The Oswestry Disability Index (Version 2.1a)
8
Spine www.spinejournal.com E83 HEALTH SERVICES RESEARCH SPINE Volume 40, Number 2, pp E83-E90 ©2015, Lippincott Williams & Wilkins DOI: 10.1097/BRS.0000000000000683 Study Design. A cross-sectional study on baseline data. Objective. To translate the Oswestry Disability Index (ODI) version 2.1a into the Dutch language and to validate its use in a cohort of patients with chronic low back pain in secondary spine care. Summary of Background Data. Patient-reported outcome measures (PROMs) are commonly accepted to evaluate the outcome of spine interventions. Functional status is an important outcome in spine research. The ODI is a recommended condition-specific patient-reported outcome measure used to evaluate functional status in patients with back pain. As yet, no formal translated Dutch version exists. Methods. The ODI was translated according to established guidelines. The final version was built into the electronic web-based system in addition with the Roland Morris Disability Questionnaire, the numeric rating scale for pain severity, 36-Item Short Form Health Survey Questionnaire for quality of life, and the hospital anxiety and depression scale. Baseline data were used of 244 patients with chronic low back pain who participated in a combined physical and psychological program. Floor and ceiling effects, internal consistency, and the construct validity were evaluated using quality criteria. Results. The mean ODI (standard deviation) was 39.6 (12.3); minimum 6, maximum 70. Most of the participants (88%) were moderately to severely disabled. Factor analysis determined a 1-factor structure (36% explained variance) and the homogeneity of ODI items is shown (Cronbach α = 0.79). The construct validity From the *Departments of Research and †Orthopedics, Sint Maartenskliniek, GM Nijmegen, The Netherlands; ‡Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Science, University of Oxford, Nuffield Orthopaedic Centre, Oxford, United Kingdom; §Achmea Health Insurance Company, AW Zeist, The Netherlands; and ¶Department of Neurosurgery, Leiden University Medical Center, RC Leiden, The Netherlands. Acknowledgment date: April 25, 2014. First revision date: September 5, 2014. Second revision date: October 8, 2014. Acceptance date: October 26, 2014. The manuscript submitted does not contain information about medical device(s)/drug(s). No funds were received in support of this work. Relevant financial activities outside the submitted work: royalties, grants, payment for lectures. Address correspondence and reprint requests to Miranda L. van Hooff, MSc, Department of Research, Sint Maartenskliniek, Box 9011, 6500 GM Nijmegen, The Netherlands; E-mail: [email protected] L ow back pain (LBP) has the largest global burden of disease 1 and is associated with a substantial amount of morbidity. Functional status is an important outcome in research evaluating surgical and nonsurgical interventions for LBP 2,3 and to assess patients’ progress in routine clini- cal practice. Limitations in functional status (disability) as assessed by patient-reported outcome measures (PROMs) is widely accepted 4 and the Oswestry Disability Index (ODI version 2.1a) 5,6 is commonly used as a PROM. The ODI has been translated into various languages. 7–22 Recently, based on international consensus, the ODI is included as a PROM in the International Consortium for Health Outcomes Measure- ment standard set for LBP. 3,23 Prior to its use, the questionnaire should be translated to the native language of users and should have undergone a cross-cultural adaptation and validation process. A multistep approach is recommended to reach equivalence between the original and the target language. 24,25 A systematic search of literature and a discussion with the initial developer of the ODI revealed that, as yet no formal Dutch version 2.1a exists. The objectives of this study were (1) to translate and adapt the ODI version 2.1a into the Dutch is supported as all (6:6) the a priori hypotheses were confirmed. Moreover, the ODI and Roland Morris Disability Questionnaire, showed a strong significant correlation ( r = 0.68, P < 0.001) and an overlap: mean difference of −18 (95% limits of agreement: −44 to 8). Conclusion. The Dutch ODI version 2.1a is a valid and valuable tool for the measurement of functional status and disability among Dutch patients with chronic low back pain. This translated condition- specific patient-reported outcome measure version is recommended for use in future back pain research and to evaluate outcome of back care in the Netherlands. Key words: low back pain, Oswestry Disability Index, outcome measure, outcome, validity, surgery, functional status, Roland Morris Disability Questionnaire, patient-reported outcome measure, outcome assessment, condition-specific questionnaire, cross- cultural adaptation, quality, spine, care. Level of Evidence: 4 Spine 2015;40:E83–E90 The Oswestry Disability Index (Version 2.1a) Validation of a Dutch Language Version Miranda L. van Hooff, MSc,* Maarten Spruit, MD, PhD ,† Jeremy C.T. Fairbank, MA, MD, FRCS,‡ Jacques van Limbeek, MD, PhD ,§ and Wilco C.H. Jacobs, PhD¶ Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The Oswestry Disability Index (Version 2.1a)
Spine www.spinejournal.com E83
HEALTH SERVICES RESEARCH
SPINE Volume 40 , Number 2 , pp E83 - E90 ©2015, Lippincott Williams & Wilkins
DOI: 10.1097/BRS.0000000000000683
Study Design. A cross-sectional study on baseline data. Objective. To translate the Oswestry Disability Index (ODI) version 2.1a into the Dutch language and to validate its use in a cohort of patients with chronic low back pain in secondary spine care. Summary of Background Data. Patient-reported outcome measures (PROMs) are commonly accepted to evaluate the outcome of spine interventions. Functional status is an important outcome in spine research. The ODI is a recommended condition-specifi c patient-reported outcome measure used to evaluate functional status in patients with back pain. As yet, no formal translated Dutch version exists. Methods. The ODI was translated according to established guidelines. The fi nal version was built into the electronic web-based system in addition with the Roland Morris Disability Questionnaire, the numeric rating scale for pain severity, 36-Item Short Form Health Survey Questionnaire for quality of life, and the hospital anxiety and depression scale. Baseline data were used of 244 patients with chronic low back pain who participated in a combined physical and psychological program. Floor and ceiling effects, internal consistency, and the construct validity were evaluated using quality criteria. Results. The mean ODI (standard deviation) was 39.6 (12.3); minimum 6, maximum 70. Most of the participants (88%) were moderately to severely disabled. Factor analysis determined a 1-factor structure (36% explained variance) and the homogeneity of ODI items is shown (Cronbach α = 0.79). The construct validity
From the * Departments of Research and † Orthopedics, Sint Maartenskliniek, GM Nijmegen, The Netherlands ; ‡ Nuffi eld Department of Orthopaedics, Rheumatology, and Musculoskeletal Science, University of Oxford, Nuffi eld Orthopaedic Centre, Oxford, United Kingdom ; § Achmea Health Insurance Company, AW Zeist, The Netherlands; and ¶ Department of Neurosurgery, Leiden University Medical Center, RC Leiden, The Netherlands.
Acknowledgment date: April 25, 2014. First revision date: September 5, 2014. Second revision date: October 8, 2014. Acceptance date: October 26, 2014.
The manuscript submitted does not contain information about medical device(s)/drug(s).
No funds were received in support of this work.
Relevant fi nancial activities outside the submitted work: royalties, grants, payment for lectures.
Address correspondence and reprint requests to Miranda L. van Hooff, MSc, Department of Research, Sint Maartenskliniek, Box 9011, 6500 GM Nijmegen, The Netherlands; E-mail: [email protected]
Low back pain (LBP) has the largest global burden of disease 1 and is associated with a substantial amount of morbidity. Functional status is an important outcome
in research evaluating surgical and nonsurgical interventions for LBP 2 , 3 and to assess patients’ progress in routine clini-cal practice. Limitations in functional status (disability) as assessed by patient-reported outcome measures (PROMs) is widely accepted 4 and the Oswestry Disability Index (ODI version 2.1a) 5 , 6 is commonly used as a PROM. The ODI has been translated into various languages. 7–22 Recently, based on international consensus, the ODI is included as a PROM in the International Consortium for Health Outcomes Measure-ment standard set for LBP. 3 , 23
Prior to its use, the questionnaire should be translated to the native language of users and should have undergone a cross-cultural adaptation and validation process. A multistep approach is recommended to reach equivalence between the original and the target language. 24 , 25
A systematic search of literature and a discussion with the initial developer of the ODI revealed that, as yet no formal Dutch version 2.1a exists. The objectives of this study were (1) to translate and adapt the ODI version 2.1a into the Dutch
is supported as all (6:6) the a priori hypotheses were confi rmed. Moreover, the ODI and Roland Morris Disability Questionnaire, showed a strong signifi cant correlation ( r = 0.68, P < 0.001) and an overlap: mean difference of − 18 (95% limits of agreement: − 44 to 8). Conclusion. The Dutch ODI version 2.1a is a valid and valuable tool for the measurement of functional status and disability among Dutch patients with chronic low back pain. This translated condition-specifi c patient-reported outcome measure version is recommended for use in future back pain research and to evaluate outcome of back care in the Netherlands. Key words: low back pain , Oswestry Disability Index , outcome measure , outcome , validity , surgery , functional status , Roland Morris Disability Questionnaire , patient-reported outcome measure , outcome assessment , condition-specifi c questionnaire , cross-cultural adaptation , quality , spine , care . Level of Evidence: 4 Spine 2015;40:E83–E90
The Oswestry Disability Index (Version 2.1a) Validation of a Dutch Language Version
Miranda L. van Hooff , MSc, * Maarten Spruit , MD, PhD , † Jeremy C.T. Fairbank , MA, MD, FRCS , ‡ Jacques van Limbeek , MD, PhD , § and Wilco C.H. Jacobs , PhD ¶
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
SPINE140559_LR E83SPINE140559_LR E83 11/12/14 1:38 PM11/12/14 1:38 PM

HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
E84 www.spinejournal.com January 2015
language and (2) to investigate the validity and internal con-sistency of the translation in a cohort of chronic low back pain (CLBP).
MATERIALS AND METHODS
Patients Orthopedic spine surgeons of a specialized hospital for spine care recruited patients with CLBP. The patients were referred to and participated in a short, intensive two-week Combined Physical and Psychological (CPP) program, as provided by RealHealthNL Sint Maartenskliniek Nijmegen (Zevenheuvelenweg, Berg en Dal, The Netherlands). 26
Translation and Cross-cultural Adaptation Procedure We used a multistep approach 24 , 25 using published guide-lines 24 , 27 recommended by the American Academy of Ortho-pedic Surgeons Outcomes Committee. The fi rst step was a forward translation performed by 2 native Dutch speakers (T-1, T-2) with a background in health sciences, and famil-iar with the concepts being examined. A third native Dutch speaker (T-3) without a medical education assisted in the translation with an appreciation of the level of understanding of the typical patient that would ultimately be completing the questionnaire (naive translator). The second step was a com-parison of the translation with the original and consensus was reached in case any discrepancies existed. The versions were synthesized to 1 common Dutch version; T-123. The third step was a back translation of T-123 by 2 native English speak-ers (1 American and 1 British), both bilingual with Dutch as their second language. One was familiar with the concepts of disability and the other was a professional translator in the medical fi eld. Both carried out their back translation indepen-dently (BT-1, BT-2). The fourth step was to develop a prefi nal Dutch version by an expert committee with access to all trans-lations. The expert committee consisted of all translators, an orthopedic spine surgeon, and an independent methodologist. The committee examined the translations and discussed all parts of the questionnaire (instructions, items, and response options). The fi fth step was to test the prefi nal version in a group of 10 patients with CLBP. They were asked to complete this version and to give their comments. All fi ndings of this phase of the adaptation process (face validity) were evaluated by the expert committee before the fi nal Dutch version (ODI version 2.1a) was compiled and further tested for validity.
Evaluation of the Psychometric Properties of the Dutch ODI Version 2.1a
Procedure and Data Collection The Dutch ODI version 2.1a was built into the electronic web-based system of the CPP program, together with all other questionnaires. Outcome assessment is a routine part of the program and patients are systematically followed over time. 28 Therefore, we were able to extract all relevant pretreatment data from the database. All measures, except the ODI, have previously been validated in CLBP samples.
Self-report Measures
Oswestry Disability Index (Version 2.1a) The ODI was originally developed in 1980 (version 1) 5 and slightly modifi ed in 1989 (version 2.1), 29 which is regularly used today. 30 A single word change in the introductory state-ment has led to the 2.1a version. 31 This ODI version measures the impact of LBP on the patients’ functional ability in 10 domains of activities in daily life (“pain intensity,” “personal care,” “lifting,” “walking,” “sitting,” “standing,” “sleeping,” “sex life,” “social life,” and “travelling”). Each domain or item consists of 6 statements (score, 0–5) and is scored by the patient in reference to his/her current functional status. The total score is a sum of all completed items and expressed as a percentage of the maximum score. 6 To avoid confusion with percentages as mathematical expressions the percentage is referred to as a total score, ranging from 0 to 100, with higher scores indicating higher disability. 11
To validate the Dutch ODI, we used several measures: (1) Roland Morris Disability Questionnaire (RMDQ; score 0–24), 32 with higher scores indicating higher disability; (2) numeric rating scale (NRS pain ; score 0–100) 33 with higher scores indicating higher levels of pain severity; (3) health-related quality of life measured with the 36-Item Short Form Health Survey Questionnaire (SF-36), 34 consisting of 2 sum-mary scores of 8 subscales: Physical Component Score and Mental Component Score (both scores 0–100); and (4) hospital anxiety and depression scale (HADS) containing 2 subscales to screen for disturbance of symptoms of anxiety (HADS-A and HADS-D; both scores 0–21). 35
Procedure and Criteria “Floor and ceiling effects” 36 were determined by calculating the number of individuals obtaining the lowest (0–10) or the highest (90–100) ODI scores. We included range of 10 points referring to the minimal clinically important difference, 37 which is widely used to report a clinically relevant difference between assessments. Floor and ceiling effects are considered to be present if more than 15% of the patients achieved the extreme ends. 36
To examine “internal consistency,” an exploratory fac-tor analysis with a varimax rotation was conducted to deter-mine whether the items form 1 predefi ned factor covering the overall scale. 36 A factor analysis with a principal component technique was chosen as the aim was to explore an underly-ing construct rather than to reduce the number of items. 38 To test the factorability, interitem correlations of the 10 items of the ODI were inspected and the signifi cance level of the Bartlett test of sphericity and the Kaiser-Meyer-Olkin mea-sure of sampling adequacy were calculated. A signifi cant Kaiser-Meyer-Olkin measure of sampling adequacy value of more than 0.6 was considered acceptable. 38 , 39 The number of factors was determined by visual inspection of the screen plot, the percentage of unique variance ( > 5%), eigenvalues more than 1, and factor interpretability. Only items with fac-tor loadings more than 0.40 (20% explained variance) were retained and items with cross-loadings on more than 1 factor
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
SPINE140559_LR E84SPINE140559_LR E84 11/12/14 1:38 PM11/12/14 1:38 PM
HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
Spine www.spinejournal.com E85
within 0.20 of the primary loading were dropped because of inadequate discrimination. Moreover, Cronbach α was calcu-lated. A Cronbach α between 0.70 and 0.95 indicates good internal consistency. 36
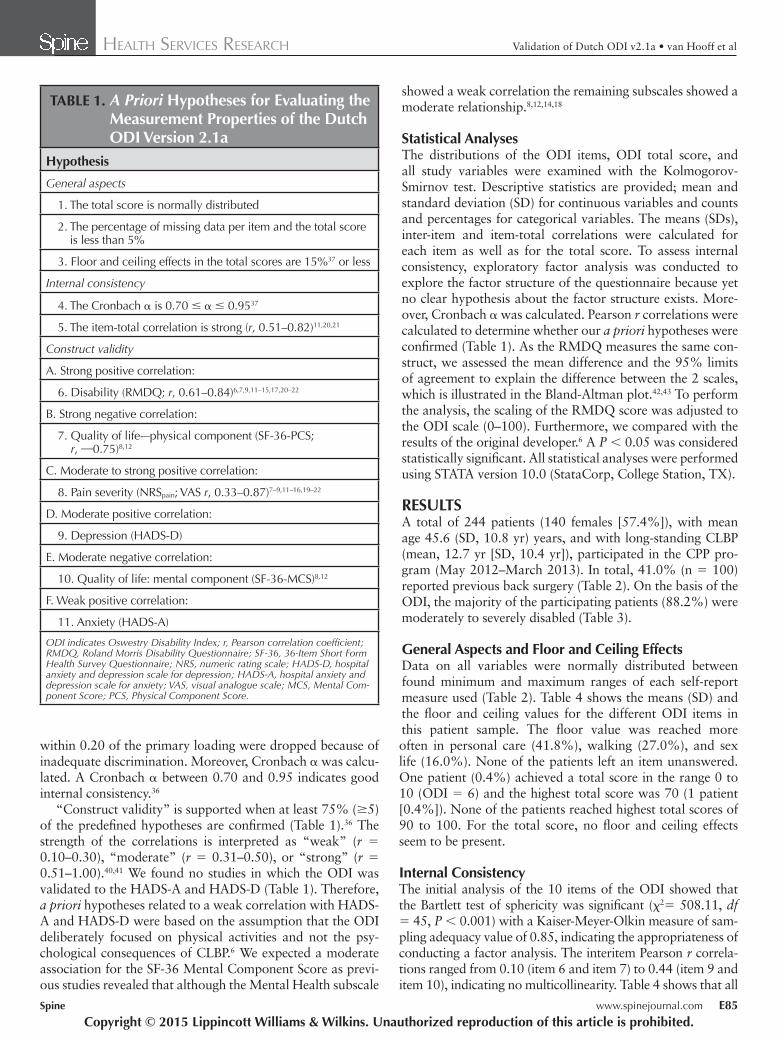
“Construct validity” is supported when at least 75% ( ≥ 5) of the predefi ned hypotheses are confi rmed ( Table 1 ). 36 The strength of the correlations is interpreted as “weak” ( r = 0.10–0.30), “moderate” ( r = 0.31–0.50), or “strong” ( r = 0.51–1.00). 40 , 41 We found no studies in which the ODI was validated to the HADS-A and HADS-D ( Table 1 ). Therefore, a priori hypotheses related to a weak correlation with HADS-A and HADS-D were based on the assumption that the ODI deliberately focused on physical activities and not the psy-chological consequences of CLBP. 6 We expected a moderate association for the SF-36 Mental Component Score as previ-ous studies revealed that although the Mental Health subscale
showed a weak correlation the remaining subscales showed a moderate relationship. 8 , 12 , 14 , 18
Statistical Analyses The distributions of the ODI items, ODI total score, and all study variables were examined with the Kolmogorov-Smirnov test. Descriptive statistics are provided; mean and standard deviation (SD) for continuous variables and counts and percentages for categorical variables. The means (SDs), inter-item and item-total correlations were calculated for each item as well as for the total score. To assess internal consistency, exploratory factor analysis was conducted to explore the factor structure of the questionnaire because yet no clear hypothesis about the factor structure exists. More-over, Cronbach α was calculated. Pearson r correlations were calculated to determine whether our a priori hypotheses were confi rmed ( Table 1 ). As the RMDQ measures the same con-struct, we assessed the mean difference and the 95% limits of agreement to explain the difference between the 2 scales, which is illustrated in the Bland-Altman plot. 42 , 43 To perform the analysis, the scaling of the RMDQ score was adjusted to the ODI scale (0–100). Furthermore, we compared with the results of the original developer. 6 A P < 0.05 was considered statistically signifi cant. All statistical analyses were performed using STATA version 10.0 (StataCorp, College Station, TX).
RESULTS A total of 244 patients (140 females [57.4%]), with mean age 45.6 (SD, 10.8 yr) years, and with long-standing CLBP (mean, 12.7 yr [SD, 10.4 yr]), participated in the CPP pro-gram (May 2012–March 2013). In total, 41.0% (n = 100) reported previous back surgery ( Table 2 ). On the basis of the ODI, the majority of the participating patients (88.2%) were moderately to severely disabled ( Table 3 ).
General Aspects and Floor and Ceiling Effects Data on all variables were normally distributed between found minimum and maximum ranges of each self-report measure used ( Table 2 ). Table 4 shows the means (SD) and the fl oor and ceiling values for the different ODI items in this patient sample. The fl oor value was reached more often in personal care (41.8%), walking (27.0%), and sex life (16.0%). None of the patients left an item unanswered. One patient (0.4%) achieved a total score in the range 0 to 10 (ODI = 6) and the highest total score was 70 (1 patient [0.4%]). None of the patients reached highest total scores of 90 to 100. For the total score, no fl oor and ceiling effects seem to be present.
Internal Consistency The initial analysis of the 10 items of the ODI showed that the Bartlett test of sphericity was signifi cant ( χ 2 = 508.11, df = 45, P < 0.001) with a Kaiser-Meyer-Olkin measure of sam-pling adequacy value of 0.85, indicating the appropriateness of conducting a factor analysis. The interitem Pearson r correla-tions ranged from 0.10 (item 6 and item 7) to 0.44 (item 9 and item 10), indicating no multicollinearity. Table 4 shows that all
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
TABLE 1. A Priori Hypotheses for Evaluating the Measurement Properties of the Dutch ODI Version 2.1a
Hypothesis
General aspects
1. The total score is normally distributed
2. The percentage of missing data per item and the total score is less than 5%
3. Floor and ceiling effects in the total scores are 15% 37 or less
Internal consistency
4. The Cronbach α is 0.70 ≤ α ≤ 0.95 37
5. The item-total correlation is strong ( r , 0.51–0.82) 11 , 20 , 21
Construct validity
A. Strong positive correlation:
6. Disability (RMDQ; r , 0.61–0.84) 6 , 7 , 9 , 11–15 , 17 , 20–22
B. Strong negative correlation:
7. Quality of life-–physical component (SF-36-PCS; r , — 0.75) 8 , 12
C. Moderate to strong positive correlation:
8. Pain severity (NRS pain ; VAS r , 0.33–0.87) 7–9 , 11–16 , 19–22
D. Moderate positive correlation:
9. Depression (HADS-D)
E. Moderate negative correlation:
10. Quality of life: mental component (SF-36-MCS) 8 , 12
F. Weak positive correlation:
11. Anxiety (HADS-A)
ODI indicates Oswestry Disability Index; r , Pearson correlation coeffi cient; RMDQ, Roland Morris Disability Questionnaire; SF-36, 36-Item Short Form Health Survey Questionnaire; NRS, numeric rating scale; HADS-D, hospital anxiety and depression scale for depression; HADS-A, hospital anxiety and depression scale for anxiety; VAS, visual analogue scale; MCS, Mental Com-ponent Score; PCS, Physical Component Score.
SPINE140559_LR E85SPINE140559_LR E85 11/12/14 1:38 PM11/12/14 1:38 PM
HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
E86 www.spinejournal.com January 2015
items are similarly associated with the total score. The screen plot of eigenvalues, the percentage of variance, and the num-ber of eigenvalues more than 1 indicated a 1-factor solution. Because of a 1-factor solution, no rotation could be performed. This factor with an eigenvalue of 2.8 explains 35.6% of the total variance ( Table 4 ). The Cronbach α was 0.79 and the item-total correlations ranged from 0.48 (for item 7; “sleep-ing”) to 0.68 (for items 9 and 10; “social life” and “travel-ling”) ( Table 4 ), confi rming the internal consistency of the ODI in our patient sample.
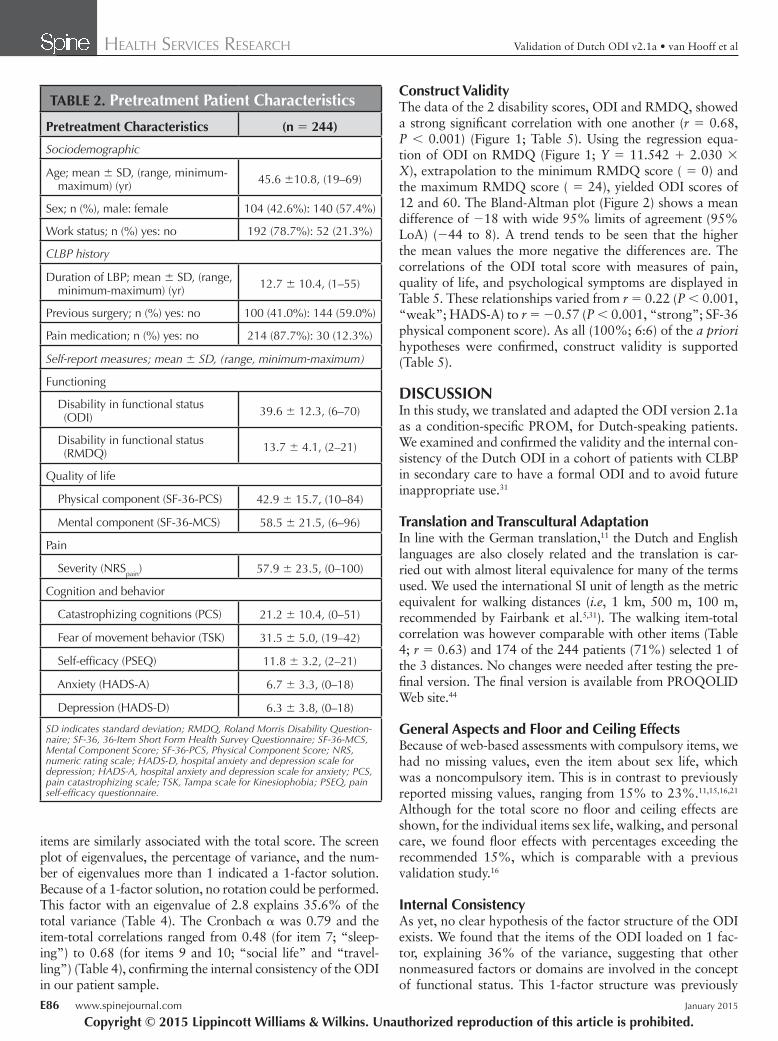
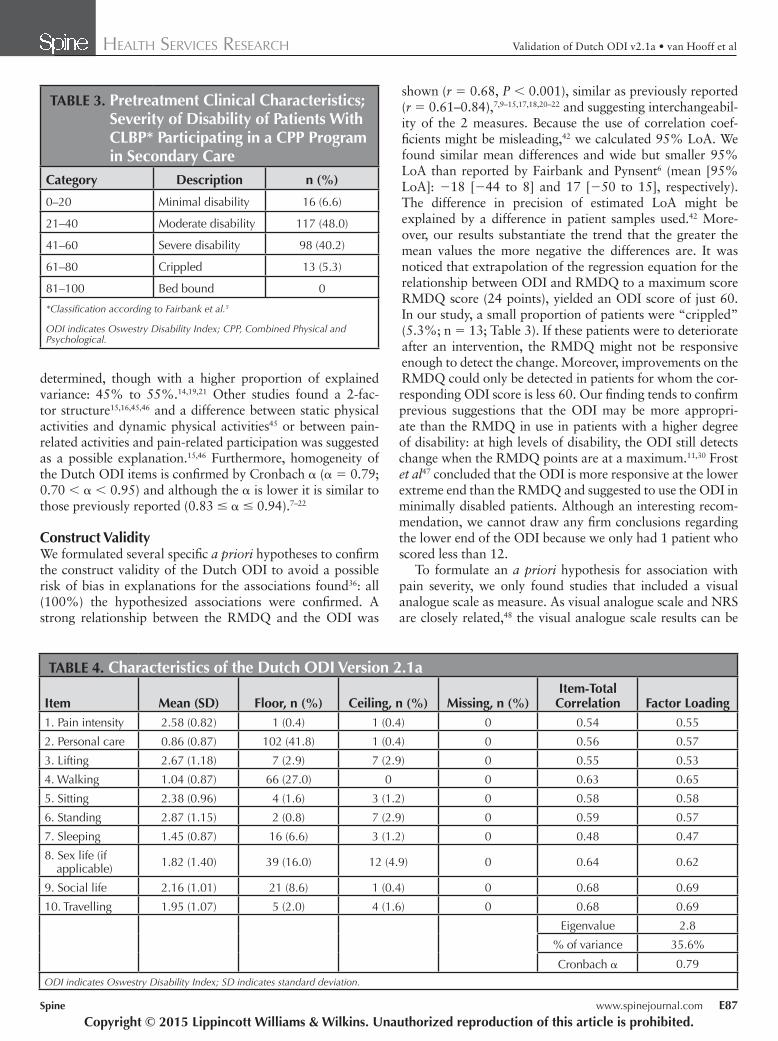
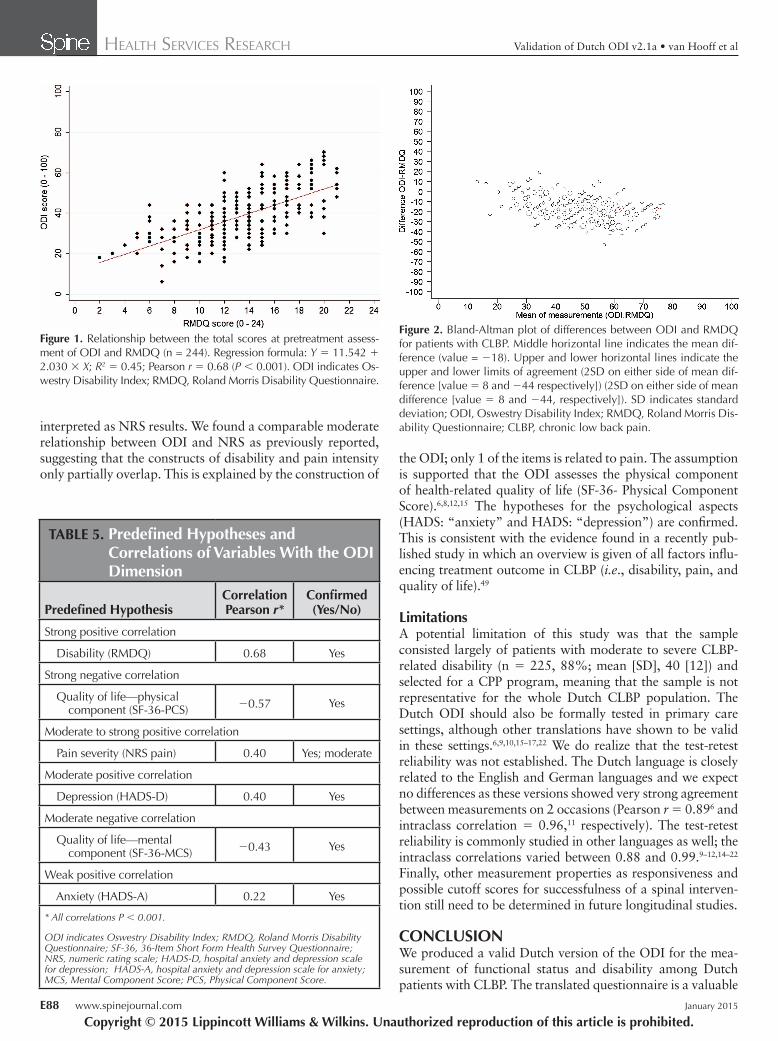
Construct Validity The data of the 2 disability scores, ODI and RMDQ, showed a strong signifi cant correlation with one another ( r = 0.68, P < 0.001) ( Figure 1 ; Table 5 ). Using the regression equa-tion of ODI on RMDQ ( Figure 1 ; Y = 11.542 + 2.030 × X ), extrapolation to the minimum RMDQ score ( = 0) and the maximum RMDQ score ( = 24), yielded ODI scores of 12 and 60. The Bland-Altman plot ( Figure 2 ) shows a mean difference of − 18 with wide 95% limits of agreement (95% LoA) ( − 44 to 8). A trend tends to be seen that the higher the mean values the more negative the differences are. The correlations of the ODI total score with measures of pain, quality of life, and psychological symptoms are displayed in Table 5 . These relationships varied from r = 0.22 ( P < 0.001, “weak”; HADS-A) to r = − 0.57 ( P < 0.001, “strong”; SF-36 physical component score). As all (100%; 6:6) of the a priori hypotheses were confi rmed, construct validity is supported ( Table 5 ).
DISCUSSION In this study, we translated and adapted the ODI version 2.1a as a condition-specifi c PROM, for Dutch-speaking patients. We examined and confi rmed the validity and the internal con-sistency of the Dutch ODI in a cohort of patients with CLBP in secondary care to have a formal ODI and to avoid future inappropriate use. 31
Translation and Transcultural Adaptation In line with the German translation, 11 the Dutch and English languages are also closely related and the translation is car-ried out with almost literal equivalence for many of the terms used. We used the international SI unit of length as the metric equivalent for walking distances ( i.e , 1 km, 500 m, 100 m, recommended by Fairbank et al. 5 , 31 ). The walking item-total correlation was however comparable with other items ( Table 4 ; r = 0.63) and 174 of the 244 patients (71%) selected 1 of the 3 distances. No changes were needed after testing the pre-fi nal version. The fi nal version is available from PROQOLID Web site. 44
General Aspects and Floor and Ceiling Effects Because of web-based assessments with compulsory items, we had no missing values, even the item about sex life, which was a noncompulsory item. This is in contrast to previously reported missing values, ranging from 15% to 23%. 11 , 15 , 16 , 21 Although for the total score no fl oor and ceiling effects are shown, for the individual items sex life, walking, and personal care, we found fl oor effects with percentages exceeding the recommended 15%, which is comparable with a previous validation study. 16
Internal Consistency As yet, no clear hypothesis of the factor structure of the ODI exists. We found that the items of the ODI loaded on 1 fac-tor, explaining 36% of the variance, suggesting that other nonmeasured factors or domains are involved in the concept of functional status. This 1-factor structure was previously
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
TABLE 2. Pretreatment Patient Characteristics
Pretreatment Characteristics (n = 244)
Sociodemographic
Age; mean ± SD, (range, minimum-maximum) (yr) 45.6 ± 10.8, (19–69)
Sex; n (%), male: female 104 (42.6%): 140 (57.4%)
Work status; n (%) yes: no 192 (78.7%): 52 (21.3%)
CLBP history
Duration of LBP; mean ± SD, (range, minimum-maximum) (yr) 12.7 ± 10.4, (1–55)
Previous surgery; n (%) yes: no 100 (41.0%): 144 (59.0%)
Pain medication; n (%) yes: no 214 (87.7%): 30 (12.3%)
Self-report measures; mean ± SD, (range, minimum-maximum)
Functioning
Disability in functional status (ODI) 39.6 ± 12.3, (6–70)
Disability in functional status (RMDQ) 13.7 ± 4.1, (2–21)
Quality of life
Physical component (SF-36-PCS) 42.9 ± 15.7, (10–84)
Mental component (SF-36-MCS) 58.5 ± 21.5, (6–96)
Pain
Severity (NRS pain ) 57.9 ± 23.5, (0–100)
Cognition and behavior
Catastrophizing cognitions (PCS) 21.2 ± 10.4, (0–51)
Fear of movement behavior (TSK) 31.5 ± 5.0, (19–42)
Self-effi cacy (PSEQ) 11.8 ± 3.2, (2–21)
Anxiety (HADS-A) 6.7 ± 3.3, (0–18)
Depression (HADS-D) 6.3 ± 3.8, (0–18)
SD indicates standard deviation; RMDQ, Roland Morris Disability Question-naire; SF-36, 36-Item Short Form Health Survey Questionnaire; SF-36-MCS, Mental Component Score; SF-36-PCS, Physical Component Score; NRS, numeric rating scale; HADS-D, hospital anxiety and depression scale for depression; HADS-A, hospital anxiety and depression scale for anxiety; PCS, pain catastrophizing scale; TSK, Tampa scale for Kinesiophobia; PSEQ, pain self-effi cacy questionnaire.
SPINE140559_LR E86SPINE140559_LR E86 11/12/14 1:38 PM11/12/14 1:38 PM
HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
Spine www.spinejournal.com E87
determined, though with a higher proportion of explained variance: 45% to 55%. 14 , 19 , 21 Other studies found a 2-fac-tor structure 15 , 16 , 45 , 46 and a difference between static physical activities and dynamic physical activities 45 or between pain-related activities and pain-related participation was suggested as a possible explanation. 15 , 46 Furthermore, homogeneity of the Dutch ODI items is confi rmed by Cronbach α ( α = 0.79; 0.70 < α < 0.95) and although the α is lower it is similar to those previously reported (0.83 ≤ α ≤ 0.94). 7–22
Construct Validity We formulated several specifi c a priori hypotheses to confi rm the construct validity of the Dutch ODI to avoid a possible risk of bias in explanations for the associations found 36 : all (100%) the hypothesized associations were confi rmed. A strong relationship between the RMDQ and the ODI was
shown ( r = 0.68, P < 0.001), similar as previously reported ( r = 0.61–0.84), 7 , 9–15 , 17 , 18 , 20–22 and suggesting interchangeabil-ity of the 2 measures. Because the use of correlation coef-fi cients might be misleading, 42 we calculated 95% LoA. We found similar mean differences and wide but smaller 95% LoA than reported by Fairbank and Pynsent 6 (mean [95% LoA]: − 18 [ − 44 to 8] and 17 [ − 50 to 15], respectively). The difference in precision of estimated LoA might be explained by a difference in patient samples used. 42 More-over, our results substantiate the trend that the greater the mean values the more negative the differences are. It was noticed that extrapolation of the regression equation for the relationship between ODI and RMDQ to a maximum score RMDQ score (24 points), yielded an ODI score of just 60. In our study, a small proportion of patients were “crippled” (5.3%; n = 13; Table 3 ). If these patients were to deteriorate after an intervention, the RMDQ might not be responsive enough to detect the change. Moreover, improvements on the RMDQ could only be detected in patients for whom the cor-responding ODI score is less 60. Our fi nding tends to confi rm previous suggestions that the ODI may be more appropri-ate than the RMDQ in use in patients with a higher degree of disability: at high levels of disability, the ODI still detects change when the RMDQ points are at a maximum. 11 , 30 Frost et al 47 concluded that the ODI is more responsive at the lower extreme end than the RMDQ and suggested to use the ODI in minimally disabled patients. Although an interesting recom-mendation, we cannot draw any fi rm conclusions regarding the lower end of the ODI because we only had 1 patient who scored less than 12.
To formulate an a priori hypothesis for association with pain severity, we only found studies that included a visual analogue scale as measure. As visual analogue scale and NRS are closely related, 48 the visual analogue scale results can be
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
TABLE 3. Pretreatment Clinical Characteristics; Severity of Disability of Patients With CLBP* Participating in a CPP Program in Secondary Care
Category Description n (%)
0–20 Minimal disability 16 (6.6)
21–40 Moderate disability 117 (48.0)
41–60 Severe disability 98 (40.2)
61–80 Crippled 13 (5.3)
81–100 Bed bound 0
*Classifi cation according to Fairbank et al . 5
ODI indicates Oswestry Disability Index; CPP, Combined Physical and Psychological.
TABLE 4. Characteristics of the Dutch ODI Version 2.1a
Item Mean (SD) Floor, n (%) Ceiling, n (%) Missing, n (%)Item-Total Correlation Factor Loading
1. Pain intensity 2.58 (0.82) 1 (0.4) 1 (0.4) 0 0.54 0.55
2. Personal care 0.86 (0.87) 102 (41.8) 1 (0.4) 0 0.56 0.57
3. Lifting 2.67 (1.18) 7 (2.9) 7 (2.9) 0 0.55 0.53
4. Walking 1.04 (0.87) 66 (27.0) 0 0 0.63 0.65
5. Sitting 2.38 (0.96) 4 (1.6) 3 (1.2) 0 0.58 0.58
6. Standing 2.87 (1.15) 2 (0.8) 7 (2.9) 0 0.59 0.57
7. Sleeping 1.45 (0.87) 16 (6.6) 3 (1.2) 0 0.48 0.47
8. Sex life (if applicable) 1.82 (1.40) 39 (16.0) 12 (4.9) 0 0.64 0.62
9. Social life 2.16 (1.01) 21 (8.6) 1 (0.4) 0 0.68 0.69
10. Travelling 1.95 (1.07) 5 (2.0) 4 (1.6) 0 0.68 0.69
Eigenvalue 2.8
% of variance 35.6%
Cronbach α 0.79 ODI indicates Oswestry Disability Index; SD indicates standard deviation.
SPINE140559_LR E87SPINE140559_LR E87 11/12/14 1:38 PM11/12/14 1:38 PM
HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
E88 www.spinejournal.com January 2015
the ODI; only 1 of the items is related to pain. The assumption is supported that the ODI assesses the physical component of health-related quality of life (SF-36- Physical Component Score). 6 , 8 , 12 , 15 The hypotheses for the psychological aspects (HADS: “anxiety” and HADS: “depression”) are confi rmed. This is consistent with the evidence found in a recently pub-lished study in which an overview is given of all factors infl u-encing treatment outcome in CLBP ( i.e ., disability, pain, and quality of life). 49
Limitations A potential limitation of this study was that the sample consisted largely of patients with moderate to severe CLBP-related disability (n = 225, 88%; mean [SD], 40 [12]) and selected for a CPP program, meaning that the sample is not representative for the whole Dutch CLBP population. The Dutch ODI should also be formally tested in primary care settings, although other translations have shown to be valid in these settings. 6 , 9 , 10 , 15–17 , 22 We do realize that the test-retest reliability was not established. The Dutch language is closely related to the English and German languages and we expect no differences as these versions showed very strong agreement between measurements on 2 occasions (Pearson r = 0.89 6 and intraclass correlation = 0.96, 11 respectively). The test-retest reliability is commonly studied in other languages as well; the intraclass correlations varied between 0.88 and 0.99. 9–12 , 14–22 Finally, other measurement properties as responsiveness and possible cutoff scores for successfulness of a spinal interven-tion still need to be determined in future longitudinal studies.
CONCLUSION We produced a valid Dutch version of the ODI for the mea-surement of functional status and disability among Dutch patients with CLBP. The translated questionnaire is a valuable
interpreted as NRS results. We found a comparable moderate relationship between ODI and NRS as previously reported, suggesting that the constructs of disability and pain intensity only partially overlap. This is explained by the construction of
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Figure 1. Relationship between the total scores at pretreatment assess-ment of ODI and RMDQ (n = 244). Regression formula: Y = 11.542 + 2.030 × X ; R 2 = 0.45; Pearson r = 0.68 ( P < 0.001). ODI indicates Os-westry Disability Index; RMDQ, Roland Morris Disability Questionnaire.
TABLE 5. Predefi ned Hypotheses and Correlations of Variables With the ODI Dimension
Predefi ned HypothesisCorrelation Pearson r*
Confi rmed (Yes/No)
Strong positive correlation
Disability (RMDQ) 0.68 Yes
Strong negative correlation
Quality of life—physical component (SF-36-PCS) − 0.57 Yes
Moderate to strong positive correlation
Pain severity (NRS pain) 0.40 Yes; moderate
Moderate positive correlation
Depression (HADS-D) 0.40 Yes
Moderate negative correlation
Quality of life—mental component (SF-36-MCS) − 0.43 Yes
Weak positive correlation
Anxiety (HADS-A) 0.22 Yes
* All correlations P < 0.001.
ODI indicates Oswestry Disability Index; RMDQ, Roland Morris Disability Questionnaire; SF-36, 36-Item Short Form Health Survey Questionnaire; NRS, numeric rating scale; HADS-D, hospital anxiety and depression scale for depression; HADS-A, hospital anxiety and depression scale for anxiety; MCS, Mental Component Score; PCS, Physical Component Score.
Figure 2. Bland-Altman plot of differences between ODI and RMDQ for patients with CLBP. Middle horizontal line indicates the mean dif-ference (value = − 18). Upper and lower horizontal lines indicate the upper and lower limits of agreement (2SD on either side of mean dif-ference [value = 8 and − 44 respectively]) (2SD on either side of mean difference [value = 8 and − 44, respectively]). SD indicates standard deviation; ODI, Oswestry Disability Index; RMDQ, Roland Morris Dis-ability Questionnaire; CLBP, chronic low back pain.
SPINE140559_LR E88SPINE140559_LR E88 11/12/14 1:38 PM11/12/14 1:38 PM

HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
Spine www.spinejournal.com E89
tool and the authors recommend this translated 2.1a version as a condition-specifi c PROM for use in future back pain research purposes and to evaluate outcome of back care. The offi cial version is implemented and used in the Dutch Spine Surgery Registry in the Netherlands.
11. Mannion AF , Junge A , Fairbank JC , et al. Development of a Ger-man version of the Oswestry Disability Index. Part 1: cross-cultural adaptation, reliability, and validity . Eur Spine J 2006 ; 15 : 55 – 65 .
12. Lue YJ , Hsieh CL , Huang MH , et al. Development of a Chinese version of the Oswestry Disability Index version 2.1 . Spine (Phila Pa 1976) 2008 ; 33 : 2354 – 60 .
13. Vogler D , Paillex R , Norberg M , et al. Cross-cultural validation of the Oswestry Disability Index in French . Ann Readapt Med Phys 2008 ; 51 : 379 – 85 .
14. Monticone M , Baiardi P , Ferrari S , et al. Development of the Italian version of the Oswestry Disability Index (ODI-I): a cross-cultural adaptation, reliability, and validity study . Spine (Phila Pa 1976) 2009 ; 34 : 2090 – 5 .
15. Payares K , Lugo LH , Morales V , et al. Validation in Colombia of the Oswestry Disability Questionnaire in patients with low back pain . Spine (Phila Pa 1976) 2011 ; 36 : E1730 – 5 .
16. Pekkanen L , Kautiainen H , Ylinen J , et al. Reliability and validity study of the Finnish version 2.0 of the Oswestry Disability Index . Spine (Phila Pa 1976) 2011 ; 36 : 332 – 8 .
17. Denis I , Fortin L . Development of a French-Canadian version of the Oswestry Disability Index: cross-cultural adaptation and vali-dation . Spine (Phila Pa 1976) 2012 ; 37 : E439 – 44 .
18. Vigatto R , Alexandre NM , Correa Filho HR . Development of a Brazilian Portuguese version of the Oswestry Disability Index: cross-cultural adaptation, reliability, and validity . Spine (Phila Pa 1976) 2007 ; 32 : 481 – 6 .
19. Valasek T , Varga PP , Szoverfi Z , et al. Reliability and validity study on the Hungarian versions of the Oswestry Disability Index and the Quebec Back Pain Disability Scale . Eur Spine J 2013 ; 22 : 1010 – 8 .
20. Joshi VD , Raiturker PP , Kulkarni AA . Validity and reliability of English and Marathi Oswestry Disability Index (version 2.1a) in Indian population . Spine (Phila Pa 1976) 2013 ; 38 : E662 – 8 .
21. Miekisiak G , Kollataj M , Dobrogowski J , et al. Validation and cross-cultural adaptation of the Polish version of the Oswestry Dis-ability Index . Spine (Phila Pa 1976) 2013 ; 38 : E237 – 43 .
22. Vincent JI , Macdermid JC , Grewal R , et al. Translation of Oswes-try Disability Index into Tamil with cross-cultural adaptation and evaluation of reliability and validity(section sign) . Open Orthop J 2014 ; 8 : 11 – 9 .
23. ICHOM Working Group LBP. Low Back Pain Flyer & Data Collec-tion User Manual. International Consortium for Health Outcomes Measurement (ICHOM). 2014. Available at: http://www.ichom.org/wp-content/uploads/2014/08/LBP-Reference-Guide-8.20.14-TP.pdf. Accessed September 1, 2015.
24. Beaton DE , Bombardier C , Guillemin F , et al. Guidelines for the process of cross-cultural adaptation of self-report measures . Spine (Phila Pa 1976) 2000 ; 25 : 3186 – 91 .
25. Acquadro C , Conway K , Hareendran A , et al. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials . Value Health 2008 ; 11 : 509 – 21 .
26. van Hooff ML , van der Merwe JD , O’Dowd J , et al. Daily function-ing and self-management in patients with chronic low back pain after an intensive cognitive behavioral programme for pain man-agement . Eur Spine J 2010 ; 19 : 1517 – 26 .
27. Guillemin F , Bombardier C , Beaton D . Cross-cultural adaptation of health-related quality-of-life measures: literature review and pro-posed guidelines . J Clin Epidemiol 1993 ; 46 : 1417 – 32 .
28. van Hooff ML , Spruit M , O’Dowd JK , et al. Predictive factors for successful clinical outcome 1 year after an intensive combined phys-ical and psychological programme for chronic low back pain . Eur Spine J 2014 ; 23 : 102 – 12 .
29. Baker D , Pynsent P , Fairbank J . The Oswestry Disability Index revisited . In: Roland M , Jenner J , eds. Back Pain: New Approaches to Rehabilitation and Education . Manchester, England : Manches-ter University Press ; 1989 : 174 – 86 .
30. Roland M , Fairbank J . The Roland-Morris Disability Question-naire and the Oswestry Disability Questionnaire . Spine (Phila Pa 1976) 2000 ; 25 : 3115 – 24 .
31. Fairbank JC . Use and abuse of Oswestry Disability Index . Spine (Phila Pa 1976) 2007 ; 32 : 2787 – 9 .
➢ Key Points
The Dutch version of ODI 2.1a is a valid and valu-able tool to measure functional outcome in spine care. Factor analysis suggested a 1-factor structure. The Dutch ODI showed a strong correlation with
the NRS pain severity as well as the Dutch RMDQ and the physical component of SF-36. The Dutch ODI is recommended as a condition-
specifi c PROM for use in future Dutch back pain research and to evaluate outcome of back care. The Dutch ODI is implemented in the Dutch
Spine Surgery Registry for the spine society in the Netherlands.
Acknowledgements The authors thank the multidisciplinary team at RealHealthNL, who were responsible for the assessments of the participants in the CPP program. They also thank Frank Laumen (EasyFile) for his support in building and managing the electronic web-based system, including the database.
References 1. Murray CJ , Vos T , Lozano R , et al. Disability-adjusted life years
(DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010 . Lancet 2012 ; 380 : 2197 – 223 .
2. McCormick JD , Werner BC , Shimer AL . Patient-reported out-come measures in spine surgery . J Am Acad Orthop Surg 2013 ; 21 : 99 – 107 .
3. ICHOM . Standard Set for Low Back Pain . 2014 . Available at: http://www.ichom.org/project/low-back-pain/ . Accessed September 1, 2014.
4. Poolman RW , Swiontkowski MF , Fairbank JC , et al. Out-come instruments: rationale for their use . J Bone Joint Surg Am 2009 ; 91 ( suppl 3 ): 41 – 9 .
5. Fairbank JC , Couper J , Davies JB , et al. The Oswestry Low Back Pain Disability Questionnaire . Physiotherapy 1980 ; 66 : 271 – 3 .
6. Fairbank JC , Pynsent PB . The Oswestry Disability Index . Spine (Phila Pa 1976) 2000 ; 25 : 2940 – 52 .
7. Boscainos PJ , Sapkas G , Stilianessi E , et al. Greek versions of the Oswestry and Roland-Morris Disability Questionnaires . Clin Orthop Relat Res 2003 ; 40 – 53 .
8. Grotle M , Brox JI , Vollestad NK . Cross-cultural adaptation of the Norwegian versions of the Roland-Morris Disability Questionnaire and the Oswestry Disability Index . J Rehabil Med 2003 ; 35 : 241 – 7 .
9. Yakut E , Duger T , Oksuz C , et al. Validation of the Turkish version of the Oswestry Disability Index for patients with low back pain . Spine (Phila Pa 1976) 2004 ; 29 : 581 – 5 .
10. Lauridsen HH , Hartvigsen J , Manniche C , et al. Danish version of the Oswestry Disability Index for patients with low back pain. Part 1: cross-cultural adaptation, reliability and validity in two different populations . Eur Spine J 2006 ; 15 : 1705 – 16 .
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
SPINE140559_LR E89SPINE140559_LR E89 11/12/14 1:38 PM11/12/14 1:38 PM

HEALTH SERVICES RESEARCH Validation of Dutch ODI v2.1a • van Hooff et al
E90 www.spinejournal.com January 2015
32. Roland M , Morris R . A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain . Spine (Phila Pa 1976) 1983 ; 8 : 141 – 4 .
33. Jensen MP , Karoly P . Pain-specifi c beliefs, perceived symptom sever-ity, and adjustment to chronic pain . Clin J Pain 1992 ; 8 : 123 – 30 .
34. Ware JE Jr , Sherbourne CD . The MOS 36-Item Short Form Health Survey (SF-36). I. Conceptual framework and item selection . Med Care 1992 ; 30 : 473 – 83 .
35. Spinhoven P , Ormel J , Sloekers PP , et al. A validation study of the hospital anxiety and depression scale (HADS) in different groups of Dutch subjects . Psychol Med 1997 ; 27 : 363 – 70 .
36. Terwee CB , Bot SD , de Boer MR , et al. Quality criteria were pro-posed for measurement properties of health status questionnaires . J Clin Epidemiol 2007 ; 60 : 34 – 42 .
37. Ostelo RW , Deyo RA , Stratford P , et al. Interpreting change scores for pain and functional status in low back pain: towards inter-national consensus regarding minimal important change . Spine 2008 ; 33 : 90 – 4 .
38. Beavers AS , Lounsbury JW , Richards JK , et al. Practical consider-ations for using exploratory factor analysis in educational research . Pract Assess Rese Eval [A peer-reviewed electronic journal] 2013 ; 18 : 1 – 13 .
39. Pett MA , Lackey NR , Sullivan JJ . Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research . Thousand Oakes, CA : Sage Publications ; 2003 .
40. Cohen J . Statistical Power Analysis for the Behavioral Sciences . 2nd ed. Hillsdale, NY : Lawrence Earlbaum Associates ; 1988 .
41. Cohen J . A power primer . Psychol Bull 1992 ; 112 : 155 – 9 .
42. Bland JM , Altman DG . Statistical methods for assessing agreement between two methods of clinical measurement . Lancet 1986 ; 1 : 307 – 10 .
43. Bland JM , Altman DG . Comparing methods of measurement: why plotting difference against standard method is misleading . Lancet 1995 ; 346 : 1085 – 7 .
44. PROQOLID . Patient-Reported Outcome and Quality of Life Instru-ments Database—Oswestry Disability Index (ODI), [Mapi Research Trust] . 2014 . Available at: http://www.proqolid.org/instruments/oswestry_disability_index_odi . Accessed September 1, 2014.
45. Guermazi M , Mezghani M , Ghroubi S , et al. The Oswestry Index for Low Back Pain translated into Arabic and validated in a Arab population . Ann Readapt Med Phys 2005 ; 48 : 1 – 10 .
46. Osthus H , Cziske R , Jacobi E . Cross-cultural adaptation of a Ger-man version of the Oswestry Disability Index and evaluation of its measurement properties . Spine (Phila Pa 1976.) 2006 ; 31 : E448 – 53 .
47. Frost H , Lamb SE , Stewart-Brown S . Responsiveness of a patient-specifi c outcome measure compared with the Oswestry Disability Index v2.1 and Roland and Morris Disability Questionnaire for patients with subacute and chronic low back pain . Spine (Phila Pa 1976) 2008 ; 33 : 2450 – 7 .
48. Von Korff M , Jensen MP , Karoly P . Assessing global pain severity by self-report in clinical and health services research . Spine (Phila Pa 1976) 2000 ; 25 : 3140 – 51 .
49. van Hooff ML , van Loon J , van Limbeek J , et al. The Nijmegen decision tool for chronic low back pain. Development of a clinical decision tool for secondary or tertiary spine care specialists . PLoS One 2014 ; 9 : e104226 .
Copyright © 2015 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
SPINE140559_LR E90SPINE140559_LR E90 11/12/14 1:38 PM11/12/14 1:38 PM