
the effects of music and nature sounds on cancer pain and
220
Title Page THE EFFECTS OF MUSIC AND NATURE SOUNDS ON CANCER PAIN AND ANXIETY IN HOSPICE CANCER PATIENTS by LING-CHUN CHIANG Submitted in partial fulfillment of the requirements For the degree of Doctor of Philosophy Dissertation Advisor: Marion Good, PhD, RN, FAAN Frances Payne Bolton School of Nursing CASE WESTERN RESERVE UNIVERSITY January, 2012
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of the effects of music and nature sounds on cancer pain and

Title Page
THE EFFECTS OF MUSIC AND NATURE SOUNDS ON CANCER PAIN AND
ANXIETY IN HOSPICE CANCER PATIENTS
by
LING-CHUN CHIANG
Submitted in partial fulfillment of the requirements
For the degree of Doctor of Philosophy
Dissertation Advisor: Marion Good, PhD, RN, FAAN
Frances Payne Bolton School of Nursing
CASE WESTERN RESERVE UNIVERSITY
January, 2012

ii
Committee Signature Page
CASE WESTERN RESERVE UNIVERSITY
SCHOOL OF GRADUATE STUDIES
We hereby approve the thesis/dissertation of
Ling-Chun Chiang
Candidate for the Doctor of Philosophy degree*:
Marion Good, PhD, RN, FAAN
Barbara J. Daly, PhD, RN, FAAN
Christopher J. Burant, PhD
Deforia Lane, PhD, MT-BC
August 29, 2011
*We also certify that written approval has been obtained for any proprietary material
contained therein.

iii
Copyright © 2012 by Ling-Chun Chiang
All rights reserved

iv
Dedication
This dissertation is dedicated to those patients and their families who participated in my
study by showing me their bravery and generosity to life.
v
Table of Contents Title Page ............................................................................................................................. i Committee Signature Page .................................................................................................. ii Dedication .......................................................................................................................... iv Table of Contents ................................................................................................................ v List of Tables ...................................................................................................................... ix List of Figures ..................................................................................................................... x Acknowledgement ............................................................................................................. xi Abstract ............................................................................................................................ xiii Chapter One Introduction ................................................................................................... 1
Problem ........................................................................................................................... 3 Significance..................................................................................................................... 5 Intervention ..................................................................................................................... 6 Conceptual Framework ................................................................................................... 7 Summary of Literature .................................................................................................. 10 Assumptions .................................................................................................................. 11 Hypotheses .................................................................................................................... 11 Research Questions ....................................................................................................... 11 Conclusion .................................................................................................................... 12
Chapter Two Review of Literature .................................................................................... 13 Cancer Pain ................................................................................................................... 13
Pathophysiology and mechanisms of cancer pain. ................................................... 13 Cancer pain in hospice patients. ................................................................................ 21 Cultural issues. .......................................................................................................... 26
Anxiety .......................................................................................................................... 29 Pathophysiology and mechanisms of anxiety. .......................................................... 31 Anxiety in hospice cancer patients. .......................................................................... 32 Cultural issues. .......................................................................................................... 36
Cancer Pain and Anxiety ............................................................................................... 39 Music for Pain and Anxiety .......................................................................................... 40
Mechanisms of music for pain and anxiety. ............................................................. 41 Effects of music on pain. .......................................................................................... 42 Effects of music on pain in cancer and hospice patients........................................... 44

vi
Effects of music on anxiety. ...................................................................................... 45 Selection of music. .................................................................................................... 47
Nature Sounds ............................................................................................................... 49 Combination of Music and Nature Sounds ................................................................... 51 Threats to Internal Validity ........................................................................................... 53 Summary of Literature Review ..................................................................................... 57
Chapter Three Method ...................................................................................................... 58 Design ........................................................................................................................... 58 Sampling ....................................................................................................................... 61
Sample size estimation. ............................................................................................. 61 Inclusion and exclusion criteria. ............................................................................... 61
Setting ........................................................................................................................... 62 Experimental Interventions ........................................................................................... 64
Music......................................................................................................................... 64 Nature sounds............................................................................................................ 65 Combination of music and nature sounds. ................................................................ 66 Equipment. ................................................................................................................ 66
Measures ....................................................................................................................... 67 Cancer pain. .............................................................................................................. 67 Anxiety. ..................................................................................................................... 69 Demographic measures. ............................................................................................ 71 Types of music and nature sounds generally liked. .................................................. 71 Experience with complementary and alternative therapies. ..................................... 71 Length of time and reasons for independent listening. ............................................. 72
Potentially Confounding Variables ............................................................................... 73 Analgesic and anxiolytics intake. ............................................................................. 73 Environmental disturbances. ..................................................................................... 74 Religious chanting box. ............................................................................................ 74
Procedure ...................................................................................................................... 75 Protection of Human Subjects ...................................................................................... 80 Data Management ......................................................................................................... 81 Data Cleaning................................................................................................................ 82 Assumptions of Statistical Tests ................................................................................... 82 Data Analysis ................................................................................................................ 84

vii
Hypotheses testing. ................................................................................................... 84 Research questions. ................................................................................................... 86
Summary ....................................................................................................................... 86 Chapter Four Results......................................................................................................... 88
Sample........................................................................................................................... 88 Demographic characteristics. .................................................................................... 89 Experience with complementary and alternative therapies. ..................................... 90 Primary sites of cancer. ............................................................................................. 92 Cancer pain and anxiety in hospice patients. ............................................................ 93
Medication Usage ......................................................................................................... 95 Analgesics and Anxiolytics Used by Participants ......................................................... 95 Pain and Anxiety Pretests and Posttests ........................................................................ 96 Correlations ................................................................................................................... 97 Hypothesis Testing ........................................................................................................ 99 Participants’ Suggestions ............................................................................................ 105 Summary ..................................................................................................................... 109
Chapter Five Discussion ................................................................................................. 110 Summary of the Study ................................................................................................ 110 Comparison with the Literature ................................................................................... 111
The effect of music on pain...................................................................................... 111 The effect of nature sounds on pain. ....................................................................... 114 The effect of nature sounds on anxiety. .................................................................. 115 The effect of the combination on pain and anxiety. ................................................ 115 Preferences for music, nature sounds, and combination. ........................................ 116 Length of independent listening.............................................................................. 117 Relationship between pain and anxiety. .................................................................. 118
Rationale for the Outcomes of Music, Nature Sounds, and Combination .................. 118 Limitations .................................................................................................................. 121 Implications for Theory .............................................................................................. 123 Implications for Research ........................................................................................... 124 Implications for Practice ............................................................................................. 126 Conclusion .................................................................................................................. 127
Appendix A ..................................................................................................................... 129 Appendix B ..................................................................................................................... 130

viii
Appendix C ..................................................................................................................... 148 Appendix D ..................................................................................................................... 166 Appendix E ..................................................................................................................... 167 Bibliography ................................................................................................................... 168

ix
List of Tables Table 1 Example of Sequence for Assigning Treatment Conditions to Room 59
Table 2 Data Points Table 78
Table 3 Orthogonal Contrasts Table 85
Table 4 Demographic Characteristics of the Participants 91
Table 5 Experience with Complementary and Alternative Therapy 92
Table 6 The Primary Sites of Cancer 93
Table 7 Participants Analgesics and/or Anxiolytics “in Effect” During Each Test 96
Table 8 Pain and Anxiety Pretests and Posttests at Each Test 97
Table 9 Correlations between Pain and Anxiety Pretests and Posttests 98
Table 10 Effect Sizes of Pain and Anxiety by Groups 100
Table 11 Types of Music, Nature Sounds Liked at Onset of the Study 103
Table 12 Intervention Liked by the Participants 105
Table 13 Types of Music and Nature Sounds Selected by Participants by Day 106
Table 14 Minutes of Independent Intervention Use Between Testing Times 107
Table 15 Adjusted R Square between Pain and Anxiety Pretests and Posttests
by Day 108

x
List of Figures Figure 1 The Conceptual Framework of this experimental Study 2
Figure 2 Conceptual-empirical Structure 8
Figure 3 Equipment Used in This Study 67
Figure 4 The Study Procedure 79
Figure 5 Pain Posttests by Groups 100
Figure 6 Anxiety Posttests by Groups 102

xi
Acknowledgement
Such a work cannot be done by a person alone. Many thanks to God and those
people who have stood behind me to complete this rewarding life journey.
However, first and foremost, I would like to thank the members of my dissertation
committee: my committee Chair and former advisor, Dr. Marion Good, for her
inexhaustible patience and invaluable guidance and assistance to be my mentor
scholarly, professionally, and personally; Dr. Barbara Daly, my current advisor and
committee member, my sincere gratitude for sharing her expertise and wisdom in
palliative care and ethics which provided an encouraging and steady path of clarity
to many complex issues; Dr. Christopher Burant for his optimism and reassurance
when I faced numerous challenges; and Dr. Deforia Lane for her unstinting
generosity in sharing her expertise and dedication to music therapy.
This study was also made possible by the support of several thoughtful
individuals in Taiwan. I sincerely appreciate Dr. Chi-Chun Chin, an associate
professor of the College of Nursing at Kaohsiung Medical University, for her
substantial assistance in the IRB process. In addition, the head nurses and staff
nurses at Kaohsiung Medical University Hospital and St. Joseph Hospital,
especially Yu-Wen Huang and Hsiao-Wen Su, for trusting in me to refer their
patients. Finally, Jung-Chun Chang and Chen-Ping Tseng for sharing their
thoughts from different perspectives and making me feel welcomed during the
data collection process.
I would like to express my love and gratitude to my family. To my parents,

xii
Kuan-Shun Chiang and Hsing-Tzu Liang, for giving me their steadfast support and
teaching me the value of education; my sister, Dr. Ling-Yu Lenny Chiang-Hanisko
and brother-in-law, Jerry Hanisko, for being available for me no matter how busy
they were; my brother, Ling-Chieh Chiang, for taking care of our parents and
helping with the family farm in my absence; and my husband, Matthew McManus,
for bringing his greatest love and patience to me and making my life complete.
My appreciation also goes to my dearest friends, Dr. Jung-Ying Tan, for being
my close friend and sensitive guiding companion who helped me share the passion
for life and strive for perfection during the challenging demands of research and
writing, and to Dr. Emily Liu, Dr. Wariya Muensa, and Dr. Tsai-Yi Au, who kept
me energized and rejuvenated through their unconditional friendship.
This educational journey could not have been possible without the support of
my colleagues at the School of Nursing, HungKuang University (HKU). I would
like to express my gratitude for the financial support provided by HKU and the
Ministry of Education, Taiwan in granting the University Faculty Scholarship
Award. I would also like to thank to Dr. Katherine Jones and Dr. Noreen Brady for
the scholarship support and the enriching opportunities to work at Sara Cole Hirsh
Institute. Finally, I would like to acknowledge the generous funding I received
from Oncology Nursing Society Foundation / Purdue Pharma Trish Greene Pain
Assessment and Management Research Grant and the Sigma Theta Tau
International Alpha Mu Chapter Research Award.

xiii
The Effects of Music and Nature Sounds on Cancer Pain and Anxiety in Hospice Cancer Patients
Abstract
by
LING-CHUN CHIANG
Cancer has been the leading cause of death in Taiwan. Cancer patients who receive
hospice care frequently suffer from pain and anxiety during the dying process. Analgesics
are needed but their side effects can increase suffering and decrease quality of life. The
purpose was to test the effectiveness of sedative music, nature sounds, and the
combination of music and nature sounds for cancer pain and anxiety in hospice cancer
patients in Taiwan. The conceptual framework was based on the Good and Moore middle
range theory of acute pain. A four-group randomized controlled trial using cluster and
adaptive randomization was used with 117 cancer patients in hospice units of two large
hospitals in Taiwan. Participants in the intervention groups listened to music, nature
sounds, or a combination of both for 20 minutes once a day for three days, using MP3
players and earphones or speakers. Participants in the control group lay or sat quietly for
20 minutes, but received a CD of their choice when the data collection process was
completed. The choices of sedative music included classical, piano, harp, religious, easy
listening, Chinese, and Taiwanese music. Nature sounds and the combination of sedative
music and nature sounds were selected from commercially available CDs in Taiwan.
Cancer pain and anxiety were measured before and after each treatment with 100-mm
visual analogue scales. Data were analyzed by multiple regression repeated measures
ANCOVA, using contrasts. The results showed that while controlling for Day 1 pretests,

xiv
the three intervention groups had significantly less pain and anxiety than the control
group, p < .001. Music and combination had medium to large effect sizes on pain and
anxiety. Nature sounds had small to large effect sizes for pain and small to medium for
anxiety. Participants selected Taiwanese folk music and forest sounds most frequently
and used the interventions independently for an average of four hours. Recommendations
are to test the interventions for four or more days and to extend the study to home hospice
settings. Staff nurses can use music, nature sounds, and combination for pain and anxiety
in hospice patients along with analgesics.
1
Chapter One
Introduction
Cancer pain and anxiety have not been managed well among hospice cancer patients
(Bonica, 1990; Chiu, Hu, & Chen, 2000; Lawrie, Lloyd-Williams, & Taylor, 2004;
McCarthy, Phillips, Zhong, Drews, & Lynn, 2000). When patients are in the advanced
cancer stage and during the dying process, cancer pain and anxiety may become more
complicated and difficult to manage with current medication. Undertreated cancer pain
and anxiety often have a reciprocal effect, and both may exacerbate other physical
symptoms and psychosocial distress (Lancee, et al., 1994). Unresolved or undermanaged
cancer pain and anxiety in hospice patients may result in decreased quality of life (S. S.
Hwang, Chang, & Kasimis, 2002; Kutner, Bryant, Beaty, & Fairclough, 2006).
Furthermore, seeing the loved one dying in agony may cause family caregivers to suffer
from emotional distress that may result in a prolonged grieving process and even physical
or psychosocial disorders (McPherson & Addington-Hall, 2004). These consequences
may either directly or indirectly increase healthcare system cost.
Music can touch a person on physical, psychosocial, emotional, and spiritual levels
(Munro & Mount, 1978). Incorporating music into nursing care may attenuate suffering
from physical symptoms, psychosocial and emotional distress, and spiritual or religious
concerns in hospice cancer patients (V. T. Chang, et al., 1998; Chibnall, et al., 2002; Hills,
et al., 2005; Lo, et al., 2002). Studies on the use of music in clinical settings have
demonstrated that it is an effective nonpharmacological adjuvant for reducing suffering
from postoperative pain (Good et al., 1999; Locsin, 1981; Voss et al., 2004), cancer pain
(Beck, 1991; Gallagher & Steele, 2001; Krout, 2001, 2003; Zimmerman, Pozehl, Duncan,

2
& Schmitz, 1989), and anxiety in hospice cancer patients (Gallagher & Steele, 2001;
Krout, 2003). In Taiwan, a few research studies of the effect of music have been
conducted for managing postoperative pain (S. L. Hwang, Chang, Lee, Ko, & Chu, 1996;
D. F. Lee, 1995; Yao, 1998), cancer pain (S. H. Huang, 2000; S. T. Huang, 2006; Hung,
2003; Y. J. Lee, 2000a; P. I. Peng, 2005) and anxiety in cancer patients (Hung, 2003;
Peng, 2005). However, none of these studies were conducted with Taiwanese hospice
cancer patients near the end of life and none were focused on using music for both pain
and anxiety relief.
In addition to music, nature sounds may have some beneficial effect on pain and
anxiety. This may be especially true in Taiwan, where nature sounds are closely
connected to people’s daily lives, but are not usually heard in the hospital setting. Gentle
nature sounds may offer a sense of peace to dying patients (Schrodeder-Sheker, 1994).
No studies of nature sounds were found in Taiwan. Therefore, the purpose of this study
was to test the effectiveness of sedative music, nature sounds, and the combination of
sedative music and nature sounds in relieving cancer pain and anxiety among hospice
cancer patients in Taiwan (Figure 1). It was hypothesized that these three interventions
would decrease cancer pain and anxiety among hospice cancer patients. The results of
this study may not only contribute to the body of nursing knowledge, but also may
improve the quality of life at the end of life among hospice cancer patients.
Figure 1. The Conceptual Framework of this Experimental Study
Music Nature Sounds Combination
Cancer Pain
Anxiety
_
_

3
Problem
Cancer has been the leading cause of death in Taiwan for the past two decades. An
estimated 80% of the world population receives inadequate treatment for cancer pain
relief (A. L. Taylor, Gostin, & Pagonis, 2008). About 75% to 81% of hospice patients
suffer from pain during the dying process (Bonica, 1990; Chiu, et al., 2000; H.-C. Hsu,
Hu, Chuang, Chiu, & Chen, 2002). During the last three days of life, more than 40% of
cancer patients were reported to be in serious pain (McCarthy, et al., 2000). Unfortunately,
cancer pain among hospice patients is not managed well and is frequently associated with
anxiety (Kerrihard, Breitbart, Dent, & Strout, 1999; Massie & Holland, 1987). Before
1990, hospice care was not available for cancer patients who were in the terminal stage.
Today, National Health Insurance in Taiwan covers hospice care for cancer patients who
have less than six months to live. Yet, managing symptoms that hospice cancer patients
encounter remains a major challenge for healthcare professionals (M. B. Chen, et al.,
2004; M. L. Chen & Tseng, 2006). Cancer pain and anxiety have been reported to be the
most common symptoms that hospice patients experience (Newell, Swanson-Fisher,
Girgis, & Ackland, 1999; J.-S. Tsai, Wu, Chiu, Hu, & Chen, 2006).
Anxiety, a common symptom experienced by cancer patients, can be associated with
fear of pain, the dying process, and death (Newell, et al., 1999; Portenoy, Payne, &
Jacobsen, 1999). Multiple research studies indicated that 66% to 77% of terminally ill
cancer patients reported moderate to severe anxiety between admission to hospice care
and the day before death ((M. L. Chen & Tseng, 2006; Ewing, et al., 2004; Georges,
Onwuteaka-Philipsen, van der Heide, van der Wal, & van der Maas, 2005; J.-S. Tsai, et
al., 2006). Anxiety is less easily identified clinically because it is frequently
4
overshadowed by other symptoms, overlooked by healthcare professionals, and
underreported by hospice cancer patients.
Unresolved or undermanaged cancer pain and anxiety in hospice patients may result
in unwanted symptoms, decreased quality of life, and increased distress during the dying
process (Lancee, et al., 1994). In palliative care settings, when patients have more
symptoms, their family caregivers have a higher level of burden and emotional distress
(Andrews, 2001). For example, in interviews conducted after a patient has died, the
family members reported that their loved one had moderate to severe pain more than 50%
of the time during the final three days of life. They said that watching their loved one
dying in agony made them feel emotionally traumatized (The SUPPORT Principal
Investigators., 1995). Caregivers may have a higher risk of a prolonged grieving process
and negative physical and psychosocial sequalae (Hudson, 2003). These may require
health-related treatments or consultations, which may increase costs in the healthcare
system. Moreover, being unable to manage patients’ symptoms and seeing their suffering
may increase stress in healthcare professionals and increase the possibility of early
attrition from the healthcare system (N. Payne, 2001).
In order to manage cancer pain and anxiety, prescribed opioids are primarily used in
healthcare settings. However, hospice patients may suffer from undesired side effects
from medication and refuse to take it in the amount needed to reduce their pain. Studies
have shown that cancer patients have multiple barriers to pain management in terms of
their attitudes and knowledge. They worry about addiction and tolerance from taking
opioid medication, are afraid of the unmanageable side effects, and fear they are not
being a “good” patient (Hodes, 1989; Jacox, et al., 1994; Sun, et al., 2007; Ward, et al.,

5
1993). In Taiwan, cancer patients reported similar misconceptions and were reluctant to
take the amount of medication they needed (C. C. Lin, 1998, 2000; C. C. Lin & Ward,
1995). Opioid analgesics in Taiwan can be quite costly and may be less accessible than
nonpharmacological adjuvants (Bureau of National Health Insurance, 2008), even though
they are recommended (Miaskowski, et al., 2009). Music can be added to enhance the
effect of analgesics and anxiolytics medication in hospice patients. Music usually has no
side effects. Unfortunately, few studies of using music for managing cancer pain or
anxiety have been done in Taiwan and most healthcare professionals do not recognize
music as an available and effective nonpharmacological adjuvant. Hence, the lack of
music in hospice settings may decrease the opportunity for cancer patients to receive
better quality of care.
Significance
The significance of the findings from the proposed study is fourfold. First, the
findings will be important to improve hospice cancer patients’ physical comfort and
decrease emotional distress in the end-of-life process. Second, the results will expand
nursing knowledge of the effectiveness of nonpharmacological adjuvants by adding a
Taiwanese cultural perspective. Third, since nursing is a profession that provides patients
with holistic care, the use of music, nature sounds, and the combination of music and
nature sounds may add to the cancer patients’ pleasure during the terminal stage of their
illness. Fourth, the results of this study will provide knowledge and evidence to extend
the middle range theory of a balance between analgesia and side effects from acute
postoperative pain to cancer pain in a hospice population.

6
Intervention
Music, nature sounds, and the combination of music and nature sounds are the
interventions that were tested in this study. In order for music to have a therapeutic effect,
matching the music to the health-related purpose is very important (Guzzetta, 1989).
Multiple researchers have used relaxing or sedative music with cancer or hospice patients
and have reported its effectiveness in decreasing cancer pain (Beck, 1991; Gallagher,
Lagman, Walsh, Davis, & Legrand, 2006; Gallagher & Steele, 2001; S. H. Huang, 2000;
S. T. Huang, 2006; Krout, 2001; Y. J. Lee, 2000a; Reinhardt, 1999; Zimmerman, et al.,
1989) and anxiety (Bailey, 1983; Gallagher, et al., 2006; Gallagher & Steele, 2001;
Horne-Thompson & Grocke, 2008; Hung, 2003; S.-Y. Li, 2007; P. I. Peng, 2005).
Therefore, sedative music was used in this study. Sedative music is characterized as
having a rate of 60-80 beats per minute (bpm), a sustained melodic quality, a general
absence of strong rhythms or percussion, controlled volume and pitch, and no lyrics
(Gaston, 1951; Good, 1995). Sedative music may facilitate relaxation of the body
because when muscles relax, there is increased blood flow, the relaxation response is
related to better oxygenation of the tissues, and a sense of calm and reduced pain
perception occurs (Gaston, 1951; Standley, 1986). Sedative music may also stimulate the
release of hormones, such as endorphins, to alleviate pain (Goldstein, 1985). Furthermore,
music may reduce pain and anxiety through distraction; that is, by focusing the mind
away from the pain and anxiety toward a more pleasurable stimulus (McCaffrey & Good,
2000; Standley, 1986).
Nature sounds, on the other hand, are not well studied. Schrodeder-Sheker (1994)
suggested that gentle sounds from Mother Nature, such as wind, ocean waves, sounds of

7
streams, rain, and birds can offer a peaceful sense and have healing power for dissolving
fears, lessening the burden, sorrows, pain, and emotional wounds in the dying process
and may help the dying patients to relax. Since Taiwan is an island, the majority of
people have their life experience closely associated with the mountains and the ocean.
From the researcher’s personal experience, some Taiwanese patients expressed that they
missed the sounds from the Nature while hospitalized. Sounds of wind, ocean, or the
songs of birds may allow these hospitalized hospice patients to feel a connection with and
embraced by what they are accustomed to hearing in their daily lives, and thus, create a
sense of being at home. Whether or not nature sounds decrease the cancer pain and
anxiety is a gap in knowledge that will be addressed in this study.
Conceptual Framework
The conceptual framework is based on Good and Moore’s (1996) middle-range
theory of acute pain: a balance between analgesia and side effects. The theory prescribes
patient participation, multimodal therapies, and attentive care from nursing actions for
pain relief and to reduce side effects of opioid analgesics. One proposition of the theory is
that multimodal therapies consisting of both pharmacological and nonpharmacological
methods will reduce pain. Nonpharmacological interventions, such as music, imagery,
massage, or cold, were proposed to contribute to decreases in acute pain (Good, 2009).
In the theory of a balance between analgesia and side effects developed by Good and
Moore (1996), music is proposed as a nonpharmacological adjuvant to reduce pain. This
study is expected to extend the theory by supporting that music not only reduces cancer
pain near the end of life, but also alleviates anxiety during that time. Furthermore, the
effect of nature sounds and the combination of music and nature sounds will be studied
8
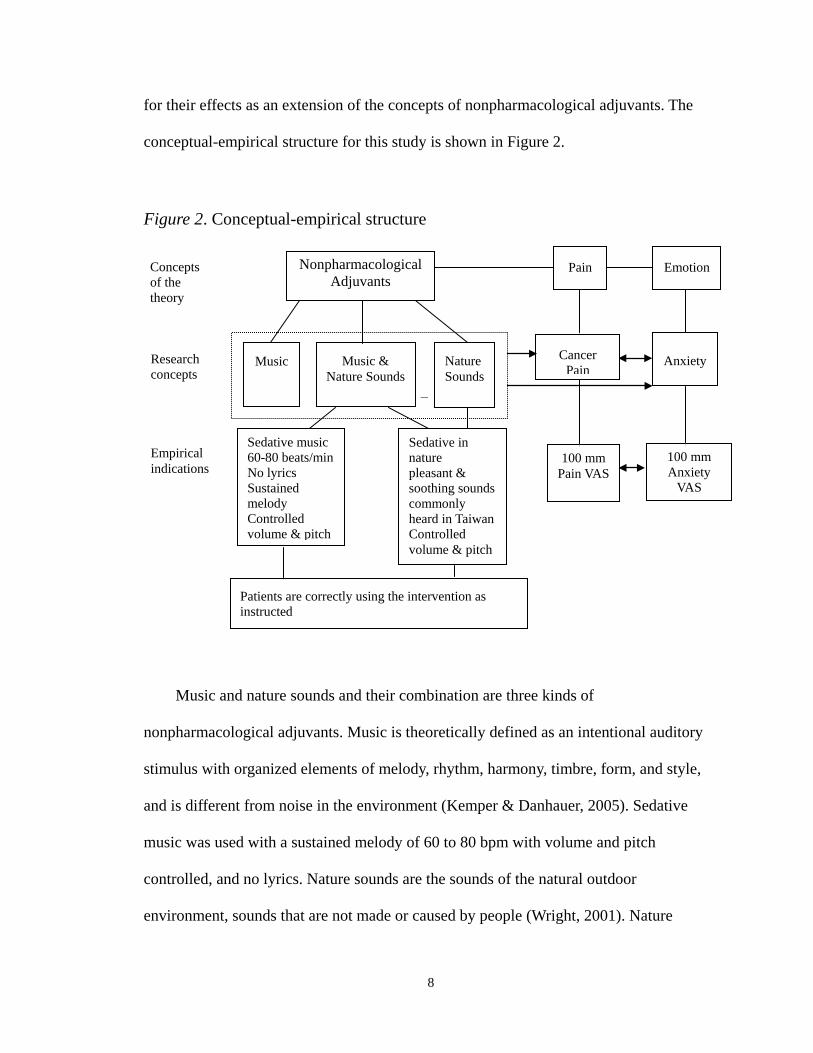
for their effects as an extension of the concepts of nonpharmacological adjuvants. The
conceptual-empirical structure for this study is shown in Figure 2.
Figure 2. Conceptual-empirical structure
Music and nature sounds and their combination are three kinds of
nonpharmacological adjuvants. Music is theoretically defined as an intentional auditory
stimulus with organized elements of melody, rhythm, harmony, timbre, form, and style,
and is different from noise in the environment (Kemper & Danhauer, 2005). Sedative
music was used with a sustained melody of 60 to 80 bpm with volume and pitch
controlled, and no lyrics. Nature sounds are the sounds of the natural outdoor
environment, sounds that are not made or caused by people (Wright, 2001). Nature
-
100 mm Pain VAS
100 mm Anxiety
VAS
Concepts of the theory
Research concepts
Empirical indications
Nonpharmacological Adjuvants
Pain Emotion
Cancer Pain
Anxiety Music Nature Sounds
Music & Nature Sounds
Sedative music 60-80 beats/min No lyrics Sustained melody Controlled volume & pitch
Patients are correctly using the intervention as instructed
Sedative in nature pleasant & soothing sounds commonly heard in Taiwan Controlled volume & pitch
9
sounds, including wind, ocean waves, streams, birds, frogs, and insects, with volume and
pitch controlled, were also expected to produce relaxation or distraction. The combination
of sedative music and nature sounds is a combination of both individual modalities.
Cancer pain is a kind of pain that is associated with the potentially life-threatening
condition of cancer. It is also called malignant pain and can be categorized as acute or
chronic (International Association for the Study of Pain., 1994). When pain is associated
with the dying process, it is sometimes called “total pain,” which involves a variety of
physical noxious stimuli and affective or emotional discomforts. The pain is related to
interpersonal conflicts, and to fear and nonacceptance of one’s own dying (Saunders,
1976). In hospice patients, pain may no longer be a simple physical discomfort, but may
be accompanied by increasing levels of emotional distress associated with pain and dying,
such as anxiety. Cancer pain was measured before and after listening to 20 minutes of the
intervention and measured on a single 100-mm horizontal visual analogue scale (VAS).
Anxiety is a kind of emotion. Spielberger (1972) proposed differences between trait
and state anxiety. Trait anxiety, or anxiety proneness, often remains stable when
encountering stressors, while state anxiety is situational anxiety, and reacts to stressful
situations differently (Spielberger, 1983). For hospice cancer patients, having pain with
multiple symptoms and knowing they are close to death can be perceived as stressful or
threatening, which results in increased state anxiety. Therefore, state anxiety is used in
this study and defined as “the emotional reaction or pattern of response that occurs in an
individual who perceives a particular situation as personally dangerous or threatening”
(Spielberger, 1972, p. 489). Anxiety will be measured before and after 20 minutes of the
intervention on a single 100-mm horizontal VAS.

10
Summary of Literature
To date, there are only six studies in Taiwan that have tested the effectiveness of
music for pain and anxiety in cancer patients. Five of them were master’s theses with
only brief descriptions of the music intervention used to relieve pain or psychological
distress in cancer patients (S. H. Huang, 2000; Hung, 2003; Y. J. Lee, 2000a; S.-Y. Li,
2007; P. I. Peng, 2005). All of these studies had a small sample size (ranging from 20 to
60 participants), used quasi-experimental design or single group pre-post test design, and
were guided by nursing faculty who might not have had previous experience in using
music as a nursing intervention. Three of these studies did not use sedative music (S. H.
Huang, 2000; Y. J. Lee, 2000a; P. I. Peng, 2005). The sixth study was a dissertation that
tested the effectiveness of sedative music for cancer pain relief (S. T. Huang, 2006). This
study had a larger sample size of cancer patients (N = 126), but only some were in
hospice. It was guided by experienced faculty and a music therapist, and was conducted
in the southern part of Taiwan. Therefore, studies to test the effect of music on multiple
time points for reducing pain and anxiety in hospice cancer patients are needed.
Currently, only five studies have explored nature sounds to help adult patients to
undergo medical and surgical procedures (Dickhaus, et al., 2003; Diette, Lechtzin,
Haponik, Devrotes, & Rubin, 2003; Tsuchiya, et al., 2003), sleep (Williamson, 1992), and
anxiety (Golletz, 1997). Two previous studies conducted in the United States reported the
effectiveness of a videotape containing the sounds of streams and birds along with scenes
of nature on decreasing pain and anxiety during medical and surgical procedures (Diette,
et al., 2003; Tsuchiya, et al., 2003). Another study reported that ocean sounds increased
the quality of sleep in patients who had coronary artery bypass graft surgery (Williamson,

11
1992). However, no similar studies were found in Taiwan.
Assumptions
1. Around-the-clock analgesics are prescribed, but may be insufficient to relieve
pain in hospice cancer patients.
2. Anxiolytic medications are prescribed to patients with signs and symptoms of
anxiety.
3. Patients are able to express their perceptions of pain and anxiety.
Hypotheses
1. Hospice cancer patients who listen to sedative music, nature sounds, or sedative
music combined with nature sounds will have less cancer pain than those who
do not when controlling for baseline.
2. Hospice cancer patients who listen to sedative music, nature sounds, or sedative
music combined with nature sounds will have less anxiety than those who do
not when controlling for baseline.
Research Questions
1. What types of music and nature sounds are generally liked by Taiwanese
hospice cancer patients?
2. How much did Taiwanese hospice cancer patients like their assigned
intervention (music, nature sounds, and the combination of sedative music with
nature sounds)?
3. How many minutes were music, nature sounds, and the combination of sedative
music with nature sounds independently used between testing times?
4. What is the relationship between anxiety and cancer pain in hospice cancer

12
patients?
Conclusion
Cancer pain and anxiety have been the most common symptoms experienced by the
hospice cancer patients. Current pharmacological regimens are primarily used for
managing these symptoms, but may cause unwanted side effects. Based on the Good and
Moore acute pain theory (Good & Moore, 1996), this study tested the effect of sedative
music, nature sounds, and the combination of sedative music and nature sounds for
reducing cancer pain and anxiety on hospice cancer patients in Taiwan. A randomized
controlled trial with cluster and adaptive randomization was used to test the effects of
these interventions in hospice cancer patients, and to extend the acute pain theory.
13
Chapter Two
Review of Literature
The literature review begins with a description of the pathophysiology and
mechanisms of cancer pain, anxiety, and then cancer pain and anxiety in hospice patients;
it also includes culture issues. Second, the literature describing music and nature sounds
is reviewed. Third, the research on effects of music and nature sounds on cancer pain and
anxiety in hospice patients is presented. Finally, the threats to internal validity and
methods to control for these threats are addressed.
Cancer Pain
Cancer pain is defined as a subjective feeling of an unpleasant sensory and
emotional experience associated with the growth and/or the treatment of cancer. The
sensory and affective components of pain may affect one another and exacerbate pain
(Paice & Fine, 2006). Pain associated with cancer may result from tumor infiltration of
structures such as nerves, bone, or soft tissues. Cancer pain can also be a result of
treatments that injure or sensitize tissues, such as chemotherapy, radiotherapy, and
surgery. Cancer pain can be classified based on duration pathophysiology. The duration of
three kinds of cancer pain are: acute pain (duration < 3 months), chronic pain (duration >
3 months), and breakthrough pain (or incidental pain) which occurs on movement.
Pathophysiologically, cancer pain is classified as visceral pain, somatic pain, and
neuropathic pain (de Leon-Casasola & Lema, 2003; R. Payne, 1987).
Pathophysiology and mechanisms of cancer pain. Visceral pain is common in
cancer patients and results from infiltration, compression, distension, or stretching of
thoracic, abdominal, or pelvic viscera (de Leon-Casasola & Lema, 2003; R. Payne, 1987).

14
Visceral pain has some important properties. First, visceral pain cannot be evoked from
all viscera because some viscera lack afferent innervations. Most solid viscera, such as
liver, kidney, and lung parenchyma, are not sensitive to pain. For example, cutting the
intestine does not cause pain, whereas stretching the bladder is painful (Cervero & Laird,
1999). Second, visceral pain is diffuse and poorly localized and can be referred to other
locations. Because the pain is often referred to distant, superficial, and somatic structures,
it becomes difficult to determine the exact source of the pain. This is known as a
viscerosomatic reflex. For example, patients with hepatic tumors may complain of
shoulder pain when the diaphragm receives pressure from an enlarged organ and the
pressure exceeds the pain threshold (Cervero & Laird, 1999; de Leon-Casasola & Lema,
2003). Third, visceral pain is accompanied by motor and autonomic reflexes, so nausea,
vomiting and lower-back muscle tension usually accompany pancreatic, colon, and renal
cell cancer (Cervero & Laird, 1999; Cervero & Morrison, 1986). Patients describe
visceral pain as gnawing, cramping, pressure-like, or deep squeezing (National
Comprehensive Cancer Network, 2008).
Somatic pain is usually caused by the activation of pain receptors in either the
cutaneous or deep tissues, such as musculoskeletal or connective tissues. Common causes
of somatic cancer pain include postsurgical incisional pain, bone metastasis, and pain
accompanying myofascial or musculoskeletal inflammation or spasm (R. Payne &
Gonzales, 2004). Depending on the involved tissues, somatic pain can be either localized
or not localized. This type of pain is frequently described as stabbing, throbbing, burning,
pricking, dull, or aching (National Comprehensive Cancer Network, 2008).
Neuropathic pain is more complex than visceral or somatic pain. Neuropathic pain

15
results from injury to the peripheral or central nervous system as a consequence of tumor
compression or infiltration of peripheral nerves, nerve roots, the spinal cord, or the brain.
Additionally, trauma or chemical injury to peripheral nerves from surgery, radiation, or
chemotherapy may also result in this neuropathic pain (de Leon-Casasola & Lema, 2003;
T. S. Jensen & Gottrup, 2003; R. Payne, 1987). For example, metastatic or
radiation-induced brachial or lumbosacral plexopathies, epidural, spinal cord, and/or
cauda-equina compression, postherpetic neuralgia, and chemotherapy-induced (vinca
alkaloids or platinol compounds) neuropathies are commonly associated with neuropathic
pain (R. Payne & Gonzales, 2004). Neuropathic pain has the qualities of burning, sharp,
tingling, ringing, shooting, or electric shock sensations (T. S. Jensen & Gottrup, 2003;
National Comprehensive Cancer Network, 2008).
Central pain is a type of neuropathic pain that is caused by a lesion or dysfunction in
the central nervous system (Boivie, 2006). It usually involves second- or third-order
neurons and produces hyperalgesia (de Leon-Casasola & Lema, 2003), which is
abnormal sensitivity to both pain and temperature and is manifested by an increased
response to noxious or even non-noxious stimuli (T. S. Jensen & Gottrup, 2003). Even
gentle pressure or a light brush on the skin, or cold and heat stimuli can evoke
excruciating pain. Central pain is associated with neoplastic lesions along the
spinothalamic tract, thalamic or cerebral cortex projections, postherpetic neuralgia, and
phantom limb syndrome (de Leon-Casasola & Lema, 2003).
Sympathetic pain, another type of neuropathic pain, occurs in cancer patients. It
occurs after pathologic fractures, thrombosis due to hypercoaguable states, and
lymphedema of the extremities (de Leon-Casasola & Lema, 2003). Sympathetic pain is
16
associated with dysregulation of the autonomic nervous system and is typified by
constant burning and allodynic pain (Pasero, Paice, & McCaffery, 1999). Moreover,
sympathetic pain may involve sudomotor and vasomotor changes, edema, and coldness
of the affected area (de Leon-Casasola & Lema, 2003).
Despite different causes and classifications of cancer pain, the body’s responses to
noxious stimuli are a series of electrical and chemical events that result in four processes,
known as transduction, transmission, modulation, and perception (Wilkie, 1995). The
first pain process is transduction, in which one form of energy is converted to another.
Transduction is also known as receptor activation (Pasero, et al., 1999). It is a process in
which external or internal noxious stimuli, induced by mechanical, thermal or chemical
sources are converted to electrophysiological activity in primary afferent nociceptors
(PANs) (Beaulieu & Rice, 2003; Besson & Chaouch, 1987). These pain receptors are
located on the terminals of the primary afferent sensory neurons that are responsible for
transmitting sensory information from peripheral tissues to the spinal cord.
Primary sensory neurons can be divided into two major fibers, myelinated A fibers
and smaller-diameter, unmyelinated C fibers. Two types of larger-diameter myelinated A
fibers, A-α and A-β fibers, are low-threshold afferents that receive non-noxious stimuli of
light pressure, soft touch, and vibration from skin, muscle and joints (Djouhri, Bleazard,
& Lawson, 1998). Transmission of noxious information, however, is to the smaller
myelinated A-δ and unmyelinated C fibers, which are specialized sensory neurons that
transmit nociceptive signals (Besson & Chaouch, 1987).
In cancer patients, transduction may begin with nerve fiber damage. For example,
rapid growth of tumor masses may exert pressure on nerve fibers or encircle and constrict
17
peripheral nerves, a nerve plexus, a nerve root, or the spinal cord, and result in nerve
tissue injury (Coyle & Foley, 1987). Antitumor therapies, such as surgery, radiation and
chemotherapy, may also cause nerve damage (Coyle & Foley, 1987). Tumor infiltration
of somatic or visceral tissues also may press on nerves and produce noxious signals
(Coyle & Foley, 1987).
Damage to both normal and cancerous cells produces chemicals that cause nerve
fibers to become activated (Wall, 1988). Phospholipids and other substances are released
to the intracellular space and initiate the arachidonic acid cascade, in which leukotrienes
and prostaglandins are synthesized (Fields, 1987). These endogenous molecules not only
sensitize the primary afferent fibers, but also stimulate substance P to be released from
the distal terminal of PAN (Wilkie, 1995). Substance P dilates nearby blood vessels,
produces edema, and causes release of histamine from mast cells (Bonica, 1990).
Additionally, cell damage results in an inflammatory response. Chemicals are
released or leak out of the cell. For example, bradykinin, histamine, and potassium are
inflammatory exudates, while serotonin is released from platelets and norepinephrine is
released from nerve injury (Bonica, 1990; Fields, 1987). Other inflammation-associated
factors released from damaged tissue include protons (Bevan & Geppetti, 1994; Caterina,
et al., 2000), endothelins (Nelson & Carducci, 2000), and nerve growth factor (McMahon,
1996). If there are sufficient concentrations of these chemicals present in the milieu of the
PAN, they initiate the transduction process.
The second pain process is transmission, in which the transducted and generated
information in the PAN is transmitted to and through the central nervous system (CNS) to
the brain, where pain is perceived (Beaulieu & Rice, 2003). Nociceptive signal

18
transmission is accomplished in three steps, (1) projection to the CNS, (2) processing
within the dorsal horn of the spinal cord, and (3) transmission to the brain. The PAN will
fire an action potential. These nociceptive signals will traverse along the sensory nerve
fiber and through the dorsal root into the dorsal horn of the spinal cord, where it will then
be sent to the brain (Fields, 1987).
Once the dorsal horn of the spinal cord receives the nociceptive signal,
neurotransmitters from the afferent nerve fibers are either released into the synaptic cleft
or bound to receptors in the dorsal horn (Bonica, 1990). These neurotransmitters include
excitatory amino acids (fast transmitters), fluoride-resistant acid phosphatase, and
peptides (slow transmitters). Neural cells (interneurons) excited by the afferent nerve
fibers’ input then release other neurotransmitters, such as gamma-aminobutyric acid
(GABA) and glycine, to influence the transmission process within the dorsal horn
(Bonica, 1990).
The transmission process involves laminae I, II and V of the dorsal horn of the
spinal cord. There are projection cells in lamina I, some projection cells and interneurons
in lamina II, and wide dynamic range (WDR) neurons in lamina III (Fields, 1987). The
projection cells in lamina I send axons to the supraspinal sites, such as the thalamus,
brainstem and cerebellum, and receive excitatory and inhibitory messages from these
sites (Jones, 1992; Wilkie, 1995). The interneurons in lamina II are responsible for
communication with other lamina II cells located within one or two spinal segments, and
with dendrites from cells located in laminae I, III, IV and V (Fields, 1987). The WDR
neurons in lamina V receive direct input from both nociceptive and non-nociceptive
fibers, and then contact cells located in laminae I, II, III and IV via dendritic projections.

19
The WDR neurons then project information to the brainstem and the thalamus (Besson &
Chaouch, 1987; Fields, 1987). Furthermore, since the WDR neurons have large receptive
fields and receive noxious input from both somatic fibers and visceral organs, the WDR
neurons are believed to be associated with referred pain (Cervero, 1985).
Finally, projection cells in the dorsal horn propagate nociceptive stimuli to the
thalamus and brain through several pathways, including the spinothalamic tract (STT),
the spinoreticular tract (SRT), the spinomesencephalic tract (SMT), the spinocervial tract,
the second-order dorsal column tract (SDCT) and the spinohypothalamic tract (Burstein,
Cliffer, & Giesler, 1987; Willis, 1989). After the thalamus receives nociceptive input
from the spinal cord, it projects the signals from the ventrobasal and posterior thalamic
nuclei to the primary somatosensory cortex for sensory discrimination of pain location,
intensity, quality and pattern. In addition, the central lateral and thalamic submedialnuclei
project to the prefrontal for affective responses to pain such as fear, anxiety and suffering,
and to the motor cortex for behavioral responses to pain (Bonica, 1990; Burstein, et al.,
1987; Fields, 1987).
The third pain process is modulation. This includes both enhancement and inhibition
of nociceptive transmission and occurs mostly in the dorsal horn of the spinal cord
(Beaulieu & Rice, 2003; Fields & Heinricher, 1985). Modulation consists of interactions
among peripheral inputs, interneurons, and descending inhibitory systems. The major
neurotransmitters responsible for excitatory transmissions are glutamate, aspartate,
substance P, purines, cytokines, and capasaicin (Dickenson, 1996). The major
neurotransmitters for inhibitory are norepinephrine, 5-HT, GABA, glycine, acetylcholine,
opioids, galanin, somatostatin, neuropeptide Y, neurotensin, adenosine, and cannabinoids

20
(Beaulieu & Rice, 2003).
Descending inhibition of pain is a critical function of modulation. Fields and
Basbaum (1989) proposed that the descending opioid-related pain inhibitory system
involves several centers to generate analgesia. The system includes the midbrain
periaqueductal grey (PAG), the rostral ventral medulla (RVM), and the superficial layers
of the dorsal horn in the spinal cord. When certain conditions occur, such as pain, the
midbrain PAG receives nociceptive inputs from the frontal cortex and hypothalamus, and
projects to neurons in the RVM. The rostral ventral medulla neurons sequentially project
to and control transmission of noxious impulses in the superficial dorsal horn. With
stimulation, both PAG and RVM produce analgesia from the release of endogenous
opioids peptides. The peptides are distributed in the pain inhibitory system. As a result,
pain is modulated (Fields & Basbaum, 1989).
Multiple receptor systems are involved in the pain inhibiting process, including
norepinephrine, serotonin, GABA, glycine, adenosine and cannabinoids (Beaulieu &
Rice, 2003). The major site for producing analgesia is at the opioid receptors in the spinal
cord. Four types of endogenous opioid peptides, endorphin, enkephalin, dynorphin, and
nociceptin, work with their receptors, μ, δ, κ and opioid receptor-like (ORL-1),
respectively. These receptors are located in laminae I and II of the dorsal horn of the
spinal cord (Beaulieu & Rice, 2003; Wick, et al., 1994).
Pain perception is the fourth process of pain. Nociceptive input is recognized in the
brain as an unpleasant sensory experience with affective, defensive, and perceptive
components (Beaulieu & Rice, 2003). The somatosensory cortex in the parietal lobe of
the brain receives noxious input from the somatosensory thalamus and is the center for

21
sensory perception, including pain location, duration, quality, pattern, and intensity
(Bushnell & Apkarian, 2006). The affective component of pain is processed through the
limbic system. In the limbic system, the anterior cingulate cortex receives nociceptive
input from the insular cortex and the thalamus and transmits it to the prefrontal cortex
where the affective dimension of pain is processed (Bushnell & Apkarian, 2006; Kanda,
et al., 2003). Sensory and affective components of pain perception are highly modulated
by cognitive factors. These cognitive factors include attention and previous experience of
pain. Both can alter pain perception. In addition, pain perception can be a very
individualized process in other cultural groups (Wilkie, 1995). For example, Chinese
people may not respond verbally or behaviorally when a noxious stimulus presents
because of their religious beliefs or their stoic cultural background.
Cancer pain in hospice patients. A review of multiple studies suggests that patients
with advanced cancer have more pain than those in earlier stages of the disease
(Thielking, 2003). Cancer patients admitted or referred to hospice care are in an advanced
stage of illness and need symptom control; pain is the most prevalent symptom (Potter,
Hami, Bryan, & Quigley, 2003; Stromgren, et al., 2004; Swanwick, Haworth, & Lennard,
2001; Tang, 2003). Researchers have found that 64% to 93% of hospice cancer patients
experienced moderate to severe pain upon arriving at the hospice setting (Kutner, Kassner,
& Nowels, 2001; W. L. Peng, Wu, Sun, Chen, & Huang, 2006; Potter, et al., 2003;
Stromgren, et al., 2004; Swanwick, et al., 2001). One study indicates that 89% of hospice
cancer patients (N = 245) experienced an average of seven breakthrough pain episodes
daily in addition to ongoing pain (Zeppetella, O'Doherty, & Collins, 2000). As the
hospice cancer patients become close to death, the prevalence of pain increases (W. L.

22
Peng, et al., 2006).
Cancer pain in hospice patients is not only a reflection of underlying
biophysiological factors, but is also influenced by psychological and social factors. When
cancer patients are admitted to a hospice program for palliative care, progression of the
disease leads to a number of diverse pain syndromes. Usually, the location of neoplastic
growth plays a key role in the pain experience of cancer patients (Caraceni & Weinstein,
2001). For example, patients with head and neck cancer and those with gynecological and
prostate cancer suffered significantly more moderate to severe pain than patients with
other primary sites (Vainio & Auvinen, 1996). About 43% of patients (N = 1,112)
suffered from mixed types of cancer pain, such as somatic and neuropathic pain, or
somatic and visceral pain (Caraceni & Portenoy, 1999). Since hospice cancer patients are
in the advanced stage of disease, they may have bone metastases, neuropathic pain, or
mixed pain pathophysiology, which can result in greater severity of pain and declining
performance status (Ger, Ho, Sun, Wang, & Cleeland, 1999; Stromgren, et al., 2004).
Cancer pain is associated with accumulation of comorbidities and debility in hospice
patients, especially in the elderly. Older people have a higher prevalence of cancer
(National Cancer Institute, 2008). Although studies found that different age groups have
similar pain intensity and incidence, age is an important biological factor in the
experience of pain for patients with advanced cancer (C.-C. Lin, Lee, Chiang, Tan, &
Huang, 2006; Mercadante, Ferrera, Villari, & Casuccio, 2006; Vigano, Bruera, &
Suarez-Almazor, 1998). Among cancer patients who are older than 60 years, the
prevalence of painful comorbidities increases at least two times when three or more
comorbid illnesses are involved (Crook, Rideout, & Browne, 1984; C. W. Given, Given,

23
Azzouz, Kozachik, & Stommel, 2001). Comorbid symptoms not only complicate pain
intensity, but also interfere with effective cancer pain treatment, and patients are less
likely to achieve effective pain control (Meuser, et al., 2001). For example, alterations in
body composition, metabolic rate, hepatic mass, and blood flow due to aging and
comorbidities in older cancer patients may increase risk for adverse events from
therapeutic agents. For example, there is an increased risk of peptic ulcer when
nonsteroidal anti-inflammatory drugs (NSAIDs) are used for pain management. In
addition, opioids have adverse effects. The amount of opioid anagelsia may require lower
dosage and careful adjustment to prevent toxicities and side effects of opioids
(Mercadante, et al., 2006; Vigano, et al., 1998).
Cancer pain-related debility also contributes to greater perceived disability,
compromised function, and low activity among hospice cancer patients (B. Given, Give,
Azzouz, & Stommel, 2001). The debility that results from cancer pain limits patients’
ability to receive pain treatment. For example, hospice patients in the end stage of illness
frequently have difficulty swallowing or physically reaching their medications (Coluzzi
& Farirbairn, 1999; Janjan, Delclos, Crane, Ballo, & Cleeland, 2003). These difficulties
may result in changing the route of medication administration and limiting the dosage of
opioids when the cancer patients really need more relief. Furthermore, impaired
communication capacity, agitation, delirium, and the high dose of opioids that is needed
( > 120 mg oral morphine equivalent/day) may prevent accurate pain assessment in
hospice cancer patients (Morita, Tei, & Inoue, 2003).
Research studies on the interplay of psychological factors in hospice cancer patients
are relatively limited. Hospice cancer patients have higher prevalence and incidence of

24
pain when death is imminent. A number of studies have documented the association
between cancer pain and emotional distress. High levels of pain intensity are associated
with significantly higher levels of mood disturbance, frustration, anger, and exhaustion
(Poulos, Gertz, Pankratz, & Post-White, 2001). Patients with cancer pain reported higher
levels of uncertainty than those without, and higher levels of cancer pain severity and
interference are associated with lower levels of hope (T.-H. Hsu, Lu, Tsou, & Lin, 2003).
Cancer patients with pain reported higher scores of depression, anxiety, and hostility than
those without (Zimmerman, Story, Gaston-Johansson, & Rowies, 1996). Female patients
in advanced stage cancer are particularly vulnerable to feelings of helplessness and
hopelessness in association with higher levels of pain (Sela, Bruera, Conner-Spady,
Cumming, & Walker, 2002; Spiegel, Sands, & Koopman, 1994).
Patients’ concerns and misconceptions about pain are major barriers to effective pain
management (Ward, Hughes, Donovan, & Serlin, 2001; Weiss, Emanuell, Fairclough, &
Emanuel, 2001). Common concerns reported by hospice cancer patients include fears of
addiction, concerns about side effects, the idea that “good” patients do not complain
about pain, and negative experiences with cancer pain management (Schumacher, et al.,
2002; Weiss, et al., 2001). These concerns may prevent hospice patients from receiving
adequate pain management and may result in unnecessary suffering during the dying
process. Researchers reported that patients with higher barrier scores were more likely to
have inadequate pain management than patients with lower barrier scores (Ward, et al.,
2001). Inadequate pain management, in turn, has been associated with poorer quality of
life, concern for suffering, patients’ desire for hastened death, and suicide (Arnold, Artin,
Person, & Griffith, 2004; Filiberti, et al., 2001; Mystakidou, Parpa, Katsouda, Galanos, &
25
Vlahos, 2005).
Although pain is a private event, it influences and can be influenced by the social
environment. As hospice cancer patients become increasingly ill at the end of life, their
dependence on family, friends, and healthcare providers to provide care and relief from
symptoms and distress increases. In order to effectively advocate and care for these
patients, caregivers must understand their patient’s experience. However, studies show
that family caregivers of cancer patients overestimate the patient’s symptoms, particularly
pain intensity (Clipp & George, 1992; Ferrell, Chohen, Rhiner, & Rozek, 1991; Yeager,
Miaskowski, Dibble, & Wallhagen, 1995). Moreover, when patients’ pain ratings were
higher than their caregivers’ rating, they had significantly higher levels of anger and
fatigue, poorer psychological and interpersonal well-being, and lower quality of life than
patients in congruent dyads (Miaskowski, Zimmer, Barrett, Debble, & Wallhagen, 1997).
Healthcare professionals in hospice settings are often not able to adequately manage
cancer pain because they have insufficient knowledge and attitudes, and because
interdisciplinary collaboration is less than it should be. In addition, these barriers vary
between medical specialties. When hospice cancer patients were cared for by primary
care physicians, their average pain level was significantly higher than that of patients who
received care from oncologic physicians. The researchers suggest that this finding may be
related to the physicians’ knowledge of pain management and their utilization of
resources for hospice cancer patients (Nowels & Lee, 1999). Researchers of two studies
found that hospice nurses had higher scores on their overall knowledge of pain
management than nurses who work in the hospital oncology unit and nononcology units.
However, even the hospice nurses struggled with understanding the pharmacology of

26
medications, especially the use of opioids to manage cancer pain (Hollen, Hollen, &
Stolte, 2000; Rushton, Eggett, & Sutherland, 2003). Other researchers reported that lack
of nurse-physician collaboration may result in more difficulties in pain management in
hospice cancer patients (Ishikawa, Kawagoe, Kashiwagi, & Yano, 2007). These authors
found that when nurses and physicians did not collaborate well, there were also fewer
specific efforts such as routine team meetings and regular educational seminars for
discussing pain control. As a result, hospice cancer patients were less likely to receive
scheduled orders in prescribing opioid analgesics and other alternative/complementary
medicine for pain management.
Cultural issues. Taiwanese people embrace and are nurtured in the traditional
Chinese culture and beliefs. Chinese culture is heavily influenced by Confucian
philosophy that encourages people to be stoic, starting in early childhood, and to view
public expression of pain as a sign of weakness (C. C. Lin, 2001; T. Y. Lin, 1983; Wills &
Wootton, 1999). In Chinese culture, a cancer diagnosis is viewed as taboo, so that
Chinese cancer patients often feel stigmatized and ashamed of the illness (T. K. Chung,
French, & Chan, 1999; C. C. Lin, et al., 2000). Within the Confucian belief system, pain
is defined as a hurt or an unpleasant feeling, yet an essential element of daily life, a “trial”
or a “sacrifice” (Creel, 2000). Therefore, when a person suffers with pain, he or she
would rather endure the pain and not report it to a clinician until the pain becomes
unbearable. Such beliefs and perceptions are likely to compromise Chinese cancer
patients’ willingness to express their pain to healthcare providers for adequate pain
management.
Fatalism, which is profoundly present in Chinese culture, also negatively affects

27
pain expression and desire for treatment (M. C. Chang, Chang, Chiou, Tsou, & Lin, 2002;
Wang, et al., 1997). A majority of Chinese people believe in Taoism and Buddhism (The
National Science Council, 2004) and are also brought up with Confucianism. In such
beliefs, pain is an essential element of life, and to live with pain is to see and understand
the world as it really is (L. M. Chen, Miaskowski, Dodd, & Pantilat, 2008). Patients who
reported more fatalistic beliefs had more fears that pain represents a sign of cancer
progressing, more pain-related functional interference, less analgesic usage, and higher
psychological distress (M. C. Chang, et al., 2002; C. C. Lin, et al., 2000; Wang, et al.,
1997).
Additionally, within the beliefs of Taoism, pain occurs if Chi (energy) or blood
circulation is blocked. The blockage of Chi or blood circulation can be caused by not
only physical illness such as tumors, but also by psychological unbalance such as feeling
unsafe, or displaying excessive vigilance, suspiciousness, and delusion. To relieve pain,
the blockage of Chi or blood must be removed and the person needs to maintain harmony
with the universe (Y. C . Chen, 2001).
In Buddhist belief, pain and suffering are powers that are unwanted, but nevertheless
exist. Pain is a part of this life and manifests in a combination of physical, emotional,
mental, and spiritual forms (Tu, 1987). However, it is also believed that pain occurs due
to a barrier in the last life. Only if the person faces the pain calmly, without becoming
emotionally distressed, can he/she attain greater states of being in this life (Smith-Stoner,
2003). Traditional Chinese herbal medicine, acupuncture, acupressure, and Tai Chi are
believed to be helpful for Chi balance and blood circulation. Religious chanting or
breathing techniques can calm a person’s emotional distress so that pain becomes

28
endurable. Hence, complementary and alternative medicine therapies are important for
Taiwanese cancer patients. They have a higher preference and better acceptance for
nonpharmacological methods of pain management than those without a Chinese cultural
background (Balducci, 2005).
Additionally, because of the Chinese cultural beliefs, pain management was not
prioritized and valued in Taiwan until 1960 to 1970. Pain management has been included
in the curriculum among medical schools in Taiwan since then. However, many medical
doctors still have limited knowledge about pain medications, misconception of opioid
analgesics, and have disseminated their misconceptions to their patients (C.-H. Hong,
2007). For example, Chen and colleagues (2006) found that some physicians still
prescribed Meperidine to cancer patients, even though it is not recommended by the
World Health Organization (WHO) or American Pain Society (APS) because of its
short-acting duration, painful injection site, and the risk of neurotoxicity (Miaskowski, et
al., 2009; World Health Organization, 1996). They also reported 11.7% of cancer patients
received only PRN drugs for pain. Recently, the first cancer pain management guideline
was published by the Taiwan Cooperative Oncology Group (Taiwan Cooperative
Oncology Group, 2007). However, it is not known how the guidelines are carried out in
clinical practice.
Nurses receive limited and fragmented knowledge about pain management from
pharmacology and medical-surgical courses in basic nursing educational programs. One
group of Taiwanese researchers used a structured questionnaire to test beliefs and
knowledge of cancer pain and opioid analgesics in senior nursing students (N = 188).
They found that the correct response rate on average was 47.9% and these students had a

29
serious knowledge deficiency in pain management, especially in pharmacological
knowledge (Y.-H. Lai, Chen, Chang, Cheng, & Wei, 2000). Another group of Taiwanese
researchers reported that 63.2% of oncology nurses (N = 95) did not know how to assess
pain adequately. More than one-third of these nurses were concerned about patients
becoming drug addicted. Less than one-third of the nurses implemented
nonpharmacological intervention for pain management. These researchers recommended
that nurses receive better knowledge of analgesics and pain management (L.-C. Hsu,
Ling, Lai, & Chen, 2002). As a result, lack of knowledge in pain management and
misconceptions about opioid analgesics among doctors and nurses present significant
barriers to cancer pain management.
In summary, the current difficulties in controlling cancer pain in hospice patients are
biophysiological, psychological, and social in origin. The biophysiological issues include
the advanced stage of cancer involvement and impaired physical function. The
accumulation of comorbidities and debility are age-related. The psychological issues
include cancer-pain-induced psychological disturbance and emotional distress, and
concerns and misconceptions about pain management in hospice cancer patients and their
families. Socially, issues include a lack of understanding and congruent pain reporting
among patients, family and friends, and lack of adequate knowledge, facilitating attitudes,
and interdisciplinary collaboration in cancer pain management among hospice
professionals. Finally, culturally related beliefs in Taiwan also contribute a unique
dimension to cancer pain assessment and management in hospice cancer patients.
Anxiety
Anxiety in cancer patients is unpleasant subjective feelings of tension, fear,

30
irritability, and apprehension associated with the perception of a threat. Anxiety is an
evolutionarily maintained and is an unconditioned response that starts in the brain as the
activation of the hypothalamic-pituitary-adrenal axis. It results in other responses such
defensive behaviors, autonomic arousal, hypoalgesia, and potentiation of somatic reflexes
(LeDoux, 1996). Anxiety is an affective feeling, but can have cognitive, behavioral, and
somatic manifestations. Cognitively, patients may worry excessively or have difficulty
concentrating. Behaviorally, anxious patients may exhibit avoidant or compulsive
tendencies. Somatic symptoms of anxiety include muscle tension, restlessness, sleep
disturbance, and fatigue. Intense anxiety or panic can be manifested in more pronounced
symptoms such as palpitations, shaking, shortness of breath, chest pain or discomfort,
nausea, dizziness, numbness, lightheadedness, or feelings of choking. The physical
manifestations of anxiety are often more prominent than the psychological features and
frequently overlap with symptoms of cancer and the treatment effects (Tremblay &
Breitbart, 2001).
The common causes of anxiety in hospice cancer patients may result from
situational stressors, symptom-related events, drug-associated problems, metabolic
disturbances, and psychiatric disorders (Fisch, 2006). Pain, palpitations, and nausea are
common causes of anxiety in hospice cancer patients (Fisch, 2006). For example, patients
with lung cancer or metastasis to the lung can experience dyspnea that results in
increased anxiety (Chan, Richardson, & Richardson, 2005; Henocha, Bergmanb,
Gustafssona, Gaston-Johanssona, & Danielsona, 2007). Researchers in Taiwan have
shown that cancer patients (N = 151) with anxiety measured on the Hospital Anxiety and
Depression Scale (HADS) also had significantly higher emotional symptoms scores,

31
distress, and sadness, than patients without anxiety (M. L. Chen & Tseng, 2006). Anxiety
in palliative cancer patients also led to more difficulty falling asleep, less restorative sleep,
and nightmares (Mercadante, Girelli, & Casuccio, 2004).
Patients with advanced disease encounter situations that contribute to anxiety. They
have fears of disability, disfigurement, dependency, and a painful death (Georges, et al.,
2005). Anxious hospice cancer patients may also fear suffering, of the unknown after
death, of loneliness, of personal extinction, and of loss of autonomy. Unfinished business
can also weigh heavily on hospice cancer patients (Cicirelli, 2006; Conte, Weiner, &
Plitchik, 1982). Cancer patients have experienced levels of anxiety starting with their
cancer diagnosis. Upon entering the hospice care setting, cancer patients’ anxiety
commonly increases as they become aware that their medical treatments have been
ineffective in halting the disease and that their life expectancy is now limited. Symptoms
of anxiety frequently intensify when patients perceive that death is imminent (Cassileth,
Lusk, & Walshm, 1986; Sherif, Jehani, Saadani, & Andejani, 2001).
Pathophysiology and mechanisms of anxiety. Optimal activity in the anxiety
circuits is associated with a normal readiness to respond to situations and a flexible and
motivated state of being. Life-threatening challenges induce anxiety and result in the
permanent imprinting of the full emotional memory of the experience in the emotional
circuits through the amygdala. Associated cues are stored via the declarative memory
circuits that include the hippocampus. This center allows for associated cues to trigger
emotional memories of the trauma and bring them to conscious awareness (Davis, 1992).
The amygdala registers emotional stimuli and develops emotional memories. The
central nucleus of the amygdala has been proposed to mediate the anxiety response. The

32
various symptoms of anxiety depend on the output pathways of the central nucleus
(Davis, 1992). For example, the amygdala mediates conditioned or unconditioned stimuli,
projects directly to the lateral hypothalamus, and results in the activation of the
sympathetic autonomic nervous system that then induces tachycardia, galvanic skin
response, pallor, pupil dilation, and blood pressure elevation (Davis, 1992).
The medial prefrontal cortex is reciprocally connected with the amygdala for
cognitive control of the anxiety response. It allows self-imposed regulation of affect and
modulation of autonomic and neuroendocrine functions (Barkley, 1997). However, if the
challenge increases, control shifts from the prefrontal executive centers to primordially
lower centers such as the amygdala, where behaviors are guided by the previous
anxious/traumatic experiences (Arnsten, 1998).
Several neurotransmitters mediate the different components of anxiety, including
excitatory amino acids such as glutamate, inhibitory amino acids such as GABA, and
monoaminergic neurotransmitters such as catecholamines and indoleamines (Sinha,
Mohlman, & Gorman, 2004). Norepinephrine mediates emotionally traumatic memories
as they become imprinted in the amygdala through the β-adrenergic receptors.
Dopamine-1 in the amygdala mediates conditioned fear to facilitate declarative memory
associations through the hippocampus (Lamont & Kokkinidis, 1998). The currently
available pharmacological treatments for anxiety such as benzodiazepines and
serotonin-1A agonists, are focused on these neurotransmitters to relieve symptoms of
anxiety (Breitbart, Chochinov, & Passik, 2004; Jackson & Lipman, 2004).
Anxiety in hospice cancer patients. Fear of death in hospice cancer patients is a
frequent cause of situational or state anxiety. Researchers have studied fear of death or

33
death anxiety in relation to age, gender, spirituality/religion, and culture. Increased death
anxiety has been inconsistently related to age in numerous research studies. In an early
study, the researchers found that death anxiety scores were not significantly different
between 230 graduate students and elders in a senior center and nursing homes. Their
ages ranged from 30 to 82 years (Conte, et al., 1982). This was also true in cancer
patients. Researchers investigated 124 Taiwanese advanced cancer patients and reported
75.8% of these patients showed mild to moderate anxiety. However, age was not
associated with anxiety (L.-Y. Tsai, Ku, Chang, & Lai, 2001).
Researchers of one review article attempted to clarify the relationship between age
and fear of death. The researchers reviewed 49 articles that were focused on elders who
were older than 50 years and were hospitalized or lived in the community or in nursing
homes. The reviewer reported that death anxiety decreased from middle age to older age,
but stabilized during the final decades of life. They suggested that age is not a reliable
predictor of death anxiety in elderly populations (Fortner & Neimeyer, 1999). A later
study conducted in Taiwan (N = 224) found the severity of death fear in cancer patients
decreased after being admitted to the hospice, but older people ( > 65 years) presented a
significantly higher level of death fear than younger people at two days before death (J.-S.
Tsai, Wu, Chiu, Hu, & Chen, 2005). These findings are similar to a study (N = 192)
conducted in the United States (Cicirelli, 2006). However, other studies found that fear of
death tends to be greater among younger than older people (Thorson & Powell, 2000; K.
G. Wilson, et al., 2007). With the inconsistent findings of the relationship between the
age and death anxiety, age will be a factor to consider controlling for when studying the
effect of music on anxiety in hospice cancer patients.

34
There were also inconsistent findings in studies of gender differences in death
anxiety. Researchers in the United States and in Taiwan reported that there was no
difference in the level of death anxiety between males and females in both older adults
(Conte, et al., 1982; Fortner, Neimeyer, & Ryharezyk, 2000) and cancer patients (L.-Y.
Tsai, et al., 2001). However, other researchers reported that women had higher anxiety
levels when they were close to death (Harding, Flannelly, Weaver, & Costa, 2005;
Neimeyer & David, 1995). The authors suggest that one possible reason may be that men
tend to avoid thoughts of death and dying to a greater extent than women. That is, men
may deal with intrusive thoughts of their mortality more defensively than women deal
with theirs and women have a greater tendency to admit to having troubled feelings
(Wong, Reker, & Gesser, 1994). Therefore, gender will also be considered as a factor to
control for in the study when analyzing anxiety.
The relationship between spirituality or religious beliefs and death anxiety has also
provided mixed findings. Three research groups reported that in hospice cancer patients,
reports of being more religious were significantly associated with lower death anxiety
(Grumann & Spiegel, 2003; Pevey, Jones, & Yarber, 2008; L.-Y. Tsai, et al., 2001). They
reasoned that this was because religion may be comforting to dying hospice patients by
offering a relationship between God and the dying that gives hope of life after death
(Pevey, et al., 2008). These findings may not be true in Taiwan. Two thirds of the
Taiwanese population has either Buddhist or Taoist beliefs. These religious belief systems
can promote fear of death. For example, if ideas of anticipated judgement and
punishment are at the core of one’s belief system, one’s death anxiety may increase and
sometimes may become unbearable (Gonda & Ruark, 1984).

35
Multiple researchers have investigated spirituality or compared both religious beliefs
and spirituality in relation to anxiety in terminally ill patients. Religious belief is defined
as a particular institutionalized or personal system of belief and practices related to the
divine. It pertains to participation in organized rituals and practices (King, Speck, &
Thomas, 1995; Mytko & Knight, 1999). Spirituality is defined as individuals thinking
about the meaning of their existence and interpreting their inner values (Chao, 1998).
Although religious beliefs and spirituality are different, they may coexist and are not
necessarily mutually exclusive (Mytko & Knight, 1999). In some studies, spirituality was
negatively correlated with anxiety, indicating that hospice cancer patients with spiritual
beliefs had less anxiety than those without (C.-C. Li, Yu, & Hwang, 2006; McCoubrie &
Davies, 2006; Wittmann, Volimer, Schweiger, & Hiddemann, 2006). In other studies,
spiritual well-being was reported to be needed by hospice cancer patients (Hampton,
Hollis, Lloyd, Taylor, & McMillan, 2007; C.-C. Li, et al., 2006; Williams, 2006). In two
studies, hospice cancer patients reported that spiritual well-being helped them to
transform uneasy feelings, regrets, and sorrow into positive attitudes and peaceful
thoughts, and also helped them to search for meaning and enhanced natural acceptance
(Ando, Morita, Lee, & Okamoto, 2008; C.-C. Li, et al., 2006). In three studies,
researchers compared religion and spirituality among patients with advanced cancer. The
terminally ill cancer patients reported that spirituality was more important and
meaningful, and decreased their anxiety and fear of death better than their religious
beliefs (Grumann & Spiegel, 2003; Hampton, et al., 2007; McCoubrie & Davies, 2006).
However, no similar study was found in Taiwan, where the religious beliefs are different
from those in the United States.

36
Medications, such as bronchodilators, corticosteroids and β-adrenergic receptor
stimulants, are commonly used for chronic respiratory conditions in hospice care settings
and these drugs may cause anxiety, irritability, and tremulousness (Bruera, et al., 1995;
Levy & Catalino, 1985). Metabolic conditions, including hyperglycemia, hypoglycemia,
organ failure, electrolyte imbalance, nutritional failure and infection, which frequently
occur in hospice cancer patients, may lead to symptoms of anxiety (Massie, Holland, &
Glass, 1983). Finally, patients with a history of psychiatric disorders can have anxiety in
palliative care settings that results in delirium, depressive disorders, panic, posttraumatic
stress, phobias, and a generalized anxiety disorder (Fisch, 2006). In this study, opioid
analgesics used by the hospice cancer patients were documented and treated as a
potentially confounding variable for possible statistical control when analyzing both pain
and anxiety. Patients who are critically ill with diagnosed metabolic disturbances were
excluded from the study. Patients with present untreated psychiatric symptoms were also
be excluded from the study.
Cultural issues. Chinese patients, especially men, are reluctant to express or discuss
their feelings (Y. F. Tsai, 2007). Expressing personal feelings, such as anxiety, to anyone
outside of the family in the Chinese culture usually is considered showing personal
weakness and is inappropriate or culturally unacceptable (T. Y. Lin, 1983). However,
family members may be the communication bridge to initiate talking about the anxious
feelings of the hospice cancer patient to healthcare professionals. Familialism and filial
piety play the key role in this context. Familialism is considered the most important and
fundamental collectivist value (D. T. Tsai & Lopez, 1997). In Confucian teaching, the
family is always to be considered before the individual. Chinese people are closely bound

37
to their families. Personal feelings and thoughts are only shared within the family
(Wellish, et al., 1999). Family members are expected to care for each other and are
perceived as the most satisfying sources of support (G. K. Hong, 1989; Lan, 2002).
The traditional Chinese belief of filial piety accompanies familialism and has been
considered as the soul of traditional Chinese culture and the most important social value
for promoting caring relationships between children and parents (Yu, 1983). The
traditional expectation is that since parents take responsibility to help their children
through life, adult children, especially the males, are obligated to protect, take care of,
and respect their parents (Holroyd, 2003). As a result, the emotional expression and some
physical symptoms of anxiety of the hospice cancer patients may be observed by the
family members. The son may be the representative of the patient initially to
communicate with the healthcare professionals.
The question is raised as to whether Taiwanese patients will report anxiety to the
researcher. Severity of anxiety in Taiwanese cancer patients increased with the stages of
chemotherapy in one study. Researchers reported that the severity of anxiety (0 – 100 mm
VAS) in 32 cancer patients increased from mild anxiety (25 + 25.2) mm before
chemotherapy to moderate anxiety (40.1 + 26.0) mm on the third day (T.-W. Huang, et al.,
2001). Researchers of three other studies reported that hospitalized cancer patients on
average had moderate anxiety (P.-Y. Chen, et al., 1999; Hung, 2003; P. I. Peng, 2005).
One of these researchers used the State Anxiety Inventory to examine 25 patients with
hematological malignant cancer before using music for anxiety and reported that the
average of these patients’ anxiety was 49.9 points (SD = 9.25) (P. I. Peng, 2005).
Researchers of the other two studies of patients in different stages of cancer used the

38
Hospital Anxiety and Depression Scale (0 – 7 points = mild anxiety, 8 – 10 = moderate
anxiety, 11 – 21 = severe anxiety). One researcher reported that the average anxiety level
was clinically significant at 7.24 points (SD = 4.94) in 34 patients before using music for
anxiety; only 2 patients were using anxiolytics (Hung, 2003). The other research group
reported that the average anxiety was 7.78 points (SD = 3.37) in a correlational study of
90 cancer patients. The use of anxiolytics was not reported (P.-Y. Chen, et al., 1999).
Therefore, despite cultural norms, Taiwanese cancer patients do report mild to moderate
anxiety in research studies.
Although some studies have shown that people who are more religious have lower
death anxiety, researchers have pointed out that if one’s religious belief relates to an
anticipatory judgement and punishment after death, death anxiety may increase and
sometimes may become unbearable (Dezutter, et al., 2009; Gonda & Ruark, 1984). Even
though no research study was found in this area, researchers of one earlier study (N = 333)
in the US reported that strong belief in afterlife contributed to higher death anxiety
(Osarchuk & Tatz, 1973). As a result, it is assumed that religious beliefs may lead to
higher death anxiety among the Taiwanese hospice cancer patients than those who have
other religious beliefs. Unfortunately, death anxiety in the Chinese culture involves not
only religious beliefs but also a mixture of local folklore, superstition, and magical belief
systems, which may contribute to higher levels of anxiety among hospice cancer patients
(Yick & Gupta, 2002). For example, Buddhists believe in reincarnation. Depending on
the deeds people have done in this life, they may be punished by being reincarnated into
unfortunate and miserable people in the next life, or even become animals. They may be
tortured in the next life (Hsing Yun, 1983). Taoists believe that after death, the person’s

39
spirit/soul will go through ten gates in the Nether World and be judged by King Yian-Luo,
the Master of Hell. Based on records in the “Birth-and-Death Notebook,” the spirit/soul
may be punished in the underworld for the misdeeds or may be rewarded and go to
Heaven (D. K. Chung, 1995; S. Li, 1993).
In summary, anxiety in hospice cancer patients is caused by unpleasant subjective
feelings of tension, fear, irritability, and apprehension associated with the perception of a
threat. These affective feelings can have cognitive, behavioral, or somatic manifestations.
The common causes of anxiety in hospice cancer patients may result from situational
stressors, symptom-related events, drug-associated problems, metabolic disturbances, and
psychiatric disorders. Anxiety may have different influences on hospice cancer patients
depending on gender, age, and spiritual or religious beliefs. Furthermore, Chinese cultural
beliefs may influence Taiwanese hospice cancer patients to not express their anxiety to
people outside of the family. Furthermore, patients who have Buddhist or Taoist beliefs
may be more anxious about death than those who do not. Therefore, when hospice cancer
patients hesitated to express their anxiety at the first meeting with the researcher, she
talked with the families to determine the patients’ levels of anxiety. If anxiety was not
identified, the hospice cancer patients marked the level of their anxiety as “no anxiety”
on the anxiety VAS. If anxiety was identified, they marked their anxiety level on the
anxiety VAS.
Cancer Pain and Anxiety
Cancer pain and anxiety are common problems for patients in hospice, and patients
with pain seem to be at increased risk for anxiety compared with those without pain
(Thielking, 2003). It has been demonstrated that anxiety and cancer pain are highly

40
correlated in patients receiving palliative care (M. L. Chen & Tseng, 2006; D. K. Payne
& Massie, 2000). Cancer patients with more severe or breakthrough pain reported
significantly more anxiety and depression than those with mild or no pain (M.-L. Chen,
Chang, & Yeh, 2000; P.-Y. Chen, et al., 1999; L.-Y. Tsai, et al., 2001). Furthermore,
anxiety reduced patients’ tolerance for physical pain and substantially impeded overall
function (Noyes, Holt, & Massie, 1998). Researchers reviewed 165 patients who suffered
from chronic pain and reported that anxiety was negatively associated with coping with
chronic pain (McCracken & Gross, 1993). In addition, cancer pain and anxiety were
shown to have a significant impact on the desire for death or hastened death in hospice
cancer patients (Mystakidou, Rosenfeld, et al., 2005). Therefore, providing music and
nature sounds in addition to opioid medication may help hospice cancer patients to have
better pain relief and less anxiety.
Music for Pain and Anxiety
The healing power of music for pain and anxiety has been described in eastern and
western literature. In eastern countries, Chinese culture has been the mainstream. The use
of music for treating illness and other health conditions was documented in the Book of
Odes as early as the 10th century BC in China. The five tones used in Chinese music are
thought to resemble the five elements (metal, wood, water, fire, and earth) that the
Chinese people believe will keep them physically and mentally balanced, and reduce
their physical discomfort and psycho-emotional distress (Chuang, 2004). During and after
World War II, physicians in the west used music to distract injured soldiers from their
pain while they recovered from surgery and to calm soldiers who were suffering from
shell shock (Wigram, Pedersen, & Bonde, 2002). Our nursing pioneer, Florence

41
Nightingale (1969), recognized that different types of music resulted in different effects.
She indicated that wind instruments with continuous sound or an “air” had soothing
effects and would be beneficial to the sick, while music played on a piano-forte could
produce the reverse effect.
Music has been viewed as a science and an art because of its scientific structures
known as the elements of music and the aesthetic results from combining those elements
(Wigram, et al., 2002). Music is comprised of five major elements: pitch (frequency),
volume (intensity), timbre (tone color), interval, and rhythm (tempo or duration) (Alvin,
1975). The effect and the character of a piece of music depends on the relationships
among these elements (Chlan, 2006). For example, a high pitch with fast rhythm and high
volume may tense muscles, trigger body movement, or produce uncomfortable feelings.
In contrast, a low pitch with slow rhythm and steady volume may help people to relax
and slow down. The combination of the elements may be interpreted as consonance (a
combination producing a pleasant acoustical sensation) or dissonance (a combination
leading to an unpleasant sensation), and is strongly associated with training and culture
(Valentinuzzi & Arias, 1999). For example, jazz music may be perceived as consonance
by African Americans, but may be perceived as dissonance by Taiwanese people (Chiang
& Good in preparation; Good et al., 2000).
Mechanisms of music for pain and anxiety. When a person listens to music, the
sound waves are transmitted via the ossicles in the middle ear to the cochlear fluid in the
inner ear. The basilar membrane of the cochlea is the resonance region and responds to
various vibration frequencies. The cilia of hair cells are the sensory receptors that turn
these vibration frequencies into electrical signals and directly connect to the acoustic

42
nerve endings. The auditory nerves carry these signals to the auditory cortex in the
temporal lobe. The primary auditory cortex receives inputs and is involved in music
perception of pitch and melody, which is influenced by personal experiences. The
secondary auditory cortex further processes the interpretation of music patterns of
harmony, melody, and rhythm (Weinberger, 2004).
Multiple brain regions respond to music stimuli. Researchers found that pleasant
emotional responses to music evoke activity in the limbic system, thalamus, amygdala,
hippocampus, medial prefrontal cortex, midbrain, e.g., periaqueductal grey (PAG), and
ventral striatum, e.g., the nucleus accumbens (NAc) (Blood & Zatorre, 2001). The limbic
system, amygdala, hippocampus, and medial prefrontal cortex are associated with
emotion, anxiety response, and pain perception. When these regions are activated by
reward or positive motivation, the dopamine and opioid systems are also activated (Bardo,
1998; Berridge & Robinson, 1998; Gardner & Vorel, 1998). Both PAG and NAc are rich
in opioid receptors and are modulated by endorphin and enkephalin (endogenous opioids
peptides) (Bardo, 1998). Activation of PAG and NAc modulates pain transmission and
perception via the descending opioid-related pain inhibitory system (Fields & Basbaum,
1989). Thus, the perceptions of pain and anxiety are altered.
Effects of music on pain. The majority of current published randomized controlled
trials that used music for reducing pain were during medical or surgical procedures (55%)
and for postoperative pain (28%) (Cepeda, Carr, Lau, & Alvarez, 2006). Because the
purposed study is based on these studies tested on adult postoperative patients, the
literature review begins by focusing on this area.
Eleven studies testing the effect of music on postoperative pain were reviewed. Most

43
of the studies were conducted in the United States (Good, 1995; Good, Anderson, Ahn,
Cong, & Stanton-Hicks, 2005; Good, et al., 2001; Good, et al., 1999; Mullooly, Levin, &
Feldman, 1988; Nilsson, Rawal, Unestahl, Zetterberg, & Unosson, 2001; Voss, et al.,
2004), while two were conducted in Taiwan (Good & Chin, 1998; S. L. Hwang, et al.,
1996), and one each in South Korea (M. Good & Ahn, 2008) and in Phillippines (Locsin,
1981). Eight studies were pre- and posttest randomized controlled trials, while three
studies used quasi-experimental design (Good & Ahn, 2008; S. L. Hwang, et al., 1996;
Locsin, 1981). The sample size had a wide range, from 24 subjects (Locsin, 1981) to 500
subjects (Good, et al., 1999). The amount of time that postoperative patients listened to
music ranged from 15 minutes once for two days (Good & Chin, 1998) to 30 minutes
every two hours for 48 hours (Locsin, 1981).
Researchers of nine studies asked the participants to select the type of music they
preferred, while the participants in the other two studies did not select the type of music
(Mullooly, et al., 1988; Nilsson, et al., 2001). The majority of the researchers preselected
the music offered to participants, except one researcher who asked the subjects to bring
their own music (Locsin, 1981). The five types of music that were offered in seven of
these studies were the same (Good, 1995; Good & Ahn, 2008; Good et al., 2005; Good &
Chin, 1998; Good et al., 2001; Good et al., 1999; Voss et al., 2004). They were first used
in Good’s dissertation study (1992, 1995). However, the study conducted in South Korea
added some culturally specific music, offering both American and Korean music (Good
& Ahn, 2008).
Researchers of eight of the 11 studies reported that music reduced pain, while two
studies showed that music reduced pain on Day 2 but not Day 1 (Good & Chin, 1998;

44
Mullooly, et al., 1988), and one study showed that music did not reduce pain during the
first postoperative ambulation (Good, 1995). A researcher conducted systematic review of
42 randomized controlled trials to examine the effect of music on anxiety and pain in
surgical patients. She reported that pain was measured in 22 studies, and 13 of them (59%)
had significant findings on reducing pain (Nilsson, 2008).
Effects of music on pain in cancer and hospice patients. Music has been found to
be effective in decreasing cancer pain in six studies, that were conducted in the United
States (Beck, 1991; Curtis, 1986; Gallagher, et al., 2006; Gallagher & Steele, 2001; Krout,
2001; Zimmerman, et al., 1989), three in Taiwan (S. H. Huang, 2000; S. T. Huang, 2006;
Y. J. Lee, 2000a), and one in Germany (Reinhardt, 1999). Three studies were two-group
randomized controlled trials (S. T. Huang, 2006; Reinhardt, 1999; Zimmerman, et al.,
1989), one study had crossover design (Beck, 1991), one had a two-group
quasi-experimental design (Y. J. Lee, 2000a), and four studies had single group design
(Gallagher, et al., 2006; Gallagher & Steele, 2001; S. H. Huang, 2000; Krout, 2001).
Most of these studies had sample sizes of less than 100 (N = 9 to 80), and three had
a larger sample, from 126 to 345 participants (Gallagher, et al., 2006; Gallagher & Steele,
2001; S. T. Huang, 2006). The amount of time that cancer patients listened to music
ranged from 15 minutes only once (Curtis, 1986) to 45 minutes twice a day for three days
(Beck, 1991). The three studies conducted by music therapists ranged from a single
session once (Krout, 2001) to multiple sessions each with different lengths of time
(Gallagher, et al., 2006; Gallagher & Steele, 2001), and minutes spent on each session
were not specified. All the researchers reported significant effects of music for pain. Two
studies used the same participants as the control group (Beck, 1991; S. H. Huang, 2000).

45
Three studies had one-group pre- and posttest designs (Gallagher, et al., 2006; Gallagher
& Steele, 2001; Krout, 2001). The results from studies with quasi-experimental or single
group designs may be biased since they did not have a control group to detect whether or
not the effect was really from the treatment. The studies with small sample sizes or with
unequal numbers of music sessions would be more likely to be biased as well. Some of
the studies were conducted more than 10 years ago. Since then, the context, medication,
and technology used for treatment and care have changed and the results may be
outdated.
Effects of music on anxiety. Sixteen studies explored the effects of music on
anxiety in a variety of situations: for stress management (Hanser, 1985), after acute
myocardial infarction (White, 1999), after surgery (Good, 1992; Voss, et al., 2004; Yao,
1998), in short-term waiting for day surgery (Cooke, Chaboyer, Schluter, & Hiratos,
2005), while undergoing root canal treatment (H. -L. Lai, et al., 2008), during dressing
change (D. F. Lee, 1995), during delivery (S.-C. Chang & Chen, 2005; Liu, 2002), in
institutionalized elderly (Y. J. Lee, 2000b), in patients receiving mechanical ventilation
(O. K. A. Lee, Chung, Chan, & Chan, 2005), in abused women in shelters
(Hernandez-Ruiz, 2005), and during medical procedures (Bally, Campbell, Chesnick, &
Tranmer, 2003; Smolen, Topp, & Singer, 2002; Yilmaz, et al., 2003). A researcher
conducted systematic review of 42 randomized controlled trials to examine the effect of
music on anxiety and pain in surgical patients. She reported that anxiety was measured in
24 studies and 12 of them had significant findings on reducing anxiety (Nilsson, 2008).
Seven studies were reviewed for the effect of music on reducing anxiety in cancer or
hospice patients. Three were conducted in the United States (Bailey, 1983; Gallagher, et

46
al., 2006; Gallagher & Steele, 2001), three were done in Taiwan (Hung, 2003; S.-Y. Li,
2007; P. I. Peng, 2005), and one was in Australia (Horne-Thompson & Grocke, 2008).
Researchers of three studies used a two-group randomized controlled design
(Horne-Thompson & Grocke, 2008; Hung, 2003; P. I. Peng, 2005), two studies had
one-group pre- and posttest design (Gallagher, et al., 2006; Gallagher & Steele, 2001),
one study had a quasi-experimental design (S.-Y. Li, 2007), and another study had a
randomized comparative group design with no control group (Bailey, 1983).
Among the cancer and hospice patients, the sample sizes ranged from 21 to 345
participants, and the length of the music sessions varied from 25 minutes once (Bailey,
1983) to 30 minutes daily for seven days (Hung, 2003). Studies conducted by music
therapists ranged from 20 to 40 minutes once (Horne-Thompson & Grocke, 2008) to
multiple sessions without specifying length of time for each session (Gallagher, et al.,
2006; Gallagher & Steele, 2001). Although researchers of all seven studies reported that
anxiety was significantly reduced by listening to music, the studies without a control
group, with a small sample size, or with an unequal number of music sessions would be
more likely to be biased.
Related effects of music in hospice and cancer patients included improved mood (D.
S. Burns, 2001; Cassileth, Vickers, & Magill, 2003) and relaxation (S. J. I. Burns, Harbuz,
Hucklebridge, & Bunt, 2001; Curtis, 1986; Krout, 2001), and increased quality of life in
dying patients (Halstead & Roscoe, 2002; Hilliard, 2003). In palliative care settings, staff
members reported that music seemed most effective in the areas of patient satisfaction,
stress reduction, anxiety reduction, and patient receptivity to pain and other physical
discomfort (Gallagher, Huston, Nelson, Walsh, & Steele, 2001). Researchers who studied

47
music thanatology (defined as a prescriptive harp vigil) found that after listening to 25 to
95 minutes of harp music, dying hospice patients (N = 65) showed decreases in agitation,
wakefulness, and breathing effort (Freeman, et al., 2006). Music was also found to
facilitate the process of connecting psychological and spiritual well-being for patients in
palliative care (Salmoon, 2001). In two qualitative studies, researchers reported that
music was able to help dying patients to decrease depressive symptoms and social
isolation, increase communication and self-expression, stimulate reminiscence and life
review, and enhance relaxation (Clements-Cortes, 2004; Porchet-Munro, 1988). Kemper
and Danhauer (2005) stated that using music in end-of-life care can also create supportive
interactions between the dying patients and their loved ones. They explained that
increased communication and expression through music listening may be less threatening
than with verbal expression.
Selection of music. In order to decrease cancer pain and anxiety in hospice cancer
patients, the investigator chose selections of music that she thought were likely to have a
relaxing effect or distract patients from pain and anxiety. First, she asked participants to
choose music they liked or found familiar. Research has shown that preferred music is
more distracting (Parente, 1976) and produces better therapeutic effects than music that is
not preferred (Bruya & Severtsen, 1984). Preferred music reduced pain (Hekmat & Hertel,
1993), negative emotional states (Labbe, Schmidt, Babin, & Pharr, 2007), and increased
relaxation (Stratton & Zalanowski, 1984).
Second, the investigator chose sedative music. Researchers reported that tempo,
typically measured in beats per minute (bpm), is the element predominantly related to an
arousal effect, and that slow or meditative music induced a relaxing effect (Bernardi,

48
Porta, & Sleight, 2006). Other researchers reported that respiratory rate was changed by
the tempo of the music and that increased tempo resulted in muscle tension and other
physical responses (Khalfa, Roy, Rainville, Bella, & Peretz, 2008). Sedative music also
distracts people’s attention and was moderately correlated with alpha rhythm (Borling,
1981). Sedative music is characterized by 60 to 80 beats per minute in tempo, with a
general absence of strong rhythms or sudden high-pitch sounds (Gaston, 1951; Good,
1992).
Third, the investigator chose music that was culturally sensitive for Taiwanese
hospice cancer patients. Researchers compared cultural differences in music preference
for pain relief among three ethnic groups: Caucasians, African Americans, and Taiwanese.
They found that Caucasians frequently chose orchestra music, African Americans
preferred jazz, and Taiwanese selected harp music (Good, et al., 2000). Others found in
South Korea indicated that when both United States and Korean music were offered, 62%
of the postoperative women chose Korean music for reducing pain (Good & Ahn, 2008).
Researchers who were educated in the United States tested Good’s music (1992) in their
studies and reported that Taiwanese patients chose Western harp and piano music for pain,
but none chose jazz (Good & Chin, 1998). Good and Chin (1998) asked Taiwanese
participants to recommend other types of music they preferred, and they suggested
Buddhist hymns and Taiwanese popular songs. Another researcher reported that 50
Taiwanese elderly people preferred Chinese orchestra music and found it relaxing, but
also chose Western music (harp music was the most preferred) from Good’s study (1992,
1995) (Hui-Ling. Lai, 2004). A third researcher offered a choice of Taiwanese and
American music (from Good’s study) and reported that about two-thirds of the

49
participants chose Taiwanese music (S. T. Huang, 2006). Multiple studies conducted in
Taiwan also demonstrated that while most Taiwanese participants were offered different
types of music, while the majority of them selected Taiwanese or Chinese folk or popular
songs or religious music (Buddhist hymns) for relaxation purposes (S. H. Huang, 2000; S.
L. Hwang, et al., 1996; H. H. Lin, Chen, Kuo, Want, & Huang, 2007; H.-C. Wu & Chou,
2008). Therefore, culturally specific music was included in this study to reduce cancer
pain and anxiety hospice cancer patients.
Nature Sounds
Nature sounds are the sounds produced by natural phenomena, such as wind, rain,
ocean, streams, animals, and birds. Human beings are closely attached to the natural
world and contact with nature is beneficial to health (Frumkin & Louv, 2007). Wilson
(1984), a biologist and sociobiological theorist, described that the intimate emotional
connection human beings have to other living organisms as the concept of biophilia. He
hypothesized that humans possess a genetically based tendency to focus on and respond
to life and lifelike processes in the environment. An environment rich in biodiversity is
preferred by human beings. Expanding on this theory, other researchers suggested that an
affinity for nature may go beyond living things, including nature scenes and sounds
(Heerwagen & Orians, 1993).
Although human beings are closely bonded with nature, the therapeutic use of nature
sounds is understudied. Five studies that focused on the effect of nature sounds were
found (Dickhaus, et al., 2003; Diette, et al., 2003; Golletz, 1997; Tsuchiya, et al., 2003;
Williamson, 1992). Four of them were conducted in the United States, while one study
was done in Japan (Tsuchiya, et al., 2003). Three studies were conducted during clinical

50
procedures for flexible bronchoscopy (Diette, et al., 2003), rectal distention process
(Dickhaus, et al., 2003), and general anesthesia (Tsuchiya, et al., 2003). One study was
conducted on postoperative patients for sleeping problems (Williamson, 1992). The other
was an unpublished doctoral dissertation and conducted on undergraduate students for
managing anxiety and anger (Golletz, 1997). All the studies used a quasi-experimental
design to compare group differences. Sample size ranged from 29 to 128 adult
participants. Nature sounds used included ocean sounds (Golletz, 1997; Williamson,
1992), sounds of streams (Diette, et al., 2003; Golletz, 1997; Tsuchiya, et al., 2003), birds
singing (Diette, et al., 2003; Tsuchiya, et al., 2003), and soft wind (Tsuchiya, et al., 2003).
Researchers of one study did not report the type of relaxing nature sounds they used
(Dickhaus, et al., 2003). Researchers of these studies found that nature sounds were
effective in reducing pain (Diette, et al., 2003), decreasing anxiety and anger (Dickhaus,
et al., 2003; Golletz, 1997), lowering blood pressure and heart rate (Tsuchiya, et al.,
2003), and improving sleep experience (Williamson, 1992).
Nature sounds have effects similar to that of music. That is, nature sounds also have
different tempos, pitch, and rhythm. For example, birds singing may have a higher pitch
than the sounds of frogs. Larger ocean waves repeat in slow, rolling tempo with more
bass frequencies, while smaller lake waves lap sand and rocks in a much faster manner.
Sounds of streams often have a continuous rhythm, and sounds of rain may create a
playful rhythm. Moreover, personal preference will also play a key role. For example,
some people may feel that a thunderstorm has a relaxing effect, but others may feel
frightened by it. Therefore, the selection of nature sounds for testing in this study took
pitch, tempo, and rhythm into consideration. Nature sounds were selected if they are

51
sedative or generally slow in nature and with a general absence of strong rhythms or a
sudden high pitch.
Since Taiwan is an island with shores, mountains, and forests, using ocean waves
and birds singing are culturally appropriate. These sounds are also recommended by other
researchers (Dossey, 1995; Rhiner, Ferrell, Ferrell, & Grant, 1993). Other nature sounds
familiar to Taiwanese people were also selected, including the sounds of frogs, sounds of
nature night life, and sounds of forests. However, the sounds of stream and winds were
not used. Sounds of streams have been found to trigger the urge to urinate in listeners
(Diette, et al., 2003) and might have potentially caused discomfort for the hospice cancer
patients. Sounds of the wind in Chinese culture are traditionally associated with sadness,
loneliness, and negative feelings, so these were also not included in the nature sounds
used in the study.
Combination of Music and Nature Sounds
The combination of music and nature sounds consists of sedative music and nature
sounds. English and Chinese language studies that focused exclusively on testing the
combination of music and natures sounds were not found. Four studies conducted in
foreign countries used the combination of music and nature sounds as only one of the
types of music intervention (Harikumar, et al., 2006; Hung, 2003; S. Y. Lin, 2003;
Sorensen & Tybjerg, 2004).
A combination of music and nature sounds was used as one choice of music in a
randomized controlled trial of patients undergoing colonoscopies in India. The
researchers indicated that they used a soothing mixture of soft instrumental music with
nature sounds in the study, and it was the second preferred type of music (23%) chosen

52
by patients in the study (N = 78). They reported that patients who were in the music
group received less midazolam and had a lower discomfort score than those who did not
(Harikumar, et al., 2006).
The second study was done in Denmark with 30 psychiatric patients who suffered
from anxiety and distress. The researchers used a commercially made program
(MusiCure) to treat these psychiatric patients. They reported that 87% of the patients
experienced a positive effect from the treatment. They calmed down and some of them
fell asleep. However, the patients were assigned to treatment and control groups by
nurses based on their clinical judgement, and the number and length of treatments were
varied in each patient (Sorensen & Tybjerg, 2004).
The other two studies were master theses conducted in Taiwan. One researcher
provided the combination of music and nature sounds as one of the music choices for 11
pediatric cancer patients during chemotherapy to control for nausea and vomiting. The
study result did not reach a statistically significant level between treatment and control
groups. The researcher did not report the number of children who chose the combination,
so the effect of using a combination of music and nature sounds is unknown (S. Y. Lin,
2003). Another researcher also included the combination of music and nature sounds as
an option 16 adult cancer patients. Although she reported that five patients selected the
combination, it is not clear whether or not the combination was effective in decreasing
anxiety and depression and improving sleep quality (Hung, 2003).
Researchers argued that music frequently can be highly subjective. They suggested
the use of nature sounds with music may be more adequate since it crosses all language,
social, and cultural barriers (Harikumar & Kumar, 2007). Therefore, the criteria for

53
selecting the combination of music and nature sounds will be sedative in nature and with
a general absence of strong rhythms or sudden high pitch in music and nature sounds.
After reviewing studies of nature sounds and the combination of music and nature
sounds, several gaps were found. Researchers of these studies did not provide a definition
of nature sounds. Studies were generally done in a small sample size without
randomization design. Most of them used nature sounds or the combination of music and
nature sounds only as one type of music selection available to patients. The types of
nature sounds and the combination of music and nature sounds lacked variety. Some
studies included a combination of nature sounds and a picture of nature scenery, so the
pure effects of nature sounds and the combination of music and nature sounds were not
clear. Although studies provided statistically significant evidence on effects of these two
interventions on procedural pain, anxiety, and sleep experience in other population, the
effect of nature sounds and the combination of music and nature sounds on cancer pain
and anxiety in hospice cancer patients remain unknown. As a result, this investigator will
define and provide criteria for nature sounds and the combination of nature sounds in the
study. Nature sounds and the combination of music and nature sounds will be separated
to two intervention groups in order to examine the effect of these two interventions.
Threats to Internal Validity
Threats to internal validity can occur in experimental designs and may result in
biased outcomes. History is an event that happens between the beginning of the treatment
and the posttest that can produce the observed outcome in the absence of that treatment
(Shadish, Cook, & Campbell, 2002, p. 56). For example, if a family member of a study
participant turned on the television, or a cell phone rings during the treatment, it may

54
influence the effect of the intervention. To prevent or minimize this problem, the
researcher will ask the family member to leave the room and come back after the
intervention is done, and turn off the television and the cell phone during the intervention
session. A sign was posted on the door of the patient’s room to help prevent unexpected
disturbances. Opioid analgesics and anxiolytics prescribed during the data collection
period are also a threat to history. The name, route, dose, frequency, time given, and
whether medication was “in effect” were recorded and controlled statistically.
Maturation is the natural changes that could occur even without the treatment, such
as growing older or gaining more knowledge or experience (Shadish, et al., 2002). The
hospice cancer patients in the study may become weaker as their illness progresses, and
this will affect their ability to actively listen to the tape and to express pain and anxiety
accurately. It would be difficult to control for the progress of their illness, so maturation
was minimized by randomization.
Attrition or experimental mortality refers to participants who drop out of the study
during the data collection period (Shadish, et al., 2002). Hospice cancer patients may
have a higher experimental mortality rate than other populations because their life
expectancy is less than six months when entering hospice care. Attrition can also happen
when the participants transfer to other units or healthcare facilities. Participants in the
control group may not like to wait for three days to receive the treatment and decide to
drop out early. If participants in one treatment group dropped out more than those in the
other groups, the outcome would be influenced by the group number differences.
Therefore, in order to have a sufficient sample size in each group, more participants were
recruited and randomized to until each group had 31 participants in it. The data collected

55
from participants who dropped out of the study was analyzed as a separate group and
compared to those who completed the data collection process. The attrition rate and
reasons for dropout from the study were recorded and reported.
Instrumentation occurs when using the same instrument for repeated measurements.
That is, when taking the same measurement twice, the second score will be influenced by
the first score (Shadish, et al., 2002). Pain and anxiety was measured with 100-mm VAS
scales three times in this study, and participants may have become familiar with the scale.
The participants may have changed their score after the treatment, and the change of the
pain score may not be due to the treatment effect. To minimize the threat of
instrumentation, pretest and posttest measures were presented to the participants on
separate pages to reduce the chance of memory of previous scores biasing response. The
use of randomization also controlled for the threat of instrumentation.
Selection bias occurs when participants are allocated purposefully into groups
(Shadish, et al., 2002). If the participants are assigned to groups based on their choice or
based on the researcher arrangement, selection bias may occur. For example, participants
may choose the combination group because they consider that music with nature sounds
represents a double dose of treatment, and believe that the combination would be more
helpful for their pain and anxiety than the other treatment group. The use of
randomization may help to minimize selection bias to ensure that participants assigned to
each group are comparable.
Diffusion of treatments may occur when participants in the control group have
access to the real or similar treatment (Shadish, et al., 2002). In this study, interventions
were shared between participants if participants in the same room were assigned to

56
different groups. This was minimized by arranging it so that participants who shared the
same room were in the same group. Unit nurses and physicians were told not to take the
MP3 players to other patients.
Compensatory equalization occurs when the treatment provides desirable outcomes
and the healthcare professional cannot tolerate the inequality. They might insist the
control group also receive treatment or provide other treatment than usual care (Shadish,
et al., 2002). For example, the staff nurse may provide other treatment, such as massage,
to those participants in the control group. In order to minimize these threats to internal
validity, healthcare providers were told not to change their usual care and to which group
the participants were assigned. The control group was provided with a CD on the fourth
day, so the healthcare providers ensured that every participant was provided with a
treatment.
Compensatory rivalry is when participants in the control group try to demonstrate
that they are able to do well even with no treatment (Shadish, et al., 2002). For example,
when participants in the control group know that they are assigned to the control group,
they may try to use other methods, such as meditation or self-guided imagery, to show
that their pain and anxiety can also be decreased even with no treatment. The researcher
told the control group that they would be in the data collection phase first and then
receive interventions on the fourth day. To minimize this threat, the control group
received music, nature sounds, or a combination of music and nature sounds based on
their preference when the data collection was completed.
Resentful demoralization can occur among participants in the control group. They
may feel resentful and demoralized because of receiving no or less treatment, so they
57
react by withdrawing from the study, becoming angry, or it may affect their ratings of
pain and anxiety (Shadish, et al., 2002). For example, if the participants in the control
group notice that they are not receiving any treatment, they may decide to withdraw from
the study. Therefore, the researcher told the control group that they would be in the data
collection phase first and then receive an intervention on the fourth day. To minimize the
chance that participants in the control group might find out they were in the control group,
clustered randomization of conditions to rooms was used rather than using simple
randomization at a personal level.
Summary of Literature Review
Cancer pain and anxiety are multidimensional phenomena and are difficult to be
managed effectively by current treatments. Their reciprocal effect may result in decreased
quality of end-of-life in hospice cancer patients. Music has been identified as a
nonpharmacological intervention to reduce pain and anxiety in different populations.
However, studies reviewed had limitations, including lack of randomization, small
sample sizes, and outdated methods. Additionally, nature sounds and the combination of
nature sounds may be culturally preferred by Taiwanese people, but are understudied in
current research. As a result, the study used sedative music and explored nature sounds
and the combination of music and nature sounds in hospice cancer patients to reduce
cancer pain and anxiety. Threats to validity were controlled by randomization, study
design, and statistical tests.

58
Chapter Three
Method
In this chapter, the methodology of the proposed study is presented. The study
design and randomization procedure are described first, followed by the sampling setting.
The experimental intervention, measures, potentially confounding variables, procedure,
and protection of human subjects are described. Finally, the procedures used for data
management, screening, and analysis plan are provided.
Design
A four-group, pre- and posttest experimental design with repeated measures was
used to study the effect of music and nature sounds on cancer pain and anxiety.
Participants in the treatment groups listened to 20 minutes of their assigned intervention
between the pretest and the posttest measures, once a day for three continuous days.
Participants in the control group rested in bed or in a chair for 20 minutes between the
pretest and posttest measures at the same time points. A convenience sample was selected
from two hospice units in two hospitals in Kaohsiung, Taiwan. One had 20 beds, and the
other had 11 beds. The first hospice unit contained eight patient rooms: three single
rooms, four 2-bed rooms, and two 4-bed rooms. The second hospice unit contained five
patient rooms: three single rooms and two 4-bed rooms. The single and 2-bed rooms are
for those who were willing to pay for them. The 4-bed rooms sometimes had both males
and females staying in the same rooms.
The randomization scheme was a combination of cluster randomization of existing
groups (rooms) and adaptive randomization to equalize the number of participants in each
group. Treatments were randomized to rooms (Friedman, Furberg, & DeMets, 1998;

59
Kalish & Begg, 1985). This was expected to prevent diffusion of treatments within the
2-bed and 4-bed wards. The investigator used an online randomization program
(Randomization.com) with a block size of four for ten blocks, one for each room, to
generate a sequence for assigning treatment condition to room: control (CT), music alone
(MU), nature sounds alone (NS), or the combination (CB) ( Table 1).
Table 1.
Example of Sequence for Assigning Treatment Conditions to Room
Block (Room) Sequences 1 2 3 4 5 6 7 8 9 10
1 CB NS MU CT NS CT MU CB CB NS 2 CT MU CB NS MU CT MU CT NS CB 3 MU CB NS CT NS MU CT CB CB NS 4 MU CT MU CB NS CT NS CB CT MU
Note. More sequences were run using Randomization.com than are shown in this example.
According to hospital protocol, cancer patients who were admitted to the hospice
were assigned rooms by the Chief Resident (CR) in the Department of Family Medicine
assigned to the hospice. The CR assigned patients to the wards based on information in
the computer system. Hospital protocol specifies that newly admitted patients are
assigned by gender to the room with the least number of patients. Due to the availability
of beds, both male and female patients may be assigned to the same room upon the
agreement of the patient and family.
The investigator used the randomization scheme initially to randomly assign
treatment conditions to all rooms in the hospice (Table 1). For each sequence in the table,
treatment conditions were printed on pieces of paper that were folded and sealed in

60
brown opaque envelopes. The ten brown envelopes (without numbers) in each sequence
were shuffled by the committee chair of the investigator and placed in sealed white
envelopes. The white envelopes were also shuffled and numbered sequentially by the
investigator’s committee chair. The investigator selected the white envelope marked “1”
and blindly selected one brown envelope from the white envelope to randomly assign
treatment conditions to rooms in Taiwan. If at any time there were no study participants
in a room, the investigator blindly selected one brown envelop from the same white
envelope. The process was repeated until all brown envelopes have been used in the
white envelope marked “1.” Then, as rooms become empty, the white envelop marked “2”
was used.
As new cancer patients were admitted to the hospice rooms and referred to the
investigator, she would approach them about the study. Patients would not be told the
treatment condition before consent so as to not bias their willingness to participate;
however, they were told that the treatments were randomly assigned to rooms, that is, by
chance, like rolling a dice.
The randomization program (Randomization.com) with a block size of four for 10
blocks was used five times in order to generate sequences for assigning room to treatment
conditions. This procedure not only ensured the blindness of room assignment, but also
increased the likelihood that all conditions would be assigned and experimental group
sizes would approach similarity. The Chief Residents were not told the treatment
assignments, and the treatment assigned to each room changed over time; therefore, the
rooms and newly admitted patients were assigned to rooms blindly and by chance.

61
Sampling
The sampling frame was cancer patients who had pain and anxiety and received
hospice care in two large hospitals in southwest Taiwan. A convenience sample was
selected from the Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUH)
and St. Joseph Hospital (SJH) in Kaohsiung City, which has a population of 1.5 million
people. The KMUH has a 20-bed hospice unit and a hospice collaborative care program,
while the SJH has an 11-bed hospice unit. All patients were diagnosed with terminal stage
cancer and had an expected life expectancy of less than six months.
Sample size estimation. Sample size was calculated for achieving a power of .80
and an alpha of .05, in four groups with three repeated measures. A medium effect size of
f = .25 (Cohen, 1992) was used based on a randomized controlled trial of patients with
chronic pain that also used a one-dimension VAS pain measure and three groups
(Siedlecki & Good, 2006). The effect size f was .26, which was calculated on the basis of
adjusted mean differences in post-treatment scores between three groups (M1 = 5.95, M2
= 5.84, M3 = 7.01; SDpooled = 2.01). Based on power analysis, using the G-power 3.0.10
program (Faul, Erdfelder, Lang, & Buchner, 2007), a sample size of 124 patients (31 per
group) was calculated.
Inclusion and exclusion criteria. Included were persons who (1) had at least one
documented cancer pain score in the past 24 hours; (2) had a regularly scheduled (versus
prn) analgesic schedule to control for fluctuations in pain that occur with prn schedules;
(3) were oriented to person, place, and time, and in the researcher’s judgment were of the
physical and mental status that would enable the individual to participate in the study; (4)
were cognitively intact to understand and follow study procedures; (5) could read and

62
speak Chinese, Taiwanese, or English, and (6) were at least 18 years of age, because the
music was designed for adults. Both genders were included in the study. At the bedside,
two additional screening questions were asked: whether the person liked to listen to
music and whether they felt it was appropriate to listen to music while they were sick and
in the hospital. Patients who answered “yes” to both questions and met the other criteria
were included.
Excluded were patients who had (1) delayed developmental status documented on
the chart; (2) difficulty hearing; and (3) severe visual deficiency to control for inability to
mark the VAS scales. The subject screening form is shown in Appendix A.
Setting
Kaohsiung Medical University Chung-Ho Memorial Hospital is one of the largest
hospice settings in the southern area of Taiwan. Approximately 400 patients were
admitted to the hospice unit in 2008 and 2009, and the average occupancy rate of beds
was about 85 % (Personal conversation with the unit head nurse, 9/28/2010). The KMUH
also has a hospice collaborative care program. This program provided hospice care to
cancer patients who were staying in other units of the KMUH while waiting for a bed
available in the hospice unit. Patients who were in the hospice collaborative care program
received care from both the unit and the hospice team. The average length of stay in the
hospice unit was 12 days. The major reason for discharge from the hospice unit was death
or in the active dying process because some people believe that they should die at home
in order to bring good luck to their offspring. The information about the length of stay
and the major reason for discharge from the collaborative care program were not
available for the researcher to collect.

63
St. Joseph Hospital is a large hospital and the first to provide hospice care in
Kaohsiung. Approximately 200 patients were admitted to the hospice unit in 2008 and
2009; the average occupancy rate was about 65 %. The average length of stay in the
hospice unit was 12 days (Personal conversation with the unit head nurse, 12/20/2010).
The major reason for discharge was death or in the active dying process. In both hospice
sites, staff nurses assessed pain regularly, but not anxiety.
In Taiwan, all hospitals are regulated by the Department of Health and receive
reimbursement from the National Health Insurance Program. These hospice units are
accredited annually by the Taiwan Academy of Hospice Palliative Medicine annually.
Therefore, many factors are similar across all the hospice units in the country. These
included the settings, forms used, medical treatments, medication management,
composition of the hospice care team and their hospice care-related education, and the
nurse-patient ratio. In addition, the accreditation committee requires that at least one
caregiver (either a family member or a nurse’s aide) is with the patient at the bedside at
all times. Other family members are encouraged to visit the patient before 10 p.m. Most
visitors come to the unit in the morning or in the evening.
Neither hospice units had music therapists to provide music therapy to the patients.
Although some nurses may have had some knowledge of nonpharmacological therapies
from their continuing education programs, music is not widely used as a therapy for
hospice patients. Patients in the unit could listen to music by request. Three CD players
were available in the KMUH hospice unit, while the SJH only had one CD player. Some
CDs were available in both hospice units and were either purchased by the nursing staff
or donated by the families or religious groups. Patients also could bring their own music

64
device and borrow music CDs from the unit.
Experimental Interventions
The experimental interventions were music, nature sounds, and music combined
with nature sounds. These interventions were selected and/or edited by the investigator
and were saved on the investigator’s laptop according to the intervention group and
choices offered. There were separate folders for different types of music, nature sounds,
or the combination of music and nature sounds. Each intervention played for a similar
amount of time. Because of the limited availability, there was less variety in types of
nature sounds and combination of music and nature sounds compared to music only.
To choose music for the study, participants who were assigned to each group
listened to 20-second excerpts of their assigned intervention: eight different types of
music, five types of nature sounds, or five types of combined music and nature sounds.
The selections that were offered as choices were chosen by the investigator and evaluated
for appropriateness by the dissertation committee chair, Marion Good, PhD, RN, FAAN,
and a professional music therapist, Deforia Lane, PhD, MT-BC.
Music. The music was expected to reduce pain and anxiety through distraction
and/or relaxation and fulfilled several criteria: it was nonvocal and generally sedative,
with a rate of 60 to 80 bpm, low volume, and included minimal strong rhythms or
percussion (Gaston, 1951; Good, 1992). Eight types of music were selected for this study:
orchestra, piano, harp, religious music (Christian or Buddhist), Chinese music, Taiwanese
music, and easy listening music. Orchestra, piano, and harp music were selected from
Good et al.’s music tapes (Good, et al., 2010; Good, et al., 1999) because they were liked
by Taiwanese people (Good & Chin, 1998) and were effective in populations with
65
postoperative patients (Good, et al., 2010; Good & Chin, 1998; Good, et al., 1999; Voss,
et al., 2004), nonmalignant chronic pain (Siedlecki & Good, 2006), and cancer pain (S.-T.
Huang, Good, & Zauszniewski, 2010). Some Christian music selected from Good’s
religious music collection (Good, et al., 2010) was labeled Christian religious music.
Buddhist religious music was selected from CDs familiar to Taiwanese people, suggested
by Taiwanese patients (Good & Chin, 1998), found effective for Taiwanese cancer
patients (S. T. Huang, 2006), and culturally appropriate for this population. Easy listening
music, Chinese music, and Taiwanese music were selected as preferred music by
Taiwanese patients in several previous studies (S. H. Huang, 2000; Y. C. Huang, 2003;
H-C. Wu, 2007). Therefore, these four types of music plus Buddhist religious music were
selected by the investigator based on the same criteria of nonvocal, generally sedative, 60
to 80 beats per minute, and with minimal strong rhythms, loud sections, or percussion.
The music selected for this study is shown in Appendix B.
Nature sounds. Nature sounds were expected to produce distraction and/or
relaxation and thereby decrease cancer pain and anxiety. No studies have provided
detailed instruction or description for selecting nature sounds for clinical use. Taiwanese
people live close to nature and the sea. Nature sounds selected for this study included
those thought to be familiar to them. The nature sounds included that of birds singing,
ocean waves, frogs, night life of nature, and forests. These sounds were commercially
produced by Wind Records from sounds collected in Taiwan. The nature sounds selected
for this study are shown in Appendix B. The nature sounds were generally sedative in
nature with minimal loud sections, strong rhythms, or sudden high-pitch sounds.

66
Combination of music and nature sounds. The combination of music and nature
sounds was based on the same criteria for selecting music and nature sounds. The music
in the combination condition was that used on commercially produced CDs of music and
nature sounds and was composed by Taiwanese musicians. No studies were found that
focused on this type of intervention. The types of music and sounds were taken from
commercially available CDs by Wind Records. The combination of music and nature
sounds selected for this study is shown in Appendix B. These included piano with bird
songs, sounds from night life and new age music with sounds of ocean waves, the forest,
and frogs. The nature sounds were collected in Taiwan and are familiar to Taiwanese
people.
The researcher told the control group that they were in the data collection phase first
and then would receive interventions on the fourth day to avoid the threat to internal
validity of resentful demoralization in this group. During the intervention period, the
control group was asked to stay in their beds or chairs in a comfortable position for 20
minutes once a day for three days. On the fourth day they were invited to select one
commercially made CD of sedative music, nature sounds, or the combination, to listen to
and keep. The selections of these CDs are shown in Appendix B with asterisks by the
CDs’ names.
Equipment. The equipment used in this study included an MP3 player, headset, and
a speaker. The Transcend MP330 MP3 player was selected for its small size, light weight,
easy use, and 2-year warranty. The YongLe clip-on headsets and the Sonpre Capsule
S020 speakers were chosen for their small size, light weight, easy use, and relatively
good sound transmission. All the equipment was marked with stickers with information

67
on them so that the investigator could organize and keep track of the devices. The stickers
had the investigator’s name, contact phone number, and an identifying letter to match all
the equipment in the set. The equipment sets were put in 4.5 x 6-inch plastic pouches
with paper clips that the participants could use to attach the pouches onto their bed sheets
or pillow cases when they listened to the intervention (Figure 3).
Figure 3.
Equipment Used in This Study
a. b.
Figure 3. Equipment used in the study is shown individually and labeled by numbers in picture (a) and assembled in the pouch in picture (b). In picture (a), number 1 is a 4.5 x 6-inch plastic pouch with a zipper shown on the left side and a binder clip on top; number 2 is the MP3 player; number 3 is the clip-on headset; number 4 is the speaker; and number 5 is the USB connector cable to connect the MP3 player and the speaker.
Measures
Cancer pain. Cancer pain in this study was defined as a subjective feeling of an
unpleasant sensory and emotional experience associated with the growth and/or treatment
of a tumor. Cancer pain was measured with the one-dimensional Pain VAS scale, a
100-mm horizontal line anchored by “no pain” and “most pain imaginable.” When using
the 100-mm Pain VAS with Taiwanese hospice cancer patients, these descriptive words
were set in the same horizontal direction as the Chinese written language, from left to
1 2
3
4
5

68
right. That is, “no pain” was placed on the left side and “most pain imaginable” was on
the right side. The investigator explained to participants that it is a ruler-like instrument to
measure their current cancer pain. Participants were asked where they had pain at the
time of measurement. If multiple pain locations were identified, participants were
instructed to mark the location of the most severe current pain on a diagram of the human
body, and to mark the VAS at the point representing the most severe pain. The Pain VAS
was scored by measuring in millimeters the distance from the side marked “no pain” to
the center of the mark made by the participant. Possible scores ranged from 0 to 100 mm.
Higher scores indicated greater pain intensity (M. McCaffery & Pasero, 1999). In the
event that patients were alert but could not use their hands to make a mark, the
investigator would have used her index finger as a pointer on the 100-mm Pain VAS scale.
She would have put her index finger at the “no pain” end as the start point and then
moved it slowly toward to the “most pain imaginable” end. When the patient said “stop”
at the correct level, the researcher would have put the tip of a pen on the VAS scale by the
tip of the researcher’s index finger and ask the patient again if it was the correct pain
level. If the patient had answered “yes,” the researcher would mark the Pain VAS scale at
the exact place indicated. If the patient had answered “no,” the researcher would resume
the process until the correct level was determined. However, no participants required this
assistance.
The one-dimension Pain VAS has support for test-retest reliability in multiple
studies. In one longitudinal study of chronic pain, researchers reported the test-retest
reliability of the Pain VAS over three different time intervals from two weeks to four
months. Reliability ranged from .55 to .84, with a median of .81 (M. P. Jensen, Turner,

69
Romano, & Fisher, 1999). In a systematic review of 164 articles focused on the reliability
and validity of pain instruments in adult cancer patients, four studies supported the
test-retest reliability of the Pain VAS. The time interval ranged from five minutes to one
week. The average test-retest reliability was .80. The Pain VAS was sensitive enough to
detect change in cancer pain across different times or treatments in 11 studies. In support
of concurrent validity, the Pain VAS had strong associations (r > .70) with other pain
intensity measures in 13 studies. However, Jenson reported two studies with a correlation
with other pain rating scales that were less than .70, but did not provide citations (2003).
Construct validity of the Pain VAS was reported as strong, r = .85, p < .001, with a
Numeric Rating Scale (NRS) in 50 cancer patients (Paice & Cohen, 1997). Concurrent
validity of the Pain VAS with the Brief Pain Inventory (BPI) Pain Interference subscale
(N = 388) was good in oncology medical (r = .71, p < .01) and surgical patients (r = .73,
p < .01) (Tittle, McMillan, & Hagan, 2003).
The Pain VAS scale was used before and after each the scheduled tests of the
interventions. The intervention and control conditions were provided to participants three
times, i.e., once a day for three days. Thus, the Pain VAS scale was marked by each
participant a total of six times. The Pain VAS is shown in Appendix C.
Anxiety. Anxiety in this study was defined as an unpleasant subjective feeling
associated with the perception of a threat. Anxiety was measured with the Anxiety VAS
scale. The Anxiety VAS is a 100-mm horizontal line anchored at either end by descriptive
words of “no anxiety” and “most anxiety imaginable.” When using the 100-mm Anxiety
VAS with Taiwanese hospice cancer patients, these descriptive words were set in the
same horizontal direction as Chinese written language, from left to right. That is, “no

70
anxiety” was placed on the left side and “most anxiety imaginable” was on the right side.
The investigator would explain to participants that anxiety can be a worrisome, uneasy, or
restless feeling, and the scale is a ruler-like instrument to measure their current anxiety.
Participants were instructed to mark the line at the point representing the intensity of their
anxiety at that time. The Anxiety VAS was scored by measuring in millimeters the
distance from the side marked “no anxiety” to the center of the mark made by the
participant. Possible scores range from 0 to 100 mm. Higher scores indicated greater
anxiety intensity. In the event that patients were alert but could not use their hands to
make a mark, the investigator would have used her index finger as a pointer on the
100-mm Anxiety VAS scale, in the same manner she was prepared to do for the Pain VAS
scale; however, no patients required this assistance either.
Test-retest reliability of the Anxiety VAS scale was supported by studies in the
United States and Taiwan. In the United States, Voss (2001) used the Anxiety VAS with
10 cardiac patients and reported a 15-minute interval test-retest reliability correlation of r
= .82. In Taiwan, researchers used the Anxiety VAS in 32 cancer patients with a
three-hour interval and reported the test-retest reliability correlation of r = .92 (T.-W.
Huang, et al., 2001). Validity of the Anxiety VAS was examined by multiple researchers.
The Anxiety VAS was found to have a strong positive correlation (r = .70) with the
State-Trait Anxiety Inventory (STAI) in Elliott’s study of 56 patients with acute ischemic
heart disease (1993), and with the STAI in women in a specialist breast clinic ( r = .78, p
< .01) (Davey, Barratt, Butow, & Deeks, 2007). The Anxiety VAS was moderately
correlated with the STAI in ten postoperative cardiac patients (r = .41) (Voss, 2001). The
anxiety VAS was moderately correlated with STAI scores in 685 preoperative patients (r

71
= .55, p < .01) (Kindler, Harms, Amsler, Ihde-Scholl, & Scheidegger, 2000). In Taiwan,
one researcher tested the concurrent validity of the Anxiety VAS with the STAI in
patients with hematological malignancy and reported moderate to strong correlations of r
= .59 to .74 for trait and state anxiety, respectively (P. I. Peng, 2005). The Anxiety VAS
scale was used before and after the assigned intervention or control condition twice a day
for three days for a total of six times. The Anxiety VAS is shown in Appendix C.
Demographic measures. The demographic measures included age, gender, race/
ethnic background, primary language used, primary religious belief, education, marital
status, number of children and significant others, cigarette and alcohol intake, and income.
The information was recorded from the hospital record (Appendix C).
Types of music and nature sounds generally liked.
To measure the types of music and nature sounds that the participants generally liked, the
question was asked at the bedside after consent was obtained. The researcher read a list of
22 types of music and nature sounds that she believed familiar to Taiwanese people.
Participants answered “yes,” “no,” or “don’t know” to respond to each item, and the
researcher checked off the answers. If the participant liked a type of music that was not
on the list, the answer was put in the space of “other.” The purpose of asking about the
types of music and nature sounds Taiwanese cancer patients like was to explore the types
of music and nature sounds Taiwanese hospice cancer patients prefer. The findings could
provide information for music and nature sounds selections for future hospice patients
(Appendix C).
Experience with complementary and alternative therapies. Participants were
asked about their experience with complementary and alternative therapies. There were

72
14 of these therapies the researcher believed were familiar to Taiwanese people.
Participants answered whether or not they had experienced any of these therapies and
whether they were using them currently. The purpose was to understand what other
nonpharmacological therapies the participants have used. If they were currently using any
of these therapies, it could be a potentially confounding variable and might need to be
statistically controlled as a covariate (Appendix C).
The investigator asked the participants at the end of the final visit whether or not
they liked the assigned intervention (music, nature sounds, and the combination) and
provided their comments about the study. The participants answered this question by
using a five-point Likert type scale (1 = disliked; 5 = liked very much). Because nature
sounds and the combination of music and nature sounds were relatively novel
interventions, this would serve as the basis for one of the research questions to be
answered. The findings would contribute to future use of these interventions on different
populations and trigger further research studies.
Length of time and reasons for independent listening. Participants who were
assigned to the treatment groups were encouraged to use the intervention independently
between tests to possibly reduce their pain and/or anxiety between the treatment sessions.
The researcher checked the MP3 player before each pretest to record the information
about the length of time the patient listened. For example, every song had its length of
time. The researcher had listed each song in sequence and included the playing time of
each song in the MP3 players. At the end of each treatment period, the researcher
accessed the name of the last song played and recorded the song’s name on the data
collection instrument. Before the pretest of the next treatment period, the researcher

73
checked the song’s name on the MP3 player and asked the participant if the MP3 player
was used between treatment sessions. The song’s name was recorded on the data
collection instrument, and the researcher would know from the sequence how many and
which songs were played between tests. The minutes were calculated by adding the
minutes of all the songs that had been played. In addition, patients were asked about the
reasons for independent listening. The findings were expected to provide a better
understanding about the length of time and the reasons for patients to use the intervention
(Appendix B).
Potentially Confounding Variables
Analgesic and anxiolytics intake. Medication may reduce the intensity of cancer
pain and anxiety and become a confounding variable. The use of analgesics and
anxiolytics, including name, route, frequencies, dose, time given, and if “in effect” at the
time of the tests were recorded from the patient’s chart by the researcher daily. “In effect”
was defined as the medication’s duration of effectiveness; for example, when morphine is
administered to a patient, the medication is in effect for four to six hours in the patient’s
system. The hospice cancer patients took prescribed analgesics around the clock for
symptom control in accordance with the WHO three-step analgesic ladder (Taiwan
Cooperative Oncology Group, 2007). The use of both scheduled and prn drugs was
recorded in the nurses’ notes and the researcher extracted these data daily and recorded
them on the data collection instrument. Pain medicine was categorized into three groups,
weak opioids, strong opioids, and nonopioids. Currently available and frequently
prescribed weak opioid analgesics in both hospice units included Codeine, Tramadol,
Darvocet, and Ultracet; the strong opioids Morphine, Fentanyl, MST Contin, and

74
Temgesic; and the nonopioids Acetaminophen, Baclofen, Cataflam, Celecoxib,
Chlorzoxzone, Clonazepam, Etoricoxib, Ibuprofen, Ketorolac, Mefenamic, Naproxen,
Neurontin, Steroids, Tegretal, Tofranil, and Urogen (Taiwan Cooperative Oncology
Group, 2007).
Although the Cochrane review of anxiolytics for hospice cancer patients reported
that there was no sufficient evidence to determine whether current methods of
pharmacological management of anxiety are beneficial or harmful to terminally ill
patients, medications such as anxiolytics, antidepressants, and antipsychotics have been
frequently prescribed for patients with anxiety or other symptoms in hospice (Jackson &
Lipman, 2004). The anxiolytics available in Taiwan included Alprazolam, Lorazepam,
Bromazepam, Chlordiazepoxide, Flunitrazepam, Estaxolam, Britielam, Midazolam,
Clonidine, Triazolam, and Zolpidem (Taiwan Cooperative Oncology Group, 2007).
Therefore, the use of analgesics and anxiolytics was recorded and were considered as
potentially confounding variables (Appendix C).
Environmental disturbances. During the tests, disturbances could be a potentially
confounding variable. The participants might have been disturbed by routine care and
treatment, visitors, phone calls, and electronic devices. This was prevented as described
in the procedure section.
Religious chanting box. Based on the researcher’s personal experience and her
observation as a nurse, people who are Buddhists or Taoists sometimes listen to chanting
music played by a religious chanting box, especially during the dying process. Listening
to the religious chanting box was considered history that could threaten the validity of the
study. A religious chanting box might have from six to more than 20 chanting music

75
selections, with and without scripture. It is believed that by listening to the chanting box,
the person is able to clear the mind and cleanse the soul, and eventually go to the Eastern
Wonderland or Heaven. Some patients listen to the music chanting box periodically,
while some patients and/or their families prefer to play it 24 hours a day for continuous
blessing. Although some of the music in the chanting box is monotone and slow in tempo,
some of the music contains varied rhythms, sudden high pitch sounds, and relatively fast
tempos (faster than 80 bpm). Therefore, the music chanting box may produce a different
effect and become a confounding variable for the study. As a result, those patients who
used the music chanting box and wanted to participate in the study were asked to refrain
from listening to it during the three days they were in the study. Those patients who were
assigned to the music group were able to select Buddhist music as one of the choices.
Those who were not willing to temporarily stop listening to the music chanting box were
excluded or dropped from this study.
Procedure
Case Western Reserve University Cancer Institutional Review Board (IRB), the
Kaohsiung Medical University Chung-Ho Memorial Hospital, and St. Joseph Hospital
provided IRB approval to conduct this study. The investigator received permission from
the head nurse of the units and set up a meeting to explain the study purpose and
procedures to all members of the medical and nursing staff and obtained their cooperation
during the data collection period. The staff nurses in the hospice unit screened patient
charts for eligibility. After preliminary identification of potential participants, the staff
nurse requested the patients’ permission for the investigator to talk with them. The
investigator completed the screening process at the bedside. Each eligible participant was

76
invited to participate and was asked to provide informed written consent. Once enrolled,
the demographic data were collected from the chart and at the bedside. First, participants
were asked questions about the kinds of music and nature sounds they liked, and then
were told their group assignment. Participants who were assigned to the intervention
groups then listened to 20-second excerpts of each kind of music, nature sounds, or the
combination of music and nature sounds. Then they selected one type of music, nature
sounds, or the combination they liked and found the most relaxing. The first visit with the
participant was completed (Day 0).
An MP3 player with the type of intervention they selected was provided to the
participants the next day (Day 1). The investigator scheduled adequate time with the
participant to provide the first intervention. She also checked with the primary nurse to
make sure the scheduled time was appropriate to avoid interruption during either patient
care or the intervention session.
The investigator instructed participants on the use of the MP3 player (start, stop, and
volume) and the headsets or speakers. If family caregivers were present in the room with
the participant, they were also taught to use the MP3 player to help the participant listen
to the music at times other than the scheduled time. Then, the investigator explained the
use of the VAS scales, demonstrated their use, and allowed time for practice. Participants
in the control group received similar instruction and practice on using the VAS scales.
Since the control group was in a separate room from the treatment groups, they did not
receive intervention until Day 4. The scheduled intervention test was 20 minutes once a
day to minimize the burden on the hospice cancer patients. The scheduled intervention
testing was carried out for three continuous days.

77
Before delivering the intervention, the researcher checked the name of the song on
the MP3 player and recorded the name of the song on the data collection instrument.
Participants were asked to rate their pain and anxiety levels on the pretest VAS scales.
They were instructed to lie in their bed or sit in their chair in a comfortable position. The
investigator assisted those in the intervention group with putting on the headset or setting
up the speakers, making sure the MP3 player was functioning, and adjusting the volume
to a comfortable level. She drew the curtain around the patient’s bed and stayed outside
of the curtain in the room during the intervention. Family members of all patients in the
room were asked to go out for a break and come back after the session. If they chose to
stay, they were asked not to talk to the participant and to stay outside of the curtain with
the investigator. Those patients and family who shared the same room and were not in the
study were asked not to talk during the intervention. After the intervention session,
participants were asked to rate their pain and anxiety levels again on the posttest VAS
scales.
In order to provide intervention integrity, the time selected for testing the
intervention were after routine care and treatment was completed. The participants’
primary care nurses were asked to schedule their work before or after the intervention,
but to consider the priority of the care and treatment. While providing the intervention or
control condition, interruptions from visitors who wished to see the participant were
avoided. Upon the agreement of the patients, the door of their room had an appropriate
sign to help prevent unexpected disturbances. Phone lines in the patients’ room were
temporally disconnected and the television was turned off by the investigator.
Participants who were assigned to intervention groups were given the opportunity to

78
change the type of music, nature sounds, or the combination of music and nature sounds
within their assigned group. For example, participants in the music group could select
piano music on the first day, change to religious music on the second day, and listen to
orchestra music on the third day. However, they were not permitted to change to a
different intervention, e.g., from music to nature sounds. The investigator encouraged
participants to use the MP3 players between tests as needed for pain and anxiety. The
investigator recorded time and reasons for the extra use of the intervention by asking the
participants, their family members, or their primary care nurses before the treatment each
day. She also checked the MP3 player for the song’s name and recorded it on the data
collection instrument. If the intervention was used by the participants, minutes of
independent listening time were calculated by summing the time listed for each song on
the MP3 player. Table 2 shows the data points.
Table 2.
Data Points Table
Day 0 Day 1 Day 2 Day 3
Demographic X
Type of MU/NS liked X
100-mm Pain VAS Xox xox xox
100-mm Anxiety VAS Xox xox xox
Minutes of Independent Intervention Use X X
Liked Assigned Intervention X
Note. MU = Music; NS = Nature Sounds; X = measure; O = treatment; xox = pretest, 20 min treatment, posttest
Those in the control group rated their pain and anxiety on the pretest VAS scales, for
20 minutes resting in their beds with the curtains drawn or sitting in their chairs quietly,

79
and rated their pain and anxiety again on the respective VAS scale for the posttest. Their
families received the same instruction as the intervention group. After the three-day data
collection period, participants in the control group were asked to select one commercial
CD of music, nature sounds, or the combination of music and nature sounds that the
intervention was selected from in the study, and they could keep the CD for personal use.
To help them to decide what CD they would like to have, they listened to the 20-second
excerpts first, then chose the CD that the 20-second excerpt was from. The procedure of
the study is shown in Figure 4.
Figure 4. The Study Procedure
Figure 4. VAS = Visual Analogue, CD = Compact Disk.
Patients assigned to room by administration
Screening
Recruitment
Demographic and Baseline
Pretest of Pain and Anxiety VAS
20 min Combination
20 min Music
20 min Nature sounds
20 min rest in bed or chair quietly
QD for 3 days
Posttest of Pain and Anxiety VAS
Select one CD to keep Listen to intervention as desired
Room randomly assigned to condition
Combination Music Nature sounds Control
80
Protection of Human Subjects
The Belmont report establishes the ethical principles relevant to the protection of
human subjects for research. These include respect for human dignity (right to
self-determination and full disclosure), beneficence (freedom from harm and
exploitation), and justice (fair treatment and privacy) (The National Commission for the
Protection of Human Subjects of Biomedical and Behavioral Research., 1979). The
investigator gave every participant oral and written descriptions of the research purpose,
procedures, risks, benefits, and assurances of privacy, anonymity, and confidentiality.
Participants had the chance to ask questions and were given answers. They were
informed that they could voluntarily choose to participate or not, and that they had the
right to withdraw from the study at any time without affecting their care.
Participants were asked to return the informed consent form to the investigator, and
those who signed the form were given a copy of it in the same day. The investigator kept
a list of the names, bed number, and study IDs of all patients who met the inclusion
criteria and who returned consent for participating in the study. The study IDs did not
reflect hospital ID. The list was used to identify participants during the study. This list
was locked in a separate drawer from the other data. When the data collection and
analysis were completed, this list was shredded. Each data collection form with the date
and ID number was prenumbered. All data collection forms were stored in a locked
cabinet to keep the information confidential. Data coding instructions were included
within the data collection instrument.
Although side effects rarely occurred when using music and nature sounds
interventions, caution was still necessary. In past studies, some participants did not like

81
music nature sounds or the music/nature sounds selected by the investigator (Bruya &
Severtsen, 1984; Hui-Ling. Lai, 2004). Therefore, during screening in the present study,
patients were asked whether or not they liked music/nature sounds and whether or not
they think listening to music/nature sounds is appropriate. This was done as part of
screening for eligibility. Those who did not like music/nature sounds or felt that listening
to them was not appropriate while they were sick in the hospice unit, or those who had an
uncomfortable response to music or nature sounds in the past, were excluded from this
study. Participants who disliked the music/nature sounds that they originally chose were
invited to change the type of music/ nature sounds within the categories of the assigned
intervention or withdraw from the study.
Some contraindications, such as musicogenic epilepsy and hypersensitivity to sound
are rare, but could happen during any study (Brust, 2001; Kaplan, 2003; Wieser,
Hungerbuhler, Siegel, & Buck, 1997). Musicogenic epilepsy is a neurological condition
in which the patient has seizures that are induced by certain sounds or music.
Hypersensitivity to sound is a condition in which sound becomes painful and produces
headaches in some patients (Allen & Good, 2000; Wieser, et al., 1997). The screening
questions assessed for those who have had uncomfortable responses in the past. If the
condition had unexpectedly happened, the music would be turned off immediately, a safe
environment would be created, and medical treatment would have been summoned. No
incidents of this nature occurred during the study
Data Management
Although the investigator was the only data collector, a clear instruction was written
on the data collection instrument to keep the data collection process consistent and

82
confidential. The investigator checked the completeness of the data before leaving the
patient’s room to avoid any missing data (Roberts, Anthony, Madigan, & Chen, 1997).
Data were coded and entered into the investigator’s computer. The questionnaire was
stored in a locked cabinet and only the investigator and research-related personnel had
access to these files. After all the entered data were double-checked again and errors were
corrected by the investigator, the data set was saved in a computer as well as on two
backup portable hard drives with password protection.
Data Cleaning
The investigator proofread the original data collection form against the entered
computer data file to ensure accuracy of the data file. Frequencies, descriptive statistics,
and graphic representations of the variables were used to identify errors in the data file.
For example, unusually small or large, or out-of-range scores on a given variable would
be examined for potential errors in coding. If errors were found, the original data
collection form was pulled and the miscoded data were corrected immediately
(Tabachnick & Fidell, 2007).
Assumptions of Statistical Tests
Repeated measures analysis of variance (RM ANOVA) has four major statistical
assumptions. First, samples in each group should be independent. Since the rooms were
randomly assigned to the four groups and patients were assigned to rooms by someone
who was blind to the room assignment of groups, they were considered to be independent.
Second, the dependent variables in each group are normally distributed. This assumption
was checked by using frequencies (numeric) for the skewness and kurtosis and graphs
(plots and histograms) of the dependent variables for each treatment group (Field, 2005;

83
Tabachnick & Fidell, 2007). To support multivariate normality, the skewness should be <
|3| and the kurtosis should be < |8 − 20|(Curran, West, & Finch, 1996). In a large
sample with continuous variables, skewed distribution generally is not expected, although
opioid medication may result in a negative skew. Normality will be met based on central
limit theorem (Tabachnick & Fidell, 2007).
Third, homogeneity of variance-covariance matrices tests whether the
variance-covariance matrices of the different groups are equal. A nonsignificant result of
Levene’s test represents homogeneity of variance matrices among groups. Box’s M test
would be used to test homogeneity of covariance matrices. A nonsignificant result of
Box’s M test means that the matrices among groups are the same. When violation of
homogeneity occurs, a more stringent alpha level will be used. If the violation is
moderate, the alpha level will be set as .025; if the violation is severe, the alpha level will
be .01 (Field, 2005; Tabachnick & Fidell, 2007). Sphericity is the equality of variances of
the differences between treatment levels in a repeated-measure ANOVA and is considered
as a part of the assumption of homogeneity of variance in between-group ANOVA. A
nonsignificant Mauchly’s test for sphericity means that the variances of the differences
between conditions are equal. If Mauchly’s test is significant, the Greenhouse-Geisser
correction should be used. If the Greenhouse-Geisser estimate is greater than .75, the
Huynh-Feldt correction should be used. However, if the Greenhouse-Geisser estimate is
less than .75, the Greenhouse-Geisser correction should be used (Field, 2005).
Fourth, linearity of the relationships among dependent variables is assumed.
Pearson’s correlations (numeric) and bivariate scatterplots (graphic) were used for the
linear relationships among continuous variables. Bivariate regression was also used to

84
examine the relationship between two continuous variables by adding a line of fit
correlation coefficient squared (R2) linear, R2 quadratic, and R2 cubic to partial plots and
check for 2% differences between these lines. Violation of linearity could reduce the
power of the statistical tests. The skewed variables would not be transformed because by
doing so, the meaning of the variable would be changed (Tabachnick & Fidell, 2007).
Data Analysis
Descriptive analysis was used for demographic data, types of music liked, experience
with complementary/alternative therapy, minutes of independent use of the intervention
between tests, outcome variables, and each variable in the set to examine the
characteristics of participants, variability, central tendency, dispersion, and normality. The
reasons that participants withdrew from the study were described. The pain and anxiety
scores of those who withdrew were compared to those who remain in the study. Based on
the previous studies in which music or nature sounds decreased cancer pain and anxiety,
this study used one-tailed test with a significance level of .05 (Diette, et al., 2003; Golletz,
1997; S. T. Huang, 2006).
Pearson’s product moment correlations and Spearman’s correlation were used to
identify the covariates. Possible covariates included age, gender, those with pain
medications and anxiolytics “in effect” during treatment, and pain and anxiety at each
pretest. Therefore, if the correlation between the potential covariate and pain and anxiety
scores was higher than r = .30 (p < .05), they were used as covariates (Cook & Campbell,
1979; Tabachnick & Fidell, 2007).
Hypotheses testing. Hypotheses 1 and 2 were tested using a priori orthogonal
contrasts (Table 3). Contrast 1 compared the three intervention groups to the control

85
group. Contrast 2 compared the music and nature sounds groups to the combination
group. Contrast 3 compared the music group to the nature sound group. Additionally, the
polynomial contrast tests were also used for trends over time in six pre-posttest measures
(Field, 2005).
Table 3.
Orthogonal Contrasts Table
Contrasts MU NS CB CT
Contrast 1 1/3 1/3 1/3 -1
Contrast 2 1/2 1/2 -1 0
Contrast 3 1 -1 0 0
Note. MU = Music; NS = Nature sounds; CB = Combination; CT = Control
To test Hypothesis 1, that hospice cancer patients who listened to sedative music,
nature sounds, and sedative music combined with nature sounds will have less cancer
pain than control when controlling for baseline, repeated-measures analysis of covariance
(RM ANCOVA) across the three pain posttests while controlling for the Day 1 pretest and
any identified covariates was used. To test Hypothesis 2, proposing that hospice cancer
patients who listened to sedative music, nature sounds, and sedative music combined with
nature sounds will have less anxiety than control when controlling for baseline,
repeated-measures analysis of covariance (RM ANCOVA) across the three anxiety
posttests while controlling for Day 1 pretest and any identified covariates was used. For
these two hypotheses, sedative music, nature sounds, and sedative music combined with
nature sounds were independent variables, while the pain and anxiety scores at posttests
were dependent variables.

86
Research questions. To answer Research Question 1 about what types of music and
nature sounds are generally liked by the Taiwanese hospice cancer patients, frequencies
were obtained for the 22 categories on the list used on day 0. To answer Research
Question 2 about how much Taiwanese hospice cancer patients liked their assigned
intervention, music, nature sounds, and the combination of sedative music with nature
sounds, frequencies were obtained for the single question at the end of the study. To
answer Research Question 3 about how many minutes music, nature sounds, and the
combination of sedative music with nature sounds were used independently between
testing times, frequencies were obtained for the single question at the end of the study. To
answer Research Question 4 about the relationship between cancer pain and anxiety in
hospice cancer patients, the relationship between cancer pain and anxiety pretests and
posttests scores were analyzed at Day 1, Day 2, and Day 3 with multiple regression
analysis in the Statistic Program of Social Science (SPSS). Since both pain and anxiety
scores are continuous variables, three primary statistical assumptions for regression,
adequate variance, absence of influential cases, and linearity were tested prior to using
the regression technique. When using pain and anxiety scores in regression, one can be
the independent variable while the other can be the dependent variable; and the results
not only presented the relationship between cancer pain and anxiety, but also provided the
explained variance between these two variables.
Summary
The effect of music, nature sounds, and the combination of music and nature sounds
on cancer pain and anxiety in 123 hospice cancer patients were examined by a
randomized four-group, pre-post test experimental design with repeated measures.

87
Participants in the experimental groups listened to 20 minutes of the assigned
intervention once a day for three days, while those in the control group in their beds or
chairs quietly for the same length of time. Cancer pain and anxiety were measured by
100-mm VAS scales, before and after the intervention at three time periods. Whether or
not the participants liked the assigned intervention was asked at the end of the study. Data
were analyzed by RM ANCOVA, frequencies, Pearson’s product moment correlations,
and regression.

88
Chapter Four
Results
This chapter provides the results of the four-group randomized controlled clinical
trial to determine the effect of music, nature sounds, and the combination of music and
nature sounds on pain and anxiety in hospice cancer patients. The sample, the settings,
and descriptive data are described. Then, the results of hypothesis testing are presented.
The four research questions are then analyzed. Finally other descriptive findings are
presented.
Sample
The sample consisted of 117 terminal cancer patients, 64 men and 53 women, aged
from 21 to 87. They were chosen from the cancer patients in two hospice units of two
large hospitals in Kaohsiung, Taiwan, Kaohsiung Medical University Hospital (KMUH)
and St. Joseph Hospital (SJH). The two hospice units were compared in terms of seven
criteria, admissions, discharges, length of stay, occupancy rate, nurses’ age, and years of
experience in the hospital and hospice. The KMUH hospice unit had significantly more
admissions, discharges and a higher occupancy rate than SJH, but there was no
significant difference in length of stay between both units, and no significant difference
in the nurses’ ages and years of working in hospital or hospice (Appendix D).
Between October 1, 2010 and May 8, 2011, a total of 309 patients were screened for
eligibility. There were 150 patients who did not meet the inclusion criteria, and 159
eligible patients who were invited to participate in the study. A total of 123 patients
agreed and signed the consent, and 36 declined. The refusal rate was 22.64%; two thirds
were male (n = 24, 66.67%). The reasons for refusal were: too weak or too tired (n = 13),

89
did not want to sign the consent form or their families did not want them to sign (n = 6),
were not in the mood for music (n = 5), were not interested in this study (n = 4), did not
like music (n = 2), only wanted to listen to the chanting box (n = 2), did not want to be
disturbed (n = 2), only wanted Japanese music (n = 1), and wanted to spend more time
with family (n = 1).
Participants were randomly assigned to one of four groups: three treatment groups
that received music (n = 30), nature sounds (n = 34), or the combination of music and
nature sounds (n = 29), and a control group that received usual care (n = 30). Three
participants died before the data collection was completed. Three participants’ condition
deteriorated and requested to withdraw from the study. The attrition rate was 4.88%.
Because all 123 participants were tested on Day 1, that number was used for the
descriptive data. There were 119 participants on Day 2 and 117 on Day 3, which is the
sample size used for the repeated measures analyses. Using Chi-square, there were no
significant differences in number of participants among four groups on each day.
Demographic characteristics. Ages ranged from 21 to 87 years with a mean of
60.54, SD = 14.74 years, and a median of 60. The majority were male (55.3%), married
(69.9%), Taiwanese (95.1%), primarily spoke Taiwanese (80.5%), had no regular income
(65.8%), and did not use a chanting box (90.2%). Two-thirds had never smoked (n = 82,
66.7%). Of the 41 smokers, all quit smoking an average of 1.9 years ago (SD = 3.82), but
they had smoked a mean of 1.31 packs per day (SD = 1.09) for 32.56 years (SD = 14.20)
before they quit. Nearly three-fourths (n = 89, 72.4%) did not drink alcohol. Of the 34
alcohol users, 13 participants drank socially and 21 participants drank daily. Using
90
Chi-square, gender, cigarette usage and alcohol usage were significantly different among
the four groups (Table 4). The control group had more males, smokers, and alcohol users.
Participants had an average of 3 children, M = 2.75, SD = 1.65, with a range of zero
to nine. The number of significant others ranged from one to eleven people, M = 2.41, SD
= 1.72, and 49 had more than one. The significant others included children (n = 69),
spouse (n = 59), siblings (n = 21), parents (n = 10), in-laws (n = 7), partner (n = 5),
friends (n = 3), and grandchildren (n = 2). The reasons for discharge from the hospice
unit after participating in the study were that participants died (n = 56), went home for
continuous care (n = 38), were transferred to another facility for continuous care (n = 17),
and were discharged against medical advice (n = 6).
Experience with complementary and alternative therapies. All participants were
asked whether they had experience with each of 14 complementary and alternative
therapies and whether they were currently using them (Table 5). Only eight types of
complementary and alternative therapy had been used by the participants. Herbal
remedies were the most frequently used, followed by massage, and a few had used
acupuncture or aromatherapy. Eighty three (67.48%) of them had used complementary/
alternative therapy in the past, but only 20 participants (22.73%) were still using the
complementary/ alternative therapy. Chi square indicated no significant differences
among the groups.

91
Table 4.
Demographic Characteristics of the Participants (N = 123)
Groups Χ2
Total MU (n=30) NS
(n=34) CB (n=29) CT
(n=30)
Characteristics n % n % n % n % n % Gender 8.72*
Male 68 55.3 14 11.4 19 15.5 12 9.7 23 18.7 Female 55 44.7 16 13.0 15 12.2 17 13.8 7 5.7
Primary language used 3.69 Taiwanese 99 80.5 24 19.5 29 23.6 20 16.3 26 21.1 Chinese 24 19.5 6 4.9 5 4.1 9 7.3 4 3.3 Religion 17.61
Folklore cultural beliefs 41 33.3 4 3.3 15 12.2 10 8.2 12 9.8 Buddhism 36 29.3 10 8.1 4 3.3 11 8.9 8 6.5 Taoism 23 18.7 9 7.2 9 7.3 4 3.3 4 3.3 Christian 16 13.0 6 4.9 3 2.4 3 2.4 4 3.3 None 5 4.1 1 0.8 1 0.8 1 0.8 2 1.6 Catholic 2 1.6 0 - 2 1.6 0 - 0 -
Education 20.41 Self study (0 yr) 6 4.9 3 2.4 2 1.6 1 0.8 0 - Elementary (1-6 yrs) 43 35.0 11 8.9 14 11.4 6 4.9 12 9.8 Junior high (7-9 yrs) 20 16.3 5 4.1 5 4.1 3 2.4 7 5.7 Senior high(10-12 yrs) 31 25.2 6 4.9 10 8.1 13 10.6 8 6.5 College (13-16 yrs) 22 17.9 4 3.3 3 2.4 6 4.9 3 2.4 Master (17-19 yrs) 1 0.8 1 0.8 0 - 0 - 0 -
Marital status 12.21 Never married 8 6.5 0 - 1 0.8 4 3.3 3 2.4 Married 86 69.9 26 21.1 23 18.7 21 17.1 17 13.8 Widowed 14 11.4 3 2.4 4 3.3 3 2.4 4 3.3 Divorced 15 12.2 2 1.6 6 4.9 1 0.8 6 4.9
Race 7.57 Taiwanese 117 95.1 28 22.8 34 27.6 3 2.4 29 23.6 Chinese 5 4.1 1 0.8 0 - 26 21.1 1 0.8 Mainlander 1 0.8 1 0.8 0 - 0 - 0 -
Income 6.36 No income 81 65.8 20 16.3 25 20.3 18 14.6 18 14.6 No stable income 2 1.6 0 - 0 - 1 0.8 1 0.8 < 10,000 NT 1 0.8 0 - 1 0.8 0 - 0 - Do not care to provide 39 31.7 10 8.13 8 6.50 10 8.1 11 8.9
Cigarette usage 9.85* No 82 66.7 22 17.9 26 21.1 21 17.1 13 10.6 Yes 41 33.3 8 6.5 8 6.5 8 6.5 17 13.8
Alcohol usage 14.02*
No 89 72.4 24 19.5 24 19.5 25 20.3 16 13.0 Yes, socially 21 17.1 5 4.1 8 6.5 1 0.8 7 5.7 Yes, daily 13 10.6 1 0.8 2 1.6 3 2.4 7 5.7
Note. MU = Music; NS = Nature sounds; CB = Combination of music and nature sounds; CT = Control. * p < .05

92
Table 5.
Experience with Complementary and Alternative Therapy (N = 123)
Past Experience Current Usage No Yes No Yes
Therapy n % n % n % n % Acupuncture 115 93.5 8 6.5 6 4.88 2 1.63 Acupressure 122 99.2 1 0.8 1 0.8 0 - Aromatherapy 118 95.9 5 4.1 1 0.8 4 3.25 Art therapy 123 100 0 - Biofeedback 123 100 0 - Chi Kung 123 100 0 - Guided imagery 122 99.2 1 0.8 1 0.8 0 - Healing touch 123 100 0 - Herbal remedy 68 55.3 55 44.7 50 40.65 5 4.1 Hypnosis 122 99.2 1 0.8 1 0.8 0 - Massage 112 91.1 11 8.9 2 1.63 9 7.32 Music therapy 123 100 0 - Chiropractic 123 100 0 Dietary 122 99.2 1 0.8 1 0.8 0 Never used 40 32.52
Primary sites of cancer. Because all hospice cancer patients had multiple sites of
metastases, only the primary cancer site was recorded (Table 6). Of the 123 participants,
the most frequent sites were colon/rectal (n = 20), lung (n = 18),
nasopharyngeal/esophagus area (n = 14), oral cavity (n = 13), and liver (n = 13). Two
participants had multiple metastases at the first visit to their doctors and “unknown
original sites” was documented in their medical record.

93
Table 6.
The Primary Sites of Cancer (N = 123)
Cancer Type n % Colon/Rectal 20 16.3 Lung 18 14.6 Nasopharyngeal/Laryngeal/Esophagus 14 11.4 Liver 13 10.6 Oral 13 10.6 Kidney/Ureter/Bladder 8 6.5 Breast 7 5.7 Cervical/Uterine 7 5.7 Digestive/Gastrointestinal 6 4.9 Pancreas 5 4.1 Prostate 3 2.4 Hematological/Blood 2 1.6 Thyroid 2 1.6 Unknown primary 2 1.6 Brain 1 0.8 Ovarian 1 0.8 Spine 1 0.8
Cancer pain and anxiety in hospice patients. Pain was assessed and documented
regularly by staff nurses at least every four to six hours daily in both hospice units. A pain
event was documented in the medical record when a patient complained about pain and
nursing assessment and intervention were provided. The investigator obtained
information about pain from the medical record during the 24 hours prior to the test of the
intervention on Day 1. The range of the number of documented pain events in the 24
hours preceding the Day 1 pretest was from 1 to 17 with an average of 3.24 (SD = 2.07)
times. The highest pain score in the 24 hours previous to the Day 1 pretest ranged from
3 – 10 points (0 – 10 scale) with an average of 5.32 points (SD = 1.86). The lowest pain
score in the previous 24 hours ranged from 0 – 6 points (0 – 10 scale) with an average of
1.26 points (SD = 1.25). Only 33 participants had a documented breakthrough pain event;

94
the breakthrough pain scores ranged from 5 to 10 with an average pain of 8.18 points (SD
= 1.45).
All the breakthrough pain events that were documented in the medical records were
“described as at an intolerable point.” Most of the records stated that the breakthrough
pain had a sudden onset, while two said the pain increased gradually. The possible causes
included position change (n = 4), dressing change (n = 1), drinking or eating (n = 2), and
unknown reason (n = 14). The locations of the breakthrough pain in the body were
abdomen (n = 13), legs (n = 4), back (n = 3), whole body (n = 2), face (n = 2), oral cavity
(n = 1), neck (n = 1), arms (n = 1), and waist (n = 1). The symptoms other than pain
included abdominal distension (n = 3), cold sweating (n = 2), stiffness of the whole body
(n = 2), and shortness of breath (n = 1). These participants were crying (n = 3), moaning
(n = 3), and feeling angry (n = 1). No participants were having breakthrough pain at the
time of testing.
Unfortunately, the staff nurses did not assess and document anxiety regularly in both
hospice units. Only eight of 123 medical records contained documented anxiety events.
There were no documented records of anxiety disorders or anxiety events in the past 24
hours. Of the eight most recent anxiety events prior to the Day 1 pretest, six were related
to thoughts of death, dying, and the unknown underworld after death. Four were related
to pain and shortness of breath. Two said they were anxious about the ghosts who visited
them during the night and in their dreams. One said that pain was related to the progress
of cancer on his face. Some participants reported more than one cause of their anxiety.

95
Medication Usage
One of the inclusion criteria was that hospice cancer patients were taking prescribed
analgesics around the clock for pain control. All participants had opioid medication “in
effect” during the tests: weak or strong opioids or both. Many also had non-opioid pain
medication along with the opioids. Anxiolytics were prescribed only on an as-needed
basis and only a small percentage of participants were receiving them (Table 7).
Chi-square analysis indicated no significant differences among the groups in analgesics
and anxiolytics “in effect” at each test.
Analgesics and Anxiolytics Used by Participants
The most frequently used weak opioid was Ultracet, followed by Codeine, Tramadol,
and Darvocet. Four strong opioids were prescribed. Nearly two-thirds of the participants
received Morphine and one-third received Durogesic. Many had non-opioid pain
medication along with the opioids to reduce inflammatory pain. The most frequently
non-opioids used were steroids, Tegretal, and Acetaminophen. Three major types of
anxiolytics were Alprazolam, Lorazepam, and Fluoxetin. Frequencies of those with
analgesics and anxiolytics each day are in Appendix E.

96
Table 7.
Participants with Analgesics and/or Anxiolytics “in Effect” During Each Test
MU NS CB CT X2
Medication n % n % n % n % p
Day 1 (N=123) n = 30 n = 34 n = 29 n = 30 Weak opioid 6 20.0 13 38.2 10 34.5 5 16.7 5.27 .15 Strong opioid 25 83.3 22 64.7 23 79.3 24 80.0 3.73 .29 Non-opioid 20 66.7 24 70.6 15 51.7 20 66.7 2.73 .44 Anxiolytics 4 13.3 5 14.7 3 10.3 5 16.7 0.53 .91 Day 2 (N=119) n = 30 n = 31 n = 29 n = 29 Weak opioid 8 26.7 12 38.7 8 27.6 5 17.2 3.47 .32 Strong opioid 25 83.3 21 67.7 23 79.3 23 79.3 2.37 .50 Non-opioid 17 56.7 22 71.0 16 55.2 19 65.5 2.15 .54 Anxiolytics 4 13.3 4 12.9 3 10.3 5 17.2 0.61 .90 Day 3 (N=117) n = 29 n = 31 n = 28 n = 29 Weak opioid 7 24.1 12 38.7 8 28.6 5 17.2 3.68 .30 Strong opioid 24 82.8 21 67.7 22 78.6 23 79.3 2.16 .54 Non-opioid 19 65.5 22 71.0 16 57.1 19 65.5 1.25 .74 Anxiolytics 4 13.8 4 12.9 4 14.3 5 17.2 0.25 .97 Note. MU = Music; NS = Nature sounds; CB = Combination of music and nature sounds; CT = Control; The n in each column represents the number of participants who received the medication; some participants were taking more than one analgesic and/or anxiolytics. Pain and Anxiety Pretests and Posttests
Cancer pain and anxiety were measured by the 100-mm Pain and Anxiety VAS
before and after each 20-minute test. The majority had average pain and anxiety scores of
less than 30 mm, except for the combination group in which Day 1 pretest pain and
anxiety and Day 2 pretest anxiety were a little greater (Table 8). The standard deviations
for both pain and anxiety were small and closely clustered about the mean, although the
standard deviations for anxiety was wider than that of pain. Using analysis of variance
analyses, there were no significant group differences in pain or anxiety at each pretest.

97
Table 8.
Pain and Anxiety Pretests and Posttests at Each Test (N = 117)
MU NS CB CT Variable M SD M SD M SD M SD F p
Day 1 n = 29 n = 31 n = 28 n = 29 Pain pretest 29.41 7.12 29.29 7.79 31.50 9.06 28.93 8.04 .66 .58 Pain posttest 23.72 6.71 25.65 8.67 24.89 7.12 27.86 8.53 .31 .82 Anxiety
pretest 28.55 13.21 28.45 11.38 32.93 14.98 27.62 11.02 .92 .43
Anxiety posttest 24.90 11.58 26.16 10.77 27.64 12.40 26.86 10.56 .18 .91
Day 2 n = 29 n = 31 n = 28 n = 29 Pain pretest 28.17 9.34 26.03 8.25 29.57 9.42 28.45 5.71 2.16 .10 Pain posttest 22.66 8.44 22.90 7.69 24.57 7.72 28.31 6.41 .77 .51 Anxiety
pretest 27.10 13.95 26.65 10.92 30.07 13.13 27.17 9.95 1.21 .31
Anxiety posttest 22.21 10.69 23.39 9.88 24.14 9.87 27.31 10.85 .13 .95
Day 3 n = 29 n = 31 n = 28 n = 29 Pain pretest 22.62 7.28 23.61 8.27 27.00 8.68 29.31 6.19 1.09 .35 Pain posttest 17.31 6.38 20.52 7.31 22.04 6.30 28.21 7.06 .44 .72 Anxiety
pretest 22.21 10.09 23.19 9.80 25.29 9.12 27.66 10.87 .37 .77
Anxiety posttest 17.34 7.82 20.68 9.52 20.64 8.33 26.83 10.98 .82 .48
Note. MU = Music; NS = Nature sounds; CB = Combination of music and nature sounds; CT = Control. Pain and anxiety were measured by the 100-mm Pain and Anxiety VAS scales.
Correlations
Pearson’s product moment correlations and Spearman’s correlation were used to
identify possible covariates. Those proposed included age, gender, pain and anxiety at
pretests, and pain medications and anxiolytics “in effect” during treatment. These
variables were used as covariates if the data were obtained before the pretest on Day 1
(Tabachnick & Fidell, 2007) and if correlations were greater than r = .30 (p = .05). Using
Pearson’s product moment correlations, age and gender were not correlated with pain and
anxiety post tests at r > .30, so age and gender were not used as covariates. Spearman’s
correlation was used to test the relationship between pain medications and anxiolytics “in

98
effect” during treatment and the dependent variables. The results showed that there were
no significant correlations between pain medications and anxiolytics “in effect” and pain
and anxiety posttests. Therefore, the analgesics and anxiolytics were not treated as
covariates.
Day 1 pain pretest was strongly and positively correlated with posttests for Day 1
pain and anxiety, and Day 2 pain. Day 1 pain pretest was moderately and positively
correlated with posttests for Day 2 anxiety, and Day 3 pain and anxiety. The correlations
with Day 1 pretests ranged from r = .41 to .70, p < .001. Day 1 anxiety pretest was
strongly and positively correlated with posttests for Day 1 and Day 2 pain and anxiety
posttests, and Day 3 anxiety. The correlations ranged from .47 to .94, p < .001. Although
Day 2 pain and anxiety pretests, and Day 3 pain and anxiety pretests were all strongly
correlated with the pain and anxiety posttests, they were measured after the treatment was
initially given. Therefore, only Day 1 pain pretest and anxiety pretest were used as
covariates (Table 9).
Table 9.
Correlations between Pain and Anxiety Pretests and Posttests
Day 1 Day 2 Day 3 Pain Anxiety Pain Anxiety Pain Anxiety Pre Post Pre Post Pre Post Pre Post Pre Post Pre Post Day 1 (N=123) Pain pretest - .70 .58 .51 .67 .52 .50 .42 .68 .48 .53 .41 Pain posttest - .52 .59 .60 .66 .49 .54 .62 .63 .54 .54 Anxiety pretest - .94 .65 .55 .85 .74 .63 .47 .78 .63 Anxiety posttest - .60 .59 .81 .78 .59 .52 .78 .71 Day 2 (N=119) Pain pretest - .88 .83 .74 .83 .62 .73 .57 Pain posttest - .75 .79 .83 .76 .73 .68 Anxiety pretest - .91 .70 .55 .89 .73 Anxiety posttest - .69 .64 .92 .88 Day 3 (N=117) Pain pretest - .86 .78 .67 Pain posttest - .72 .76 Anxiety pretest - .90 Anxiety posttest - Note. Pre = Pretest; Post = Posttest; all correlations between tests had a significant level, p < .001.

99
Hypothesis Testing
Hypothesis 1 was tested using a priori reverse Helmert contrasts with
repeated-measures analysis of covariance (RM ANCOVA) across the three pain posttests,
while controlling for Day 1 pain pretest. The results showed that pain was significantly
different among four groups, F(5.98, 223.38) = 4.36, p < .001. Contrast #1 indicated that
while controlling for Day 1 pretest pain, the pain posttests were significantly lower in the
music, nature sounds, and combination groups, taken together, than in the control group,
p < .001, 95% CI [4.08, 8.09]. However, contrast #2 indicated no significant differences
in pain when comparing the individual groups, music and nature sounds, taken together,
to the combination group, p = .66, 95% CI [-1.68, 2.63]. Contrast #3 showed no
significant difference in pain when comparing the two individual groups, music and
nature sounds, p = .13, 95% CI [-0.55, 4.28]. The observed power for the contrasts was
1.0. Post-hoc analyses of RM ANCOVA were conducted with a Bonferroni adjustment
controlling for Day 1 pain pretest. Each treatment group had significantly lower pain
across the three tests than the control group. Hypothesis 1 was supported.
HO 1: Hospice cancer patients who listen to sedative music, nature sounds, or sedative
music combined with nature sounds will have less cancer pain than those who do not
when controlling for baseline.
On Day 1 medium effect sizes were found for music and the combination, while a
small effect size was found for nature sounds. On Day 2 all three interventions had
medium effect sizes. On Day 3, all three intervention s had large effect sizes (Table 10).
Thus across the three days, pain in the control group remained the same as the pretest,

100
while the effect sizes for the music and combination groups increased from Day 2 to Day
3 and for the nature sounds group they increased each day (Figure 5).
Table 10.
Effect Sizes of Pain and Anxiety by Groups
MU CB NS Symptom Day Partial η2 ES Partial η2 ES Partial η2 ES Pain 1 .08 M .09 M .03 S
2 .10 M .07 M .09 M 3 .34 L .18 L .21 L
Anxiety 1 .07 M .11 M .02 S 2 .09 M .11 M .06 M 3 .23 L .18 L .12 M
Note. MU = Music, CB = Combination of music and nature sounds, NS = Nature sounds, ES = Effect size, S = Small, M = Medium, L = Large Figure 5. Pain Day 1 Pretests and Three Posttests by Group (N = 117)
Figure 5. Day1pre = Day 1 pretest; The three pain posttests mean scores were compared by treatment groups on Day 1, Day 2, and Day 3. The posttest means were adjusted by Day 1 pain pretest score.
15
17
19
21
23
25
27
29
31
Day1pre Day 1 Day 2 Day 3
100
mm
Pai
n VA
S
Music
Nature Sounds
Combination
Control
101
Hypothesis 2 was tested using a priori reverse Helmert contrasts with
repeated-measures analysis of covariance (RM ANCOVA) across the three anxiety
posttests, while controlling for Day 1 anxiety pretest. The results showed that anxiety was
significantly different among four groups, F(5.42, 202.50) = 4.04, p = .001. Contrast #1
indicated that while controlling for Day 1 pretest anxiety, the anxiety posttests were
significantly lower in the music, nature sounds, and combination groups, taken together,
than in the control group, p < .001, 95% CI [3.57, 7.53]. However, contrast #2 indicated
no significant differences in pain when comparing the individual groups, music and
nature sounds, taken together, to the combination group, p = .25, 95% CI [-3.37, 0.89].
Contrast #3 showed no significant difference in pain when comparing the two individual
groups, music and nature sounds, p = .10, 95% CI [-0.39, 4.37]. The observed power for
the contrasts was 1.0. Post-hoc analyses of RM ANCOVA were conducted with a
Bonferroni adjustment controlling for Day 1 anxiety pretest. Each treatment group had
significantly lower anxiety across the three tests than the control group. Hypothesis 2 was
supported.
HO 2: Hospice cancer patients who listen to sedative music, nature sounds, or sedative
music combined with nature sounds will have less anxiety than those who do not when
controlling for baseline.
For anxiety, on Day 1 medium effect sizes were found for music and the
combination, while a small effect size was found for nature sounds. On Day 2 all three
interventions had medium effect sizes. On Day 3 music and combination had large effect
sizes, while the nature sounds continued to have a medium effect size (Table 10). Thus
across the three days anxiety in the control group remained essentially the same as the
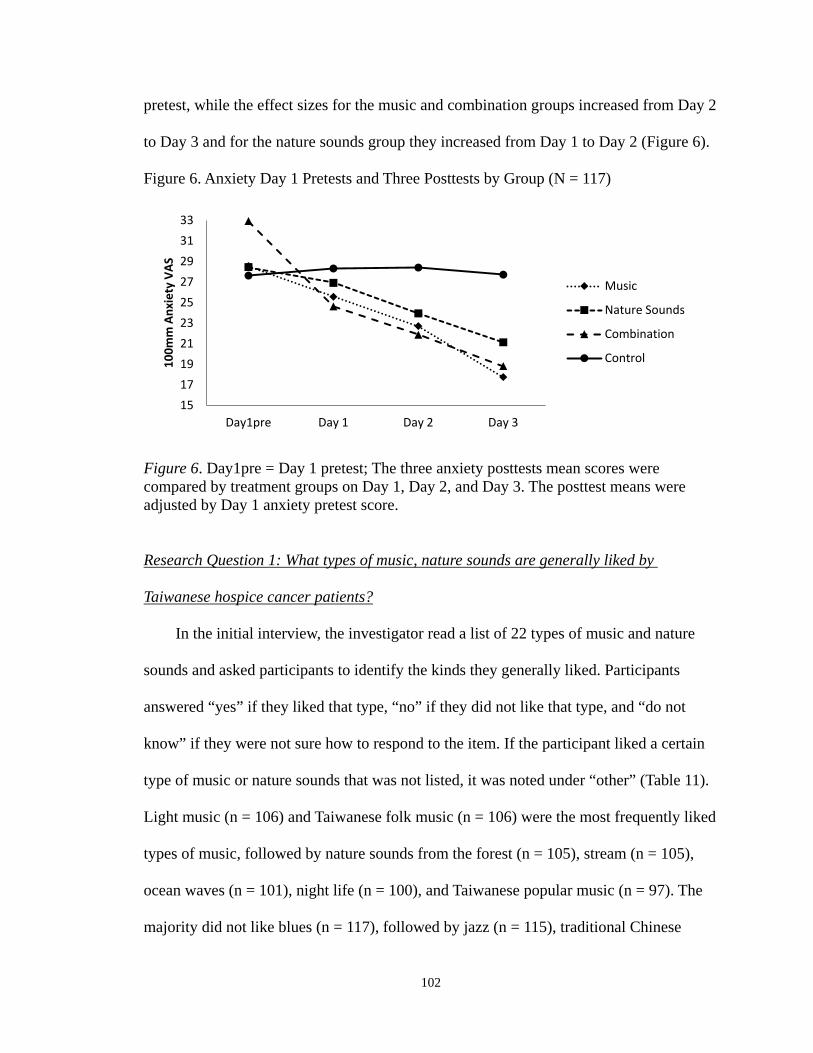
102
pretest, while the effect sizes for the music and combination groups increased from Day 2
to Day 3 and for the nature sounds group they increased from Day 1 to Day 2 (Figure 6).
Figure 6. Anxiety Day 1 Pretests and Three Posttests by Group (N = 117)
Figure 6. Day1pre = Day 1 pretest; The three anxiety posttests mean scores were compared by treatment groups on Day 1, Day 2, and Day 3. The posttest means were adjusted by Day 1 anxiety pretest score.
In the initial interview, the investigator read a list of 22 types of music and nature
sounds and asked participants to identify the kinds they generally liked. Participants
answered “yes” if they liked that type, “no” if they did not like that type, and “do not
know” if they were not sure how to respond to the item. If the participant liked a certain
type of music or nature sounds that was not listed, it was noted under “other” (Table 11).
Light music (n = 106) and Taiwanese folk music (n = 106) were the most frequently liked
types of music, followed by nature sounds from the forest (n = 105), stream (n = 105),
ocean waves (n = 101), night life (n = 100), and Taiwanese popular music (n = 97). The
majority did not like blues (n = 117), followed by jazz (n = 115), traditional Chinese
Research Question 1: What types of music, nature sounds are generally liked by
Taiwanese hospice cancer patients?
15 17 19 21 23 25 27 29 31 33
Day1pre Day 1 Day 2 Day 3
100m
m A
nxie
ty V
AS
Music
Nature Sounds
Combination
Control
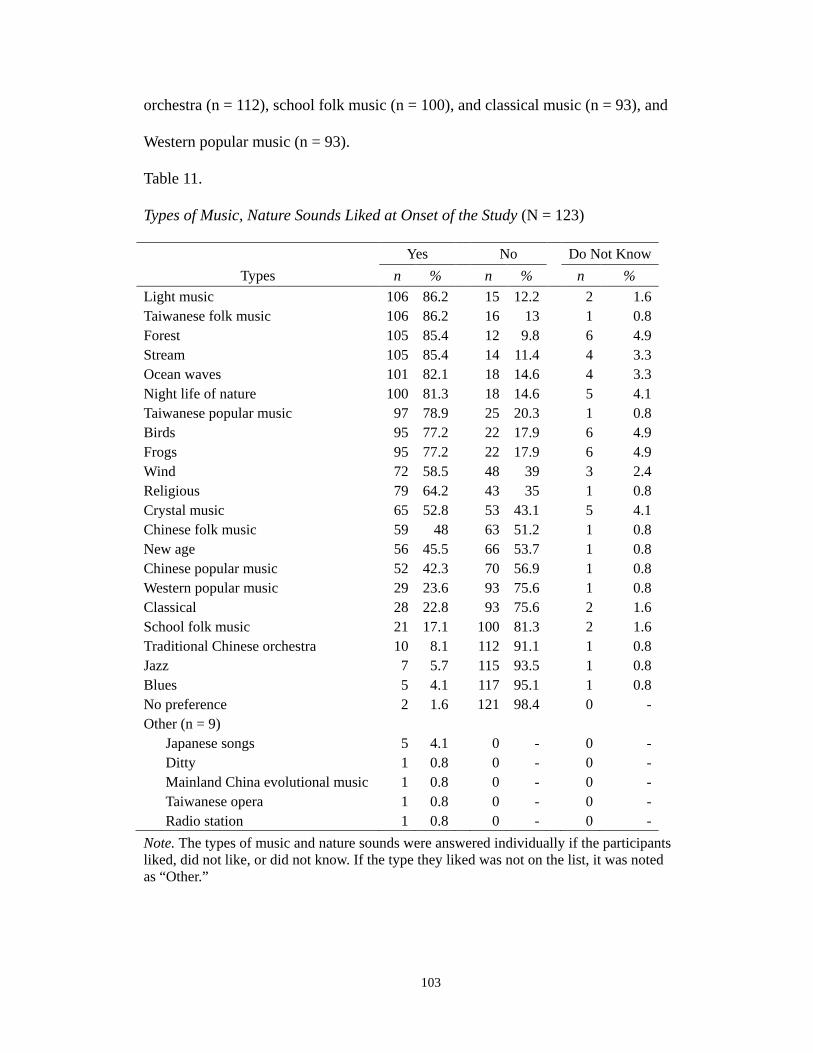
103
orchestra (n = 112), school folk music (n = 100), and classical music (n = 93), and
Western popular music (n = 93).
Table 11.
Types of Music, Nature Sounds Liked at Onset of the Study (N = 123)
Yes No Do Not Know Types n % n % n %
Light music 106 86.2 15 12.2 2 1.6 Taiwanese folk music 106 86.2 16 13 1 0.8 Forest 105 85.4 12 9.8 6 4.9 Stream 105 85.4 14 11.4 4 3.3 Ocean waves 101 82.1 18 14.6 4 3.3 Night life of nature 100 81.3 18 14.6 5 4.1 Taiwanese popular music 97 78.9 25 20.3 1 0.8 Birds 95 77.2 22 17.9 6 4.9 Frogs 95 77.2 22 17.9 6 4.9 Wind 72 58.5 48 39 3 2.4 Religious 79 64.2 43 35 1 0.8 Crystal music 65 52.8 53 43.1 5 4.1 Chinese folk music 59 48 63 51.2 1 0.8 New age 56 45.5 66 53.7 1 0.8 Chinese popular music 52 42.3 70 56.9 1 0.8 Western popular music 29 23.6 93 75.6 1 0.8 Classical 28 22.8 93 75.6 2 1.6 School folk music 21 17.1 100 81.3 2 1.6 Traditional Chinese orchestra 10 8.1 112 91.1 1 0.8 Jazz 7 5.7 115 93.5 1 0.8 Blues 5 4.1 117 95.1 1 0.8 No preference 2 1.6 121 98.4 0 - Other (n = 9)
Japanese songs 5 4.1 0 - 0 - Ditty 1 0.8 0 - 0 - Mainland China evolutional music 1 0.8 0 - 0 - Taiwanese opera 1 0.8 0 - 0 - Radio station 1 0.8 0 - 0 -
Note. The types of music and nature sounds were answered individually if the participants liked, did not like, or did not know. If the type they liked was not on the list, it was noted as “Other.”
104
Participants in the intervention groups (MU, NS, and CB) were asked how much
they liked the intervention they received on the third day after marking the posttest. The
question had a five-point Likert type rating scale (1 = disliked very much; 2 = disliked; 3
= neutral; 4 = liked; 5 = liked very much). Eighty eight participants answered the
question and the mean score was 4.40 (SD = 0.7). More than half of the participants (n =
46) liked their intervention very much, more than one-third (n = 31) liked it, and a few
rated it as neutral (Table 12). The music group rated their intervention the highest, M =
4.79, SD = 0.41; the combination group was next, M = 4.64, SD = 0.49; and the nature
sounds group was third, M = 3.81, SD = 0.70. There was a significant difference in liking
the intervention among three intervention groups, F(2, 85) = 27.85, p < .001. A
Bonferroni adjustment showed that the music group liked the intervention significantly
more than the nature sounds group, p < .001, 95% CI [0.64, 1.34], so did the combination
group compared to the nature sounds group, p < .001, 95% CI [0.48, 1.19]. However,
there was no significant difference in liking the intervention between the music group and
the combination group.
Research Question 2: How much did Taiwanese hospice cancer patients like their
assigned intervention?

105
Table 12.
Intervention Liked by the Participants
Total MU
(n = 29) NS (n = 31) CB
(n = 28)
Rating Amount liked n % n % n % n % F 5.55***
3 Neutral 11 12.5 0 - 11 12.5 0 - 4 Liked 31 35.2 6 6.8 15 17 10 11.4 5 Liked very much 46 52.3 23 26.1 5 5.7 18 20.5
Note. The Likert type rating scale is from 1 to 5, but 1 (disliked very much) and 2 (disliked) were not rated by the participants. MU = Music; NS = Nature sounds; CB = Combination of music and nature sounds; CT = Control. *** p < .001
The types of the assigned intervention that were selected by the participants were
recorded on daily basis (Table 13). Because the participants in the intervention groups
were allowed to change different types of music/nature sounds, some decided to listen to
a different type of music/nature sounds on either Day 2 or Day 3. In the music group,
Taiwanese music was the most frequently selected, followed by easy listening music and
Buddhist music. The most frequently selected nature sounds were forest and then ocean
waves in the nature sounds and the combination groups. In the combination group, none
of the participants selected the music with frogs or night life sounds. On Day 2, five
participants in the music group changed their selection, two in the combination group,
and one in the nature sounds group. On Day 3, seven participants in the nature sounds
group changed their selection, four the combination group, and two in the music group.
Participants’ Suggestions
Twenty three participants provided their suggestions for use of the intervention after
they completed the study. Of these, seven (30.43%) said that the nature sounds were a
little bit monotonous. They suggested having a broader selection of nature sounds and/or

106
combining several types of nature sounds together. Four (17.39%) suggested including
Japanese music among the selections. Three suggested that the intervention should be
provided to more people for a longer period of time. Three participants and their families
suggested that the investigator provide the title of the CD so they could use the same
music when they were discharged from the hospital. Three participants’ families wished
the intervention could be provided for the family, so the family could relax from the
stress of taking care of their loved ones and could remember them after they die. One
participant wanted to listen to music with lyrics. One suggested including Taiwanese
music played on a harp, while one suggested having Taiwanese music combined with
nature sounds.
Table 13.
Types of Music and Nature Sounds Selected by Participants by Day
Day 1 Day 2 Day 3 Type n % n % N %
Music n = 30 n = 30 n = 29 Taiwanese 12 12.9 11 12.2 11 12.5 Easy listening 6 6.5 2 2.2 4 4.5 Christian 4 4.3 4 4.4 2 2.3 Harp 3 3.2 3 3.3 3 3.4 Buddhist 2 2.2 5 5.6 5 5.7 Chinese 2 2.2 2 2.2 2 2.3 Orchestra 1 1.1 1 1.1 0 - Piano 0 - 2 2.2 2 2.3 Nature sounds n = 34 n = 31 n = 31 Forest 20 21.5 20 22.2 13 14.8 Ocean 9 9.7 8 8.9 8 9.1 Birds 4 4.3 0 - 1 1.1 Frogs 1 1.1 2 2.2 7 8.0 Night life 0 1 1.1 2 2.3 Combination n = 29 n = 29 n = 28 Forest 19 20.4 20 22.2 16 18.2 Birds 5 5.4 3 3.3 2 2.3 Ocean 5 5.4 6 6.7 10 1.4 Frogs 0 - 0 - 0 - Night life 0 - 0 - 0 - Note. MU = Music; NS = Nature sounds; CB = Combination of music and nature sounds; CT = Control. Participants could change to different types of music/nature sounds; some chose a different type on Day 2 and/ or Day 3.

107
The length of time that the hospice patients listened to the interventions
independently between tests was measured in minutes and is presented in Table 14.
Between Day 1 and Day 2, the range was from 21 to 569 minutes with a mean of 250.58
minutes (SD = 126.39). Between Day 2 and Day 3, was from 29 minutes to 568 minutes
with a mean of 234.65 minutes (SD = 124.76). There was a statistically significant
difference among three intervention groups between Day 1 and Day 2, F(2, 88) = 19.32,
p < .001 and between Day 2 and Day 3, F(2, 81) = 12.06, p < .001. Taken together, the
music and the combination groups listened to the intervention significantly longer than
the nature sounds group at both times, M = 293.04, SD = 50.18, p < .001, CI [170.61,
415.48], M = 214.68, SD = 50.63, p < .001, CI [91.14, 338.22] minutes longer
respectively. The minutes of independent intervention use between testing times were not
significantly correlated with the pain and anxiety posttests across each days.
Research Question 3: How many minutes were music, nature sounds, and the
combination of sedative music with nature sounds independently used between
testing times?
Table 14.
Minutes of Independent Intervention Use Between Testing Times
Day 1 to Day 2 Day 2 to Day 3 n M SD n M SD
Music 29 314.62 128.42 29 300.34 125.03 Nature Sounds 33 159.45 67.90 29 161.55 73.21 Combination 29 290.24 117.98 26 251.92 122.77 Note. a Between Day 1 and Day 2, one participant withdrew and one did not find time to listen to the intervention. b Between Day 2 and Day 3, two participants withdrew and five did not find time to listen.

108
The Reasons for Independent Use
The participants had a variety of reasons for using the intervention independently
between tests. The main reason on Day 1 and Day 2 was that they wanted to relax (n =
83). Other reasons were that they liked the intervention (n = 46), felt pain (n = 15), were
curious about the collection in the MP3 player (n = 7), felt anxious (n = 6), could not
sleep (n = 2), and tried to kill time (n = 1). Between Day 2 and Day 3, the main reason
was also that they wanted to relax (n = 79). Other reasons were that they liked the
intervention (n = 51), felt pain (n = 9), felt anxious (n = 6), were curious about the
collection in the MP3 player (n = 5), wanted to sleep (n = 3), and tried to kill time (n = 1).
Pain and anxiety pretests and posttests were positively and strongly correlated with
one another at a significant level at each test: Day 1 pretest r = .58, Day 1 posttest, r = .59,
Day 2 pretest r = .83, Day 2 posttest, r = .79, Day 1 pretest r = .78, Day 1 posttest, r = .76,
p < .001. To determine the amount of variation in anxiety that was related to pain,
miltuple regression was used: pain was the independent variable and anxiety was the
dependent variable. The results showed that Day 2 pain accounted for the most variation
in Day 2 anxiety, followed by Day 3 and then Day 1, p < .001 (Table 15).
Research Question 4: What is the relationship between cancer pain and anxiety in
hospice cancer patients?
Table 15.
Adjusted R Square between Pain and Anxiety Pretests and Posttests by Day
Adjusted R2
Day 1 Day 2 Day 3 Pain pretest – Anxiety pretest .34 .68 .61
Pain posttest – Anxiety posttest .35 .62 .58

109
Summary
Pretest pain and anxiety in the 123 participants in two hospice units was ≦ 32 mm
and was not significantly different among the music, nature sounds, combination, or
control group, nor were most demographic characteristics. The control group had more
males, smokers, and alcohol users, but correlations between demographic and dependent
variables were < .30. Day 1 pain and anxiety pretests were used as covariates. Orthogonal
a priori reversed Helmert contrasts with repeated measured ANCOVA and pretest control
indicated that pain and anxiety posttests were significantly lower in the music, nature
sounds, and combination groups together, than the control group. Comparison of each
intervention group with the control group supported these findings with some increased
effect sizes over time. Contrast #2 and #3 were not significant for either variable. Light
music, Taiwanese folk songs, the sounds of the forest and the stream were most
frequently liked types of music and nature sounds at the onset of the study by the
participants. The majority of participants liked their intervention very much. The most
frequently selected music was Taiwanese music, while the most frequently selected
nature sounds was the sounds of the forest. The minutes of independent intervention use
were significantly different among three treatment groups and the music and combination
groups listened to the intervention significantly longer than the nature sounds group
between the two time periods, with longer listening by those in the music and
combination groups than the nature sounds group at both times. Pain and anxiety in
hospice cancer patients were positively, strongly, and significantly correlated.

110
Chapter Five
Discussion
This chapter presents a summary of the study, the comparison of the findings from
this study with the literature, and the rationale for differences in the findings. The
limitations of the study and implications of the findings for theory, research, and practice
are then discussed.
Summary of the Study
Cancer has been the leading cause of death in Taiwan for more than 20 years.
Cancer patients who receive hospice care frequently suffer from pain and anxiety. The
purpose of the study was to test the effects of sedative music, nature sounds, and the
combination of music and nature sounds on cancer pain and anxiety in hospice cancer
patients in Taiwan. A middle-range theory of acute pain was used as the conceptual
framework because it proposed using nonpharmacological modalities for pain
management (Good & Moore, 1996). A four-group randomized controlled trial with
repeated measures was conducted in two hospice units (N = 117). Participants in the
intervention groups listened to the assigned intervention and the control group rested in
the bed or the chair quietly for 20 minutes per day for three continuous days. Pain and
anxiety were measured on 100 mm VAS scales before and after the test and were
positively, strongly, and significantly correlated.
The results showed that while controlling for the Day 1 pain and anxiety pretests,
participants in the intervention groups had significantly less pain and anxiety than those
in the control group. Music and combination had medium effect sizes on both Days 1 and
2, which increased to large effect sizes by Day 3. For pain, nature sounds resulted in a

111
small effect size on Day 1, which increased to a medium effect size on Day 2, and a large
effect size on Day 3. For anxiety, nature sounds resulted in a small effect size on Day 1
which increased to a medium effect size on Days 2 and 3. The participants reported they
liked light music, Taiwanese folk songs, and sounds of the forest and sounds of the
stream most frequently when surveyed at the onset of the study. Among the choices
offered to the intervention groups the most frequently selected were Taiwanese music and
the sounds of the forest. The majority liked their intervention very much. Independent use
of the interventions between testing times averaged nearly four hours, and was
significantly longer in the music and combination groups than in the nature sounds group.
Comparison with the Literature
The effect of music on pain. Music effectively decreased pain in hospice cancer
patients in contrast to findings of a few studies of post-operative pain (Good, 1995; L. K.
Taylor, Kuttler, Parks, & Milton, 1998) and procedural pain (Bally, et al., 2003;
Kwekkeboom, 2003). These findings were consistent with 19 previous studies of seven
different types of pain. Music was effective in decreasing post-operative pain (Good &
Ahn, 2008; Good, et al., 2010; Good, et al., 2005; Good, Anderson, Stanton-Hicks, Grass,
& Makii, 2002; Good & Chin, 1998; Good, et al., 1999; Locsin, 1981; Mullooly, et al.,
1988; Voss, et al., 2004), labor pain (Phumdoung & Good, 2003), cancer pain (Beck,
1991; Gallagher, et al., 2006; Gallagher & Steele, 2001; S.-T. Huang, et al., 2010; S. H.
Huang, 2000; Krout, 2001; Zimmerman, et al., 1989), chronic pain (R. McCaffery &
Freeman, 2003; Siedlecki & Good, 2006).
Music was provided for 20 minutes daily for three days, and pain was significantly
reduced. Compared to other randomized controlled trials, the three days in hospice

112
patients was shorter than three previous longitudinal studies. Siedlecki and Good (2006)
had participants with chronic pain to listen to one hour of music for seven days;
McCaffery and Freeman (2003) asked the elderly who had osteoarthritis pain to listen to
20 minutes of music for 14 days. Lai and Good (2006) had older adults who had sleeping
problems to listen music for 45 minutes each night for three weeks. All researchers of
these studies reported decreased pain or increased sleep quality, but two studies showed
that the effect of music continued to increase as time went on (R. McCaffery & Freeman,
2003) and sleep (Hui-Ling Lai & Good, 2006). The effects of the present study were
consistent with these studies, although the length of time and days were varied. Thus,
based on this literature, it is possible that when patients with chronic symptoms listen to
music for more than one day, the music may have a cumulative effect.
In present study, music had medium to large effect sizes on pain. There were small
to medium effect sizes on pain following abdominal surgery (Good, et al., 2010; Good, et
al., 2005; Good, et al., 2002), medium effect sizes on cancer pain (S.-T. Huang, et al.,
2010) and chronic pain (Siedlecki & Good, 2006), and a large effect size following open
heart surgery (Voss, et al., 2004). In two studies the participants listened to music 15
minutes for two days (Good, et al., 2005; Good, et al., 2002), and in two others the
participants listened for 30 minutes of music one time (S.-T. Huang, et al., 2010; Voss, et
al., 2004), while in one study the participants listened to music for one hour a day for
seven days (Siedlecki & Good, 2006). The effect sizes in these studies varied and
therefore may be influenced by the types of pain, the sample size, and the timing and the
types of music provided in the study.

113
The effect of music on anxiety. Music effectively decreased anxiety in hospice
cancer patients, in contrast to the findings of two studies of medical procedures (Bally, et
al., 2003; Yilmaz, et al., 2003). However, the finding was consistent with 15 previous
studies of eight different patient populations. Music was effective in decreasing anxiety
before or after surgery (Bringman, Giesecke, Thorne, & Bringman, 2009; Cooke, et al.,
2005; Pandmanabhan & Hildreth, 2005; Voss, et al., 2004), in the intensive care unit (O.
K. A. Lee, et al., 2005; White, 1999), during cesarean delivery (S.-C. Chang & Chen,
2005), during kangaroo care (H. -L. Lai, et al., 2006), dental procedure (H. -L. Lai, et al.,
2008), and in shelters for abused women (Hernandez-Ruiz, 2005). Music also decreased
anxiety in cancer patients (Bailey, 1983) and hospice patients (Gallagher, et al., 2006;
Gallagher & Steele, 2001; Horne-Thompson & Grocke, 2008; Nakayama, Kikuta, &
Takeda, 2009).
Music was provided 20 minutes daily for three days in the present study and it
significantly decreased anxiety. Of nine randomized controlled trials, researchers of eight
studies provided a single music session ranged from 20 to 60 minutes (S.-C. Chang &
Chen, 2005; Cooke, et al., 2005; Horne-Thompson & Grocke, 2008; H. -L. Lai, et al.,
2008; O. K. A. Lee, et al., 2005; Padmanabhan & Hildreth, 2005; Voss, et al., 2004;
White, 1999). Only one study was found in which the participants listened to music for
60 minutes daily for three consecutive days (H. -L. Lai, et al., 2006). The researchers
reported that maternal anxiety significantly improved daily. Based on the findings from
that study and the present study, it is possible that when patients with an ongoing
condition listening to music for more than one day, music may have an accumulated
effect.

114
Music has a medium to large effect sizes on anxiety. Few researchers reported the
effect size of music on anxiety. There was a medium effect size on anxiety in patients
undergoing dental procedures (H. -L. Lai, et al., 2008), and a large effect sizes on
mothers during kangaroo care (H. -L. Lai, et al., 2006) and following open heart surgery
(Voss, et al., 2004). Music was provided for 30 minutes once to 19 post operative patients
(Voss, et al., 2004), 60 minutes once to 22 dental patients (H. -L. Lai, et al., 2008), and 60
minutes a day for three days to 15 new mothers (H. -L. Lai, et al., 2006). Voss et al. (2004)
provided a choice among six types of music for cardiac surgery patients, while no choice
was provided to the dental patients (piano) and the mothers (lullaby). The differences in
effect sizes among these studies may be influenced by the sample size, the sources of
anxiety, the length of music listening, and the type of music.
The effect of nature sounds on pain. There are fewer studies of the effect of nature
sounds. Only one previous study with a quasi-experimental design showed that listening
to sounds of streams reduced pain during the flexible bronchoscopy procedure (Diette, et
al., 2003). There are no known studies of the effect of nature sounds on cancer pain and
none at the end of life. Thus the findings of this study provide new information that
nature sounds significantly lowered pain across three posttests compared to the control
group. Nature sounds had a small effect size on Day 1, a medium effect size on Day 2,
and a large effect size on Day 3. Researchers of the previous studies only provided one
type of nature sounds to their participants, while a choice among five different types of
nature sounds were offered to participants in this study. Choice among a variety of
selections may satisfy individual preferences, which may be based on familiarity with the
nature sounds offered. Although nearly one-third of participants in the nature sounds

115
group felt “neutral” about how much they liked the intervention and a few felt the sounds
were a little bit monotonous, the majority did not offer negative comments and reported
that they liked the sounds they received.
The effect of nature sounds on anxiety. In this sample of hospice cancer patients,
nature sounds were effective in lowering anxiety across the three daily posttests and the
effect sizes increased from small to medium. Few studies have explored the effect of
nature sounds on anxiety. The results are in contrast to one study that found no effect on
patients undergoing flexible bronchoscopy (Diette, et al., 2003). The results were
consistent with two studies, one in college students (Golletz, 1997) and one in adults
receiving medical procedures (Dickhaus, et al., 2003). However, none of the three
previous studies randomized their subjects, and the types and severity of anxiety in
previous studies is probably different from hospice cancer patients who have anxiety
associated with pain and dying. Therefore, the findings in this study add new information
to current knowledge of the effect of nature sounds on anxiety.
The effect of the combination on pain and anxiety. No studies were found of the
effect of the combination on pain and anxiety. Four previous studies used the
combination of music and nature sounds as only one of the types of music intervention on
patients during colonoscopy for discomfort and anxiety (Harikumar & Kumar, 2007), on
psychiatric patients for anxiety and distress (Sorensen & Tybjerg, 2004), on pediatric
cancer patients for chemotherapy induced nausea and vomiting (S. Y. Lin, 2003), and on
adult cancer patients for anxiety, depression and sleep quality (Hung, 2003). None of the
researchers reported the effect of the combination in their study since the combination of
music and nature sounds was only one of the choice of the music intervention. As a result,

116
the findings of the study provided new information that the combination of music and
nature sounds significantly reduced both pain and anxiety in hospice cancer patients, and
that the effect sizes increased from medium effect sizes to large. The hospice cancer
patients listened to 20 minutes of the combination daily for three days that pain and
anxiety decreased daily. Like music, it is possible that when patients listen to the
combination of music and nature sounds for more than one day, it may have a cumulative
effect.
Preferences for music, nature sounds, and combination. The top three types of
music the participants selected during the survey at the start of the study were Taiwanese
music, easy listening music, and religious music (either Christian or Buddhist). Few
studies have asked this question of participants, and it was done to gain information about
preferences to offer in the future. A researcher in Taiwan asked the elderly people about
their musical preferences and reported that Chinese orchestral music was the most
preferred music among the other six music selection (Hui-Ling. Lai, 2004). Also Ahn
conducted a pilot study where she asked patients their favorite type of music from a list
(Good & Ahn, 2008). Many investigators simply reported the participants choice between
the few types of music offered for testing. The top choices of Taiwanese folk music and
easy listening music found in this study were consistent with previous studies (Good &
Chin, 1998; S.-T. Huang, et al., 2010; S. H. Huang, 2000; Y. C. Huang, 2003; H-C. Wu,
2007).
The participants in the music group liked their intervention more than those in the
nature sounds group or the combination group. They also listened to music independently
between testing times the longest, nearly a half hour longer than the combination group
117
and more than two hours than the nature sound group. This may imply that the
participants in the music group actually obtained the types of music they liked. The
preselected music in this music collection may be culturally appropriate and may have
offered sufficient choice for hospice cancer patients in Taiwan, except that some would
have liked to have heard Japanese music.
For nature sounds, all the sounds were liked by nearly all participants at onset of the
study. This is interesting, considering that after listening for three days, fewer people
seemed to like them. The nature sounds group had the lowest score on the amount they
liked the intervention they received and listening time was nearly two hours less than in
the music and the combination groups. In the initial survey, nearly all participants in both
the nature sounds and the combination groups chose the sounds of forest, followed by the
sounds of ocean waves and birds. The musical component in the combination may have
made nature sounds more enjoyable than nature sounds alone, and nearly two-thirds of
participants in the nature sounds group liked their intervention.
Length of independent listening. The independent use of music, nature sounds, and
combination between testing times indicated that the music and the combination groups
listened significantly longer than the nature sounds group. One study recorded the length
of independent listening to music in postoperative patients: it ranged from 15 to 480
minutes with a mean of 156 minutes, or two and a half hours, which is shorter than in the
present study (Good, 1992). Between the testing times, the music group listened nearly
five hours, the combination group listened more than four hours, and the nature sounds
group listened more than two hours. Nearly all participants used the intervention
independently because they wanted to relax and more than half used the intervention

118
because they liked the intervention. The long hours of independent use of the intervention
may imply that the preselected music, nature sounds, and combination have a soothing
effect that help participants to relax and are enjoyable when listening to them. Longer
listening may also be because the equipment was portable and easy to use, so participants
were able to listen to music or nature sounds in other places rather than only in their room.
They were often able to reach and operate the equipment by themselves. Hospice cancer
patients may have less energy to perform physical activity or they may be less interested
in the available TV programs, so the intervention provided an alternative leisure for them
and also relieved their symptoms.
Relationship between pain and anxiety. In this study, pain and anxiety were
positively, strongly, and significantly correlated. The findings were consistent with other
studies in palliative care (M. L. Chen & Tseng, 2006; D. K. Payne & Massie, 2000).
Cancer pain and anxiety often have a reciprocal effect, and both may exacerbate other
physical symptoms and psychosocial distress (Lancee, et al., 1994). Since pain in these
hospice units was generally managed to be at a low level, the anxiety may reflect the
good control of the pain.
Rationale for the Outcomes of Music, Nature Sounds, and Combination
Music, nature sounds, and the combination of music and nature sounds were found
to have significant effects in hospice cancer patients in this study. The findings may be
because the interventions were preferred and generally liked and the sedative effect of
music and nature sounds helped them in relaxation and distraction. Research has shown
that preferred music can produce better therapeutic effects and more distraction than

119
music that is not preferred (Bruya & Severtsen, 1984; Parente, 1976). Slow and sedative
music increases a relaxing effect (Bernardi, et al., 2006; Stratton & Zalanowski, 1984).
When a person listens to preferred music or sounds, pleasant emotional responses
evoke activity in the limbic system, amygdale, hippocampus, and medial prefrontal
cortex, which are associated with emotion, anxiety response, and pain perception (Blood
& Zatorre, 2001). The dopamine and opioid system are also activated to alter the
perceptions of pain and anxiety (Bardo, 1998). Thus, when hospice cancer patients can
choose from among the preselected music or nature sounds, they are then able to listen to
music that they prefer, which may have contributed to the significant effects.
There was no significant difference in pain and anxiety between the music and the
nature sounds group, which may have been influenced by the similar selection criteria:
sedative in nature and with volume control and no sudden high pitched sounds. However,
there were descriptive differences between the two groups. The music group liked the
intervention most and they listened longest between testing times. The nature sounds
group liked their intervention least and had a shorter listening time between tests. Perhaps
this was because the music had been developed and tested more. Three of the music types
had been shown to be liked and effective in Taiwanese people (Good & Chin, 1998; S.-T.
Huang, et al., 2010), while the other five types of music were selected based on the
suggestions of these and other Taiwanese researchers (S. H. Huang, 2000; Y. C. Huang,
2003). Conversely, the nature sounds intervention had only been tested for pain and
anxiety in few studies and there were fewer recordings and less information available for
selecting among them. Further music consists of a variety of rhythms, timbre, and
intervals, while the nature sounds offered consisted of one type of sound throughout the

120
listening time. Finally, participants were randomly assigned to the nature sounds and
some may not have liked them as much as they liked music, but were willing to give it a
try.
There was also no significant difference in pain and anxiety between the
combination group and the individual intervention groups. One might expect that
combining two interventions would be more effective than using single modalities. The
combination included a variety of music with the sounds of nature. However, it was not
more effective than the single interventions. This finding may be influenced by the
similarity of the interventions, which were selected based on same criteria, sedative, 60 to
80 beats per minute, with no sudden high pitch and volume. The three interventions
probably increased relaxation and distraction, but there may be a limit to the body’s
autonomic response to relaxation and the interventions (Personal communication with M.
Good, 8/17/2011).
The effect sizes were mainly medium to large in hospice patients, and were larger
than those in a study of postoperative pain (Good, et al., 1999). The reason may be that
pain and anxiety in hospice patients were lower and more consistent than in previous
studies. This may due to the policy of the hospice units that patients’ pain should be
controlled to less than 3 points on a 0 to 10 scale after patients are admitted to the unit.
The pain of postoperative patients decreases with wound healing and is controlled with
diminishing amounts of opioid in patient controlled analgesia.
Pretest VAS anxiety levels in the hospice cancer patients were much lower than
pretests in two previous studies (S.-C. Chang & Chen, 2005; Voss, et al., 2004). Further,
pain and anxiety were strongly correlated and pain was controlled to less than 30 mm;

121
good pain control plus the effects of consistent opioid intake may be why anxiety in the
hospice cancer participants was lower than the participants in the previous studies. The
types of anxiety and the intensity of pain may also have influenced the anxiety scores.
Limitations
The results are reflective of effects of interventions designed for hospice patients in
southern Taiwan, and because participants were not randomly selected from the
population, they are not generalizable beyond the sample itself. Other hospice patients
may have had different responses to the interventions: those who did not have the
opportunity to be invited to participate and those who were excluded by the criteria or did
not want to participate. Most participants had mild pain and anxiety and the effects might
have been different if these symptoms were more severe.
It is not possible to blind conscious participants to auditory interventions.
Participants were told the purpose of the study in the consent form and that they would be
randomly assigned to receive music, nature sounds, the combination, or data collection
first (control). Therefore, participants in all groups might have responded to the pain and
anxiety VAS scales in accordance with their knowledge of the investigator’s expectations.
However, the control group may not have responded as a control because they were not
told they were in a control group. They were told they were in a delayed intervention
group and they would receive an intervention after three days of data collection.
Patients in the control group might have been resentful if they had been without an
intervention for weeks and if they knew others in the study received theirs earlier, but this
was avoided in a short 3-day study with randomization to rooms rather than to
individuals.

122
Compensatory equalization might have occurred if the nurses saw that some patients
had an MP3 player while some did not and if the nurses could not tolerate the inequality.
They may unconsciously compensated by giving participants in the control group extra
attention or other treatment (Shadish, et al., 2002). To minimize this threat of internal
validity, the staff nurses were told in their orientation and reminded of the need to do their
usual care. They had previous experience with researchers collecting data in the unit, and
were used to following the researcher’s instructions. They did not know the method of
random assignment to rooms, so if they noticed that patients did not have an MP3 pouch
in the bedside, they might have assumed that those patients were not participants. On the
other hand, nurses might have seen the investigator collecting data at the bedside of
someone in the control group and might have guessed that they were controls. Thus
precautions were taken to minimize the threats to validity, but undocumented possibilities
may have existed.
The randomization scheme was a combination of cluster randomization of
conditions to rooms and adaptive randomization. Treatments were randomized to rooms
to prevent diffusion of treatments in the 2-bed and 4-bed wards. Because random
assignment does not always balance the groups on all variables, the control group had
more males, smokers and alcohol drinkers, although these were not different among four
groups. A limitation of the randomization scheme was that the group size could vary. This
occurred if a participant stayed in a room for a long time, so there was low turnover in
that group and if there was higher turnover in other rooms/groups because the hospice
kept admitting new patients who were then recruited. For example, the nature sounds
group had greater turnover and more participants than the other groups, although there

123
was no significant difference in group size.
Two major problems in data collection were difficulties of getting consent in hospice
cancer patients and recruiting sufficient numbers. These problems were similar to those
of another researcher of cancer patients in Taiwan (S. T. Huang, 2006). There were
problems of insufficient strength to sign the consent, past experiences in signing
documents, and family reluctance to sign. It was not clear whether the refusal of patients
or families was related to the cultural background or personal reasons, or both.
Another problem was slow referral from the staff nurses. The staff nurses in the
hospice units were very busy and frequently had little time to refer possible patients to
the investigator. To improve the accrual rate, the investigator participated in their
morning meetings and asked the primary care nurses about potential participants and
whether they could refer them to the study. During the last three months of the data
collection period, the staff nurses may have felt more familiar with the study. In addition,
some said they had heard positive feedback from patients or families or saw that the
interventions had an observable effect on some of the participants, so they began to refer
potential participants more actively. Due to the slow progress of recruitment, a second
hospice unit in another hospital was added to increase the sample size.
Implications for Theory
The Good and Moore (1996) middle range theory of acute pain, a balance between
analgesic and side effects, proposes that nonpharmacological interventions, such as music,
will reduce acute pain. This study extended the theory to terminally-ill hospice cancer
patients; it supported music as an adjuvant modality to reduce not only cancer pain but
also alleviate anxiety. The findings also extend the domain of nonpharmacological

124
adjuvants to include nature sounds and the combination of music and nature sounds,
which also reduced pain and anxiety. Further, the interventions were carefully chosen for
their familiarity to the Taiwanese population. The results support the effectiveness of this
cultural adaptation. Considering patients’ cultural preferences for music is important
when using music in a specific locality (Good, et al., 2000). This is the first study of
nature sounds thought to be culturally appropriate in people a specific place; in this case
it was people in the island of Taiwan.
Implications for Research
It is recommended that future studies be conducted with longer use of the
interventions to determine whether the effects would continue to improve pain and
anxiety over four or more days in hospice cancer patients. In addition to only hospice and
hospice collaborative care cancer patients, the interventions may be beneficial to cancer
patients who receive hospice home care. A study can examine the feasibility and test the
effects of carrying the interventions from the hospice unit to the home for ongoing
self-care.
Although more varieties of music, nature sounds, and combination were offered to
select from than in previous studies, the choices can be expanded further, based on the
preferences and suggestions from the present study. It is recommended that for older
Taiwanese patients, Japanese music and the sounds of streams be offered. Questions
about how much they liked the intervention can be asked and brief verbal suggestions and
comments can be recorded.
In future studies, it is recommended that a pilot study be conducted for the effect of
these interventions on sleep in hospice cancer patients, followed by a randomized

125
controlled trial that includes sleep as an outcome variable along with pain and anxiety. In
this study, pain and anxiety were the only two outcome variables of interest. However, a
few participants also used their assigned intervention for sleep. Music has been shown to
be effective for sleep in Taiwanese cancer patients (Hung, 2003) and older adults
(Hui-Ling Lai & Good, 2006; Y. J. Lee, 2000b). Sedative music, nature sounds, and the
combination may be useful in providing a relaxing effect and sleep in some of the hospice
cancer patients.
A qualitative design or component of a randomized controlled trial could be used to
obtain verbal descriptions of the perceptions and experiences of music, nature sounds,
and the combination. This may provide more insight into the meaning of the music or
nature sounds to the person, their relaxing or distracting effects, and the scene and the
memories in the patient’s mind. Such insight may help researchers to select music or
nature sounds that are familiar to people in the participant’s age range and can be used for
those who are unable to express themselves but may benefit from listening to music and
nature sounds.
The family members of the hospice cancer patients suffer from the physical burden
of taking care of their family and the emotional stress from deterioration and anticipated
loss of their loved one. Some family members wished that the intervention could be
provided for them too. Therefore, it is recommended that studies be conducted with the
family members to test the effectiveness of the interventions. A longitudinal design can
also be used to follow up the effect of the interventions on the family members during
their grieving process after the patient dies.

126
This study was conducted in two hospice units in the southern Taiwan. The
interventions that were effective in one part of this country may not necessarily be
effective in other hospice units in different cities. The study can be replicated in other
hospice units with the same study design and interventions to explore the similarities and
differences among hospice units in Taiwan.
Implications for Practice
Music, nature sounds, and the combination of both were effective in decreasing pain
and anxiety in hospice cancer patients. A total of 18 types of music and nature sounds (8
for music, 5 each for nature sounds and combination) were preselected for the middle
aged hospice cancer patients in Taiwan to choose from and were then provided to
participants. Nature sounds and the combination were preselected based on the
suggestions from researchers who conducted studies in other countries. Nurses can use
the music and nature sounds tested in this study as a starting point to treat their hospice
cancer patients for pain and anxiety (See Appendix B for selections used). It is also
recommended that nurses in the hospice unit consider patients’ preferences, age, and
cultural background when selecting music, nature sounds, or combination choices for
their patients.
Interventions were provided by a MP3 player, a clip-on headset or a small speaker
(Figure 3). Hospice cancer patients frequently bring many personal belongings which
occupy most of their bedside table. When space is limited, a traditional CD or audio tape
player is too big for the bedside table and is not portable when patients want to move
around. It is recommended that nurses use small MP3 players, place all the equipment in
a small pouch (Figure 3), and clip it to the side of the patient’s pillow case, put in the

127
pocket of their jacket, or hung on the IV stand. This increases the mobility of the hospice
patient rather than occupying limited space on the bedside table. It is recommended that
nurses provide small speakers with enough volume for the participants to hear but low
enough that it would not disturb other patients in the same room. This will avoid the
burden of earphones or ear buds in patients’ ears. The capacity of all MP3 players
currently in the market is large enough to store more songs than the traditional CDs or
audiotapes. It is recommended that nurses consider portable, light weight, and easy to use
equipment when selecting a device to play music and nature sounds in hospice settings.
This study provided a detailed description of the method used to select music, nature
sounds, and the combination, the audio device selection, and the instruction and
delivering of the intervention to hospice patients. The findings of this study could easily
be incorporated in practice. It is recommended that nurses can use the information
presented here to develop an instruction manual for hospice patients in their working
environment.
Conclusion
Music, nature sounds, and the combination if both reduced pain and anxiety, which
is consistent with most studies. The sample size, design, length of the intervention, types
of interventions available for choice, and equipment were possible contributors to the
medium to large effect size in this study. The interventions provided were generally liked
and frequently used for relaxation purpose by the hospice cancer patients. Sedative
effects plus having preferred music and nature sounds may increase the relaxing and
distracting effects and contribute to decreased pain and anxiety. Studies with longer use
of the intervention, expanding the study to home hospice and family members, providing

128
more types of music and nature sounds, and collecting qualitative information are
recommended for future research. This study contributed new knowledge by using an
innovative randomization scheme, including a delayed-start control group, providing
various music/nature sounds selections, and using current media technology. Staff nurses
can select cultural and age appropriate music and nature sounds and offer choices to
hospice patients. Portable, light weight and easy to use equipment will facilitate their use
for pain and anxiety along with medication. Nurses can develop an instruction manual
based on the procedure and the findings of the study for their hospice settings.

129
Appendix A
Date: ____________ (yy/m/d) Medical Record # ___________
The Effects of Music/Nature Sounds on Cancer Pain and Anxiety in Hospice
Patients Inclusion and Exclusion Criteria Form
CONFIDENTIAL
NOTE:If all of the responses are marked with a *, the person is not eligible to be in this study
Inclusion & Exclusion Criteria Yes No
1. Documented cancer pain at least one in past 24 hours *___ 2. Regularly scheduled (versus prn) analgesics *___ 3. A physical and mental status that would enable the individual to participate in the study *___ 4. Cognitively intact (oriented to person, place, and time) *___ 5. Understand Chinese, Taiwanese, or English *___ 6. At least 18 years of age *___ 7. Documented delayed developmental status *___ 8. Hearing difficulty *___ 9. Severe vision deficiency *___ 10. Known history of musicogenic epilepsy or hypersensitivity to sound *___
Note. *= Not eligible
Music and nature sounds related screening questions 1 Would you like to listen to recorded music or nature sounds while you are here? Yes___ *No___ 2 Do you feel it is appropriate to listen to recorded music or nature sounds while
you are sick and in the hospice center? Yes___ *No___
Eligible Yes___ *No___ Consented Yes___ *No___
Participation status
Agree to participate the study……………………………………………………………Group# ___________ Reason for refusal………………………………………..……………….......................................___________ 1. Not interested 2. Too tired to participate in the study 3. Too much going on in the life 4. Has already in another study 5. Do not want to be bothered 6. Had known musicogenic epilepsy or hypersensitivity to sound (circle the one) 7. No reason 8. Other (specify) _____________________________________________________________

130
Appendix B
Selections of Music, Nature Sounds, and Combination
Music – Chinese
Selection CD Artist 1 I only care about you Dream in the Afternoon Unknown 2 Dream a life time for love Piano and Violin- Dream a life Time
for Love Unknown
3 Bamboo ballad 童話 童畫 巴洛克獨奏家樂團 4 What is in front of my
home? 童話 童畫 巴洛克獨奏家樂團
5 The dream of the red chamber
Dream in the Afternoon Unknown
6 Look back again Piano and Violin- Dream a life time for love
Unknown
7 Love me or love me not Piano and Violin- Dream a life time for love
Unknown
8 Forget who I am 純真年代—橄欖樹 Trio 最好的時光三重奏 9 The forgotten moments 被遺忘的時光 Trio 最好的時光三重奏 10 Drinking with the past Piano and Violin- Dream a life time for
love
11 Like your tenderness 純真年代—橄欖樹 Trio 最好的時光三重奏 12 Daily blue 中國交響世紀—浮世戀情 1 俄羅斯國家交響樂團 13 It’s over 中國交響世紀—戀戀琴聲 1 俄羅斯國家交響樂團 14 Sea waves 中國交響世紀—流金歲月 1 俄羅斯國家交響樂團 15 Another unforgettable love
affair 被遺忘的時光 李哲藝&林天吉&歐陽慧
擩 16 Falling flowers 中國交響世紀—浮世戀情 2 上海交響樂團 17 Could it be a flower 中國交響世紀—浮世戀情 2 上海交響樂團 18 What west wind says 中國交響世紀—浮世戀情 2 上海交響樂團 19 Farewell 中國交響世紀—浮世戀情 2 上海交響樂團 20 Lady Meng-Jiang 中國交響世紀—大地春夢 上海交響樂團 21 Flowing water 中國交響世紀—浮世戀情 2 上海交響樂團 22 So much to say 中國交響世紀—流金歲月 1 中央歌劇芭蕾舞劇院交響
樂團 23 Farewell, Cambridge
(Re-edit) 中國交響世紀—流金歲月 2
中央歌劇芭蕾舞劇院交響
樂團 24 Home sickness Dream in the Afternoon Unknown 25 Dream and poem Dream in the Afternoon Unknown 26 Pieces of autumn poem
(Re-edit) 中國交響世紀—流金歲月 1 中央歌劇芭蕾舞劇院交響
樂團

131
Music – Easy Listening
Selection CD Artist 1 The unforgetting heart The Unforgetting Heart Michael Hoppe 2 Vaya con dios Guitar by Candlelight* Gray Bartlett 3 If I fell/My life Counting the Ways* Ed Gerhard 4 Lake of heart Crystal Glory* Sheng-Di Wang 5 Imagine Guitar by Candlelight Gray Bartlett 6 Quietness Crystal Glory Sheng-Di Wang 7 Moving like a could Chinese Massage for Heart* Xu-Dong Wang 8 Waltz for the lonely Guitar by Candlelight Gray Bartlett 9 Under the moonlight Crystal Glory Sheng-Di Wang 10 Maria Elena Counting the Ways Ed Gerhard 11 Pacifying your heart Chinese Massage for Heart Xu-Done Wang 12 The rose Guitar by Candlelight Gray Bartlett 13 Not a dream Sleep for Body and Mind* Xu-Dong Wang, Jian-Min
Wang 14 Thoughts Crystal Glory Sheng-Di Wang 15 Vincent Guitar by Candlelight Gray Bartlett 16 Wild mountain thyme Counting the Ways Ed Gerhard 17 Printless Crystal Glory Sheng-Di Wang 18 Love me tender Guitar by Candlelight Gray Bartlett 19 Cavatina Guitar by Candlelight Gray Bartlett 20 Renouncement The Unforgetting Heart Hoppe, Michael 21 Clear mirror Crystal Glory Sheng-Di Wang 22 Song of silence Crystal Innocence* Sheng-Di Wang 23 Can’t help falling love Counting the Ways Ed Gerhard 24 Childhood memories The Unforgetting Heart Michael Hoppe 25 Deep thinking Crystal Glory Sheng-Di Wang 26 Let it be me Guitar by Candlelight Gray Bartlett 27 The water is wide Counting the Ways Ed Gerhard 28 To you my friend Guitar by Candlelight Gray Bartlett 29 To all the girls Guitar by Candlelight Gray Bartlett 30 Spring tract Mirror of Water Wang Shun 31 The music of the night Guitar by Candlelight Gray Bartlett
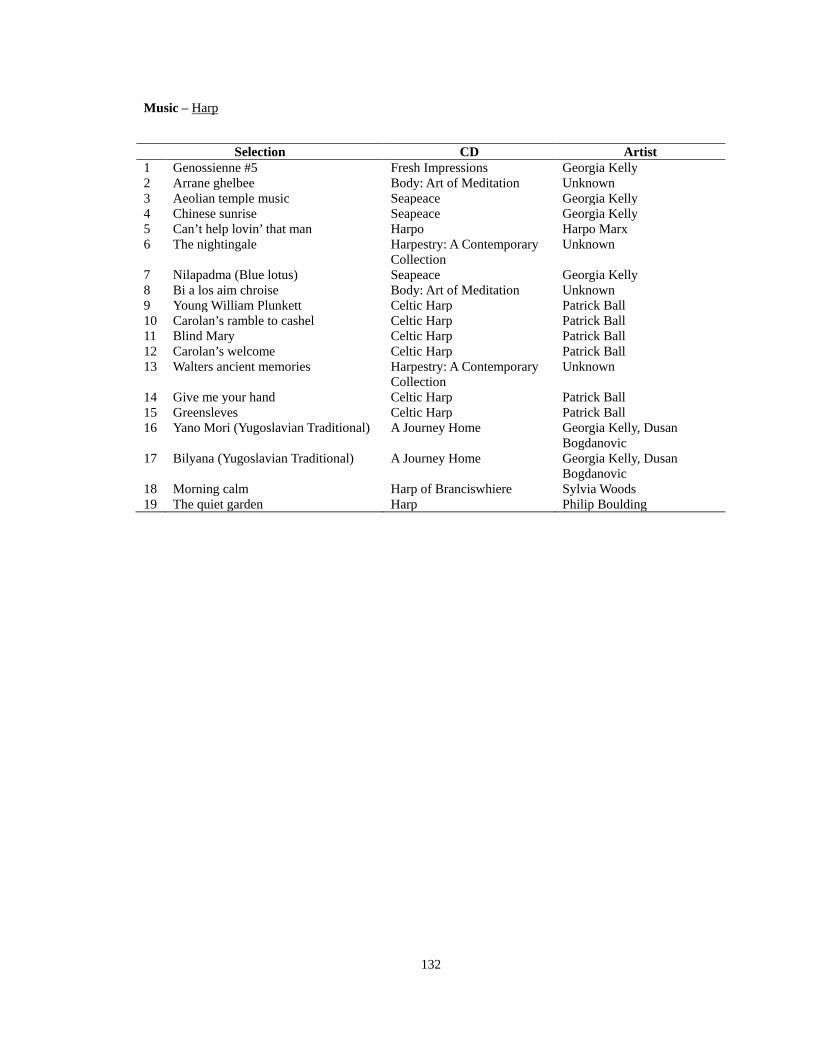
132
Music – Harp
Selection CD Artist 1 Genossienne #5 Fresh Impressions Georgia Kelly 2 Arrane ghelbee Body: Art of Meditation Unknown 3 Aeolian temple music Seapeace Georgia Kelly 4 Chinese sunrise Seapeace Georgia Kelly 5 Can’t help lovin’ that man Harpo Harpo Marx 6 The nightingale Harpestry: A Contemporary
Collection Unknown
7 Nilapadma (Blue lotus) Seapeace Georgia Kelly 8 Bi a los aim chroise Body: Art of Meditation Unknown 9 Young William Plunkett Celtic Harp Patrick Ball 10 Carolan’s ramble to cashel Celtic Harp Patrick Ball 11 Blind Mary Celtic Harp Patrick Ball 12 Carolan’s welcome Celtic Harp Patrick Ball 13 Walters ancient memories Harpestry: A Contemporary
Collection Unknown
14 Give me your hand Celtic Harp Patrick Ball 15 Greensleves Celtic Harp Patrick Ball 16 Yano Mori (Yugoslavian Traditional) A Journey Home Georgia Kelly, Dusan
Bogdanovic 17 Bilyana (Yugoslavian Traditional) A Journey Home Georgia Kelly, Dusan
Bogdanovic 18 Morning calm Harp of Branciswhiere Sylvia Woods 19 The quiet garden Harp Philip Boulding

133
Music –Orchestral
Selection Composer/ CD Artist 1 Symphony #6 Pastorale Beethoven Cleveland Orchestra 2 Clair de lune Debussy Philadelphia Orchestra 3 Air on the G string from Suite #3 in D Bach Bach Festival Chamber 4 Nocturne from a midsummer night’
dream Mendelssohn Cleveland Orchestra
5 Greensleaves Traditional from World Hits
Mantovanil
6 Symphony #1 second movement Brahms London Philharmonic 7 Pachebel: Canon Pachehel English Chamber Orchestra 8 Valse triste Sibelius Berglund Philharmonic 9 Romanze Eine Klein Nachtmusik Mozart Liszt Ferenc Chamber
Orchestra 10 Reverie Debussy Philadelphia Orchestra 11 The swan Classics by candlelight Unknown 12 Wind Serenade No.12, c miinor, K.388 Mozart Effect – Sleep Harnoncourt; Wiener
Mozart-Blaser 13 Piano Concerto, No.24, c minor,K.491 Mozart Effect – Sleep Daniel Barenboim: Berlin
Philharmonic Orchestra 14 Clarinet Concerto, A Major, K.622 Mozart Effect – Sleep Kam, Faerber 15 Horn Concerto, E-flat, K.495 Mozart Effect – Sleep Pyatt, Marriner 16 Serenade In G Major _Eine Kleine
Nachtmusik_ Romance_ Andante Time life classics for kids St. Petersburg Musical Theatre
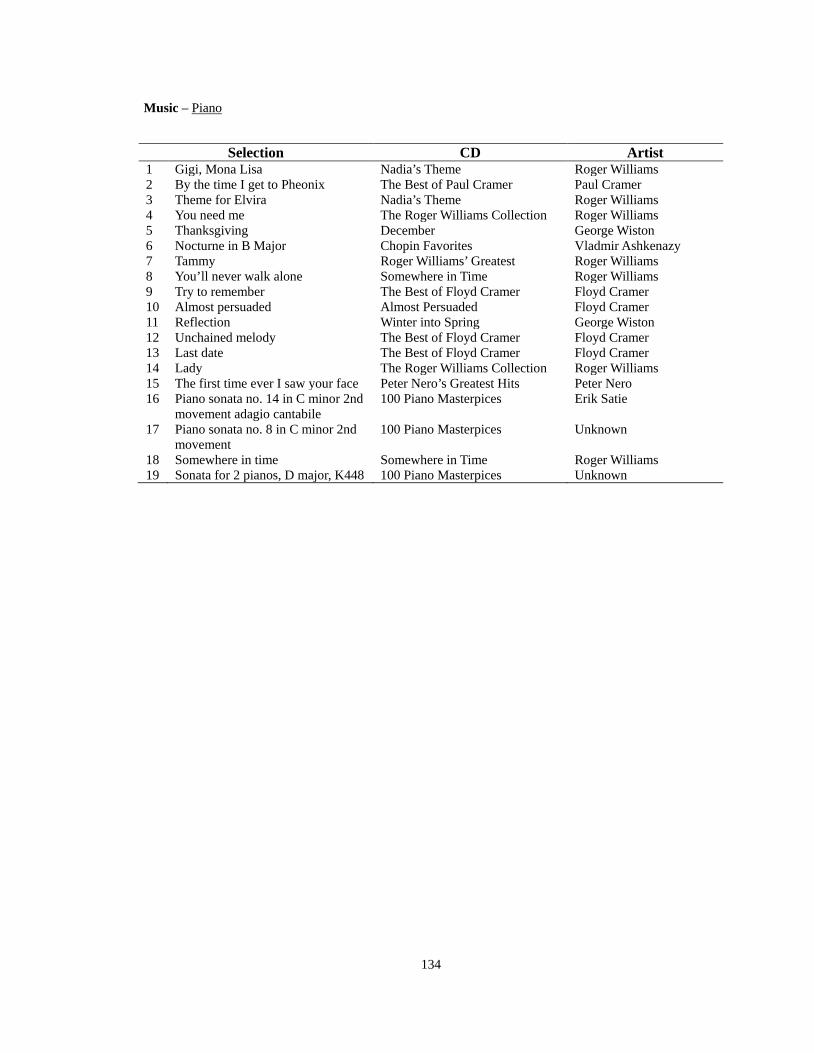
134
Music –
Piano
Selection CD Artist 1 Gigi, Mona Lisa Nadia’s Theme Roger Williams 2 By the time I get to Pheonix The Best of Paul Cramer Paul Cramer 3 Theme for Elvira Nadia’s Theme Roger Williams 4 You need me The Roger Williams Collection Roger Williams 5 Thanksgiving December George Wiston 6 Nocturne in B Major Chopin Favorites Vladmir Ashkenazy 7 Tammy Roger Williams’ Greatest Roger Williams 8 You’ll never walk alone Somewhere in Time Roger Williams 9 Try to remember The Best of Floyd Cramer Floyd Cramer 10 Almost persuaded Almost Persuaded Floyd Cramer 11 Reflection Winter into Spring George Wiston 12 Unchained melody The Best of Floyd Cramer Floyd Cramer 13 Last date The Best of Floyd Cramer Floyd Cramer 14 Lady The Roger Williams Collection Roger Williams 15 The first time ever I saw your face Peter Nero’s Greatest Hits Peter Nero 16 Piano sonata no. 14 in C minor 2nd
movement adagio cantabile 100 Piano Masterpices Erik Satie
17 Piano sonata no. 8 in C minor 2nd movement
100 Piano Masterpices Unknown
18 Somewhere in time Somewhere in Time Roger Williams 19 Sonata for 2 pianos, D major, K448 100 Piano Masterpices Unknown

135
Music – Religious-Buddha
Selection CD Artist 1 Enlightenment 古箏佛讚(十二)照人清涼 閻愛華 2 Respondance 古箏佛讚(十二)照人清涼 閻愛華 3 Compassion 古箏佛讚(十二)照人清涼 閻愛華 4 Freshness 古箏佛讚(十二)照人清涼 閻愛華 5 Walking with breeze Mirror of water 王珣 6 Cool breeze in summer Mirror of water 王珣 7 般若波羅蜜多心經 古箏佛讚(六)心經* 王珣 8 南無本師釋迦牟尼佛 古箏佛讚(六)心經 王珣 9 雲水禪心 古箏佛讚(七)雲水禪心 王珣 10 靈山梵音 古箏佛讚(七)雲水禪心 王珣 11 Deep woods of Zen 古箏佛讚(七)雲水禪心 王珣 12 禪院鐘聲 古箏佛讚(七)雲水禪心 王珣 13 佛門鐘聲 古箏佛讚(七)雲水禪心 王珣

136
Music – Religious_Christian
Selection CD Artist 1 我寧願有耶穌 Piano for quiet time Vol. 2 Unknown 2 明亮的天路 Piano for quiet time Vol. 1 Unknown 3 歌頌救贖主 Piano for quiet time Vol. 2 Unknown 4 至善聖靈 Piano for quiet time Vol. 1 Unknown 5 今來就主 Piano for quiet time Vol. 2 Unknown 6 靠恩得救 Piano for quiet time Vol. 1 Unknown 7 AveMaria Unknown 8 你總要依靠寶血 Piano for quiet time Vol. 2 Unknown 9 讚慕美地(甜蜜的變奏曲) Piano for quiet time Vol. 1 Unknown 10 為將我們將從罪就贖 Piano for quiet time Vol. 2 Unknown 11 面對面 Piano for quiet time Vol. 1 Unknown 12 向高處行 Piano for quiet time Vol. 2 Unknown 13 雖然四面狂風大作 Piano for quiet time Vol. 1 Unknown 14 When you walk through the dark hold your
head high Unknown
15 暫時旅住世上 Piano for quiet time Vol. 1 Unknown 16 看那!快樂的家 Piano for quiet time Vol. 2 Unknown 17 歸我更美家鄉 Piano for quiet time Vol. 1 Unknown 18 萬古盤石 Piano for quiet time Vol. 2 Unknown 19 在天國相見 Piano for quiet time Vol. 1 Unknown 20 我貧窮之福到寶貴之城 Piano for quiet time Vol. 2 Unknown 21 我有最好朋友 Piano for quiet time Vol. 1 Unknown 22 結束世上苦難 Piano for quiet time Vol. 2 Unknown 23 How great thou art Unknown 24 向前直往錫安 Piano for quiet time Vol. 2 Unknown 25 永遠的榮耀 Piano for quiet time Vol. 1 Unknown 26 寶血大權能 Piano for quiet time Vol. 2 Unknown
27 荒蕪之地變玫瑰園 Piano for quiet time Vol. 1 Unknown 28 聖哉聖哉 我知誰掌管明天 至好朋友就是耶
穌 Good’s Tape- Inspirational Unknown
29 Jesus is my shepherd Good’s Tape- Inspirational Unknown 30 與主接近 Piano for quiet time Vol. 2 Unknown

137
Music – Taiwanese
Selection CD Artist 1 No one understand what I feel 純真年代-海海人生 Trio 最好的時光三重奏 2 June Jasmine 純真年代-海海人生 Trio 最好的時光三重奏 3 Wife 純真年代-海海人生 Trio 最好的時光三重奏 4 Little Egret 璀璨西灣 巴洛克獨奏家樂團 5 When I open the door to my
heart The Unforgettable Love Affair Trio 最好的時光三重奏
6 A white peony 中國交響世紀-台灣幻想曲 1 Chinese Orchestra 7 The flower in raining night 中國交響世紀-台灣幻想曲 1 Chinese Orchestra 8 The crying of homeless birds 中國交響世紀-台灣幻想曲 1 Chinese Orchestra 9 Moonlight sorrow 中國交響世紀-台灣幻想曲 1 Chinese Orchestra 10 Life 純真年代-海海人生 Trio 最好的時光三重奏 11 Dream of riverside 純真年代-海海人生 Trio 最好的時光三重奏 12 The taste of love The Unforgettable Love Affair Trio 最好的時光三重奏 13 The gloomy night Faraway on a Moonlit Night Stamic Quartet/New Prague
Trio 14 Red in the snow 中國交響世紀-戀戀情深-2 中央歌劇芭蕾舞劇院交響
樂團 15 Pillow for couple 中國交響世紀-戀戀情深-2 中央歌劇芭蕾舞劇院交響
樂團 16 Love like thread and needle 中國交響世紀-戀戀情深-2 中央歌劇芭蕾舞劇院交響
樂團 17 Recalling the past The Unforgettable Love Affair Trio 最好的時光三重奏 18 Faraway on a moonlit night Faraway on a moonlit night Stamic Quartet/New Prague
Trio 19 When the gong’s sound raises 中國交響世紀-台灣幻想曲 2 北京中央交響樂團 20 The unforgettable love affair 中國交響世紀-台灣幻想曲 2 北京中央交響樂團 21 Weeding broken net 中國交響世紀-台灣幻想曲 2 北京中央交響樂團 22 Raining night with autumn wind 中國交響世紀-台灣幻想曲 2 北京中央交響樂團 23 Nocturne of southern city 中國交響世紀-台灣幻想曲 2 北京中央交響樂團 24 Awaiting your early return
(Re-edit) 中國交響世紀-台灣幻想曲 2 北京中央交響樂團
25 Lovesick when the spring breeze blew (Re-edit)
中國交響世紀-台灣幻想曲 2 北京中央交響樂團

138
Nature Sounds – Birds
Selection CD Artist 1 晨曦霧影(Re-edit) 最近的天堂-生態現場 廖東坤 2 議論-小彎嘴/山紅頭(Re-edit) 最近的天堂-生態現場 廖東坤 3 晨鳥之歌(Re-edit) 森林狂想曲 吳金黛 4 Wild birds in Taiwan-1 (Re-edit) 野鳥鳴唱 風潮唱片 5 Wild birds in Taiwan-2 (Re-edit) 野鳥鳴唱 風潮唱片 6 Wild birds in Taiwan-3 (Re-edit) 野鳥鳴唱 風潮唱片 7 Wild birds in Taiwan-4 (Re-edit) 野鳥鳴唱 風潮唱片 8 晨鳥之歌-2 (Re-edit) 野鳥鳴唱 風潮唱片 9 最近的天堂鳥之生態 (Re-edit) 野鳥鳴唱 風潮唱片 10 Wild birds in Taiwan-5 (Re-edit) 野鳥鳴唱 風潮唱片 11 Wild birds in Taiwan-6 (Re-edit) 野鳥鳴唱 風潮唱片 12 Wild birds in Taiwan-7 (Re-edit) 野鳥鳴唱 風潮唱片 13 Wild birds in Taiwan-8 (Re-edit) 野鳥鳴唱 風潮唱片

139
Nature Sounds – Forests
Selection CD Artist 1 Monterey magic (Re-edit) The Blue Mountains Experience Unknown 2 Rivers run deep (Re-edit) Body: Art of Meditation Unknown 3 Wenworth falls (Re-edit) The Blue Mountains Experience Unknown 4 Mountain Life (Re-edit) The Blue Mountains Experience Unknown 5 Spirits of the forests (Re-edit) The Blue Mountains Experience Unknown 6 Sounds of the forest (Re-edit) Forest Mitsuhiro 7 Poem of the forest (Re-edit) Forest Mitsuhiro 8 Forest sonata (Re-edit) Forest Sonata 吳金黛 9 Sleeping forests (Re-edit) Forest Sonata 吳金黛 10 Song of autumn stream (Re-edit) 青蛙四季唱遊 風潮唱片 11 Winding (Re-edit) 最近的天堂-生態現場 廖東坤

140
Nature Sounds – Frogs
Selection CD Artist 1 早春的太魯閣山林(Re-edit) 青蛙四季唱遊 風潮唱片 2 陽明山的春之夢幻(Re-edit) 青蛙四季唱遊 風潮唱片 3 拜訪溪頭竹林的春天(Re-edit) 青蛙四季唱遊 風潮唱片 4 阿里山的四月(Re-edit) 青蛙四季唱遊 風潮唱片 5 池畔(Re-edit) 最近的天堂-生態現場 廖東坤 6 初夏的嘉義農場(Re-edit) 青蛙四季唱遊 風潮唱片 7 嘉南平原的青蛙精靈(Re-edit) 青蛙四季唱遊 風潮唱片 8 虎山溪的夏天(Re-edit) 青蛙四季唱遊 風潮唱片 9 樹蛙之歌(Re-edit) 森林狂想曲 吳金黛 10 花東稻田之歌(Re-edit) 青 四季唱遊 風潮唱片 11 石門水庫大頭蛙的秋天(Re-edit) 青蛙四季唱遊 風潮唱片 12 擁擠(Re-edit) 最近的天堂-生態現場 廖東坤 13 發現水窪(Re-edit) 最近的天堂-生態現場 廖東坤 14 溫泉鄉的青蛙(Re-edit) 青蛙四季唱遊 風潮唱片 15 台灣青蛙之一(Re-edit) 青蛙四季唱遊 風潮唱片 16 群蛙暢鳴 1 (Re-edit) 青蛙四季唱遊 風潮唱片 17 群蛙暢鳴 2 (Re-edit) 青蛙四季唱遊 風潮唱片 18 群蛙暢鳴 3 (Re-edit) 青蛙四季唱遊 風潮唱片 19 群蛙競鳴 Frogs chirping (Re-edit) 青蛙四季唱遊 風潮唱片
141
Nature Sounds – Night Life
Selection CD Artist 1 Dusk(Re-edit) 夜的節目單 風潮唱片 2 Country evening breeze(Re-edit) 夜的節目單 風潮唱片 3 Starry night(Re-edit) 夜的節目單 風潮唱片 4 Silvery hills(Re-edit) 夜的節目單 風潮唱片 5 Summer night of Shan-Ping(Re-edit) 青蛙 四季唱遊 風潮唱片 6 Autumn night of Fu-Shan(Re-edit) 青蛙 四季唱遊 風潮唱片 7 The beginning of winter in
Wu-Lai(Re-edit) 青蛙 四季唱遊 風潮唱片
8 Free time(Re-edit) 最近的天堂 生態現場 廖東坤 9 Ano Nuevo(Re-edit) 腦內革命 Unknown 10 Hot summer (Re-edit) 夜的節目單 風潮唱片 11 In the night(Re-edit) 夜的節目單 風潮唱片 12 Night lullaby (Re-edit) 夜的節目單 風潮唱片 13 Nocturnal(Re-edit) 夜的節目單 風潮唱片 14 Dream(Re-edit) 夜的精靈 風潮唱片

142
Combination – Ocean
Selection CD Artist 1 三貂角 Shandau corner (Re-edit) 台灣海聲實錄 吳金黛 2 九棚(Re-edit) 台灣海聲實錄 吳金黛 3 和平島 Peace island (Re-edit) 台灣海聲實錄 吳金黛 4 戲水 Play in the ocean (Re-edit) 台灣海聲實錄 吳金黛 5 流星的夜空 Night of shooting stars (Re-edit) On the Beach Unknown 6 海之聲 1 Ocean sounds-1 (Re-edit) On the Beach Unknown 7 海之聲 2 Ocean sounds-2 (Re-edit) On the Beach Unknown 8 海之聲 3 Ocean sounds-3 (Re-edit) On the Beach Unknown 9 海之聲 4 Ocean sounds-4 (Re-edit) On the Beach Unknown 10 海之聲 5 Ocean sounds-5 (Re-edit) On the Beach Unknown 11 白砂枋山四草(Re-edit) 台灣海聲實錄 吳金黛 12 豐濱 Fengbin (Re-edit) 台灣海聲實錄 吳金黛 13 都蘭 Sulan (Re-edit) 台灣海聲實錄 吳金黛 14 龜山島+蘭嶼(Re-edit) 台灣海聲實錄 吳金黛

143
Combination – Birds
Selection CD Artist 1 Poem of forest Forest Mitsuhiro 2 Fragrance of wind Daydream in the grove 廣橋貞紀子 3 Green Air Daydream in the grove 廣橋貞紀子 4 Sensitive Plants It’s Summer Time 螢火蟲 5 Breeze of cloud Daydream in the grove 広橋貞紀子 6 Fog festival-the other side of the forest Forest Mitsuhiro 7 Autumn Breeze 三顆貓餅乾 繪本音樂專輯 8 Morning visit Forest Mitsuhiro 9 Dots of sunlight Songbirds 吳金黛 10 Songs of water birds Songbirds 吳金黛 11 Morning songs 森林狂想曲 吳金黛 12 Love song for birds 森林狂想曲 吳金黛 13 Nature song of birds-1 (Re-edit) The Nature- Birds Unknown 14 Nature song of birds-2 (Re-edit) The Nature- Birds Unknown 15 Nature song of birds-3 (Re-edit) The Nature- Birds Unknown

144
Combination – Forests
Selection CD Artist 1 Beyond The Reef(Re-edit) 腦內革命 Unknown 2 Overture-The Mist(Re-edit) 最近的天堂 林海 3 Point Lobos(Re-edit) 腦內革命 Unknown 4 Your Warm Shaded Forest(Re-edit) MIND art of meditation Various Artists 5 Summer dream(Re-edit) Sea Relieving Stress –On the
Beach 6 Spirits of forests(Re-edit) Daydream in the grove 廣橋真紀子 7 Natures Creation (Re-edit) The Blue Mountains
Experience Ken Davis
8 Shining waves(Re-edit) 春物語 Mitsuhiro 9 Monterey Magic(Re-edit) 腦內革命 Unknown 10 Rivers Run Deep(Re-edit) Body Art of Meditation Various Artists 11 New green of forest(Re-edit) 春物語 Mitsuhiro 12 Greensleves(Re-edit) 腦內革命 Unknown 13 Tranquil Garden (Re-edit) The Blue Mountains
Experience Ken Davis
14 Falling leaves(Re-edit) 山居歲月 螢火蟲 15 Morning, subtropical(Re-edit) 森林狂想曲 吳金黛 16 Water path(Re-edit) 森林狂想曲 吳金黛 17 Sleeping forests(Re-edit) 森林狂想曲 吳金黛 18 Tree of hope(Re-edit) 山居歲月 螢火蟲 19 Misty Morning (Re-edit) Isotonic sound- Rain Unknown 20 Southern dreamer-Forests(Re-edit) The Unforgetting Heart Michael Hoppe` 21 The Wind through the rainforests
(Re-edit) 最近的天堂 小莊

145
Comibnation – Frogs
Selection CD Artist 1 Gabriel’s oboe(Re-edit) Into the Mist David Agnew 2 Song for Sarah(Re-edit) Touching Beauty Michael Hoppe` 3 Summer of 300 years(Re-edit) Touching Beauty Michael Hoppe` 4 Summer dusk Summer Mitsuhiro 5 Summer shadow Summer Mitsuhiro 6 Spring finally Spring Mitsuhiro 7 Looking at each other(Re-edit) Looking at Each Other 黃愛蓮 8 Autumn(Re-edit) 青蛙四季唱遊 風潮唱片 9 Invitation from autumn Autumn Mitsuhiro 10 Autumn sky Autumn Mitsuhiro 11 Brown avenue(Re-edit) Autumn Mitsuhiro 12 The smell of happiness(Re-edit) Moon Light, lavender Cincin Lee 13 Dancing snow on the
hills(Re-edit) Winter Unknown

146
Combination – Night Life
Selection CD Artist 1 Evening(Re-edit) 夜的精靈 風潮唱片 2 Sunshine, silence(Re-edit) 山居歲月 螢火虫 3 A Night Banquet With Pan(Re-edit) 最近的天堂 彭靖 4 Autumn night Autumn Mitsuhiro 5 And, again Autumn Mitsuhiro 6 Starry night(Re-edit) 夜的精靈 風潮唱片 7 An Encounter(Re-edit) 最近的天堂 楊錦聰 8 Ano Nuevo Body: Art of Meditation unknown 9 Afro Cuban Lullabye(Re-edit) Body: Art of Meditation unknown 10 Silver hills(Re-edit) 夜的精靈 風潮唱片 11 Dream(Re-edit) 夜的精靈 風潮唱片 12 Secrete garden(Re-edit) 風和 日麗 螢火虫 13 Lightning Isotonic Sound-Rain Unknown 14 Dancing in the night(Re-edit) 夢的延長線 范宗沛 15 Norwegian lakes and woods(Re-edit) Fantasia of Tuscany Cincin Lee 16 Cloud, and the sky Summer Mitsuhiro 17 Sea of clouds(Re-edit) It’s Summer Time 螢火蟲

147
Combination – Ocean
Selection CD Artist 1 Gymnopedie No. 1&3(Re-edit) MIND art of meditation Various Artists 2 White Sand On the Beach Unknown 3 Playing in the ocean My Ocean 吳金黛 4 Blue horizon Isotonic Sound Sea 高垣直美 5 Lighten Up Ocean Dreams Dean Evenson 6 My ocean My Ocean 吳金黛 7 Tall ships 腦內革命 Unknown 8 Yellows tone 腦內革命 Unknown 9 Summer dream On the Beach Unknown 10 Deep blue My Ocean 吳金黛 11 Missing the far away On the Beach Unknown 12 Deeper Sanctuary Ocean Dreams Dean Evenson 13 Night of shooting stars On the Beach Unknown 14 Recalling the Past Voyage to Paradise Matthew Lien 15 Lapping on the beach Summer Mitsuhiro 16 Ocean watching My Ocean 吳金黛 17 Lightly Salted Ocean Dreams Dean Evenson 18 Light of dusk My Ocean 吳金黛 19 Smooth Drifting Ocean Dreams Dean Evenson 20 Island of star My Ocean 吳金黛 21 Sand print My Ocean 吳金黛 22 Coral dance(Re-edit) 海洋嬉遊記 吳金黛

148
Appendix C
The Effects of Music/Nature Sounds on Cancer Pain and Anxiety in Hospice Patients Demographic Data Questionnaire
CONFIDENTIAL
NOTE: Code missing data: 999; N/A: 888; not able to answer(NAA): 777 1. Admission Date (yy/m/d)..………………………………………..……………2. Date of withdrawal (yy/m/d)…………………………….…………………….______________
______________
3. Primary reason for withdrawal……………..…………………………..........______________ 1. Died 2. Condition deteriorated 3. Not interested 4. Too tired to participate in the study 5. Too much going on in their life 6. Does not want to be bothered 7. Did not like the intervention (MU, NS, CB) 8. No reason 9. Other (specify ___________________________________________________)
4. Date discharged from the unit (yy/m/d)…………………………………….______________ 5. Reason for discharge ………………………………..………...........................______________
1. Died 2. AAD (Against Advise Discharge) 3. Transfer to other facility for continuous care 4. Go home for continuous care 5. Other (Specify ___________________________________________________)
6. Using Chanting box………..……………………………………….……………..______________ 1. No 2. Yes, once in a while (< 8 hours per day) 3. Yes, sometimes (>8 hours but < 16 hours per day) 4. Yes, usually (>16 hours but < 24 hours) 5. Yes, always (24 hours continuous listening)

149
7. Age (Day of birth: _______________yy/m/d)....…………..…..……..……….._____________
Obtained from the chart:
8. Gender ..………………………………………………..………….....…………….._____________ 1. Male 2. Female
9. Primary language used ……………………………………..............................._____________ 1. Chinese 2. Taiwanese 3. English
10. Primary religious belief ………………………………………………………….._____________ 1. None 2. Folklore cultural beliefs 3. Buddhism 4. Taoism 5. Christian 6. Catholic 7. Other (Specify ________________________________________________)
11. Years of education ……………………………………..…………………………_____________ 1. Self study (0 years) 2. Elementary (1-6 years) 3. Junior High School (7-9 years) 4. Senior High School/ Vocational High School (10-12 years) 5. College or University (2-year/3-year/4-year/5-year program) (13-16 years) 6. Masters degree (17-19 years) 7. Doctorate (≧ 20 years)
12. Marital status ………………………………………………................................._____________ 1. Never married 2. Married 3. Widowed 4. Divorced 5. Separated
13. Number of children ………………..……………………………………………._____________
14. Use of cigarettes …………………………………………………………………_____________ 1. No 2. Yes
i. Have used for __________years, but stopped for __________years ii. Have used for __________years, ______ Pack Per Day (PPD)

150
15. Use of alcohol …………………………………………………………………….______________ 1. No 2. Yes
i. Drink occasionally ii. Drink ________ Glass Per Day (GPD)
16. Type of cancer (Original) …………………………..…………………………..______________ 1. Unknown primary 2. Liver 3. Colon/Rectal 4. Lung 5. Breast 6. Digestive/Gastrointestinal 7. Ovarian 8. Cervical 9. Pancreas 10. Prostate 11. Laryngeal 12. Nasopharyngeal 13. Bone 14. Esophagus 15. Brain 16. Sarcoma 17. Hematological/Blood 18. Skin 19. Lymphoma 20. Kidney/Bladder 21. Other cancer (Specify __________________________________________)
17. Documented pain events in past 24 hours (times) ……………………....______________ 18. Documented highest pain score in past 24 hours ……………………...______________ 19. Documented lowest pain score in past 24 hours … ..……………..……..______________ 20. The most recent documented breakthrough pain event (yy/m/d)………..______________
Description ____________________________________________________________________________________________________________________________________________________
21. The most recent documented pain score ………………..…………………..______________ 22. Documented anxiety disorder ________________________________________________ 23. Documented anxiety events in past 24 hours (times)……………………..______________ 24. Documented highest anxiety score in past 24 hours ……………………..______________ 25. Documented lowest anxiety score in past 24 hours ………………………______________ 26. The most recent documented anxiety event (yy/m/d)…….………….........______________
Description ____________________________________________________________________________________________________________________________________________________
27. The most recent documented anxiety score …………..…………………..______________

151
Obtain from interview
28. Race /Ethnic background……………………………………………..............______________
:
1. Chinese 2. Taiwanese 3. Hakkanese 4. Aboriginal 5. Mainlander 6. Indonesian 7. Thai 8. Vietnamese 9. Philippine 10. Caucasian 11. Other (Specify ___________________________________________________)
29. Number of significant others………………………………………………….______________
(Circle all applied, but record the total number of significant others) 1. Spouse 2. Partner 3. Sibling (Specify _______________________________________________) 4. Friend (Specify _______________________________________________) 5. Spiritual mentor 6. Other (Specify ________________________________________________)
30. Monthly income ………………………………………………………………….._____________
1. No income at all 2. No stable income 3. <10,000 NT 4. 10,001 – 20,000 NT 5. 20,001 – 30,000 NT 6. 30,001 – 40,000 NT 7. 40,001 – 50,000 NT 8. 50,001 – 60,000 NT 9. >60,001 NT 10. Do not care to provide

152
* 777-NAA; 888-N/A; 999-Missing 31. Types of music liked(Ask every music type, do not leave blank)
Ask: Please tell me what types of music you like, do not like, or not sure.
Music types NO (0) Don’t Know (1) YES (2)
a. No preference
b. Classical
c. Jazz
d. Blues
e. New age
f. English popular music
g. Religious
h. Crystal music
i. Light music
j. Traditional Chinese orchestra
k. Chinese folk music
l. Chinese popular music
m. Taiwanese folk music
n. Taiwanese popular music
o. School folk music
p. Birds
q. Ocean waves
r. Frogs
s. Night life of nature
t. Forest
u. Wind
v. Stream
w. Other _________________

153
* 777-NAA; 888-N/A; 999-Missing
32. Experience with complementary and alternative therapy (Ask every therapy on the list, do not leave blank)
Complementary/Alternative Therapy No (0) Yes (1) Currently use No(0), Yes(1)
a. Acupuncture
b. Acupressure
c. Aromatherapy
d. Art therapy
e. Biofeedback
f. Chi Kung
g. Guided imagery
h. Healing touch / Therapeutic touch
i. Herbal remedy
j. Hypnosis
k. Massage
l. Music therapy
m. Chiropractic
n. Never used
o. Other _____________________________
p. Other _____________________________
q. Other _____________________________
r. Other _____________________________

154
VAS Example
Explain scales:
PAIN
The line is the pain scale. It is a line that goes from “no pain” to “the most pain imaginable.” If you are having a lot of pain right now, you will make your mark closer to the right end. If you are not having much pain, you will make your mark closer to the left end. I want you to mark how much pain you are having on the line of the scale. (show scale to the participant)
Bad examples
No Pain Most Pain Imaginable
Good example
No Pain Most Pain Imaginable
Please use one slash that cross the line at the point that shows how much pain you are having now. Make your mark like this: l . You may mark anywhere on this line now.
Pain Scale
Practice
No Pain Most Pain Imaginable

155
STUDY ID _________
Day 1 Time _____ Pretest
This line is a pain scale. It is a line that goes from “no pain” to “the most pain imaginable.” If you are having a lot of pain right now, you will make your mark closer to the left end. If you are not having much pain, you will make your mark closer to the right end. I want you to mark how much pain you are having right now on the line of the scale. (show scale to the participant)
33.
Please use one slash that cross the line at the point that shows how much pain you are having now. Make your mark like this: . You may mark anywhere on this line now.
PAIN Scale
Score _____
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. This line is an anxiety scale. It is a line that goes from “no anxiety” to “the most anxiety imaginable.” If you are having a lot of anxiety right now, you will make your mark closer to the left end. If you are not having much anxiety, you will make your mark closer to the right end.
34.
Please use one slash that cross the line at the point that shows how much anxiety you are having now. Make your mark like this: . You may mark anywhere on this line now.
ANXIETY Scale
Score _____
No Anxiety Most Anxiety Imaginable
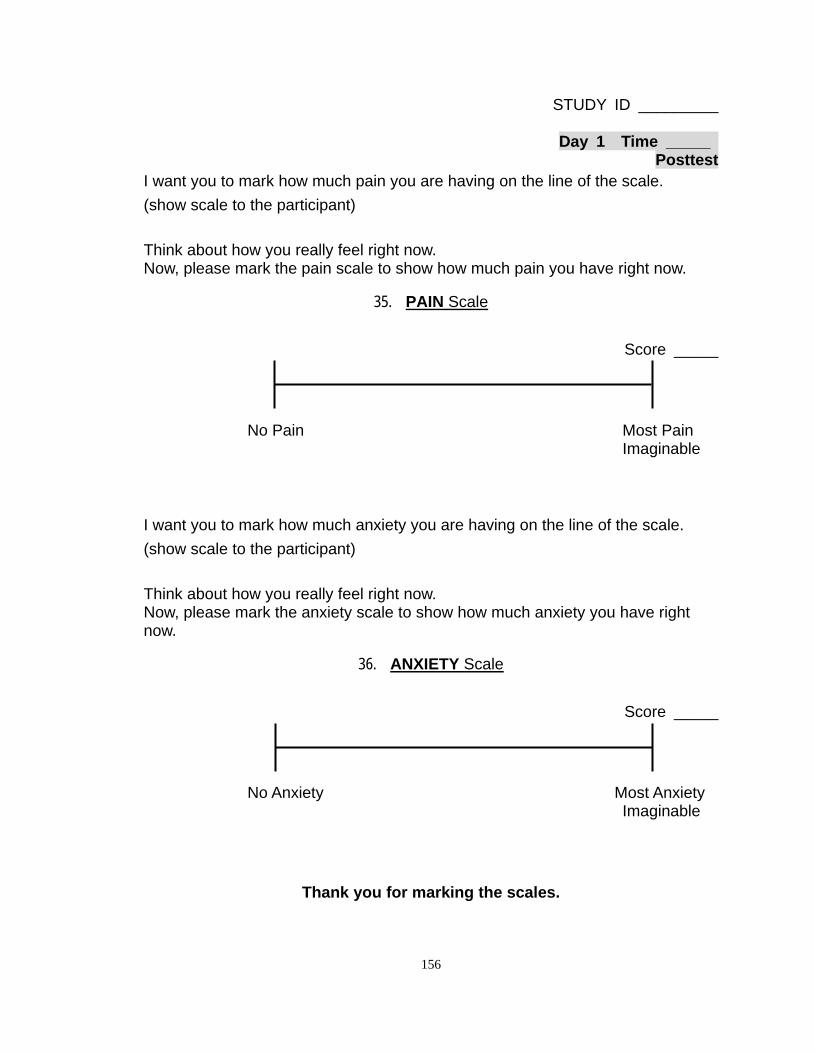
156
STUDY ID _________
Day 1 Time _____ Posttest
I want you to mark how much pain you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the pain scale to show how much pain you have right now.
35.
Score _____
PAIN Scale
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the anxiety scale to show how much anxiety you have right now.
36.
Score _____
ANXIETY Scale
No Anxiety Most Anxiety Imaginable
Thank you for marking the scales.

157
STUDY ID _________
Day 2 Time _____ Pretest
This line is a pain scale. It is a line that goes from “no pain” to “the most pain imaginable.” If you are having a lot of pain right now, you will make your mark closer to the left end. If you are not having much pain, you will make your mark closer to the right end. I want you to mark how much pain you are having right now on the line of the scale. (show scale to the participant)
37.
Please use one slash that cross the line at the point that shows how much pain you are having now. Make your mark like this: . You may mark anywhere on this line now.
PAIN Scale
Score _____
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. This line is an anxiety scale. It is a line that goes from “no anxiety” to “the most anxiety imaginable.” If you are having a lot of anxiety right now, you will make your mark closer to the left end. If you are not having much anxiety, you will make your mark closer to the right end.
38.
Please use one slash that cross the line at the point that shows how much anxiety you are having now. Make your mark like this: . You may mark anywhere on this line now.
ANXIETY Scale
Score _____
No Anxiety Most Anxiety Imaginable

158
STUDY ID _________
Day 2 Time _____ Posttest
I want you to mark how much pain you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the pain scale to show how much pain you have right now.
39.
Score _____
PAIN Scale
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the anxiety scale to show how much anxiety you have right now.
40.
Score _____
ANXIETY Scale
No Anxiety Most Anxiety Imaginable
Thank you for marking the scales.

159
STUDY ID _________
Day 3 Time _____ Pretest
This line is a pain scale. It is a line that goes from “no pain” to “the most pain imaginable.” If you are having a lot of pain right now, you will make your mark closer to the left end. If you are not having much pain, you will make your mark closer to the right end. I want you to mark how much pain you are having right now on the line of the scale. (show scale to the participant)
41.
Please use one slash that cross the line at the point that shows how much pain you are having now. Make your mark like this: . You may mark anywhere on this line now.
PAIN Scale
Score _____
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. This line is an anxiety scale. It is a line that goes from “no anxiety” to “the most anxiety imaginable.” If you are having a lot of anxiety right now, you will make your mark closer to the left end. If you are not having much anxiety, you will make your mark closer to the right end.
42.
Please use one slash that cross the line at the point that shows how much anxiety you are having now. Make your mark like this: . You may mark anywhere on this line now.
ANXIETY Scale
Score _____
No Anxiety Most Anxiety Imaginable

160
STUDY ID _________
Day 3 Time _____ Posttest
I want you to mark how much pain you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the pain scale to show how much pain you have right now.
43.
Score _____
PAIN Scale
No Pain Most Pain Imaginable I want you to mark how much anxiety you are having on the line of the scale. (show scale to the participant) Think about how you really feel right now. Now, please mark the anxiety scale to show how much anxiety you have right now.
44.
Score _____
ANXIETY Scale
No Anxiety Most Anxiety Imaginable (Intervention group only) 45. How much did you like the assigned intervention? (circle the number)
1 2 3 4 5 Disliked Liked Very Much
46. Have you had any problem or comment being in the study?
_____________________________________________________________________
Thank you for marking the scales and being in the study.

161
47. Intervention used between testing times
Intervention (circle one) MU/ NS/ CB
Start song (a) Ending song (b) Total minutes used
(c) Reason for use (d)
1. Day 1 treatment Treatment 1
2. Day 1 to Day 2 Reason
3. Day 2 treatment Treatment 2
4. Day 2 to Day 3 Reason
5. Day 3 treatment Treatment 3
Reason for use
0. Regular treatment 1. Feel pain 2. Feel anxious 3. Want to relax 4. Like the intervention 5. _______________ 6. _______________ 7. _______________ 8. _______________
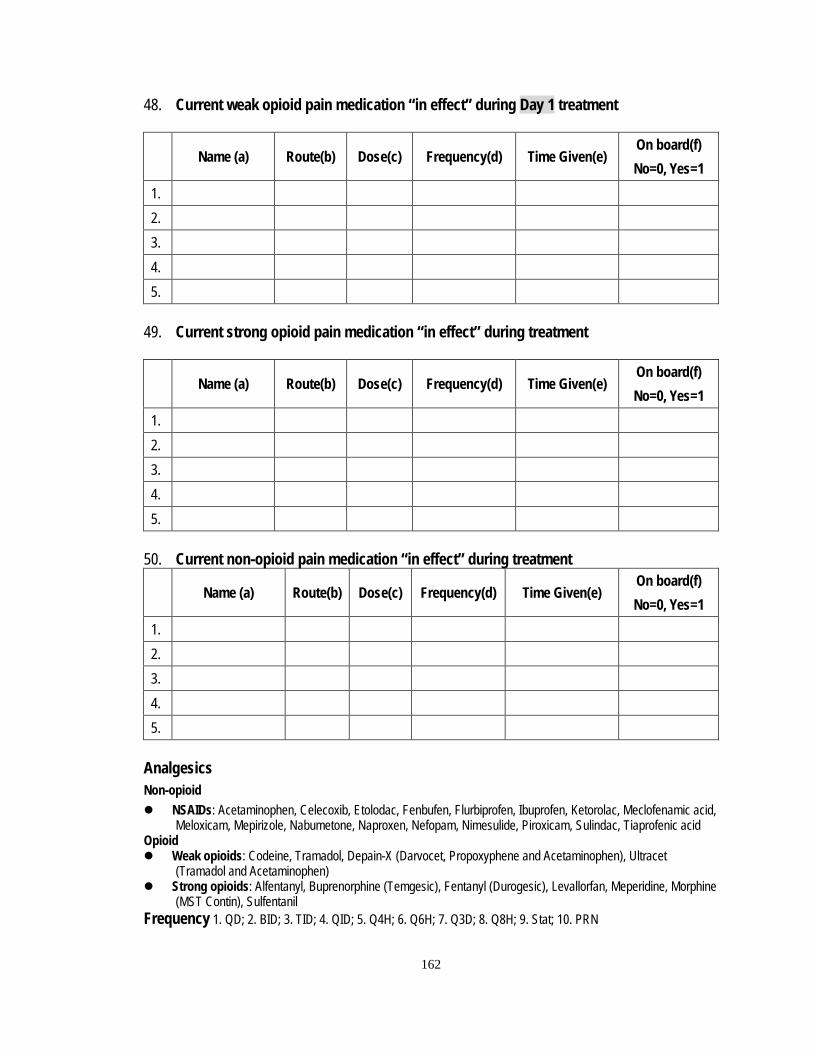
162
48. Current weak opioid pain medication “in effect” during Day 1 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
49. Current strong opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
50. Current non-opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
Analgesics Non-opioid NSAIDs: Acetaminophen, Celecoxib, Etolodac, Fenbufen, Flurbiprofen, Ibuprofen, Ketorolac, Meclofenamic acid,
Meloxicam, Mepirizole, Nabumetone, Naproxen, Nefopam, Nimesulide, Piroxicam, Sulindac, Tiaprofenic acid Opioid Weak opioids: Codeine, Tramadol, Depain-X (Darvocet, Propoxyphene and Acetaminophen), Ultracet
(Tramadol and Acetaminophen) Strong opioids: Alfentanyl, Buprenorphine (Temgesic), Fentanyl (Durogesic), Levallorfan, Meperidine, Morphine
(MST Contin), Sulfentanil Frequency 1. QD; 2. BID; 3. TID; 4. QID; 5. Q4H; 6. Q6H; 7. Q3D; 8. Q8H; 9. Stat; 10. PRN

163
51. Current weak opioid pain medication “in effect” during Day 2 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
52. Current strong opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
53. Current non-opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
Analgesics Non-opioid NSAIDs: Acetaminophen, Celecoxib, Etolodac, Fenbufen, Flurbiprofen, Ibuprofen, Ketorolac, Meclofenamic acid,
Meloxicam, Mepirizole, Nabumetone, Naproxen, Nefopam, Nimesulide, Piroxicam, Sulindac, Tiaprofenic acid Opioid Weak opioids: Codeine, Tramadol, Depain-X (Darvocet, Propoxyphene and Acetaminophen), Ultracet
(Tramadol and Acetaminophen) Strong opioids: Alfentanyl, Buprenorphine (Temgesic), Fentanyl (Durogesic), Levallorfan, Meperidine, Morphine
(MST Contin), Sulfentanil Frequency 1. QD; 2. BID; 3. TID; 4. QID; 5. Q4H; 6. Q6H; 7. Q3D; 8. Q8H; 9. Stat; 10. PRN
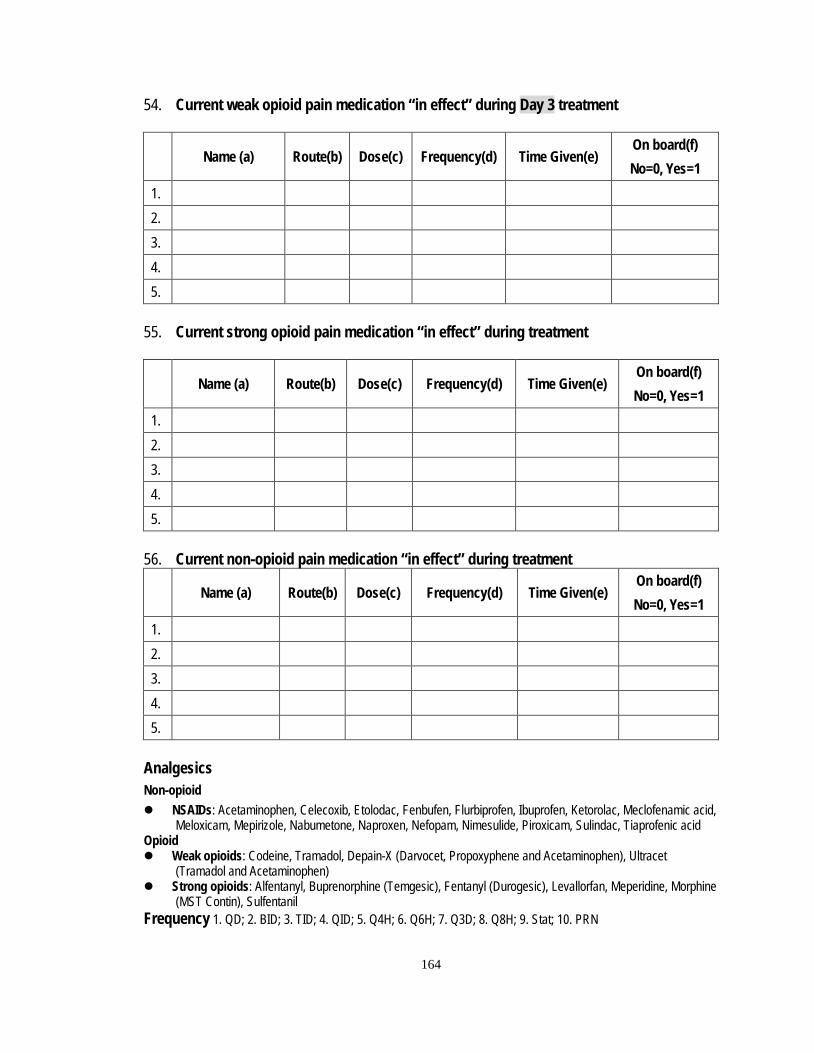
164
54. Current weak opioid pain medication “in effect” during Day 3 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
55. Current strong opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
56. Current non-opioid pain medication “in effect” during treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
Analgesics Non-opioid NSAIDs: Acetaminophen, Celecoxib, Etolodac, Fenbufen, Flurbiprofen, Ibuprofen, Ketorolac, Meclofenamic acid,
Meloxicam, Mepirizole, Nabumetone, Naproxen, Nefopam, Nimesulide, Piroxicam, Sulindac, Tiaprofenic acid Opioid Weak opioids: Codeine, Tramadol, Depain-X (Darvocet, Propoxyphene and Acetaminophen), Ultracet
(Tramadol and Acetaminophen) Strong opioids: Alfentanyl, Buprenorphine (Temgesic), Fentanyl (Durogesic), Levallorfan, Meperidine, Morphine
(MST Contin), Sulfentanil Frequency 1. QD; 2. BID; 3. TID; 4. QID; 5. Q4H; 6. Q6H; 7. Q3D; 8. Q8H; 9. Stat; 10. PRN

165
57. Current anxiolytics medication “in effect” during Day 1 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
58. Current anxiolytics medication “in effect” during Day 2 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
59. Current anxiolytics medication “in effect” during Day 3 treatment
Name (a) Route(b) Dose(c) Frequency(d) Time Given(e) On board(f) No=0, Yes=1
1.
2.
3.
4.
5.
1. Benzodiazepines: Alprazolam (Xanax), Diazepam (Valium), Chlordiazepoxide (Librium, Librax, Libritabs), Lorazepam
(Ativan), Clorazepate (Azene), Oxazepam (Serax) 2. Buspirone (BuSpar) 3. Tricyclics (TCAs): amitriptyline (Elavil), clomipramine (Anafranil), doxepin (Sinequan), imipramine, (Tofranil),
nortriptyline (Pamelor), protriptyline (Vivactil), trimipramine (Surmontil) 4. SSRIs: citalopram (Celexa), fluvoxamine (Luvox), paroxetine (Paxil), fluoxetine (Prozac), sertraline (Zoloft)
Frequency 1. QD; 2. BID; 3. TID; 4. QID; 5. Q4H; 6. Q6H; 7. Q3D; 8. Q8H; 9. Stat; 10. PRN

166
Appendix D
Comparison of Two Hospice Units
KMUH SJH
Variable n M (SD) n M (SD) t P
Admission (n/month) - 30.71 (4.39) - 16.5 (2.23) 7.61 < .001 Discharge (n/month) - 30.57 (5.50) - 16.86 (3.72) 5.46 < .001 Length of stay (days) - 13.18 (2.08) - 14.69 (4.18) - .85 .41 Occupancy rate (%/month) - 83.23 (4.91) - 70.37 (5.30) 4.71 .001 Age of RN (years) 18 34.89 (6.06) 12 31.67 (4.74) 1.55 .13 Experience in hospital (years) 18 10.89 (7.41) 12 6.67 (4.31) 1.97 .06 Experience in hospice (years) 18 6.33 (2.03) 12 6.67 (4.31) - .25 .81
Note. KMUH = Kaohsiung Medical University Hospital; SJH = St. Joseph Hospital; RN = Registered nurse. The variables were measured from October, 2010 to April 2011.

167
Appendix E
Frequency of Participants with Analgesics and Anxiolytics
Day 1 Day 2 Day 3 Medication n % n % n %
Weak opioids n = 39 n = 37 n = 37 Codeine 5 12.82 4 10.81 4 10.81 Darvocet 1 2.56 2 5.41 2 5.41 Tramadol 2 5.13 3 8.11 3 8.11 Ultracet 31 79.49 28 75.68 28 75.68 Strong opioids n = 116 n = 116 n = 115 Durogestic 33 28.45 36 31.03 36 31.30 Morphine 77 66.38 76 65.52 76 66.09 MST 3 2.59 3 2.59 3 2.61 Temgesic 3 2.59 1 0.86 0 - Non-opioids n = 136 n = 133 n = 129 Acetaminophen 23 16.91 21 15.79 19 14.73
Beclofen 2 1.47 2 1.50 2 1.55 Cataflam 3 2.20 4 3.01 3 2.33 Celecoxib 9 6.62 9 6.77 9 6.98
Chlorzoxzone 7 5.15 5 3.76 4 3.10 Clonazepam 2 1.47 2 1.50 2 1.55 Etoricoxib 1 0.74 1 0.75 2 1.55
Ibuprofen 1 0.74 1 0.75 1 0.78 Ketorolac 5 3.68 5 3.76 4 3.10 Mefenamic acid 1 0.74 1 0.75 1 0.78 Naproxen 1 0.74 2 1.50 1 0.78 Neurontin 6 4.41 6 4.51 6 4.65 Steroids 46 33.82 45 33.84 45 34.88 Tegretal 23 16.91 23 17.29 23 17.83 Tofranil 5 3.68 5 3.76 6 4.65 Urogen 1 0.74 1 0.75 1 0.78 Anxiolytics n = 35 n =30 n = 30 Alprazolam 16 45.71 14 46.67 14 46.67 Fluoxetine 5 14.29 1 3.33 1 3.33 Lorazepam 14 0.40 15 0.50 15 0.50
Note. MST = Morphine Sulfate ; the n represents the number of participants who received the drug and one participant could received more than one drug.
168
Bibliography
Allen, J., & Good, M. (2000). Music during crisis. American Journal of Nursing, 100(12),
24AA,24CC-24FF.
Alvin, J. (1975). Music Therapy. New York: Basic Books.
Ando, M., Morita, T., Lee, V., & Okamoto, T. (2008). A pilot study of transformation,
attributed meanings to the illness, and spiritual well-being for terminally ill cancer
patients. Palliative and supportive care, 6(4), 335-340.
Andrews, S. C. (2001). Caregiver burden and symptom distress in people with cancer
receiving hospice care. Oncology Nursing Forum, 28(9), 1469-1474.
Arnold, E. M., Artin, K. A., Person, J. L., & Griffith, D. L. (2004). Consideration of
hastening death among hospice patients and their families. Journal of Pain and
Symptom Management, 27(6), 523-532.
Arnsten, A. F. (1998). The biology of being frazzled. Science, 280(5370), 1711-1712.
Bailey, L. M. (1983). The effects of live music versus tape-recorded music on
hospitalized cancer patients. Music Therapy, 3(1), 17-28.
Balducci, L. (2005). Supportive care of elderly patients with cancer. Supportive Cancer
Therapy, 2(4), 225-228.
Bally, K., Campbell, D., Chesnick, K., & Tranmer, J. E. (2003). Effects of
patient-controlled music therapy during coronary angiography on procedural pain
and anxiety distress syndrome. Critical Care Nurse, 23(2), 50-58.
Bardo, M. T. (1998). Neuropharmacological mechanisms of drug reward: Beyond
dopamine in the nucleus accumbens. Critical reviews in neurobiology, 12(1-2),
37-67.

169
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions:
Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65-94.
Beaulieu, P., & Rice, A. S. C. (2003). Applied physiology of nociception. In D. J.
Rowbotham. & P. E. Macintyre. (Eds.), Clinical pain management: Acute pain
(pp. 3-16). New York: Oxford University Press Inc.
Beck, S. L. (1991). The therapeutic use of music for cancer-related pain. Oncology
Nursing Forum, 18(8), 1327-1337.
Bernardi, L., Porta, C., & Sleight, P. (2006). Cardiovascular, cerebrovascular, and
respiratory changes induced by different types of music in musicians and
non-musicians: the importance of silence. Heart, 92(4), 445-452.
Berridge, K. C., & Robinson, T. E. (1998). What is the role of dopamine in reward:
Hedonic impact, reward learning, or incentive salience? Brain Research Reviews,
28(3), 309-369.
Besson, J. M., & Chaouch, A. (1987). Peripheral and spinal mechanisms of nociception.
Physiological Reviews, 67, 67-186.
Bevan, S., & Geppetti, P. (1994). Protons: Small stimulants of capsaicin-sensitive sensory
nerves. Trends in Neuroscience, 17(12), 509-512.
Blood, A. J., & Zatorre, R. J. (2001). Intensely pleasurable responses to music correlated
with activity in brain regions implicated in reward and emotion. Proceedings of
the National Academy of Sciences of the United States of America, 98(20),
11818-11823.
Boivie, J. (2006). Central pain. In S. B. McMahon. & M. Koltzenburg. (Eds.), Wall and
Melzack's textbook of pain (5th ed., pp. 1057-1074). Philadelphia: Elsevier.

170
Bonica, J. J. (1990). The management of pain. In J. J. Bonica (Ed.), Cancer Pain.
Philadelphia: Lea and Febiger.
Borling, J. E. (1981). The effects of sedative music on alpha rhythms and focused
attention in high-creative and low creative subjects. Journal of Music Therapy,
18(2), 101-108.
Breitbart, W., Chochinov, H. M., & Passik, S. D. (2004). Psychiatric symptoms in
palliative medicine. In D. Doyle., G. Hanks., N. I. Cherny. & K. C. Sir. (Eds.),
Oxford textbook of palliative medicine (pp. 746-771). New York: Oxford
University Press.
Bringman, H., Giesecke, K., Thorne, A., & Bringman, S. (2009). Relaxing music as
pre-medication before surgery: A randomized controlled trial. Acta
Anaesthesiologica Scandinavica, 53, 759-764. doi:
10.1111/j.1399-6576.2009.01969.x
Bruera, E., Moyano, J., Seifert, L., Fainsinger, R. L., Hanson, J., & Suarez-Almazor, M.
(1995). The frequency of alcoholism among patients with pain due to terminal
cancer. Journal of Pain & Symptom Management, 10(8), 599-603.
Brust, J. C. (2001). Music and the neurologist. A historical perspective. Annals of the New
York Academy of Sciences, 930, 143-152.
Bruya, M. A., & Severtsen, B. (1984). Evaluating the effects of music on
electroencephalogram patterns of normal subjects. Journal of Neurosurgical
Nursing, 16(2), 96-100.
Bureau of National Health Insurance. (2008). National Health Insurance regulation of
medication. Taipei, Taiwan: Bureau of National Health Insurance.

171
Burns, D. S. (2001). The effect of the bonny method of guided imagery and music on the
mood and life quality of cancer patients. Journal of Music Therapy, 38, 51-65.
Burns, S. J. I., Harbuz, M. S., Hucklebridge, F., & Bunt, L. (2001). A pilot study into the
therapeutic effects of music therapy at a cancer help center. Alternative Therapies
in Health and Medicine, 7(1), 48-56.
Burstein, R., Cliffer, K. D., & Giesler, G. J., Jr. (1987). Direct somatosensory projections
from the spinal cord to the hypothalamus and telencephalon. Journal of
Neuroscience, 7(12), 4159-4164.
Bushnell, M. C., & Apkarian, A. V. (2006). Representation of pain in the brain. In S. B.
McMahin. & M. Koltzenburg. (Eds.), Wall and Melzack's textbook of pain (5th ed.,
pp. 107-124). Philadelphia: Elsevier.
Caraceni, A., & Portenoy, R. K. (1999). An international survey of cancer pain
characteristics and syndromes. Pain, 82(3), 263-274.
Caraceni, A., & Weinstein, S. M. (2001). Classification of cancer pain syndromes.
Oncology 15(12), 1627-1640.
Cassileth, B. R., Lusk, E. J., & Walshm, W. P. (1986). Anxiety levels in patients with
malignant disease. The Hospice Journal, 2(2), 57-69.
Cassileth, B. R., Vickers, A. J., & Magill, L. A. (2003). Music therapy for mood
disturbance during hospitalization for autologous stem cell transplanatation: A
randomized controlled trial. Cancer, 98, 2723-2729.
Caterina, M. J., Leffler, A., Malmberg, A. B., Martin, W. J., Trafton, J., Petersen-Zeitz, K.
R., et al. (2000). Impaired nociception and pain sensation in mice lacking the
capsaicin receptor Science, 288(5464), 306-313.
172
Cepeda, M., Carr, D. B., Lau, J., & Alvarez, H. (2006). Music for pain relief. Cochrane
Database of Systematic Reviews, 4, 1-51.
Cervero, F. (1985). Visceral nociception: Peripheral and central aspects of visceral
nociceptive systems. Philosophical Transactions of the Royal Society of London.
Series B. Biological Sciences, 308, 325-337.
Cervero, F., & Laird, J. M. A. (1999). Visceral pain. Lancet, 353, 2145-2148.
Cervero, F., & Morrison, J. F. B. (1986). Visceral sensation (Vol. 67). New York:
Elsevier.
Chan, C. W. H., Richardson, A., & Richardson, J. (2005). A study to assess the existence
of the symptom cluster of breathlessness, fatigue and anxiety in patients with
advanced lung cancer. European Journal of Oncology Nursing, 9(4), 325-333.
Chang, M. C., Chang, Y. C., Chiou, J. F., Tsou, T. S., & Lin, C. C. (2002). Overcoming
patient-related barriers to cancer pain management for home care patients. A pilot
study. Cancer Nursing, 25(6), 470-476.
Chang, S.-C., & Chen, C.-H. (2005). Effects of music therapy on women's physiologic
measures, anxiety, and satisfaction during cesarean delivery. Research in Nursing
& Health, 28(6), 453-461.
Chang, V. T., Thaler, H. T., Polyak, T. A., Kornblith, A. B., Lepore, J. M., & Portenoy, R.
K. (1998). Quality of life and survival: the role of multidimensional symptom
assessment. Cancer, 83(1), 173-179.
Chao, C. S. (1998). Psychiatric mental health nursing and spiritual care. Journal of
Nursing, 45(1), 16-21.
Chen, C.-H., Liu, T.-W., Tsai, L.-Y., Liu, I.-P., Hsu, T.-H., & Tang, S. T. (2006).

173
Appropriateness of cancer pain management for non-hospice terminally ill cancer
patients in Taiwan. Journal of the Chinese Oncology Society, 22(1), 1-29.
Chen, L. M., Miaskowski, C. A., Dodd, M., & Pantilat, S. (2008). Concepts within the
Chinese culture that influence the cancer pain experience. Cancer Nursing, 31(2),
103-108.
Chen, M.-L., Chang, H.-K., & Yeh, C.-H. (2000). Anxiety and depression in Taiwanesese
cancer patients with and without pain. Journal of Advanced Nursing, 32(4),
944-951.
Chen, M. B., Hsieh, L. F., Lin, H. L., Lee, S. C., Lin, C. R., & Tsai, S. L. (2004).
Predicting factors on quality of life in cancer patients. VGH Nursing, 21(4),
352-362.
Chen, M. L., & Tseng, H. C. (2006). Symptom clusters in cancer patients. Supportive
Care in Cancer, 14(8), 825-830.
Chen, P.-Y., See, L.-C., Wang, C.-H., Lai, Y.-H., Chang, H.-K., & Chen, M.-L. (1999).
The impact of pain on the anxiety and depression of cancer patients. Formosan
Journal of Medicine, 3(4), 373-382.
Chen, Y. C. (2001). Chinese value, health and nursing. Journal of Advanced Nursing,
36(2), 270-273.
Chibnall, J. T., Videen, S. D., Duckro, P. N., Miller, D. K., Chibnall, J. T., Videen, S. D.,
et al. (2002). Psychosocial-spiritual correlates of death distress in patients with
life-threatening medical conditions. Palliative Medicine, 16(4), 331-338.
Chiu, T. Y., Hu, W. Y., & Chen, C. Y. (2000). Prevalence and severity of symptoms in
terminal cancer patients: A study in Taiwan. Supportive Care in Cancer, 8(4),

174
311-313.
Chlan, L. (2006). Music intervention. In M. Snyder & R. Lindquist (Eds.),
Complementary/Alternative Therapies in Nursing (pp. 79-92). New York:
Springer.
Chuang, I. (2004). Music therapy. Taipei, Taiwan: Psychological Publishing
Chung, D. K. (1995). Taoism. In J. Beversluis. (Ed.), A sourcebook for earth's community
of religions (2nd ed., pp. 85-86). Grand Rapids, MI: CoNexus Press.
Chung, T. K., French, P., & Chan, S. (1999). Patient-related barriers to cancer pain
management in a palliative care setting in Hong Kong. Cancer, 22(3), 196-203.
Cicirelli, V. G. (2006). Fear of death in mid-old age. The Journal of Gerontology, 61B(2),
75-81.
Clements-Cortes, A. (2004). The use of music in facilitating emotional expression in the
terminally ill. American Journal of Hospice & Palliative Care, 21(4), 255-260.
Clipp, E. C., & George, L. K. (1992). Patients with cancer and their spouse caregivers:
Perceptions of the illness experience. Cancer, 69(4), 1074-1079.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159.
Coluzzi, P. H., & Farirbairn, B. S. (1999). The management of pain in terminally ill
cancer patients with difficulty swallowing. American Journal of Hospice &
Palliative Care, 16(6), 731-737.
Conte, H. R., Weiner, M. B., & Plitchik, R. (1982). Measuring death anxiety: Conceptual,
psychometric, and factor-analytic aspects. Journal of Personality and Social
Psychology, 43(4), 775-785.
Cook, T. D., & Campbell, D. T. (1979). Quasi-experimentation Design and Analysis

175
Issues for Fields Settings. Boston: Houghton Mifflin Company.
Cooke, M., Chaboyer, W., Schluter, P., & Hiratos, M. (2005). The effect of music on
preoperative anxiety in day surgery. Journal of Advanced Nursing, 52(1), 47-55.
Coyle, N., & Foley, K. M. (1987). Prevalence and profile of pain syndromes in cancer
patients. In D. B. McGuire. & C. H. Yarbro. (Eds.), Cancer pain management (pp.
21-46). Philadelphia: Saunders.
Creel, H. G. (2000). Confucius and the Chinese way. New York: Peter Smith Publisher.
Crook, J., Rideout, E., & Browne, G. (1984). The prevalence of pain complaints in a
general population. Pain, 18(3), 299-314.
Curran, P. J., West, S. G., & Finch, J. F. (1996). The robustness of test statistics to
nonormality and specification error in confirmatory factor analysis.
Psychological Methods, 1(1), 16-29.
Curtis, S. L. (1986). The effect of music on pain relief and relaxation of the terminally ill.
Journal of Music Therapy, 23(1), 10-24.
Davey, H. M., Barratt, A. L., Butow, P. N., & Deeks, J. J. (2007). A one-item question
with a Likert or Visual Analog Scale adequately measured current anxiety.
Journal of Clinical Epidemiology, 60(4), 356-360.
Davis, M. (1992). The role of the amygdala in fear-potentiated startle: Implications for
animal models of anxiety. Trends in Pharmacological Sciences, 13(1), 35-41.
de Leon-Casasola, O. A., & Lema, M. J. (2003). Cancer pain. In T. J. Healy. & P. R.
Knight. (Eds.), Wylie and Churchill-Davidson's a practice of anesthesia (7th ed.,
pp. 1255-1265). London: Arnold Publishers.
Dezutter, J., Soenens, B., Luyckx, K., Bruyneel, S., Vansteenkiste, M., Duriez, B., et al.
176
(2009). The role of religion in death attitudes: distinguishing between religious
belief and style of processing religious contents. Death Studies, 33(1), 73-92.
Dickenson, A. H. (1996). Pharmacology of pain transmission and control. In J. Campbell.
(Ed.), Pain 1996 - An updated review. Refresher courses syllabus (pp. 113-122).
Seattle: ISAP Press.
Dickhaus, B., Mayer, E. A., Firooz, N., Stains, J., Conde, F., Olivas, T. I., et al. (2003).
Irritable bowel syndrome patients show enhanced modulation of visceral
perception by auditory stress. American Journal of Gastroenterology, 98(1),
135-143.
Diette, G. B., Lechtzin, N., Haponik, E., Devrotes, A., & Rubin, H. R. (2003). Distraction
therapy with nature sights and sounds reduces pain during flexible bronchoscopy:
a complementary approach to routine analgesia. Chest, 123(3), 941-948.
Djouhri, L., Bleazard, L., & Lawson, S. N. (1998). Association of somatic action
potential shape with sensory receptive properties in guinea-pig dorsal root
ganglion neurones. Journal of physiology, 513(Pt 3), 857-872.
Dossey, B. M. (1995). Peaceful deathing and death. In B. M. Dossey. (Ed.), Holistic
nursing : A handbook for practice (2nd ed., pp. 429-454). Gaithersburg, MD
Aspen Publishers.
Elliott, D. (1993). Comparison of three instruments for measuring patient anxiety in a
coronary care unit. Intensive & Critical Care Nursing, 9(3), 195-200.
Ewing, G., Todd, C., Rogers, M., Barclay, S., McCabe, J., & Martin, A. (2004).
Validation of a symptom measure suitable for use among palliative care patients
in the community: CAMPAS-R. Journal of Pain and Symptom Management,
177
27(4), 287-299.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible
statistical power analysis program for the social, behavioral, and biomedical
sciences. Behavior Research Methods, 39, 175-191.
Ferrell, B. R., Chohen, M. Z., Rhiner, M., & Rozek, A. (1991). Pain as a metaphor for
illness pat II: Family caregivers' management of pain. Oncology Nursing Forum,
18(8), 1315-1321.
Field, A. (2005). Discovering statistics using SPSS (2nd ed.). Thousand Oaks, CA: SAGE
Fields, H. L. (1987). Pain. New York: McGraw-Hill.
Fields, H. L., & Basbaum, A. I. (1989). Endogenous pain control mechanisms. In P. D.
Wall. & R. Melzack. (Eds.), Textbook of pain (2nd ed., pp. 206-217). New York:
Churchill Livingstone.
Fields, H. L., & Heinricher, M. M. (1985). Anatomy and physiology of a nociceptive
modulatory system. Philosophical Transactions of the Royal Society of London.
Series B. Biological Sciences, 308(1136), 361-374.
Filiberti, A., Ripamonti, C., Vittorio Ventafridda, A. T., De Conno, F., Contiero, P., &
Tamburini, M. (2001). Characteristics of terminal cancer patients who committed
suicide during a home palliative care program. Journal of Pain and Symptom
Management, 22(1), 544-553.
Fisch, M. J. (2006). Depression/Anxiety. In E. Bruera., I. J. Higginson., C. Ripamonti. &
C. F. v. Gunten. (Eds.), Textbook of palliative medicine (pp. 675-687). London:
Hodder Arnold.
Fortner, B. V., & Neimeyer, R. A. (1999). Death anxiety in older adults: A quantitative

178
review. Death Studies, 23(5), 387-411.
Fortner, B. V., Neimeyer, R. A., & Ryharezyk, B. (2000). Correlates of death anxiety in
older adults:A comprehensive review. In A. Tomer. (Ed.), Death attitudes and the
older adult: Theories, concepts, and applications (pp. 95-108). Philadelphia:
Taylor & Francis.
Freeman, L., Caserta, M., Lund, D., Rossa, S., Dowdy, A., & Partenheimer, A. (2006).
Music thanatology: Prescriptive harp music as palliative care for the dying patient.
American Journal of Hospice & Palliative Care, 23(2), 100-104.
Friedman, L. M., Furberg, C. D., & DeMets, D. L. (1998). Fundamentals of Clinical
Trials (3rd ed.). New York: Springer Science+Business Media, LLC.
Frumkin, H., & Louv, R. (2007). The powerful link between conserving land and
preserving health The Land Trust Alliance special anniversary report, 2007.
Washington, DC: The Land Trust Alliance.
Gallagher, L. M., Huston, M. J., Nelson, K. A., Walsh, D., & Steele, A. L. (2001). Music
therapy in palliative medicine. Supportive Care in Cancer, 9(3), 156-161.
Gallagher, L. M., Lagman, R., Walsh, D., Davis, M. P., & Legrand, S. B. (2006). The
clinical effects of music therapy in palliative medicine. Supportive Care in Cancer,
14(8), 859-866.
Gallagher, L. M., & Steele, A. L. (2001). Developing and using a computerized database
for music therapy in palliative medicine. Journal of Palliative Care, 17(3),
147-154.
Gardner, E. L., & Vorel, S. R. (1998). Cannabinoid transmission and reward-related
events. Neurobiology of disease, 5(6), 502-533.

179
Gaston, E. T. (1951). Dynamic music factors in mood change. Music Education Journal,
37(4), 42-44.
Georges, J.-J., Onwuteaka-Philipsen, B. D., van der Heide, A., van der Wal, G., & van der
Maas, P. J. (2005). Symptoms, treatment and "dying peacefully" in terminally ill
cancer patients: A prospective study. Supportive Care in Cancer, 13(3), 160-168.
Ger, L.-P., Ho, D.-T., Sun, W.-Z., Wang, M.-S., & Cleeland, C. S. (1999). Validation of
the Brief Pain Inventory in a Taiwanese population. Journal of Pain and Symptom
Management, 18(5), 316-322.
Given, B., Give, C. W., Azzouz, F., & Stommel, M. (2001). Physical functioning of
elderly cancer patients prior to diagnosis and following initial treatment. Nursing
Research, 50(4), 222-232.
Given, C. W., Given, B., Azzouz, F., Kozachik, S., & Stommel, M. (2001). Predictors of
pain and fatigue in the year following diagnosis among elderly cancer patients.
Journal of Pain and Symptom Management, 21, 456-466.
Goldstein, A. (1985). Music/endorphin link. Brain/Mind Bulletin, 11(4/5), 1.
Golletz, D. V. (1997). Uses of nature stimuli in relaxation therapy for anxiety and anger.
doctoral dissertation, University of Washington, Seattle.
Gonda, T. A., & Ruark, J. E. (1984). Dying dignified. The health professional's guide to
care. Menlo Park, CA: Addison Wesley
Good, M. (1992). Comparison of the effects of relaxation and music on postoperative
pain. doctoral dissertation, Case Western Reserve University, Cleveland.
Good, M. (1995). A comparison of the effects of jaw relaxation and music on
postoperative pain. Nursing Research, 44(1), 52-57.

180
Good, M. (2009). Pain: A balance between analgesia and side effects. In S. J. Peterson &
T. S. Bredow (Eds.), Middle Range Theories (2nd ed., pp. 63-81). Philadephia:
Lippincott Williams & Wilkins.
Good, M., & Ahn, S. (2008). Korean and American music reduces pain in Korean women
after gynecologic surgery. Pain Management Nursing, 9(3), 96-103.
Good, M., Albert, J. M., Anderson, G. C., Wotman, S., Cong, X., Lane, D., et al. (2010).
Supplementing relaxation and music for pain after surgery. Nursing Research,
59(4), 259-269.
Good, M., Anderson, G. C., Ahn, S., Cong, X., & Stanton-Hicks, M. (2005). Relaxation
and music reduce pain following intestinal surgery. Research in Nursing & Health,
28(3), 240-251.
Good, M., Anderson, G. C., Stanton-Hicks, M., Grass, J. A., & Makii, M. (2002).
Relaxation and music reduce pain after gynecologic surgery. Pain Management
Nursing, 3(2), 61-70.
Good, M., & Chin, C. C. (1998). The effects of Western music on postoperative pain in
Taiwan. Kaohsiung Journal of Medical Sciences, 14(2), 94-103.
Good, M., & Moore, S. M. (1996). Clinical practice guidelines as a new source of
middle-range theory: focus on acute pain. Nursing Outlook, 44(2), 74-79.
Good, M., Picot, B. L., Salem, S. G., Chin, C. C., Picot, S. F., & Lane, D. (2000).
Cultural differences in music chosen for pain relief. Journal of Holistic Nursing,
18(3), 245-260.
Good, M., Stanton-Hicks, M., Grass, J. A., Anderson, G. C., Lai, H. L., Roykulcharoen,
V., et al. (2001). Relaxation and music to reduce postsurgical pain. Journal of

181
Advanced Nursing, 33(2), 208-215.
Good, M., Stanton-Hicks, M., Grass, J. A., Cranston Anderson, G., Choi, C.,
Schoolmeesters, L. J., et al. (1999). Relief of postoperative pain with jaw
relaxation, music and their combination. Pain, 81(1-2), 163-172.
Grumann, M. M., & Spiegel, D. (2003). Living in the face of death: Interviews with 12
terminally ill women on home hospice care. Palliative and supportive care, 1(1),
23-32.
Guzzetta, C. E. (1989). Effects of relaxation and music therapy on patients in a coronary
care unit with presumptive acute myocardial infarction. Heart & Lung, 18(6),
609-616.
Halstead, M. T., & Roscoe, S. T. (2002). Restoring the spirit at the end of life: Music as
an interevention for oncology nurses. Clinical Journal of Oncology Nursing, 6,
332-336.
Hampton, D. M., Hollis, D. E., Lloyd, D. A., Taylor, J., & McMillan, S. C. (2007).
Spiritual needs of persons with advanced cancer. American Journal of Hospice &
Palliative Medicine, 24(1), 42-48.
Hanser, S. B. (1985). Music therapy and stress reduction research. Journal of Music
Therapy, 22(4), 193-206.
Harding, S. R., Flannelly, K. J., Weaver, A. J., & Costa, K. G. (2005). The influence of
religion on death anxiety and death acceptance. Mental Health, Religion &
Culture, 8(4), 253-261.
Harikumar, R., & Kumar, S. (2007). Colonscopy and the role of music therapy: How to
go about an ideal protocol. World Journal of Gastroenterology, 13(23),

182
3272-3273.
Harikumar, R., Raj, M., Paul, A., Harish, K., Kumar, S. K., Sandesh, K., et al. (2006).
Listening to music decreases need for sedative medication during colonoscopy: A
randomized, controlled trial. Indian Journal of Gastroenterology, 25(1), 3-5.
Heerwagen, J. H., & Orians, G. H. (1993). Humans, habitats, and aesthetics. In S. R.
Kellert. & E. O. Wilson. (Eds.), The biophilia hypothesis (pp. 138-172).
Washington DC: Island Press.
Hekmat, H. M., & Hertel, J. B. (1993). Pain attenuating effects of preferred versus
non-preferred music interventions. Psychology of Music, 21(2), 163-173.
Henocha, I., Bergmanb, B., Gustafssona, M., Gaston-Johanssona, F., & Danielsona, E.
(2007). Dyspnea experience in patients with lung cancer in palliative care.
European Journal of Oncology Nursing, 12(2), 86-96.
Hernandez-Ruiz, E. (2005). Effect of music therapy on the anxiety levels and sleep
patterns of abused women in shelters. Journal of Music Therapy, 42(2), 140-158.
Hilliard, R. E. (2003). The effects of music therapy on the quality and length of life of
people diagnosed with terminal cancer. Journal of Music Therapy, 40(2), 113-137.
Hills, J., Paice, J. A., Cameron, J. R., Shott, S., Hills, J., Paice, J. A., et al. (2005).
Spirituality and distress in palliative care consultation. Journal of Palliative
Medicine, 8(4), 782-788.
Hodes, R. L. (1989). Cancer patients' needs and concerns when using narcotic analgesics.
Advances in Pain Research and Therapy, 11, 91-99.
Hollen, C. J., Hollen, C. W., & Stolte, K. (2000). Hospice and hospital oncology unit
nurses: a comparative survey of knowledge and attitudes about cancer pain.

183
Oncology Nursing Forum, 27(10), 1593-1599.
Holroyd, E. E. (2003). Chinese family obligations toward chronically ill elderly members:
Comparing caregivers in Beijing and Hong Kong. Qualitative Health Research,
13(3), 302-318.
Hong, C.-H. (2007). The development of pain management in Taiwan: Ten years review
of history Retrieved October 23, 2008,
from http://www.pain-manage.org.tw/normal/p24.htm
Hong, G. K. (1989). Application of cultural and environmental issues in family therapy
with immigrant Chinese Americans. Journal of Strategic and Systemic Therapies,
8(3), 14-21.
Horne-Thompson, A., & Grocke, D. (2008). The effect of music therapy on anxiety in
patients who are terminally ill. Journal of Palliative Medicine, 11(4), 582-590.
Hsing Yun. (1983). Reincarnation in Buddhism Retrieved March 10, 2009,
from http://www.fgs.org.tw/master/masterA/library/buddhist-book/08-5.htm
Hsu, H.-C., Hu, W.-Y., Chuang, R.-B., Chiu, T.-Y., & Chen, C.-Y. (2002). Symptoms in
the elderly with terminal cancer - A study in Taiwan. Formosan Journal of
Medicine, 6(4), 465-473.
Hsu, L.-C., Ling, C.-C., Lai, Y.-H., & Chen, M.-L. (2002). Assessment and management
of cancer pain and its related factors by the oncology nurse. New Taipei Journal of
Nursing, 4(2), 29-38.
Hsu, T.-H., Lu, M.-S., Tsou, T.-S., & Lin, C. C. (2003). The relationship of pain,
uncertainty, and hope in Taiwanese lung cancer patients. Journal of Pain and
Symptom Management, 26(3), 835-842.

184
Huang, S.-T., Good, M., & Zauszniewski, J. A. (2010). The effectiveness of music in
relieving pain in cancer patients: A randomized controlled trial. International
Journal of Nursing Studies, 47(11), 1354-1362.
Huang, S. H. (2000). Effects of music therapy on relieving pain and symptom distress
among hospice cancer patients. master's thesis, Taipei Medical University,
Taipei, Taiwan.
Huang, S. T. (2006). The effects of music on cancer pain. doctoral dissertation, Case
Western Reserve University, Cleveland.
Huang, T.-W., Lai, Y.-H., Chen, A.-l., See, L.-C., Chang, C.-S., & Hsiang, C.-Y. (2001).
The effects of back massage on fatigue and anxiety during chemotherapy.
Formosan Journal of Medicine, 5(4), 369-378.
Huang, Y. C. (2003). Physiological and psychological effects of music therapy among
nursing home residents. Fu-Jen Journal of Medicine, 1(1), 47-57.
Hudson, P. (2003). A conceptual model and key variables for guiding supportive
interventions for family caregivers of people receiving palliative care. Palliative
and supportive care, 1(4), 353-365.
Hung, H. J. (2003). Effects of music therapy on anxiety, depression and sleep quality of
the cancer patients. mater's thesis, Kaohsiung Medical University, Kaohsiung,
Taiwan.
Hwang, S. L., Chang, Y., Lee, M. B., Ko, W. J., & Chu, S. H. (1996). Effect of music
therapy on reducing stress for post-open heart surgery patients in intensive care
unit. Tzu Chi Medical Journal, 8(1), 47-54.
Hwang, S. S., Chang, V. T., & Kasimis, B. (2002). Dynamic cancer pain management

185
outcomes: the relationship between pain severity, pain relief, functional
interference, satisfaction and global quality of life over time. Journal of Pain &
Symptom Management, 23(3), 190-200.
International Association for the Study of Pain. (1994). Classification of chronic pain
Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms (2nd ed.).
Seattle: IASP Press.
Ishikawa, H., Kawagoe, K., Kashiwagi, M., & Yano, E. (2007). Nurse-physician
collaboration in pain management for terminally ill cancer patients treated at
home in Japan. Journal of Palliative Care, 23(4), 255-261.
Jackson, K. C., & Lipman, A. G. (2004). Drug therapy for anxiety in palliative care.
Cochrane Database of Systematic Reviews(1), 1-8.
Jacox, A., Carr, D. B., Payne, R., Berde, C. B., Breitbart, W., Cain, J. M., et al. (1994).
Management of cancer pain. Clinical practice guideline No. 9. AHCPR
Publication No. 94-0592. Rockville, MD: Agency for Health Care Policy and
Research, U. S. Department of Health and Human Services, Public Health
Service.
Janjan, N. A., Delclos, M., Crane, C., Ballo, M., & Cleeland, C. (2003). Palliative
radiotherapy. In E. Bruera. & R. K. Portenoy (Eds.), Cancer pain: Assessment and
management (pp. 279-310). New York: Cambridge University Press.
Jensen, M. P. (2003). The validity and reliability of pain measures in adults with cancer.
The Journal of Pain, 4(1), 2-21.
Jensen, M. P., Turner, J. A., Romano, J. M., & Fisher, L. D. (1999). Comparative
reliability and validity of chronic pain intensity measures. Pain, 83(2), 157-162.

186
Jensen, T. S., & Gottrup, H. (2003). Assessment of neuropathic pain. In T. S. Jensen., P. R.
Wilson. & A. S. C. Rice. (Eds.), Clinical pain management: Chronic pain (pp.
113-124). New York: Oxford University Press Inc.
Jones, S. L. (1992). Anatomy of pain. In R. S. Sinatra., A. H. Hord., B. Ginsberg. & L. M.
Preble. (Eds.), Acute pain: Mechanisms & managment (pp. 8-28). St. Louis, MO:
Mosby.
Kalish, L. A., & Begg, C. B. (1985). Treatment allocation methods in clinical trials: A
review. Statistics in Medicine, 4, 129-144.
Kanda, M., Mima, T., Oga, T., Matsuhashi, M., Toma, K., Hara, H., et al. (2003).
Transcranial magnetic stimulation (TMS) of the sensorimotor cortex and medial
frontal cortex modifies human pain perception. Clinical Neurophysiology, 114(5),
860-866.
Kaplan, P. W. (2003). Musicogenic epilepsy and epileptic music: a seizure's song.
Epilepsy & Behavior, 4(5), 464-473.
Kemper, K. J., & Danhauer, S. C. (2005). Music as therapy. Southern Medical Journal,
98(3), 282-288.
Kerrihard, T., Breitbart, W., Dent, R., & Strout, D. (1999). Anxiety in patients with cancer
and human immunodeficiency virus. Seminars in Clinical Neuropsychiatry, 4(2),
114-132.
Khalfa, S., Roy, M., Rainville, P., Bella, S. D., & Peretz, I. (2008). Role of tempo
entrainment in psychophysiological diffferentiation of happy and sad music.
International Journal of Psychophysiology, 68(1), 17-26.
Kindler, C. H., Harms, C., Amsler, F., Ihde-Scholl, T., & Scheidegger, D. (2000). The
187
visual analog scale allows effective measurement of preoperative anxiety and
detection of patients' anesthetic concerns. Anesthesia and Analgesia 90(3),
706-712.
King, M., Speck, P., & Thomas, A. (1995). Theroyal free interview for religious and
spiritual beliefs: Development and standardization. Psychological Medicine, 25(6),
1125-1134.
Krout, R. E. (2001). The effects of single-session music therapy interventions on the
observed and self-reported levels of pain control, physical comfort, and relaxation
of hospice patients. American Journal of Hospice & Palliative Care, 18(6),
383-390.
Krout, R. E. (2003). Music therapy with imminently dying hospice patients and their
families: Facilitating release near the time of death. American Journal of Hospice
& Palliative Care, 20(2), 129-134.
Kutner, J. S., Bryant, L. L., Beaty, B. L., & Fairclough, D. L. (2006). Symptoms distress
and quality of life assessment at the end of life: The role of proxy response.
Journal of Pain and Symptom Management, 32(4), 300-310.
Kutner, J. S., Kassner, C. T., & Nowels, D. E. (2001). Symptom burden at the end of life:
Hospice providers' perceptions. Journal of Pain and Symptom Management, 21(6),
473-480.
Kwekkeboom, K. (2003). Music versus distraction for procedural pain and anxiety in
patients with cancer. Oncology Nursing Forum, 30(3), 433-440.
Labbe, E., Schmidt, N., Babin, J., & Pharr, M. (2007). Coping with stress: The
effectiveness of different types of music. Applied Psychophysiol and Biofeedback,

188
32(3-4), 162-168.
Lai, H.-L. (2004). Music preference and relaxation in Taiwanese elderly people. Geriatric
Nursing, 25(5), 286-291.
Lai, H.-L., Chen, C.-J., Peng, T.-C., Chang, F.-M., Hsieh, M.-L., Huang, H.-Y., et al.
(2006). Randomized controlled trial of music during kangaroo care on maternal
state anxiety and preterm infants' responses. International Journal of Nursing
Studies, 43(2), 139-146.
Lai, H.-L., & Good, M. (2006). Music improves sleep quality in older adults. Journal of
Advanced Nursing, 53(1), 134-144; discussion 144-136.
Lai, H.-L., Hwang, M.-J., Chen, C.-J., Chang, K.-F., Peng, T.-C., & Chang, F.-M. (2008).
Randomised controlled trial of music on state anxiety and physiological indices in
patients undergoing root canal treatment. Journal of clinical Nursing, 17(19),
2654-2660.
Lai, Y.-H., Chen, S.-C., Chang, L.-I., Cheng, S.-Y., & Wei, L.-L. (2000). Beliefs about
and knowledge of cancer pain and narcotic analgesics and related factors in
undergraduate student nurses. New Taipei Journal of Nursing, 2(2), 5-15.
Lamont, E. W., & Kokkinidis, L. (1998). Infusion of the dopamine D1 receptor antagonist
SCH 23390 into the amygdala blocks fear expression in a potentiated startle
paradigm. Brain Research, 795(1-2), 128-136.
Lan, P.-C. (2002). Subcontracting filial piety: Elder care in ethnic Chinese immigrant
families in California. Journal of Family Issues, 23(7), 812-835.
Lancee, W. J., Vachon, M. L., Ghadirian, P., Adair, W., Conway, B., & Dryer, D. (1994).
The impact of pain and impaired role performance on distress in persons with

189
cancer. Canadian Journal of Psychiatry, 39(10), 617-622.
Lawrie, I., Lloyd-Williams, M., & Taylor, F. (2004). How do palliative medicine
physicians assess and manage depression. Palliative Medicine, 18(3), 234-238.
LeDoux, J. (1996). The emotional brain: The mysterious underpinnings of emotional life.
New York: Simon & Schuster.
Lee, D. F. (1995). Effects of music therapy on burn patients regarding pain level,
physiological responses and psychological perception during change dressing.
master thesis, National Taiwan University, Taipei, Taiwan.
Lee, O. K. A., Chung, Y. F. L., Chan, M. F., & Chan, W. M. (2005). Music and its effect
on the physiological responses and anxiety levels of patients receiving mechanical
ventilation: a pilot study. Journal of Clinical Nursing, 14, 609-620.
Lee, Y. J. (2000a). Effects of music therapy on pain level, physiological responses and
psychological perception of cancer patients. master thesis, Chang Gung
University, Taipei county, Taiwan.
Lee, Y. J. (2000b). Effects of music therapy on sleep quality and emotional status for
institutionalized elders. master thesis, National Taipei College of Nursing,
Taipei, Taiwan.
Levy, M. H., & Catalino, R. B. (1985). Control of common physical symptoms other than
pain in patients with terminal disease. Seminars in Oncology, 12(4), 411-430.
Li, C.-C., Yu, P.-J., & Hwang, S.-L. (2006). Spiritual well-being of caring. Taiwan
Journal of Hospice Palliative Care, 11(1), 59-74.
Li, S.-Y. (2007). Exploring the effects of music therapy on anxiety in breast cancer
patients during chemotherapy. Master thesis, Fu-Ying University, Kaohsiung,

190
Taiwan.
Li, S. (1993). The funeral and Chinese culture. Journal of Popular Culture, 27(2),
113-120.
Lin, C.-C., Lee, Y.-W., Chiang, L.-C., Tan, J.-Y., & Huang, T.-W. (2006). The relationship
between the degree of fatigue and the demographic differences of patients with
cancer while receiving cancer-related treatment. Bulletin On Hungkuang Institute
Of Technology, 48, 47-57.
Lin, C. C. (1998). Enhancing management of cancer pain: contribution of the internal
working model. Cancer Nursing, 21(2), 90-96.
Lin, C. C. (2000). Barriers to the analgesic management of cancer pain: a comparison of
attitudes of Taiwanese patients and their family caregivers. Pain, 88(1), 7-14.
Lin, C. C. (2001). Congruity of cancer pain perceptions between Taiwanese patients and
family caregivers: relationship to patients' concerns about reporting pain and
using analgesics. Journal of Pain & Symptom Management, 21(1), 18-26.
Lin, C. C., Wang, P., Lai, Y. L., Lin, C. L., Tsai, S. L., & Chen, T. T. (2000). Identifying
attitudinal barriers to family management of cancer pain in palliative care in
Taiwan. Palliative Medicine, 14(6), 463-470.
Lin, C. C., & Ward, S. E. (1995). Patient-related barriers to cancer pain management in
Taiwan. Cancer Nursing, 18(1), 16-22.
Lin, H. H., Chen, H. M., Kuo, T. F., Want, C. Y., & Huang, C. H. (2007). Effects of music
on anxiety and stress in hemodialysis patients. The Kaohsiung Journal of Nursing,
24(2), 1-16.
Lin, S. Y. (2003). A preliminary study: The influence of music therapy on

191
chemotherapy-induced acute nausea and vomiting of cancer children. master
thesis, National Defense Medical Center, Taipei, Taiwan.
Lin, T. Y. (1983). Psychiatry and Chinese culture. Western Journal of Medicine, 139(6),
862-867.
Liu, Y. H. (2002). Effects of music therapy on women's pain perception and anxiety
during labor. master thesis, Kaohsiung Medical University, Kaohsiung, Taiwan.
Lo, R. S., Woo, J., Zhoc, K. C., Li, C. Y., Yeo, W., Johnson, P., et al. (2002). Quality of
life of palliative care patients in the last two weeks of life. Journal of Pain &
Symptom Management, 24(4), 388-397.
Locsin, R. (1981). The effect of music on the pain of selected post-operative patients.
Journal of Advanced Nursing, 6, 19-25.
Massie, M. J., & Holland, J. C. (1987). Consultation and liaison issues in cancer care.
Psychiatric Medicine, 5(4), 343-359.
Massie, M. J., Holland, J. C., & Glass, E. (1983). Delirium in terminally ill cancer
patients. American Journal of Psychiatry, 140(8), 1048-1050.
McCaffery, M., & Pasero, C. (1999). Pain: Clinical Manual (2nd ed.). St. Louis, MO:
Mosby.
McCaffery, R., & Freeman, E. (2003). Effect of music on chronic osteoarthritis pain in
older adults. Journal of Advanced Nursing, 44(5), 517-524.
McCaffrey, R. G., & Good, M. (2000). The lived experience of listening to music while
recovering from surgery. Journal of Holistic Nursing, 18(4), 378-390.
McCarthy, E., Phillips, R. S., Zhong, Z., Drews, R. E., & Lynn, J. (2000). Dying with
cancer: Patients' function, symptoms, and care preferences as death approaches.

192
Journal of American Geriatrics Society, 48(5), S110-S121.
McCoubrie, R. C., & Davies, A. N. (2006). Is there a correlation between spirituality and
anxiety and depression in patients with advanced cancer? Supportive Care in
Cancer, 14(4), 379-385.
McCracken, L. M., & Gross, R. T. (1993). Does anxiety affect coping with chronic pain?
The Clinical Journal of Pain, 9(4), 253-259.
McMahon, S. B. (1996). NGF as a mediator of inflammatory pain. Philosophical
Transactions of the Royal Society of London. Series B. Biological Sciences,
351(1338), 431-440.
McPherson, C. J., & Addington-Hall, J. M. (2004). Evaluating palliative care: Bereaved
family members' evaluations of patients' pain, anxiety and depression. Journal of
Pain & Symptom Management, 28(2), 104-114.
Mercadante, S., Ferrera, P., Villari, P., & Casuccio, A. (2006). Opioid escalation in
patients with cancer pain: The effect of age. Journal of Pain and Symptom
Management, 32(5), 413-419.
Mercadante, S., Girelli, D., & Casuccio, A. (2004). Sleep disorders in advanced cancer
patients: Prevalence and factors associated. Supportive Care in Cancer, 12(5),
355-359.
Meuser, T., Peitruck, C., Radbruch, L., Stute, P., Lehmann, K. A., & Grond, S. (2001).
Symptoms during cancer pain treatment following WHO-guidelines: A
longitudinal follow-up study of symptom prevalence, severity and etiology. Pain,
93(3), 247-257.
Miaskowski, C. A., Bair, M., Chou, R., D'Arcy, Y., Hartrick, C., Huffman, L., et al. (Eds.).

193
(2009). Principles of analgesic use in the treatment of acute pain and cancer pain
(6th ed.). Glenview, IL: American Pain Society.
Miaskowski, C. A., Zimmer, E. F., Barrett, K. M., Debble, S. L., & Wallhagen, M. (1997).
Differences in patients' and family caregivers' perceptions of the pain experience
influence patient and caregiver outcomes. Pain, 72(1-2), 217-226.
Morita, T., Tei, Y., & Inoue, S. (2003). Impaired communication capacity nd agitated
delium in the final week of terminally ill cancer patients: Prevalence and
identification of research focus. Journal of Pain and Symptom Management, 26(3),
827-834.
Mullooly, V. M., Levin, R. F., & Feldman, H. R. (1988). Music for postoperative pain and
anxiety. Journal of New York State Nurses Association, 19(3), 4-7.
Munro, S., & Mount, B. (1978). Music therapy in palliative care. Canadian Medical
Association Journal, 119(9), 1029-1034.
Mystakidou, K., Parpa, E., Katsouda, E., Galanos, A., & Vlahos, L. (2005). Pain and
desire for hastened death in terminally ill cancer patients. Cancer Nursing, 28(4),
318-324.
Mystakidou, K., Rosenfeld, B., Parpa, E., Katsouda, E., Tsilika, E., Galanos, A., et al.
(2005). Desire for death near the end of life: the role of depression, anxiety and
pain. General Hospital Psychiatry, 27(4), 258-262.
Mytko, J. J., & Knight, S. J. (1999). Body, mind and spirit: Towards the integration of
religious and spirituality in cancer quality of life research. Psycho-Oncology, 8(5),
439-450.
Nakayama, H., Kikuta, F., & Takeda, H. (2009). A pilot study on effectiveness of music

194
therapy in hospice in Japan. Journal of Music Therapy, 46(2), 160-172.
National Cancer Institute. (2008, April 15). Complete and limited-duration cancer
prevalence estimates. SEER cancer statistics review 1975-2005. Retrieved
Feburary 2, 2009, from http://srab.cancer.gov/prevalence/statistics.html
National Comprehensive Cancer Network. (2008). Clinical practice guidelines in
oncology: Adult cancer pain [v.1.2008] Retrieved January 3, 2009,
from http://www.nccn.org/professionals/physician_gls/PDF/pain.pdf
Neimeyer, R. A., & David, V. B. (1995). Death anxiety. In H. Wass. & R. A. Neimeyer.
(Eds.), Dying: Facing the facts (3rd ed., pp. 49-58). New York: Taylor & Francis.
Nelson, J. B., & Carducci, M. A. (2000). The role of endothelin-1 and endothelin receptor
antagonists in prostate cancer. British Journal of Urology International, 85(Suppl
2), 45-48.
Newell, S., Swanson-Fisher, R. W., Girgis, A., & Ackland, A. (1999). The physical and
psycho-social experiences of patients attending an outpatient medical oncology
department: A cross-sectional study. European Journal of Cancer Care, 8, 73-82.
Nightingale, F. (1969). Notes on nursing. Mineola, NY: Dover Publications.
Nilsson, U., Rawal, N., Unestahl, L. E., Zetterberg, C., & Unosson, M. (2001). Improved
recovery after music and therapeutic suggestions during general anaesthesia: a
double-blind randomised controlled trial. Acta Anaesthesiologica Scandinavica,
45(7), 812-817.
Nowels, D., & Lee, J. T. (1999). Cancer pain management in home hospice settings: A
comparison of primary care and oncologic physicians. Journal of Palliative Care,
15(3), 5-9.

195
Noyes, R., Holt, C. S., & Massie, M. J. (1998). Anxiety disorders. In J. C. Holland (Ed.),
Psycho-oncology (pp. 548-559). New York: Oxford University Press.
Osarchuk, M., & Tatz, S. J. (1973). Effect of induced fear of death on belief in afterlife.
Journal of Personality and Social Psychology, 27(2), 256-260.
Padmanabhan, R., & Hildreth, A. L. (2005). A prospective, randomized controlled study
examining binaural beat audio and pre-operative anxiety in patients undergoing
general anaesthesia for day case surgery. Anaesthesia, 60, 874-877.
Paice, J. A., & Cohen, F. L. (1997). Validity of a verbally administered numeric rating
scale to measure cancer pain intensity. Cancer Nursing, 20(2), 88-93.
Paice, J. A., & Fine, P. G. (2006). Pain at the end of life. In B. R. Ferrell. & N. Coyle.
(Eds.), Textbook of palliative nursing (2nd ed., pp. 131-153). New York: Oxford
University Press.
Pandmanabhan, R., & Hildreth, A. L. (2005). A prospective, randomized controlled study
examining binaural beat audio and pre-operative anxiety in patients undergoing
general anaesthesia for day case surgery. Anaesthesia, 60, 874-877.
Parente, J. A. (1976). Music preference as a factor of music distraction. Perceptual and
Motor Skills, 43, 337-338.
Pasero, C., Paice, J. A., & McCaffery, M. (1999). Basic mechanisms underlying the
causes and effects of pain. In M. McCaffery. & C. Pasero. (Eds.), Pain: Clinical
manual (2nd ed., pp. 15-34). St. Louis, MO: Moscy Inc.
Payne, D. K., & Massie, M. J. (2000). Anxiety in palliative care. In H. M. Chochinov. &
W. Breitbart. (Eds.), Handbook of psychiatry in palliative medicine (pp. 63-74).
New York: Oxford University Press.

196
Payne, N. (2001). Occupational stressors and coping as determinants of burnout in female
hospice nurses. Journal of Advanced Nursing, 33(3), 396-405.
Payne, R. (1987). Anatomy, physiology, and neuropharmacology of cancer pain. Medical
Clinics of North America, 71(2), 153-167.
Payne, R., & Gonzales, R. G. (2004). Pathophysiology of pain in cancer and other
terminal diseases. In D. Doyle., G. Hanks. & N. Cherry. (Eds.), Oxford textbook of
palliative medicine (3rd ed., pp. 288-298). New York: Oxford University Press
Inc.
Peng, P. I. (2005). Effectiveness of music therapy on anxiety and physiological responses
for patients with hematologic malignancy. master thesis, Chang Gung
University, Linko, Taiwan.
Peng, W. L., Wu, G. J., Sun, W. Z., Chen, J. C., & Huang, A. T. (2006). Multidisciplinary
management of cancer pain: a longitudinal retrospective study on a cohort of
end-stage cancer patients. Journal of Pain & Symptom Management, 32(5),
444-452.
Pevey, C. F., Jones, T. J., & Yarber, A. (2008). How religion comforts the dying: A
qualitative inquiry. Omega - Journal of Death & Dying, 58(1), 41-59.
Phumdoung, S., & Good, M. (2003). Music reduces sensation and distress of labor pain.
Pain Management Nursing, 4(2), 54-61.
Porchet-Munro, S. (1988). Music therapy in support of cancer patients. Recent Results in
Cancer Research, 108, 289-294.
Portenoy, R. K., Payne, D., & Jacobsen, P. (1999). Breakthrough pain: Characteristics and
impact in patients with cancer pain. Pain, 81, 129-134.

197
Potter, J., Hami, F., Bryan, T., & Quigley, C. (2003). Symptoms in 400 patients referred
to palliative care services: Prevalence and patterns. Palliative Medicine, 17,
310-314.
Poulos, A. R., Gertz, M. A., Pankratz, V. S., & Post-White, J. (2001). Pain, mood
disturbance, and quality of life in patients with multiple myeloma. Oncology
Nursing Forum, 28(7), 1163-1171.
Reinhardt, U. (1999). Investigations into synchronisation of heart rate and musical
rhythm in a relaxation therapy in patients with cancer pain. Forschende
Komplementarmedizin, 6(3), 135-141.
Rhiner, M., Ferrell, B. R., Ferrell, B. A., & Grant, M. M. (1993). A structured nondrug
intervention program for cancer pain. Cancer Practice, 1(2), 137-143.
Roberts, B. L., Anthony, M. K., Madigan, E. A., & Chen, Y. (1997). Data management:
cleaning and checking. Nursing Research, 46(6), 350-352.
Rushton, P., Eggett, D., & Sutherland, C. W. (2003). Knowledge and attitudes about
cancer pain management: A comparison of oncology and nononcology nurses.
Oncology Nursing Forum, 30(5), 849-855.
Salmoon, D. (2001). Music therapy as psychospiritual process in palliative care. Journal
of Palliative Care, 17(3), 142-146.
Saunders, C. M. (1976). The challenge of terminal care. In T. Symington & R. L. Carter
(Eds.), Scientific Foundations of Oncology. London: Heinemann.
Schrodeder-Sheker, T. (1994). Music for the dying: A personal account of the new field of
music -Thanatology -- History, theories, and clinical narratives. Journal of
Holistic Nursing, 12(1), 83-99.

198
Schumacher, K. L., West, C., Dodd, M., Paul, S. M., Tripathy, D., Koo, P., et al. (2002).
Pain management autobiographies and reluctance to use opioids fro cancer pain
management. Cancer Nursing, 25(2), 125-133.
Sela, R. A., Bruera, E., Conner-Spady, B., Cumming, C., & Walker, C. (2002). Sensory
and affective dimensions of advanced cancer pain. Psycho-oncology, 11(1), 23-34.
Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and
quasi-experimental designs for generalized causal inference. Boston: Houghton
Mifflin.
Sherif, T., Jehani, T., Saadani, M., & Andejani, A. W. (2001). Adult oncology and
chronically ill patients: Comparison of depression, anxiety and caregivers' quality
of life. Eastern Mediterranean Health Journal, 7(3), 502-509.
Siedlecki, S. L., & Good, M. (2006). Effect of music on power, pain, depression and
disability. Journal of Advanced Nursing, 54(5), 553-562.
Sinha, S. S., Mohlman, J., & Gorman, J. M. (2004). Neurobiology. In R. G. Heimberg., C.
L. Turk. & D. S. Mennin. (Eds.), Generalized anxiety disorder: Advances in
research and practice (pp. 187-216). New York: Guilford Press.
Smith-Stoner, M. (2003). How Buddhism influences pain control choices. Nursing, 33(4),
17.
Smolen, D., Topp, R., & Singer, L. (2002). The effect of self-selected music during
colonoscopy on anxiety, heart rate, and blood pressure. Applied Nursing Research,
15(3), 126-136.
Sorensen, T. E., & Tybjerg, J. (2004). Treatment of psychiatric patients suffering from
anxiety using MusiCure - A pilot study Retrieved March 16, 2009,

199
from http://www.musicahumana.dk/documents/00022.pdf
Spiegel, D., Sands, S., & Koopman, D. (1994). Pain and depression in patients with
cancer. Cancer, 74(9), 2570-2578.
Spielberger, C. D. (1972). Anxiety: Current trends in theory and research: I. New York:
Academic Press.
Spielberger, C. D. (1983). Manual for the State-trait Anxiety Inventory (STAI). Menlo
Park, CA: Mind Garden, Inc.
Standley, J. M. (1986). Music research in medical/dental treatment: meta-analysis and
clinical applications. Journal of Music Therapy, 23(2), 56-122.
Stratton, V. N., & Zalanowski, A. H. (1984). The relationship between music, degree of
liking, and self-reported relaxation. Journal of Music Therapy, 21(4), 184-192.
Stromgren, A. S., Groenvold, M., Petersen, M. A., Goldschmidt, D., Pedersen, L., Spile,
M., et al. (2004). Pain characteristics and treatment outcome for advanced cancer
patients during the first week of specialized palliative care. Journal of Pain &
Symptom Management, 27(2), 104-113.
Sun, V. C., Borneman, T., Ferrell, B., Piper, B., Koczywas, M., & Choi, K. (2007).
Overcoming barriers to cancer pain management: an institutional change model.
Journal of Pain & Symptom Management, 34(4), 359-369.
Swanwick, M., Haworth, M., & Lennard, R. F. (2001). The prevalence of episodic pain in
cancer: A survey of hospice patients on admission. Palliative Medicine, 15(1),
9-18.
Tabachnick, B. G., & Fidell, L. S. (2007). Using Multivariate Statistics (5th ed.). Boston:
Pearson Education.
200
Taiwan Cooperative Oncology Group. (2007). Cancer pain management guideline.
Miaoli, Taiwan: National Health Research Institutes.
Tang, S. T. (2003). Determinants of hospice home care use among terminally ill cancer
patients. Nursing Research, 52(4), 217-225.
Taylor, A. L., Gostin, L. O., & Pagonis, K. A. (2008). Ensuring effective pain treatment:
A national and global perspective. JAMA, 299(1), 89-91.
Taylor, L. K., Kuttler, K. L., Parks, T. A., & Milton, D. (1998). The effect of music in the
postanesthesia care unit on pain levels in women who have had abdominal
hysterectomies. Journal of PeriAnesthesia Nursing, 13(2), 88-94.
The National Commission for the Protection of Human Subjects of Biomedical and
Behavioral Research. (1979). The Belmont Report: Ethical Principles and
Guidelines for the protection of human subjects of research. Regulations and
Ethical Guidelines Retrieved April 27, 2009,
from http://ohsr.od.nih.gov/guidelines/belmont.html
The National Science Council. (2004, December 19, 2008). Religion and culture in
Taiwan. Taiwan Social Change Survey Retrieved January 9, 2009,
from http://www.ios.sinica.edu.tw/sc/cht/5-a8.php
The SUPPORT Principal Investigators. (1995). A controlled trial to improve care for
seriously ill hospitalized patients: The Study to Understand Prognoses and
Preferences for Outcomes and Risls of Treatment (SUPPORT). JAMA, 274(20),
1591-1598.
Thielking, P. D. (2003). Cancer pain and anxiety. Current Pain & Headache Reports, 7(4),
249-261.

201
Thorson, J. A., & Powell, F. C. (2000). Death anxiety in younger and older adults. In A.
Tomer. (Ed.), Death attitudes and the older adult: Theories, concepts, and
applications (pp. 123-136). Philadelphia: Taylor & Francis.
Tittle, M. B., McMillan, S. C., & Hagan, S. (2003). Validating the brief pain inventory for
use with surgical patients with cancer. Oncology Nursing Forum Online, 30(2),
325-330.
Tremblay, A., & Breitbart, W. (2001). Psychiatric dimensions of palliative care.
Neurologic Clinics, 19(4), 949-966.
Tsai, D. T., & Lopez, R. A. (1997). The use of social support by elderly Chinese
immigrants. Journal of Gerontological Social Work, 29(1), 77-93.
Tsai, J.-S., Wu, C.-H., Chiu, T.-Y., Hu, W.-Y., & Chen, C.-Y. (2005). Fear of death and
good death among the young and elderly with terminal cancers in Taiwan. Journal
of Pain & Symptom Management, 29(4), 344-351.
Tsai, J.-S., Wu, C.-H., Chiu, T.-Y., Hu, W.-Y., & Chen, C.-Y. ( 2006). Symptom patterns of
advanced cancer patients in a palliative care unit. Palliative Medicine, 20(6),
617-622.
Tsai, L.-Y., Ku, N.-P., Chang, T.-Y., & Lai, Y.-H. (2001). Anxiety, depression and related
factors in cancer patients with pain. New Taipei Journal of Nursing, 3(1), 23-33.
Tsai, Y. F. (2007). Gender differences in pain and depressive tendency among Chinese
elders with knee osteoarthritis. Pain, 130(1-2), 188-194.
Tsuchiya, M., Asada, A., Ryo, K., Noda, K., Hashino, T., Sato, Y., et al. (2003). Relaxing
intraoperative natural sound blunts haemodynamic change at the emergence from
propofol general anaesthesia and increases the acceptability of anaesthesia to the

202
patient. Acta Anaesthesiologica Scandinavica, 47(8), 939-943.
Tu, W. M. (1987). A Chinese perspective of pain. Acta Neurochirurgica, 38, 147-151.
Vainio, A., & Auvinen, A. (1996). Prevalence of symptoms among patients with advanced
cancer: An international collaborative study. Journal of Pain and Symptom
Management, 12(1), 3-10.
Valentinuzzi, M. E., & Arias, N. E. (1999). Human psychophysiological perception of
musical scales and nontraditional music. IEEE Engineering in Medicine and
Biology Magazine, 18(2), 54-60.
Vigano, A., Bruera, E., & Suarez-Almazor, M. E. (1998). Age, pain intensity, and opioid
dose in patients with advanced cancer. Cancer, 83(6), 1244-1250.
Voss, J. A. (2001). Measurement of anxiety and pain in critucally ill patients. Paper
presented at the Midwest Nursing Research Society, Cleveland, OH.
Voss, J. A., Good, M., Yates, B., Baun, M. M., Thompson, A., & Hertzog, M. (2004).
Sedative music reduces anxiety and pain during chair rest after open-heart surgery.
Pain, 112(1-2), 197-203.
Wall, P. D. (1988). Neurological mechanisms in cancer pain. Cancer Surveys, 7(1),
127-140.
Wang, K. Y., Ho, S. T., Ger, L. P., Wang, J. J., Cherng, C. H., & Lin, C. C. (1997). Patient
barriers to cancer pain management: from the viewpoint of the cancer patients
receiving analgesics in a teaching hospital of Taiwan. Acta Anaesthesiologica
Sinica, 35(4), 201-208.
Ward, S. E., Goldberg, N., Miller-McCauley, V., Mueller, C., Nolan, A., Pawlik-Plank, D.,
et al. (1993). Patient-related barriers to management of cancer pain. Pain 52(3),
203
319-324.
Ward, S. E., Hughes, S., Donovan, H., & Serlin, R. C. (2001). Patient education in pain
control. Supportive Care in Cancer, 9(3), 148-155.
Weinberger, N. M. (2004). Music and the brain. Scientific American, 16(3), 36-43.
Weiss, S. C., Emanuell, L. L., Fairclough, D. L., & Emanuel, E. J. (2001). Understanding
the experience of pain in terminally ill patients. Lancet, 357(9265), 1311-1315.
Wellish, D., Kagawa-Singer, M., Reid, S. L., Lin, Y.-J., Nishikawa-Lee, S., & Wellish, M.
(1999). An exploratory study of social support: A cross-cultural comparison of
Chinese-, Japanses-, and Anglo-American breast cancer patients.
Psycho-Oncology, 8(3), 207-219.
White, J. M. (1999). Effects of relaxing music on cardiac autonomic balance and anxiety
after acute myocardial infarction. American Journal of Critical Care, 8(4),
220-230.
Wick, M. J., Minnerath, S. R., Lin, X., Elde, R., Law, P. Y., & Loh, H. H. (1994).
Isolation of a novel cDNA encoding a putative membrane receptor with high
homology to the cloned mu, delta, and kappa opioid receptors. Brain research.
Molecular brain research, 27(1), 37-44.
Wieser, H. G., Hungerbuhler, H., Siegel, A. M., & Buck, A. (1997). Musicogenic epilepsy:
review of the literature and case report with ictal single photon emission
computed tomography. Epilepsia, 38(2), 200-207.
Wigram, T., Pedersen, I. N., & Bonde, L. O. (2002). A comprehensive guide to music
therapy. Philadelphia: Jessica Kingsley Publishers.
Wilkie, D. J. (1995). Neural mechanisms of pain: A foundation for cancer pain

204
assessment and management. In D. B. McGuire., C. H. Earbro. & B. R. Ferrell.
(Eds.), Cancer Pain Management (2nd ed., pp. 61-87). Sudbury, MA: Jones and
Bartlett Publishers.
Williams, A. L. (2006). Perspectives on spirituality at the end of life: A meta-summary.
Palliative and supportive care, 4(4), 407-417.
Williamson, J. W. (1992). The effects of ocean sounds on sleep after coronary artery
bypass graft surgery. American Journal of Critical Care, 1(1), 91-97.
Willis, W. D. (1989). The origin and destination of pathways involved in pain
transmission. In P. D. Wall. & E. Melzack (Eds.), Textbook of pain (2nd ed., pp.
112-127). New York: Churchill Livingstone.
Wills, B. S., & Wootton, Y. S. (1999). Concerns and misconceptions about pain among
Hong Kong Chinese patients with cancer. Cancer Nursing, 22(6), 408-413.
Wilson, E. O. (1984). Biophilia: The bond with other species. Cambridge, MA: Harvard
University Press.
Wilson, K. G., Chochinov, H. M., Skirko, M. G., Allard, P., Chary, S., Gagnon, P. R., et al.
(2007). Depression and anxiety disorders in palliative cancer care. Journal of
Pain & Symptom Management, 33(2), 118-129.
Wittmann, M., Volimer, T., Schweiger, C., & Hiddemann, W. (2006). The relation
between the experience of time and psychological distress in patients with
hematological malignancies. Palliative and supportive care, 4(4), 357-363.
Wong, P. T., Reker, G. T., & Gesser, G. (1994). Death attitude profile-Revised. In R. A.
Neimeyer (Ed.), Death anxiety handbook: Research, instrumentation, and
application (pp. 121-148). Washington, DC: Taylor & Francis.

205
World Health Organization. (1996). Cancer pain relief: With a guide to opioid availability,
cancer pain relief and palliative care. In T. W. E. Committee (Ed.), WHO
Technical Report Series (2nd ed.). Geneva: World Health Organization.
Wright, J. (Ed.) (2001) Collins Cobuild English dictionary for advanced learners (3rd
ed.). Glasgow: HarperCollins Publishers.
Wu, H.-C. (2007). The effects of listening to music on anxiety reduction for mechanically
ventilated patients. Unpublished master thesis, Kaohsiung Medical University,
Kaohsiung, Taiwan.
Wu, H.-C., & Chou, F.-H. (2008). Effectiveness of music therapy in reducing
physiological and psychological anxiety in mechanically pentilated Patients The
Journal of Nursing, 55(5), 35-44.
Yao, C. C. (1998). Effects of music therapy on state anxiety in open-heart surgery
patients during weaning ventilator. master thesis, National Defense Medical
Center, Taipei, Taiwan.
Yeager, C. A., Miaskowski, C. A., Dibble, S. L., & Wallhagen, M. (1995). Differences in
pain knowledge and perception of the pain experience between outpatients with
cancer and their family caregivers. Oncology Nursing Forum, 22(8), 1235-1241.
Yick, A. G., & Gupta, R. (2002). Chinese cultural dimensions of death, dying, and
bereavement: Focus group findings. Journal of Cultural Diversity, 9(2), 32-42.
Yilmaz, E., Ozcan, S., Basar, M., Basar, H., Batislam, E., & Ferhat, M. (2003). Music
decreases anxiety and provides sedation in extracorporeal shock wave lithotripsy.
Urology, 61(2), 282-286.
Yu, L. C. (1983). Patterns of filial belief and behavior within the contemporary

206
Chinese-American family. International Journal of Sociology of the Family, 13(2),
17-36.
Zeppetella, G., O'Doherty, C. A., & Collins, S. (2000). Prevalence and characteristics of
breakthrough pain in cancer patients admitted to a hospice. Journal of Pain and
Symptom Management, 20(2), 87-92.
Zimmerman, L., Pozehl, B., Duncan, K., & Schmitz, R. (1989). Effects of music in
patients who had chronic cancer pain. Western Journal of Nursing Research, 11(3),
298-309.
Zimmerman, L., Story, K. T., Gaston-Johansson, F., & Rowies, J. (1996). Psychological
variables and cancer pain. Cancer Nursing, 19(1), 44-53.




















