
The Effect of Instructional Intervention about Competency ...
27
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4 123 The Effect of Instructional Intervention about Competency-Based Nursing Education on academic’s knowledge, planning skills, and their acceptance during COVID Pandemic. Azza Fathi Ibrahim (*1) , Magda Atiya Gaber (2) , Shadia Ramadan Morsy (1) (1) Nursing Education Department, Faculty of Nursing, Alexandria University, Egypt (2) Department of Nursing Administration, Faculty of Nursing, Zagazig University, Egypt *Correspondence Email: [email protected] Abstract Nursing professionals are at the forefront of the pandemic management of COVID-19 all over the world. Egypt almost suffers from a severe shortage of nursing staff. Thus, Egyptian nursing educators are obligated to edivorp the nursing students with essential competencies for approaching nursing work, mainly in such difficult situations. Therefore, Competency-based nursing education (CBNE) is an inevitable as an educational delivery option in nursing colleges as required by the Egyptian government. The current study aimed at determining the effect of CBNE instructional intervention on nursing academics' knowledge, planning skills, and acceptance to follow CBNE during the COVID pandemic in Egypt. A quasi-experimental design was operated at the Faculty of Nursing, Alexandria University. The study subjects comprized 84 academics (nursing educators from all the faculty departements) who were selected convpeopeine and dovided into control and exppromental groups. ehp CBNE triple-section assessment sheet was developed and used for data collection. Results revealed that there was a higher improvement in the experimental group’s scores than control group regarding CBNE knowledge, planning skills, and their acceptance to follow CBNE during COVID eierpnop, after the conduction of the CBNE instructional intervention. Thus, there was a statistically significant difference between the experimental and control groups after such intervention in favor of the experimental group. In conclusion, CBNE awareness, understanding and acceptance to follow it during the current risk time of COVID, among nursing academics are urgent Recommendation: the CBNE scheme requires a comprehensive understanding. Interdisciplinary healthcare contributions should be carried out to develop a CBNE model in nursing field. Further studies: Assessment of CBNE implementation progress in Egyptian colleges, Evaluate of the effect of the CBNE program on Egyptian nursing students' achievement, engagement, and patients' satisfaction. Key words: Competency-based nursing education, academics, students, COVID-19 pandemic, instructional intervention, Egypt. Introduction: Competency-based education (CBE) is an educational delivery option that proves to be effective in meeting nursing students' essential competencies for approaching nursing practice. Nursing and its shortage in Egypt needs expert professional educational preparations to equip competent nursing students, fundamentally, in healthcare crisis situations, like COVID-19 pandemic. But, there is still considerable confusion about the concept of competence, competency, and competency based education, competency-based nursing education (CBNE) particularly in nursing. Correspondingly, curriculum, teaching strategies and evaluation frameworks in CBNE still need clarifications, explanations and application. (Western Governor's University 2016, Dashash et al, 2020, Englander et al., 2013, Brownie et al, 2018) Consistently, validity and reliability of such an educational paradigm have to be explored, comprehended and practiced, mainly in the developed countries. Nursing curricula require an inevitable improvement in competencee development during the Corona crisis that is ii the same time, already, required from the Ministry of higher education by the Egyptian government. (National Authority for Quality Assurance and Accreditation of Education , 2017, Brownie et al, 2018, Ramoset al., 2019, Gravina 2017, Lucey 2018, Bohain et al., 2014) All health sectors and ihpministry of health or ihp ministry of higher education in Egypt have approved the critical nursing role in
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of The Effect of Instructional Intervention about Competency ...

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
123
The Effect of Instructional Intervention about Competency-Based Nursing
Education on academic’s knowledge, planning skills, and their acceptance
during COVID Pandemic.
Azza Fathi Ibrahim(*1), Magda Atiya Gaber(2), Shadia Ramadan Morsy(1)
(1) Nursing Education Department, Faculty of Nursing, Alexandria University, Egypt
(2) Department of Nursing Administration, Faculty of Nursing, Zagazig University, Egypt
*Correspondence Email: [email protected]
Abstract
Nursing professionals are at the forefront of the pandemic management of COVID-19 all over the world. Egypt almost suffers from a severe shortage of nursing staff. Thus, Egyptian nursing
educators are obligated to edivorp the nursing students with essential competencies for approaching
nursing work, mainly in such difficult situations. Therefore, Competency-based nursing education
(CBNE) is an inevitable as an educational delivery option in nursing colleges as required by the
Egyptian government. The current study aimed at determining the effect of CBNE instructional
intervention on nursing academics' knowledge, planning skills, and acceptance to follow CBNE during the COVID pandemic in Egypt. A quasi-experimental design was operated at the Faculty of
Nursing, Alexandria University. The study subjects comprized 84 academics (nursing educators
from all the faculty departements) who were selected convpeopeine and dovided into control and
exppromental groups. ehp CBNE triple-section assessment sheet was developed and used for data
collection. Results revealed that there was a higher improvement in the experimental group’s scores
than control group regarding CBNE knowledge, planning skills, and their acceptance to follow
CBNE during COVID eierpnop, after the conduction of the CBNE instructional intervention. Thus,
there was a statistically significant difference between the experimental and control groups after
such intervention in favor of the experimental group. In conclusion, CBNE awareness,
understanding and acceptance to follow it during the current risk time of COVID, among nursing
academics are urgent Recommendation: the CBNE scheme requires a comprehensive understanding. Interdisciplinary healthcare contributions should be carried out to develop a CBNE
model in nursing field. Further studies: Assessment of CBNE implementation progress in Egyptian
colleges, Evaluate of the effect of the CBNE program on Egyptian nursing students' achievement,
engagement, and patients' satisfaction.
Key words: Competency-based nursing education, academics, students, COVID-19 pandemic, instructional intervention, Egypt.
Introduction:
Competency-based education (CBE) is an
educational delivery option that proves to be
effective in meeting nursing students' essential
competencies for approaching nursing practice.
Nursing and its shortage in Egypt needs expert
professional educational preparations to equip
competent nursing students, fundamentally, in
healthcare crisis situations, like COVID-19
pandemic. But, there is still considerable
confusion about the concept of competence, competency, and competency based education,
competency-based nursing education (CBNE)
particularly in nursing. Correspondingly,
curriculum, teaching strategies and evaluation
frameworks in CBNE still need clarifications,
explanations and application. (Western
Governor's University 2016, Dashash et al,
2020, Englander et al., 2013, Brownie et al,
2018) Consistently, validity and reliability of
such an educational paradigm have to be
explored, comprehended and practiced, mainly
in the developed countries. Nursing curricula
require an inevitable improvement in competencee development during the Corona
crisis that is ii the same time, already, required
from the Ministry of higher education by the
Egyptian government. (National Authority for
Quality Assurance and Accreditation of
Education , 2017, Brownie et al, 2018, Ramoset
al., 2019, Gravina 2017, Lucey 2018, Bohain et
al., 2014) All health sectors and ihp ministry of
health or ihp ministry of higher education in
Egypt have approved the critical nursing role in
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
124
Egypt, which needs empowerment and
reforming. Therefore, as a national strategy,
developing and implementation of Competen-
cy-Based Education (CBE) among healthcare
colleges and particularly, in the nursing field
becomes an important national need in Egypt.
(National Authority for Quality Assurance and
Accreditation of Education, 2017,Brownie et
al., 2018, Watson, et al., 2002, El Tawil 2021, Wu and Martin, 2019)
The concept of competency firstly appears
in the third quarter of the past decade within the
work of Robert White in 1959 in his article
about work motivation theory. In 1971, the
competency term was used in recruitment in
Human Resource Management (HRM) David
Clarence McClelland in 1975 presents the
criteria or competencies needed for a specific
job. McCalland developed a list of
competencies that are needed for each job in HRM which are called model for superior
performance. (Spady 1977, Perry and Hamm
2017, Mahapatro 2010, Stern 2010)
Descriptions and definitions of
Competence, competency, performance or
learning outcomes, and competency-based
nursing education are almost confused.
(Brownie et al., 2018, Wu and Martin, 2019,
Pijl-Zieber et al., 2014) There are many various
ways of thinking about the concept of competency and several interpretations of its
meaning, particularly in vocational work. But,
all terms in the current study were handled
them on an academic basis. Hager and Gonczi
in 1996, Austin in 2019, Bates in 2020, Fukada
in 2018, Brownie et al., in 2018, Wu and
Martin, in 2019, Salman et al, in 2020 reported
that competency describes that the people have
a chain of required characteristics involving
attitudes or values, knowledge, skills and
capabilities such as critical thinking, leadership, and communication skills that allow them to do
any task successfully. Or, it is the person’s
aptitudes to execute something successfully or
efficiently. From Greek views, competency
means the quality to be capable, or having skills
and abilities to do something. Thus, the
academic utilization of the competency concept
was developed in vocational education then,
spreading to all types of schools and colleges’
education. The competency concept has
appeared through knowledge application, not
acquisition. Competency entails a group of
knowledge, skills, attitudes that the learners
obtain and develop through their teaching-
learning experiences, training, and then, into the
profession. Consequently, the competency
concept built the personal abilities, and traits
that were equipped by the students to be
competent professionals. Competency refers to a cluster of cognitive, affective, and behavioral
abilities that were explained in cognitivin,
humanism, behaviorism, and social learning
theories. (Hager and Gonczi, 1996, Austin,
2019, Bates, 2020, Fukada, 2018, Brownie et
al., 2018, Wu and Martin, 2019, Salman et al,
2020, Mulder et al., 2006, , Jung et al. 2020,
and Koster 2017) Competency is translated into
the ability to confirm the link between the
theory and the practice, in which the students
develop multiple personal features and
attributes.
For competence term, it refers to the level
which comes after competency. When the
student can link all his\her abilities and
attributes with certain professional situations,
after learning acquisition, the competence takes
place. The concept of competence or
competencies is a more precise term than competency because competence is more
directpr to a certain function or a specific job
than competency. The students have to tie their
abilities and characteristics with the learning
knowledge, skills, and attitudes to fit certain
functions in a particular practical situation.
(Jung et al. 2020, and Koster 2017, Wilcox
2012, Hager and Gonczi 1996). Competence in
nursing translates the students' abilities with the
learning content into scientific awareness in
work situation and life-long learning
management for professional application. (Fukada, 2018, Austin 2019, Lucey 2018,
Garneau et al, 2017, Koster et al, 2017) After
learning and training, students can transfer
knowledge into practice and can develop
competencies along the course to manage
certain tasks for professional success.
Competence passes through certain phases
(Unconscious incompetence, conscious
incompetence, conscious competence, and
Unconscious competence). Moreover, to
acquire certain competencies, you will step by step follow hierarchy levels of competency

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
125
(basic, competent, advanced, and expert)
Furthermore, competency has many types such
as administrative, technical, people, and core
competencies. For each professional discipline,
there is a unique group of competencies
involved and achieved in its profession.
(Brownie et al., 2018, Wu and Martin, Fukada,
2018, Austin 2019, Lucey 2018, Garneau et al,
2017, Koster et al, 2017) Therefore, competence is a leading force for observed
effective professional action.
Performance and learning outcome are
the end obvious results of competency and
competence. Smith, in 1993, Kennedy et al., in
2009, Blömeke et al., in 2013, Brownie et al., in
2018, Wu and Martin in 2019 documented that
Performance\Learning outcome is a specific
statement of what the student is able to do as a
result of teaching experience in a measurable
way. It describes exactly what a student will be able to carry out after the course of education in
an observable and measurable manner.
Therefore, the competence can be measured
through observing or assessing its learning
outcomes which are accomplished and observed
by the students. Educators have to understand
and determine all competencies for each course
and its related learning outcomes for each
competency that closely relies upon the
professional attributes and performance in the
workplace. (Jung et al., 2020, Weeks et al., 2017, Bates 2020) Accordingly, learning
outcomes are the origins for an assessment and
evaluation process of the program
competencies.
In consistencep with Dreyfus, there are
five phases for acquiring competencies for
professional work that are: novice, advanced
beginner, competence, proficiency, and
expertise. Through such a gradual developed
skill scale, the student's competencies in
practice are developed and enhanced. (Blömeke et al., 2013, Bates 2020, Gravina 2017, Fukada,
2018, Nyoni and Botma 2019, Koster et al,
2017) Consequently, it is a significant shift in
the nursing educational paradigm, to be focused
on job requirements, not academic ones. Hence,
there are six phases to develop a competency-
based curriculum as the following: 1-
Determine the needed attributes among
graduates. 2-Obviously define the essential
competencies and their performance outcomes.
3-Specify indicators for each developed
competency and learning transfer. 4- Choose
teaching-learning and training activities with fit
instructional strategies. 5- Choose suitable
assessment instruments that assess the student's
advance of mastery with details. 6- Plan ie
overall assessment program.(Albanese et al,
2010, Frank et al, 2010, and Sistermans 2020,
Getha-Taylor, 2013, Fukada 2018, Japanese Nursing Association 2005, American Nurses
Association, 2006)
Competency-based nursing education is
the main target of the current study. All over
the world, and mainly in Arabian countries, in
nursing colleges, there is necessitating
transferring from the traditional educational
system to CBNE. According to Garneau et al,
in 2017, Gravina, in 2017, and Jung in 2020,
who discussed that CBNE is an instructional
system in which a performance-based learning
process is used in nursing education that reflects to which extend the nurse students
demonstrate their level of accomplishment on
subject-area. In another word, it is an
educational system structured to allow students
to demonstrate their learning according to their
abilities and attributes in nursing with their pace
and under authentic assessment with high
quality and validation. The study schedules in
CBNE curricula are planned in a flexible
individualized manner with extra hours, online,
blended learning interactions, open labs, and with continuous reality practice to fit students'
differences and needs, regardless of the time.
CBNE focuses on students' achievement and
the learning they obtained, not the credit hours
of course time. Nursing students have their full
self-dependency and responsibility about their
learning place, nature, time, and content used.
(Garneau et al, 2017, Gravina, 2017, and Jung
2020) If the students gain the required
competencies in a limited time, this will meet
work needs, save time, and money for students, teachers, and institutions.
The National Authority for Quality
Assurance and Accreditation of Education in
2017 in Egypt discussed that the nurses play an
essential role in the promotion, maintenance
and restoration of health. Thus, the Egyptian
healthcare district found it is a necessity to
prepare competent nurses with expert
competencies in the nursing field. Those
competencies are highly required to enable

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
126
nurses to carry out their vital roles such as
health promoters, educators, counselors, care
coordinators, case managers, and researchers.
(Bates 2020, Brownie et al., 2018, Jung et al.,
2020, National Authority for Quality Assurance
and Accreditation of Education 2017)
Consequently, Five Competence-Domains are
developed and included in the competence-
based National Academic Reference Standards for Nursing Education by the National
Authority for Quality Assurance and
Accreditation of Education 2017: Domain 1:
Professional and Ethical Practice, Domain 2:
Holistic Patient-Centered Care, Domain 3:
Managing People, Work Environment, and
Quality, Domain 4: Informatics and
Technology, Domain 5: Inter-professional
Communication. Since 1991 there hivp eppe
many trials to develop specific competency
domains in nursing education, in Egypt. (The
National Authority for Quality Assurance and Accreditation of Education 2017, Salem et al.,
2018, Brownie et al., 2018) Nowadays,
incorporating, carrying out, and evaluating
CBNE nationally and internationally, is a hope
in nursing colleges. In line with Fastre et al, in
2014, it is important to give the nurse students
the assessment criteria and the learning skills
during their training with specific performance
criteria. Therefore, assessment criteria in
implementing the CBNE ought to be
performance criteria that are present in the checklist, rubrics, and rating scales. (Fastre et
al, 2014, Fan et al, in 2015) All nursing courses
in the program should be revised, mainly for
clinical parts, to involve a content that parallels
professional needs and standards with detailed
statements of performance. Consequently, the
CBNE curricula of each course can be easily
comprehended, implemented, and evaluated.
But, literature is still limited to give details
about such valuable systems and how to operate
it effectively, in Egypt, mainly in risk situations, like in the era of COVID-19.
Nurses are the soldiers who stay for and
carryout patient care every minute, hour, and
day that exposp them to death and illness.
Healthcare quality and success can't be
established without competent nurses.
Therefore, in Egypt, the ministry of higher
education put a clear vision to incorporate
CBNE in the nursing curricula that allow
nursing students to demonstrate mastery in
nursing practice and professional competencies
through their work performance and against any
healthcare risks. (Brownie et al., 2018, Salem et
al., 2018, Western Governor's University 2016,
Englander et al., 2013, Ramos et al, 2020,
Dashash et al, 2020) The ministry of higher
education obligated all universities to start
incorporation of CBE planning in all courses in
Bachelor programs in 2018-2020. The COVID-19 pandemic situation started in 2019-2020,
parallel with the starting point of CBE, in
Egypt, which is a valuable and beneficial
coincidence. Therefore, academic staff’s
orientation and training for preparing courses in
a form of CBE National Framework requires
rapid organization, planned time, preparations
and guidance. (National Authority for Quality
Assurance and Accreditation of Education
2017, Wallace et al, 2021, Lucey 2018, Inter-
professional Education Collaborative 2016)
During the pandemic era, Egyptian colleges competed in preparing the academics
for using of online platforms and E-educational
shifting as approaches to deal with the
unanticipated crisis of Corona pandemic. Such
methodologies used to adjust the students'
situation of abrupt confinement of the crisis. At
the same time, all colleges in Egypt start to
incorporate CBE system and enhance all
academics for shifting with the current policies
and the current academic situation. Therefore,
CBNE faced many challenges, some of those challenges are: 1) academics resistance and
unawareness for planning, integrating and
implementing of CBNE, 2) the gap between
theory and practice for tailoring all nursing
subjects according to professional standards and
work market needs, 3) shifting of student’s
clinical procedures to be competencies nature,
4) clinical environment preparations for the
settled competencies and 5) COVID-19 risks in
the work place and so on. (Blömeke et al, 2013,
Essa, et al, 2021, Albanese et al, 2010, Ramos et al, 2020) Nursing students' ie hiers training
is ultimately beneficial in the past, nowadays
and forever, which is still necessitated.
(Blömeke et al, 2013, Essa, et al, 2021, Ramos
et al, 2020, Gravina 2017, Wu et al,
2019)Therefore, CBNE is inevitable and
beneficial in the crisis situation because the
healthcare system needs expert and proficient
nursing students with proper attributes and
competencies to face any healthcare crisis. But

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
127
CBNE should be planned and implemented by
trained academics that can plan, operate,
manage, and accept it and keep nursing students
safe. Conversely, still, in Egypt, nursing
academics at many of nursing colleges, need
comprehensive and well planned instructional
sessions about CBNE to be incorporated and
executed in nursing curricula in the current
pandemic crisis. (National Authority for Quality Assurance and Accreditation of
Education 2017, Ramos et al, 2020, Gravina
2017, Wu et al, 2019, Hussien et al, 2020)
Obviously, academic staff resistance is
anticipated. Some nursing academics may find
CBNE is risky approach for nursing students.
And others may find it the only solution to
promote nursing students’ qualifications,
against any healthcare risks. Therefore,
provision of CBNE guidance and orientation to
nursing academics will correct any conflict.
Significance of the study In Egypt, CBNE should be assumed
broadly, correctly and strictly according to the
Ministry of higher education requirements and
to effectively equip our nurses with fit
competencies against any healthcare risks.
Using of professional standards in planning for
CBNE system under the light of National
Qualification Framework 2017 (National
Authority for Quality Assurance and
Accreditation of Education 2017) and
integrating the competencies and its measurable outcomes, in the fluency of nursing
education(curricula, teaching strategies,
student’s evaluation and its policies or rules), is
a crucial issue for nursing academics. CBNE
orientation, training, guidance, support and
instructional interventions are essentially and
mostly required for nursing academics,
particularly, in the COVID era. Nowadays,
there is minimal evidence about provision and
support nursing academics with such guidance
or training in Egypt, mainly in a form of experimental trial. Establishment of such
educational interventions for nursing academics
will help them in successfully and
constructively spreading of CBNE culture and
strengthenoei CBNE nursing academics'
knowledge, skills and acceptance to follow it.
CBNE will prepare nursing students to be
competent mainly, against pandemic situations.
CBNE finds some resistance among academics
that can be resolved by their guidance and
awareness about CBNE. Proper realization of
CBNE value in preparing our nursing students'
competencies, among academics, especially,
during crisis situations is a beneficial step for
nursing education. Accordingly, the current
study aimed at determining the effect of CBNE
instructional intervention on nursing academics'
knowledge, planning skills, and acceptance regarding implementing CBNE during the
COVID pandemic.
Theoretical framework
Staff development is an essential process
in the educational organization. Construction of
educational and training or orientation
instruction for the employees (nursing
academics), essentially, during crisis time, has a
worthy impact on their achievement progress
and work success. Mel Kleiman (2000) put a
framework for the employee training and orientation construction for knowledge,
management skills and their attitudes regarding
any new mission in the risk situation. Anxiety,
fear and restlessness during the crisis, enhance
preparedness and initiation of the employee. It
is a grassroots for employee educational trials
that helps them to gain cooperation, positive
thinking, motivation and work loyalty,
particularly in risk conditions.
Research hypotheses: The following hypotheses were
developed:
*H1: Nursing academics who receive
CBNE instructional intervention will have higher scores in their knowledge regarding
CBNE than those who do not receive such
intervention.
*H2: Nursing academics who receive
CBNE instructional intervention will have
higher scores in their planning skills for CBNE
than those who do not receive such
intervention.
*H3: Nursing academics who receive
CBNE instructional intervention will have
higher scores in their acceptance to follow CBNE during the COVID pandemic than those
who do not receive such intervention.
Materials & method
Research design: a quasi-experimental
research design was operated.
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
128
Setting: This study was conducted at the Faculty of Nursing, Alexandria University in
Egypt. CBNE instructional intervention was
conducted at the College council venue (it was
prepared well for experimental group only for
four days). The control group was selected from
all nine scientific nursing departments in the
college, namely: Medical& Surgical Nursing,
Critical Care and Emergency Nursing, Pediatric Nursing, Obstetric and Gynecological Nursing,
Gerontological Nursing, Psychiatric and Mental
Health Nursing, Community Health Nursing,
Nursing Administration and Nursing Education
Departments.
Study subjects: involved nursing
acadenics who have a doctoral degree, and they
are involving in the planning of nursing
program’ and course’s spisification
development in the faculty (lecturers, assisstant
professors and professors).
The minimal sample size that was estimated
based on Epi info program is 76.
Therefore, conveniently the study sampling
recruitment reaches 84 nursing academics, as
follow:
Group A: A convenopei sample of 42
nursing academics who wpdp assigned as an
expreomental group because they regostered and attendpr the CBNE instructional
intervention after announcement in the
Nursing Faculty.
Group B: A convenopei sample of 42nursing
academics who assigned as a control group
and accepter to participate into the study and
not regostered or attend the CBNE
instructional intervention. Group B was
selected convenoently from all the nine
scientific nursing departments, by
proportionate random sampling approach from each department. The researchers
recruited the control group sample number
until it became approximately equal to the
experimental group.
Tools: a triple section evaluation sheet was developed by the researchers which included
three parts for data collection:
a. Part one: CBNE knowledge test: that was developed by the researchers after a
thorough review of the related literature,
(Dashash et al, 2020, Page 2020, Ramos-
Morcillo et al, 2020, Brownie et al, 2018,
Lucey 2018, National Authority for Quality
Assurance and Accreditation of Education
2017, Gravina 2017, Inter-professional
Education Collaborative 2016, Englander et
al, 2013) to determine nursing academics'
knowledge about CBNE. It comprised
eleven Multiple Choice Questions (MCQ)
about major and significant content of the
CBNE in terms of; major concepts,
components, stages, levels, principles and hazards or benefits of such system during
COVID pandemic. Those questions were
followed by three open ended questions
about; CBNE domains in the NARS 2017,
justifications about hazards or benefits of
implementing CBNE during COVID era.
Scoring for MCQs was dependent on the
right answer that took one and wrong one
that took zero. For open ended questions,
the scoring was dependent on the number of
nursing academics' responses for each open
ended question. Analysis and interpretation of the open question’ responses followed the
process of grouping of similar responses and
deriving a specific number of items for each
question.
b. Part two: CBNE planning skills rubric: that was developed by the researchers after a
thorough review of the related literature,
(Page 2020, Austin 2019, Lucey 2018,
Gravina 2017, Inter-professional Education
Collaborative 2016, Albanese et al, 2010) to
determine nursing academics' CBNE planning skills. It included six higher
planning skills, in terms of: developing
competencies statements for each domain in
NARS 2017, developing learning outcomes
for each competency, filling nursing
bachelor program specification template,
filling course specification template, and
filling program competencies\learning
outcomes\courses matrix, and mechanics,
grammar and understanding. Each planning
skill rated against four points rating scale; which is; poor = 1, inadequate= 2, adequate
= 3, and exemplary = 4. Six is the minimum
scoring which represents poor CBNE
planning skills performance. Above 6 to 12
is indicated inadequate CBNE planning skill
performance. In between 12 to 18 is showed
adequate CBNE planning skill performance.
From 18 to 24 is the maximum scoring
which represents excellent CBNE planning
skills performance.

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
129
c. Part three: CBNE acceptance scale: It
was developed by the researchers based on a
thorough review of related literature
(Wallace et al, 2021, Dashash et al, 2020,
Page 2020, Austin 2019, Lucey 2018,
Gravina 2017, Inter-professional Education
Collaborative 2016, Morris et al, 2012,
Sangwan et al, 2012, Fieger 2012, Albanese
et al, 2010). The scale was designed to assess and measure nursing academics'
attitude, value and satisfaction toward using
the CBNE that represented their acceptance
to follow such oncoming system, during the
COVID crisis in their nursing faculty. This
scale included 30 statements; ten for the
attitude, ten for the value and ten for the
satisfaction. Each statement is rating against
five points rating scale; that are ranging
from strongly disagree= 1, to strongly agree
= 5. The total score is 150. Above 75
represents high level of acceptance for following CBNE among nursing academics.
Below 75 denotes their low level of
acceptance.
Additionally, Academic’s profile sheet is
attached.
The three parts of study tool were checked
for its face and content validity by five experts
in the fields of Medical & Surgical Nursing,
Psychiatric and Mental Health Nursing, Community Health Nursing, Nursing
Administration and Nursing Education
Departments, and accordingly, essential
modifications were done. Moreover, the three
parts of the study tool were statistically checked
for reliability as follows: part one and three
were tested by Cronbach Alpha Coefficient
Statistical Test for internal consistency for its
items that denoted = 0.74 to 0.77, and 0.68 to
0.73 respectively. Part two was tested by inter-
rater reliability by Cohen's Kappa Coefficient Statistical Test to check its scores consistency
when used by three different raters. This part
indicated K =0.69 in such reliability, with 95%
confidence interval.
Data collection procedure:
A pilot study was established on ten
nursing academics that were excluded from the
study sample, using the study tool with the
developed CBNE templates (program
specification, course specification and program
learning outcomes/courses matrix) that were
evaluated by part two of the study tool, and thus
significant changes were nirp. The current
study passed into four phases: pre-test,
planning, conduction and post-test:
Pre-test phase: both study groups received
and filled the study tool with the developed
CBNE templates (program specification,
course specification and program learning
outcomes/courses matrix) before conducting
the CBNE instructional intervention, with
the presence of the researchers to guide the
nursing academics in answering them. (for
control group, they filled the study tool on
individualized bases and for the experimental group, they received the study
tool, half an hour before the instructional
intervention and on group bases)
Planning phase: Based on ihp pre-test
phase and a thorough review of the related
literature, CBNE instructional intervention
was planned and developed including aim,
objectives, contents, active teaching
strategies (such as discussion, brain
storming, demonstration and presentation).
Pictures, illustrative PowerPoint, descriptive diagrams, templates of program, course
specifications, program and course matrix
and handouts were developed. The content
of the instructional intervention was
checked and reviewed for content validity
by a jury of three experts in nursing
education, and administration departments.
The jury scientifically investigated the
instructional intervention content and
decided if it includes typical elucidations
and interpretations with explanation about CBNE outlines for concepts, definitions,
features, rational, levels, development,
implementation, student’s assessment,
writing competency and learning outcomes
statements, program and course
specification, policies and barriers, during
COVID crisis. Additionally, the jury ensures
the content details representation to the
evidences and theories or literature that
related CBNE and NARS 2017.
Arrangements and announcement about the
CBNE instructional intervention were established with student’s affair department.

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
130
Registration and venue preparation were
prepared by the researchers and the quality
unit and academic affairs.
Conduction phase: the developed CBNE
instructional intervention was implemented
with the experimental group only who
received theoretical and application parts
through four days and 16 hours (4 for each
day). Examples, explanations, questions and justifications were delivered during the
CBNE instructional intervention using the
flip chart, presentation, and discussion or
demonstrations. Each nursing academic in
the experimental group received two
teaching sessions in one day with half an
hour break, on two sequential days.
Post-test phase: the study tool with the
developed CBNE templates (program
specification, course specification and
program learning outcomes/courses matrix) were used again with both study groups.
The scores of the three parts of the study
tool before and after CBNE instructional
intervention for both study groups were
calculated, compared, and then, the
difference between both groups ’scores was
estimated. Thus, the effect of the developed
CBNE intervention during the pandemic era
with nursing academics was determined.
Part one and part three of the study tool
were filled by self-reporting methodology,
while, part two was filled by the researchers after observing and evaluating the CBNE
planning skills of nursing academics when
filling the CBNE templates, (program
specification, course specification and
program learning outcomes/courses matrix).
Ethical considerations: Written agreements
were obtained from the ethical committee,
for conduction of the study. Also, written
informed consents were taken from the
nursing academics in the study sample after full description of the purpose and the
method of the study. The nursing academics
were ascertained that they participated in the
study with their full voluntary decision.
Additionally, they were reassured that all
their answers were used with a confidential
approach. Also, anonymity was ascertained,
by avoiding the participants putioei their
names on the study tool. Moreover, the
participants were ensured that they can
withdraw from the study at any time of the
study phases.
Data Analysis:
The collected data was fed to the
computer, coded, investigated and arranged and presented. Statistical Packages for the Social
Sciences (SPSS) version 20.0 for Windows
(Office 2010) were employed for calculating
and revealed the study findings. Number,
percentage, mean and standard deviation were
used for descriptive data. Chi-square was used
for test of significance with P values.
Results:
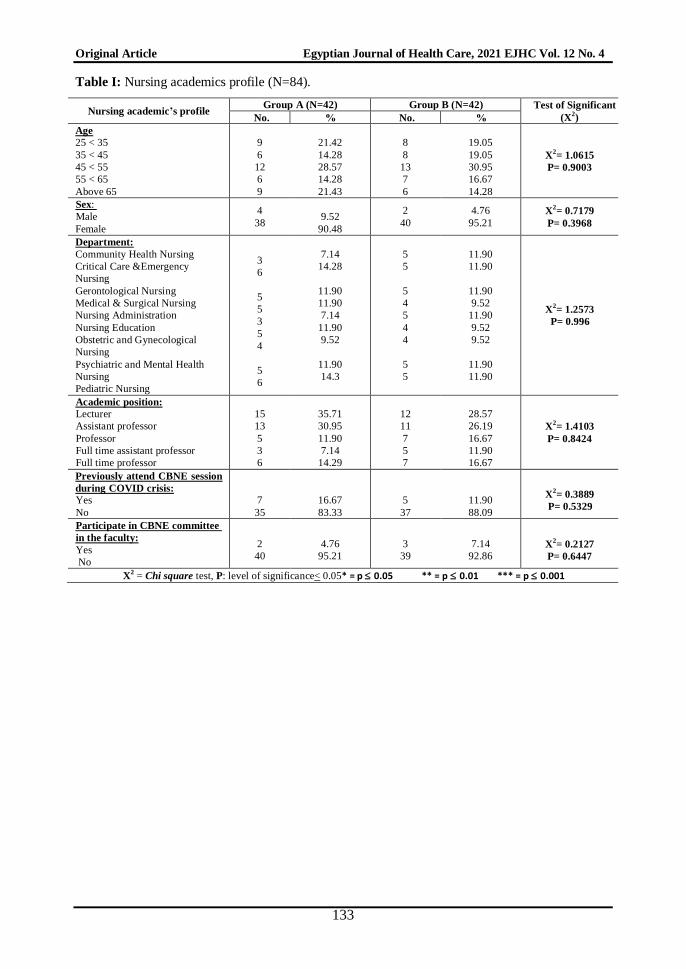
Table I clarifies that approximately one
third of both groups (28.57%, 30.95 %) were in between 45, and 55yearsold and almost eiih io
ihpn (90.48%, 95.21%) were females. It is
obvious that all college departments were
representative in both study groups, just about
equally. Nearly one third of both groups, for
group A (35.71%, 30.95 %) and for group B
(28.57%, 26.19%); are lecturers and assistant
professors, respectively. Almost both groups
did not attend any CBNE educational sessions
during COVID crisis and likewise, the majority
of both did not participate in any CBNE
committee in the faculty. Generally, there was no apparent statistically significant difference
among both study groups as regards their
profile, and the level of significance < 0.05.
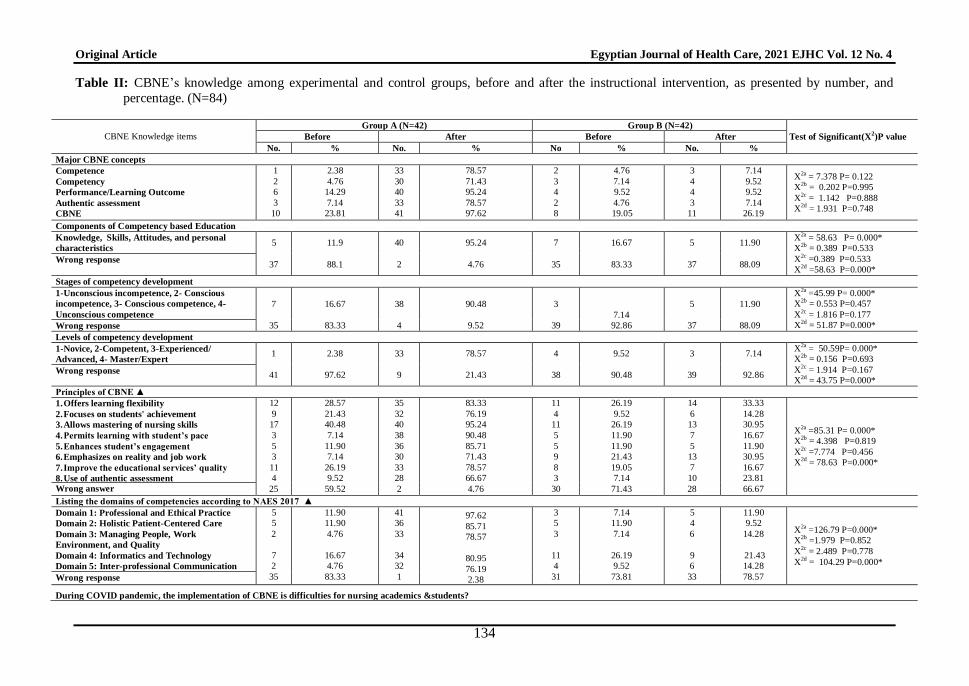
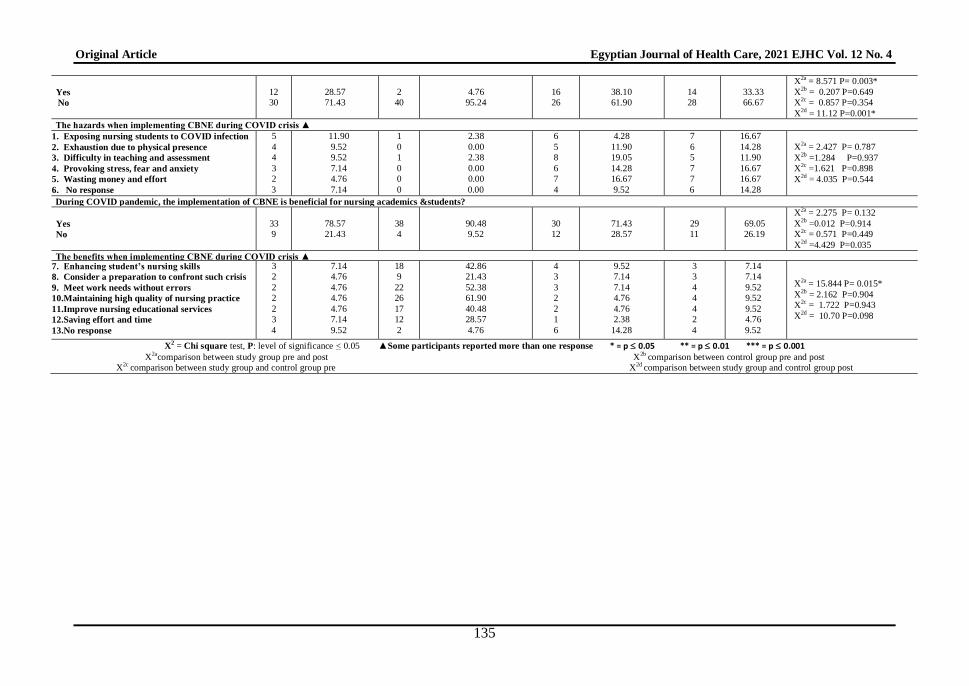
Table II illustrates a hoihpd
improvement in the experimental group 's
knowledge about CBNE before and after the
instructional intervention than the control
group, regarding all knowledge tests
.Concerning, identifying the CBNE’ major
concepts among group A before conducting the
instructional intervention, minimal percentages (2.38%, 4.76%, 14.29%, 7.14%, and 23.81) of
them mentioned those concepts correctly. But,
after conducting the instructional intervention,
academics in group A approved an apparent
improvement in understanding and reporting
those major concepts, so, their percentages
became high (78.57%, 71.43%, 95.24%,
78.57%, and 97.62). tui, group B, did not show
any improvement in identification of those
CBNE’ major concepts before, and after
conducting the instructional intervention,
respectively.

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
131
In relation to ihp CBNE components,
stages and levels of development, few
percentages of group A (11.9%, 16.67%, and
2.38 %) reported right answers, before
conducting the intervention, however, after
conducting it, great percentages of them
(95.24%, 90.48%, 78.57%) documented right
answers. On the other hand, group B, did not
indicate any progress in awareness of those CBNE items before and after conducting the
instructional intervention.
Pertaining to CBNE principles and
domains, the majority of both groups (59.52%,
83.33% for group A and 71.43%, 73.81% for
group B) provided wrong answers before
conducting the instructional intervention.
However, after conducting the instructional
intervention, those percentages among group A
became very minimal (4.76%, 2.38%), while,
in-between group B, those percentages
approximately dpnioeprthe same (66.67%, 78.57%). This result denoted that almost all of
experimental group didn’t have any wrong
answers about the CBNE principles and
domains but the control group still, has wrong
answers about such items.
For subjects' awareness io ihp CBNE
difficulties among academics and students,
about two thirds of both groups A & B
(71.43%, 61.90%), before, conducting the
instructional intervention reported that CBNE has no difficulties. But, after conducting the
instructional intervention, these percentages
became (95.24%, 66.67%) in favor of the
experimental group who approve their refusal
that CBNE has any difficulties for academics or
students.
The study groups mentioned some CBNE
difficulties according to their point of views; in
terms of: Exposing nursing students to COVID
infection, they are Exhaustion due to
continuous physical presence, Difficulty in teaching and assessment, Provoking stress, fear
and anxiety and wasting money and effort.
With reference to the subjects' awareness
if CBNE benefits, for academics and students,
the majority of both groups A & B (78.57%,
71.43%), before, conducting the instructional
intervention, reported that CBNE is beneficial.
But, after conducting the instructional
intervention, these percentages became
(90.48%, 69.05%) in favor of experimental
group who admire their complete agreement
that CBNE is beneficial for academics and
students.
The groups mentioned some CBNE
benefits according to their points of view; in
terms of Enhancing students nursing skills,
Consider a preparation to confront such i crisis,
Meet work needs without errors, Maintaining
high quality of nursing practice, Improve nursing educational services, and Saving effort
and time
Generally, it was observed that there was a
statistically significant difference between both
groups particularly, after conducting the CBNE
instructional intervention for almost all items in
the knowledge test and P = 0.000. The CBNE
instructional intervention showed a significant
and effective influence in improving group A’
CBNE knowledge.
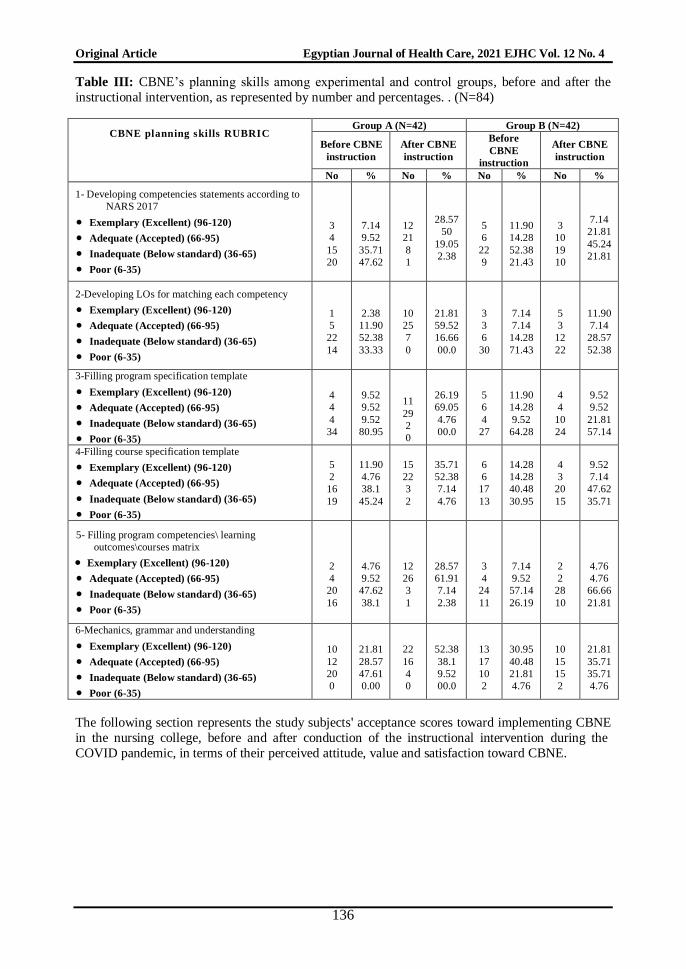
Table III denotes that both study groups
have inadequate CBNE’s planning skills scores, before the instructional intervention. But, after
the instructional intervention, the experimental
group showed an apparent progress in all
CBNE’s planning skill in all rubric items,
while, the control group showed no
improvement. For example, regarding,
developing competencies’ statements according
to NARS 2017, it was observed that there was
significant percentages of group A (28.57%,
50%) ihii have an excellent and accepted
skill scores, after the CBNE instructional intervention which were poor and inadequate
before the CBNE instructional intervention. On
the other hand, and with a comparison with
group B, they have poor and inadequate skill
scores before and after conduction of CBNE
instructional intervention, unlike group A.
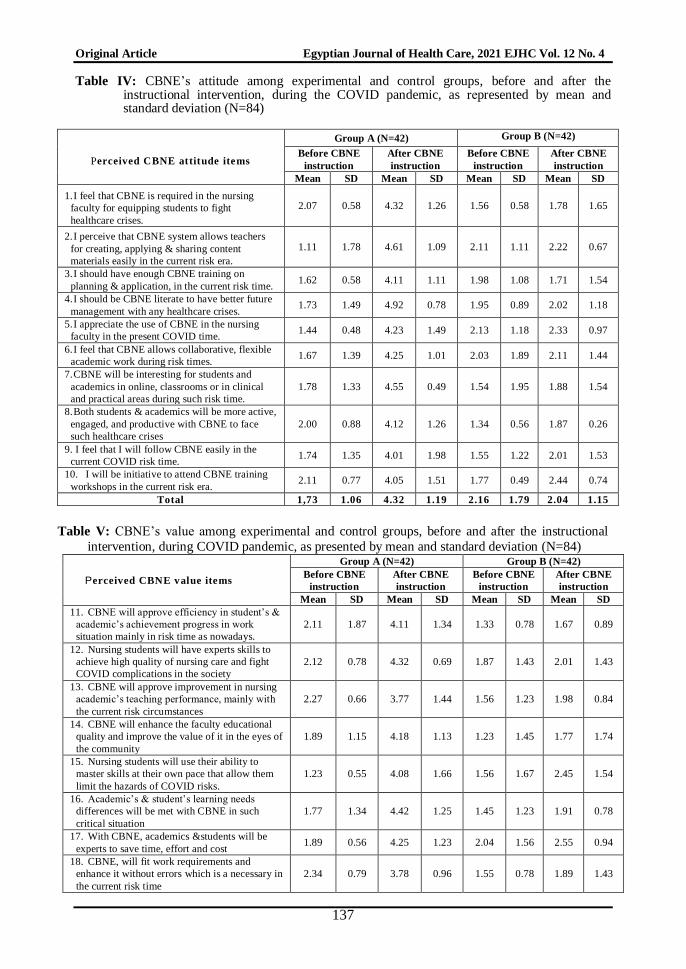
a. Perceived attitude toward CBNE
As regards table IV, it reveals the CBNE’s
attitude scores among experimental and control
groups during COVID era. According to the
scale’s mean scoring, above 2.5 mean scores indicated CBNE positive attitude and below 2.5
mean scores denoted a CBNE negative attitude
during COVID era. Therefore, it was clear that
both study groups have CBNE negative attitude
before conduction of CBNE instructional
intervention during COVID era. While, after
conduction of CBNE instructional intervention
during COVID circumstances, group A mean
scores were improved and became above 2.5

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
132
for all subscale items, but group B has no
improvement and continued approximately the
same.
Perceived CBNE value
Concerning table V, oi clarifies the
CBNE’s value scores among experimental and
control groups during COVID pandemic.
According to the scale’s mean scoring, above
2.5 mean scores indicated high CBNE value perception and below 2.5 mean scores denoted
low CBNE value perception during COVID era.
Therefore, it was obvious that both study
groups have low perception of CBNE value
before conduction of CBNE instructional
intervention during COVID era. While, after
conduction of CBNE instructional intervention
during COVID era, group A mean scores were
improved and became above 2.5 for all subscale
items, but group B has no improvement and
sustained almost the same.
Perceived satisfaction toward CBNE Table VI elucidates the CBNE’s
satisfaction score levels among experimental
and control groups during COVID pandemic.
Inconsistency, with the scale’ scoring, above
2.5 mean scores show pr high CBNE
satisfaction, and below 2.5 mean scores
indicated low satisfaction level regarding
CBNE during COVID era. Consequently, it was
understandable that both study groups have low
CBNE satisfaction level before conduction of
CBNE instructional intervention during COVID era. While, after conduction of CBNE
instructional intervention during COVID era,
group A mean scores were improved and
became above 2.5 for all subscale items, but
group B has no improvement and continued
approximately the same.
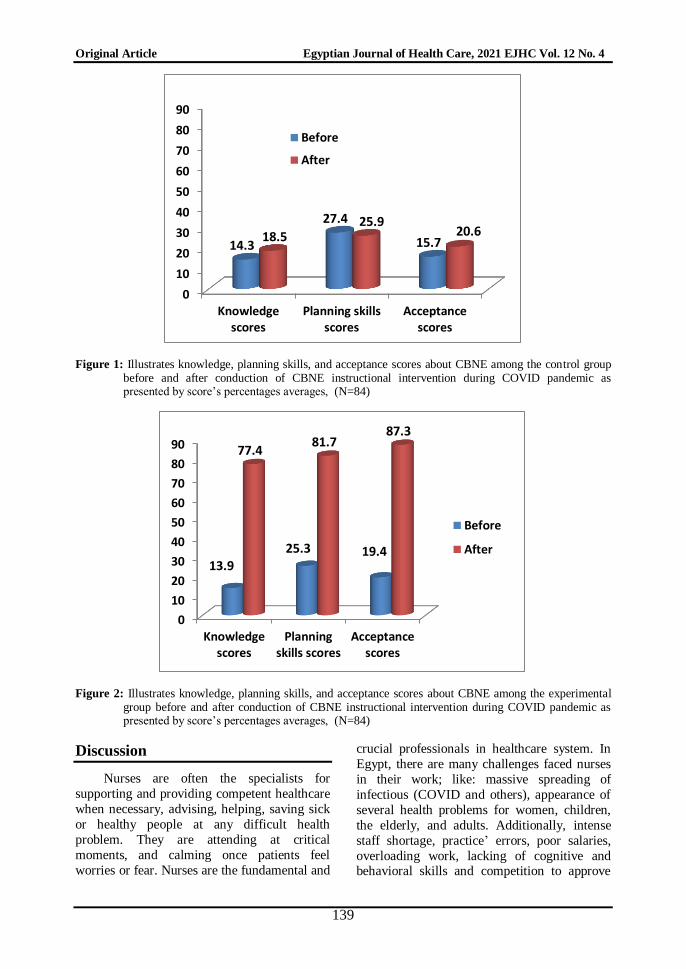
Figure 1 shows knowledge, planning
skills, and acceptance scores about CBNE
among the control group before and after
conduction of CBNE instructional intervention
during COVID pandemic as presented by
score’s percentages averages. They have
limited scores before the intervention and after
intervention; their scores approximately still the
same. Figure 2 clarifies knowledge, planning
skills, and acceptance scores about CBNE
among the experimental group before and after
conduction of CBNE instructional intervention
during COVID pandemic as presented by
score’s percentages averages. The improvement
is obviously observed which approves the
effectiveness of the CBNE instructional
intervention among academics at knowledge,
skills and attitude levels.
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
133
Table I: Nursing academics profile (N=84).
Nursing academic’s profile Group A (N=42) Group B (N=42) Test of Significant
(X2) No. % No. %
Age
25 < 35
35 < 45
45 < 55
55 < 65
Above 65
9
6
12
6
9
21.42
14.28
28.57
14.28
21.43
8
8
13
7
6
19.05
19.05
30.95
16.67
14.28
X2= 1.0615
P= 0.9003
: Sex
Male
Female
4
38
9.52
90.48
2
40
4.76
95.21
X2= 0.7179
P= 0.3968
Department:
Community Health Nursing
Critical Care &Emergency
Nursing
Gerontological Nursing
Medical & Surgical Nursing
Nursing Administration
Nursing Education
Obstetric and Gynecological
Nursing
Psychiatric and Mental Health
Nursing
Pediatric Nursing
3
6
5
5
3
5
4
5
6
7.14
14.28
11.90
11.90
7.14
11.90
9.52
11.90
14.3
5
5
5
4
5
4
4
5
5
11.90
11.90
11.90
9.52
11.90
9.52
9.52
11.90
11.90
X2= 1.2573
P= 0.996
Academic position:
Lecturer
Assistant professor
Professor
Full time assistant professor
Full time professor
15
13
5
3
6
35.71
30.95
11.90
7.14
14.29
12
11
7
5
7
28.57
26.19
16.67
11.90
16.67
X2= 1.4103
P= 0.8424
Previously attend CBNE session
during COVID crisis:
Yes
No
7
35
16.67
83.33
5
37
11.90
88.09
X2= 0.3889
P= 0.5329
in CBNE committee Participate
in the faculty:
Yes
No
2
40
4.76
95.21
3
39
7.14
92.86
X2= 0.2127
P= 0.6447
X2 = Chi square test, P: level of significance< 0.05* = p 0.05 ** = p 0.01 *** = p 0.001
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
134
Table II: CBNE’s knowledge among experimental and control groups, before and after the instructional intervention, as presented by number, and
percentage. (N=84)
CBNE Knowledge items
Group A (N=42) Group B (N=42)
Test of Significant(X2)P value Before After Before After
No. % No. % No % No. %
Major CBNE concepts
Competence
Competency
Performance/Learning Outcome
Authentic assessment
CBNE
1
2
6
3
10
2.38
4.76
14.29
7.14
23.81
33
30
40
33
41
78.57
71.43
95.24
78.57
97.62
2
3
4
2
8
4.76
7.14
9.52
4.76
19.05
3
4
4
3
11
7.14
9.52
9.52
7.14
26.19
X2a = 7.378 P= 0.122
X2b = 0.202 P=0.995
X2c = 1.142 P=0.888
X2d = 1.931 P=0.748
Components of Competency based Education
Knowledge, Skills, Attitudes, and personal
characteristics 5
37
11.9
88.1
40
2
95.24
4.76
7
35
16.67
83.33
5
37
11.90
88.09
X2a = 58.63 P= 0.000*
X2b = 0.389 P=0.533
X2c =0.389 P=0.533
X2d =58.63 P=0.000* Wrong response
Stages of competency development
1-Unconscious incompetence, 2- Conscious
incompetence, 3- Conscious competence, 4-
Unconscious competence
7
35
16.67
83.33
38
4
90.48
9.52
3
39
7.14
92.86
5
37
11.90
88.09
X2a =45.99 P= 0.000*
X2b = 0.553 P=0.457
X2c = 1.816 P=0.177
X2d = 51.87 P=0.000* Wrong response
Levels of competency development
1-Novice, 2-Competent, 3-Experienced/
Advanced, 4- Master/Expert 1
41
2.38
97.62
33
9
78.57
21.43
4
38
9.52
90.48
3
39
7.14
92.86
X2a = 50.59P= 0.000*
X2b = 0.156 P=0.693
X2c = 1.914 P=0.167
X2d = 43.75 P=0.000* Wrong response
Principles of CBNE ▲
1. Offers learning flexibility
2. Focusse on students' achievement
3. Allows mastering of nursing skills
4. Permits learning with student’s pace
5. Enhances student’s engagement
6. Emphasizes on reality and job work
7. Improve the educational services’ quality
8. Use of authentic assessment
12
9
17
3
5
3
11
4
25
28.57
21.43
40.48
7.14
11.90
7.14
26.19
9.52
59.52
35
32
40
38
36
30
33
28
2
83.33
76.19
95.24
90.48
85.71
71.43
78.57
66.67
4.76
11
4
11
5
5
9
8
3
30
26.19
9.52
26.19
11.90
11.90
21.43
19.05
7.14
71.43
14
6
13
7
5
13
7
10
28
33.33
14.28
30.95
16.67
11.90
30.95
16.67
23.81
66.67
X2a =85.31 P= 0.000*
X2b = 4.398 P=0.819
X2c =7.774 P=0.456
X2d = 78.63 P=0.000*
Wrong answer
Listing the domains of competencies according to NAES 2017 ▲
Domain 1: Professional and Ethical Practice
Domain 2: Holistic Patient-Centered Care
Domain 3: Managing People, Work
Environment, and Quality
Domain 4: Informatics and Technology
Domain 5: Inter-professional Communication
5
5
2
7
2
35
11.90
11.90
4.76
16.67
4.76
83.33
41
36
33
34
32
1
97.62
85.71
78.57
80.95
76.19
2.38
3
5
3
11
4
31
7.14
11.90
7.14
26.19
9.52
73.81
5
4
6
9
6
33
11.90
9.52
14.28
21.43
14.28
78.57
X2a =126.79 P=0.000*
X2b =1.979 P=0.852
X2c = 2.489 P=0.778
X2d = 104.29 P=0.000*
Wrong response
During COVID pandemic, the implementation of CBNE is difficulties for nursing academics &students?
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
135
Yes
No 12
30
28.57
71.43
2
40
4.76
95.24
16
26
38.10
61.90
14
28
33.33
66.67
X2a = 8.571 P= 0.003*
X2b = 0.207 P=0.649
X2c = 0.857 P=0.354
X2d = 11.12 P=0.001*
The hazards when implementing CBNE during COVID crisis ▲
1. Exposing nursing students to COVID infection
2. Exhaustion due to physical presence
3. Difficulty in teaching and assessment
4. Provoking stress, fear and anxiety
5. Wasting money and effort
6. No response
5
4
4
3
2
3
11.90
9.52
9.52
7.14
4.76
7.14
1
0
1
0
0
0
2.38
0.00
2.38
0.00
0.00
0.00
6
5
8
6
7
4
4.28
11.90
19.05
14.28
16.67
9.52
7
6
5
7
7
6
16.67
14.28
11.90
16.67
16.67
14.28
X2a = 2.427 P= 0.787
X2b =1.284 P=0.937
X2c =1.621 P=0.898
X2d = 4.035 P=0.544
During COVID pandemic, the implementation of CBNE is beneficial for nursing academics &students?
Yes
No 33
9
78.57
21.43
38
4
90.48
9.52
30
12
71.43
28.57
29
11
69.05
26.19
X2a = 2.275 P= 0.132
X2b =0.012 P=0.914
X2c = 0.571 P=0.449
X2d =4.429 P=0.035
The benefits when implementing CBNE during COVID crisis ▲ 7. Enhancing student’s nursing skills
8. Consider a preparation to confront such crisis
9. Meet work needs without errors
10. Maintaining high quality of nursing practice
11. Improve nursing educational services
12. Saving effort and time
13. No response
3
2
2
2
2
3
4
7.14
4.76
4.76
4.76
4.76
7.14
9.52
18
9
22
26
17
12
2
42.86
21.43
52.38
61.90
40.48
28.57
4.76
4
3
3
2
2
1
6
9.52
7.14
7.14
4.76
4.76
2.38
14.28
3
3
4
4
4
2
4
7.14
7.14
9.52
9.52
9.52
4.76
9.52
X2a = 15.844 P= 0.015*
X2b = 2.162 P=0.904
X2c = 1.722 P=0.943
X2d = 10.70 P=0.098
X2 = Chi square test, P: level of significance < 0.05 ▲Some participants reported more than one response * = p 0.05 ** = p 0.01 *** = p 0.001
X2acomparison between study group pre and post X2b comparison between control group pre and post
X2c comparison between study group and control group pre X2d comparison between study group and control group post
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
136
Table III: CBNE’s planning skills among experimental and control groups, before and after the
instructional intervention, as dppresented by number and percentages. . (N=84)
CBNE planning skills RUBRIC Group A (N=42) Group B (N=42)
Before CBNE
instruction
After CBNE
instruction
Before
CBNE
instruction
After CBNE
instruction
No % No % No % No %
1- Developing competencies statements according to
NARS 2017
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
3
4
15
20
7.14
9.52
35.71
47.62
12
21
8
1
28.57
50
19.05
2.38
5
6
22
9
11.90
14.28
52.38
21.43
3
10
19
10
7.14
21.81
45.24
21.81
2-Developing LOs for matching each competency
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
1
5
22
14
2.38
11.90
52.38
33.33
10
25
7
0
21.81
59.52
16.66
00.0
3
3
6
30
7.14
7.14
14.28
71.43
5
3
12
22
11.90
7.14
28.57
52.38
3-Filling program specification template
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
4
4
4
34
9.52
9.52
9.52
80.95
11
29
2
0
26.19
69.05
4.76
00.0
5
6
4
27
11.90
14.28
9.52
64.28
4
4
10
24
9.52
9.52
21.81
57.14
4-Filling course specification template
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
5
2
16
19
11.90
4.76
38.1
45.24
15
22
3
2
35.71
52.38
7.14
4.76
6
6
17
13
14.28
14.28
40.48
30.95
4
3
20
15
9.52
7.14
47.62
35.71
5- Filling program competencies\ learning
outcomes\courses matrix
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
2
4
20
16
4.76
9.52
47.62
38.1
12
26
3
1
28.57
61.91
7.14
2.38
3
4
24
11
7.14
9.52
57.14
26.19
2
2
28
10
4.76
4.76
66.66
21.81
6-Mechanics, grammar and understanding
Exemplary (Excellent) (96-120)
Adequate (Accepted) (66-95)
Inadequate (Below standard) (36-65)
Poor (6-35)
10
12
20
0
21.81
28.57
47.61
0.00
22
16
4
0
52.38
38.1
9.52
00.0
13
17
10
2
30.95
40.48
21.81
4.76
10
15
15
2
21.81
35.71
35.71
4.76
The following section represents the study subjects' acceptance scores toward implementing CBNE
in the nursing college, before and after conduction of the instructional intervention during the
COVID pandemic, in terms of their perceived attitude, value and satisfaction toward CBNE.
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
137
Table IV: CBNE’s attitude among experimental and control groups, before and after the instructional intervention, during the COVID pandemic, as dppresented by mean and standard deviation (N=84)
Perceived CBNE attitude items
Group A (N=42) Group B (N=42)
Before CBNE
instruction
After CBNE
instruction
Before CBNE
instruction
After CBNE
instruction
Mean SD Mean SD Mean SD Mean SD
1. I feel that CBNE is required in the nursing
faculty for equipping students to fight
healthcare crises.
2.07 0.58 4.32 1.26 1.56 0.58 1.78 1.65
2. I perceive that CBNE system allows teachers
for creating, applying & sharing content
materials easily in the current risk era.
1.11 1.78 4.61 1.09 2.11 1.11 2.22 0.67
3. I should have enough CBNE training on
planning & application, in the current risk time. 1.62 0.58 4.11 1.11 1.98 1.08 1.71 1.54
4. I should be CBNE literate to have better future
management with any healthcare crises. 1.73 1.49 4.92 0.78 1.95 0.89 2.02 1.18
5. I appreciate the use of CBNE in the nursing
faculty in the present COVID time. 1.44 0.48 4.23 1.49 2.13 1.18 2.33 0.97
6. I feel that CBNE allows collaborative, flexible
academic work during risk times. 1.67 1.39 4.25 1.01 2.03 1.89 2.11 1.44
7. CBNE will be interesting for students and
academics in online, classrooms or in clinical
and practical areas during such risk time.
1.78 1.33 4.55 0.49 1.54 1.95 1.88 1.54
8. Both students & academics will be more active,
engaged, and productive with CBNE to face
such healthcare crises
2.00 0.88 4.12 1.26 1.34 0.56 1.87 0.26
9. I feel that I will follow CBNE easily in the
current COVID risk time. 1.74 1.35 4.01 1.98 1.55 1.22 2.01 1.53
10. I will be initiative to attend CBNE training
workshops in the current risk era. 2.11 0.77 4.05 1.51 1.77 0.49 2.44 0.74
Total 1,73 1.06 4.32 1.19 2.16 1.79 2.04 1.15
Table V: CBNE’s value among experimental and control groups, before and after the instructional
intervention, during COVID pandemic, as presented by mean and standard deviation (N=84)
Perceived CBNE value items
Group A (N=42) Group B (N=42)
Before CBNE
instruction
After CBNE
instruction
Before CBNE
instruction
After CBNE
instruction
Mean SD Mean SD Mean SD Mean SD
11. CBNE will approve efficiency in student’s &
academic’s achievement progress in work
situation mainly in risk time as nowadays.
2.11 1.87 4.11 1.34 1.33 0.78 1.67 0.89
12. Nursing students will have experts skills to
achieve high quality of nursing care and fight
COVID complications in the society
2.12 0.78 4.32 0.69 1.87 1.43 2.01 1.43
13. CBNE will approve improvement in nursing
academic’s teaching performance, mainly with
the current risk circumstances
2.27 0.66 3.77 1.44 1.56 1.23 1.98 0.84
14. CBNE will enhance the faculty educational
quality and improve the value of it in the eyes of
the community
1.89 1.15 4.18 1.13 1.23 1.45 1.77 1.74
15. Nursing students will use their ability to
master skills at their own pace that allow them
limit the hazards of COVID risks.
1.23 0.55 4.08 1.66 1.56 1.67 2.45 1.54
16. Academic’s & student’s learning needs
differences will be met with CBNE in such
critical situation
1.77 1.34 4.42 1.25 1.45 1.23 1.91 0.78
17. With CBNE, academics &students will be
experts to save time, effort and cost 1.89 0.56 4.25 1.23 2.04 1.56 2.55 0.94
18. CBNE, will fit work requirements and
enhance it without errors which is a necessary in
the current risk time
2.34 0.79 3.78 0.96 1.55 0.78 1.89 1.43

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
138
Perceived CBNE value items
Group A (N=42) Group B (N=42)
Before CBNE
instruction
After CBNE
instruction
Before CBNE
instruction
After CBNE
instruction
Mean SD Mean SD Mean SD Mean SD
19. In CBNE, nursing academics will use many
teaching methodology, assessment
authenticity which strengthen their
qualifications
1.74 1.56 3.66 1.11 1.45 0.73 2.51 1.11
20. CBNE will add positive effects ii the
reputation of nursing field. 1.95 0.86 4.34 0.78 2.11 0.47 2.32 0.89
Total 1.93 1.01 4.09 1.16 1.62 1.13 2.11 1.16
Table VI: CBNE’s satisfaction among experimental and control groups, before and after the
instructional intervention, during COVID pandemic, as presented by mean and standard
deviation. (N=84)
Perceived CBNE’s satisfaction level
Group A (N=42) Group B (N=42)
Before
CBNE
instruction
After CBNE
instruction
Before
CBNE
instruction
After CBNE
instruction
Mean SD Mean SD Mean SD Mean SD
21. I appreciate that CBNE can be used easily and
with flexibility with distance precautions 1.31 0.69 3.67 0.94 1.11 0.34 1.77 0.56
22. I feel that with CBNE nursing academics and
students' need will be recognized & understood,
even in current crisis.
1.67 1.08 4.16 1.89 1.45 1.11 1.22 0.44
23. I appreciate that in CBNE, we will use blended
teaching & online platforms which will fit
COVID precautions
1.69 1.16 3.88 1.11 1.93 0.83 2.18 0.68
24. I anticipate that CBNE will upgrade academics
potentials which idp required in crises era 2.17 1.67 4.56 1.34 1.22 0.75 1.45 1.22
25. I have a confidence in authentic assessment ier
in CBNE ensures competency achievement that
we need oe crisis situations
1.90 0.78 4.78 0.86 1.26 1.14 2.12 1.34
26. I appreciate that in CBNE, teachers can identify
strengths & defects of teaching, in such crisis
era
1.45 1.11 3.67 1.11 1.85 1.44 1.67 0.89
27. I appreciate that in CBNE, nursing students will
attain enough chances for training, even with
COVID restrictions.
1.67 1.11 4.22 1.21 1.67 1.56 1.45 1.33
28. CBNE develop students' problem-solving skills
that help them deal with any crisis. 2.11 1.45 3.89 0.89 1.45 0.72 1.34 1.11
29. CBNE helps students to be self-dependent,
clinical judgers, even with any crisis. 2.09 0.89 4.44 1.54 2.44 1.07 1.55 1.45
30. CBNE improves students' soft & hard skills that
permitted them to manage efficiently at risks. 1.56 1.21 3.78 1.45 2.12 0.67 2.11 0.78
Total 1.76 1.16 4.11 1.23 1.65 0.96 1.69 0.98
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
139
Figure 1: Illustrates knowledge, planning skills, and acceptance scores about CBNE among the control group before and after conduction of CBNE instructional intervention during COVID pandemic as presented by score’s percentages averages, (N=84)
Figure 2: Illustrates knowledge, planning skills, and acceptance scores about CBNE among the experimental group before and after conduction of CBNE instructional intervention during COVID pandemic as presented by score’s percentages averages, (N=84)
Discussion
Nurses are often the specialists for
supporting and providing competent healthcare
when necessary, advising, helping, saving sick
or healthy people at any difficult health
problem. They are attending at critical
moments, and calming once patients feel
worries or fear. Nurses are the fundamental and
crucial professionals in healthcare system. In
Egypt, there are many challenges faced nurses
in their work; like: massive spreading of
infectious (COVID and others), appearance of
several health problems for women, children,
the elderly, and adults. Additionally, intense
staff shortage, practice’ errors, poor salaries,
overloading work, lacking of cognitive and behavioral skills and competition to approve
0
10
20
30
40
50
60
70
80
90
Knowledgescores
Planning skillsscores
Acceptancescores
14.3
27.4
15.7 18.5 25.9
20.6
Before
After
0
10
20
30
40
50
60
70
80
90
Knowledgescores
Planningskills scores
Acceptancescores
13.9 25.3 19.4
77.4 81.7
87.3
Before
After

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
140
accepted quality and image of nursing serveries
nationally and internationally, considered a
great challenges. Therefore, upgrading of
nursing education has become urgent. Nursing
student’s preparation becomes necessitate and
national need. (Brownie et al., 2018, Ramos et
al., 2019, Watson, et al., 2002, El Tawil 2021,
Wu and Martin, 2019)
There are many nursing education programs in Egypt affiliated to two isolated
governmental ministries: 1- ehp Ministry of
Health and Population (MoHP) covers
secondary nursing schools and technical and
associate nursing institutes which awarded a
diploma and associate certificates, and 2-the
Ministry of Higher Education (MoHE) which
covers the graduate and postgraduate levels of
nursing programs that provided bachelors and
post-graduation certificates. Since 2017, the
government has a vision to implement CBE
allover Egyptian universities and in all specialties. Egyptian government stressed on
the importance of implementing CBE in
nursing and medical education as vital health
specialties. (National Authority for Quality
Assurance and Accreditation of
Education2017, Brownie et al, 2018, Ma et al.,
2012, Technical Institutes Directorate 2017)
Particularly, CBNE has created growing
thoughtfulness, attention, and argument among
healthcare academics and professionals since
the beginning of the current decade, particularly in the developed countries. (Frank
et al. 2010, Blömeke et al, 2013, Brownie et al,
2018, Salman et al, 2020) CBNE system
becomes the necessitated educational approach
in the bachelor nursing program as strong
means to close the gap between theory and
practice as a foundation for professional
practice. (Boyle et al, 2016, Fukada, 2018,
Garneau et al, 2017, Frank et al. 2010)
Egyptian academic community has a great
struggle and competition to prepare their graduates with such approach which allows
efficiency, expertise, and proficiency in the
clinical practice. Hence, to follow such crucial
system, preparation of nursing academics by fit
training intervention is essential.
According to the revealed results in the
current study, after providing the CBNE
instructional intervention, group A approved
apparent improvement in acquiring CBNE
related knowledge than group B whom have no
observed progress in such variable. Group A
reported such progress regarding CBNE
concepts, components, stages, levels,
principles, and identifying NARS 2017’
domains of competencies. Therefore, and
matching with the first research hypothesis,
there is significant statistical difference between experimental and control groups as
regards gaining the CBNE knowledge in favor
of experimental group, after conducting of
CBNE instructional intervention. The CBNE
approve clear effectiveness in changing
academic’s knowledge that will have a
wrathful reflection on their achievement in the
future. Such educational programs required for
the academics if there is any curricular change.
Ahmed and Sayed in 2021conducted a study in
Assuit, Egypt, and reported that competency
based education is necessitated to build educator’s understanding toward new
knowledge, concepts and awareness with the
change agent introduced in the collage. Also,
the authors added that the educators need
numerous formats of training, containing
workshops, seminars, visits, case studies,
coaching, and mentoring. (Ahmed and Sayed in
2021) supporting to this view, Kang and
Pavlova in 2019discusses that to develop
academic work identity, theories, models,
principles, processes, and concepts of the related content of training, they should acquire
deep, clear, accurate and comprehensive details
about any induced subject or reform.
Academic’s education or instruction trials must
be included all review and backgrounds which
can improve trainee’s comprehension and then,
academic motivation and commitment will take
place. In the same line, and additionally, Zhang
et al., in 2017 illustrated that teachers and
academics need wide range of knowledge and
understanding with the training content as a grass root for professional development which
enable them integrate such knowledge into
practice and easily reaching the organization’
target. (Kang and Pavlova 2019, Zhang
et al., 2017) The academics should use
theoretical part with the practical part, together,
thus, knowledge base is necessary to achieve
the application into reality.

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
141
The major goal of CBNE is to translate all
content of teaching into doing. Similarly,
CBNE, particularly in a crucial field like
nursing, needs knowledge capitalizing, and
integrate acquired knowledge into learning
experiences building. Likewise, CBNE
flexibility should be understood well by
nursing academics through recognizing that
CBNE methodology obligates the students to be accountable for achieving performance
outcomes of competencies with no certain time
or certain place for such achievement. CBNE
has a wide range of concepts, principles,
features and components that should be
clarified with academics for allowing them
having effective planning and implementation.
(Zineb et al, 2017, Ahmed and Sayed, 2021,
Brownie et al. 2018) Therefore, any
educational program for academics should
provide great considerations for the bulk of
knowledge which is the fundamental ground for any training instruction.
Moreover, the CBNE instructional
program showed positive effects on subject’s
awareness about the benefits and difficulties of CBNE. Before conducting the intervention
both groups reported some CBNE benefits and
difficulties, but after the intervention, the most
of experimental group only, mentioned the
benefits without difficulties. It can be due to
their understanding of CBNE components and
how they can manage any difficulty easily.
Similarly to these views, Ahmed and Sayed in
2020 discussed that professional educators have to fit lot of professional potentialities in
their teaching career which allow them to
assess and manage any sufferings or problems.
(Ahmed and Sayed 2020, Ahmed and Sayed
2021)CBNE have many benefits that upgrade
the abilities of teachers and students, and if
there are any limitations, it can be due to
organization, fund, training, and timing or
polices, and limitations are not related to the
system itself.
Contradictory to the previous results, Friedler, in 2018 and Guo, &Qiu, in 2019,
Ahmed and Sayed in 2021, and Nyoni& Botma
in 2019 found that the CBE training program
has many obstacles and misunderstanding may
hinder the effectiveness of the CBE
implementation. Those obstacles can be
regarding the compliance to integrate
knowledge with application, restrictive rules,
regulation and policies, staff resistance, rigid
organizational culture and language difficulties,
limited economic preparations and
infrastructure presence and environmental
aspects. The didactic concepts of CBE requires
action and interaction instructional trials for
establishing the target of competence through
people participation to close the gap between theory and practice in a vital field like
healthcare and nursing practice. (Friedler,
2018, Guo, &Qiu, 2019, Ahmed and Sayed
2021, Nyoni& Botma in 2019) CBNE has great
benefits and influences in the colleges of
applied science because it allows joining the
subjects with the needs of professional
standards and work market that enforce the
nations for educational, political, economic,
and reproduction advances.
With referring to the finding in the current
study and after providing the CBNE instructional intervention, group A showed
apparent improvement than group B in
executing the CBNE planning skills in terms
of: Developing competencies statements
according to NARS 2017, Developing LOs for
matching each competency, Filling program
specification template, Filling course
specification template, and Filling program
competencies\ learning outcomes\ courses
matrix, plus their mechanics, grammar and
understanding skills were better. Group B has no noticed improvement in such skills.
Consequently, and corresponding with the
second research hypothesis, there is significant
statistical difference between experimental and
control groups as regards performing the
CBNE planning skills in favor of experimental
group. It is clear that the planning phase is the
huge phase in conduction any educational
projects. In CBNE, the planning phase
includes; planning for planning, planning for
implementation and planning for evaluation that are clear in its program and course
specifications or curricular matrix. Parallel to
such result, Zineb et al, in 2017discussed that
CBE curriculum is established and planned
using many different teachers’ skills. CBE
requires a comprehensive reform of practical or
clinical training systems and processes in the
faculty for staff and students plus the
environment at all. Such reform is clearly
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
142
noticed and followed through accurate and
valid planning process. Likewise, in healthcare
and nursing fields, Wuet al, in 2019,
Sistermans in 2020 and Ahmed& Sayed in
2021detected that the teachers should be have
the basic planning skills that enable them to
plan suitable and feasible curricula. They have
to be responsible for demonstrating the skills in
writing the competencies and its learning outcomes. Flexibility and objectivity or
authenticity of the CBE should be noticed in
the curricular plan through the teaching
methodology, assessment tools and time table.
Representation of subjects for each competency
should be apparent in the curricular matrix.
Accordingly, CBE planning skills have to be
acquired by the teachers through effective and
comprehensive training. (Wu et al, 2019,
Sistermans 2020, Ahmed& Sayed 2021) each
competency should be settled with its learning
outcomes, teaching strategies, and assessment\ evaluation tools. Similarly, for each
competency the academics should plan for its
concepts, learning activities, clinical or
practical skills and put descriptions if needed.
Dissimilar to the previous finding, there
are many references explained many obstacles
and challenges that observed during the
planning for CBNE, particularly among
nursing academics and in nursing schools.
Bates in 2020, Bohain, and Hofman, in 2014,
Englander et al, in 2013, Frank et al, in 2010, Fukada in 2018, Pijl-Zieber et al, in 2013,
Salman et al, in 2020, and Watson et al, in
2002, mentioned that there are some
challenging and difficult aspects in the
planning for application of CBNE. One of the
areas that include the major troubles is
planning for assessment and evaluation in
which there is a serious lacking of instruments
that are valid, objective, and reliable for
competency measurement. Another aspect is
planning for competency courses quality assurance that entails some problems to
determine the criteria for operationalizing the
competencies and its LOs with limited models
or benchmarking examples. Additionally, some
challenges are raised when conductingng
curriculum planning with insufficient clear data
and vague terms of competency
implementation and its requirements in the
clinical settings, which could be unclear in
course specification. Furthermore, some
troubles appear in tailoring the teaching
methodology with fit teachers and various
learning styles of the nursing students. In
addition, there is an observable lacking of
CBNE studies about planning and evaluation
that may be a great source for academics
guidance and support. These planning skills
problems are provoking confusion and exhaustion among nursing academics. Also, in
the area of instructional planning for CBNE
teaching strategies, there is a challenge to plan
and tailor all college services to enhance
nursing student’s full independency in learning
competencies. (Bates 2020, Bohain, and
Hofman, 2014, Englander et al, 2013, Frank et
al, 2010, Fukada 2018, Pijl-Zieber et al, 2013,
Salman et al, 2020, and Watson et al, 2002)
Nursing is a vital disciple and needs close
supervision and support CBNE planning that
will be a huge beneficial shifting for nursing education advancement.
As regard the last finding in the current
study, and after conducting the CBNE
instructional intervention, group A gain high
scores and has apparent progress than group B
in CBNE acceptance scores during COVID
pandemic, in terms of: attitude, value and
satisfaction about the oncoming CBNE system
in the nursing collage. Group B has no noticed
improvement in such scores. Thus, and
matching with the third research hypothesis, there is significant statistical difference
between experimental and control groups as
regards CBNE acceptance scores during
COVID pandemic in favor of experimental
group. Academics in both groups were having
low scores in CBNE acceptance (attitude, value
and satisfaction), during COVID pandemic
before the instructional intervention. But, after
the intervention, the improvement was clear
with the experimental group only which
reflected the great role of CBNE instructional intervention and to which extend the awareness
and understanding of CBNE system may affect
positively to change ones’ attitude, value and
satisfaction, even during healthcare crises.
Nursing academics’ CBNE acceptance has a
major importance to help them in oncoming
smoothly implementing and following such
system successfully. Staff feelings may be the
most crucial domain to be changed and will
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
143
support staff compliance and adherence to
CBNE requirements during risk situation. In
Egypt, because, COVID crisis is coming
parallel in the same time with CBNE
preparation and planning in all Egyptian
colleges, some nursing educators may have
some fear about assuming the clinical training
or coming to college during COVID risk. But,
currently the study provided an evidence that the guidance and educational trials with the
staff can change their feelings positively, even
they are facingrisks. Congruent to such finding,
Harerimana and Beer in 2013, Satoh et al 2020,
Ramos-Morcillo in 2020 and Wallace in
2021found and clarified that the nurse
educators had positive attitude and perceptions
toward utilization and following CBNE,
because they found a great benefit for
themselves and for nursing students
academically and practically, during healthcare
risks. Authors mentioned that the lacking of nursing academic’s training can be a
considerable reason for their negative feedback
and perception toward such system and may
aggravate their worries toward the pandemic
situation. Therefore, staff orientation and
guidance about CBNE strategies, rules,
principles, evaluation and implementation is
necessitated, particularly with any healthcare
risks. Nursing academics should have positive
professional attitudes, acceptance and
contentment with work behaviors including using of innovative teaching strategies,
audiovisuals, evaluation tools, and curricular
management approaches. Mainly, with CBNE
as a valuable direction for nursing practice,
nurse educators have to be initiative, motivated
and gratified and be sure that CBNE is a
methodology for dealing with COVID
emergency, not a source of fear or anxiety.
(Harerimana and Beer 2013, Satoh et al, 2020,
Ramos-Morcillo 2020, Wallace in 2021)
Dissimilarly with the previous results and discussions, Salem et al, in 2018 and Ramos-
Morcillo in 2020declared that the nurse
educators have some stresses and sufferings
due to integration of CBNE quality
requirements and safety of themselves and
students in nursing practice, mainly during
clinical risk time. These stresses may affect
negatively on their attitude to follow and
adhere to CBNE methodology effectively,
particularly with COVID restrictions. CBNE
and quality measurement needs certain
standards, attributes, and preparation to
graduate expert nurses, but COVID crisis may
put some hinders. In the same time, nursing
academics requires specific acceptable
performance and hope that the nursing students
meet professional expectations, fundamentally
with CBNE. Similarly, numerous governing and accreditation organizations still need credit
hours with restricted rules and use performance
examinations for nursing graduates in using of
CBNE. Hence, qualifies nurses will face any
healthcare risks competently and the credit
hours system will be more supportede,
specially, by licensure boards by CBNE in
recruitment and license exams. (Salem et al, in
2018 and Ramos-Morcillo in 2020, Fukada
2018, Pijl-Zieber et al, 2013, Salman et al,
2020)
Furthermore, and oppositely to the current study finding, Brownie et al, 2018, Khaled in
2011and Wallace in 2021 highlighted that
particularly, in Egypt and Africa, nursing
educators found an apparent obstacle in
offering adequate facilities and equipment's in
clinical nursing practice with CBNE. Most
hospitals have a severe shortage of training
requirements. Besides, lacking training chances
and preparations of nursing educators for
competency-based teaching approaches, plus
COVID infection’ fears may produce barriers in CBNE implementation in Egypt.
Correspondingly, Bhutta et al, in 2010,
Nicholas in 2012, Satoh et al 2020, Ramos-
Morcillo in 2020 and Wallace in 2021and
Brownie et al, 2018 clarified that the nursing
curricula are mostly out-of-date and needed
modifications to match the professional
situations. Lacking of curriculum development
models is considered a remarkable challenge
among curricula developers in CBNE,
essentially with some challenges as COVID situation. The governmental view to improvee
the capacity of Egyptian nursing education and
its position between healthcare professionals is
allowing Egypt to determine the indicators of
healthcare quality and advances in the
healthcare system. Such view came in excellent
time, to face healthcare crisis competently and
confidently. Moreover, nursing academics will
find some troubles in following the authentic
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
144
student’s assessment which is a basic
component of CBNE and may raise some
confusion and restlessness among them. Morris
et al, in 2012, Brannick et al, in 2011and
Dashash reported that identification and
deciding of competencies' scores are very
difficult to be determined even with a checklist
in objective structured clinical examination
scores (OSCE) or in clinical or demonstration area, particularly in the COVID circumstances.
A judgment for a student's passing or failing
may be unreliable and may not determine if the
skill is ideally achieved and the competency
outcome is established or not. (Brownie et al,
2018, Khaled 2011, Wallace 2021, Bhutta et al,
2010, Nicholas 2012, Satoh et al 2020, Ramos-
Morcillo 2020)Many references illustrated that
competency assessment standardization in
CBNE is still not clear that may be a cause for
nursing students and educator’s dissatisfaction.
Therefore, to overcome the previous challenges, that may hider nursing academics
cooperation in CBNE, and affect negatively in
their acceptance to such valuable system during
the crisis time, the researchers suggested and
implemented the CBNE intervention. It
designed for encouraging and instructing
nursing academics and leaders about CBNE
development process, and curricular
establishment. Orientation and training are
essential steps for CBNE success among
nursing educators and within emergency situations. The curriculum committee and all
academics should participate in the refining of
the nursing courses to match the professional
requirements. Nursing curricula should be
updated to match the CBNE and work market
needs. Curriculum and program planning for
various self-directed instructional strategies
that parallel nursing students' pace and progress
of mastery are necessary. Accordingly, clinical
and practical preparation with enough facilities,
resources, and training opportunities are required to implement effective CBNE in
Egypt, during such emergency era.
Conclusion
CBNE instructional intervention among
nursing academics in Faculty of Nursing, Alexandria, Egypt, showed significant value
and positive impact in improving their CBNE
knowledge, planning skills and acceptance,
particularly during COVID pandemic. CBNE
concepts of competence, competency, and
authentic assessment are comprehended during
the intervention and inherited in their
organizational culture which is detected after
the intervention among experimental group.
Nursing academics have been equipped to plan
and implement the CBNE approach effectively
with nursing students during CORONA risk that was clearly reflected in their planning
skills scores, after the educational intervention.
Accordingly, CBNE awareness and
understanding among nursing academics is
clearly detected, by such educational trials
which is a necessary for nursing students
during the current pandemic time. There are
scarce experimental trials or research evidences
in such significant issue, consequently, the
incorporation, carrying out, and evaluation of
CBNE awareness among nursing educators
need continuous in-service training programs. It is a crucial issue that will be assumed in
Egypt to meet higher education, government,
and community benefits for nursing education
and nursing workforce advancement at all.
Recommendations and further studies:
There is a chronic and severe shortage in
the nursing workforce in Egypt, mainly, during
COVID pandemic. At the same time, there is a
growing in chronic and acute diseases for
adults, women, and children, and healthcare
community needs. Therefore, upgrading in the
nursing education approach is inevitable to be
CBNE. This instructional scheme requires a
comprehensive understanding of related
concepts, implementation, and evaluation
among nursing academics. Guidance is a great help for nursing academics in implementing
CBNE in Egypt. Based on the current study’
results, interdisciplinary healthcare
contributions should be carried out to develop a
comprehensive and valid insight or model
about CBNE. Teamwork among nursing
specialties and other healthcare professions
should cooperate to develop valid, reliable, and
declarative assessment tools for competency
measurement. Obtaining all literature views
about CBNE may help to implement it successfully and overcomee any challenges or
healthcare crises that may confront such
educational scheme, mainly in Egypt.
Consequently, the present review highlighted

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
145
some thoughts for further studies such as (1)
Assessment of CBNE implementation progress
in Egyptian colleges. (2) Evaluate the effect of
CBNE program on nursing students'
achievement, engagement, and patients'
satisfaction. (3) Replication the current study
among nursing students and academics and
evaluate achievement and compliance, mainly
during healthcare risks. (4) Using valid competency assessment tools for effective
nursing student performance. (5) Integrating
and assessing CBNE curricula in nursing
courses. (6) Using blended learning in CBNE
to decrease the consequences of COVID risk
on nursing students.
Conflicts Of Interest Disclosure
The authors declare that they have no
conflicts of interest.
References
Ahmed A, Sayed K. (2021) An extensive model
for implementing competency-based training in technical and vocational
education and training teacher training
system for Assiut-Integrated Technical
Education Cluster, Egypt. The Journal of
Competency-Based Education; 6 (2) e01245
Ahmed, A., & Sayed, K. (2020). Development of
competency-based training system in
Assiut-ITEC: A case study. Competency-
based Education, 5,
e01217. https://doi.org/10.1002/cbe2.1217
Albanese, M. A., Mejicano, G., Anderson, W. M., & Gruppen, L. (2010). Building a
competency-based curriculum: The agony
and the ecstasy. Advances in Health
Sciences Education, 15(3), 439–454.
Available
at: https://doi.org/10.1007/s10459-008-
9118-2. Retrieved in March 2021
American Nurses Association. (2006) Translation
Supervisor Kamiizumi K. Nursing: Scope &
Standards of Practice. International Nursing
Review; 29:12-20. Japanese.
Austin Z. (2019). Competency and Its Many
Meanings. Pharmacy 7, 37;
doi:10.3390/pharmacy7020037
Bates T. (2020). What is the difference between
competencies, skills, and learning outcomes
– and does it matter?
Bhutta ZA, Chen L, Cohen J, Crisp N, Evans T,
Fineberg H. (2010) Education of health
professionals for the 21st century: a global
independent Commission. 3;
375(9721):1137–8. Available at:
https://doi.org/10.1016/S0140-6736(10)60450-3 PMID:20362799
retrieved in February 2021
Blömeke S, Troitschanskaia OZ, Kuhn C, Fege J.
(2013) Modeling and Measuring
Competencies in Higher Education; Tasks
and Challenges. PROFESSIONAL AND
VET LEARNING. Sense Publishers,
Rotterdam, the Netherlands. 12-43, ISBN:
978-94-6091-867-4
Bohain, P., & Hofman, W. H. (2014). Perceived
effects of competency-based training on the
acquisition of professional skills. International Journal of Education, 36, 81–
89.http://dx.doi.org/10.1016/j.ijedudev.2013
.11.003.
Boyle J, Connolly M, MacKay T. (2016)
Systematic Reviews and Meta-Analyses.
Educational & Child Psychology 33(3): 76–
91.
Brannick, M.T., Erol-Korkmaz, H.T., Prewett,
M. (2011) A systematic review of the
reliability of objective structured clinical
examination scores. Med. Educ. 45, 1181–1189.
Brownie S, Rossiter R. (2018) Supporting the
nationally mandated transition to
competency-based nursing curricula in
Egypt. ICN Regional Conference 1-18
Available at:
https://ecommons.aku.edu/eastafrica_fhs_so
nam/208
Brownie SH M, Docherty C, Al-Yateem N,
Gadallah MH, Rossiter R. (2018)
Developing a national competency-based curriculum for technical nurses in Egypt.
EMHJ; 24 (9), 922-932
Dashash M, Almasri B, Takaleh E, Halawah AA,
Sahyouni A. (2020) Educational perspective
for the identification of essential
competencies required for approaching
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
146
patients with COVID-19. East Mediterr
Health J; 26 (9) P: 1011-1017. Available at:
https://doi.org/10.26719/emhj.20.111
Retrived in Iuly 2021
Dreyfus SE. (2004) the five-stage model of adult
skill acquisition. Bull Sci Technol Soc,
24(3):177-181.
El Tawil N. (2021) 'Egypt's population growth
has to be cut to 400K yearly so we can feel the impact of public spending': Pres. Sisi.
Egypt Today. Available
at:https://www.egypttoday.com/Article/1/98
679/Egypt-s-population-growth-has-to-be-
cut-to-400K Retrieved in February 2021
Englander, R., Cameron, T., Ballard, A.J.,
Dodge, J., Bull, J. & Aschenbrener, C.A.
(2013). Toward a common taxonomy of
competency domains for the health
professions and competencies for
physicians. Academic Medicine, 88(8),
1088–1094.
Essa H, Elkazeh E, Zewil M, Hassan L. (2021)
Effect of COVID-19 Pandemic on the
Competencies of Academic Staff of Nursing
Faculties Regarding their Use of Online
Applications in Teaching / Learning Tasks.
DOI: 10.21608/TSNJ.2021.170822
Fan J, Wang Y, Chao La2Jane S, Hsu L. (2015).
Performance evaluation of nursing students
following competency-based education.
Nurse Education Today; 35(1) 97-103
Fastre ,́ G. M., van der Klink, M., Amsing-Smit P., & van Merrie¨nboer, J. J. G. (2014)
Assessment criteria for competency-based
education: a study in nursing education.
Instr Sci; 42:971–994. DOI
10.1007/s11251-014-9326-5
Fieger F. (2012) Measuring student satisfaction
from the Student Outcomes Survey.
National Centre for Vocational Education
Research. Commonwealth of Australia.
Available at:
https://www.researchgate.net/publication/313701724_Measuring_Student_Satisfaction_
from_the_Student_Outcomes_Survey
retrieved in June 2020
Frank J et., al. (2010) Competency-based medical
education: theory to practice. Medical
Teacher 32: 638–645 DOI:
10.3109/0142159X.2010.501190
Frank, J. R., Snell, L. S., Ten Cate, O., Holmboe,
E. S., Carraccio, C., Swing, S. R., et al.
(2010). Competency-based medical
education: Theory to practice. Medical
Teacher, 32(8), 638–45. Available
at: https://doi.org/10.3109/0142159X.2010.
501190. Retrieved in March 2021
Friedler, A. (2018). Teachers training micro-
learning innovative model: Opportunities
and challenges. 2018 Learning With
MOOCS (LWMOOCS), Madrid, pp. 63–
65. https://doi.org/10.1109/LWMOOCS.201
8.8534647
Fukada M. (2018) Nursing Competency:
Definition, Structure, and Development.
Yonago Acta Medica;61:001–007
Garneau, A.; Lavoie, P.; Grondin, M. (2017).
Dichotomy and dialogue in
conceptualizations of competency in health professionals’ education. J. Nurs. Educ.
Pract, 7, 18–26.
Getha-Taylor, Heather; Hummert, Raymond;
Nalbandian, John; Silvia, Chris
(2013). Competency model design and
assessment: findings and future
directions. Journal of Public Affairs
Education. 19 (1): 141–
171. doi:10.1080/15236803.2013.12001724
. JSTOR 23608938. S2CID 116247757
Gough, D. (2007), “Weight of evidence: a framework for the appraisal of the quality
and relevance of evidence”, Research
Papers in Education, 22 (2) 213-28.
Gravina EW. (2017) Competency-Based
Education and Its Effect on Nursing
Education: A Literature Review. Teaching
and Learning in Nursing 12, 117–121
Guo, G., & Qiu, B. (2019). Investigation and
research on vocational education teachers'
competencies based on smart learning
environment. 2019 10th International Conference on Information Technology in
Medicine and Education (ITME), Qingdao,
China, pp. 415–
418. https://doi.org/10.1109/ITME.2019.00
099
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
147
Hager P, Gonczi A. (1996). What is competence.
Medical Teacher, 18(1)
Hallinger P. (2013) A conceptual framework for
systematic reviews of research in
educational leadership and management.
Journal of Educational Administration, 51
(2)126-149
Harerimana A, Beer J (2013) Nurse educators’
utilization of different teaching strategies in a competency-based approach in Rwanda.
Africa Journal of Nursing and Midwifery 15
(1) 2013 pp. 29–41
http://www.wgu.edu/about_WGU/competency-
based-education. Retrieved in October 2020
https://doi.org/10.1007/s12564-020-09658-6
Retrieved in January 2021
Hussien R, Elkayal M, Shahin M. (2020)
Emotional Intelligence and Uncertainty
among Undergraduate Nursing Students
during the COVID-19 Pandemic Outbreak:
A Comparative Study. The Open Nursing Journal, 14, 220-231. DOI:
10.2174/1874434602014010220, 2020, 14,
220-231
Interprofessional Education Collaborative.
(2016). Core competencies for
interprofessional collaborative practice:
2016 update. Retrieved
from https://hsc.unm.edu/ipe/resources/ipec
-2016-core-competencies.pdfRetrieved in
February 2021
Japanese Nursing Association. (2005) International competency standards
framework for generalist nurses. Nursing
White Paper. 170-8. Japanese.
Jung JH, Kim HJ, Kim J. (2020). Comparison of
Nursing Performance Competencies and
Practical Education Needs Based on
Clinical Careers of Operating Room Nurses:
A Cross-Sectional Study. Healthcare 2020,
8, 136; doi:10.3390/healthcare8020136
Kang, R., Pavlova, M. (2019). Development of
TVET Teachers' Career Identity through Teacher Education and Training Programs
for the purposes of including ESD in
Classroom Practices. www.tvet-
online.asia Issue, 14, 1–11.
Kennedy D, Hyland A, Ryan N. (2009) Learning
outcomes and competencies. Available at:
https://www.researchgate.net/publication/28
5264101 Retrieved in March 2021
Khaled A. (2011) Egypt: Ailing nursing colleges
promised to rescue. University World News,
Africa Edition. Available at: http://www.
universityworldnews.com/article.php?story
=20110114223638291 retrieved in March 2021
Koelemay M. et al. (2016) Quick Guide to
Systematic Reviews and Meta-analysis Eur
J Vasc Endovasc Surg, 51, 309e309
Koster, A.; Schalekamp, T.; Meijerman, I. (2017)
Implementation of competency-based
pharmacy education. Pharmacy, 5, 10.
Loke A, Guo C, Molassiotis A. (2021)
Development of disaster nursing education
and training programs in the past 20 years
(2000–2019): A systematic review. Nurse
education today, 99; 104809
Lucey, C.R.(2018). Achieving competency-based,
time-variable health professions education.
Proceedings of a conference sponsored by
Josiah Macy Jr. Foundation in June 2017.
New York, NY: Josiah Macy Jr.
Foundation.
Ma C, Fouly H, Li J, D’Antonio P. (2012) The
education of nurses in China and Egypt.
Nurs Outlook, 60(3):127–133.e1. Available
at:
https://doi.org/10.1016/j.outlook.2011.08.002 PMID:22000692 retrieved in March 2020
Mahapatro BB, (2010). Human resource
management. New Age International (P)
Ltd., Publishers, ISBN (13) : 978-81-224-
2943-5
Massachusetts Department of Higher Education
Nurse of the Future Competencies
Committee. (2007). Nurse of the Future
Nursing Core Competencies, version 2.
Boston: Massachusetts Department of
Higher Education. Available at: http://www.mass.edu/currentinit/currentinit
NursingNurseFutureComp.asp. Retrieved in
January 2021

Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
148
Mel Kleiman (2000). What happens if you don’t
train them and they stay? Occupational
Health and Safety, 69 (1), pp. 18, 70
Morris, M.C., Gallagher, T.K., Ridgway, P.F.
(2012) Tools used to assess medical
student’s competence in procedural skills at
the end of a primary medical degree: a
systematic review. Med. Educ. Online 17,
1–9.
Mulder, M., Weigel T, Collins K. (2006). The
concept of competence concept in the
development of vocational education and
training in selected EU member states. A
critical analysis. Journal of Vocational
Education and Training, 59, 1, 65-85.
National Authority for Quality Assurance and
Accreditation of Education. (2017) National
Academic Reference Standards (NARS)
Nursing Education, 2nd edition. Egypt.
Available at: http://naqaae.eg/wp-
content/uploads/2014/10/nursing.pdf Retrieved in May 2020
Nicholas PK, Corless IB, Fulmer H, Meedzan N.
(2012) Preparing nursing students for
education in the global village. MCN Am J
Matern Child Nurs. 37(6):367–72.
Available at:
https://doi.org/10.1097/NMC.0b013e31825
8a9e1 PMID:23073249 Retrieved in
January 2021
Nyoni Ch, Botma Y. (2019) Implementing a
competency-based midwifery program in Lesotho: A gap analysis. 34, 72-78
Oducado R, Estoque H. (2021) Online Learning
in Nursing Education during the COVID-19
Pandemic: Stress, Satisfaction, and
Academic Performance. Journal of Nursing
Practice, 4 (2) 143-153 ISSN: 2614-3488
(print); 2614-3496
Page M. et al. (2020) PRISMA 2020 statement:
updated guidelines for reporting systematic
reviews and meta-analyses. MONASH
University. 26th Cochrane Colloquium, 2019, Santiago, Chile.
Perry R, Hamm J. (2017). An Attribution
Perspective on Competence and Motivation:
Theory and Treatment Interventions.
Published thesis. Department of
Psychology, University of Manitoba,
Winnipeg, MB, Canada; 5-37
Pijl-Zieber, E. M., Barton, S., Konkin, J.,
Awosoga, O., & Caine, V. (2013).
Competence and competency-based nursing
education: Finding our way. Nurse
Education Today, 34, 676–678. Available
at:
http://dx.doi.org/10.1016/j.nedt.2013.09.007. Retrieved in October 2020
Ramos-Morcillo A, Leal-Costa C,Moral-García
J, Ruzafa-Martínez M. (2020) Experience of
Nursing Students during the Abrupt Change
from Face-to-Face to e-Learning Education
during the First Month of Confinement Due
to COVID-19 in Spain. Int. J. Environ. Res.
Public Health, 17, 5519;
doi:10.3390/ijerph17155519
Salem OA, Aboshaiqah AE, Mubaraki MA,
Pandaan IN. (2018) Competency-Based
Nursing Curriculum: Establishing the Standards for Nursing Competencies in
Higher Education. Open Access Library
Journal, 5, e4952, ISSN Online: 2333-9721,
ISSN Print: 2333-9705
Salman M, Ganie SH A, Saleem I. (2020). The
concept of competence: a thematic review
and discussion. European Journal of
Training and Development. DOI:
10.1108/EJTD-10-2019-0171
Sangwan A, Sangwan A, Punia P. (2021)
Development and Validation of an Attitude Scale towards OnlineTeaching and Learning
for Higher Education Teachers.
TechTrends; 65:187–195 Available at:
https://doi.org/10.1007/s11528-020-00561-
wretrieved in June 2020
Satoh M, Fujimura A, Sato N. (2020)
Competency of Academic Nurse Educators
SAGE Open Nursing 6: 1–11, DOI:
10.1177/2377960820969389
Sistermans IJ. (2020) Integrating competency-
based education with a case-based or problem-based learning approach in online
health sciences. Asia Pacific Education
Review 21:683–696. Available at:
Smith, B. (1993): Building managers from the
inside out competency-based action
Original Article Egyptian Journal of Health Care, 2021 EJHC Vol. 12 No. 4
149
learning, in Journal of Management
Development, 12, 1: 43-8
Spady WG. 1977. Competency-based education:
A bandwagon in search of a definition. Educ
Res 6 (1):9–14
Stern D. (2010). Study of competencies and
competency-based human resource
management: exploring practices and
perspectives of selected senior human resource leaders/practitioners and thought
leaders. Published thesis. College of
Education, Pennsylvania State University,
Available at
https://etda.libraries.psu.edu/files/final_sub
missions/1425 Retrieved in October 2020
Technical Institutes Directorate. Overview of
nursing in Egypt. Cairo: Ministry of Health
and Population; 2017.
Wallace SH, Kaulback M, Hunt K, Baker M.
(2021) Nursing student experiences of
remote learning during the COVID-19 pandemic. Nursing Forum and independent
voice for nurses, Wiley Periodicals LLC.
DOI: 10.1111/nuf.12568
Watson R, Stimpson A, Topping A, Porock D.
(2002) Clinical competence assessment in
nursing: a systematic review of the
literature. Journal of Advanced Nursing
39(5), 421–431
Weeks, K.; Coben, D.; Lum, G.; Pontin, D.
(2017). Developing nursing competence:
Future-proofing nurses for the changing practice requirements of 21st-century
healthcare. Nurse Educ. Pract; 27, A3–A4
Western Governor's University (2016).
Competency-based education: higher
education for the 21st-century student.
Available at:
Wilcox Y. (2012) An Initial Study to Develop
Instruments and Validate the Essential
Competencies for Program Evaluators
(ECPE). The faculty of the graduate school
of the University of Minnesota; published thesis. 1-149 available at
https://conservancy.umn.edu/bitstream/hand
le/11299/132042/Wilcox_umn_0130E_128
86.pdf?sequence=1&isAllowed=y
Retrieved in February 2021
Wu W, Martin BC, Ni C. (2019) A Systematic
Review of Competency-Based Education
Effort in the Health Professions: Seeking
Order Out of Chaos. Health Policy Reform
Concepts Methodology Tools Appl. 1410–
36. In Handbook of Research on
Competency-Based Education in University Settings. DOI: 10.4018/978-1-5225-0932-
5.ch018
Zineb, A. H., Soumia, B., Souad, A., Karim,
G. (2017). The application of the
competency based approach to assess the
training and employment adequacy
problem. International Journal of Education
(IJE), 5(1), 1–18. https:// doi. org/ 10. 5121/
ije.2017.5101




















