The Use of Checklists Among New Graduate Nurses in a ...
12
The Use of Checklists Among New Graduate Nurses in a Surgical Intensive Care Unit to Improve Patient Safety and Outcomes Kathryn S. Dippel, RN, MSN, AGACNP-BC ¦ Lorraine Duli, RN, MSN ¦ Maureen Keckeisen, RN, MN, CNS New graduate nurses (NGNs) in the intensive care unit have trouble learning standards of care essential to patient safety and outcomes. Two checklists were developed to help NGNs learn to consistently practice to the unit standards of care during orientation. NGNs were more consistently able to practice to the standards of care compared to a control group that had not utilized the checklists. Preceptors noticed modest improvements in the abilities of NGNs to practice to the standards of care. I t is essential that nursing care be held to the highest standard to maintain patient safety and achieve positive outcomes. This includes regular assessment and care of intravenous (IV) drips and IV access, vital signs monitoring and emergency equipment, invasive devices, and hemo- dynamic monitoring systems as well as preparation for shift change to ensure a smooth handoff. In the transplant/ surgical intensive care unit (ICU) in a large academic med- ical center, the new graduate nurses (NGNs) are expected to master difficult medical concepts and operate multiple complex devices after 12 weeks of orientation. Based on staff feedback, preceptor evaluation, and direct observa- tion, it became clear that recent cohorts of NGNs were not consistently practicing to the unit standards of care. For example, NGNs would often fail to change expired central line dressings and IV tubing, which would put pa- tients at risk for serious infectious complications. This was observed to be an issue across multiple NGN cohorts, and so it was determined that there was opportunity to reexam- ine the unit-based NGN orientation program. Discussion with unit leadership, preceptors, and former cohorts of NGNs revealed that although NGNs were trained how to complete the tasks necessary to practice to the unit standard of care, they were not provided with any standard- ized method with which to reliably remember to complete these tasks. Experienced nurses complete these tasks from memory gained through years of repetition; however, it is not reasonable to expect the same of NGNs being oriented to the ICU environment. Rationale According to Patricia Benner’ s novice to expert theory, NGNs are classified as “novices” and are by nature task-oriented and rely on rules to guide their actions. They lack the abil- ity to prioritize tasks to focus the overall clinical picture of the patient (Benner, 1982). NGNs often become entirely focused on remembering to complete tasks and conse- quently forget to pay attention to more important external demands, such as subtle changes in vital signs. Their ability to think critically is extremely limited, and they are unable to develop these skills until they master routine tasks (Benner, 1982). The use of checklists in an ICU NGN orientation pro- gram is an ideal way to provide a standardized tool for NGNs to help them learn to practice to the standards of care. The tasks that must be completed to meet these stan- dards, though seemingly mundane, are critical to maintain- ing patient safety, high-quality care, and patient/family sat- isfaction. In a healthcare system where reimbursement is closely linked to patient outcomes and satisfaction, it is es- sential for NGNs to be provided with standardized tools that ensure they can practice to the standards of care by the time they have completed orientation. Available Knowledge Checklists have long been incorporated as common prac- tice in the aviation industry to ensure the safety and oper- ability of complex systems. The integration of checklists 3.0 ANCC Contact Hours Kathryn S. Dippel, RN, MSN, AGACNP-BC, is a former Staff Nurse, Trans- plant/Surgical Intensive Care Unit, Ronald Reagan UCLA Medical Center, Los Angeles, California. She is now a Critical Care Nurse Practitioner at California Pacific Medical Center, San Francisco, California. Lorraine Duli, RN, MSN, is the Unit Educator, Transplant/Surgical Intensive Care Unit, Ronald Reagan UCLA Medical Center, Los Angeles, California. Maureen Keckeisen, RN, MN, CNS, is the former Clinical Nurse Special- ist, Transplant/Surgical Intensive Care Unit, Ronald Reagan UCLA Medi- cal Center, Los Angeles, California. She retired in June 2019. The authors have no conflicts of interest to disclose. ADDRESS FOR CORRESPONDENCE: Kathryn S. Dippel, 252 McDonnel Road, Alameda, CA 94502 (e‐mail: [email protected]). DOI: 10.1097/NND.0000000000000810 JNPD Journal for Nurses in Professional Development • Volume 38, Number 1, 7–18 • Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved. Journal for Nurses in Professional Development www.jnpdonline.com 7 Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of The Use of Checklists Among New Graduate Nurses in a ...

JNPD Journal for Nurses in Professional Development • Volume 38, Number 1, 7–18 • Copyright © 2021Wolters Kluwer Health, Inc. All rights reserved.
The Use of Checklists AmongNew Graduate Nurses in a SurgicalIntensive Care Unit to ImprovePatient Safety and Outcomes
3.0 ANCCContactHours
Kathryplant/SLos AnCalifor
LorrainCare U
Maureist, Tracal Cen
The au
ADDRRoad,
DOI: 1
Journ
Kathryn S. Dippel, RN, MSN, AGACNP-BC ¦ Lorraine Duli, RN, MSN ¦Maureen Keckeisen, RN, MN, CNS
New graduate nurses (NGNs) in the intensive care unit havetrouble learning standards of care essential to patient safetyand outcomes. Two checklists were developed to help NGNslearn to consistently practice to the unit standards of careduring orientation. NGNs were more consistently able topractice to the standards of care compared to a control groupthat had not utilized the checklists. Preceptors noticedmodest improvements in the abilities of NGNs to practice tothe standards of care.
I t is essential that nursing care be held to the higheststandard tomaintain patient safety and achieve positiveoutcomes. This includes regular assessment and care of
intravenous (IV) drips and IV access, vital signs monitoringand emergency equipment, invasive devices, and hemo-dynamic monitoring systems as well as preparation for shiftchange to ensure a smooth handoff. In the transplant/surgical intensive care unit (ICU) in a large academic med-ical center, the new graduate nurses (NGNs) are expectedto master difficult medical concepts and operate multiplecomplex devices after 12 weeks of orientation. Based onstaff feedback, preceptor evaluation, and direct observa-tion, it became clear that recent cohorts of NGNs werenot consistently practicing to the unit standards of care.For example, NGNs would often fail to change expiredcentral line dressings and IV tubing, which would put pa-tients at risk for serious infectious complications. This was
n S.Dippel, RN,MSN, AGACNP-BC, is a former Staff Nurse, Trans-urgical Intensive CareUnit, Ronald Reagan UCLAMedical Center,geles, California. She is now a Critical Care Nurse Practitioner atnia Pacific Medical Center, San Francisco, California.
eDuli, RN,MSN, is the Unit Educator, Transplant/Surgical Intensivenit, Ronald Reagan UCLA Medical Center, Los Angeles, California.
en Keckeisen, RN, MN, CNS, is the former Clinical Nurse Special-nsplant/Surgical Intensive Care Unit, Ronald Reagan UCLA Medi-ter, Los Angeles, California. She retired in June 2019.
thors have no conflicts of interest to disclose.
ESS FORCORRESPONDENCE: Kathryn S. Dippel, 252McDonnelAlameda, CA 94502 (e‐mail: [email protected]).
0.1097/NND.0000000000000810
al for Nurses in Professional Development
Copyright © 2021 Wolters Kluwer H
observed to be an issue across multiple NGN cohorts, andso it was determined that there was opportunity to reexam-ine the unit-based NGN orientation program.
Discussion with unit leadership, preceptors, and formercohorts of NGNs revealed that although NGNs were trainedhow to complete the tasks necessary to practice to the unitstandard of care, they were not provided with any standard-ized method with which to reliably remember to completethese tasks. Experienced nurses complete these tasks frommemory gained through years of repetition; however, it isnot reasonable to expect the same of NGNs being orientedto the ICU environment.
RationaleAccording to Patricia Benner’s novice to expert theory, NGNsare classified as “novices” and are by nature task-orientedand rely on rules to guide their actions. They lack the abil-ity to prioritize tasks to focus the overall clinical picture ofthe patient (Benner, 1982). NGNs often become entirelyfocused on remembering to complete tasks and conse-quently forget to pay attention to more important externaldemands, such as subtle changes in vital signs. Their abilityto think critically is extremely limited, and they are unableto develop these skills until they master routine tasks(Benner, 1982).
The use of checklists in an ICU NGN orientation pro-gram is an ideal way to provide a standardized tool forNGNs to help them learn to practice to the standards ofcare. The tasks that must be completed to meet these stan-dards, though seemingly mundane, are critical to maintain-ing patient safety, high-quality care, and patient/family sat-isfaction. In a healthcare system where reimbursement isclosely linked to patient outcomes and satisfaction, it is es-sential for NGNs to be provided with standardized toolsthat ensure they can practice to the standards of care bythe time they have completed orientation.
Available KnowledgeChecklists have long been incorporated as common prac-tice in the aviation industry to ensure the safety and oper-ability of complex systems. The integration of checklists
www.jnpdonline.com 7
ealth, Inc. All rights reserved.

into the standard workflow in aviation reduces variabilityand the risk of human error bymeticulously listing each ac-tion that is required to be performed for each stage of flight.It has been previously argued that the use of checklists inhealth care can similarly elevate quality and safety (Clay-Williams & Colligan, 2015). This is especially apparent inthe ICU setting, where the extreme complexity of patientcare makes it impossible for healthcare professionals toprovide care safely and effectively without the use of stan-dardizedmemory aids, such as checklists (Gawande, 2007).
Clay-Williams and Colligan (2015) discuss the conceptof a “normal checklist,” which helps to standardize perfor-mance and organize a series of tasks that are too long to bememorized reliably, especially in an environment whereinterruptions are common. In the airline industry, check-lists are such a seamless part of the workflow that theircompletion does not impose additional burden upon staff.Given the unpredictable and diverse nature of caring forhuman beings, the use of checklists in health care havebeen argued as best used asmemory aids for simple, standard-ized, and time-critical tasks (Clay-Williams & Colligan, 2015).
Checklists have already been successfully implementedin a variety of settings in health care. The implementationof a checklist was found to increase the rate of a successfuland timely implementation of a therapeutic hypothermiaprotocol in one ICU (Avery et al., 2015). Another meta-analysis concluded that the use of a surgical safety check-list can improve patient outcomes, team communication,and safety (Lyons & Popejoy, 2014). In the multicenter Key-stone ICU Project conducted in Michigan, a simple five-itemchecklist was integrated into standard practice during cen-tral line insertion to reduce the prevalence of central line-associated bloodstream infections (CLABSI). Results dem-onstrated that the use of this checklist reduced rates ofCLABSIs by 66% (Pronovost et al., 2006). The results of thisstudy were so compelling that the Agency for HealthcareResearch and Quality expanded this intervention to 1,100ICUs nationwide, demonstrating a 40% CLABSI reduction(Agency for Healthcare Research and Quality, 2012). Fi-nally, the use of a checklist during morning rounds in anICU increased the appropriate implementation of 14 bestpractice guidelines, increased throughput, and resulted inan earlier initiation of physical therapy (Byrnes et al., 2009).
There has been less research conducted on the effec-tiveness of checklists used in NGN orientation programs.One study conducted in a surgical ICU in 2007 utilized skillschecklists to evaluate NGN readiness to progress to subse-quent stages in their orientation (Chesnutt & Everhart,2007). However, these checklists were designed to ensurethat NGNs had received training and mastered certain skills,rather than focused on completion of specific daily tasks.Most of the research regarding NGN orientation programimprovement initiatives involves preceptor developmentand training (Hickerson et al., 2016; Senyk & Staffileno,
8 www.jnpdonline.com
Copyright © 2021 Wolters Kluwer
2017). One review evaluated various strategies utilized inthe literature to develop critical thinking skills in NGNsand concluded that preceptors were critical to developingthe critical thinking skills of NGNs, regardless of strategyused (Schuelke & Barnason, 2017). The study also notedthat preceptors have little formalized training in educationand require significant support from management to besuccessful (Schuelke & Barnason, 2017).
Specific AimsThe aim of this study was to assess if the use of two check-lists, one designed for use at the beginning of the shift andone to be used at the end of the shift, compared to the pre-vious practice of using no checklists, demonstrated an in-crease in NGNs’ perceived ability to consistently practiceto the unit standards of care. A secondary aimwas to assessif preceptors felt that the use of the checklists improved theNGNs’ ability to practice to the standards of care.
METHODSContextConsideration of the contextual elements of the transplant/surgical ICU’s unique NGN program was critical to the de-velopment and deployment of the beginning- and end-of-shift checklists. The transplant/surgical ICU NGN orienta-tion is an approximately 12-week program that combinesdidactic and clinical learning. During the first several weeksof orientation, the focus is to build on basic nursing skillsand learn about the unit standards of care. Half of the NGNsbegin their training on day shift, whereas the other half be-gins on night shift. At approximately Week 6 of orientation,the two groups switch shifts to have the opportunity toexperience both the day and night shift workflows. Theorientation timeline and structure are tailored to theneeds of each NGN as much as possible to ensure thatthey are safe and competent ICU nurses by the time theycomplete orientation.
In the initial 2–3 weeks of orientation, the NGNs areassigned one low-complexity patient who does not requiremultiple interventions. Based on preceptor feedback andNGN level of comfort, the NGNs are gradually exposedto more complex patients and equipment. At Weeks 6–8,the NGNs begin to take two patients at a time or “paired”patients. For the remainder of their orientation, theywill fo-cus on “pairs” and high-acuity one-to-one patient assign-ments. In the latter half of the orientation, the goal is for in-creased independence of the NGN and a shift of the role ofa preceptor from that of a partner to that of an observerand resource.
The NGN is paired with an average of four preceptorsover the course of their orientation, although this numbercan increase because of staffing needs and unexpected ab-sences. The NGN is formally evaluated by the preceptors
January/February 2022
Health, Inc. All rights reserved.

every shift, utilizing standardized evaluation forms. Theseforms are specific to orientation week and provide guid-ance for both the preceptor and the NGN of what skills, ex-periences, and level of independence the NGN should beachieving at the specific point in their orientation. Theseevaluations also help unit leadership to tailor patient as-signments based on the NGN’s needs.
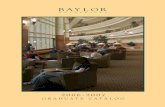
InterventionsTwo checklists were developed, one that was designed tobe completed at the beginning of the shift and one to becompleted at the end of the shift. The beginning-of-shiftchecklist includes important items that should be com-pleted as part of the nurse’s initial assessment of the patient
FIGURE 1. Beginning-of-shift checklist. This figure is available in color onlin
Journal for Nurses in Professional Development
Copyright © 2021 Wolters Kluwer H
(see Figure 1). This checklist was ideally to be completedbefore noon/midnight of each shift. Items on the beginning-of-shift checklist were grouped into themes of tasks thatare generally completed at the same time. The end-of-shift checklist was designed to prompt the NGN to reassessthe patient and roomprior to handoff to ensure that the up-coming shift change went smoothly (see Figure 2). Theitems in each checklist were not required to be completedin any specific order.
The development of the checklists was a collaborativeeffort on behalf of transplant/surgical ICU preceptors, for-mer NGNs, the unit clinical nurse specialist, and the uniteducator. Each preceptor in the transplant/surgical ICUwas e-mailed draft copies of each checklist, and their
e (www.jnpdonline.com).
www.jnpdonline.com 9
ealth, Inc. All rights reserved.

FIGURE 2. End-of-shift checklist. This figure is available in color online (www.jnpdonline.com).
feedback was elicited. Unit preceptors provided feedbackabout the checklist content as well as their recommenda-tions on how they should be integrated into practice. For-mer NGNs provided feedback about the specific tasks theystruggled to remember during their own orientation. In ad-dition, the transplant/surgical ICU nurse leadership groupreviewed the checklists during their monthly meeting, andfeedbackwas given regarding content, appearance, and de-ployment of the checklists.
Unit preceptors were essential to facilitating the integra-tion of the checklists into the orientation program. Prior tothe NGN group receiving the checklists, unit preceptorswere educated about the required use of the checklistsby the NGNs and the purpose of the study. This was done
10 www.jnpdonline.com
Copyright © 2021 Wolters Kluwer
both in person and via e-mail, with the goal of not onlyinforming the staff but also eliciting further feedback andgenerating buy-in.
The fall 2018 surgical ICU NGN cohort was composedof eight nurses. At approximately Week 4 of their orienta-tion, the group was educated in person and via e-mailabout the purpose of both checklists as well as how to uti-lize them properly. The NGNs then received digital copiesof the checklists and were instructed to begin utilizingthem in their practice. Additional copies were kept on theunit in case an NGN forgot to bring the checklists to a shift.
Each orientee was required to complete the beginning-of-shift checklist by 1200/0000 of each shift and the end-of-shift checklist by 1900/0700 of each shift. They and their
January/February 2022
Health, Inc. All rights reserved.

preceptors were required to sign each checklist to verifythat each item had been addressed and the checklistshad been completed on time. It was expected that NGNswould forget to address certain items, and the hope wasthat their memory would be triggered upon referencingthe checklist. It was encouraged that when this occurred,the NGN would make a note at the bottom of the checklistto improve for the next shift.
The checklists were not released until Week 4 of orien-tation, because it was believed by unit preceptors andleadership that if they were deployed at Week 1 of orienta-tion, they would serve as more of a distraction than a tool.The NGNs receive a significant amount of paperwork dur-ing the first several weeks of orientation, and it wasthought that the checklists would have been lost amongthe deluge. Furthermore, during the initial weeks of orien-tation, the NGNs are already overwhelmed by developinga working relationship with their preceptors, learning thebasic unit routine, and learning how to navigate the elec-tronic medical record.
MeasuresThe fall 2018 NGN group received an identical survey atWeeks 4, 8, and 12 of their orientation. The survey wascomposed of eight Likert-style scale questions designedto assess how frequently orientees remembered to com-plete items on the checklists. Answer choices included al-ways, often, sometimes, seldom, and never. Another surveywas sent to preceptors at Weeks 4 and 12 of orientation,which consisted of the 10 questions. The first eight ques-tions contained the exact same content and were phrasedalmost identically to the questions in the survey sent tothe NGNs. However, instead of requiring a self-assessment,the questions were designed to assess preceptors’ observa-tions of the NGNs’ ability to complete certain tasks on a rou-tine basis. The last two questions of the preceptor surveymeasured preceptors’ level of agreement with a statement,with answer options including strongly agree, agree, neitheragree nor disagree, disagree, and strongly disagree. Thesetwo questions were designed to evaluate preceptor opinionof the overall effectiveness of the checklists as a teachingtool. All responses were anonymous.
To understand if the use of the checklists alone im-proved the fall 2018 NGN cohort’s confidence in their abil-ity to complete certain routine tasks, a control group wasestablished utilizing the cohort of nurses who had com-pleted the unit orientation approximately 1 month priorand had never been exposed to the checklists during theirorientation. They were asked to complete the same surveythe fall 2018 NGN cohort completed at Week 12 of theirorientation. This group was still quite early in their practiceand struggling to manage their time while safely caring forcritically ill patients. Thus, it was hypothesized that thisgroup would have a similar perception of their own ability
Journal for Nurses in Professional Development
Copyright © 2021 Wolters Kluwer H
to consistently practice to the unit standards of care whencompared to the fall 2018 NGN group.
AnalysisThe data were analyzed using independent t tests to com-pare means between different survey responses. Indepen-dent t tests compared NGN survey results obtained atWeek 4 andWeek 8 as well asWeek 4 andWeek 12. In ad-dition, t-test analysis was used to compare responses fromthe control group and fall 2018 NGN cohort survey resultsat Weeks 4, 8, and 12. Finally, preceptor responses fromWeek 4 and Week 12 were compared. To understand themagnitude of differences between the groups, we calcu-lated effect size using Cohen’s d.
Ethical ConsiderationsIt is a priority of the transplant/surgical ICU unit leadershipthat every member of each NGN cohort be given everypossible opportunity to succeed during their orientation.It was felt that it would be unfair to allow some membersof the NGN cohort to have access to a training tool whiledenying others a potentially useful resource. As a result,the entire fall 2018 NGN cohort was given access to thechecklists, with the hope that they would be a valuable ad-dition to their training. This study was exempt from reviewand approval by the institutional review board given thecomplete anonymity of results reporting. Each survey par-ticipant was provided with a standardized letter notifyingthem of the purpose of the study, risks, and assurance thatthe results of the study would not identify the participants.The authors have no conflicts of interest to disclose.
RESULTSAll eight of the NGNs participating in the fall 2018 orienta-tion responded to theWeek 4 andWeek 12 surveys,whereasseven responded to the Week 8 survey. The NGN cohort(n = 7) who had recently completed the transplant/surgicalICU orientation program without use of the checklists com-pleted the same survey and served as the control group.Fourteen nurse preceptors were assigned to the new grad-uate cohort during the fall of 2018. Of these 14 preceptors,7 responded to theWeek 4 survey and 13 responded to theWeek 12 survey. Participating preceptors had 3–10 yearsof clinical experience in the transplant/surgical ICU.
When comparing survey response means with inde-pendent t tests, results did not show significant differencesin patterns of response. However, a statistically significantcomparisonwas seen between the fall 2018 NGN responseto the survey question assessing critical vital signs monitor-ing safety checks and emergency equipment setup atWeek 4 versusWeek 12 (p = .033). A statistically significantcomparison was also seen between the fall 2018 NGN re-sponse to the question assessing end-of-shift patient read-iness for shift change at Week 4 versus Week 8 (p = .045).
www.jnpdonline.com 11
ealth, Inc. All rights reserved.

The relative lack of statistical significance was likely be-cause of the small sample size; however, results did dem-onstrate multiple medium to large effect sizes when com-paring survey responses (given in Cohen’s d metric), indi-cating that if these effect sizes were seen in a study with alarger sample size, the comparisons could potentially havebeen statistically significant (see Table 1).
ByWeek 12 of orientation, eachmember of the fall 2018NGN cohort perceived that they “always” or “often” prac-ticed to all aspects of the unit standards of care outlinedin the checklists, indicating an overall improved level ofconfidence in their ability to practice to the unit standardsof care (see Table 1). This was especially apparent in theareas of vital signs monitoring, emergency equipment, andhemodynamic monitoring (Survey Questions 3 and 8),where 100% of the NGNs indicated they “always” practicedto the standard of care in these areas by Week 12. Whencomparing the survey responses from these two questionsat Week 4 and Week 12, the effect size was calculated tobe d = 1.32 (Question 3) and d = 1.03 (Question 8).
The control group had the added advantage of complet-ing orientation approximately 4 weeks prior to being sur-veyed, yet their survey responses reflected an interestingdifference in their perception of compliance with stan-dards of care as compared to the Week 12 survey re-sponses of the fall 2018 NGN cohort. The control groupdemonstrated an overall lesser degree of perceived com-pliance with the standards of care in the areas of IV drip
TABLE 1 Results From Comparisons by t Test
SurveyQuestion
NGN Cohort
Week 4 vs. Week 8 Week4vs.Wee
p d p1 .17 0.76 .33
2 .85 0.10 .64
3 .22 0.66 .033
4 .12 0.86 .07
5 .40 0.46 .60
6 .74 0.18 .08
7 .15 0.80 .11
8 .045 1.15 .25
9
10
Note. NGN = new graduate nurse.
12 www.jnpdonline.com
Copyright © 2021 Wolters Kluwer
management, IV access, vital signs monitoring, emergencyequipment, hemodynamic monitoring, and end-of-shift IVdrip and drain reconciliation (see Table 2). A medium ef-fect size (d = 0.56) was calculated when comparing re-sponses involving vital signs monitoring and emergencyequipment, and a large effect size (d = 0.86) was calculatedwhen comparing responses involving hemodynamic mon-itoring. The control group did demonstrate a slightly higheraverage level of perceived compliance with practice stan-dards related to feeding tube maintenance, tube feedingadministration, Foley catheter care, and preparation of thepatient for shift handoff. In regard to Foley catheter care, amedium to large effect size was calculated (d = 0.74) whencomparing the fall 2018 NGN and control group responses.Importantly, in all standards of care directly related to criticalpatient safety checks, the fall 2018 NGN cohorts’ perceivedability to comply with the unit standards of care was higherthan the control group.
When the fall 2018 NGN cohort was surveyed at Week12 of orientation, two additional free response questionswere included, eliciting both positive and negative feedbackabout the checklists. Most of the feedback regarding thechecklists was positive, with the checklist being regarded asuseful, but best as a temporary tool to be used during training(see Table 3).
Results indicate that preceptor perception of the NGNs’ability to “always” and “often” complete the tasks addressedin the checklists differed significantly from theNGNperception
NGN Control vs.NGN Cohort Preceptors
k12 Control vs.Week 12Week 4 vs.Week 12
d p d p d0.50 .89 0.08 .41 0.40
0.24 .85 0.10 .60 0.25
1.32 .30 0.56 .60 0.19
0.97 .79 0.14 .63 0.18
0.28 .17 0.74 .20 0.62
1.03 .17 0.86 .77 0.14
0.86 .47 0.38 .86 0.08
0.61 .64 0.25 .85 0.09
.35 0.45
.52 0.31
January/February 2022
Health, Inc. All rights reserved.

TABLE 2 Fall 2018 NGN Cohort Weeks 4, 8, and 12 and Control Group Survey Results
Survey Question Answer Choice
Fall 2018NGNCohortWeek 4(n = 8)
Fall 2018NGNCohortWeek 8(n = 7)
Fall 2018NGNCohortWeek 12(n = 8)
ControlNGNCohort(n = 7)
IV drip and IVaccess management
NGNQuestion 1:At the beginning of my shift, I assesswhere each drip is infusing, if the drips have adequatevolume, if any IV tubing or drip is expired and ensurethat for each drip the drug concentration/dosingweight is correctly programmed in the pump.
Always OftenSometimes SeldomNever
50% 50%0% 0%0%
85.7%14.29%0% 0%0%
75% 25%0% 0%0%
71.43%28.57%0% 0%0%
NGNQuestion 2:At the beginning of my shift, I checkto see what central lines and peripheral IV’s thepatient has, note their location, ensure their patency,and check if any of the dressings are soiled or expired.
Always OftenSometimes SeldomNever
37.5%62.5% 0%0% 0%
42.86%57.14%0% 0%0%
62.5%37.5% 0%0% 0%
57.14%42.86%0% 0%0%
Vital signs monitoring and emergency equipment
NGNQuestion 3:At the beginning of my shift, I checkmy alarm parameters, make sure that nothing issilenced, and check that the ambu bag is set up andready for use.
Always OftenSometimes SeldomNever
37.5%37.5%12.5%12.5% 0%
57.14%42.86%0% 0%0%
100% 0%0% 0%0%
28.57%57.14%14.29%0% 0%
Invasive devices
NGNQuestion 4:At the beginning of my shift, I checkthat myNGT/Dobhoff tape is not soiled or expired, thetube feed bag is filled with only 4 hours worth of tubefeeds, the tube feed bag is not expired, and the NGTsuction is set up correctly and functioning.
Always OftenSometimes SeldomNever
25% 50%25% 0%0%
57.14%42.86%0% 0%0%
62.5%37.5% 0%0% 0%
85.71%0%14.29%0% 0%
NGNQuestion 5:At the beginning of my shift, I checkthat the Foley bag is not touching the floor, there is nodependent tubing, the bag is not more than⅔ full, andthe statlock is intact/not soiled.
Always OftenSometimes SeldomNever
71.43%14.29%14.29%0% 0%
85.71%14.29%0% 0%0%
75% 25%0% 0%0%
100% 0%0% 0%0%
Hemodynamic monitoring
NGN Question 6: At the beginning of my shift, I leveland zero my hemodynamic lines, check at least oneNIBP to ensure correlation, ensure that the pressurebag is adequately inflated, and ensure that there isenough saline in the pressure bag.
Always OftenSometimes SeldomNever
62.5%37.5% 0%0% 0%
71.43%28.57%0% 0%0%
100% 0%0% 0%0%
71.43%28.57%0% 0%0%
Shift change preparation
NGN Question 7: At the end of my shift, I make surethat my room(s) is clean and organized, that I haveordered replacement IV drips if necessary, discard anyIV bags that are older than 24 hours, and that I haveemptied the drains/Foley/rectal tube.
Always OftenSometimes SeldomNever
50%37.5%12.5% 0%0%
85.71%14.29%0% 0%0%
87.5%12.5% 0%0% 0%
71.43%28.57%0% 0%0%
NGN Question 8: At the end of my shift, I make surethat my patient is clean, their central line/drain/surgical dressings are intact, and their linens/chucksare clean.
Always OftenSometimes SeldomNever
50%37.5%12.5% 0%0%
100% 0%0% 0%0%
75% 25%0% 0%0%
85.71%14.29%0% 0%0%
Note. NGN = new graduate nurse; IV = intravenous; NIBP = non-invasive blood pressure; NGT = nasogastric tube.
Journal for Nurses in Professional Development www.jnpdonline.com 13
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 3 Fall 2018 NGN Open-EndedChecklist Feedback
• “Very helpful for a new nurse. Helps to organize anoverwhelming amount of new information!”
• “Nice to have the checklist especially when it’s a busy shiftit’s a good tool to reference to ensure everything is done tomaintain safety”
• “Very helpful, help me make all of these standards anautomatic part of my routine. I do them without reallythinking about them as much as before.”
• “I found the checklist to be very helpful in reminding me ofsomething I may have forgotten and writing it down to makesure I would not forget them again!”“Helps me remember what things I need to do for everypatient before I leave! #WWTCS (what would the checklistsay).”
• “…it can be time consuming at the end of the shift to fill out,so I think this a good, temporary measure to learn thestandards.”
• “Honestly, I thought the checklists were a great way tomemorize the things we needed to do. It laid out in a niceway what preceptors would tell us, but perhaps we couldforget. I like how it was rolled out in the middle of theorientation process.”
Note. NGN = new graduate nurse.
of their own compliance. No statistically significant differenceswere seen when comparing survey responses at Week 4 andWeek 12. Preceptors’ perception of each NGN’s ability to “al-ways” complete the tasks addressed in the checklists did in-crease modestly between Weeks 4 and 12 in the areas of IVdrip and IV access management, invasive devices, and shiftchange preparation (see Table 4). For example, preceptor sur-vey responses indicated that betweenWeeks 4 and 12, the fall2018 NGN cohort more consistently practiced to the unit stan-dard of care in the areas of IV drip and IV accessmanagement,with responses of “always” increasing from 28.57% to 38.46%and 28.57% to 30.77%, respectively. However, by comparison,NGN survey results in these same areas demonstrated an in-crease in “always” responses from 50% to 75% and 37.5% to62.5%, respectively.When comparing the preceptor survey re-sponses betweenWeek 4 andWeek 12, only in the area of Fo-ley catheter management was a greater than medium effectsize seen (d = 0.62).
The survey administered to the preceptors at Weeks 4and 12 included two additional questions. The results fromthe first question indicated a decreased level of agreementwith the statement “Using the checklists helps my orienteeremember critical safety checks and adhere to the eightICU standards of care” between Week 4 and Week 12.The results from the second question indicated an in-creased overall level of agreement with the statement“The checklists help guide my teaching” from Week 4 toWeek 12. In the survey administered at Week 12, the pre-ceptors were also given the opportunity to provide open-ended feedback (see Table 5).
14 www.jnpdonline.com
Copyright © 2021 Wolters Kluwer
DISCUSSIONSummaryTwo simple checklists helped to progressively increaseNGNs’ perceived level of confidence in their ability topractice to the unit standards of care during orientation.Their perceived ability to practice to these standards wasbetter in tasks related to critical safety checks than a controlgroup who had not utilized the checklists during orienta-tion and were surveyed after practicing independently for4 weeks. Interestingly, preceptors observed NGNs werenot practicing to the standard of care as regularly as theNGNs seemed to believe.
InterpretationAlthough overall results indicate that the NGN cohorts’ per-ception of their ability to practice to the standards of careincreased betweenWeek 4 andWeek 12, there were someareas where NGN confidence decreased between Week 8and Week 12 of orientation. This may be a result of devel-opmental milestones, changes in the primary preceptor,caring for progressively more complex patients, andtransitioning from low acuity to much higher acuity 1:1 pa-tients during the transplant/surgical ICU orientation. TheNGNs also switch from day to night shifts (and vice versa)andmust learn new shift workflows. Finally,midway throughorientation, more experienced preceptors help the NGNtransition from task-based nursing care to more complexcritical thinking. For the NGN, this may present new chal-lenges and may cause simple tasks to be forgotten ordeprioritized. These challenges may also affect an expertpreceptor’s expectations of the new graduate and assess-ment of their competence.
The fall 2018 NGN cohort that utilized the beginning-and end-of shift checklists during their orientation perceivedthat they were more consistently able to practice to the unitstandards compared to a control group who completed ori-entation without using the checklists. These results supportthe use of the checklist as amemory aid to reinforce practicestandards. It is important to note, however, that this wasnot the case in the areas of invasive device managementand shift change preparation. This is likely partially becausethe control group was surveyed approximately 4 weeks af-ter ending their orientation, and so they had additional timeto develop their knowledge and skills on the unit.
Preceptors’ perception of the NGNs’ ability to routinelypractice to the unit standards of care did not consistentlytrend upward over the course of orientation. In fact, atWeek 12 of orientation, significant percentages of precep-tors were still selecting “sometimes” or “seldom” as answerchoices across all survey questions, whereas all fall 2018NGN responses at week 12 were “often” or “always.” Thisindicates a certain level of disagreement between the NGN
January/February 2022
Health, Inc. All rights reserved.

TABLE 4 Preceptor Open-Ended Checklist Feedback
Survey Question Answer Choice
PreceptorSurvey Week4 (n = 7)
PreceptorSurvey Week12 (n = 13)
IV drip and IVaccess management
Preceptor Question 1: At the beginning of the shift, my orienteechecks which lumen each drip is infusing into, ensures that foreach drip the drug concentration/dosing weight is correctlyprogrammed, checks if the drips have adequate volume, andchecks if any IV tubing or drip is expired.
Always OftenSometimes SeldomNever
28.57% 71.43%0% 0% 0%
30.77% 38.46%30.77% 0% 0%
Preceptor Question 2: At the beginning of the shift, my orienteechecks to see what central lines and peripheral IVs the patienthas, notes their location, ensures their patency, and checks tosee if any of the dressings are soiled or expired.
Always OftenSometimes SeldomNever
28.57% 57.14%14.29% 0% 0%
38.46% 38.46%15.38% 7.69%0%
Vital signs monitoring and emergency equipment
Preceptor Question 3: At the beginning of the shift, my orienteechecks the alarm parameters, makes sure that nothing issilenced, and checks that the ambu bag is set up and ready foruse.
Always OftenSometimes SeldomNever
28.57% 42.86%28.57% 0% 0%
23.08% 38.46%38.46% 0% 0%
Invasive devices
Preceptor Question 4: At the beginning of the shift, my orienteechecks that the NGT/Dobhoff tape is not soiled or expired, thetube feed bag is filledwith only 4 hours worth of tube feeds, thetube feed bag is not expired, and the NGT suction is set upcorrectly and functioning.
Always OftenSometimes SeldomNever
0% 85.71%14.29% 0% 0%
30.77% 23.08%30.77% 15.38%0%
Preceptor Question 5: At the beginning of the shift, my orienteechecks that the Foley bag is not touching the floor, there is nodependent tubing, the bag is not more than ⅔ full, and thestatlock is intact/not soiled.
Always OftenSometimes SeldomNever
0% 71.43%28.57% 0% 0%
38.46% 38.46%23.08% 0% 0%
Hemodynamic monitoring
Preceptor Question 6: At the beginning of the shift, my orienteelevels and zeros the hemodynamic lines, checks at least oneNIBP to ensure correlation, ensures that the pressure bag isadequately inflated, and ensures that there is enough saline inthe pressure bag.
Always OftenSometimes SeldomNever
71.43% 14.29%14.29% 0% 0%
61.54% 23.08%15.38% 0% 0%
Shift change preparation
Preceptor Question 7: At the end of the shift, my orienteemakes sure that the room is clean and organized, they orderreplacement IV drips if necessary, they discard any IV bags thatare older than 24 hours, and they empty my drains/Foley/rectaltube.
Always OftenSometimes SeldomNever
14.29% 71.43%14.29% 0% 0%
46.15% 23.08%23.08% 7.69%0%
Preceptor Question 8: At the end of the shift, my orienteemakes sure that the patient is clean, the central line/drain/surgical dressings are intact, and the linens/chucks are clean.
Always OftenSometimes SeldomNever
14.29% 71.43%14.29% 0% 0%
38.46% 8.46%15.38% 7.69%0%
Checklist value
Preceptor Question 9: Using the checklists helps my orienteeremember critical safety checks and adhere to the eight ICUstandards of care.
Strongly agreeAgree Neitheragree nor disagreeDisagree Stronglydisagree
57.14% 42.86%0% 0% 0%
53.85% 15.38%23.08% 7.69%0%
(continues)
Journal for Nurses in Professional Development www.jnpdonline.com 15
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 4 Preceptor Open-Ended Checklist Feedback, Continued
Survey Question Answer Choice
PreceptorSurvey Week4 (n = 7)
PreceptorSurvey Week12 (n = 13)
Preceptor Question 10: The checklists help guide my teaching. Strongly agreeAgree Neitheragree nor disagreeDisagree Stronglydisagree
14.29% 42.86%42.86% 0% 0%
38.46% 30.77%23.08% 7.69%0%
Note. IV = intravenous; ICU = intensive care unit; NIBP = non-invasive blood pressure; NGT = nasogastric tube.
and preceptor perceptions of NGNs’ ability to consistentlypractice to the unit standards of care.
These response differences are likely partially becausepreceptors change approximately halfway through orien-tation. Although a preceptor may orient an NGN for the full12 weeks, it will never be the same NGN the entire time.Newer (3–5 years of experience) preceptors also tend toprecept at the beginning of orientation, and more experi-enced preceptors (5+ years of experience) take over inthe later part of the orientation. As a result, many of the pre-ceptors who completed the Week 4 survey did not com-plete the Week 12 survey and vice versa, contributing toresult variation. Finally, a preceptor may orient severaldifferent NGNs over several weeks, so in certain cases,when responding to the survey, a preceptor had to generalizetheir responses to account for multiple NGN performances.
In the latter half of orientation, there is less focus placedupon task completion and more on developing overallclinical competence. If the NGN has been able to masterthe skills outlined in the checklists, this should lead to animprovement in critical thinking and perceptual skills.The preceptor may also be less likely to observe theNGN perform the tasks outlined in the checklists, insteadchoosing to step out of the room during these times to let
TABLE 5 Preceptor Open-Ended ChecklistFeedback
• “Even after several reminders, my orientee did not utilize herchecklist until the end of the shift.”
• “This checklist is very thorough and helpful. I think that it’s agreat way for orientees to keep track of a lot of little details/tasks that are actually very important to safe patient care.”
• “I feel like this could be a great resource for some orientees,but for those that are already too task-oriented, this checklistperpetuated the bad habit.”
• “It is very helpful as a preceptor and also to the orientee.”• “I think it’s a good reminder for preceptors for the first fewweeks of orientation but as it progressed, I noticed myorientees and I did not really utilize the checklist.”
• “At times, my orientee forgets or is too busy to fill out thechecklist. Orientee feels the checklist is another task to addon top of the other tasks she must do.”
16 www.jnpdonline.com
Copyright © 2021 Wolters Kluwer
the NGNpractice independently. Finally, more experiencedpreceptors tend to train the NGNs during the second half ofthe orientation, and it is likely that they do not prioritize taskcompletion when orienting the NGN. These preceptors areclassified as proficient or expert according to Benner’smodel and, as a result, are less tied to rules and guidelinesto provide excellent care (Benner, 1982). It is possible thatthese nurses may not fully understand the difficulties theNGNs face practicing to the standard of care without a stan-dardized memory aid.
The comments submitted in the surveys indicate thatpreceptors believed the checklist was useful; however, itwas difficult to motivate the NGN to complete the checkliston time, if at all. In addition, survey feedback and in-personfeedback indicated that although the checklist was usefulfor some, there were certain NGNs whose progress wasimpeded by checklist use. In the task-oriented state ofthe “advanced beginner,” some of the NGNswere observedto focus too much on the checklists. This became an issuelater in orientationwhen theywere required to develop crit-ical thinking skills and move beyond simply completingtasks successfully.
LimitationsBased on the study results, several limitations were identi-fied. First, because of the task-focused nature of the firstportion of orientation, it may have been useful to releasethe checklists earlier in the orientation program. Second, thesmall sample size of both the NGN and preceptor groupslimits the significance of the results. To understand whetherthe implementation of the checklists truly improves theNGNorientation process, it would be important to studymul-tipleNGNcohorts. A third limitationwas that the participatingpreceptors varied between theWeek 4 andWeek 12 surveys,which made it difficult to truly understand the relationshipbetween NGN survey results and preceptor survey results.The varying experience levels of each preceptor and dif-ferent teaching styles undoubtedly impacted their percep-tion of each NGN’s progress, as well. Finally, the controlgroup of NGNs who had recently completed orientationhad been working independently for several weeks prior
January/February 2022
Health, Inc. All rights reserved.

to completing the survey. As a result, this groups’ level ofconfidence in their ability to practice to the standards ofcare is likely influenced by the extra time they had beenin practice. This makes it difficult to validate the relation-ship between their survey responses and the responsesof the intervention NGN group at Week 12.
Lessons LearnedIt became clear that for implementation of the checklists tobe successful, generating preceptor buy-in regarding theimportance of the checklists was essential. Although pre-ceptors generally agreed it could be a useful tool, therewas no widespread agreement that it was an essential tool.Future successful implementation would require buy-infrom not only preceptors but also unit leadership and unitstaff. Presenting the results of this study to the transplant/surgical ICU nursing leadership, to unit practice council,and at staff meetings will be instrumental in generating dis-cussion and interest as well as critical support from all unitstakeholders, thereby ensuring every opportunity to fullyembed the checklists into the orientation program.
In addition, preceptor feedback demonstrated that of-ten the NGNwould not use the checklists on time or some-times not at all, which indicated that they were not user-friendly. To streamline daily use of the checklists, it wouldbe worthwhile to consider embedding the beginning- andend-of-shift checklist content within the electronic medicalrecord. The completion of each item on the checklists couldbecome part of the standard charting workflow within aunit, with checklist items integrated within the same task listcontaining pending medications, laboratories, and woundcare. The NGN would not have to remember to bring thechecklists to each shift and would not have to carry addi-tional pieces of paper around with them during their shift.The checklist’s efficiency and ease of use would be furtherincreased if checklist item completion would autopopulatecertain areas of charting, such as assessment of invasive devices.
ConclusionsThe integration of checklists into an NGN orientation pro-gram in the ICU is a simple, easy-to-use, and low-cost inter-vention with a potential to greatly improve the orientationprocess. These checklists create a standardized trainingmethod in which to teach NGNs to integrate unit standardsof care into their daily practice. The use of beginning- andend-of-shift checklists for NGN orientation can be easilycustomized for other contexts, such as medical surgical
Journal for Nurses in Professional Development
Copyright © 2021 Wolters Kluwer H
wards. Suggested next steps would be to deploy thechecklists across multiple cohorts of NGNs to gather alarger sample size, which would allow for a more mean-ingful statistical analysis.
ReferencesAgency for Healthcare Research and Quality. (2012). AHRQ patient
safety project reduces bloodstream infections by 40 percent.https://psnet.ahrq.gov/resources/resource/25037
Avery, K. R., O’Brien, M., Pierce, C. D., & Gazarian, P. K. (2015). Useof a nursing checklist to facilitate implementation of therapeutichypothermia after cardiac arrest. Critical Care Nurse, 35(1),29–37. 10.4037/ccn2015937
Benner, P. (1982). From novice to expert. The American Journal ofNursing, 82(3), 402–407. 10.2307/3462928
Byrnes, M., Schuerer, D., Schallom, M. E., Sona, C., Mazuski, J. E., Taylor,B. E., McKenzie, W., Thomas, J., Emerson, J., Nemeth, J. L., Baily, R.A., Boyle, W. A., Buchman, T. G., & Coopersmith, C. M. (2009).Implementation of a mandatory checklist of protocols and objec-tives improves compliance with a wide range of evidence-basedintensive care unit practices. Critical Care Medicine, 37(10),2775–2781. 10.1097/CCM.0b013e3181a96379
Chesnutt, B. M., & Everhart, B. (2007). Meeting the needs of graduatenurses in critical care orientation: Staged orientation program insurgical intensive care. Critical Care Nurse, 27(3), 36–40. http://ccn.aacnjournals.org/content/27/3/36.full.pdf+html
Clay-Williams, R., & Colligan, L. (2015). Back to basics: Checklists inaviation and healthcare. BMJ Quality & Safety, 24, 428–431. 10.1136/bmjqs-2015-003957
Gawande, A. (2007). Annals of medicine: The checklist. The New Yorker,https://www.newyorker.com/magazine/2007/12/10/the-checklist
Hickerson, K. A., Terhaar, M. F., & Taylor, L. A. (2016). Preceptor sup-port to improve nurse competency and satisfaction: A pilot studyof novice nurses and preceptors in a pediatric intensive care unit.Journal of Nursing Education and Practice, 6(12), 57–62. 10.5430/jnep.v6n12p57
Lyons, V. E., & Popejoy, L. L. (2014). Meta-analysis of surgical safetychecklist effects on teamwork, communication, morbidity, mortal-ity, and safety.Western Journal of Nursing Research, 36(2), 245–261.10.1177/0193945913505782
Pronovost, P., Needham, D., Berenholtz, S., Sinopoli, D., Chu, H.,Cosgrove, S., Sexton, B., Hyzy, R., Welsh, R., Roth, G., Bander,J., Kepros, J., & Goeschel, C. (2006). An intervention to decreasecatheter-related bloodstream infections in the ICU. The NewEngland Journal of Medicine, 335(26), 2725–2732. 10.1056/NEJMoa061115
Schuelke, S., & Barnason, S. (2017). Interventions used by nurse pre-ceptors to develop critical thinking of new graduate nurses: A sys-tematic review. Journal for Nurses in Professional Development,31(1), E1–E7. 10.1097/NND.0000000000000318
Senyk, J., & Staffileno, B. (2017). Reframing nursing preceptor de-velopment: A comprehensive approach to improve education,standardize processes, and decrease costs. Journal for Nursesin Professional Development, 33(3), 131–137. 10.1097/NND.0000000000000343
www.jnpdonline.com 17
ealth, Inc. All rights reserved.

TEST INSTRUCTIONS• Read the article. The test for this nursing continuing professionaldevelopment (NCPD) activity is to be taken online at www.nursingcenter.com/CE/JNPD. Tests can no longer be mailed or faxed.• You'll need to create an account (it's free!) and log in to access MyPlanner before taking online tests. Your planner will keep track of allyour Lippincott Professional Development online NCPD activities foryou.• There's only one correct answer for each question. A passing score forthis test is 7 correct answers. If you pass, you can print your certificateof earned contact hours and access the answer key. If you fail, you havethe option of taking the test again at no additional cost.• For questions, contact Lippincott Professional Development:1-800-787-8985.• Registration deadline is December 6, 2024.
PROVIDER ACCREDITATIONLippincott Professional Development will award 3.0 contact hours for thisnursing continuing professional development activity.
Lippincott Professional Development is accredited as a provider ofnursing continuing professional development by the American NursesCredentialing Center's Commission on Accreditation.
This activity is also provider approved by the California Board ofRegistered Nursing, Provider Number CEP 11749 for 3.0 contact hours.Lippincott Professional Development is also an approved provider ofcontinuing nursing education by the District of Columbia, Georgia, andFlorida, CE Broker #50-1223. Your certificate is valid in all states.
Payment: The registration fee for this test is $27.95.DISCLOSURE STATEMENTThe authors and planners have disclosed that they have no financialrelationships related to this article.
For more than 131 additional continuing professional development articles related to Safety topics,go to www.NursingCenter.com/ce.
INSTRUCTIONSThe Use of Checklists Among New Graduate Nurses in a Surgical Intensive Care Unit to Improve Patient Safety and Outcomes
18
www.jnpdonline.comCopyright © 2021 Wolters Kluwer
January/February 2022
Health, Inc. All rights reserved.