The Physical Activity Patterns of European Youth with Reference to Methods of Assessment
21
Sports Med 2006; 36 (12): 1067-1086 REVIEW ARTICLE 0112-1642/06/0012-1067/$39.95/0 2006 Adis Data Information BV. All rights reserved. The Physical Activity Patterns of European Youth with Reference to Methods of Assessment Neil Armstrong and Joanne R. Welsman Children’s Health and Exercise Research Centre, University of Exeter, Exeter, UK Contents Abstract ................................................................................... 1067 1. Physical Activity Guidelines for Youth ..................................................... 1068 2. Measurement Issues ..................................................................... 1069 3. Subjective Measures of Physical Activity ................................................... 1070 4. Objective Measures of Physical Activity ................................................... 1073 4.1 Doubly Labelled Water .............................................................. 1073 4.2 Indirect Calorimetry ................................................................. 1074 4.3 Direct Observation .................................................................. 1074 4.4 Heart-Rate Monitoring ............................................................... 1075 4.5 Pedometry ......................................................................... 1079 4.6 Accelerometry ..................................................................... 1081 5. Conclusions ............................................................................ 1082 This article reviews the habitual physical activity of children and adolescents Abstract from member countries of the European Union in relation to methods of assessing and interpreting physical activity. Data are available from all European Union countries except Luxembourg and the trends are very similar. European boys of all ages participate in more physical activity than European girls and the gender difference is more marked when vigorous activity is considered. The physical activity levels of both genders are higher during childhood and decline as young people move through their teen years. Physical activity patterns are sporadic and sustained periods of moderate or vigorous physical activity are seldom achieved by many European children and adolescents. Expert committees have produced guidelines for health-related physical activity for youth but they are evidence-informed rather than evidence-based and where there is evidence of a relationship between physical activity during youth and health status there is little evidence of a particular shape of that relationship. The number of children who experience physical activity of the duration, frequency and intensity recommend- ed by expert committees decreases with age but accurate estimates of how many girls and boys are inactive are clouded by methodological problems. If additional insights into the promotion of health through habitual physical activity during
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of The Physical Activity Patterns of European Youth with Reference to Methods of Assessment

Sports Med 2006; 36 (12): 1067-1086REVIEW ARTICLE 0112-1642/06/0012-1067/$39.95/0
2006 Adis Data Information BV. All rights reserved.
The Physical Activity Patterns ofEuropean Youth with Reference toMethods of AssessmentNeil Armstrong and Joanne R. Welsman
Children’s Health and Exercise Research Centre, University of Exeter, Exeter, UK
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10671. Physical Activity Guidelines for Youth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10682. Measurement Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10693. Subjective Measures of Physical Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10704. Objective Measures of Physical Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1073
4.1 Doubly Labelled Water . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10734.2 Indirect Calorimetry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10744.3 Direct Observation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10744.4 Heart-Rate Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10754.5 Pedometry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10794.6 Accelerometry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1081
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1082
This article reviews the habitual physical activity of children and adolescentsAbstractfrom member countries of the European Union in relation to methods of assessingand interpreting physical activity. Data are available from all European Unioncountries except Luxembourg and the trends are very similar. European boys ofall ages participate in more physical activity than European girls and the genderdifference is more marked when vigorous activity is considered. The physicalactivity levels of both genders are higher during childhood and decline as youngpeople move through their teen years. Physical activity patterns are sporadic andsustained periods of moderate or vigorous physical activity are seldom achievedby many European children and adolescents. Expert committees have producedguidelines for health-related physical activity for youth but they areevidence-informed rather than evidence-based and where there is evidence of arelationship between physical activity during youth and health status there is littleevidence of a particular shape of that relationship. The number of children whoexperience physical activity of the duration, frequency and intensity recommend-ed by expert committees decreases with age but accurate estimates of how manygirls and boys are inactive are clouded by methodological problems. If additionalinsights into the promotion of health through habitual physical activity during

1068 Armstrong & Welsman
youth are to be made, methods of assessment need to be further refined andrecommended guidelines re-visited in relation to the existing evidence base.
This article reviews the physical activity patterns empirically based guidelines that can be used byof youth from member countries of the European clinicians in their counselling, as well as by policyUnion (EU). Relevant studies for review were locat- makers with responsibility for youth health promo-ed through computer searches of MEDLINE, tion.”[6] A systematic review of the scientific paedia-SportDiscus and personal databases, supplemented tric literature relating physical activity to bloodwith an extensive search of bibliographies of ac- lipids,[7] blood pressure,[8] body fatness,[9] skeletalcessed studies and through personal contacts with health[10] and psychological health[11] was presentedcolleagues in other European countries. Where data to the predominantly North American members offrom specific countries were sparse, embassies were the conference and the following guidelinesrequested to provide appropriate contacts within emerged:their home countries. • All adolescents should be physically active daily
Physical activity is defined as a complex set of or nearly every day, as part of play games, sports,behaviours that encompass any bodily movement work, transportation, recreation, physical educa-produced by skeletal muscles that result in energy tion or planned exercise, in the context of family,expenditure.[1] The habitual physical activity of chil- school and community activities.dren and adolescents is extremely difficult to assess • Adolescents should engage in three or more ses-and interpret in the context of promoting health. sions per week of activities that last 20 minutes orMore than 30 different methods of assessing physi- more at a time and that require moderate tocal activity have been identified but the reliability, vigorous levels of exertion. Moderate to vigorousobjectivity and validity of many of these methods activities were defined as those that require athave not been established with children and adoles- least as much effort as brisk or fast walking.[12]
cents.[2,3] Several expert committees have publishedIn the first guideline, in contrast with previous
guidelines for young people’s physical activity butguidelines, the intensity and duration of activity was
the scientific rationales underlying the recommen-not emphasised. The rationale was that daily weight-
dations have been challenged.[4] To evaluate thebearing activities, of even brief duration, during
physical activity of European youth, we thereforeadolescence are critical for enhancing bone develop-
need to consider both measurement techniques andment that affects skeletal health throughout life, and
current physical activity guidelines.that substantial daily energy expenditure is expectedto reduce risks of obesity, and may also have other1. Physical Activity Guidelines for Youthpositive health effects. The rationale for the secondguideline was that regular participation in continu-The earliest formal physical activity guidelinesous moderate to vigorous physical activity duringfor youth were provided by the American College ofadolescence enhances psychological health, in-Sports Medicine (ACSM) who developed an opin-creases high-density lipoprotein cholesterol and in-ion statement on the amount of physical activitycreases cardiorespiratory fitness. Although otherneeded for optimal functional capacity and health.physical activity guidelines were published, mainlyThe ACSM based their proposals on guidelines forin North America,[13,14] internationally the ICCadults and recommended that children and adoles-guidelines informed youth physical activity studiescents should achieve 20–30 minutes of vigorousthroughout the 1990s.exercise each day.[5] In 1993, an International Con-
sensus Conference on Physical Activity Guidelines In 1998 in England, the Health Education Au-for Adolescents (ICC) was convened “to develop thority (UKHEA) commissioned a similar series of
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of European Youth 1069
reviews of the scientific paediatric literature to those • a relationship where significant health benefitscan be gained only in the lower part of thethat informed the ICC.[15] Following a consensusphysical activity scale;conference of principally British scientists, different
• a relationship where significant health benefitsrecommendations for the physical activity of youngcan be gained only in the upper part of thepeople were proposed, although they were foundedphysical activity scale;on the same evidence base as the ICC. The primary
• an S-shaped curve, which suggests that there is arecommendation was that all young people shouldthreshold value somewhere on the scale.participate in physical activity of at least moderateHe explored the scientific paediatric literatureintensity for 1 hour per day and that young people
linking physical activity with cardiovascular, skele-who currently do little activity should participate intal and psychological health seeking dose-responsephysical activity of at least moderate intensity for atrelationships or threshold values and demonstrated
least half an hour per day. A secondary recommen-that where there is evidence of a relationship be-
dation was that at least twice a week, some of these tween physical activity during youth and health sta-activities should help to enhance and maintain mus- tus there is hardly any evidence of a particularcular strength and flexibility and bone health.[15] The pattern of that relationship. He stated that there areUKHEA Conference’s primary recommendation different patterns of relationships for differentshifted the emphasis from vigorous to moderate health outcomes and that there is only marginalintensity physical activity, and from sustained peri- evidence to support the guidelines proposed by ex-ods of activity to activity accumulated over a day. pert committees, which tend to be ‘evidence-in-
formed’ rather than ‘evidence-based’. Twisk[4] con-In 2005, a panel of experts from North Americacluded that based on scientific evidence, the currentsystematically evaluated evidence of the effects ofguidelines are as valid as stating that every increasephysical activity on several health and behaviouralin physical activity can have some beneficial healthoutcomes in US school-age youth and concludedeffects for young people. He suggested that thethat they should participate daily in ≥1 hour ofadvantage of this ‘guideline’ is that the goal is muchmoderate to vigorous physical activity that is devel-easier to achieve and probably leads to the same
opmentally appropriate, enjoyable and involves ahealth benefits as satisfying the guidelines proposed
variety of activities.[16] However, at the time of by expert committees.writing, no published study of European youth hasadopted this recommendation and the UKHEA rec-
2. Measurement Issuesommendation has been the most influential in theconclusions drawn from recent studies of youngpeople’s physical activity. Physical activity assessment techniques must be
socially acceptable, should not burden the child withTwisk[4] critically reviewed the confusion in thecumbersome equipment and should only minimallyfield of physical activity guidelines for youth. Heinfluence the person’s normal physical activity pat-elegantly argued that before guidelines can be devel-tern. Ideally the intensity, duration, frequency andoped, the pattern of the possible relationship(s) be-mode of activity should be monitored and, if a truetween physical activity and health status must bepicture of habitual physical activity is required,
considered. He discussed hypothetical dose-re-some account should be taken of day to day varia-
sponse relationships between physical activity and tion. Although empirical evidence is not available,health such as: Bar-Or[17] has recommended a minimum monitoring• a linear dose-response relationship where every period of 3 days, whereas others[3,18,19] have suggest-
increase in physical activity level will have simi- ed 4–9 days as appropriate depending on the mea-lar health consequences; surement instrument used.
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1070 Armstrong & Welsman
Habitual physical activity is a behaviour, but it occupational activity, making up a greater propor-can only occur as a result of skeletal muscle activity tion of total physical activity in children.that is supported by energy expenditure. Physical Self-administered questionnaires are less accu-activity is therefore interrelated with energy expen- rate than those administered by an interviewer[23]
diture; however, it may cause an elevation in meta- and large discrepancies have been demonstrated be-bolic rate that persists long after cessation of observ- tween the two methods.[24,25] It is difficult to ascer-able movement. Different techniques may therefore
tain at what age children become able to producebe measuring different dimensions of physical activ-
meaningful questionnaire data but it has been sug-ity and this could, at least in part, account for the
gested that children under the age of 12 years cannotoften weak relationships between different measure-
recall activities accurately and are unable to quantifyment techniques used on the same children and
the time-frame of activity.[26]
adolescents. To interpret adequately the habitualPhysical activity diaries have been reported to bephysical activity of European youth, measurement
superior to retrospective questionnaires,[27,28] butissues must be considered and the data evaluated insome studies[24,29] have found that the quality ofthe context of the methodology used.completed diaries is inconsistent with children. Dia-ry measures place a heavy burden on the subjects[20]
3. Subjective Measures of and keeping a diary may in itself influence physicalPhysical Activity activity habits.[30] Saris[31] concluded that physical
activity diaries were unsuitable for use with childrenSelf-report of physical activity is the most widely <15–16 years of age.
used method in epidemiological research due to the Proxy reports are sometimes used to assess theease and low costs of implementation. Self-report physical activity of children <10 years of age, whomethods include retrospective questionnaires, inter- would have difficulty completing a questionnaire,view-administered recall, activity diaries and mail
and they are normally provided by parents or teach-surveys. Proxy reports by parents and/or teachers
ers. The validity of proxy reports is limited especial-have been employed in studies with children and
ly when they concern activities outside the home orsome studies have estimated the level of physical
school.[32,33] For example, Harro[34] observed paren-activity through self-report of surrogate measures
tal report of activity to provide values 1.8 timessuch as sports participation. Considerable demands
higher than physical activity estimated from heart-are placed on the child’s cognitive abilities to recall
rate recordings of the same children.specific events from the past and Sallis[20] has point-
Several research teams have attempted, on theed out actual behaviour is not directly assessed bybasis of self-report data, to classify activities accord-self-reports and the data obtained are “memories ofing to their estimated energy expenditure usingthe behaviour of interest that have decayed, beenphysiological data from other studies and often ex-filtered through perceptions and biases, and havetrapolated from data on adults.[35,36] This approach isbeen tainted by competing memories, social desira-fraught with inaccuracies due to the methodologicalbility and misunderstanding of instructions.”[20]
limitations of directly determining the energy chil-Children are less time-conscious than adults anddren expend in specific activities. The use of adulttend to engage in physical activities at sporadicenergy costs of activities to estimate energy expen-times and intensities rather than consistentditure in children introduces substantial errors. Inbouts.[21,22] The self-recall of the intensity, frequen-young children, energy costs may be underestimatedcy and duration of bouts of activity by children isby up to 40% using adult values. At 10 years of age,therefore even more problematic than with adults.the underestimation is about 20% decreasing toThe problem is further confounded by leisure time
activity, which is more difficult to quantify than about 5% at 16 years.[37,38]
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of European Youth 1071
Self-report and objective measures of physical mark,[68,69] Lithuania,[50,70] Cyprus,[71] Latvia,[50,72]
Czechoslovakia,[73] the Czech Republic,[74,75] Mal-activity should be compared cautiously. Childrenta,[55] Slovenia,[76,77] Slovakia,[70] Estonia[78,79] andhave been reported to overestimate their recall ofThe Netherlands.[29,80] There are no data on youngvigorous physical activity[39] and ‘dramatic discrep-people from Luxembourg. Levels of physical activi-ancies’ have been reported between self-reportedty cannot be confidently compared across studies,and objectively measured estimates of vigorousbut age- and gender-related trends are consistent andphysical activity.[40] However, when moderate-in-we will use a large WHO multinational survey totensity physical activity is considered, children tendillustrate general trends.to underestimate their level of physical activity com-
pared with objective measures.[41,42] The probable Several multinational WHO surveys of youngexplanation for this is that moderate activity tends to people’s physical activity have been carriedbe sporadic, non-planned, less memorable and quan- out.[50,51,55,70] The first in 1983/84 involved four EUtifiable, and therefore less likely to be collected by countries and the latest in 2001/02 included childrenself-report methods.[43] Ekelund et al.,[44] however, and adolescents from 22 EU countries. The surveyscompared the use of heart-rate monitoring and activ- have selected samples representative of nationality diaries in 30 15-year-old adolescents and report- populations and provide across-country insights intoed no significant difference between methods in the physical activity of European youth. A potentialtime spent in moderate to vigorous physical activity weakness in national comparisons, however, is that(MVPA). They concluded that heart-rate monitoring the time of year the questionnaires were adminis-and activity diaries are comparable for group assess- tered varied between countries, although it was quitement of total daily energy expenditure and its com- tightly defined within countries.ponents, and for estimating time spent in MVPA. The 2001/02 survey[55] involved 22 EU countriesHowever, the activity diary underestimated time and 115 981 young people aged 11, 13 or 15 years.spent in MVPA for inactive subjects and conse- The national sample sizes varied from 1980 in Maltaquently overestimated highly active subjects. Kem- to 14 372 in the UK. The German sample of 5650per[45] attempted to validate physical activity mea- participants was regional and selected from Berlin,sures during the first 4 years of the Amsterdam Hessen, North Rhine-Westphalia and Saxony. TheGrowth Study by relating mean daily heart-rate data were collected from October 2001 to Junemeasures and mean pedometer counts to the mean 2002. This survey cannot be compared directly withresults of a habitual physical activity interview. the earlier reports as it introduced revised questionsNone of the calculated correlation coefficients ex- that focused on physical activity of at least moderateceeded r = 0.20 and he concluded that the various intensity, carried out at school and/or in free timemethods for assessing physical activity should be during both the previous week and a typical week.considered to measure different aspects of physical The participants were provided with a definition ofactivity. physical activity as “any activity that increases your
heart rate and makes you get out of breath some ofThe use of self-report techniques is common inthe time. Physical activity can be done in sports,studies of children’s physical activity; however, inschool activities, playing with friends, or walking toanything but large studies with high statistical pow-school. Some examples of physical activity are run-er, the data need to be interpreted cautiously. Studiesning, brisk walking, rollerblading, biking, dancing,of generally non-representative samples of youngskateboarding, swimming, soccer, basketball, foot-people are widely available and data have emergedball and surfing.”[55]
from Belgium,[46,47] Ireland,[48,49] Austria,[50,51] theUK,[52,53] Italy,[54,55] Spain,[51,56] Finland,[28,57] Hun- The methodology was informed by the UKHEAgary,[50,51] Greece,[58,59] France,[60,61] Sweden,[62,63] physical activity guidelines[18] and based on thePoland,[50,51] Germany,[64,65] Portugal,[66,67] Den- screening measure developed by Prochaska et al.[81]
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1072 Armstrong & Welsman
0
10
20
30
40
50
60
70a
b
0
10
20
30
40
50
60
70
No.
of c
hild
ren
(%)
Irelan
d
Austri
a
Sloven
ia
Lithu
ania
Scotla
nd
Finlan
d
Englan
d
Czech
Rep
Poland
Malt
a
Wale
s
Nethe
rland
s
Sweden
Greec
e
Denm
ark
Hunga
ry
Latvi
aSpa
in
Estonia
Portu
gal
Germ
any
Italy
Belgium
Franc
e
11 years13 years15 years
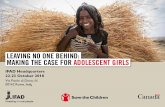
Fig. 1. Percentage of (a) boys and (b) girls meeting the primary UK Health Education Authority guideline on physical activity.[55]
so that the participants were asked to “add up all the response categories for both questions were 0 days,1 day, 2 days… 7 days and scores were calculated bytime you spend in physical activity each day.” Theaveraging the results of the two items with a score offirst question asked about physical activity under-≥5 classifying the respondent as meeting the recom-taken in the previous week, and the second about amendation of >60 minutes of moderate activity atypical week as follows: (i) over the past 7 days, onday on most days.how many days were you physically active for at
least 60 minutes per day?; and (ii) over a typical or The data suggest that about one-third of youngusual week, on how many days are you physically people meet the UKHEA primary recommendationactive for a total of at least 60 minutes per day? The (figure 1). There are, however, wide variations
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of European Youth 1073
across countries and although across-country com- derived from indirect calorimetry for subjects livingparisons must be made cautiously, in Austria, Fin- in metabolic chambers.[83] It provides a powerfulland, Malta, Wales, Greece, Hungary, Latvia, Esto- tool for the accurate measurement of daily energynia, Portugal, Germany, Italy, Belgium and France expenditure but it has several limitations. The iso-<20% of 15-year-old girls self-reported meeting the topes are expensive and difficult to obtain, accuraterecommendation. Comparisons within countries are dietary records must be kept and the data onlymore secure and in all countries more boys than girls provide a measure of total daily energy expenditurereported being physically active for 60 minutes a (TDEE) over the study period. Studies generallyday at least five times a week, although the gender have very small sample sizes and no information isdifferences were small in some countries (e.g. provided on the participants’ physical activity pat-among 15-year-olds, 1% in The Netherlands and 5% terns, therefore making it impossible to identifyin Italy) but marked in others (e.g. among 15-year- activity of moderate or vigorous intensity.olds, 25% in Malta and 22% in Wales). In all coun- In DLW studies, physical activity is usually ex-tries, except boys in France and the Czech Republic, pressed as the physical activity level (PAL) or thefewer 15-year-olds than 11-year-olds met the activity-related energy expenditure (AEE). James etUKHEA criterion and in France and the Czech al.[84] defined PAL as the index TDEE over basalRepublic more 13-year-olds than 15-year-olds met metabolic rate (BMR). TDEE and BMR are used tothe guideline. calculate AEE as (0.9 × TDEE) – BMR, assuming a
The findings that physical activity declines with diet-induced thermogenesis of 10%. Normal levelsage and that girls are less likely to be physically of PAL and AEE for children are the subject ofactive than boys are remarkably consistent across ongoing debate.European countries. There is no evidence to indicate Davies[85] reviewed TDEE data on children agedmajor differences in the level of physical activity of 1–6 years and concluded that there was a consistentyouth living in Europe compared with those living pattern across the three laboratories, which had gen-in North America.[50,55]
erated the world database on 225 children. His re-view revealed that TDEE was, on average, 20%4. Objective Measures ofbelow current international recommendations. HePhysical Activitypostulated that this was probably due to changes inlevels of habitual physical activity.
4.1 Doubly Labelled Water Hoos et al.[86] systematically reviewed the litera-ture and combined data from 17 studies, includingDoubly labelled water (DLW) is recognised asstudies of European children,[87,88] with the aim ofthe reference method or ‘gold standard’ for theconstructing a reference line for PAL and AEE as aassessment of energy expenditure in free-living sub-function of age and gender. The children were agedjects. This technique assesses energy expenditure byfrom 3 to 16 years and whereas there was no genderestimating carbon dioxide production using isotopedifference in PAL values, boys had higher AEEdilution during a minimum of 3 days.[82] However, itvalues than girls. Low values were found in youngshould be noted that energy expenditure is a physio-children increasing to adult values with age. Hoos etlogical consequence of physical activity and the twoal.[89] explained this as a function of adults’ higherare distinct constructs, which limits attempts to usebody mass and less time spent sleeping. They sug-DLW to validate measures of physical activity. Forgested that as children grow older, they sleep lessexample, physical activity may cause an elevation inand spend more time on physical activities, resultingmetabolic rate that persists long after cessation ofin higher PAL and AEE values.observable movement.
The DLW technique has low reactivity and it DLW has been used quite extensively to validateappears to be accurate to within 5% relative to data other methods of estimating energy expenditure.
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1074 Armstrong & Welsman
Accelerometers have been reported to provide sig- (9.16MJ) at 8 years of age to 3901 caloriesnificant relationships with TDEE, PAL and AEE in (16.31MJ) at 17 years of age. Girls’ ‘heat produc-6-[89] and 9-year-old children,[88] although O’Connor tion’ increased from 2223 calories (9.29MJ) at 9et al.[90] found no significant correlation between years of age to 3214 calories (13.43MJ) at 17 yearsDLW measures and either accelerometer or activity of age. Although difficult to interpret, her resultsdiary estimates of energy expenditure. Emons et indicated that boys had a higher ‘heat production’ atal.[91] showed heart-rate monitoring to overestimate all ages studied.DLW determined TDEE by about 12% in 8- to Recent technology has allowed the introduction9-year-old children. Livingstone et al.[92] described a of portable, lightweight metabolic systems; howev-FLEX HR technique, which uses an individually er, despite this advance, the equipment is still toodetermined heart rate measured in conjunction with cumbersome to use indirect calorimetry with chil-oxygen uptake (VO2), that can be used to distin- dren under free-living conditions.guish between resting and AEE. Resting metabolicrate is substituted for periods when the heart rate 4.3 Direct Observationfalls below the FLEX HR. Using this technique,
The assessment of physical activity through thethey accurately predicted group DLW estimates ofuse of direct observation has inherent appeal andTDEE in 7- to 15-year-olds.recent technological advances permitting complexobservational codes to be entered, stored and4.2 Indirect Calorimetryanalysed by microcomputers have stimulated re-search into children’s activity patterns using directIndirect calorimetry has been used to validateobservation techniques. Sirard and Pate[2] criticallyheart-rate monitoring, pedometry and accelerome-reviewed seven direct observation systems and con-try. Emons et al.[91] compared 24-hour energy ex-cluded that all seven techniques attained satisfactorypenditure determined during a 1-day stay in a calo-inter-observer agreement (84–99%) among simulta-rimeter with energy expenditure estimated fromneous observations of the same child.continuous heart-rate monitoring and demonstrated
Direct observation is, however, labour-intensive,that heart-rate monitoring overestimated energy ex-time consuming and therefore costly. Events studiedpenditure by about 10%. Eston and his col-must be observable and codeable and observers orleagues[93,94] investigated energy expenditure duringvideo cameras need to be in the same environmenta series of activities with 8- to 10-year-old childrenas the subject. The extent to which even well trainedusing indirect calorimetry, heart-rate monitoring,observers affect subject behaviour (subject reactivi-accelerometry and pedometry. Across all activities,ty) is problematic. Puhl et al.[96] reported that 16.6%both heart rate and accelerometry counts wereof the children in their study reacted to the observ-strongly correlated with VO2 and the results alsoers. Direct observation can capture valuable short-suggested that pedometry offers potential for largeterm patterns and sudden changes in children’sstudies of young people’s physical activity.physical activity,[22] but it is normally impossible toHistorically, Bedale’s[95] analysis of ‘heat pro-follow a child for a full day[19,97] and few long-termduction’ during selected activities was probably thedirect observation studies have been undertakenfirst attempt to classify the daily energy expenditurewith children.of European children. Her work was limited by the
available technology as she used Douglas bags to The series of studies by Sleap andcollect expired air, which she subsequently analysed Warburton[98-100] of English children appear to befor oxygen and carbon dioxide content using a the most comprehensive direct observation studiesHaldane apparatus. Bedale[95] reported her results in of the physical activity of European youth. Theyterms of ‘total heat production in 24 hours’ and observed 93 girls and 86 boys aged 5–11 years, onconcluded that boys’ values rose from 2191 calories separate occasions, during school break times, lunch
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of European Youth 1075
times and physical education lessons. Further obser- of storing minute by minute data for several daysvations were undertaken on one weekday evening and therefore allow long duration monitoring ofand one 4-hour period on either a weekend or during physical activity. However, the activity patterns ofa school vacation. In total, each child was observed young children are characterised by very shortfor an average of 418 minutes. During this time, bursts of MVPA and therefore shorter recordingchildren were engaged in MVPA for 29.3% of total intervals may be required in some circumstances;time observed. Twenty one percent of children re- this will reduce the overall duration of monitoring.corded at least one sustained 20-minute period of Telemetry systems are used widely, but they are notMVPA. Ninety five percent of children engaged in without problems and heart rate traces often needat least one 5-minute period of MVPA and no signif- individual editing because of electrical interferenceicant differences in MVPA were observed between causing spuriously high or low datapoints.[18,101]
boys and girls. Sleap and Warburton[100] concluded The interpretation of heart-rate data is complexthat their results were disturbing since preadolescent and Harro and Riddoch[18] have identified 24 differ-children appeared to be engaging in very little sus- ent methods of data reduction. This makes directtained, playful physical activity during their free comparisons between studies very difficult. Gener-time outside of school. ally, heart rate has been used to either estimate
energy expenditure or to provide ‘thresholds’ equat-4.4 Heart-Rate Monitoring ing to moderate and/or vigorous physical activity.
The direct prediction of children’s daily energyHeart-rate monitoring provides an objective esti-expenditure from heart rate[29,103] is fraught withmate of physical activity that is based on the as-problems[101] and more recent studies have tended tosumption that children who spend longer periods ofrely on the FLEX HR technique.[92] Numerous heart-time with elevated heart rates are generally morerate indices or thresholds can be found in the litera-active than those whose heart rate remains in theture. Some investigators[31,104] have suggested thelower ranges. Heart-rate monitoring is accepted as ause of a heart-rate threshold corresponding to 50%reliable and valid measure of physical activity overof each individual’s peak VO2; however, as thisextended time periods but it is an indirect measurerequires individual calibration of each subject, it is athat indicates the relative stress placed on the cardio-burdensome technique in large studies. Other re-respiratory system.[101,102] Several other factors be-searchers have defined moderate and vigorous activ-side physical activity can influence heart rate, par-ity as brisk walking and jogging, respectively, andticularly during low-intensity physical activity. Ex-directly determined the heart rate corresponding toamples include anxiety, emotional stress, fatigue,these activities to use as a threshold.[101,102] Severalbody position, active muscle group, type of musclestudies have used a threshold of 140 beats/min tocontraction, training status, level of fitness, fooddefine moderate physical activity.[18,101]
intake, state of hydration, ambient temperature andhumidity.[101] Despite the problems with its assessment and
interpretation, heart-rate monitoring has providedA number of self-contained, computerised telem-valuable insights into young people’s physical activ-etry systems have been developed for the unobtru-ity patterns. Bradfield et al.[105] appear to have beensive monitoring of heart rate. Typically, these sys-the first to continuously monitor the heart rates oftems consist of a lightweight transmitter that is fixedEuropean boys and, following calibration of heartto the chest with electrodes or a belt, and a receiver/rates against VO2, they reported the mean energymicrocomputer that is worn as a watch on the wrist.expenditure of 54 7- to 10-year-old boys as 9.2 kJ/They are socially acceptable, they permit freedom ofmin during lunchtime and play periods. Seliger etmovement, they are not immediately noticeable, andal.[73] monitored the heart rates of 11 12-year-oldtherefore should not unduly influence the child’sCzech boys for 24 hours and reported that heart ratesnormal activity pattern. Some systems are capable
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1076 Armstrong & Welsman
>150 beats/min were rare and only fleetingly en- ical activity (equivalent to brisk walking) as generat-countered. They noted that “the daily activity heart ing a heart rate ≥140 beats/min and vigorous physi-rate response implied that very little circulation re- cal activity (equivalent to jogging) as generating asponse was required to support the daily activity”, heart rate ≥160 beats/min.but they did not describe their method of monitoring For the purpose of this review, these data havein any detail. been merged and re-analysed in three categories: (i)
Saris[29] developed an eight-level heart-rate inte- first school (mean age 7.2 years; 93 girls, 95 boys);grator that stored heart rates within appropriate (ii) middle school (mean age 11.0 years; 263 girls,ranges over periods of 24 hours. He subsequently 271 boys); and (iii) high school (mean age 13.3used the instrument in a bi-annual analysis of 217 years; 265 girls, 220 boys). Specific details of sam-boys and 189 girls from The Netherlands over a pling procedures are available in the original papers6-year period beginning when the children were 6 but the participants were generally representative ofyears old. Saris[29] reported that, at all ages, boys had the South of England. The boys in each categorya higher total energy expenditure and spent more spent a significantly greater percentage of time withtime above an exercise intensity equivalent to 50% their heart rate ≥140 and 160 beats/min than theof peak VO2, than girls. corresponding girls.
Verschuur and Kemper[103,106,107] used Saris’ In total, 305 of the high-school children and 114heart-rate integrator to annually monitor Dutch chil- of the middle-school children also had their heartdren for 48 hours over a 4-year period, beginning at rates monitored on a Saturday. The high-school girlsage 12–13 years. The daily energy expenditure of spent significantly less time above the 140 beats/mingirls in relation to body mass was found to decrease threshold than high school boys. No significant dif-from 12–13 to 17–18 years of age. Boys’ daily ferences were detected between middle-school boysenergy expenditure in relation to body mass was and girls.almost constant from age 12–13 to 14–15 years and
To provide a more comprehensive picture ofthen decreased to 17–18 years of age. Boys demon-
young people’s physical activity patterns, the num-strated significantly higher energy expenditures than
ber of 5-, 10- and 20-minute periods with heart rategirls at ages 12–13 and 14–15 years.
sustained ≥140 and 160 beats/min was determined.By the end of the 1980s, heart-rate monitoring Five-minute periods of moderate physical activity
technology had advanced to the point where unob- were common, particularly among the younger chil-trusive telemetry systems allowed monitoring over dren, where 93% of the boys and 78% of the girlsseveral days. Studies of European children and ado- achieved at least one 5-minute period of moderatelescents that have employed heart-rate monitoring physical activity per day. Eighty two percent ofover at least a 3-day period and from which relevant older (high- plus middle-school) boys and 63% ofdata can be extracted have been summarised and older girls achieved a daily 5-minute period of mod-collated in table I. erate physical activity, but 34% of older boys and
Over a 10-year period and in a series of studies 47% of older girls did not experience a singleArmstrong and his associates[21,102,108-110,113,115-117] 10-minute period of moderate physical activity overmonitored the heart rates of 1227 young people aged 3 days of monitoring. Ten-minute periods of moder-5–16 years from South West England over three ate physical activity were more common among theschooldays. To interpret their data, they exercised first school children, but 11% of boys and 31% of98 young people, aged 5–16 years, at various speeds girls failed to raise their heart rate ≥140 beats/minon a horizontal treadmill and noted that, regardless for a sustained 10-minute period. Twenty-minuteof age, brisk walking and jogging elicited steady- periods of either moderate or vigorous physical ac-state heart rates of about 140 and 160 beats/min, tivity were sparse in all age groups, illustrating thatrespectively. They therefore defined moderate phys- sustained periods of physical activity do not
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of E
uropean Youth
1077
2006 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2006; 36 (12)
Table I. Habitual physical activity of European youth measured over at least 3 days using heart rate monitoring
Study Participants Physical activity Outcomesmeasure
Armstrong et al.[102] 163 girls, 103 boys; aged 4d HR monitoring Boys had HR >139 bpm for significantly greater percentage of time than girls11–16y; England (6.2% vs 4.3%) during 3 weekdays and a Saturday, boys (n = 92) 5.6% vs girls
(n = 120) 2.6%. A significant negative correlation with age was found with girls(weekday r = –0.27, Saturday r = –0.21), but not with boys. 51.5% of girls and35.9% of boys did not exhibit a single 10 min sustained period with HR >139bpm over 3 weekdays. On Saturday the corresponding figures were 70.7% ofboys and 93.3% of girls
Armstrong and Bray[108] 11 girls, 13 boys; aged 10–11y; 6d HR monitoring Children spent 8.8% of time with HR >139 bpm and 3.6% of time with HR >159England bpm. 33.4% of children did not exhibit a single 10 min sustained period with HR
>139 bpm and 62.5% did not exhibit a single 10 min sustained period with HR>159 bpm. No significant differences were detected between boys and girls
Armstrong and Bray[21] 65 girls, 67 boys; aged 10.7y; 4d HR monitoring No significant gender differences in time spent with HR >139 bpm during 3England weekdays (boys 9.4% vs girls 8.2%) or a Saturday (16 boys [5.2%] vs 23 girls
[6.0%]). Boys spent significantly more time with HR >159 bpm during weekdays(4.5% vs 3.5%) but not during Saturdays (1.8% vs 1.8%). 25% of girls and 19%of boys did not exhibit a single 10 min sustained period with HR >139 bpmduring weekdays. On Saturday the corresponding figures were 75% of boysand 65% of girls
Biddle et al.[109] 20 girls and 26 boys; aged 3d HR monitoring No significant gender differences in time spent with HR >139 bpm during 312.2y; England weekdays, but boys spent significantly more time with their HR >159 bpm
(2.7% vs 1.9%). 45.9% of boys and 34.3% girls did not sustain a single 10 minperiod with HR >139 bpm. The corresponding figures for 10 min periods withHR >159 bpm were 64.9% of boys and 91.4% of girls
Riddoch et al.[104] 22 girls and 23 boys; aged 2–4d HR monitoring No significant gender difference in daily time spent with HR >50% VO2peak
11–16y; Northern Ireland (boys, 24 min; girls, 17 min). Boys spent significantly more time than girls withHR >70% VO2peak (8 vs 4 min). Younger boys engaged in significantly moretotal activity than older boys and in more vigorous activity than younger girls. Asignificant negative correlation (r = –0.48) was found between age and totalactivity in boys but not in girls
McManus and 100 girls, 100 boys; aged 3d HR monitoring Boys spent significantly more time than girls with HR >139 bpm (9.1% vs 7.3%)Armstrong[110] 11.1y; England and HR >159 bpm (4.3% vs 3.0%). 22% of boys and 30% of girls did not
sustain a single 10 min period with HR >139 bpm and 49% of boys and 57% ofgirls did not sustain a single 10 min period with HR >159 bpm
Falgairette et al.[111] 34 girls, 30 boys; aged 6–11y; 7d HR monitoring Daily HR and percentage of HR reserve varied little with age, although thereFrance was a tendency for a decrease in girls. PA was higher during weekdays than
weekend days
Continued next page

1078A
rmstrong &
Welsm
an
2006 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2006; 36 (12)
Table I. Contd
Study Participants Physical activity Outcomesmeasure
Sallo and Silla[112] 29 girls, 25 boys; aged 7y; 4d HR monitoring The children spent 7.9% of monitored time with HR >139 bpm. No genderEstonia differences were detected. 55% of girls and 64% of boys did not exhibit a 10
min sustained period with HR >139 bpm
Welsman and 31 girls, 26 boys; aged 6–9y; 3d HR monitoring Boys spent significantly more time than girls with HR >139 bpm (11.1% vsArmstrong[113] England 8.7%) and HR >159 bpm (4.7% vs 3.3%). 23% of boys and 31% of girls did not
exhibit a 10 min sustained period with HR >139 bpm, corresponding figures forHR >159 bpm were 69% of boys and 83% of girls. Time with HR >139 and 159bpm declined significantly with age in both boys and girls
Gavarry et al.[114] 38 girls, 28 boys; aged 11–16y; 7d HR monitoring 32% of the children were classified as active according to ACSM[5] guidelines.France No gender differences were noted, but PA decreased with age
Manios et al.[59] 22 girls, 17 boys; aged 6y; 3d HR monitoring Children from urban areas had significantly longer activity intervals than thoseGreece from rural areas. The time spent in activity intervals was significantly longer
during weekdays than weekend days
Welsman and 22 girls, 17 boys; aged 5–7y; 3d HR monitoring Boys spent significantly more time than girls with HR >139 bpm (13.6% vsArmstrong[115] England 8.5%) and HR >159 bpm (6.1% vs 2.9%). 32% of girls did not exhibit a 10 min
sustained period with HR >139 bpm, although all boys did so. Correspondingfigures for HR >159 bpm were 77% of girls and 53% of boys
Armstrong et al.[116] 98 girls, 104 boys; aged 3d HR monitoring In the first year of the study, 76.2% of boys and 73.5% of girls accumulated 3011–13y; England min with HR >139 bpm. In the final year the figures were 44.4% and 31.6% for
boys and girls, respectively. At age 11y, 22.1% of boys and 29.6% of girls didnot experience a single 10 min sustained period with HR >139 bpm at age 13ythe figures were 28.4% and 51.9% for boys and girls, respectively. PA declinedwith age with a consistent gender difference reflecting the lower PA of girls
Welsman and 40 girls, 42 boys; aged 14–15y; 4d HR monitoring 67.3% of the boys and 59.5% of the girls accumulated a daily 30 min with HRArmstrong[117] England >139 bpm. 28.8% of boys and 54.8% of girls did not experience a single 10
min sustained period with HR >139 bpm
Ekelund et al.[118] 40 girls, 42 boys; aged 14–15y; 3d HR monitoring No gender differences were observed in time spent engaged in MVPA, butSweden boys’ activity energy expenditure (total-sedentary energy expenditure) was
significantly higher than girls
Sleap and Tolfrey[42] 36 girls, 43 boys; aged 10.6y; 4d HR monitoring Girls accumulated 105 min with their HR >120 bpm and 38 min >140 bpm.England Corresponding data for boys were 118 min and 50 min. Boys spent significantly
more time with HR >140 bpm than girls
Vermorel et al.[61] 29 girls, 31 boys; aged 12–16y; 5d HR monitoring Mean DEE increased significantly with age in boys, but not in girls. PA level didFrance not vary with gender and age. Mean DEE was 21% higher on non-schooldays
in the active children but 7% lower in the sedentary children
ACSM = American College of Sports Medicine; bpm = beats/min; DEE = daily energy expenditure; HR = heart rate; MVPA = moderate to vigorous physical activity; PA = physicalactivity; VO2peak = peak oxygen uptake.

Physical Activity of European Youth 1079
characterise young people’s physical activity pat- Pedometers are relatively simple motion sensorsterns. Less than 3% of boys were reported to experi- that record the acceleration and deceleration ofence the equivalent of a daily 20-minute period of movement in one direction[120] and are normallyvigorous physical activity. Of the 641 girls moni- used to estimate mileage walked or the number oftored for 3 weekdays and the 195 girls monitored on steps taken over a period of time. Six days of pe-a Saturday, not a single girl experienced the dometer data have been reported as adequately relia-equivalent of a daily 20-minute period of vigorous ble for research into children’s physical activity withphysical activity. the inclusion of both weekday and weekend scores
recommended.[121] Disadvantages of pedometry in-In what appears to be the only longitudinal studyclude the inability to measure intensity or pattern ofof 3-day heart-rate monitoring, Armstrong et al.[116]
assessed annually the physical activity patterns of 98 activities performed, record counts during cycling orgirls and 104 boys, aged 11 years at the onset of the increases in energy expenditure due to carrying ob-study. Sustained 10- or 20-minute periods of moder- jects or walking/running uphill. Ankle-mounted pe-ate or vigorous physical activity were not character- dometers overcome the problem of recording duringistic of the physical activity patterns and both mea- cycling, but ankle pedometers are less reliable thansures declined with age with a consistent gender waist-mounted pedometers[120] and most recentdifference reflecting the lower physical activity pedometry studies have used waist-mounted instru-levels of girls. Using multilevel modelling, they ments.demonstrated age and gender differences in time There are no well accepted guidelines for youngspent above 139 and 159 beats/min. Seventy six people for the number of steps that equate to 1 hourpercent of 11-year-old children accumulated a daily of moderate physical activity per day and recom-30 minutes with their heart rate >139 beats/min, but mendations for adults (e.g. 10 000 steps per day) areby age 13 years 44% of the children met this target. likely to be too low for children. RecommendationsThe decline in the percentage of girls being particu- for appropriate step counts during childhood andlarly marked (from 74% to 32%). adolescence should take into account factors such as
Most, but not all (see table I) heart-rate monitor- age, stature and stride length. Predictions and pro-ing studies have reported boys to be more physically motion of daily moderate physical activity engage-active than girls. Boys appear to engage in moderate ment during youth based on pedometer counts perand vigorous, sustained periods of physical activity day should therefore be made with caution.[122]
more often than girls, but this type of activity doesNevertheless, Rowlands et al.[123] provide a de-
not appear to be characteristic of European youth’stailed examination of the use of pedometry and
physical activity patterns. Studies consistently showsuggest that as pedometers are inexpensive, re-usa-
a decline in physical activity with age, at leastble, objective and non-reactive they are useful tools
during the teen years. Children tend to be morefor large scale studies and well suited to the assess-
active during schooldays than at weekends.ment of children’s physical activity.
Pedometry studies of European youth that have4.5 Pedometryassessed physical activity over a minimum of 3 days
As almost all forms of physical activity require have been collated in table II. The measurements aremovement of the trunk or limbs, the assessment of less precise than with other objective measures of‘movement’ is appealing. The most common physical activity, but the large sample sizesmechanical device for measuring movement is the strengthen the results. Findings are very consistentpedometer, which was first used in this context by across the countries surveyed and show that boys areLauter,[119] although Leonardo da Vinci designed a more active than girls at all ages from 7 to 18 years.pedometer to measure distance by counting steps Two recent large Swedish studies[124,125] across thesomewhat earlier.[33] age range 7–14 years indicate that girls’ activity
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1080A
rmstrong &
Welsm
an
2006 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Sp
orts M
ed
2006; 36 (12)
Table II. Habitual physical activity of European youth measured over at least 3 days using pedometry
Study Participants Physical activity measure Outcomes
Verschuur et al.[126] 215 girls, 195 boys; 3d pedometer monitoring Boys spent significantly more time on ‘heavy activities’ than girls. Boys’ median
aged 13–14y; The 99 min, girls’ median 1 min
Netherlands
Skalik et al.[125] 58 girls, 68 boys; aged 7d accelerometer and Mean DEE in PA was 9.7 kcal/kg/d in girls and 11.2 kcal/kg/d in boys. In all
16–18y; Czech pedometer monitoring regions boys had a higher level of PA. 17% of girls failed to reach 6 kcal/kg/d
Republic, Poland and
Sweden
Vincent et al.[127] 324 girls, 356 boys; 4d pedometer monitoring The 12-year-old boys in the most active tertile accumulated more steps than
aged 7–12y; Sweden the 7-year-old boys. In the least active tertile the younger boys accumulated
more steps than the older boys. In both the most active and the least active
tertiles the younger girls accumulated more steps than the older girls
Loucaides et al.[71,128] 127 girls, 129 boys; 4d pedometer monitoring in Urban schoolchildren were significantly more active in winter than rural
aged 11–12y; Cyprus winter schoolchildren and rural schoolchildren were more active in the summer. Boys
4d pedometer monitoring in acquired significantly higher mean daily step counts than girls in winter
summer
Raustorp et al.[124] 435 girls, 457 boys; 4d pedometer monitoring Boys were significantly more active than girls across all age groups. For both
aged 7–14y; Sweden boys and girls the most active age groups were 10-year-olds. With the
exception of 10-year-olds, activity levels were quite stable among children aged
7–11y but there tended to be a drop-off in step counts among adolescents in
the 13–14y age groups
Cardon and De 41 girls, 51 boys; aged 6d pedometer monitoring Mean daily step counts were significantly higher in boys than in girls (16 628 ±
Bourdeaudhuij[122] 6–13y; Belgium 3527 steps vs 13 002 ± 3644 steps). Daily step counts during the week did not
differ significantly from the weekend step count. Step counts were significantly
higher in younger children regardless of gender
DEE = daily energy expenditure; PA = physical activity.

Physical Activity of European Youth 1081
declines with age, although the decline in boys’ approaches used to calibrate the devices againstphysical activity with age may not commence until directly measured energy expenditure. They report-the early teens. ed that the cut points (counts per minute) used to
define the boundaries of young people’s moderate (34.6 Accelerometry metabolic equivalents [METs]) and vigorous (6
METs) physical activity varied substantially for aAccelerometers are more sophisticated motion given accelerometer, even though most studies had
sensors than pedometers and they record movement included similar activities in the protocol. They ac-through piezo-electric transducers and microproces- knowledged that calibration should be fit for pur-sors that convert recorded accelerations to a quanti- pose with, for example, studies using accelerome-fiable digital signal referred to as ‘counts’. Acceler-
ters to examine the impact of activity on obesityometers are normally attached to a belt at the hip and
relating counts to energy expenditure. However,relative to heart-rate monitors they are less burden-
they suggested that for studies where the purpose issome to children. Accelerometers provide an objec-to characterise or track physical activity behaviour,tive, non-reactive and re-usable technique withthe most appropriate accelerometer measure may bewhich to assess habitual physical activity but theythe raw counts.are insensitive to cycling, locomotion on a gradient
Relatively few accelerometry studies of the phys-or other activities with limited torso movement.[2,3]
ical activity of European youth have been published,Early accelerometers were uniaxial, but morebut those located that have monitored activity overrecent models measure movement in three planesat least 3 days are collated in table III.(triaxial). Trost[3] critically reviewed uniaxial and
triaxial models and stated that they “provide compa- The most substantial study of European chil-rable assessments of free-living physical activity in dren’s physical activity using accelerometry waschildren.” He noted that triaxial models tend to be carried out as part of the European Youth Heartbigger than uniaxial models and that this is impor- Study.[43] Subjects aged 9 and 15 years were recruit-tant in field-based studies where children are more ed to broadly represent children either side of puber-likely to wear a device that is unobtrusive. They can, ty. Data were collected from well defined popula-however, be worn underneath clothes when necessa- tions from four countries and 2185 children hadry and do not prevent participation in common activ- their physical activity assessed over either 4 daysities and sports. Trost concluded that the develop- (70%) or 3 days (30%).ment of a compact and highly reliable three-dimen-
The results confirmed significant gender differ-sional accelerometer remains a research priority.ences in physical activity with 9-year-old boys beingThere are a number of commercial accelerome-21% more active than girls and 15-year-old boysters on the market and Sirard and Pate[2] have tabu-being 26% more active than similarly aged girls.lated available studies of young people’s physicalGender differences in time spent in activity of atactivity where accelerometry has been comparedleast moderate intensity were even more markedwith energy expenditure (determined by DLW or(20% and 36% difference, respectively). Similarly,indirect calorimetry) and direct observation of activ-9-year-old children of both genders were considera-ity. Correlation coefficients across the various mod-bly more active than 15-year-olds (27% more activeels ranged from r = –0.09 to r = 0.95.in boys, 32% in girls). The age difference was evenThe calibration of accelerometer output to esti-more marked with time spent in moderate activitymate the physical activity of children and adoles-(94% more active in boys, 129% more active incents is, however, a challenge. Freedson et al.[129]
girls). Ninety seven percent of 9-year-old childrenrigorously reviewed calibration studies of the fouraccumulated 60 minutes of moderate activity asaccelerometers used most frequently to assess phys-
ical activity in this population and critiqued the recommended by the UKHEA,[15] but fewer boys
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1082 Armstrong & Welsman
(82%) and, particularly, girls (62%) achieved this atage 15 years.
Riddoch et al.[43] commented on the remarkableconsistency of the results across Denmark, Portugal,Estonia and Norway. Physical activity levels andage and gender differences were mirrored across thefour countries despite the wide differences in geog-raphy, socio-economic circumstances, culture andclimate. The authors suggested that physical activityhabits in children may be determined by biologicalfactors as much as by environmental factors, a con-cept supported by others.[136-138]
Other accelerometry studies of the physical activ-ity of European youth provide further support forgender differences;[132,135] however, Santos et al.[133]
observed that the time spent in MVPA by Portu-guese children increased with age in direct contrastwith the findings of the European Heart Study[43]
whose study contained a large Portuguese samplecovering the same age range.
5. Conclusions
The habitual physical activity of children andadolescents is difficult to assess and interpret in thecontext of promoting health. Several methods ofassessing physical activity are available but all haveweaknesses. Nevertheless, despite the lack of preci-sion, self-report surveys of large representative sam-ples have provided informative overviews of youngpeople’s level of activity and more objective meth-ods have allowed insights in the patterns of physicalactivity during the progression through childhoodand adolescence. Data are available from all Euro-pean Countries except Luxembourg, although ob-jective studies have been mainly centred in specificcountries, principally Estonia, Sweden, France, Por-tugal, The Netherlands and the UK. Trends in differ-ent countries are very similar and European boysappear to participate in more physical activity thanEuropean girls, with the gender difference beingmore marked in comparisons of vigorous physicalactivity. The physical activity levels of both gendersdecline as they move through adolescence. Physicalactivity patterns are sporadic and sustained periods
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)
Tab
le I
II. H
abitu
al p
hysi
cal a
ctiv
ity o
f E
urop
ean
yout
h m
easu
red
over
at
leas
t 3
days
usi
ng a
ccel
erom
etry
Stu
dyP
artic
ipan
tsP
hysi
cal a
ctiv
ityO
utco
mes
mea
sure
Rau
dsep
p an
d P
all[1
30]
23 g
irls,
19
boys
; ag
ed4d
acc
eler
omet
erB
etw
een-
day
repr
oduc
ibili
ty o
f ac
cele
rom
eter
mon
itorin
g w
as h
ighe
r be
twee
n si
mila
r8–
9y;
Est
onia
mon
itorin
gda
ys o
f th
e w
eek
(wee
kday
s or
wee
kend
day
s).
Sho
rt-t
erm
sta
bilit
y of
PA
dur
ing
late
child
hood
was
mod
erat
eS
kalik
et
al.[1
25]
58 g
irls,
68
boys
; ag
ed7d
acc
eler
omet
er a
ndM
ean
DE
E in
PA
was
9.7
kca
l/kg/
d in
girl
s an
d 11
.2 k
cal/k
g/d
in b
oys.
In
all r
egio
ns,
16–1
8y;
Cze
chpe
dom
eter
mon
itorin
gbo
ys h
ad a
hig
her
leve
l of
PA
. 17
% o
f gi
rls f
aile
d to
rea
ch 6
kca
l/kg/
dR
epub
lic,
Pol
and
and
Sw
eden
Nils
son
et a
l.[131
]6
girls
, 10
boy
s; a
ged
4d a
ccel
erom
eter
Chi
ldre
n ac
cum
ulat
ed >
60 m
in o
f at
leas
t m
oder
ate
activ
ity e
very
day
7.5y
; S
wed
enm
onito
ring
Gue
rra
et a
l.,[1
32]
93 g
irls,
64
boys
; ag
ed3d
acc
eler
omet
erB
oys
enga
ged
in s
igni
fican
tly m
ore
MV
PA
per
day
. 94
% o
f bo
ys a
nd 7
9% o
f gi
rlsS
anto
s et
al.,
[133
]8–
16y;
Por
tuga
lm
onito
ring
accu
mul
ated
at
leas
t 60
min
of
MV
PA
per
day
. T
he t
ime
spen
t in
MV
PA
incr
ease
dM
ota
et a
l.[134
]ac
ross
age
gro
ups
in b
oth
boys
and
girl
sM
alla
m e
t al
.[135
]95
girl
s, 1
20 b
oys;
5d a
ccel
erom
eter
In g
ener
al,
girls
did
less
phy
sica
l act
ivity
tha
n bo
ysag
ed 7
–10.
5y,
Eng
land
mon
itorin
gR
iddo
ch e
t al
.[43]
2185
chi
ldre
n; a
ged
94d
acc
eler
omet
erB
oys
wer
e m
ore
activ
e th
an g
irls
at a
ge 9
y an
d at
age
15y
. 9-
year
-old
s w
ere
mor
ean
d 15
y, D
enm
ark,
mon
itorin
gac
tive
than
15-
year
-old
s. W
ith r
espe
ct t
o tim
e sp
ent
in m
oder
ate-
inte
nsity
act
ivity
,P
ortu
gal,
Est
onia
and
gend
er d
iffer
ence
s in
fav
our
of b
oys
wer
e ap
pare
nt a
t ag
e 9
and
15y.
At
9y,
97.4
% o
fN
orw
aybo
ys a
nd 9
7.6%
of
girls
acc
umul
ated
60
min
of
mod
erat
e in
tens
ity a
ctiv
ity.
At
age
15y,
81.9
% o
f bo
ys a
nd 6
2.0%
of
girls
did
so
DE
E =
dai
ly e
nerg
y ex
pend
iture
; M
VP
A =
mod
erat
e to
vig
orou
s ph
ysic
al a
ctiv
ity;
PA
= p
hysi
cal a
ctiv
ity.

Physical Activity of European Youth 1083
6. Sallis JF, Patrick K, Long BJ. Overview of the internationalof either moderate or vigorous physical activity areconsensus conference on physical activity guidelines for ado-
not part of the lifestyle of most European children. lescents. Pediatr Exerc Sci 1994; 6: 299-3027. Armstrong N, Simons-Morton B. Physical activity and bloodIt is well documented that the number of young
lipids in adolescents. Pediatr Exerc Sci 1994; 6: 381-405people who experience physical activity of the type,8. Alpert BS, Wilmore JH. Physical activity and blood pressure in
duration, frequency and intensity recommended by adolescents. Pediatr Exerc Sci 1994; 6: 361-809. Bar-Or O, Baranowski T. Physical activity, adiposity, and obesi-expert committees decreases with age, but accurate
ty among adolescents. Pediatr Exerc Sci 1994; 6: 348-60estimates of how many girls and boys can be classi-10. Bailey DA, Martin AD. Physical activity and skeletal health in
fied as inactive according to current recommenda- adolescents. Pediatr Exerc Sci 1994; 6: 330-4711. Calfas KJ, Taylor WC. Effects of physical activity on psycho-tions are clouded by methodological inconsisten-
logical variables in adolescents. Pediatr Exerc Sci 1994; 6:cies. For example, arguably the two most important 406-23recent contributions to the European youth physical 12. Sallis JF, Patrick K. Physical activity guidelines for adolescents:
a consensus statement. Pediatr Exerc Sci 1994; 6: 302-14activity literature are the studies by Riddoch et al.[43]
13. Cale L, Harris J. Exercise recommendations for young people:and Currie et al.[55] Both studies were rigorouslyan update. Health Educ J 2001; 101: 126-38
designed and executed with large well defined sam- 14. Pate RR, Trost SG, Williams CA. Critique of existing guidelinesfor physical activity in young people. In: Biddle S, Sallis J,ples. Data were collected from the same four Euro-Cavill N. editors. Young and active? London: Health Educa-pean countries, Estonia, Portugal, Norway and Den- tion Authority, 1998: 162-76
mark, at the same time. Riddoch et al.,[43] using 15. Biddle S, Sallis J, Cavill N. Young and active? London: HealthEducation Authority, 1998accelerometry, reported 81.9% of 15-year-old boys
16. Strong WB, Malina RM, Blimkie CJR, et al. Evidence basedand 62.0% of 15-year-old girls satisfied the guide- physical activity for school-age youth. J Pediatr 2005; 146 (6):lines of the UKHEA expert committee,[15] whereas 732-7
17. Bar-Or O. Pediatric sports medicine for the practitioner. NewCurrie et al.,[55] using self-report methods, notedYork: Springer-Verlag, 1983
27.9% and 18.5% of 15-year-old boys and girls, 18. Harro M, Riddoch C. Physical activity. In: Armstrong N, vanrespectively, to satisfy the same criterion. Mechelen W. editors. Paediatric exercise science and
medicine. Oxford: Oxford University Press, 2000: 77-84Trends describing the physical activity patterns19. Janz KF, Witt J, Mahoney LT, et al. The stability of children’s
of European youth are consistent but to obtain addi- physical activity measured by accelerometry and self-report.Med Sci Sports Exerc 1995; 27: 1326-32tional insights into the role of physical activity in
20. Sallis JF. Self-report measures of children’s physical activity. Jpromoting health during childhood and adolescence,Sch Health 1991; 61: 215-9
methods of assessment need to be further refined 21. Armstrong N, Bray S. Physical activity patterns defined bycontinuous heart rate monitoring. Arch Dis Child 1991; 66:and recommended guidelines regularly re-visited in245-7relation to the increasing evidence base.
22. Bailey RC, Olson J, Pepper SL, et al. The level and tempo ofchildren’s physical activities: an observational study. Med SciSports Exerc 1995; 27: 1033-41Acknowledgements
23. Montoye HJ, Taylor HL. Measurement of physical activity inpopulation studies: a review. Hum Biol 1984; 56: 195-216This review was supported by a grant from the European
24. Watson AWS, O’Donovan DJ. Influences of level of habitualUnion. The authors have no conflicts of interest that areactivity on physical work capacity and body composition ofdirectly relevant to the content of this review.post pubertal school boys. Q J Exp Physiol 1977; 62: 325-32
25. Wessel JA, Montoye HJ, Mitchell H. Physical activity assess-ment by recall method. Am J Public Health 1965; 55: 1430-6References
26. Pate RR. Physical activity assessment in children and adoles-1. Casperson CJ, Powell K, Christenson G. Physical activity, exer-cents. Crit Rev Food Sci Nutr 1993; 33: 321-6cise and physical fitness: definitions and distinctions of health-
27. Baranowski T, Dworkin RJ, Cieslik C, et al. Reliability andrelated research. Public Health Rep 1985; 100: 126-31validity of self report of aerobic activity: family health report.2. Sirard JR, Pate RR. Physical activity assessment in children andRes Q 1984; 55: 309-17adolescents. Sports Med 2001; 31: 439-54
28. Telama R, Viikari J, Valimaki I, et al. Atherosclerosis precur-3. Trost SG. Objective measurement of physical activity in youth:sors in Finnish children and adolescents leisure time physicalcurrent issues, future directions. Exerc Sport Sci Rev 2001; 29:activity. Acta Paediatr Scand 1985; 318: 169-8032-6
29. Saris WHM. Aerobic power and daily physical activity in chil-4. Twisk JWR. Physical activity guidelines for children and ado-dren. Meppel (The Netherlands): Kripps Repro, 1982lescents. Sports Med 2001; 31: 617-27
5. American College of Sports Medicine. Physical fitness in chil- 30. Salonen JT, Lakka T. Assessment of physical activity in popula-dren and youth. Med Sci Sports Exerc 1988; 20: 422-3 tion studies: validity and consistency of the methods in the
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1084 Armstrong & Welsman
Kuopio ischemic heart disease risk factor study. Scand J Sports 52. Heartbeat Wales. Welsh youth health survey 1986. Cardiff:Sci 1987; 9: 89-95 Heartbeat Wales, 1986
31. Saris WHM. Habitual physical activity in children: methodolo- 53. Riddoch C. Northern Ireland health and fitness survey. Belfast:gy and findings in health and disease. Med Sci Sports Exerc Sports Council for Northern Ireland and Department of Health1986; 18: 253-63 and Social Services, 1990
32. Murphy JK, Alpert BS, Christman JV, et al. Physical fitness in 54. Marella M, Colli R, Faina M. Evaluation de l’aptitude physique:children: a survey method based on parental report. Am J Eurofit, batterie experimentagle. Rome: Scuola Dello Sport,Public Health 1988; 78: 708-10 1986
33. Saris WHM. The assessment and evaluation of daily physical 55. Currie C, Roberts C, Morgan A, et al., editors. Young people’sactivity in children: a review. Acta Paediatr Scand 1985; 318: health in context. Copenhagen: World Health Organisation,37-48 2004
34. Harro M. Validation of a questionnaire to assess physical activi-56. Cantera-Garde MA, Devis-Devis J. Physical activity levels ofty of children ages 4-8 years. Res Q Exerc Sport 1997; 68:
secondary school Spanish adolescents. Eur J Phys Educ 2000;259-685: 28-44
35. Bouchard C, Tremblay A, Leblanc C, et al. Method to assess57. Silvennionen M. Relations between different kinds of physicalenergy expenditure in children and adults. Am J Clin Nutr
activity and motive types among Finnish comprehensive and1983; 37: 461-7upper secondary school pupils. Scand J Sports Sci 1984; 6:36. Durnin JVGA, Lonergan ME, Good J, et al. A cross-sectional72-82nutritional and anthropometric study, with an interval of 7
58. Bouziotas C, Koutedaiks Y. A three year study of coronary heartyears on 611 young adolescent school children. Br J Nutrdisease risk factors in Greek adolescents. Pediatr Exerc Sci1974; 32: 169-792003; 15: 9-1837. Sallis JF, Buono MJ, Freedson PS. Bias in estimating caloric
59. Manios Y, Kafatos A, Markakis G. Physical activity of 6-year-expenditure from physical activity in children. Sports Medold children: validation of two proxy reports. Pediatr Exerc Sci1991; 11: 203-91998; 10: 176-8838. Torun B. Inaccuracy of applying energy expenditure rates of
adults to children. Am J Clin Nutr 1983; 38: 813-4 60. Deheeger M, Rolland-Cachera MF, Fontvielle AM. Physicalactivity and body composition in 10 year old French children:39. Sallis JF, Saelens BE. Assessment of physical activity by self-linkages with nutritional intake? Int J Obes 1997; 21: 372-9report; status, limitations and future directions. Res Q Exerc
Sports 2000; 71: S1-14 61. Vermorel M, Vernet J, Bitar A, et al. Daily energy expenditure,40. Pate R, Freedson P, Sallis J, et al. Compliance with physical activity patterns, and energy costs of the various activities in
activity guidelines: prevalence in a population of children and French 12–16-y-old adolescents in free living conditions. Eur Jyouth. Ann Epidemiol 2002; 12: 303-8 Clin Nutr 2002; 56: 819-29
41. Epstein LH, Paluch RA, Kalakanis LE, et al. How much activity 62. Engstrom LM. Physical activity of children and youth. Actado youth get? A quantitative review of heart-rate measured Paediatr Scand 1980; 283: 101-5activity. Pediatrics 2001; 108: E44 63. Sunnegardh J, Bratteby LE, Sjolin S, et al. The relation between
42. Sleap M, Tolfrey K. Do 9-to-12-yr-old children meet existing physical activity and energy intake of 8 and 13 year oldphysical activity recommendations for health? Med Sci Sports children in Sweden. In: Binkhorst RA, Kemper HC G, SarisExerc 2001; 33: 591-6 WHM, editors. Children and exercise XI. Champaign (IL):
43. Riddoch CJ, Andersen LB, Wedderkopp N, et al. Physical Human Kinetics, 1985: 183-93activity levels and patterns of 9- and 15-yr-old European 64. Fuchs R, Semmer NK, Lippert P, et al. Patterns of physicalchildren. Med Sci Sports Exerc 2004; 36: 86-92 activity among German adolescents: the Berlin-Bremen study.
44. Ekelund U, Yngve A, Sjostrom M. Total daily energy expendi- Prev Med 1988; 17: 746-63ture and patterns of physical activity in adolescents assessed by
65. Rutenfranz J, Berndt I, Knauth P. Daily physical activity inves-two different methods. Scand J Med Sci Sports 1999; 9:tigated by time budget studies and physical performance ca-257-64pacity of schoolboys. Acta Paediatr Belg 1974; 28: 79-86
45. Kemper HCG. The Amsterdam growth study. Champaign (IL):66. Guerra S, Duarte J, Mota J. Physical activity and cardiovascularHuman Kinetics, 1995
disease risk factors in schoolchildren. Eur Phys Educ Rev46. Deforce B, Lefevre J, De Boudeaudhuig I, et al. Physical fitness2001; 7: 269-81and physical activity in obese and non-obese Flemish youth.
67. Ribeiro J, Guerra S, Pinto A, et al. Overweight and obesity inObes Res 2003; 11: 434-41children and adolescents: relationship with blood pressure and47. Guillaume M, Lapidus L, Bjorntorp P, et al. Physical activity,physical activity. Ann Hum Biol 2003; 30: 203-13obesity and cardiovascular risk factors in children: the Belgi-
68. Andersen LB, Schelin B. Physical activity and performance in aum Luxembourg child study II. Obes Res 1997; 5: 549-56random sample of adolescents attending school in Denmark.48. Hussey J, Gormley J, Bell C. Physical activity in Dublin chil-Scand J Med Sci Sports 1994; 4: 13-8dren aged 7-9 years. Br J Sports Med 2001; 35: 268-73
69. Hasselstrom H, Hansen SE, Frobert K, et al. Physical fitness and49. O’Sullivan SO. The physical activity of children: a study ofphysical activity during adolescence as predictors of cardio-1603 Irish school children aged 11-12 years. Ir Med J 2002;vascular disease risk in young adulthood: Danish youth and95: 78-81sports study: an eight year follow-up. Int J Sports Med 2002;50. Currie C, Hurrelmann K, Settertobulte W, et al. Health and23: S27-31health behaviour among young people. Copenhagen: World
Health Organisation, 2000 70. King A, Wold B, Tudor-Smith C, et al., editors. The health of51. King AJC, Coles B. The health of Canada’s youth. Ottawa: youth: a cross national survey. Copenhagen: World Health
Ministry of Health and Welfare, 1992 Organisation, 1996
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

Physical Activity of European Youth 1085
71. Loucaides LA, Chedzoy SM, Bennett N, et al. Correlates of 91. Emons HJG, Groenenboom DC, Westerterp KR, et al. Compari-physical activity in a Cypriot sample of sixth-grade children. son of heart rate monitoring combined with indirect calorime-Pediatr Exerc Sci 2004; 16: 25-36 try and the doubly labelled water method for the measurement
of energy expenditure in children. Eur J Appl Physiol 1992;72. Aberberga-Augskalne L. Individual growth patterns and physi-65: 99-103cal fitness in Riga schoolchildren. Acta Medico-Historica
Rigensia 2002; 25: 65-76 92. Livingstone MBE, Coward AW, Prentice AM, et al. Dailyenergy expenditure in free-living children: comparison of heart73. Seliger VS, Trefny S, Bartenkova S, et al. The habitual physicalrate monitoring with the doubly labelled water method. Am Jactivity and fitness of 12 year old boys. Acta Paediatr BelgClin Nutr 1992; 56: 343-521974; 28: 54-9
93. Eston RG, Rowlands AV, Ingledew DK. Validity of heart rate,74. Naul R, Telema R, Rychtecky A. Physical fitness and activepedometry, and accelerometry for predicting the energy cost oflifestyle of Czech, Finnish and German youth. Acta Univ Carolchildren’s activity. J Appl Physiol 1998; 84: 362-71Kinanthrop 1997; 33: 5-16
94. Louie L, Eston RG, Rowland AV, et al. Validity of heart rate,75. Telema R, Naul R, Nupponen H, et al. Physical fitness, sportingpedometry and accelerometry for estimating the energy cost oflifestyles and Olympic ideals: cross-cultural studies on youthactivity in Hong Kong Chinese boys. Pediatr Exerc Sci 1999;sport in Europe. Schorndorf: Verlag Karl Hofmann, 200211: 229-3976. Jurak G, KovacM, Strel J. How Slovenian primary school pupils
95. Bedale EM. Energy expenditure and food requirements of chil-spend their summer holidays. In: Jurak G, editor. Sports activi-dren at school. Proc R Soc (London) 1923; 94: 368-404ties of Slovenian children and young people during their
summer holidays. Ljubljana: University of Ljubljana, 2003: 96. Puhl J, Greaves K, Hoyt M, et al. Children’s activity rating scale23-38 (cars): description and calibration. Res Q Exerc Sport 1990;
61: 26-3677. Jurak G, KovacM, Strel J, et al. How Slovenian secondary97. Armstrong N, Welsman JR. Young people and physical activity.school children spend their summer holidays. In Jurak G,
Oxford: Oxford University Press, 1997editor. Sports activities of Slovenian children and young peo-ple during their summer holidays. Ljubljana: University of 98. Sleap M, Warburton P. Physical activity levels of 5-11 year oldLjubljana, 2003: 39-58 children in England determined by continuous observation.
Res Q Exerc Sport 1992; 63: 238-4578. Raudsepp L, Liblik R, Hannus A. Children’s and adolescents’physical self-perception as related to moderate to vigorous 99. Sleap M, Warburton P. Physical activity levels of preadolescentphysical activity and physical fitness. Pediatr Exerc Sci 2002; children in England. Br J Phys Educ Res Suppl 1994; 14: 2-614: 97-106 100. Sleap M, Warburton P. Physical activity levels of 5-11-year-old
79. Sallo M, Viru A. Aerobic capacity and physical activity in 4 to children in England: cumulative evidence from three direct10-year-old children. Biol Sport 1996; 13: 211-9 observation studies. Int J Sports Med 1996; 17: 248-53
80. Kemper HCG. Growth, health and fitness of teenagers. Med 101. Armstrong N. Young people’s physical activity patterns asSport Sci 1985; 20: 1-202 assessed by heart rate monitoring. J Sports Sci 1998; 16: S9-16
81. Prochaska JJ, Sallis JF, Long BA. A physical activity screening 102. Armstrong N, Balding J, Gentle P, et al. Patterns of physicalmeasure for use with adolescents in primary care. Arch Pediatr activity among 11 to 16 year old British children. BMJ 1990;Adolesc Med 2001; 155: 554-9 301: 203-5
82. Ainslee PN, Reilly T, Westerterp KR. Estimating human energy 103. Verschuur R, Kemper HCG. Habitual physical activity in Dutchexpenditure. Sports Med 2003; 33: 683-98 teenagers measured by heart rate. In: Binkhorst RA, Kemper
HCG, Saris WHM, editors. Children and exercise XI. Cham-83. Saris WHM. New developments in the assessment of physicalpaign (IL): Human Kinetics, 1985: 194-202activity in children. In: Coudert J, Van Praagh E. editors.
Pediatric work physiology. Paris: Masson, 1992: 107-14 104. Riddoch C, Mahoney C, Murphy N, et al. The physical activitypatterns of Northern Irish schoolchildren ages 11 to 16 years.84. James WPT, Ferro-Luzzi A, Waterlow JC. Definition of chronicPediatr Exerc Sci 1991; 3: 300-9energy deficiency in adults: report of a working party of the
international dietary energy consultancy group. Eur J Clin Nutr 105. Bradfield RB, Chan H, Bradfield NE, et al. Energy expenditures1988; 42: 969-81 and heart rates of Cambridge boys at school. Am J Clin Nutr
1971; 24: 1461-685. Davies PSW. Total energy expenditure in young children. Am JHum Biol 1996; 8: 183-8 106. Verschuur R, Kemper HCG. Habitual physical activity. Med
Sport Sci 1985; 20: 56-6586. Hoos MB, Gerver WJM, Kester AD, et al. Physical activitylevels in children and adolescents. Int J Obes 2003; 27: 605-9 107. Verschuur R, Kemper HCG. The pattern of daily physical
activity. Med Sport Sci 1985; 20: 169-8687. Bratteby LE, Sandhagen B, Fan H, et al. Total energy expendi-ture and physical activity as assessed by the doubly labeled 108. Armstrong N, Bray S. Primary schoolchildren’s physical activi-water method in Swedish adolescents in whom energy intake ty patterns during autumn and summer. Bull Phys Educ 1990;was underestimated by 7-d diet records. Am J Clin Nutr 1998; 26: 23-667: 905-11 109. Biddle S, Mitchell J, Armstrong N. The assessment of physical
88. Ekelund U, Sjostrom M, Yngve A, et al. Physical activity activity in children: a comparison of continuous heart rateassessed by activity monitor and doubly labeled water in monitoring, self-report and interview techniques. Br J Physchildren. Med Sci Sports Exerc 2001; 33: 275-81 Educ Res Suppl 1991; 10: 4-8
89. Hoos MB, Plasqui G, Gerver WJM, et al. Physical activity level 110. McManus A, Armstrong N. Patterns of physical activity amongmeasured by doubly labeled water and accelerometry in chil- primary schoolchildren. In: Ring FJ, editor. Children in sport.dren. Eur J Appl Physiol 2003; 89: 624-6 Bath: University Press, 1995: 17-23
90. O’Connor J, Ball EJ, Steinbeck KS, et al. Measuring physical 111. Falgairette G, Bedu M, Fellmann N, et al. Bioenergetic profileactivity in children: a comparison of four different methods. in 144 boys aged from 6 to 15 years with special reference toPediatr Exerc Sci 2003; 15: 202-15 sexual maturation. Eur J Appl Physiol 1991; 62: 151-6
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)

1086 Armstrong & Welsman
112. Sallo M, Silla R. Physical activity with moderate to vigorous Ilmarinen J, Valimaki I. editors. Children and sport. Newintensity in preschool and first grade schoolchildren. Pediatr York: Springer-Verlag, 1984: 255-61Exerc Sci 1997; 9: 44-54
127. Vincent SD, Pangrazi RP, Raustorp A, et al. Activity levels and113. Welsman JR, Armstrong N. Physical activity patterns of 5 to body mass index of children in the United States, Sweden and
11-year-old children. In: Armstrong N, Kirby BJ, Welsman JR, Australia. Med Sci Sports Exerc 2001; 35: 1367-73editors. Children and exercise XIX: promoting health and
128. Loucaides CA, Chedzoy SM, Bennett N. Pedometer-assessedwell-being. London: E and FN Spon, 1997: 139-44physical (ambulatory) activity in Cypriot children. Eur Phys
114. Gavarry O, Bernard T, Giacomoni M, et al. Continuous heart Educ Rev 2003; 9: 43-55rate monitoring over 1 week in teenagers aged 11-16 years. Eur
129. Freedson P, Pober D, Janz KF. Calibration of accelerometerJ Appl Physiol 1998; 77: 125-32output for children. Med Sci Sports Exerc 2005; 37 (11 Sup-
115. Welsman JR, Armstrong N. Physical activity patterns of 5-topl.): S523-30
7-year-old children and their mothers. Eur J Phys Educ 1998;3: 145-55 130. Raudsepp L, Pall P. Reproducibility and stability of physical
activity in children. Pediatr Exerc Sci 1998; 10: 320-6116. Armstrong N, Welsman JR, Kirby BJ. Longitudinal changes in11-13-year-olds’ physical activity. Acta Paediatr 2000; 89: 131. Nilsson A, Ekelund U, Yngve A, et al. Assessing physical775-80 activity among children with accelerometers using different
time sampling intervals and placements. Pediatr Exerc Sci117. Welsman JR, Armstrong N. Physical activity patterns in secon-2002; 14: 87-96dary school children. Eur J Phys Educ 2000; 5: 147-57
132. Guerra S, Santos P, Ribeiro JC, et al. Assessment of children’s118. Ekelund U, Poortvleit E, Nilsson A, et al. Physical activity inand adolescent’s physical activity levels. Eur Phys Educ Revrelation to aerobic fitness and body fat in 14-to-15 year-old2003; 9: 75-85boys and girls. Eur J Appl Physiol 2001; 85: 195-201
119. Lauter S. Zur genese der fettsucht. Dtsch Arch Klin 1926; 150: 133. Santos P, Guerra S, Ribeiro JC, et al. Age and gender-related315-65 physical activity: a descriptive study in children using acceler-
ometry. J Sports Med Phys Fitness 2003; 43: 85-9120. Saris WHM, Binkhorst RA. The use of pedometer and actome-ter in studying daily physical activity in man: part II -validity 134. Mota J, Santos P, Guerra S, et al. Differences of daily physicalof pedometer and actometer measuring the daily physical activity levels of children according to body mass index.activity. Eur J Appl Physiol 1977; 37: 229-35 Pediatr Exerc Sci 2002; 14: 442-52
121. Rowe DA, Mahar MT, Raedeke TD, et al. Measuring physical 135. Mallam KM, Metcalf BS, Kirby J, et al. Contribution of timet-activity in childhood with pedometers: reliability, reactivity abled physical education to total physical activity in primaryand replacement of missing data. Pediatr Exerc Sci 2004; 16: schoolchildren: cross-sectional study. BMJ 2003; 327: 592-3343-54
136. Berman N, Bailey R, Barstow TJ, et al. Spectral and bout122. Cardon G, De Bourdeaudhuij I. A pilot study comparing pedom-detection analysis of physical activity patterns in healthy,eter counts with reported physical activity in elementaryprepubertal boys and girls. Am J Hum Biol 1998; 10: 289-97schoolchildren. Pediatr Exerc Sci 2004; 16: 355-67
137. Perusse L, Trembley A, Le Blanc C, et al. Genetic and environ-123. Rowlands AV, Eston RG, Ingledew DK. Measurement of physi-mental influences on level of habitual physical activity andcal activity in children with particular reference to the use ofexercise participation. Am J Epidemiol 1989; 129: 1012-22heart rate and pedometry. Sports Med 1997; 24: 258-72
138. Rowland TW. The biological basis of physical activity. Med Sci124. Raustorp A, Pangrazi RP, Stahle A. Physical activity level andSport Exerc 1998; 30: 392-9body mass index among schoolchildren in south eastern Swe-
den. Acta Paediatr 2004; 93: 400-4
125. Skalik K, Fromel K, Sigmund E, et al. Weekly physical activityCorrespondence and offprints: Prof. Neil Armstrong, Chil-in secondary school students (a comparative probe into Czech,
Polish and Swedish conditions). Gymnica 2001; 31: 21-6 dren’s Health and Exercise Research Centre, St Luke’sCampus, University of Exeter, Exeter, EX1 2LU, UK.126. Verschuur R, Kemper HCG, Besseling CWM. Habitual physical
activity and health in 13 and 14 year old teenagers. In: E-mail: [email protected]
2006 Adis Data Information BV. All rights reserved. Sports Med 2006; 36 (12)