Tribally Based Suicide Prevention Programs: A Review of Current Approaches
24
7ULEDOO\ %DVHG 6XLFLGH 3UHYHQWLRQ 3URJUDPV $ 5HYLHZ RI &XUUHQW $SSURDFKHV Puneet Chawla Sahota, Sarah Kastelic Wicazo Sa Review, Volume 29, Number 1, Spring 2014, pp. 77-99 (Article) 3XEOLVKHG E\ 8QLYHUVLW\ RI 0LQQHVRWD 3UHVV DOI: 10.1353/wic.2014.0000 For additional information about this article Access provided by University Of Pennsylvania (2 Jan 2015 20:54 GMT) http://muse.jhu.edu/journals/wic/summary/v029/29.1.sahota.html
Transcript of Tribally Based Suicide Prevention Programs: A Review of Current Approaches

Tr b ll B d d Pr v nt n Pr r : R vf rr nt ppr h
Puneet Chawla Sahota, Sarah Kastelic
Wicazo Sa Review, Volume 29, Number 1, Spring 2014, pp. 77-99 (Article)
P bl h d b n v r t f nn t PrDOI: 10.1353/wic.2014.0000
For additional information about this article
Access provided by University Of Pennsylvania (2 Jan 2015 20:54 GMT)
http://muse.jhu.edu/journals/wic/summary/v029/29.1.sahota.html
77
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
I n t R o D u C t I o n
Suicide is a major health challenge in American Indian/Alaska Native (AI/AN) communities, particularly among the youth. In 2004, suicide was the second leading cause of death for AI/ANs of all age groups. Among individuals between ten and fourteen years old, 13.5% of deaths were from suicide, which is nearly twice the national rate of 7.2%.1 Many factors contribute to the high prevalence of suicide in AI/AN communities, including individual factors (mental illness, sub-stance abuse, feelings of hopelessness or isolation, impulsive behavior, and a history of violence, substance abuse, or family history of mental illness) and group factors (historical trauma, poverty, unemployment, and geographic isolation).2
Actions are needed at both the federal and tribal levels to prevent suicide, and some initial important steps have been taken. To address the challenges of youth suicide in Indian Country, a bill titled 7th Generation Promise: Indian Youth Suicide Prevention Act of 2009 was incorporated into health care reform legislation enacted in March 2010 (Patient Protection and Affordable Care Act, 2010).3 This legislation authorizes two demon-stration projects aimed at preventing youth suicide in AI/AN commu-nities. To assist tribes in preventing youth suicide, the Substance Abuse and Mental Health Services Administration (SAMHSA) within the U.S. Department of Health and Human Services (DHHS) published
tribally Based suicide Prevention Programsa review of Current approaches
P u n e e t C h a w l a S a h o t a a n d S a r a h K a s t e l i c

78
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
a detailed guide in 2010.4 The guide, To Live to See the Great Day That Dawns: Preventing Suicide by American Indian and Alaska Native Youth and Young Adults, is an excellent resource.
Below, we present fifteen policy and practice recommendations for further supporting tribally based suicide prevention efforts. By “trib-ally based” we mean efforts that are tailored to the unique contexts of in-dividual tribes and Native communities, which may include adaptations of mainstream programs or newly designed local suicide prevention programs, such as those based on spiritual or cultural traditions. The aim of this project was to review the range of approaches being used in tribally based suicide prevention programs and make recommendations about how policy makers, tribal communities, health care providers, and other service providers might better support locally tailored efforts to prevent suicide. As we describe in the next section, our goal in this paper was not to capture an exhaustive list of strategies being used in tribally based suicide prevention programs. Rather, we reviewed exist-ing literature and consulted a select group of key informants in order to broadly describe the landscape— the commonalities and distinctive elements of these strategies— at a level of detail necessary to identify practice and policy change recommendations for a tribal leader and program staff audience. While these recommendations are targeted to supporting suicide prevention efforts in AI/AN communities, we also believe they have broader relevance for other community- based suicide prevention programs.
P A P e R D e v e L o P M e n t A n D
R e s e A R C h M e t h o D s
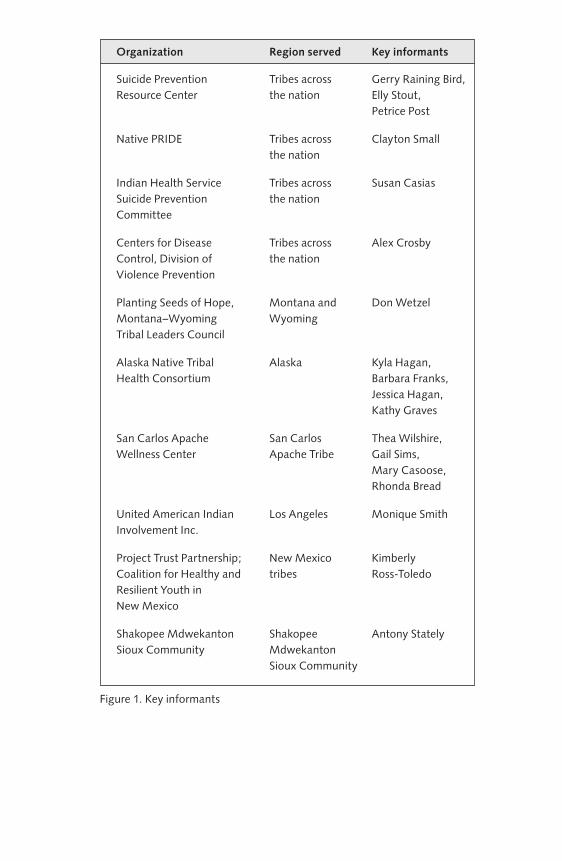
We developed this paper in collaboration with expert, key informant interviewees. For a list of the organizations and individuals who were interviewed or consulted by e- mail, please see Figure 1. This paper was originally intended to be a white paper for tribal leaders, not an aca-demic research paper. Our initial goal was to write a paper for tribal communities that would review existing academic literature on suicide prevention and develop resulting recommendations about best practices and policies specifically for tribal governments. However, the initial lit-erature review and conversations with experts in the field revealed that many successful tribal suicide prevention programs were not included in published academic articles, and that there was a need for publications about culturally appropriate tribal strategies. For this reason, we sought to review the landscape of tribally based suicide prevention programs. We conducted this broad review by reading published academic litera-ture and “gray” literature (i.e., policy reports, white papers, program brochures, Web sites) as well as interviewing and corresponding with key informants working in the field of tribal suicide prevention.

79
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
In reflecting on key informants’ comments, we felt that there was a great deal of important information shared which was not already available in the academic literature. We also felt that this information would be useful to a broad audience that would include not only tribal leaders but also mental health care providers, policy makers, commu-nity advocates, researchers, and other interested stakeholders. For this reason, we decided to submit our paper for publication in an academic journal. At that point in the work, we wrote to the key informants and shared with them our intention to publish the paper. One key infor-mant asked not to be named or quoted in the study due to her organi-zation’s policy on publishing. All other key informants reviewed and approved their quotes, as noted below. Because our original goal was simply to conduct a literature review, we did not seek approval from an Institutional Review Board for this study. Thus, this article is a review paper that discusses specific tribally based approaches to suicide pre-vention documented in the literature and shared with us by key infor-mants working in the field.
Our research procedure was as follows: First, we reviewed the published academic literature and gray literature in tribal suicide pre-vention. Second, we developed a set of general questions (see below) for seeking input about suicide prevention in Indian Country. We then distributed this call for comments broadly to e- mail Listservs of diverse stakeholders, including tribal leaders, researchers, mental health pro-fessionals, and federal agency staff working with tribal communities. We also solicited feedback at meetings of two advisory councils of diverse tribal leaders: the AI/AN Health Research Advisory Council to DHHS and the Suicide Prevention Task Force of the National Congress of American Indians. In addition, input was sought from the Indian Health Service (IHS) Suicide Prevention Committee. Finally, we sought feedback from specific types of stakeholders that were not represented in the initial response to the call for comments (e.g., an urban Indian community, IHS behavioral health staff). We then fol-lowed up with each of the commenters who provided detailed feed-back, requesting telephone interviews and complementary written ma-terials (e.g., brochures, PowerPoint presentations, news articles about their programs). We asked key informants’ permission to interview them by telephone and to take notes on a laptop during the interviews. Each key informant was provided with the option to be identified or remain anonymous in any resulting writings.
Our interview procedure was based on the “responsive interview-ing” method developed by Herbert and Irene Rubin.5 In responsive in-terviewing, the interviewee is treated as a “conversational partner”6 with unique experiences, so new interview questions are written for each interviewee. Following this principle, specific interview questions were formulated for the interviewees based on early correspondence with
Organization Region served Key informants
Suicide prevention Tribes across gerry Raining Bird, Resource Center the nation Elly Stout, petrice post
native pRIDE Tribes across Clayton Small the nation
Indian Health Service Tribes across Susan Casias Suicide prevention the nation Committee
Centers for Disease Tribes across Alex Crosby Control, Division of the nation Violence prevention
planting Seeds of Hope, Montana and Don Wetzel Montana–Wyoming Wyoming Tribal Leaders Council
Alaska native Tribal Alaska Kyla Hagan, Health Consortium Barbara Franks, Jessica Hagan, Kathy graves
San Carlos Apache San Carlos Thea Wilshire, Wellness Center Apache Tribe gail Sims, Mary Casoose, Rhonda Bread
United American Indian Los Angeles Monique Smith Involvement Inc.
project Trust partnership; new Mexico Kimberly Coalition for Healthy and tribes Ross- Toledo Resilient Youth in new Mexico
Shakopee Mdwekanton Shakopee Antony Stately Sioux Community Mdwekanton Sioux Community
Figure 1. Key informants

81
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
them and the suicide prevention programs with which they worked. Questions that were commonly asked included:
1. Could you please describe your suicide prevention program?
2. What lessons have you learned about successful approaches to suicide prevention?
3. Do you have any data about the efficacy of your program?
4. What do you think is the best way to evaluate suicide prevention programs in tribal communities?
5. What policy and practice recommendations do you have related to suicide prevention in Indian Country?
Question 4 is mainly addressed in a previously published com-plementary paper on evaluating tribally based suicide prevention pro-grams. Responses to the other questions were used in the development of this paper. In applying Rubin and Rubin’s concept of a “conversational partner,” we concluded that the relationship between the interviewer and interviewee should be one of trust and reciprocity. We believe that the interviewer and interviewee are equal parties who cocreate the re-sults of the interview. For this reason, we felt that interviewees should be able to review and edit our interpretations of their perspectives. Rubin and Rubin also suggest that interviewees be provided with the opportunity to edit their quotes or to review a researcher’s writings in an early stage.7 They argue that interviewee review helps to ensure the accuracy and thoroughness of research reports. This has been our ex-perience as well. We view interviewees’ feedback and editing as a way of validating our research results because the interviewees are experts on the programs with which they work. It is our impression that using the “responsive interviewing” method increased our research credi-bility in Indian Country.
During each interview, Puneet Chawla Sahota took detailed notes on a laptop while the key informants talked. Those notes were then coded for key themes.8 According to LeCompte and Schensul, coding is defined as follows:
At the most general level, coding simply means organizing data in terms of a framework that [researchers] can use to support the results and conclusions they reach at the end of their study. At a more specific level, coding can mean actually reading through interviews . . . and assigning to sentences or paragraphs of text . . . codes representing concepts, categories, or themes.9

82
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
In this project, both interview notes and correspondence with key in-formants were coded. Specific quotes from key informants were then grouped together under common themes which emerged from the cod-ing process. Those themes were used to structure this paper. Themes related to evaluating tribally based suicide prevention programs are de-scribed in a complementary paper.10
All key informants were sent the first draft of this paper with sections highlighted that were taken from their comments and/or pro-gram materials. They were offered the opportunity to review and edit their quotes and any text about their programs. This type of key in-formant review was important because written program materials may not always be consistent with actual program implementation. We had follow- up phone conversations and e- mail exchanges with key infor-mants when necessary to negotiate revised text. Quotes from the key informants are interspersed with information from the literature review throughout the sections below. Key informants’ quotes are also refer-enced in the endnotes.
The process used in the development of this paper reflects our broader belief that both research and policy development should be tribally driven. In our work, we seek to support AI/AN communities in developing a proactive, data- driven policy agenda, and we conduct trib-ally driven policy research ourselves. As such, we hold that Indigenous knowledge and approaches to research are as valuable as academic or scientific research studies. Because we respect and value the knowledge of AI/AN people, we believe our interviewees should be able to influ-ence how their knowledge is portrayed in our writings. We also have found that key informants are more comfortable sharing their knowl-edge when they are assured they will be able to review early publica-tion drafts. As a result, the information we are able to obtain is more accurate and validated by the informant review process. The process of discussing our initial writings with key informants sometimes results in clarification of their thoughts and new insights, both for us and for them. During the review of previous papers, our key informants have com-mented that they gained new perspectives on their own work by reading and reflecting on our portrayals of it. Exchanges with our key informants have also helped us build ongoing, trusting relationships with them that have sometimes led to other collaborations beyond our papers.
All individuals contacted agreed to be interviewed, and many of them shared written materials with us pertaining to their programs. For a list of the key informants and their organizational affiliations, see Figure 1. Eighteen informants’ comments were included in this paper. Twenty key informants were consulted in interviews or by e- mail for our project, but not all informants’ comments were pertinent to this paper. Other informants’ comments are included in a complementary paper about evaluating tribally based prevention programs. Given the

83
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
relatively small number of key informants, our results are not quantifi-able or generalizable throughout Indian Country. Rather, we present a snapshot of some current, tribally based approaches to suicide preven-tion. Our review of program strategies is not exhaustive, and we did not attempt to include all possible strategies in this paper.
R e s u L t s : P o L I C y A n D P R A C t I C e
R e C o M M e n D A t I o n s
Given the diverse cultures of tribal nations, as well as the differing contributors to suicide in various communities, suicide prevention pro-grams are likely to be most effective when they address local contexts. While strategies may differ from community to community, there are some commonalities. Clearly identifying the common elements as well as distinct aspects of tribally based strategies serves tribal communities seeking to develop and/or increase the effectiveness of their own strate-gies. This review of tribally based suicide prevention programs might also inform future research questions and data collection for program evaluation. Finally, policy makers and funders (both public and private) might benefit from a survey of the field such as that presented here. A more comprehensive survey could be undertaken in the future to parse out factors with the greatest impact within and across programs.
Below, we provide a number of policy and practice recommenda-tions for supporting tribally based suicide prevention programs. These recommendations are taken from the interviews and review of the litera-ture. Each recommendation is supported by detailed explanations of cur-rent approaches being used in tribally based suicide prevention programs. We have organized the recommendations by topic. We begin with those that could apply at both the federal and tribal levels, and then delineate some specific suggestions for tribes and other AI/AN communities.
Supporting Tribal Development of Suicide Prevention Programs
1. increase funding and technical support for tribally based suicide prevention programs, including those based on local cultural and spiri-tual practices. Locally developed programs are promising precisely be-cause they are tailored to the unique needs of each community. Unlike suicide prevention programs developed for use in the general U.S. popu-lation, culturally based programs emphasize the strengths of AI/AN communities. Dr. Clayton Small, who developed the suicide prevention program Native HOPE (Helping Our People Endure), said:
Most of the mainstream suicide prevention programs I’m aware of focus on risk factors and protective factors. This

84
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
is important information, but if you weren’t depressed at the beginning of the [mainstream suicide prevention] training, you are at the end. These programs don’t focus on strengths and culture, just problems. To be success-ful, you have to focus on how Native Americans can use strengths to overcome barriers. . . . Our curriculum [Native HOPE] does that. Cultural activities are incor-porated throughout the process. You’re proud to be an Indian in the program. You won’t find that in mainstream programs.11
Native HOPE is a peer- counseling curriculum for Native youth focused on suicide prevention and related risk factors. Dr. Small also commented that for tribes to be able to develop their own programs based in culture and strengths, they will require increased funding. Tribes face myriad health concerns and have limited resources, but yet are increasingly seeking to take over the delivery of their own health care. The nation- to- nation relationship between tribes and the United States includes a federal trust responsibility to provide adequate re-sources for health care in AI/AN communities. Such funding should in-clude resources for the local development of tribal plans and programs for suicide prevention.
In addition to funding for supporting program development, tribes also need resources for evaluation. Program evaluation is important for establishing effective approaches in suicide prevention programs that are specific to Native communities, and for collecting data that can be used in advocacy and applications for program funding. In a comple-mentary paper, we have provided a detailed discussion of strategies for evaluating tribally based suicide prevention programs.12 Here, we simply note that increased funding for evaluation is critical and that AI/AN communities need technical assistance, training, and staff sup-port to increase their capacity for evaluating their own suicide preven-tion programs. Federal agencies can play an important role in provid-ing such trainings and technical assistance.
2. Provide flexible budget line items for supporting cultural activities and norms. New tribal suicide prevention programs need to become integrated in and build trust with the community. One strategy for doing so is to participate in cultural activities and honor tribal mem-bers in traditional ways. Don Wetzel Jr., the former project director for Planting Seeds of Hope, a suicide prevention program at the Montana–Wyoming Tribal Leaders Council, negotiated a small amount of flexible funding within a grant for these types of activities.13 His project used this funding to help support travel to access behavioral health services

85
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
for the family of an individual who attempted suicide, as well as to buy gifts for traditional healers. He commented that a small flexible budget item, on the order of $2,000, would help tribal suicide prevention pro-grams become established in their communities. It can be very helpful for both federal and private funders to provide support for community norms such as buying food for events or supporting cultural traditions such as gift- giving.
3. increase funding for areas with greater need. Communities with a higher prevalence of suicide should proportionally receive greater funding in any increases of resources beyond what is currently pro-vided for suicide prevention programs. Rather than basing funding formulas on population size alone, we recommend placing weight on the rates of suicide attempts/completions in determining resource al-location. Kimberly Ross- Toledo, executive director of the Coalition for Healthy and Resilient Youth in New Mexico, pointed out that at the state level, funding is often allocated by population size, so rural com-munities with higher rates of suicide do not receive adequate resources in relation to their need.14 In New Mexico, these rural communities in-clude substantial American Indian populations. Ideally, these commu-nities would receive proportionally greater funding for suicide preven-tion programs because of their high rates of suicide.
Increase Collaboration
4. increase collaboration and coordination among federal agencies and tribes. Several federal agencies are engaged in suicide prevention efforts in Indian Country, including IHS, SAMHSA, the Centers for Disease Control and Prevention (CDC), the Bureau of Indian Education (BIE), and the Bureau of Indian Affairs (BIA). It has been a challenge for many tribes to determine which resources are available from which federal agencies and how to access them. A common theme in our in-terviews was that federal agencies should coordinate more with one an-other in working with tribes to improve efforts in education, outreach, training, and data collection. Such coordination efforts have begun, as is evident in the recent IHS/BIA/BIE/SAMHSA Action Summit for Suicide Prevention, which was held August 1–4, 2011, in Scottsdale, Arizona. For broader federal agency collaboration efforts, the White House Domestic Policy Council, which is charged with coordinat-ing various federal policies and programs, could perhaps have a role. Dr. Monique Smith, former administrative clinical director of United American Indian Involvement Inc. in Los Angeles, said that collabora-tions between federal agencies could include joint yearly trainings for tribes.15 These trainings would provide tribes with the latest federal

86
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
data on suicide prevalence and incidence in Indian Country, including among subgroups, such as veterans. Updates could also be provided on the specific activities of federal agencies related to suicide prevention. Finally, technical assistance and tools for preventing suicide in their local communities could also be shared with tribes. The recent Action Summit for Suicide Prevention, which was jointly sponsored by several federal agencies, might serve as a foundation for such future trainings.
Federal agencies should also collaborate in data collection related to suicide prevention in AI/AN communities, as was recommended by a round table of experts convened by the Suicide Prevention Action Network16 and our interviewees. For example, the types of data collected by the IHS, the CDC, and the Veteran’s Administration are different, and if tribes were made aware of those different data sources, they might be able to better use that information for education and advocacy.17 Dr. Smith noted that suicide- related data are sensitive for individual tribes and that aggregate data by region or even for Indian Country overall would be useful for federal agencies, including the BIA and BIE, to share with AI/AN communities and health care providers.
To help facilitate the collection of data on suicide in Indian Country, IHS has encouraged AI/AN communities who have access to the IHS Resource and Patient Management System (RPMS) to use the suicide reporting form application in that program.18 RPMS is the health information system used by IHS and is composed of more than sixty applications, including a behavioral health system, which con-tains the suicide reporting form.19 The suicide reporting form is used by IHS to collect data about suicide attempts and completions. The availability of the RPMS suicide surveillance tool promotes a standard-ized and systematic documentation of suicide events. Suicide data can be analyzed locally through RPMS reports and exported nationally so that IHS can develop a better understanding of this important public health problem.
The suicide reporting form includes a variety of variables, and access to the resulting data is limited to IHS and tribal health staff.20 Individual health care facilities regularly export these data to the IHS Office of Information Technology, National Programs in Albuquerque, New Mexico. Exported data does not include patient identifiers, and tribes can choose whether or not to export their RPMS behavioral health system data. Not all IHS supported health care facilities use the suicide reporting form, and IHS is attempting to increase awareness of it.21 Tribally run health care programs that do not use RPMS currently do not have access to the suicide reporting form.
Thus, collaboration among federal agencies and with tribes could result in a number of benefits: more accurate and timely data on sui-cide in Indian Country; better access to those data for tribes; more co-ordinated education and outreach to tribes; and more effective use of

87
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
limited federal resources through coordination of suicide prevention programs by different agencies.
5. increase collaboration among tribes, states, and counties for devel-oping services and collecting data. Tribes may benefit from collaborat-ing with the states in which they are located. These collaborations can help tribes and states make the best use of limited resources. For example, the San Carlos Apache Tribe is located within several counties and mul-tiple state behavioral health service areas, which affects their ability to respond to suicide crises, according to Dr. Thea Wilshire, clinical co-ordinator of the San Carlos Apache Wellness Center.22 To deal with this challenge, she and other tribal behavioral health staff have worked with all the relevant counties to create a cross- county crisis plan so that indi-viduals at risk for suicide receive the services they need. The tribe has also collaborated with the Arizona governor’s office, state department of behavioral services, and other tribes on coordinating services. Finally, tribal behavioral health staff have provided cultural sensitivity training for off- reservation crisis response teams to help them understand how to best help an Apache individual with suicidal ideation.23
Data collection is another important area in which states and tribes could productively collaborate. For example, both states and tribes commonly rely on death certificates in their data collection on suicide and other forms of violent death. AI/AN individuals have been racially misclassified on death certificates more frequently than have members of other racial groups, which is a significant issue that has been identified by the National Center for Health Statistics.24 Coordination between states and tribes in data collection may help to improve this problem.25 In addition, tribes may need to share data with state public health departments in some cases if they wish to have that informa-tion included in national databases. For example, the CDC coordinates a national surveillance system, the National Violent Death Reporting System, which collects information on homicides, suicides, and other firearm injuries. There are currently eighteen states included in the system, and tribal data must be submitted through these states’ pub-lic health departments. Tribes are not independently included in the system at this time, although they are sovereign governments and should be treated equally with states. Under current policy, however, tribal data are included only through collaboration with the partici-pating states. Tribal Epidemiology Centers (Epi Centers) can serve as liaisons between state public health departments and tribes. Tribal Epi Centers are part of the partnership between the CDC and the IHS.26 Epi Centers collect disease surveillance data and develop disease con-trol and prevention programs.
Data collection on suicide attempts, not just completions, also needs improvement. Such data could be gleaned from hospitalization

88
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
records and emergency department visits related to suicide attempts.27 Recommendations from the Institute of Medicine and the National Strategy for Suicide Prevention have also mentioned the need for more data on nonfatal suicidal behavior.28 Tribes may benefit from collabo-ration with neighboring counties and states in collecting these data, particularly when tribal citizens seek health care at hospitals outside of IHS and the tribe’s jurisdiction. Finally, tribes could also work with one another to evaluate their suicide prevention programs. Dr. Antony Stately, director of mental health, chemical health, and employee as-sistance programs at the Shakopee Mdewakanton Sioux Community, suggested that tribes could form partnerships and then jointly apply for grants to fund suicide prevention programs and evaluations. These types of partnerships “would facilitate cross- site evaluations,” or evaluations which include more than one tribe’s data, according to Dr. Stately.29 Such tribal collaborations “could help [grant] dollars go further and help tribes get the data that they need for future funding efforts,” Dr. Stately said.
6. expand the use of tele- behavioral health through coordinated, collaborative efforts. One challenge in Indian Country is expanding access to behavioral health services. Tele- behavioral health is begin-ning to be used to address this issue. In tele- health, video conferencing is used to provide face- to- face contact between patients and mental health care providers in different locations. In his recent testimony to the Senate Committee on Indian Affairs, Randy Grinnell, deputy direc-tor of IHS, noted that increasing bandwidth and telecommunications infrastructure is a necessary prerequisite to expanding tele- behavioral health services in AI/AN communities.30 The IHS is updating this in-frastructure using funding from the American Recovery and Reinvestment Act of 2009.31
Tele- health can be used to provide counseling sessions, psychiatric consultations on medication, and other kinds of behavioral health ser-vices. In the IHS, more than fifty sites, including both tribal and federal facilities, are either actively using tele- health–based behavioral health ser-vices or are planning to do so.32 As part of the Methamphetamine and Suicide Prevention Initiative, IHS has also funded a new National Tele- Behavioral Health Center of Excellence.33 The IHS Albuquerque Area Office is establishing this center in partnership with the University of New Mexico and the University of Colorado, both of which have pro-grams in tele- health. The National Tele- Behavioral Health Center of Excellence is focusing on developing business models, billing practices, and policies around tele- behavioral health that might ultimately be ex-panded throughout the IHS. Tele- behavioral health efforts could be coor-dinated at regional and national levels in order to make the best use of re-sources. For example, several small AI/AN communities could partner in

89
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
order to have an adequate volume of cases to collectively hire a psychia-trist who would provide services to them all via tele- health connections.34
Recommendations for AI/AN Communities
7. build community- wide plans and collaborations for suicide pre-vention. Suicide prevention efforts are most successful when there is a broad, holistic effort involving the whole community.35 Many AI/AN communities have limited resources, but they can still build broad- based coalitions between existing community groups. From our interviewees’ descriptions of their communities’ suicide prevention programs, we learned that effective community plans involve collabo-ration between elected tribal leaders and different community depart-ments and organizations, including tribal primary care and behavioral health systems; IHS; emergency medical services; police and fire de-partments; schools; youth groups; religious leaders; and traditional cul-tural and spiritual leaders. A comprehensive community- based suicide prevention program might include behavioral health screening or other clinic- based components, school- based prevention programs and edu-cation, training for mental health professionals and other community members on identifying and assisting individuals at risk for suicide, and cultural or spiritual activities.36
For example, the San Carlos Apache Tribe’s suicide prevention program includes ASIST (Applied Suicide Intervention Skills Training) and safeTALK (Safe Tell, Ask, Listen, and KeepSafe) trainings for com-munity members and tribal staff; community education; a Gathering of Native Americans training; wellness promotion events, such as har-vest festivals, movie nights, and softball tournaments; wellness camps and retreats; and efforts to revitalize traditional culture and language to support resilience of tribal youth.37 The Tribe has also built a suicide prevention task force, which is a community coalition of diverse stake-holders to help plan and implement suicide prevention activities. A key principle of the San Carlos Apache Tribe’s efforts is to focus on increas-ing the resilience and strength of tribal members, rather than just re-ducing risk factors for suicide, according to tribal health staff who were interviewed, including Dr. Thea Wilshire (clinical coordinator of the San Carlos Apache Wellness Center), Dr. Gail Sims (program manager), Mary Casoose (prevention team leader), and Rhonda Bread (recreation technician).38 Their plan also includes targeted programs for groups at higher risk for suicide, such as veterans; lesbian, gay, bisexual, and trans-gender individuals; and individuals recovering from substance abuse.
Dr. Clayton Small’s program, Native HOPE, also involves a process of developing a comprehensive strategic action plan that is community- wide. This plan includes “the formation of a youth council, implement-ing talking circles/support groups, peer- to- peer video presentations

90
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
with positive messages, presentations to school boards/tribal councils, and ongoing ‘booster’ prevention/leadership activities at least once per month.”39 Dr. Small emphasized the importance of programs for youth that are community- and school- based— in other words, in settings out-side the clinic. Providing trainings in these settings will improve Native youths’ access to suicide prevention programs.
8. consider implementing a tribal mental health code and/or a central-ized suicide attempt and completion reporting system. Coordination and collaboration between tribal departments is important for collect-ing accurate data on suicide attempts and completions, as well as for ensuring that the individuals at risk receive the services they need. For example, if tribal police are called to a situation with a suicidal indi-vidual, they would ideally coordinate with the tribal behavioral health department to refer that individual for services immediately. Dr. Thea Wilshire suggested that tribes consider adopting a centralized suicide reporting system, where all tribal departments and staff would report if they identified individuals with suicidal ideation.40 Suicide completions would also be included in the system. Having a centralized system can help to ensure that individuals at risk receive services. Such a system can also facilitate better tribal data collection on suicide attempts and completions, which could then inform development and improvement of suicide prevention programs.
The White Mountain Apache Tribe has developed a unique centralized suicide reporting system. The Tribe partnered with Johns Hopkins University to formalize the reporting process and to interpret data collected through the surveillance system. A recent journal article authored by tribal and university partners described the establishment of the surveillance system:
In 2001, a cluster of suicides among youths on the Apache reservation led the Tribal Council to enact a resolution to mandate tribal members and community providers to re-port all suicidal behavior (ideations, attempts, and deaths) to a central data registry. The resulting surveillance system is the first of its kind, gathering data from both community- based and clinical settings.41
Collection of data from community settings and involvement of commu-nity members in reporting suicidal behavior are key innovations in the White Mountain Apache Tribe’s surveillance system. Suicidal behavior that does not result in hospitalization or an emergency room visit will not be documented in data collection efforts that are strictly hospital based. For this reason, community- based data collection is critical for getting an accurate picture of suicidal behavior. Importantly, the White

91
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
Mountain Apache Tribe’s surveillance system not only includes deaths by suicide, but also suicidal ideation and attempts. Behaviors reported to the system include “suicidal ideation, attempts, deaths . . . binge drink-ing, drug use, and cutting.”42 The White Mountain Apache Tribe has worked with Johns Hopkins University to train a team of Apache case managers who follow up on all reported incidents. These case managers evaluate youths’ risk for suicide, and then refer youth and their fami-lies to behavioral health services.43 Original reporting forms collected through the White Mountain Apache Tribe’s suicide surveillance sys-tem are stored on the reservation and may not be removed.
In addition to centralized reporting, a tribal mental health code could include procedures for how police should deal with individuals with suicidal ideation. Without a separate police code and procedure, individuals posing a danger to themselves may be charged with assault/battery or disorderly conduct and then be imprisoned for significant lengths of time when they have not committed a crime and urgently need behavioral health services, Dr. Wilshire said.44
9. develop a prioritized tribal health agenda that addresses issues un-derlying suicide. Given that many tribes have limited resources, find-ing creative ways to use those resources is important. One strategy is for tribal leaders to develop a list of their health priorities, and then to target applications for funding accordingly.45 This kind of coordinated approach is suggested by the suicide prevention toolkit developed for First Nations in Canada by the First Nations Centre, National Aboriginal Health Organization, and the report of the Advisory Group on Suicide Prevention, Health Canada, Acting on What We Know: Preventing Youth Suicide in First Nations.46 There are multiple angles from which suicide pre-vention could be approached. Dr. Alex Crosby (medical epidemiologist, Division of Violence Prevention, CDC) commented that addressing is-sues underlying suicide, such as violence and substance abuse, can enable tribes to make an impact on multiple health priorities at the same time.47
Communities might also consider strategically working on im-proving intermediate outcomes related to suicide prevention. Some of these could include screening and treatment rates of depression and substance abuse, according to Kimberly Ross- Toledo.48 Other interme-diate outcomes could include pride in cultural identity and a stronger sense of community belonging. These and other measures of success and well- being of urban AI/AN youth were identified by Portland, Oregon, AI/AN community members in the project Practice- Based Evidence: Building Effectiveness from the Ground Up.49
10. invest in and develop positive activities and centers for youth. Many of our interviewees approach suicide prevention from a strengths- based perspective: they focus on building youths’ capacity for resilience

92
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
and overcoming obstacles, rather than just educating youth about suicide specifically.50 For example, tribes could invest in positive activities for youth related to culture, such as traditional arts and crafts and language classes. Interviewees also commented on the importance of youth cen-ters. Dr. Clayton Small said it was important to invest in local Boys and Girls Clubs.51 Planting Seeds of Hope hosts a basketball camp for youth, and includes life skills training and suicide prevention education as part of that.52 The San Carlos Apache tribe offers year- round activities for youth through the Young Warriors program, which is sponsored by and under the oversight of the San Carlos Apache Wellness Center, accord-ing to Dr. Wilshire.53 This program includes several weeks of sleepover and day camps for youth. High school seniors are trained to help youth during the summer programs, and forty- five youth mentors, who are college- aged Apache young adults, serve as the primary camp staff. The Young Warriors program also includes before- and after- school pro-gramming in tribal schools, as well as in- class support and mentoring by thirty full- time Apache youth mentors. During the enrollment process, youth are screened for suicidal ideation, and those identified as at- risk are provided with counseling on- site in the Young Warrior program. Thus far, among the forty- two youth identified as actively suicidal and pro-vided with counseling, there have been no suicide attempts.54
11. Restrict access to lethal means when possible. For youth at risk of suicide, restricting their access to firearms, dangerous prescription drugs, and other means of death may be a useful suicide prevention strategy. As an example, Kyla Hagan, program manager in the Wellness and Prevention Department of the Division of Community Health Services at the Alaska Native Tribal Health Consortium (ANTHC), described the Gun Safe Project conducted in six rural Alaska communi-ties by three tribal health organizations (ANTHC, Yukon- Kuskokwim Health Corporation, and Bristol Bay Area Health Corporation) and the Harborview Injury Prevention Center.55 Locking gun cabinets were in-stalled in all homes that had guns in two phases: an “early” group and a “late” group (one year later). The project team returned one year and eighteen months after installation, and interviewed community mem-bers about safe gun storage practices. They found that the percent-age of homes where all guns were stored in a locked location increased from 7% to 65% in the “early” group after one year. Similar results were found in the “late” group as well at the eighteen- month follow- up.56 Lethal- means restriction can also be implemented at the pharmacy level: for instance, limits could be placed on the amount of prescription drugs given to patients at one time.
12. consider adapting mainstream suicide prevention programs by making cultural modifications. There are a number of suicide preven-

93
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
tion trainings and educational curricula that have been developed for the general U.S. population, including ASIST and QPR. QPR stands for “question, persuade, and refer” and is a training program to help individuals recognize the warning signs of suicide and refer at- risk indi-viduals to appropriate services. These and other programs can be modi-fied so that they are more culturally relevant to AI/AN communities, as our interviewees pointed out.57 It may be easier for some communities to use these culturally adapted programs rather than creating their own suicide prevention program from scratch. Consultation with program developers can help to maintain the fidelity of a suicide prevention pro-gram even when cultural adaptations are made.58
AI/AN behavioral health professionals and communities have worked with the creators of QPR and ASIST to make cultural modifica-tions that better tailor these trainings to Native communities.59 The QPR program has specific videos for different populations, including AI/AN communities, that use actors from similar backgrounds. ASIST includes role- play scenarios and simulations that can be made more specific to Native communities. For example, a suicide attempt scenario located on a bridge could be changed to train tracks, a mesa, or other geographical features specific to a particular community.60 For communities with sig-nificant numbers of individuals for whom English is a second language, it may be helpful to develop a handout with key terms defined, according to Dr. Kathy Graves, director of behavioral health and rural services at ANTHC. She noted that terms like “ambivalence” were not clear to some Alaska Native participants in suicide prevention trainings.61
The format and time allotted for trainings may also need to be modified for AI/AN communities. More time may be required to accom-modate rich discussions about broader contexts in the community re-lated to suicide. AI/AN training participants may also need more time and preparation for scenarios and role-plays that might remind them of their own experiences, Dr. Kathy Graves noted.62 She reflected on a training she conducted in a rural Alaskan community where there had been a re-cent suicide. In that training, a few participants had posttraumatic stress reactions to role- play scenarios. Dr. Graves and her colleagues encour-aged the individuals with posttraumatic stress to complete the training if they could, but also advised them to refrain from participating in any parts that might be too close to their own painful experiences.
Another strategy for working with diverse groups is to have dis-cussions throughout the training about whether the presented material is consistent with local cultural values, according to Kyla Hagan.63 She said these types of discussions are very productive, particularly when there are elders in the room. Another way to respect and include elders is to invite them to serve as facilitators for debriefings during suicide pre-vention trainings. Barbara Franks, program associate with suicide pre-vention programs at ANTHC, commented that in ANTHC’s training

94
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
for trainers, during which individuals will learn how to run their own suicide prevention trainings, an elder will be asked to “stand by during the lunch hour, so that if people have problems with the content of the course they can talk to her for guidance or support.”64 She was con-cerned that Alaska Native people might not feel comfortable offering criticisms during the course, but wanted to provide them with a way to deal with any internal conflicts they might experience in the training. She also tries to provide opportunities for one- on- one conversation with herself and other trainers. Spirituality is important in many AI/AN communities, so beginning and ending trainings with prayer can also help to make them more culturally appropriate.65
13. include spiritual and cultural components in any suicide preven-tion program. Suicide is viewed in many AI/AN communities not just as a mental health concern but as a spiritual issue as well.66 For this reason, suicide prevention programs may need to include spiritual components and can benefit from the involvement of community spiritual leaders (both traditional and Christian) and traditional healers. Interviewees commented that the blessings of elders and spiritual leaders can make it easier to speak about suicide and may increase the acceptance of sui-cide prevention programs in AI/AN communities. For example, Mary Casoose sought permission from elders before beginning to speak about suicide prevention at the San Carlos Apache Tribe.67 Dr. Clayton Small suggested that tribal leaders take an active role in promoting cultural and spiritual approaches. He said, “We need tribal leaders to advocate for culture- based and spirit- driven (healing) suicide prevention programs.”68
14. Provide support for suicide survivors and opportunities for them to be involved in suicide prevention activities. Programs specifically involving suicide survivors can be an important part of tribal suicide prevention plans, according to Susan Casias, cochair of the IHS Suicide Prevention Committee.69 The stories told by survivors can also be power-ful parts of community education and awareness programs.70 Providing support for survivors is also important for preventing suicide contagion (several suicides happening in sequence). Survivors close to an individual who completed suicide may be at increased risk for suicide attempts themselves.71 More information on creating a community plan to prevent suicide contagion is available from the CDC.72
15. support and training for behavioral health providers. AI/AN com-munities face many behavioral health challenges, in part because of his-torical trauma. As a result, behavioral health care providers are often overwhelmed and can become traumatized themselves from hearing many painful stories.73 They can also begin to feel helpless, which af-fects their ability to assist their clients and proactively refer them to

95
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
other resources, according to Kimberly Ross- Toledo.74 Extra support for these providers and cultural competency training can help them to avoid burnout. Kimberly Ross- Toledo pointed out that providers unfamiliar with AI/AN communities may feel particularly ineffective if they are unable to help their clients. She said that training and edu-cation on AI/AN community culture may help these providers to de-velop more effective strategies and feel more capable in their jobs.75 On the Red Lake Indian Reservation, behavioral health staff debrief with one another proactively when they see a colleague becoming stressed. Self- care is encouraged as part of the workplace environment, and staff regularly check in with one another, particularly when there have been traumatic events in the community.76
C o n C L u s I o n
Suicide is a major health challenge for AI/AN communities, which are developing unique and creative local prevention programs. Supporting programs is critical: while there are common factors underlying sui-cide throughout Indian Country, the context and culture of each com-munity is unique. We have provided a number of policy and practice recommendations that we hope will increase support for tribally based suicide prevention programs. Although the suicide epidemic in Indian Country is daunting, there is hope for the future because of tireless ef-forts by AI/AN communities and their allies in suicide prevention.
a u t h o r b i o g r a p h i e s
Puneet Chawla Sahota, MD, PhD, is a resident physician in psy-chiatry and a visiting scholar in anthropology at the University of Pennsylvania. In 2009–10, she was a postdoctoral fellow at the National Congress of American Indians Policy Research Center, where she conducted a national study of suicide prevention approaches used in American Indian/Alaska Native communities.
Sarah Kastelic, PhD, is the deputy director of the National Indian Child Welfare Association. She worked at the National Congress of American Indians from 1998 to 2010, and served as the founding di-rector of the NCAI Policy Research Center from 2003 to 2010. She is Alutiiq and an enrolled member of the Native Village of Ouzinkie.
N o t e s
We thank all the individuals (listed in Figure 1) who served as key informants and contributed their expertise to this paper. In addition, Bobbi Jo Bruce pro-
vided insightful comments and advice in the preparation of this paper. We also are grateful to Ahniwake Rose, Dr. Rose Weahkee, Cara Cowan Watts,

96
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
N o t e s
and Kathy Hughes for helping to dis-tribute the call for comments. Emily R. White Hat provided valuable assistance in manuscript preparation and format-ting. The work described here was conducted at the National Congress of American Indians Policy Research Center, and was supported by grant funding from the Association of American Indian Physicians and the Nathan Cummings Foundation. This paper does not necessarily represent the views of these funders.
1 Centers for Disease Control and Prevention, “Deaths: Leading Causes for 2004,” National Vital Statistics Report 56, no. 5 (Novem-ber 2007): 1–95, available at http://www.cdc.gov/nchs/data/nvsr/nvsr56/nvsr56_05.pdf.
2 Dale Walker, Patricia Silk Walker, and Douglas Bigelow, “Native Adolescent Suicide Cofactors: Prevention and Treatment Best Practices” (presentation in Rapid City, S. Dak., July 26–27, 2006), available at http://www.onesky center.org/pp/presentations.cfm; U.S. Department of Health and Human Services (DHHS), To Live to See the Great Day That Dawns: Preventing Suicide by American Indian and Alaska Native Youth and Young Adults, DHHS Publication SMA (10)- 4480, CMHS- NSPL- 0196 (Rockville, Md.: Center for Mental Health Services, Sub-stance Abuse and Mental Health Services Administration, 2010), available at http://www.sprc.org/ library/Suicide_Prevention_Guide.pdf.
3 Patient Protection and Affordable Care Act, Pub. L. No. 111–148, 124 Stat. 119 (2010).
4 U.S. DHHS, To Live to See the Great Day That Dawns, 1.
5 Herbert Rubin and Irene Rubin, Qualitative Interviewing: The Art of Hearing Data (Thousand Oaks, Calif.: Sage, 2005), 34.
6 Ibid.
7 Ibid., 71.
8 Margaret LeCompte and Jean Schensul, Analyzing and Interpreting Ethnographic Data (Walnut Creek, Calif.: AltaMira Press, 1999), 45.
9 Ibid.
10 Puneet Chawla Sahota and Sarah Kastelic, “Culturally Appropri-ate Evaluation of Tribally Based Suicide Prevention Programs: A Review of Approaches,” Wicazo Sa Review 27 (Fall 2012): 99–127.
11 Clayton Small, interview with Puneet Chawla Sahota, Febru-ary 18, 2010.
12 Sahota and Kastelic, “Culturally Appropriate Evaluation of Trib-ally Based Suicide Prevention Programs.”
13 Don Wetzel Jr., interview with Puneet Chawla Sahota, Febru-ary 24, 2010.
14 Kimberly Ross- Toledo, interview with Puneet Chawla Sahota, March 1, 2010.
15 Monique Smith, interview with Puneet Chawla Sahota, April 29, 2010.
16 Strategies to Improve Non- fatal Suicide Attempt Surveillance: Recom-mendations from an Expert Roundtable (Washington, D.C.: Suicide Prevention Action Network USA, 2006), available at http:// c.ymcdn.com/sites/safestates .site- ym.com/resource/resmgr/imported/SPANsurveillance06 .pdf.
17 Smith, interview.
18 B. Bruning, D. Grenier, and W. Wisdom, “Health Informa-tion Technology and Behavioral Health Care: Opportunities and Challenges” (presentation in St. Paul, Minn., August 4, 2009).

97
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
N o t e s
19 Ibid.
20 Ibid.
21 Ibid.
22 Thea Wilshire, Gail Sims, Mary Casoose, and Rhonda Bread, interview with Puneet Chawla Sahota, February 10, 2010.
23 Wilshire, Sims, Casoose, and Bread, interview.
24 E. Arias, W.S. Schauman, K. Eschbach, P. D. Sorlie, and E. Backlund, “The Validity of Race and Hispanic Origin Re-porting on Death Certificates in the United States,” Vital and Health Statistics 2, no. 148 (2008): 1–23.
25 Alex Crosby, interview with Puneet Chawla Sahota, February 2, 2010.
26 For more information about Tribal Epidemiology Centers, see http://www.cdc.gov/omhd/populations/aian/AIANEpiCntrs.htm.
27 Crosby, interview.
28 S. K. Goldsmith, T. C. Pellmar, A. M. Kleinman, and W. E. Bunney, eds., Reducing Suicide: A National Imperative (Washington, D.C.: National Academies Press, 2002); U.S. Public Health Ser-vice, National Strategy for Suicide Prevention: Goals and Objectives for Action (Rockville, Md.: U.S. De-partment of Health and Human Services, 2001).
29 Antony Stately, interview with Puneet Chawla Sahota, May 25, 2010.
30 Randy Grinnell, written testimony, Senate Committee on Indian Affairs, Oversight Hearing on the Preventable Epidemic: Youth and the Urgent Need for Mental Health Care Resources in Indian Country, 111th Cong. 2nd sess., 2010, available at http://www .hhs.gov/asl/testify/2010/03/t20100325a.html.
31 American Recovery and Reinvest-ment Act of 2009, Pub. L. No. 111–5, 123 Stat. 115 (2009).
32 Grinnell, written testimony, Sen-ate Committee on Indian Affairs.
33 Ibid.
34 Ibid.
35 Small, interview.
36 Phil A. May, Patricia Serna, Lance Hurt, and Lemyra M. DeBruyn, “Outcome Evaluation of a Public Health Approach to Suicide Prevention in an American Indian Tribal Nation,” American Journal of Public Health 95, no. 7 (2005): 1238–44.
37 Wilshire, Sims, Casoose, and Bread, interview.
38 Ibid.
39 Small, interview.
40 Wilshire, Sims, Casoose, and Bread, interview.
41 B. Mullany, A. Barlow, N. Goklish, F. Larzelere- Hinton, M. Cwik, M. Craig, and J. Walkup, “To-wards Understanding Suicide Among Youths: Results from the White Mountain Apache Tribally Mandated Suicide Surveillance System, 2001–2006,” American Journal of Public Health 99, no. 10 (2009): 1840.
42 Novalene Goklish, written testi-mony, Senate Committee on Indian Affairs, Oversight Hearing on the Preventable Epidemic, available at http://www.gpo.gov/fdsys/pkg/CHRG- 111shrg58331/html/CHRG- 111shrg58331.htm.
43 Ibid.
44 Wilshire, Sims, Casoose, and Bread, interview.
45 Crosby, interview.

98
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
N o t e s
46 National Aboriginal Health Orga-nization, Assessment and Planning Tool Kit for Suicide Prevention in First Nations Communities (Ottawa: First Nations Centre of NAHO, 2005), available at http://www .naho.ca/documents/fnc/english/FNC_SuicidePreventionToolkit .pdf; Health Canada, Advisory Group on Suicide Prevention Report, Acting on What We Know: Preventing Youth Suicide in First Nations (Ottawa: Health Canada, 2005), available at http://www.hc- sc .gc.ca/fniah- spnia/alt_formats/fnihb- dgspni/pdf/pubs/suicide/prev_youth- jeunes- eng.pdf.
47 Crosby, interview.
48 Ross- Toledo, interview.
49 Barbara Friesen, Kris Gowen, Pa-chida Lo, Abby Bandurraga, Terry Cross, and Cori Matthew, Literature Support for Outcomes in Evaluating Culturally- and Community- Based Pro-grams Indicators of Success for Urban American Indian/Alaska Native Youth: An Agency Example (Portland, Ore.: Practice- Based Evidence Project, Research and Training Center on Family Support and Children’s Mental Health, Portland State University, 2010), available at http://www.rtc.pdx.edu/PDF/pbPBELiteratureOutcomes.pdf.
50 Ross- Toledo, interview; Small, interview; Wetzel, interview.
51 Small, interview.
52 Wetzel, interview.
53 Wilshire, Sims, Casoose, and Bread, interview.
54 Thea Wilshire, e- mail communi-cation to Puneet Chawla Sahota, June 3, 2010.
55 Kyla Hagan, Barbara Franks, and Jessica Hagan, interview by Puneet Chawla Sahota, February 24, 2010.
56 D. Grossman, H. Stafford, T. Koepsell, R. Hill, K. Hagan,
and W. Jones, “Improving Firearm Storage in Alaska Native Villages: A Randomized Trial of House-hold Gun Lockers” (unpublished MS, 2010).
57 Ger RainingBird, Elly Stout, and Petrice Post, interview with Puneet Chawla Sahota, Febru-ary 24, 2010; Kathy Graves, inter-view with Puneet Chawla Sahota, February 20, 2010.
58 U.S. DHHS, To Live to See the Great Day That Dawns, 61.
59 RainingBird, Stout, and Post, interview.
60 Arizona Suicide Prevention Coalition, ASIST: Applied Suicide Intervention Skills Training, Tips for Trainers (Phoenix: Arizona Sui-cide Prevention Coalition, 2009), available at http://www .sprc.org/grantees/statetribe/ 2010/1D%20Post.pdf.
61 Graves, interview.
62 Ibid.
63 Hagan, Franks, and Hagan, interview.
64 Ibid.
65 Hagan, Franks, and Hagan, inter-view; Small, interview.
66 Small, interview; Wetzel, inter-view; Wilshire, Sims, Casoose, and Bread, interview.
67 Wilshire, Sims, Casoose, and Bread, interview.
68 Small, interview.
69 Susan Casias, interview with Puneet Chawla Sahota, May 4, 2010.
70 Hagan, Franks, and Hagan, interview.
71 U.S. DHHS, To Live to See the Great Day That Dawns, 38.

99
SP
RI
NG
2
01
4
W
IC
AZ
O
SA
R
EV
IE
W
N o t e s
72 P. W. O’Carroll, J. A. Mercy, and J. A. Steward, “CDC Recommen-dations for a Community Plan for the Prevention and Contain-ment of Suicide Clusters,” Mor-bidity and Mortality Weekly Report 37, no. 6 (1988): 1–12, available at http://www.cdc.gov/mmwr/preview/mmwrhtml/00001755 .htm.
73 A. Allick, L. Perkins, and J. Kennedy, “Behavioral Health
Approaches to Addressing Communities After Red Lake” (presentation in St. Paul, Minn., August 6, 2009).
74 Ross- Toledo, interview.
75 Ibid.
76 Allick, Perkins, and Kennedy, “Behavioral Health Approaches to Addressing Communities After Red Lake.”




















