The epidemiology of measles in England and Wales since the 1994 vaccination campaign
16
The epidemiology of measles in England and Wales since the 1994 vaccination campaign N Gay, M Ramsay, B Cohen, L Hesketh, P Morgan-Capner, D Brown, E Miller Summary The incidence of measles in England and Wales has fallen since the national vaccination campaign in November 1994, in which 92% of children aged 5 to 16 years were vaccinated. A total of 148 confirmed cases with onsets in the 18 months from January 1995 to June 1996 have been ascertained. Notified cases did not provide a reliable measure of incidence: 11 343 suspected cases were notified in the same period, 6426 (57%) of whom were tested for salivary antibody. Only 90 (1.4%) of cases tested were confirmed. Many confirmed cases occurred in small clusters; 12 imported cases were identified. The pattern of small, local clusters is what would be expected from the introduction of imported cases into a population with herd immunity. Serological surveillance showed that the campaign produced a significant fall in the proportion of 5 to 16 year old children with low levels of measles antibody: the proportion with levels <50mIU/ml fell from 8.4% to 2.1%; the proportion with levels <100mIU/ml fell from 15.7% to 6.6%. About 15% of 2 to 4 year old children had antibody levels <100mIU/ml before and after the campaign. The addition of a routine second dose of measles vaccine (as measles, mumps, and rubella vaccine) to the vaccination schedule will provide another opportunity to immunise these children before they start school. The two dose vaccination programme should maintain the herd immunity of the population and the elimination of endemic measles transmission. Key words: immunisation – measles – preventive health services – salivary diagnosis – seroepidemiological methods Introduction A national campaign of measles and rubella vaccination took place in the United Kingdom in November 1994 to prevent an epidemic of measles that had been predicted to occur in 1995 1,2 . All children aged 5 to 16 years (5 to 18 years in Scotland) were offered the combined vaccine and 92% of the 7.1 million eligible children in England were vaccinated 3 . Such high coverage was expected to lead to the interruption of endemic measles transmission 1 . Since the campaign, the PHLS has enhanced surveillance of measles by offering to test saliva specimens from all cases of measles notified to the Office for National Statistics (ONS) – formerly the Office of Population Censuses and Surveys (OPCS). In addition, serological surveys to determine the prevalence of measles antibody in children aged 2 to 16 years were performed both before and after the campaign. We report data from these surveillance programmes, which provide insights into the epidemiology of measles in England and Wales since the vaccination campaign. Methods Incidence of measles Confirmed cases of measles were ascertained from three sources: cases notified to ONS that were confirmed by the detection of measles specific IgM antibody in saliva specimens at the Enteric and Respiratory Virus Laboratory, PHLS The epidemiology of measles in England and Wales since the 1994 vaccination campaign N Gay, M Ramsay, B Cohen, L Hesketh, P Morgan-Capner, D Brown, E Miller R17–21 Mumps surveillance in England and Wales supports introduction of two dose vaccination schedule N Gay, E Miller, L Hesketh, P Morgan-Capner, M Ramsay, B Cohen, D Brown R21–6 The epidemiology of rubella in England and Wales before and after the 1994 measles and rubella vaccination campaign: fourth joint report from the PHLS and the National Congenital Rubella Surveillance Programme E Miller, P Waight, N Gay, MaRamsay, J Vurdien, P Morgan- Capner, L Hesketh, D Brown, PaTookey, C Peckham R26–32 Correction: Editorial: innovations for the new year S Handysides R32 Volume 7 Review Number 2 7 February 1997 ISSN 1350-9349 Correspondence to: Editor CDR, PHLS Communicable Disease Surveillance Centre, 61 Colindale Avenue, London NW9 5EQ Tel: 0181 200 6868 Fax: 0181 200 7868 Telex: 8953942 Public Health Laboratory Service CDR REVIEW © 1997 Communicable Disease Review
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The epidemiology of measles in England and Wales since the 1994 vaccination campaign
The epidemiology of measles in England andWales since the 1994 vaccination campaignN Gay, M Ramsay, B Cohen, L Hesketh, P Morgan-Capner, D Brown, E Miller
SummaryThe incidence of measles in England and Wales has fallen since the nationalvaccination campaign in November 1994, in which 92% of children aged 5 to16 years were vaccinated. A total of 148 confirmed cases with onsets in the18 months from January 1995 to June 1996 have been ascertained. Notified cases didnot provide a reliable measure of incidence: 11 343 suspected cases were notified inthe same period, 6426 (57%) of whom were tested for salivary antibody. Only 90(1.4%) of cases tested were confirmed. Many confirmed cases occurred in smallclusters; 12 imported cases were identified. The pattern of small, local clusters iswhat would be expected from the introduction of imported cases into a populationwith herd immunity. Serological surveillance showed that the campaign produceda significant fall in the proportion of 5 to 16 year old children with low levels ofmeasles antibody: the proportion with levels <50mIU/ml fell from 8.4% to 2.1%; theproportion with levels <100mIU/ml fell from 15.7% to 6.6%. About 15% of 2 to4 year old children had antibody levels <100mIU/ml before and after the campaign.The addition of a routine second dose of measles vaccine (as measles, mumps, andrubella vaccine) to the vaccination schedule will provide another opportunity toimmunise these children before they start school. The two dose vaccinationprogramme should maintain the herd immunity of the population and theelimination of endemic measles transmission.
Key words: immunisation – measles – preventive health services – salivarydiagnosis – seroepidemiological methods
IntroductionA national campaign of measles and rubella vaccination took place in the UnitedKingdom in November 1994 to prevent an epidemic of measles that had beenpredicted to occur in 19951,2. All children aged 5 to 16 years (5 to 18 years inScotland) were offered the combined vaccine and 92% of the 7.1 million eligiblechildren in England were vaccinated3. Such high coverage was expected to leadto the interruption of endemic measles transmission1.
Since the campaign, the PHLS has enhanced surveillance of measles byoffering to test saliva specimens from all cases of measles notified to the Office forNational Statistics (ONS) – formerly the Office of Population Censuses andSurveys (OPCS). In addition, serological surveys to determine the prevalence ofmeasles antibody in children aged 2 to 16 years were performed both before andafter the campaign. We report data from these surveillance programmes, whichprovide insights into the epidemiology of measles in England and Wales sincethe vaccination campaign.
MethodsIncidence of measlesConfirmed cases of measles were ascertained from three sources: cases notifiedto ONS that were confirmed by the detection of measles specific IgM antibodyin saliva specimens at the Enteric and Respiratory Virus Laboratory, PHLS
The epidemiology of measlesin England and Wales sincethe 1994 vaccinationcampaign
N Gay, M Ramsay, B Cohen,L Hesketh, P Morgan-Capner,D Brown, E Miller
R17–21
Mumps surveillance inEngland and Wales supportsintroduction of two dosevaccination schedule
N Gay, E Miller, L Hesketh,P Morgan-Capner, M Ramsay,B Cohen, D Brown
R21–6
The epidemiology of rubellain England and Wales beforeand after the 1994 measlesand rubella vaccinationcampaign: fourth joint reportfrom the PHLS and theNational Congenital RubellaSurveillance Programme
E Miller, P Waight, N Gay,MaRamsay, J Vurdien, P Morgan-Capner, L Hesketh, D Brown,PaTookey, C Peckham
R26–32
Correction: Editorial:innovations for the new year
S HandysidesR32
Volume 7
Review Number 2
7 February 1997
ISSN 1350-9349
Correspondence to: Editor CDR, PHLS Communicable Disease Surveillance Centre, 61 Colindale Avenue, London NW9 5EQ Tel: 0181 200 6868 Fax: 0181 200 7868 Telex: 8953942 Public Health Laboratory Service
CDR REVIEW
© 1997
Communicable Disease Review
Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R18
0
100
200
300
400
500
600
700
800
95908580757065601955
Year
Not
ifica
tions
(th
ousa
nds)
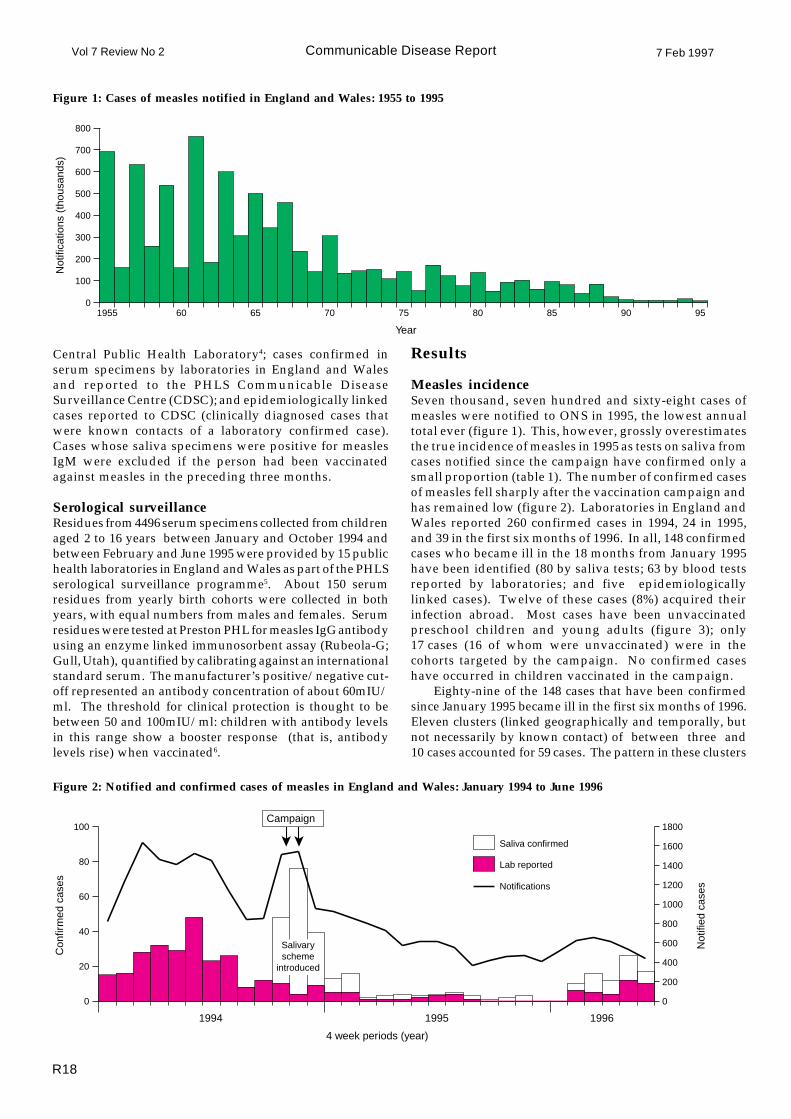
Figure 1: Cases of measles notified in England and Wales: 1955 to 1995
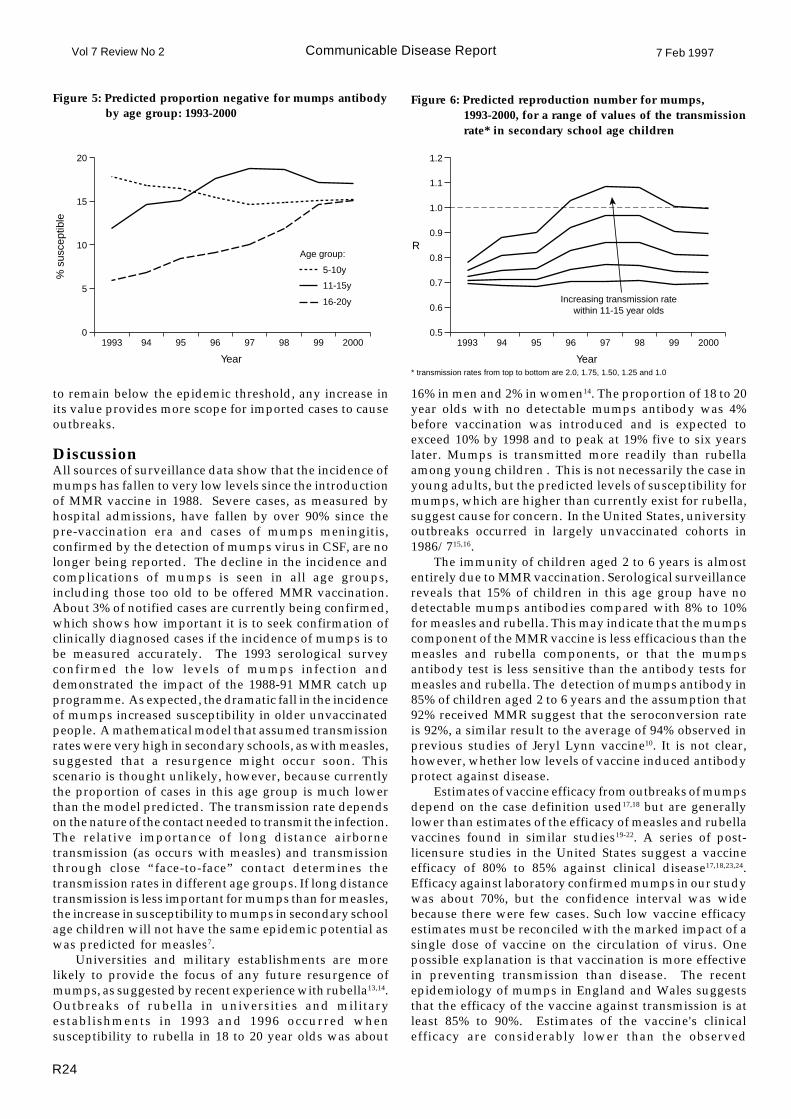
Figure 2: Notified and confirmed cases of measles in England and Wales: January 1994 to June 1996
Results
Measles incidenceSeven thousand, seven hundred and sixty-eight cases ofmeasles were notified to ONS in 1995, the lowest annualtotal ever (figure 1). This, however, grossly overestimatesthe true incidence of measles in 1995 as tests on saliva fromcases notified since the campaign have confirmed only asmall proportion (table 1). The number of confirmed casesof measles fell sharply after the vaccination campaign andhas remained low (figure 2). Laboratories in England andWales reported 260 confirmed cases in 1994, 24 in 1995,and 39 in the first six months of 1996. In all, 148 confirmedcases who became ill in the 18 months from January 1995have been identified (80 by saliva tests; 63 by blood testsreported by laboratories; and five epidemiologicallylinked cases). Twelve of these cases (8%) acquired theirinfection abroad. Most cases have been unvaccinatedpreschool children and young adults (figure 3); only17 cases (16 of whom were unvaccinated) were in thecohorts targeted by the campaign. No confirmed caseshave occurred in children vaccinated in the campaign.
Eighty-nine of the 148 cases that have been confirmedsince January 1995 became ill in the first six months of 1996.Eleven clusters (linked geographically and temporally, butnot necessarily by known contact) of between three and10 cases accounted for 59 cases. The pattern in these clusters
Central Public Health Laboratory4; cases confirmed inserum specimens by laboratories in England and Walesand reported to the PHLS Communicable DiseaseSurveillance Centre (CDSC); and epidemiologically linkedcases reported to CDSC (clinically diagnosed cases thatwere known contacts of a laboratory confirmed case).Cases whose saliva specimens were positive for measlesIgM were excluded if the person had been vaccinatedagainst measles in the preceding three months.
Serological surveillanceResidues from 4496 serum specimens collected from childrenaged 2 to 16 years between January and October 1994 andbetween February and June 1995 were provided by 15 publichealth laboratories in England and Wales as part of the PHLSserological surveillance programme5. About 150 serumresidues from yearly birth cohorts were collected in bothyears, with equal numbers from males and females. Serumresidues were tested at Preston PHL for measles IgG antibodyusing an enzyme linked immunosorbent assay (Rubeola-G;Gull, Utah), quantified by calibrating against an internationalstandard serum. The manufacturer’s positive/negative cut-off represented an antibody concentration of about 60mIU/ml. The threshold for clinical protection is thought to bebetween 50 and 100mIU/ml: children with antibody levelsin this range show a booster response (that is, antibodylevels rise) when vaccinated6.
0
20
40
60
80
100
0
200
400
600
800
1000
1200
1400
1600
1800
Saliva confirmed
Lab reported
Notifications
4 week periods (year)
Con
firm
ed c
ases
Not
ified
cas
es
Salivaryscheme
introduced
Campaign
1994 1995 1996

Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R19
Number Number (%) Number (%)Week notified notified tested confirmed
Table 1 Cases of measles confirmed by the detection ofsalivary antibody in cases notified to ONS:November 1994 to June 1996
Figure 3: Age distribution of 148 confirmed cases of measlesin England and Wales: January 1995 to June 1996
DiscussionEnhanced surveillance of measles has shown an extremelylow incidence of confirmed infections since the nationalmeasles and rubella vaccination campaign in November1994. In all, 148 cases with onset between January 1995and June 1996 have been confirmed. Investigation of 6426cases notified since January 1995 using saliva tests hasconfirmed the diagnosis of measles in only 90 (1.4%).These data represent a dramatic fall from the incidencebefore the campaign7. Effective surveillance of measleswould be impossible without such microbiologicalsupport. Studies to investigate the causes of cases notifiedbut not confirmed as measles are planned. These studieswould test specimens from cases for a range of infectionsincluding rubella, parvovirus B19, human herpes virus 6,Epstein Barr virus, cytomegalovirus, enteroviruses, andgroup A streptococci.
The low incidence of measles gives added importanceto the specificity of the laboratory tests. If only 1% ofnotified cases are due to measles, even a confirmatory testwith 99% specificity would produce equal numbers oftrue and false positive results8. To monitor the occurrenceof false positive diagnoses obtained from saliva tests, anadditional IgM test was performed on serum if a suitablespecimen was available8. Twenty-two of the 26 salivapositive cases tested were positive for measles IgM inserum and four were negative, confirming theexceptionally high specificity of the saliva test8.
The confirmed cases detected by surveillance do notinclude all measles infections. The proportion of measlescases that are notified cannot be measured easily, but anestimate of 63% was made in the pre-vaccination era9.Using this figure we estimate that saliva specimens areobtained from 36% of all measles cases (57% of notifiedcases provide a specimen). Almost all true cases testedwould be identified as measles because of the highsensitivity of the salivary assay10. Taking into account theadditional cases that are reported by laboratories, as manyas 50% of all measles infections may be detected by thesurveillance system.
Figure 4: Proportions of serum residues with low levels ofmeasles antibody before and after MR campaign,by age
1994 44–52 2823 1462 (51.8) 114 (7.8)
1995 01–13 2777 1720 (61.9) 27 (1.6)
1995 14–26 2018 1242 (61.5) 5 (0.4)
1995 27–39 1524 885 (58.1) 9 (1.0)
1995 40–52 1449 771 (53.2) 6 (0.8)
1996 01–13 1962 970 (49.4) 13 (1.3)
1996 14–26 1613 838 (52.0) 30 (3.6)
0
5
10
15
20
50-99 mlU/ml
0-49 mlU/ml
19951994199519941995199419951994
Age group (years)
2-4 5-9 10-14 15-16
% o
f spe
cim
ens
0
10
20
30
40Vaccinated
Unvaccinated
40+35-3930-3425-2920-2415-1910-145-90-4
Age group (years)
Confir
med c
ase
s
was of initial transmission between young adults, andsubsequent transmission to unvaccinated preschool children.Three clusters were associated with universities (Essex8 cases, Hertfordshire 4, and Merseyside 8). Five importedcases were identified in 1996; three from Greece, and onefrom each of Germany and Pakistan. One was the index casefor the university outbreak in Essex, one produced twosecondary cases, and no confirmed secondary cases werereported in association with the other three.
Serological surveillanceThe measles/rubella vaccination campaign has made asignificant impact on the susceptibility of the target cohorts(figure 4). The proportion of 5 to 16 year olds withmeasles antibody levels <50mIU/ml fell by 74% from8.4% (150/1796) in 1994 to 2.1% (40/1868) in 1995(p<0.0001): the proportion of the same age group withmeasles antibody levels <100mIU/ml fell by 58% from15.7% (282/1796) in 1994 to 6.6% (124/1868) in 1995(p<0.0001). There was no significant difference in antibodyprevalence between the sexes. Measles antibody levels in2 to 4 year olds were similar in both years (p=0.31): 15.3%(127/832) were <100mIU/ml. (All p values were calculatedusing the chi squared test.)

Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R20
Serological surveillance confirms that the MRcampaign has reduced the susceptibility of children ofschool age. The level of susceptibility is sufficiently lowfor the population to possess herd immunity; mathematicalmodels2 suggest that the reproduction number R (thenumber of secondary cases infected by a typical primarycase) is not greater than 0.7, well below R=1, values abovewhich represent loss of herd immunity. In this situation,elimination of endemic measles would be expected. Somelocal outbreaks would continue to occur as a result oflimited secondary spread from imported cases but theherd immunity of the population would preventwidespread transmission. Imported cases would beexpected to account for a proportion 1-R of all cases11, ie30% with R=0.7.
The pattern of small, local outbreaks of measlesobserved in England and Wales since 1995 is consistentwith this interpretation. It is, however, often impossible toidentify the primary case in an outbreak, despite intensiveinvestigation. Although surveillance should pick upresidents who acquire infection abroad, there are difficultiesin confirming cases in foreign visitors. Short term visitorsmay be infectious while in England and Wales but notbecome ill before returning home. Visitors who do becomeill may not present to health services. These problemsmay be exacerbated by a surveillance system that reliesprimarily on obtaining a specimen of saliva some weeksafter the illness. The proportion of cases that are confirmedmay be considerably lower for imported cases than forcases acquired in England and Wales. This may explainwhy only 8% of confirmed cases were acquired abroad,rather than the 30% predicted by the model.
The increased number of cases seen in the first half of1996, which may be due to an increase in the number ofimported cases, shows how the epidemiology of measlesin England and Wales depends on external influences.Measles epidemics occurred in Germany12 and Greece(DriStelios Triantios, personal communication) in the firsthalf of 1996; four of the five confirmed importations in1996 came from these two countries. The sources ofimported cases will vary from year to year in line withepidemic cycles in other countries. Genotyping of measlesvirus may help to find the source of imported cases13,14.The only way to minimise the effect of importations is tomaintain high levels of immunity throughout thepopulation.
The need to introduce a routine second dose of MMRvaccine for preschool children to build on the success ofthe campaign is highlighted by the high proportion ofchildren aged 2 to 4 years with low antibody levels. Thisaddition to the routine vaccination programme will reducethe level of susceptibility in future cohorts of schoolchildrenby providing a second opportunity to immunise childrenwho do not respond or who miss the first dose of MMRvaccine15. The coverage of the second dose in vaccinatedand unvaccinated children will be monitored in theCOVER/Körner statistics16 and the impact on susceptibilityidentified by serological surveillance. The two dosevaccination programme should maintain the herdimmunity of the population and the elimination of endemicmeasles transmission.
AcknowledgementsWe thank the staff at Ashford, Birmingham, Bristol,Cambridge, Cardiff, Carlisle, Exeter, Gloucester, Leeds,Manchester, Norwich, Preston, Reading, Rhyl, and Tootingpublic health laboratories for providing the serum residuesfor serological surveillance; general practitioners forassisting with the collection of saliva specimens; and JoeRowlatt for help with data management.
References1. Ramsay ME, Gay NJ, Miller E, Rush M, White JM,
Morgan-Capner P, et al. The epidemiology of measles inEngland and Wales: rationale for the 1994 nationalvaccination campaign. Commun Dis Rep CDR Rev 1994;4: R141-6.
2. Gay NJ, Hesketh LM, Morgan-Capner P, Miller E.Interpretation of serological surveillance data for measlesusing mathematical models: implications for vaccinestrategy. Epidemiol Infect 1995; 115: 139-56.
3. Salisbury DM, Horsley SD. Measles campaign. BMJ1995; 310: 1334.
4. Brown DW, Ramsay ME, Richards AF, Miller E. Salivarydiagnosis of measles: a study of notified cases in theUnited Kingdom, 1991-3. BMJ 1994; 308: 1015-7.
5. Morgan-Capner P, Wright J, Miller CL, Miller E.Surveillance of antibody to measles, mumps and rubellaby age. BMJ 1988; 297: 770-2.
6. Calvert N, Cutts FT, Irving R, Brown DW, Marsh J, MillerE. Measles immunity and response to revaccinationamong secondary school children in Cumbria. EpidemiolInfect 1996; 116: 65-70.
7. Ramsay ME, Brown DW. Measles data are reliable. BMJ1996; 311: 810.
8. Ramsay ME, Cohen BJ, Brown DW. Serum IgM testingis needed in all cases of suspected measles. BMJ 1996;313: 231.
9. Fine PEM, Clarkson JA. Measles in England and Wales.II. The impact of the measles vaccination programme onthe distribution of immunity in the population. Int JEpidemiol 1982; 11: 15-25.
10. Perry KR, Brown DW, Parry JV, Panday S, Pipkin C,Richards A. The detection of measles, mumps andrubella antibodies in saliva using antibody captureradioimmnuoassays. J Med Virol 1993; 40: 235-40.
11. Gay NJ. A model of long term decline in diseasetransmissibility: implications for the incidence of hepatitisA. Int J Epidemiol 1996; 25: 854-61.
12. Robert Koch Institut. Masernerkrankungswelle in denneuen Bundeslandern. Epidemiologisches Bulletin1996;190-2.
13. Rota JS, Heath JL, Rota PA, King GE, Celma ML, CarabanaJ, et al. Molecular epidemiology of measles virus:identification of pathways of transmission andimplications for measles elimination. J Infect Dis 1996;173: 32-7.
14. Jin L, Richards A, Brown DW. Development of a dualtarget-PCR for detection and characterization of measlesvirus in clinical specimens. Mol Cell Probes 1996; 10: 191-200.
15. CDSC. A second dose of MMR vaccine for children in theUnited Kingdom. Commun Dis Rep CDR Wkly 1996; 6: 259.

Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R21
P Morgan-Capner, director, PHLS North West.
Address for correspondenceNigel GayImmunisation DivisionPHLS Communicable Disease Surveillance Centre61 Colindale AvenueLondon NW9 5EQtelephone 0181 200 6868 ext 3401fax 0181 200 7868email [email protected]
Mumps surveillance in England and Wales supports introductionof two dose vaccination scheduleN Gay, E Miller, L Hesketh, P Morgan-Capner, M Ramsay,
B Cohen, D Brown
SummarySentinel surveillance in general practice and laboratoryreports to the PHLS Communicable Disease SurveillanceCentre show that the incidence of mumps has fallen tovery low levels since vaccination against measles, mumps,and rubella was introduced in 1988. Hospital admissionsfor mumps show a 92% decline compared with the pre-vaccination era, to a rate of 0.2 per 100 000 population peryear. Serological surveillance has shown an increase inthe proportion of school age children who have nodetectable antibody to mumps, which is consistent withthe reduction in mumps virus transmission. Theproportion of children aged 11 to 15 years with nodetectable antibody is expected to peak at 19% in 1997.Mathematical models suggest that this increase insusceptibility is unlikely to allow a large resurgence ofmumps in the short term but that school outbreaks maybecome more common. Outbreaks in universities andmilitary establishments are possible in the medium term.Analysis of efficacy data for mumps vaccine indicates thatmumps is unlikely to be eliminated with a single dose ofvaccine at current coverage rates. A second dose ofvaccine,which is now being offered to preschool children,will reduce morbidity and should eventually eliminatemumps if coverage is high enough.
Key words: immunisation – mumps – preventive healthservices – salivary diagnosis – seroepidemiologicalmethods
IntroductionImmunisation against mumps was introduced in Englandand Wales in October 1988 as one component of thecombined measles, mumps, and rubella (MMR) vaccineoffered to all children aged 12 to 15 months. In addition,all preschool children were offered MMR vaccine in athree year catch up programme. Some districts extendedthe programme to children aged 5 to 10 years1,2. Coverage
by the end of the second year of life has exceeded 90%since 1991 and is currently 92%3. This paper evaluates theimpact of the first seven years of MMR vaccination on theincidence of mumps and the population's immunity anddiscusses the implications for future vaccine policy.
MethodsData on the incidence of clinically diagnosed mumps inEngland and Wales were obtained from reports fromsentinel surveillance practices to the Royal College ofGeneral Practitioners (RCGP) and notifications to theOffice of Population Censuses and Surveys (OPCS). Theincidence of laboratory confirmed mumps infection wasmonitored through reports to the PHLS CommunicableDisease Surveillance Centre (CDSC) from PHLS andNational Health Service hospital laboratories in Englandand Wales. Since November 1994, saliva specimens havebeen requested from all notified cases of mumps in Englandand Wales and tested for mumps specific IgM antibodyusing a capture radioimmunoassay at the PHLS Entericand Respiratory Virus Laboratory4. Vaccination historiesof laboratory confirmed cases were obtained from generalpractice or district records. Hospital admission rates formumps before the introduction of MMR vaccine5 werecompared with data from Hospital Episode Statistics (HES)available for England since 1988/9. Computeriseddischarge data obtained from patient administrationsystems in hospitals in North Thames Region wereanalysed for the period April 1993 to March 1994.
The age specific prevalence of antibodies to mumpsbefore and after the introduction of MMR vaccination wasmonitored through the PHLS serological surveillanceprogramme6. Since 1986, residues of serum specimenssubmitted for microbiological investigation to sentinelPHLS laboratories in England have been collected inspecified age groups. These residues do not come from arandom sample of the population, but should representthe population in terms of exposure to mumps. Results ofseroprevalence studies of other infections using samplesobtained in this way have consistently reflected expectedepidemiological trends. Results of radial haemolysis testson serum residues collected in 1986/7 have been reported
16. White JM, Rush M, Leon S, Ramsay ME. COVER/Körner95-1 (April to June 1995): vaccination coverage statisticsfor children up to 2 years old in the United Kingdom.Commun Dis Rep CDR Rev 1995; 5: R186-7.
N Gay, mathematical modeller, M Ramsay, consultantepidemiologist, E Miller, head, Immunisation Division,PHLS Communicable Disease Surveillance Centre.B Cohen, clinical scientist, D Brown, director,Enteric and Respiratory Virus LaboratoryPHLS Central Public Health Laboratory.L Hesketh, medical laboratory scientific officer,Preston Public Health Laboratory.

Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R22
Results
RCGP reportsThe introduction of MMR vaccine in October 1988 wasfollowed by an immediate and sustained reduction in thefour weekly incidence of clinically diagnosed mumpscases reported to the RCGP (figure 1). The annual incidencein 1995 was 17 per 100 000 compared with 160/100 000 in1989. The incidence fell in all age groups but the fall wasmost marked in children aged 0 to 14 years.
NotificationsMumps notifications fell sharply and remained low afterMMR vaccination was introduced. The annual incidencein 1995 was 4.0/100 000, with about 50 notifications perweek compared with about 400 per week in 1989.
Laboratory confirmed casesThe number of laboratory reports received by CDSC hasdeclined sharply since 1989 to fewer than 50 each year(figure 1). The tests used to confirm cases are virus isolationand detection of virus specific IgM or a four fold rise inIgG titre. A report of a single high IgG titre is notconsidered to represent a confirmed case. The ages of 50out of the 53 confirmed cases reported between January1993 and December 1995 were known. Only 19 (38%) werechildren aged under 15 years (7 of these were aged 0 to 4years, 10 were 5 to 9 years, and 2 were 10 to 14 years),compared with 67% for the period 1975-815.
Since the national salivary diagnosis scheme was setup in November 1994, 46% (1333/2868) of the notifiedcases of clinically diagnosed mumps have been tested formumps specific IgM antibody, and antibody was detectedin 40 (3%). Acute mumps was diagnosed in 39, and theother had been vaccinated recently. Fourteen of the 39acute cases had a history of vaccination: they comprisedfive of the six cases overall aged 1 to 4 years, six of theeight aged 5 to 9 years, two of the five aged 10 to 14 years,and one whose age was not known. Thus 11/14 confirmedcases aged 1 to 9 years had been vaccinated. Assuming92% coverage with MMR vaccine in these cohorts3, vaccineefficacy was estimated by the screening method to be 68%(95% confidence interval -14 to 91)11,12.
previously6, but residues negative on radial haemolysishave been retested using an enzyme linked immunosorbentassay (ELISA) if sufficient serum was left over. Serumresidues from 3535 people aged 1 to 24 years (about 150 ofeach year group), submitted to nine public healthlaboratories (PHL) in 1993 were tested for IgG antibody tomumps using an ELISA (Biowhitaker), whose sensitivityand specificity are comparable with the radial haemolysis/ELISA procedure used for the 1986/7 specimens (ACharlett, unpublished). The proportions that wereantibody negative in different age groups up to the year2000 were predicted assuming that the proportion negativein each birth cohort did not subsequently change, in otherwords, that these cohorts did not acquire antibodiesthrough infection or vaccination. The proportion of newcohorts remaining antibody negative was assumed toequal the proportion observed in 2 to 6 year olds in 1993,as vaccination coverage of these cohorts was similar.
The age specific antibody prevalence data wereinterpreted using mathematical models7. For this analysisthe presence of antibody was taken to indicate immunity,and nondetection to indicate susceptibility. The modelswere used to show whether the expected levels ofsusceptibility would exceed the threshold above which anepidemic could occur. This was achieved by calculatingthe reproduction number, R, (the number of secondaryinfections produced by a typical primary case) from thepredicted age specific levels of susceptibility and thetransmission rates between and within different agegroups7,8. If R<1 the population has herd immunity; ifR>1 the potential exists for an epidemic7,8. The size ofsuch a potential epidemic was estimated to be twice thenumber of infections required to reduce R to 17,9. Themorbidity associated with an epidemic was estimatedusing the age specific rates of complications per infection10.The sensitivity of the predictions to the transmission ratein secondary school age children was investigated as ithas been for measles7,9. We applied values for thetransmission rate from one to two times the transmissionrate in primary school age children; all were consistentwith the epidemiology of mumps before vaccination wasintroduced. Details of the parameter estimation will bepublished elsewhere.
Figure 1: Mumps incidence (RCGP) and number ofconfirmed cases reported to CDSC: 1962-95
Figure 2: Isolates of mumps virus from CSF reported toCDSC: 1980-95
Labo
rato
ry r
epor
ts a
ndG
P c
onsu
ltatio
n ra
tes
0
500
1000
1500 Laboratory reports
GP consultation rates
Year
per 100 000 population
70 75 80 85 901965
MMR vaccineintroduced
950
10
20
30
40
50
>4 years
1-4 years
9594939291908988878685848382811980
Year
Num
ber
of c
ases
MMR vaccineintroduced

Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R23
Figure 4: Proportion of serum residues negative for mumpsantibody by age in 1993 compared with a baselineprofile *
Figure 3: Proportion of serum residues negative for mumpsantibody by age: 1986/7 and 1993
0
20
40
60
80
Baseline
1993 data
2018161412108642
Age (years)
% a
ntib
ody
nega
tive
No evidenceof vaccination
or infection
ReceivedMMR at
15 months
Targeted inpre-schoolcatch up
May havereceived
ad hoc MMRvaccination
represent antibody acquired by infection or vaccination.Children aged 2 to 6 years in 1993 would have beeneligible for MMR vaccine at 12 to 15 months; 15.5% ofthem (113/730) were antibody negative. Children aged 7to 9 years in 1993 were the cohorts targeted by the preschoolcatch up programme; 19.2% (84/437) of them wereantibody negative in 1993 compared with 61.7% (612/992) in the baseline (p<0.0001). In children aged 10 to 13years 14.9% (89/599) were antibody negative in 1993compared with 23.9% (311/1303) in the baseline (p<0.0001)and this smaller difference may be due to the ad hocadministration of MMR vaccine during the catch upprogramme. The similarity of profiles in those aged over13 years is evidence of lack of infection and vaccination inthese birth cohorts; 7.9% (71/900) of 14 to 19 year oldswere antibody negative in 1993 compared with 7.6% (154/2014) in the baseline profile (p=0.88).
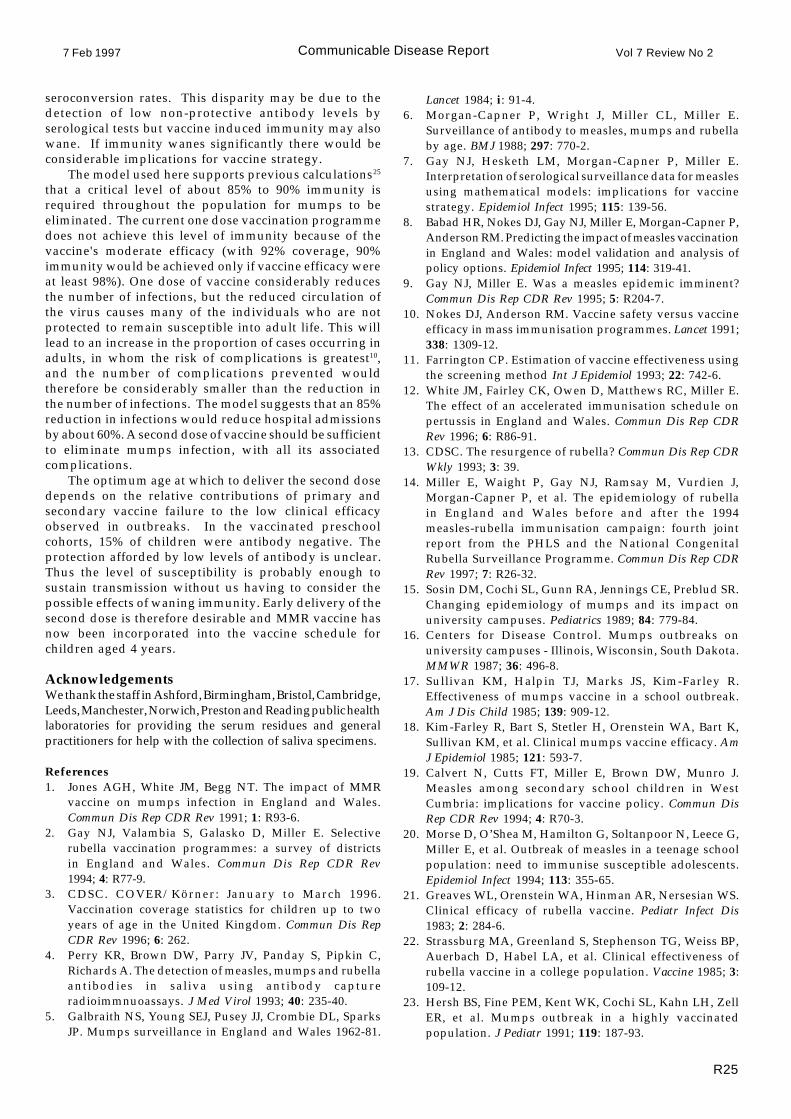
Mathematical modellingFigure 5 shows the proportion of children who arepredicted to be antibody negative in different age groupsup to the year 2000. The proportion of children up to 10years of age who are antibody negative stabilises at 15%.The proportion of antibody negative 11 to 15 year oldspeaks at 19% in 1997 and falls gradually to 15%.Seronegativity in 16 to 20 year olds continues to rise foranother five years as the most susceptible cohorts passthrough this age group.
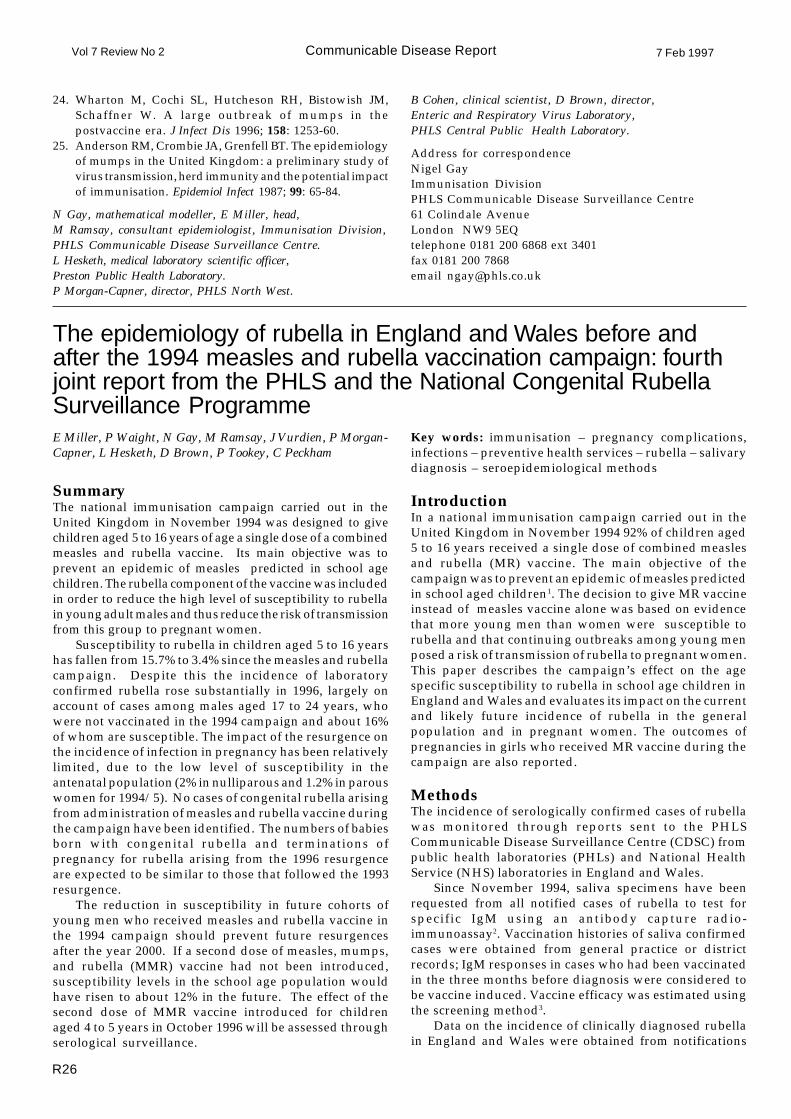
Figure 6 shows changes in R from 1993 to 2000. Rincreases as a result of increasing susceptibility in olderage groups. The value of R remains below the epidemicthreshold (R=1) at most transmission rates. If we assumea transmission rate in children of secondary school agetwice that in primary school children, however, R wouldexceed one in 1997/8. The resulting epidemic couldresult in over 100 000 infections and over 500 hospitaladmissions. This model also predicted that most cases atthe present time would have been in 11 to 15 year olds,however, which is not supported by evidence fromlaboratory confirmed cases. Models that better reflect theobserved age distribution suggest that a major resurgencein secondary schools will not occur. Although R is expected
Cases of mumps meningitis/encephalitis confirmedby the detection of mumps virus in cerebrospinal fluid(CSF) reported to CDSC between 1980 and 1995 are shownin figure 2. Seventeen of the 28 cases aged 1 to 4 yearsreported since January 1989 were children aged 12 to 24months who had received MMR vaccine containing theUrabe mumps strain two to five weeks earlier. No viruspositive mumps meningitis cases in recent MMR vaccineeshave been reported since the Jeryl Lynn strain replacedthe Urabe strain in MMR vaccines in September 1992. Nocases of mumps meningitis in which wild virus has beenisolated from CSF have been reported to CDSC in any agegroup since 1992.
Hospital admissionsThe number of hospital admissions for mumps in Englandfell when MMR vaccine was introduced from 623admissions in the year to March 1989 to 79 in the year toMarch 1991. The annual admission rate for mumps hasnow levelled off at around 0.2 per 100,000, a 92% reductioncompared with an average annual admission rate forEngland and Wales of 2.6 per 100 000 over the period1962-815. An age distribution of cases admitted to hospitalwas unavailable from HES data. Computerised PAS datafor the North Thames region showed a total of 14admissions due to mumps for the year to March 1994 - anannual rate of 0.2 per 100 000. Only five of the 14 admissionswere of children under 15 years of age compared with 66%of admissions before MMR vaccine was introduced5.
Serological surveillanceThe proportions of people aged 3 to 20 years in 1993 and1986/7 in whose serum no mumps antibody was detectedare shown in figure 3. The proportion in whom no antibodywas detected fell at ages 2 to 6 years as a result ofvaccination, but rose at ages 9 to 20 years as a result ofreduced exposure to infection. Figure 4 compares the 1993profile with a baseline profile - the profile expected if noone in any age group had acquired mumps antibody sinceMMR vaccination was introduced (calculated by ageingthe prevaccination profile, the smoothed 1986/7 data, byfive years). The difference between the two profiles must
0
10
20
30
40
50
60
1986/7
1993
19-2017-1815-1613-1411-129-107-85-63-4
Age group (years)
% a
ntib
ody
nega
tive
(* profile expected if there had been no acquisition of mumps antibody in any age groupsince the introduction of MMR vaccination).
Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R24
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
20009998979695941993
Year
R
Increasing transmission ratewithin 11-15 year olds
Figure 6: Predicted reproduction number for mumps,1993-2000, for a range of values of the transmissionrate* in secondary school age children
Figure 5: Predicted proportion negative for mumps antibodyby age group: 1993-2000
0
5
10
15
20
16-20y
11-15y
5-10y
20009998979695941993
Year
% s
usce
ptib
le
Age group:
to remain below the epidemic threshold, any increase inits value provides more scope for imported cases to causeoutbreaks.
DiscussionAll sources of surveillance data show that the incidence ofmumps has fallen to very low levels since the introductionof MMR vaccine in 1988. Severe cases, as measured byhospital admissions, have fallen by over 90% since thepre-vaccination era and cases of mumps meningitis,confirmed by the detection of mumps virus in CSF, are nolonger being reported. The decline in the incidence andcomplications of mumps is seen in all age groups,including those too old to be offered MMR vaccination.About 3% of notified cases are currently being confirmed,which shows how important it is to seek confirmation ofclinically diagnosed cases if the incidence of mumps is tobe measured accurately. The 1993 serological surveyconfirmed the low levels of mumps infection anddemonstrated the impact of the 1988-91 MMR catch upprogramme. As expected, the dramatic fall in the incidenceof mumps increased susceptibility in older unvaccinatedpeople. A mathematical model that assumed transmissionrates were very high in secondary schools, as with measles,suggested that a resurgence might occur soon. Thisscenario is thought unlikely, however, because currentlythe proportion of cases in this age group is much lowerthan the model predicted. The transmission rate dependson the nature of the contact needed to transmit the infection.The relative importance of long distance airbornetransmission (as occurs with measles) and transmissionthrough close “face-to-face” contact determines thetransmission rates in different age groups. If long distancetransmission is less important for mumps than for measles,the increase in susceptibility to mumps in secondary schoolage children will not have the same epidemic potential aswas predicted for measles7.
Universities and military establishments are morelikely to provide the focus of any future resurgence ofmumps, as suggested by recent experience with rubella13,14.Outbreaks of rubella in universities and militaryestablishments in 1993 and 1996 occurred whensusceptibility to rubella in 18 to 20 year olds was about
16% in men and 2% in women14. The proportion of 18 to 20year olds with no detectable mumps antibody was 4%before vaccination was introduced and is expected toexceed 10% by 1998 and to peak at 19% five to six yearslater. Mumps is transmitted more readily than rubellaamong young children . This is not necessarily the case inyoung adults, but the predicted levels of susceptibility formumps, which are higher than currently exist for rubella,suggest cause for concern. In the United States, universityoutbreaks occurred in largely unvaccinated cohorts in1986/715,16.
The immunity of children aged 2 to 6 years is almostentirely due to MMR vaccination. Serological surveillancereveals that 15% of children in this age group have nodetectable mumps antibodies compared with 8% to 10%for measles and rubella. This may indicate that the mumpscomponent of the MMR vaccine is less efficacious than themeasles and rubella components, or that the mumpsantibody test is less sensitive than the antibody tests formeasles and rubella. The detection of mumps antibody in85% of children aged 2 to 6 years and the assumption that92% received MMR suggest that the seroconversion rateis 92%, a similar result to the average of 94% observed inprevious studies of Jeryl Lynn vaccine10. It is not clear,however, whether low levels of vaccine induced antibodyprotect against disease.
Estimates of vaccine efficacy from outbreaks of mumpsdepend on the case definition used17,18 but are generallylower than estimates of the efficacy of measles and rubellavaccines found in similar studies19-22. A series of post-licensure studies in the United States suggest a vaccineefficacy of 80% to 85% against clinical disease17,18,23,24.Efficacy against laboratory confirmed mumps in our studywas about 70%, but the confidence interval was widebecause there were few cases. Such low vaccine efficacyestimates must be reconciled with the marked impact of asingle dose of vaccine on the circulation of virus. Onepossible explanation is that vaccination is more effectivein preventing transmission than disease. The recentepidemiology of mumps in England and Wales suggeststhat the efficacy of the vaccine against transmission is atleast 85% to 90%. Estimates of the vaccine's clinicalefficacy are considerably lower than the observed
* transmission rates from top to bottom are 2.0, 1.75, 1.50, 1.25 and 1.0
Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R25
seroconversion rates. This disparity may be due to thedetection of low non-protective antibody levels byserological tests but vaccine induced immunity may alsowane. If immunity wanes significantly there would beconsiderable implications for vaccine strategy.
The model used here supports previous calculations25
that a critical level of about 85% to 90% immunity isrequired throughout the population for mumps to beeliminated. The current one dose vaccination programmedoes not achieve this level of immunity because of thevaccine's moderate efficacy (with 92% coverage, 90%immunity would be achieved only if vaccine efficacy wereat least 98%). One dose of vaccine considerably reducesthe number of infections, but the reduced circulation ofthe virus causes many of the individuals who are notprotected to remain susceptible into adult life. This willlead to an increase in the proportion of cases occurring inadults, in whom the risk of complications is greatest10,and the number of complications prevented wouldtherefore be considerably smaller than the reduction inthe number of infections. The model suggests that an 85%reduction in infections would reduce hospital admissionsby about 60%. A second dose of vaccine should be sufficientto eliminate mumps infection, with all its associatedcomplications.
The optimum age at which to deliver the second dosedepends on the relative contributions of primary andsecondary vaccine failure to the low clinical efficacyobserved in outbreaks. In the vaccinated preschoolcohorts, 15% of children were antibody negative. Theprotection afforded by low levels of antibody is unclear.Thus the level of susceptibility is probably enough tosustain transmission without us having to consider thepossible effects of waning immunity. Early delivery of thesecond dose is therefore desirable and MMR vaccine hasnow been incorporated into the vaccine schedule forchildren aged 4 years.
AcknowledgementsWe thank the staff in Ashford, Birmingham, Bristol, Cambridge,Leeds, Manchester, Norwich, Preston and Reading public healthlaboratories for providing the serum residues and generalpractitioners for help with the collection of saliva specimens.
References1. Jones AGH, White JM, Begg NT. The impact of MMR
vaccine on mumps infection in England and Wales.Commun Dis Rep CDR Rev 1991; 1: R93-6.
2. Gay NJ, Valambia S, Galasko D, Miller E. Selectiverubella vaccination programmes: a survey of districtsin England and Wales. Commun Dis Rep CDR Rev1994; 4: R77-9.
3. CDSC. COVER/Körner: January to March 1996.Vaccination coverage statistics for children up to twoyears of age in the United Kingdom. Commun Dis RepCDR Rev 1996; 6: 262.
4. Perry KR, Brown DW, Parry JV, Panday S, Pipkin C,Richards A. The detection of measles, mumps and rubellaantibodies in saliva using antibody captureradioimmnuoassays. J Med Virol 1993; 40: 235-40.
5. Galbraith NS, Young SEJ, Pusey JJ, Crombie DL, SparksJP. Mumps surveillance in England and Wales 1962-81.
Lancet 1984; i: 91-4.6. Morgan-Capner P, Wright J, Miller CL, Miller E.
Surveillance of antibody to measles, mumps and rubellaby age. BMJ 1988; 297: 770-2.
7. Gay NJ, Hesketh LM, Morgan-Capner P, Miller E.Interpretation of serological surveillance data for measlesusing mathematical models: implications for vaccinestrategy. Epidemiol Infect 1995; 115: 139-56.
8. Babad HR, Nokes DJ, Gay NJ, Miller E, Morgan-Capner P,Anderson RM. Predicting the impact of measles vaccinationin England and Wales: model validation and analysis ofpolicy options. Epidemiol Infect 1995; 114: 319-41.
9. Gay NJ, Miller E. Was a measles epidemic imminent?Commun Dis Rep CDR Rev 1995; 5: R204-7.
10. Nokes DJ, Anderson RM. Vaccine safety versus vaccineefficacy in mass immunisation programmes. Lancet 1991;338: 1309-12.
11. Farrington CP. Estimation of vaccine effectiveness usingthe screening method Int J Epidemiol 1993; 22: 742-6.
12. White JM, Fairley CK, Owen D, Matthews RC, Miller E.The effect of an accelerated immunisation schedule onpertussis in England and Wales. Commun Dis Rep CDRRev 1996; 6: R86-91.
13. CDSC. The resurgence of rubella? Commun Dis Rep CDRWkly 1993; 3: 39.
14. Miller E, Waight P, Gay NJ, Ramsay M, Vurdien J,Morgan-Capner P, et al. The epidemiology of rubellain England and Wales before and after the 1994measles-rubella immunisation campaign: fourth jointreport from the PHLS and the National CongenitalRubella Surveillance Programme. Commun Dis Rep CDRRev 1997; 7: R26-32.
15. Sosin DM, Cochi SL, Gunn RA, Jennings CE, Preblud SR.Changing epidemiology of mumps and its impact onuniversity campuses. Pediatrics 1989; 84: 779-84.
16. Centers for Disease Control. Mumps outbreaks onuniversity campuses - Illinois, Wisconsin, South Dakota.MMWR 1987; 36: 496-8.
17. Sullivan KM, Halpin TJ, Marks JS, Kim-Farley R.Effectiveness of mumps vaccine in a school outbreak.Am J Dis Child 1985; 139: 909-12.
18. Kim-Farley R, Bart S, Stetler H, Orenstein WA, Bart K,Sullivan KM, et al. Clinical mumps vaccine efficacy. AmJ Epidemiol 1985; 121: 593-7.
19. Calvert N, Cutts FT, Miller E, Brown DW, Munro J.Measles among secondary school children in WestCumbria: implications for vaccine policy. Commun DisRep CDR Rev 1994; 4: R70-3.
20. Morse D, O’Shea M, Hamilton G, Soltanpoor N, Leece G,Miller E, et al. Outbreak of measles in a teenage schoolpopulation: need to immunise susceptible adolescents.Epidemiol Infect 1994; 113: 355-65.
21. Greaves WL, Orenstein WA, Hinman AR, Nersesian WS.Clinical efficacy of rubella vaccine. Pediatr Infect Dis1983; 2: 284-6.
22. Strassburg MA, Greenland S, Stephenson TG, Weiss BP,Auerbach D, Habel LA, et al. Clinical effectiveness ofrubella vaccine in a college population. Vaccine 1985; 3:109-12.
23. Hersh BS, Fine PEM, Kent WK, Cochi SL, Kahn LH, ZellER, et al. Mumps outbreak in a highly vaccinatedpopulation. J Pediatr 1991; 119: 187-93.
Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R26
24. Wharton M, Cochi SL, Hutcheson RH, Bistowish JM,Schaffner W. A large outbreak of mumps in thepostvaccine era. J Infect Dis 1996; 158: 1253-60.
25. Anderson RM, Crombie JA, Grenfell BT. The epidemiologyof mumps in the United Kingdom: a preliminary study ofvirus transmission, herd immunity and the potential impactof immunisation. Epidemiol Infect 1987; 99: 65-84.
N Gay, mathematical modeller, E Miller, head,M Ramsay, consultant epidemiologist, Immunisation Division,PHLS Communicable Disease Surveillance Centre.L Hesketh, medical laboratory scientific officer,Preston Public Health Laboratory.P Morgan-Capner, director, PHLS North West.
B Cohen, clinical scientist, D Brown, director,Enteric and Respiratory Virus Laboratory,PHLS Central Public Health Laboratory.
Address for correspondenceNigel GayImmunisation DivisionPHLS Communicable Disease Surveillance Centre61 Colindale AvenueLondon NW9 5EQtelephone 0181 200 6868 ext 3401fax 0181 200 7868email [email protected]
The epidemiology of rubella in England and Wales before andafter the 1994 measles and rubella vaccination campaign: fourthjoint report from the PHLS and the National Congenital RubellaSurveillance Programme
SummaryThe national immunisation campaign carried out in theUnited Kingdom in November 1994 was designed to givechildren aged 5 to 16 years of age a single dose of a combinedmeasles and rubella vaccine. Its main objective was toprevent an epidemic of measles predicted in school agechildren. The rubella component of the vaccine was includedin order to reduce the high level of susceptibility to rubellain young adult males and thus reduce the risk of transmissionfrom this group to pregnant women.
Susceptibility to rubella in children aged 5 to 16 yearshas fallen from 15.7% to 3.4% since the measles and rubellacampaign. Despite this the incidence of laboratoryconfirmed rubella rose substantially in 1996, largely onaccount of cases among males aged 17 to 24 years, whowere not vaccinated in the 1994 campaign and about 16%of whom are susceptible. The impact of the resurgence onthe incidence of infection in pregnancy has been relativelylimited, due to the low level of susceptibility in theantenatal population (2% in nulliparous and 1.2% in parouswomen for 1994/5). No cases of congenital rubella arisingfrom administration of measles and rubella vaccine duringthe campaign have been identified. The numbers of babiesborn with congenital rubella and terminations ofpregnancy for rubella arising from the 1996 resurgenceare expected to be similar to those that followed the 1993resurgence.
The reduction in susceptibility in future cohorts ofyoung men who received measles and rubella vaccine inthe 1994 campaign should prevent future resurgencesafter the year 2000. If a second dose of measles, mumps,and rubella (MMR) vaccine had not been introduced,susceptibility levels in the school age population wouldhave risen to about 12% in the future. The effect of thesecond dose of MMR vaccine introduced for childrenaged 4 to 5 years in October 1996 will be assessed throughserological surveillance.
Key words: immunisation – pregnancy complications,infections – preventive health services – rubella – salivarydiagnosis – seroepidemiological methods
IntroductionIn a national immunisation campaign carried out in theUnited Kingdom in November 1994 92% of children aged5 to 16 years received a single dose of combined measlesand rubella (MR) vaccine. The main objective of thecampaign was to prevent an epidemic of measles predictedin school aged children1. The decision to give MR vaccineinstead of measles vaccine alone was based on evidencethat more young men than women were susceptible torubella and that continuing outbreaks among young menposed a risk of transmission of rubella to pregnant women.This paper describes the campaign’s effect on the agespecific susceptibility to rubella in school age children inEngland and Wales and evaluates its impact on the currentand likely future incidence of rubella in the generalpopulation and in pregnant women. The outcomes ofpregnancies in girls who received MR vaccine during thecampaign are also reported.
MethodsThe incidence of serologically confirmed cases of rubellawas monitored through reports sent to the PHLSCommunicable Disease Surveillance Centre (CDSC) frompublic health laboratories (PHLs) and National HealthService (NHS) laboratories in England and Wales.
Since November 1994, saliva specimens have beenrequested from all notified cases of rubella to test forspecific IgM using an antibody capture radio-immunoassay2. Vaccination histories of saliva confirmedcases were obtained from general practice or districtrecords; IgM responses in cases who had been vaccinatedin the three months before diagnosis were considered tobe vaccine induced. Vaccine efficacy was estimated usingthe screening method3.
Data on the incidence of clinically diagnosed rubellain England and Wales were obtained from notifications
E Miller, P Waight, N Gay, M Ramsay, J Vurdien, P Morgan-Capner, L Hesketh, D Brown, P Tookey, C Peckham

Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R27
collated by the Office for National Statistics (ONS)(formerly the Office of Population Censuses and Surveys(OPCS)) and from the Medical Officers of SchoolsAssociation (MOSA).
The impact of rubella vaccination on the incidence ofrubella in pregnancy was monitored through serologicallyconfirmed cases, pregnancies terminated because ofrubella, and notifications to the National CongenitalRubella Surveillance Programme (NCRSP)4. Women whohave received rubella vaccine during or shortly beforepregnancy are also reported to and followed up by theNCRSP.
The age specific prevalence of antibodies to rubellabefore and after the MR campaign was assessed throughthe PHLS serological surveillance programme5. FromJanuary to October 1994, 15 PHLs in England and Walescollected residues of 1750 serum specimens submitted bychildren aged 5 to 16 years for microbiologicalinvestigation. A further 1846 specimens were collectedfrom children aged 5 to 16 years by the same laboratoriesfrom February 1995 to June 1995. Both sets of specimenswere tested for rubella antibodies at Preston PHL usingradial haemolysis; those that gave equivocal results wereretested by latex agglutination. Results for the two sets ofspecimens were compared with results from the PHLSserological surveillance programme in earlier years5,6.
The effect of the selective rubella vaccinationprogramme for schoolgirls and adult women has beenmonitored since 1984 by collating the results of rubellaantibody tests carried out on pregnant women by sixsentinel laboratories in England6,7. All six laboratoriesrecord the age and parity (number of previous deliveries)of the women screened and three also record ethnic origin.The rubella antibody results of 147 900 women screenedduring pregnancy during 1994 and 1995 are reported.
ResultsRubella incidenceSerologically confirmed and notified casesThe incidence of serologically confirmed rubella has risensubstantially since late 1995, predominantly in peoplewho were ineligible for vaccination in the MR campaign,routine MMR, or selective rubella vaccination programmes(figure 1). Several outbreaks in universities, with somelimited spread to the neighbouring communities, werereported in the 1996 resurgence. MOSA reported twooutbreaks in boarding schools affecting boys aged 13 to 18years; one of the outbreaks occurred in a school that haddeclined to take part in the MR campaign.
Ninety-seven per cent of the confirmed cases reported inthe first half of 1996 whose ages were recorded (2324/2384)were aged 17 years and over and 1917 (82%) of these were
Figure 1 Serologically confirmed laboratory reports of rubella, England and Wales: 1984 to July 1996
0
20
40
60
80
0
20
40
60
80
MMR vaccineintroduced
Pregnant women
Age 1-14 years
4-weekly periods
1984 85 86 87 88 89 90 910
200
400
600
800
92 93 94 95 96
MR vaccinationcampaign
Others
Num
ber
of la
bora
tory
rep
orts
Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R28
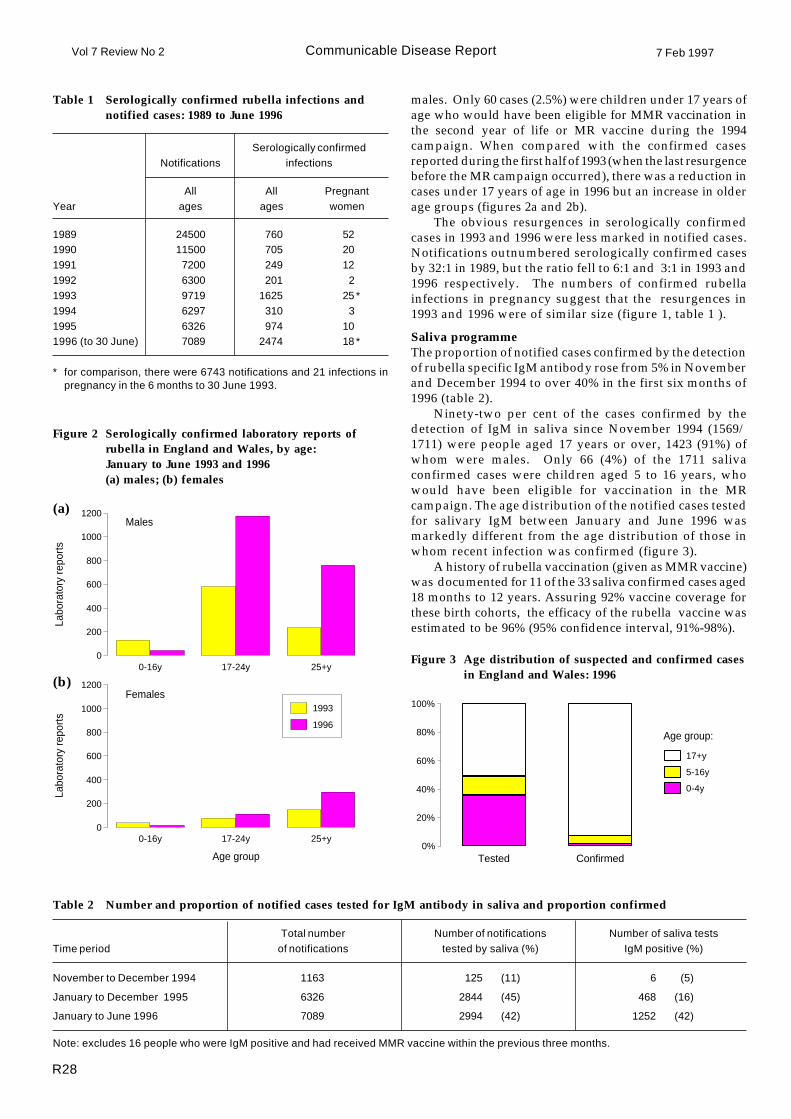
Table 1 Serologically confirmed rubella infections andnotified cases: 1989 to June 1996
Table 2 Number and proportion of notified cases tested for IgM antibody in saliva and proportion confirmed
Total number Number of notifications Number of saliva testsTime period of notifications tested by saliva (%) IgM positive (%)
November to December 1994 1163 125 (11) 6 (5)
January to December 1995 6326 2844 (45) 468 (16)
January to June 1996 7089 2994 (42) 1252 (42)
Note: excludes 16 people who were IgM positive and had received MMR vaccine within the previous three months.
Figure 3 Age distribution of suspected and confirmed casesin England and Wales: 1996
Tested Confirmed0%
20%
40%
60%
80%
100%
17+y
5-16y
0-4y
Age group:
males. Only 60 cases (2.5%) were children under 17 years ofage who would have been eligible for MMR vaccination inthe second year of life or MR vaccine during the 1994campaign. When compared with the confirmed casesreported during the first half of 1993 (when the last resurgencebefore the MR campaign occurred), there was a reduction incases under 17 years of age in 1996 but an increase in olderage groups (figures 2a and 2b).
The obvious resurgences in serologically confirmedcases in 1993 and 1996 were less marked in notified cases.Notifications outnumbered serologically confirmed casesby 32:1 in 1989, but the ratio fell to 6:1 and 3:1 in 1993 and1996 respectively. The numbers of confirmed rubellainfections in pregnancy suggest that the resurgences in1993 and 1996 were of similar size (figure 1, table 1 ).
Saliva programmeThe proportion of notified cases confirmed by the detectionof rubella specific IgM antibody rose from 5% in Novemberand December 1994 to over 40% in the first six months of1996 (table 2).
Ninety-two per cent of the cases confirmed by thedetection of IgM in saliva since November 1994 (1569/1711) were people aged 17 years or over, 1423 (91%) ofwhom were males. Only 66 (4%) of the 1711 salivaconfirmed cases were children aged 5 to 16 years, whowould have been eligible for vaccination in the MRcampaign. The age distribution of the notified cases testedfor salivary IgM between January and June 1996 wasmarkedly different from the age distribution of those inwhom recent infection was confirmed (figure 3).
A history of rubella vaccination (given as MMR vaccine)was documented for 11 of the 33 saliva confirmed cases aged18 months to 12 years. Assuring 92% vaccine coverage forthese birth cohorts, the efficacy of the rubella vaccine wasestimated to be 96% (95% confidence interval, 91%-98%).
0-16y 17-24y 25+y0
200
400
600
800
1000
1200
Labo
rato
ry re
port
s
Males
0-16y 17-24y 25+y0
200
400
600
800
1000
1200
1993
1996
Labo
rato
ry re
port
s
Females
Age group
(b)
(a)
Figure 2 Serologically confirmed laboratory reports ofrubella in England and Wales, by age:January to June 1993 and 1996(a) males; (b) females
Serologically confirmedNotifications infections
All All PregnantYear ages ages women
1989 24500 760 521990 11500 705 201991 7200 249 121992 6300 201 21993 9719 1625 25 *1994 6297 310 31995 6326 974 101996 (to 30 June) 7089 2474 18 *
* for comparison, there were 6743 notifications and 21 infections inpregnancy in the 6 months to 30 Junei1993.
Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R29
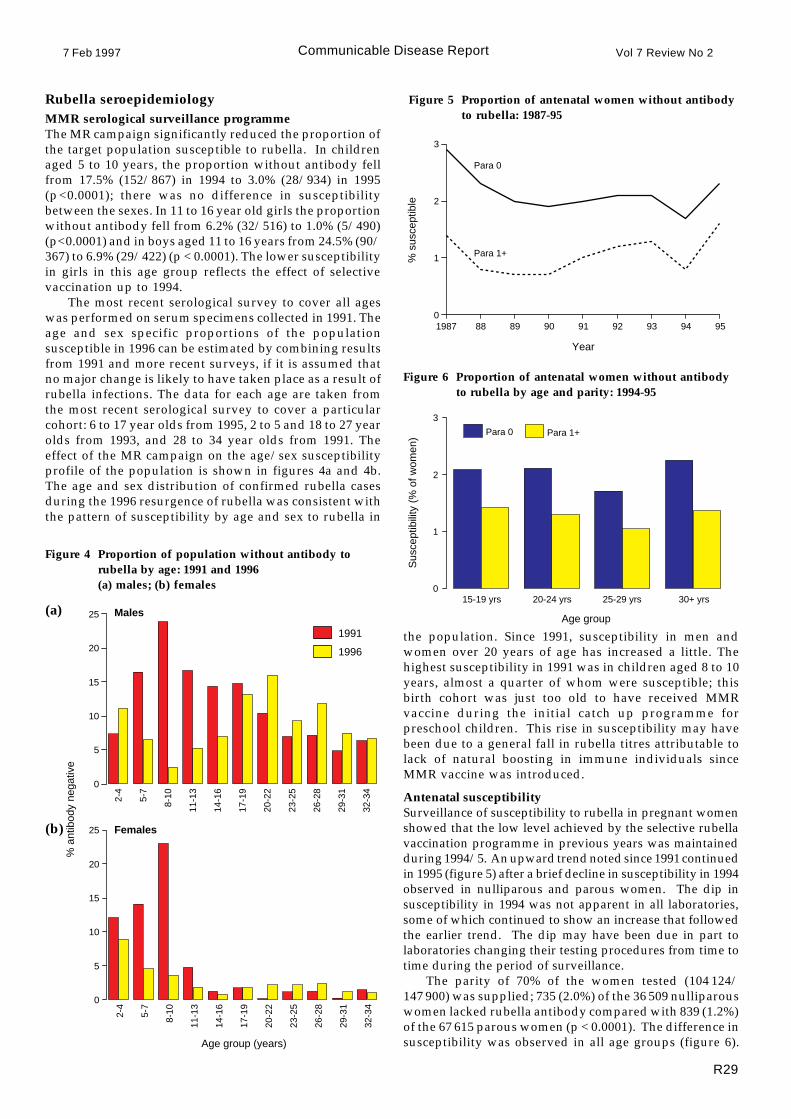
Rubella seroepidemiologyMMR serological surveillance programmeThe MR campaign significantly reduced the proportion ofthe target population susceptible to rubella. In childrenaged 5 to 10 years, the proportion without antibody fellfrom 17.5% (152/867) in 1994 to 3.0% (28/934) in 1995(p<0.0001); there was no difference in susceptibilitybetween the sexes. In 11 to 16 year old girls the proportionwithout antibody fell from 6.2% (32/516) to 1.0% (5/490)(p<0.0001) and in boys aged 11 to 16 years from 24.5% (90/367) to 6.9% (29/422) (p < 0.0001). The lower susceptibilityin girls in this age group reflects the effect of selectivevaccination up to 1994.
The most recent serological survey to cover all ageswas performed on serum specimens collected in 1991. Theage and sex specific proportions of the populationsusceptible in 1996 can be estimated by combining resultsfrom 1991 and more recent surveys, if it is assumed thatno major change is likely to have taken place as a result ofrubella infections. The data for each age are taken fromthe most recent serological survey to cover a particularcohort: 6 to 17 year olds from 1995, 2 to 5 and 18 to 27 yearolds from 1993, and 28 to 34 year olds from 1991. Theeffect of the MR campaign on the age/sex susceptibilityprofile of the population is shown in figures 4a and 4b.The age and sex distribution of confirmed rubella casesduring the 1996 resurgence of rubella was consistent withthe pattern of susceptibility by age and sex to rubella in
Figure 4 Proportion of population without antibody torubella by age: 1991 and 1996(a) males; (b) females
(a)
(b)
Figure 5 Proportion of antenatal women without antibodyto rubella: 1987-95
1987 88 89 90 91 92 93 94 950
1
2
3
Year
Para 0
Para 1+
% s
usce
ptib
le
Age group
15-19 yrs 20-24 yrs 25-29 yrs 30+ yrs0
1
2
3
Para 0 Para 1+
Sus
cept
ibili
ty (
% o
f wom
en)
Figure 6 Proportion of antenatal women without antibodyto rubella by age and parity: 1994-95
0
5
10
15
20
25
1991
1996
0
5
10
15
20
25
Age group (years)
Males
Females
% a
ntib
ody
nega
tive
2-4
5-7
8-10
11-1
3
14-1
6
17-1
9
20-2
2
23-2
5
26-2
8
29-3
1
32-3
4
2-4
5-7
8-10
11-1
3
14-1
6
17-1
9
20-2
2
23-2
5
26-2
8
29-3
1
32-3
4
the population. Since 1991, susceptibility in men andwomen over 20 years of age has increased a little. Thehighest susceptibility in 1991 was in children aged 8 to 10years, almost a quarter of whom were susceptible; thisbirth cohort was just too old to have received MMRvaccine during the initial catch up programme forpreschool children. This rise in susceptibility may havebeen due to a general fall in rubella titres attributable tolack of natural boosting in immune individuals sinceMMR vaccine was introduced.
Antenatal susceptibilitySurveillance of susceptibility to rubella in pregnant womenshowed that the low level achieved by the selective rubellavaccination programme in previous years was maintainedduring 1994/5. An upward trend noted since 1991 continuedin 1995 (figure 5) after a brief decline in susceptibility in 1994observed in nulliparous and parous women. The dip insusceptibility in 1994 was not apparent in all laboratories,some of which continued to show an increase that followedthe earlier trend. The dip may have been due in part tolaboratories changing their testing procedures from time totime during the period of surveillance.
The parity of 70% of the women tested (104 124/147 900) was supplied; 735 (2.0%) of the 36 509 nulliparouswomen lacked rubella antibody compared with 839 (1.2%)of the 67 615 parous women (p < 0.0001). The difference insusceptibility was observed in all age groups (figure 6).
Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R30
Congenital rubellaYear of
birth syndrome infection only Unclassified
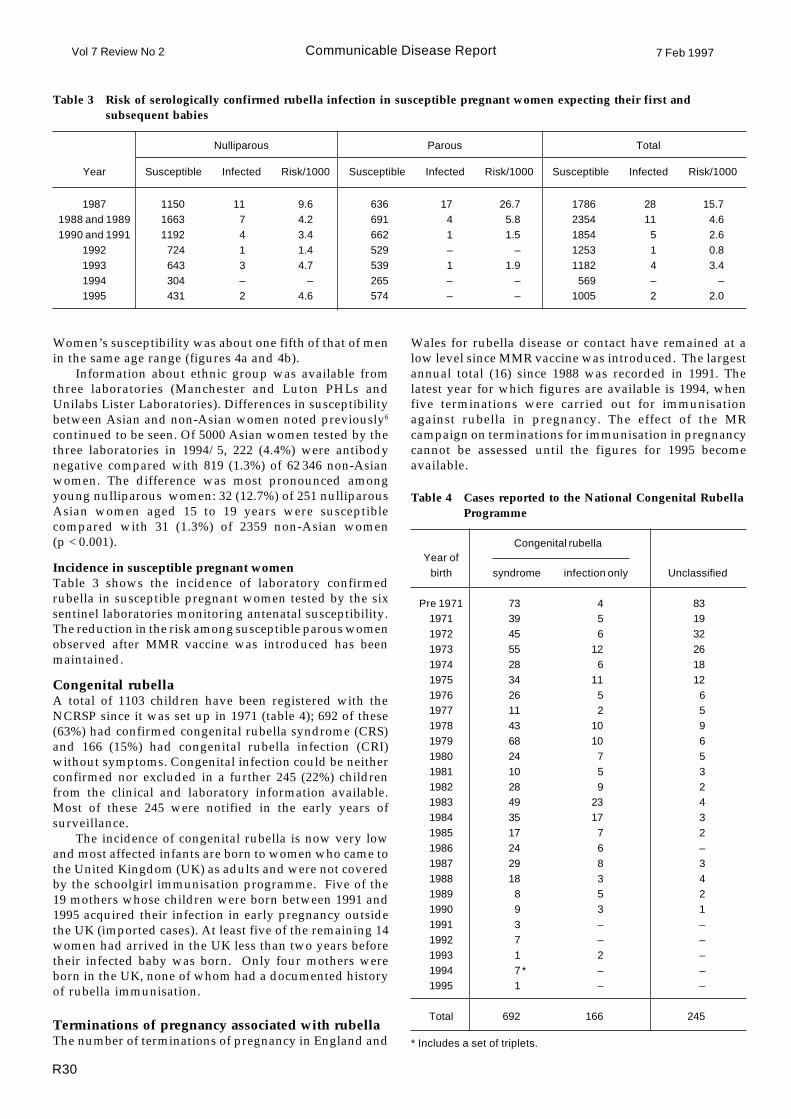
Table 4 Cases reported to the National Congenital RubellaProgramme
Pre 1971 73 4 831971 39 5 191972 45 6 321973 55 12 261974 28 6 181975 34 11 121976 26 5 61977 11 2 51978 43 10 91979 68 10 61980 24 7 51981 10 5 31982 28 9 21983 49 23 41984 35 17 31985 17 7 21986 24 6 –1987 29 8 31988 18 3 41989 8 5 21990 9 3 11991 3 – –1992 7 – –1993 1 2 –1994 7* – –1995 1 – –
Total 692 166 245
* Includes a set of triplets.
Nulliparous Parous Total
Year Susceptible Infected Risk/1000 Susceptible Infected Risk/1000 Susceptible Infected Risk/1000
1987 1150 11 9.6 636 17 26.7 1786 28 15.71988 and 1989 1663 7 4.2 691 4 5.8 2354 11 4.61990 and 1991 1192 4 3.4 662 1 1.5 1854 5 2.6
1992 724 1 1.4 529 – – 1253 1 0.81993 643 3 4.7 539 1 1.9 1182 4 3.41994 304 – – 265 – – 569 – –1995 431 2 4.6 574 – – 1005 2 2.0
Table 3 Risk of serologically confirmed rubella infection in susceptible pregnant women expecting their first andsubsequent babies
Women’s susceptibility was about one fifth of that of menin the same age range (figures 4a and 4b).
Information about ethnic group was available fromthree laboratories (Manchester and Luton PHLs andUnilabs Lister Laboratories). Differences in susceptibilitybetween Asian and non-Asian women noted previously6
continued to be seen. Of 5000 Asian women tested by thethree laboratories in 1994/5, 222 (4.4%) were antibodynegative compared with 819 (1.3%) of 62 346 non-Asianwomen. The difference was most pronounced amongyoung nulliparous women: 32 (12.7%) of 251 nulliparousAsian women aged 15 to 19 years were susceptiblecompared with 31 (1.3%) of 2359 non-Asian women(p < 0.001).
Incidence in susceptible pregnant womenTable 3 shows the incidence of laboratory confirmedrubella in susceptible pregnant women tested by the sixsentinel laboratories monitoring antenatal susceptibility.The reduction in the risk among susceptible parous womenobserved after MMR vaccine was introduced has beenmaintained.
Congenital rubellaA total of 1103 children have been registered with theNCRSP since it was set up in 1971 (table 4); 692 of these(63%) had confirmed congenital rubella syndrome (CRS)and 166 (15%) had congenital rubella infection (CRI)without symptoms. Congenital infection could be neitherconfirmed nor excluded in a further 245 (22%) childrenfrom the clinical and laboratory information available.Most of these 245 were notified in the early years ofsurveillance.
The incidence of congenital rubella is now very lowand most affected infants are born to women who came tothe United Kingdom (UK) as adults and were not coveredby the schoolgirl immunisation programme. Five of the19 mothers whose children were born between 1991 and1995 acquired their infection in early pregnancy outsidethe UK (imported cases). At least five of the remaining 14women had arrived in the UK less than two years beforetheir infected baby was born. Only four mothers wereborn in the UK, none of whom had a documented historyof rubella immunisation.
Terminations of pregnancy associated with rubellaThe number of terminations of pregnancy in England and
Wales for rubella disease or contact have remained at alow level since MMR vaccine was introduced. The largestannual total (16) since 1988 was recorded in 1991. Thelatest year for which figures are available is 1994, whenfive terminations were carried out for immunisationagainst rubella in pregnancy. The effect of the MRcampaign on terminations for immunisation in pregnancycannot be assessed until the figures for 1995 becomeavailable.

Communicable Disease Report7 Feb 1997 Vol 7 Review No 2
R31
Rubella vaccination in pregnancy study: reportsassociated with the MR campaignNine young women who had been vaccinated at the ages14 to 16 years during the MR campaign in England,Scotland, and Wales were reported to the RubellaVaccination in Pregnancy study, five prospectively andfour retrospectively. The rubella status in all cases wasunknown at the time of vaccination. Vaccination occurredbetween 11 and 86 days after their last menstrual periods.The nine pregnancies resulted in eight live births and oneintrauterine death. All eight live-born babies were negativefor rubella specific IgM antibody at birth and viral studieson the baby who died in utero were negative.
The five prospective notifications include theintrauterine death, which occurred at 32 weeks gestation.Necropsy revealed no abnormalities but the cord waswrapped around the baby’s neck at delivery. Three babieswere normal at birth and the other had a cystic hygroma.
The remaining four reports were made retrospectively:two were reported after abnormal findings were made byultrasound (one with Down’s syndrome and another with acleft lip); a third baby, born at 33 weeks gestation, had severeintrauterine growth retardation with mild pulmonarystenosis; the fourth was reported to be normal at birth.
A doctor who suffered a needlestick injury whileadministering vaccine when she was 16 weeks pregnantwas also reported. Her baby was normal at birth, andpermission to take blood for IgM testing was refused.
Although the reported cases showed an extremely highrate of morbidity, this was largely attributable to the selectivenature of the retrospective reports (adverse outcomes aremore likely to be reported than normal outcomes). No caseof congenital rubella infection was reported to have arisenas a result of the administration of MR vaccine.
DiscussionAlthough a substantial resurgence of rubella has occurred inadults, it has not spread to preschool children (in whomMMR vaccine coverage exceeds 90%) or to those covered bythe MR campaign (92% of whom were vaccinated). Spread topregnant women has been limited by their high level ofimmunity and the rarity of cases in children, who wereformerly a major source of infection for mothers. The impacton births of babies with congenital rubella and terminationsof pregnancy for rubella has yet to be established but, asjudged by the impact of the 1993 resurgence, a substantialincrease is not expected. The increase in the ratio of confirmedto notified cases in 1996 compared with 1993 suggests thatpart of the increase in laboratory reports in 1996 is attributableto more thorough investigation of suspected cases.Laboratory confirmed infections in pregnancy, whoseascertainment is unlikely to have changed, suggest that the1996 and 1993 resurgences were of similar size.
Many of the confirmed cases of rubella in young adultsin 1996 occurred in association with outbreaks in residentialestablishments such as university campuses, where thepotential for transmission is high. University outbreakshave become commoner as the proportion of men aged 18 to20 years who are susceptible has increased. Since MMRvaccine was introduced this proportion has risen from 13%to 16%, but it is expected to fall to 7% by the year 2000 whenthe cohorts vaccinated in the MR campaign reach this age.Outbreaks of the current size are not expected to occur
thereafter. Without the campaign, susceptibility in 18 to 20year old men would have risen to over 20%, as the cohort ofboys who were too old to have received MMR vaccine in theinitial catch up programme reached this age.
Surveillance of susceptibility in pregnant womencontinues to provide the main source of information onthe extent of rubella vaccination in adult women. Thedifference in susceptibility between nulliparous andparous pregnant women of the same age is evidence of thecontinuing successful implementation of the postpartumvaccination programme. This opportunity for vaccinationis particularly important for women who enter the UKafter school age, since efforts to vaccinate them beforetheir first pregnancy appear to be largely unsuccessful, asshown by the tenfold difference in susceptibility betweennulliparous Asian and non-Asian women aged under 20years. This higher susceptibility rate in young Asianwomen has been shown previously to be associated withrecent immigration to the UK for marriage. It reflects theabsence of an opportunity for school immunisation ratherthan a higher rate of vaccine refusal by members of thisethnic group8. The disproportionately high number ofcases of congenital rubella born to women who haverecently entered the UK illustrates the importance ofvaccinating these women before they become pregnant,possibly with the help of district immunisationcoordinators. Few women born in the UK are vaccinated(or become infected) between leaving school and becomingpregnant for the first time: the level of susceptibility in 12to 16 year old girls in 1991 (1.9%) was similar to that innulliparous women aged 15 to 19 years in 1994/5 (2.0%).The schoolgirl programme has been discontinued sincethe school age cohort was vaccinated in the 1994 MRcampaign. In 1995, 3.2% of girls aged 5 to 10 years weresusceptible, a level that vindicates the decision to abandonthe school rubella vaccination programme, which achieveda similar level in 12 to 16 year old girls in 1994 (3.0%). Itwill be important, however, to continue to monitorsusceptibility in future school age cohorts to ensure thatthe current low levels of susceptibility are maintained.
Accurate information about the age specific incidenceof infection is essential to interpret the epidemiologicalimpact of vaccination. Clinical diagnosis of rubella isinaccurate and surveillance has to be based on laboratoryconfirmed infections, but reluctance to take blood fromchildren to investigate rashes means that an excess oflaboratory confirmed cases in adults is to be expectedwhatever the true age specific incidence of disease.Salivary diagnosis has been shown to be an acceptablenon-invasive method for confirming rubella in childrenand has allowed the true extent of infection in differentage groups to be documented9. The ability to ascertaintrue cases in children provided an opportunity to estimatethe efficacy of the rubella component of MMR vaccine inpreventing clinically apparent disease. The estimate of96% obtained using the screening method is higher thanthe estimates of efficacy for the measles and mumpscomponents of MMR vaccine obtained using similarmethods10,11 and accords with the antibody persistencedata obtained in 4 to 5 year old children who receivedMMR vaccine during the second year of life12.
Relying on a single dose of rubella vaccine (as MMR atage 15 months) would leave about 12% of each cohort

Communicable Disease ReportVol 7 Review No 2 7 Feb 1997
R32
susceptible to rubella (assuming 92% coverage and 96%efficacy). Susceptibility among nulliparous women wouldeventually rise to 12%, a sixfold increase on current levels.Mathematical models suggest that 12% susceptibilitythroughout the population would not be sufficient tosustain endemic rubella transmission13. Some secondarytransmission from imported cases would be inevitable,however, exposing susceptible pregnant women to somerisk of infection. The future risk of exposure amongpregnant women would depend on the number of importedcases and the extent of secondary transmission in thegeneral population. Their current low risk of exposurewould need to fall by a factor of six to compensate for thesixfold rise in susceptibility to prevent the number ofinfections arising currently in pregnancy from increasing.
A second dose of rubella vaccine, given as MMR, wasintroduced into the UK immunisation schedule in October1996 and is being offered to all children before they startschool at 4 to 5 years of age. This second vaccinationopportunity should protect the 4% who remain susceptibleafter the first dose, and will provide another opportunityto immunise the 8% who are not vaccinated at 15 months.The uptake of vaccine in this latter group will be crucial indetermining the effect of the second dose. The COVER/Körner programme14 will monitor the uptake of thepreschool dose of MMR vaccine and show what proportionof children receive one or both doses. The overall impactof the two dose MMR vaccination programme on thesusceptibility of children as they enter school will bemonitored by serological surveillance.
AcknowledgementsWe thank staff in the following laboratories for providingdata on antenatal rubella susceptibility: James Nash, AshfordPHL; Charles Ashley, Bristol PHL; Steve Adcock, LutonPHL; Alan Blackley, Manchester PHL; Colin Woodward,Leeds PHL; Jane Sellwood and Geoff Pinney, Reading PHL;Brian Shipton, Unilabs Lister Laboratories. We thank generalpractitioners for helping to collect saliva specimens andPaddy Farrington for help with the statistical analysis.
References1. Gay NJ, Hesketh LM, Morgan-Capner P, Miller E.
Interpretation of serological surveillance data for measlesusing mathematical models: implications for vaccinestrategy. Epidemiol Infect 1995; 115: 139-56.
2. Perry KR, Brown DW, Parry JV, Panday S, Pipkin C,Richards A. The detection of measles, mumps, and rubellaantibodies in saliva using antibody captureradioimmunoassays. J Med Virol 1993; 40: 235-40.
3. Farrington CP. Estimation of vaccine effectiveness usingthe screening method. Int J Epidemiol 1993; 22: 742-6.
4. Dudgeon JA, Peckham CS, Marshall WC, SmithellsiRW.National Congenital Rubella Surveillance Programme.Health Trends 1973; 5: 75-9.
5. Morgan-Capner P, Wright J, Miller CL, Miller E.Surveillance of antibody to measles, mumps, and rubellaby age. BMJ 1988; 297: 770-2.
6. Miller E, Tookey PA, Morgan-Capner P, Hesketh LM,Brown DW, Waight PA, et al. Rubella surveillance toJune 1994: third joint report from the PHLS and theNational Congenital Rubella Surveillance Programme.Commun Dis Rep CDR Rev 1994; 4: R146-52.
7. Miller CL, Miller E, Waight PA. Rubella susceptibilityand the continuing risk of infection in pregnancy. BMJ1987; 294: 1277-8.
8. Miller E, Waight PA, Rousseau SA, Hambling MH,Rushton P, Ellis D, et al. Congenital rubella in the Asiancommunity in Britain. BMJ 1990; 301: 1391.
9. CDSC. Surveillance of rubella since the MR vaccinationcampaign. Commun Dis Rep CDR Wkly 1995; 5: 81.
10. Gay N, Miller E, Hesketh L, Morgan-Capner P, RamsayiM,Cohen B, et al. Mumps surveillance in England and Walessupports introduction of two dose vaccine schedule.Commun Dis Rep CDR Rev 1997; 7: R21-6.
11. Brown DW, Ramsay ME, Richards AF, Miller E. Salivarydiagnosis of measles: a study of notified cases in theUnited Kingdom, 1991-3. BMJ 1994; 308: 1015-7.
12. Miller E, Hill A, Morgan-Capner P, Forsey T, Rush M.Antibodies to measles, mumps, and rubella in UKchildren 4 years after vaccination with different MMRvaccines. Vaccine 1995; 13: 799-802.
13. Anderson RM, Grenfell BT. Quantitative investigationsof different rubella vaccination policies for the control ofcongenital rubella syndrome (CRS) in the UnitedKingdom. Journal of Hygiene 1986; 96: 305-33.
14. CDSC. COVER/Körner: January to March 1996. Vaccinationcoverage statistics for children up to two years of age in theUnited Kingdom. Commun Dis Rep CDR Wkly 1996; 6: 262.
E Miller, head, P Waight, principal scientist, N Gay, mathematicalmodeller, M Ramsay, consultant epidemiologist, J Vurdien,information assistant, Immunisation Division,PHLS Communicable Disease Surveillance Centre.P Morgan-Capner, director PHLS North West.L Hesketh, medical laboratory scientific officer,Preston Public Health Laboratory.D Brown, director, Enteric and Respiratory Virus Laboratory,PHLS Central Public Health Laboratory.P Tookey, research fellow, C Peckham, head of Epidemiology andBiostatistics Unit, Department of Paediatric Epidemiology,Institute of Child Health.
Address for correspondencePauline Waight, Immunisation DivisionPHLS Communicable Disease Surveillance Centre61 Colindale AvenueLondon NW9 5EQTelephone: 0181 200 6868 ext 3407Fax: 0181 200 7868e-mail [email protected].
Correction: Editorial: innovations for the new year(S Handysides)
The four apparent orphan references, 6 to 9, may be reunited with their parent text by inserting “use multiple sourcesof data6-9,” after the first clause of the last sentence on page R1 of CDR Review No 1 published on 10 January 1997. Thesentence should have read, “Papers that illustrate the interdependency of the two disciplines, use multiple sources ofdata6-9, and employ novel methods of handling data and approaching problems are particularly welcomed”.
The views expressed in the Communicable Disease Report are those of individual contributors and not, necessarily, those of the PHLS.
PHLS 1997.