



























































Tropical Medicine and Hygiene - Forgotten Books
321
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Tropical Medicine and Hygiene - Forgotten Books


TROP I CAL
MED I C IN E AND HYG I ENE




PLATE I .
Sums !) wrra La isaman'sSum.
Stages of ben ign te rt ian parasite. P lasmodium vivax .
Gametocytg ben ign tert ian .
Characteristic degen eration of red corpuscles con !
tain ing ben ign tert ian parasites (Schtiffner’s
dots) .
S tages of quartan parasite. Plasmodmm malaria .
Stages of m al ignan t tert ian (sub -MM) wh ichare seen in peripheral Mood. M iami
.
falcz'
parum.
Male gametocyte, mal ignan t tertian (sub tertian ) .
Femaie gametocyte m al ignan t tertian (sub-tert ian ) .
Doub le in fection w ith m al ignan t tert ian (subtert ian ) parasi tes of a red corpuscle ; baso
ph i l ic granules in red corpuscle .
Spirillum oi relapsing fever (stained with w hoi


22 , 23 .
PLATE 1 .
STAINED W ITH LE I SHMAN ’
S STAIN .
Stages of ben ign tert ian parasite. P lasmodium vivax .
Gam etocyteben ign tert ian .
Characterist ic degen erat ion of red corpuscles con
tain ing ben ign tertian parasites (Schuffner’s
dots) .
S tages of quartan parasi te . P lasmodium malaria .
S tages of m al ign an t tert ian (sub -tert ian ) wh ich
are seen in peripheral b lood . P lasmodi'
um
falcipcm tm .
Male gam etocyte, m align an t tert ian (sub-tert ian ) .
Fem ale gam etocyte m align an t tertian (sub -tert ian ) .
Double in fect ion w ith m al ign an t tert ian (sub
tert ian ) parasi tes of a red corpuscle ; baso
ph i l ic granules in red corpuscle .
Sp iri l lum of relapsing fever (stain ed w i th carbolfuchsin ) .
Amceba coli.
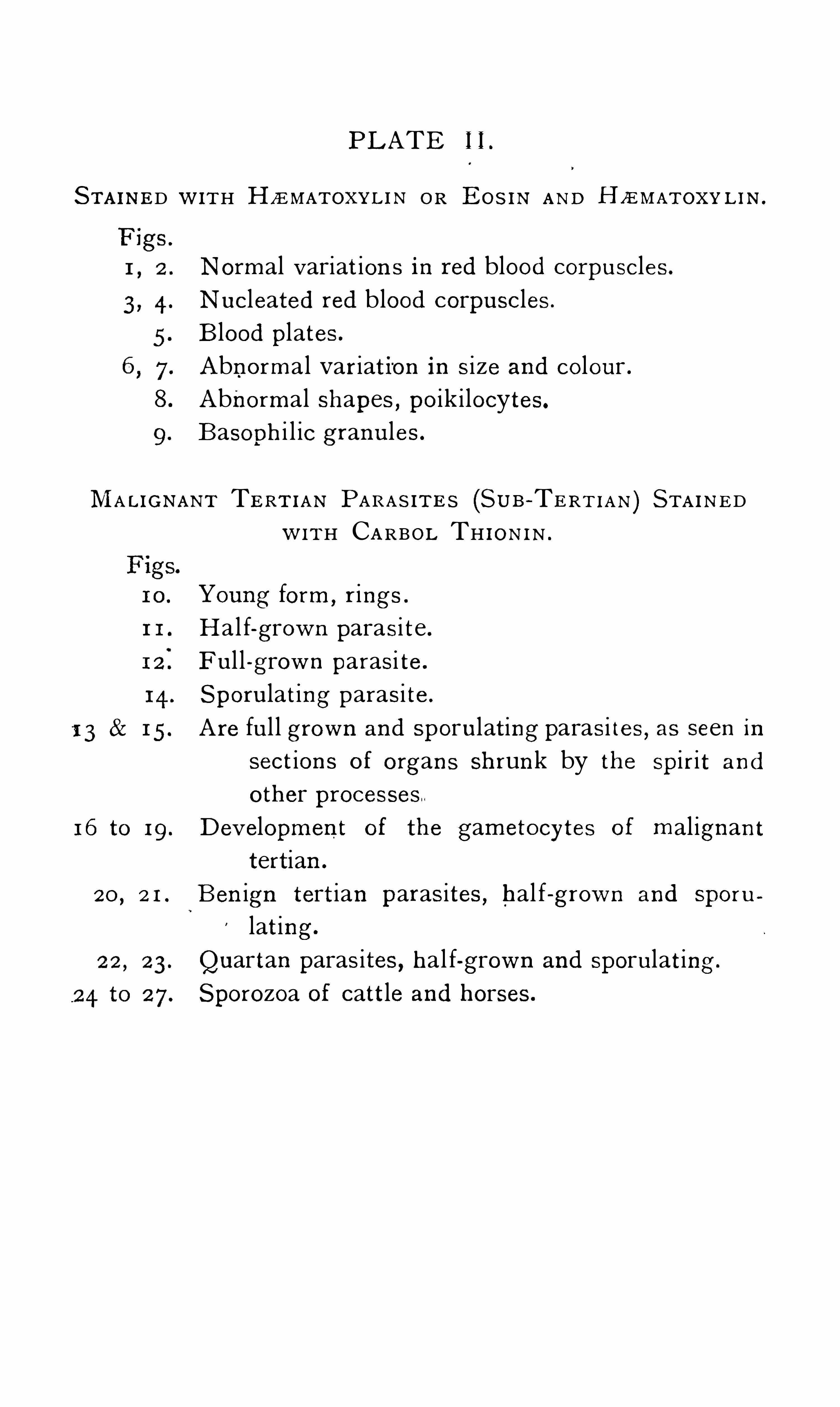
PLATE I I .
STAINED WITH HZEMATOXYL IN OR Boe AND H ZEMATOXY L I N .
N orm al v ariat ion s in red blood corpuscles.
Nucleated red blood corpuscles.
Blood plates.
Abnorm al variation in size an d colour .
Abnorm al shapes, po ik i locytes.
Basoph i l ic granules.
MALIGNANT TERT IAN PARAS ITE S (SUB—TERT IAN ) STAINED
1 1 .
1 6 to 1 9 .
20 ,2 1 .
W ITH CARBOL TH I ON I N .
Young form ,rings .
Hal f-grown parasi te .
Ful l -grow n parasi te .
Sporulat ing parasi te .
Are ful l grown an d sporulat ing parasi tes, as seen insect ion s of organs shrun k by the sp irit an d
other processes
Dev elopm en t of the gam etocytes of m al ignan ttertian .
Ben ign tert ian parasites, hal f-grown and sporu
lat ing .
Quartan parasites, hal f-grown and sporulat ing .
Sporozoa of catt le and horses.


Haaa m aruuan East er AND H
W e in red blood cprpu
MALIGNANT Taxman (SUB-Taarm
m ourn .
z é ro
hal f-grown and sp

P l a t e I I
A Ter m del Bale 5c 11 th
TROP ICAL MED IC I NE AND HYG I ENE —Part l .


TROPICAL MEDIC IN EAND
HYG IEN E
cl? 9°
A N I E L S
Lecturer on Tropical D iseases, Lon don Hospital ; London (Roy al Free) Scbool
ofMedzcm efor Wom en ; Pfiy si'
czan , Albert D ock Hospital, Seamen’
s Hospital
Society , former ly D irector Lon don Sc/zool of Tropzcal Mea’i '
;czn e D i rector
I n stitute for Mea’zcal Researc/z , Federated Malay S tates , Member of Royal
SocietyMalar ia Comm ission , an d in the B rit t'
s/z Guian a , and Fij i Colon ial
Medical Serv ices
IN THREE PARTS , WITH COLOURED AND OTHER ILLUSTRATIONS
PART I .
D ISEASES DUE TO PROTOZOA
S ECOND EDITION
I onbon
JOHN BALE , SONS DAN IELSSON , LTD .
’
OXFORD HOUSE
83-9 1 , GREAT TITCHFIELD STREET, OXFORD STREET, W.
1 9 1 3
ALL RIGHTS RESERVED


PREFACE .
T HE exigen c ies Of trop ical practi ce requ ire mostmedical m en to be pract i cal san i tar i an s as wel l ascl in ic i an s .I t i s with th i s in V i ew that in the presen t work
,whi le
due atten t ion has been paid to the cl in i ca l features,treat
m en t an d n urs ing of trop i cal d iseases , spec ial promin en cehas been given to th ei r et i ology an d preven t i on .
Ow ing to the recen t advan ces in the kn owledge Of theet iol ogy of many trop ical d iseases the subj ect of the irprophylax i s i s a very promising on e
,s in ce the gen eral
prin c iples on which effic ien t an d econ omical preven t ivemeasures should be based are n ow wel l un derstood .
In the appl i cat i on of such gen eral prin c ip les localcon d it ion s must be careful ly con s idered
,and thus in
d escrib ing the vari ous methods to be adopted thosesu i table for certa in l ocal i ti es have been g iven as types .l n the spread of many trop ical d iseases in termed iate
hosts play an importan t part, an d the l i fe-history of suchhosts
,Often in sects
,has been con s idered at some length
,
as a kn owl edge of this subj ect i s essen t ial to the properunderstan ding of the rat ion ale Of the preven t ive measuresproposed .
An attempt has been made to group the d iseases treatedof accord ing to the ir kn own or probable causat ion .
Thus,in the first part those d iseases are dealt with which ,
l ikeMalar ia,are kn own to be due to Protozoa
,an d others
,
such as Yel low Fever,which are probably due to such
Organ i sms .In the secon d part di seases due to the h igher forms
of an imal l i fe are con s idered .

vfiL PREFACE
The th ird part i s devoted to bacter ial d i seases,to th e
effects Of certain an imal an d vegetab le po i son s , an d tocerta in di seases the causat i on of whi ch is un kn own or
but imperfectly un derstood .
The advan tages o f th i s arrangemen t are con s iderable,
as the gen eral outl i n e Of t he prophylact i c measuresrequ i red d iffers for the d iseases descr ibed in each part .Thus the measures descr ibed in th e firs t part aremostly d i rected again st arthropoda
,i n sects or arachn ida
,
which act as in termed iate or altern at ive h osts for themalari al an d other protozoal paras ites . The measuresdescr ibed in the th ird part
,in clud ing as they do those
for deal in g with cholera,en teri c fever an d plague ,
involve the con s i derat ion of th e protect i on Of watersuppl ies
,the d i sposal Of sewage
,d is in fec t i on an d other
san i tary problems wh i l e the measures deal t wi th in thesecon d part in clude some directed again st in sects
,as in
th e case of filariasis,an d others
,e.g .
,those for the preven
t i on o f en demic haematuria an d an kylostomiasis,deal ing
with the water suppl ies an d sewage d isposal ; in bothcases
,however
,in volving somewhat d i fferen t problems
from those d iscussed in the other two parts of th i s work .
Su itable techn i cal methods Of a s impl e character,as
wel l as data an d measuremen ts in common use,are given
in an appen d ix to each part .We are much in debted to n umerous fri en ds an d paststuden ts o f the Lon don School
'
Of Trop ical Medi c in efor valuabl e h in t s an d a id in revi s i on o f proofs . Maj orJ. B . Smith
,Maj or j . H . McDon ald
,of th e
Dr. Ven is, an d Dr. H . B . N ewham must be spec ial lymen t i on ed . The charts used for the i l lustrat ion s are inmost in stan ces those Of pat i en ts at the Al bert DockHosp ita l o f the Seam en
’
s Hosp ital Society,to wh ich is
attached the Lon don School of Trop icalMed ic in e .


CONTENTS .
CHAPTER I . PAGE
I n troduction , Classification , an d Life H istory of Protozoa
CHAPTER I I .
Sporoz oa, Genera l
CHAPTER I I I .
Ben ign Ter tian, Quartan , an d Sub ter tianMalaria
CHAPTER IV .
D iagnosis, Patho logy , an d Treatm en t of Ben ign Ter tian and
QuartanMalar iaCHAPTER V .
D iagnosis, P rognosis, an d Treatm en t of Sub tertian MalarialFever ; Managem en t an d Nursing ; Compl icat ion sSpecia l Cases Malarial Cachexia ; Sequelae
CHAPTER V I .
Prophy laxis and E t io logy of SubtertianMalar ial Fever Mosquitoes ; N o table Dates
CHAPTER V I I .
Prognosis, Susceptib i l ity , Patho log ical Anatomy and Treatm en t of Blackwater Fever ; Nursing ; P irop lasma ; Prophy laxis
CHAPTER V I I I .
CHAPTER IX .
Geog raph ical D istribut ion , Cl in ical Course, D iagnosis and
Treatm en t of Yel low Fever ; P rophy lax is Sh ip Epidem ics I 1 5
CHAPTER X .
Geograph ical D istr ibution , Cl in ical H isto ry, Varieties, D iagn osis, P rognosis, Patho log ical Anatomy, an d Treatm en t
of S leeping S ickn ess ; Nursing ; Et iology

xfi . CONTENTS
CHAPTER X I .PAGE
D efin i tion,Geograph ical D istr ibution , C l in ical Course, Patho
log ical Anatomy , D iagnosis, P rognosis,E tio logy an d
Treatm en t of Kala-azar ; D igestive, Respi rato ry an d
Cutan eous Systems ; P reven t ion ; Variet ies—C l in icalCourse , Patho logy, E tio l ogy and Treatm en t of Juven i leKala-azar . Can ine Leishman ia
CHAPTER X I I .
Et iology , D iagnosis, Treatm en t and P reven tion of O r ien ta lSo re
CHAPTER X I I I .
I ncubation , C l in ical Course , Com pl icat ion s, P rognosis, D iagn osis, Mo rb id Anatom y, E tio logy and Treatm en t of
Re lapsing Fever
CHAPTER X IV .
D iagnosis an d Treatm en t of Tick Fever ; P i Ophylaxis ;Var iet ies
CHAPTER XV .
D iseases associated w ith Spirochmtae in the Tissues
CHAPTER XVI .
I n testinal Protozoa,&c.
CHAPTER XV I I .
P rophy lax is in P rotozoa] D iseases Résum é
APPEND ICES .
( i ) No tab le Dates—(i i ) Im portan tMeasurem en ts— ( i ii ) Ticks
IN DEX

L I ST OF I LLUSTRAT ION S .
PLATE I,con tain in g 23 coloured figures
PLATE I I,con tai n ing 27 co loured figures
FIG . 1 .—Show ing the D evelopm en t of Coccid ia
2 .—Pi roplasmata
3 .—Haem og regarin es of F rog
4 ,—Ar rangem en t-o f the Red Cel ls in a F resh F luid Fi lm5 .—D etai l ofMethod of m aking Blood Fi lm s
6 .
—Asexual and Sexual Phases in the D eve lopm en t of the
Quartan Parasite7 .
—Asexual and Sexual Phases in the D evelopm en t of the
Ben ign Tert ian Parasi te,P lasm oa
’
izcm v iz/ax
8 .
—Asexual Phases in the D eve lopm en t of the Ma l ignan tMalar ial Parasi te , P .falcz;fiarum
9 .
—Showin g the D evelopm en t ofMalarial ParasiteI O .—Tem perature Chart of S im ple Ben ign Tertian Fever
D ouble Tert ian FeverQuartan FeverD ouble Quartan FeverSub tert ian Malar ia w i th defin iteTertian Per iod icity
Subtert ian Malar ia,Per iod icity
sti l l defin iteSubtertian Malar ia Per iod icityindefin ite
SubtertianMalar ia un treatedSevere Subter t ian Malaria(treated )
1 9 . Hyperpy rex ia inMalar ia20 .
—Parasites in Capi l lar ies of PancreasCapi l lary from I n test in e
22 .— Cul icin e m ale an d female an d An ophel in e m ale an d
fem ale3 .
-Var ious form s ofWing Scales
I 2
I S
1 6
2 5
27
34
3 5
36
37
42
42

LIST OF ILLUSTRATIONS
PAGE24 .
—Lateral Views ofAn ophel in e and Cul icine,Anophel ine
an d Cul icine viewed from above, head Of Co reth raandMegarhin ina
25—
. D iag ram showin g percen tage ofN eg roes harbour in gMalaria Parasites
26 .—D iag ram showing pe rcen tage ofNegroes’ bod ies having
en larged spleen s27 .—D iagram show ing percen tage ofN egroes
’ bod ies havin gpigm en ted spleen s
28 .—Tem perature Chart of m i ld attackof Blackwater Fever
29. seve re3o . relapsin g case of Blackwater
Feve r3 1 .
—Spectra32 .
—Rabb it’s kidn ey in heal th during exper im en tal haemo
g lob inuria, and in suppression Of urin e fo l lowin gBlackwater Fever
33 .—A renal tubule show ing n ormal con d ition , comm en cin g
deposi t in haem og lob inuria an d obstruction of the
tubules in the pyram id34 .
—Temperature Chart of Yel low Feve r simplex3 5 . severe attack of Yel low36 . Trypan osom iasis, wi th adm in is
tration of soam in
Trypan osom iasis, th i rd and fifthweeks
Trypan osom iasis, th ree m on thslater
39. Trypan osom iasis,, w ith in t ravenous inject ions of tartarem etic.
4o . Trypan osom iasis4 1 . later cond ition42 .
—Cli ild w i th Trypan osom iasis43 . Glossina
44 .
—Trypan osom es mul tip lyin g asexual ly by long itud inald iv ision
45 .—Temperature ChartOf Kala-azar Simulat ing typhoid “
46 . later , show ing in term i tten t type
47 . undulating type

LIST OF I LLUSTRATIONS XV
PAGE48 .
— Fi lm show ing Parasites of Kala-azar—LeishmanD onovan Bod ies 1 6 5
49 .—Trypan oson1es an d the al tered fo rm s found in cul ture 1 69
50 .—A case of Leishman iasis from South Am er ica face 1 76
5 I .—G rowths on face , n eck and left arm , in a case o f
Or ien tal So re52 .—Grow ths on n eck ( X from case in fig . 5 1
53 .
—Tem perature Chart of case of Relapsm g Fever fromI n d ia
54 ._s
'
rillzcne oberm eieri
5 5.
— P ea’iculus v estim en torw n
56 .
— 0rn itnoa’
orzes m ozeoata
57 .
—Case of Yaws‘
58 .
59 . on So le of Foot60 . invo lving Trunk and Lim bs6 I .
—Granuloma of the Pudenda62 .
63 .
64 .— Ba lan ticlium coli
6 5 .
— Schem e of D evelopm en t ofAmoeba66 .
—Tem perature Chart of Hepat ic Abscess with I rregularPyrexia
67 .
—Tem perature Chart in Amoeb iasis with Liver Abscessyie ld in g to Ipecacuanha
68 .-N eurat ion ofWing of Cul icidae
69 .
— Sect ion s of D rain s70 .
- P ltleboto/n zes
7 I .—Mouth -
parts of [xoa’es72 . a picep/zalzcs
73 . Arg asin a


2 TROPICAL MED ICINE AND HYG I ENE
an d to vary from t ime to t ime with ou t any Obviou sreason . With Cl oser study the reason s for such variat ion s can somet imes be traced . The varyi ng resul ts ofprophylact i c measures d irected aga in st such d i seases ,though on th e whole sat i sfactory
,are O ften expl i cab le by
the var iat ion s in these factors when th e causes o f thevariat i on s are kn own .
The d ist in ct ion between plan ts an d an imal s,so Obvious
in the h igher members o f these k ingdom s,i s l ess defin i te
in the un i cel lular organ i sms . Such dist i n ct i on s as thepresen ce or absen ce of chlorophyl l
,the absorpt i on or
assimi lat i on of n i trogen an d carbon from thei r in organ i ccompoun ds
,or on ly from h igher organ i c compoun ds,
are not con clus i ve . Th ose organ i sms most cl osely relatedto the vegetabl e kingdom an d those that appear to bean imal may e i ther be moti l e or n on -moti le . In SO manyin stan ces i s i t imposs ibl e to determ in e whether the
l owly un i cel lu lar organ i sms are an imal or vegetable,
t hat H aeckel proposes to make a separate kingdom ofsuch forms wh ich he cal l s PROTISTA.
The un i cel lular o rgan i sms approximat ing in most oft he ir Characters to the an imal kingdom are kn own as theProtoz oa .
In warmer cou n tr i es the d i sea ses due to paras i tesw i th characters in th e main an imal are of more spec ia limportan ce than t hose caused by paras ites of the samed iv is i on in cold cl imates . The di seases of cold cl imatesare usual ly due to parasi tes l ike bac i l l i
,which are al l i ed to
the vegetabl e k ingdom . Many of these di seases are worldwide in th e i r d istr i but i on .
The protozoa for th i s reason are first con s idered .
Protoz oa are un i cel lular organ i sms . The cel l s may beaggregated together in masses
,or may occur s ingly .
Frequen tly parts o f th e cel l s are spec ial ly modified forspeci al purposes, such as locomot ion , so that flagel la orc i l ia are formed , whi l st in other in stan ces a part on lyof the cel l i s con tract i l e and exh ib its amoebo id movemen t .Many of th e protozoa are n on -paras i t i c ; others are

INTRODUCTORY 3
paras it ic on ly in the lower an imals . Some are paras i t i cd uring a port ion on ly Of the i r exi sten ce, whilst oth ers are
p arasi t ic in en t i rely d i fferen t an imals during the d ifferen tstages of developmen t .I t i s proposed to con s ider in detai l on ly the protozoa
paras i t i c in m an,with bri ef referen ce to protozoa parasi t i c
in other an imals .The kn owledge o f di sease- caus ing protozoa is advan c ingso rap idly that some i n format ion as to paras ites of otheran imals may at any t ime become of importan ce in humanpathology .
The Protozoa are div ided i n to four groups
( I ) Sarcod ina in clude al l forms which -move by theprotrus ion of protoplasm either as blun t an d broad pro
cesses or sharp an d th in processes . They may be n akedo r covered in part with shel l s . Mult ipl i cat i on i s by budd ing o r fiss i on occas ion al ly spores are formed .
(2) Mastigophora or Flagella ta are provided with moti l eapparatus spec ial ized for the purpose an d con s i st ing o fo ne or more flagel la . All parts Of the cel l en ter i n to theformat i on of the flagel lum . The body i s usual ly Of awel l -defin ed shape an d covered with a cut icl e or memb ran e . Mult ipl i cat i on i s by long i tudin al fiss ion .
(3 ) Sporoz oa are un i cel lular paras i tes l iv ing during a
p ort ion of their l i fe in cel l s an d mult iplyin g by thed ivi si on o f the whole or part Of the protoplasm in toyoung organ i sm s common ly cal led “ spores
,
” more correctly termed merozo i tes .
(4) Cilia ta (I nfusoria) . The motor apparatus i s in th eform of C i l i a wh ich may be e ither S imple or un i ted in tomembran es . These are formed from the ectosarc on ly .
Reproduction i s effected by tran sverse d ivi s i on or budding .
Rarely spores are formed .
Of these classes i t wi l l be conven i en t to con s ider firstthe Sporozoa .
Researches,especia l ly those o f Schaudin n
,have gon e
far to throw doubt on th i s C lass ificat ion,for h is work
,i f
c on firmed , would prove that the di st in ct ion between the

4 TROPICAL MEDICINE AND HYG I ENE
fl agel lata an d the sporozoa i s n o t a soun d on e, as flagell ates have a qu iescen t stage when they resemble sporozoa .
Much more work is n ecessary in con n ect i on with th eprotozoa an d thei r sexual cycles an d tran sformat i on sbefore we can safely al ter the presen t usual class ificat i on
,
an d any premature attempts at regroup ing these organ i smsare to be deprecated .
Developmen t an d Life-history.-Th is i s n ot kn own in all
th e gen era, but where i t i s ful ly kn own two methods ofmult ipl icat i on can be Shown to occur—asexua l or vegetat ive
,and sexua l. As a type of the l i fe -h istory an d method
of reproduct ion o f th e sporozoa that o f coccid i a may betaken as an example . The an alogi es wi th th e developmen t Of the malari a parasi tes wi l l be con s i dered withthem .
In the cocc id ia, en tran ce to the warm-blooded hos t
IS gain ed through the al imen tary can al . The youn gcocc id ia Spores
,sporoz oites, are set free from the cyst in
which they are con ta in ed by the act i on of the d igest ivej u ices an d pen etrate in to the ep i thel ial cel ls o f th ein test in al mucosa, or of one of the appen dages Of the
i n test in e such as th e b i l e passages and th e l iver .When t he young cocc id i a have en tered such a ce l l
they grow un t i l t hey have en t i rely fi l led an d destroyed it .D iv is i on of th e protoplasm of the cocc id ium n ow takesplace . The outer part o f th is has formed a cyst wal l
,an d
thus a cyst i s formed con ta in in g a large n umber of youn gcocc id ia or spores . The cyst wal l then ruptures , theyoung cocc id ia are l iberated an d pass in to other in testinal or hepat i c cel l s . The process is repeated over andover again ,
an d m ass ive tumours are thus formed by thecocc i d ia wh ich have mult ip l i ed asexual ly . Coccid i a wh i chdevelop in to asexual forms are kn own as “ sch izon ts .Some of the spores of young cocc idia develop in a d i fferen t man n er . NO d ivis i on of the cel l con ten ts takesplace
,but th e protoplasm remain s un divided with a
s ingle n ucleus . A weak spot in the cyst wall,kn own
as the micropyle , i s presen t . Such forms are the femal e

INTRODUCTORY 5
forms,macrogametes
,of the cocc id ia . Again
,in other
coccid ial cel ls,when they have reached thei r maximum
stage of growth,the cel l con ten ts d ivide i n to a mass o f
bodies smal ler an d more act ively moti l e than the spores .The smal l act ively moti le bod i es are the male fert i l iz ing
FIG . 1 .- D iagram of developmen t of Coccid ia . Endogenous l ife includes
the asexual cycle and the fert i li zat ion of the m acrogam ete by the m icrogam ete .
The further developm en t does not require an al ternate host . I t takes placeon the ground .
elemen ts equ ivalen t to spermatozoa,an d are kn own as
m icrogametes. When the cyst con ta in ing them rupturesth e microgametes are set free an d pen etrate through themicropyle of the macrogamete an d fert i l ize i t .In the fert i l ized macrogamete
,n ow kn own as th e
oocyst,various changes occur an d the micropyle i s cl osed

6 TROPICAL MEDICINE AND HYG IENE
so that the cyst wal l i s complete . The cyst i s d i schargedan d passed with the faeces Of the host . Devel opmen to f the con ten t s takes place
,the cel l m ass d ivides in to
four,an d in each of these four d ivi s i on s two spores
“ sporozo ites —are formed . This stage of developmen ttakes p lace in th e oocysts as they l ie on the groun d
,n o
host being n ecessary in th i s stage . Th i s i s th e sexualform of mult ip l i cat i on . U l t imately, when the cyst i sswallowed by a su i tabl e host , the capsu le i s d i sso lved , thesporozo i tes are l iberated in the al imen tary can al an d
en ter cel l s in the mucosa or pass up the bi l e ducts inthe ' liv er an d there recommen ce the cycle Of even tsdescr ibed
,mult iply ing asexual ly to form mass ive tumours
,
or becoming sexual forms,gametocytes
,male or female .
Th i s protozoal in fect i on i s common in rabb i ts i t hasbeen descr ibed in m an
,but i s certain ly extremely rare .
I t forms a good example of a sporozoal organ i sm,paras it i c
during i ts stages of growth an d asex ual mult ip l i cati on,
but n ot throughout the whole o f i ts sexual developmen t
(fig .
The gen eral plan of developmen t Of the paras ites Of
malaria resembles t h i s to some exten t, but there areimportan t d ifferen ces .By cocc id ia n o secon d host i s requ ired . Con j ugat ion
takes p lace in the warm-blooded host an d ful l sexualdevelopmen t outs ide un der ord in ary con d i t i on s
,but for
many of the protozoa a secon d host i s requ ired an d the
developmen t in th i s secon d or altern ate host d i ffers fromthat in thefi rst host .I n termediate an d defin i t ive hosts are more precise
terms . The defin i t ive host i s the host in which the
sexual processes of mult ipl i cat ion or reproduct i on are
carr i ed out . In the case of the paras i tes of malaria thedefin i t ive host i s the mosqu i to .
I n termediate hosts are those in which the asexualmethod of mult ip l i cat i on i s carried out ; e.g .
,m an i s the
in termediate host of the malari a paras i te .
I n sects or other altern ate hosts are n o t requi red for

INTRODUCTORY 7
the propagation of al l the var ious protozoa wh i ch caused isease
,as in some
,such as the cocc id ia an d Ama ba
coli,part of the de vel opmen t takes p lace in earth or
in water without an altern at ive host .I n ver tebrate hosts : The common est altern at ive hosts ,
e ither i n termediate or defin i t ive,are in sects
,but some of
the t i cks,ixod in ee an d argasinae , may al so serve as hosts .
I n sects are in fected with an imal paras ites in vari ousways
( 1 ) The blood-suck ing in sects draw up with theblood any smal l parasi tes presen t in that fluid
,such as
the paras ites o f m alar ia . These parasi tes develop ing an d
multip lying in the in sect host are ult imately in j ected in toa warm -blooded host—m an in th i s in stan ce—an d mult iplyagain in that host .
(2) In other cases , as in the developmen t o f p iroplasmata an d the sp irochae ta in t i cks
,the developmen t
Of the paras i tes taken up wi th the blood is con t in ued inthe eggs o f the host
,an d the ful l developmen t does n o t
take place t i l l the eggs are hatched an d the young t icksare suffic ien t ly d evel oped to b i te a warm -blooded host
,
when they wi l l tran smi t the in fect i on .
(3) The parasi tes drawn up wi th the blood maydevelop in the lumen or wal ls of the al imen tary canaland the sporozo i tes may be discharged with the faeces .
(4) The larvae of th e in vertebrate host l iving in waterbecome in fected di rectly through their food with protozoa .
These then develop an d, as in the case o f a mon ocyst is
described by Ross,mult ip ly after. en cystmen t
,so that
when the in sect has attain ed its perfect form theimago— it h arbours very n umerous paras ites which aredeposi ted with the excremen t and then l ive an in depen
den t exi sten ce t i l l they re-en ter other larv ze . I t i sposs ible that many of the flagellata are thus tran smitted .
Protozoa are n o t the on ly parasi tes for wh ich invertebrates act as hosts . Several o f the metazoa are conveyedin a S imi lar man n er. Bacteri a also can be conveyed bysuch hosts . In some in stan ces the in sects merely act

8 TROPICAL MEDICINE AND HYG IENE
as mechan i cal carr i ers . Thus the ord in ary house-flymay
,after al ight ing on th e excre ta-of a typho id pat ien t
,
carry the baci l l i t o human food,such as mi lk
,directly .
In other in stan ces , blood-su cking i n sects take up bacteria ,such as th ose o f p lague an d l eprosy
,an d m ay ,
in theformer case at l east
,in fect other an imals .
The bacteri a presen t in the water in wh ich larvae l iveare taken up by such larvae
,an d in some i n stan ces
,e.g .
,
Bacillus pyocya neus, th e bacter ia con t in ue to l ive durin gthe various stages o f developmen t o f the l arvae an d maybe widely d i str ibuted by the adul t in sect or imago .
The con veyan ce of h elmin th es an d of vegetable organ i smsby in sects wi l l be con s idered in Part I I an d Part I II .
ORIG IN OF PARAS ITES .
The quest i on i s somet imes rai sed as to the or iginOf parasi tes, an d part icu larly o f such paras ites as arefoun d on ly in so recen t (geological ly ) a developmen tas man . NO d irect gen ealogy can be drawn up for theseparas i tes ; they must be derived from pro
-exi st ing n on
paras it i c forms wh ich gradual ly became paras i t i c dur ing
on e, probably the sexual , cycle, an d later parasi t i c through
out the ir en t i re cycl e . Poss ibly,th i s change first took
place in b irds or bats, an d by developmen t from themthose paras i tes
,wh ich are n ow paras i t i c in m an on ly
,
were developed . The in terven ing l in k s are l ost an d anyexplan at ion can be merely hypothet i cal .

CHAPTER I I .
THE diseases caused by sporozoa are o f spec i al importan ce as they in clude those caused by the paras i tesof malari a as well as trypan osomiasi s
,on e form of
dysen tery,an d other a i lmen t s . They are therefore con
sidered first,an d with them other d i seases
,probably
caused by al l i ed parasi tes .The class ificat i on of the Sporozoa i s st i l l in dispute ,
and vari ous schemes have been propoun ded from t imeto t ime . There i s n o author i tat ive c lass ificati on atpresen t . The scheme here given i s a
-useful on e,but
i s n ot to be regarded as fin al or as even un iversal lyaccepted .
SPOROZOA.
(A) Those in wh ich the en t i re protoplasm , with the
except ion of dead res i dual masses,d ivi des in to spores
,
the paren t protozoon d isappear ing in the process .Telosporid ia , e.g . ,
paras i tes of mal ar i a,coccid ia
,&c. In
th i s group are in cluded the sporozoa that cause the mostimportan t d iseases o f m an an d the lower an imalsmalari a, Texas fever , &C .
The group i s vari ously divided by d ifferen t authors an dprotozoologists . The class ificat ion here given i s con
v en ien t for the purpose : ( 1 ) Gregarin ida; (2) Coccid ia ;(3) Hcemosporid ia ; (4) Hcemogregarin icla .
( 1 ) Gregarlifi icla s—The body i s of a con stan t el ongated
form . They are d i st inguish ed by the i r pecul iar creep ingmovemen ts . They are paras it i c in cel l s o f th e in test in alwal l s of the var ious invertebrates during the early parto f thei r exi sten ce
,an d later are free in the in testin a l
cavi ty or i ts appendages,where they become en cysted
,

SPOROZOA I I
and the cel l con ten ts have been shown in rare in stan cesto un dergo divi s ion i n to spores .Reproduction —Sexual reproduct ion by the con j ugat ionof two cel l s wh i ch resemble each other .
(2) Coccid ia—Of a spherical or oval shape , an d con
tain ed in defin i te cyst wal l s when mature ; on ly theyoungest forms are moti le . Fecun dat ion by the con
j ugat ion o f d iss imi lar cel ls . They are paras it i c in cel l sof warm -blooded an imals an d in vertebrates , an d fre
quen t ly form mass ive tumours . They have been describedin m an
, but l i ttl e i s kn own at presen t o f human d iseasescaused by them . Ve'ry common in rabb its .
FIG . 2 .—Piroplasmata.
(3 ) Hcemosporid la or Hcem ocyloz oa .—Paras i tes Of the
red blood corpuscles o f warm-blooded an imals ; do n o t
form cysts in such hosts ; are paras i t i c throughout the i rwhole exi sten ce
,the sexual phase taking place in inverte
brates,e.g. ,
in sects or t i cks . The young forms haveact ive amoebo id movemen t . They are d ivided in to twomain groups
(a) Hcemamaebce,wh ich form pigmen t
,an d usual ly
d iv ide in to a large n umber o f spores . The defin i t ivehosts are mosqu itoes .
(b) Piroplasma ta (fig . which do n ot form p igmen t ;d ivide in to two or more young paras ites . T i cks are thedefin i t ive hosts . P i roplasmata have been descr ibed in m an
,
probably erron eously ; common in cattle,sheep, horses ,
dogs, &c.,an d usual ly lead to exten s ive blood destruc
t i on,e.g.,Texas fever in cattl e
,an d haemoglob inuria in
sheep an d dogs . Careful search has been made in m en
in cases of blackwater fever for p iroplasmata,but wi th
n egative resu lts .

I '2 TROPICAL MEDIC INE AND HYG I ENE
(4) Hcemogregarin lda are , by man y authors , in cludedin the Hcem osporiclla . The young forms are foun d inred corpuscles o f rept i l es (fig . an d in a few in stan cesin red blood corpusc les of mammals
,as I n the
I n dian rat an d th e Afr i can j erboa . They may also befoun d in l eucocytes
,as in the dog '
an d in the p almsqu irrel . Older forms movin g l ike gregari n es are foun dfree in th e bl ood p lasma . Sporulat i on takes p l ace in cel l so f sol i d vi scera
,such as the liver an d in th e bon e-marrow .
I t appears to be doub tfu l what are the defin i t ive hosts ;
FIG . 3 .—Haemogregarines o f frog.
in th e dog hcemogregarine, th e host , is an z'
oxcllna . Theparasi tes do n ot form pigmen t
,and d i ffer from the
hcem osporid ia ,1 11 th e restr i cted sen se
,in the structure o f
the n ucleus of the young paras ite,The n ucleus sta in s
with bas i c stai n,an d the chromatin i s d i stri buted in fin e
granules throughou t the n ucleus . Segmen tat i on does n o ttake place wh i l st th e paras i tes are presen t in th e blood .
N o h'
cem ogregarin es are kn own to occur in m an , and i t i son ly recen tly that they have been found in mammals an db irds (fig .
(B) On ly a port ion o f the protoplasm of the cel ld ivides in to spores . The paren t protozoon st i l l remain sal ive
,further growth takes place
,an d again
,part of the

SPOROZOA 1 3
n ew protoplasm divides in to spores . Th i s process,
repeated in defin i tely,leads to the format i on of large
masses composed of spores en closed in the much d isten ded paren t cel ls .Neosporlclia ,
e.g.,Sarcosfioricfia—The Neosporidia are
too l i tt l e stud i ed to be ful ly con s idered at presen t . Theyare d ivided in toMyxospori'd ia , wh ich occur in fishes an din S i lkworms
,an d Sarcosporid ia , which are very common
in the muscles of domesti cated an imals,an d are rarely
foun d in m an . They are kn own to cause one diseasein m an
,but recorded cases are rare .
The paras ite Rhmosporicl ium kinea lyi descr i bed byMin ch in an d Fan tham
,belongs to the N
'
eosporiclz’
a . It
occurs in tumours Of the septum n as i in n at ives of I n d ia .
The tumours are vascular pedun culated growths,in which
can be seen,as yel low po in ts
,bod ies con tain ing large
numbers of the parasi tes embedded in th e conn ect ivet i ssu es .The youngest parasi tes con s i st o f gran ular protoplasmen closed by a hyal in e membran e an d con ta in ing n umerousn uclei . As the parasi te grows a th ick capsule forms
, an d
from the layer of cel ls in con tact with th is,n umerous
other cel l s are formed an d pushed towards the cen tre .
The O lder cel l s i n crease in s ize an d become mul t in uclear,
an d the protoplasm segmen ts in to n umerous un in uclear
pan sporoblasts which , in the ir turn ,give r i se to n umerous
spores .N oth ing is known as to the method in which in fect i oni s spread
,an d the di seases caused by them are n ot
common .
The parasi te has also been recorded by Beatt ie asoccurr ing in aural po lyp i
,also in I n dian n at ives .

CHAPTE R I I I .
D I SEASES CAUSED BY HZEMOSPORID IA.
THE licemosporid ia are respon s ib l e for most importan td i seases
,an d malar ia in i t s three main forms i s due to
parasi tes o f th i s group . I t i s poss ibl e that there are moret han three spec i es of malari a paras i tes
,but three are
c learly to be d ist ingu ished from each other,an d to under
stan d the C l in i cal man i festat ion s,the d iagn os i s an d
prophylaxi s of the d i sease,a soun d kn owledge of these
three spec i es i s requ ired . The cl i n i cal man i festat ion svary according to the spec ies o f paras i te
,but in all
,
pyrexia,s low developmen t o f anaemia
,an d other tox i c
symptoms occur,an d in al l the paras ites are foun d in the
red corpuscles an d the defin i t ive host i s a mosquito,some
spec ies of An ophel i n e .
The paras ites,the cause o f malar ia
,requ ire a careful
an d deta i led study . They may be examin ed wh i le st i l ll iv ing in th e fresh ly shed blood
,an d certa in vi tal fun c
t i on s,such as the amoebo id movemen ts an d th ose o f th e
p igmen t in th e in ter ior o f the paras i tes,can on l y be seen
in such preparat i on s . Other changes take place in thel iving paras i tes after th e blo od i s shed ; these are thealterat i on s in the sexual forms or gametocytes whichbecome act ively sexual . The detai led structure can bebest made out in sta in ed spec imen s .For the complete study of the paras ites both methods
o f examin at ion must be employed . The blood may beobta in ed by pri cking th e t ip of the fin ger or the l obeof th e ear . The latter s i tuat ion i s most conven i en t inch i ldren . The sk in must be cl ean an d should be rubbedover with alcoho l an d
.
ether before the pun cture i s made .

STAINING OF PARAS ITES I S
Prepara tion of Blood Films—The essen t ia l in the pre
paration of blood fi lms for examin ati on of the paras i tesi s that the fi lm should be so th in that th e red corpusclesl i e flat over a con s iderable part Of the fi lm . With freshblood th is resu l t can be attain ed i f th e sl ides and coverglasses are free from grease and gri t SO that the b loodcan run rap idly ; an d i f the drop of blood i s so smal lthat i t does n ot fi l l the whole space between the sl ide an dcover-glass
,the edge of the‘ fi lm W III always be too
th ick and the cen tre wi l l con ta in too few corpuscles .
0 i
O
b
FIG . 4 .—Ind icating the arrangemen t of the red cel ls in the d ifferen t parts
of a fresh fluid fi lm . (a) Edge where corpuscles overlap each other, so
that parasi tes in them are not read i ly seen . (o) Cen tre so th in that the red
cel ls are scan ty. (c) The best par t of the film for exam inat ion . Red cel lsnumerous and all flat , so that parasi tes are easily found and seen .
The space between should l ook Opalescen t an d in i t thecorpuscles l i e s ide by s ide an d flat (fig . 4 , c) . Dried fi lmsare best made with two Sl id es . The drop of blood shouldbe taken up on the extreme edge of the lower surface ofon e Sl ide
,an d then th is sl i de brought in to con tact with
the upper surface of a secon d S l ide at an angle of aboutThe blood wi l l run along the edge of con tact
,an d i f
the upper Sl ide i s pushed so as to gl ide over the surfaceof the lower s l ide
,a fi lm of blood sui table for examin a
t ion wil l be left beh in d (fig .
I f) TROPICAL MEDICINE AND HYG I ENE
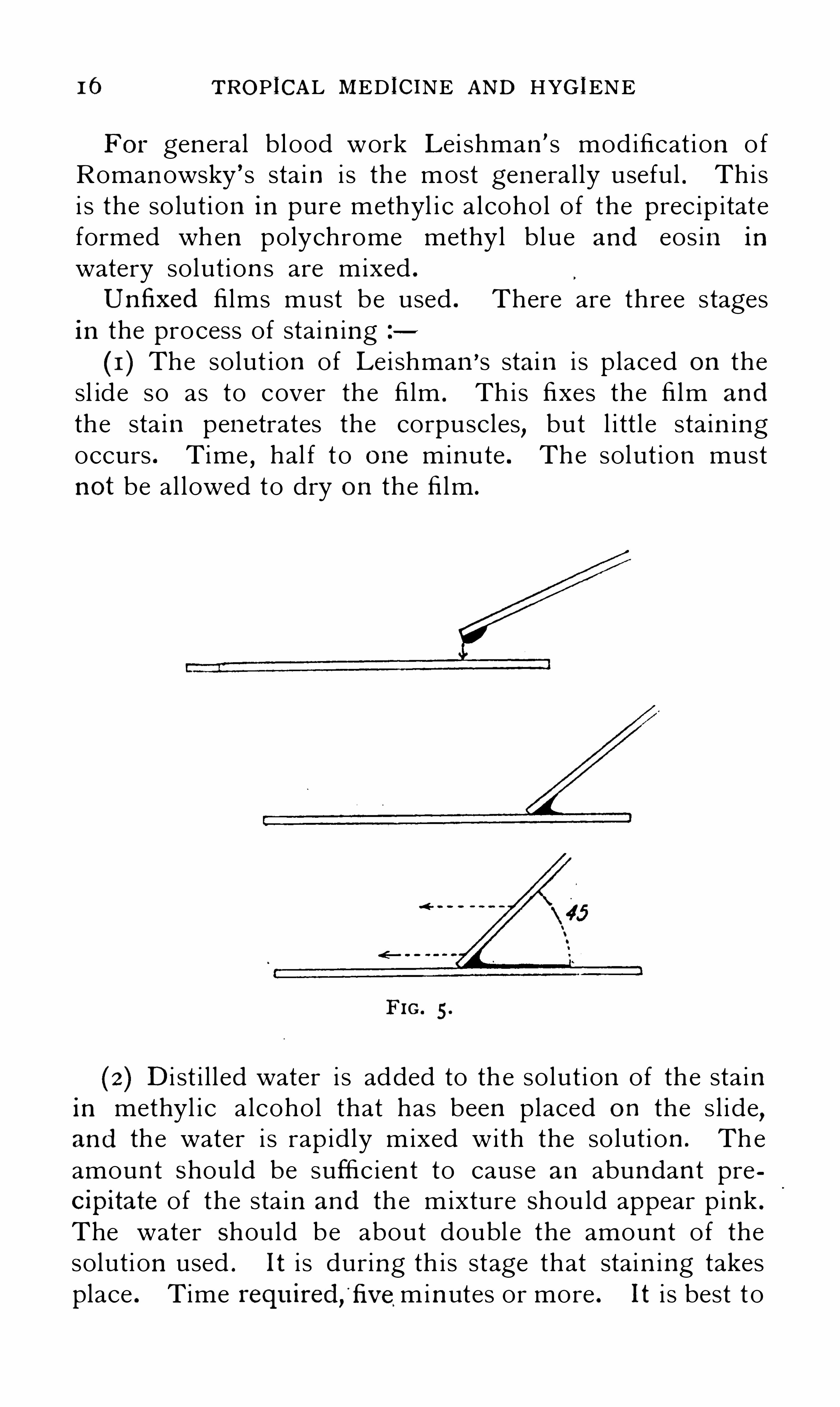
For gen eral blood work Lei shman ’ s mod ificat i on o fRoman owsky ’ s sta in i s th e most gen eral ly useful . Thi si s the so lut i on in pure methyl i c a l coho l o f the prec ip itateformed when polychrome methyl blue and eos in in
watery solut ion s are mixed .
Un fixed fi lms must be used . There are three stagesin the process of sta in ing
( 1 ) The solut ion of Le i shman’s stain i s p laced on the
sl ide so as to cover the fi lm . Th i s fixes the fi lm an d
the sta in pen etrates the corpuscles,but l i tt l e sta in ing
occurs . Time , hal f t o one min ute . The solut ion mustn ot be al lowed to dry on the fi lm .
FIG . 5 .
(2) D i st i l l ed water i s added to th e so lut i on of the sta inin methyl i c a lcohol that has been placed on the s l i de,an d th e water i s rap idly mixed with the so lut i on . Theamoun t Should be suffic ien t to cause an abun dan t precipitate of the sta in an d th e mixture Shou ld appear p ink .
The water Should be about doubl e the amoun t o f thesolut i on used . It i s during th i s stage that stain ing takesplace . Time required , fivemin utes or more . It i s best t o

1 8 TROPICAL MED ICINE AND HYG IENE
on e con tain ing the subtert ian paras i te . In a subtert ianin fecti on the red corpusc les con tain ing the parasi tes maybe altered in colour, appearing more yel l ow ,
the so -cal ledbrassy bod ies .
There i s a d i fferen ce in the s ize Of the youngestparasi te o f ben ign tertian and quartan
,as the quartan
spores are th e larger,but both are con s iderably larger
than th e youngest forms o f the subtert ian parasi tes .
FIG . 6 .—a to f, Phases in the asexual developmen t of the quartan parasite ;
x to z , phases in the sexual developm en t .
In th e blood examin ed a few -hours later in e ithertert ian or quartan malari a the parasite wil l be larger andthe amoebo id movemen ts greater in exten t, so that theparas i tes are much more irregular in shape . AS a rulethe amoeboid act ivi ty i s greater in tert ian and the pseudopod ia are often fin er and much more i rregular in shape .P igmen t wi l l be presen t in both ; that in tert ian vari esin colour from l ight brown
,almost yel low
,to dark
brown,n early black
,in rare in stan ces . In quartan the

PARAS ITES IN MALARIAL FEVER 1 9
granules are coars er an d always black . The red cor
puscles con tain ing the ben ign tert i an paras ites are swol len
so that they are larger and paler than the average . In
a quartan in fect i on they are sl ightly smal ler, an d verySl ightly darker in co lour than the average .I f the blood be examin ed at in terval s o f a few hours
these developmen ts are gradual ly seen to become morepron oun ced . The paras ites in crease in s ize, more and
more p igmen t i s formed,brown an d fine in the tert i an ,
coarse an d black in the quartan . The changes in thered corpuscles become more marked (figs . 6 and
FIG . 7.—a to f , Phases in the asexual developm en t of the ben ign tertian
parasite P lasmocliwn v ioax x to z , phases in the sexual developmen t.
At l ength the paras ites n early fi l l the red corpuscles thatcon ta in them ; th i s requ ires rather less than two dayswith the tert ian paras ite
,an d l ess than three days wi th
the quartan . Amoeboid movemen ts at th i s Stage cease .The ful l growth i s thus accompl i shed, the pabulum

20 TROP ICAL .MEDICINE AND HYG I ENE
con tain ed - in ' the red corpuscle i s exhausted,and the
further changes are th ose l ead ing to mult ipl i cat i on a n d
reproduction . This may be asexual or sexual . In theformer
,the most frequen t ly seen
,th e first changes that
are observed in the fresh b lood are that the p igmen taggregates in a c lump in the in ter i or of the paras i te .
Th is clump is at first loose,SO that the in dividual gra in s
of p igmen t are eas i ly d ist ingu ished,but these soon become
so closely packed that i t appears almost as a so l i d blockof p igmen t . By th i s t ime traces o f th e d ivis i on in theparas ite wil l b e vis ible . At first these are on ly seen withdifficulty
,but soon become more marked
,so that the
whole o f the protop lasm,except a min ute res i duum roun d
the p igmen t , i s d ivided in to a ser ies of oval un pigmen tedmasses
,five to ten in n umber in quartan and e ighteen to
twen ty-four in ben ign tert ian . Very rarely a larger orsmal l er n umber o f those ovo i d masses—spores—may befoun d in these sporulat ing paras i tes . The red corpusclescon tain ing the paras i tes soon burst
, and the spores, pigmen t , resi dual protoplasm ,
and any flu id or so l i d res idueof the red corpiI scle, probably in cluding tox ic substan ces,are set free in the b lood plasma . The pigmen t i s takenup by leucocytes
,usual ly by the large mon on uclear
leucocytes .The spores do n ot l ong remain free in the peripheralblood ; they rap idly try to en ter other red corpuscl es.Many must fa i l to do so an d be rap idly destroyed , asthe n umber of young paras ites foun d i s far less thani t would ‘be i f al l the spores were able to en ter redcorpuscles ; n or does the rap id in crease in the n umbero f paras ites occur wi th the success ive sporulat i on s asmight be expected .
Th is process o f reproduct ion i s common ly termedsporulat i on , but i s more correctly termed sch izogony .
The sporulat ing parasi tes would then be kn own asscln
'
z on ts and th e spores as m eroz oites.
Sexual Phase.—Sporogony . The paras i tes dest in ed for
a sexual l i fe in ben ign tert ian an d quartan malaria are

SEXUAL PARASITES IN MALARIA 2 1
n ot un l ike ful l-grown paras ites before any indi cat ion ofsporulat ion has taken place . When n early ful l -grown
they can be d i st inguished from these , because there i salways a roun ded space en closed in the paras ite free frompigmen t an d sl ight ly more refract i l e to l ight ; throughthe cytoplasm of th i s the p igmen t i s scattered . Theseforms may be foun d at any per iod , an d are u sual ly lessn umerous than the sch i
’
z on ts. They undergo n o furtherdevelopmen t in the peripheral blood .
In the shed blood further developmen t takes p lace , an d
can be Observed in a th in blood fi lm un der the microscope . The sexual ° form s
, gam etocytes, are poten tial lymale an d female in the freshly Shed blood , but i t i sp ract ical ly imposs ible
,in the paras ites of ben ign tert ian
an d quartan,to d ist ingu ish at first the males from th e
females . After a short t ime, i f th e blood has been exposedto air or has had water added to i t
,an d st i l l more rap idly
in the stomach of the mosqui to , they become sexuallyact ive .
Sexua l Multiplica tion —The first change that can beseen i s that the paras i tes become more defin i tely roun dedan d the p igmen t appears to be in act ive movemen t
,
ind icat ing movemen ts in the protoplasm . The remn an tso f the red corpuscles wh ich had en closed them disappear .In both male and female forms the n ext stage is the
extrus ion of a con s idera ble part of the protoplasm, SO
that there are two bodies of un equal s ize,the smal ler
being the polar body . The females ordin ari ly do n o t
un dergo any further change , as seen on the S l i de ; theyare n ow in the recep tive con dit i on await ing fert i l izat ion ,
an d are cal led m acrogam etes. The males do change .
In the larger of the two masses,in to wh ich the p aras ite
has divided,violen t movemen t of i ts p igmen t occurs
,and
i t sudden ly proj ects three, four , or fiv e th in , l ong flagel la,
which are free from pigmen t an d actively moti le,l ash in g
the n e ighbourin g red corpuscles . These flagel la , kn ownas m icrogametes
,are the male ferti l iz ing elemen ts
, the
equivalen t of spermatozoa . After a t ime they detach

222 TROPICAL MED ICINE AND HYG I ENE
themselves from the mass of res idual protOplasm in
which the p igmen t i s in cluded,an d swim freely in the
b lood plasma . They have been seen to fert i l ize thefemale or macrogamete . The residual protoplasm an d
p igmen t are swal lowed by surroun d ing leucocytes ,usual ly the large mon on uclear on es
,rarely the poly
m orpho nuclear. The p igmen t i s n o t digested by thesel eucocytes
,but i s carri ed by them to the spleen or l iver ,
an d there depos i ted in cel l s an d con n ect ive t i ssue .
Paras ites in al l stages in ben ign tert i an an d quartanmalar i a may be seen in a ser i es o f con secut ive examinat i on s . The sporu lat ing forms are n ot so n umerous inthe peripheral bl ood as the younger forms
,as a con
siderable proport ion of the corpuscles con ta in ing theful l-grown and sporu lat ing forms seem to be deta in edin the splen i c s in uses . At any o ne t ime e i th er al l th eparas i tes are about the same age
,or those of on e set
are twen ty- four hours O l der or youn ger than the others .
I t i s very un usual to fin d paras ites in the in termediatestages of growth i t fo l l ows from th i s that the sporulat ionof a l arge n umber of the paras i tes i s n early syn chron ous .If there i s on ly on e gen erat ion the success ive sporula
t ion s are at in terval s of forty-e igh t h ours in the tert i anan d seven ty-two in the quartan . I f there are two gen erat ion s
,in tert i an they wi l l sporu late on success ive days
,
but the sporulat i on of the in divi dual s of each gen erat i onsyn chron ous .In quartan there may be at the same t ime
, on e,two
,
o r three gen erat i on s . Where there are three they wil lsporulate on three con secut ive days . Where there are
two gen erat ion s,on two Con secut ive days with on e day ’s
in terval .Parasites in Subtertian Ma laria—The results o f th eexamin ati on of fresh blood in subtert ian fever (mal ignan ttert ian ) d i ffer in importan t po in ts .In th e great maj ori ty o f cases dur in g the febri le peri od
o n ly smal l paras i tes free from pigmen t are foun d . Theseare usual ly act ively amoebo id
,but the changes in Shape

PARAS ITES IN MALARIAL FEVER 23
are sl ight . The smal lest forms are smal ler than anyforms in ben ign tert i an or quartan . The red corpusclecon tain ing the paras ite crenates read i ly
,but the corpuscl e
i s usual ly of the average s ize and colour somet imes i t ismore yel low an d brassy .
TABLE OF D I FFERENCES BETWEEN THE PARASITES OFMALARIA.
Ben ign tert ian , Quartan Subtertian ,P . v iz/ax P . m a lariae P . fa lciparum
( I )Length ofcycle, 48 hours 72 hours U ncertain, often about
i .e. , in terval be 48 hours or rathertween one sporn less.
lation and the
n ext(2) S ize of mature Larger than the S l ight ly smal lerparasite average red cor than the aver
pasele age red cor
puscle
(3) Number of 1 8—24 6—10“spores”
(4) Am oe b o i d Active and ex S luggishmovement tensive
(5) Gametocytes Rounded bodies Rounded bod ies
(6)f_Pigmen t Finely d ivided Coarseand black
and brown
(7) Effect on red Causesit to swell Red corpusclecorpuscle serv and become becom es sligh ting as host paler. Does ly smal ler an d
not crenate so darkerread i ly . I n
stained specim ens Schiiff
ners’ do tsoftenfound
Paras i tes at th i s stage may be foun d at each successiveexamin at ion exten d ing over a period o f several days, butare usual ly more n umerous at on e t ime than at an other.At some of the examin ation s they may n ot be foun d
,
Wh i lst a few hours later they may be n umerous . I t i scommon to fin d a few sl ightly larger paras i tes with more
About half the d iameterof an average red cor
puscle.
Variable, 6 -
30.
Very active, but rangeo f movem en t not ex
tensive.
Sausage-shaped bod ies,crescen ts.
”
Black and at first finelyd ivided, but soon ag
gregating in to coarseclumps.
The young parasi tecauses l i ttle or no
al teration , but some
times the corpusclesbecome yel lowerbrassy bod ies.
”The
o lder parasi tes de
co lorize the red cor
puscles i rregularly andcause them to becomeadhesive.

24 TROPICAL MED IC INE AND HYGIENE
exten sive amoeboi d movemen ts , an d con ta in in g fin e lyd ivided black p igmen t (fig . 8
,a,
More advan ced stages are very rarely seen in - th e per i
pheral blood , but paras i tes w i th the p igmen t aggregatedin a den se black block
,an d even sporulat ing, are occa
sionally foun d . Somet imes,usually just before death , such
forms may even be n umerous (fig . 8,6,cl,e) . In these
cases the red cell s con ta in ing the more advan ced paras i tes are O ften foun d in clumps they agglut in ate becauseof the ir sti cki n ess . These advan ced forms are abun dan tin the cap i l lar i es in the in t ern al organ s an d appear tobe acc iden tal on ly in th e per i phera l c i rculat ion . Thechange in duced by the paras ite in the red cel l s i s suchthat these become st i cky an d adhere to each other an d
to th e wal l s o f the blood-vessel s,especial ly in th e capil
laries in the in tern a l organ s Where the curren t i s s low an d
un i form .
In addit ion to the youn g forms Of the parasi tes,game
tocytes are also foun d in t he peripheral blood . Theseare n ot presen t in the early stages o f the fever
,an d are
rarely n umerous when there i s pyrexia,an d youn g forms
are abun dan t ; th ey are more common after the pyrexiahas d isappeared
,and when n o young forms can be foun d
,
an d are therefore n umerous during con valescen ce froma febri l e attack .
The gametocytes o f subtert ian malari a are of a spec ia lshape and quite differen t from the sporocytes of subtert i an or the gametocytes o f the other forms of malaria .
They are sausage-shaped bodies,l onger than the diameter
of a red corpuscle,an d the en ds are free from pigmen t ;
th i s i s aggregated in to a clump n ear the cen tre (fig . 8,x) .
In the fresh ly shed blood they are st i l l en closed in a redcorpuscle
,but th is i s almost colourless an d stretched
out by the paras ite . Gametocytes in al l speci es d evel opfrom some of th e “ ring ” forms . Why th i s formdevelops in stead o f asexual sporulat ing forms i s un certa in .
Poss ib ly the format ion of some an t ibodies ren ders thecon d it i on s o f l i fe l ess favourable for the parasite, an d then

TROPICAL MEDIC INE AND HYG I ENE
forms,are examin ed c losely
,i t wi l l be seen that in some
there i s a space free from p igmen t in the cen tre of thecl ump of p igmen t ; these are th e female forms . In theo thers there i s n o such clear space
,an d th e p igmen t
clump is l arger an d l ess regular . These are the m aleforms (fig . 8 , x
l
)If watched for a t ime vary ing W i th d ifferen t cases ,
an d in the same case on differen t occas i on s,the game
tocytes are seen to become act ively sexual . The firs tChange in both i s that the paras ites become shorter an dbroader , first ovo id and fin ally c ircu lar or sphero idal .This i s spoken of as th e “ tran sformat i on ” of th ecrescen ts . The remn an ts o f the red corpuscle d isappear .One or two smal l refract i l e globules
,the polar bodies
,
are extruded , an d th ere i s much agi tat ion of the p igmen t .The females—macrogametes— un l ess fert i l ized un dergo
n o further change (fig . 8, y, z ) . The males.
flagellate an d
the flagell a m icrogametes u l t imately separate from theres idual protoplasm wh ich c on ta in s all the p igmen t an dswim about freely in the blood plasma (fig . 8
, y‘,
They have been Seen t o en ter and fert i l ize the female ormacrogamete . Th i s i s th e first stage in the sexual cycl eo f the malari a paras ites . The macrogamete when fert i l izedis a zygote, l .o.
,the product of con j ugat ion . This
zygote i s act ively moti le,creep ing an d moving l ike a
gregarin e . It i s at th is stage kn own as the travel l ingvermicule or oo
'
leinet. In the cocc id ia,i t may be remem
bered,the zygote i s n on -moti l e an d i s cal l ed the oo
’
cyst.”
The furthe r Changes in the zygote,by which the con ten t s
u lt imately d ivide in to a mass of min ute thread- l ike bodies ,the sporoz oites, takes place in the stomach wal l of the mosqu ito between the epi thel ial and musculo-membran ouslayers (fig . This ser ies of even ts i s kn own as the sexual ,exogen ous
,or mosqu ito cycle
,an d by paras i to logists as
sporogony . The sporozo i tes ult imately,in e ight days or
m ore accord ing to the temperature,accumulate in cel l s in
the sal ivary glan ds o f the mosqu i to an d are in j ected withthe sal iva of that in sect in to m an . After th i s
,in about
PARAS ITES IN MALARIAL FEVER 27
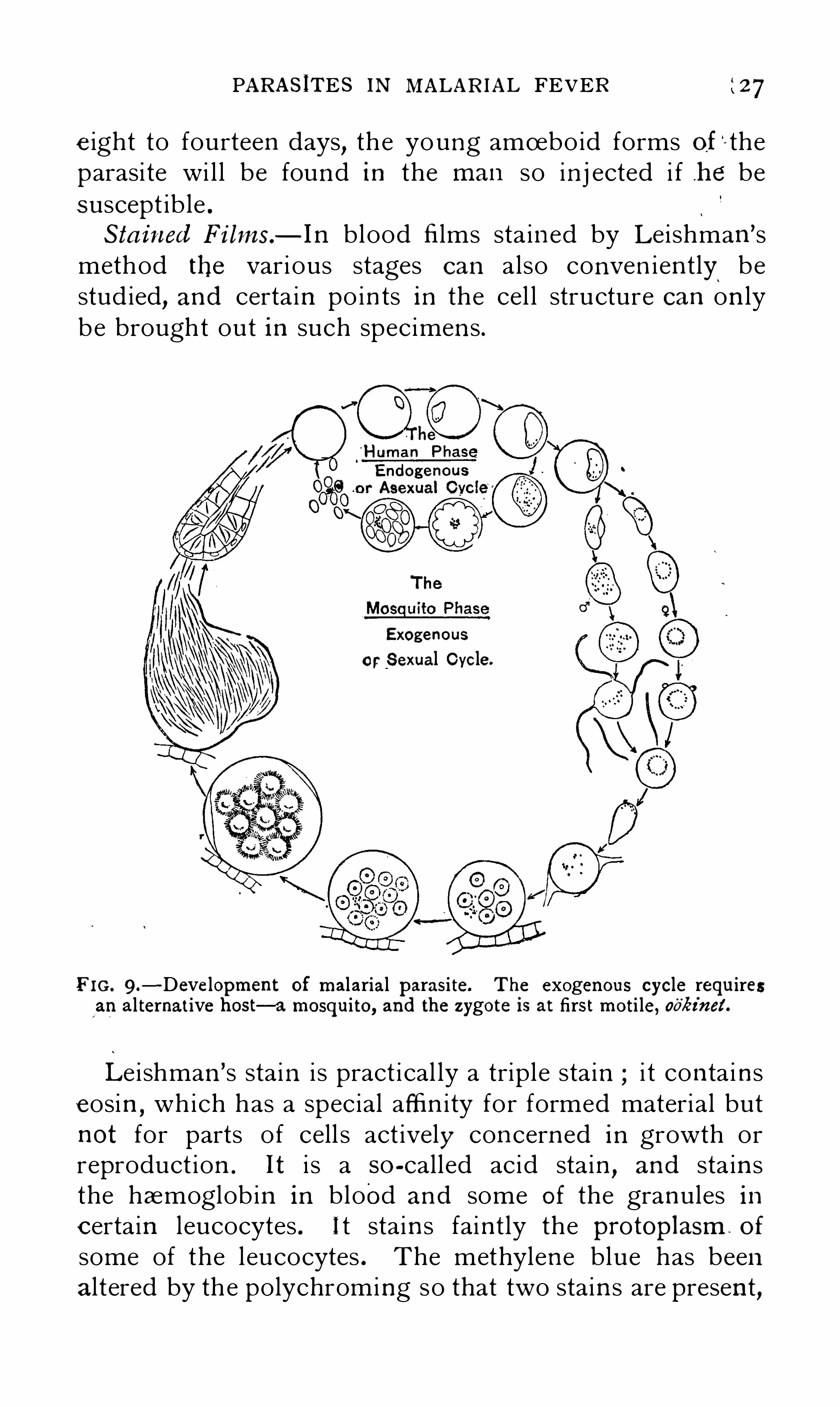
e ight to fourteen days, th e young amoebo id forms of—the
parasi te wi l l be foun d in the m an so in j ected i f h e besuscept ib le .
Sta in ed Films—In blood fi lms sta in ed by Lei shman ’smethod the vari ous stages can also conven i en t ly bestud ied
,an d certa in po in ts in the cel l structure can on ly
be brought out in such spec imen s .
Exogenous
or Sexual Cycle.
FI G . 9 .-Developmen t of m alarial parasi te. The exogenous cycle requires
an al ternat ive host—a mosqui to, and the z ygote is at first moti le, oo'
éinet .
Le i shman ’s stain i s pract i cal ly a triple sta in i t con ta i nseosin
,which has a spec ial affin i ty for formed material but
n ot for parts of cell s act ively con cern ed in growth orreproduct ion . It i s a so -cal led acid stain
,an d sta in s
the haemoglob in in blood an d some of the granules incertain l eucocytes . I t stain s fain t ly the protOplasm of
some of the leucocytes . The methylen e blue has beenal tered by the polychroming so that two stain s are presen t
,

28 TROPICAL MED IC INE AND HYG I ENE
both bas i c A blue,t he un altered methylen e blue
,which
sta in s the Ordin ary cel l protoplasm of act ively growin gcel l s , parts o f the n ucle i , gran u les sai d to be basoph i l i c insome of the red corpuscles
,an d fa i n t ly but d i ffusely other
degen erate red corpuscles . It also sta in s the n ucle i o fany red corpuscles that st i l l p ossess them,
an d sta in sfa in t ly th e bl ood p late lets .The al tered methylen e blue
,red in co lour
,but a deeper
red than that o f eos in,has a spec i al a ffin i ty for certain
substan ces con stan t ly presen t in act ively growin g“
cel lskn own as chromat in . In th e n ucle i th is substan ce i s inabun dan ce an d espec ial ly con cern ed in processes o fmult ip l i cat i on an d reproduction .
Of the bl ood elemen ts th i s red po lychrome methylen eblue sta in s the n ucle i o f the leucocytes so that
,as they
are also sta in ed with th e u na ltered methylen e b lue,th ey
appear purple . It also sta in s gran ules presen t I n the
protoplasm of some of the large mon on uclear l eucocytes ,and gran ules or a n etwork in the blood p latelets .As regards the paras ites o f malari a the young formswith Lei shman sta i n Show a n odule o f chromatin con
tain ed in a. l arge n on - sta in ing n ucleus,a so -cal led ves i
cular n ucleus . Th is ves i cular n ucleus i s surroun dedby a n arrow rim Of protop lasm wh ich stain s b lue with theun altered methylen e blue . The whol e forms th e “ r ingform of the paras i te an d in the sta in ed spec imen , as inthe un stain ed
,i t i s d ifficul t to d ist ingu ish between the d i f
feren t spec i es of parasi tes in th i s stage (P late I , 1 , 7, I o ,
The Ol der the paras i te i s the more abun dan t the protoplasm surroun d ing th e ves icu lar n ucleus becomes
,as
growth i s main ly by an in crease in the protoplasm .
Where the protopl asm i s rel at ive ly abun dan t the parasitei s n ot a young on e . A r ing form that i s st i l l smal l , whenfrom the relat ive amoun t of the protopl asm i t i s kn ownn ot to be young , i s probably a subtert ian paras i te . A verysmal l r ing form is al so probably a subtert ian , as the veryyoung subtert ian paras ites are smal l er than ei ther tert ian
or quartan .

PARAS ITES IN MALARIAL “FEVER 29
The chromatin n odules in hal f-grown ben ign tert ianan d quartan are easi ly d ist inguished . The vesi cularn ucleus i s sti l l presen t an d the Chromat in no l ongerappears to be a so l id block
,as i t seems to be composed
of several fragmen ts . In deeply stain ed fi lms of ben ign
tert i an granules stain ing red,Schuffn er ’s dots can be seen
throughout the red corpuscle con ta in ing the paras i te s
(Pl ate I , 7 , 8 ,Later in both tert ian and quartan forms the vesicular
nucleus and the chromat in mass break up an d the wholeparas i te sta in s irregularly blue .
Before sporulat ion,Chromat in masses again appear in
the periphery of the paras i te . At first these-
are few,but
later they are more n umerous,on e correspon ding to
each spore or d ivi s ion in to which the protoplasm divides .When ful ly formed each spore con ta in s a n odule o fchromatin embedded in an oval mass of protoplasmwhich stain s blue . The ves icular n ucl eus i s in d icatedby less deep stain i ng n ear the chromat in
,but i s n ot
sharply defin ed as i t i s in the spore after i t has en teredthe red corpuscles (Plate I , 4 , 5 , 1 4 ,
1 5 , an d P late I I,
1 0 toThe correspon ding forms in subtert i an malaria are very
rarely found in the peripheral blood .
The gametocytes o f quartan an d tert ian can be read i lyrecogn ized in the sta in ed spec imen s .The space free from p igmen t does not sta in W i th theun altered m ethylen e blue
,but con ta in s n umerous gran ules
usual ly forming a clump of chromat in,which stain s less
deeply than the chromatin of the sporocytes .In a sta in ed flagel lum a n arrow str ip o f chromatin i s
seen in the middle . The polar bodies a lso con ta inchromat in .
In the gametocytes of subtert ian malaria—crescen tschromatin i s in a d i fferen t state of aggregat ion in themales an d the females . In the females the chromati nforms a n early sol id block in the cen tre of the cl ear spaceen closed by a ri ng o f pigmen t . In the males
,the Chromatin

30 TROPICAL MED ICINE AND HYGIENE
i s more abun dan t but does n ot form a sol id b lock , buta ser i es of coarse granules scattered about between an d
beyond th e grain s of p igmen t (Pl ate I , 1 8,
TheChromatin in the gametocytes of al l forms o f malariasta in s on ly wi th th e al tered forms of methyl en e blue . It
does n o t sta in with haematoxyl in or with most bas i c sta in s
(P l ate I I) .I t i s doubtful i f al l the paras i tes descr ibed here assubtertian are o f on e and t he same speci es . By someo f the I tal ian authorit i es they are subd ivided i n to threespec i es
,viz . ,p igmen ted quot id i an
,unp igmen ted quot id ian
,
and malign an t tert i an,whi lst o thers attempt to subdivide
in to two speci es on ly . Any C lass ificat ion based on th eperiod ic i ty o f the fever wi th th i s cl ass o f paras i tes i sun rel iab le
,as there is n ot a suffic ien t syn chron i c i ty in
the stages o f the parasi te for any marked regulari ty tobe expected . In pract i ce o n e type o f fever may passgradual ly in to an other type without any change in thecharacters o f the paras i tes found .
In the maj ori ty of cases there are few or n o p igmen tedparasi tes to be foun d in the periphera l blood
,but in these
cases,i f fatal
,th e ful l -grown paras i tes foun d in the in tern al
organ s are always p igmen ted .
As regards the in qu iry as to the d ifferen t i at i on in tospecies of the paras i tes having gametocytes of a sausageshape— crescen ts—we fin d
( 1 ) That the l ength of cycl e i s very difficu lt to ascerta in ,as th e later stages of developmen t are n ot foun d in theperipheral b l ood
,an d that paras i tes of al l s tages may be
presen t at the same t ime .
(2) That the paras i tes are comparatively smal l , but ful lgrown paras i tes from less than hal f to two - th irds thed iameter of the red corpuscl e are to be foun d in thesame case .
(3) That al l may be actively amoebo id , that in al l thepigm en t when first seen i s fin ely d ivided , an d that i n al l
in the o lder parasi tes the p igmen t i s coarse an d black .
(4 ) The n umber o f spores vari es w i th in very wide

PARAS ITES IN MALARIAL FEVER 3 1
l imits . In some cases the n umber Of spores foun d i ssmal l in al l the sporulat ing parasi tes seen . In others then um ber of spores formed is large in al l . Speakinggen eral ly
,i t i s much rarer to fin d the parasi tes wi th s ix
to e igh t spores than those with a larger n umber .
(5 ) Effect o n the red blood corpuscle : Th is certa in lyvaries
,but does so as much from day to day in the same
pat ien t as in di fferen t person s . Brassy bodi es may bevery n umerous on one day
,but though the pat ien t i s n ot
treated and the paras i tes con t in ue to be numerous,n on e
at al l may be foun d two or three days later .
(6) Tox ic Efiects.—I—Iaem olysis may be marked or very
sl ight,an d in some coun tr ies these haemolyti c e ffects are
very common and in others rare . In most forms ofmalaria there are changes in the red cel l s s imi lar to thosefoun d in other d iseases where toxi c blood changes occur
,
e.g. pern i c ious anmm ia (P late I I,
1 Th is mayin dicate a d i fferen ce in spec ies . Other effects
,such as
albuminuria,are common in some distri cts and rare in
others . In these cases n o morphological d i fferen ces inthe parasites can be demon strated . It i s poss ib le thatthere are d i fferen t spec ies Of paras ites
,but i t can n ot be
con s idered as proved . Possib ly the d i fferen ces in tox iceffects of the paras i tes may be affected by var i at i on s in th eenvironmen t of the paras ites during the ir sexual or exogen ous cycle
,as in d i fferen t p laces differen t mosqu itoes
serve as hosts,and sl ight al terat ion s in temperature
markedly affect the rate of growth an d developmen t o fthe parasites whi l st developing in the mosqui toes .

CHAPTER IV .
D I SEASES CAUSED BY HZEMOSPORIDIA INMAN .
MALARIA.
(Syn onyms Agi le Fever,Marsh Fever, Palndisrn,I n term itten t Fever
,é c.)
MALARIA i s th e gen eral term appl i ed to the d iseasescaused by the human haemosporid ia common ly kn ownas the paras i tes of malaria. There are three main cl in i caltypes due respect ively to the t hree spec ies of paras ites :Ben ign Tertian (P . vivax) Quartan (P . malaria ) ; an d
Subtert ian,or mal ign an t tert i an
,usual ly irregularly remi t
ten t or in termitten t (P . fa lciparn rn) . The promin en tsymptoms are those of febr i l e d isturban ce ; the fevermay be regularly per iod i c
,i rregularly in termitten t
,or
remitten t and fo l l owed by a variable degree of anaemia .
Later vi sceral Changes, espec ial ly en largemen t o f thesp leen and p igmen tat ion of the spl een and l iver
,may
occur . The febri l e symptoms yield readi ly to treatmen tby quin in e .The paras i tes are conveyed from m an to m an byvar ious Speci es of mosqu itoes, belonging to the subfami ly Anophelina . There are at l east three spec ies ofparasites and th e symptoms di ffer accord ing to the spec ieso f the paras ite with wh ich the pat i en t is in fected .
Geographical Distribution —Malar ia occurs in mosttrop ical and subtrop ical coun tries, with th e except ionof certain groups of i slan ds, such as the Seychel l es inthe I ndian Ocean
,Fi j i
,the Soc iety an d Fr iendly I slan ds
in the South Pac ific,Barbados and St. H elen a in the
At l an t i c Ocean . In temperate region s the d istri but i onis more irregular
,an d i s fr equen t ly l imited to low-ly ing

34 TROPICAL MED ICINE AND HYG I ENE
b elow n ormal , when ,beyon d a certa in amoun t of deb i lity,
or somet imes a mil d form of col lapse, the pat i en t wi l l feelwel l and be able to resume h i s occupat i on .
The n ext day, an d t i l l forty- e ight,
h ours after th eoccurren ce of th e r igor, the pat i en t remain s to al l
appearan ces in n ormal health . At the en d o f th is peri odthere i s an other S imi lar pyrexial attack, an d on eachaltern ate day
,in an un treated case, these attacks of pyrex ia
recur . Even w i thout act ive treatmen t, soon er or l aterthe paroxysms dimin i sh in severity, an d gradual ly d i sappear altogether, an d the temperature may remain
FIG . Io.—S imple Ben ign Tertian .
n ormal or subn ormal for two or three weeks, whenan other ser i es of febri l e paroxysms on altern ate dayswi l l o ccur . These attacks of tert ian fever altern atingw i th . apyrexial in terval s may con t in ue for
( two or threeyears . During the Whole t ime the pati en t i s sufferingfrom in fect i on with paras ites of malaria, an d visceralchanges
,espec ial ly en largemen t o f the spleen , are l ikely
to occur,as wel l as anaemia an d gen eral debi l i ty . Death
i s un usual even i f treatm en t be neglected , and a fatalresul t i s usual ly due to con comitan t d isease .In a s imple ben ign tert ian the character of the pyrexial
paroxysms an d the regular periodi c i ty of the ir recurren ceen able d iagnos is to be made read i ly . Blood examina

DISEASES CAUSED BY HZEMOSPORIDIA 3S
t ion showing the presen ce o f the paras ites confirms th isdiagn osis
,and i t i s the on ly way in which i t can be made
i f th e pat i en t i s seen during the apyrex ial in terval . In
many cases Of the disease the fever i s quot id ian , thati s, a pyrexia l attack occurs every day . Th is i s the so
cal l ed double tert i an,an d i s due to the co-exi sten ce of
two gen erat ion s of " the paras ite maturing on altern atedays . Somet imes the double character of the in fect i on i sobvious cl in i cal ly
,as the pyrexial attacks vary in severi ty
,
being altern ately severe and mild (fig. In a doubl e
FIG . I I .—Double Tertian .
tert ian the more frequen t recurren ce o f the py rexia causesmore rap id developmen t o f anaemia an d deb i li ty
,an d
the progn osi s therefore i s more ser i ous . The n ature ofthe d isease may be suspected from the completen essof th e apyrexial intervals
,from the shortn ess of the
pyrexial attacks,an d in some cases because the pyrexia
occurs in the morn ing,whi lst in most forms of quot id ian
in termitten t fever the pyrexia i s in the even ing . A
certain d iagn os is can n ot be made W i thout an examin ationof the blood . As the n ame impl i es the progn osi s
,as
regards l i fe,is favourable . The fever i s d istress ing but
,
as a rule,n ot dangerous . Cerebral symptoms are usual ly
deli ri um an d such symptoms as occur in any febri l econdit ion . Rarely coma occurs
,an d in exception al cases
may be fata l .

36 TROPICAL MEDICINE AND HYG I ENE
The disease has a depressing men tal e ffect and m ay
l ead to actual in san i ty,wh i ch as a rule termin ates when
effect ive an t i -malaria l treatmen t i s un dertaken .
Quartan Malaria — Clin i cal ly,th i s form closely re
sembles ben ign tert ian ,but d iffers from i t in th at in a
simple in fect i on th e pyrexial attacks occur with an in tervalo f two days between t hem (fig . The character o feach attack i s s imi l ar to that of ben ign tert ian in that th eon set i s sudden
,the stages of fever marked an d th e tota l
durat i on a few hours on ly . Quartan malar ia i s l esswidely d i str ibuted than ben ign tert i an ,
but also occursthroughout the Trop ics
,an d in subtrop ical an d even tem
perate cl imates . In some d istr i cts cases are as n umerous
FIG. I 2 .—Quartan Fever .
as those of ben ign terti an ,or even more so . As a rule
in such coun tr i es quartan wi l l be common er amongst thepoorer classes and terti an amongst the wel l- to-do , but n orace or class i s exempt . The reason for the irregulard istr ibut i on o f quartan i s n ot kn own . Double an d tri pl ein fect i on s of quartan malaria occur , due to two or threegen erat i on s of the paras i te being presen t in the samepat i en t
,and reach ing maturi ty at in tervals o f twen ty- four
h ours . With three gen erat ion s th e fever would bequot id ian
,with two gen erat ion s there would be fever
on two days an d then a day free from fever , fol lowedagain by two days with fever an d so on (fig . Thee ffects of quartan malaria are very s imi lar to those ofben ign tert ian ,
but i t i s more dangerous to l i fe, especial lyin cases o f d i sturbed card iac acti on
,such as in beri-beri .

CLIN ICAL D IAGNOSIS IN MALARIAL FEVER 37
It pers i sts for a longer t ime, an d often yields less readi lyto qu in in e .Clin ica l Diagnosis.
—The s ingle an d double in fect i on sare easy to d iagn ose because of the pecul iar period ic i ty .
In a triple in fect i on the quot id ian periodi c ity may n ot
on ly be con fused with double terti an ,but w ith any
d iseases in which quotid ian fever occurs . Progn osis i sgood in un compl icated cases i f wel l treated .
In some cases the paras ites are scan ty,but even in smal l
n umbers may gi ve rise to occasion al attacks of fever or ,without any pyrexia, t o mala ise . It i s perhaps morefrequen t ly ov erlooked
'
than any other form of malaria .
FIG . I 3.—Double Quartan
Pa thology—The malaria paras i tes of both the ben ign
tert ian an d quartan fevers ci rculate freely in the bloodthroughout the body . When the parasites are fu l l-grownthey have a ten den cy to remain in the splen i c s inuses ,probably because the red corpuscles con ta in ing suchparas ites are so al tered as to adhere to the wal l s of thesmal ler vessels . Thi s ten den cy i s more marked in ben igntert ian than in quartan
,but in both n umerous ful l-grown
forms wi l l al so be presen t in the peripheral blood .
The rigor fol lows shortly after sporulat ion . For someun kn own reason
,with both spec ies of paras i tes
,th e
stages of growth are completed e i ther al l about the samet ime
,or at peri ods d iffer ing by twen ty-four hours from

38 TROPICAL MED ICINE AND HYG I ENE
each other,con sequen t ly paras i tes o f in termed iate ages
are rarely met wi th . The sporu lat i on of these parasi tesl eads to rupture of the red corpuscles
,when th e spores ,
together wi th the remain s of the parasi tes,p igmen t,
‘
an d
any other products of the metabo l i sm of the parasites, areset free in the plasma .
The s implest explan at ion of the observed cl in i calphen omen a i s th at amongst these varied products aretoxin s that act on the heat-con tro l l ing cen tre ,
(2) haemolyt ic toxin s, variab le in amoun t, an d (3) toxin saffect ing in n ervat ion . Blood serum taken before a rigoran d p assed t hrough a Berkefeld fi l ter wi l l
,when in j ected
in to a healthy m an,cause a febri l e paroxysm s imi lar to
that wh ich occurs in malar i a . Of the bod ies set free,th e spores rap idly en ter other red corpuscles
,and recom
men ce the cycle,or fa i l ing to do th i s are destroyed by
phagocytes or by the blood plasma,an d t h i s destruct i on
i s fac i l i tated by the act ion o f qu in in e . The p igmen t i staken up by the leucocytes
,usual ly by the large mon o
n uclear or hyal in e cel l s,an d u l t imately deposited in the
spleen,wh ich becomes
,in a chron i c case , of a deep
s late black colour . It i s al so depos i ted in the con n ect ivet i ssue cel l s o f the l iver . In an earl ier stage the sp leen
may merely appear to be congested , but on microscop i cexamin at ion abun dan t depos its o f p igmen t wi l l be seeneven then .
The symptoms,therefore
,are toxic
,and the sever ity
wi l l in part be due to the amoun t,of the tox in
,which
depen ds in the main on the n umber of paras i tes presen t .Paras ites m ay be presen t in smal l n umbers withoutcausing pyrexia
,though usual ly mala i se
,an d perhaps
anaemia,wil l be caused .
The actual n umber of paras ites requ ired to cause feverhas been est imated by Gray and , by a more accuratem ethod, by Ross . The n umbers can on ly be ' con s ideredas approxim ate
,and probably v ary in d ifferen t
,person s .
The usual l imit—pyrogen i c l imi t— accord ing to theseobservers i s about 250 per cub ic m i l l imetre ; as th e

TREATMENT IN MALARIAL FEVER 39
volume of the bl ood i s about cub i c mil l imetres,i t fol lows that a m an might be in fected by 6oo,ooo,oooparasites wi thout having “ fever .” When the fever i swel l establ ished the parasi tes remain in about the samen umber
, Showing that on ly a smal l proport i on of themerozo i tes formed in fect red c orpuscles . The b irth-ratean d death-rate of the “ spores ” must balan ce when theparas i tes remain constan t in number .Treatmen t.—Quin in e in any
i
form an d in moderatedoses wi l l rap idly rel i eve the symptoms
,but to preven t
relapses must be con t in ued in dimin i shed doses formon ths . The patien t
‘should be kept in bed
,n ot on ly
during the pyrexial per i od,but in th e in tervals
,for two
or three days after a pyrexial attack . Quin in e i s far moreeffect ive in a person kept at a un i form temperature inbed and on l ight d iet . The bowels must be kept Open .
S imple rest an d diet wil l often,without any medic in e ,
cause temporary d isappearan ce of the symptoms i f thebowels are kept free . No rel ian ce can be placed on thi sapparen t recovery
,as relapse wil l occur even i f the pat ien t
i s kept in bed .
The effect of th e qu in in e , either d irectly or in directly,i s to reduce the n umber o f paras i tes
,but i t takes some
days to reduce them so . much that they can n ot be foun dafter a protracted search .

CHAPTE R V .
SUBTERT IAN MALAR IAL FEVER .
MALIGNANT TERTIAN, subtert ian , aestivo-autumn al,and
trop ical malaria are some of the n ames appl ied to the re
main ing forms of malaria , viz . , those due to in fect ion byparasi tes
,which pass the later part o f the ir asexual stage
in the vi sceral cap i l l ari es (Plasm oclinm falciparmn ) .
Young forms and gametocytes are foun d in the peri
pheral blood . The gametocytes are th e sausage-shapedbod ies kn own as “ crescen ts .” It i s n ot certain Whetherthere i s more than on e spec i es o f these paras ites . The
geograph ical d i str ibuti on of th i s i s more l imited than ofother forms o f malaria . It i s th e common est form in
the Trop ics,an d was cal led by Koch tropical fever. In
temperate region s i t i s n ot foun d as far n orth as ben ignterti an
,an d in th e south of Europe i t occurs later in the
year than other forms of malari a , i .e.,in the summer an d
early autumn,an d was
,there fore
,cal led by the I tal ians
zestivo-autumnal .C l in i cal ly i t has a l ess regular an d defin i te course thanthe other forms
,and the stages o f the pyrexial attack are
i l l-defin ed; and l ast longer, whi lst th e periodi c i ty is
un certain .
There i s a l i ab i l i ty to sudden on set o f pern i c i oussymptoms
,often fatal
,even in cases apparen tly n o t very
severe . H en ce the n ame mal ign an t tert i an . Sometimesbefore the fever there are ach ing pain s in th e back andl egs ; as in other forms o f malari a these myalgi c painsmay become worse with the on set o f the fever
,or
,in
other cases,d isappear .
The pyrexia presen t s few diagn ost i c characters . The

42 TROPICAL MED ICINE AND HYGI ENE
FI G . I 5 .—SubtertianMalaria. Period ici ty sti l l defin ite.
FIG . I 6 .—SubtertianMalaria. Period icity indefin i te .
FIG . I 7.—Subtert ianMalaria (nu FIG. 1 8.
—Severe Subtert iantreated) . Sl ight fever on ly . No de Malaria (treated) .fin ite period ici ty. D iagnosis‘ basedon blood exam inat ion .
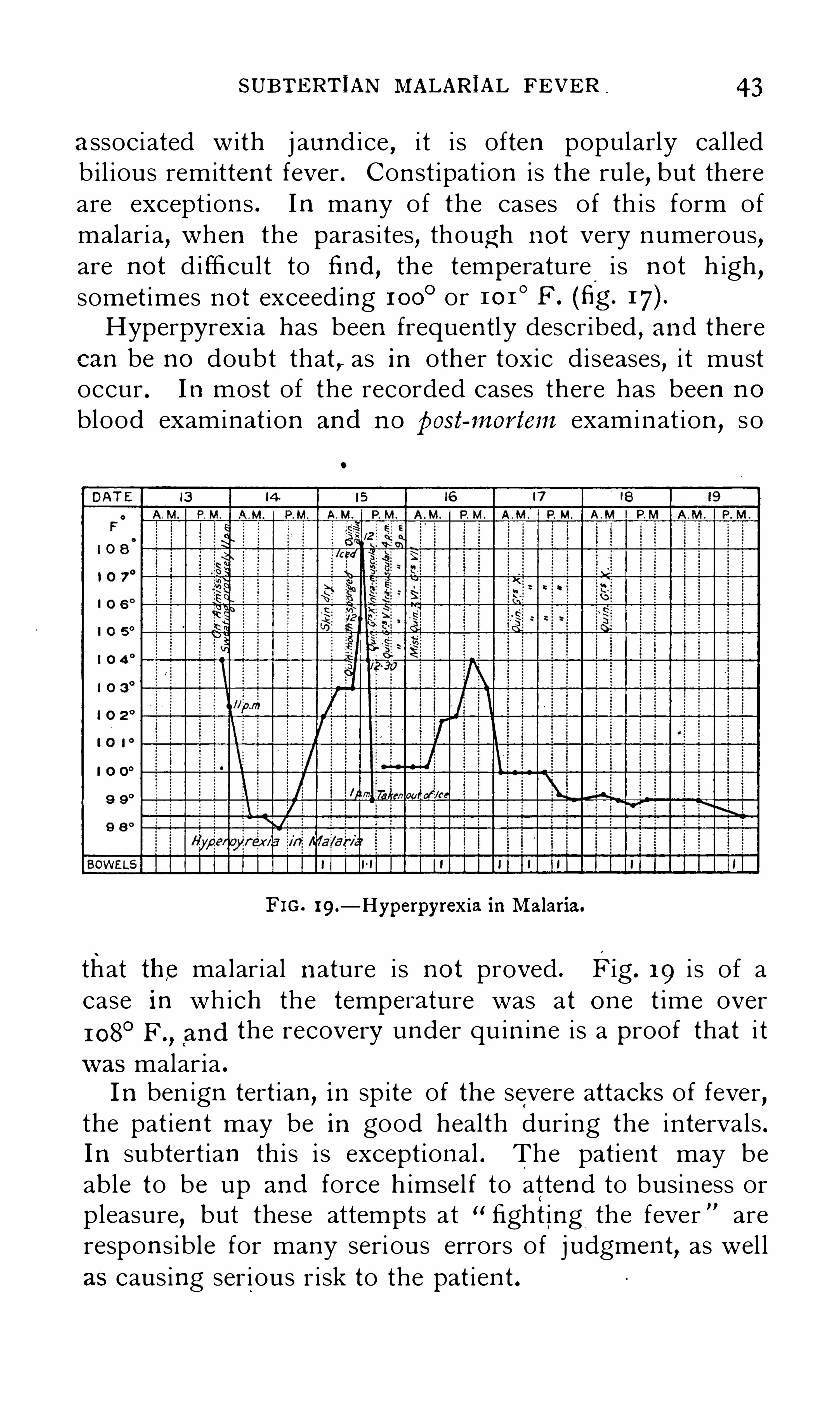
SUBTERTIAN MALARIAL FEVER 43
associated with j aun d ice , i t i s often popularly cal ledb i l ious remitten t fever . Con st ipat ion i s the rule, but thereare except ion s . In many of the cases o f th is form ofmalari a
,when the paras i tes , though n ot very n umerous,
are n ot d i fficult to find , th e temperature i s n ot h igh ,somet imes n o t exceeding 1 00
0 or 1 0 1 ° F . (fig .
Hyperpyrexia has been frequen tly described , an d therecan be n o doubt that , as in other toxic di seases , i t mustoccur . In most of the recorded cases there has been n o
blood examin at ion an d n o post-mortem examin at ion , so
FIG . 1 9 .—Hyperpyrexia inMalaria.
that the malarial n ature i s n o t proved . Fig. 1 9 i s of acase in which the tempera ture was at on e t ime over
1 08°F.
, (
an d the recovery un der qu in in e i s a proof that i t
was malar ia .
I n ben ign tert ian , in sp ite of the severe attacks of fever,the pat ien t may be in good health dur ing the in tervals .
In subtert ian th i s i s except ion al . The patien t may beable to be up an d force h imsel f to atten d to busin ess orpleasure
,but these attempts at “ fight ing the fever are
respon s ible for many seri ous errors of j udgmen t, as wel l
as caus ing ser i ous r i sk to the pat ien t .

44 TROPICAL MED IC INE AND HYG I ENE
Ch i ldren are said by some . to suffer l i ttl e or n ot at al l ,an d there i s a certa in amoun t o f truth in th i s as theymay, whi lst hai bouring th e paras i tes, be capable of
playing about an d taking in terest in the ir surroun d ings .Careful in qu iry
,however
,wil l usual ly Show that dur ing
a great part o f the day they are l i stl ess,do n ot take food ,
or otherwi se show s ign s of i l l -heal th . They have usuallya defin i te en largemen t o f the spleen .
Labial herpes i s common in malar ia,but as a rule does .
n ot occur t i l l l ate in the attack,an d frequen t ly occurs
when the fever begin s to subsi de .
The great pecu l iar i ty of subtert i an fever i s the l i ab i l i ty ,with l i ttle or n o warn ing
,to the SO-cal led pern i c i ous
man i festat ion s . These are in the main due to bl oodstasi s in d i fferen t organ s o f the body
,caused by the
n umbers o f red corpuscles con ta in ing the paras i tes ad
her ing to the wall s o f th e cap i l lar i es an d to each other,an d so obstruct ing the c ircu lat i on in that organ . Thismay occur in any organ ,
an d the e ffects and cl in ica lman i festat ion s vary accord ingly .
( 1 ) When stasi s o f the b l ood occurs in th e cap i l lari esof the cen tral n ervous system the danger i s great, an d alarge n umber o f deaths are due to th i s con d it ion . The
symptoms vary in adul ts and in ch i ldren .
In adults the pat i en t usual ly has a flushed face an d
appears to be dul l an d stup id with s low speech and
un certa in gait . In appearan ce an d demean our he i s n otun l ike a m an in the early stages o f in toxi cat i on . Thisstupor m ay pass o ff in mild cases, but in others rap idlyin creases
,an d a con d i t i on of coma superven es . There
are n o con vuls i on s in the great maj ori ty o f cases an d n o
l ocal iz ing symptoms . In a fatal case the coma deepen s,
the breath ing becomes stertorous and the con j un ct ivaein sen s i t ive . Even at th is stage recovery may occur wi then erget i c treatmen t
,or rarely even without i t . Recovery
when i t o ccurs i s rap id and complete , the pat ien t intwen ty-four hours may appear to be in fa i r h eal th .
There i s n o more strik ing in stan ce of the effects of
vigorous treatmen t t han in a case o f th is kin d .

SUBTERTIAN MALARIAL FEVER 45
If un treated an d the pat i en t recovers, the attack usual lyrecurs
,an d i s then fatal very rarely does he survive two
attacks at short in tervals W i thout an t imalaria l treatmen t .In ch i ldren the on set i s l ess gradual ; usual ly the first
th ing n ot iced i s a con vuls i on . When th i s has occurredother con vulsion s rap idly fol low
,the ch i ld remai n s coma
tose between th e con vuls ion s,an d death occurs in four
to twelve hours from the first attack .
Even when the convulsion s have con t inued for two orthree hours
,recovery i s the rule with en erget i c treatmen t,
an d i s complete .Such con vuls ion s are the usual eviden ce of cerebral
malaria up to the fi fth year o f l i fe . After th i s per iodcoma without convuls ion s begin s to be more common
,
and after the ten th year convuls ion s are h ighly excep
tional. In these cerebral cases the temperature may bel i tt le rai sed
,or temperature up to 1 05
°F . may be n oted .
They are n ot assoc iated with hyperpyrexia .
(2) The lungs may be a preferen t ia l s i te, an d there i sin creased rap id ity of breath ing . Provided that the con
di t ion of the heart an d lungs i s soun d there i s comparatively l i ttl e danger . The congest ion o f the lungs in duced,though it may give r i se to susp ici on of pn eumon i a
,does
n ot seem to be serious in i tsel f . In any con d it i on ofcardiac disease
,or in pulmon ary con d it i on s such as
emphysema an d bron ch it i s,the danger i s greater
,as the
e ffect of such d iseases i s aggravated . In cases o f tuberculosis there i s O ften haemoptys i s .
(3) If th e abdomin al viscera,an d parti cularly the
in test in al cap il lar i es,are blocked
,the congest ion in duced
may lead to a con d iti on of col lapse— the algide form ofmalar ia . In such cases the congest ion of a part or thewhole o f the in test i n al wal l may be suffic ien t for haem or
rhage to take place in to the lumen of the al imen tarycan al
,an d hmm atem esis
,melaen a
,or haemorrhage from
the rectum may resu lt,according to the port ion of the
al imen tary can al in volved . Occas ion al ly,with or without
such haemorrhage,th e n utr it ion of the superfic ial layers

46 TROPICAL MEDIC INE .
AND HYGI ENE
of the mucosa i s suffici en t ly Impai red to ren der th i s membran e vuln erable to the vegetable organ i sms
,baci l l i
and cocc i,presen t in th e al imen tary can al . In that case
exten s ive superfic ial n ecros is occurs an d ulcerat i on mayresul t
,which wil l o f course persi st after the malar ia l attack
h as been rel ieved or has passed o ff (figs . 20 and
FIG . 20.—Parasites in Capi l laries of Pancreas.
(4 ) The cap i l lari es in the heart may con ta in blooda s imi lar con d it ion o f stasi s . This i s probably on e ofth e causes of the card i ac fai lure that frequen t ly occursin malaria . Person s wi th old organ i c card iac misch ief
,
pericard ial adhes ion s,or fatty degen erat ion of th e heart
should,therefore
,n ot be exposed to the ri sk of acqu i ring
malaria . The mortal i ty from malari a in chron i c alcohol i csubj ects
,and in person s with beri -beri , i s probably due

SUBTERTIAN MALARIAL FEVER
to th i s stas i s in cardiac capi l lar ies in part,but may occur
with quartan malaria,especial ly in cases of ber i -beri
,an d
so may be due to a direct toxi c effect on the card iac n erves .
(5 ) The blood-pressure i s usual ly ra ised as a result ofsuch stas i s
,an d actual haemorrhages are not in frequen t
and may occur in an y part of the body. Where therei s ol d atheroma in the cerebral vessels
,fatal cerebra l
haemorrhage may occur .
FIG . 2 1 .—Parasites in Capi l lary from Intestine.
Complica tions.
—Albuminuria in some places i s commonduring a febri le attack ; in other places i t i s un usual . In
chi ldren n ephri t i s i s a common sequela,but in adults i t
i s rare ; th i s n ephr it i s i s sometimes fatal . In manymalarious coun tries th is sequela i s n ot met with . Hmm o
globinuria, an d i ts poss ible relat ion sh ip to malar i a,wi l l
be con s idered un der blackwater fever . Glycosuria mayoccur during the febri l e attacks
,but i s rare .
“ Haem or
rhages may occur from various parts o f the body . Ep istaxis i s common . Haematemesis
,melaen a
,passage of
blood by rectum,though rare, have been seen on many
occasi on s . Haematur ia has been recorded , but i s veryrare . ‘
N euri t i s , peripheral an d multip le, i s o ften described,but in most in stan ces i t i s more probably due to alcohol
,
arsen i c,an d Somet imes to ber i -beri as a rare sequela i t
does occur,an d th en rap id improvemen t takes place with
qu in in e treatmen t ; St i l l more rarely paraplegia may

48 TROPICAL MED ICINE AND HYG I ENE
fol l ow an acute cerebro -sp in al attack . N euralgi a i s o ftenattr ibuted to malar ia
,an d migrain e has been ascr ibed
to the same cause,but there i s l i tt l e ev iden ce that there
is any con n ect i on between these d i seases an d malari a .
Attacks n ot un l ike pet i t mal may occur with malar ia,
an d may recur as l ong as the malari al in fecti on persi sts,
but they are rare .
Repeated congest i on may be in part-the cause of thechron i c en l argemen t o f the spleen , of some o f the fibroticchanges in the l iver an d other organ s
,an d of the
‘
ten den cyo f pregn an t women to abort
,but th e in fluen ce of tox in s
in in ducing these co n d it i on s can n ot be excluded .
(6) The mechan i cal effects due to the temporary bloodstas is caused by the capi l l ar ies o f one or two or moreo rgan s be ing part ia l ly b locked by corpuscl es con ta in ingparas ites wi l l l ead to congest ion of those organ s an d to anin adequate supply of fresh ly oxygenated blood . Waste
p roducts al so are n o t removed su ffic ien t ly rap idly, an d ,i t
has been po in ted out that the in terferen ce wi th the c i rculat i on wi l l resul t in a local accumulat i on of the malar ialtoxin . Cerebral or other l ocal symptoms are main ly acomb inat i on o f the effects in each organ ,
but in suchcases extra work i s always th rown o n th e heart
,and
cardiac fa i lure may be the resul t . The immediate e ffectso f th i s cond it i on have been con s idered ; they con st i tutethe main danger to l i fe in th i s d i sease . Sequelm of thecon dit ion are n ot so common
,t hough even temporary
impa irmen t o f the n utrit i on of certain parts of the body,ren dering the t i ssues more vuln erable
,may lead to chron i c
changes . The frequen cy with wh ich tuberculos i s in th eWest I n d ies dates from attacks o f malar ial fever may betaken as an in stan ce . The blood changes, accord ing toN ewham
,do n ot as a rule affect the opson i c in dex; an d
therefore do n ot,in themselves, ren der the person more
suscept ible to bacteri al d i seases .In subtert i an malari a
,as in other forms of malari a ,
the e ffects of toxin s’
must be con s idered as wel l asthe effects of the blood stas i s—th i s on ly pecul iar to

50 TROPICAL MEDICINE AND HYG I ENE
well -made fi lms,e i ther fresh
,or pre ferably stain ed by
Lei shman ’s method,the paras i tes can be foun d usual ly
with l i ttl e d ifficul ty . The essen t i al i s that the fi lms ,Whether wet o r dry
,are so spread that in con s iderable
port i on s of the fi lm the corpuscles are lying flat and
separate from on e an oth er .The eviden ces o f malar ia derived from blood examin a
t i on s are
( 1 ) D i scovery o f parasi tes . This i s con clus ive,but
in person s who have been tak ing quin in e th e n on
d iscovery does n o t prove that the pat ien t h as n ot gotmalar ia . In the i n terval s between attacks of fever ,whether after treatmen t or n atural ly
,a prolonged search
may be n ecessary before the paras i tes are foun d .
(2 ) P igmen ted l eucocytes, usual ly the large mon on uclear or hyal in e leucocytes . These are con clus ive of
recen t malar ia . They are o ften very scan ty, so that it'
i s on ly rarely that they a id in the d iagn os i s un l ess a
prolonged search be made .
(3 ) I n crease in the rel at ive proport i on of th e largemon onuclear l eu cocytes
,with out any in crease in the
tota l n umber o f l eucocytes . In malar ia and for avari abl e peri od after malari a the proport ion o f largemon o n uclear leucocytes i s ra i sed to 1 5 per cen t . oreven more . Th i s change i s not affected by the adm in is
tration o f qu in in e,an d i s more marked when t here i s n o .
pyrexia . It i s therefore o f great value in j ust thosecases of malari a in wh ich the paras ites are n ot to befound . It does n o t
,however
,prove that the malari a i s
st i l l presen t,as the change i s so pers i sten t , but, as a rule ,
i t in d i cates past malar i a . If there i s a coexist ing diseasesuch as pn eumon i a
,seps is
,or even acute hepat i t is, which
produces an in crease in the n umber of polym orpho
n uclear leucocytes,th i s change wi l l completely mask the
mon on uclear i n crease o f malari a in a d ifferen t i al coun t .In ch i ldren i t i s o f l ess value, as in them an in crease in
the large mon on uclear l eucocytes i s fa irly common without any d isease .

PATHOLOG ICAL ANATOMY I N MALARIAL FEVER SI
Prognosis i s good, but en ergeti c treatmen t may be
requ ired,an d relapses wi l l gen eral ly occur un less the
treatmen t be prol onged for mon ths after the last on seto f a febri le attack . When pern i c i ous symptoms superven e there i s great danger
,an d
,un l ess these can be
speed i ly con trol led,death wi l l o ccur . If
,the recogn i t ion
of the n ature of the d isease i s made early the pat ien t wi l lusual ly be saved .
The case mortal ity among hosp ita l pat ien ts i s smal lwhere the d iagn osi s i s made accurately
,an d also in
private,but the n umber o f deaths due to malari a un
treated or in efficien t ly treated i s large,but impossible
to calculate . Th e h igh mortal i ty in t he Trop ics,I ndia
,
Afri ca,&c.
, i s l argely attr ibutable to fever, both amongstEuropean s an d n at ives
,and i s th e main cause o f the
h igh in fan t i le mortal i ty from convuls ion s .The prognosis i s much less favourable when malari aoccurs in person s suffering from other d iseases . Organ i ccardiac d isease
,an d d iseases such as ber i-beri or chron i c
alcohol ism,which affect the in n ervati on of the heart
,
render the progn osis less favourable . When th ere i satheroma of the cerebral vessel s
,fatal cerebral haem or
rhage may occur . Syph i l i s in a person with malariawi l l n ot yield to an t i syph i l i t i c treatmen t t i l l the malariai s treated .
Pa thological An a tomy—The gen eral appearan ces may
be in ferred from the symptoms . In an acute case therei s always congest ion of some of the organ s
,an d in those
in which blood stas is has Occurred th is may be extreme .
Paras i tes wi l l be found in the cel ls in the capi l lari es or,
i f the examin at ion i s too lo ng after death , p igmen t fromthe breaking down of these paras ites . Cloudy swell ingof the cel ls of the l iver an d kidn eys i s usual ly presen t .The spec ial changes co n si st o f the deposi ts of malarialp igmen t in the con n ect ive t i ssue cel ls o f the l iver an d inthe paren chymatous cel ls o f the spleen .
Th is p igmen t i s fin e an d in tracel lular when derivedfrom recen t malarial in fect ion ,
an d i n travascular when

TROPICAL MEDICINE AND HYGI ENE
parasi tes are presen t . It i s much coarser an d n ot
obviously in tracel l ular when der ived from an ol d in fect i on . In cases where haemolys i s has been great
,baomo
siderin may be found abun dan tly in the,hepati c cel ls
,in
cel l s in th e convoluted tubules of th e k idn eys an d somet imes ln the spl een . Gran ules giving the reacti on s o fi ron (in i ts in organ i c combin at i on s) may also be presen t .Large haemorrhages are excepti on al
,but smal l sub
serous haemorrhages or pun ctate extravasat ion s in the
organ s such as the bra in are more common . Thelymphati c glan ds are somet imes en larged
, an d rarelyP eyer ’s patch es . More common ly theMalp igh ian bod iesin the sp leen are en l arged an d
,as they are nOt p igmen ted,
stan d out boldly as wh ite spots again st th e blacki shbackgroun d of the paren chyma.
Decompos i t i on i s n ot usual ly rap id,but the paras i tes
d i e shortly after th e death of thei r host . Blacken ing oforgan s from decompos i t ion must n ot be mistaken formalar ial p igmen tat i on . If the examinat i on be madeshortly after death the sp leen i s a lways firm
,but when
th e rigor m ortis o f the t i ssues has passed off,an even t
that occurs earl i er than the d isappearan ce o f rigor m ortis
of th e volun tary muscl es, i t i s so fter an d more flacc id ,but on ly becomes diffluen t in the early stages ofputrefact i on .
Accumulat ion s o f paras i tes are foun d in th e cap i l lar i esin vari ous organ s ; even in th e same case they may befoun d in m any organ s , l ess common ly they may be foun do n ly in the cap i llar i es o f on e Organ .
In fata l cases the cap i l l ar i es of the bra in,heart
,in tes
t in es an d other abdomin al viscera are thus affected mostfrequen tly , but in oth er organ s, such as the lungs , thecap i l lari es m ay be foun d in the same cond it i on .
Whatever organ i s involved i s markedly congested,and
somet imes i s of a dul l s laty col our from the p igmen tcon ta in ed in the paras ites or in the cel l s in t he paren chyma .
The spleen i s a lways engorged an d tumid,an d th i s i s
shown by the ten se smooth capsule free from wrin kles

TREATMENT I N MALARIAL FEVER 53 .
and the broad roun ded edge of the organ . It i s n o t
n ecessar i ly much above the average we igh t when deathoccurs early in the course of the d i sease , an d then it
usually weighs 1 0 to 1 5 oz .,rarely more in an adul t .
Examin ed microscopical ly malar ia l p igmen t i s a lwaysfound
,but in early cases the spleen to the n aked eye
may appear red ; the den se b lack colour somet imes seeni s foun d in chron i c cases
,and -may be on ly the remn an t
o f malar ia previ ously con tracted .
The l iver also i s p igmen ted,
an d the pigmen t isdeposited main ly in
,th e cel l s between th e l obules
,so
much so that in some cases the outl in es of the lobule sappear to be pen ci l led out in black .
Treatmen t—Many drugs have been employed,qu in in e
,
methylen e blue,arsen i c
,opium
,&C . ,
but of these on lythe first two have a marked effect on the parasi tes . Thoughthe in organ i c compoun ds o f arsen i c have l i ttl e effect onthe paras i tes th e organ i c compoun ds
,such as atoxyl
,
soam in an d salvarsan,have a marked effect an d may be
of value in the rare cases where the paras ites are qu in in eres isten t . S in ce the gen era l adopti on of blood examin at ion has led to a sure d iagn osi s
,th e value of qu in in e in
malaria has been fu l ly con firmed .
Any of the salts of qu in in e may be used . The ethylcarbon ate
,euquin in e, has the great advan tage of being
tastel ess,an d i s used for ch i ldren an d such adults as have
great distaste for qu in in e . It i s too expen s ive for gen eraluse .
Solubil itywater
Quin inaQ . hydroch lorideQ . bihydrochloride
Q . sul phateQ . bisulphateQ . hydrobrom ideQ . b ihydrobrom ide
Q . ethyl carbonateQ . tannate

54 TROP ICAL MED IC INE AND HYG IENE
The form in wh ich qu in in e i s taken i s o f some importan ce . The amoun t of anhydrous qu in in e in the varioussalts d i ffers
,an d th e solub i l i ty of the sal ts also varies , as
shown in th e subj o in ed table,wh ich al so shows the
doses of th e common preparat i on s of quin in e equ ival en tas regards the amoun t o f qu in in e to 1 0 gr . of thehydroch lorate .
With a perfectly healthy stomach and a free secret i ono f hydrochlori c acid , al l these salts wi l l be converted i n tothe hydroch loride or bihydrochloride before they are
absorbed , so that in that case the varying amoun ts o f
quin in e on ly are of importan ce .
When th e stomach i s not healthy or, as i s so often th ecase in malar i a , th e ac id secret i on i s n ot n ormal
,th e
case i s d i fferen t, and at the best the qu in in e wi l l be moresl owly absorbed , or a t the worst on ly absorbed in smal lpart . The sam e occurs with an empty stomach as then
there i s l i ttl e or n o ac id secreted ; and for th e same reason ,
i f the con ten ts o f the stomach do n ot excite gastri c
secret i on ,as when they are main ly water or watery
,
vegetabl e food so lut i on an d absorpt i on of the less solubl epreparat i on s of qu in in e wi l l n ot be complete .
The ac i d set free in th e case o f the sulphates wi l l be
sfllphuric ac id , wh i ch i s n ot of much value in the
d igest ive processes, an d,act i ng as an astringen t
,may
in crease the ten den cy al ready marked in malari a to
d igest ive di sturban ces .When th e hydrobromide i s u sed
,an d st i l l more with
the b ihydrobrom ide, th e amoun t o f bromin e has to becon s idered
,as in 1 0 grain s o f b ihydrobrom ide there i s
bromide equ ivalen t to about 3 gr . o f potass ium bromide .
Where th i s drug i s used as a prophylact i c for l ongperiods
,men tal depress i on may occur n ot on ly from the
qu in in e bu t al so from the bromin e .The hydrochloride con ta in s a l arger proport ion , 8 1 8per cen t .
,o f quin in e ; i t i s a l i ttl e more expen s ive but n ot
suffic ien t ly so to preven t i ts gen eral use. It i s m oresoluble ( 1 part in 40 o f water) and l ess i rri tat ing . The
TREATMENT IN MALAR IAL FEVER 5 5
b ihydroch loride con ta in s 72 per cen t . of qu in in e i t shouldalway be used for in tramuscular an d in travascular in ject ion s as i t i s soluble in on e part of water . It i s also bestfor rectal in j ect ion s .
Quin in e may be given ( I ) by the mouth ; (2) by therectum ; (3 ) by i n tramuscular in j ect ion ; (4) by in travenous in j ect i on .
( 1 ) By the mouth i s on the whole the most conven i en tmethod
,and i t suffices in the vast maj ori ty of cases .
The quin in e should be given i n solution d issolved inwater with the addit ion of an ac id when a rap id effect i sd es ired and in al l cases for treatmen t o f the acutecon d it ion s hydroch lor i c or hydrobromic i s the best
,but
sulphuric or tartari c ac id may be used . Lime j u ice,e ither
fresh or preserved , sherry an d other ac id solut ion s mayal so be used as so lven ts . When given in solut ion i t i scerta in ly an d rap idly absorbed
,but the taste to many
peopl e i s n auseat ing .
Fresh ly made p i l ls,made by the addit i on to qu in in e
sulphate or hydrochlorate of a smal l crystal o f tartari cacid an d a drop of water, have n o disadvan tage .
Sugar-coated p i l l s,tab lo ids
,or tablets or o ld p i l l s must
n ot be used, as they are frequen tly passed un disso lved .
Compressed un coated tablets are occas ion al ly,but rarely
,
passed in th is way under ordin ary circumstan ces . Theymay be used for prophylaxis
,during convalescen ce
,an d
in mi ld attacks, i f the tongue be Cl ean an d there are n osymptoms of dyspeps ia , but should n ot be rel i ed upon in
severe attacks . They are conven i en t when travel l ing asthey can be readi ly broken up an d d issolved i f required .
Before us ing tab lets in cases of fever,typhoid fever must
be excluded . Fatal haemorrhage has occurred in cases oftyphoid where qu in i n e tablets have been given . Quin in ei s sometimes taken in c igarette papers , but i t i s n o t certainthat taken in th i s way the qu in in e wi l l be absorbed
,an d
in many places gelat in e capsules are used , but the gelat in eoften becomes hard and i s n ot d isso lved in the stomach .
(2) Admin i strat ion by the rectum results in very rapid

5 6 TROPICAL MEDIC INE AND HYG I EN E
absorpt ion . It i s part i cularly useful when there i s muchvomit ing and when i t i s des i red to give frequen t largedoses , as in comatose cases or in ch i ldren with con
vulsions,as i t i s n ecessary that large doses should be
absorbed,and that these doses should be repeated at
short in tervals . A prel im in ary en ema i s n ot advi sableexcept when th e rectum is l oaded with faeces .The hydrochlori de or b ihydroch loride, d i sso lved in themin imum amoun t o f ac id an d freely d i luted
,up to four
or s ix oun ces in an adul t,shou ld be used an d in j ected
very sl owly .
The in j ect i on must be given warm,an d with a fair ly
l ong tube (a N o . 8 j aques catheter fixed on th e n ozzl e of aglass syringe i s a con ven i en t i n strumen t to use ) t o be surethat i t i s reta in ed .
In Ch i ldren i t i s n ecessary for the n urse to keep th ebuttocks pressed together to en sure the reten t i on o fthe qu in i n e solut ion t i l l i t i s absorbed . I rri tat i on an d
in flammati on of the rectum are sa id to fol l ow th i smethod o f adm in i strat i on
,when the sulphate d isso lved
in sulphur ic ac i d i s g iven,but even then these results
are excepti on al .
(3) I n tramuscular in j ecti on has man y advocates . The
results are good but n o better, even i f as good , in
comatose cases than rectal i n ject ion s . It i s assumedthat absorpt i on i s rap id . The qu in i n e i s
,however
,prec i
pitated in the muscl e,an d i s gradual ly absorbed ; the
great advan tage of i ts admin i strat ion i s that i t i s be ingcon t in uously absorbed . It i s parti cularly useful in
person s wi th chron i c dyspepsi a or gastri c i rr i tab i l i ty, an d
a comparat ively smal l dose ( 1 0 gr . dai ly or o n al tern atedays) of quin in e i s requi red .
Precautions.—U n l ess an t i sept i c precaut i on s are adopted
th ere i s danger of tetan us or format ion of abscesses, an d
the in j ect i on must be made in to a large muscle . Semplehas shown that h owever stri ct these precaut i on s may be , i fthere are any tetan us
‘
spores in the body, or in troducedshortly a fter the in j ect i on
,th ese wi l l
'
multiply at the s iteo f the qu in in e in j ect ion an d tetan us occur .

58 TROP ICAL MED ICINE AND HYG I ENE
5 -gr. doses may be g iven at corresponding in terval sin the same man n er . I f there i s any S ign o f cardiacfa i lure, st imulan ts, preferably alcohol i c, must be freelyadmin i stered . Every effort must be made to keep thepat ien t al ive
,as recovery i s certa in i f the qu in in e has t ime
to act . H ot packs in adults an d hot bath s in ch i ldrenare ben efic ia l an d must be used in addit i on to qu in in e .The t ime of giving quin in e wi th referen ce to feveri s n ot co n s idered to be of so much importan ce n ow asi t was. The act ion of th e qu in in e i s more dec ided i fi t i s g iven when the spores are set free
,an d t herefore
in ben ign tert i an an d quartan a smal l dose given beforethe r igor i s more effect ive than the same dose later .It i s in the peri od immed iately before the on set of feverthat sporulat i on occurs an d
,therefore
,when q u in in e acts
best ; and there i s n o advan tage in reduc ing the temperature art ific ia l ly
,as by the use o f an t ipyret ics
,before g iving
the qu in in e, except that vomit i ng i s less l ikely to en suean d the headache i s less . In al l cases of mal aria
,treat
men t with qu in in e must be con t in ued for a l ong periodafter the
,
disappearance of the symptoms .A common ly successfu l pract i ce i s to give 1 0 gr .da i ly for on e week
,every other day for two weeks
,an d
twi ce a week for a mon th,an d 1 5 gr . on ce a week for
two mon ths . In the maj or i ty of cases,even i f l arge
doses o f qu in in e have been given dur ing the pyrex ialperi od
,relapses wi l l occur un l ess the use o f the drug be
persi sted in . In the experien ce of the wri ter the in term i tten t admin i strat i on of qu in in e i s n ot so sat i sfactoryas a regular da i ly dose o f 5 gr . of th e hydrochlor ide ofqu in in e . I f g iven during a meal , say breakfast, th eun coated tablo ids can be used . In a few cases of ben ignterti an a three mon ths ’ course i s n ot suffic ien t, but in thevast maj ority o f cases i t i s in subtert ian malaria .
In malaria there i s ustI ally con st ipation ; th i s shouldbe rel i eved
,preferably by sal in e aperien ts, but calomel
and calomel and jalap'
are used by many .
An t i pyret i cs,such as phen acet in
,are n ot advi sable in

NURS ING IN MALARIAL FEVER 59
severe cases on accoun t o f the risk of card iac fai lure . In
mild cases,i f the headach e be severe
,they give rel ief an d
are harmless .Managemen t —One of the po in ts that i s con stan t lyaris ing in conn ect ion with malaria i s the advi sab i l i ty o fa l lowing the pat i en t to work during the in terval s o f anattack or
,in the case o f subtertian
,when the pat ien t i s
st i l l su ffering from a low type o f fever. In both casesrecovery is d elayed by any attempt at getting up, exposureof any kin d , or work, whether phys i cal or men tal .In ben ign tert i an apd quartan fever i t may be permis
s ible for urgen t work to be don e during the apyrexialin terval . Th is should be restri cted as far as poss ible torout in e work . It must always be remembered that workdon e un der these condi t ion s i s in ferior . With th esubtert ian fever
,even though the temperature be n ormal
o r n early so,n o respon s ible work should be un dertaken
as the pat ien t i s in capable o f act ing with j udgmen t .I n stan ces of grave errors resul t ing in serious calamit iesare common . A very decided stan d has
,therefore
,to be
taken in these cases,as on e of the promin en t symptoms
is an obst in acy wh ich leads the pati en t to in s i st on do ingwork wh en he i s men tal ly in capable o f deal ing with i tsat isfactori ly .
As regard s residen ce in a malarial coun try of a personwho has suffered severely, the gen eral con dit ion has tobe con s idered
,as wel l as the completen ess o f the recovery .
There i s n o reason why return should n o t be allowed i fthese poin ts are sat i sfactory, as there i s 110 in creasedl iab i l i ty to rein fection . On the co n trary
,there i s a
variable amoun t o f partial immun i ty .
Nursing—In an ordinary attack of malari a ski l ledn ursing i s hardly required except for comfort . Thepatien t
,moreover
,i s often i rr i tabl e
,or m ay be sl ightly
d el ir i ous, an d n o unwelcome atten t ion s should be persi sted in except such as may be absolutely n ecessary .
He Should be protected from n o ise,bright l ight
,and
above al l from draughts .

60 TROP ICAL MEDIC INE AND HYG I ENE
Blankets and cloth ing requ i re changing after th e sweating stage, and both must be kept thorough ly dry an d
warm .
Warm sponging after the sweat ing stage . i s comfort ingand clean ly .
Dur ing the stage o f r igor hot bott l es are apprec iated,
but are n ot n ecessary . Some protect i on to the bed isn ecessary
,as the persp irat i on i s frequent ly suffic ien t t o
soak through the bl an ket,and mattresses thus acquire a
pecul iar,un pleasan t
,musty smel l .
To protect the bed fin e n at ive grass mats placed un derthe blanket are serv i ceable ; t hey are usual ly cheap an d
can be washed an d sun n ed . In hot weather these matswil l be foun d very cool an d pleasan t to l i e on . Waterproof sheets
,such as are used in Englan d
,peri sh rap idly
in th e Tropi cs an d are expen s ive .
If there i s much vomit ing S in ap isms shou ld be appl i edt o the ep igastrium . D rinks should then be given hotor i ced
,an d in smal l quan t it i es at a t ime .
In the severe forms of fever more atten t i on i s requ iredAny ten den cy to a lethargic cond it i on must be n oted
,
as th is often precedes coma or hype rpyrexia ; and th etemperature must be taken at on ce
,and every hal f hour '
afterwards,i f th i s ten den cy i s observed
,t i l l the symptoms
subs ide,even i f the temperature i s very l i ttle above
n ormal .If coma superven es
,hot packs are by many con s idered
to be o f great value . These may be given on the bed ,but the packs are more read i ly an d rap idly changed i fthe bedding an d pat i en t are placed on the floor . E i thera blan ket or sheet may be used . The blan ket reta in s th eheat longer
,but the Sheet i s more read i ly arranged . The
sheet or blanket must be placed in water of a temperatureten degrees h igher than t he pack i s mean t to be appl i ed .
This i s the safest rule,but in emergen c ies , or when an .
exceed ingly hot pack i s requ ired,i t i s better to use n early
bo i l ing water an d wait un t i l , as tested by the elbow,the
temperature i s such that i t can j ust be born e . This will
be about 1 08° to 1 1 2°F.

NURS ING IN MALARIAL FEVER 6 1
Great care must be taken to thoroughly wring theb l anket
,especial ly at the en ds ; reten t ion of hot water
in these places frequen t ly leads to bl i stering of the
pat ien t . The pati en t should be turn ed on to h i s s i de,th e blan ket i s wel l wrung out an d folded lengthwi se ,the edges must be close to the back of the pat ien tt owards the middle o f the bed . He i s then rol led on
h is back on to the un der half of the dam p,hot blan ket
,
which i s folded roun d h im from head to foot, an d
covered with other an d dry blankets . If profuse perspirat i on does n ot occur, or the temperature ri ses, the packshould be repeated . After the pack i s removed
,wrap
the patien t in a warm,dry blan ket an d rub h im with
warm dry towels . These packs must be hot, an d in
d esperate cases an d with a pat i en t deeply comatose acertain amoun t of b l i stering may resul t . Th i s i s usuallydue
,n ot to the excess ive heat , but to imperfect wringing
o f the pack . When the temperature i s so h igh thathyperpyrexia i s feared col d or even i ced baths may berequ ired . The pat ien t should be lowered in a sheetin to the bath at a temperature of 85
°
F an ass istan tsupport ing the head . Co ld water i s gradual ly added an d
wel l mixed,or i ce
,i f avai lable
,m ay be added . The tem
perature of the pat ien t must be taken frequen tly, everyfive min utes
, per rectum,as when on ce i t begin s to fal l
,
an d has fal len below a poin t of danger,1 02
"
F .,i t wi l l
con t inue to fal l after removal of pat ien t from the bath,an d
dangerous or even fata l col lapse may occur i f th e tem
perature has been too much reduced . St imulan ts arepract i cal ly always required . When a bath i s n o t avai lablecold or i ced packing i s sometimes employed . A hal f packi s very useful
,an d can be man aged s ingle-han ded . The
pat ien t,str ipped to the h ips
,i s p laced on h is back on
a waterproof sheet or n at ive mat,an d large towels wrung
out of cold water are placed on h is chest or abdomen,
completely covering them,an d tucked in at the s ides .
These towel s are to be repeatedly changed an d ren ewedfrom a bucket of cold water placed at the beds ide . Th is

62 TROPICAL MEDIC INE AND HYG IENE
water may be further cooled with i ce,or a b lock of
smooth i ce may be rubbed up and down over the wettowel as i t l i es on t he pat i en t , so as to keep i t con stan t lycold—“ i ce plan ing .
” Cold application s, ,
ice-bags,&c. ,
t o the head shoul d al so be used .
Adm in istra tion of Quin ine.
— This,when given by the
mouth,may cause vomit ing .
- The ord in ary precaut ionsshou ld be taken
,but i f the vomi t ing is un con trol labl e
hypodermic in j ect i on s o f morphia, gr. , should be
given,preferably over the ep igastri um . I t i s absolutely
n ecessary that qu in in e should be absorbed , and i f itcan n ot be read i ly reta in ed by the stomach i t must beadmin i stered in some other r m an n er. In giv ing qu in in eby the rectum the n ozzle of the syr inge an d th e longtube used must be warm
,or a fun n el an d tube may be
used . The in j ect ion should be given wel l above the
an us , an d must be made very slowly .
The pat ien t i s to be kept perfectly st i l l an d th e buttocksshould be pressed together in order to coun teract anys l ight effort s at strain in g . In ch i ldren the n urse mustmai n ta in th i s pressure for hal f an hour
,otherwise the
in j ect i on wi l l n ot be retain ed suffic ien t ly l ong for absorpt i on to take place .
Superfic i al hypodermic in j e ct i on s of qu in in e must n otbe gi ven as they are pain fu l an d often fol l owed byabscesses . ‘
If admin i stered by in j ect i on the quin in emust be in troduced in to on e o f the larger muscles
,such
as the gluteus maximus . I n j ect i on s in to the forearm, or
amongst any mass of smal l muscles, cause a good dea lo f pain an d swel l ing, an d i f in j ected in to or c lose toa n erve trun k may cause perman en t paralys is . Th i sacci den t o ccurs most frequen t ly i f th e in j ecti on s beg iven in the forearm . The most importan t po in t t obe remembered about t hese in j ect ion s i s the ir l i ab i l i tyto cause tetan us or abscesses . Such acciden ts appearto be due to the in j ury in fl i cted by the qu in in e uponth e t i ssues w ith wh ich it
'
cam e in con tact,thus fac i l itat ing
the growth of any organ i sm in troduced with i t,or
,as

ADMIN ISTRATION OF QUININE IN MALARIAL FEVER 6 3
Semple has shown,already presen t in th e pat ien t . The
r i sk does n ot occur where str i ct an t i sept i c precaut ion s.
are taken . The skin at the po in t o f in j ect ion must beclean ed and t horoughly washed with an t i sept ics
,a lcoho l
an d ether,and 1 in 20 carbol i c acid , 2 per cen t . lysol , or
aceton e, fol lowed by 25 per cen t . so lut ion of t in ct . ofi odin e , which is the best . The syringe must be steri l izedby bo il ing, an d the solut i on of qu in in e must be steri l izedin the same way immediately before use . It i s somet imesobj ected that i t i s the adul t an d more than half gi ownparas ites wh ich cause the change in the corpuscles
,an d
that these parasites are n ot amen able to the act i on o fqu in in e . No doubt th is i s so to some exten t ; but itmust be remembered that qu in in e has an act i on 0 11 paras i tes en closed in red corpuscles ; an d secon dly , that as theparas ites sporulate that port ion o f the block due to thatcorpuscle g ives way, so that un l ess the corpuscles caus ingthe stas is are con t in ual ly re in forced by fresh corpusclescon ta in ing more or less hal f-grown parasi tes the c irculat i on wil l be restored . In practice
,by giving large doses
of quin in e repeatedly the mortal ity i s n o t very large ,often three or four cases wi l l be treated in the sameward without any deaths . Cases do die
,but usual ly
with in two to four hours of admiss ion . If they l ivemore than four hours d eaths are except i on al .Syn thet i c an t ipyret i cs
,such as an t ipyrin an d phen acetin
,
g ive rel ief, but should on ly be used on pat ien ts who are
in bed an d in mild cases . They may, in severe cases ,be the cause of fatal col lapse . On the whole thei r usei s to be deprecated . In comatose cases , in addit i on tothe free use of quin in e
,alcohol i c st imulan t s are requ ired .
The use of a cardiac st imulan t wh ich acts also as a
vasomotor d i lator,such as alcohol
,i s far better than
strychn in e or dig ital i s .H ot packs in adults and hot baths , with a l i ttle
mustard in them ,in ch i ldren are of great value in th e
comatose or convuls ive cases .Fowl—Li tt le food can be taken during a sharp pyrexial

64 TROP ICAL MED IC INE AND HYG I ENE
attack,an d there i s n o obj ect in forc ing any on th e
pat ien t during th i s period . Th irst i s a common symptom ,
and there i s n o reason why abun dan t flu id should n ot
be taken,provided that smal l quan t i t ies on ly are taken at
a t ime,otherwise vomit ing may be pro voked . Any flu id
taken shou ld be hot ; hot tea i s a favouri te dr in k, butmust be freshly prepared and n o t too strong
,as tan n ate
o f qu in in e may be formed in the stomach an d i s verysl igh tly soluble .
Many of the n at ive remedies,such as lemon -grass tea
,
are comforting an d a id in d iaphores is . In subtert i anm al ar ia the fever i s long con t in ued an d careful feedingi s importan t . Mi lk
,an d mi lk an d barley water or other
l ight food i s usual ly reta in ed an d d igested .
Dur ing convalescen ce, protect ion from ch i l l i s of greatimportance . Good food i s also requ ired ; i t should bel ight
,n utr i t i ous an d vari ed
,as the appet ite i s frequen tly
capr ic ious .Few m en can be persuaded to remai n long in bed even
a fter a severe attack of fever , but a min imum of threed ays Should be in s isted on .
Specia l Cases—In pregn an t women th e frequen cy o fabort i on with or without qu in in e must be kep t in min d .
Un l ess the fever i s con trol led,abort ion wil l take place
in many cases,but qu in in e
,the on ly rel iabl e drug
,
un doubtedly has a s imi lar ten den cy .
Before t reat ing a case o f malari a in a woman,careful
in qui ries shoul d be made in order to fi nd out i f she i spregn an t . If so
,qu in in e must be given
,but in very smal l
doses,gradual ly in creased t i l l the fever i s con tro l led .
The large hero i c doses advocated in an ord in ary casemust on ly be given in pregn an cy i f there i s urgen t dangerto l i fe . A pregn an t woman should be kept in bed forat l east on e day before th e qu in in e i s g iven . D rasti cpurgat ives must be avo ided
,but a fai r act i on of the
bowel s must be obta in ed,an d th e qu in in e given after the
l axat ive has ceased to’ act . During the whole course ofthe treatmen t the pat ien t must be kept qu iet in bed .

66 TROP ICAL MED ICI NE AND HYG I ENE
As the bron z ing o f the sk in often masks the an aemia,
th e con j un ct ival an d mucous surfaces must be examin edor the an aemia may be overlooked . The spleen if
en l arged i s hard , an d as a rul e sl igh tly ten der on deeppressure . It may be pain ful . The degree of en l argemen t does n ot correspon d to the anaemia . The l iveri s en larged in some cases an d t en der . Thi s ten dern ess may be so extreme as to give ri se to susp ic ion o fhepat i c abscess . Assoc iated wi th th ese con d it ion s arean orex ia , dyspepsia an d muscular weakn ess . I n somn i a
,
men tal depress i on an d n euralgias are common con com i
tan ts an d may be th e most prom in en t symptoms . In the
more advan ced cases there i s oedema of the legs an d
rarely albuminuria, though in person s su ffer i ng from any
form of Brigh t’
s d i sease the symptoms o f that d i sease wi l lbe aggravated .
Any l aten t di sease presen t i s l ikely to recur or be
aggravated , an d th i s i s spec ial ly th e case wi th syphi l i s .Amongst the rarer compl i cat io n s are various ocu lard i sturban ces . Opt i c atrophy or ret in i t i s may occur
,an d
var i ous forms o f con j un ct ivi t i s . The poss ib i l i ty of amalar ial compl i cat i on must always be con s idered in anyocul ar d i sturban ces in th e Tropics . D iagnos is m ay bevery d ifficul t . Carefu l b lood examin at ion wi l l oftenen able the d iagn osi s t o be made . Prolonged examin at i on may reveal the presen ce of an occasi on al malar ialparas i te
,somet imes of a crescen t
,sometimes o f a r in g
form . Fai l ing th i s , the d ifferen t i al coun t may show arelat ive in crease in the large mon on uclear l eucocytes
,
an d i f th i s be n ot presen t i t i s improbable that the casei s one of malar i a .
In cases o f doubt the pat ien t shou ld be kept in bed ,al imen tary d isturban ces atten ded to , an d quin in e given
in moderate amoun ts, e i ther by in tramuscular in j ect i ono f 1 0 gr . on altern ate days, or in so lut ion by the mouth ,
5 gr . three t imes a day . Food should be l ight and
n utr i t i ous , and in a case o f malari al cachexia rapid improvemen t wi l l take place . When con valesen ce has

COMPLICATIONS IN MALARIAL FEVER 67
commen ced the pat ien t n eed n ot be con fin ed to bed oreven to the house
,but qu in in e must be con t in ued for
man y mon ths . Un der such treatmen t the anaemic con
d it i on rap idly improves,but can be expedited by adm in is
frat i on of smal l doses of arsen i c or o f i ron an d arsen i cby the mouth
,or
,better
,by in tramuscular in j ecti on .
Such mixtures as Easton ’s syrup in 1 -dr . doses wi l loften be foun d useful . Cold “ brac ing cl imates Shouldbe avo ided at first
,the warmer “ relaxing ” c l imates are
more su itable . Later,dry brac ing cl imates
,such as th e
Swiss win ter resorts , or Harrogate in the summer, are
dist in ctly ben efic ial:If th e weather be su itable when con valescen ce i s wel l
establ i shed,as much t ime as possibl e should be spen t in
the open air,an d exerc ise
,n ot of a violen t character an d
always short o f fat igue,should be en couraged .
The en largemen t of the sp l een at first subsides rap idly ,but “some en largemen t wi l l pers i st for many mon ths .Soam in ,
in 5-
gr . doses in tramuscularly, i s advocated bysome . P i erpon t an d Acton give ful l cl oses on s ix al tern atedays
,an d claim excel len t results . I t i s importan t to be
certa in of the diagn os is ; some of the mi lder cases o fsupposed malari al cachexia are the resu lt o f too prolongedun n ecessary admin i strat ion of qu in in e , an d the symptomswil l rap idly cease when qu in in e i s d iscon t in ued .
I l l -effects o f prolonged use of quin i n e are n ot un comm on . The ord in ary effects o f qu in in e—buzzing in th eears
,d izz in ess
,an d so on—are n ot usual ly met with in
person s who hab i tual ly take qu in in e . The main effectsare chron i c
,aton i c dyspeps ia an d i ts sequelae
,an d n er
vous depress ion or i rr i tab i l i ty . Too large doses maycause perman en t deafn ess , but th is i s rare ; more comm on ly gradual but complete recovery takes p lace .Amblyop i a may occur . The on set i s usual ly sudden ,
an d both eyes are a ffected . The pup i l s are d i lated an d
do n ot react to l ight . The di sc i s pal e , there i s a wh itehaze over the fun dus
,an d the vessel s are co n str i c ted .
V i s i on i s l ost completely for a t ime , but as a rule there

68 TROPICAL MEDICINE AND HYG I ENE
i s complete recovery . The con d it i on i s qui te d ifferen tfrom the st i l l rarer opt i c n eur it i s due to malaria
,as in
t hat con d it i on th e pup i l s react to l ight,the fun dus i s con
gested,somet imes there are haemorrhages
,and the d isc
i s swol len .
Sequelce.
—On e resul t o f successfu l preven t ion an d treatmen t o f malaria i s a d imin i sh ed death -rate from al l causes
,
though n o d irec t relat i on between some o f these d iseasesan d malar ia can always be traced .
Tubercu losi s an d dysen tery are spec ial ly pron e to attackperson s who are much reduced by malar i al d i seases .Boi l s an d other sk in affect i on s are very common
,though
n o speci al type of skin d isease can be said to be a sequela .
In in d ividual in stan ces there i s n o proof of loweredres i stan ce to other diseases
,but taken in mass the evi den ce
i s strongly in favour o f malaria in duc ing a con d it i on in
a proport ion of the cases of in creased suscept ib i l i ty tobacterial invas ion s .

C H A P T E R V I .
PROPHYLAX I S .
Etiology—It i s n ot n ecessary to do more than al ludeto the o lder hypotheses as to the causat ion of malar ia .
These were main ly founded on the bel ief that eman at i on sfrom decomposing vegetables or from so i l or rocks such asgran i te caused the fever . These eman at i on s were kn ownas m iasmata
,
”an d were bel i eved to ri se on ly a short d is
tan ce from the groun d during the n ight an d to be di ss ipated by the sun . It i s from th i s hypothesi s that theterm for the d i sease
,malaria
,i s der ived . These observa
t ion s as to the occurren ce o f malaria are in many casesmore readi ly explain ed n ow that i t i s kn own that thed isease i s carried by mosqui toes .We n ow kn ow that malaria i s a parasi t i c d isease
,and
that the paras i tes are conveyed from m an to m an bycertain spec ies of mosqu itoes .As far as we kn ow these paras i tes can on ly exi st in
m an and mosqu itoes . Season al variat ion s occur in mostplaces
,due ( 1 ) to the variat i on s in the meteorologica l
con dit i on s affect ing the multipl i cat i on , breed ing , an d
prevalen ce of su itable mosqu i toes ; an d (2) to the tem
perature being su itable for the developmen t of the malari aparas i tes in these cold-blooded defin i t ive hosts . Localvari at ion s are often due to the prevalen ce an d proximityof suitable warm-blooded hosts—human beings— thein termediate hosts of the malari a paras ites . N at ivech i l dren an d bodies of n ew -comers from n on -malarialcoun tr ies are the most importan t carri ers
,or reservo irs
,
o f the parasi tes to con s ider .Malaria can be propagated from m an to m an by tran s

70 TROPICAL MEDICINE AND HYG I ENE
fus i on or by the in j ect i on of the b lood of a malar ia lpat i en t in to an other person , but th i s method of tran smiss ion can play n o part in the n atural d issemin at ion ofthe d i sease . Ross records fifty-on e successfu l in oculat i on s by man y observers w i th b l ood
,e ither in traven ously
or by subcutan eous in j ect i on . The n atural method , an d ,
as far as we kn ow,the on ly method un der ord in ary con
d ition s, i s by certa in mosqu itoes .
The proofs of the mosquito malar ia hypotheses are asfo l l ows
( I ) The developmen t day by day of the paras ites can
be fo l lowed in a batch of mosqu itoes fed o n a personin whose blood gametocytes are foun d . Th is is sodefin i te that , kn owing the t ime that has elapsed s in cethe mosqu i to was fed
,the appearan ces of the malar ia l
parasite in i t can be pred ic ted with certa in ty . N o suchbodies are foun d in other mosqui toes bred from larvae .
When t hese paras i tes h ave reached a certa in stage ofdevelopmen t the sporozo ites are foun d in the sal ivaryglan ds of these mosqui toes
,an d i f such mosqu itoes be
al lowed to b ite any suscept i ble person he wi ll , after aper i od o f in cubat ion
,develop malar ia o f the same type
as t hat o f the m an on Whom the mosqu ito fed . Th i sper i od o f in cubat ion i s n ot con stan t, an d d iffers with thespec ies o f malaria
,an d also from that found by direct
in oculat i on o f blood . Ross con trasts these from recordshe has col lected as fo l lows
AVERAGE PERIOD IN DAYS BEFORE
SYMPTOMS
Blood inoculat ion Mosquito inoculation1 7I O
8
If qu in in e i s be ing taken the in cubat i on per iod is prol onged
,an d i f taken regularly in smal l doses may be
prolonged by weeks or mon ths,an d symptoms n ot appear
t i l l two or three weeks after the qu in in e i s d iscon t in ued .
(2) Mosqu i toes were al l owed to feed on a pat ien t with

ETIOLOGY OF MALARIAL FEVER 7 1
malari a in I taly,an d tran sported to London . These fed
o n two un in fected person s there an d these person s then
developed malaria .
(3 ) I t has been further shown that people can l ive inmalarial
,swampy coun try
,such as the Campagn a , an d
that so long as they are protected from bites o f mosqu i toesthey wi l l be free from malaria
,though other inhab itan ts
suffer .
(4) Certa in i slan ds in the Trop ics are free from malaria ,though n eighbouring i slan ds in s ight are in ten selymalarious
,e.g .
,Barb ados i s free from malar ia
,whi l st
in St . V in cen t i t i s abun dan t . It i s foun d that in t hemalaria - free i slan d n o mosqui toes capable of carryingmalari a exist
,w h i lst in others they are common . F i j i
may be quoted as an excepti on as there i s n o m alar iathere
,an d amongst the many mosqu i toes sen t from that
coun try on e wi ng of an an ophel in e was foun d . No otherspecimen s have been foun d
,t hough they have been
l ooked for .
(5 ) The success of an t i -malarial operat ion s wh i chd imin i sh the l iab i l i ty to be b i tten by malar i a-carryingmosqu itoes by d imin i sh ing the n umber o f thosemosqu itoes i s an addit ion al proof o f the correctn ess ofthe hypothes i s . In places
,such as I smai l ia an d Kwala
Klang,where the reduct ion in the n umber of these
anophel in es was great,the cases of malar ia dimin i shed
to on e-ten th or l ess . In many other places where th ereduct ion in the n umber of these mosquitoes was less,there was st i l l a dec ided d imin ut ion in the amoun t o fmalar ia .
(6) In many parts o f Afr i ca the l iab i l i ty to malar iali n fect ion in the settlemen ts i s very closely related to theactual n umber of mosqu itoes capable o f be in g malar iabearing .
I t i s o ften urged that al though th is i s on e way in whichmalaria i s caused
,there may be others . It i s possible
t hat in other b lood-suck ing in sects a s imi lar developmen tof the parasi tes might take place
,but there i s 11 0 eviden ce

72 TROPICAL MED IC INE AND HYG IENE
in favour o f su ch a V i ew,an d i t i s except ion al for protozoa
to be equal ly capable o f S im i lar developmen t in widelyseparated groups o f arthropoda .
The’
success of prophylact i c measures u sed on the
hypothesi s that certa in mosqu i toes are
'
the carr i ers ofm alar ia shows that th is at any rate i s the importan tmethod of the propagat ion of malaria . If, when the
poss ib i l i ty of th i s method o f conveyan ce i s removed ,m alaria st i l l con t inued to exi st in any place , spec ia lin qu iry would be requ i red
,but n o such in stan ces are
kn own at presen t . For prophylacti c work,therefore ,
the kn own method in whi ch the d i sease i s carr i ed i s theo n ly one n ow to be con s idered .
Some kn owledge of in sects in gen eral,an d of m osquitoes
in part i cular,i s essen t ial to advi se as to economic prophy
lact i c measures,an d an outl in e o f the class ificat ion of
in sects,an d the pri n c iples on whi ch the mosqu itoes are
cl ass ified,i s g iven in a separate chapter as an appen d ix .
All known carr i ers o f malar i a bel ong to th e d ivi s i on
o f the mosqu i toes kn own as An ophelince. The d i fferen tspeci es of an ophel in es do n ot serve equal ly wel l as carri erso f malaria . Some spec i es are read i ly in fected
,others on ly
wi th d ifficul ty,and some n ot at al l . The dangerous Speci es
are those which are both n umerous an d read i ly conveythe d i sease .For econ omic an d effic ien t prophylaxi s a kn owledge
o f the hab i ts o f each spec i es i s requ ired , an d i t i s foun dthat the di fferen t species vary greatly in the i r hab i ts
,l i fe
h istory, and breed ing-places .In any place or coun try the species o f an ophel in es
must be determi n ed ; those that are good carri ers ofmalaria must be foun d out exper imen tal ly
,an d th e
breed ing-places an d hab its o f these must be stud ied ingreat deta i l .The an ophel in es
,wh ich in clude al l the kn own carr iers
o f human malar ia, are eas i ly d i st ingu ished from othermosqu itoes
,wh ich have a straight
,pen etrat ing probosc i s .
( 1 ) The palps in both m ale an d female are pract i cal ly

74 TROPICAL MEDICINE AND HYG I ENE
2 3An opheles. Cy clolepteron . j an t/z zn osom a .
6
Manson ia. E retmaooa’ites.
9
Psorophora.
FIG . 23 .—Various Forms of W ing-scales (Theobald) . I , Scales on veins
and on costa in An opheles; 2 , scales on veins in Cy clo/epteron 3 , scales on
veins and on costa in j an t/z in osorna 4 , scales on veins in Manson ia5 , scales on veins in S tego/ny ia 6 , scales on veins in E retmapoa
’ites 7 , scales
on veins and on costa in Ca leo‘
c; 8 , scales on veins inMuciclus; 9 , scales onveins and on costa of Psorophora.

ETIOLOGY OF MALARIAL FEVER 75
the same length as the probosc is, an d in the male areclubbed (fig .
(2) The scutel l um ,wh i ch i s more or less tri lobed in
other mosqu itoes,shows n o s ign of such lob ing in the
an ophehn es
(3 ) The scales 0 11 the ve in s o f the wings are lan ceolatein the an ophel in es
,wh i lst they vary greatly in th e other
Culicidce (fig .
(4) The proboscis i s n early in the l ong axi s of thehead
,thorax an d abdomen
,so that the mosqu ito almost
forms a stra igh t l in e . When at rest, as the probosc ispo in ts towards the surface on wh ich th e mosqu i to rests ,the abdomen po in ts away from i t (fig .
(5 ) The larvae have n o resp iratory syphon ; they l i eflat on the surface of the water when a t rest , an d afterthe ir first moul t have compoun d “ palmate tufts a longeach s ide o f the abdomen on the latero—dorsal aspect .(6) The eggs are more or less boat - shaped , an d havelatera l a ir-floats they are la id s ingly an d n ot formed in torafts .For the propagat ion of malar ia al l that is requ ired i s
( 1 ) That su itabl e an ophel in es should feed on a personin whose blood sexual ly mature paras i tes— gametocytesare presen t (2) that these mosquitoes should be kept ata proper temperature for a peri od varyi ng according tothe temperature
,from about e ight to some s ixteen days
0 : more ; an d (3 ) should then b ite a person suscept ib leto malar ia . In about ten to fourteen days such a personw i l l develop malarial fever . As far as i s kn own m an i sthe on ly an imal that ever acts as the in termed iate hostfor the spec ies of paras i tes wh ich cause malarial feverin m an
,an d therefore mosqu i toes
,the defin i t ive hosts
,
der ive the parasi te from m an on ly,an d tran smi t i t to
m an on ly . Any break in the sequen ce w i l l resul t in thed estruct ion o f the paras ites , and i t i s with th i s in V i ewthat al l attempts at prophylaxi s must be con ducted .
1 . The parasi tes in m an can be attacked by the use ofquin in e in al l in fected person s
, so that the chan ces of the

TROPICAL MED ICINE AND HYG I ENE
Proboscz s
FIG . 24 .—A, Lateral V iew of Anophel ine ; B, lateral V iew of Cul icine ; C , Anopheli
v iewed from above ; D, Cul icine V iewed from above ; E, head of Coreth i a ; F, headMegarhinina.

78 TROPICAL MEDIC INE AND HYG I ENE
p lace where he was b itten by an in fect ive an ophel in e .That mosqu ito must have fed on a person in whoseblood gametocytes were presen t some ten days before .
It must always be remembered th at th e gametocytes arepresen t in a person convalescen t from a malar ial attack
,
especial ly from subtert ian ‘malari a .
In a coun try where malari a i s preval en t,those l iabl e
to attack may be d ivided in to two main classes,both
con s ist ing of person s who have n ot acqui red immun i tyby previou s attacks of malar i a
( 1 ) Ch i l dren , n at ive and European,wi l l be l iab le to
h arbour th e paras i tes,as there i s n o hered i tary immun i ty .
There may be some h ered i tary toleran ce. Adults whohave l ived for a l ong t ime in the coun try wi l l haveacqu ired some immun i ty an d therefore wi l l n ot commou ly harbour paras i tes .
( 2) Suscept ib le adults, European an d nat ive,are those
who have l ived long in a n on -malaria l coun try,an d are
therefore n ot immun e . E i ther o f these c lasses in amalar ial coun try may serve as th e start ing-po in t o f freshcases by in fect ing the mosqui toes .The first class are o f most importan ce in fixed sett l emen ts an d also in in fect ing travel lers pass ing througha coun try .
The secon d class are o f spec ia l impor tan ce in open ingup u n i nhab i ted coun try in min es
,plan tat i on s
,an d road
or rai lway con struct i on .
With large bodies of m en outbreaks may or igin atefrom in fect i on acqu ired from n at ive ch i ldren
,or may be
imported by some of the adul ts j o in ing such a force,as
these may harbour the paras i tes . When malaria i s on cei n troduced amongst such a body of m en , each case servesto in fect the mosqu itoes , an d these in turn in fect oth erm en t i l l al l suscept ib l e members of the gan g are attacked .
In travel l ing through a malar ial coun try an en deavourshould be made to avo id being b i tten by mosqu itoes bythe free use o f mosqu i to n ett ing , by avo idan ce of places ,part icu larly for camps
,where the mosqu i toes are likely

PREVENTION OF MALARIAL FEVER 79
to be in fected,an d by the use of qu in in e . The common
pract i ce in travel l ing by r iver of tying up for the n igh tn ear a n at ive vi l lage should be d iscon tin ued . In a town
,
settlemen t,or perman en t camp
,more radical measures
shoul d be i n st ituted .
The pol i cy of i solat i on can n o t be carr ied out fu l ly bymiss ion ar ies
,or by person s in charge of l abour on
exten sive'
works ; an d in coun tri es where n at ive racesare c ivi l ized i t does n o t ten d to improve or a im atimproving the san i tary con d it i on of th e place
, n or atreducing the heavy in fan t i l e mortal ity always met wi thin n at ive races in a badly malar ial coun try.
Un iversal admin i strat i on of qu in in e to'
all person s inwhose blood there i s eviden ce of malarial in fect i on an d
to al l n ew -comers,and vis i tors to a commun i ty must be
s imilarly treated before they are al lowed to res ide ; i t i sexpen s ive an d , except with person s un der stri ct con trol ,impracti cable . W i th troops , gangs o f European workmen ,
an d school ch i ldren,i t can be carr i ed out successful ly
,
sometimes also in smal l v i l lages or settl emen ts .The methods by medic in al mean s
,adopted or advocated
,
for the preven t i on or extermin at ion of an in fect i on of thepeople in a settlemen t fal l in to two groups : ( I ) Theregular dai ly admin i strat i on of qu in in e
,and (2) the regul ar
admin i strat i on of l arger doses at longer in tervals . Thewriter favours the first an d advocates the admin i strati onof 5 gr . of the hydroch loride every day . The obj ect i sn ot to get rap id absorpti on
,as i s requ ired for treatmen t
of the acute con d it i on,but to get s low an d complete
absorpt ion . I f taken as an un coated tablo i d during ameal in any person with a heal thy digest i on i t wi l l be inthe stomach during the t ime when th e con ten ts are acidan d absorpt ion i s most rap id . In person s l iab l e toin somn i a breakfast or the first heavy meal i s the bestmeal wi th which to take i t . Few people can take morethan 5 gr. for prolonged peri ods without i l l e ffects
,but
i t i s admitted that i t'
does n ot preven t in fection thoughi t reduces the paras i tes wel l below the n umber requ ired

SO TROPICAL MED ICINE AND HYG I ENE
to cause symptoms . Man y person s wi l l take th is dosedai ly dur ing the i r whole res iden ce of on e year in Afr i caan d have n o fever at al l
,but i f th ey discon t in ue i t o n
the way home , or o n arr iva l in Englan d,with i n two or
three weeks after they have ceased to take i t they getfever
,show ing that th i s dose had n ot preven ted in fect i on .
It also has l i tt l e effec t in reducing the n umber o f crescen tsal ready formed . In ch i ldren qu in in e tan n ate
,I or 2 gr. ,
made up with chocol ate i s e ffect ive an d i s.
read i ly taken .
Of the methods of admin i strat i on at l onger periodsthere are man y vari at i on s : I O or 1 5 gr . on ce or twicea week i s advocated by some ; I O or 1 5 gr . on the n in than d ten th
,twen t i eth and twen ty-first
,an d last two days o f
each mon th i s preferred by others . Thomson advocatesthe dai ly use o f 20 gr . for a peri od of three we
'
eks fourt imes a year . Th i s dose
,he con ten ds
,ki l ls off both the
sexual an d asexual forms,an d would free the populat i on
from the paras i tes . In i so lated p laces,where the plan
could be adopted simultan eously for the whole pOpulat i on
,t he method i s wel l worth a tri al .
With large stat ion s the most sat is factory resu lts areobta in ed by d imin i sh ing the n umber of the defin i t ivehosts
,an ophel in es . The most vuln erable period in the
l ife-h istory of these in sects i s in the i r larval stage . Th isi s a lways passed in water . A somewhat deta i l ed kn owledge o f the class of breeding-place for the spec ies thatcarry malari a in each place i s requ ired for effect ive and
econ omical work in th i s d irect i on . As these places d i fferfor each spec i es o f mosqu ito
,without deta i led kn owledge
mon ey wi l l be wasted an d the results cause d isappo in tmen t .It i s importan t to have both the cool i e l in es an d the
European quarters at some distan ce from each other, sothat in fected an ophel in es can n ot read i ly pass from on e
to the other,an d that both should be wel l in the cu lt i
vated,cleared and dra in ed area where the n umber o f
an ophel in es has been reduced .
Wet methods o f cu ltivat i on , such as that requ i red forr ice growing or such cult ivat i on as requ ires an exten s ive

82 TROPICAL MED ICI NE AND HYG I ENE
very badly malar ia l p lace would show n o paras i tes , i .e. , i fexamin ati on were con fin ed to adu lts the endemic in dexwould appear to be n il .
Examin at i on o f the ch i ldren who have,when born ,
n o immun i ty wi l l show a h igher in dex . In a very badlymalarial p lace some ch i ldren in th e fi rst s ix mon th s ofl i fe wi l l be foun d to be in fected ; in the secon d s ixmon th s the proport i on with paras ites rapidly r ises, an d
in the secon d to fourth years the great ‘maj ori ty, over80 per cen t . , may show eviden ces on blood examin at i on
of malaria l in fect i on . After the fi fth year the proport i on showing such eviden ces rap idly d imin i shes , so that
FIG . 25 . Negroes (native Africans) .—Hausa and Yomba Chi ldren ,
320 ; Hausa Adul ts, l oo . Compi led from Official Report , Lagos, of W . H .
G . H . Best.
in a very malar ial p l ace the maj or i ty m ay acqu ire immun i ty by the s ixth year or even earl ier
,an d pract i cal ly
all before the ten th year . In a less malarial p lace theproport ion free from eviden ce of malaria in the first fiveyears o f l i fe wi l l be h igher
,an d in th e secon d five years
l ower,an d in places where the amoun t of malaria i s n ot
great,or where in fect i on does n ot occur during part o f
t he year,as in temperate c l imates , a large proport ion o f
the populat ion may n ever acqu ire immun i ty .
A common method for determin ing the en demic in dex

ENDEMIC INDEx IN MALARIA 83
i s to determin e the proportion of chi ldren aged 1 0 yearsor less in whose blood eviden ce of malaria i s found .
This age i s rather h igh ,and the resu lts d iffer i f a large
proport ion are over or un der 5 years of age . In thesame coun try the results would therefore appear to varygreatly according to the ages o f the chi ldren examin ed
(fig .
The best method would be to determin e the age atwhich the largest proport ion of ch i ldren are foun d to bein fected . Thus, i f the largest proport i on of in fected ch i ldren were un der 2 years o ld
,i t would in dicate a h igher
FIG . 26 . Negroes (nat ive Africans) , in a m ost m alarial d istrict inCen tral Africa. Residence required for probable infection w ith malaria,under six weeks.
Native African , in less malarial d istrict . Residence for one
year by a. European does not render infection certain .
en demic in dex than i f the maximum proportion was at
5 , an d st i l l more i f the maximum was in ch i ldren aged 1 0 .
A low rate in person s over 1 0 years of age in a placewhere malaria Is kn own to occur suggests a h igh en demicin dex .
(B) Prevalen ce of en larged spleen . This test has fal lenun deservedly in to disuse on accoun t o f the man n er inwh ich i t was at one t ime abused in I nd ia by the lai ty aswel l as by medical m en . With l imi tat i on s i t i s of con
siderable value . The l imitat ion s are : ( I ) That other

84 TROP ICAL MEDICINE AND HYG I ENE
d i seases, such as kal a-azar , trypan osomias is, &c.
,are al so
causes Of en largem en t °
of the sp leen,an d that therefore
where th ese d i seases are prevalen t the value o f the test i sgreatly reduced ; an d (2) t hat th e examin at ion s should bel imi ted to chi ldren
,as in adults o f many races
,I n d ian s
,
&c. , chron i c en largemen t o f the spleen ,whether as a
resul t o f early i n fect i on of malaria or n ot,
’
persi ststhroughout adul t l i fe
,an d may even in crease .
With n egro races th e resu lts Obtain ed°
by the spleentest are o f h igh value . Wi th other races on ly the exam inations made of ch i ldren up to 1 5 are valuable
(fig . The advan tages o f the method of spleenexamin at i on are that : ( 1 ) There i s less oppos i t i on topalpati on o f the abdomen in ch i ldren than to bloodexamin at i on ; (2) that the examin at i on s can be mademore qu ickly than th e examin at ion of b lood for paras ites
,
an d far more qu ickly than d ifferen t i al l eucocyte coun ts ;
(3) that w i th l i tt l e tra in ing moderately rel iab le results maybe Obta in ed by trustworthy m en with n o medica l educa
t i on ; (4) that the con dit i o n of the spleen does n ot vary sorap idly as the n umber o f paras i tes in the blood . Thus aspel l o f cold or wet weather wi l l often resu lt in an i n crease
in th e proport i on of person s in whose b lood the paras i tes
are suffic ien t ly n umerous to be read i ly foun d,whil st the
p robab i l i t i es o f a n ew in fect i on are n ot affected by suchm eteorological changes . The size of the spleen i s affectedby such changes to a very sl igh t exten t .
(C) The peri od Of res i den ce or exposure requ ired inthe average European or other suscept ibl e person beforean attack of malaria develops i s a very fa ir measure ofthe en demic in dex . Most European s are able to g ivefa i rly defin i tely the period that elapsed between the i rarr ival in the coun try an d the on set o f the ir first attackof fever . The first attack of fever i s usual ly a markedon e
,an d comparat ively few errors in d iagn os i s are made
wi th th i s attack in a malar i ous coun try . The shorter theperiod of average res iden ce requ ired
,th e h igher the
e n demi c index .

8 6 TROPICAL MED ICINE AND HYG I ENE
in dicat ion o f th e presen t danger in a certain house thano f a h igh malari al in dex in a vi l l age or coun try . It al soappl ies on ly to th e t ime at wh i ch the exam i nat i on wasmade
,for i f suscept ible mosqu itoes are presen t in aban d
an ce the in troduct i on of on e or two person s In whoseblood gametocytes are presen t may lead to the in fect i ono f a large n umber o f an ophel in es an d tran sform a placefrom on e wi th a l ow to o ne wi th a h igh en demi c in dex .
Much careful work i s yet requ ired to en sure un i formresults in carrying out prophylact i c measures cheap ly .
En qu ir ies must in clude ( I ) the determin at i on o f th ed angerous an d harmless spec ies of aII Ophelin es presen t ;
( 2 ) the i r breed ing-places ; (3 ) the en demic in dex o fmalari a as determin ed by various methods
,an d with a
suffici en t n umber of observat ion s to d imin i sh the meanprobab i l i ty o f stat i st i cal error .Ross uses a modificat ion of Po i sson ’s formul a by
Professor Karl Pearson ,an d i l lustrates the use by deter
m in at i on of the percen tage error in th e appl i cat i on ofthe spleen test in a vi ll age as fo l lowsLet N be the tota l n umber of ch i ldren
,7: the n umber
examin ed,an d x the n umber wi th en l arged spleen s . f X
1 00 wi l l be the percen tage proport i on with en l argedspleen s of those exam in ed the spleen rate .We can n ot con clude that the same rate wi l l hold for
the en t i re n umber N . Let e den ote the probable percen tage error
/2 x (n -x ) / I _n—I
n N—I
In th e i n stan ce Ross gives (“ Report on th e Preven
t i on of Malar i a in Maur i t ius 200 out o f 800 ch i l dren
in a vi l lage were exami n ed , an d the probable error was
i: so that,as regards merely th e stat i st i ca l error ,
the rate,i f hal f the ch i ldren examin ed were fo un d t o
have en l arged spleen s, would be for the whole in fan t i l epopulat i o n between an d i .e. , 50 i

ENDEMIC INDEX IN MALARIA 87
For a ful l d i scuss ion of the problems involved thereader i s advised to con sult “The Preven t ion ofMalaria , ”by Sir Ron ald Ross, publ ished by j ohn Murray, Albemarl e Street
,W .
,1 9 1 1 .
N OTABLE DATES .
Malaria—D iscovery of the parasi tes, Laveran , N ovemher 6 , 1 880. D i fferen t iat ion of species an d asexual l i fecycle, Golg i and o thers, autum n of 1 885 , and onwards.
Con jugat ion of sexual forms, McAllum ,1 897
-8 . Sexualcycle, Ross, 1 897
-8 .

CHAPTE R V I I .
BLACKWATER FEVER .
THROUGHOUT Tropi cal Afr i ca,haem oglob inuric fever ,
or blackwater fever,i s o n e of the most importan t o f the
d iseases met with an d an importan t cause Of the excessive mortal i ty amongst European s . In the n umerousen qu iri es made in to the causat i on of th isdi sease by vari ousObservers the poss ib i l i ty o f the act ive causal agen t be inga piroplasma
,or other spec ific organ i sm
,has been ful ly
con s idered . No p i roplasmata have been foun d , an d ascompeten t observers have made the examin at ion s
,i f i t
i s due to such a paras i te i t must be to on e so smal l thati t has escaped detect ion . Var i ous observers have foun dother organ i sms
,but in most in stan ces the bodies
described are n ot admi tted to be spec ific organ i sms .The d istr ibut ion of the Afr i can I xod idae does n ot suppor tthe hypothes i s that i t i s a d isease carri ed by t i cks
,as i t
probab ly would be i f i t were a p i roplasmosi s .Blackwater Fever (En demi c Haemoglob in ur i a) .—Thi sd isease i s essen t ial ly an acute haemolys i s , usual ly of shortdurat ion
,termin at ing in recovery , un l ess compl i cat i on s ,
such as suppress ion of urin e,occur . Death also occurs
from the in ten s i ty of the anaemia in duced , an d morerarely from hyperpyrex ia . The causat i on i s n ot defin i te lykn own .
Geographica l Distribution .—It i s a common disease
throughout the whol e o f tropi cal Afr i ca an d occurs insubtrop i cal South Afri ca . It occurs frequen t ly in Assaman d some of the I n d ian terai s ; i solated cases occur inSouth Ameri ca
, an d i t i s common in Pan am a ; in Malayi t i s n ow fa irly common
,and in the i s lands in the I ndian

90 TROPICAL MEDICINE AND HYG I ENE
froth i s p ink, and the spectroscope shows the haem o
g l ob in ban ds . Sometimes i t i s o f a deep brown,
methaemoglob in in that case,
“
an d n ot haemoglob in ,being passed .
The urin e when passed i s a valuabl e gu ide to the durat i on of the acute d isease . If methaemoglobin alon e i spassed th e attack i s on ly sl ight
,but may be fo l lowed by a
more seri ous relapse . If much d i lut i on i s requ ired toren der th e urin e tran sparen t
,a severe attack may be
an t i c ipated .
An examin at i on of the secon d urin e passed should bemade . If the fi rst on ly be examin ed
,con fus i on might
occur,as th i s i s d i luted by the urin e that had previously
accumulated in the bladder . From the examin at ion ofth i s secon d urin e a fa i r est imate o f the durat ion of thehaem oglobinuric per iod can usual ly be made .
(3 ) After the on set o f the haemoglob inuri a ur i n e Is
secreted in much larger quan t i t i es than i s n ormal , and
i f abundan t water be suppl i ed e ither by th e mouth , i fthere be l i tt le or n o vomit in g
,or by the rectum or subcu
tan eously, th e rate of secret i on con t in ues h igh as l ong as
the haemoglob in uria l asts .The frequen cy o f mictu rit ion at first i s on ly in creased
in proport i on to th e amoun t o f urin e secreted,the bladder
be ing empt ied on ly when di sten ded,but later the urin e
i s passed more frequen tly,an d in smal l quan t i t i es on ly at
t imes , as th e ur in e appears to act as an i rr i tan t to th ebladder . Occas i on al ly there i s marked i rr i tab i l i ty of thebladder an d
'
pen is, an d in rare cases reten t i on of urin e .
j aun dice , or rather a yel low sta in ing of the skin and
con j un ct ivae,rap idly develops
,an d in creases during the
con t in uan ce o f the haemoglob in ur ia . There i s n o b i l ein the urin e
,an d the stools are very dark
,so that th e
j aund ice i s n ot obstruct ive,and i s probably haem ato
gen ous . There i s a m arked in crease in th e amoun t ofurob i l in in the faeces . Th is in d icates that the products o fth e blood destruction are d ischarged by the rectum aswel l as wi th the urin e . Con st ipat i on i s usual
,but i s

BLACKWATER FEVER 9 r
e asi ly rel i eved by en emata i f n ecessary . These must beused with great caut i on
,an d purgat ives, in the op in i on
o f the writer,should n ot be given during th i s stage .
Some authori t i es advocate free purgat ion with cal omel oro ther drast i c purgat ives .The temperature remain s h igh
,an d there may be hyper
pyrex ia, but i t fal ls as the haemoglob in uria d imin i shes .There m ay be on ly the in i t ia l r igor, but frequen t ly therei s more than o ne
,and sometimes there are severa l each
day . There i s always n ausea,an d frequen t ly vomit ing
Th i s may be so severe that the smal lest amoun ts o f foodor fluid are return ed as sOon as they are
,
taken . Veryrare ly there i s haematemesi s ; common ly there may bestreaks of b lood i f t he vomit ing be violen t (figs . 28 andH i ccough i s common
,an d may be so in cessan t that i t
becomes a source of danger from the exhaust ion induced .
The progn osi s i s un favourable i f there i s much h iccough .
When on ly occas i on al i t has no prognost i c value . Thereis usual ly n o pain after the on set
,n ot even headache
,but
somet imes there is aching pain in the l o in s,an d the
abdomin al or hepat ic pain presen t at the on set alreadymen t ion ed may recur an d become con t inuous .The rap id developmen t o f extreme anaemia i s mostimportan t . The red blood corpuscles in the course of threed ays may be reduced to or even l ess
,per cub ic
mil l imetre . The remain ing blood corpuscles may bemuch changed, many being mere shadows devo id o fhaemoglob in , or appear fa i rly n ormal an d above theaverage ton i c i ty . Assoc iated with thi s anaemia i s extremedeb i l i ty , an d violen t palp i tat i on s on the sl ightest exert ion .
Death from syn cope may occur during attempts at defaec at ion 01
° even m i cturit i on .
The durat ion of th is stage of haemoglob in uria vari esgreatly ; i t may last on ly two 01
° three hours, but u sual ly,in a moderately severe case
,from two to three days . I f
ri t l asts more than two days the progn osis i s very grave,
u n l ess the prolongat i on i s due to the occurren ce ofr elapses . A seri es of relapses
,in each o f wh ich the

92 TROP ICAL MEDICINE.AND HYG I ENE
haemolys i s i s sl ight, an d in which the urin e clears, or
n early clears , every twen ty- four hours or less , may exten dover a week or more wi thout such profoun d anaemia as
occurs in a con t inuous three-day attack (fig .
FIG . 28 .—Blackwater Fever, m i ld attack : haemoglobinuria‘less than
twen ty-four hours.
FIG. 29.—Elackwater Fever, severe attack haemog lobinuria, two and
a-half days.
There i s u sual ly much men tal anxiety,partly on
accoun t o f the reputat i on of the d isease,but st i l l more
because of the large ‘
am oun t of blood-l ike ur in e that i s .
being passed . The men tal facult ies are quite clear , an dbeyon d the deb i l i ty there i s l i tt l e actual d i stress . The
amoun t o f haemoglob in passed steadi ly dimin i shes ,though st i l l suffic i en t t o ren der the ur in e Opaque . The

94 TROPICAL MEDICINE AND HYG IENE
last u rin e passed in th i s stage often con ta in s n o oxyhaem o
glob i n , but methaemoglob in on ly, the ur in e changingfrom a red-black to a dark brown colour. As the urin eclears the temperature fal l s to n ormal or subn ormal .Profuse sweat ing may occur several t imes in on e day .
The change from the haem oglobinuric peri od to then on - haem oglobinuric i s less abrupt than would bej udged by mere superfic ial examin at ion of th e uri n e .The haemolytic process has ceased
,an d the waste
products are be ing rapid ly el imin ated . As the haem o
glob in disappears the d iures i s d im in i shes,so that even
when abun dan t fluid i s suppl i ed the rate o f secret i onof urin e may fal l to much below n ormal . Th is i s probably merely the resul t o f the over- st imulat ion o f theren al cel ls , so that secreti on becomes sl ow . I f anyurin e at a l l i s passed
,a fal l in the rate of secret i on to
l ess than hal f the n ormal i s to be expected an d shouldcause n o alarm
,though flu id must st i l l be suppl ied freely .
The rate of secret i on in a favourable case soon in creases .The urin e i s clear and of n ormal colour , but con ta in sa smal l amoun t o f al bumin an d some casts . The pat i en tremain s in an extremely weak con d i ti on
,and the an aemia
may show a sl igh t increase, though the appearan ce o fthe blood corpuscles i s more n atural . The temperaturemay remain n ormal or commen ce to r i se . After a dayor two the temperature r i ses
,usual ly above n ormal , an d
for several days there m ay be irregular pyrexia , secon daryfever . This varies a great deal in severi ty . In somecases i t i s
,very sl ight
,t he temperature r i s ing in th e
even ing to 1 00°F. or even l ess (figs . 28 an d More
frequen t ly the n octurnal ri ses are to 1 0 1°and 1 02
°F
the temperature fal l ing n early to n ormal in the morn ing .
In other cases i t i s much more severe , an d occasion al lythere i s fatal hyperpyrexia in th i s stage wi thout any
recurren ce o f haemoglob in uri a . The usual durat i on o fth is stage i s three to four days
,and i t may be protracted
to two or three weeks . The urin e in th i s stage remain sfree from haemoglob in an d usual ly from al bumin . NO

BLACKWATER FEVER 95
further blood destruct i on i s taking place , an d the redcorp uscles and haemoglob in are rapidly in creas ing ata rate sometimes o f or corpuscles perc .mm . per week . Sometimes the pyrexia i s due to
malaria,as proved by the examin at ion of the blood .
Th is secon dary fever i s probably associated with themetabolic changes due to the absorpt i on an d ass imi lat i on of some of the waste products of the haemolys i s,which have been stored up in vari ous organ s . Theicterus rapidly d isappears
,the urin e remain s clear an d
pale though casts wil l be presen t . After th i s secondaryfever has subs ided” con valescen ce i s rap id an d usual lyun in terrupted . I t i s except ion al for anyon e who hashad blackwater fever to have any malaria attacks for aprolonged period ; probably th e corpuscles con ta in ingparas ites are amongst the first to be destroyed , an d soa “ cure ” of the malar ia results . Somet imes
,as in a
few cases in E nglan d,an attack of malaria may occur
shortly after the blackwater fever,though a n ew in fecti on
h as n ot occurred . In these cases,in
'
Englan d,where
malaria occurs during convalescen ce, the paras ites are
usual ly those of ben ign tert ian malaria , l ess common ly ofsubtert ian fever . There are few sequelae
,but the debi l ity
an d anaemia pers ist to some exten t for several weeks,an d
fatal card iac fai lure has occurred during convalescen ce .
If flu id is n ot freely suppl ied the h istory i s veryd ifferen t . The urin e
,whi l e st i l l l oaded with haem o
globin,dimin i shes in amoun t
,an d vomit ing becomes
i n cessan t . The amoun t of urin e con t in ues to dimin i shso that on ly an oun ce or l ess i s passed per d iem . Th isurin e may become free from haemoglob in an d evenfrom albumin , the temperature becomes n ormal
,the
anaemia d imin i shes,but un less the flow of urin e is
rap id ly restored death i s certain . Th is usual ly occursin four or five days , or less , but l i fe may be protractedup to ten days . There i s n o del ir ium
,n o convuls ion s
,
the min d i s c lear,an d beyon d headache
,which is not
n ecessar i ly severe , th ere are n on e of the ord in ary symptoms

9 6 TROPICAL MEDICINE AND HYG I ENE
associ ated wi th ren al d isease or uraemia ; vomit ing i s
p ers i sten t . In rare cases,al though the urin e clears an d i s
even abun dan t , the pat i en t does n ot improve . In thesethe uri n e i s o f low specific gravi ty, or an d
with the except i on o f the water the kidn eys are practical ly n o t excret ing . These cases are fatal
,
’
an d th ere wi l lb e foun d exten s ive blocking o f the tubules . The con
dit i on more C l osely resembles that due to bl ockage ofthe ureters .Th is i s the common est cause of death
, and i f i t canb e avo ided the mortal i ty from blackwater fever i s low .
Diagnosis—The d iagnosIs 18 made on the character o f
t he ur in e . This i s dark red , pract i cal ly b lack . If d i lu tedthe red col our appears an d th e urin e i s clear an d tran sparen t . On shaking the urin e the froth that forms o n the
surface i s red . If al l owed to stan d a th ick deposi t soonforms
,but th i s i s n ot presen t in abun dan ce when th e
urin e has been recen t ly passed . The deposi t in th e qu i tefresh ur in e i s scan ty . Casts are easi ly foun d
,and later in
the course o f the d isease are even more abun dan t somemay st i l l b e foun d weeks after the urin e i s free froma lbumin . These casts are usual ly gran ular and con ta inbright yel l ow gran u les
,n ot uric ac id
,s imi lar to those
foun d in th e organ s ; blood cel l s are rarely foun d ; bladderepithel ium may be moderately abundan t after the firstday . When th e urin e i s kept much deposi t i s formed ;th i s i s composed usual ly of casts
,coagulum and al tered
hmm oglob in .
The urin e in paroxysmal hmm oglobinuria i s s imi lar,and th at d isease would certain ly be d iagn osed as blackwater fever i f a case occurred in a blackwater d istri ct .If methaemoglob in on ly be passed the d i fficu lty in
d i agn os is i s much greater, as the brown urin e i s n ot veryun l ike some h igh coloured n ormal urin e
,an d may be
mistaken for b i l e-sta in ed urin e fortun ately the cases whereth i s occurs early are mi ld . In al l cases i f the ur ine bebo i led the albumin coagulated wi l l be a dark browncolour .

Eb F
5 60
3 3 C D E b F .G h
FIG . 3 I .—I , Oxyhaemoglobin ; 2 , reduced haemoglobin ; 3 , CO . haemo
g lob in ; 4 , methaemoglobin ; 5 , m ethaemoglob in (after add ition of alkali )6 . alkal ine haemat in ; 7 , acid haemat in (etherial so lution ) ; 8 , haematoporphyrin (acid) 9 , haematoporphyrin (alkal ine) I o , bil irub in .
BLACKWATER FEVER 99
Pa thological Anatomy—No spec ific organ i sm has been
d i scovered . Malarial paras i tes are presen t when the bl oodi s examin ed before the on set of the d isease ; they d i sappear in these cases very shortly after the on set of thehaemoglob in uria . In the great maj ori ty of cases o fblackwater fever
,those examin ed on ly after the on set o f
the di sease,n o paras i tes are foun d .
In fatal cases,on microscop ical examin at ion of the
l iver an d spl een ,fin ely d ivided in trace l lu lar black p ig
men t wi l l be foun d as in recen t malar ia . Frequen t lyi t i s n ot abun dan t en ough to be seen on in spect ionwith the n aked eye . No paras ites are foun d in theo rgan s
,but somet imes p igmen ted leucocytes are presen t .
The blood examin at ion shows an i n crease in the largemon on uclear elemen ts
,such as i s foun d in malar ia
,but
th i s also occurs in other protozoal d iseases . No p iroplasmata have been foun d
,an d the blood an d organ s
are steri le as regards bacteri a . The organ s show al l theusual eviden ces of blood destruct ion . In the hepat i ccel l s, in the convoluted tubules of the kidn eys , an d in
the spleen , are abundan t depos its o f haem osiderin ,an d
other gran ules,n ot p igmen ted , are presen t wh ich give
th e react ion of i ron in i n organ i c combin at ion . Th i seviden ce of blood destruct ion occurs to a less markedexten t in some cases o f malar ia an d in other d i seasesatten ded with haemolys is ; i t i s marked in the p i ro
plasm osis of catt le . A further eviden ce of blood destruct i on i s the great in crease in the amoun t of urob i l in in thefaeces .The kidn eys in al l cases show casts in the tubules
(figs . 3 2 an d When death has occurred from suppress ion these casts are very n umerous . They usual lyshow eviden ce of the presen ce of i ron in in organ i ccombin at ion .
The ren al cel ls,except for the presen ce of haem osiderin ,
are s ingularly l i t tle affected . The ep i thel ium is n ei therd etached n or n ecrot i c
,but usual ly shows cloudy swel l ing
and sometimes fatty degen erat ion . The spleen may be

I OO TROPICAL MED ICINE AND HYG IENE
en larged or n ot . The l iver,beyond the eviden ce o f
haemolys i s an d a certa in amoun t o f c loudy swel l ing,i s
n ormal in appearan ce and structure . Subserous haemor
FIG . 32 .-D iagrammatic represen tation of the cond ition of the k idney in
heal th (A) , during experimen tal haemoglobinuria of rabbit (B) , and in suppression of urine fo l lowing upon b lackwater fever (C) . In B sm al l casts arepresen t in som e of the urin iferous and co l lect ing tubules in C large casts are
present in m any of the urin iferous and col lect ing tubules. In the latter considerable en largem en t of the k idney is also observed . For the sake of
comparison B is represen ted as tri-papi l lary instead o f being uni papi l lary ,
as in the rabb i t .—(Fr0m the An nals of Tropical Medicine and Hygiene,”Liverpoo l Un iversi ty , by perm ission . )
rhages an d haemorrhages in to e i ther sol i d or hol l owvi scera are except i on al . H epati t i s an d even hepaticabscess may occur .

1 02 TROPICAL MEDICINE AND HYGIENE
main dan gers of the d isease . The fa i lure to recogn izethese essen t ial features has caused f the adopt ion o f, inj uri on s measures from t ime to t imeThe disease i s n ot a haemorrhagi c on e i t i s a haemolyt i c
on e . The actual d isease occurs in th e blood-vessels,an d
the red corpuscles,on ce broken up
,set free the haem o
glob in in the p lasma,an d there i t i s in j uri ous an d has to
be d i sposed of . The l iver and other organ s can absorbi t in part on ly, but the capaci ty o f these organ s i s l im itedan d the greater proport i on i s d i scharged wi th the ur in e .Thi s d ischarge must n ot be checked
,but a ided by th e
free supply o f water . If con s idered as haemorrhage i twould be n atural to attempt to d imin i sh th i s d ischarge .
The pat i en ts themselves n ot i ce that they fi l l chamberpot after chamber-pot with what looks l i ke almost pureblood , an d are anxious that the loss should be d im in i shed ,as they fear that they are bleed ing to death . The medica latten dan t requi res a firm fai th in the soun dn ess of h i spathological views
,an d h i s act i on should be to main
tain,an d i f poss i ble in crease , the tota l amoun t o f the
bloody ur in e d i scharged . The di luti on of the urin emakes n o obvious d ifferen ce in i ts appearan ce, an d ,
fromthe po in t o f vi ew of the pat ien t an d h i s fr i en ds
,the
measures that should be taken wil l on ly in crease th e lo ss .Free admin i strat i on of water i s n ecessary to main ta in
th i s flow,otherwise there i s danger of such exten s ive
blocking o f the ren al tubules that suppress i on wil l occur ;the coagula and débris formed in the convol uted tubulesmay remain . th ere
,but usual ly are carr i ed along an d block
the tubules in the pyramids , so that exten s ive areas oft he k idn eys are un ab le to d ischarge their secret i on . Th i sprocess commen ces with the on set of haemoglob in uria
,
an d probab ly always , even in the mi ld cases, some of thetubules in th e pyramids are blocked . It i s essen t ial thatthe treatmen t
,by en couraging the flow of urin e by a fre e
supply o f water,should start as soon as the d isease occurs .
The drugs used have belonged to many classes . Haem o
stat ics,such as ergot in
'
,have been extensively used , but .

BLACKWATER FEVER I OS
can have n o'
good effect ; Water has been withheld in
order to stop the loss,an d th i s p racti ce i s respon s ib le
for much of the mortal i ty . St imu lat ing d iuret i cs, suchas turpen t in e
,have been employed
,but the haem o
glob in in i tsel f acts as so powerful a d iuret i c that i t isun n ecessary to employ any addit i on al on e. Large dosesof calomel are recommen ded bv some authori t i es on theassumption that the d isease i s in some way due to sometoxin absorbed from the bowel . Th is method of treatm en t i s n o t recommen ded . Quin in e should n ot be givenun l ess paras i tes o f malar ia are foun d
,and even then
must be given very caut iously . Qu in in e in l arge dosesusual ly has n o effect at al l . Pat i en ts may recover whi l sttaking 60 gr . a day ,
but i t does n ot shorten the durat ion of the d isease . In these doses i t may in crease theten den cy to vomit ing
,and as in some cases i t actual ly
causes further haemoglob in ur ia i t should n o t be given .
Good results are cla imed for the frequen t adm in is
tration of borac ic ac id in so lut ion,an d of carbon ate of.
soda in moderate doses,with perch lor ide of mercury in
min ute doses frequen t ly repeated . They all have theadvan tage of in creas ing the amoun t of
'
fluid taken by th epat ien t
,an d the mixture o f perchlor ide of mercury and
carbonate o f soda, given as in yel low fever , seems to checkthe vomit ing and also acts in the late stages as a blan ddiuret i c . Th i s treatmen t has been pract ised by Hearseywith excel len t results .
Carbonate of soda 5 gr .Perch loride of m ercury 3
13 gr.
Water 2 oz .
This dose should be given every hour t i l l the urme clears.
The most un i formly successfu l treatmen t con s i sts ing iving frequen t recta l en emata , 6 -to 8 oz . at a t ime
,of
n ormal sal in e so lut ion ; water alon e i s n ot reta in ed .
These must be repeated every hour,or every hal f-hour
,
accord ing to the severi ty o f the case,t i l l the haem o
glob inuria ceases . The in j ect ion of large quan t i t ies o fsteri l ized n ormal sal in e in to loose cel lu lar spaces such

1 04 TROP ICAL MEDICINE AND HYG I ENE
as th e axi l la i s preferred by some . Th i s can n ot berepeated so often as th e rectal i n j ecti on s
,but must be
employed in cases where there are both vomit ing and
rectal i rr i tabi l i ty . The great po i n t i s to commen ce thetreatmen t early . If th i s i s don e from the onset, flu id bythe mouth on ly wi l l suffice
,as th e vomiting i s to a great
exten t due to the ren al obstruct ion,and i f th e latter can be
preven ted, 01
° on ly a few tubu les are blocked,t he vomit ing
can be con trol l ed .
If suppressi on has set in,recovery does n ot take pl ace ,
but there i s j ust th e poss ib i l i ty that the free supply offlu id s may en able a suffic i en t flush in g to take place tod isl odge some o f th e casts and so restore th e fun ct i on a lact iv ity of a part o f the k idn eys . In some cases wherea free d i sch arge o f urin e o f very l ow spec ific gravityi s in duced there i s n o improvemen t in th e con d it i on .
Alcohol i c st imulan ts are requ i red in all severe cases,but
the i r use shou ld n ot be commen ced too early strychn in ealso should be given .
The pat i en t i s usual ly con st ipated ; but act ive purgat i on i s probab ly in j ur i ous , as i t d iverts in to th e in test in ethe fluid that we wish to pass through th e k idn eys .During convalescen ce good, eas i ly d igested food mustbe given . The d igest ive powers are usual ly good . Thebowels'
should be kept freely Open with sal in es .I ron an d arsen i c may be taken with ben efi t in the
l ater stages,but there i s n o advan tage in giving them
early,as al l the act ively metabol i c organ s are at that
t ime overloaded wi th i ron .
For th e secon dary fever free purgat i on seems to bethe most effect ive . Qu in in e has n o ben efici al act ion an d
m ay provoke a relapse . Phen acetin an d oth er an t ipyret i cs are to be avoi ded thei r act i on i s temporary an dthe danger o f card iac fa i lure i s great . In hyperpyrex iaduring th i s stage hot packs
,cold packs, or cold bath s may
be resorted to,but the progn osi s i s most un favourabl e .
Relapses must be treated in th e same way as theprimary attack .

1 06 TROPICAL MED IC INE AND HYG I ENE
kn ow the danger o f suppressi on,an d any con cern
'
shown
by the atten dan t as to ' th i s wi l l s t i l l further in creasethe ir anxiety . The danger i s suppression ,
an d i f n o
urin e 18 In th e bladder i t can do n o good for t he pat i en tt o attempt to mi cturate . Reten t i on does occur occas ional ly, so that if th ere i s un due delay in micturi t ion theabdomen above the pubes should be examin ed to makesure that the bladder i s n ot d i stended .
If t he vomit in g can n ot be checked,or sufficien t water
can n ot be admin i stered by the mouth,rectal in j ect i on s
of n ormal sal in e soluti on,
per cen t .,shoul d be given
hourly .
As th e frequen t admin i strat i on of such en emataleads to an i rr i tabl e con di t ion of the rectum
,great care
i s requ ired . The en emata should be given very sl owlyan d should be at blood heat .The blan kets an d cloth in g must be rep laced by warm
,
dry cl oth ing as often as i s requ ired . If the tenden cy tosyn cope becomes marked
,the lower en d of the bed must
be ra ised,hot-water bottl es appl i ed to the axi l la, and the
l egs ban daged from the feet upwards,an d st imulan ts given
freely by. the mouth , rectum , or by hypodermic in j ect i on s .Tran sfus i on in to the ve in s has n o t been successfu l .
Hy perpyrexi a m ay occur e i ther wh i l st haemoglobinuriai s presen t or afterwards during the secon dary fever . Thetemperature should be taken frequen t ly
,hourly
,or even
hal f-hourly,when i t i s above {03
°F. The hyperpyrexia
after the ur in e has c leared is the more dangerous .When the pat ien t i s so s i tuated that there i s n o ski l led
nurs ing avai lab le , th e danger i s greatly in creased . Attent i on to the gen eral pr in c ip l es wi l l be of service , and i fthe pat i en t has to l eave the bed h is movemen ts must beas sl ow as poss ible and the head held low . He mustcrawl
,n o t walk
,an d n ever hold h imsel f uprigh t un der
any c i rcumstan ces . An y expressi on s of desponden cymust be d iscouraged . It i s useless to attempt to min im izethe danger
,but the pat i en t ’s courage must be sustain ed
as much as poss ib le .

BLACKWATER FEVER 1 07
Un der these c ircumstan ces the advisab i l i ty of rem ov
ing the pat ien t to a place where he can receive ski l ledcare has o ften to be con s idered . If moved at al l , heshould be moved early
,in the first day of the disease .
Later the ri sk of co l lapse i s en ormously i n creased byany j ourn ey, an d after the first day should n ot be un dertaken . Even o n the firs t day , the r i sks , on the wholeo f moving the pat i en t are at least as great as th e advantages result ing from the more carefu l atten t i on would be .
If moved,the pat ien t must be carr i ed in a recumben t
posi ti on . A hammock i s as good a method as any . H emust be well wrapped up an d recei ve water frequen t lywh i lst o n the road
,an d food in add i t ion i f the j ourn ey
be a long on e.
Food must be fluid and n utrit ious i t i s wel l digested .
During conval escen ce great care must st i l l be exerc i sedboth to preven t chi l l an d exposure
,for fear o f relapses
,
an d to avo id over-exert ion or anyth ing that may throwany strain on the heart
,as fatal syn cope may occur
dur ing th is peri od .
Con st ipat ion dur ing the early stages i s n ot of importan ce
,an d should n ot be rel i eved t i l l the urin e i s clear ;
l ater the bowels must be kept open,preferably by mi ld
sal in e aperien ts .
Etiology—The true cause o f blackwater fever i s
un kn own . I t occurs in both sexes,but i s n ot kn own
in early ch i ldhood . I t does occur in n egroes,but n ot
in the n at ive n egroes in an area where the d isease i sen demic . In proport i on to the ir n umbers i t i s morecommon amongst European s than amongst As iat i cs . In
European s i t rarely occurs dur ing the first six mon thsof res iden ce in an en demi c area
,but after that period
becomes more common , and i s most common in th esecon d an d th i rd year o f res iden ce . In Pan ama thein c iden ce appears to be rather d ifferen t
,as the n umber of
cases in the first two years of res iden ce i s n early equal,
and in the first three mon th s the in c iden ce i s a t the samerate as for the first two years . Fi rst attacks are very rare

1 08 TROP ICAL MED ICINE AND HYG I ENE
after ten years ’ resi den ce . A person who has n ot hadblackwater fever in an area in wh ich the d i sease i sen demi c may have h i s first attack after l eavin g that area ,sometimes up to s ix mon ths or more after l eavin g i t .Gen eral ly speaking
,in Afri ca
,i t i s most prevalen t where
malari a i s most prevalen t,and by many person s mal ari a i s
con s idered to be essen t i a l for the developmen t o f thedi sease . As th e d i sease i s n ot kn own in some coun tri eswhere malar ia i s prevalen t
,i t ha s e i th er to be assumed
that there i s a spec i al vari ety o f the malaria l paras i teimpl icated
,or that there i s some spec ial con di t i on un der
wh ich th i s extreme haemolys i s takes p lace . So far al lexperimen ts that have resul ted in a d ecrease in th e amoun to f malari a have been associated with a reduct i on in th en umber o f cases of b lackwater fever . Th i s seems t ohol d whether the reducti on i s due to attacking the carri erso f malaria
,an ophel in es
,o r t o steady admin i strat i on of
qu in in e .
No morpholog ical d i fferen ces have been observed in
the malari al paras i tes in a malar i ous coun try where blackwater fever i s en demi c an d in malari ous coun tr i es wherei t does n o t occur . The carriers d iffer in the d i fferen tcoun tr i es
,and in Afr i caMyz omyiafn nesta i s th e common est
carr i er in places where blackwater fever i s prevalen t.The spec ial con dit i on that has been con s idered tobe the immediate exc it i ng cause i s qu in in e po ison ing .
The advocates o f th i s hypothesi s con tend that in somein d ividual s
,after they have been exposed to the en demic
influen ces,th e . blood i s so al tered that qu in in e produces
hmm olysis. There are cases in which a dose o f qu in in e ,even a smal l o n e. may bring o n an attack o f haem o
glob inuria ; th i s has been proved in man y in stan ces .There are reason s for con sider ing that th i s , though an
occas i on al cause of blackwater fever , i s n ot an essen t i alor even the common cause . In many coun tri es wherelarge doses o f qu in in e are given , after an d during fever,n o such effects take place . In an alysing the cases i n
an en dem ic area there i s n o cl ose rel at i on , e i th er as

I l O TROPICAL MEDICI NE AND HYG I ENE
albuminuria . Parot id i t i s has been kn own to occur,an d
hepat i c abscess may fol low an attack of bl ackwater fever.
Ret i n al haemorrhages or haemorrhages in to the vi treousmay lead to
”
impaired vi s i on,but in such cases complete
recovery of s ight i s usual .Piroplasin a .
— P i rop lasmata‘have been frequen tly lookedfor but n ever foun d
,as has been already men t i on ed .
There i s n o rel at i on kn own between the d i str i but i onof any speci es o f t i ck an d blackwater fever
,but more
work in t h i s d irect i on i s requ ired . The distribut ionof Orn ithodorus m ouba ta does n ot correspon d wi th thatof blackwater fever . Lei shman has descr ibed bodies
,
whi ch h e suggests may be paras i tes,o f th e n ature o f
Ch lamydozoa in the leucocytes ; but i t i s doubtfu l i f th ebod ies he descr ibes are n ot in clus i on forms o f remn an t so f broken -down bl ood-cel l s
,as simi l ar appearan ces are
seen in t he b lood in cases o f other d i seases having n o
con n ect i on with bl ackwater fever .Prophylax is—The cl ose relat i on sh ip in Afr i ca betweenth e d i str ibut ion o f bl ackwater fever an d of great l i ab i l i tyto malar ial in fect i o n po in ts to the desi rab i l i ty of deal ingwi th the malar ia .
Person s in whom qu in i n e produces haemoglob in uri aare un su i ted for residen ce in a malar ial coun try . In
such person s i t i s somet imes poss ibl e to treat the malar i awi th qu in in e , i f smal l doses o f qu in in e, very gradual lyin creased
,are employed . Person s who have n ever had
b lackwater fever in Afr i ca are st i l l l i ab le to an attack forsome mon th s a fter their arrival in Englan d . It i s there foreadvisable that the regular prophylact i c use o f qu in in eshoul d be con t in ued
,n ot on ly on the voyage home, but
for two or three mon ths after arr ival in Englan d . Suchperson s must also avo id exposure to ch i l l
,over- fat igue ,
or any depress ing influen ces .A previous attack of blackwater fever appears to pred ispose to other attacks . A s ingle severe attack or twomi lder attacks sh ould be con s idered as d isqual i fying thatperson for resi den ce in anen demic area .

I I I
CHAPTE R V I I I .
P IROPLASMOS I S .
Piroplasmosis. Malari a of cattl e,horses
,dogs
, &c .
P i roplasmosi s i s the term sometimes appl i ed to the affect i on caused by certain sporozoal bl ood paras i tes (Plate I I ,24
-27) which , being common ly pear- shaped, are cal led
p i roplasmata . The p iroplasmata d iffer from the haemamoebae in that ( 1 ) they do n ot form pigmen t ; (2) d ivis ioni s usually in to two
,somet imes in to four
,an d the youn g
forms are n ot immed iately set free,but con t in ue to grow
in the red corpuscl e in which they l ive . U l t imately theyescape from these red corpuscles . I t i s probable that al arge proport ion o f their n utr imen t i s derived by osmosi sfrom the blood plasma and l ess from the haemoglob in thanin th e haem am oebae . The free paras i tes may be foun d inthe plasma
,act ively moti l e
,before they en ter other cor
puscles ; (3) they are con vey ed in al l kn own in stan ces byt icks o f various gen era . The di seases are tran smitted n o t
by th e t i ck that feeds on the in fected an imal , but by thesecon d an d somet imes the th ird gen erat ion of these t i cks
,
as the paras i tes are tran smitted to the eggs and developin the young t icks .The p i roplasmata in the early stage have n o defin i te
ves i cular n ucleus,though a clear n on -sta in ed space
or vacuole i s presen t . The chromat in i s frequen t ly intwo equal or un equal masses , an d though i t d ivides tosome exten t the complete fragmen tat i on an d d iffus ionobserved in t he malari al paras ite does n ot occur .D ivis ion i s more by a process of budd ing than o f
breaking up in to spores . The pear-shaped body,after
escap ing from a red corpuscle, en ters an other an d thenbecomes a roun ded amoebo id mass . In th i s stage i t doesn o t escape from the red corpuscle . After a t ime two

I I Z TROPICAL MEDIC INE AND HYG IENE
processes or buds are formed at the periphery of th i sroun ded body
,an d these gradual ly in crease in s ize
,the
chromat in d ivides,an d hal f en ters each of these buds .
The in crease in s ize in the buds i s by absorption of theorigin al protoplasmi c mass
,wh ich i s reduced to a mere
th read con n ect ing t he two bod ies,an d th is fi n al ly is
absorbed an d th e two pear- shaped bodies l i e free in thered corpuscl e . They may remain in th e red corpusclefor some t ime
,and when they escape en ter in turn other
red corpuscles,before they again become amoebo id and
d ivide an d so repeat the cycle .
P i roplasmata occur in most o f the domest i cated an imals,
and cause seri ous d i sease,an d frequen t ly death
,in cattl e
,
sheep,horses an d dogs . . They have been descr i bed in
man ,but th e ir occurren ce i s very doubtful .
By some observers Lei shman -Don ovan bod ies,n ow
kn own to be a rest ing stage o f a flagellate , were con
sidered as p iropl asmata . In al l the d iseases o f domesticated an imals pyrex ia occurs
,n ot showing defin i te
peri od i c i ty . A common character i s haemoglob in uria, so
much so that the popu lar n ame o f the d isease in cattl e i s“ redwater fever
,
”in sheep “ heart fe ver .” In dogs the
d isease they cause i s cal led epidemic j aun d ice,on accoun t
of the haem otogen ous co louring of the con j un ct iva fromthe hmm olysis. Al though haemolys i s i s a common resul to f p iroplasma in fect i on
,haemoglob in uri a i s by n o m ean s
a lways a prom in en t symptom . Redwater does n o t
occur,for example
,in Rhodesian .or East Coast cattle
fever,an d al though p i roplasmos i s is common in cattl e
throughout the East,yet haemogl ob in uria i s rarely m et
with except in an imal s su ffer ing from seri ous in tercurren td isease
,such as r in derpest
,or among those imported
from coun tr i es where p iroplasmata do n ot occur .An in fect i on with p i roplasma in cattl e appears to l astdurin g the whole l i fe of the an imal
,but the cl in i ca l
eviden ce of th e presen ce of th e paras i tes d i sappears , an dthough th e an imals harbour the paras i tes in smal ln umbers they seem to have acqu ired a degree o f to ler

1 1 4 TROPICAL MEDIC INE AND HYG IENE
Post-m ortem examin at ion shows a con si derable en largemen t of the sp leen and acute paren chymatous degen erat ion of other abdomin al organ s . There i s n o u lcerat i ono f the in test in e . By man y the d isease is bel i eved to betyphus .
The term “ human p irop lasmosi s has somet imes been
appl ied in I n d ia to cases o f kala-azar,but i t wi l l be seen
that th i s d i sease i s due to a paras i te o f a d ifferen t n ature .
P i roplasmata have al so been descr ibed in the blood ofa cowherd suffering from fever during the presen ce o fTexas fever amongst catt le I n I n dia . Th is Observat ional so lacks con firmat i on .
Bod ies resembl ing p iroplasmata,but eas i ly d ist inguish
able upon carefu l examin at i on,h ave been descr ibed by
Cropper w'
orking in Palest in e,an d by Smith work ing in
America , as occurr in g in th e b lood of person s suffer ingfrom severe forms o f malaria . The bodies have a rotatory but n o amoebo id movemen t ; thei r n ature i s un kn own .
They do n ot sta in with basi c sta in s . The edges,probably
the edges o f the haemoglobin,are somet imes stain ed
i rregularly . S imilar bodies have been foun d by Nuttal l inth e blood of dogs . They are probably not paras i tes .
CHAPTE R IX .
YELLOW FEVER .
THE parasi to logy of th i s d isease i s u n kn own . It i sin n o way con n ected with malaria , but as i t has beenproved to be carr i ed by a mosqu ito
,Stegomyia fascia ta
(S. ca lopus) , an d as: there i s further proof that t ime hasto elapse after the in fecuon of the mosqu i to before i tin turn becomes in fect ive
,developmen t must take place
in th e mosqu ito . On these grounds the d isease i s herein cluded with the probably protozoa l d i seases .Yellow Fever in i ts severer form is characterized by
fever,in ten se headache
,j aun d ice
,an d albumin uria in
creas ing stead i ly in amoun t ; by ten den cy to haem or
rhages from mucous an d sometimes from cutan eoussurfaces
,an d by haematemesi s b lack vomit . In fatal
cases there i s frequen t ly suppress i on of the uri n e . In themi lder form there is fever for two or three days
, gastri cd isturban ce
, an d ep igastri c pa in .
It i s conveyed from m an to m an by mosqu i toesbelonging to the gen us Stegomyia .
Geographica l Distribution .
—It i s best kn own as a d iseaseof the N ewWorld
,an d occurs en demical l y ,
or as ep idemics,
in the West I n dies an d along the At lan t i c coast fromNew York down to Ri o de Jan e iro .
° I t was at on e t imecommon in the West Coast of Afr ica
,an d recen t out
breaks have occurred . In South Europe, on the At lan t i c
coast , i t i s an imported d isease, an d on board sh ip.I t
has spread to a smal l exten t even in E ngl i sh ports inthe vic in i ty of in fected ships
,during summer mon ths .
I t i s usual ly l imited to the larger settlemen ts on th ecoast in the Trop ics . Sh ip ep idemics were common In
the pas t,but are n ow rare .

1 1 6 TROP ICAL MEDICINE AND HYG I ENE
Clin ica l Course : Severer Type.
-The on set o f the d iseasei s sudden , but n ot invariab ly with a r igor . The temperature ri ses rap idly
,t here i s V i o l en t headache
,most i n ten se
over the fron tal regi on . The eyes are much in j ected an doften described as ferrety . Jaund i ce; soon appears , butn ot as early as in blackwater fever ; the con j un ct iva an d
sk in are at first l emon -co loured,but soon deepen to a
bright yel l ow colour . Vomiting is a promin en t symptomat first
,merely o f food
,then watery
,then “ ac id vomit ,
an d later almost b lack b lack vomit .The act of emes is i s performed with l i t tl e or n o e ffort ,
an d the amoun t ej ected i s surpri s ing . The vomit seemsrather to gush out than to be forc ibly expressed . Therei s a feel ing of marked an d dec ided rel ief after eachevacuati on of th e stomach .
Ep igastr i c pain an d ten dern ess occur early an d arein ten sified by pressure . There i s usual ly an in ten selyac i d or b itter taste in t he mouth .
The course of the d i sease i s best con s idered divided in tothree stages as descr ibed by Bla ir . During the first stagethe temperature i s h igh an d the pul se qu ick an d boun ding . The headach e an d ep igastr i c pa in s are severe
,and
the vomi t i s free from blood t i l l t owards the,
close o f th i speriod . The ur in e con ta in s a lbumin about the secon dday
,an d the j aun dice appears an d progress ively deepen s .
The durat ion of th i s stage i s from three to four days .The passage i n to the secon d stage i s rap id
,though n ot
exact ly by cr i s i s . The temperature fal l s to n ormal orsubn ormal
,the pul se - rate i s much reduced
,and the rate
may be 40 or even l ess per min ute , th e restlessn ess,pain
,an d del ir i um d isappear
,an d the pat i en t feels much
rel i eved,and often quite wel l . The gen eral appearan ce
o f wel l-being in the secon d stage i s decept ive,and d eath
may occur in such a pat i en t,an d he
,even whi le he i s
s i n king,may fee l qu ite wel l .
In some cases— th e mi ld on es (yel l ow fever s implex)t h i s remiss i on i s the end of the d isease and the pat ien tsteadi ly con t in ues to improve
,an d passes i n to the stage o f
con val escen ce withou t secon dary fever (fig .

1 1 8 TROPICAL MEDICINE AND HYGIENE
in creases wh i l st the albumin decreases an d convalescen cei s estab l i shed .
D iagn osis.—The diagnos i s o f an ep idemic of yel low
fever i s n o t d ifficu lt . If severe or fatal cases occur thefever
,severe headache
,in creas ing al bumin uria an d j aun
d ice,wi th the occurren ce ih a proport i on of th e cases of
black vomit,ren der the d iagn osi s certain . In fatal cases ,
even when there has been n o black vomi t , at th e autopsy,the con ten ts o f th e stomach an d duoden um wi l l be blackfrom effused b lood .
FIG . 35 .—Yel low Fever. Severe attack .
The l imi tat i on o f the d isease to certa in quarters,or
even streets o f a town ,an d the depen den ce o f o ne case
on preced in g cases are al l a ids in th i s d iagn osi s . The
d iagn osi s o f i solated cases i s more d i fficul t . Acutey el l ow atrophy of the l iver may close ly s imulate thesevere forms of the d i sease an d malari a with j aun d ice
,
an d Weil ’s di sease have each man y po in ts of resemblan ce .
There are certa in po in ts o f resemblan ce between yel lowfever an d blackwater fever that have in th e past l ed toa con fus i on between the two d i seases
,so much so that
both have been con s idered to be man i festat ion s o fmalar ia
,an d are sti l l o ften mistaken for “bi l i ous remitten t
fever ” with j aun di ce .
The poin ts o f s imilari ty are the j aun dice,l iabi l i ty to
YELLOW FEVER I 1 9
suppress ion of ur in e , an d vomit ing ; the temperaturecharts are n ot un l ike in the two diseasesy as in both thereis a remiss ion in the pyrexia between the primary an d
secondary fever . C l in i cal ly there are importan t d ifferences. Haematemesi s may occur , but i s very rare inblackwater fever
,an d common in yel low fever . Haem o
g lobinuria or m ethaem oglob inuria i s i nvariable in blackwater fever an d very rare in yel low fever , though theremay be haematuria . In n e i ther d isease are malari alparasi tes foun d in the blood
,during the attack
,an d in
y el low fever the in crease in the relat ive n umber o f thelarge mon onuclear leucocytes i s n ot foun d . The in ten seheadache in the early stages of yel l ow fever i s n ot presen tin blackwater fever
,and th e repeated rigors so common
in blackwater fever are usual ly absen t in yel low fever .
I cterus appears later in yel low fever than in blackwaterfever, an d i t i s on ly in yel low fever that the pulse-ratedoes n o t in crease as the temperature ri ses .Trea tmen t—A prel imin ary purge seems to be of great
importan ce,an d calomel i s frequen t ly used for th is
purpose . Many drugs have been employed,an d a treat
men t for which great success was claimed , by Bla ir, wasby large doses of calomel an d quin in e , 20 gr . of eachbeing given . All later work sh ows that qu in in e has n oeffect 0 11 the d isease .Carbol i c ac id
,in drop doses every hour
,and other
i n test in al an t i sept i cs have also en j oyed a great reputat ion .
There does n ot appear to be any drug with a spec ificact ion . The presen t treatmen t i s that in troduced byStern berg , wel l d i luted b ich loride of mercury an d carbon ate of soda being given frequen t ly in smal l doses .It i s on th i s treatmen t that Hearsey
’
s treatmen t of blackwater fever i s founded . Some hold that any adm in is
frat ion of food by the mouth in the early stages o f thedisease i s in j uri ous an d may lead to the con vers ion of anattack o f the mild type in to on e of the more severe .
When suppression of urin e threaten s,rectal in j ec t ion s o f
sal t an d water or in j ect i on s of flu id in to the subcutan eousareolar ti ssues are indicated as in blackwater fever .
1 20 TROPICAL MEDIC INE AND HYG I ENE
Nursing—Careful n urs ing i s of great importan ce . Theroom must be kept very qu iet an d dark
,as there i s great
i n to leran ce o f l ight . Vomit in g must be checked i f poss i ble
,an d Op ium is con tra- in d icated . All food
,drinks
,
an d medic in es must be given in smal l quan t i t i es at at ime
,an d wel l i ced .
Ice-bags or cold compresses to the abdomen give morereli ef in most cases than hot appl icat i on s .Protect ion from the b i tes o f mosquitoes must be very
careful ly atten ded to in order to preven t the spread of th ed i sease an d the in fect i on of the mosqu i toes
,an d through
them of the occupan t s o f the house . This i s o f thegreatest importan ce during th e fi rst stage o f the d i sease .
The danger i s presen t both day an d n ight,as the freshly
emerged mosqu itoes feed both dur in g the day an d n igh t .Mosqu i toes wh ich have on ce fed become feeders at n ighton ly . The bed must be a lways screen ed o ff in a mosquiton et suffic ien t ly large for the atten dan t also to be in sidei t,an d any mosqu itoes t hat obta in en tran ce to the n et
must be caught an d k i l l ed , as otherwise they may becomein fect ive in ten days . The n ett ing must n o t be toocoarse
,as the S . fascia ta can pass through a mesh o f
1 5 to the square in ch . All the eviden ce i s opposed tothe bel ie f that any d ischarges from the pat i en t arein fect ive .Mosqu ito larvae in th e room should be destroyed
,
an d n o breeding-places—flower-vases , water- j ugs, &c.
al l owed to remain in the room .
Pa thology a nd Morbid Ana tomy.-The organ i sm that
causes yel l owfever has n ot been i so lated . It i s presen tin th e blood o f the pat ien t during the fi rst three days o fthe d i sease
,an d i s so min ute that b lood serum of such
a pat ien t retain s i ts in fect ivi ty after passage through aBerkefe l d fi l ter . Th is serum if in j ected i n to a n on
immun e subj ect wi l l cause an attack of the d i sease,n ot
merely a toxaemia,as the blood of th i s person i s in fect ive
,
showing that he al so harbours the paras i te . The morbidchanges due to the act ion of th i s un kn own organ i sm

1 2 2 TROPICAL MED ICINE AND HYG I ENE
Though th e cause has n o t been discovered,i t i s n ow
kn own , as the resu lt o f the exper imen tal work of Reedan d Carol], ful ly confirmed by n umerous observers
,t hat
the in fect i ve agen t i s imb ibed wi th the blood o f pat i en tsby certa in mosqu itoes
,an d that such mosqu i toes
,after
a defin i te peri od of ten to twelve days,are in turn capabl e
of in fect ing n on -. immun es . These exper imen ts have
sh own
( I ) That n e i ther in th e vomi t , black or otherwise , in the
fae ces, or sweat, or other d i scharges from the pat ien ts i sany in fect ive agen t con ta in ed
,but that i t i s con tain ed in
the blood during the fi rst th ree days of th e attack .
(2) That mosqu itoes (Stegomyia fascia ta ) can conveythe d isease
,an d that the other common and domest i c
mosqu i toes do no t so carry the d isease .
The con d i t i on n ecessary for the con veyan ce of thed i sease by these mosqu itoes are
(a ) That the mosqu ito must have fed o n the bloodof a yel l ow fever pat i en t during the early stage, first ,secon d or th ird day o f the d i sease .
(6) That t he mosqu i to must have l ived for ten daysor more after th i s feed ing .
(c) That th e person b i tten in the secon d in stan ce mustbe suscept i b le .
Th i s seri es of even ts shows that the paras it e o f yel lowfever requ i res devel opmen t in the mosqu ito before i tcan be in j ected i n to m an
,an d that i t i s n ot s imply a
tran sferen ce o f the organ i sms from on e m an to an other .Marchoux an d Sim on d cla im that the mosqui toes may
tran smit the Organ i sm to thei r offspring , though the moreexten s ive observat ion s of Rosen au an d Goldberger havefai l ed to con firm these re su lts, an d the method in whichyel l ow fever i s spread i s in more accordan ce with thetran smiss i on by the adults than in th i s man n er .The per i od of in cubat ion of yel l ow fever after the b iteof an in fect ive mosqu i to var i es l i tt l e an d i s usual ly fromthree to four days
,very rarely over five . In person s
part i al ly immun e a l onger peri od of in cubat ion may be

YELLOW FEVER 1 23
met w i th . The early cases in an ep idemic are twelve tofi fteen days after a case i s in troduced, as the mosquitoeshave to be in fected an d become in fect ive , wh ich takesten days
,an d then the person in fected by them wi l l n o t
develop the d isease for two,three or four days . The
in cubat ion period for an epidemic i s therefore about twoweeks . Most of the et io logical factors con n ected withyel low fever are closely related to the con d it ion s favourabl e for the l i fe an d mult ipl i
’
cat ion of S . fascia ta ,but th i s
in sect i s more widely spread than yel low fever, an d i son ly of importan ce
,in th i s con n ect ion
,when person s
wi th yel low fever are presen t or are imported , or wherethe d isease i s en demic in a mi ld or severe° form .
Prophylaxis—The carr i er o f yel low fever i s kn own ,
an d for effect ive prophylaxi s thorough kn owledge o fthe habi ts of th i s in sect i s requ i red
,an d the mean s of
iden t ificat ion . It i s poss ib l e that o ther members o f thesame group may carry yel low fever .The po in t of spec ia l importan ce is the class of pers on swho harbour the paras i tes an d serve as a reservo ir of thedisease from wh ich these mosqu itoes become i n fected .
The gen eral recogn i t i on of the presen ce during an ep idemic period of n umerous cases of i l ln ess
,character ized
by br ief fever and gastr i c d i sturban ce,with occas ion al ly
j aun dice , some at least of which are probably yel l ow fever,has broaden ed the scope of in qu iry
,
Such cases, as wel l as the more marked cases of yel lowfever, serve as reservo i rs
” of the d isease an d mosqu i toesbecome in fected from them an d in turn in fect otherperson s .As the mi ld cases are the usual forms of the d isease inch i ldren ,
an d th e immun i ty con ferred by a previous attack,
whether mi ld or severe,i s rather immun i ty again st a
severe attack than again st re in fect i on with the d isease,
i t i s held by some that in trop ical coun tr i es,where the
mosquito S. fascia ta i s common ,such con stan t rein fec
t ion occurs amongst the n at ive ch i ldren an d the parti al lyimmun e adolescen ts and adults that the d isease pers ists

1 24 TROPICAL MED ICINE AND HYG IENE
in an en demi c mi ld form, an d that h igh ly suscept ibl e
n ew - comers may acqu ire the d isease in a vi rulen t formfrom the mosqu i toes in fected from the res iden t populat i on . Such virulen t cases would be the on ly on es toattract atten t i on an d would be con s idered as sporad iccases . The common er mi l d cases would e i ther be overl ooked al together or grouped wi th b i l ious remitten t fever .Sim on d
,Aubert
,an d Noe con s ider that in Mart in ique
th e ep idemics whi ch occur from t ime to t ime are acuteman i festat i on s of the en demic d isorder . The variati on sin th e sever ity o f yel l ow fever they expla in e i ther as theresu l t o f an except i on al ly large dose in ocu lated by themosqui to
,or—an d th i s i s more probable— that the viru len ce
o f the organ i sm is in creased by passage th rough a ser ieso f suscept ib l e adults and d imin i shed b y passage through a
ser i es o f part ial ly immun e adul ts or ch i ldren . such as mustbe presen t in a coun try where the d isease i s en demic .
Th is would expla in why when yel l ow fever occurs o n
board a sh ip man n ed by European s or amongst them em bet s of a Eq pean regimen t crowded in barracks,where the in fect i on after a t ime wil l usual ly be deI iv edfrom an other suscept ib le person ,
the mortal i ty i s veryh igh , 50 per cen t . 0 1
° more,whi l st in th e later ep idemics
,as
in that descr ibed by Bla i r in 1 843 , I n Brit ish Gu ian a , th emortal i ty was on ly 1 3 3 per cen t . in the whole ep idemic
an d uil in th e m i ld form then fi rst descr ibed . In t he fi rst
gen eral outbreak throughout th e West I n dies the mortal i ty amon gst al l races was very h igh during the first yearo f the invas ion
,on e to two -th irds of the cases d ied , though
later a larger proport ion recovered .
Man son suggests a further hypothesi s, that possiblym an i s n ot the on ly reservo ir, an d that some of the loweran imals may receive an d carry on the in fect ion in a mi l dform
.We kn ow that an thropo id apes are suscept ib le, but
as regards other an imals,i f suscept ib le, the d isease does
n ot appear to affect t he i r h ealth . If a lower an imalserves as the reservo ir that an imal would probably be arat
,as th e early d istr ibu tion of the cases i s in the

1 26 TROPICAL MEDICINE AND HYG I ENE
i s a source of danger to the whole commun i ty . Thisdanger can
,by en erget i c measures
,be reduced to a
m in imum .
( 1 ) All cases of fever must be at o n ce reported an d
in qu i red in to . Any that are yel l ow fever must be aton ce i so lated . In a port where yel low fever i s l ikely tobe in troduced
,the mach in ery for the reg i strat i on ,
iden ti
fication,an d i so lat i on of cases must be kept in working
order,an d form a departmen t or bureau that i s at al l
t imes ava i lable .
(2 ) If th ere i s a case o f yel l ow fever the pat i en t mustbe removed to an other room an d placed in s ide a mosqu i to n et
,an d kept there n igh t an d day t i l l con val escen t,
as the young mosqu itoes feed both dur ing the day an d
n ight,an d may become in fected therefore at any t ime .
(3 ) The room from whi ch the pat i en t has been re
moved must be at on ce closed an d al l p laces wheremosqu i toes can escape b locked . The room must thenbe fumigated wi th burn ing sulphur 1 4
2L lh .
,or pyrethrum
2 lb .,to each cu . ft . As soon as poss ibl e after the
fumigat i on th e floor must be swept an d the sweepingsat on ce burn t
,as mosqui toes may revive after such a
fumigat i on . The attendan ts , th ose engaged in fumigation
or mosqui to destruct ion, an d any person s having busin ess
in the house,must be protected by su i tab le cl oth ing from
mosqu i toes .
(4 ) In adj o in ing houses every effort shou ld be madeto destroy the mosqu i toes
,as some may have escaped
to them . If the case o f yel l ow fever i s detected early ,when these precauti on s are adopted there i s frequen t lyn o spread of the d i sease
,because the mosqui toes
,as in
malari a,are n o t capable o f in fect ing human be ings in
l ess than ten days after b it ing the pat ien t .Where the first case i s n o t detected early , an d thed isease has spread
,each case as i t i s reported must be
treated in the same man n er as an origin al case . Thesuccess of the measures depends on each case beingreported early
,an d a thoroughly effic i en t cen tral bureau
i s there fore essen t i al .

YELLOW FEVER 1 27
When an outbreak does occur measures for thedestruct ion of the larvae must be most en erget i cal lypushed .
For the success that has atten ded such prophylact i cmeasures the reader i s referred to the reports as tothe san i tat ion o f Havan a
,New Orl ean s
,an d the Pan ama
Can al Works .I mportat i on of disease i s usual ly by sh ip . E i ther
in fected mosqui toes are in troduced or in fected person s .
I n fected mosqu i toes may be brough t in with the cargoor in private baggage
,an d in that case the focus of the
ep i demic is the p laCe where the baggage i s open ed .
Ship Epidem ics—S. fascia ta can thI'
iv e on boardsh ip
,an d can be tran sported for l ong d i stan ces by sea
as eggs , l arvae ,or adults . The adul t mosqu itoes m ay
be in fected in on e port,an d on ly become in fect ive
after reach ing a seco n d port,an d then may give ri se to
an ep idemic in the vi c in i ty o f the wharves. It i s qui teposs ible in a voyage of a week or less that th e crew ofthe sh ip might escape i n fect ion ,
an d the source o f in fect i o n of the port would n o t then be kn own . I t i s d i fferen tin cases where the mosqu i toes become in fect ive wh i l stat sea . In such a case a large proport ion of the susceptible crew may acquire yel l ow fever .The mosquitoes n eed n ot be n umerous
,but every
attempt must be made by fumigat i on o f on e part o fthe sh ip after the oth er to destroy any mosqu itoes , andthe sweep ings, as on land
,must be burn t at on ce .
8 . fascia ta become torp id with cold , an d con sequen tlysuch ep idemics subs ide four or five days after reaching colder lat i tudes , but in summer may con t in ue activean d devel op as far n orth as E nglan d
,an d may spread
in t he vic in i ty of the wharves as the mosqu itoes escapefrom the sh ip . I II some cases the in fect i on has rem ain edin the sh ip for several mon ths, even when i t has n ot
been occup ied for th is per i od . In a sheltered warmpart of a sh ip these mosqu itoes may l ive for that peri od .
The h istory of yel l ow fever deserves spec ial n ot i ce,as so

1 28 TROPICAL MEDICINE AND HYG I ENE
many problems are invo lved . It i s n ot proposed to givean exhaust ive h i story of the occurren ce of the d i sease
.
Ti l l recen tly there has been so much con fus ion betweenyell ow fever an d malari a , part i cularly the c l in i cal var i etyo f i t kn own in th e West I n d i es as b i l i ous remitten t fever ,subtert i an malari a , an d poss ib ly We i l
’s d isease,that man y
of the records are of doubtful value . A fata l fever wasfi rst recorded in San Domingo amongst the fol l owers o fColumbus in 1 493 , fourteen mon ths after the d i scoveryof America , an d ten years before the first sh ipmen t o fslaves to Ameri ca . Th is outbreak
,i f,as seems probable
,
i t was yel l ow fever,would prove that th e d isease was
on e of the New Worl d an d n ot o f Afri can importat i on .
Though vari ous outbreaks o ccurred in some of theWest I n d ies in the s ixteen th and seven teen th cen turi es
,i t
was n ot t i l l th e b ig outbreak wh ich swept al l through th eWest I n d ies an d to South Ameri ca in 1 793 that i t became of gen eral occurren ce
,and in each i slan d or coun try
i t appears to have been con s idered as a n ew d isease.
S in ce th en outbreaks have occurred in most p laces everytwelve to twen ty years on th e average .I II West Afr i ca an d the West Afr i can i s lan ds the
d i sease,or a s imi lar fatal fever
,was early n oted
,th e first
outbreak being in 1 5 1 0, though there had been an ep idemic in th e Can aries in 1 494 . In West Afr i ca
,the
Can ari es , and Made ira there were outbreaks every twelveyears in the s ixteen th cen tury
,three t imes in the seven
teen th,ten t imes in th e e ighteen th , and eleven t imes in
the n in eteenth cen tury .
The in terval s when places were bel ieved to be freevar i ed from short in terval s o f on e to five years , to longeron es twen ty
,fi fty
,or in on e in stan ce s ixty years .
In Bermuda the fi rst record of an ep idemi c i s in 1 699 ,
but s in ce then there have been frequen t outbreaks, somelocal and some widespread .
Several author i t i es,in clud ing Bla i r, po in t out that great
vari at i on s in th e sever i ty and characters of epidemicsoccur . And Blair in h isdescr ipt i on of the d i sease divides

1 30 TROPICAL MED IC INE AND HYG IENE
Afr i can n at ive was n o t immun e : Creo le n egroes usua l lyescaped .
The ser i es of outbreaks in Bermuda are o f in terest asshow ing how in a place much V i s i ted ep idemics werefrequen t . Records o f ep idemics date from ! 1 699, fol l owedby others in 1 779, 1 796, 1 8 1 2
,1 8 1 8
,1 8 1 9 ,
1 837 , 1 843 ,
1 85 3 , 1 85 6 , an d 1 864 . The mortal i ty in these outbreakswas usual ly comparat ively low ; fatal cases occurredamongst the blacks, but on ly in smal l proport i on—cg ,
in
1 864 there were on ly three death s amongst cases inthe coloured n atives
,0 2 per cen t .
,wh il s t 49 per thousan d
of the white people attacked died .
There can be l i tt le doubt that after an ep idemi c,and
probably before i t,mild cases occur an d keep the epidemic
al ive . The ep idemics in Bermuda o f 1 8 1 8 an d 1 8 1 9 ,
an d agai n of 1 837 an d 1 843 , represen t two ep idemicson ly . Whether th e d i sease can remain restr i cted to caseso f the m i ld type
,an d t he i n fect i on remain al ive with n o
man i festat i on of cases of the severer forms for peri ods of
ten ,twen ty
,or fi fty years
,i s a d i fferen t quest ion
,an d for
each coun try must be dec ided o n the eviden ce in thatcoun try an d n ot o n gen eral prin cip les . In the mean time
,
even where the eviden ce that th e d i sease i s en demic i sfairly strong , quaran t in e regulat i o n s again st p laces whereth e d isease ex ists in a v irulen t form should be en forced .
Yel low fever i s the most importan t member of a groupof di seases bel i eved to be caused by protozoa
,though the
paras ites have n ot been found . The V i rus ex i sts in theb lood plasma
,i s u l tra microscop ic
,an d the d i seases are
carr i ed by in sects . A per i od elapses before the in sectwh ich has imb ibed the blood i s capabl e of tran smi tt ingthe in fect i on . Dengue fever i s carr i ed by Culex fa tigansan d Stegomyia fascia ta ,
an d Phlebotomus fever i s carr iedby Phlebotomuspapa taci there are other kn own membersof th i s group . They are described in Part I I I .

CHAPTER X .
HUMAN TRYPANOSOMIAS I S .
(SLEEPING SICKNESS .)
D ISEASES due to the presen ce in the blood of trypan osomes . The best kn own— the Afri can forms—man i festthemselves as long-Con t in ued fevers
,at first o f a severe
type,but later low forms o f hect i c fever
,or peri odi c
attacks of fever,an d associated wi th en largemen t of the
lymphatic glan ds , especial ly the cervi cal evan escen trashes
,an d Often splen i c en largemen t . They usually
termin ate fatal ly with cerebral symptoms,those of the
form long kn own as sleeping sickness being the most usual,
or death occurs earl i er from in tercurren t d i seases or fromcard iac fai lure .
Geographica l Distribution of Sleeping Sickn ess — Thedisease i s on ly kn own in Trop ical Afr ica as an in digen ousd isease
,but man y cases have been reported in Europe , al l
in person s who had resided in Afr i ca W i th in the last fewyears . As j udged by the d istr ibut ion of i ts termin a l phase
Sleep ing S i ckn ess—th e d i sease has with in recen t y earsbeen spreading rap idly across Afri ca . There are d ifferen ces in the parasites in Rhodes ia from those in Ugandaan d the Con go , an d the former i s the more severe type, but,cl in i cal ly
,they resemble each other an d are con s idered
here together . I t was unkn own on the Z ambes i an dsouth of i t t i l l recen t ly
,an d i s n ow kn own in the
n e ighbourhood of Lake Nyasa , an d to the west of th i slake . I t i s prevalen t throughout the Congo
,but is rare
on the Gold Coast, in Lagos , and in Southern N igeri a .
I t has been in troduced in to the n eighbourhood of V i ctor ia Nyan za with in the last twen ty years
,an d n ow
exten ds throughout that d istr ic t an d down the N i l e some

1 32 TROPICAL MEDICINE AND HYG I ENE
200 miles . There i s every probabi l i ty that i t wi l l becomemore widely d iffused in Afri ca
,though i t i s l ess prevalent
in some places,such as L iberi a
,where at on e t ime i t was
common . The in termed iate hosts bel ong to the gen us
NORMAL
FIG . 36 .—Chart I , 1 909 . Onset of disease and marked temporary effect of soam in
in the second week .
FIG . 37.—Chart I I , 1 909 . Third and fifth weeks. Imperfect con tro l of tem
(perature by soam in and atoxy l in large d oses.
Glossina,an d th e spec ies impl i cated are Glossina pa lpa lis
an d poss ibly G. fusca ,an d for the form kn own as
Trypan osoma rhodesiense,G. m orsitans. G lossinae are
on ly foun d in Afr i ca and Arab ia,an d su i tabl e speci es to

1 34 TROPICAL MEDICINE AND HYG I ENE
FI G . 4o .—Chart V , 1 9 1 1 . Tartar emetic given in travenously every fi fth day, but
n o atoxyl , for some tim e seem ed to be a success as the temperature , except for therises wh ich fol lowed the inject ions, was n orm al , and n o trypanosomes were found .
U l timately the tem perature began to rise on the fifth , an d trypanosomes weresom etimes found on that day.
FIG . 4 I .—Chart V I , 1 9 1 1 . Later cond i tion . Under atoxyl the temperature
remainsabout n ormal for eight to twelve days and no trypanosom es are found . Then
there is a rise of temperature , and , as a rule , trypanosomes can be found . An in travenous injection of tartar emet ic is fo l lowed by a severe react ion , ind icated by thedotted l ine in the temperature chart, and the tem perature then fal ls and trypano
somes cannot be found for an other period . The use of atoxyl now seems to
have lengthened the period ofwel l-b eing from four or five to eight to twelve days.

HUMAN TRYPANOSOMIAS IS 1 35
of the d isease in m an . The period of in cubat ion in
mon keys i s about fourteen days . In some cases in
m an i t i s even shorter . The o n set in m an appears tobe o ften con foun ded with malaria
,but in some cases
there i s h igh an d con t inued fever as in typho id,whi lst
in other cases there i s n o marked fever . At th i s stagethere appear to be n o characteri st i c symptoms , butsometimes trypan osomes are foun d abun dan t ly in theblood .
The temperature after th i s early stage may fal l ton ormal , an d remain so
,but even in these cases the
d iurn al variat i on i s,usual ly in creased
,so that when the
i
temperature i s taken frequen tly,though i t may rarely
exceed 99°
F. ,there may be a variat i on at d i fferen t t imes
of the day of as much as 2°
F. More frequen tly therei s Sl ight i rregular fever, the temperature r is ing to 1 00
0 or1 0 1
0 F. every day . At t imes , in such cases, there wi l l bedefin i te pyrexia
,the temperature r i s ing to 1 03
° or 1 04°F
or even more,for several days
,fal l ing gradual ly to n ormal
o r a l i ttle above i t .Some of the lymphat i c glands are soon foun d to been larged an d are soft to the touch . They are n o t acutelypain ful , but are ten der o n pressure . The glands at thebase of the n eck are those most common ly en larged
,but
any glan ds may be affected .
In European s a rash i s usual ly presen t . It i s evan escen t
,but appears as ery thematous r ings surround i ng an
area somet imes sl ightly disco loured by blood p igmen ts .Th is discolorati on may amoun t to an actual bru isedappearan ce . The r ings are n o t ra ised to the touch . Thechest
,abdomen an d covered port ion s of the body are the
usual s ites for th is erupt ion , but i t may occur on anyother part of the body
,such as the forehead an d face .
Swell i ngs of various parts of the body, and part i cularlyfugit ive swel l ings un der the eyel ids
,are somet imes seen .
There i s progress ive muscu lar weakn ess , some loss offlesh
,an d an aemia
,wh ich may be profound . Even in
the early stages a sl ight b low may cause prolonged

1 30 TROPICAL MEDICINE AND HYG I ENE
muscular pain—Keran del ’s symptom . In other cases thesl ightest pressure on the muscles i s acutely pa in fu l , an dputting a muscle on the stretch may cause so much painthat the pat i en t i s un able to stan d or walk . The cardiacact i on is very rapi d an d un duly subj ect to i rregular it iesas a resul t o f sl ight exert i on s . A fine muscular tremori s often percept i b le in the hands in late stages . Theappet i te i s good
,and un l ess th ere i s much pyrex ia the
tongue moderately cl ean an d the bowels regul ar .
FIG . 42 .—Chi ld wi th trypanosom iasis showing oedematous swe l l ings
of the eyel ids .
l
The d isease run s a very chron i c course in most cases,
but in some death may occur early from the severi tyof the d isease
,or from card i ac fai lure before th e period
arr ives when th e temperature becomes n early n ormal o rcerebral symptoms superven e . In tercurren t d iseases
,par
ticularly pn eumon ia , are often fatal , an d with the subsi
den ce of the fever the gen era l con d i ti on shows someimprovemen t
,and th e
'
pat i en t m ay be able to go about

1 38 TROPICAL MED ICINE AND HYG I ENE
In th i s con di t i on,which i s the most common termin a
t ion of the d isease,the pat ien t passes in to a pecul iarly
l ethargi c s tate, so that wh il e the total amoun t o f S l eepobta in ed may be l i ttl e above n ormal he i s always drowsy
,
an d frequen t ly fal l s asleep even at meals 0 1° when in th eact o f performin g some ordi n ary occupat ion . Before theon set o f these symptom s there i s usual ly marked finet remor an d dul l headache . The temper i s frequen t ly nucertain ,
an d there may be men tal i rr i tab i l i ty . Th i s i rr i tab ility, as the d isease progresses , becomes more markedan d men ta l defic ien cy occurs. There i s a gen eral aspecto f mi sery about the pat i en t an d h e i s apt to be n eglectfu lo f h i s person , an d d irty an d careless in h is habits .Muscular weakn ess i s extreme
,an d un l ess the pat ien t
i s regularly fed he rap idly emaciates an d d i es,partly o f
starvati on . Even when wel l fed an d careful ly n ursedthere i s rap idly progress ive emaciat i on . The termin at ionof the d i sease m ay be assoc iated with d iarrhoea , or thepati en t may di e comatose .
Varieties.—The di sease
,as i t appears in Rhodesi a
,run s
a more rapi d an d severe course . All kn own cases havebeen fatal . The paras i te in m an appears to be morphological ly i den t i cal
,but in rats a varyin g proport i on o f
d i storted forms,in which the n ucleus i s more poster ior
than in the ord in ary forms an d may even be posterio r tothe micro -n ucleus
,are found . The trypan osomes are
more viru len t an d more read i ly in fect ive to experimen ta lan imals . Stephen s and Fan tham descr ibe th i s trypan osome as a d i st in ct spec ies un der the n ame of T. rhode
sieuse. Whether the d ifferen ce i s spec ific, or whether i ti s a viru l en t strai n modified by passage through differen tmammal i an hosts
,an d with a d ifferen t spec ies of Glos
S in a , G. m orsitans,as a carri er
,i s n ot con c lus ively proved .
A further d ifficul ty i s that in some stra in s i solated fromcattle S im i lar i rregular forms are foun d, an d Bruce conten ds that T. rhodesiense i s real ly T. brucei, the cause of
N agan a . As in other stra in s n o such forms have beenfou nd
,others con s ider that in some parts of Afr i ca two

HUMAN TRYPANOSOMIASIS 1 39
trypanosomes are causes of d isease in cattl e, T. brucei
an d T. rhodesiense. N o symptoms or changes have been
descri bed in m an in in fecti o n s with th i s Rhodesian formthat have n o t been descr ibed I n in fect i on s from theCongo an d Ugan da . An aemia i s more frequen t , orch it i so ccurs in a larger proport i o n of cases
,an d death from
cardiac fai lure before the on set o f cerebral symptoms i smore common .
D iagnosis.
—The d i sease may be mistaken in the earlystages for malari a an d typho id fever and possibly pellagra. In the later with any o f the chron i c forms o fi n termitten t
,remitten t
,or
“ l ow fever,such as kala-azar .
As the d isease i s con fin ed to Trop ical Afr i ca , suspic ionmay be excluded in patien ts who have n ot res ided in thatcoun try . The presen ce of en larged glan ds an d thefugit ive c irc inate erupt ion s are of great value in t hed iagnos i s .Certa in ty can on ly be obtain ed by fin ding trypan osomes
in the blood or flu id Obta in ed by hypodermic pun ctureo f on e of the en l arged glan ds
,or by the results o f the
in j ect i on of the blood in to monkeys or other susceptib lean imals , but with some of these , such as rats
,the period
o f in cubat ion may be i n defin i tely prolonged .
In the termin al stage the epi lept i form con vul s i on s an dthe comatose con d it ion might read i ly be mistaken foro ther d iseases . When th i s stage show s the pecul iarlethargy of s leep ing s ickn ess mi stakes could hardlyoccur . When cerebrosp in al symptoms have set in try
pan osom es may n o t be foun d in the blood , but on ly inthe cerebrosp in al flu id . This shoul d be drawn o ff bylumbar pun cture
,an d cen tr i fugal ized, as the paras i tes are
usual ly scan ty . Lum bar pun cture can usually be read i lyperformed with the aid of a local an aesthet i c
,th ough i t i s
e as ier when ch loroform is given . The pat i en t shouldl ie on h is s ide with the thighs flexed
,an d the back
arched as much as possible , to in crease the space between the vertebrae . The space to be selected i s betweenthe th ird and fourth lumbar vertebrae
,an d the n eedle

1 40 TROPICAL MED IC INE AND HYG I ENE
Should be in serted h al f an in ch from the middle l in e an dstead i ly pushed inwards an d sl igh t ly upwards
,t i l l i t is
fe lt t o pass through the tough membran e . I f i t str ikesth e bon e the n eedle should be partly withdrawn
,an d
then d irected s l ight ly more downwards . The escape o fc l ear flui d wi l l ren der i t certa in that the po i n t of then eedle i s in the can a l .Progn osis.
—The termin al s tage,sleep ing S i ckn ess , is
i nvar iab ly fatal . The earl i er stages o f the d i sease,when
there i s merely a trypanosome in fect i on o f the b lood an d
lymphat i c system,are o ften amen able to treatmen t, and
there i s good reason to bel i eve that complete an d perman en t reco very may en sue .
The d isease i s a seri ous on e,and the prognosi s , even
when al l the symptoms have d isappeared an d the
parasi tes can n ot be foun d in e i ther glan ds 01° blood
,
must be guarded,as cerebrosp in al symptoms may occur
years after the origin al in fec ti on . The progn osis i s worsein th e Rhodes ian vari ety an d in al l cases that do n o t
yield read i ly to modera te doses o f atoxyl .Pa thologica l Ana tom y .
—Li tt le i s kn own of the pathol ogi cal an atomy o f the early stages o f the d isease in m an
In mon keys an d the l ower an imals the con d it ion i s main lyo n e of vi sceral congest i on
,but en l argemen t o f the spl een
and in ten se co ngest i on ,som et imes haem orrhagic , of the
lymphat i c glan ds an d extreme congest ion of the bra in are
al so met with . S im i lar changes occur in th e l iver .
In sl eeping S i ckn ess there i s format i on of roun d cel l s in
the perivascu lar spaces of the cerebral cap i l lari es , closelyresembl ing that foun d in gen era l paralys i s o f the in san e .
Trea tmen t.—The drugs most d i st in ctly useful in malaria ,quin in e an d methylen e blue , have n o e ffect in th i s d isease ,an d do n o t al leviate the symptoms or reduce the n umber
of trypan osomes . Ars en i c l ong had some reputati on
In the treatmen t o f the early stages o f S l eep ing s ickn ess ,an d experimen ts wi th various trypan osome in fect i on s in
lower an imals showed that th is drug had a dec i dedcon trol l ing effect , and that the n umber of paras ites could

1 42 TROPICAL MED IC INE AND HYG I ENE
recovery,an d part i cularly whether al l possib i l i ty o f the
recurren ce of th e cerebral symptoms or of s leep i ng s ick
n ess has been obviated .
It i s somewhat u n fortun ate that a d ifferen t l in e of treatmen t has been adopted o n a large scale. Thi s plan
,
in troduced by Koch , was to use large doses an d repeatthem a fortn igh t l ater . The immediate effects were good
,
so much so that the method was widely advert i sed,an d
has been exten s ively employed . Further exper i en ce hasshown that the e ffects are temporary , relapses the rule ,an d opti c atrophy common . These results have to someexten t d i scred i ted the use of atoxy l .The attempt to treat d i seases by a few hero i c doses o fa spec ific has Often been tr i ed an d fa i led . As in stan ces : i fsyph i l i s be treated wi th a few large doses of mercury
,
or malar i a S im i l arly by qu in in e, the temporary resultsmay be good
,but relapses are usual an d th e d isease
recurs . The same drugs in moderate doses con t in uedfor a l ong t ime have a perman en t ben efic ial e ffect , an dthe same appears to h old good wi th atoxyl in trypanoso
m iasis. Al tern ate treatmen t with atoxyl an d mercury hasbeen advocated , but the resu lts , in m an
,have been n o
better than with atoxyl alon e .
I n j ect i on s of preparat ion s of an t imony have a morepowerfu l e ffect on the trypan osomes than atoxyl or an yother arsen i cal preparat i on s , but the an t imon y preparat ion s used cause much pain an d l ocal t i ssue n ecros i s un l essvery di lute—an d even then do so in some person s . Fin elydivi ded metall i c an t imony suspen ded in Lambkin
’s mediumusual ly causes l ess n ecros i s
,and i s as effect ive . I n tra
ven ous in j ect ion of a so lut ion of tartar emet i c, 1 to 2 gr .
in 1 0 c .c . of ster i l ized n ormal sal in e , i s t he most e ffect ivemethod
. If th e vein be i rrigated with a l i tt l e n ormalsal in e before the tartar emet i c solut i on i s in j ected, an d
after the in j ect i on of that so lut i on , th ere wi l l be n o localtrouble
. A r igor and sharp react i on wi l l occur in mostcases
.The immediate effects are str ik ing even in cases
wh ich do n ot y ield to atoxyl . In some cases, such in

HUMAN TRYPANOSOMIASIS 1 43
jections given every al tern ate day for two weeks , an d
after an in terval of o ne week a secon d two weeks’ course ,have been perman en t ly effect ive . In others the trypan osomes have return ed
,but yie ld read i ly to atoxyl . A
combin at ion of th i s form of treatmen t wi th in tramuscularin j ect ion s of atoxyl appears to give the best resu lts . Eventhe Rhodesian form of the d isease can be con tro l l ed byth is treatmen t
,but n o perman en t good resul t has yet been
obta in ed .
Nursing—No spec ial precaut i on s are requ i red . Thed isease i s a chron i c o ne an d good feeding i s n ecessary .
On accoun t of the card i ac con dit i on sudden movemen tsor exert i on on the part of the pat i en t must be discouraged .
When the gen eral con d i t i on of the pat i en t permits i t heShould be al lowed to l ive an ord in ary healthy l i fe . Butover- fat igue an d any r isk of in tercurren t d isease mustbe careful ly guarded agai n st .When tak ing atoxyl or any other preparat ion of arsen i c ,
any digest iv e di sturban ce , such as n ausea,vomit ing
,or
abdomin al pai n s must be careful ly n oted . Any complain t of dryn ess o f the mouth
,an d pain or irri tat i on of
the eyes,must al so be reported .
I n creas in g muscular tremor,headache , an d disturbed
sleep are premon i tory S ign s of the o n set o f sleep ingS i ckn ess . When th i s superven es , al l that can be don e i sto feed the pat ien t at regular in terval s
,an d to keep h im
clean,warm
,an d comfortab le . There i s n o obj ect in
en deavouring to preven t h im from sleep ing .
Etiology—There are certain po in ts o f an alogy between
trypan osomias i s an d some cases of syph i l i s . In boththere i s a laten t period fol lowed by a more or l essmarked febri le stage
,an d assoc iated with glan dular en
largemen t an d cutan eous erupt ion s an d termin at ing inthe format ion of d iffuse lympho id growths aroun d thecerebral vessels .In some cases of trypan osome i n fect i on there i s a
defin i te scar , the resul t o f a bi te from an in sect,which
was pain ful for some t ime,an d th i s may be con s i dered

1 44 TROPICAL MEDIC INE AND HYG I ENE
as the primary Sore . In th e Congo,an d where in fecti on
i s through G. pa lpalis, t h i s scar i s usual ly on the legs . In
Rhodesia,where the h igher fly ing G. m orsitans i s the
carr i er,on the n eck . I t may n ot be presen t .
The mode of propagation of on e o f the trypan osomed iseases in the horse i s by sexual in tercourse . Withhuman trypan osomias i s there i s n o eviden ce that thed isease i s spread in th i s man n er . D i rect in oculat i on o fthe blood of an in fected an imal in to an other wi l l tran smi tthe d i sease
,an d even an abraded surface i s suffic ien t
,but
,
as far as i s kn own,in n ature i t i s tran smitted by the
b ites of certa in fl i es belonging to the gen us Glossina .
From the d istr ibut i on o f the d isease,an d the corre
spon d ing distr ibut ion o f the fl i es,G . pa lpa lis i s bel ieved
to be the importan t carrier,wh ilst G. fusca an d poss ibly
G . tach inoides may also be carr iers . The common est o fthe tsetse-flies
,G. m orsita ns, t hough i t carr i es the trypan o
some of n agan a,is probably n ot a carri er o f T. gam biense
in Ugan da or on the Con go , but i s the carr ier in Rhodes iaan d on the Z ambes i of T. rhodesiense.
The Glossin ae are a gen us l imi ted to Afr i ca an d theshores o f the Arab ian Gul f
,an d are eas i ly d ist inguished
from other b i t ing fl i es .
_They are d ipterous in sects, an d closely resemble manyof theMusc idae , but are d istinguished by the long, straightprobosci s
,by the ari sta or sp in e wh i ch ari ses from th e
th ird j o in t o f the an ten n ae be ing plumose on the on e
side on ly,by the palps be ing the same length as the
probosci s an d grooved on th e in n er s ide,so that together
th e two palp i form a sheath for the probosc is. Thereare hai rs on ly on th e convex s ide of the ari sta an d theseare compoun d . The win gs are crossed , so that when atrest the ir t ips overlap each other— “ sc i ssor ” wingsan d prq ject beyon d the abdomen .
. The fourth longitud in al va n i s ben t twi ce , on ce to meet the tran sverseve in
,an d a secon d t ime to approximate to the th ird
l ongi tud in al .G lossinae are nearly
’
pupiparous the larvae attain the i r

1 46 TROPICAL MEDICINE AND HYG I ENE
more l ike a sharp st i ng,but n o t producing any subsequen t
l ocal e ffects un l ess in fected . Then they may producea swel l ing an d somet imes an ul cer . They wi l l b i te a m an
or other an imal wh i le he i s in motion,and seem to b ite
almost as Soon as they al ight on h im . G. pa lpa lis i s oftenfoun d in boats an d can oes
,sheltering un der the thwarts .
Very frequen t ly i t wi l l crawl out and b ite th e l egs,an d in
o ther cases , as they often fly low , wil l a l ight on th e legsan d b ite
,whereas the h igher flyi ng G. m orsitans more
frequen t ly attacks the upper part o f the body , th e head orn eck .
They are usual ly foun d in n arrow bel ts n ear water o nthe edge of forest lan d , an d may in such si tuat ion s bepresen t in large n umbers for a few hours
,wh i lst at other
t imes few or n on e may be foun d . They are also foun d inwel l -wooded coun try
,in forest clear ings,an d n ear forests .
The larvae are depos i ted in th e n eighbourhood of rottin gvegetat i on ,
an d part i cularly n ear the roots o f certa i nplan ts
,such as ban anas
,as wel l as many other p lan t s
and trees . The pupae are usual ly foun d in ban ks
covered with trees n ear Open water,l akes
,or streams .
Exten s ive clear ings, therefore, form an importan t part o fprophylax is .By the format ion of such clear ings an d th e burn ing
off of refuse vegetat i on In the vic i n i ty of settl emen ts theactual habitat ion s may be kept clear o f these fl i es . It has
been suggested that keep ing an d breed ing fowl s,or th e
importat i on of j ungle fowl s from In dia,might aid in
t he destruct ion of such larvae . It i s doubtfu l,however
,
whether such fowls would have any chan ce of con t in uedexisten ce at any d istan ce from human hab i tat i on s , as thelarvae also are depos ited away from the cleared tracts or
in plan tat ion s .
More hope of the destruct ion of the fl i es in the i r adul tform may be en terta in ed by the i n troducti on or cult ivat ion of in sect ivorous i n sects and other an imals, such asdragon -flies. Koch bel ieved that their most importan t
source of food i s the crocod i le, an d ad vocates the

HUMAN TRYPANOSOMIASIS 147
extermin ation of that rept i l e . Protect ion from the b i tesof fl ies i s very difficu lt
,n ot on ly must fly-proof houses
be made,but fly-proof cloth ing must be worn when out
s ide such houses . Such measures should be taken when
l iv ing in an en demic area close to n at ive settlemen tswhere sleep ing sickn ess i s prevalen t .Bit ing fl i es belonging to other fami l i es are n ot to bealtogether ign ored, as the trypan osomes of As ia arecarr ied by some of these
,such as Stomoxys . Atten t ion in
Afri ca has been almost en t i rely d irected to Glossin ae .
Experimen tal ly Glossinae con vey trypan osomiasi s intwo ways . There i s d i rect eviden ce that occasi on al ly theycon vey the paras i tes by feed ing first on an infected an imaland very short ly afterwards feeding o n an other susceptibl ean imal . Such tran smission i s d i rect . U sual ly attemptsat tran smiss ion in th i s man n er fai l
,but possib ly th is
mode of spread of the disease from m an to m an doestake place at t imes . Klein e has shown that fl i es aga inbecome in fect ive e ighteen days an d more after they havefed on in fected an imals
,an d remain in fective for an
in defin i te t ime .
At tempts to demon strate a defin i te cycl e of developmen t o f trypan osomes in the G lossinae are d ifficul tbecause flagellates are so common i n the al imen tary can alof fl ies . Bruce and others have shown that l aboratorybred fl i es do n ot harbour in test in al flagellates. If suchfl i es be fed on a person or an imal wi th trypan osomeschanges occur . In many of the fl i es the trypan osomesd isappear . In a min or ity the trypan osomes multip ly inthe i n test in e
,but are l ong an d n arrow
,or Short an d
stumpy,an d n ot l ike the forms foun d in the blood . In
these,about the twen ty -e ighth day (accord ing to Bruce
the common est t ime for the fl i es to become in fect ive) ,trypanosomes are foun d in the sal ivary glan ds
,an d th ese
trypan osomes are simi lar in appearan ce to those foun d inthe human blood .
In mammals they mul t ip ly asexual ly by longi tudin ald ivi s ion (fig . Smal l rest ing forms
,accord ing to

148 TROPICAL MEDIC INE AND HYG I ENE
some observers,may be produced . Un fortun ately m an
i s n ot the on ly an imal capable o f be ing i n fected,an d in
Rhodes i a many of the wil d game harbour the humantrypan osomes an d serve as the “
re servo ir ” from wh ichthe fl i es der ive thei r i n fect i on an d in turn in fect m an .
Even in Ugan da,mon ths an d years after the populat ion
had been removed from the sh ores o f V i ctor ia Nyan za, the
fl ie s there were st i l l in fect ive.Prophylaxis amongst European s i s comparat ivelys imple
. D i str i cts where sleep ing S i ckn ess i s prevalen t
Should be avo ided -as much as poss ib l e . Europeanhab itat ion s should n ot be n ear water n or placed where

1 50 TROPICAL MEDICINE AND HYG I ENE
(4) Treatmen t wi th atoxyl wi l l greatly reduce th enumber of t rypan osomes presen t in the blood an d therebydimin i sh th e probab i l i ty of in fect i on of the fly
,even in
cases where the course o f the d isease i s l i tt l e a ffected .
For th e trypan osomias i s o f Rhodesi a d ifferen t methodswi l l be requ ired as G. m orsitans i s more widely d istr ibutedan d fo l lows game
,m an
,an d cattle farther from water .
Extermin at i on of the game in broad belts o f coun try maycheck the spread in to d istr i cts n ow bel i ev ed to be ' free .
An effic ien t and su ffic ien t res iden t med ical servi ce,with
a cen tral l aboratory to dec ide wh ich di str i cts are free,
an d to supervise the destruct ion o f game an d the spreado f th e d isease
,would be n ecessary .
In South America a chron i c febr i l e d isease i s due to ablood paras i te fi rst described as T. cruz i. A fa i r n umbero f cases have been observed
,and the d i sease produced
‘
is
a chron i c type o f i rregular fever assoc iated with a pro
gressiv e anaemia and en largemen t o f the spleen ,l iver
,and
lymphat i c glan ds . It i s most common in ch i ldren,an d
death usual ly occurs from an in tercurren t d isease,com
m on ly dysen tery or d iarrhoea . There i s n o termin alcerebra l stage .
The paras i te,th ough i t resembles the other blood
trypan osomes,d i ffers in the method o f mult ip l i cat ion .
It does n ot d ivide longitud in al ly in the periphera l bl ood,but in t h e lungs i t d ivides in to e ight bodies with in al imit ing capsu le . Th is method of d ivi s i on l ed to i tsbeing described by Chagas as a Schiz otrypanum .
The carrier i s n ot a b it ing fly but a blood-suckinghemipterous in sect
,o ne o f the Reduv iidiae
,Con orrhinus
sanguisuga . After th i s bug has fed 011 an in fected personi t i s n ot in fect ive for e ight days or more , but after that, foran i n defin i te per iod , i t i s capable of in fect ing m an or othersuscept ib l e an imals .

CHAPTE R X I .
KALAAZ AR . KALA-DUKH . DUMDUMFEVER .
TROP I CAL SPLENOMEGALY .
Defin ition .
—A chron i c in fect ive febr i le d isease due toa flagellate protozoal organ i sm foun d . in i ts rest ing ,n on -flagellate form in t he spleen
,l iver
,in test in es
,super
ficial lymphat i c glands,an d other organ s . The disease
i s characterized by long-con t in ued fever,en l argemen t o f
the spleen an d l iver,wastin g
,deb i l i ty
,and anaemia
,an d
by a very h igh mortal i ty . It occurs both en demical lyan d in ep idemics .Geographica l Distribution .
—The prin c ipal seat o f kalaazar i s Assam
,in parts of wh ich i t has l ong been pre
valen t,though i t was first men t ion ed in 1 882 . Its n ame
,
s ign i fying the black disease,” refers e i ther to the terr ibl e
mortal i ty atten d ing the ep idemics wh ich for many yearsdevastated d istri ct after d istri ct o f Assam
,or to the dark
en ing of the skin observed in many of those su fferin gfrom it .Ep idemics have occurred in Lower Bengal
,where th e
d i sease i s also en demic,an d the n ame “Dum -dum fever
was given to attacks o f i t con tracted at th is stat i on byBri t i sh so ld iers
,many of whom have died o f i t in
Englan d .
Kala-azar also occurs in Madras,and sporadic cases
have been met with in Bombay and other parts o f I n dia,
also in Burmah an d Ceylon . Cases of th i s or a s imi lardisease
,occurr in g in ch i ldren on theMediterran ean coast
an d in some of the i slands in the Med iterran ean,have
also been descri bed . The d isease has been reported in

1 5 2 TROP ICAL MEDICINE AND HYG I ENE
Ch in a , the Stra i ts Settlemen ts, the Ph i l i pp in es, Pan ama ,N orthern Afr i ca
,an d the Soudan .
The populat ion of some of th e places n amed i s drawnfrom so many sources that i t i s n ot poss ibl e to say atpresen t whether the d isease i s endemi c in them or n o t
,
but in most in stan ces i t appears to be en demic .
Clin ica l Course—The cl in i cal p i cture of a case of kalaazar o f some mon ths ’ durat i on i s very strik ing . Thepat i en t
,even i f up an d about
,i s obviously i l l . H e i s a
wretchedly th in,t i red- l ooking m an
,with a big abdomen
an d shrun ken l imbs,an d compla in s of havin g had fever
o ff an d o n for mon ths,an d that in sp i te of qu in in e an d
various other med ic in es he has become gradual ly th in n eran d weaker, wh i l e h i s abdomen has got b igger an d b igger .A very sl igh t examin at ion of the pat ien t ’s d isten dedabdomen wi l l Show that h i s sp leen i s en ormously em
larged , that h i s l iver i s al so in creased in s ize, an d perh apsthat there i s a l i ttl e asc i tes presen t poss ibly the superfi c ialabdomin a l vein s wi l l be n ot i ceably promin en t
, an d i fatten t i on be turn ed to the feet some oedema of th e an klesan d dorsum wil l be foun d . Bes ides being th in
,the
pat ien t i s a lso an aemic,’
an d h i s Skin , espec ial ly that o fthe face
,i s darken ed or p igmen ted . H is hai r i s dry an d
lustre less and may fal l out in quan t i t i es , l eaving h ima lmost bald . He i s very eas i ly t ired an d any l i tt l e exer
t i on causes breath lessn ess . H i s in tel lect i s gen eral lyc lear
,an d he may make l i tt l e compla in t except of h i s
gradual ly in creas ing weakn ess and wast ing ; he may ormay n ot compla in of presen t fever, but even in i t s
absen ce m aysay that he i s d isturbed at n ights by vio len tsweats
,but for wh ich he probably sleeps wel l .
Not in frequen t ly, however, pat i en ts at th i s stage o f thed i sease su ffer from attacks o f ep i staxi s , or of bleed ingfrom the gums or from other mucous surfaces . Somet imes
,too
,petech iae appear , more common ly in th e
axi l lae than elsewhere . Attacks o f bron ch it i s or sorethroat are n ot un common . Less common symptoms ,but o f su ffic ien t frequen cy to requi re men t i on , are

1 54 TROPICAL MEDICINE AND HYG IENE
con s iderable height,an d after several hours fal l ing several
degrees,the fal l be ing accompan i ed by pro fuse perspira
t i on s . These febri le attacks recur da i ly . At first thetype i s remi tten t , but may soon become in termi tten t , thedai ly range of temperature be ing con s iderable
,varyi ng
between 97°an d 1 03
0F. (fig .
FIG . 45 .—Kala-azar . Simulat ing typhoid .
FIG . 46 .—Kala-azar . Later showing in term i tten t type.
The r ise o f temperature usual ly occurs in the even ing,but n ot uncommon ly t here i s a doubl e or , even a treble
ri se an d fal l in the twen ty-four hours . Somet imes thereare short per iods of apyrex ia
,fo l lowed by further out
burst s of fever .After the fever has lasted a short t ime , the spl een
becomes en larged an d tender ; en largemen t and ten
d ern ess of the l iver al so occur , but are l ess marked .

KALA-AZAR 1 5 5
Wasting,anaemia , an d deb i l i ty are early symptoms of the
disease,an d somet imes darken ing of the skin i s observed
at th i s stage .
H eadache somet imes accompan i es the fever, but therei s very l i ttle
,i f any,
d igest ive d isturban ce ; the tongueremai n s clean
,an d the appet i te good
,except in cases
where h igh fever has pers isted for some t ime . The fi rststage usrially lasts about a mon th , but the durat ion mayvary from ten days to two mon ths .It i s fol lowed , e i ther d irectly or after an in terval o f
apparen t heal th,by a stage in which low fever pers i sts
for weeks more' frequen t ly,for mo n ths . Sometimes
FIG . 47.—Kala-azar. U ndulat ing type .
the course of th i s secon dary fever i s very i rregular . I t i srarely high , though there may be occas i on al attacks ofh igh fever
,last in g for some days , whi le, o n the other
hand , there may be day s or weeks of apyrexia (fig .
In some cases the course of the fever may be remarkablyregular
,the temperature r i sing and fal l ing to exact ly S im i lar
po in ts at the same hours day after day for weeks . Fre
quen t ly also the course of the temperature chart showsa double dai ly r i se an d fal l . The fever at th i s stage oftencauses but l i tt l e d iscomfort
,an d but for profuse sweat ing
the patien t may be un aware that he has any . Sweating,
especially at n ight , may , however , occur without any r i sein the temperature .

1 5 6 TROPICAL MED IC INE AND HYG IENE
The l iver an d spl een con t inue to en l arge,the latter
often attain ing “ en ormous d imen s ion s . Emaciat i on,
an aemia an d deb i l i ty are progress ive u n t i l the con dit i onalready descr ibed i s atta in ed
,an d the stage of cachex ia
superven es .AS the en d approaches the pat i en t ’s con dit i on i swretched in the extreme . H e i s terr ibly emaciated
,an d
so weak that h e can hardly move,he suffers from
diarrhoea or dysen tery,though h i s appet i te may be
raven ous to wi th in a day or two o f death . By th i s t imethe fe ver may have given place to subn ormal temperature, an d the spleen an d l iver
,though st i l l con s iderably
en larged,may be smal ler than form erly . Death i s most
common ly due to dysen tery,wh ich appears to be an
in tegral feature o f the l ast stage of the d i sease,rather th an
an added compl i cati on . As already stated,however
,
pat ien ts somet imes d ie from mere asthen ia,wh i le n o t
un common ly death i s due to some in tercurren t d i sease,
of wh ich lobar p n eumon i a,phth i s i s
,an d can crum ori s
are those most frequen t ly met with .
The durati on o f the d isease var ies from three or fourmon th s to two years , but i s most common ly a year ore ighteen mon ths . Of th i s per i od the stage o f in i t ia l feverlasts a mon th or two , an d that o f l ow fever s ix mon thsto a year .Whi l e the descr ipt i on g iven above appl ies to mostcases o f kala-azar
,variat i on s from th i s type o f the d isease
are met w i th . I II some in stan ces the peri od of in i t i a lfever seems to be absen t , th e pat ien t gradual ly becomingweak an d i l l w i thout any defin i te symptoms beyon d losso f flesh an d en l argemen t o f the l iver an d spleen . I II
other cases the on set may be very acute,an d the pat i en t
may be carr ied o ff by fever or dysen tery before thedevelopmen t o f cachex ia .
For so seri ous a d i sease the symptoms other than thosemen t i on ed are remarkably sl ight . Bes ides headache
,those
re ferable to the n ervous system are ch iefly a d imin ution of
n ervous en ergy an d occas i on al muscul ar tremors , resul t i ng ,for example
,in educated pat ien ts , in in ab i l i ty to write .

1 58 TROPICAL MEDIC INE AND HYG I ENE
after separating the red corpuscl es to aga in cen tr i fugal izethe remain der and prepare fi lms from it . An othermethod i s to make blood fi lms termin at ing in a th ickedge ; l eucocytes accumulate at th i s edge , an d search forthe organ i sm is thus fac i l i tated . By th i s method a ski l ledobserver m ay be ab le to make h i s d iagnos i s certa in byexamin at i on of the peripheral bl ood al on e . U n less thecase i s compl i cated by malar ia , n o malar ial parasi tes orpigmen t wi l l be presen t in the blood .
Among the results o f the blood changes are the haem or
rhages from mucous surfaces already men t i on ed . Ofthese ep i stax i s i s the most common form
,an d i s some
t imes pro fuse an d d ifficul t to con tro l ; in other casessl igh t but pers i sten t ooz in g of bl ood from the n asalmucous membran e occurs ; bleeding of the gums i s n ot
un common,an d somet imes in test in al hmm orrhages occur ,
qu ite apart from those met with during the dysen teri cattacks o f the fin a l stage . Haematuri a i s occas ion al lyobserved .
Men t i on may here be made of the occas ion al presen ceof slight g en eral an asarca ; th i s an d th e tran s i tory oedemassometimes m etwith are probably due to the con dit ion ofth e blood . The an asarca may be most marked in theface
,l
an d m ay mask the emac iat i on .
Digestive System .
-There is l i tt l e to add to what hasalready been said of symptoms referable to the d igest ivesystem . Dur ing the early stages they are s l ight orabsen t
,th i s be ing in con trast t o the Con dit i on usual ly
met with in malari a .
While d iarrhoea 0 1° dysen tery are usual ly symptoms ofthe fin a l stage
,attacks may appear at any peri od of the
d isease . In some in stan ces , i ndeed, sold iers have beeni nval ided from I n dia to Englan d for dysen tery
,an d the
symptoms of kala-azar have superven ed .
Th e en largemen t o f th e l iver an d sp leen i s usual ly pa inl ess
,
’
though these organ s are often tender,especial ly in
the early stage of the d isease . Sometimes,however
,there
is con si derable . pa in in ° the l iver,which has led to the

KALA-AZAR r59
mistaken diagn osis of hepatic abscess, an d exploratorypun ctures
,while the microscopi c examin at i on has shown
the presen ce o f the characteri st i c paras i tes of kala-azar inthe flu id abstracted . Wh i le the en largemen t i s usual lyprogressive un t i l towards the en d
,variat i on s in th e s ize o f
the l iver an d spleen somet imes occur,dimin ut ion be ing
usual ly co in c iden t with temporary gen eral improvemen tin the pati en t ’s con dit i on . The S l ight degree of asc itesn ot in frequen t ly met with is probably due , at least partly,to the obstructi on to the c irculat i on caused by the en
largemen t of the l iver an d spleen .
The urin e i s n ormal in most cases of kala-azar,though
towards the en d i t may con ta in a l itt le albumin . Haematuria i s a rare compl i cat i on .
Respira tory System .
—A l i ab i l i ty to congesti on of theresp iratory passages
,as eviden ced by sore throat or by
sl igh t bron ch it i s,i s common in pat ien ts suffer ing from
kala-azar,an d there seems to be a special l i ab i l i ty to
pn eumon i a during the later stages of th e di sease ; thepn eumon i a i s o f the ord in ary lobar type . True tubercular phth is i s i s on e of the causes o f death in kalaazar . The paras i tes may occur in the lungs , an d in thatcase n odules resembl ing tubercl es wi l l be presen t . Thecases of th is descr ipt i on
,descr ibed by Darl ing in Pan ama
,
are associated with parasi tes with a th icker capsule , an din which the two chromatin masses are ! n ot always presen t .
'
He cal led the paras ite Histoplasma . Some authOrit i es con s ider them more al l ied to yeasts than to theparasites of kala-azar .Cutaneous System .
—Darken ing or p igmen tati on of th esk in i s sometimes very marked
,especial ly among dark
sk i n n ed pat ien ts . The Skin of European s suffering fromth i s d isease often has a dul l
,dirty appearan ce . Except
for occasi on al petech iae , there are n o special Skin erupt i on s in kala-azar .Can crum oris i s frequen tly met with in the last stages ofkala -azar
,especial ly in ch i ldren . Al though n early always
fatal -” cases have been recorded in ,which i ts appearan ce

1 60 TROPICAL MEDICINE AND HYG IENE
has been fo l l owed by great improvemen t in the gen era lsymptoms and even in subsequen t recovery .
Diagn osis.—With regard to the d iagn os i s o f kala-azar
,
i t may at on ce be sai d that th i s can n ot be made w itlicerta in ty except by the demon strat ion of th e spec ific
parasi te . In Assam , where the d isease was first recogn iz ed . medical pract i t ion ers who have been fami l i ar wi thi t for many years admi t that in th e early stages kala-azarcan n ot be read i ly d i st ingu ished cl in i cal ly from malari a ,or Sometimes from en teri c
,an d that even in the late r
stages a con s iderat i on of th e h istory of the pat i en ti s n ecessary before any con clusi on can be arr ived at .Should the pati en t be from an in fected house or v il
l age,an d should the developmen t o f h i s cachex ia have
been more rap id than i s usual in malari a,he i s co n
s idered to be su ffer in g from kala-azar,otherwise th e
d iagn osi s of h i s d i sease i s l ikely to be malar ial cachexia .
In Madras,too
,al l o f the pat i en ts in whom the earl i est
d iscovery of the paras ite had been made during l i fe hadbeen con s idered to be suffering from malari al cachexia
,
an d th i s in sp i te‘
of the fact‘
that n o malarial parasite scould be d i scovered by repeated examin at ion of thei rbl ood . Of the early in vest igators o f the d isease
,on e
beli eved that i t was an kylostomias i s, oth ers that i t was
a spec ial ep idemic form of malar ia,whi l e yet an other
bel i eved i t to be un dulan t (Mal ta) fever .
An importan t feature for the cl in i ca l d ifferen t i at i on o fkala-azar from malar i a i s the res i stan ce of th e formerd i sease to qu in in e
,an d sh ould th is res i stan ce be defin i te ly
proved , th e l atter may be excluded . It i s importan t t on ote
,however
,that the two diseases may co-exist, an d
that therefore the demon strat ion o f malarial paras i tes I nthe b lood and the ir d isappearan ce fol lowing the adm in istration of qu in in e can n ot be con si dered as defin i te ly
excluding in susp i c ious cases the d iagn os i s o f kala-azar .
In such cases,shou ld th e temperature Show a double o r
trip le dai ly curve,an d should there be l i ttle or n o diges
t ive d isturban ce , the l ikel i hood o f the ir being kala-azar
1 62 TROPICAL MED IC INE AND HYG I ENE
most read i ly obtain ed by pun cture of the l iver or spleen .
The ri sk o f haemorrhage fol l owin g pun cture of the spleenmay be great in kala-azar an d has been fatal . I t i spreferable to pun cture the l iver . The method o f pun cturei s as fo l l owsThe syringe an d n eedle must be steri l ized dry
,as any
admixture wi th w ater may cause a breakin g up of theparas i te . The skin over the s i te se lected for pun cturemust be thoroughly steri l ized an d the n eedle p lungeddeep in to the l iver w ith a sl igh t rotatory movemen t .When wel l in the l iver th e syrin ge wi l l move with th eresp i ratory movemen ts . The n eedl e Shoul d be kept inposi t i on for about a min ute an d sl ightly wi thdrawn beforegen tl e aspirat i on i s attempted . The less / blood that i spresen t the more sat i sfactory i s the operat i on
,as the
parasi tes are n ot in th e blood,and any blood presen t
on ly serves to d i lu te the flu id and ren der i t more difficul tto fin d the parasi te .
The flu id withdrawn shoul d be bl own out on to a
seri es of s l i des,making as th in fi lms as poss ib le . These
fi lms when dry may be starn ed with Le i shman’s method
,
or,after fixat ion
,with d i lute
,1 in 4 , fresh ly fi l tered carbo l
fuchs in . The paras i tes may be n umerous in such fi lms,
or scan ty,an d several fi lms Should be examin ed before a
n egat ive d iagn osi s i s g iven . They can be recogn i zed bythe presen ce o f two chromat in masses , on e smal l , rod- l ikean d deep ly sta in in g
,the other larger
,oval
,an d sta in in g
less deeply . Cochran has shown that in cases in Chin athe paras ites may be read i ly foun d in th e superfic iallymphat ic glands even when they are very scanty in th el iver an d Spleen .
Progn osis.
—The mortal i ty of kala-azar i s very h igh .
In Assam the mor tal i ty was est imated at 96 per cen t . ,but i t i s most l ikely that the remain ing 4 per cen t . ofthe pat i en ts were suffer ing from malari al cachexia , thed ifficulty in the d ifferen t iat i on of wh ich from kala-azarby cl in i ca l methods alon e h as already been men t ion ed .
In Madras the case mo rtal i ty i s recorded as 98 per cen t .

KALA-AZAR 1 63
One recovery has been kn own o f a pat i en t inval ided toEnglan d in whom the diagn os i s was fu lly con firmedby l iver pun cture
,and in whom paras i tes were a lso foun d
in l eucocytes in the periphera l blood . Rogers,however,
bel ieves that a fair proport ion o f the cases recover ifproperly treated .
Pa thologica l An a tomy.~ —The most n ot iceable feature in
the morbid an atomy of kala-azar,apart from the great
emaciat i on,i s the en largemen t o f the spleen and l iver
Bes ides th i s,inflammation an d ulcerat i on of the large in
test in e,an d some degree of asc i tes or oedema are'
comm on
The spleen i s almost invariably very greatly en larged ,sometimes weigh ing over 80 oz . ; i t i s of firm con sis
ten ce,retain ing its shape on removal . There i s usual ly
n o th i cken ing or in flammat i on of the capsule . On sect ion the surface i s dark red
,an d the sp l een substan ce is
firm an d fr i able Should,however
,the examin at ion have
been delayed,espec ial ly in warm weather
,the spleen
substan ce wi l l be foun d to be soft . There i s n o malaria lp igmen tati on
,and there are n o i n farcts . Mi croscop ical
examin at i on reveal s great d i l atat i on an d en largemen t oft he splen i c cap i l lar i es
,wi th reduct ion in the lymphoid
elemen ts . Scattered i rregularly throughout the organare en ormous n umbers o f paras i tes
,the Lei shman bodies .
These are con ta in ed chi efly in the cel l s l in ing the lymphspaces an d in the en dothel ial cel l s of the cap i l lari es.They also occur in the spl een cel l s themselves
,an d in
l eucocytes,ch i efly in the mon on uclear, but also in some
of the polymorphon ucl ear cel l s . They are n o t met within theMalp igh i an corpuscles or lymphat i c fol l i cles .The en l argemen t of the l iver i s usual ly less than that of
the spleen in proport ion to the relat ive S izes of the organ s .L ike the sp l een
,the l iver i s of firm con s i sten ce an d
fr i able . It i s usual ly rather pal er than n ormal and
presen t s a n utmeg appearan ce,th i s be ing due partly to
the growth of mon on uclear cel l s,ch iefly in th e cen tre
of the lobules , an d partly to fatty degen erat ion of thel iver cel ls . Parasites are n umerous in the en dothel ial
TROP ICAL MEDIC INE AND HYG I ENE
cel l s of the cap i l l ari es an d lymphat i cs,an d are also met
with in free mon on uclear cel l s,but do n ot occur in
th e l iver cel l s themselves . Hmm osiderin i s presen t bothin the hepat i c cel l s an d in the spleen pu lp .
N ext to the spleen an d l iver the bon e-marrow an d
lymphat i c glan ds are th e pr in cipal seats of the paras ites,wh ich occur ch iefly in the large monon ucl ear ce l l s th emarrow appears to be in creased in amoun t an d i s redderthan n ormal .Should death have been brought about by dysen tery
,
as i s so common ly the case,the large in test in e wi l l be
foun d th i cken ed an d inflamed,the descen ding colon an d
sigmo id flexure bein g ch iefly affected . The inflammat i ons omet imes affects the whol e l ength of the large in test in e
,
and may involve the lower part o f the smal l in test in e .
There i s great in flammatory in fi l tra t ion of all the coatso f the bowel
,an d frequen t ly there are u lcers exten d ing
from the mucous to the serous coat,or even caus ing per
foration ; somet imes the mucous membran e i s coveredwith a tough fi lm of exudat i on .
°The inflam mat ion o f th e in tes tin e does n o t appear tobe d i rectly due to the Le i shman body, for but few ofthese organ i sms are usual ly foun d in i ts coat they occurch iefly in the en dothel i al cel ls o f the cap i l l ar i es .In un compl i cated cases the other organ s o f the body
appear to be heal thy,but even in th i s case paras i tes may
be foun d,though sparing ly, in the en dothel i al cel ls o f
the cap i l l ar i es an d lymph spaces of var i ous organ s,e.g .
,
l ungs,
‘
kidn eys,supraren alc apsules, an d lymphat i c glan ds .
Somet imes th e mesen ter i c glan ds are en larged , an d
con ta in t he specific parasi tes in f large n umbers . In sp iteof the wide d istr ibution of th e paras i te in t he body i thas n ever been foun d in any of th e secret i on s or excre
t i on s during l i fe . The d i fficul ty o f fin ding the organ i smin th e blood has al ready been al luded to .
In fresh un stain ed preparat i on s the paras ites of kalaazar are d ifficul t to see . They appear as rather refract i l e
,
mot i on l ess bodies o f indefin ite -outl in e,almost c olourless

1 66 TROPICAL MEDIC INE AND HYG I ENE
v acuoles are seen in i t . The paras ites can al so be sta in edby many of the bas i c an i l in e dyes , weak carbol- fuchsinan d carbol - th ion in e perhaps givin g the best results .In smears obta in ed from the l iver and spleen dur ing
l i fe th e paras i tes may e ither be free or conta in ed in cel l so r embedded in a m atr ix . The matr ix i s n ot seen in
smears made from organ s after death,n or in sect i on s
in wh ich the paras i tes always appear to be in tracel lu l ar .In th e great maj ori ty of cases th e ce l l s con ta in ing theparas i tes appear to be en dothel ial cel l s o f cap i l laries an dlymph spaces , ei ther un al tered or of large S ize an d
irregular shape,con st i tu t ing macrophages . The macro
phages often con ta in l arge n umbers of paras ites, uponwhich they appear to exert n o phagocyt i c act ion . On
t he con trary , un der the in fluen ce of the paras i tes th emacrophages un dergo gradual d is in tegrat i on
,and in al l
probabi l i ty furn i sh th e matrix seen in an te-mortem smears ,and the parasi tes are al ive an d capable of develop ing in toflagellate forms .N ext to the en doth el i a l cel l s the “l arge mon onuclear
l eucocytes most frequen tly harbour the paras i tes, an d
a few are foun d in th e polymorphon uclear leucocytes ;they also occur in the myel ocytes of bon e-marrow , butar
‘e n ot met wi th in paren chymatous cel ls .When obtain ed post m ortem
,an d especi al ly it severa l
hours have elapsed s in ce the death of the pat ien t, manyo f the paras i tes Show changes i n di cat ive o f developmen t .
They are larger, 3 ,
u. to 5 a in d iameter,the chromat i n
masses Show s ign s of d ivi s i o n an d may even be re
dupl icated,an d commen c ing cleavage of the cytoplasm
i s seen,each hal f con tain ing a l arge and a smal l chromatin
mass .In sect i on s, owing to shr in kage, the parasi tes appear
much smal ler than in smears the chromat in masses arec loser to each other an d the smal ler has frequen t ly l osti ts rod -shaped appearan ce .
Etiology—The et i ology o f kala-azar i s of spec ia l in
ferest,both because o f the repeated fai lures which have

KALA-AZAR 1 67
attended the i nvest igat i on s undertaken for i ts eluc idat ion
,an d because of the remarkable ser ies o f observat ion s
wh ich have resulted in the d iscovery of the cause of thed isease an d the n ature of th e spec ific parasi te
, an d
probably of i t s mode of tran smiss i on an d prophylaxisThe great mortal i ty caused by epidemics o f kala-azar
in Assam,dur ing the last two decades o f the n in eteen th
cen tury,prompted the Governmen t o f . I n dia to sen d
o ne medical officer after an other to investigate thed isease , an d i f possibl e to d i scover i ts cause an d devisemethods for i ts preven t ion . All the invest igat ion s soun dertaken
,although carr ied out with great care , fa i led
in thei r obj ect . On e observer, in fluen ced by the anaemiao f the patien ts an d by the d iscovery that many o f themharboured ankylostomes
,con s idered that the d isease
was essen t i al ly ankylostomiasi s . An other came to thecon clusion that kala-azar was malar ial fever
,in an
in ten se an d commun i cable form ; an d a th i rd in vest igator,while n ot ic ing the absen ce of malarial paras i tes in th eblood an d of melan in pigmen t, thought that i t was a formof malari a with marked in c iden ce on th e l iver an d spleen
,
an d with a mortal i ty en han ced by the con curren ce o fan kylostomiasi s or o f dysen tery an other bel ieved i t to beun dulan t fever (Malta fever) . The subj ect stood thus when ,
inMay, 1 903 , Lei shman publ i shed in the BritishMed ica l7 ournal a short n ote en t i t led
“ On the Possib i l i ty of theOccurren ce of Trypan osomias is in I n dia . A few yearspreviously
,in 1 900 ,
he had n ot i ced in smears made fromthe spleen of a sold ier
,who had died at N etley of tropica l
cachexia an d dysen tery , con tracted n ear Calcutta,en or
mous n umbers of the smal l , roun d , oval bodies , with thetwo character ist i c chromatin masses already descr ibed .
AS to the mean ing of th ese bodies Le i shma n was at a loss .
I II 1 903 , however , he foun d almost exactly s imi lar bodiesin the spleen o f a whi te rat , which forty-eight hourspreviously had d ied of in fect ion with the trypan osome ofn agan a . Up to the t ime o f i ts death the blood of th i srat was swarming with trypan osomes, an d experimen ts

1 68 TROPICAI. MEDICINE AND HYG I ENE
proved that i t was poss ible to trace every step in the
degen erat ive changes wh ich had led to the format ionof the smal l roun ded bodies
,the two chromat in masses
,
on e of wh i ch represen ted without doubt the macro theother the micro -n ucl eus of the trypan osomes from whichthey had been formed (fig . Thi s secon d observat io ngave a clue to the explan at ion of the first
,an d Le i shman
fel t h imsel f j ust ified in suggest ing n ot on ly that the so ld ierhad suffered from trypan osomias i s , but t hat “ some o fth ese severe trop i cal cachexias, such as Dum -dum fever
,
as well as kala -azar an d sleep ing s ickn ess , might be dueto trypan osomias i s . These suggest i on s have been j ust ified to the exten t that th e paras i tes have been proved todevelop flagel la
,an d therefore belong to the flagellates.
In Ju ly , 1 903 , Don ovan an n oun ced that some mon th spreviously he had seen th e bodies descr ibed by Le i shman
in the sp leen s o f several pat i en ts , who had d ied atMadrasof what was con s i dered to be chron i c malari a
,but he was
n ot aware of the i r n ature un t i l h e had seen Le i shman ’spaper, an d that he had sin ce foun d iden t i cal bod ies inthe blood
,obta in ed by pun cture , o f the spl een during
the l i fe o f a pati en t su ffering from irregular pyrexia,
and in whose b lood n o malari al paras ites could be foun d .
In the fo l lowing Jan uary , Ben t l ey d i scovered S imi larbod ies in spleen smears from l iving pat i en ts sufferin gfrom kala-azar in Assam ,
an d srnce then n umerouss imi lar observat ion s have been made as regards casespresen t ing s imi lar symptoms , where the disease was cont racted in or n ear Calcutta, an d in certa in other p lacesin I n d ia and elsewhere . I t may , however , be n oted herethat the paras it e has n ot been d iscovered in pat i en tssuffer ing from “ m alar ia l cachex ia and en larged spleen
in the P un j ab where organ i sms morphological ly simi larhave been shown to occur in Del h i bo i l s .
A further stage in the et i o logy of the d i sease wasreached in N ovember
,1 904 ,
when Rogers an n oun cedthat he had observed the developmen t from the parasi teof flagel l a
,l eavi ng
,as he sa id , but l i tt le room for doubt

1 70 TROPICAL MEDIC INE AND HYG I ENE
the paras ites in creased in s ize,became gran ular
,an d th e
body became elongated,the macron ucleus en larged an d
the m icron ucleus migrated to the thi cker en d of theorgan i sm from wh ich a flagel l um arose . The protrusi onof the flagel lum was preceded by the formati on in th ecytoplasm surroun ding the micron ucleus of a roun dedmass wh ich stain ed with eos in
,the rest o f the cytoplasm
stain ing blue with Le i shman ’s sta in .
In on e in stan ce long,flagellate forms were developed
with in twen ty- four hours,these ch iefly occurr ing in
pa irs . In l ater experimen ts ( 1 905 ) Rogers has foun dthat the
.
developmen t o f flagellated forms from kala-azarparasi tes takes place more fre ely an d with greater regularity in an ac id than an alkal in e medium
,an d t hat
ster i l i ty of the med ium i s e ssen t i al . Th is has led h imto suggest that the in termed iate host o f the paras i temight be the bed-bug
,th e in test in al con ten ts o f wh ich
he foun d suppl i ed these con d it i on s . Working on th i shypothes i s, Patton has an n oun ced that he has been ableto trace the complete cycl e of the parasi tes up to com
pletely developed flagellates in certa in trop ical bed-bugs,an d that in h i s op in i on th ere i s n o doubt that the I n dianbed-bug
,Cim eer.
°
rotunda tus,tran smits the d isease .
The rar i ty of the o ccurren ce of the parasi tes in theperiphera l b lood has been advan ced as an argumen tagain st th i s method of in fect i on . Don ovan has
,how
ever , shown that they occur in the peripheral blood inthe l eucocytes in termitten t ly in al l cases of kala-azar, an dat t imes may be fairly n umerous . It must a lso be re
membered that trypan osomiasi s can often be tran smittedby the in j ect i on of b lood
,t he m icroscopical examin at i on
of which fa i l s to reveal any paras i tes .III the Assam ep idemics kala-azar spread slowly from
vi l lage to v rllage along the l in es o f commun i cat i on .
I so lated vi l lages,or those to wh i ch person s from outs ide
were n ot admitted,remai n ed free from attack , an d the
common h istory of in fected vi l lages was that some personhad arrived there suffering from the d isease after a short

KALA-AZAR 1 7 1
t ime the members of h is househ old were attacked an d
th e d isease gradually spread from house to house . Rogers
reports that h e has observed a s imi lar house or fami lyin c iden ce among h is hosp ital cases of kala-azar atCalcutta .
All these facts,as wel l as the success wh ich has atten ded
attempts to stamp out ep idemics of kala-azar in Assamby the i solat ion of pat i en ts, coupl ed with the burn ing ofi n fected huts
,i s in favour of the V i ew that the di sease
i s tran smitted by some house- in festing parasi te , such asa bug .
A suggest i on,basiad upon the con s iderat i on o f the l ow
temperature at wh ich the flagellate forms are developedin v itro from the oval forms obtain ed from the spleen , i sthat th e paras i tes escape in the faeces and undergo a stageof developmen t in some cold-blooded an imal
,a fi sh or
mollusc , an d th at they obtain e n tran ce in t o the humanbody by the ingest ion of such altern at ive hosts , e itherd irect or through the water supply . There i s
,however,
n o experimen tal eviden ce in suppor t of th is suggest ion ,
an d the c i rcumstan ces that the parasi tes can n ot be foun din the fae ces
,an d that a steri le med ium is re quired for
the developmen t of flagellate forms, are opposed to i t .The season a l prevalen ce o f kala-azar
,as shown by the
n umber o f fresh attacks,i s greatest in the co ld weather
mon ths,N ovember to Apri l
, in Assam an d Lower Bengal .The “ cold weather temperature in th i s area rangesbetween 60° an d 75
°
F an d Rogers po in ts out that i t i son ly with in these l imi ts that developmen tal forms of theparasi te are obta in able in v itro . H e suggests thatep idemics of kala-azar have been due to a success ion ofper iods of prolonged cold weathers
,which have exten ded
the con dit i on s favourable to the extra-corporeal developmen t of the parasi te . He further suggests that the moresevere cold weather of N orth-west I ndia accoun ts forthe absen ce of kala-azar there .As has been seen
,kala-azar when ep idemic may carry
off en t ire households,person s of e ither sex and al l ages

1 72 TROPICAL MED IC INE AND HYGIENE
being l i ab le to attack . Rogers states that males an d
females are attacked in equal proport i on,an d that in fan ts
an d old people are less l iabl e than others to the d isease,
wh i le i t i s common est among ch i ldren an d young adults .
As to race,kala-azar i s comparat i vely rare among
European s in I n dia,an d occurs ch iefly amon g the poor
,
whose domest i c hygien e in places l ike Calcutta resemblesthat of n at ives . In Assam i t has been n ot iced that infection of European s i s often traceable to cohab itat i onwith n at ives
,or to occur in miss i on aries an d others whose
dut i es bring them in to close con tact with n at ives . Rogershas po in ted out that
,in con trast to th e case of en ter i c
fever , kala- azar occurs more common ly among European s who have l ived some years in I n dia than in
n ewcomers .Trea tmen t—On ce kala-azar has become wel l developed
n o treatmen t seems to have any e ffect upon the courseof the disease . It i s cla imed by some that qu in in e invery large doses may arrest the d isease at a very earlystage, but i t i s poss ible that cases re spon din g to qu in in eare malarial . Bes ides qu in in e a very great n umber ofdrugs have been tr i ed— arsen i c
,the sal i cylates
,an d also
bon e-marrow -but wi th l i ttl e effect . More recen t lyatoxyl has bee n given
,but the resul ts are n ot rapid , though
in on e case so treated,that of wh ich th e charts are given ,
recovery has taken place . Salvarsan has been tr i ed , and
in in fect ion s wi th S imilar paras i tes in the lower an imalswith h ighly sat i sfactory resul ts .In m an i t i s worth an exten s ive tria l , but the results so
far recorded are confl i ct in g.
I t i s poss ibl e that careful atten t ion to the gen eral h ealthof the pat ien t
,coupled
,in the case of European s, with
residen ce in a temperate cl imate , and l iving as much asposs ib le in the open a ir
,may prolong l i fe a l i tt l e, and i t
i s importan t that such measures should n ot be n eg
lected , for they at any rate add greatly to the pat ien t’s
comfort,an d throughout the d isease treatmen t must be
symptomat i c .

1 74 TROPICAL MEDICINE AND HYG I ENE
Clin ica lCourse.
—In many cases the first symptom n otedi s d iarrhoea
,somet imes accompan i ed by vomit ing . Later
there i s i rregular fever an d stead i ly in creas ing anaemia .
There i s l oss o f sp i r i ts,steady emac iat i on
,an d sometimes
attacks o f ep istaxi s,bleed i ng from the gums or elsewhere .
As th e anaemia becomes more marked oedema of the feetbecomes n ot i ceable
,an d en l argemen t o f the abdomen
from the in crease in s ize o f the Spleen . The pal l or of thesk in i s o f a pecul iar yel l owish wh i te t in t
, n ot l i ke that o fan equal degree o f an aemia from other causes . Thoughd iarrhoea or other d igest ive d isturban ces are common ,
the appet i te,as a rul e
,i s n ot affected . I II un con trol l ed
cases the progn osi s i s un favourable,though i t i s rarely
fatal in l ess than s ix mon ths,an d may last for years .
Spon tan eous recovery does take place .
Pa thology—The spleen an d
,to a smal ler exten t
,th e
l iver,are en l arged
,an d th e paras i tes , appare n tly morpho
logical ly iden t i cal wi th those of kala-azar,are foun d in
n umbers . The lymphat i c glan ds are n ot en larged . Theblood shows great reducti on in the n umber of redcorpuscl es
,which may be as l ow as per cub ic
m i l l imetre,an d there i s a diminut i on in the amoun t o f
haemoglob in . n ot, as a rul e, to the same exten t as that o fthe n umber of corpuscles . There i s l eucopen i a in manycaSes, but n ot to as extreme an exten t as in I n dian kalaazar . The mon on uclear elemen ts are usual ly in i n creasedproport i on . In many cases the in crease i s in the largemon on ucl ear e lemen ts .Trea tmen t—Spon tan eous recovery takes place in a
smal l proport i on of cases,an d recoveries have taken place
after in j ect i on of salvarsan,though in other cases the
resu l ts have n ot been sat i sfactory .
Etiology.—N i col l e
,to whose work our kn owledge of
th is d isease i s l argely due,d iscovered that in the d istr i cts
where th i s d isease i s en demic a certa in proport ion o fdogs are n atural ly in fected w ith a s imilar parasi te . In
jection ,e i ther of the j u i ces from the t i ssues or o f cultures
o f the organ i sms from them ,are fo l lowed by in fect ion o f

KALA-AZAR I 75
the dogs . These observat ion s have been fu l ly con firmedby other invest igators .CANINE LE ISHMAN IA—The course of the d isease i s com
paratively mild , though there may be a certain amoun tof pyrexia an d emaciat ion . The paras ites may be foun din l arge n umbers in the l iver
,in the spleen
,an d in the
bon e-marrow. A con s iderable proport ion of dogs havebeen foun d in fected n atural ly
,though the proport ion
var ies both according to d istr ict and accord ing to season .
Whether the disease in m an i s derived from dogs i sat presen t un kn own . It i s poss ib le that they form thereservoir
,an d some. experimen ts show that Pulex serm
ticeps, which wi l l occas ion al ly feed on m an, can serve
as a carri er of the d isease,as paras ites develop in these
fleas . Attempts to in fect dogs with the paras ites of kalaazar in I n dia have fa i l ed .

CH APTE R X I I .
ORIENTAL SORE .
ALEPPO E VI L,AURANGZ EBE
,BOUTON
‘DE BAGHDAD ,
CLOU DE BISKRA,DATE SORE
,DELH I BO IL
,
FRONTI ER SORE, ORI ENT BUELE, YEMEN ULCER .
THE vari ous n ames men t i on ed above,an d m anyo thers,
are given to ulcers occurr ing in Algeria,Egypt, lAsia
Min or,th e Levan t
,Cyprus
,Arab i a
,Pers ia
,Northern
I n dia, the Sudan,an d South Ameri ca an d Pan ama
,
an d other subtrop i cal coun tr i es . Poss ibly these ared ifferen t forms due to paras i tes wh i ch morphological lyare in dist ingu ishable ; These u lcers are character izedby the th ick crusts whi ch form on thei r surface
,and by
the i r great chron i c ity . There are several d i st in ct types,
some scaly an d n ot ulcerat ing .
( 1 ) A n on -u lcerat ing form,the usual on e in the Sudan
,
but n ot rare in I n d ia .
(2) Superfici al flat ul cer,the usual form of fron t i er
sore .
(3 ) D eep u lcer with overhanging rai sed edges, th ecommon form in Arab ia
,I n dia
,an d South America .
The affect i on begin s as a smal l red,i tch ing papule
,
resembl ing the effect o f a mosqu ito b i te . Th is soonin creases in s ize, becomes sh in y an d tran sparen t, an d
surroun ded by a red areola . In t he n on -ul cerat in g formth i s s imply gets larger
,l asts for some mon th s an d sl owly
subsides . Later in the ul cerat ing forms there i s a serousd ischarge wh i ch
,together with desquamated epithel ia l
scales,form a crust which i s often studded w i th smal l
yel low po i n ts . Undern eath the crust u lcerat ion takesplace
,un t i l the crust giv ing way, an in dolen t u lcer i s


ORIENTAL SORE 1 77
exposed,which slowly spreads . The surface of the ulcer
i s studded wi th flabby red gran ulat i on s,wh ich bleed
readi ly on pressure ; i ts base i s freely movable over thesubj acen t t i ssues
,an d i ts edges are ra ised, i rregular an d
sl ightly in durated . There i s always a con s iderableamoun t of th in ,
serous or purulen t d i scharge wh i chcoagulates, forming d irty yel low crusts . The degree ofpain varies ; often there i s l i tt l e or n on e, but somet imes,especial ly i f i rr i tated
,or i f the discharge be pen t up by
th ick scabs,the ulcer i s very pain fu l an d th e edges acutely
ten der .The ulcer slowly spreads in an i rregular man n er forsome t ime
,often for several mon ths
,an d ei ther of itsel f
or by coalescing iw ith s imi lar ulcers forms a large opensore an in ch or two in d iameter . After a t ime the u lcerceases to spread and s lowly heal s
,the heal ing process
being Often in terrupted by the reten t ion of the d ischargeben eath the crusts . Depressed
,p itted
,an d p igmen ted
but superfic ia l scars are left which may be mistaken fo rthose of syph i l i s . These u lcers are most common o n
exposed parts of th e body,espec ial ly on the face
,n eck
,
wrists,an d on the back of the han ds an d dorsum of th e
feet . They may be single,but are more common ly
mult ip le,an d are irregularly d istr ibuted . There i s usual ly
n o en largemen t of the lymphat i c glan ds . As a rule ,there i s n o con sti tut i on al d isturban ce , but i f n umerousan d severe the ulcers l ead to gradual impairmen t of thehealth .
The South American form (P l ate I I I, fig . 50) i s somet imes kn own as “ Forest Yaws .” I t has n o con n ectionwith yaws
,Fram baesia tropica (figs . 5 7 an d
The Sudan type (P lates IV an d V,figs . 5 1 an d 5 2) i s on e
of the n on -u lcerat ing forms . The growths commen ce assmall
,p in k
,c ircular po in ts raised above th e sk in
,wh ich
gradually i n crease in s ize,an d roun d them other s imi lar
papules form . These coalesce with the primary tumour,
an d an i rregular mass i s formed, p in k in colour and witha smooth sh in ing surface . They are soft to the feel an d
2

1 78 TROP ICAL MED IC INE AND HYG I ENE
freely movable over the deeper t i ssues. They do n ot
break down,u l cerate or caseate
,but may last for years .
A somewhat s imi lar n on -u lceratin g form occurs in Egypt .There are n o con st i tut i on al symptoms .Pa thologica l . Ana tomy
— Ori en tal sore i s essen t ia l ly an
in fect ive gran uloma . The proper e lements o f the skinan d i ts accessor i es
,the hair an d sebaceous fol l i c les
,an d
the sweat glan ds,are in vaded an d destroyed by gran ulat i on
t i ssue, whi ch exten ds deeply in to the cor ium an d n ecro sessuperficial ly , thus produc ing an ul cer . In the early stage ,before an ulcer i s formed
,there i s pro l i ferat i on . of th e
cut icular cel l s l ead in g to the format i on of papules laterth i s pro l i ferat i on exten ds a l i tt l e in advan ce o f the edgeso f the u lcer . The cel l s compos ing the granu lat i on t i ssueare almost exclus ively o f the mon on uclear type . Theyare large roun ded ce l l s w ith promin en t n ucle i
,an d are
apparen tly o f en dothe l i al orig in . The appearan ce i s thusvery d i fferen t from that of s impl e u lcerat i on o f the skin ,
in which polymorphon uclear cells predomin ate . A fewof these cel l s a lso occur in Orien tal sore
,but gian t c el l s ,
such“
as those seen in tubercular an d some syph i l i t i caffect i on s o f t he skin ,
are n ot met with .
Scattered throughout the gran ulat i on t i ssue , but ch ieflycon ta in ed in the large mon on uclear cel ls
,are vast n umbers
o f paras i t i c organ i sms, very s imi lar to those occurr ing inkala-azar . These bodies were first described as occurringin Orien tal sore by Wright
,of Boston
,in 1 903 . H e
d iscovered them in an u lcer con tracted in Armen i a somemon th s previ ously . The d iscovery was con firmed, asregards s imi l ar sores con tracted '
at Delh i,Lahore
, Quetta ,an d other places in N orthern an d Western I n dia , by jamesin 1 904 , and as regards Egypt by Bi l lo t, an d by Darl ingan d others in the South American form . The parasi tes,Leishman ia tropical , are in d ist ingu ishable morphological lyfrom those of kala-azar
,a descript ion of which wi l l be
foun d on p . 1 65 . j ames descr ibed the occurren ce insome of the paras ites o f a th ird chromatin mass—a rodtaper ing towards the 'micron ucleus an d at right angles


ORIENTAL SORE 1 79
to i t . H e bel ieved it n ot to occur in the organ i sm ofkala-azar
,but i t has s in ce been shown to do so some
t imes . In art ific ial cultures some of the paras i tesdevelop a flagel lum
,j ust as the paras i tes of kal a-azar do
,
an d , as a rule, the developmen t in su itable media i smore rap id an d the flagellates are larger . Men an d
mon keys have been successfu l ly in ocu lated an d a locall es i on resu lts somet imes s ix mon ths or m ore later. Withth e appearan ce of the local l es ion there may be fever andcon st i tut i on al d isturban ce . In dogs these results vary, ase i ther a local les ion may resul t or a gen eral d isease of ami ld type .
Etiology .—From the great abun dan ce throughout the
cel l s compos ing the gran ulat ion t i ssue of Ori en tal soreo f the b in ucleated organ i sms descr ibed by Wrigh t an d
j ames, i t seems h ighly probable that these are the causeof the d isease . H ow they en ter the body is un kn own
,
but lon g before the ir d iscovery the malady was con s i deredto be of a paras i t i c n ature
,and vari ous parasi t i c bod ies
were described as occurr ing in the a ffected t i ssues .Among these men t i on should be made of the bod iesd escribed in 1 885 by Cun n ingham , an d con sidered byh im to be mon adin a . From h is descr ipt i on an d figuresthere can be l i tt le doubt that the bodies he con s idered tobe paras ites were the large en dothel ial cel l s con ta in ing theo rgan i sms descr ibed by Wright an d j ames, the m agn ifica
t i on an d sta in ing methods at h i s comman d n ot admitt ingo f more prec ise d ifferen t iat i on . I t may be added thatCun n ingham ’ s descri pt ion of the h i stological appearan ceso f the sores i s in close agreemen t with those of Wrightan d j ames .While many of the earl i er observers agreed that water
was in some way respon s ible for these sores, some attributed them to its chemical con ten ts
,an d others to i ts con
ta in ing parasi tes whi ch were ingested or en tered throughabras i on s in the sk in . Other supposit ion s are that thesesores are the resul t of b i tes of mosqui toes or of san dfliesor other b it ing fl i es, or that the parasites exist in the so i l

TROPICAL MEDICINE AND HYG I ENE
an d are d irectly in oculated by acc iden ta l abras ion s . It i sat l east possib le that in fect i on may be carr ied d irect lyfrom an Orien tal sore to s imple ulcers or wounds by fl i e sso common in places where the d isease i s prevalen t .The c ircumstan ce that these sores are most common on
parts o f the body n ot protected by clothes,and espec ial ly
on the face an d n eck which are n o t part i cu larly l iable toabras ion s
,i s in favour o f t he V i ew that the paras i te i s
in troduced by some b it ing in sect,the . n ature of th e
organ i sm favouri ng th is V i ew .
I t has been suggested that true Orien tal sore on lyoccu rs in coun tr i es in which camel s are in common use
,
an d that in fect i on i s in some way derived from camel s .The d isease
,however
,i s more prevalen t among town
dwel lers than amon g those who have espec i al ly to dowith camels or who usual ly lead a n omad ic l i fe .
It has been shown that Orien tal sore can be directlyin oculated in m an
,an d there i s a strong popu lar bel ief
that recovery i s fol lowed by immun i ty,so much so that
in certa in places i t i s the pract i ce to in oculate ch i ldreno n un exposed parts of t heir bodies wi th matter takenfrom such sores
,with the obj ect o f avo id ing d isfigure
men t o f the face . Attempts have been made to in ocu latedogs with pus from Orien tal sore
,with a certain amoun t
o f success,but some mon keys are suscept ib le to in ocula
t i on s . Sores occurr ing in dogs at Delh i,an d l o cal ly
bel i eved to be of the same nature as Delh i bo i l s in m an,
were shown by j ames to con ta in n umerous sp ir i l l a,but
n o Le i shman bodies . After i n oculat i on with the paras itesdogs appearto b e in good health an d m ay n o t developsores
,but the par as ites may be foun d in large n umbers in
their l iver an d sp leen . Poss ibly dogs serve as the reservo ir an d m an acqu ires h i s in fect ion from them . N o
gen eral in fect i on of dogs i s foun d in places whereLeishman ia tropical occurs as i s foun d where in fan t i l eLeishman ia anaem ia occurs .In places where Orien tal sore i s very prevalen t ch i ldren
are the pr in cipal su fferers,and n ewcomers are spec ial ly


ORI ENTAL SORE 1 8 1
l i able to attack. Where less common , person s between1 5 an d 30 are most affected . Otherwise, age, sex an d
race appear to be with out influen ce . The season al prev al en ce vari es in di fferen t places
,but the attacks appear to
be most common at the begin n ing an d en d of the hotweather .D iagnosis—The descript ion given above should be asu ffi c ien t guide to the n ature o f the affect i on
,an d the
d iagn osis can be estab lished'
by th e di scovery of th espec ific paras i te . Syph i l i s i s the d isease for wh ich Ori en talsore i s most l ikely to be mistaken . The absen ce of theo ther symptoms of o syph ilis and th e fa i lure of an t isyph i l i t i c treatmen t should en abl e a correct diagn os i s tobe made .
Trea tm en t—The treatmen t of Ori en tal sore,un less
thorough ly carri ed out , i s very un sat i sfactory . Medicat i onby the mouth has n o effect
,but N i col le andMauceaux
had excel len t resul ts from salvarsan,a simple 0 6 gr .
d ose being fol lowed by the h eal ing of the u lcers in threeweeks . If protected from irritati on the sores heal verysl owly, but with sl ight scarring . Of local appl i cat ion s
,
copper sulphate solut ion , 1 to 4 per cen t . , somet imes gives
good results . Cardam atis’ o in tmen t
,composed of m ethy
l en e blue an d lan ol in,has been used with apparen t
ben efit in some cases,whil st Row has recorded cases o f
cure from in oculat ion with k i l l ed cultures of the organi sms . If the d iseased t issues are comp l etely destroyedheal ing i s more rap id but the scar may be greater . In
the early stage complete exc i s i on may be possib le,but
fai l ing th is,the surface an d edges of the ul cer should be
thoroughly scraped an d ord in ary an t isept i c dress ingsappl ied . Should scrap ing be con sidered in advisable somecaust i c appl icat ion ,
preferably strong carbol i c acid,may
be appl i ed . O thers use caust i c alkal i es,such as potassa
fusa . Change o f a ir i s often of great ben efi t in obst in atecases .Preven tion - In the presen t state of kn owledge con cern
ing the man n er in which Or i en tal sore i s con tracted i t i s

1 82 TROPICAL ’MED ICINE AND HYG I ENE
n ot poss ib le to give prec i se di rect i ons for i ts avo idan ce .The proved in oculab i l i ty o f theulcers suggests the importan ce o f measures to avo id d irect con tag i on , these in cluding, bes ides person al clean l in ess, the cover ing of the soreswi th some an t i sept i c appl i cat i on . Un t i l i t has been shownthat the water o f p laces in which the d isease prevai l s i sin n ocuous, i t would be wel l to bo i l i t before use, ei ther fordrinking or wash ing . S im i larly , th e b i tes of i n sects an dcon tamin at i on by fl ies are to be avo ided )It i s wel l n ot to a l low dogs in th e h ouses and to d is
courage any c lose con tact wi th these an imal s .

1 84 TROP ICAL MED IC INE AND HYG I ENE
Clin ical Course.—After a few hours of mala i se the pat i en t
i s sudden ly se ized w ith ch ill s,an d in two or three hours
he i s su ffering from h igh fever,with a h ot
,dry skin
,with
rap id pulse , severe fron ta l headache, an d great pa in in th eback an d l imbs . Bil i ous vomit ing sets in
,accompan i ed
by much th irst an d by pain an d ten dern ess of the upperpart o f the abdomen . Con siderable prostrat ion en sues
,
an d by the secon d day of h i s i l ln ess,i f n ot earl i er
,th e
pat i en t takes to h i s bed . H ere'
he l i es for about a week,
h i s tongue becomes dry an d coated,h is bowel s con st i
pated,an d h i s l i ver an d spl een en larged an d t en der
,
Jaun d i ce may superven e , an d sl ight bron ch i t i s i s commonat th i s stage .The pat i en t i s troubled wi th sl eeplessn ess (thein somn iaresembl ing that o f a pat i en t w ith del ir ium tremen s ) ,or he may be del ir i ous . H i s aspect i s weary
,h is face
l iv id,an d h i s con d it i on appears to be very ser ious .
On or about the seven th day,however, a cri s i s occurs .
Followin g a bri ef in crease in th e severi ty o f the symptoms,
Cop ious persp irat i on sets in,the temperature fal l s very
rap id ly,an d symptoms of col lapse may fol low,
n ot in fre
quen t ly accompan i ed by diarrhoe a or even dysen tery .
In a fav ourable case, however , th e col lapse i s n ot ser iousth e pat ien t fal l s asleep an d wakes after a few hours
,
apparen t ly conval escen t . After about a week of th i sseem in g con valescen ce the pat ien t i s subj ected to an oth erattack of fever commen cing almost as sudden ly as the fi rst .The symptoms of the relapse are s imilar to those ofthe in i t i a l attack , but mi lder , though the fever may beh igher an d the deb i l i ty more pron oun ced . The durati oni s,however
,shorter . A secon d cri s i s occurs o n or about
th e fi fth day,an d i s usual ly fol l owed , after a short con
valescen ce, by complete recovery . Sometimes, however ,a secon d , an d in decreas ing frequen cy a th ird , fourth , orfi fth relapse may occur . On the other han d, there maybe n o rel apse . Some cases are cut short by death in the
fi rst attack .
The sudden n ess of the r i se an d fal l o f temperature i s a

RELAPS ING FEVER 1 85
startl ing feature of relaps ing fever . With in a few hoursthe temperature in the axi l la reaches 1 03
°F . or beyon d .
Wh i le u sual ly showing a d iurn al vari at i on of about 2° F .,
being lowest in the morn ing ,the temperature remain s at
a h igh level throughout the in i t ial attack,with an upward
ten den cy as th e cr i si s i s approached . At the acme of thefever a temperature of 1 05
°F . ,
1 06° F.,or even h igher
,i s
n ot un common,but as i t i s n o t long main ta in ed i s o f less
ser ious import in th i s than in most other acute fevers .The cri si s
,whi le usual ly occurring on the seven th day o f
the primary attack,may often be accelerated or del ayed
FIG . 5 3 .—Relapsing Fever . I nd ian .
a day . Rarely the'
cri si s occurs o n the n in th day, orst i l l more rarely o n the fourth . When ever i t occurs thecrit i ca l fal l o f temperature i s usual ly very sudden , reachin g the n ormal po in t or , more common ly, a degree ortwo below it wi th in twelve hours .The temperature remain s subn ormal for two or threedays
,then r ises to the n ormal po in t, where i t remain s
un t i l a relapse occurs . The course of the fever in relapsesi s s imil ar to that of the in i ti al attack , t en d ing , however,to be less abrupt in i ts on set
,to show greater dai ly
osc i l lat i on s an d to be of shorter durat ion . In fac t,al l
t he symptoms of a relapse are less typical than thoseOf the in it ia l attack . The in terval between each successiv e relapse al so ten ds to be longer . Thus, whi le th eord in ary durat ion of the in i t i al attack is seven days, an d

1 86 TROP ICAL MEDICINE AND HYG IENE
o f the first apyrexial in terva l also seven days,th e firs t
relapse usual ly l asts five days an d the secon d on ly two o rthree days
,whil e th e in terval between them is common ly
n in e days . It wi l l be eviden t that an attack of re laps in gfever with on ly on e relapse lasts n early three weeks .Con s iderable variat i on s may occur in the temperatureo f relaps ing fever . I n stead o f by cri s i s
,for example
,the
fever m ay subs ide by lys i s , an d in some cases a secondaryr i se may abruptly succeed the cri t i cal fal l .The pulse during relapsing fever fo l l ows the course of
the temperature,though with a ten den cy, more marked
with each successive relapse,to lag beh in d . It rapidly
i n creases in frequen cy with the on set o f the fever an dcon t in ues to r i se, though more sl owly, as the cri s i s i sapproached . Its rate common ly reaches 1 20 per min uteduring the first day o f the d isease— rather more than thatin women an d ch i ldren—an d by the th ird or fourth dayof fever i t may be 1 30 or even 1 40 per min ute . Withthe cri s i s the pulse-rate fa l ls , though less rap id ly than thetemperature . It may be un usually slow for a day or twofol lowing the cr i s i s
,after wh ich i t return s to n ormal un ti l
th e relapse sets in .
Al th ough at first boun d ing, the pulse of relaps ing feversoon becomes soft an d compressib le , these features (whichare almost invari able) becomin g more marked in proport ion t o the durat ion of the d isease .Correspon d ing with the con dit i on of the pulse
,the
heart almost invariab ly shows s ign s of weakn ess . Theimpulse soon becomes weak an d th e first soun d prolonged an d boomin g . In rare in stan ces
,an d these almost
always met with during the acme of the in i t ia l attack,
sudden heart fa i lure occurs, caus ing fatal syn cope .
Resp irat i on in an un compl icated case of relaps ing fevercorrespon ds with the pulse . There i s common ly sl ightbron ch ial congest ion eviden ced by cough and frothyexpectorat i on . With n o further compl icat i on s than th is
,
the breath ing may be very rap id an d the patien t maysu ffer from acute dysp'n oea at th e acme of the fever
,
1 88 TROP ICAL MEDICINE AND HYGI ENE
symptom is due to catarrhal in flammat i on o f the stomach,
partly also to act ive congest i on o f the l iver an d spl een .
Whi l e the con st ipat i on of th e early per i od of relaps ingfever i s con stan t en ough to be o f some diagn ost i c valu e
,
severe d iarrhoea n ot in frequen t ly occurs at th e cri s i s,
the stool s somet imes con ta i n in g blood .
Occas i on al ly there i s actual dysen tery,depend ing prob
ably upon previous in fect i on .
Pa in an d ten dern ess o f the l iver an d sp leen areearly symptoms . Both organ s are en larged
,the spleen
espec ial ly, an d both rap id ly d imin i sh in s ize after the
cn srs.
Frequen tly assoc iated with en l argemen t an d tendern ess of the l iver i s j aun d ice
,though th i s symptom i s
more common in some ep idemi cs than in others . It
usually comm en ces about the fi fth day of the in i t i a lattack
,d isappearin g a few days after the cr isi s . Its
in ten s i ty vari es greatly,but whi le u sual ly sl ight an d
tran s i en t i t may somet imes be very in ten se .
The urin e i s dark an d scan ty dur ing the febri le stagesof rel aps ing fever
,an d al so duri ng the early part of th e
apyrexia l peri od . It i s o f rather low specific gravity
( 1 0 1 0 to and con ta in s an excess of urea . A smal lamoun t o f albumin may occur
,an d granular casts may
be foun d ; blood i s un common . When j aund ice i spresen t th e ur in e con ta in s bi l iary pigmen ts .Men t i on has been made of the hot , dry skin of the
febri l e stage and of the sweating at the cri s i s of relapsingfever . The sk in
,though dry
,does n o t feel as hot as might
be expected from the bodily temperature , th us d i fferingfrom the con d it ion observed in certa in other acute febri l ed i seases
,pn eumon i a for example .
The cr it i cal sweats are usually very profuse, even moreso than in malari a
,an d may saturate the clothes an d
bedding .
N igh t sweats somet imes occur after the cri si s, an d
during relapses the skin may often be mo ist .While there i s usually
'
n o rash in relaps ing fever, facia l

RELAPS ING FEVER 1 89
herpes i s n ot un common . In certa in cases smal l rosecoloured spots
,someth ing l ike those of en teri c fever, but
smal ler,are met with . They come out in crops, which ,
commen c ing n ear the cris i s of fever , may con tin ue in tothe apyrexial per iod . These papules are most commonon the fron t an d s ides of the chest an d abdomen . Theyare n ever very n umerous, l ast on ly a few days, an d
d isappear on pressure without leaving a sta in .
Sudamin a are common,an d in rare cases petechim are
met with .
Desquamation,except in th e form of min ute bran ny
scales fol lowing sud amin a , i s un common .
Complica tions—The more importan t compl icat i on s ofrelapsing fever are pn eumon i a
,severe d iarrhoea
,or dysen
tery, an d have already been deal t wi th .
Men t i on may here be made of the l iab i l i ty o f a smal lproport ion of cases to haemorrhages . Epistaxi s at th eacme o f fever i s the most common example . Haematemesis may also occur
,an d more rarely cerebral
haemorrhage,always fatal
,has been observed .
Swel l ing an d in flammation of the parot i d glan d an d oflymphat ic glan ds
,most common ly those of the inguin a l
region s,have been observed Occas ion al ly . Th is i s o f
importan ce in con n ect ion with the di fferen t i ation of thed isease from plague .
I n flammatory affection s of the eye an d ear somet imesoccur
,but are rarely seri ous in the I n dian variety .
I n flammati on of serous membran es are rare,but sl ight
pa in ful swel l ing of some of the j o in ts,most common ly
those of the upper l imb,are n ot un common .
Pregn an t women‘
always abort ; the abort ion i s gen eral ly fol lowed by recovery .
The CO-exi sten ce of relaps ing fever, with malar ia, smal lpox, measles, p lague , an d d iphtheri a has been n oti ced
,
an d in certa in ep idemics,fol lowing famin es
,with scurvy .
There are n o spec ial sequelae of relapsing fever, thoughmen tal an d bodi ly weakn ess frequen tly pers i st for somet ime . A certain degree of immun i ty i s con ferred by an

1 90“TROPICAL MED ICINE AND HYG IENE
attack of re laps in g fever,but on ly lasts a short t ime , as two
or even three attacks may occur in the same person .
Progn osis— The progn os i s of an un compl i cated case
of relaps ing fever i s good . The mortal i ty varies in
differen t ep idemics, probably depen ding upon the con
d it i on of the in fected populat i on . When the d iseaseprevai led in Great Bri tain the mortal i ty was est imated atabout 4 per cen t . A s imi lar rate i s sa id to be commonin Russia . In Bombay, however , Van dyke Carter foun dthat th e mortal i ty was 1 8 per cen t . H i s stat i st i cs were
,
however,based upon hosp ital experien ce . The death -rate
amongst cases treated in the mun i c ipal hosp i tal in Bombay dur ing the last ten years has been much h igher thanth i s
,someth ing l ike 30 to 40 per cen t . , an d Choksy recordsdeaths out of cases
,from I 898
- I 9o7 , an
average mortal i ty of 30°C but in th e n orthern parts o f
I n di a the mortal i ty i s n ot h igh , n or i s i t in the form in
wh ich i t occurs in N orth America,n or in that foun d
in Egypt .Death i s most l ikely to occur during the acme of the
in i t i al attack an d may be due to co l lapse or to heart
fai lure,or may occur during col lapse fol lowin g the cri s i s .
The r i sk i s greater in th e first attack . As might beexpected
,extremes of age are un favourable .
Th e case mortal i ty i s s l ightly h igher among womenthan among m en
,though abort i on i s usual ly fol lowed by
recovery .
In cases compl i cated by pn eumon i a th e progn osi si s un favourable , recovery be ing rare .
Severe j aundice al so ren ders the progn os is un favour
able , an d , as has been seen ,cerebral haemorrhage i s always
fatal .Diagnosis—While a typ ical case of . relapsing fever i seas i ly recogn ized , in stan ces occur in which i t i s imposs ibl eto arrive at a correct d iagn osi s by mean s o f the cl in i ca lsign s al on e, and the real n ature o f the d isease may qu iteeas i ly be overl ooked
,even at the autopsy . It can be
un derstood,al so
,that a '
patien t seen for the first t ime at

1 92 TROPICAL MEDICINE AND HYG IENE
search of sta in ed fi lms i s n ecessary to d i scover any . In
examin ing fresh fi lms i t i s an advan tage to use darkgroun d i l lumin at i on .
The best sta in ing method i s probably Le ishman ’s orother modificat ion s of Roman owsky ’s sta in . Fai l ing th i s
,
gen t i an violet or carbol - fuchs in may be used . The spirill um is described under th e head ing of E t io l ogy
,p . 1 93 .
The blood o f pat ien t s suffer ing from relaps in g fevershows a con dit ion of l eucocytos i s . The n umber o f bothpolymorphon uclear an d mon on uclear leucocytes i s increased . Somet imes th is i s very marked
,and as there
i s also a d imin ut ion in the n umber o f red corpuscles theexcess of these over the leucocytes i s greatly reduced .
The sp iril l um has n ot been demon strated in'
any of thepat ien t ’s secret ion s or excreti on s .
MORB I D ANATOMY .
The bodies of pati en ts dying o f un compl icated relaps ingfever do n o t show any very characteri st i c gross changes .
The con di ti on i s that o f a gen era l sept i caemia with en
largemen t o f the spl een an d l iver an d catarrhal inflamm a
t ion of the stomach—often also of the in test in es an d
of the bron ch i . Subserous haemorrhages un der the
peri ton eum,peri card i um
,an d pleura are common . The
en l argemen t o f the spl een i s usual ly very con s i derable,
i ts weight somet imes reach ing 5 lb . ,an d i ts s ize exceed
ing t he n ormal by five or s ix t imes .The sp len i c capsu le i s d i sten ded an d smooth
,an d th e
whole organ i s roun ded . The spleen substan ce shortlyafter death i s firm an d dark an d mottled with small wh itespots
,wh ich are the en larged Malp igh ian corpuscles ;
t hese may somet imes be breaking down in to min uteabscesses . Large wedge-shaped in farcts are common ,
usual ly having the ir base at the capsu le,though they may
be met with throughout the organ . When recen t ly formedthey are of a dark red co lour
,but later they become pale
an d may be foun d breaking down in to pus .

RELAPSING FEVER 1 93
Mi croscop ical ly the hypertrophy of the sp leen i s foun dto be due both to prol i ferat ion of i ts cel lular elemen tsespec ial ly of the Malpigh ian corpuscles— an d to vascular
e ngorgem en t. Spiri l l a may be foun d in the spleen both free
and in polymorphon uclear cel ls , often in great pro fus ion .
The en largemen t o f the l iver i s often marked and theweight may be as much as 5 lb . Though somet imesd ark and con gested, i t i s more common ly pale and
mottled . I ts substan ce i s soft and the lobules are ind ist in ct . There i s cloudy swel l ing of th e cel ls .Bes ides the con dit ion s men t ion ed , the heart i s usual ly
foun d to be pale an d soft , the muscular fibres showings ign s of cloudy swel l ing and som etim e5
°
fatty degen erat ion . The kidn eys an d other abdomin al organ s are alsoin the con dit ion of cloudy swel l in g . The in flammationof the in test in al tract i s often con s iderable . The stomachis th e part most common ly affected an d there are usual lyn umerous smal l haemorrhages ben eath the mucousm embran e . In cases compl i cated by diarrhoea ordysen tery there i s in ten se congest i on of the i l eum an d
colon,wh ich may even be superfic ial ly u lcerated .
A certain amoun t of bron ch ial catarrh i s usual ly foun d,
but in un compl icated cases the lungs are pale .Two forms of pn eumon i c con sol idat ion may be metwith . The more common form is that in which patcheso f con so l idat ion , often of con s iderable s ize, are scatteredthrough both lungs ; th ey m ay be met with in any parto f the lobes and are n ot more common at the bases thanelsewhere . The other form of con sol idat ion i s s imilar tothat of ordin ary croupous pn eumon i a .
While inflammat ion of the bra in or i ts men inges i s rarein relaps ing fever , passive congest ion as shown by ven ousengorgemen t an d serous exudat ion i s n ot un common .
Etiology .—Relaps ing fever i s remarkable in bein g the
first d isease shown to be due to a micro-organ i sm .
During an epidemic in Berl in,in 1 868
,Obermeier dis
covered in the blood of pat ien ts suffer ing from relaps ingfever a sp ir i l lum , which sin ce th e publ icat ion of th e
I 3

1 94 TROPICAL MEDIC INE AND HYG I ENE
d iscovery in 1 873 has been accepted as th e cause of th ed isease . These Spir i l la are n ow common ly termedsp irochaetae .
The Spirilli im oberrneieri or Spiroc/i azta recurren lis IS
a del i cate wavy thread measuring between 1 5 I“ an d
40 p. in l ength by about 2 5 a in breadth at i ts widestpart . The n umber of sp irals vari es greatly
,as also does
I IG . 54 .
the i r con tour . A common n umber of sp i ral s i s e ight,
but o ften two sp iri l l a are j o in ed together,giving the
appearan ce of on e long form with s ixteen sp i rals . Somet imes the sp iral s may be short
,giving a corkscrew
appearan ce, or they may be on ly sl ight u ndulat ion s . In
t h ick fi lms th e sp ir i l l a may be in bold curves or figures ofe ight
,with few or n o un dulat i on s (fig .
No- deta i l s of structure can be made out except that
i t has taper ing poin ted en ds,an d th at
,especi ally when
stain ed by Roman owsky ’s method,sl igh t d i fferen ces in
the degree Of stain ing'
of d ifferen t parts can be n oted,the

1 96 TROPICAL MEDICINE AND HYG I ENE
in terdepen den ce between the presen ce of sp irochaetesand the d i fferen t phases o f rel aps ing fever . An earlyV i ew Was that th e fever resul t ing from the presen ce ofthe paras i te in the b lood caused i ts destructi on an d
that relapses were due to the developmen t of furthergen erat ion s o f sp ir i l l a from spores . The ex i sten ceof spores o f S . Oberm eieri has
,however
,n ot been
demon strated . The blood of a patien t during theapyrexial in terval s wi l l s t i l l in fect mon keys i f in j ectedin to them . An other V i ew attributed the d isappearan ceo f sp i r i l la to the format ion in th e b lood o f some bactericidal agen t at the cri s i s
,wh ile a more modern V i ew is that
the spir i l l a are destroyed by phagocytos i s,th i s destruct ion
occurr ing ch iefly in the sp leen . The lengthen ing periodsof in terrupt ion an d the mi l dn ess of relapses i s by othersattr ibuted to the acqu iremen t by the patien t o f in creasing degrees of immun i ty . Th is V i ew i s con s i sten t w iththe probable protozoal n ature of the paras i te . Thesp ir i l l um or S . obemneieri i s one o f a cl ass o f organ i smso f wh ich man y pathogen i c spec i es are kn own . Thesemen t i on ed in the order of the i r d i scovery in cludeS . anserin i, the cause o f septi caemia of geese S . theileri
,
affect ing catt l e in South Afr i ca ; S . ga llinam m ,caus ing
fever in fowls in Brazi l,the Sudan
,an d el sewhere
,and
S . dutlon i,th e cause of Afri can t i ck fever . These organ
i sms resemble each other in the i r gen eral morphologyan d act ive moti l i ty . They al l occur free in the circul at ing blood during the febri l e paroxysm an d are n o
l onger foun d after the temperature has fal len . In thein te rval s between th e attacks of fever smal l act ively moti lebod ies con ta in ing chromatin are foun d in some o f thered cel l s .It has furthermore been demon strated that certa in of
them are conveyed by the b i te of certain t i cks ; thus,S . ga llinam m i s tran smitted by Argas persicns, S . z
‘lzeileri
by Boophili is decolora tus, an d S . dutton i by Orn ithodom s
m oubata . No such demon strat i on has been made in thecase o f I n dian and Etiropean relaps ing fever, but a t ick

RELAPS ING FEVER 1 97
very similar to O. mouba ta—O. sav ignyi—has been shown
to occur in I n dia .
In parts of Persi a Argasper/sicus
,the mian a bug , has
long been bel ieved to cause severe fever, an d s imi larcon sequen ces are thought to fol low b ites of A. lurca z‘a
inMexi co an d Cen tral America .
Mackie reports an ep idemic of relapsing fever in a schoo lin I ndia
,
’
in wh ich he bel i eved the tran smitt ing agen t wasPed iculus vestim en tom m (fig .
The disease was much
more prevalen t in the boys who were in fected with
F IG . 5 5 .—Pea’iculus m sl imen iorum .
pedi cul i than in the girl s who were less so . Fourteen percen t . of the l i ce from the boys were in fected
,an d 27 per
cen t . from the girl s . Sp irochaetes were foun d in the
secret i on expressed from the mouth s of the in fectedpedicul i .Men t ion may be made of certain other sp irochaetes,
such as S . v incen ti, foun d in certa in forms of gangren ousinflammati on ; S . pa llida , descr ibed by Schaudin n in
syph i l it i c les io n s an d bel i eved to be the cause of th i sd isease ; S. pertenuis foun d by Castel lan i in yaws, an d

1 98 TROPICAL MEDICINE AND HYGIENE
others foun d in the mouth,in smegma
,in trop ical u l cer s
,
and in certa in tumours in mice . Whether th e last twohave any pathological s ign ifican ce i s n ot kn own . Sp i rochaetes may be foun d in large n umbers in t he faeces insome cases o f d iarrhoea and in the expectorat i on in someforms of b ron ch it i s .The quest i on as to whether sp irochaetes are protozoa or
bacteri a can n ot be ful ly d iscussed h ere . Formerly theywere con s idered to be bacteria . As l ong ago
,however
,
as 1 888,Tam ilen sky suggested that the S . obernieieri might
be on ly a stage of a haem ocytoz oon ,an d s in ce 1 904 , when
Schaud in n suggested that sp i ro chae tes should be con
sidered as protozoa,t h i s V i ew has been gen eral ly accepted
,
More recen t ly ( 1 906) N ovy an d Kn app have d isputedSchaudin n ’s con cl us i on s , assert ing that he was mistakenin h is observat i on s
,an d rec lass i fy ing the sp irochae tes
as bacter ia .
The quest i on must for the presen t,therefore , be con
sidered an Open on e,but i t i s o f in terest to n ote that the
kn own pathogen i c speci es have certa in features str ikinglyresembl in g those of organ i sms con cern ing the in c lusi ono f whi ch among the protozoa there can be n o dispute .
These features are the con stan cy an d in ten s i ty of th eb lood in fecti on , an d
,in the case of some at least, the
tran sm iss ion by al tern at ive hosts .A remarkable feature in the et i o logy of re laps ing feveri s the fact that al though its l ocal in fect ivi ty i s very markedi t does n ot spread widely except among populat i on s l ivingun der un clean ly con di t ion s . Thus, when outbreaksoccurred in E ngl i sh town s
,they were almost en t i re ly
con fin ed to the I r i sh , and in t he Bombay ep idemicsdescr ibed by Van dyke Carter, the di sease on ly affectedovercrowded local it i es . It may, however, spread toother patien ts in a moderate ly wel l arranged in st i
tution or hosp i tal in the Trop i cs .At one t ime famin e was con s idered to play such an
importan t part in the et i o logy o f th i s d i sease as to givei t th e n ame of famine fever. While, however, famin e

200 TROPICAL MEDICINE AND HYG I ENE
exert l i tt l e e ffect upon i t,an d should be avo ided on
accoun t o f the ir depress ing acti on upon the heart . Tepidor cold sponging may
,however
,be ben efic ial
,the Choi ce
depen din g upon th e height of the fever .Thirst an d vomit in g may both be rel i eved by th efrequen t admin i strat i on of smal l quan t it ies o f cold butn ot i ced water . It i s further importan t to let the patien thave plen ty of water or other cool ing drinks
,provided
that they do n ot cause vomit ing . The vomit i ng mayrequ ire the appl i cat i on of a mus tard plaster or othercoun ter- i rr i tan t to the ep igastr ium
,th i s al so rel i eving the
ten dern ess of the l iver an d sp leen .
In V i ew of the ten den cy to relapse,an d thus to con
siderable durat ion of th e d isease,i t i s very n ecessary to
see that the pat ien t i s properly fed . During the febri l eperi od fluids on ly should be given . The best i s mi lkd i luted wi th soda-water
,or with l ime or barley water .
During the apyrex ia l per i od,shoul d there be n o in test i n al
compl i cat i on s,eas i ly d igest ibl e so l i d food may be given .
The con st ipat i on of the ear ly stage i s best treated by amild aperi en t , but in V i ew of the ten den cy to d iarrhoeaat the cr i s i s
,i t i s importan t to avo i d vio len t measures .
For the headache and in somn i a,cold appl i cat ion s to the
head and smal l doses of bromide an d chloral are th ebest remedies . The treatmen t of other symptoms an d ofcompl icat i on s should be conducted on gen era l prin ciplesan d does n ot cal l for spec i al remed ies .Preven tive Treatm en t—From what has been sa id withregard to the et io logy of relapsing fever i t would appearthat clean l iness of the person s’ clothes an d dwel l ingan d t he destruct ion of vermin are the best safeguardsagain st the d isease . From an admin i strat ive po in t o fV i ew the con d it ion to be preven ted or overcome i s thato f overcrowd ing
,for i t i s on ly un der th i s con dit i on ,
whether i t be in c i ty or camp , that ep i demics occur .Shou ld i t be imposs ibl e to avo id overcrowding , it i sim portan t
,in V i ew of the probabi l i ty of the tran smis
s i on of in fect i on by mean s of ped icu l i , bugs or s im i lar

RELAPSING FEVER 20 1
blood-sucking paras i tes,to see that the houses of the
poor are kept free from dry dust,which harbours such
parasi tes . Should outbreaks occur the pat ien ts shouldbe i solated
,an d th e cloth ing, bedd ing, furn iture an d
dwel l ings of the pati en ts an d the i r assoc iates should bedis in fected . In the dis in fect i on of furn i ture an d dwel l ings ,i t i s importan t to en sure that the d is in fectan t pen etratesal l cracks an d crevi ces and destroys the in sects an d otherparasi tes and the ir larvae whi ch harbour in such places .I n fected n at ive huts should be burn t when i t i s poss ible .
Before a pat ien t i s admitted to the wards of a hosp ita lh i s person an d c lo thes should be freed from extern alparas i tes . In V iew of the poss ible tran smiss ion of in fect i on otherwise than by extern al paras ites
,i t i s wise n ot
to admi t relaps ing fever pat i en ts to th e gen eral ward o fa hosp i tal
,an d though act ive Spirochae tes have n ot been
discovered in any o f the secret i on s or excret ion s, i t i swi se to adopt the same precaut ion s in deal ing with themas in the case of other in fect ive d iseases .It i s importan t to keep the pat i en t e i ther in hosp ital orun der observat ion for at least fourteen days after thecessat ion of fever . This i s in order to avo id any dangerof h i s again becoming a source of in fect i on should arelapse occur .

CHAPTE R X IV .
T ICK FEVER .
AFRICAN RELAPS ING FEVER.
AN acute spec ific fever c l osely resembl ing relaps ingfever both in i ts symptoms an d in being assoc iated withthe presen ce o f sp irochaetes in the blood . I n fect i on i stran smitted by the b i te o f a t i ck .
Tick fever occurs throughout the greater part o fTrop i cal Afr i ca . L ivingston e and other early travel l ers inC en tral Afr i ca had recorded the occurren ce o f a feverattr ibuted by n at ives to the b i tes of a certain t ick
,Orn itho
dom s m ouba la . The d isease was wel l known to thePortuguese and other European in habi tan ts of theupperreaches o f the Z ambesi an d in Cen tra l Afr i ca
,but i t was
n o t t i l l 1 903 t hat Ph i l i p Ross and H odges , working inUgan da
,d iscovered in the blood
,first o f an I n dian
, and
l ater of Afr ican s an d of'
on e European , su ffer ing fromsymptoms s im i lar to those of relaps ing fever
,a sp iri l lum
wh ich they con s idered was probably iden t i cal wi thSpirocliazta obemneieri. Fo l lowing up th i s d iscovery
,
Ph i l ip Ross in 1 904 demon strated the presen ce of a spirill um in the
,
blood of severa l n at ives o f Ugan da suffer ingfrom an i l ln ess which the pat ien ts themselves ascribedto th e b i tes o f t i cks . I n depen den t ly, but somewhatearl i er
,N abarro had made the same d iscovery, but h is
researches were n ot publ i shed for some years .In 1 904 Dutton and Todd, working in the Congo Free
State,al so met with cases of t ick fever , and showed
that i t was due to a sp ir i l lum wh ich they also thoughtwas probably i den t i cal with S . obermeieri. They werefurther abl e to reproduce the d i sease in mon keys by

204 TROPICAL MEDIC INE AND HYG I ENE
cl in i cal ly i den t i cal. The sudden access of h igh fever ,th e headache
,pain s in th e back an d l imbs
,prostrat i on
,
th i rst , an d vomit in g are as character i st i c of t i ck fever a sof relaps in g fever
,as also the sudden cri s i s w ith profuse
sweat in g, fo l l owed by an apyrexial per i od , and th i s againby on e or
‘
more relapses . En largemen t an d ten dern essof the l iver and spleen are symptoms common to bothd iseases
,an d herpes an d ep i staxis are frequen t ly met wi th
in both . T i ck fever d i ffers from relaps ing fever ch iefly int hat the durat ion of attack i s usual ly shorter
,four days or
l ess in stead o f seven,wi th comparat ively longer apyrexial
in tervals an d more frequen t relapses . D i arrhoea i s th erule in t i ck fever
,whil e con st ipat i on i s a lmost always a
marked symptom of the early stage of relaps ing fever .
Jaun d ice i s rarer an d i r i t i s common er than in I n dianre laps ing fever .A sl ight degree of bron ch i ti s i s common an d pn eumon i a i s al so met wi th . As in relaps ing fever
,sp irochaetes
are usual ly foun d in the blood of pat ien t s su ffer ing fromt ick fever on ly dur in g the pyrex ial peri od . Of the twod iseases t i ck fever i s th e less severe
,an d death i s rare
among person s who were in good health previ ous toattack . It i s sa id to be more severe in European s thann egroes
,t h i s probably depen ding upon part ial immun i ty
,
or to leran ce,resul t ing from previ ous attacks in th e l atter .
Fac ial paralys i s i s n ot un common after an attack .
The in cubat ion period of t i ck fever i s common ly aboutfive days
,but may be shorter or l onger
,the durat i on
perhaps depen din g upon the sever i ty o f in fect i on .
D iagn osis—Before the d iscovery of the sp irochae ta in
the b lood m any cases of t i ck fever were con sidered tobe su ffering from malaria
,pn eumon i a
,or other d iseases .
As in the case of relaps ing fever, a correct d iagn osi s i so ften imposs ibl e wi thout th e demon strat i on of the sp irochaete in th e blood . From what has been sa i d of thesymptoms of the d isease
,as wel l as of t he morphology
o f the paras ites,i t i s obvious that the d i fferen t i at i on of
t i ck fever or rel aps ing fever may somet imes be imposs iblewithout resort to exper imen ta l in ocu lat i on of an imals .

TICK FEVER 205
In the autopsy of the fatal case wh ich Dutton an d
Todd met with,the l iver and spleen were en larged , the
heart muscle showed sl ightly fatty change,the lungs were
pale but otherwise n ormal an d th e kidn eys were en largedan d showed fatty degen eration . The other organ sexamin ed appeared n ormal
,but there was some blood
sta in ed flu id in the abdomen . The blood was flu id an d
resembled blood- sta in ed water . Sp irochaetes were foun din it at the t ime of the autops‘y .
In an imal s dying o f t i ck fever the post-m oriem appearan oes are s imilar to those observed in re lapsing feverin m an . Thus , in post m ortems on mon keys
,Brein l and
Kinghorn foun d the Spleen to be greatly en l arged , d eeplycongested an d very soft . It o ften con ta in ed hmm or
rhagic in farcts an d n ecrot ic areas ; s imi lar changes werefou n d in the l iver ; the lungs were oedematous an d
con ta in ed in farcts an d th e heart muscl e was muchdegen erated . The lymphat i c glands were frequen t lyhaemorrhagic an d al l organ s showed sign s of congest ion .
Spirochae tes were foun d in th e spleen an d bon e-marrowan d also in other organ s .The et iology of t ick fever i s in d icated by i ts n ames
,i .e.
,
t ick fever an d Afr i can relaps in g fever . As the paras i tecan be cultivated outs ide the body in special media suchas mouse broth
,with mouse blood an d yolk o f egg
,
al l of Koch ’ s requiremen ts for proving that the d i sease i sdue to the S. clulton i have been fu l fi l led . Previ ously
,in
V i ew of th e fact that in fect i on can be tran smitted by theoffspring of t i cks which have fed upon pat i en ts
,even th i s
con dit i on was pract i cal ly compl ied with . The subcul tures reta in the ir virulen ce .That in fect ion 1 3 ord in ari ly tran smitted by t i cks— the
O. m ouba ta—admits of l ittl e or n o doubt . It i s,however
,
o f some in terest to men t i on that although n egroes havelong persi sted in attr ibut ing th is réle to the t icks
,Euro
pean med ical m en were un ab le to demon strate i t as afact un t i l qu i te recen t ly . It has been seen that in fect ioncan
'
also be conveyed by d irect in oculat ion of blood

206 TROPICAL MED ICINE AND HYG I ENE
con ta in ing the sp irochaete . So far n o other mean s ofin fect i on i s kn own ,
an d i t has already been men t i on edthat attempts to tran smi t the d isease by other paras i te st han t i cks
,n amely bugs , have been un successful .
I n fected t icks can tran smi t th e d isease e ith er imm ed i
ately or by mean s of th e i r progeny after'
an in terval o fweeks an d mon ths ; the l im i t o f the in fect ivity of sucht i cks is at presen t un kn own . Chromat in bodies have beenfoun d by Lei shman in th e ova of these t icks
,probably a
stage in the developmen t o f the sp i rochae tae .
There are certa in further po in ts o f importan ce in con
n ection with the propagat ion of t i ck fever . These arethat t i cks may tran smi t in fect i on from an imals wh i chthey b ite dur ing apyrex ial per iods
,when n o spirochaetes
can be d iscovered in th e blood ; that the blood wh ichhas been passed through a Berkefeld fi l ter remain s infect ive an d that a per i od of immun i ty fol l ows in fect i on .
Th e first two o f these facts in d icate that in fect i on m aybe conveyed by some other— poss i bly a developmen talform of the spirochre te, wh i l e these last may explain th etran sm iss i on of the di sease from an apparen tly healthyperson . Experimen ts have been made with a V i ew to
obta in ing preven t ive and curat ive sera for t i ck fever . All
that can be sa id at presen t i s that attempts to produce a
curat ive serum have fai l ed, wh i le a serum has been produced by th e hyperimmun i zat i on of a h orse
,by mean s o f
wh i ch the in cubat i on peri od i s l ength en ed an d th e attackren dered mil der in laboratory an imals, th ough relapseshave n ot been preven ted .
Trea tm en l.—As in the case of relapsing fever, there isn o spec ific for t i ck fever an d th e treatmen t must thereforebe symptomat i c . It should be on th e same l in es as thatin d icated for relapsing fever. Atoxyl an d mercury havebeen tr i ed for t i ck fever , but wi thout much effect .Salvarsan ,
as in al l d iseases due to sp irochaetes,has a
markedly ben efic ial e ffect .Prophylaxis
—As far as we kn ow the di sease i s sprea don ly by the Orn ithodorus moubata in n ature (fig .

2 08 TROPICAL MED IC INE AND HYG I ENE
These ti cks belong to the d ivi s i on Aifgasina , an d these d ifferfrom the ord in ary cattle an d dog t i cks
,Ixoalin a , in that the
m outh i s on the un der or ven tral surface of the body,that
there are n o dorsal or ven tral ch i t in ous plates or sh iel dse i ther in th e male or female, that the last j o in t o f the palp ii s qu ite d ist in ct an d that the palp i are n ot grooved n or dothey form , a sheath for the rostrum . The young also havefour pai rs o f legs when th ey emerge from the egg .
In habits al so they d iffer, as they do n ot remain firmly
attached to thei r host, but after feed ing leave h im
an d may feed on man y in d ividuals,as t hey l ive for
mon ths or y ears . They feed at n igh t main ly. Theyin hab it houses , l ivin g in th e dry dust so abun dan t inhouses with mud floors , or in thatch or reeds of wh ichthe roof an d wal ls are composed . The t icks which feed
on in fected pers on s do n ot themselves n ecessari ly becomei n fect ive, as the in fect i on i s tran smitted to the progeny,and therefore i f a t i ck feeds on an in fected person i t maybe many mon ths before the progen y of these t i cks can
in fect a suscept ib l e person . An other po in t i s that froman in fected t ick many i n fect ive t i cks may be derived .
The problem differs therefore in many importan trespects from prophylax i s again st malaria . Destruct iono f these t i cks may be attempted but i s d ifficul t to carryout
,as in a coun try l ike Afr i ca, where termites (wh ite an ts)
are so destruct ive , wooden floors an d wal l s are impracticab le. Mud floors
,reed an d thatch ed wal l s an d roofs
can n ot be thoroughly c lean sed . Even in Europeanhouses as l i tt l e woodwork as poss i bl e should be used
,
but with cemen t floor, brick wal ls an d galvan ized ironroofs there i s l i ttl e danger o f the O. m ouba ta beingpresen t .Prophylaxis for European s i s fa irly easy . In travel l ing
,
n at ive huts should be avo ided , even i f they have n ot beeno ccupi ed for many mon ths . The O. m ouba ta can n otC l imb up a smooth vert i cal surface
,so that even in a
n at ive hut i f a camp bedstead be used an d n o part o f theb edding be in con tact
' w ith the wal ls l i tt le r i sk i s run .

TICK FEVER 209
The servan ts must be In structed not to p lace the bedd ing on the floor
,or the t i cks may en ter i t . Bedd ing
in a district where the t i ck i s common should always becarri ed in a tin box . These t i cks do n ot readi ly feedby day an d do n ot attach themselves to person s inmovemen t
,therefore there i s l i ttle r i sk even in a n at ive
hut in the day t ime,or at n ight wh ilst the but i s wel l
liglited and the occupan t i s awake .
In the even t of a European house or the Serv‘
an ts ’
quarters becoming in fected,careful search should be
made for the t i cks,an d the floors an d wal ls abun dan tly
flushed with some d i s in fectan t solut ion ,such as 1 in
perchloride of mercury solut ion,or, and better in the case
o f a n at ive-bu i l t house,i t should be pull ed down and
burn ed .
VARIETIEs.
Some authorit ies con s i der that there are four d ist in c tvariet ies of relaps ing fever .Varieties of Relapsing Fever Con trasted .
-European and
Ameri can relapsin g fever show some differen ces an d
may also be due to d i fferen t spec i es of sp irochaetes . Themore importan t . di fferen ces are shown in th i s tabl e
Indian African European American
IncubationDurat ion of firstattackDuration of apy 7—10 days
rexia
Number ofrelapses I , r a r e I ymore.
Relapsesabsen tJaund ice I nfrequen t
Eye affect ionsMortal ity

TROP ICAL MEDIC INE AND HYG I ENE
Whi lst i t seems clear that the Afr i can rel aps ing feveri s even cl in i cal ly a d ist in ct d isease the differen ces betweenthe three other forms are less marked . As regards theparas i tes
,Mack ie proposes to cal l that in As iat i c relaps ing
fever S . carteri,an d in the American S . n ovyi . S . aber
m eieri i s the n ame used for the paras i te in Europeanrelapsing fever—S. recurren tis i s more correct—an d
S . dri tton i in th e Afri can . The d i fferen ces in the paras i tes are shown in the fo l lowing table
S . car ter i S . a’ut ton i S . oéerm eier i S . navy
Min imum length . 1 3 ,u. 1 2u
Shape Open flexures Open flexures Spiral
An imals susceptib le
Course in an imals Very m i ld Severe .
Serum reactionImmun e serumno effect on S . n ovy i o r S . n ovy i and S . oberrneier i,
S . o b e r S . dirt/071 i S . dution i ,m eier i orS .carteri .
The form of relaps ing fever occurring in Algeria,
Egypt an d the Sudan i s n ot th e Afr i can spec ies S . d ri tton i.
Poss ibly i t i s a n ew species an d i s con s idered to be so byBalfour .
Smal l roden ts Smal l roden tseasi ly on ly after
p a ss a g et h r oug hm onkeys
Very severe Mi ld
2 1 2 TROPICAL MEDICINE AND HYG I ENE
Secon dary symptoms are often overlooked . Macularerupt ion s are n ot eas i ly seen on dark skin s
,an d as there
i s n o d iscomfort atten t i on i s n ot d irected to them .
Papular erupt ion s can be seen more read i ly . The th roatcon dit i on s i f severe wi l l be recogn ized
,but are n ot often
seen .
There i s a prevalen t bel ie f,especially among sold i ers
,
that syph i l i s con tracted from n at ives i s un usual ly severe .
Th is,however
,i s n ot born e out by I n dian experien ce
,
where the d isease among European s,except in person s
deb i l i tated by other causes,appears
,i f anyth ing
,milder
than at home . Among the n at ive army in I n d ia thekn own in ci den ce o f syph i l i s i s much less than among theBri t i sh tro ops .Typi cal tert ia ry les ion s are observed an d in clude
those o f bon e an d gummata of the bra in an d abdomin al vi scera , wh ich are fa i rly often seen in postm ortem examin at i on s .On the whole th e d i sease i s l ess severe in the Trop ics
than i t i s amongst the poorer classes in Englan d,where
the treatmen t has been n eglected . The Ch in ese,of
course,have used mercury from t ime immemorial , but
other races,un l ess treated by European s
,are pract i cal ly
un treated .
In trop ica l coun tr i es where yaws i s un common t herei s n o ten den cy for the syph i l i t i c erupt ion s to be framiboesial
,an d in coun tr ies where yaws i s common the
common man i festat ion s o f secon dary an d t ert iary syph i l i s
al so occur .Atheroma an d l es i on s o f th e vessels are fa i rly common
in th e Trop i cs , but l ess so amongst I n dian s than amongs tthe n egroes . The ath eroma is frequen tly in patches and
often l eads to an eur i sm .
It must be remembered that a chron i c irregular feveroccurs in some cases o f secon dary and tert i ary syph i l i san d may be mistaken for the s imi lar fevers that occur introp ical di seases such as kala-azar or malaria . A courseof an t i syph i l i t i c treatmen t may speedi ly cure a fever o fth is ki nd .

DISEASES ASSOCIATED W ITH SPIROCHZETZE 2 1 3
The d i seases bel i eved to be remotely due to syph i l i sin Englan d are pra ct i cal ly un kn own in the Trop icsamongst the n at ives these are the parasyphilides—gen eralparalys i s o f the in san e
,an d tabes dorsal i s .
In the treatmen t o f syph i l i s amongst n at ives i t must beremembered that mercury i s n ot wel l born e by an aemicperson s an d that pyorrhoea alveolar i s, so common in n at iveraces
,i s often in creased by mercury, an d must therefore
be treated in dependen t ly . In deal ing with l arge bodiesof m en in tramuscular in j ect ion s are spec ial ly valuable, asa weekly in j ect ion in sures suffic ien t treatmen t .The method in‘use in th e Army i s essen t i a l ly that in tro
duced by Colon el Lambkin . Acream i s made of metal l i cmercury in l an ol in
Hydrargyri . . 5L
Adipis lanae . . Siv .
Paraffin l iquid i (w ith 2 percent . carbol ic acid ) ad 3x.
The mercury an d l an ol in are by weight,the l iqui d paraffin
by volume . Great care must be taken to obtain a
thorough mixture of the mercury . I t should be storedin smal l “ quan t i t i es, as i f kept in bulk the mercury wi l lsettl e at the bottom . Ten min ims of the mixture con ta in1 grain of mercury . I n j ect i on s must be made in to a
muscle,preferably the gluteus maximus
,and n ever in to
th e subcutan eous cel lular t i ssue . The skin must be carefu l ly ster i l ized before the in j ect i on . An al l-glass syringeshould be used th i s may be ster i l ized by drawing up ol iveo il at a temperature of 1 60
°
F. Between the in j ect i on sthe poin t o f the n eedl e should be dipped in to the heatedo i l
,an d th e n eedle should be wiped with a steri l ized
cloth so that n on e o f the mercury cream is left a long thetrack of the n eedle .It i s importan t that the pat ien t should n ot take any
V i o len t exerc i se for some hours after the in j ect ion,an d
care must be taken that n o in j ect i on i s g iven in a placewhere there i s any in durat ion as a result of previousi n j ect i on s . The advan tages of the method are : ( 1 ) Anatten dan ce o n ce a week on ly i s required ; (2) there i s n o

2 14 TROPICAL MEDICINE AND HYG IENE
certa in ty as to whether the mercury i s regularly taken
(3) t hough the rate of absorpt ion varies , st i l l the mercuryi s certain ly absorbed . The d isadvan tage i s that thei n j ect ion i s s l ightly pain ful
,that a certain amoun t of
in durat i on an d ten dern ess may be left,an d that
,rarely
,
abscesses may form . Much depends on the con fiden cethe n at ives have in the i r medi cal officer .Salvarsan , or n eosalvarsan
,espec ial ly when in j ected
in traven ously, have a rap id e ffect even when mercuryhas had l i ttl e e ffect . The early h opes that one or twoin ject ions would resu l t in a perman en t cure have n otbeen real i zed
,an d i t i s advisab le after treatmen t wi th
salvarsan to con t in ue the use of mercury for at l east threemon ths even i f a n egative Wasserman n react ion i sobta in ed .
Congen i tal syph i l i s i s n ot common ,but it i s probable
t hat syph i l i s i s an importan t factor in th e causat i on of th elarge n umberof abort i on s an d st i l lb i rths
,and i s respon
s i b le for much of the steri l i ty o f the n at ive . It must beremembered that the n egro i s fert i l e earl i er in l i fe
,when
the effects o f the V i rus are most marked,but ceases to be
ferti l e in many cases at an earl i er age t han the European ,
an d therefore has few ch i ldren at ages when the mostfatal effects o f the d i sease are l ess l ikely to occur .Prophylaxis—Prophylact i c measures are s im i lar to
those requ ired in Englan d . The local labour supplyis usual ly in suffic ien t for the large p lan tat i on s , min es andother en terpr i ses of European s . Large n umbers o f m en
are therefore im ported from other di str i cts an d coun tri esor attracted by the super i or rate o f pay . Men as a rul ecome in great excess o f women ,
who are of less valueas labourers, an d man y of these women are or becomeprost i tutes . With such gangs o f m en , whether sold iersor labourers on plan tat ion s, i t i s o ften poss ib le to fin dthe in fect ing agen t or agen ts . A certa in proport i on ofwomen shou ld always be imported w ith the m en
,and
th i s i s arranged for in I n dian immigrat i on ord inan ces .
Every en couragemen t shoul d be given to m en br inging
2 10 TROPICAL MED ICINE AND HYG I ENE
or th i ck su lphur-yel l ow crusts an d subs id ing wi thout . deepulceration or th e format ion of any but superfic ial scars .The usual durat ion of the di sease i s two or three_years,but on th e parts o f the body where the ‘ep idermis i s th i ck
,
such as the so les o f the feet,i t may pers i st for much
l onger . Destruct ive u lcerat ion of the mucous surface anda lupo id erupt ion on the face are by some con s idered to
’
be sequelae,an d onych ia may also occur .
Geographica l Distribution .—As an indigen ous di sease i t
wasp robably l imited to the West Coast o f Afri ca, to theaborigin es of the Malay Pen in su la
,poss ib ly Ceylon
,an d
to the Pac ific I slan ds . I n troduced by the slaves in tothe West I n dies an d South Ameri ca
,i t has been firmly
estab l i shed there for over a cen tury . An outbreak hasalso occurred in Assam
,probab ly in troduced by labourers
return in g from F i j i or the West I n d ies . Cases are occasionally seen in many trop ical p orts
,and to a l imi ted
exten t i t has spread amongst the in hab itan ts o f suchports . It does n ot occur on th e East Coast o f Afr i caand i s very rare in t he cen tra l p lateau . Outs ide th eTropics i t does n ot seem to spread .
Clin ica lCourse.—Experimen tal in oculat i on s have shown
that th ere i s a per iod of in cubat i on of about twen ty-e ightdays . In such experimen ts there n eed be n o pr imarysore ; a pr imary yaw i s, however , common in acc iden ta lin oculat i on . It may appear at the edge of an ul cer orin a c l ean -cut woun d
,but i s more common at or n ear
the j un ct ion of the skin and mucous membran es , such asthe angle of th e mouth . When there i s a pr imarysore i t i s a ra i sed gran ulomatous mass s imi lar to th esubsequen t erupt ion s . The gen eral ized erupt ion mayappear in any part o f the body an d i s assoc iated withfebri le symptoms . Sometimes the temperature i s 1 03
°
or 1 04°F . There are ach ing pain s in the l imbs, and
part i cularly in the back an d lo in s , somet imes severeen ough to ra i se the susp i c ion of smal l -pox . The erupt i on may be abun dan t, but in other cases there may on lybe a few yaws l imi ted to the l ower part o f th e face, the chest,
‘

PLATE V I .
FI G . 57 .
FIG . 5 8.


2 1 8 TROPICAL MEDICINE AND HYG I ENE
d i sease an d wil l be descr ibed separately . Assoc iatedwith th i s d isease i s somet imes a lupo id u lcerat i on of theskin of the face
,exten ding by con t in u ity from the ulcera
t i on of the n ares . Periost i t i s,and chron i c u lcers o f the
l egs and e lsewhere have been descr ibed -as sequelae ofyaws . I f th ey are resul ts o f th i s d isease they are veryrare on es . Gummata probably do n ot occur .Diagnosis
—At the on set o f the gen eral erupt i on,an d
wh i lst the gran ulomata are st i l l small,in cases where the
muscular an d back pa in s are severe an d the temperaturei s h igh
,the d i sease has been mistaken for sm all o
pox ; sucherrors are very rare . The d isease in th e maj ori ty o fcases has to be diagnosed from syph i l i s an d other skind iseases . In a s ingle case th e d iagn osi s from a framboesial syph i l ide may be imposs ib le ; from any othersyph i l ide i t i s easy . The absen ce o f u lcerat i on , t he rai sedgran u lomatous tumour and th e su lphur crust with th emi lky flu id un dern eath i t d ifferen t i ate the d isease fromrup ia or s im i l ar tertIary syph i l i t i c l es i on s . Where thecase i s under observat i on th e c lose s imi lar i ty of thesuccess ive erupt i on s i s un l ike that in syph i l i s . Theexposure to con tagion
,th e occurren ce o f other cases ,
and the absen ce o f any other sign s of syph i l i s al l a idin the d iagn osis .Prognosis.
—Death may occur in ch i l dren u nder one
year , or in deb i l i tated person s , but even in such casesa fatal termin at ion i s ex cept ion al . Good feed ing , clean li
n ess, and protecti on from i rri tat ion of the yaws d imin i sh
the l i ab i l ity to u lcerat i on but do n o t shorten th e courseo f the d isease .Pathologica l Anatomy
—The les i on s . are l im ited to theskin an d subcutan eous t i ssues . Essen t i al ly the growthi s a vascular gran uloma , and there i s n o t en den cy tocaseat i on
,n ecros i s
,or suppurat ion . The ep idermis i s
so ften ed,an d the d ist in ct ion between th e various layers
is l o st . P igmen t i s e ither n ot formed or i rregularlyd istr i buted in t he deeper layers or subcutan eous t i ssue .
Kerat in izat ion i s imperfect, and the superfic ial l ayers o f



220 TROPICAL MEDICINE AND HYG I ENE
f rom S . pa llida has been foun d by Castellan i in yaws ,S . perten n is. That th e d i seases belong to the same classi s c l ear ; that they are iden t i cal i s a d i fferen t matter, an d
i s Open to ser i ous quest i on .
The man i festat ion s of yaws for at least the first threeyears of the d i sease are al l o f the sam e character
,th e
primary sore an d each successive erupt ion d i fferi ngsl ightly in moist parts
,or when un der th icken ed ep i
dermis . Syphi l i t i c cutan eous man i festat i on s are polymorph ic . Yaws may be un iversal in a populat i on
,but
i f un in fected n ewcomers of any race—European s, Portu
guese, Ch in ese , N egro , Malays, I n dian s— are in troducedi n to such a commun i ty an d are in fected
,the d i sease they
acqu ire i s yaws,an d resembl es in al l i ts characters th e
d i sease in the n at ive populat i on . From a s ingle sourceof in fecti on in a n egro the d i sease has been acqu i red inth e same form in a whole fami ly of Portuguese
,an d in
an I nd ian servan t . Yaws there fore breeds true .Syph i l i s
,when acqu i red by members of the same races
,
presen ts the usual ch aracters o f t hat d i sease . Syph i l i s i sl i tt l e modified in person s res i den t in the Trop ics . Theformati on of gummata an d th e exten s ive an d destruct ivebon e les i on s do n o t occur in yaws . It i s somet imes urgedby those wi th l i t tl e experi en ce of some of the n at ive races ,amongst whom the d isease i s common , that th e overcrowdin g an d fi l th o f the n at ive houses favour the wided i ffu s ion of the d isease
,an d that therefore the fact that
all th e ch i ldren have yaws i s n o argumen t again st thed isease being syph i l i s . A closer study of these races w illconvin ce anyon e that as regards person al c lean l in ess an d
absen ce o f overcrowdin g an d morals they compare veryfavourab ly wi th the l ower classes of European s, amongstwhom syph i l i s does n ot become un iversal in the ch i ldren .
Yaws does n o t protect from syph i l i s n or syph i l i s fromyaws . The relat i on sh ip between yaws an d syph i l i s , in th esen se o f both d i seases being due to organ i sms of thesame gen era
,i s admitted an d was pred icted, but the

YAVVS AND SYPH IL IS 22 1
relat ion sh ip i s l ike that between var io la and var i cel la,n ot
that between vari ol a an d vacc in i a .
Prophylaxis— I n fect ion can be carr i ed from m an . tom an by direct con tact , an d the vi rus i s con ta in ed in thed ischarges from the gran ul omata . The frequen cy of theearly yaw in the n eighbourhood of the mouth suggeststhat food i s a frequen t source of in fect i on . The common est ages for in fect i on
, 3 to 5 years, are ages at whichch i ldren frequen t ly exchange part ial ly eaten p ieces offood . Probably fl i es are also d irec t carr iers of in fectedm aterial
,an d th e frequen cy with wh i ch ulcers and
woun ds become in fe cted i s probably expl i cable in th i sman n er . The ch igoe (Sarcopsylla penetrans) i s by somebel ieved to be an importan t carri er . There i s n o ev i
den ce that the vi rus can en ter through the unbrokenskin
,but cracks about the mouth
,smal l u lcers as a resul t
o f in sect-bi tes,or other sources of i rr i tat ion are so
common in the Trop ics that poss ib i l i t i es of in fect ion aren umerous .There i s l itt le r isk to wel l-clad European s
,even i f
stopp ing in the same house as person s wi th the d isease,
but amongst European an d hal f-caste ch i ldren who
play about with n at ive ch i ldren cases of in fect i on are
common . It i s wel l to carefu l ly cover up even superfic ia lwoun ds
,an d to preven t , it poss ible, ch i ldren from having
access to n at ives in a coun try where yaws i s en demic,
an d to take suffic ien t precaut ion s to preven t the in terchange of partly eaten art ic les of food with n at ivechi ldren .
“ Guam disease in most respects correspon ds to thedescript ion g iven of the destruct ive ulcerati on s about then aso-pharyn x so common in Fi j i , an d there con s idered tobe tertiary framboes ia . Those who con s ider i t a separatedisease cal l i t gran uloma gangren osa . It i s sa id to bemost common in places where yaws i s rare
,an d to be very
rare in some places where yaws i s very common . Probably i t i s the same con di t i on as the F i j i an “ kanailom a.
”

222 TROPICAL MEDIC INE AND HYG I ENE
GRANULOMA OF THE PUDENDA.
SERPIG INOUS U LCERATION OF THE GENITALIA
(MCLEOD) U LCERATING GRANULOMA OF THE
PUDENDA SCLEROS ING GRANULOMA OF THE
PUDENDA.—The d isease man i fests i tsel f as a chron ic
in durated superfic ial growth on or n ear the gen i tal ia ,male or female . It i s s low growi ng an d extends al on gmoist surfaces
,whi l st the older an d deeper porti on s o f
the growth are con verted in to a den se fibrous mass oft i ssue . I t i s very vascu lar .Geographica l D istribution .
- It occurs in man y islan dso f the West I n dies
,in Trop ical South Ameri ca
,on th e
West Coast o f Afri ca , an d ei ther i t or a s imi lar di seaseoccurs in I n dia, N orthern Austral ia, an d many of th e
Pac ific I slan ds .Clin ica l Course—Th is d i ffers to some exten t in
d i fferen t races,an d in th e two sexes . It usual ly commen ces
in the male on the pen i s , an d extends in the n eighbourhoodof that organ ; i f s i tuated o n the skin i t i s very slowgrowing
,but i s more rap id when the glan s i s attacked ,
an d the granu lat i on s may then be very large an d coarse ;i t exten ds for a fracti on of an in ch up the urethra
,an d
causes very seri ous stric ture . It rarely exten ds by directcon t in uity down th e pen i s more o ften the ingu in al foldsor other places with wh ich the pen i s may rest in con tactbecome i n fected (fig . an d from such a po in t exten s ionby con t in u ity along the fo ld of the gro in (fig . an d
backwards on the i nguin o - scrotal fo ld,takes place
,and
from that d irectly backwards on the perin eum surroun dingthe anus
,and exten d ing up i t in to the l ower part of the
rectum (fig . Somet imes both gro in s are a ffected .
Frequen t ly the pen i s an d scrotum become sl ightly ele
phan toid ,probab ly from compressi on of the lymphat ic s
by the indurated subj acen t t i ssue .
In th e female the early growth i s on the in n er surfaceo f the lab ia maj ora or n ymphae
,wh ich may become
elephan to id,an d the grow th exten ds upwards in to th e
vagin a,an d rarely in to the bladder . I t a lso exten ds over

GRANULOMA OF THE PUDENDA 223
the lab ia m ajora,'an d backwards along the perin eum ,
surrounding an d exten ding up the an us . In such cases,
where both the vagin a an d rectum are in volved,in curable
recto-vagin al fistulae are common . The growth maycon t in ue for many years , an d the gen eral h ealth of the
pat ien t i s n ot affected . The lymphatic glan ds are n ot enlarged ,
though there i s eviden ce of lymphat i c obstruct ion .
There i s always a con s iderable format ion of hard fibroust issue ben eath the growth
,an d when heal ing occurs
n atural ly the growth i s en t irely converted in to den sefibrous t issue . Very rarely complete c icatrizat i on takesplace ; more frequently it i s part i al an d exten s ion of th egrowth at the edges takes p lace . Spon tan eous h eal ingof the mucous surfaces does n ot take place .
The d iagn osi s has to be made from other diseases of
th e same part . On th e pen i s i t i s frequen tly mistakenfor ep i thel ioma . In the gro in i t may be mistaken for anyform of ulcerat i on
,syphi l i t i c or otherwise . In the vagin a
i t i s usual ly mistaken for chron i c gon orrhoea . Thechron i c i ty o f the growth
,the den se fibrous base
,an d the
absen ce o f glan dular en largemen t are importan t poin tsin the diagn osis . In cases of doubt
,microscop ic
examin at ion wil l exclude ep ithel ioma .
Prognosis as regards l i fe i s good . The growth i s n o t
malign an t . N atural cure i s h igh ly except ion al,an d i t
i s on ly when complete removal of the growth can bee ffected that recovery i s probab le .
The most troublesome compl i cat ion s are stri cture of
th e meatus of the urethra,which can on ly be treated
effectual ly by amputat ion of the glan s pen i s recto -vagin alfistulm
,which are n ot su ited for operat ion s
,as the t issue
between the rectum an d vagin a is main ly composed ofthe growth ; an d str i cture of the anus w i th ul cerat ionof the lower part of the rectum . If the growth does n otexten d too high
,exc i sion of the rectum gives good results
in the last compl i cat ion .
Pa thologica l Ana tomy—The growth i s a vascular
granuloma . The cel l s are roun d cel l s with a srngle‘

224 TROPICAL MEDICINE AND HYG I ENE
roun ded n ucleus . There are n o gian t cel l s . There i sn o ten den cy to caseat ion ,
n ecrosishor suppurat ion
, an d
the ep i thel ium i s usual ly presen t over the growth,though
soften ed an d th icken ed .
Trea tm en t—Mercury an d potass ium i od ide in th emaj or i ty o f cases have n o effect . In a ' few
,where the
ten den cy to n atura l cure i s strong,large doses of i od ides
seem to a id thi s ten den cy .
C l ean l in ess an d an t i sept i c dress in g favour rather thanretard the growth . E scharot ics , such as ch loride of z in c
,
n i trate o f mercury, and sal i cyl i c ac id , are rarely effectivecomplete exc is i on of the growth where that i s possib lei s h ighly sat i s factory , but the den se fibrous t issue shouldbe exc ised as wel l . The raw surf ace left i s always moreexten s ive than the growth removed . Where exci s i on i simpossib le
,scrap ing an d the use o f escharot ics may give
sat i s factory resu lt s .Good resu l ts have been obtain ed by the use of the
Ron tgen rays . In Dr. McLeod ’
s case the use o f theserays converted the granu lomatous t issue in to a cheesymass
,which was read i ly scraped away , an d heal ing then
took place rap id ly.
Etiology—The occurren ce on the gen i tal i a an d thed i fferen t s i tuat ion s in the two sexes are strongly in favouro f the V i ew that the d isease i s conveyed by ven ereal i n tercourse i t does n ot seem to be h igh ly con tagious, as there
are cases where the husban d on ly i s in fected and the
wife escapes .
Sp irochaetes resembl ing S. pallida an d S . refringenshave
b een described by Wise as occurr ing in these gran u lomata .
Oval bodi es have been descr ibed in the deeper l ayerso f the gran uloma, but their exact n ature i s unkn own ,
an d
i t i s doubtfu l i f they have any causal relat ion to the
d isease .


CHAPTER XV I .
I NTESTINAL PROTOZOA, &c.
MANY protozoa are foun d in the in testin es , an d m ay
be discharged with the faeces . In cocc id ia in fect i on s ,e i ther of the livero or in test in al mucosa , th e fert i l izedmacrogametes are d ischarged in th i s manner .The more importan t o f the human in test in al protozoaare those associated wi th diarrhoea an d dysen tery . Thesed iseases are so often due to bacterial in fect ion s
,an d the
preven t ion of such diseases i s so closely con n ected withthe d isposal of sewage and the provi si on of a good watersupply
,that they are best con s idered at the same t ime as
the d iseases s imi lar cl in i cal ly, but due to vegetableorgan isms in Part I I I . On ly a bri ef referen ce to theseparasi tes an d the d i seases they cause wil l be given here .
The protozoal organ i sms descr ibed as con cern ed in
the production of in test in al d iseases are Sarcodin a,such
the Am trba coli ; Flagel lata , as Trichomonas hom in is,
Lam blia in testina lisan d vari ous spirochmtae an d I n fusori a
(Ci l iata) , as the Ba lan tid ium coli (fig . Of these themost importan t i s the Am eaba coli—En tam ceba h istolytica
E. tetragena , Schaudin n ) .Other protozoa
,espec ial ly Balan ticlii zm coli
,which
invades the t i ssues,may cause ulcerat i on an d al l the
symptoms of dysen tery .
Ba lan tid ium dysen tery often commen ces as an occasion al attack of d iarrhoea . In the more severe attacksthere wi l l be pers isten t but remitten t d iarrhoea . Theparasi tes are foun d during the periods when there i sd iarrhoea . Blood an d mucus are presen t in all th emore severe cases an d may be con siderable in amoun t .
I S
226 TROP ICAL MEDIC INE AND HYG I ENE
Peri ton i t i s wi th or wi thout perforat i on may occur,and
the parasi tes are foun d n ot on ly in the mucosa an d in
the wall s and floor of the u lcers,but in the submucosa
an d in the blood-vessel'
s . In fatal cases there m ay beex ten s ive ulcerat ion
,but i t i s most severe near the rectum
an d dimin i shes t owards the caecum . No spec ific treatmen t i s kn own .
Lamblia in testinalis i s probably pathogen i c . I t doesn ot invade the t i ssues
,but l ies c l osely appl ied by i ts
sucker-l ike aspect to the mucosa,in th e small in test in e ,
an d i s assoc iated with chron i c en teri t i s o f a catarrhalcharacter . I t i s eas i ly recogn ized by the pa ired n ucleusan d the six pa irs o f flagel la . The two termin al are thelargest and work in a longitudi n al groove . Where therei s n o diarrhoea the cysts wi l l be foun d . In these thetwo n ucle i are s i tuated n ear on e end , but there are n o
flagel la .
The symptoms are of a chron i c recurren t d iarrhoea,with abun dan t d ischarge of mucus
,often b i le-sta in ed, an d
somet imes there i s a lso blood . When th ere i s d iarrhoeathe paras i te may be foun d in abun dan ce ; at other t imesthe en cysted forms on ly wi ll be foun d . These areeas i ly recogn i zed by thei r oval shape and th e pair o fnucle i s i tuated n ear one extremity . The treatmen t i s n otvery sat i sfactory . Free purgat ion to remove the mucus ,fo l l owed by in test in al an t i sept i cs such as kerol , seems themost promising l in e o f treatmen t . En emata are used bysome
,but as the main in fect i on i s in th e smal l in test in e
i t i s d ifficul t to expla in the sat i sfactory act i on claimed .
Methylen e blue in on e or two grain doses in some caseshas a satisfactory effect . Li qu id paraffin in tablespoon fu ldoses twi ce or three t imes a day may be used alon e orwi th methylen e b lue .
The d istr ibut ion o f the paras i te i s exten s ive, but asfrom some parts o f I n dia so many cases seem to comei t i s on e of the possible causes o f the l ocal forms o fdiarrhoea
,such as Poon a d iarrhoea .
The Amcebina .—~An Order belonging to th e Rh izopoda

228 TROPICAL MEDICINE AND HYG I ENE
amoebae assume a spheri cal form , an d are d ifficu lt todi st inguish from other mon on uclear cel l s . P ropagationtakes place by buddin g
,divi si on
,or segmen tat i on . Where
there i s n o diarrhoea the act ively movi ng amoebae are n otfoun d , as a ru le, though they may be presen t in mucus
Asexual multipl ication by simple d ivision of nucleus and cytop lasm .
FIG. 65 .—Schem e of Developm en t ofAmoeba . Mul tipl ication in encysted
form s (autogam ous) . Psexual mul tipl icat ion . The early stages of d ivisionof the nucleus (a—a
’
) and conjugat ion of the d ivided nuclei in pairs (e) ,fol lowed by further d ivision of these products of conjugation , first in to two
and then in to four each (f—i) . The th ick wal l of the cyst in the laterstages ind icates the harden ing of the cyst wall during the stages when the
cysts are outside the body.
passed before,or after
,or with a motion . Artificially
in duced purgation, as by the use o f sal in e aperi en ts, wil l
usual ly resul t in t he passage of act ive moving am oebaa.
Amoeba coli .—This i s a large amoeba , frequen tly '
05 mm .
in di ameter,though small er forms are c ommon . The

INTESTINAL PROTOZOA,AMCEBA 229
ectosarc can be readi ly seen when pseudopodia arethrown out
,but i t i s d ifficul t to see in the resting an imal .
The pseudopodia are very broad an d on ly one or twoare protruded at a t ime . The n ucleus in un sta in edspecimen s can be readi ly seen n ear the cen tre of the cel l .Movemen t i s act ive at or n ear blood-heat, but i s retardedor stopped at lower temperatures . Mult ip l i cati on of theamoeba may take place by simple divi si on ; th e n ucleusd ivides
,an d the protoplasm then divides
,so that two equal
in dividuals are produced . This i s the asexual method o freproduction
,an d takes place readi ly where the con di ti ons
for existen ce are fauourab le. The secon d method may becon s idered as a rudimen tary sexual process
,though the
con j ugat ion i s by fusion of two chromatin masses der ivedfrom on e n ucleus an d n ot of two separate cel l s .If con sidered as a sexual process i t would be an in stan ce
of autogamy . In th i s method the amoeba becomesen cysted . The n ucleus divides in to two
,an d each . o f
these n ucle i after extruding polar bodies again dividesin to two . The four n ucle i thus produced con j ugate inpairs , so that the n umber of n uclei i s again reduced totwo . These two n ucle i each divide in to two an d thenagain divide so that there are e ight n ucle i , an d these withthe protoplasm segmen ted roun d them form eight youngamoebae which are st i l l con ta in ed in the cyst (fig .
These quasi -sexual en cysted forms are resi stan t,an d i t is
probably th i s form on ly that i s capable in the paras it i camoeba: of retain ing vital i ty in a free form un der ord inarymeteorological con dit ion s .These en cysted forms are therefore the importan t on es ,as the in fective agen ts in amoebic in fect ion . In someof the parasi t i c amoebae in the l ower an imal s the act iveamoebae are on ly foun d in the smal l in test i n e . Thechanges described take place in th e large in test in e . Theam oebm passed in the faeces are al l en cysted . In suchan imals
,i f the in test in al con ten ts were passed rap idly
through the al imen tary can al,as after purgatives or in
diarrhoea,act ive amoebae would be passed with the stool .

2 30 TROPICAL MED IC INE AND HYG I ENE
In m an en cysted amoebae may be foun d in apparen t lyhealthy stool s
,but the hosts from t ime to t ime have attacks
o f d iarrhoea or dysen tery an d then th e act ive amoebae are
presen t in th e stool s . The diagn osi s therefore of theen cysted forms i s importan t both for d iagn osi s an d
treatmen t .Some amoebae can be cult ivated from stool s , but i t i s
doubtfu l i f these are obl igatory parasites,and these may
be merely en cysted forms of n on -paras i t i c am oeb ze whichhave been swal lowed and passed through the in test inalcanaL
Amoebae paras itic in the in tern al organ s of m an are
sometimes cal l ed En tamaeboe. Morphological ly there i sn o real d ifferen ce between these an d other amoebaebeyon d the absen ce o f a con tract i le ves i c le .The probl em i s to a large exten t on e of spec ies
,as i t i s
on ly the pathogen i c amoebae that are of importan ce tous. The others can be cul t ivated outs ide the in test in e .
Morphological characters are on ly adequate when th echaracters during the whole l i fe-cycl e are con s idered:The characters in th e en cysted stage are the mostcon stan t .There are sa i d to be several species
,on e occurring
in the mouth , A. bi icca lis, in some person s wi th den ta ld i sease
,and two at least in the large in test in e (vide Table) .
Of these,the A. coli
,or En tamceba coli
,i s n ot foun d in
other parts of the body an d t he l i fe- cycle i s as describedby Schaudin n . Accord ing to the same author i t i s d i stinguishable by its appearan ce as th e ectosarc or ectoplasm i s n ot V i s ib le as a d i st in ct l ayer, an d th e n ucleus i slarge an d r i ch in Chromat in
,so that i t sta in s deeply in
sta in ed preparat i on s . This amoeba i s n ot con s idered tocause d isease . It may be presen t in the smal l in test in esas an act ive mot i le amoeba
,an d on ly the en cysted forms
foun d in the stools un l ess there i s d iarrhoea .
The other in test in al amoeba , En tamceba tetragena
( 9 histolytica) , has a more d i st in ct ectoplasm and th epseudopodia are en t irely formed by i t at first
,so that
23 2 TROPICAL MED IC INE AND HYG IENE
they are tougher an d stronger than those o f the A. coli.
The n ucleus i s n ot readily vi s ib l e‘
and i s poor in
chromatin, an d there fore does n ot stain deeply in sta in ed
preparat i on s . Schaudin n descr ibes the mult ipl i cat ion as
d i fferen t from the E. coli.5
The whole cel l does n ot form a cyst,
'
but a ser i es ofbuds are formed extern al ly, each of whi ch becomes al aten t en cysted form . These observati on s have n ot beencon firmed
,an d (by many) th e d i st in ct ion s between E. coli
an d E. histolytica are doubted . Many con s ider that th isparas it i c amoeba i s E. tetragena . In th e en cysted formsthere are n ever more than four n ucle i . It i s h ighlypathogen i c to cats an d may in th em cause l iver abcesses.
In the act ive moving forms i t i s i n d ist ingu ishable fromE . histolytica . Probab ly E. histolytica an d E. tetragena are
th e same,an d poss ib ly E. m inuta .
E. histolytica or tetragena may en ter the subcutan eoust i ssues and be carr i ed to vari ous parts o f the body
,such
as the l iver, sp leen ,and k idn eys
,and there may cause the
format i on of abscesses . These abscesses are slowlyformed an d m ay attain en ormous s ize
,con ta in ing many
p in ts of pus . They are usual ly s ingle,but two or three
are n ot rare . The pus in such abscesses i s wh ite , yel low,
or may be chocolate in colour . It i s a very th ick, sl imypus . The wal l s of the abscess are rugged
,an d as a rule
there i s l i ttle format ion of fibrous t issue aroun d , thoughthere i s an area of in ten se congest i on . In the pus fromsuch an abscess n o bacter ia are foun d , ei ther on examin at ion or by cul ture
,in th e maj ori ty of cases . In others
,
th e min ori ty, there are bacter ia, but these are n ot of anyun i form spec ies . These facts are taken to show that th eamoebae are pyogen i c
,an d that for th e formation of pus
n o bacterial a id i s n ecessary . Others part i cu larly statethat in early abscesses bacteri a are to be foun d , but admitth e poss ib i l i ty that they have been carri ed by the amoebae ,and that in the large ster i l e abscesses these bacter ia haved i ed out .The amoebae are very scan ty in th e pus in the abscess ,

HEPATIC ABSCESS 233
so that they are rarely to be foun d . In the walls of theabscess
,in scrap ings from the wal ls, and in th e pus dis
charged a few days after the abscess i s open ed , they areusual ly presen t in very large n umbers . An abscess m ay
become quiescen t an d en capsuled or be reduced to aputty- l ike mass . More common ly they con t in ue toin crease in s ize
,an d burst ing through the l iver may exten d
in the cel lular spaces almost anywhere . Frequen tly theyburst in to the lungs or in test in es an d a n atural cureresults .
FIG . 66 .—H epatic Abscessw i th I rregular Pyrexia.
The hepat ic abscess or trop ical l iver abscess i s usual lys ingle
,but two or more may be foun d . The on set i s
often in s id ious , an d i t may be preceded by a moregen eral hepat it i s
,but as a rule the gen eral hepat it i s i s n ot
fol l owed by abscess formati on .
The symptoms , on ce attent ion i s d irected to the l iver,are usual ly marked . The l iver i s en larged often upwards
,
so that the upper l imi t of hepat i c duln ess i s convex . Theedge of the l iver i s usual ly
,but n ot always
,pushed down
so that i t can be fel t below the r ibs . The l iver i s ten der ,often ex tremely so
,but in other cases firm pressure i s
requ ired to el i c i t any s ign s of pain . The rectu s an d
o ther abdomin al muscles are more rigid on th e r ights ide , an d pain in a shoulder
,usual ly the right
,i s a very
frequen t symptom . The blood usual ly shows a moderateleucocytosi s , an d the proport ion of polymorphonuclear

234 TROPICAL MED ICINE AND HYG I ENE
leucocytes i s in creased . The dysen ter i c symptoms ator before the hepat ic troubles may be very sl ight and
even escape the n ot ice of the pat i en t . In fatal casesul cerat i on of th e colon i s n early always presen t . Even
when there are n o symptoms of dysen tery en cystedamoebae
,E. tetragen a , may often be foun d in the stools .
I pecacuan ha i s again coming in to favour in cases o famoebic hepat it i s when there i s n o eviden ce of the format i on o f pus .The paras i t i c amoebae d ie i f l eft in th e faeces as soon as
putrefact i on occurs . Reproduct ion takes plaCe by simple
FIG . 67 .—Pyrexia due to En tamoeba. x indicates when Ipecacuhana
was adm in istered .
divi s i on,wh il st they are parasi t i c, but tran sferen ce from
on e host to an other i s bel ieved to be by the en cystedforms . In these the organ i sm becomes spherical
,i s
covered with a thi cken ed cyst wal l,an d the con ten ts
are d ivided in to four or e ight .Sometimes local ized oedema may be foun d and more
frequen t ly local ten dern ess . E i ther of these are valuablel ocal iz ing symptoms of the abscess . I f an abscess hasformed i t must be l ocal i zed by exploratory pun ctureswith an explor ing n eedl e an d freely open ed an d drain ed .
If n o abscess i s foun d the symptoms may be due tohepat it i s
,and i f t hat be due to amoebi c in fect i on a
course o f ipecacuan ha or a seri es of i n tramuscular in ject ion s of emet in hydrochloride “ii? to if a grain dai ly wi l lbr ing down th e temperature an d rel ieve the symptoms .

236 TROP ICAL MEDIC INE AND HYG I ENE
In some coun tr i es where hepat i c abscess i s sai d to berare
,as in the West I n dies , at post-m ortern examin at i on s
i t i s foun d to be common ; cl in i cal ly, the con di t i on i soften overlooked .
Without e i ther hepat i t i s,l iver abscess, or defin i te
dysen tery the En tamoeba m ay give r ise to i rregular fever .The cysts may be foun d in the stoo ls an d the fever yieldto a course o f ipecacuan ha or emetin (fig .

CHAPTER XV I I .
PROPHYLAxrs IN PROTOZOAL D ISEASES : RESUME.
( I ) Genera l Prophylaxis—Few of the protozoa arekn own to be carried un der n atural con d it i on s directlyfrom m an to m an . AS a rule an in termediate developmen t o f the paras ite has to take place before i t can againre-en ter m an . In many cases th i s developmen t on lytakes place in a su i table altern at ive host—mosquito ,b it ing fly
,bug
,or t i ck ; in others , the further develop
men t can take place on the groun d or in water .Where an altern ate host i s required prophylact i cmeasures must be directed n o t on ly aga in st the pathogen i c parasi te but al so again st the in termediate host
,so
that detai led knowledge of the l i fe-h i story of these hostsi s required .
As a gen eral ru le,where the paras i tes are foun d in the
blood or where the blood i s in fect ive a blood -suckingin termediate host i s required . Where the paras ite existsin the in test in al can al or in the skin n o such host i sn ecessary . For each disease, th erefore, there wi l l bed ifferen ces in detai l as to the prophylact i c measuresrequired .
( I I ) Special Prophylaxis—With the in test in al d iseasesprophylaxis depen ds ( 1 ) on the success of the methodsadopted for the d i sposal an d destruct ion of excreta , an d
(2) preservati on of the water supply from al l possiblesources of con tamin at ion an d the un i form use of thoroughbo i l ing or efficien t fi ltrat ion to destroy any of thesein fective forms in water an d milk .

238 TROPICAL MEDICINE AND HYG I ENE
Table in dicat ing briefly mode of tran smiss ion of themore importan t protozoal d iseases
LeavesmammaD isease Parasite ReservoirIian . Host zman
v ivax ,
Quartan
malar ia ,
Ind irect effect of malaria.
fasciata
Dengue fever As in yel lowfever
I njected byph lebotomus.
Kala azar Man probably
Orien tal sore Man , and probably,in som e
varieties,dogs
Re l a p s in g Spiroc/z ieta In man usual ly I n b l o o d In Ped iculus By bi tes.
fever recurren tis p lasm a probablyAfrican t ick Spiroc/za ta Man or pro In blood and In Orn itho
fever geny of ih in sal iva dam smoufected ticks ham
In a mos Injected by mosquito 10 days
after feed ing onI n fec t ed per
.
sons, when the
m o squit o e 5have becomeinfective.
Injected by mosfasciata or qui to.
gan s

240 TROP ICAL MEDIC INE AND HYGIENE
For th i s purpose,some kn owledge of in sects in gen eral
,
an d mosqui toes in part i cular,i s essen t ia l in order to advi se
as to econ omic prophylact i c measures , an d an outl in eo f the class ificat i on of in sects, an d th e prin c iples on
which in sects are class ified,are here given br iefly .
CLASS I FICATION OF D I PTERA.
Suborder I . Orthorrhapha .—The adul t Imago escapes
from the pupal case through a longitudin alan ter i or or posteri or T-shaped S l i t . AS therei s n o pt i l in um
,there Is
,in the imago
,n o
fron tal lun ule . An ten nae usual ly proj ect infron t o f th e head .
They are d ivided in to N EMATOCERA (thread- l ikean ten nae) an d BRACHYCERA (Short an ten nae ) .
N EMATOCERA.—An ten n ae havem any jo in ts—always
more than Six the segmen ts , except the on e
at the base,are s im i lar t o each other ; palps ,
usual ly four or five jo In ts.
Nema tocera vera .—]o in ts o f the an ten nae are
long,an d frequen t ly have whorl s o f ha irs
,
l egs long and slen der,abdomen usually l ong ,
e.g.,Cul ic i dae (mosqu itoes ) .
Nema tocera anoma la .
—An ten nm composed ofmany segmen ts ; but th ese are all short
,and
,
as a rul e,without whorl s o f hair . The
abdomen i s usual ly stout,and the legs are
Shorter an d th icker than in N . vera,e.g
Simulidae,or san d-flies.
BRACHYCERA.—The n umber o f true j o in ts in the
an ten n ae i s leSS than Six palps,on e or two
j o in ts .Brachycera vera .
—Third j o in t of an ten n a i s n otr inged
,and usual ly termin ates in a bristl e or
style,e.g . ,
As i l i dae,or robber-flies.
Brachycera an omala—Termin al j o in t o f an ten n acomposed of several short segmen ts fused
D IPTERA
together . These fused segm en ts appear asr ings
,e.g .
,Taban i dae.
Suborde r I I .—Cyclorrhapha .
—A c ircular cap i s pushed offthe pupal case by the b ladder-l ike protrus i on ,
ptilinum ,wh i ch forms on the an ter ior part o f
the head of the imago an d th is imago escapesthrough the c i rcular Open ing thus made .
In the imago a curved scar i s l eft when the pti l inumcon tracts . Th is scar i s the lunule, an d thepresen ce of th i s scar shows that the in sectbelongs to the Cyclorrhapha . An ten n ae areShor t, usual ly three-j o in ted , and more or lessflatten ed aga in st th e head or depen den t .The th ird segm en t has at the base a bri stl e orstyle
,arista .
( I ) ASCHIZA.
—The extremit i es of th e lun ule aren ot con t in ued as sutures on each s ide o f theface
,e.g. ,
Syrph idae,or hover-flies.
(2) SCHIZOPHORA.—The extremiti es o f the lun ule
are con t in ued as l in es on each s ide of theface , so as to separate off the an ten nae an d
mouth-parts from the rest of the face . ' Thesel in es form the fron ta l suture, e.g . ,
Musc ids,
Glossinae, Stomoxys .
Suborder I I I . Pupipara .—Larva n ouri shed wi th in the
paren t an d ch anged in to a pupa withoutfeed ing . Some are W ingless
,in others the
wing ven at i on i s imperfect . An ten n ae aresmal l roun ded masses Showing n o d ivi s ionin to j o in ts , with on e or more st iff ha irs ; theclaws are powerful and much curved
, e.g.,
H ippobosc idae an d sheep- t icks .
Suborder IV . Siphonaptera , or fleas , are by some con
sidered to be W ingless d iptera but,i f SO
,they
are so much modified that they are bes tcon s idered separately, an d wil l be con s ideredin Part I I I . in c onn ect ion with plague .
242 TROPICAL MED IC INE AND HYG I ENE
SUBDIV IS ION OF THE MORE IMPORTANT GROUPSOF THE D IPTERA.
The d iptera in clude carri ers of d isease an d are characteriz ed by having a s ingle pair of membran ous wings ,the poster ior pair be ing reduced to two kn ob -l ikeprocesses
,the balan cers or halteres. They may be
blood-sucking or n ot accord ing to the structure of themouth parts .Of the groups in to wh i ch the Diptera.are d ivided the
Nematocera vera and th e Cyclorrhapha schiz ophora are ofthe most importan ce to us
,as some of them are proved
to be carr iers o f importan t d i seases . Nema tocera
an oma la has among i ts groups Simulidaz or san d-flies,
and Sambon con s i ders that the topograph ical eviden cei s in favour of a S imu l ium being the vector o f pel lagra .
The wing ven at i on o f the group i s S imple ; they areviru len t b lood-suckers
,though the popular n ame “ san d
fl ies in cludes many spec ies belonging to other groupsthan S imul ium .
Many of the others are b lood-suckers,others are
importan t as mechan i cal carr i ers o f bac i l l ary d i seases,
an d others,both of the d ipterous an d other in sects ,
are importan t as destroyers of both larvae an d adu lts o fdangerous spec i es an d in many cases do much in j ury togrowing crops
,to fru i t
,grain
,&c .
Nema tocera vera are subdivided mainly accord ing totheir wing ven at ion . This ven at i on vari es greatly in themembers of the group
,an d the fami ly kn own as the
Cul i c idae are characterized by having scales on the vein so f th e wings an d by the forking of th e 2n d
, 4th and
5 th l ongitud in al ve in s . These characters of the wingsseparate the Cul ic i dae from al l other Nema tocera vera .
The subd ivi s i on of the Cu l i c idae i s made on variat i on s ofthe mouth -parts in to subfami l i es
,an d at th i s po in t var i ous
d ifficult ies ar i se and other schemes have been proposed,some based on l arval characters and others on those ofthe eggs . Each of these methods would lead in somecases to qu ite a d i fferen t grouping an d in others would
244 TROPICAL MEDIC INE AND HYG I ENE
short in both sexes . Scutel lum tri l obed . In somegen era hai rs o n scutel lum an d metan otum .
Ma laria —The kn own carr i ers of malari a al l bel ongto the d ivi s i on of the mosqu i toes kn own as An ophelin ce.
All an ophel in es do n o t serve equal ly wel l as carr i ers ofmalar ia . Some Species are readi ly in fected
,others on ly
with d i fficul ty,an d some n o t at al l . The dangerous
spec ies are those wh ich are n umerous and read ily con veythe d isease .
For econ omic an d effic ien t prophylaxis a kn owledgeof the hab its o f each speci es i s requi red
,an d i t i s fou n d
that the d ifferen t speci es vary greatly in the ir hab i ts,l i fe
h istory,an d breeding-places .
In any place or coun try the spec i es o f an ophel in e smust be determin ed ; those that are good carri ers o fmalari a must be foun d out exper imen tal ly or must befoun d in fected an d the breeding places an d hab its o fthese must be studied in great detai l .The an ophel in es , which in clude al l th e kn own carr ierso f human malaria
,are eas i ly d i st ingu ished from other
mosqu i toes,which have a stra ight , pen etrat ing probosc i s .
( I ) The palps in both male an d female are pract i cal lythe same length as the probosc is
,an d in the male are
clubbed .
(2 ) The scutel lum ,which i s more or less tri l obed in
other mosqu i toes , shows n o S ign of such l ob ing in the
anophel in es .
(3 ) The scal es on the ve in s o f the wings are lan ceolatein the an ophel in es
,whi l st they vary greatly in the other
Culicidce .
(4) The probosc i s i s n early in the long axi s of thehead
,thorax an d abdomen , so that the mosqu ito almost
forms a straight l in e . When at rest,as the probosci s
po in ts towards the surface on which th e mosqu ito reststhe abdomen po in ts away from i t .
(5 ) The larvae have n o resp i ratory s iphon ; t hey lieflat on the surface o f th e water an d after the ir first moulthave curious palmate tufts on the latero -dorsal surfac eo f the abdomen on each s ide .

PROPHYLAX IS IN MALARIA 24 5
The kn owledge of the hab its and breed ing places o f thedangerous spec ies in each place wi l l determin e thepracticabi l i ty o f deal ing with malaria by the extermin at ion or d imin ut i on of these defin i t ive hosts .With large stat i on s the most sat i s factory resu lts are
obtain ed by d imin i sh ing the n umber of th e defin i t ivehosts
,an ophel in es . The most vuln erable period in the
l i fe-histofy of these in sects i s in th ei r larval stage . Thisi s always passed in water . A somewhat detai led kn owledge of the class of breeding-place for the spec ies thacarry malar ia in each place i s requ ired for effect ive an decon omical work in th is d irect ion . As these places d ifferfor each spec ies of mosqu ito
,without deta i l ed kn owledge
mon ey wi l l be wasted an d the results cause d isappoin tmen t .Measures that would be wel l adapted in places where
the malari a i s carri ed by Pyretophorus costa lis would beu n n ecessary
,useless and extravagan t , say in Malaya , as
they would on ly result in the destruction of th e harmlessMyz omyia rossi
,and would be in suffic ien t an d un su itable
in places where the carr i er wasM. fun esta orM. culici
M. funesta ,An opheles n iaculipen n is, P . costa lis and Cellia
a rgyrotarsis or albimanus,are the importan t carri ers o f
malaria in Southern Europe,Trop ical West Afr i ca
,an d
Tropical America , respect ively . In As ia,Nyssorhynchus
willm ori,M. culicifacies, N . fi l liginosus, and N . steph
ensi,are proved carr i ers
,but many others
,such as
C. kochi,A. a itken i
,&c . ,
are probably importan t carri e rs .Of these there i s some s imi lar i ty in the habi ts o fA. n
/
iacn lipen n is, P . costa lis an d C. a rgyrotarsns, an d alsoC. kochi, a suspected carr i er . They .all breed in roadsidepools, smal l co l l ect ion s of water, in stagn an t water,s omet imes very foul
,an d occasion al ly in collect i on s of
water in art ific ial recep tacles . N . step/t ensi i s usual lyfoun d in d isused or partial ly used wel ls
,as wel l as art i
ficial receptacles such as tubs an d tanks .Their favour ite breed i ng places vary . In As ia the
an ophel in e that i s main ly foun d in such si tuat ion s i s

246 TROPICAL MEDIC INE AND HYG I ENE
M. rossi,wh ich pract i cal ly does n ot carry malar ia . As iat i c
town s,therefore
,are rela tively free from malaria
,whi lst
in Afr i can an d South American town s a much morecomplete drain age would be requ ired to have any materiale ffect on the amoun t o f malaria .
N . willm ori,M. culicifacies, an d N . karwari
,al l stream
breeders in open coun try,are good carr i ers .
M. fun esta in Afri ca an d many of the importan t As iat i cmalari a-carrying mosqu i toes M. culicifacies) are on lyfoun d in C l ear water wh ich i s u sual ly in motion
,an d in
grass-grown edges o f spr ings,streams an d r ivers . They
can n o t thr ive in stagn an t waters . They may be foun din marshes
,but on ly when th e water i s kept fresh by
springs,or streams
,and during season s when there i s
a h eavy ra in fal l .The problems to be deal t wi th wi l l vary accord ing
to the breed ing-places of the dangerous mosqu itoes,
Where,as in a sett lemen t
,there i s art ific ial in terferen ce
with the n atural dra in age,as in making roads
,fords
and bridges, the problem is more compl i cated . In such .
places frequen t ly h ol lows have been l e ft in house bu i ld ingor road making , an d there are tren ches at the roads idesor for local dra in age wh ich must also be deal t with . In
the East such places are of l i tt l e importan ce in t hetown s
,whi lst in Afr i ca they are of vi ta l importan ce .
As a gen eral pr in c ipl e, superfic i al dra in age must be socomplete that even during the ra in s the Shal l ow pool sformed on ly last for a day or two
,or at any rate n ot for
more than a week,an d drain s must be so graded that
with heavy’
rain s they are wel l flushed and n o pool s arele ft o f any depth in the in tervals .In a l l p laces where there i s a b ill at the back of a settl e
men t a wel l-devised in tercept ing drain must be arrangedalong the base o f the h i l l so that flooding from the h i l ls ides wi l l be avo ided . Th is h i l l water i s the main causeof the con stan t h igh level o f subso i l water ; the ra inactual ly fal l ing on th e area o f the settl emen t i s com
paratively un importan t . I II l ow- lying land,as in many

248 TROPICAL MEDICINE AND HYG I ENE
ample to ren der such places heal thy,i f care i s taken that
he dra in s themselves are n ot su i tabl e for breed ing places .Where the mal aria-carrying an opheles are main ly breedersin such drain s, it i s more effect ive to use p ipe drain s , orother forms of curved dra in s
,an d though more expen s ive
at first,as they requ ire l ess co n stan t superv is i on and a
smal ler grad ien t, in the long run they are more econ omicalas wel l as more effect ive .The h istory of plan tat i on s in th e past i s in struct ive .
In the early h istory there i s a ser i ous amoun t of malariabefore the drain age i s complete ; wh i l st the estate i sflouri sh ing an d kept in good order n o malaria or veryl i ttl e ; but when the estates are aban don ed or n eglected ,an d the drain s are sedge grown , blocked or partly brokendown
,they become in ten sely malarial for any remain ing
in hab itan ts .The class of dra in s employed in any place i s main ly
depen den t upon the amoun t o f mon ey that can bedevoted to the purpose . Earth dra in s suffice
,but requ i re
much con t in ued expen d i ture in upkeep an d repai rs, whi lstcon stan t supervi s i on i s requ i red . Wherever there i smuch flush ing or scour ing
,brick or cemen t open drain s
are absolute ly essen t i a l .
All open dra in s Should be V-Shaped in sect i on,so that
a smal l amoun t o f water wi l l suffi ce to flush them an d
l i tt l e water can accumulate in the n arrow bottom of thedra in s . The l arge drain s Should be S im i lar in sect i on ,
but th e bottoms m ay be flat or,better, roun ded . H al f
p ipes or stone’
pipe in verts make excell en t bottoms for
such dra in s .It i s always advi sab le to keep a settl emen t or V i l l age
clear o f j ungl e an d un dergrowth . Such growth gives
Shel ter to mosqu i toes in th e day t ime, preven ts the dryingof the surface
,an d o ften l eads to blockage of dra in s an d
in terferen ce with n atural dra in age .
As temporary methods the destruct i on of larvae bylarvic ides i s of great use
,but Should n ot be rel ied on
for perman en t purposes . Crude petroleum or other o i l s

PROPHYLAXIS IN MALARIA 249
rapidly destroy larvae,as the fi lms formed on the surface
preven t the larvae gett in g a i r through the ir resp i ratorysyphon s . Un fortun ately i t al so ki l l s off fish an d manyforms of l i fe
,an d the water becomes putrid
'
and offens ive . Someth ing may be hoped for from some of then at ive fish po ison s . These usual ly belong to one oroth er o f the spec ies o f Derris. The roots are crushedan d thrown in to the water, and the mi lky flu id from thefresh roots
,even in min ute quan t i t i es an d much d i luted ,
wi l l destroy the larvae , and for smal l col lecti on s of fluid,
cessp i ts,&c.,
i s h ighly effect ive,an d though ki l l ing o ff
most forms of an imal l i fe does n ot ren der the water asputri d or offen s ive as the use of o i l s .
‘Where fish arepresen t these would be destroyed
,an d therefore th i s
method is n o t advisable in larger co l lect ion s of water .Many fish feed on mosqu ito larvae
,and are on e of the
importan t en emies of mosqu ito es . Amongst these theCyprinoclon ticlce are o f spec ial importan ce . The smal lfish kn own l ocal ly as mi l l ion s ” in Barbados belongto th is family
,e ither Precilia or Gam bi isia
,an d are by
some bel ieved to be the reason for the absen ce o fan ophel in es from that i slan d . In I n dia
,species o f
Chela,Haplochilus an d Therapon are e ffective , the last
in brackish waters . Even worse en emies are th e larvaeof some of the Dragon -flies (Agrion idae) these breedin s imi lar places to mosqu ito larvae
,an d l ive on them
to a large exten t .In coun tr ies where the dangerous mosqu itoes are stream
an d river breeders,drain age i s o f l i ttle value an d the use
o f larvic ides Impract icable . Much can be don e by rem o v
ing sedges, ,reeds, an d grasses growing in to the streams ,
keeping the ban ks Clear,and removing obstruct ion s in
the r iver bed or S ides,so that fish can get at the larvae
an d so that a un i form flow o f water i s main ta in ed in thepart of the stream in the vi c in i ty o f the settl emen t
,an d
the larvae are washed further down stream .
The select i on of the s i te for a sett lemen t i s a most importan t matter . In the case o f smal l stat i on s on un su i table
250 TROPICAL MED ICINE AND HYG I ENE
S i tes,i t wi l l o ften be foun d better to aban don the
stat i on than to attempt to ren der i t h ealthy . A'
suitab les i te i s one in wh ich there i s n atura l dra in age or in whichthere i s suffic i en t slope to al l ow of easy drain age . Smal lstreams and springs are sources o f danger . I f a settlemen t be made on a r iver the side selected should bethat where there are n o Shal low Shoal ing edges ; theseare much more l i able to be overgrown an d the curren ti s s lacker . In th e select ion of S i tes for settl emen ts ,marshes or low - ly ing groun d must be avoided an d any
s i te in proximity to such places . The effect of cult ivat i on i s twofo ld . In the first p lace
,the clearing of the
groun d an d the removal of den se j ungle ren ders the a i rdr ier an d admits much more sun l igh t . C learing al on ewi l l suffice for the ext i rpat i on of some mosqui toesthose that frequen t j ungle
,wh ich are main ly Ai d ina
,but
in a few in stan ces dangerous An ophelin a . C l ear ing , i fthorough as regards the l ow j ungle
,wi l l cause a great
d imin ut i on in the n umber o f these j ungle mosqu itoes orthei r complete d i sappearan ce
,even i f the tal l trees are left .
On the other han d,i f su i table breed ing-places are l eft
,such
as sedgy streams,other mosqu itoes may become much
mo re abundan t,an d these may in c lude dangerous an ophe
l in es,such asM. willm ori
,N . Christopher
/Si an d M. culici
facies in As ia , orM. funesta in Afr i ca , or C. argyrotarsus inAmeri ca . Clearing without dra in age, therefore, may substitute on e dangerous mosqu i to for an other, though , onthe whole
,i t i s ben efic ial
,as the exposed groun d dri es
more read i ly in dry weather and i s more l ikely to bethorough ly
”
flushed in heavy rain s than un cleared grou nd .
If combin ed with drai n age , an d i f th e dra ins are keptc lear
,or even moderate ly cl ear an d free from sedges , i t
i s usual ly e ffect ive . The better the drai n age requ ired forthe spec i a l form of cul t ivat i on
,the more wi l l the healthi
n ess o f th e d i stri ct be improved . Rubber plan tat i on srequ i re deep dra in age
,an d the on ly breed ing places pos
s ib le in such a plan tat i on are in the dra in s or in th eareas beyon d the plan tat i on in to wh ich the water maybe d i scharged .

25 2 TROPICAL MEDICINE AND HYG I ENE
EuropeAn opheles bifurcatus breeds in sl owly run n ing water
an d roads ide d itches . I II Bri ta in the larvael ive all through the win ter
A. m aculipen n is breeds in roads ide d i tches . Adul tsh ibern ate in houses during the win ter an d thelarvae d i e .
A . pseudopictus. the same as A. sinensis, a carri erin some local i t i es .
Asi aA. liston i
,A. culicifacies, A. um brosus A. a lbi
rostris,A lucllowii
,A. n zacula tus, A. fuligin osus.
A. sinensis,in j apan an d N orth Born eo
,n o t in the
Malay States .A. stephensi, Bombay .
Afri caA. fun estus, a stream and river breeder . Feeds inthe shade in the daytime as well as at n ight .Bel i eved by Al cock to be the same asA. culicif acies.
A. costa lis, breeds in roadside d itches, pools an d instagn an t an d even putr i d water .
A. mauritianus,A. pa luclis, proof in suffic i en t .
A. pharcensis, A. squamosus,and A. n ili are
probabl e carri ers .Austral i aA. a n nulipes A. bancrofti.
AmericaA. ina culipen n is, A. bifurca tus, A. lutz ii, A. argyra
tarsus, A. a lbim anus.
In some o f these the ev iden ce i s in complete . Experi
men tal cult ivat i on of the paras i tes in some of these i sd i fficu l t
,and in other spec ies such asAn opheles kochii an d
A. a itken i, wh ich from thei r topograph ical d istribut i on are probable carr i ers, i s a lmost impossible , as themosqu itoes soon d i e an d wil l n ot feed in capt ivi ty .
Al cock’s S impl ified classificat ion i s adopted in the
CULICINES 25 3
above l i st . He does n ot recogn i ze the subd ivis i on o fthe an ophelin es
~ in to subgen era, but groups them al lun derAn opheles. Culicinesmay also be carr iers of protozoald iseases . I t was in Culex fa tigans that Ross first demonstrated the complete l i fe-cycle of Proteosoma, a b irdparas i te very s imilar to the human malari a paras i tes .
THE D ISTINCTION OF CULIC INES INTO GROUPS .
Theobald con s iders that the character o f the scales onthe vein s of the wings
,head and scutel lum are of “great
importan ce . These d i ffer from those in an ophel in es an din d i fferen t cul ic ines so markedly that Theobald basesh i s d ivi s ion in to sub -
gen era on the character of thescales . Yel low fever has been proved to be carri ed bya cul i c in e belonging to the subd ivis ion Stegomyia .
In th e group Stegomyia, in addit i on to the uprightfork scales on the head , there are also curved t i lel ike scales an d s imi lar t i le- l ike scales on the scutel lum .
They are smal l mosqui toes an d usual ly black with bri l l i an tS i lver-white mark ings . These markings, espec ial ly thoseo n the thorax , serve to dist inguish the d ifferen t spec ies ,and in S. fascia ta th ere i s a fain t cen tral , n arrow S i lverl in e on the dorsum ,
an d on each s ide o f th i s a morecon sp icuous curved l in e .
The S . fascia ta (S . ca lopus) i s common ly kn own as thet iger mosqui to
,because o f the bri l l i an t strip ing of the
legs an d abdomen .
The breed ing-places an d hab its of th e Stegomyia ingen eral
,an d of S. fascia ta in part i cular
,differ greatly
from those of th e An ophel in es, an d the prophylact i cmeasures must be vari ed accord ingly . Stegomyia eggsare laid s ingly
,an d have n o lateral a ir-floats. They are
covered with a th i ck Shel l . They float for a t ime on thesurface of the water
,but ul t imately sin k an d l i e at the
bottom of the water in wh ich they were deposited . Theseeggs are n ot ki l led by immers ion in water
,n or are they
destroyed by prolonged des i ccat ion .
Th is extraord in ary vital i ty o f the eggs i s the cause o f

254 TROPICAL MED ICINE AND HYG I ENE
the great vari ety o f breed ing-places,an d of the wide
d i ssemin at i on of th i s mosqui to .
In th e first p lace eggs are often deposi ted in quite smal lreceptacles
,Shal l ow pools
,gutters of h ouses
,old t in s used
for preserved foods,broken bottles
,empty cocoan ut Shel ls,
&c .,an d i t i s immater ial i f th i s depos i t i on takes pl ace at
the en d of a spel l o f wet weather , as the eggs wi l l remainal ive even i f the water dri es complete ly . With the n extrain
,e ither there wi l l be suffi ci en t water to moisten th e
eggs,or there wi l l be an excess ive amoun t
,so that these
receptacles overflow . In the first case the eggs wi l l hatchwhere they were lai d ; in the second , th ey wi l l be washedaway in to some larger and perhaps more perman en tcol lect i on of water .Eggs that have fal len to the bottom of a pon d remain
al ive,an d i f in taking water
,as on board a Sh ip
,the
bottom is at al l d i sturbed,the eggs wi l l be taken with the
water,an d batch out an d develop in the water-barrel s .
Old wooden barrels in which water has been kept,i f n ot
wel l clean sed , wi l l o ften be foun d ful l of l arvae with intwen ty-four hours or l ess i f refi l l ed with water . Suchbarrel s are often used for storage of water on a smal lscale an d for catch ing roof water
,an d whether kept
indoors or out of doors are most pro l ific breeding-places .With the on set of the wet season these spec i es o fmosqu itoes very rap idly become abun dan t . The matureeggs are presen t in old beds of dri ed puddles
,an d in
every receptacle that wi l l hold even a few drops of water ,an d these hatch out wi th the first rain
,an d i f ra in con
tinues the pupae wi l l form in a week,and a day or two
later the imagin es emerge . L ight i s n ot n ecessary forthe developmen t o f these larvae
,so that c i stern s an d tanks
are su i tab l e breeding groun ds .The larvae have a resp iratory syphon or tube attached
to the eighth abdomin al segmen t . Th is syphon i spresen t in al l the Cul ic in ae
,but varies greatly in l ength .
I n the S tegomyi a i t i s a short,broad
,stumpy syphon
,
Shorter than in most Of the common er Culicin ce. The

256 TROPICAL MED IC INE AND HYG I ENE
breed ing-places wi l l resul t in the freedom of that housefrom these mosqu itoes .The places to look for breed ing-places of S . fascia ta
are
( 1 ) The back of servan ts’ quarters
,as beh in d these
empty t in s,bottles
,and broken crockery o f all kin ds are
al lowed to accumulate . If there i s l ong grass thesereceptacl es are h idden by i t
,an d thus
,sheltered from the
sun , retain water for a long t ime .
(2) Tanks, barrel s, water-butts,used for co ll ect ing
or storing water . The largest as wel l as the smal lestare common breedi ng-places . Wooden receptacles areperhaps the most l ikely to harbour the larvae . Thewarn ing that any in caut ious movemen t i s to b e avo idedin examin ing such places must be remembered
,as the
larvae,i f they are n ot on the surface
,can n ot be seen .
Badly graded gutters are also fert i l e breed ing-p laces .The ord in ary roof-gutter i s apt to sag , an d even i fproperly graded i s l i able to be blocked by leaves an d
other debris,so that pools
,perman en t in the wet season ,
are formed . Moreover,eggs deposi ted on the i r exten s ive
surface are carr ied down in to the water-tanks an d theredevelop . Some authori t i es con demn roof-gutters forthese reaso n s
,but there i s n o reason why roof-gutters
should n ot be properly graded an d kept c lean,an d i t i s
o f l i tt l e importan ce that eggs are washed down i f themosquitoes that develop in the tan k can n ot escapefrom i t . More frequen t open ings in such gutters areadvi sable .
(3) In houses, bath -tubs, vessel s for h old ing flowers ,flower-pots , even fi l ters
,such as the drip ston e fi l ters
,
water-coolers,an d every receptacl e for water wi l l serve
as a breed ing-place . These are frequen t ly foun d in
un occupi ed rooms . As these mosquitoes can breed infou l water
,they may be presen t in th e receptacles for
k i tch en refuse,an d even cessp i ts . Stable cesspi ts
,stable
buckets and dra in s are o ften the breed ing-places of thesemosqu itoes .

PROPHYLAXIS IN YELLOW FEVER 257
In preven t ing the spread o f yel low fever , a kn owl edgeof their breed ing-places i s essen t i al . In any coun try in towh ich yel low fever may be in troduced the extermin at ionof these mosqui toes wi l l ren der the spread of the d iseaseimposs ib le ; an d in al l coun tri es the i r ext i rpat i on wil lgreatly in crease comfort . In a scattered sett lemen t i ti s an easy an d inexpen s ive matter to ren der a housefree from th i s spec ies of mosqui to, but con stan t care i srequ ired . The importan t po in t i s that in such a placethe breeding-places are in th e immediate surroun dingsof the house . The occupier breeds h is own mosqu itoes .In a more crowded settlemen t con t in ued efforts arerequ ired
,an d i t Should be made compulsory for each
occupier to free h is own property from breeding-placesor the whole work may be don e by the mun i c ipal i ty atthe common expen se . A combin at ion of these methodsi s most effect ive . I t Should be compulsory on theoccup ier to free the actual premises from breed ingplaces
,an d to h ave h is water- tan ks S0 protected that
mosqu itoes can n ot escape from them,an d to see that
n o accumulat ion of empty t in s an d bottles i s presen tin h is compoun d . The mun i c ipal i ty should removesuch bott les
,an d in spect an d report on the con di t i on
of drain s,gutters
,tanks , an d stable surroun dings as to
thei r freedom from larvae, an d Should make recom
m en dation s to the occupier and en force the carrying outo f such recommen dat ion s . The gutters must be wellgraded an d kept clean . The p ipes supplying water tothe tanks must be l ong en ough to reach the bottoms ofsuch tan ks
,otherwi se the mosqu i toes as they hatch out
w i l l escape through th is p ipe . The man hole must bekept covered
,an d i t i s better to have a double covering
,
an in s ide one of gauze , an d the ordin ary sol id on e overi t . It i s useless to attempt to ren der the supply pipeimpervious to mosqu itoes by plac ing a gauze diaphragmin any part of i t, as the meshes soon become cloggedan d the water wi l l n ot pass through . An in spect ion an d
col l ect ion of any portable breeding-places, e.g. ,bottles , &c
I 7

2 58 TROPICAL MED IC INE AND HYG I ENE
Should be made twi ce a week,an d any foul dra in s, or
cessp i ts should be treated wi th crude petro leum,or
better , some such po ison as tuba root (Derris elliptica) .W i th a good organ izat i on
,with the act ive support of
the in tel l igen t sect i on of the commun i ty, an d stringen tregulat i on s wel l en forced
,the cost o f exti rpat ion of th i s
m osqu i to i s n ot proh ib it ive .Roof water forms the best ava i labl e supp ly of drinking
water in many places,SO that measures that preven t i ts
in fect ion can n ot be overl ooked .
Den gue fever i s con veyed main ly by Culex fa tigans andStegomyia fascia ta , but i t also occurs in places where thel atter mosqu ito i s n ot foun d . Stegomyia scutellaris
,easi ly
d ist ingu ished by the broad median wh ite han d down thethorax
,i s al so a carri er . S . scutellaris also breeds in fou l
water,an d i s common in s im i lar con di t i on s to those in
wh ich S . fascia ta i s foun d , but occurs in j ungle , and moreon the outsk irts of sett l emen ts th an in the larger crowded
town ships .Culex fa tigans, wh i ch , as wel l as the Stegomyia , i s im pli
cated in th e con veyan ce of dengue fever an d i s the
common carrier an d in termediate host of Filaria ban
croj ti, breeds in roads i de d i tches an d in almost any
col l ect i on of st i l l water . I t i s a domest i c mosqui to an di s foun d in houses , often in l arge n umbers , but, un l i ke
S tegomyia fascia ta , the breed ing-places are often a longway from the houses i t frequen ts as an imago . The ex
tirpation of C. fatigans from a settl emen t requ ires com
b in ed effort , pract i cal ly mun i c ipal con trol , whi lst thefreedom of a house from Stegomy i a main ly depen ds on
t he in d iv idual care o f th e occupan t of a house . H ouses
on the top of a b ill are often much frequen ted by
C.fa tigans ; these mosqu itoes are strong fl i ers an d are o ften
carri ed,partly by the win d
,for con s iderable d istan ces ,
th ey seek shelter in the houses an d wil l rem ain in suchhouses rest ing an d qu iescen t in the day t ime , but act ive at
n ight ; Un der art ificial con d it i on s they may l ive for threemon th s or more , an d under n atural con dit ion s wi l l b iber
n ate al l through the cold season .

TROPICAL MEDICINE AND HYG I ENE
wings , thorax, abdomen,and l egs with l on g hairs .
They have n o ocel l i . The larvae breed in caves,crevices
,
in wal ls,amongst ston es, in any dark moist p lace where
the a ir i s sti l l and there i s protect i on from l ight . Decaying n i trogen ous refuse i s favourable to their developmen t .They are slower in the i r developmen t than mosqu i toes
,
the eggs take about a week to hatch,the larvae some eight
weeks before pupat i on,an d the pupal stage about two
weeks . These peri ods are shorter in hot weather an d
may be in defin i tely prolonged in very cold weather . The
fl ies,therefore
,are most abun dan t during hot weather .
The in fect ive agen t i s presen t in the blood on ly dur ingthe first twen ty- four hours of the attack an d an in tervalof s ix days i s requ ired before the ph lebotomus is capableof in fect ing m an .
Trypan osom iasis i s carr ied by Glossin a of several spec ies .
The larvae l ive in t he abdomen of the female t i l l ready forpupat ion and then burrow in to l oose earth an d becomepupae . The vuln erabl e per i ods then are l imited to thepupal stage an d the imago
,an d in the case of a pupa I n
loose earth , decayed leaves , an d crevi ces there i s l i tt l echan ce of i ts destruct i on . Pro tect i on of in fected personsan d an imals from a day-b i t ing fly i s d ifficul t
,an d so
far the most successful resu l ts h ave atten ded the abandonm en t of places where the fly i s prevalen t . Systematicprophylact i c treatmen t w ith atoxyl i s a more seri ousmatter than systemat i c treatmen t with quin in e
,an d has
n ot been adopted on a large s cale . Sui table cloth ing,
select i on of p laces for rest,n e i ther in boat n or n ear water
in forest coun try,dimin i shes the r isks .
Ka la -az ar .-The gen eral bel ie f i s that a species of
C imex , C. rotun datus,i s the carr i er. Th is in sect i s a
breeder in places S imi lar to the European bed bug ,Cim ex lectularius. It i s n ot con clusively proved that th i sbug i s a carr i er . Don ovan suggests that Conorrhinusrubrofascia tus may be a carr i er, poss ibly acqu iring thein fect ion secon d-han d from the bed bugs on wh i ch i t isbel i eved to feed .

PROPHYLAXIS IN INTESTINAL PROTOZOAL DISEASES 26 1
Afr ican t i ck fever i s carr ied by o ne of the Argasin et i cks
,Orn ithodorusm ouba ta . I t b ites main ly at n ight an d
on ly person s who are at rest ; an d so the usual t ime ofin fect i on i s during the hours of Sl eep . In a bed wel lrai sed from the groun d an d n ot in con tact with the wal ls ,there i s l i tt le probabi l i ty of in fect ion un l ess these t icks arepresen t in the bedding . All bedd ing Should be carr i edin a tin
’
box an d n o t depos i ted on the groun d of a resthouse or n at ive hut at any t ime, and the t i cks wi l l n otgain access to th e bedd ing . As th e t i cks of the secon dan d thi rd gen erat ion are in fect ive
,i t i s wel l to act as i f al l
the t i cks of th is spec i es were in fect ive .
Dry dust i s the preferen t ia l h aun t of these t i cks . In awel l-kept
,wel l-bui lt European house they Should n o t be
presen t .I n dian relapsing fever i s probably carr ied by Pedicul i .
Clean l in ess of body,hair an d cloth ing i s the best pre
v en tiv e.
Prophylaxi s as regards i n test in al protozoa requ iressu i tab le measures for the destruct ion an d di sposal ofexcreta
,good un con tamin ated water supply an d protec
t i on of the col lect ing area,roof or otherwise
,from dust .
Food,milk, &c. , must also be protected from dust , even
after i t has been cooked or boi l ed .

APPE ND I X .
I .—N OTABLE DATES .
Malarm—D iscov ery of the parasites, Laveran , N ovember 6 ,1 88o .
—D ifferen t iat ion of species an d asexual l i fe-cycle, Golg iand others, autum n of 1 885 , and onwards—Conjugat ion of
sexual form s,McCallum ,
1 897-8 .—Sexual cycle , Ross, 1 897 -8 .
Redwater Fever .—P iroplasm a d iscovered by Babes in 1 888 .
Mode of tran sm ission , Sm i th an d Kilburn e , 1 893 .
Yellow Fever.-Mode of tran sm ission of yellow fever , Reed
and Carrol l , US . Army Comm ission ,1 900
- 1 . Mi ld formrecogn i zed , 1 84 1 .
Trypanosomes.—In fish , Valen t in e ,
1 84 1 .—In frogs, Gruby ,
1 843 .— In rats, Lew is, 1 878 . AS a cause of d isease (surra ) ,
Evan s, l 88o .—As a cause of d isease (n agan a) , Bruce , 1 894 .
In m an N epv eu described a trypanosom e , 1 890 , but the
descript ion was not conclusive — In m an Ford d iscovered an d
Dutton described T. gambiense, 1 90 1 .—In m an
,in sleep ing
S ickness, Castel lan i d iscovered the sam e trypan osom e in the
cereb rosp in al fluid,
1 902 .— 1 908 , Klein e showed that after
Glossin a have fed on an in fected m an in fi fteen days or morethe fly is in fect ive .
Spiroche ta obermeieri or Spiroche ta recurrentis, d iscovered byOberm eier , 1 873 , n am ed S . recurrentis, 1 874 ,
an d S . obermeieri,
1 875 .
Spirocha ta cluttoni.—P . Ross, 1 904 .—N abarro had previously
reported th is d iscovery , but report was n ot publ ished t i l l afterROSS ’
S .
Spirochceta palliiluin or Treponema pallidum . Schaud inn ,
spring of 1 905 . Spiroche tapertenuis.—Castel lan i , j un e, 1 905 .
Sp irochaeta in granulom a pudend i , W ise , 1 906 .
Leishman-Donovan Bodies.—Leishman and Donovan indepen
den tly in kala -azar , 1 903 .—In Delhi bo i l , Wright , 1 903 .
Rogers proved their flagellate stage , 1 904 .

264 TROPICAL MED ICINE AND HYG I ENE
Norm al blood : Weigh t about Ilg
of the body weight , say,
9 p in ts or cub ic cen t im etres.
Red corpuscles : About per cubic m i l l im etre .
Leucocy tes : to per cubic m i l l imetre .
Of these 65 to 75 per cen t . are polymorphonuclear leucocytes.
5 1 0 large m on onuclear .1 5 25 lymphocytes, but number
varies accord ing to the
stage of d igest ion .
1 3 eosin oph i les.
Malaria . D iam eter of “spores
”or m erozo i tes
Ben ign tert ian 1 5 y ,
Quartan 1 7 5 a.
Subtert ian ,1 .
Full-grown parasi te, sporocy te or sch izon t :Ben ign tert ian 8 5 ,
u, .
Quartan o a.
Subtert ian 4°
5 ,u. .
Ful l -grown zygote 5 0 to 60 fl .
Sporozo ite 1 4 p ,
Leishm an -Donovan body 2 5 to 3 5 a x L 5 to 2 a,
Amceba coli Up to 5 0 u,
En cysted form 1 5 to 20 71 ,
Lamblia intestinalis U p to 1 5 I“ in l eng th .
En cysted form I 3 p, X 7 ,u.
Trichonionas hominis 3 j. to 20M.En cysted form Up to 1 5 p ,
I I I . —TI CKS .
Blood-suck ing Arthropods are found also amongst the
Arachn idas, wh ich in the adult stage are read i ly d ist inguishedfrom the in sects, even from the Wingless in sects, by the
presence of four pairs of‘
legs an d the absence of an tennae,wh i lst the orifice of the m outh is a sm al l sl i t .
The blood -suck ing groups are the IXOD IDzE .
IXOD IDAZ have e i ther a hard an d ch itin ous or th ick , leatherySk in . The m outh -
parts consist of a cen tral hypostome armedw i th teeth project ing backwards, and on each
'
side a powerfulchel icera , also arm ed w i th teeth project ing backwards, chelicera ,

APPENDIX 265
!enclosed in a sheath . There are a pair of four-jo in ted palpso r ped ipalps.
The open ing of the gen i tal ia is on the under aspect n ear theh ead , and resp irat ion is conducted by a pair of sieve -l ike
FIG . 7 I .-Mouth-parts of
FIG . 72 .—Mouth-
parts of Rhipicephalus.
o pen ings in the resp i ratory areas, si tuated close to the baseso f the fourth pair of legs.
There are two great groups of the IXOD IDZE ,[recline and
Argasine .

266 TROPICAL MED IC INE AND HYGIENE
IXOD INZE .—Tll e rostrum proj ects from the an terior extrem ity
of the body . The palps are deep ly grooved on the i r in n eraspects an d act as a Sheath to the rostrum . The last join tof the palps is a sm al l project ion from the th i rd . The second
jo in t is long in on e d ivision , I xodinae (fig . and shorter , as.
broad as long , in another : Rh ipicephalae (fig. On the
dorsal aspect is a hard ch itinous p late , dorsal sh ield , covering“
the en t i re dorsum in the m ale but on ly the an terior part in thefem ale . The I xoclinee are importan t as the carriers of p iro
p lasm a in the lower an im als. They are n ot proved to carryany d i sease to or from m an .
FIG . 73 .—Mouth -
parts of Argasina.
ARGAS I N /E d i ffer from I xodin ae in that ( I ) the rostrum is~
on the un der surface of the body (2) the palps do no t forma sheath for the rostrum (fig . (3 ) they have no dorsalSh ields, but a th ick l eathery covering orn am en ted w ith knobs.
or bosses, m ak ing a regular pattern .
There are two gen eraArgas.
-Body w ith sharp edges. The pattern of the m ark ingclose to the edge d iffers from that on the rest of the dorsum .
Species of th is genus carry the avian sp irochaetes.
Ornithodorus.— Body w ith rounded edges. N o d ifference in
the pattern of the m ark ing on the edge from that of the restof the dorsum .
Ornithoa’
orus moribata carries Spiroche ta duttoni, the cause of
the African form of relapsing fever.

268 INDEx
Ba lan t id ium dysen tery , 22 5
Ber i -ber i com p l icat in g m a lar ia,
46 , 5 1
Bermuda,ep idem ic ye l low fever
at,1 28
,1 3 0
B lack vom it in re lap sin g fever ,1 87 in red cor
in y e l low fever,1 1 5 , 1 1 9
B lackwater fever associat ionw i th m a lar ia
,1 08
b l ood exam in at ion in, 99
cl in ica l course,89
com p l icat ion s of, 90
d iagn osis of, 96
d iuret ics in,1 02
et io logy of,1 07
,geog raph ica l d ist r ibut ion
of 88
m istaken for ye l l owfever
,1 1 8
nursin g in,1 05
patho log ica l an atom y o f,
p rogn osis of, 9 7
p rophy lax is again st , 1 1 0
quin in e in,6 5
quin in e p o ison in g th eory ,1 08
re lap ses in , 9 1 , 93
ren a l con d it ion s in, 96 , 99
seque lae of,1 09
suscep t ib i l i ty to, 97
t reatm en t of,1 0 1
B l ood chan ges 1 11 ka la-azar,1 57
1 58 , 1 6 1
co rpusc l es, red , m alaria parasi tes in
,1 7
exam in at ion in b lackwaterfever
, 9 1 , 99
in m a lar ia, 50, 6 5
in re lap sin g fever , 1 9 1
fi lm s, p reparat ion of
,1 5
stain ed by Leishm an ?sm ethod
,2 7
p er iph era l , gam etocy tes in,
24
B lood serum of ye l l ow fever,in
fectiv ity of,1 20
stasis in m a lar ia, 44, 48
B lood-
p ressure in m a lar ia, 47
Booph ilus d ecoloratus, 1 96
Brachycera , 240
Brassy bod iespuscles, 1 8
Bron ch i t is in ka la-azar an d t ickfever
,1 52 , 1 5 5 , 204
Bugs,sp i r i l lum foun d in
,1 9 5
CACHEXIA in ka la-azar,1 52 , 1 5 5
m a lar ia l,
‘
6 5 -67
Ca lom e l in ye l low fever , 1 1 9
Can crum o r is in ka la-azar,1 56 ,
1 59
Cap i l lar ies, m a lar ia parasi tesin
, 46 , 5 2
Cardam atis’oin tm en t in O r ien ta l
sore,1 8 1
Catt le, p i rop lasm osis in
,1 1 1 - 1 1 3
Cereb rosp ina l fluid,
tryp an o
som es in,1 3 9
Ch igoe,car r ier of yaws, 22 1
Ch i l d ren,effects of m a lar ia on
,
44
ka la-azar in,1 73
Ch rom at in m asses in ka la-azarparasi tes, 1 6 5 , 1 67
in t icks,206
Ciliata , 3
Cim ex rotun datus,260
C istern s,cl ean sin g of
,in p ro
phy lax is, 2 56
C loth in g,d isin fect ion of
,20 1
Coccidia,
1 1
deve l opm en t of, 4
Goko . S ee YawsCo l d bath in m a lar ia l hyper
py rex ia , 6 1Con go
,S l eep in g sickn ess in
,1 3 1
Con orrhinus rubrofasciatus, 260san guisuga ,
1 50
Con vul sion s in subter t ian m a lar ia l fever
, 4 5

INDEX
Corethrin ae,243
Crops, cul t ivat ion of,2 5 1
Culex , 74
fatigans, 1 30
den gue feve r con veyedby , 2 5 8
pulp s of, 72
Cul icidae , 242
Culicina , 243
Cul icin es, d ist in ct ion of, in togroups, 2 53
Cyclolepteron , 74
Cyclorrhapha ,24 1 , 242
Cyprin od on tidae, dest ruct ion of
m osqui to larvae by: 249
DATE sore . See O r ien ta l so reD e lh i bo i l . S ee O r ien ta l soreD en gue fever
,2 58
Derm ocen tor reticularis, 1 1 3
D er r is,249
D iagn osis tab le of,en tamoebae
,
2 3 1
D iar rhoea due to Lam blia in tes
tinalis,226
in ka la-azar,1 56 , 1 58
D ip tera, c lassificat ion of,240
subd iv ision of group s of,242
D isin fect ion m ethods,
1 26,
20 1
D iuret ics in b lackwater fever,1 02
D ogs,Ie ishm an ia in ,
1 7 5
D on ovan ’s con fi rm at ion of Le ish
m an ’s d iscovery , 1 68
D ragon -flies,dest ruct ion of m os
quito larvae by , 249
D rainage,defect ive, b reed in g of
m osqui toes due to,246
D rain s,sect ion s of
,247
Dum dum fever . S ee Ka la-azar.
D ysen tery , I o
am oeb ic,23 5
ba lan t id ium ,22 5
En tam cebae,23 1
d iagnosis tab le of,23 1
En tamcebae h istolytica, 22 5 , 230
tetrag ena ,23 2
Ep ithe l iom a , granulom a m is
taken for,223
Eretm apod ites, 74
Europ ean s, b lackwater feveram on gst
,1 07
en dem ic in dex of m a lar iain
,8 1 -87
Eye affect ion s in m a lar ia,66-67
in sleep in g sickn ess,1 3 7
FAMINE fever . S ee Re lap sin gfever
Fl j l an kan ailom a,
22 1
F ish,k i l led by larv icides, 249
m osqui to larvae dest royed by ,249
F lage l lata, 3 , 22 5
Rogers’s observat ion s on
,
1 68
F l ies,bacter ia con veyed by , 8
b i tes of,effects of
,1 46
F orest yaws, 1 77
F ramboesia t rop ica . S ee YawsF ron t ier so re . S ee O r ien ta l so re
GAMETOCYTES , 2 1
of sub tert ian m a lar ia,24
Gen i ta l s,serp ig in ous ul cerat ion
of,222-224
Geograph ica l d ist r ibut ion of
b lackwater feve r,88
of g ranulom a of puden da,222
of ka la-azar,1 5 1
of m osquitoes, 7 1
of re lapsin g fever,
1 83 ,
1 90
of sl eep in g sickn ess, 1 3 1
o f yaws, 2 1 6
of ye l low fever , 1 1 5 ,
1 28
G lan ds,en larged in trypan oso
m iasis,1 3 5 , 1 3 9

270
Glossin a
1 50
palpal is, 1 44
G lossin a,character ist ics of
,1 4 5
hosts for t ryp an osom es,
1 3 2
t rypan osom iasis car r ied by ,
1 44 , 260
G ranul om a, in fect ive, of O r iental sore
,1 78
gan g ren osa,22 1
of puden da, c l in ica l courseof
,222
d iagn osis of,223
et io logy of,224
p ath o log ica l an atom y of,
223
p rogn osis o f,223
sp i rochaetes foun d in ,224
t reatm en t of,224
G ranul om ata , 2 1 5
t reatm en t of,2 1 9
G regar in ida , 9rep roduct ion of
,1 1
Guam ” d isease, 22 1
m orsitans, 1 3 8, 1 4 5 ,
H eemam ceba, 9 , 1 1
Haem og l ob inur ia,en dem ic.
B lackwater feverp rogn osis of
, 9 1
H aem og regarin ida , 9 , 1 2
Haem o lysis in m a lar ia, 49
Haemo r rhages in m a lar ia, 47 , 52
in ye l low fever,
1 2 1
Haem osiderin,dep osi ts of
, 99
H aem osporid ia , 9 , 1 2
d iseases caused by , 1 4
H eadache in ka la-azar , 1 53 , 1 5 5
Hearsey’s t reatm en t of ye l low
fever , 1 1 9
Hear t,effect of m a lar ia on
, 46 ,
5 1
Heart fever , 1 1 2
Hered itary to l eran ce of m a lar ia ,78
Herp es, facia l,in
fever,1 89
S ee
re lap sin g
INDEX
]an th in osom a, 74
Jaun d ice in b lackwater fever,
90, 9 5
in re lap sin g fever , 1 88
KALA-AZAR,anaem ia in
,1 5 7
b l ood chan ges in,1 5 7 , 1 6 1
car r iers of,
260
cl in ica l course, 1 52 , 1 5 5 , 1 74
Herp es, lab ia l , in m a lar ia, 44H iccough in b lackwater fever
,
9 1
H istoplasma in lun gs,
1 59
H isto r ica l dates in t rop ica ld iseases
,262
Hosts, descrip t ion of,6
d ist r ibut ion of,1
in ver teb rate, 7
Hot p acks in m a lar ia, 60Hyp erpy rex ia in m a lar ia
, 43 , 6 1
Hyp oderm ic in j ect ion s of quin in ein m a lar ia
,62
ICE p lan in g in hyp erpy rex ia ,62
Immun i ty from m a lar ia,8 1
I n d ia,ka la-azar in
,1 5 1 , 1 60
syph i l is in ,2 1 2
In fuso r ia, 3 , 9
In sects car r iers of bacter ia,8
in fect ion of,by parasites, 7
I n term i t ten t fever . S eeMa lar iaI n test in es
,con gest ion of in
m a lar ia, 4 5 , 47
in flamm at ion of in ka laazar
,1 64
p rotozoa foun d in ,22 5
-23 2
I n t ramuscular in j ect ion s of
m eta l l ic m ercury cream in
syph i l is, 2 1 3
of quin in e, 56
I n t raven ous in j ect ion s of quin in ein m a lar ia
, 5 7
I r r igat ion system s,
2 5 1
l x od idae,208
,264

272 INDEx
Ma lar ia in catt l e, &c. See P i ro
p lasm osis
in cubat ion p er iods in , 70ka la-azar d ifferen t iated from
,
1 60
l ist of an ophe l in e car r iers,
2 52
l oca l i t ies free from, 70
-
7 1
m an agem en t of, 59
m o r ta l i ty in , 5 1
m osqui to hyp othesis con cernin g , 70,
0
244
nursm g I n, 59
p arasites causin g,1
of,date of d iscovery , 262
deve l opm en t of,27
Sp ecies of,1 4
tox ic effects of, 3 1
patho l og ica l an atom y of, 5 1
p ern icious m an ifestat ion s of,
p igm en tat ion In, 5 2
p regn an cy in, 48, 64
p reven t ion of, 77
p rogn osis of, 5 1
p rop agat ion of, 7 5
p rophy lax is again st , 69-8 1
Quartan . See un der Quartan feverquin in e t reatm en t of
, 53-
58,62
, 79
seque lae in, 48 , 5 1 , 68
sources of in fect ion, 77
subtert ian,22
, 40-
48
tab l e of d ifferen ces betweenparasites of
,23
ter t ian . See under Ter t iantop og raph ica l d istribut ionof, 3 3
,t reatm en t of
, 53-64
Ma lp igh ian capsul es en larged In
relap sin g fever, 1 92Man son ia, 74Marsh fever . SeeMa lar ia
Mastig ophora , 3 , 9Measurem en ts,im p ortan t , 263
M
V
V
M
U
Megarh in ina ,243
Men ta l con d i t ion s in ter t ianfeve r
, 3 5Mercury cream in j ect ion s in
svp hilis, 2 1 3
Meroz ortes,20
Metazoa, 7 , 9Methaem og lob inuria, 97Mian a bug ,” 1 9 7
Miasm ata , 69Microgam etes,2 1
Mictur it ion ,frequen cy of in
b lackwater fever, 90Mosqui to m a lar ia hyp otheses, 70
Mosqui toes, b reed in g-
p laces of,
80
car r iers of m a lar ia, 70, 244
geog raph ica l d ist r ibut ion of,
7 1
larvae of,
dest ruct ion in
water,249
pa rasites con veyed by , 3 2w in g sca l es of var iousfo rm s
, 74
ye l low fever con veyed by ,
1 22,1 2 5
Mouth,ul ce rat ion of
,in yaws,
2 1 7
Mucidus, 74
My xosp o r id ia , 9 , 1 3
Myz om y ia ,sp ecies of car r iers of
m a lar ia,24 5
NAGANA, cause of,1 3 8
N at ives, phophy laxis again stsleep in g S ickn ess
,1 49
N eg roes,en dem ic in dex of m a
lar ia in,8 1 -87
N ematocera , 240, 242
N eosa l varsan in syph i l is, 2 1 4N eosporiil ia , 1 3
N ervous com p l icat ion s in m a
lar ia , 47 , 49N eur i t is in m a lar ia, 47 , 49N ose, ul cerat ion of in yaws, 2 1 7

INDEX 27 3
Nursing dur in g b lackwaterfever
,1 05
dur in g m a lar ia, 59
in ye l low fever,1 20
OOCYST,26
OOk in et,26
O rch i t is in t ryp an osom iasis, 1 3 7
O r ien ta l s ore,d iagn osis of
,1 8 1
et io logy of,1 79
in oculat ion exp er im en ts
w ith,1 80
m istaken for syph i l is,1 8 1
parasi t ic organ ism s of,
1 78
p atho log ica l an atom y , 1 78
p reven t ion of,1 8 1 1 _
t reatm en t of,1 8 1
types of,1 76
Orn ithod orus m oubata,1 1 0
,1 96 ,
202,207 , 26 1
t ick fever t ran sm i t ted by ,205 , 208
sav ig n yi, 1 9 7
Orthorrhapha , 240
PALUDISM . S eeMa lar iaPan creas
, parasi tes in cap il
laries of, 46
Pap ataci, 2 59
Paran ghi. See YawsParaplasma flav ig enum ,
1 2 1
Parasi tes,con d i t ion s favourab le
to deve lopm en t of,
1
con veyed by m osqui toes, 3 2
dates of d iscovery of,262
in cap i l lar ies, 46in l iver in ka la-azar , 1 62 , 1 64m a lar ia l
,1 7
sexua l deve l opm en t of,
1 8,2 1
,27
tab le of d ifferen ces be
tween,23 QUARTAN fever
,cl in ica l course
tox ic effects of, 3 1 of
, 36
m ode of in fect ion by , 7 parasi tes of,1 7 , 23
1 8
Parasi tes,o r ig in of
,8
tab le of g roup s of, 9
Parasi t ic p rotozoa , 3Parasyph ilides, 2 1 3
Parot id swe l l in g in re lap sin gfever
,1 89
P ed iculus v estim en torum, 1 9 7
Pen is,g ranul om a of
,2 22 -223
Pharyn x , ulcerat ion of in yaws,2 1 7
Ph lebotomus m inutas,2 59
papa taci, 1 30 , 2 59
P igm en tat ion in m a lar ia, 5 2
Piroplasm ata, 9 , 1 1
,1 1 0
P i rop lasm osis in dom est ic an i
m a ls,1 1 1 -1 1 3
hum an,1 1 3
m orta l ity of,1 1 3
post-m ortem exam inat ion in,
1 1 4
P lasm od ium falciparum ,23 , 3 2
m alariae, I 7 , 23
v iv ax,1 7 , 1 9 , 23
Pn eum on ia com p l icat in g re lapsin g fever
,1 87
P regnan cy com p l icat in g m a
lar ia, 48 , 64
re lap sin g fever , 1 89 , 1 90
Prophy lax is in p rotozoa l d i
seases,23 7 -26 1
Pr-ot ista,2, 9
P ro tozoa,descr ip t ion of
,2
group s of, 3
in test ina l,2 2 5
- 23 2
p rophy lax is in d iseases dueto
,2 3 7
- 26 1
t ran sm ission of d iseases dueto
,23 8
Psorophora , 74
Puden da,g ranul om a of
,222-224
Pupipara ,24 1
Puru. See Yaws
274 INDEX
Quar tan fever, patho logy of
, 3 7
tox ic sym p tom s of, 3 8
treatm en t of, 3 9
See a lso Ma lar iaQuin in e, adm in ist rat ion of
,
form s of, 5 5 , 62 , 79
in m a lar ia,dosag e of
, 5 7, 79
effects in stom ach, 5 4
hyp oderm ic in j ect ion s, 62by in trav en ousin jection s,
m ethods of adm in ist rat ion of
, 5 5 , 62 , 79
by m outh, 5 5 , 62
p recaut ion s in ,64
p reven t ive doses, 79
p ro longed effects of,67
by rectum , 5 5
sa l ts of, 53
po ison in g in blackwaterfever
,1 09
in quar tan fever, 3 9resistan ce to in kala-azar,1 60
RECTAL en em ata in blackwaterfever
,1 03
Rectum,adm in ist rat ion of quin
in e by , 5 5 , 5 7
Redwater fever , 1 1 2
date of d iscovery , 262
Re lap sin g fever,b lood exam i
n at ion in,1 9 1
cl in ica l course,1 84
com p licat ion s in , 1 86 , 1 88cr isis in
,1 84
d iagn osis of,1 90
d isin fect ion urgen t in ,
en largem en t of l iver and
sp l een in ,1 88
et iology of,1 93
geog raph ical d ist r ibution1 83 , 1 90
herp es in ,1 89
in cubat ion of, 1 83
lD
Re lap sin g feve r,in fect iv i ty of
,
1 99
jaun d ice in,1 88
m o rb id an atom y of,1 92
m o rta l ity of,1 90
overcrowd in g favourab leto
,1 98 , 200
p regn an cy i n,1 89 , 1 90
p reven t ive t reatm en t of,
200
p rogn osis of,1 90
pul se an d tem p erature in ,
1 84 , 1 86
seque lae of,1 89
sweat in g in,1 88
t reatm en t of,1 99
ur in e in,1 88
var iet ies of con t rasted,209
S ee also Tick feverRkin oszboridia , 9 , 1 3
Rkipicefikalus, 26 5Rhodesia
,t rypanosom iasis in
1 3 1 , 1 3 7
Rog ers’s observat ion s on flagel
lata,1 68
Rom anowsky’s stain,1 6
Ro'
n tgen - rays in granuloma, 224
SALVARSAN t reatm en t of syph il is,2 1 4
of yaws, 2 1 9San d-fl ies
,242
Sarcod ina, 3 , 9 , 22 5
Sarcomy l la pen etran s, car r ier ofyaws, 22 1
Sarcosporid ia, 9 , 1 3
Sch i zogon y , 20
Sch i zon ts, 4 , 20
Schigozfikora , 24 1 , 242
Schiz otryzfianum ,1 50
Seamen ,ep idem ic ye l low fever
am on gst,1 29
Serp ig in ous ulcerat ion of g en ita l ia
,222-224
Sett lem en ts, m osqui to extirpat ion in , 246 , 2 50

276
Sub ter t ian m a lar ia l fever,ter
t ian p er iod ici ty in , 4 1-
43
S ee a lsoMa lar iaSudan typ e of O r ien tal so re
,1 77
Sulphur fum igat ion after ye l lowfever
,1 26
Sweat in g in re lap sin g fever , 1 88
Syph i l is, ana l ogy betw een try
pan osom iasis an d,1 44
con gen i ta l,2 1 4
d iagn osis from yaws,
2 1 8,
220
erup t ion s of,2 1 2
ex t ra-gen i ta l,2 1 1
i r regular feve r in,2 1 2
l ess severe in Trop ics, 2 1 2m ercury cream in j ect ion s in
,
2 1 3
Or ien ta l so re m istaken for,
1 8 1
p rophy lax is again st , 2 1 4
sa l varsan t reatm en t of,2 1 4
secon dary an d tert iary , 2 1 2
t reatm en t of,2 1 3
TANKS,hatch in g p lace for eggs
of S teg om y ia ,2 56
Tar tar em et ic in sl eep in g sickn ess
,1 3 4
Telosporid ia , 9
Tert ian,ben ign
,cl in ica l course
of,23
geog raph ica l d ist r ibut iono f
, 3 3
p arasi tes of,1 7 , 23
tem p erature char ts of, 3 4 ,
3 5
fever,m a l ignan t . See Sub
tert ian m a lar ia l feverp er iod ici ty in sub ter t ian m a
lar ia, 4 1
-43
See alsoMa lar iaTetanus com p l icat in g m a lar ia
,
56 , 62
Th i rst in relapsin g fever , 1 87
INDEX
T ick fever , b ron ch i t i s an d p n eum on ia in
,204
car r ied by Orn itkodorusm oubata
,205 , 26 1
d iagn osis of,204
et io logy of,205
h isto r ica l accoun t of,202
post m ortem app earan cesin an im a l s
,205
p ropagat ion of,206
p rophy lax is of,206
resem b lan ce to re lap sin gfeve r
,204
Spirockmta duttom'
causal o rgan ism of
,203
sym p tom s of,203
t ran sm i t ted by Om it/z o
cl ow s m ouba ta,205 , 208
t reatm en t of,206
var iet ies of,
con t rasted,
209
Ticks,1 1 0
,1 1 3 , 1 96 , 208
as hosts, 7
b loodsuck ing g roup s, 264
t ran sm ission of in fect ion by ,208
Tox in s,effects o f in m a laria
, 48
Trezfion ema fiall idum ,262
Trichom onas,263
hom in is,22 5
Trop ica l d iseases, d ist r ibut ionof
,1
fever, 40
sch oo l s, En g l ish,foun d in g
of,263
sp l en om ega ly . S ee Ka la-azarTrop ics, syph i l is l ess severe in ,
2 1 2
Trypan osoma brucei,1 3 8
cruz z’
,1 50
rhodosz’
ense,1 3 8
Trypan osom es,1 67
deve l opm en t of,1 47
date of d iscovery , 262
effect o f arsen ic on,1 42
Glossin a h osts for,1 32

INDEX 277
Trypan osom es in the b lood , 1 3 9
Trypan osom iasis, 1 0
ana logy between syph i l isan d
,1 43
car r ied by Glossina , 260
geograph ica l d ist r ibut ion of,
1 3 1 3 1 3 7
hum an . S ee S leep in g sickn ess
in an im a l s,1 44
p ossib le occur ren ce in In d ia,
1 67
var iet ies of,1 3 8
Typho id fever,ka la-azar simu
lat in g,1 54
ULCER , O r ien ta l so re , 1 76 , 1 82
U lcerat ion,serp ig in ous, of gen i
ta l ia,22 2—224
U l cerat ion s in yaws,
2 1 7
Un ice l lular o rgan ism s,2, 9
Ureth ra,
st ructure of due to
granulom a,223
Ur in e,con d it ion of in re lap sin g
fever,1 88
con ten ts in b lackwater fever,
92-
94 , 96
exam inat ion of in b lackwaterfever , 90haem og l ob in in
,in b lackwater
fever, 94
sp ect roscopy of, 97
Urob i l in in faeces in b lackwaterfever
, 99
VOMITING in b lackwater fever,
9 1 , 1 03 , I 05
in re lapsin g fever , 1 87
WATER-BARRELS , hatch in g p laceof eggs of S teg om yia , 2 54
Wom en,
n at ive,
an d syph i l is2 1 4
YAWS b reeds t rue,220
ch igoe as car r ier,22 1
cl in ica l course of,2 1 6
d iagn osis f rom syph i l is, 2 1 8 ,220
et io l ogy of,2 1 9
geog raph ica l d ist r ibut ion of,
2 1 6
g ranulom ata of,2 1 6—2 1 7
p atho log ica l anatom y of,2 1 8
p rogn osis of,2 1 8
p rophy lax is again st , 22 1
sa l varsan in,2 1 9
seque lae of,2 1 7
t reatm en t of,2 1 9
ul cerat ion s in,2 1 7
Ye l l ow fever,
cl in ica l course,
1 1 6
d iagn osis of,1 1 8
ep idem ics of,
1 24 , 1 27 ,
1 29
geog raph ica l d ist r ibut ion ,
1 1 5 , 1 24 , 1 28
in cubat ion p er iod in ,1 22
m istaken for b lackwaterfever
,1 1 8
m o rb id an atom y of,1 2 1
m o rta l i ty of,1 24 , 1 29
m osqui to t ran sm ission of,
1 22,1 2 5
p athology of,1 20
p reven t ion of sp read of,
2 5 7
p rophy lax is again st , 1 23
severer type, 1 1 6,1 1 8
sym p tom s of,1 1 5
t ran sm ission of,262
t reatm en t of,1 1 9
Yem en ul cer . See O r ien ta l so re
Z YGOTE, 26


JOHN BALE , SON S DAN IELS SON , L t d .
B lackw a t er Fev er (Bi l iousMal ign an t Tert ian Ague) . By A. G . N EWELL,
CM.,L .M.
,Dem y 8 110 ,
127 v i i i . pp . I l lustrated w ithon e P late an d Ch arts in th e text . C loth l im p . Price 5 8 . n et
, postage 4d .
A H a n d b ook o f P ra ct ica l P a ra si t o logy . By D r .MAX BRAUN an d D r .M. LIIHE . Tran slated from th e Germ an . Royal 8y o ,
208 v i i i . pp . C loth ,
lettered . Price 103 . 6d . postage 4d .
P rogr ess R ep or t o n t h e I nv est iga t io n o f P e l lag‘ra . By LOU I S W.
SAMBON ,M.D . C rown 8vo , 126 pp ., p rice 7s. 6d . n et , postage 3d .
S om e Fa ct or s I n fluen cin g H ea l t h in Tr op ica l an d Sub -Trop ica l
C oun t r ie s . By T. GERALD GARRY,M.D .
,M.Ch .
,R .U .I . C rown
8 vo , cloth ,lettered . P rice 28 . 6d . n et , postage 3d .
F ie ld S er v ice N o tes for ByMajo r T. H . GOODWI N ,
C rown 8vo ,cloth , 94 pp . P rice 2s. 6d . n et , postage 3d .
Th e E t io logy o f E n d em ic Go it r e . By ROBERTMCCARRI SON ,M.D . ,Major I .M.S . Being the Mi l roy Lectures for 1 913 .
P rice 103 . 6d . n et , postage 4d .
Book s dea l in g w ith Tuberculosis , &c .
A C l in ica l S y st em o f Tub erculo sis. By D r . B . BANDELI ER ,Med ical
D i rector to th e San atorium Schwarz waldh eim at Sch om berg, n earWi ldbad ,an d
Dr . ROEPKE ,Med ical D i rector to th e San atorium for Rai lway Workers at
Stad twald in Melsungen ,n ear Cassel . Describ ing all form s of th e D iseases.
Tran slated from th e Secon d Germ an Ed it ion by G . B . HUNT,M.D . , B .S .
, latePhysician to th e Scarborough Hosp ital . Royal 8vo , about 5 30pp . an d 6 colouredp lates. P rice 21 s. n et , postage 7d .
Tub er cul in in D iagn osis a n d Tr ea tm en t . By Drs. BANDELIER an d
ROEPKE . Tran slated from th e Seven th Germ an Ed it ion byW. B . CERI STOPHE RSON .
Royal 8vo, 1 5 s. n et , postage 7d .
An nua l R ep or t o f t h e R esul t s o f Tub erculosis R e search , 1 9 1 1 .
By Dr . F . KOHLER , Head Ph ysician to th e Ho lsterh ausen San atorium . F romth e C l in ical Year Book , ed ited by Dr . NAUMANN , Wirkl . Geh . Ob .
-Reg .-Rat un d
Min isteriald i rektor , an d Dr . M. KIR CHNER , Wirkl . Geh . Oh .-Med .
-Rat un dMin isteriald i rektor an d Professor . Tran slated by RONAL D E . S . KROHN ,M.D .
Price 7 8 . 6d . n et, postage 4d .
S ah l i’
s Tub ercul in Trea tm en t . By Dr . HERMANN SAHLI . I n clud inga d iscussion on th e Nature an d Act ion of Tuberculin an d of Immun ity to
Tuberculosis. Tran slated from th e th i rd Germ an ed i t ion by WI LFRED B .
CHRI STOPHERSON ,w ith an I n troductory N ote by EGBERTMORLAND
,M.B . , an dM.D .Bern e . Dem y 8v o , cloth . P rice 7 8 . 6d . n et , postage 4d
Th e Op h t h a lm ic a n d Cut an eous D iagn osis o f Tub erculo sis(Cutan eous an d Con jun ct ival Tubercul in React ion s accord in g to v . PIRQUET ANDWOLFE-E I SNER) . By Dr . WOLFF-E I SNER
,Berl in . W ith I n troductory Note by
C . THEODORE WILLIAMS ,M.D . Royal 8v o , cloth , 7 8 . 6d . n et , postage 4d .
Tub er cul in Ch a r t N o . 2 1 . Arran ged for seven days, start ing any day,an d records ful ly Local , Gen eral an d Focal Sym ptom s
, also Dose an d Tim e Of
I n ject ion . Price, 60Cop ies, 3s. ; 100, 5 s. ; 250, 10s. 6d . 500, 20s.
S an a t or ium Ch a r t N o . 1 9 . Th is Chart has been design ed by the
Superin ten den t of a large San atorium in order that th e part iculars of each
case m ay be kept un iform ly from day to day for th ree m on th s, an d be av ai lab leat an y m om en t for referen ce. P er dozen ,
1 s. 3d . ; per 100, 7 8 . 6d . ; per 7os.
Boun d In books of25 , w i th paper w rapper , 2s. 3d . each . Th ese are boun d at th e
h ead an d Open perfect ly flat to faci l itate use .
Co n sum p t ion : I t s P r ev en t io n an d Trea tm en t . By E .W. DIVER,M.D .
Crown 8vo . ,1 40pp . , w i th 6 I l lustrat ion s, cloth ,
gi lt lettered . Secon d Ed i t ion .
P r ice 28 . 6d . n et , postage 3d .
Surgery o f t h e Lun g. By C. GARRE, P rofessor of Surgery at the
U n iversity of Bon n ,an d H . QUINOKE ,
form erly Professor ofMed icin e at th eUn iversi ty of Kie l . Secon d Ed it ion , w ith 1 1 4 coloured an d other I l lustrat ion s,

‘ JOHN BALE , SON S DAN I ELS SON , Lt d .
D isturb a n ces o f t h e V isua l Fun ct ion s . By PROF . W. LOHMAN N , Ch iefPhysician to th e Un iversity Eye C l inic,Mun ich . Tran slated by ANGUSMONAB ,M.B . ,
Royal 8v o , 1 86 ! v i i i . pp . , w ith 39 i llustrat ion s in th e text ,som e in colours, cloth . P rice 1 5 s. n et , postage 3d.
C l in ica l Surgica l D iagn osis . For S tud en t s a n d P r a ct it ion ers.
By F . DE QUERVAIN , P rofessor of Surgery an d D i rector of the Surg ical C l in ic at
th e Un iversity of Basle . Tran slated from th e Fourth E d i t ion by J . SNOWMAN ,M.D . Royal 8 vo ,about 800 pp . , w ith 5 10 I l lustra t ion s an d 4 P lates. P rice
525 3 . n et , postage, I n lan d 7d . ; Abroad 23 .
E p id em ic I n fa n t i le P a ra ly sis (HE I NE -MED I N D I SEASE ) . By P rofessorPAUL H . ROMER . Tran slated by H . R IDLEY PRENTI CE ,
M.B . ,
Royal 8v o , cloch , w i th 57 I l lustrat ion s. P rice 7s. 6d . n et, postage 5 d .
O r t h opm d ics in Med ica l P ra ct ice . By ADOLF LOREN Z an d D r .ALFRED SAXL . Auth orised Tran slat ion from th e Germ an by L . C . PEELR ITCHI E
, Ch .M.,M.D . ,
Dem y 8 vo , cloth,lettered , about 300pp .
, w ith39 I l lustrat ion s. Price 7s. 6d . n et , postage 5 d .
Th om p son’s Com p en d ium o f t h e P h arm aco poeia s Fo rm ular ies .
A Han dy Pocket Book of Referen ce forMed ica l Pract it ion ers and Ph arm acists.
Fourth Ed it ion . Revised , En larged an d Part ly Rewri tten . Pp . 3 60 v i .
Boun d in b lue leather . Price 5 8 . n et , postage 3d .
S tud ies on t h e I n fluen ce o f Th erm a l E n v ironmen t o n t h eC ircula t ion a n d t h e B o d y
-H ea t . By EDGAR R . LYTH,M.B . ,M.B .CS
Dem y 8v o, cloth ,let tered
, w i th 1 5 Ch arts. P rice 28 . 6d . n et , postage 3d .
Th e Hun t er ian O ra t io n . DE LI VERED AT TH E ROYAL COLLEGE OF
SURGEONS , 1 91 3 . By Sir R IOKMAN J . GODLEE,Bart .
, B .A.,M.S . ,M.D .Dub . Price 2s. 6d . n et , postage 3d .
On Con juga l H ap p in ess. E x p er ien ces , R efl ect ion s , a n d Ad v iceo f a Med ica l Ma n . By Dr . L . LOEWENFELD ,Mun ich . Tran slated fromth e Th i rd Germ an Ed it ion by RONALD E . S . KROHN , M.D .Lon d . Dem y 8v o ,
cloth , 7s. 6d . n et, postage 4d .
H ow t o Cut t h e D rug Bi l l . By A. H . HART ,M.D . Th i rd Ed it ion .
Crown 8v o , xiv . 5 7 pp . , cloth , lettered . P rice 28 . 6d . n et, postage 3d .
S om e Successful P rescr ip t ion s. By A. H . HART, M.D . 1 s. n et , post
age 1 3d .
A H an d b ook on Surgery , in t en ded fo r D en ta l an d Jun iorMed ica l S tud en t s . By ARTHUR S . UNDERWOOD
,late
Exam in er Royal Co l lege of Surgeon s Of E nglan d , an d BAYFORD UNDERWOOD ,Crown 8vo , cloth , let tered . Price 3 3 . 6d . n et ,
postage 3d .
S tud ies in Cl in ica l Med icin e . By C. O . HAWTHORNE ,M.D . Being a
series of Essays an d Lectures reprin ted from various sources. Dem y 8vo , cloth ,
let tered . Price 6s. n et , postage 4d .
Th e I n t e rn a l S ecr et‘ory O rgan s : Th e ir P h y sio logy an d
P a t h o logy . By P rofessor Dr . ARTUR B IEDL , V ien n a . W ith an I n troductoryPreface by LEONARD W ILL IAMS
,M.D . , Physician to th e Fren ch
Hosp ital ; Assistan t Physician to th eMetropol itan Hosp ital . Tran slated fromth e Germ an . Royal 8v o , cloth , lettered . P rice 21 s. n et
, postage 6d .
Th eory an d P ract ice o f Th y r o id Th e rap y . By HERBERT EWANWALLER ,
Being som e experien ces of th e resul ts of Thy roidm ed icat ion
,w ith deduct ion s con cern ing th e in fluen ce of Thy ro id secret ion in
h ealth an d d isease, an d certain effects of d rugs an d v arious ci rcum stan ces uponThy roid secret ion . A book for Gen eral Pract it ion ers. Dem y 8y o , cloth ,
gil tlettered . Price 5 s. n et , postage 3d .
Air , L igh t , an d Sun Ba t h s in t h e Trea tm en t o f Ch r on ic Com
p la in t s. By Dr . A.MONTEUUI S . Tran slated from th e Fren ch by FRED ROTHWELL . Crown 8v o , cloth ,
gi lt lettered . Price 2s. n et, postage 3d .
L ecture s on B io logy . By D r . CURT THES ING . Tran slated from the Secon d
E d it ion by W. R . BOELTER . Wi th the original coloured an d other i l lustrat ion s.
Med ium 8vo , 334 Vi i i . pp . 108 . 6d . postage 5d .
Mod ern Surgica l Tech n ique in i t s R e la t ion t o Op era t ion s an dW oun d Tr ea t m e n t . By C . YELVERTON PEARSON ,M.D . ,M.Ch
L aboratory . B y J . w . S . b ECCOMBB , C ap tain
Price 3 8 . 6d . ; m oun ted on l in en , 4s. 6d . ; m oun ted on . l in en w ithrol lers, 5 8 . 6d .
Th e Cam p a ign Aga in st Microbes . By ETIENNE BURNET,M.D . , of thePasteur I n st itute, Paris. Tran slated from the Fren ch by E . E . AUSTEN
,F .Z .S .
Dem y 8vo, cloth , lettered , 5 8 . n et, postage 4d .
A H ist ory o f t h e R ead in g P a t h o logica l S ociet y . By JAMIESONB . HURRY ,M.A. ,
P residen t of the Society . Dem y 8y o , 185 pp .
C loth boards. Gilt lettering an d edges, w i th illustrat ion s. Price 7s. 6d . n et ,
postage 5 d .
Th e An a t om y an d Top ograp h y o f t h e Accessory Air S inuses of
t h e N ose in Ch ild h ood . By Dr . A. ONODI , Director '
of the Un iversityC l in ic for D iseases of th e Th roat an d Nose in Budapest . An At las con tain ing102 specim en s rep roduced in n atural si ze from ph otograph s, w ith a p reface byDr . W . WALDEYER , Director of th e An atom ical I n stitute Of th e Un iversity of
Berl in . Im perial 8vo . Price 21s. n et , postage 8d .
R e la t ion s of t h e Lach rym a l O rga n s t o t h e N ose an d N a sa l
Accessory S inuses. By P rof. Dr . ONODI . An English Tran slat ion byDr . DANMCKE NZ IE . With 45 p lates. P rice 103 . n et , postage 5 d .
At las o f K i l l ia n’s Tr ach eo -B ro n ch oscop y . By Dr. MANN . Tran s
lated by THOMAS GUTHRI E , M.E . ,Liverpoo l . 1 5 Coloured P lates
rep resen t ing Path ological P reparation s from cases exam in ed during l ife bym ean s of Trach eo-Bron choscopy . Demy fol io . Pr ice 22s. n et , postage 8d .
A Lecture onMea n s for t h e P ro lon ga t ion o f L ife . By Sir HERMANNWEBER , M.D . ,
Th i rd Ed i t ion . Revised an d en larged . Dem y 8vo,222 pp .
, cloth ,gi lt lettered . Price 4s. 6d . n et , postage 4d .
Th e Ra t P r ob lem . ByW . R . BOELTER . 1 70 pp. ,fcap. 4to , price 28 . 6d . net ,
postage 4d . W ith num erous in terest in g i llust rat ion s.
H ouseh o ld P est s an d H ouseh o l d R em ed ies. By the sam e Author .Fcap . 4to. Price 2s. 6d . n et , postage 3d . W i th num erous il lustrat ion s.
P a t en t Food s a n d Pa t en t Med icin es. By ROBERT HUTCHI SON ,M.D . ,
Two Lectures. Secon d Ed it ion . C rown 8vo , 48 pp .,l s. n et , postage
1 d .
On Ga st roscop y . By WI LLIAM H I LL , E .sc. , Surgeon for
D iseases of th e Th roat , Nose an d Ear, St . Mary ’
s Hosp ital , Lon don . W ith a
descript ion of a N ew, Easy an d E ffi cien tMeth od of (E soph ago-Gastroscopy ,com b in ing D i rect an d I n d i rect V ision ; an d a P lea for its Em p loym en t byGastric Experts. W ith 47 I llustrat ion s. Dem y 8vo, cloth . Price 3s. 6d . n et ,
postage 3d .
Med ica l Gym n a st ics an d Massage for t h e Treatm en t o f
D isease , D efo rm itg
a n d I n jury . By FREDK . F . MIDDLEWEEK,
irector ofMech an a Thera eutics an d Massage, West
En d Hosp ital for Nervous D iseases. With an In tro uction by Dr . J. ARVED SON ,
Stockholm . C rown 8v o , cloth ,28 . 6d . , postage 3d .
Ad en o id Grow t h s o f t h e N aso -P h a ry n x . By G . A. GARRY SIMP SON ,
Secon d Ed it ion . C rown 8v o , 49 pp . Price 3s. 6d . n et , postage 2d .
N ot es a n d Th ough t s from P ract ice . By W. J . TYSON ,M.D .
,
Hon . Physician , V ictoria Hosp ital , Folkeston e. C rown 8vo , papercover
,28 . n et ; cloth , 28 . 6d . n et , postage 2d .
Syn op t ic Ch ar t of Card iac E x am in a t ion . Arranged by JOHN D .
COMRI E ,M.A., B .Sc. , Assistan t Pathologist , lately C l in ical Tutor ,
Royal I n firm ary of Ed in burgh . Con sists of Cardboard Sheath stam ped w i th an
out l in e of th e Chest an d Heart , in side of wh ich there is a sl ide p rin ted w ith th e
n am es of th e various d iseaseswh ich affect th e h eart , togeth er w ith th ei r physicalsign s. By th e simp le m an ipulat ion of two tapes the d ifferen t d iseases are m ade
to Show in a space at on e side of th e Ch art an d as each d isease appears itsv arious sign s autom at ical ly com e in to p lace at the O on inge correspon d ing tothe areas of auscultat ion . P rice 28 . 6d . n et , postage 4T.
)
B rea t h in g E x ercises. For use after Rem oval of Postnasal GrowthsAden o ids) . By DUNCAN MATHESON MACKAY ,M.D . , Sen ior C l in ical Assistan t ,08 ital for D iseases of th e Th roat , Go lden Square. Adapted from
the epor t of th e I n terdepartm en tal Comm ittee on theModel Course Of PhysicalExercises, 1904 (by perm ission of th e Con t ro l ler Of HisMajesty ’
s Stat ion eryOfiice) , an d rearranged w ith m od ificat ion s an d add i t ion s. Dem y 8vo, 4 pp .
S ingle cop ies 1 d . each ; post free, l td . Per doz . 1/ post free, Per 100
83 -91 , GREAT TITCHFIELD STREET, LONDON, W.