The Effect of a Community Action Intervention on Adolescent Smoking Rates in Rural Australian Towns:...
9
Preventive Medicine 32, 332–340 (2001) doi:10.1006/pmed.2000.0823, available online at http://www.idealibrary.com on The Effect of a Community Action Intervention on Adolescent Smoking Rates in Rural Australian Towns: The CART Project 1 Lynne Hancock, B.Sc. (Hons), Ph.D.,* , ² ,2 Rob Sanson-Fisher, BPsych (Hons), MClinPsych, Ph.D.,² , ‡ Janice Perkins, BPsych (Hons), Ph.D.,² , ‡ Afaf Girgis, B.Sc. (Hons), Ph.D.,‡ Peter Howley, BMath (Hons)(Stats),§ and Margot Schofield, B.A., Dip.Sc., MClinPsych, Ph.D. ¶ *Hunter Centre for Health Advancement, Newcastle, Wallsend 2287, New South Wales, Australia; ²Faculty of Medicine and Health Sciences and §Health Services Research Group, University of Newcastle, Australia; ‡NSW Cancer Council Cancer Education Research Program, Newcastle, Australia; and ¶ School of Health, University of New England, Armidale, New South Wales, Australia compliance with legislation should be carefully moni- Background. This paper describes one outcome of a tored. q 2001 American Health Foundation and Academic Press randomized controlled trial of community action for Key Words: consumer participation; smoking; smok- cancer prevention, Cancer Action in Rural Towns. The ing cessation; adolescent behavior; self-report. aims are to [1] explore the effectiveness of community action in decreasing adolescent smoking in rural Aus- tralian towns; and [2] describe the relationship be- INTRODUCTION tween adolescent smoking rates and demographic vari- ables. Smoking-related disease is recognized as one of the Methods. In 1992, 20 rural Australian towns were se- major preventable health problems in the Western lected. Community action involved formation of com- munity committees and utilization of access-point net- world today [1,2]. While over the past 3 decades the works to initiate and maintain intervention strategies. overall rates of smoking for adults have declined [3], Cross-sectional surveys of smoking behaviors for all smoking rates have continued to rise in the adolescent Year 9 and Year 10 students (13–16 years) in each town population [4–7]. were conducted pre- and posttest. The main outcome The overall rise in adolescent smoking rates has been measure was self-reported smoking in the past 4 weeks. attributed to several factors, including targeted adver- SUDAAN software was used to look at differences be- tising [7,8] and increased disposable income for pur- tween treatment. chase of cigarettes [9]. In recent years, there has been Results. The results showed strong secular trends a greater increase in adolescent smoking of females toward increased adolescent smoking, regardless of compared to males [10]. Australian rates of adolescent treatment group, particularly for females. There was smoking have followed trends found in international no significant intervention effect. data [4–7]. Repeated national stratified surveys of Conclusions. Increasing adolescent smoking rates smoking by Australian school students showed that, found in this and other studies highlight that the defin- while in 1984 there were no differences in daily smoking itive strategy to stem the adolescent smoking epidemic rates between males and females, in 1990 there were has not been found. Hope may remain for recent legisla- more females smoking daily than males, although tive strategies, but rigorous evaluation is essential, and males continued to smoke more cigarettes [4,5]. Interventions aimed at reducing adolescent smoking have often been school-based, educational, and peer- 1 The CART (Cancer Action in Rural Towns) project was a collabora- support approaches [11,12] or mass media campaigns tive project jointly funded by the National Health and Medical Re- search Council (Australia) and the NSW Cancer Council (Australia) [12–14], which have achieved a limited population ef- (Rob Sanson-Fisher, Principal Investigator). fect. More recently, strategies such as legislating to re- 2 To whom reprint requests should be addressed at Hunter Centre duce access and availability have been introduced [15– for Health Advancement, Locked Bag 10, Wallsend 2287, New South 17], although the results of these strategies have yet Wales, Australia. Fax: 61–2–49246–209. E-mail: lhancock@doh. health.nsw.gov.au. to be fully tested. One potentially promising strategy 332 0091-7435/01 $35.00 Copyright q 2001 by American Health Foundation and Academic Press All rights of reproduction in any form reserved.
Transcript of The Effect of a Community Action Intervention on Adolescent Smoking Rates in Rural Australian Towns:...

Preventive Medicine 32, 332–340 (2001)doi:10.1006/pmed.2000.0823, available online at http://www.idealibrary.com on
The Effect of a Community Action Intervention on AdolescentSmoking Rates in Rural Australian Towns: The CART Project1
Lynne Hancock, B.Sc. (Hons), Ph.D.,*,†,2 Rob Sanson-Fisher, BPsych (Hons), MClinPsych, Ph.D.,†,‡Janice Perkins, BPsych (Hons), Ph.D.,†,‡ Afaf Girgis, B.Sc. (Hons), Ph.D.,‡
Peter Howley, BMath (Hons)(Stats),§ and Margot Schofield, B.A., Dip.Sc., MClinPsych, Ph.D.¶
*Hunter Centre for Health Advancement, Newcastle, Wallsend 2287, New South Wales, Australia;†Faculty of Medicine and Health Sciences and §Health Ser
sn
compliance with legislation should be carefully moni-
‡NSW Cancer Council Cancer Education Re¶School of Health, University of New Engla
Background. This paper describes one outcome of arandomized controlled trial of community action forcancer prevention, Cancer Action in Rural Towns. Theaims are to [1] explore the effectiveness of communityaction in decreasing adolescent smoking in rural Aus-tralian towns; and [2] describe the relationship be-tween adolescent smoking rates and demographic vari-ables.
Methods. In 1992, 20 rural Australian towns were se-lected. Community action involved formation of com-munity committees and utilization of access-point net-works to initiate and maintain intervention strategies.Cross-sectional surveys of smoking behaviors for allYear 9 and Year 10 students (13–16 years) in each townwere conducted pre- and posttest. The main outcomemeasure was self-reported smoking in the past 4 weeks.SUDAAN software was used to look at differences be-tween treatment.
Results. The results showed strong secular trendstoward increased adolescent smoking, regardless oftreatment group, particularly for females. There wasno significant intervention effect.
Conclusions. Increasing adolescent smoking rates
found in this and other studies highlight that the defin-itive strategy to stem the adolescent smoking epidemichas not been found. Hope may remain for recent legisla-tive strategies, but rigorous evaluation is essential, and1 The CART (Cancer Action in Rural Towns) project was a collabora-tive project jointly funded by the National Health and Medical Re-search Council (Australia) and the NSW Cancer Council (Australia)(Rob Sanson-Fisher, Principal Investigator).
2 To whom reprint requests should be addressed at Hunter Centrefor Health Advancement, Locked Bag 10, Wallsend 2287, New SouthWales, Australia. Fax: 61–2–49246–209. E-mail: [email protected].
332
vices Research Group, University of Newcastle, Australia;earch Program, Newcastle, Australia; andd, Armidale, New South Wales, Australia
tored. q 2001 American Health Foundation and Academic Press
Key Words: consumer participation; smoking; smok-ing cessation; adolescent behavior; self-report.
INTRODUCTION
Smoking-related disease is recognized as one of themajor preventable health problems in the Westernworld today [1,2]. While over the past 3 decades theoverall rates of smoking for adults have declined [3],smoking rates have continued to rise in the adolescentpopulation [4–7].
The overall rise in adolescent smoking rates has beenattributed to several factors, including targeted adver-tising [7,8] and increased disposable income for pur-chase of cigarettes [9]. In recent years, there has beena greater increase in adolescent smoking of femalescompared to males [10]. Australian rates of adolescentsmoking have followed trends found in internationaldata [4–7]. Repeated national stratified surveys ofsmoking by Australian school students showed that,while in 1984 there were no differences in daily smokingrates between males and females, in 1990 there weremore females smoking daily than males, althoughmales continued to smoke more cigarettes [4,5].
Interventions aimed at reducing adolescent smokinghave often been school-based, educational, and peer-support approaches [11,12] or mass media campaigns[12–14], which have achieved a limited population ef-
fect. More recently, strategies such as legislating to re-duce access and availability have been introduced [15–17], although the results of these strategies have yetto be fully tested. One potentially promising strategy0091-7435/01 $35.00Copyright q 2001 by American Health Foundation and Academic Press
All rights of reproduction in any form reserved.

CART ADOLESC
to encourage populations to engage in cancer preventivebehaviors is a community action approach [17,18],which requires multiple intervention componentsacross multiple access-points with community partici-pation integral to program implementation and mainte-nance. The community organization approach used inthe Minnesota Heart Health Program appeared to havesome success in decreasing adolescent smoking rates[19], although the evaluation design of this project wasless than rigorous, therefore restricting the confidencewith which the results can be interpreted [20–23]. TheCOMMIT study, which aimed to evaluate the effect ofa range of standardized intervention components onadult smoking rates, had a moderate degree of successin reducing community smoking rates for light to mod-erate smokers [24,25]. The results of these two inter-ventions could encourage some optimism that a commu-nity action approach may be successful in reducingadolescent smoking.
This paper describes one of the outcomes of a random-ized controlled trial of community action for cancer pre-vention, Cancer Action in Rural Towns (CART). Theprimary aim of the CART project was to evaluate theeffectiveness of a community action program in increas-ing community rates of preventive and screening behav-iors relating to breast, cervical, smoking-related, andskin cancer in rural Australian towns. The aims of thispaper are to:
1. explore the effectiveness of a community action
program in decreasing adolescent smoking rates in ru- ral towns of Australia; and2. describe the relationship between adolescentsmoking rates pre- to posttest and selected demo-graphic and process variables.
METHOD
Design
In 1992, 20 towns in rural Australia (population5,001–15,000 adults) were selected for inclusion in theCART project. A matched pairs design was used, withtowns matched on several variables. A computer pro-gram was created which gave each possible pair oftowns a “matching score” based on the following vari-ables:
• demographic structure which included age distri-bution, country of birth, occupation, education levels,and non-English-speaking background, from 1986 Aus-
tralian Bureau of Statistics Census data [25];• population density as an isolation index, calculatedas postcode population divided by area of postcode [25];
• average summer temperature, obtained from theAustralian Meteorological Service.
ENT SMOKING 333
The variables for town matching were chosen followingextensive consultation with statistical and methodolog-ical experts both in Australia and overseas. [26]
Each possible pair of towns was ranked according tothis matching score from the most similar pair of townsdown to the least similar pair. Town pairs were thenselected by working down the ranking list starting fromthe best-matched pair. Town pairs were rejected if :
• geographical position of both towns did not coincide(coastal or inland);
• towns were within 100 km of each other;• one town in the pair was within 50 km of a town
in a pair already selected.
One town from each pair was randomly allocated toeither intervention or control condition. The design andmatching process are detailed in another publicationby this group [27]. Baseline data collections were con-ducted from February to March 1993 and from Febru-ary to March 1994. Follow-up occurred from Februaryto March 1997.
The CART Intervention
The community action intervention involved the for-mation of community committees and the utilization ofaccess-point networks to initiate and maintain inter-vention strategies within each town. The approach usedin the CART intervention was developed with referenceto similar projects [18,22,27] and through consultationwith identified experts in the field, local health promo-tion workers, and lay people. The research team ap-proach to towns was standardized. This involved, firstthe appointment of an external community facilitatorto act as a link between the community and the researchteam. Next, an extensively advertised open-invitationcommunity meeting was held in each town, which ledto the formation of a CART steering committee. Mobili-zation occurred mainly through key community access-points (health care providers, community organiza-tions, media, retailers, schools, and workplaces); and acommunity-recruited liaison officer was recruited as aresource for achieving program targets. Standard strat-egy packages were developed preimplementation andprogressively refined throughout intervention imple-mentation. These were provided to encourage similaractivities in each town. However, it was expected fromthe outset that flexibility would be the key to securingand maintaining community involvement. Conse-
quently, activities and time frames varied considerablybetween communities. Additionally, introduction of theintervention was staggered across the 10 towns, fromJune 1993 to March 1994. The CART interventionmodel has been previously described in detail [27].
K
334 HANCOCCART Adolescent Smoking Activities
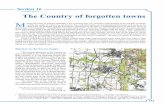
Figure 1 summarizes the types of anti-smoking activ-ities that were conducted in towns. The target for ado-lescent smoking activities was to reduce communityprevalence of adolescent smoking by 5% (from 25 to20%). The Project team recommended that 60% of theprogram effort in adolescent smoking be directed toretailers, 20% to community organizations (such assporting groups), 10% to the media, and 10% to schools.The strategies recommended for implementation intowns were identified through consideration of the rele-vant literature, past work by this group, and extensive
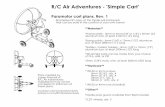
consultation with experts in the field and were seenas having a highreducing adolescention program [11,2Figure 2 describ
FIG. 1. Summary of anti-smoking a
ET AL.
10 CART towns, according to access point. The numberof “crosses” denotes a crude qualitative indicator ofnumber and “size” of activities undertaken within eachtown. This is a comparative indicator rather than abso-lute. As can be seen, overall activity varied a little be-tween towns and considerably between access points.
Evaluation Procedure and Sample
All Year 9 and Year 10 students (13–16 years) fromall secondary schools in each rural town were invitedto participate in cross-sectional surveys of smoking be-haviors, pre- and posttest. The survey methodology was
the same for Time 1 (1993–1994) and Time 2 (1997).as staggered overnting community-lly distant towns.-sectional surveys
At Time 1, however, data collection wprobability of achieving success int smoking within a community ac- 2 years, given the logistics of impleme
wide interventions in 10 geographica8,35].es the level of activity in each of the Permission for conduct of both cross
ctivities conducted in CART towns.

335
C
FIG. 1—was obtained through the University of Newcastle Hu-man Research Ethics Committee and the NSW Depart-ment of School Education.
Principals of all 29 secondary schools in the 20 townswere approached to assist in the data collection. Activeparent consent was sought through letters distributedby the schools. All participating Year 9 and 10 students(13–16 years) in each school were surveyed using a self-report questionnaire. This age group was used becausepast studies have found that most smokers begin smok-ing by the time they reach their midteens [27,28], withapproximately 25% of school children age 15 smokingregularly [29].
Teachers were responsible for distribution and collec-tion of surveys. Teachers were provided with standardinformation packages outlining when and how surveysshould be completed, which included overheads to usewhen explaining to students how the survey shouldbe done. Scannable forms were used to ensure ease ofcompletion. Surveys were completed under exam-like
conditions within school hours, on a specified date ateach school. Teachers were instructed to distribute thequestionnaires in the first class of the data collectionday. Questionnaires were returned to the research teamby prepaid mail.ontinued
Measures
The questionnaire included demographic and smok-ing status questions. While the reliability of adolescentself-report of smoking has sometimes been questioned[30], it was assumed that the deception rate would besimilar for Time 1 and Time 2 [4,6,7]. At Time 1, anexploratory study failed to show a significant effect forreal threat of biochemical validation of smoking statuson student’s smoking self-report, and validation of self-report was not logistically feasible, given the con-straints of geographical distance [31].
Items used in the questionnaire were similar to thoseused in past published studies of this type [4–7,28]and underwent an iterative critical review process withclinicians and identified experts. The questions of rele-vance to this paper were as follows.
Time 1 and time 2.
CART ADOLESCENT SMOKING
• Demographics (age, gender, school year);• Smoked in the past 4 weeks (yes, no);• Amount smoked in the past 4 weeks (none, only a
couple, less than one packet, more than one packet);

K
336 HANCOC• Rules about smoking at home (such as can smokeanywhere, can smoke only in certain rooms, not allowedto smoke at all).
Time 2 only.
• Perceived change in number of signs in the commu-nity about legal age to buy tobacco;
• Perceived change in ease of purchase of tobacco;• Awareness of CART;• Awareness of school anti-smoking activities.
Analyses
The main outcome measure was self-report of smok-ing in the 4 weeks prior to survey. Surveys containingobviously “nonsensical” responses answers (such as70,000 cigarettes smoked per day, indicating that thelegal age of purchase of cigarettes was below 10 or above21 years, or scribbling over the survey) were deletedfrom analyses. Although weekly smoking and havingever smoked were also assessed, these variables arenot reported here, as the results were very similar tothose for monthly smoking. Additionally, monthlysmoking was considered the most reasonable indicatorof current smoking behavior for a group of adolescents,
who are likely to be sporadic smokers [10]. Tables weregeneracal redentsfor TimFIG. 2. Level of activity for community
ET AL.
SUDAAN software was used to consider differencesbetween treatment groups (intervention/control) totake into account the potential design effects caused bybetween-town variation [28,32]. SUDAAN incorporatesthe sampling design when calculating proportions andstandard errors. The design was a two-stage clustersample, with town being the primary sampling unit,selected with replacement, as matching on demograph-ics was part of the selection process.
To ensure that the potential confounding variablesof age, gender, and school year did not influence theestimate of the intervention effect, logistic regression,using SUDAAN, was undertaken to determine the sta-tistical significance of the treatment effect on smokingrates, while including these possible confounders [32].
Additionally, the possible predictors of smoking wereexplored for Time 2 only, using a variable for the rulesabout smoking at home and a composite variable whichtook into account students’ report of the level of anti-smoking activities in the community or at school in thepast 2 years. The “rules” variable represented whetherthe student indicated that they were subject to a “nosmoking” rule at home, independent of their smokingstatus. Responses to the questions on having observedposters promoting nonsmoking, talks to parents about
not smoking, and other school anti-smoking activitiesositer cal-gistic
in the past 2 years were used to generate the compted, based on surveys that didn’t have nonsensi-“awareness” variable. SUDAAN was again used fosponses, for the number and percentage of stu-culating standard errors of proportions and the loin each town who had smoked in the past 4 weeks,
e 1 and Time 2, by demographic variables. regression [32].
quit smoking promotion in CART towns.

E
CART ADOLESCRESULTS
Sample
At Time 1, the consent rate for school participationwas 97% (28 of 29 schools participated). At Time 2, 25of the 28 Time 1 schools agreed to be resurveyed (89%),with no school from Town 4 agreeing to be resurveyed.
Table 1 details the consent rate for individual schools.At Time 1, the consent rate for students varied betweenschools from 11 to 100%, with overall consent being75%. A total of 4,141 students (49.7% female) were sur-veyed in the 20 towns. The average age was 14.6 years(males 5 14.5, females 5 14.6 years). After excludingthose who gave nonsensical responses, the sample sizereduced to 3,973 for Time 1.
At Time 2, the consent rate for students varied be-tween schools from 18 to 87%, with an overall consent
rate of 69%. A total of 3,733 students (52.8% female)13 16.8 (113) 20.2 (84) 15.0 (80) 36.9 (65)14 20.8 (886) 25.9 (798) 21.8 (780) 32.9 (596)
2 11 793 80 71
Total 28 75 75 69 69
a Odd numbers are intervention towns.b Estimate only.
15 29.9 (936) 30.7 (753) 28.8 (848) 33.0 (642)16 32.2 (143) 37.1 (105) 32.4 (170) 40.5 (116)17 42.9 (7) 100.0 (1) 33.3 (3) 50.0 (4)
Table 2 details sample sizes overall, and by town pair,gender, school year, and age, according to study Timeand treatment group. Those returning nonsensical re-sponses have been deleted from these samples.
Smoking Prevalence
Table 2 also details prevalence of self-reported smok-ing in the past 4 weeks, overall, by town pair, gender,age, and school year, according to treatment group andstudy time. This table illustrates an increase in thepercentage of students reporting smoking, from Time 1to Time 2, for both control and intervention treatments,with the intervention group showing a greater overallincrease. In particular, girls showed an increase of 5.5%(SE 5 3.0%) in control towns and 10.5% (SE 5 3.2%)in intervention towns. This difference of 5% betweencontrol and intervention towns was not statistically sig-nificant (P 5 0.2).
Treatment Effect on Smoking
were surveyed in 19 towns. The average age was 14.5years (males 5 14.6, females 5 14.5 years). After ex-cluding those who gave nonsensical responses, the sam-ple size was reduced to 3,230 for Time 2.
TABLE 1
Consent Rate for Schools and Towns, Time 1 and Time 2
Consent rate, Consent rate,Codes Time 1 (%) Time 2 (%)
Towna School School Town School Town
1 1 92 92 87 872 1 67 67 84 843 1 78 78 78 784 1 93 93 — —5 1 51 51 81 816 1 96 94 83 77
2 84 367 1 75 77 42 45
2 90 598 1 74 74 72 729 1 57 57 46 46
10 1 81 83 — 14b
2 100 7411 1 90 90 85 8512 1 47 47 74 7413 1 96 96 38 3814 1 90 90 84 8415 1 85 85 18 1816 1 57 64 50 60
2 89 8417 1 34 34 80 8018 1 97 99 82 63
2 100 4819 1 73 77 72 59b
2 94 —20 1 42 38 25 59
NT SMOKING 337
TABLE 2
Percentage of Students Reporting Smoking in the Past 4 Weeks,by Town Pair, Gender, School Year and Age, According to Study
Time and Treatment (with Sample Sizes)
Percentage smoking (sample size)
Control Intervention
Time 1 Time 2 Time 1 Time 2
Overall 25.5 (2,085) 28.6 (1,777) 25.6 (1,888) 34.0 (1,453)Town pair
1 28.9 (201) 32.0 (244) 28.9 (388) 28.7 (216)2 26.4 (159) — 36.2 (199) 37.0 (216)3 29.7 (212) 44.8 (163) 25.9 (112) 34.5 (171)4 24.5 (94) 18.6 (102) 16.0 (212) 34.2 (114)5 29.2 (284) 45.8 (48) 18.0 (100) 27.6 (98)6 26.4 (178) 24.4 (283) 26.9 (279) 38.1 (260)7 25.0 (312) 24.6 (305) 20.1 (159) 39.1 (69)8 16.1 (137) 18.2 (137) 32.2 (143) 48.5 (33)9 30.4 (263) 27.0 (267) 32.6 (46) 39.0 (100)10 14.7 (245) 33.3 (228) 20.0 (250) 26.1 (176)
GenderMale 25.3 (1,042) 25.3 (801) 24.8 (937) 30.2 (625)Female 25.8 (1,033) 31.3 (967) 26.5 (948) 37.0 (813)
School year9 20.1 (1,107) 27.0 (929) 24.7 (1,001) 34.0 (695)10 31.6 (978) 30.6 (833) 26.6 (887) 33.7 (750)
Age
Table 3 shows the results of the logistic regression,calculated using SUDAAN, exploring the association ofage, gender, school year, study time, and treatmentgroup to reported smoking in the past 4 weeks, after

K
338 HANCOCexcluding the interaction of treatment and study time.The logistic regression model failed to indicate thetreatment group as a significant predictor of havingsmoked in the past 4 weeks (P 5 0.2). Age and studytime were the only statistically significant variables(P , 0.001, P 5 0.01, respectively), with the proportionhaving smoked in the past 4 weeks increasing withincreasing age and at Time 2.
Awareness of Anti-smoking Campaigns at Time 2
Only 2,588 students answered at least one of thequestions regarding anti-smoking campaigns at Time2. Of these students, the proportions indicating anawareness of anti-smoking activities in the past 2 yearswere 74.6 and 70.8% for the intervention and controlgroups, respectively. The relationship between aware-ness of campaigns and treatment group was not statisti-cally significant (P 5 0.5).
Of the students who were aware of the anti-smokingcampaigns, 30.1% had smoked in the past month,whereas of those who weren’t aware, 28.6% had smokedin the past month. The relationship between havingsmoked and awareness of the campaigns was not statis-tically significant (P 5 0.5).
Rules about Smoking at Home at Time 2
There were 2,571 students who responded to thequestion regarding the existence of a nonsmoking ruleat home. Of those students who indicated that theywere not permitted to smoke at home, 31.0% reportedsmoking in the past month, whereas 30.6% of the stu-dents who reported no specific rule against smoking athome reported smoking in the past month. This differ-ence was not statistically significant (P 5 0.9).
Predictors of Smoking at Time 2
A logistic regression which explored the predictors of
having smoked in the past month at Time 2 by incorpo- rating age, treatment group, and whether the studentwas not allowed to smoke at home found no statisticallysignificant treatment effect (P 5 0.1) nor any effect dueto whether they were not allowed to smoke at home.TABLE 3
Logistic Regression Analyses, Using SUDAAN, ExploringTreatment Effect on Reported Smoking in the Past 4 Weeks
Independent variables Odds Lower Upperand effects ratio 95% limit 95% limit
Age 1.34 1.19 1.52*
Gender 5 male 0.83 0.68 1.00School year 5 9 1.05 0.81 1.36Study time 5 1 0.77 0.64 0.94*Treatment 5 intervention 1.11 0.88 1.40* Significant (P , 0.05)
ET AL.
DISCUSSION
This paper describes one of the outcomes of a random-ized controlled trial of community action for cancer pre-vention, CART, in 20 rural towns of Australia. The re-sults indicate that a community action program had nosignificant effect upon the increasing rates of adoles-cent smoking in rural Australian communities.
There are a few methodological issues which shouldbe discussed before the details of the findings of thisstudy are considered, such as reduced sample sizes atTime 2, nonsensical responses, accuracy of self-report,and process measures. At Time 2, despite the fact thatthe same methods were used as at Time 1 and a newcross-sectional survey was conducted, overall consentrates were somewhat lower than for Time 1 (69% com-pared to 75%). There were over 600 fewer studentssurveyed at Time 2 than at Time 1. In particular, fewerboys took part in the survey at Time 2. While it isdifficult to interpret how this may have affected theresults of the study, it should be noted that smokingrates did not increase as much for boys as for girls. Thiscould be an indication that fewer boys who smokedanswered the survey or that males had a higher decep-tion rate, rather than a true difference.
A second issue was that about 10% of the surveysreturned contained nonsensical responses (such as70,000 cigarettes smoked per day). These surveys weredeleted from analyses. However, it is difficult to knowwhether all responses by these students were nonsensi-cal. Adolescents have been confirmed as a difficultgroup to survey [30] and this type of unusable data iscommon. Similar rates of nonsensical responses wereobtained at both study times and for intervention andcontrol groups, so it does not appear that a systematicbias occurred. It must be acknowledged that no valida-tion of self-report for smoking status was applied tothese data. Although adolescent smoking report isknown to be potentially inaccurate [30,31], it was as-sumed that the deception rate would be similar for Time1 and Time 2 [4,6,7]. At Time 1, an exploration of “realthreat of validation” for a similar sample found no sig-nificant effect of this treatment on self-reported smok-ing rates, so a bogus pipeline strategy was not used inthe main surveys. The logistics of validation at distancewere not feasible for this study.
Although process measures were not fully exploredin this paper, of note is the finding that there were nosignificant effects on smoking self-report at Time 2 forawareness of anti-smoking activities (a composite ofresponses to the questions on having observed posters
promoting nonsmoking, talks to parents about notsmoking, and other school anti-smoking activities inthe past 2 years) or for the existence of rules aboutnot smoking at home. Although not explored here, theresults of a survey of school principals supports this
E
ACKNOWLEDGMENTS
CART ADOLESC
finding in that no significant differences were foundbetween treatment groups for principal report of schoolanti-smoking activities in the past 2 years. Therefore,it appears that many similar activities were occurringin control towns and schools as happened in CARTtowns and schools.
The results demonstrated a strong secular trend forincreased rates of smoking among adolescents for allcommunities regardless of treatment group. This find-ing concurs with recent Australian studies [6,7] whichfound that adolescent smoking had increased between1990 and 1993, and with data from the United States[33] and the United Kingdom [34]. The CART projectemployed state-of-the-art best practice principles inrecommending community strategies for reducing ado-lescent smoking [35]. It appears that a much more in-tensive strategy than a diffuse community-based inter-vention may be needed. However, the amount of effortdevoted to adolescent smoking research coupled withthe ever-increasing adolescent smoking rate highlightsthe fact that the definitive strategy has yet to be found[35]. Recent legislative solutions, where people under18 years of age are not legally able to obtain cigarettes[17], have yet to be fully tested. The results of the CARTproject demonstrate the importance of rigorously evalu-ating strategies for reducing adolescent smoking. It isrecommended that compliance with recently introducedlegislation in regard to selling tobacco to minors alsobe rigorously monitored, so that scientific conclusionscan be made about this approach.
The design of the CART project was ambitious andensured that the effectiveness of the mobilization ofcommunity resources to preventing cancer was as rigor-ously evaluated as resources and current scientific prac-tice would allow [23]. Results for other outcomes of thistrial suggest that community action approaches mayhave credence for selected health behaviors and targetgroups. For CART adult smoking outcomes, when dif-ferences in quit rate, uptake rate, and net effect werecompared for intervention versus control condition, inall cases the difference favored an intervention effect.However, the effect was not large enough to achievesignificance except for male quitters, where there wasa significant difference in the proportion of smokersquitting at follow-up (intervention–control) of 7.1%(95% CI: 0.6, 13.7) [36]. Also, for CART cervical cancerscreening rates, the results indicated that under-screened women were more likely and overscreenedwomen were less likely to have a Pap test after theCART intervention, indicating that a community action
program can be effective in increasing cervical cancerscreening rates [37]. However, given the failure to ob-serve a positive intervention effect, the CART projectteam could not recommend community action as a toolfor decreasing adolescent smoking.NT SMOKING 339
Our sincere appreciation is extended to all those community mem-bers and NSW Cancer Council staff who were involved in the CARTproject. Many thanks to the schools and teachers who helped us withdata collection.
REFERENCES
1. Australian Cancer Society. National Cancer Prevention Policy1993. Sydney: The Australian Cancer Society, 1993.
2. World Health Organization European Collaborative Group. Aninternational controlled trial in the multifactorial prevention ofcoronary heart disease. Int J Epidemiol 1974;3(3):219–24.
3. McAlister A, Puska P, Salonen JT, Tuomilehto J, Koskela K.Theory and action for health promotion: illustrations from theNorth Karelia Project. Am J Public Health 1982;72(1):43–50.
4. Hill D, Willcox S, Gardner G, Houston J. Tobacco and alcoholuse among Australian secondary school children. Med J Aust1987;146:125–30.
5. Hill D, White V, Pain M, Gardner G. Tobacco and alcohol useamong Australian secondary school children in 1987. Med JAust 1990;152:124–30.
6. Hill D, White VM, Williams RM, Gardner GJ. Tobacco and alcoholuse among Australian secondary school students in 1990. MedJ Aust 1993;158:228–34.
7. Hill D, White V, Segan C. Prevalence of cigarette smoking amongAustralian secondary school students in 1993. Aust J PublicHealth 1995;19(5):445–9.
8. Pierce JP, Choi WS, Gilpin EA, Farkas AJ, Berry CC. Tobaccoindustry promotion of cigarettes and adolescent smoking.JAMA 1998;279(7):511–5.
9. Kaufman JS, Jason LA, Sawlski LM, Halpert JA. A comprehen-sive multi-media program to prevent smoking among black stu-dents. J Drug Educ 1994;24:95–108.
10. Waldron I, Lye D. Relationship between teenage attitudes to-wards women’s rights, sex roles and marriage and family. WomenHealth 1990;16(3–4):23–36.
11. Lynagh M, Schofield MJ, Sanson-Fisher RW. School health pro-motion programs over the past decade: a review of the smoking,alcohol and solar protection literature. Health Promot Int1997;12(1):43–60.
12. Secker-Walker RH, Worden JK, Holland RR, Flynn BS, DetskyAS. A mass media programme to prevent smoking among adoles-cents: costs and cost effectiveness. Tob Control 1997;6(3):207–12.
13. Flynn BS, Worden JK, Secker-Walker RH, Pirie PL, Badger GJ,Carpenter JH. Long-term responses of higher and lower riskyouths to smoking prevention interventions. Prev Med1997;26(3):389–94.
14. Worden JK, Flynn BS, Solomon LJ, Secker-Walker RH, BadgerGJ, Carpenter JH. Using mass media to prevent cigarette smok-ing among adolescent girls. Health Educ Q 1996;23(4):453–68.
15. Murray DM, Prokohov AV, Harty KC. Effects of a statewide anti-smoking campaign on mass media messages and smoking beliefs.Prev Med 1994;23:54–66.
16. Jones, T. Regulatory mechanisms to inhibit adolescent smoking.University of Newcastle.
17. Green LW, Kreuter MW. Health promotion as a public health
strategy for the 1990s. Ann Rev Public Health 1990;11:319–34.18. Kinne S, Thompson B, Chrisman NJ, Hanley JR. Communityorganization to enhance the delivery of preventive health ser-vices. Am J Prev Med 1989;5(4):225–9.
19. Kelder SH, Perry CL, Klepp KL, Lytle LL. Longitudinal tracking

340 HANCOCK
of adolescent smoking, physical activity and food choice behav-iors. Am J Public Health 1994;84(7):1121–6.
20. Prokhorov AV, Perry CL, Kelder SH, Klepp KI. Lifestyle valuesof adolescents: Results from Minnesota Heart Health Youth Pro-gram. Adolescence 1993;28(111):637–47.
21. Perry CL, Kelder SH, Murray DM, Klepp KL. Community widesmoking prevention: long-term outcomes of the Minnesota HeartHealth program and the Class of 1989 study. Am J PublicHealth 1992;82(9):1210–6.
22. Hancock L, Sanson-Fisher RW, Redman S, Burton R, Burton L,Butler J, et al. Community action for health promotion: a reviewof methods and outcomes 1990–1995. Am J Prev Med 1997;13(4):229–39.
23. COMMIT Research Group. Community intervention trial forsmoking cessation (COMMIT): I Cohort results from a four-yearcommunity intervention. Am J Public Health 1995;85:183–92.
24. COMMIT Research Group. Community intervention trial forsmoking cessation (COMMIT): II Changes in adult cigarettesmoking prevalence. Am J Public Health 1995;85(2):193–200.
25. Australian Bureau of Statistics. Population and housing census,1986. Canberra: Australian Bureau of Statistics, 1987.
26. Sanson-Fisher R, Redman S, Hancock L, et al. Developing meth-odologies for evaluating community-wide health promotion.Health Promot Int 1996;11(3):227–36.
27. Hancock L, Sanson-Fisher R, Redman S, Burton R, Burton L,Butler J, et al. Community action for cancer prevention: overviewof the Cancer Action in Rural Towns (CART) project, Australia.Health Promot Int 1996;11(4):277–90.
28. Knight J, Bowman J, Considine R, Sanson-Fisher R, Redman S.The adolescent project: reducing adolescent smoking and unsafe
ET AL.
drinking in rural towns in the Hunter area of NSW. Health Pro-mot J 1994;4(1):54–6.
29. Armstrong BK. The epidemiology and prevention of cancer inAustralia. Aust NZ J Surg 1988;58:179–87.
30. Patrick DL, Cheadle A, Thompson DC, Diehr P, Koepsell T, KinneS. The validity of self-reported smoking: a review and meta-analysis. Am J Public Health 1994;84(7):1086–93.
31. Hodgetts J, Hancock L, Sanson-Fisher R. Enhancing self-reportof adolescent smoking: the effect of anonymity and threat ofbiochemical validation. Forthcoming.
32. Shah BV, Barnwell BG, Hunt PN, LaVange LM. SUDAAN user’smanual: professional software for survey data analysis for multi-stage sample designs. Release 6.0. Research Triangle Park (NC):Research Triangle Institute, 1992.
33. Lynch B, Bonnie R, editors. Growing up tobacco free: preventingnicotine addiction in children and youths. Washington: NationalAcademy Press, 1994.
34. Thomas M, Holroyd S, Goddard E. Smoking among secondaryschool children in 1992. Her Majesty’s Stationery Office, 1993.
35. Paul CL, Sanson-Fisher RW. Experts’ agreement on the relativeeffectiveness of 29 smoking reduction strategies. Prev Med1996;25:517–26.
36. Hancock L, Sanson-Fisher R, Perkins J, McClintock A, HowleyP, Gibberd R. The effect of community action program on adultquit smoking rates in rural Australian towns: the CART proj-ect. Forthcoming.
37. Hancock L, Sanson-Fisher R, Perkins J, Corkrey R, Burton R,Reid S. The effect of community action intervention on cervicalcancer screening rates in rural Australian towns: the CART proj-ect. Forthcoming.