
The effect of exercise on pQCT parameters of bone structure and strength in postmenopausal women—a...
13
REVIEW The effect of exercise on pQCT parameters of bone structure and strength in postmenopausal women—a systematic review and meta-analysis of randomized controlled trials I. Polidoulis & J. Beyene & A. M. Cheung Received: 29 December 2010 / Accepted: 22 June 2011 /Published online: 3 August 2011 # International Osteoporosis Foundation and National Osteoporosis Foundation 2011 Abstract Summary Inconsistent study findings of exercise on areal bone density highlight the need to include parameters of bone geometry and volumetric bone density measurements. Using a systematic review and meta-analysis, we found a decrease in bone loss through the maintenance of cortical and trabecular volumetric bone mineral density (BMD). Studies with longer exercise durations and larger sample sizes are needed. Introduction Exercise has long been recommended to prevent age-related loss of bone mass in postmenopausal women. However, inconsistent study findings on the effect of exercise on BMD preservation have highlighted the importance of extending the evaluation of bone to include the parameters of bone geometry. We conducted both a systematic review and meta-analysis of the effects of exercise on bone geometry and volumetric BMD in postmenopausal women. Methods We searched MEDLINE, PubMed, and EMBASE from 1950 to April 2009 and included prospective, randomized controlled trials of healthy postmenopausal women where the intervention involved exercise or sport and outcomes included quantitative or peripheral quantita- tive computed tomography bone parameters. Outcome variables included: total volumetric BMD, cortical volu- metric BMD (CvBMD), trabecular volumetric BMD (TrvBMD), total bone mineral content, cortical BMC, total bone area, cortical area, polar stress–strain index, and bone strength index. Results Six studies satisfied our inclusion and exclusion criteria. Lower extremity exercises resulted in small (∼0.9%) but significant improvements in TrvBMD of the distal tibia (p = 0.0006) and in CvBMD of the tibial shaft (p =0.0007). Studies with longer durations of exercise (12 months) and those in early postmenopausal women showed significant changes in CvBMD at the tibial shaft. Conclusions We conclude that exercise in postmenopausal women may decrease bone loss by maintaining cortical and trabecular volumetric BMD. To better understand the effect of exercise on bone geometric structure and strength, more studies of longer duration and larger sample sizes are needed. Keywords Bone geometry . Exercise . Postmenopausal . pQCT . Women Introduction Exercise plays an important role in the development and maintenance of bone mass and strength [1–3]. A key outcome in the majority of studies examining the effect of exercise on bone strength has been areal bone mineral density (aBMD) I. Polidoulis Department of Family & Community Medicine, University of Toronto, The Scarborough General Medical Mall, 309-3030 Lawrence Avenue East, Scarborough, Ontario M1P 2T7, Canada e-mail: [email protected] J. Beyene Department of Public Health Sciences, University of Toronto, Population Health Sciences, Research Institute, Hospital for Sick Children, 555 University Avenue, Toronto, Ontario M5G 1X8, Canada e-mail: [email protected] A. M. Cheung (*) University Health Network/Mount Sinai Hospital, Eaton North Wing, 7th Floor Room 7EN221, 200 Elizabeth Street, Toronto, Ontario M5G 2C4, Canada e-mail: [email protected] Osteoporos Int (2012) 23:39–51 DOI 10.1007/s00198-011-1734-7
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The effect of exercise on pQCT parameters of bone structure and strength in postmenopausal women—a...
REVIEW
The effect of exercise on pQCT parameters of bone structureand strength in postmenopausal women—a systematic reviewand meta-analysis of randomized controlled trials
I. Polidoulis & J. Beyene & A. M. Cheung
Received: 29 December 2010 /Accepted: 22 June 2011 /Published online: 3 August 2011# International Osteoporosis Foundation and National Osteoporosis Foundation 2011
AbstractSummary Inconsistent study findings of exercise on arealbone density highlight the need to include parameters ofbone geometry and volumetric bone density measurements.Using a systematic review and meta-analysis, we found adecrease in bone loss through the maintenance of corticaland trabecular volumetric bone mineral density (BMD).Studies with longer exercise durations and larger samplesizes are needed.Introduction Exercise has long been recommended to preventage-related loss of bone mass in postmenopausal women.However, inconsistent study findings on the effect of exerciseon BMD preservation have highlighted the importance ofextending the evaluation of bone to include the parameters ofbone geometry. We conducted both a systematic review andmeta-analysis of the effects of exercise on bone geometry and
volumetric BMD in postmenopausal women.Methods We searched MEDLINE, PubMed, and EMBASEfrom 1950 to April 2009 and included prospective,randomized controlled trials of healthy postmenopausalwomen where the intervention involved exercise or sportand outcomes included quantitative or peripheral quantita-tive computed tomography bone parameters. Outcomevariables included: total volumetric BMD, cortical volu-metric BMD (CvBMD), trabecular volumetric BMD(TrvBMD), total bone mineral content, cortical BMC, totalbone area, cortical area, polar stress–strain index, and bonestrength index.Results Six studies satisfied our inclusion and exclusioncriteria. Lower extremity exercises resulted in small (∼0.9%)but significant improvements in TrvBMDof the distal tibia (p=0.0006) and in CvBMD of the tibial shaft (p=0.0007). Studieswith longer durations of exercise (12 months) and those inearly postmenopausal women showed significant changes inCvBMD at the tibial shaft.Conclusions We conclude that exercise in postmenopausalwomen may decrease bone loss by maintaining cortical andtrabecular volumetric BMD. To better understand the effect ofexercise on bone geometric structure and strength, morestudies of longer duration and larger sample sizes are needed.
Keywords Bone geometry . Exercise . Postmenopausal .
pQCT.Women
Introduction
Exercise plays an important role in the development andmaintenance of bonemass and strength [1–3]. A key outcomein the majority of studies examining the effect of exercise onbone strength has been areal bone mineral density (aBMD)
I. PolidoulisDepartment of Family & Community Medicine,University of Toronto,The Scarborough General Medical Mall,309-3030 Lawrence Avenue East,Scarborough, Ontario M1P 2T7, Canadae-mail: [email protected]
J. BeyeneDepartment of Public Health Sciences, University of Toronto,Population Health Sciences, Research Institute,Hospital for Sick Children,555 University Avenue,Toronto, Ontario M5G 1X8, Canadae-mail: [email protected]
A. M. Cheung (*)University Health Network/Mount Sinai Hospital,Eaton North Wing, 7th Floor Room 7EN221,200 Elizabeth Street,Toronto, Ontario M5G 2C4, Canadae-mail: [email protected]
Osteoporos Int (2012) 23:39–51DOI 10.1007/s00198-011-1734-7

as measured by dual-energy X-ray absorptiometry (DXA)[4–7]. Compared to non-exercising controls, these studies inpostmenopausal women have shown two key benefits ofexercise on bone which are: measurable increases in aBMD[5, 8] and a reduction in the loss of bone mineral [6, 7].
Several systematic reviews have been published suggestingthat exercise slows age-related decline of aBMD by approxi-mately 1% per year in postmenopausal women [9, 10].However, aBMD accounts at best for 60–70% of the variancein ultimate strength of bone tissue [11]. Inconsistent studyfindings have highlighted the limitations of using aBMDalone to determine the effect of exercise on bone health [2, 3].These findings have led researchers to expand their assess-ment of bone strength and fracture risk to also includeparameters of bone geometry [12]. Whereas quantitativecomputed tomography (QCT), peripheral QCT (pQCT), andmagnetic resonance imaging allow for geometric measure-ment of bones, DXA has limitations with respect to theassessment of bone geometric structure and the arrangementof the bone mineral in the cortical vs. the trabecularcompartments [12]. DXA is a two-dimensional technique thatrequires a number of assumptions not as yet tested acrossvarious populations and treatment groups [12]. Bone geomet-ric structure, measured by three-dimensional imaging usingCT, is an important determinant of bone fragility independentof bone density [13] and adds measurably to the prediction offracture risk as indicated by aBMD alone [5–8, 11].
The purpose of this study was to critically evaluate,through systematic review and meta-analysis, the effect ofexercise on bone geometry and cortical and trabecularvolumetric BMD in postmenopausal women as reported inrandomized controlled clinical trials.
Methods
Study selection
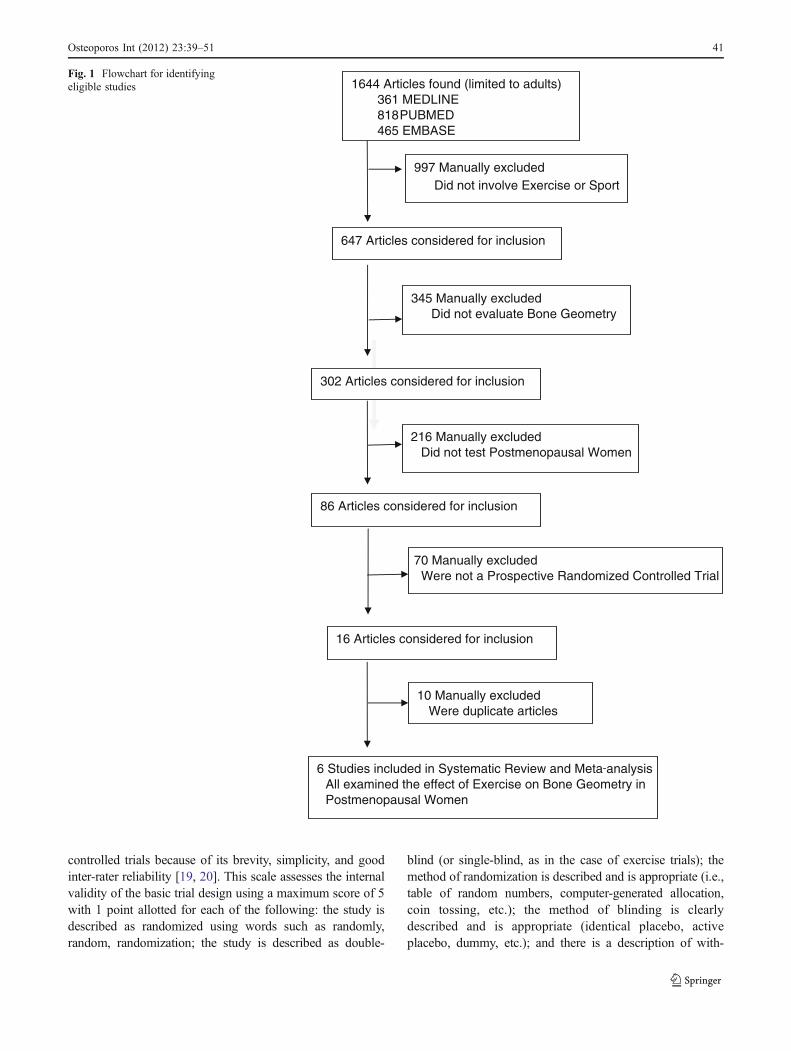
With the help of two professional librarians, we conductedsystematic searches of MEDLINE and PUBMED from1950 to April 2009 and EMBASE from 1980 to April 2009.Our aim was to identify prospective, randomized controlledtrials on the effect of exercise on QCT and pQCTparameters of bone geometry and volumetric BMD inpostmenopausal women (Fig. 1). Our search strategy usedtwo groups of terms using an AND strategy. We combinedexercise-related search terms including: exercise, exercisemovement techniques, motor activity, physical activity,physical capacity, physical performance, or sports; withbone parameter search terms that included: bone or bones,microarchitecture, geometry, structure, histomorphometry,histomorphology, histology, or QCT. We limited our searchto human studies and excluded studies in children, men,
and patients with secondary osteoporosis. We includedprospective, randomized controlled trials of healthy post-menopausal women where the intervention involved exer-cise or sport and the outcome included QCT or pQCTparameters of bone. We excluded trials that studied disease-specific patient populations. We did, however, include onetrial which studied elderly men and women with a historyof stroke because this trial included only stable, ambulatory,community-dwelling individuals with minimal residualstroke deficits who were able to walk independently andexercise [14]. As exercise is an intervention that is difficultto blind, we did not require that the investigators or thestudy participants be blinded to the intervention.
Data extraction and collection
The following variables were assessed: study population;age; race; years since menopause; duration of exerciseintervention; sample size; compliance with exercise; type,frequency, and intensity of exercise; type, precision, andreliability of outcome measuring device(s); bone sitesmeasured; statistical power; use of confidence intervals;consideration for contamination; intention-to-treat; qualityof studies; and similarity of baseline characteristics betweenthe exercise and control groups.
Our primary outcomes were geometric and bone strengthparameters as measured by pQCT. The pQCT parameterswere total volumetric BMD, trabecular volumetric BMD(TrvBMD), cortical volumetric BMD (CvBMD), total bonemineral content, cortical BMC, total bone area, cortical area(CoA), polar stress–strain index, and bone strength index.These outcomes were assessed at four different bone sites:the distal radius, radial shaft, distal tibial, and tibial shaft.
In studies where the investigators included osteoporosismedications such as alendronate [15] or hormone replacementtherapy [16], that treatment arm was excluded from ouranalysis and only data from the exercise and the controlgroups were utilized. In studies where there were more thanone exercise group [17, 18], either the combined effect of thedifferent exercise groups was used [17] where possible or onlydata from the resistance exercise group was used [18] as mostof these studies examined the effect of resistance exercise. Inthe study that included postmenopausal women with strokewith minimal residual effects [14], only data from the non-paretic side of these women were used. Data were collected ina standardized format with our outcome variables collected aspercent difference between the baseline and endpoint valuesfor the exercise groups and the control groups.
Study quality
Two independent reviewers assessed the quality of the studies.We used the Jadad [19] quality scale for randomized,
40 Osteoporos Int (2012) 23:39–51
controlled trials because of its brevity, simplicity, and goodinter-rater reliability [19, 20]. This scale assesses the internalvalidity of the basic trial design using a maximum score of 5with 1 point allotted for each of the following: the study isdescribed as randomized using words such as randomly,random, randomization; the study is described as double-
blind (or single-blind, as in the case of exercise trials); themethod of randomization is described and is appropriate (i.e.,table of random numbers, computer-generated allocation,coin tossing, etc.); the method of blinding is clearlydescribed and is appropriate (identical placebo, activeplacebo, dummy, etc.); and there is a description of with-
1644 Articles found (limited to adults)361 MEDLINE
PUBMED818 465 EMBASE
997 Manually excludedDid not involve Exercise or Sport
647 Articles considered for inclusion
345 Manually excludedDid not evaluate Bone Geometry
302 Articles considered for inclusion
216 Manually excludedDid not test Postmenopausal Women
86 Articles considered for inclusion
16 Articles considered for inclusion
10 Manually excludedWere duplicate articles
6 Studies included in Systematic Review and Meta analysisAll examined the effect of Exercise on Bone Geometry inPostmenopausal Women
70 Manually excludedWere not a Prospective Randomized Controlled Trial
Fig. 1 Flowchart for identifyingeligible studies
Osteoporos Int (2012) 23:39–51 41
Tab
le1
Overview
ofrand
omized
controlledtrialsinclud
edin
system
atic
review
Year/author/jo
urnal
Study
popu
latio
nDurationof
exercise
Sam
plesize
Percentage
compliancewith
exercise
(%)
Detailsof
exercise
interventio
nOutcomemeasurementdevice/site(s)
measured
2002
/Cheng
etal./
Bon
eFinnish
wom
en,50–5
7years,<5years
postmenop
ause
12mon
ths
12Exercisers
50Highim
pact,prog
ressive,
upper
andlower
body
exercises,and
abdo
minal
andlow
back
exercises,
duratio
nno
tspecified
pQCT—SeimensSom
atom
DR:prox
imal
femur,prox
imal
tibia,midfemur,25
%of
tibialshaft
15Con
trols
Con
trols:maintainedpre-stud
ylevelof
activ
ity
2003
/Uusi-Rasiet
al./
Bon
eFinnish
wom
en,50
.2–
56.6
years,1–
5years
postmenop
ause
12mon
ths
37Exercisers
67Highim
pact,prog
ressivelower
body
exercise,50
min,3tim
esperweek
DXA—Norland
XR-26:
L-spine,R
prox
imal
femur,no
ndom
inant
distal
radius
39Con
trols
Con
trols:maintainedpre-stud
ylevelof
activ
itypQ
CT—XCT30
00:R-tibialmidshaft,
R-distaltib
ia
2004
/Chanet
al./A
rchives
ofPhysicalMedicine
andRehab
ilitatio
n
Chinese
wom
en,50
.4–
57.7
years,1–
10years
postmenop
ause
12mon
ths
54Exercisers
84Low
impact,no
n-prog
ressive
Tai
Chi
Chu
n,50
min,5tim
esperweek
DXA—Norland
XR-36:
nond
ominant
prox
imal
femur,lumbarspine
54/49Con
trols
Con
trols:maintainedpre-stud
ylevelof
activ
ity
pQCT—Densiscan
2000
:no
ndom
inant
ultradistaltib
ia,no
ndom
inantdistal
tibialdiaphy
sis
2004
/Liu-A
mbroseet
al./Jou
rnal
ofClin
ical
Densitometry
Canadianwom
en,
75–8
5years
6mon
ths
(25weeks)
28(avg
)Resistance
exercisers
85Resistanceexercise:prog
ressive,
high
intensity
upperandlower
body,andtrun
kexercises,
50min
grou
pexercise,twice
perweek
DXA—Holog
ic45
00:totalhip,
femoral
neck,trochanter
34(avg
)Agility
exercisers
Agilityexercise:training
oflower
body
forbalance,
coordinatio
nandreactio
ntim
e,50
min
grou
pexercise,twice
perweek
pQCT—XCT54
0:Ldistal
tibia
at10
%site,Ltib
ialshaftat
50%
site,Ldistal
radius
at10
%site,Lradial
shaftat
30%
site
28(avg
)Con
trols
Con
trols:sham
exercises(stretching
andrelaxatio
n)
2006
/Karinkantaet
al./O
steopo
rosis
Internationa
l
Finnish
wom
enliv
ing
inTam
pere,70
–79
years
12mon
ths
111Alltypes
ofexercisers
67Highim
pact,prog
ressiveexercise,
45min,3tim
esperweek:
resistance
training
(low
erbo
dyandback)vs.
balance/jumping
training
(low
erbo
dy)
vs.combinatio
ntraining
(resistance
andbalancetraining
onalternate
weeks)
DXA—Norland
XR-26:
Rprox
imal
femur
36Con
trols
Con
trols:maintainedpre-stud
ylevel
ofactiv
ity
pQCT—XCT30
00:Rdistal
tibia,R
tibialmidshaft,Rdistal
radius,R
radial
midshaft
2006
/Panget
al./O
steopo
rosis
Internationa
l
Canadianwom
en,
stable,am
bulatory
with
historyof
stroke,
minim
alresidu
aldeficits,
5mon
ths
(19weeks)
9/11
Exercisers
85Low
impact,prog
ressive,
lower
body
exercise,1h,
3tim
esperweek:
aerobicexercise,static
anddy
namic
balance,
functio
nalexercises
pQCT—XCT20
00:no
n-paretic
distal
tibia,no
n-paretic
tibialshaft
42 Osteoporos Int (2012) 23:39–51

drawals and dropouts. A point is deducted if the method ofrandomization is described and is not appropriate (i.e.,alternate allocation, date of birth, hospital, chart numbers,etc.). A point is also deducted if the study is described asdouble-blind but the blinding method is not appropriate (i.e.,comparison of tablet vs. injection, no double dummy, etc.).The Jadad scale has been shown to discriminate wellbetween low-quality studies (2 points or less) and high-quality studies (3 points or more) [19, 20]. In cases whererandomization and blinding were in question, we contactedthe authors [4, 17] for clarification.
Meta-analysis
We followed published guidelines for the meta-analysis ofrandomized controlled trials [21, 22]. We calculated theweighted pooled mean percent difference (and 95%confidence intervals) between the exercise and non-exercise groups using RevMan 4.1 (The Cochrane Collab-oration, Oxford, England, 2000). Weighting was assignedaccording to the inverse of the variance. Heterogeneity wastested using the Cochrane Q test and quantified by the I2
statistic [23]. The I2 statistic was used to select theappropriate pooling method: fixed effects models wereused for I2 less than 50% and random effect models for I2
greater than 50%.We contacted all authors [15–17] who reported the
standard deviation (SD) of the baseline values and the finalvalues separately, but not the standard deviation of thedifference. One of the authors [16] was unable to providethis data so we excluded this study from the meta-analysisbut not from the systematic review. Data from this studywould have contributed to only two of the endpoints in ourmeta-analysis, namely CvBMD of the tibial shaft and CoAof the tibial shaft.
To test the robustness of our meta-analytic results, weconducted sensitivity analyses by excluding lower qualitytrials using a Jadad score of 2 as the cutoff. We alsoperformed subgroup analyses to examine the potentialeffect of the duration of the exercise intervention (5–6 months [14, 18] vs. 12 months [4, 15, 17]) and yearssince menopause (1–10 years [4, 15] vs. more than 10 years[17, 18]) on our outcomes.
Results
Systematic review
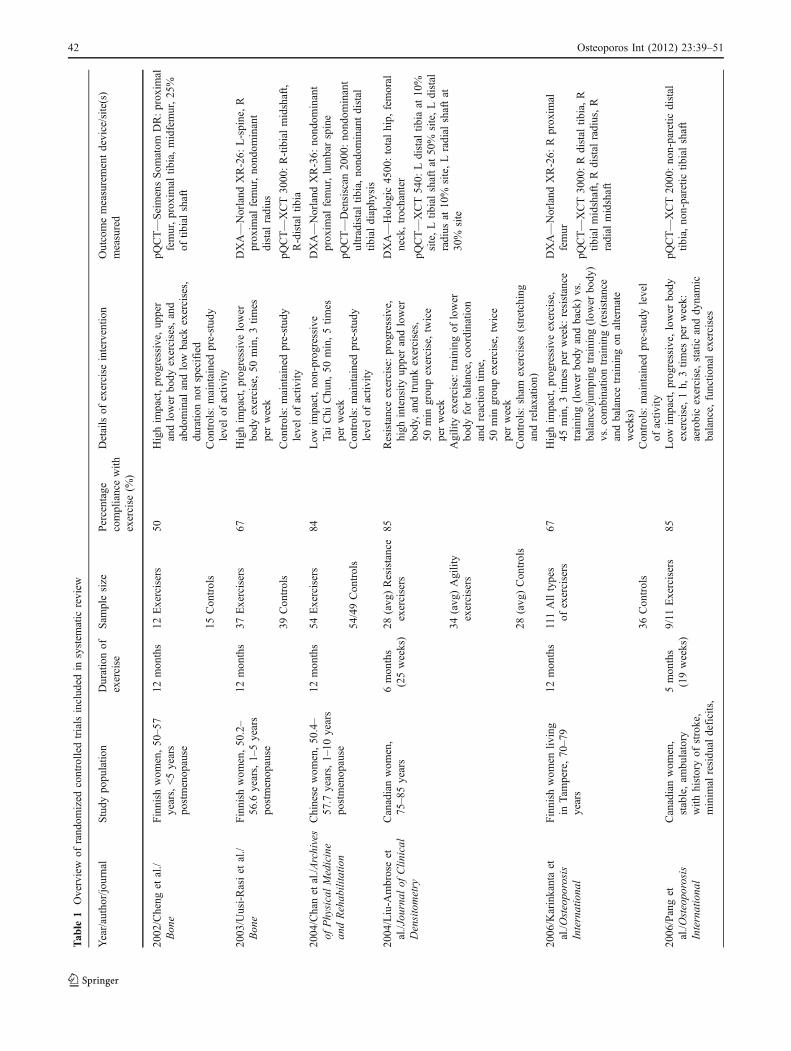
Our systematic search of the literature yielded six random-ized controlled trials with a total of 287 exercisingpostmenopausal women and 182 controls [4, 14–18](Fig. 1 and Table 1). All studies used pQCT rather thanT
able
1(con
tinued)
Year/author/jo
urnal
Study
popu
latio
nDurationof
exercise
Sam
plesize
Percentage
compliancewith
exercise
(%)
Detailsof
exercise
interventio
nOutcomemeasurementdevice/site(s)
measured
55.1–7
4.3years
6/10
Con
trols
Con
trols:seated
upperbo
dyexercises
for1h,
threetim
esperweekor
electrical
stim
ulationto
wrist
extensorsifthey
had
<20
°of
activ
ewristextension
Avg
average,
Lleft,Rrigh
t,pQ
CTperiph
eral
quantitativecompu
tedtomog
raph
y,DXAdu
al-energyX-ray
absorptio
metry
Osteoporos Int (2012) 23:39–51 43
QCT. The average age of the study participants was65.8 years, (range 50–85 years) and the average durationof the exercise intervention was 9.7 months (range 5–12 months). The studies were carried out in three differentcountries (two in Canada, three in Finland, and one in HongKong). There were notable variations between the studies interms of average age of participants, years since meno-pause, sample size (range 9–111 among exercise groups),outcome measures, exercise intensity, duration (5 to12 months), compliance (50–85%), and type of exercise(very low impact such as Tai Chi Chun to high-impactexercise).
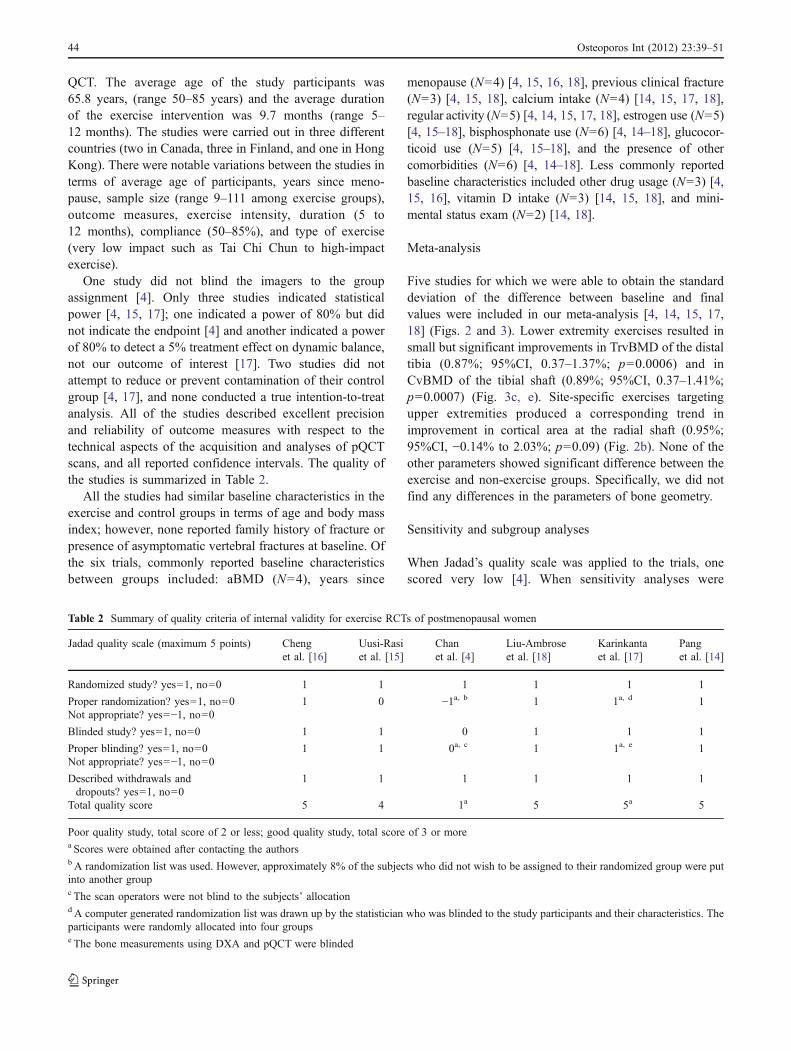
One study did not blind the imagers to the groupassignment [4]. Only three studies indicated statisticalpower [4, 15, 17]; one indicated a power of 80% but didnot indicate the endpoint [4] and another indicated a powerof 80% to detect a 5% treatment effect on dynamic balance,not our outcome of interest [17]. Two studies did notattempt to reduce or prevent contamination of their controlgroup [4, 17], and none conducted a true intention-to-treatanalysis. All of the studies described excellent precisionand reliability of outcome measures with respect to thetechnical aspects of the acquisition and analyses of pQCTscans, and all reported confidence intervals. The quality ofthe studies is summarized in Table 2.
All the studies had similar baseline characteristics in theexercise and control groups in terms of age and body massindex; however, none reported family history of fracture orpresence of asymptomatic vertebral fractures at baseline. Ofthe six trials, commonly reported baseline characteristicsbetween groups included: aBMD (N=4), years since
menopause (N=4) [4, 15, 16, 18], previous clinical fracture(N=3) [4, 15, 18], calcium intake (N=4) [14, 15, 17, 18],regular activity (N=5) [4, 14, 15, 17, 18], estrogen use (N=5)[4, 15–18], bisphosphonate use (N=6) [4, 14–18], glucocor-ticoid use (N=5) [4, 15–18], and the presence of othercomorbidities (N=6) [4, 14–18]. Less commonly reportedbaseline characteristics included other drug usage (N=3) [4,15, 16], vitamin D intake (N=3) [14, 15, 18], and mini-mental status exam (N=2) [14, 18].
Meta-analysis
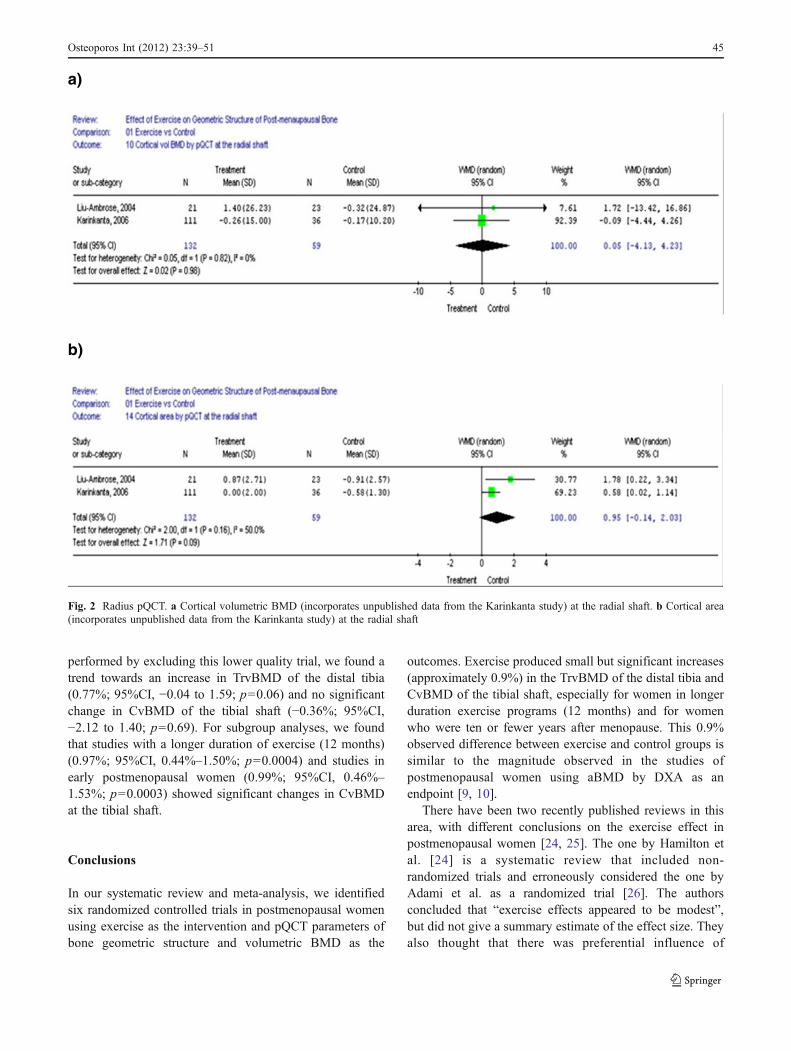
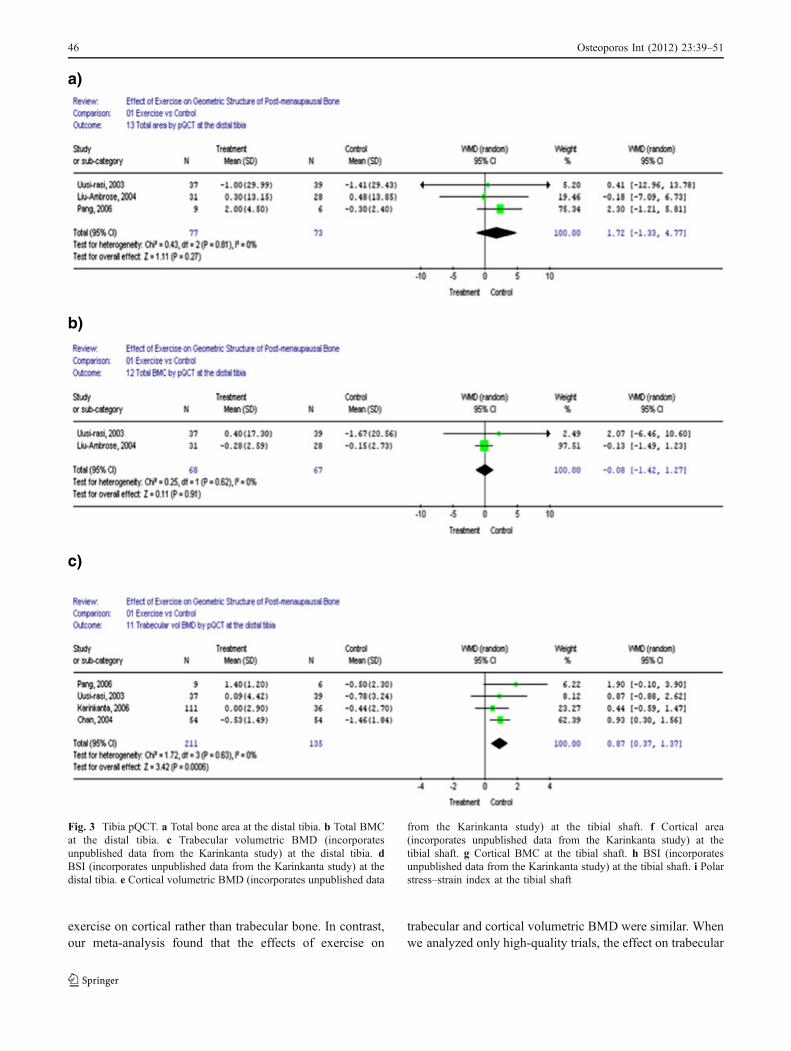
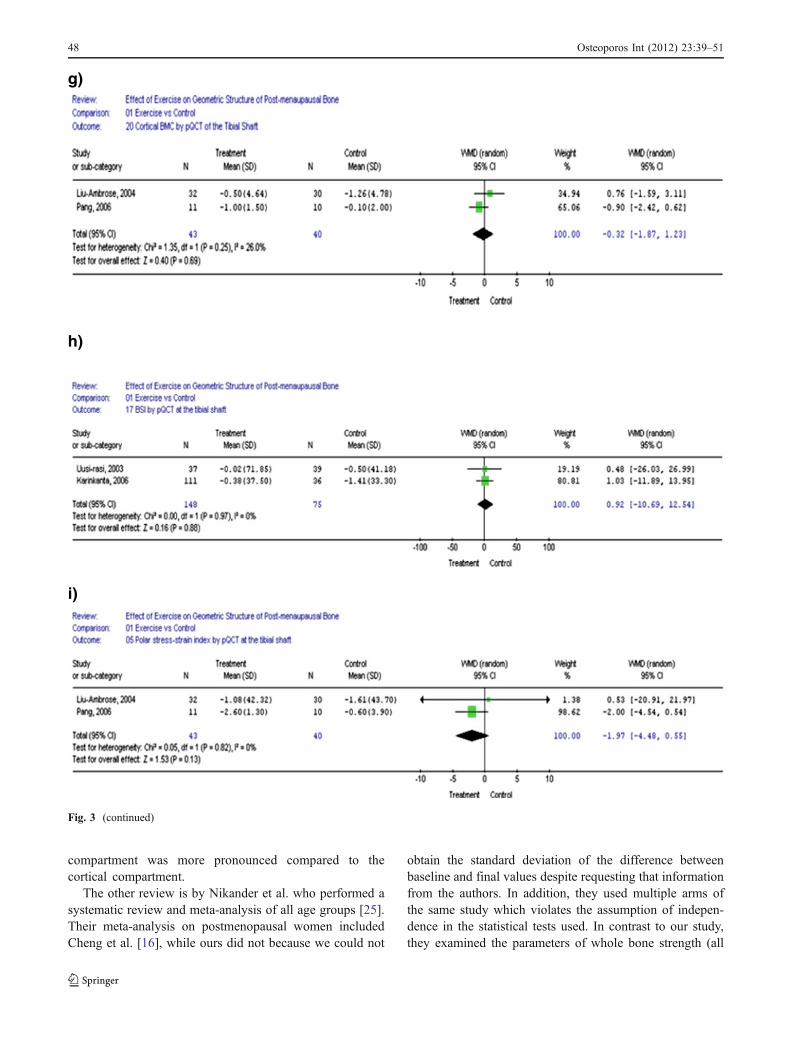
Five studies for which we were able to obtain the standarddeviation of the difference between baseline and finalvalues were included in our meta-analysis [4, 14, 15, 17,18] (Figs. 2 and 3). Lower extremity exercises resulted insmall but significant improvements in TrvBMD of the distaltibia (0.87%; 95%CI, 0.37–1.37%; p=0.0006) and inCvBMD of the tibial shaft (0.89%; 95%CI, 0.37–1.41%;p=0.0007) (Fig. 3c, e). Site-specific exercises targetingupper extremities produced a corresponding trend inimprovement in cortical area at the radial shaft (0.95%;95%CI, −0.14% to 2.03%; p=0.09) (Fig. 2b). None of theother parameters showed significant difference between theexercise and non-exercise groups. Specifically, we did notfind any differences in the parameters of bone geometry.
Sensitivity and subgroup analyses
When Jadad’s quality scale was applied to the trials, onescored very low [4]. When sensitivity analyses were
Table 2 Summary of quality criteria of internal validity for exercise RCTs of postmenopausal women
Jadad quality scale (maximum 5 points) Chenget al. [16]
Uusi-Rasiet al. [15]
Chanet al. [4]
Liu-Ambroseet al. [18]
Karinkantaet al. [17]
Panget al. [14]
Randomized study? yes=1, no=0 1 1 1 1 1 1
Proper randomization? yes=1, no=0 1 0 −1a, b 1 1a, d 1Not appropriate? yes=−1, no=0Blinded study? yes=1, no=0 1 1 0 1 1 1
Proper blinding? yes=1, no=0 1 1 0a, c 1 1a, e 1Not appropriate? yes=−1, no=0Described withdrawals anddropouts? yes=1, no=0
1 1 1 1 1 1
Total quality score 5 4 1a 5 5a 5
Poor quality study, total score of 2 or less; good quality study, total score of 3 or morea Scores were obtained after contacting the authorsb A randomization list was used. However, approximately 8% of the subjects who did not wish to be assigned to their randomized group were putinto another groupc The scan operators were not blind to the subjects’ allocationd A computer generated randomization list was drawn up by the statistician who was blinded to the study participants and their characteristics. Theparticipants were randomly allocated into four groupse The bone measurements using DXA and pQCT were blinded
44 Osteoporos Int (2012) 23:39–51
performed by excluding this lower quality trial, we found atrend towards an increase in TrvBMD of the distal tibia(0.77%; 95%CI, −0.04 to 1.59; p=0.06) and no significantchange in CvBMD of the tibial shaft (−0.36%; 95%CI,−2.12 to 1.40; p=0.69). For subgroup analyses, we foundthat studies with a longer duration of exercise (12 months)(0.97%; 95%CI, 0.44%–1.50%; p=0.0004) and studies inearly postmenopausal women (0.99%; 95%CI, 0.46%–1.53%; p=0.0003) showed significant changes in CvBMDat the tibial shaft.
Conclusions
In our systematic review and meta-analysis, we identifiedsix randomized controlled trials in postmenopausal womenusing exercise as the intervention and pQCT parameters ofbone geometric structure and volumetric BMD as the
outcomes. Exercise produced small but significant increases(approximately 0.9%) in the TrvBMD of the distal tibia andCvBMD of the tibial shaft, especially for women in longerduration exercise programs (12 months) and for womenwho were ten or fewer years after menopause. This 0.9%observed difference between exercise and control groups issimilar to the magnitude observed in the studies ofpostmenopausal women using aBMD by DXA as anendpoint [9, 10].
There have been two recently published reviews in thisarea, with different conclusions on the exercise effect inpostmenopausal women [24, 25]. The one by Hamilton etal. [24] is a systematic review that included non-randomized trials and erroneously considered the one byAdami et al. as a randomized trial [26]. The authorsconcluded that “exercise effects appeared to be modest”,but did not give a summary estimate of the effect size. Theyalso thought that there was preferential influence of
a)
b)
Fig. 2 Radius pQCT. a Cortical volumetric BMD (incorporates unpublished data from the Karinkanta study) at the radial shaft. b Cortical area(incorporates unpublished data from the Karinkanta study) at the radial shaft
Osteoporos Int (2012) 23:39–51 45
exercise on cortical rather than trabecular bone. In contrast,our meta-analysis found that the effects of exercise on
trabecular and cortical volumetric BMD were similar. Whenwe analyzed only high-quality trials, the effect on trabecular
a)
b)
c)
Fig. 3 Tibia pQCT. a Total bone area at the distal tibia. b Total BMCat the distal tibia. c Trabecular volumetric BMD (incorporatesunpublished data from the Karinkanta study) at the distal tibia. dBSI (incorporates unpublished data from the Karinkanta study) at thedistal tibia. e Cortical volumetric BMD (incorporates unpublished data
from the Karinkanta study) at the tibial shaft. f Cortical area(incorporates unpublished data from the Karinkanta study) at thetibial shaft. g Cortical BMC at the tibial shaft. h BSI (incorporatesunpublished data from the Karinkanta study) at the tibial shaft. i Polarstress–strain index at the tibial shaft
46 Osteoporos Int (2012) 23:39–51

d)
e)
f)
Fig. 3 (continued)
Osteoporos Int (2012) 23:39–51 47
compartment was more pronounced compared to thecortical compartment.
The other review is by Nikander et al. who performed asystematic review and meta-analysis of all age groups [25].Their meta-analysis on postmenopausal women includedCheng et al. [16], while ours did not because we could not
obtain the standard deviation of the difference betweenbaseline and final values despite requesting that informationfrom the authors. In addition, they used multiple arms ofthe same study which violates the assumption of indepen-dence in the statistical tests used. In contrast to our study,they examined the parameters of whole bone strength (all
g)
h)
i)
Fig. 3 (continued)
48 Osteoporos Int (2012) 23:39–51

derived variables) such as bone strength index and sectionmodulus and concluded that exercise did not have an effecton bone strength in adults.
The six trials we reviewed had small sample sizes and werequite heterogeneous in terms of duration of exercise, type andintensity of exercise, compliance, and methodological quality.Due to the limited number of studies, we did not performfunnel plots to detect publications bias. Instead, we used theJadad scale to assess the quality of the clinical trials. One studyscored ≤2 on the Jadad quality scale for randomized controlledtrials. Even in studies with higher quality scores, baselinecharacteristics varied widely between the exercise and controlgroups, and there were issues of potential contamination of thecontrol group, the statistical methods used, and adequacy ofvitamin D and calcium supplementation.
Current research suggests a positive association betweenvitamin D supplementation and exercise performance [27–31] as well as BMD [28]. Only three of the studies in oursystematic review assessed vitamin D intake [14, 15, 18]. Inthe Liu-Ambrose trial [18], the daily dosage of vitamin Dsupplementation in the exercise group averaged 892.9 IU(SD=265.2), whereas in the control group, the daily dosageof vitamin D averaged 638.9 IU (SD=404.3). Thedifference in the dosage of vitamin D supplementationmay have affected the outcomes of the study. While calciumsupplementation was more consistently reported in thestudies (four out of five), differences in average dailycalcium intake of 1,164.3 mg (SD=529.7 mg) in theexercise group compared to 750.0 mg (SD=312.6 mg) inthe control group can potentially affect the results of thestudy. In general, trials with methodological flaws canexaggerate a treatment effect [32–34]. For example, theChan trial had the lowest quality score according to Jadad’scriteria primarily due to inappropriate randomization andabsence of blinding [4]. By excluding this study, the resultsof our meta-analyses were significantly altered.
Overall, we did not find any significant changes in bonegeometry. This may be because the total sample size of 287exercisers was too small for the effect size that we were tryingto measure. Changes in bone geometry may not be aspronounced as changes in bone mass and may require a largersample size and longer duration of exercise to observesignificant results.
Implications for the future
Our systematic review and meta-analysis gave us a betterunderstanding of the overall effects of exercise on bone inpostmenopausal women. We showed that site-specificexercise benefits bone in postmenopausal women, moreso at usually loaded bone sites (such as TrvBMD of thedistal tibia and CvBMD of the tibial shaft) than at usuallynon-loaded sites (such as CvBMD and cortical area at the
radial shaft). This beneficial effect is more pronounced inearly postmenopausal women. Future trials assessing theeffects of exercise on bone health need to control forbaseline characteristics such as age, gender, baselinevitamin D levels, prior history of fractures and falls,estrogen and bisphosphonate use, and level of physicalactivity, as well as other variables associated with age-related bone loss among postmenopausal women.
Conducting randomized controlled trials to assess theeffectiveness of exercise presents specific challenges forinvestigators. For example, assessing the effects of exerciseon BMD and bone geometry requires long-term lifestylechanges among study participants, compliance with theexercise program, and regular monitoring to ensure adher-ence to study protocols. Therefore, to gather accurate data,study participants must also be relatively healthy, motivatedto exercise; and the exercises must be challenging, yet,progressive and safe to perform. This means that inves-tigators also need to focus on implementing methods [35–37] that manage these challenges, and that they reportcompliance with exercises in order that study resultsapproach the true effect of the intervention.
Based on our analysis, exercise in postmenopausalwomen decreases bone loss by maintaining cortical andtrabecular volumetric BMD. More research is still neededto further explore the effects of exercise on bone health, andspecifically bone geometry. In particular, trials that focus onthe common fragility bone sites of postmenopausal women,which are the wrist, hip, spine, and proximal humerus [38]will provide us with a greater understanding of the effect ofexercise on bone loss and fracture risk in the postmeno-pausal patient.
When it comes to reducing the public health burden offractures with a safe, easy to implement, widely availableintervention with other potential health benefits [39],exercise may be one of the most cost-effective interventionswe have—but the type of exercise, intensity, frequency, andduration of activity that produces the best results has notbeen fully explored [40, 41]. Further research is still neededto determine the most effective types of exercise to reducefragility fracture risk in the pre-, peri-, and postmenopausalyears.
Acknowledgments We wish to sincerely thank the librarians of TheScarborough Hospital, General Division, Scarborough, Ontario,Canada, Deborah Lambert, and Judy Ng and the librarian of theDepartment of Family & Community Medicine, University ofToronto, Toronto, Canada, Rita Shaughnessy for their assistance withthe literature searches, as well as Zoe Agnidis for her assistance in thepreparation of this manuscript. We also wish to thank Debra Butt andConor McDermott for their guidance, inspiration, and support in theproduction of this paper. Dr. A.M. Cheung is funded by the CanadianInstitutes of Health Research/Institute of Gender and Health SeniorScientist Award and the University of Toronto/University HealthNetwork Lillian Love Chair in Women’s Health.
Osteoporos Int (2012) 23:39–51 49
Conflicts of interest None.
References
1. Asikainen TM, Kukkonen-Harjula K, Miilunpalo S (2004)Exercise for health for early postmenopausal women: a systematicreview of randomised controlled trials. Sports Med 34:753–778
2. Bérard A, Bravo G, Gauthier P (1997) Meta-analysis of theeffectiveness of physical activity for the prevention of bone loss inpostmenopausal women. Osteoporos Int 7:331–337
3. Martyn-St JM, Carroll S (2008) Meta-analysis of walking forpreservation of bone mineral denisty in postmenopausal women.Bone 43:521–531
4. Chan K, Qin L, Lau M, Woo J, Au S, Choy W, Lee K, Lee S(2004) A randomized, prospective study of the effects of Tai ChiChun exercise on bone mineral density in postmenopausalwomen. Arch Phys Med Rehabil 85:171–722
5. Kemmler W, Engelke K, Weineck J, Hensen J, Kalender WA(2003) The Erlangen fitness osteoporosis prevention study: acontrolled exercise trial in early postmenopausal women withlow bone density-first-year results. Arch Phys Med Rehabil84:673–682
6. Snow CM, Shaw JM, Winters KM, Witzke KA (2000) Long-termexercise using weighted vests prevents hip bone loss in postmen-opausal women. J Gerontol 55A:M489–M491
7. Stengel SV, Kemmler W, Pintag R, Beeskow C, Weineck J, LauberD, Kalender WA, Engelke K (2005) Power training is moreeffective than strength training for maintaining bone mineraldensity in postmenopausal women. J Appl Physiol 99:181–188
8. Kerr D, Ackland T, Maslen B, Moron A, Prince R (2001)Resistance training over 2 years increases bone mass in calcium-replete postmenopausal women. J Bone Miner Res 16:175–181
9. Kelley GA, Kelley KS, Tran ZV (2002) Exercise and lumbarspine bone mineral density in postmenopausal women: a meta-analysis of individual patient data. J Gerontol 57:M599–M604
10. Wolff I, Van Croonenborg J, Kemper HCG, Kostense PJ, TwiskJWR (1999) The effect of exercise training programs on bonemass: a meta-analysis of published controlled trials in pre- andpostmenopausal women. Osteoporos Int 9:1–12
11. Dougherty G (1996) Quantitative CT in the measurement of bonequantity and bone quality for assessing osteoporosis. Med EngPhys 18:557–568
12. Bouxsein ML, Karaski D (2006) Bone geometry and skeletalfragility. Curr Osteoporos Rep 4:49–56
13. Dalle Carbonare L, Valenti MT, Bertoldo F, Zanatta M, Zenari S,Realdi G, Lo Cascio V, Giannini S (2005) Bone microarchitectureevaluated by histomorphometry. Bone Struc Health Dis 36:609–616
14. Pang MYC, Ashe MC, Eng JJ, McKay HA, Dawson AS (2006) A19-week exercise program for people with chronic strokeenhances bone geometry at the tibia: a peripheral quantitativecomputed tomography study. Osteoporos Int 17:1615–1625
15. Uusi-Rasi K, Kannus P, Cheng S et al (2003) Effect of alendronateand exercise on bone and physical performance of postmenopaus-al women: a randomized controlled trial. Bone 33:132–143
16. Cheng S, Sipila S, Taafe DR, Puolakka J, Suominen H (2002)Change in bone mass distribution induced by hormone replace-ment therapy and high-impact physical exercise in post-menopausal women. Bone 31:126–135
17. Karinkanta S, Heinonen A, Sievanen H, Uusi-Rasi K, Pasanen M,Ojala K, Fogelholm M, Kannus P (2006) A multi-componentexercise regimen to prevent functional decline and bone fragility
in home-dwelling elderly women: randomized, controlled trial.Osteoporos Int 18:453–462
18. Liu-Ambrose TY, Khan KM, Eng JJ, Heinonen A, McKay HA(2004) Both resistance and agility training increase cortical bonedensity in 75- to 85-year-old women with low bone mass. J ClinDensitom 7:390–398
19. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM,Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reportsof randomized clinical trials: is blinding necessary? Control ClinTrials 17:1–12
20. Brouwers MC, Johnston ME, Charette ML, Hanna SE, Jadad AR,Browman GP (2005) Evaluating the role of quality assessment ofprimary studies in systematic reviews of cancer practice guide-lines. BMC Med Res Methodol 5:8
21. DeAngelis CD (2008) Instructions for authors. JAMA 299:82122. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF,
Group ftQ (2008) Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement.Lancet 354:1896–1900
23. Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003)Measuring inconsistency in meta-analyses. BMJ 327:557–560
24. Hamilton CJ, Swan VJ, Jamal SA (2010) The effects of exerciseand physical activity participation on bone mass and geometry inpostmenopausal women: a systematic review of pQCT studies.Osteoporos Int 21:11–23
25. Nikander R, Sievänen H, Heinonen A, Daly RM, Uusi-Rasi K,Kannus P (2010) Targeted exercise against osteoporosis: asystematic review and meta-analysis for optimising bone strengththroughout life. BMC Med 8:47
26. Adami S, Gatti D, Braga V, Bianchini D, Rossini M (1999) Site-specific effects of strength training on bone structure andgeometry of ultradistal radius in postmenopausal women. J BoneMiner Res 14:120–124
27. Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E,Dietrich T, Dawson-Hughes B (2005) Fracture prevention withvitamin D supplementation: a meta-analysis of randomizedcontrolled trials. JAMA 293:2257–2264
28. Bunout D, Barrera G, Leiva L, Gattas V, Pia de la Maza M,Avendano M, Hirsch S (2006) Effects of vitamin D supple-mentation and exercise training on physical performance inChilean vitamin D deficient elderly subjects. Exper Gerontol41:746–752
29. Cranney A, Horsley T, O’Donnell S, et al. (2007) Effectivenessand safety of vitamin D in relation to bone health. Evid RepTechnol Assess 1–235
30. Mezquita-Raya P, Munoz-Torres M, De Dios LJ, Luna V, Lopez-Rodriguez F, Torres-Vela E, Escobar-Jimenez F (2001) Relationbetween vitamin D insufficiency, bone density, and bone metab-olism in healthy postmenopausal women. J Bone Miner Res16:1408–1415
31. Trivedi DP, Doll R, Khaw KT (2003) Effect of four monthly oralvitamin D3 (cholecalciferol) supplementation on fractures andmortality in men and women living in the community: randomiseddouble blind controlled trial. BMJ 326(7387):469
32. Moher D, Jadad AR, Tugwell P (1996) Assessing the quality ofrandomized controlled trials. Int J Tech Assess Health Care12:195–208
33. Moher D, Pham B, Jones A, Cook DJ, Jadad AR (1998) Doesquality of reports of randomised trials affect estimates ofintervention efficacy reported in meta-analyses? Lancet 352:609–613
34. Schulz KF, Chalmers I, Hayes RJ, Altman DG (1995) Empiricalevidence effects in controlled trials of bias: dimensions ofmethodological quality associated with estimates of treatment.JAMA 273:408–412
50 Osteoporos Int (2012) 23:39–51

35. Irwin ML, Tworoger SS, Yasui Y et al (2004) Influence ofdemographic, physiologic, and psychosocial variables on adher-ence to a yearlong moderate-intensity exercise trial in postmen-opausal women. Prev Med 39:1080–1086
36. Resnick B, Magaziner J, Orwig D, Zimmerman S (2002) Evaluatingthe components of the exercise plus program: rationale, theory andimplementation. Health Educ Res 17:648–658
37. Ryan RM, Deci EL (2007) Active human nature: self-determination theory and the promotion and maintenance ofsport, exercise, and health. In: Hagger MS (ed) Intrinsicmotivation and self-determination in exercise and sport. HumanKinetics Europe Ltd., Pudsey, pp 1–19
38. Riggs BL, Melton LJ (1995) The worldwide problem ofosteoporosis: insights afforded by epidemiology. Bone 17:S505–S511
39. Seeman E (2002) An exercise in geometry. J Bone Miner Res 17(3):373–380
40. Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, BirgeSJJ (1988) Weight-bearing exercise training and lumbar bonemineral content in postmenopausal women. Ann Intern Med108:824–828
41. Jiang Y, Zhao J, Rosen C, Geusens P, Genant HK (1999)Perspectives on bone mechanical properties and adaptive responseto mechanical challenge. J Clin Densitom 2:423–433
Osteoporos Int (2012) 23:39–51 51




















