The Global Fund and the re-configuration and re-emergence of ‘civil society’: Widening or...
17
This article was downloaded by: [Anuj Kapilashrami] On: 17 April 2012, At: 01:39 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Global Public Health: An International Journal for Research, Policy and Practice Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rgph20 The Global Fund and the re- configuration and re-emergence of ‘civil society’: Widening or closing the democratic deficit? Anuj Kapilashrami a & Oonagh O'Brien b a Global Public Health Unit, University of Edinburgh, Edinburgh, UK b Institute for International Health and Development, Queen Margaret University, Edinburgh, UK Available online: 13 Jan 2012 To cite this article: Anuj Kapilashrami & Oonagh O'Brien (2012): The Global Fund and the re- configuration and re-emergence of ‘civil society’: Widening or closing the democratic deficit?, Global Public Health: An International Journal for Research, Policy and Practice, 7:5, 437-451 To link to this article: http://dx.doi.org/10.1080/17441692.2011.649043 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and- conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Global Fund and the re-configuration and re-emergence of ‘civil society’: Widening or...

This article was downloaded by: [Anuj Kapilashrami]On: 17 April 2012, At: 01:39Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Global Public Health: An InternationalJournal for Research, Policy andPracticePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rgph20
The Global Fund and the re-configuration and re-emergence of‘civil society’: Widening or closing thedemocratic deficit?Anuj Kapilashrami a & Oonagh O'Brien ba Global Public Health Unit, University of Edinburgh, Edinburgh,UKb Institute for International Health and Development, QueenMargaret University, Edinburgh, UK
Available online: 13 Jan 2012
To cite this article: Anuj Kapilashrami & Oonagh O'Brien (2012): The Global Fund and the re-configuration and re-emergence of ‘civil society’: Widening or closing the democratic deficit?,Global Public Health: An International Journal for Research, Policy and Practice, 7:5, 437-451
To link to this article: http://dx.doi.org/10.1080/17441692.2011.649043
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,

demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012
The Global Fund and the re-configuration and re-emergence of ‘civilsociety’: Widening or closing the democratic deficit?
Anuj Kapilashramia* and Oonagh O’Brienb
aGlobal Public Health Unit, University of Edinburgh, Edinburgh, UK; bInstitute forInternational Health and Development, Queen Margaret University, Edinburgh, UK
(Received 24 March 2011; final version received 2 October 2011)
The past decade has witnessed a tremendous growth in the scale and policyinfluence of civil society in global health governance. The AIDS ‘industry’ inparticular opens up spaces for active mobilisation and participation of non-stateactors, which further crystallise with an ever-increasing dominance of globalhealth initiatives. While country evaluations of global initiatives call for a greaterparticipation of ‘civil society’, the evidence base examining the organisation,nature and operation of ‘civil society’ and its claims to legitimacy is very thin.Drawing on the case of one of the most visible players in the global response toHIV epidemic, the Global Fund to Fight AIDS, Tuberculosis and Malaria, thisarticle seeks to highlight the complex micropolitics of its interactions with civilsociety. It examines the nature of civil society actors involved in the Fund projectsand the processes through which they gain credibility. We argue that theimposition of global structures and principles facilitates a reconfiguration ofactors around newer forms of expertise and power centres. In this context, thenotion of ‘civil society’ underplays differences and power dynamics betweenvarious institutions and conceals the agency of outsiders under the guise ofautonomy of the state and people.
Keywords: Global Fund to Fight AIDS, TB and Malaria; civil society; AIDSindustry; global health initiatives; democratic deficit
Introduction
In recent years, civil society organisations have come to play a prominent role in
global health governance (Altman 1994, Frenk et al. 1997, Altman 1999, Dodgson
et al. 2002, Loewenson 2003). A growing involvement in global health initiatives
(GHI) has facilitated their role in decision-making, through membership in
consultative forums and implementing programmes as a direct recipient of grants.
Their increasing share in the aid market is accompanied by a growing legitimacy that
has enabled their movement beyond support services into the realm of provisioning
and financing.
The introduction of GHI and their interaction with the AIDS ‘industry’ opens up
spaces for active participation and mobility of civil society at large and the ‘affected’
communities in particular with national and international agencies seeking civil
society representation and participation in disease control programmes. The
rationale for this is built on three premises: (1) addressing the democratic deficit
*Corresponding author. Email: [email protected]
Global Public Health
Vol. 7, No. 5, May 2012, 437�451
ISSN 1744-1692 print/ISSN 1744-1706 online
# 2012 Taylor & Francis
http://dx.doi.org/10.1080/17441692.2011.649043
http://www.tandfonline.com
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

within structures of global governance by ensuring wider and more democratic
representation of people’s voices, particularly those most affected (Anderson and
Rieff 2004, Scholte 2004); (2) comparative edge over the government in delivering
services given its outreach and presence in the very communities the programmes
target (Doyle and Patel 2008); and (3) balancing the growing influence of markets
and reinforcing public interest role of states (Labonte 1998, Dodgson et al. 2002).
A significant body of literature exists around approaches to decentralise
governance and devolve power to the civil society (Shah 1999, McCoy and Shuping
2000). Central to this is the concept of ‘participation’. Although mainstreaming of
participation gained prominence during the 1990s, Hickey and Mohan (2004, p. 3)
draw attention to its ‘longer and more varied genealogy in development thinking’.
Much of this history is traced by Nelson and Wright (1995), who discuss the myriad
ways the concept is incorporated into national/international policy as well as
development work: ‘from a simple representative presence, through contributors of
casual cheap or free labour to being politically co-opted legitimizers of a policy’
(1995, p. 2). Initially welcomed as an innovative response to lengthy and top-down
planning processes, participatory approaches have been criticised since their ‘boom’
period (Neef 2003) on various accounts: their increasing institutionalisation,
compatibility with ‘top-down planning systems’ without necessarily changing
‘prevailing institutional practices of development’ (Mosse 2001, p. 17), the lack of
attention given to processes of political power and its potential to ‘tyrannise’
development debates with unsatisfactory evidence of effectiveness (Cooke and
Kothari 2001). Notwithstanding this ‘growing backlash’, Hickey and Mohan argue
that ‘participation has actually deepened and extended its role, albeit unevenly, in
theory, policy and practice’ (2004, p. 3). They discuss ways in which people who are
subjectivised are continually devising innovative strategies for expressing their agency
in development arenas. Tied intrinsically to the success of development policies,
Mosse (2004) argues the ways in which participation allows communities and
supporting actors to constantly translate and interpret different sets of interest,
actively contributing to stabilise and establish order.
However, there is remarkably little debate about the nature of agencies whose
involvement is sought in the name of ‘participation’ of civil society, the kind of
organising and expertise required, and the processes of political action with which
they establish ‘order’.
These questions gain particular significance in relation to the organisation of
the Global Fund to Fight AIDS, TB and Malaria, hereafter referred to as the
Fund, given its strong commitment to and recognition of the critical role played by
civil society in its ‘design and development’ (Fund website accessed in February
2011). The Fund reflects an assemblage of diverse discourses. Prominent and
distinctive among these is the international human rights discourse whereby civil
society’s demand for greater participation of the affected communities ‘to make
services more efficient and responsive to local needs’ helped crystallise the form of
the Fund (Fund website). Recent evaluations of the performance of the Fund have
highlighted the continued dominance of national governments in policy-making
and implementation thereby reinforcing the need for a greater involvement of civil
society, particularly within country-level governance in the recipient countries
(Winters 2008, Bhattacharya and Dasgupta 2009). The Fund is regarded as a
438 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

finance mechanism which levers funds to mitigate the impact of the three diseases.
It makes a strong commitment to (1) inclusiveness and partnership, (2) quality
assurance through conditions and precedents, and (3) performance-funding based
on clear and measurable outputs (Fund website).
In this article, we examine the processes set off by the Fund protocol and
commitment, and its implication for civil society participation. Such examination
will be situated within a broad framework which alludes to the following questions:
how does the Fund re-constitute the civil society actors in the AIDS ‘industry’ and
how do the actors in turn respond to this new form of organising?
We begin by discussing the features of AIDS ‘industry’ to present an account of
its increasingly plural nature and the main constituencies involved in the national
response to the epidemic in India. The bulk of this article, however, examines the
disciplinary regime of the Fund, the challenges faced by the civil society actors within
the industry and the ways in which they interact with the Fund to reinforce their
legitimacy and credibility.
Research methodology
This article presents an ethnographic account of field studies undertaken as part of a
doctoral research to understand the discourse and practice of public�private
partnerships through an examination of the country-level governance of the Fund
in India (Kapilashrami 2010).
Using critical ethnography and a case study approach, the research involved an
intensive period of field studies between 2007 and 2009 carried out in five Indian
states: four categorised as high prevalence, legitimising concentrated presence of
donors and Fund grants, and the fifth, Delhi, epicentre of ministries, donors and
Fund governance. Diverse sources of data included observation of meetings; a short-
term consultancy; documentary analysis of record of meetings, and performance
reports; and 70 in-depth interviews carried out with individuals at various levels of
Fund governance. Interviews were conducted in two official languages: English and
Hindi, both of which the researcher has fluency in. All but two respondents in the
health facility could speak either of the two languages. On these two occasions, the
researcher was assisted by other facility staff. Interview transcripts and field notes
were used to develop key themes and categories based on which relevant data were
coded, examined for additional links, commonalities and contrasting perspectives
(constant comparison) in order to develop a coherent interpretation of the processes
and written as narratives or ‘emerging stories’. The final stage of analysis
triangulated multiple information sources, and adopted an iterative process of
testing and retesting of ideas and assumptions (analytic induction).
This article draws on quotes from interviews with staff of civil society and
government partners, and front line staff at antiretroviral treatment (ART) clinics,
where appropriate. Through the case study we examine the tensions and challenges
faced by a network of people living with HIV/AIDS (PLHA) and the wider
consortium of civil society actors in the Fund organisation. Although there are
several independent networks of PLHA in India, the focus of investigation was one
with high visibility in international and national fora and the Fund projects in India.
Global Public Health 439
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012
The nature of AIDS ‘industry’
The usage of the term ‘industry’ to refer to the HIV/AIDS sector is not new. Cindy
Patton (1991), for instance, in her pioneering work ‘Inventing AIDS’ highlighted the
dominance of funded and professionalised care and education programmes in
addressing the AIDS epidemic in the USA. She argued that the medical and
technological solutions reliant on ‘experts’ and volunteers that were characteristic of
the then emerging government funded professionalised AIDS services contrasted
sharply with the earlier politicised and self-empowering AIDS activism initiated by
gay and intravenous drug-taking communities.
During the last two decades, with intensified processes of globalisation and
proliferation of non-state actors in global governance, the industry has shaped as an
unprecedented ‘private-public industrial complex around a single disease’ (Rennie
2008). This complex is characterised by fluctuating figures, dominance of large
pharmaceutical and philanthropic corporations led development and research
(Altman 1997), escalating prominence within donor agendas (MacKellar 2005)
and a disproportionate worldwide spending, as some would argue, at the expense of
other diseases or wider health sector development (Shiffman 2008, Liese and
Schubert 2009). This new global order has also witnessed a transition in the role of
the business sector, earlier seen as an adversary to fair pricing of drugs particularly
antiretroviral, from supplier to a ‘partner’ in expanding access to medicines, building
new markets through infrastructural support and prevention and treatment
programmes (Kettler et al. 2003, Caines et al. 2004).
The industry comprises a wide range of players � national governments,
international agencies, community-based organisations working with or representing
specific ‘communities’ that are identified or, who have begun to self identify in the
course of their interactions with the AIDS industry (See Khanna 2009), as ‘high risk’
or ‘vulnerable populations’. This language of ‘community’ and the growth of
community-based politics was accompanied by a near universalisation and
internationalisation of identities around HIV status, sexuality, drug use and sex
work (Altman 1994, 1999) evidenced by categories such as Men Having Sex with
Men, Drug Users and Commercial Sex Workers.
These diverse players, as active agents in the industry, are required to organise in
a particular fashion, speak a particular language that exudes acronyms around
services and specific communities or ‘target populations’, engage in similar practices
and generate shared meanings. This enables their movement within the industry
(across constituencies) to more influential and rewarding positions.
A distinctive feature in the landscape of AIDS politics is the emergence of the
AIDS movement, a ‘movement’ around an identity based on the embodiment of the
illness. Historically, the feminist health movement has been at the forefront of
challenging the bio-medical hegemony over patient’s bodies, putting patient�provider
interaction centre stage of medical ethics. However, the AIDS movement is the first
social movement to engage with bio-medicine in a manner that transforms the
affected ‘victims’ into ‘activist experts’ (Epstein 1996).Highly significant for the cultural redefinition of interactions between medical or
technical experts and patients or lay consumers, the AIDS movement is not perceived
as merely a ‘disease constituency’ advocating for greater resource allocation and
treatment but, as Steven Epstein (1996, p. 8) puts it, an alternative basis of expertise.
440 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

The movement(s) is itself broad based and includes organisations or networks that
represent ‘communities’ stigmatised on the basis of their status or practices defined
as ‘high risk’ in the bio-medical understanding of the epidemic. While a spectrum of
NGOs and activists representing alternative, often criminalised, sexualities andbehaviours have been at the forefront, the notion of ‘people living with HIV/AIDS’
has been central to the organisation of the movement(s).
Building on the perceived strength of community organising around AIDS, the
international agencies (for example, the WHO Global Programme on AIDS and the
UNAIDS) facilitated the formation of international and transnational networks
around the PLHA identity, formally adopted at the 1994 Paris Summit (Altman
1999). The earlier writings by Fisher (1997) raise caution around the inherent bias of
international networks reflected in their concentration in metropolis, the heavyreliance on global telecommunications and information, and the nature of
organisations that derived legitimacy through such interactions. Exploration of
these tensions is central to the focus of this article.
Finally, the national response to the epidemic in India is structured as a vertical
(top-down) disease control programme administered by the federal government.
With a separate organisational structure, administration and budget provision, the
AIDS programme enjoys certain functional independence from the wider public
health system. It is led by the national AIDS control organisation (NACO), a projectmanagement organisation under the Ministry of Health and Family Welfare, which is
responsible for formulation of policy, technical guidance, evaluation research and
procurement of test kits, drugs and equipments. It implements the HIV policy
through its state divisions officiated by senior bureaucrats, and NGOs sub-
contracted to deliver support programmes for the community. More recently the
NACO has entered into newer forms of partnerships, which see the corporate sector
and NGOs as co-recipients of the Fund grant.
Case study: The disciplining regime of the Fund
The grant from the Fund has enabled running of parallel projects set up with each
annual call for proposals. Each Fund round is for five years implemented in twophases of two and three years each. The rounds commence in sequence but run
parallel, so much so that at any given time up to five rounds are running
simultaneously, each with a different objective, partnership arrangement and funding.
New opportunities and complex configurations
The annual bidding process presents itself as an opportunity for stakeholders
representing diverse constituencies to enter into new relationships, form new entities
and participate in the national policy processes. It also facilitates movement of
leading international organisations into India and large national organisations from
other fields into the AIDS industry. This was evident from an increased number of
international NGOs such as AIDS Alliance and Engender Health registering theirIndia offices and playing a leading role as recipients of Fund grants (Kapilashrami
2010).
With Fund’s emphasis on inclusion of the ‘voices of the affected’, participation of
PLHA became key to successful bids. The network, with its existing national and
Global Public Health 441
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

international links was a convenient site for much of the development work around
HIV. While some networks emerged in the wake of the Fund, the existence of others,
often women’s networks and other grassroots groups, was threatened. Visits to the
ART clinics revealed their peripheral role in the organisation and delivery of the
programme, where they were often seen managing patient queues and highlighting
the shortcomings in delivery of care. Their invisibility from the Fund governance, a
significant platform for planning and decision-making for the national AIDS
programme, also limited their visibility in the industry and thus their ability to
make claims on country wide resources (Kapilashrami 2010).
The network was registered in 1997 with an explicit mandate to preserve, protect
and promote rights of PLHA (Yepthomi 1998). It is led by a governing body and a
national secretariat and operates through network offices at the state, district and
block level. Different accounts on the genesis and growth of the network emerged
during the research. According to Yepthomi (1998) the network is the outcome of a
national workshop organised by NACO, at which certain PLHA were assigned the
task of networking.
With its president as a distinguished member of national committees, the network
has a strategic presence in different Fund rounds through partnerships with
government as well as NGOs. It implements prevention programmes for the state
divisions of NACO and is also a member of a civil society consortium � the first non-
government principal recipient of the Fund grant for India � for which it was
responsible for seven of the nine deliverables that were the consortium’s mandate. As
part of the consortium, which also comprises national and international NGO and
corporate representatives, the network is mandated to set up networks in each
district to ensure treatment adherence and support for PLHA. The field studies
involved visits to 10 network offices (and their intervention sites) across five states.
Interventions at the district level network
District level networks (DLN) are established in districts as part of the Fund grant
with the objective to reach out to PLHA’s in the community and thereby expand the
network’s membership. These are meant to serve as the first point of contact and
main service delivery point for PLHA offering a range of services including
counselling (to encourage testing and adherence), support group meetings, nutri-
tional supplements and referrals to ART centres.
Formally registered as a society (under the Society Registration Act), each DLN
has a separate governance and organisational structure, which comprises of a board
and project staff. The infrastructure usually comprises of four or five rooms each run
as a dedicated unit, distinguished by the Funder’s name mounted on a nameplate at
the entrance of each room, for the respective agency whose project is being
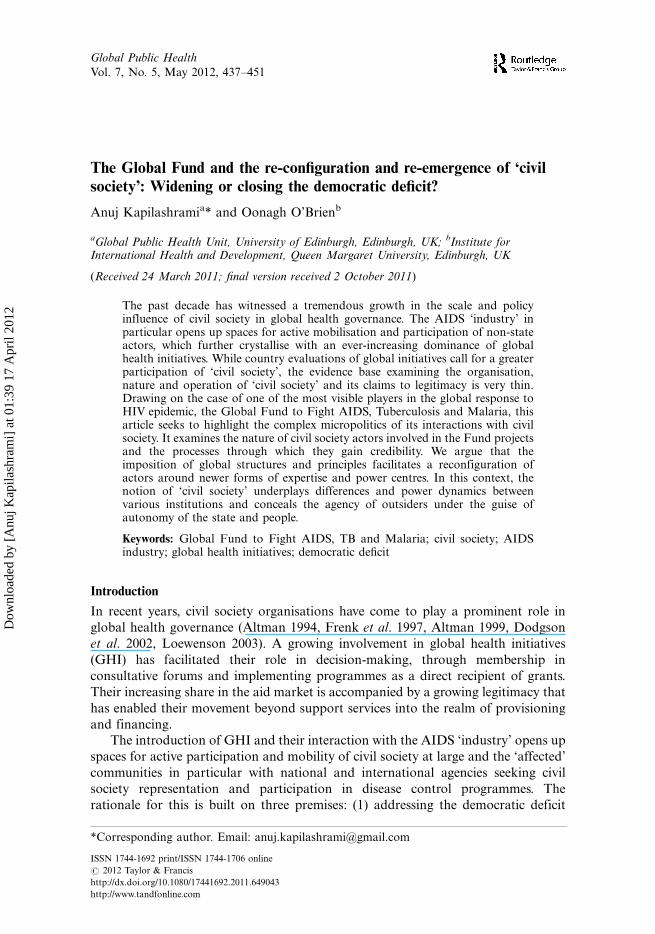
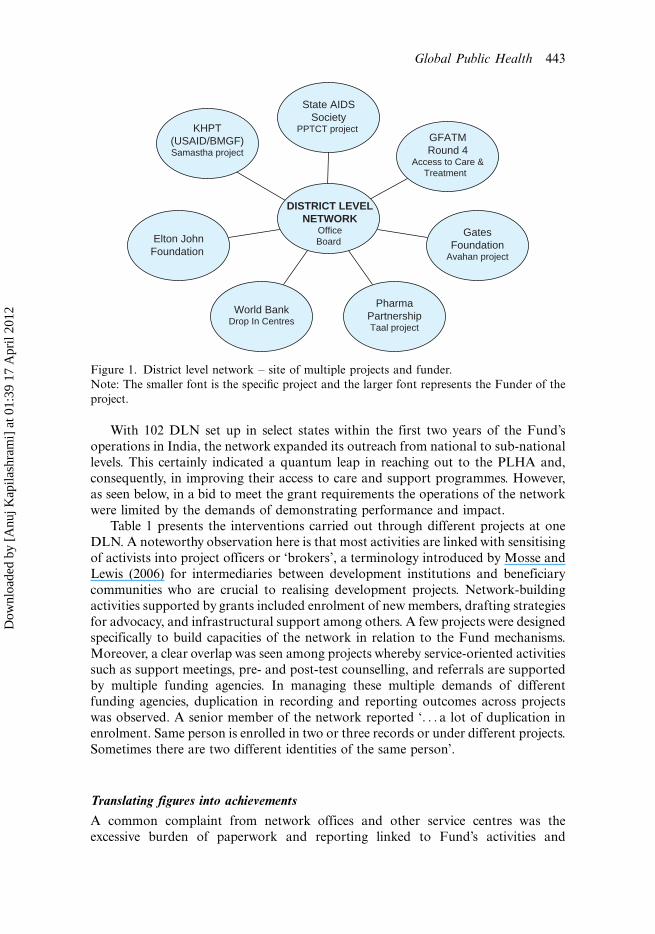
implemented. Figure 1 gives a glimpse into the myriad interventions triggered by
the HIV at one of the sites visited. Typically, each DLN had on an average five to six
projects being implemented. Of these, the Fund, with concurrent open rounds, had a
prominent presence, for example, access to care and treatment projects under round
four and six, prevention of parent to child transmission as sub-recipients of NACO
and drop in centres under round two. In addition, they received funds for different
projects directly from other funding agencies.
442 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012
With 102 DLN set up in select states within the first two years of the Fund’s
operations in India, the network expanded its outreach from national to sub-national
levels. This certainly indicated a quantum leap in reaching out to the PLHA and,
consequently, in improving their access to care and support programmes. However,
as seen below, in a bid to meet the grant requirements the operations of the network
were limited by the demands of demonstrating performance and impact.
Table 1 presents the interventions carried out through different projects at one
DLN. A noteworthy observation here is that most activities are linked with sensitising
of activists into project officers or ‘brokers’, a terminology introduced by Mosse and
Lewis (2006) for intermediaries between development institutions and beneficiary
communities who are crucial to realising development projects. Network-building
activities supported by grants included enrolment of new members, drafting strategies
for advocacy, and infrastructural support among others. A few projects were designed
specifically to build capacities of the network in relation to the Fund mechanisms.
Moreover, a clear overlap was seen among projects whereby service-oriented activities
such as support meetings, pre- and post-test counselling, and referrals are supported
by multiple funding agencies. In managing these multiple demands of different
funding agencies, duplication in recording and reporting outcomes across projects
was observed. A senior member of the network reported ‘. . . a lot of duplication in
enrolment. Same person is enrolled in two or three records or under different projects.
Sometimes there are two different identities of the same person’.
Translating figures into achievements
A common complaint from network offices and other service centres was the
excessive burden of paperwork and reporting linked to Fund’s activities and
KHPT(USAID/BMGF)Samastha project
Elton JohnFoundation
World BankDrop In Centres
PharmaPartnershipTaal project
GatesFoundation
Avahan project
GFATMRound 4
Access to Care &Treatment
State AIDSSociety
PPTCT project
DISTRICT LEVELNETWORK
OfficeBoard
Figure 1. District level network � site of multiple projects and funder.
Note: The smaller font is the specific project and the larger font represents the Funder of the
project.
Global Public Health 443
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012
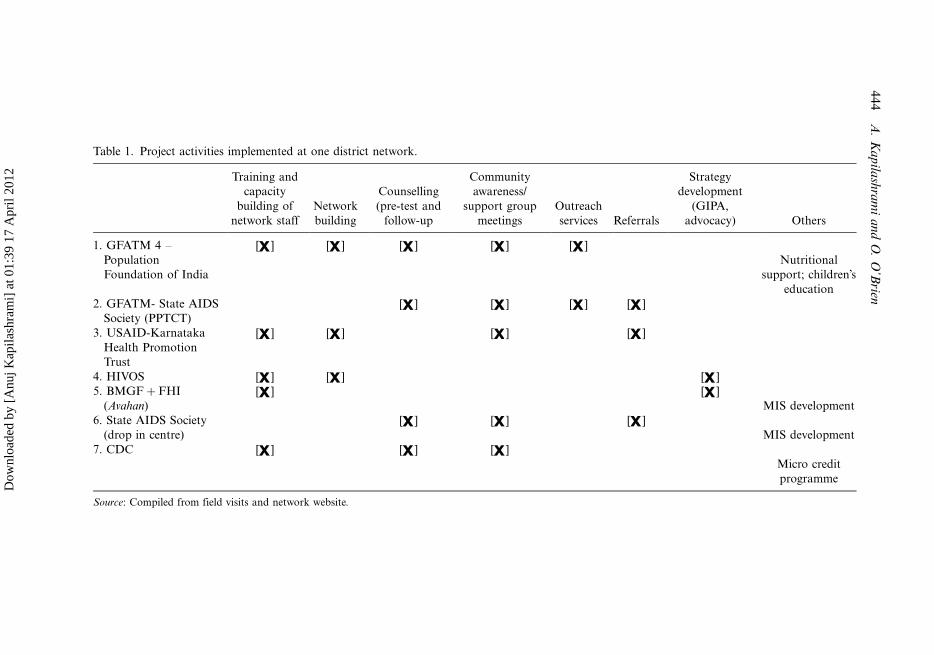
Table 1. Project activities implemented at one district network.
Training and
capacity
building of
network staff
Network
building
Counselling
(pre-test and
follow-up
Community
awareness/
support group
meetings
Outreach
services Referrals
Strategy
development
(GIPA,
advocacy) Others
1. GFATM 4 �Population
Foundation of India
[ ] [ ] [ ] [ ] [ ]
Nutritional
support; children’s
education
2. GFATM- State AIDS
Society (PPTCT)
[ ] [ ] [ ] [ ]
3. USAID-Karnataka
Health Promotion
Trust
[ ] [ ] [ ] [ ]
4. HIVOS [ ] [ ] [ ]
5. BMGF�FHI
(Avahan)
[ ] [ ]
MIS development
6. State AIDS Society
(drop in centre)
[ ] [ ] [ ]
MIS development
7. CDC [ ] [ ] [ ]
Micro credit
programme
Source: Compiled from field visits and network website.
44
4A
.K
ap
ilash
ram
ia
nd
O.
O’B
rien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

deliverables. An innovative and distinct feature of the Fund programmes is its claim
to technology centred management of information. Network offices are therefore
equipped with computers and computerised management information systems
(CMIS) along with software training for staff. Besides the electronic database, staff
is required to maintain extensive registers and forms for every interaction and
activity performed. This implies that at any given point the project staff in the
network unit maintained between six and seven registers: a master register of all
PLHA enrolled, record of every individual counselled, all support meetings
organised, peer educator trainings held, each person followed up on treatment,
peer educator’s working registers and other similar records. This information is then
entered into cumbersome computer databases accessible to the state and national
network office. Additionally, progress reports are generated at the end of each
month both by the state and the network head office, collating the information
from different districts, for quarterly submissions to the Fund.
To handle this workload, there were at least five project staff for each Fund grant:
network officer, social worker, peer counsellor, outreach worker and accountant.
Visits to the DLN also revealed an abundance of training programmes, offered by
multiple partner agencies � international and national � often as deliverables of the
Fund rounds, to build capacities of the project staff. Participation in multiple
trainings resulted in continuous absence of the majority of staff, leaving one or two
individuals to manage records and databases alongside their other responsibilities
including home visits, counselling and other provisions. Counsellors reported not
finding time to counsel because they were required to fill in for other staff while they
are away on training programmes. Likewise, the social workers were reportedly
‘overburdened by the task of record keeping owing to the very poor education levels
and skills of the PLHA’.Despite this thrust on capacity and skill building, senior members of the network
and other government and non-government partner agencies frequently observed
that capacities of the DLN staff were insufficient to cope with the scale and nature of
interventions they engaged with. This also emerged as a barrier in effective
documentation, as a senior staff at the state network highlighted:
All are NGOs working in two or three districts. Suddenly we are expected to cover somany districts and achieve high targets. Through the Fund we have MoU with 22districts and four more are due this month. This is the scale we are talking about and theState network is not adequate to support or supervise.
The network was also crucial for the success of interventions or deliverables of other
consortium partners, enabling their access to subjects (PLHA) for training- and skill-
building programmes or operational research. As a result, district network staff
working on the fund projects were constantly responding to demands of the state
network offices as well as the consortium partners. A network staff stated:
It was very hectic. By the time we started one study, the concept of the next was sent by[the partner NGO] responsible for 8 operational research in the first phase of the Fundprogramme.
Global Public Health 445
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

Most participants highlighted the stress on reporting and evaluation linked to the
‘performance-based’ funding arrangements of the Fund and its focus on time-bound
outputs, ironically perceived as a ‘healthy’ habit of GHIs adding value to
international health by raising standards in disease control efforts (Buse and
Harmer 2007). However, the project staff is under constant pressure to meet the
deliverables or outputs against which the performance is measured. For instance,
reported monthly targets included ‘30 new enrolments’, ‘four support group meetings
per taluka (block)’, ‘1000 peer treatment educators trained by 2010’ among others.
Pressure to meet targets in a competitive and uncertain environment resulting from
multiple projects has led the different constituencies in making counter-claims on the
achievements of one project vis-a-vis the other. The formats, registers and
operational research studies thus become crucial sites for establishing the organisa-
tional relevance to the Fund as well as staff competence in the project. These, in turn,
legitimise claims on the next cycle of the grant and re-organisation of key people in
the project cycle. This was evident from the movement of the project staff (outreach
workers, counsellors, social workers) from the network to other NGOs or from one
project to a relatively better funded project within the network.
In this environment of competition, it is imperative to maintain institutional
sustainability in order to successfully bid for programmes. Since the DLNs rely on
project funding, for two to five years, there is a constant lookout for new funders and
projects. A senior member of the network observed that:
. . . project driven network units can be threatening to the overall objective of theprogramme. Somewhere in filling the forms to meet enrolment numbers and maintainrecords, the network has diverted from its objectives and lost its vision. Most networksare worried only about getting new funding.
Towards sustainability
The network’s partnership with a pharmaceutical company to dispense antiretroviral
and opportunistic infection drugs at subsidised costs can be regarded as one such
attempt by the network towards maintaining institutional sustainability. Stating its
rationale as filling the treatment deficit created by the overburdened public health
system and unaffordable private sector, the network’s website refers to it as ‘a
partnership to bail out persons in private ART facility’. A project officer of the
network presented the model as:
. . .offer[ing] entire package . . . there is also a positive living centre [another service runby the consortium], so a doctor is available to visit. For CD4 count, x-rays, blood reportand other tests we have established links through them and with a private clinic. Butpeople prefer to get CD4 done from government itself because it is free while outside itcosts around 570/-.
The model, although heralded as a ‘one-stop-treatment-shop’ providing treatment
literacy, all types of counselling, peer support and referrals, was heavily reliant on
either the public or private health facility for laboratory tests and hospital
admissions. Project officers in the state AIDS societies and the medical staff at the
public ART centres expressed their resentment with regards to the potential
deception of patients who were charged for a service that was available in the public
446 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

hospitals for free. It was not clear to what extent the initiative addressed the
treatment deficit. On the contrary, a senior bureaucrat at the state AIDS society
highlighted the resulting duplication of services:
They [the network] have started their own drug distribution centres, their ownopportunist(ic) infection treatment, their doctors . . .But for investigations, they sendthem to public health facility. Why duplicate?
The challenge posed by competing activities proposed across the Fund rounds was afrequently emerging theme across the narratives of civil society actors. For example,
in an initiative under Fund round 2, the government entered into a partnership with
a leading organisation working on HIV to offer low cost drugs through price
negotiations with the pharmaceutical. The launch of this initiative was soon followed
by federal government’s decision to introduce free antiretroviral through the national
programme. This became a major hindrance for the organisation and impacted its
performance, compelling the staff to ‘sell’ its programme by making claims that
quality of drugs and treatment provided was better in comparison with thegovernment facility. A senior member of the consortium implementing the
programme elaborated on this dilemma stating how the ‘. . .government roll out
became a big challenge for this project. Why would anyone come here and pay for
drugs when there is a roll out?[. . .]. But we have tried to do our best and managed to
achieve numbers simply by focusing on issues of quality.’
Discussion and conclusion
Impact on ‘civil society’: Widening or shrinking spaces?
The AIDS epidemic has given voice and visibility to non-state actors as organisers,
implementers and advocates. From the very onset of the epidemic, they have been atthe forefront of promoting prevention, care and treatment. Their contribution
ranged from addressing stigma and generating awareness in the communities to
importing antiretrovirals when none existed as part of the national programme. The
power and legitimacy derived by ‘civil society’ in AIDS politics is especially evident
from the global human rights discourse that underpins the creation of the Fund.
However, prior to the Fund the national programme was structured around a
centralised state that sought out NGOs to play an active role in addressing the
epidemic in the community. In doing so, the NGOs extended the state authority. Theentry of the Fund and the authority of its protocol, which mandates civil society’s
involvement as principal recipient and performance-based funding arrangements,
have transformed this equation.
Firstly, these arrangements have transformed the nature of the relationship
between the state and the civil society. As a direct recipient of the grant, the civil
society enjoys a certain level of autonomy from the state. While this suggests a shift
in power dynamics and accountability flows, the state continues to exercise its
authority as a funder for other projects. In the absence of clear definition of roles,line of authority and arbitration, the role of the State in implementing national
programmes and regulating private interests is reduced. Several structures and
mechanisms are put in place to ‘coordinate’ efforts and ‘oversee’ implementation of
projects arising from partnership arrangements. However, there is a failure to
Global Public Health 447
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

regulate the dominance of targets and there is no mechanism of arbitration in case of
failure in meeting substantive goals. The duplication and tensions born out of
competing activities and limited funds and clients, as demonstrated in the case study,
has been counterproductive to the programme.
Secondly, the translocal and transnational connections facilitated by the Fund
entail opportunities as well as threats. On one hand, the Fund may offer the network(and some Southern NGOs) greater visibility and leverage in their efforts to influence
national policy and work with national governments. In the case of the network
illustrated earlier, the Fund facilitated its expansion from metropolis to smaller (and
often poorer) districts, which could be suggestive of a greater and improved access of
PLHA to health services and ART treatment. On the other hand, the network is
exposed to direction or control by funding and associated conditionalities. Failure to
maintain computerised records or detailed registers is understood as a marker of
technical ‘inefficiency’ and ‘non-performance’ and often results in disbanding of
certain activities and withholding of small grants to local NGOs and network. Many
writers have observed how donor dependency of NGOs redirects accountability away
from its grass-roots constituencies towards funders (Tandon 1994, Fisher 1997), in
the process making ‘brokers’ out of project staff and ‘clients’ or ‘customers’ out of
the constituencies they represent. Their vulnerabilities as beneficiaries of funding
from both State and the Fund can make them less critical of the positions taken on
programme priorities and strategies and serve as intermediaries to facilitate and
provide organisation assistance and access to the ‘local’.While the concept of ‘local’ remains central to the legitimacy derived by
networks, the case study highlights the growing professionalisation, with over-
whelming focus on targets and recruitments suggesting a depoliticisation of critical
voices, which through training and skill-building sessions with PLHA (members) and
staff of DLN are assimilated and adjusted to the policies of the Fund. The trail of
paper work and extensive reporting requirements of the elite governance mechanisms
of the Fund have transformed the political and organisational culture and diverted
attention from the core mandate of advocacy networks. While the network (and
other non-state) actors have served as important agents of public education
and strengthened their networks by enrolling members, little attention is given to
how enrolment is translated into tackling stigma, discrimination and other human
rights violations or enabling access to drugs and services.
This apparent transition from critical to increasingly technical discourses in order
to fit in with formalised models and frameworks of mainstream development
agencies has also changed the very nature of ‘expertise’. For instance, the cadre ofcommunity workers who are the main links with the community (generating
awareness on treatment through community education and home visits) are
encouraged to work voluntarily, whereas employees with professional degrees and
computer skills are increasingly sought to fill up network positions. Moreover, the
environment of inequities instilled through different pay scales for differently funded
projects (though with overlapping objectives) within the network has also resulted in
increasing discontent among workers, and a high project-specific turnover, affecting
their community links.
Thirdly, the imposition of global structures and ideas on local systems facilitates
a reconfiguration of non-state actors around newer forms of expertise and power
centres. This is made possible as the Fund facilitates the entry of organisations that
448 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

enjoy a certain level of credibility on the basis of their: (1) access to resources
(including expertise) to translate ‘innovative’ project ideas into successful bids, (2)
international standing and links with the government and (3) ability to generate the
support of the ‘beneficiaries’ (in this case, the PLHA). Organisations privileged
within the Fund organisation included international organisations whose registration
as Indian entities, and national organisations whose genesis or movement into the
AIDS industry could be traced around the same time as the launch of the Fund.
Scholte (2004) reflects on the inherent bias and tendency of global governance
agencies to reach out mainly to Northern, urban elite, English-speaking civil society
professionals, which fails to engage wider and often more marginalised constitu-
encies (See also Fisher 1997).
Likewise, in this study, some local and marginal groups seemed to remain at the
mercy of the government for minimal grants to run care centres or provide ad-hoc
group counselling at the treatment centres. However, the realisation and success of
interventions proposed to the Fund necessitated support and participation of PLHA.
The network and other community-based organisations therefore become crucial to
the Fund organisation acting as ‘interpretive communities’ (Mosse 2004) required to
socially sustain the model of partnerships through a constant act of tying in supporters
and reproduce its underlying ideas on volunteerism including greater involvement of
PLHA. A valued partner, as the network, is required to continually recruit support
(through an expanding membership) to stabilise the Fund organisation and its
dominant narratives � country driven, inclusive and participatory governance.
This also necessitates a re-visit of our understanding of the civil society: who are
the civil society actors whose participation is sought and how do hierarchies get
reproduced through these arrangements? Amoore and Langley (2004) have argued
that the term ‘civil society’ enables a dishonest creation of an idealised space where a
large collection of individuals and organisations are assumed to pool their interests
to secure optimal outcomes. This metaphorical notion of civil society underplays
differences and power relations between CSOs and confers unfounded legitimacy on
policy decisions and the actions of international agencies and global governance
strategies. This results in reinforcing rather than challenging the ‘democratic deficit’
of the international systems (Anderson and Rieff 2004).The Fund attributes the successful launch of its first round to ‘grassroots
activism’ and the critical role played by both ‘Northern and Southern civil society
members in creating, funding and governing the Fund’ (Fund website). However, the
analysis highlights how the elite fund governance: annual calls for grant proposals
and performance-based grant-making instil a competitive environment and system-
atically re-configure actors around newer forms of expertise and power centres. It
also facilitates the entry and increasing dominance of international and corporate
actors in country-level governance of disease programmes, thereby concealing the
agency of outsiders under the notion of civil society participation.
References
Altman, D., 1994. Power and community: organizational and cultural responses to AIDS.London: Taylor & Francis, 1�36.
Altman, D., 1999. Globalisation, political economy and HIV/AIDS. Theory and Society, 28(4), 559�564.
Global Public Health 449
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

Amoore, L. and Langley, P., 2004. Ambiguities of global civil society. Review of InternationalStudies, 30, 89�110.
Anderson, K. and Rieff, D., 2004. ‘Global civil society’: a sceptical view. In: H. Anheier,M. Glasius, and M. Kaldor, eds. Global civil society. London: Sage, 26�39.
Bhattacharya, S. and Dasgupta, R., 2009. A tale of two global health programmes. AmericanJournal of Public Health, 99, 1176�1184.
Buse, K. and Harmer, A., 2007. Seven habits of highly effective global public-private healthpartnerships: practice and potential. Social Science & Medicine, 64, 259�271.
Caines, K., Buse, K., Carlson, C., de Loor, R.M., Druce, N., Grace, C., Pearson, M., Sancho,J., and Sadanandan, R., 2004. Assessing the impact of global health partnerships. London:DFID Health Resource Centre.
Cooke, B. and Kothari, U., 2001. The case for participation as tyranny. In: B. Cooke and U.Kothari, eds. Participation: the new tyranny? London: Zed, 1�15.
Dodgson, R., Lee, K., and Drager, N., 2002. Global health governance: a conceptual review.LSHTM/WHO Discussion Paper No. 1.
Doyle, C. and Patel, P., 2008. Civil society organisations and global health initiatives: problemsof legitimacy. Social Science and Medicine, 66, 1928�1938.
Epstein, S., 1996. Impure science: AIDS, activism and the politics of knowledge. Berkeley:University of California Press.
Fisher, W.F., 1997. Doing good? The politics and antipolitics of NGO practices. AnnualReview of Anthropology, 26, 439�464.
Frenk, J., Sepulveda, J., McGuiness, M., and Knaul, F., 1997. The future of world health: thenew world order and international health. British Medical Journal, 314, 1404�1412.
Hickey, S. and Mohan, G., 2004. Participation as transformation. In: S. Hickey andG. Mohan, eds. Participation: from tyranny to transformation? London: Zed Books.
Kapilashrami, A., 2010. Understanding public private partnerships: the discourse, the practice,and the system wide effects of GFATM. A case of the HIV management in India. Thesis(PhD). Queen Margaret University, UK.
Kettler, H., White, K., and Jordan, S., 2003. Valuing industry contributions to public-privatepartnerships for health. Geneva: IPPPH.
Khanna, A., 2009. Taming of the shrewed Meyeli Chhele: a political economy ofdevelopment’s sexual subject. Development, 52, 43�51.
Labonte, R., 1998. Healthy public policy and the WTO: a proposal for an international healthpresence in future world trade/investment talks. Health Promotion International, 13,245�256.
Liese, B.H. and Schubert, L., 2009. Official development assistance for health � how neglectedare neglected tropical diseases? International Health, 1, 141�147.
Loewenson, R., 2003. Civil society influence on global health policy: an annotated bibliography.Zimbabwe: WHO Civil Society Initiative and Training and Research Support Centre.
Mackellar, L., 2005. Priorities in global assistance for health, AIDS and population.Population and Development Review, 31, 293�312.
McCoy, D. and Shuping, S., 2000. Organisation, integration and decentralization: keyrequirements for an HIV response but easier said than done! International conference onAIDS, 9�14 July 2000, 13: abstract no. ThPeD5745.
Mosse, D., 2001. People’s knowledge, participation and patronage. In: B. Cooke andU. Kothari, eds. Participation: the new tyranny? London: Zed Books.
Mosse, D., 2004. Is good policy unimplementable? Reflections on the ethnography of aidpolicy and practice. Development and Change, 35, 639�671.
Mosse, D. and Lewis, D., eds., 2006. Development brokers and translators. The ethnography ofaid and agencies. Bloomfield, CT: Kumarian Press.
Neef, A., 2003. Participatory approaches under scrutiny: will they have a future? QuarterlyJournal of International Agriculture, 42 (4), 489�497.
Nelson, N. and Wright, S., 1995. Participation and power. In: N. Nelson and S. Wright, eds.Power and participatory development. London: Intermediate Technology Publications, 1�18.
Patton, C., 1991. The AIDS service industry: the construction of ‘victims,’ ‘volunteers,’ and‘experts’. In: C. Patton, ed. Inventing AIDS. New York: Routledge, 5�23.
450 A. Kapilashrami and O. O’Brien
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012

Scholte, J.A., 2004. Civil society and democratically accountable global governance.Government and Opposition, 39, 211�233.
Shiffman, J., 2008. Has donor prioritisation of HIV/AIDS displaced aid for other healthissues? Health Policy and Planning, 23, 95�100.
Tandon, R., 1994. Civil society, the state and the role of NGOs. In: I. Serrano, ed. Civil societyin the Asia-Pacific region. Washington, DC: CIVICUS, 117�136.
Winters, D.J., 2008. Country coordinating mechanisms: partnership and leadership. Geneva:GFATM. Global Fund Implementer Series. 25-6-2009.
Yepthomi, T., 1998. From darkness to light. International Conference on AIDS. 12, 916(abstract no. 43355).
Global Public Health 451
Dow
nloa
ded
by [
Anu
j Kap
ilash
ram
i] a
t 01:
39 1
7 A
pril
2012