed Consent (IC) and the Challenges around Cultural Consent
The ethical principle of Informed Consent offers protection to both research
participants and researchers in case of litigation (National Research Council 2014,
Murphy, Dingwall 2001, Heller 2011, Murphy, Dingwall 2007). However, the
protection of researchers against litigation is only possible if the researchers can
demonstrate that they have acted in the best interest of participants. Hence,

123 | P a g e
researchers should give all essential information and opportunity for invited subjects to
navigate around the complex decisions of participating in research (National Research
Council 2014). Doctors and nurses in the hospitals usually informed patients who met the
inclusion criteria if they would speak with me.
I gave potential participants a copy of the Participants Information Sheet explained
the study to them in the local dialect and allowed time for participants to contemplate and
process the information and ask questions before committing to take part (Cameron, Murphy
2007, RCN 2011). I relied on the services of research assistants in the hospitals to sign as
witnesses after observing that I had gone through the normal Informed consent process
properly. I stressed to all potential participants that their taking part in the study was
voluntary and will not affect their care or relationship with hospital staff.
Also, I assured participants of confidentiality and anonymity to their participation,
responses to questions and protection of their data. I notified participants of their right not to
answer every question or withdraw from the study at any point without having to give a
reason. I told participants that they could withdraw their data even after their interview, in
which case the data will be destroyed (deleted from all records). However, participants could
not withdraw their data after it had been analysed or once I had returned to the UK. Hence, I
gave participants a Ghana telephone number, purposely acquired for the study and told them
when I would leave the country so that participants could make contact if they had any
concerns.
I faced practical challenges around cultural differences in what constitutes consent
and the process of obtaining it. Most Ghanaian perceive more questioning, asking for more
information and documentation to indicate distrust. Consequently, some potential participants
required me to show them my trust by merely taking their word seriously as a guarantee or
consent without any documentation or signature. Some potential participants felt

124 | P a g e
uncomfortable and did not understand why I should call a witness or asked them to
sign a piece of paper when they had willingly offered to take part in the study. They
thought I did not trust them. Moreover, some participants were sceptical and feared
that they were signing a piece of paper that would implicate them in a problem.
Interestingly, even some of the study participants who had high education had
the notion that trust is best shown by taking peoples’ word for what they say. These
dynamics highlight the importance of tailoring consent to the characteristics of a
context (Oakes 2002). I assured these participants of my trust and explained to them
the necessity to illustrate to the University supervisors and governing institutions that
I followed due processes. Nonetheless, some participants had strong sentiments of
mistrust and refused to participate in the study. Others felt offended to sign the
consent form. Because of these challenges and complexities, some participants took
part in the study through verbal and not written consent. However, their verbal
consent was captured as part of the interview recordings.
3.16 Observations: The Dynamics of Doctor-Patient versus Herbalist-Patient Relationships
The primary method of data collection in Grounded theory is through
interviewing of participants. However, a background observational data is vital in
enhancing the richness and understanding of the context of a Grounded theory study
(Charmaz 2014, Charmaz 2006, Charmaz, Mitchell 2007).
In any social context, usually what people say may differ from their actions
and how they explain their actions to each other (Charmaz, Mitchell 2007). Hence, the
information that researchers capture from participants during interviews may not
directly reflect the behaviour of participants in practice. The observational data was,
125 | P a g e
therefore, crucial in providing an understanding of participants behaviour and real-time
interaction with staff in the hospitals and the herbal clinics.
In contrast to ethnographic observation which focuses on describing the settings,
structures and topics of interest, the Grounded theory researcher focuses on the phenomenon
of interest, as well as the processes and interactions related to the phenomenon (Charmaz
2014, Charmaz 2006, Charmaz, Mitchell 2007). Grounded theory researchers have selectivity
over the scenes that they observe and then systematically direct their attentions towards them
across different settings to gain more knowledge (Charmaz 2014, Charmaz 2006, Charmaz,
Mitchell 2007). The observations for this study were focused on participants actions,
interactions and behaviours in the context of the study. The observations enriched the data
and provided an understanding of the relationships and context within which the patients
sought help outside the hospital and their reported trust in Traditional Healers.
I conducted a total of 20 hours of observations (10 in each visit) of staffs’ interactions
and engagement with patients at the hospitals and herbal clinics. The observation data was
integrated with the interview data for the analysis. The observations were conducted during
the times when I was not conducting interviews or looking for a potential participant. I
documented the observations as part of the field notes immediately it was possible to do so
and ensured they accurately reflected the dynamics at the sites (Emerson et al. 2011,
Wolfinger 2002).
I did not want to make staff suspicious, apprehensive or alter their approach of doing
things. Hence, I took the field notes away from the clinics and staffs, sometimes when I got
home. I was worried that staffs’ awareness or impression that I was writing what goes on in
the clinics could jeopardise the maintenance of my access or encouraged staffs to act
artificially and to modify their practices and behaviours. Moreover, multiple activities and
interactions were happening at the same time. Hence, I could not observe and document

126 | P a g e
everything carefully. I used Emerson’s et al. (2011) ‘Salience Hierarchy’, in writing
field notes to focus on observations that struck me as most noteworthy exciting and
telling. For example, I found it interesting in documenting how staff showed care and
communicated with their patients, and the following are examples from a hospital and
an herbal clinic.
I remained vigilant to capture opportunities where staffs had direct interactions
with patients and how they communicated and supported the patients. The hospitals
appeared very busy with large numbers of patients, staffs and relatives. There was no
appointment system, and usually, clinics were full by 8 am as many patients come
very early from very far. Also, the doctors saw patients based on tier ticket number,
which staffs issued to patients as registration on their arrival. Most doctors were
usually late to the clinics with nurses unable to tell their whereabouts or provide
I was sitting at the corridor with patients who were waiting for the doctor. A
patient came out from a clinic room, walked to me and asked me ‘’ mepa wo
kyɛo, ɛhe na yɛ gye aduro’’ (please where do we collect medicine or where is
the pharmacy). I told the patient that I was new and directed her to the
receptionist. The receptionist asked the patient ‘’ how many times have you
come to this hospital? Every patient knows the pharmacy. Before the patient
could respond, the receptionist asked her to walk through the corridor, and she
would find it (OFN, SRH, 18/05/16).
On a different occasion in the herbal clinic, I was sitting outside with many
patients and some relatives. One of the security men came and asked whether
they got their medicine. One patient said to the security that he was relaxing
and would go and collect his medicine later. The security willingly went to
collect the medicine and brought them to the patient (OFN, HC, 20/05/16).

127 | P a g e
information to patients. It appeared this had become the norm and the receptionist did not
seem obligated to apologise to the patients.
Also, the relationship between hospital staffs and patients was very paternalistic, non-
interactive and patients appeared very mindful and unsure of how they should behave at
times. Most patients looked anxious and frustrated facially and based on their body language.
Some of them would take a walk to the main hospital entrance or ''roadside'' and come back
later to check whether the doctor had come to the clinic. Others asked me what the time was,
and it appeared they were concerned that they might miss their transport to their village.
Some clinic staffs shouted aloud to patients, warned them to keep quiet or face the
consequence of not being seen by the doctors.
Doctors and nurses usually told patients what to do rather than engaging with them in
any meaningful discussion and allowing them time to ask questions or voice concerns. Some
patients appeared anxious and upset but unable to express them in front of the nurses.
Occasionally, two patients would be talking and then stop abruptly as soon as they see staff
coming close to them or passing. Some patients were observed to go out of the consultation
room and then come back to clarify the instructions that the doctor or the nurse previously
gave them. These could be as simple as how they can locate a department. Such patients
appeared frightened at the thought that the nurse will not take it kindly with them and would
treat them like children. On one occasion, the nurse said to a patient “where was your ear
when I was talking, you did not listen, and now you are coming back to disturb”. Staffs also
had an influence on which the patient was seen first.
Usually, patients who were related to doctors or nurses in some capacity had the
advantage to bypass other patients to see the doctor, sometimes almost immediately. I
observed how the nurses quickly made doctors aware if someone who knows them or has a
high-status in society arrives. The doctor will then ask the nurse to allow that patient to come

128 | P a g e
in immediately. The lack of trust for doctors was evident to me right from the onset.
Some patients refused to talk to me, thinking I was a doctor or a member of staff.
These patients feared that whatever they share with me may have consequences on
them later.
Furthermore, most of the doctors and nurses did not give much attention to
privacy and confidentiality. At times, more than one doctor and nurses share some
clinics. Some staffs who did not work in the clinic usually visit for a chat with the
clinic staffs in the presence of patients, sometimes interrupting the consultation.
Clinic staffs discussed patients’ condition amongst themselves, across the room
without any reservation. However, some doctors and nurses were liked by patients for
their patience and helpfulness. Most patients preferred to see doctor “F’’ who was
very experienced and had returned to the clinic after retirement. Doctor “F’’ appeared
to be patient and showed more consideration to patients. Interestingly, both patients
and other staffs had high respect for doctor “F’’, and my experience in meeting him
was one of warmth and support.
Contrary to the hospitals, the situation in the herbal clinics was calmer and
peaceful as patients behaved with more spontaneity. Although patients waited for
sometimes before seeing the Traditional Healers, they appeared happy. Both staffs
and patients were comfortable and relaxed without any sense of rush or hurry. Even at
times when there were more patients, it appeared the patients themselves did not
notice or pay any attention. Patients, relatives and some staffs sat under a parasol,
played local games and interacted friendlily with each other. The playing of local
music was familiar to all the Traditional clinics, and people appeared they were
enjoying the songs. Strikingly, staffs in the herbal clinics actively supported patients
and would usually ask patients and relatives if they needed water or a seat. Staffs
129 | P a g e
supported patients in carrying their luggage, transferring into cars and running the errands to
the local shop for them.
The patients were freer and showed no reservations in talking to me or participating in
the interview. There was more interaction amongst patients, and the staffs frequently assured
patients that the Traditional healer would see them soon. The herbalist themselves had very
calm personalities and showed personal concern and care for patients. It was not a surprise
that some participants described the atmospheres of the Traditional clinic to a community or
family. There was a sense of belonging, compassion and trust.
3.17 Confidentiality and Sensitivity to Participants and Their Data
Confidentiality is an ethical obligation or principle which I complied by adhering to
the UK Data Protection Act 2018, and its equivalence in Ghana (Dovi 2013, Asante 2016,
The Government of Ghana 2012). As part of confidentiality to participants, I conducted the
interviews in quiet rooms away from other peoples and did not share the interview schedules
and participants responses with staffs. In a specific Herbal clinic, I allowed the herbalist to
listen to the first part of an interview to gain his trust and maintain continued access to the
clinic. However, this was done with the full permission of the patient. Also, the transcription
of all interviews was performed by me. Additionally, I observed confidentiality by limiting
access to data for supervisors only and appropriately managing the storage of data (Fathalla,
Fathalla, 2004; Melton 1997, RCN 2011).
The digital audio recorder for the interviews was protected with a password, and the
interviews were transferred immediately, or at the earliest possibility onto a password-
protected University of Surrey computer shared drive for backup. I also securely stored a
copy of the data on an encrypted USB stick as a backup. The consent forms which had
participants names were separately locked in a cabinet at the University of Surrey in a card

130 | P a g e
access room. Furthermore, I preserved the confidentiality and anonymity of
participants by using interview codes and pseudonyms in the transcripts, analysis,
reporting the findings and presenting and documenting participants’ demographic data
(RCN, 2011).
Unlinking the data this way made it impossible to associate participants with
any information or excerpts in reports (Fathalla, Fathalla, 2004, Melton 1997, RCN
2011). The storage of the research data will last for least 10yrs and administration
data for 6yrs following their last access before destruction by the policies of the
University of Surrey. Ethics in research surpass merely seeking formal approval;
instead, researchers should be sensitive to ethical issues throughout their study
(Creswell 2012). I prioritised the participants’ welfare always and remained vigilant
and sensitive to feelings of distress or discomfort. I was able to demonstrate
closeness, authenticity, empathy and deep sensitivity to the culture and traditions of
participants because of my familiarity with the socio-cultural settings (James 1992,
Broom, Kirby 2013).
I usually wore the local “Tie-Dye cloths and presented in a manner that was
congruent with the culture. The sensitivity to participants also allowed them to
emotionally and physically express themselves without any prejudice or rush.
Although I showed much sensitivity to participants, they always had the potential to
be emotionally upset. Hence the counselling team or service of Techiman Holy
Family and Sunyani Regional Hospitals were made aware of the study and stood
ready to offer support to participants if necessary.

131 | P a g e
3.18 Researcher’s Safety and Risk minimisation
Although Ghana is a safe and democratic country, the foreign office offers
some specific advice that travellers should ensure adherence. Some of this
information was to avoid carrying or displaying large sums of money in public,
travelling at night and attending informal gatherings or parties in unfamiliar locations alone.
All interviews were conducted at the hospitals and herbal clinics during the day to ensure
safety. Also, the timing of the interviews made it easy for participants to access support from
the hospitals if they become distressed. I always had my mobile phone switched on (vibration
during interviews) and made sure that family members were aware of my schedules or
itinerary for the day and the approximate time of returning home.
3.19 In-field reflexivity and Emotional Labour
In-field reflexivity relates to the dynamics of how researchers collect data in the
context (Neumann, Neumann 2015), using verbal and nonverbal communication, social
characteristics and socio-cultural orientations (Neumann, Neumann 2015, Pillow 2003). In-
field reflexivity extends to the emotional dynamics of the researcher's connection, sensitivity,
experiences and interactions with the participants and context, and their potential impact
(Coffey 1999; Allan 2018; Hochschild 2012).
The field is an interaction with actual persons during interviews, observations or data
collection in which we make deliberate decisions (Neumann, Neumann 2015, Wheeler 2013,
Neuman 2005). Although my familiarity with the culture and language helped in establishing
report and relationships, I had to maintain a sensible balance and judgement (Hammersley,
2007). Some participants did not understand why I would ask them to elaborate or clarify
their responses since I understood the language. However, it was vital for me to understand
the meaning of words in the sense that the participants used them or understood

132 | P a g e
them(Lofland, Lofland 2006, Starks, Trinidad 2007, Charmaz 2014). I felt the
constant compulsion of wanting to identify with participants. Equally, I had to ensure
that the doctors' interest and views did not influence the study. I found this
challenging as explicitly disagreeing with their opinions could jeopardise continuing
access and their support to me (Pollner 2010).
I continuously adapted to the environment and situations to maintain the trust
of participants, doctors, the herbal practitioners and negotiated their implicit and
explicit demands. Gestalt psychologists or traditions describe such dynamics or
situational interactions in the field, framed in accordance to the situation, context and
people involved as contact mechanism or patterns (Neumann, Neumann 2015,
Clarkson, Mackewn 1993). I was susceptible to the confluence type contact
mechanism in which through spending time with people, one develops the inclination
to agree with them (Neumann, Neumann 2015, Clarkson, Mackewn 1993). I
displayed confluence behaviour as a way of trying to avoid conflict in the field.
Confluence behaviour can impede researchers from asking specific vital
questions if they are uncomfortable to participants or can potentially jeopardise their
relationships with the participants (Clarkson, Mackewn 1993, Neumann, Neumann
2015). For example, I shielded my views and avoided partisan conversations to
preserve the trust of participants, doctors and herbalists. My interaction with
participants and their context has given me a deeper understanding of how the
perception of healthcare vary across communities and the need to avoid imposing a
system of health model in any society. I have become more appreciative to how we
experience healthcare in the UK after listening to participants accounts of their
experiences in the hospitals.
133 | P a g e
Furthermore, my experience and interaction involved negotiating and dealing with
sensitive emotions. Although the emotional connection to participants and setting was
positive (Coffey 1999), it could equally be demanding and deleterious to the researcher
(Hochschild 2012, Allan, Arber 2018). The researchers can suffer emotional stress, especially
in dealing with sensitive issues or participants with heightened emotions (Lee-Treweek,
Linkogle 2000, Dickson-Swift et al. 2008, Dickson-Swift et al. 2009). Hearing sensitive
issues and observing deplorable institutional cultures can induce negative feelings in
researchers (Allan, Arber 2018). Researchers can develop anger, frustration, sadness,
disappointment, injustice, embarrassment and even numbness (Coffey 1999, Allan, Arber
2018). Some participants gave upsetting accounts on longer queuing and waiting time in the
hospitals, anxiety and lack of systems for redress. I felt my inability to support participants on
these practical concerns was inappropriate.
Equally, I did not have access to professional emotional support during the fieldwork.
My empathetic emotions presented me to participants as ''human'' and encouraged
participants to trust me and openly share their stories (Halpern, 2001). Being privy to these
participants situations strengthened my identification and understanding with their
experiences and to represent their voices correctly. It was essential to deal with these
emotions properly and not allow them to impede the progress of the research (Pillow 2003,
Finlay 2002). Some people deal with such feeling through emotional labour in which they
express positive or desirable emotion to the encounter or situation (Brotheridge, Grandey
2002, Ashforth, Humphrey 1993, Hochschild 2012, Morris, Feldman 1996).
Emotional labour, therefore, manages impressions or feelings to create a publicly
accessible expression (Hochschild 2012, Gardner, Martinko 1988, Ashforth, Humphrey
1993). The practice of emotional labour can cover significant issues and be catastrophic to
employees or researchers (Hochschild 2012, Brotheridge, Grandey 2002). I differ from

134 | P a g e
labelling my experience of managing the emotional situation and challenges in the
field as “emotional labour’’ as described often in the text (Hochschild 2012,
Brotheridge, Grandey 2002, Ashforth, Humphrey 1993). My emotions were
culturally genuine, and I did not engage in a “large-scale’’ emotional work to show
emotions or superficially act emotions and empathy (Down et al. 2006).
Researchers are recommended to be open and honest in discussing or
managing psychological risks at all phases of the research to avoid burnout and not
see them as a weakness (Hochschild 2012, Allan, Arber 2018). Initially, I shielded my
emotions from supervisors for the concern to avoid the perception of weakness or
allowing emotions to obstruct the study. However, they were quick to notice the
emotional intensity of the early interviews and observations. They offered me support
and practical advice to take breaks or time out, enjoy some recreation and continue to
share my feelings with them. The relationship between my supervisors and myself
grew until it became normal for me to openly share and discuss my feelings at the
supervisory meeting, through emails and at any opportunity. I was able to share the
sensitive issues in the field and how they were coming back to my memory during the
transcription and analysis of the interviews. I also was able to share the frustrations at
work and impact the death of my parents were having on my studies.
3.20 Data Analysis
In this section, the methods and procedures are discussed that were used in
analysing the data. I describe how I transcribed, coded and developed categories from
the data using the iterative and constant comparison method. The coding was done at
three stages: Open coding using the line-by-line method, Focused coding to form
categories and Theoretical coding to lift substantive categories to more conceptual

135 | P a g e
levels of theory development. As the analysis progressed through these phases, categories
subsumed more data, developed and related to their properties and increased their theoretical
power.
3.21 Transcribing the Interviews
Transcription of data is an essential part of the preliminary stages of data analysis in
transforming the audio recorded interviews or raw data into a standardised format to facilitate
a more detail analysis (Babbie 2015, Bowling 2009, Kvale 2008). My transcription of the
data was not arbitrary but an interpretive and selective process (Davidson 2009) which
reflected the research aims and objectives (Duranti 2006). Using an earpiece connection, I
listened to each interview prior, during, and after transcription into Microsoft word
document. The transcribing of the interviews took an average of three hours for a typical
interview of about forty minutes long.
However, the process helped me in becoming more habituated with the data and
checking the accuracy of the transcripts (Richards 2014, Rapley 2011, Dey, 2003). I followed
the same process or approach to transcribe each interview data verbatim to ensure
consistency (Hesse-Biber, Leavy 2010) and to gain accurate transcript content reflecting
participants narrations (Beech et al., 2012). My transcription followed the denaturalised
approach, which captures only the main spoken words and responses (Lapadat 2000, Jaffe,
2007; Oliver et al., 2005). However, I ensured that the context of the interviews and all
memory points were preserved and reflected in the transcripts. My supervisors read samples
of the transcripts but were unable to listen to the interviews and to check for accuracy
because of their lack of familiarity with the local dialect.

136 | P a g e
3.22 Open, Focused and Theoretical Coding of the Data
I commenced the coding by reading, reflecting and noting on the transcripts and
throughout the analysis to become more absorbed in the data before the in-depth
analysis (Neuman 2005, Dey 1999, Harding 2013). I identified some initial catchy
codes and impressions that facilitated the subsequent analysis. My initial reflection on
the data was that participants seemed to speak negatively about doctors’ behaviour
and positive about the Traditional Healers behaviour around cultural practices. As the
foundation of analysis, coding classifies or categorises data segments with a label that
stays firmly to the data and concurrently encapsulates the essence of each piece of
data to interpret the accounts of a social phenomenon meaningfully. (Charmaz, 2014,
Dey, 2003, Burgess, 2003)
The methods of constant comparison were used throughout the analysis to
compare codes and categories with each other and with data and preserved more
analytic categories which had fitter and power to subsume more data (Dey 2012, Dey
1993, Charmaz 2014). After the manual line-by-line coding using Microsoft word
tracking and commenting system, I transferred all the data and codes into NVivo
qualitative analysis software which facilitated the sorting, managing and organising a
large amount of data with ease.
Again, the software provided an audit trail of the analysis, my thoughts, and
allowed me to revisit them quickly. I was able to write memos and description of
categories (nodes in NVivo) and linked them to the data. The software also facilitated
my ability to interrogate the data more rigorously through comparison, shifting,
reorganisation, relabelling and word frequency search. The salient line-by-line codes
were transferred to NVivo as nodes and tested against large sums of data.
137 | P a g e
Coding focuses on possibilities in the data to define a range of variations in the
phenomenon which is under investigation and not the accuracy of data fit into the
labels or codes (Charmaz 2014). Respectively, I focused on the various dimensions of
the participants' account of their motivations and experiences of using Traditional Healers.
Some of the initial emerging ideas that I saw in the data was how participants referred to
Traditional Medicine as something they share with Traditional Healers because the ancestors
gave it to them all. Participants talked about Traditional Healers as people who represented
their ancestors and could be trusted for their goodwill and intentions.
Although the coding of the data was iterative, it followed a sequential progression
from Open coding, through Focused coding and to Theoretical coding (Charmaz 2014). Open
coding is the initial coding of the data. I used the line-by-line approach for the open coding
(Charmaz 2014) and attached a label to each line of the transcripts using Microsoft Word
commenting and track changes system.
The following are samples of excerpts from 72-year-old male participants who had prostate
cancer and how I coded them using line-by-line open coding.
Line-by-line coding was still guided by the research and analytic interest (Dey 1999; Dey
2003; Harding 2013, Charmaz 2014). I consciously focused on actions and their scope of
encapsulating more data in the next phase of the analysis. Although line-by-line coding
The truth is that I was thinking a lot and even now, I am still thinking, although I have
hope after the herbalist spoke to me (Code: Being encouraged)
They are very free; they joke with me and encourage me to be strong and do (Code: being
jovial).
They did not hide anything from me, they let me know what they are doing and want to do
(Code: Openness)

138 | P a g e
usually generates a copious amount of provisional codes, the process ensures the researchers’
thorough engagement, interrogation and submersion in the data. The intense data habituation
was useful for me in identifying and defining new and implicit meanings such as power,
inequalities, emotional management and potential concepts which I later explored
analytically (Charmaz 2014, Dey 2003, Rapley 2011).
I reduced the number of provisional line-by-line codes by re-coding the first
and second codes of each transcript, comparing, evaluating, and combining codes
based on their fit to the data, usefulness and capability to accommodate for more data.
The initial or open coding also involved the incorporation of in-vivo codes which
refer to the terms, language or symbolism that participants used to describe their
experiences (Charmaz 2014). These codes were essential in preserving the views and
meanings of the participants in the coding process. I used in-vivo codes to construct
aggregate terms and statements of participants’ thoughts, beliefs and action. The
following extracts from the interviews provide examples of in-vivo codes.
Both Nyantah and Boasiako used these words to discuss how they protected
their self-image by concealing their health condition from their community and
relatives. I used these In-vivo codes to generate ideas and concepts about how the
“I was afraid that I could not just jump to wash my clothes in public” (Nyantah,
female, 58, cervical cancer),
“I do not think it is necessary to let people know when you are not well. You would be
washing your cloth in public, and this is not a good thing’’ (Boasiako, male, 25, skin
cancer?).

139 | P a g e
herbalists related to the participants, understood their concerns and protected their self-
esteem. I integrated in-vivo codes into the coding process and tested for their salience to the
data and theoretical or conceptual significance through constant comparison and analytic
examination.

140 | P a g e
Focused coding is the next primary phase in coding after the initial coding
(open coding) to form more conceptual codes or categories and to move towards an
analytic process and advance the theoretical direction (Charmaz 2014). Through the
method of constant comparison, evaluation and coding of the open codes, I was able
to decide which initial codes made the most analytic sense, subsumed more data, and
elevated them to focused codes (Charmaz 2014). For example, I combined some of
the line-by-line codes by Feseini to form the focused codes or categories. The
following is an example of how I developed focused codes from the initial line-by-
line codes.
Figure 7 example of Open line-by-line codes

141 | P a g e
Developing focus codes from Line-by-line codes
Furthermore, through constant comparison, I was able to test how these codes were fitting to
the data, understand their properties, refined and used them to interrogate, examined and
categorised extensive data (Holtslander, Duggleby 2009, Charmaz 2014). Equally, I
combined some Focused codes and dropped those that did not have much fit or relevance to
the data. I elevated the most salient Focused codes into higher categories which had more
conceptual or abstract power to create the theory (Charmaz 2014). For example, raising the
Focused code “Sense of Community’’ to a conceptual category in this study meant paying
attention to why participants talked about their familiarity with the Traditional Healers and
how they lived in the same community or neighbourhood and shared ancestry and traditions.
Comparing this focused category with participants’ description of the cultural divide,
power difference and foreign-like attitude of the conventional doctors, I was able to raise the
category to a more conceptual level, i.e. “Placing trust in one's community and identity''.
Focused coding was followed by theoretical coding to analytically raise the substantive
categories to a higher conceptual or abstract level (Charmaz 2014). Theoretical coding is an
emergent process of conceptualising the relationships between the substantive categories
Line-line codes
Always funny,
always laughing with me,
being jovial,
encouraging friendship,
making jokes
Focused code (Category)
Being Friendly and Jovial

142 | P a g e
(Glaser 1992) or the application of analytical patterns to substantive categories to
augment their conceptual abstraction (Glaser 2005, Stern 1980, Dey 2003, Charmaz
2014). These substantive categories are linkable to existing theories.
In practice for me, theoretical coding was an intellectual exercise which I
achieved by reading related literature, having a discussion with supervisors and
thinking analytically about the data. I was cautious to avoid any theoretical imposition
on the study, and this was facilitated by my supervisors to continually emphasising
the need to allow the data to dictate the theoretical direction. Hence, I remained open
to change and to refine the theoretical codes.
The application of axial coding was not suitable for the Constructivist
Grounded theory. I did not employ the rigid application of an analytic frame around
the data as that would have limited or constrained my ability to exercise flexibility,
tolerance to ambiguity and innovation (Charmaz 2014). The application of such a pre-
set structure limits the emergence of categories and exploration by forcing the data
into a specific paradigm. However, I still developed sub-categories and properties of
categories and showed the conceptual relationship or links between them by following
emergent leads from data collection, analysis and experiences that the categories
represent.
Right from the onset of the analysis and throughout the analysis, I applied
constant comparison by comparing codes and categories with themselves and with
data. The use of constant comparison ensured that my analysis started from specific
instances in the data and remained close to the data while moving to a more general
abstract category (Urquhart 2013; Charmaz 2014; Creswell 2012). By continually
asking the theoretical question of the data, I was able to engage and interrogate the
data thoroughly. For example, the codes: we are one, respecting the culture, cultural

143 | P a g e
training, reputation, ancestral connection, lacking cultural communication and hoping in the
Traditional healers were compared with each other and with codes of other interviews.
It was identified that these codes had similarities in their expressions of trust in the
Traditional healer and contributed to developing the theoretical code of trust. The constant
comparison helped in identifying commonalities and differences in the manner the
participants constructed or talked about their experiences. Also, such a comparative
evaluation of codes and categories with each other and with the data helped to unearth their
analytic distinction and fit (Glaser, Strauss 2009, Charmaz 2014). I remained theoretically
sensitive to facilitate theoretical comparison but ensured that any existing theory that came
into mind was tested for their fit and not imposed on the data.

144 | P a g e
Box 3, Comparison of the focused codes of Fuseini and Yamoah and how
they developed into Substantive Categories

145 | P a g e
3.23 Memo Writing
Successive writing of memos encourages engaging with the data, generating current
ideas, analytical codes, and increasing the level of abstraction (Charmaz 2014, Lempert
2007). A memo is the notes of the rational conversation or interrogation with the data where
researchers find their voice and facilitate an analytic jump (Charmaz 2014, Gibbs 2015,
Lempert 2007). Analytical memos were used to express ideas about the data and to track the
patterns and emerging categories and concept. Using NVivo software facilitated memos
writing on the interview, codes and categories. Also, memos were used to describe the
meaning and boundaries of categories and how they related to each other. For example, I
used a memo to describe the category of quality time as not being rushed, giving enough time
for consultation, allowing time for questions and involving participants in the discussion.
Although the centrality of memo writing is in building theoretical categories or
concepts (Charmaz 2014, Glaser 1992), memo writing is encouraged throughout the research
process. I wrote down my thoughts, momentary idea, feelings, challenges, setback and
feedback. Some analytic insights occurred to me randomly, even in the middle of the night.
Also, sometimes while driving, and they were written down as soon as it was possible.
Theoretical insights can arise at any time, even away from the data, and the researcher should
document them as soon as possible (Goulding 2001, Lempert 2007, Gibbs 2015, Charmaz
2012). Although memos ideally should have a caption reflecting a category or a concept
(Lempert 2007, Charmaz 2014), it was not practical for me to write memos neatly and
promptly always. The important thing was to ensure that ideas and reflections were noted
down so that I could visit them in the analytic or research process.

146 | P a g e
3.24 Developing Categories
Categories are conceptual ideas which help in categorising or classifying and
comparing essential differences and similarities (commonalities) of the phenomenon
through abstracting of salient features from the immense details and complexity of the
data (Dey 2003). A category must have an analytic context, relate to other categories
and have broader conceptual relations while at the same time reflecting the empirical
material or data (Dey 2003, Charmaz 2014). The categories that I developed were
assessed for their abstraction power while at the same time, ensuring that they link
closely to the data and the context of the study using the constant comparison method.
The approach of constant comparison allowed me to compare categories continuously
to themselves and to the data to access their emergent or fit and relevance to the data.
Constructivist Grounded theory categories encourage the explanation of categories
concerning their contextual or socio-environment origin (Charmaz 2014).
Hence, the categories for the study needed to reflect the socio-cultural context,
environment and the phenomenon that I was investigating. For example, the central or
analytical core categories of “Placing trust in one’s community and identity”,
“Finding Solace in Therapeutic Hospitality and Conviviality” and “Aiming to Avoid
Upset and Manage Emotions” closely aligned with the context of the indigenous
communities and practices in Ghana and the phenomenon of Traditional healing or
medicine. The process of category formation is an analytical process which allowed
me to assess how the data support or contradict the initial codes and their theoretical
contribution to the findings of the study (Dey 2003, Glaser 1992, Strauss,
Corbin,1990).
Using iterative coding and constant comparison, I identified commonalities
and divergences and created core properties fitting to all categories that I lifted from

147 | P a g e
the initial open and focused coding. In practice, the formation of categories was using the
method of constant comparison and elevating some focused codes that had more conceptual
or analytical power. These codes also had fit to the data (able to subsume more extensive
data) and relevance to context and phenomenon of the study. The focused codes were lifted
to the next higher level called categories.
Again, using constant comparison, memo writing and conceptual thinking, I
developed core or analytic categories and generated various aspects or patterns of the core
categories from the data but with conceptual relevance and power to compare to extant
theories for theoretical contribution (Glaser 1992, Charmaz 2014). Moreover, the approach is
evident in Strauss and Corbin (1990) through the concept of unifying all categories around a
central core which explains other categories in more detail through relationships with the core
properties (See Figure 8 for analytical core category and subcategories). Charmaz (2014),
underscores involving in the process, creating a balance between core categories and
theoretical statements about the categories, including memo integration. For example, in the
main category of trusting communities, I wrote the following description or statements.
Participants see themselves and the Traditional Healers as one community with a collective
identity. They expressed these identities in a shared language, community relationship and
accountability to each other, shared tradition and shared reputable values or sensibility.
Although most participants trusted the Traditional Healers and thought the Traditional
Healers provided a hospitable service, there was an unusual case in which a participant spoke
unfavourably about Traditional Healers. This participant was disappointed by paying money
to a Traditional Healers and not seeing an effective treatment outcome, which may explain
his dissatisfaction. Although the participants trusted the institution of Traditional healing, he
felt that charlatans had infiltrated the system.

148 | P a g e
3.25 Theory Development
From the interpretive perspective, a theory is a conceptual interpretation and
understanding of the relationships (pattern and connection) in an investigated or
examined phenomenon instead of seeking causality (Thornburgh, Charmaz 2012,
Charmaz, 2014). The Constructivist Grounded theory focuses on generating a theory
outside of a theoretical framework through iterative inductive and constant
comparison data analysis. Constructivist Grounded theory allows researchers the
flexibility and freedom to gain knowledge about any aspects of participants
experience and life (Charmaz 2014). The use of iterative, constant comparison and
coding led to the development of the analytical categories and their sub-categories.
Through data interpretation and comparison of the analytical categories to existing
theories and concepts, I developed a theory of abstraction that was not initially
explicit or obvious in the data.
In this study, the broad theoretical categories that I developed were Trust and
Hospitality. I focused my attention on how these categories explained the participants’
motivation to use Traditional Healers. In the process, I developed a theory of the
Figure 8 Sample of analytical core category and subcategory

149 | P a g e
intricacies of the relationship between participants and the Traditional Healers. The theory
also shows how these relationships influence the participants’ trust and perception of
hospitality in herbal clinics. I analysed hospitality through the process of analysing
participants’ language about how Traditional Healers created a welcoming atmosphere at
their clinics, exhibited friendliness, listened with attention, lifted participants spirit, boosted
their hope, provided quality time to participants and managed participants’ emotions. These
practices were what the participants appreciated the most, and hence, the practice of
hospitality encourage participants to use Traditional Healers.
Also, I analysed trust and how it forms the foundation of the relationship between
indigenous Ghanaian communities and Traditional healers, and how trust influences
participants’ preference to use traditional healers instead of Conventional doctors.
Participants justified their trust in the Traditional healers based on the universal language,
tradition and the Traditional healers’ reputation and accountability towards their community.
The theory of “ Community of Us’’ which I developed represent the fabric of identities and
subtilities of trust in most Ghanaian indigenous communities and how they influenced
participants’ motivation to use Traditional Healers.
3.26 Post field Reflexivity
In general, the post field phase involves reflexivity about the processes that usually
occur after the data production (or collection) period (Neumann, Neumann 2015). While
Neumann and Neumann (2015) describe this phase as textual situatedness, Mauthner, Doucet
(2003) and Mauthner et al. (1998) emphasise post field reflexivity in the analysis,
interpretation and conclusions of a study. Researchers decisions on the method of analysis
and process of interpretation is a reflexive exercise through which they make sense and find
meaning (Mauthner et al. 1998, Mauthner, Doucet 2003). The decisions that I continued to

150 | P a g e
make on the study after the fieldwork were not arbitrary but reflected the institutional,
departmental, supervisory and personal perspectives. These included the books and literature
that I read, the analysis software that I used, feedback and recommendation from
supervisors, colleagues and other academic staffs and how I used them.
Moreover, decisions were made on the portions of data selected and
interpreted as evidence to support the line of argument. Devine (1999) was right to
mention how researchers enter the post-field or analysis phase wearing blinders of
pre-conceived ideas, assumptions, and the planned trajectory of the research. Many
authors argue for openly acknowledging and discussing elements that may have
influenced their post field activities as part of strengthening the validity and
credibility of the study (Mauthner, Doucet 2003, Neumann, Neumann 2015, May
1998). Some elements influenced and directed my thoughts and actions directly or
indirectly in the post field activities.
3.27 Considerations for Rigour and Credibility
A qualitative researcher should not consider or assess the rigour of their work
base on reliability, validity and generalisability, typically required for quantitative
research (Yardley 2000, Noble, Smith 2015). Instead of directly applying these
assessments to judge qualitative studies, we should explain the terms within the
framework of qualitative studies or use equivalent terminologies (Yardley 2000,
Noble, Smith 2015, Charmaz 2014, Glaser, Strauss 2009 ). The credibility of a
qualitative study is vital in assessing its rigour and quality (Noble, Smith 2015,
Corbin, Strauss 2008; Beck 1993, Glaser, Strauss 2017). Credibility is an indication
that the findings of a study are trustworthy and believable by reflecting the
participants’, the researcher’s and audience’s experience and a product of credible

151 | P a g e
interpretation of data in a manner that stands out as one of the many possible and plausible
interpretations from the data (Corbin, Strauss 2008).
Also, the credibility of a study is a measure of its reliability and validity, which we
should address more appropriately in qualitative studies as true value, consistency and
confirmability (Noble, Smith 2015). Similarly, these elements can be addressed as sensitivity
to context, commitment and rigour, and transparency and coherence (Yardley 2000). It is
essential for qualitative researchers to openly acknowledge multiple realities, and their
personal and subjective biases (true values) (Noble, Smith 2015) and remain sensitive to
participant perspective, socio-cultural settings and ethical consideration (sensitivity to
context) (Yardley 2000). Reflexivity is critical in boosting consistency, conformability or
traceability and overall credibility of a study (Beck 1993, Noble, Smith 2015, Yardley 2000).
Using reflexivity, I was able to openly recognise existing background preconceptions,
professional and academic experiences and asked questions of emerging codes or categories.
I maintained objectivity by being aware and situating myself throughout the collection and
analysis of the data.
The use of Constructivist Grounded theory approach meant the study was a version of
my story about participants’ account of social processes, social actions and situations
(Charmaz 2014). By following and documenting the analytic process of grounded theory and
ensuring transparency, I amplified the credibility of my study (Watson 2000). I ensured
transparency in the research findings through the acknowledgement and documentation of
interactions and dynamics, challenges, and the possible influence of my background and
empathy with participants and their potential influence on both the data collection and
analysis. Moreover, I maintained transparency by thoroughly documenting observational
field notes, audio recording interviews, keeping interviews transcripts and revisiting them for
clarity and accuracy, attending monthly supervisions and writing of memos (Beck 1993).

152 | P a g e
Also, I maintained credibility using constant comparison approach to unveiling
similarities and differences in how participants constructed their experiences and
identified an unusual case.
Furthermore, instead of reliability, a qualitative study should aim to achieve its
equivalence such as dependability, consistency or trustworthiness, and commitment
and rigour ((Morse 2015, Noble, Smith 2015, Yardley 2000). The dependability of a
study is concerned with the ability of another researcher to obtain the same or
comparable results if they retrace the study (Morse 2015) which is achievable through
the ‘trustworthiness’ of the appropriate use of methods, transparency and clarity of
researcher’s decision and audit trail (Noble, Smith 2015). The Constructivist
Grounded Theory approach does not strongly recommend the notion to achieve
reliability or dependability on the basis that we examine phenomenon with regards to
participant’s context, making it unlikely for another researcher to achieve the same
results (Charmaz 2014).
However, qualitative research should have some level of dependability or
consistency to make the findings usable to guide changes in behaviour or health
literature used by third sector organisations. Charmaz (2014) prefers the term
resonance, which focuses on whether the analytical categories portray the full reality
of participants and offer a more in-depth understanding or explanation into their world
of experience. I achieved dependability through in-depth engagement and interaction
with my study through methodological awareness, data collection and detail analysis
of data. Also, I used multiple methods (interviews and observations) and sites
(hospitals and herbal clinics) to collect data and thoroughly engaged in the study
context during both visits. The dependability of Constructivist Grounded theory

153 | P a g e
depends on how close, relevant, and reflective the theory is to the context and phenomenon of
the investigation.
The categories and the theory development were relevant and closely related to the
context and the phenomenon that I studied and derived from the accounts or data from
participants. Again, I achieved dependability in the study through the conducting, listening
and transcribing the interviews, painstakingly reading and annotating transcripts and carefully
scrutinising the data through the analysis and coding process. These activities helped me to
be more immersed and habituated with the data. Qualitative research attracts criticism for
lacking transferability or generalisability due to small sample sizes and lack of control over
individual variables (Blaikie 2010). However, the quality of a study corresponds to be
applicability. If the study is accepted to meet the test of quality, then equally, it should be
considered applicable as well (Corbin, Strauss 2008). The findings of such a study should fit
the context, provide enough insight, understanding and work in various situation or
populations to bring about a preferred outcome (Noble, Smith 2015, Yardley 2000).
However, some qualitative researchers often argue against generalisation as pointless
and impractical because of the complexities of social environments which do not operate with
consistency (Guba, Lincoln 1989). Such a view is congruent to the Constructivist approach,
which rejects the thought of predicting human experience with one universal set of ideas
(Guba, Lincoln 1989). The aim of my study was not to achieve generalisation but to generate
a theory that is relevant to a phenomenon and its context (Charmaz 2014, Yardley 2000,
Noble, Smith 2015).
However, such a theory can serve as a useful guide for studies with similar
characteristics. Using both purposeful and theoretical sampling in this study produced a depth
in the data and thick findings (Guba, Lincoln 1989, Noble, Smith 2015). Thick data and
description of findings enable interested parties to judge the degree to which the finding

154 | P a g e
would transfer to their area of interest (Morse 2015). I purposely selected participants
who had relevant experience in using Traditional healers and in a context where the
Traditional healers are predominant and interwoven with the socio-cultural traditions.
Also, the categories and sub-categories that I developed were relevant to the
phenomenon and the contest of participants experience.
3.28 Summary of Chapter
I have described theoretical paradigms that underpin Grounded theory or
Constructivist Grounded theory and how they influenced my methodological
orientation. I have described Grounded theory and Constructivist Grounded theory
and my justification for choosing it. I have discussed the fit of the research design and
methods for my study objectives and research questions to be answered. Moreover, I
have described the Constructivist Grounded theory method, its key concepts, and how
I applied them in my study. I also discussed Constructivist Grounded theory
methods’ relationship with literature pre-data and during the analysis. Also, I
described the recruitment process, participants selection, negotiation of various
accesses (formal and Informal), and how I sustained them throughout the data
collection period.
Furthermore, I described the procedures and methods that I employed to
analyse the data that were suitable for Constructivist Grounded theory approach and
how that led to the developing of categories and the substantive theory. Moreover, I
talked about how my study achieved the standard of credibility, dependability and
applicability.

155 | P a g e
CHAPTER FOUR: FINDINGS
4.1 Chapter Overview
I have divided the findings chapter into three main sections which provide evidence
from participants interview accounts and observation of their context of interaction with
Traditional Healers and doctors to substantiating the core categories developed from the data
analysis. These categories are: 'Placing trust in one's community and Identity'', ''Finding
Solace in the therapeutic hospitality'' and conviviality'', ‘‘Aiming to avoid upset and manage
emotions''.
''Placing trust in one's community and identity'' presents participants' accounts of how
they identified with their community, shared socio-cultural values and interaction with
Traditional Healers and how these elements facilitate participants trust for the Traditional
Healers. The category of ''Placing trust in one's community and identity’’ also shows how
participants' accounts generally signified a lack of trust in the conventional doctors. The lack
of trust in the doctors was because of the participants perceived that the doctors were
dissociated from the local communities and represented a cultural divide, power, and
inequality. The category of ''Finding solace in therapeutic hospitality and conviviality''
describes participants encounter and experience with the Traditional Healers in the herbal
clinics against their experiences with doctors and nurses in the hospitals. The third section on
''Aiming to avoid upset and manage emotions'' reports on participants’ description of their
feeling of reassurance that the Traditional Healers would protect their privacy which enabled
them to trust the Traditional Healers than the conventional doctors. Also, the participants
obtained emotional security and comfort that the Traditional Healers will keep their
information safe.

156 | P a g e
4.2. Power Disparity and Lack of Trust
Many participants' accounts indicated a lack of trust in most doctors and
hospital institutions because of the perception that their practices brought a cultural
divide and revived distant colonial memories. Although most participants were
unlikely to have had a direct experience of colonial administration, they know of it
through oral history. A typical example is the Cape Coast and Elmina Castle, which
are sanctuaries of some appalling memories of the slave trade. Many participants
opposed the colonialist idea and did not trust many things they considered as colonial
legacy or representation. Most participants were concerned with the colonialist era
legacies such as cultural adulteration, the impact of western education, and the power
of the elite. They perceived these colonial depictions to be present in the hospital
environment and their interactions with the Conventional doctors.
Many participants viewed these legacies as the causes of the power difference
between themselves and the doctors. Such participants perceptions about doctors
hindered the formation of trustful relationships between participants and doctors.
Although many participants expressed a lack of trust for the doctors, they continued to
use their services, possibly because they were dependent on the doctors. Yamoah and
Kisiwaa perceived the conventional doctors to endorse everything “white’’ or
“Whiteman’’: related as superior to the indigenous as indicated in the excerpts below.
“The problem with the doctors is that they are very proud and think everything White is right
and everything Black is wrong’’ (Yamoah, male, 31, liver cancer?).
“What I want to say is that you people with White education should not think the herbalist is
not good. The hospitals do not like it if you come to the Traditional Healers; they think you
are stupid or something. The doctors always think they are superior to everyone, and that is
not a good thing’’ (Kisiwaa, female, 50, cervical cancer).

157 | P a g e
Most participants used the words “White’’, “Whiteman’’ or “White medicine’’ as a
metaphor to describe some doctors as symbols of power, superiority, control, elitism and
wealth. The word in general also defines behaviours and practices that are foreign and
differing to the Ghanaian culture and identity. Most of the unprivileged population think the
rich and powerful do not respect the culture, and local norms and values because of their
education and expensive lifestyle, a symbolic reflection of colonial influence (Mathiot et al.
2011).
In Yamoah’s view, some doctors exalted everything that originates from Europe and
America over anything local. These may range from simple products such as food and
clothing to more advanced products and institutions. These products or institutions are
coincidentally mostly accessible and affordable to the higher class. Some people of such
high calibre or rank do not usually identify themselves closely with the indigenous culture
and people. Instead, they prefer to identify themselves with modern and sophisticated
European culture and life. My observations in both the hospitals and the Traditional Healers
clinics highlighted the notion that the doctors were interested in European and American
products and lifestyle than the local ones.
I observed in the hospitals that all the doctors usually dressed in cute shirts, trousers,
dresses, shoes, expensive watches, and a white coat. Such a manner of dressing up was
different from the way most of the patients and the local community dress up. The local
community and most of the patients wore something made from the locally produced tie-and-
dye material. Also, all the doctors that I met had beautiful and big vehicles and had parking
spaces allocated to them. Some of the doctors frequently travel to Europe and America for
holidays and enthusiastically shared their experiences with other staffs in the presence of
patients.
In contrast, I observed that the Traditional Healers, their staff, and patients dressed in the
local apparel. These include “tie-and-dye”, “Fugu”, ‘’ahenema’’ (local slippers made from
goatskin) which mean the children of a king. There were a few staff and patients dressed in
what others would consider as European dressing but remained moderate and showed no
sense of extravagance and wealth (OFN, CP, HC,2015/2016).

158 | P a g e
From the observation, we can see why patients felt that the hospital doctors
were not interested in what happens in the local community or considered them less
relevant. From my experience of growing up and working in Ghana as a nurse,
doctors and nurses generally do not use the locally produced costume or cultural
regalia. Also, some doctors import brand-new cars from Europe and America and use
items that people have imported from these countries. The ownership of a private
vehicle is a sign of wealth in Ghana, and doctors are usually able to afford some of the
most expensive cars. Hence, most people in Ghana see doctors as members of the
upper class who are apathetic to indigenous items. However, it is difficult to know
with certainty whether the doctors’ interest, acquisition and use of foreign items were
by necessity or just luxury. For example, although the use of a white coat by doctors
is an adoption from the European culture, it has become part of the doctors’ uniform
in Ghana and possibly necessary for identification.
Although it is unlikely that all doctors in Ghana have such attitude in them,
most participants expressed such feeling about them. Such a feeling is also generally
prominent among most of the ordinary Ghanaian population, who are usually rural or
agrarian with low education and low income.
Kisiwaa’s quote above commenced with a note of caution to doctors and
people who receive western education or in the position of power not to undermine
Traditional Healers recklessly:
“What I want to say is that you people with white education should not think
the herbalist is not good.”
My experience and observation at both the hospital and the herbal settings
indicated strong power dynamics between doctors and the Traditional Healers. Most
Traditional Healers expressed outrage at what they perceived to be a shift in power
against them in favour of the doctors. Some Traditional Healers spoke to me about

159 | P a g e
how they felt that the doctors had always undermined them and the socio-cultural traditions
of their communities. My observation field notes express some of the contentions between
Traditional Healers and the doctors. Sometimes, the tension between the Traditional Healers
and the doctors was shown in how some Traditional Healers had a suspicion that I was a
doctor or connected with doctors and had the ulterior motive of exposing their practices. At
one of the herbal clinics, the Traditional Healer asked me to show evidence that I was a
student and had no affiliation with any conventional institution or not a doctor in Ghana.
Some herbal clinic staff told me how they feel doctors are arrogant and think that they are
more important than anyone. They also talked about how doctors pretend that they can cure
all illnesses. Some Traditional Healers and their staffs expressed concern about how the
doctors undermine the community traditions and ancestral legacies. The following was an
observation note from one of the herbal clinics that I visited:
Sometimes, the Traditional Healers expressed their tension with the doctors through their
reaction and suspicion towards me. Some of the Traditional Healers had the suspicion that I
had links with doctors at the local hospitals. In one of the herbal clinics, the staff asked me to
wait to speak to the herbalist for permission before I could do anything in the clinic or speak
to any patients. The staffs were not prepared to discuss anything with me until the herbalist
had established my identity and had permitted them to allow me to operate in the clinic. A
member of staff described how they (clinic staff) could only trust people who trust them or
believe in them. The staff was upset and mentioned that the doctors should stay away from
the clinic and not attempt to defame their name. At that time, I sensed that the staff thought I
was a doctor or affiliated to the local hospital. The herbalist asked me ‘’ How do I know that
you are a student and just doing research? These days we must be careful about doctors as
they just want to tarnish our image to our people”. I reiterated to him that I was a student
from the UK and doing the research as part of my studies and not in any way linked to the
local hospitals or doctors. The herbalist asked me to show some evidence that I was a student
and not a doctor. I showed him the recruitment materials and the introductory letter from my
supervisor as they had the university logos on them to prove that I had come from the UK
(OFN, HC, June 2016)
The Traditional Healer and his staff showed their resentment to doctors and how
doctors were not welcome to their premises. Possibly, the Traditional Healer may have
instructed his staff not to discuss any issues with potential doctors or hospital staff until they

160 | P a g e
could ascertain their identity. Traditional Healer only allowed me to operate in his
clinic when he was satisfied that I was not a doctor. Initially, the staffs in the clinic
identified me as a doctor. Hence, they saw a perfect opportunity to show their
bitterness and dislike to me in response to their perceived general behaviours of
doctors towards Traditional Healers. The staff felt the doctors do not trust them, and
hence they should also not trust the doctors. The clinic was on the lookout for any
undercover work from the doctors that may expose how they work and pitch it against
Conventional Medicine.
Traditional Healers see the resentments from doctors as a real threat to their
very livelihood, survival, and dignity in society. In this respect, some Traditional
Healers exercised caution to validate my identity and to establish that I had no links
with the doctors before allowing me access to their facilities (see Chapter 3.9, 3.15 for
indications of distrust). Equally, the doctors openly expressed their concerns about the
Traditional Healers during my interactions with them and reported that the Traditional
Healers have no education or understanding in treating illness and are preventing
people from using conventional medicine.
Some doctors expressed anger about the fact that some Traditional Healers
addressed themselves as doctors. The doctors thought the Traditional Healers were
undermining their arduous work to become doctors. Similarly, some doctors spoke
openly with me that the herbalists do not have the requisite knowledge or
qualifications and are 'charlatans. Such a powerful language of condemnation
emphasised the level of resentment that doctors had for Traditional Healers. Most
doctors mentioned how they could not understand why some patients would visit the
Traditional Healers. In their view, the herbalists' assurances to the public that they can

161 | P a g e
treat illnesses were false. Kisiwaa's accounts suggest the doctors sometimes criticised the
Traditional Healers in from of the patients.
However, Kisiwaa felt that the doctors’ assessments and criticism of the Traditional
Healers were not fair as the Traditional Healers do much work in the community and care for
the vulnerable people. Furthermore, Kisiwaa found it unacceptable that some doctors criticise
patients who visit the herbalists instead of the hospital. Some participants saw such doctors as
oblivious to the cultural practices in the indigenous communities. Moreover, many
participants viewed the doctors’ behaviour of using inaccessible language and perceived lack
of sensitivity to tradition, whether deliberate or from ignorance as culturally inappropriate,
suggesting their socio-cultural disconnect and power inequality.
Possibly, the participants, through their narratives, were addressing the power balance
by telling stories about their bad experiences with Conventional doctors. Some participants
came across during the interviews as wanting to pass a message to the doctors. These
participants expressed their resentment and dissatisfaction to the inequality and cultural
detachment that the doctors represent. This category of power and lack of trust shows how
most participants lacked trust in the doctors because they perceived the doctor to have
westernised standings and detachment from the indigenous cultural values.
Most participants felt the doctors exercised and reflected colonial supremacy over
ordinary people because of the power and privileges they enjoy in society. Many participants
viewed western culture and education as features of a cultural divide, the revival of colonial
memories and the creation of power imbalance between the average population and the elite.
On the contrary, most participants trusted the Traditional Healers because they saw the
Traditional Healers as people who shared a similar identity with them and have the necessary
cultural sensitivity, humility and understanding required in the community.

162 | P a g e
4.3 Placing Trust in One’s Community and Identity
“Trust shapes all aspects of human life. Whatever matters to human beings,
Trust is the atmosphere in which it thrives… When it is damaged, the community as a
whole suffers, and when it is destroyed, societies falter and collapse” (Bok 1979,
page 69).
One cannot overstate the importance of trust in all dimensions of human life
and activity, and the functioning of society depends on trust to a greater extent (Bok,
1979). Tradition and strong familial and community bonds give clear moral
guidelines for the development of good character and smooth functioning of most
Ghanaian communities (Utley, 2016). Most Ghanaian communities require trust as a
fundamental character or value from their members or institutions. However, the
problem in societies or communities is more of trustworthiness than trust as even the
person who is most willing to trust will still look for signs of trustworthiness in others
before placing trust in them (Gambetta 2008, Hardin, 2006).
Socio-cultural identities, and relationships and appropriate standard
behaviours are the essential fabric of the Ghanaian indigenous communities. This core
category, ‘Placing trust in one’s community and identity’, encapsulate the
fundamentally shared community values, relationships, and the Traditional Healers
behaviours’ that made them trustworthy amongst most of the participants.
4.3.1 Tradition: Participants shared Ancestral and Cultural Connection with Traditional
Healers
Most participants reported trusting in the Traditional Healers because they shared the same
traditional identities with them. Participants trust in the Traditional Healers generally
appeared to be part of the way they showed conformity to their traditional identity and
revered the community's ancestral authority. Most Ghanaian communities consider people
who distance themselves from indigenous traditions and moral values as arrogant and

163 | P a g e
disrespectful. This interview extract from Barwuah identifies the importance of ancestral
heritage and how community elders sustain and perpetuate it to future generations:
''Our ancestors gave the Traditional Healers to us for the benefit of the community and all of
us. Our ancestors and grandfathers pass on Traditional Medicine to the Traditional Healers
when they are about to die. When they are about to die, they would call someone in the
family, and they [grandfathers] would hand over their herbal knowledge to them'' (Barwuah,
male, 74, prostate cancer).
Barwuah highlighted how the elders or grandparents would call on a family member
that they consider apt and then pass on the healing knowledge to them. The approach
establishes the notion that people do not gain herbal knowledge through personal merit but as
a favour from their ancestors and elders. The elders can transfer their knowledge and power
to their successor before they die. Also, the elders can gradually transfer their power to their
successor by training them. The elders usually train their successor when they sense the
possibility of death due to age, ill-health or communication from the ancestors of their
intention to take them home. A common belief in most communities in Ghana is the notion
that elders can see the spiritual world and communicate with ancestral spirits.
Fremah's narrative below reflects the importance of cherishing the Traditional Healers
because of a shared historical connection with the ancestors who usually are responsible for
passing on traditional healing as a gift to families and community members. Participants
cherishing of the Traditional Healers leads to placing trust in them.
''I believe that we should never throw away Traditional Medicine. It is our past (our history)
and a gift from our ancestors so I will continue to use it” (Fremah, female, 31, cervical
cancer).
Fremah's beliefs in Traditional Medicine represent trust in Traditional Healers and
the ancestors who are responsible for the Traditional Healers’ knowledge. The expression 'we
do not throw away' is part of a famous Ghanaian axiom that implores people to avoid
distancing themselves from their traditions and native identity. In this sense, Fremah saw
Traditional Healers as part of her tradition, history and represented a gift from the ancestors.
Fremah emphasised her commitment to continuing to trust the Traditional Healers and use

164 | P a g e
their services. Most Ghanaian indigenous communities broadly encourage their
members to honour what the ancestors have left behind for the good of their
communities. These communities believe that the ancestors have preserved their
character in the Traditional Healers, which earn the Traditional Healers the credibility
of trust.
Some participants felt that they could trust the Traditional Healers because the
Traditional Healers receive training that reflected the society’s tradition and moral
standards. Thus, the community values and traditions instilled in the Traditional
Healers through training conferred to them a positive reputation which people can
trust. Both Boampong and Abrafi described how the Traditional Healers receive
community-based training and learning of ethical values:
“Somebody can start learning from a very young age and get all the wisdom before he or she
can work as herbalist’’ (Abrafi, female, 41, cervical cancer).
“Well, my experience is that the herbalist is very well trained. They have not trained abroad,
or in any institution, they are trained in the community and know the people in the
community. They are outstanding’’ (Boampong male, 76, prostate cancer).
Abrafi described how the training of the trainee Traditional Healer continue
until the elders are satisfied that they have acquired the required wisdom to practice as
Traditional Healers. Most Ghanaian believe that the training of the Traditional
Healers involves a rigorous personality, identity and character training. Abrafi's
description about the Traditional Healers acquisition of wisdom before commencing
their practice has a link with the Ghanaian adage that says ''efie nyansa nko, ena
sukuu nyansa nko.'' The literal meaning of this idiom is that the wisdom obtained
from home is different and better than the wisdom obtained from the school.
The elders usually use this idiom to caution those who have detached or are
contemplating to detach themselves from their culture because of academic prowess
and primarily encourage people to seek relevant soft cultural values. Boampong used

165 | P a g e
the word outstanding in describing the Traditional Healers character and reputation.
Traditional Healers appear to epitomise respect, selflessness, community solidarity,
humility and equality, which are all necessary building blocks of most Ghanaian communities
(Utley 2016). The training of the Traditional Healers in the local communities meant the
Traditional Healers receive first-hand knowledge of their community values and a buffer
against cultural adulteration. Also, the community training of the Traditional Healers
enhances their integration, building of community bonds and learning of the skills that
prepare them for community life.
On the contrary, most participants reported the lack of trust for doctors because of the
western system of education that doctors receive. Many participants felt that the medical
education system does not provide doctors with culturally rooted or relevant training. Instead,
most doctors were reported to receive knowledge and medical training that is devoid of
compassion, character and traditional values that the local community espouses:
“I agree that the doctors know about drugs (medical knowledge) and they are trained in
medicine, but they can learn something from the herbalist. They can learn about our culture
and how to behave appropriately (Buruwa, female, 30, cervical cancer?).
Buruwa acknowledges the importance of the expert medical knowledge of doctors but
implores them not to let that knowledge become detrimental to their behaviour. Given these
concerns, some authors have argued that the governments of Africa should ground and tailor
Africa's teaching and education in its culture and values (Ocheni, Nwankwo 2012).
4.3.2 Participants Shared Language with the Traditional Healers
Most participants expressed trust in the Traditional Healers because they shared a
common language with them. Many participants described how they could understand and
communicate satisfactorily with the Traditional Healers, in contrast to the conventional
doctors who often used English. Majority of the participants did not speak English and

166 | P a g e
signalled their preference to speak in “Twi’’ which is a familiar local language that
everyone could speak in the community.
Aborampah showed the difference between the languages used by the doctors and Traditional
Healers and how they influenced trust and power relations:
“Sometimes, you may not even understand what the doctors are saying. For example, I do not
understand some of the languages that they use. They speak the White man's language
because they have all become ‘, White men and women’. The herbalist speaks our language,
and we can understand each other. If you understand what someone is saying, then you can
also contribute or feel you have power” (Aborampah, male, 73, prostate cancer).
Aborampah expressed the lack of trust in the doctors because he could not
understand what the doctors discussed with him in the hospital. Furthermore,
Aborampah felt he was powerless in doctors’ presence and unable to identify with
them and contribute to the clinical encounter. Many authors describe how language
can be used as a power dynamic to distance others from an interaction (Luhmann
2018, Garrett 2010, Giles, Ogay 2013). Most doctors often used English and medical
terms which were unfamiliar to the local population. Aborampah’s used of the
statement '' the doctors’' language'' as a way of distancing himself and the local
population from such a language. It seems Aborampah expected to be involved in the
exchange of communication with doctors but felt unable to do so because of his lack
of understanding of the doctors' language.
Many Ghanaians refer to English as the ''White man's language'' and those
with European or American cultural attachments as ''Whites''. In a profound sense,
Aborampah was expressing his lack of trust in the doctors because of their use of a
foreign language which he interpreted to illustrate power inequality, elitism and loss
of cultural attachment. Aborampah felt that the language barrier between himself and
his doctor meant he was unable to ask questions or have a full picture of his situation
and what he needed to do.

167 | P a g e
Contrary, Aborampah's account unveiled his trust in the Traditional Healers because
of his ability to understand and identify with the Traditional Healers in a common language.
Aborampah called the local language ''our language'', thus invoking a sense of collectiveness,
inclusiveness, and trust for the Traditional Healers because of the shared language. Some
studies have shown how people who are fluent with a common language were more likely to
be accepted and trusted by their intra-groups and have a personal sense of identification with
the group (Sanchez et al. 2012). Similarly, ethnic communities perceive someone who speaks
the ethnic community's language as showing respect to them.
Such respect can lead to substantial interaction and bonding, which are essential to
trust. Aborampah described how his shared language with the Traditional Healers provided
him with a sense of power and ability to contribute to the therapeutic discussions. Other
participants (e.g. Akomeah, female, 28, cervical cancer; Aboagyewaa, female, 56, breast
cancer; Asabia, female, 41, cervical cancer? and Kisiwaa, female, 50, cervical cancer)
expressed a feeling of frustration at their inability to understand the language that the doctors
used. They expressed a profound lack of parity between themselves and the doctors because
of the language barrier, and hence they found it challenging to trust the doctors.
In Akomeah’s view, the doctors’ use of English during the therapeutic encounter and
interaction was deliberately designed to prevent her from understanding her situation.
''The herbalists speak to you in your language so that you can understand. They do not
behave like the doctors who sometimes do not want you to hear or understand them.
Traditional Healers do not speak to you in English” (Akomeah, female, 28, cervical cancer).
The Traditional Healers spoke to participants in a common language in contrast to the
doctors who spoke an unfamiliar language. Most participants thought the doctors used the
English language and complex medical expressions deliberately to sabotage and alienate
them from the discussions about their illness. Most participants thought the doctors used
English to maintain their power, inequity and exclusivity over them.

168 | P a g e
The following is a sample of my observations in a Gynaecology-Oncology
clinic in one of the hospitals
I usually spent part of my day in the Gynaecology clinic where doctors and nurses will
introduce me to potential participants for recruitment. Since I was not a member of staff, I
usually sat outside the main consultation room. At about 13:00 hours, a porter brought a
patient in a wheelchair from the emergency room. During the consultation, the doctors
shouted to me “This case is vulvar cancer, would you be interested?” I answered yes, and the
doctor continued to speak to me in English across the room in the presence of the patients.
He told me that the condition had spread to most of the patient’s private parts because the
patient does not always come for review. The doctor expressed his suspicion that the patient
may have been visiting a herbalist for treatment and only comes to the hospital in an
emergency (OFN. 19 October 2015 Hospital Clinic).
Such a conversation can cause anxiety to patients as they are not familiar nor
understand the English language which the doctor used. Equally, the patient could be
uncomfortable because she did not understand what the doctor was discussing with me.
Probably, the doctor may be aware that it was not appropriate to be telling me in more detail
about the patient’s condition and potential behaviour. Hence, the doctor’s' use of English
could be an attempt to stop the patient from understanding the conversation. The observation
substantiates why most patients reasonably believed that doctors sometimes do not want them
to hear the contents of their discussions. This observation was in contrast with the herbal
clinic where the herbalists spoke to the patients in the local language (Twi). Also, the
herbalists usually conducted a consultation with the patients alone. They did not speak to any
staff or others about the patients’ condition.
However, it appeared that many of the participants had accepted the culture of
disempowerment. They were unable to ask the doctors to speak in the local dialect during the
consultation. The doctors' training focuses on enhancing their medical and academic
knowledge and not the dynamics of local communities. Hence, doctors may not always be
aware and sensitive to how their behaviour may contradict the socio-cultural environment in
which they practice. However, it is not clear whether patients would hold the same

169 | P a g e
unfavourable views about doctors if they were able to speak English and understand the
medical terminologies, or if the doctors were to speak in the local language
4.3.3 Perception of Familiarity, Goodwill and Accountability
“Whoever wants to win trust must take part in social life and be in a position to build the
expectation of others into his self-presentation’’ (Luhmann 2018, page 69).
The quote suggests how familiarity forms the basis of trust, and hence those interested
in a trust must show themselves as a social identity and interact with their communities.
People who isolate themselves from their communities are not in the position to build trust
since they do not make themselves available for others to know them. Most Ghanaian
communities have close familiarity and a sense of mutual help, collective responsibility and
reciprocal obligation (Utley 2016, Uzzell et al. 2012). The familiarity and close social
relations in these communities strengthen the members' sense of goodwill and accountability
towards each other.
Many of the participants indicated that they trust the Traditional Healers because they
had relationships, interactions and neighbourhood bond with the Traditional Healers. Most
participants trusted the Traditional Healers because of familiarity; for example, Fremah
conveyed how she lived in the same village as the Traditional Healer
“I know about the man because he lives in the village with us for many years and has always
treated people who are sick. He is part of our community” (Fremah, female, 31, cervical
cancer).
In this account, Fremah trusted the Traditional Healer because he was not a stranger
but a member of the community. In the Ghanaian context, to know somebody denotes a
knowledge about their character, behaviour, and whether they are trustworthy. Fremah's
cohabitation in the same village with the Traditional Healer gave her the confidence to trust
him. The expression that the Traditional Healers are part of ''our community'' broadly means

170 | P a g e
the Traditional Healers are more than mere residents of the community. The local
expression is ''Kuromane papa'', which means a genuine and engaging community
member. The implication is that Traditional Healers are part of the everyday routine
life and cultural practices of the community.
Most Traditional Healers in Ghana fulfil their community's expectation for its
members and contribute to community life through their participation in ceremonial
activities. These include funerals, marriages, festivals and practical community
improvement activities. Most participants trusted the Traditional Healers because of
the Traditional Healers active interaction and engagement with them ordinarily on a
day-to-day basis in the community. Fremah described how the Traditional Healers
had always shown goodwill towards the people in the community by treating their
illnesses. Participants' seemed to have an implied assumption that the Traditional
Healers have goodwill and responsibility towards them. Communities in Ghana
usually label people who have apathy and lack involvement in the communities as
‘‘Kuromane bonee'' which broadly means non-engaging or lousy community
members. People perceive such members of the community to have ulterior motives
or hidden agendas and lack goodwill and accountability towards their community.
Akoto described her relationship with the Traditional Healers as one “like a
family’’, an indication of familiarity and relationship, accountability and goodwill.
“The thing is, your farm maybe next to the herbalist farm, and you always say hello to each
other and share a boundary. We are like a family to them'' (Akoto, female, 47, cervical
cancer).
Akoto compared the extent of her relationship with the Traditional Healers to
that of family. This comparison is an indication of trust based on good personal
knowledge and frequently repeated interactions. These interactions included living

171 | P a g e
and farming in the same locality and routinely greeting each other and promoting the feeling
of being part of a family.
Most Ghanaians may consider people who may not share blood relations with them as
family, based on sound and trusting relationships. The sense of family is an indication of
trust, security and accountability to each other. Hence, Akoto, in a profound sense, was
perhaps implying that the Traditional Healers were worthy of trust and would behave in a
manner that considers her best interest.
In both the account of Akoto and Fremah, there was a perception of trustworthiness
and goodwill in the Traditional Healers' behaviour which are an essential aspect of the
Traditional Healers image in the community (McCroskey, Teven 1999, Choi, Stvilia 2015).
Goodwill is the participants’ perception of the Traditional Healers intention towards them.
There is an implicit assumption that the goodwill of health professional towards patients
should always primarily be caring (McCroskey et al. 2006). Most participants appeared to
know the Traditional Healers at the community or neighbourhood level and had the
confidence that the Traditional Healers have goodwill towards them. Other participants
(Aboagyewaa, female, 56, leg ulcer/skin cancer?; Abrafi, female, 41, cervical cancer;
Yamoah, male, 31, liver cancer?; Boampong, male, 76 prostate cancer and Akoto, female, 47,
cervical cancer) shared similar views of how they could trust their Traditional Healers
because they knew them in the community.
Aboagyewaa felt the Traditional Healers have a mutual responsibility for the kindness
and support that the communities had given to them and would reciprocate them.
''The Traditional Healers remember all good things that people in the community have done
for them, the things that others have given to them and want to pay back and show their
gratitude” (Aboagyewaa, female, 56, leg ulcer/skin cancer).
Most Traditional Healers benefit from support, prestige and status as part of their
quintessence of the traditional and ancestral moral values in their communities.

172 | P a g e
Consequently, the communities require the Traditional Healers to show some
responsibility to abide by specific moral standards of behaviour and honour some
obligations to the community. Many participants trusted the Traditional Healers to
reciprocate the privileges they received during their training and show some gratitude
to the community. Thus, the privileges and respect that the Traditional Healers enjoy
required them to behave ethically towards the community. Aboagyewaa was
convinced that the Traditional Healers would try their best to show some appreciation
to the generosity that they receive from their communities.
In contrast, the participants described the conventional doctors negatively. For
example, Opambuor gave a displeasing description of the doctors' lack of connection
with the communities in which they worked:
“Doctors come from many places in the country or anywhere in the world to work in our
communities. They do not know us because they are not from here and hence everything to
them is about business or transaction that will earn them money” (Opambuor, male, 68,
prostate cancer).
Opambuor found it challenging to trust the doctors because of his perception
that the doctors lacked lineage, accountability and goodwill towards the local
population. In Ghana, most doctors are non-natives of the communities in which
they work and have the flexibility to transfer to another community or hospital or look
for opportunities elsewhere. Based on the lack of lineage or strong bonds to these
local communities, Opambuor felt the doctors had no sense of moral responsibility
towards them or equally did not have any incentive to show goodwill towards the
population. Opambuor felt the main ambitions of doctors were to acquire wealth, and
they lacked the credibility of committing to the local communities as the Traditional
Healers do.
Most participants’ perception of the doctors' lack of credibility may
influence how they relate and listen to doctors. Some participants may not see the

173 | P a g e
need to listen to doctors if they perceive the doctors not to have goodwill towards them or
interact with sincerity (McCroskey, Teven 1999, Choi, Stvilia 2015). My experience of
practising in Ghana as a nurse was that most doctors lived in exclusive and expensive
locations from the average population, making the doctors inaccessible to most people apart
from the usual brief interactions in the hospitals. Equally, most doctors did not seem to
respect the local community’s moral standards or show secure moral attachment to the
communities. Doctors acted on a simple matter of legal and professional principles which
did not agree with the local traditions regarding the therapeutic encounter.
Most participants described how they could trust the Traditional Healers because of
their goodwill. The Traditional Healers’ goodwill was seen through the acts of compassion,
which corroborated their credibility and trustworthiness (Choi, Stvilia 2015, McCroskey,
Teven 1999). Most of the participants (e.g., Fremah, Boasiako, Akoto, Fuseini, Abrafi,
Nyamekye and Husain) believed that the Traditional Healers motive for serving their
communities and reaching out to the vulnerable was compassion without any ulterior
motives. These participants described how the Traditional Healers demonstrated their
compassion through the willingness to assist the rural population. Some Traditional Healers
also visit patients who cannot attend the clinic at home to provide them with the support that
they need. Boasiako emphasised the vital role of the Traditional Healers in supporting the
vulnerable in their communities.
“As for them, they are ’our own’ people; they go everywhere to help our mothers and fathers
who are in remote villages. Therefore, I think it is good’’ (Boasiako, male, 35, skin cancer?).
Boasiako was convinced that the Traditional Healers would do everything in their
capacity to attend to the remote communities to support the vulnerable. The context in which
Boasiako used the word ''our own'' in the local dialect entails a sense of oneness and shared
identity between himself and the Traditional Healers. Such a conception of oneness with the
community possibly motivates the Traditional Healers to have the compassion to attend to the

174 | P a g e
places where doctors usually would not go. Husain described how some Traditional
Healers show compassion by visiting and supplying treatments to their patients at
home:
“If you are very sick and cannot even go out, the herbalist will come to your house to treat
you or give you the medicine; they will come and see how you are getting on because their
aim is you becoming strong again” (Husain, male, 56, liver cancer)
In Hussain’s view, the Traditional Healers do not work for profit gain but are
motivated by seeing the sick person become healthy again. Moreover, most
Traditional Healers usually would go to the remote communities where there are no
doctors or doctors would not usually visit or stay. By implication, Husain had
concerns about the lack of such practices of compassion in conventional medical
institutions or from doctors. Most doctors usually prefer to work in cities where they
can access more opportunities and career progression. However, it is also possible that
most doctors have the restrictions of regulation and professional codes which may
limit their flexibility to offer low-level services such as visiting patients at home. It is
unknown whether the Traditional Healers will still offer such a soft and flexible
service if their relationships with participants were guided and regulated by law and
professional codes like doctors.
4.3.4 Participants Perceptions of the Traditional Healers Reputable Virtues
“A good name is better than riches’’. Proverbs 22:1, Bible
Most participants trusted the Traditional Healers because of the impression
that the Traditional Healers have reputable virtues. These essential virtues included
how Traditional Healers showed dignity and respect to patients, demonstrated
reliability to their communities and the successful treatment stories of the Traditional
Healers. Majority of the participants' trusted the Traditional Healers because of the
dignity that they showed them (e.g. Asenso, Ohemaa, Kyeremaa, Pinaman, Assifuah

175 | P a g e
and Abrafi). For most participants, respect and dignity included the health professional
acceptance, tolerance and consideration to their cultural values and identities when
interacting with them. Pinaman described how the hospital treated her with lack of respect
and dignity; she believed such behaviours would not happen in the traditional setting:
“I was lying on a trolley with no cover, the room was cold, and they will not even bother to
give you something to cover your nakedness while men were coming in and going out. In the
same manner, the doctor will take your clothes without even saying sorry or minding who is
around, and they would be looking at your whole body. Our fathers, the traditional healers
have manners, and their eyes are opened; they will not expose people nakedness. They have
respect for our culture and us. It is very disrespectful to look at someone nakedness”
(Pinaman, female, 40, Vulvar cancer).
Pinaman felt the doctors treated her with ignominy, leaving her on a trolley
uncovered. Similarly, Pinaman was concerned about the doctor's behaviours of sometimes
exposing patients without asking permission or taking precaution for dignity. Pinaman
perceived such behaviours of hospital doctors as disrespectful and entirely against the cultural
prerogatives. Contrary, Pinaman described how Traditional Healers have manners and treated
patients with respect and dignity. In Ghana, covering and protecting one's private parts is a
crucial cultural imperative: a moral high ground. Hence, most participants perceived
Traditional Healers of showing show respect and dignity by not exposing patients' body or
doing it with precaution. Pinaman felt the Traditional Healers would not look at someone's
nakedness or expose their bodies. Kyeremaa expressed her trust that the Traditional Healers
would not put their hands inside her or do any of the uncomfortable and invasive procedure
that the hospital doctors carry out:
“They do not put things inside you or call people to see what they are doing’’ (Kyeremaa,
female, 32, cervical cancer).
Kyeremaa described her confidence in the Traditional Healers that they would not
intrude, people, intimate privacy, expose their intimate body parts and would always treat
patients with dignity. Most participants perceived the Traditional Healers as sensitive to their
needs around dignity and took the necessary precaution to maintain them. However, the
176 | P a g e
Traditional Healers do not usually conduct the invasive procedures, and hence it was
not possible in this study to know how the Traditional Healers would behave if they
had to carry out such investigations. According to most of my study participant,
Traditional Healers seem to consider dignity during examinations and did not invite
others to the room. The Traditional Healers not calling others to come into the room
when they are dealing with patients, may not necessarily be adherence to patients'
dignity. Traditional Healers do not usually have many trainees at any one point in
time who may need to be around during examinations of patients. The participants in
this study may have been shocked by conventional practices in modern medicine.
Most participants gave the impression that they trusted the Traditional Healers
because of their reliability and continuity of care. Majority of the participants felt they
could depend on the Traditional Healers most of the time to act on their interest
irrespective of prevailing adverse conditions. Most participants expressed the feeling
of an existing implicit ''moral contract' in the community between them and the
Traditional Healers.
“The man used to live a bit far away from my house but used to see me every day or at least
every other day no matter what the weather conditions were. On the days that he could not
see me, he will tell my husband to call and tell him how I am doing’’ (Fremah, female, 31,
cervical cancer).
Noticeably, Fremah could always count on the Traditional Healers
unconditional and continuity of care. The symbolism 'weather conditions' as used by
Fremah is like ''rain or shine'' which was used by Barwuah. Ghanaians use both
allegories to express the commitment to do something even in an uncomfortable
situation.
“You can call them in the night or anytime and if you need them then they would come to you
in shine or rain’’ (Barwuah, male, 74, prostate cancer).

177 | P a g e
Primarily, Fremah and Barwuah emphasised the Traditional Healers loyalty and
commitment to honour their obligation to their patients even under challenging conditions.
Patients or relatives could request to see the Traditional Healers at any time, and the
Traditional Healers would usually respond favourably. Such a practice is not different in my
experience of residing in Ghana where it was common to call the Traditional Healers in the
night to see a sick person in the community. In contrast, both my experience of previously
living and working in Ghana as a nurse and during the data collection for this study at the
hospitals showed that most encounters between patients and doctors were transitory and brief
without recurrence. Most doctors kept their contact and address private and have little or no
interaction with patients outside the hospitals or working hours.
Also, there was a lack of continuity of care, as most patients saw different doctors at
each visit. The responsibility of the doctors to patients was usually a legal contract, ending at
the hospital with no long-term moral attachment. Most participants demonstrated the lack of
trust in doctors because of the perception of the doctor’s unreliability to provide continuity of
care, a representation of the lack of ‘moral contract’ between doctors and patient. Most
participants primarily trusted the Traditional Healers because of the perception that the
Traditional Healers were reliable and committed to them no matter the situation. The
following observation is a reinforcement of the concerns that some patients had about the
lack of continuity of care.
I observed in the hospitals that different doctors conducted consultations on different days.
Hence, patients had to see any doctor who was available or scheduled to review patients on
the day of their visit. Some doctors in the hospitals were student doctors on rotation and
followed a rota system which required them to move between wards and clinics. Also, some
doctors moved between hospitals as part of their orientation program or because they were
doing locum work. I observed how sometimes the patients spoke among themselves trying to
ascertain which doctor was on duty at the clinic. The patients appeared to prefer some
doctors. However, they had no control on consistency on which doctor would see them.
In contrast, the herbal clinics were managed by the same herbalists with a few other staff.
Some of the staff have worked in herbal clinics for many years. Most of the patients appeared
to see the same staffs at every visit and hence felt familiar and comfortable with them (OFN,
CP, HC, 2015/2016).

178 | P a g e
The frequent moving and changing of doctors made it impossible for patients to see
the same doctors regularly or form a therapeutic relationship with them. The patients
interpreted the situation in the hospitals as a lack of care towards them. Also, the patients'
inability to see the same doctors regularly may force them to repeat to the doctors what they
may have already discussed or said before. However, most herbal clinics had been managed
by the same herbalist and staff for many years, and the patients had formed long term
therapeutic relationships with them.
Some participants trusted the Traditional Healers because of the widespread success
stories from their own experiences or other people's encounters. Many of the participants had
experienced a successful treatment of some illnesses from the Traditional Healers or were
aware of the Traditional Healers reputation in treating certain illnesses. In the excerpt below,
Abrafi described the success story and experience of her sister’s treatment with a Traditional
Healers:
“I remember that my sister was playing volleyball and had a fracture of the left leg. It was an
herbalist who put it together, and within two weeks, she was out of bed” (Abrafi, female, 41,
cervical cancer).
Abrafi expressed trust in the Traditional Healers for swiftly and successfully
treating her sister when she fractured her leg. Most Ghanaian indigenous communities
think the herbalists are competent and would successfully treat fractures or chronic
diseases than the doctors (Aries et al. 2007, Solagberu 2005). The chronicity of cancer
for most of my study participants may have contributed to their choice for the
Traditional Healers. However, there was no evidence of the Traditional Healers
successfully treating cancer in Ghana. Furthermore, some participants (e.g. Yamoah,
Benewaa and Akoto) trusted the Traditional Healers for their ability to treat the
conditions which were perceived to have supernatural dimension to them.

179 | P a g e
“Traditional Medicine helps us regarding these things, diseases that the doctor has no
medicine or are not caused by physical [causes]” (Benewaa, female, 43, cervical cancer).
Most participants trusted the Traditional Healers for their inherent recognition of supernatural
influence on human endeavours and the possession of spiritual authority to treat both the
physical and spiritual aspects of an illness. Some studies in Ghana and other parts of Africa
found that the perception of a spiritual association with cancer influences patients to choose
Traditional Healers (Yarney et al. 2013, Ezeome, Anarado 2007, Bazzano et al. 2008).
Although many participants were not specific that their condition had spiritual inference,
many of them assumed the possibility since they did not see a favourable treatment response
from the hospitals. Most Ghanaians have received successful treatments from doctors, but
this does not form part of the community discourse as people do not generally look for
testimonies before attending the hospital. However, some participants trusted the doctors in
emergencies. Barwuah, for example, thought the doctors were useful in dealing with acute
and life-threatening conditions:
“The hospital medicines are good when you want something to happen immediately. They are
suitable for only emergencies. In an emergency, they stop the problem quickly but leave it
there and do not cure it’’ (Kyeremanteng, male, 70, prostate cancer?).
Kyeremanteng trusted the hospitals and doctors’ ability to treat emergency conditions.
Although they were unable to provide a long-term solution, consequently, some participants
mentioned how they would go to the hospital to get a diagnosis and subsequently go for
treatment from the Traditional Healers. For example, accident victims immediately attended
the hospitals for doctors to stop their bleeding and later left for the Traditional Healers (Aries
et al. 2007). Also, in an emergency, the sick person may not necessarily have many choices
apart from going to the hospital accident and emergency department.

180 | P a g e
4.4 Finding Solace in Therapeutic Hospitality and Conviviality
The paradigm’s shift within the healthcare industry to emphasise on patient
experience and perspective makes customer service a logical partner and complementary
resource for healthcare providers (Steele et al. 2015, Suess, Mody 2017). Therapeutic
hospitality and conviviality describe the amicable between participants and
Traditional Healers within the herbal clinic context. Most participants described how
Traditional Healers treated them respectfully and established friendly relationships
with them. Many participants thought the Traditional Healers showed interest in them
by listening to them, giving them the necessary attention and providing
encouragement to them. Thus, the Traditional Healers created the right atmosphere
for the therapeutic interaction by focusing on the social aspects of the therapeutic
encounter and treating the participants as whole human beings rather than as diseased
bodies.
4.4.1. Being Reassured by the Friendly and Jovial Manner of the Traditional Healers
Most participants recognised the importance of their health professional being
friendly towards them and not being rigidly and overly professional. In the following
excerpt, Akomeah described how the Traditional Healers treated him like a friend:
“As I said earlier, the herbal practitioners or clinics treat people or me well. They are jovial
and treat you like their friend. You may not have visited them before, but they treat you in a
friendly way before attending to you” (Akomeah, female, 28, cervical cancer).
Akomeah described how the Traditional Healers exhibited hospitality and
conviviality towards her during the therapeutic encounter with an array of functional
interactions. Most participants thought the Traditional Healers presented themselves
as cheerful, humorous, friendly and informal. Traditional Healers may create a joke
and laughter to relieve any anxiety and tension that their patients may be
experiencing. Akomeah described the hospitable and convivial behaviours of

181 | P a g e
Traditional Healers as being treated well. Akomeah’s quote shows how the Traditional
Healers friendly interaction was indiscriminate and extended to all patients, including those
visiting for the first time. Likewise, other participants (e.g., Nkrumah, male, 70, prostate
cancer & Boasiako, male, 35, skin cancer?) shared similar experiences:
“Even the receptionist told me that. Oh, brother, you look worried is everything ok and I said
yes. She smiled and started talking to me about yesterday’s football and what team I support,
and before I realised, I was in a good mood and cheerful. When I went to the out-Outpatient
Department, they talked and smiled at me, and I even forgot that I was sick. Everyone was
friendly, so there was no stress. That was my experience” (Boasiako, male, 25, skin cancer?).
The receptionist pleasantly and informally addressed Boasiako as a brother and
consequently lowered the threshold of any real or perceived hierarchical protocol in their
relationship between herself and Boasiako. Equally important, the receptionist smiled and
discussed everyday activities with Boasiako. The behaviour of the receptionist was like what
some researchers have termed as 'symbiotic niceness'. Symbiotic niceness is a situation in
which both nurses and patients construct therapeutic relationships in psychosocial palliative
care with mutual niceness (Li 2004). The concept describes how nurses and patients
presented themselves as friendly people to facilitate therapeutic relationships (Li 2004).
Also, Boasiako described how the receptionist smiled and commenced discussing an
everyday subject with him to allay his anxiety. The introduction of casual discussion on
mundane life occurrences is an essential part of friendliness that can progress to a more
significant discussion (Hunt 1991). Consequently, Boasiako figuratively was able to take his
attention away from his illness and stress because of the receptionist friendly behaviour.
Being friendly and informal is a necessary manoeuvre in creating the prospect for health
professionals and patients to form appropriate therapeutic rapport that can foster useful
therapeutic encounter (Jarrett 1998). Through the friendly and jovial relationship, Traditional
Healers and participants built a trusting relationship for their mutual benefits. However, the
Traditional Healers friendliness and happiness may also be a way that the Traditional Healers

182 | P a g e
induced compliance and exerted power over their patients. Some participants co-
constructed the friendly encounter or therapeutic hospitality by either responding to
the Traditional Healers or sharing their jokes. The excerpt below from Yamoah serves
as an illustration:
“I was even practically making jokes with them, and they did not take it as an offence’’
(Yamoah, male, 31, liver cancer?).
Yamoah felt comfortable and at ease to make jokes in return to the clinic's
staffs' behaviour and was astonished that they did not become offended. Hence, the
initial impression or behaviour of a health professional can influence the therapeutic
relationships and encounters by encouraging a positive response from the patients
(James 1986, Jarrett 1998)
4.4.2 Participants perception of Traditional Healers interest in them
Most participants thought the Traditional Healers were interested in their lives
and hence conversed with them about a wide range of social and personal matters of
importance. In the data extract below, Nkrumah, a 70-year-old man with prostate
cancer, shared his experience:
“Also, some of the herbalists, you become their customer, the moment they see you, they treat
you as if you have gone to them many times. Even if it is your first time, they take their time to
find out more about you and the diseases and even the places you have visited before unlike
the nurses and some of the doctors” (Nkrumah, male, 70, prostate cancer).
Most participants described the Traditional Healers by discussing conventional
doctors or drawing the comparison with the manner of them. Some authors refer to
this as contrasting rhetoric in which the participants try to reveal the positive aspect of
Traditional Healers or Traditional Medicine by simple discussing their negative
feelings about the conventional doctors (Hargreaves 1981, Coffey 1996, Mylonas
2014, Titley 2013). According to Nkrumah, the Traditional Healers casually showed
interest in participants routine activities and previous encounters. Traditional Healers

183 | P a g e
wanted patients to feel at home and genuinely cared about their entire personhood and
welfare. Also, Nkrumah described how the Traditional Healers find out in more detail
about the patient's condition and concerns and any places they have visited for treatment.
In contrast, Nkrumah viewed the doctors and nurses as uninterested in their patients'
previous therapeutic encounters, whether in another Conventional or Traditional Healers
setting and focus on the now. The following data extract from Aborampah, a 73-year-old man
with prostate cancer echoes Nkrumah’s view:
''Oh, you do not have to queue, they talk and chat with you as because they have known you
for a long time or you are from the same village. Traditional Healers do not talk only about
the disease to make you feel you are sick. Instead, they welcome you well and explain
everything to you’’ (Aborampah. male, 73, prostate cancer).
Strategically, the vivacity of the Traditional Healers preceded the discussions about
the patient's sickness. Most participants valued simple warm-up interaction, such as receiving
culturally specific greetings on their arrival at the clinic or encounter with staffs. Exchanging
of wellbeing greetings is very much part of the initial proceedings of social encounters in the
Ghanaian culture. From this perspective, the Traditional Healers may be adhering to the
cultural requirements of their communities. Perchance, they know how to talk to patients and
put them at ease and to deliberately divert their patients' attention from the disease and
anxiety. In either case, most participants felt that the Traditional Healers showed that they
have an interest in their entire wellbeing.
Notably, participants desired their health care professionals to show interest in the
entirety of their life. Such a desire did not appear to preclude participants fundamental
objective of getting a cure for their illness. Most participants preferred the process and the
trajectory to cure to be considerate of their broader needs and feelings. Aborampah wanted
the health care professionals to recognise him as a person not treat him like a disease. The
following field note observation explains how the Traditional Healers welcomed and initiated
a conversation with their patients as part of their hospitality.

184 | P a g e
Traditional Healer: Welcome Madame (Mother).
Patient: Thank you.
Traditional Healer: How are you?
Patient: I am fine, thank you.
Traditional Healer: Where have you come from?
Patient: I came from [name of the village]
Traditional Healer: Oh, I know that place very well because my sister lives there with her husband. I am
visiting them this weekend.
Patient: you are coming at the right time because of the season; you can bring a lot of food and fruits
back with you. ….(OFN, HC, 17/06/16)
“I observed most Traditional Healers having chitchat with their patient at the
beginning and the end of their encounter as a matter of standard routine. Such
behaviour or practice appeared to help the Traditional Healers to introduce to patients
their planned transaction steadily and bring it politely to a close. Other participants”
(Duffie, female, 42, cervical cancer; Boasiako, male, 25, skin cancer; Yamoah, male,
31, liver cancer; Ohemaa, female, 71, cervical cancer) shared similar experiences of
the herbalist talking to them on routine matters and showing interest in them.
In contrast, many participants did not think that such was the case in the
conventional medicine settings, as shown in the extract from Ohemaa:
“Hahaha, I cannot read, I cannot write, I did not go to school, they give you a paper and say
go to the pharmacy and get drugs or buy and you do that. They do not ask you a question
because they cannot spend their time talking to you alone, so you must do what they say’’
(Ohemaa, female, 71, cervical cancer).
Ohemaa's described her interaction with the doctor at the hospital as brief and
one-way precise instructions (Berry 2006) in which she had to obey without
questioning. Interestingly, Ohemaa blamed herself based on her lack of education, and
the situation in the hospital, which may have contributed to the doctors’ lack of

185 | P a g e
interest and engagement with her. In contrast, Traditional Healers or staff showed interest
through their compassionate manner and consideration to the needs of most participants.
E.g., Boasiako described the support that he received from the Traditional Healers:
“I do not know what kind of training he gives to his people, but they are very
hospitable and helpful. They understand everyone, or at least I can only speak for myself that
they showed understanding and empathy” (Baosiako, male, 25, skin cancer).
Boasiako felt that the Traditional Healers or staffs were supportive to him and
described the elements of this support as hospitable, helpful, understanding and empathy. It
seems Traditional Healers responded to their patients’ emotional or psychological needs by
showing warm, tolerance and empathy with them. Equally, the Traditional Healers or staffs
provided physical assistance to their patients, such as getting them a seat to sit on; getting
them water to drink and making sure, they were comfortable. I observed in the herbal clinic
that the staffs showed willingness and promptness to help both visitors and patients:
A man got out of a taxi with her daughter and headed towards the clinic entrance. He
was indicated that they were coming to the clinic. The man appeared weak and strolled. The
daughter, however, could not support him because she was carrying two full big bags, which
appeared heavy. The security person got up to help immediately he saw the man and the
daughter. He took the bags from the daughter and asked them to wait where they were. The
security man took the bags to the clinic and came back to support the man also to the clinic.
The daughter was very grateful and commented on how the staffs are always helpful during a
casual conversation at the communal area (OFN: HC, 10 June 2016).
“The security person acted responsively and offered to help the patient to carry her
bags to the clinic. The patient's daughter shared her gratitude to the security staff with me and
indicated that the practice was common in the clinic”.

186 | P a g e
4.4.3 Being Listen to and Giving Attention
Most participants felt the Traditional Healers showed hospitality to them by giving
them attention, listening to them and engaging them in dialogue. Additionally, most
participants thought the Traditional Healers could see them within a reasonable time of their
arrival to the clinic, allocate to them enough consultation time, and did not make them
feel rushed. Majority of participants feel they do not receive such hospitality or
attention in the conventional medical facilities.
In the following excerpts, Yamoah shared his experience with the Traditional Healer as
commendable.
''When I went there, they took their time, no rush. The herbalist asked me all
the necessary questions and allowed me to ask questions, and he answered them. The
doctors in the hospital should learn to listen when we ask the question even if they are
stupid because that is the only way you can help somebody, the only way you can help
me. The herbalist had the time for all my questions. Here or any herbal clinic that
you go, the truth is that they care about you, their medicine may not even be good,
but you would love to go there because they listen to you as human beings'' (Yamoah,
Male, 31, liver cancer)
The Traditional Healer allocated enough time to listen and asked questions to
gain an understanding of Yamoah's disease and concerns. Yamoah felt the Traditional
Healer did not judge his intellectual capacity but allowed enough time and opportunity
to talk regardless of whether what he had to say was pertinent or not. Yamoah
highlighted the need for doctors or conventional health professional to listen to their
patients even if what they may be saying is not medically plausible. In Yamoah's view,
the only way one could help with his condition appropriately was for that person to
take the time to listen to his concerns.
Yamoah does not view health-seeking to be influenced by the quality of
treatment alone but also how one is made to feel like a human by health care
professionals. Yamoah described how the medicine that the Traditional Healers
provide may be less effective but would still attract the visit of many people because of
187 | P a g e
the kind of the human experience that they may receive. Other participants, (e.g., Duffie,
female, 42, cervical cancer and Abrafi, female, 41, cervical cancer) described similar
experiences with the Traditional Healers of how they take their time to listen.
Data from Abrafi draws a clear distinction between the situation in the hospital and the herbal
clinic:
‘They have time for you (emphasised). Until you are ok and have asked your entire questions
or talk about anything, you want they would engage with you. There is no rush at all.
Sometimes the herbalist would take about 30 minutes to one hour to see one person. In the
hospitals, it is very different, you queue, and you are just part of the numbers or statistics.
Sometimes you would go at 8 am and would only see the doctor at say 3-4 pm. nobody would
even tell you what is happening. You could sit there like a tree while people walk pass you up
and down. The doctors would not explain anything to you. They would only tell you to take
this take your prescription and go. They have no time or interest in you. It is whom you
know’’ (Abrafi, female, 41, cervical cancer).
Again, in this quote, Abrafi used contrastive rhetoric to discuss her experience in the
herbal clinics and the hospital. Abrafi described how the herbalist gave her enough time to
exhaust all her questions and discussed any issues she wanted by drawing a comparison with
the doctors' behaviour. Although it might be a hyperbole that the herbalist allowed between
thirty minutes to one hour for consultation, my observations back the reported fact that the
Traditional Healers in this study gave time and attention to their patients. I observed that the
Traditional Healers did not seem to work under pressure or fast pace. In contrast, Abrafi
characterised the hospitals with longer waiting times, short section times, lack of attention to
patients and lack of information or updates about the doctors' schedule. In my experience of
working in Ghana, doctors are very autonomous and have a limited sense of accountability to
any subordinate or associate staff.
It appeared in the hospitals that most doctors did not inform the nurses or health care
assistants of their schedule. Hence, the nurses were unable to update patients of the doctors
whereabout or what time they would be coming to the clinic. They leave patients unattended

188 | P a g e
or ''walk past'' them and avoided interaction, interruption or questions. Therefore,
patients usually must wait until anytime the doctors arrived.
Moreover, Abrafi mentioned the idea of '' whom you know'' to symbolise how
the privileged few, e.g., those who know the staffs, have wealth or rank high in
society do not encounter the same challenges. In the hospitals, I observed that people
with the right class or connections had due attention and were prioritised by the
doctors and usually bypassed others. The following observations substantiate the
assertions of most participants about the difficulties they encountered in the hospitals.
“I arrived at the hospital at 8 am, and the corridor to the clinics and
consulting rooms were already full of patients. At 10 am, I asked the reception when
the doctors would be coming to see the patients. The reception told me that she does
not know. Sometimes they come at 10 am, sometimes at 11 am and sometimes at noon.
It all depends on which doctor is on duty. Nurses and other staff are moving around;
some would go to the clinic rooms and come out. Patients were anxiously waiting, but
no one tells them anything’’ (OFN, CP, 2015)
There was no specific clinic schedule as it was dependent on the doctor on
duty. Most doctors came to the clinic late and had limited time to see patients, which
could explain why they were straightforward in their approach and avoided
conversations or questions that might delay them. The following is an illustration of
how the doctor discounted Yamoah's question and the suggestion.
“The doctor said he was going to do a malaria test, and I asked him why he was not going to
add typhoid test. Instead of him explaining to me why he does not want to add typhoid test, he
asked me whether I am the doctor” (Yamoah, male, 31, liver cancer).
Unfortunately, the doctor saw Yamoah’s suggestion for other investigations
to be carried out as unequivocally challenging his authority and expertise. The doctor,
instead of explaining things to Yamoah, quickly curtailed Yamoah’s suggestion and

189 | P a g e
asserted his authority as the one who makes all the clinical decision. From my personal
experience and field observations, most conventional doctors in Ghana view any quizzing
from their patients as a lack of trust or a challenge on their expertise and authority. Doctors
and the Biomedicine turn to see themselves as the repository of medical knowledge and
hence monopolise and influence most medical decision and policies (Nettleton 2013, Rose
2007). The sequel of such a notion in Ghana is that most of the indigenous population and
participants of my study felt they had no legitimate right to question what the conventional
doctors perceived as the best treatment or cause of action.
However, the situation is transforming, especially for the population who have had
western education and culture. Yamoah was a teacher, and hence, it was not surprising that he
wanted to contribute to the decision about his care. However, the situation in Ghana differs
from developed countries where patients have more power, choice, and input into their care.
Such behaviours between the conventional doctors and the rest of the population is not a
social contract, instead is a facsimile of power and knowledge dynamics in the society. On
the other hand, most participants explained how they felt comfortable and able to converse
freely and asked the Traditional Healers questions without feeling intimidated.
4.4.4 Feeling Relaxed
Most participants gave an account of experiencing a friendly atmosphere at the herbal
clinics. They described the herbal clinics as loose and lacking rigidity and restriction. Most
participants associated the Traditional Healers clinics with softness, easiness and a homely
ambience where they could relate to both the staff, other patients and freely express
themselves naturally without the fear of judgment (Parr 1997). Most participants considered
the herbal clinic staff as open-minded people who allowed them to be spontaneous and
natural. Authors describe such liberal environments of social relatedness and sense of safety
as “effective sanctuaries’’, “haven of sociality’’, “shelter’’, and “convivial space’’ (Nayak

190 | P a g e
2017, Butterfield, Martin 2016, Moore et al. 2013, Glover, Parry 2009). The interview
excerpt and observation below are illustrations of the prevailing atmosphere in the herbal
clinic:
“Well, you can see for yourself, there is the music playing with a calm atmosphere. I could
not complain in any way. They are real community people, and I enjoy it here. I am not
saying this because I am here, I am an elder and I cannot lie, I say it as it is. Sometimes you
look at the way the nurses handle some people or patients in the hospital; you are sure such a
person would not come back again if they had the choice” (Boampong, male, 76, prostate
cancer)
“I observed that radio was music; some patients and relatives were sitting outside around
some tables with a parasol. Some people were playing the “Oware game’, some were
chatting and laughing, while others were enjoying the music and relaxing’’ (OFN, HC,
2016).
The people around the clinic seemed happy from their facial and outward
expressions. Some of them were laughing and talking with each other while others
were playing the local game “Oware .’ Boampong’s instant reaction when I asked him
to share his experience of using Traditional Healer was to point to the open
interactions that were taking place around him. He referred to the people around him
and the clinic as ‘’community people’’. Boampong was implying that the people in
the clinic, both staff and patients were free and got on well with each other. Although
Boampong mentioned that he enjoys coming to the clinic, it is unlikely that he meant
this be literally. Quite contrary; he may be referring to the feeling of liberty and
hospitality that he receives at the clinic not feeling tense about visiting the clinic.
Boampong mentioned his age to substantiate the credibility of his views. There is a
general conception in Ghana that the senior citizens have experience, wisdom, and
character, and they would always tell the truth. In effect, people can trust or believe
them, to be honest.
Contrary to the experience in the Traditional Healers clinic, Boampong
expressed dissatisfaction with the rigidity, atmosphere of surveillance and

191 | P a g e
judgemental attitude in the conventional hospitals. Indeed, the sophistication of conventional
health facilities may require structuring, monitoring and controlling of some of their practices
and environments from patients for safety purposes (Curtis et al. 2009). Most of these
hospitals did not offer much hospitality to their patients; instead, they focused on procedures
and processes, leaving most patients frightened and unable to be themselves. Boampong
believed that most people are unlikely to go back to the hospitals if they have a choice.
Nearly, all participants (e.g. Akoto, female, 47, cervical cancer; Fremah, female, 31, cervical
cancer; Fuseini, male, 72, prostate cancer; and Nyamekye, female, 29, uterine cancer) uttered
similar concerns about the tense hospital atmosphere and their inability to be themselves or
voice their opinions for fear of repercussion such as not being treated by the doctors.
4.4.5 Feeling of Lifting the Spirit and Boosting Hope
Most Traditional Healers offered another aspect of welcoming attitude and
atmosphere to their patients by giving them hope and encouragement that their situation is
under control. As part of hospitality and excellent customer care, some professionals
exercise emotional labour of presenting themselves as enthusiastic, capable and having things
under control all times (Hochschild 2012). Similarly, as cultural practice in Ghana, elders and
healers are required to maintain their composure and show emotional strength under
challenging circumstances to offer hope and support to the rest of the populace.
Consequently, healers are usually careful to avoid the sick person or their families, perceiving
them as weak or negative.
The following observation in a herbal clinic was a demonstration of how the
Traditional Healers gave hope to their patients through conversation.
I observed that the Traditional Healers appeared very calm in their demeanour and
approach to patients and seemed to not talk about the severity and potential consequences of
patients’ condition. Instead, they seemed to downplay the illnesses of their patients and offer
them hope and encouragement. While I was in one of the herbal clinics, a woman brought her
father for treatment. The receptionist asked the older man to sit down. The receptionist told
the older man that his facial appearance was not good, as he appeared worried. The older

192 | P a g e
man said to the receptionist that he has been suffering from the disease for a long time. The
receptionist then informed the older man that he would recover soon. The receptionist
reassured him that all the other patients that he sees around were once in comparable
situations, and now they are all doing very well. The herbalist told the older man that he
would do everything possible for him so he should not worry. In a brief time, the older man
appeared cheerful from his facial expression and demeanour (OFN, HC, 2016).
The herbalist and his staff appeared to focus their conversation on the positive
outcomes and testimonies of others and not on the current situation or what can go
wrong. Most herbalists gave their patients hope and encouragement by talking about
their achievements and their ability to treat illnesses. Some of the herbal clinic staff
also pointed to other patients to emphasise the herbalists' ability to treat illnesses. I
was a bit surprised that the herbal clinics did not appear to tell patients about the
severity of their conditions or discussed the potential or possible adverse outcomes.
Although most participants accepted that they were very unwell and current
condition was severe, they maintained some optimism within their heart: light at the
end of the tunnel. Even those at the advanced stages of their illness appeared to keep
their hope and optimism alive and welcomed the Traditional Healers reinforcement of
their hopes and aspirations. Most participants reported that Traditional Healers
provided them with inspiration and expectation by using encouraging and uplifting
words and maintaining the right demeanour of reassurance. Fordjour expressed how
he maintained his hope because of the hopeful presentations of the Traditional
Healers.
“I am hopeful because they gave me hope. They have not given up on me; they keep
encouraging me that it would be ok, so I also have the hope that it would be ok. If the person
looking after you have not declared you hopeless, then it means you are not going to die. If
you are not supported but made to feel that your condition is worse, then you will die
tomorrow’’ (Fordjour, male, 61, prostate cancer?).
Health professionals have the power to influence the moods and motivations
of patients through their interactions and choices of words (Fallowfield 1993).
Fordjour's feeling was that the Traditional Healers had not relinquished their

193 | P a g e
positivity towards him or declared his condition as dismal, and hence there was no reason for
him to give up. The attitude of the Traditional Healers influenced Fordjour to have
confidence in himself and hoped for a favourable treatment outcome. Similarly, the assurance
from the Traditional Healers positively affected Fordjour's wellbeing, security and recovery.
In contrast, patients can misconstrue any nihilism from a health care professional as a sign of
doom or impending death. Fordjour believed that people would die sooner or have their
condition deteriorate if they get the signal that their condition is hopeless.
Perhaps, this is one of the reasons for most Traditional Healers maintaining a positive
attitude, at least in the presence of patients. Other participants (Yamoah, male, 31, liver
cancer; Adomako, female, 80, cervical cancer; Abrafi, female, 41, cervical cancer and
Ohemaa; female, 71 cervical cancer) shared similar experiences that the Traditional Healers
spoke to them in a way that gave them the impetus for the future. Adomako described how a
receptionist in an herbal clinic offered her hope that her condition would improve:
“The woman at the reception perchance thought I was anxious and said mama, now that you
have come here you will be ok. Many people with significant problems come here and see
their lives change. You must be hopeful that you will get better (Adomako, female, 80,
cervical cancer).
The receptionist may have observed Adomako’s possible expressions of the feelings
of worry and anxiety and spoke to her hearteningly. The receptionist was strikingly aware
that most of the patients who come to the clinic could be worried and anxious because of
their vulnerability and situation. Therefore, she appears to watch out for signs and facial
expressions of anxiety and intervenes appropriately. The receptionist comforted Adomako
that her case was minor compared to the severe conditions that the herbalist can treat. Most
participants shared similar experiences in their accounts. They described how they became
uplifted because of the words of encouragement they received from the Traditional Healers.
The Traditional Healers thus provided a positive mood stimulus for their patients.
194 | P a g e
4.5. Aiming to Avoid Upset and Manage Emotions
’Words are singularly the most powerful force available to humanity…. Words have energy
and power with the ability to help, to heal, to hinder, to hurt, to harm, to humiliate and to
humble’’ Yehuda Berg (Toler 2019, chapter 1, page 9)
The theme “Aiming to avoid upset and Manage Emotions “describes the
participant’s perception of how the Traditional Healers negotiated within the socio-cultural
conventions to avoid upsetting or exacerbating their feelings and manage their emotions.
Many participants described how Traditional Healers discussed their condition and sensitive
issues with them by using a euphemism to protect their emotions. For example, “Yade bɔne’
which means a deadly disease. In a more profound sense, the term is a description of a
deadly disease and used usually to discuss diseases such as cancer and HIV/AIDS by most
people in Ghana. In parallel, most participants themselves used nondisclosure and secrecy as
a way of avoiding upsetting themselves, their families, and protecting their self-image.
4.5.1 Euphemising: Softening and Placating Participants Situation
Euphemising was most participants’ description of how Traditional Healers
used the appropriate moments and culturally acceptable words to discuss participants’
situation to avoid upsetting them and managed their emotions. Most Ghanaians
believe that openly discussing death, misfortunes or severe illnesses or referring to
their actual names can upset the victims. Also, this can lead to the illness or condition
occurring, reoccurring or perpetuating. Most participants felt the Traditional Healers
understood the socio-cultural requirements and complexities around severe or
terminal illnesses and their emotional impact on people, as shown in the excerpt from
Serwaa.
’The herbalist would know how to tell you when there is something wrong with you so that
you do not become upset. Some of the doctors are so blunt’ (Serwaa, female, 52, breast
cancer ).

195 | P a g e
Serwaa felt that the Traditional Healers were mindful of the time, place and moments
to deliver tragic or unpleasant information to their patient to prevent upsetting them or at least
curtailing the impact on them. Most Ghanaians consider some severe diseases as misfortunes;
hence, they treat such sicknesses with the same weight of spirituality and use indirect or
subtle words to discuss them.
Discussing these diseases softly and at the right moment, diffuses their intensity and
manages and protects the emotions of the people affected. Furthermore, identifying the right
moment to deliver shocking news is a cultural imperative in Ghana. For example, messengers
of sad news would usually hold off until the right time, and the setting is ready without
rushing. Such people are usually skilful and would sometimes behave as if their visit is
routine, ensuring that the recipients of their message have eaten, have had their shower and
are comfortable before sharing the shocking news. Serwaa’s analogy emphasised how
Traditional Healers choose the right time and environment to discuss sensitive and disturbing
issues to safeguards participants' emotions.
On the contrary, most participants described doctors as causing upset to them by
being abrupt and direct with their language. In the following excerpt, Nana Hussain, a 56-
year-old man with liver and lung cancer, became upset and expressed grievance with the
doctor for not adhering to the socio-cultural decorum;
“When I met him, he said Nana, there is a problem, I said to him, but the other doctor said
there was no problem. He kept quiet and said I am afraid you have your liver and lung
damaged. You have liver cancer, and you must reduce smoking and drinking; otherwise, it
will kill you soon. He was very blunt, and I do not think a doctor should say things like you
will die, that alone can kill me’’ (Hussain, male, 54, liver and lung cancer).
Hussain was concerned that the doctor was forthright with him in discussing the
possible negative outcome of his disease. Death and dying have acute sensitivity in most
Ghanaian communities. Respectively, people handle a conversation about death and dying
with extreme sympathy and compassion. People use subtle words such as ''Wawhire

196 | P a g e
Akwa/kra'' (he has lost his life or soul), Wafiri Mu (he has left or gone), and ''Wadane
atɔ’ (he has turned away) to talk about dying or say someone has died as a way of
respecting and showing empathy.
Therefore, Hussain did not find it promising for the doctor to say to him that
he would die, although the doctor was merely stating the obvious. Instead, Hussain
expected the doctor to appreciate that directly referring to death was inappropriate
culturally and showed disregard to his sentiment. Hussain wished the doctor had
ensured that their conversation was not charged emotionally or caused nervousness to
him. Most participants found conventional doctors to be too direct in dealing with
daunting issues with their patients. The doctors appear to consider the legal and
professional implications of their communication more than the culturally agreed
ways of breaking the unwelcome news.
However, precisely and indifferently delivering sad news have distressing and
abiding consequences on the recipient (Fallowfield 1993). Unfortunately, weak
sensitivity to cultural practices hinders most doctors from managing such situations
appropriately (Fallowfield 1993). Given the manner that the hospitals were busy, it
may be possible that the doctors bluntly delivered terrible news because they do not
have enough time to spend with each patient and prepare them gradually for the sad
news.
4.5.2 Concealing: A Non-Disclosure of Participants Illness
Another way in which participants tried to avoid upsetting themselves and
others was through demanding concealment from health professionals, keeping their
condition to themselves, and not disclosing it to their families or relatives.
Concealing, in most contexts, involves the notion or elements of silence and secrecy
(Carlisle et al. 2013, Brennan 2017, Lavers 2012). Hence, my study participants

197 | P a g e
primarily wanted their health care professional to keep their situation secret and not expose it
to others. Urging or adhering to secrecy was a way in which most participants tried to protect
their image, avoid being a burden on loved ones and not causing upset to themselves or close
family.
Most participants described their ardent desire for health care professionals to keep
their information confidential and not to pass them on, even to their partners without their
permission. The following extract illustrated the unhappiness of some participants when
doctors discussed their information with others without their approval.
“They do not care who is there or what would happen when they have said told them about
your illness. You see, I could come to the hospital with my wife, but it does not mean I want
my wife to know what is wrong, so the doctor should check with me before passing
information to them. However, for them, they talk without consideration to your feelings”
(Yamoah, male, 31, liver cancer).
Yamoah expected the doctor to conceal his illness and became upset that the doctors
did not observe such confidentiality. Instead, the doctor shared Yamoah’s information with
Yamoah’s wife without getting permission or considering the possible consequences of such
an action. In this case, the doctor may have presumed that it was right to tell Yamoah’s
spouse about his condition without Yamoah’s permission. In my experience of working in
Ghana as a nurse, caring for patients was a collective family responsibility. Most health
professionals considered it acceptable to give some degree of information to families to
enable them to carry out their duties or care for their loved ones.
Regardless of what may have motivated the doctor to share the information, Yamoah
deemed such a practice unseemly in certain situations. Yamoah, for some personal reasons,
did not want his wife to know of his situation. Maybe, Yamoah wanted to protect his wife’s
emotions or avoid upsetting her. Granting the current legal liberation and proliferation in
Ghana and heightened awareness of western practices, at least in theory, adhering to patient
confidentiality and seeking consent concerning sharing of patients’ information is essential.

198 | P a g e
However, my observation suggests that the doctors sometimes unintentionally and
unconsciously discussed patients with their colleagues without cautiousness.
In my observation, the doctors always saw their patients in a room and sometimes allowed
relatives in the room but not strangers. The relatives turn to be in the consulting room on the
doctor or patient’s request o because of a need for a relative to support the doctor physically
or offer language interpretation. Also, most consultants share their clinics or consulting
rooms with their associates, subordinates, and nurses (OFN, CP, 2015/2016).
The hospitals were busy and had limited spaces compared to traditional
settings. It was, therefore, difficult to conclude whether both the Traditional Healers
and Conventional Medical Practitioners were acting based on resources they had or on
their understanding of the local culture. Yamoah felt that the Traditional Healers’
stealth their patient's condition and information and unlikely to discuss or share the
information with other people. A portion of Boasiako’s interview expounds this
assertion;
“When you see the herbalist, I think everything is kept a secret, so you are free to discuss
your feelings and whatever that you want. The doctors would be discussing your disease with
staffs, and when they are talking to you, they do not care who is around they talk and before
you know a healthcare assistant or a nurse is taking your problem to people that you
probably do not want them to know” (Boasiako, male, 25, skin cancer?).
Boasiako felt that the herbalist would keep his information secret, giving him
the confidence and security to discuss his feelings and concerns freely. In contrast,
Boasiako shared his concerns about the possible lack of confidentiality to his
information with the doctors. He feared that his information with the doctors might
end up in the public or wrong domain. Moreover, most participants regarded non-
disclosure or concealment as part of the process of minimising their shame and
gaining control over managing their self-presentation and personal identity (Golthan
2009).
Majority of participants kept their situation to themselves to avoid
disconcerting themselves from the possible attitude and reaction from other people.

199 | P a g e
Some participants were afraid that people whom they may discuss their situation would cause
them upset by stigmatising or treating them with contempt. The following quote illustrates
the dilemma of patients about their condition. However, they resolved to keep their condition
to themselves, as much as possible and as long, as necessary.
“I was afraid that I could not just jump to wash my clothes in public. We are in Ghana, and
you must be careful and sure whom you discuss your disease or situation. Some people will
even laugh at you or take advantage of you trusting them to isolate or stigmatise you. As it
was stated earlier, it was not supposed to be shared with anyone. It was to be kept personal.
It was not supposed to be on the news or the topic of discussion at a gathering or in people's
home. The next day the blood was coming, was yielding in clots. Therefore, I had no choice
but to tell someone which I did, and they brought me to the hospital” (Nyantah, female, 58,
cervical cancer).
Although Nyantah did not feel settled about her condition, she wanted to keep it
secret from others. She used the metaphor of washing one’s clothes in public to imply
making public of something that should be private. Nyantah felt that one should avoid or
exercise caution in disclosing their illness because of the possible undesirable upshots and
upset. Nyantah described some of the possible ramifications of revealing her condition to
others to include ridicule, isolation, stigmatisation and becoming the topic of discussion in
the neighbourhood or people’s home. Nyantah thought that people could take advantage of
her susceptibility to treat her abysmally if they were aware of her illness.
As a result, Nyantah was determined to keep everything to herself at least until it was
no longer possible. Most participants (e.g., Boampong, male, 76, prostate cancer, Boasiako
male 25, skin cancer? and Nyamekye; female, 29, uterine cancer) strongly felt that they
needed to keep their situation to themselves to protect their own emotions and image.
In the excerpts below, Boasiako was concerned that others might patronise and consider him
inadequate if they know of his troubles:
“I put specific barriers sometimes between my friend and me so that they do not go
and tell people that maybe I am going to die or something like that. I do not think it is
necessary to let people know when you are not well. You would be washing your cloth in
public, and this is not a good thing. Also, some people would even look down on you.
Because they think you are inadequate in some way, you are sad and suffering, that is the

200 | P a g e
way they will treat you. I do not want to be pitied because that can be patronising”
(Boasiako, male, 25, skin cancer?).
Boasiako kept some secrets about his illness from friends for the fear that his
friends might tell others about his illness or assume that he was going to die and lead
to people treating him with contempt. Also, Boasiako did not want people to pity him
or think he was suffering. He felt that people who view him in this way were likely to
treat him with pity. Boasiako felt that some form of commiserating could be a
cunning way in which people may belittle and make him feel defective. Boasiako kept
things secret to avoid feeling distressed and upsetting from his friends’ potential
behaviour or reaction and that of others who may get to know of his situation.
Furthermore, most participants tried their sickness to themselves and not tell
others, especially their significant others as they did not want to inconvenience or
burden them. They felt that their relatives or families would feel obliged to look after
them once they know the situation.
“I did not tell anyone because I did not want to be a burden on my family. The thing is that
when you tell them then, they feel obliged to help because they cannot look at you to suffer.
You end up letting them stop their own business. They may not be able to tell you that you are
a nuisance, but you know it yourself that you are becoming a burden to them” (Nyantah
Female, 58, cervical cancer).
Nyantah expressed the fact that he did not want to upset her family by
becoming a burden on them. She did not want her family to feel the onus to support or
care for her. The Ghanaian society regards supporting a sick relative as a moral and
cultural responsibility. People consider families who fail to meet such an expectation
as spiteful. Hence, families usually feel the pressure to honour the duty of supporting
their sick relatives to maintain or earn their reputation in society. Offering such
support sometimes require families to adjust or halt their commitments. In effect, the
socio-cultural contract leaves families with no option other than to provide support
once they are aware of the situation, and Nyantah did not want to put her family under

201 | P a g e
such pressure. Nyantah described how she felt her relatives or families might consider her as
a nuisance and offer their help reluctantly. Nyantah seemed very perceptive to such family
frictions and dynamics that can arise. Nyanta’s account reveals the tension that patients go
through in negotiating for family help and trying not to upset them.
4.6 Chapter Summary
The findings chapter has described and conceptualised how the study participants articulated
their motivations to use Traditional Healers and their experiences with the Traditional
Healers in contrast to their lack of trust in conventional doctors. The chapter has shown how
shared community and socio-cultural identities formed the foundation of participants’ trust in
Traditional Healers. Also, the well-established reputation of the Traditional Healers served as
a motivation and influenced participant help-seeking behaviours. In contrast, participants
expressed the lack of trust in conventional doctors as they perceived them as a symbolism of
power, inequality and cultural detachment. The chapter described how participants found
solace in their experience of the therapeutic hospitality and conviviality in using the
Traditional Healers or Traditional Medicine. Besides, the chapter shows how Traditional
Healers used euphemisms to protect the participant’s emotions and how participants
themselves tried very much to conceal their illness and expected their health professional to
do the same.

202 | P a g e
4.7 The theory of “Community of Us.”
Figure 9 The Developed Substantial Theory
The theory of ''Community of Us'' shows community identities and tradition as the fabric of
trust in indigenous communities in Ghana. The Theory explains how the placement of trust in
one’s community and identity underpinned the motivation of people living with cancer to use
Traditional Healers and influenced their therapeutic encounter in the herbal clinics or the
traditional health sector. The trust that people living with cancer had for the Traditional
Healers was enshrined in the notion of ''Us', which represents people living with cancer,
Traditional Healers and their community identities. The shared identities create a sense of

203 | P a g e
oneness between the people living with cancer, the Traditional Healers and their
communities. People living with cancer shared identities of trust with Traditional Healers
include the shared traditional or ancestral connection, local language identity, familiarity in
community and neighbourhood interaction, and perception of goodwill and reputation of
Traditional Healers. The '' Us'' is also a sense of collective moral sensibility or rightness
which is inherently known to those who share in the common identities and confer trust to
them on the basis that they will act according to the known standards. Traditional Healers
are members of the ''Us'', and hence people living with cancer could trust them to do the right
thing and act in their best interest.
The'' Us' 'excluded ''Them'' or ''They'' as doctors or conventional medical practitioners who
did not share in the trusting identities or ''Us'', and hence could not be trusted by people
living with cancer. Doctors spoke in English, had wealth and power and did not interact with
the local traditions. They were considered as ''White'', a symbolic representation of cultural
detachment, elitism, and colonial or post-colonial supremacy or influence. People living with
cancer did not see doctors as people who have the sensibility and goodwill towards them and
excluded them ideologically as outsiders who could not be trusted.

204 | P a g e
CHAPTER FIVE: DISCUSSION
5.1 Chapter Overview
Congruous with Constructivist Grounded theory approach, the participants'
accounts were analysed against the backdrop of the social construction of knowledge.
The focus of the analysis was on people living with cancer’ motivation and
experiences of using Traditional Healers in Ghana. Also, the focus was on how the
motivations and experiences influenced participants health-seeking behaviours
concerning their current diagnosis. The literature review showed that socio-economic
elements such as affordability, availability and accessibility to Conventional Medicine
influence the use of Traditional Healers in Ghana
My study highlighted the subtleties of trusting communities and identities and
the importance of relationships and convivial interactions. These elements
underpinned the trust which formed the foundational motivation of people living with
cancer for using Traditional Healers in the Brong-Ahafo region of Ghana.
This chapter discusses the key findings of my study and how they influence
participants’ motivations to use Traditional Healers for help-seeking regarding their
illness in response to the research question. The findings of the study are also situated
in the broader theoretical context of literature. I demonstrate how my study advances
and to add to the existing body of knowledge around patients use of Traditional
Healers in Ghana. The following are the synopsis of the key finding of my study.
My study findings identified how people living with cancer in Ghana
conceptualised their motivation and experiences for using Traditional Healers as a
relationship of trust. The relationship of trust was significant and comforting to
participants in their help-seeking behaviour concerning health. Participants trusted the
Traditional Healers because of how they saw and experienced the Traditional Healers
as members of their local communities. The Traditional Healers were well-integrated
205 | P a g e
into the socio-cultural and historical traditions in the community, with collective community
identities and understandings. People living with cancer and Traditional Healers shared these
community and socio-cultural dynamics of trust. These sociocultural dynamics include
ancestral connection shared everyday language, familial goodwill and local accountability,
and the known reputation of Traditional Healers in the community. Participants local
interconnections of shared identities and trust with the Traditional Healers gave them the
perception of the equal footing of power and equality. These smoothed participants
relationships with Traditional Healers and influenced their preference to use them
[Traditional Healers].
In contrast to the trusting relationships with Traditional Healers, most of my study
participants were left feeling they could not trust the hospital doctors. Most participants
reported little or no trust in these doctors. Most participants felt the doctors were detached
from their patients and sometimes expressed contempt to the socio-cultural and indigenous
values or identities of trust. Some participants described doctors as “Whites ‘or their
behaviour and practices as “whiteness’’. The description designate inequalities, power
imbalance, lack of cultural attachment and lack of respect for socio-cultural prerogatives.
These characterisations of doctors reported by my participants were broadly a symbolic
representation of colonial and post-colonial incursion and adulteration of local customs.
Similarly, many participants in my study did not trust doctors because they found the
doctors' behaviour was culturally and even medically inappropriate. These culturally
inappropriate behaviours include how they treated patients with a rush during consultations
and insensitivity to their dignity. Also, the participants reported a lack of continuity of care.
Most participants saw different doctors each time they visited the hospitals. I did not recruit
conventional doctors to my study or explored their views. Hence it is not possible to explain
their behaviour and whether they feel this is an accurate reflection of themselves.

206 | P a g e
Moreover, my study identified people living with cancer and how they
conceptualised their interactions and experiences with the Traditional Healers as one
of therapeutic conviviality and hospitality. My interviews and observations found that
the interaction between participants and Traditional Healers during the therapeutic
encounter was informal and friendly. Also, many participants described the provision
of human and quality time in which participants felt the Traditional Healers did not
rush them in consultations. Instead, many participants felt the Traditional Healers
listened to them and manifested interest in the entirety of their being. Equally, many
participants felt the Traditional Healers created a relaxed atmosphere in their clinics
or consultation. The relaxed atmosphere allowed participants to be open and have the
freedom to be themselves without any anxiety.
Although trust appeared in the study as an element in participants' community
and a source of influence on their health-seeking decisions and behaviours, there are
certain inherent risks which may not always be immediately apparent to the
participants. The trust in Traditional Healers could prevent participants from seeking
appropriate or advanced medical help early or not doing so at all (Helman 2007).
Such a failure to seek help promptly from appropriately trained professionals can lead
to worsening or deterioration of patients' condition and treatment outcome. Moreover,
there is the risk of harm from the treatments from Traditional Medicine as most of
them are not standardised or regulated and lack records of efficacy and safety (Davis
et al. 2012, Langlois-Klassen. 2007).
In Ghana, most patients turn to use both Conventional and Herbal treatment
without any communication with their doctors. The lack of dialogue can lead to
potential drug interaction and danger to patients' life (Langlois-Klassen et al. 2007).
Furthermore, there had been many documented instances across the globe regarding

207 | P a g e
the contamination of Traditional Medicine with metals and dangerous minerals with toxicity
and harmful effects on consumers (Garvey et al. 2001, Obi et al. 2006, Ernst 2002, Annan et
al. 2010, Au et al. 2000, Adewale et al. 2016, Teschke et al. 2014). Hence, the whole concept
of Traditional Medicine and Traditional Healers need more research and regulation. Such
attention would ensure that patients who use these medications and services receive the right
protection from potential harm and abuse.
Furthermore, trust potentially played a role even in how participants interacted with
the researcher during the data collection and responded to the interview questions. It is
possible that some participants behaved and responded in a manner that would safeguard the
trust that they had for their communities, Traditional healers and their ancestors. Equally,
some participants could potentially use the interview as an opportunity to express their
general dissatisfaction with the doctors and not give a balanced view or responses (Cook,
Hardin et al. 2005, Hardin 2006, Luhmann 2018, Misztal 2013).
Despite the awareness of the risk, safety, and ethical implications, the researcher
intended to represent the views and voices of the participants as accurately as possible. At
the same time, the researcher acknowledges that the findings of the study were not a
comprehensive reflection of every context.
Conviviality and hospitality also involved the feeling of hope and the lifting of spirits.
Many participants felt that the Traditional Healers offered them encouragement and
reassurance that their condition is under control. Traditional Healers were reported to offer
reassurances through their talk and cultural demeanour of calmness, softness and apparent
resilience. In contrast, most participants described their unhappiness with the judgemental,
regimented and potentially punitive experience in the hospitals. My study found that
participants were mostly anxious and cautious about what they said and how they behaved for
fear of potential repercussions with hospital staffs. Also, participants felt the doctors and
208 | P a g e
nurses were unfriendly, unhelpful and did not engage with them in a meaningful
manner and therefore engendered a sense of distrust.
Furthermore, people living with cancer experiences in using the Traditional
Healers also embodies the Traditional Healers’ ability to negotiate within the
indigenous culture. Traditional healers achieve this through appropriateness in
behaviour, management of participants’ emotions, and avoiding upset of participants.
The study found that most participants faced a substantial emotional challenge from
their illnesses and felt the traditional healers had the skills, cultural knowledge and
sensitivity to manage and support them emotionally. Traditional Healers were
reported to achieve this through their method of indirect delivery of sensitive
messages.
Most participants described how the Traditional Healers knew how to tell
them and inform them about sensitive situations. Traditional Healers were able to
choose the right environment and suitable conditions to deliver crucial information
using the appropriate euphemisms, indirect and softer language (cultural telling).
Most participants described positive feelings towards such behaviour and considered
the Traditional Healers as showing thoughtfulness and sensitivity to their emotions,
congruent with the local cultural norms.
Similarly, as part of managing the emotions of participants was the practice of
keeping things to oneself or concealment. Concealment was a complex dynamic in
which participants reported how Traditional Healers sensitively avoided upsetting
participants by keeping participants information secret. Most participants wanted to
keep their illnesses secret from family, relatives and the community, and expected
their health professional to do the same. Most participants reported trust in the
Traditional Healers to keep their illness secret and not disclose to others compare to
209 | P a g e
the doctors or hospital staffs. Many of my study participants trusted the Traditional Healers
because they believed and had experienced from them the cultural understanding of keeping
their information about their illnesses secret from family and the public.
Some participants described this as ''keeping to oneself” or “not washing one's clothes
outside in public'' to avoid stigmatisation or ridicule from people. Some participants also kept
their illness information secret to avoid burdening the family. They did not want to put
unintended pressure on their family to provide support for them. However, the participants
did not address their illness like cancer. Hence, their fear of stigmatisation related to their
general condition, appearance and symptoms.
In contrast, participants described doctors as insensitive to their emotions and
disclosing sensitive information about their illnesses bluntly and directly. I observed how
some doctors delivered information to patients in the presence of other doctors, nurses and
healthcare assistants. Such behaviour of doctors appeared as a very grey area as some of
these staffs who were usually present when the doctors shared patients’ information were
staff in the hospitals or clinics. It was not clear whether it was necessary or in patients’
interest for the doctors to share the information with these staffs. However, most doctors also
delivered the news to the patient in front of relatives or partners. Many participants perceived
such behaviour by doctors as hurting their emotional well-being and causing them a great
deal of upset.
The following is a discussion of the key findings concerning people living with
cancer’ construction of the complexities of trust, hospitality and emotion management. The
discussion also includes how these shaped their help-seeking behaviour concerning their
symptoms and health condition and motivations for using the Traditional Healers and their
subsequent experiences of the therapeutic encounters. I begin the discussions by looking at

210 | P a g e
the term “White’’ or “Whiteness’’ as used by most participants to denote power,
inequality and cultural detachment and how participants showed distrust toward
''whiteness''.
This chapter also discusses the importance of traditional and community
identities as elements of trust espoused by participants and as their motivation for
using the Traditional Healers. Also, I discuss the critical elements of the interaction of
conviviality and hospitality that explain participants' motivation in using Traditional
Healers services. Furthermore, I discuss the dynamics of emotional management and
avoidance of upset and how both participants and Traditional Healers achieved it. I
discuss these critical findings alongside the contrast of what happens during the
medical encounter with the hospital doctors.
5.2 Trusting Identities: People Living with cancer’ Relationships and Motivations for Using
Traditional Healers
In the study, participants described their motivation for using the Traditional
Healers services based on their relationships and perception of trust in the Traditional
Healers and identity. The participants reported socio-cultural relationships and
perceptions of trustworthiness as a cornerstone of their motivation to use Traditional
Healers. Social trust is the barometer for the perception or level of trustworthiness of
people or an institution (O'neill 2002, Sztompka, 1999, Heckscher, 2015, Mackie,
2001). Social trust forms the foundation and stability of indigenous Ghanaian
communities and their smooth functioning.
In most Ghanaian indigenous communities, social trust, and the general
community’s opinion about the character and performance of health providers
influence the relationships that the community members or individuals usually have

211 | P a g e
with these providers. My study identified that most participants had positive views about
Traditional Healers and trusted them. Participants trusted the Traditional Healers as they
matched up to the socio-cultural signals of trust in their indigenous communities. Hence, my
study participants primarily had social trust for people and institutions in their communities
who shared in these identities of trust. In most Ghanaian communities, members are
encouraged to trust community members, the traditional institutions and values that form the
fabrics of the communities. My study participants considered Traditional Healers as part of
the traditional institutions and members of the local communities. Consequently, most
participants perceived the Traditional Healers to be trustworthy and were willing to trust
them regarding medical help for their illness.
In contrast, most participants could not place trust in the doctors because they did not
form part of the community or social circle of trusting identities known to most participants.
My findings are consistent with Mackie’s (2001) analysis of the Eurobarometer data on trust,
a European community survey. In this survey, he observed that people always rated their
country and populations as more trustworthy than the other countries or people of other
nationalities. However, this study did not explain the reasons why its participants selected
their countries population as more trustworthy over other countries. My study was unique or
different in the sense that participants did not base their social trust indiscriminately on
simple physical or sociological membership of the local communities. Instead, my study
participants trusted the Traditional Healers based on the Traditional Healers active and
meaningful engagement and membership, attachment and submission to the socio-cultural
traditions and values of the communities.
Although beyond the scope of this PhD, social psychology has long been concerned
about how social categorisation or dynamics function to accentuate inter-category or in-group
similarities and intra-category or intra-group disparities (Kruglanski, Higgins 2007, Brewer
212 | P a g e
2007, Turner et al. 1979, Tajfel, Turner 1986, Tajfel 2010). Generally, people have a
preference for their in-groups or a group in which they share a similar identity. Such
preference can lead to in-group favouritism or acceptance and often distrust and
dislike of out-groups which leads to out-group derogation or rejection (Kruglanski,
Higgins 2007, Brewer 2007, Turner et al. 1979, Tajfel, Turner 1986, Tajfel 2010).
The doctors’ exclusion from the social trust by participants of my study was
both an ideological and practical sense. Most doctors were reported to not come from
the local communities. Also, they lived in expensive and isolated and secluded parts
of the towns from the rest of the local communities. Hence, participants did not
consider them as community members. Ideologically and in a more profound sense,
doctors were not considered as part of the local communities because they had
minimal or no interaction and contact with the local people. Doctors were not seen to
be engaged with the socio-cultural traditional and values. Interestingly, some
conventional doctors were in-group members, either Ghanaians or community
residents. Nonetheless, they were still perceived as out-group members by many
participants because they did not speak the local language or abide by the local
customs and had elite statuses.
Many researchers emphasise the importance of trust in healthcare
professionals and how trust influences the effectiveness of therapeutic encounters and
relationships (Lagenspetz 1992, Rhodes, Strain 2000). The therapeutic relationship
between most of my study participants and their health care professional was
influenced by social trust.
Many of them appeared to report an excellent therapeutic relationship with the
Traditional Healers and expressed satisfaction with their services. In contrast, there
was a note of dissatisfaction regarding their relationship with the doctors. Trust

213 | P a g e
influences patients’ behaviour and attitude towards treatment reception, adherence and
sharing of sensitive information that can affect treatment outcomes (Lagenspetz 1992,
Rhodes, Strain 2000, Hall et al. 2002, Hall et al. 2001).
A trusting relationship prevents patients-physician disputes and leads to increased
satisfaction and continuity of care, as patients usually stay longer with the physician they
trust (Lagenspetz 1992, Rhodes, Strain 2000, Hall, et al. 2002, Hall, et al. 2001). Most of my
study participants were vulnerable because of the nature and the stage of their illnesses. Their
accounts reflected a preference for the Traditional Healers whom they could trust to have
their holistic interest at heart and to give them a loving and continuous care. Many
participants in my study knew their Traditional Healers. They had lived in the same
community with them for many years. Hence, they had experienced continuity of care by the
same Traditional Healers.
However, as noted above, the social trust or trust in individual and institutions in
indigenous communities are not arbitrary but based on trusting identities and identification to
specific socio-cultural requirements. In the following sections, I discuss the participants’
expressions or conceptualisation of trust in the findings. These are broadly linked with
theoretical concepts of trust and how they influenced and motivated participants to use
Traditional Healers services.

214 | P a g e
Figure 10: Participants model of placing trust in their communities
5.2.1 Whiteness: Power, Inequality and Lack of Trust
Most participants reported distrust in the hospital doctors they visited or
encountered during their current condition and treatment for cancer. Most participants
described their lack of trust in the doctors because of their experience of the doctors’
behaviours and practices. The attitude of doctors was described as representing of
power, contempt and detachment from the local sociocultural standards. These
behaviours and practices included the doctors’ use of the English language as the
primary mode of communication, their western education and perceived attachment to
European or western culture. Most of my study participants, therefore, referred to the
doctors and their practices as “oburoni’’. The term is translated as “white’’ or

215 | P a g e
“Whiteman’’ to denote power, economic and class inequalities which were intrinsic to
colonialism in the colonial era with a strong history within Ghana.
The symbolism was also universal in most participants’ accounts to describe the elite
in a society whose behaviours and practices were discordant with the local culture and
identity. Foucault conceptualises power as a social relationship or relational dynamics
(Foucault 1988, Foucault, Rabinow 1991). Luhmann (2018), sees power as a communication
medium that in addition to language can transmit and regulate choices in society. Both
conceptualisations contradict the traditional discourse or perspective of power which involves
one’s ability to impose their will on others or exercise a sovereign or absolute control over
them (Nunkoo, Gursoy 2012, Stein, Harper 2003, Luhmann 2018).
My study participants’ use of Traditional Healers in conjunction with conventional
medicine signified empowerment as they were able to make treatment choices and demand
more respectful patient care. Many of my study participants had the freedom to choose
between the Traditional Healers and the doctors. They could avoid the hospitals if they were
dissatisfied with their treatment or the behaviour of the medical staff. These dynamics were
reflections of power as sociocultural therapeutic interactions and relationships or a medium of
engagement.
In this sense, power exists and functions in a set of relationships, the medium of
communications and social institutions (Luhmann 2018, Stein, Harper 2003). Power has its
expression in these relationships and institution through dependency or interdependency and
inequalities created by social and functional stratification (Luhmann 2018). Doctors and the
medical profession enjoy institutional and professional power because of the vital services
they provide to the public and the unique set of skills and expertise they hold. Hence, the
power of doctors outweighed the power of my study participants as their condition or
sicknesses made them dependent on the hospitals and the doctors. Also, the hospitals

216 | P a g e
participating in my study were public or government-funded hospitals where doctors'
pay did not relate to any specific performance. Hence, doctors during my observations
did not seem to have incentives to raise their standards of behaviour and interactions
with my study participants to encourage the continued use of their services.
It was observed that most doctors came to the clinic late and gave little
attention to patients. Some of these were related to doctors performing other duties in
the wards and working under pressure. However, there were some occasions that the
other clinical staffs did not know why the doctors were not in the clinic or know what
they were doing. There was a common knowledge that most doctors worked in private
clinics or hospital and considered that a priority over their work in the public sector. It
is not clear whether data from private hospitals where doctors are more dependent on
the number of patients and their experience for their remunerations would have
altered the power balance in the doctor-patient relationship.
Equally, there is a possibility that the Traditional Healers provided excellent
service because they depended on my study participants for their reputation, income
and existence. Some authors acknowledge how power disparity and dependence
undercut trust as the trustor may not have any hope of influencing the trustee or the
power holder (Hardin 2001, Bachmann 2001, Cook et al. 2005). Some authors argue
that trust and power tend to operate concurrently and hence any theoretical analysis of
trust amongst social actors should be considered simultaneously with power and
inequality (Bachmann 2001, Hardin 2001, Cook et al. 2005, Stein, Harper 2003,
ÖUberg, Svensson 2010). Using Goldthorpe analysis of social class and occupation,
doctors will fall into the category of the upper echelon of society, giving them wealth,
opportunities, and power over my study participants (Goldthorpe, McKnight 2006,
Giddens, Sutton 2013).

217 | P a g e
Most doctors in Ghana have affluence and access to the best opportunities in contrast
to my study participants who were at the lower strata of the socio-economic scale. Most
participants were unable to trust doctors because of the socio-economic inequalities, which
they associated with the influence of western education and practices. Such inequalities were
a symbolic representation of the power of the colonial past and cultural contempt or
detachment. Many of my participants described how the doctors have contempt for anything
local and assume superiority for things that originate from the ‘West or America’ (e.g.
Kisiwaa, female, 50, cervical cancer and Yamoah, male, 31, liver cancer, see details in
chapter 4.2 power disparity and lack of trust).
Although it is unlikely that all doctors in Ghana have such attitudes, participants’ lack
of trust in the doctors was prominent and widespread. However, participants continued to use
both traditional and conventional medicine in parallel to meet their needs. Perhaps, the lack
of trust in the doctors was not a rejection of western medicine but a rejection of its cultural
disconnection and seemingly reported contemptuous attitude towards traditional standards.
5.2.2 Trust as a Traditional Identity and Shared Sensitivity
The study found that most participants shared traditions or traditional identities with
Traditional Healers formed the basis of their close relationships, a bond of trust, and
motivation to use the Traditional Healers for therapy. Many participants trusted the
Traditional Healers and had the confidence that the Traditional Healers understood or were
part of the local socio-cultural values and will behave in a manner that was matching with
these values. Some authors conceptualise trust as the confidence or believe that people or
institutions will act rightly or appropriately even in a future situation and broadly in the best
interest of the trustor based on a common established standard (Misztal 2013, Heckscher
2015, Luhmann 2018). Most of my study participants believed that the Traditional Healers
would act in their best interest because of the Traditional Healers understanding of a shared

218 | P a g e
rightness or sensibility. Shared rightness is a collective understanding of what both
the trustor and the trustee inherently consider as appropriate behaviour towards each
other (Heckscher 2015).
The mutual understanding provides both the trustor and the trustee the
assurance that each party will act according to an acceptable standard (Heckscher
2015, Giddens, Sutton, 2013). Although my study participants did not pinpoint, or
they were unable to say what precisely this shared sensibility was, they found its
expression in the local traditions and values. Thus, the shared traditional identities of
values and practices reinforce most participant’s perception of a shared rightness with
the Traditional Healers. Most of the participants of my study and traditional healers
lived in orthodox communities or neighbourhoods. These neighbourhoods had
traditional collective identities as the basis of rightness, morality and framework of
behaviours. Equally, the Traditional Healers and my study participants were
normatively bounded by this common tradition or socio-cultural morality as the
foundation of their behaviours in the communities. They, therefore, had the basis for
trusting each other as in any trusting relationship, both the trustor and the trustee
should have a collective understanding of what is right to form the basis of a
reasonable demand and expectation in the relationship (Heckscher 2015).
Many participants of my study displayed their confidence and trust in the
traditional healers because of the Traditional Healers attachment and understanding of
the local cultural and traditional values. These traditional values formed the basis or
framework of appropriate behaviour. Hence, they demonstrated and expressed a sense
of shared rightness in the notion that they and Traditional Healers have the same mind
as the ancestors and will help each other per the ancestral instructions. An example of
such expression is the excerpts from Kyeremeh below.

219 | P a g e
“We are one people with Traditional Healers. It is like we have the same mind from the
ancestors to help each other. They will always obey the ancestors who gave them their gift to
help their people, and that is why I believe them’’ (Kyeremeh, male, 44, prostate cancer?).
Most of my participants acknowledged the ancestors as the providers or basis of
traditional or socio-cultural identities and framework for moral behaviour or rightness.
Primarily, they perceived the Traditional Healers to have the same mind as the ancestors and
hence will act or behave appropriately as intended by the ancestors. In contrast, there was a
complete cultural dissonance or lack of any shared traditional framework as the basis for my
study participants to trust doctors in the hospitals. Most participants expressed the lack of a
sense of common ancestry or tradition and consequently lacked any basis of shared rightness
for doctors to act appropriately.
In other words, many participants could not be confident that the doctors will behave
appropriately because of their perceived lack of understanding of the inherently shared
accepted standards of the local community or socio-culturally expected behaviour. Some of
the participants for my study thought the doctors had ulterior motives or motives of
accumulating wealth and not necessarily the welfare of the local communities. Many
participants thought doctors were not morally bound or have the obligations to behave per the
ancestral instruction and therefore had the versatility in how they chose to behave. Durkheim
(2012, 2013) described social-cultural rightness as a normative obligation in which trust
emanates from shared values and faith that communities or societies reaffirm through rituals
and ceremonies.
Most indigenous Ghanaian communities achieve traditional morality or rightness by
inculcating in their members and encouraging them to believe and submit to the ancestors or
their symbolic traditions as the supreme authority and moral consciousness. My study found
that most participants trusted the Traditional Healers as a matter of showing their
commitment and deference to the ancestral or traditional authorities, which the Traditional

220 | P a g e
Healers symbolise. In this case, participants were motivated to use the Traditional
Healers for therapy. Many participants felt the Traditional Healers were linked to
traditional ancestral identities or authorities. Such a motivation echoes with the
concept of trust as a commitment and deference to traditional authority and identity
(Tyler, DeGoey 1996, Tyler 2001, Braithwaite, Levi 2003).
The participants showed their identification or validated their identity with the
authorities and the indigenous communities where they belong. Generally, people
trust authorities established from their culture, families or communities and assume
that such authorities will do what is right for them (Tyler, DeGoey 1996, Tyler 2001,
Braithwaite, Levi 2003). In Ghana, deference trust and commitment to ethnic
authorities is prominent and reflect many aspects in society, including voting patterns
and voters’ behaviour in which people vote along their ethnic lines (Adjei 2013,
Hoffman, Long 2013).
Possibly, deference trust in authorities may change when the authorities fail to
live up to the required standards or fulfil their promises. However, my study is
different in the sense that the relationship between participants and the Traditional
Healers have a strong and unwavering anchorage of the ancestors who are the
ultimate authority that the participants must respect. Hence, my study participants
deference to the Traditional Healers motives equals to the motives of the ancestors,
which is the bedrock of the trust that the participants had for the Traditional Healers.
Also, many participants appeared more concerned about expressing their
identities or identification with the ancestors whom the Traditional Healers symbolise
and not focused on any tangible rewards from the Traditional Healers. Although most
participants did not focus on tangible results, they were convinced of the general
goodwill of Traditional Healers towards them. They expected the Traditional Healers

221 | P a g e
decisions and actions to broadly be favourable to their best interest by reflecting the
community and ancestral values. Most of my study participants used the Traditional
Healers or continued to use them even when they were not getting any cure or treatment
benefits. Such participants behaviour suggest that their motivation was not on treatment
outcome but deference and identification to their traditional identities and authorities. Such
insight contrasts with the traditional notion that treatment-seeking only focus on the possible
treatment outcome.
Most of the participants reported seeing traditional healers as part of their ingroup and
embodiment or representation of traditional morality and authority figures. Even participants
who were not regularly using the services of the traditional healers expressed a generalised
trust in the Traditional Healers and described how the Traditional Healers would not falter in
performing their moral responsibilities. Most of my study participants gave the impression
that they were committed to holding on and continuously trusting their traditions and
traditional values. Participants used idiom such as “Yento Amamre Nkwene’’ (“we do not
throw away tradition”) to emphasise the importance and pride in trusting and sticking to
one’s traditional identity.
In describing their experiences with traditional healers, most participants pointed to
the trustworthiness of the ancestors who are the real source of the traditional healers’
knowledge. Most participants took pride in their ancestral origin and trusted their ancestors
because they believe the ancestors fought in the past against the enemies and preserved the
local lands and identities. Also, many participants thought it was honourable to continue to
trust the Traditional Healers as the symbolism of the ancestors who used herbal medicine for
centuries before the advent of conventional medicine.
Equally unique to my study was the suggestion from the participants that any act of
distancing or showing contempt to the Traditional Healers was tantamount to condescension

222 | P a g e
towards ancestral or traditional authorities and undermines participants own identity.
Durkheim (2018), used the concept of mechanical and organic solidarity to describe the basis
of trust for traditional authorities. While mechanical solidarity is usually the result of
fear of punishment and pressure of conformity or identification, organic solidarity or
trust is a function of societal roles, responsibilities and a shared moral decorum
(Durkheim 2018). In this study, participants’ accounts and my observations did not
suggest that participants’ trust for the Traditional Healers was because of fear or
pressure to conform. Instead, my study participants felt proud of their traditions and
willingly submitted to the Traditional Healers who are part of its symbolism of the
ancestors and local traditions.
However, this does not rule out the possibility of at least an implicit pressure
on my study participants to positively appraise Traditional Healers in conformity to
trusting and respecting tradition. Some authors describe how indigenous communities
can sometimes use pressure and the possibility of severe punishment to inculcate their
values into the people (Heckscher 2015, Sztompka 1999). Generally, the traditional
healers and the healing service they provide in Ghana, even in the indigenous
communities, are continuously transitioning from their original premise of serving the
community interest alone to a means of livelihood (Yeboah 2000).
These changes make it difficult to take at phase values that all Traditional
Healers were serving the interest of participants. Few participants expressed concern
about the lack of control, monitoring and supervision of Traditional Healers and the
possible infiltration of fake healers who may have selfish motives from the traditional
moral standards. Perhaps, my study participants’ trust for the Traditional Healers
provided comfort to participants and helped simplify the complexities involved in
participants seeking treatment for their serious illnesses

223 | P a g e
On the contrary, most participants of my study did not feel they had a shared sense of
rightness or subscribe to the same moral principle with the hospital doctors and hence did not
express the same feeling of trust about them. Although doctors in Ghana may not be so close
to their communities or take an interest in the traditional standards, this alone may not be
enough to suggest that they will or do not act in the interest of patients. At least, in principle,
doctors vow to care and to act in the interest of their patients' and communities following
their professional code of ethics. In the Ghanaian context, doctors need to be aware of the
cultural and community dynamics of care to avoid both the direct and indirect criticisms and
clash with the social-cultural expectation.
Almost, all the participants had low socioeconomic status and education and found it
challenging to communicate with highly educated doctors. These could influence the
participants’ ability to feel trust for doctors whom they considered as upper class. It was not
possible to compare my study participants behaviour or accounts with the rest of the
population who may have higher education or better access to conventional medicine. In
other words, my study did not uncover the extent of the influence of socio-economic status in
participants’ behaviour and whether wealthy participants would have had a different level of
trust in doctors and Traditional Healers
5.2.3 Trust as a Shared Language and Identity
Here, the study discusses another way that my study participants conceptualised trust
as a shared language identity and how it influences the relationships and motivations of
participants in using the Traditional Healers services. The study found that the participants’
trust for the Traditional Healers were anchored in the identity of a common language and
understanding. Most participants mentioned that they could understand what the Traditional
Healers told them and felt they were able to contribute to the therapeutic discussions and

224 | P a g e
conversations with Traditional Healers in contrast to hospital doctors. Many authors
acknowledge the critical role of a common language and understanding in the formation and
development of trust (Bacharach, Gambetta 2001, Gambetta 2008, Sanchez et al.
2012, Saha et al. 2000). Most of my study participants identified with the local dialect
“Twi’’ which served as one of the critical elements of trusting identity that connected
them with the Traditional Healers and their communities. I observed in the hospitals
that even doctors who understood and spoke “Twi’’ fluently did not speak it routinely
or regularly and found it comfortable to speak in English.
The accounts of my study participants suggested that they considered
communication or a shared language with the traditional healers as a resource or
something more than just a medium of exchanging words or handling the therapeutic
encounter. Instead, the language signified participants’ identity and identification with
the local socio-cultural or ancestral traditions, belongingness and empowerment,
which the Communication Accommodation Theory supports (Garrett 2010, Giles,
Ogay 2013). In my study, most participants perceived their shared language (Twi)
with Traditional Healers as an expression of identity and identification to their
indigenous groups, communities and values that can be trusted.
In other words, language forms the foundation of expressing collective
identities, trust and conveys a more profound sense of familiarity and belongingness
(Garrett 2010, Giles, Ogay 2013). The Communication Accommodation Theory
acknowledges the importance of sociocultural and sociohistorical context in which
communications or individuals embody. According to this theory, our personal and
sociocultural identities are inherent in our communications and not just the immediate
situation. The theory emphasises the notion that communication or language is not

225 | P a g e
just an exchange of facts, information or even emotions but a salient category of identity and
membership negotiation and validation to a group (Giles, Ogay 2013).
In this respect, language is a code, abstract or a systematic knowledge base that is
deeper than just the ordinary instances of expression (Giles, Ogay 2013). For most
participants, language formed a fundamental part of their collective identity and whom they
could trust. Most participants expressed a shared identity around the local language using
inclusion words such as “Omo Ka Ye Kasa’’, meaning “they [Traditional Healers] speak our
language”, to invoke collectiveness and how language connected them with the traditional
healers. In contrast, most participants’ inability to understand and smoothly communicate
with doctors led to their expression of lack of trust in the hospital doctors. Ghana was a
British colony, and English is an official language and continues to dominate in public and
academic life or institutions. For my study participants, the use of English was an expression
of power and socio-cultural demarcation or distancing and served as a means of alienating the
lower class.
The Communication Accommodation Theory and Luhmann’s conceptualisation of
power as a communication medium emphasise power as robust language code which can
create identity or identification, set criteria for inclusion and exclusion and defines power and
limitations for people (Giles, Ogay 2013, Luhmann 2018, Garrett 2010). Many participants
saw the doctors’ dominant use of English for interaction as barring, disempowering and
undermining or disrespecting of their linguistic identity and that of the local communities.
Similarly, people can use language as the means for creating, projecting or reflecting,
harmonising or concentrating and routinising or normalising power in society (Reid, Ng
1999).
Many doctors in Ghana use the English language in clinics and from my observations,
even when patients are present. Doctors’ dominant use of the English language may not be

226 | P a g e
intended to exclude participants but a matter of convenience and blindness to cultural
values. Peculiar to my study is participants perceived extension of the use of the
English language by the doctors as an emphasis on “whiteness’’ or reflection of
colonial representations in the form of power, inequality and detachment from the
locally shared identities. Superficially and in practice, as reported by participants, at
least in the hospitals, it appeared that doctors used language to exclude my study
participants. However, one can construe that the participants also used the criteria and
power of language to exclude doctors from the local identity and to define doctors’
level of trustworthiness based on how they related to the local dialect. In other words,
both my study participants and the reported behaviour of doctors was an exercise of
power and identity of languages in diverse ways.
5.2.4 Trust in the Familiar and Habits in Communities
Most of my study participants conceptualise trust in their accounts as
familiarity and habits. Many of them and their use of the services of the Traditional
Healers was based on the relationships of familiarity, habits and perceived Traditional
Healers accountability and goodwill. My study identified a connection between the
participants’ trust in the Traditional Healers and their communities and local
neighbourhoods’ relationships of familiarity and the principles of accountability and
continuity. Familiarity can develop into an encapsulated self-interest account of trust,
which is the notion of the trustor that the trustee will act favourably towards them as it
is within their interest to do so (Hardin 2006). Does familiarity breed trust? Gulati’s
(1995) assessment of the relationship between familiarity and trust found that
familiarity increases with repeated encounters and interactions and leads to trust in
which parties suspend equity as the basis of forming alliances.

227 | P a g e
In such repeated encounters and close working relationships, the interest of each party
builts into the other. Hence it becomes necessary and comfortable for the parties to act
appropriately without any legal or written commitments (Gulati 1995). Many authors in their
conceptualisation of trust identified the tendency for people to trust a familiar person,
situation or environment than a stranger (Hardin 1993, Luhmann 2018, Sztompka 1999,
Hechter, Kanazawa 1993, Heckscher 2015).
Similarly, most of my study participants familiarity or active engagement and
community interaction with the Traditional Healers assured them that their self-interest
encapsulates in the Traditional Healers interest. In other words, many participants trusted that
the Traditional Healers would not behave in a manner that would ruin this community
connection and statuses accord to them. However, my study was different in identifying that
the participants tie their interest to the moral framework and goodwill of the ancestors which
the Traditional Healers were inherently required to obey. Most of my study participants
assumed that the Traditional Healers were responsible or accountable to them and their
communities because of the strong relations and community identity bonds that they had with
them.
Also, many of my study participants acknowledged familiarity as a form of security.
Familiarity reduced the complexity and uncertainty and gave participants the incentive to
trust Traditional Healers. Luhmann (2018) in conceptualising trust, discussed the foundation
for building trust as the presentation of the self or groups through social identity and
interaction. In this respect, those who want to be trusted or are interested in the trust must
make themselves familiar through community and social interaction (Luhmann 2018,
Heckscher 2015). Doing so allows the trustee to understand the basis and dynamics of trust in
their environments and build the expectation of others into their self-presentation (Luhmann

228 | P a g e
2018). My study participants had opportunities for contact with the Traditional
Healers through networks of local groups and activities through which they built and
developed trust.
Furthermore, trust relationships and accountability are found to flourish in a
social context or structural conditions of relative persistence, re-encounters and
mutual dependence. Some authors refer to these re-encounters and repeated cycle of
events as trust in “habits “ (Durkheim 2012, Misztal 2019, Gulati 1995, Gilson 2006,
Wuthnow 2004, Misztal 2013). My study participants trusted in the protection and
comfort of the reliability of the familiar and predictable stable routines, reputation and
tacit memories of traditions or socio-cultural identities. Trust in the familiar is like
trust in habits which built on past experiences and avoidance of risk in dealing with
the unforeseen situation (Misztal 2019, Misztal 2013). Hence, trusting in habits or the
familiar is a disposition that offers predictability, provides security, continuity and
strength to face uncertainties and complexities of social life, particularly in vulnerable
and unsettled situations (Latour 2013, Misztal 2019).
The community and neighbourhood activities as focus of interaction provided
a repeated cycle of events, familiarity and interdependence for my study participants
and traditional healers. Through these interactions, my study participants and
Traditional Healers had developed predictable expectations, obligations and
accountability towards each other in terms of reciprocity. Perhaps, participants used
this as a mechanism to guard against the desperate situation they were in because of
their advanced cancer with little available treatment and the threatening situation of
the hospital and the doctors. Many participants, therefore, trusted the Traditional
Healers and the more comfortable situation of the ‘habits’ and comfort available at the

229 | P a g e
Traditional clinics which provided them with hope and were unavailable in the hospital
setting.
On the contrary, my study participants expressed a lack of trust in doctors because
they felt they did not know the doctors well enough or have a well-established relationship
with them. Most participants in my study considered doctors as mere community residents
and not members of the community because of their lack of lineage or attachment to these
communities. Hence, some participants felt that doctors could leave the communities without
justification. They perceived doctors to have less responsibility towards them and the
community. Doctors unstable behaviour caused a sense of the lack of continuity of care.
Also, most participants had concerns that the doctors, unlike the Traditional Healers, were not
living in the communities to provide continuity of care and interaction.
Conceptualising familiar trust as trust in habit contribute to continuity and stability of
social life and relationship (Latour 2013, Misztal 2019). According to Latour (2013),
predictability of habit helps to create a social order in dealing with the perception of
discontinuity and unreliability. Predictability of situations appeared essential to my study
participants and gave them some level of control, safety, certainty and normality. Habits play
an essential role in fostering trust by increasing familiarity and serving as the basis for
continuity and predictability for my study participants in negotiating the complexities and
uncertainties in societies.
The participants of the study had very little chance of getting to know their doctors,
predict the possible occurrences and prevailing situation in the hospitals. They could not even
guarantee that they would be seeing a doctor that they have previously met and unable to trust
doctors for continuity. Most of my study participants did not attend hospital regularly and
were seen by different doctors who conducted the clinics on different days, making it difficult
for participants to get to know the doctors intimately.

230 | P a g e
5.2.5 Reputational Trust: Reputable Characteristics of the Traditional Healers
In this section, I focused the discussions on how participants conceptualised
their trust in the Traditional Healers as reputation. Reputational trust served as a
motivation for participants to use the Traditional Healers for treatment. Collectively,
Traditional Healers or Traditional healing as an institution has built a sturdy
reputation over generations in most Ghanaian communities. Most participants’
accounts showed that they mostly had become aware of and ascribed reputation to the
Traditional Healers based on cumulative community knowledge and the testimony
and experiences of others. Often, authors conceptualise reputation as records of past
deeds (Ensminger 2001, Good 2000, Misztal 2013), perception of integrity and
dependability (Giddens 1991), or evaluation or opinion of others of a social institution
(Goffman 2009).
Hence, reputational trust is usually based on our historical experiences or
knowledge (Sztompka 1999, Good 2000) and involves multiple attestation and events
(Misztal 2013). In this study, some participants expressed trust in the Traditional
Healers reputation or important characteristics without any apparent explanations.
Respectively, some participants ascribed the reputational qualities to Traditional
Healers collectively or as a social institution and not in an individual Traditional
Healers. In this sense, the Traditional Healers enjoyed what some authors describe as
identity reputation or trust in which an individual’s trustworthiness depends as their
identity with a profession or institution (Gambetta 2008, Pettit 1995, Hausman 1997,
Bacharach, Gambetta 2001).
In other words, we select and judge people or events according to
preconceived concepts and reputations as defined by our culture and society

231 | P a g e
(Goffman 2009). Possibly, my study participants were biased in ascribing reputation to the
Traditional Healers based on the information and opinions that their tradition and
communities had given them. Equally, some participants were quick to talk negatively about
doctors, even when they have not received any harsh treatment from doctors. Such
behaviours suggest that participants may have formed their opinions about the doctors based
on the wider sociological and cultural discourse of doctors lacking reputation.
Although Traditional Healers or Traditional healing as an institution have established
a reputation that my study participants could trust, there was no guarantee or certainty that
individual Traditional Healers would take this reputation seriously and will act appropriately.
In this sense, my study participants trusted the traditional healers based on the assumption
that the Traditional Healers will remain trustworthy to maintain or keep their reputable image
and moral status. However, many of the participants who had recently visited the Traditional
Healers and those recruited from the Traditional Healers clinic sounded positive about the
individual Traditional Healers. Participants expressed satisfaction of quality of services they
had received or were receiving from the Traditional Healers. Few participants had concerns
about individual Traditional Healers and possibility of infiltration into the profession by those
who had not the genuine call to the profession as in the excerpts below
In most Ghanaian indigenous communities, people consider reputation as a precious
asset, and the process of acquiring it is arduous and protracted. Once people obtain a
reputation, they must work hard to protect and preserve it because of its fragility and ease to
lose. The nature and closeness of most Ghanaian indigenous communities in which people
“Traditional Medicine , there have many benefits, but the only thing is that
a Whiteman will say the proliferation of traditional quack practitioners who
are not real ones’’ (Kyeremeh, male. 44, prostate cancer?).

232 | P a g e
know each other and aware of almost all incidents in their neighbourhood suggest
how quickly a person’s reputation can deteriorate. Unsurprisingly, many authors have
the view that trust rooted in reputation requires the relentless and constant effort of
permanent confirmation, through self-presentation in social interaction (Goffman
2010, Goffman 2017).
It appeared that the Traditional Healers are in a web of a reputation built
individually as well as collectively in most indigenous communities. Traditional
Healers cannot afford to breach such a reputation because of the implications it would
have on their profession. The reputational trust dynamics are consistent with Hardin
(2006) encapsulated interest concept of trust. The encapsulated interest concept
applies to healthcare institutions and professionals. The reputation and trust of
healthcare professionals and their organisations depend on how they relate or behave
toward patients. Congruently, my study participants trusted the traditional healers
because they believed that it was in the best interest of the Traditional Healers to
behave appropriately by the community expectation for their reputation.
In contrast, most participants suggested that they did not feel that it was within
the interest of doctors to behave in a manner that warrants trust and reputation. Most
participants thought that the doctors did not stand to lose relations, community
prestige and reputation if they misbehave. Hence doctors had little incentive to act
appropriately. Arguably, doctors also have a reputation, although not based on the
same things as measured in the Traditional Healers and not generally discussed at the
community level to influence popular opinion. Participants’ accounts did not suggest
that doctors lack reputation regarding their professional competence and performance.
Participants concerns were more on the softer side of care or soft interactional skills
which has become paramount in most organisation.

233 | P a g e
In this respect, Sztompka (1999) argues against considering reputation as generically
constituting the same elements in every society. In her view, reputation is culturally specific,
and hence the credential or reputable characteristics and their measurements may vary across
cultures and even over time as societies transform (Sztompka 1999). Most participants
considered the traditional healers’ training to be focused on character or behaviour
development, relevant to local requirements and insulated from western influence and
adulteration. Participants equated the training of Traditional Healers to training in wisdom.
Many participants related this wisdom to the socio-cultural traditions and values such as
respect for the elderly, compassion for the vulnerable and the sick, greeting even strangers,
having time for people and participating in local festivals and contributing to community life.
Many participants considered wisdom as more important than academic knowledge
and necessary to navigate through the complexities of communal issues. Traditional Healers,
therefore, earned a reputation from the nature of their training. In contrast, most participants
perceived the doctors’ training as devoid of culturally relevant values, wisdom, and character
development and instead focused on academic prowess. The accounts of most participants
highlighted the importance of grounding and contextualising medical education in Africa and
Africa’s education in its culture. Doing so would ensure maximum acceptance amongst the
public and patients, and thus maximise the benefits and usage (Ocheni, Nwankwo 2012,
Tervalon, Murray-Garcia 1998).
Moreover, participants reported compassionate behaviours from the Traditional
Healers as a form of reputation. As pointed out by Sztompka (1999), reputation required
some level of consistency of past deeds and reliability or commitment to a principled way of
life. The findings revealed that most Traditional Healers did not just count on their past
reputation but committed to continuously supporting the vulnerable in their communities. My
study participants attributed the Traditional Healers’ commitment to charity and respected

234 | P a g e
them for that. While it is difficult to ascertain the exact motives of Traditional
Healers’ compassionate behaviour, money cannot be ruled out entirely. Traditional
Healers advertise their products and services with enthusiasm and charge for their
services. Even so, most participants thought the Traditional Healers showed
compassion by allowing flexibility of payments.
In contrast to the traditional setting, many participants expressed a lack of trust
in doctors because doctors were thought to be unwilling to work in remote
communities. However, my study participants may not be aware or appreciate the
professional code of conduct that guides and restricts the work of the doctors. Most of
the time, doctors in Ghana are legally allowed and remunerated to cover a particular
geographical jurisdiction and unable to provide some of the softer care that the
Traditional Healers may be able to provide. Also, an element of my study participants
perceived reputational trust in the Traditional Healers was around the issues of dignity
in a sociocultural context.
The participants of the study expressed satisfaction in the Traditional Healers’
observance of their dignity and privacy and found it inappropriate that some doctors
exposed their intimate body areas. Doctors were more likely than the Traditional
Healers to perform procedures involving probing or exposing my study participants
intimate body parts. Some participants understood the nature of the doctors’
procedures or investigations but thought the doctors could still have maintained some
decorum and asked for permission. Although it was not known whether Traditional
Healers would maintain privacy and dignity if they were involved in specific
procedures, the findings suggest that they were conscious of the cultural and ethical
prerequisite of privacy and adhered to them. I observed at the traditional settings that
most of the Traditional Healers conducted their consultation and clinic activities with

235 | P a g e
only the patient in a room and called for an assistant when necessary. It appeared that the
Traditional Healers did not share any therapeutic or ''professional discussion'' they had with
my study participants with even the other clinic staff.
In contrast, it was observed that the doctor's consultation and ward rounds did not
appear private as other doctors and other medical staffs formed part of the ward rounds.
Similarly, doctors sometimes stayed or worked from the same office in which the
consultation may be taking place. A forty-year-old female participant, known as Pinaman,
described how hospital staffs treated her with no dignity and left her naked on a trolley in a
room which was accessible to other members of staff. In conjunction, my findings were
consistent with the notion that the Traditional Healers have an excellent reputation for
treating certain diseases. Most studies identified Traditional Healers as more capable in
treating fractures and other conditions perceived to have spiritual causes (Awusabo-Asare,
Anarfi 1997, Abel, Busia 2005, Bazzano et al. 2008, Aries et al. 2007, Solagberu 2005). For
example, Abrafi described how the herbalist was able to fix her sister’s fracture within two
weeks (Abrafi, female, 41, cervical cancer, details in chapter 4.3.4, Traditional Healers
reputation).
The finding of my study is consistent with studies that show that the perception of a
spiritual link with the manifestations of disease affected patients’ choice for traditional
healers (Yarney et al. 2013, Ezeome, Anarado 2007, Bazzano et al. 2008). Both Helman
(2007) and Nettleton (2013) discussed the cultural and sociological conceptualisations and
understanding of health and illness in contrast to the dominant biomedical approach
extensively. The western biomedical concept of disease is dualistic and reduces the
complexities of human health to a simple organ pathology or bodily malfunction.
Consequently, the biomedical approach to treatment focuses on the alleviating physical pain

236 | P a g e
and restoring bodily function (Wade, Halligan 2004; Dick 2010, Hewson 1998;
Nettleton 2013, Helman 2007).
Most indigenous populations in Ghana believe in the concept of misfortune or
a supernatural influence on how certain illnesses occur. Some participants in my study
thought the traditional healers could deal with the supernatural influences on illnesses.
For example, Benewaa described how the doctors could only treat physically caused
diseases in contrast to the Traditional Healers. The latter are capable of treating
diseases which people perceive to have spiritual causation (Benewaa, female, 43,
cervical cancer, detail in Chapter 4.3.4, Traditional Healers reputation). Although not
all participants were specific that their condition had a spiritual cause, many of them
assumed the possibility since they had not received favourable treatment from the
conventional doctors. When it comes to medical emergencies, however, most of my
participants reported trust in the doctors rather than the Traditional Healers. For
example, Nyamekye described how doctors could deal with people who are bleeding
or have collapsed:
Most participants of my study viewed the doctors as lacking the wisdom’’
(knowledge and skill) to continue to treat chronic diseases or make long-standing
conditions. These participants thought the doctors had the requisite skills for acute
cases and saw the hospital as a place with the sophisticated equipment to stabilise the
acutely unwell but not for continuity of care or treatment of chronic diseases.
''If you collapse or something, then they will take you to doctor to fix you. They can stop
bleeding or emergencies, they stopped my bleeding but could not help me, they could
not continue, that is where their wisdom is, so you need ''dunsinii'' (local medicine man)
to look after you. (Nyamekye, Female, 29, cervical cancer).

237 | P a g e
5.3 Conviviality Interaction and Convivial Therapeutic Landscape
Conviviality and hospitality describe and answers the research question on the
participants' experiences and interactions during their encounter with the Traditional Healers
or when using their services. The discussions cover the quality of participants interactions
with Traditional Healers. Also, it covers the atmosphere of participants encountered with
Traditional Healers. These are contrasted with participants experience in hospital clinics. For
Gilroy (2004), the phrase convivial culture subsumes the humdrum nature of daily
encounters, the boisterous everyday interaction of the diverse cultural traditions in a location.
The interviews and observation data showed that the Traditional Healers were friendly to
patients, showed interest in them, listened attentively to them, and ensured a relaxed
atmosphere or space for the encounter. These gave my study participants a sense of emotional
and physical security.
The term conviviality is often politicised and identified with various political
implications, aspirations and strategies of fostering multiculturalism, social cohesion and
diversity in the broader society (Wise, Velayutham 2014, Wise, Velayutham 2009, Meissner,
Vertovec 2015, Vertovec 2007), through regular transient social or public space encounters
(Crouch 2003, Karner, Parker 2011, Neal et al. 2013). Principally, the concept is used to
express new forms of urban citizenship in which the deep cultural dynamics, belongingness
and identities of people may be hybridised or neglected for a superficial good (Nayak 2017,
Gilroy 2004, Askins 2016).
Nonetheless, the concept of conviviality or convivial culture has implications on
healthcare indices, patients experience and relationship between patients and health
professionals (Probyn 2015, Hall, 2013). In this study, conviviality is more than a simple
superficial engagement or getting on with people. The experience of conviviality for my
238 | P a g e
study participants was essential and symbolic of their sense of identity, security,
belongingness, affection and recognition of their socio-cultural norms which were lacking in
the hospitals. Although Conventional medicine has moved or is moving to a more
patient-centred approach, my study participants could not see this in how doctors
treated them. My study participants described their interaction and encounter with the
Traditional Healers or their clinics with words such as pleasantness, helpfulness and
friendliness.
The friendliness of the Traditional Healers seemed to help with the lowering
and or removing of both real and potential hierarchy between themselves and my
study participants, putting participants at ease and creating the conditions for
participants to co-construct and reciprocate the friendly encounter. My study
participant accounts described how the Traditional Healers and the herbal clinic staff
engaged in-jokes and laughter with them, helping to relax the atmosphere and to take
their minds away from their illnesses. Also, the nature of the herbal clinics
contributed to the pleasant experiences of the study participants as it offered a haven
from severe illness and disability where social relationships and networks are
available for support.
The concept of Conviviality space or Landscape looks at how the nature of the
herbal clinics' environments contributed to the convivial interactions and experiences
of participants. Gesler (2003) first posited the term therapeutic landscape to find an
explanation of why specific environments seemed to support healing or have a sense
of healing effect. He conceptualised therapeutic landscapes as spaces where the
physical environment, social conditions and human perception combine to produce an
atmosphere conducive to healing and promotion of health (Gesler 2003, Gesler1996).
Since then, several authors have developed related concepts of environments or places

239 | P a g e
of free social interaction as ''effective sanctuaries'', ''havens of sociality'', ''shelter'' and
''convivial space'' (Nayak 2017, Butterfield, Martin 2016, Moore et al. 2013, Glover,
Parry 2009).
Again, the concept has been broadened to include the relationships and social
networks of interaction that offers security and belongingness or inclusion in a health facility
or social space (Smyth 2005, Wakefield, McMullan 2005). The findings of my study
resonate with studies that found elements of conviviality as an essential element between
health professional and patients or between other professionals and their customers
(Hochschild 2012, Li 2004, Hunt 1991).
In Hochschild (2012), flight attendants were duty-bound to show conviviality during
flights to signal safety and to maintain an accepted interaction and social order. Li (2004)
used the term symbiotic niceness to describe the mutual, reciprocal or co-production of
conviviality between palliative care nurses and patients. Similarly, palliative care nurses in
Hunt’s (1991) study used conviviality to facilitate their communication and work with the
terminally ill patients and their families. However, these studies, (Hochschild 2012, Hunt
1991, Li 2004) had their participants in professions that have explicitly stipulated codes of
conduct for their members, which reflected their behaviours.
In other words, the behaviours of the nurses and the flight attendants may be
components of their professional training which functions to maintain orderliness, provide
reassurance, and advance personal, professional and organisational aspiration (Hochschild
2012, Ashforth, Humphrey 1993, Brotheridge, Grandey 2002, Morris, Feldman 1996). Many
authors describe such professional behaviours as paid emotional labour or impression
management in which conviviality relates to the industry of work (Hochschild 2012,
Ashforth, Humphrey 1993, Brotheridge, Grandey 2002, Morris, Feldman 1996).
240 | P a g e
Unlike the previous researches on conviviality, my study focused on the
experiences of patients (participants) in using the traditional healers’ services. The
Traditional Healers were mostly not bound by any strict or explicit professional code
of conduct or standards. Hence, the issue of impression management to comply with
any organisational or professional code in the strictest sense was unlikely. Also, the
participants did not signal any feeling that the friendly behaviours and interactions of
traditional healers were artificial or simulated. My observations of the behaviour of
Traditional Healers and their staff felt very natural and consistent with the
participants’ accounts. Although the Traditional Healers did not have any written code
of conduct for their practice, they were more likely to behave by the socio-cultural
standards of their communities by being friendly or convivial to study participants.
From my observation and as reported by participants, the Traditional Healers behaved
by the shared socio-cultural norms and values.
The Traditional Healers charged a fee for their services, and hence, it was
difficult to rule out their impressionistic behaviour to attract customers. In any case,
my study participants appreciated the pleasant experience that they received from the
Traditional Healers and used it in conceptualising their experiences with the
Traditional Healers. There is always the question of whether the Traditional Healers
were intentionally using their pleasant and friendly manner of interaction as a
distracting technique for participants, and to hide or manage their own emotion.
However, such an essential interactional and enabling skills of jokes and banter
usually happened before the actual clinical or consultation engagement and put the
participants at ease and facilitate the encounter. Both my observation and participants
accounts show that the Traditional Healers listened professionally and attentively
during the consultations, gave advice, allowed questions and double-checked that the

241 | P a g e
participants were satisfied and knew what to do or aware of the date for their next
appointments.
From the participants ‘perspective, the convivial spaces have various aspects or are
characterised by looking comfortable and relaxed. Most participants depicted Traditional
Healers or the clinics as discounting rigidity, restriction, surveillance and judgemental
attitude. Instead, participant’s accounts suggested that the Traditional Healers offered an
environment of easiness and homely ambience. Such an environment encouraged
spontaneity, natural interaction and appeared to have a positive therapeutic effect on my
study participants’ total wellbeing. Some participants expressed the sense of freedom and
belongingness in the Traditional clinics using words such as “nipa baako’’ meaning “one
people’’ and “abusua Baako’’ meaning one community or family. Per my observation, most
of the Traditional clinics had local music playing in the background and local games
available as the entertainment for patients who would be waiting.
However, there are concerns that such relaxed and unchecked atmospheres or spaces
can mask addressing the essential therapeutic and cultural needs of patients (Nayak 2017,
Gilroy 2004). There was no evidence in my study to suggest that the socio-cultural dynamics
of interaction in the Traditional clinics compromised care. For example, some of the
participants showed me the treatment or medicines that had been given to them to take home
and mentioned when they had to come back for their follow up appointment.
In contrast, the participants’ thought the doctors, or the hospitals, were inflexible,
judgemental, controlling and tied to procedures and processes. The strict procedural
approaches in the hospital prevented the hospital or doctors from engaging and resolving any
participant’s issues or concerns. Also, most participants could not act naturally and thought
they had to be mindful of their behaviours for fear of negative aftermath. Some potential
participants in the hospitals refused to speak to me or take part in the interviews in case I was

242 | P a g e
a doctor or a hospital staff. Many participants appeared and described how they
usually felt anxious and afraid to talk or even ask questions.
There was undoubtedly an elevated level of anxiety and uneasiness for
participants to freely have a conversation for fear that staff would not listen to them,
overhear them and shout at them. Some participants described their inability to
complain or raise concerns as doing so could turn against them and influence the level
of service they may receive from the staff. My observation supported most of my
study participants’ assertions about the nature of the hospital environment. For
example, some participants were sceptical about me because I appeared close to the
clinical staff who were offering me support with recruitment. Understandably, certain
places in the hospital required strict control as regulatory standards and guidelines
(Curtis et al. 2009).
However, my study participants concern was the actual human interaction and
mood or entertaining atmosphere of the environment and not the physical space
limitations. Doctors need to ensure that patients feel comfortable and natural to
discuss or share their feelings in an open, confidential and friendly space as this is not
only of socio-cultural importance but also has a positive therapeutic outcome.
5.4 Holistic Support and Quality Human Time
My participant's accounts indicated how the Traditional Healers showed
interest in their entirety and wellbeing through broadly asking them questions about
themselves and allowing quality human time to listen to them without a rush. The
Traditional Healers allowed the necessary time during the therapeutic encounter to
engage with participants and to demonstrate their interest in all aspects and activities
of participants and not just their medical condition. Per participants’ accounts, the

243 | P a g e
Traditional Healers engaged them in discussions that encompassed a wide range of
participants’ social and personal routine life. Such engagement laid the foundation
and facilitated a meaningful therapeutic interaction and encounter between the Traditional
Healers and the study participants (Hunt 1991, Li 2004).
As per the observation and most participants’ accounts, the holistic view of care also
related to the Traditional Healers empathy, understanding and provision material help or
support to participants. It was observed that the traditional or herbal clinic staffs helped
patients and relatives to carry bags, gave them water, seats, and assisted them to walk and
transfer from vehicles. The approach and the manner of interaction and support used here by
the Traditional Healers resonate with the concept of Holism and patient-centred care which
contrasts with the biomedical model of care (Mead, Bower 2000). Both the concept of holism
and patient or person-centred care acknowledge the socio-cultural, psychospiritual and
biophysical context of a person and how this interconnectedly affect their wellbeing
(Kolcaba, 1997, Kolcaba, 2003, Stewart 2003).
From this perspective, supporting patients should not only focus on their medical
needs but all related aspects of their lives. Presumably, many doctors inhabited in the
biophysical and only concerned about treating physical illness or body malfunction. The
Traditional Healers engaged in the therapeutic encounter with cultural greetings, ordinary
everyday conversations, physical support and comfort. The Traditional Healers and their staff
demonstrated an understanding of the socio-cultural context and dynamics of participants and
indicated that they were interested in participants as whole persons. Required and inherent in
the Ghanaian culture is the practice of exchanging in cultural and welfare greeting at the
beginning of any encounter and helping the sick or the vulnerable. Hence, it is difficult to
ascertain the motives of the Traditional Healers behaviour, whether they were merely
adhering to the culture or broadly interested in their patient’s total welfare.

244 | P a g e
Perhaps, the Traditional Healers were culturally fitting in their greetings and
therefore created the trusting atmosphere at the start of the interaction. In doing so, the
Traditional Healers created a therapeutic landscape of interaction by ensuring a
trusting atmosphere. The Traditional Healers appropriate interacting practices and
behaviour seemed to consider participants needs beyond their treatment. Hence,
patients felt cared for and safe. The doctors’ approach was in sharp contrast to the
Traditional Healers. The doctors straight away discussed the patient’s illness and told
them what to do next without any consideration to other impacts that their illnesses
may be having on them. Most participants felt that doctors and other hospital staff
were not interested in any aspects of their life and were not interested in allowing
them to discuss anything else. In the hospitals, the provision of physical support such
as transferring, feeding, and cleaning, appeared to be the responsibilities of
participants’ family and relatives.
In conjunction, participants expressed their encounter, and interaction with the
Traditional Healers as quality time in which the Traditional Healers listened, paid
attention and allowed enough time for consultation. The participants described how
the traditional healers did not rush them during the consultation. The participants’
accounts and supported observations showed that the Traditional Healers consultation
and interaction with participants were controlled, slower-paced and took more time
than the hospitals. The Traditional Healers appeared very patient and listened to
participants with undivided attention and allowed questions and showed no hurry
during the consultation. On this basis, most participants thought the Traditional
Healers were in a better position to understand and support them than doctors because
of the attention and time they gave to them. The concept of time: clock time and

245 | P a g e
human time, primarily influence the quality of human interaction and therapeutic experiences
(Hall, 1989, Gell 1992, Fabian 2014, Helman 2007).
The concept of time exhibited by the Traditional Healers was more of human or
quality time in which, it would appear the Traditional Healers focused on my study
participants satisfaction and experience of the consultation or the therapeutic encounter. The
Traditional Healers, congruent with most Ghanaian indigenous communities operated in
human times where encounters were not limited or regulated by clock time. The findings
suggest that my study participants preferred their health professional to give them attention
and quality human and interactive time rather than rigid schedules, appointments and rush
that they encountered at the hospital. However, this concept of time may not always be
applicable or appropriate and can cause dissatisfaction for patients who may be required to
wait longer before their consultation time.
Similarly, some Traditional Healers may not appreciate a patient who would be taking
all their time. Although my observation and participants' accounts did not reveal any such
dissatisfaction, it was possible that they were potentially being controlled. On the contrary,
the doctors or hospitals operated with a concept of time in which scheduled clock time
regulated all activities (Hall, 1989, Munn 1992, Gell 1992, Fabian 2014, Helman 2007). My
study participants characterised their experiences of clock time in the hospital or with the
doctors as haste of consultation, longer waiting times, lack of time, lack of attention or
listening. Most participants had to fit their lives into a tight and rigid hospital or doctors’
appointment regimes.
Many participants lived in remote communities and had to commence their journeys
in the early morning. Some of the participants start their journey the day to their
appointment. Equally, the doctors operated with a tight busy schedule, which did not allow
for enough clinic consultation times and flexibility. The question always arises whether it is
246 | P a g e
ever possible for the doctors or hospitals to operationalise time in the same way as the
Traditional Healers. The hospitals were far busier with many patients in comparison to the
Herbal clinics and had regulated time activities. While it may not be possible for
doctors to allow the same amount of time for patients in the hospital, it was possible
to make a little time more human and quality for their patients.
5.5 Protecting Feelings and Avoiding Distress
One of the findings of my study is participants expression of how the
Traditional Healers negotiated within the indigenous culture to manage, protect and to
mitigate participants’ emotions. This part of the discussion focusses on the nuances
between participants and Traditional Healers relationship and interactions, which
supported and protected participants’ emotions and intended to avoid distressing
them. The study identified the work of protecting feelings and avoidance of upsetting
participants through appropriate cultural telling or communication. Cultural telling
involved the Traditional Healers use of euphemism or softer language, adoption of
appropriate cultural demeanour and message of hope to interact and discuss
participants’ situation.
Several studies have highlighted the psychological and emotional difficulties
that confront people with cancer and other chronic diseases and the importance of
managing the psychosocial aspects appropriately throughout the disease trajectory
(Yarney et al. 2013, Probst et al. 2013, Lawton 1998, Clegg-Lamptey et al. 2009,
Charmaz 1997, Copp 1999, Wanchai et al. 2010). Cancer and chronic illness can
bring a sense of shame, loss of personal dignity, low self-image or disfigurement and
loss of independence (Goffman 2009). Likewise, patients also suffer from anxiety,
uncertainty, shock and fear of the possible consequences of the illness especially

247 | P a g e
regarding cancer (Clegg-Lamptey et al. 2009, Yarney et al. 2013, Wanchai et al. 2010, Miller
et al. 1998).
However, the level of support, if at all, that exists for the emotional needs of people
living with cancer who attend hospitals in Ghana is limited or lacking (Clegg-Lamptey et al.
2009, Opoku et al. 2012, Yarney et al. 2013). Most previous researches in Ghana
acknowledge that the Traditional Healers provide their services in congruence with the
Ghanaian culture which supports the emotions of people with cancer and chronic disease
patients’ better than conventional medicine (Wanchai et al. 2010, Clegg-Lamptey et al. 2009,
Yarney et al. 2013). However, these previous studies did not explain how traditional healers
specifically support the psychosocial and emotional experience of patients who have cancer
and other chronic illnesses. My study reveals some of the behaviours of Traditional Healers
and people living with cancer themselves in preventing upset and managing emotions which
the study discusses
5.5.1 Cultural Telling and Disclosure
Participants’ accounts showed that the Traditional Healers appeared to use softer
languages or words in talking to participants about sensitive issues to avoid distressing them
or exacerbating their existing emotional distresses. Many participants mentioned how
Traditional Healers were knowledgeable and competent in delivering bad news. Most
Traditional Healers understood how, when and where to discuss or tell their patients about an
uncomfortable situation. The behaviour of the Traditional Healers could be seen in the use of
euphemism, symbolism or “softer language’’ to show compassion and understanding to
participants. Most participants preferred the Traditional Healers method of using euphemism
or symbolic language as a coping mechanism in which they were supported to

248 | P a g e
psychologically distance themselves from the consequences of their illness
(Mccallum, Mcglone 2011).
Becker (2007, 2010) in expounding on his concept of death and denial, talked
about the trepidations and unpleasant existential threats of illnesses and how people
go through the trajectory by emotionally shunning or disconnecting from the situation.
The nature and possible advanced stages of the illnesses of my study participants
mean they were likely to have a similar sense of anxiety, emotional concerns and
possible existential threats. Most of my participants’ accounts suggested that they did
not want the doom or sensitive aspect of their illnesses repeated or discussed with
them candidly. Also, the indigenous Ghanaian culture generally does not permit the
open discussion or naming of death, misfortunes and certain diseases.
Openly discussing such situations can upset those with the condition and their
families who believe that such conversations may lead to bad luck. Such beliefs
highlight the need to be sensitive to the weight and complexities of discussing severe
diseases such as cancer with patients and family. For example, Yamoah (31, male,
liver cancer, chapter 4.5.1 softening and placating ) was confident that the traditional
healers would deliver lousy news appropriately. In contrast, nana Hussain (54, male,
liver and lung cancer, chapter 4.5.1 softening and placating ) became very upset and
concerned that the doctors told him directly and in plain language about the
possibility of him dying in a not too distant future. I navigated around this complexity
by not asking participants to name or tell me what illness they had or the doctor’s
prognosis of their illness. Most participants described their illness as very unwell,
awful disease or something serious without necessary mentioning the word cancer.
Although I was aware of the exact diagnosis of some participants who were
identified by hospital doctors and nurses, I referred to participants’ illness in the

249 | P a g e
words that they chose and to show my respect for them and avoid upsetting them. In other
words, I behaved in a culturally appropriate way with a respectful demeanour which enables
the participants to talk with me despite their worries about who I was initially. The traditional
Healers’ use of euphemisms was consistent with studies that identified the use of metaphors
to discuss sex or sex organs during medical encounters (Mbugua 2007), symbolism to discuss
the progressive disintegration and deterioration of unbounded bodies (Lawton 1998), and
euphemisms to describe tumours and cancers (Abu-Saad Huijer et al. 2009).
Again, the findings of my study are consistent with studies that have emphasised the
importance of using socio-culturally appropriate methods of communication to avoid causing
upset, distress or aggravation (Doumit, Abu-Saad 2008, Levine 1966). Doumit and Abu-
Saad’s (2008) termed such an approach as tactful communication, while Levine (1966)
referred to it as double layered communication which allows for vagueness, ambiguity and
interpretation. However, there are concerns that the use of euphemisms can become a
superficial strategy for impression management, avoidance, displacement or denial from
reality (McGlone, Batchelor 2003, Liszka 1990, McGlone et al. 2006).
Additionally, euphemisms or metaphors may serve the purpose of saving or
preventing the loss of face of the Traditional Healers and not the patients’ (Keith, Burridge
1991, Allan, Burridge 2006). In other words, the style of vague communication may afford
the Traditional Healers some latitude to avoid blame and not be held responsible in case there
is an unsuccessful treatment outcome, or something goes wrong. While these criticisms are
valid, there was no suggestion from my findings or participants’ accounts that the traditional
healers’ behaviour in managing participants’ emotions were simulated or intended for this
purpose. Instead, the Traditional Healers appeared to acknowledge the cultural necessities,
language traditions and the immediate contextual environment in breaking or discussing
important news.

250 | P a g e
The timings and method of delivering sad news or discussing sensitive issues
are paramount in most Ghanaian indigenous communities. For example, supposed
wise people who can gauge the right moments and use euphemistic or symbolic
languages are usually sent to deliver shocking news such as death and misfortunes to
diffuse the intensity and impact of the message for the receivers of such news. Many
authors agree to the relevance of such a communication approach and its implications
on patients’ emotional experience, treatment satisfaction and outcomes (Arora 2003,
Beck et al. 2002, Ong et al. 1995, Stewart et al. 2000, Baile, Aaron 2005, Tayler,
Ogden 2005, Mccallum, Mcglone 2011).
On the contrary, the account of most participants of my study showed
dissatisfaction of how doctors used the direct or straight-to-the-point approach in
discussing or breaking sad news (Mccallum, Mcglone 2011, Tayler, Ogden 2005).
Most of my study participants considered such an approach unacceptable, insensitive
and culturally inappropriate. However, several authors acknowledge that achieving
the skills of cultural communication to manage emotions is a complex process which
cannot take place in a vacuum (Ackerson, Viswanath 2009, Demers, Viswanath 1999,
Simpson et al. 1991, Tayler, Ogden 2005).
Hence, such awareness cannot be expected to arise from theoretical
knowledge in the classrooms of medical schools without continuous and intentional
community engagement (Simpson et al. 1991, Tervalon, Murray-Garcia 1998).
Broadly, the Traditional Healers have an advantage in this sense of having their
training in the communities and learning the community values and acceptable
behaviours. Similarly, the approach of cultural telling and disclosure involved the
Traditional Healers hopeful and encouraging communication to participants. My
study participants described how Traditional Healers offered them hope and not used

251 | P a g e
pessimistic or despondent words. The data shows that some Traditional Healers reassured
participants that their illness was not beyond redemption, even in the most advanced disease
stage.
Although superficially, most study participants may appear to believe what the
Traditional Healers told them, it cannot be taken at face value that they believed the
Traditional Healers could heal them. Most Traditional Healers did not explicitly tell the
participants that they could heal them, and hence, most participants expressed their hope in a
general and immeasurable sense. Such behaviour could also be a way in which my study
participants exercised their denial of the seriousness of their illness. Traditional Healers use
of hopeful and encouraging word helped the participants to live in a state of denial. Hence,
they did not question the Traditional Healers about their illnesses as they preferred remaining
in the dark as a coping strategy. The quote below is an example of how the Traditional
Healers offered hope to the participants;
Most participants expressed how the Traditional Healers gave them hope and
discounted the gloomy and pessimistic information they received from the doctors. The
traditional healer's language offered most participants a sense of hope, confidence, security
“He (Traditional Healer ) told me that I would not lose my life. The doctors said
that because they (Doctors) do not know how to treat such disease, all they know
is”kukuku’’ (inpatient or lack of patience). He (Traditional Healer) said it was
good that I have brought it to him. He told me that there is sore in my womb and
under and hence, he was going to give me some treatment that would help to
resolve this, so I should not worry’’ (Nyantah, female, 58, cervical cancer)

252 | P a g e
and positive emotional outlook although participants’ reports of treatment outcomes
were primarily of symptom relief and appetite boosting rather than of actual healing
of their illness. In my experience of living and working in Ghana, tradition required
elders to demonstrate both emotional and physical composure in a challenging
situation and not to show weakness. Although there was no suggestion from my study
participant’s accounts or my observation that this was the case for the Traditional
Healers, it is conceivable that the Traditional Healers were acting superficially to
appease and validate their status and function in society. Possibly, the Traditional
Healers were required to reassure participants and to hide the truth of the seriousness
of their illness.
The findings of my study echo the view found by previous research, e.g.
Fallowfield (1993) that health professionals are vital in motivating patients through
their choice of words, composure and actions. My findings suggest the traditional
healers understood the impact of their attitude on the emotions of participants. The
caution is that such a community or cultural demands, although they enhance the
reputation and sense of control of Traditional Healers, can be unhelpful to their
patient's mental health and wellbeing (Hochschild 2012, Brotheridge, Grandey 2002).
Although the traditional healers’ behaviour may be a cultural prerequisite, there was
no hint that they were under pressure to behave in the manner that they did. Indeed,
the traditional healers in my study appeared to have a genuine sense of care and
support to ensure that participants remain positive and hopeful in their situation. The
study observed in the herbal clinics that the Traditional Healers appeared to not be
under pressure and had things under control through their facial expression of smile
and demeanour of soft calm and gentle approach.

253 | P a g e
5.5.2 Keeping It to Oneself and Not Washing One’s Clothes in Public
Keeping it to oneself and non-disclosure of information by both the
participants and the traditional healers was a means of protecting participant’s emotion. My
study participants expressed their confidence and trust in the Traditional Healers to keep their
information secret and not upset them. Most participants themselves concealed their
condition from their families to avoid upsetting their families and themselves. Studies support
how a culture of emotion control and awareness in the form of non-disclosure helps to protect
the image and emotion of patients and families (Copp 1999, Glaser, Strauss 2017).
In both studies (Copp 1999, Glaser, Strauss 2017), the dynamics of information
sharing, and control was used by patients and other stakeholders as protection or power to
protect and define the status of the terminally ill. Most participants referred to the information
secrecy as “not washing one's clothes in public or outside’’, “Yensi ntoma wo abonten’’.
Hence, most participants wanted a health professional to keep their condition secret and not
reveal it even to families to avoid indignity, emotional distress and loss of control or
independence (Probst et al. 2013, Charmaz 2002). Many participants had concerns about the
doctors’ lack of confidentiality and protection and the assumption that it was accepted to
share information with participants’ family or other staff members.
Many participants, therefore, expressed confidence and openness to disclose and
discuss their feelings in more detail with the Traditional Healers because of their culturally
appropriate behaviour regarding the confidentiality of information about the illness. Also, the
Traditional Healers offered a safe place for participants to discuss issues which are so
sensitive for participants and needed handling with the utmost delicacy. The practice of non-
disclosure protected the participants’ emotions by shielding them from potential public
ridicule, judgment and opprobrium. The socio-cultural concept of helping or supporting a
sick relative is a massive moral responsibility in Ghana to the extent that the society regards
people who fail to meet such obligation with contempt.

254 | P a g e
Although such a cultural practice can be helpful, it can equally put pressure on
participants to suffer in silence, to remain independent and not be a nuisance or
inconvenience to their family. Some participants felt that telling their families about
their illness would put the family under enormous pressure to adjust their life routines
to look after them. Most participants appreciated the invaluable support from their
partners or families but had legitimate concerns that their physical and economic
incapacity and dependency may put their relationships under strain. My study
participants’ feelings highlighted the adverse effects of chronic illnesses and their
significant impact on relations and social interactions, sometimes leaving divisions
even within families (Charmaz 2002).
My study found that the participant's decision to hide their situation from
families came with difficulty and involved some participants changing their life
routines and social relationships which radically impacted on their very self, life and
financial situation. Managing and protecting emotions was an essential cultural
prerogative for both the traditional healers and the participants.
5.6 Summary of Chapter
In this chapter, I have discussed the main findings of the study and how they
compare to relevant theories and findings of other studies. I have shown how trusting
identities of participants and Traditional Healers influence participants motivation to
use the services of the Traditional Healers. I have discussed the experience of
participants in seeking Traditional Healers as one of conviviality, hospitality and
emotional management through the perspective of socio-cultural understanding and
standards. The discussion has helped to answer the research question or fulfilled the

255 | P a g e
study objective of exploring participants ‘motivations and experiences of using Traditional
Healers.
The chapter has highlighted the contrast of the lack of trust for the conventional
doctors because of their lack of “ shared identity’’ with the participants and how they
symbolise power and inequality in society. “Community of Us’’ the grounded theory from
this study encompasses participants share of identity, trust and convivial interaction with
Traditional Healers and how that affects their motivation and experience in using Traditional
Healers in Ghana.

256 | P a g e
CHAPTER SIX: CRITIQUE OF STUDY AND CONTRIBUTION TO KNOWLEDGE
6.1 The Study Contributions to Knowledge
This study has shown the complexities and subtleties of community identities
of trust and relationships and how they influence participants health-seeking
behaviours. The research has shown that the motivations of people living with cancer
to use Traditional Healers or Traditional Medicine in Ghana are more profound than
we currently know through other researches as lack of availability, affordability and,
accessibility to conventional medicine. Instead, the study establishes that the socio-
cultural community dynamics of trust which have their expressions in a shared
tradition or ancestry, language, familiarity and established reputational characteristics
influence the motivation of people living with to use Traditional Healers in the Brong-
Ahafo region of Ghana.
In other words, people living with cancer have a shared community identity
with Traditional Healers or saw Traditional Healers as an active integral part of their
socio-cultural history and values. These shared identities formed the basis of the trust
that people living with cancer had for Traditional Healers or their motivation to use
the Traditional Healers. These add to the existing body of knowledge.
Equally, the study has shown that some people living with cancer in the
Brong-Ahafo region of Ghana have a generalised lack of trust in hospital doctors.
Most people living with cancer had the perception that the doctors did not share in the
local communities’ trusting identities. Instead, they were detached and sneering to the
local community trusting identities. This finding reflects and may explain why most
Ghanaian indigenous population use the Traditional Healers for their health-seeking
regarding illnesses.

257 | P a g e
Moreover, the study explored the experiences of people living with cancer in their
therapeutic encounter with Traditional Healers in the Brong- Ahafo Region of Ghana. The
research has shown that people living with cancer conceptualised their therapeutic contact
and interaction with the Traditional Healers as friendly, informal and relaxed following their
community socio-cultural propriety. Therefore, the study highlights the importance of good
patient-health professional relationships and interaction, which is based on community socio-
cultural understanding. The study has shown that such relationships enhance patients’
experience, openness and feeling of liberty to discuss their condition and concerns health
professional.
The study adds to the current literature by showing that people living with cancer are
not only interested in the outcome of their treatment but also how their health professional
related to them in the therapeutic encounter and illness trajectory. The study has shown how
patients’ socio-cultural identities impinge on the perception of health and health-seeking
behaviours for illness and symptoms. Most people living with cancer in the study wanted
their health professionals to recognise their broader socio-cultural identity needs during the
therapeutic encounter and treat them with respect, dignity and friendliness. The study has
highlighted how patients and health professionals trusting relationship in indigenous
communities is linked with shared identities. The study adds to the knowledge that health
professional should endeavour to understand the cultural environment in which they practice
and align their practices and behaviour to it.
Furthermore, the study has shown how people living with cancer received emotional
and psychological support from Traditional Healers in the Brong Ahafo region of Ghana. The
pieces of literature had already demonstrated that chronic disease patients prefer Traditional
Healers to conventional doctors because of the emotional and psychological support they
receive from Traditional Healers. However, there was no evidence of how Traditional
258 | P a g e
Healers provided such psychological support. The study adds to the body of
knowledge by emphasising the importance for health professionals to be sensitive and
adopt a culturally appropriate language of communication in speaking to people living
with cancer. The study has also shown how important it is for health professionals to
maintain their patients' information confidential, even from close relatives. The study
has shown that the legal and professional requirements for conventional doctors to be
straight and direct to their patient is not generically applicable to indigenous
communities. Some indigenous communities have different understanding and
manner of dealing with sensitive and complex issues. The study has shown how the
perception and understanding that some indigenous communities in Ghana have about
certain illnesses are associated with heightened emotions for both patients and their
families, which require additional skills from health professionals to handle. The
study shows the vital role or potential role of Traditional Healers in maximising
psychological care for patients in Ghana.
Moreover, the study adds to the body of knowledge that chronic disease
patients prefer to seek help from Traditional Healers for symptom management and
palliative care. Thus, Traditional Healers are better in managing chronic diseases,
while conventional doctors are competent in managing emergencies or acute
conditions. Most participants appeared happy with the manner that the Traditional
Healers managed their condition over a prolonged period and revisited the Traditional
Healers on a regular occasion. Even those who attended the hospitals still attended the
Traditional Healers for long term or palliative management of their illness.
The principal aim of the study was to develop a substantive theory or
conceptual understanding of people living with cancer’ motivation and experiences of
using Traditional Healers in the chosen context. The theory of “Community of Us”

259 | P a g e
developed from participants accounts explains how people living with cancer see themselves
and the Traditional Healers as “Us’’, or people who share a standard traditional or ancestral
connection and community identities of trust. The study has shown how most patients trusted
health professionals whom they considered as part of the “Us’’ identity as they believe such
people would act towards them according to a shared rightness or sensibility. The study
shows how community identities formed the basis or measure of one’s trustworthiness in
indigenous communities
On the contrary, the concept shows how people living with cancer excluded the
hospital doctors from the ’Us’’ identities and categorised them as detached from the
community and showed distrust to them. The study has shown how people merely residing in
a community does not make them members or part of the ‘’Us’’ unless they share in the
community identities of trust.
6.2 Strength of the Study
The use of constructivist Grounded Theory (CCG) methodology has led to the
development of in-depth participants’ knowledge and understanding of their motivation and
experiences in using Traditional Healers in the context of the Brong-Ahafo region of Ghana.
The transparency of the researcher was important in this study as the researcher pre-field
biography, and clinical experience had the potential to influence the interview or data
collection and its analysis (Li, Arber 2006; Jack 2008).
However, the use of pre-field, in-field and post-field reflexivity was a strength to the
study by allowing the researcher to openly acknowledge and examine his own bias and deal
with them in a balanced manner. The potential biographical and professional, and academic
reflection allowed for the appropriate scrutiny of all the research thoughts and activities and
ensured they were not imposed on the process or outcome of the study. These provided a

260 | P a g e
balance to ensure that my decisions were not based on preformed ideas. Instead, they
were based on the context and the participants' view.
Furthermore, my understanding of the local culture and fluency in the local
dialect helped in navigating the complexities of the setting and asking the interview
questions appropriately to sustain participants engagement and honest responses.
Hence, the dialogue between myself and the participants reflects the phenomenon and
the context of the study. Also, the study has the strength of interviewing patients from
both the herbal clinics and hospitals which provided a broader perspective and a
balanced view of patients who have used or were using Traditional Healers. The
multiple data sources ensured that the findings were a more representative view of the
phenomena.
6.3 Limitations and Requirement for Future Research
One of the limitations of this research is the small number of participants
involved in the study (n=35). Hence, one should exercise caution in the interpretation
of the data. We should acknowledge the difficulty in generalising any of the findings
and conclusions. Also, the study collected data from only two hospitals in the region
which dealt with only gynaecology and prostate cancer cases. Hence, the accounts of
participants were not a complete reflection or representation of all types of people
living with cancer or patients in the region. Equally, the lack of records in the herbal
clinics hindered the ability to confirm the diagnosis of participants recruited in these
clinics. I relied on the staff in these clinics and their descriptions of patients’ condition
as a diagnosis of cancer. Also, the participants themselves in both the hospitals and
the herbal clinics did not discuss their cancer diagnosis explicitly. Hence, the study
cannot claim that all participants were people living with cancer. The findings do not

261 | P a g e
claim to be a representation of the experiences of people living with cancer in the entire
region.
As acknowledged in most social researches, the study represents an instant of what
takes place. Hence, the assumption is that a different reconstruction of the reality is possible
at contrasting times and various sites. The findings of the study cannot be generalised to the
whole community or another context. However, the study still has relevance and applicability
in a similar context.
Moreover, most participants of the study had low socioeconomic status. So, it was not
possible to compare the study participants behaviour or accounts with the rest of the
population who may have higher education or better access to Conventional medicine. It was
not possible to compare the study participants behaviour or accounts with the rest of the
population who may have higher education or better access to Conventional medicine.
In other words, the study did not uncover the extent of the influence of socio-
economic status in participants’ behaviour and whether wealthy participants would have had
a different level of trust in doctors’ or Traditional Healers. It is possible that patients who
have formal or western-style education, live in the city and have money may have had their
views changed regarding the socio-cultural values and unlikely to trust or use Traditional
Healers. It would be interested in exploring in future the views of patients who have moved
from the village to the city to understand how their views have transitory.
The study did not interview doctors or Traditional Healers, and hence, it was not
possible to clarify some of the assertions or impression that the study participants have
created about them. It would be interesting to know in future the findings of studies that
would consider the Traditional Healers and doctors as their participants.

262 | P a g e
6.4 Recommendations for practice policy and education
The study did not offer criticism to any existing policies or lack of it but aimed
to conceptualise the motivations and experiences of people living with cancer who use
Traditional Healers. However, the findings of the study are significant to augment the
effective functioning of health delivery systems among the indigenous populations of
Ghana and similar settings. This section discusses the recommendations regarding the
relevance of the study to practice or the practical implications of the study on
improving practice and local delivery of healthcare. Also, the section discusses the
significance of the study to the development of health policies and regulatory
frameworks that acknowledge and reflect the active use of Traditional Healers in
some communities of Ghana. Such policies would position Traditional Medicine
alongside Conventional Medicine with the appropriate recognition of safety standards
and oversight. Additionally, the section discusses the importance of the study to how
Conventional Medical Education is designed and delivered in Ghana. Furthermore,
The section discusses the relevance of the study to research development to maximise
safety and innovation in Traditional Medicine.
6.4.1 Recommendations for Practice
Many patients in the study had concerns that Conventional Medical
Practitioners were unfriendly, paid them no attention or respected their cultures
during the therapeutic encounter. Friendly and cordial relationships, cultural greetings
and use of the local dialect were vital to enhancing patients experience of the
therapeutic encounters and building trust. Hence, Conventional Medical Practitioners
should have the necessary skill to interact with their patients at a human level. Such a
manner of interaction should occur at both the community level and in the hospitals.
Conventional Medical Practitioners should try to learn these cultural skills through

263 | P a g e
engagements and interactions with the local communities, social groups and activities.
Equally, the hospital authorities should create engagement opportunities between
health professionals and the communities. This approach will help health professionals to
understand the populations' cultural priorities and expectations during the therapeutic
encounter. Such a culturally appropriate approach of interactions and engagements will
enable patients to identify with the health care system and the hospital environment. Also,
such practices would encourage patients to feel comfortable to discuss their concerns with
health professionals and inform them of any herbal treatments they may be using. Such
conversations would allow doctors the opportunity to give the right advice to patients on
safety and potential drug interactions in using Traditional Healers.
Furthermore, the study revealed many participants and Traditional Healers lack of
trust and suspicion for doctors and the Conventional Medical System. The lack of trust, as
reported, was deepened by the dichotomy and lack of dialogue between Conventional
Medical Practitioners and Traditional Healers. Accordingly, both Conventional Medical
Practitioners and Traditional Healers should be willing to set aside their ideological and
practical differences and work together for the best interest of their local communities. Such
collaboration would be difficult but possible with the appropriate policy backing and
stakeholders involvement. Also, the local community leaders can take the initiative to create
forums of communication to facilitate engagement between Conventional Medical
Practitioners and the Traditional Healers. These practical engagements and interactions
would encourage open discussions and help to build the necessary trust for collaboration
between Conventional Medical Practitioners and Traditional Healers. The collaboration
between Conventional Medical Practitioners and Traditional Healers would ensure continuity
of care and safety for patients who use the Traditional Healers.
264 | P a g e
6.4.2 Recommendation for Policy
The findings of the study showed that the Traditional Healers and
Conventional Medical Practitioners function independently without a system of
collaboration. The lack of collaboration does not allow oversight and development of
safety systems for Traditional Healers (Boateng et al. 2016, Owoahene-Acheampong,
Vasconi 2010). The government should develop policies and strategies of integration
between Traditional Healers and Conventional Medical Practitioners wherever
possible. The policies of integration can help to improve the safety, efficacy and raise
the standard profile of Traditional Healers (Griffiths 2009, Robinson 2006).
Conventional Medical facilities can use their expertise to support the Traditional
Healers and to make it safer for patients who would like to continue to use them.
Equally, Conventional Medicine Practitioners can point patients who prefer
Traditional Medicine to the appropriate Traditional Healers who have the requisite
skills and accreditation to practice.
The government of Ghana and Conventional Health Care Systems currently
legally tolerate Traditional Healers or Traditional Medicine. However, there is no
formal accreditation or regulation of the entire Traditional healing system. The lack of
regulation and standards for Traditional Healers is a concern to patients' safety.
Consequently, there is no system of holding Traditional Healers accountable for
medical negligence or harms to patients unless in cases of a criminal offence. The
broader policy initiatives around the recognition of Traditional Healers, training, and
standardisation should be set out by the Central government and serve as the basis for
local guidelines. The government of Ghana made some previous attempts to introduce
and enforce the registration of Traditional Healers. Unfortunately, the complexity of
Traditional healing, the difficulty of bringing Traditional Healers together and the
lack of government's motivation to enforce such policies and regulations have led to

265 | P a g e
their abandonment. The government should have the political will to introduce policies that
would ensure appropriate oversight of Traditional Healers as has been done in China, Hong
Kong and India (Griffiths 2009, Robinson 2006). In these countries, Traditional Healers are
trained, recognised, regulated, and to some varying extends integrated into the Primary
Health care system (Griffiths 2009, Robinson 2006).
Similarly, the policies in Ghana should ensure that the Traditional Healers have the
training, knowledge and skills before accrediting them to practice. The appropriate standard
and process of accreditation will protect patients' safety and the quality of care that they
receive from Traditional Healers. It would also be simpler and more feasible to hold
Traditional Healers professionally and legally accountable.
Furthermore, although Traditional Healers were found to play a significant
role in supporting the healthcare of indigenous communities, there is the danger of delaying
patients from seeking appropriate and advanced health support. Hence, the government
should have a clear policy and guidelines on what minor ailments Traditional Healers can
treat. (Griffiths 2009, Robinson 2006). Equally, the government should develop guidelines
for referral to the appropriate health facilities for cases beyond the Traditional Healers’
expertise.
Traditional Healers have trust and respect in indigenous communities and can
play a vital role in expanding Primary Health Care in these communities where Conventional
Health Practitioners are lacking. The government should develop strong Primary Health Care
policies that would involve Traditional Healers and existing indigenous facilities in health
delivery. These policies should offer standardised training in first aid, infection prevention,
health promotion practices, hygiene, treatment of minor ailments and guidance on patient
referral to hospitals. For example, the Global Network for Women's and Children Health
Research in Argentina, Guatemala, India, Kenya, Pakistan and Zambia found a reduction in
266 | P a g e
maternal-child death and postpartum haemorrhage using community interventions
(Pasha et al. 2010). Other studies have highlighted the use of Traditional birth
attendance, and community trained health workers and Traditional healers to improve
Primary Health (Pasha et al. 2010, Bahl et al. 2010, Sibley, Sipe 2006). Such an
inclusive approach would maximise the expertise and existing facilities of Traditional
Healers through Primary Health Care and minimise the risk of delay or unsafe
treatments.
6.4.3 Recommendation for Education
The study has shown that the Traditional Healers were educated in their
communities and involved in community or neighbourhood life. In contrast,
Conventional Medical Practitioners are trained in western style institution and have
no practical involvement in their local communities. The current western-style
education system or institutions provide the training of doctors and nurses without any
community input or considerations. The current policy on Patients Charter in Ghana
talks about the importance of patient-professional partnership and user involvement
(Ghana Health Service 2017). However, some authors argue that the policy is a latent
document for health professional while patients and the public are not aware of it
(Yarney et al. 2016).
The current medical training or education are confined to western-style
institutions and lack cultural trust, sensitivity and community relevance.
Conventional Medical Practitioners must-have cultural sensitivity, humility and
understanding of the needs and the dynamics of the communities in which they work.
Hence, universities and medical institutions should design their curriculum and
training programs to reflect the Ghanaian cultural traditions such as Traditional
Medicine and the dynamics of local communities. Practically, these curricula should

267 | P a g e
allow Conventional Medical Practitioners to spend time in the communities and with
Traditional Healers as part of their training to gain more community understanding of
illnesses and to win the trust of the populations.
Moreover, the curriculum and training should incorporate lessons on history,
tradition, culture and their relevance on health decisions and behaviours. Such an approach is
imperative for doctors to acquire the necessary skills to negotiate and function effectively
within the communities that they serve after their training.
It is equally essential that Traditional Healers are also supported to gain some level of
education and training to improve the safety and quality of their practice. Ghana has no
formal education or training and accreditation for Traditional Healers. Hence, there is no way
of measuring or standardising a minimum level of skills and knowledge required for them to
practice safely. The current lack of consistency in the criteria of how people become
Traditional Healers and minimum knowledge and skillset for Traditional Healers encourage
the proliferation of treatments which may have serious safety implication for users (Adusei
et al. 2019)
Also, the current open system may allow imposters who may defraud patients and
make their conditions worse. Traditional Healers who have the right treatments, skills and
knowledge may still lack knowledge in hygienic preparation of their products and accurate
dosing. To protect patients and to make Traditional Medicine safer for them, there should be
some minimum qualification, formal training and registration of Traditional Healers. Primary
Health Care (PHC) and public health professionals can organise informal workshops,
engagement programs, and seminars to support Traditional Healers to acquire these essential
skills and knowledge. The government and other stakeholders should support the creation
incentives such as given special recognition to Traditional Healers who participate in these
workshops.

268 | P a g e
6.4.4 Recommendation for Research
The evidence of the efficacy and safety of most Traditional Medicines in Ghana has not
appropriately been investigated or verified. The only source of the claim of their safety,
efficacy and potency to treat specific ailments usually come from the individual patient
account and the Traditional Healers themselves. The government should ensure the
involvement of educational and medical institution in researching to establish the efficacies,
safety and appropriate dosages of these medicines. Researching into Traditional Medicine can
also help to eradicate the potentially dangerous and harmful elements of Traditional Medicine
to patients. Equally, efficacious and safe Traditional Medicine can be a source of revenue for
the government and reduce the cost of specific treatments in Ghana.
6.5 Conclusion
The study has shown the complexities of health-seeking behaviours of people living with
cancer in the Brong-Ahafo region of Ghana. The findings of the study have been theoretically
positioned and compared to the relevant literature, focusing on health-seeking behaviours in a
socio-cultural context. Previous studies have found socioeconomic statuses of people and
their inability to access Conventional Medicine as the motivations for using Traditional
Healers.
However, this study has found deeper and shared trusting community socio-cultural
traditions, beliefs and identities as the motivations for using Traditional Healers by people
living with cancer. These trusting identities include the language traditions, neighbourhood
and community goodwill and accountability, ancestral connections, and community
reputational characteristics. The trusting identities enabled a positive experience for people
living with cancer in their therapeutic encounters with Traditional Healers.
In contrast, participants experienced Conventional Medicine based on western and
modern scientific philosophy and education. The operations and practices of Conventional
269 | P a g e
systems of health and its professionals did not conform to the socio-cultural trusting identities
in the communities. Most Conventional Health professionals did not speak the local dialect,
engage in neighbourhood interactions, nor had the standard of reputation that the community
and culture expected of them. Hence, people living with cancer did not feel they had the basis
for trusting Conventional Health professionals.
The theory of the” Community of Us” shows the foundation of the trusting
relationship between Traditional Healers and people living with cancer and how that trust
affects their motivation to use the Traditional Healers for therapeutic reasons. The theory was
developed from the trusting community identities and shared cultural traditions and beliefs
between people living with cancer and Traditional Healers.
These reciprocal and shared trusting relationships unified the Traditional Healers and
people living with cancer together as " Community of Us "and created a sense of oneness
with each other. The sense of trust and collectiveness was a motivation for people living with
cancer to use Traditional Healers as they behaved with cultural sensitivity and a shared
rightness. However, the "Community of Us" had boundaries and exclusions, and mostly
excluded Conventional doctors who did not share the same cultural identities and therefore,
not the same level of trust. Doctors were perceived with having a “whiteness" or an
exemplification of a colonial past. These include cultural detachment and power, which was
associated with post-colonial histories and socioeconomic inequalities.
The theory has implications on designing health programmes and systems in Ghana
and highlights the importance and necessity of trust in health professionals and the health
system. Also, the study has shown how health-seeking behaviours among people living with
cancer are influenced by their trust in health professional. However, the components of trust
are culturally dynamic and vary in context. Hence, the study has shown the need for health
policies, strategies, planning and education to broadly reflect their socio-cultural context. In
270 | P a g e
practice, such an approach would make the health system relevant and identifiable to the
target populations.
Furthermore, the study has identified the importance of health professionals having
cultural competence and sensitivity to the local communities in which they work. Moreover,
many people in the Ghanaian indigenous communities’ trust in Traditional Healers for
therapeutic purposes. Hence, any bespoke health delivery approach in Ghana must integrate
Traditional Healers to ensure patients who access Traditional Healers are doing so safely and
under the right regulations and standards.
6.6 Dissemination of Findings
Part of the findings of the study has already been presented at the British
Medical Sociology Conference (2016 and 2019) and the Qualitative Health Research
Network Conference (2019). I am currently writing drafting a paper for publication.
The regional health director of the Brong-Ahafo region of Ghana has shown interest
in the study and would like to know the findings. A summary of the findings and
recommendation will be sent to him. Also, the recruitment hospitals are interested to
know the findings. I am keeping all the necessary contacts and hoping to do these
presentations in Ghana by next year.

271 | P a g e
REFERENCE
ABEKAH-NKRUMAH, G. (2006). Information for health improvements; Prospects and
challenges facing the Ghanaian health sector, Conference of the Ghana Library Association.
Accra, pp. 14-15
ABEL, C. and BUSIA, K., 2005. An exploratory ethnobotanical study of the practice of
herbal medicine by the Akan Peoples of Ghana. Alternative Medicine Review, vol. 10, no. 2,
pp. 112-122
ABOTCHIE, P.N. and SHOKAR, N.K., 2009. Cervical cancer screening among college
students in Ghana: knowledge and health beliefs. Int Journal Gynaecology Cancer. vol. 19,
no. 3, pp. 412-600
ABRAMS, D. and HOGG, M.A., 2006. Social identifications: A social psychology of
intergroup relations and group processes. Routledge.
ABU-SAAD HUIJER, H., ABBOUD, S. and DIMASSI, H., 2009. Palliative care in
Lebanon: Knowledge, attitudes and practices of nurses. International Journal of Palliative
Nursing, vol. 15, no. 7, pp. 346-353.
ACKERSON, L.K. and VISWANATH, K., 2009. The social context of interpersonal
communication and health. Journal of Health Communication, vol. 14, no. S1, pp. 5-17.
ADEWALE, O.B., ONASANYA, A., ANADOZIE, S.O., ABU, M.F., AKINTAN, I.A.,
OGBOLE, C.J., OLAYIDE, I.I., AFOLABI, O.B., JAIYESIMI, K.F., AJIBOYE, B.O. and
FADAKA, A.O., 2016. Evaluation of acute and subacute toxicity of aqueous extract of
Crassocephalum Rubens leaves in rats. Journal of Ethnopharmacology, vol. 188, pp. 153-
158.

272 | P a g e
ADDO-FORDJOUR, P., ANNING, A.K., BELFORD, E.J.D. and AKONNOR, D., 2008.
Diversity and conservation of medicinal plants in the Bomaa community of the Brong Ahafo
Region, Ghana. Journal of Medicinal Plant Research, vol. 2, no. 9, pp. 226-233.
ADJEI, J.K., 2013. Ethnicity and Voting Behaviour in the Ashanti and Volta Regions of
Ghana: A Cramp in the Wheel of a Fledgling Democracy. Journal of Global Initiatives:
Policy, Pedagogy, Perspective, vol. 7, no. 1, pp. 1.
ADJEI, P., AKPALU, A., LARYEA, R., NKROMAH, K., SOTTIE, C., OHENE, S. and
OSEI, A., 2013. Beliefs on epilepsy in Northern Ghana. Epilepsy & Behaviour, vol. 29, no. 2,
pp. 316-320.
ADUSEI-MENSAH, F., HAARANEN, A., KAUHANEN, J., TIKKANEN-KAUKANEN,
C., HENNEH, I.T., GANU, D., AMETSETOR, E.S.E., OLALEYE, S.A. and EKOR, M.,
2019. Post-Market Safety and Efficacy Surveillance of Herbal Medicinal Products from
Users Perspective: A Qualitative Semi-Structured Interview Study in Kumasi, Ghana. Int J
Pharm Pharmacol 2019; 3: 136 vol. 3080, no. 2.
AGYEMANG-DUAH, W., MENSAH, C.M., PEPRAH, P., ARTHUR, F. and ABALO,
E.M., 2019. Facilitators of and barriers to the use of healthcare services from a user and
provider perspective in Ejisu-Juaben Municipality, Ghana. Journal of Public Health vol. 27,
no. 2, pp. 133-142.
AIKINS, A.D., BOYNTON, P., ATANGA, L.L., 2010. Developing effective chronic disease
interventions in Africa: insights from Ghana and Cameroon. Globalization and Health, vol. 6,
no. 1, pp. 6.
ALLAN, H.T. and ARBER, A., 2018. Emotions and reflexivity and health and social care
field research. Cham, Switzerland: Palgrave Macmillan.
ALLAN, K. and BURRIDGE, K., 2006. Forbidden words: Taboo and the censoring of
language. Cambridge University Press.

273 | P a g e
ALTHEIDE, D. and JOHNSON, J., 1994. Criteria for Assessing Interpretive Validity in
Qualitative Research. In: N.K. DENZIN and Y.S. LINCOLN eds., The handbook of
qualitative research CA: Thousand Oaks, Sage
.
ALVESSON, M. and SKÖLDBERG, K., 2017. Reflexive methodology: New vistas for
qualitative research. Sage.
AMEGBOR, P.M., 2017. Understanding usage and preference for health care therapies in a
Ghanaian context: A pluralistic perspective. Norsk Geografisk Tidsskrift - Norwegian Journal
of Geography, vol. 71, no. 5, pp. 288-300
AMIRA, O. and OKUBADEJO, N., 2007. Frequency of complementary and alternative
medicine utilization in hypertensive patients attending an urban tertiary care centre in
Nigeria. BMC Complementary and Alternative Medicine, vol. 7, no. 1, pp. 30.
ANNAN, K., KOJO, A., CINDY, A., SAMUEL, A.N. and TUNKUMGNEN, B., 2010.
Profile of heavy metals in some medicinal plants from Ghana commonly used as components
of herbal formulations. Pharmacognosy Research, 01 Jan, vol. 2 (1), pp. 41-44.
ANDERSON, B.O., CAZAP, E., EI SAGHIR, N.S., YIP, C., KHALED, H.M., OTERO, I.V.
ADEBAMOWO, C.A., BADWE, R.A. and HARFORD, J.B., 2011. Optimisation of breast
cancer management in low-resource and middle-resource countries: executive summary of
the Breast Health Global Initiative consensus, 2010. The Lancet Oncology, vol. 12, no. 4, pp.
387-398.
ANDERSON, E., 2013. Streetwise: Race, class, and change in an urban community.
University of Chicago Press.
ANKU-TSEDE, O., 2013. The Media and the Offence of Criminal Libel in Ghana: Sankofa.
The Journal of Law, Policy and Globalization, vol. 9, pp. 26-34.
ARIES, M.J.H., JOOSTEN, H., HARRY, H., WEGDAM, H.H.J. and VAN DER GEEST, S.,
2007. Fracture treatment by bonesetters in central Ghana: patients explain their choices and
experiences. Tropical Medicine and International Health, vol. 12, no.4 pp. 564-574; 564

274 | P a g e
ARORA, N.K., 2003. Interacting with cancer patients: the significance of physicians’
communication behaviour. Social Science & Medicine, vol. 57, no. 5, pp. 791-806.
ASANTE, J.Y., 2016. Data Protection and Electronic Human Resource Systems (E-Hrs): A
Case Study of Valley View University, Oyibi-Ghana. University of Ghana Digital
Collection-UG Space.
ASASE, A., AKWETEY, G.A. and ACHEL, D.G., 2010. Ethnopharmacological use of
herbal remedies for the treatment of malaria in the Dangme West District of Ghana. Journal
of Ethnopharmacology, vol. 129, no. 3, pp. 367-376; 367.
ASEWEH ABOR, P., ABEKAH-NKRUMAH, G. and ABOR, J., 2008. An examination of
hospital governance in Ghana. Leadership in Health Services, vol. 21, no. 1, pp. 47-60
ASHFORTH, B.E. and HUMPHREY, R.H., 1993. Emotional labour in service roles: The
influence of identity. Academy of Management Review, vol. 18, no. 1, pp. 88-115.
ASKINS, K., 2016. Emotional citizenry: everyday geographies of befriending, belonging and
intercultural encounter. Transactions of the Institute of British Geographers, vol. 41, no. 4,
pp. 515-527.
ATKINSON, P., 2012. Discourse, Descriptions and Diagnosis: Reproducing Normal
Medicine In: M. LOCK and D. GORDON eds., Biomedicine examined, Springer Science &
Business Media, pp. 180.
ATKINSON, P., 1992. Understanding ethnographic texts. Sage Publications, Inc.
ATKINSON, P., COFFEY., A., DELAMONT, S. LOFLAND, J. and LOFLAND, L., 2007.
Handbook of ethnography. London: Sage.
AU, A.M., KO, R., BOO, F.O., HSU, R., PEREZ, G. and YANG, Z., 2000. Screening
Methods for Drugs and Heavy Metals in Chinese Patent Medicines. Bulletin of
Environmental Contamination and Toxicology, vol. 65, no. 1, pp. 112-119.

275 | P a g e
AWUSABO-ASARE, K. and ANARFI, J., 1997. Health-seeking behaviour of persons with
HIV/AIDS in Ghana. Health Transit Rev. vol. 7 Suppl, pp. 243-56
AWUSABO-ASARE, K., ANARFI, J. and AGYEMAN, D.K., 1993. Women's control over
their sexuality and the spread of STDs and HIV/AIDS in Ghana. Health Transition Review,
pp. 69-84.
AZIATO, L. and CLEGG-LAMPTEY, J.N.A., 2015. Breast Cancer Diagnosis and Factors
Influencing Treatment Decisions in Ghana. Health Care for Women International, vol.36,
no.3, pp. 543-557
BABBIE, E.R., 2015. The practice of social research. 12th ed.Nelson Education.
BACHARACH, M. and GAMBETTA, D., 2001. Trust in signs. In: K.S. COOK ed., Trust in
society New York: Russell Sage Foundation, New York, pp. 148-184.
BACHMANN, R., 2001. Trust, power and control in trans-organizational relations.
Organization Studies, vol. 22, no. 2, pp. 337-365.
BADU APPIAH, I., 2011. Doctors’ perception of, and attitudes towards traditional herbal
medicine in Ghana. The University of Brighton, Institute of Postgraduate Medicine (Thesis)
BAHL, R., S. QAZI, G.L. DARMSTADT and J. MARTINES. Why is the continuum of care
from home to health facilities essential to improve perinatal survival? Anonymous Seminars
in perinatology, 2010.
BAILE, W.F. and AARON, J., 2005. Patient-physician communication in oncology: past,
present, and future. Current Opinion in Oncology, vol. 17, no. 4, pp. 331-335.
BAZZANO, A.N., KIRKWOOD, B.R., TAWIAH-AGYEMANG, C., OWUSU-AGYEI, S.
ADONGO, P.B., 2008. Beyond symptom recognition: care-seeking for ill newborns in rural
Ghana. Trop Med Int Health. Vol. 13, no. 1, pp. 123-8

276 | P a g e
BBC., 2018, BBC News - Ghana country profile - Overview. Available from: bbc.co.uk
BEAUCHAMP, T.L., 1982. Ethical issues in social science research. Baltimore: John
Hopkins University Press.
BECK, C.T., 1993. Qualitative research: the evaluation of its credibility, fittingness, and
auditability. Western Journal of Nursing Research, vol. 15, no. 2, pp. 263-266.
BECK, R.S., DAUGHTRIDGE, R. and SLOANE, P.D., 2002. Physician-patient
communication in the primary care office: a systematic review. The Journal of the American
Board of Family Practice, vol. 15, no. 1, pp. 25-38.
BECKER, E., 2010. Birth and death of meaning. Simon and Schuster.
BECKER, E., 2007. The denial of death. Simon and Schuster.
BEECH, N., ARBER, A. and FAITHFULL, S., 2012. Restoring a sense of wellness
following colorectal cancer: a grounded theory. Journal of Advanced Nursing, vol. 68, no. 5,
pp. 1134-1144
BERGE, P.L., LUCKMANN, T., 1967. The social construction of reality. New York:
Anchor.
BERKES, F., 1993. Traditional ecological knowledge in perspective. In: I. JULIAN ed.,
Traditional ecological knowledge: Concepts and cases Ottawa: Canadian Museum of Nature
and International Development Research Centre, pp. 1-9.
BERRY, D., 2006. Health Communication. Buckingham: McGraw-Hill Education.
BHAT, Z.A., 2012. Traditional Medicine s in drug discovery. Journal of Pharmacy
Research, vol. 5, no. 5, pp. 2457-2459
BIERLICH, B., 1995. Notions and treatment of guinea worm in Northern Ghana. Social
Science & Medicine, vol. 41, no. 4, pp. 501-509.

277 | P a g e
BIGNANTE, E., 2015. Therapeutic landscapes of traditional healing: building spaces of well-
being with the traditional healer in St. Louis, Senegal. Social & Cultural Geography, vol. 16,
no. 6, pp. 1-16
BOATENG, M.A., DANSO-APPIAH, A., TURKSON, B.K. and TERSBøL, B.P., 2016.
Integrating biomedical and herbal medicine in Ghana “experiences from the Kumasi South
Hospital: a qualitative study. BMC Complementary and Alternative Medicine, vol. 16, no. 1,
pp. 189.
BODEKER, G. and ONG, C., 2005. World Health Organization Global Atlas of Traditional,
Complementary, and Alternative Medicine. World Health Organization.
BOK, S., 1979. Lying: Moral choice in public and private life. Vintage.
BONSI, S., 1980. Modernization of native healers: implications for health care delivery in
Ghana. Journal of the National Medical Association, vol. 72, no. 11, pp. 1057-1063.
BOON, H., STEWART, M., KENNARD, M.A., GRAY, R., SAWKA, C., BROWN, J.B.,
MCWILLIAM, C., GAVIN, A., BARON, R.A., AARON, D. and HAINES-KAMKA, T.,
2000. Use of Complementary/Alternative Medicine by Breast Cancer Survivors in Ontario:
Prevalence and Perceptions. Journal of Clinical Oncology, vol. 18, no. 13, pp. 2515-2521.
BOUDIAB, D.L. and KOLCABA, D. K, 2015. Comfort Theory: Unravelling the
Complexities of Veteransʼ Health Care Needs. Advances in Nursing Science, vol. 38, no. 4,
pp. 270-278
BOULWARE, L.E., COOPER, L.A., RATNER, L.E., LAVEIST, T.A. and POWE, N.R.,
2016. Race and trust in the health care system. Public Health Reports.
BOWEN, G., 2008a. Grounded theory and sensitizing concepts. International Journal of
Qualitative Methods, vol. 5, no. 3, pp. 12-23.
278 | P a g e
BOWEN, G., 2008b. Naturalistic inquiry and the saturation concept: a research note.
Qualitative Research, vol. 8, no. 1, pp. 137-152
BOWLING, A., 2009. Research methods in health: investigating health and health services.
3rd ed. Maidenhead: Open University Press
BRAHMI, S.A., EL M'RABET F, Z., BEN BRAHIM, Z., AKESBI, Y., AMINE, B.,
NEJJARI, C., EL MESBAHI, O., 2011. Complementary medicine uses among Moroccan
patients with cancer: a descriptive study. Pan African Medical Journal, vol. 10, no, 2011,
pp. 36.
BRAITHWAITE, V. and LEVI, M., 2003. Trust and governance. Russell Sage Foundation.
BRAVO, P., EDWARDS, A., BARR, P.J., SCHOLL, I., ELWYN, G. and MCALLISTER,
M., 2015. Conceptualising patient empowerment: a mixed-methods study. BMC Health
Services Research, vol. 15, no. 1, pp. 252.
BRAY, F., FERLAY, J., SOERJOMATARAM, I., SIEGEL, R.L., TORRE, L.A. and
JEMAL, A., 2018. Global cancer statistics 2018: GLOBOCAN estimates of incidence and
mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians,
vol. 68, no. 6, pp. 394-424.
BRENNAN, J., 2017. Stealth breeding: bareback without consent, Journal of Psychology &
Sexuality, vol. 8, no. 4, pp. 318-333.
BREWER, M.B., 2007. The social psychology of intergroup relations: Social categorization,
ingroup bias, and outgroup prejudice. In: A.H. KRUGLANSKI Tory ed., Social Psychology:
Handbook of Basic Principles Guilford Press, pp. 695-711.
BRINKMANN, S. and KVALE, S., 2015. Interviews: Learning the craft of qualitative
research interviewing. Sage Thousand Oaks, CA.

279 | P a g e
BROOM, A., WIJEWARDENA, K., SIBBRITT, D., ADAMS, J., NAYAR, K.R., 2010. The
use of traditional, complementary and alternative medicine in Sri Lankan cancer care: Results
from a survey of 500 cancer patients. Public Health, vol. 124, no. 4, pp. 232-237.
BROOM, A., KIRBY, E., 2013. The end of life and the family: hospice patients’ views on
dying as relational. Sociology of Health & Illness, vol. 35, no. 4, pp. 499-513.
BROTHERIDGE, C.M. and GRANDEY, A.A., 2002. Emotional labour and burnout:
Comparing two perspectives of “people work”. Journal of Vocational Behaviour, vol. 60, no.
1, pp. 17-39.
BRUCE, J. C., 2002. Marrying modern health practices and technology with traditional
practices: issues for the African continent. International Nursing Review, vol. 49, no. 3, pp.
161-167
BRUCE, S., 2005. What Is Spirituality? New Directions for Teaching and Learning, vol. 104,
pp. 3-13.
BRUNDTLAND, G.H., 1987. World Commission on environment and development: our
common future. Oxford University Press.
BRUNER, J.S., 1990. Acts of meaning. Harvard University Press.
BRYANT, A. and CHARMAZ, K., 2019. The SAGE handbook of current developments in
grounded theory. SAGE Publications Limited.
BRYANT, A., CHARMAZ, K., 2010. Grounded theory in historical perspective: An
epistemological account. In: A. BRYANT and K. CHARMAZ eds., Handbook of grounded
theory London: Sage, pp. 31-57.
BRYANT, A. and CHARMAZ, K., 2007. Grounded Theory Methods and Practices. In: A.
BRYANT and K. CHARMAZ eds., The Sage handbook of grounded theory London: Sage.
BRYMAN, A., 2012. Social research methods. Oxford university press.

280 | P a g e
BUOR, D., 2003. Analysing the primacy of distance in the utilization of health services in the
Ahafo-Ano South District, Ghana. International Journal of Health Plann Manage. Vol. 18,
no. 4, pp. 293-311
BURFORD, G., BODEKER, G., KABATESI, D., GEMMILL, B. and RUKANGIRA, E.,
2000. Traditional Medicine and HIV/AIDS in Africa: a report from the International
Conference on Medicinal Plants, Traditional Medicine and Local Communities in Africa (a
parallel session to the Fifth Conference of the Parties to the Convention on Biological
Diversity, Nairobi, Kenya, . Journal of Alternative Complementary Medicine. Vol. 6, no. 5,
pp. 457-71.
BURGESS, R.G., 2003. Field research: A sourcebook and field manual. Routledge.
BURRELL, G., MORGAN, G., 2017. Sociological paradigms and organisational analysis:
Elements of the sociology of corporate life. Routledge.
BUSIA, K., 2005. Medical provision in Africa–Past and present. Phototherapy Research, vol.
19, no. 11, pp. 919-923.
BUTTERFIELD, A., MARTIN, D., 2016. Affective sanctuaries: understanding Maggies as
therapeutic landscapes. Landscape Research, vol. 41, no. 6, pp. 695-706
CAMERON, L. and MURPHY, J., 2007. Obtaining consent to participate in research: the
issues involved in including people with a range of learning and communication disabilities.
British Journal of Learning Disabilities, vol. 35, no. 2, pp. 113-120.
CARLISLE, R., CHOI, J., BAZAN-PEREGRINO, M., LAGA, R., SUBR, V., KOSTKA, L.,
ULBRICH, K., COUSSIOS, C. and SEYMOUR, L.W., 2013. Enhanced tumour uptake and
penetration of virotherapy using polymer stealthing and focused ultrasound. Journal of the
National Cancer Institute, vol. 105, no. 22, pp. 1701

281 | P a g e
CASSILETH, B.R. and VICKERS, A.J., 2004. Massage therapy for symptom control:
outcome study at a major cancer centre. Journal of Pain and Symptom Management, vol. 28,
no. 3, pp. 244-249.
CASTILLO-MONTOYA, M., 2016. Preparing for interview research: The interview protocol
refinement framework. The Qualitative Report, vol. 21, no. 5, pp. 811-831.
CASTLE, S.E., 1994. The (Re)negotiation of Illness Diagnoses and Responsibility for Child
Death in Rural Mali. Medical Anthropology Quarterly, vol. 8, no. 3, pp. 314-335.
CHAMBERLAIN-SALAUN, J., MILLS, J., USHER, K., 2013. Linking symbolic
interactionism and grounded theory methods in research design: From Corbin and Strauss’
assumptions to action. SAGE Open, vol. 3, no. 3, pp. 2158-2440
CHARMAZ, K., 2014. Constructing grounded theory. 2nd ed. Sage
CHARMAZ, K., 2012. The power and potential of grounded theory. Medical Sociology
Online, vol. 6, no. 3, pp. 2-15.
CHARMAZ, K., 2006. Constructing grounded theory: A practical guide through qualitative
research. London: Sage.
CHARMAZ, K., 2002. The self as a habit: The reconstruction of self in chronic illness.
OTJR: Occupation, Participation and Health, vol. 22, no. 1, suppl.
CHARMAZ, K., 1997. Good days, bad days: the self in chronic illness and time. New
Brunswick: Rutgers University Press
CHARMAZ, K. and MITCHELL, R., 2007. Grounded Theory in Ethnography, In A.
COFFEY, P. ATKINSON, S., DELAMONT., LOFLAND, J., LOFLAND, L., eds., The
handbook of ethnography London: sage publications, inc, pp. 161-172.
CHARMAZ, K. and MITCHELL, R.G., 1996. The myth of silent authorship: Self, substance,
and style in ethnographic writing. Symbolic Interaction, vol. 19, no. 4, pp. 285-302

282 | P a g e
CHEN, Z., GU, K., ZHENG, Y., ZHENG, W., LU, W. and SHU, X.O., 2008. The use of
complementary and alternative medicine among Chinese women with breast cancer. Journal
of Alternative & Complementary Medicine, vol. 14, no. 8, pp. 1049-1055.
CHOI, W. and STVILIA, B., 2015. Web credibility assessment: Conceptualization,
operationalization, variability, and models. Journal of the Association for Information
Science and Technology, vol. 66, no. 12, pp. 2399-2414.
CLARKE, A., 2012. Feminism, Grounded Theory, and Situational Analysis Revisited. In: S.
HESSE-BIBER ed., Handbook of feminist research: theory and praxis Second edition. Ed.
Los Angeles; London: Thousand Oaks, California: SAGE Publications.
CLARKE, A., 2005. Situational analysis grounded theory after the postmodern turn.
Thousand Oaks, Calif.; London: Thousand Oaks, Calif; London: SAGE.
CLARKE, A., MONTINI, T., 1993. The many faces of RU486: Tales of situated knowledge
and technological contestations. Science, Technology, & Human Values, vol. 18, no. 1, pp.
42-78.
CLARKSON, P., MACKEWN, J., 1993. Clarkson: Fritz Perls. Sage.
CLEGG-LAMPTEY, J., DAKUBO, J. and ATTOBRA, Y.N., 2009. Psychosocial aspects of
breast cancer treatment in Accra, Ghana. East African Medical Journal, vol. 86, no.7
CLEGG-LAMPTEY, J., DAKUBO, J. and ATTOBRA, Y., 2009. During treatment in
Ghana? A pilot study. Ghana Medical Journal, vol. 43, no. 3.
COFFEY, A., 1999. The ethnographic self: Fieldwork and the representation of identity.
Sage.
COFFEY, A., 1996. Making sense of qualitative data: complementary research strategies. P.
ATKINSON ed., Thousand Oaks: Sage Publications
.

283 | P a g e
COHEN, L., MANION, L. and MORRISON, K., 2011. Research methods in education. 7th
ed. London: Routledge
COLEMAN, J.S., 1994. Foundations of social theory. New ed. ed. Cambridge, Mass.;
London:
COLEMAN, J.S., 1988. Social capital in the creation of human capital. American Journal of
Sociology, vol. 94, pp. S95-S120.
COLOMBO, C., MOJA, L., GONZALEZ-LORENZO, M., LIBERATI, A. and MOSCONI,
P., 2012. Patient empowerment as a component of health system reforms: rights, benefits and
vested interests. Internal and Emergency Medicine, vol. 7, no. 2, pp. 183-187.
COOK, K.S., 2001. Trust in society. New York: Russell Sage Foundation
COOK, K.S., HARDIN, R. and LEVI, M., 2005. Cooperation without trust? R. HARDIN
and M. LEVI eds., New York: Russell Sage Foundation.
COPP, G., 1999. Facing impending death: experiences of patients and their nurses. London:
London: Nursing Times Books.
CORBIN, J., STRAUSS, A., 2008. Basics of qualitative research: Techniques and procedures
for developing grounded theory
.
CORBIN, J., STRAUSS, A., 2014. Basics of qualitative research. Sage.
COUGHLIN, S.S., EKWUEME, D.U., 2009. Breast cancer as a global health concern.
Cancer Epidemiology, vol. 33, no. 5, pp. 315-318
COUPLAND, N. and JAWORSKI, A., 1997. Relevance, accommodation and conversation:
Modelling the social dimension of communication. Multilingual, no. 16, pp. 235-258.
CRESWELL, J.W., 2012. Qualitative inquiry and research design: Choosing among five
approaches—3rd ed. Sage publications.

284 | P a g e
CRESWELL, J.W. and CRESWELL, J.D., 2017. Research design: Qualitative, quantitative,
and mixed methods approach. Sage publications.
CROTTY, M., 1998. The foundations of social research: Meaning and perspective in the
research process. Sage.
CUDMORE, H. and SONDERMEYER, J., 2007. Through the looking glass: being a critical
ethnographic researcher in a familiar nursing context. Nurse Researcher, vol. 14, no. 3.
CUNNINGHAM, A.B., 2001. Applied Ethnobotany, People, Wild Plant Use and
Conservation. London: Earth scan.
CURTIS, S., GESLER, W., PRIEBE, S. and FRANCIS, S., 2009. New spaces of inpatient
care for people with mental illness: A complex ‘rebirth ‘of the clinic. Health & Place, vol.
15, no. 1, pp. 340-348.
DAKE, F.A., 2018. Examining equity in health insurance coverage: an analysis of Ghana’s
National Health Insurance Scheme. International Journal for Equity in Health, vol. 17, no. 1,
pp. 85.
DALABA, M.A., WELAGA, P., ODURO, A., DANCHAKA, L.L. and MATSUBARA, C.,
2018. Cost of malaria treatment and health-seeking behaviour of children under-five years in
the Upper West Region of Ghana. (Research Article). PLoS ONE, vol. 13, no. 4, pp.
e0195533
DARKO, I.N., 2009. Ghanaian Indigenous Health Practices: The use of Herbs.
Researchgate.Net.
DASGUPTA, P., 2008. Trust as a commodity. In: D. GAMBETTA ed., Trust: Making and
breaking cooperative relations Oxford UK: Basil Blackwell, pp. 49-72.

285 | P a g e
DAVIDSON, C., 2009. Transcription: Imperatives for qualitative research. International
Journal of Qualitative Methods, vol. 8, no. 2, pp. 35-52.
DAVIS, E.L., OH, B., BUTOW, P.N., MULLAN, B.A. and CLARKE, S., 2012. Cancer
Patient Disclosure and Patient-Doctor Communication of Complementary and Alternative
Medicine Use: A Systematic Review. The Oncologist, vol. 17, no. 11, pp. 1475-1481
DAWES, R.M., VAN, D.K. and ORBELL, J.M., 1990. Cooperation for the benefit of us—
Not me, or my conscience. In: J.J. MANSBRIDGE ed., Beyond Self Interest Chicago, IL, US:
University of Chicago Press, pp. 97-110.
DEBAS, H.T., LAXMINARAYAN, R. and STRAUS, E.S., 2006. Complementary and
Alternative Medicine. In: T.D. JAMISON, J.G. BREMAN, and A.R. MEASHAM. Eds.,
Disease Control Priorities in Developing Countries, 2nd Edition ed. Oxford University Press,
New York: world bank, pp. 1281-1291;
DE-GRAFT AIKINS, A., 2005. Healer shopping in Africa: new evidence from a rural-urban
qualitative study of Ghanaian diabetes experiences. British Medical Journal, vol. 331, no.
7519, pp. 737-742
DEMERS, D. and VISWANATH, K., 1999. Mass media, social control, and social change:
A macrosocial perspective. Iowa State University Press.
DENNIS, A. and SMITH, G., 2015. Interactionism, Symbolic. Elsevier Ltd.
DENZIN, N.K. and LINCOLN, Y.S., 2011. The SAGE handbook of qualitative research.
Sage.
DEVINE, F., 1999. Sociological research methods in context. Macmillan International
Higher Education.

286 | P a g e
DEY, I., 2012. Grounding grounded theory: Guidelines for qualitative inquiry—Crane
Library at the University of British Columbia.
DEY, I., 2003. Qualitative data analysis: A user-friendly guide for social scientists.
Routledge.
DEY, I., 1999. Grounding grounded theory: Guidelines for qualitative inquiry. Academic
Press San Diego, CA.
DEY, I., 1993. Qualitative Data Analysis: A user-friendly guide for social scientists. London:
Routledge.
DEZIN, N.K. and LINCOLN, Y.S., 2013. The landscape of qualitative research.
DICK, S., 2010. The future of Tradition: An Ethnographic and Comparative Study of Social
Preference and Medicine in Rural Ghana. Seattle:
DICKSON-SWIFT, V., JAMES, E.L., KIPPEN, S. and LIAMPUTTONG, P., 2009.
Researching sensitive topics: Qualitative research as emotion work. Qualitative Research,
vol. 9, no. 1, pp. 61-79.
DICKSON-SWIFT, V., JAMES, E.L., KIPPEN, S. and LIAMPUTTONG, P., 2008. Risk to
researchers in qualitative research on sensitive topics: Issues and strategies. Qualitative
Health Research, vol. 18, no. 1, pp. 133-144.
DIXON, J., TENKORANG, E.Y. and LUGINAAH, I., 2011. Ghana's National Health
Insurance Scheme: helping the poor or leaving them behind? Environment and Planning-Part
C, vol. 29, no. 6, pp. 1102
DODD, N., 1994. The sociology of money: economics, reason & contemporary society.
Continuum Intl Pub Group.
DOUGLAS, M., 2003. Purity and danger: An analysis of concepts of pollution and taboo.
Routledge.

287 | P a g e
DOUMIT, M.A.A., ABU-SAAD, H.H., 2008. Lebanese cancer patients: Communication and
truth-telling preferences. Contemporary Nurse, vol. 28, no. 1-2, pp. 74-82.
DOVE, N., 2008. A Return to Traditional Health Care Practices: A Ghanaian Study. Journal
of Black Studies.
DOVI, S., 2013. Data Protection Act: Privacy and Security in the Information Age. The
Yaounde Conference.
DOWN, S., GARRETY, K. and BADHAM, R., 2006. Fear and loathing in the field:
emotional dissonance and identity work in ethnographic research. M@ N@ Gement, vol. 9,
no. 3, pp. 95-115.
DRAUCKER, C.B., MARTSOLF, D.S., ROSS, R. and RUSK, T.B., 2007. Theoretical
Sampling and Category Development in Grounded Theory. Qualitative Health Research, vol.
17, no. 8, pp. 1137-1148.
DURANTI, A., 2006. Transcripts, like shadows on a wall. Mind, Culture, and Activity, vol.
13, no. 4, pp. 301-310.
DURKHEIM, E., 2018. The division of labour in society. In: Inequality. Routledge, pp. 55-
64.
DURKHEIM, E., 2013. Professional ethics and civic morals. Routledge.
DURKHEIM, E., 2012. Moral education. Courier Corporation
.
DYE, C., BOERMA, T., EVANS, D., HARRIES, A., LIENHARDT, C., MCMANUS, J.,
PANG, T., TERRY, R. and ZACHARIAH, R., 2013. The world health report 2013:research
for universal health coverage.
EDWIN, A.K., 2010. Is routine human papillomavirus vaccination an option for Ghana?
Ghana Med Journal, vol. 44, no. 2, pp. 70-5.

288 | P a g e
EL HUSSEIN, M.T., KENNEDY, A.and OLIVER, B., 2017. Grounded theory and the
conundrum of literature review: Framework for novice researchers. The Qualitative Report.
ELSTER, J., 2015. Explaining social behaviour: More nuts and bolts for the social sciences.
Cambridge University Press.
EMERSON, R.M., FRETZ, R.I. and SHAW, L.L., 2011. Writing ethnographic fieldnotes.
University of Chicago Press.
ENSMINGER, J., 2001. Reputations, trust, and the principal-agent problem. In: K.S. COOK
ed., Trust in society New York: Russell Sage Foundation, pp. 185-201.
ERNST, E., 2002. Heavy metals in traditional Indian remedies. European Journal of Clinical
Pharmacology, vol. 57, no. 12, pp. 891-896
ERNST, E., 1998. The prevalence of complementary/Alternative medicine in cancer.
International Journal of American Cancer Society, vol. 83, no. 4, pp. 777-782.
EVANS-ANFOM, E., 1986. Traditional Medicine in Ghana: practice, problems and
prospects. Accra: Academy of Arts and Sciences Copac.
EZEOME, E.R. and ANARADO, A.N., 2007. Use of complementary and alternative
medicine by cancer patients at the University of Nigeria Teaching Hospital, Enugu, Nigeria.
BMC Complement Alternative Medicine, vol. 7, no 1, pp. 28
FABIAN, J., 2014. Time and the other: How anthropology makes its object. Columbia
University Press.
FABRICANT, D.S. and FARNSWORTH, N.R., 2001. The value of plants used in
Traditional Medicine for drug discovery. Environmental Health Perspectives, vol. 109, no.
Suppl 1, pp. 69.

289 | P a g e
FALLOWFIELD, L., 1993. Giving sad and bad news. The Lancet, vol. 341, no. 8843, pp.
476-478.
FARNES, C., BECKSTRAND, R.L. and CALLISTER, L.C., 2011. Help‐seeking behaviours
in childbearing women in Ghana, West Africa. International Nursing Review, vol. 58, no. 4,
pp. 491-497
FATHALLA, M.F. and FATHALLA, M.M., 2004. A practical guide for health researchers.
World Health Organization, Regional Office for the Eastern Mediterranean.
FAULKNER, P. and SIMPSON, T., 2017. The philosophy of trust. Oxford University Press.
FENNY, A.P., ASANTE, F.A., ENEMARK, U. and HANSEN, K.S., 2015. Malaria care-
seeking behaviour of individuals in Ghana under the NHIS: Are we back to the use of
informal care? BMC Public Health, vol. 15, no. 1, pp. 370.
FENTRESS, J. and WICKHAM, C., 1992. Social memory. Blackwell Oxford.
FETTERMAN, D.M., 2019. Ethnography: Step-by-step. SAGE Publications, Incorporated.
FETTERMAN, D.M., 2009. Ethnography: Step-by-step. Sage Publications.
FINK, M., HARMS, R. and MÖLLERING, G., 2010. Introduction: A strategy for
overcoming the definitional struggle. The International Journal of Entrepreneurship and
Innovation, vol. 11, no. 2, pp. 101-105.
FINLAY, L., 2002. Negotiating the swamp: the opportunity and challenge of reflexivity in
research practice. Qualitative Research, vol. 2, no. 2, pp. 209-230.
FOUCAULT, M., 1988. The Final Foucault. J.W. BERNAUER and D.M. RASMUSSEN
eds., Cambridge: Mit Press Cambridge, MA.
FOUCAULT, M. and RABINOW, P., 1991. The Foucault reader. Reprinted ed. London:
Penguin Books

290 | P a g e
FROWE, I., 2005. Professional trust. British Journal of Educational Studies, vol. 53, no. 1,
pp. 34-53.
GAMBETTA, D., 2008. Trust: Making and breaking cooperative relations. Oxford UK:
Basil Blackwell.
GAMBETTA, D., HAMILL, H., 2005. Streetwise: How taxi drivers establish customer's
trustworthiness. Russell Sage Foundation.
GARDNER, W.L., MARTINKO, M., 1988. Impression management in organizations.
Journal of Management, vol. 14, no. 2, pp. 321-338.
GARRETT, P., 2010. Communication accommodation theory. In: Attitudes to Language
Cambridge: Cambridge University Press, pp. 105-120.
GARVEY, G.J., HAHN, G., LEE, R.V.and HARBISON, R.D., 2001. Heavy metal hazards of
Asian traditional remedies. Taylor & Francis.
GEERTZ, C., 2017. The interpretation of cultures. New York: Basic books.
GELL, A., 1992. The anthropology of time: Cultural constructions of temporal maps and
images.
GERRISH, K., LACEY, A., 2010. The research process in nursing. John Wiley & Sons.
GESLER, W., 1996. Lourdes: healing in a place of pilgrimage.
GESLER, W.M., 2003. Healing places. Rowman & Littlefield.
GESSLER, M.C., MSUYA, D.E., NKUNYA, M.H.H., SCHÄR, A., HEINRICH, M. and
TANNER, M., 1995. Traditional healers in Tanzania: sociocultural profile and three short
portraits. Journal of Ethnopharmacology, vol. 48, no. 3, pp. 145-160

291 | P a g e
Ghana Health Service., 2017. The Patients Charter. Available from: ghanahealthservice.org.
Ghana Health Service., 2013. Ghana Health Service: your health-our concern. Available
from ghanahealhservice.org
Ghana Tourism Authority., 2019. The Brong-Ahafo Region. Available from:
https://www.ghana.travel/places-to-visit/regions/.
GIBBS, G.R., 2015. A Discussion with Prof Kathy Charmaz on Grounded Theory. University
of Huddersfield Repository.
GIDDENS, A., 1991. Modernity and self-identity: Self and society in the late modern age.
Stanford university press.
GIDDENS, A., 1990. The consequences of modernity. Cambridge: Cambridge: Polity Press
in association with Blackwell.
GIDDENS, A., SUTTON, P., 2013. Sociology. Cambridge: Polity Press.
GILES, H., OGAY, T., 2013. Communication accommodation theory. In: Bryan, Whaley,
Wendy and Samter eds., Explaining communication: Contemporary theories and exemplars
New York: Routledge, pp. 293-310.
GILGUN, J.F., 2013. Design and Analysis in Qualitative Research Twin city: University of
Minnesota
GILROY, P., 2004. After Empire: Melancholia or convivial culture? London, Routledge.
GILSON, L., 2006. Trust in health care: theoretical perspectives and research needs. Journal
of Health Organization and Management, vol. 20, no. 5, pp. 359-375.
GIRARDET, H. and ROBERTSON WINN, D., 1994. Profile of a traditional healer: Dr Oku
Ampofo Herbalgram 31. 46-51, 58. Ethnobotany, Medicines, Potential, Deforestation,
Review,

292 | P a g e
GLASER, B., 2009. Jargonizing: Using the grounded theory of vocabulary. Sociology Press.
GLASER, B., 2007. Remodelling grounded theory. Historical Social Research, Supplement,
no. 19, pp. 47-68.
GLASER, B., 2005. The grounded theory perspective III: Theoretical coding. Sociology
Press.
GLASER, B. Constructivist grounded theory? Forum, Qualitative Sozialforschung/Forum:
Qualitative Social Research, 2002.
GLASER, B., 2001. The grounded theory perspective: Conceptualization contrasted with
description. Sociology Press.
GLASER, B., 1998. Doing grounded theory: Issues and discussions. Sociology Press.
GLASER, B., 1992. Basics of grounded theory analysis: Emergence vs forcing. Sociology
Press.
GLASER, B. and J. HOLTON. 2004, Remodelling grounded theory Anonymous Forum
Qualitative Sozialforschung/Forum: Qualitative Social Research, vol.5,no.2, pp.11-21
GLASER, B., STRAUSS, A., 2017. Awareness of dying. Routledge.
GLASER, B. and STRAUSS, A., 2009. The discovery of grounded theory: Strategies for
qualitative research. Transaction Publishers.
GLOVER, T.D. and PARRY, D.C., 2009. A third place in the everyday lives of people living
with cancer: Functions of Gilda's Club of Greater Toronto. Health and Place, vol. 15, no. 1,
pp. 97-106.

293 | P a g e
GOBAH, F.K. and ZHANG, L., 2011. The national health insurance scheme in Ghana:
prospects and challenges: cross-sectional evidence. Global Journal of Health Science, vol. 3,
no. 2, pp. p90
GOFFMAN, E., 2017. Interaction ritual: essays in face-to-face behaviour. London:
Routledge.
GOFFMAN, E., 2010. Relations in public: microstudies of the public order. New
Brunswick, N.J., London: Transaction.
GOFFMAN, E., 2009. Stigma: Notes on the management of spoiled identity. Simon and
Schuster.
GOLDTHORPE, J.H. and MCKNIGHT, A., 2006. The economic basis of social class.
Mobility and Inequality: Frontiers of Research from Sociology and Economics, pp. 109-136.
GOOD, D., 2000. Individuals, interpersonal relations, and trust. In: D. GAMBETTA ed.,
Trust: Making and breaking cooperative relations Oxford UK: Department of Sociology,
University of Oxford., pp. 31-48.
GOULDING, C., 2005. Grounded theory, ethnography and phenomenology: A comparative
analysis of three qualitative strategies for marketing research. European Journal of
Marketing, vol. 39, no. 3/4, pp. 294-308.
GOULDING, C., 2001. Grounded Theory: A Magical Formula or a Potential Nightmare.
Marketing Review, vol. 2, no. 1, pp. 21.
Government of Ghana., 2015. Brong-Ahafo.[accessed Oct 2014] Available from
ghana.gov.gh
GOVINDA RAJ, R., OBUOBI, A., ENYIMAYEW, N., ANTWI, P. and OFOSU-AMAAH,
S., 1996. Hospital autonomy in Ghana: the experience of Korle Bu and Komfo-Anokye
Teaching hospitals. Boston, MA, Data for Decision Making Project, Harvard School of
Public Health.
294 | P a g e
GOZUM, S., TEZEL, A. and KOC, M., 2003. Complementary alternative treatments used by
patients with cancer in eastern Turkey. Cancer Nursing, vol. 26, no. 3, pp. 230-236.
GRANT, M.J. and BOOTH, A., 2009. A typology of reviews: an analysis of 14 review types
and associated methodologies. Health Information & Libraries Journal, vol. 26, no. 2, pp.
91-108.
GRAY, D.E., 2013. Doing research in the real world. Sage.
GRIFFITHS, S., 2009. Development and regulation of traditional Chinese medicine
practitioners in Hong Kong. Perspect Public Health, vol. 129, no. 2, pp. 64-67.
GUBA, E. and LINCOLN, Y., 1994. Competing paradigms in qualitative research. In: D,
Norman., K., Yvonna., S. Lincoln. Ed., Handbook of qualitative research, CA: Sage,
Thousand Oaks, CA.
GUBA, E. and LINCOLN, Y., 1989. Fourth generation evaluation. Sage
.
GUEST, G., BUNCE, A. and JOHNSON, L., 2006. How many interviews are enough? An
experiment with data saturation and variability. Field Methods, vol. 18, no. 1, pp. 59-82.
GULATI, R., 1995. Does familiarity breed trust? The implications of repeated ties for
contractual choice in alliances. Academy of Management Journal, vol. 38, no. 1, pp. 85-112
GYASI, R.., AGYEMANG-DUAH, W., MENSAH, C.M., ARTHUR, F., TORKORNOO, R.
and AMOAH, P.A., 2017. Unconventional medical practices among Ghanaian students: A
university-based survey.
GYASI, R., MENSAH, C. and SIAW, L., 2015. Predictors of Traditional Medicine s
Utilisation in the Ghanaian Health Care Practice: Interrogating the Ashanti Situation. Journal
of Community Health, vol. 40, no. 2, pp. 314-325

295 | P a g e
HALL, E., 2013. Making and gifting belonging: creative arts and people with learning
disabilities. Environment and Planning A, vol. 45, no. 2, pp. 244-262.
HALL, E., 1989. The dance of life: the other dimension of time. Paperback. Ed. New York:
Anchor Books.
HALL, M., CAMACHO, F., DUGAN, E., BALKRISHNAN, R., 2002. Trust in the medical
profession: conceptual and measurement issues. Health Services Research, vol. 37, no. 5, pp.
1419-1439.
HALL, M., DUGAN, E., ZHENG, B. and MISHRA, A., 2001. Trust in physicians and
medical institutions: what is it, can it be measured, and does it matter? The Milbank
Quarterly, vol. 79, no. 4, pp. 613-639.
HALLBERG, L.R., 2006. The “core category” of grounded theory: Making constant
comparisons. International Journal of Qualitative Studies on Health and Well-Being, vol. 1,
no. 3, pp. 141-148.
HALPERN, J., 2001. From detached concern to empathy: humanizing medical practice.
Oxford University Press.
HAMER, J.H., 1994. Identity, process, and reinterpretation. The past made present and the
present made past. Anthropos, pp. 181-190.
HAMMERSLEY, M. and ATKINSON, P., 2007. Ethnography: Principles in practice.
Routledge.
HAMPSHIRE, K., OWUSU, S.A., 2012. Grandfathers, Google, and Dreams: Medical
Pluralism, Globalization, and New Healing Encounters in Ghana. Medical Anthropology, vol.
32, no. 3 pp. 247-265.
HAMPSHIRE, K., HAMILL, H., MARIWAH, S., MWANGA, J. and AMOAKO-SAKYI,
D., 2017. The application of Signalling Theory to health-related trust problems: The example

296 | P a g e
of herbal clinics in Ghana and Tanzania. Social Science & Medicine, vol. 188, no, 2017, pp.
109-118.
HANDBERG, C., THORNE, S., MIDTGAARD, J., NIELSEN, C.V. and LOMBORG, K.,
2015. Revisiting Symbolic Interactionism as a Theoretical Framework Beyond the Grounded
Theory Tradition. Qualitative Health Research, vol. 25, no. 8, pp. 1023-1032
HARDICRE, J., 2014. An overview of research ethics and learning from the past. British
Journal of Nursing, vol. 23, no. 9, pp. 483-486.
HARDIN, R., 2006. Trust. Cambridge: Cambridge: Polity.
HARDIN, R., 2001. Conceptions and explanations of trust. In: K.S. COOK ed., Trust In
Society New York, NY, US: Russell Sage Foundation, pp. 3-39
HARDIN, R., 1993. The street-level epistemology of trust. Politics & Society, vol. 21, no. 4,
pp. 505-529.
HARDING, J., 2013. Qualitative data analysis from start to finish. Sage.
HARGREAVES, A., 1981. Contrastive Rhetoric and Extremist talk: Teachers, Hegemony
and the Educationist Context; In L., Barton., WALKER, S.(Eds) Schools, Teachers and
Teaching, Falmer Press.
HASAN, S.S., AHMED, S.I., BUKHARI, N.I. And LOON, W.C.W., 2009. Use of
complementary and alternative medicine among patients with chronic diseases at outpatient
clinics. Complementary Therapies in Clinical Practice, vol. 15, no. 3, pp. 152-157.
HAUSMAN, D.M., 1997. Trust in game theory. Phil Papers.
HECHTER, M. and KANAZAWA, S., 1993. Group solidarity and social order in Japan.
Journal of Theoretical Politics, vol. 5, no. 4, pp. 455-493.

297 | P a g e
HECKSCHER, C.C., 2015. Trust in a complex world: enriching community. First edition.
Ed. Oxford: Oxford University Press.
HEIMER, C.A., 1999. Solving the problem of trust. American Bar Foundation.
HELLER, K.J., 2011. The Nuremberg military tribunals and the origins of international
criminal law. Oxford: Oxford University Press on Demand.
HELMAN, C., 2007. Culture, health and illness. 5th ed. London: Hodder Arnold
HENRY, S.G., FRANCIS, A. and KOFI, A., 2013. Ethnobotanical survey of medicinal plants
used for the treatment of diarrhoea and skin ulcer in the Brong Ahafo region of Ghana.
Journal of Medicinal Plants Research, vol. 7, no. 44, pp. 3280-3285
HENWOOD, K., PIGEON, N., 2003. Grounded theory in psychological research.
HESSE-BIBER, S.N. and LEAVY, P., 2010. The practice of qualitative research. Sage
.
HEVI, J., 1989. In Ghana, conflict and complementarity. Hastings Centre Report, vol. 19,
no.4, pp.
HEWSON, M.G., 1998. Traditional healers in southern Africa. Annals of International
Medicine, vol. 128, no. 12 Pt 1, pp. 1029-34
HIRSCH, F., 2005. Social limits to growth. Routledge.
HOCHSCHILD, A.R., 2012. The managed heart: Commercialization of human feeling. Univ
of California Press.
HOFFMAN, B.D., LONG, J.D., 2013. Parties, ethnicity, and voting in African elections.
Comparative Politics, vol. 45, no. 2, pp. 127-146.
HOFSTEDE, G., 1991. Cultures and organizations: Software of the mind. McGaw-Hill,
London.

298 | P a g e
HOLLWAY, W., JEFFERSON, T., 2000. Doing qualitative research differently: Free
association, narrative and the interview method. Sage
.
HOLTON, J.A., 2007. The coding process and its challenges. The SAGE Handbook of
Grounded Theory, pp. 265-289.
HOLTSLANDER, L.F. and DUGGLEBY, W.D., 2009. The hope experience of older
bereaved women who cared for a spouse with terminal cancer. Qualitative Health Research,
vol. 19, no. 3, pp. 388-400.
HOOD, J.C., 2007. Orthodoxy vs power: The defining traits of grounded theory. In: A.
BRYANT and K. CHARMAZ eds., The Sage handbook of grounded theory London: Sage,
pp. 151-164.
HOROWITZ, R. and GERSON, K., 2002. Observation and interviewing: options and choices
in qualitative research. In: M Tim ed., Qualitative Research: An International Guide to Issues
in Practice London: Sage.
HOSKING, G., 2014. Trust: A history. OUP Oxford.
HOWARD-PAYNE, L., 2016. Glaser or Strauss? Considerations for selecting a grounded
theory study. South African Journal of Psychology, vol. 46, no. 1, pp. 50-62.
HSU, E., 2008. Medical pluralism. International Encyclopaedia of Public Health, vol. 4, pp.
316-321.
HUNT, M., 1991. Being friendly and informal: reflected in nurses', terminally ill patients' and
relatives' conversations at home. Journal of Advanced Nursing, vol. 16, no. 8, pp. 929-938.
IRWIN, K., BERTRAND, J., MIBANDUMBA, N., MBUYI, K., MUREMERI, C.,
MUKOKA, M., MUNKOLENKOLE, K., NZILAMBI, N., BOSENGE, N. and RYDER, R.,
1991. Knowledge, attitudes and beliefs about HIV infection and AIDS among healthy factory

299 | P a g e
workers and their wives, Kinshasa, Zaire. Social Science Medicine, vol. 32, no. 8, pp. 917-
930
JACKSON, J.G., CLARKE, J.H. and RASHIDI, R., 2001. Introduction to African
civilizations. New York: Citadel Press: Kensington Pub. Corp.
JAFFE, A., 2007. Variability in transcription and the complexities of representation, authority
and voice. Discourse Studies, vol. 9, no. 6, pp. 831-836.
JAMES, N., 1992. Care organisation physical labour, emotional labour. Sociology of Health
& Illness, vol. 14, no. 4, pp. 488-509.
JAMES V., 1986. Care and work in nursing the dying: a participant study of a continuing
care unit. [accessed, Dec 2015]. Available from: ethos.bl.uk.
JANES, C.R., 1999. The health transition, global modernity and the crisis of Traditional
Medicine: the Tibetan case. Social Science & Medicine, vol. 48, no. 12, pp. 1803-1820.
JARRETT, N.J., 1998. 'Comfortable ‘conversation: nurse-patient communication in the
cancer care context.
JEMAL, A., BRAY, F., CENTER, M.M., FERLAY, J., WARD, E. and FORMAN, D., 2011.
Global cancer statistics. CA Cancer Journal for Clinician, vol. 61, no. 2, pp. 69-90
JEMAL, A., CENTER, M.M., DESANTIS, C. and WARD, E.M., 2010. Global Patterns of
Cancer Incidence and Mortality Rates and Trends. Cancer Epidemiology Biomarkers &
Prevention, vol. 19, no. 8, pp. 1893-1907.
Joanna Briggs Institute, 2015. Joanna Briggs Institute reviewers’ manual: 2015
edition/supplement. Methodology for JBI Scoping Reviews. Adelaide: The Joanna Briggs
Institute.
JOHNSTON, S.L., 2002. Native American Traditional and Alternative Medicine. Annals of
the American Academy of Political and Social Science, vol. 583, pp. 195-213.

300 | P a g e
KAKUTE, P.N., NGUM, J., MITCHELL, P., KROLL, K.A., FORGWEI, G.W., NGWANG,
L.K. and MEYER, D.J., 2005. Cultural barriers to exclusive breastfeeding by mothers in a
rural area of Cameroon, Africa. Journal of Midwifery & Women's Health, vol. 50, no. 4, pp.
324-328.
KEESING, R.M. and STRATHERN, A., 1998. Cultural anthropology: a contemporary
perspective. 3rd ed, M. ROGER., A. KEESING, eds., Fort Worth; London: Harcourt Brace
College Publishers
KEITH, A. and BURRIDGE, K., 1991. Euphemism and dysphemism: language used as
shield and weapon.
KENNY, M. and FOURIE, R., 2015. Contrasting classic, Straussian, and constructivist
Grounded Theory: Methodological and philosophical conflicts. The Qualitative Report, vol.
20, no. 8, pp. 1270-1289
KINCHELOE, J.L. and STEINBERG, S.R., 2008. Indigenous knowledge in education:
Complexities, dangers, and profound benefits. In: N.K. DENZIN, Y.S. LINCOLN and L.T.
SMITH eds., Handbook of critical and indigenous methodologies Sage Thousand Oaks, CA,
pp. 135-156.
KING, A. and HOPPE, R.B., 2013. “Best practice” for patient-centred communication: a
narrative review. Journal of Graduate Medical Education, vol. 5, no. 3, pp. 385-393.
KINGHAM, T.P., ALATISE, O.I., VAN DERPUYE, V., CASPER, C., ABANTANGA,
F.A., KAMARA, T.B., OLOPADE, O.I., HABEEBU, M., ABDULKAREEM, F.B. and
DENNY, L., 2013. Treatment of cancer in sub-Saharan Africa. Lancet Oncology, vol. 14, no.
4, pp. 158.
KLEINMAN, A., 1980. Patients and healers in the context of culture: An exploration of the
borderland between anthropology, medicine, and psychiatry. Univ of California Press.

301 | P a g e
KLUFIO, G.O., 2004. A review of genitourinary cancers at the Korle-Bu teaching hospital
Accra, Ghana. West African Journal of Medicine, vol. 23, no. 2, pp. 131-4.
.
KNIGHT, J., 2001. Social norms and the rule of law: Fostering Trust in a socially diverse
society. In: K.S. COOK ed., Trust in Society New York, NY, US: Russell Sage Foundation,
pp. 354-373
KOFFMAN, J., 2006. The language of diversity: controversies relevant to palliative care
research. European Journal of Palliative Care, vol. 11, no. 1, pp. 18-21.
KOLCABA, K., 2003. Comfort theory and practice: a vision for holistic health care and
research. Springer Publishing Company.
KOLCABA, R., 1997. The primary holisms in nursing. Journal of Advanced Nursing, vol.
25, no. 2, pp. 290-296.
KPOBI, L., SWARTZ, L. and KEIKELAME, M.J., 2018. Ghanaian traditional and faith
healers' explanatory models for epilepsy. Epilepsy & Behaviour, vol. 84, pp. 88-92
KRAMER, R.M., BREWER, M.B. and HANNA, B.A., 1996. Collective trust and collective
action. In: R.M. KRAMER and T.R. TYLER eds., Trust in organizations: Frontiers of theory
and research CA: Thousand Oaks CA: Sage Publications, pp. 357-389.
KRUGLANSKI, A.W. and HIGGINS, E.T., 2007. Social psychology handbook of basic
principles. 2nd ed. New York: Guilford Press
KUHN, T.S., 1970. The structure of scientific revolutions. University of Chicago Press
KUUIRE, V.Z., BISUNG, E., RISHWORTH, A., DIXON, J. and LUGINAAH, I., 2016.
Health-seeking behaviour during times of illness: a study among adults in a resource-poor
setting in Ghana. Journal of Public Health, vol. 38, no. 4, pp. 545-553
KVALE, S., 2008. Doing interviews. Sage.
302 | P a g e
KWANSA, B.K., 2010. Complex negotiations: ‘spiritual’ therapy and living with HIV in
Ghana. African Journal of AIDS Research, vol. 9, no. 4, pp. 449-458
KWOK, C. and SULLIVAN, G., 2006. Influence of traditional Chinese beliefs on cancer
screening behaviour among Chinese-Australian women. Journal of Advanced Nursing, vol.
54, no. 6, pp. 691-699.
LAGENSPETZ, O., 1992. Legitimacy and trust. Philosophical Investigations, vol. 15, no. 1,
pp. 1-21.
LAIRD, S., 2002. The 1998 children's act: Problems of enforcement in Ghana. British
Journal of Social Work, vol. 32, no. 7, pp. 893-905.
LAMBERT, V., GLACKEN, M. and MCCARRON, M., 2011. Employing an ethnographic
approach: key characteristics. Nurse Researcher, vol. 19, no. 1.
LANDY, D., 1977. Medical systems in a transcultural perspective. In: D. LANDY ed.,
Culture, disease and healing: studies in medical anthropology. New York: Macmillan.
LANGLOIS-KLASSEN, D., KIPP, W., JHANGRI, G.S. and RUBAALE, T., 2007. Use of
traditional herbal medicine by AIDS patients in Kabarole District, western Uganda. The
American Journal of Tropical Medicine and Hygiene, vol. 77, no. 4, pp. 757-763
LANGLOIS-KLASSEN, D., KIPP, W. and RUBAALE, T., 2008. Who is talking?
Communication between health providers and HIV-infected adults related to herbal medicine
for AIDS treatment in western Uganda. Social Science & Medicine, Jul, vol. 67, no. 1, pp.
165-176.
LAPADAT, J.C., 2000. Problematizing transcription: Purpose, paradigm and quality.
International Journal of Social Research Methodology, vol. 3, no. 3, pp. 203-219.
LAST, M. and CHAVUNDUKA, G.L., 2018. The professionalisation of African medicine.
Manchester University Press.

303 | P a g e
LATOUR, B., 2013. An inquiry into modes of existence. Harvard University Press.
LAVERS, C., 2012. Stealth warship technology. London: London: Adlard Coles Nautical.
LAWTON, J., 2002. The dying process: patients' experiences of palliative care. Routledge.
LAWTON, J., 1998. Contemporary hospice care: the sequestration of the unbounded body
and ''dirty dying''. Sociology of Health & Illness, vol. 20, no. 2, pp. 121-143
LAYTON, R., 1971. Patterns of informal interaction in Pellaport. In: F.G. BAILEY ed., Gifts
and Poison. New York: Schocken Books, pp. 97-118.
LEACH, E., 1973. Structuralism in social anthropology. Structuralism: An Introduction, pp.
37-56.
LEE-TREWEEK, G. and LINKOGLE, S., 2000. Danger in the field: Risk and ethics in social
research. Psychology Press.
LEMPERT, L.B., 2007. Asking questions of the data: Memo writing in the grounded theory
tradition. The Sage Handbook of Grounded Theory, pp. 245-264.
LEVINE, D.N., 1966. Wax & gold: Tradition and innovation in Ethiopian culture.
University of Chicago Press.
LEWIS, I.M., 2002. Ecstatic religion: a study of shamanism and spirit possession.
Routledge.
LEWIS-BECK, M., BRYMAN, A.E., LIAO, T.F., 2004. The sage encyclopaedia of social
science research methods. CA: Sage Publications.
LI, S., 2004. ‘Symbiotic niceness’: constructing a therapeutic relationship in psychosocial
palliative care. Social Science & Medicine, vol. 58, no. 12, pp. 2571-2583.

304 | P a g e
LINCOLN, Y., LYNHAM, S. and GUBA, E., 2011. Paradigmatic controversies,
contradictions, and emerging confluences revisited. In: N.K. DENZIN and Y.S. LINCOLN
eds., The Sage handbook of qualitative research CA: Thousand Oaks, Sage, pp. 97-128.
LINDAN, C., ALLEN, S., CARAEL, M., NSENGUMUREMYI, F., VAN DE PERRE, P.,
SERUFILIRA, A., TICE, J., BLACK, D., COATES, T. and HULLEY, S., 1991. Knowledge,
attitudes, and perceived risk of AIDS among urban Rwandan women: relationship to HIV
infection and behaviour change. Vol. 5, no. 8, pp. 993-1002
LISZKA, J.J., 1990. Euphemism as transvaluation. Language and Style, vol. 23, no. 4, pp.
409-424.
LOFLAND, J., LOFLAND, L.H., 2006. Analysing social settings. Wadsworth Publishing
Company Belmont, CA
LOMBORG, K. and KIRKEVOLD, M., 2003. Truth and validity in grounded theory–a
reconsidered realist interpretation of the criteria: fit, work, relevance and modifiability.
Nursing Philosophy, vol. 4, no. 3, pp. 189-200.
LONG, T. and JOHNSON, M., 2007. Research ethics in the real world: issues and solutions
for health and social care. Elsevier Health Sciences.
LORD, K., IBRAHIM, K., KUMAR, S., RUDD, N., MITCHELL, A.J.and SYMONDS, P.,
2012. Measuring Trust in Healthcare Professionals—A Study of Ethnically Diverse UK
Cancer Patients.
LUHMANN, N., 2018. Trust and power. John Wiley & Sons.
MACHA, J., HARRIS, B., GARSHONG, B., ATAGUBA, J.E., AKAZILI, J.,
KUWAWENARUWA, A. and BORGHI, J., 2012. Factors influencing the burden of health
care financing and the distribution of health care benefits in Ghana, Tanzania and South
Africa. Health Policy and Planning, vol. 27, no. suppl_1, pp. i46-i54.

305 | P a g e
MACIONIS, J. and GERBER, L., 2010. Sociology, seventh Canadian edition. Don Mills:
Pearson Education, Canada.
MACKIE, G., 2001. Patterns of social trust in Western Europe and their genesis. In: K.
COOK ed., Trust in society Russell Sage Foundation, New York, NY, pp. 245.
MANGOMA, J.F., CHIRENJE, M.Z., CHIMBARI, M.J. and CHANDIWANA, S.K., 2006.
An Assessment of Rural Women's Knowledge, Constraints and Perceptions on Cervical
Cancer Screening: The Case of Two Districts in Zimbabwe. African Journal of Reproductive
Health vol. 10, no. 1, pp. 91-103.
MAO, J., PALMER, C., HEALY, K., DESAI, K. and AMSTERDAM, J., 2011.
Complementary and alternative medicine use among cancer survivors: a population-based
study. Journal of Cancer Survivorship, vol. 5, no. 1, pp. 8-17.
MARTIN, M., 1981. Native American medicine: thoughts for post-traditional healers. Jama,
vol. 245, no. 2, pp. 141-143.
MARTIN, V.B., 2006. The Postmodern Turn: Shall classic grounded theory take that detour?
A review essays. The Grounded Theory Review: An International Journal, vol. 5, no. 2/3, pp.
119-129.
MASSON, J., 2002. Qualitative interviewing: asking, listening and interpreting. In: M. Tim
ed., Qualitative Research in Action London: Sage.
Mathiot, Gervais and Gervais., 2011. Elitism. In: B. BADIE, Berg-Schlosser and L.
MORLINO eds., International Encyclopaedia of Political Science ed. Thousand Oaks, CA:
Sage.
MAUTHNER, N.S., DOUCET, A., 2003. Reflexive accounts and accounts of reflexivity in
qualitative data analysis. Sociology, vol. 37, no. 3, pp. 413-431.

306 | P a g e
MAUTHNER, N.S., PARRY, O. and BACKETT-MILBURN, K., 1998. The data are out
there, or are they? Implications for archiving and revisiting qualitative data. Sociology, vol.
32, no. 4, pp. 733-745.
MAY, T., 1998. Reflections and reflexivity. In: T.W. MAY ed., Knowing the Social World
Buckingham: Open University.
MAYER, R.C., DAVIS, J.H., SCHOORMAN, F.D., 1995. An integrative model of
organizational trust. Academy of Management Review, vol. 20, no. 3, pp. 709-734.
MBUGUA, N., 2007. Factors inhibiting educated mothers in Kenya from giving meaningful
sex-education to their daughters. Social Science & Medicine, vol. 64, no. 5, pp. 1079-1089
MCCALLUM, N.L. and MCGLONE, M.S., 2011. Death Be Not Profane: Mortality Salience
and Euphemism Use. Western Journal of Communication, vol. 75, no. 5, pp. 565-584
MCCANN, T. and CLARK, E., 2003. Grounded theory in nursing research: Part 1 -
Methodology. Nurse Researcher, vol. 11, no. 2, pp. 7-18.
MCCROSKEY, J.C., RICHMOND, V.P. and MCCROSKEY, L.L., 2006. An introduction to
communication in the classroom: The role of communication in teaching and training. Allyn
& Bacon.
MCCROSKEY, J.C. and TEVEN, J.J., 1999. Goodwill: A re-examination of the construct
and its measurement. Communications Monographs, vol. 66, no. 1, pp. 90-103.
MCGLONE, M.S. and BATCHELOR, J.A., 2003. Looking out for number one:
Euphemism and face. Journal of Communication, vol. 53, no. 2, pp. 251-264.
MCGLONE, M.S., BECK, G. and PFIESTER, A., 2006. Contamination and camouflage in
euphemisms. Communication Monographs, vol. 73, no. 3, pp. 261-282.
MCINTYRE, D., GARSHONG, B., MTEI, G., MEHEUS, F., THIEDE, M., AKAZILI, J.,
ALLY, M., AIKINS, M., MULLIGAN, J. and GOUDGE, J., 2008. Beyond fragmentation

307 | P a g e
and towards universal coverage: insights from Ghana, South Africa and the United Republic
of Tanzania. Bulletin of the World Health Organization, vol. 86, no. 11, pp. 871-876
MEAD, N. and BOWER, P., 2000. Patient-centredness: a conceptual framework and review
of the empirical literature. Social Science and Medicine, vol.4, no.7, 1087-1110
MEISSNER, F. and VERTOVEC, S., 2015. Comparing super-diversity. Ethnic and Racial
Studies, vol. 38, no. 4, pp. 541-555.
MELTON, L.J., 1997. The Threat to Medical-Records Research. New England Journal of
Medicine, vol. 337, no. 20, pp. 1466-1470.
MENA, M., WIAFE-ADDAI, B., SAUVAGET, C., ALI, I.A., WIAFE, S.A., DABIS, F.,
ANDERSON, B.O., MALVY, D. and SASCO, A.J., 2014. Evaluation of the impact of a
breast cancer awareness program in rural Ghana: a cross-sectional survey. International
Journal of Cancer. Vol. 134, no. 4, pp. 913-24.
MERTENS, D.M., 2014. Research and evaluation in education and psychology: Integrating
diversity with quantitative, qualitative, and mixed methods. Sage publications.
MESSICK, D.M., KRAMER, R.M., 2001. Trust as a form of shallow morality. In: K.S.
COOK ed., Trust In Society New York, NY, US: Russell Sage Foundation, pp. 89-117
MILLER, M., BOYER, M.J., BUTOW, P.N., GATTELLARI, M., DUNN, S.M. and
CHILDS, A., 1998. The use of unproven methods of treatment by cancer patients. Supportive
Care in Cancer, vol. 6, no. 4, pp. 337-347.
MILLIKEN, P.J. and SCHREIBER, R., 2012. Examining the nexus between grounded theory
and symbolic interactionism. International Journal of Qualitative Methods, vol. 11, no. 5, pp.
684-696.
MISZTAL, B., 2019. Trust in Habit: A Way of Coping in Unsettled Times. In: M. SASAKI
ed., Trust In Contemporary Society Social Sciences: Brill, pp. 41-59.

308 | P a g e
MISZTAL, B., 2013. Trust in modern societies: The search for the bases of social order.
John Wiley & Sons.
MOELLERING, A., SAMUILOVA, M., KUNDACINA, J., 2011. National profile of
migration of health professionals – Ghana. Brussels, Belgium: MOH Professional-Mobility
of health professionals
MOH., 2000. Ministry of Health. Medium-Term Health Strategy towards Vision 2020. Accra:
MOH.
MÖLLERING, G., 2005. Rational, institutional and active trust: just do it. In: k. BIJLSMA-
FRANKEWA and R.K. WOLLTHUIS eds., Trust under pressure: Empirical investigations
of trust and trust-building in uncertain circumstances. Edward Elgar Publishing, pp. 30.ss
MOORE, A., CARTER, B., HUNT, A., SHEIKH, K., 2013. I am closer to this place, Space,
place, and notions of home in lived experiences of hospice daycare. Health and Place, vol.
19, pp. 151-158
MORRIS, J.A., FELDMAN, D.C., 1996. The dimensions, antecedents, and consequences of
emotional labour. Academy of Management Review, vol. 21, no. 4, pp. 986-1010.
MORSE, J.M., 2015. Critical analysis of strategies for determining rigour in qualitative
inquiry. Qualitative Health Research, vol. 25, no. 9, pp. 1212-1222.
MORSE, J.M., 2010. Sampling in grounded theory. The SAGE Handbook of Grounded
Theory, pp. 229-244.
MOSHABELA, M., BUKENYA, D., DARONG, G., WAMOYI, J., MCLEAN, E.,
SKOVDAL, M., DDAAKI, W., ONDENG’E, K., BONNINGTON, O. and SEELEY, J.,
2017. Traditional healers, faith healers and medical practitioners: the contribution of medical
pluralism to bottlenecks along the cascade of care for HIV/AIDS in Eastern and Southern
Africa. Sex Transmission Infection, vol. 93, no. Suppl 3, pp.

309 | P a g e
MOSHABELA, M., ZUMA, T., GAEDE, B., 2016. Bridging the gap between biomedical
and traditional health practitioners in South Africa. South African Health Review, vol. 2016,
no. 1, pp. 83-92.
MOUNCE, H.O., 2000. Pragmatism. Nursing Philosophy, vol. 1, no. 1, pp. 80-81.
MOUSTAKAS, C., 1994. Phenomenological research methods. Sage.
MOYER, C.A., ADONGO, P.B., ABORIGO, R.A., HODGSON, A., ENGMANN, C.M.,
DEVRIES, R., 2014. “It is up to the woman’s people”: how social factors influence facility-
based delivery in Rural Northern Ghana. Maternal and Child Health Journal, vol. 18, no. 1,
pp. 109-119.
MUNN, N.D., 1992. The cultural anthropology of time: A critical essay. Annual Review of
Anthropology, vol. 21, no. 1, pp. 93-123.
MURPHY, E., DINGWALL, R., 2007. Informed consent, anticipatory regulation and
ethnographic practice. Social Science & Medicine, vol. 65, no. 11, pp. 2223-2234.
MURPHY, E., DINGWALL, R., 2001. The ethics of ethnography. Handbook of
Ethnography, vol. 339, pp. 351.
MUSARA, T.M., 1991. Interview with a traditional healer. In: M.A. MERCER and S.J.
SCOTT eds., Tradition and transition: NGOs respond to AIDS in Africa, Baltimore,
Maryland: Johns Hopkins School of Public Health, Institute for International Programs, pp.
29-34.
MWAKA, A.D., OKELLO, E.S., ORACH, C.G., 2015. Barriers to biomedical care and use
of Traditional Medicines for treatment of cervical cancer: an exploratory qualitative study in
northern Uganda. European Journal of Cancer Care, vol. 24, no. 4, pp. 503-513
MYERS, C.D., WALTON, T., SMALL, B.J., 2008. The Value of Massage Therapy in
Cancer Care. Haematology/Oncology Clinics of North America, vol. 22, no. 4, pp. 649-660

310 | P a g e
MYLONAS, Y., 2014. Crisis, austerity and opposition in mainstream media discourses of
Greece. Critical Discourse Studies, vol. 11, no. 3, pp. 305-321.
NAGELKERK, J., 1994. Nursing in Ghana. Journal of Nursing Administration, vol. 24, no.
9, pp. 17-18.
NARTEY, Y., HILL, P.C., AMO-ANTWI, K., NYARKO, K.M., YARNEY, J., COX, B.,
2016. Cervical cancer in the Greater Accra and Ashanti regions of Ghana. Journal of Global
Oncology, vol. 3, no. 6, pp. 782-790.
National Research Council., 2014. Proposed revisions to the common rule: for the protection
of human subjects in the behavioural and social sciences. Washington, District of Columbia:
The National Academies Press.
NAYAK, A., 2017. Purging the nation: race, conviviality and embodied encounters in the
lives of British Bangladeshi Muslim young women. Transactions of the Institute of British
Geographers, vol. 42, no. 2, pp. 289-302.
NDUBANI, P., HÖJER, B., 1999. Traditional healers and the treatment of sexually
transmitted illnesses in rural Zambia. Journal of Ethnopharmacology, vol. 67, no. 1, pp. 15-
25.
NEBA, N.E., 2011. Traditional health care system and challenges in developing
ethnopharmacology in Africa: Example of Oku, Cameroon. Studies on Ethno-Medicine, vol.
5, no. 2, pp. 133-139.
NEE, V., INGRAM, P., 1998. Embeddedness and beyond: institutions, exchange, and social
structure. The New Institutionalism in Sociology, vol. 19, pp. 45.
NEE, V., SANDERS, J., 2001. Trust in ethnic ties: Social capital and immigrants. In: K.S.
COOK ed., Trust in society New York: Russell Sage New York, pp. 374-392.
NEILL, S.J., 2000. Acute childhood illness at home: the parents’ perspective. Journal of
Advanced Nursing, vol. 31, no. 4, pp. 821-832.

311 | P a g e
NETTLETON, S., 2013. The sociology of health and illness. 3rd ed. ed. Cambridge:
Cambridge: Polity.
NEUMAN, L., 2005. Social research methods: Quantitative and qualitative approaches.
Allyn and Bacon.
NEUMANN, C.B., NEUMANN, I.B., 2015. Uses of the Self: Two Ways of Thinking about
Scholarly Situatedness and Method. Millennium-Journal of International Studies, vol. 43, no.
3, pp. 798-819
NGOKWEY, N., 1994. The president's illness: Culture, politics, and fetishism in Benin.
Culture, Medicine & Psychiatry, vol. 18, no. 1, pp. 61-81
NGOM, P., DEBPUUR, C., AKWEONGO, P., ADONGO, P., BINKA, F.N., 2003. Gate-
Keeping and Women's Health Seeking Behaviour in Navrongo, Northern Ghana. African
Journal of Reproductive Health / La Revue Africaine De La Santé Reproductive, vol. 7, no. 1,
pp. 17-26
NKYEKYER, K., 2000. Pattern of gynaecological cancers in Ghana. East African Medical
Journal vol. 77, no. 10, pp. 534-8.
NORTHOUSE, L.L., NORTHOUSE, G.P., 1998. Health communication: strategies for
health professionals. Stamford, Conn.: Appleton & Lange.
NOYES, J., HANNES, K., BOOTH, A., HARRIS, J., HARDEN, A., POPAY, J., PEARSON,
A., CARGO, M., PANTOJA, T., 2015. Qualitative research and Cochrane reviews.
NUNKOO, R., GURSOY, D., 2012. Residents’ support for tourism: An identity perspective.
Annals of Tourism Research, vol. 39, no. 1, pp. 243-268.
OAKES, J.M., 2002. Risks and wrongs in social science research: An evaluator's guide to the
IRB. Evaluation Review, vol. 26, no. 5, pp. 443-479.

312 | P a g e
OBI, E., AKUNYILI, D.N., EKPO, B. and ORISAKWE, O.E., 2006. Heavy metal hazards of
Nigerian herbal remedies. Elsevier.
O'BRIEN, K.S., SOLIMAN, A.S., ANNAN, K., LARTEY, R.N., AWUAH, B. and
MERAJVER, S.D., 2012. Traditional Herbalists and Cancer Management in Kumasi, Ghana.
Journal of Cancer Education, vol. 27, no. 3, pp. 573-9.
OCHENI, S., NWANKWO, B.C., 2012. Analysis of colonialism and its impact in Africa.
Cross-Cultural Communication, vol. 8, no. 3, pp. 46.
OCLOO, J.E. and FULOP, N.J., 2012. Developing a ‘critical ‘approach to patient and public
involvement in patient safety in the NHS: learning lessons from other parts of the public
sector. Health Expectations, vol. 15, no. 4, pp. 424-432.
OHMAGARI, K., BERKES, F., 1997. Transmission of Indigenous Knowledge and Bush
Skills Among the Western James Bay Cree Women of Subarctic Canada. Human Ecology,
vol. 25, no. 2, pp. 197-222.
OKOROH, J., ESSOUN, S., SEDDOH, A., HARRIS, H., WEISSMAN, J.S., DSANE-
SELBY, L., RIVIELLO, R., 2018. Evaluating the impact of the national health insurance
scheme of Ghana on out of pocket expenditures: a systematic review. BMC Health Services
Research, vol. 18, no. 1, pp. 426.
OKYEREFO, M., FIAVEH, D., 2017. Prayer and health-seeking beliefs in Ghana:
Understanding the 'religious space' of the urban forest. Health Sociology Review, vol. 26, no.
3, pp. 308-320.
OLIVER, D.G., SEROVICH, J.M., MASON, T.L., 2005. Constraints and opportunities with
interview transcription: Towards reflection in qualitative research. Social Forces, vol. 84, no.
2, pp. 1273-1289.
OLIVIER, J., SHOJO, M., WODON, Q., 2014. Faith-inspired Health Care Provision in
Ghana: Market Share, Reach to the Poor, and Performance. The Review of Faith &
International Affairs, vol. 12, no. 1, pp. 84-96

313 | P a g e
O'NEILL, O., 2002. A question of trust: The BBC Reith Lectures 2002. Cambridge University
Press.
ONG, L.M., DE HAES, J.C., HOOS, A.M., LAMMES, F.B., 1995. Doctor-patient
communication: a review of the literature. Social Science & Medicine, vol. 40, no. 7, pp. 903-
918.
OPOKU, S.Y., BENWELL, M., YARNEY, J., 2012. Knowledge, attitudes, beliefs, behaviour
and breast cancer screening practices in Ghana, West Africa. Pan African Medical Journal,
vol. 11, no. 1
OREAGBA, I.A., OSHIKOYA, K.A., AMACHREE, M., 2011. Herbal medicine uses among
urban residents in Lagos, Nigeria. BMC Complement Alternative Medicine vol.11, no 1, pp.
117
O'REILLY, K., 2008. Key concepts in ethnography. Sage.
ORLIKOWSKI, W.J. and BAROUDI, J.J., 1991. Studying information technology in
organizations: Research approaches and assumptions. Information Systems Research, vol. 2,
no. 1, pp. 1-28.
OSUJIH, M., 1993. Exploration of the frontiers of traditional practices: basis for development
of alternative medical healthcare services in developing countries. Journal of the Royal
Society of Health, vol. 113, no. 4, pp. 190-194
ÖUBERG, P., SVENSSON, T., 2010. Does power drive out trust? Relations between labour
market actors in Sweden. Political Studies, vol. 58, no. 1, pp. 143-166.
OWOAHENE-ACHEAMPONG, S. and VASCONI, E., 2010. Recognition and integration of
traditional medicine in Ghana: A perspective. Institute of African Studies Research Review,
vol. 26, no. 2, pp. 1-17.

314 | P a g e
PALTIEL, O., AVITZOUR, M., PERETZ, T., CHERNY, N., KADURI, L., PFEFFER, R.M.,
WAGNER, N. and SOSKOLNE, V., 2001. Determinants of the Use of Complementary
Therapies by Patients With Cancer. Journal of Clinical Oncology, vol. 19, no. 9, pp. 2439-
2448.
PARR, H., 1997. Mental health, public space, and the city: questions of individual and
collective access. Environment and Planning D: Society and Space, vol. 15, no. 4, pp. 435-
454.
PASHA, O., GOLDENBERG, R.L., MCCLURE, E.M., SALEEM, S., GOUDAR, S.S.,
ALTHABE, F., PATEL, A., ESAMAI, F., GARCES, A. and CHOMBA, E., 2010.
Communities, birth attendants and health facilities: a continuum of emergency maternal and
newborn care (the Global Network's EmONC trial). BMC Pregnancy and Childbirth, vol. 10,
no. 1, pp. 82.
PATTERSON, R.E., NEUHOUSER, M.L., HEDDERSON, M.M., SCHWARTZ, S.M.,
STANDISH, L.J., BOWEN, D.J .and MARSHALL, L.M., 2002. Types of alternative
medicine used by patients with breast, colon, or prostate cancer: predictors, motives, and
costs. The Journal of Alternative & Complementary Medicine, vol. 8, no. 4, pp. 477-485
PATTON, M.Q., 2002. Qualitative research and evaluation methods. New ed. Newbury
Park, California: Sage.
PATWARDHAN, B., MASHELKAR, R.A., 2009. Traditional Medicine -inspired
approaches to drug discovery: can Ayurveda show the way forward? Drug Discovery Today,
vol. 14, no. 15–16, pp. 804-811.
PELTZER, K., PREEZ, N.F., RAMLAGAN, S., FOMUNDAM, H., 2008. Use of traditional
complementary and alternative medicine for HIV patients in KwaZulu-Natal, South Africa.
BMC Public Health. Vol. 8, no 1, pp. 255
PETTIT, P., 1995. The cunning of trust. Philosophy & Public Affairs, vol. 24, no. 3, pp. 202-
225.
315 | P a g e
PILLOW, W., 2003. Confession, catharsis, or cure? Rethinking the uses of reflexivity as
methodological power in qualitative research. International Journal of Qualitative Studies in
Education, vol. 16, no. 2, pp. 175-196.
POLLNER, M., 2010. Mundane reason: Reality in everyday and sociological discourse.
Cambridge University Press.
POPE, C., MAYS, N., 2008. Qualitative research in health care. John Wiley & Sons
PORTER, S., 1997. The patient and power: Sociological perspectives on the consequences of
holistic care. Health & Social Care in the Community, vol. 5, no. 1, pp. 17-20.
POST-WHITE, J., KINNEY, M.E., SAVIK, K., GAU, J.B., WILCOX, C. and LERNER, I.,
2003. Therapeutic massage and healing touch improve symptoms in cancer. Integrative
Cancer Therapies, vol. 2, no. 4, pp. 332-344
PROBST, S., ARBER, A., FAITHFULL, S., 2013. Malignant fungating wounds – The
meaning of living in an unbounded body. European Journal of Oncology Nursing, vol. 17,
no. 1, pp. 38-45.
PROBYN, E., 2015. Outside belongings. Routledge.
PUTNAM, R.D., LEONARDI, R., NANETTI, R.Y., 1994. Making democracy work: Civic
traditions in modern Italy. Princeton university press.
PYTLIKZILLIG, L.M., KIMBROUGH, C.D., 2016. Consensus on conceptualizations and
definitions of trust: Are we there yet? In: Interdisciplinary Perspectives on Trust, Springer,
pp. 17-47.
RAMALHO, R., P. ADAMS, P. HUGGARD and K. HOARE. Literature review and
constructivist grounded theory methodology Anonymous Forum Qualitative
Sozialforschung/Forum: Qualitative Social Research, 2015.

316 | P a g e
RAPLEY, T., 2011. Some pragmatics of data analysis. In: D. SILVERMAN ed., Qualitative
research Sage London, pp. 273-290.
RCN., 2011. Research ethics: RCN guide for Nurses. RCN [accessed, Nov 2014]. Available
from: http://www.rcn.org.uk/__data/assets/pdf_file/0007/388591/003138.pdf.
REID, S.A., NG, S.H., 1999. Language, power, and intergroup relations. Journal of Social
Issues, vol. 55, no. 1, pp. 119-139.
REYES-GARCÍA, V., 2010. The relevance of traditional knowledge systems for
ethnopharmacological research: theoretical and methodological contributions. Journal of
Ethnobiology and Ethnomedicine, vol. 6, pp. 32.
RHODES, R. and STRAIN, J.J., 2000. Trust and transforming medical institutions.
Cambridge Quarterly of Healthcare Ethics, vol. 9, no. 2, pp. 205-217.
RICHARDS, L., 2014. Handling qualitative data: A practical guide. Sage.
RICHARDSON, M.A., SANDERS, T., PALMER, J.L., GREISINGER, A., SINGLETARY,
S.E., 2000. Complementary/Alternative Medicine Use in a Comprehensive Cancer Center
and the Implications for Oncology. Journal of Clinical Oncology, vol. 18, no. 13, pp. 2505-
2514
ROBINSON, N., 2006. Integrated traditional Chinese medicine
ROGOFF, B., 1990. Apprenticeship in thinking: cognitive development in a social context.
New York; Oxford: Oxford University Press Copac.
ROSE, N., 2007. The politics of life itself: biomedicine, power and subjectivity in the twenty-
first century. Princeton, N.J. ; Oxford: Princeton University Press.
ROSE, N., 2001. The Politics of Life Itself. Theory, Culture & Society, vol. 18, no. 6, pp. 1-
30

317 | P a g e
ROUSSEAU, D.M., SITKIN, S.B., BURT, R.S. and CAMERER, C., 1998. Not so different
after all: A cross-discipline view of trust. Academy of Management Review, vol. 23, no. 3, pp.
393-404.
RUBIN, H.J. and RUBIN, I.S., 2011. Qualitative interviewing: The art of hearing data. Sage.
RYAN, G.W., 1998. What do sequential behavioural patterns suggest about the medical
decision-making process? Modelling home case management of acute illnesses in a rural
Cameroonian village. Social Science & Medicine, vol. 46, no. 2, pp. 209-225.
SAHA, S., BEACH, M.C. and COOPER, L.A., 2008. Patient centeredness, cultural
competence and healthcare quality. Journal of the National Medical Association, vol. 100,
no. 11, pp. 1275-1285.
SAHA, S., TAGGART, S.H., KOMAROMY, M., BINDMAN, A.B., 2000. Do patients
choose physicians of their own race? Health Affairs, vol. 19, no. 4, pp. 76-83
.
SALISU, A. and PRINZ, V., 2009. Health care in Ghana. Austria: Austrian Red Cross.
SANCHEZ, D.T., CHAVEZ, G., GOOD, J.J., WILTON, L.S., 2012. The Language of
Acceptance. Journal of Cross-Cultural Psychology, vol. 43, no. 6, pp. 1019-1033
SANKARANARAYANAN, R., SWAMINATHAN, R., 2011. Cancer, International Agency
for Research on. 2011. Cancer survival in Africa, Asia, the Caribbean and Central America.
International Agency for Research on Cancer
SARPONG, N., LOAG, W., FOBIL, J., MEYER, C.G., ADU‐SARKODIE, Y., MAY, J.,
SCHWARZ, N.G., 2010. National health insurance coverage and socioeconomic status in a
rural district of Ghana. Tropical Medicine & International Health, vol. 15, no. 2, pp. 191-197
SATO, A., 2012. Revealing the popularity of Traditional Medicine in light of multiple
recourses and outcome measurements from a user's perspective in Ghana. Health Policy and
Planning, vol. 27, no. 8, pp. 625-637

318 | P a g e
SAWADOGO, W.R., SCHUMACHER, M., TEITEN, M., DICATO, M. and DIEDERICH,
M., 2012. Traditional West African pharmacopoeia, plants and derived compounds for cancer
therapy. Biochemical Pharmacology, vol. 84, no. 10, pp. 1225-1240.
SCHWANDT, T.A., 2001. Dictionary of qualitative inquiry. Sage Publications.
SEALE, C., 1999. The Quality of Qualitative Research. Clive Seale ed., London: England,
SAGE Publications Ltd.
SEIDMAN, I., 2012. Interviewing as qualitative research: A guide for researchers in
education and the social sciences. Teachers college press
SENDELL, P., 1997. Some Discontinuities in the enculturation of Mistassini Cree children.
In: G.D. SPINDLER ed., Education and cultural process: anthropological approaches 3rd
ed. Prospect Heights, Ill.: Waveland Press, pp. 560
SHUKLA, S., SINCLAIR, A.J., 2009. Becoming a traditional medicinal plant healer:
divergent views of practicing and young healers on traditional medicinal plant knowledge
skills in India. Ethnobotany Research & Applications, vol. 7, pp. 39-51
SIBLEY, L.M. and SIPE, T.A., 2006. Transition to skilled birth attendance: is there a future
role for trained traditional birth attendants? Journal of Health, Population, and Nutrition, vol.
24, no. 4, pp. 472.
SILVERMAN, D., 2000. Doing qualitative research: a practical handbook. Thousand Oaks,
CA; London: SAGE.
.
SIMPSON, M., BUCKMAN, R., STEWART, M., MAGUIRE, P., LIPKIN, M., NOVACK,
D., TILL, J., 1991. Doctor-patient communication: the Toronto consensus statement. BMJ:
British Medical Journal, vol. 303, no. 6814, pp. 1385.
SMITH, M.E., DANN, G., DELFENDAHL, B., FRANCILLON, G., GREENWOOD, D.J.,
HUGHES, D.T., JAFARI, J., MANNING, F.E., NARAYAN, S. and NASH, D., 1982. The
319 | P a g e
Process of Sociocultural Continuity [and Comments and Replies]. Current Anthropology, vol.
23, no. 2, pp. 127-142.
SMYTH, F., 2005. Medical geography: therapeutic places, spaces and networks. Progress in
Human Geography, vol. 29, no. 4, pp. 488-495
.
SOLAGBERU, B.A., 2005. Long bone fractures treated by traditional bonesetters: a study of
patients' behaviour. Tropical Doctor. Vol. 35, no. 2, pp. 106-8
SOSA, E., 1993. Putnam's pragmatic realism. The Journal of Philosophy, vol. 90, no. 12, pp.
605-626.
STARKS, H. and TRINIDAD, S.B., 2007. Choose your method: A comparison of
phenomenology, discourse analysis, and grounded theory. Qualitative Health Research, vol.
17, no. 10, pp. 1372-1380.
STEELE, J.R., JONES, A.K., CLARKE, R.K., SHOEMAKER, S., 2015. Health Care
Delivery Meets Hospitality: A Pilot Study in Radiology
STEIN, S.M. and HARPER, T.L., 2003. Power, trust, and planning. Journal of Planning
Education and Research, vol. 23, no. 2, pp. 125-139.
STERN, P.N., 1980. Grounded theory methodology: Its uses and processes. Image, vol. 12,
no. 1, pp. 20-23.
STEWART, M., 2003. Patient-centred medicine: transforming the clinical method. Radcliffe
Publishing.
STEWART, M., MEREDITH, L., BROWN, J.B., GALAJDA, J., 2000. The influence of
older patient-physician communication on health and health-related outcomes. Clinics in
Geriatric Medicine, vol. 16, no. 1, pp. 25.
STRAUSS, A., CORBIN, J., 1998. Basics of qualitative research: Procedures and techniques
for developing grounded theory.

320 | P a g e
STRAUSS, A., CORBIN, J.M., 2012. Basics of qualitative research: techniques and
procedures for developing grounded theory. 3rd ed. Thousand Oaks, Calif. ; London: Sage.
STRAUSS, A., CORBIN, J.M., 1990. Basics of qualitative research: Grounded theory
procedures and techniques. Sage Publications, Inc
.
STRUTHERS, R., ESCHITI, V.S., PATCHELL, B., 2004. Traditional indigenous healing:
Part I. Complementary Therapies in Nursing and Midwifery, vol. 10, no. 3, pp. 141-149
SUESS, C., MODY, M., 2017. Hospitality health capes: A conjoint analysis approach to
understanding patient responses to hotel-like hospital rooms.
SWANTZ, L.W., 1990. The Medicine Man Among the Zaramo of Dar Es Sallam. Nordic
Africa Institute
SZTOMPKA, P., 1999. Trust a sociological theory, UK, Cambridge University Press.
TABI, M., POWELL, M. and HODNICKI, D., 2006. Use of traditional healers and modern
medicine in Ghana. International Nursing Review, Mar, vol. 53, no. 1, pp. 52-58
TABI, M. and SOO, F., 2003. HIV infection of women in developing countries. International
Nursing Review, vol. 50, pp. 40-50.
TABUTI, J.R., LYE, K.A. and DHILLION, S.S., 2003. Traditional herbal drugs of
Bulamogi, Uganda: plants, use and administration. J Ethnopharmacology, vol. 88, no. 1, pp.
19-44
TAJFEL, H., 2010. Social identity and intergroup relations. Cambridge University Press.
TAJFEL, H. and TURNER, J., 1986. The social identity theory of intergroup behaviour. In:
S. WORCHEL and W.G. AUSTIN eds., Chicago: Nelson-Hall Chicago:

321 | P a g e
TAYLER, M. and OGDEN, J., 2005. Doctors’ use of euphemisms and their impact on
patients’ beliefs about health: an experimental study of heart failure.
TERAWAKI, K., SAWADA, Y., KASHIWASE, Y., HASHIMOTO, H., YOSHIMURA, M.,
SUZUKI, M., MIYANO, K., SUDO, Y., SHIRAISHI, S., HIGAMI, Y., YANAGIHARA, K.,
KASE, Y., UETA, Y. and UEZONO, Y., 2014. New cancer cachexia rat model generated by
implantation of a peritoneal dissemination-derived human stomach cancer cell line.
American Journal of Physiology-Endocrinology and Metabolism, Feb, vol. 306, no. 4, pp.
373-387.
TESCHKE, R., WOLFF, A., FRENZEL, C. and SCHULZE, J., 2014. Review article: herbal
hepatotoxicity – an update on traditional Chinese medicine preparations.
TERVALON, M. and MURRAY-GARCIA, J., 1998. Cultural humility versus cultural
competence: a critical distinction in defining physician training outcomes in multicultural
education. Journal of Health Care for the Poor and Underserved, vol. 9, no. 2, pp. 117-125
.
The Government of Ghana., 2012. The Data Protection Act (843) Protecting the Privacy of
the Individual and personal data.
The World Bank., 2015. Overview: The World Bank In Ghana. Data.worldbank.org
THOM, D.H., HALL, M. and PAWLSON, L.G., 2004. Measuring patients’ trust in
physicians when assessing quality of care. Health Affairs, vol. 23, no. 4, pp. 124-132.s
THOMAS, A., MENON, A., BORUFF, J., RODRIGUEZ, A.M. and AHMED, S., 2014.
Applications of social constructivist learning theories in knowledge translation for healthcare
professionals: a scoping review. Implementation Science, vol. 9, no. 1, pp. 54.
THOMPSON, C., 1999. Qualitative research into nurse decision making factors for
consideration in theoretical sampling. Qualitative Health Research, vol. 9, no. 6, pp. 815-828
THOMPSON, N., 2000. Theory and practice in health and social care. Changing Practice in
Health and Social Care. Sage, London, pp. 62-72.

322 | P a g e
THORNE, S. and DARBYSHIRE, P., 2005. Land mines in the field: A modest proposal for
improving the craft of qualitative health research. Qualitative Health Research, vol. 15, no. 8,
pp. 1105-1113.
TITLEY, G., 2013. Budgetjam! A communications intervention in the political-economic
crisis in Ireland. Journalism, vol. 14, no. 2, pp. 292-306.
TOLER, S., 2019. The Power of Positive Words: What You Say Makes a Difference. Harvest
House Publishers.
TOVEY, P., DE BARROS, N.F., HOEHNE, E.L., CARVALHEIRA, J.B.C., 2006. Use of
Traditional Medicine and globalized complementary and alternative medicine among low-
income cancer service users in Brazil. Integrative Cancer Therapies, vol. 5, no. 3, pp. 232-
235.
TRACY, K., 2013. Discourse and Identity, Language or Talk; In B. WHALEY and W.
SAMTER eds., Explaining communication: Contemporary theories and exemplars
Routledge.
TSEY, K., 1997. Traditional Medicine in contemporary Ghana: A public policy analysis.
Social Science & Medicine, vol. 45, no. 7, pp. 1065-1074.
TURNER, J.C., BROWN, R.J and TAJFEL, H., 1979. Social comparison and group interest
in ingroup favouritism. European Journal of Social Psychology, vol. 9, no. 2, pp. 187-204.
TWUMASI, P.A., 2005. Medical Systems in Ghana: A Study in Medical Sociology. Team,
Ghana Publishing Corporation.
TYLER, T., 2001. Why do people rely on others? Social identity and social aspects of trust.
In: K.S. COOK ed., Trust in Society New York, NY, US: Russell Sage Foundation, pp. 285-
306

323 | P a g e
TYLER, T. and BLADER, S., 2013. Cooperation in groups: Procedural justice, social
identity, and behavioural engagement. Routledge.
TYLER, T., DAWES, R.M., 1993. Fairness in groups: Comparing the self-interest and social
identity perspectives. Psychological Perspectives on Justice: Theory and Applications, pp.
87-108.
TYLER, T. and DEGOEY, P., 1996. Trust in organizational authorities: The influence of
motive attributions in willingness to accept decisions. In: R.M. KRAMER and T. TYLER
eds., Trust in Organisation Thousand Oaks, CA: Sage Publications.
TYLER, T. and HUO, Y.J., 2001. Trust and the rule of law: A law-abidingness model of
social control. New York: Russell Sage.
TYLOR, E.B., 2010. Primitive Culture. London, Bradbury, Evans and Co Printers.
Whitefriars
URQUHART, C., 2013. Grounded theory for qualitative research: A practical guide. Sage.
UTLEY, I., 2016. Ghana-Culture Smart! The Essential Guide to Customs & Culture.
Plymouth, UK: Kuperard.
UZZELL, D., VASILEIOU, K., MARCU, A.and BARNETT, J., 2012. Whose Lyme is it
anyway? Subject positions and the construction of responsibility for managing the health
risks from Lyme disease. Health and Place, vol.8, no.5, pp.1101-1109
VALSECCHI, M.G. and STELIAROVA-FOUCHER, E., 2008. Cancer registration in
developing countries: luxury or necessity? The Lancet Oncology, vol. 9, no. 2, pp. 159-167SS
VAN DEN BOOM, G., NSOWAH-NUAMAH, N. and OVERBOSCH, G.B., 2004.
Healthcare Provision and Self-medication in Ghana. Jel Classification, vol. 111, pp. H51.
324 | P a g e
VAN DER GEEST, S., 1997. Is there a role for Traditional Medicine in basic health services
in Africa? A plea for a community perspective. Tropical Medicine and International Health,
vol. 2, no. 9, pp. 903-11
VAN MAANEN, J., 2011. Tales of the field: On writing ethnography. University of Chicago
Press.
VANDEBROEK, I., VAN DAMME, P., VAN PUYVELDE, L., ARRAZOLA, S., and DE
KIMPE, N., 2004. A comparison of traditional healers’ medicinal plant knowledge in the
Bolivian Andes and Amazon. Social Science & Medicine, vol. 59, no. 4, pp. 837-849.
VERHOEF, M.J., BALNEAVES, L.G., BOON, H.S., VROEGINDEWEY, A., 2005.
Reasons for and characteristics associated with complementary and alternative medicine use
among adult cancer patients: a systematic review. Integrative Cancer Therapies, vol. 4, no. 4,
pp. 274-286
VERTOVEC, S., 2007. Super-diversity and its implications. Ethnic and Racial Studies, vol.
30, no. 6, pp. 1024-1054.
WADE, D.T. and HALLIGAN, P.W., 2004. Do biomedical models of illness make for good
healthcare systems. BRITISH Medical Journal, vol. 329, no. 7479, pp. 1398-401.
WAKEFIELD, S. and MCMULLAN, C., 2005. Healing in places of decline: (re)imagining
everyday landscapes in Hamilton, Ontario.
WALSHAM, G., 2006. Doing interpretive research. European Journal of Information
Systems, vol. 15, no. 3, pp. 320-330.
WANCHAI, A., ARMER., JM, and STEWART, BR, 2010. Breast cancer survivors'
perspectives of care practices in Western and alternative medicine. Oncology nursing forum,
vol, 37, no,4 494-500

325 | P a g e
WARREN, D.M., SLIKKERVEER, L.J., BROKENSHA, D.,Dechering, W H J C., 1995. The
cultural dimension of development: indigenous knowledge systems. London: Intermediate
Technology Publ.
WATSON, J., 2000. Male bodies: Health, culture, and identity. Open Univ Pr.
WEINRICH, S.P., WEINRICH, M.C., 1990. The effect of massage on pain in cancer
patients. Applied Nursing Research, vol. 3, no. 4, pp. 140-145
WHEELER, G., 2013. Gestalt reconsidered: A new approach to contact and resistance.
Gestalt Press.
WHO., 2013 Traditional Medicine strategy: 2014-2023. Geneva World Health Organization.
WHO., 2012. REGIONAL STRATEGY FOR TRADITIONAL MEDICINE IN THE WESTERN
PACIFIC 2011-2020. Geneva: World Health Organisation.
WHO., 2004. WHO guidelines on safety monitoring of herbal medicines in
pharmacovigilance systems. Geneva: World Health Organization
WHO., 2002. Traditional Medicine Strategy, 2002-2005. Geneva: World Health
Organisation.
WHO: Global Cancer Observatory., 2018 Cancer Population Facts Sheet (GLOBACON
Cancer Statistics).
WILLIAM, M., KUFFOUR, G., EKUADZI, E., YEBOAH, M., ELDUAH, M. and
TUFFOUR, P., 2014. Assessment of psychological barriers to cervical cancer screening
among women in Kumasi, Ghana, using a mixed-methods approach. African Health Sciences,
vol. 13, no. 4, pp. 1054-1061
WILLIAMS, M.S., 2014. A Qualitative Assessment of the Social-Cultural Factors That
Influence Cervical Cancer Screening Behaviours and the Health Communication Preferences
of Women in Kumasi, Ghana. Journal of Cancer Education, vol.29, no.5, pp.555-562

326 | P a g e
WILLIAMS, M.S. and AMOATENG, P., 2012. Knowledge and beliefs about cervical
cancer screening among men in Kumasi, Ghana. Ghana Medical Journal vol. 46, no. 3, pp.
147-51
WILLIG, C., 2013. Introducing qualitative research in psychology. McGraw-hill Education
(UK).
WIREDU, E.K., ARMAH, H.B., 2006. Cancer mortality patterns in Ghana: a 10-year review
of autopsies and hospital mortality. BMC Public Health. Vol. 6, no 1, pp. 159
WISE, A. and VELAYUTHAM, S., 2014. Conviviality in everyday multiculturalism: Some
brief comparisons between Singapore and Sydney. European Journal of Cultural Studies,
vol. 17, no. 4, pp. 406-430.
WISE, A. and VELAYUTHAM, S., 2009. Everyday multiculturalism. Springer.
WOLCOTT, H.F., 1999. Ethnography: A way of seeing. Rowman Altamira
.
WOLFINGER, N.H., 2002. On writing fieldnotes: collection strategies and background
expectancies. Qualitative Research, vol. 2, no. 1, pp. 85-93.
World Bank., 2013. Country Overview-Ghana. Worldbank.org
WUTHNOW, R., 2004. Trust as an aspect of social structure. In: J.C. ALEXANDER, G.T.
MARX and C.L. WILLIAMS eds., Self, Social Structure, and Beliefs: Explorations in
Sociology Berkeley: Univ of California Press, pp. 145-167.
YARNEY, L., BUABENG, T., BAIDOO, D. and BAWOLE, J.N., 2016. Operationalization
of the Ghanaian patients charter in a peri-urban public hospital: voices of healthcare workers
and patients. International Journal of Health Policy and Management, vol. 5, no. 9, pp. 525.
327 | P a g e
YARNEY, J., DONKOR, A., OPOKU, S.Y., YARNEY, L., AGYEMAN-DUAH, I.,
ABAKAH, A.C. and ASAMPONG, E., 2013. Characteristics of users and implications for
the use of complementary and alternative medicine in Ghanaian cancer patients undergoing
radiotherapy and chemotherapy: a cross-sectional study. BMC Complement Alternative
Medicine vol. 13, pp. 16
YEBOAH, T., 2000. Improving the provision of traditional health knowledge for rural
communities in Ghana. Health Libraries Review, vol. 17, no. 4, pp. 203-208.
YOUNG, R.A. and COLLIN, A., 2004. Introduction: Constructivism and social
constructionism in the career field. Journal of Vocational Behaviour, vol. 64, no. 3, pp. 373-
388.
ZARGER, R.K. and STEPP, J.R., 2004. Persistence of Botanical Knowledge among Tzeltal
Maya Children. Current Anthropology, vol. 45, no. 3, pp. 413-418.
ZHANG, X., 1999. Traditional Medicine Worldwide—The Role of Who. Drug Information
Journal, vol. 33, no. 1, pp. 321-326.

328 | P a g e
APPENDIXES
Appendix 1 CASP Appraisal Tool

329 | P a g e

330 | P a g e

331 | P a g e

332 | P a g e

333 | P a g e
Appendix 2: Participants Information sheet
s
334 | P a g e

335 | P a g e
Appendix 3: Consent form
336 | P a g e

337 | P a g e
Appendix 4 Interview Schedule

338 | P a g e
Appendix 5: Risk assessment

339 | P a g e

340 | P a g e

341 | P a g e
Appendix 6: Ethics Approval Certificate, University of Surrey

342 | P a g e

343 | P a g e
Appendix 7 Ethics Approval Certificate, Ghana

344 | P a g e

345 | P a g e
Appendix 8: Scientific Research Approval certificate, Ghana
Copyright © 2022 FDOKUMEN




















