
The Rational Clinical Examination Does This Patient Have Hypertension? How to Measure Blood Pressure
8
The Rational Clinical Examination tihypertensive drrg treatment, can lead to reduced CVD and mortality.to,ll STANDARDS FOR MEASURING BP The "gold" standard for instantaneous BP measurement is the intra-arterial or direct BP (delermined by arigid-walled catheter). The standard for clinical prac- tice is the so-called casual cuff or indi- rect BP. Guidelines for Diagnosing Hypertension Cardiovascular disease risk rises monotonically with BP, revealing no cut point below which risk is minimal and above which CVD will definitely occur. Terms used to indicate the degree ofBP elevation now emphasize the importance of what was previously termed mild hy- pertension and the long-recognized greater predictive value ofelevated sys- tolic BP12 (Table 1). Risk for future CVD is predicted by even a single careful BP reading.ls-ls However, BP is rather vari- able and often decreases with observa- tion so that, in accord with statigtical expectations, risk relates more closely to mean BP over several visitsl3 (al- though brief, severe BP elevation can also be catastrophic, eg, with cocaine overdose). Therefore, we could define the "treatable BP level" as that mean clinical BP above which treatment has been shown in randomized controlled trials to do more good than harm. The largest of these trials used drug treat- ment vs placebo after finding a consis- tent or average entry BP from two to three visits ofgreater than or equal to 160 mm Hg systolic (tested only in the elderly) with or without diastolic BP elevation,l6 or greater than or equal to 90 mm Hg diastolic (tested in the young and in the elderly).11 In the future, in- dividualZed assessments of absolute risk incorporating other relevant informa- tion, such as age, sex, concomitant risk factors, and coexisting target organ dam- age, along with the patient's tolerance for risk and history of drug side effects may replace arbitrary cut points in de- termining when BP elevation becomes treatable.T At present, a diagnosis of hypertension reflects a consensus re- garding the office BP level above which CVD risk worsens importantly, about 140/90 mm Hg. A detailed conceptual analysis ofhy- pertension is beyond the scope of this article, but has been addressed thought- fuliy by Jennings and Netsky.l? How to Measure Clinical BP Meticulous technique in indirect aus- cultatory BP measurement is manda- tory for research, for diagnosis, and for optimal clinical care of hypertensive pa- tients. Published procedurai guidelines show general uniformity.3-5'r8-20 The ac- curacy and reliability of BP measure- ment will be increased by following the widely accepted procedures recom- mended by the American Heart Asso- ciation (Table 2, Figure 1). Blood pres- sure is customarily measured after ob- taining the medical history as part of the "vital sign" determination at the be- ginning of the physical examination. At each visit, two or more readings should be obtained and averaged from the same The Fational Clinical Examination section editors: David L. Simel. lVD. MHS. Durham Veterans Affairs N.4edical Center and Duke University l\,4edical Center, Durham, NC; Drummond Fennie, N,4D, Deputy Edltor (WeSt), JAMA. Does This Patient Have Hypertension? How to Measure Blood Pressure Richard A. Reeves, MD FRCPC CLINICAL SCENARIO ls This Patient's Blood Pressure Really Elevated? A 46-year-old man who has recently moved to your neighborhood presents with a painful ankle sprain. Before he leaves, you decide to check his blood pressure (BP) and obtain an initial read- ing of 1641102 mm Hg. He denies having high BP previously. WHY IS ACCURATE BP MEASUREMENT IMPORTANT? Elevated arterial BP, or hyperten- sion, is important because it is common, it is clinically silent, it leads to cardio- vascular disease (CVD), and it decreases life expectancy. Because surveys find that approximately 207o1 3 of North American adults have an elevated BP (systolic BP >140 mm Hg and/or dias- tolic BP =90 mm Hg) or are taking an- tihy-pertensive medication, physicians are advised to check all patients peri- odically for BP elevation.s-? On the other hand, overestimation of BP can errone- ously label people as hypertensive and potentially result in unnecessary dietary restrictions, exposure to potential side effects from drug treatment, medica- tion expense. and adverse socioeconomic effects.s,e Fortunately, measuring BP is an easy and safe diagnostic procedure that, when followed by appropriate an- From the Division of Clinical Pharmacology, Depart- ment of Medicine, and the Clinical Epidemiology Unit, Sunnybrook Health Sciences Centre, University of Toronto (Ontario). Dr Reeves is now with Bristol-Myers Squibb Pharmaceutical Fiesearch Institute, Princeton, NJ, Reprint requests to Bristol-lvlyers Squibb Pharma- ceutical Research Institute, PO Box 4000, Princeton, NJ 08543 (Dr Reeves). JAMA, April 19, 1995-Vol 273, No. 15 Does This Patient Have Hypertension?-Reeves 121'l
-
Upload
independent -
Category
Documents
-
view
7 -
download
0
Transcript of The Rational Clinical Examination Does This Patient Have Hypertension? How to Measure Blood Pressure
The Rational Clinical Examination
tihypertensive drrg treatment, can leadto reduced CVD and mortality.to,ll
STANDARDS FOR MEASURING BP
The "gold" standard for instantaneousBP measurement is the intra-arterial ordirect BP (delermined by arigid-walledcatheter). The standard for clinical prac-tice is the so-called casual cuff or indi-rect BP.
Guidelines for DiagnosingHypertension
Cardiovascular disease risk risesmonotonically with BP, revealing no cutpoint below which risk is minimal andabove which CVD will definitely occur.Terms used to indicate the degree ofBPelevation now emphasize the importanceof what was previously termed mild hy-pertension and the long-recognizedgreater predictive value ofelevated sys-tolic BP12 (Table 1). Risk for future CVDis predicted by even a single careful BPreading.ls-ls However, BP is rather vari-able and often decreases with observa-tion so that, in accord with statigticalexpectations, risk relates more closelyto mean BP over several visitsl3 (al-though brief, severe BP elevation canalso be catastrophic, eg, with cocaineoverdose). Therefore, we could definethe "treatable BP level" as that meanclinical BP above which treatment hasbeen shown in randomized controlledtrials to do more good than harm. Thelargest of these trials used drug treat-ment vs placebo after finding a consis-tent or average entry BP from two tothree visits ofgreater than or equal to160 mm Hg systolic (tested only in theelderly) with or without diastolic BPelevation,l6 or greater than or equal to
90 mm Hg diastolic (tested in the youngand in the elderly).11 In the future, in-dividualZed assessments of absolute riskincorporating other relevant informa-tion, such as age, sex, concomitant riskfactors, and coexisting target organ dam-age, along with the patient's tolerancefor risk and history of drug side effectsmay replace arbitrary cut points in de-termining when BP elevation becomestreatable.T At present, a diagnosis ofhypertension reflects a consensus re-garding the office BP level above whichCVD risk worsens importantly, about140/90 mm Hg.
A detailed conceptual analysis ofhy-pertension is beyond the scope of thisarticle, but has been addressed thought-fuliy by Jennings and Netsky.l?
How to Measure Clinical BP
Meticulous technique in indirect aus-cultatory BP measurement is manda-tory for research, for diagnosis, and foroptimal clinical care of hypertensive pa-tients. Published procedurai guidelinesshow general uniformity.3-5'r8-20 The ac-curacy and reliability of BP measure-ment will be increased by following thewidely accepted procedures recom-mended by the American Heart Asso-ciation (Table 2, Figure 1). Blood pres-sure is customarily measured after ob-taining the medical history as part ofthe "vital sign" determination at the be-ginning of the physical examination. Ateach visit, two or more readings shouldbe obtained and averaged from the same
The Fational Clinical Examination section editors:David L. Simel. lVD. MHS. Durham Veterans AffairsN.4edical Center and Duke University l\,4edical Center,Durham, NC; Drummond Fennie, N,4D, Deputy Edltor(WeSt), JAMA.
Does This Patient Have Hypertension?How to Measure Blood Pressure
Richard A. Reeves, MD FRCPC
CLINICAL SCENARIO
ls This Patient's Blood PressureReally Elevated?
A 46-year-old man who has recentlymoved to your neighborhood presentswith a painful ankle sprain. Before heleaves, you decide to check his bloodpressure (BP) and obtain an initial read-ing of 1641102 mm Hg. He denies havinghigh BP previously.
WHY IS ACCURATE BPMEASUREMENT IMPORTANT?
Elevated arterial BP, or hyperten-sion, is important because it is common,it is clinically silent, it leads to cardio-vascular disease (CVD), and it decreaseslife expectancy. Because surveys findthat approximately 207o1 3 of NorthAmerican adults have an elevated BP(systolic BP >140 mm Hg and/or dias-tolic BP =90 mm Hg) or are taking an-tihy-pertensive medication, physiciansare advised to check all patients peri-odically for BP elevation.s-? On the otherhand, overestimation of BP can errone-ously label people as hypertensive andpotentially result in unnecessary dietaryrestrictions, exposure to potential sideeffects from drug treatment, medica-tion expense. and adverse socioeconomiceffects.s,e Fortunately, measuring BP isan easy and safe diagnostic procedurethat, when followed by appropriate an-
From the Division of Clinical Pharmacology, Depart-ment of Medicine, and the Clinical Epidemiology Unit,Sunnybrook Health Sciences Centre, University ofToronto (Ontario). Dr Reeves is now with Bristol-MyersSquibb Pharmaceutical Fiesearch Institute, Princeton,NJ,
Reprint requests to Bristol-lvlyers Squibb Pharma-ceutical Research Institute, PO Box 4000, Princeton,NJ 08543 (Dr Reeves).
JAMA, April 19, 1995-Vol 273, No. 15 Does This Patient Have Hypertension?-Reeves 121'l
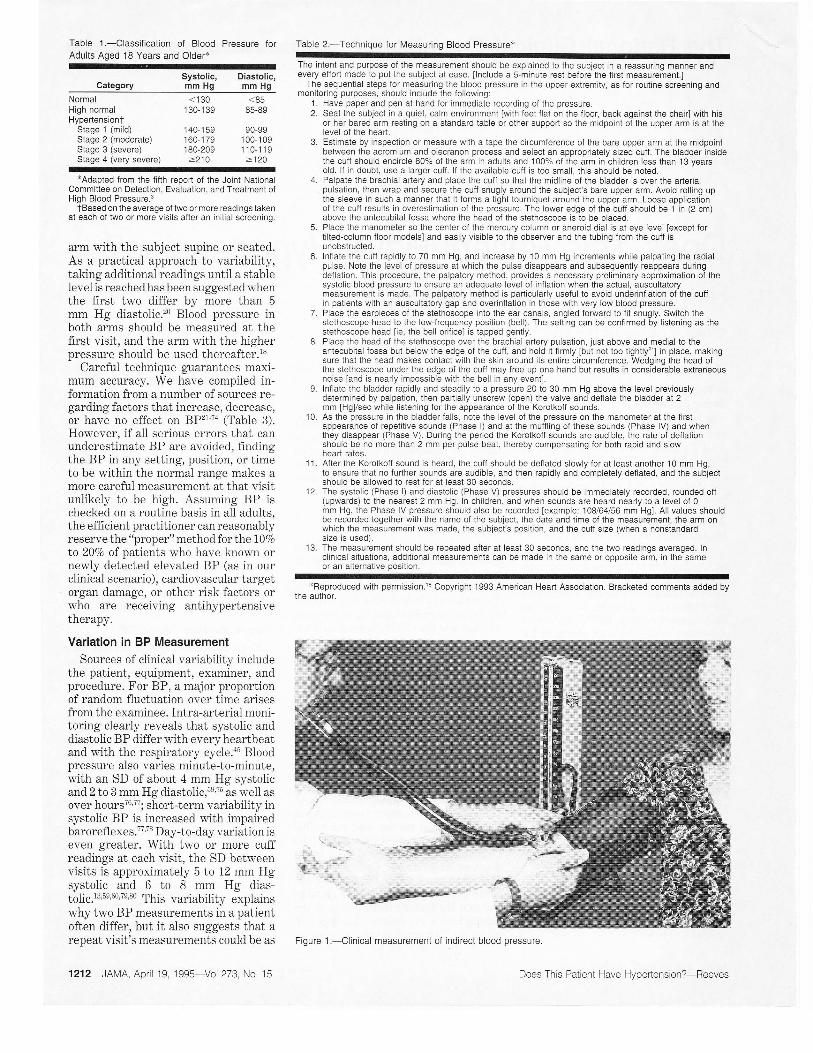
Table 1.-Classification of Blood Pressure forAdults Aged 18 Years and Older+
CategorySystolic, Diastolic,mm Hg mm Hg
Table 2.-Technique for Measuring Blood Pressure*
The intent and purpose of the measurement should be explained to the subject in a reassuring manner andevery eifort made to put the subject at ease. ilnclude a s-minute rest before the firsi measuremenl.l
The sequeniial steps for measuring the blood pressure in the upper extremity, as for routine screening andmonitoring purposes, should include the following:
1. Have paper and pen at hand for immediate recording of the pressure.2. Seat the subject in a quiet, calm environment [with feet flat on the floor, back against the chair] with his
or her bared arm resting on a standard table or other support so the midpoint of the upper arm is al thelevel of the heart.
3. Estimate by inspection or measure with a tape the circumference of the bare upper arm at the midpoinlbetween the acromium and olecranon process and select an appropriately sized cuff. The bladder insidethe cuff should encircle 80% of the arm in adults and 100% of the arm in children less than 13 yearsold. lf in doubt, use a larger cuff. lf the available cuff is too small, this should be noted.
4. Palpate the brachial artery and place the cutf so that the midline of the bladder is over the anerialpulsation, then wrap and secure the cutf snugly around the subject's bare upper arm. Avoid rolling uplhe sleeve in such a manner that it forms a tight tourniquet around the upper arm. Loose applicationof the cufl results in overestimation of the pressure. The lower edge of the cuff should be 1 in (2 cm)above the antecubital fossa where the head of the stethoscooe is to be Dlaced.
5. Place the manometer so the center of the mercury column or aneroid dial is at eye level [except fortilted-column floor modelsl and easily visible to the observer and the tubing from the cuff isunobstructed.
6. Inflate the cuif rapidly to 70 mm Hg, and increase by 10 mm Hg increments while palpating the radialpulse. Note the level of pressure at which the pulse disappears and subsequently reappears duringdeflation. This procedure, the palpatory method, provides a necessary preliminary approximation of thesystolic blood pressure to ensure an adequate level of intlation when the actual, auscultatorymeasurement is made. The palpatory method is particularly useful to avoid underinflation of the cuffin patients wilh an auscultatory gap and overinflalion in those with very low blood pressure.
7. Place the earpieces of lhe stethoscope into the ear canals, angled foMard to fit snugly. Switch thestethoscope head to the low-frequency position (bell). The setting can be confirmed by listening as thestethoscope head lie, the bell orifice] is tapped gently.
8. Place the head of the stethoscope over the brachial artery pulsation, just above and medial to theaniecubital lossa but below the edge of the cuff, and hold it lirmly lbut not too tightly'zll in place, makingsure that the head makes contact with the skin around its enlire circumference. Wedging the head olihe stethoscope under the edge of the cufl may {ree up one hand but results in considerable extraneousnoise land is nearly impossible with the bell in any eventl.
9. Inflate the bladder rapidly and steadily to a pressure 20 to 30 mm Hg above the level previouslydetermined by palpation, then partially unscrew (open) the valve and deilate the bladder at 2mm [Hg]/sec while listening lor the appearance ot the Korotkoff sounds.
10. As the pressure in the bladder falls, note the level o{ the pressure on the manometer at the firstappearance of repetitive sounds (Phase l) and at the muffling oi these sounds (Phase lV) and whenthey disappear (Phase V). During the period the Korotkoff sounds are audible, the rate of deflationshould be no more than 2 mm per pulse beat, thereby compensating for both rapid and slowheart rates.
1 1 . Aiter the Korotkolf sound is heard, the cuff should be def lated slowly {or at least another 1 0 mm Hg,to ensure that no fufther sounds are audible, and then rapidly and completely deflated, and the subjectshould be allowed to rest for at least 30 seconds.
12. The systolic (Phase l) and diastolic (Phase V) pressures should be immediately recorded, rounded otf(upwards) io the nearest 2 mm Hg. ln children, and when sounds are heard nearly to a level of 0mm Hg, the Phase IV pressure should also be recorded lexample: 108/64/56 mm Hg]. All values shouldbe recorded together with the name ol the subject, the date and time of the measurement, the arm onwhich the measurement was made, the subject's position, and the cuff size (when a nonstandardsize is used).
13. The measurement should be repeated aiter at least 30 seconds, and the two readings averaged. Inclinical situations, additional measurements can be made in the same or opposite arm, in the sameor an alternative position.
xReproduced with permission.le Copyright 1993 American Heart Association. Bracketed comments added bythe author.
Figure 1.-Clinical measurement of indirect blood pressure.
NormalHigh normalHypertensiont
Stage 1 (mild)Stage 2 (moderate)Stage 3 (severe)Stage 4 (very severe)
< 1301 30-1 39
1 40-1 591 60-1 791 80-209>210
<8585-89
90-991 00-1 09110-119>120
*Adaoted from the liith reoort of the Joint NationalCommittee on Detection, Evaluation, and Treatment ofHigh Blood Pressure.3
tBased on the average oftwo or more readings iakenat each of two or more visits after an initial screenino.
arm with the subject supine or seated.As a practical approach to variability,taking additional readings until a stablelevel is reached has been suggested whenthe first two differ by more than 5mm Hg diastolic.zo Blood pressure inboth arms should be measured at thefirsl visit, and the arm with the higherpressure should be used thereafter.l8
Careful technique guarantees maxi-mum accuracy. We have compiled in-formation from a number of sources re-garding factors that increase, decrease,or have no effect on BP21-74 (Table 3).However, if all serious errors that canunderestimate BP are avoided, findingthe BP in any setting, position, or timeto be within the normal range makes amore careful measurement at that visitunlikely to be high. Assuming BP ischecked on a routine basis in all adults,the efficient practitioner can reasonablyreserve the "proper" metho d for the l}Voto 207a of oatients who have known ornewly detected elevated BP (as in ourclinical scenario), ca1'diovascular target,organ damage, or other risk factors orwho are receiving antihypertensiveInerapy.
Variation in BP MeasurementSources of clinical variability include
the patient, equipment, examiner, andprocedure. For BP, a major proportionof random fluctuation over time arisesfrom the examinee. Intra-arLerial moni-toring clearly reveals that systolic anddiastolic BP differ with every heartbeatand with the respiratory cycle.as Bloodpressure also varies minute-to-minute,with an SD of about 4 mm Hg systolicand 2 to 3 mm Hg diastolic,ss,?5 as well asover hours76,?7; short-term variability insystolic BP is increased with impairedbarorefl exes.77'?8 Day-to-day variation iseven greater. With two or more cuffreadings at each visit, the SD belweenvisits is approximately 5 to 12 mm Hgsystolic and 6 to 8 mm Hg dias-t01ic,13,5e,60,?e'80 This variability explainswhy two BP measurements in a patientoften differ, but it also suggests that arepeat visit's measurements could be as
1212 JAIVA, April 19, 1995-Vol 273, No. 15 Does This Patient Have Hvoertension?-Reeves
much as l5ll2 mm Hg higher or lowerthan today's result about 57o of the time.The greater magnitude ofthe between-vs within-visit variability is the reasonwhy more visits are recommended toachieve greater diagnostic precisionrather than more replications at a visit.In reality, the return BP reading in ourclinical scenario will likely be lower, pos-sibly much lower, because of our pa-tient's present distress, unfamiliaritywith the physician and the physician'soffice procedures, and "regression to themean" (discussed herein).
Arrhy-thmias, particularly atrial fibril-lation, cause beat-to-beat cardiac out-put to vary substantially and increaseinterobserver variation in measuredBP.81 With atrial fibrillation, probablythe best one can do is to deflate the cuffslowly while attempting to ascertainwhen most of the contractions are re-sulting in audible Korotkoff sounds (theapproximate systolic BP) and when thesounds have all but ceased yet still occurinfrequently (the approximate diastolicBP), or one can average several read-ings.ts'zo Because Korotkoff sounds gen-erated by occasional premature beats(and the subsequent beat) are urirepre-sentative of the day's mean BP level,lhey should be ignored.22
Examiners can introduce random er-rors. Under ideal conditions, simulta-neous BP readings by independent ob-servers lypically correlate above r=0.95with mean absolute differences of lessthan 2 mm Hg systolic and less than 1
mm Hg diastolic.82 However. even inresearch settings, careful BP readingsobtained just a few minutes apart showdistressingly high variation (eg, SD of 7mm Hg systolic and 5 mm Hg dias-tolicls'54,61). In routine medical practice,physicians and nurses often measure BPfar less carefully: differences of 10/8mm Hg are common.83'84 \Afhite et al85
performed intra-arterial BP recordingin 48 hypertensive patients and foundthe humbling result that two ausculta-tory automatic monitors showed lessoverall discrepancy and fewer widelydiscrepant readings than did experienced clinicians using the standardmethod.
Environmental problems (eg, noisefrom construction work next door) ordeficient equipment (eg, an inadequatelydamped, "bouncy" mercury column, rem-edied by tightening the knurled nut atthe column's top22) may also be expectedto decrease precision.
Accuracy of BP Measurernent
Accuracy, or validity, refei:s to agree-ment with the tr"uth and reguires notonlyprecision but also foeedomfrom sys-tematic error (ie, bias). In cr nical BP
JAMA, April 19, 1995-Vol 273, No. 5
Table 3.-Factors Alfecting the lmmediate Accuracy of Office BP*
Magnitude,SBP/DBP, mm Hg Reference
ExamineeSoft Korotkoff sounds
lncreases Recorded BP
DBP Assumed
Missed auscultatory gap DBP (rare, huge)
Pseudohypertension 2 to 98/3 to 49
"White coat" reactionTo physician 11 to28/3to 15
To nonphysician 1 to 12/2lo 7 27,31,32
Paretic arm (due to stroke)
Pain, anxiety May be large
Acute smoking
Acute caffeine I t/c
Acute elhanol ingestion
Distended bladder 15/10
Talkinq; signing 38; 39
Setting, equipmentEnvironmental noise Assumed
Leaky bulb valve >2 DBP
Blocked manometer vents 2to10 41
Cold hands or stethoscooe Not stated
ExaminerExpectation bias Probably <10 In theory
lmpaired hearinq
ExaminationCutf too narrow -g to +10/2 to ICutf not centered
Cutf over clothing 5to50Elbow too low
Cuft too loose Not stated
Too short rest period Varied estimates
Back unsupported 6to10 49,50
Arm unsupported 1 to7l5to'11 clToo slow deflation -1 to+2/5too 52, 53
Too fasl deflation DBP only 52. 53
Parallax error 2lo 4 By author
Using phase lV (adult) 6 DBP
Too rapid remeasure 52,54
Cold season (vs warm) 6/3to 10 55-57
measurement, we look through a seriesofdark glasses, fruther considered herein:(1) the indirect BP may not reflect theconcurrent intra-arterial BP; (2) the cufftechnique may be incorrectly perforrned;and (3) a perfectly executed indirect (oreven direct) BP reading at a parbicularmoment may not represent the patient'saverage clinic BP nor the average BPthroughout the day's activities, as ad-dressed in the section on ambulatory BPmonitoring. Finally, to interpret even aperfect BP reading requires consider-ation of the whole patient because fac-tors other than BP strongly influencethe risk for CVD events.
Indirect BP vs Direct BP.-Indirectauscultatory BP correlates well with thesimultaneous intra-arterial value (r=0.94to 0.98).86 However, the Korotkoff phaseI sounds do not appear until 15 to 4mm Hg below the 'irect systolic BP,whereas at phase V the sounds disap-
pear 3 to 6 mm Hg above the true di-astolic BP in adu1ts.45'85'86
If these technical differences appliedequally lo all patients, they wouid bemerely academic; clinical importancearises when an individual patient pos-sesses an unusual discrepancy. Such pa-tients are often elderly (where false el-evation is termed "pseudohyperten-sion"23'2,8?8e) or obese,a6 but otherwiseunexplained extreme false elevations incuff BP may also occur.e0 Pseudohyper-tension might seem at first glance to bea variant of normal BP. However, mostpatients actually have chronic hyper-tension,el on which is superimposed afurther faise BP elevation. Although ithas been claimed that pseudohyperten-sion can be suspected in an older personif "Osier's sign" (while feeling the radialpulse, occlude the brachial artery by cuffinflation or by direct pressure using theother thumb;if the radial artery remains
Does This Patient Have Hvoertension?-Reeves 12'|3
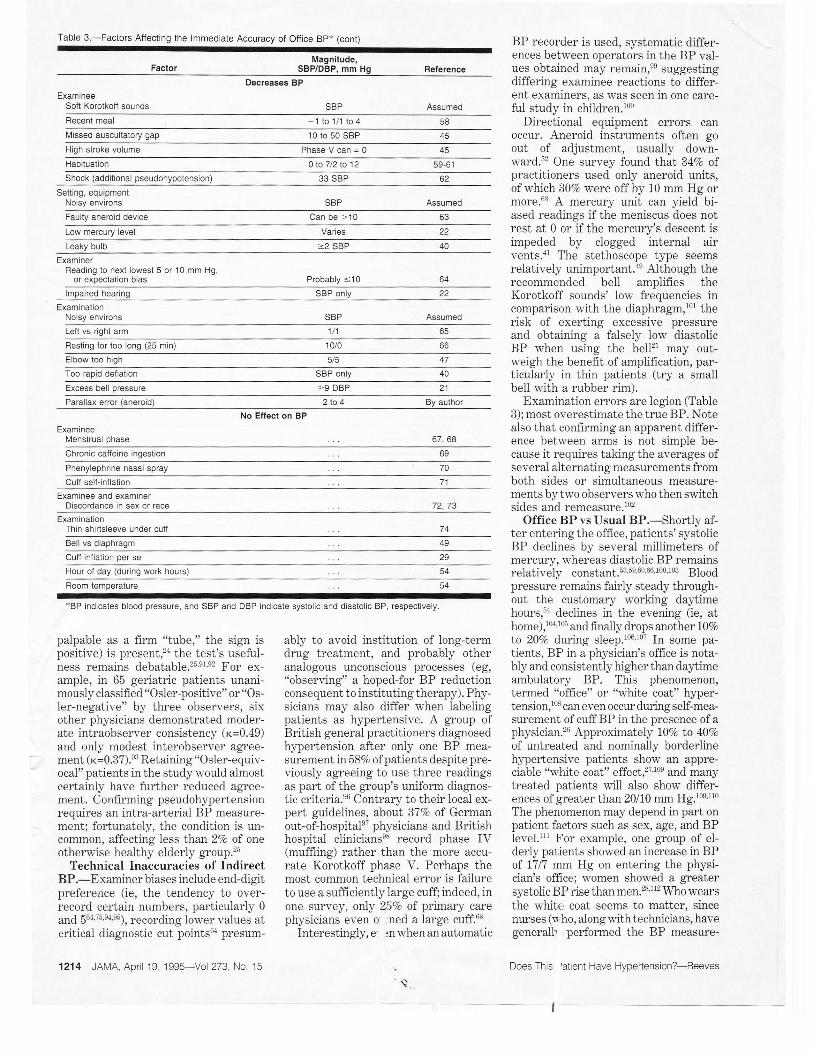
Table 3.-Factors Affecting the lmmediate Accuracy of Otfice Bp* (cont)
Magnitude,FACTOT SBP/DBP, MM Hg
BP recorder is used, systematic differ-ences betv'een operators in the BP val-ues obtained may remain,ee suggestingdiffering examinee reactions to differ-ent examiners, as was seen in one care-ful study in children.loo
Directional equipment enors canoccur. Aneroid instruments often goout of adjustment, usually down-ward.;2 One survey found that 347o ofpractitioners used only aneroid units,of which 307o werc off by 10 mm Hg ormore.63 A mercury unit can yield bi-ased readings if the meniscus does notrest at 0 or if lhe mercury's descent isimpeded by clogged internal airvents.ar The stethoscope type seemsrelatively unimportant.le Although therecommended bell amplifies theKorotkoff sounds' low frequencies incomparison with the diaphragm,1o1 therisk of exerting excessive pressureand obtaining a falsely low diastolicBP when using the bell2l may out-rveigh the benefit of amplification, par-ticularly in thin patients (try a smallbell with a rubber rim).
Examination errors are legion (Table3); most overestimate the true BP. Notealso that confirming an apparent differ-ence between arms is not simple be-cause it requires taking the averages ofseveral aiternating measurements fromboth sides or simuitaneous measure-ments by two observers who then switchsides and remeasure.lo2
Office BP vs Usual BP.-Shortly af-ter entering the office, patients'systolicBP declines by several millimeters ofmercury, whereas diastolic BP remainsrelatively constant.s3'5s'60'66'100'103 Bloodpressure remains fairly steady through-out the customary working day'timehours,sa declines in the evening (ie, athome),1u'105 and finally drops another L07o
to 20Va during sleep.to0'tor In some pa-tients, BP in a physician's office is nota-bly and consistently higherthan daytimeambulatory BP. This phenomenon,termed "office" or "white coat" hyper-tension,l08 can even occw during self-mea-surement of cuff BP in the presence of aphysician.'6 Approximately l\Vo to 40Vo
of untreated and nominally borderlinehypertensive patients show an appre-ciable "white coat" effect,2?Joe and manytreated patients will also shorv differ-ences of greater than 20110 mm Hg.tos'ttoThe phenomenon may depend in part onpatient factors such as sex, age, and BPlevel.lrr For example, one group of el-derly patients showed an increase in BPof l7l7 mnr Hg on entering the physi-cian's office; \l''omen showed a greatersystolic BP rise than men.%'112 Who wearsthe white coat seems to matter, sincenurses (u.'ho, alongwithtechnicians, havegenerall. perfor"rned the BP measure-
Does This 'atient Have Hypertension?-Reeves
Reterence
Decreases BP
ExamineeSoft Korotkolf sounds Assumed
Recent meal 1to1/1to4Nilissed auscultatory gap 10 to 50 SBP
High stroke volume PhaseVcan=0Habituation 0 to 7/2 to 12
Shock (additional pseudohypotension) 33 SBP
Setting, equipmentNoisy environs Assumed
Faulty aneroid device Can be >10
Low mercury level
Leaky bulb =2 SBP
ExaminerReading to next lowest 5 or '10 mm Hg,
ur E^pELLduvil urdr Probably <10
lmpaired hearing SBP only
ExaminationNoisy environs Assumed
Left vs right arm 1/1
Resting for too long (25 min)
Elbow too high
Too rapid defiation SBP only
Excess bell pressure =9 DBP 21
Parallax error (aneroid) 2lo 4 By author
No Effect on BP
ExamineeMenstrual phase 67, 68
Chronic caffeine ingestion
Phenylephrine nasal spray
Cuff sell-inflation 71
Examinee and examinerDiscordance in sex or race 72,73
ExaminationThin shirtsleeve under cutf 74
Bell vs diaphragm
Cuff inflation per se
Hour of day (during work hours)
Foom temperature
xBP indicates blood pressure. and SBP and DBP indicate systolic and diastolic BP. respectively
palpable as a fir'm "tube," the sign ispositive) is present,2a Lhe test's useful-ness remains debatable.25e1 e2 For ex-ample, in 65 geriatric patients unani-mously classified "Osler-positive" or "Os-ler-negative" by three observers, sixother physicians demonstraled moder-ate intraobserver consistency (r=0.49)and only modest interobserver agree-ment ( r=0.37).et Retaining "Osler-equiv-ocai" patients in the study would almostcertainly have further reduced agree-ment. Confirming pseudohypertensionreouires an intra-arterial BP measure-ment; fortunately, the condition is un-common, affecting less than 2Vo of oneotherwise healthy elderly group.25
Technical Inaccuracies of IndirectBP.-Examiner biases include end-digitprefereoce (ie, the tendency to over-record certain numbers, particuiarly 0
and 56r"i5 e4'e5), recording lower values alcritical diagnostic cut points6r presum-
1214 JAMA, April 19, 1995-Voi 273, No 15
ably to avoid institution of long-termdrug treatment, and probably otheranalogous unconscious processes (eg,"observing" a hoped-for BP reductionconsequent to instituting therapy). Phy-sicians may also differ when labelingpatients as hypertensive. A group ofBritish general practitioners diagnosedhl,pertension after only one BP mea-surement in 587a ofpatients despite pre-viously agreeing to use three readingsas part ofthe group's uniform diagnos-tic criteria.e6 Contrary to their local ex-pert guidelines, about 37Vo of Germanout-of-hospitale7 physicians and Britishhospital clinicianseE record phase IV(muffling) rather than the more accu-rate Korotkoff phase V. Perhaps themost common technical error is failureto use a sufficiently large cuff; indeed, inone survey, only 25Vo of primary carephysicians even 0 ned a large cuff.63
Interestingly, e :n when an automatic

Figure 2.-How to calibrate a porlable aneroid ma-nometer against a mercury unit: (1) Disconnect bothbulbs from the cuffs. Reconnect the aneroid bulbidialassembly to the mercury unit's cuff (already con-nected to the column). Applying a few drops of waterto the metal connector will lacilitate its insertion intothe rubber tubing. Close the aneroid assembly valve.Roll the cufi up loosely so that it is held by its Velcrostrips. lf necessary to prevent unrolling, frrst wrap thecuff around a sturdy large bottle or other surrogate"arm," or simply use a steady handgrip. (2) Graduallyand steadily inflate the cuff unlil the mercury columnrises to about 90 mm Hg. Holding the dial near thecolumn, compare the two readings. (3) Obtain repeatreadings at several other pressures, eg, 1 60 mm Hg,22Q mm Hg, 40 mm Hg. Modification for wall-mounted aneroid devices: Remove and set aside theaneroid cuff by disconnecting its tubing from its metalconnector. Leave the dial tubing connector stillcoupled. Slightly inflate the mercury unit's cuff, andpinch the bulb tubing closed (fingers or clamp). Re-move the bulb and replace it with the hvo coupledconnectors running to the aneroid dial. Roll up thecuff. Squeeze the rolled-up cuff by hand to proceedas outlined in steps (2) and (3).
ments used for entry to lhe large clinicaltrials) seem to evoke a smaller BP in-crease than physicians.2xtlil
THE ISSUE OF PREDICTION
BP Now vs BP Later
Systematic (and therefore at least par-tially predictable) changes in BP be-tween visits occur for several reasons.As examinees (volunteers or patients)become more familiar with the exam-iner, environment, and procedure (in-cluding BP self-measurement26), BP de-creases by 0 to 7 mm Hg systolic and 2to 12 mm Hg diastolic.5e 6r This habitu-ation may be more marked in patientswith anxiety trait.']4 An additional andprobably more importanl factor,ll5 re-gression to the mean, represents thetendency for any unusually high (or low)reading to fall closer to the populationmean when repeated. These phenom-ena are distinguishable fuom a true "pla-cebo" effect since they can occur in theabsence of placebo treatment.l3';e 116 SomeBP changes likely represent currentlyunappreciated systematic influences; forexample, a systematic reduction in BPof about 6 mm Hg occurs during warmvs coid seasons.55-57
JAMA, April 19, 1995-Vol 273, No. 15
Major outcome trials of antihyperten-sive pharmacotherapy have used two tothree BP readings taken at each oftwoor more visits not only to increase pre-cision (by "averaging out" minute-to-minute and between-day random fluc-tuations), but also to partially controi forregression to the mean and habituation.In practice, following the same multivisitprotocol helps enswe that published trialresults will be appiicable to individualpatients. (A fuither refinement, usednaturally by many experienced clinicians,is to conduct fi.nther follow-up visits whenthe BP is hovering near a diagnostic cutpoint. Patients whose true values are farfrom this threshold labove or be]owl logi-cally need fewer visits for confident clas-sification.117) In practice, the interval be-tween visits should take into account boththe BP level and the patient's clinicalstatus. The Joint National Committee3recommends remeasurement within 1
month for BP initially in the range of160 to 179 mm Hg systolic or 100 to 109mm Hg diastolic (ie, stage 2), within 2months for stage 1, within 1 week forstage 3, and immediate evaluation forstage 4.
Relative Risk of Casual BP Elevationfor Persistent Hypertension
Given high random variation, how welldoes the finding of a single elevaled BPpredict later definite hlpertension? Ca-sual BP, paiticularly systolic BP at onevisit, is predictive of later BP eievationin young men,118 medicai students,lleadults,l3 and children.l20 (Tracking cor-relations vary widely; for example, r=0.2to 0.7, depending on the population, tech-nique, and foilow-up interval.) In a largeprospective study,121 one diastolic BP read-ing greater than or equal to 90 mm Hgpredicted a later definite diagnosis ofhy-ner-tension in 69Vo of men ar'd 49Vo ofwomen; any BP elevation warants care-ful follow-up. Looked at the other way,however, about one third to one half ofsubjects with initially elevated BP willultimately prove not to have hlperten-sion. In practice, regression to the meanguarantees that many individuals withinitially elevated BP are really normo-tensive.T5 For example, among subjectswith four diaslolic BP measurements attwo entry visits averaging between 95 to104 mm Hg in a mild hypertension trialin Australia,lz 287o proved to have anaverage diastolic BP less than 90 mm Hgduring the next 4 years on placebo. In acareful screening program, similar dias-tolic BP reductions were seen in the 105
to 114 mm Hg stratum from the first tosecond screen, and approximately IjVoofsubjects with diastolic BP greater thanor equal to 115 mm Hg were normoten-sive (<90 mm Hg) at the next visit.rl6
Therefore, using the mean of several vis-its' BP readings improves the ability topredict not only future h;pertensionl2obut also CVD sequelae.ls Because he maybe normotensive, the patient in our casescenario should not be told that he ishypertensive at this initial visit,a but heshould be carefully followed up.
ls a High BP Value Ever Normal?
In normotensive subjects, aerobic ex-ercise, which is generaily accepted to begood for health, causes systolic BP toincrease moderately while diastolic BPchanges little.123'12r Since increased BPforms part of the "fight or flight" re-sponse, pain (eg, a lacerated finger) andother stresses (eg, pulmonary edema)predictably raise BP, sometimes to ex-treme values. These reactive elevationsof BP do not indicate the presence of"hypertension" ifthe BP returns to nor-mal levels at rest.
How Do I lmprove My Technique?Checking one's equipment periodically
is mandatory to preserve accuracy.rs An-eroid devices should be recalibrated atleast every 6 months. The recommendedapproach invoives inserting a Y-connec-tor somewhere in the pressurized pathbetween bulb and mercurTr column andattaching the aneroid device. An alter-native method not requiring a Y-connec-tor is given in Figure 2. Although one canmeasure arm circumference in each pa-tient to select an appropriately sized cuff,one can more efficienbly mark the limit ofar.rn circumference directly on each cuffby drawing a line in indelible ink at adistance from the free bladder end equalto twice the measured bladder width.
Tape recordings can help standardizeobservers' identiflrcation of Korotkoffsounds.&,lz5 Alternatively, iocate a two-headed stethoscope (and a second set ofears attached to a willing expert brain)for hands-on training. Initial formal train-ing in the technique of BP measurementis necessary, but in addition, periodic re-view of technique and retraining asneeded are recommended.a Retrainingcan increase accuracy,er but may beneeded every 1 to 2 months for optimaleffect,126 a frequency probably practicalonly in research settings. Atriai fibrilla-tion requires a modified technique (dis-cussed earlier). When faced with softKorotkoff sounds, have the subject el-evate the arm and then open and closethe fist several times; inflate the cuff,lower the arm (with fuither inflation as
needed), and listen again. In this situa-tion, as permitted by some guidelines,amore rapid deflation after determinationofthe systolic BP until the vicinity ofthediastolic BP will minimize attenuation ofthe Korotkoff sounds arising from ve-
Does This Patient Have Hvoertension?-Reeves 1215

nous congestion without altering the mea-sured 8P.53 Appllrng the cuff with itstubing emerging at the tople will elimi-nate extraneous noises generated if tub-ing contacts the stethoscope.
For research purposes, random-zerosphygmomanometers will reduce butstill not eliminate observer bias. FullyauNomatic devices, if other-w-ise techni-cally accurate, should eliminate certainhuman foibles (eg, end-digit preferenceeaand seiective recording of "desirable"readings). Statisticai monitoringsa to de-tect end-digit preference ol excessivevariability followed by mandatory re-training should be helpful.
In praetice, the grossest error, notchecking BP at" all, remains a commonfailing even among cardiovascular sub-specialists.12? Most measurement errorscould be obviated ifpractitioners wouidonly follow the published recommenda-tions1e,128-132. a1as, many do not.63,e6-e8
Other Ways to Measure BP
Lacking the ability to hear properly,both systolic and diastolic BP (as notedby Janeway, among others) can be de-termined by palpation to within about10 mm Hg.133 Palpated systolic BP isabout 7 mm Hg lorver than the auscul-tatory value.i3a
Potential lmprovements in theDiagnosis of Hypertension
Elevated BP during aerobic exercisetesting in subjects normotensive at resthas some predictive value for subsequentdefinite hypertension (relative risk from2.3 to approximately 7).t23'124,\35 BecauseBP is so variable during daily activity,ambulatory BP monitoringl36-138 oughtto provide a better estimate of whole-day target organ exposure. AmbulatoryBP monitoring correlates better withcoexisting target organ damage13s and aretrospective follow-up study suggestedimproved prediction for subsequentCVD.13e However, some patients cannottolerate ambulatory BP monitoring andaccurale measurements are not alwayspossible (eg, rn'ith marked arrhythmiaor obesity).140 Although appropriatestudies have begun,lar no data yet existto show that adding ambulatory BPmonitoring results in clinical benefit, andissues such as cost-effectiveness re-main,t36
Self-measurement of BP1a2 is also un-der active study. Concurrent accuracy,E2the meaning of differences in measure-ments at home and at work,la3 and con-cerns about selective reporting remain.When patients bring in their own, usu-ally lower home BP readings, be certainto explain that only antihypertensivetreatment of resting BP readings is ofproven value, that daytime BP is rou-
1216 JAMA, April 19, 1995-Voi 273, No. 15
tinely higher than evening BP, and thatcardiac involvement may relate moreclosely to worktime BP.1a Although theappeal of self-monitoring includes po-tentially desirable psychological andcompliance effects, any benefit remainsquestionablelaz; a L-yeat trial of homeBP monitoring found no difference intreatment, attained BP, or risk factorreduction.la5
THE BOTTOM LINE
Hypertension remains one of the mostprevalent and most important publicheaith problems. Measurement of BPhas rvon its place in the recommendedperiodic health examination because hy-pertension is common, clinically silent,dangerous, and treatable. Accuratelymeasuring BP by the indirect methodrequires minimal equipment combinedwith a willingness to make the effort; allhealth care oractitioners should read and
r ri rfollow published guidelines.'E Attentionto proper teehnique plus an apprecia-tion of the inherent variability of BPshould yield an accurate diagnosis inmost patients. Occasional patients wilhsuspected pseudohypertension or whitecoat syndrome may benefit from ancil-lary technology such as echocardiogra-phy or ambulatory BP monitoring tooptimize diagnostic decision making.Converseiy, in the far more common,otherwise low-risk patient, yearly BPreadings will suffice to exclude the pres-ence of severe or long-standing un-treated hypertension. The patient in ourclinical scenario would be served wellby a return visit in a few weeks forrepeat BP measurement.s whereas im-mediately labeling him as hypertensivewould be incorrect and, by causing himunnecessary concern, could be an im-mediate disservice.
Following expert treatment guidelinesconstitutes the physician's final respon-sibility, tying a proper diagnosis andproven therapy together to benefit thepatient.
Dr Reeves was supported by a Career Awardfrom the Pharmaceutical Manufacturers Associa-tion of Canada0{edical Research Council of CanadaCombined Program.
Reterences
1. Dept of National Health and Welfare. Muin, Find-ings Reytott ofthe Canarlio,n Blood Pressure Sttr-uey. Ottawa, Ontario: Minister of National Healthand Welfare; 1989:1.2. Hlpertension Detection and Follor-up Program.The Hypertension Detection and Follow-up Pro-gram: a progress report. Circ Res. 19?7;40(supplI):I-106-I-109.3. Joint National Committee. The fifth report ofthe Joint National Committee on Detection, Evalu-ation, and Treatment of High Blood Presswe(JNC V). Arch Intenz i.{ed. 1993;153:154-183.4. Hayres RB, Lacourciere Y, Rabkin SW, et al.Report ofthe Canadian Hypertension Society Con-sensus Conferenee, 2: diagnosis of hypertension in
adults. Caz Med Assoc J.1993i149:409-418.5. Zanchetti A, Chalmers JP, Arakawa K, et al.The 1993 guidelines for the management of mildhJpertension: memorandum from a WHO/ISH meet-ing. H y peft en sion. 1993;22:392- 403.
6. Swales JD, Ramsay LE, Coope JR, et al. Treat-ing mild hlpertension, agreement from the largetrials: report of the British Hypertension SocietyWorking P arty. B M J. 1989;298:694-698.7. Jackson R, Barham P, Bills J, et al. Managementof raised blood pressure in New Zealand: a discus-sion document. BMJ. 1993:.307 :707 -110.8. Haynes RB, Sackett DL, Taylor DW, GibsonES, Johnson AL. Increased absenteeism from workafLer detection and labeling of hyperlensive pa-tients. N Erzgl J Med. 1978;299:741-744.9. Lefebrre RC, Hursel' KG, Carleton RA. Label-ing ofpafticipants in high blood pressure screeningprograms: implications for blood cholesterol screen-ings. Arc lt I tttent M ed,. 1988; 148: 1993- 1997.
10. MacMahon SW, Cutler JA, Furberg CD, PayneGH. The effects ofdr-ug treatment for hyperbensionon norbidity and mortalityfrom cardiovascular dis-ease: a review ofrandomized controlled trials. ProgC cLrdiouas c Dis. 1986;29:99-1 18.11. Collins R, Peto R, MacMahon S, et al. Bloodpressure, stroke, and coronary heart disease, part2, short-term reductions in blood pressure: over-view of randomized dnrg trials in their epidemio-logical context. Lancet. 7990;335:827 -838.12, Kannel WB. Some lessons in cardiovascular epi-demiology from Framinghzm. Am J Carrliol.7976;37:269-282.13. Gordon T, Sorlie P, Kannel WB. Problems inthe assessment ofblood pressure: the FraminghamStudy. Izt J Epiclemiol. 7976;5:327 -334.14. Waaler HT. Specificity and sensitivity of bloodpressure measurements. J EpidemioL CommunityH e a I t h. 1980 tB 4:52- 58.15. Fujii I, Ueda K, Omae T, et al. Natural historyof borderline hypertension in the Hisayama com-munity, Japan-I: the relative prognostic impor-tance of transient variability in blood pressure.J Chronic Dls. 1984;37:895-902.16. Beard K, Bulpitt C, Mascie-Taylor H, O'MalleyK, Sever P, Webb S. Management of elderly pa-tients with sustained hlpertension. B M J. 7992;304:412-476.17. Jennings D, Netsky MG. Essential hlperten-sion: a sign in search of a disease. Can Med, AssocJ. 199l;144:973-979.18. Perloff D, Grim C, l'lack J, et al. Human bloodpressure deterrnination by sphygmomanometry.C ir cuLation. 7993;88:2460 -247 0.19. Petrie JC, O'Brien ET, Littler WA, de Swiet M.Recommendations on blood pressue measuement.B M J. 1986:293:61I -615.20. American Society of Hlpertension. Recommen-dations for routine blood pressure measurement byindirect cuff sphygmomanometry. Am J Hgper-tens. 7992:5:207-209.21. Londe S, Klitzner TS. Auscultatory blood pres-su)'e measurement: effect of pressure on the headof the stethoscope. West J Med. 1984;141:193-195.22. Frohlich ED, Grim C, Labarthe DR, MaxwellMH, Perloff D, Weidman WH. Recommendationsfor human blood pressure determination by sphyg-momanometers: report of a special task force ap-pointed by the steering committee, AHA. Hyper-lenslon. 1 988;1 1:210a-227a.23. Spence JD, Sibbald WJ, Cape RD. Pseudohy-pertension in the elderl;*. Clitt. Sci MoL Med. !978;55(suppl 4):399s-402s.24, Messerli FH, Ventura HO, Amodeo C. Osler'smaneuver and pseudohypertension. N Erzgl J Med.1985;312:1548-1551.25. Kuwajima I, Hoh E, Suzuki Y, Matsushita S,Kuramoto K. Pseudohypeftension in the elderly.J H g p eft e n s. 7990;8:429 -432.26. Mengden T, Battig B, Edmonds D, et al. Self-measured blood pressures at home and duing con-sulting hours: are there any differences? J Hyper-ten s SUWL i990;8:S15-S19.27. Pickering TG, James GD, Boddie C, HarshfieldGA, Blanl< S, Laragh JH. How common is white
Does This Patient Have Hvoertension?-Reeves

coat hJ?ertension? J AMA. 7988;259:225-228.28. Shimada K, Ogura H, Kawamoto A, Matsubaya-shi K, Ishida H, Ozawa T. Noninvasive ambulatoryblood presswe monitoring during clinic visit in el-derly hypertensive patients. CI'in Etp Hgpeftens.i990;12:151-170.29. Mancia G, Parati G, Pomidossi G, Grassi G,Casadei R, Zanchetti A. Alerting reaction andrise in blood presswe during measurement byphysician and nurse. Hgpertension. 1987;9:209-275.30. Kenny RA, Brennan M, O'Malley K, O'Brien E.Blood presure measurements in borderline hyper-tension. J Hypefiezs. 1987;5(suppl):483-485.31, Laughlin KD, Sheroard DJ, Fisher L. Com-parison of clinic and home blood pressure levels inessential hyperlension and variables associated withclinic-home differenees. J Chronic Dis. 1980;33:197-206.32. Porchet M, Bussien JP, Waeber B, NussbergerJ, Brmner HR. Unpredictability of blood pressuresrecorded outside the clinic in the treated hlper-tensive patient. J Cardioaasc Pharm.acol. 7986;8:aet 99F
33. Yagi S, Ichikawa S, Sakamaki T, Takayama Y,Murata K. Blood pressure in the paretic ams ofpatients with stroke. N EngL J Med.7986;315:836.34. Benowitz NL, Kult F, Jacob PI. Influence ofnicotine on cardiovascular and homonal effects ofcigrette smoking. CLin Plta:rmacol Th,er. 1984;36:74-8t.35. Robertson D, Wade D, Workman R, WoosleyRL. Tolerance to the humoral and hemodl'namieeffects of caffeine in man- J Clitt Inaest. 1981;67:.11 11-11 17.
36. Potter JF, Watson RDS, Skan W, Beevers G.The pressor and metabolic effects ofalcohol in nor-motensive subjects. Hypaftension. 1986;8:625-631.37. Fagius J, Karhuvaara S. Spnpathetic activityand blood pressure increases with bladder disten-sion in humans. Hgpertension. 1989;14:511-517.38. Lynch JJ, Thomas SA, Long JM, Malinow KL,Friedmann E, KatcherAH. Blood pressure changeswhile talking. Isr J Med. Scl. 1982;18:5?5-579.39. Malinow KL, Lpch JJ, Foreman PJ, Fried-mann E, Thomas SA. Blood pressure increases whilesigning in a deaf population. Pq/cft.osom Med,.1986;48:95-101.40. Conceicao S, Ward MK, Kerr DNS. Defects insphygmomanometers: an important source of errorin blood pressure recordirg. BMJ. 1976;1:886-888.41. Shaw A, Deehan C, Lenihan JMA. Sphygmo-manometers: enors due to blocked vents. BMJ.1979;1:789-790.42. Steinfeld L, Alexander H, Cohen ML. Updat-ing sphygmomanometry. Am J Cardtol. 7974133:107-110.43. Russell AE, Wing LMH, Smith SA, et al. Op-timal size of cuffbladder for indirect measurementof aiterial pressure in adults. J Hypettens. 1989;7:607-613.44. Maxwell MH, Waks AU, Schroth PC, KaramM, Dornfeld LP. Erlor in blood-pressure measure-ment due to incorrect cuff size in obese patients.Lancet- 7982;2:33-36.45. Webb CH. The measurement of blood pressureand its interpretation. Primary C are. 7980;7 :637 -oal.46. Trout KW, Bertrand CA, Williams MH. Mea-suement of blood pressurein obese persons. /AMA.1956;162:970-9?1.47. Mitchell PL, Parlin RW, Blackburn H. Effect ofvertical displacement of the arm on indirect blood-presswe measuement. N Engl J Med,. 7964;277:
48. Neussle WF. The importance of a tight bloodpressure cl:fr, Am Heart J.1956;52:905-907.49. Cushman WC, Cooper KM, Horne RA, Mey-drech EF. Effect of back support and stethoscopehead on seated blood pressure determinations. AmJ Hypertens. 7990;3:240-247.50. Viol GW, Goebel M, Lorenz GJ, Ing TS. Seatingas a variable in clinical blood pressure measure-ment. Am Heaft J. 1979:98:813-814.51. Silverberg DS, Shemesh E, Iaina A. The un-
JAMA, April .19, 1995-Voi 273, No. 15
supporLed arm: a cause offalsely raised blood pres-sure readings. BMJ. 7977 ;2:7337.52. Thulin T, Andersson G, Schersten B. Measure-ment of blood pressure: a routine test in need ofstandardization. Postgrad Med J. 7975;51.:390-39153. King GE. Influence of rate of cuff inllation anddeflation on observed blood pressure by sphygmo-manometry. Am Heart J. 1963;65:303-306.54. Canner PL, Borhani NO, Oberman A, et al. TheHypertension Prevention T?ial: assessment of thequality ofblood pressure measurements. Am J ETti-demio l. 7997;734:37 9 -392.55. Izzo JL, Larzabee PS, Sander E, Lillis LM.Hemodl'namics of seasonal adaptation. Am J Hy-p eft en s. \990 ;3:405 - 407 .
56. Kunes J, Tremblay J, Bellavance F, Hamet P.Influence of environmenta"l temperatue on the bloodpressule 0f h)?eftensive patients in Montreal. ArzJ Hypertens. 799I;4:422-426.5?. Giaconi S, Palombo C, Genovesi-Ebert A, Ma-rabotti C, Volterrani D, Ghione S. Long-term re-producibility and evaluation of seasonal influenceson blood pressure monitoring. J Hgpertens. 1988;6(suppl 4):564-S66.58. Mader SL. Effects of meals and time of day onpostural blood pressure responses in young andelderly subjects. Arch Intenz M ed. 1989;149:27 57 -2760.59. Armitage P, Rose GA. The variability of mea-surements of casual blood pressure, I: a laboratorysttdy. CLin Sci. 1966;30:325-335.60. Watson RDS, Lumb R, Young MA, Stallard TJ,Davies P, Littler WA. Variation in cuffblood pres-sure in untreated outpatients with mild hypeiten-sion: implications for initiating antihypertensivetreatment. J Hgpertetzs. 1987 ;5:207 -277.61. Shepard DS. Reliability of blood pressure mea-surements: implications for designing and evaluat-ing programs to control hy-pertension. J ChronicDis. 1981;34:191-209.62. CohnJN. Blood pressure measurement in shock:mechanism of inaccuracy in auscultatory and pal-patory mefhods. JAMA. 1967 ;I99i972-976.63. McKay DW, Campbell NR, Parab LS, Chocka-lingam A, Fodor JG. Clinical assessment of bioodpressure. J Hum Hgpettens. 1990;4:639-645.64. Patterson HR. Sources of error in recordingthe blood pressure ofpatients with hypertension ingeneral practice. BMJ. 19M;289:7667-1664.65. Hashimoto F, Hunt WC, Hardy L. Differencesbetx'een right and left arn blood pressures in theelderly. West J Med. 198l;741:189-192.66. van Loo JM, Peer PG, Thien TA. Twenty-fiveminutes between blood pressure readings: the in-fluence on prevalence rates of isolated systolic hy-pertension. J Hgpertens. 1986;4:631-635.67. von Eiff AW, Plotz EJ, Beck KJ, Czemik A.The effect of estrogens and progestins on bloodpressure regulation of normotensive women. Anz../Ob stet Gynecol. 1971;109:887-892.68. PolefroneJM, Maauck SB. Effects of menstr"ualphase and parental history of hypertension on car-diovascular response to cognitive ehallenge. Psy-chosom Med.. 1988;50:23-36.69. Myers MG, Reeves RA. The effect of caffeineon daytime ambulatory blood pressure. Atn J Hy-Ir eli erc. 799 7;4: 427 - 43].70. Myers MG,IazzetLa JJ. Intranasally adminis-tered phenylephrine and blood pressure. Can MedAssoc J. 1982;127:365-368.71. Veerman DP, van Montfrans GA, KaremakerJM, Wieling W. In{lating one's ou'n cuff does notincrease self-recorded blood pressure. J Hgper"tetzs.1992;6(suppl 4):S77-S78.72. Kraus JF, Conley A, Hardy R, Sexton M, SweezyZ. Relationship of demographic characteristics ofinterviewers to blood pressure measurements,J Communitg Hea.lth. 1982;8:3-72.73. Reeves RA, Lewis JE, Hebed PC, KernermanY, Revah A. Gender, status and'white coat'phe-nomenon in family practice. Clin Inuest Med.799I;14(suppl A):A69.74. Holleman DR, Westman EC, McCrory DC,Simel DL. The effect of sleeved arms on oscillo-metric blood pressure measurement. J Gen Intent,
Med. 1993;8:325-326.75. Hypertension Detection and Follow-up Pro-gram. Variability ofblood pressure and the resultsof screening in the Hyaeftension Detection andFollow-up Program. J Ch.ronic Dis. 1978;31:651-667.76. Di Rienzo M, Parati G, Pomidossi G, Veniani M,Pedotti A, Mancia G. Blood pressure monitoringover short day and night times camot predict 24-hour average blood pressule. J Hypertens.7985;3:343-349.77. Mancia G, Parati G, Pomidossi G, Casadei R, DiRienzo M, Zanchetti A. Arterial baroreflexes andblood pressure and heart rate variabilities in hu-mans. Hypet"tensiorz. 1986;8:147-153.78. Watson RDS, Stallard TJ, Flinn RM, LittlerWA. Factors determining direct aiterial pressuleand its variability in hypeftensive man. H!/perten-sioiz. 1980;2:333-341.79. Reeves RA. A review of the stability of am-bulatory blood pressure: impiications for diagnosisof hlpertension. Clin Inuest Med. 1997;74:251-255.80. Reeves RA, Leenen FHH, Jolmer CD. Repro-ducibility of nurse-measured, exercise and ambu-latory blood pressure and echocardiographic leftventricular mass in borderline hlpertensi0n. ,/ Fly-p et'te ns. !992110'.7249 -1256.81. Sykes D, Dervar R, Mohanamban K, et al. Mea-suring blood pressure in the elderly: does atrialfibrillation increase obsen er variability? BMJ.1990;300:162-163.82. O'Brien E, Mee F, Atkins N, O'Malley K. In-accuracy of seven popular sphygmomanometers forhome measurement ofblood pressute. J Hgpertett s.
1990;8:621-63,1.83. Scherwitz LW, Evans LA, Hennrikus DJ, Vall-bona C. Procedures and discrepancies ofblood pres-sure measurements in two community health cen-Iers. Med, Care. 1982;20:727-738.84. Neufeld PD, Johnson DL. Observer enor inblood pressure measwement. Cun Med Assoc J.1986;135:633-637.85. White WB, Lund-Johansen P, Omvik P. As-sessment of four ambulatory blood pressule moni-tors and measurements by clinicians versus intra-arterial blood pressure at rest and during exercise.Am J Cardiol. 1990165:60-66.
86. Blank SG, West JE, Mliller FB, et al. Widebandexternal pulse recording during cuff deflation: anew technique for evaluation of the arterial pres-sure pulse and measurement of blood pressure.C i rc u I al i on. 1988;77:1 297-1305.87. Taguchi JT, Suwangool P. Pipe-stem brachialarteries: a cause of pseudohypertension. JAMA.19741228:733.88. Wallace CT, Carpenter FA, Evins SC, Mahaf-fey JE. Acute pseudohypertensi\.e ensis. Anesthe-sio Io g y. 197 5;43:588-589.89. Keenan WF. Pseudohl'pertension mimicking ahypedensive emergency. J.A,\[ A. L98I;246:1088.90. Saklayen MG. Pseudohlpertension in a youngu.oman. An. J Med. 7988;84:794-795.91. O'Rourke M, Kelly R. Osler's maneuver andpseudohypertension. N Ettgl J Med. 1985;313:1300.92. Tifft CP. Are the days of the sphygmomanom-eter past? Arclz Intern Med. 1988;148:518-519.93. Hla KM, Samsa GP, Stoneking HT, FeussnerJR. Observer variabilit)' of Osler's rnaneuver indetection of pseudoh)?ertension. / C lirz E pidemiol.1991;44:513-518.94. Hla KM, Vokaty KA, Feussner JR. Observererrorin systolic blood pressure measurement in theelderly: a case for automatic recorders? Arch In-tent M ed. 1986',1 46:237 3-237 6.
95, Padfield PL, Jyothinagaram SG, Watson DM,Donald P, McGinley IM. Problems in the measure-ment ofblood pressure. J Hunt Hgpertetzs. 1990;4(suppl 2):3-7.96. Smith TD, Clayton D. Individual variation be-tv/een general practitioners in labellirg of hyper-tension. BM,/. 1990;300:?4-75.97. Weiland SK, Keil U, Spelsberg A, et al. Diag-nosis and management of h;pertension by physi-cians in the Federal Republic of Germany. J Hy-n ertetz s. 7997 :9:1.37 -734.
Does This Patient Have Hyperlension?-Reeves 1217
98. Wilkinson LS, Perry IJ, Shinton RA, BeeversDG. An emerging consensus among clinicians ontreating mild hypertension but persistent uncer-tainty as to how blood pressure should be mea-sured. J,R ColL Phgs.ici,ans Lond. lggl;25:776-179.99. Bruce NG, Cook DG, Shaper AG. Differencesbetween observers in blood pressure measurementwith an automatic oscillometric recorder, J Hgper-tens SuMl. 1990;8:S11-S13.100. Burke GL, Webber LS, Shear CL, Zlnkgra|SA, Smoak CG, Berenson GS. Sources ofenor inmeasurement ofchildren's blood pressure in a largeepidemiologic study: Bogalusa Heart Study. JC hr onic Dis. 1987;40:83-89.101. Abella M, Formolo J, Penney DG. Comparisonof the acoustic properties of six popular stetho-scopes. ,/ Acozr.sl Soc Am. 7992;97:2224-2228.102. Sapira JD. The vital signs. In: Sapira JD, ed.The At-t and, Science of Bed,side Dtagnosis. Balti-more, Md: Urban & Schwarzenberg; 1990:85-104.103. Wietlisbach V, Rickenbach M, Burnand B,Hausser D, Gutzwiller F. Combiningrepeated bloodpressure measurements to obtain prevalences ofhigh blood pressure. Acta Med, Scand Suppl.7988;728:165-168.104. Millar-Craig MW, Bishop CN, Raftery EB.Circadian variation of blood pressure. Loncet. 1978;I:795-797.105. Gould BA, Hornung RS, Cashman PMM,Raftery EB. Ambulatory blood pressure-directand indirect. In: Weber MA, Drayer JIM, eds. Arz-bulatory Blood, Pressure Monitoing, New York,NY: Springer-Verlag NY Inc; 1984:9-19.106. LittlerWA, Honou AJ, Carter RD, Sleight P.Sleep and blood pressure. B M J. 197 5;7:346-347.107. Millar-Craig MW, Mann S, BalasubramanianV, Raftery EB. Blood pressure circadian rhythm inessential hyperLension. CI'in Sci MoI Med..1978',55:391s-393s.108. Kleinert HD, Harshfield GA, Pickering TG, etal. What is the value of home blood pressure mea-surement in patients with mild hypertension? Ilg-p ertensi.on. 7984;6:57 4-57 8.109. Omstein S, Markerb G, Litchfield L,ZempL.Evaluation of the DINAMAP blood pressure moni-tor in an ambulatory primary care setling. J FamP r a ct. 7988;26:517 -527.110. Myers MG, Reeves RA. White coat phenom-enon in patients receiving antihypertensive therapy.Am J Hypet"tens. 1991;4:844-849.111. Silagy CA, McNeil JJ, McGrath BP. Isolatedsystolic hypertension: does it really exist on am-bulatoryblood pressure monitoring? Clin Exp Phnr-macol P hy siol. 1990;17:203-206.112. Imai Y, Nakatsuka H, Ikeda M, et al. A ooss-sectional survey of home blood pressure in a ruralcommunity in northern Japan. C\irt Erp Hyper-tezs. 1990;12:1095-1106.
113. Ellis PJ, Marshall E, Ellis SJ. Which bloodpressure? Lancet. 1,988;2:902-903.114. McGrady A, Higgins JT Jr. Effect ofrepeatedmeasurements ofblood pressure on blood pressurein essential h;perbension: role ofanxiety. J BehnuMed. 1990;13:93-101.115. Haynes RB, Logan AG, Flanagan PT, MilneBJ. The effect of patient 'familiarity' with bloodpressue assessme',t on lhe accuracy of follow-upreadings. J Hypertens. 1983;1:91-94.116, H)?erlension Detection and Follow-up Pro-gTam Cooperative Group. Blood presswe studies ln14 communities: a two-stage screen for hyperten-slon. J AM A. 797 7 ;237 :2385-2397.117. Perry HM Jr, Miller JP. Diffrculties in diag-nosing hypertension: implications and alternatives.J Hgpettens. 1992;10:887-896.ll8. Rabkin SW, Mathewson FA, Tate RB. Rela-tionship ofblood pressure in 20- to 39-year-old mento subsequent blood pressure and incidence of hy-pertension over a 3O-year observation period. Cir-culation. 1982;65:291-300.119. Thomas CB, Duszynski KR. Blood presswelevels in young adulthood as predictors of hyper-tension and the fate of the cold presscr test. "rolzzsHopkins Med J. L982;157:93-100.120. Shear CL, Burke GL, Freedman DS, Beren-son GS. Value of childhood blood pressure mea-surements and famil;' history in predicting futureblood pressure status: results from 8 years offollow-up in the Bogalusa Heart Study. Pediatri.cs. 1986;77:862-869.121. Trembath CR, HicknerJM, Bishop SW. Inci-dental blood pressure elevations: a MIRNETproject. J Fam Procl. 1991;32:378-38i.122, Management Committee. The Australiantherapeutic trial in mild hypertension. Lancet. 1980;7:7261-1287.123. Dlin RA, Hanne N, Silverberg DS, Bar-Or O.Follou-up of nomotensive men with exaggeratedblood pressure response to exercise. Am Heat't J-1983;106:316-320.124. Guenera G, Melina D, Colivicchi F, Santoliq-uido A, Folli G. Abnormal blood pressure responseto excercise in borderline hypertension: a two-yearfollow-up study. Anz J Hgpefiens. 799I;4:27 l-27 3.125. Rose GA. Standardisation of observers inblood-pressure measurement. Lancet. 1965;1:673-67 4.126. Bruce NG, Shaper AG, Walker M, Wanna-methee G. Obsener bias in blood pressure studies.J Hgpeftens. 1988;6:375-380.127. Warshaw LJ. Physicians: check that blood pres-sur e. J AM A. 7989;262:17 7 5-17 7 6.128. Campbell NR, Chockalingam A, Fodor JG,McKay DW. Accurate, reproducible measurementof blood pressure. Can Med A.ssoc J.7990;143:19-24.129. O'Brien ET, O'Malley K. ABC of blood pres-stre measurement: the observer. BMJ. 1979:2:77 5-
776.130. O'Brien ET, O'Malley K. ABC of blood pres-sure measurement: the sphygmomanometer. BMJ.1979;2:851-853.131. O'Brien ET, O'Malley K. ABC of blood pressuremeasurement: the patient. B M J. 1979;2:920-927.132. O'Brien ET, O'Malley K. ABC of blood pres-sure measurement: technt qrc. B M J. 1979;2:982-9U.133. Segall HN. A note on the measurement ofdiastolic and systolic blood pressure by the palpa-tion ofarterial vibrations (sounds) over the brachialaytery. Can Med, Assoc.r. 1940;42:311-313.134. Scordo K. Using radial artery palpation tomonitor blood pressure. Dimens Cr[t Care Nurs-7983;2:75-79.135. Wilson NV, Meyer BM. Early prediction ofhypertension using exercise blood pressure. PreoMed. 7981;10:62-68.136. Reeves RA, Myers MG. Ambulatory bloodpressue monitoring: an emerging technology. ClinItt uest Med. 1991;14:198-201.137. Health and Public Policy Committee, Ameri-can College of Physicians. Automated ambulatoryblood pressure monlbonng. Ann Intetn Med.1986;704:275-278.138. National High Blood Pressure Education Pro-gram Coordinating Committee. National High BloodPressue Education Program Working Group re-port on ambulatory blood pressure morttLoing. ArchI ntent M e d. 1990 ;750 :227 0 -2280.139. Perloff D, Sokolow M, Cowan R. The prog-nostic value ofambulatory blood pressures. JAMA.1983;249:2792-2798.140. Reeves RA. Patient and environmental fac-tors affecting ambulatory blood pressure monitor-ing. Clin Inuest Med. 1997114:278-223.141. Clement DL, the Steering Committee. Offtceversus ambulatory recordings of blood pressure(OvA): a European multicenter study. J HypeftensSzppl. 1990;8:S39-M1.142. Canadian Coalition for High Blood PressurePrevention and Control. Recommendations on self-measurement ofblood pressure. Can Med Assoc J.1988:138:1093-1096.143. Pickering TG, James GD. Some implications ofthe differences between home, clinic and ambula-tory blood pressure in normotensive and hyper-tensive patients. J Hypertens Szppl. 1989;7:565-s72.144. Devereu RB, Pickering TG, Harshfield GA,et al. Left ventricular hypertrophy in patients withhlpertension: importance of blood pressrre responseto regularly recurring stress. Circulation. 7983;68:470-476.r45. Midanik LT, Resnick B, Hurley LB, Smith EJ,McCarthy M. Home blood pressure monitoring formild hypertensives. Public Health Rep. 1991;106:85-89.
1218 JAlVlA, April 19, 1995-Vol 273, No. .15
Does This Patient Have Hypertension?-Reeves




















