The effect of armed conflict on spontaneous abortions in Benghazi–Libya
292
Transcript of The effect of armed conflict on spontaneous abortions in Benghazi–Libya


14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS, GYNECOLOGY & INFERTILITY (COGI)
Editors Z. Ben-Rafael B.C.J.M. Fauser R. Frydman
NOVEMBER 17-20, 2011
PARIS, FRANCE
ISBN 978 88 6521 054 3
All rights reserved. No part of this publication may be reproduced,stored in a retrieval system, or internet communication system
or transmitted in any form, or by any means, electronic,mechanical, photocopying, recording or otherwise, without
the prior permission, in writing, from the publisher.© Copyright 2012 MONDUZZI EDITORIALE S.r.l.
Via Meucci, 15/17 – 43015 Noceto (PR) – ItalyMONDUZZI EDITORIALE S.r.l.
Via B. Eustachi, 12 – 20129 Milano – ItalyPhone (+) 39-02-20404031 – Fax (+) 39-02-20404044
www.monduzzieditore.ite-mail: [email protected]
Layout: ESN – Rastignano – Bologna – ItalyPrinted in February 2012 by EB.O.D. – Milano – Italy

Contents
Preface .............................................................................................................. 11
INFERTILITY & ART ........................................................................................... 13
The effectiveness of immunotherapy with paternal lymphocytes in patients with at least two IVF cycles .......................................... 15R. Barini, I.N. Machado, Y. Klimesch, S.B.S. Lima, M.C. Vicentini
Robotic coelioscopy versus vaginal route for simple hysterectomy .................... 19M. Carbonnel, S. Roy, H.T. N’guyen, H. Abbou, J.M. Ayoubi
A novel approach for treating infertile patients with diminished ovarian reserve (DOR) ............................................................. 23G. Carlomagno, S. Roseff, S. Harter, RN, S. Murphy Cohen, ARNP, V. Unfer
Impact of rh-FSH on sperm DFI in idiopathic oligoasthenospermia .................... 27N. Colacurci, M.D. D’Eufemia, V. Auletta, P. De Franciscis, M.G. Monti, C. Trotta, E. La Verde, D. Mele
Pregnancy rate of gonadotrophin therapy and laparoscopic ovarian electrocautery in polycystic ovary syndrome resistant to clomiphene citrate: a comparative study ........................................................ 31M. Ghafarnejad, N. Arjmand, Z. Khazaee
Premature ovarian failure in a woman with a balanced 15; 21 translocation – a case report ......................................................................... 37S. Hosseini, M. Vahid Dastjerdi, Z. Asgari, H. Samiee
Male obesity and sperm parameters in infertility ................................................ 41L. Jamshidi
Upper age limit for access to ART: never-ending discussions? ........................... 45H. Konecna, T. Kucera, S. Suda
Classifi cation of utero-vaginal malformations ................................................... 51L.V. Adamyan, Z.N. Makiyan, A.A. Stepanian
Female genital organ's malformations: new hypothesis of embryo-morphogenesis ....................................................... 55Z. Makiyan
6
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Association of expanded Natural Killer cells subsets in women with recurrent gestational failure ....................................................... 59R. Ramos-Medina, Á. García-Segovia, M. Tejera-Alhambra, Á. Aguarón, B. Alonso, M. Rodríguez-Mahou, J. Gil , J. A. León, P. Caballero, S. Sánchez-Ramón
The effect of bromocriptine and cyclodynon on the clinical symptoms and prolactin levels in women of reproductive age with hyperprolactinemia ..................................................... 65L. Suturina, L. Kolesnikova, L. Popova
Sperm recovery in patients with non-mosaic Klinefelter syndrome: a comparative study ......................................................................... 69H. Terada, T. Sugiyama, S. Mugiya, S. Ozono
Co-occurrence of polycystic ovary syndrome with depression and anxiety symptoms ..................................................................... 73Xin Li, Fulong Wang, Johnna Wu, Fang Fang,Yi Jin
Cryopreservation of a small number of human spermatozoa with home-made Strawtop: 3 years experience ................................................. 77Songguo Xue, Qiuping Peng, Shaofeng Cao, Qiao Yu, Jiqiang Si, Yanping Kuang
Sucrose pretreatment vitrifi cation yields 100% survival rate of mouse and human eggs ................................................................................. 81Songguo Xue, Qiuping Peng, Qiao Yu, Qifeng Lyu, Shaofeng Cao, Yanping Kuang
FETOMATERNAL MEDICINE ............................................................................. 85
Types of fi stula and their management in a referral center in Saudi Arabia .................................................................................................. 87G. Al-Shaikh, K. Perveen, M. Moazin, A. Al-Badr
Determination of the early immunological changes in patients with pregnancy loss .......................................................................... 91F. Aliyeva, A. Poletayev, A. Amirova, N. Shahbazova, X. Tahmazi
Challenges in implementing humanized birth practices in a highly specialized and university affi liated hospital .................................... 95R. Behruzi, M. Hatem, L. Goulet, W. Fraser
Placenta praevia: our experience ......................................................................101M. Brandão, J. Casanova, M.M. Sampaio, T. Oliveira, R.M. Rodrigues
The infl uence of bacterial vaginosis on preterm rupture of membranes ...............105E. Bylykbashi, I.V. Bylykbashi, E. Kosturi, O. Janushaj, A. Zhaka, E. Treska

7
November 17-20, 2011 Paris, France
The impact of periodontitis in the preterm birth and body size of newborns ...............................................................................109L. Muhametaj, E. Bylykbashi, M. Muhametaj, A. Manaj, M. Xhelili
Pre-pregnant body mass indexin women with gestational diabetes mellitus and pregnancy outcome ......................................113S. De Carolis, A. Botta, F. Macrì, F. Stifani, L. Casarella, S. Garofalo, C. Martino, V.A. Degennaro, S. Moresi, G. Del Sordo, E. Di Pasquo, D. Pitocco
Controversies in the introduction of antenatal ultrasonography in rural Tanzania ......................................................117E. Firth, P. Mlay, R. Walker, P.R. Sill
Maternal status and recent patterns of double and triple deliveries in Spain .............................................................125V. Fuster Siebert, J. Román-Busto
The infl uence of mode of delivery in neonatal complications in breech presentation ...............................................................129S. Latifi -Hoxha, M. Hoxha, Sh. Bajraktari Ponosheci, N. Berisha, B. Skenderi
Waist circumference in relation to prediction of delivery outcomes ..................133E. Mehrabi, M. Ebrahimi Mameghani, M. Kamalifard, P. Yavari Kia
Effect of melatonin on the oxidative metabolism of colostrum phagocytes of diabetic women .....................................................139I. Calderon, G. Morceli, C. Hara, R. Volpato, M. Rudge, A. Honorio-França, E. França
The role of dydrogesterone in threatened abortion ............................................143A. Bimbashi, E. Ndoni, R. Hoxhallari
Our experience in management of severe preeclampsia ...................................149E. Ndoni, A. Bimbashi, A. Dokle
Fetal growth and birth weight: the need for clinical decision support software .....................................................................155R. Santos, C. Santos, J. Bernardes, R. Cruz-Correia
Endothelin-1 system polymorphisms in preeclampsia and gestational hypertension .......................................................161A. Seremak-Mrozikiewicz, M. Barlik, K. Drews
TNF-α concentrations in maternal and umbilical cord plasma and the perinatal outcome ....................................................................165J. Zegarska, K. Borowska-Mackowiak, J. Kłyszejko-Molska, M. Socha, M. Gruszka, P. Krepska, B. Wolski, W. Szymanski, M. Grabiec

8
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
GYNECOLOGY ................................................................................................171
The effect of armed confl ict on spontaneous abortions in Benghazi – Libya .....................................................173Z.A. Bodalal, K. Agnaeber
Peculiarities of HRT for women with obesity ....................................................181G. Alimbayeva, I. Kuznetzova, M. Yakokutova
Complications of meshes in combination with surgery for uterovaginal prolapse ..............................................................185E. Athanassiou, T. Tantanasis, X. Giannoulis, N. Tsambazis, A. Loufopoulos
Pregnancy after gigantic bilateral ovarian teratoma ...........................................189M. Brandão, S.V. Soares, P. Reis, M. Rodrigues, T. Oliveira, R.M. Rodrigues
Primary bilateral Burkitt´s lymphoma of the ovary ............................................193A.M. Coelho, A.M. Sousa, F. Passos, M. Bernardino, I. Santana, A.F. Jorge, J. Cabeçadas
Retrospective study of laparoscopic assisted vaginal hysterectomy (LAVH) for benign gynecological disorders ..................................197R. Condeço, L. Barros, S. Barreto, C. Leitão, M.C. Silva, R. Mira
The cyst of Nuck: clinical case and review of the literature ...............................203A. Cubal, J. Carvalho, F. Azevedo
Body composition in users of levonorgestrel-releasing intrauterine system ...........................................................................................207N. Dal´Ava, L. Bahamondes, M.V. Bahamondes, A. de Oliveira Santos, I. Monteiro
Can promestriene be used even in oncology patients? ......................................213L. Del Pup, D. Postruznik
Postpartum echographic diagnosis of ganglioneuroblastoma – a case report ..................................................................................................219O. Eremina, Y. Boykova, E. Shifman, I. Shevelev, V. Korolishin, A. Gus
Impact of capsule rupture in stage I clear cell carcinoma of the ovary ......................................................................223H. Kajiyama, M. Mizuno, E. Yamada, H. Matsumura, F. Kikkawa
Improvement of postoperative care after major abdominal gynecologic surgery ..............................................................227E. Kallfa, G. Hyska, E. Belaj , A. Delilaj , S. Xinxo, V. Grori, V. Mulliqi F. Lauszus, O. Gliozheni
Evaluation of the ovarian malignancies' occurrence in patients with previous IVF treatment .............................................................231A. Koumousidis, A. Kotelis, A. Daskalakis, I. Kaniaris, M. Kontoyannis, V. Sanoulis, D. Ftoulis, Ch. Tsarmaklis, Ch. Katsetos

9
November 17-20, 2011 Paris, France
Can infl ammation take part in development and progression of endometrial hyperplasia? ....................................................237Ye. Kovalenko, T. Tatarchuk, A. Kubyshkin, T. Filonenko
The expression and characterization of endoglin in uterine leiomyosarcoma ...............................................................................241H. Matsumura, K. Shibata, E. Yamada, M. Mizuno, H. Kajiyama, T. Senga, F. Kikkawa
A rare case of invasive vaginal carcinoma associated with complete uterine prolapse ......................................................245M.M. Melo, E. Gonçalves, A.R. Neiva, A. Almeida, J. Mesquita, A. Carvalho, D. Magalhães, J. Maia
Is adjuvant chemotherapy necessary for stage IA ovarian clear cell carcinoma? ...........................................................................251M. Mizuno, H. Kajiyama, E. Yamada, H. Matsumura, F. Kikkawa
Comparing Metformin and Pioglytazone in polycystic ovary ...........................255N. Navali, S.Tagavi
An explorative study upon factors that contribute to contraceptive-seeking behaviour among married Sudanese women in Khartoum, Sudan ..............................................................261T. Parekh, J. Parr
Lynch Syndrome – a case report .......................................................................267A.M. Sousa, A.M. Coelho, M. Bernardino, A.S. Gomes, A.F. Jorge, I. Claro
An ovarian tumor with origin in an appendiceal cancer – a case report ..................................................................................................271A.M. Sousa, A.M. Coelho, M. Bernardino, A.S. Gomes, A.F. Jorge, R. Rego
Breast cancer and hot fl ashes treatment ...........................................................275C. Tomás, M. Rodrigues, A. Relva, L. Canelas, F. Romão, MJ. Botica, M. Vieira
Charged particle therapy for recurrence of gynecologic cancer, 9 case reports ..................................................................281E. Yamada, K. Shibata, H. Kajiyama, M. Mizuno, H. Matsumura, F. Kikkawa
Single site laparoscopic surgery for complex cases in benign gynecology .......................................................................................285J. Ybanez-Morano, R.P. Rivera, J.O. Fuentes, M.C. Vicencio, M. A. Panaligan
Physiologic and pathologic changes in veins during pregnancy. What to be afraid of? ...........................................................289E. Yupatov, L. Maltseva, I. Ignatyev, E. Fomina, M. Nyukhnin, S. Sokolov, A. Zaitsev


Preface
Dear Friends and ColleaguesOver the years, the fi eld of Obstetrics, Gynecology & Infertility has undergone enor-
mous expansion in clinical and basic data, as well as that of fi eld-related technology. The intention of the 14th COGI Congress was to search for answers even when
evidence is lacking, and to reach current conclusions to ongoing debates in the fi elds through evidence-based medicine. The Congress functions as an exclusive forum for international experts to share and compare experiences, in order to outline ap-propriate treatment.
The 14th COGI in Paris had 2,200 participants from 101 countries (increase of 20%), 720 accepted abstracts and 18 supporting companies, which shows the growing importance of COGI in Europe and worldwide. In addition, a “Position Paper” on the treatment of osteoporosis in women under 70 years of age has been developed by a group of experts.
We would like to thank the authors of these chapters for their contribution to the success of the Congress.
Zion Ben-RafaelEditorFounder and Chairman of the COGI Congress

INFERTILITY & ART

© 2012 Monduzzi Editoriale | Proceedings Code: 72
The effectiveness of immunotherapy with paternal lymphocytes in patients with at least two IVF cycles
R. Barini, I.N. Machado, Y. Klimesch, S.B.S. Lima, M.C. VicentiniAllovita – Laboratory Immunology of Reproduction, Campinas-SP, Brazil
SUMMARYObjective: To describe our experience with the immunotherapy with pater-
nal lymphocytes (IPL) for couples with implantation failure in at two previous cycles of IVF. Materials/Methods: Retrospective analysis of all couples who were referred to our laboratory for IPL after two or more IVF cycles negative for serum levels of the hormone chorionic gonadotropin (βHCG). The rate of viable pregnancies after the IPL in further IVF cycles was considered suc-cess rate of pregnancy. Results: 25 couples were included in this study with a mean women age of 35.7 years (± 3.56). The number of cycles of IVF before immunotherapy with paternal lymphocytes ranged from 2 to 6 cycles. The suc-cess rate of pregnancy was 63% (14/22) after new IVF cycles and 68% (17/25) when spontaneous pregnancies were included. Conclusion: Couples who had undergone at least two previously failed IVF cycles before the IPL seemed to benefit with this immunotherapy, suggesting that IPL is a valuable adjuvant therapy for them.
INTRODUCTIONRecent technological developments in assisted reproduction techniques have
enabled many couples to accomplish the dream of having children. However, fail-ure to conceive despite normal appearing embryo transfer cycles may still occur. Many underlying causes of this unsuccessful in vitro fertilization treatment were postulated.
In 1953 Peter Medawar formulated the fi rst hypothesis that embryo behaves like one graft since has both maternal and paternal antigens, being therefore likely theo-ries rejection and immunological tolerance originated in maternal organism (alloim-

16
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
mune) (Guerin et al., 2009; Porcu-Buisson et al., 2007). In the embryo implantation process, cells of the villous cytotrophoblast has extra features to express nonclas-sical HLA molecules (HLA-G). Uterine natural killer cells recognize the HLA-G as the cytotrophoblast and the block does not own, promoting a Th2-type immune response favorable to successful pregnancy (Choudhury and Knapp, 2000; Van Mourik et al., 2009). Thus, there are some data suggesting that successful implanta-tion may be directly linked to the balance between Th1 and Th2 (Kwak-Kim et al., 2003; Kalu et al.; Saito et al., 2010).
According to these data, patients with repeated pregnancy loss and failure of embryo implantation in IVF cycles have abnormal immunological response (NG et al. 2002; Yokoo et al,. 2006; Kalu et al., 2008). Besides having a high level of natural killer cells (NK) and cytotoxic also have an inversion in the balance of Th1 and Th2 cytokines (NG et al., 2002; Kwak-Kim et al.,2003; Yokoo et al., 2006; Kalu et al.,2008; Chernyshov et al.,2010) The prevalence of Th1 immune response leads to the release of IL-2, IL - 12, interferon gamma (INF γ) and tumor necrosis factor alpha (TNF), induce infl ammatory reactions and cytotoxic via IL - 2, IFN gamma and TNF alpha, promoting a deleterious effect on pregnancy, specifi cally in the cells of the villi primary trophoblast by inducing apoptosis and rejection of the embryo (Raghupathy et al., 2000; NG et al., 2002; Kwak-Kim et al., 2003; Kalu et al., 2008; van Mourik et al., 2009; Boomsma et al., 2009; Winger et al., 2010; Saito et al., 2010).
In vitro fertilization (IVF) treatment is expensive and emotional stressing. Cou-ples usually inquire as to what reason is for the implantation failures and if there is something else it can be done. Based on the above theoretical etiologies, one treat-ment option is to consider the immunotherapy with paternal lymphocytes (IPL). The ILP is available as adjuvant therapy as it appears to reverse the function of immuno-logical changes to a predominance of Th2-type immune tolerance thereby allowing embryo implantation and subsequent development of gestational increasing rates in assisted fertilization.
The aim of this study was to report our experience with the immunotherapy with paternal lymphocytes (IPL) for couples with implantation failure in at two previous cycles of IVF.
MATERIAL AND METHODSIt was carried out a retrospective analysis of all couples who were referred to
our laboratory from January 2009 to March 2011 for IPL after two or more IVF cycles negative for serum levels of the hormone chorionic gonadotropin (βHCG). The treatment (IPL) was administered intradermally every 21 days, totaling 3 doses. After a positive post-treatment crossmatch test, the couples were allowed to further attempts to pregnancy. The rate of viable pregnancies was considered success rate of pregnancy.
17
November 17-20, 2011 Paris, France
RESULTSA total of 25 couples were included in this study with a mean women age of 35.7
years (± 3.56). The number of cycles of IVF before immunotherapy with paternal lymphocytes ranged from 2 to 6 cycles. The success rate of pregnancy was 63% (14/22) after new IVF cycles and 68% (17/25) when spontaneous pregnancies were included.
CONCLUSIONSOur study demonstrated that couples who had undergone at least two previously
failed IVF cycles before the IPL seemed to benefi t with this immunotherapy, sug-gesting that IPL is a valuable adjuvant therapy for them.
With the introduction of immunotherapy with paternal lymphocytes by Dr. Alan Beer in 1981 (Beer et al., 1981), it appears as a therapeutic option also in patients with repeated implantation failure in IVF cycles. In agreement with the results pre-sented here, previous published results have reported that the rate of successful pregnancy could be increased by active immunotherapy – IPL (Check et al., 2005; Wegener et al., 2006; Margalioth et al., 2006).
REFERENCES1. BEER AE,QUEBBEMAN JF, AYERS JW, HAINES RF. Major histocompatibility complex antigens,
maternal and paternal immune responses, and chorionic habitual abortions in humans. Am J Obstet Gynecol 141:987- 999; 1981.
2. BOOMSMA CM, KAVELAARS A, EIJKEMANS MJC, LENTIES EG, FAUSER BCJM, HEIJNEN CJ, MACKLON NS. Endometrial secretion analysis identifi es a cytokine profi le predictive of pregnancy in IVF. Human Reproduction 24(6):1427 – 1435; 2009.
3. CHECK J H, LISS M L, DIANTINO A, DUROSEAU M. Lymphocyte immunotherapy can improve pregnancy outcome following embryo transfer (ET) in patients falling to conceive after two previous ET. Exp Obstret Gynecol 32 (1):21-2; 2005.
4. CHERNYSHOV PV, SUDOMA O I, DONS’KOI V B, KOSTYUCHYK A A, MASLIY V Y. Elevated NK Cell Cytotoxicity, CD 158a Expression in NK Cells and Activated T Lymphocytes in Peripheral Blood of Women with IVF Failures. American Journal of Reproductive Immunology; 64:58-67, 2010.
5. CHOUDHURY SR, KNAPP L A. Human Reproductive failure I: Immunological factors. Human Reproduction Update 7 (2): 113-134; 2000.
6. GUERIN LR, PRINS JR, ROBERTSON AS. Regulatory T – cells and immune tolerance in pregnancy new target for infertility treatment? Human Reproduction Update; 15 (5): 517- 535; 2009.
7. KALU E, BHASKARAN S, THUM MY, VISHWANATHA R, CROUCHER C, SHERRIFF E, FORD B, BANSAL AS. Serial Estimation of Th1:Th2 cytokines profi le in Women undergoing In – Vitro fertilization – embryo transfer. American Journal of Reproductive Immunology; 59: 206 – 211; 2008.
8. KWAK-KIM JYH, CHUNG-BANG HS, NG SC, NTRIVALAS EI, MANGUBAT CP, BEAMAN KD, BEER AE, GILMAN-SACHS A. Increased T helper 1 cytokine responses by circulating T cells are present in women with multiple implantation failures after IVF. Human Reproduction 18 (4):767 – 773; .2003.

18
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
9. MARGALIOTH EJ, BEN-CHETRIT A, GAL M, ELDAR-GEVA T. Mini Review – Developments in Reproductive Medicine. Investigation and treatment of repeated implantation failure following IVF-ET. Human Reproduction21 (12):3036 – 3043; 2006.
10. NG SC, GILMAN – SACHS A, THAKER P, BEAMAN KD, BEER AE, KWAK-KIM J. Expression of intracellular Th1 and Th2 cytokines in women with recurrent spontaneous abortion, implantation failures after IVF/ET or normal pregnancy. American Journal of Reproductive Immunology; 48: 77 – 86; 2002.
11. PORC U – BUISSON G, LAMBERT M, LYONNET L, LOUNDOU A, GAMERRE M, CAMOIN-JAU L, DIGNAT – GEORGE F, CAILLAT-ZUCMAN S, PAUL P. Soluble MHC Class I chain-related molecule serum levels are predictive markers of implantation failure and successful term pregnancies following IVF. Human Reproduction; 22 (8): 2261 – 2266; 2007.
12. RAGHUPATHY R, MAKHSEED M, AZIZICH F, OMU A, GUPTA M, FARHAT R. Cytokine production by maternal lymphocytes during normal human pregnancy and in unexplained recurrent spontaneous abortion. Human Reproduction; 15 (3):713 – 718; 2000.
13. SAITO S, NAKASHIMA A, SHIMA T, ITO M. Th1/Th2/Th17 and regulatory T-cell paradigm in pregnancy. American Journal of Reproductive Immunology; 63: 601 – 610; 2010
14. VAN MOURIK MSM, MACKLON NS, HEIJNEN CJ. Embryonic implantation: cytokines, adhesion molecules, and immune cells in establishing an implantation environment. Journal of Leukocyte Biology; 85; 2009.
15. WEGENER S, SCHNURSTEIN K, HANSCH S, BOLZ M, BRIESE V, SUDIK R, WEGENER R, BUSECKE A, MÜLLER H. Immunotherapy with paternal lymphocytes for recurrent miscarriages and unsuccessful in vitro fertilization treatment. Transfus Med Hemother 33: 501 – 507; 2006.
16. WINGER EE, REED JL, ASHOUSH S, AHUJA S, EL-TOUKHY T, TARANISSI M. Treatment with adalimumab (Humira®) and intravenous immunoglobulin improves pregnancy rates in women undergoing IVF. American Journal of Reproductive Immunology; 61: 113 – 120; 2009.
17. YOKOO T, TAKAKUWA K, OOKI I, KIKUCHI A, TAMURA M, TANAKA K. Alteration of Th1 and Th2 cells by intracellular cytokine detection in patients with unexplained recurrent abortion before and after immunotherapy with husband’s mononuclear cells. Fertility and Sterility; 85 (5): 1452 – 1458; 2006.
© 2012 Monduzzi Editoriale | Proceedings Code: 112
Robotic coelioscopy versus vaginal route for simple hysterectomy
M. Carbonnel, S. Roy, H.T. N’guyen, H. Abbou, J.M. AyoubiService de Gynécologie Obstétrique, Hôpital Foch, Suresnes. Faculté de Médecine Paris Ouest, Paris, France
ABSTRACTThis prospective study carried out from March 2010 to August 2011 has been de-
signed to compare two techniques used for simple hysterectomy: vaginal hysterec-tomy (HV) and robot-assisted coelioscopic hysterectomy (RH). Thirty-four patients were included in the RH group, and 22 in that undergoing HV. Compared with the VH group, both anaesthesia and intervention durations were signifi cantly longer in the RH group while the duration of hospital stay was shorter; blood loss and D1 and D2 pain assessed by visual analogue scale were also signifi cantly reduced. No dif-ference between groups was found 8 weeks post-surgery regarding complications, duration of work leave, return to normal life, and sexual life. Robotic coelioscopy in simple hysterectomy may provide some benefi ts over vaginal access. Randomized prospective studies and defi nition of specifi c indications are necessary, however, to confi rm these results.
INTRODUCTIONLaparoscopic hysterectomy is the easiest and the most frequently used technique
for simple hysterectomy; but this procedure is also invasive and may have com-plications (1). Vaginal hysterectomy (VH) is less invasive and adequate in obese patients but it presents some diffi culty in nulliparas or in patients with large uterus or adherences (1). Coelioscopy is less invasive and easier than the vaginal route in patients with adherences and nulliparas; in addition, compared with the vaginal or the coelio-assisted vaginal procedure, it causes less pain and reduces the length of postoperative hospital stay (1-3). Robotic hysterectomy (RH) is a novel technique that potentializes the benefi ts of coelioscopy. Considering the widespread use of the vaginal procedure in our country, we decided to perform a comparative evaluation of the two techniques.

20
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
METHODSThis was a single-centre prospective study comparing all vaginal and robot-as-
sisted coelioscopic simple hysterectomies carried out from March 2010 to August 2011 in Foch Hospital (Suresnes, France).
Population characteristics, durations of anaesthesia, surgical procedure and hos-pital stay, per- and postoperative complications, blood loss, and analgesic consump-tion were extracted from patients’ medical fi les. Immediately post-surgery, patients were given a questionnaire meant to record the intensity of pain using a visual ana-logue scale (VAS), and the time of colonic transit restoration. A questionnaire was also to be completed at Month 2 for the evaluation of the duration of work leave, return to normal activity, sexual life, satisfaction, complications, and mid-term pain.
RESULTSFifty-six patients were included: 34 in the RH group and 22 in the VH group.
Patients were comparable in terms of age, BMI, history of laparotomy, conserva-
RH
( =34)
mean ± SD
VH
( =22)
mean ± SD
p
Anaesthesia duration (min) 208 ± 8.8 114.5 ± 10.1 < 0,0001
Operative duration (min) 137.9 ± 7.9 73.2 ± 9.7 < 0,0001
Console management duration
(min)
106 ± 7.2
Blood loss (ml) 44 ± 8.9 135.3 ± 30 < 0,01
Laparoconversion 0 (0%) 1 (4.5%) NS
Transfusion 0 (0%) 1 (3CGR) (4.5%)
Total morphine consumption
(mg)
9.4 ± 1.7 6.9 ± 1.5 0,3
Hospital stay duration (days) 3.5 ± 0.2 4.3 ± 0.2 0,01
VAS D0 4 ± 0.4 4.7 ± 0.6 0.3
VAS D1 2.7 ± 0.4 4.5 ± 0.5 0.002
VAS D2 1.9 ± 0.4 3.5 ± 0.5 0.007
Tab. 1 - Results.

21
November 17-20, 2011 Paris, France
tive and non-conservative hysterectomy, and uterine weight. Indications were also comparable (fi broma, adhenomyosis) except for Benjamin’s syndromes (14RH / 1 VH). The number of lifetime pregnancies was higher in the VH group (2.9 ± 0.7 vs. 1.7 ± 0.4). Compared with data of VH group, the results displayed in Table I show longer operative and anaesthesia durations, reduced blood loss and pain at D1 and D2, and a shorter hospital stay in the RH group. No difference between groups was observed in terms of complications: 1 case of pain related to arm compression, and 1 of digestive injury in the RH group; 2 haemorrhages in the VH group. Duration of work leave, return to normal activity, satisfaction and sexuality were not different at Month 2. More pain was reported however in the group having undergone VH.
CONCLUSIONBenefi ts of RH versus coelioscopy have been described previously (4,5), especially
regarding blood loss, complications and duration of hospital stay. But few studies have compared this technique to the vaginal route (6-8). Our observations are in accordance with their results (reduced blood loss, shorter hospital stay, less complications). Our study is the fi rst with an evaluation of postoperative pain; this parameter appears to be improved by the robotic technique. Nevertheless, the use of such surgical procedure remains restricted due to its related cost and duration of installation
REFERENCES1. Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, van Voorst S, Mol BW, Kluivers
KB. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev, Jul 8(3), 2009.
2. Ghezzi F, Uccella S, Cromi A, Siesto G, Serati M, Bogani G, Bolis P. Postoperative pain after laparo-scopic and vaginal hysterectomy for benign gynecologic disease: a randomized trial. Am J Obstet Gynecol, Aug; 203(2):118.e1-8, 2010.
3. Gendy R, Walsh CA, Walsh SR, Karantanis E. Vaginal hysterectomy versus total laparoscopic hys-terectomy for benign disease: a metaanalysis of randomized controlled trials. Am J Obstet Gynecol, May; 204(5):388.e1-8, 2011.
4. Payne TN, Dauterive FR. A comparison of total laparoscopic hysterectomy to robotically assisted hys-terectomy: surgical outcomes in a community practice. J Minim Invasive Gynecol,15(3):286-91, 2008.
5. Boggess JF, Gehrig PA, Cantrell L, Shafer A, Mendivil A, Rossi E, Hanna R. Perioperative outcomes of robotically assisted hysterectomy for benign cases with complex pathology. Obstet Gynecol, 114(3):585-93, 2009.
6. Matthews CA, Reid N, Ramakrishnan V, Hull K, Cohen S.Evaluation of the introduction of robotic technology on route of hysterectomy and complications in the fi rst year of use. Am J Obstet Gynecol, 203(5):499.e1-5. 2010.
7. Landeen LB, Bell MC, Hubert HB, Bennis LY, Knutsen-Larson SS, Seshadri-Kreaden U. Clinical and cost comparisons for hysterectomy via abdominal, standard laparoscopic, vaginal and robot-assisted approaches.S D Med, 64(6):197-9, 201, 203 passim. 2011-10-17.
8. Wright KN, Jonsdottir GM, Jorgensen S, Einarsson JI. A Comparison of Abdominal, Laparoscopic, Vaginal, and Robotic Hysterectomies: Surgical Outcomes and Operative Cost in a Single Institution Journal of Minimally Invasive Gynecology, Volume 17, Issue 6, Supplement, Page S23, 2010,


© 2012 Monduzzi Editoriale | Proceedings Code: 113
A novel approach for treating infertile patients with diminished ovarian reserve (DOR)
G. Carlomagno1, S. Roseff2, S. Harter, RN2, S. Murphy Cohen, ARNP2, V. Unfer1
2Palm Beach Center for Reproductive Medicine, Florida USA; 1AGUNCO Obstetrics and Gynecology Center, Rome Italy
SUMMARYOvarian reserve (OR) decreases throughout life and has a physiological limit
around the age of 50. The diagnosis of diminished ovarian reserve (DOR) is based on menstrual cycle day 2-4 follicle-stimulating hormone (FSH) and estradiol levels, antral follicle counts, and anti-mullerian hormone (AMH) titers. In particular, FSH levels increase and AMH levels decrease with age, providing diagnostic criteria across the reproductive spectrum.
In the clinical IVF practice, it is crucial to improve stimulation protocols in order to obtain higher quality oocytes and embryos, and this is of the ut-most importance especially for DOR patients. In the present study, we aimed to evaluate the effect of two well-known compounds, myo-inositol and melatonin, on serum AMH levels. Indeed, several studies have suggested that AMH is a predictor of IVF outcome. 11 patients (35.40± 5.1 years old, mean±SD) diag-nosed with DOR were selected and treated with a combination of 2g of myo-inositol and 3mg of melatonin (Inofolic®Plus, Lo.Li.pharma, Roma; Italy) once daily for one month. After treatment, patients showed a significant increase in AMH levels. AMH levels increased from 0.58±0.16 ng/ml at baseline to 1.24±0.25ng/ml (p<0.05).
Obtaining high quality oocytes is essential for a positive IVF outcome, particu-larly for patients with diminished ovarian reserve. In the present study, we presented preliminary evidence that daily administration of a combination of 2g of myo-ino-sitol and 3mg of melatonin can positively impact serum AMH levels. This, in turn, might result in more positive IVF outcomes.

24
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
INTRODUCTIONThe anti-mullerian hormone (AMH) belongs to the transforming growth factor-β
superfamily. In the female, AMH production is FSH dependent1 and it is performed at the level of the granulosa cells from pre-antral and small antral follicles. One of its role is to inhibit the initiation of premature follicle growth and decrease the sensitivity of follicles to FSH 2; 3; 4;. AMH levels decrease with age from adulthood toward menopause, reflecting the size of the ovarian follicle pool5. Therefore, AMH has been proposed as a marker for detection of diminished ovarian reserve6.
A woman’s ovarian reserve (OR) decreases throughout her life and has a phys-iological limit around the age of 50. A premature depletion of that reserve is classifi ed as premature ovarian failure (POF) and affects 1% of women before the age of 40 and 0.1% below the age of 30 7. Natural POF can occur due to a diminished ovarian reserve (DOR). The diagnosis of DOR is based on menstrual cycle day 2-4 follicle-stimulating hormone (FSH) and estradiol levels, antral fol-licle counts, and AMH titers. In particular, FSH levels increase and AMH levels decrease with age. Thus, it is possible to defi ne a threshold for normal and ab-normal levels for both hormones at different ages, providing diagnostic criteria across the reproductive spectrum.
In the clinical IVF practice, DOR patients require special attention. In particular, it is crucial to improve the current stimulation protocols in order to obtain higher quality oocytes and embryos.
In the present study, we aimed to evaluate the effect of two well-known com-pounds previously shown to improve oocyte quality, myo-inositol and melatonin, on serum levels of AMH. Indeed, several studies have suggested that AMH is one of the best predictors of IVF outcome, including the chances of successful pregnancy 8.
MATERIALS AND METHODSPatients were recruited at the Palm Beach Center for Reproductive Medicine
(Wellington, Florida, USA). Patients were diagnosed with DOR according to com-monly used criteria: menstrual cycle day 2-4 FSH and estradiol levels, antral follicle counts, and AMH titers.
Patients were considered ineligible for this study if they were diagnosed with polycystic ovarian syndrome, or had abnormal peripheral chromosomal abnormali-ties. They were also considered ineligible if they had a history of illicit drug or tobacco use or had ovarian surgery within 90 days of signing the consent form.
In total, 11 patients (35.40± 5.1 years old, mean±SD) were selected and treated with a combination of 2g of myo-inositol and 3mg of melatonin (Inofolic® Plus, Lo.Li.pharma, Roma; Italy) once daily for one month.
AMH baseline levels were evaluated before treatment using a standard ELISA blood assay; blood sampling was repeated and analyzed after 30 days of treatment.

25
November 17-20, 2011 Paris, France
AMH titers were analyzed by Unilab of Dade (Ft. Lauderdale, FL, USA). Data were analyzed by Student’s t test and are reported as MEAN ± SD.
RESULTSAfter 30 days of treatment with Inofolic® Plus, patients showed a signifi cant in-
crease in AMH levels compared to baseline. AMH levels increased from 0.58±0.16 ng/ml at baseline to 1.24±0.25ng/ml after 1 month of Inofolic® Plus administration (p<0.05, tab. 1).
CONCLUSIONFailure of IVF cycles is a serious public health issue due to both the high costs as-
sociated with therapy and its strong psychological implications for patients. There-fore, obtaining high quality oocytes is essential, particularly for patients with dimin-ished ovarian reserve.
AMH has a crucial role in oogenesis: it inhibits the initiation of premature follicle growth and decrease the sensitivity of follicles to FSH 2; 3; 4. Therefore, AMH serum levels are a predictor of IVF outcome. In the present study, we show for the fi rst time that daily administration of a combination of 2g of myo-inositol and 3mg of melatonin can positively impact on serum AMH levels. This, in turn, might result in more positive IVF outcomes.Recent evidence has shown that myo-inositol and melatonin can be used in ovarian stimulation protocols to obtain high quality oocytes and reduce the overall dosage of rFSH administrated 9-12; this ob-servation, together with our data, strongly suggests that the same approach could be successfully used in clinical practice to effi ciently stimulate patients diagnosed with DOR.
Fig. 1 - AMH levels after 30 days of treatment with 2g of myo-inositol and 3mg of melatonin.

26
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
REFERENCES1. TAIEB, J, et al., FSH and its second messenger cAMP stimulate the transcription of human anti-
Mullerian hormone in cultured granulosa cells. Mol Endocrinol; 25: 645-655, 2011.2. GRUIJTERS, MJ, et al., Anti-Mullerian hormone and its role in ovarian function. Mol Cell Endocrinol;
211: 85-90, 2003.3. VISSER, JA and AP THEMMEN, Anti-Mullerian hormone and folliculogenesis. Mol Cell Endocrinol;
234: 81-86, 2005.4. KNIGHT, PG and C GLISTER, TGF-beta superfamily members and ovarian follicle development.
Reproduction; 132: 191-206, 2006.5. VAN ROOIJ, IA, et al., Serum antimullerian hormone levels best refl ect the reproductive decline with
age in normal women with proven fertility: a longitudinal study. Fertil Steril; 83: 979-987, 2005.6. VISSER, JA, et al., Anti-Mullerian hormone: a new marker for ovarian function. Reproduction; 131:
1-9, 2006.7. COULAM, CB, SC ADAMSON, and JF ANNEGERS, Incidence of premature ovarian failure. Obstet
Gynecol; 67: 604-606, 1986.8. LEKAMGE, DN, et al., Anti-Mullerian hormone as a predictor of IVF outcome. Reprod Biomed
Online; 14: 602-610, 2007.9. PAPALEO, E, et al., Myo-inositol may improve oocyte quality in intracytoplasmic sperm injection
cycles. A prospective, controlled, randomized trial. Fertil Steril; 91: 1750-1754, 2009.10. UNFER, V, et al., Myo-inositol rather than D-chiro-inositol is able to improve oocyte quality in
intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. Eur Rev Med Pharmacol Sci; 15: 452-457, 2011.
11. RIZZO, P, E RAFFONE, and V BENEDETTO, Effect of the treatment with myo-inositol plus folic acid plus melatonin in comparison with a treatment with myo-inositol plus folic acid on oocyte quality and pregnancy outcome in IVF cycles. A prospective, clinical trial. Eur Rev Med Pharmacol Sci; 14: 555-561, 2010.
12. UNFER, V, et al., Effect of a supplementation with myo-inositol plus melatonin on oocyte quality in women who failed to conceive in previous in vitro fertilization cycles for poor oocyte quality: a prospective, longitudinal, cohort study. Gynecol Endocrinol 2011.
© 2012 Monduzzi Editoriale | Proceedings Code: 139
Impact of rh-FSH on sperm DFI in idiopathic oligoasthenospermia
N. Colacurci, M.D. D’Eufemia, V. Auletta, P. De Franciscis, M.G. Monti, C. Trotta, E. La Verde, D. MeleDepartment of Gynaecology, Obstetrics and Reproductive Sciences, Second University of Naples, Naples, Italy
SUMMARYIn a prospective study the effects of rh-FSH treatment on sperm DNA fragmenta-
tion in men with idiopathic oligoasthenoteratozoospermia (iOAT) was evaluated. One hundred-sixty men with sperm count less than 10x106 spermatozoa/mL and forward motility <25%, normal serum levels of FSH, LH and T, and no other causes of infertility were included. The patients were randomized into two groups: 80 men were treated on alternate days for 90 days with injections of 150 IU rh-FSH and 80 men received non antioxidants-vitamin supplements. No signifi cant differences were observed between the two groups as regards sperm parameters and hormone values. The DFI reduced signifi cantly (p<0.05) after rh-FSH therapy, did not change in the control group. When basal DFI was > 15%, rh-FSH treatment signifi cantly increased DFI (p<0.01) only in patients undergone rh-FSH therapy.
INTRODUCTIONThe standard analysis of sperm count, motility and morphology has traditionally
been used as indicator of male fertility potential (1, 2). Nevertheless, the conven-tional semen parameters do not allow a full evaluation of the reproductive capability in infertile men (3). The sperm obtained from subjects with poor seminal quality shows several morphological and functional alterations along with high percent-ages of spermatozoa with anomalies in DNA integrity (4). Sperm DNA fragmenta-tion has been demonstrated to negatively affect the reproductive outcome both in spontaneous cycles and in assisted reproduction settings (5) and the sperm DNA fragmentation levels have been found signifi cantly higher in idiopathic oligoasthe-nospermic infertile men as compared with the levels observed in fertile donors (6).
To date, a limited number of small uncontrolled studies have examined potential
28
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
treatments to reduce sperm DNA damage. Since FSH plays an important role in the spermatogenic process, iOAT has been treated with FSH administration showing confl icting results (8). Previous experiences (9) emphasized that FSH administra-tion induces an increase of the pregnancy rate in iOAT male candidates for ICSI, but it doesn’t affect signifi cantly the number and the motility of spermatozoa. Moreover a previous study (2) showed that rhFSH treatment can increase sperm DNA conden-sation in idiopathic infertile men. The aim of our study was to investigate the effects of rhFSH treatment on sperm DNA fragmentation in men with iOAT.
MATERIAL AND METHODSThe study involved 160 oligoasthenospermic men with normal hormonal levels
(FSH >1 <7 IU/L, LH >1 <8 IU/L, T >3 <10 ng/mL), sperm count less than 10x106 spermatozoa/mL and forward motility <25%, and no other causes of infertility. The patients were randomized into two groups: 80 men were treated on alternate days for 90 days with injections of 150 IU rh-FSH (group A) and 80 men received non antioxidants-vitamin supplements (group B). Serum hormone levels and DFI as-sessed with TUNEL assay were evaluated at baseline and after 90 days. Considering DFI ≤ 15% as normal, two subgroups of patients were identifi ed: A1 (66 patients) and B1 (60 patients) with DFI > 15%, A2 (12 patients) and B2 (17 patients) with DFI < 15%. Results are means ± SD. One way analysis of variance and Mann-Whitney U-test were used to evaluate the differences between groups for normally and not-normally distributed data, respectively. Analysis of paired data within a group was performed by the paired Student t test or the Wilcoxon signed-rank test. Statistical signifi cance was set at p<0.05.
RESULTS Baseline clinical and hormonal characteristics were not signifi cantly different be-
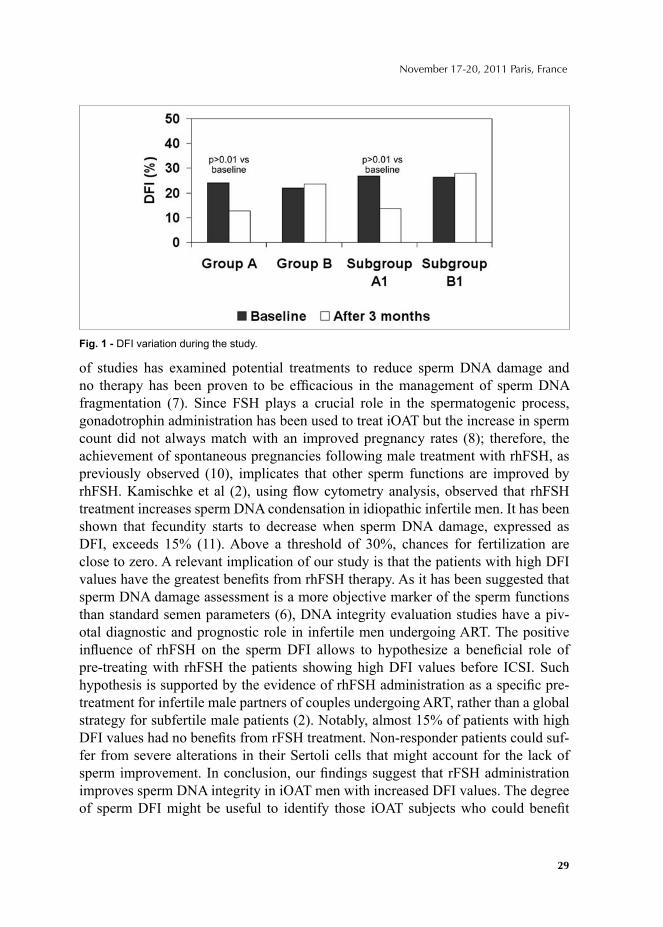
tween the study and the control group. In group A 78 patients and in group B 77 patients completed the study. No signifi cant differences were observed between the study and the control group as regards sperm count, sperm concentration, motility, and the percentage of normal sperm forms. The DFI detected by TUNEL was simi-lar between the group A and B at the time of the enrollment (24.0±9.3 vs 22.1±9.1), a statistically signifi cant reduction was observed after rhFSH therapy (12.8±7.2 vs 23.7±10.2, p<0.05), while in the control group no signifi cant variation occurred after the study period (Figure 1). DFI signifi cantly increased (p<0.01) as compared with the baseline values in the subgroup A1 while no signifi cant variation occurred in group B1 (fi gure 1).
CONCLUSIONThe present study shows that 90 days of rFSH administration improve sperm
DNA integrity in men with iOAT by reducing DFI values. To date, a limited number
29
November 17-20, 2011 Paris, France
of studies has examined potential treatments to reduce sperm DNA damage and no therapy has been proven to be effi cacious in the management of sperm DNA fragmentation (7). Since FSH plays a crucial role in the spermatogenic process, gonadotrophin administration has been used to treat iOAT but the increase in sperm count did not always match with an improved pregnancy rates (8); therefore, the achievement of spontaneous pregnancies following male treatment with rhFSH, as previously observed (10), implicates that other sperm functions are improved by rhFSH. Kamischke et al (2), using fl ow cytometry analysis, observed that rhFSH treatment increases sperm DNA condensation in idiopathic infertile men. It has been shown that fecundity starts to decrease when sperm DNA damage, expressed as DFI, exceeds 15% (11). Above a threshold of 30%, chances for fertilization are close to zero. A relevant implication of our study is that the patients with high DFI values have the greatest benefi ts from rhFSH therapy. As it has been suggested that sperm DNA damage assessment is a more objective marker of the sperm functions than standard semen parameters (6), DNA integrity evaluation studies have a piv-otal diagnostic and prognostic role in infertile men undergoing ART. The positive infl uence of rhFSH on the sperm DFI allows to hypothesize a benefi cial role of pre-treating with rhFSH the patients showing high DFI values before ICSI. Such hypothesis is supported by the evidence of rhFSH administration as a specifi c pre-treatment for infertile male partners of couples undergoing ART, rather than a global strategy for subfertile male patients (2). Notably, almost 15% of patients with high DFI values had no benefi ts from rFSH treatment. Non-responder patients could suf-fer from severe alterations in their Sertoli cells that might account for the lack of sperm improvement. In conclusion, our fi ndings suggest that rFSH administration improves sperm DNA integrity in iOAT men with increased DFI values. The degree of sperm DFI might be useful to identify those iOAT subjects who could benefi t
Fig. 1 - DFI variation during the study.
30
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
from rFSH therapy. The possible impact of this treatment on the male fertility and on the fertilizing capability of spermatozoa in ART and therefore on the pregnancy rate, needs to be evaluated.
REFERENCES1. Cavallini G. Male idiopathic oligoasthenoteratozoospermia. Asian J Androl. 8:143-57. 2006.2. Kamischke A. rhFSH for treatment of male idiopathic infertility: a randomized, double-blind, pla-
cebo-controlled, clinical trial. Hum Reprod. 13:596–603. 1998 .3. Saleh RA. Increased sperm nuclear DNA damage in normozoospermic infertile men: a prospective
study. Fertil Steril. 78:313–8. 2002.4. Seli E. Spermatozoal nuclear determinants of reproductive outcome: implications for ART. Hum
Reprod Update. 11 (4):337-49. 2005.5. Evenson D. Meta-analysis of sperm DNA fragmentation using the sperm chromatin structure assay.
Reprod Biomed Online. 12 (4):466-72. 2006.6. Liu CH. DNA fragmentation, mitochondrial dysfunction and chromosomal aneuploidy in the sper-
matozoa of oligoasthenoteratozoospermic males. J Assist Reprod Genet. 21:119-26. 20047. The Practice Committee of the American Society for Reproductive Medicine. The clinical utility of
sperm DNA integrity testing. Fertil Steril. 90 (3): 178-180. 2008.8. Attia AM. Gonadotrophins for idiopathic male factor subfertility. Cochrane Database Syst Rev.
(4):CD005071. 2007.9. Caroppo E. rhFSH as a pretreatment for idiopathic oligoasthenoteratozoospermic patients undergo-
ing intracytoplasmic sperm injection. Fertil Steril. 80:1398-403. 200310. Zalata AA. FSH receptor polymorphism and seminal anti-Müllerian hormone in fertile and infertile
men. Androl. 40:392-7. 2008.11. Spano M. Sperm chromatin damage impairs human fertility. The Danish First Pregnancy Planner
Study Team. Fertil Steril. 73: 43–50. 2000.
© 2012 Monduzzi Editoriale | Proceedings Code: 203
Pregnancy rate of gonadotrophin therapy and laparoscopic ovarian electrocautery in polycystic ovary syndrome resistant to clomiphene citrate: a comparative study
M. Ghafarnejad, N. Arjmand, Z. KhazaeeDepartment of Obstetrics & Gynecology, Tehran University of Medical Sciences, Tehran, Iran
Background: Polycystic ovary syndrome (PCOS) is a common cause of ovu-lation insuffi ciency and then infertility. Therapeutic options to induce ovulation in anovulatory PCOS patients are clomiphene citrate, metformin, tamoxifen, dopamine agonists (bromocriptin), Gonadotrophin and laparoscopic ovarian electrocautery (LOE). Gonadotrophin and LOE are important options in anovu-latory clomiphene citrate resistant patients with PCOS. Literature data regarding compare of the effi cacy of these two treatments are few. Therefore we aimed to study the pregnancy rates of these treatments in infertile clomiphene citrate-resistant patients with PCOS.
Methods: A randomized clinical trial study was carried out in infertile clomi-phene citrate-resistant patients with PCOS, referred to infertility clinic of Mirza Koochackhan Hospital affi liated to Tehran University of Medical Science in Tehran, Iran, between 2003 and 2008.
Results: A total of 100 patients women were randomly allocated in two groups. There were no differences in age and pimary and secondary infertility duration. In LOE treatment group, eight cases (16%) were pregnant and all delivered at term. In gonadotrophin treatment 14 cases (28%) were pregnant, 10 cases (20%) delivered at term but four cases aborted. The cost in gonadotrophin treatment was signifi cantly more than laparoscopic ovarian diathermy (p<0.001). In logistic regression analysis, age, BMI, cost and kind of treatment had no signifi cant effect on pregnancy rate.
Conclusions: Pregnancy and abortion rate in gonadotrophin treatment was more than LOE but the difference was not signifi cant.
Keywords: Polycystic ovary syndrome, gonadotrophin, laparoscopic ovarian electrocautery, pregnancy.

32
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
INTRODUCTIONAffecting 10- 15% of couples, infertility refers to failure in pregnancy after one
year of relation without any contraception (1-2). Almost 80- 95% of young healthy couples get pregnant during the fi rst year of engage. Among those 43% of infertile couples seeking for a solution, 24% ask for a special option of treatment (1-3). It is possible to induce ovulation in almost all the cases with anovulatory infertility (1- 3); the problem which involves half of all the infertile women (1- 4). Polycystic ovary syndrome (PCOS) is one of the major causes for anovulation (4, 5), consid-ered as the most common endocrinology disorder in women presenting with a va-riety of clinical symptoms. Clomiphene citrate remains the treatment of fi rst choice in subjects with PCOS (1-3) inducing ovulation in 80% of them if selected properly (6- 8). 20 – 22% of the treated women don’t give any response to clomiphen while there is also a difference between ovulation and gestation in such cases (9). In ad-dition, a mild increase (5- 8%) in multiple gestation rate is reported as the adverse effect of ovulation induction by Clomiphene (10, 11).
Laparoscopic ovarian cauterization not only affects successful ovulation rate but brings a better hormonal balance in serum by lowering LH, androgen, and DHEA; such reduction of intra- ovarian synthesized androgen leads to production of func-tional follicles (12). Exogenous gonadotropin products for induction of ovulation are available in three forms of urinary, extracted urinary and recombinant com-pound. HMG is extracted from menopausal women’s urine of which each ampoule contains 75 mg of LH and FSH equally injected intramuscular in cases of ovulation failure induced by clomiphen (1- 3). It is hardly possible to induce a single follicle to ovulate and thus multi gestation and ovarian hyperstimulatory syndrome (OHSS) occurs in many cases of PCOS treated with such option (1- 4). Hypogonadotropic hypogonadism is the main indication for administration of these exogenous com-pounds; this condition does not respond to clomiphen and other similar medications.
Laparoscopic ovarian electrocautery (LOE) has been compared to induction of ovulation by gonadotropin compound in literature; but to our knowledge, there is not such an assessment in Iran; the society with its national, cultural and economic issues which is experiencing an increasing incidence of infertility and its presented treating options.
The aim of this study is to compare the successful rate of laparoscopic ovarian electrocautery and gonadotropin for ovulation induction and pregnancy in women with POCS resistant to clomiphen.
METHODS AND MATERIALSIn a randomized clinical trial, infertile clomiphene citrate-resistant patients with
PCOS, referred to infertility clinic of Mirza Koochackhan Hospital of Tehran Uni-versity of Medical Science in Tehran, Iran, entered the study between 2003 and
33
November 17-20, 2011 Paris, France
2008. Inclusion criteria were as following: age of 20 to 30, clinically, laboratory, and transvaginal sonographically (TVS) diagnosed PCOS which have been resistant to clomiphen (no ovulation after administration of 150 mg of clomiphen citrate during 5th to 9th days of cycle for 2- 3 cycles), and normal semen analysis (sperm count> 20 million per milliliter, morphology> 30% and motility> 50%) in spouse men; while tubal conditions and male problems were considered as exclusion criteria.
Under a general anesthesia, cauterization was performed using a 100 watt cutting fl ow followed by a 30 watt coagulation fl ow for 2- 4 seconds. Dependant to the size of ovary, 5- 15 sites were pointed in a nearly 5 millimeter depth. Cold serum was used to diminish temperature of operation sites in order to avoid post- op adhesions. Spontaneous ovulation was assessed by 21th day measurement of progesterone. Values more than 3 ng/ dl but lower than 7ng/ dl were considered as ovulation with luteal phase insuffi ciency, while those values more than 7 ng/ dl were representative of optimal ovulation. Β- HCG and sonography were used to diagnose pregnancy in case of retarding period. The patients were then followed for 4 month.
In patients under gonadotropin treatment, clomiphen citrate (50 mg BD/ 100 mg every day) was administered between 5th and 9th days of cycle followed by injection of single dose gonadotropin daily. Transvaginal sonography was used to assess intra ovarian growing follicles for numbers and sizes; if at least two follicles sizing > 18 mm were seen in TVS, 10’000 units HCG is injected. The cases had intercourse two days after injection of HCG. Β-HCG> 10 U/L were considered as positive test of pregnancy in association
with sensed fetal heart rate (FHR) in seventh week of gestation. Abortion was de-fi ned as loss of pgestation product under 20th week of pregnancy.
Data were analyzed by SPSS version 6, using fi sher's exact test, Mann-Whitney test, Logistic regression, and chi square test and values were considered signifi cant at p< 0.05.
The patients fi lled an informed consent and ethical and research committee of Tehran University of Medical Sciences approved the study for medicolegal issues.
RESULTSA total of 100 women at the age of pregnancy were randomly allocated in two
groups. There were no differences in age, BMI, primary and secondary infertility du-ration. In LOE treatment group, eight cases (16%) were pregnant and all delivered at term while in group receiving gonadotrophin treatment, 14 cases (28%) got pregnant with 10 cases (20%) delivered at term but 4 cases (8%) were aborted. Among 18 full- term pregnancy outcomes, 8 cases (44.4%) were in while 10 (55.6%) were embedded in gonadotropin treated patients representing no signifi cant difference (p> 0.05).
10 of 50 patients (20%) had a serum level of progesterone more than 7 ng/ dl during the fi rst month after operation but no pregnancy was achieved; 10 patients (20%) in the second month had progestron level of more than 7 ng/ dl of which 2

34
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
cases (20%) got pregnant; in third month 12 patients of remained 48 had ovulation with no gestation while fi nally in the fourth month, 13 patients of 48 got ovulation which 6 of them led to gestation. It was not possible to evaluate ovulation in those patients receiving gonadotropin as a treatment for induction.
The cost for gonadotrophin induction of ovulation was signifi cantly more than laparoscopic ovarian diathermy (p < 0.001). In logistic regression analysis, age, BMI, cost, and type of treatment had no signifi cant effect on pregnancy rate.
DISCUSSIONOur study constituted of 50 patients in each group of treatment; in laparoscopic
group, we had 8 full- term pregnancy (16%) while in gonadotropin receiving patients, 14 cases (28%) succeed to pregnancy, 10 (20%) of them reaching to full term and the rest 4 (8%) led to an abortion. Among all these full term pregnancy, 8 (44.4%) were under the laparoscopic treatment while other 10 (55.6%) were embedded in gonado-tropin territory; no differences were observed signifi cantly between these two groups of successful pregnancy in terms of gestation rate and duration of pregnancy.
Farquhar et al., reported a 52 % and 62% of ovulation in laparoscopic ovarian cauterization and gonadotropin induction of ovulation, respectively (13); they have had a successful experience of gestation as much as 17 % and 24% in former and the latter group. Kaya and collegues in 2005 couldn’t conclude a signifi cant differ-ence between 35.3 % and 33.3% in ovulation rate of infertile women undergoing laparoscopic ovarian cauterization and gonadotropin medicating, respectively (14).
Kovacs didn’t report many advantages for either of these over each other in terms of pregnancy rate or cost of treatment, while he has recommended cauterization for treating infertile PCOS women as a second line option due to its potential benefi ts whenever the patient is recognized resistant to clomiphen (15).
The same controversy is seen between Balen’s study in 2007 and Unlu’s report in 2006; Balen et al., has reported no differences for rate of pregnancy (16) while Unlu reported lower costs and better regulation of menstrual cycle (17).
Although Farquhar has reported no signifi cant differences for pregnancy outcome between two groups of PCOS receiving gonadotropin and undergoing laparoscopic cauterization, evidence of higher costs in gonadotropin treating patients were compat-ible to Kaya (14), Kovacs (15), and Unlu (17). But our logistic regression analysis showed no signifi cant differences when age, BMI, and type of treatment is considered.
We didn’t observe any complications for general anesthesia or surgery and mul-tiple gestation or OHSS in LEC and gonadotropin group, respectively. Farquhar et al., in 2002 reported no complication related to cauterization or developing OHSS (13). Kaya didn’t report any complications like adhesion due to laparoscopy (14). Ballen reported although some but mild complications in cauterization including ovary injury, pelvic adhesions, and anesthetic issues (16).
Farquhar in 2008 reported less occurrence of multiple gestation in cauterization
35
November 17-20, 2011 Paris, France
group compared to gonadotropin induced patients (OR: 0.13, CI 95%: 0.03- 0.52) while the cauterization had been associated with long term risks for function failure in ovary (18); there was also no difference in terms of abortion (OR: 81%, CI 95%: 0.36- 1.86) between these two groups. Besides, in Farquhar’s opinion, less direct and indirect costs could be related to LOE (19).
It seems that less abortion but less pregnancy rate occurs in LOE group. This however is not signifi cant. Our study could not assess the rate of ovulation in go-nadotropin receiving group as the patients weren’t cooperated to participate in such setting. In association with small population size, this is going to need further stud-ies for a better result.
CONCLUSIONPregnancy and abortion rate in infertile women of PCOS receiving gonadotro-
phin as a treatment for induction of ovulation seems to be more than LOE.
REFERENCES1. Berek JS. Berek & Novak's Gynecology. 14th ed. Philadelphia: Lippincott Williams & Wilkins;
2005. 2. Speroff L, Fritz MA, editors. Clinical Gynecologic Endocrinology and Infertility. 7th ed. Philadel-
phia: Lippincott Williams & Wilkins; 2005. p. 1175-205. 3. Speroff L, Fritz MA, editors. Clinical Gynecologic Endocrinology and Infertility. 7th ed. Philadel-
phia: Lippincott Williams & Wilkins; 2005. p. 474-86. 4. Van Santbrink EJ, Hop WC, Fauser BC. Classifi cation of normogonadotropic infertility: polycystic
ovaries diagnosed by ultrasound versus endocrine characteristics of polycystic ovary syndrome. Fertil Steril 1997; 67(3):452-8.
5. Franks S, Adams J, Mason H, Polson D. Ovulatory disorders in women with polycystic ovary syn-drome. Clin Obstet Gynaecol 1985; 12(3):605-32.
6. Hack M, Brish M, Serr DM, Insler V, Salomy M, Lunenfeld B. Outcome of pregnancy after induced ovulation. Follow-up of pregnancies and children born after clomiphene therapy. JAMA 1972; 220(10):1329-33.
7. Asch H, Greenblatt RB. Update on the safety and effi ciency of clomiphene citrate as a therapeutic agent. J Reprod Med 1976; 17:175-80.
8. Ahlgren M, Källén B, Rannevik G. Outcome of pregnancy after clomiphene therapy. Acta Obstet Gynecol Scand 1976; 55(4):371-5.
9. Kettel LM, Roseff SJ, Berga SL, Mortola JF, Yen SS. Hypothalamic-pituitary-ovarian response to clomiphene citrate in women with polycystic ovary syndrome. Fertil Steril 1993; 59(3):532-8.
10. Schenker JG, Yarkoni S, Granat M. Multiple pregnancies following induction of ovulation. Fertil Steril 1981; 35(2):105-
11. Wu CH. Less miscarriage in pregnancy following Tamoxifen treatment of infertile patients with luteal phase dysfunction as compared to clomiphene treatment. Early Pregnancy 1997; 3(4):301-5.
12. Amin AF, Abd el-Aal DE, Darwish AM, Meki AR. Evaluation of the impact of laparoscopic ovarian drilling on Doppler indices of ovarian stromal blood fl ow, serum vascular endothelial growth factor, and insulin-like growth factor-1 in women with polycystic ovary syndrome. Fertil Steril 2003; 79(4):938-41.
36
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
13. Farquhar CM, Williamson K, Gudex G, Johnson NP, Garland J, Sadler L. A randomized controlled trial of laparoscopic ovarian diathermy versus gonadotropin therapy for women with clomiphene citrate-resistant polycystic ovary syndrome. Fertil Steril 2002; 78(2):404-11.
14. Kaya H, Sezik M, Ozkaya O. Evaluation of a new surgical approach for the treatment of clomiphene citrate-resistant infertility in polycystic ovary syndrome: laparoscopic ovarian multi_ needle intervention. J Minim Invasive Gynecol 2005; 12(4):355-8.
15. Kovacs GT, Clarke S, Burger HG, Healy DL, Vollenhoven B. Surgical or medical treatment of polycystic ovary syndrome: a cost-benefi t analysis. Gynecol Endocrinol 2002; 16(1):53-5.
16. Balen AH. Surgical Management of the Polycystic Ovarian Syndrome. 2nd ed. Human Press; 2007. p. 415-20.
17. Unlu C, Atabekoglu CS. Surgical treatment in polycystic ovary syndrome. Curr Opin Obstet Gynecol 2006; 18(3):286-92.
18. Farquhar C, Lilford RJ, Marjoribanks J, Vandekerckhove P. Laparoscopic 'drilling' by diathermy or laser for ovulation induction in anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev 2007; (3):CD001122.
19. Farquhar CM, Williamson K, Brown PM, Garland J. An economic evaluation of laparoscopic ovarian diathermy versus gonadotrophin therapy for women with clomiphene citrate resistant polycystic ovary syndrome. Hum Reprod 2004; 19(5):1110-5.
© 2012 Monduzzi Editoriale | Proceedings Code: 227
Premature ovarian failure in a woman with a balanced 15; 21 translocation – a case report
S. Hosseini, M. Vahid Dastjerdi, Z. Asgari, H. Samiee Arash University Hospital, Department of Obstetrics & Gynecology, Tehran University of Medical Sciences, Tehran, Iran
ABSTRACTIntroduction: The diagnosis of Premature Ovarian Failure (POF) with concomi-
tant fi ndings of the Robertsonian translocation between 15 and 21 chromosomes is evaluated here. The aforementioned karyotypic aberration has never been reported in the context of premature ovarian failure before.
Case presentation: We hereby present a case of premature ovarian failure in a 27-year-old infertile Kurdish Iranian woman with a Robertsonian 15; 21 translocation.
Conclusion(s): The diagnosis of premature ovarian failure of unknown etiolo-gy, but with karyotypic evidence of a balanced autosomal translocation, suggests the possible role of autosomal genes in the pathogenesis of ovarian follicular attrition.
INTRODUCTIONA signifi cant family history of early menopause is found in about 5% of cases
with POF [1]. To determine the underlying basis of POF, genetic causes with a range of proposed loci are currently under investigation. One out of every 900 babies is born with a Robertsonian translocation (sited for the fi rst time in 1964 by Gustavs-son, Ingemar), showing that this translocation is the most common, signifi cant and recurrent structural rearrangement known in human being.
CASE PRESENTATIONOur case, who was an Iranian Kurdish 27-year-old woman under evaluation for
infertility, had secondary amenorrhea from the age of 24. She received hormonal re-placement for the past 3 years which resulted in cyclical bleeding but she remained
38
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
anovulatory. The Karyotype of the proband showed a translocation between chro-mosomes 21 and 15:45,XX,t (21; 15).
She had regular menstruation cycles from the age of 13 until 21 years of age. Her height and weight fell in the 90th and 50th percentile respectively and she had a body mass index of 21 kg/m².
Her arm span to height and upper to lower segment ratios were both normal.Regarding pubertal status, she was Tanner V for pubic hair and Tanner IV for breast.
Her genitalia were normal and she had no virilized or dysmorphic features. Her intel-lectual capacity was in the normal range and she had a full-time career as a teacher.
No positive family history was noted regarding premature menopause, infertility and subfertility, smoking, chemotherapy, radiation or autoimmune diseases. Results of cytogenetic and molecular studies by Polymerase Chain Reaction (PCR) tech-niques for fragile X mutations or premutations were negative.
Serum anti-thyroid, anti-ovarian and anti-adrenal antibodies were absent. Estra-diol level was 32pg/ml and serum anti mullerian hormone was 0.34μg/L. She de-nied any history of pelvic infl ammatory or sexually transmitted diseases. No sign of pelvic surgery was seen, too. An ultrasound examination of the pelvis revealed a normal uterus measuring 68 × 29 mm, and the right and left ovaries were 24 × 20 and 23 × 21 mm, respectively. One selectable antral follicle (4.6mm) was also seen.
Hysterosalpingogram (the infertility center's routine request) confi rmed a normal uterine and tubal anatomy. Hormonal evaluation showed elevated FSH (25 IU/ml) and LH (22 IU/ml) levels. Her TSH, testosterone and prolactin were within normal limits.
DISCUSSIONPremature ovarian failure is a pretty common description in the context of balanced
X: autosomal translocations. Chromosomal imbalance can increase oocyte atresia be-cause after meiosis is initiated, X inactivation is not operative in germ cells [2].
It is possible that translocations like X monosomy (Turner syndrome) lead topremature ovarian failure through causing aberrations in pairing or X-inactivation
during folliculogenesis [2] not by interrupting specifi c genes which are important in ovarian development.
The most common ROBs apparently have the same breakpoints and arise mainly during oogenesis, predominantly during the meiosis [3]. During chromosomal pair-ing and condensation, failure at checkpoints (specifi c locations along chromosomes) provokes germ cell death. Chromosome dynamics may be sensitive to structural changes, while modifying by translocations, might provoke apoptosis at meiotic checkpoints [2]. Robertsonian translocation between chromosomes 13 and 14 has recently been reported in a 19- year- old Japanese woman with secondary amenor-rhea [4]. There are four autosomal translocations in women with premature ovarian failure, 46 XX,t (2; 11), 45,XX,t (13; 14)[4], 46,XX,t (2; 15)[1; 5], and mosaicism
39
November 17-20, 2011 Paris, France
45,XX,ROB (13; 21)(q10; q10)/46,XX in 55% of the cells [6]. An about 5-year ear-lier menopause is described in trisomy 21 [7], therefore, a critical balance of ‘‘de-terminant’’ genes within this chromosome may infl uence the reproductive lifespan.
CONCLUSIONAs trisomy 21 is described in association with reduced ovarian reserve [3], the present translocation risk for such an eventuality is especially escalated. In ad-
dition, given the reduced ovarian reserve, although fertility prognosis with these karyotype gametes remains suboptimal, this feature has an increased risk of con-ceiving a fetus with trisomy 15 and monosomy 21 or 15. To minimize the risk of fetal aneuploidy, donor egg IVF provides a reassuring alternative.
Based on our medical -e- search of English and Persian articles, there seems to be no previously published report identifying a Robertsonian translocation between 15 and 21 chromosomes accompanied by either early menopause or reduced ovarian reserve.
This fi nding merits widespread exploration to fi nd whether 15; 21 translocation results in disruption of ovarian folliculogenesis or follicular atresia and an early decline in ovarian follicles.
However, some aspects of this case will be clarifi ed after the Human Genome Project is very completed.
ConsentThe Patient gave her informed consent for the case report to be published.
Competing InterestsAuthors have no confl icts of interest to declare. Authors have fulfi lled all condi-
tions required for authorship. The authors have no previous publication similar to this study.
We acknowledge our colleagues' efforts in Shariati Infertility Center.
Authors' contributionsAll authors analyzed and interpreted patients' data. The fi rst author was the ma-
jor contributor in writing the manuscript. All authors read and approved the fi nal manuscript.
REFERENCE LIST1. Burton KA, Van EE CC, Purcell Kim, Winship Inger, Shelling AN. Autosomal translocation associ-
ated with premature ovarian failure. J Med Genet 2000 May 1; 37(5): e2.2. Schlessinger D, Herrera L, Crisponi L, Mumm S, Percesepe A, Pellegrini M, et al. Genes and trans-
locations involved in POF. Am J Med Genet 2002; 111(3):328-33.3. Kummer N, Martin JR, Pal L. Diminished ovarian reserve in a woman with a balanced 13; 21 trans-
location. Fertil Steril 2009 Mar; 91(3):931.

40
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
4. Kawano Y, Narahara H, Matsui N, Miyakawa I. Premature ovarian failure associated with a Robert-sonian translocation. Acta Obstet Gynecol Scand 1998; 77(4):467-9.
5. Van Montfrans JM, Dorland M, Oosterhuis GJE, Van Vugt JMG, Rekers-Mombarg LTM, Lambalk CB. Increased concentrations of follicle-stimulating hormone in mothers of children with Down's syndrome. Lancet 1999; 353(9167):1853-4.
6. Bandyopadhyay R, McCaskill C, Knox-Du Bois C, Zhou Y, Berend SA, Bijlsma E, et al. Mosaicism in a patient with Down syndrome reveals post-fertilization formation of a robertsonian translocation and isochromosome. Am J Med Genet 2003; (2).
7. Cosgrave MP, Tyrrell J, McCarron M, Gill M, Lawlor BA. Age at onset of dementia and age of menopause in women with Down's syndrome. J Intellect Disabil Res 1999; 43(6):461-5.
© 2012 Monduzzi Editoriale | Proceedings Code: 240
Male obesity and sperm parameters in infertility
L. JamshidiNursing Department, Hamedan branch, Islamic Azad University, Hamedan, Iran
SUMMARYIntroduction: Fertility can be negatively affected by obesity. In men, obesity is
associated with low testosterone levels. The aim of this study is assess the effect of male obesity on sperm parameters. Material and Methods: on presentation, all men reported their weight and height and fi lled out an intake form that includes ques-tions regarding factors that affect male infertility. Body mass index (BMI) was di-vided into three groups: normal, overweight, and obese. Sperm parameters reviewed included sperm concentration and progressively motile sperm count. Results: the incidence of oligozoospermia increased with increasing BMI. The prevalence of a low progressively motile sperm count was also greater with increasing BMI. In men with less than normal fat percent, had the lowest sperm count (10*68.88). In massively obese individuals, reduced spermatogenesis associated with severe hypo-testosteronemia may favor infertility. Conclusions: much more attention should be paid to the impact of obesity on fertility in both women and men.
INTRODUCTIONIt is believed that with the increasing prevalence of sedentary life styles and di-
etary changes, obesity is emerging as an important cause of adverse health out-comes, including male infertility. Male factors alone constitute 25%–30% of all cases of infertility, and they contribute to another 30% in combination with female factors. Obesity was recently proposed for addition to this list (Jensen et al, 2004). Recently, the prevalence of male obesity in the Iran was reported to be 53.8 % (Janghorbani et al 2007). It is possible that the increasing prevalence of overweight and obesity accounts for a portion of the trend, albeit a widely debated one, of de-creasing sperm counts over recent decades. Although complicated by varying sam-ple sizes and methodologies for the assembled data, it has been estimated that sperm counts have been decreasing by as much as 1.5% each year in the United States, a

42
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
fi nding similar to those for other Western countries and not present in other regions where obesity is less prevalent (Swan et al, 2000). These fi ndings suggest a possible link between life style changes, obesity, semen quality, and possibly male fertility (Jensen et al, 2004).In fact, both total and free blood testosterone levels are shown to be decreased in obese men. Total body fat, intra-abdominal fat, and subcutaneous fat have all been associated with low levels of total and free testosterone (Strain et al, 1982; Haffner et al; Tsai et al, 2004). However, there is consistent enthusiasm in the literature, with considerable circumstantial support, for the hypothesis that alterations of sperm parameters associated with obesity can be attributed to inap-propriate suppression of the hypothalamic-pituitary-gonadal axis by elevated estro-gens derived from peripheral aromatization, and resulting decreased testosterone production refl ected in low levels of circulating testosterone and intratesticular tes-tosterone. The role of estrogen in male reproductive health was highlighted with the growing public concerns that exposures to environmental chemicals with estrogenic activity may impact human reproductive health (Oliva et al, 2001). Obese men have been shown to exhibit higher levels of circulating estradiol and/or elevated estra-diol/ testosterone ratios in multiple studies (Jensen, 2004; Fejes, 2006).
MATERIALS AND METHODSA single semen sample was collected from each man. None of the men had previ-
ous surgery. Sperm parameters reviewed included sperm concentration and progres-sively motile sperm count. Patient height (m) and weight (kg) were recorded on the day of semen collection. BMI was calculated for each patient as kg/m2. BMI is recognized as the measure of overall obesity. The criteria for underweight, normal-weight, overweight, and Classes I, II, and III obesity used in the present study were based on BMI (weight/height2) [ kg/m2] ) and were consistent with the defi nitions set forth by the WHO and the National Heart, Lung, and Blood Institute as follows: underweight <18.5, normal-weight 18.5 to 24.9, overweight 25 to 29.9, Class I obe-sity 30 to 34.9, Class II obesity 35 to 39.9, and Class III obesity ≥40 kg/m2. Sperm concentration and percent motility was evaluated according to World Health Orga-nization guidelines (WHO,1999). Sperm morphology scores were determined by the Tygerberg "strict" criteria system (Kruger et al, 1986, 1988; WHO, 1999). The total number of normal-motile spermatozoa (NMS) for each patient semen speci-men was calculated as NMS = volume x concentration x %motility x %morphology.
RESULTSA total of 450 semen specimens were analyzed as described. The mean age of the
study population was 34.6 ± 0.3 years. There was no signifi cant difference in patient ages among the different BMI groups. Among the 450 patients, 10.2% (54 of 526).Were excluded because of the presence of a male factor known to affect fertility.

43
November 17-20, 2011 Paris, France
The incidence of oligozoospermia increased with increasing BMI. The prevalence of a low progressively motile sperm count was also greater with increasing BMI. Negative relationship between BMI and NMS. ANOVA revealed a signifi cant dif-ference (P <.05) in the total number of normal-motile sperm cells among the 3 dif-ferent BMI groups. The NMS per BMI group was as follows: normal, 18.6 x 106 cells; overweight, 3.6 x 106 cells; and obese, 0.7 x 106 cells.
The average percentage of fat samples was 17.63 percent. In people with normal body fat percentage, had the highest sperm count (10 ×90.74) in men with less than normal fat percent, had the lowest sperm count (10 ×68.88).In massively obese individuals, reduced spermatogenesis associated with severe hypotestosteronemia may favors infertility. Moreover, the frequency of erectile dysfunction increases with increasing body mass index.
CONCLUSIONSRecent population-based studies suggest an elevated risk for sub fertility among
couples in which the male partner is obese and an increased likelihood of abnormal semen parameters among heavier men. Male factor infertility is associated with a higher incidence of obesity in the male partner. Obese men exhibit reduced andro-gen and SHBG levels accompanied by elevated estrogen levels. Among a sample of 1558 Danish military recruits, several semen parameters were correlated with body mass index, with less favorable values refl ecting spermatogenesis observed in individuals with either above or below the BMI range of 20–25 kg/m2 (Jensen et al, 2004). After correction for multiple factors, including exposures, illnesses, and abstinence period prior to sample collection, sperm concentration and total count per ejaculate among men with BMI. 25 kg/ m2 were reduced by 26.1% and 23.9%, respectively, when compared to the reference group with BMI between 20 and 25 kg/m2. The frequency of sperm density less than 20 million/ml was 29% among the overweight men compared to 21.7% in the normal weight reference group. Re-ductions in these measures were similar among the subjects with BMI less than 20 kg/m2, such that total sperm count and sperm concentration exhibited an inverted U-shaped distribution relative to BMI. Kort et al described the relation between sperm parameters and BMI in a generally overweight selection of subjects. An index of semen quality appeared to exhibit a decline with increasing BMI, as did the number of normal sperm per ejaculate. In his study, the total number of normal spermatozoa correlated negatively with body mass index in 520 semen analyses. The total number of normal motile spermatozoa differed statistically according to weight group (BMI, 25 kg/m2 518.6 6 106; BMI $ 25 kg/m2 and, 30 kg/m2 5 3.6 6 106; and BMI $ 30 5 0.7 6 106, P,.05, ANOVA) (Kort et al, 2005). Additional features of male obesity that may contribute to an increased risk for infertility are altered retention and metabolism of environmental toxins, altered lifestyle factors,

44
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
and increased risks for sexual dysfunction. Neither reversibility of obesity-asso-ciated male infertility with weight loss nor effective therapeutic interventions has been studied yet.Much more attention should be paid to the impact of obesity on fertility in both women and men.
REFERENCES 1. Haffne r SM, Valdez RA, Stern MP, Katz MS. Obesity, body fat distribution and sex hormones in
men. Int J Obes Relat Metab Disord. 17: 643 –649. 1993. [Medline].2. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight
and obesity among US children, adolescents, and adults, 1999–2002. JAMA. 291: 2847 –2850. 2004.[Abstract/Free Full Text].
3. Hilton I. Kort, Joe B. Massey, Carlewe W. Elsner, et al, Impact of Body Mass Index Values on Sperm Quantity and Quality, Journal of Andrology, Vol. 27, No. 3, May/June 2006.
4. Janghorbani M, Amini M, Walter C. Willett, Gouya M.M, Delavari AR, Alikhani S, First Nationwide Survey of Prevalence of Overweight, Underweight, and Abdominal Obesity in Iranian Adults, Obesity. 15, 2797–2808; 2007.
5. Mokdad AH, Serdula MK, D ietz WH, Bowman BA, Marks JS, Koplan JP. The spread of the obesity epidemic in the United States, 1991–1998. JAMA. 282: 1519 –1522. 1999.[Abstract/Free Full Text].
6. Oliva A, Spira A, Multigner L. Contr ibution of environmental factors to the risk of male infertility. Hum Reprod. 16: 1768 –1776. 2001.[Abstract/Free Full Text].
7. Slama R, Eustache F, Ducot B, Jensen TK, Jorgens en N, Horte A et al. Time to pregnancy and semen parameters, a cross-sectional study among fertile couples from four European cities. Hum Reprod. 17: 503 –515.2002. [Abstract/Free Full Text].
8. Strain GW, Zumoff B, Kream J, Strain JJ, Deucher R, Rosenfel d RS, Levin J, Fukushima DK. Mild hypogonadotropic hypogonadism in obese men. Metabolism. 31: 871 –875. 1982.[CrossRef][Medline].
9. Swan SH, Elkin EP, Fenster L. The question of declining sperm density revisited: an analysis of 101 studies published 1934–1996. Environ Health Perspect. 108: 961 –966.2000. [Medline].
10. Tsai EC, Matsumoto A M, Fujimoto WY, Boyko EJ. Association of bioavailable, free, and total tes-tosterone with insulin resistance, infl uence of sex hormone-binding globulin and body fat. Diabetes Care. 27: 861 –868.2004. [Abstract/Free Full Text].
11. World Health Organization Laboratory. Manual for the Examination of Human Semen and Sperm-Cervical Mucus Interaction. 4th ed. Cambridge, MA: Cambridge University Press; 1999.
© 2012 Monduzzi Editoriale | Proceedings Code: 299
Upper age limit for access to ART: never-ending discussions?
H. Konecna1, T. Kucera2, S. Suda3
1Faculty of Health and Social Studies, University of South Bohemia, Ceske Budejovice, Czech Republic; 2Faculty of Science, Charles University, Prague, Czech Republic; 3Pedagogical Faculty, University of South Bohemia, Ceske Budejovice, Czech Republic
SUMMARYThe Czech Republic (CR) is preparing a new act to regulate ART. The goal of the
study was to fi nd a generally acceptable limit refl ecting specifi cities of the country. Design: Qualitative analysis of discussions with laymen, speeches of the Parlia-ment members, expert texts. Results: The main arguments of laymen and experts concerned the inviolability of the person’s right to make decisions about his or her life and on the other hand the interests of the child brought into the world by an elderly mother. Nobody argued the protection of the oocyte donors. No respondent considered a limit for men. Conclusions: Our research team argues for an upper age limit of 45 years for a woman.
INTRODUCTIONThe CR is preparing a new act to regulate ART. The new bill differs from the
preceding Act particularly by introduction of upper age limit for the woman for ac-cess to ART; the old Act did not restrict the access; there was only a recommenda-tion of the ethical commission of the Czech expert association not to treat women over 47 years. The fi rst bill of the new Act contained the age limit of 55 years. It is known and generally recognized that IVF in the case of women over 42 years has low chance of success [1],[2] and that donor oocytes must be used. The CR does not have great problems to acquire either sperm or oocyte donors. The goal of the study was to ascertain whether age limits are needed, and if yes, then to fi nd an interdisciplinary-acceptable limit refl ecting the Czech situation.
MATERIAL AND METHODSQualitative analysis of discussions with statements of leaders of foreign patient
46
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
organizations from 8 European countries, interviews with 11 MPs and their speech-es with comments to the draft act at the Parliament sessions, discussions with lay-men (about 100 persons) as well as the research of political and expert texts.
RESULTS AND DISCUSSIONThe Universal Declaration of Human Rights (1948) states: “Men and women of
full age, without any limitation due to race, nationality or religion, have the right to marry and to found a family.” The entry of reproduction technologies is already re-fl ected by the Charter on Sexual and Reproductive Rights (1996): “All persons shall be entitled to protection from and information on any harmful effects of reproductive health care technology on their health and well-being.” as well as by the opinion of the European Society of Human Reproduction and Embryology (ESHRE) [3]. Sub-jects included in the 3rd-party reproduction are: a) person(s) asking for medical help to implement their parent intentions; b) future child; c) gamete donor; d) medical team; e) society.
a) The inviolability of the right to decide about the life of person(s) asking for medical help to implement their parent intentions was the main argument of all dis-cussers not to set age limits or to set them in suffi cient range [4]. The upper age limit was substantiated in this way in the fi rst draft bill too; the Ministry of Health add-ed that its proposal refl ected purely medical aspects. Also most leaders of foreign patient organizations objected to the limits; typical statements went: “We do not like the age limit because they are arbitrarily. We want the clinics, both public and private, to make an individual assessment of each couple's potential to succeed.” It must be added that these were the statements of patient leaders from countries where oocyte donation is forbidden or where there is lack of oocytes. Another argu-ment objecting the limits consisted of the fact that older patients pay for the therapy themselves, so it does not concern anybody else. Is unrestricted access to the thera-py benefi cial to all patients? The discussion concerns the arguments whether older women should be given preferential treatment in waiting lists, or whether younger women should be preferred; whether childless couples should be preferred to the detriment of couples having children already, or whether the patients' origin should be considered (national vs. foreign)[5]. The patients undergoing therapy are in a bad emotional situation; they usually do not look at risks. One of the most diffi cult steps is to terminate the therapy. It is therefore essential to have the feeling that they have done everything they could to succeed; but without a reasonable age limit, the chances are "optically" always open, the suffering has no foreseeable time horizon. High age limit is against the patients’ interests; it does not allow them to be freed by reconciling themselves with their situation, and ART becomes a "never-ending story". Both patient organizations and expert circles start demanding the system to respond in some way [6], [7].
b) The interest of the future child was the main argument for introduction of suf-
47
November 17-20, 2011 Paris, France
fi ciently low age limits; “the child has the right to a mother, not to a grandmother” – the usual formulation of the argument against motherhood at a higher age. This argumentation led also in the parliament discussion to reduce the originally pro-posed age limit from 55 years to 49 years. It was interesting that the discussions did not include considerations of introducing age limit for men. The basic ESHRE document [3] refl ects the Convention on the Rights of the Child when it states: „In natural conception, the intentional parents are responsible for the health and well-being of the child. They should provide reasonable care up to the age when the child reaches adulthood. Moreover, given the fact that they initiate the project by which the child comes into existence, they should be able to handle his or her care without constant support from others.“ The increasing life expectancy, personal maturity, couple stability and fi nancial security of older persons often constitute arguments defending parenthood at a higher age. But are they cogent arguments? Parenthood is an extraordinarily challenging role, both mentally and physically [8],[9]. Although the couple may be in excellent condition when deciding about parenthood, the out-looks for the future are not very optimistic; the health condition of women and men starts worsening markedly at about 45 years of age [10]. Therefore the age differ-ence between the adopted child and the adoptive parent in substitutive family care in the CR is recommended to be 20-40 years. Particularities of age are refl ected also by the discussion on increasing age of retirement or by projects called Genera-tion 50+. Stability of partnership at a higher age is not sure either: „The share of divorced men in higher age has considerably grown; in the age group of 45 – 49 years from 8,7% in the year of 1989 to 12,7% in the year of 2001, and in the age group of fi fty-year old and older men from 8,4% to 13,6% from the total number of men divorced in the relevant calendar years. The trends for women are similar, but the shares are lower” [11].
c) The parenthood of older couples depends on oocyte donors. The bill sets the age of the donor at 18-35 years, i.e. the age when the donor herself often has not fulfi lled her own parenthood plans. The donors undergo the same procedures as the recipients. The procedures are physically and psychically demanding and are not without risks. The discussers including experts in the fi led of assisted reproduction surprisingly did not mention donor as an essential element. Nothing is known about long-term health consequences of oocyte donorship at repeated donor cycles yet. Ethicists generally agree that basic expenses should be compensated to the donors: “Oocyte donors should receive reimbursement for all direct and indirect costs of the procedure and should receive a compensation for the time lost and inconve-nience suffered during the treatment” [12], but nobody knows adequate amount of the compensation. We do not doubt that altruism is a frequent motive of donorship but we are very sceptical as for the signifi cance of this partial motive with regard to other motives of most donors. Our scepticism is supported also by the current British discussion about the amount of compensation of oocyte donors. In some

48
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
countries, oocyte donorship is forbidden. “When the scarcity of oocytes intensifi es (and this will be the case if somatic cell nuclear transfer becomes possible without good alternative treatment), there is a serious risk that respect for ethical principles will dwindle.” [12]. The Convention on Biomedicine states: „Removal of organs or tissue from a living person for transplantation purposes may be carried out solely for the therapeutic benefi t of the recipient and where there is no suitable organ or tissue available from a deceased person and no other alternative therapeutic meth-od of comparable effectiveness”; donorship should be perceived as expression of the deepest human solidarity with a suffering person. What about the origin of de-sire for parenthood? Two main concepts compete here – the biologically oriented concept and the psycho-socially oriented one. In a situation when people postpone parenthood for the time when it is problematic from biological perspective, the bio-logically oriented theories lose force. Motivation for parenthood is a set of a lot of partial motives [13],[14],[15]; a great part of those partial motives can be fulfi lled also in another way. And at a higher age, not all parenthood motives can be fulfi lled any more even by assisted reproduction. Besides, parenthood as a reliable path to happiness is questioned by more and more studies [16],[17],[18]. We conclude the analysis of the donors’ situation ESHRE [12] by a quotation: “... the principle of proportionality, which requires that the risks for research subjects are in proportion to the expected benefi ts for science and society.”
d) When the discussions about the age limits for access to ART mentioned the medical team of the CARs, it was related to their fi nancial profi t. The physicians sometimes refuse legal regulation arguing that the body creating the law does not know the practice; they consider their own expert evaluation of a specifi c situation and recommendation of expert associations to be suffi cient. The argument seems reasonable, but its implementation has some weak points: „Firstly, there are seldom sanctions attached to violations of guidelines, making professional guidelines less powerful than statutes. Secondly, the most controversial issues are not medical is-sues and, consequently, the physicians have no special expertise to decide these matters…. Finally, the experience shows clearly that this solution fails... a consid-erable number of practitioners are simply ignoring the guidelines.”[19]. ART dif-fers markedly from other medical specializations: it does not solve current health situation of the patients but their psycho-social future. But the physicians are often not aware or do not admit this task: “The physician carries joint responsibility for the welfare of the child because of his or her causal and intentional contribution to the parental project.”[3]. More and more lawsuits are accusing physicians of inad-equate therapy; is the vision of suits submitted by children of older couples stating that the physician did not suffi ciently consider their interests too unrealistic? But if the parenthood of older parents is socially (by law) designated as common and safe, the physicians get into an extraordinarily diffi cult situation: when they refuse the therapy, they can be prosecuted for not having provided the therapy; they can

49
November 17-20, 2011 Paris, France
defend the refusal very diffi cultly. When they do not refuse the therapy, they can be prosecuted for the consequences of the therapy.
e) Thinking of the impacts on the society was characterized by the statements like “the society will then have to care for the orphans” or “all that is completely outside, I do not want to live to see it.” The draft bill was explained by the ministry as focused only on medical, not on psycho-social aspects, and other experts did not deal with impacts on the society to much either. The Act is an important document, substantially infl uencing the opinion of the society about what is and is not stan-dard, what is and is not common, usual, safe or desirable [20],[21]. We consider it completely improbable that people would view unrestricted age limit or high limit as a reserve for absolutely exceptional situations (in the context of relatively easy access to therapy and good availability of donor oocytes); so from this perspec-tive, the high age limit is confusing and will very probably lead to further increase of number of people postponing parenthood to the highest levels of reproductive age and consequently seeking help of assisted reproduction. The seemingly simple solution - preventive programs focused on informing the young people on biologi-cal limits of fertility - has no effect, according to our experience: parenthood is not postponed due to ignorance of biological limits but - among other things - due to unrealistic visions of success rate, risks and consequences of ART [22]. From this point of view, the ESHRE defi nition of infertility as “a disease of the reproductive system defi ned by the failure to conceive after 12 months of regular unprotected sexual intercourse” completed in common practice by defi nition of fertility as oc-currence of menstruation is maybe confusing too. Why the “take home baby rate” constitutes the criterion of ART success rate then?
CONCLUSIONSThe opinions of our research team on age restriction of access to the therapy by
assisted reproduction (even for paying patients) were changing during the analyses; the age limit was gradually descending. Considering the broad context of the prob-lem, we agreed on a limit of 45 years for a woman. We recommend also completing the defi nition of infertility with the ability to carry a healthy baby to term and to deliver it. The research goes on; we are dealing for example with the man's age for access to the therapy.
Supported by GACR P407/10/0822 and MSM 0021620831
REFERENCES1. CHAMBERS, G.M., HO, M.T., SULLIVAN, E.A. Assisted reproductive technology treatment
costs of a live birth: an age-stratifi ed cost–outcome study of treatment in Australia. MJA 2006; 184 (4): 155-158. 2006.
2. Centers for Disease Control and Prevention (2007). ART – Success rates. USA.
50
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
3. ESHRE Task Force on Ethics and Law 13: the welfare of the child in medically assisted reproduc-tion (2007). Hum. Reprod. (2007) 22 (10): 2585-2588. 2007.
4. BOIVIN, J., PENNINGS, G. Parenthood should be regarded as a right. Arch Dis Child 2005; 90:784-785. 2005.
5. PENNINGS, G. Distributive Justice in the Allocatin of Donor Oocytes. Journal of Assisted Repro-duction and Genetics, Vol. 18, No. 2, 2001, 56-63. 2001.
6. DILL, S. (2010). Facing failure: fi nding new strenght. IFFS Munich 2010.7. GURGAN, T. What to do after IVF/ICSI failure. IFFS Munich 2010. 8. KONECNA,H., BUBLEOVA,V., JANKU, V. Reprodukční zdraví 2009. Praha 2009.9. FEENEY, J.A., HOHAUS, L., NOLLER, P., ALEXANDER, R.P. Becoming Parents. Exploring the
Bonds between Mothers, Fathers and Their Infants. CUP 2001.10. Ročenka Všeobecné zdravotní pojišťovny za rok 2010. 11. http://www.rozveduse.cz/news/rozvody-podle-veku-rozvadenych-manzelu-/12. ESHRE Task Force on Ethics and Law 12: Oocyte donation for non-reproductive purposes. Human
Reproduction Vol.22, No.5 pp. 1210–1213, 2007. 13. KONECNA, H. Motivy k rodičovství. Československá psychologie 54, 2, 126-137. 2010.14. SILKE, D., NTEBALENG, M., JOHANNES, M., VAN DER SPUY ZEPHNE. Motives for
parenthood among couples attending a level 3 infertility clinic in the public health sector in South Africa. Hum. Reprod. (2008) 23 (2): 352-357. 2007.
15. STÖBEL-RICHTER,Y., BEUTEL, M. E., FINCK,C., BRÄHLER,E. The “wish to have a child“, childlessness and infertility in Germany. Hum. Reprod. (2005) 20(10):2850–2857. 2005.
16. McLANAHAN,S., ADAMS, J. The effects of children on adults’ psychological well-being. Social Forces, 68(1), 124-146. 1989.
17. TWENGE, J.M., CAMPBELL, W.K., FOSTER, C.A. Parenthood and marital Satisfaction. Journal of Marriage and Family, 65(3), 574-583. 2003.
18. EVENSON, RJ, SIMON, RW. Clarifying the Relationship Between Parenthood and Depression. Journal of Health and Social Behavior, 2005 (46) no. 4, 341-358. 2005.
19. PENNINGS, G. International evolution of legislation and guidelines in medically assisted reproduction. Repr. BioMedicine Online (2009) 18 (suppl. 2): 15-18. 2009.
20. HACKING, I. (1995). The looping effects of human kinds. In: Sperber, D., Premarck, D., Premarck, A., J. (eds.): Causal cognition – a multidisciplinary debate. Chapter 12, pp. 351 – 383. Cambridge: Harvard University. 1995.
21. SULLEROT, E. Krize rodiny. Praha: Karolinum. 1998.22. HEWLETT, S.A. Creating a Life. Professional Women and the Quest for Children. New York: Talk
Miramax Books. 2002.
© 2012 Monduzzi Editoriale | Proceedings Code: 667
Classifi cation of utero-vaginal malformations
L.V. Adamyan, Z.N. Makiyan, A.A. StepanianFederal State Institution “Scientifi c Center of Obstetrics, Gynecology and Perinatology”, Moscow, Russia
SUMMARYWe had a systematic literature review of contemporary female genital anomaly
classifi cations, that found in PubMed, Medline [1-7].Since 1992 to 2011 we had operated 1492 patients with various utero-vaginal
malformations: (312) patients with utero-vaginal aplasia (MRKH syndrome), cervi-co-vaginal atresia (64), partial vaginal aplasia (230), uterus duplex (246), bicornu-ate uterus (210) and unicornuate uterus (145), septate uterus (285). According of our opinion, the optimal surgical treatment depends on clinical data and exactly diagnosed anatomical defects. We proposed an update clinico-morphological classi-fi cation, allows to optimize surgical correction of uterovaginal malformations. This classifi cation consist seven classes, and 23 basic groups of uetro-vaginal malforma-tions, fallopian tubes defects.
INTRODUCTIONAn ideal classifi cation system should be based on clinical data, aetiopathogen-
esis, morphological defects and will suggest the appropriate surgical and therapeutic strategy [3, 5, 7].
MATERIALS AND METHODSDuring the period 1992-2011 we had operated 1492 female patients with various
uterovaginal anomalies, patients aged 17 to 42 years.Clinical investigations included the following general clinical diagnostic labo-
ratory tests, ultrasound examination, laparoscopy, hysteroscopy, and 124 patients were examined with magnetic resonance imaging.
52
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
RESULTSSurgical correction of uterine and vaginal malformations depends of: patient`s
complaints, clinical manifestations (infertility, miscarriage, abdominal pain, men-strual disfunction, sexual problem, etc.) and genital organ`s anatomy.
The differential diagnosis of utero-vaginal malformations morphology had evalu-ated with ultrasound examination, MRI, laparoscopy, hysteroscopy and consecutive histological examination of the excised material (in cases of rudimentary uterine horn, rudimentary uterus removed).
All patients were operated according diagnosed anatomical defects (utero-vaginal malformations) and their complaints.
For 246 patients with utero-vaginal aplasia (MRKH syndrome), performed con-struction of neovagina - laparoscopic assisted peritoneal colpopoesis. After op-eration revealed adequate length of neovagina (8-12 cm) and normal lubrication. During operation we detected 3 variants of persistant mullerian ducts (rudimental uterine horns), with (or without) functional endometrial cavity. In 17,9% (44) cases with abdominal pain, had removed functional rudimental horns.
Surgical treatment of cervicovaginal aplasia depends of there morphological vari-ants. In 23 cases with functional uterus, and aplasia of cervical canal, made the reconstructive operation – utero-vaginal anastomosis. In 41 cases of functional rudi-mental uterus, with complete cervical and vaginal aplasia – performed laparoscopy, hysterectomy; following peritoneal colpopoesis.
All (230) patients with partial vaginal aplasia and hematocolpos, hematometra had operated, performed the vaginoplasty and laparoscopy.
Operative treatment of patients with unicornuate uterus (145) depends of abdomi-nal pain, infertility. Functional rudimentary horn with endometrial cavity removed in 60%(87) cases laparoscopically, other patients had unfunctional horns.
Duplicated uterus had symmetric and asymmetric forms, and 4 variants. Patients with asymmetric duplicated uterus and vagina, with partially aplasia of hemyvagina (asymmetric form), complaints of acute pelvic pain and operated for vaginoplasty, draining of hematocolpos,.
Patients with incomplete intrauterine septum (163) had pregnancy loss in 96,7%; with complete uterine septum (122) had premature delivery in 50% cases before op-eration. Hysteroscopic dissection of uterine septum and adequate treatment appears to gate succecfull pregnancy in 56,8% (162).
Four patients with bicornuate uterus and miscarriage, had laparoscopic Strassman`s metroplasty, 66 patients - underwent laparoscopic correction of other infertile factors (adhesions, synechia, endometriosis, policistic ovary) and 140 - had nonoperative treatment.
The systematic analysis of all clinical cases, allows to upgrade morphological classifi cation of uterovaginal malformations:
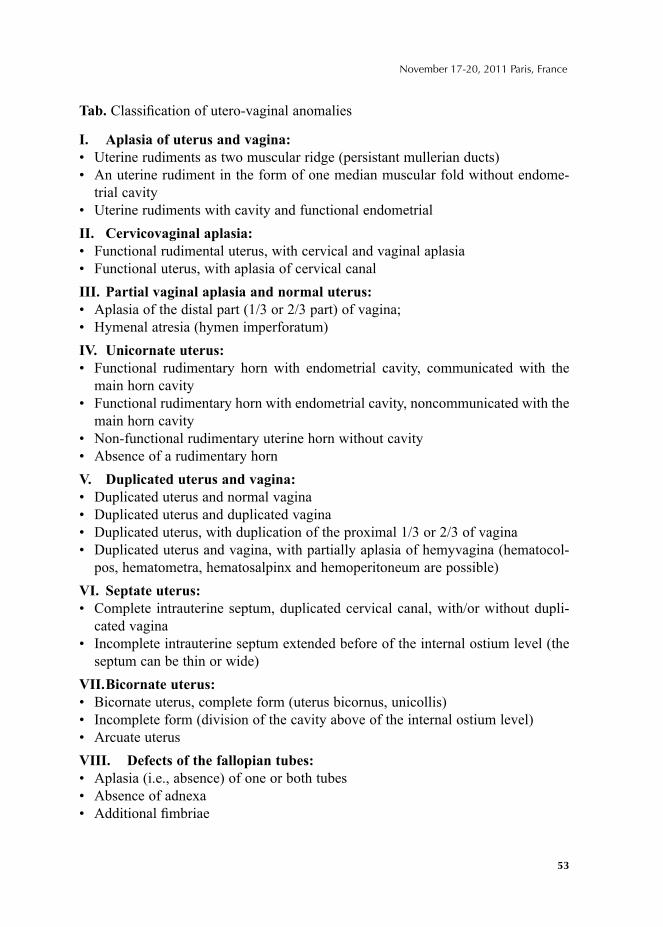
53
November 17-20, 2011 Paris, France
Tab. Classifi cation of utero-vaginal anomalies
I. Aplasia of uterus and vagina:• Uterine rudiments as two muscular ridge (persistant mullerian ducts)• An uterine rudiment in the form of one median muscular fold without endome-
trial cavity• Uterine rudiments with cavity and functional endometrialII. Cervicovaginal aplasia:• Functional rudimental uterus, with cervical and vaginal aplasia• Functional uterus, with aplasia of cervical canalIII. Partial vaginal aplasia and normal uterus: • Aplasia of the distal part (1/3 or 2/3 part) of vagina; • Hymenal atresia (hymen imperforatum)IV. Unicornate uterus:• Functional rudimentary horn with endometrial cavity, communicated with the
main horn cavity• Functional rudimentary horn with endometrial cavity, noncommunicated with the
main horn cavity• Non-functional rudimentary uterine horn without cavity• Absence of a rudimentary hornV. Duplicated uterus and vagina:• Duplicated uterus and normal vagina • Duplicated uterus and duplicated vagina • Duplicated uterus, with duplication of the proximal 1/3 or 2/3 of vagina • Duplicated uterus and vagina, with partially aplasia of hemyvagina (hematocol-
pos, hematometra, hematosalpinx and hemoperitoneum are possible)VI. Septate uterus: • Complete intrauterine septum, duplicated cervical canal, with/or without dupli-
cated vagina • Incomplete intrauterine septum extended before of the internal ostium level (the
septum can be thin or wide)VII. Bicornate uterus:• Bicornate uterus, complete form (uterus bicornus, unicollis)• Incomplete form (division of the cavity above of the internal ostium level)• Arcuate uterusVIII. Defects of the fallopian tubes:• Aplasia (i.e., absence) of one or both tubes• Absence of adnexa• Additional fi mbriae

54
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
CONCLUSIONClinico-morphological classifi cation of utero-vaginal malformations necessary
for correct precisive diagnosis of anatomical defects, allows to perform optimal surgical correction and improves reproductive results.
REFERENCES1. Acién P, Acién MI. The history of female genital tract malformation classifi cations and proposal of
an updated system.// Hum Reprod Update. 2011 Jul 4. [Epub ahead of print] PMID: 21727142.2. Acién P, Acién MI, Sánchez-Ferrer ML. Complex malformations of the female genital tract. New
types and revision of classifi cation.// Hum Reprod 2004; 10:2377-2384.3. Adamyan L.V., Kurilo L.F., Okulov A.B., Bogdanova E.A., Stepanian A.A., Glybina T.M., Makiyan
Z.N. Systematization of female genital malformations.// Probl. of Repr., Moscow, Russia, 2010, v.3, pp.10-14.
4. Peter A. Lee, MD, PhDa,b, Christopher P. Houk, MDc, S. Faisal Ahmed. Consensus Statement on Management of Intersex Disorders.// Pediatrics Vol. 118 No. 2 August 2006, pp. e488-e500.
5. Buttram V.C., Gibbons W.E. (1979) Mullerian anomalies: a proposed classifi cation (an analysis of 144 cases).// Fertil Steril 32, 40–46.
6. Nistal M., García-Fernández E., Mariño-Enríquez A., Serrano A., Regadera J., González-Peramato P. Usefulness of gonadal biopsy in the diagnosis of sexual developmental disorders.// Actas Urol Esp. 2007; 31(9):1056-1075.
7. Sánchez-Ferrer ML, Acién MI, Sánchez del Campo F, Mayol-Belda MJ, Acién P. Experimental con-tributions to the study of the embryology of the vagina.// Hum Reprod 2006; 21:1623-1628.
© 2012 Monduzzi Editoriale | Proceedings Code: 668
Female genital organ's malformations: new hypothesis of embryo-morphogenesis
Z. MakiyanFederal State University Scientifi c Center of Obstetrics, Gynecology and Perynathology, Moscow, Russia
SUMMARYLiterature review about 126 full articles and original monographies, revealed a
lot of publication about Mullerian theory controversies, and induced authors create new embryological hypothesis [2, 3, 4, 5, 6, 7, 8, 9, 11, 13].
Clinico-morphological analysis of various female genital malformations compar-atively with embryological datas allowed to formulate new hypothesis [10].
INTRODUCTIONThe famous German scientifi c professor Johannes Peter Muller suggested embry-
ological theory about utero-vaginal morphogenesis 150 year ago, based on investi-gation of human emryos with simple light microscopy devices. According original Mullerian theory: “Fallopian tubes, Uterus and Vagina formes by fusion of pair paramesonephral (Mullerian) ducts, so Vestibulum vaginae derivates from Sinus Urogenitalis [1]. Mesonephral ducts completely reduced in female embryos, but derivates ductus seminipherus in male embryos”.
Contemporary “Mullerian theory” seams to be different: Fallopian tubes, uterus and proximal 1/3 of Vagina formes by paramesonephral (Mullerian) ducts, and distal 2/3 of vagina. Vestibulum Vagina derivates from urogenital sinus [12]. Perhaps it coused, of the contemporary embryological investigations made on laboratory rats and mouses.
MATERIALS AND METHODSClinical examination and surgical correction of 452 patients with various utero-
vaginal malformations (345 patients) and disorders of sex development (107) per-formed since 1998 to 2011: MRKH syndrome – 23; Duplicated Uterus and Vagina – 36; Duplicated Uterus and Vagina with partial aplasia of hemyvagina – 30; Bicor-nuate Uterus – 48; Unicornuate Uterus – 22; Vaginal aplasia – 39; Cervico-vaginal
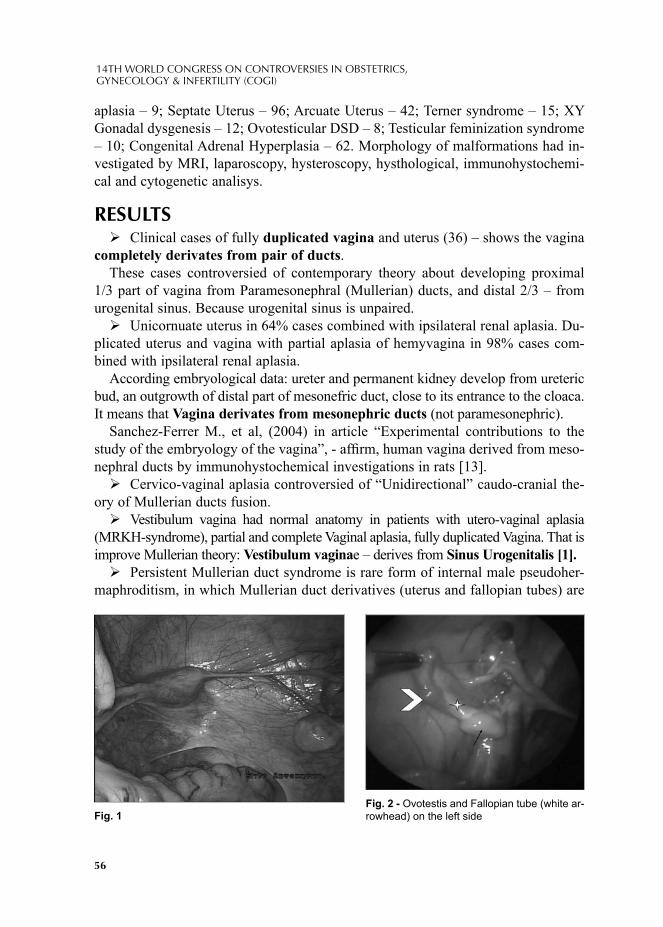
56
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
aplasia – 9; Septate Uterus – 96; Arcuate Uterus – 42; Terner syndrome – 15; XY Gonadal dysgenesis – 12; Ovotesticular DSD – 8; Testicular feminization syndrome – 10; Congenital Adrenal Hyperplasia – 62. Morphology of malformations had in-vestigated by MRI, laparoscopy, hysteroscopy, hysthological, immunohystochemi-cal and cytogenetic analisys.
RESULTSClinical cases of fully duplicated vagina and uterus (36) – shows the vagina
completely derivates from pair of ducts. These cases controversied of contemporary theory about developing proximal
1/3 part of vagina from Paramesonephral (Mullerian) ducts, and distal 2/3 – from urogenital sinus. Because urogenital sinus is unpaired.Unicornuate uterus in 64% cases combined with ipsilateral renal aplasia. Du-
plicated uterus and vagina with partial aplasia of hemyvagina in 98% cases com-bined with ipsilateral renal aplasia.
According embryological data: ureter and permanent kidney develop from ureteric bud, an outgrowth of distal part of mesonefric duct, close to its entrance to the cloaca. It means that Vagina derivates from mesonephric ducts (not paramesonephric).
Sanchez-Ferrer M., et al, (2004) in article “Experimental contributions to the study of the embryology of the vagina”, - affi rm, human vagina derived from meso-nephral ducts by immunohystochemical investigations in rats [13].Cervico-vaginal aplasia controversied of “Unidirectional” caudo-cranial the-
ory of Mullerian ducts fusion. Vestibulum vagina had normal anatomy in patients with utero-vaginal aplasia
(MRKH-syndrome), partial and complete Vaginal aplasia, fully duplicated Vagina. That is improve Mullerian theory: Vestibulum vaginae – derives from Sinus Urogenitalis [1].Persistent Mullerian duct syndrome is rare form of internal male pseudoher-
maphroditism, in which Mullerian duct derivatives (uterus and fallopian tubes) are
Fig. 1Fig. 2 - Ovotestis and Fallopian tube (white ar-rowhead) on the left side
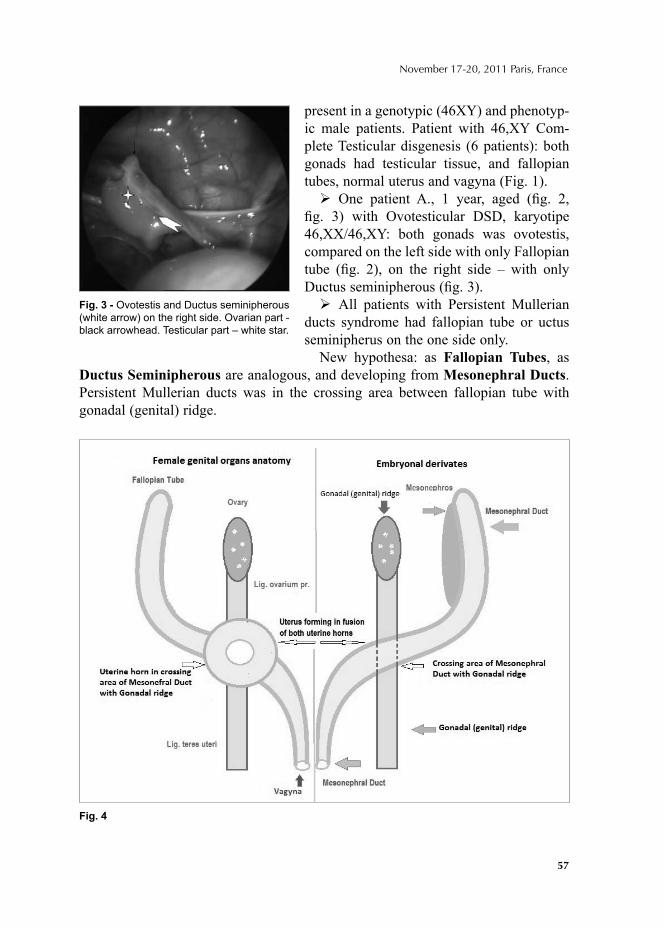
57
November 17-20, 2011 Paris, France
present in a genotypic (46XY) and phenotyp-ic male patients. Patient with 46,XY Com-plete Testicular disgenesis (6 patients): both gonads had testicular tissue, and fallopian tubes, normal uterus and vagyna (Fig. 1). One patient A., 1 year, aged (fi g. 2,
fi g. 3) with Ovotesticular DSD, karyotipe 46,XX/46,XY: both gonads was ovotestis, compared on the left side with only Fallopian tube (fi g. 2), on the right side – with only Ductus seminipherous (fi g. 3). All patients with Persistent Mullerian
ducts syndrome had fallopian tube or uctus seminipherus on the one side only.
New hypothesa: as Fallopian Tubes, as Ductus Seminipherous are analogous, and developing from Mesonephral Ducts. Persistent Mullerian ducts was in the crossing area between fallopian tube with gonadal (genital) ridge.
Fig. 3 - Ovotestis and Ductus seminipherous (white arrow) on the right side. Ovarian part - black arrowhead. Testicular part – white star.
Fig. 4

58
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
CONCLUSIONNew hypothesa (fi g. 4):
• Ovary, ovarian ligamentum proprium and ligamentum teres uteri - derives from Gonadal (genital) ridge.
• Fallopian tubes and Vagina derives from Mesonephral ducts • Uterine horns forms in crossing area of Gonadal (genital) ridge with Mesone-
phral ducts. Normal uterus forms by fusion of both uterine horns together.• Vestibulum Vaginae completely derives from Urogenital Sinus (according orig-
inal Mullerian theory). Comparative data of original Mullerian theory and new hypotesa see in tabl. Tabl.
Mullerian theory.png
REFERENCES1. Müller I.P. Anatomie des Menschen, 1931, Berlin, p. 272-275.2. Müller P.P., Musset R., Netter A. et al. Etat du haut appereil urinaire chez les porteuses de
malformations uterines, Etude de 133 Presse Med 1967; 75:1331–1336.3. Adamyan L.V., Makiyan Z.N. Urogenital anomalies – new look on embryogenesis.// Materials of
International congress “New technology in gynecology”, 2001, p. 329-341, Russia, Moscow. 4. Acien P., Acien M., Sanchez-Ferrer M. Complex malformations of the female genital tract. New
types and revision of classifi cation. Human Reprod 2004; 19:10. 5. Acién P., Susarte F., Romero J., Galán J., Mayol M.J., Quereda F.J., Sánchez-Ferrer M. Complex
genital malformation: ectopic ureter ending in a supposed mesonephric duct in a woman with renal agenesis and ipsilateral blind hemivagina. Eur J Obstet Gynecol Reprod Biol. 2004; In press.
6. Chang A.S., Siegel C.L., Moley K.H., Ratts V.S., Odem R.R. Septate uterus with cervical duplication and longitudinal vaginal seprum: a report of fi ve new cases. Fertil Steril 2004; 81:4:1133-1136.
7. Engmann L., Schmidt N.J., Benadiva C. An anusual variation of a unicornuate uterus with normal eternal uterine morphology. Fertil Steril 2004:82:4:950-953.
8. Fatum M., Rojansky N., Shushan A. Septate uterus with cervical duplication: rethinking the development of mullerian anomalies. Gynecol Obstet Invest 2003; 55:3:186-188.
9. Giraldo J.L., Habana A., Duleba A.J., Dokras A. Septate uterus associated with cervical duplication and vaginal septum. J Am Assoc Gynecol Laparosc 2000; 7:2:277-279.
10. Makiyan Z.N. “Female genital anomaly: systematization and surgical treatment”, doctor of medicine dissertation, 2011, Moscow, Russia.
11. Shapiro E., Huang H., McFadden D.E., Mash R.J., Eliza N.G., Lepor H. The prostatic utricle is not a Mullerian duct remnant: immunonistochemical evidence for a distinct urogenital sinus origin. J Urology 2004; 172:4: Part 2:Suppl.:1753-1756.
12. Sadler T.W. “Langman`s Medical Embryology”. Williams&Wilkins USA, 2000; p. 215.13. Sanchez-Ferrer M., Acien P., Sanchez Del Campo, Mayol-Belda M.J., Acien M. Experimental
contributions to the study of the embryology of the vagina. Human Reprod Embryol 2006; 21:6.
© 2012 Monduzzi Editoriale | Proceedings Code: 523
Association of expanded Natural Killer cells subsets in women with recurrent gestational failure
R. Ramos-Medina1*, Á. García-Segovia2*, M. Tejera-Alhambra1, Á. Aguarón3, B. Alonso1, M. Rodríguez-Mahou1, J. Gil 1, J. A. León3, P. Caballero2, S. Sánchez-Ramón1
*RRM and AGS have equally contributed to this workDepartments of Clinical Immunology1 and Gyneco logy3, Hospital General Universitario Gregorio Marañón, Madrid, Spain; Clinica Tambre2, Madrid, Spain
SUMMARYBlood expansion of Natural Killer (NK) cells (CD3- CD56+/CD16+) has been re-
ported in women with recurrent miscarriages (RM) and implantation failures (IF) compared to fertile women. NK cells play a key role in embryo implantation and pregnancy success, whereas NK expansions are involved in the pathophysiology of recurrent gestational failure (RGF).
We propose to study the association of circulating %NK cells in women with RPL. Our results show that NK cells did not vary across the menstrual cycle. NK were signifi cantly higher in women with RGF (p=0.001) than in controls. Using Receiver Operating Characteristic (ROC) curves, the cut-off value for blood NK cells was 12% with 34% sensitivity and 76% specifi city for RM and IF. Women with NK>12% presente more frequently pregnancy losses (p< 0.0001) than those with ≤12% NK cells. Multivariate analysis disclosed that NK is an independent risk factor for RGF. A cut-off of 12% baseline NK defi nes a subgroup of RGF women of putative immune alterations.
INTRODUCTIONSpontaneous pregnancy loss is a surprisingly common occurrence. Whereas ap-
proximately 15% of all clinically recognized pregnancies result in spontaneous loss, there are many more pregnancies that fail prior to being clinically recognized. Only 30% of all conceptions result in a live birth (1).This clinical problem affecting up to 10% of couples in occidental countries. Recurrent spontaneous abortion (RSA),
60
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
defi ned by three or more consecutive spontaneous abortions, which has numerous causes and clinical presentations and may occur during any stage of pregnancy, have been frequently explained with an immunological pathomechanism (2). At present, there exist a small number of etiologies for recurrent gestational failure (RGF). These include parental chromosomal abnormalities, anatomic factors, autoimmune diseases, endocrine disorders, infections, etc. After evaluation for these causes, ap-proximately half of all cases remain unexplained (1). There are two known inde-pendent risk factors for RGF: the age of the mother and the number of previous pregnancy losses (3). However, there is no surrogate marker that could help to de-fi ne those women at risk of pregnancy loss in the next gestation. Thus, the search of biological predictive markers is critical. Natural killer (NK) cells constitute the predominant leukocyte population in uterine mucosa from embryo implantation and considerable effort has been made to investigate the phenotype and functions of NK cells at implantation and during pregnancy. Dysregulation of NK cells has been associated with reproductive pathologies, such as recurrent miscarriages (RM), in-fertility, and pre-eclampsia. In women with these conditions, NK cell parameters, either in absolute numbers or in proportion (%), subsets, functional activity such as cytotoxicity or secretory cytokine profi le, receptor or gene expression, have been extensively investigated in peripheral, endometrial or decidual NK cells (4).
MATERIALS AND METHODSStudy population
Women with a history of repeated implantation failure (IF) (n=110) and recurrent miscarriage (RM) (n=84) who were consecutively studied at the Clinical Immunol-ogy Unit at Hospital General Universitario Gregorio Marañón and Clinica Tambre comprise the study group. Normal fertile women (n=55) here included as controls (Table 1). All medical charts were reviewed prospectively by the same person on the
Study Group Control Group
(n=55) RM (n=84) RIF (n=110)
P value*
Age (years) 30.14±6.2 35.92±3.62 37.60±3.36 <0.0001
Nº of Fetal Losses 0 3.41±1.46 2.85±1.78 -
Nº of IVF 0 0 5.06±2.57 -
%NK 9.55±4.46 12.76±5.34 12.91±6.32 0.001
%NKT 5.09±2.70 5.53±4.54 4.23±3.22 NS
*Significance between control and study group. NS statistically not significant
Tab. 1 - Age, infertility history and immunological variables of women with recurrent miscarriage (RM), recurrent implantation failure and control groups.*Signifi cance between control and study group. NS sta-tistically not signifi cant.

61
November 17-20, 2011 Paris, France
basis of clinical manifestations, obstetrical exams, immunologic markers, and treat-ments. Gestational age was determined by combination of prenatal ultrasonography, physical examination of uterine height and menstrual history.
Quantifi cation of peripheral NK cells subsetsWhole blood samples (100 μl and 1x106 cells respectively) were labeled with
fl uorescence-conjugated (FITC) anti-human CD69 mAb (BD Biosciences), PE an-ti-human CD16mAb (BD Biosciences), PerCP anti-human CD3mAb (BD Biosci-ences) and APC anti-human CD56 (BD Biosciences), for the surface staining during 20 minutes at room temperature (RT) in dark. In the next step, red blood cells were lysed by the addition of 2 mL of lysing solution (FACSTM-Lysing Solution) (Becton Dickinson), incubated for 15 minutes in dark, and then removed and washed with 2 mL phosphate-buffered saline (PBS). In the last step, a four-color analysis was car-ried out using FACScalibur fl ow cytometer (Becton Dickinson), using a CellQuest research and FlowJo softwares.
Statistical analysis Proportions were compared using the 2 test or Fisher exact test for expected
values below 5. Quantitative variables were expressed as means±standard error of the mean and compared by using the Student t test ANOVA or non-parametric Wil-coxon rank sum test. Receiver operating characteristic (ROC) curves were used to select the optimal cut-off values of signifi cant variables for predicting the develop-ment of pregnancy loss based on the optimum sensitivity and specifi city. Data were analyzed with SPSS software (Chicago, Illinois). A p value of 0.05 was considered statistically signifi cant.
RESULTS AND CONCLUSIONSIn our cross-sectional study of NK proportion; in RGF patients and controls, we
found that the %NK cells were signifi cantly higher in women with RM and/or IF (p=0.001) than in the control group (Table 1 and Figure 1). Higher proportions of women in the RGF group (p=0.002) had NK cells >12% than the control group. Using ROC curves, statistically chosen cut-off value for NK cells in our population was 12% of total lymphocytes, with sensitivity for the occurrence of pregnancy loss of 34%, and specifi city: 76%. Using this level, a greater numbers of subjects with NK>12% presented pregnancy loss (p<0.0001) than those with ≤ 12% NK cells.
By Cox multiple regression analysis, NK cells were independently associated with increased risk of pregnancy loss after adjustment for age. Patients with NK cells >12% had 2.7-fold (hazard ratio, HR 95% CI: 1.38-5.48) higher risk for hav-ing pregnancy loss.
We show for the fi rst time that %NK is an independent risk factor for RGF. We concluded that a cut-off of 12% baseline NK cells defi nes a subgroup of RGF
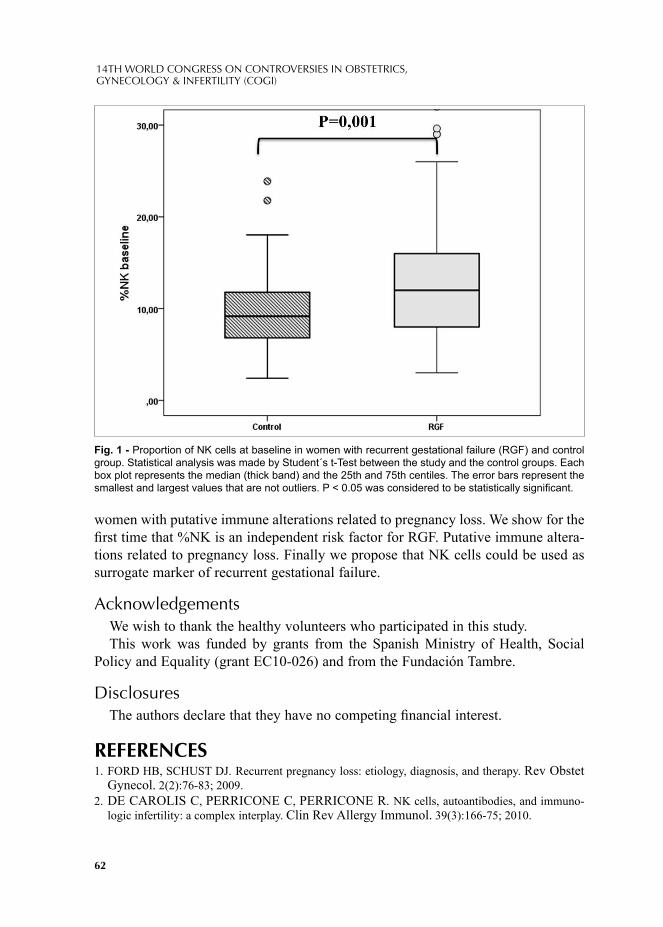
62
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
women with putative immune alterations related to pregnancy loss. We show for the fi rst time that %NK is an independent risk factor for RGF. Putative immune altera-tions related to pregnancy loss. Finally we propose that NK cells could be used as surrogate marker of recurrent gestational failure.
AcknowledgementsWe wish to thank the healthy volunteers who participated in this study.This work was funded by grants from the Spanish Ministry of Health, Social
Policy and Equality (grant EC10-026) and from the Fundación Tambre.
DisclosuresThe authors declare that they have no competing fi nancial interest.
REFERENCES 1. FORD HB, SCHUST DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet
Gynecol. 2(2):76-83; 2009.2. DE CAROLIS C, PERRICONE C, PERRICONE R. NK cells, autoantibodies, and immuno-
logic infertility: a complex interplay. Clin Rev Allergy Immunol. 39(3):166-75; 2010.
Fig. 1 - Proportion of NK cells at baseline in women with recurrent gestational failure (RGF) and control group. Statistical analysis was made by Student´s t-Test between the study and the control groups. Each box plot represents the median (thick band) and the 25th and 75th centiles. The error bars represent the smallest and largest values that are not outliers. P < 0.05 was considered to be statistically signifi cant.
63
November 17-20, 2011 Paris, France
3. Professor L REGAN, Miss M BACKOS, and DR R RAI. The Investigation and Treatment of Couples with Recurrent First-trimester and Second-trimester Miscarriage. Green-top Guideline No. 17Royal College of Obstetricians and Gynaecologists. April 2011.
4. KWAK-KIM J, GILMAN-SACHS A. Clinical implication of natural killer cells and reproduc-tion. Am J Reprod Immunol. 59(5):388-400; 2008.

© 2012 Monduzzi Editoriale | Proceedings Code: 583
The effect of bromocriptine and cyclodynon on the clinical symptoms and prolactin levels in women of reproductive age with hyperprolactinemia
L. Suturina1,2, L. Kolesnikova1, L. Popova2
1Scientifi c Centre of the Family Health and Human Reproduction Problems, Siberian Branch, Russian Academy of Medical Sciences, Irkutsk, Russia; 2Irkutsk State Medical Academy of Postgraduate Education, Irkutsk, Russia
SUMMARYThis article presents the fi ndings of a three month prospective open-label con-
trolled trial comparing the effi cacy of bromocriptine (2,5 mg twice daily) (group 1, n=24) with the cyclodynon (40 mg 1 once daily) (group 2, n=24) effi cacy in 48 women of reproductive age who have non-neoplastic hyperprolactinemia. As a result of treatment, in both groups of women there was signifi cant decrease in se-rum prolactin concentration compared with the baseline values. In addition to this a comparable decrease in the frequency of psycho-emotional and menstrual disorders was observed. In the cyclodynon group we registered higher effi cacy in the manage-ment of mastalgia and less frequent adverse effects.
INTRODUCTIONHyperprolactinemia is one of the increasingly common problems of gyneco-
logical endocrinology. It is found in 15 - 30% of women with secondary amen-orrhea and oligomenorrhea. Besides, hyperprolactinaemia is present in 30-70% of female patients with galactorrhea and/or infertility. Dopamine receptor agonists (eg, bromocriptine, quinagolide, cabergoline) are the main agents used to manage pathological hyperprolactinemia, and their effi cacy has been thoroughly studied. For example, prolactin decreasing is achieved in 60-100% of female patients used dopamine agonists, and normalization of menstrual cycles - in 70-100%. Ovula-tory function was restored in 52-80% of hyperprolactinemic women, followed by pregnancy in 80-91% of patients. On the other hand, use of one of the fi rst genera-
66
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
tion dopamine agonists—bromocriptine, a semisynthetic ergot alkaloid derivative, which is the "gold standard" of treatment,-- is also associated with a series of side effects (up to 65%) that are the reason for discontinuation of treatment in 5-10% of female patients [3,5,6].
Data from previous studies show that, as a rule, there is a lower incidence of ad-verse reactions in the use of phytotherapeutics, than in the use of pharmaceuticals. It is known that the extract of Vitex agnus-castus, also called Vitex, Chasteberry, or Monk's Pepper, has dopaminergic properties. Clinical effi cacy of a Vitex agnus castus-based phytotherapeutic agent (Cyclodynon®) in women with non-neoplastic hyperprolactinemia, premenstrual syndrome, and mastopathy has been shown in a number of uncontrolled trials [1, 4]. However, there is insuffi cient data on the com-parative effectiveness of phytotherapeutical agents and synthetic dopamine agonists in women with hyperprolactinemia [2].
The objective of the study was to compare the effects of bromocriptine and Vi-tex agnus castus-based phytotherapeutic agent (Cyclodynon®) on prolactin secretion and clinical symptoms in women of reproductive age with non-neoplastic hyperp-rolactinemia.
MATERIAL AND METHODSThe study involved a total of 48 female patients of reproductive age with non-
neoplastic hyperprolactinemia. The exclusion criteria were as follows: a pituitary micro and macroadenoma, thyroid dysfunction, pregnancy, lactation, obesity and use of medicines that effect prolactin levels within three months prior to this trial. To achieve the objective women were assigned to two treatment groups: one group received Bromocriptine (Gedeon Richter, Hungary) (2.5 mg twice daily) (group 1, n=24), the other group - Cyclodynon (Bionorica AG, Germany) (40 mg once daily) (group 2, n = 24) for 3 months. The patients of both groups were comparable in the incidence and the structure of the causes of primary and secondary infertility, menstrual disorders, galactorrhea, age (26.6 ± 3.7 years in group 1 and 26.3 ± 2.9 years in Group 2, р > 0.05), body mass index (21.7 ± 3.0 and 22.6 ± 3.9 kg/mg, respectively, р > 0.05) and the severity of hyperprolactinemia (782 ± 55 and 600 ± 55 mU/ml, respectively, р > 0.05, while the reference range was 72—480 mU/ml).
A questionnaire survey, analysis of medical documentation, and overall clinical and gynecological examination of female patients were carried out in both groups. Instrumental methods included pelvic ultrasound scan performed by the Aloka-650 ultrasound scanner, and thyroid and breast ultrasound scans. All women underwent either computed tomography or magnetic resonance imaging of the pituitary gland and nearby area. Blood samples for hormonal testing were collected in the morning, between 8-9 a.m., on the 5- 9th days of the menstrual cycle or if there was a delay of menstruation, at any time. The concentrations of PRL (prolactin) were measured by
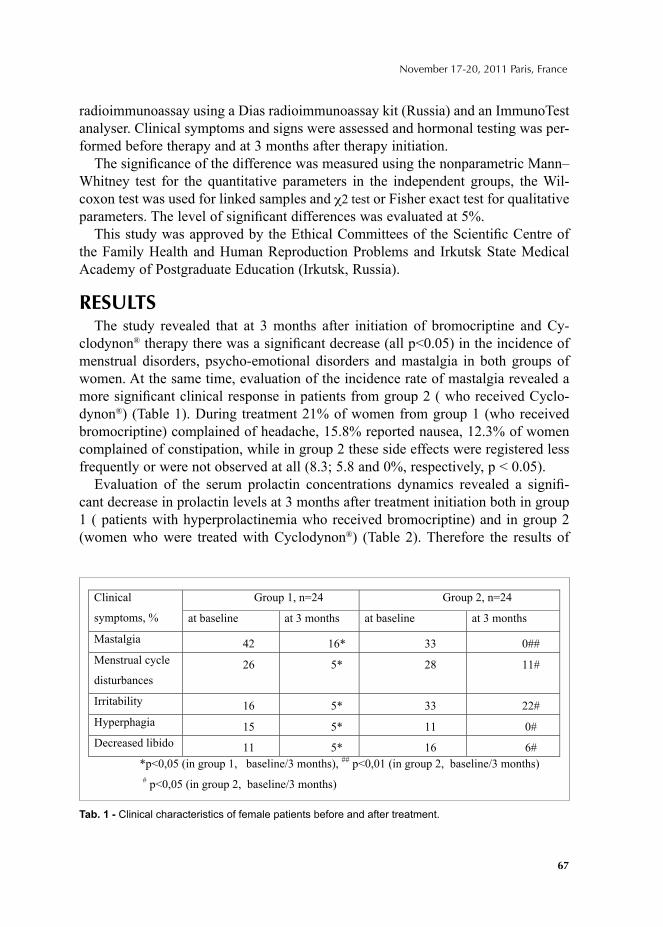
67
November 17-20, 2011 Paris, France
radioimmunoassay using a Dias radioimmunoassay kit (Russia) and an ImmunoTest analyser. Clinical symptoms and signs were assessed and hormonal testing was per-formed before therapy and at 3 months after therapy initiation.
The signifi cance of the difference was measured using the nonparametric Mann–Whitney test for the quantitative parameters in the independent groups, the Wil-coxon test was used for linked samples and χ2 test or Fisher exact test for qualitative parameters. The level of signifi cant differences was evaluated at 5%.
This study was approved by the Ethical Committees of the Scientifi c Centre of the Family Health and Human Reproduction Problems and Irkutsk State Medical Academy of Postgraduate Education (Irkutsk, Russia).
RESULTSThe study revealed that at 3 months after initiation of bromocriptine and Cy-
clodynon® therapy there was a signifi cant decrease (all р<0.05) in the incidence of menstrual disorders, psycho-emotional disorders and mastalgia in both groups of women. At the same time, evaluation of the incidence rate of mastalgia revealed a more signifi cant clinical response in patients from group 2 ( who received Cyclo-dynon®) (Table 1). During treatment 21% of women from group 1 (who received bromocriptine) complained of headache, 15.8% reported nausea, 12.3% of women complained of constipation, while in group 2 these side effects were registered less frequently or were not observed at all (8.3; 5.8 and 0%, respectively, р < 0.05).
Evaluation of the serum prolactin concentrations dynamics revealed a signifi -cant decrease in prolactin levels at 3 months after treatment initiation both in group 1 ( patients with hyperprolactinemia who received bromocriptine) and in group 2 (women who were treated with Cyclodynon®) (Table 2). Therefore the results of
Group 1, n=24 Group 2, n=24 Clinical
symptoms, % at baseline at 3 months at baseline at 3 months
Mastalgia 42 16* 33 0##
Menstrual cycle
disturbances
26 5* 28 11#
Irritability 16 5* 33 22#
Hyperphagia 15 5* 11 0#
Decreased libido 11 5* 16 6#
*p 0,05 (in group 1, baseline/3 months), ##
p 0,01 (in group 2, baseline/3 months)
# p 0,05 (in group 2, baseline/3 months)
Tab. 1 - Clinical characteristics of female patients before and after treatment.
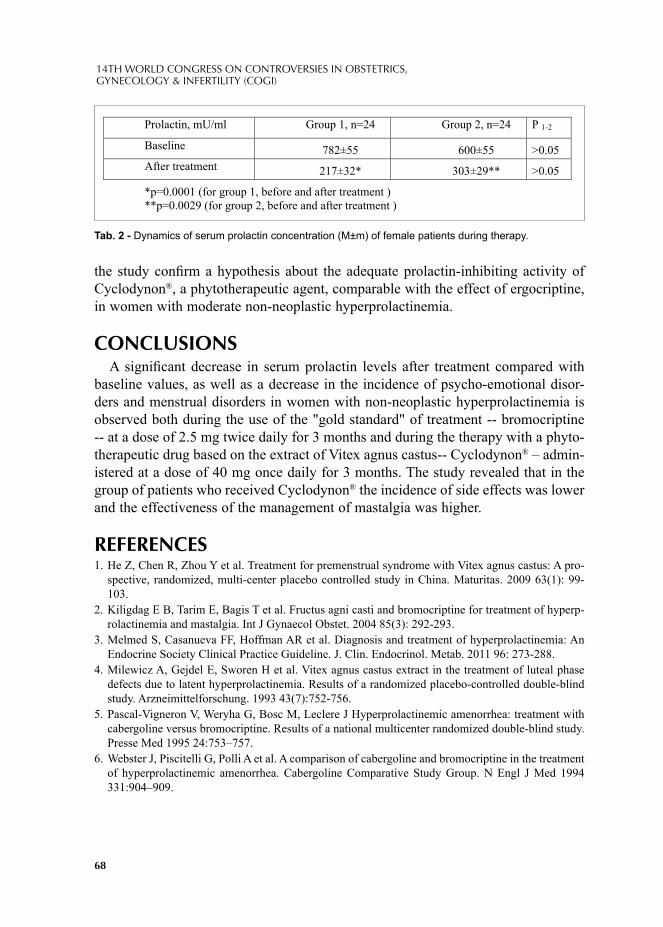
68
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
the study confi rm a hypothesis about the adequate prolactin-inhibiting activity of Cyclodynon®, a phytotherapeutic agent, comparable with the effect of ergocriptine, in women with moderate non-neoplastic hyperprolactinemia.
CONCLUSIONSA signifi cant decrease in serum prolactin levels after treatment compared with
baseline values, as well as a decrease in the incidence of psycho-emotional disor-ders and menstrual disorders in women with non-neoplastic hyperprolactinemia is observed both during the use of the "gold standard" of treatment -- bromocriptine -- at a dose of 2.5 mg twice daily for 3 months and during the therapy with a phyto-therapeutic drug based on the extract of Vitex agnus castus-- Cyclodynon® – admin-istered at a dose of 40 mg once daily for 3 months. The study revealed that in the group of patients who received Cyclodynon® the incidence of side effects was lower and the effectiveness of the management of mastalgia was higher.
REFERENCES 1. He Z, Chen R, Zhou Y et al. Treatment for premenstrual syndrome with Vitex agnus castus: A pro-
spective, randomized, multi-center placebo controlled study in China. Maturitas. 2009 63(1): 99-103.
2. Kiligdag E B, Tarim E, Bagis T et al. Fructus agni casti and bromocriptine for treatment of hyperp-rolactinemia and mastalgia. Int J Gynaecol Obstet. 2004 85(3): 292-293.
3. Melmed S, Casanueva FF, Hoffman AR et al. Diagnosis and treatment of hyperprolactinemia: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011 96: 273-288.
4. Milewicz A, Gejdel E, Sworen H et al. Vitex agnus castus extract in the treatment of luteal phase defects due to latent hyperprolactinemia. Results of a randomized placebo-controlled double-blind study. Arzneimittelforschung. 1993 43(7):752-756.
5. Pascal-Vigneron V, Weryha G, Bosc M, Leclere J Hyperprolactinemic amenorrhea: treatment with cabergoline versus bromocriptine. Results of a national multicenter randomized double-blind study. Presse Med 1995 24:753–757.
6. Webster J, Piscitelli G, Polli A et al. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. Cabergoline Comparative Study Group. N Engl J Med 1994 331:904–909.
Prolactin, mU/ml Group 1, n=24 Group 2, n=24 P 1-2
Baseline 782±55 600±55 >0.05
After treatment 217±32* 303±29** >0.05
*p=0.0001 (for group 1, before and after treatment )
**p=0.0029 (for group 2, before and after treatment )
Tab. 2 - Dynamics of serum prolactin concentration (M±m) of female patients during therapy.
© 2012 Monduzzi Editoriale | Proceedings Code: 596
Sperm recovery in patients with non-mosaic Klinefelter syndrome: a comparative study
H. Terada, T. Sugiyama, S. Mugiya, S. OzonoDepartment of Urology, Hamamatsu University School of Medicine, Shizuoka, Japan
SUMMARYWe investigated factors that predict successful microdissection sperm extraction
(MD-TESE) in men with non-mosaic Klinefelter syndrome and the infl uence of preoperative hormonal therapy on the sperm retrieval rate. From June 2008 to Oc-tober 2010, 78 MD-TESE attempts were made in 16 patients. Patients with serum follicle stimulating hormone (FSH) and luteinizing hormone (LH) levels <25 mIU/ml and testosterone >300 ng/dl received hormonal therapy with human chronic go-nadotropin. The success rate for retrieval was 25% (4/16 patients) using MD-TESE, and this procedure followed by intracytoplasmic sperm injection led to one birth. Age, hormonal therapy, and LH, FSH and testosterone levels were not predictors of sperm retrieval. We conclude that MD-TESE is an effective technique in men with non-mosaic Klinefelter syndrome and that these men can father a child, despite concerns regarding genetic risks.
KEY WORDSChromosomal anomaly, Klinefelter syndrome, TESE-ICSI
INTRODUCTIONKlinefelter syndrome is a common genetic condition that was fi rst described in
1942.1. Affected non-mosaic men are azoospermic and have been labeled as infer-tile. Men with Klinefelter syndrome account for 3% of infertile men and 11% of men with azoospermia and one in 500-1000 male newborns 1,2. The fi nding that men with non-mosaic Klinefelter syndrome have potential fertility has been aided by developments in assisted reproduction techniques. We investigated the preopera-

70
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
tive factors that predict successful microdissection sperm extraction (MD-TESE) in men with non-mosaic Klinefelter syndrome and the infl uence of hormonal therapy on the sperm retrieval rate. Herein, we present our experience in 16 patients with Klinefelter syndrome who underwent TESE procedures.
MATERIALS AND METHODSFrom June 2008 to October 2010, a total of 78 MD-TESE attempts were made
in 16 patients with non-mosaic Klinefelter syndrome. Patients with serum follicle stimulating hormone (FSH) and luteinizing hormone (LH) levels <25 mIU/ml and testosterone level >300 ng/dl received hormonal therapy with human chronic go-nadotropin (hCG). Treatment with hCG was initiated at a dose of 3000 IU once a week for eight weeks and titrated upward until a response of serum testosterone before TESE. The infl uences of hormonal therapy and age on sperm retrieval were analyzed.
RESULTSThe overall success rate for retrieval was 25% (4/16 patients) using MD-TESE.
Combined with ICSI, this led to the birth of one child. Attempts at ICSI are continu-ing in the 3 other cases. Hormonal therapy using hCG did not affect sperm retrieval rates, with normal baseline testosterone ³250 ng/dl. The 4 patients with successful sperm retrieval were 26-42 years old and the 12 patients in whom retrieval was unsuccessful were 25-42 years old. Therefore, age had no effect on the success rate. Clinical parameters such as LH, FSH and testosterone levels were also not predictive of the success of sperm retrieval in patients with non-mosaic Klinefelter syndrome.
CONCLUSIONSKlinefelter syndrome have hypergonadotropic hypogonadism with a sex-chromo-
some anomaly. Affected non-mosaic men are azoospermic and have been labeled as infertile. The genotypic abnormality results from a meiotic nondisjunction event that results in a 47,XXY genotype in up to 80% of non-mosaic cases; however, up to 3% of men with this syndrome are mosaic 46,XX/47,XXY.4 The extra chromosome is inherited from the mother or father at an approximately equal rate.5 The pheno-typic appearance of a male with Klinefelter syndrome varies widely, but enlarged breasts, sparse facial and body hair, and small, fi rm testes are common.
Mosaic patients occasionally have sperm in their ejaculate,6 but men with non-mosaic Klinefelter syndrome have been considered to be sterile.1
The fi rst pregnancy using surgical sperm retrieval in a patient with non-mosaic Klinefelter syndrome was published in 1996 7 and the fi rst birth using ICSI was reported in 1997 8. Physical features, biochemistry (serum testosterone, FSH, LH),
71
November 17-20, 2011 Paris, France
and testicular volume have been investigated as factors associated with the success rate of surgical sperm retrieval. A study in 20 patients found that a signifi cantly larger testicular volume and the serum testosterone level were markers of success 7. However, in the current study, serum testosterone levels and age did not differ between patients with and without successful sperm retrieval. Theoretically, the po-tential for sperm retrieval should decrease with age as hyalinization of seminiferous tubules progresses. Thus, the concern for maintenance of fertility in young men with Klinefelter syndrome must be balanced with the possible psychosocial benefi ts of testosterone replacement through early androgen replacement therapy.
We conclude that MD-TESE for men with non-mosaic Klinefelter syndrome fol-lowed by ICSI is a viable assisted reproduction technique, and does not depend on the age of the man.
REFERENCES1. FORESTA C, GALEAZZI C, BETTELLA A, MARIN P, ROSSATO M, GROLLA A, FERLIN
A. Analysis of meiosis in intratesticular germ cells from subjects affected by classic Klinefelter’s syndrome. J Clin Endocrinol Metab 84, 3807-3810, 1999.
2. KLINEFELTER JR HF, REIFENSTEIN JR EC, ALBRIGHT F. Syndrome characterized by gynecomastia, aspermatogenesis without A-Leydigism and increased excretion of follicle stimulating hormone. J Clin Endocrinol Metab 2, 615-627, 1942.
3. FRIEDLER S, RAZIEL A, STRASSBURGER D, SCHACHTER M, BERN O, RON-EL R. Outcome of ICSI using fresh and cryopreserved-thawed testicular spermatozoa in patients with non-mosaic Klinefelter’s syndrome. Hum Reprod 16, 2616-2620, 2001.
4. HARARI O, BOURNE H, BAKER G, GRONOW M, JOHNSTON I. High fertilization rate with intracytoplasmic sperm injection in mosaic Klinefelter’s syndrome. Fertil Steril 63, 182-184, 1995.
5. THOMAS NS, HASSOLD TJ. Aberrant recombination and the origin of Klinefelter syndrome. Hum Reprod Update 9, 309-317, 2003.
6. COZZI J, CHEVRET E, ROUSSEAUX S, PELLETIER R, BENITZ V, JALBERT H, SELE B. Achievement of meiosis in XXY germ cells: study of 543 sperm karyotypes from an XY/XXY mosaic patient. Hum Genet 93, 32-34, 1994.
7. STAESSEN C, COONEN E, VAN ASSCHE E, TOURNAYE H, JORIS H, DEVROEY P, VAN STEIRTEGHEM A, LIEBAERS I. Preimplantaion diagnosis for X and Y normality in embryos from three Klinefelter's patients. Hum Reprod 11, 1650-1653, 1996.
8. BOURNE H, STERN K, CLARKE G, PERTILE M, SPEIRS A, BAKER HW Delivery of normal twins following the intracytoplasmic injection of spermatozoa from a patient with 47,XXY Klinefelter’s syndrome. Hum Reprod 12, 2447-2450, 1997.

© 2012 Monduzzi Editoriale | Proceedings Code: 629
Co-occurrence of polycystic ovary syndrome with depression and anxiety symptoms
Xin Li1, Fulong Wang2, Johnna Wu2, Fang Fang1,Yi Jin1
1Obstetrics and Gynecology Hospital of Medical Center, Fudan University, Shanghai, China; 2Institute for Nutritional Sciences, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences, Graduate School of the Chinese Academy of Sciences, Shanghai, China
SUMMARYObjective:We studied the psychological characteristics in PCOS women and
whether its endocrinometabolic profi les are associated with depressive and anxiety symptoms.
Methods:100 PCOS aged 19-40 years were recruited in and performed an-thropometric measurements,endocrinometabolic profi les,self-Rating Depression Scale(SDS) and self-Rating Anxiety Scale(SAS).
Results:The SDS and the SAS scores of the PCOS women were both signifi -cantly higher than norm. 27% PCOS women were ascertained depressive symp-toms and 15% were ascertained anxiety symptoms. 14% PCOS women had both depression and anxiety symptoms. However,no relationship was found between the SDS or SAS scores and body mass index, HOMA-IR and free androgen index (p<0.05).
Conclusion:Although no clear association was found of depression and anxiety symptoms with endocrinometabolic profi les, mild to midrange depression and anxi-ety symptoms distinguished women with PCOS.
INTRODUCTIONPCOS is the most widespread endocrine disorders among females, the preva-
lence of which is now between 6.5% to 8%[1] and the morbidity is still increasing. Recently, some groups have reported that PCOS is often accompanied by emotional disorders[2] such as depression and anxiety symptoms, while no corresponding data-can be found in China.

74
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
SUBJECTS AND METHODSThe subjects were consecutive early PCOS patients selected from Endocrinology
Department of Obstetrics and Gynecology Hospital of Medical Center of Fudan Uni-versity in the period between September 2009 and October 2010, according to diag-nostic criteria revised by ASRM and ESHRE. The patients in line with the above cri-teria but undergoing pharmacological treatment were excluded,the fi nal 100 PCOS patients recruited aged between 19 to 40 with an average age of 25.47 yrs.
SDS: a self-rating scale made by Zung in 1965[3], whose score is independent of factors such as age, gender and fi nancial status etc.. The scale has 20 items with a full mark of 80. The scores of the subjects were converted to standard scores. Adjusting to Chinese norm, a score of 53~59 is classifi ed as mild, while 60~69 is classifi ed as moderate and over 69, severe.SAS: a self-rating scale made by Zung in 1971, the form and evaluation method of which are similar to SDS. The only dif-ference is that in SAS, 50 is the threshold rather than 53 in SDS. The questionnaire was accomplished independently by patients after they apprehended the meaning of the scales and was collected on the spot. Specially-assigned person were in charge of the data assessments and family history preservation. 10 ml elbow venous blood was taken and centrifugated to be stored at -20 before measuring LH, FSH, TT, PRL,E2,DHEAS and 17-OHP etc. Elbow venous blood was taken to test FPG, FINS and F after overnight(10~12h) fasting. HOMA-IR was carried out to evaluate insu-lin resistance. FAI was used as determinant of androgen activity. Taken individu-ally, according to Chinese norm, PCOS patients with a standard SDS score equal or greater than 53 were classifi ed as depression group and otherwise asymptom group. Similarly, patients with a standard SAS score equal or greater than 50 were categorized as anxiety group and otherwise asymptom group. Measurement data was labeled x(s) and skewed distribution data was analysed after natural logarithms conversion.One way ANOVA was used to investigate the differences between the various groups. The Pearson's correlation was used to analyse the correlation be-tween the variables. Student's T-test was used to investigate the difference between our data and the Chinese norm. Chi-Square Test was used to compare ratio. The statistical software package SPSS version 13 was used for analysis of results.
RESULTS The standard SDS score of PCOS patients was 46.0(9.9), compared with the
41.9(10.6) of norm, demonstrating a statistic signifi cance(t=4.06,P<0.001) and its SAS counterpart scored 40.7(9.2) in comparison with the norm 37.2(12.6), which is also statistically signifi cant(t=43.69,P<0.001). Of the 100 PCOS patients, there were 28 cases in symptoms group(14 with both symptoms, 14 with either symptoms) and 72 cases in asymptom group.Patients in symptoms group scored more than asymptom group in both scales and the difference was signifi cant(p<0.001). The
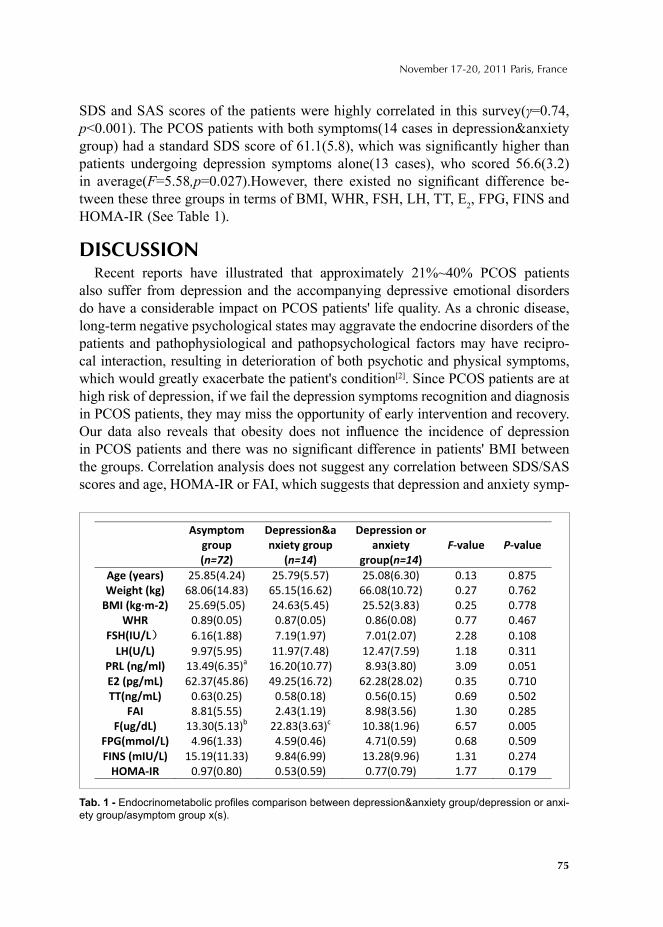
75
November 17-20, 2011 Paris, France
SDS and SAS scores of the patients were highly correlated in this survey(γ=0.74, p<0.001). The PCOS patients with both symptoms(14 cases in depression&anxiety group) had a standard SDS score of 61.1(5.8), which was signifi cantly higher than patients undergoing depression symptoms alone(13 cases), who scored 56.6(3.2) in average(F=5.58,p=0.027).However, there existed no signifi cant difference be-tween these three groups in terms of BMI, WHR, FSH, LH, TT, E2, FPG, FINS and HOMA-IR (See Table 1).
DISCUSSIONRecent reports have illustrated that approximately 21%~40% PCOS patients
also suffer from depression and the accompanying depressive emotional disorders do have a considerable impact on PCOS patients' life quality. As a chronic disease, long-term negative psychological states may aggravate the endocrine disorders of the patients and pathophysiological and pathopsychological factors may have recipro-cal interaction, resulting in deterioration of both psychotic and physical symptoms, which would greatly exacerbate the patient's condition[2]. Since PCOS patients are at high risk of depression, if we fail the depression symptoms recognition and diagnosis in PCOS patients, they may miss the opportunity of early intervention and recovery.Our data also reveals that obesity does not infl uence the incidence of depression in PCOS patients and there was no signifi cant difference in patients' BMI between the groups. Correlation analysis does not suggest any correlation between SDS/SAS scores and age, HOMA-IR or FAI, which suggests that depression and anxiety symp-
Tab. 1 - Endocrinometabolic profi les comparison between depression&anxiety group/depression or anxi-ety group/asymptom group x(s).
76
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
toms in PCOS patients are not directly connected with factors such as clinical course, obesity, hyperinsulinemia and hyperandrogenism. The etiology of PCOS depression is probably independent of clinical features like obesity, infertility, acne and poly-trichosis, which is consistent with Kristen Farrell's conclusion based on his review of 127 papers on the emotional disorders in PCOS patients in 2010[2].
In summary, the etiology of PCOS is elusive and the symptoms are complicated for its association with various systems and pathogenesis. While the reproduction dysfunction and endocrine and metabolic disorders of the PCOS patients should be valued, more attention should be paid to the development of patients' emotional disorders.
REFERENCES 1. Azziz R. Controversy in clinical endocrinology:diagnosis of PCOS: the Rotterdam criteria are
premature. J Clin Endocrinol Metab 2006,91:781-785.2. Kristen Farrell, Michael H, Antoni. Insulin resistance, obesity, infl ammation, and depression in
PCOS:biobehavioral mechanisms and interventions. Fertility and Sterility, 2010,94(5):1565-1574. 3. Zung WWK.A self-rating depression scale. Arch Gen Psychiatry,1965; 63-70.
© 2012 Monduzzi Editoriale | Proceedings Code: 633
Cryopreservation of a small number of human spermatozoa with home-made Strawtop: 3 years experience
Songguo Xue, Qiuping Peng, Shaofeng Cao, Qiao Yu, Jiqiang Si, Yanping KuangDepartment of Assisted Reproduction, Shanghai 9th People’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
SUMMARYThe purpose of this study is to develop a novel method for the cryopreserva-
tion of a small number of human spermatozoa. The effi ciency of it’s clinical application was also evaluated.
INTRODUCTIONIn clinical medical practice, cryopreservation of spermatozoa from testicular
sperm extraction (TESE), percutaneus epididymal sperm aspiration (PESA) or oligozoospermic patients is need in order to avoid the surgical sperm extrac-tion which can negative consequences upon testicular function or the failure of surgical sperm extraction which can results in cancellation of the treatment cycle. Our group have invented a new method for cryopreservation of single human sperm(microdrop, thawing in warm oil) which has good survival rate
(1)
. Now conventional cryopreservation of spermatozoa from TESE,PESA or oligo-zoospermic patients is straw method,which need centrifuge and washing,which may result in damage to sperm
(2)
. So we try to cryopreserve a small number of human spermatozoa by modifi ed method for cryopreservation of single human sperm(microdrop, thawing in warm oil).
MATERIALS AND METHODSHome-made Strawtop (Fig 1, similar to Cryoleaf and Cryotop) was used for
spermatozoa loading and oil bath was ued for spermatozoa thawing (Fig 2). spermatozoa from TESE, PESA or oligozoospermic patients was centrifugal
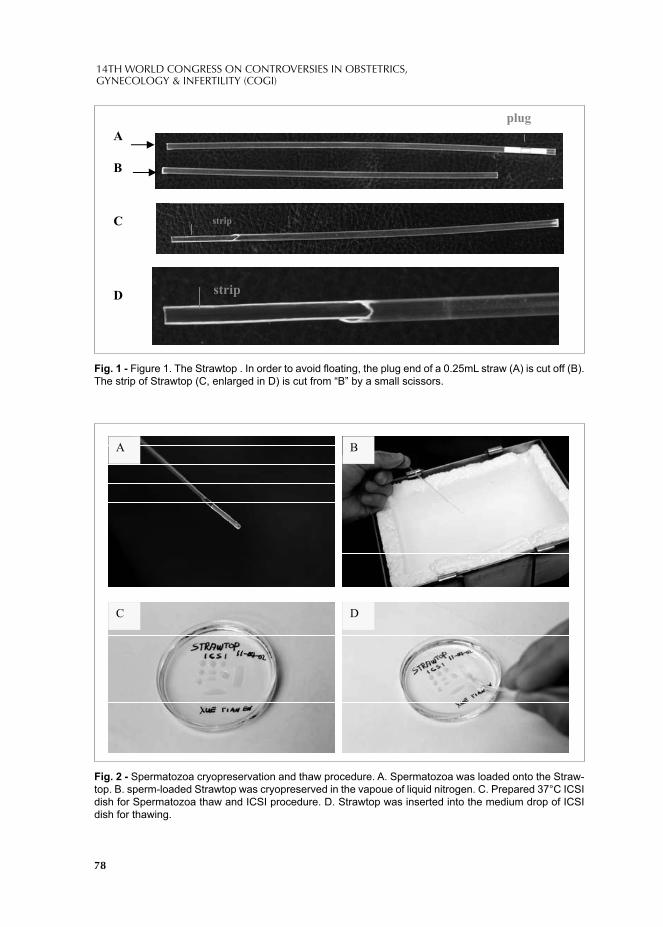
78
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
B
Aplug
C strip
dD strip
A B
C D
Fig. 1 - Figure 1. The Strawtop . In order to avoid fl oating, the plug end of a 0.25mL straw (A) is cut off (B). The strip of Strawtop (C, enlarged in D) is cut from “B” by a small scissors.
Fig. 2 - Spermatozoa cryopreservation and thaw procedure. A. Spermatozoa was loaded onto the Straw-top. B. sperm-loaded Strawtop was cryopreserved in the vapoue of liquid nitrogen. C. Prepared 37°C ICSI dish for Spermatozoa thaw and ICSI procedure. D. Strawtop was inserted into the medium drop of ICSI dish for thawing.
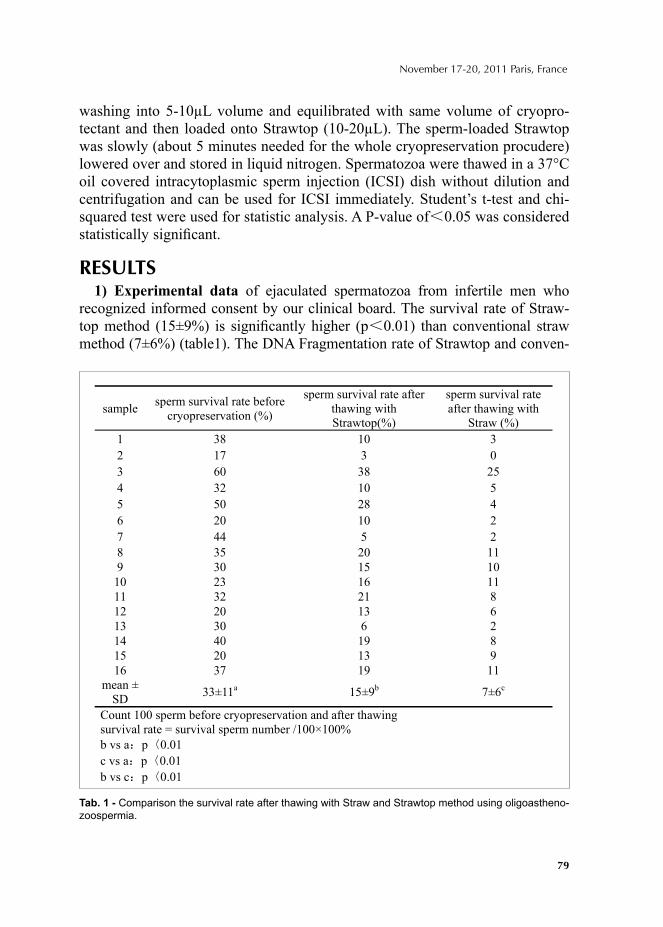
79
November 17-20, 2011 Paris, France
washing into 5-10μL volume and equilibrated with same volume of cryopro-tectant and then loaded onto Strawtop (10-20μL). The sperm-loaded Strawtop was slowly (about 5 minutes needed for the whole cryopreservation procudere) lowered over and stored in liquid nitrogen. Spermatozoa were thawed in a 37°C oil covered intracytoplasmic sperm injection (ICSI) dish without dilution and centrifugation and can be used for ICSI immediately. Student’s t-test and chi-squared test were used for statistic analysis. A P-value of 0.05 was considered statistically signifi cant.
RESULTS1) Experimental data of ejaculated spermatozoa from infertile men who
recognized informed consent by our clinical board. The survival rate of Straw-top method (15±9%) is signifi cantly higher (p 0.01) than conventional straw method (7±6%) (table1). The DNA Fragmentation rate of Strawtop and conven-
Tab. 1 - Comparison the survival rate after thawing with Straw and Strawtop method using oligoastheno-zoospermia.
using oligoasthenozoospermia
sample sperm survival rate before cryopreservation (%)
sperm survival rate after thawing with Strawtop(%)
sperm survival rate after thawing with
Straw (%) 1 38 10 3 2 17 3 0 3 60 38 25 4 32 10 5 5 50 28 4 6 20 10 2 7 44 5 2 8 35 20 11 9 30 15 10 10 23 16 11 11 32 21 8 12 20 13 6 13 30 6 2 14 40 19 8 15 20 13 9 16 37 19 11
mean ± SD 33±11a 15±9b 7±6c
Count 100 sperm before cryopreservation and after thawing survival rate = survival sperm number /100×100% b vs a p 0.01 c vs a p 0.01 b vs c p 0.01
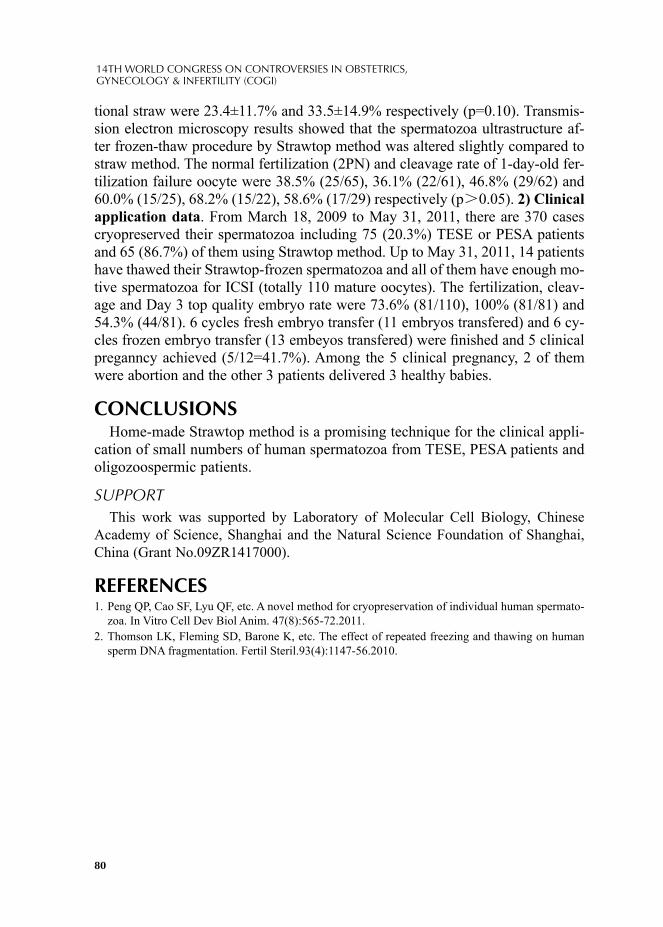
80
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
tional straw were 23.4±11.7% and 33.5±14.9% respectively (p=0.10). Transmis-sion electron microscopy results showed that the spermatozoa ultrastructure af-ter frozen-thaw procedure by Strawtop method was altered slightly compared to straw method. The normal fertilization (2PN) and cleavage rate of 1-day-old fer-tilization failure oocyte were 38.5% (25/65), 36.1% (22/61), 46.8% (29/62) and 60.0% (15/25), 68.2% (15/22), 58.6% (17/29) respectively (p 0.05). 2) Clinical application data. From March 18, 2009 to May 31, 2011, there are 370 cases cryopreserved their spermatozoa including 75 (20.3%) TESE or PESA patients and 65 (86.7%) of them using Strawtop method. Up to May 31, 2011, 14 patients have thawed their Strawtop-frozen spermatozoa and all of them have enough mo-tive spermatozoa for ICSI (totally 110 mature oocytes). The fertilization, cleav-age and Day 3 top quality embryo rate were 73.6% (81/110), 100% (81/81) and 54.3% (44/81). 6 cycles fresh embryo transfer (11 embryos transfered) and 6 cy-cles frozen embryo transfer (13 embeyos transfered) were fi nished and 5 clinical preganncy achieved (5/12=41.7%). Among the 5 clinical pregnancy, 2 of them were abortion and the other 3 patients delivered 3 healthy babies.
CONCLUSIONSHome-made Strawtop method is a promising technique for the clinical appli-
cation of small numbers of human spermatozoa from TESE, PESA patients and oligozoospermic patients.
SUPPORTThis work was supported by Laboratory of Molecular Cell Biology, Chinese
Academy of Science, Shanghai and the Natural Science Foundation of Shanghai, China (Grant No.09ZR1417000).
REFERENCES1. Peng QP, Cao SF, Lyu QF, etc. A novel method for cryopreservation of individual human spermato-
zoa. In Vitro Cell Dev Biol Anim. 47(8):565-72.2011. 2. Thomson LK, Fleming SD, Barone K, etc. The effect of repeated freezing and thawing on human
sperm DNA fragmentation. Fertil Steril.93(4):1147-56.2010.
© 2012 Monduzzi Editoriale | Proceedings Code: 634
Sucrose pretreatment vitrifi cation yields 100% survival rate of mouse and human eggs
Songguo Xue, Qiuping Peng, Qiao Yu, Qifeng Lyu, Shaofeng Cao, Yanping KuangDepartment of Assisted Reproduction, Shanghai 9th People’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
SUMMARYTwo step method, including equilibration solution and vitrfi cation solution, is
the most popular technique for oocyte vitrifi cation in the published paper. But the survival rate is sig nifi cantly different among different IVF centers and the effi ciency is extensively controversial. The purpose of this study is to develop a stable and effi cient method for oocyte vitrifi cation.
INTRODUCTIONSome kind of open loading system, for example Cryotop and Cryoleaf or else,
and aboved mentioned two step vitrifi cation method is the most widely used protocol for human eggs vitrifi cation in clinical practice. But the survial rate is signifi cantly different from about 75% to 100% and the effi ciency was extensively controversial(1). Liu(2) and A. Van Soom(3) demonstrated that 0.3 M sucrose treatment will cause artifi cial compaction of the volume of eggs and embryos and have no det-rimental effect on their developmental competence. In this study, we aim to improve the eggs vitrifi cation effi ciency by sucrose pretreatment induced volume reduction.
MATERIALS AND METHODSHome-made Strawtop (Fig 1, similar to Cryotop and Cryoleaf) was used for eggs
loading. In our IVF center, we use Strawtop for embryos vitrifi cation from the year of 2006 and the survival rate is abot 98% with more than 4000 embryos thawed data. 434 Kunming mouse oocytes (a kind of widely used Chinese strain mouse) were used in this study. We compared the survival rate (SR), cleavage rate (CR),
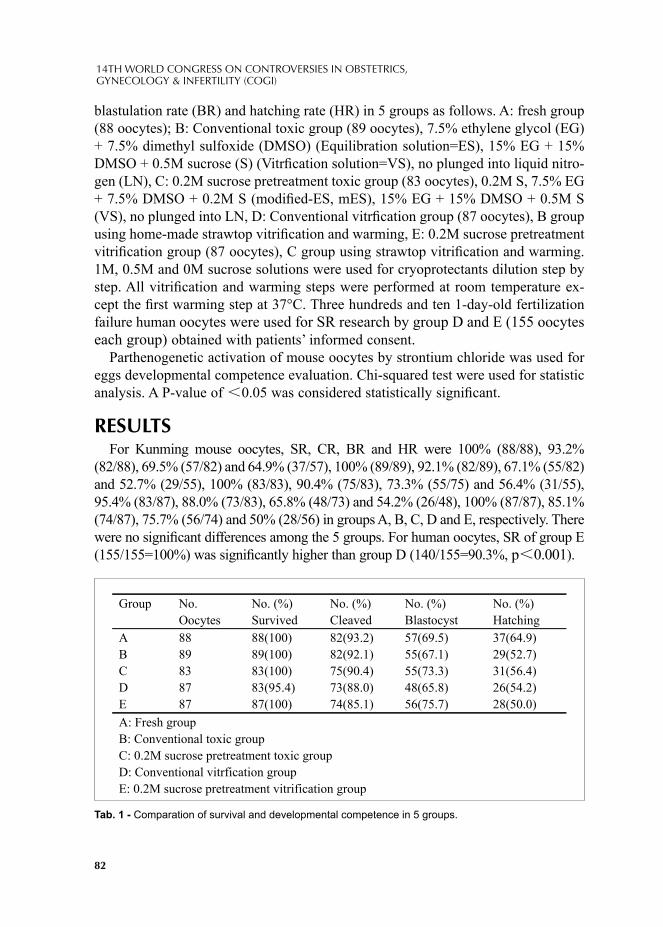
82
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
blastulation rate (BR) and hatching rate (HR) in 5 groups as follows. A: fresh group (88 oocytes); B: Conventional toxic group (89 oocytes), 7.5% ethylene glycol (EG) + 7.5% dimethyl sulfoxide (DMSO) (Equilibration solution=ES), 15% EG + 15% DMSO + 0.5M sucrose (S) (Vitrfi cation solution=VS), no plunged into liquid nitro-gen (LN), C: 0.2M sucrose pretreatment toxic group (83 oocytes), 0.2M S, 7.5% EG + 7.5% DMSO + 0.2M S (modifi ed-ES, mES), 15% EG + 15% DMSO + 0.5M S (VS), no plunged into LN, D: Conventional vitrfi cation group (87 oocytes), B group using home-made strawtop vitrifi cation and warming, E: 0.2M sucrose pretreatment vitrifi cation group (87 oocytes), C group using strawtop vitrifi cation and warming. 1M, 0.5M and 0M sucrose solutions were used for cryoprotectants dilution step by step. All vitrifi cation and warming steps were performed at room temperature ex-cept the fi rst warming step at 37°C. Three hundreds and ten 1-day-old fertilization failure human oocytes were used for SR research by group D and E (155 oocytes each group) obtained with patients’ informed consent.
Parthenogenetic activation of mouse oocytes by strontium chloride was used for eggs developmental competence evaluation. Chi-squared test were used for statistic analysis. A P-value of 0.05 was considered statistically signifi cant.
RESULTSFor Kunming mouse oocytes, SR, CR, BR and HR were 100% (88/88), 93.2%
(82/88), 69.5% (57/82) and 64.9% (37/57), 100% (89/89), 92.1% (82/89), 67.1% (55/82) and 52.7% (29/55), 100% (83/83), 90.4% (75/83), 73.3% (55/75) and 56.4% (31/55), 95.4% (83/87), 88.0% (73/83), 65.8% (48/73) and 54.2% (26/48), 100% (87/87), 85.1% (74/87), 75.7% (56/74) and 50% (28/56) in groups A, B, C, D and E, respectively. There were no signifi cant differences among the 5 groups. For human oocytes, SR of group E (155/155=100%) was signifi cantly higher than group D (140/155=90.3%, p 0.001).
Group No.
Oocytes
No. (%)
Survived
No. (%)
Cleaved
No. (%)
Blastocyst
No. (%)
Hatching
A 88 88(100) 82(93.2) 57(69.5) 37(64.9)
B 89 89(100) 82(92.1) 55(67.1) 29(52.7)
C 83 83(100) 75(90.4) 55(73.3) 31(56.4)
D 87 83(95.4) 73(88.0) 48(65.8) 26(54.2)
E 87 87(100) 74(85.1) 56(75.7) 28(50.0)
A: Fresh group
B: Conventional toxic group
C: 0.2M sucrose pretreatment toxic group
D: Conventional vitrfication group
E: 0.2M sucrose pretreatment vitrification group
Tab. 1 - Comparation of survival and developmental competence in 5 groups.
83
November 17-20, 2011 Paris, France
CONCLUSIONSSucrose pretreatment vitrifi cation method was a promising technique for Kunming
mouse vitrifi cation. More research need to be performed on human mature oocytes developmental competence for this method.
SUPPORTThis work was supported by Laboratory of Molecular Cell Biology, Chinese
Academy of Science, Shanghai and the Natural Science Foundation of Shanghai, China (Grant No.09ZR1417000).
REFERENCES1. Cobo A, Diaz C. Clinical application of oocyte vitrifi cation: a systematic review and meta-analysis
of randomized controlled trials. Fertil Steril. 96(2):277-85.2011.2. Liu JL, Sung LY, Barber M, etc. Hypertonic medium treatment for localization of nuclear material in
bovine metaphase II oocytes. Biol Reprod. 66(5):1342-9. 2002.3. Van Soom A, Ysebaert MT, Vanhoucke-De Medts A, etc. Sucrose-induced shrinkage of in vitro
produced bovine morulae: effect on viability, morphology and ease of evaluation. Theriogenology. 46(7):1131-47.1996.
FETOMATERNAL MEDICINE


© 2012 Monduzzi Editoriale | Proceedings Code: 31
Types of fi stula and their management in a referral center in Saudi Arabia
G. Al-Shaikh1, 2, K. Perveen2, M. Moazin3, A. Al-Badr2
1 King Saud University, King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia; 2 Women's Specialized Hospital, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia; 3 Department of Surgical Specialties, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia
SUMMARYA retrospective chart review of all fi stula cases referred to the urogynecology
department of King Fahad Medical City, Riyadh, Saudi Arabia, from January 2005 to July 2011, to review their causes, management, and outcome. Medical records were reviewed and analyzed. Fourteen genitourinary fi stula cases were identifi ed; eight (57.1 %) cases of vesicovaginal fi stula, three (21.4 %) cases of vesicouterine fi stula, and three (21.4 %) cases of vesicocervical fi stula. Mean age was 41 (± 9.5) and mean parity was 7 (± 4). Out of the 14 cases, 10 (71.4 %) were obstetrical surgi-cal complications, of which 7 (50 %) were complications of cesarean sections. Ten cases (77 %) cured after primary surgical repair, two (15.4 %) after secondary repair and one after tertiary repair. Most genitourinary fi stulae were iatrogenic obstetric caused, unlike causes of fi stulae in developing or developed countries.
INTRODUCTIONUrogenital Fistula has been an anguish condition for centuries, they are attributed
to prolonged and obstructive labor or obstetric trauma in developing countries, [1, 2,
3] however, hysterectomy or pelvic surgery, irradiation and gynecologic malignancy accounts for vast majority of cases in the developed world. [4, 5, 6]
Vesicovaginal fi stula (VVF) remains the most common variety. Vesicouterine (VUF) and vesicocervical (VCF) fi stula were considered rare, [7] but incidence is ris-ing in recent decades, [8] because of the increasing rates of lower segment caesarian section (CS). [9] Other uncommon causes include; instrumental delivery in previous cesarean, [10] placenta percreta, [11] uterine artery embolization [12] and pelvic trauma. [13]
The objective of our study was to evaluate cases of urogenital fi stula referred to our department, with respect to etiology, types, management and outcome.

88
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
MATERIAL AND METHODSA retrospective descriptive study of all urogenital fi stula cases seen from Decem-
ber 2004 to July 2011, at the Urogynecology Department, King Fahd Medical City (a tertiary care referral center), Riyadh, Saudi Arabia. Rectovaginal and other unre-lated fi stulae were excluded. Research and ethical committee approval was granted prior to data collection. Medical records of all urogenital fi stula patients were identi-fi ed through medical coding system, reviewed and analyzed.
All patients were diagnoses after detailed history and physical examination. Fur-ther investigations include urine culture and sensitivity, kidney function test, intrave-nous pyelogram, cystoscopy and examination under anesthesia. Diagnoses were con-fi rmed radiologically (cystogram, CT scan and MRI) and endoscopically in all cases. Conservative management was tried for all except those who presented later than couple of months. Surgical approach was chosen based on type and location of the fi stula, accessibility, surgeon’s expertise, and preference. Bladder was repaired in two layers, using absorbable suture, adhering to principles of successful closure, omen-tum or peritoneum was interposed as graft when appropriate. Trans-urethral Foley catheter drainage was continued for two to three weeks and antibiotic used only if there is evidence of urinary tract infection. Cystogram (or MRI if indicated) was done to confi rm healing, prior to removing the catheter. Procedures were performed by a primary urogynecologist, assisted by two urologists and a urogynecologist.
RESULTSDuring the study period, 14 cases of genitourinary fi stula were identifi ed, eight
(57.1 %) cases of VVF, three (21.4 %) cases of VUF, and three (21.4 %) cases of VCF. The mean age was 41 (± 9.5) and the mean parity was 7 (± 4).
Out of the 14 cases, 10 (71.4 %) were obstetrical surgical complications, of which 7 (50 %) were complications of CS. Three VVF cases were caused by complica-tion of repeat CS, and one case following cervical cerclage at 22 weeks for twin pregnancy. The remaining 4 cases were complications of different types of hyster-ectomies (Table 1). All cases of VUF were complication of repeat CS with 3rd or 4th repeat CS. Concerning VCF, one was a complication of repeat CS (3rd), one after vaginal birth after cesarean and one after primary CS in 2nd stage of labor, with blad-der injury and vaginal extension. Six (46 %) underwent surgical repair though an abdominal approach, 4 (30.7 %) had robotic repair and 3 (23 %) had vaginal repair. Ten cases (77 %) cured after primary surgical repair and 2 (15.4 %) after secondary repair; one after failed abdominal approach and the other after failed robotic repair. One patient had 2 failed abdominal repairs followed by a vaginal repair. A single case (7.1 %) of VUF resolved with catheter drainage for four weeks and remained dry after removal of the catheter. On follow up, all cases were considered cured, by history, physical examination and radiologic confi rmation.
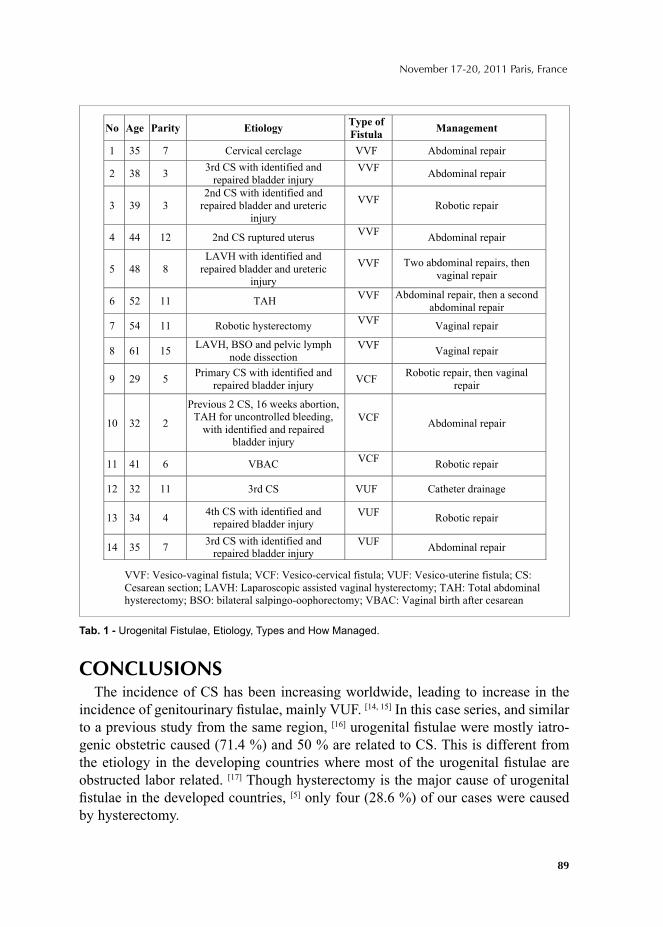
89
November 17-20, 2011 Paris, France
CONCLUSIONSThe incidence of CS has been increasing worldwide, leading to increase in the
incidence of genitourinary fi stulae, mainly VUF. [14, 15] In this case series, and similar to a previous study from the same region, [16] urogenital fi stulae were mostly iatro-genic obstetric caused (71.4 %) and 50 % are related to CS. This is different from the etiology in the developing countries where most of the urogenital fi stulae are obstructed labor related. [17] Though hysterectomy is the major cause of urogenital fi stulae in the developed countries, [5] only four (28.6 %) of our cases were caused by hysterectomy.
o Age Parity Etiology Type of
Fistula Management
1 35 7 Cervical cerclage VVF Abdominal repair
2 38 3 3rd CS with identified and
repaired bladder injury VVF
Abdominal repair
3 39 3
2nd CS with identified and
repaired bladder and ureteric
injury
VVF Robotic repair
4 44 12 2nd CS ruptured uterus VVF
Abdominal repair
5 48 8
LAVH with identified and
repaired bladder and ureteric
injury
VVF Two abdominal repairs, then
vaginal repair
6 52 11 TAH VVF Abdominal repair, then a second
abdominal repair
7 54 11 Robotic hysterectomy VVF
Vaginal repair
8 61 15 LAVH, BSO and pelvic lymph
node dissection VVF
Vaginal repair
9 29 5 Primary CS with identified and
repaired bladder injury VCF
Robotic repair, then vaginal
repair
10 32 2
Previous 2 CS, 16 weeks abortion,
TAH for uncontrolled bleeding,
with identified and repaired
bladder injury
VCF Abdominal repair
11 41 6 VBAC VCF
Robotic repair
12 32 11 3rd CS VUF Catheter drainage
13 34 4 4th CS with identified and
repaired bladder injury VUF
Robotic repair
14 35 7 3rd CS with identified and
repaired bladder injury VUF
Abdominal repair
VVF: Vesico-vaginal fistula; VCF: Vesico-cervical fistula; VUF: Vesico-uterine fistula; CS:
Cesarean section; LAVH: Laparoscopic assisted vaginal hysterectomy; TAH: Total abdominal
hysterectomy; BSO: bilateral salpingo-oophorectomy; VBAC: Vaginal birth after cesarean
Tab. 1 - Urogenital Fistulae, Etiology, Types and How Managed.
90
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
REFERENCES1. HILTON P. Vesico-vaginal Fistula in Developing Countries. Int J Gynecol Obstet; 82(3):285-95,
2003.2. WALL LL, ARROW SMITH SD, BRIGGS ND, BROWNING A AND LASSEY A. The Obstetric
Vesicovaginal Fistula in Developing World. Obstetrics Gynecology Surv; 60(7 Suppl 1):S53-S51, 2005.
3. RATHEE S, NANDAS S. Vesicovaginal Fistula A 12 Year Old Study. J Indian Med Assoc; 93(3): 93– 94, 1995.
4. MIOR JC. Vesicovaginal Fistula as seen in Britain. J Obstet Gynecol Brit Commonwealth; 80(7):598 – 602, 1973.
5. CORTESSE A, COLAU A. Vesicovaginal Fistula. Ann Urol; 38(2) 52 – 66, 2004.6. HADLEY HR. Vesicovaginal Fistula. Curr Urol Rep; 3(5): 401-7, 2002.7. IBACHIE GC, NJOKU O. Vesico-uterine Fistula; Br J. Urol: 57 438 – 439, 1985.8. SHING KY, TAK YL. Vesicouterine Fistula. An updated Review. Int. Urogynecol J; 9:252 – 256,
1998.9. JOZWIK M, JOZWIK M. Clinical Classifi cation of Vesicouterine Fistula. Int. J. Gynecol Obstet;
70:353 – 7, 2000.10. Pelosi MA 3rd, Pelosi; MA. Vesicouterine Fistula: A Rare Complication of Vaginal birth after
Caesarean Section. Obstet Gynecol; 87 (1): 160-2, 1996.11. KRYSIEWICZ S, AUH YH, KAZAM E. Vesico-Uterine Fistula associated with placenta percreta.
Urol Radial; 10: 213–15, 1988.12. SULTANA CJ, GOLDBURG J, AIZENMAN L, CHON JK. Vesicouterine Fistula after Uterine
Artery Embolization: a Case Report. Am J Obstet Gynecol; 187(6):1726-7, 2002.13. KUMAR A, VAIDYANATHAN S, SHARMA SK, SHARMA AK, GOSWAMI AK. Management
of Vesicouterine Fistulae – A Report of Six Cases. Int J Gynecol Obstet; 26(3):453-7, 1998.14. PORCARO AB, ZICARI M, ZECCHINI ANTONIOLLI S, PIANON R, MONACO C,
MIGLIORINI F, LONGO M, COMUNALE L. Vesicouterine fi stulas following cesarean section: report on a case, review and update of the literature. Int Urol Nephrol; 34(3):335-44, 2002.
15. MEEKS RODNEY G, ROTH TED M. Vesicovaginal and urethrovaginal fi stula. In: Rock JA, Thompson JD (ed). Te Linde's Operative Gynaecology, 10th ed. Philadelphia, PA: J.B Lippincot, 2003; 973–5.
16. AL-BADR A, MALABARY O, AL-JASSER A, ZIMMERMAN V. Common genitourinary fi stulae at a referral hospital in Saudi Arabia. Pelviperineology; 29: 110-112, 2010.
17. WALL LL, KARSHIMA JA, KIRSCHNER C, ARROWSMITH SD. The obstetric vesicovaginal fi stula: characteristics of 899 patients from Jos, Nigeria. Am J Obstet Gynecol; Apr; 190(4):1011-9, 2004.
© 2012 Monduzzi Editoriale | Proceedings Code: 47
Determination of the early immunological changes in patients with pregnancy loss
F. Aliyeva1, A. Poletayev2, A. Amirova1, N. Shahbazova1, X. Tahmazi1
1 Scientifi c Research Institute of Obstetrics and Gynecology (Department of Obstetrics and Gynecology), Baku, Azerbaijan; 2 Medical Research Center "Immunculus" (Immunology and Reproduction Biology Laboratory) Moscow, Russia
SUMMARYThe main aim of the study was to determine the immunological changes of the
level of 12 auto antibodies in blood at the pregnant women with pregnancy loss risk and women with the pregnancy loss in past with using ELIP-test-12 method. The scientifi c research work was carried out in 112 patients, which were divided in two groups. The 46 no pregnant patients with pregnancy loss in past were included in Group 1. The 66 pregnant women with the risk of pregnancy loss were included in Group 2. As a result of research, it was found that the the rate of changes of auto antibodies is different and depending on cause of pregnancy loss. The main immunological markers of ELIP-test-12 at pregnancy loss are anti-HCG AB, AB againist collagen, B-2-GP-1 AB, AB againist insulin, anti-sperm (SPR) AB. The determination of immune system changes with using ELIP-test-12 method give the opportunity to fi nd some disorders before early clinical symptoms were manifested and also to help with providing of more extended investigations to the patients.
INTRODUCTIONAt this time pregnancy loss is very actual problem. It is very diffi cult to know
the main reason of pregnancy loss and this pathology could be repeated during next pregnancy in the future. (1,3) Also it is not easy to determine another factors of this condition, the effectiveness of the carried out treatment to the patients. The statistic information about the rate of repeated pregnancy loss after two loss cases is 24%, after three – 30%, after four – 40%. ELİP-test-12 is the method for determination of the concentration of embryotoxic auto antibodies in the blood. It is possible to evaluate the condition of general and reproductive health at the early stage of diseases before any clinical signs will have a place. (2,4,5)
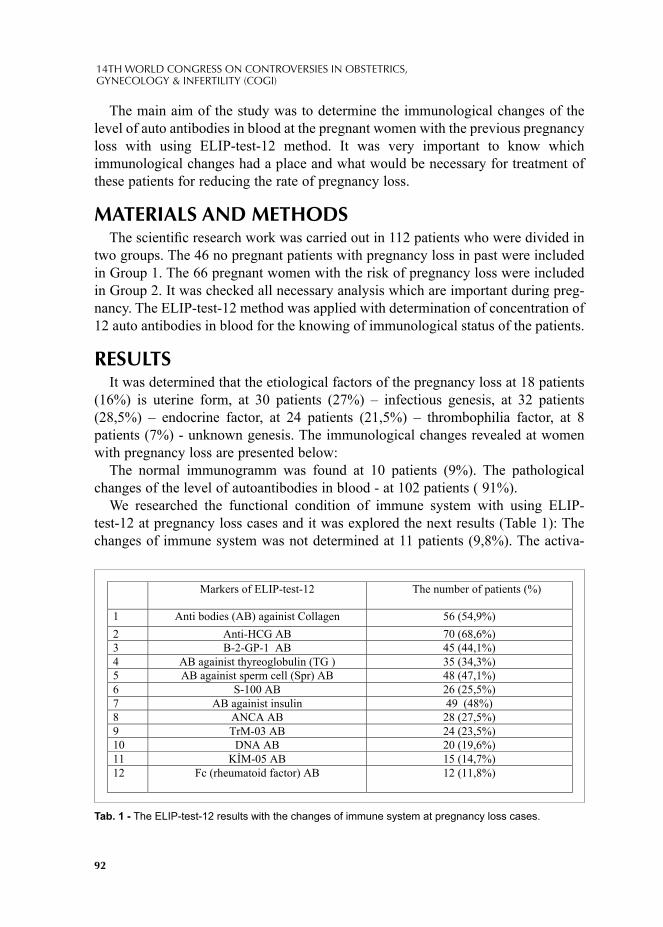
92
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The main aim of the study was to determine the immunological changes of the level of auto antibodies in blood at the pregnant women with the previous pregnancy loss with using ELIP-test-12 method. It was very important to know which immunological changes had a place and what would be necessary for treatment of these patients for reducing the rate of pregnancy loss.
MATERIALS AND METHODSThe scientifi c research work was carried out in 112 patients who were divided in
two groups. The 46 no pregnant patients with pregnancy loss in past were included in Group 1. The 66 pregnant women with the risk of pregnancy loss were included in Group 2. It was checked all necessary analysis which are important during preg-nancy. The ELIP-test-12 method was applied with determination of concentration of 12 auto antibodies in blood for the knowing of immunological status of the patients.
RESULTSIt was determined that the etiological factors of the pregnancy loss at 18 patients
(16%) is uterine form, at 30 patients (27%) – infectious genesis, at 32 patients (28,5%) – endocrine factor, at 24 patients (21,5%) – thrombophilia factor, at 8 patients (7%) - unknown genesis. The immunological changes revealed at women with pregnancy loss are presented below:
The normal immunogramm was found at 10 patients (9%). The pathological changes of the level of autoantibodies in blood - at 102 patients ( 91%).
We researched the functional condition of immune system with using ELIP-test-12 at pregnancy loss cases and it was explored the next results (Table 1): The changes of immune system was not determined at 11 patients (9,8%). The activa-
Markers of ELIP-test-12 The number of patients (%)
1 Anti bodies (AB) againist Collagen 56 (54,9%)
2 Anti-HCG AB 70 (68,6%)
3 B-2-GP-1 AB 45 (44,1%)
4 AB againist thyreoglobulin (TG ) 35 (34,3%)
5 AB againist sperm cell (Spr) AB 48 (47,1%)
6 S-100 AB 26 (25,5%)
7 AB againist insulin 49 (48%)
8 ANCA AB 28 (27,5%)
9 TrM-03 AB 24 (23,5%)
10 DNA AB 20 (19,6%)
11 K M-05 AB 15 (14,7%)
12 Fc (rheumatoid factor) AB 12 (11,8%)
Tab. 1 - The ELIP-test-12 results with the changes of immune system at pregnancy loss cases.
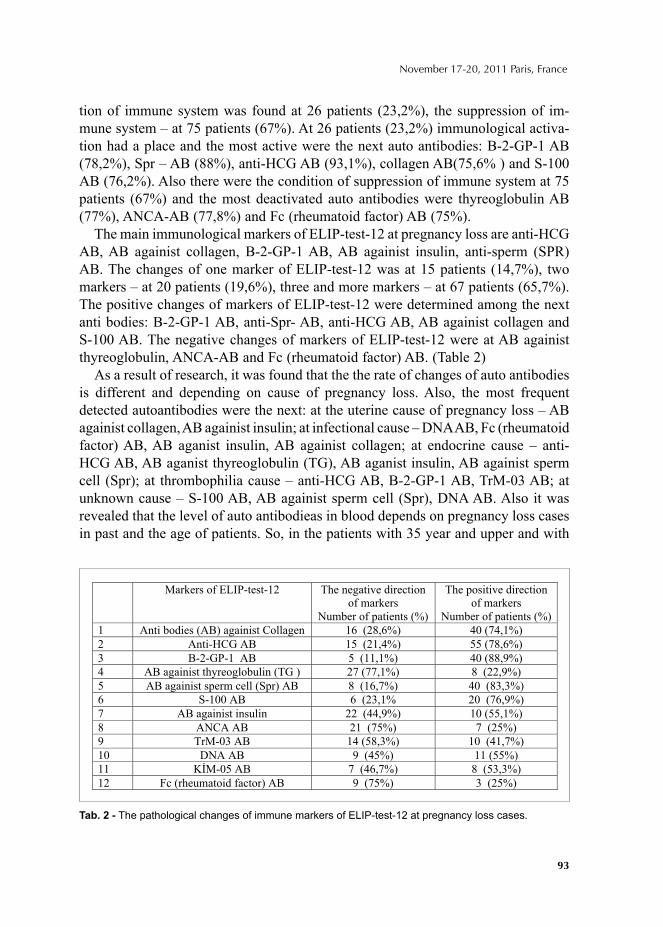
93
November 17-20, 2011 Paris, France
tion of immune system was found at 26 patients (23,2%), the suppression of im-mune system – at 75 patients (67%). At 26 patients (23,2%) immunological activa-tion had a place and the most active were the next auto antibodies: B-2-GP-1 AB (78,2%), Spr – AB (88%), anti-HCG AB (93,1%), collagen AB(75,6% ) and S-100 AB (76,2%). Also there were the condition of suppression of immune system at 75 patients (67%) and the most deactivated auto antibodies were thyreoglobulin AB (77%), ANCA-AB (77,8%) and Fc (rheumatoid factor) AB (75%).
The main immunological markers of ELIP-test-12 at pregnancy loss are anti-HCG AB, AB againist collagen, B-2-GP-1 AB, AB againist insulin, anti-sperm (SPR) AB. The changes of one marker of ELIP-test-12 was at 15 patients (14,7%), two markers – at 20 patients (19,6%), three and more markers – at 67 patients (65,7%). The positive changes of markers of ELIP-test-12 were determined among the next anti bodies: B-2-GP-1 AB, anti-Spr- AB, anti-HCG AB, AB againist collagen and S-100 AB. The negative changes of markers of ELIP-test-12 were at AB againist thyreoglobulin, ANCA-AB and Fc (rheumatoid factor) AB. (Table 2)
As a result of research, it was found that the the rate of changes of auto antibodies is different and depending on cause of pregnancy loss. Also, the most frequent detected autoantibodies were the next: at the uterine cause of pregnancy loss – AB againist collagen, AB againist insulin; at infectional cause – DNA AB, Fc (rheumatoid factor) AB, AB aganist insulin, AB againist collagen; at endocrine cause – anti-HCG AB, AB aganist thyreoglobulin (TG), AB aganist insulin, AB againist sperm cell (Spr); at thrombophilia cause – anti-HCG AB, B-2-GP-1 AB, TrM-03 AB; at unknown cause – S-100 AB, AB againist sperm cell (Spr), DNA AB. Also it was revealed that the level of auto antibodieas in blood depends on pregnancy loss cases in past and the age of patients. So, in the patients with 35 year and upper and with
Markers of ELIP-test-12 The negative direction
of markers
Number of patients (%)
The positive direction
of markers
Number of patients (%)
1 Anti bodies (AB) againist Collagen 16 (28,6%) 40 (74,1%)
2 Anti-HCG AB 15 (21,4%) 55 (78,6%)
3 B-2-GP-1 AB 5 (11,1%) 40 (88,9%)
4 AB againist thyreoglobulin (TG ) 27 (77,1%) 8 (22,9%)
5 AB againist sperm cell (Spr) AB 8 (16,7%) 40 (83,3%)
6 S-100 AB 6 (23,1% 20 (76,9%)
7 AB againist insulin 22 (44,9%) 10 (55,1%)
8 ANCA AB 21 (75%) 7 (25%)
9 TrM-03 AB 14 (58,3%) 10 (41,7%)
10 DNA AB 9 (45%) 11 (55%)
11 K M-05 AB 7 (46,7%) 8 (53,3%)
12 Fc (rheumatoid factor) AB 9 (75%) 3 (25%)
Tab. 2 - The pathological changes of immune markers of ELIP-test-12 at pregnancy loss cases.

94
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
pregnancy loss in past were found the changes of 3-4 markers of auto antibodies level in blood with using ELIP-test-12 method. Also, at those patients the level of autoantibodies changed from -42 to +87 at ELIP-test-12 results. The determination of immune system changes with using ELIP-test-12 method give the opportunity to fi nd some disorders before early clinical symptoms were manifested and also to help with providing of more extended investigations to the patients.
CONCLUSIONAt the research work it was determined that the main immunological markers
of ELIP-test-12 at pregnancy loss were anti-HCG AB, AB againist collagen, B-2-GP-1 AB, AB againist insulin, anti-sperm (SPR) AB. The fi rst changes of immune system could be found at placental insuffi ciency and trombophilia disorders with using ELIP-test-12 in patients with pregnancy loss cases. The using of ELIP-test-12 method is the fi rst step of diagnostics of main immunological changes in patients with pregnancy loss in past and at 80% of cases it will be possible to determine the pathology. Also it is possible to carry out necessary treatment in depending on im-munological changes which could be found by using ELIP-Test-12 method.
REFERENCE1. Facchinetti F, Marozio L, Frusca T, Grandone E, Venturini P, Tiscia GL, Zatti S, Benedetto C. Am J
Obstet Gynecol. 2009 Jan; 200(1):46.e1-5. Epub 2008 Oct 9.Maternal thrombophilia and the risk of recurrence of preeclampsia. Mother-Infant Department, Unit of Gynecology and Obstetrics, Faculty of Medicine and Surgery, University of Modena and Reggio Emilia, Italy. [email protected]
2. Chong P., Matz W. The immunology of pregnancy loss. The female Patient, Vol 20, feb 1995. P. 1-43. Matzner W., Chong P., Xu G., Ching W. The comparative assessment of fl owing cytofl uometria
and microtoxicity for the determination of effectiviness of aloimmune theraphy at the patients with pregnancy loss. Am J Reprod Immunol; vol. 33, 1995; pp 10-13.
4. Phadungkiatwattana P, Sirivatanapa P, Tongsong T. J Med Assoc Thai. 2007 Oct; 90(10):1981-5.Outcomes of pregnancies complicated by systemic lupus erythematosus (SLE). Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand. [email protected]
5. The diagnostics with using technology “Immunculus”. http://www.center-akusherstva.ru/index.php?option=com_content&task=view&id=1545&Itemid=573.
© 2012 Monduzzi Editoriale | Proceedings Code: 83
Challenges in implementing humanized birth practices in a highly specialized and university affi liated hospital
R. Behruzi1, M. Hatem2, L. Goulet3, W. Fraser4
1McGill University, Department of Family Medicine, Montreal, Canada; 2,3Université de Montréal, Department of Social and Preventive Medicine, Montreal, Canada; 4Université de Montréal, Department of Obstetrics & Gynaecology, Montreal, Canada
SUMMARYA signifi cant proportion of high-risk pregnancies and low obstetric risk women
are currently referred to or seeking care in the tertiary level hospitals, therefore, it is crucial to explore the factors that infl uence the childbirth experience in these hos-pitals. The purpose of our study was to explore the facilitating factors and barriers in the provision of humanized obstetrical care in a highly specialized, university-affi liated hospital in Quebec, Canada. A single case study design was chosen. The fi nding shows that a high level of expertise, a pain free birth, as well as caring and family-centered model of care all are necessary to ensure the provision of human-ized care in a highly specialized institution. The humanization of birth practices in highly specialized hospitals should meet all the physiological, as well as psycho-logical aspects of birth care. This includes respect for the fears, beliefs, values, and needs of women and their families.
INTRODUCTIONDuring the past decades, giving birth has been an increasingly medicalized proce-
dure in most of countries and humans have basically been replaced by machines in order to bring more security to procedures to reduce the associated risks. (Hausman, 2005) The appropriate use of the medical interventions clearly save the life of moth-ers and babies; however, there are some concerns that medical intervention rates have increased around the world which suggests that they are not always necessary. A recent Canadian Perinatal Survey showed that cesarean births and epidural anal-gesia were 26.3% and 57.3% respectively, about 90.8% of women reported having

96
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
electronic fetal monitoring (EFM) during labour, and 62.9% reported having con-tinuous use of EFM. (Dzakpasu, et al., 2008) Davies’ study (2002) also showed that the use of EFM varied between 84.4% and 99.3% in the studied hospitals in Canada. (Davies, et al., 2002) The inductions accounted for 20% of all in-hospital births in Canada in 2006 and 2007,(Kirkey, 2009) and an even higher induction rate (25%) was reported by the Society of Obstetricians and Gynecologists of Canada (Canada, 2003) and Canadian Perinatal Survey (44%).(CPSS, 2008)
Considering the fact that the highly specialized environment of a hospital has its own rules, regulations, standards, and technology, any change in the provision of care in such environment needs to study the complex structural, cultural, social, historical, and political context of hospital. This study aimed to explore the orga-nizational and cultural dimensions of a highly specialized and university affi liated hospital which would act as barriers or facilitators for birth practices ensuring hu-manizing care in a highly specialized hospital, in the province of Quebec.
METHODSA single case study design was chosen for this study. The study sample included
17 professionals and administrators from different disciplines, and 157 women who gave birth in the hospital. Ethical approval for the study was obtained from the Research Ethical Committee of Université de Montréal and the Hospital. All the participants were informed about the nature of the research project, and a written consent was obtained before holding any interview. The data was collected through interviews, fi eld notes, participant observations, questionnaire, documents, and ar-chives, from November 2007 to March 2008. The investigator observed the birth practices and deliveries of six normal and four high-risk women and invited these ten women to a 45-60 minutes interview. The women were invited to express their childbirth experience or views on the characteristics of care in their institution and the humanization of care, as well. All 157 women participants fi lled out a question-naire comprised of four parts and 94 multiple choice and open-ended questions. The open-ended questions allowed women to elaborate theirs satisfaction and comments about the care they received during the perinatal period. Semi-structured interviews were accomplished with 11 professionals from multidisciplinary team and 6 ad-ministrators in the hospital. Documents of different natures such as administrative documents, proposals, progress reports, internal records and newspaper clipping were used for this study whilst respecting the administrators’ approval. The SPSS software (version 17) and descriptive statistic were used to analyze the responses collected in the questionnaire. The qualitative inductive and deductive content an-alyses were performed by help of the QDA Miner software (version 3.2.3) and use of Organizational culture model theory introduced by Allaire and Firsirotu. (Allaire & Firsirotu, 1984)
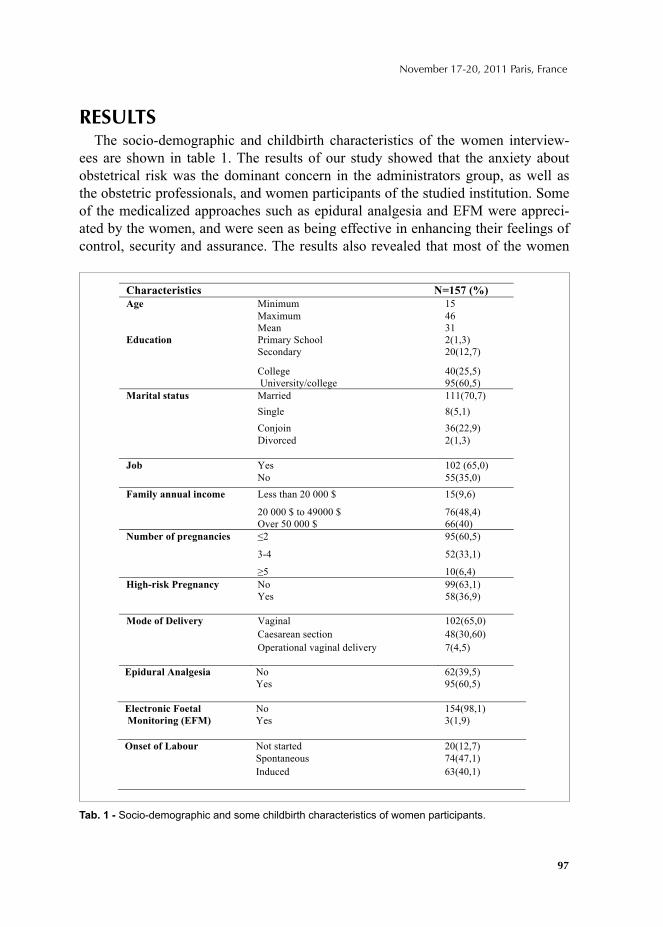
97
November 17-20, 2011 Paris, France
RESULTSThe socio-demographic and childbirth characteristics of the women interview-
ees are shown in table 1. The results of our study showed that the anxiety about obstetrical risk was the dominant concern in the administrators group, as well as the obstetric professionals, and women participants of the studied institution. Some of the medicalized approaches such as epidural analgesia and EFM were appreci-ated by the women, and were seen as being effective in enhancing their feelings of control, security and assurance. The results also revealed that most of the women
Epidural Analgesia No Yes
62(39,5) 95(60,5)
Electronic Foetal
Monitoring (EFM)
No Yes
154(98,1) 3(1,9)
Not started 20(12,7)
Spontaneous 74(47,1)
Onset of Labour
Induced
63(40,1)
Characteristics =157 (%)
Minimum 15
Maximum 46
Age
Mean 31 Primary School 2(1,3) Secondary 20(12,7)
College 40(25,5)
Education
University/college 95(60,5)
Married 111(70,7)
Single 8(5,1)
36(22,9)
2(1,3)
Marital status
Conjoin
Divorced
Job
Yes
No
102 (65,0)
55(35,0)
Family annual income Less than 20 000 $ 15(9,6)
20 000 $ to 49000 $ 76(48,4) Over 50 000 $ 66(40)
2 95(60,5)
3-4 52(33,1)
umber of pregnancies
5 10(6,4)
High-risk Pregnancy No Yes
99(63,1) 58(36,9)
Vaginal 102(65,0)
Caesarean section 48(30,60)
Mode of Delivery
Operational vaginal delivery 7(4,5)
Tab. 1 - Socio-demographic and some childbirth characteristics of women participants.

98
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
were satisfi ed with the care they received during their perinatal period in the tertiary hospital. The women’s satisfaction was mainly related to the care they received by health care providers of the hospital. Being in good hands and having competent healthcare providers, being humanly attended and receiving good service were con-sidered as important facilitating factors for the provision of a humanized birth care in the hospital. Undergoing a painless childbirth was considered as a humanistic care approach by women, as it relieved women’s pain and suffering, and allowed them to live through a better child birthing experience. The presence of competent professionals who were able to provide a caring and humane manner of assistance during labour and delivery, as well as giving confi dence to the women was shown to be an important factor in the provision of humanized birth care.
Our fi ndings also showed that many of the components of the external and the internal environment of a highly specialized hospital can act as facilitators or ob-stacles for the ‘humanization of birth’ practice (Table2). The greatest facilitating factors found were related to the structure of the institute including its caring and family-centered model of care, its fl exible companionship and visiting rules, and its free accommodation for parents in the hospital, in case baby had to remain in the hospital for a longer period. The individuals of the institution and the profes-sionals desires to tailor the medicalized aspect of care with the humanized care ap-proach, and to provide a pain free birth for women who demand it were important components of humanized birth in the studied hospital. The cultural competency of individuals to adapt to multiculturalism; and fi nally, the hospital’s culture and ideologies in dealing with the patients’ spiritual and religious beliefs, and valuing family were the others facilitating factors towards humanization of birth.
The fi ndings of the present study also showed many of barriers in offering hu-manized birth care practice in the studied hospital. These were found to be factors relating to the shortage of care providers, specially psychiatrists and midwives, as well as a lack of choice of a health care provider or continuity of care. Other barriers showed to be the hospital discharge rules, its professional environment and the lack of suffi cient communication among them. The training environment of the hospital and the exceeded number of care providers caused lack of continuity of care. The physical environment restrictions such as double occupancy of rooms and lack of privacy for women and families were considered a major obstacle for humanization of birth. The other barriers were the language communication diffi culties between women and care providers and much valuing medical performance by all the study participants.
CONCLUSIONAny change in policy proposed by health care decision makers in the highly
specialized hospitals should be brought about with sensitivity to women’s view. In order to explore the facilitating factors and barriers present toward the humanization
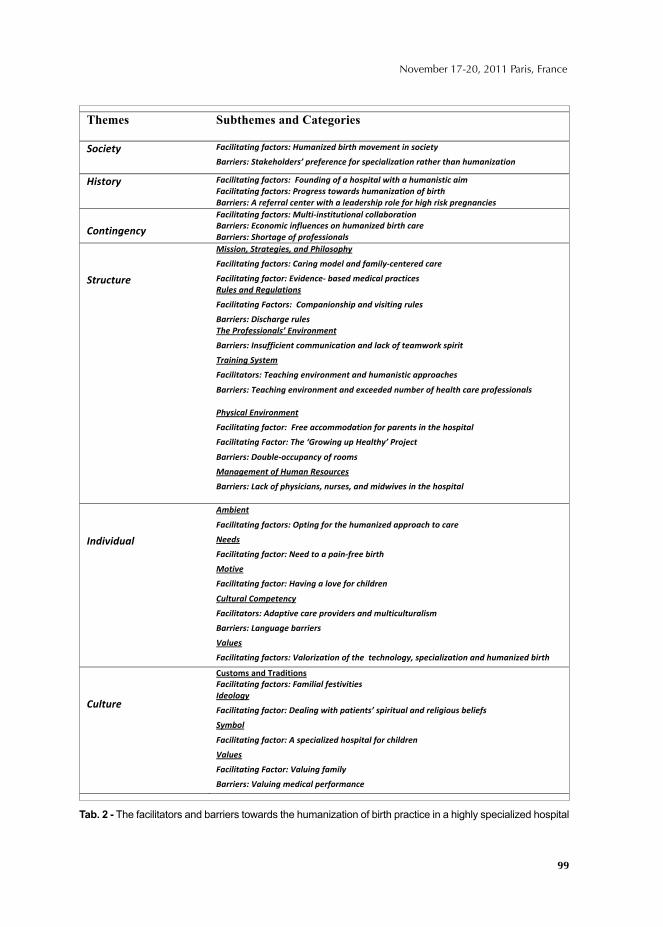
99
November 17-20, 2011 Paris, France
Themes Subthemes and Categories
Tab. 2 - The facilitators and barriers towards the humanization of birth practice in a highly specialized hospital

100
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
of birth care, the terms of risk, risk reduction, and risk management within such a setting must de redefi ned. Imposing an organization of care in the highly specialized hospitals with the philosophy of humanized birth, modifi cation of the rules and reg-ulations in order to provide continuity of care, evolving the mechanisms of budget allocation to the hospitals for reassuring fi nancial and hiring human resources and proposing closer cooperation in professional levels, all could promote the organiza-tion of care with regards to humanized birth care.
REFERENCES1. Allaire, Y., & Firsirotu, M. (1984). Theories of Organizational Culture',. Organizational Studies,
5(3), 193-226.2. Canada, H. (2003). Canadian Perinatal Health Report: Ottawa: Minister of Health.3. CPSS (2008). What Mother Says: The Canadian Maternity Experiences Survey.4. Davies, B., Hodnett, E., Hannah, M., O'Brien-Pallas, L., Pringle, D., & Wells, G. (2002). Fetal health
surveillance: a community-wide approach versus a tailored intervention for the implementation of clinical practice guidelines. CMAJ, 167(5), 469-474.
5. Dzakpasu, S., Kaczorowski, J., Chalmers, B., Heaman, M., Duggan, J., & Neusy, E. (2008). The Canadian maternity experiences survey: design and methods. Journal of Obstetrics and Gynaecology Canada, 30(3), 207-216.
6. Hausman, B. L. (2005). Risky business: framing childbirth in hospital settings. J Med Humanit, 26(1), 23-38.
7. Kirkey, S. (2009). Specialists want doctors to reduce c-section rate. National Post. http://www.nationalpost.com/news/story.html?id=1695536.
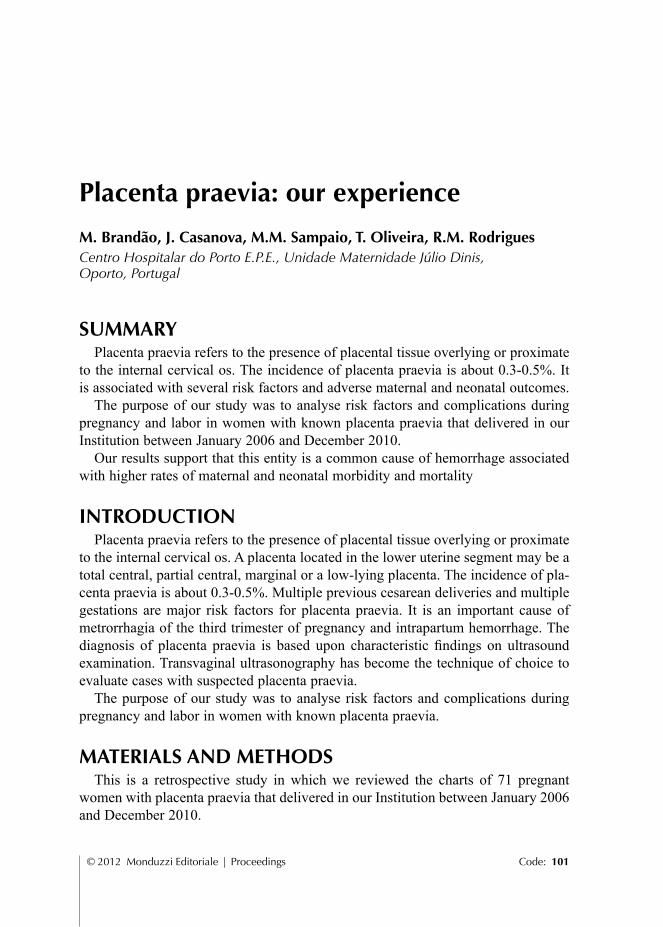
© 2012 Monduzzi Editoriale | Proceedings Code: 101
Placenta praevia: our experience
M. Brandão, J. Casanova, M.M. Sampaio, T. Oliveira, R.M. RodriguesCentro Hospitalar do Porto E.P.E., Unidade Maternidade Júlio Dinis, Oporto, Portugal
SUMMARYPlacenta praevia refers to the presence of placental tissue overlying or proximate
to the internal cervical os. The incidence of placenta praevia is about 0.3-0.5%. It is associated with several risk factors and adverse maternal and neonatal outcomes.
The purpose of our study was to analyse risk factors and complications during pregnancy and labor in women with known placenta praevia that delivered in our Institution between January 2006 and December 2010.
Our results support that this entity is a common cause of hemorrhage associated with higher rates of maternal and neonatal morbidity and mortality
INTRODUCTIONPlacenta praevia refers to the presence of placental tissue overlying or proximate
to the internal cervical os. A placenta located in the lower uterine segment may be a total central, partial central, marginal or a low-lying placenta. The incidence of pla-centa praevia is about 0.3-0.5%. Multiple previous cesarean deliveries and multiple gestations are major risk factors for placenta praevia. It is an important cause of metrorrhagia of the third trimester of pregnancy and intrapartum hemorrhage. The diagnosis of placenta praevia is based upon characteristic fi ndings on ultrasound examination. Transvaginal ultrasonography has become the technique of choice to evaluate cases with suspected placenta praevia.
The purpose of our study was to analyse risk factors and complications during pregnancy and labor in women with known placenta praevia.
MATERIALS AND METHODSThis is a retrospective study in which we reviewed the charts of 71 pregnant
women with placenta praevia that delivered in our Institution between January 2006 and December 2010.
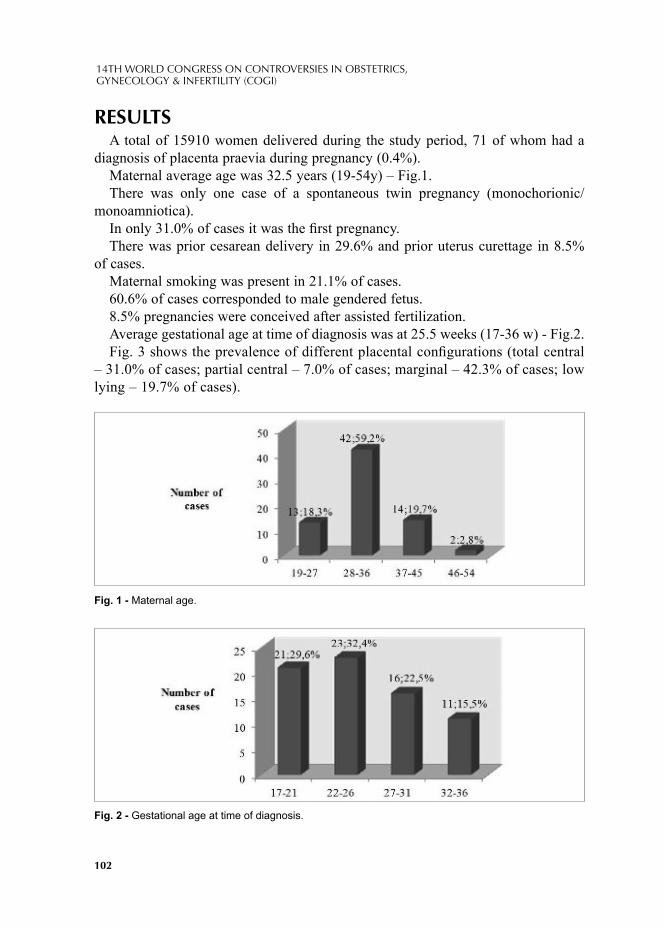
102
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
RESULTSA total of 15910 women delivered during the study period, 71 of whom had a
diagnosis of placenta praevia during pregnancy (0.4%).Maternal average age was 32.5 years (19-54y) – Fig.1. There was only one case of a spontaneous twin pregnancy (monochorionic/
monoamniotica).In only 31.0% of cases it was the fi rst pregnancy.There was prior cesarean delivery in 29.6% and prior uterus curettage in 8.5%
of cases.Maternal smoking was present in 21.1% of cases.60.6% of cases corresponded to male gendered fetus.8.5% pregnancies were conceived after assisted fertilization.Average gestational age at time of diagnosis was at 25.5 weeks (17-36 w) - Fig.2.Fig. 3 shows the prevalence of different placental confi gurations (total central
– 31.0% of cases; partial central – 7.0% of cases; marginal – 42.3% of cases; low lying – 19.7% of cases).
Fig. 1 - Maternal age.
Fig. 2 - Gestational age at time of diagnosis.
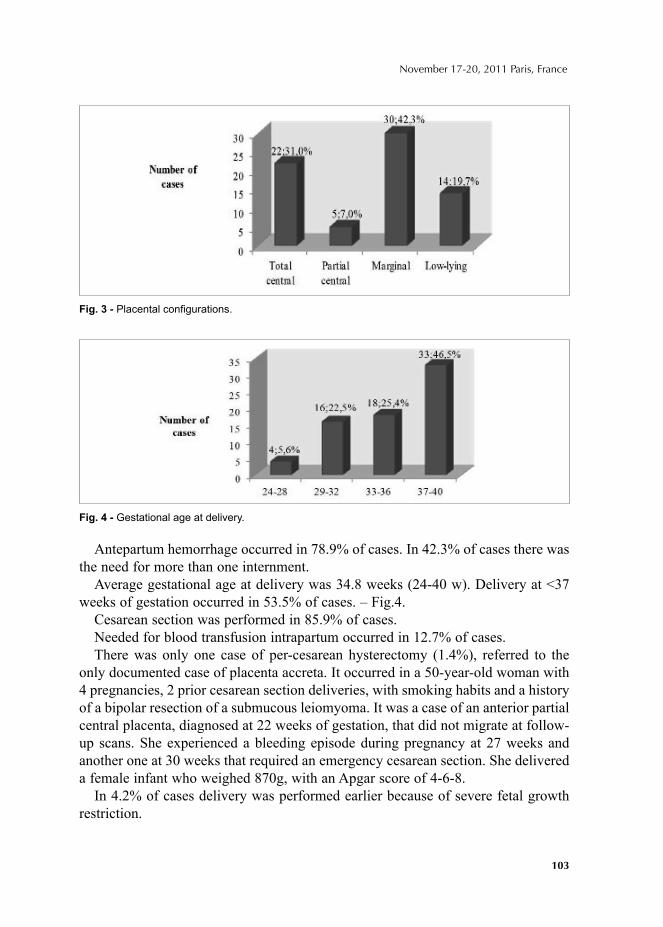
103
November 17-20, 2011 Paris, France
Antepartum hemorrhage occurred in 78.9% of cases. In 42.3% of cases there was the need for more than one internment.
Average gestational age at delivery was 34.8 weeks (24-40 w). Delivery at <37 weeks of gestation occurred in 53.5% of cases. – Fig.4.
Cesarean section was performed in 85.9% of cases.Needed for blood transfusion intrapartum occurred in 12.7% of cases.There was only one case of per-cesarean hysterectomy (1.4%), referred to the
only documented case of placenta accreta. It occurred in a 50-year-old woman with 4 pregnancies, 2 prior cesarean section deliveries, with smoking habits and a history of a bipolar resection of a submucous leiomyoma. It was a case of an anterior partial central placenta, diagnosed at 22 weeks of gestation, that did not migrate at follow-up scans. She experienced a bleeding episode during pregnancy at 27 weeks and another one at 30 weeks that required an emergency cesarean section. She delivered a female infant who weighed 870g, with an Apgar score of 4-6-8.
In 4.2% of cases delivery was performed earlier because of severe fetal growth restriction.
Fig. 3 - Placental confi gurations.
Fig. 4 - Gestational age at delivery.
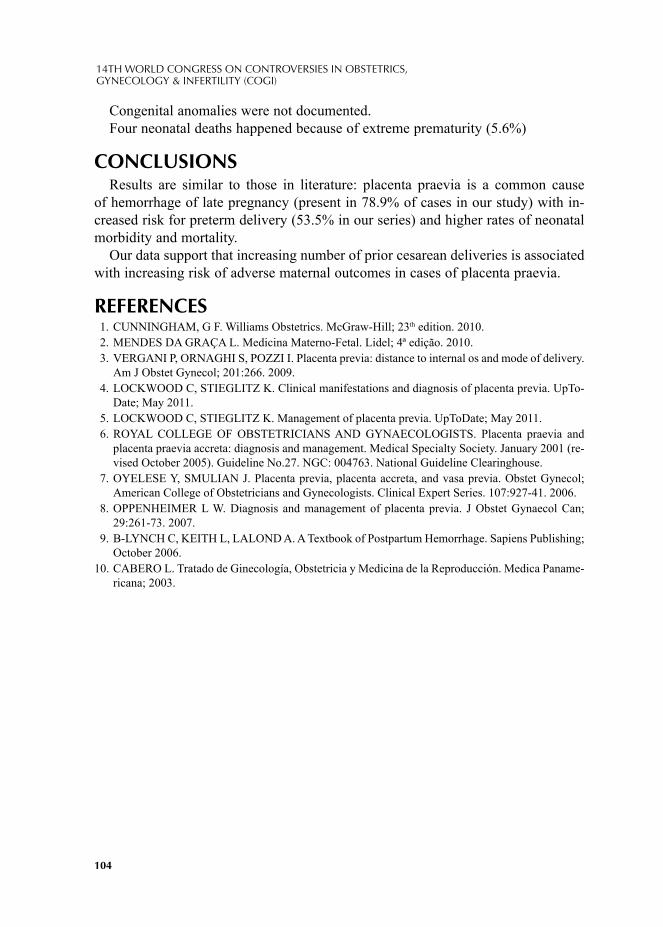
104
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Congenital anomalies were not documented.Four neonatal deaths happened because of extreme prematurity (5.6%)
CONCLUSIONSResults are similar to those in literature: placenta praevia is a common cause
of hemorrhage of late pregnancy (present in 78.9% of cases in our study) with in-creased risk for preterm delivery (53.5% in our series) and higher rates of neonatal morbidity and mortality.
Our data support that increasing number of prior cesarean deliveries is associated with increasing risk of adverse maternal outcomes in cases of placenta praevia.
REFERENCES1. CUNNINGHAM, G F. Williams Obstetrics. McGraw-Hill; 23th edition. 2010.2. MENDES DA GRAÇA L. Medicina Materno-Fetal. Lidel; 4ª edição. 2010.3. VERGANI P, ORNAGHI S, POZZI I. Placenta previa: distance to internal os and mode of delivery.
Am J Obstet Gynecol; 201:266. 2009.4. LOCKWOOD C, STIEGLITZ K. Clinical manifestations and diagnosis of placenta previa. UpTo-
Date; May 2011.5. LOCKWOOD C, STIEGLITZ K. Management of placenta previa. UpToDate; May 2011.6. ROYAL COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS. Placenta praevia and
placenta praevia accreta: diagnosis and management. Medical Specialty Society. January 2001 (re-vised October 2005). Guideline No.27. NGC: 004763. National Guideline Clearinghouse.
7. OYELESE Y, SMULIAN J. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol; American College of Obstetricians and Gynecologists. Clinical Expert Series. 107:927-41. 2006.
8. OPPENHEIMER L W. Diagnosis and management of placenta previa. J Obstet Gynaecol Can; 29:261-73. 2007.
9. B-LYNCH C, KEITH L, LALOND A. A Textbook of Postpartum Hemorrhage. Sapiens Publishing; October 2006.
10. CABERO L. Tratado de Ginecología, Obstetricia y Medicina de la Reproducción. Medica Paname-ricana; 2003.
© 2012 Monduzzi Editoriale | Proceedings Code: 105
The infl uence of bacterial vaginosis on preterm rupture of membranes
E. Bylykbashi1, I.V. Bylykbashi1, E. Kosturi2, O. Janushaj3, A. Zhaka2, E. Treska4
1”Bylykbashi Clinic”, ”Queen Geraldine” Maternity, Department of Ob-Gyn, Tirana, Albania; 2”Bylykbashi Clinic”, Department of Family Physician, Tirana, Albania; 3”Bylykbashi Clinic”, Tirana, Albania 4”Queen Geraldine” Maternity, Tirana, Albania
SUMMARY Premature rupture of membranes(PROM), yet has a considerable rate among peri-
natal complications. The aim of our study was to assess the correlation between the presence of bacterial vaginosis (BV) and its impact on the above mentioned event. We conducted a study on a group of 354 women, who had a term delivery. We ex-cluded all women with cardinal causes for such event. The remaining, underwent further examinations, for the detection of BV, including Gardnerella, Chlamydia Trachomatis, Trichomonas Vaginalis, Mycoplasma Hominis, Ureaplasma Urealyti-cum, by taking vaginal smears. 65% of the women developing PROM, had at least one of the major causes responsible for the above event. The 35% remaining,were screened for bacterial vaginosis. 75% had at least one of the microorganisms previ-ously mentioned. Therefore, we can affi rm that there is a good evidence, proving the infl uence of BV on PROM, and the benefi ts from screening, in foreseeing the risk of such complication.
INTRODUCTIONPremature rupture of membranes, is a serious event, as there is a considerable
risk of developing chorioamniotis or sepsis, which will as well affect the health of the offspring.
The objective of our study is to analyze the correlation between bacterial vagino-sis and premature rupture of the membranes.[1]
Bacterial vaginosis is a result of an imbalanced naturally occurring bacterial fl ora and is often confused with yeast infection. It is a quantitative alteration of normal
106
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
fl ora, in which lactobacilles are substituted with anaerobes, Mycoplasma Hominis ect.[2][3]. The most common sign of such infection are abnormal homogeneous off-white vaginal discharge with unpleasant smell, without irritation, pain or ery-thema. In clinical practice, BV is diagnosed through the use of Amsel criteria:1. Thin, white, yellow homogeneous discharge, 2. Clue cells on microscopy, 3. pH of vaginal fl uid >4.5, 4. Release of a fi shy odor by adding alkali – 10% potassium hydroxide(KOH.)[4]
In pregnant women, BV causes the membranes to be fragile, thanks to the pres-ence of specifi c enzymes as sialidases (neuraminidases), that enhance the ability of microorganisms to invade and destroy tissue, as well as galactosidase or cytokines like interleucine-1. Elevated levels of these enzymes, have been detected in more than 80% of fl uid specimen taken from women with BV.[5][6][7][8]
Our study involved a group of women who had a term delivery, and chose to study swabs from the ones who had a PROM in absence of any cardinal causes to justify such complication.
MATERIAL AND METHODSTo determine if there was a correlation between BV and PROM we studied a
group of 354 women who had a term delivery. We considered term delivery, preg-nancies which ended after the 37th week of gestation.
The diagnosis of BV, were based not only on Amsel criteria, but as well on the Gram-stained vaginal smear, with the Haylson criteria or the Nugent criteria; - Grade 1 = Normal – Lactobacillus predominate- Grade 2 = Intermediate – mixed fl ora with some lactobacilli present, but Gardnerella
also present- Grade 3 = BV – predominantly Gardnerella. Few or absent lactobacilli.[9]
RESULTSPROM was present in 52/354 (14%). In 65% (34/52) we identifi ed one of the
major causes responsible for PROM; hypertension, polihydramnion, multiple preg-nancies ect. The remaining 18 women (35%) were screened for bacterial vaginosis as mentioned above. Of these 18 women, 13 meaning 74% had at least one of the microorganisms previously mentioned.
CONCLUSIONSThe study we conducted, shows a good evidence proving the infl uence of bacte-
rial vaginosis on premature rupture of membranes. Based on the above results, we strongly support the application of routine screen-
ing for bacterial vaginosis during pregnancy. This way we can foresee the risk of developing a premature rupture of membranes.[10]
107
November 17-20, 2011 Paris, France
The sooner we diagnose a bacterial vaginosis, the sooner we can act and start the right therapy. [11]
REFERENCES1. MARTIUS J, ESCHENBACH DA. The role of bacterial vaginosis as a cause of amniotic fl uid
infection, chorioamnionitis and prematurity - a review. Arch Gynecol Obstet. 1990; 247(1):1-13. 2. TERRI WARREN, RN (2010). "Is It a Yeast Infection?". Retrieved 2011-02-23.3. FERRIS DG, NYIRJESY P, SOBEL JD, SOPER D, PAVLETIC A, LITAKER MS (March 2002).
"Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candi-diasis". Obstetrics and Gynecology 99 (3): 419–425.
4. AMSEL R, TOTTEN PA, SPIEGEL CA, CHEN KC, ESCHENBACH D, HOLMES KK (1983). "Nonspecifi c vaginitis. Diagnostic criteria and microbial and epidemiologic associations". Am. J. Med. 74 (1): 14–22.
5. ROBERTON, A. M., WIGGINS, R., HORNER, P. J., GREENWOOD, R., CROWLEY, T., FER-NANDES, A., BERRY, M., CORFIELD, A. P. (2005). A Novel Bacterial Mucinase, Glycosulfatase, Is Associated with Bacterial Vaginosis. J. Clin. Microbiol. 43.
6. CAUCI, S., THORSEN, P., SCHENDEL, D. E., BREMMELGAARD, A., QUADRIFOGLIO, F., GUASCHINO, S. (2003). Determination of Immunoglobulin A against Gardnerella vaginalis He-molysin, Sialidase, and Prolidase Activities in Vaginal Fluid: Implications for Adverse Pregnancy Outcomes. J. Clin. Microbiol. 41: 435-438.
7. CAUCI, S., GUASCHINO, S., DRIUSSI, S., De SANTO, D., LANZAFAME, P., QUADRIFOGLIO, F. (2002). Correlation of Local Interleukin-8 with Immunoglobulin A against Gardnerella vaginalis Hemolysin and with Prolidase and Sialidase Levels in Women with Bacterial Vaginosis. The Jour-nal of Infectious Disease 185: 1614-1620.
8. WENNERHOLM UB, HOLM B, MATTSBY-BALTZER I, et al. Interleukin-1 alpha, interleukin-6 and interleukin-8 in cervico/vaginal secretion for screening of preterm birth in twin gestation. Acta Obstet Gynecol Scand. 1998; 77(5):508-14.
9. NUGENT RP, KROHN MA, HILLIER SL (1991). "Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation". J. Clin. Microbiol. 29 (2): 297–301.
10. SIMOEOS JA, GIRALDO PC, CECATTI JG, CAMARGO RPS, FAUNDES A. Association between perinatal complications and bacterial vaginosis in Brazilian pregnant women. Int J
11. HAUTH JC, GOLDENBERG RL, ANDREWS WW, DUBARD MB, COOPER RL. Reduced incidence of preterm delivery with metronidazole and erythromycin in women with bacterial vaginosis. N Engl J Med. 1995; 333(26):1732-6.

© 2012 Monduzzi Editoriale | Proceedings Code: 106
The impact of periodontitis in the preterm birth and body size of newborns
L. Muhametaj1, E. Bylykbashi2, M. Muhametaj3, A. Manaj3, M. Xhelili1
1“Apex” Clinic, Tirana, Albania; 2“Bylykbashi” Clinic, Tirana, Albania; 3“Manaj” Clinic, Tirana, Albania
Objective: The aim of our study was to assess the relation between periodontitis, preterm birth and perinatal morbidity.
Materials and methods: We conducted the present observational retrospective cohort study among 230 women. Women which had other known prematurity risk factors, such as: age < 18, multiple gestations, DM, hypertension, corticosteroid use before our study ect. were left out of the study.
Results: Clinical measures of periodontal health were determined in all subjects, including sulcus/probing depth (PD), gingival recession and periodontal clinical at-tachment loss (CAL).
57 of 230 women resulted with periodontitis. Of these 57, 15 had premature rup-ture of membranes vs. 6/173 pregnant women with normal oral fl ora.
The use of H-square test to determine periodontitits and premature birth correla-tion was 8.1,which means a high statistical signifi cance, p=0.004.
Conclusions: Periodontitis is present in 10 up to 30% of all pregnancies. In our study it was present in 26% of all women included in the study. Therefore, we can affi rm that it is one of the main causes of preterm-premature rupture of membranes and a proper treatmen is the best solution for this pathology. Early diagnosis, can prevent premature birth and this way can reduce morbidity, mortality and fi nancial costs due to prematurity.
INTRODUCTIONPeriodontitis is an infective disease which affects more than 23% of women be-
tween 30 – 54 years. In absence of a regular oral hygene, periodontal bacteria acu-mulate, forming a very well organised structure known as “the bacterial biofi lm”:the bacteria possess a plethora of virulence factors, including lipopolysaccharide (LPS), that may cause direct destruction to the periodontal tissues or stimulate the host to activate a local infl ammatory and even general response by disseminating systemati-

110
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
cally to the fetal-placental unit via blood circulation and this way induce pregnancy complication. (1)(2)(3)(7).
Collins and colleagues found that infections like periodontitis, could act like source of bacteria and infl ammatory mediators. Maternal infection with these peri-odontal pathogenes have a strong impact on fetal growth and viability (4)(5)(6).
Preterm birth and low birth weight are worldwide leading perinatal problems and have evident public health implications, due to the fact that their incidence doesn’t decrease in spite of the many attempts at their prevention. (8)(9)(10)(14)(15)(16)
Periodontitis is a chronic infection by anaerobic gram-negative organisms and may produce local and systemic infection, so a possible association between peri-odontitis and adverse pregnancy outcomes has been suggested. During the second trimester of pregnancy, the proportion of Gram – negative anaerobic bacteria in dental plaque increases respect to aerobic bacteria. (5)
Fusobacterium nucleatum and other subspecies coming from the oral fl ora, have been found in the amniotic fl uid of women with preterm births. (12) The Gram – negative bacteria associated with pregressive disease can produce a variety of bioactive mol-ecules that may directly affect the host (5). Periodontitis shares some risk factors with preterm births and low birth weight. It’s probable that maternal periodontitis may inter-act synergically with other maternal risk factors to induce preterm births.(6)(15)(16).
METHODSWe conducted the present observational retrospective cohort study among 230
pregnant women. Clinical measures of periodontal health were determined in all subjects. Women with other know risk factors for premature birth, were left out of the study. Premature labour was defi ned as the occurrence of regular and persistent uterine contractions before the 37th week of gestation. Maternal morbidity was con-sidered to be present if there was the presence of endometritis and/or infection of a surgical wound that required hospital admission.
RESULTSOur study showed a signifi cant correlation between periodontitis and preterm
births, 15/57 with periodontitis had premature rupture of membranes vs. 6/173 with normal fl ora, which means 3 times more frequent in women with periodontitis.
Incidence of prematurity in Albania varies from 6 to 11.7 %. Neonatal mortality varies from 0.7 to 2.4%. The use of H-square test to determine periodontitits and pre-mature birth correlation was 8.1 which means a high statistical signifi cance p=0.004.
Periodontitis is a frequent pathology, present in 10-36% of pregnant women, in our study 26%.
On the other hand, children born from mothers in initial periodontitis had signs of hypotrophia in 17.9% whereas the ones from mothers with established periodontitis were hypotrophic in 82% of cases.

111
November 17-20, 2011 Paris, France
CONCLUSIONSFrom our study, we can affi rm that there is a strong correlation between the pres-
ence of periodontitis and high risk for prematurity and low birth weight. This as-sociation does not imply causality, as some underlying mechanisms might cause predisposition to both conditions. Other studies with better methodological quality will be necessary to confi rm that periodontitis in pregnant women is an independent risk factor for adverse pregnancy outcomes.
This study, shows the importance of detecting this pathology in order to prevent preterm birth, low birth weight, and that the best way to prevent complications is to have a good oral hygene.
REFERENCE1. Darveau RP, Tanner A, Page RC. The microbial challenge in periodontitis. Periodontol 2000 1997;
14:12–32.2. Miller WD. The human mouth as a focus of infection. Dental Cosmos 191; 33 :689–713.3. Collins JG, Smith MA, Arnold RR, Offenbacher S. Effects of Escherichia coli and P orphyromonas gingi-
valis lipopolysaccharide on pregnancy outcome in the golden hamster. Infect Immun 1994; 62(10):4652–5. 4. Collins JG, Windley HW 3rd, Arnold RR, Offenbacher S. Effects of a Porphyromonas gingivalis
infec tion on infl ammatory mediator response and pregnancy outcome in hamsters. Infect Immun 1994; 62(10):4356–61.
5. Offenbacher S, Katz V, Fertik G, et al. Periodontal infection as a possible risk factor for preterm low birth weig ht. J Periodontol 1996; 67(supplement 10):1103–13.
6. Mokeem SA, Molla GN, Al-Jewair TS. The prevalence and relationship between periodontal dis-ease and pre-term low birth weigh t infants at King Khalid University Hospital in Riyadh, Saudi Arabia. J Contemp Dent Pract 2004; 5(2):40–56.
7. Goepfert AR, Jeffcoat MK, Andrews WW, et al. Periodontal disease and upper genital tract infl am-mation in early spontaneous preterm birth. Obstet Gynecol 2004; 104(4):777–83.
8. Radnai M, Gorzo I, Nagy E, Urban E, Novak T, Pal A. A possible association between preterm birth and early periodontitis: a pilo t study. J Clin Periodontol 2004; 31(9):736–41.
9. Canakci V, Canakci CF, Canakci H, et al. Periodontal disease as a risk factor for pre-eclampsia: a case-control study. Aust N Z J Obstet Gynaecol 2004; 44(6):568–73.
10. Jarjo ura K, Devine PC, Perez-Delboy A, Herrera-Abreu M, D’Alton M, Papapanou PN. Markers of periodontal infection and pret erm birth. Am J Obstet Gynecol 2005; 192(2):513–9.
11. Dasanayake AP. Poor periodontal health of the pregnant woman as a risk factor for low birt h weight. Ann Periodontol 1998; 3(1):206–12.
12. Offenbacher S, Lieff S, Boggess KA, et al. Maternal periodontitis and prematurity, I: obstetric out-come of prematurity and growth restriction. Ann Periodontol 2001; 6(1):164–74.
13. Offenbacher et al., "Periodontitis : A potential risk factor for spontaneous preterm birth" Compendium of Continuing Education in Dentistry (1999) 19(1):32-3
14. Jeffcoat MK, G eurs NC, Reddy MS, Cliver SP, Goldenberg RL, Hauth JC. Periodontal infection and preterm birth: results of a prospective study. JADA 2001; 132(7):875–80.
15. World Health Organization. Oral health surveys: Basic methods. Geneva: World Health Organization; 1987.
16. Lopez NJ, Smith PC, Gutierrez J. Higher risk of preterm bi rth and low birth weight in women with peri odontal disease. J Dent Res 2002; 81(1):58–63.

© 2012 Monduzzi Editoriale | Proceedings Code: 531
Pre-pregnant body mass indexin women with gestational diabetes mellitus and pregnancy outcome
S. De Carolis1, A. Botta1, F. Macrì1, F. Stifani1, L. Casarella1, S. Garofalo1, C. Martino1, V.A. Degennaro1, S. Moresi1, G. Del Sordo1, E. Di Pasquo1, D. Pitocco2
1Dept. Obstetrics and Gynaecology, Catholic University of Sacred Hearth Rome, Italy; 2Dept. Internal Medicine, Catholic University of Sacred Hearth Rome, Italy
SUMMARYThis study is about the effects of Gestational Diabetes on pregnancy outcome.
The pre-pregnant body mass index (BMI) was considered and we found a corre-lation with fetal weight. No differences in term of Cesarian section, rate of pre-eclampsia, week of delivery and rate of intrauterine growth restriction between the two groups were found. No statistically signifi cant correlation between the total gestational weight gain and the pregnancy outcome was found. The same results in the different therapy groups were observed. Our study highlighted that a normal pre-pregnant BMI is an important requirement to obtain a good obstetric outcome in women affected by GDM.
INTRODUCTIONGestational diabetes mellitus (GDM) is defi ned as an impared glucose tolerance
with fi rst onset or fi rst diagnosis during pregnancy.It is the most frequent metabolic pregnancy complication associated with an increased risk of maternal and neonatal morbidities. The prevalence of the disease is about 4% of all pregnancies, with variations between 1% and 14% depending on the population studied and diagnos-tic tests used. The diagnosis is obtained by the sistematical application of an oral glucose tolerance test (OGTT) in women otherwise considered healty. Like other forms of hyperglycemia, GDM is characterized by higher insulin levels that are not suffi cient to maintain fasting and post-prandial blood glucose levels in a normal range. This is due both to an increased insuline resistance that physilogicallyoccures
114
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
in pregnancy and to a beta-cellular disfuction caused by mechanisms that are still not fully understood.(1) So, we can consider GDM as a manifestation of insuline resistance.The main risks for development of GDM are: maternal body mass index (BMI), belonging to a high-prevalence ethnic group, family history of fi rst-degree relatives with diabetes, age>25, previous large for gestational age (LGA) newborn and previous GDM. Women who develop GDM also have an increased prevalence of obesity and metabolic syndrome. In the last decade, an increased incidence was described in parallel with the increase in obesity: so we have to consider obesity and GDM as two related conditions.(2)
It’s well know that GDM is an important determinant of a bad pregnancy out-come, but different studies have demonstrated that also obesity alone during preg-nancy is considered a high-risk status. Obese women have higher rate of early mis-carriage and congenital anomalies, they are predisposed to have pregnancy-induced hypertension, gestational diabetes, thromboembolism, macrosomia, and spontane-ous intrauterine demises in the latter half of pregnancy. Instrument or Cesarean sec-tion delivery were required more often than in average-weight women. Irrespective of the delivery mode, children born to obese mothers have a higher incidence of macrosomia and associated shoulder dystocia. In addition to being large at birth, children born to obese mothers are also more susceptible to obesity in adolescence and adulthood. Prevention is the best way to prevent this problems(3-4). Mater-nal anthropometric parameters, such as pregestational BMI and gestational weight gain, have repeteadly been shown to be independent determinants of the size of the offspring. As pregnancy is the worst time to lose weight, women with a high BMI should be encouraged to lose weight prior to conceiving. During preconcep-tion counseling, they should be educated about the complications associated with a high BMI if scientifi c evidences have demonstrated that also an excessive weight gain during pregnancy can infl uence the pregnancy outcome itself.(5-6)
Since obesity and GDM are often related, many studies, in order to investigate the prognostic role of anthropometric parameters, were performed. The aim of our study is to evaluate the infl uence of pre-pregnant BMI on the obstetric outcome in diabetic women.
MATERIALS AND METHODSOne hundred-ninetyfi ve patients with 184 singleton pregnancies (10 twin preg-
nancies and 1 triple pregnancy) complicated by GDM were followed in our tertiary referral center from January 2009 to February 2011. Women were divided into two groups: patients with BMI ≥25 and patients with BMI< 25. The following param-eters from clinical history, medical records and reports of delivery room were col-lected: mother’s age, pre-pregnancy BMI and total gestational weight gain, time, mode and indication to delivery, labour results (miscarriages, intrauterine deaths, neonatal weight, birth weight percentile, presence of congenital abnormalities), in-
115
November 17-20, 2011 Paris, France
cidence of preeclampsia and kind of insulin regimen taken during pregnancy. We considered the pregnancy and neonatal outcome, respectively in women with a BMI <25 Kg/m2 and in women with a BMI ≥25 Kg/m2. 81 patients were treated with Regular Insulin therapy, 99 patients with Aspart Insulin, 4 with Metformin and 11 only with a diet strategy.
Gestational age was defi ned on the basis of the last maternal menstrual date con-fi rmed by early ultrasound examination. Preterm birth was defi ned as a delivery occurred before the 37 th gestational week. Intrauterine death was defi ned as a fetal loss occured> 20 weeks of gestation. We defi ned: macrosoma a newborn infant with a birth weight ≥4000g; Large for Gestational Age (LGA) a birth weight ≥90°Pc and Small for Gestational Age (SGA) a birthweight ≤10° Pc considering the birth weight in relation to the birth gestational week and according to a national standard curve for singleton birth. Polydramnios was defi nded as a amniotic fl uid quantity >95° pc for the gestational age. We calculated total gestational weight gain as the difference between maximum recorded weight gain during pregnancy and self-re-ported pre-pregnancy weight.
No subject had taken drugs that may have affected the metabolism for at least 3 months before the enrollement or had had desease known to affect pregancy and fetaloutcme. Informed consent was obtain from each patient and the study protocol was approved by our Institutional Review Board.
Data were stored and analyzed using SPSS software (Statistical Packagefor Social Science, release 6.0; SPSS, Inc., Chicago, IL) on an IBMcompatiblecomputer. Dis-tribution of the data was tested by the Kolmogorov-Smirnov test to verify whether the samples followed a normaldistribution. The absolute differences between the two groups were comparedusing the Student’s t test, whereas the nonparametric tests wereapplied to biochemical data that violated the assumption of normality.A two-tailed P<0.05 was considered statistically signifi cant. All data are presentedas mean ± SD.
RESULTS AND CONCLUSIONSIn the population affected by GDM a preterm delivery rate of 30.2% and a Cesar-
ian section rate of 53.3% were found. A birth weight percentile ≥ 90° occurred in 22 cases (10.7%) while intrauterine growth restriction occurred in 9 cases (4.3%). We observed polydramnios in 7 cases (3.4%) and fetal malformations in 3 cases (1.5%).
Considering the pregnancy outcome on the basis of pre-pregnant BMI, we found that the patients with a BMI < 25 Kg/m2 had statistically signifi cant lower birth weight (2919.63±509 vs.3127.85±583; p value=0.004) and lower birth weight per-centile than those women with a BMI ≥25 Kg/m2 (46.04±22.0 vs.60.36±25.0; p value<0.001). A statistically signifi cant correlation between BMI ≥25 Kg/m2 and a birth weight pecentile ≥90° was found. No differences in term of Cesarian section, rate of preeclampsia, week of delivery and rate of intrauterine growth restriction

116
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
between the two groups were found. No statistically signifi cant correlation between the total gestational weight gain and the pregnancy outcome was found.
We didn’t fi nd any correlation among the four different therapy groups, in terms of birth weight, birth weight percentile and week of delivery.
According with other scientifi c evidences,our study highlighted that a normal pre-pregnant BMI is an important requirement to obtain a good obstetric outcome in women affected by GDM. A pre-pregnancy overweight is an indipendent predictor of high birth weight and recent studies documented that obese non-diabetic women have higher daytime and nocturnal glucose than normal-weight women despite a controlled diet (7). At the same time, it’s well known that GDM is the most impor-tant determinant of fetal growth. In women affected by both these conditions, the rate of LGA newborn is increased despite a strict control of the weight gain during pregnancy. Further investigations are necessary to evaluate the specifi c role of BMI and GDM on the pregnancy and neonatal outcome and the relative risk of each fac-tor (overweight, GDM or both) must be considered.
In conclusion outpatient pre-conceptional counseling and weight evaluation is important in order to improve the pregnancy outcome.
REFERENCES1. METZGER BE, BUCHANAN TA, COUSTAN DR, DE LEIVA A, DUNGER DB, HADDEN DR,
HOD M, KITZMILLER JL, KJOS SL, ET AL. Summary and recommendations on the fi fth interna-tional workshop-conference on gestational diabetes Diabetes Care 30(suppl. 2): S251-S260,2007.
2. FORSBACH-SANCHEZG.,TAMEZ-PEREZH H.E.,VAZQUEZ-LARA J.; Diabetes and pregnan-cy; archives of; edial research 36 291-299; 2005.
3. SIMMONS D: Diabetes and obesity in pregnancy; Best Pract. Res ClinObstetGynaecol; 25 (1); 25-36; 2011.
4. VAN EERDEN P.; Obesity in pregnancy; S d Med; Spec no; 46-50; 2011.5. CLAUSEN T; BURSKI T.H. et al.; Maternal anthropometric and metaboli factors in the fi rst half
of pregnancy and risk of neonatal macrosomia in term pregnancies. A prospective study; European journal of endocrinology; 153; 887-894; 2005.
6. KABALL C.; WERLER MM; Pre-pregnant body mass index, weight gain and the risk of delivering large babies among non-diabetic mothers; Int J GynaecolObstet; 97 (2); 100-104; 2007.
7. HARMON KA; GERARD L.; JENSEN DR et al; Continuous glucose profi le in obese and normal-weight pregnant women on a controlled diet: metabolic determinants of fetal growth; Diabetes Care; 34 (10); 198-204; 2011.
© 2012 Monduzzi Editoriale | Proceedings Code: 196
Controversies in the introduction of antenatal ultrasonography in rural Tanzania
E. Firth1, P. Mlay2, R. Walker3, P.R. Sill4
1School of Medicine, Sheffi eld University, UK; 2Department of Obs & Gynae, KCMC, Moshi, Tanzania; 3Department of Medicine, North Tyneside General Hospital, North Shields, UK; 4Department of Obs & Gynae, Wansbeck Hospital, Northumberland, UK
SUMMARYThis study explored pregnant women’s beliefs, expectations and experiences of
the newly introduced antenatal ultrasound service in BomaNg’ombe, Tanzania. 25 semi-structured interviews and 41 questionnaires were completed with pregnant women aged 18 years, May-June 2010. Thematic analysis was performed. Despite varied levels of knowledge about ultrasound, most women desired a scan. Some enjoyed seeing the baby, and several believed ultrasound would increase antena-tal care (ANC) attendance. However many women over-estimated the capacity of ultrasound. Signifi cant fears of ultrasound being invasive, and causing disability or even death were also present. One-sixth of questionnaire respondents did not want a scan. Despite this, no woman had declined a scan. Numerous interviewees believed scans were obligatory. We recommend that research on attitudes towards new medical technology should be conducted at early stages, education campaigns may be necessary, as is an informed consent policy is crucial to reduce fears and protect autonomy.
INTRODUCTIONIn 2009 BomaNg’ombe District hospital, Northern Tanzania, began a pilot of rou-
tine antenatal ultrasound. Antenatal ultrasound is recognised as the most accurate method for calculating estimated date of delivery (EDD).1 Whilst widely established in the developed world, it is a newer concept in many developing countries such as Tanzania. It has been recognised that medical technology should be introduced cau-tiously in resource-poor settings, with attention to social, cultural and political ac-

118
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
ceptability2,3. In fact, research into the acceptability of antenatal ultrasound is largely Euro-American and Australian. Only Nigerian4-7 and Botswanan8 studies represented the views and experiences of pregnant African women before this Tanzanian study.
Maternal mortality in Tanzania is estimated at 950 deaths per 100,000 births9, double that of the average maternal mortality rates for developing countries10. In this context, timely uptake of ultrasound and of antenatal care, are each potentially life-saving. Ultrasonography may positively or negatively affect the timely atten-dance at antenatal clinics (ANC). Understanding the views of pregnant women to-wards ultrasound scans is therefore of crucial importance.
MATERIALS AND METHODSAll participants were pregnant women, aged 18 and over, who attended
BomaNg’ombe ANC, where a pilot of routine ultrasound had begun in 2009. 25 semi-structured interviews and 41 questionnaires were completed during May and June 2010. Two questionnaires were created: Questionnaire I (completed n=36) for women who had not previously undergone an ultrasound examination and Question-naire II (completed n=5) for women who had. Two physicians acted as interview interpreters, one of whom translated questionnaires between Swahili and English. Questionnaires were offered to all consecutive patients at ANCs during the research period. Consecutive patients attending clinic with the working physician during the research period were invited to be interviewed. Consent for interviews was gained via signature (n=20) or thumb print (n=5). Completion of a questionnaire acted as consent; all were anonymous. No patients declined participation. Interviews were recorded via note-taking, due to ethical restrictions on audio recording. This study was endorsed by the Leeds University, and the Kilimanjaro Christian Medical Cen-tre ethical committees, and ratifi ed by the Hai District Medical Offi cer.
Thematic analysis of interviews was performed continuously throughout re-search, allowing an emergent design. Questionnaire data was then cross-analysed. Non-represented groups included women <18 years, and those not attending ANC. Illiterate women were represented in interviews, but not in questionnaires. Transla-tions from the study were verifi ed by an independent, non-medical translator.
RESULTSPast experience of ultrasound, and timing of ANC visits: The majority of in-
terviewees and questionnaire participants (77%), had never undergone a prior an-tenatal ultrasound examination (Figure 2). Interview participants made their fi rst ANC visit from 12–40+ weeks [5 interviewees (20%) did not know when]. Only 9 (36%) interviewees confi rmed their 1st attendance was <24 weeks (Figure 1). En-suring women attend clinic between 12-24 weeks gestations for accurate ultrasound examination, may prove diffi cult.
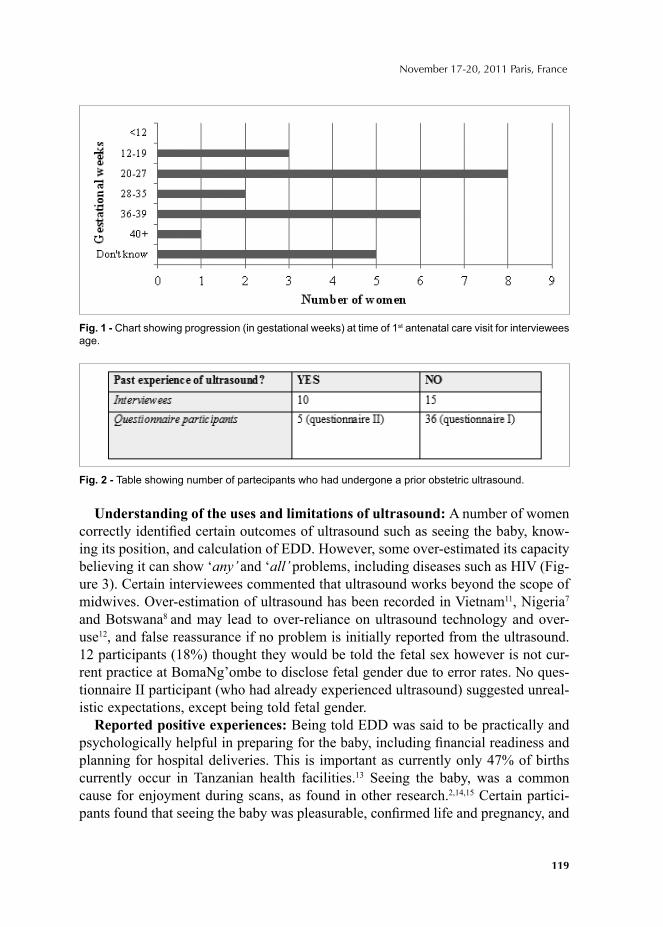
119
November 17-20, 2011 Paris, France
Understanding of the uses and limitations of ultrasound: A number of women correctly identifi ed certain outcomes of ultrasound such as seeing the baby, know-ing its position, and calculation of EDD. However, some over-estimated its capacity believing it can show ‘any’ and ‘all’ problems, including diseases such as HIV (Fig-ure 3). Certain interviewees commented that ultrasound works beyond the scope of midwives. Over-estimation of ultrasound has been recorded in Vietnam11, Nigeria7 and Botswana8 and may lead to over-reliance on ultrasound technology and over-use12, and false reassurance if no problem is initially reported from the ultrasound. 12 participants (18%) thought they would be told the fetal sex however is not cur-rent practice at BomaNg’ombe to disclose fetal gender due to error rates. No ques-tionnaire II participant (who had already experienced ultrasound) suggested unreal-istic expectations, except being told fetal gender.
Reported positive experiences: Being told EDD was said to be practically and psychologically helpful in preparing for the baby, including fi nancial readiness and planning for hospital deliveries. This is important as currently only 47% of births currently occur in Tanzanian health facilities.13 Seeing the baby, was a common cause for enjoyment during scans, as found in other research.2,14,15 Certain partici-pants found that seeing the baby was pleasurable, confi rmed life and pregnancy, and
Fig. 1 - Chart showing progression (in gestational weeks) at time of 1st antenatal care visit for interviewees age.
Fig. 2 - Table showing number of partecipants who had undergone a prior obstetric ultrasound.
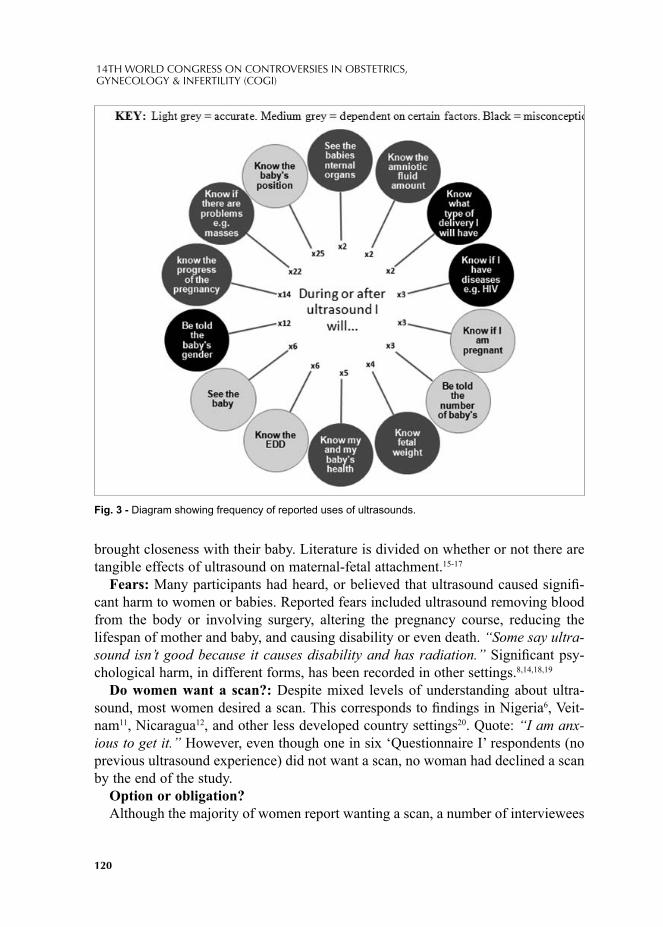
120
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
brought closeness with their baby. Literature is divided on whether or not there are tangible effects of ultrasound on maternal-fetal attachment.15-17
Fears: Many participants had heard, or believed that ultrasound caused signifi -cant harm to women or babies. Reported fears included ultrasound removing blood from the body or involving surgery, altering the pregnancy course, reducing the lifespan of mother and baby, and causing disability or even death. “Some say ultra-sound isn’t good because it causes disability and has radiation.” Signifi cant psy-chological harm, in different forms, has been recorded in other settings.8,14,18,19
Do women want a scan?: Despite mixed levels of understanding about ultra-sound, most women desired a scan. This corresponds to fi ndings in Nigeria6, Veit-nam11, Nicaragua12, and other less developed country settings20. Quote: “I am anx-ious to get it.” However, even though one in six ‘Questionnaire I’ respondents (no previous ultrasound experience) did not want a scan, no woman had declined a scan by the end of the study.
Option or obligation?Although the majority of women report wanting a scan, a number of interviewees
Fig. 3 - Diagram showing frequency of reported uses of ultrasounds.

121
November 17-20, 2011 Paris, France
also thought that ultrasound scans were obligatory at ANC. This may be a reason for why no-one has yet declined to undergo a scan since the programme started in 2009 despite 6 (17%) of ‘Questionnaire I’ participant saying they did not want a scan, and signifi cant fears about the effects of ultrasound. Equally it may be that health professionals explain the procedure appropriately before ultrasound examinations which changes the mind of women who were previously unsure. Allowing women to fully understand the purpose, limitations and procedure of ultrasound, and choice to accept or decline is part of gaining fully informed consent. The World Health Organisation emphasised the need for fully informed consent before antenatal ul-trasounds as early as 1984.21 Nonetheless, suboptimal informed consent has been documented world-wide.6,7,11,14-16,19,22
Impact of ultrasound on ANC attendance: Most interviewees said that ultra-sound availability made ANC seem more appealing to them, and that they thought it would increase attendance at clinics by other women. In this way, ultrasound could potentially increase timely attendance at ANC, an idea supported by Hofmeyr2. This hypothesis does depend on the timing requirements for accurate ultrasound being met, and cannot necessarily be generalised to women not wanting ultrasound (6 (17%) completing ‘Questionnaire I’), or women not already attending ANC (not included in this study).
CONCLUSIONSResearch on attitudes towards new medical technology should be conducted at
early stages of implementation. An improved informed consent policy is needed to facilitate understanding of the purpose, procedure and limitations of ultrasound, and to protect autonomy.20,23 Training sonographers and ANC staff in counselling wom-en about ultrasound, and providing written materials for women are key interven-tions.24 Dispelling misconceptions about harm, and explaining the correct gestation at which to attend ANC for ultrasound scanning would be priorities. Radio, village theatre, schools and print media have been successfully employed in African coun-tries to relay messages about obstetric health.25 Similar methods could be utilised to educate about ultrasound. Further research on the impact of ultrasound on ANC uptake and maternal mortality is required.
REFERENCES1. KALISH RB, CHERVENAK FA. Sonographic determination of gestational age. The Ultrasound
Review of Obstetrics and Gynecology 2005; 5(4): 254–2582. HOFMEYR GJ. Routine ultrasound examination in early pregnancy: is it worthwhile in low-in-
come countries? Ultrasound Obstet Gynecol 2009; 34(4): 367–373. DAAR AS, THORSTEINSDOTTIR H, Martin DK, Smith AC, Nast S, Singer PA. Top ten biotech-
nologies for improving health in developing countries. Nat Genet 2002; 32(2): 229–232.4. EKELE BA, MAAJI SM, BELLO SO, MORHASON-BELLO IO. Profi le of Women Seeking Fetal
Gender at Ultrasound in a Nigerian Obstetric Population. Ultrasound 2008; 16(4): 199-202.

122
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
5. ENAKPENE CA, MORHASON-BELLO IO, MARINHO AO, ADEDOKUN BO, KALEJAIYE AO, SOGO K et al. Clients' reasons for prenatal ultrasonography in Ibadan, South West of Nigeria. BMC Women's Health 2009; 9(1): 12
6. OCHIE K, UGWU AC. Access to Obstetric Ultrasonography in Some Rural Settings in Nigeria: Results of a Sample Survey. European Journal of Scientifi c Research 2009; 36(2): 246-250
7. UGWU AC, OSUNGBADE EO, ERONDU FO. Maternal Perspectives of Prenatal Sonogram in a North-Eastern Population in Nigeria. Libyan Journal of Medicine 2009; 4(4): 140-142
8. TAUTZ S, JAHN A, MOLOKOMME I, GÖRGEN R. Between fear and relief: how rural pregnant women experience foetal ultrasound in a Botswana district hospital. Soc Sci Med 2000; 50(5): 689-701
9. UNICEF. Tanzania, United Republic of: Statistics. 2010. [Online] Available from: http://www.unicef.org/infobycountry/tanzania_statistics.html [Accessed 21/07/10]
10. WHO, UNICEF, UNFPA & World Bank 2007, Maternal Mortality in 2005: Estimates developed by WHO, UNICEF, UNFPA, and the World Bank, WHO, Geneva, Switzerland.
11. GAMMELTOFT T. Sonography and Sociality: Obstetrical Ultrasound Imaging in Urban Vietnam. Med Anthropol Q 2007; 21(2): 133-153
12. HARRIS RD, MARKS WM. Compact Ultrasound for Improving Maternal and Perinatal Care in Low-Resource Settings: Review of the Potential Benefi ts, Implementation Challenges, and Public Health Issues. J Ultrasound Med 2009; 28(8): 1067–1076
13. NATIONAL BUREAU OF STATISTICS Dar Es Salaam, Tanzania, United Republic of Tanzania and ORC MACRO Calverton, MARYLAND, USA. 2005. Chapter 9: Maternal and Child Health, in Tanzania: Standard DHS, 2004-2005. [Online] Available from: http://www.measuredhs.com/pubs/pub_details.cfm?ID=566 [Accessed 17/01/10]
14. HARRIS G, CONNOR L, BISITS A, HIGGINBOTHAM N. “Seeing the Baby": Pleasures and Dilemmas of Ultrasound Technologies for Primiparous Australian Women. Med Anthropol Q 2008; 18(1): 23-47
15. BASHOUR H, HAFEZ R, ABDULSALAM A. Syrian Women's Perceptions and Experiences of Ultrasound Screening in Pregnancy: Implications for Antenatal Policy. Reprod Health Matter 2005; 13(25): 147-154
16. EKELIN M, CRANG-SVALENIUS E, DYKES A-K. Developing the P30R-U scale to measure parents’ expectations, experiences and reactions to routine ultrasound examinations during preg-nancy. J Reprod Infant Psyc 2008; 26(3): 211–228
17. SPARLING JW, SEEDS JW, FARRAN DC. The relationship of obstetric ultrasound to parent and infant behaviour. Obstet Gynecol 1998; 72(6): 902-7
18. LARSSON A-K, SVALENIUS EC, MARSÁL K, DYKES A-K. Parental level of anxiety, sense of coherence and state of mind when choroid plexus cysts have been identifi ed at a routine ultrasound examination in the second trimester of pregnancy: a case control study. J Psychosom Obst Gyn 2009; 30(2): 95–100
19. EKELNIN M, SVALENIUS EC, LARSSON A-K, NYBERG P, MARSAL K, DYKES AK. Paren-tal expectations, experiences and reactions, sense of coherence and grade of anxiety related to rou-tine ultrasound examination with normal fi ndings during pregnancy. Prenat Diagn 2009; 29(10): 952–959
20. NIGENDA G, LANGER A, KUCHAISIT C, ROMERO M, ROJAS G, AL-OSIMY M et al. Wom-ens' opinions on antenatal care in developing countries: results of a study in Cuba, Thailand, Saudi Arabia and Argentina. BMC Public Health 2003; 3(1):17
21. WORLD HEALTH ORGANISATION (WHO) Diagnostic ultrasound in pregnancy: WHO view on routine screening. The Lancet 1984; 2: 361
22. LALOR JG, DEVANE D. Information, knowledge and expectations of the routine ultrasound scan. Midwifery 2007; 23(1): 13–22
123
November 17-20, 2011 Paris, France
23. PROUD J. Ultrasound for midwives: a guide for midwives and other health professionals. Hale, Cheshire: Books for Midwives Press; c1994
24. CASH R, MANOGARAN M, SROKA H, OKUN N. An Assessment of Women’s Knowledge of and Views on the Reporting of Ultrasound Soft Markers During the Routine Anatomy Ultrasound Examination. J Obstet Gynaecol Can 2010; 32(2): 120-5
25. ENGENDERHEALTH, United Nations Population Fund. Obstetric fi stula needs assessment re-port: fi ndings from nine African countries. New York, NY: EngenderHealth; 2003. [Online] Avail-able from: http://www.engenderhealth.org/res/offc/mac/obs-fi s/index.html [06/02/2011].


© 2012 Monduzzi Editoriale | Proceedings Code: 198
Maternal status and recent patterns of double and triple deliveries in Spain
V. Fuster Siebert, J. Román-BustoDep. of Zoology and Physical Anthropology Complutense University of Madrid & GEPS, Madrid, Spain
SUMMARYDemographic indicators for multiple deliveries considering the maternal country
of birth are analyzed for the 1996-2009 period. For the Spanish, double deliveries continued to rise up through 2009, while cases of triplets have declined since 2001. Data proved to be signifi cant for fi rst time Spanish mothers over 25, while for the non Spanish, this occurred only for mothers 40 or older. In case of mothers with one or more previous children, differences remained signifi cant among the Spanish. Double deliveries were more frequent, mainly for Spanish mothers, in cases of high education and professional qualifi cation. Greater rates of double deliveries in cities were observed, but no clear geographic pattern was found. These results indicate a bias in the demand for reproductive treatments which is associated with higher cul-tural and economic status. (Paper supported by Project reference CGL2008-03737).
INTRODUCTIONWorldwide, twinning rates declined throughout the 1960s and the 70s, especially
in Western Europe. Decreasing endogamy and demographic changes affecting age at maternity and parity as well as urbanization have been used as arguments to explain the fall in twinning rates [1]. Beginning in the 80s several European countries have shown an increase in the frequency of multiple deliveries with the use of assisted reproductive treatments [2, 3], an increase which occurred in Spain after 1990 [4].
The aim of this paper is to infer indirectly through socio-demographic indica-tors whether the incidence of multiple deliveries in Spain may indicate a variable demand for reproductive treatments.
MATERIAL AND METHODSDigital individual records (one per delivery) provided by the Spanish National
Institute of Statistics contained bio-demographic information regarding newborns
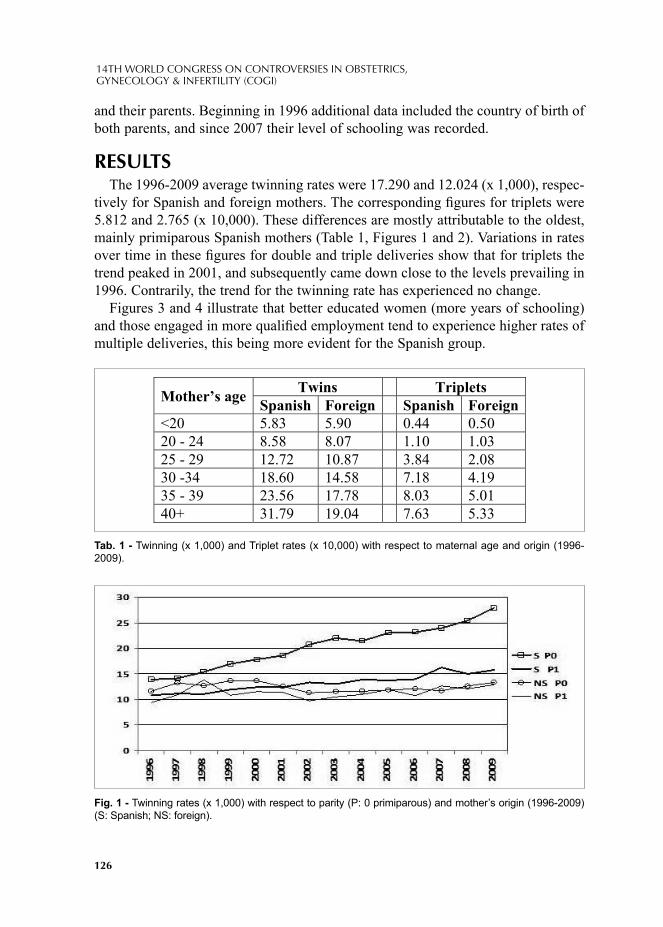
126
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
and their parents. Beginning in 1996 additional data included the country of birth of both parents, and since 2007 their level of schooling was recorded.
RESULTSThe 1996-2009 average twinning rates were 17.290 and 12.024 (x 1,000), respec-
tively for Spanish and foreign mothers. The corresponding fi gures for triplets were 5.812 and 2.765 (x 10,000). These differences are mostly attributable to the oldest, mainly primiparous Spanish mothers (Table 1, Figures 1 and 2). Variations in rates over time in these fi gures for double and triple deliveries show that for triplets the trend peaked in 2001, and subsequently came down close to the levels prevailing in 1996. Contrarily, the trend for the twinning rate has experienced no change.
Figures 3 and 4 illustrate that better educated women (more years of schooling) and those engaged in more qualifi ed employment tend to experience higher rates of multiple deliveries, this being more evident for the Spanish group.
Mother’s age Twins Triplets Spanish Foreign Spanish Foreign
<20 5.83 5.90 0.44 0.50 20 - 24 8.58 8.07 1.10 1.03 25 - 29 12.72 10.87 3.84 2.08 30 -34 18.60 14.58 7.18 4.19 35 - 39 23.56 17.78 8.03 5.01 40+ 31.79 19.04 7.63 5.33
Tab. 1 - Twinning (x 1,000) and Triplet rates (x 10,000) with respect to maternal age and origin (1996-2009).
Fig. 1 - Twinning rates (x 1,000) with respect to parity (P: 0 primiparous) and mother’s origin (1996-2009) (S: Spanish; NS: foreign).
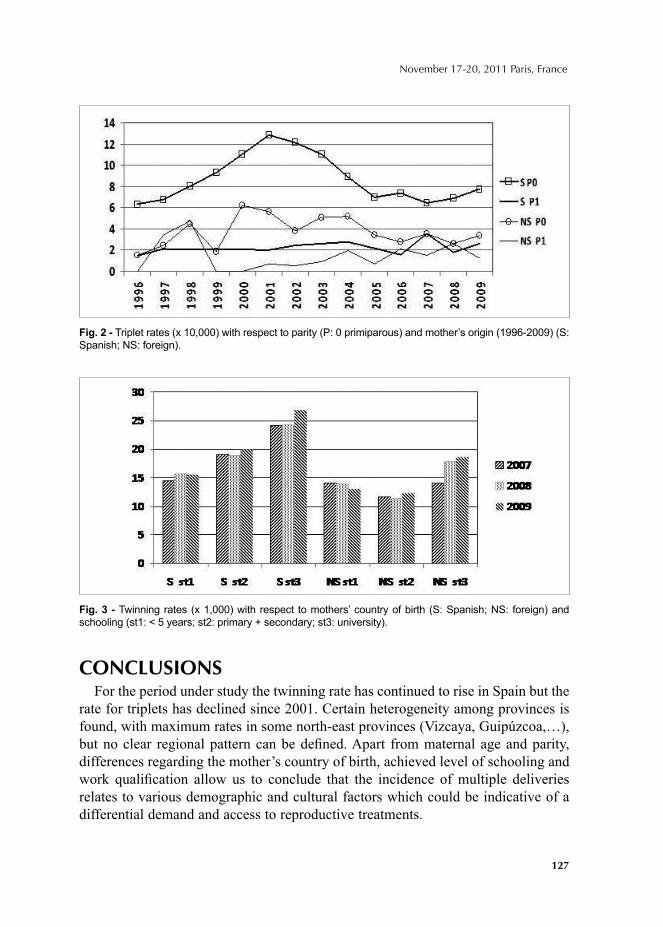
127
November 17-20, 2011 Paris, France
CONCLUSIONSFor the period under study the twinning rate has continued to rise in Spain but the
rate for triplets has declined since 2001. Certain heterogeneity among provinces is found, with maximum rates in some north-east provinces (Vizcaya, Guipúzcoa,…), but no clear regional pattern can be defi ned. Apart from maternal age and parity, differences regarding the mother’s country of birth, achieved level of schooling and work qualifi cation allow us to conclude that the incidence of multiple deliveries relates to various demographic and cultural factors which could be indicative of a differential demand and access to reproductive treatments.
Fig. 2 - Triplet rates (x 10,000) with respect to parity (P: 0 primiparous) and mother’s origin (1996-2009) (S: Spanish; NS: foreign).
Fig. 3 - Twinning rates (x 1,000) with respect to mothers’ country of birth (S: Spanish; NS: foreign) and schooling (st1: < 5 years; st2: primary + secondary; st3: university).
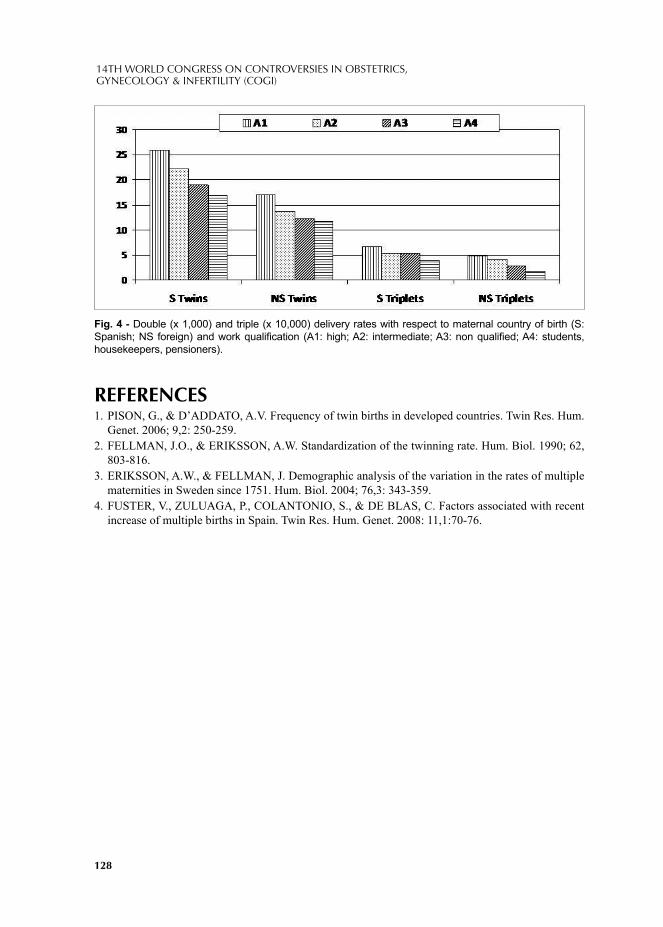
128
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
REFERENCES1. PISON, G., & D’ADDATO, A.V. Frequency of twin births in developed countries. Twin Res. Hum.
Genet. 2006; 9,2: 250-259.2. FELLMAN, J.O., & ERIKSSON, A.W. Standardization of the twinning rate. Hum. Biol. 1990; 62,
803-816.3. ERIKSSON, A.W., & FELLMAN, J. Demographic analysis of the variation in the rates of multiple
maternities in Sweden since 1751. Hum. Biol. 2004; 76,3: 343-359.4. FUSTER, V., ZULUAGA, P., COLANTONIO, S., & DE BLAS, C. Factors associated with recent
increase of multiple births in Spain. Twin Res. Hum. Genet. 2008: 11,1:70-76.
Fig. 4 - Double (x 1,000) and triple (x 10,000) delivery rates with respect to maternal country of birth (S: Spanish; NS foreign) and work qualifi cation (A1: high; A2: intermediate; A3: non qualifi ed; A4: students, housekeepers, pensioners).
© 2012 Monduzzi Editoriale | Proceedings Code: 587
The infl uence of mode of delivery in neonatal complications in breech presentation
S. Latifi -Hoxha, M. Hoxha, Sh. Bajraktari Ponosheci, N. Berisha, B. SkenderiUniversity Clinical Centre of Kosovo, Clinics for Obstetrics and Gynecology, Pristine, Kosovo
SUMMARYThe aim of this study was to compare the risk for neonatal complications in
breech presentation according to mode of delivery. Study was designed as retro-spective study of pregnancies with breech presentation in Clinic of Obs&Gyn of the University Clinical Centre of Kosovo (2008-2009). Neonatal complications were compared in 413 pregnancies delivered by caesarean section with 388 vaginal births. The cases with congenital anomalies, multiple pregnancies, foetuses >3800g was excluded from the study. The outcome was expressed through Odds Ratio, with confi dence interval 95%. Planned cesarean section signifi cantly reduced the risk for IVH, birth trauma and neonatal death, but not signifi cantly for perinatal asphyxia, early neonatal infections, sepsis, RDS, and CPAP requirement.
KEY WORDNeonatal complications, breech presentation, mode of delivery, birth weight, cae-
sarian sections, vaginal delivery
INTRODUCTIONIn breech presentation, both the mother and the baby are at higher risk for appear-
ance of complications, compared with the birth with head presentation.Pre-emptive Caesarean section has been promoted since the publication of the
Term Breech Trial in 2000 (1). The published trial indicated that there were serious differences in short-term neonatal morbidity, from 0.4 for deliveries via Caesarean section to 5.1 for vaginal deliveries (2).

130
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
This controversial trial made a dramatic impact on practice and raised further questions beyond its scope. Rapid change in clinical practice occurred in many lo-cations, although not universally, as some desired more evidence and others were reticent to accept the trials results as conclusive.
By 2003–2004, a number of countries had started to question the results of the Term Breech Trial. Further re-analysis and follow-up indicated that at fi ve years, there was very little difference in neonatal outcome. Maternal outcome was not sig-nifi cantly changed, as there was no increase in maternal mortality for either vaginal or Caesarean section delivery.
MATERIALS AND METHODSStudy was designed as retrospective study of pregnancies with breech presenta-
tion in Clinic of Obstetrics and Gynaecology of the University Clinical Centre of Kosovo (2008-2009). Neonatal complications were compared in 413 pregnancies delivered by caesarean section with 388 vaginal births. The cases with congenital anomalies, multiple pregnancies, foetuses >3800g was excluded from the study. The outcomes were analysed by t-test and the risk scale was expressed through Odds Ratio, with confi dence interval 95%.
The study was done in the Clinic of Obstetrics and Gynaecology of the Universi-ty Clinical Centre of Kosovo. It included 801 pregnancies with breech presentation delivered between the year 2008 and 2009. The cases with congenital anomalies, multiple pregnancies, foetuses >3800g was excluded from the study. All patients who met the selection criteria (n=801) were divided in to groups: pregnancy who delivered by cesarean section (study group, n=415) and pregnancy who delivered by vaginal delivery (control group, n=388). The study was designed as retrospective study for comparison of neonatal complications between study and control group. Obstetrics fi les were reviewed and data from breech pregnancies was collected. De-pending on the mode of delivery, the following parameters were recorded: gesta-tional age, average APGAR-score at fi rst and fi fth minutes, birth weight, and par-ity. From the neonatal parameters we analyzed: intraventricular hemorrhage (IVH), perinatal asphyxia, early neonatal infection, sepsis, respiratory distress syndrome (RDS), the requirement for continuous positive airway pressure (CPAP), birth trau-ma and neonatal death.
Gestational age was determined from the fi rst day of last menstruation and con-fi rmed by an expert of neonatology after birth. Apgar score was evaluated and care given by an expert neonatologist. Perinatal asphyxia was determined based on the APGAR-score in 5 min., gas-analysis of the newborn, neurological signs - convul-sions in the fi rst 24 hours, multi-systemic dysfunction of vital organs. Early neo-natal infection was diagnosed based on clinical criteria and laboratory tests (blood analysis, C-reactive protein - CRP, positive blood culture) in fi rst 3 days of life. Sepsis was diagnosed based on clinical criteria and laboratory confi rmation. IVH
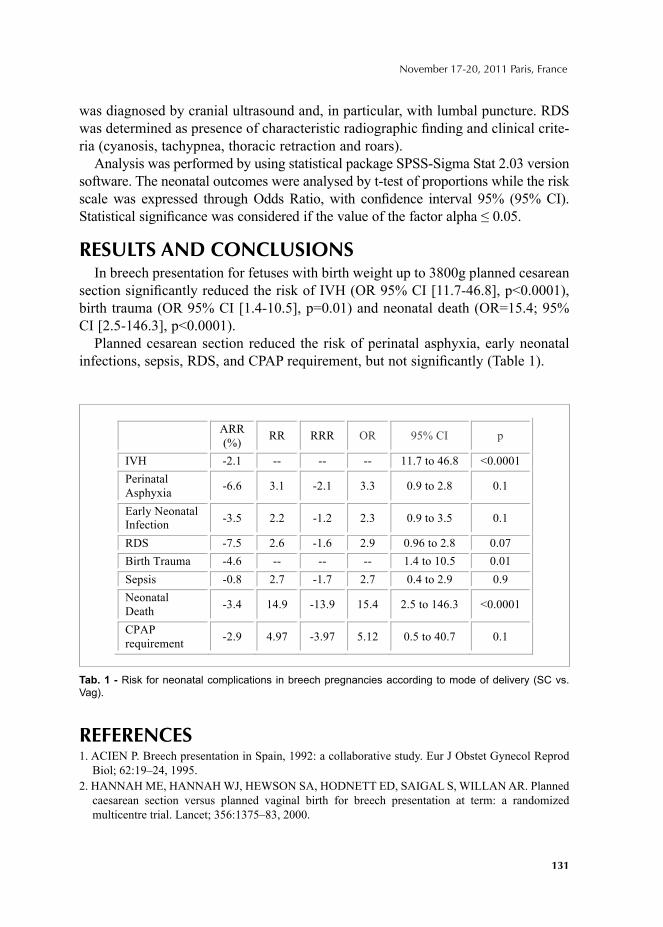
131
November 17-20, 2011 Paris, France
was diagnosed by cranial ultrasound and, in particular, with lumbal puncture. RDS was determined as presence of characteristic radiographic fi nding and clinical crite-ria (cyanosis, tachypnea, thoracic retraction and roars).
Analysis was performed by using statistical package SPSS-Sigma Stat 2.03 version software. The neonatal outcomes were analysed by t-test of proportions while the risk scale was expressed through Odds Ratio, with confi dence interval 95% (95% CI). Statistical signifi cance was considered if the value of the factor alpha ≤ 0.05.
RESULTS AND CONCLUSIONSIn breech presentation for fetuses with birth weight up to 3800g planned cesarean
section signifi cantly reduced the risk of IVH (OR 95% CI [11.7-46.8], p<0.0001), birth trauma (OR 95% CI [1.4-10.5], p=0.01) and neonatal death (OR=15.4; 95% CI [2.5-146.3], p<0.0001).
Planned cesarean section reduced the risk of perinatal asphyxia, early neonatal infections, sepsis, RDS, and CPAP requirement, but not signifi cantly (Table 1).
REFERENCES1. ACIEN P. Breech presentation in Spain, 1992: a collaborative study. Eur J Obstet Gynecol Reprod
Biol; 62:19–24, 1995. 2. HANNAH ME, HANNAH WJ, HEWSON SA, HODNETT ED, SAIGAL S, WILLAN AR. Planned
caesarean section versus planned vaginal birth for breech presentation at term: a randomized multicentre trial. Lancet; 356:1375–83, 2000.
ARR
(%) RR RRR OR 95% CI p
IVH -2.1 -- -- -- 11.7 to 46.8 <0.0001
Perinatal
Asphyxia -6.6 3.1 -2.1 3.3 0.9 to 2.8 0.1
Early Neonatal
Infection -3.5 2.2 -1.2 2.3 0.9 to 3.5 0.1
RDS -7.5 2.6 -1.6 2.9 0.96 to 2.8 0.07
Birth Trauma -4.6 -- -- -- 1.4 to 10.5 0.01
Sepsis -0.8 2.7 -1.7 2.7 0.4 to 2.9 0.9
Neonatal
Death -3.4 14.9 -13.9 15.4 2.5 to 146.3 <0.0001
CPAP
requirement -2.9 4.97 -3.97 5.12 0.5 to 40.7 0.1
Tab. 1 - Risk for neonatal complications in breech pregnancies according to mode of delivery (SC vs. Vag).

132
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
3. SCHINDL M, BIRNER P, REINGRABNER M, JOURA E, HUSSLEIN P, LANGER M. Elective cesarean section vs. spontaneous delivery: a comparative study of birth experience. Acta Obstet Gynecol Scand; 82(9):834-40, 2003.
4. ZANARDO V, SIMBI AK, FRANZOI M, SOLDÀ G, SALVADORI A, TREVISANUTO D. Neonatal respiratory morbidity risk and mode of delivery at term: infl uence of timing of elective caesarean delivery. Acta Paediatr; 93(5):643-7, 2004.
5. GOFFINET F, CARAYOL M, FOIDART JM, ALEXANDER S, UZAN S, SUBTIL D, BRÉART G; PREMODA Study Group. Is planned vaginal delivery for breech presentation at term still an option? Results of an observational prospective survey in France and Belgium. Am J Obstet Gynecol; 194(4):1002-11, 2006.
© 2012 Monduzzi Editoriale | Proceedings Code: 369
Waist circumference in relation to prediction of delivery outcomes
E. Mehrabi1, M. Ebrahimi Mameghani2, M. Kamalifard3, P. Yavari Kia4
Department of Midwifery, Tabriz Branch, Islamic Azad University, Tabriz, Iran
Background and Objective: using BMI as a simple index for prediction gesta-tional and delivery outcomes is extensively consolidated at the literature but there are limited studies on the other obesity indexes particularly abdominal obesity ones such as waist circumference (WC) during pregnancy. This study was aimed to in-vestigate the prediction value of maternal early pregnancy BMI and WC in relation to delivery outcomes.
Material and Method: in this prospective study, demographic and obstetric his-tory as well as measurement of weight, height and waist circumference of 1140 nuliparous pregnant women delivered singleton babies were measured based on standard methods by a trained assessor at 1st trimester of pregnancy in Tabriz health care centers. BMI was estimated and obesity was defi ned based on WHO defi ni-tion. Abdominal obesity was defi ned as WC equal to 88 cm and more. Delivery out comes were recorded after delivery by following the subjects.
Results: mean BMI and WC among nulliparous women at 1st trimester of preg-nancy was 24.32 (kg/m2) and 81.84 cm, respectively. Signifi cant correlation was found between early pregnancy BMI and WC (r=0.84, P<0.001). Likelihood of ce-sarean delivery was more common among overweight and obese women and also in women with abdominal obesity (BMI 25-30 and ≥30kg/m2 or WC ≥88cm), {OR= 1.91, CI 95%: 1.36 - 2.68}, {OR= 17.28, CI95% 8.98 - 33.23} and {OR= 2.43, CI95% 1.73 - 3.41}. Macrosomia rate was higher in the overweight, obese women and those with high WC {OR= 3.23, CI95%: 1.12 - 8.59}, {OR= 12.12, CI95%: 4.64 - 31.68} and {OR= 9.28, CI95%: 2.76 - 31.21} in comparison with women who had normal BMI and WC. Obese women were more likely to have postpartum hemorrhage {OR= 4.28, CI95% 1.94 - 9.45}, {OR= 2.06, CI95% 1.03 - 4.12} com-pared with normal weight women, respectively.
Conclusion: results of this study reveals that abdominal obesity as well high BMI of early pregnancy could predict delivery out comes.
Key words: body Mass Index, Waist Circumference, delivery out comes.

134
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
INTRODUCTIONObesity is an important public health problem worldwide, and its prevalence is
increasing in both developed and developing nations with changes in dietary habits and activity level.1-11 Anthropometric measurements taken in the antenatal period can predict increased risk of gestational diabetes, preeclampsia, eclampsia, fetal macrosomia, post-term delivery and cesarean section.12 Although obesity is de-fi ned as a condition of excessive body fat, it is usually assessed clinically by BMI, obtained by dividing weight by height squared.13Aspregnancy progresses, this in-dex is infl uenced by gestational weight gain in lean tissues, thus limiting its use in pregnancy.14 Abdominal adiposity used only, measured by WC, is frequency used outside of pregnancy as a risk factor for diabetes and cardiovascular disease.15 In pregnancy, however it is seldom used to predict risk, probably because it is believed to be unduly infl uenced by the increasing volume.Among the various standardized sites for measuring waist circumference, the minimal waist, being most distant from growing uterus, is likely to be less infl uencedThis study was aimed to investigate the prediction value of maternal early pregnancy BMI and WC in relation to deliv-ery outcomes.
METHODSThis prospective study was carried out on 1140 nulliparous pregnant women
at 1st trimester of pregnancy. Sampling technique was stratifi ed sampling.The re-searcher measured standing height (stature) without shoes, heel against the wall and head in the plan to the nearest centimeter using the height measure stadiom-eter. Weight (with light clothing) was measured to the nearest 100 g by vertical scale (Seca, Germany) calibrated at the central health care offi ce. Then BMI was calculated. Waist circumference was measured by placing a tape measure around the bare abdomen just above the hip bone without compressing the skin.Delivery type, macrosomia and postpartum hemorrhage were recorded in the questionnaire through following participants during pregnancy and postpartum period. Includ-ing Criteriawerebeing nulliparous and at 1st trimester of pregnancy, without hyper emesis gravidarom, without special diet, no history of recurrent spontaneousabor-tion, uterine surgery, molar pregnancies, any disease and willingness to participat-ing. Excluding Criteria were the client withdraws of the study, disproportionate weight gain over pregnancy.
RESULTS AND CONCLUSIONWe compared differences in mean BMI and WC among women with and without
complications using independed 2-tailed t test (Table1). We used logistic regression anal-ysis to examine the associations between WC and BMI withdelivery outcomes(Table2). A normal WC and BMI were used as the reference category (OR, 1.00).

135
November 17-20, 2011 Paris, France
Overweight and obesity diagnosis using simple indicators such as BMI, is exten-sively consolidated at the literature and association between early pregnancy maternal BMI and most of pregnancy-delivery complications was confi rmed in a number of studies. WC was proposed in the 1990s by Han et al, is used to identify individuals with overweight and obesity.14Nevertheless evidence due to WC studies in relation to delivery outcomes are rare.Results showed gestational hypertension, preeclampsia and gestational diabetes were more common among overweight and obese women at early pregnancy vs women with normal BMI and WC. In addition mean BMI and WC in individuals with gestational hypertension, preeclampsia and gestational dia-betes were signifi cantly higher compared with those without these complications (p≥ 0.001). According to present study results, obesity in term of high BMI and WC were found to be signifi cantly associated with greater odds for cesarean, macrosomia and postpartum hemorrhage. Similar trends were found for abdominal obesity.
Delivery outcomes N BMI) kg/m2)
SEM**
± Mean
WC) kg/m2)
SEM ± Mean
Positive 282 0.33±26.24 0.64±85.63
Negative 666 0.12 ±23.71 0.31±81.00 Cesarean delivery
P*
--- 0.0001 0.0001
Positive 126 1.10±28.28 1.50±90.05
Negative 834 0.13 ±24.34 0.30±82.14 Macrosomia
P --- 0.0001 0.0001
Positive 53 0.77±26.91 1.41±86.84
Negative 595 0.13±24.32 0.30±82.12 Postpartum
hemorrhage P --- 0.0001 0.002
P*: P Value SEM
**:Standard error of mean
*Odds Ratio (Confidence interval 95%)
OR (CI 95%) *
Gestational
complications
WC 88cm BMI 30 kg/m
2.43(1.73 - 3.41) 17.28(8.98 - 33.23) Cesarean
9.28(2.76, 31.21) 12.12(4.64, 31.68) Macrosomia
2.06(1.03 - 4.12) 4.28(1.94, 9.45) Postpartum
hemorrhage
Tab. 1 - Compare mean of BMI & WC among women with pregnancy-delivery complications.
Tab. 2 - Association between early pregnancy BMI and WC and delivery outcomes.
136
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
In the same studies also it was reported that, cesarean, macrosomia and postpar-tum hemorrhagewere signifi cantly more common among over weight and obese pregnant women vs women with healthy BMI (P<0.05).16-17-18 Another study fi nd-ing confi rmed that mean BMI and WC were signifi cantly higher in subjects with mentioned outcomes (P≤0.002).15,19Similar fi nding were reported by a number of research which are in agreement with the results of our research regarding BMI.17,20-
23Finally, results of this study reveals that abdominal obesity as well high BMI of early pregnancy could predict delivery out comes.
REFERENCES1. No authors listed. National Task Force on the Prevention and Treatment of Obesity. Overweight,
obesity, and health risk. Arch Intern Med. 2000; 160:898-904.2. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight,
overweight, and obesity. JAMA. 2005; 293:1861-7.3. Seidell JC, Flegal KM. Assessing obesity: classifi cation and epidemiology. Br Med Bull. 1997;
53:238-52.4. No authors listed. Obesity: preventing and managing the global epidemic. Report of a WHO
Consultation. World Health Organ Tech Rep Ser. 2000; 894: 1-253. 5. Bell AC, Ge K, Popkin BM. Weight gain and its predictors in Chinese adults. Int J Obes Relat
Metab Disord. 2001; 25: 1079-86. 6. Popkin BM, Doak CM. The obesity epidemic is a worldwide phenomena. Nutr Rev. 1998; 56:106-
14.7. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US
adults, 1999-2000. JAMA. 2002; 288:1723–7.8. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight
and obesity among US children, adolescents, and adults, 1999-2002. JAMA.2004; 291:2847-50.9. Rennie KL, Jebb SA. Prevalence of obesity in Great Britain. Obes Rev. 2005; 6:11-2.
10. Hodge AM, Dowse GK, Bareeboo H, Tuomileho J, Alberti KG, Zimmet PZ. Incidence, increasing prevalence, and predictors of change in obesity and fat distribution over 5 years in the rapidly developing population of Mauritius. Int J Obes Relat Metab Disord. 1996; 20:137- 46.
11. Azizi F, Azadbakht L, Mirmiran P. Trends in overweight, obesity and central fat accumulation among Tehranian adults between 1998-1999 and 2001-2002: Tehran lipid and glucose study. Ann Nutr Metab. 2005; 49:3- 8.
12. Cnattingius S, Bergstrom R, Lipworth L, Kramer MS. Pre-pregnancy weight and the risk of adverse pregnancy outcomes. N Engl J Med 1998, 338:147-52.
13. World Health Organization. Physical status: the use and interpretation of anthropometry. Geneva: World Health Organization,1995.
14. Nucci LB, Schmidt MJ, Duncan BB, Fuchs SC, Fleck ET, Santos Britto MM. Nutritional status of pregnant women: prevalence and associated pregnancy outcomes. Rev Saude Publica 2001, 35; 502-7.
15. Wendland E, Bartholow Douncan B. Serrate Mengue S, Bertoldi Nucci L, Ines Schmidt M.(2007).Waist circumference in the prediction of obesity-related adverse pregnancy out comes. Cod.Saude publica,Rio de janeiro,23(2); 391-398,fev,2007.
16. Margaret E, Samuels K, Edmund F, Funai M, Catalin B, Errol N et al.(2007).pregnancy body mass index, hypertensive disorders of pregnancy, and long – term maternal mortality. American journal of Obstetric &Genecology,197(5),490.

137
November 17-20, 2011 Paris, France
17. Bhattacharya SO, Campbell D, Liston W, Bhttacharya SI.(2007).Effect of Body Mass Index on pregnancy outcomes in nulliparous women delivering singleton babies. BMC Public Health journal,7,168.
18. Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW, Regan L, Robinson S.(2001). Maternal obesity and pregnancy outcome: a study of 287 213 pregnancies in London. International Journal of Obesity 25, 1175-1182.
19. Sattar N, Clark P, Holmes A, Lean MEJ, Walker I, Greer IA.(2001). Antenatal Waist Circumference and Hypertension Risk. Obstetric and Gynecology Journal 97(2), 268-271.
20. Heinrich CD, Hansen M, McCulloch A, Archer L. (2009).The Association of Prepregnancy Body Mass Index and Adverse Maternal and Perinatal Outcomes.Colorado Department of Public Health and Environment. Health watch.No69:1-6.
21. Omanwa k, Zimmer M, Tlolka j, Wytrychowska E, Maciejewska J, Drys A.(2006).Is low pre-preg-nancy body mass index a risk factor for preterm birth and low neonatal birth weight?.Ginecol Pol journal. 77(8),618.
22. Spinillo A, CapuzzoE, PiazziG, FerrariA, MoralesV, Di Mario M.(1998). Risk for spontaneous preterm delivery by combined body mass index and gestational weight gain patterns. Acta Obstetric and Gynecology Journal. 77(1):32-36.
23. Kalkwarf, heidi J.(1991).Maternal weight gain and risk of preterm delivery:Effect on neonatal mortality and public health impact.Unpublished Ph.D. thesis of Cornel (New York)University.

© 2012 Monduzzi Editoriale | Proceedings Code: 415
Effect of melatonin on the oxidative metabolism of colostrum phagocytes of diabetic women
I. Calderon1, G. Morceli1, C. Hara2, R. Volpato2, M. Rudge1, A. Honorio-França2, E. França2
1PG - Program in Gynecology, Obstetrics and Mastology, Botucatu Medical School, São Paulo State University (UNESP), Brazil; 2Institute of Biological and Health Science - Federal University of Mato Grosso, Pontal do Araguaia, Mato Grosso, Brazil
SUMMARYAim: the aim of this study was verifi ed the ability of melatonin hormone to modu-
late the oxidative metabolism of colostral phagocytes from diabetic mothers. Meth-ods: bas ed on 100g-OGTT and glucose profi le analysis subjects were allocated into two groups: Non-diabetic (ND-10) and Diabetic (DM- 8). Cells were separated by a Ficoll-Paque gradient and the oxidative metabolism was availablethought super-oxide release by colostrum phagocytes using the cytochrome C method. Results: melatonin hormone increased superoxide release by colostrum phagocytes of ND and decreased theserelease in colostrum phagocytes of DM mothers. Conclusion: the results suggest that the melatonin hormone can modulate the oxidative metabo-lism of phagocytes and an existence of relationship between control of glucose me-tabolism and melatonin action in colostrum phagocytes.
KEYWORDSColostrum, phagocytes, superoxide, melatonin, diabetes.
INTRODUCTIONHuman milk present among soluble and cellular components that are important
to nutrition and immunological defense of human infants, as lipids, carbohydrates, proteins, cells and hormones (Honorio-França et al, 2001, França et al, 2010, França et al, 2011, Morceli et al, 2011). Melatonin hormone produced by pineal gland is
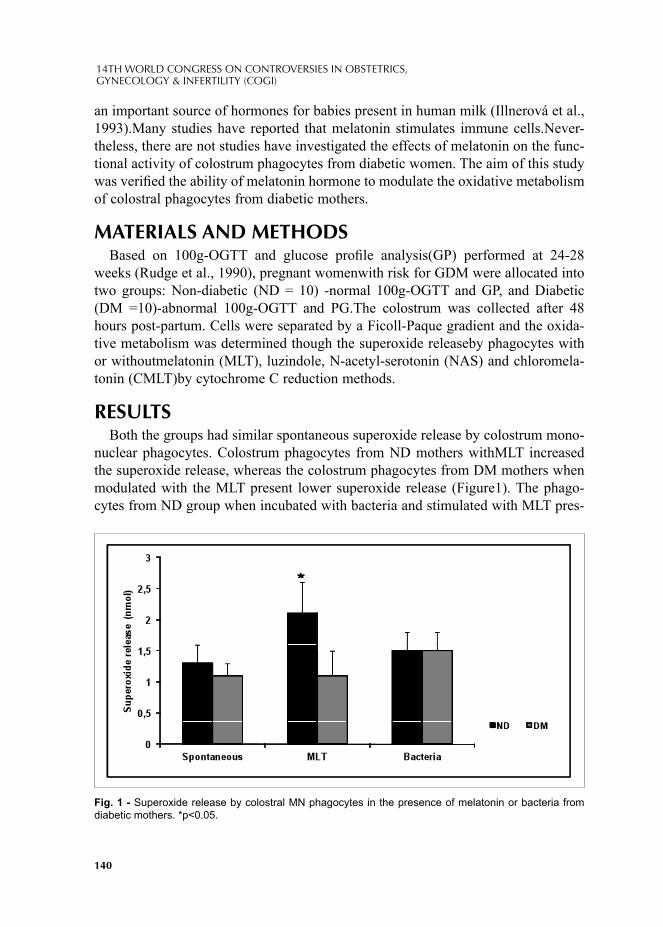
140
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
an important source of hormones for babies present in human milk (Illnerová et al., 1993).Many studies have reported that melatonin stimulates immune cells.Never-theless, there are not studies have investigated the effects of melatonin on the func-tional activity of colostrum phagocytes from diabetic women. The aim of this study was verifi ed the ability of melatonin hormone to modulate the oxidative metabolism of colostral phagocytes from diabetic mothers.
MATERIALS AND METHODS Based on 100g-OGTT and glucose profi le analysis(GP) performed at 24-28
weeks (Rudge et al., 1990), pregnant womenwith risk for GDM were allocated into two groups: Non-diabetic (ND = 10) -normal 100g-OGTT and GP, and Diabetic (DM =10)-abnormal 100g-OGTT and PG.The colostrum was collected after 48 hours post-partum. Cells were separated by a Ficoll-Paque gradient and the oxida-tive metabolism was determined though the superoxide releaseby phagocytes with or withoutmelatonin (MLT), luzindole, N-acetyl-serotonin (NAS) and chloromela-tonin (CMLT)by cytochrome C reduction methods.
RESULTSBoth the groups had similar spontaneous superoxide release by colostrum mono-
nuclear phagocytes. Colostrum phagocytes from ND mothers withMLT increased the superoxide release, whereas the colostrum phagocytes from DM mothers when modulated with the MLT present lower superoxide release (Figure1). The phago-cytes from ND group when incubated with bacteria and stimulated with MLT pres-
*
Fig. 1 - Superoxide release by colostral MN phagocytes in the presence of melatonin or bacteria from diabetic mothers. *p<0.05.

141
November 17-20, 2011 Paris, France
ent high superoxide release. In both groups, the luzindole decreased superoxide release, whereas the NAS increased this anion release. The CMLT not stimulated the superoxide release by colostrum phagocytes (Figure 2).
CONCLUSIONThe melatonin hormone can modulate the functional activity of colostrum phago-
cytes and these results suggest a relationship between control of glucose metabo-lism and melatonin action in colostrum phagocytes.
SUPPORTThis research received grants from Fundação de Amparo à Pesquisa de São Paulo
(FAPESP-No. 2008/09187-8; No. 2009/01188-8) and Fundação de Amparo à Pes-quisa de Mato Grosso (FAPEMAT No. 735593/2008; No 453387/2009).
REFERENCES1. FRANÇA EL, BITENCOURT RV, FUJIMORI M, MORAIS TC, CALDERON IMP, HONORIO-
FRANÇA AC. Human colostral phagocytes eliminate enterotoxigenicEschechia coli opsonized by colostrums supernatant. J. MicrobiolImmunolInfec44,1-7; 2011.
2. FRANÇA, E L, NICOMEDES, TR, CALDERON, HONORIO-FRANÇA, AC. Time-dependent al-terations of soluble and cellular components in human milk. BiolRhythm Res 41, 333-47; 2010.
3. HONORIO-FRANÇA AC, LAUNAY P, CARNEIRO-SAMPAIO MMS, MONTEIRO RC. Colos-tral neutrophils express Fc alpha receptors (CD89) lacking gamma chain association and mediate noninfl ammatory properties of secretory IgA. J LeukocBiol 69, 289-96; 2001.
*
*
*
*
*
*
Fig. 2 - Superoxide release by colostral MN phagocytes from diabetic mothers, in the presence of bacteria and treated with melatonin (MLT), luzindole (antagonist), N-acetyl serotonin precursor of melatonin (NAS) and chloromelatonina (CMLT - agonist). *p<0.05.
142
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
4. ILLNEROVÁ H, BURESOVÁ M, PRESL J. MELATONIN RHYTHM IN HUMAN MILK. J.Clin. Endocrinol. Metab.77, 838-41; 1993.
5. MORCELI, G., FRANÇA, E.L., MAGALHÃES, V.B., DAMASCENO, D.C., CALDERON, I.M.P., HONORIO FRANÇA, A.C. Diabetes induced immunological and biochemical changes in human colostrum. Acta Paediatr. 100, 550-6; 2011.
6. RUDGE MVC, PERAÇOLI JC, BEREZOWSKI AT, CALDERON IMP & BRASIL MAM. The oral glucose tolerance test is a poor predictor of hyperglycemia during pregnancy. Braz J Med Biol Res. 23, 1079-1089; 1990.

© 2012 Monduzzi Editoriale | Proceedings Code: 430
The role of dydrogesterone in threatened abortion
A. Bimbashi1, E. Ndoni1, R. HoxhallariUniversity Hospital of Obstetrics and Gynecology “Koço Gliozheni”, “Fertilitas” Clinic, Tirana, Albania
SUMMARYObjective: The aim of this study is to determine if the use of dydrogesterone can
improve the pregnancy outcome in cases with threatened abortion during the fi rst trimester of pregnancy.
Material and methods: We included pregnant women presenting with vaginal bleeding during the fi rst trimester of pregnancy, from January 1, 2010 until January 1, 2011. Women were randomized to receive either dydrogesterone 10 mg twice a day or conservative therapy, for at list one week or until they had 48 hours without bleeding. They were followed until delivery or abortion in UHOG "Koço Gliozheni".
Results: Pregnant women were randomized to have dydrogesterone (76 patients) or conservative management (70 patients). The treatment was considered successful if the pregnancy continued beyond 24 weeks of gestation. The incidence of abor-tion resulted signifi cantly lower (p=0.042) in the dydrogesterone group (6.7%) com-pared with the group who received conservative treatment (14.2%).
Conclusion: Dydrogesterone can reduce the incidence of pregnancy loss in threatened abortion during the fi rst trimester in women.
INTRODUCTIONThreatened abortion is defi ned as vaginal bleeding in early pregnancy in the pres-
ence of closed cervix and ultrasound confi rmed an intrauterine gestational sac with a fetal heartbeat. Threatened abortion is a common complication, occurring in about 20% of all clinically recognised pregnancies, and is associated with a 10-14% risk of full miscarriage7.
Cytokines are known to play an important role in implantation. An imbalance in cytokine production occurs in early pregnancy loss. A strong association exists between maternal T helper-1 (Th1-type) immunity and pregnancy loss, whereas a
144
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
shift towards T helper-2 (Th2-type) cytokine response has been observed in suc-cessful pregnancy.
Protocols developed for the management of threatened abortion include conser-vative management and hormonal therapy. Based on data from several studies that indicate an increasing risk of fi rst trimester miscarriage with declining serum pro-gesterone levels, hormonal therapy is based on progesterone administration6. Pro-gesterone realizes the decidualisation of endometrium, cellular immuno-regulation (shifting toward Th2 synthesis, synthesis of PIBF – Progesterone Induced Blocking Factor), and prevents uterine contractions1,5.
Recent data indicate that dydrogesterone that corrects Th1/Th2 imbalance, shift-ing toward Th2 production, could help prevent that threatened abortion ends in a full miscarriage1,2-4.
Dydrogesterone is an orally active, highly selective progestogen that is similar to endogenous progesterone, but which has a better bioavailability1. In addition, it does not alter coagulation parameters, blood lipids or glucose/insulin parameters, is not hepatotoxic and does not cause an increase in body temperature11. Preclinical studies indicated no mutagenic, teratogenic or carcinogenic potential of dydroges-terone, and pharmacovigilance data do not provide evidence for congenital malfor-mations associated with dydrogesterone use during pregnancy12.
MATERIALS AND METHODSIn this study we have prospectively recruited pregnant women, presenting in
UHOG “Koço Gliozheni” in Tirana, with vaginal bleeding during the fi rst-trimes-ter of pregnancy, from January 1, 2010 until January 1, 2011. Inclusion criteria: pregnant women with clinical diagnosis of threatened abortion, after the ultrasound confi rmation of a singleton viable pregnancy. Exclusion criteria included patients with recurrent abortions, multiple pregnancies, molar pregnancies, uterine anoma-lies (congenital or acquired that distort the uterus), cervical incompetence, thrombo-philia, or patients with chronic diseases under medication. The gestational age was calculated from the fi rst day of their last menstrual period.
Women were randomized in two groups: to receive either dydrogesterone 10 mg twice a day or conservative therapy for at list one week or until they had 48 hours without bleeding. They were followed until delivery or abortion in UHOG “Koço Gliozheni”. The treatment was considered successful if the pregnancy continued beyond 24 weeks of gestation.
RESULTS AND CONCLUSIONSA total of 146 women in both groups were randomised to have dydrogesterone
treatment (10mg twice a day) or conservative management.In the dydrogesterone group (group A) were included 76 pregnant women, with
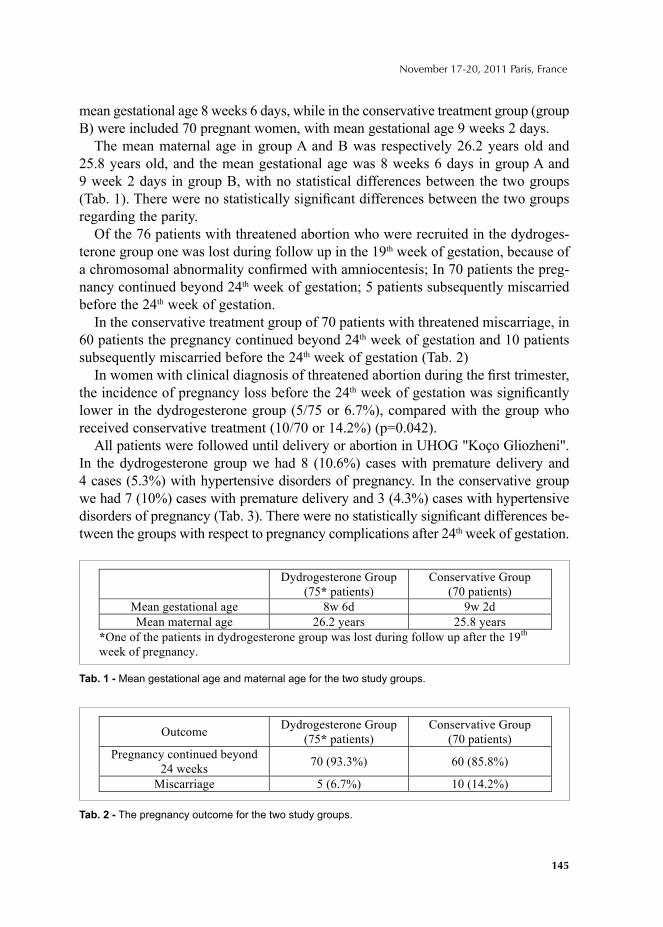
145
November 17-20, 2011 Paris, France
mean gestational age 8 weeks 6 days, while in the conservative treatment group (group B) were included 70 pregnant women, with mean gestational age 9 weeks 2 days.
The mean maternal age in group A and B was respectively 26.2 years old and 25.8 years old, and the mean gestational age was 8 weeks 6 days in group A and 9 week 2 days in group B, with no statistical differences between the two groups (Tab. 1). There were no statistically signifi cant differences between the two groups regarding the parity.
Of the 76 patients with threatened abortion who were recruited in the dydroges-terone group one was lost during follow up in the 19th week of gestation, because of a chromosomal abnormality confi rmed with amniocentesis; In 70 patients the preg-nancy continued beyond 24th week of gestation; 5 patients subsequently miscarried before the 24th week of gestation.
In the conservative treatment group of 70 patients with threatened miscarriage, in 60 patients the pregnancy continued beyond 24th week of gestation and 10 patients subsequently miscarried before the 24th week of gestation (Tab. 2)
In women with clinical diagnosis of threatened abortion during the fi rst trimester, the incidence of pregnancy loss before the 24th week of gestation was signifi cantly lower in the dydrogesterone group (5/75 or 6.7%), compared with the group who received conservative treatment (10/70 or 14.2%) (p=0.042).
All patients were followed until delivery or abortion in UHOG "Koço Gliozheni". In the dydrogesterone group we had 8 (10.6%) cases with premature delivery and 4 cases (5.3%) with hypertensive disorders of pregnancy. In the conservative group we had 7 (10%) cases with premature delivery and 3 (4.3%) cases with hypertensive disorders of pregnancy (Tab. 3). There were no statistically signifi cant differences be-tween the groups with respect to pregnancy complications after 24th week of gestation.
Dydrogesterone Group
(75* patients)
Conservative Group
(70 patients)
Mean gestational age 8w 6d 9w 2d
Mean maternal age 26.2 years 25.8 years
*One of the patients in dydrogesterone group was lost during follow up after the 19th
week of pregnancy.
Outcome Dydrogesterone Group
(75* patients)
Conservative Group
(70 patients)
Pregnancy continued beyond
24 weeks 70 (93.3%) 60 (85.8%)
Miscarriage 5 (6.7%) 10 (14.2%)
Tab. 2 - The pregnancy outcome for the two study groups.
Tab. 1 - Mean gestational age and maternal age for the two study groups.
146
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Progesterone Induced Blocking Factor (PIBF) is an immunomodulatory proges-terone-dependent protein that alters the Th1/Th2 ratio, shifting toward Th2 produc-tion, with immunoprotective properties. Th1 response, that is considered harmful immunologic response is subject to down-regulation. In this way, PIBF creates an immunoprotective environment8,9.
Appropriate values of progesterone are essential for a successful pregnancy; if progesterone fails to stimulate lymphocites for the production of PIBF, the equi-librium shifts toward the harmful response mediated by Th1, increasing the risk of miscarriage3,5,6.
Mechanisms by which progesterone alters the immune system are: (1) induction of asymmetric anticorps (considered as embryo-protective) production, which bind poorly with antigens, not activating the cascade of complement; (2) up regulation of Th2 activity, that activates protective cytokines and blocks the harmful response of Th1; and (3) down regulation of TH1 activity that prevents the release of TNFα dhe IL-26,10.
The results of this study indicated that dydrogesterone can reduce the incidence of pregnancy loss during the fi rst trimester in women with clinical diagnosis of threatened abortion.
Anyway, further clinical trials and in vitro studies should be carried out to con-fi rm the effect of dydrogesterone in reversing the imbalance of Th1/Th2 in women with threatened abortion, resulting in higher percentage of positive outcome in preg-nant women with this clinical diagnosis.
REFERENCES1. Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR, Schweppe KW, Thijssen JH.
Classifi cation and pharmacology of progestins. Maturitas 61: 171-180; 2008. 2. Liu F, Luo SP. Effect of Chinese herbal treatment on Th1- and Th2-type cytokines, progesterone and
beta-human chorionic gonadotropin in early pregnant women of threatened abortion. Chin J Integr Med 15:353-8; 2009.
3. Raghupathy R, Kalinka J. Cytokine imbalance in pregnancy complications and its modulation. Front Biosci 13:985-94; 2008.
4. Kalinka J, Szekeres-Bartho J. The impact of dydrogesterone supplementation on hormonal profi le and progesterone-induced blocking factor concentrations in women with threatened abortion. Am J Reprod Immunol 53: 166-171; 2005.
Pregnancy complications Dydrogesterone Group
(75* patients)
Conservative Group
(70 patients)
Premature Delivery (< 37weeks) 8/75(10.6%) 7/70 (10%)
Hypertensive disorders of
pregnancy 4/75 (5.3%) 3/70 (4.3%)
Tab. 3 - The pregnancy complications after 24th week gestation.
147
November 17-20, 2011 Paris, France
5. Daily CA, Laurent SL, Nunley WC. The prognostic value of serum progesterone and quantitative hCG in early human pregnancy. Am J Obstet Gynecol 171: 380-384; 1994.
6. Arck PC, Rücke M, Rose M, Szekeres-Bartho J, Douglas AJ, Pritsch M, Blois SM, Pincus MK, Bärenstrauch N, Dudenhausen JW, Nakamura K, Sheps S, Klapp BF. Early risk factors for miscar-riage: a prospective cohort study in pregnant women. Reprod Biomed Online 17: 101-113; 2008.
7. C. Everett, Incidence and outcome of bleeding before the 20th week of pregnancy: prospective study from general practice. BMJ, 315 (1997), pp. 32–34.
8. Szekeres-Bartho J, Wegmann TG. A progesterone-dependent immunomodulatory protein alters the Th1/Th2 balance. J Reprod Immunol 31: 81-95; 1996.
9. Kelemen K, Bognar I, Paal M, Szekeres-Bartho J. A progesterone-induced protein increases the synthesis of asymmetric antibodies. Cell Immunol 167: 129-134; 1996.
10. Polgár B, Nagy E, Mikó E, Varga P, Szekeres-Barthó J. Urinary progesterone-induced blocking factor concentration is related to pregnancy outcome. Biol Reprod 71: 1699-1705; 2004.
11. Picolet H, Girard P, Nemoz C, Boissel JP. Effects of dydrogesterone on hydroelectrolytic metabo-lism: a randomized double-blind study. Gynecol Endocrinol 4:219–24; 1990.
12. Queisser-Luft A. Dydrogesterone use during pregnancy: overview of birth defects reported since 1977. Early Hum Dev 85:375–7; 2009.

© 2012 Monduzzi Editoriale | Proceedings Code: 431
Our experience in management of severe preeclampsia
E. Ndoni, A. Bimbashi, A. DokleUniversity Hospital of Obstetrics and Gynecology “Koço Gliozheni”, Tirana, Albania
SUMMARYObjective: To evaluate the maternal and perinatal outcome in expectant versus
immediate management in severe preeclampsia.Materials and methods: In this study were included 52 patients with severe pre-
eclampsia in 27-34 weeks’ gestation. 26 patients were treated immediately and 26 patients were managed expectantly. We analyzed maternal and perinatal outcome.
Results: In the group managed immediately, we had 6 cases (23%) with HELP syndrome, 1 case with renal insuffi ciency, 3 cases (11.5%) with eclampsia, 4 cas-es (15.4%) with placental abruption, 1 case with postpartum haemorrhage. In ex-pectant management group, resulted 2 cases (7.7%) with HELP syndrome, 2 cases (7.7%) with eclampsia, 2 cases (7.7%) with placental abruption. Perinatal outcome in immediate management resulted: mean birthweight at delivery 1506g, perinatal mortality 61.5%, IUGR fetuses 57%, and respiratory distress was notice in 16 cases (61.5%), neonatal jaundice in 16 cases (61.5%) and IVH in 2 cases (7.7%). In ex-pectant management: mean birthweight at delivery was 1608g; perinatal mortality was 30%, IUGR fetuses 57%, respiratory distress syndrome was notice in 12 cases (46%), neonatal jaundice in 21 cases (80%) and IVH in 3 cases (11.5%).
Conclusion: No statistically signifi cant differences in relation to maternal out-come were found between two groups, but we found a statistically signifi cant de-crease of perinatal mortality (p=0.026) in expectant management group.
INTRODUCTIONPreeclampsia is a multiorgan disorder usually associated with raised blood pres-
sure and proteinuria that is unique to pregnancy. Preeclampsia is often associated with signifi cant maternal and neonatal morbidity and mortality, especially when it is severe and occurs before term. The prevalence of preeclampsia is estimated at 6-8%

150
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
of all pregnancies1 while the severe preeclampsia is found to affect about 1-2% of all pregnancies.4
The cure for preeclampsia is delivery of the baby and placenta. Although delivery is always appropriate for the mother, it may not be optimal for the premature fetus. Some obstetricians prefer early delivery in order to prevent the development of serious maternal complications. This can result in delivery of a very premature baby and more neonatal complications. Others prefer to be conservative and to delay delivery in order to reduce the neonatal mortality and morbidity as a result of premature delivery, but this could place the mother at risk of multisystem organ failure. The main objective of expectant management is to allow the baby more time in utero so that the risk of respiratory distress syndrome or other complications due to prematurity could be reduced.
MATERIALS AND METHODSIn this study were included 52 patients with severe preeclampsia in 27-34 weeks’
gestation, hospitalized in Pathology of Pregnancy Clinic, in the University Hospital of Obstetrics & Gynecology “Koço Gliozheni”.
Based on the Magpie Trial, preeclamsia was defi ned as: diastolic blood pressure ≥110 mmHg on 2 occasions or systolic blood pressure ≥170 mmHg on 2 occasions plus ≥3+ proteinuria; or diastolic blood pressure ≥100 mmHg on 2 occasions or systolic blood pressure ≥150 mmHg on 2 occasions plus ≥2+ proteinuria plus at least two signs or symptoms of imminent eclampsia; or, highest diastolic blood pressure whist on antihypertensive ≥100 mmHg or highest systolic blood pressure whist on antihypertensive ≥150 mmHg plus ≥2+ proteinuria plus at least two signs or symptoms of imminent eclampsia.3
26 patients were treated immediately (use of corticosteroids followed by delivery after 48h), and 26 patient were managed expectantly (use of corticosteroids followed by deliv-ery only for specifi c maternal and fetal indications). Expectant management consisted of monitoring the patients by checking blood pressure, pulse rate, respiratory rate, abdomi-nal examination, fetal heart, CTG and proteinuria daily. Intravenous fl uids and urinary output were monitored daily and a full blood count cell, renal function, liver function and ultrasonography were performed at least twice weekly. For each group we analyzed maternal complications as eclampsia, HELLP syndrome, renal failure, placental abrup-tion, postpartum haemorrhage etc. Also we analyzed perinatal outcome as birthweight, perinatal mortality, IUGR fetuses, respiratory distress syndrome, neonatal jaundice and intraventricular haemorrhage (IVH). Another variable that we analyzed was the mode of delivery (vaginal versus caesarean section) in relation to maternal and perinatal outcome.
RESULTSIn the group managed immediately, we had these results regarding the maternal
outcome: 6 cases (23%) with HELP syndrome, 1 case with renal insuffi ciency, 3 cases (11.5%) with eclampsia, 4 cases (15.4%) with placental abruption, 1 case with
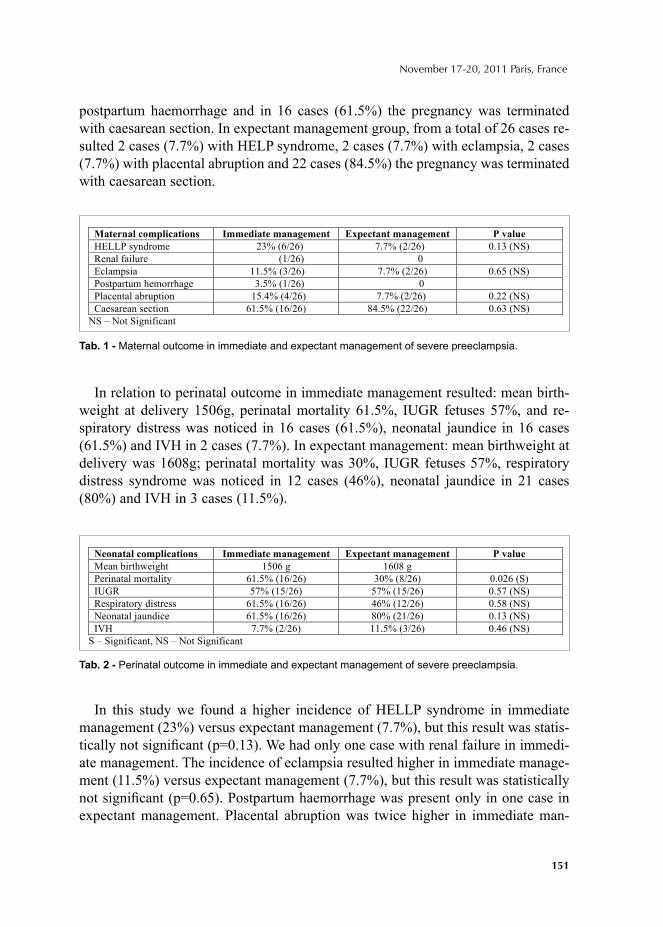
151
November 17-20, 2011 Paris, France
postpartum haemorrhage and in 16 cases (61.5%) the pregnancy was terminated with caesarean section. In expectant management group, from a total of 26 cases re-sulted 2 cases (7.7%) with HELP syndrome, 2 cases (7.7%) with eclampsia, 2 cases (7.7%) with placental abruption and 22 cases (84.5%) the pregnancy was terminated with caesarean section.
In relation to perinatal outcome in immediate management resulted: mean birth-weight at delivery 1506g, perinatal mortality 61.5%, IUGR fetuses 57%, and re-spiratory distress was noticed in 16 cases (61.5%), neonatal jaundice in 16 cases (61.5%) and IVH in 2 cases (7.7%). In expectant management: mean birthweight at delivery was 1608g; perinatal mortality was 30%, IUGR fetuses 57%, respiratory distress syndrome was noticed in 12 cases (46%), neonatal jaundice in 21 cases (80%) and IVH in 3 cases (11.5%).
In this study we found a higher incidence of HELLP syndrome in immediate management (23%) versus expectant management (7.7%), but this result was statis-tically not signifi cant (p=0.13). We had only one case with renal failure in immedi-ate management. The incidence of eclampsia resulted higher in immediate manage-ment (11.5%) versus expectant management (7.7%), but this result was statistically not signifi cant (p=0.65). Postpartum haemorrhage was present only in one case in expectant management. Placental abruption was twice higher in immediate man-
Maternal complications Immediate management Expectant management P value
HELLP syndrome 23% (6/26) 7.7% (2/26) 0.13 (NS)
Renal failure (1/26) 0
Eclampsia 11.5% (3/26) 7.7% (2/26) 0.65 (NS)
Postpartum hemorrhage 3.5% (1/26) 0
Placental abruption 15.4% (4/26) 7.7% (2/26) 0.22 (NS)
Caesarean section 61.5% (16/26) 84.5% (22/26) 0.63 (NS)
NS – Not Significant
p g p p
eonatal complications Immediate management Expectant management P value
Mean birthweight 1506 g 1608 g
Perinatal mortality 61.5% (16/26) 30% (8/26) 0.026 (S)
IUGR 57% (15/26) 57% (15/26) 0.57 (NS)
Respiratory distress 61.5% (16/26) 46% (12/26) 0.58 (NS)
Neonatal jaundice 61.5% (16/26) 80% (21/26) 0.13 (NS)
IVH 7.7% (2/26) 11.5% (3/26) 0.46 (NS)
S – Significant, NS – Not Significant
Tab. 2 - Perinatal outcome in immediate and expectant management of severe preeclampsia.
Tab. 1 - Maternal outcome in immediate and expectant management of severe preeclampsia.

152
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
agement (15.4%) versus expectant management (7.7%). Caesarean section rate was higher in expectant management. These results indicate that there was not a signifi -cant increase of maternal complications in expectant management.
Regarding the perinatal outcome we found a perinatal mortality signifi cantly low-er (p=0.026) in expectant management group. In addition, we noticed an increase of mean birthweight, a decrease of respiratory distress syndrome, an increase of the presence of neonatal jaundice in expectant management, but these changes were statistically not signifi cant.
CONCLUSIONSPreeclampsia is the leading cause of iatrogenic preterm birth. The management
of severe preeclampsia continues to present a challenge for the obstetricians. Ag-gressive management with delivery may result in a high neonatal mortality and morbidity; meanwhile expectant management may result in an increase of maternal complications. The decision between delivery and expectant management depends on fetal gestational age, fetal status, and severity of maternal condition. Cases with severe preeclampsia remote from term should be followed in specialized tertiary hospital.
In our study we did not found statistically signifi cant differences in relation to maternal outcome between immediate management group and expectant manage-ment group, but we found a statistically signifi cant decrease of perinatal mortality (p=0.026) in expectant management group.
We found in the literature two randomised trials for the management of severe preeclampsia. Odendaal et al have showed a decrease in neonatal complications (33% vs. 75%) and no increase in maternal mortality.8 Also Odendaal et al8 and Sibai et al9 reported that expectant management with antenatal steroid administra-tion, and appropriate maternal and fetal surveillance, should be recommended in pregnancies between 28 and 32 weeks.
The major problem with expectant management in developing countries is the need of resources to monitor the mother and fetus intensively. Expectant management is recommended in patients with severe preeclampsia remote from term, after proper selection of patients and careful monitoring.10,11 The obstetricians should balance the risk of maternal morbidity in expectant management against the risk of perinatal mor-bidity and mortality as result of fetal prematurity in immediate management.
REFERENCES1. ACOG technical bulletin. Hypertension in pregnancy. Number 219-January 1996 (replaces no. 91,
February 1986). Committee on Technical Bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 1996; 53:175-83.
2. Tuffnell DJ, Jankowicz D, Lindow SW, Lyons G, Mason GC, Russell IF, Walker JJ. outcomes of severe pre-eclampsia/eclampsia in Yorkshire 1999/2003. BJOG 2005; 112:875–80.
153
November 17-20, 2011 Paris, France
3. Magpie Trial Follow Up Study Management Group. The Magpie Trial Follow Up Study: outcome after discharge from hospital for women and children recruited to a trial comparing magnesium sulphate with placebo for pre-eclampsia. BMC Pregnancy Childbirth. 2004.
4. Brown MA, Buddle ML. What’s in a name? Problems with the classifi cation of hypertension in pregnancy. Journal of Hypertension 1997; 15:1049–54.
5. Sibai BM. Magnesium sulfate prophylaxis in preeclampsia: Lessons learned from recent trials. Am J Obstet Gynecol. Jun 2004; 190(6):1520-6.
6. Churchill D, Duley L. Interventionist versus expectant care for severe pre-eclampsia before term. Cochrane Database of Systematic Reviews 2002, Issue 3.
7. Friedman SA, Schiff E, Lubarsky SL, Sibai BM. Expectant management of severe preeclampsia remote from term. Clin Obstet Gynecol 1999; 42:470-8.
8. Odendaal HJ, Pattinson RC, Bam R, Grové D, Kotze TJ. Aggressive or expectant management for patients with severe preeclampsia between 28-34 weeks’ gestation: a randomized controlled trial. Obstet Gynecol 1990; 76:1070-5.
9. Sibai BM, Mercer BM, Schiff E, Friedman SA. Aggressive versus expectant management of severe preeclampsia at 28 to 32 weeks’ gestation: a randomized controlled trial. Am J Obstet Gynecol 1994; 171:818–22.
10. Hall DR, Odendaal HJ, Kirsten GF, Smith J, Grové D. Expectant management of early onset, severe pre-eclampsia: perinatal outcome. Br J Obstet Gynecol 2000; 107:1258-64.
11. Haddad B, Deis S, Goffi net F, et al. Maternal and perinatal outcomes during expectant management of 239 severe preeclamptic women between 24 and 33 weeks’ gestation. Am J Obstet Gynecol 2004; 190:1590-5.
12. Sibai BM, Akl S, Fairlie F, Moretti M. A protocol for managing severe preeclampsia in the second trimester. Am J Obstet Gynecol 1990; 163:733-8.
© 2012 Monduzzi Editoriale | Proceedings Code: 527
Fetal growth and birth weight: the need for clinical decision support software
R. Santos1,2, C. Santos2, J. Bernardes2, R. Cruz-Correia2
1Centro Hospitalar do Alto Ave, Guimarães, Portugal; 2CINTESIS, Faculty of Medicine, University of Porto, Porto, Portugal
SUMMARYHealth Information Systems (HIS) are growing. Their role is to both facilitate the
processing of an ever increasing amount of health related information and to opti-mize workfl ows, in order to provide better care. This last characteristic, arguably the most important, is often neglected by lack of planning and communication with the professionals involved in the process being changed by the HIS or its component implementation. The software must be able to better provide a (correct) task, but also to respond to healthcare professional’s needs and expectations. Fetal growth and birth weight is often used to classify pregnancy or new born risk, because its extremes are often associated with pathological conditions. This classifi cation is diffi cult, and multiple reference tables were created for this purpose. Several tools may be provided by software to alleviate correct risk classifi cation, reference cre-ation and validation. We provide a rationale to the creation of such clinical decision support software, arguably the most important step for health related software ac-ceptance and success.
INTRODUCTIONNew technologies have been steadily introduced in healthcare over the years.
Particularly, health information Systems (HIS) adoption is usually driven by a need for process change or optimization, either driven by patients, healthcare profes-sionals or other stakeholders. Barriers are common to these changes 1, but several success stories and the methodology to overcome diffi culties were published 2-4. It is important to understand that the rate of adoption of a computerized system will be dependent on the perceived need for that change, the difference in workfl ow (how much of it will be different) and the benefi ts gained. These benefi ts may be eco-nomical, enhanced clinical performance, reduced bureaucratic time for healthcare

156
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
professionals, etc. 5. In this scope, any change in HIS should be thoroughly planned having in mind not only the technical performance and correctness of the change, but also all factors involved in care delivery, including its need, workfl ow optimi-zation, the changes implemented and their consequences, the impact on healthcare professionals satisfaction, and both improvements and setbacks not directly related to the problem addressed by the change (e.g. an electronic prescription service cre-ated for resource optimization that also allows for better clinical performance, di-minishing prescription errors but also taking more time from doctors and nurses, due to complexity).
Although it is fairly intuitive that changes in healthcare should be driven by such carefully planned approaches, this is often not the case 6, and approaches such as evidence based ones are even rarer 7. The rationale for the development of health-care related software, specifi cally, is often overlooked. Our goal is to describe a healthcare problem that needs solving and illustrate how a computer program may help in this task, creating the rationale for its development and effectively planning for its success.
The problem of fetal growth and birth weightBefore the sixties, a child born weighting less than 2500g was considered pre-
mature. A seminal study by Lubchenko et al 8 stated that certain newborns do not achieve their full growth potential, and originated a search for identifi cation and classifi cation of this pathological condition. With this paper it was produced the fi rst table of reference values for birth weight, by gestational age (GA). These kinds of reference values are, in the present day, widely known and used to monitor fetal growth and to classify risk in fetuses and newborns, defi ning normal and abnormal weight, considering their gestational age. This leads to the defi nition of fetal growth restriction (FGR). The 10th percentile of the references is frequently used 9 to iden-tify Small for Gestational Age fetuses (SGA), and warrant further investigation, in order to distinguish constitutionally small fetuses from growth restricted ones. This is not an easy task, as multiple factors contribute to determine a newborn’s weight.
There are several reference tables/charts used for this purpose, some of which are over 40 years old 8,10. If we were to defi ne the 10th percentile as a cutoff for further investigation (or tighter surveillance) of any given pregnancy, it would yield, at 37 GA weeks and according to different authors: 2340g in Doubilet et al. 11, 2392g in Babson at al. 10, 2405g in Yudkin et al. 12, 2541g in Alexander et al 13. Depending on the table used, it is possible that a value can be considered normal in some cases but abnormal in others.
Besides the inherent differences related to geographical localization and genetic heritage, other variables infl uencing birth weight have been identifi ed as signifi cant-ly contributing to determine the full growth potential of a fetus and, thus, contribute to enhanced sensibility and specifi city when using fetal weight to defi ne and further
157
November 17-20, 2011 Paris, France
investigate pathology. Sex was one of the fi rst recognized variables affecting growth potential 10, but other characteristics have been identifi ed, such as race, maternal weight, parity and tobacco use 14,15. Curves constructed with multivariable sets have been identifi ed as more accurate to predict perinatal mortality 16.
To further complicate matters, the method used to extrapolate fetal weight is usu-ally based in ultrasound biometry, by the use of a few standardized measurements on the fetus. The problem is there are over 30 formulae described, and none has been considered superior, mainly because the method is itself highly imperfect, with errors that may range upwards of 20% of birth weight, with a median absolute error of about 6% 17,18.
These problems are of paramount importance, yet frequently doctors are unaware of them, and tend to trust values outputted in ultrasound and corresponding reported centiles 19. There is the need to validate the ultrasound techniques, formulas and ref-erences used to the population in which it is used and, yet, this is often disregarded, as it involves profound knowledge in the subject (clinical, theoretical, and statisti-cal) applied to large samples of the population. This is not easily achieved.
The software and its roleSoftware may aid in the integration of these concerns in everyday practice, by
alleviating knowledge on the basics of the problem, such as statistical knowledge, making the process of validation and classifi cation of fetuses more complete and correct, yet more transparent on its mechanics.
Reference validation: As reference values may not be the same across different countries or even regions, it is necessary to choose the right reference values to which will be compared the ones obtained by the ultrasound operator or the scale, if we are measuring a newborn. The reference values used should be such that, once plotted enough values, the distribution of the actual measurements across the refer-ence curve would be consistent with the plotted centiles (i.e. about 10% of values would be below the 10th percentile, for instance), excluding systematic measure-ment errors. By having a reference table or a set of tables from which to choose, and the ability to access a data fi le in a predefi ned format, or even data entered directly, the software could calculate the centile values for each gestational age and compare them to those we choose.
Multivariate table: By changing some parameters in a regression equation, such as mother weight, parity and smoking status, it is possible to better predict the range of normal values to a given fetus 14,16. By optionally allowing input of these variables, the software could further aid in the detection of abnormal growth patterns. Variables such as fetus sex and mother race further change the reference values, as these frequently produce measurements that are statistically different. With the possibility of storing and using multiple tables, a simple piece of software could easily change the compari-son reference, hence producing enhanced diagnostic sensitivity and specifi city.

158
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Reference values output: Having all algorithms necessary to statistically compare reference values for birth weight, the software could even produce them. Although this would require, at least, hundreds of subjects, and to the extent of thousands, if data were to be properly collected and validated (i.e. scanned for errors), the process of making the table could be quite streamlined by software. The outputted tables/reference values could be used to compare regions, make audits, etc. The raw data could contribute to continuously audit and update a region or country tables, with transmission of anonym data.
Data validation: A set of tools may be introduced to aid in the diffi cult tasks of identifying errors of raw data on birth weight, or to prevent the input of improbable values. Random errors are usual in these kinds of data 20, which are better extracted automatically.
System integration: Instead of merely creating a single standalone product, the code could be used to integrate data from other sources or to act as a module for other developers, namely in the ultrasound reporting business.
CONCLUSIONNo drug enters the market without being submitted to numerous trials. This same
care should exist in software development, which serves an important function in healthcare delivery. Health informatics can greatly improve healthcare, but it is nec-essary to develop products that are respectful of the current paradigm and bring improvement to all intervenient.
We have shown how software may help in the reference values for birth weight problem, helping doctors understand the problem, enhancing clinical performance, reducing errors in related data input and analysis and allowing for better research of the issue by providing data easily compiled for this purpose. We have presented the grounds for the development of this useful tool, in a clinically understandable and relevant manner. This is the fi rst step to a successful approach to the software development, one which is not often taken or understood, in order to produce a tool that improves healthcare delivery.
By involving clinical staff early in the development of software products in healthcare, different views on the same problem may lead to a better and more real-istic approach of a useful solution.
REFERENCES 1. Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal Health Records: Defi nitions,
Benefi ts, and Strategies for Overcoming Barriers to Adoption. Journal of the American Medical Informatics Association 2006; 13:121-6.
2. Andreen DL, Dobie LJ, Jasperson JC, Lucas TA, Wubbenhorst CL. The conversion to electronic hospital notes at Mayo Clinic. Overcoming barriers and challenges. J Healthc Inf Manag 2010; 24:57-64.
159
November 17-20, 2011 Paris, France
3. Oliver A. Public-sector health-care reforms that work? A case study of the US Veterans Health Administration. The Lancet; 371:1211-3.
4. Scott JT, Rundall TG, Vogt TM, Hsu J. Kaiser Permanente's experience of implementing an electronic medical record: a qualitative study. BMJ 2005; 331:1313-6.
5. Haux R. Health information systems - past, present, future. International Journal of Medical Informatics 2006; 75:268-81.
6. Alexander G, Staggers N. A systematic review of the designs of clinical technology: fi ndings and recommendations for future research. ANS Adv Nurs Sci 2009; 32:252-79.
7. Kitchenham BA, Dyba T, Jorgensen M. Evidence-based software engineering. In: Software Engineering, 2004 ICSE 2004 Proceedings 26th International Conference on; 2004 23-28 May 2004; 2004. p. 273-81.
8. Lubchenco L, Hansman C, Dressler M, Boyd E. Intrauterine growth as estimated from liveborn birth-weight data at 24 to 42 weeks of gestation. Pediatrics 1963; 32:793.
9. Battaglia FC, Lubchenco LO. A practical classifi cation of newborn infants by weight and gestational age. J Pediatr 1967; 71:159-63.
10. Babson SG, Behrman RE, Lessel R. FETAL GROWTH. Liveborn Birth Weights for Gestational Age of White Middle Class Infants. Pediatrics 1970; 45:937.
11. Doubilet PM, Benson CB, Nadel AS, Ringer SA. Improved birth weight table for neonates developed from gestations dated by early ultrasonography. J Ultrasound Med 1997; 16:241-9.
12. Yudkin PL, Aboualfa M, Eyre JA, Redman CWG, Wilkinson AR. New birthweight and head circumference centiles for gestational ages 24 to 42 weeks. Early Human Development 1987; 15:45-52.
13. Alexander G, Himes J, Kaufman R, Mor J, Kogan M. A United States national reference for fetal growth. Obstet Gynecol 1996; 87:163 - 8.
14. Gardosi J, Mongelli M, Wilcox M, Chang A. An adjustable fetal weight standard. Ultrasound in Obstetrics and Gynecology 1995; 6:168-74.
15. Vielwerth SE, Jensen RB, Larsen T, Greisen G. The impact of maternal smoking on fetal and infant growth. Early Human Development 2007; 83:491-5.
16. Gardosi J, Clausson B, Francis A. The value of customised centiles in assessing perinatal mortality risk associated with parity and maternal size. BJOG: An International Journal of Obstetrics & Gynaecology 2009; 116:1356-63.
17. Dudley NJ. A systematic review of the ultrasound estimation of fetal weight. Ultrasound Obstet Gynecol 2005; 25:80-9.
18. Anderson NG, Jolley IJ, Wells JE. Sonographic estimation of fetal weight: comparison of bias, precision and consistency using 12 different formulae. Ultrasound Obstet Gynecol 2007; 30:173-9.
19. Zhang J, Merialdi M, Platt LD, Kramer MS. Defi ning normal and abnormal fetal growth: promises and challenges. Am J Obstet Gynecol 2010; 202:522-8.
20. Platt RW. The effect of gestational age errors and their correction in interpreting population trends in fetal growth and gestational age-specifi c mortality. Seminars in Perinatology 2002; 26:306-11.

© 2012 Monduzzi Editoriale | Proceedings Code: 539
Endothelin-1 system polymorphisms in preeclampsia and gestational hypertension
A. Seremak-Mrozikiewicz, M. Barlik, K. DrewsDivision of Perinatology and Women’s Diseases; University of Medical Sciences; Poznan, Poland
Endothelin (ET) is a paracrine hormone (21 amino-acid peptide) and a potent vasoconstrictor synthesized mainly by endothelium of blood vessels. Three differ-ent isoforms of endothelin family (ET-1, ET-2 and ET-3) encoded by separate genes have been recognized. The best known is ET-1 which is involved in cell prolif-eration, acid-alkali balance, infl ammation processes, hemostasis and cardiovascular system function. ET-1 is synthesized through multiple proteolytic steps in a process regulated by endothelin-1 converting enzyme (ECE-1) localized mainly in endothe-lial cells.
ECE-1 protein is an integral membrane part and its activity is probably regulated by vascular endothelial growth factor, interleukin-1 and tumor necrosis factor alpha which increase ET-1 and ECE-1 mRNA expression. ECE-1 is also recognized as an part of ET-1 and both elements are known as endothelin-1 system. Recently, three different isoforms of ECE-1 (ECE-1a, -1b and -1c) have been described (differing only in their N-terminal regions), from which the ECE-1a isoform is suggested to have regulatory function because of the presence of potential binding sites for nu-merous transcription factors.
It is believed that ET-1 and ECE-1 are very important agents of the development of preeclampsia (PE). Any changes in ECE-1 activity and quantity may infl uence the proper evolution of feto-placental unit and the development of preeclampsia. Pathogenesis of preeclampsia is explained by endothelium damage of spiral ar-teries during trophoblast invasion to the vessel wall. At the beginning of normal pregnancy trophoblast changes the muscle layer of the spiral arteries to modulate low-resistant system which assures proper perfusion of the placenta. Endothelin-1 system controls the process of angiogenesis, blood-fl ow regulation and evolution of utero-placental unit. In PE normal trophoblast invasion is limited only to decidual part of spiral arteries leading to the placental anoxia and endothelial damage. These
162
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
changes are connected with imbalance of vasodilatator and vasoconstrictor levels. During this pathological process, an increase of tromboxan A2 and endothelin-1 as well as decrease of nitric oxide concentrations in plasma have been occur. The impair balance between vasoactive factors, especially disturbances in endothelin-1 secretion which start in the early stage of pregnancy, intensify during the second half of pregnancy and are manifested clinically by preeclampsia symptoms.
Considering multifactorial background of PE, especially including the genetic variants, it was hypothesized that many genetic polymorphisms are involved in its pathogenesis. Attempts have been made to correlate the presence of genetic poly-morphisms with blood pressure levels in preeclamptic pregnant women. Recent studies show that polymorphisms of ET-1 and ECE-1 genes may affect ET-1 sys-tem and suggest that conditioned by genetic polymorphisms changes in this system could take part in the development of preeclampsia.
In our study we decided to evaluate the correlation between polymorphisms of ET-1 (Lys198Asn) and ECE-1 (Thr341Ile) genes and the risk of gestational hyper-tension (GH) and preeclampsia. There were no statistically signifi cant differences in genotype frequencies of ET-1 Lys198Asn and ECE-1 Thr341Ile gene polymorphic variants between hypertensive pregnant women and the control group. There were also no remarkable differences between GH and PE groups when compared to the controls. Additionally, we have analyzed the ECE-1 and ET-1 variant localization of both Thr341Ile ECE-1 and Lys198Asn ET-1 investigated polymorphisms. Parallel presence of both Thr341Ile ECE-1 and Lys198Asn ET-1 variant localisation showed a higher occurrence rate of ECE-1 CT/ET-1 GT heterozygotic genotypes in the con-trol group than in the whole study or GH and PE groups.
The last step involved the analysis of the connection of blood pressure with particular genotypes of investigated polymorphisms. In preeclamptic women, the higher systolic blood pressure value was observed in GG Lys198Asn ET-1 genotype carriers than in patients with at least one mutated T allele (GT and TT). The lowest blood pressure level was connected with the mutated TT Lys198Asn ET-1 genotype presence. In connection to the Thr341Ile ECE-1 gene polymorphism, the systolic blood pressure was slight higher in CC genotype carriers than in carriers of mutated T allele (CT + TT). Also, the analysis of genotypes coexistence showed that in PE women the lowest blood pressure level was connected with the TT mutated geno-types of Lys198Asn ET-1 gene polymorphism presence.
Results of our study suggest lack of direct correlation of Lys198Asn ET-1 and Thr341Ile ECE-1 gene polymorphisms with the risk of gestational hypertension and preeclampsia in studied population of Polish women. High prevalence of ECE-1 CT/ET-1 GT heterozygote genotypes of both Thr341Ile ECE-1 and Lys198Asn ET-1 polymorphisms in healthy pregnant subjects compared to GH and PE groups sug-gests a protective role of mutated alleles in the development of PE. The carrier of mutated TT genotype of Lys198Asn ET-1 polymorphism is probably connected

163
November 17-20, 2011 Paris, France
with lower systolic blood pressure level in preeclamptic women. To the best of our knowledge, this study is the fi rst to monitor the signifi cance of Thr341Ile ECE-1 polymorphism in relation to PE in Polish pregnant women. Although the weakness of this study is a small group of preeclamptic women and lack of measurement of ET-1 and ECE-1 activity, this research presents up-to-date problem concerning ge-netic markers involved in the development of PE. Our study is also a confi rmation of an important role of several substances involved in angiogenesis and vascular tense regulation which occur to be very signifi cant factors in many obstetric condi-tions. Additional studies are needed to establish the role of analyzed polymorphisms in the etiology of gestational hypertension and preeclampsia.
Endothelial injury, remarkable in the second phase of PE, is evidently linked with endothelin-1 system disturbances. Thus, researches correlated to this problem cover the changes of ET-1 and ECE-1 activity. In the study made by Słowiński et al., there was notably higher ET-1 level in serum from PE women (30 subjects, 24-36 weeks gestation) compared to 125 healthy pregnancies. The study of Baksu et al. revealed that not only increased ET-1 concentration but also decreased concentration of nitric oxide and impaired balance of those two substances play an signifi cant pathogenetic role in PE development. On the other hand, Ajne et al. analyzed ECE-1 activity and concentration in women with PE and showed higher ECE-1 synthesis in hyperten-sive patients compared to healthy pregnant women.
Furthermore, the changes of ET-1 and ECE-1 concentration observed in pre-eclamptic women could be conditioned by different polymorphic variants of the genes coding for these elements. In PE, the ET-1 released from maternal endothe-lium is augmented, contrary to endothelium in placental vessels, where decreasing level of ET-1 is suggested to be one of the compensation forms of disturbances in utero-placental fl ow. These signals show a association among genetic variants of ECE-1 and impairment of endothelial functions and allow to recognize the endo-thelin-1 system as the essential initiating point leading to the cardiovascular system lesions which could also be involved in pathomechanism of preeclampsia.
REFERENCES1. Słowiński T, Neumayer HH, Stolze T [et al.]. Endothelin system in normal and hypertensive preg-
nancy. Clin Sci (Lond). 2002, 103, 446-449.2. Baksu B, Davas I, Baksu A [et al.]. Plasma nitric oxide, endothelin-1 and urinary nitric oxide and
cyclic guanosine monophosphate levels in hypertensive pregnant women. Int J Gynaecol Obstet. 2005, 90, 112-117.
3. Ajne G, Wolff K, Fyhrquist F [et al.]. Endothelin converting enzyme (ECE) activity in normal pregnancy and preeclampsia. Hypertens Pregnancy. 2003, 22, 215-224.
4. Funalot B, Courbon D, Brousseau T [et al.]. Genes encoding endothelin-converting enzyme-1 and endothelin-1 interact to infl uence blood pressure in women: the EVA study. J Hypertens. 2004, 22, 739-743.
5. López-Jaramillo P, Casas JP, Serrano N. Preeclampsia: from epidemiological observations to mo-lecular mechanisms. Braz J Med Biol Res. 2001, 34, 1227-1235.

164
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
6. Escudero C, Puebla C, Westermeier F [et al.]. Potential cell signaling mechanisms involved in dif-ferential placental angiogenesis in mild and severe pre-eclampsia. Curr Vasc Pharmacol. 2009, 7, 475-485.
7. Kaufmann P, Black S, Huppertz B. Endovascular trophoblast invasion: implications for the patho-genesis of intrauterine growth retardation and preeclampsia. Biol Reprod. 2003, 69, 1-7.
8. Myatt L, Webster RP. Vascular biology of preeclampsia. J Thromb Haemost. 2009, 7, 375-384.9. Gilbert JS, Ryan MJ, La Marca BB [et al.]. Pathophysiology of hypertension during preeclampsia:
linking placental ischemia with endothelial dysfunction. Am J Physiol Heart Circ Physiol. 2008, 294, 541-550.
10. Rossi GP, Pitter G. Genetic variation in the endothelin system: do polymorphisms affect the therapeutic strategies? Ann N Y Acad Sci. 2006, 1069, 34-50.
© 2012 Monduzzi Editoriale | Proceedings Code: 658
TNF-α concentrations in maternal and umbilical cord plasma and the perinatal outcome
J. Zegarska1, K. Borowska-Mackowiak1, J. Kłyszejko-Molska1, M. Socha1, M. Gruszka2, P. Krepska1, B. Wolski1, W. Szymanski1, M. Grabiec1
1Department of Obstetrics and Gynecology of the Nicolas Copernicus University in Torun, Collegium Medicum in Bydgoszcz, Poland; 2Department of Laboratory Medicine of the Nicolas Copernicus University in Torun, Collegium Medicum in Bydgoszcz, Poland
SUMMARYThe aim of our study was to evaluate the diagnostic value of umbilical cord and
maternal plasma TNFα concentrations in the presence or absence of the early onset neonatal infection and other severe complications of infl ammation. Study design: 80 mothers and their neonates were enrolled to our study. Maternal blood was collected during the active phase of labor and umbilical cord blood was collected immedi-ately after delivery. Prospectively antepartum and intrapartum data were collected. We collect also all information concerning neonatal outcomes. Results: Higher level of TNF-α in delivering women blood was associated with neonatal infection (130,1 vs. 78,75 pg/ml; p=0,0462). There were no signifi cant differences in TNF-α levels in umbilical cord plasma between healthy and infected neonates in both preterm and term neonates. Nevertheless high level of TNFα in umbilical blood was correlated with severe early onset infection and other perinatal disorders. All (seven) neonates with level of TNF-α in umbilical cord plasma higher than 750 pg/ml had severe complications, including periventricular leukomalacia. Conclusions: High level of TNFα in maternal plasma correlates with severity of neonatal infection. High level of TNFα in umbilical cord plasma correlates with the presence of other severe peri-natal disorders.
INTRODUCTIONPreterm birth and neonatal infection still are the major clinical challenges for
today’s medicine. There is a lot of studies supporting the association between in-

166
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
trauterine infection, preterm birth, early-onset neonatal infection and other neonatal disorders including periventricular leukomalacia (PLV) and cerebral palsy (1,2). El-evated level of proinfl ammatory cytokines in amniotic fl uid as well as in fetal, neo-natal and maternal plasma has been reported to be associated with an increased risk for neonatal morbidity. TNFα is thought to be a pregnancy-threatening cytokine (3). Higher level of TNFα was observed in preterm deliveries caused by chorioamnion-itis and there are some studies suggesting that TNFα is responsible for preterm labor (4).There are some researches that prove increased production of TNFα after LPS stimulation (5). Local production of TNFα induces synthesis of other proinfl am-matory cytokines such as IL-1, IL-6 and may lead to fetal damage. Some authors suggest that high level of TNFα together with other cytokines such as IL-1β, IL-6 can be considered as a marker of perinatal infection or infl ammation. According to these fi ndings high level of TNFα may suggest a high risk of serious fetal disease and damage including PLV which may lead to cerebral palsy (6,7). There are no reference level for TNFα concentration in umbilical plasma and furthermore the noticed levels vary widely from one studies to another. The aim of our study was to evaluate the diagnostic value of umbilical cord and maternal plasma TNFα concen-trations in the presence or absence of the early onset neonatal infection (EONI) and other severe complications of infl ammation
MATERIALS AND METHODSThis research was performed at the Obstetrics Department of the Nicolaus Co-
pernicus University in Torun, CM in Bydgoszcz, with the approval of the Bioethical Commission of the Nicolaus Copernicus University in Torun. All pregnant women delivering at our department during four months period were offered to enroll our study. After we collected all blood samples we divided all patient to four groups as follow: term non-infected, term infected, preterm non-infected and preterm in-fected. At the end we chose from all group 20 patients by chance, so our study population consist of 80 women and their newborns. We excluded from enrollment: 12 mothers and their babies whose cord blood sample was too small to determine the study markers, 2 multiple pregnancies and 1 baby with lethal abnormalities. The fi nal population enrolled to this study was 65 delivering women and their new-borns. A sample of maternal blood was collected during the active phase of labor and the same amount of umbilical cord blood was collected immediately after de-livery. All samples were centrifuged, aliquoted and stored in small aliquots at -70° C until analysis. Maternal and umbilical cord blood level of TNF-α was measured by enzyme-linked immunosorbent assay kits (Bender MedSystems GmbH Human TNF-α ELISA test). We collect prospectively maternal demographic, antepartum and intrapartum data including age, parity, co-existing diseases, pregnancy-related diseases, medications during pregnancy, group B streptococcus colonization, anti-biotic treatment, mode of delivery, duration of pregnancy, duration of active phase
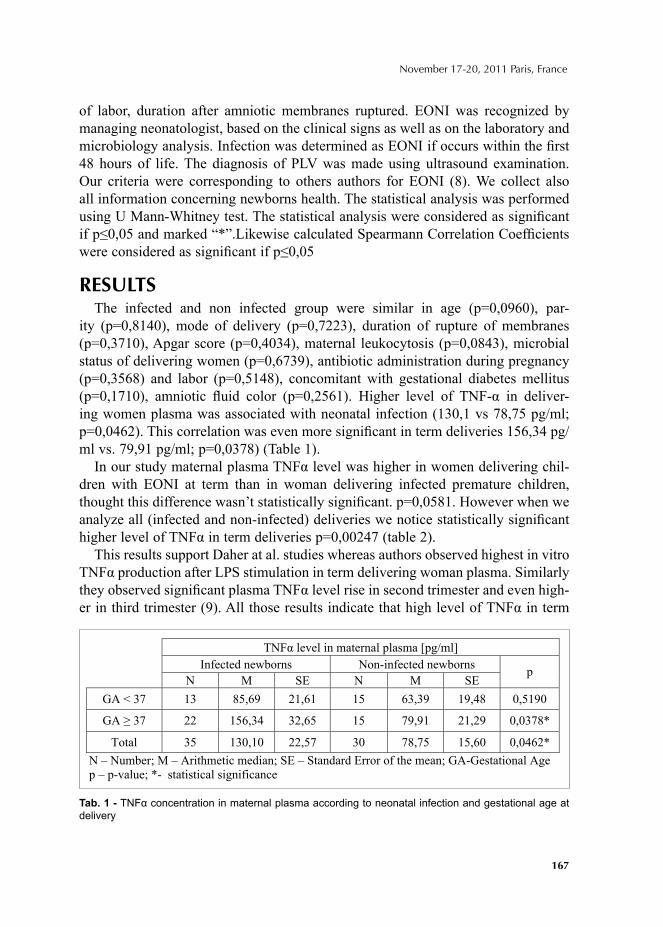
167
November 17-20, 2011 Paris, France
of labor, duration after amniotic membranes ruptured. EONI was recognized by managing neonatologist, based on the clinical signs as well as on the laboratory and microbiology analysis. Infection was determined as EONI if occurs within the fi rst 48 hours of life. The diagnosis of PLV was made using ultrasound examination. Our criteria were corresponding to others authors for EONI (8). We collect also all information concerning newborns health. The statistical analysis was performed using U Mann-Whitney test. The statistical analysis were considered as signifi cant if p≤0,05 and marked “*”.Likewise calculated Spearmann Correlation Coeffi cients were considered as signifi cant if p≤0,05
RESULTSThe infected and non infected group were similar in age (p=0,0960), par-
ity (p=0,8140), mode of delivery (p=0,7223), duration of rupture of membranes (p=0,3710), Apgar score (p=0,4034), maternal leukocytosis (p=0,0843), microbial status of delivering women (p=0,6739), antibiotic administration during pregnancy (p=0,3568) and labor (p=0,5148), concomitant with gestational diabetes mellitus (p=0,1710), amniotic fl uid color (p=0,2561). Higher level of TNF-α in deliver-ing women plasma was associated with neonatal infection (130,1 vs 78,75 pg/ml; p=0,0462). This correlation was even more signifi cant in term deliveries 156,34 pg/ml vs. 79,91 pg/ml; p=0,0378) (Table 1).
In our study maternal plasma TNFα level was higher in women delivering chil-dren with EONI at term than in woman delivering infected premature children, thought this difference wasn’t statistically signifi cant. p=0,0581. However when we analyze all (infected and non-infected) deliveries we notice statistically signifi cant higher level of TNFα in term deliveries p=0,00247 (table 2).
This results support Daher at al. studies whereas authors observed highest in vitro TNFα production after LPS stimulation in term delivering woman plasma. Similarly they observed signifi cant plasma TNFα level rise in second trimester and even high-er in third trimester (9). All those results indicate that high level of TNFα in term
TNF level in maternal plasma [pg/ml]
Infected newborns Non-infected newborns
N M SE N M SE p
GA < 37 13 85,69 21,61 15 63,39 19,48 0,5190
GA 37 22 156,34 32,65 15 79,91 21,29 0,0378*
Total 35 130,10 22,57 30 78,75 15,60 0,0462*
N – Number; M – Arithmetic median; SE – Standard Error of the mean; GA-Gestational Age
p – p-value; *- statistical significance
Tab. 1 - TNFα concentration in maternal plasma according to neonatal infection and gestational age at delivery
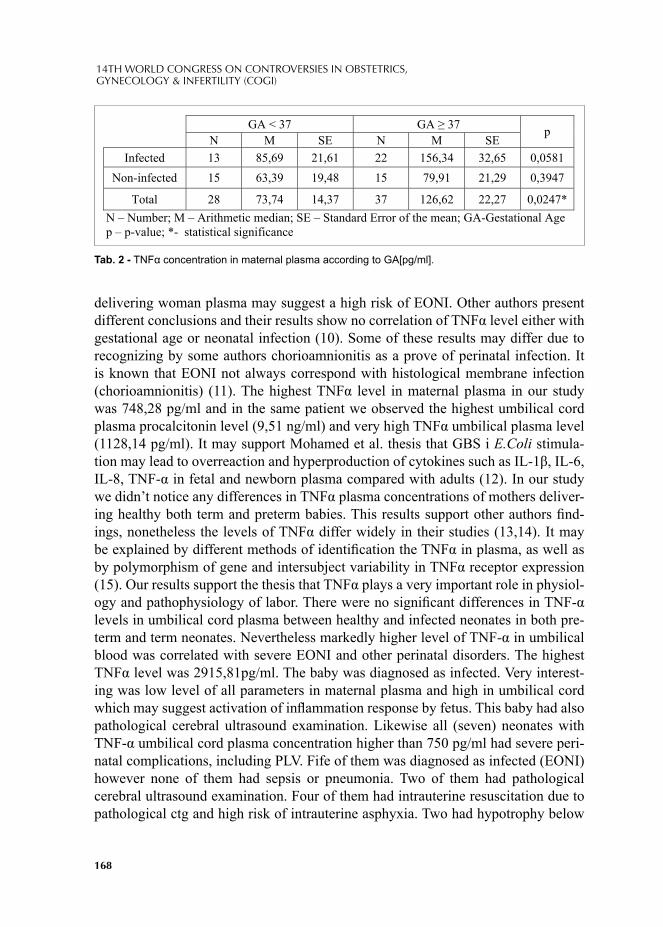
168
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
delivering woman plasma may suggest a high risk of EONI. Other authors present different conclusions and their results show no correlation of TNFα level either with gestational age or neonatal infection (10). Some of these results may differ due to recognizing by some authors chorioamnionitis as a prove of perinatal infection. It is known that EONI not always correspond with histological membrane infection (chorioamnionitis) (11). The highest TNFα level in maternal plasma in our study was 748,28 pg/ml and in the same patient we observed the highest umbilical cord plasma procalcitonin level (9,51 ng/ml) and very high TNFα umbilical plasma level (1128,14 pg/ml). It may support Mohamed et al. thesis that GBS i E.Coli stimula-tion may lead to overreaction and hyperproduction of cytokines such as IL-1β, IL-6, IL-8, TNF-α in fetal and newborn plasma compared with adults (12). In our study we didn’t notice any differences in TNFα plasma concentrations of mothers deliver-ing healthy both term and preterm babies. This results support other authors fi nd-ings, nonetheless the levels of TNFα differ widely in their studies (13,14). It may be explained by different methods of identifi cation the TNFα in plasma, as well as by polymorphism of gene and intersubject variability in TNFα receptor expression (15). Our results support the thesis that TNFα plays a very important role in physiol-ogy and pathophysiology of labor. There were no signifi cant differences in TNF-α levels in umbilical cord plasma between healthy and infected neonates in both pre-term and term neonates. Nevertheless markedly higher level of TNF-α in umbilical blood was correlated with severe EONI and other perinatal disorders. The highest TNFα level was 2915,81pg/ml. The baby was diagnosed as infected. Very interest-ing was low level of all parameters in maternal plasma and high in umbilical cord which may suggest activation of infl ammation response by fetus. This baby had also pathological cerebral ultrasound examination. Likewise all (seven) neonates with TNF-α umbilical cord plasma concentration higher than 750 pg/ml had severe peri-natal complications, including PLV. Fife of them was diagnosed as infected (EONI) however none of them had sepsis or pneumonia. Two of them had pathological cerebral ultrasound examination. Four of them had intrauterine resuscitation due to pathological ctg and high risk of intrauterine asphyxia. Two had hypotrophy below
GA < 37 GA 37
N M SE N M SE p
Infected 13 85,69 21,61 22 156,34 32,65 0,0581
Non-infected 15 63,39 19,48 15 79,91 21,29 0,3947
Total 28 73,74 14,37 37 126,62 22,27 0,0247*
N – Number; M – Arithmetic median; SE – Standard Error of the mean; GA-Gestational Age
p – p-value; *- statistical significance
Tab. 2 - TNFα concentration in maternal plasma according to GA[pg/ml].

169
November 17-20, 2011 Paris, France
5 percentile. All 7 mothers had elevated C-reactive protein concentration and leu-kocytosis, All of them had antibiotic therapy. One of two children without infection had hypotrophy and was delivered by cesarean section due to acute, severe hypoxia. The second baby without infection was born healthy, without any worrying syn-drome, apart from fact that the delivery was performed 17 days after PPROM (the baby girl was born in 34 weeks of pregnancy with 10 Apgar score). The mother had high C-reactive protein level and was administered antibiotic till delivery. All this fact may suggest that this two children wasn’t fi nd as infected thanks to arresting the infl ammation by antibiotics. All children in this group needed short and long-term follow up focused especially on their nervous system. This clinical analysis of new-borns with extremely high TNFα level may suggest that high umbilical cord plasma TNFα level may be linked to PLV (which is strongly joined to perinatal infection), and intrauterine growth restriction (IUGR) (16).
CONCLUSIONSHigh level of TNFα in maternal plasma correlates with severity of neonatal in-
fection. High level of TNFα in umbilical cord plasma correlates with the presence of other severe perinatal disorders. More investigations are needed to prove the role of maternal and umbilical cord blood level of TNFα in prediction of perinatal complications.
REFERENCES1. ROMERO R, EREZ O, ESPINOZA J. Intrauterine Infection, Preterm Labor, and Cytokines. J Soc Gynecol
Investig 2005; 12(7)463-5.2. KADHIM H, TABARKI B, VERELLEN G, DE PREZ C, RONA AM, et al. Infl ammatory cytokines in the
pathogenesis of periventricular leukomalacia. Neurology. 2001; 56(10):1278-84.3. SILEN ML, FIRPO A, MORGELLO S, LOWRY SF, FRANCUS T. Interleukin-1 alpha and tumor necrosis
factor alpha cause placental injury in the rat. Am J Pathol. 1989; 135(2):239-44.4. ROMERO R, MAZOR M, WU YK, AVILA C, OYARZUN E, MITCHELL MD. Bacterial endotoxin and tumor
necrosis factor stimulate prostaglandin production by human decidua. Prostaglandins Leukot Es-sent Fatty Acids. 1989; 37(3):183-6.
5. VINCE G, SHORTER S, STARKEY P, HUMPHREYS J, CLOVER L, WILKINS T, et al. Localization of tumour necrosis factor production in cells at the materno/fetal interface in human pregnancy. Clin Exp Neurol. 1992; 88(1):174-80.
6. GOTSCH F, ROMERO R, KUSANOVIC JP, MAZAKI-TOVI S, PINELES B, EREZ O, et al. The fetal Infl amma-tory Response Syndrome. Clinical Obstetrics & Gynecology. 2007; 50(3):652-83.
7. LEVITON A. Preterm birth and cerebral palsy: is tumor necrosis factor the missing link? Dev Med Child Neurol. 1993; 35(6):553-8.
8. KALINKA J, KRAJEWSKI P, SOBALA W, et al. The association between maternal cervicovaginal proin-fl ammatory cytokines concentrations during pregnancy and subsequent early-onset neonatal infec-tion. J. Perinat Med 2006; 34:371-377
9. DAHER S, FONSECA F, RIBEIRO OG, MUSATTI CC, GERBASE-DELIMA M. Tumor necrosis factor during pregnancy and at the onset of labor and spontaneous abortion. Eur J Obstet Gynaecol Reprod Biol. 1999; 83(1):77-9.

170
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
10. KAZIMIERCZAK IA, KORZENIEWSKI J, GRYBOŚ M. Ocena zagrożenia zakażeniem wrodzonym u noworodków w oparciu o wartości cytokin: IL-1á, IL-6 i TNFŕ w surowicy krwi i płynie owodniowym ciężarnych oraz we krwi pępowinowej noworodków. Ginekol Pol. 2003; 74(4):297-302.
11. DØLLNER H, VATTEN L, HALGUNSET J, RAHIMIPOOR S, AUSTGULEN R. Histologic chorioamnionitis and umbilical serum levels of pro-infl ammatory cytokines and cytokine inhibitors. Br J Obstet Gynaecol. 2002; 109(5):534-9.
12. MOHAMED MA, CUNNINGHAM-RUNDLES S, DEAN CR, HAMMAD TA, NESIN M. Levels of pro-infl ammatory cytokines produced from cord blood in-vitro are pathogen dependent and increased in comparison to adult controls. Cytokine. 2007; 39(3):171-7.
13. LAHAM N, BRENNECKE SP, BENDTZEN K, RICE GE. Tumour necrosis factor a during human pregnancy and labour: maternal plasma and amniotic fl uid concentrations and release from intrauterine tissues. Eur J Endocrinol. 1994; 131(6):607-14.
14. BECKMANN I, VISSER W, STRUIJK PC, VAN DOOREN M, GLAVIMANS J, WALLENBURG HC. Circulating bioactive tumor necrosis factor-alpha, tumor necrosis factor-alpha receptors, fi bronectin, and tumor necrosis factor-alpha inducible cell adhesion molecule VCAM-1 in uncomplicated pregnancy. Am J Obstet Gynecol. 1997; 177(5):1247-52.
15. FORTUNATO SJ, MENON R, LOMBARDI SJ. Role of tumor necrosis factor-α in the premature rupture of membranes and preterm labor pathways. Am J Obstet Gynecol.2002; 187(5):1159-62.
16. BARTHA JL, ROMERO-CARMONA R, COMINO-DELGADO R. Infl ammatory cytokines in intrauterine growth retardation. Acta Obstet Gynecol Scand. 2003; 82(12):1099-102.
GYNECOLOGY

© 2012 Monduzzi Editoriale | Proceedings Code: 17
The effect of armed confl ict on spontaneous abortions in Benghazi – Libya
Z.A. Bodalal1, K. Agnaeber2
1 Faculty of Medicine, Libyan International Medical University, Benghazi, Libya; 2Head of Maternity Ward, Al-Jamhouria Hospital, Benghazi, Libya DGO, MRCOG, FRCOG, CCST
ABSTRACTThis paper will study the effect of armed confl ict and civilian instability on the
spontaneous abortion rates and cesarean birth rate. Data from the offi cial records of patients admitted to the gynecological department of Al-Jamhouria hospital (the main maternity hospital in the largest city in Eastern Libya) were used in this study, for both informative and comparative purposes. A statistical analysis was done us-ing professional software, namely SPSS (through t-tests, binomial tests and binary logistic regression). It was found that there was a signifi cant increase in the rate of spontaneous abortion (compared to the same period in the previous year). Also, there was a signifi cant decrease in the age of patients admitted to the OT as well as a signifi cant decrease in the admission of foreign nationals. Moreover, there was an increase in the rate of cesarean births. The possible implications of these fi gures are further discussed in the paper. It was concluded that the armed confl ict had caused an increase in both the spontaneous abortion rate as well as the cesarean birth rate. Future research should deal with the long term impact of the confl ict on the general health of the people and proper social, psychological and marital support should be given to the mothers who had suffered from such an abortion.
INTRODUCTIONIn February of 2011, confl ict erupted in Libya between government forces and
rebels in the city of Benghazi. This spread further to include all of eastern Libya as well as large areas of the rest of the country. Fighting was intense during the periods of February and March, especially on March 19th, 2011 when the government troops reached the city of Benghazi.
174
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Libya has not witnessed a war on its land since its independence in 1951, about 60 years ago. Moreover, the country was undergoing a recent economic boom and the people were hence taken by surprise when the fi ghting started. A great amount of stress was placed on the population especially in rebel-held territories such as Benghazi.
The most vulnerable sections of society are women and children. Pregnant wom-en in particular are very prone to being negatively infl uenced as a result of the hos-tile environment currently present. This paper aims at studying the impact of this stress on spontaneous abortions in Benghazi, through studying the cases admitted to the operating theatre (OT) of Al-Jamhouria hospital. This hospital receives the vast majority of obstetrical cases and the majority of Benghazi’s children are delivered there. A statistical analysis is done and the various parameters are studied and pre-sented in the results section.
In addition, the importance of these numbers will be discussed and elaborated upon based on previous literature. Moreover, in the conclusion, the main fi ndings are summarized and a number of recommendations will be made.
METHODOLOGYHospital records were obtained from Al-Jamhouria Hospital in Benghazi, Libya
for the period of February to May for both 2010 and 2011. These months, in par-ticular, were chosen because they witnessed the most intense period of the confl ict, especially February and March. A total sample size of 2255 cases was documented and of those cases, 1162 were in 2010 and 1093 in 2011.
The records of the OT rooms in the hospitals were input into our calculations. These cases included all the procedures carried out, most prominently spontaneous abortions. In addition to the procedures, age and nationality was also recorded. A comparison was made between the two years in order to determine whether or not there was a statistically signifi cant increase. The binomial test was used in order to compare proportions of spontaneous abortion between the two years. As for the age, the Student’s T-test was done to determine the signifi cance between the average ages of patients in both years. A χ2 test was done to determine the signifi cance of the distribution of cases across the months. Last but not least a binomial test was done to determine the signifi cance in the proportion of foreign nationals and also to test for the signifi cance in the increase of cesarean section rates. All statistical tests were done using PASW (SPSS) 18 Statistical software.
RESULTSThe number of spontaneous abortions in 2010 was recorded at 739 cases,
forming 63.54% of OT cases. In 2011 however, there were 815 cases of spon-taneous abortion, comprising 74.45% of OT cases. Using the binomial test, the
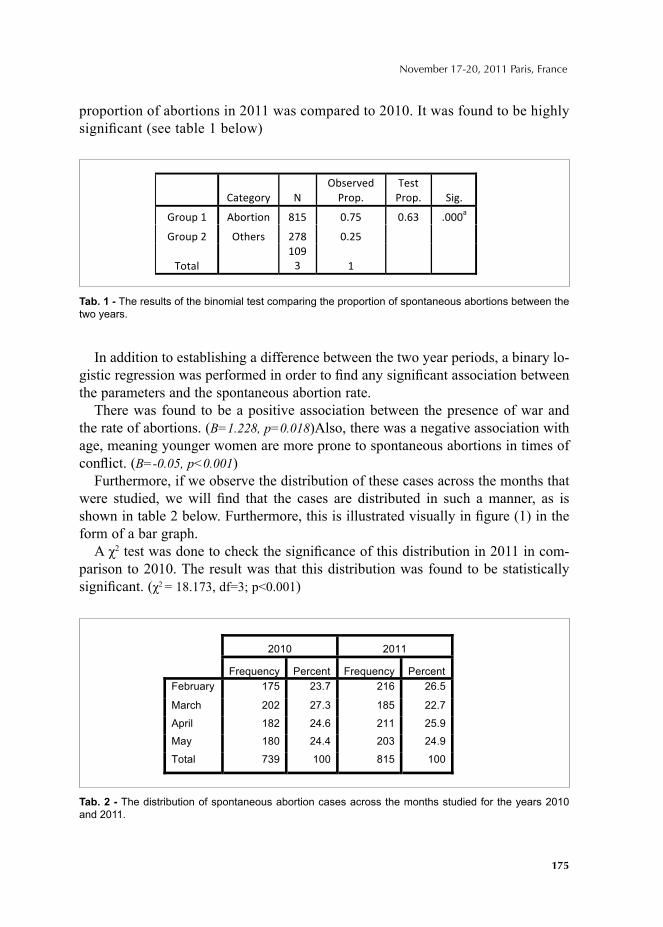
175
November 17-20, 2011 Paris, France
proportion of abortions in 2011 was compared to 2010. It was found to be highly signifi cant (see table 1 below)
In addition to establishing a difference between the two year periods, a binary lo-gistic regression was performed in order to fi nd any signifi cant association between the parameters and the spontaneous abortion rate.
There was found to be a positive association between the presence of war and the rate of abortions. (B=1.228, p=0.018)Also, there was a negative association with age, meaning younger women are more prone to spontaneous abortions in times of confl ict. (B=-0.05, p<0.001)
Furthermore, if we observe the distribution of these cases across the months that were studied, we will fi nd that the cases are distributed in such a manner, as is shown in table 2 below. Furthermore, this is illustrated visually in fi gure (1) in the form of a bar graph.
A χ2 test was done to check the signifi cance of this distribution in 2011 in com-parison to 2010. The result was that this distribution was found to be statistically signifi cant. (χ2 = 18.173, df=3; p<0.001)
Tab. 1 - The results of the binomial test comparing the proportion of spontaneous abortions between the two years.
Tab. 2 - The distribution of spontaneous abortion cases across the months studied for the years 2010 and 2011.
2010 2011
Frequency Percent Frequency Percent
February 175 23.7 216 26.5
March 202 27.3 185 22.7
April 182 24.6 211 25.9
May 180 24.4 203 24.9
Total 739 100 815 100

176
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The average age of patients admitted to the OT in 2010 was 34.23 (±8.67) while the average age for 2011 was 33.30 (±7.73). The difference between the years was approximately 0.93 years and is statistically signifi cant (t=-3.865; p<0.001; 95% CI -1.46 - -0.46).
In addition, there was a signifi cant decrease in the proportion of foreign nation-als admitted to the operation theatre. In 2010, foreign nationals constituted 3.2% of admission but in 2011, that number decreased to 1.9%. Using the binomial test, this decrease was found to be statistically signifi cant (p=0.007).
Cesarean sections increased signifi cantly from 24.75% in 2010 to 26.05% in 2011 (p<0.05 ).
DISCUSSIONThe results show that there was a signifi cant increase in spontaneous abortion
cases between 2010 and 2011. Moreover, when we look at the monthly distribution of cases, we will see that all the months have increased incidences of abortions, apart from March. One main hypothesis is that the main trend for the month of March was a shift towards premature births. This will be covered in upcoming re-search to be proved in a statistical manner.
Armed confl ict in general exacerbates social factors contributing to maternal stress and adverse pregnancy outcomes.[1] This increase in negative pregnancy out-comes has been proven in other incidences of war, such as in the Congo civil war [1], among Gulf war veterans [2][3] and even in the early 20th century Europe[4]. Even in peace times, psychological stress has been shown to negatively affect the reproductive outcomes of women in high stress professions such as medicine. [5]
However, armed confl ict in and of itself, is rarely the cause of the abortion. Rath-er, it is the amount of stress placed on the mother during her pregnancy that can
Fig. 1 - A comparison of the percentage of spontaneous abortion cases distributed across the months under observation.
177
November 17-20, 2011 Paris, France
infl uence the outcome. The etiology and mechanism through which stress and preg-nancy interact has been thoroughly researched [6] where some papers have even made a direct link between the two [7] and hence the topics is not included within the scope of the paper.
A great number of these abortions would have become viable full term babies had it not been for the confl ict. These cases are still not reported as death in global mortality statistics. [8] [9] The fact that the average age of admission into the OT decreased signifi cantly during the confl ict may also implicate the increased stress in targeting a younger subset of pregnant women.
Foreign nationals and Libyans alike were displaced during the confl ict and many fl ed to neighbouring Egypt and then to their home countries. As a result of the exo-dus of foreigners, we see the signifi cant decrease in the proportion of their admis-sion into the OT of the hospital.
C-sections are carried out in Libya regularly and now form approximately 26% of all births. This value is high compared to the goals set out by US in its “Healthy People 2010” plan aiming at a rate of 15% or lower. [10] In the hospital’s defense, Al-Jamhouria takes on high-risk cases and US hospitals that did the same also had similar cesarean rates.
During the making of this paper, we didn’t differentiate between miscarriage, stillbirths and intrapartum deaths and hence included them all under the umbrella of “spontaneous abortions”. This was done for two main reasons; the fi rst being a lack of data on the gestational age for some cases and more importantly for the recent muddling of the delineation between the three defi nitions.
Confusion over the defi nition of stillbirth, intrapartum death, and miscarriage, when collecting reports in and out of facilities, makes consistent registration chal-lenging. Stillbirth may refer to late fetal death, which is a death after 28 weeks ges-tation or at least 1000 grams birth weight or it may include early fetal death, which is a death after 22 weeks gestation or at least 500 grams birth weight. Thirty years ago, the minimum gestational age for classifi cation as a stillbirth was 28 weeks. The defi nition has become progressively inclusive by decreasing the minimum required gestational age. These different measures of stillbirth have had a signifi cant impact on infant mortality estimates. [11]
The fact that spontaneous abortions have signifi cantly increased during this pe-riod of time will place a further burden on the medical system. The loss of a fetus causes women to experience intense emotional distress. [12] The loss or prospect of losing a baby may also be the fi rst major loss in a woman's life. If she is vulner-able to the development of depressive illness then this major life event may be the precipitating factor. [13] These “major life events” pose a great risk for antenatal and post-natal depression. [14]
The importance of antenatal depression has been largely under-recognized with the focus of research and treatment programs on postnatal depression. Yet results

178
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
from previous literature indicate that antenatal depression is the strongest risk factor for postnatal depression. [15]
When comparing women who reported a history of pregnancy loss and infertility with mothers who reported no fertility problems, signifi cant differences were found in life satisfaction, depression and self-esteem. Women reporting previous preg-nancy loss (regardless of motherhood status) or infertility problems also reported signifi cantly less satisfaction with life and more depressive symptoms than women with no fertility problems. [16]
There is also a possibility that the mother may fall into a cycle of stressful preg-nancies after an abortion. Previous research shows that during a pregnancy that follows an abortion, the mother experiences general state anxiety during the second and third trimesters. [17]
According to descriptive studies of pregnancy following miscarriage and other types of perinatal loss, for some women the subsequent pregnancy is perceived as threatening and involves heightened vulnerability, anxiety, and guarded emotions related to uncertainty about its outcome [17].
This apprehension should not be underestimated since it falls under the major two worries listed in Cambridge Worry Scale (CWS). The major worries referred to the process of giving birth (CWS mean value 2.26) and the possibility that something might be wrong with the baby (1.99), followed by coping with the new baby (1.57), going to hospital (1.29) and the possibility of going into labour too early (1.28). [18]
Abortions were also found to place a strain on the marriage of the would-be parents. Fetal loss may be a signifi cant source of additional stress in a relationship and, although the majority of couples are able to adjust to a loss and may even grow closer; there may be a subgroup whose relationships are particularly vulnerable to this major stress. Couples with an unstable relationship before the pregnancy and those with other risk factors for breaking up may fi nd themselves unable to sustain their relationship after a miscarriage or stillbirth. It also is possible that having a live birth is protective to the marital relationship, rather than miscarriage which increases dissolution rates. [19]
An even greater amount of stress is placed on the relationship if the abortion occurs in the later stages of pregnancy. Although it is well recognized that parents form attachments very early after conception, later losses allow for an even longer period for attachment and therefore may cause more psychological trauma and a longer duration of psychological stress. [20] Moreover, the differences in coping mechanisms between the man and woman may cause misunderstandings. [21] [22]
CONCLUSIONS A number of conclusions have been reached in this study:i) The armed confl ict in Libya played a signifi cant role in the increase of abortion
rates in Benghazi.

179
November 17-20, 2011 Paris, France
ii) Patients admitted in the time of crisis are signifi cantly younger.iii) Foreign nationals left Libya in massive numbers and that changed their pro-
portion among patients.iv) The rate of cesarean births has increased.
RecommendationsIn the light of the above, the authors would like to make the following recommenda-
tions:i) Further research is needed in the case of the Libyan confl ict and its impact on
the healthcare system, particularly low birth weight and preterm births. These stud-ies need to focus on both the short and long-term effects that this crisis has had on the general health of the people all across Libya.
ii) A social support system needs to be provided to the women who have suffered spontaneous abortions in this period and special attention needs to be paid to them to avoid future psychological pathologies. [22]
iii) Bereavement counseling should also be provided to those couples in order to help maintain the strength of their relationship.
AcknowledgementsThe authors would like to thank the nursing staff of the labour room at Al-Jama-
hiriya Hospital (with special regards to Midwife Majda Al-Kwairi and Nurse Intisar Al-Shteiti) for their cooperation, consultation and patience. The authors owe a debt of gratitude to Dr. Bridget Stirling for her time and effort in helping to provide us with a wider access to scientifi c literature.
REFERENCES1. Ahukaa OL, Chabikuli N, Ogunbanjoc GA “The effects of armed confl ict on pregnancy outcomes in
the Congo.” International Journal of Gynecology & Obstetrics Volume 84, Issue 1, January 2004, Pages 91-92.
2. Maconochie N, Doyle P, Davies G et al “Reproductive health of Gulf War veterans.” BMC Public Health 2003, 3:4.
3. Doyle P, Maconochie N, Ryan M “Reproductive health of Gulf War veterans” Phil. Trans. R. Soc. B (2006) 361, 571–584.
4. “War wastage and the birth rate.” BMJ April 15th, 1916.5. Katz VL, Miller NH, Bowes WA Jr “Pregnancy complications of physicians, In Women and
Medicine.” [Special Issue]. West J Med 1988 Dec; 149:704-707.6. Nakamura K, Sheps S, Arek P “Stress and reproductive failure: past notions, present insights and
future directions.” J Assist Reprod Genet (2008) 25:47–62.7. Arck PC, Rose M, Hertwig K, Hagen E, Hildebrandt M, Klapp BF “Stress and immune mediators
in miscarriage.” Hum Reprod 2001; 16:1505–11.8. Lawn JE, Cousens S, Zupan J “4 million neonatal deaths: when? Where? Why?” Lancet 2005,
365(9462):891-900.

180
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
9. Stanton C, Lawn JE, Rahman H, Wilczynska-Ketende K, Hill K “Stillbirth rates: delivering estimates in 190 countries.” Lancet 2006, 367(9521):1487-1494.
10. Moore M, “Increasing cesarean birth rates: a clash of cultures?” Journal of Perinatal Education, 14(4), 5–8, doi: 10.1624/105812405X72276.
11. Kelley M, Rubens C “Global report on preterm birth and stillbirth (6 of 7): ethical considerations.” BMC Pregnancy and Childbirth 2010, 10(Suppl 1):S6.
12. Corney RT, Horton FT. “Pathological grief following spontaneous abortion.” Am J Psychiatry 1974; 131: 825-847.
13. Freidman T, “Women's experiences of general practitioner management of miscarriage.” Journal of the Royal College of General Practitioners, 1989, 39, 456-458.
14. Newton R, Webster P et al “Psychosocial stress in pregnancy and its relation to the onset of premature labour.” British Medical Journal, 1979, 2, 411-413.
15. Leigh B, Milgrom J “Risk factors for antenatal depression, postnatal depression and parenting stress.” BMC Psychiatry 2008, 8:24 doi:10.1186/1471-244X-8-24.
16. Schwerdtfeger K, Shreffl er K “Trauma of pregnancy loss and infertility for mothers and involun-tarily childless women in the contemporary United States.” J Loss Trauma. 2009; 14(3): 211–227. doi:10.1080/15325020802537468.
17. Woods-Giscombé C, Lobel M, Crandell J “The impact of miscarriage and parity on patterns of maternal distress in pregnancy.” Res Nurs Health. 2010 August; 33(4): 316–328. doi:10.1002/nur.20389.
18. Petersen J, Paulitsch M, Guethlin C, Gensichen J and Jahn A “A survey on worries of pregnant women - testing the German version of the Cambridge Worry Scale.” BMC Public Health 2009, 9:490 doi:10.1186/1471-2458-9-490.
19. Gold K, Sen A, Hayward R “Marriage and cohabitation outcomes after pregnancy loss.” Pediat-rics. 2010 May; 125(5): e1202–e1207. doi:10.1542/peds.2009-3081.
20. Leon, I. “Helping families cope with perinatal loss.” Glob Lib Womens Med. 2008 [Accessed July 15th, 2011].
21. Alderman L, Chisholm J, Denmark F, Salbod S. “Bereavement and stress of a miscarriage: as it affects the couple.” Omega 1998; 37(4):317–327.
22. Beutel M, Willner H, Deckardt R, Von Rad M, Weiner H. “Similarities and differences in couples’ grief reactions following a miscarriage: results from a longitudinal study.” J Psychosom Res 1996; 40 (3):245–253.
23. Manca D, Bass M “Women's experience of miscarriage.” Can Fam Physian 1991; 37:1871-1877.
© 2012 Monduzzi Editoriale | Proceedings Code: 32
Peculiarities of HRT for women with obesity
G. Alimbayeva,¹ I. Kuznetzova,² M. Yakokutova³¹National Medical University, Almaty, Kazakhstan; ²Russian Medical Academy of Post Graduated Education, Moscow, Russia; ³Clinic of Russian Medical Academy of Post Graduated Education, Moscow, Russia
SUMMARY HRT should be safe for women with any risks. Our goal was to fi nd optimal HRT
for women with obesity. 25 women with mean BMI 34,7±2,1 kg/m² and HOMA index 4,79±1,24 (mean age 48,7±0,7 yo) with menopausal symptoms were inves-tigated. Methods used: metabolic profi le, US examination, Paypel biopsy. After 6 months was found decreasing of triglycerides levels (р<0,05). It was positive result that should be widely used in practice.
KEY WORDSHRT, obesity, metabolic disorders.
INTRODUCTIONWomen at risk regarding hyperplasia and endometrial cancer who have excessive weight and metabolic disorders cause a particular problem in menopausal transition (1, 2). Planning hormonal therapy for such patients, it is necessary to select a progestagen component which able to provide the best protection for the endometrium (3, 4); while doing so it is desirable to administer it continuously in perimenopause. At the same time, the effect of this progestagen on metabolism should be minimal. Compliance with these conditions is not a simple task. During premenopause the continuous combined regimen of HRT is frequently unacceptable because of poor cycle control, and as called ‘strong’ progestagens could provide a negative effect on carbohydrate and lipid metabolism due to the partial androgenic activity (5). The problem can be partially solved by using non-oral administration of HRT agents.
182
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The goal of study was to fi nd optimal HRT for women with obesity and meta-bolic disorders.
MATERIAL AND METHODSThe study included 25 patients with menopausal symptoms, obesity and meta-
bolic disorders. The average age was 48.7±0.7 years. All patients had obesity; BMI was 34.7±2.1 kg/m2 and HOMA index 4,79±1,24
RESULTSThe patients have been observed since the period of premenopause for abnormal
uterine bleedings; and ordinary endometrial hyperplasia was established by biopsy. LNG-IUD was used for treatment of endometrial hyperplasia. Later estrogen defi -ciency was confi rmed by an elevation of FSH level. From the insertion of LNG-IUD to the initiation of HRT with TDE was not less than a year gap. By the moment of the appearance of menopausal symptoms only 1 (3,3%) had spotting. In all pa-tients according to the ultrasound endometrium did not exceed 3,0±0,1 mm. Pipelle biopsy was performed in all patients. The morphological data revealed in 100% decidual reaction of stroma with atrophy of endometrial glands.
The parameters of lipid and carbohydrate metabolism were characterized by marked deviations. The increasing of the LDL, triglycerides and a decrease of HDL plasma levels determined the increased risk of heard and vessels diseases. Insulin resistance was confi rmed for 83.3% of patients. The effectiveness of HRT therapy with TDE was observed in 100% of patients after 6 months of treatment. The endo-metrium sizes during LNG-IUD+TDE therapy were within the range of 3,0±0.8 mm and did not exceed 5 mm in any patient. The biopsy of the endometrium performed after 6 months of therapy revealed similar morphological picture obtained before adding the patch (endometrial atrophy and decidual reaction of the stroma).
The biochemical parameters of lipid metabolism did not change, but the level of triglycerides: was reduced from 2.2±0.31 mmol/l as baseline to 1.8±0.12 mmol/l after 6 months (р<0.05). The parameters of carbohydrate metabolism had an insig-nifi cant tendency toward improvement, but the tendency was not signifi cant.
CONCLUSIONThe complex therapy with TDE/ LNG-IUD women with menopausal symptoms
and previous endometrial hyperplasia and obesity/metabolic disorders resulted in a signifi cant reduction of all menopausal symptoms. The local use of LNG provided endometrium protection and the minimal infl uence on metabolism.
REFERENCES1. Kaaks R, Lukanova A and Mindy S. Kurzer. Obesity, Endogenous Hormones, and Endometrial Cancer
Risk / a systematic review. - Cancer Epidemiology Biomarkers & Prevention Vol. 11. - 1531-1543.- 2002.
183
November 17-20, 2011 Paris, France
2. Buckler H. The menopause transition: endocrine changes and clinical symptoms. J. British. Menop. Soc. 2005.Vol. 11, № 2. P. 61-65.
3. Wildemeersch D., Dhont M. Treatment of non atypical and atypical endometrial hyperplasia with a levonorgestrel-releasing intrauterine system. - Am J Obstet Gynecol 188(5):1297-1298, May 2003.
4. Bhattacharya S., Middleton L.J., Tsourapas A. et al. Hysterectomy, endometrial ablation and Mirena for heavy menstrual bleeding: a systematic review of clinical effectiveness and cost-effectiveness analysis. Health Technology Assessment 2011; 15(19).
5. Kwok S, Selby PL, Mc Elduff P et al. Progestogens of varying androgenecity and cardiovascular risk factors in postmenopausal women receiving oestrogen replacement therapy. Clin Endocrinol 2004; 61:760–7.


© 2012 Monduzzi Editoriale | Proceedings Code: 57
Complications of meshes in combination with surgery for uterovaginal prolapse
E. Athanassiou, T. Tantanasis, X. Giannoulis, N. Tsambazis, A. Loufopoulos2nd Department of Obstetrcics & Gynecology University of Thessaloniki, Ippocration General Hospital, Thessaloniki, Greece
SUMMARYThe use of meshes in the last 15 years has revotionalized the surgical treatment
of women with uterovaginal prolapsed. However complications have arisen some annoying for the woman and some life threatening fortunately not so often. Women with prolapse of the uterus, with elongated cervix, with cystocele and with or with-out incontinence can benefi t from such operation. There is however a question for the more appropriate procedure for similar conditions. Is vaginal hysterectomy more appropriate in combination with mesh or amputation of the cervix (Manchester re-pair)? The latter is more minimal and perhaps this relates to fewer complications. In this preliminary study we try to determine which procedure is best for women with uterovaginal prolapsed.
INTRODUCTIONUterovaginal prolapse is common in up 35% of women age over 50 and can be
accompanied by urine incontinence. Uterovaginal prolapsed can be divided in two categories: a-prolapse of the body of the uterus grade I, II and III and b-elongation of the cervix. Both conditions can be accompanied with cystocele grade I, II and III.
Defi nitions: Grade I prolapsed means that the protruding organ (uterus or cer-vix) is behind the introitus. Grade II the uterus can be viewed externally without separating the labia minora or can be seen when the patient in lithotomy position is coughing. Finally grade III means that the organ is permanently outside the labia minora (total prolapsed). Similarly in cystocele grade I there just some protrusion of the anterior vaginal wall, in grade II the protrusion can be seen when the patient is coughing and in grade III the protrusion can be seen behind the labia minora.
Incontinence of urine can be mild (on occasions of high stress), moderate (more often but not interfering with social life) or severe (continuous leakage disturbing social life)
186
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The degree of cystocele and prolapsed do not always correspond to the urine incontinence in direct relation (i.e. a woman can have a small cystocele and severe incontinence).
Meshes are used to reinforce the anterior vaginal wall so that cystocele can be repaired more effi ciently. They have been used for more than 100 years. Synthetic materials (polypropylene) have been used since 1996. The complications are divid-ed in 7 categories: vaginal with no exposure, vaginal with small < 1 cm exposure, vaginal with large > 1 cm exposure, urinary tract compromise or perforation, gas-trointestinal tract compromise or perforation, skin or muscular complications and fi nally patient compromise. Each is dividing in four sub-categories: asymptomatic for the patient but seen in clinical examination, symptomatic, infection and abscess formation.
Surgery: Vaginal hysterectomy is the preferred method of hysterectomy for be-nign uterine disease. This is more true in the case of uterine prolapsed in which anterior vaginal compartment requires simultaneous repair.
The Manchester procedure has the advantage of leaving the uterus in patients with cervical elongation in women wishing to do so. It is also less invasive less traumatic and requires less operating time. The operation consists of amputation of the elongated cervix, followed by suturing of the ligated cardinal ligaments to the anterior cervical remnant. This removes the elongated cervix from the vagina and simultaneously rotates the cervix posteriorly and elevates the uterine corpus ante-riorly and increases the functional vaginal length. Although there appear to be no signifi cant differences in complication rates compared with vaginal hysterectomy the only exception is cuff abscess formation in 5% of vaginal hysterectomy patients. On the other hand in Manchester procedure there is a 4,3% prolapsed recurrence as compared with vaginal hysterectomy.
MATERIALS AND METHODSIn order to compare the complications of the meshes we collected data from
the 2nd Department of Obstetrics & Gynecology in Ippocration Hospital in Thessa-loniki, Greece between March 2008 and March 2011. We found 38 women (group A) who had vaginal hysterectomy for prolapsed uterus grade II and III and anterior mesh and 55 women (group B) with prolapsed uterus grade I and II and elongated cervix who had Manchester repair and anterior mesh. In all women the mesh used was polypropylene.
RESULTSIn group A we found 8 (21%) complications and in group B 4 (7, 2%) complica-
tions. This difference is statistically signifi cant. The main complication in group A was erosion of the anterior vaginal wall and in group B reccurence of cystocele and prolapse of the body of the uterus.

187
November 17-20, 2011 Paris, France
DISCUSSIONThe combination of Manchester repair with mesh is associated with fewer com-
plications in comparison with the vaginal hysterectomy with mesh in women with similar grade of prolapse. It is possible that factors contribute to that result are the length of the operation time and the traumatized tissue which are less in Manchester repair. Another point is that despite vaginal hysterectomy there can still be pro-lapsed vault which is not known how to predict so more conservative surgery may be more effective in terms of mesh complications. This study is preliminary and ongoing for more results.
REFERENCES1. Bernard T.Haylen, Robert M.Freeman et al, An International Urogynecological Association (IUGA)/
International Continence Society (ICS) joint terminology and classifi cation of the complications related directly to the insertion of prostheses (meshes, implants, tapes) & grafts in female pelvic fl oor surgery, Int urogynecol. J., 22:3-15, 2011.
2. Kate Moore, Urogynecology: Evidenced-Based Clinical Practice, London, Springer, 20063. Fiona Reid, Uterine prolapsed-preservation or excision?, Ethics/Education, Elsevier, 1:176-179,
2011.4. Hampel C., Naumann G., et al, Management of complications after sling and mesh implantations,
Urologe A, 48:496-509, 2009.

© 2012 Monduzzi Editoriale | Proceedings Code: 102
Pregnancy after gigantic bilateral ovarian teratoma
M. Brandão, S.V. Soares, P. Reis, M. Rodrigues, T. Oliveira, R.M. RodriguesCentro Hospitalar do Porto E. P. E., Unidade Maternidade Júlio Dinis, Oporto, Portugal
SUMMARYThe mature cystic teratoma of the ovary is a tumour comprising more than a sin-
gle cell type derived from more than one germ layer. They are bilateral in 10-15% of the cases, causing therapeutic and fertility problems in young women.
We report a case of a 27-year-old woman who underwent an ovary-conserving intervention for bilateral teratomas, resulting in successful preservation of ovarian function.
INTRODUCTIONThe mature cystic teratoma of the ovary is a tumour comprising more than a
single cell type derived from more than one germ layer. More than 80% appears in fertile age and are of the most frequent benign tumours in women younger than 40 years. They are bilateral in 10-15% of the cases, causing therapeutic and fertility problems in young women. They can suffer malignant transformation in 1–3% of the cases, with survival rates of 25% in the fi rst year of diagnosis. Usually they are asymptomatic, but they can suffer a pedicle torsion, rupture or rapid growth and become symptomatic. The best diagnostic method is the transvaginal ultrasonogra-phy, at the expense of its characteristic pattern: “white ball” (hair and sebum) in the corner of a cyst or fi lling whole tumour, long white lines and echogenic dots in cyst fl uid and shadowing. Defi nitive diagnosis is made at the time of surgical excision.
MATERIALS AND METHODSA 27-year-old caucasian woman (gravida 1, para 1), presented at consultation
with complaints of deep dyspareunia with 6 months evolution. She had menarche at sixteen, oral contraception use and regular menstrual cycle.
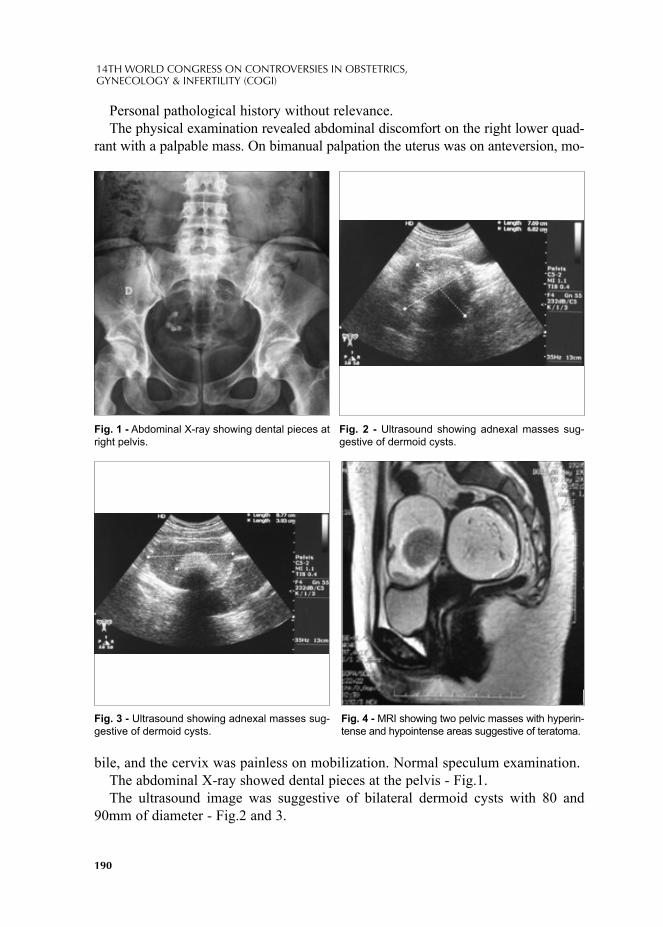
190
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Personal pathological history without relevance.The physical examination revealed abdominal discomfort on the right lower quad-
rant with a palpable mass. On bimanual palpation the uterus was on anteversion, mo-
bile, and the cervix was painless on mobilization. Normal speculum examination. The abdominal X-ray showed dental pieces at the pelvis - Fig.1.The ultrasound image was suggestive of bilateral dermoid cysts with 80 and
90mm of diameter - Fig.2 and 3.
Fig. 1 - Abdominal X-ray showing dental pieces at right pelvis.
Fig. 3 - Ultrasound showing adnexal masses sug-gestive of dermoid cysts.
Fig. 2 - Ultrasound showing adnexal masses sug-gestive of dermoid cysts.
Fig. 4 - MRI showing two pelvic masses with hyperin-tense and hypointense areas suggestive of teratoma.

191
November 17-20, 2011 Paris, France
The magnetic resonance imaging showed expansive lesions on the pelvis with 89x76x50mm and 67x69x61mm at median position that rise probably from the right and left ovaries respectively, with T1 and T2 images suggestive of teratoma - Fig.4 and 5.
The patient was submitted to laparot-omy, through a Pfannenstiel incision, with excision of the two large adnexal masses and bilaterally preservation of
the remaining ovarian tissue.The fi nal histology confi rmed the in-
tra-operatory histological diagnosis of bilateral mature cystic teratoma. After surgical intervention patient kept regular menstrual cycles using condom as
contraception method for 24 months. Spontaneous pregnancy occurs 38 months after intervention. She is now 15
weeks pregnant.
CONCLUSIONSThis is a case of bilateral symptomatic teratoma in a young woman with one child.The transvaginal ultrasonography is the fi rst option for the diagnosis of adnexal
masses with high sensitivity (53–100%) and specifi city (94-100%) for dermoid cyst, and a better cost effectiveness ratio than computed tomography scan or magnetic resonance imaging.
The surgical intervention required bilateral excision of the adnexal masses (con-servative cystectomy) and it was a challenge procedure, because the cystic terato-mas involved almost all the ovarian tissue.
It was preserved the maximum of the macroscopic “normal” ovarian tissue to avoid infertility and premature menopause.
We were able to conclude that the intervention was well succeeded, because the pa-tient was asymptomatic and capable of spontaneous pregnancy, following the surgery.
REFERENCES1. BEREK, JS. Berek & Novak´s Gynecology, 14th Edition, Lippincott Williams & WilKins, 2007.2. SPEROFF L, FRITZ MA. Clinical Gynaecologic Encocrinology and Infertility, 7th edition, Lip-
pincott Williams & WilKins, 2005.3. HIDLEBAUGH DA, VULGAROPULOS S, ORR RK. Treating adnexal masses. Operative lapa-
roscopy vs. Laparotomy, J Reprod Med. Sep; 42(9):551-8, 1997. 4. YAMAUCHI H, TAKAHASHI A, HIRAKATA T. Bilateral ovarian teratomas successfully treated
by ovary-conserving technique, Pediatr Int. Apr; 48(2):181-4, 2006.
Fig. 5 - MRI showing the uterus squeezed by the two masses.
192
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
5. TALERMAN A. Germ cell tumours of the ovary. In: Blaustein's Pathology of the Female Genital Tract, Kurman RJ (Ed), Springer Verlag, New York; p.849. 1994.
6. SMITH HO, BERWICK M, VERSCHRAEGEN CF. Incidence and survival rates for female malig-nant germ cell tumors. Obstet Gynecol; 107:1075. 2006.
7. AYHAN A, BUKULMEZ O, GENC C. Mature cystic teratomas of the ovary: case series from one institution over 34 years. Eur J Obstet Gynecol Reprod Biol; 88:153. 2000.
8. DISAIA PJ, CREASMAN WT. Germ cell, stromal and other ovarian tumors. In: Clinical Gyneco-logic Oncology, 7th, Mosby-Elsevier; p.381. 2007
9. PATEL MD, FELDSTEIN VA, LIPSON SD. Cystic teratomas of the ovary: diagnostic value of sonography. AJR Am J Roentgenol; 171:1061. 1998.
10. TONGSONG T, LUEWAN S, PHADUNGKIATWATTANA P. Pattern recognition using transab-dominal ultrasound to diagnose ovarian mature cystic teratoma. Int J Gynaecol Obstet; 103:99. 2008.
© 2012 Monduzzi Editoriale | Proceedings Code: 135
Primary bilateral Burkitt´s lymphoma of the ovary
A.M. Coelho1, A.M. Sousa1, F. Passos1, M. Bernardino1, I. Santana1, A.F. Jorge1, J. Cabeçadas2
1Departament of Gynecology, Instituto Português de Oncologia de Lisboa Dr Francisco Gentil, Lisbon, Portugal; 2Department of Laboratorial Diagnosis, Instituto Português de Oncologia de Lisboa Dr Francisco Gentil, Lisbon, Portugal
SUMMARYPrimary malignant lymphoma of the ovary is a rare disease (1.5% of all ovarian
neoplasms). We report a case of a 23-year-old Caucasian patient presenting with two months history of painful pelvic distension and a bilateral ovarian tumor. Full investigation fails to reveal evidence of another disease location. She underwent hysterectomy with bilateral salpingo-oophorectomy complicated by severe hemor-rhage. Ovaries were substituted by fragile solid tumors weighing 1787gr and 1050gr. Histological and immunohistochemical studies supported the diagnosis of Burkitt´s lymphoma. The confi rmation of this highly aggressive subtype of lymphoma is re-quired to defi ne the specifi c chemotherapeutic regimen.
INTRODUCTIONOvarian involvement by lymphoma as part of a generalized disease is well rec-
ognized, but ovarian involvement as an initial presentation of lymphoma, without detectable extraovarian disease, is a rare reported event.
We report a case of Burkitt´s lymphoma initially presenting with a bilateral ovarian mass.
CASE REPORTA 23-year-old primiparous woman, with no relevant antecedents, presented to
our Institution with a two months history of painful pelvic distension, metrorrhagia, nausea and vomiting, nocturnal fever (38ºC) and weight loss (10Kg).
On bimanual pelvic examination, a large, fi rm and irregular abdomino-pelvic mass, the size of a 20-week gravid uterus was noted, more prominent on the right side. No lymph nodes were palpable.
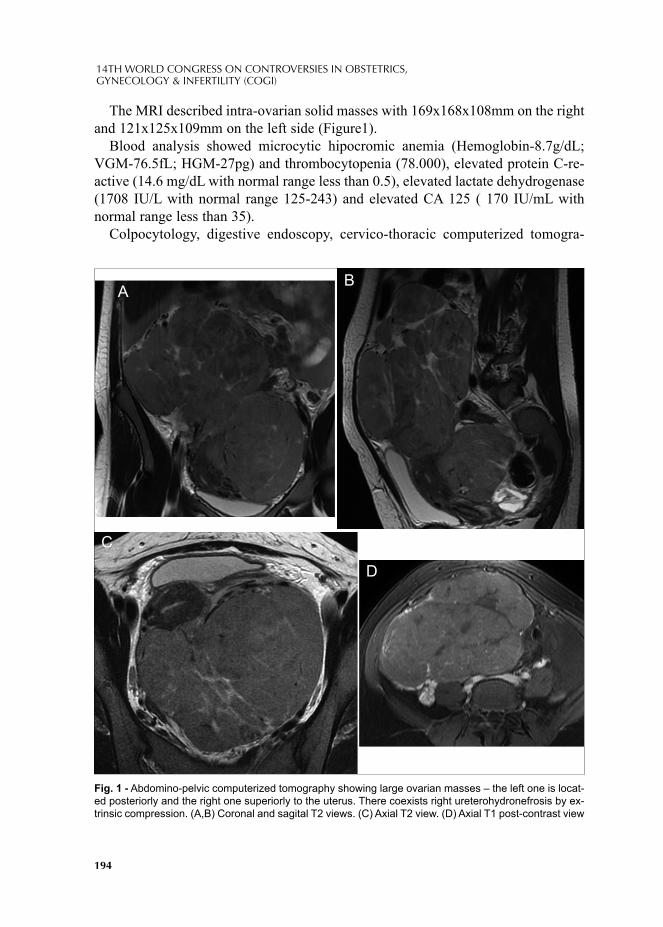
194
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The MRI described intra-ovarian solid masses with 169x168x108mm on the right and 121x125x109mm on the left side (Figure1).
Blood analysis showed microcytic hipocromic anemia (Hemoglobin-8.7g/dL; VGM-76.5fL; HGM-27pg) and thrombocytopenia (78.000), elevated protein C-re-active (14.6 mg/dL with normal range less than 0.5), elevated lactate dehydrogenase (1708 IU/L with normal range 125-243) and elevated CA 125 ( 170 IU/mL with normal range less than 35).
Colpocytology, digestive endoscopy, cervico-thoracic computerized tomogra-
Fig. 1 - Abdomino-pelvic computerized tomography showing large ovarian masses – the left one is locat-ed posteriorly and the right one superiorly to the uterus. There coexists right ureterohydronefrosis by ex-trinsic compression. (A,B) Coronal and sagital T2 views. (C) Axial T2 view. (D) Axial T1 post-contrast view
AB
C
D

195
November 17-20, 2011 Paris, France
phy, lumbar puncture, mielogram and bone marrow biopsy failed to document he-matologic disease.
We performed an exploratory laparotomy. Both ovaries were substituted by fragile solid tumors weighing 1787gr (20x18x18cm) on the right and 1050gr (19x15x7cm) on the left side. Hysterectomy with bilateral salpingo-oophorectomy was complicat-ed by severe hemorrhage, consumption coagulopathy and respiratory insuffi ciency. A 3cm residual tumor was left on the peritoneal surface of the colon.
Histologically, a lymphoid proliferation of small round cells of difuse growth was observed, with a high nucleo-cytoplasmic ratio. The mitotic index was high creating the typical starry-sky pattern. Immunohistochemical data supported the diagnosis of Burkitt´s lymphoma (CD20+, CD10+, Ki-67 100%). (Figure 2) Fluorescence in situ hybridization (FISH) detected a break in the c-Myc gene, arising from the transloca-tion and deregulation of the c-myc gene on chromosome 8.
Having no bone marrow or central nervous system involvement on postsurgical staging evaluation, the patient started multiagent COP chemotherapy according to LMB-95 protocol, which consisted on vincristine 1mg/m2 on day 1 and cyclophos-phamide 0.3g/m2 on day 1 intravenously and oral prednisolone 60mg/m2 on day 1. Additionally she received anti-CD20 antibody (Rituximab). On day 8 she started COPADM (cyclophosphamide 1000mg/m2/day days 2-4, vincristine 2mg days 1 and 6, doxorubicin 60mg/m2 day 2, prednisolone 60mg/m2/day on days 1-5, metho-trexate 3g/m2 day 1, methotrexate intrathecal 15mg days 2 and 6, ara-C 40mg days 2 and 6) complicated by severe post-lumbar puncture headache. Granulocyte colony-stimulating factor (G-CSF) was initiated after this course.
As computed and positron emission tomography suggested disease progression, confi rmed by biopsy and fl ow cytometry, the patient underwent consolidation treat-ment with CYM (methotrexate 3g/m2 day 1, ara-C 100mg/m2/day for 24-hour infu-sion days 2-6, intrathecal methotrexate 15mg day 2, intrathecal ara-C 40mg day 7) followed by Rituximab suspension and CYVE (high doses of ara-C and etoposide) as a cytoreductive trial actually in course.
DISCUSSIONPrimary ovarian lymphoma (POL) is a rare disease, accounting for 0.5% of all
non-Hodgkin´s lymphomas and 1.5% of all ovarian neoplasms.1 The origin of these rare tumors is controversial. The malignant transformation of benign lymphoid infi l-trates seen in up to 50% of normal ovaries, as suggested by Monterroso et al., may contribute to explain their pathogenesis.2
Differential diagnosis between primary or secondary malignant lymphoma is sometimes diffi cult, especially in advanced cases. According to Fox and Langley criteria3 proposed in 1976, we can exclude a secondary origin if 1) the lymphoma is clinically confi ned to the ovary and full investigation fails to reveal evidence of another location, if 2) the peripheral blood and bone marrow do not contain any
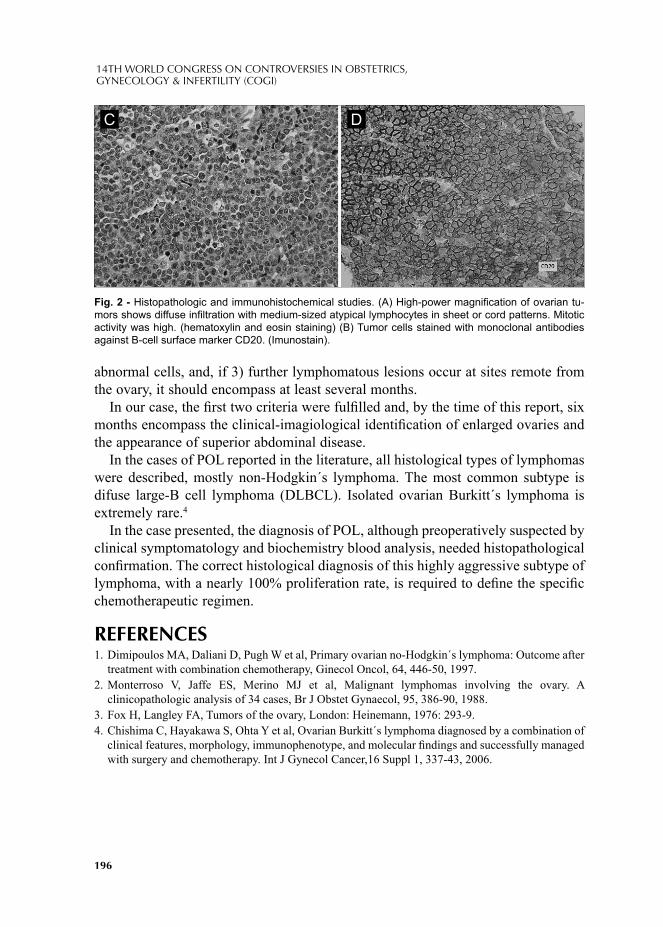
196
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
abnormal cells, and, if 3) further lymphomatous lesions occur at sites remote from the ovary, it should encompass at least several months.
In our case, the fi rst two criteria were fulfi lled and, by the time of this report, six months encompass the clinical-imagiological identifi cation of enlarged ovaries and the appearance of superior abdominal disease.
In the cases of POL reported in the literature, all histological types of lymphomas were described, mostly non-Hodgkin´s lymphoma. The most common subtype is difuse large-B cell lymphoma (DLBCL). Isolated ovarian Burkitt´s lymphoma is extremely rare.4
In the case presented, the diagnosis of POL, although preoperatively suspected by clinical symptomatology and biochemistry blood analysis, needed histopathological confi rmation. The correct histological diagnosis of this highly aggressive subtype of lymphoma, with a nearly 100% proliferation rate, is required to defi ne the specifi c chemotherapeutic regimen.
REFERENCES1. Dimipoulos MA, Daliani D, Pugh W et al, Primary ovarian no-Hodgkin´s lymphoma: Outcome after
treatment with combination chemotherapy, Ginecol Oncol, 64, 446-50, 1997. 2. Monterroso V, Jaffe ES, Merino MJ et al, Malignant lymphomas involving the ovary. A
clinicopathologic analysis of 34 cases, Br J Obstet Gynaecol, 95, 386-90, 1988.3. Fox H, Langley FA, Tumors of the ovary, London: Heinemann, 1976: 293-9.4. Chishima C, Hayakawa S, Ohta Y et al, Ovarian Burkitt´s lymphoma diagnosed by a combination of
clinical features, morphology, immunophenotype, and molecular fi ndings and successfully managed with surgery and chemotherapy. Int J Gynecol Cancer,16 Suppl 1, 337-43, 2006.
Fig. 2 - Histopathologic and immunohistochemical studies. (A) High-power magnifi cation of ovarian tu-mors shows diffuse infi ltration with medium-sized atypical lymphocytes in sheet or cord patterns. Mitotic activity was high. (hematoxylin and eosin staining) (B) Tumor cells stained with monoclonal antibodies against B-cell surface marker CD20. (Imunostain).
C D
© 2012 Monduzzi Editoriale | Proceedings Code: 140
Retrospective study of laparoscopic assisted vaginal hysterectomy (LAVH) for benign gynecological disorders
R. Condeço, L. Barros, S. Barreto, C. Leitão, M.C. Silva, R. MiraHospital Dona Estefânia – CHLC, Lisboa, Portugal
SUMMARYThe purpose of this retrospective observational study was to evaluate the indica-
tions, operative data and complications of LAVH for benign conditions. The 42 patients included were evaluated regarding age, vaginal deliveries, previous ab-dominal surgery, uterine and adnexal pathology, intra-operative and post-operative complications, uterus weight, blood loss and number of days of hospitalization.
The commonest indication for hysterectomy was uterine fi broids (80%), and the most frequent complaint was menorrhagia. The medium operative time was 167 minutes and the uterine weight ranged from 69 to 500g. There was one case of accidental incision of rectum (2%), and 3 conversions to laparotomy for technical diffi culties (7%). There were no signifi cant post-operative complications.
LAVH is a safe and effi cient surgery to manage benign gynecological disorders, and an alternative to consider when vaginal hysterectomy is expected diffi cult.
INTRODUCTIONHysterectomy is the most frequently performed major gynecologic
procedure annually throughout the world (1). This surgical procedure is in-dicated in several common gynecologic problems and it may be total or sub-total, with or without adnexectomy. The surgical approach for hysterectomy may be abdominal (AH), vaginal (VH), laparoscopic (LH), laparoscopic as-sisted vaginal hysterectomy (LAVH) or with robotic assistance (2).
Traditionally, abdominal hysterectomy has been used for gynecologi-cal malignancies and for enlarged uterus. Vaginal hysterectomy was origi-nally used for uterine prolapsed, but is now also used in other disorders, when the uterus is approximately normal size (3).
198
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The fi rst laparoscopic hysterectomy was performed by Harry Reich in 1988 (4). Laparoscopic hysterectomy may be classifi ed as Total Laparoscopic Hysterectomy (TLH) if the uterine arteries are ligated and the vagina is opened laparoscopically, or LAVH when the upper blood supply of the uterus is ligated laparoscopically, fol-lowed by a vaginal hysterectomy (5).
A Cochrane review in 2010 of 34 studies comparing the various approaches for hysterectomy concluded that VH should be preferred whenever possible. When VH is not possible, LH may avoid the need for AH, with benefi ts such as speedier return to normal activities, lower intraoperative blood loss, smaller drop in haemoglobin, shorter hospital stay, and fewer wound or abdominal wall infections at the cost of more urinary tract (bladder or ureter) injuries and longer operation time. The au-thors also stated that the length of the surgery increases as the extent of the surgery performed laparoscopically increases (3).
Regarding the comparison of LAVH and TLH, Twijnstra in 2009 showed an ad-vantage of TLH with respect to blood loss, with comparable length of surgery and complication rates (5). The authors stated that LAVH should only be indicated in cases of VH when additional surgery is needed (adhesions, endometriosis, adnexal pathology).
The objective of our study was to analyze the laparoscopic assisted vaginal hys-terectomies performed in our department regarding the indications for choosing the procedure, operative data and outcome.
MATERIAL AND METHODSRetrospective observational study carried out in the Department of Obstetrics and
Gynecology of the Dona Estefânia Hospital in Lisbon.The authors included all the patients that underwent LAVH during a period of 24
month, from January 2009 to December 2010, representing a group of 42 women.The patients undergoing LAVH were identifi ed from operating room diaries.The medical records of the patients were reviewed and the factors analyzed in-
cluded age, vaginal deliveries, previous abdominal surgery, indication for operation, surgery time, intra-operative and postoperative complications, haemoglobin drop, time of hospitalization, uterus weight and histopathology.
RESULTSThe patient average age was 47 years old, (range 31 – 67). Five women were
nuliparous (11,9%), with the remainder varying from 1 to 3 vaginal deliveries.There was history of previous abdominal surgery in 20 women (47,6%), being
the most frequent cesarean section, followed by tubal ligation, adnexectomy, appen-dectomy and cholecystectomy.

199
November 17-20, 2011 Paris, France
The main indication for operation was uterine fi broids and the most frequent com-plaint was menorrhagia. The indications for surgery are listed in the graphics 1 and 2.
The surgery performed varied regarding adnexectomy, depending on the exis-tence of suspected lesions and the patient choice to keep or remove the ovaries. There were also 3 cases of abdominal hysterectomy resulting from the conversion of laparoscopic to abdominal approach because of intraoperative complications. The procedures are listed in the table 1.
The mean operating time was 167 minutes, ranging from 105 to 330 minutes.The average uterine weight was 217g (range 69-500g).Histopathologically the most frequent diagnosis was fi broids in 33 cases (78.5%).
The histopathological results are depicted in table 2.Intraoperatively there were 3 unplanned conversions to laparotomy, two of the
cases because of dense adhesions, one of them associated with ovarian endome-triosis, and in one case the conversion was due to inability to control haemostasis.
One patient had an intraoperative bowel injury, occurred in the vaginal step. The
Graphic 1 - Preoperative diagnosis. Graphic 2 Preoperative symptoms.
Surgery º
LAVH + adnexectomy 20
LAVH without adnexectomy 18
LAVH + unilateral adnexectomy 1
Abdominal hysterectomy (post conversion) 3
Tab. 1 - Surgeries performed.
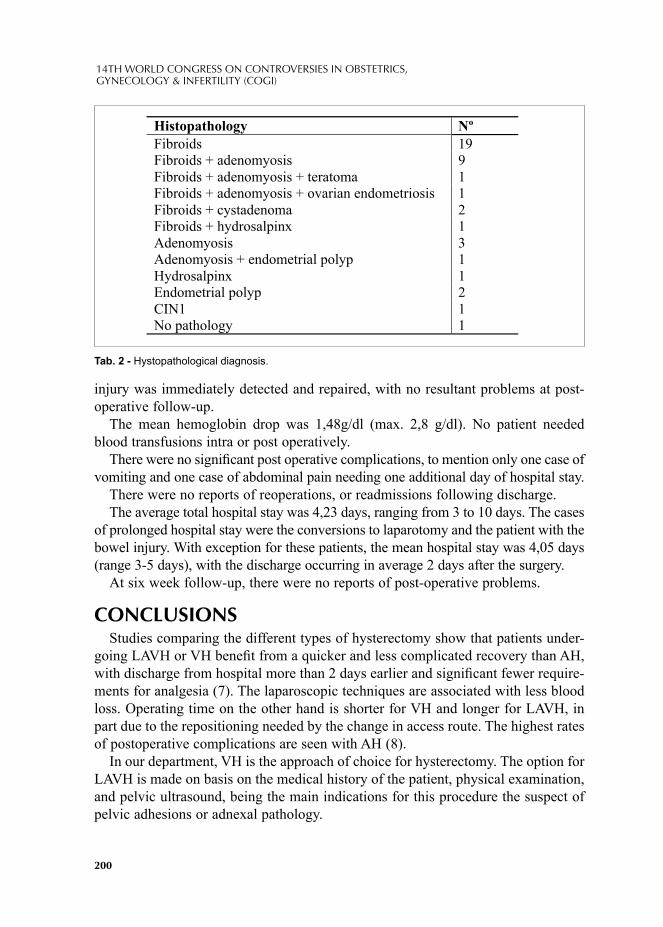
200
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
injury was immediately detected and repaired, with no resultant problems at post-operative follow-up.
The mean hemoglobin drop was 1,48g/dl (max. 2,8 g/dl). No patient needed blood transfusions intra or post operatively.
There were no signifi cant post operative complications, to mention only one case of vomiting and one case of abdominal pain needing one additional day of hospital stay.
There were no reports of reoperations, or readmissions following discharge.The average total hospital stay was 4,23 days, ranging from 3 to 10 days. The cases
of prolonged hospital stay were the conversions to laparotomy and the patient with the bowel injury. With exception for these patients, the mean hospital stay was 4,05 days (range 3-5 days), with the discharge occurring in average 2 days after the surgery.
At six week follow-up, there were no reports of post-operative problems.
CONCLUSIONSStudies comparing the different types of hysterectomy show that patients under-
going LAVH or VH benefi t from a quicker and less complicated recovery than AH, with discharge from hospital more than 2 days earlier and signifi cant fewer require-ments for analgesia (7). The laparoscopic techniques are associated with less blood loss. Operating time on the other hand is shorter for VH and longer for LAVH, in part due to the repositioning needed by the change in access route. The highest rates of postoperative complications are seen with AH (8).
In our department, VH is the approach of choice for hysterectomy. The option for LAVH is made on basis on the medical history of the patient, physical examination, and pelvic ultrasound, being the main indications for this procedure the suspect of pelvic adhesions or adnexal pathology.
Tab. 2 - Hystopathological diagnosis.
Histopathology º
Fibroids 19
Fibroids + adenomyosis 9
Fibroids + adenomyosis + teratoma 1
Fibroids + adenomyosis + ovarian endometriosis 1
Fibroids + cystadenoma 2
Fibroids + hydrosalpinx 1
Adenomyosis 3
Adenomyosis + endometrial polyp 1
Hydrosalpinx 1
Endometrial polyp 2
CIN1 1
No pathology 1

201
November 17-20, 2011 Paris, France
In the author’s opinion, such as is shown in the literature, the purpose of laparo-scopic hysterectomy (LAVH and TLH) is not to replace VH, but rather to increase the capacity to perform minimal invasive surgery for more extended indications, such as the presence of ovarian tumors, adhesions, endometriosis or previous pelvic surgery, avoiding the need of laparotomy (6). Whenever possible, VH should be the procedure of choice, however, for patients with more complex pathology, the choice between LAVH and AH will depend on the surgeon´s experience (3, 7).
In our study, the main intra-operative complication of LAVH was the risk of con-version to laparotomy, but post-operatively this procedure had few minor complica-tions. Regarding the operative time, it should be noted that in our department great part of the surgeries are performed by residents who are in the learning curve, what results in prolonging the operative time.
Nowadays, the indication for LAVH is questioned, and probably this procedure should be considered a step in the learning curve for TLH (5). However, for sur-geons familiar with the procedure, LAVH is a safe and effi cient surgery to manage benign gynecological disorders, and an alternative to consider when vaginal hyster-ectomy is expected diffi cult.
REFERENCES1. GARRY R.; Health economics of hysterectomy, Best Pract Res Clin Obstet Gynaecol, 19: 451-465;
20052. PAPADOPOULOS M. S.; Hysterectomy – Current Methods and Alternatives for Benign Indications;
Obstetrics and Gynecology International; article ID 356740; Vol. 20103. NIEBOER T. E.; Surgical approach to hysterectomy for benign gynaecological disease; Cochrane
Database Syst Rev.; 20104. REICH H.; Laparoscopic Hysterectomy; Surg Laparosc. Endosc.; Vol.2:85-88; 19925. Twijnstra A.R.H.; Twenty-fi rst century laparoscopic hysterectomy: should we not leave the vaginal
step out? Gynecol Surg, Vol 6:311-316; 2009 6. SESTI F.; Laparoscopically Assisted Vaginal Hysterectomy Versus Vaginal Hysterectomy for
Enlarged Uterus; JSLS; vol 12:246-251; 2008 7. MCCRACKEN G.; Comparison of Laparoscopic-assisted Vaginal Hysterectomy, Total Abdominal
Hysterectomy and Vaginal Hysterectomy; Ulster Med J; 75(1):54-58; 20068. MULLER A.; Hysterectomy- A comparison of Approaches; Dtsch Arztebl Int; 107(20): 353-9; 2010


© 2012 Monduzzi Editoriale | Proceedings Code: 148
The cyst of Nuck: clinical case and review of the literature
A. Cubal, J. Carvalho, F. AzevedoCentro Hospitalar Tâmega e Sousa EPE, Penafi el, Portugal
SUMMARYThe canal of Nuck consists in an evagination of parietal peritoneum through the
inguinal canal, which usually obliterates in the eighth month of embryonic devel-opment. When this doesn’t occur, the channel can allow the passage of liquid or abdominal viscera, forming a cyst or a hernia, respectively.
This is more frequent in childhood; few cases are described in adult women.In this paper we report a case of a cyst of the canal of Nuck in a 37-year old
female. The diagnosis was made by physical examination and ultrasound, and was confi rmed by histology after surgery.
In conclusion, the cyst of the canal of Nuck should always be considered in the differential diagnosis of a groin lump in female patients.
INTRODUCTIONIn the sixth month of female embryonic development occurs an evagination of
the parietal peritoneum through the inguinal canal, towards the ipsilateral labia ma-jora – processus vaginalis (1). The portion of the processus vaginalis which is lo-cated within the inguinal canal is called "the canal of Nuck" (2). It is usually short and narrow, and obliterates in the eighth month of development (3). However, it can persist after birth, closing later (4). When the canal remains open, pathological situations may occur (5): if the opening is narrow and only allows the passage of peritoneal fl uid, it forms a cyst/hydrocele; if the opening is wider, it may give way to the abdominal organs with herniation (6).
CLINICAL CASEA 37 year-old female noticed the appearance of a painless swelling in the region of the
right labium majora, which was progressively growing. There were no other symptoms or history of trauma, previous surgery or signifi cant changes in gynecological history.

204
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Physical examination revealed a mass in the region of the right labia majora, with about 2.5 cm of greatest diameter, without skin changes. On palpation the swelling was painless, mobile, soft consistency, regular borders and without pulsatility.
Ultrasound revealed a simple cystic formation, elongated, with a narrowing in the region adjacent to the cranial inguinal canal; there was no evidence of intestinal contents.
Considering the fi ndings of physical examination and ultrasound, we decided to perform surgery with excision of the cyst and closure of its cranial top. Surgical specimen consisted of a 2cm cyst, with mucinous content, wrapped in a membra-niform tissue. Histology showed a cyst lined by cubical and columnar epithelium; immunocytochemistry showed cells positive for calretinin (a marker of mesothelial cells). These histological and immunocytochemical results are compatible with a cyst of the canal of Nuck.
There were no signifi cant incidents during recovery after surgery. After 6 months it was conducted a surgical correction of the scar, since the patient was not satisfi ed with the aesthetic result.
DISCUSSIONThe canal of Nuck cyst is more common in infants and children; there are few
descriptions of this entity in adult women (6). Its appearance can be explained by de novo permeabilization of the canal or any condition that increases an unknown pre-existing cyst (7). In some published cases, there were found histological changes in the epithelium, as endometriosis (5), angiomyofi broma (8) and adenocarcinoma (9).
When there is any visceral content associated with the cyst, it is considered that there is a hernia, a situation that occurs in 40% of cases; 15-20% contain ovary, sometimes with the fallopian tubes (2).
The canal of Nuck cyst typically presents as a painless mass in the inguinal or labial region. It is not accompanied by gastrointestinal symptoms. The occurrence of pain raises the suspicion of incarcerated hernia or abscess.
The differential diagnosis of inguinolabial tumours should include not only the cyst of Nuck as well as hernia, lymph node, abscess, lipoma, leiomyoma and sarcoma (6,7).
Physical examination should be performed in the supine position and also stand-ing. If the swelling disappears in the supine position it is more likely to correspond to a hernia. On transillumination a cyst is translucent, but sometimes a hernia con-taining bowel may also be translucent and therefore this test is not pathognomonic. In the presence of herniated bowel sounds can be heard on auscultation.
As the defi nitive diagnosis cannot be fully evident by history and physical exami-nation, ultrasound is usually performed, since it is an easy and very sensitive exam (2,6). On ultrasound the cyst of Nuck is presented as a simple cyst of anechogenic content, sometimes oval. If pressure is applied to the probe, its backward course through the inguinal canal can be evidenced (10).
205
November 17-20, 2011 Paris, France
Sometimes it may be needed a MRI study for a more accurate picture (11). In this examination, the cyst appears hypointense on T1-weighted images and hyperintense on T2-weighted images (10).
Treatment is usually surgical resection of the cyst and ligation of the neck of the processus vaginalis to prevent recurrence (6). There are some cases of successful laparoscopic treatment (12).
Final diagnosis is pathological (6). In conclusion, the cyst of Nuck canal is part of the differential diagnosis of a
swelling in the inguinolabial region in women. The clinical history and physical ex-amination are helpful in establishing the diagnosis. Ultrasound confi rms the cystic nature of the mass, but it may be necessary to supplement the study with MRI. The treatment is surgical, allowing the defi nitive histological diagnosis.
REFERENCES1. KHANNA PC, PONSKY T, ZAGOL B et al. Sonographic appearance of canal of Nuck hydrocele.
Pediatr Radiol 2007; 37:603–6062. HUANG CS, LUO CC, CHAO HC et al. The presentation of asymptomatic palpable movable mass
in female inguinal hernia. Eur J Pediatr 2003; 162:493–4953. JEDRZEZWSKY G, STANKIEWICZ A, WIECZOREK AP. Uterus and ovary hernia of the canal
of Nuck. Pediatr Radiol 2008; 38:1257-12584. ANDERSON CC, BROADIE TA, MACKEY JE et al. Hydrocele of the canal of Nuck: ultrasound
appearance. Am Surg 1995; 61:959–9615. BRANNINGAM A, JOYCE MR, O’CONNELL PR, PIERCE C, RYAN JD. Haematoma in a hy-
drocele of the canal of Nuck mimicking a Richter’s hernia. Hernia 2009; 13: 643-6456. DE MEULDER F, HUBENS G, RAMET J, WOJCIECHOWSKY M. Female hydrocele of the
canal of Nuck: a case report. Eur J Pediatr 2006; 165: 193-1947. CAVIEZEL A et al. Female hydrocele: the cyst of Nuck. Urol Int 2009; 82:242–2458. LASKIN WB, FETSCH JF, TAVASSOLI FA: Angiomyofi broblastoma of the female genital tract:
analysis of 17 cases including a lipomatous variant. Hum Pathol 1997; 28: 1046–1055.9. MESKO JD, GATES H, et al: Clear cell adenocarcinoma of the vulva arising in endometriosis: a
case report. Gynecol Oncol 1988; 29: 385–391.10. ERDOGMUS B, GOKGOZ AT, SAFAK AA, YAZICI B. Hydrocele of the Canal of Nuck: Sono-
graphic and MRI Appearances. Ultrasound 2007; 35: 531-532.11. PARK SJ, LEE HK, HONG HS et al. Hydrocele of the canal of Nuck in a girl: ultrasound and MR
appearance. Br J Radiol 2004; 77: 243–244.12. YEN CF, WANG CJ, LIN SL, et al: Laparoscopic closure of patent canal of Nuck for female indi-
rect inguinal hernia. J Am Assoc Gynecol Laparosc 2001; 8: 143–146.

© 2012 Monduzzi Editoriale | Proceedings Code: 152
Body composition in users of levonorgestrel-releasing intrauterine system
N. Dal´Ava1, L. Bahamondes1, M.V. Bahamondes1, A. de Oliveira Santos2, I. Monteiro1
1HUMAN REPRODUCTION UNIT, Department of Obstetrics and Gynecology; 2 Department of Radiology, School of Medicine, University of Campinas (UNICAMP), Campinas, Brazil
SUMMARY Introduction: The objective was to evaluate body composition (BC) in levonorg-
estrel-releasing intrauterine system (LNG-IUS) users and compared to TCu380A intrauterine device (IUD) users. Methods: A prospective study was conducted with 76 users of both contraceptive methods. Women were paired by age (± 2 years) and body mass index (BMI; kg/m²) (±2). It was evaluated weight and % lean mass and % fat mass at baseline and at one year of use. Results: The mean (±SEM) age was 34,4 (±7.5) and 33.9 (±8.0) years old, BMI was 25.3 (± 4.1) and 25.9 (± 4.1) in LNG-IUS and TCu380AIUD users, respectively, without signifi cance between groups. There was a signifi cant increase in weight of 2,9% in LNG-IUS group when compared values at baseline and at one year of use. LNG-IUS users showed a fat percentage increased (p=0,0009) at 12 months. Conclusions: It was observed an increase in body weight in both groups up to the 1st year of use, while the LNG-IUS users presented increase of fat mass.
Key Words: Body composition; fat mass; levonorgestrel-releasing intrauterine system.
INTRODUCTIONWomen utilize contraceptive methods for a prolonged time during life and many
of them choose methods for long duration [1]. The levonorgestrel-releasing intra-uterine system (LNG-IUS) is a long-lasting progestin intrauterine method. It is ap-proved for use in more than 113 countries and it is utilized for more than 10 mil-lion women [2]. It is highly effective, economic, long-lasting (5 years), and with
208
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
few side effects [2,3]. The main mechanism of action included interference with ovulation, effects upon cervical mucus and sperm penetration and suppress the en-dometrial proliferation, leading to amenorrhea [3,4]. Nevertheless, serum estradiol (E2) levels during use are similar to those found during the follicular phase of the menstrual cycle [5,6].
Additionally, levonorgestrel (LNG) derives from 19-nortestosterone and is, being able to cause anabolic effects over lean mass [7]. Changes in body weight is one of the reasons of discontinuing contraceptive methods, including the LNG-IUS [8-10]. In a study of 94 women with adenomyosis who used the LNG-IUS for up to 3 years, 28.7% reported weight gain of more than 2 kg [11]; however, on the contrary, weight increase was not observed when compared up to 5 years. LNG-IUS users increase an average of 4 kg and TCu380A IUD users had an increase of 4.9 kg [12].
Although E2 levels of LNG-IUS users had shown to be similar to the values ob-served at follicular phase of the menstrual cycle, the concern with use of progestin contraceptives for a long time still indicates the need for knowledge about the ef-fects on BMD. As far as we know, there are no prospective studies which evaluated body composition (lean mass and fat mass) among LNG-IUS users and there are still doubts about weight variation during use. This study aimed to evaluate body composition in users of the LNG-IUS and compared to TCu380A IUD users at baseline and after one year of use.
METHODSThis prospective study was carried out at the Human Reproduction Unit, De-
partment of Obstetric and Gynecology, School of Medical Sciences, University of Campinas (UNICAMP). The study was approved by the local Institutional Review Board and all of the participants signed an informed consent form before enter the study. Women with desire of contraception, between 18 and 45 years of age who initiated the use of either the LNG-IUS (Mirena®, Bayer Oy, Turku, Finland) or a TCu380A IUD (Optima, Injefl ex, Sao Paulo, Brazil) was recruited between October 2009 and May 2010. Women from both groups were paired by age (±2 years) and BMI (kg/m²) (±2) at the beginning of the study.
Women were excluded if they were breastfeeding or had been breastfeeding in the 6 months before enrollment in the study, corticosteroids, thiazide diuretics or drugs for the treatment of thyroid disease. Women with eating disorders like bulimia and anorexia and chronic diseases including diabetes mellitus, chronic renal failure, hyper- or hypothyroidism, hyper- or hypoparathyroidism, hepatitis, cancer or pitu-itary diseases were also excluded.
For the study, 76 women were included, consisting of 38 users of LNG-IUS and 38 TCu380A IUD users paired by age and BMI. The LNG-IUS and TCu380A IUD users were evaluated at the beginning of the study and returned for the 2nd evalua-tion at 12 months.
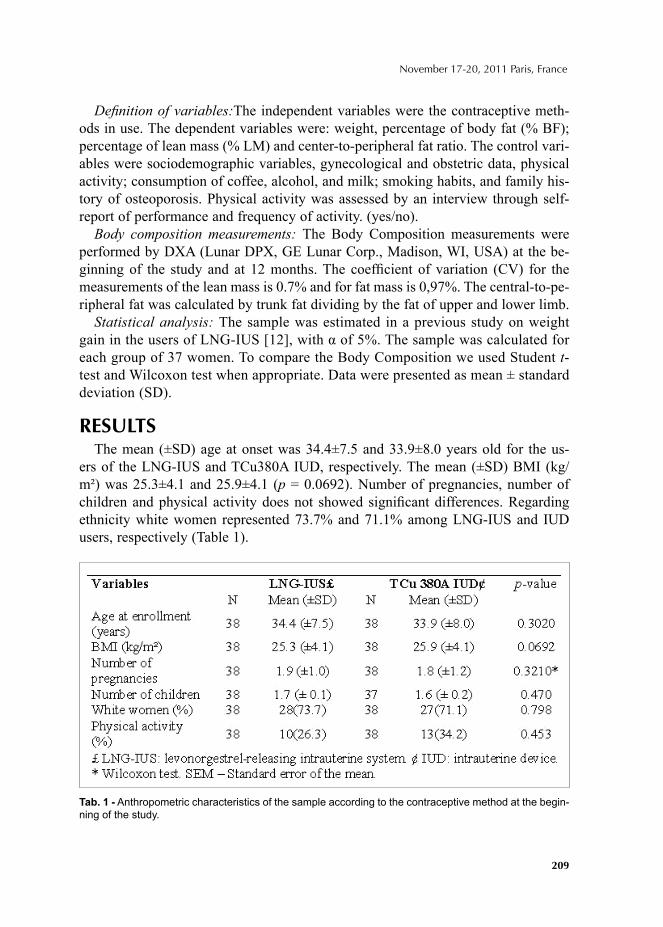
209
November 17-20, 2011 Paris, France
Defi nition of variables:The independent variables were the contraceptive meth-ods in use. The dependent variables were: weight, percentage of body fat (% BF); percentage of lean mass (% LM) and center-to-peripheral fat ratio. The control vari-ables were sociodemographic variables, gynecological and obstetric data, physical activity; consumption of coffee, alcohol, and milk; smoking habits, and family his-tory of osteoporosis. Physical activity was assessed by an interview through self-report of performance and frequency of activity. (yes/no).
Body composition measurements: The Body Composition measurements were performed by DXA (Lunar DPX, GE Lunar Corp., Madison, WI, USA) at the be-ginning of the study and at 12 months. The coeffi cient of variation (CV) for the measurements of the lean mass is 0.7% and for fat mass is 0,97%. The central-to-pe-ripheral fat was calculated by trunk fat dividing by the fat of upper and lower limb.
Statistical analysis: The sample was estimated in a previous study on weight gain in the users of LNG-IUS [12], with α of 5%. The sample was calculated for each group of 37 women. To compare the Body Composition we used Student t-test and Wilcoxon test when appropriate. Data were presented as mean ± standard deviation (SD).
RESULTS The mean (±SD) age at onset was 34.4±7.5 and 33.9±8.0 years old for the us-
ers of the LNG-IUS and TCu380A IUD, respectively. The mean (±SD) BMI (kg/m²) was 25.3±4.1 and 25.9±4.1 (p = 0.0692). Number of pregnancies, number of children and physical activity does not showed signifi cant differences. Regarding ethnicity white women represented 73.7% and 71.1% among LNG-IUS and IUD users, respectively (Table 1).
Tab. 1 - Anthropometric characteristics of the sample according to the contraceptive method at the begin-ning of the study.
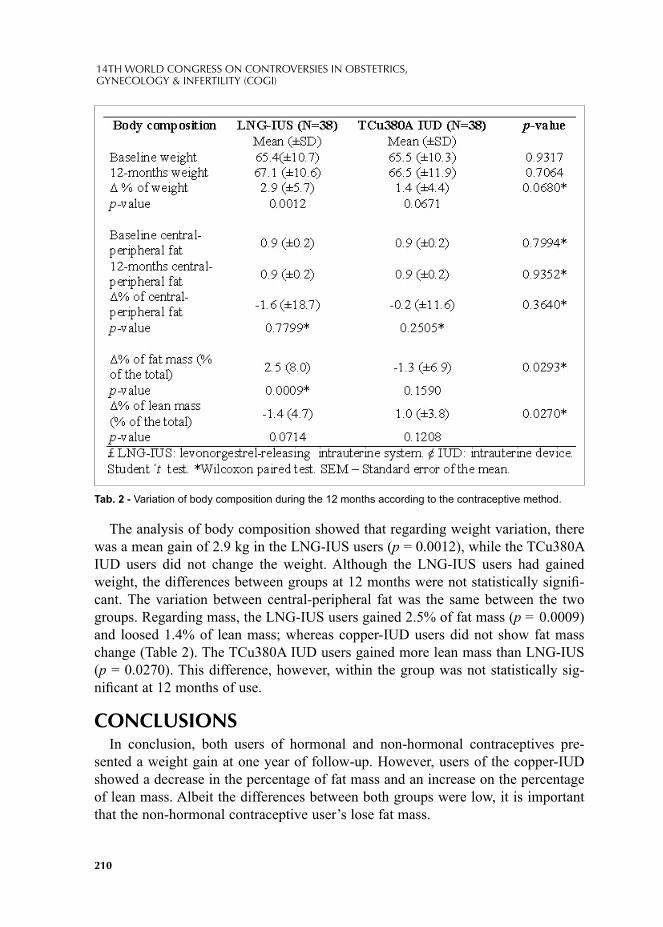
210
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The analysis of body composition showed that regarding weight variation, there was a mean gain of 2.9 kg in the LNG-IUS users (p = 0.0012), while the TCu380A IUD users did not change the weight. Although the LNG-IUS users had gained weight, the differences between groups at 12 months were not statistically signifi -cant. The variation between central-peripheral fat was the same between the two groups. Regarding mass, the LNG-IUS users gained 2.5% of fat mass (p = 0.0009) and loosed 1.4% of lean mass; whereas copper-IUD users did not show fat mass change (Table 2). The TCu380A IUD users gained more lean mass than LNG-IUS (p = 0.0270). This difference, however, within the group was not statistically sig-nifi cant at 12 months of use.
CONCLUSIONSIn conclusion, both users of hormonal and non-hormonal contraceptives pre-
sented a weight gain at one year of follow-up. However, users of the copper-IUD showed a decrease in the percentage of fat mass and an increase on the percentage of lean mass. Albeit the differences between both groups were low, it is important that the non-hormonal contraceptive user’s lose fat mass.
Tab. 2 - Variation of body composition during the 12 months according to the contraceptive method.
211
November 17-20, 2011 Paris, France
REFERENCES1. Bahamondes L, Espejo-Arce X, Hidalgo MM, Hidalgo-Regina C, Teatin-Juliato C, Petta CA. A
cross-sectional study of the forearm bone density of long-term users of levonorgestrel-releasing intrauterine system. Hum Reprod. 2006; 21:1319-2006.
2. ESHRE Capri Workshop Group. Intrauterine devices and intrauterine systems. Hum Reprod Up-date 2008; 14:197-208.
3. Beatty MN, Blumenthal PD. The levonorgestrel-releasing intrauterine system: safety, effi cacy, and patient acceptability. Therapeutics and Clinical Risk Management 2009; 5: 561-574.
4. Bahamondes MV, Monteiro I, Castro S, Espejo-Arce, Bahamondes L. Prospective study of the forearm bone mineral density of long-term users of levonorgestrel-releasing intrauterine system. Hum Reprod. 2010; 0:1-7.
5. Luukkainen T, Lähteenmäki P, Toivonen J. Levonorgestrel-releasing intrauterine device. Ann Med 1990; 22:85-90.
6. Hidalgo MM, Hidalgo-Regina C, Bahamondes MV, Monteiro I, Petta CA, Bahamondes L. Serum levonorgestrel levels and endometrial thickness during extended use of the levonorgestrel-releasing intrauterine system. Contraception 2009; 80:84-89.
7. Balasch J. Sex steroids and bone: current perspectives. Hum Reprod 2003; 9(3):207-222.8. Westhoff C, Jain JK, Milson I, Ray A. Changes in weight with depot medroxyprogesterone acetate
subcutaneous injection 104mg/0,65ml. Contraception 2007; 75(4):261-7.9. Bahamondes L, Del Castillo S, Tabares G, Arce XE, Perrotti M, Petta CA. Comparision of weigth
increase in users of Depot Medroxyprogesterone acetate and copper IUD up to 5 years. Contracep-tion 2001; 64(4):223-5.
10. Berenson AB, Rahman M. Changes in weight, total fat, percent body fat, and central-to-peripheral fat ratio associated with injectable and oral contraceptive use. Am J Obstet Gynecol 2009; 200:329.e1-329.e8.
11. Sheng J, Zang WY, Zang JP, Lu D. The LNG-IUS study on adenomysis: a 3-year follow-up study on the effi cacy and side effects of the use of levonorgestrel intrauterine system for the treatment of dysmenorrhea associated with adenomysis. Contraception 2009; 79:189-193.
12. Yela DA, Monteiro I, Bahamondes LG, Castillo SD, Bahamondes MV, Fernandes A. Variação de peso em usuárias de sistema intra-uterino liberador de levonorgestrel, DIU T-Cobre e acetato de medroxiprogesterona no Brasil. Rev Assoc Med Bras 2006; 52(1):32-6.

© 2012 Monduzzi Editoriale | Proceedings Code: 162
Can promestriene be used even in oncology patients?
L. Del Pup1, D. Postruznik2
1Oncological Gynecology, National Cancer Institute, Aviano, PN, Italy; 2MD Ob Gyn Scientifi c Advisor, Monaco, Montecarlo
SUMMARYVaginal estrogens use is controversial in gynecology oncology patients. Vaginal
promestriene is not signifi cantly absorbed and estrone-sulfate (E1S) is a reliable marker of its impact on overall estrogenicity. Matherial and methods: E1S was measured before and after one month of vaginal promestriene treatment (10 mg/day) in 17 patients suffering from severe vaginal dryness and dyspareunia using the very sensitive and precise liquid chromatography-tandem mass spectrometry (LC-MS/MS) Results: Estrone sulfate plasma levels, did not change signifi cantly [me-dia 533 (22-2920) to 374 (81-856) pg/ml] (p=0.85). With promestriene use vaginal lubrication [3 (2-4) to 5 (4-8)] (p= 0.008) and dyspareunia improved [6.4 (6-8) to 3 (2-5)] (p=0.007) and mean vaginal pH decreased [5.5 (4.8-6.2) to 4.4 (4.2-5.4)] (p= 0.043). Conclusion: plasma estrone sulfate levels did not change signifi cantly using promestriene which was effective to cure vaginal dryness and dyspareunia and to restore vaginal trophism in oncology patients.
INTRODUCTIONVaginal estrogens use is controversial in gynecology oncology patients as they are
more likely to suffer from severe vaginal atrophic symptoms, so they more frequent-ly need it, but, at the same time, most of them have an estrogen sensitive neoplasm and fear for its possible systemic effect (1-4). Vaginal hypoestrogenism is important to be treated, expecially from the colposcopist perspective, because it alters prop-er low genital tract cancer early diagnosis. ASCUS ratio is increased but diagnosis of ASCUS in hypoestrogenic women is less likely to be associated with dysplasia. A correct diagnosis and an effi cient treatment can be obtained with a short-time promestriene treatment before cytological and colposcopic follow-up as it makes the Squamo-Columnar Junction (SCJ) diffi cult or impossibile to be seen (5).

214
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Vaginal conjugated equine estrogens and estradiol signifi cantly increase systemic estrone levels as reported by Labrie F et al 2009 (6) who found relevant increase in serum estrogen measured with mass spectrometry in postmenopausal women. After a week of daily treatment with vaginal estrogen applications in the 20 patients inves-tigated the E2 mean fold increase was 5.4- fold after daily application of 1 g (0.625 mg) CEE (conjugated equine estrogens) cream or 25 mcg E2 tablets while the E1 fold increase resulted of about 500% and 150% for CEE and with E2 tablets. On the contrary promestriene is not signifi cantly absorbed as confi rmed by long term and wide clinical experience and by literature (7-10). Promestriene is a stable estradiol diether derivative that is incapable of crossing the vaginal malpighian epithelium and with an effi cient action that is limited to the vaginal atrophy without stimulating the endometrium or affecting the gonadotrophins or estrogen plasma levels.
Estrone-sulfate (E1S) is the most abundant estrogen precursor, it is more stable and it has an extended half-life so that it is considered as a better marker of overall estrogenicity (11). In order to confi rm and to precisely measure the poor vaginal promestriene absorption, E1S was measured by very sensitive liquid chromatogra-phy-tandem mass spectrometry (LC-MS/MS) in oncology patients suffering from severe vaginal dryness and dyspareunia.
MATHERIAL AND METHODSE1S was measured before and after one month vaginal promestriene treatment
(10 mg/day) in seventeen patients suffering from severe vaginal dryness and dys-pareunia referred to the gynecological endocrine- oncological service of the Gyne-cological Oncology department of the National Cancer Institute of Aviano, Porde-none, Italy. They were informed of the aim of the study and of benefi ts and risks of promestriene. Two patients were withdrawn during the study: one started a therapy with letrozole and the other died, unrelated with the treatment. Of the eligible pa-tients, six had cervical cancer, four endometrial cancer, three ovarian cancer and two vulvar cancer. The median age of the patients was 48 years (range 26-66). At the visits before and after the vaginal lubrication and dyspareunia were evaluated subjectively using a visual analogue scale. Atrophy was evaluated with the colpos-copy, also using Lugol solution, cytology and vaginal pH.
RESULTS AND DISCUSSIONOne month only promestriene treatment signifi cantly relieved all subjective and
objective parameters assessed in these highly symptomatic patients. At the same time systemic absorption were negligible which is of outmost importance for oncologi-cal gynecological patients and reassuring for them and for their physician. (Tab 1) Estrone sulfate plasma levels, did not change signifi cantly [media 533 (22-2920) to 374 (81-856) pg/ml] (p=0.85). All patients improved with the one month promes-

215
November 17-20, 2011 Paris, France
triene treatment both subjectively and objectively. Vaginal lubrication [3 (2-4) to 5 (4-8)] (p= 0.008) and dyspareunia improved [6.4 (6-8) to 3 (2-5)] to (p=0.007). Col-poscopic evaluation of atrophy also improved and mean vaginal pH decreased [5.5 (4.8-6.2) to 4.4 (4.2-5.4)] (p= 0.043). Colposcopy was more reliable and intracervical procedures were feasible and more tolerated after estrogenization of the cervix which made low genital tract early diagnosis more effective in the non hysterectomized patients. Vaginal cytology revealed four ASCUS before treatment and only one after promestriene treatment.
There was a high interindividual variability mostly of basal E1S levels the lesser and higher value differed ten times. The variation of individual E1S systemic levels after the one month treatment were negligible. This is further reassuring if we con-sider that topical estrogen can escape into the general circulation, in the fi rst 2 to 4 weeks of treatment, because of rapid absorption through a thin atrophic vaginal mu-cosa and all these patients had a highly symptomatic vaginal atrophy. Then absorp-tion is reduced till it is no clinically relevant once vaginal thickening has occurred (12-14). So if there was no effect after the fi rst month an even lesser absorption thereafter is expected.
The only plasma estrogen measured was E1S in our study, but this estrogen was
Tab. 1
Tab 1 Before After p
Estrone Sulfate
levels (pg/ml)
533 (22-2920) 374 (81-856) 0.85
Vaginal
lubrication
3 (2-4) 5 (4-8) 0.008
Dyspareunia 6.4 (6-8) 3 (2-5) 0.007
Vaginal pH 5.5 (4.8-6.2) 4.4 (4.2-5.4) 0.043
ASCUS 4 1

216
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
chosen because it is considered as a “reservoir”, an important marker for assessing the women’s overall “estrogenicity” (11). As compared to both E1 and E2 precur-sors, estrone sulfate (E1S) is present at 10-50 fold higher plasma concentration that enables its more sensitive quantifi cation with a better inter-assay variation. Futher-more it is characterized by a prolonged half-life that makes its measurement in-dependent from the blood sampling time and from the problems associated to the diurnal variations suffered by E1 and E2. (15-16). Measurement of E1S with the accurate and sensitive mass spectrometry makes these study interesting if compared with the previous studies performed with RIA assay.
This study was limited by the small number of patient, but it was highly diffi cult to enroll oncologic gynecology patients, some of them had a contraindication for local estrogens like endometrial cancer, and all of them are scared about using es-trogens. We choose to limit the study to highly symptomatic patients and to assess multiple subjective ad objective parameters and E1S dosing, before and at the end of treatment, only in those who used promestriene daily all the month.
CONCLUSIONVaginal promestriene is very effective to cure vaginal dryness and dyspareunia
in oncology patients while plasma estrone sulfate levels did not change signifi cant-ly. The effi cacy and safety data are in line with previous literature on promestri-ene. This is by our knowledge the only work performed in the subset of oncology patients and with the reliable measurement of E1S with mass spectrometry. This results, although preliminary, help to confi rm and reassure even the general post-menopausal women that promestriene is a safe and effective therapy.
REFERENCES1. Piccoli R., Mandato V.D., Lavitola G., Acunzo G., Bifulco G., Tommaselli G.A., Attianese W., Nappi
C. Atypical squamous cells and low squamous intraepithelial lesions in postmenopausal women: Implications for management. European Journal of Obstetrics & Gynecology and Reproductive Biology 2008; 140: 269–274.
2. Suckling JA, Kennedy R, Lethaby A, Roberts H Local oestrogen for vaginal atrophy in postmenopausal women (Review) Cochrane Database Syst Rev. 2006 Oct 18; (4):CD001500.
3. Ponzone R, Biglia N, Jacomuzzi ME, Maggiorotto F, Mariani L, Sismondi P. Vaginal oestrogen therapy after breast cancer: is it safe? Eur J Cancer 2005; 41:2673–2681.
4. Trinkaus M., Chin S., Wolfman A., Simmons C, Clemons M. Should Urogenital Atrophy in Breast Cancer Survivors Be Treated with Topical Estrogens? The Oncologist 2008; 13:222–231.
5. The Endogenous Hormones and Breast Cancer Collaborative Group Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies, J Natl Cancer Inst 2002; 94: 606-616.
6. Labrie F., Cusan L., Gomez J.L., Côté I., Bérubé R., Bélanger P., Martel C., and Labrie C. Effect of one-week treatment with vaginal estrogen preparations on serum estrogen levels in postmenopausal women Menopuase 2009; 16(1): 30-36 Wolff J.P., Cachelou R., Gueritée N., Absence of systemic hormonal effects in an oestradiol diether topically active on the vaginal mucosa, Maturitas 1982; 4: 239–246.

217
November 17-20, 2011 Paris, France
7. Wolff J.-P.,Cachelou R. and Gueritee N. Absence of systemic hormonal effects in an oestradiol diether topically active on the vaginal mucosa. Maturitas 1982; 4 :239-246.
8. Borrelli A.L., Casolaro A.M., Espósito G., Berlingieri D., Attività biologica del promestriene sul tratto genitale della ratta castrata, Minerva Ginecol1990; 42(11): 467—472.
9. Belaish J., Thomas J.L., Becker, Lumbroso M. Esperienza francese ed europea con il promestriene. In: Bottiglioni F. Il cimaterio femminile. Torchio de Ricci 1988: 29-44.
10. Campana G., Di Francesco G. Menopausal syndrome: clinical experiences with promestriene. Ann Ost Med Pren 1976; 3: 1-9.
11. Corona G., Elia C., Casetta B., Da Ponte A. Del Pup L., Ottavian E., Toffoli G. Liquid chromatography tandem mass spectrometry assay for fast and sensitive quantifi cation of estrone-sulfate. Clinica Chimica Acta 2010; 411: 574–580.
12. Pschera B., Hjerpe A., Carltröm K. Infl uence of the maturity of the vaginal epithelium upon the absorption of vaginally administered estradiol-17 and progesterone in postmenopausal women. Gy-necol. Obstet. Invest 1989; 27: 204-208.
13. Fraser IS, Wang Y. New delivery systems for hormone replacement therapy. In Wren BG, ed. Prog-ress in the Management of the Menopause. Carnforth, UK: Parthenon Publishing, 1997: 58–67
14. Rigg LA, Hermann H, Yen SC. Absorption of estrogens from vaginal creams. N Engl J Med 1978:298: 195–197.
15. Pasqualini JR, Chetrite GS. Recent insight on the control of enzymes involved in estrogen forma-tion and transformation in human breast cancer. J.Steroid Biochem.Mol.Biol. 2005; 93:221-36.44.
16. Crandall CJ, Guan M, Laughlin GA et al. Increases in serum estrone sulfate level are associated with increased mammographic density during menopausal hormone therapy. Cancer Epidemiol.Biomarkers Prev. 2008; 17:1674-81.

© 2012 Monduzzi Editoriale | Proceedings Code: 184
Postpartum echographic diagnosis of ganglioneuroblastoma – a case report
O. Eremina1, Y. Boykova1, E. Shifman1, I. Shevelev2, V. Korolishin2, A. Gus1
1V.I.Kulakov Research Center for Obstetrics, Gynecology and Perinatology, Moscow, Russian Federation; 2N.N.Burdenko Neurosurgery Institute Moscow, Russian Federation
SUMMARYThere are few reports of long-term outcome survivors of pelvic neuroblastoma
during pregnancy and postpartum period. We present a case of 31-year-old pregnant woman with an uneventful history. Her pregnancy was terminated at 36 weeks of gestation because of placental abruption. Occasionally during echographic screen-ing a large retroperitoneal tumor was revealed, it was treated with surgical resection, chemotherapy, and radiation. Conclusion: echography should be a routine proce-dure at the postpartum in every obstetrical department. In case of unknown pelvic masses during postpartum, a color Doppler and Power fl ow should be used to make a differential diagnosis.
INTRODUCTIONGanglioneuroblastoma is a malignant tumor of neural tissue. This tumor is diag-
nosed in children 2-4 years, 41% of cancers in infants diagnosed within the fi rst 3 months of life, after 10 years its frequency is about 10% and it is very rare in adults [2,3,4]. No publications were found about this tumor during pregnancy and in post-partum. We present a case of 31-year old woman with large undiagnosed neuroblas-toma, diagnosed only after C-section.
MATERIALS AND METHODSThe patient was referred to our Center at 36 weeks of gestational age because of
massive vaginal bleeding. It was her second pregnancy, somatic and gynecologic history were common. Her previous delivery was terminated by C-section because of labor dystocia. This time an abruptio placentae was diagnosed and urgent c-section was performed, the girl, 2800 g, 7-8 Apgar score was delivered. No surgical
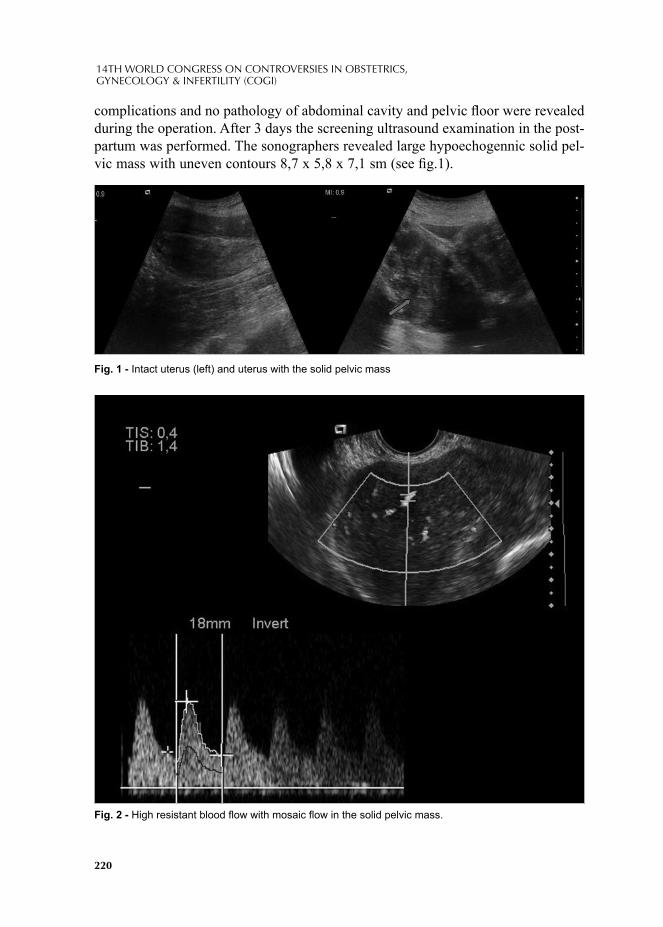
220
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
complications and no pathology of abdominal cavity and pelvic fl oor were revealed during the operation. After 3 days the screening ultrasound examination in the post-partum was performed. The sonographers revealed large hypoechogennic solid pel-vic mass with uneven contours 8,7 х 5,8 х 7,1 sm (see fi g.1).
Fig. 2 - High resistant blood fl ow with mosaic fl ow in the solid pelvic mass.
Fig. 1 - Intact uterus (left) and uterus with the solid pelvic mass
221
November 17-20, 2011 Paris, France
No other pathology of pelvic fl oor was found. The differential diagnosis was conducted between intraligamentar myoma, parametral hematoma and unknown retroperitoneal tumor. Color Doppler and Power fl ow revealed an intensive, high resistant blood fl ow, with several mosaic color areas (fi g.2).
A large retroperitoneal tumor was suspected. An additional MR-imaging with contrast was performed. It revealed a large retroperitoneal tumor with vertebral in-vasion in L5-S1 (fi g.3).
The patient was consulted by neurosurgeons, they recommended to suppress the lactation and in 3 months neurosurgical curative operation was made. Pathomorpho-logical diagnosis was ganglioneuroblastoma. After the operation 4 cycles of a chemo-therapy protocol and radiation were conducted and in 6 months during the screening examination sonographers revealed a recurrent retroperitoneal tumor 7*6*7 sm. At present we plan 2 cycles of chemotherapy and dynamic monitoring of the patient.
DISCUS SIONNeuroblastoma derives from neuroectodermal cells. There are several theories of
its pathogenesis, the main theory is the malignant transformation of residual micro-scopic neuroblastic nodules, which results from a failure of these cells to respond adequately to the normal signals that stimulate differentiation or apoptosis [1]. Usually, in children it is located in the adrenal medulla. While in adults, the more common sites are retroperitoneum (30%) followed by adrenal, pelvis and mediasti-num[5], other rare sites include head and neck, mesentery, thoracic spine, epidural space, liver and extremities [6]. There are several perinatal risk factors of this tu-
Fig. 3 - MR scan of the tumor..

222
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
mor: maternal anemia during, neonatal respiratory distress and low (below or equal to 7) 1-min Apgar score [7]. We did not fi nd in literature special publications about neuroblastoma during pregnancy. N.Watanabe et al. [8] described the pregnancy after treating the tumor during the childhood. Authors suggest that long-term female survivors of childhood pelvic neuroblastoma might develop complications during pregnancy due to the negative effects of the tumor or prior radiation therapy. In our patient an abruption placentae occurred, but we can’t associate it with the presence of neuroblastoma.
Usually the revealing of a solid mass in the pelvic fl oor in the postpartum period is associated with postcesarean or postnatal complications In the presented case a combination of the methods allowed to exclude postoperative complications such as haematoma or fi broma and helped us to precise the type of the mass and its lo-calization. The diagnosis of a neuroblastic tumor in an adult patient is very rare [1], both clinicians and pathologists think about another neoplasms (for example, sacral tumors). In our case pelvic MRI showed tumor localization and revealed its origin from the spinal cord.
CONCLUSIONTo conclude, an echography during postpartum period should be a routine proce-
dure. Sometimes it helps to precise the origin of the mass and to correct the treat-ment of the patient. Routine echography and a color Doppler application gives much additional information in performing a differential diagnosis of unknown pel-vic masses during postpartum.
REFERENCES1. Then C, Ebelt K, Langer A, Mayr D, Schmidmaier R, Oduncu F. Neuroblastoma in a 55-year-old
patient: a case report. // Case Rep Oncol. 2010 Sep; 3(3):458-62. Epub 2010 Dec 4.2. Surveillance, Epidemiology, and End Results (SEER) Program, National Cancer Institute, Division
of Cancer Prevention and Control, Surveillance Program, Cancer Statistics Branch, registry data 1975 - 2000 www. seer. cancer. gov. Accessed September 15, 2008
3. London WB, Boni L, Simon T, Berthold F, Twist C, Schmidt ML, Castleberry RP, Matthay KK, Cohn SL, De Bernardi B. The role of age in neuroblastoma risk stratifi cation: the German, Italian, and children's oncology group perspectives. Cancer Lett. 2005; 228:257-266
4. Zerrweck-López C, Quijano-Orvañanos F. et al. Neuroblastoma in the adult. Case report. Cir Cir. 2009; 77:397-401.
5. Ohtaki Y, Ishii G Adult neuroblastoma arising in the superior mediastinum. // Interact Cardiovasc Thorac Surg. 2011 Aug; 13(2):220-2. Epub 2011 Mar 9.
6. Ouakaa-Kchaou A, Khalfallah T Liver neuroblastoma in an adult. // Tunis Med. 2010 Sep; 88(9):682.7. Bluhm E, McNeil DE, Cnattingius S Prenatal and perinatal risk factors for neuroblastoma. // Int J
Cancer. 2008 Dec 15; 123(12):2885-90.8. Watanabe N, Tsutsui J, Kakiuchi S Intra-Abdominal Bleeding during Pregnancy, Preterm Delivery,
and Placental Polyp in a Long-Term Survivor of Neuroblastoma: A Case Report. // Obstet Gynecol Int. 2009; 2009:564567. Epub 2009 Dec 6.
© 2012 Monduzzi Editoriale | Proceedings Code: 254
Impact of capsule rupture in stage I clear cell carcinoma of the ovary
H. Kajiyama1, M. Mizuno1, E. Yamada1, H. Matsumura1, F. Kikkawa1
1Department of Obstetrics and Gynecology, Nagoya University Graduate School of Medicine, Japan
SUMMARYIntroduction: We analyzed stage I clear cell carcinoma of the ovary (CCC)
patients to estimate the survival impact of the capsule status. Materials and Methods: Survival analyses on 224 patients with stage I CCC were evaluated the recurrence-free survival (RFS) and overall survival (OS). Results: There was no signifi cant difference in both the OS and DFS of CCC patients between IA and IC(ir) (intraop-erative capsule rupture). In contrast, CCC patients at IC(non-ir) {IC excluding for IC(ir)} showed a poorer OS and DFS than those at IC(ir). Conclusion: This suggests that CCC patients other than those with intraoperative capsule rupture show a con-siderable risk of for mortality.
INTRODUCTIONClear cell carcinoma of the ovary (CCC) has been recognized as a distinct histo-
logical entity in the World Health Organization (WHO) classifi cation of EOC since 1973 1. Most CCC cases are assigned to stage IC because the tumor capsule is ruptured either before or during surgery regardless of capsule surface involvement or positive cytology of ascites 2, 3. There have been few reports involving a com-prehensive investigation of the relation between the capsule status and prognosis of CCC patients.
In the present study, we retrospectively analyzed a large number of CCC patients to estimate the survival impact of the capsule status in stage I CCC patients.
MATERIALS AND METHODSA variety of malignant ovarian tumors have been accumulated by the Tokai Ovar-
ian Tumor Study Group, consisting of Nagoya University Hospital and affi liated institutions cooperating under the central pathological review system since 1986. Of
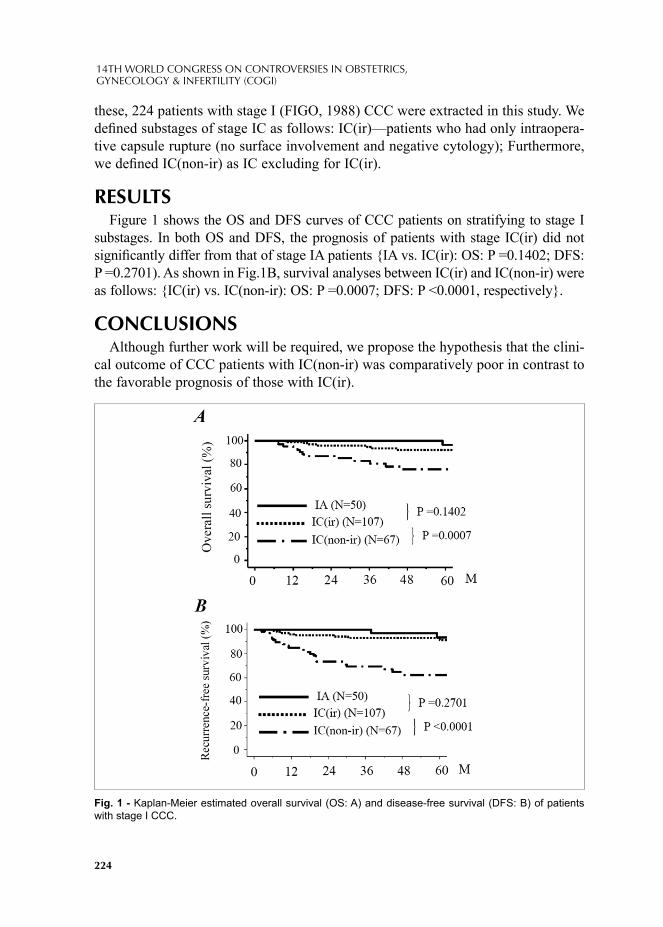
224
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
these, 224 patients with stage I (FIGO, 1988) CCC were extracted in this study. We defi ned substages of stage IC as follows: IC(ir)—patients who had only intraopera-tive capsule rupture (no surface involvement and negative cytology); Furthermore, we defi ned IC(non-ir) as IC excluding for IC(ir).
RESULTSFigure 1 shows the OS and DFS curves of CCC patients on stratifying to stage I
substages. In both OS and DFS, the prognosis of patients with stage IC(ir) did not signifi cantly differ from that of stage IA patients {IA vs. IC(ir): OS: P =0.1402; DFS: P =0.2701). As shown in Fig.1B, survival analyses between IC(ir) and IC(non-ir) were as follows: {IC(ir) vs. IC(non-ir): OS: P =0.0007; DFS: P <0.0001, respectively}.
CONCLUSIONSAlthough further work will be required, we propose the hypothesis that the clini-
cal outcome of CCC patients with IC(non-ir) was comparatively poor in contrast to the favorable prognosis of those with IC(ir).
Fig. 1 - Kaplan-Meier estimated overall survival (OS: A) and disease-free survival (DFS: B) of patients with stage I CCC.

225
November 17-20, 2011 Paris, France
REFERENCES1. Rusell P BP. Surgical Pathology of the Ovaries. Churchill Livingstone, New Yolk 1989.2. Kennedy AW, Biscotti CV, Hart WR, Webster KD. Ovarian clear cell adenocarcinoma. Gynecol
Oncol 1989; 32:342-9.3. Suzuki S, Kajiyama H, Shibata K, Ino K, Nawa A, Sakakibara K, Matsuzawa K, Takeda A,
Kinoshita Y, Kawai M, Nagasaka T, Kikkawa F. Is there any association between retroperitoneal lymphadenectomy and survival benefi t in ovarian clear cell carcinoma patients? Ann Oncol 2008; 19:1284-7.


© 2012 Monduzzi Editoriale | Proceedings Code: 257
Improvement of postoperative care after major abdominal gynecologic surgery
E. Kallfa1, G. Hyska2, E. Belaj2, A. Delilaj2, S. Xinxo3, V. Grori1, V. Mulliqi F. Lauszus4, O. Gliozheni1
1Department of Gyneacology Universitary Hospital for Obstetrics and Gynecology “Koço Gliozheni” Tirana, Albania; 2Department of Intensive Care Universitary Hospital for Obstetrics and Gynecology “Koço Gliozheni” Tirana, Albania; 3Institute of Public Health, Tirana, Albania; 4Herning Hospital MIDT Julland Denmark
SUMMARYAbdominal surgery plays a major role in the treatment of various benign and ma-
lignant gynaecologic disorders, for example, uterine fi broid, endometriosis, ovarian cyst, uterine cancer, and ovarian cancer. In this regard, hysterectomy and removal of ovarian cysts or ovarian tumour are the commonly performed procedures. Frequent-ly, gynecologic patients undergo multiple procedures during their surgery. This is especially the case for the patients with cancer.
There is widespread belief that intestinal stasis (paralytic ileus), a temporary in-hibition of bowel motility, follows all abdominal surgery. The exact cause of this clinical phenomenon is unknown, but it has been proposed that stimulation of pain fi bres, excessive sympathetic tone, and the release of inhibitory neurotransmitters from the gut wall are mechanisms involved (Kelly 1997). Gynecologists have tra-ditionally withheld postoperative oral intake until the return of bowel function as evidenced by a presence of bowel sound, a passing of fl atus/stool, and a feeling of hungry. There has been concern that early oral intake would result in vomiting and severe paralytic ileus with subsequent aspiration pneumonia, wound dehiscence (break down), and anastomotic leakage (leakage of surgically created connection between parts of the intestine) (Fanning 2001). This belief has become a surgical dogma, despite the lack of supporting scientifi c evidence.
Several clinical benefi ts of giving food and fl uids soon after surgery have been proposed in the literature. Following surgery, optimal nutritional status and mainte-nance of bowel function contribute signifi cantly to wound healing (Windsor 1988; Deitch 1991). Early oral intake has also been suggested to be an effective alternative
228
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
in postoperative stress ulcer prophylaxis as it helps maintaining strength of bowel mucosa. A risk of sepsis is reduced because of decreased bacterial colonization and decreased translocation through defects on the bowel mucosa into blood circula-tion in patients receiving early oral intake (Deitch 1991). Furthermore, psychologi-cal impact of oral fl uids and food following surgery was considered and improved sense of well being is observed in the patients who eat sooner (Schilder 1997). The psychological aspect also has a signifi cant role in the entire postoperative recovery process. Cost saving, which appears to be an important issue in many countries or health care systems, is another potential advantage of early feeding scheme as the patients in this group tend to have a shorter length of hospital stay. Currently, there is an ongoing Cochrane systematic review on early enteral nutrition after colorectal surgery to determine whether there is evidence that early enteral nutrition following colorectal surgery is of clinical benefi t (Beier-Holgersen 2003).
INTRODUCTIONTo assess the effects of early versus delayed (traditional) initiation of oral intake
of food and fl uids and pain control after major abdominal gynecologic surgery.
METHODS Based on the Danish experience and the Cochrane controlled trials register we
decided to implement in our Hospital a cohort retrospective study that compared the effect of early versus delayed initiation of oral intake of food and fl uids and pain control after major abdominal gynecologic surgery. During the 8 month period of study from March 2011 to October 2011, 114 patients who underwent major abdom-inal gynecological surgery in University Hospital for Obstetrics and Gynecology “Koço Gliozheni” Tirana, Albania were included in this study. The study consists of a total of 114 women, 53 from early feeding group and 61 from delayed group.
RESULTSThe groups are well balanced regarding the age, parity, BMI, and indications of
the abdominal gynecologic surgery. The mean difference of day stay in hospital is 1.52 days CI95 % -0,23 to 3.2 p>0.05. There is a signifi cant difference regarding the nausea and vomiting in the control group versus early intake group (respectively d= 0.19 CI 95 % 0,02 to 0.37 p < 0.01, d= 0.16 CI 95% 0,01 to 0.31 p <0.01). The dif-ference of proportion regarding the motility < 12 h is 0.71 with CI 95 % from 0.59 to 0.82 P < 0.05. The difference in mobilization < 24 h in early intake group versus the control group is 0. 55 with a CI 95 % from 0.43 to 0.66 p < 0.05. The difference of proportion regarding the fl atus in the early intake group versus the control group is 0.48 with a CI 95 % from 0.34 to 0.62 P < 0.05. The proportion of removal of the urethral catheter within 24 h in the early intake group is higher than in the control

229
November 17-20, 2011 Paris, France
group ( difference = 0.03 with CI 95 % from -0.14 to 0.2 p > 0.05. ). There was no signifi cant difference in abdominal distension, need for postoperative nasogastric tube placement, febrile morbidity (the illness characterised by fever with other asso-ciated symptoms), wound complications, and pneumonia between the study groups.
CONCLUSIONSThe fi ndings from this study have demonstrated the safety of the early postopera-
tive feeding approach in women undergoing major abdominal gynecologic surgery. There is a signifi cant reducing of the symptoms of nausea, vomiting. This procedure accelerate the mobilization and fl atus within 24 h and intestinal motility within 12 h. However, does not reduce the length of stay in hospital signifi cantly. Control of postoperative pain with combination of Ibuprofen Arginine and Paracetamol shows that is very effective.
REFERENCES1. Singh G, Ram RP, Khanna SK. Early postoperative enteral feeding in patients with nontraunatic
intestinal perforation and peritonitis. Journal American College Surgery 1998; 187:142-6.2. Cutillo G, Maneschi F, Franchi M, Giannice R, Scambia G, Benedetti-Panici P. Early feeding
compared with nasogastric decompression after major oncologic gynecologic surgery: a randomized study. Obstet Gynecol 1999; 93:41-5.
3. Fanning J, Yu-Brekke S. Prospective trial of aggressive postoperative bowel stimulation following radical hysterectomy. Gynecol Oncol 1999; 73:412-4.
4. Kraus K, Fanning J. Prospective trial of early feeding and bowel stimulation after radical hysterectomy. American Journal Obstet Gynecol 2000; 182:996-8.
5. MacMillan SL, Kammerer-Doak D, Rogers RG, Parker KM. Early feeding and the incidence of gastrointestinal symptoms after major gynecologic surgery. Obstet Gynecol 2000; 96:604-8.
6. Johnson C, Casto C, Krammer J, Drake J.Postoperative feeding: A clinical review.7. Obstet Gynecol Surv. 2000; 55(9):571-573.8. Amatyakul P, Suprasert P. Length of hospital stay after major gynecologic operation: a comparison
between traditional and early oral feeding. Dissertation thesis for the diploma in Obstetrics and Gynecology, The Royal Thai College of Obstetricians and Gynecologists 2001.
9. Fanning J, Andrews S. Early postoperative feeding after major gynecologic surgery: evidence-based scientifi c medicine. American Journal Obstet Gynecol 2001; 185:1-4.
10. Ghosh K, Downs LS, Padilla LA, MurrayKP, Twiggs LB, Letourneau CM, Carson.11. LF. The implementation of critical pathways in gynecologic oncology in a managed.12. care setting: A cost analysis. Gynecol Oncol. 2001; 83(2):378-382.13. Lewis SJ, Egger M, Sylvester PA, Thomas S. Early enteral feeding versus "nil by mouth" after
gastrointestinal surgery: systematic review and meta-analysis of controlled trials. British Medical Journal 2001; 323:773-6.
14. Taguchi A, Sharma N, Saleem R, Sessler D, Carpenter R, Seyedsadr M, Kurz A. Selective postoperative inhibition of gastrointestinal opioid receptors. New England Journal Medicine 2001; 345:935-40.
15. Steed HL, Capstick V, Flood C, Schepansky A, Schulz J, Mayes DC. A randomized controlled trial of early versus "traditional" postoperative oral intake after major abdominal gynecologic surgery. American Journal Obstet Gynecol 2002; 186:861-5.
230
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
16. Pearl ML, Frandina M, Mahler L, Valea FA, DiSilvestro PA, Chalas E. A randomized controlled trial of a regular diet as the fi rst meal in gynecologic oncology patients undergoing intraabdominal surgery. Obstet Gynecol 2002; 100:230-4.
17. Asao T, Kuwano H, Nakamura J-I, Morinaga N, Hirayama I, Ide M. Gum chewing enhances early recovery from postoperative ileus after laparoscopic colectomy. J Am Coll Surg 2002; 195:30–2. CrossRef, PubMed, Web of Science® Times Cited: 43.
18. Beier-Holgersen R, Andersen HK, Lewis SJ, Thomas S, Han-Geurts I. Early enteral nutrition within 24h of colorectal surgery versus later commencement of feeding for postoperative complications (Protocol for a Cochrane Review). Cochrane Database of Systematic Reviews 2003, Issue 3.
19. Behm B, Stollman N. Postoperative ileus; etiologies and interventions. Clin Gastroenterol Hepatol 2003; 1:71–80. CrossRef, PubMed.
20. Mangesi L, Hofmeyr GJ. Early compared with delayed oral fl uids and food after caesarean section (Cochrane Review). Cochrane Database of Systematic Reviews 2003, Issue 2.[Art. No.: CD003516. DOI:
21. Delaney C, Weese J, Hyman N, Bauer J, Techner L, Gabriel K, Du W, Schmidt W, Wallin B. Phase III trial of alvimopan, a novel, peripherally acting, Mu opioid antagonist, for postoperative ileus after major abdominal surgery. Dis Colon Rectum 2005; 48:1114-29.
22. Wu L, Griffi th P. Early postoperative feeding and abdominal gynecological.23. surgery. Br J Nurs. 2005; 14(1):42-46.24. Charoenkwan K, Palapinyo C. Early solid food after cesarean section and postoperative ileus. Int
J Gynecol Obstet 2005; 90:144–5. CrossRef, PubMed, ChemPort, Web of Science® Times Cited: 125. Martindale RG, Maerz LL. Management of perioperative nutrition support. Curr.Opin Crit Care 2006; 12(4):290-294.26. Schuster R, Grewal N, Greaney GC, Waxman K. Gum chewing reduces ileus after elective open
sigmoid colectomy. Arch Surg 2006; 141:174–6. CrossRef, PubMed, Web of Science® Times Cited: 20.
© 2012 Monduzzi Editoriale | Proceedings Code: 268
Evaluation of the ovarian malignancies' occurrence in patients with previous IVF treatment
A. Koumousidis, A. Kotelis, A. Daskalakis, I. Kaniaris, M. Kontoyannis, V. Sanoulis, D. Ftoulis, Ch. Tsarmaklis, Ch. Katsetos Tzaneio Hospital, General Hospital of Piraeus, Pireas, Attiki, Greece
SUMMARYIntroduction: Ovarian cancer affects mostly more than fi fty years old women,
with history of fatty diet, previous breast or colon cancer, subfertility, nulliparity and positive for malignancies family history. Researchers support the multiple, un-successful under IVF treatment, efforts to be an etiologic factor for the disease. Ma-terial and methods: We searched the web, using several keywords, and found lots of interesting articles. Results: Low cancer risk was found after IVF treatment in some studies, while other researchers observed higher malignancy rate in IVF-patients comparing to the risk in the general population. We noticed that this controversy is attributed to the lack of a systematic and worldwide-accepted classifi cation in the cancer patients, who have undergone IVF treatments, in terms of several factors: age, body-weight, parity, positive for malignancies history. Conclusions: If we clas-sify the IVF-candidate women in terms of their personal and family history, we will fi nd a way out of this controversy and eventually, minimize the various potential long-term complications.
INTRODUCTION Ovarian cancer affects mostly more than 50 years old women, with medical his-
tory of fatty diet, previous breast or colon cancer, subfertility (1), nulliparity (2) and a positive for malignancies family history. Researchers support the multiple, unsuc-cessful under IVF treatment, efforts to be another etiologic factor for the disease. Induction of ovulation is most frequently used to restore ovulation in anovulatory patients with the aim of inducing unifollicular growth and release of a mature oo-cyte. Controlled ovarian hyperstimulation exposes the ovaries to supraphysiological

232
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
levels of gonadotropins, resulting in multiple follicular development for assisted conception (3). Does this ovarian stimulation increase the chance of an ovarian neo-plasia, as a risk factor for this malignancy? The widely known Fathalla’s incessant ovulation hypothesis suggests that the epithelial ovarian carcinoma results from the repeated ovulations, where the cumulative effects of each minor trauma to the ovar-ian epithelium can lead to malignant transformation (4). And, if this happens, what is the complex of a possible interplay of the potential cofactors that involve, to-gether with the previous IVF exposure, towards the development of the carcinoma?
MATERIAL AND METHODS We searched the web (data-warehouse: articles, forums, case reports, etc., data-
mining: Sequence Analysis, Association Rules, Classifi cation, Clustering, Forecast-ing) for related issues, using several keywords such as “ART/IVF/cancer/malignan-cies/borderline tumors” etc. and we extracted many articles as well as we entered and examined several forums, lots of blogs and a variety of case reports (: we focused mainly on cases with tumors surgically extracted at least fi ve years after previous IVF treatment(s)). We investigated the several cited aspects and their analysis on the issue in question and found an adequate number of interesting articles with some-times totally opposed opinions. All the above data-warehouse became a very useful tool in our hands so as to be able to proceed in the basic Online Analytical Process-ing- OLAP (measures: data with mean values, categorization/dimensions (like age, obesity, parity, previous breast or colon cancer, etc.) (5)), in data-mining, such as the Association Rules (method for discovering interesting relations between variables within large databases -(6)), the Sequence Analysis (comparison of sequences in or-der to fi nd similarities, identifi cation of intrinsic sequence features or sequence dif-ferences, etc. –(7)), the Classifi cation (identifying the sub-population to which new observations belong –(8)), the Clustering (assignment of a set of observations into subsets (called clusters) so that observations in the same cluster are similar in some sense -(9)), the Forecasting (process of making statements about events whose ac-tual outcomes (typically) have not yet been observed –(10)) for ovarian cancer cases after previous IVF treatment. All this statistical procedure was particularly valuable in forming an integrated icon for the matter in question and furthermore, in creating a proper strategy for taking correct decisions on the application of any needed IVF therapy in our patients (for subfertility treatment), accompanied at the same time by a deep scientifi c interest on the minimization of the ovarian cancer’s occurrence.
RESULTS We have to mention that the extraction of several information was based on a
web-material, which we found scientifi cally interesting, using several criteria such as the quality and the traffi c of the website, the impact factor of many medical web-
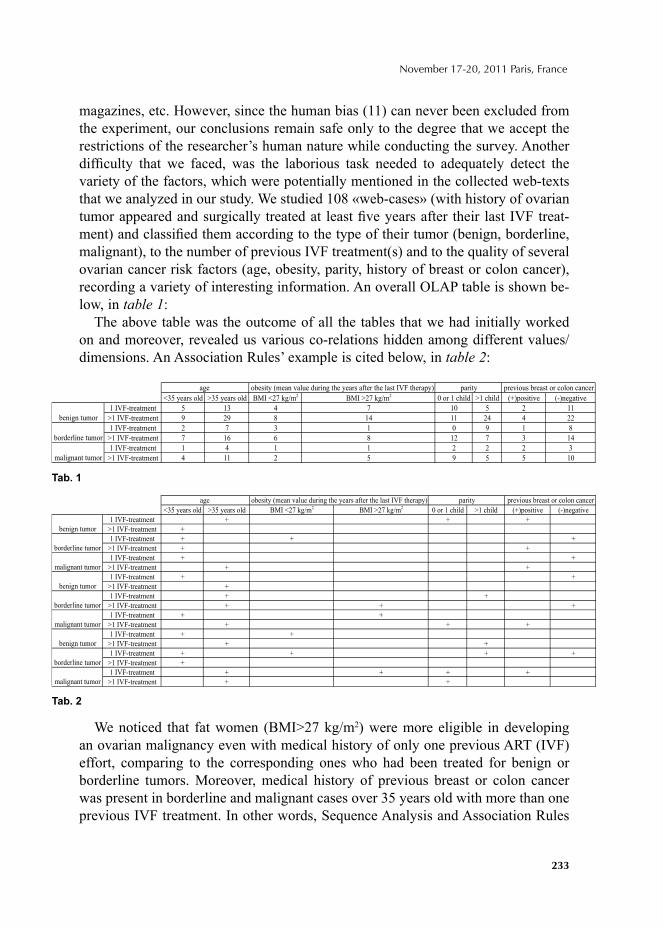
233
November 17-20, 2011 Paris, France
magazines, etc. However, since the human bias (11) can never been excluded from the experiment, our conclusions remain safe only to the degree that we accept the restrictions of the researcher’s human nature while conducting the survey. Another diffi culty that we faced, was the laborious task needed to adequately detect the variety of the factors, which were potentially mentioned in the collected web-texts that we analyzed in our study. We studied 108 «web-cases» (with history of ovarian tumor appeared and surgically treated at least fi ve years after their last IVF treat-ment) and classifi ed them according to the type of their tumor (benign, borderline, malignant), to the number of previous IVF treatment(s) and to the quality of several ovarian cancer risk factors (age, obesity, parity, history of breast or colon cancer), recording a variety of interesting information. An overall OLAP table is shown be-low, in table 1:
The above table was the outcome of all the tables that we had initially worked on and moreover, revealed us various co-relations hidden among different values/dimensions. An Association Rules’ example is cited below, in table 2:
We noticed that fat women (BMI>27 kg/m2) were more eligible in developing an ovarian malignancy even with medical history of only one previous ART (IVF) effort, comparing to the corresponding ones who had been treated for benign or borderline tumors. Moreover, medical history of previous breast or colon cancer was present in borderline and malignant cases over 35 years old with more than one previous IVF treatment. In other words, Sequence Analysis and Association Rules
<35 years old >35 years old BMI <27 kg/m2 BMI >27 kg/m2 0 or 1 child >1 child (+)positive (-)negative
1 IVF-treatment 5 13 4 7 10 5 2 11
>1 IVF-treatment 9 29 8 14 11 24 4 22
1 IVF-treatment 2 7 3 1 0 9 1 8
>1 IVF-treatment 7 16 6 8 12 7 3 14
1 IVF-treatment 1 4 1 1 2 2 2 3
>1 IVF-treatment 4 11 2 5 9 5 5 10malignant tumor
age obesity (mean value during the years after the last IVF therapy) parity previous breast or colon cancer
benign tumor
borderline tumor
<35 years old >35 years old BMI <27 kg/m2 BMI >27 kg/m2 0 or 1 child >1 child (+)positive (-)negative
1 IVF-treatment + + +
>1 IVF-treatment +
1 IVF-treatment + + +
>1 IVF-treatment + +
1 IVF-treatment + +
>1 IVF-treatment + +
1 IVF-treatment + +
>1 IVF-treatment +
1 IVF-treatment + +
>1 IVF-treatment + + +
1 IVF-treatment + +
>1 IVF-treatment + + +
1 IVF-treatment + +
>1 IVF-treatment + +
1 IVF-treatment + + + +
>1 IVF-treatment +
1 IVF-treatment + + + +
>1 IVF-treatment + +
age obesity (mean value during the years after the last IVF therapy) parity previous breast or colon cancer
malignant tumor
benign tumor
borderline tumor
malignant tumor
benign tumor
borderline tumor
malignant tumor
benign tumor
borderline tumor
Tab. 1
Tab. 2

234
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
helped us to evaluate properly the observations and proceed further in the suitable Clustering and Classifi cation, tools that are essential in the forecasting and the safe selection of the IVF candidates.
The medical literature presents to us huge controversies concerning the issue «ovarian malignancies’ occurrence in patients with previous IVF treatment». On the one hand, a signifi cantly low cancer risk was found after IVF in several stud-ies (12, 13), while on the other hand, many researchers have observed a higher rate of malignancy in IVF patients compared with the known risk in the general population (14). Furthermore, several studies attribute the above increased risk to the ovarian pathology that causes both infertility and ovarian malignancies and, at the same time, other scientifi c efforts are focused on fi ndings proving higher rate of borderline tumors (15) rather than of other types of ovarian can-cer in ART-treated patients. We noticed that this extended spectrum of scientifi c attitude towards this controversial theme is mainly attributed to the lack of a systematic and a worldwide-accepted classifi cation (low and high risk for cancer patients, undergoing IVF treatment) according to several risk factors for malig-nancies like age, body weight, parity, positive for malignancies family history, etc. Studies, concerning each of these factors and their coactions in the potential future malignant ovarian behavior after IVF exposure, must precede any further data-processing of the above mentioned research in order the latter to become scientifi cally fertile.
CONCLUSIONS We strongly support that an integrated approach on the matter in question must
be followed, by applying on the one hand the principles of Audit (16) in the exist-ing wide-accepted studies (meta-analysis, cohort, etc.), so as a reasonable assurance that the collected information is free from material error to be provided, while on the other hand, new surveys must be conducted on the basis of a proper classifi ca-tion, concerning the risk factors that may involve in the development of the ovarian malignancy. By reviewing previous research and by conducting new surveys under a correct and satisfying classifi cation, like the one mentioned above, a scientifi c order will be established in the sector of the IVF treatment, minimizing at the same time its various potential complications such as the new emerging ovarian cancer cases. Only if we classify the IVF-candidate women according to their personal (age, obesity, parity, medical history of previous cancer, etc.) and family (breast or ovarian cancer, colon malignancies, etc.) history in low and high risk for future can-cer development patient-categories, we will fi nd a way out of this great controversy and we will eventually minimize the several potential long-term complications, such as borderline or general ovarian tumors, in IVF treatment through adequately informing/consulting our general population.
235
November 17-20, 2011 Paris, France
REFERENCES1. VENN A., WATSON L., LUMLEY J., GILES G., KING C., HEALY D., «Breast and ovarian can-
cer incidence after infertility and in vitro fertilization.» Lancet, 346: 995 - 1000 :1995.2. MODAN B., RON E., LERNER-GEVA L., BLUMSTEIN T., MENCZER J., RABINOVICI J., et
al., «Cancer incidence in a cohort of infertile women.» Am J Epidemiol, 147:1038-42:1998.3. MAHDAVI A., PEJOVIC T., NEZHAT F., « Induction of ovulation and ovarian cancer: a critical
review of the literature», Fertil Steril., 85(4): 819-26: 2006.4. FATHALLA MF., «Incessant ovulation--a factor in ovarian neoplasia?», Lancet, 2(7716):163
:1971.5. http://en.wikipedia.org/wiki/OLAP6. http://en.wikipedia.org/wiki/Association_rules7. http://en.wikipedia.org/wiki/Sequence_analysis8. http://en.wikipedia.org/wiki/Statistical_classifi cation9. http://en.wikipedia.org/wiki/Cluster_analysis
10. http://en.wikipedia.org/wiki/Forecasting11. http://en.wikipedia.org/wiki/Human_error_assessment_and_reduction_technique12. POTASHNIK G., LERNER-GEVA L., GENKIN L., CHETRIT A., LUNENFELD E., PORATH
A., «Fertility drugs and risk of breast and ovarian cancers: results of a long-term follow-up study.» Fertil. Steril., 71: 853-9: 1999.
13. DOYLE P., MACONOCHIE N., BERAL V., «Cancer incidence following treatment for infertility at a clinic in the UK.» Hum Reprod, 17: 2209-13: 2002.
14. KASHYAP S., MOHER D., FUNG MF., ROSENWAKS Z., «Assisted reproductive technology and the incidence of ovarian cancer: a meta-analysis.», Obstet Gynecol, 103: 785-94: 2004.
15. NESS RB., CRAMER DW., GOODMAN MT., «Infertility, fertility drugs, and ovarian cancer: a pooled analysis of case-control studies.», Am J Epidemiol, 155: 217-24: 2002.
16. http://en.wikipedia.org/wiki/Audit

© 2012 Monduzzi Editoriale | Proceedings Code: 304
Can infl ammation take part in development and progression of endometrial hyperplasia?1 Ye. Kovalenko, 2 T. Tatarchuk, 1 A. Kubyshkin,1 T. Filonenko1Crimea State Medical University, Simferopol, Ukraine; 2 Institute of Pediatrics, Obstetrics and Gynecology Academy of Medical Sciences, Kiev, Ukraine
Summary. In investigation include 107 patients, which were classifi ed into four groups: normal endometrium (n=18), simple hyperplasia (n=41), complex hyper-plasia without atypia (n=36), complex hyperplasia with atypia (n=12). Local in-fl ammatory cytokines, nonspecifi c proteinases and their inhibitors together with immunohistochemical analysis of common leukocyte antigen CD45+ expression in endometrium was investigated. It was showed that endometrial hyperplasia is associated with the formation of infl ammation in the endometrium. Our results indicate the important role of infl ammation in the development of hyperplastic processes in the endometrium, which can be interpreted such as «infl ammation associated with endometrial hyperplasia» or «endometrial hyperplasia - related infl ammation».
INTRODUCTIONA key factor in the development of hyperplastic processes in the endometrium is
the formation of hyperestrogenemia [1], but more and more researchers pay atten-tion to other mechanisms that may underlie the pathogenesis of this disease. At the same time more attention paid to the study of cellular markers, which take part in infl ammation for the characterization of endometrial hyperplastic processes. In last time actively studied the role of cytokines, matrix metalloproteinases, proteinases from active leukocytes and tissue proteinase inhibitors in the development of endo-metrial hyperplasia [2-4].
In our study infl ammatory cytokines, nonspecifi c local proteinases and their in-hibitors together with immunohistochemical analysis of common leukocyte antigen CD45+ expression in endometrium was investigated to estimate signifi cance of their changes in formation and transformation of endometrial hyperplasia.
238
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
MATERIALS AND METHODSIn investigation include 107 patients who underwent endometrial curettage and/or
hysteroscopy, which were classifi ed into four groups: normal endometrium (NE, n=18) as the control group, simple hyperplasia (sHP, n=41), complex hyperplasia without atypia (cHP, n=36), complex hyperplasia with atypia (cAHP, n=12). Histopathologic classifi cation of endometrial hyperplasia was based on the "International Society of Gynecological Pathologists" criteria. Paraffi n-embedded sections from clinical endo-metrial tissue samples were subjected to immunostaining for CD45+ using antihuman monoclonal antibody to common leukocyte antigen CD45+ (Clone 2B11 + PD7/26) and EnVision™ FLEX+, High pH (DAKO), Code K8024 visualization system, em-ploying a scoring method of the immunohistochemical staining frequency [5]. For either tissue samples examined under an Olympus microscope CX41.
Uterine fl ushing’s for investigation of cytokines and proteolytic enzymes were performed by slowly intrauterine injecting and aspirating 3-4 ml of warm normal saline through a pediatric Foley catheter.
The level of cytokines IL-1β, IL-6 and TNF-α in uterine fl ushing’s investigated by standard ELISA method. The elastase-like (ELA) and trypsine-like (TLA) activi-ties and level of acid-stable inhibitors (ASI) and acid-nonstable antitrypsine activ-ity (ATA) in uterine fl ushing’s were measured by enzyme methods with specifi c synthetic substrates. All results were recalculated to 1 mg of intrauterine fl ushing protein. Total protein were measured by Lowry.
Distribution of the patients' characteristics was presented as mean (SD) for con-tinuous variables, and frequency (%) for categorical variables including immuno-histochemical staining. The Student and Mann-Whitney test was used to compare the mean or median values. A p-value <0.05 was considered statistically signifi cant.
RESULTSThe obtained results showed that the usual histological examination of endome-
trial tissues were stained with eosin and hematoxylin were detected morphological characteristics of chronic infl ammatory process in the endometrium in 67% of pa-tients with simple and complex hyperplasia.
In this connection, we studied endometrial tissue by immunohistochemical analy-sis with the detection of common leukocyte antigen CD45+ expression to determine the severity of infl ammatory process. All patients with endometrial hyperplasia were detected cells expression of CD45+. The number of these cells increased dur-ing the transition from simple to complex hyperplasia, including complex atypical hyperplasia (Fig. 1). So, if in normal endometrium stroma were detected only 4,2 ± 1,2% of cells expressing CD45+, in the simple hyperplasia the percentage of CD45+
increased to 19,9 ± 0,9% (p <0.001), while the complex hyperplasia reached 31,2 ± 2,1% (p <0.001) CD45+ in epithelial space and in the glands lumen. The maximum

239
November 17-20, 2011 Paris, France
level of CD45+ expression 57,8 ± 2,4 % (p <0.001) was observed in cAHP. Thus, there is a clear association between expression common leukocyte antigen, which determines the pool of infl ammatory infi ltration in the endometrial tissue, and with different types of hyperplasia.
Study of local cytokine levels showed that they are also specifi cally refl ect the nature of the infl ammatory process in the endometrium. The level of IL-1β more than in 3 times higher in simple hyperplasia and more than in 20 times higher in complex hyperplasia than in control. In atypical hyperplasia level of IL-1β more than 2 times higher than in women with cHP without atypia. A similar changes characterize IL-6, which in sHP in 5 times higher, in cHP in 10 times higher, and in cAHP in 15 times higher than in control women. More less changes detected in the level of TNF-α. In patients with sHP TNF-α increased in 2 times, in cHP in 2, 5 times and in cAHP in 3 times compared with control.
The formation of a endometrial hyperplasia also led to an increase of proteo-lytic activity in the uterine fl ushing’s. Thus, the activity of elastolytic enzymes sig-nifi cantly increased in 7.5 times in sHP and in 8-9 times in both forms of complex hyperplasia. The level of TLA was signifi cantly elevated in the 2.5 - 3 times in all types of hyperplasia. Antitrypsin activity that characterizes the ability to inhibit trypsin-like proteinase in uterine lavage fl uid did not signifi cantly change. After a slight increase in the sHP take part reduction to its control values in complex en-dometrial hyperplasia. At the same time, acid-stable proteinase inhibitors, which are locally secreted, signifi cantly decreased in 2-3 times in simple and complex hyperplasia and not determined in complex cAHP. Reaction in proteinases and their inhibitors in endometrial hyperplasia should be noted the development of an imbal-ance which is manifested by an increase in the activity of proteases and relative or absolutely defi ciency of proteinase inhibitors development.
Conclusions. It can be assumed that endometrial hyperplasia is associated with the formation and development of infl ammation in the endometrium, which can take part in the development, progression and transformation of endometrial hyperplastic process. It should be noted that in last years important role is given to infl ammation which associated with tumor growth [6], and which is described as one of the com-
Fig. 1 - Immunohistochemical staining for CD45+ expression (×200). (A) Simple hyperplasia (B) Complex hyperplasia without atypia (C) Complex hyperplasia with atypia. EnVision™ FLEX+, High pH visualization system.
240
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
mon hallmarks of cancer [7]. It was showed that "cancer-related infl ammation" may affect the genetic tumor tissue restructuring and stimulate the processes of invasion and metastasis. The results which obtained in our work indicate the important role of infl ammation in the development of hyperplastic processes in the endometrium, which can be interpreted such as «infl ammation associated with endometrial hyper-plasia» or «endometrial hyperplasia-related infl ammation».
Assessment of the severity of infl ammatory changes in the endometrium by the level of cytokines, proteases and their inhibitors in uterine lavage fl uid and leu-kocyte infi ltration by the level of CD45+ expression can be used as criteria of the formation of infl ammatory changes in the endometrium during hyperplasia develop-ment, criteria for assessing the prognosis of endometrial hyperplasia, and also esti-mation the risk factor of endometrial malignancy and the effi ciency of the treatment.
REFERENCES1. AMANT F., MOERMAN P., NEVEN P., et al. Endometrial cancer. Lancet.: 366: 491- 505: (2005).2. KOVALENKO YE., KUBYSHKIN A., LITVINOVA S. Role of nonspecifi c proteolytic enzymes
and their inhibitors in endometrial hyperplasia development. 14 World Congress of Gynecological Endocrinology.: Firens: N.531 (2010).
3. KOVALENKO YE., KUBYSHKIN A., LITVINOVA S., FOMOCHKINA I. Pathology of female reproductive system, infertility and role of proteolytic enzymes and their inhibitirs. 6-th international congress of pathophysiology.: Montreal.: P049: (2010).
4. BOURBOULIA D., STETLER-STEVENSON W.G. Matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs): Positive and negative regulators in tumor cell adhesion. Semin. Cancer Biol.: 20: 161-168: (2010).
5. DABBS D. J. Diagnostic immunohistochemistry. London: Churchill Livingstone, (2006). 6. COLOTTA F., ALLAVENA P., SICA A., et al. Cancer-related infl ammation, the seventh hallmark of
cancer: links to genetic instability. Carcinogenesis.:30 (7):1073–1081: (2009). 7. HANAHAN D., ROBERT A. WEINBERG. Hallmarks of Cancer: The Next Generation. Cell.:144
(5): 646-674: (2011).
© 2012 Monduzzi Editoriale | Proceedings Code: 363
The expression and characterization of endoglin in uterine leiomyosarcoma
H. Matsumura1, K. Shibata1, E. Yamada1, M. Mizuno1, H. Kajiyama1, T. Senga2, F. Kikkawa1
1Department of Obstetrics and Gynecology, 2 Division of Cancer biology; Nagoya University Graduate School of Medicine, Japan
SUMMARYRecently, it was reported that endoglin (CD105) expression was signifi cantly
associated with worse survival in several cancers. In this study, we evaluated the role of endoglin in uterine leiomyosarcoma. We examined the assocication between endoglin expression and outcomes in 22 uterin uterine leiomyosarcoma. Endog-lin positive group had a signifi cantly worse overall survival and progression free survival than endoglin negative group. Additionally, to study the biological role of endoglin, we knocked-down endoglin in uterine leiomyosarcoma cell line. Endoglin knockdown has negative effect on migration, invasion, MMP-9 anctivity and VEGF secretion. Investigation of endoglin may lead to a new strategy of uterine leiomyo-sarcoma therapy.
INTRODUCTIONUterin leiomyosarcoma is a rare but highly malignant tumor. Complete surgical
excision is the standard initial treatment. But there is no established standard adju-vant therapy.
Endoglin (CD105) is a transmembrane glycoprotein that is strongly expressed on vascular endothelial cells and on several other cell types. It is an accessory receptor of the transforming growth factor-β (TGF-β) receptor. Endoglin can modu-late TGF-β signaling and has an important role in angiogenesis. Endoglin knockout mice die in utero owing to defects in vasculogenesis, and mutations in endoglin result in the human vascular disease, hereditary hemorrhagic telangiectasia.
Recently, it was reported that endoglin was associated with pregnancy-induced hypertension, ischemic heart disease and several cancers. In this study, we evaluated the role of endoglin in uterine leiomyosarcoma.
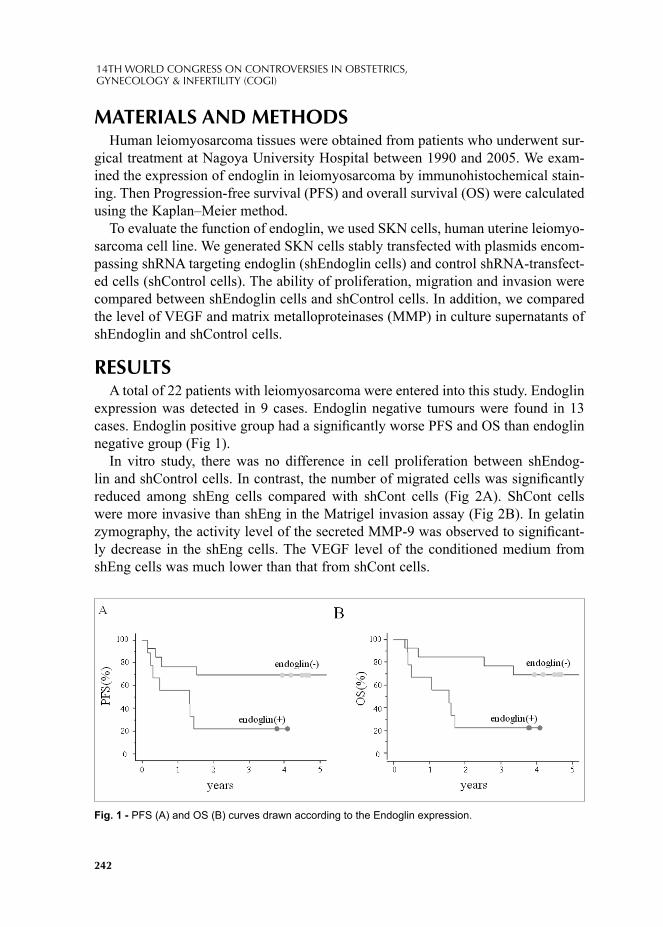
242
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
MATERIALS AND METHODSHuman leiomyosarcoma tissues were obtained from patients who underwent sur-
gical treatment at Nagoya University Hospital between 1990 and 2005. We exam-ined the expression of endoglin in leiomyosarcoma by immunohistochemical stain-ing. Then Progression-free survival (PFS) and overall survival (OS) were calculated using the Kaplan–Meier method.
To evaluate the function of endoglin, we used SKN cells, human uterine leiomyo-sarcoma cell line. We generated SKN cells stably transfected with plasmids encom-passing shRNA targeting endoglin (shEndoglin cells) and control shRNA-transfect-ed cells (shControl cells). The ability of proliferation, migration and invasion were compared between shEndoglin cells and shControl cells. In addition, we compared the level of VEGF and matrix metalloproteinases (MMP) in culture supernatants of shEndoglin and shControl cells.
RESULTSA total of 22 patients with leiomyosarcoma were entered into this study. Endoglin
expression was detected in 9 cases. Endoglin negative tumours were found in 13 cases. Endoglin positive group had a signifi cantly worse PFS and OS than endoglin negative group (Fig 1).
In vitro study, there was no difference in cell proliferation between shEndog-lin and shControl cells. In contrast, the number of migrated cells was signifi cantly reduced among shEng cells compared with shCont cells (Fig 2A). ShCont cells were more invasive than shEng in the Matrigel invasion assay (Fig 2B). In gelatin zymography, the activity level of the secreted MMP-9 was observed to signifi cant-ly decrease in the shEng cells. The VEGF level of the conditioned medium from shEng cells was much lower than that from shCont cells.
Fig. 1 - PFS (A) and OS (B) curves drawn according to the Endoglin expression.
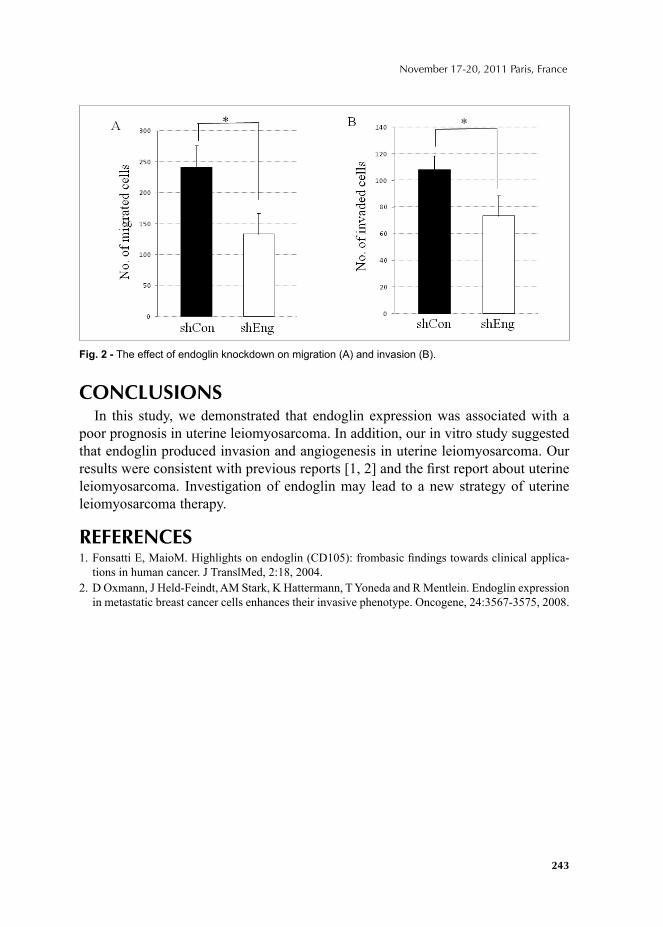
243
November 17-20, 2011 Paris, France
CONCLUSIONSIn this study, we demonstrated that endoglin expression was associated with a
poor prognosis in uterine leiomyosarcoma. In addition, our in vitro study suggested that endoglin produced invasion and angiogenesis in uterine leiomyosarcoma. Our results were consistent with previous reports [1, 2] and the fi rst report about uterine leiomyosarcoma. Investigation of endoglin may lead to a new strategy of uterine leiomyosarcoma therapy.
REFERENCES1. Fonsatti E, MaioM. Highlights on endoglin (CD105): frombasic fi ndings towards clinical applica-
tions in human cancer. J TranslMed, 2:18, 2004.2. D Oxmann, J Held-Feindt, AM Stark, K Hattermann, T Yoneda and R Mentlein. Endoglin expression
in metastatic breast cancer cells enhances their invasive phenotype. Oncogene, 24:3567-3575, 2008.
Fig. 2 - The effect of endoglin knockdown on migration (A) and invasion (B).

© 2012 Monduzzi Editoriale | Proceedings Code: 372
A rare case of invasive vaginal carcinoma associated with complete uterine prolapse
M.M. Melo, E. Gonçalves, A.R. Neiva, A. Almeida, J. Mesquita, A. Carvalho, D. Magalhães, J. MaiaUnidade Local de Saúde do Alto Minho – Hospital De Santa Luzia, Viana do Castelo, Portugal
Summary: Primary cancer of the vagina constitutes 1-2% of all malignant genital tract tumors in women. A a standardized therapy is not established due to it’s rarity and lack of clinical experience. To our knowledge, few cases have been previously reported that assess the clinical experience of primary vaginal carcinoma associ-ated with vaginal prolapse. We present a case report of a 81-year-old female with invasive carcinoma of the anterior wall of the vagina associated with long standing third degree uterovaginal prolapse. The patient was confi rmed to be in an advanced stage – FIGO stage III. Radiation was the main therapy implemented on the present case. Vaginal cancer treatment was controversial previously and current review of literature suggests radiotherapy for advanced stage vaginal carcinoma associated with genital prolapse. Due to early invasion of bladder or rectum and particularly in older patients primary radiotherapy is very common.
INTRODUCTIONCarcinoma of the vagina is considered the rarest of primary gynecological neo-
plasms. It represents 1-3% of gynecological malignancies and it is usually seen in the age group of 60-80 years (its incidence peaks during 60s) [1,2,8,10]. Squamous lesions represent the majority of cases, approximately 85% of all vaginal carcino-mas [11]. Bacterial infection, trauma (especially from pessary use or prolapse) and HPV exposure are suggested to be the main predisposing factors [9].
The most common clinical presentation is genital bleeding. However, urinary tract disturbances and pelvic pain may occur [1]. Based on scarcity of this neoplasm, therapeutic management of this entity is still controversial. Various approaches may be implemented according to invasiveness of tumor and prognostic factors. Radia-

246
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
tion represents the most common therapeutic modality for invasive carcinoma, al-though surgery may be implemented in early tumor stage [1,2].
Genital prolapse associated with primary carcinoma of the vagina is even more uncommon. There are few published cases of combined uterine prolapse and vagi-nal carcinoma and, of our knowledge, none located on anterior wall of the vagina. In this study, the authors report a rare case of primary invasive carcinoma of the anterior wall of the vagina associated with long standing third degree uterovaginal prolapse.
CASE REPORTA 81-year-old patient, gravid 3, para 3, was referred from a primary care unit
with long term third degree uterovaginal prolapse associated with pelvic pain, pallor weight loss and asthenia which have appeared 4 weeks prior. She had presented with complaints of vulvar foreign body sensation for several years along with occasional blood stained discharge and diffi culty in micturition for the last 6 months. Her past medical history included 3 previous pregnancies with 3 normal spontaneous vaginal deliveries and pulmonary emphysema. Without family history of cancer syndromes. On gynecologic examination there was a third degree uterovaginal prolapse with second degree cystocele and fi rst degree rectocele. An extensive exophytic ulcer-ated lesion, with about 5x5cm occupied the middle anterior and right lateral vaginal wall. There was no macroscopical involvement of the cervix with the closest inter-space between the cervix and the vaginal tumor being approximately 3,5cm (Fig.1).
Fig. 1 - Uterovaginal prolapse and exophytic ulcerated lesion.
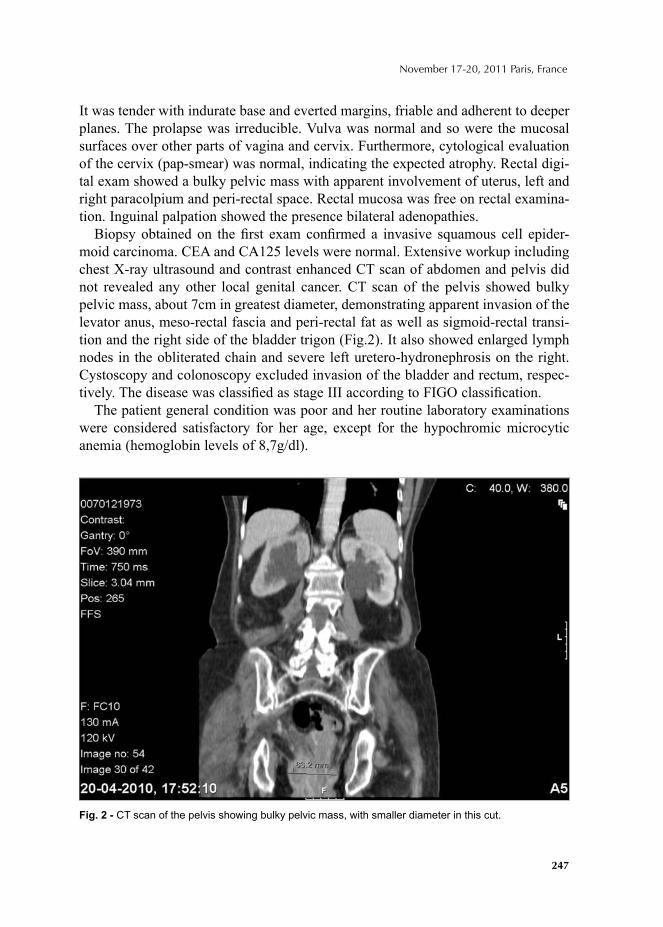
247
November 17-20, 2011 Paris, France
It was tender with indurate base and everted margins, friable and adherent to deeper planes. The prolapse was irreducible. Vulva was normal and so were the mucosal surfaces over other parts of vagina and cervix. Furthermore, cytological evaluation of the cervix (pap-smear) was normal, indicating the expected atrophy. Rectal digi-tal exam showed a bulky pelvic mass with apparent involvement of uterus, left and right paracolpium and peri-rectal space. Rectal mucosa was free on rectal examina-tion. Inguinal palpation showed the presence bilateral adenopathies.
Biopsy obtained on the fi rst exam confi rmed a invasive squamous cell epider-moid carcinoma. CEA and CA125 levels were normal. Extensive workup including chest X-ray ultrasound and contrast enhanced CT scan of abdomen and pelvis did not revealed any other local genital cancer. CT scan of the pelvis showed bulky pelvic mass, about 7cm in greatest diameter, demonstrating apparent invasion of the levator anus, meso-rectal fascia and peri-rectal fat as well as sigmoid-rectal transi-tion and the right side of the bladder trigon (Fig.2). It also showed enlarged lymph nodes in the obliterated chain and severe left uretero-hydronephrosis on the right. Cystoscopy and colonoscopy excluded invasion of the bladder and rectum, respec-tively. The disease was classifi ed as stage III according to FIGO classifi cation.
The patient general condition was poor and her routine laboratory examinations were considered satisfactory for her age, except for the hypochromic microcytic anemia (hemoglobin levels of 8,7g/dl).
Fig. 2 - CT scan of the pelvis showing bulky pelvic mass, with smaller diameter in this cut.

248
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The patient received external pelvic radiotherapy with 20 applications of 30cGy/day (total dose of 600cGy), with good immediate response. Despite that, three months later it has shown a signifi cant clinical worsening and signifi cative increase in invasive growth.
Four months after the diagnosis she was again hospitalized for superfi cial and deep venous thrombosis of left femoral vein. At that time the CT scan of thorax, abdomen and pelvis showed a signifi cant increase in pelvic tumor with distal in-volvement of urethers and consequent bilateral uretero-hydronephrosis, multiple liver metastases, osteolytic metastasis of the iliac bone and right basal pulmonary micronodules also suggestive of metastasis. There was also involvement of the right external iliac vein by this neoplasm, giving rise to external iliac and right common femoral vein thrombosis. She was discharged on the 9th day of hospitalization. Pa-tient died fi ve months after the diagnosis.
DISCUSSIONVaginal ulcer associated with long stand genital prolapse need careful evalua-
tion for underlying carcinoma. There is a paucity of information on the etiology and management of squamous cell vaginal cancer due to the rarity of the disease. Most vaginal tumors are metastatic in nature with primary focus in the cervix or endometrium [11]. So, the appropriate diagnosis of primary vaginal carcinoma is based on exclusion of concomitant gynecologic cancer and no recurrence after at least 5 years prior to gynecological cancer. [1]. Thus, genital tumors which extend to vagina and reach outer ostium of cervix or those with vulva or urethra involve-ment are generally classifi ed as cervical carcinomas or primary vulva and urethral cancers, respectively [1,2].
The management of vaginal cancer depends upon its prognostic factors, i.e. size, location, and extent of tumor, patient’s age, clinical staging and histological clas-sifi cation [1,2], but radiotherapy is generally the most preferred modality of treat-ment for invasive vaginal cancers [1,2]. Treatment planning is important, thereby considering the extent, volume and location of tumor as critical variables related to radiation techniques and doses to be used.
There have been reported extremely rare cases of vaginal carcinoma with genital prolapse [1,3-8] and, to our knowledge, a case referring to a lesion of the anterior wall of the vagina has not been published in the most current literature. Tumors usually occur in the upper third of the vagina in about 50% of cases, with more than one-half of them arising from the posterior vaginal wall [12]. It has been established clinically that the prolapsed uterus, although exposed to constant mechanical irrita-tion, is remarkably free from the risk of cancer [3]. However, when present, vaginal carcinoma usually presents as an ulcerative lesion. It is believed that continued irri-tation and chronic infl ammation of the exposed vagina and underlying cancer lesion contributes to these ulcerative lesions [8].

249
November 17-20, 2011 Paris, France
The clinical stage of the primary malignancy is quite often more advanced in elderly patients because of delay in recognize warning symptoms and signs and avoidance medical-gynecological examination.
In our case, patient had a history of genital prolapse of more than 10 years’ dura-tion, long before any lesion could be noted, suggesting that neoplasia appeared after the prolapse. The fi rst complaint is usually vaginal discharge with or without bleed-ing, sign that was present in our case too.
Still, no consensus exists regarding the proper treatment of this particular cancer, partly because of the rarity of the disease. Current review of literature suggests ra-diotherapy for advanced stage vaginal carcinoma associated with genital prolapse. Because of the poor prognosis with radiation alone (predominantly local failures) [13], some investigators advocate the combined use of radiation and concurrent chemotherapy (as used for cervical or vulvar cancer) in woman with high-risk dis-ease (eg, stage III or IV, or tumor size larger than 4cm) [14]. Based on the large size and upper location of tumor and patient’s age, primary radiotherapy was con-sidered the most appropriate approach by the authors; chemotherapy has not been made because of poor clinical condition of the patient. Uterovaginal prolapse or its complications such as ulceration, bleeding or urinary retention will not change the management guidelines in advanced stage vaginal carcinoma with prolapse. Radio-therapy also causes fi brosis in the parametrial tissue with a possible retraction of the prolapsed uterus.
Advanced stage is associated with high morbidity and fi ve year survival is 42% if diagnosed in stage III, according to the latest FIGO statistics. The treatment choice should be considered particularly for patients with advanced stage disease in their later years in such a way that the treatment may only be marginally different with respect to survival, but signifi cantly different in the impact of quality of life.
REFERENCES1. BATISTA TP, MORAIS JA, REIS TJ, MACEDO FI (2009) A rare case of invasive vaginal carci-
noma associated with vaginal prolapse. Arch Gynecol Obstet 280:845-848. Doi: 10.1007/s00404-099-1016-1
2. BENEDET JL, BENDER H, JONES HIII, NGAN HY, PECORELLI S (2000) FIGO staging clas-sifi cations and clinical practice guidelines in the management of gynecologic cancers. Int J Gynecol Obstet 70(2):209-262. Doi: 10.1016/S0020-7292(00)00300-3
3. IAVAZZO C, VOGIAS G, VECCHINI G, KATSOULIS M, AKRIVOS T (2006) Vaginal carci-noma in a completely prolapsed uterus. A case report. Arch Gynecol Obstet 275(6):503-5056. Doi: 10.1007/s00404-006-0284-2
4. KARATEKE A, TUGRUL S, YAKUT Y, GURBUZ A, CAM C (2006) Management of a case of primary vaginal cancer with irreducible massive uterine prolapse - a case report. Eur J Gynaecol Oncol 27(5):528-530
5. RESALLA S, MURIA EF, RIBEIRO JU (1994) Carcinoma of the vagina associated to genital pro-lapse in nullipara patient: case report. J Bras Ginecol 104(3):63/65
250
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
6. RAO K, KUMAR NP, GEETHA AS (1989) Primary carcinoma of the vagina with uterine prolapse. J Indian Med Assoc 87(1):10-12.
7. GUPTA N, MITTAL S, DALMIA S et al (2007) A rare case of primary invasive carcinoma of va-gina associated with third degree uterovaginal prolapse. Arch Gynecol Obstet 276:563-564. Doi: 10.1007/s00404-007-0415-4.
8. GHOSH SB, TRIPATHI R, MALA YM et al (2008) Primary invasive carcinoma of vagina with third degree uterovaginal prolapse: a case report and review of literature. Arch Gynecol Obstet 279(1):91-93. Doi: 10.1007/s00404-008-0815-0.
9. TRAN PT, SU Z, LEE P et al (2007) Prognostic factors for outcomes and complications for primary squamous cell carcinoma of the vagina treated with radiation. Gynecol Oncol 105:641.
10. JEMAL A, SIEGEL R, XU J, WARD E (2010) Cancer statistics. CA Cancer J Clin 60:277.11. ELKAS JC, BEREK JS. Vaginal cancer. Up to date.12. GRIGSBY PW (2002) Vaginal Cancer. Curr Treat Options Oncol 3:125.13. FONSECA AM, PEREYRA EA, VALENTE SE et al (1988) Colposcopic cytologic and histologic
fi ndings in patients with uterine prolapse of second and third degree. Arq Bras Med 62(4):273-275.14. BEREK JS, HACKER NF (Eds). Practical Gynecologic Oncology, 3rd ed, Lippincott Williams &
Wilkins, Philadelphia, 2000.
© 2012 Monduzzi Editoriale | Proceedings Code: 393
Is adjuvant chemotherapy necessary for stage IA ovarian clear cell carcinoma?
M. Mizuno1, H. Kajiyama1, E. Yamada1, H. Matsumura1, F. Kikkawa1 1Department of Obstetrics and Gynecology, Nagoya University Graduate School of Medicine, Japan
SUMMARYThis study was designed to evaluate the outcomes associated with the inclu-
sion or exclusion of adjuvant therapy following comprehensive surgery in pa-tients with stage I clear cell carcinoma (CCC). Median follow-up was 64 months. Among total of 184 patients with stage I CCC, there were 41, 93 and 50 in sub-stages IA, intraoperative capsule ruptured IC (rupture-IC), and all other IC, re-spectively. The 5-year recurrence-free survival (RFS) were 97.6, 87.8, and 70.4% p<0.001, respectively. There was no signifi cant difference between adjuvant chemotherapy(AC) and no therapy groups in RFS (IA 93.8% vs. 100%, rupture-IC 86.6%vs. 94.1).AC was not also demonstrated as signifi cant prognostic factor in multivariate analysis. The routine adjuvant chemotherapy may be unnecessary for patients with at least stage IA.
INTRODUCTIONSeveral studies have found that postoperative chemotherapy improves re-
currence-free survival (RFS) in patients with early-stage epithelial ovarian car-cinoma1. Conversely, some authors advocated not administering any adjuvant treatment following comprehensive surgery in patients with stage IA and grade 1 disease1,2. Advanced clear cell adenocarcinoma (CCC) is resistant to most treat-ments, thus, even stage I is treated as a high-grade tumor. Recently, some reports on stage IA CCC have shown decent prognosis3. The effi cacy of treating stage I with adjuvant therapy has yet to be established.
This study retrospec tively evaluated whether a large number of patients with CCC benefited from adjuvant therapy followed by comprehensive surgical staging.
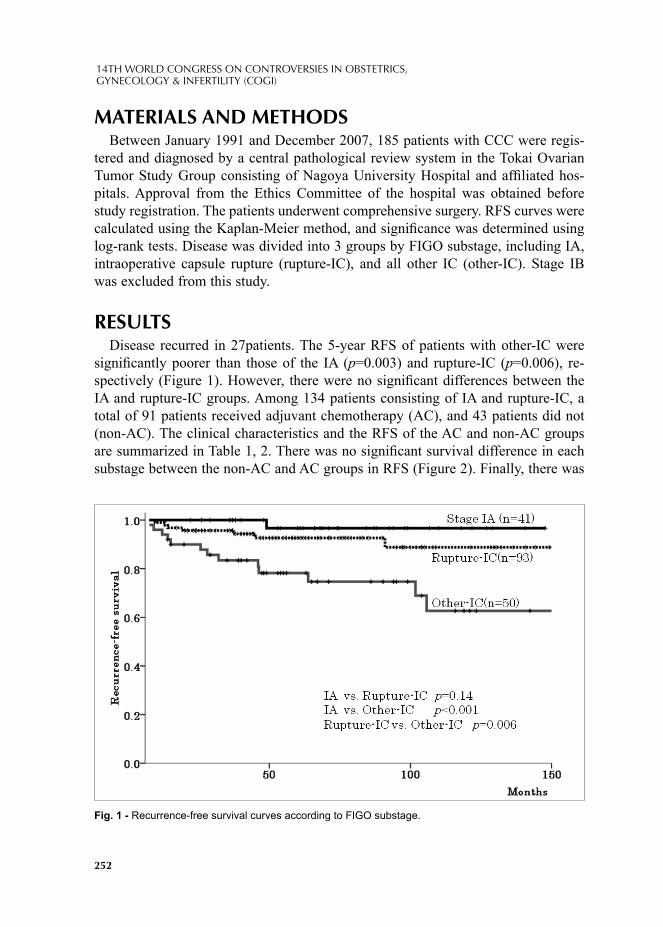
252
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
MATERIALS AND METHODSBetween January 1991 and December 2007, 185 patients with CCC were regis-
tered and diagnosed by a central pathological review system in the Tokai Ovarian Tumor Study Group consisting of Nagoya University Hospital and affi liated hos-pitals. Approval from the Ethics Committee of the hospital was obtained before study registration. The patients underwent comprehensive surgery. RFS curves were calculated using the Kaplan-Meier method, and signifi cance was determined using log-rank tests. Disease was divided into 3 groups by FIGO substage, including IA, intraoperative capsule rupture (rupture-IC), and all other IC (other-IC). Stage IB was excluded from this study.
RESULTSDisease recurred in 27patients. The 5-year RFS of patients with other-IC were
signifi cantly poorer than those of the IA (p=0.003) and rupture-IC (p=0.006), re-spectively (Figure 1). However, there were no signifi cant differences between the IA and rupture-IC groups. Among 134 patients consisting of IA and rupture-IC, a total of 91 patients received adjuvant chemotherapy (AC), and 43 patients did not (non-AC). The clinical characteristics and the RFS of the AC and non-AC groups are summarized in Table 1, 2. There was no signifi cant survival difference in each substage between the non-AC and AC groups in RFS (Figure 2). Finally, there was
Fig. 1 - Recurrence-free survival curves according to FIGO substage.
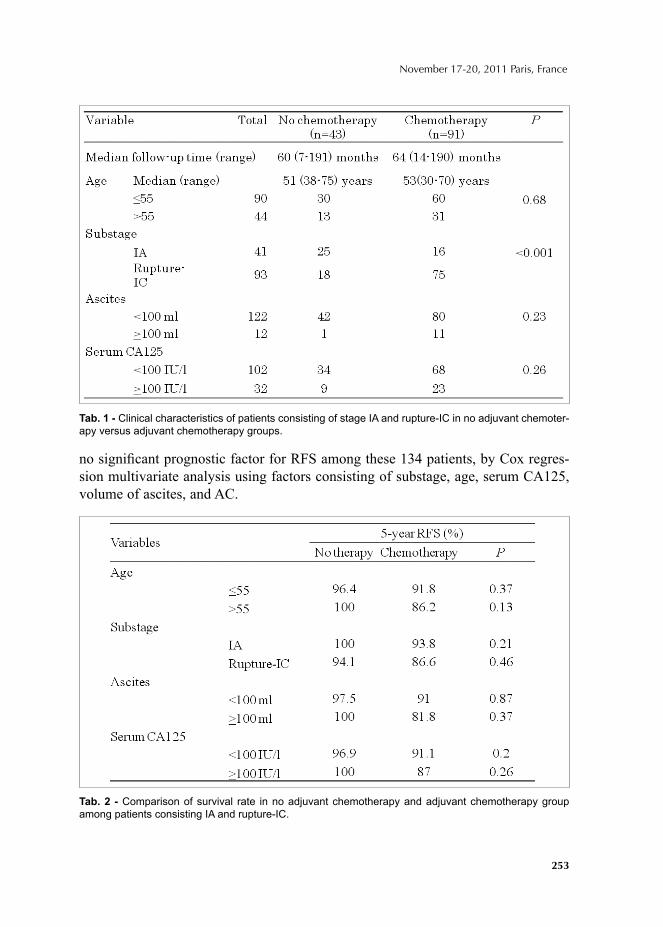
253
November 17-20, 2011 Paris, France
no signifi cant prognostic factor for RFS among these 134 patients, by Cox regres-sion multivariate analysis using factors consisting of substage, age, serum CA125, volume of ascites, and AC.
Tab. 1 - Clinical characteristics of patients consisting of stage IA and rupture-IC in no adjuvant chemoter-apy versus adjuvant chemotherapy groups.
Tab. 2 - Comparison of survival rate in no adjuvant chemotherapy and adjuvant chemotherapy group among patients consisting IA and rupture-IC.

254
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
CONCLUSIONSIs impossible to lead to a defi nite conclusion precluding AC for Stage I CCC by
this retrospective study. However, these results indicate that AC does not contribute to the improving prognosis of stage IA or rupture-IC CCC. For histologically con-fi rmed CCC, the routine AC after comprehensive surgical staging may be unneces-sary for patients with at least stage IA.
REFERENCES1. Trimbos JB, Vergote I, et al. Impact of adjuvant chemotherapy and surgical staging in early-stage
ovarian carcinoma: European Organization for Research and Treatment of Cancer-Adjuvant Chemotherapy in Ovarian Neoplasm trial. J Natl Cancer Inst. 95(2):113-125, 2003.
2. Young RC, Walton LA, et al. Adjuvant therapy in stage I and stage II epithelial ovarian cancer. Results of two prospective randomized trials. N Engl J Med.; 322(15):1021-1027.,1990.
3. Chan JK, Teoh D, et al. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecol Oncol.; 109(3):370-376. 2008.
Fig. 2 - Recurrence-free survival curves in patients with stage IA according to adjuvant chemotherapy.
© 2012 Monduzzi Editoriale | Proceedings Code: 429
Comparing Metformin and Pioglytazone in polycystic ovary
N. Navali, S.TagaviTabriz University of Medical Sciences, Women's Reproductive Health Research Center, Tabriz, Iran
Objective: The aim of this study is to compare therapeutic effects of Metformin and Pioglitazone in Polycystic ovary syndrome (PCOS).
Methods: In a randomized clinical trial, 100 women with PCOS, were recruited during one year period in an educational hospital in Tabriz, Iran. These patients were randomized into two groups of 50 patients receiving either Metformin pill, 500 mg TDS, or Pioglitazone pill, 15 mg BID, for six months. Clinical and laboratory fi ndings were compared between the two groups at the baseline and at the end of the study.
Results: Pregnancy frequency was higher in Metformin group amelioration of menstrual cycles, hirsutism, and laboratory tests, including FBS, hyperinsulinemia, oral glucose tolerance test, 2hpps and insulin, free testosterone and prolactin was signifi cant in both groups. The change of serum total cholesterol and HDL was not signifi cant in the Pioglitazone group.
Conclusion: According to our results, Metformin is superior to Pioglitazone due to better infl uence on pregnancy and lipid profi le.
Key words: Polycystic Ovary Syndrome, Metformin, Pioglitazone
INTRODUCTIONPolycystic ovary syndrome (PCOS) is the most common endocrine disorder in
reproductive ages, the most common cause of infertility due to ovulatory disorder and makes up 73% of the causes of hirsutism in this age group1-2. The diagnosis of the disease is made according to the Netherland criteria when at least two of the three criteria mentioned below exist: polycystic ovaries detected by ultraso-nography, irregular menstrual bleeding, hyperandrogenism3-4. PCOS‘s etiology is complicated and still unknown, but there is some kind of insulin resistance due to changes of two types of cytochrome p450 producing genes. So far, we conducted a study comparing therapeutic results of Metformin and Pioglitazone, two antidia-
256
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
betic drugs with different structures and mechanisms of actions1-4-5. In addition, due to the probable genetic basis of the disease, the effect of these two drugs may vary in our area. So, comparison of the effectiveness of these two drugs in PCOS patients seems necessary which may help us choosing the more effective and convenient drug in controlling clinical and vitro signs of PCO.
METHODS & MATERIALSIn a randomized clinical trial in an educational and health center of Tabriz Uni-
versity of Medical Sciences in Iran, during 12 months period between 2008/11 and 2009/11, 100 women with PCO were randomly divided into two groups of 50 pa-tients and treated with Metformin or Pioglitazone for six months. Clinical and labo-ratory changes in the two groups were compared. In Pioglitazone group, 6 people withdrew the study due to weight gain during the few weeks beginning the study, which were replaced with six other patients.
Metformin with dose of 1500 mg per day in three divided doses or Pioglitazone 15 mg bid, were administered for 6 months. Clinical and laboratory parameters, including pattern of menstrual cycles, hirsutism, and FBS, hyperinsulinemia, oral glucose tolerance test(GTT), 2hpps and insulin, free testosterone and prolactin were determined and measured at the baseline and at the end of the six months period. Fertility rate was also studied in patients who had this desire.
This study has been approved by the Ethical Committee of Tabriz University of Medical Sciences.
After collecting data, all were interred SPSS software and analyzed. In this re-search, statistical and descriptive analysis, and statistical indices like mean, median and Chi-square and independent t-test were used to compare the means. It should be mentioned that P less than 0.05 is considered to be meaningful.
RESULTSMean age of Metformin group patients was 26.8±4.5 year and in Pioglitazone
group patients was 28.8±5.2 year (P=0.051). Mean BMI of Metformin group pa-tients was 27.9±0.9 and in Pioglitazone group patients was 27.8±0.7 (P=0.449). Mean gravidity of Metformin group patients was 0.3±0.7 and in Pioglitazone group patients was 0.2±0.4 (P=0.394).
Forty four percent of Metformin group patients and 34% of Pioglitazone group patients had primary infertility, 30% of Metformin group patients and 38% of Pio-glitazone group patients had secondary infertility, 10% of Metformin group patients and 12% of Pioglitazone group patients were single and 16% of patients in both groups were fertile.
Skin rash was observed in 4% of Metformin group patients, Galactorrhea in 12% of Metformin group patients and alopecia was found in 4% of patients in both groups.

257
November 17-20, 2011 Paris, France
Ten and three patients of Metformin and Pioglitazone groups were pregnant at the end of study respectively. So the frequency of pregnancy was signifi cantly more prevalent in Metformin group patients than in Pioglitazone group (P=0.037).
Frequency(%) of Irregular menstrual cycles, hirsutism, Abnormal GTT and Hy-perinsulinemia at baseline and at the end of study is showed in table 1. Laboratory fi ndings of patients at baseline and at the end of study is showed in table 2.
DISCUSSIONIn our study, we evaluated and compared the results of treatment with Metformin
and Pioglitazone in PCOS for six months. At the end of the study, normalized cy-cles, improved hirsutism, glucose tolerance test, hyperinsulinemia, free testosterone and prolactin, were seen in both groups. In Pioglitazone group, incontrast of Metfor-min group, HDL and total cholesterol changes were not signifi cant and triglyceride level of serum was signifi cantly increased at the end of the study.
Frequency of pregnancy in Metformin group was signifi cantly higher. In a meta-analysis study, Pillai et al(2007) investigated all the studies conducted
in this fi eld and fi nally concluded that the information in this fi eld is not suffi cient for a defi nite decision. Low number of samples and inconvenient methods of studies in this fi eld, in addition to the low number of these studies have been mentioned as the main constraints6.
In our study, we showed that Pioglitazone has no desirable effect on lipid profi le and especially the level of serum triglycerides. On the other hand, at the baseline, 6 cases of Pioglitazone group withdrew the study complaining of weight gain. This is one of the major constraints for using Pioglitazone. Moreover, the frequency of pregnancies in Metformin recipients group was signifi cantly higher. This may be due to the low dose of Pioglitazone used because of the lack of similar study in our patients- and fear of complications. Since ovulation and pregnancy probability is greater with higher dose of Pioglitazone, low rate of pregnancy in Pioglitazone group can be explained.
Tab. 1 - Frequency (%) of Irregular menstrual cycle, hirsutism, Abnormal GTT and Hyperinsulinemia at baseline and the end of study.
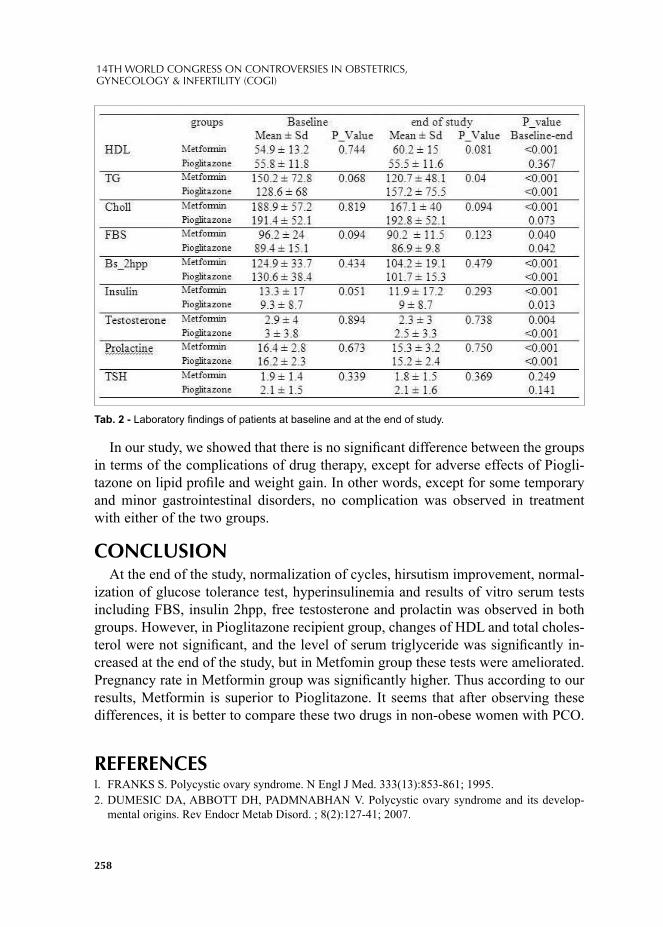
258
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
In our study, we showed that there is no signifi cant difference between the groups in terms of the complications of drug therapy, except for adverse effects of Piogli-tazone on lipid profi le and weight gain. In other words, except for some temporary and minor gastrointestinal disorders, no complication was observed in treatment with either of the two groups.
CONCLUSIONAt the end of the study, normalization of cycles, hirsutism improvement, normal-
ization of glucose tolerance test, hyperinsulinemia and results of vitro serum tests including FBS, insulin 2hpp, free testosterone and prolactin was observed in both groups. However, in Pioglitazone recipient group, changes of HDL and total choles-terol were not signifi cant, and the level of serum triglyceride was signifi cantly in-creased at the end of the study, but in Metfomin group these tests were ameliorated. Pregnancy rate in Metformin group was signifi cantly higher. Thus according to our results, Metformin is superior to Pioglitazone. It seems that after observing these differences, it is better to compare these two drugs in non-obese women with PCO.
REFERENCESl. FRANKS S. Polycystic ovary syndrome. N Engl J Med. 333(13):853-861; 1995. 2. DUMESIC DA, ABBOTT DH, PADMNABHAN V. Polycystic ovary syndrome and its develop-
mental origins. Rev Endocr Metab Disord. ; 8(2):127-41; 2007.
Tab. 2 - Laboratory fi ndings of patients at baseline and at the end of study.
259
November 17-20, 2011 Paris, France
3. FULGHESU AM, ANGIONI S, FRAU E. Ultrasound in polycystic ovary syndrome the measuring of ovarian stroma and relationship with circulating androgens: results of a multicentric study. Hum Reprod. 22(9):2501-2508; 2007.
4. HARWOOD K, VUGUIN P, DIMARTINO-NARDI J. Current approaches to the diagnosis and treatment of polycystic ovarian syndrome in youth. Horm Res. 68(5):209-217; 2007.
5. VELAZQUEZ EM, MENDOZA S, HAMER T. Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy. Metabolism. 43:647-654; 1994.
6. PILLAI A, BANG H, GREEN C.Metformin and glitazones: do they really help pcos patients? J Fam Pract. 56(6):444-45; 2007.

© 2012 Monduzzi Editoriale | Proceedings Code: 465
An explorative study upon factors that contribute to contraceptive-seeking behaviour among married Sudanese women in Khartoum, Sudan
T. Parekh, J. ParrUniversity of Leeds, Leeds, UK
SUMMARYThe contraceptive prevalence rate (CPR) among married Sudanese women is es-
timated at 7.6%. Reports suggest that poor accessibility and cost of services are major infl uential factors. However, contraceptive use among Sudanese populations is under-researched. This study therefore, explores and identifi es key factors that contribute to contraceptive-seeking behaviour. Semi-structured interviews were un-dertaken with 30 participants. Thematic data analysis reveals that 83% of respon-dents gave importance to the role of men in the decision to use a contraceptive.
INTRODUCTIONFamily planning (FP) and contraceptive use is essential in reducing a rapidly
growing population rate, and is also a key intervention to prevent risks directly associated with maternal mortality.1,2 In Sudan there is a striking relationship be-tween unplanned pregnancies, high parity and maternal mortality ratio (MMR).1,3,4 National surveys report that MMR is 638 and 2,005 per 100,000 live births for the north and south of Sudan respectively.5,6 The estimated CPR among married Sudanese women aged 15-49 years is 7.6%, one of the lowest reported CPRs in the East Mediterranean region.7 A number of underreported maternal deaths and an increasingly large internally displaced population conceal the reality of the current situation in Sudan.7,8
There are multiple benefi ts of contraceptive use, it empowers women to be in control of their pregnancies and plan them so that there is suffi cient time between each birth (birth spacing).9,10 Population-reports-indicate that women who have in-tervals for at least 27 months between each birth can signifi cantly-reduce risks of
262
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
maternal deaths.11,12 This can be achieved through the use of modern contraceptive methods. Despite the integration of FP in the current reproductive health (RH) pro-gramme, the use of modern contraceptives in Sudan is far from targets set by the government.13 Previous reports have identifi ed that the decision to use contraception is largely determined by a range of factors.1,2,13
The purpose of this research is to-gain-an in-depth understanding-of-the-use-and-access-of contraceptive methods-among-married-Sudanese women, aged-16-49-years, in Khartoum. It is hoped that exploration of attitudes, beliefs and perceptions of married women and service providers will enable policy-makers and stakehold-ers of existing FP programmes to improve services in a manner that will increase modern contraceptive use amongst the population.
MATERIALS AND METHODSA qualitative research design was adopted, ethical approval was granted by the
University of Leeds and the Federal Ministry of Health of Khartoum (MoH). In-formed consent was gained from all participants in either written or verbal form before they participated in the study.
The study was undertaken in the capital state of Sudan, Khartoum, in June 2010. Semi-structured interviews (SSIs) were carried out with health workers (HW) and married Sudanese women. A focus group discussion (FGD) was also undertaken with HWs to explore the quality of service provision offered to married women.
Participants were divided into three groups; service users (SUs), non-service us-ers (NSUs) and HWs. Purposive and convenient sampling techniques were adopted to recruit all participants who met the inclusion criteria (table 1). A snowballing sampling method was specifi cally adopted to recruit NSUs.
A total of 30 participants were recruited in the study. Secondary data collec-tion, participant observation and informal interviews enabled triangulation, thus
Tab. 1 - Inclusion criteria for participant recruitment.

263
November 17-20, 2011 Paris, France
improving the credibility of fi ndings. Pilot interviews were undertaken to ensure the appropriateness of questions within the socio-cultural context of Sudan. Each interview was recorded using a dictaphone; a separate dictaphone was used to re-cord informed verbal consent. Two female translators were hired, one translator was present in the SSIs and FGD conducted, whilst the other confi rmed the accuracy of translations made. The ‘three stage approach to thematic content analysis (TCA)’ was adopted to analyse the data. The themes were then analysed and compared with fi ndings from existing literature.
RESULTS AND DISCUSSIONFrom the sample population, it was also found that 86% of married women inter-
viewed were Muslim and 60% of women were currently housewives. There was no signifi cant difference between the age of marriage and average number of children between SUs and NSUs. The average age of marriage among SUs and NSUs is 20 and 19.5 respectively. In addition, the average number of children per SU and NSU was 3.9 and 4.1 respectively.
According to respondents, approval of spouse, social infl uences and religious be-liefs were major factors that contribute to contraceptive-seeking behaviour. Married Sudanese women currently using contraceptives indicated that fi nancial constraints and current medical illness motivated contraceptive-seeking behaviour. Traditional family planning methods and poor knowledge were major factors accountable for poor modern contraceptive awareness within the communities. Subsequently, ob-servations demonstrated that lack of time in consultations prevented patients from receiving suffi cient information upon various contraceptive methods available to them. The majority of reasons for contraceptive use were justifi ed by religious be-liefs. Data comparison revealed that 86% of total respondents conceived within fi rst 12 months of being married, respondents claimed that ‘contraceptive use before conceiving a child shows ignorance to Allah’s gifts’. Method of choice is also re-stricted by religious beliefs as SUs claimed that Islam prohibits condom use as ‘it reduces the pleasure’ and results in dissatisfaction for the male partner.
From the total study population, 83% of participants gave importance to the role of men in the decision to use contraceptive methods. The majority of HWs claimed ‘receiving approval from the woman’ spouse is most important’, 5 HWs claimed that women are advised to seek permission from their spouse before they attend FP clinic. If however, the spouse still disapproved, 50% of HWs claimed that they would not prescribe the contraceptive to the client. Although this may be an effec-tive strategy to increase the role of men in FP, it seems to be creating a negative impact upon women’s autonomy. Many NSUs also expressed the belief that ‘taking contraceptives would result in divorce’. Ironically, the RH policy 2010 formulat-ed, states that women should have free-will over any decision regarding their own health. 15

264
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
Participant observations reveal that women commonly attended appointments alone, on many occasions; contraceptives were hidden in a disguised container to prevent confl ict amongst partners. In addition to this, the possibly of facing disap-proval led 30% of SUs to also purchase contraceptive methods such as the oral contraceptive pill (OCP) over-the-counter in local pharmacies. Although, the avail-ability of contraceptive methods in pharmacies may seem promising, purchasing methods without receiving counselling upon potential risks associated can result in unexpected health outcomes.
Contrary to expectations, this study did not fi nd a signifi cant difference in the age or level of education between SUs and NSUs. Results from a national survey demonstrated a positive correlation between low CPRs and low literacy rates.6 The fi ndings strongly contradict this as there was little variation in the level of education between SUs and NUs. Evidence upon whether socio-economic status affects the use of contraception is inconclusive, as the socio-economic statuses of participants were not recorded. Furthermore, cost and access to services were not considered as barriers to contraceptive use, however the study was undertaken in a predominantly urban population, therefore may not represent women from rural areas, who may fi nd these factors as signifi cant contributors to decision-making.
CONCLUSIONOn the basis of this study, it is clear that the majority of factors that contribute
to contraceptive-seeking behaviour are pre-determined by deep-rooted cultural and/or religious beliefs of married Sudanese women. Attempting to achieve changes in negative attitudes towards modern contraceptives is a timely process. However, increased involvement of social agents to raise awareness of the benefi ts of modern contraceptives may facilitate this change. It is recommended that current educa-tional campaigns focus particularly upon raising awareness of modern contracep-tives and increase involvement of men in FP. Involvement of community religious leaders in planning and implementing initiatives in existing FP programmes would be an effective strategy to remove concerns that religion prohibits contraceptive use.
REFERENCES1. WHO, UNICEF, UNFPA, The World Bank. Maternal Mortality in 2005 [online]. 2007. World
Health Organisation. Available from: www.who.int/WHOSIS/mme_2005.pdf2. STROVER J, ROSS J. How contraceptive use affects maternal mortality. Health Policy and
Initiative, USAID. 1-12, 2008. 3. WHO. Primary Health Care: no more than ever. The world health report [online].2008.World
Health Organisation. Available from: www.who.int/whr/2008/whr08_en.pdf4. Population Action International. A Measure of Commitment. Women’s Sexual and Reproductive
risk. Index for Sub Saharan Africa. Centre for the study of adolescence and population action international, 4-8, 2008.
265
November 17-20, 2011 Paris, France
5. Sudan Household Survey and Millennium Development Goal indicators. Summary of Findings [online]. 2006. Available from: www.irinnews.org/pdf/pn/SHHSreport.pdf
6. Sudan 1989/1990: Results from the demographic and health survey. Studies in Family Planning, 23(1), pp. 66-70, 1991.
7. WHO. East Mediterranean Regional Health System Observatory. Health System Profi le: Sudan [online]. 2006. World Health Organisation. Available from: www.emro.who.int/HealthSystemObservatory/PDF/Sudan/Full%20Profi le.pdf
8. SHOKAI TB, GADIR KA, ELABBASI M, ELBASHIR IA, SALIH M, ELTIGANI L. The National Reproductive Health Policy. Sudan Government of National Unity. Federal Ministry of Health. 2010.
9. NORTON M, GRIFFIN J. Birth Spacing, a call for action. Birth intervals of three years or longer for infant and child health [online]. 2003. USAID. Available from: www.usaid.gov/our_work/global_health/pop/techareas/birthspacing/index.html
10. MEHTA S. Contraception and Women’s Health. Int J Gynaecol Obstet,46, pp.165-171, 1994.11. Sudan Population Consensus, Central Bureau of Statistics Khartoum, 2008.12. Population Council. Annual Report. Strengthening Local Resources, Sudan [online]. 2004.
Available from: www.popcouncil.org/about/ar40/srl.html13. Khartoum State Ministry of Health. Plans and Strategies of Health Services in Khartoum State.
Unpublished, 2003.

© 2012 Monduzzi Editoriale | Proceedings Code: 576
Lynch Syndrome – a case report
A.M. Sousa1, A.M. Coelho1, M. Bernardino1, A.S. Gomes1, A.F. Jorge1, I. Claro2 1Serviço de Ginecologia; 2 Serviço de Gastrenterologia e Clínica de Risco Familiar. Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E, Lisboa, Portugal
SUMMARYLynch Syndrome (LS) is an autosomal dominant disease caused by germline
pathogenic mutations in one of the DNA mismatch repair (MMR) genes, most of-ten MLH1 and MSH2. LS patients have a high risk of developing colorectal cancer (CRC) and several other extracolonic malignancies, especially endometrial cancer (EC). LS is also the most common cause of hereditary endometrial cancer.
INTRODUCTIONLS or hereditary non-polyposis colorectal cancer, is caused by pathogenic germ-
line mutations in one of the DNA MMR genes MLH1, MSH2, MSH6, or PMS2. This syndrome is characterized by a high risk of early onset colorectal cancer and several other extracolonic malignant tumors, especially EC.1 Since this syndrome does not display a characteristic phenotype, the diagnosis is based on the careful harvesting of family history of malignancy. The clinical diagnosis of LS is based on Amsterdam criteria (Table 1), fi rst published in 19912 and revised in 1999.3 The last criteria include non-colonic tumors in addition to CRC. In these families genetic testing is indicated, and nearly 90% of all mutations identifi ed are located in MLH1 and MSH2 genes, being MSH6 and PMS2 genes less frequently involved.
CASE REPORTWe report a case of a 31-year-old woman presenting with metrorrhagia and pain in
the left fl ank. She had been submitted to a colonic polypectomy four years ago. The histological diagnosis of this polyp was unknown. The family medical history revealed: mother with CRC at age 31, father with an urothelial tumor at age 55, paternal grand-mother with endometrial carcinoma at age 60 and paternal aunt with an ovarian tumor at age 50. (Figure 1).
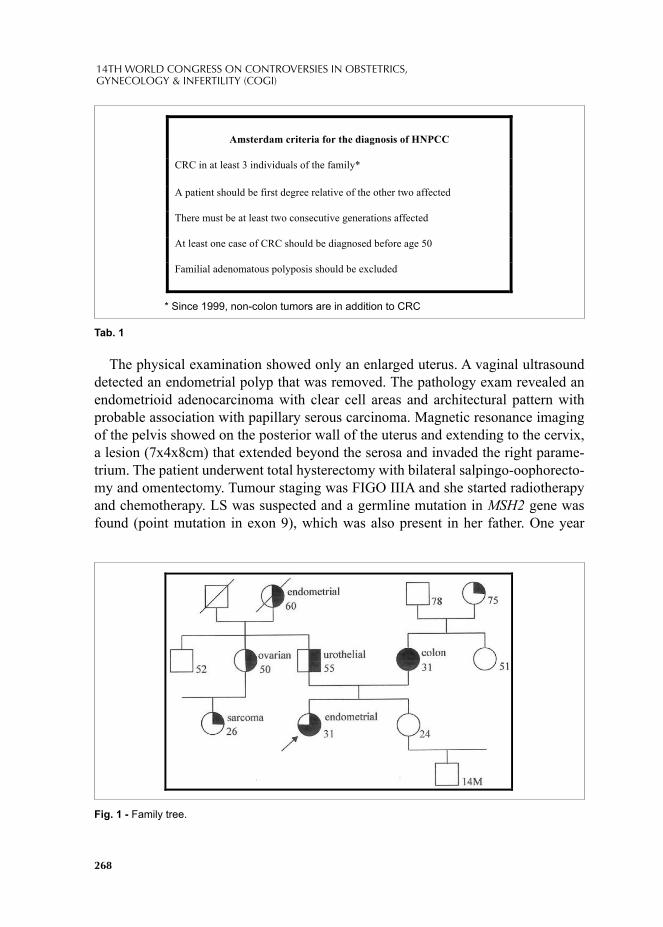
268
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
The physical examination showed only an enlarged uterus. A vaginal ultrasound detected an endometrial polyp that was removed. The pathology exam revealed an endometrioid adenocarcinoma with clear cell areas and architectural pattern with probable association with papillary serous carcinoma. Magnetic resonance imaging of the pelvis showed on the posterior wall of the uterus and extending to the cervix, a lesion (7x4x8cm) that extended beyond the serosa and invaded the right parame-trium. The patient underwent total hysterectomy with bilateral salpingo-oophorecto-my and omentectomy. Tumour staging was FIGO IIIA and she started radiotherapy and chemotherapy. LS was suspected and a germline mutation in MSH2 gene was found (point mutation in exon 9), which was also present in her father. One year
Tab. 1
Fig. 1 - Family tree.
Amsterdam criteria for the diagnosis of H PCC
CRC in at least 3 individuals of the family*
A patient should be first degree relative of the other two affected
There must be at least two consecutive generations affected
At least one case of CRC should be diagnosed before age 50
Familial adenomatous polyposis should be excluded
* Since 1999, non-colon tumors are in addition to CRC

269
November 17-20, 2011 Paris, France
later, during a colonoscopy a tubular adenoma with low grade dysplasia was ex-cised. Three years later similar adenoma was excised.
The patient has been followed also in the Familial Risk Clinic. The family carri-ers of this mutation are now under surveillance for LS associated cancers.
DISCUSSIONIn LS lifetime risk of EC is estimated between 27 and 71%4 and EC may be the
presenting tumor. Currently genetic testing is proposed in women with EC if their family history fulfi lls the Amsterdam II criteria. However not all women with LS associated cancer fulfi ll these criteria.1 A recent study suggest that use of immuno-histochemistry in women of any age with at last one fi rst-degree relative with LS associated cancer would identify more cases of LS and be cost-effective compared with Amsterdam II criteria.4
A specifi c surveillance of carriers of pathogenic mutations of MMR genes associ-ated with HNPCC is performed with colonoscopy every 1 to 2 years, beginning at age 20 to 25 years or 10 years earlier than the earliest colon cancer in the family5 and given the high rate of metachronous tumors, individuals with LS and colon can-cer should be advised to pursue a subtotal colectomy with ileorectal anastomosis.1
For surveillance of the endometrium gynaecological examination and hysteros-copy with aspiration biopsy is indicated beginning at age 30-35 every 1 to 2 years5.
Ovarian cancer screening should include transvaginal ultrasound with doppler eval-uation and determination of serum CA 125 also beginning at age 30-35 and every 1 to 2 years.5 Data regarding prophylactic gynecological surgery are still insuffi cient but total hysterectomy with bilateral salpingo-oophorectomy should be considered after completion of childbirth.6
The impact of screening for extracolonic tumors in LS on mortality remains un-known, and is generally personalized to the family history, however gyneacologic surveillance is a standard procedure.1 Upper digestive endoscopy is indicated when there is family history of gastric cancer.5
Urine cytology and ultrasound are indicated when there is family history of uri-nary tract cancer.5
It is important to identify endometrial cancer patients with LS because colorectal cancer surveillance is necessary to decrease CRC incidence and improve survival of patients and their at-risk relatives. Equally, surveillance for endometrial cancer is widely undertaken in all women with this disease.
REFERENCES1. Gala M, Chung. Hereditary Colon Cancer Syndromes. Semin Oncol 2011; 38: 490-499. 2. Vasen HF, Mecklin JP, Khan PM, Lynch T. The International Collaborative Group on
Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC). Dis Colum Rectum 1991; 34: 424-425.

270
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
3. Vasen HF, Watson P, Mecklin JP, Lynch HT. New Clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch Syndrome) proposed by the International Collaborative Group on HNPCC. Gastroenterology 1999; 116: 1453-1456.
4. Kwon JS, Scott JL, Gilks CB et al. Testing women with endometrial cancer to detect Lynch Syndrome. J Clin Oncol 2011; 2): 2247-2252. Epub 2011 May 2.
4. Vasen HF, Moslein G, Alonso A, et al. Guidelines for the clinical management of Lynch syndrome (hereditary non-polyposis cancer). J Med Genet 2007; 44: 353-362.
5. Schmeler KM, Lynch HT, Chen LM et al. Prophylactic surgery to reduce the risk of gynecologic cancers in the Lynch Syndrome. N Engl J Med 2006; 354: 261-269.
© 2012 Monduzzi Editoriale | Proceedings Code: 577
An ovarian tumor with origin in an appendiceal cancer – a case report
A.M. Sousa1, A.M. Coelho1, M. Bernardino1, A.S. Gomes1, A.F. Jorge1, R. Rego2
1Serviço de Ginecologia do Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E; 2Serviço de Anatomia Patológica Instituto Português de Oncologia de Lisboa Francisco Gentil, E.P.E, Lisboa, Portugal
SUMMARYPrimary appendiceal cancers are rare. The age-adjusted rate in the United States is
approximately 0.12 cases per 1,000,000 persons per year1. Appendiceal cancers com-monly spread to the ovaries and may, initially, be diagnosed by gynecological surgeons. A 43-year-old woman underwent hysterectomy with bilateral salpingo-oophorectomy, omentectomy and appendectomy for an ovarian mass. The pathologist reported a muci-nous adenocarcinoma of the appendix with metastatic spread to both ovaries. This case illustrates how an appendiceal cancer can mimic an ovarian one. Differential diagnosis is determinant for adequate treatment and survival rates are distinct.
INTRODUCTIONApproximately 7% of lesions clinically presenting as primary ovarian tumors are
of metastatic origin2. Secondary tumors account for 17.4%-30% of all ovarian ma-lignancies3. The mean age of patients at the time of diagnosis is 57 years2. The most common primary origins for metastatic ovarian tumors are colon, stomach, breast, and genitourinary tract2. Metastases from cancers of the appendix are occasional-ly encountered2. The most common presenting symptoms are abdominal pain and swelling but some patients were asymptomatic at the time of diagnosis. Seidman et al defends that all bilateral tumors or unilateral tumors <10 cm are metastatic, uni-lateral tumors ≥15 cm are primary, and unilateral tumors with sizes between 10 cm and 15 cm are indeterminate5,6. Appendiceal spread to the ovary has predominantly a bilateral involvement but, when unilateral, the most common involved ovary is the right one3,4. Serum CEA and CA-125 are elevated in most cases (> 2.5 U/ml and > 35 U/ml, respectively) 1.

272
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
CASE REPORTWe report a case of a 43-year-old woman who presented to our Institution with
a two months history of abdominal pain, distension and weight loss. There was no signifi cant past medical history. On physical examination an enlarged and tender uterus was observed. CEA and CA-125 were elevated (26.7 U/ml and 58 U/ml, respectively). Resonance scan showed a mass on the right ovary with 16x8x18cm compressing part of the sigmoid, ascending colon and the last ileal loop. On com-puted tomography peritoneal implants and aortic lymph node enlargement were also identifi ed. Given the suspicion of ovarian tumor, the patient underwent total hys-terectomy with bilateral salpingo-oophorectomy, omentectomy and appendectomy, having been left with residual tumor in peritoneum and mesos. The pathologist re-ported a mucinous adenocarcinoma of the appendix extending through all the layers of the appendiceal wall to the regional fat with metastatic spread to both ovaries.
The ovarian capsules were intact. There was extrinsic invasion of outer half of the myometrium and bilateral fallopian tubes. Cytology of ascites was negative for neoplastic cells. During the postoperative period, the patient developed a right sub-frenic abscess needing surgical drainage. The patient was then proposed to systemic chemotherapy (Folfox) and peritonectomy followed by intraperitoneal chemohyper-thermia.
CONCLUSIONSThe ovary is a preferential site for metastic disease. The highest survival rates of
appendiceal cancer occur in patients with carcinoid tumors, intermediate survival rates in patient with colonic type adenocarcinoma, and the lowest survival rates in patients with signet ring type mucinous carcinomas1. The accurate diagnosis of secondary ovarian tumors is always crucial since the misinterpretation of such tu-mors may cause signifi cant adverse consequences for patients. In many cases of metastatic disease to the ovaries, there is a known history of malignancy. Suspicion of metastatic disease to the ovaries usually depends on a detailed clinical history. Nonetheless, an ovarian tumor may occasionally be the initial manifestation of dis-ease, especially in cancers of the gastrointestinal tract. Primary appendiceal cancer is diagnosed in 0.9–1.4% of appendectomy specimens1. Appendiceal cancers com-monly spread to the ovary and may be detected initially by gynecologic surgeons at the time of exploratory laparotomy for ovarian tumor removal. Optimal surgical treatment includes appendectomy and, often right hemicolectomy, as well as resec-tion of sites of metastatic disease. The addition of hemicolectomy to appendectomy in specifi c cases generally confers a 5-year survival advantage of 20–30%1. A num-ber of studies have emphasized the importance of performing appendectomy as part of the surgical staging of epithelial ovarian cancer1,7. Appendiceal metastasis occur in a low percentage of patients with early stage epithelial ovarian cancer and up to

273
November 17-20, 2011 Paris, France
half of patients with advanced disease. In patients with more advanced epithelial ovarian cancer, the appendix may be grossly involved by metastatic ovarian cancer, and appendectomy is required to obtain optimal surgical debulking prior to chemo-therapy.
This case supports the need for appendectomy in patients undergoing surgery for presumed ovarian cancer, but for an additional reason. Although primary ap-pendiceal cancer is extremely rare, it commonly spreads to the ovary, and gyneco-logic surgeons are often involved in the initial surgical evaluation of these patients. Particularly in patients with bilateral ovarian tumors and a frozen section diagnosis of mucinous carcinoma, the appendix should be removed and inspected intraopera-tively. If histologic examination reveals adenocarcinoma involving the mucosa of the appendix, appropriate surgical staging should be undertaken, and a right hemi-colectomy performed when appropriate.
This case illustrates how an appendicular cancer can mimic an ovarian one. Dif-ferential diagnosis is determinant for adequate treatment.
REFERENCES1. Dietrich CS, DeSimone CP, Modesitt SC, DePriest PD, Ueland FR, Pavlik EJ, Kryscio R, Cibull M,
Huhd W, Partridge E, Numnum TM, Schilder J, Higgins RV, van Nagell JR, Primary appendiceal cancer: Gynecologic manifestations and treatment options, Gynecologic Oncology 104 (2007) 602–606.
2. Koyama T, Mikami Y, Saga T, Tamai K, Togashi K, Secondary ovarian tumors: spectrum of CT and MR features with pathologic correlation, Springer Science+Business Media, LLC 2007.
3. Kir G, Gurbuz A, Karateke A, Kir M, Clinicopathologic and immunohistochemical profi le of ovarian metastases from colorectal carcinoma, World J Gastrointest Surg 2010 Abril 27; 2(4): 109-116.
4. McCluggage WG, Wilkinson N, Metastatic neoplasms involving the ovary: a review with an emphasis on morphological and immunohistochemical features, Histopathology 2005, 47, 231–247.
5. Jung ES, Bae JH, Lee A, Yeong Choi J, Park JS, Lee KY, Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classifi cation Algorithms using Tumor Size and Laterality, J Korean Med Sci 2010; 25: 220-5.
6. Khunamornpong S, Pojchamarnwiputh S, Settakorn J, Siriaunkgul S, Primary and metastatic mucinous adenocarcinomas of the ovary: Evaluation of diagnostic approach using tumor size and laterality, Gynecol Oncol, 2006 Apr; 101 (1).
7. Timofeev J, Galgano MT, Stoler MH, Lachance JA, Modesitt SC, Jazaeri AA, Appendiceal Pathology at the Time of Oophorectomy for Ovarian Neoplasms, Obstetrics & Gynecology 2010 December, vol. 166.

© 2012 Monduzzi Editoriale | Proceedings Code: 604
Breast cancer and hot fl ashes treatment
C. Tomás, M. Rodrigues, A. Relva, L. Canelas, F. Romão, MJ. Botica, M. VieiraServiço de Ginecologia e Obstetricia, Hospital Garcia de Orta, Almada, Portugal
INTRODUCTION Breast cancer is one of the most frequent women’s cancers worldwide. In Por-
tugal it accounted for 30% of all malignant tumors in 2001. Its treatment includes any combination of surgery, chemotherapy and radiation therapy. For women with cancers positive for the estrogen or the progesterone receptor (or both) hormone suppression is an additional option. Hormone suppression therapies are used for the treatment of breast cancer in the adjuvant and metastatic settings alike. Blocking uptake of estrogen at the receptor level or suppressing estrogen and progesterone production therefore becomes a goal of treatment. This kind of treatment is for pre- and postmenopausal women and it’s done with Tamoxifen, Fulvestrant and Aroma-tase Inhibitors. However, side effects are frequently reported by patients as a cause of therapy discontinuation. Therapies that target estrogen production are associated with hormone-deprivation symptoms, most commonly hot fl ashes. Information from clinical trials has revealed that approximately 25% of women do not adhere to the life-saving therapy and that this percentage increases to 50% for women not in clinical trials, due to those side effects, mainly caused by Tamoxifen. To improve treatment adherence, quality of life, and, ultimately, life-saving, researchers must identify strategies to reduce the frequency and severity of hot fl ashes in women treated for breast cancer, chiefl y those who are in premenopausal.
Nearly 25% of all women with breast cancer are premenopausal at the time of diag-nosis. Premenopausal women who receive adjuvant chemotherapy for early breast can-cer may undergo premature menopause, as consequence of ovarian damage due to chemotherapy, and it reaches about 40% of 40-year-old and close to 100% of 50-year-old women. Women with chemotherapy-induced menopause experience more frequent and severe symptoms, such as hot fl ashes, than women undergoing natural menopause. This might occur because the process of menopause, which occurs naturally over sev-eral years, is compressed into weeks or months. In addition to hot fl ashes, and for both
276
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
pre- and postmenopausal women, frequently reported side effects include more vaginal discharge, loss of interest in sex, dyspareunia, insomnia due to night sweats, dysuria and urinary incontinence, arthralgia, weight gain and hair thinig.
Hot fl ashes are commonly defi ned as recurring transient episodes of fl ushing and sweating, with a sensation of heat often accompanied by palpitations or anxiety, with objective signs of cutaneous vasodilatation. The frequency, duration and inten-sity of hot fl ushes can vary widely, occurring anywhere from several times a month to every hour, and lasting anywhere from a few seconds to several minutes, with an intensity ranging from mild, moderate and severe to very severe. Hot fl ushes dur-ing the day tend to be associated with problems of social anxiety, discomfort and managing day to day activities, whereas night sweats tend to be associated with sleep disruption and its consequences. Breast cancers survivors were 5.3 times more likely to experience these menopausal symptoms than women in general population.
Hormonal replacement therapy with estrogen is highly effective in treating vaso-motor symptoms associated with menopause; however it is contraindicated in wom-en with breast cancer or history of it. Non-hormonal therapies tend to be preferred but the effi cacy and acceptability of treatment limit their use.
Despite the large variety of pharmacological options, the initial assessment of hot fl ashes should include onset, baseline number and severity, effect on measures of qual-ity of life such as sleep and work, and day known patterns or triggers. Often, patterns emerge and links can be made with triggers such as caffeine, smoking and alcohol. Re-duction of these risk factors is recommended. It is sometimes helpful to review lifestyle interventions such as dressing in layers, use of cotton clothing and bedding and the car-rying of cold drinks avoiding spicy food, and keeping a lower room temperature.
Non-hormonal medications for hot fl ashes have received a signifi cant amount of attention over the past 20 years, but show a range of bothersome side-effects. There are also nonpharmacologic interventions that have been evaluated for the manage-ment of hot fl ushes in oncology and other populations.
There is growing evidence that cognitive behavioral therapy (CBT) and physi-cal exercise can have a positive impact on symptoms in naturally occurring meno-pause. They are potentially useful treatments among women with breast cancer undergoing treatment-induced premature menopause. Cognitive behavioral therapy focuses on the relationship between thoughts, feelings and behavior and is aimed primarily at stress reduction and it is expected to lead to signifi cant reductions in menopausal symptoms via cognitive restructuring and stress management. In what concerns to exercise, Swedish women indicated that regular vigorous exercise at least 3 hours per week is associated with signifi cantly lower risk of hot fl ushes. Although CBT and physical exercise have been shown favorable effects in women undergoing natural menopause, the intervention have not yet been investigated in the context of menopausal symptoms experienced by breast cancer patients under-going treatment-induced menopause. Another non-medical treatments are popular,

277
November 17-20, 2011 Paris, France
including acupuncture, hypnosis and yoga, although the lack of studies to prove their effi cacy on the management of hot fl ushes. Randomized trials with signifi cant duration should be conducted to identify effective strategies for those who not want or cannot tolerate pharmacologic therapies.
In what concerns to pharmacologic agents, there are a few which have shown varying degrees of effi cacy for treating hot fl ashes: SSRIs (selective serotonin reup-take inhibitor), clonidine, gabapentin, megestrol and oxybutynin. Trials provide evidence for effi cacy but some adverse effects might restrict use for some women.
Clonidine is a central active alpha agonist that reduces vascular reactivity and norepinephrine release. Transdermical patches of 0,1mg of clonidine were found to reduce the frequency of hot fl ashes in 20% and the severity in about 10%. In another trial, Pandaya et al concluded that 0,1mg of clonidine, during 8 days, decreased the frequency in those patients in 38% than for the placebo group (20%) with benefi t also noted in measures of intensity and duration. Patients experienced signifi cant adverse effects including mouth dryness, constipation, itchiness, and drowsiness.
Estrogen withdrawal is associated with decreasing levels of serotonin and an in-crease in serotonin receptors in the hypothalamus. Maybe for that, SSRIs (selective serotonin reuptake inhibitor) antidepressants have also shown some effi cacy in managing hot fl ashes in menopausal women and in the breast cancer population too. Venlafaxine selectively inhibits reuptake of serotonin, norepinephrine, and dopa-mine. Loprinzi et al conducted a randomized placebo controlled trial of venlafaxine in 191 breast cancer survivor with hot fl ashes. After 4 weeks, benefi t was seen in the 75mg dose group, with 63% of participants reporting more than 50% reduction in hot fl ashes, and no additional benefi t was seen by increasing the dose to 150 mg as side effects daily group had more side effects, including mouth dryness, decreased appetite, nausea, and constipation. However, some of the SSRIs antidepressants produce the response by blocking the effi cacy of an active tamoxifen metabolite, endoxifen, which use the same CYP2D6 pathway in the liver. Data suggests that both venlafaxine and citalopram are least likely to affect CYP2D6 activity, unlike paroxetine and fl uoxetine should be avoided, as they are potent inhibitors.
The anticonvulsivant gabapentin has been studied for hot fl ashes management. Pandya et al showed that after 8 weeks, 300mg of gabapentin take into a modest reduction of 20% in hot fl ashes, but with 900mg e reduction of approximately 46%. Oxybutynin is an antimuscarinic agent and, with 2,5 mg once or twice daily, was observed to reduce hot fl ashes in about 70% of patients who had been refractory to other treatments; side effects are generally mild and well tolerated.
So, to manage the hot fl ashes in premenopausal women with history of breast can-cer, the authors follow an adapted version of the Treatment Algorithm for Hot Flashes, based on the experience of the London Regional Cancer Program (fl uxogram 1).
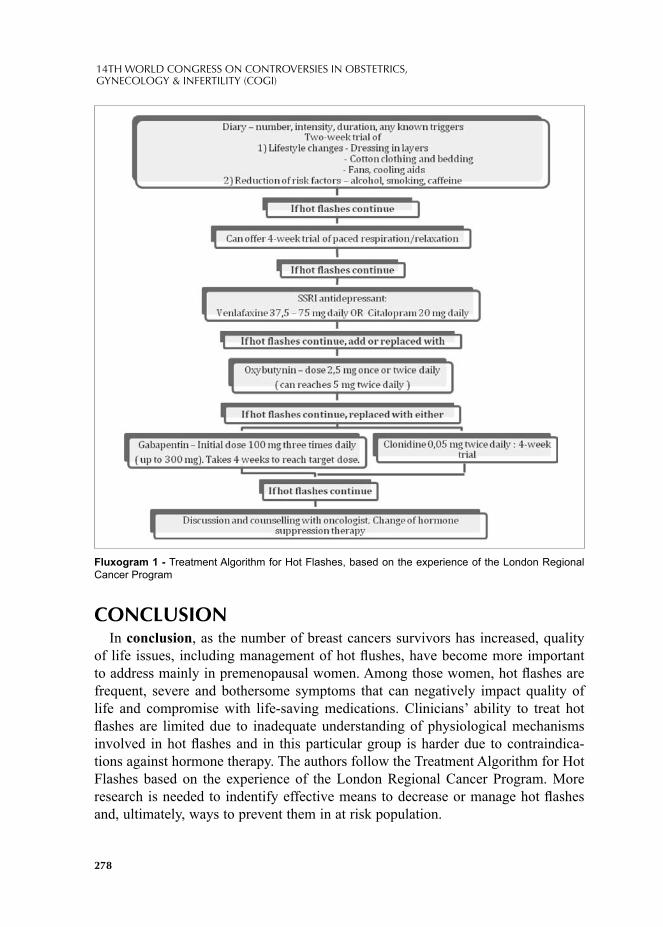
278
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
CONCLUSIONIn conclusion, as the number of breast cancers survivors has increased, quality
of life issues, including management of hot fl ushes, have become more important to address mainly in premenopausal women. Among those women, hot fl ashes are frequent, severe and bothersome symptoms that can negatively impact quality of life and compromise with life-saving medications. Clinicians’ ability to treat hot fl ashes are limited due to inadequate understanding of physiological mechanisms involved in hot fl ashes and in this particular group is harder due to contraindica-tions against hormone therapy. The authors follow the Treatment Algorithm for Hot Flashes based on the experience of the London Regional Cancer Program. More research is needed to indentify effective means to decrease or manage hot fl ashes and, ultimately, ways to prevent them in at risk population.
Fluxogram 1 - Treatment Algorithm for Hot Flashes, based on the experience of the London Regional Cancer Program

279
November 17-20, 2011 Paris, France
REFERENCES1. Mar Fan; N. Houédé-Tchen, I Chemerynsky; et al. Menopausal symptoms in women undergoing
chemotherapy-induced and natural menopause: a prospective controlled study. Annals of Oncology 2010; 21:938-987.
2. L. Klingman, J. Younus; Management of hot fl ashes in women with breast cancer. Current Oncology 2010; 17.
3. Oldenhave A; et al; Impact of climacteric on well-being. A survey based on 5231 women 39 to 60 years old. Am J Obstet Gynecol 1993; 168:172-80.
4. Atlanta, GA. Cancer Facts Figures 2000 - Amercian Cancer Society.5. Shanafelt TD; Barton DL; et al; Pathopysiology and treatment of hot fl ashes. Mayo Clin Proc 2002,
77 (11); 1207-18.6. Duijts S; Oldenburg H; et al; Congitive behavioral therapy and pyisical exercise for climacteric
symptoms in breast cancer patients experiencing treatment-induced menopause: design of a multicenter trial. BMC Women’s health, 2009, 9:15.
7. Hoda D; Perez DG; Loprinzi CL. Hot fl ashes in breast cancer survivors. Breast J 2003; 9: 431-438.8. Loprinzi CL, Kugler JW, Sloan JA, et al. Venlafaxine in management of hot fl ashes in survivors of
breast cancer: a randomised controlled trial. Lancet 2000; 356:2059–63.9. Stearns V, Johnson MD, Rae JM, et al. Active tamoxifen metabolite plasma concentrations after
coadministration of tamoxifen and the selective serotonin reuptake inhibitor paroxetine. J Natl Cancer Inst 2003; 95:1758–64.
10. Boekhout, A.H.; et al; Symptoms and treatment in cancer therapy-induced early menopause. Oncologist 2006, 11, 641–654. doi: 10.1634/theoncologist.11-6-641
11. Kelly, C.M., Juurlink, D.N., Gomes, T., Duong-Hua, M., Pritchard, K.I., Austin, P.C., & Paszat, L.F. Selective serotonin reup take inhibitors and breast cancer mortality in women receiving tamoxifen: A population based cohort study. BMJ 2010; 340, c693.
12. Shanafelt TD, Barton DL, Adjei AA, Loprinzi CL. Pathophysiology and treatment of hot fl ashes. Mayo Clin Proc. 2002; 77(11):1207–1218.
13. Kaplan, M; Mahon, S et al; Putting Evidence Into Practice: Evidence-Based Interventions for Hot Flashes Resulting From Cancer Therapies. Clinical Journal of Oncology Nursing, 2010; 15, 149-157.
14. Otte, JL; et al; Comparison of Subjective and Objective Hot Flash Measures Over Time Among Breast Cancer Survivors Initiating Aromatase Inhibitor Therapy. Menopause. 2009; 16(4): 653–659.

© 2012 Monduzzi Editoriale | Proceedings Code: 636
Charged particle therapy for recurrence of gynecologic cancer, 9 case reports
E. Yamada1, K. Shibata1, H. Kajiyama1, M. Mizuno1, H. Matsumura1, F. Kikkawa1 1Department of Obstetrics and Gynecology, Nagoya University Graduate School of Medicine, Japan
SUMMARYCharged particle radiotherapy has higher biological effi ciency in tumor cell treat-
ment. This study was to evaluate the effi cacy and toxicity of the therapy for lo-cally recurrent gynecologic cancer. Nine patients who underwent charged particle radiotherapy for recurrence of gynecologic cancer, one corpus, three cervical and fi ve ovarian cancers, were included. The median follow-up periods were 25 months (range; 9-67 months). Five cases resulted CR just after treatment and 2 cases are NED in latest status. Treatment related toxicities, pelvic fraction and intestinal per-foration were seen in two cases. Although we experienced a few cases with severe toxicities, the outcome is suffi ciently encouraging to continue the therapy in patients with recurrent chemoresistant cancer for its favorable result in local control.
INTRODUCTIONCharged particle radiotherapy using proton and heavier ion was fi rst proposed
for clinical application in 1946. It has more effective dose distribution due to Bragg peak, an enhanced reactive biological effectiveness (RBE), a lesser dependence of radiosensitivity on position in the cell-cycle and an enhanced oxygen enhancement ratio (OER). These characteristics allow for higher biological effi ciency in tumor cell treatment, and have been started to be used to treat many kinds of cancers. To date, more than 60 protocols have been established and phase I/II and II trials have been conducted in many facilities. Tumor types of the existing protocols are vari-ous, such as pelvic recurrence of rectal cancers hepatocellular carcinoma and bone/soft tissue sarcoma. Most of the protocols show favorable results. In gynecologic fi elds, we encounter cases of local recurrence which are surgically unresectable, resulting in salvage chemotherapy. Therefore, a more potent treatment is necessary
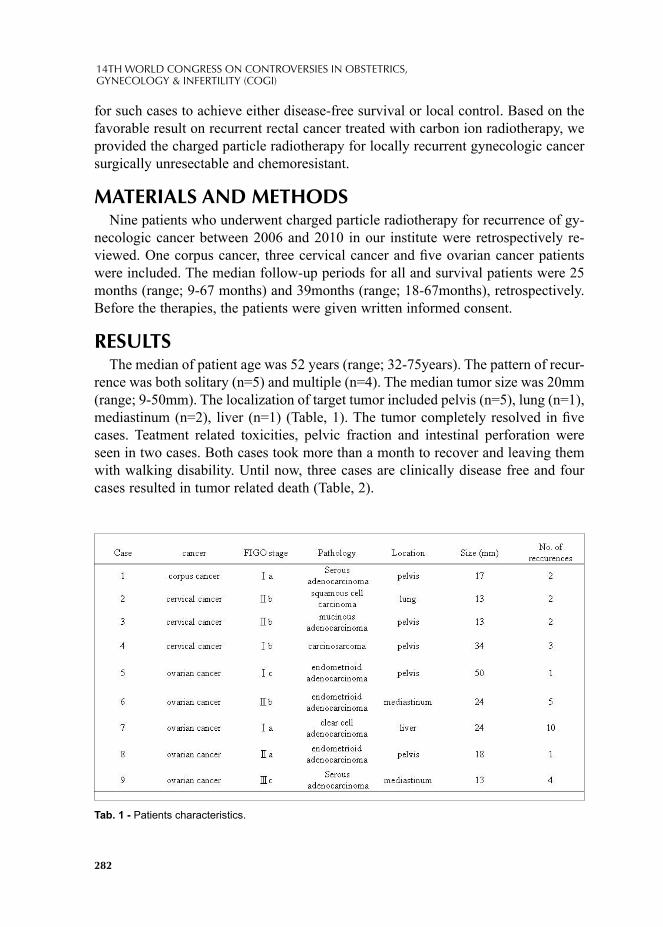
282
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
for such cases to achieve either disease-free survival or local control. Based on the favorable result on recurrent rectal cancer treated with carbon ion radiotherapy, we provided the charged particle radiotherapy for locally recurrent gynecologic cancer surgically unresectable and chemoresistant.
MATERIALS AND METHODSNine patients who underwent charged particle radiotherapy for recurrence of gy-
necologic cancer between 2006 and 2010 in our institute were retrospectively re-viewed. One corpus cancer, three cervical cancer and fi ve ovarian cancer patients were included. The median follow-up periods for all and survival patients were 25 months (range; 9-67 months) and 39months (range; 18-67months), retrospectively. Before the therapies, the patients were given written informed consent.
RESULTSThe median of patient age was 52 years (range; 32-75years). The pattern of recur-
rence was both solitary (n=5) and multiple (n=4). The median tumor size was 20mm (range; 9-50mm). The localization of target tumor included pelvis (n=5), lung (n=1), mediastinum (n=2), liver (n=1) (Table, 1). The tumor completely resolved in fi ve cases. Teatment related toxicities, pelvic fraction and intestinal perforation were seen in two cases. Both cases took more than a month to recover and leaving them with walking disability. Until now, three cases are clinically disease free and four cases resulted in tumor related death (Table, 2).
Tab. 1 - Patients characteristics.

283
November 17-20, 2011 Paris, France
CONCLUSIONSThe charged particle radiotherapy is a promising tool for cancer treatment due to
its effectiveness and contribution to local control especially in the chemoresistant recurrence of gynecologic tumors. Although we experienced a few cases with se-vere toxicities, the outcome is suffi ciently encouraging to continue the therapy in patients with recurrent chemoresistant cancer for its favolable result in local control. More experience is necessory to determine which cases are more suitable with bet-ter local control and acceptable complication.
REFERENCES1. Nawa A, Kikkawa F., et al. Carbon beam therapy in recurrent ovarian cancer.: Ann Oncol.; 19(1):192-
4.,2007 2. Okada T, Tsujii H., et al. Carbon ion radiotherapy: clinical experiences at National Institute of Ra-
diological Science (NIRS).: J Radiat Res (Tokyo). 51(4):355-64.,20103. Matsushita K, Tsujii H., et al. The effects of carbon ion irradiation revealed by excised perforated
intestines as a late morbidity for uterine cancer treatment.; Surg Today. 36(8):692-700., 2006
Tab. 2 - Patients outcomes.

© 2012 Monduzzi Editoriale | Proceedings Code: 643
Single site laparoscopic surgery for complex cases in benign gynecology
J. Ybanez-Morano1, R.P. Rivera2, J.O. Fuentes2, M.C. Vicencio2, M. A. Panaligan2
1Medical Director, Women’s Health Specialists of Wheeling Hospital, Department of Obstetrics and Gynecology, Wheeling, West Virginia, USA; 2Department of Obstetrics and Gynecology, The Medical City Hospital, Metro Manila, Philippines
SUMMARYInnovations in various laparoscopic approaches have allowed significant ad-
vances in benign gynecologic cases. Using single site laparoscopic techniques in even complex cases have improved patient outcomes. This innovative tech-nique improves surgical management of persistent pelvic pain from severe adenomyosis, treatment of chronic endometriosis and control of dense pelvic adhesions secondary to pelvic inflammatory disease. The patient benefits with shortened hospital stays and markedly reduced convalescent times. Patient sat-isfaction has also been observed by aesthetic advantages from well-hidden in-cision placement.
INTRODUCTIONSince the introduction of reduced-site access, milestones have been achieved with
management of complex benign gynecological cases. Single site laparoscopic sur-gery has allowed signifi cant advances in surgical techniques for minimally invasive gynecological surgery. The advancements have been utilized to enhance anatomi-cal access, to shorten hospital stay, to minimize convalescent time, and to improve greater patient satisfaction.
METHODSSingle site laparoscopic surgery using a trans-umbilical approach has been used
to accomplish various procedures, which previously required full abdominal lapa-rotomy incisions. These three cases presented report the ability to address three common complex procedures encountered in practice using this new approach. The
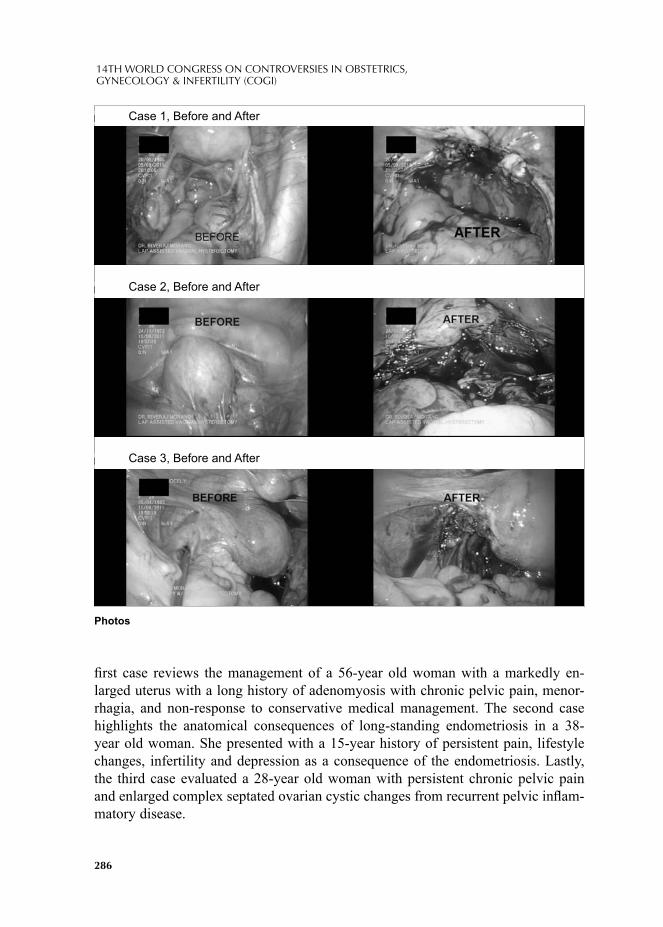
286
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
fi rst case reviews the management of a 56-year old woman with a markedly en-larged uterus with a long history of adenomyosis with chronic pelvic pain, menor-rhagia, and non-response to conservative medical management. The second case highlights the anatomical consequences of long-standing endometriosis in a 38-year old woman. She presented with a 15-year history of persistent pain, lifestyle changes, infertility and depression as a consequence of the endometriosis. Lastly, the third case evaluated a 28-year old woman with persistent chronic pelvic pain and enlarged complex septated ovarian cystic changes from recurrent pelvic infl am-matory disease.
Case 1, Before and After
Case 2, Before and After
Case 3, Before and After
Photos
Case 1, Before and After
Case 2, Before and After
Case 3, Before and After

287
November 17-20, 2011 Paris, France
RESULTSThe use of single site surgery allowed the surgeon to visualize anatomical land-
marks more readily, to facilitate better anatomical access, to shorten patient hospi-talization and to decrease signifi cantly patient recovery time. The patients stayed overnight for observation and discharged to home the following day. Patients re-turned to work in less than two weeks and had minimal scars with the umbilical incision of less than 2 cm in length.
CONCLUSIONSingle site laparoscopic surgery has improved surgical technique and anatomical
access. Furthermore, the patient has more benefi ts with shortened hospital stays, di-minished pain complaints and reduced convalescent time. Furthermore, the patients describes better aesthetic surgical outcomes from the single 1-2 cm scar, well hid-den in the umbilical folds.

© 2012 Monduzzi Editoriale | Proceedings Code: 652
Physiologic and pathologic changes in veins during pregnancy. What to be afraid of?
E. Yupatov1,2, L. Maltseva1, I. Ignatyev3, E. Fomina3, M. Nyukhnin1, S. Sokolov2, A. Zaitsev2
1Kazan State Medical Academy, 2Kazan Center for Medical Research and reconstractive Technologies, 3 Interregional Clinics and Diagnosys Center, Russian
SUMMARYDifferent changes is happening in women organism during pregnancy. One of the
most important is changes in venous compartment which contain 75% of circulation blood volume. This changes concerns to changes of venous diameter, fl ow velocity, formation of thrombotic masses. Hence several complications of pregnancy con-nected with alteration of blood fl ow occur. It could be preeclampsia, threatening abortions, thrombotic events. There is no problems to make a right diagnosys when this changes of veins are visible. Our study shows serious alterations of fl ow veloc-ity and it`s impact to pregnancy in women with no visible varicose veins which refers to C0 of CEAP.
INTRODUCTIONDuring pregnancy the risk of thrombotic complication is very high. The reason
for such complications are different pathological changes in veins, in 80 % of cases the reason for this changes is chronic venous disease (CVD) [1]. The major factors of development of CVD during pregnancy are hypercoagulability, increased venous stasis, decreased venous outfl ow, aorto-caval compression syndrome, hypodynamia, weakness of vessel`s wall, wich includs a connective tissue disorders and smooth musculature, also disfunction and damage of endothelium of veins, venous valves, alteration of microcirculation [2,3,4].
The goal of our research was investigation of changes in venous compartment of low extremities, pelvis and kidneys depending on trimester of pregnancy and its impact on current pregnancy.

290
14TH WORLD CONGRESS ON CONTROVERSIES IN OBSTETRICS,GYNECOLOGY & INFERTILITY (COGI)
MATERIALS AND METHODSWe have examined 115 pregnant women in I, II, III trimesters of pregnancy for
the period from 2009-2011. 92,2 % of patients has had specifi c "venous" complaints without visual changes of superfi cial veins: a pain in gastrocnemius muscle, pain through altered veins, oedema of low extremities, swelling, burning pain. In 7,8% of pregnant women has had visual varicosities of veins of low extremities and vulva.
Mean age of patients was 29,5 years. Among them was 9,5 % multipara, 9 of women with varicose veins had one pregnancy.
There were two phases in our research. During the fi rst phase all women have passed clinical evaluation by obstetrician and gynecologist and laboratory study. In the second phase all women underwent duplex ultrasonography of venous hemody-namics of low extremities, pelvis and kidneys with ATL HDI 5000 SonoCT (Philips), Voluson 730 Expert (GE), Vivid 7 (GE) machines. In the evaluation protocol follow-ing vessels were included: v.cava inferior, common iliac vein, internal iliac veins, common, superfi cial, and deep femoral veins, popliteal, tibial posterior veins, large and small subcutaneous veins, racemose veins, arcuate and vulvar veins, renal veins, and intralobular and segmental veins of kidneys. Duplex ultrasonography was con-ducted fasting, in supine left-side rotation position with application of hydrodynami-cal test of Valsalva. Valsalva maneuver were short-term (3-4 sec) and low intense. For the complete characteristic of venous system B and M modes were used. The patency of vessels, condition of valves with assessment sladge in valve sinuses.
At the presence of chronic intravascular dissemination syndrome markers we pre-scribed low molecular weight heparins and diosmin in dosage 600 mg under control of hemostasis.
RESULTS AND CONCLUSIONDuring pregnancy the venous system of women is exposed to different changes.
According to this conditions, as we could fi nd during our research the diameter of veins of low extremities and pelvis are increased. As our data shows the diameter of common femoral vein increases 1,5 fold to the time of third trimester, the diameter of popliteal vein - is increased 1,4 fold. The diameter of racemose veins is increased 1,13 fold. Besides, on a background of increase of venous diameter, tonico-elastic charachteristics of vessels are reduced, what causes valve insuffi ciency and at the end venous stasis.
Important changes occurs in kidneys venous fl ow. In general, venous fl ow of kid-neys depends on a level of morphological changes in parenchyma of organ. During pregnancy the diameter of renal veins is increased, and fl ow velocity parameters of renal veins is reduced. It is known, that in conditions of venous stasis develops venous hypertension which causes renal hypoxia.
The important component of CVD is retrograde venous fl ow. For the moment
291
November 17-20, 2011 Paris, France
there is no one opinion, what refl ux velocity duration considers to be pathological, however it is considered, that already presence of minimal refl ux testifi es to an in-consistency of the valves.
One of components infl uencing work of venous valves, is sladge - the ultrasonic phenomenon of presence of echopositive elements in valve sinuses. According to modern data it is necessary to allocate 3 degrees of sladge. So 1 degree sladge is physiological, refl ects that fact, that the area of valve sinuses is most thrombogenic a zone. 2 degree sladge is estimated as pathological and considers as prethrombotic condition. 3 degree sladge is ascertaining of thrombosis. With increase of term of pregnancy the diameter of low extremities, pelvic and renal veins is increased, with increase of refl ux fl ow velocity, and it`s duration. This specifi ed changes that on a background of damage of endothelium results in activation of prothrombotic activ-ity and starts appearance of thrombi in venous valve sinuses.
The outcomes of our study is that already in the fi rst trimester the varicose of pelvic and low extremities veins is being formed. This varicose transforma-tion is physiological reaction which is not complicating current pregnancy.
Occurrence of venous complaints even in С0 stage of CEAP is accompanied with refl ux in pelvic and low extremities veins, which leads to alteration of venous valve function and following complications of pregnancy: by pyelonephritis-53% of cases, alteration of maternal-fetal blod fl ow-32% cases, threatening abortion - 24 % of cases.
In the pregnant women with CVD the diameter of renal veins increases with infringement of fl ow velocity which leads to formation of renal hypoxia, and ob-stetrics complications.
An early ultrasonic marker of formation of thrombotic process is sladge in ve-nous valve sinuses of low extremeties.
REFERENCES1. DANILENKO-DIXON DR, HIET JA, SILVERSTEIN MD, YAWN BP,PETTERSON TM, LOHSE
CM, et al. Risk factors for deep veinthrombosis and pulmonary embolism during pregnancy orpost partum: a population-based, case-control study. Am JObstet Gynecol 2001; 184:104–0. (Level II-3)
2. GORDON MC. Maternal physiology. In: GABBE SG, NIEBYL JR and SIMPSON JL, editors. Ob-stetrics: normal and problem pregnancies. 5th ed. Philadelphia (PA): Churchill Livingstone; 2007. p. 55–84. (Level III)
3. MACKLON NS, GREER IA, BOWMAN AW. An ultrasoundstudy of gestational and postural changes in the deepvenous system of the leg in pregnancy. Br J ObstetGynaecol 1997; 104:191–7. (Level III)
4. WHITTY JE, DOMBROSWKI MP. Respiratory diseases in pregnancy.In: GABBE SG, NIEBYL JR and SIMPSON JL, editors.Obstetrics: normal and problem pregnancies. 5th ed.Philadelphia (PA): Churchill Livingstone; 2007. p. 939–63.(Level III)