
The use of referenced-EEG (rEEG) in assisting medication selection for the treatment of depression
12
The use of referenced-EEG (rEEG) in assisting medication selection for the treatment of depression Charles DeBattista a, * , Gustavo Kinrys b , Daniel Hoffman c , Corey Goldstein d , John Zajecka d , James Kocsis e , Martin Teicher f , Steven Potkin g , Adrian Preda g , Gurmeet Multani h , Len Brandt i , Mark Schiller j , Dan Iosifescu k , Maurizio Fava l a Stanford University School of Medicine, Department of Psychiatry and Behavioral Sciences, 401 Quarry Road, Stanford, CA 94305, USA b Cambridge Health Alliance,101 Station Landing, Suite 2100, Medford, MA 02155, USA c CNS Response Inc, 85 Enterprise, Suite 410, Aliso Viejo, CA 92656, USA d Rush University Medical Center, Department of Psychiatry,1700 W. Van Buren Street, 5th Floor, Chicago, IL 60612-3824, USA e New York Presbyterian Hospital, Payne Whitney Clinic, Box 140, 525 East 68th Street, New York, NY 10021, USA f Department of Psychiatry, Harvard Medical School, Developmental Biopsychiatry Research Program, McLean Hospital,115 Mill Street, Belmont, MA 02478-9106, USA g UCI School of Medicine, Department of Psychiatry and Human Behavior,101 City Center Drive, Building 3, Rt 88, Room 310 e BIC, Irvine Hall, Orange, CA 92868, USA h Shanti Clinical Trials, 1880 East Washington Street, Colton, CA 92324, USA i 28911 Via Hacienda, San Juan Capistrano, CA 92675, USA j Mind Therapy Clinic, 2299 Post Street, Suite 104A, San Francisco, CA, USA k Massachusetts General Hospital, Depression Clinical and Research Program, 50 Staniford Street, Suite 401, Boston, MA 02114, USA l Depression Clinical and Research Program, Massachusetts General Hospital, 55 Fruit Street, Bulfinch 351, Boston, MA 02114, USA article info Article history: Received 17 March 2010 Received in revised form 10 May 2010 Accepted 11 May 2010 Keywords: Resistant depression Biomarkers Antidepressants QEEG rEEG Response prediction abstract Objective: To evaluate the efficacy of rEEG Ò -guided pharmacotherapy for the treatment of depression in those circumstances where rEEG and STAR*D provided different recommendations. Materials and methods: This was a randomized, single-blind, parallel group, 12 center, US study of rEEG- guided pharmacotherapy vs. the most effective treatment regimens reported in the NIH sponsored STAR*D study. Relatively treatment-resistant subjects 18 years who failed one or more antidepressants were required to have a QIDS-16-SR score 13 and a MADRS score 26 at baseline. All subjects underwent a washout of all current medications (with some protocol-specified exceptions) for at least five half-lives before receiving a QEEG and rEEG report. Subjects randomized to rEEG were assigned a regimen based on the rEEG report. Control subjects who had failed only SSRI’s in their current episode were randomized to receive venlafaxine XR. Control subjects who had failed antidepressants from 2 classes of antidepressants were randomized to receive a regimen from Steps 2e4 of the STAR*D study. Treatment lasted 12 weeks. The primary outcome measures were change from baseline for self-rated QIDS-SR16 and Q-LES-Q-SF. Results: A total of 114 subjects were randomized and 89 subjects were evaluable. rEEG-guided phar- macotherapy exhibited significantly greater improvement for both primary endpoints, QIDS-SR16 (6.8 vs. 4.5, p < 0.0002) and Q-LES-Q-SF (18.0 vs. 8.9, p < 0.0002) compared to control, respectively, as well as statistical superiority in 9 out of 12 secondary endpoints. Conclusions: These results warrant additional studies to determine the role of rEEG-guided psycho- pharmacology in the treatment of depression. If these results were confirmed, rEEG-guided pharma- cotherapy would represent an easy, relatively inexpensive, predictive, objective office procedure that builds upon clinical judgment to guide antidepressant medication choice. Ó 2010 Published by Elsevier Ltd. 1. Objectives of the study and background The treatment of major depressive disorder (MDD) remains a great challenge for clinicians. Many depressed patients do not respond to acute treatment (Rush, 2007). Even with multiple medications administered sequentially, many patients do not respond adequately * Corresponding author. Tel.: þ1 650 723 8324; fax: þ1 650 723 8331. E-mail address: [email protected] (C. DeBattista). Contents lists available at ScienceDirect Journal of Psychiatric Research journal homepage: www.elsevier.com/locate/psychires 0022-3956/$ e see front matter Ó 2010 Published by Elsevier Ltd. doi:10.1016/j.jpsychires.2010.05.009 Journal of Psychiatric Research xxx (2010) 1e12 Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment of depression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009
-
Upload
michellenmeyer -
Category
Documents
-
view
1 -
download
0
Transcript of The use of referenced-EEG (rEEG) in assisting medication selection for the treatment of depression

The use of referenced-EEG (rEEG) in assisting medication selection for thetreatment of depression
Charles DeBattista a,*, Gustavo Kinrys b, Daniel Hoffman c, Corey Goldstein d, John Zajecka d,James Kocsis e, Martin Teicher f, Steven Potkin g, Adrian Preda g, Gurmeet Multani h, Len Brandt i,Mark Schiller j, Dan Iosifescu k, Maurizio Fava l
a Stanford University School of Medicine, Department of Psychiatry and Behavioral Sciences, 401 Quarry Road, Stanford, CA 94305, USAbCambridge Health Alliance, 101 Station Landing, Suite 2100, Medford, MA 02155, USAcCNS Response Inc, 85 Enterprise, Suite 410, Aliso Viejo, CA 92656, USAdRush University Medical Center, Department of Psychiatry, 1700 W. Van Buren Street, 5th Floor, Chicago, IL 60612-3824, USAeNew York Presbyterian Hospital, Payne Whitney Clinic, Box 140, 525 East 68th Street, New York, NY 10021, USAfDepartment of Psychiatry, Harvard Medical School, Developmental Biopsychiatry Research Program, McLean Hospital, 115 Mill Street, Belmont, MA 02478-9106, USAgUCI School of Medicine, Department of Psychiatry and Human Behavior, 101 City Center Drive, Building 3, Rt 88, Room 310 e BIC, Irvine Hall, Orange, CA 92868, USAh Shanti Clinical Trials, 1880 East Washington Street, Colton, CA 92324, USAi 28911 Via Hacienda, San Juan Capistrano, CA 92675, USAjMind Therapy Clinic, 2299 Post Street, Suite 104A, San Francisco, CA, USAkMassachusetts General Hospital, Depression Clinical and Research Program, 50 Staniford Street, Suite 401, Boston, MA 02114, USAlDepression Clinical and Research Program, Massachusetts General Hospital, 55 Fruit Street, Bul!nch 351, Boston, MA 02114, USA
a r t i c l e i n f o
Article history:Received 17 March 2010Received in revised form10 May 2010Accepted 11 May 2010
Keywords:Resistant depressionBiomarkersAntidepressantsQEEGrEEGResponse prediction
a b s t r a c t
Objective: To evaluate the ef!cacy of rEEG!-guided pharmacotherapy for the treatment of depression inthose circumstances where rEEG and STAR*D provided different recommendations.Materials and methods: This was a randomized, single-blind, parallel group, 12 center, US study of rEEG-guided pharmacotherapy vs. the most effective treatment regimens reported in the NIH sponsoredSTAR*D study. Relatively treatment-resistant subjects !18 years who failed one or more antidepressantswere required to have a QIDS-16-SR score !13 and a MADRS score !26 at baseline. All subjectsunderwent a washout of all current medications (with some protocol-speci!ed exceptions) for at least!ve half-lives before receiving a QEEG and rEEG report. Subjects randomized to rEEG were assigneda regimen based on the rEEG report. Control subjects who had failed only SSRI’s in their current episodewere randomized to receive venlafaxine XR. Control subjects who had failed antidepressants from !2classes of antidepressants were randomized to receive a regimen from Steps 2e4 of the STAR*D study.Treatment lasted 12 weeks. The primary outcome measures were change from baseline for self-ratedQIDS-SR16 and Q-LES-Q-SF.Results: A total of 114 subjects were randomized and 89 subjects were evaluable. rEEG-guided phar-macotherapy exhibited signi!cantly greater improvement for both primary endpoints, QIDS-SR16 ("6.8vs. "4.5, p< 0.0002) and Q-LES-Q-SF (18.0 vs. 8.9, p< 0.0002) compared to control, respectively, as wellas statistical superiority in 9 out of 12 secondary endpoints.Conclusions: These results warrant additional studies to determine the role of rEEG-guided psycho-pharmacology in the treatment of depression. If these results were con!rmed, rEEG-guided pharma-cotherapy would represent an easy, relatively inexpensive, predictive, objective of!ce procedure thatbuilds upon clinical judgment to guide antidepressant medication choice.
" 2010 Published by Elsevier Ltd.
1. Objectives of the study and background
The treatmentofmajordepressivedisorder (MDD) remainsagreatchallenge for clinicians. Many depressed patients do not respond toacute treatment (Rush, 2007). Even with multiple medicationsadministered sequentially, many patients do not respond adequately
* Corresponding author. Tel.: #1 650 723 8324; fax: #1 650 723 8331.E-mail address: [email protected] (C. DeBattista).
Contents lists available at ScienceDirect
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
0022-3956/$ e see front matter " 2010 Published by Elsevier Ltd.doi:10.1016/j.jpsychires.2010.05.009
Journal of Psychiatric Research xxx (2010) 1e12
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

to pharmacotherapy (Warden et al., 2007). The Sequenced TreatmentAlternatives to Relieve Depression (STAR*D) (Rush et al., 2006),a landmark study of more than 4000 MDD subjects, observed a 50%response to citalopram. For citalopram failures, only an additionalresponse of around 25% was observed when switched either to twoother classes of antidepressants or cognitive behavior therapy. Inaddition, many patients who achieve remission are unable to sustainit (Trivedi et al., 2009; Rush et al., 2006).
The pharmacotherapy of MDD in clinical practice rests largelyon clinical judgment and a trial-and-error method. Such a methodhas many problems. Patients may be exposed to multiple ineffec-tive medication trials associated with adverse effects that some-times are substantial in nature. In addition, each of these trials cantake eight weeks or longer. As a result, the duration of illness andsuffering is prolonged. Furthermore a longer duration of thedepressive episode may be associated with a poorer long-termprognosis (Altamura et al., 2008).
Unlike other areas of medicine, psychiatry has lackedbiomarkers that can help guide pharmacotherapy with similarreliability as bacterial assays (Rosenblatt, 1991) that guide antibiotictreatment or histological and genetic tests that guide chemo-therapy (Dunn and Demichele, 2009; Tutt and Ashworth, 2008).While a number of potential biomarkers are being evaluated forguiding antidepressant pharmacotherapy including genomics(Lohoff and Ferraro, 2010; Lin and Chen, 2008) functional imaging(Evans et al., 2006; Leuchter et al., 1997) and other sensitivity/speci!city markers (Gordon et al., 2007) cost or access limit theapplication of most of these technologies in clinical practice.
The electroencephalogram (EEG) may also have a role in pre-dicting treatment response in depression. Early work in quantita-tive EEG (QEEG) in depression (Henriques and Davidson, 1990,1991) reported a frontal asymmetry described as hypoactivationof the left frontal area. Other work (Bruder et al., 2008) found anassociation between EEG alpha power asymmetry and clinicalresponse to selective serotonin receptor inhibitors (SSRI). Anotherplacebo-controlled study (Cook et al., 2002) examined EEG abso-lute and relative power, along with cordance, to !nd regionalchanges that might be associated with a response to depressiontreatment in 51 adults. Medication responders showed decreases inprefrontal cordance as early as 48 h after startingmedication. Theseresults suggested that the prefrontal region might play a role inpredicting response to antidepressants.
Subsequent work in depression led to a large multicenter trial(n$ 375) (Leuchter et al., 2009) that examined a frontal quantitativeEEG (QEEG) biomarker’s ability to predict response to the SSRIescitalopram after one week of treatment. Subjects were subse-quently randomized to remain on treatment or crossed over toalternative treatment. Seventy-!ve (75) subjects remained on esci-talopram and 52% responded to therapy after 49 days. In thesesubjects, the QEEG biomarker predicted response with a 74% accu-racy, demonstrating that changes in asymmetry composite EEGindex oneweek into pharmacological treatment can be predictive ofpositive response to SSRI medication at the end of treatment.
Referenced-EEG (rEEG) differs from a standard QEEG in that itreferences the QEEG to a normative and then symptomatic database.By comparing the QEEG in a given patient to QEEGs in a database ofpatients who have been tried on and responded to a speci!c medi-cation, rEEG may be able to predict response to a wide number ofmedications. rEEG may thus have the advantage of providing treat-ment predictions before medication is started. It also may providepredictions for several medication classes beyond SSRIs.
rEEG is based upon the work of Suf!n and Emory (1995) whoreported correlations between particular EEG data and medicationclass response in samples of patients with affective and attentionalsymptoms. Theenergywithin frequencybands (e.g., delta 1.5e3.5 Hz,
theta 3.5e7.5 Hz, alpha 7.5e12.5 Hz and beta 12.5e25.5 Hz) andcoherence (a measure of the cross correlation of recording siteswithin a frequency band) were among the elements utilized to clas-sify participants. These authors extended this model by creatinga database from patients seen in clinical practice. Since the !rstpublication of this work (Suf!n and Emory, 1995) the database hasexpanded; it currently contains un-medicated EEG’s frommore than1800 patients and it compares those EEG’s to a FDA-approvednormative age-corrected database. For these same 1800# patients,they also collected the outcomes (average length of time is 405 days)of more than 17,000 medication trials/intervals (positive, negative orneutral) from which they built a usable database of 74 biomarkerscurrently referred to as referenced-EEG. It provides a very largecollection of outcome data allowing calculation of statistical corre-lation between the biomarkers found in a patient’s EEG and thetreatment response predictions to many medications based onpatients who had triggered similar EEG biomarkers.
Small, preliminary studies have suggested a potential role in theuse of rEEG-guided medication selection for depression. A small,prospective, randomized, controlled study of rEEG enrolled andcompleted 25 weeks of follow-up on two groups of treatment-resistant depressed patients (n$ 6 Control; n$ 7 Experimental) ata VA hospital (Suf!n et al., 2007). The trial used rEEG to guideprescribing of psychotropic medications while the control groupreceived essentially treatment as usual. Results indicated that sixout of seven rEEG subjects received ratings of moderate to markedimprovement, in contrast to a single subject in the control group.When unblinded that same subject was treated successfully withthe medication that was predicted to be effective by the rEEG.
Another pilot study (DeBattista et al., 2008) was conducted tocompare rEEG-guided pharmacotherapy with the TexasMedicationAlgorithm Project (TMAP) (Trivedi et al., 1998) algorithm forpatients with treatment-resistant depression. This small (n$ 18),10-week study found that rEEG-guided therapy resulted in statis-tically greater change from baseline scores for the Quick Inventoryof Depressive Symptomatology-Self Report-16 (QIDS-SR16) and theQuality of Life Enjoyment and Satisfaction Questionnaire-ShortForm (Q-LES-Q-SF) than TMAP-guided therapy. It also found that!ve subjects in the TMAP group received a successful TMAP therapythat was predicted by their pre-treatment rEEGs.
Pilot studies using rEEG in eating disorders (Schiller et al., 2004;Greenblatt et al., 2008) and substance abuse (Shaffer et al., 2005;Schiller, 2008) demonstrated similar promising results.
For the study presented here, a control group was chosen tore"ect the most effective treatments that were found in the STAR*Dstudy (Rush et al., 2006). The published ef!cacy rates of the STAR*Dpharmacotherapies provided a clear comparison against which tomeasure rEEG-guided therapy.
The objective of this study was to more rigorously andcomprehensively evaluate the utility of rEEG in guiding pharma-cotherapy in a larger group of patients with major depression inthose circumstances where rEEG and STAR*D provided differentrecommendations.
2. Materials and methods
2.1. Study participants
Subjects were recruited at 12 centers across the US from twobasic strata: (1) subjects with depression treatment failure afterone or more SSRIs in the current episode, and (2) those with failureafter at least two classes of antidepressants in the current episode.Current episode was de!ned as a current unsuccessfully treateddepressive episode, following a previously achieved remission(back to baseline or symptom-free), for four or more months.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e122
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

Subjects may have been on medication during remission. If thesubject never achieved remission, but simply responded orimproved and then had a worsening of symptoms, the currentepisode included the previous unresolved episode. The researchdesign, protocol, and informed consent for each site were reviewedby either a local or central IRB. All patients signed an informedconsent as required by the Helsinki Declaration.
Subjects were 18 years or older and were required to speak andread English. Each subject was required to have, as a primarydiagnosis, major depressive disorder (MDD) as de!ned by theDiagnostic and Statistical Manual of Mental Disorders, FourthEdition (DSM-IV) (American Psychiatric Association, 1994). Con!r-mation of diagnosis was made using the MINI InternationalNeuropsychiatric Interview (MINI), English Version 5.0 (Sheehanet al., 1992e2006). Subjects were also required to have a Mont-gomery-Åsberg Depression Rating Scale (MADRS) (Carmody et al.,2006a) score of >26 at screening and a QIDS-SR16 (Carmodyet al., 2006b) score of !13 at both screening and at the time theQEEG was obtained. The MADRS information was collected directlyfrom each patient using a web-based version of MADRS providedby Concordant Rater Systems, Boston, MA (Concordant RaterSystems Products and Services, 2009). MADRS scores were calcu-lated by the web-based version and provided to the study site forreview. Suicidality scores of !ve or higher were reported immedi-ately to the site personnel and investigator.
Potential subjects were excluded for medically relevant condi-tions such as closed head injury with unconsciousness, craniotomy,cerebral metastases, cerebrovascular accident, current diagnosis ofseizure disorder, bipolar disorder, schizophrenia, dementia, mentalretardation, or major depressionwith psychotic features; substanceabuse, acute or chronic pain requiring prescription pain medica-tion, pregnancy and lactation. Subjects with the intent to becomepregnant, who had previous electroconvulsive therapy (ECT)treatments, or use of depot neuroleptics in the last 12 months werealso excluded.
All subjects had amedicationwashout for aminimumof!ve half-lives of each current medication. Prior to washout, however, if therewere any concerns about patient safety during washout, then thesubject would be excluded from the trial. Washout medicationsincludedprescription drugs, drugs of abuse, recreational drugs, over-the-counter drugs, food supplements, vitamins, caffeine, alcohol,and nicotine. Most anti-hypertensive drug half-lives are shortenough that the washout period doesn’t adversely affect a patient’shealth. Certain medications were not required to be washed out:thyroxine, insulin, oral contraceptives, and hormones. Blood pres-sure medications were washed out provided that a substitute, shorthalf-lifemedication such as hydrochlorthiazide, could be used safely.
After the washout period a drug-free quantitative EEG (QEEG)was obtained. After the QEEG but prior to randomization, subjectscould be excluded for a variety of EEG-related !ndings that wereprospectively de!ned by the protocol. One such !nding was whenthe EEG revealed a physiologic abnormality, which was thought tobe related to a neurological condition (e.g., seizures or spaceoccupying lesions). Also, EEG !ndings that indicated a low abnor-mality led to exclusion from the study. The low abnormalitydesignation was given to a rEEG report when the EEG failed toreveal any abnormality that was signi!cant enough to !nda biomarker that allowed for a clear medication prediction. Inaddition to physiological and low abnormalities, there were a verysmall number of cases where a rEEG report did not !nd strongcorrelations for any of the drugs that were currently used by therEEG database. These few cases were due to the limitations of anevolving technology. Therefore, patients who needed medicationsthat were not yet represented in the current rEEG database did nothave a strong prediction on the rEEG report. As a result, subjects
who had rEEG reports that were not strongly predictive for anymedication were excluded from the trial. In some situations, therEEG report revealed one or more predictions the subject had usedpreviously but which failed to achieve ef!cacy. These subjects werealso excluded as it was considered unethical to follow the rEEGknowing the medications were ineffective for that patient. The lastEEG-related exclusion, which occurred before randomization,occurred when the rEEG report for a given subject indicateda treatment that was substantially the same regardless of whetherthe subject was in the control or experimental treatment group.This situation was de!ned as “equivalency”. Had these equivalentsubjects been randomized, they would have received the sametreatment in either group which would have confused the differ-ences between rEEG-guided therapy and control-guided therapy,required a larger sample size, and created a less ef!cient study.Therefore, the study design team chose to exclude these “equiva-lent” subjects to maintain an ef!cient and clear difference betweentreatments in each group.
2.2. Design
This was a randomized, controlled, single-blind, parallel group,multicenter study of rEEG-guided therapy. The control therapy wasbased on a treatment algorithm that was designed to use the mosteffective medications reported in the STAR*D study (Rush et al.,2006). Twelve sites across the United States participated. Eachinvestigator, sub-investigator, and study coordinator was trainedeither during an investigator’s meeting or during a teleconferencethat reviewed the background of rEEG, rEEG interpretation andprotocol administration. QEEG technicians were required to followstandardized collection guidelines (CNS Response Inc, 2009) oncompatible QEEG machines that permitted valid comparisons tothe databases. Each QEEG technicianwas required to submit at leastone sample EEG recording to con!rm their ability to produce a 20-min artifact-free EEG and to upload the report to a secure FTPwebsite and to con!rm the sponsor’s ability to process therecording.
2.2.1. Screening visitThe study began for each subject with informed consent fol-
lowed by con!rmation of minimum entry criteria for MADRS (!26)and QIDS-SR16 (!13), diagnosis of non-psychotic MDD, evaluationof the inclusion/exclusion criteria, urine drug screen, vital signs,drug history, physical exam, psychiatric history, serum laboratoryevaluation, and an optional electrocardiogram (ECG) if one had notbeen done within 6 months. Baseline ratings were also obtained onthe following scales: Clinical Global Impressions of Severity (CGI-S)(Guy, 1967), Q-LES-Q-SF (Rucci et al., 2007) and Patient HealthQuestionnaire (PHQ-9) (Kroenke et al., 2001).
Subjects were classi!ed into two major strata (A and B) and 2sub-strata (1 and 2) as follows:
Stratum A: SSRI failures in the current episode:Sub-Stratum A1: subjects who failed only 1 SSRI.Sub-Stratum A2: subjects who failed !2 SSRIs.
Stratum B: Multiple class failures in the current episode:Sub-Stratum B1: subjects who failed 2 antidepressants in 2classes.Sub-Stratum B2: subjects who failed !3 antidepressants in!2 classes.
2.2.2. Washout period/QEEG visitSubjects who were quali!ed to continue in the study began
a washout period prior to receiving the drug-free QEEG. This
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e12 3
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

washout period consisted of at least !ve half-lives for each drug thesubject was taking at the time of the screening visit. After washout,subjects returned to the site for the QEEG visit. The QIDS-SR16 wasperformed to determine if the subject still quali!ed (score !13) forstudy entry and if not, the subject was asked to return to the clinicwithin 2 months to re-evaluate eligibility once again. Once thesuccessful washout and an eligible QIDS-SR16 were con!rmed,a QEEG was performed by a quali!ed EEG technician and uploadedto the secure rEEG website. If the QEEG recording was inadequatefor a rEEG report, the QEEG was repeated.
2.2.3. Randomization processThis study design was parallel and used two treatment groups
randomized in a 1:1 ratio. A randomization schedule, preparedprior to enrollment of the !rst subject, identi!ed for each stratumthe treatment group assignments (either rEEG or control) in blocksof four. Randomization was centrally performed after a rEEG anda control treatment plan was established for each subject for eachtreatment group (see Section 2.3 below) and “equivalency” wasevaluated.
2.3. Treatment groups
The experimental group received rEEG-guided therapy, whichwas based on the rEEG report. Medication switching based on therEEG report was permitted up to eight weeks after initiatingtreatment.
The control group received therapy using a treatment algorithmthat was based on the most effective medications reported in theSTAR*D study (Rush et al., 2006). The Stratum A control treatmentwas limited to venlafaxine XR, which had the highest response ratein the STAR*D trial. The Stratum B control treatments consisted ofoptions that were similar to those offered in STAR*D (i.e., Steps2e4) but the options were ranked by their reported ef!cacy rates sothe subject would receive the most effective STAR*D treatmentpossible.
2.4. Endpoint measures
The co-primary endpoints for this study were: the QIDS-SR16depression scale and the Q-LES-Q-SF quality of life scale. Thesecondary endpoint measures were the CGI-severity scale, the CGI-improvement scale (Guy, 1967), the MADRS, and PHQ-9.
2.5. Schedule of assessments
The primary measures (QIDS-SR16 and Q-LES-Q-SF) werecollected at screening, the QEEG visit, and weeks 2, 4, 6, 8, 10, and12. The secondary measure CGI-I was collected at each post-treat-ment visit (weeks 2, 4, 6, 8, 10, and 12). The other secondarymeasures (CGI-S, MADRS and PHQ-9) were collected at screeningand at week 12.
2.6. Statistical analysis
The study populations were de!ned as follows. Randomizedpopulation: all subjects who were randomized in the trial, whetheror not they received study medication. Safety population:randomized subjects who received at least one dose of studymedication. Modi!ed intent-to-treat (MITT) population: random-ized subjects who received at least one dose of study medicationand had valid data to calculate the baseline and post-baselinevalues for the primary endpoints. Per protocol (PP) population: allMITT subjects who were treated according to the protocol withoutsigni!cant protocol violations or lack of compliance.
The protocol-de!ned analysis for the primary endpointmeasures (QIDS-SR16 and Q-LES-Q-SF) was mean change frombaseline at week 12 in the PP population. Secondary analyses of thePP population were as follows: QIDS-SR16 response (50% reduc-tion), QIDS-SR16 remission (score %5), mean change in MADRSscores, MADRS response (50% reduction), MADRS remission (score%12), mean change in CGI-I scores, percent subjects with CGI-Iscore of 2 or 1 (much or very much improved), percent subjectswith CGI-I score of 1 (very much improved), mean change in PHQ-9score, PHQ-9 response (50% reduction), PHQ-9 remission (score%5), and mean change in CGI-S score. Negative mean change frombaseline results represent a clinical improvement for all endpointsexcept for the Q-LES-Q-SF re"ecting a clinical improvement witha positive mean change from baseline. The same analyses wereperformed for the MITT population and the results are presentedwhere appropriate. Statistical signi!cance for the two primaryoutcome measures is de!ned as p-value %0.05, using two-tailedanalysis, with no adjustments for multiplicity.
The ef!cacy variables that were measured at multiple timepoints during the trial (QIDS-SR16, Q-LES-Q-SF, CGI-I) wereanalyzed using a mixed model repeated measures analyses withthe two strati!cation factors, site and prior treatment failure(s)(Stratum A and Stratum B) included in the models. The exceptionsto this approach were those variables that were collected only atscreening and at week 12 (MADRS, PHQ-9, and CGI-severity) whichwere evaluated using analysis of covariance (ANCOVA).
3. Results
3.1. Patient disposition
As shown in the patient "ow diagram (Fig. 1), a total of 465subjects consented to be screened for the study. Due to inclusion/exclusion criteria speci!ed by protocol, 269 of these subjects wereexcluded prior to randomization for: washout failure (n$ 21),physiologic abnormalities on the EEG (n$ 7), low abnormality onthe rEEG report (n$ 25), no strong prediction by rEEG (n$ 10),previous failure of rEEG-guided medications (n$ 8), equivalency(n$ 54), and other exclusion criteria (n$ 144) such as bipolar, OCD,alcoholism, suicidality, manic disorder, thyroid, positive drugscreen, labs, EKG, low MADRS or QIDS, or current episode medi-cations did not qualify for the protocol. Another 82 (out of 465)subjects were excluded prior to randomization for non-protocol-related reasons such as: withdrawn consent (n$ 40), unusableQEEG (n$ 1), no reason given (n$ 12), investigator retirement(n$ 5), and the sponsor stopped the study (n$ 24). A total of 114subjects were randomized (57 rEEG, 57 control). Stratum A (SSRIfailures) consisted of 44 subjects and Stratum B (multiple classfailures) consisted of 70 subjects. Of the 114 randomized subjects,three subjects failed to receive at least one dose of study medica-tions, leaving 111 subjects in the Safety Population. A total of 13subjects were lost to follow up after receiving study medicationand 19 subjects prematurely terminated due to: adverse events(AEs) (4), lack of ef!cacy (3), withdrawal of consent (6), and otherreasons (6). Eighty-two (82) subjects completed all 12 weeks oftreatment. The MITT population consisted of 104 randomizedsubjects who received at least one dose of study medication, anddelivered valid data for the primary endpoints. Fifteen (15) MITTsubjects did not ful!ll all protocol criteria and were excludedfrom the PP population for: non-compliance with medicationinstructions (n$ 11); medication problems such as failure to usea speci!ed medication (n$ 1) or use of a drug that was speci!-cally prohibited by protocol (n$ 1); or, due to an error prior torandomization which allowed the subject to be randomizedwhen he/she should have been excluded from treatment due to
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e124
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

inclusion/exclusion criteria (n$ 2). The PP population, therefore,consisted of 89 MITT subjects who completed at least two weeksof treatment, delivered primary endpoint data and ful!lled allprotocol criteria. Out of the 89 PP subjects analyzed for ef!cacy,40 subjects were in the rEEG group and 49 subjects were in theSTAR*D group.
3.2. Demographic and background characteristics
This study population was on average 44 years old, 63% femaleand 66% Caucasian. These characteristics were similarly repre-sented in both the rEEG and control treatment groups (see baselinedemographic, clinical, and psychiatric characteristics of random-ized subjects, Table 1). The treatment groups were also similar withrespect to the mean number of central nervous system (CNS)medication failures in the current episode (1.6 vs.1.4) and the meannumber of all previous CNSmedication failures (4.3 vs. 3.9) for rEEGand control, respectively.
3.3. Ef!cacy results
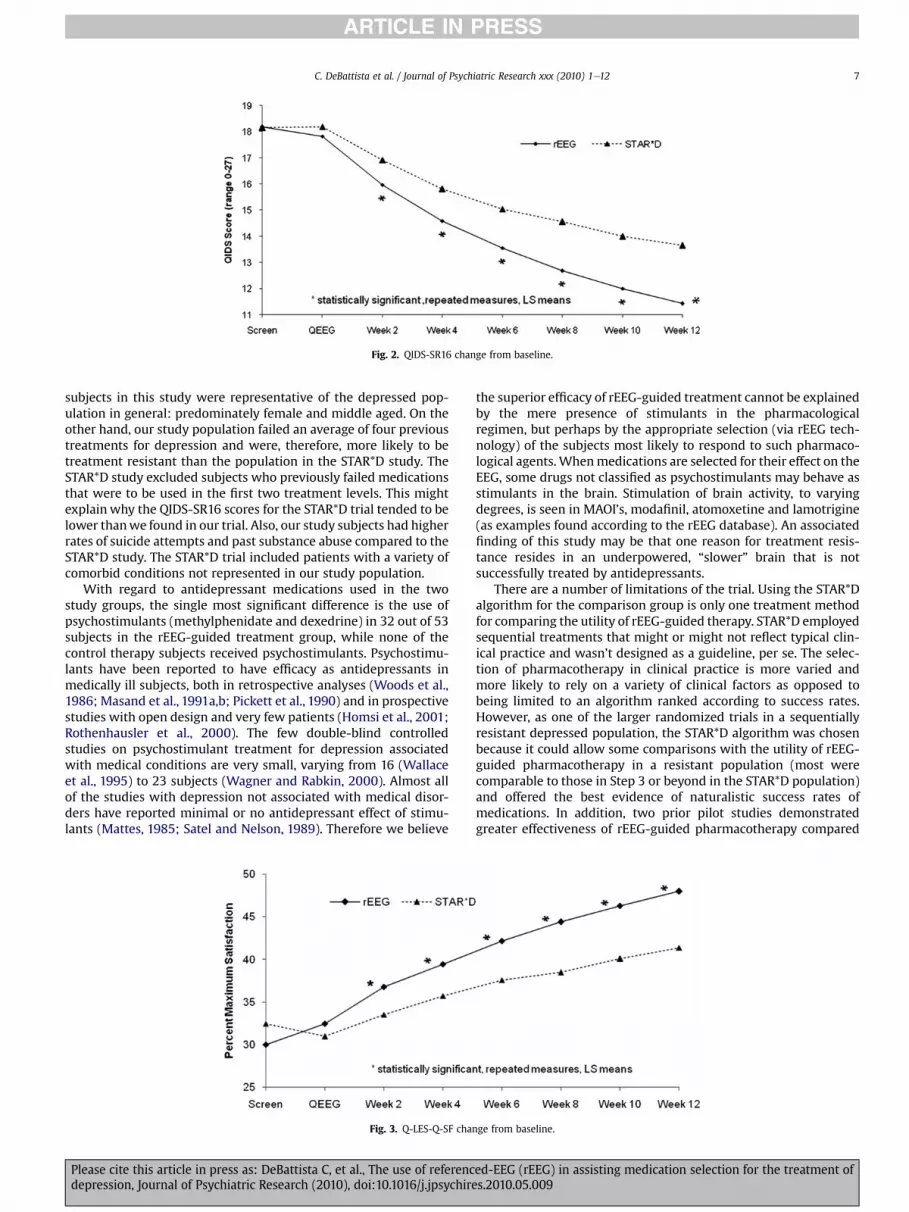
The ef!cacy results for the primary endpoints are presentedin Table 2 and Figs. 2 and 3. Per protocol subjects treated in the
rEEG-guided group exhibited signi!cantly greater improvement inmean change from baseline scores for both primary endpoints:QIDS-SR16 ("6.8 vs. "4.5, p< 0.0002) and Q-LES-Q-SF (18.0 vs. 8.9,p< 0.0002) compared to control-guided therapy, respectively. TheMITT population results for the primary endpoints are alsoprovided in Table 2, and are signi!cantly in favor of rEEG-guidedtreatment over control.
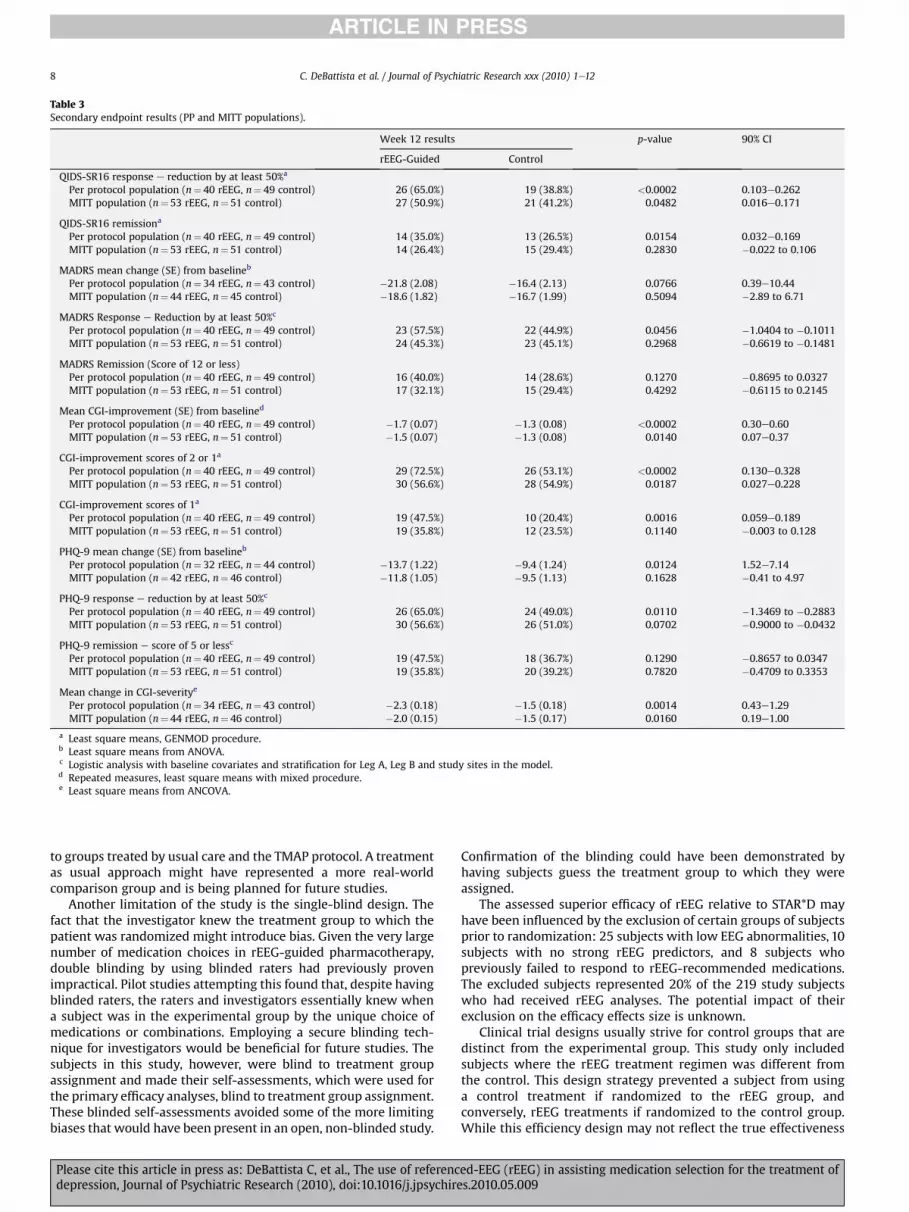
The ef!cacy results for the secondary endpoints for both the PPand MITT populations are presented in Table 3.
In the PP population, using the QIDS-SR16 response andremission endpoints, rEEG-guided therapy demonstrated statisti-cally signi!cant improvement over control-guided therapy. For theglobal assessments, the CGI-improvement scores at each visitdemonstrated that rEEG-guided therapy signi!cantly exceededcontrol-guided therapy on all analyses (CGI-I scores of 2 or 1, andCGI-I scores of 1), and the CGI-S change from baseline at week 12was statistically superior to control as well. For the web-basedMADRS, the analysis of MADRS responders was statistically greaterthan control, however, the change from baseline and remissionanalyses were not statistically greater in the rEEG-guided group.For the PHQ-9, analyses of change from baseline and response,subjects in the rEEG-guided therapy exhibited statistically greaterimprovement compared to the control group. The PHQ-9 remission
Assessed for Eligibility
(n=465)
Excluded from randomization (n=351) due to:
Protocol Inclusion/Exclusion Criteria:21 - washout failure7 - physiologic abnormality on EEG25 - low abnormality in rEEG report10 - no strong prediction by rEEG report8 - previous failure of rEEG-recommended meds54 - rEEG recommendation no different than control144 - other protocol inclusion/exclusion criteria:
(bipolar, OCD, alcoholism, suicidality, manic disorder, thyroid, positive drug screen, labs, EKG, low MADRS or QIDS, or current episode medications did not qualify)
Other Reasons:12 - no reason given5 - investigator retired24 - sponsor stopped the study40 - withdrew consent (includes lost-to-follow-up)1 - unable to obtain a usable QEEG
Randomized Population (n=114)
Allocated to rEEG-guided therapy (n= 57)
Safety Population (received medication)
(n=55)
Failed to pick up prescription (n=2)
Allocated to control therapy (n=57)
Safety Population (received medication)
(n=56)
Failed to pick up prescription (n=1)
Lost to follow-up (n=5)
Discontinued intervention due to:
Adverse Events (n=1)
Lack of Efficacy (n=2)
Withdrew Consent (n=4)
Other (n=4)
Modified ITT Population (n=53)
Per-Protocol Population (n=40)
Lost to follow-up (n=8)
Discontinued intervention due to:
Adverse Events (n=3)
Lack of Efficacy (n=1)
Withdrew Consent (n=2)
Other (n=2)
Modified ITT Population (n=51)
Per-Protocol Population (n=49)
Fig. 1. Patient "ow diagram.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e12 5
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

endpoint failed to detect a difference between treatment groups. Intotal, 9 of the 12 secondary endpoint analyses in this studydemonstrated signi!cant improvement for subjects in the rEEGgroup compared to control.
From week 2 to week 12, rEEG-guided therapy demonstratedsigni!cant superiority with both an increasing level of separationon the QIDS-SR16 and Q-LES-Q-SF (see Figs. 2 and 3) as well as anincreasing signi!cance level on these measures. In addition, theincreasing separation was statistically signi!cant for QIDS-SR16between groups when comparing each week to the next (p< 0.005,2 tailed test, df$ 4).
3.4. Exposure and tolerability
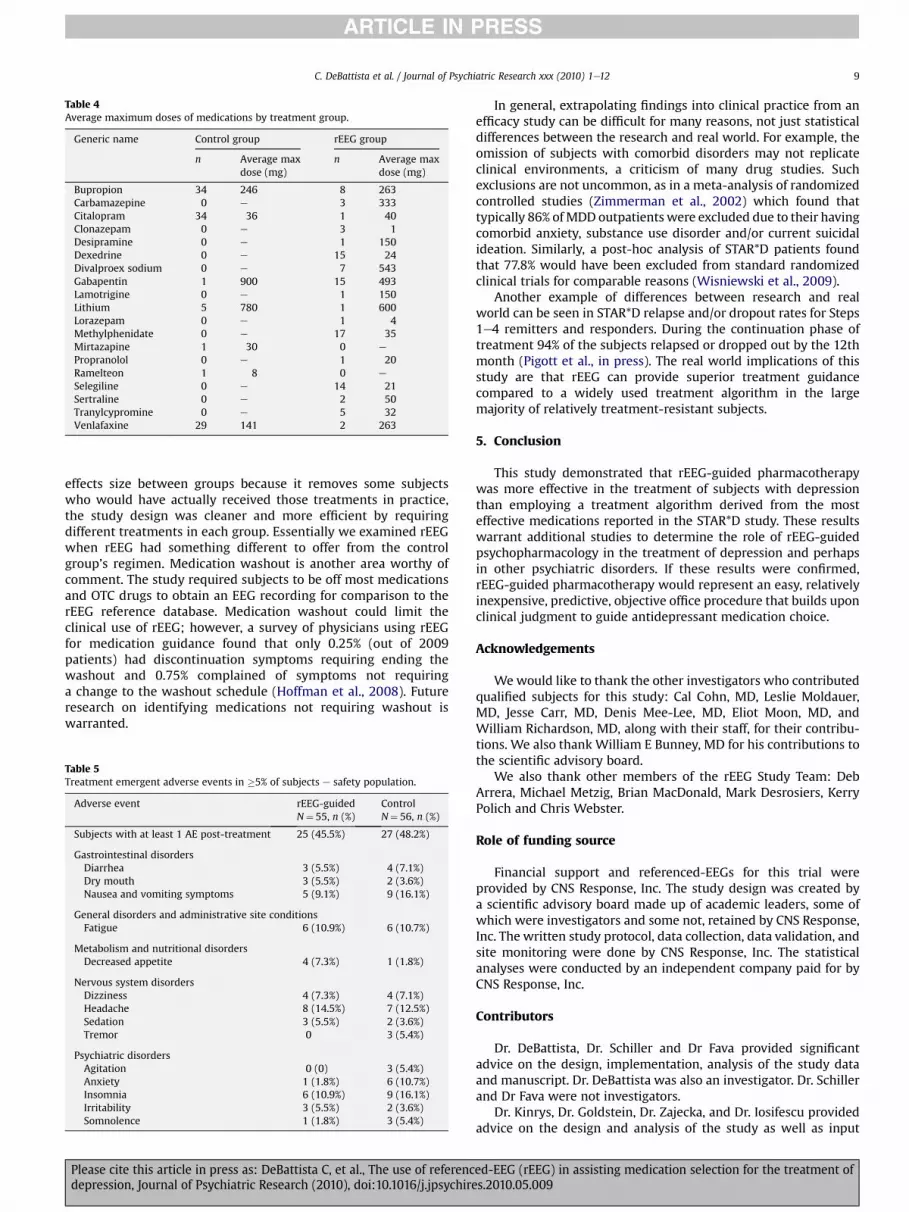
Medications and average maximum doses used for treatment inthe rEEG and control groups are presented in Table 4. Not presentedare the combinations of medications used by subjects. The tablereveals the variety of medications used in the rEEG group comparedto the antidepressant therapy used by the control group.
Treatment emergent AEs occurred in 45.5% of the subjects in therEEG-guided treatment group and 48.2% of the subjects in theSTAR*D-guided treatment group (Table 5). The most frequentlyreported AEs (in >10% of subjects) in either the rEEG-guided orcontrol-guided treatment groups were nausea and vomitingsymptoms (9.1% vs. 16.1%), fatigue (10.9% vs. 10.7%), headache(14.5% vs. 12.5%), anxiety (1.8% vs. 10.7%), and insomnia (10.9% vs.16.1%), respectively. The AEs that were at least 5% greater in onegroup vs. the other were: nausea and vomiting symptoms werefewer (9.1% vs. 16.1%); decreased appetite was higher (7.3% vs. 1.8%);agitation was lower (0 vs. 5.4%); anxiety was lower (1.8% vs. 10.7%)insomnia was lower (10.9% vs. 16.1%) and tremor was lower (0 vs.5.4%) for subjects in the rEEG group compared to control, respec-tively. No serious adverse events were reported in this study. Noneof these AEs were new or different from typically reported sideeffects in the drug’s package insert.
4. Discussion
Referenced-EEG-guided pharmacotherapy appeared to be moreeffective in treating depressed patients than treatment based onthe most effective medications used in the STAR*D study. Theresults appeared to be consistent for the co-primary outcomemeasures (QIDS-SR16 and Q-LES-Q-SF), and across 9 of the 12secondary outcome measures. The secondary endpoints includingQIDS-SR16, Q-LES-Q-SF, MADRS, CGI-I, CGI-S, and PHQ-9 wereanalyzed for change from baseline, response, and remission. Nearlyall analyses revealed signi!cant improvements for the rEEG groupover the control group. Only the remission analyses of QIDS-SR16pre-post, MADRS, and PHQ-9 failed to achieve statistical superi-ority. The secondary endpoint superiority of rEEG over controlprovides clinically relevant support for favoring rEEG-guidedpharmacotherapy. For example, the magnitude of improvement onthe QIDS-SR16 response rate was 65% for rEEG compared to only38.8% for control. Likewise, the secondary measures on the Q-LES-Q-SF were also quite consistent in supporting the ef!cacy of therEEG-guided pharmacotherapy. In addition, the week-to-weekanalysis showing statistically increasing separation from week toweek suggests that rEEG’s superiority in reducing patients’depressive symptoms might have continued had the trialcontinued.
Relative to the STAR*D trial this study population had someimportant similarities and differences. Like STAR*D the randomized
Table 1Baseline demographic, clinical, and psychiatric characteristics of randomizedsubjects.
Characteristics rEEG-guidedn$ 57
Controln$ 57
Demographic characteristicsSexMale, n (%) 22 (38.6%) 20 (35.1%)Female, n (%) 35 (61.4%) 37 (64.9%)
Age (years)Mean (SD) 45.6 (13.6) 43.2 (11.4)Median 48.4 45.3MineMax 18e70 18e62
Weight (lbs)Mean (SD) 183.8 (45.5) 176.2 (50.4)Median 178.0 165.0MineMax 94e304 97e308
RaceCaucasian, n (%) 36 (63.2%) 39 (68.4%)Asian, n (%) 1 (1.8%) 3 (5.3%)Hispanic, n (%) 11 (19.3%) 7 (12.3%)Black, n (%) 6 (10.5%) 5 (8.8%)Paci!c Islanders, n (%) 1 (1.8%) 0Other, n (%) 2 (3.5%) 3 (5.3%)
Number of previously failed CNS medicationsIn the current episode 1.6 1.4All previous CNS meds 4.3 3.9
Psychiatric historyAge of !rst psychiatric episode (years) 29.5 24.2Age of !rst depressive episode (years) 29.7 26.1Psychiatric hospitalizations, n (%) 17 (30.4%) 11 (21.2%)Suicide attempts, n (%) 17 (30.4%) 11 (21.2%)History of substance abuse, n (%) 16 (28.6%) 11 (21.2%)Subjects with comorbid psychiatric illnesses,n (%)
20 (35.7%) 14 (26.9%)
Study duration (days)Mean (SD) 116.8 (32.2) 107.2 (32.1)Median 122.0 113.0MineMax 23e190 19e168
Table 2Primary endpoint results (PP and MITT populations).
Baseline (screening) Week 12 change from baseline p-value 90% CI
Mean scores (SE) Least square meansa (SE)
rEEG-guided Control rEEG-guided Control
Per protocol n$ 40 n$ 49 n$ 34 n$ 44QIDS-SR16 (PP) 18.2 (0.50) 18.2 (0.45) "6.8 (0.35) "4.5 (0.38) <0.0002 1.52e2.99Q-LES-Q-SF (PP) 30.0 (2.18) 32.4 (2.18) 18.0 (1.06) 8.9 (1.14) <0.0002 "11.21 to "6.81
Modi!ed ITT n$ 53 n$ 51 n$ 45 n$ 46QIDS-SR16 (MITT) 18.3 (0.44) 18.0 (0.45) "5.7 (0.30) "4.2 (0.34) <0.0002 0.84e2.17Q-LES-Q-SF (MITT) 29.8 (1.94) 32.6 (2.10) 14.1 (0.92) 8.0 (1.05) <0.0002 "8.17 to "4.07
a Repeatedmeasures, two-tailed, mixed procedure with covariance structure including strati!cation (Leg A, Leg B) and study sites in themodel. PP (per protocol population).MITT (modi!ed intent-to-treat population).
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e126
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009
subjects in this study were representative of the depressed pop-ulation in general: predominately female and middle aged. On theother hand, our study population failed an average of four previoustreatments for depression and were, therefore, more likely to betreatment resistant than the population in the STAR*D study. TheSTAR*D study excluded subjects who previously failed medicationsthat were to be used in the !rst two treatment levels. This mightexplain why the QIDS-SR16 scores for the STAR*D trial tended to belower thanwe found in our trial. Also, our study subjects had higherrates of suicide attempts and past substance abuse compared to theSTAR*D study. The STAR*D trial included patients with a variety ofcomorbid conditions not represented in our study population.
With regard to antidepressant medications used in the twostudy groups, the single most signi!cant difference is the use ofpsychostimulants (methylphenidate and dexedrine) in 32 out of 53subjects in the rEEG-guided treatment group, while none of thecontrol therapy subjects received psychostimulants. Psychostimu-lants have been reported to have ef!cacy as antidepressants inmedically ill subjects, both in retrospective analyses (Woods et al.,1986; Masand et al., 1991a,b; Pickett et al., 1990) and in prospectivestudies with open design and very few patients (Homsi et al., 2001;Rothenhausler et al., 2000). The few double-blind controlledstudies on psychostimulant treatment for depression associatedwith medical conditions are very small, varying from 16 (Wallaceet al., 1995) to 23 subjects (Wagner and Rabkin, 2000). Almost allof the studies with depression not associated with medical disor-ders have reported minimal or no antidepressant effect of stimu-lants (Mattes, 1985; Satel and Nelson, 1989). Therefore we believe
the superior ef!cacy of rEEG-guided treatment cannot be explainedby the mere presence of stimulants in the pharmacologicalregimen, but perhaps by the appropriate selection (via rEEG tech-nology) of the subjects most likely to respond to such pharmaco-logical agents. Whenmedications are selected for their effect on theEEG, some drugs not classi!ed as psychostimulants may behave asstimulants in the brain. Stimulation of brain activity, to varyingdegrees, is seen in MAOI’s, moda!nil, atomoxetine and lamotrigine(as examples found according to the rEEG database). An associated!nding of this study may be that one reason for treatment resis-tance resides in an underpowered, “slower” brain that is notsuccessfully treated by antidepressants.
There are a number of limitations of the trial. Using the STAR*Dalgorithm for the comparison group is only one treatment methodfor comparing the utility of rEEG-guided therapy. STAR*D employedsequential treatments that might or might not re"ect typical clin-ical practice and wasn’t designed as a guideline, per se. The selec-tion of pharmacotherapy in clinical practice is more varied andmore likely to rely on a variety of clinical factors as opposed tobeing limited to an algorithm ranked according to success rates.However, as one of the larger randomized trials in a sequentiallyresistant depressed population, the STAR*D algorithm was chosenbecause it could allow some comparisons with the utility of rEEG-guided pharmacotherapy in a resistant population (most werecomparable to those in Step 3 or beyond in the STAR*D population)and offered the best evidence of naturalistic success rates ofmedications. In addition, two prior pilot studies demonstratedgreater effectiveness of rEEG-guided pharmacotherapy compared
Fig. 2. QIDS-SR16 change from baseline.
Fig. 3. Q-LES-Q-SF change from baseline.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e12 7
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009
to groups treated by usual care and the TMAP protocol. A treatmentas usual approach might have represented a more real-worldcomparison group and is being planned for future studies.
Another limitation of the study is the single-blind design. Thefact that the investigator knew the treatment group to which thepatient was randomized might introduce bias. Given the very largenumber of medication choices in rEEG-guided pharmacotherapy,double blinding by using blinded raters had previously provenimpractical. Pilot studies attempting this found that, despite havingblinded raters, the raters and investigators essentially knew whena subject was in the experimental group by the unique choice ofmedications or combinations. Employing a secure blinding tech-nique for investigators would be bene!cial for future studies. Thesubjects in this study, however, were blind to treatment groupassignment and made their self-assessments, which were used forthe primary ef!cacy analyses, blind to treatment group assignment.These blinded self-assessments avoided some of the more limitingbiases that would have been present in an open, non-blinded study.
Con!rmation of the blinding could have been demonstrated byhaving subjects guess the treatment group to which they wereassigned.
The assessed superior ef!cacy of rEEG relative to STAR*D mayhave been in"uenced by the exclusion of certain groups of subjectsprior to randomization: 25 subjects with low EEG abnormalities, 10subjects with no strong rEEG predictors, and 8 subjects whopreviously failed to respond to rEEG-recommended medications.The excluded subjects represented 20% of the 219 study subjectswho had received rEEG analyses. The potential impact of theirexclusion on the ef!cacy effects size is unknown.
Clinical trial designs usually strive for control groups that aredistinct from the experimental group. This study only includedsubjects where the rEEG treatment regimen was different fromthe control. This design strategy prevented a subject from usinga control treatment if randomized to the rEEG group, andconversely, rEEG treatments if randomized to the control group.While this ef!ciency design may not re"ect the true effectiveness
Table 3Secondary endpoint results (PP and MITT populations).
Week 12 results p-value 90% CI
rEEG-Guided Control
QIDS-SR16 response e reduction by at least 50%a
Per protocol population (n$ 40 rEEG, n$ 49 control) 26 (65.0%) 19 (38.8%) <0.0002 0.103e0.262MITT population (n$ 53 rEEG, n$ 51 control) 27 (50.9%) 21 (41.2%) 0.0482 0.016e0.171
QIDS-SR16 remissiona
Per protocol population (n$ 40 rEEG, n$ 49 control) 14 (35.0%) 13 (26.5%) 0.0154 0.032e0.169MITT population (n$ 53 rEEG, n$ 51 control) 14 (26.4%) 15 (29.4%) 0.2830 "0.022 to 0.106
MADRS mean change (SE) from baselineb
Per protocol population (n$ 34 rEEG, n$ 43 control) "21.8 (2.08) "16.4 (2.13) 0.0766 0.39e10.44MITT population (n$ 44 rEEG, n$ 45 control) "18.6 (1.82) "16.7 (1.99) 0.5094 "2.89 to 6.71
MADRS Response e Reduction by at least 50%c
Per protocol population (n$ 40 rEEG, n$ 49 control) 23 (57.5%) 22 (44.9%) 0.0456 "1.0404 to "0.1011MITT population (n$ 53 rEEG, n$ 51 control) 24 (45.3%) 23 (45.1%) 0.2968 "0.6619 to "0.1481
MADRS Remission (Score of 12 or less)Per protocol population (n$ 40 rEEG, n$ 49 control) 16 (40.0%) 14 (28.6%) 0.1270 "0.8695 to 0.0327MITT population (n$ 53 rEEG, n$ 51 control) 17 (32.1%) 15 (29.4%) 0.4292 "0.6115 to 0.2145
Mean CGI-improvement (SE) from baselined
Per protocol population (n$ 40 rEEG, n$ 49 control) "1.7 (0.07) "1.3 (0.08) <0.0002 0.30e0.60MITT population (n$ 53 rEEG, n$ 51 control) "1.5 (0.07) "1.3 (0.08) 0.0140 0.07e0.37
CGI-improvement scores of 2 or 1a
Per protocol population (n$ 40 rEEG, n$ 49 control) 29 (72.5%) 26 (53.1%) <0.0002 0.130e0.328MITT population (n$ 53 rEEG, n$ 51 control) 30 (56.6%) 28 (54.9%) 0.0187 0.027e0.228
CGI-improvement scores of 1a
Per protocol population (n$ 40 rEEG, n$ 49 control) 19 (47.5%) 10 (20.4%) 0.0016 0.059e0.189MITT population (n$ 53 rEEG, n$ 51 control) 19 (35.8%) 12 (23.5%) 0.1140 "0.003 to 0.128
PHQ-9 mean change (SE) from baselineb
Per protocol population (n$ 32 rEEG, n$ 44 control) "13.7 (1.22) "9.4 (1.24) 0.0124 1.52e7.14MITT population (n$ 42 rEEG, n$ 46 control) "11.8 (1.05) "9.5 (1.13) 0.1628 "0.41 to 4.97
PHQ-9 response e reduction by at least 50%c
Per protocol population (n$ 40 rEEG, n$ 49 control) 26 (65.0%) 24 (49.0%) 0.0110 "1.3469 to "0.2883MITT population (n$ 53 rEEG, n$ 51 control) 30 (56.6%) 26 (51.0%) 0.0702 "0.9000 to "0.0432
PHQ-9 remission e score of 5 or lessc
Per protocol population (n$ 40 rEEG, n$ 49 control) 19 (47.5%) 18 (36.7%) 0.1290 "0.8657 to 0.0347MITT population (n$ 53 rEEG, n$ 51 control) 19 (35.8%) 20 (39.2%) 0.7820 "0.4709 to 0.3353
Mean change in CGI-severitye
Per protocol population (n$ 34 rEEG, n$ 43 control) "2.3 (0.18) "1.5 (0.18) 0.0014 0.43e1.29MITT population (n$ 44 rEEG, n$ 46 control) "2.0 (0.15) "1.5 (0.17) 0.0160 0.19e1.00
a Least square means, GENMOD procedure.b Least square means from ANOVA.c Logistic analysis with baseline covariates and strati!cation for Leg A, Leg B and study sites in the model.d Repeated measures, least square means with mixed procedure.e Least square means from ANCOVA.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e128
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009
effects size between groups because it removes some subjectswho would have actually received those treatments in practice,the study design was cleaner and more ef!cient by requiringdifferent treatments in each group. Essentially we examined rEEGwhen rEEG had something different to offer from the controlgroup’s regimen. Medication washout is another area worthy ofcomment. The study required subjects to be off most medicationsand OTC drugs to obtain an EEG recording for comparison to therEEG reference database. Medication washout could limit theclinical use of rEEG; however, a survey of physicians using rEEGfor medication guidance found that only 0.25% (out of 2009patients) had discontinuation symptoms requiring ending thewashout and 0.75% complained of symptoms not requiringa change to the washout schedule (Hoffman et al., 2008). Futureresearch on identifying medications not requiring washout iswarranted.
In general, extrapolating !ndings into clinical practice from anef!cacy study can be dif!cult for many reasons, not just statisticaldifferences between the research and real world. For example, theomission of subjects with comorbid disorders may not replicateclinical environments, a criticism of many drug studies. Suchexclusions are not uncommon, as in a meta-analysis of randomizedcontrolled studies (Zimmerman et al., 2002) which found thattypically 86% ofMDD outpatientswere excluded due to their havingcomorbid anxiety, substance use disorder and/or current suicidalideation. Similarly, a post-hoc analysis of STAR*D patients foundthat 77.8% would have been excluded from standard randomizedclinical trials for comparable reasons (Wisniewski et al., 2009).
Another example of differences between research and realworld can be seen in STAR*D relapse and/or dropout rates for Steps1e4 remitters and responders. During the continuation phase oftreatment 94% of the subjects relapsed or dropped out by the 12thmonth (Pigott et al., in press). The real world implications of thisstudy are that rEEG can provide superior treatment guidancecompared to a widely used treatment algorithm in the largemajority of relatively treatment-resistant subjects.
5. Conclusion
This study demonstrated that rEEG-guided pharmacotherapywas more effective in the treatment of subjects with depressionthan employing a treatment algorithm derived from the mosteffective medications reported in the STAR*D study. These resultswarrant additional studies to determine the role of rEEG-guidedpsychopharmacology in the treatment of depression and perhapsin other psychiatric disorders. If these results were con!rmed,rEEG-guided pharmacotherapy would represent an easy, relativelyinexpensive, predictive, objective of!ce procedure that builds uponclinical judgment to guide antidepressant medication choice.
Acknowledgements
Wewould like to thank the other investigators who contributedquali!ed subjects for this study: Cal Cohn, MD, Leslie Moldauer,MD, Jesse Carr, MD, Denis Mee-Lee, MD, Eliot Moon, MD, andWilliam Richardson, MD, along with their staff, for their contribu-tions. We also thank William E Bunney, MD for his contributions tothe scienti!c advisory board.
We also thank other members of the rEEG Study Team: DebArrera, Michael Metzig, Brian MacDonald, Mark Desrosiers, KerryPolich and Chris Webster.
Role of funding source
Financial support and referenced-EEGs for this trial wereprovided by CNS Response, Inc. The study design was created bya scienti!c advisory board made up of academic leaders, some ofwhich were investigators and some not, retained by CNS Response,Inc. The written study protocol, data collection, data validation, andsite monitoring were done by CNS Response, Inc. The statisticalanalyses were conducted by an independent company paid for byCNS Response, Inc.
Contributors
Dr. DeBattista, Dr. Schiller and Dr Fava provided signi!cantadvice on the design, implementation, analysis of the study dataand manuscript. Dr. DeBattista was also an investigator. Dr. Schillerand Dr Fava were not investigators.
Dr. Kinrys, Dr. Goldstein, Dr. Zajecka, and Dr. Iosifescu providedadvice on the design and analysis of the study as well as input
Table 4Average maximum doses of medications by treatment group.
Generic name Control group rEEG group
n Average maxdose (mg)
n Average maxdose (mg)
Bupropion 34 246 8 263Carbamazepine 0 e 3 333Citalopram 34 36 1 40Clonazepam 0 e 3 1Desipramine 0 e 1 150Dexedrine 0 e 15 24Divalproex sodium 0 e 7 543Gabapentin 1 900 15 493Lamotrigine 0 e 1 150Lithium 5 780 1 600Lorazepam 0 e 1 4Methylphenidate 0 e 17 35Mirtazapine 1 30 0 e
Propranolol 0 e 1 20Ramelteon 1 8 0 e
Selegiline 0 e 14 21Sertraline 0 e 2 50Tranylcypromine 0 e 5 32Venlafaxine 29 141 2 263
Table 5Treatment emergent adverse events in !5% of subjects e safety population.
Adverse event rEEG-guidedN$ 55, n (%)
ControlN$ 56, n (%)
Subjects with at least 1 AE post-treatment 25 (45.5%) 27 (48.2%)
Gastrointestinal disordersDiarrhea 3 (5.5%) 4 (7.1%)Dry mouth 3 (5.5%) 2 (3.6%)Nausea and vomiting symptoms 5 (9.1%) 9 (16.1%)
General disorders and administrative site conditionsFatigue 6 (10.9%) 6 (10.7%)
Metabolism and nutritional disordersDecreased appetite 4 (7.3%) 1 (1.8%)
Nervous system disordersDizziness 4 (7.3%) 4 (7.1%)Headache 8 (14.5%) 7 (12.5%)Sedation 3 (5.5%) 2 (3.6%)Tremor 0 3 (5.4%)
Psychiatric disordersAgitation 0 (0) 3 (5.4%)Anxiety 1 (1.8%) 6 (10.7%)Insomnia 6 (10.9%) 9 (16.1%)Irritability 3 (5.5%) 2 (3.6%)Somnolence 1 (1.8%) 3 (5.4%)
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e12 9
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

on the manuscript. Dr. Kinrys and Dr. Goldstein were also investi-gators. Dr. Zajecka a sub-investigator. Dr. Iosifescu was not aninvestigator.
Dr. Hoffmanwas Chief Medical Of!cer over the rEEG Study Teamat CNS Response, Inc. He coordinated with all advisors to thedesign, implementation, and analysis of the study data. He was notan investigator.
Dr. Kocsis and Dr. Teicher provided advice into the analysis ofthe study as well as input into the manuscript. Both wereinvestigators.
Dr. Potkin and Dr. Preda provided input into the manuscript.Both were investigators.
Dr. Multani provided review of the manuscript. He was also aninvestigator.
Mr. Brandt provided advice into the design of the study andapproval of the manuscript.
Con!ict of interestDr. DeBattista has received research support in the last 5 years
from: GSK, Wyeth, Lilly, Cephalon, Cyberonics, Neuronetics,Novaritis, AstraZeneca, Forest, CNS Response, Medtronics, Boer-hinger, ANS, P!zer, Neuropace, Brain Resources. Dr. DeBattista hasreceived support as a speaker/consultant in the last 5 years from:Lilly, GSK, P!zer, Cephalon, Wyeth, BMS, AstraZeneca, Cyberonics,Corcept, Forest. Dr. DeBattista is a stock holder in: CorceptTherapeutics.
Dr. Kinrys has received research support from: Astra-Zeneca,Bristol-Myers Squibb Company, Cephalon, Elan Pharmaceuticals, EliLilly & Company, Forest Pharmaceuticals Inc., GlaxoSmithkline,Sano!/Synthelabo, Sepracor Inc., P!zer Inc, UCB Pharma, Wyeth-Ayerst Laboratories. Dr. Kinrys has served as an Advisor and/orConsultant to: Astra-Zeneca, Cephalon, Eli Lilly & Company, ForestPharmaceuticals Inc., GlaxoSmithkline, Janssen Pharmaceutica,P!zer Inc, Sepracor Inc., UCB Pharma, Wyeth-Ayerst Laboratories.Dr. Kinrys has received speaking support from: Astra-Zeneca, ForestPharmaceuticals Inc., GlaxoSmithkline, Sepracor Inc., Wyeth-AyerstLaboratories.
Dr. Martin H. Teicher has received (throughout his lifetime)research support from: NIMH, NIDA, NARSAD, Tourette’s SyndromeAssociation, Scottish Rite Schizophrenia Research Program,ADAMHA, USPHS, LiteBook, CNS Response, BioBehavioral Diag-nostic Co., Kodak, GlaxoSmithKline, Wyeth-Ayerst, OPTAx SystemsInc., Sepracor, SunBox, Ambulatory Monitoring Inc., Copley Phar-maceuticals, Glaxo-Welcome, Sandoz andMead Johnson. Dr MartinH. Teicher has spoken with support from the following companies:BioBehavioral Diagnostic Co., Bristol-Myers Squib, Glaxo-Welcome,Optax Systems Inc., Upjohn, Cell-tech, Cephalon, J & J Pharmaceu-ticals and Eli Lilly. Dr. Martin H. Teicher has served on the Scienti!cAdvisory Board of the following companies: OPTAx Systems Inc.and BioBehavioral Diagnostic Co. and has received consulting feesfrom these companies. He has also received consulting fees fromMDCI, Copley Pharmaceuticals, Watson Pharmaceuticals, Sention,Sepracor and Ambulatory Monitoring Inc. Dr. Martin H. Teicherholds 13 US Patents and has received patent royalties for inventionslicensed through McLean Hospital to Sepracor, Optax Systems Inc,and BioBehavioral Diagnostic Co.
Dr. Maurizio Fava has received research support (over his life-time) from the following companies: Abbott Laboratories,Alkermes, Aspect Medical Systems, Astra-Zeneca, BioResearch,BrainCells, Inc., Bristol-Myers Squibb Company, Cephalon, ClinicalTrial Solutions,LLC, Eli Lilly & Company, Forest Pharmaceuticals Inc.,Ganeden, GlaxoSmithKline, J & J Pharmaceuticals, Lichtwer PharmaGmbH, Lorex Pharmaceuticals, NARSAD, NCCAM, NIDA, NIMH,Novartis, Organon Inc., PamLab, LLC, P!zer Inc, Pharmavite, Roche,Sano!-Aventis, Shire, Solvay Pharmaceuticals, Inc., Synthelabo,
Wyeth-Ayerst Laboratories. Dr. Maurizio Fava has consulted (overhis lifetime) to the following companies: Abbott Laboratories,Amarin, Aspect Medical Systems, Astra-Zeneca, Auspex Pharma-ceuticals, Bayer AG, Best Practice Project Management, Inc, Bio-Marin Pharmaceuticals, Inc.,Biovail Pharmaceuticals, Inc.,BrainCells, Inc, Bristol-Myers Squibb Company, Cephalon, ClinicalTrials Solutions,LLC, CNS Response, Compellis, Cypress Pharma-ceuticals, Dov Pharmaceuticals, Eisai, Inc., Eli Lilly & Company, EPIXPharmaceuticals, Euthymics Bioscience, Inc., Fabre-Kramer, Phar-maceuticals, Inc., Forest Pharmaceuticals Inc., GlaxoSmithKline,Grunenthal GmBH, Janssen Pharmaceutica, Jazz Pharmaceuticals, J& J Pharmaceuticals, Knoll Pharmaceutical Company, Labopharm,Lorex Pharmaceuticals, Lundbeck, MedAvante Inc., Merck, Methyl-ation Sciences, Neuronetics, Novartis, Nutrition 21, Organon Inc.,PamLab, LLC, P!zer Inc, PharmaStar, Pharmavite, Precision HumanBiolaboratory, PsychoGenics, Psylin Neurosciences, Inc., RidgeDiagnostics, Inc., Roche, Sano!-Aventis, Sepracor, Schering-Plough,Solvay Pharmaceuticals, Inc., Somaxon, Somerset Pharmaceuticals,Synthelabo, Takeda, Tetragenex, TransForm Pharmaceuticals,Inc., Transcept Pharmaceuticals, Vanda Pharmaceuticals Inc,Wyeth-Ayerst Laboratories. Dr. Maurizio Fava has spoken/pub-lished (over his lifetime) with support from the followingcompanies: Adamed, Co., Advanced Meeting Partners, AmericanPsychiatric Association, American Society of Clinical Psychophar-macology, Astra-Zeneca, Belvoir, Boehringer-Ingelheim, Bristol-Myers Squibb Company, Cephalon, Eli Lilly & Company, ForestPharmaceuticals Inc., GlaxoSmithKline, Imedex, Novartis, OrganonInc., P!zer Inc, PharmaStar, MGH Psychiatry Academy/Primedia,MGH Psychiatry Academy/Reed-Elsevier, UBC, Wyeth-AyerstLaboratories. Dr. Maurizio Fava has equity in the followingcompany: Compellis. Dr. Maurizio Fava has the following rolyal-ties/patents: patent applications for SPCD and for a combination ofazapirones and bupropion in MDD, copyright royalties for theMGH CPFQ, SFI, ATRQ, DESS, and SAFER.
Dr. James H. Kocsis has received research support from: NIMH,NIDA, Burroughs Wellcome Trust, Pritzker Consortium, Astra-Zeneca, Sano! Aventis, Forest, Novartis, CNS Response, Roche. Dr.James H. Kocsis has spokenwith support from: P!zer,Wyeth, Astra-Zeneca. Dr. James H. Kocsis has served on an advisory board for:P!zer and Wyeth.
Dr. Corey Goldstein has received research support from: Astra-Zeneca, Boehringer-Ingelheim, Bristol-Myers Squibb/Otsuka, CNSResponse, Inc., Cyberonics, Eli Lilly, GlaxoSmithKline, McNeil,National Institute of Mental Health, Novartis, PamLab, P!zer,Takeda. Dr. Corey Goldstein has spoken with support from: Astra-Zeneca, Eli Lilly.
Dr. John Zajecka has received research support from: AstraZe-neca, Boehringer-Ingelheim, Bristol-Myers Squibb/Otsuka, CNSResponse, Inc., Cyberonics, Eli Lilly, GlaxoSmithKline, McNeil,National Institute of Mental Health, Novartis, PamLab, P!zer,Takeda. Dr. John Zajecka has served as consultant to: AbbottLaboratories, Bristol-Myers Squibb, Eli Lilly, Novartis, Otsuka,PamLab, P!zer, Takeda, Wyeth-Ayerst. Dr. John Zajecka has spokenwith support from: Abbott Laboratories, AstraZeneca, Bristol-MyersSquibb, Covidien, Cyberonics, Eli Lilly, GlaxoSmithKline, PamLab,P!zer, Wyeth-Ayerst. Dr. John Zajecka is a trustee of Cheryl T.Herman Charitable Foundation.
Dr. Hoffman is an employee of CNS Response, Inc. and holdsstock in the company. Over his lifetime, Dr. Hoffman has spokenwith support from: Wyeth, Forest Laboratories, Cephalon, Eli Lilly,P!zer, GlaxoSmithKline.
Mr. Brandt is a former employee of CNS Response, Inc and holdsstock in the company.
Dr. Mark Schiller has served as consultant to CNS Response, Inc.Dr. Mark Schiller owns stock in CNS Response, Inc.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e1210
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

Dr. Adrian Preda has received research support (over his life-time) from: Astra-Zeneca, NARSAD, NIMH. Dr. Adrian Preda hasspoken/published (over his lifetime) with support from thefollowing companies: American Psychiatric Association, UC Irvine.
Dr. Iosifescu has received research support from Aspect MedicalSystems, Forest Laboratories and Janssen Pharmaceutica. Dr. Iosi-fescu has been a consultant for Forest Laboratories, Gerson Lehr-man Group and P!zer, Inc. Dr. Iosifescu has been a speaker for EliLilly & Co., Forest Laboratories, P!zer, Inc and Reed-Elsevier.
Dr. Steven Potkin received grant support, funding, or has beena paid consultant to the following companies in the past year thatconduct scienti!c or medical research and/or make medicationrelated to Psychiatric and Neurodegenerative disorders: AstraZe-neca AB, Bioline, Bristol-Myers Squibb, Ceregene, Cortex, Dai-nippondSumitomo, Elan Corporation plc, Eli Lilly and Company,Forest Laboratories, Janssen Pharmaceutica, Minster Pharmaceuti-cals, Novartis Pharmaceuticals Corporation, Schering Plough/Merck, Otsuka Pharmaceuticals, P!zer Pharmaceuticals, SolvayPharmaceuticals, Roche Laboratories, Wyeth Research, and Vanda.Dr. Steven Potkin has received grant support, funding or has beena consultant to the following funding agencies, universities anduniversity af!liates, as well as professional organizations thatconduct medical or scienti!c research related to Psychiatric andNeurodegenerative disorders: American Psychiatric Association,Alzheimer’s Association, Brigham and Women’s Hospital, HarvardMassachusetts General Hospital, ISCTM, NIH (NIAAA, NIBIB, NCRR),the University of California, San Francisco and the University ofSouthern California.
Mr. Brandt is a former employee of CNS Response, Inc.All other authors declare no con"icts of interest.
References
Altamura A, Dell'osso B, Vismara S, Mundo E. May duration of untreated illnessin"uence the long-term course of major depressive disorder? EuropeanPsychiatry 2008;23(2):92e6.
American Psychiatric Association. DSM-IV, diagnostic and statistical manual ofmental disorders. 4th ed. American Psychiatric Association; 1994.
Bruder GE, Sedoruk JP, Steward JW, McGrath PJ, Quitkin FM, Tenke CE. EEG alphameasures predict therapeutic response to an SSRI antidepressant: Pre and posttreatment !ndings. Biol. Psychiatry 2008;63(12):1171e7.
Carmody TJ, Rush AJ, Bernstein I, Warden D, Brannan S, Burnham D, et al. TheMontgomery Asberg and the Hamilton ratings of depression: a comparison ofmeasures. Eur. Neuropsychopharmacol. 2006a;16(8):601e11.
Carmody TJ, Rush AJ, Bernstein IH, Brannan S, Husain MM, Trivedi MH. Makingclinicians lives easier: guidance on use of the QIDS self-report in place of theMADRS. Journal of Affective Disorders 2006 October;95(1e3):115e8.
CNS Response, Inc. CNS response [online]. Available from: http://cnsresponse.com/doc/CNSR_rEEG_Intro_Guide_to_EEG_Recording_v2.0_Mar2009.pdf (accessed19.12.09).
Concordant Rater Systems. Products and Services. [Online]. Available from: http://www.concordantrater.com/index.php (accessed 19.12.09).
Cook IA, Leuchter AF, Morgan M, Witte E, Stubbeman WF, Abrams M, et al. Earlychanges in prefrontal activity characterize clinical responders to antidepres-sants. Neuropsychopharmacology 2002;27(1):120e31.
DeBattista, C., Hoffman, D., Schiller, M., Iosifescu, D., 2008. Referenced-EEG (rEEG)guidance of medications for treatment resistant depressed patients e a pilotstudy. Poster #228. US Psychiatric and Mental Health Congress, 2008 Oct.
Dunn L, Demichele A. Genomic predictors of outcome and treatment response inbreast cancer. Molecular Diagnosis and Therapy 2009;13(2):73e90.
Evans K, Dougherty D, Pollack M, Rauch S. Using neuroimaging to predict treatmentresponse in mood and anxiety disorders. Annals of Clinical Psychiatry 2006;18(1):33e42.
Gordon E, Liddell B, Brown K, Bryant R, Clark C, Das P, et al. Integrating objectivegene-brain-behavior markers of psychiatric disorders. Journal of IntegrativeNeuroscience 2007;6(1):1e34.
Greenblatt, J., Sussman, C., Jameson, M., Kasumova, G., 2008. Referenced-EEG!
guided medication predictions in treatment-refractory eating disorder patients.Poster presentation, American Psychiatric Association Annual Meeting.
Guy W. Clinical global impressions. In: ECDEU assessment manual for psycho-pharmacology, revised. Rockville: US Dept of Health, Education, and Welfare,National Institute of Mental Health; 1967.
Henriques JB, Davidson RJ. Left frontal hypoactivation in depression. Journal ofAbnormal Psychology 1991;100:535e45.
Henriques JB, Davidson RJ. Regional brain electrical asymmetries discriminatebetween previously depressed and healthy control subjects. Journal ofAbnormal Psychology 1990;99:22e31.
Hoffman, D.A., DeBattista, C., Schiller, M., 2008. Medication washout: imposingdiscontinuation or a diagnostic and therapeutic tool? Poster #230, US Psychi-atric and Mental Health Congress, San Diego, CA, October, 2008.
Homsi J, Nelson KA, Sarhill N, Rybicki L, LeGrand SB, Davis MP, et al. A phase II studyof methylphenidate for depression in advanced cancer. American Journal ofHospice and Palliative Care 2001;18(6):403e7.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depressionseverity measure. Journal of General Internal Medicine 2001;16:606e13.
Leuchter A, Cook I, Uijtdehaage S, Dunkin J, Lufkin R, Anderson-Hanley C, et al. Brainstructure and function and the outcomes of treatment for depression. Journal ofClinical Psychiatry 1997;58(Suppl. 16):22e31.
Leuchter AF, Cook IA, Marangell LB, Gilmer WS, Burgoyne KS, Howland RH, et al.Comparative effectiveness of biomarkers and clinical indicators for predictingoutcomes of SSRI treatment in major depressive disorder: results of the BRITE-MD study. Psychiatry Research 2009;169:124e31.
Lin E, Chen PS. Pharmacogenomics with antidepressants in the STAR*D study.Pharmacogenomics 2008;9(7):935e46.
Lohoff FW, Ferraro TN. Pharmacogenetic considerations in the treatment ofpsychiatric disorders. Expert Opinion in Pharmacotherapy 2010;11(3):423e39.
Masand P, Pickett P, Murray GB. Psychostimulants for secondary depression inmedical illness. Psychosomatics 1991a;32(2):203e8.
Masand P, Murray GB, Pickett P. Psychostimulants in post-stroke depression. Journalof Neuropsychiatry and Clinical Neurosciences 1991b;3(1):23e7.
Mattes JA. Methylphenidate in mild depression: a double-blind controlled trial.Journal of Clinical Psychiatry 1985;46:525e7.
Pickett P, Masand P, Murray GB. Psychostimulant treatment of geriatric depressivedisorders secondary to medical illness. Journal of Geriatric Psychiatry andNeurology 1990;3(3):146e51.
Pigott, H.E., Leventha, A.M., Alter, G.S., Boren, J.J. The current status of antidepres-sants’ ef!cacy and effectiveness research. Psychotherapy and Psychosomatics,in press.
Rosenblatt JE. Laboratory tests used to guide antimicrobial therapy. Mayo ClinicProceedings 1991;66(9):942e8.
Rothenhausler HB, Ehrentraut S, von Degenfeld G, Weis M, Tichy M, Kilger E, et al.Treatment of depression with methylphenidate in patients dif!cult to weanfrom mechanical ventilation in the intensive care unit. Journal of ClinicalPsychiatry 2000;61(10):750e5.
Rucci P, Rossi A, Mauri M, Maina G, Pieraccini F, Pallanti S, et al. Validity and reli-ability of quality of life, enjoyment and satisfaction questionnaire, short form.Epidemiologia e Psichiatria Sociale 2007;16(1):82e9.
Rush A, Trivedi M, Wisniewski S, Nierenberg A, Stewart J, Warden D, et al. Acute andlonger-term outcomes in depressed outpatients requiring one or severaltreatment steps: a STAR*D report. American Journal of Psychiatry 2006;163(11):1905e17.
Rush AJ. Limitations in ef!cacy of antidepressant monotherapy. Journal of ClinicalPsychiatry 2007;68(Suppl. 10):8e10.
Satel SL, Nelson JC. Stimulants in the treatment of depression: a critical overview.Journal of Clinical Psychiatry 1989;50:241e9.
Schiller, M.J., Emory, W.H., Suf!n, S.C., 2004. rEEG! e in the treatment of eatingdisorders. Poster, NCDEU Conference.
Schiller, M.J., 2008. Referenced EEG-guided pharmacotherapy of dually-diagnosedpatients. Poster presentation, College on Problems in Drug Dependence AnnualMeeting.
Shaffer, J.H., Milner, J.E., Schiller, M.J., 2005. rEEG-guided pharmacotherapy forseverely ill dually-diagnosed patients. Poster presentation, American Psychi-atric Association Annual Meeting.
Sheehan D, Janavs J, Baker R, Lecrubier Y, Hergueta T, Weiller E. MINI internationalneuropsychiatric interview, English version 5.0. Sheehan DV & Lecrubier Y;1992e2006.
Suf!n SC, Emory WH, Gutierrez G, Arora G, Schiller MJ, Kling A. A QEEG databasemethod for predicting pharmacotherapeutic outcome in refractory majordepressive diisorders. Journal of American Physicians and Surgeons 2007;12(4):104e8.
Suf!n SC, Emory WH. Neurometric subgroups in attentional and affective disordersand their association with pharmacotherapeutic outcomes. Clinical Electroen-cephalography 1995;26(2):76e83.
Trivedi MH, Pigott T, Stegman K, Key T, O’Neal B, Baker S, et al. TMAP proceduralmanual: depression module, physician algorithm implementation manual.Physician’s manual. Dallas: University of Texas Southwestern Medical School;1998.
Trivedi MH, Thase ME, Osuntokun O, Henley DB, Case M, Watson SB, et al. Anintegrated analysis of olanzapine/"uoxetine combination in clinical trials oftreatment-resistant depression. Journal of Clinical Psychiatry 2009;70(3):387e96.
Tutt A, Ashworth A. Can genetic testing guide treatment in breast cancer? EuropeanJournal of Cancer 2008;44(18):2774e80.
Warden D, Rush A, Trivedi M, Fava M, Wisniewski S. The STAR*D Project results:a comprehensive review of !ndings. Current Psychiatry ReportS 2007;9(6):449e59.
Wagner GJ, Rabkin R. Effects of dextroamphetamine on depression and fatigue inmen with HIV: a double-blind, placebo-controlled trial. Journal of ClinicalPsychiatry 2000;61(6):436e40.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e12 11
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009

Wallace AE, Kofoed LL, West AN. Double-blind, placebo-controlled trial of methyl-phenidate in older, depressed, medically ill patients. American Journal ofPsychiatry 1995;152:929e31.
Wisniewski SR, Rush AJ, Nierenberg AA, Gaynes BN, Warden D, Luther JF, et al. Canphase III trial results of antidepressant medications be generalized to clinicalpractice? A STAR*D report. American Journal of Psychiatry 2009;166:599e607.
Woods SW, Tesar GE, Murray GB, Cassem NH. Psychostimulant treatment ofdepressive disorders secondary to medical illness. Journal of Clinical Psychiatry1986;47(1):12e5.
Zimmerman M, Mattia JI, Posternak MA. Are subjects in pharmacological treatmenttrials of depression representative of patients in routine clinical practice?American Journal of Psychiatry 2002;159:469e73.
C. DeBattista et al. / Journal of Psychiatric Research xxx (2010) 1e1212
Please cite this article in press as: DeBattista C, et al., The use of referenced-EEG (rEEG) in assisting medication selection for the treatment ofdepression, Journal of Psychiatric Research (2010), doi:10.1016/j.jpsychires.2010.05.009




















