The role of theory-driven graphic warning labels in motivation to quit: a qualitative study on...
11
RESEARCH ARTICLE Open Access The role of theory-driven graphic warning labels in motivation to quit: a qualitative study on perceptions from low-income, urban smokers Erin L Mead 1,2* , Joanna E Cohen 3 , Caitlin E Kennedy 4 , Joseph Gallo 5 and Carl A Latkin 1 Abstract Background: Use of communication theories in the development of pictorial health warning labels (graphic warning labels) for cigarette packaging might enhance labels’ impact on motivation to quit, but research has been limited, particularly among low socioeconomic status (SES) populations in the U.S. This qualitative study explored perceptions of theory-based graphic warning labels and their role in motivation to quit among low-income smokers. Methods: A cross-sectional qualitative study was conducted with 25 low-income adult smokers in Baltimore, Maryland, who were purposively sampled from a community-based source population. Semi-structured, in-depth interviews were conducted from January to February 2014. Participants were asked about the motivational impact of 12 labels falling into four content categories: negative depictions of the health effects of smoking to smokers and others, and positive depictions of the benefits of quitting to smokers and others. Data were coded using a combined inductive/deductive approach and analyzed thematically through framework analysis. Results: Labels depicting negative health effects to smokers were identified as most motivational, followed by labels depicting negative health effects to others. Reasons included perceived severity of and susceptibility to the effects, negative emotional reactions (such as fear), and concern for children. Labels about the benefits of quitting were described as motivational because of their hopefulness, characters as role models, and desire to improve family health. Reasons why labels were described as not motivational included lack of impact on perceived severity/susceptibility, low credibility, and fatalistic attitudes regarding the inevitability of disease. Conclusions: Labels designed to increase risk perceptions from smoking might be significant sources of motivation for low SES smokers. Findings suggest innovative theory-driven approaches for the design of labels, such as using former smokers as role models, contrasting healthy and unhealthy characters, and socially-oriented labels, might motivate low SES smokers to quit. Keywords: Graphic warning labels, Health communication, Behavioral theories, Smoking cessation, Motivation, Low- income adults, Qualitative research * Correspondence: [email protected] 1 Department of Health, Behavior and Society, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD, USA 2 Tobacco Center of Regulatory Science, Department of Behavioral and Community Health, University of Maryland School of Public Health, College Park, MD 20742-2611, USA Full list of author information is available at the end of the article © 2015 Mead et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Mead et al. BMC Public Health (2015) 15:92 DOI 10.1186/s12889-015-1438-6
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The role of theory-driven graphic warning labels in motivation to quit: a qualitative study on...

Mead et al. BMC Public Health (2015) 15:92 DOI 10.1186/s12889-015-1438-6
RESEARCH ARTICLE Open Access
The role of theory-driven graphic warning labelsin motivation to quit: a qualitative study onperceptions from low-income, urban smokersErin L Mead1,2*, Joanna E Cohen3, Caitlin E Kennedy4, Joseph Gallo5 and Carl A Latkin1
Abstract
Background: Use of communication theories in the development of pictorial health warning labels (graphicwarning labels) for cigarette packaging might enhance labels’ impact on motivation to quit, but research has beenlimited, particularly among low socioeconomic status (SES) populations in the U.S. This qualitative study exploredperceptions of theory-based graphic warning labels and their role in motivation to quit among low-incomesmokers.
Methods: A cross-sectional qualitative study was conducted with 25 low-income adult smokers in Baltimore,Maryland, who were purposively sampled from a community-based source population. Semi-structured, in-depthinterviews were conducted from January to February 2014. Participants were asked about the motivational impactof 12 labels falling into four content categories: negative depictions of the health effects of smoking to smokersand others, and positive depictions of the benefits of quitting to smokers and others. Data were coded using acombined inductive/deductive approach and analyzed thematically through framework analysis.
Results: Labels depicting negative health effects to smokers were identified as most motivational, followed bylabels depicting negative health effects to others. Reasons included perceived severity of and susceptibility to theeffects, negative emotional reactions (such as fear), and concern for children. Labels about the benefits of quittingwere described as motivational because of their hopefulness, characters as role models, and desire to improvefamily health. Reasons why labels were described as not motivational included lack of impact on perceivedseverity/susceptibility, low credibility, and fatalistic attitudes regarding the inevitability of disease.
Conclusions: Labels designed to increase risk perceptions from smoking might be significant sources of motivationfor low SES smokers. Findings suggest innovative theory-driven approaches for the design of labels, such as usingformer smokers as role models, contrasting healthy and unhealthy characters, and socially-oriented labels, mightmotivate low SES smokers to quit.
Keywords: Graphic warning labels, Health communication, Behavioral theories, Smoking cessation, Motivation, Low-income adults, Qualitative research
* Correspondence: [email protected] of Health, Behavior and Society, Johns Hopkins UniversityBloomberg School of Public Health, Baltimore, MD, USA2Tobacco Center of Regulatory Science, Department of Behavioral andCommunity Health, University of Maryland School of Public Health, CollegePark, MD 20742-2611, USAFull list of author information is available at the end of the article
© 2015 Mead et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.

Mead et al. BMC Public Health (2015) 15:92 Page2of11
BackgroundGlobally, the U.S. ranks among the highest in income in-equality among high-income countries [1], and incomeinequality continues to grow [2]. The association be-tween socioeconomic inequality and increased mortalitycan be partially explained by greater prevalence of riskbehaviors, including smoking [3,4]. In the U.S., low so-cioeconomic status (SES) smokers are less likely to at-tempt to quit and achieve cessation for ≥6 monthscompared to higher SES smokers [5,6]. Smoking preva-lence is highest in low SES neighborhoods, which maybe due to targeted marketing [7-9] and the use of smok-ing as a coping mechanism for stress and as a shared be-havior that fosters norms favorable toward smoking andsignificant barriers to quitting [10,11]. In Baltimore,Maryland, for example, smoking prevalence is 58% insome low SES neighborhoods [12]. Moreover, the globalfiscal crisis of 2008 contributed to increased smokingprevalence among the unemployed in the U.S., thus in-creasing health inequities [13]. Public health interven-tions that effectively promote cessation among low SESsmokers are needed to help close the health equity gap,particularly in light of the growing socioeconomic in-equality in the U.S.Research has shown that motivation to quit is associ-
ated with making quit attempts [14-16]. The term mo-tivation conveys both an emotional component and arational, cognitive component that weighs the benefitsand risks of changing behavior [14]. Individuals can beintrinsically motivated—that is, by inherent desires toachieve internal rewards, such as improved health or en-joyment—and extrinsically motivated—that is, by desiresto achieve rewards or avoid punishments from externalsources, including social influences [17,18]. One ap-proach to increase motivation and change behavior istheorized by the extended parallel process model, whichposits that individuals are motivated to act through fearif they perceive a high level of risk from their engage-ment in an unhealthy behavior, specifically that they aresusceptible to severe, negative consequences [19]. If theybelieve that they have the ability to change their behav-ior (perceived self-efficacy) and the behavioral changewill reduce their risk of negative outcomes (perceived re-sponse efficacy), they are motivated to engage in thehealthier behavior. According to this theory, then, to-bacco control messaging that aims to increase smokers’motivation to quit should contain both threat and effi-cacy messages to increase risk perceptions and efficacybeliefs.One policy approach used by many countries to mo-
tivate cessation is graphic warning labels, which are pic-torial health warning labels on cigarette packagingdescribing the dangers of tobacco use [20,21]. Labelshave largely relied on fear appeals to increase smokers’
risk perceptions using depictions of the negative effectsof smoking [20]. Studies in several countries have exam-ined the vividness of pictures and the portrayal of in-ternal vs. external health effects [20], but little work hasexplicitly compared messages about the effects to othersto messages about the effects to smokers [22]. Labelsportraying the effects to others may be important giventhat social concern for others is a significant motivatingfactor for smokers to quit [23]. They may also provide asource of extrinsic motivation to quit smoking by invok-ing social influence. Moreover, limited research on la-bels’ influence on efficacy beliefs has found very littleimpact, likely due to the lack of theory-driven efficacymessages [24-26].Exploring the role of graphic warning labels on motiv-
ation to quit among low SES smokers might be particu-larly important given the evidence of a health knowledgegap [27,28]. According to the health knowledge gap hy-pothesis, high SES individuals are able to more easilyand rapidly obtain health information than low SES indi-viduals, and this gap is linked to health disparities[27-29]. Although research has shown that graphicwarning labels are more effective than text-only labelsregardless of SES [30], the effectiveness of specific typesof content (such as testimonial vs. didactic information)might differ by socioeconomic factors [31,32].As a first step to address these gaps in the literature,
this qualitative study explored perceptions of graphicwarning labels and their influence on motivation to quitamong low-income, urban smokers. To examine whatcontent might play a bigger role in motivation, we devel-oped and compared theory-based labels that variedbased on: depictions of the effects of smoking or quittingto smokers and others, level of threat from smoking,and efficacy messages.
MethodsFrom January to February 2014, semi-structured in-depthinterviews were conducted with 25 low-income smokerswho had participated in a quantitative survey on tobaccouse, attitudes and communication channels in Baltimore,Maryland. Inclusion criteria were aged ≥18 years,smoked ≥100 cigarettes in lifetime, and smoked ciga-rettes in the past 30 days at the time of the quantita-tive study. We purposively sampled from the pool ofsurvey participants for an adequate distribution bygender and age group (18–39 and ≥40 years) to cap-ture variations among younger and older middle-agedsmokers who may have different health concerns. Allindividuals who were approached agreed to participatein this qualitative study.Recruitment for the survey occurred in low-income
neighborhoods through street outreach and word-of-mouth by trained staff from the Lighthouse Studies at

Mead et al. BMC Public Health (2015) 15:92 Page3of11
Peer Point, a community-based research center thatworks with low SES populations with a high prevalenceof injection drug use and HIV [33]. This population waschosen because of its high smoking prevalence and sig-nificant barriers to cessation; unpublished data fromthree studies showed smoking rates of 83-88%.
ProceduresTwelve graphic warning labels were developed using(whenever possible) the warning statements mandated byU.S. law and either existing labels (from the U.S., Canada,Brazil, and Australia) or pictures (Table 1). Labels also in-cluded the U.S. Quitline number. The labels fell into oneof four content categories: negative depiction of the healtheffects of smoking to the smoker (n = 4) and others (childor adult non-smoker; n = 4), and a positive message aboutquitting for the smoker (n = 2) and others (n = 2).The labels were designed to portray different levels of
threat and convey efficacy messages following the ex-tended parallel process model and social cognitive the-ory [19,38]. Based on previous categorization [22], labelswith a vivid picture of the negative effects were catego-rized as high threat, nonvivid picture of the negative ef-fects as low threat, and positive picture about quitting asno threat. Following social cognitive theory [38], the effi-cacy messages were in text format placed to the right ofthe picture and designed to increase self-efficacy to quit(confidence in ability to quit successfully), response effi-cacy of quitting (effectiveness of quitting on improvinghealth), and response efficacy of the Quitline (effective-ness of the Quitline to aid in cessation). The labels andinterview guide were developed and finalized throughpilot testing with five participants and Lighthouse staff.Participants were asked about their cognitive and
affective reactions to each label (such as what was themain message of the label and how it made them feel)and which labels were most likely to motivate them to quit.Data on age, gender, race, marital status, educational level,employment status, income, smoking, and quitting behav-ior were also collected. The Johns Hopkins BloombergSchool of Public Health Institutional Review Board ap-proved this study. Interviews took place in a private officeat the Lighthouse, were audio-recorded, and lasted 1–2hours. Participants provided written informed consent andwere compensated $25. The lead author (ELM), who istrained in qualitative interviewing and analysis, conductedall recruitment, interviews, and data analysis.
Data analysisTranscripts were analyzed using the framework method,a type of thematic analysis using a matrix structure tosystematically reduce qualitative data [39]. The lead au-thor developed the coding scheme using a deductive andinductive approach based on the interview guide as well
as emerging themes from the data and with input fromtwo co-authors (CEK and JEC). The lead author con-ducted analytic memoing to reflect on emerging themesand issues, including deviant cases. Codes were thengrouped into broader categories, such as a category forcodes related to motivation to quit. Next, the data werecharted into the framework matrix to provide accuratesummaries by participant, category, and label. For ex-ample, responses were summarized for all codes withinthe motivation category for each participant and label.Broader themes were developed by comparing codes andcategories within and across cases with special attentionto deviant cases. The framework approach and matrixstructure allowed for the data to be kept within therich context of each case, facilitated the identificationof patterns, and included references to specific tran-script lines, thus enhancing rigor and transparency[39]. This study adheres to the RATS guidelines forreporting qualitative studies (http://www.biomedcen-tral.com/authors/rats).
ResultsTwelve men and 13 women participated and were onaverage 45 years old (Table 2). Most were AfricanAmerican (n = 22) and earned less than $10,000 in theprevious year (n = 16). Many had not completed highschool (n = 12). Most reported smoking everyday (n =23), and many smoked less than one pack per day (n =11). Fourteen participants reported that they had evertried to quit, and many had made at least one attempt inthe previous 12 months (n = 11) and were currently try-ing to quit (n = 8).
Role in motivation to quitParticipants were asked about the labels’ influence ontheir motivation to quit. They most often identified la-bels depicting the negative consequences of smoking tosmokers, regardless of whether the label portrayed highor low threat, because of the influence on their risk per-ceptions (perceived severity and susceptibility):
Because you look at which way you going… Yougoing to [get] a messed up heart and you going toyour throat cancer or whatever he got. And oh, myGod, that [label #2] speak for itself. That one speakfor itself. (man, 47 years).
I have to say, this kinda changes your mind, but aftergoing outside smoking a cigarette,… you won’t beenjoying it as much after this… I mean, you know it’sharming you, but you don’t know it’s harming [you] tothis [extent]… [When] you actually see a heart likethis, you just be like, “Wow”. You know what I’msaying? It really makes you think. (man, 31 years).

Table 1 Characteristics of the graphic warning labels
Label # Label image Content category Origin
1 Negative consequences of smoking to smokers Adapted from Canada, 2012
2 Negative consequences of smoking to smokers Adapted from Brazil, 2009 [34]
3 Negative consequences of smoking to smokers Adapted from Canada, 2012 [35]
4 Negative consequences of smoking to smokers Adapted from U.S., 2012 (proposed) [36]
5 Negative consequences of smoking to others1 Adapted from Australia, 2011 [37]
Mead et al. BMC Public Health (2015) 15:92 Page4of11

Table 1 Characteristics of the graphic warning labels (Continued)
6 Negative consequences of smoking to others1 Adapted from U.S., 2012 (proposed) [36]
7 Negative consequences of smoking to others1 Adapted from U.S., 2012 (proposed) [36]
8 Negative consequences of smoking to others1 Adapted from Brazil, 2009 [34]
9 Benefits of quitting for smokers Created using purchased image, 2014
Mead et al. BMC Public Health (2015) 15:92 Page5of11
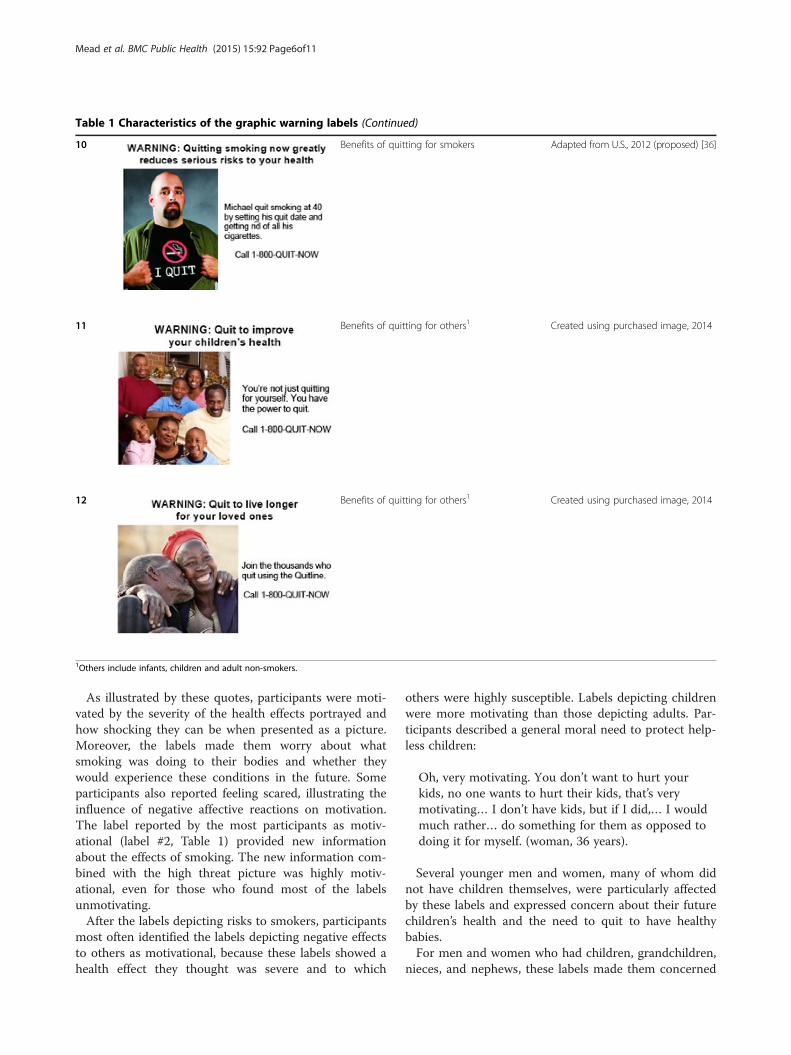
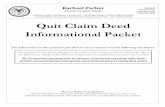
Table 1 Characteristics of the graphic warning labels (Continued)
10 Benefits of quitting for smokers Adapted from U.S., 2012 (proposed) [36]
11 Benefits of quitting for others1 Created using purchased image, 2014
12 Benefits of quitting for others1 Created using purchased image, 2014
1Others include infants, children and adult non-smokers.
Mead et al. BMC Public Health (2015) 15:92 Page6of11
As illustrated by these quotes, participants were moti-vated by the severity of the health effects portrayed andhow shocking they can be when presented as a picture.Moreover, the labels made them worry about whatsmoking was doing to their bodies and whether theywould experience these conditions in the future. Someparticipants also reported feeling scared, illustrating theinfluence of negative affective reactions on motivation.The label reported by the most participants as motiv-ational (label #2, Table 1) provided new informationabout the effects of smoking. The new information com-bined with the high threat picture was highly motiv-ational, even for those who found most of the labelsunmotivating.After the labels depicting risks to smokers, participants
most often identified the labels depicting negative effectsto others as motivational, because these labels showed ahealth effect they thought was severe and to which
others were highly susceptible. Labels depicting childrenwere more motivating than those depicting adults. Par-ticipants described a general moral need to protect help-less children:
Oh, very motivating. You don’t want to hurt yourkids, no one wants to hurt their kids, that’s verymotivating… I don’t have kids, but if I did,… I wouldmuch rather… do something for them as opposed todoing it for myself. (woman, 36 years).
Several younger men and women, many of whom didnot have children themselves, were particularly affectedby these labels and expressed concern about their futurechildren’s health and the need to quit to have healthybabies.For men and women who had children, grandchildren,
nieces, and nephews, these labels made them concerned

Table 2 Characteristics of the interview participants(N=25)
Characteristics n (%)1
Age in years (mean ± standard deviation) 45 ± 11
Age range in years 22 – 61
Age group
< 40 years 10 (40)
≥ 40 years 15 (60)
Race
African American 22 (88)
Caucasian 3 (12)
Gender
Male 12 (48)
Female 13 (52)
Marital status
Single 12 (48)
Married/partnered 12 (48)
Separated 1 (4)
Level of education
Less than high school 12 (48)
High school or GED2 completed 11 (44)
Some college, college completed or higher 2 (8)
Employment status
Employed full time 1 (4)
Unemployed 7 (28)
Unable to work or retired 16 (64)
Student 1 (4)
Personal pre-tax income from previous year
Less than $10,000 16 (64)
$10,000 – 29,999 6 (24)
$30,000 – 49,999 1 (4)
Not applicable 2 (8)
Smoking frequency
Once a week or a few times a week 2 (8)
Everyday 23 (92)
Cigarette packs smoked per day3
Less than 1 pack 11 (44)
1 pack 7 (28)
More than 1 pack 7 (28)
Ever tried to quit 14 (56)
≥1 quit attempt in the previous 12 months4 11 (79)
Currently trying to quit4 8 (57)1Frequency and percentage reported unless otherwise noted.2General Educational Development (GED).3On days that they smoked.4Only among participants who reported ever trying to quit (n=14).
Mead et al. BMC Public Health (2015) 15:92 Page7of11
about their health: “My grandson have asthma real badand he was hospitalized three times. So that made mepick [these labels]… I want to be around, healthy. I wantto see my grandchildren graduate from school, get mar-ried or whatever” (woman, 52 years). Participants werenot only concerned about the effect of secondhandsmoke on the children, but also felt concern for theirown health and a desire to live longer for the children.Several participants described these labels as encour-aging them to think about how their future poor healthand premature death would negatively impact their fam-ilies emotionally: “Sometimes it’s too late and then youactually see more pain from them than you actually go-ing through” (woman, 22 years).Different patterns emerged by participants’ quitting
behaviors. Most participants who were currently tryingto quit or had never tried to quit identified both types ofnegative labels (effects to smokers and others) as motiv-ational. In contrast, participants who were not currentlytrying to quit but had tried in the past were only moti-vated by the labels depicting their own risk.Overall, participants were more motivated by the
negative labels than the positive labels about the benefitsof quitting. However, several participants said the posi-tive labels were very motivational, with a relatively equalmixture of people motivated by the benefits of quittingfor smokers, others, and both. Participants stated theselabels were motivational because they showed hopefulmessages about people who quit and the benefits ofquitting. They viewed some characters as role modelsfor quitting and its benefits. In addition, participants re-ported that quitting for others was a highly motivationalmessage and discussed their family members as aninspiration:
[My husband’s] the one with the secondhand smoke.And I know I love him so much – that’s why I beentrying to cut down… I don’t want to… [make] hishealth bad because of my smoking. So I’m reallythinking. (woman, 46 years).
Notably, none of the positive labels were motivating toparticipants who had made a quit attempt, but they weremotivating to participants currently trying to quit orwho had never tried to quit.
Factors inhibiting role in motivationParticipants also described why the labels failed to mo-tivate them and why the labels might fail to motivateothers. The most significant factor discussed was thatthe labels failed to influence their perceived severity andsusceptibility. For several participants, the positive labelsabout the benefits of quitting did not depict serioushealth conditions, which they considered necessary for

Mead et al. BMC Public Health (2015) 15:92 Page8of11
motivation. When discussing the negative labels aboutthe consequences of smoking, several participants indi-cated that smokers think they are unlikely to get thehealth conditions:
Even smoking, drinking, whatever, drugs, whateverthey are doing, [older people] tend to think that if Istop now, all these ailments are going to come up allof a sudden. So I don’t think the picture would reallyaffect a lot of people if they been smoking for a longperiod of time because they think, ‘I’ve been smokingall this time and nothing happened yet.’(woman, 52 years).
Another inhibiting factor was that some participantsdoubted the labels’ credibility. They questioned the cred-ibility of the characters pictured on the positive labels,saying, for example, that they were actors or real peoplewho did not actually quit. A few participants alsodoubted the validity of the text, distrusting that smokingcaused the health conditions or that quitting would im-prove health.Even when believed, several participants reported that
improving health and avoiding disease was not sufficientmotivation and they could still fall sick. As one olderman (aged 60 years) said, “It’s not an ad that I would ad-here to… It’s like I’ve always thought: if you’re going toget [a disease], you’re going to get it; if you’re not, you’renot.” As described by another older man (aged 55 years),this fatalism could affect multiple aspects of individuals’lives: “A lot of people just don't… want to try to betterthemselves. You got some people that just don't want toquit. Doesn't matter. ‘Whatever's going to happen is go-ing to happen’”. For these participants, the health threatportrayed by the labels was not motivational.Some participants also described labels as unmotivat-
ing because the characters did not have inspirationalstories or did not correspond to the text, they had nodesire to emulate the characters who quit, and the char-acters were not similar to them. For the labels aboutquitting for others, some participants said these labelsdid not apply to them because they did not currentlyhave children (or did not plan to have future children)and were not family-oriented people.Three participants reported that none of the labels
were motivational, and each may represent different sub-sets of the smoker population. An older man (aged61 years) described a high level of intrinsic motivation toquit, such that the labels provided very little extrinsicmotivation. He was motivated to quit to improve hishealth and had reduced his smoking. He was somewhatmotivated by the positive labels because he wanted tolook healthy like the characters and stated quitting forothers was a good message. A younger man (aged
39 years), who had never made a quit attempt, alsoexpressed a lot of concern about his health and was mo-tivated to quit both to be healthier and make his familyhappy. However, he said he was unable to overcome hisnicotine addiction – in other words, he had low self-efficacy to quit. He discussed how the labels made himthink about quitting sooner, but could not motivate himto quit at the moment.Lastly, a younger woman (aged 39 years) was not mo-
tivated by the labels because she had no desire to quit.She expressed a somewhat fatalistic attitude as well aslow perceived risk from smoking, describing doubts thatsmoking would kill her and, if it does, “so be it”. She wasinitially somewhat motivated by label #11 because itshowed quitting as a family activity, but then becamedistrustful of the characters’ credibility. Overall, she wasaccepting of her decision to smoke and what it mightlead to: “Because I’m at the point in my life that I’m go-ing to do what I want to do, and I already know whatI’m doing to myself and I got to live with that. That’s thetruth I decide in me. That’s the truth I got to live with”.This quote illustrates the limited impact that labels mayhave on smokers with little desire to quit.
DiscussionThis qualitative study contributes to the graphic warninglabel literature by exploring low-income, urban U.S.smokers’ perceptions of theory-based labels and the la-bels’ role in their motivation to quit smoking. We foundthat participants were most motivated by labels portray-ing the negative consequences of smoking (negative la-bels), especially consequences to smokers; high and lowthreat labels were both motivational. The threat por-trayed in a message—characterized by severity of andsusceptibility to health conditions—intrinsically moti-vates action through fear and by increasing individuals’perceptions of their risk [19]. Indeed, we found that per-ceived severity, feelings of susceptibility, and negativeemotional reactions—such as fear and concern forothers—were major reasons why participants were moti-vated by the negative labels. These findings are consist-ent with other research showing that vivid depictions ofnegative effects promote cessation-related attitudes andbehaviors [20,22].Some negative labels failed to motivate participants be-
cause of low perceived susceptibility. Research hasshown that smokers have an optimistic bias regardingtheir cancer risk compared to nonsmokers and othersmokers [40], and increasing perceived vulnerability canincrease motivation to quit [41]. Vivid pictures that con-vey high threat, depictions of conditions commonly ex-perienced by smokers with a progression to moreserious outcomes, and use of characters who are highlysimilar to smokers and portrayed as susceptible to

Mead et al. BMC Public Health (2015) 15:92 Page9of11
conditions are some ways in which labels could be de-signed to enhance perceived susceptibility.Participants were also motivated by the positive labels
about the benefits of quitting because of their hopeful-ness, use of characters as role models, and depiction ofthe benefits for their and their families’ health and emo-tional wellbeing. These findings illustrate the potentialfor self-efficacy and response efficacy messages on labelsto motivate quitting. Our prior work showed that partic-ipants vicariously experienced characters’ quit successesportrayed on the labels, and these experiences played arole in their self-efficacy beliefs [Mead, Cohen, Kennedy,Gallo and Latkin: The influence of graphic warning la-bels on efficacy beliefs and risk perceptions: a qualitativestudy with low-income, urban smokers, submitted].Using a narrative format to enhance vicarious experi-ences and overcome message resistance [42], labels canshare the testimonials of ex-smokers who were able toquit and potentially increase self-efficacy and motivation.However, formative research is needed to develop realis-tic models to avoid doubts about their credibility. To in-crease motivation through response efficacy messages,labels can describe how quitting reduces risk to promotemessage acceptance. To address the critique that posi-tive labels did not portray a significant threat, labelscould show someone whose health improved after quit-ting (on the back of the pack) contrasted with someonewho did not quit and experienced deteriorating health(on the front of the pack).Notably, participants who had made a quit attempt
were most motivated by labels about their own risks ofsmoking, rather than risks to others, and not motivatedby positive labels. Individuals at different stages of theprocess towards behavior change are motivated by differ-ent factors [43]. For example, smokers who are not readyto quit may be motivated by messages providing new in-formation and allowing them to experience negativeemotions about smoking. Indeed, participants reportedthese factors as motivating characteristics of the labels.Using stages of change theory and audience segmenta-tion techniques [43], labels can be designed to targetsmokers by readiness to quit, including those who areseemingly unmotivated to quit, such as helping smokersweigh the pros and cons of quitting.Socially-oriented messages are an untapped potential
avenue for future messaging. Our finding that smokerswho never tried to quit were motivated by messagesabout effects to others is consistent with other evidenceshowing they are more likely to attempt to quit if theyperceive that others desire them to quit [15]. Labels canutilize this social concern to provide extrinsic motivationfor quitting and better target smokers who have nevermade a quit attempt. For some smokers, social concernmay be the only motivational label message, as
exemplified by the younger woman who was partly moti-vated by a label about family support for quitting.“Fatalistic” attitudes regarding health were present in a
subset of participants. Contrary to the extended parallelprocess model, threat messages did not appear to be suf-ficient to motivate action in this group. The participantslive within economically deprived areas in which smok-ing might be considered lower risk than other risks, suchas injection drug use, HIV, and violence. When examin-ing labels’ effectiveness, future work should considersuch attitudes and contextual factors that may influencethe impact of labels. Research is needed to examine whatfactors other than risk perceptions might motivatesmokers holding fatalistic attitudes.There are several strengths and limitations to this
study. We used purposive sampling of smokers whowere recruited from low-income, urban neighborhoods.Although the community-based, low-income, predomin-antly African-American sample allowed for the partici-pation of an understudied population, the transferabilityof the findings to other populations might be limited.However, the findings might be relevant beyond thepopulation studied, including populations in other coun-tries, because evidence-based theories were used in thedesign and analysis of labels. For example, future workmight test socially-oriented labels among cultures thatare less individualistic and more community-oriented.High SES smokers were not included because the focusof the study was on low SES populations as there hasbeen insufficient research on persons with low SES andsmoking. The qualitative methodology allowed for an in-depth exploration of smokers’ perceptions of the motiv-ational aspects of labels, but the cross-sectional designprecludes conclusions about the causal relationship be-tween labels and smokers’ motivations and behaviors.
ConclusionsThe role of graphic warning labels in risk perceptions,self-efficacy beliefs, and response efficacy beliefs were re-ported as motivators for cessation in this population oflow-income, urban smokers. Our findings suggest mul-tiple avenues for the design of future labels that mightpromote smoking cessation. Labels portraying negativeeffects of smoking, socially-oriented messages, and bene-fits of quitting are potential approaches to motivate ces-sation. Differences in the perceptions of labels thatemerged by quit attempt history suggests includingwarning labels that address smokers’ readiness to quitmight enhance effectiveness. Several factors that mightinfluence the impact of labels, such as low perceived sus-ceptibility, quit attempt history, and fatalistic attitudes,should be examined and addressed in future work. Byusing evidence-based theories to design and studygraphic warning labels, these findings are a first step

Mead et al. BMC Public Health (2015) 15:92 Page10of11
towards promoting smoking cessation among low SESand minority populations through graphic warning labels.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsELM specified the research question, designed the qualitative study, collectedand analyzed the interviews, and drafted the manuscript. JEC made substantialcontributions to the research design. JEC and CEK contributed to the dataanalysis. All authors contributed to the interpretation of the data and providedintellectually important contributions and revisions to the manuscript.All authors read and approved the final manuscript.
AcknowledgementsWe thank Dr. Melissa Davey-Rothwell and the Lighthouse staff for theirinsight and assistance throughout this study. Also, we sincerely thank theparticipants for their time.
FundingThe data collection was supported by the National Institute on Drug Abuse atthe National Institutes of Health and the Food and Drug Administration Centerfor Tobacco Products (grant numbers R01DA032217-04 and R01DA032217-04S);and by the National Institute of Allergy And Infectious Diseases at the NationalInstitutes of Health, The Johns Hopkins Center for AIDS Research (grant number1P30 AI094189). The agencies were not involved in any technical aspect of thestudy. Funding for Open Access provided by the UMD Libraries Open AccessPublishing Fund.
Author details1Department of Health, Behavior and Society, Johns Hopkins UniversityBloomberg School of Public Health, Baltimore, MD, USA. 2Tobacco Center ofRegulatory Science, Department of Behavioral and Community Health,University of Maryland School of Public Health, College Park, MD 20742-2611,USA. 3Department of Health, Behavior and Society, Institute for GlobalTobacco Control, Johns Hopkins University Bloomberg School of PublicHealth, Baltimore, MD, USA. 4Department of International Health, JohnsHopkins University Bloomberg School of Public Health, Baltimore, MD, USA.5Department of Mental Health, Johns Hopkins University Bloomberg Schoolof Public Health, Baltimore, Maryland, USA.
Received: 29 October 2014 Accepted: 15 January 2015
References1. Central Intelligence Agency. The World Factbook, 2013–14. Washington, DC:
Central Intelligance Agency; 2013.2. OECD. An overview of growing income inequalities in OECD countries:
Main findings. In: Divided We Stand: Why Inequality Keeps Rising. Paris,France: OECD Publishing; 2011. p. 21–45.
3. Nandi A, Glymour MM, Subramanian SV. Association among socioeconomicstatus, health behaviors, and all-cause mortality in the United States.Epidemiology. 2014;25(2):170–7.
4. Shaw BA, McGeever K, Vasquez E, Agahi N, Fors S. Socioeconomicinequalities in health after age 50: are health risk behaviors to blame?Soc Sci Med. 2014;101:52–60.
5. Centers for Disease Control and Prevention. Quitting smoking among adults–-United States, 2001–2010. Morb Mortal Wkly Rep. 2011;60(44):1513–9.
6. Barbeau EM, Krieger N, Soobader MJ. Working class matters: socioeconomicdisadvantage, race/ethnicity, gender, and smoking in NHIS 2000. Am JPublic Health. 2004;94(2):269–78.
7. Hackbarth DP, Silvestri B, Cosper W. Tobacco and alcohol billboards in 50Chicago neighborhoods: market segmentation to sell dangerous productsto the poor. J Public Health Policy. 1995;16(2):213–30.
8. Brown-Johnson CG, England LJ, Glantz SA, Ling PM. Tobacco industrymarketing to low socioeconomic status women in the USA. Tob Control.2014;23(e2):e139–46.
9. Seidenberg AB, Caughey RW, Rees VW, Connolly GN. Storefront cigaretteadvertising differs by community demographic profile. Am J Health Promot.2010;24(6):e26–31.
10. Dragano N, Bobak M, Wege N, Peasey A, Verde PE, Kubinova R, et al.Neighbourhood socioeconomic status and cardiovascular risk factors: amultilevel analysis of nine cities in the Czech Republic and Germany.BMC Public Health. 2007;7:255.
11. Stead M, MacAskill S, MacKintosh A-M, Reece J, Eadie D. “It’s as if you’re lockedin”: qualitative explanations for area effects on smoking in disadvantagedcommunities. Health Place. 2001;7(4):333–43.
12. LaVeist T, Thorpe Jr R, Mance G, Jackson J. Overcoming confounding of racewith socio-economic status and segregation to explore race disparities insmoking. Addiction. 2007;102 Suppl 2:65–70.
13. Gallus S, Ghislandi S, Muttarak R. Effects of the economic crisis on smokingprevalence and number of smokers in the USA. Tob Control. 2015;24(1):82–8.
14. Borland R, Yong HH, Balmford J, Cooper J, Cummings KM, O’Connor RJ,et al. Motivational factors predict quit attempts but not maintenance ofsmoking cessation: findings from the International Tobacco Control FourCountry project. Nicotine Tob Res. 2010;12 suppl 1:S4–11.
15. Clark MA, Kviz FJ, Crittenden KS, Warnecke RB. Psychosocial factors andsmoking cessation behaviors among smokers who have and have not evertried to quit. Health Educ Res. 1998;13(1):145–53.
16. Lee HS, Catley D, Harris KJ. Improving understanding of the quitting process:psychological predictors of quit attempts versus smoking cessationmaintenance among college students. Subst Use Misuse. 2014;49(10):1332–9.
17. Curry SJ, Grothaus L, McBride C. Reasons for quitting: intrinsic and extrinsicmotivation for smoking cessation in a population-based sample of smokers.Addict Behav. 1997;22(6):727–39.
18. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsicmotivation, social development, and well-being. Am Psychol. 2000;55(1):68–78.
19. Witte K, Allen M. A meta-analysis of fear appeals: implications for effectivepublic health campaigns. Health Educ Behav. 2000;27(5):591–615.
20. Hammond D. Health warning messages on tobacco products: a review.Tob Control. 2011;20(5):327–37.
21. Azagba S, Sharaf MF. The effect of graphic cigarette warning labels onsmoking behavior: evidence from the Canadian experience. Nicotine TobRes. 2013;15(3):708–17.
22. Hammond D, Thrasher JF, Reid JL, Driezen P, Boudreau C, Santillan EA.Perceived effectiveness of pictorial health warnings among Mexican youthand adults: a population-level intervention with potential to reducetobacco-related inequities. Cancer Causes Control. 2012;23 suppl 1:57–67.
23. McCaul KD, Hockemeyer JR, Johnson RJ, Zetocha K, Quinlan K, GlasgowRE. Motivation to quit using cigarettes: a review. Addict Behav. 2006;31(1):42–56.
24. Cismaru M, Lavack AM. Tobacco warning labels and the protectionmotivation model: implications for Canadian tobacco control policy. CanPublic Pol. 2007;33(4):477–86.
25. Schneider S, Gadinger M, Fischer A. Does the effect go up in smoke? Arandomized controlled trial of pictorial warnings on cigarette packaging.Patient Educ Couns. 2012;86(1):77–83.
26. Romer D, Peters E, Strasser AA, Langleben D. Desire versus efficacy insmokers’ paradoxical reactions to pictorial health warnings for cigarettes.PLoS One. 2013;8(1):e54937.
27. Beacom AM, Newman SJ. Communicating health information todisadvantaged populations. Fam Community Health. 2010;33(2):152–62.
28. Viswanath K, Finnegan Jr JR. The knowledge gap hypothesis: twenty-fiveyears later. In: Burleson BR, Kunkel A, editors. Communication Yearbook.Volume 19, edn. Thousand Oaks, CA US: Sage Publications, Inc; 1996.p. 187–227.
29. Viswanath K, Breen N, Meissner H, Moser RP, Hesse B, Steele WR, et al.Cancer knowledge and disparities in the information age. J HealthCommun. 2006;11 suppl 1:1–17.
30. Cantrell J, Vallone DM, Thrasher JF, Nagler RH, Feirman SP, Muenz LR, et al.Impact of tobacco-related health warning labels across socioeconomic, raceand ethnic groups: results from a randomized web-based experiment. PLoSOne. 2013;8(1):e52206.
31. Thrasher JF, Arillo-Santillan E, Villalobos V, Perez-Hernandez R, Hammond D,Carter J, et al. Can pictorial warning labels on cigarette packages addresssmoking-related health disparities? Field experiments in Mexico to assesspictorial warning label content. Cancer Causes Control. 2012;23 suppl 1:69–80.
32. Thrasher JF, Villalobos V, Szklo A, Fong GT, Perez C, Sebrie E, et al. Assessingthe impact of cigarette package health warning labels: a cross-countrycomparison in Brazil, Uruguay and Mexico. Salud Publica Mex.2010;52(suppl2):S206–215.

Mead et al. BMC Public Health (2015) 15:92 Page11of11
33. Tobin KE, Kuramoto SJ, Davey-Rothwell MA, Latkin CA. The STEP into Actionstudy: a peer-based, personal risk network-focused HIV prevention interventionwith injection drug users in Baltimore, Maryland. Addiction. 2011;106(2):366–75.
34. Instituto Nacional de Câncer (Brazil): Brazil: Health warnings on tobaccoproducts, 2009. Rio de Janeiro, Brazil: Ministério da Saúde, Instituto Nacional deCâncer; 2008. [http://www.tobaccolabels.ca/wp/wp-content/uploads/2013/12/Brazil-2008-Health-Warnings-on-Tobacco-Products-Report-English.pdf]
35. Decima Research. Testing of health warning messages and healthinformation messages for tobacco products. Decima Research Inc.: Canada;2009. [http://www.tobaccolabels.ca/wp/wp-content/uploads/2013/12/Canada-2009-Testing-of-Health-Warning-Messages-and-Health-Information-Messages-for-Tobacco-Products-Government-Report.pdf]
36. U.S. Food and Drug Administration. Experimental study of graphic cigarettewarning Labels, final results report, December 2010 - [required warnings forcigarette packages and advertisements; research report] re FDA-2010-N-0568–0006. 2011(6/27). Rockville, MD: Center for Tobacco Products, FDA; 2010 [http://www.tobaccolabels.ca/wp/wp-content/uploads/2013/12/USA-2010-Experimental-Study-of-Graphic-Cigarette-Warning-Labels-Final-Results-Report-FDA.pdf]
37. Parr V, Ell P, Gagg K. Market testing of new health warnings and informationmessages for tobacco product packaging: phase 3 refinement of healthwarnings. Qualitative formative research report. Australia: GfK Blue Moon;2011. [http://www.health.gov.au/internet/publications/publishing.nsf/Content/gmtp3]
38. Bandura A. On the functional properties of perceived self-efficacy revisited.J Manage. 2012;38(1):9–44.
39. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the frameworkmethod for the analysis of qualitative data in multi-disciplinary healthresearch. BMC Med Res Methodol. 2013;13:117.
40. Weinstein ND, Marcus SE, Moser RP. Smokers’ unrealistic optimism abouttheir risk. Tob Control. 2005;14(1):55–9.
41. Copeland AL, Brandon TH. Testing the causal role of expectancies insmoking motivation and behavior. Addict Behav. 2000;25(3):445–9.
42. Kreuter MW, Green MC, Cappella JN, Slater MD, Wise ME, Storey D, et al.Narrative communication in cancer prevention and control: a framework toguide research and application. Ann Behav Med. 2007;33(3):221–35.
43. Prochaska JO, Redding CA, Evers KE. The transtheoretical model and stagesof change. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior andHealth Education: Theory, Research, and Practice. 4th ed. San Francisco, CA:Jossey-Bass; 2008. p. 97–121.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit