
The societal and organizational contexts of culturally sensitive mental health services: Findings...
11
The Societal and Organizational Contexts of Culturally Sensitive Mental Health Services: Findings from an Evaluation of Bilingual/ Bicultural Psychiatric Programs Orlando Rodriguez, Ph.D. Johanna Lessinger, Ph.D. Peter Guarnaccia, Ph.D. Abstract The Hispanic mental health literature focuses mostly on cultural and clinical issues. This paper argues that researchers and practitioners concerned with mental health services for Hispanics and other minority groups need to pay more attention to the societal and organizational contexts that facilitate or impede the development of effective culturally sensitive psychiatric programs. Utilizing data from an evaluation of three New York psychiatric programs for seriously mentally ill (SMI) Hispanic patients, the paper discusses societal and organizational factors that influenced the pro- grams' development. Among societal forces were the significance of Hispanics as a voting bloc, the political organization of Hispanic mental health professionals, the philosophy of ethnic assimilation in American society, prevailing views about the place of cultural knowledge in psychiatric treatment, and fiscal crises, and the shortage of Hispanic mental health professionals. Among organizational factors, hospital administrative support and program leadership mediated the effects of societal forces upon the programs, while ethnic competition and lack of coordination between the program and other organizational units acted as barriers to the programs' development. The findings are relevant to any innovative mental health service in an organizational setting. Introduction Since the mid-1970s, when the idea first gained currency that mental health services were not responsive to the social and cultural needs of minorities, great progress has been made in the provi- sion of services to minority groups, especially the Hispanic mentally ill. In many cities with large Address correspondence to Orlando Rodriguez, Ph.D., Director, Hispanic Research Center, Fordham University, Thebaud Hall, Bronx, NY 10458. Johanna Lessinger, Ph.D., is with the Hispanic Research Center, Fordham University. Peter Guarnaccia, Ph.D., is with the Department of Human Ecology and the Institute for Health Care Policy and Aging Research, Rutgers University. This study was supported in part by Grant MH30569 from the Division of Services Research, National Institute of Mental Health, and by Contract C-003234 from the New York State Office of Mental Health. The opinions are those of the authors and do not reflect the policies or views of the U.S. Department of Health and Human Services or the New York State Office of Mental Health. BilinguaUBicultural Psychiatric Programs RODRIGUEZ, LESSINGER, GUARNA CCIA 213
Transcript of The societal and organizational contexts of culturally sensitive mental health services: Findings...
The Societal and Organizational Contexts of Culturally Sensitive Mental Health Services: Findings from an Evaluation of Bilingual/ Bicultural Psychiatric Programs Orlando Rodriguez, Ph.D. Johanna Lessinger, Ph.D. Peter Guarnaccia, Ph.D.
Abstract The Hispanic mental health literature focuses mostly on cultural and clinical issues. This paper
argues that researchers and practitioners concerned with mental health services for Hispanics and other minority groups need to pay more attention to the societal and organizational contexts that facilitate or impede the development of effective culturally sensitive psychiatric programs. Utilizing data from an evaluation of three New York psychiatric programs for seriously mentally ill (SMI) Hispanic patients, the paper discusses societal and organizational factors that influenced the pro- grams' development. Among societal forces were the significance of Hispanics as a voting bloc, the political organization of Hispanic mental health professionals, the philosophy of ethnic assimilation in American society, prevailing views about the place of cultural knowledge in psychiatric treatment, and fiscal crises, and the shortage of Hispanic mental health professionals. Among organizational factors, hospital administrative support and program leadership mediated the effects of societal forces upon the programs, while ethnic competition and lack of coordination between the program and other organizational units acted as barriers to the programs' development. The findings are relevant to any innovative mental health service in an organizational setting.
Introduction Since the mid-1970s, when the idea first gained currency that mental health services were not
responsive to the social and cultural needs of minorities, great progress has been made in the provi-
sion of services to minority groups, especially the Hispanic mental ly ill. In many cities with large
Address correspondence to Orlando Rodriguez, Ph.D., Director, Hispanic Research Center, Fordham University, Thebaud Hall, Bronx, NY 10458.
Johanna Lessinger, Ph.D., is with the Hispanic Research Center, Fordham University. Peter Guarnaccia, Ph.D., is with the Department of Human Ecology and the Institute for Health Care Policy and Aging
Research, Rutgers University. This study was supported in part by Grant MH30569 from the Division of Services Research, National Institute of
Mental Health, and by Contract C-003234 from the New York State Office of Mental Health. The opinions are those of the authors and do not reflect the policies or views of the U.S. Department of Health and Human Services or the New York State Office of Mental Health.
BilinguaUBicultural Psychiatric Programs RODRIGUEZ, LESSINGER, GUARNA CCIA 213
numbers of Hispanics, mental health services have been especially created for Hispanic clients, and Hispanic professionals have been hired to deliver these services. In the last two decades, clinicians and social scientists have seriously examined ways in which the organization and delivery of clinical services - - therapies, assessments, and their organization - - should be modified to concord with Hispanic culture.
As a result, there now exists a modest but significant literature that purports to show professionals how to provide psychiatric services for Hispanics. 18 For the most part, this literature focuses on the nature of culturally sensitive clinical practice. This paper argues that the Hispanic mental health literature and, in general, the professionals involved in the practice of culturally sensitive mental health treatment tend to ignore the politico-econonfic and organizational contexts that facilitate or impede the effectiveness of bilingual/bicultural psychiatric programs. Utilizing data from an evalua- tion of three New York psychiatfc programs for seriously mentally ill (SMI) Hispanic patients, 9 we enumerate and discuss societal and organizational factors that influenced the planning, implementa- tion, and development of the programs. Although the focus is on the need for hospital and program administrators to address politico-economic and organizational issues in developing Hispanic psychi- atric programs, the findings have implications for any innovative mental health treatment in an orga- nizational setting.
Research Background Most of the literature on culturally sensitive psychiatric treatment for Hispanics addresses clinical
issues, with a primary focus on what cultural knowledge the therapist needs to acquire in order to engage the patient and provide effective diagnosis and treatment. Much of the literature thus presup- poses and is stated in terms of the cultural content of the interaction between therapist and patient.I~ In the Hispanic mental health literature, the concept of culture usually denotes the norms, values, and beliefs guiding everyday interactions. This approach views culture as the subjective expression of group attributes. H Some anthropological approaches view culture more critically, by examining norms and values within and as products of their broader sociopolitical and organizational contexts.tZ-~5 This paper utilizes the former, more restrictive definition of culture in order to emphasize the lack of attention paid to broader contextual factors in the Hispanic mental health fiterature on clinical services. This literature ignores the fact that for most Hispanic patients, therapy typically takes place in an organizational setting such as an inpatient ward, an outpatient clinic, or a community mental health center. In such settings, team treatment is required, involving the skills of the practitio- ners of several mental health disciplines as well as those of administrative mad paraprofessional staff.
Marcos and Gil have observed that mental health service providers are generally not trained in policy-making, a6 This observation is also applicable to how mental health providers generally view culturally sensitive treatment. Organizational factors have been given greater attention with respect to the issue of Hispanic undemtilization of mental health services, namely, how to organize psychiatric services to increase the probability that Hispanics will contact them when in need of treatment? 72z This segment of the literature provides some guidance to the approach taken in this paper.
The research literature also provides some orientation to the societal and organizational contexts of mental health practice. Societal factors have received considerable attention in attempts to understand the configuration of mental health services. An example is Mechanic's recent review of socioeco- nomic forces affecting mental health policy z3 and Elpers' discussion of political constraints upon administrators of county mental health systems. 24 It is rare, however, to find societal contexts as a factor in attempts to understand microlevel phenomena, as this paper undertakes.
Organizational issues have also received wide attention in the mental health literature. Attention has been called to how the structure of mental health service organizations affects service delivery z5~6
214 The Journal of Mental Health Administration 19:3 Fall 1992
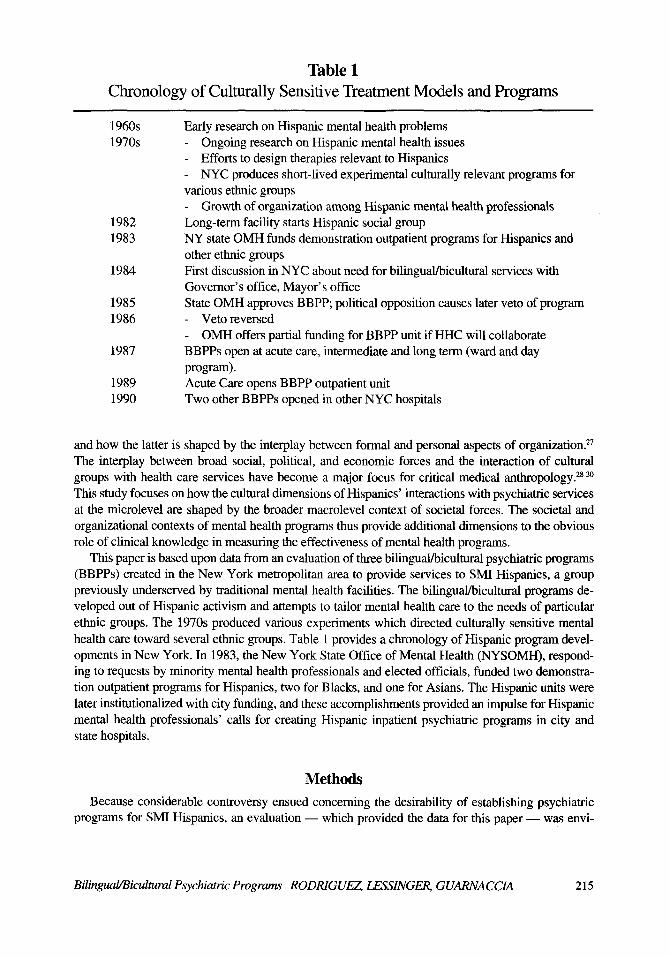
Table 1 Chronology of Culturally Sensitive Treatment Models and Programs
1960s 1970s
1982 1983
1984
1985 1986
1987
1989 1990
Early research on Hispanic mental health problems Ongoing research on Hispanic mental health issues Efforts to design therapies relevant to Hispanics NYC produces short-lived experimental culturally relevant programs for
various ethnic groups Growth of organization among Hispanic mental health professionals
Long-term facility starts Hispanic social group NY state OMH funds demonstration outpatient programs for Hispanics and other ethnic groups First discussion in NYC about need for bilingual/bicultural services with Governor's office, Mayor's office State OMH approves BBPP; political opposition causes later veto of program
Veto reversed OMH offers partial funding for BBPP unit if HHC will collaborate
BBPPs open at acute care, intermediate and long term (ward and day program). Acute Care opens BBPP outpatient unit Two other BBPPs opened in other NYC hospitals
and how the latter is shaped by the interplay between formal and personal aspects of organization. 27 The interplay between broad social, political, and economic forces and the interaction of cultural groups with health care services have become a major focus for critical medical anthropology? 8-3~ This study focuses on how the cultural dimensions of Hispanics' interactions with psychiatric services at the microlevel are shaped by the broader macrolevel context of societal forces. The societal and organizational contexts of mental health programs thus provide additional dimensions to the obvious role of clinical knowledge in measuring the effectiveness of mental health programs.
This paper is based upon data from an evaluation of three bilingual/bicultural psychiatric programs (BBPPs) created in the New York metropolitan area to provide services to SMI Hispanics, a group previously underserved by traditional mental health facilities. The bilingual/bicultural programs de- veloped out of Hispanic activism and attempts to tailor mental health care to the needs of particular ethnic groups. The 1970s produced various experiments which directed culturally sensitive mental health care toward several ethnic groups. Table 1 provides a chronology of Hispanic program devel- opments in New York. In 1983, the New York State Office of Mental Health (NYSOMH), respond- ing to requests by minority mental health professionals and elected officials, funded two demonstra- tion outpatient programs for Hispanics, two for Blacks, and one for Asians. The Hispanic units were later institutionalized with city funding, and these accomplishments provided an impulse for Hispanic mental health professionals' calls for creating Hispanic inpatient psychiatric programs in city and state hospitals.
Methods Because considerable controversy ensued concerning the desirability of establishing psychiatric
programs for SMI Hispanics, an evaluation - - which provided the data for this paper - - was envi-
Bilingual/Bicultural Psychiatric Programs RODRIGUEZ LESSINGER, GUARNA CCIA 215

sioned by NYSOMH and program advocates as a way of assessing the feasibility of bilingual/bicul- tural programs. The evaluation was to answer four questions: Could culturally sensitive programs for Hispanics be implemented in public institutions? Were the culturally sensitive programs that were developed replicable in other institutions or settings? Could assessment methods be developed that were responsive to cultural and linguistic variability? Could effective culturally sensitive treatment approaches be developed?
To address these questions, qualitative research was needed to encompass the details, the complex- ity, and occasional ambiguity involved in the creation of experimental programs. Since the concepts of language and culture are also central to social anthropology, anthropological methods of unobma- sive but intensive observation and open-ended interviewing were adopted. Three types of qualitative data were collected: observations of interactions among patients and staff; program documents such as descriptions of services; and unstructured interviews with patients, staff, hospital and program administrators, government mental health officials, and program advocates. These observations were the basis for emerging conceptualizations concerning the societal and organizational factors focused upon in this paper. In addition, following Schatzman and Strauss's methodological guidelines, 31 the interviews with officials and administrators provided confirmatory evidence for emerging hypothe- ses. For example, remarks by program staff suggesting that the hospital was protecting the program from budget-cutting personnel shifts suggested the concept of organizational mediation of societal forces. Follow-up interviews with hospital administrators provided confirmatory evidence of the concept.
Quantitative data were also collected to develop profiles of each facility in terms of patient popula- tion characteristics and program and patient outcome measures. However, the quantitative data were used mainly to address questions concerning the programs' effectiveness, an issue outside this paper's focus. In keeping with the evaluation's goals, to examine culturally sensitive treatment in practice, an experimental design was not undertaken. Furthermore, the resources available for the evaluation precluded comparisons with mainstream wards. Undoubtedly, such an examination would have en- hanced the study.
The methods, used over a three-year period at the three institutions, produced richly detailed data on how the bilingual/biculmral programs operated day to day; on the philosophies that motivated the staff; on the perceptions of administrators, mental health officials, and Hispanic professionals who advocated the programs; and on the practical problems attendant in creating new programs within large institutions. The methods were particularly useful in clarifying tile social context - - interperson- al, organizational, and societal - - in which the programs developed.
Findings: Political and Organizational Contexts of Developing Programs The discussion of findings below synthesizes those organizational features and politico-economic
contexts assessed to be important predictors of the effectiveness of Hispanic psychiatric programs. Figure 1 depicts a model of how politico-economic and organizational factors affected the programs. The specific factors depicted are not meant to comprise an exhaustive list; they are those found to be most salient in the analysis. Among societal factors that impinged upon the programs' development were politics, ideologies, and economic forces. Organizational factors have their locus in the wider administrative unit of which the program is a component, in this case a city or state hospital. In this conceptualization, organizational factors have two types of functions. One function is to mediate the effects of societal forces upon programs, as exemplified by administrative decisions about how bud- get cuts would affect the programs. The second function is to impede or facilitate the programs' development. To complement the model, the figure also includes the extent of staff knowledge about
216 The Journal of Mental Health Administration 19:3 Fall 1992
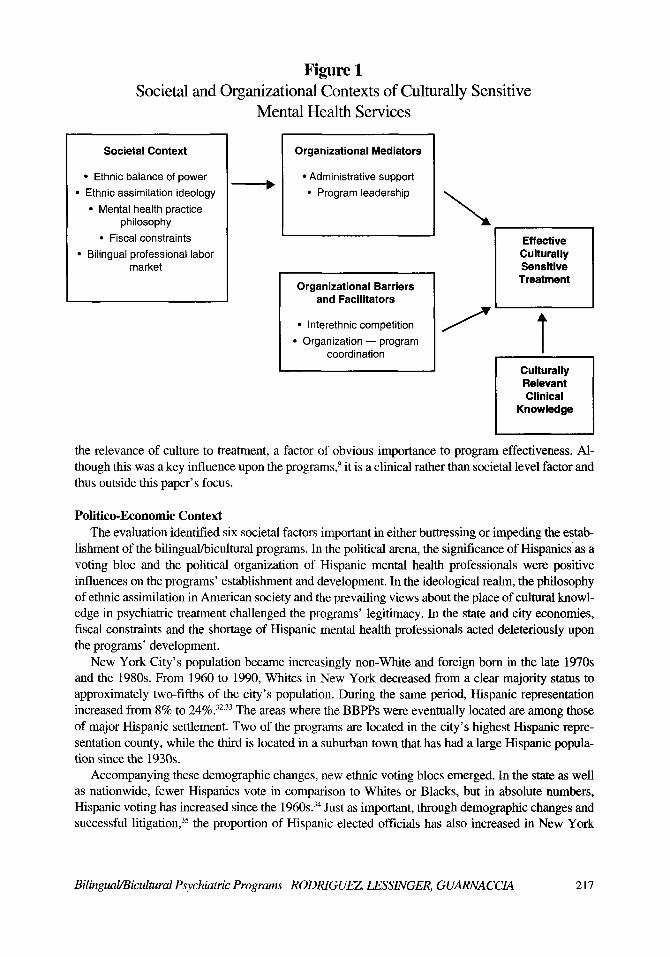
Figure 1 Societal and Organizational Contexts of Culturally Sensitive
Mental Health Services
Societal Context
�9 Ethnic balance of power
�9 Ethnic assimilation ideology �9 Mental health practice
philosophy
�9 Fiscal constraints
�9 Bilingual professional labor market
r,-
Organizational Mediators
�9 Administrative support
�9 Program leadership
Organizational Barriers and Facilitators
�9 Interethnic competit ion
�9 Organization - - program coordination
Effective Culturally Sensitive
Treatment
T Culturally Relevant Clinical
Knowledge
the relevance of culture to treatment, a factor of obvious importance to program effectiveness. Al- though this was a key influence upon the programs, 9 it is a clinical rather than societal level factor and thus outside this paper' s focus.
Politico-Economlc Context The evaluation identified six societal factors important in either buttressing or impeding the estab-
lishment of the bilingual/bicultural programs. In the political arena, the significance of Hispanics as a voting bloc and the political organization of Hispanic mental health professionals were positive influences on the programs' establishment and development. In the ideological realm, the philosophy of ethnic assimilation in American society and the prevailing views about the place of cultural knowl- edge in psychiatric treatment challenged the programs' legitimacy. In the state and city economies, fiscal constraints and the shortage of Hispanic mental health professionals acted deleteriously upon the programs' development.
New York City's population became increasingly non-White and foreign born in the late 1970s and the 1980s. From 1960 to 1990, Whites in New York decreased from a clear majority status to approximately two-fifths of the city's population. During the same period, Hispanic representation increased from 8% to 24%. 32,33 The areas where the BBPPs were eventually located are among those of major Hispanic settlement. Two of the programs are located in the city's highest Hispanic repre- sentation county, while the third is located in a suburban town that has had a large Hispanic popula- tion since the 1930s.
Accompanying these demographic changes, new ethnic voting blocs emerged. In the state as well as nationwide, fewer Hispanics vote in comparison to Whites or Blacks, but in absolute numbers, Hispanic voting has increased since the 1960s. 34 Just as important, through demographic changes and successful litigation, 35 the proportion of Hispanic elected officials has also increased in New York
Bilingual/Bicultural Psychiatric Programs RODRIGUEZ LESSINGER, GUARNA CCIA 217
City and other areas. 36 For politicians, Hispanic voters became a force to be courted or placated, possibly in an effort to offset African American electoral strength and to prevent the emergence of an African American/Hispanic coalition. The three Hispanic programs, as well as their predecessors, form part of mental health officials' recognition of growing Hispanic voting strength.
An additional factor which set New York apart from many other cities in the United States was the relatively large number of Hispanics working in the mental health field. In addition to the large numbers of Hispanics working as aides in local hospitals, there were also a significant number of Hispanic psychiatrists, psychologists, and social workers in city and state hospitals and in mental health government agencies. An initially ad hoc group of Hispanic professionals had taken on a formal identity through the Association of Hispanic Mental Health Professionals (AHMHP), based in New York City. The AHMHP urged the need for bilingual/bicultural mental health services, using as evidence findings from reports on Hispanic concerns commissioned by the city and state. When the proposal to form one or more BBPPs was made, these health workers and administrators, many with considerable seniority, were influential in putting together a feasible plan, in winning support for it at the state, city, and institutional levels, and then in helping to staff and oversee the units formed.
In ideological terms, the attempt to form the BBPPs touched off resistance and controversy, which were reflections of the larger debates going on in U.S. society. Some saw such wards as institutions promoting racial/ethnic discrimination. Others argued that BBPPs would be unfair because they provided services for one marginalized population but not for others such as African Americans or Haitian Americans. As discussed below, this issue was salient at the organizational level. Still others, among them some Hispanics, argued that the wards would be a form of ghettoization, offering Hispanics second-class care under the guise of ethnic sensitivity. Still another group felt that part of Hispanic patients' mental health profile was a failure to assimilate; Hispanic wards were thus seen as denials of the American ideology of ethnic assimilation into the mainstream.
Those who supported the formation of the programs pinpointed language as the major barrier to access. They also argued that the combination of Hispanic culture with marginalized immigrant status creates special forms of psychic distress which standard psychiatric practice may misinterpret. Propo- nents of the BBPPs thus argued that any psychiatric unit for Hispanics needed the help of staff who were not only bilingual but also Hispanic, in order to decode the patient's mental states and to communicate fully with patients and their families.
A different form of resistance came from a few professionals who rejected the implied critique of existing mental health care involved in the concept of culturally sensitive care. This group, while acknowledging the language problems of Hispanics and other ethnic minorities, felt that the BBPPs' philosophical basis was specious because conditions such as schizophrenia were not mediated by culture but were universal. This form of antagonism had no direct relationship to ethnic tensions or economic concerns but stemmed from adherence to an anticultural stance within U.S. psychiatry. The power of this viewpoint is exemplified by one program's reaction to a recurring theme in evaluation reports: that the programs lacked a theory of the relevance of cultural knowledge to clinical practice. In the evaluation's first year, administrators dismissed this as irrelevant because they deemed the program's philosophy to be the elimination of language (and not cultural) barriers to treatment. However, by the third year of the evaluation, when the program had overcome hostility from adminis- trators in other units, the program had labeled itself "bicultural." Another indication of positive change lies in the fact that by the end of the evaluation, two other Hispanic BBPPs had been initiated in city hospitals (see Table 1).
The ethnic balance of power favored the programs' creation, while ideological opposition was eventually overcome. In contrast, state and city fiscal crises and the shortage of Hispanic mental health professionals in the labor market created serious obstacles to the programs' development. The evaluation period was marked by waves of cuts in both city and state health budgets, all of which had
218 The Journal of Mental Health Administration 19:3 Fall 1992
a cumulative impact on the BBPPs. Although BBPP units were often protected from direct cuts by sympathetic administrators, the units were still integral parts of large public institutions which were floundering to maintain services with less money and smaller staffs. All the programs suffered from chronic staff shortages, and often struggled with shortages of equipment and supplies and poor physical plant maintenance. Some BBPPs went without key staff for long periods, because hiring freezes or wage caps made it impossible to fill job slots. Additionally, in a job market where profes- sionally trained bilinguals are in great demand, the programs could not completely rely on bilingual personnel. The proportion of nonbilingual staff was approximately 20-25% of all professionals. The programs often experienced personnel losses as bilingual staff took other positions, usually in nongovernmental facilities.
The resulting working conditions both demoralized and exhausted the staff and contributed to rapid turnover among professionals. As a result, it was more difficult for program administrators to create innovative programming, lest they burden staff further. Consequently, none of the New York BBPPs went as far as they might have in exploring culturally sensitive assessment and treatment methods. The experience of the New York BBPPs suggests that situations of budgetary crisis are severely detrimental to the establishment of such programs, which need extra time, effort, and money and which presuppose a period of staff training and consolidation.
Organizational Context
A distinction was made earlier between organizational factors that mediated societal influences upon the programs, and those that, like politico-economic forces, impeded or facilitated the programs' development. Among organizational mediators, the analysis identified hospital administration sup- port for the program and program administrators' leadership. Interethnic competition and lack of coordination between the program and other hospital units acted as barriers to the programs' develop- ment. The latter factor comprises several features of bureaucratic organization and is explicated in greater detail in the discussion below. Organizational barriers and facilitators are examined first.
The issue of all-Hispanic staffing for the BBPPs was particularly inflammatory in a city where public health institutions form one of the major sources of stable employment for members of many minority groups. Among professionals, there were suspicions that Hispanic wards would offer His- panic professionals special opportunities for advancement and promotion in experimental programs under scrutiny from NYSOMH. Only a few professionals initially grasped the idea that success of the BBPPs might lay the foundation for wards geared to Black and Asian groups as well. In fact, part of the early conflict in one of the hospitals was resolved by creating a Black ward. (The evaluation contract precluded examination of that program.) The end result was that program administrators had to devote much time to defending their programs from attacks, to the detriment of developing innova- tive treatment.
Problems of organizational coordination also impeded the programs' ability to provide culturally sensitive treatment. Innovative programming often implies the need to modify existing organizational arrangements. The organizational framework of each BBPP required coordination with other BBPP units in the hospital and with non-BBPP units, such as emergency rooms or rehabilitation units. One aspect of coordination concerned the programs' place within a hierarchy of command. For example, two of the institutions had more than one component - - in one program an inpatient ward and an outpatient department; in another an inpatient ward, a day program, and a discharge residence. This arrangement created difficulties because the program administrator had to report to two supervisors in two divisions, often receiving contradictory commands. Both facilities eventually modified the chain of command to accommodate the programs.
The creation of an innovative program often implies that other units should modify their activities to facilitate achieving the programs' objectives. In the programs evaluated, this requirement posed
Bilingual/Bicultural Psychiatric Programs RODRIGUEZ LESSINGER, GUARNA CCIA 219
serious difficulties, some of which were never resolved. For example, when one program was asked by administrators to increase its discharge rate, program staff decided to more fully utilize the hospi- tal's rehabilitation unit, participation in which is considered a sign of discharge-readiness. An imped- iment to this move was the lack of bilingual staff and materials in the rehabilitation unit. When the unit's director was asked to add bilingual materials to his unit, he dismissed the concept of bilingual- ism and biculturalism: the unit's philosophy was assimilationist. Another example concems an ambi- tious plan to link two programs, so that patients from one, a short-stay Hispanic ward, could be moved directly to the other hospital's longer stay Hispanic ward. The proposed link never materialized because of the latter hospital's need to restrict admissions.
Two important organizational factors - - administrative support and program leadership - - medi- ated the deleterious effects of fiscal crisis and political hostility faced by the programs during their creation and development. Administrative enthusiasm for the BBPP concept was present from the beginning; such enthusiasm was the prerequisite for establishing the BBPPs. In addition, however, each unit needed ongoing administrative support and supervision as the BBPPs developed. For in- stance, in one hospital the administration eventually "unitized" the ward, exempting it from the requirement to send its aides into other wards in periods of staff shortage. Administrators, alerted by the ward staff, realized that the hospitalwide policy of moving aides around damaged the BBPP's ability to maintain a full bilingual staff.
The budget cuts, which became a leitmotif during the complete evaluation period, provide an example of how administrative support mediates societal constraints. Although rumors swept through BBPP units periodically, no administrator ever proposed closing down a BBPP. With respect to other issues, however, administrative support for BBPPs was not forthcoming, or was very slow to materi- alize. Where administrative support for a BBPP was ineffective, BBPPs found themselves short of crucial supplies, unable to fill needed staff positions or unable to coordinate relationships between components or with other units in the institution.
The programs' effectiveness was not solely dependent upon administrative support, however. Internally, each BBPP needed leadership to manage hospital-program coordination, to guide the program through the period of establishment while welding staff of the newly constituted unit into a working team with a common approach. More importantly, leadership was necessary if programs were to develop the specifics of bilingual/bicultural treatment. The best leaders, like the best adminis- trators, were those able to manage both people and bureaucracies. Over the research period, evalua- tors watched units that had such leadership, and those that eventually developed it. In wards without adequate leadership, dally life was chaotic, staff responsibilities were unclear, patient programming was perfunctory or abandoned, and paperwork piled up. Tired and demoralized staff refused to take the initiative needed in order to develop their own working models of bicultural care. Rapid turnover undermined the accumulation of experience from which practical models of effective culturally based treatment might emerge.
On the other hand, good ward leadership, although never able to overcome budgetary shortages, made routine ward life run smoothly enough so that staff could concentrate on the complex tasks of administering bilingual care and bringing bicultural sensitivity to patients' problems. The conceptual and practical advances the BBPPs made took place in periods of competent ward-level leadership that was able to allocate the work load, keep patient therapy sessions running smoothly, and encourage staff initiative. The perpetual problem of each BBPP, however, was to identify and promote individu- als able to combine administrative skills with commitment to the BBPP concept.
An important aspect of program leadership is the program's relationship with the surrounding community. To varying degrees, the BBPPs mobilized community support through advisory boards composed of Hispanic mental health professionals or people from the local Hispanic community, and through the personal networks of staff members. The ideologies of Hispanic solidarity and self-help
220 The Journal of Mental Health Administration 19:3 Fall 1992
contributed to these ties. For example, in one of the programs, patients made a float for the local Hispanic Day parade. The float was widely admired, not only in the local community but throughout the hospital itself. In fact, the float was put on display for days after the parade in front of various other wards. Community ties seem an especially important adjunct to BBPP units in times of budgetary crisis, since they provide a way to mobilize resources and services through volunteer efforts and to recruit Spanish-speaking family care sponsors. The advisory boards were also in a good position to do political lobbying on behalf of BBPPs.
Conclusions and Recommendations
This paper argues that the operations of Hispanic Clinical programs are inextricably bound with the programs' social and organizational contexts. Although the discussion is geared to the creation and development of culturally sensitive psychiatric programs, it is also relevant to any innovative mental health program. It would be imprudent to claim that the study's results are generalizable to other BBPPs, since the sociopolitical context in other localities may be different from the one described in this paper. For the same reason, specific action steps to address the societal contexts cannot realistical- ly be offered. However, the results are generalizable in the sense that similar sociopolitical and organizational contexts can be predicted in other areas of the United States. The assumption that culturally sensitive mental health programs can operate as if only clinical issues are involved, or muddle through, once launched, is overoptimistic. Failures in both assessing the context of the pro- gram and conceptualizing culturally sensitive treatment could bring the whole concept of culturally oriented treatment into disrepute. Organizations or individuals advocating the establishment of BBPPs need to assess these contexts carefully in advance. The mix of conceptual and organizational issues, shaped by local history, needs to be understood if new programs are to succeed and to become part of the mental health mainstream. The discussion below outlines the basic contexts that adminis- trators and program planners need to consider in developing a new program.
Clearly, BBPPs must start with support at a variety of levels. This support, even if initially absent, can sometimes be created through persuasive argument and political maneuvering. At the state level, BBPPs need the legitimacy conferred by the state mental health agency and by professional organiza- tions comparable to the Association of Hispanic Mental Health Professionals. This support needs to be technical, political, and budgetary. Specifically, programs need to be followed for an initial two- to three-year period to see that plans are adequately implemented. Adequate funding in this initial period is imperative.
Relevant local support for a BBPP must also come from advisory boards, community groups, politicians, health workers' unions, and patient advocacy groups. As the New York experience sug- gests, ideologies of ethnic unity and self-help can be tremendously useful in mobilizing support for a BBPP, but these ideologies run the danger of provoking ethnic rivalries among those who see them- selves as excluded by ethnic particularism. Alternative ideologies of social justice, equal access, multiculturalism, and panminority empowerment can be invoked to build cross-ethnic coalitions. Similarly, advocating for culturally sensitive programs means tackling the anticultural assumptions that prevail in mental health service systems. Program advocates thus need to persuasively articulate the rationales underlying culturally sensitive care.
Once again, reference is made to the need for BBPPs to tackle the intellectual issues underlying culturally sensitive clinical practice, an important factor outside this paper's scope. Once societal and organizational contexts are addressed, effective culturally sensitive treatment depends on the degree to which staff can grapple with complex ideas such as the relationship between language and culture and the link between cultural knowledge and effective assessment and treatment. 37-39 Here, too, pro- spective BBPPs need help in creating relatively detailed assessment and treatment models to address
Bilingual/Bicultural Psychiatric Programs RODRIGUEZ, LESSINGER, GUARNA CCIA 221
questions of language and culture in depth and to provide appropriate staff training. In summary, it seems clear from the New York experience that BBPPs require major initial
commitments from their institutions if they are to succeed. The institution's administration must be visibly supportive to counter internal hostility to the BBPP idea, to facilitate the needed level of bilingual staffing and an ethnic patient roster and to promote good ward-level leadership. In a larger sense, the institution must have a certain tolerance for innovation and change since BBPPs may evolve in ways that depart from established hospital routine. Once BBPPs are established, hospital administrations need to make longer term commitments to such programs. Adequate levels of bilin- guai professional staffing and staff stability are major goals, but they cost money and organizational time. If institutions are unprepared to provide these, they are also unprepared to run BBPPs.
Acknowledgment We are grateful to Vilma Santiago-Irizarry, M.A., for her comments on this paper.
References 1. Acosta FX, Cristo MH: Development of a bilingual interpreter program: an alternative model for Span-
ish-speaking services. Professional Psychology 1981; 12(4):474-482. 2. Bluestone H, Vela RM: Transcultural aspects in the psychotherapy of the Puerto Rican poor in New
York City. Journal of the American Academy of Psychoanalysis 1982; 10:269-283. 3. Inclan J: Variations in value orientations in mental health work with Puerto Ricans. Psychotherapy 1985;
22: 324-334. 4. Rogler LH, Malgady RG, Costantino G, et al.: What do culturally sensitive mental health services mean?
The case of Hispanics. American Psychologist 1987; 42: 565-570. 5. Rogler LH, Malgady RG, Rodriguez O: Hispanics and Mental Health: A Framework for Research.
Malabar, Fla.: Robert E. Krieger Publishing Company, 1989. 6. Ruiz R: Cultural and historical perspectives in counseling Hispanics. In: Sue DW (ed.): Counseling the
Culturally Different: Theory and Practice. New York: Wiley and Sons, 1981. 7. Ruiz P, Ruiz PP: Treatment compliance among Hispanics. Journal of Operational Psychiatry 1983;
14:112-114. 8. Szapocznik J, Scopetta M, King O: Theory and practice in matching treatment to the special characteris-
tics and problems of Cuban immigrants. Journal of Community Psychology 1978; 6:112-122. 9. Rodriguez O, Lessinger J, Guarnaccia P, et al.: Final Report: Bilingual/Bicultural Psychiatric Programs
at Bronx Psychiatric Center, Lincoln Hospital, and Pilgrim Psychiatric Center, Hispanic Research Cen- ter, Fordham University, New York, 1991.
10. Sue S, Zane N: The role of culture and cultural techniques in psychotherapy, a critique and reformula- tion. American Psychologist 1987; 42:37-45.
11. Marin G, Marin BVO: Research with Hispanic Populations. Newbury Park, Calif.: Sage Publications, 1991.
12. Baer HA: Sociological contributions to the political economy of health: lessons from medical anthropol- ogists. Medical Anthropology Quarterly 1986; 17:129-131.
13. Singer M: Developing a critical perspective in medical anthropology. Medical Anthropology Quarterly 1986; 17:128-129.
14. Baer HA, Singer M, Johnson J: Introduction: toward a critical medical anthropology. Social Science and Medicine 1986; 23:95-98.
15. Singer M, Davison L, Gerdes G: Culture, critical theory and reproductive illness behavior in Haiti. Medical Anthropology Quarterly 1988; 2:370-385.
16. Marcos LR, Gill RM: Muddling through mental health policies. American Journal of Psychiatry 1983; 140:854-856.
222 The Journal of Mental Health Administration 19:3 Fall 1992

17. Bloom B: Changing Patterns of Psychiatric Care. New York: Human Sciences Press, 1975. 18. Gaviria M, Stern G: Problems in designing and implementing culturally relevant mental health services
for Latinos in the U.S. Social Science and Medicine 1980; 14B :65-71. 19. Rodriguez O: Overcoming barriers to clinical services among chronically mentally ill Hispanics: lessons
from the evaluation of the Project COPA demonstration. Hispanic Research Center Research Bulletin (11)1. New York: Fordham University, 1986.
20. Rodriguez O: Hispanics and Human Services: Help Seeking in the Inner City. Monograph No. 13. Hispanic Research Center. New York: Fordham University, 1987.
21. Scott JF, Delgado M: Planning mental health programs for Hispanic communities. Social Casework 1979; 60(8): 451-456 (October).
22. Trevino FM, Bruhn JG, Bunce H nh Utilization of community mental health services in a Texas-Mexico border city. Social Sciences and Medicine 1979; 13:331-334.
23. Mechanic D: Toward the year 2000 in U.S. mental health policy making and administration. In: Roche- fort DA (ed.): Handbook of Mental Health Policy in the United States. Greenwood, Conn.: Greenwood Press, 1989.
24. Elpers JR: Development and utilization of incentive systems for mental health operations: successful and unsuccessful knowledge utilization in California and Los Angeles. The Journal of Mental Health Admin- istration 1989; 16:9-20.
25. Clifford DL: A consideration of simple measures of organizational structure. Evaluation and Program Planning 1987; 10:231-237.
26. Sorensen JE, Zelman W, Hanbery GW: Managing mental health organizations with 25 key performance indicators. Evaluation and Program Planning 1987; 10:239-247.
27. Mechanic D: Issues in the sociology of organizations and the administration of mental health services. In: Mechanic D (ed.): Politics, Medicine and Social Science. New York: John Wiley and Sons, 1974.
28. Baer HA, Singer M, Johnson J (eds.): Special issue: toward a critical medical anthropology. Social Science and Medicine 1986; 23(2).
29. Frankenberg R (ed.): Gramsci, Marxism and phenomenology: essays for the development of critical medical anthropology. Medical Anthropology Quarterly 1988; 2(4).
30. Singer M, Baer H (eds.): Socialist health/capitalist health: is there a difference? Medical Anthropology 1989; 11(2).
31. Schatzman L, Strauss A: Field Research: Strategies for a Natural Sociology. Englewood Cliffs, N.J.: Prentice Hall, 1973.
32. The Puerto Rican New Yorker, A Recent History of their Distribution and Population Household Char- acteristics. New York: New York Department of City Planning, 1985, Table 5.
33. 1990 Census. Comparative 1980-1990 Population and Housing Data. Based on 1990 Public Law File 94-171 and the 1980 Census. New York City and Boroughs. New York: New York Department of City Planning, March 6, 1990, Table 3.
34. Schick FL, Schick R: Statistical Handbook on U.S. Hispanics. Phoenix: Oryx Press, 1991, Tables FI-1 and F1-3.
35. Lee FR: Panel approves revised plan for New York's council seats. New York Times July 26, 1991, Sec. A, p. 1.
36. Pachon HP: Politics and public policy, the Hispanic community. Vital Speeches of the Day 1988(May 15):464-466.
37. Comas-Diaz L, Griffith EEH (eds.): Clinical Guidelines in Cross-Cultural Mental Health. New York: Wiley-Interscience, 1990.
38. Lopez S, Hemandez P: When culture is considered in the evaluation and treatment of Hispanic patients. Psychotherapy 1987; 24:120-126.
39. Sue DW, Sue D: Counseling the Culturally Different: Theory and Practice. New York: Wiley- Interscience, 1988.
Bilingual/Bicultural Psychiatric Programs RODRIGUEZ, LESSINGER, GUARNA CCIA 223




















