
The 9th Asia Pacific Heart Rhythm Society Scientific Session
611
The 9 th Asia Pacific Heart Rhythm Society Scientific Session ABSTRACTS BOOK 12 -15 October 2016 Seoul, Republic of Korea
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The 9th Asia Pacific Heart Rhythm Society Scientific Session

The 9th Asia Pacific Heart RhythmSociety Scientific Session
ABSTRACTS BOOK
12 -15 October 2016 Seoul, Republic of Korea

ii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
BOARD OF TRUSTEESPresident Wee Siong TEO (Republic of Singapore)
1st Vice President Shu ZHANG (People’s Republic of China)
2nd Vice President Jonathan KALMAN (Australia)
1st Secretary General Chu-Pak LAU (Hong Kong)
2nd Secretary General Tachapong NGARMUKOS (Kingdom of Thailand)
Treasurer Wataru SHIMIZU (Japan)
Chief Editor of the Official Journal Shih-Ann CHEN (Taiwan)
Scientific Program Chair Yoshinori KOBAYASHI (Japan)
Nomination Committee Chair Masayasu HIRAOKA (Japan)
COUNTRY/REGIONAL PRESENTING MEMBERSAustralia Prash SANDERS Andrew D. MCGAVIGAN
Hong Kong Hung-Fat TSE
India Mohan NAIR Balbir SINGH
Islaminc Republic of Pakistan Zahid AWAN
Japan Ken OKUMURA Kenzo HIRAO
Kingdom of Thailand Tachapong NGARMUKOS
Malaysia Razali OMAR Soot Keng MA
Myanmar Nwe NWE
New Zealand David HEAVEN
People’s Republic of China Congxin HUANG Dejia HUANG
Republic of Indonesia Muhammad MUNAWAR Yoga YUNIADI
Republic of Korea Yong Seog OH
Republic of Philippines Giselle GERVACIO
Republic of Singapore Chi Keong CHING
Taiwan Tsu-Juey WU Chen-Chuan CHENG
Vietnam Quoc Khanh PHAM
iii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
LOCAL ORGANIZING COMMITTEE OF APHRS 2016President Young-Hoon KIM, Korea University Anam Hospital
Chairman Dong-Gu SHIN, Yeungnam University Medical Center
Vice Chairmen Moon-Hyoung LEE, Severance Hospital
Yong Seog OH, The Catholic University of Korea Seoul St. Mary's Hospital
Honorary Advisors Jeong-Gwan CHO, Chonnam National University Hospital
June Soo KIM, Samsung Medical Center
Yoon Nyun KIM, Keimyung University Dongsan Medical Center
Man Young LEE, The Catholic University of Korea Yeouido St. Mary's Hospital
Tai-Ho RHO, The Catholic University of Korea Seoul St. Mary's Hospital
Organizing Secretary Boyoung JOUNG, Severance Hospital
Jt. Organizing Secretary Hyung-wook PARK, Chonnam National University Hospital
Treasurer Nam-Ho KIM, Wonkwang University School of Medicine & Hospital
Scientific Program Committee Chair Seil OH, Seoul National University Hospital
Scientific Program Committee Co-Chairs
Tae-Joon CHA, Kosin University Gospel Hospital
Boyoung JOUNG, Severance Hospital
Jun KIM, Asan Medical Center
Sung-Hwan KIM, The Catholic University of Korea Seoul St. Mary’s Hospital
Hyung-Wook PARK, Chonnam National University Hospital
Communications Committee Chair Hui-Nam PAK, Severance Hospital
Communications Committee Co-Chair Jin-Bae KIM, Kyung Hee University Medical Center
Exhibition Committee Chair Gyo-Seung HWANG, Ajou University Medical School
Govt. Relations Committee Chair Sang-Weon PARK, Sejong General Hospital
Publication Committee Chair Gi-Byoung NAM, Asan Medical Center
Public Relations Committee Chair Seongwook HAN, Keimyung University Dongsan Medical Center
Registration & AccommodationCommittee Chairs
Jong-Il CHOI, Asan Medical Center
Kee-Joon CHOI, Korea University Medical Center
Social Activity Committee Chair Young Keun ON, Samsung Medical Center

iv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
ORAL PRESENTATION 01 (13 October)
OP 1-01 COMPARISON OF TWO-DIMENSIONAL VS. THREE-DIMENSIONAL PHASE MAPPING IN THE DETECTION OF 2 ROTORS DURING HUMAN PERSISTENT AF
Bhupesh PATHIK (Australia)
OP 1-02 KOREAN AF NETWORK GENOME-WIDE ASSOCIATION STUDY FOR EARLY-ONSET ATRIAL FIBRILLATION 3 IDENTIFIES NOVEL SUSCEPTIBILITY LOCI
Ji-Young LEE (Republic of Korea)
OP 1-03 ESOPHAGEAL ACID REFLUX CAUSES ATRIAL ELECTRICAL REMODELING AND INCREASES ATRIAL 4 ARRHYTHMOGENESIS
Li-Wei LO (Taiwan)
OP 1-04 SUDDEN ARRHYTHMIA DEATH SYNDROMES IN HONG KONG IDENTIFIED BY CLINICAL OR MOLECULAR 5 AUTOPSY OF YOUNG SUDDEN DEATH VICTIMS AND CLINICAL AND GENETIC EVALUATION OF THEIR FIRST DEGREE RELATIVES-SADS HK STUDY
Ngai Shing MOK (Hong Kong)
OP 1-05 NEW MECHANISM CONTRIBUTING TO DIABETIC CARDIOMYOPATHY INDUCED ARRHYTHMIA: 6 O-GLCNACYLATION OF CARDIAC SODIUM CHANNEL NAV1.5 PROTEIN
Peng YU (China)
OP 1-06 THE EFFECT OF LOW-LEVEL LEFT VAGUS NERVE STIMULATION ON GENE EXPRESSION AND CARDIAC 7 NEURAL REMODELING IN POSTINFARCTED HEART
Shuang ZHAO (China)
ORAL PRESENTATION 02 (13 October)
OP 2-01 WORLDWIDE PERFORMANCE OF A LEADLESS TRANSCATHETER PACEMAKER: LONG-TERM RESULTS 9 FROM THE MICRA TRANSCATHETER PACING STUDY
Calambur NARASIMHAN (India)
OP 2-02 ACUTE AND CHRONIC PERFORMANCE OF COMMUNICATING LEADLESS ANTI-TACHYCARDIA PACEMAKER 10 AND SUBCUTANEOUS IMPLANTABLE CARDIOVERTER DEFIBRILLATOR
Fleur TJONG (Netherlands)
OP 2-03 IS IMPLANTATION OF AN ATRIAL LEAD REASONABLE IN PATIENTS WITH ATRIAL FIBRILLATION?- 11 A LONG-TERM RHYTHM FOLLOW-UP STUDY
Gerhard GOEBEL (Germany)
OP 2-04 ACCESS TO MRI OF PATIENTS WITH MAGNETIC RESONANCE-CONDITIONAL PACEMAKER AND 12 IMPLANTABLE CARDIOVERTER DEFIBRILLATOR SYSTEMS: RESULTS FROM THE REALLY PROMRI STUDY
Giampiero MAGLIA (Italy)
OP 2-05 PLACEMENT OF DEFIBRILLATION COIL UNDER THE STERNUM: THE ACUTE SUBSTERNAL 13 DEFIBRILLATION (ASD) STUDY EXPERIENCE
Jian CAO (United States )
OP 2-06 HOW TO IMPLANT AN LV LEAD WHEN THERE IS NO SVC: COMBINING THE FEMORAL AND ANTIDROMIC 14 SNARE TECHNIQUES IN TWO PATIENTS
Jussi NIIRANEN (Finland)
ORAL PRESENTATION 03 (13 October)
OP 3-01 LOW ALCOHOL INTAKE AND INCIDENT ATRIAL FIBRILLATION-IS THERE A SAFE LEVEL? 16 Celine GALLAGHER (Australia)
OP 3-02 INCIDENCE OF CARDIAC ARRHYTHMIAS AND OTHER CARDIAC MANIFESTATIONS IN PATIENTS WITH 17 FABRY’S DISEASE. THE WESTERN AUSTRALIAN EXPERIENCE
David CHIENG (Australia)

v
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSOP 3-03 CARDIAC ARREST AMONG MARATHON RUNNERS-A 15 YEARS’ EXPERIENCE OF HONG KONG STANDARD 18 CHARTERED MARATHON
Kit CHAN (Hong Kong)
OP 3-04 GENDER DIFFERENCE OF RISK OF ISCHEMIC STROKE IN ATRIAL FIBRILLATION PATIENTS STRATIFIED BY 19 AGE
Ling KUO (Taiwan)
ORAL PRESENTATION 04 (13 October)
OP 4-01 HIGH DENSITY MAPPING OF ATRIAL MACRO-REENTRY. NEW INSIGHTS INTO THE RELATIONSHIP 21 BETWEEN ACTIVATION PATTERNS AND SUBSTRATE
Bhupesh PATHIK (Australia)
OP 4-03 COMPARISON OF STROKE PREDICTION PERFORMANCE OF ATRIA, CHADS2, R2CHADS2, AND CHA2DS2 22 -VASC RISK SCORES IN PATIENTS WITH ATRIAL FIBRILLATION: A NATIONWIDE COHORT STUDY IN KOREA
Daehoon KIM (Republic of Korea)
OP 4-04 CHARACTERIZATION OF FOCI AND NONRANDOM BREAKTHROUGH DURING PERSISTENT AND 23 LONG-STANDING PERSISTENT ATRIAL FIBRILLATION IN PATIENTS-STUDIES USING HIGH DENSITY (510-512 ELECTRODES) BI-ATRIAL EPICARDIAL MAPPING
Seungyup LEE (United States)
OP 4-05 HIGHER VENTRICULAR PREMATURE COMPLEX BURDEN, LOWER SYSTOLIC BLOOD PRESSURE 24 RESPONSE
Weita CHEN (Taiwan)
OP 4-06 LEFT ATRIAL APPENDAGE CONTRAST-FILLING IN HEART COMPUTED TOMOGRAMS AFTER 25 PERCUTANEOUS LEFT ATRIAL APPENDAGE OCCLUSION PROCEDURE
Yeong-Min LIM (Republic of Korea)
ORAL PRESENTATION 05 (14 October)
OP 5-01 EARLY IMPLANTATION OF PRIMARY PREVENTION IMPLANTABLE CARDIOVERTER-DEFIBRILLATORS FOR 27 PATIENTS WITH NEWLY DIAGNOSED SEVERE NON-ISCHEMIC CARDIOMYOPATHY
Aleksandr VOSKOBOINIK (Australia)
OP 5-02 ACUTE AND CHRONIC CHANGES AND PREDICTIVE VALUE OF TPTE FOR VENTRICULAR ARRHYTHMIA RISK 28 IN CARDIAC RESYNCHRONIZATION THERAPY PATIENTS
Cong XUE (China)
OP 5-03 NEGATIVE AV HYSTERESIS AND MPP 29 David O’DONNELL (Australia)
OP 5-04 DISPARITY IN UTILIZATION OF IMPLANTABLE CARDIOVERTER DEFIBRILLATORS IN ASIAN PATIENTS 30 WITH HEART FAILURE
Eugene S.J. TAN (Singapore)
OP 5-05 REVERSE VENTRICULAR REMODELLING FOLLWING AF ABLATION IN PATIENTS WITH PERSISTENT AF 31 AND SYSTOLIC DYSFUNCTION-A PROSPECTIVE RANDOMISED STUDY
Sandeep PRABHU (Australia)
OP 5-06 FIXED PULSE WIDTH TUNED WAVEFORMS REDUCE DELIVERED ENERGY AND VOLTAGE DEFIBRILLATION 32 THRESHOLDS IN PIGS WITH HEART FAILURE
Yusuke KONDO (Japan)
vi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
ORAL PRESENTATION 06 (14 October)
OP 6-01 ATRIAL REMODELING EXPLAINS DISCREPANCIES BETWEEN ACTIVATION MAPPING AND PHASE MAPPING 34 Christopher KOWALEWSKI (United States)
OP 6-02 PULMONARY VEIN ISOLATION ALONE IS AN EFFECTIVE RHYTHM CONTROL STRATEGY IN PATIENTS WITH 35 PERSISTENT ATRIAL FIBRILLATION THOSE CHANGED TO PAROXYSMAL TYPE WITH ANTIARRHYTHMIC DRUG THERAPY: A MULTI-CENTER PROSPECTIVE RANDOMIZED STUDY
Hee Tae YU (Republic of Korea)
OP 6-03 REVERSIBLE PERIESOPHAGEAL VAGAL NERVE INJURY IS COMMON AFTER AF CRYOABLATION AND 36 PREDICTS A FAVORABLE OUTCOME
Shin Huei LIU (Taiwan)
OP 6-04 LEFT ATRIAL APPENDAGE FLOW VELOCITY AND SPONTANEOUS ECHO CONTRAST IN TRANSESOPHAGEAL 37 ECHOCARDIOGRAPHY ARE PREDICTORS OF LONG-TERM SUCCESS AFTER CATHETER ABLATION FOR NON-PAROXYSMAL ATRIAL FIBRILLATION
Takashi YOSHIZAWA (Japan)
OP 6-05 A NOVEL COMPUTER SIMULATION MODEL FOR PRECISE ROTOR QUANTIFICATION EMPLOYING PHASE 38 MAPPING METHODOLOGY FOR PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION
Yenn-Jiang LIN (Taiwan)
OP 6-06 PROCEDURAL AND CLINICAL OUTCOME OF PATIENTS WITH CHEMICALLY CARDIOVERTED PERSISTENT 39 ATRIAL FIBRILLATION
Yong-Soo BAEK (Republic of Korea)
ORAL PRESENTATION 07 (15 October)
OP 7-01 ARE YOU HITTING THE BULLS EYE? ROLE OF ESMOLOL IN ELECTRICAL STORM: A CASE SERIES 41 Abhinay TIBDEWAL (India)
OP 7-02 IMPACT OF LATE GADOLINIUM ENHANCEMENT ON PATIENT OUTCOMES IN ISCHEMIC AND NONISCHEMIC 42 CARDIOMYOPATHY: A SYSTEMATIC REVIEW AND META-ANALYSIS
Anand GANESAN (Australia)
OP 7-03 A NOVEL PREDICTION MODEL FOR RISK STRATIFICATION OF PATIENTS WITH TYPE 1 BRUGADA ECG 43 PATTERN
Natarajan KUMARASWAMY (India)
OP 7-04 LIFE-THREATENING VENTRICULAR ARRHYTHMIA ASSOCIATED WITH BRUGADA-TYPE ST-SEGMENT 44 ELEVATION DUE TO ACUTE ISCHEMIA OF RIGHT VENTRICULAR OUTFLOW TRACT
Rena NAKAMURA (Japan)
OP 7-05 CORRELATION BETWEEN SCN5A GENE MUTATION AND OCCURENCE OF VENTRICULAR FIBRILLATION 45 AND SYNCOPE IN BRUGADA SYNDROME
Sunu Budhi RAHARJO (Indonesia)
OP 7-06 THE IMPACT OF EXERCISE INTENSITY IN SUDDEN CARDIAC ARREST: A NATIONWIDE COHORT STUDY 46 Young-Ah PARK (Republic of Korea)
ORAL PRESENTATION 08 (15 October)
OP 8-01 WRONG PLACED VENTRICULAR LEAD AND PATENT FORAMEN OVALE-REASON FOR HEART-LUNG 48 MACHINE?
Gerhard GOEBEL (Germany)
OP 8-02 RESTING ELECTROCARDIOGRAPHIC CHANGES AND THE NEED FOR PERMANENT PACEMAKER 49 INSERTION AFTER PERCUTANEOUS TRANSLUMINAL SEPTAL MYOCARDIAL ABLATION FOR HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY: A 16 YEAR AUSTRALIAN EXPERIENCE
Jason NOGIC (Australia )

vii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSOP 8-03 ALL SAVIORS COME IN PAIRS 50
Kantha Rao NARASAMULOO (Malaysia)
OP 8-04 SUCCESSFUL CATHETER ABLATION OF VENTRICULAR PREMATURE COMPLEXES FROM THE RIGHT 51 ATRIAL SIDE OF THE ATRIOVENTRICULAR SEPTUM
Marina ARAI (Japan)
OP 8-05 COMPLETE VA DISSOCIATION IN NARROW QRS TACHYCARDIA: ATRIOVENTRICULAR NODAL REENTRY 52 TACHYCARDIA WITH UPPER COMMON PATHWAY
Mohammad IQBAL (Republic of Korea)
OP 8-06 CATHETER ABLATION OF PERSISTENT ATRIAL FIBRILLATION IN A PATIENT WITH INTERRUPTED 53 INFERIOR VENA CAVA
Mungun-Ulzii KHURELBAATAR (Mongolia)
ORAL PRESENTATION 09 (15 October)
OP 9-01 SIGNIFICANT REDUCTION IN RADIATION DOSE FOR ATRIAL FIBRILLATION ABLATION OVER TIME: 55 A 12 YEAR SINGLE CENTRE EXPERIENCE
Aleksandr VOSKOBOINIK (Australia)
OP 9-02 P WAVE DURATION & SPECTRAL ANALYSIS OF SIGNAL AVERAGED P WAVE: CAN THIS GUIDE US IN 56 DECIDING EXTENT OF ABLATION TO BE PERFORMED DURING PULMONARY VEIN ISOLATION? A PROSPECTIVE STUDY
Subrahmanya Srinivas VARANASI (United Kingdom)
OP 9-03 CASES OF AIR EMBOLISM DURING ATRIAL ABLATION OF ATRIAL FIBRILLATION 57Hee-Soon PARK (Republic of Korea)
OP 9-04 ASSESSMENT OF LESION FORMATION AND ESOPHAGEAL INJURY BY LGE-MRI IN ATRIAL FIBRILLATION 58 ABLATION WITH A FORCE SENSING CATHETER
Mihail CHELU (United States)
OP 9-05 PREDICTOR OF NO ATRIAL REVERSE REMODELING AFTER SUCCESSFUL CATHETER ABLATION FOR 59 ATRIAL FIBRILLATION
Ryohsuke NARUI (Japan)
OP 9-06 COMPARISON OF REMOTE MAGNETIC CATHETER NAVIGATION WITH MANUAL TECHNIQUE FOR 60 CATHETER ABLATION OF ATRIAL FIBRILLATION. A SINGLE CENTER STUDY
Shiwen YUAN (Sweden)
MINI ORAL SESSION 01 (13 October)
MO 1-01 OPTIMAL DURATION AND PREDICTORS OF DIAGNOSTIC UTILITY OF PATIENT-ACTIVATED AMBULATORY 62 ECG MONITORING
Eugene S.J. TAN (Singapore)
MO 1-02 THE RATIO OF AVL/AVR IS SIMPLE IN DISTINGUISHING VENTRICULAR ARRHYTHMIAS ORIGINATED FROM 63 THE RIGHT AND THE LEFT CORONARY CUSP
Hong-Wei TAN (China)
MO 1-03 SYMPATHETIC NERVE BLOCK ATTENUATES INFLAMMATION-INDUCED ARRHYTHMIA VIA A CHOLINERGIC 64 ANTI-INFLAMMATORY PATHWAY
Hyelim PARK (Republic of Korea)
MO 1-04 ARTERIAL PH AND HEMOGLOBIN REGARDLESS OF AMIODARONE AND EMERGENT INTERVENTION ARE 65 DETERMINANTS FOR SURVIVAL ON THE RETURN OF SPONTANEOUS CIRCULATION OF THE OUT-OF HOSPITAL CARDIAC ARREST
Ki-Woon KANG (Republic of Korea)

viii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSMO 1-05 PREDICTING THE DIFFICULTY OF A TRANSVENOUS LEAD EXTRACTION PROCEDURE: VALIDATION OF THE 66 LED INDEX
Luca BONTEMPI (Italy)
MO 1-06 RISK STRATIFICATION FOR SUDDEN CARDIAC DEATH IN JAPANESE HYPERTROPHIC CARDIOMYOPATHY 67 PATIENTS WITH IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR
Miyo NAKANO (Japan)
MO 1-07 GENETIC POLYMORPHISM OF RYANODINE RECEPTOR 2 AND LEFT ATRIAL VOLTAGE IN PATIENTS 68 WITH ATRIAL FIBRILLATION
Pil-Sung YANG (Republic of Korea)
MO 1-08 CATHETER ABLATION OF VENTRICULAR TACHYCARDIA IN ARRHYTHMOGENIC RIGHT VENTRICULAR 69 CARDIOMYOPATHY-EXPERIENCE OF A TERTIARY CARE CENTER
Shibu MATHEW (Germany)
MO 1-09 TRANSVENOUS PACING USING CONVENTIONAL PACEMAKER IN PEDIATRIC PATIENTS ≤ 12 KGS: 70 TECHNIQUE AND MIDTERM RESULTS
Vivek PILLAI (India)
MO 1-10 EFFECT OF LOW-LEVEL ELECTRICAL STIMULATION OF THE AROTIC ROOT VENTRICULAR GANGLIONATED 71 PLEXI ON STRUCTURAL REMODLING IN DOGS WITH HEART FAILURE
Hong-Tao WANG (China)
MO 1-11 SAFETY AND STABILITY OF PERMANENT HIS BUNDLE PACING 72 Weijian HUANG (China)
MINI ORAL SESSION 02 (14 October)
MO 2-01 BIATRIAL MACRRENTRANT ATRIAL TACHYCARDIA AFTER ABLATION AT BACHMANN’S BUNDLE IN 74 PATIENTS WITH ATRIAL FIBRILLATION
Dae In LEE (Republic of Korea)
MO 2-02 AGE CRITERIA MODIFICATION OF CURRENT RISK SCORES PREDICTING STROKE IN PATIENTS WITH 75 ATRIAL FIBRILLATION: A NATIONWIDE COHORT STUDY IN KOREA
Daehoon KIM (Republic of Korea)
MO 2-03 IMPACT OF ATRIAL FIBRILLATION ON OUTCOMES AFTER EMERGENCY CHEST PAIN PRESENTATION 76 Daniel LANCINI (Australia)
MO 2-04 FREQUENT ACCELERATED VENTRICULAR RHYTHM 77 Hailei LIU (China)
MO 2-05 ABORTED SUDDEN CARDIAC DEATH OR SYNCOPE DUE TO LIFE THREATENING VENTRICULAR 78 TACHYARRHYTHMIA IN YOUNG KOREAN SOLDIERS
Hee Sun MUN (Republic of Korea)
MO 2-06 CARDIAC SYMPATHETIC DENERVATION AFTER FAILED RADIOFREQUENCY ABLATION 79 Ilknur CAN (Turkey)
MO 2-07 THE EFFICACY OF FREEZER MAX TO MITRAL ISTHMUS ABLATION: THREE CASE REPORTS 80 Kenji KUROKI (Japan)
MO 2-08 NON-FATAL MYOCARDIAL INJURIES AMONG MARATHON RUNNERS-A 15-YEARS EXPERIENCE OF 81 HONG KONG STANDARD CHARTERED MARATHON
Kit CHAN (Hong Kong)
MO 2-09 INCESSANT LEFT VENTRICULAR TACHYCARDIA OF UNUSUAL ETIOLOGY 82Praloy CHAKRABORTY (India)
MO 2-10 CATHETER ABLATION FOR A VENTRICULAR PREMATURE CONTRACTION TRIGGER REFRACTORY 83 ELECTRICAL STORM AND VENTRICULAR FIBRILLATION
Weichieh LEE (Taiwan)
MO 2-11 FLUOROSCOPY IMAGE INTEGRATED 3D MAPPING SYSTEM REDUCES RADIATION EXPOSURE DURING 84 ABLATION FOR PEDIATRIC CARDIAC ARRHYTHMIAS
Yoko YOSHIDA (Japan)

ix
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSMO 2-12 THE IMPACT OF FASCICULOVENTRICULAR BYPASS TRACTS ON THE DIAGNOSIS AND TREATMENT OF 85 CONCOMITANT ARRHYTHMIA AND CARDIAC DISEASE
Yong-Giun KIM (Republic of Korea)
MINI ORAL SESSION 03 (15 October)
MO 3-01 ELECTROCARDIOGRAPHIC ELECTROPHYSIOLOGICAL FEATURES OF EPICARDIAL ACCESSORY PATHWAYS 87 ABLATED WITHIN THE MIDDLE CARDIAC VEIN
Balasubramanian VIDHYAKAR (India)
MO 3-02 MECHANISTIC PROOF THAT HUMAN AF CAN BE DRIVEN BY ATRIAL TACHYCARDIAS OUTSIDE THE 88 PULMONARY VEINS
Christopher KOWALEWSKI (United States)
MO 3-03 OPTIMIZING CRT WITH NEGATIVE HYSTERESIS AND LV PRE-EXCITATION 89 David O’DONNELL (Australia)
MO 3-04 COMPARISON OF DE-NOVO VERSUS UPGRADE CARDIAC RESYNCHRONIZATION THERAPY; FOCUSED ON 90 THE UPGRADE FOR PACING-INDUCED CARDIOMYOPATHY
Hye Bin GWAG (Republic of Korea)
MO 3-05 FAILURES IN RADIOFREQUENCY CATHETER ABLATION OF PATIENTS WITH WOLFF-PARKINSON-WHITE 91 SYNDROME: AN 8-YEAR RETROSPECTIVE STUDY OF FACTORS RELATED TO FAILURE OF INITIAL RFA
Maria Blanca DE GUZMAN (Singapore)
MO 3-06 INCIDENCE AND RISK FACTORS OF ATRIAL FIBRILLATION AFTER CAVOTRICUSPID CATHETER ABLATION 92 IN PATIENTS WITH “ISOLATED” TYPICAL ATRIAL FLUTTER
Peter NOVIKOV (Russian Federation)
MO 3-07 THE PULMONARY VENOUS ANTRUM IN PATIENTS WITH PERSISTENT AF AND HEART FAILURE- 93 ELECTROPHYSIOLOGIC AND ELECTRO-ANATOMICAL ASSESSMENT
Sandeep PRABHU (Australia)
MO 3-08 LEFT ATRIAL PRESSURE RESPONSE DURING INCREMENTAL DUAL CHAMBER PACING IN THE PATIENTS 94 WITH ATRIAL FIBRILLATION: THE CONCEPT OF ADAPTATION AND STIFFNESS
Seung-Young ROH (Republic of Korea)
MO 3-09 CIRCULATING LEPTIN PREDICTS IMPROVEMENT IN COGNITIVE FUNCTION AFTER CATHETER ABLATION 95 FOR ATRIAL FIBRILLATION: 1-YEAR FOLLOW-UP DATA
Tae-Hoon KIM (Republic of Korea)
MO 3-10 IMPACT OF CHEMICAL ABLATION OF THE MARSHALL VEIN ON CREATION OF MITRAL ISTHMUS BLOCK 96Yasuteru YAMAUCHI (Japan
MO 3-11 FEASIBILITY AND CLINICAL USEFULNESS OF HIGH-RESOLUTION LEFT ATRIAL SOUND MAP AS A 97 RELIABLE GEOMETRY
Yeonghwa (Eiwa) CHUN (ZEN) (Japan
MO 3-12 LONG-TERM OUTCOMES OF CATHETER ABLATION OF ATRIAL FIBRILLATION: A MORE THAN 10 YEARS OF 98 EXPERIENCE
Yong-Soo BAEK (Republic of Korea)
YIA SESSION [BASIC] (13 October)
YIA 1-01 CAN A SODIUM CHANNEL BLOCKER CAUSE WENCKEBACH ACTION POTENTIAL CONDUCTION WITHIN 100 THE RABBIT LEFT VENTRICLE?
Guoliang LI (China)
YIA 1-02 ACUTE AND CHRONIC SUPPRESSION AND LOSS OF CIRCADIAN VARIABILITY OF CARDIAC SYMPATHETIC 101 NERVE ACTIVITY IN A CANINE MODEL OF PREMATURE VENTRICULAR CONTRACTION-INDUCED CARDIOMYOPATHY
Ricardo CARDONA GUARACHE (United States)

x
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSYIA 1-03 SEROTONIN REGULATES QT-INTERVAL: ACCELERATION OF CARDIAC REPOLARIZATION BY ENHANCED 102 KV4.3 MEMBRANE TRAFFICKING
Shanyu CUI (Republic of Korea)
YIA 1-04 ROLE OF ADJUNCTIVE ANTI-FIBROTIC THERAPY WITH TRANILAST IN REVERSING ATRIAL REMODELLING 103 IN SPONTANEOUSLY HYPERTENSIVE RATS
Shivshankar THANIGAIMANI (Australia)
YIA 1-05 MICROVESICLES FROM MESENCHYMAL STEM CELLS IMPROVES CALCIUM REGULATION BY HISTONE 104 DEACETYLASE-6 INHIBITION IN TACHYCARDIA MODEL OF HL-1 MYOCYTE
Yoo Ri KIM (Republic of Korea)
YIA 1-06 SPINAL CORD STIMULATION SUPPRESSES ATRIAL FIBRILLATION BY ACTIVATING CHOLINERGIC 105 ANTI-INFLAMMATORY PATHWAY
Zixuan DAI (China)
YIA SESSION [CLINICAL] (13 October)
YIA 2-01 UNIPOLAR AND BIPOLAR ELECTROGRAM CHARACTERISTICS OF RECURRENT CASES OF VENTRICULAR 107 ARRHYTHMIAS UNDERGOING CATHETER ABLATION
Anupam JENA (Republic of Korea)
YIA 2-02 DETERMINING THE OPTIMAL DOSE OF ADENOSINE FOR UNMASKING DORMANT PULMONARY VEIN 108 CONDUCTION FOLLOWING ATRIAL FIBRILLATION ABLATION: ELECTROPHYSIOLOGICAL AND HEMODYNAMIC ASSESSMENT. DORMANT-AF STUDY
Sandeep PRABHU (Australia)
YIA 2-03 PLASMA HOMOCYSTEINE LEVELS PREDICT EARLY RECURRENCE AFTER CATHETER ABLATION OF 109 PERSISTENT ATRIAL FIBRILLATION
Yan YAO (China)
YIA 2-04 DIFFERENTIATION BETWEEN PAPILLARY MUSCLE AND FASCICULAR VENTRICULAR ARRHYTHMIA USING 110 NOVEL ELECTROCARDIOGRAPHIC INDICES
Yaoting CHANG (Taiwan)
YIA 2-05 HEART RATE-PR INTERVAL DISSOCIATION PREDICTS CARDIOVASCULAR DEATH AND EVENTS: A NOVEL 111 MARKER OF CARDIAC AUTONOMIC DYSREGULATION
Yap-Hang CHAN (Hong Kong)
YIA 2-06 RADIOFREQUENCY CATHETER ABLATION IMPROVES THE QUALITY OF LIFE MEASURED WITH A SHORT 112 FORM-36 QUESTIONNAIRE IN ATRIAL FIBRILLATION PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Yun Gi KIM (Republic of Korea)
LATE-BREAKING TRIAL (13 October)
LBT 01-1 VIRTUAL IN-SILICO MODELING GUIDED CATHETER ABLATION VS. EMPIRICAL ABLATION FOR 115 LONGSTANDING PERSISTENT ATRIAL FIBRILLATION: MULTICENTER PROSPECTIVE RANDOMIZED STUDY
Hui-Nam PAK (Republic of Korea)
LBT 01-2 THE FIRE AND ICE TRIAL: IMPACT OF CATHETER ABLATION TECHNOLOGIES ON PATIENT 116 DEMOGRAPHIC-BASED CLINICAL OUTCOME AND HEALTHCARE COSTS
Karl-Heinz KUCK (Germany)
LBT 01-3 RIVAROXABAN FOR TREATMENT OF LEFT VENTRICLE THROMBOSIS: A CASE SERIES 117Monirah ALBABTAIN (Saudi Arabia)
LBT 01-4 ABSENCE OF REGIONAL FIBROSIS ON CARDIAC MRI IN VENTRICULAR FIBRILLATION AND 118 NON-ISCHEMIC CARDIOMYOPATHY
Aleksandr VOSKOBOINIK (Australia)

xi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
THURSDAY POSTER PRESENTATION (13 October)
BASIC/TRANSLATIONAL SCIENCEP 1-001 THE ELECTROPHYSIOLOGY MECHANISM OF CACNA1C (R1950K) CAUSE L TYPE CALDIUM CHANNEL 120 DYSFUNCTION WITH BRUGADA SYNDROME
Li FENG (China)
P 1-002 KCNH2 MUTATION IN PATIENTS WITH LONG QT SYNDROME TYPE 2 121 Daisuke FUKUMOTO (Japan)
P 1-003 SHORTER LEUKOCYTE TELOMERE LENGTH IS ASSOCIATED WITH ATRIAL REMODELING AND PREDICTS 122 THE RECURRENCE OF ATRIAL FIBRILLATION AFTER RADIO FREQUENCY ABLATION THERAPY
Kuo Li PAN (Taiwan)
P 1-004 GENERATION OF LMNA KNOCK OUT HUMAN INDUCED PLURIPOTENT STEM CELLS USING THE 123 CRISPR-CAS9 NICKASE SYSTEM
Yimin WURIYANGHAI (Japan)
P 1-005 TRANSCRIPTIONAL PROFILE AND FUNCTIONAL ANALYSIS OF AGED ATRIAL FIBRILLATION 124 Yan YAO (China)
P 1-006 GENETIC POLYMORPHISMS IN PITX2 ARE ASSOCIATED WITH ATRIAL FIBRILLATION IN A CHINESE HAN 125 POPULATION
Fengxiang ZHANG (China)
P 1-007 THE RS6584555 PLYMORPHISM IN NEURL IS ASSOCIATEDWITH THE RISK OF ATRIAL FIBRILLATION IN 126 CHINESE HAN POPULATION
Fengxiang ZHANG (China)
P 1-008 THE RS6771157 C/G POLYMORPHISM IN SCN10A IS ASSOCIATED WITH THE RISK OF ATRIAL 127 FIBRILLATION IN A CHINESE HAN POPULATION
Fengxiang ZHANG (China)
P 1-009 PLEOMORPHIC MANIFESTATIONS OF SODIUM CHANNELOPATHY IN A FAMILY 128 Praloy CHAKRABORTY (India)
P 1-010 RELATIONSHIP BETWEEN LRP6 POLYMORPHISMS AND SUDDEN CARDIAC DEATH IN PATIENTS WITH 129 CHRONIC HEART FAILURE
Qi GUO (China)
P 1-011 VARIOUS ANK2 MUTATIONS IN PATIENTS WITH INHERITED PRIMARY ARRHYTHMIA SYNDROMES 130Mari ICHIKAWA (Japan)
P 1-012 LQTS 10 IN A CHILD WITH CONGENITAL COMPLETE HEART BLOCK 131Rajnish JUNEJA (India)
P 1-013 VALIDATION OF KOREAN AF NETWORK GENETIC RISK SCORE FOR EARLY ONSET ATRIAL FIBRILLATION 132 IN THE INDEPENDENT COMMUNITY-BASED COHORT
Ji-Young LEE (Republic of Korea)
P 1-014 NON DESMOSOMAL MUTATIONS DETECTED IN JAPANESE PATIENTS WITH ARRHYTHMOGENIC RIGHT 133 VENTRICULAR CARDIOMYOPATHY
Koichiro TAKAYAMA (Japan)
ALLIED PROFESSIONALSP 1-015 SPECIALISED AF MANAGEMENT IS ASSOCIATED WITH GREATER ADHERENCE TO GUIDELINE 134 RECOMMENDED CARE
Celine GALLAGHER (Australia)
P 1-016 HOW TO OVERCOME FAILURES OF INITIAL RADIOFREQUENCY CATHETER ABLATION OF PATIENTS WITH 135 WOLFF-PARKINSON-WHITE SYNDROME: AN 8-YEAR RETROSPECTIVE STUDY
Kaung Htoo LWIN (Singapore)
P 1-017 LONG TERM HIGH PERCENTAGE RIGHT VENTRICULAR OUTFLOW TRACT SEPTAL PACING CONTRIBUTES 136 TO LEFT VENTRICULAR FUNCTIONAL REMODELING
Kuo Li PAN (Taiwan)

xii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-018 RESULTS OF REPERFUSION THERAPY FOR ACUTE ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION 137 WITH THROMBOLYTIC AGENT
Anh X. PHAM (Viet Nam)
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICESP 1-019 DETERMINANTS OF UTILIZATION OF CARDIAC RESYNCHRONIZATION THERAPY WITH OR WITHOUT 138 DEFIBRILLATOR IN CHINA
Xiaohan FAN (China)
P 1-020 PREDICTORS AND DURATION OF RECOVERY FROM ATRIOVENTRICULAR CONDUCTION DISORDERS AFTER 139 TRANSCATHETER AORTIC VALVE IMPLANTATION
Ju-Youn KIM (Republic of Korea)
P 1-021 INITIAL EXPERIENCE OF LEADLESS PACEMAKER IMPLANTATION IN CHINESE 140 Chin Pang CHAN (Hong Kong)
P 1-022 SCREENING OF SLEEP DISORDERED BREATHING BY USING A TRANSTHORACIC IMPEDANCE SENSOR IN 141 PATIENTS IMPLANTED WITH CARDIAC PACEMAKER
Kensuke FUJIWARA (Japan)
P 1-023 PERMANENT DIRECT HIS BUNDLE AND PARAHISIAN PACING: A SYSTEMATIC REVIEW 142Chiw Yeh LIM (Singapore)
P 1-024 NEW WIRE TECHNIQUE FOR VENOUS ACCESS OF DEVICE IMPLANTATION 143Narutaka OHASHI (Japan)
P 1-025 OPTIMIZING THE ATRIOVENTRICULAR DELAY PACEMAKERS 144Jane ABOULENEIN (Egypt)
P 1-026 PACING-QRS DURATION REGARDLESS OF PACING-SITE IS A MAJOR DETERMINANT FOR OCCURRENCE 145 OF PACING-INDUCED CARDIOMYOPATHY IN THE COMPLETE AV BLOCK FOR 15 YEARS FOLLOW-UP
Ki-Woon KANG (Republic of Korea)
P 1-027 BRAIN NATRIURETIC PEPTIDE CAN PREDICT THE CLINICAL COURSE OF PAROXYSMAL 146 ATRIOVENTRICULAR BLOCK
Hitoshi MORI (Japan)
P 1-029 CLINICAL INVESTIGATION OF LEFT VENTRICULAR PACING USING CORONARY SINUS IN PATIENTS WITH 147 MECHANICAL PROSTHETIC TRICUSPID VALVE REPLACEMENT
Kelan ZHA (China)
P 1-030 PRIMARY PREVENTION IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR DEVICES IN MEN AND WOMEN 148 IN A MULTI-ETHNIC SOUTHEAST ASIAN POPULATION WITH HEART FAILURE-FINDINGS FROM SHOP
Elaine BOEY (Singapore)
P 1-031 INITIAL EXPERIENCES OF WEARABLE CARDIOVERTER DEFIBRILLATOR IN OUTPATIENT SETTING 149Tamami FUJIISHI (Japan)
P 1-032 ARRHYTHMIA RISK OF HOCM PATIENTS AFTER SURGICAL MYECTOMY 150Kei MABUCHI (Japan)
P 1-033 FACTORS FOR INELIGIBILITY OF CANDIDATES FOR S-ICDS IN PATIENTS WITH BRUGADA SYNDROME 151Yu NAGANO (Japan)
P 1-034 THE ADAPTATION OF SICD SHOULD BE EVALUATED IN THE S-ICD SCREENING ECG BEFORE LEADLESS 152 PACEMAKER IMPLANTATION
Motomi TACHIBANA (Japan)
P 1-035 PREDICTION OF VENTRICULAR TACHYARRHYTHMIAS TERMINATED BY IMPLANTABLE-CARDIOVERTER- 153 DEFIBRILLATOR SHOCKS
Ngai-Yin CHAN (Hong Kong)
P 1-036 HIGH DEFIBRILLATION EFFICACY OF PERI-IMPLANT DEFIBRILLATION TESTING 154Newman Sze Yan CHENG (Singapore)
P 1-037 DEVICE AND COIL TYPE USED ACROSS ASIA DIFFERS IN THE IMPROVE SCA TRIAL 155Diego A. RODRIGUEZ (Republic of Korea)

xiii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-038 RESULTS OF THE SUBSTERNAL PACING ACUTE CLINICAL EVALUATION (SPACE) STUDY: FEASIBILITY 156 OF EXTRAVASCULAR SUBSTERNAL PACING
Peter LEONG-SIT (Canada)
P 1-039 COMPARATIVE ANALYSIS OF PREDICTED LONGEVITIES OF CARDIAC IMPLANTABLE ELECTRONIC 157 DEVICES: IMPLICATIONS FOR CLINICAL PRACTICE
Dian MUNAWAR (Australia)
P 1-040 THE INVESTIGATION OF MYOCARDIAL INJURY AFTER SUBCUTANEOUS ICD IMPLANTATION WITH 158 DEFIBRILLATION TEST IN COMPUTER SIMULATION MODEL AND CLINICAL CASES
Takayuki SHIMIZU (Japan)
P 1-041 DEFIBRILLATION THRESHOLD TESTING DURING IMPLANTABLE CARDIOVERTER DEFIBRILLATOR 159 PLACEMENT: SINGLE CENTER EXPERIENCE
Kim SUNGSOO (Republic of Korea)
P 1-042 RESULTS OF DEFIBRILLATION THRESHOLD TESTING COMPARING TRANSVENOUS, SUBCUTANEOUS 160 AND NOVEL SUBSTERNAL ELECTRODE CONFIGURATIONS IN SWINE
Amy THOMPSON (United States)
P 1-043 EFFICACY OF ICD THERAPY ON ELECTRICAL STORM 161Ying Chieh LIAO (Taiwan)
P 1-044 A COMPARATIVE STUDY OF POST MI LV DYSFUNCTION PATIENTS WITH SECONDARY VT-AAD + AICD 162 VERSUS AAD
Praveen PAI (India)
P 1-045 STUDYING ICD THERAPY WHERE ICDS ARE UNDERUTILIZED: IMPLANT RATES HIGHER THAN EXPECTED 163 IN THE IMPROVE SCA TRIAL
Balbir SINGH (India)
CATHETER ABLATIONP 1-047 SAFETY AND EFFICACY OF AF ABLATION USING HANSEN® MEDICAL SENSEI® ROBOTIC CATHETER 164 SYSTEM: LARGEST SERIES IN ASIA PACIFIC REGION
Waheed AHMAD (Australia)
P 1-048 SUCCESSFUL CATHETER ABLATION OF ATRIAL TACHYCARDIA AFTER MITRAL VALVE REPAIR BY 165 SUPERIOR TRANSSEPTAL APPROACH.
Madoka AKASHI (Japan)
P 1-049 SAFETY AND EFFICACY OF ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION IN OLDER ADULTS 166Kengo ANDO (Japan)
P 1-051 SAFETY OF CATHETER ABLATION WITH CONTACT FORCE 167Manabu FUJIMOTO (Japan)
P 1-052 LEFT ATRIAL POSTERIOR WALL ISOLATION (THE “BOX LESION PATTERN”) IN THE TREATMENT OF 168 ATRIAL FIBRILLATION: A SINGLE CENTRE EXPERIENCE
Guy FURNISS (United Kingdom)
P 1-053 INCIDENCE OF A NON-INTENTIONAL BLOCK LINE AT THE LEFT ATRIAL ROOF DUE TO SECOND- 169 GENERATION CRYOABLATION: OCCURRENCE OF A ROOF-DEPENDENT ATRIAL FLUTTER
Yuichi HORI (Japan)
P 1-054 SMART CHINA REGISTRY: INTERIM SAFETY AND EFFECTIVENESS OF PAROXYSMAL AF ABLATION 170 USING THERMOCOOL® SMARTTOUCH™ CATHETER IN CHINESE PATIENTS
Congxin HUANG (China)
P 1-055 COMPARISON OF TREATMENT EFFICACY BETWEEN HYBRID TREATMENT AND REDIOFREQUENCY 171 CATHETER ABLATION FOR ATRIAL FIBRILLATION
Jin Kyung HWANG (Republic of Korea)
P 1-056 EFFICACY AND SAFETY OF PULMONARY VEIN ISOLATION IN PATIENTS WITH ATRIAL FIBRILLATION 172 OVER 80 YEARS
Takashi IKENOUCHI (Japan)

xiv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-057 EFFECTIVENESS OF ADDITIONAL SUBSTRATE MODIFICATION IN FOR RECURRENT ATRIAL FIBRILLATION 173 PATIENTS
Takahiro ISEDA (Japan)
P 1-058 COMBINED ABLATION OF CRYOBALLOON AND RADIOFREQUENCY FOR PAROXYSMAL ATRIAL 174 FIBRILLATION
Chenyang JIANG (China)
P 1-059 CRYOBALLOON ABLATION VERSUS REMOTE MAGNETIC NAVIGATION ABLATION IN PATIENTS WITH 175 PAROXYSMAL ATRIAL FIBRILLATION: A PROSPECTIVE, CONTROLLED STUDY
Qi JIN (China)
P 1-060 IMPACT OF FREEZING DURATION ON ACUTE SUCCESS OF CRYOBALLOON-BASED PULMONARY VEIN 176 ISOLATION ACHIEVING MINIMUM TEMPERATURE
Takatsugu KAJIYAMA (Japan)
P 1-061 COMBINATION STRATEGY OF SUBSTRATE MODIFICATION IN ADDITION TO PULMONARY VEIN ISOLATION 177 WITH LINEAR ABLATION IMPROVES THE EFFICACY IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION
Dong-Hyeok KIM (Republic of Korea)
P 1-062 REDUCED LEFT ATRIAL COMPLIANCE AND ENDOCARDIAL VOLTAGE AFTER CATHETER ABLATION FOR 178 ATRIAL FIBRILLATION
Tae-Hoon KIM (Republic of Korea)
P 1-063 DURABILITY OF LEFT ATRIAL LINEAR ABLATION AND CLINICAL OUTCOME AFTER CATHETER ABLATION 179 FOR PERSISTENT ATRIAL FIBRILLATION
Tae-Hoon KIM (Republic of Korea)
P 1-064 HIGH CIRCULATING ADIPONECTIN IS ASSOCIATED WITH POOR LONG-TERM CLINICAL OUTCOME AFTER 180 CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION
Tae-Hoon KIM (Republic of Korea)
P 1-065 EVALUATION OF NEW IMAGING SOFTWARE FOR FOCAL IMPULSE AND ROTOR MAPPING IN ATRIAL 181 FIBRILLATION ABLATION PROCEDURES
Christopher KOWALEWSKI (United States)
P 1-067 RADIOFREQUENCY CATHETER ABLATION TARGETING THE VEIN OF MARSHALL IN DIFFICULT MITRAL 182 ISTHMUS ABLATION OR PULMONARY VEIN ISOLATION
Ji Hyun LEE (Republic of Korea)
P 1-068 MANAGEMENT OF DIFFICULT MITRAL ISTHMUS ABLATIONS 183Ji Hyun LEE (Republic of Korea)
P 1-069 THE CHARACTERISTICS OF PATIENTS WHO REQUIRED MINIMAL ABLATION IN NON-PAROXYSMAL ATRIAL 184 FIBRILLATION
Kwang No LEE (Republic of Korea)
P 1-070 SNORING EVENTS DURING THE CATHETER ABLATION INCREASE TOTAL PROCEDURE TIME AND CLINICAL 185 RECURRENCE RATE IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION
Yeong-Min LIM (Republic of Korea)
P 1-072 CLINICAL CHARACTERISTICS AND TYPES OF ATRIAL TACHYCARDIA OCCURRING AFTER TERMINATION OF 186 AF DURING STEPWISE ABLATION FOR PERSISTENT AF
Mayumi MASUMURA (Japan)
P 1-073 DURATION OF RADIOFREQUENCY ENERGY DELIVERY IS PREDICTIVE OF ARRHYTHMIA RECURRENCE 187 AFTER STEPWISE ABLATION FOR PERSISTENT ATRIAL FIBRILLATION
Mayumi MASUMURA (Japan)
P 1-074 CATHETER ABLATION OF PERSISTENT ATRIAL FIBRILLATION ENHANCED BY FIRM GUIDED ABLATION- 188 PROCEDURAL EXPERIENCE
Shibu MATHEW (Germany)
P 1-075 IS FLEXABILITY SIMPLE TO USE FOR 8MM-TIP ABLATION CATHETER USERS IN PULMONARY VEIN 189 ISOLATION?
Mutsuki MIYAGAWA (Japan)
P 1-076 THE ROLE OF POST-OPERATIVE LEFT ATRIAL VOLUME INDEX IN MAINTAINING SINUS RHYTHM AFTER 190 SURGICAL ABLATION IN PATIENTS WITH CHRONIC ATRIAL FIBRILATION AND CONCOMITAN MITRAL SURGERY
Larasati MUNAWAR (Indonesia)

xv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-077 A COMPARISON OF THE ATRIAL FIBRILLATION BURDEN BETWEEN RADIOFREQUENCY ABLATION AND 191 CRYOABLATION
Kazuaki NAKAJIMA (Japan)
P 1-078 BOTH LINEAR AND COMPLEX FRACTIONATED ELECTROGRAMS ABLATION IS NECESSARY IN SIGNIFICANT 192 PART OF PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION
Taku NISHIDA (Japan)
P 1-079 EFFICACY AND SAFETY OF CONTACT FORCE GUIDED CATHETER ABLATION FOR ATRIAL FIBRILLATION IN 193 THE ELDERLY PATIENTS
Kimitaka NISHIZAKI (Japan)
P 1-080 CRYOBALLOON ABLATION ACHIEVES EQUAL SUCCESS RATE COMPARED WITH RADIOFREQUENCY 194 ABLATION REGARDLESS OF FREQUENT RECURRENCE IN BLANKING PERIOD
Junichi NITTA (Japan)
P 1-081 COMPARISON OF FLUOROSCOPY USE BETWEEN CRYOBALLOON AND RADIOFREQUENCY CATHETER 195 ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION
Guodong NIU (China)
P 1-082 TRANS-ISTHMUS CONDUCTION TIME ALONE IS INSUFFICIENT FOR PREDICTING COMPLETE CONDUCTION 196 BLOCK OF CAVOTRICUSPID ISTHMUS IN TYPICAL ATRIAL FLUTTER ABLATION
Guodong NIU (China)
P 1-083 DESCRIPTION OF EP FINDINGS AT SECOND STAGE OF NON-CONCOMITANT HYBRID AF ABLATION WITH 197 THE COBRA FUSION DEVICE
Dimitrios PANAGOPOULOS (United Kingdom)
P 1-084 THE EFFECTS OF COMMON VARIANTS OF SINGLE NUCLEOTIDE POLYMORPHISMS IN YOUNG PATIENTS 198 WITH LONE ATRIAL FIBRILLATION AFTER CATHETER ABLATION
Yae Min PARK (Republic of Korea)
P 1-085 EPICARDIAL CATHETER ABLATION IN REPEATED CATHETER ABLATION FOR PERSISTENT ATRIAL 199 FIBRILLATION: A PRELIMINARY RESULT OF PROSPECTIVE RANDOMIZED CONTROLLED TRIAL
Seung-Young ROH (Republic of Korea)
P 1-086 IMPORTANCE OF THE ORDER OF ABLATION IN COMBINATION OF GANGLIONATED PLEXI ABLATION AND 200 PULMONARY VEIN ANTRAL ISOLATION
Yuichiro SAKAMOTO (Japan)
P 1-087 CLINICAL OUTCOMES OF ELECTRICAL ISOLATION OF LEFT ATRIAL APPENDAGE DURING CATHETER 201 ABLATION OF ATRIAL FIBRILLATION
Jaemin SHIM (Republic of Korea)
P 1-088 MAPPING AND ABLATION OF LEFT ATRIAL FLUTTERS AND ITS RECURRENCE 202Balbir SINGH (India)
P 1-089 REDUCED FLUOROSCOPY USE WITH REMOTE MAGNETIC CATHETER NAVIGATION COMPARED TO 203 CONVENTIONAL ABLATION IN ATRIAL FIBRILLATION ABLATION
Hooi Khee TEO (Singapore)
P 1-090 CATHETER ABLATION OF ATRIAL FIBRILLATION: A SINGLE CENTRE EXPERIENCE AND COMPARISON 204 BETWEEN REMOTE MAGNETIC NAVIGATION VERSUS CONVENTIONAL ABLATION
Joseph Jia Hong TOH (Singapore)
P 1-091 ADENOSINE TESTING DURING CRYOBALLOON ABLATION AND RADIOFREQUENCY ABLATION FOR ATRIAL 205 FIBRILLATION: A PROPENSITY SCORE MATCHED ANALYSIS
Michifumi TOKUDA (Japan)
P 1-092 ONE-YEAR OUTCOMES OF ABLATION WITH CRYOBALLOON FOR PAROXYSMAL ATRIAL FIBRILLATION: 206 NEED OF ADDITIONAL ABLATION FOR EXTRA FOCUS AND SUBSTRATE
Akira UENO (Japan)
P 1-093 HEART RATE VARIABILITY CAN PREDICT THE RECURRENCE AFTER CATHETER ABLATION FOR 207 PAROXYSMAL ATRIAL FIBRILLATION
Tadashi sWADA (Japan)
P 1-094 SIGNIFICANCE OF LOW VOLTAGE ZONES IN LEFT ATRIUM AS A SOURCE OF FOCAL FIRINGS 208Takanori YAMAGUCHI (Japan)

xvi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-095 UTILITY OF MINI ELECTRODES ON THE 8MM-TIP FOR CAVOTRICUSPID ISTHMUS ABLATION 209
Seigo YAMASHITA (Japan)
P 1-096 DOSE THE APPEARANCE OF DORMANT PULMONARY VEIN CONDUCTION PREDICT RECURRENCE OF 210 ATRIAL FIBRILLATION AFTER CATHETER ABLATION?
Kenichi YOKOYAMA (Japan)
P 1-097 STRICT SEQUENTIAL CATHETER ABLATION STRATEGY TARGETING PULMONARY VEIN AND SUPERIOR 211 VENA CAVA FOR PERSISTENT ATRIAL FIBRILLATION
Yasuhiro YOSHIGA (Japan)
P 1-098 ENDURANCE ABLATION WITH MODERATELY INCREASED RADIOFREQUENCY POWER FACILITATES 212 LONG-LASTING CIRCUMFERENTIAL PULMONARY VEIN ISOLATION AND BETTER CLINICAL OUTCOMES IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION
Hee Tae YU (Republic of Korea)
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATIONP 1-099 DECREASED STROKE VOLUME DURING AND AFTER A VENTRICULAR PREMATURE COMPLEX IS 213 ASSOCIATED WITH VENTRICULAR PREMATURE COMPLEX-RELATED SYMPTOM
Hye Bin GWAG (Republic of Korea)
P 1-100 THE UNDER-RECOGNIZED RISK OF DRUG INDUCED TORSADES DE POINTES WITH INTRAVENOUS 214 AMIODARONE:RECOGNITION AND MANAGEMENT
Vivek PILLAI (India)
P 1-101 VENTRICULAR TACHYCARDIA SECONDARY TO TAKAYASU’S ARTERITIS SUPPRESSED WITH ANTI- 215 TNF-ALPHA THERAPY
Naveen VELAGA (Singapore)
P 1-102 IMPACT OF LOW FREQUENCY PREMATURE VENTRICULAR COMPLEXES ON LONG-TERM CLINICAL 216 OUTCOME
Ting-Yung CHANG (Taiwan)
P 1-103 THE IMPACT OF EARLY REPOLARIZATION PATTERN ON THE OUTCOME OF CATHETER ABLATION OF 217 IDIOPATHIC VENTRICULAR TACHYCARDIA
Yuan HUNG (Taiwan)
P 1-104 ELECTROCARDIOGRAPHIC DIFFERENTIATION OF FASCICULAR VENTRICULAR TACHYCARDIA FROM 218 ATRIAL FLUTTER WITH RIGHT BUNDLE BRANCH BLOCK ABERRANT CONDUCTION
Minsu KIM (Republic of Korea)
P 1-105 PREVALENCE AND CLINICAL SIGNIFICANCE OF FRAGMENTED QRS COMPLEX OR J WAVE IN PATIENTS 219 WITH IDIOPATHIC VENTRICULAR FIBRILLATION
Choong-Sil SEONG (Republic of Korea)
P 1-106 CIRCADIAN DISTRIBUTION AND RELATION WITH HEART RATE IN THE DIFFERENT OVERLOAD OF 220 OUTFLOW TRACT PREMATURE VENTRICULAR CONTRACTIONS
Liang SHAN (China)
P 1-108 LEFT VENTRICULAR REMODELING PREDICT VENTRICULAR ARRHYTHMIA IN THE PATIENTS WITH ICD 221Weichieh LEE (Taiwan)
P 1-109 COMBINATION OF ADMISSION HEMOGLOBIN LEVEL AND BMI PREDICTS 3-YEAR CUMULATIVE SUDDEN 222 CARDIAC RISK IN DILATED NON-ISCHEMIC CARDIOMYOPATHY PATIENTS WITH SEVERE HEART FAILURE
Xiaofei LI (China)
P 1-110 LONG-TERM OUTCOME OF CATHETER ABLATION FOR LEFT POSTERIOR FASCICULAR VENTRICULAR 223 TACHYCARDIA WITH DEVELOPMENT OF LEFT POSTERIOR FASCICULAR BLOCK AND CHARACTERISTICS OF REPEAT PROCEDURES
Bin LUO (China)
P 1-112 VENTRICULAR ARRHYTHMIC EVENT AFTER CRT IMPLANTATION 224Hiroyasu SUGIYAMA (Japan)
P 1-113 RADIOFREQUENCY CATHETER ABLATION UTILIZING CARTOSOUND WAS EFFECTIVE FOR A CASE OF 225 IDIOPATHIC PREMATURE VENTRICULAR CONTRACTION ARISING FROM THE LEFT VENTRICULAR PAPILLARY MUSCLE
Hideshi AOYAGI (Japan)

xvii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-114 EFFICACY OF MYOCARDIAL FAT DETECTION WITH MDCT FOR SUBSTRATE-BASED ABLATION OF 226 ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY PATIENT WITH NON-MRI CONDITIONAL ICD
Hirofumi ARAI (Japan)
P 1-115 AGE RELATED RIGHT VENTRICULAR ABNORMALITY IN ARRHYTHMOGENIC RIGHT VENTRICULAR 227 CARDIOMYOPATHY
Haryadi HARYADI (Indonesia)
P 1-116 CARDIAC MRI: USEFULNESS IN PATIENTS WITH VENTRICULAR ARRHYTHMIA AND “STRUCTURALLY” 228 NORMAL HEART.
Vikas KATARIA (India)
P 1-118 ISOLATION OF LATE POTENTIALS FOR VENTRICULAR TACHYCARDIA IN A NON-INDUCIBLE PATIENT 229Masahito SUZUKI (Japan)
P 1-119 PR INTERVAL IS ASSOCIATED WITH LEFT VENTRICULAR HYPERTROPHY INSTEAD OF ENLARGED LEFT 230 ATRIUM IN PATIENTS WITH HYPERTENSION
Siyang FAN (China)
P 1-120 CHARACTERISTICS FOR DETECTED DURATION AND ETIOLOGIES IN THE CAUSE OF SYNCOPE USING 231 IMPLANTABLE LOOP RECORDER
Ritsuko KOHNO (Japan)
P 1-121 RISK PREDICTORS OF MORTALITY IN JAPANESE PATIENTS WITH CARDIOVASCULAR SYNCOPE WITHIN 232 1 YEAR
Tatsuya ONUKI (Japan)
P 1-122 HEART RATE RECOVERY AND RECOVERY OF THE BLOOD PRESSURE RATIO ON THE EXERCISE TREADMILL 233 TEST PREDICT A RECURRENT VASOVAGAL SYNCOPE REFERRED TO THE HEAD-UP TILT TABLE TEST
Ki-Woon KANG (Republic of Korea)
P 1-123 UTILITY AND SAFETY OF HEAD UP TILT TEST WITH SUBLINGUAL NITROGLYCERINE PROVOCATION IN 234 PATIENTS WITH STRUCTURAL HEART DISEASE AND SYNCOPE
Vivek PILLAI (India)
CLINICAL ELECTROPHYSIOLOGYP 1-124 THROMBOEMBOLISM AND BLEEDING RISK IN ATRIAL FIBRILLATION PATIENTS WITH LIVER CIRRHOSIS 235
Myung-Jin CHA (Republic of Korea)
P 1-125 THE ASSOCIATION OF STRUCTURE ABNORMALITIES IN REFRACTORY VENTRICULAR ARRHYTHMIA 236 ORIGINATING FROM PAPILLARY MUSCLE
Yaoting CHANG (Taiwan)
P 1-126 DEVELOPMENT AND VALIDATION OF A QUESTIONNAIRE MEASURING PATIENT KNOWLEDGE OF ATRIAL 237 FIBRILLATION IN AN ASIAN COHORT
Rebecca HOE (Singapore)
P 1-128 THE CHADS2 AND CHA2DS2-VASC SCORES ARE ASSOCIATED WITH VASCULAR CELL ADHESION 238 MOLECULE 1 (VCAM-1) IN AN INCREMENTAL MANNER
Chen-Ying HUNG (Taiwan)
P 1-129 IMPACT OF NON-DIPPING STATUS ON THE VENTRICULAR ELECTRICAL AND MECHANICAL DYSFUNCTION 239 IN PRE-HYPERTENSIVE PATIENTS
Sung Il IM (Republic of Korea)
P 1-130 IMPACT OF PERIODONTITIS ON LONG TERM CLINICAL OUTCOMES IN PATIENTS WITH ATRIAL 240 FIBRILLATION
Sung Il IM (Republic of Korea)
P 1-131 LONG DURATION OF PREMATURE ATRIAL CONTRACTIONS UNTIL DIAGNOSIS WITH ATRIAL 241 FIBRILLATION INCREASES ISCHEMIC STROKE
Dong-Hyeok KIM (Republic of Korea)
P 1-132 ANEMIA AND THE RISK OF SUDDEN CARDIAC ARREST IN GENERAL POPULATION 242In-Jung KIM (Republic of Korea)

xviii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 1-133 LIVER CIRRHOSIS IS A RISK FACTOR FOR ATRIAL FIBRILLATION: A NATIONWIDE POPULATION-BASED 243 STUDY
HyunJung LEE (Republic of Korea)
P 1-135 THE ASSOCIATION BETWEEN Γ-GLUTAMYL-TRANSPEPTIDASE LEVEL AND RISK OF ATRIAL 244 FIBRILLATION: A NATIONWIDE POPULATION-BASED STUDY
So-Ryoung LEE (Republic of Korea)
P 1-136 RELATIONSHIP BETWEEN CHRONIC COMORBIDITIES AND FAST RESTING HEART RATE IN HYPERTENSIVE 245 PATIENTS
Xiaofei LI (China)
P 1-137 PROTEINURIA DETECTED BY DIPSTICK URINE TEST PREDICTS ATRIAL FIBRILLATION: A NATIONWIDE 246 POPULATION-BASED STUDY
Woohyun LIM (Republic of Korea)
P 1-138 PROVISION OF CATHETER ABLATION PROCEDURES IN AUSTRALIA 247Jonathan LIPTON (Australia)
P 1-139 GENDER DIFFERENCE & LONG-TERM TREND OF SUDDEN CARDIAC ARREST IN POPULATION OF 248 WORKING GENERATION
Yasushi OGINOSAWA (Japan)
P 1-140 ELECTROCARDIOGRAPHIC FINDINGS OF BREAST CANCER COMPARED TO BENIGN BREAST DISEASE 249Suk-Kyu OH (Republic of Korea)
P 1-141 ECG AND CLINICAL MANIFESTATION OF PECTUS EXCAVATUM AS A BRUGADA PHENOCOPY 250Hee-Soon PARK (Republic of Korea)
P 1-142 ECG-DIAGNOSED SINUS BRADYCARDIA PREDICT ATRIAL FIBRILLATION IN GENERAL POPULATION: 251 A 10-YEAR COMMUNITY-BASED PROSPECTIVE STUDY
Jin-Kyu PARK (Republic of Korea)
P 1-143 CLINICAL IMPLICATION OF IMPAIRED FASTING GLUCOSE AND PRE-HYPERTENSION RELATED TO NEW 252 ONSET ATRIAL FIBRILLATION IN HEATHY POPULATION WITHOUT UNDERLYING DISEASES: A NATIONWIDE COHORT STUDY IN KOREA
Junbeom PARK (Republic of Korea)
P 1-144 PREDICTORS OF APPROPRIATE SHOCKS AND VENTRICULAR ARRHYTHMIAS IN A INDONESIAN PATIENTS 253 WITH BRUGADA SYNDROME
Ardian RIZAL (Indonesia)
P 1-145 RISK FOR STROKE IN KOREAN PATIENTS WITH ATRIAL FIBRILLATION: THE KOREA NATIONAL HEALTH 254 INSURANCE SERVICE DATABASE 2007 TO 2013
Mi Kyoung SON (Republic of Korea)
P 1-146 INCREASED RISK OF VENTRICULAR TACHYCARDIA AND CARDIOVASCULAR DEATH IN PATIENTS WITH 255 MYOCARDITIS DURING THE LONG-TERM FOLLOW-UP: A NATIONAL REPRESENTATIVE COHORT FROM THE NATIONAL HEALTH INSURANCE RESEARCH DATABASE
Abigail Louise TE (Taiwan)
P 1-148 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCREASES THE RISK OF NEW-ONSET ATRIAL 256 FIBRILLATION AND MORTALITY OF PATIENTS WITH ATRIAL FIBRILLATION
Pil-Sung YANG (Republic of Korea)
P 1-149 THE IMPACT OF COMORBID ATRIAL FIBRILLATION ON THE INCIDENCE AND OUTCOME OF FRACTURE 257 IN PATIENTS WITH OSTEOPOROSIS: A PROPENSITY SCORE MATCHED ANALYSIS
Pil-Sung YANG (Republic of Korea)
P 1-150 OUTCOMES OF RATE-CONTROL TREATMENT IN PATIENTS WITH ATRIAL FIBRILLATION AND HEART 258 FAILURE: A NATIONWIDE COHORT STUDY
Hee Tae YU (Republic of Korea)

xix
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
HEART FAILUREP 1-151 IMPACT OF VENTRICULAR LATE POTENTIAL TO PREDICT REVERSE REMODELING IN THE PATIENTS 259 WITH FIRST DOCUMENTED NONISCHEMIC HEART FAILURE WITH REDUCED LEFT VENTRICULAR EJECTION FRACTION
Yuya AOYAMA (Japan)
P 1-152 THE IMPORTANCE OF A CHANGE IN SERUM BILIRUBIN IN PREDICTING LEFT VENTRICULAR REVERSE 260 REMODELING AND OUTCOMES IN HEART FAILURE PATIENTS WITH CARDIAC RESYNCHRONIZATION THERAPY
Junya HOSODA (Japan)
P 1-153 FIRST DEGREE AV BLOCK AS A PARAMETER PREDICTING LONG-TERM PROGNOSIS IN PATIENTS WITH 261 ACUTE HEART FAILURE_ FROM KOREAN ACUTE HEART FAILURE REGISTRY (KORAHF REGISTRY)
Dae In LEE (Republic of Korea)
PEDIATRIC/ADULT CONGENITAL HEART DISEASEP 1-155 SUCCESSFUL CATHETER ABLATION FOR EARLY POSTOPERATIVE VENTRICULAR TACHYCARDIA IN AN 262 EBSTEIN ANOMALY PATIENT WITH CONE PROCEDURE
Kyung Jin AHN (Republic of Korea)
P 1-156 WHICH WOULD BE BETTER MEDICATION FOR POST-OPERATIVE JUNCTIONAL ECTOPIC TACHYCARDIA, 263 AMIODARONE OR NIFECALANT?
Hisaaki AOKI (Japan)
P 1-157 3 YEAR-OLD-BOY WITH HEART FAILURE DUE TO RIGHT VENTRICLE PACING FOR ATRIOVENTRICULAR 264 BLOCK, CRT WITH TRANSVENOUS LEAD WAS EFFECTIVE
Misugi EMI (Japan)
P 1-158 PREVALENCE OF ARRHYTHMIA AFTER EXTRACARDIAC CONDUIT FONTAN PROCEDURE: A SINGLE 265 INSTITUTION STUDY
Rahmalia GUSDINA (Indonesia)
P 1-159 CHARACTERISTICS AND LONG-TERM FOLLOW-UP OF YOUNG ADULTS FOLLOWING PERMANENT 266 PACEMAKER PLACEMENT FOR COMPLETE HEART BLOCK
Atul PRABHU (Taiwan)
P 1-161 ACUTE OUTCOMES FOR CRYOABLATION OF PEDIATRIC PATIENTS WITH TACHYARRHYTHMIA IN TAIWAN: 267 SINGLE CENTER REPORT
Kun-Lang WU (Taiwan)
P 1-162 CONCURRENT ANK2 AND RYR2 MUTATION IN A PATIENT WITH REFRACTORY TACHYCARDIA 268Jakyoung YOON (Republic of Korea)
P 1-163 SHORT QT INTERVAL IN YOUNG HEALHTY SUBJECTS OF AFRICAN AND CAUCASIAN RACE DURING 269 6-MINUTE WALK TEST
Tatiana DRONOVA (Russian Federation)
P 1-164 PROLONGATION OF CORRECTED QT INTERVAL PREDICTS THE RISK FOR CARDIAC DEATH IN PATIENTS 270 WITH HYPERTROPHIC CARDIOMYOPATHY
Hyungdon KOOK (Republic of Korea)
P 1-165 SUCCESSFUL CATHETER ABLATION FOR ATRIAL FIBRILLATION IN A PATIENT WITH CONGENITAL 271 MYOPATHY
Yasuki KOYANO (Japan)
P 1-166 OUTCOME OF THE MAZE PROCEDURE IN PATIENTS WITH CONGENITAL HEART DISEASES 272Sangyun LEE (Republic of Korea)

xx
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
FRIDAY POSTER PRESENTATION (14 October)
BASIC/TRANSLATIONAL SCIENCEP 2-001 THE EFFECT OF RADIOFREQUENCY ABLATION ON STEM CELLS AND SYSTEMIC INFLAMMATION IN 274 PATIENTS WITH SUPRAVENTRICULAR TACHYCARDIA
Ahmet Lutfu SERTDEMIR (Turkey)
P 2-002 HEAT SHOCK PROTEIN INDUCER GERANYLGERANYLACETONE (GGA) PROTECTS AGAINST ATRIAL 275 FIBRILLATION VIA THE PI3K PATHWAY
Eun Kyoung CHOI (Republic of Korea)
P 2-003 ETHANOL INDUCES PROLONGATION OF THE PLATEAU PHASE OF ACETYLCHOLINE-ACTIVATED K+ 276 CURRENT IN MOUSE ATRIAL CARDIOMYOCYTES
Eun Kyoung CHOI (Republic of Korea)
P 2-004 DIFFERENTIAL EFFECTS OF CARVEDILOL AND ATENOLOL ON ACETYLCHOLINE-ACTIVATED K+ 277 CURRENT: POSSIBLE ATRIAL-SPECIFIC ANTIARRHYTHMIC EFFECTS OF CARVEDILOL ON ATRIAL FIBRILLATION
Eun Kyoung CHOI (Republic of Korea)
P 2-005 RESVERATROL PROMOTES CARDIOMYOCYTE SURVIVAL AND DECREASES APOPTOSIS THROUGH 278 HIPPO-YAP SIGNALING PATHWAY
Yu-Ting HUANG (Taiwan)
P 2-007 MISSENSE MUTATION A561V-HERG CAUSES CARDIOMYOCYTE APOPTOSIS VIA ENDOPLASMIC 279 RETICULUM STRESS PATHWAY
Shuting MA (China)
P 2-008 ENHANCED CELL SURVIVAL AND PARACRINE EFFECTS OF MESENCHYMAL STEM CELLS 28 0 OVEREXPRESSING HEPATOCYTE GROWTH FACTOR PROMOTE CARDIOPROTECTION IN MYOCARDIAL INFARCTION MYOCARDIAL INFARCTION
Fengxiang ZHANG (China)
P 2-009 GANGLIONATED PLEXI STIMULATION INDUCES PULMONARY VEIN TRIGGERS AT LEFT ATRIUM- 281 PULMONARY VEIN JUNCTION CHANGING WAVE-DYNAMICS: IN SILICO MODELING STUDY
Minki HWANG (Republic of Korea)
P 2-010 THE SPATIOTEMPORAL STABILITY OF DOMINANT FREQUENCY SITES IN IN-SILICO MODELING OF 282 3-DIMENSIONAL LEFT ATRIAL MAPPING OF ATRIAL FIBRILLATION
Byounghyun LIM (Republic of Korea)
P 2-011 DOMINANT FREQUENCY ABLATION TERMINATES ATRIAL FIBRILLATION DEPENDING ON CONDUCTION 283 VELOCITY IN-SILICO 3-DIMENSIONAL MODEL OF LEFT ATRIUM
Byounghyun LIM (Republic of Korea)
ALLIED PROFESSIONALSP 2-012 BENEFITS OF RISK FACTOR MODIFICATION ON AF RECURRENCE STRATIFIED BY GENDER 284
Melissa MIDDELDORP (Australia)
P 2-013 LOW PREVALENCE OF EXTERNALIZED CONDUCTOR AND ELECTRICAL ABNORMALITIES IN RIATA LEAD 285 AFTER LONG TERM FOLLOW UP: A SINGLE CENTER EXPERIENCE
Napawan PORNNIMITTHUM (Thailand)
P 2-015 CARDIAC ARRHYTHMIAS DURING PERIOPERATIVE PERIOD OF NON-CARDIAC SURGERY 286Seiichi TANIAI (Japan)
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICESP 2-016 PATIENT EXPERIENCE WITH MINIATURIZED INSERTABLE CARDIAC MONITOR 287
Prashanthan SANDERS (Australia)
P 2-017 INFLUENCE OF PATIENT CHARACTERISTICS ON INTRATHORACIC IMPEDANCE MEASUREMENTS IN 288 CRT-D/ICD PATIENTS
Vinod SHARMA (United States)

xxi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-018 EXPLANT PROCEDURE FOR THE REVEAL LINQ INSERTABLE CARDIAC MONITOR: EXPERIENCES FROM 289 THE LINQ USABILITY TRIAL
Prashanthan SANDERS (Australia)
P 2-019 IMPACT OF AGE ON THE INSERTION PROCEDURE OF THE REVEAL LINQ™ INSERTABLE CARDIAC 290 MONITOR: RESULTS FROM A REAL-WORLD GLOBAL MULTI-CENTER REGISTRY
Atul VERMA (Canada)
P 2-020 SIMPLIFIED USE OF TELESCOPING-SUPPORT CATHETER SYSTEM FOR LEFT VENTRICULAR LEAD 291 PLACEMENT IN PATIENTS UNDERGOING CARDIAC RESYNCHRONIZATION THERAPY
Devender AKULA (United States)
P 2-021 FUNDAMENTAL ANATOMICAL INPUTS TO MOTIVATE SAFE IMPLANTATION OF A NOVEL EXTRAVASCULAR 292 ICD SYSTEM
Ryan LAHM (United States)
P 2-022 EXPERIENCE OF PERCUTANEOUS TRANSHEPATIC VENOUS ACCESS FOR ICD AND PACEMAKER 293 IMPLANTATION
Zhifu CEN (China)
P 2-023 NOVEL TECHNIQUE FOR RIGHT ATRIAL LEAD PLACEMENT IN YOUNG PATIENTS WITH SMALL RIGHT 294 ATRIUM
Dinesh CHOUDHARY (India)
P 2-024 THE CLINICAL SIGNIFICANCE OF ANATOMICAL EVALUATION USING 3D-CT FOR SUBCTANEOUS-ICD 295 IMPLANTATION JUST AFTER MITRAL VALVE REPLACEMENT WITH VENTRICULAR FIBRILLATION
Hikari HASHIMOTO (Japan)
P 2-025 ATRIAL SEPTAL AND HIGH RIGHT VENTRICULAR SEPTAL PACING IN ADVANCED AGE PATIENTS: 296 MID-TERM FOLLOW-UP ATRIAL AND VENTRICULAR LEADS PERFORMANCES
Tatsuo MISAWA (Japan)
P 2-026 CHANGES IN PULMONARY ARTERY SYSTOLIC PRESSURE FOLLOWING PACEMAKER/DEFIBRILLATOR 297 LEAD EXTRACTION
Alwaleed ALJOHAR (Saudi Arabia)
P 2-027 THE USE OF SIMPLE TRACTION VS. ADVANCED EXTRACTION TECHNIQUES IN CARDIAC DEVICES LEAD 298 EXTRACTION: IDENTIFICATION OF PREDICTORS
Alwaleed ALJOHAR (Saudi Arabia)
P 2-028 TRANSESOPHAGEAL VS. TRANSTHORACIC ECHOCARDIOGRAPHY: WHAT VISUALIZES CARDIAC DEVICE 299 LEAD VEGETATIONS BETTER?
Alwaleed ALJOHAR (Saudi Arabia)
P 2-029 PACEMAKER/DEFIBRILLATOR LEAD EXTRACTION AND THE RISK OF TRICUSPID VALVE 300 REGURGITATION
Alwaleed ALJOHAR (Saudi Arabia)
P 2-030 ENHANCED SAFETY OF TRANSVENOUS LEAD EXTRACTION IN HIGH-RISK PATIENTS: A HYBRID 301 MINIMALLY INVASIVE APPROACH
Luca BONTEMPI (Italy)
P 2-031 DOUBLE SNARE TECHNIQUE: A NEW AND SIMPLE FEMORAL APPROACH FOR LEAD EXTRACTION 302Mohammad IQBAL (Indonesia)
P 2-032 MANAGEMENT OF ANTICOAGULATION IN CARDIAC IMPLANTABLE ELECTROPHYSIOLOGICAL DEVICES 303 PERIOPERATIVE PERIOD
Junji MORITA (Japan)
P 2-033 CARDIAC RHYTHM MANAGED DEVICE INFECTIONS 304 Michio NAGASHIMA (Japan)
P 2-034 PRECLINICAL RESULTS DEMONSTRATING THE TWO-YEAR EXTRACTABILITY OF A NOVEL LEFT 305 VENTRICULAR ACTIVE FIXATION LEAD FROM THE CORONARY VEINS
Amy THOMPSON (United States)
P 2-035 TRACTION ALONE IS RARELY EFFECTIVE IN REMOVING CONTEMPORARY ICD LEADS: RESULTS FROM 306 THE ICDTEA LEAD EXTRACTION TENSILE FORCE ASSESSMENT (ICDTEA) STUDY
Pierce VATTEROTT (United States)

xxii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
CATHETER ABLATIONP 2-036 RHYTHM VS. RATE CONTROL IN PATIENTS WITH ATRIAL FIBRILLATION COMBINED WITH LEFT 307 VENTRICULAR SYSTOLIC DYSFUNCTION: A META-ANALYSIS
Jinhee AHN (Republic of Korea)
P 2-037 THE CLINICAL OUTCOME OF EARLY CARDIOVERSION IN PATIENTS WITH EARLY RECURRENCE OF ATRIAL 308 TACHYARRHYTHMIAS: THE EFFECT OF TIMING AND ATRIAL FIBRILLATION TYPE
Jinhee AHN (Republic of Korea)
P 2-038 REDUCTION OF BLOOD CHOLESTEROL ON RECURRENCE AFTER CATHETER ABLATION IN PATIENTS 309 WITH ATRIAL FIBRILLATION
Yong-Soo BAEK (Republic of Korea)
P 2-039 IMPACT OF CONTACT FORCE AS A PREDICTOR OF CLINICAL OUTCOME IN RADIOFREQUENCY ABLATION 310 Sanisara CHANDRACHAMNONG (Thailand)
P 2-040 RADIOFREQUENCY OR CRYOBALLON ABLATION FOR PAROXYSMAL ATRAIL FIBRILLATION? 311 A META-ANALYSIS AND SYSTEMATIC REVIEW
Chao-Feng CHEN (China)
P 2-041 RISK OF STROKE AFTER MYOCARDIAL INFARCTION IN PATIENT WITH OR WITHOUT ATRIAL 312 FIBRILLATION
Cheng-Hung CHIANG (Taiwan)
P 2-042 THE FEASIBILITY OF A BOX ISOLATION WITH LINEAR ABLATION IN PERSISTENT ATRIAL FIBRILLATION 314 Taishi FUJISAWA (Japan)
P 2-043 THE LEVEL OF INFLAMMATORY CYTOKINES BETWEEN RADIOFREQUENCY AND CRYOBALLOON 315 AFTER ATRIAL FIBRILLATION ABLATION
Ya-Wen HSIAO (Taiwan)
P 2-045 VIRTUAL IN-SILICO MODELING GUIDED CATHETER ABLATION VS. EMPIRICAL ABLATION FOR 316 LONGSTANDING PERSISTENT ATRIAL FIBRILLATION: MULTICENTER PROSPECTIVE RANDOMIZED STUDY
Hui-Nam PAK (Republic of Korea)
P 2-046 ACUTE PROCEDURAL OUTCOME AND PROCEDURAL PARAMETERS OF ATRIAL FIBRILLATION CATHETER 317 ABLATION USING THE NOVEL PULMONARY VEIN ABLATION CATHETER PVAC GOLD®
Jongmin HWANG (Republic of Korea)
P 2-047 SUCCESSFUL CATHETER ABLATION WITH MULTIPLE SESSIONS FOR RECURRENT ATRIAL FIBRILLATION 318 IMPROVES THE RENAL FUNCTION IN PATIENTS WITH CHRONIC KIDNEY DISEASE
Dai INAGAKI (Japan)
P 2-048 VALUE OF ADENOSINE TEST TO REVEAL DORMANT CONDUCTION OR ADENOSINE INDUCED ATRIAL 319 FIBRILLATION AFTER PULMONARY VEIN ISOLATION
Mohammad IQBAL (Republic of Korea)
P 2-049 THE CHARACTERISTICS OF PAROXYSMAL ATRIAL FIBRILLATION IN HYPERTROPHIC CARDIOMYOPATHY 320Shin KASHIMURA (Japan)
P 2-050 IMPACT OF DIFFERENT MECHANISM BETWEEN EARLY AND LATE PHASE RECURRENCE OF ATRIAL 321 FIBRILLATION AFTER CATHETER ABLATION
Nobutaka KATO (Japan)
P 2-051 DETECTION OF REAL-TIME LEFT ATRIAL APPENDAGE STAGNANT DYE STAINING DURING PULMONARY 322 VEIN ANTRAL ISOLATION
Bong-Joon KIM (Republic of Korea)
P 2-052 THE CHARACTERISTICS OF ATRIAL FIBRILLATION PATIENTS WITH PERIPROCEDURAL ORAL 323 ANTICOAGULANTS
Takehiro KIMURA (Japan)
P 2-053 LEFT ATRIAL EMPTYING FRACTION AS A PREDICTOR FOR CLINICAL OUTCOME IN PATIENTS WITH 324 ATRIAL FIBRILLATION ABLATION
Dae In LEE (Republic of Korea)
P 2-054 LEFT ATRIAL APPENDAGE CLOSURE USING LAMBRE AND WATCHMAN DEVICE: CONSECUTIVE 325 OBSERVATIONAL STUDY
Anggia LUBIS (Indonesia)

xxiii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-055 DECREASE IN B-TYPE NATRIURETIC PEPTIDE LEVELS AND SUCCESSFUL CATHETER ABLATION FOR 326 ATRIAL FIBRILLATION IN PATIENTS WITH HEART FAILURE: A CLINICAL INDICATOR OF REVERSE REMODELING
Yosuke MURASE (Japan)
P 2-056 THE COMPARISON OF LEFT ATRIAL LOW VOLTAGE ZONE BETWEEN PAROXYSMAL ATRIAL 327 FIBRILLATION (PAF) AND NON-(PAF) PATIENTS FOR ATRIAL FIBRILLATION ABLATION
Yasutsugu NAGAMOTO (Japan)
P 2-057 PATTERN OF SINUS RHYTHM RECOVERY BY CARDIOVERSION AFTER RECURRENCE DURING BLANKING 328 PERIOD IN PAROXYSMAL ATRIAL FIBRILLATION PATIENTS RECEIVING CATHETER ABLATION WAS ASSOCIATED WITH ABLATION OUTCOME
Ryo NAKAMARU (Japan)
P 2-059 QUALITY OF ANTICOAGULATION AND BLEEDING EVENT IN PATIENTS WITH NON-VALVULAR ATRIAL 329 FIBRILLATION NEWLY TREATED WITH VITAMIN K ANTAGONIST: A REVIEW OF REAL-WORLD REGISTRY [THE KORAF II]
Il-Young OH (Republic of Korea)
P 2-060 IMPACT OF CATHETER ABLATION FOR ATRIAL FIBRILLATION ON PATIENTS TAKING DABIGATRAN 330Noriyuki OHASHI (Japan)
P 2-061 THE IMPACT OF ADENOSINE-INDUCED DORMANT CONDUCTION ON RECURRENCE AFTER ATRIAL 331 FIBRILLATION ABLATION; AN ANALYSIS STRATIFIED BY TIME TO RECURRENCE
Masato OKADA (Japan)
P 2-062 GENDER DIFFERENCE IN OUTCOMES OF CATHETER ABLATION FOR ATRIAL FIBRILLATION IN JAPANESE 332 POPULATION
Masato OKADA (Japan)
P 2-063 IMPACT OF FOCAL IMPULSE AND ROTOR MODULATION ON PROCEDURAL AND CLINICAL OUTCOMES: 333 A SYSTEMATIC REVIEW AND META-ANALYSIS
Catherine O’SHEA (Australia)
P 2-064 SATISFACTION WITH VITAMIN K ANTAGONISTS IN PATIENTS WITH NON-VALVULAR ATRIAL 334 FIBRILLATION [THE KORAF II]
Hyung-Wook PARK (Republic of Korea)
P 2-065 INTERNATIONAL NORMALIZED RATIO CONTROL AND SIDE EFFECTS IN PATIENTS WITH NONVALVULAR 335 ATRIAL FIBRILLATION TAKING VITAMIN K ANTAGONIST WITH OR WITHOUT ANTIPLATELET DRUGS [THE KORAF II]
Jaeseok PARK (Republic of Korea)
P 2-066 IMPLANT SUCCESS AND SAFETY OF LEFT ATRIAL APPENDAGE CLOSURE WITH THE WATCHMAN DEVICE 336 IN AN ASIAN POPULATION: PERI-PROCEDURAL OUTCOMES FROM THE WASP REGISTRY
Karen PHILLIPS (Australia)
P 2-067 IMPACT OF MONOCYTE-TO-HIGH-DENSITY LIPOPROTEIN RATIO AS THE PREDICTOR FOR SUBSTRATE OF 337 ATRIAL FIBRILLATION
Akira SATO (Japan)
P 2-068 THE INFERIOR SHIFT OF P-WAVE AXIS IS ASSOCIATED TO LINEAR ABLATION AND CLINICAL OUTCOME IN 338 PATIENTS WITH LONGSTANDING PERSISTENT ATRIAL FIBRILLATION
Dong Geum SHIN (Republic of Korea)
P 2-069 CLINICAL OUTCOME OF ADDITIONAL CAVOTRICUSPID ISTHMUS ABLATION IN PATIENTS WITH 339 PAROXYSMAL ATRIAL FIBRILLATION AND WITHOUT ATRIAL FLUTTER: PROSPECTIVE RANDOMIZED STUDY
Dong Geum SHIN (Republic of Korea)
P 2-070 THE MORPHOLOGICAL CHARACTERISTICS OF THE VEIN OF MARSHALL UTILIZED ON THE CHEMICAL 340 ABLATION
Yuya TAKAHASHI (Japan)
P 2-071 THE SAFETY OF STOPPING ORAL ANTICOAGULATION THERAPY AFTER SUCCESSFUL ABLATION OF 341 ATRIAL FIBRILLATION
Akihiro TAKITSUME (Japan)
P 2-072 EFFECT OF VASO-VAGAL REACTION ON IMMEDIATE AND LONG-TERM OUTCOMES OF CRYOBALLOON 342 ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION
Hiroshi TASAKA (Japan)

xxiv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-073 SUBCLAVIAN VEIN PACING FOR PHRENIC NERVE MONITORING DURING CRYOBALLOON ABLATION OF 343 ATRIAL FIBRILLATION
Kenichi TOKUTAKE (Japan)
P 2-074 EARLY RECURRENCE OF ATRIAL FIBRILLATION FOLLOWING RADIOFREQUENCY CATHETER ABLATION 344 IN NATIONAL CARDIOVASCULAR CENTER HARAPAN KITA-A 3 MONTHS FOLLOW UP
Priyandini WULANDARI (Indonesia)
P 2-075 ELECTRICAL PACING FROM LEFT SUBCLAVIAN VEIN FOR PREVENTION OF LEFT PHRENIC NERVE 345 INJURY DURING CRYOBALLOON ABLATION OF ATRIAL FIBRILLATION
Mitsumi YAMASHITA (Japan)
P 2-076 ELEVATED RED BLOOD CELL DISTRIBUTION WIDTH PREDICTS RECURRENCE AFTER CATHETER 346 ABLATION FOR ATRIAL FIBRILLATION IN PATIENTS WITH HEART FAILURE: COMPARISON WITH NON-HEART FAILURE PATIENTS
Satoshi YANAGISAWA (Japan)
P 2-077 LONG-TERM OUTCOME OF CATHETER ABLATION FOR ATRIAL FIBRILLATION IN HYPERTROPHIC 347 CARDIOMYOPATHY
Takashi YOSHIZAWA (Japan)
P 2-078 SEVERE COMPLICATION DURING CATHETER ABLATION FOR ATRIAL FIBRILLATION DUE TO 348 SIMULTANEOUS SPASM OF RIGHT AND LEFT CORONARY ARTERY
Akemi ASO (Japan)
P 2-079 CLINICAL PRESENTATION OF PULMONARY VEIN STENOSIS COMPLICATING ABLATION FOR ATRIAL 349 FIBRILLATION
Yukihiro INAMURA (Japan)
P 2-080 BE CAUTIOUS. A SOFT TIP OF THE LONG SHEATH CAN BECOME DANGEROUS 350Ryusuke KIMURA (Japan)
P 2-081 PULMONARY VEIN ISOLATION USING CRYOABLATION CAN BE SAFELY PERFORMED AS A DAY-CASE 351 PROCEDURE
Edwin KOOIJMAN (New Zealand)
P 2-082 EFFICACY OF CRYOABLATION FOR PAROXYSMAL AND PERSISTENT AF IN THE MIDLAND REGION OF 352 New Zealand
Edwin KOOIJMAN (New Zealand)
P 2-083 2:1 ATRIO-VENTRICULAR BLOCK DURING CAVO-TRICUSPID ISTHMUS ABLATION 353Takuro NISHIMURA (Japan)
P 2-085 RIGHT CORONARY ARTERY OCCLUSION AFTER CAVOTRICUSPID ISTHMUS ABLATION 354Erika YAMASHITA (Japan)
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATIONP 2-086 CLINICAL PREDICTORS OF TOTAL AV BLOCK IN HYPERTROPHY OBSTRUCTIVE CARDIOMYOPATHY 355 UNDERGO ALCOHOL SEPTAL ABLATION
Haikal BALWEEL (Indonesia)
P 2-087 FEASIBILITY OF THE TRANSSEPTAL APPROACH FOR VENTRICULAR ANEURYSM RELATED 356 VENTRICULAR TACHYCARDIA MAPPING AND ABLATION
Lian CHEN (China)
P 2-088 CATHETER ABLATION OF LEFT FASCICULAR VENTRICULAR TACHYCARDIA BASED ON FRACTIONATED 357 PRESYSTOLIC PURKINJE POTENTIAL
Pradeep HASIJA (India)
P 2-091 RADIOFREQUENCY CATHETER ABLATION OF VENTRICULAR TACHYCARDIA IN STRUCTURAL HEART 358 DISEASE: SINGLE TEAM EXPERIENCE WITH FOLLOW-UP UPTO 5 YEARS
Vikas KATARIA (India)
P 2-092 COMPARISON OF REMOTE MAGNETIC NAVIGATION ABLATION AND MANUAL ABLATION OF IDIOPATHIC 359 VENTRICULAR ARRHYTHMIA AFTER FAILED MANUAL ABLATION
Mitsuharu KAWAMURA (Japan)
P 2-094 A ONE YEAR FOLLOW-UP AFTER EPICARDIAL ABLATION IN A PATIENT WITH BRUGADA SYNDROME AND 360 INFERIOR EARLY REPOLARISATION
Edward LEE (Singapore)

xxv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-095 LONG-TERM CLINICAL OUTCOMES OF CATHETER ABLATION FOR VENTRICULAR TACHYARRHYTHMIAS 361 ACCORDING TO THE SITE OF ORIGIN: LEFT VENTRICULAR END DIASTOLIC DIMENSION PREDICTS THE RECURRENCES
Kwang No LEE (Republic of Korea)
P 2-097 CATHETER ABLATION OF PARAHISIAN VENTRICULAR ARRHYTHMIAS WITH THREE QRS MORPHOLOGIES 362 ORIGINATE FROM ONE FOCUS USING IDENTIFICATION OF CHANNEL.
Yuya NAKAMURA (Japan)
P 2-098 DIVERGENT LONG-TERM OUTCOME OF CATHETER ABLATION FOR VENTRICULAR TACHYCARDIA IN 363 CARDIOMYOPATHY WITH DIFFERENT ETIOLOGIES
Ching Ju WU (Taiwan)
P 2-099 IDIOPATHIC FOCAL VT FROM BOTH PAPILLARY MUSCLES AND AVNRT IN A PATIENT WITH POST AVR 364Ramdeo YADAVE (India)
P 2-100 IDIOPATHIC VT FROM LV BASE NEAR ANTERIOR MITRAL ANNULUS 365Ramdeo YADAVE (India)
P 2-101 A CASE OF SUCCESSFUL RADIOFREQUENCY CATHETER ABLATION OF BOTH SLOW-FAST 366 ATRIOVENTRICULAR NODE REENTRANT TACHYCARDIA AND FREQUENT IDIOPATHIC PREMATURE VENTRICULAR CONTRACTION WITH IN KOCH’S TRIANGLE
Yoshiaki YUI (Japan)
P 2-103 ESTABLISHMENT OF ADDITIONAL ELECTRICAL PARAMETERS FOR SAFELY AND EFFECTIVELY 367 PERFORMING BIPOLAR RADIO-FREQUENCY ABLATION: OBSERVATIONS FROM AN EXPERIMENTAL STUDY
Osamu SAITOH (Japan)
P 2-104 CORONARY ARTERY-LEFT VENTRICULE FISTULA FOLLOWING VENTRICULAR TACHYCARDIA ABLATION 368Chihiro OTA (Japan)
P 2-105 THE CHARACTERISTIC OF EARLY REPOLARIZATION IN PATIENT WITH ACUTE MYOCARDIAL INFARCTION 369 AND SUBSEQUENT VENTRICULAR ARRHYTHMIA
Cheng-I WU (Taiwan)
CLINICAL ELECTROPHYSIOLOGYP 2-106 INTERIM RESULTS FROM NEW REDUCIBLE STUDY: A MULTICENTER, PROSPECTIVE, RANDOMIZED 370 CLINICAL TRIAL OF INVESTIGATION ON APPROPRIATE DURATION OF NOVEL ORAL ANTICOAGULANTS USE AFTER CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION IN PATIENTS WITH LOW THROMBOEMBOLIC RISK
Yong-Soo BAEK (Republic of Korea)
P 2-107 TREATMENT OF ATRIAL FIBRILLATION PATIENT WITH METOPROLOL AND AMIODARONE COMPLICATED 371 BY PSORIASIS
Miaomiao CAO (China)
P 2-108 INCIDENCE AND RISK FACTORS OF ISCHEMIC STROKE AMONG NON-VALVULAR ATRIAL FIBRILLATION 372 IN THAILAND
Thunyarat CHAIPRUCKMALAKARN (Thailand)
P 2-109 THE ANTICOGULATION THERAPY OF PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION 373 IN MACAU
Ruohan CHEN (China)
P 2-111 APIXABAN POSTMARKETING SURVEILLANCE OF KOREAN AND JAPANESE PATIENTS WITH 374 NONVALVULAR ATRIAL FIBRILLATION: BASELINE CHARACTERISTICS OF THE POOLED STUDY POPULATION
Seongwook HAN (Republic of Korea)
P 2-112 PRE-EXISTING ISCHEMIC HEART DISEASE IS A RISK FACTOR FOR CARDIAC MORTALITY IN ATRIAL 375 FIBRILLATION WITH CONTINUOUS DIGOXIN USE FOR 10-YEAR FOLLOW-UP
Ki-Woon KANG (Republic of Korea)
P 2-113 SAFETY AND EFFICACY OF NOVEL ORAL ANTICOAGULATION IN PATIENT WITH ATRIAL FIBRILLATION 376 AND PRIOR INTRACEREBRAL HEMORRHAGE
Kyu KIM (Republic of Korea)
P 2-114 FAVORABLE EFFECT OF NOVEL ORAL ANTICOAGULATION IN ATRIAL FIBRILLATION PATIENTS WITH 377 NEWLY DIAGNOSED CANCER
Kyu KIM (Republic of Korea)

xxvi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-116 XANAP: REAL-WORLD, PROSPECTIVE, OBSERVATIONAL STUDY OF PATIENTS TREATED WITH 378 RIVAROXABAN FOR STROKE PREVENTION IN ATRIAL FIBRILLATION
Young-Hoon KIM (Republic of Korea)
P 2-117 EFFICACY OF RHYTHM CONTROL AND ITS RESPONSE PREDICTORS IN PATIENTS WITH CARDIAC 379 IMPLANTABLE ELECTRONIC DEVICES & ATRIAL FIBRILLATION
Po-Lin LIN (Taiwan)
P 2-118 DIFFERENTIAL EFFECTS OF STATIN IN PREVENTING NEWLY ONSET ATRIAL FIBRILLATION BETWEEN 380 PATIENTS WITH AND WITHOUT CHRONIC KIDNEY DISEASE
Yen-Nien LIN (Taiwan)
P 2-119 AN INTERNATIONAL SURVEY OF PATIENT PERCEPTIONS OF ATRIAL FIBRILLATION, STROKE RISK, AND 381 ORAL ANTICOAGULATION TREATMENT
Gregory YH LIP (United Kingdom)
P 2-120 ATRIAL FIBRILLATION PATIENTS’ PERCEPTIONS OF ANTICOAGULATION THERAPY: COMPARING ASIA 382 WITH THE REST OF THE WORLD
Gregory YH LIP (United Kingdom)
P 2-121 PROPORTION OF THAI PATIENTS WITH ATRIAL FIBRILLATION RECEIVING WARFARIN WITH LABILE INR 383 IN EACH GROUP OF SAMETT2R2 SCORE
Komsing METHAVIGUL (Thailand)
P 2-122 ROLE OF NEW ORAL ANTICOAGULANTS(NOACs) IN LEFT ATRIAL OCCLUDER DEVICE-WATCHMAN 384 IMPLANT
Zulkeflee MUHAMMAD (Malaysia)
P 2-123 LONG-TERM SAFETY OF ORAL ANTICOAGULANT DISCONTINUATION AFTER ATRIAL FIBRILLATION 385 RADIOFREQUENCY ABLATION: SYSTEMATIC REVIEW AND META-ANALYSIS
Dian MUNAWAR (Australia)
P 2-124 NEW ORAL ANTICOAGULANT AND VITAMIN K ANTAGONIST MANAGEMENT IN PERI-PROCEDURAL 386 ATRIAL FIBRILLATION RADIOFREQUENCY ABLATION: SYSTEMATIC REVIEW AND META-ANALYSIS
Dian MUNAWAR (Australia)
P 2-125 IMPACT OF STROKE EVENTS IN JAPANESE PATIENTS WITH ATRIAL FIBRILLATION DETECTED BY 387 CARDIAC IMPLANTABLE ELECTRONIC DEVICE
Miyo NAKANO (Japan)
P 2-126 EFFICACY OF ANTIARRHYTHMIC DRUGS THERAPY IN PREVENTING AF RECURRENCE AND LONG-TERM 388 CARDIOVASCULAR PROGNOSIS IN PATIENTS WITH ASYMPTOMATIC PAROXYSMAL ATRIAL FIBRILLATION
Shingen OWADA (Japan)
P 2-127 IMPACT OF NOVEL ORAL ANTICOAGULANTS ACCORDING TO DOSAGE ON CLINICAL OUTCOMES IN ATRIAL 389 FIBRILLATION PATIENTS WITH UNDERWEIGHT
Chan Soon PARK (Republic of Korea)
P 2-128 1 OR 2 MONTHS WARFARIN THERAPY WITH LOW THROMBOEMBOLIC RISK PATIENTS AFTER 390 RADIOFREQUENCY CATHETER ABLATION OF ATRIAL FIBRILLATION: INTERIM RESULTS OF SINGLE CENTER PROSPECTIVE RANDOMIZED STUDY
Hee-Soon PARK (Republic of Korea)
P 2-129 NOAC EXPERIENCE FROM A TERTIARY GOVERNMENT HOSPITAL IN MALAYSIA 391Noel ROSS (Malaysia)
P 2-130 THE PERSISTENCE AND SAFETY OF NON VITAMIN K ANTAGONIST ORAL ANTICOAGULATION IM KOREA 392 PATIENTS WITH ATRIAL FIBRILLATION
Choong-Sil SEONG (Republic of Korea)
P 2-131 RISK FACTORS FOR THE LEFT ATRIAL APPENDAGE THROMBUS IN PATIENTS TAKING APPROPRIATE ORAL 393 ANTICOAGULATION WITH ATRIAL FIBRILLATION
Satoshi TAKAHASHI (Japan)
P 2-132 AMIODARONE, A DOUBLE EDGED SWORD: A CASE SERIES ON THE TOXIC EFFECTS OF THE DRUG 394Abhinay TIBDEWAL (India)
P 2-133 TREATMENT ADHERENCE FOR ANTICOAGULANT THERAPY IN PATIENTS WITH ATRIAL FIBRILLATION 395Steven Alviano YUWONO (Indonesia)

xxvii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
HEART FAILUREP 2-134 CLINICAL CHARACTERISTICS OF PATIENTS RESPONDING ONE YEAR AFTER CARDIAC 396 RESYNCHRONIZATION THERAPY
Young CHOI (Republic of Korea)
P 2-135 OUTCOMES OF CARDIAC RESYNCHRONIZATION THERAPY IN PATIENTS WITH ATRIAL FIBRILLATION 397 ACCOMPANIED BY SLOW VENTRICULAR RESPONSE
Jin Kyung HWANG (Republic of Korea)
P 2-136 PREDICTORS OF SUPER-RESPONDER TO CARDIAC RESYNCHRONIZATION THERAPY IN ADVANCED 398 HEART FAILURE PATIENTS
A. Hafiedz A. KARTAMIHARDJA (Indonesia)
P 2-138 TYPICAL LEFT BUNDLE BRANCH BLOCK IS ASSOCIATED WITH MORE FAVORABLE RESPONSE TO 399 CARDIAC RESYNCHRONIZATION THERAPY IN HEART FAILURE PATIENTS
Jaewon OH (Republic of Korea)
P 2-140 IMPACT OF CARDIAC RESYNCHRONIZATION THERAPY-DEFIBRILLATOR IMPLANTATION ON THE 400 ASSOCIATION BETWEEN BODY MASS INDEX AND PROGNOSIS IN PATIENTS WITH HEART FAILURE
Masaki TAKENAKA (Japan)
P 2-142 ASSOCIATION OF BASELINE BIG ENDOTHELIN-1 LEVEL WITH LONG-TERM CLINICAL OUTCOMES AMONG 401 CARDIAC RESYNCHRONIZATION THERAPY RECIPIENTS
Shengwen YANG (China)
P 2-143 LEFT VENTRICULAR DYSSYNCHRONY ASSESSMENT BY QUANTITATIVE BLOOD POOL SPECT FOR 402 PREDICTION OF CRT RESPONSE
Yuriko YOSHIDA (Japan)
PEDIATRIC/ADULT CONGENITAL HEART DISEASEP 2-144 HIGH ATRIAL DEFIBRILLATION THRESHOLD WITH INTERNAL CARDIOVERSION CAUSED BY LEFT ATRIAL 403 DILATATION IN PERSISTENT ATRIAL FIBRILLATION CASE
Satoshi AITA (Japan)
P 2-145 VARYING ATRIOVENTRICULAR BLOCKS IN A YOUNG ADULT WITH ACUTE MYOCARDITIS: 404 A CASE REPORT
Andre AWALOEI (Philippines)
P 2-146 ENDOCARDIAL CARDIAC RESYNCHRONIZATION THERAPY IN SMALL CHILDREN WITH BIVENTRICULAR 405 DYSFUNCTION AND COMPLETE ATRIOVENTRICULAR BLOCK
Misugi EMI (Japan)
P 2-147 THE CHARACTERISTICS OF THREE CARDIAC SARCOIDOSIS CASES WHO UNDERWENT CATHETER 406 ABLATION FOR VENTRICULAR TACHYCARDIA
Naotaka HASHIGUCHI (Japan)
P 2-148 EARLY DETECTION OF ACTIVE BLEEDING FROM THE SUPERFICIAL BRANCH OF THE FEMORAL ARTERY 407 AFTER CRYOBALLOON ABLATION IN A PATIENT WITH PAROXYSMAL ATRIAL FIBRILLATION
Satoshi HIGA (Japan)
P 2-149 UNUSUAL LEFT VENTRICULAR LEAD PLACEMENT FOR IMPROVED RESPONSE TO CARDIAC 408 RESYNCHRONIZATION THERAPY
Yong JI (United States)
P 2-150 A RARE CASE OF PULMONARY VEIN ISOLATION INDUCED ASYSTOLE 409Yong JI (United States)
P 2-151 CATHETER ABLATION FOR SWALLOWING-INDUCED PAROXYSMAL ATRIAL FIBRILLATION BY ECTOPIC 410 BEATS ORIGINATING FROM THE RIGHT ATRIUM
Ken KATO (Japan)
P 2-152 A CASE OF ATRIAL FIBRILLATION WITH AZYGOS CONTINUATION OF THE INFERIOR VENA CAVA 411Ryusuke KIMURA (Japan)
P 2-153 CASE REPORT OF PACEMAKER LEAD COMPLICATION DUE TO BRAIN MAGNETIC RESONANCE 412 IMAGING(MRI) SCAN
Tarlochan KLER (India)

xxviii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 2-154 BRUGADA PATTERN RESOLUTION AFTER ENDOCARDIAL ABLATION IN A PATIENT WITH BRUGADA ARVC 413 OVERLAP. A CASE REPORT IN SCN5A VARIANT BRUGADA SYNDROME
Simon BINNY (Australia)
P 2-155 PROVOCATIVE CASES-INCESSANT DOUBLE FIRE CARDIOMYOPATHY 414Adam LEE (Australia)
P 2-156 A CASE OF SCAR RELATED ATRIAL TACHYCARDIA AFTER THE SURGERY OF MITRAL VALVE PLASTY 415 WHOSE CIRCUIT COULD NOT BE IDENTIFIED WITHOUT USING 3D MAPPING
Tomoaki NAKANO (Japan)
P 2-157 ANCIENT TECHNIQUE STILL FEASIBLE? 416Kantha Rao NARASAMULOO (Malaysia)
P 2-158 A CASE OF IDIOPATHIC PREMATURE VENTRICULAR CONTRACTIONS WITH NARROW QRS DURATION 417 ORIGINATING FROM THE MIDDLE PORTION OF THE LEFT VENTRICULAR SEPTUM
Yoshimi ONISHI (Japan)
P 2-159 A CASE OF LONGER SLOW CONDUCTION ZONE IN ATP-SENSITIVE ATRIAL TACHYCARDIA ORIGINATING 418 FROM THE ATRIOVENTRICULAR ANNULUS
Maki ONO (Japan)
P 2-160 DYSPNEA FOLLOWING MAZE PROCEDURE 419Jae Yoon PARK (United States)
P 2-161 VENTRICULAR ARRHYTHMIAS INDUCTION BY PROGRAMMED ELECTRICAL STIMULATION OF THE RIGHT 420 VENTRICULAR OUTFLOW TRACT ONLY DURING TYPE 1 BRUGADA ECG MAXIMIZATION
Bich Lien NGUYEN (Italy)
P 2-162 AN UNCOMMON PROCEDURE FOR A COMMON ARRHYTHMIA:FAST PATHWAY ABLATION AFTER FAILED 421 SLOW PATHWAY MODIFICATION FOR TYPICAL AV NODE REENTRANT TACHYCARDIA
Vivek PILLAI (India)
P 2-164 TWO CASES OF PERSISTENT ATRIAL FIBRILLATION WHO BECOME SINUS TACHYCARDIA AFTER 422 PULMONARY VEIN ISOLATION AND DOMINANT FREQUENCY ABLATION
Yoshinao SUGAI (Japan)
P 2-165 TOTAL TRANSVENOUS CARDIOVETER-DEFIBRILLATOR IMPLANTATION IN A PATIENT WITH ARTIFICIAL 423 TRICUSPID VALVE REPLACEMENT
Kazuyuki TANOUE (Japan)
P 2-166 NARROW QRS TACHYCARDIA WITH SIMULTANEOUS ATRIAL AND VENTRICULAR ACTIVATION IN A 424 PATIENT WITH COMPLETE HEART BLOCK (CHB) WITH PERMANENT PACEMAKER (PPM) IMPLANTATION
Ameya UDYAVAR (India)
P 2-167 SIGNIFICANT IMPACT OF OBSTRUCTIVE SLEEP APNEA IN A PATIENT WITH AN INCESSANT FORM OF 425 VENTRICULAR TACHYCARDIA ORIGINATING FROM THE LEFT SINUS OF VALSALVA
Nobumori YAGI (Japan)

xxix
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
SATURDAY POSTER PRESENTATION (15 October)
BASIC/TRANSLATIONAL SCIENCEP 3-001 ROTIGAPTIDE DECREASES THE SUSCEPTIBILITY TO VENTRICULAR FIBRILLATION BY DECREASING 427 DIVERGENCE DURING THERAPEUTIC HYPOTHERMIA
Yu-Cheng HSIEH (Taiwan)
P 3-002 CO-LOCALIZATION OF CARDIAC SYMPATHETIC AND PARASYMPATHETIC NERVES PREDOMINANTLY AT 428 LEFT ATRIUM IN HUMAN INFANT HEART
In-Soo KIM (Republic of Korea)
P 3-003 ROTIGAPTIDE DECREASES THE INDUCIBILITY OF VENTRICULAR FIBRILLATION BY REDUCING SPATIAL 429 CONDUCTION VELOCITY HETEROGENEITY DURING THERAPEUTIC HYPOTHERMIA IN ISOLATED RABBIT HEARTS
Jiunncherng LIN (Taiwan)
P 3-004 MITIGATING ISCHEMIA/REPERFUSION INJURY: MICROVESICLES DERIVED FROM HYPOXIC HUMAN 430 MESENCHYMAL STEM CELLS IMPROVE ELECTRICAL CONDUCTION IN MOUSE, RAT, AND RABBIT MODELS
Hyewon PARK (Republic of Korea)
P 3-005 LEFT VENTRICULAR TRANSMURAL REPOLARIZATION GRADIENT IN HUMANS 431Bich Lien NGUYEN (Italy)
P 3-006 RENAL DENERVATION REGULATES THE ATRIAL ARRHYTHMOGENIC SUBSTRATES THROUGH REVERSE 432 STRUCTURAL REMODELING IN HEART FAILURE RABBIT MODEL
Ling-Hui CHIANG (Taiwan)
P 3-007 ANATOMIC CONFORMATION OF RENAL SYMPATHETIC NERVE FIBERS IN LIVING HUMAN 433 SPECIMENS
Won-Seok CHOE (Republic of Korea)
P 3-008 OBESITY CAUSES VENTRICULAR IONIC AND STRUCTURAL REMODELING AND INCREASES 434 ARRHYTHMOGENECITY IN RABBIT MODEL
Yu-Hui CHOU (Taiwan)
P 3-009 LONG-TERM GENE EXPRESSION OF CONNEXIN43 PRESERVED CONDUCTION TIME AND PREVENTED 435 ATRIAL FIBRILLATION IN RATS
Tomonori IGARASHI (Japan)
P 3-010 FRAGMENTATION AND PROLONGATION OF PARADOXICAL SLEEP PHASE WITH SYMPATHETIC 436 HYPERACTIVITY IN LEFT CORONARY ARTERY LIGATION RATS FACILITATES FETAL ARRHYTHMIA AND SUDDEN DEATH AFTER MYOCARDIAL INFARCTION
Wei-Lun LIN (Taiwan)
P 3-011 THE IMPACT OF NEURAL REMODELING FOLLOWING MYOCARDIAL INFARCTION ON INDUCIBILITY OF 437 VENTRICULAR ARRHYTHMIA IN PORCINE MODEL
Keijiro NAKAMURA (United States)
P 3-012 NEURONAL ISOFORM OF NITRIC OXIDE SYNTHASE IS UPREGULATED IN CARDIAC INTRINSIC AND 438 EXTRINSIC SYMPATHETIC AFFERENT AND EFFERENT GANGLIA FOLLOWING MYOCARDIAL INFARCTION
Keijiro NAKAMURA (United States)
P 3-013 AUTONOMIC MECHANISM OF ARRHYTHMOGENESIS IN RHEUMATOID ARTHRITIS RATS 439Yen-Ling SUNG (Taiwan)
P 3-014 DISTINCT ELECTROPHYSIOLOGICAL CHARACTERISTICS OF RIGHT VENTRICULAR OUTFLOW TRACT-A 440 CANINE MODEL STUDY
Wei-Chieh TSENG (Taiwan)
P 3-015 EFFECTS OF EXERCISE ON ARRHYTHMOGENESIS IN SPONTANEOUSLY HYPERTENSION RAT MODEL 441Chih-En WU (Taiwan)

xxx
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTS
ALLIED PROFESSIONALSP 3-016 PULSE PALPATION ON SUBJECTS WITH POOR PULMONARY FUNCTION FOR SCREENING OF CARDIAC 442 ARRHYTHMIA
Sun Hwa KIM (Republic of Korea)
P 3-017 NON-VIT K ANTAGONIST ANTICOAGULANTS VERSUS WARFARIN FOR THE INCIDENCE OF SPONTANEOUS 443 ECHO-CONTRAST IN PATIENTS WITH ATRIAL FIBRILLATION
Yun Gi KIM (Republic of Korea)
P 3-020 TORSADES DE POINTES IN LONG QT SYNDROME: A CASE REPORT 444Hengky HENGKY (Indonesia)
P 3-021 INADVERTENTLY ACHIEVED BIDIRECTIONAL CONDUCTION BLOCK OF THE LATERAL MITRAL ISTHMUS 445 BY CRYOBALLOON APPLICATIONS APPLIED AT THE LEFT ATRIAL APPENDAGE AND LEFT SUPERIOR PULMONARY VEIN
Nobuhiro NISHIYAMA (Japan)
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICESP 3-022 DOES APPLICATION AND EFFECT OF CARDIAC RESYNCHRONIZATION THERAPY DIFFER BETWEEN 446 THE USA AND ASIA? INSIGHTS FROM THE INTERNATIONAL ADVANCE CRT REGISTRY
Niraj VARMA (United States)
P 3-023 REMOTE MONITORING ENABLES SIGNIFICANTLY EARLIER DETECTION OF CARDIAC IMPLANTABLE 447 ELECTRONIC DEVICE ALERTS COMPARED TO CONVENTIONAL IN-OFFICE DEVICE CHECKS
Hui Min CHONG (Singapore)
P 3-024 EFFECTIVE REDUCTION OF INAPPROPRIATE SHOCK AFTER APPLYING LONG DETECTION INTERVAL OF 448 VENTRICULAR ARRHYTHMIA
You-Mi HWANG (Republic of Korea)
P 3-025 EVALUATION OF ARRHYTHMIC EVENT MONITORING FUNCTION OF WEARABLE CARDIOVERTER- 449 DEFIBRILLATOR IN PATIENT AT HIGH RISK OF SUDDEN CARDIAC DEATH
Yuji ISHIDA (Japan)
P 3-026 PREVALENCE OF SUBCLINICAL ATRIAL FIBRILLATION PATIENTS DETECTED BY CARDIAC IMPLANTABLE 450 ELECTRICAL DEVICE AND ASSOCIATION WITH ISCHEMIC STROKE, A SINGLE CENTER STUDY
Sirichai JAMNONGPRASATPORN (Thailand)
P 3-027 FIRST NOTIFICATION OF LEAD FAILURE IS ARRHYTHMIC EVENTS IN PATIENTS FOLLOWED BY REMOTE 451 MONITORING
Nobuhiro NISHII (Japan)
P 3-028 DEVICE-DETECTED ASYMPTOMATIC ATRIAL TACHYARRHYTHMIAS IN INDIAN HEART FAILURE PATIENTS: 452 THE ATTEND STUDY
Nayani MAKKAR (United States)
P 3-029 OBSERVATION OF IMAGEREADY™ MR CONDITIONAL PACING SYSTEM IN CHINA 453Yangang SU (China)
P 3-030 PHYSICAL ACTIVITY COULD PREDICT CARDIAC DEATH IN IMPLANTABLE CARDIOVERTER-DEFIBRRILATOR 454 AND CARDIAC RESYNCHRONIZATION THERAPY-DEFIBRILLATOR PATIENTS
Shuang ZHAO (China)
P 3-031 OUTCOMES IN PATIENTS WITH SAME DAY DISCHARGE AFTER PACEMAKER OR DEFIBRILLATOR 455 IMPLANTATION
Devender AKULA (United States)
P 3-032 THE INCIDENCE OF INFECTION AFTER CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICE: 456 DEDICATED ELECTROPHYSIOLOGY LABORATORY VERSUS SHARED CARDIAC CATHETERIZATION LABORATORY
Yong-Soo BAEK (Republic of Korea)
P 3-033 CONTRAST VENOGRAPHY BEFORE PACEMAKER AND IMPLANTABLE CARDIOVERTER DEFIBRILLATOR 457 LEAD INSERTION IMPROVES PATIENT OUTCOMES VERSUS BLIND LEAD INSERTION USING ANATOMICAL LANDMARKS
Raymond BAYAUA (Philippines)

xxxi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-034 TURN OVER PECTORAL MUSCLE FLAP TO SALVAGE IMPLANTABLE DEVICES. IS IT FEASIBLE! 458
Anoop GUPTA (India)
P 3-035 COLCHICINE REDUCED PERICARDIAL EFFUSION FOLLOWING CARDIAC RESYNCHRONIZATION THERAPY 459 IMPLANTATION: CASE REPORT
Tadashi HOSHIYAMA (Japan)
P 3-036 CHANGE OF PHYSICAL ACTIVITY AFTER INAPPROPRIATE SHOCK THERAPIES IN JAPANESE PATIENTS 460 WITH IMPLANTABLE CARDIOVERTER DEFIBRILLATOR
Yusuke KONDO (Japan)
P 3-037 A PROSPECTIVE OBSERVATIONAL COHORT STUDY: ASSESSING ICD RECIPIENTS’ DEVICE 461 UNDERSTANDING AND QUALITY OF LIFE
Paul MAGGIORE (Australia)
P 3-038 CLINICAL COURSE OF PATIENTS WITH AUTOMATIC IMPLANTABLE DEFIBRILLATORS IN JAPAN 462 -RETROSPECTIVE SINGLE CENTER STUDY
Naomi MIKI (Japan)
P 3-039 TAKOTSUBO CARDIOMYOPATHY ASSOCIATED WITH PACEMAKER IMPLANTATION 463Yuko MIKI (Japan)
P 3-040 BARRIERS TO THE UPTAKE OF PRIMARY PREVENTION INTERNAL CARDIOVERTER DEFIBRILLATOR (ICD) 464 & OUTCOMES IN A MULTI-RACIAL COHORT FOLLOWED UP IN HEART FAILURE CLINIC: SINGLE CENTRE EXPERIENCE
Aye Aye MON (Singapore)
P 3-041 DEVELOPMENT OF FREQUENT VENTRICULAR PACING IN PATIENTS WITH IMPLANTABLE CARDIAC 465 DEFIBRILLATORS
Dawn OH (Singapore)
P 3-042 REDUCTION OF INAPPROPRIATE THERAPY IN SINGLE CHAMBER VERSUS DUAL/TRIPLE CHAMBERS 466 IMPLANTABLE CARDIOVERTER DEFIBRILLATORS: A SYSTEMATIC REVIEW AND META-ANALYSIS
Vern Hsen TAN (Singapore)
P 3-043 SURVIVAL SUPERIORITY IN PATIENTS WITH DUAL CHAMBER PACEMAKER VERSUS SINGLE CHAMBER 467 PACEMAKER: A SINGLE CENTRE REVIEW
Hooi Khee TEO (Singapore)
CATHETER ABLATIONP 3-044 CATHETER ABLATION OF SUPRAVENTRICULAR TACHYCARDIA UNDER THE GUIDANCE OF THE EASTAR 468 PRINCIPLE: SIX-YEAR DATA ANALYSIS OF SINGLE CENTER
Xianfeng DU (China)
P 3-045 THE APPLICATION OF POSITIONAL REFERENCE CATHETER IN PULMONARY ARTERY IN 469 RADIOFREQUENCY ABLATION OF ATRIAL FIBRILLATION BY NAVX SYSTEM
Xianfeng DU (China)
P 3-046 QUANTITATIVE PACE MAPPING-DEVELOPMENT OF NEW METHODS TO DETERMINE SPATIAL ACCURACY 470Anand GANESAN (Australia)
P 3-047 USE OF ZERO FLUOROSCOPY FOR ELECTROPHYSIOLOGICAL INTERVENTION: THE ZEROX PILOT STUDY 471Audry LEE (Singapore)
P 3-048 ACCURACY AND REPRODUCIBILITY OF NOVEL ELECTROANATOMIC THREE-DIMENSIONAL AUTOMATED 472 MAPPING SOFTWARE (CARTO 3 SYSTEM CONFIDENSE™ MODULE) FOR THE ASSESSMENT OF THE RIGHT VENTRICULAR SUBSTRATE IN VENTRICULAR ARRHYTHMIA
Chin-Yu LIN (Taiwan)
P 3-049 THE EFFICACY OF MULTIPOLAR BASKET CATHETERS IN MAPPING THE ENTIRE LEFT ATRIUM IN HUMAN 473 PERSISTENT ATRIAL FIBRILLATION
Bhupesh PATHIK (Australia)
P 3-050 ACCESSORY PATHWAY-RELATED WALL MOTION ABNORMALITY AND LEFT VENTRICULAR DYSFUNCTION 474 IN PATIENTS WITH WOLFF-PARKINSON-WHITE SYNDROME
Jae-Sun UHM (Republic of Korea)
P 3-051 CATHETER ABLATION OF INCESSANT ATRIAL TACHYCARDIA FROM NON-PULMONARY VEIN FOCI 475Pradeep HASIJA (India)

xxxii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-052 CATHETER ABLATION OF PARA-HISIAN VERSUS NON-SEPTAL ACCESSORY PATHWAY: IMPACT OF 476 CONTACT NUMBER AND TIME DURING ENERGY-DELIVERY ON RECONNECTION
Dong-Hyeok KIM (Republic of Korea)
P 3-054 A CASE OF BIATRIAL TACHYCARDIA MIMICKING COMMON ATRIAL FLUTTER 477Keita MASUDA (Japan)
P 3-056 TRANSCATHETER ABLATION OF ATRIOVENTRICULAR NODAL REENTRANT TACHYCARDIA IN CHILDREN 478 AND ADOLESCENTS IN TAIWAN: COMPARISON OF CRYOABLATION WITH RADIOFREQUENCY ABLATION
Kun-Lang WU (Taiwan)493
P 3-057 IS IT LEFT SIDED CIRCUIT IN AVNRT? 479Ramdeo YADAVE (India)
P 3-058 REGULAR WIDE QRS TACHYCARDIA WITH BASELINE PRE-EXCITATION: WHAT IS THE MECHANISM? 480Ramdeo YADAVE (India)
P 3-059 WPW SYNDROME WITH RIGHT ATRIAL APPENDAGE TO RV ACCESSARY PATHWAY 481Ramdeo YADAVE (India)
P 3-060 POSTERO-SEPTAL ACCESSORY PATHWAY REQUIRING ABLATIONS AT BOTH THE RIGHT AND LEFT SIDED 482 POSTERO-SEPTUM; A CASE REPORT
Shu YAMASHITA (Japan)
P 3-061 TRANSSEPTAL CATHETER ABLATION OF LEFT SIDED ACCESSORY PATHWAY VIA PROBE-PATENT 483 FORAMEN OVALE WITHOUT ATRIAL SEPTAL PUNCTURE
Xu ZHOU (China)
P 3-062 CORRELATION OF DEMOGRAPHIC FACTORS AND PATIENT SYMPTOMS WITH PATIENT COMPLIANCE IN 484 FOLLOWING UP ONE MONTH AFTER ADMISSION IN AF PATIENTS IN A LOCAL SECONDARY HOSPITAL
Dylan HADI (Indonesia)
P 3-063 ABLATION OF LOW VOLTAGE ZONE HARBORING ROTOR FREQUENTLY TERMINATES ATRIAL 485 FIBRILLATION
Akira FUKUI (Japan)
P 3-064 IMPACT OF LEFT ATRIAL EJECTION FRACTION IN PATIENTS UNDERGOING CATHETER ABLATION FOR 486 PAROXYSMAL ATRIAL FIBRILLATION
Masato FUKUNAGA (Czech Republic)
P 3-065 ZERO FLUOROSCOPY ABLATION OF ATRIAL FIBRILLATION USING THE CARTO3 SYSTEM 487Tohru KAWAKAMI (Japan)
P 3-066 HEMODYNAMIC CONSEQUENCES OF DELAYED ACTIVATION OF LEFT ATRIAL APPENDAGE AFTER 488 RADIOFREQUENCY CATHETER ABLATION OF ATRIAL FIBRILLATION: FOLLOW-UP MRI STUDY
Yun Gi KIM (Republic of Korea)
P 3-067 IS THE DIFFERENCE OF LATE GADOLINIUM ENHANCEMENT IN THE LEFT ATRIUM BETWEEN PRE- 489 AND 1 YEAR POST-ABLATION ASSOCIATED WITH RECURRENCE OF ATRIAL FIBRILLATION/TACHYCARDIA?
Kwang No LEE (Republic of Korea)
P 3-068 EFFICACY OF A NON-FLUOROSCOPIC THREE-DIMENSIONAL MAPPING SYSTEM ON REDUCING 490 FLUOROSCOPY TIME IN ATRIAL FLUTTER ABLATION IN PATIENTS WITH OR WITHOUT STRUCTURAL HEART DISEASE
So-Ryoung LEE (Republic of Korea)
P 3-069 INTRACARDIAC ECHOCARDIOGRAPHY FROM INTRA LEFT ATRIUM CAN DETECT ACCURATE LEFT 491 ATRIUM ANATOMICAL INFORMATION FOR PULMONARY VEIN ISOLATION
Emi NAKANO (Japan)
P 3-071 THE RELATIONSHIP BETWEEN LEFT ATRIAL APPENDAGE MORPHOLOGY AND TRANSIENT ISCHEMIC 492 ATTACK IN PATIENTS WITH ATRIAL FIBRILLATION
Hwan-Cheol PARK (Republic of Korea)
P 3-072 THREE-DIMENSIONAL WAVEMAPPING OF HUMAN PERSISTENT ATRIAL FIBRILLATION 493Bhupesh PATHIK (Australia)
P 3-073 EXPERIENCE OF ATRIAL AND VENTRICULAR TACHYARRHYTHMIAS MAPPING WITH HIGH DENSITY 494 BASKET CATHETER IN RAMATHIBODI HOSPITAL, THAILAND
Asadayudh PHOOLPITHAYADHORN (Thailand)

xxxiii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-074 BI-ATRIAL ELECTROANATOMIC MAPPING IN PERSISTENT AF: DOES THE RIGHT ATRIUM REPRESENT 495 THE LEFT?
Sandeep PRABHU (Australia)
P 3-075 BI-ATRIAL ELECTRICAL AND STRUCTURAL REMODELLING IN HEART FAILURE: ELECTROANATOMIC 496 MAPPING IN PERSISTENT ATRIAL FIBRILLATION IN HUMANS
Sandeep PRABHU (Australia)
P 3-076 LOCALIZATION OF MITRAL ISTHMUS GAP USING NOVEL HIGH-DENSITY ENSITE AUTOMATED MAPPING 497 SYSTEM
Teerawut RUEDEEJAROONRUNG (Japan)
P 3-077 THE UTILITY OF RADIOFREQUENCY CATHETER ABLATION OF ATRIA FIBRILLATION GUIDED BY CARTO- 498 UNIVU SYSTEM
Zhonghui XIE (China)
P 3-078 THE ACCURACY AND CLINICAL APPLICABILITY OF A SENSOR BASED ELECTROMAGNETIC NON 499 FLUOROSCOPIC CATHETER TRACKING SYSTEM
Shinya YAMADA (Taiwan)
P 3-079 A CASE OF PRIMARY CARDIAC AMYLOIDOSIS WITH CATHETER ABLATION FOR PERSISTENT ATRIAL 500 FLUTTER
Kiyotaka YOSHIDA (Japan)
P 3-080 CLINICAL USEFULNESS OF CHEMICAL ABLATION IN TERMS OF TREATING ATRIAL FIBRILLATION; 501 REPRESENTATIVE TWO COMPLICATED CASES
Tomofumi NAKAMURA (Japan)
P 3-081 EFFECT OF LOW-LEVEL ELECTRICAL STIMULATION OF AORTIC ROOT VENTRICULAR GANGLIONATED 502 PLEXI ON AUTONOMIC NERVOUS SYSTEM-MEDIATED ATRIAL FIBRILLATION
Hong-Tao WANG (China)
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATIONP 3-083 ELECTROCARDIOGRAPHIC TRANSMURAL DISPERSION OF REPOLARIZATION AS A MARKER OF 503 CORONARY ARTERY DISEASE IN PATIENTS WITH NON ST ELEVATION ACUTE CORONARY SYNDROME
Raymond BAYAUA (Philippines)
P 3-084 LATE POTENTIAL PREVALENCE AND PREDICTORS IN PATIENTS WITH SERIOUS MENTAL ILLNESS 504John FITZGERALD (Australia)
P 3-085 CLINICAL VALUE OF SHORT-TERM HEART RATE VARIABILITY FOR PREDICTION OF MORTALITY IN 505 KOREANS: EFFICACY OF NONLINEAR HEART RATE DYNAMICS
Chan-Hee LEE (Republic of Korea)
P 3-086 THE IMPACT OF VLF COMPONENT IN HOLTER ELECTROCARDIOGRAMS ON FATAL VENTRICULAR 506 ARRHYTHMIA AND CARDIAC DEATH IN POST MI PATIENTS
Yoshikazu SATO (Japan)
P 3-087 CAN P WAVE SIGNAL AVERAGED ECG PREDICT ATRIAL FIBRILLATION IN PATIENTS WITH EMBOLIC 507 STROKE WITH UNKNOWN SOURCE?
Seung Yong SHIN (Republic of Korea)
P 3-088 REPOLARIZATION DISPERSION PARAMETER FOR PREDICTING INHOSPITAL MAJOR ADVERSE CARDIAC 508 EVENT IN ST ELEVATION MYOCARDIAL INFARCTION: TPEAK-TEND OR TPEAK-TEND/QT RATIO?
Erdiansyah ZULYADAINI (Indonesia)
P 3-089 COMPARISON OF INTERVAL TPEAK-TEND REDUCTION IN PRIMARY PERCUTANEUS CORONARY 509 INTERVENTION VS FIBRINOLYTIC THERAPY IN ST ELEVATION MYOCARDIAL INFARCTION
Erdiansyah ZULYADAINI (Indonesia)
P 3-090 INCREASED SUDDEN ARREST WITH CHRONIC OBSTURCTIVE PULMONARY DISEASE IN GENERAL 510 POPULATION; THE EFFECT OF AGE
Shinjeong SONG (Republic of Korea)
P 3-091 THE GENOTYPE-PHENOTYPE TRAITS OF BRUGADA SYNDROME IN BRUNEI DARUSSALAM 511Bee LAU (Brunei Darussalam)

xxxiv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-092 MALIGNANT EARLY REPOLARIZATION ASSESSMENT BY 2D SPECKLE-TRACKING ECHOCARDIOGRAPHY 512
Bich Lien NGUYEN (Italy)
P 3-093 MEASUREMENT OF MAGNETOCARDIOGRAM USING MAGNETORESISTIVE SENSOR 513Yasuhiro SHIRAI (Japan)
CLINICAL ELECTROPHYSIOLOGYP 3-095 ATRIOVENTRICULAR ACCESSORY PATHWAY ORIGINATING FROM THE SMALL CARDIAC VEIN WITH 514 RIGHT ATRIAL ORIFICE USING FLUOROSCOPY INTEGRATED 3D MAPPING SYSTEM
Kaijun CUI (China)
P 3-096 SECONDARY ONSET OF A NEW LEFT ANTERIOR PREEXCITATION AFTER SUCCESFUL ABLATION OF A 515 LEFT POSTERIOR ACCESSORY PATHWAY-LATENT PREEXCITATION: A CASE REPORT
Christophe D’IVERNOIS (France)
P 3-097 PREVALENCE OF T-WAVE INVERSION IN RIGHT PRECORDIAL LEADS OF A 12-LEAD 516 ELECTROCARDIOGRAM IN CHINESE YOUNG ATHLETES
Li FENG (China)
P 3-098 OBSERVATIONS OF DECELERATION CAPACITY AND DECELERATION RUNS ON HYPERTROPHIC 517 CARDIOMHYOPATHY PATIENTS
Houyuan HU (China)
P 3-099 SHORT ATRIOVENTRICULAR MAHAIM FIBERS IN CHINESE PATIENTS:OBSERVATIONS ON THEIR CLINICAL, 518 ELECTROCARDIOGRAPHIC, AND ELECTROPHYSIOLOGIC PROFILE
Bin LUO (China)
P 3-100 SUPRAVENTRICULAR TACHYCARDIA WITH BUNDLE BRANCH BLOCK AND ATRIOVENTRICULAR BLOCK 519Amit MALIK (India)
P 3-101 FREQUENT ATRIAL PREMATURE COMPLEXES AND ITS ASSOCIATION WITH RISK OF STROKE: 520 A META-ANALYSIS
Ho-Cheol SHIN (Republic of Korea)
P 3-102 THE RELATIONSHIP OF ELECTROCARDIOGRAPHIC CHARACTERISTICS, PRESENCE OF J-WAVES AND 521 TORSADE DE POINTES WITH HYPOTHERMIA
Minoru TAGAWA (Japan)
P 3-103 THE ATRIAL FIBRILLATION IN MACAU 522Ruohan CHEN (China)
P 3-104 A SYSTEMIC REVIEW AND META-ANALYSIS TO APPRAISE AORTIC STIFFNESS AS A PREDICTIVE TOOL 523 FOR CARDIOVASCULAR AND ALL CAUSE MORTALITY WITH EVIDENTIAL INSIGHT INTO ADDENDUM ROLE OF PULSE PRESSURE IN AF
Kashif KHOKHAR (Australia)
P 3-105 SUCCESSFUL ELECTRICAL CARDIOVERSION WITH LOW ENERGY SHOWED LESS RECURRENCE RATE IN 525 PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION
Chee Hae KIM (Republic of Korea)
P 3-106 COULD NEW-ONSET ATRIAL FIBRILLATION IN PATIENTS WITH SEVERE SEPSIS OR SEPTIC SHOCK 526 PREDICT FUTURE MORTALITY?
Wen-Yu LIN (Taiwan)
P 3-107 THE RELATIONSHIP BETWEEN THYROID-RELATED ANTIBODIES AND ATRIAL FIBRILLATION IN 527 EUTHYROID PATIENTS
Donghyun PARK (Republic of Korea)
P 3-108 ANALYSES OF ASSOCIATION BETWEEN ATRIAL FIBRILLATION AND ERYTHROCYTE DEFORMABILITY 528 USING MICROFLUIDIC EKTACYTOMETER
Kyu-Hwan PARK (Republic of Korea)
P 3-109 CAN WE ALWAYS BELIEVE WHAT WE SEE? ENTRAINMENT REMAINS IMPORTANT FOR DIAGNOSIS OF 529 ATRIAL MACRO-REENTRY IN THE ERA OF HIGH DENSITY 3D MAPPING.
Bhupesh PATHIK (Australia)
P 3-110 SURGICAL ATRIAL FIBRILLATION ABLATION DURING RHEUMATIC MITRAL VALVE AND TRICUSPID VALVE 530 SURGERY: THE FIRST CASE IN PHILIPPINE HEART CENTER
Josephine Rose SALIGAN (Philippines)

xxxv
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-111 ATRIAL DEFIBRILLATION THRESHOLD PREDICTS THE OUTCOME OF CATHETER ABLATION FOR ATRIAL 531 FIBRILLATION
Satoshi TAKAHASHI (Japan)
P 3-113 EFFICACY OF ABLATION TO LONG-STANDING ATRIAL FIBRILLATION USING STEERABLE SHEATH STEER 532 ABLATION METHOD
Taku ASANO (Japan)
P 3-114 USEFULNESS OF P-WAVE DEFLECTION IN PREDICTING CLINICAL RECURRENCE AFTER PULMONARY 533 VEIN ISOLATION IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION
Ji-Eun BAN (Republic of Korea)
P 3-115 THE EFFECT OF DIFFERENT ATRIAL FIBRILLATION ABLATION STRATEGIES ON P WAVE DURATION 534Guy FURNISS (United Kingdom)
P 3-116 PREVALENCE OF DE NOVO ATRIAL FIBRILLATION AFTER ISOLATED SURGICAL AORTIC VALVE 535 REPLACEMENT IN SEVERE AORTIC STENOSIS
You-Mi HWANG (Republic of Korea)
P 3-117 IMPACT OF QRS DURATION CHANGES DURING ERGONOVINE PROVOCATION TEST ON ARRHYTHMIC 536 COMPLICATIONS
Sung Il IM (Republic of Korea)
P 3-118 PREDICTORS OF PERMANENT ATRIAL FIBRILLATION WITH FAILED ELECTRICAL CARDIOVERSION IN 537 PATIENTS WITH LONG-STANDING PERSISTENT ATRIAL FIBRILLATION
Ji-Hyun JUNG (Republic of Korea)
P 3-119 INCIDENCE, RISK FACTORS AND CLINICAL IMPACT OF ATRIAL ARRHYTHMIAS AFTER LUNG 538 TRANSPLANTATION
Byung Gyu KIM (Republic of Korea)
P 3-120 ELECTROCARDIOGRAPHIC PARAMETERS FOR DIFFERENTIATING BETWEEN LEFT ATRIAL ROOF 539 DEPENDENT AND MITRAL ISTHMUS DEPENDENT MACROREENTRANT ATRIAL TACHYCARDIAS
Tomonori WATANABE (Japan)
HEART FAILUREP 3-122 THE MODULATING EFFECTS OF CARDIAC RESYNCHRONIZATION THERAPY ON MYOCARDIAL 540 METABOLISM IN HEART FAILURE
Chao-Feng CHEN (China)
P 3-124 CLINICAL CHARACTERISTICS, PREDICTORS, AND OUTCOMES OF EARLY OR LATE SUPER-RESPONDER 541 IN CARDIAC RESYNCHRONIZATION THERAPY OF PATIENTS WITH HEART FAILURE
Jaewon OH (Republic of Korea)
P 3-125 ELECTRICAL SUBSTRATE IN LBBB-ISCHEMIC VS. NON-ISCHEMIC-ASSESSED BY QUADRIPOLAR LV 542 LEADS
Brian WISNOSKEY (United States)
P 3-126 NON PACING AFTER CARDIAC RESYNCHRONIZATION THERAPY IMPLANTATION: A CASE REPORT 543Muhammad YAMIN (Indonesia)
P 3-127 INNER CATHETER FRAGMENTS EMBOLIZATION IN CRT IMPLANT: A CASE REPORT 544Muhammad YAMIN (Indonesia)
P 3-128 QUADRIPOLAR LEFT VENTRICULAR LEADS PROVIDE MORE VIABLE PACING SITES THAN BIPOLAR 545 EQUIVALENTS
Min GU (China)
P 3-129 IMPLANTATION EXPERIENCE WITH THE QUARTETTM QUADRIPOLAR LEFT VENTRICLE LEAD IN 546 CHINESE PATIENTS WITH HEART FAILURE
Min GU (China)
P 3-130 ACUTE AND THREE-MONTH AVAILABILITY OF VIABLE LEFT VENTRICULAR PACING SITES WITH 547 QUARTETTM LEADS IN THE CHINESE POPULATION
Min GU (China)
P 3-131 ACUITY X4 QUADRIPOLAR LEAD-FROM CONCEPT TO CLINICAL 548Lili LIU (United States)

xxxvi
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-132 CARDIAC RESYNCHRONIZATION THERAPY EPICARDIAL LEFT VENTRICULAR LEAD PLACEMENT A 549 MAJOR FACTOR TO IMPROVE RESPONDER RATE
Abhinay TIBDEWAL (India)
PEDIATRIC/ADULT CONGENITAL HEART DISEASEP 3-133 REPRODUCIBLE BILATERAL CONFINED PULMONARY VEIN FIBRILLATION IN A PATIENT WITH 550 PERSISTENT ATRIAL FIBRILLATION
Keiichi ASHIKAGA (Japan)
P 3-134 MULTIMODALITY DIAGNOSIS OF ARRHYTHMOGENIC CARDIOMYOPATHY 551Ariston BAUTISTA (Philippines)
P 3-135 RADIATION THERAPY IN MEDTRONIC MICRA® LEADLESS PACEMAKER 552Kenneth CHEW (Singapore)
P 3-136 PERSISTENT DIFFUSE DEEP T WAVE INVERSION AN ECG MANIFESTATION OF MYASTHENIA GRAVIS 553 IN CRISIS
Jose Eduardo DUYA (Philippines)
P 3-137 SUBACUTE CONTRALATERAL PNEUMOTHORAX ASSOCIATED WITH ATRIAL LEAD PERFORATION IN A 554 PATIENT WITH ON CORTICOSTEROID THERAPY
Naruya ISHIZUE (Japan)
P 3-138 SUCCESSFUL CATHETER ABLATION BY USING MULTIELECTRODE CATHETER FOR ATRIAL 555 TACHYCARDIA AFTER SURGICALLY REPAIRED TETRALOGY OF FALLOT IN A PATIENT WITH DEXTROCARDIA
Kenji KAWAMOTO (Japan)
P 3-139 A CASE OF FEVER-INDUCED BRUGADA SYNDROME WITH VENTRICULAR FIBRILLATION STORM 556 COMBINED WITH MYELODYSPLASTIC SYNDROMES
Akira KIMATA (Japan)
P 3-140 CARDIAC RESYNCHRONISATION THERAPY FOR THE TREATMENT OF PACING INDUCED 557 CARDIOMYOPATHY IN YOUNG PATIENTS
SL KUI (Singapore)
P 3-141 TACHYCARDIA-INDUCED CARDIOMYOPATHY- IS IT TRULY BENIGN? 558Takashi KUZE (Japan)
P 3-143 THE CLINICAL SIGNIFICANCE OF Β-BLOCKER ON STRESS CARDIOMYOPATHY FOR PREVENTION OF 559 TORSADES DE POINTES WITH QT PROLONGATION FROM CASE REPORT STUDY
Taito NAGAI (Japan)
P 3-144 A SUPER RESPONDER CASE AFTER DEVICE UPGRADE TO ADAPTIVE CARDIAC RESYNCHRONIZATION 560 THERAPY
Yoshiki NAGATA (Japan)
P 3-145 HEART BLOCK ! HEART BLOCK!-A DISEASE OF GREAT MIMICRY (SARCOIDOSIS) WITH CARDIAC AND 561 PULMONARY INFILTRATIONS
Choon Seong NG (Malaysia)
P 3-146 A CASE FROM MALAYSIA OF DE NOVO IDIOPATHIC CONSTRICTIVE PERICARDITIS MASQUERADING 562 RECURRENT UNSTABLE ANGINA WITH IRREGULAR HEART RHYTHM
Choon Seong NG (Malaysia)
P 3-147 A DIFFICULT POSTERO SEPTAL ACCESSORY PATHWAY-SUCCESSFUL RADIO FREQUENCY ABLATION 563 BY BIVENTRICULAR APPROACH
Oruganti SAI SATISH (India)
P 3-148 RADIOFREQUENCY ABLATION OF PLEOMORPHIC VENTRICULAR TACHYCARDIA IN 564 PHEOCHROMOCYTOMA-INDUCED CARDIOMYOPATHY
Abigail Louise TE (Taiwan)
P 3-149 A SUDDEN DETERIORATION OF VENTRICULAR PACING THRESHOLD VOLTAGE IN A PATIENT WITH 565 CARDIAC SARCOIDOSIS-A CASE REPORT
Yosuke TERUI (Japan)
P 3-150 RADIOFREQUENCY ABLATION OF AUTOMATIC JUNCTIONAL ECTOPIC TACHYCARDIA IN ADULT WITH 566 PRESERVATION OF AV NODE FUNCTION
Alexander Edo TONDAS (Indonesia)

xxxvii
The 9th Asia Pacific Heart Rhythm Society Scientific Session
CONTENTSP 3-151 PROTECTION FIELD-EFFECT TRANSISTORS SIGNALS DETECTED ON THE LEADLESS ECG IN PATIENTS 567 WITH SINGLE COIL DEFIBRILLATORS
Ameya UDYAVAR (India)
P 3-152 BUTTERFLY IN THE BROKEN HEART-A CASE OF 2 VENTRICULAR TACHYCARDIAS IN A CORRECTED 568 CONGENITAL HEART DISEASE
Wan Faizal WAN RAHIMI SHAH (Malaysia)
P 3-153 INTERFASCICULAR VENTRICULAR TACHYCARDIA-THE ONE WHICH REFUSED TO GO AWAY 569Wan Faizal WAN RAHIMI SHAH (Malaysia)
P 3-154 SUCCESSFUL CATHETER ABLATION OF LONG LASTING ACCELERATED IDIOVENTRICULAR RHYTHM IN A 570 PATIENT WITHOUT ORGANIC HEART DISEASE
Marie YOSHIKAWA (Japan)
P 3-155 A CASE WITH ELECTRICAL STORM OF ATRIOVENTRICULAR REENTRANT TACHYCARIDIA AFTER TAVI, 571 WHICH MIGHT RESULT FROM PARTIAL DAMAGE TO THE CONDUCTION SYSTEM DURING TAVI
Daisuke YOSHIMOTO (Japan)
P 3-156 DISLODGEMENT OF CIRCULAR MAPPING CATHETER ELECTRODE IN THE LEFT ATRIUM: A NEAR MISS 572Fengxiang ZHANG (China)
P 3-157 SEIZURES? PANCREATITIS? JACK IN THE BOX!-ATYPICAL PRESENTATIONS OF A RARE CONGENITAL 573 HEART DISEASE
Abhinay TIBDEWAL (India)
P 3-158 CONDUIT PUNCTURE FOR ELECTROPHYSIOLOGICAL PROCEDURES IN PATIENTS WITH FONTAN 574 CIRCULATION
Jae-Sun UHM (Republic of Korea)

ORAL PRESENTATION 01(13 October)

2
Introduction: Current mapping systems create 2D phase maps by projecting basket data onto an idealized grid of evenly spaced points (Figure, panel B). This assumes that the basket electrodes are evenly distributed in the atria, however this may not be correct. We devel-oped novel three-dimensional (3D) phase mapping software that utilizes the 3D locations of basket electrodes to project phase onto a pa-tient specific 3D surface geometry. We sought to compare differences in AF activation patterns and the prevalence of rotors using 2D vs. 3D phase mapping techniques.
Methods: 12 patients with PerAF (mean age 62±8 years, median AF duration 4.7 years [2-6]) were mapped using a Constellation catheter (Boston Scientific). In each patient one minute of AF data was exported and analyzed offline using Matlab (Version R2015a). Raw unfiltered data was subjected to sinusoidal recomposition and then phase reconstruction was performed using the Hilbert transform. Customized software was then used to create 2D and 3D phase maps based on the same data. Activation patterns seen in 2D and 3D were classified into i) Wavefronts ii) Rotors (≥2 rotations of 360°) iii) or focal sources with radial spread.
Results: Over 4,000 individual wavefront patterns were analyzed. Using 2D phase mapping, AF was characterised by highly dynamic acti-vation patterns made up of single (72.0±8.4%) and two simultaneous wavefronts (4.2±1.9%), focal activations (22.4±6.9%) and rotors (1.3±0.8%). Although rotors were seen in 8 patients during 2D phase analysis they were all transient and isolated lasting only a median of 5 [IQR 4,9] rotations. The most common (75%) site for rotor formation was the posterior left superior pulmonary vein. In 25% of cases, the rotor was located at the posterior right superior pulmonary vein.When the same data was analysed using 3D phase mapping techniques, AF was characterised by single wavefronts (79.6±7.5%), two simultaneous wavefronts (5.3±1.2%), focal activations (14.5±5.3%) and rotors (0.6±0.3%). Transient isolated rotational activity was seen in only 3 patients lasting for median 4 (IQR 4,7) rotations. The location of the ro-tors was variable in each patient; anterior roof, anterior LSPV and posterior LSPV. None of the rotors seen in 2D were seen in correspond-ing time segments in 3D and conversely none of the rotors seen in 3D were seen in 2D.
Conclusions: The prevalence of Rotors is highly dependent on the technique used to animate phase. 2D phase mapping oversimplifies spatially relationships and can create false rotors that are not present during 3D phase mapping. This has significant implications for ro-tor ablation techniques.
COMPARISON OF TWO-DIMENSIONAL VS. THREE-DIMENSIONAL PHASE MAPPING IN THE DETECTION OF ROTORS DURING HUMAN PERSISTENT AF Bhupesh Pathik1, Tomos Walters1, Pawel Kuklik2, Jichao Zhao3, Andrew Madry1, Sandeep Prabhu1, Chrishan Nalliah1, Jonathan Lipton1, Joseph Morton1, Paul Sparks1, Peter Kistler4, Jonathan Kalman1, Geoff Lee1 1Royal Melbourne Hospital, Melbourne, Australia; 2Maastricht University Medical Center, Maastricht, Netherlands; 3University of Auckland, Auckland, New Zealand; 4Alfred and Baker IDI, Melbourne, Australia
BASIC/TRANSLATIONAL SCIENCE OP 1-01

3
Introduction: Some of genetic susceptibility loci for atrial fibrillation (AF) proven by genome-wide association studies (GWAS) in European database showed ethnic difference in Asian population. We explored the novel AF susceptibility variants for early-onset AF patients (≤60 years old) among Korean patients who underwent AF catheter ablation.
Methods: We conducted a genome-wide association study (GWAS) with 672 cases (≤60 years old, Yonsei AF Ablation cohort) and 3,700 controls (Korea Genome Epidemiology Study). Association analysis was performed under an additive model of logistic regression, and replication study was conducted with 200 independent cases of Korean AF Network and 1,812 controls.
Results: 1) We validated already proven 5 genetic loci (1q24/PRRX1, 4q25/PITX2, 10q24/NEURL, 12q24/TBX5, 16q22/ZFHX3). Two novel genetic loci associated with early-onset AF were found on chromosomes 1q32.1/PPFIA4 (rs11579055, P=6.84×10-10) and 4q34.1/HAND2 (rs8180252, P=1.49×10-11) and replicated in an additional independent sample of Korean AF Network. 2) There were significant associa-tions between the novel SNP rs11579055 in 1q32.1 and European database proven loci in 1q21 (rs13376333, KCNN3; OR 4.77, 95% CI 2.40-9.50, P=9.0×10-6), and between novel rs8180252 in 4q34 and previously proven loci in 4q25 (rs4611994 proxy to PITX2; OR 12.9, 95% CI 7.33-22.68, P=7.3×10-19) in GWAS. 3) The identified loci implicate candidate genes that encode proteins related to cell-to-cell connection, hypoxic status, or long non-coding RNA.
Conclusions: We identified two novel candidate genes for early-onset AF in Korean patients who underwent catheter ablation. Both novel susceptibility loci have strong association with previously proven genes in European ancestry database.
KOREAN AF NETWORK GENOME-WIDE ASSOCIATION STUDY FOR EARLY-ONSET ATRIAL FIBRILLATION IDENTIFIES NOVEL SUSCEPTIBILITY LOCIJi-Young Lee1, Tae-Hoon Kim2, Pil-Sung Yang2, Hong-Euy Lim3, Eui-Keun Choi4, Jaemin Shim5, Eunsoon Shin6, Jae-Sun Uhm2, Jin-Seok Kim3, Boyoung Joung2, Seil Oh4, Moon-Hyoung Lee2, Young-Hoon Kim5, Hui-Nam Pak2 1Yonsei University, Seoul, Republic of Korea; 2Yonsei University Health System, Seoul, Republic of Korea; 3Korea University Guro Hospital, Seoul, Republic of Korea; 4Seoul National University Hospital, Seoul, Republic of Korea; 5Korea University Anam Hospital, Seoul, Republic of Korea; 6DNA Link Incorporation, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE OP 1-02

4
Introduction: Gastroesophageal reflux disease has been reported to associate with clinical significant AF. The study aimed to investigate the impact of esophageal acid reflux to atrial electrophysiology and AF inducibility in acid reflux rabbit model.
Methods: Twelve rabbits, randomized to acid reflux groups ([Group 1] with pylorus ligation) and control (Group 2) under general anesthe-sia with isoflurane. Electrophsiological tests were performed in both atria and ventricles at baseline (0 hour) and then hourly till 5 hours. Inducibility test was performed at baseline, 3-hour and the end of study. Atrial myocardium and esophgeal-gastric junction tissue were harvested for Trichrome and HE stain, respectively.
Results: Compared to baseline, isoflurane prolonged the ERP within Group 2 in LA (after 2 hours) and RA (after 3 hours, Figure A to D). In contrast, the ERPs shortened in LA and RA 3 hours after experiment in Group 1, compared to baseline (Figure A to D). Compared between 2 groups, the ERP differences developed earlier in LA (after 1 hour) and then RA (after 2 to 3 hours, Figure A to D). The ventricular ERPs were the same between 2 groups hourly (Figure E to H). In the end of the study, AF inducibility was higher in Group 1 than 2 (18±8% vs. 3±5%, P=0.009). HE stains showed significant mucosa break and inflammation of esophageal mucosa in lower third of esophagus due to acid reflux (Figure I). There was no difference of atrial myocardial fibrosis between 2 groups (Figure J).
Conclusions: Acid reflux causes local esophageal mucosa inflammation and leads to atrial electrical remodeling, but not structural re-modeling, which in turn increases AF inducibility.
ESOPHAGEAL ACID REFLUX CAUSES ATRIAL ELECTRICAL REMODELING AND INCREASES ATRIAL ARRHYTHMOGENESISLi-Wei Lo, Yu-Hui Chou, Shih-Huei Liu, Yamada Shinya, Ching-Liang Lu, Wei-Lun Lin, Tsung-Ying Tsai, Ling-Hui Chiang, Wen-Han Cheng, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE OP 1-03

5
Introduction: Sudden cardiac death (SCD) in young people is not uncommonly caused by Sudden Arrhythmia Death Syndromes (SADS) in overseas studies. We sought to determine the prevalence and genetic basis of SADS underlying SCD among local young victims through clinical and molecular autopsy of SCD victims and clinical and genetic evaluation of their first degree relatives (FDR).
Methods: This is a prospective study. Young SCD victims (age 5-40 years) with either an inheritable arrhythmogenic cardiomyopathy or no structural heart disease identified on clinical autopsy and a negative toxicology screening and their FDR will be recruited into study. Mo-lecular autopsy of SCD victims is done by Next Generation Sequencing (NGS) to identify pathogenic mutations in 35 SADS-related genes. All recruited FDR will undergo clinical evaluation for SADS. Mutation-specific family screening will be performed if pathogenic mutation is found in probands.
Results: As of April 2016, 17 SCD victims (M:F 13:4, mean age 26.5±7.4 years) and 46 FDR (M:F 24:22, mean age 41.0±16.6 years) were recruited into the study after 18 months of recruitment. Clinical autopsy found ARVC in 2 and structurally normal heart in 15 SCD victims. Molecular autopsy was completed in 14 SCD victims. Pathogenic or likely pathogenic mutations in DSP, DSC2, AKAP9, MYBPC3 and RYR2 genes were found in 6 SCD victims. These mutations were implicated in ARVC, ARVC, long QT syndrome, hypertrophic cardiomyopathy and CPVT respectively. 11 FDR were found to be asymptomatic carriers of known mutation of the probands. Among them only 1 with DSP mutation demonstrated phenotype of ARVC while the rest of them could not be identified by clinical evaluation.
Conclusions: This is the first local genetic and clinical study to identify SADS in young SCD victims and their FDR in Hong Kong. Prelimi-nary data suggest that SADS are not uncommonly implicated in SCD among young victims. Molecular autopsy using NGS is able to char-acterize the pathogenic genetic defects in SADS victims and facilitate the identification of mutation carriers in their FDR.
SUDDEN ARRHYTHMIA DEATH SYNDROMES IN HONG KONG IDENTIFIED BY CLINICAL OR MOLECULAR AUTOPSY OF YOUNG SUDDEN DEATH VICTIMS AND CLINICAL AND GENETIC EVALUATION OF THEIR FIRST DEGREE RELATIVES-SADS HK STUDYNgai Shing Mok1, Chloe Mak1, Ho Cheung Shum2, Nai Chung Fong1, Wai Ming Poon2, Hencher Lee1, Chi Bun Tso2, Chun Leung Lau1, Doris Ching1, Calvin Chong1, Sammy Chen1, Ying Keung Lo1, Ping Tim Tsui1 1Princess Margaret Hospital, Kowloon, Hong Kong; 2Forensic Pathology Service, Hong Kong
BASIC/TRANSLATIONAL SCIENCE OP 1-04

6
Introduction: Diabetes is a dangerous etiological factor of cardiovascular disease. Myocardial diastolic dysfunction as an early manifesta-tion of diabetic cardiomyopathy (DCM), myocardial systolic dysfunction as a late manifestation of DCM. DCM eventually caused a variety of arrhythmias, heart failure, and even cardiac sudden death. The exact mechanism of DCM inducing arrhythmias has not been illuminated, and majority considered that it was correlated with the ion channel function and expression abnormalities of in ion homeostasis.
Methods: DCM was induced in SD male rats with STZ (DM group), and control animals were given citrate buffer (Vehicle group). Cardiac systolic function and electrical function were measured by echocardiography and electrocardiogram, respectively. Ventricular arrhythmias were induced by programmed electrical stimulation in vivo. Patch clamp experiments were conducted to record Na (+) current (I (Na)) in HEK-293t cells transfected with human cardiac Na (+) channels (Nav1.5) protein. We used neonatal rat cardiac cells, cultured primary cell with high glucose medium, and simulated diabetes cell model in vitro. Protein and mRNA expression were assessed by Western blot and qRT-PCR, respectively.
Results: Rat treated with STZ displayed increased susceptibility for inducible ventricular arrhythmias and impaired left ventricle systolic function at 12 weeks when compared to Vehicle rat, which was associated with disruption of cardiac action potential conduction and de-creased Na (+) current density. In vitro and in vivo experiments, we observed that the expression of cytoplasmic Nav1.5 and the level of O-GlcNAc modification of the total protein were increased, while the expression of membranal Nav1.5 was decreased. In addition, aug-mented cytoplasmic Nav1.5 O-GlcNAc modification correlates to decreased Nav1.5 membrane trafficking and Na (+) current density.
Conclusions: Our findings clearly demonstrate that the elevated levels of O-GlcNAc modification of myocardial tissue Nav1.5 sodium channel protein may contribute to electrical disturbances of the diabetic heart, which may be a new mechanism of DCM inducing arrhyth-mia.
NEW MECHANISM CONTRIBUTING TO DIABETIC CARDIOMYOPATHY INDUCED ARRHYTHMIA: O-GLCNACYLATION OF CARDIAC SODIUM CHANNEL NAV1.5 PROTEINPeng Yu, Kui Hong
The Second Affiliated Hospital of Nanchang University, Nanchang, China
BASIC/TRANSLATIONAL SCIENCE OP 1-05

7
Introduction: Vagus nerve stimulation has been widely studied for the treatment of ventricular arrhythmias (VAs) and cardiac remodeling. The aim of this study was to study the effect of low-level left vagus nerve stimulation (LLVNS) on gene expression and cardiac neural re-modeling in postinfarcted heart.
Methods: After implanted with implantable cardioverter defibrillators (ICD) and left-cervical vagal stimulators, 17 dogs were randomly di-vided into three groups: myocardial infarction (MI) (n=7), MI+LLVNS (n=5), and sham operation (n=5). Gene expression profile was docu-mented by using affymetrix gene chip canine genome 2.0 array and real time-PCR; the level of interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α ) were measured with ELISA; the immunohistochemical staining for tyrosine hydroxylase (TH), growth-associated protein 43 (GAP43) and neurofilament (NF) were performed to assessed the density of sympathetic nerve, new axonal growth and nerve fibrils, respectively; left ventricular ejection fraction (LVEF) was measured to assess cardiac function; VAs events were detected by ICD.
Results: Three weeks after MI, compared with the MI group, dogs in MI+LLVNS group had a higher LVEF (P<0.001). A total 206 genes were involved in processes, such as immune response, apoptosis and regulation of ERK1 and ERK2 cascade, were found to be differen-tially expressed (P values <0.05 and fold change >1.5) between MI+LLVNS and MI dogs. Of the 206 genes, 55 were up-regulated and 151 down-regulated. ELISA results showed a reduction of IL-6 and TNF-α (P<0.05). LLVNS inhibited the excessive sympathetic nerve sprout-ing, decreased the density of TH-positive, GAP43-positive and NF-positive nerve (P<0.05). LLVNS significantly reduced the incidence of VAs (P<0.05).
Conclusions: The present data suggest that LLVNS regulates remodeling-related genes, prevents excessive sympathetic nerve sprouting and reverses cardiac neural remodeling without altering heart rate, which may be responsible for cardiac remodeling and VAs in postin-farcted heart.
THE EFFECT OF LOW-LEVEL LEFT VAGUS NERVE STIMULATION ON GENE EXPRESSION AND CARDIAC NEURAL REMODELING IN POSTINFARCTED HEARTShuang Zhao1, Yan Dai1, Xiaohui Ning1, Min Tang1, Yunzhou Gao2, Zeyi Li1, Yunzi Zhao1, Shu Zhang1 1State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, Beijing, China; 2Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences, School of Basic Medicine Peking Union Medical College, Beijing, China
BASIC/TRANSLATIONAL SCIENCE OP 1-06

ORAL PRESENTATION 02(13 October)

9
Introduction: Micra Transcatheter Pacing Study Group, the largest worldwide clinical trial reported 99.2% successful implantation of the device with low and stable pacing thresholds and a low rate (3.7%) of complications up to 7.7 months of follow up. Results of 12 months safety outcomes will be presented from Asia Pacific cohort.
Methods: This prospective, single-arm trial was designed to assess the safety and efficacy of the Micra VVIR leadless pacemaker (0.8 cu-bic centimeters, 2.0 grams). Patients were enrolled from 56 centers in 19 countries across 5 continents. All patients met Class I or II guideline indications for de novo ventricular pacing and were not restricted by comorbidities. The pre-specified long-term safety objective will be met if >89% of patients are free from a system or procedure related major complication at 12 months (lower boundary of the two-sided 95% confidence interval >82%). A pre-defined historical control group of 2,667 patients with transvenous pacemakers from 6 studies conducted from 2000 to 2012 will be used to compare major complication rates. Safety and trial conduct oversight are provided by an independent data monitoring committee.
Results: Of the total of 720 patients implanted with Micra, 85 patients (12%) were from Asia/Pacific countries: Australia, India, Japan, and Malaysia. The pre-specified long-term safety objective will be evaluated after all patients complete their 12-month visit with average fol-low-up duration ranging from 16.5 months to 29 months. The analysis will be done in July 2016 with results available for APHRS. Compar-ative analysis of major complication rates between Micra and the historical control cohort and results of the electrical performance of Mi-cra through 12 months will also be reported.
Conclusions: Long-term performance of the Micra transcatheter pacemaker has been evaluated in the largest transcatheter pacing co-hort to date through a globally diverse clinical trial with 12% of implanted patients from Asia/Pacific. The implications for this novel tech-nology and comparison to transvenous systems at 12 months will be discussed.
WORLDWIDE PERFORMANCE OF A LEADLESS TRANSCATHETER PACEMAKER: LONG-TERM RESULTS FROM THE MICRA TRANSCATHETER PACING STUDYCalambur Narasimhan1, Philippe Ritter2, Gabor Z. Duray3, Razali Omar4, Joseph Brugada5, Shu Zhang6, Kyoko Soejima7, Clemens Steinwender8, Mikhael El-Chami9, Aimee Laechelt10, Shufeng Liu10, Dwight Reynolds11 1CARE Hospitals, Hyderabad, India; 2CHU/Université de Bordeaux, Pessac, France; 3Medical Centre, Hungarian Defence Forces, Budapest, Hungary; 4National Heart Institute, Kaula Lumpur, Malaysia; 5Hospital Clinic I Provincial de Barcelona, Barcelona, Spain; 6Fuwai Hospital, Beijing, China; 7Kyorin University Hospital, Tokyo, Japan; 8Kepler University Hospital Linz, Linz, Austria; 9Emory University, Atlanta, United States; 10Medtronic Inc., Minneapolis, United States; 11University of Oklahoma Health Sciences Center, Oklahoma, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-01
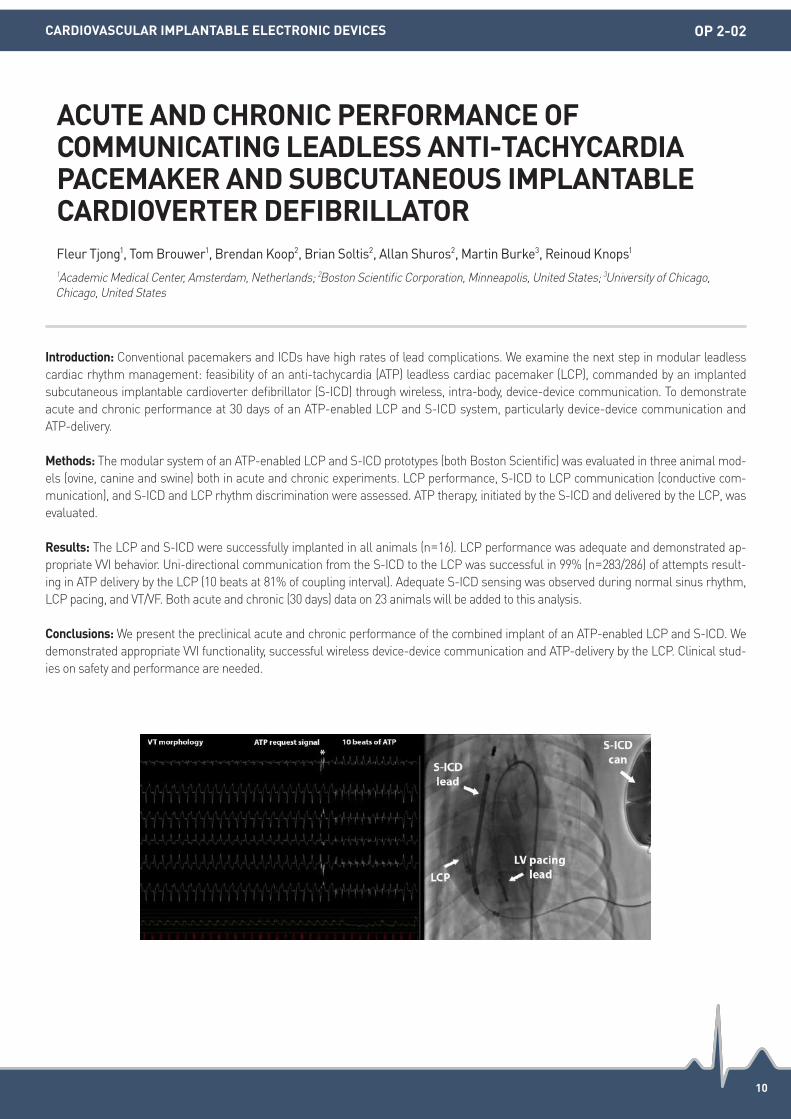
10
Introduction: Conventional pacemakers and ICDs have high rates of lead complications. We examine the next step in modular leadless cardiac rhythm management: feasibility of an anti-tachycardia (ATP) leadless cardiac pacemaker (LCP), commanded by an implanted subcutaneous implantable cardioverter defibrillator (S-ICD) through wireless, intra-body, device-device communication. To demonstrate acute and chronic performance at 30 days of an ATP-enabled LCP and S-ICD system, particularly device-device communication and ATP-delivery.
Methods: The modular system of an ATP-enabled LCP and S-ICD prototypes (both Boston Scientific) was evaluated in three animal mod-els (ovine, canine and swine) both in acute and chronic experiments. LCP performance, S-ICD to LCP communication (conductive com-munication), and S-ICD and LCP rhythm discrimination were assessed. ATP therapy, initiated by the S-ICD and delivered by the LCP, was evaluated.
Results: The LCP and S-ICD were successfully implanted in all animals (n=16). LCP performance was adequate and demonstrated ap-propriate VVI behavior. Uni-directional communication from the S-ICD to the LCP was successful in 99% (n=283/286) of attempts result-ing in ATP delivery by the LCP (10 beats at 81% of coupling interval). Adequate S-ICD sensing was observed during normal sinus rhythm, LCP pacing, and VT/VF. Both acute and chronic (30 days) data on 23 animals will be added to this analysis.
Conclusions: We present the preclinical acute and chronic performance of the combined implant of an ATP-enabled LCP and S-ICD. We demonstrated appropriate VVI functionality, successful wireless device-device communication and ATP-delivery by the LCP. Clinical stud-ies on safety and performance are needed.
ACUTE AND CHRONIC PERFORMANCE OF COMMUNICATING LEADLESS ANTI-TACHYCARDIA PACEMAKER AND SUBCUTANEOUS IMPLANTABLE CARDIOVERTER DEFIBRILLATORFleur Tjong1, Tom Brouwer1, Brendan Koop2, Brian Soltis2, Allan Shuros2, Martin Burke3, Reinoud Knops1 1Academic Medical Center, Amsterdam, Netherlands; 2Boston Scientific Corporation, Minneapolis, United States; 3University of Chicago, Chicago, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-02
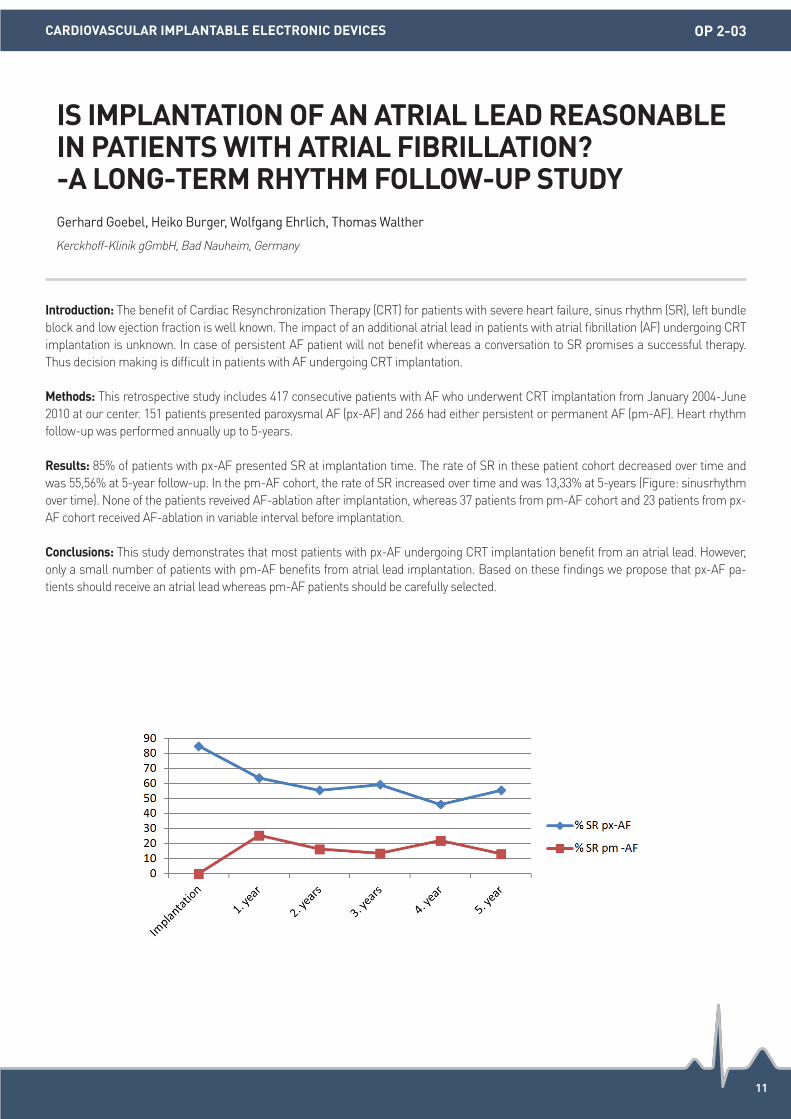
11
Introduction: The benefit of Cardiac Resynchronization Therapy (CRT) for patients with severe heart failure, sinus rhythm (SR), left bundle block and low ejection fraction is well known. The impact of an additional atrial lead in patients with atrial fibrillation (AF) undergoing CRT implantation is unknown. In case of persistent AF patient will not benefit whereas a conversation to SR promises a successful therapy. Thus decision making is difficult in patients with AF undergoing CRT implantation.
Methods: This retrospective study includes 417 consecutive patients with AF who underwent CRT implantation from January 2004-June 2010 at our center. 151 patients presented paroxysmal AF (px-AF) and 266 had either persistent or permanent AF (pm-AF). Heart rhythm follow-up was performed annually up to 5-years.
Results: 85% of patients with px-AF presented SR at implantation time. The rate of SR in these patient cohort decreased over time and was 55,56% at 5-year follow-up. In the pm-AF cohort, the rate of SR increased over time and was 13,33% at 5-years (Figure: sinusrhythm over time). None of the patients reveived AF-ablation after implantation, whereas 37 patients from pm-AF cohort and 23 patients from px-AF cohort received AF-ablation in variable interval before implantation.
Conclusions: This study demonstrates that most patients with px-AF undergoing CRT implantation benefit from an atrial lead. However, only a small number of patients with pm-AF benefits from atrial lead implantation. Based on these findings we propose that px-AF pa-tients should receive an atrial lead whereas pm-AF patients should be carefully selected.
IS IMPLANTATION OF AN ATRIAL LEAD REASONABLE IN PATIENTS WITH ATRIAL FIBRILLATION? -A LONG-TERM RHYTHM FOLLOW-UP STUDYGerhard Goebel, Heiko Burger, Wolfgang Ehrlich, Thomas Walther
Kerckhoff-Klinik gGmbH, Bad Nauheim, Germany
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-03

12
Introduction: Magnetic resonance (MR)-conditional cardiac implantable electronic devices (CIEDs) can be safely undergo MR scan. The multicenter prospective Really ProMRI study aimed at evaluating whether MR-conditional systems have actually facilitated the access to MR imaging in normal practice.
Methods: Patients either with an MR-conditional pacemaker or implantable defibrillator (ICD) system or with at least a component (device or one or more leads) from an MR-conditional system, were asked to fill in a questionnaire in case they were referred to a MR scan. The rate of prescription, denial or execution of MR examinations was evaluated in a 1-year follow-up visit.
Results: In total, 555 patients (median age [interquartile range] 72.2 [62.2-78.6]; 72% male) were enrolled in 21 Italian sites, 49% (270) with a pacemaker, 51% (285) with an ICD system. The majority of the subjects (85%) were implanted with a complete MR-conditional system. Five hundred and ten patients (92%) completed the follow-up period. A total of 37 MRI referrals were reported in 35 patients, with a conse-quent event rate of 7.0/100 patient-years [confidence interval (CI), 4.9-9.7]. Fourteen were denied, while 23 (66%; [CI, 48-81%]) were per-formed. The number of patients with MR referrals was not statistically different between pacemaker and ICD groups (21 vs. 14; P=0.178). The rate of scans performed was higher in the pacemaker subjects (19 of 23 vs. 4 of 14, P=0.003), while it was similar between patients with or without a complete MR-conditional system (19 of 30 vs. 4 vs. 7, P=0.606). Other diagnostic imaging examinations were performed: 44 X-ray, 36 CT (computed tomography), 2 PET (positive emission tomography) and 2 scintigraphy scans. No adverse events related to any diagnostic exams occurred.
Conclusions: In this study we reported a 7.0/100 patient-years event rate of MR prescriptions in CIED patients. Many examinations were denied, despite MR-conditional systems, especially in ICD patients. Regulatory and cultural changes are needed to allow wider access to MR imaging in CIED patients with MR-conditional systems.
ACCESS TO MRI OF PATIENTS WITH MAGNETIC RESONANCE-CONDITIONAL PACEMAKER AND IMPLANTABLE CARDIOVERTER DEFIBRILLATOR SYSTEMS: RESULTS FROM THE REALLY PROMRI STUDYGiampiero Maglia1, Eduardo Celentano2, Vincenzo Caccavo3, Matteo Santamaria4, Claudia Baiocchi5, Donato Melissano6, Ennio Pisanò7, Paolo Gallo8, Giuseppe Arena9, Antonio Polcino10, Luigi Padeletti11, Gaetano Senatore12, Santina Patanè13, Giovanni Licciardello14, Antonello Vado15, Daniele Giacopelli16, Alessio Gargaro16 1Ospedale Pugliese-Ciaccio, Catanzaro, Italy; 2C.D.C. Santa Maria Spa, Bari, Italy; 3E.E. Miulli, Acquaviva delle Fonti (Bari), Italy; 4Fondazione G. Paolo II, Campobasso, Italy; 5Policlinico Le Scotte, Siena, Italy; 6P.O. F.Ferrari, Casarano (Lecce), Italy; 7P.O. Vito Fazzi, Lecce, Italy; 8C.D.C. Villa dei Fiori, Napoli, Italy; 9Nuovo Ospedale Apuano Marina, Massa, Italy; 10A.O. G. Rummo, Benevento, Italy; 11A.O.U. Careggi, Firenze, Italy;
12Ospedale di Ciriè, Ciriè, Italy; 13P.O. Papardo, Messina, Italy; 14P.O. Muscatello, Augusta (Siracusa), Italy; 15S. Croce e Carlo, Cuneo, Italy;
16Biotronik Italia, Milano, Italy
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-04

13
Introduction: Subcutaneous ICD (S-ICD) is currently recommended as an alternative to transvenous ICD systems in certain patients. The S-ICD device is substantially larger in size and has defibrillation thresholds greater than transvenous ICDs. The anterior mediastinum is a potential location for a defibrillation coil that is closer in proximity to the heart. This study aims to determine if this new extravascular lead position results in improved defibrillation efficacy.
Methods: Subjects were enrolled from five international sites (UK, Hong Kong, Poland and Netherlands) and this study included subjects undergoing midline sternotomy cardiac surgery, S-ICD implant or transvenous ICD implant. A stainless tunneling tool was used to tempo-rarily insert an 8 cm defibrillation coil under the sternum using a percutaneous approach with fluoroscopic guidance. A shock vector was created using a 109 cm2 external skin patch placed at the left lateral 4th to 5th intercostal space along the midaxillary line. The ICD lead and the skin patch were connected to a conventional 35J ICD externally. Ventricular fibrillation (VF) was induced and one 35J shock from Coil to Patch was tested. Rescue shock if needed was provided by external defibrillator. After testing the ICD coil was removed. The study endpoint is successful termination of induced VF by 35J shock delivery in the substernal-lateral configuration. A one-sided 95% exact confidence interval was calculated for defibrillation success. The objective was that the lower bound of this interval be greater than 65%.
Results: Sixteen subjects (12 males; mean age: 61.6±11.8 years) were enrolled (2 coronary bypass grafting; 7 valve replacement/repair; 1 aortic aneurysm repair; 5 S-ICD, 1 transvenous ICD). Twelve subjects underwent general anesthesia. Lead tunneling was successful in all 16 subjects with mean lead placement time of 11.1±6.6 minutes and mean fluoroscopy time of 2.5±1.3 minutes. Of the 14 subjects with successfully induced VF episodes, 13 subjects (92.9%) had successful defibrillation at 35J. The primary objective of true proportion of shock success was met with a lower bound of 70.3% (>65%). One shock failure was associated with high and lateral shock coil place-ment, and an external rescue shock successfully terminated the induced VF. The mean VF duration was 18.4±5.6 seconds and shock im-pedance was 99.1±19.3 ohms.
Conclusions: Preliminary data demonstrate that substernal lead implantation is safe and feasible and provides high defibrillation success using relatively low energy.
PLACEMENT OF DEFIBRILLATION COIL UNDER THE STERNUM: THE ACUTE SUBSTERNAL DEFIBRILLATION (ASD) STUDY EXPERIENCEJian Cao1, Mark Hall2, Jacek Lelakowski3, Francis Murgatroyd4, Lucas Boersma5, Vladimir Nikolski1, Griet Wouters6, Joseph Chan7 1Medtronic, Inc., Mounds View, United State; 2Liverpool Heart and Chest Hospital, Liverpool, United Kingdom; 3The John Paul II Hospital, Krakow, Poland; 4King’s College Hospital, London, United Kingdom; 5St. Antonius Hospital, Nieuwegein, Netherlands; 6Medtronic, Inc., Maastricht, Netherlands; 7Prince of Wales Hospital, Hong Kong
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-05

14
Introduction: The superior vena cava (SVC) is congenitally absent when both the right and the left innominate veins drain directly into the coronary sinus (CS) also known as isolated persistent left superior vena cava which is an extremely rare venous anomaly. Absence of the SVC makes transvenous LV lead implantation almost impossible utilizing standard transvenous techniques. We report two patients with previously failed LV lead implantation due to congenital absence of the SVC who were successfully implanted by combining the femoral approach with the antidromic snare technique.
Methods: N/A.
Results: Case 1: An 80-year-old woman with sick sinus syndrome, the first atrial pacemaker was implanted in 2004 and an isolated per-sistent left superior vena cava (PLSVC) was noted. In 2014 a CRT implantation was attempted but the LV lead caused phrenic nerve stimu-lation or the Spacing threshold was too high. In 2015 a new attempt of a CRT implantation was planned. The RV lead was placed into the RV septum through the left axillary vein. A steerable catheter was advanced to the os of the CS through the right femoral vein. A 300 cm PCI wire was guided into the posterior vein and passed through the collaterals into the posterolateral vein and back to the right atrium. A snare catheter was introduced through the axillary vein and the PCI wire was snared. A 1,8Fr Coronary Micro-Guide catheter was ad-vanced through the femoral route over the PCI wire to protect the coronary veins as the PCI wire was snared to the subclavian pocket. Next a quadripolar LV lead was advanced over the PCI wire into the posterolateral vein using the antidromic technique. Case 2: A 54-year-old man. In 2006 a mitral valve repair was done and an isolated PLSVC noted. In 2014 he developed signs of heart failure and in 2015 a CRT-P implant was attempted. First the right ventricular lead was placed into the RV septum through the left axillary vein. LV lead im-plantation was performed as described in the previous case. Finally an atrial lead was implanted in the anterior wall of the right atrium.
Conclusions: Interventional approach and combining different tools and techniques when implanting CRT offer more possibilities when implantation with the normal catheters is not successful.
HOW TO IMPLANT AN LV LEAD WHEN THERE IS NO SVC: COMBINING THE FEMORAL AND ANTIDROMIC SNARE TECHNIQUES IN TWO PATIENTSJussi Niiranen, Mika Lehto
Helsinki University Hospital, Helsinki, Finland
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 2-06

ORAL PRESENTATION 03(13 October)

16
Introduction: The association between high alcohol intake and incident AF is well established with numerous epidemiological studies clearly delineating this relationship. However, less is known about the impact of low alcohol intake on risk of incident AF. Here, we further explored this association with a systematic review and meta-analysis.
Methods: Pubmed and Embase databases were searched up to February, 2016 using the keywords ‘atrial fibrillation’, ‘alcohol drinking’, ‘binge drink*’, ‘ethanol’, ‘risk’, ‘incidence’, ‘prevalence’, ‘dose response relationship, drug or dose’ and ‘drinking behavior’. 1,877 articles were screened to identify prospective studies that examined the impact of alcohol on AF development, were published in English and in-cluded at least three levels of alcohol intake (low, moderate and high) to ascertain a dose response. One standard drink was reported as 10-12 grams of alcohol in these studies.
Results: Nine studies encompassing 249,496 individuals were included. Mean age was 60±10.4 years and 57% were female. High alcohol intake, as classified by the highest alcohol consumption group in all of the nine studies was significantly associated with development of AF (HR 1.34, 95% CI 1.20-1.49; P<0.00001). Similarly, moderate alcohol intake was also significantly associated with AF risk overall (HR 1.11, 95% CI 1.05-1.18; P=0.0002) but subgroup analyses demonstrated that this association was significant in males but not females (HR 1.26, 95% CI 1.04-1.54, P=0.02 and HR 1.03, 95% CI 0.86-1.25, P=0.74; respectively). Up to one standard drink per day, compared to no al-cohol intake, was not significantly associated with incident AF (HR 0.95, 95% CI 0.85-1.06; P=0.37) from four studies that specifically re-ported on this category.
Conclusions: There is a dose dependent association between alcohol consumption and AF. However, up to one standard drink per day does not appear to confer an increase in risk. Gender differences are apparent but further prospective studies are required to confirm these associations.
LOW ALCOHOL INTAKE AND INCIDENT ATRIAL FIBRILLATION-IS THERE A SAFE LEVEL?Celine Gallagher, Jeroen Hendriks, Adrian Elliott, Geetanjali Rangnekar, Melissa Middeldorp, Rajiv Mahajan, Dennis Lau, Prashanthan Sanders
University of Adelaide, South Australian Health and Medical Research Institute, Adelaide, Australia
ALLIED PROFESSIONALS OP 3-01
17
Introduction: Fabry’s disease is a rare X linked lysosomal storage disorder characterized by deficiency of alpha-galactosidase A. Clinical presentation of this disorder is variable but tends to be more severe in males, including neuropathic pain, dermatologic disease, renal in-sufficiency, and cerebrovascular accidents. Cardiac involvement includes left ventricular hypertrophy, ischaemia, valvulopathy, and ar-rhythmia; and portends poorer prognosis if untreated. The aim of this study is to review the incidence of cardiac manifestations, with focus on arrhythmia, in our current cohort of patients with Fabry’s disease in Western Australia.
Methods: Patients with Fabry’s disease were derived from a centralized, state-wide database from a multi-disciplinary clinic in a tertiary hospital in Western Australia. Results of cardiac investigations were compiled-including echocardiography, cardiac MRI, Holter/event monitors, and clinical reviews. In total 25 patients with Fabry’s Disease (with 4 families) were identified.
Results: The average age of patients was 44.6±16.5. There were 13 male (52%) and 12 female (48%) patients. Ten patients (40%) are cur-rently receiving enzyme replacement therapy at the time of this study. Major non cardiac manifestations were: acroparaesthesiae (48%), keratopathy (44%), cerebrovascular events (36%), and chronic kidney disease (24%). The average age of patients with any cardiac manifes-tation was higher at 49 years, compared to patients without cardiac manifestation (30.9 years). The most common cardiac finding was left ventricular hypertrophy, found in 9 patients (36%), of which 33.3% were asymmetric in nature. 7 patients (28%) underwent Holter monitor-ing following their diagnosis, where the incidence of documented arrhythmia was paroxysmal atrial fibrillation (4%), complete heart block requiring PPM insertion (4%), and non-sustained atrial tachycardia (4%). 1 patient had an asymptomatic sinus pause at 2.8s. Other cardi-ac findings relating to Fabry’s disease include 1 patient with significant LVOT gradient, 3 patients (12%) with cardiac failure, and 2 patients (8%) with dilated aortic root. The most common valvulopathy was mild mitral regurgitation at 25%. 17 patients (68%) have surveillance MRIs, of which 23.5% had evidence of delayed gadolinium enhancement on their last scan.
Conclusions: In our patient cohort with Fabry’s disease, 76% of patients have evidence of cardiac involvement which tend to occur at a lat-er age, consistent with existing literature. The incidence of tachy- or brady-arrhythmia was 12%. Long term follow up of these patients with Fabry’s disease is essential to monitor for further cardiovascular complications.
INCIDENCE OF CARDIAC ARRHYTHMIAS AND OTHER CARDIAC MANIFESTATIONS IN PATIENTS WITH FABRY’S DISEASE. THE WESTERN AUSTRALIAN EXPERIENCEDavid Chieng, Paul Maggiore, Mark Thomas, Doug Crawford, Nik Stoyanov
Royal Perth Hospital, Perth, Australia
CLINICAL ELECTROPHYSIOLOGY OP 3-02

18
Introduction: Over the past 15 years (2002-2016), 750,960 people participated in the Hong Kong Standard Chartered Marathon, which is one of the largest marathon event in Asian Pacific Region. We aim to study the prevalence of marathon race-related sudden cardiac death.
Methods: All the Standard Chartered Marathon related hospital admissions over the past 15 years (2002-2016) were retrieved from Acci-dent and Emergency Department admission record. We reviewed the prevalence, epidemiological profile and clinical outcome of mara-thon runners admitted for cardiac arrest.
Results: Over the past 15 years, among the 750,960 marathon participants, there were 10 runners admitted for cardiac arrest (Mean age 36±13 year-old. Nine males. Five 10 kilometers runners, 4 half-marathon runners and 1 full-marathon runner). The cardiac arrest rhythms could not be retrieved in 2 patients. In the remaining 8 patients, the arrest rhythms were ventricular fibrillation (VF) (N=4), pulse-less-electrical activity (PEA) (N=3), and asystole (N=1). Seven of the ten cardiac arrest runners were successfully resuscitated. Echocar-diogram showed normal left ventricular function in 5 out of 7 patients. Only 1 out of the 7 patients had significant coronary artery disease. Among the 7 resuscitated runners, the etiologies of cardiac arrest were myocardial infarction (N=1), ischemic cardiomyopathy with ven-tricular fibrillation (VF) (N=1), idiopathic VF (N=1), malignant coronary anomaly (N=1), and idiopathic (N=3). Percutaneous coronary inter-vention was performed in one patient with myocardial infarction. Implantable cardioverter-defibrillators were implanted in two patients with resuscitated VF. Postmortem examination of the 3 deceased runners showed unrevealing finding in one and significant coronary ar-tery disease in two.
Conclusions: The incidence of cardiac arrest among Standard Chartered Marathon Runners over past 15 years was 1.3 per 100,000. The incidence of mortality was 0.4 per 100,000. In contrast to the Western data, we did not identify any patients hypertrophic cardiomyopathy. Coronary artery disease remained the commonest etiology of cardiac arrest among the Asian runners.
CARDIAC ARREST AMONG MARATHON RUNNERS-A 15 YEARS’ EXPERIENCE OF HONG KONG STANDARD CHARTERED MARATHONKit Chan1, Kuang An Wan1, Sai Chau Leung1, Ngai Shing Mok2, Natalie Leung3, Jessica, Wai Ling Poon1, Yuk Kong Lau1 1Ruttonjee and Tang Shiu Kin Hospitals, Wan Chai, Hong Kong; 2Princess Margaret Hospital, Lai Chi Kok, Hong Kong; 3Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong
CLINICAL ELECTROPHYSIOLOGY OP 3-03
19
Introduction: The CHA2DS2-VASc scheme has been used for stroke risk stratification in patients with atrial fibrillaiton (AF). Although 1 point was assigned for female sex in the scoring system, previous studies have shown inconsistent results about whether AF females had a higher risk of ischemic stroke compared to males. Thus, we compared the risk of ischemic stroke for AF males with a CHA2DS2-VASc score of 0 to that of AF females with a score of 1 (only due to female gender) stratified by age. We hypothesized that age may play an im-portant role about the stroke risk for AF males compared to females.
Methods: The present study used the “National Health Insurance Research Database (NHIRD)” in Taiwan. From year 1996-2011, a total of 9,416 males with a CHA2DS2-VASc of 0 and 6,390 females with a CHA2DS2-VASc of 1 were identified from the NHIRD to constitute the study population. Amongst these patients, we divided them in two groups by age, that is, 20-49 years and 50-64 years. The risk of ischemic stroke of males was compared to that of females in different age strata.
Results: During the follow-up, 1,167 ischemic stroke events were documented. For patients aged between 20-49 years, the annual risk of ischemic stroke was lower for AF males compared to females (0.46%/year vs. 0.64%/year) with a hazard ratio (HR) of 0.72 (95% confidence interval <CI>=0.57-0.91, P value <0.05) (Figure). On the contrary, the annual risk of ischemic stroke was higher for AF males aged 50-64 years compared to females with a HR 1.25 (95% CI=1.09-1.43, P value<0.05).
Conclusions: For young AF patients (<50 years), female gender was associated with a higher risk of ischemic stroke compared to that of males. However, for patients older than 50 years, females did not have a higher risk of ischemic stroke than males.
GENDER DIFFERENCE OF RISK OF ISCHEMIC STROKE IN ATRIAL FIBRILLATION PATIENTS STRATIFIED BY AGELing Kuo, Tze-Fan Chao, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
ALLIED PROFESSIONALS OP 3-04

ORAL PRESENTATION 04(13 October)

21
Introduction: Over the past decade improvements in 3D mapping systems have led to increasing understanding of the nature of activation patterns during complex atrial arrhythmias. However, the relationship between the activation patterns and underlying atrial substrate re-mains uncertain. The recent advent of high resolution 3D electroanatomical mapping (Rhythmia, Boston Scientific) that automatically an-notates electrograms and allows rapid acquisition of thousands of points (bipolar spacing 2 mm) provides a level of detail not previously possible. Using the Rhythmia mapping system we aimed to characterize the relationship between atrial conduction and atrial substrate during MAT. We hypothesized that atrial substrate may vary markedly between individual patients with MAT.
Methods: 16 patients with macro reentrant atrial tachycardia undergoing catheter ablation were studied. High density (HD) 3D electro-anatomical mapping was performed using a novel basket catheter with 64 electrodes and automated electrogram annotation. Bipolar ac-tivation maps were created and regional atrial conduction times calculated. Regional atrial conduction was correlated with the regional voltage map.
Results: In the 16 patients studied, 18 atrial flutter circuits were observed. Eleven (61%) had counterclockwise CTI dependent atrial flutter, 2 (11%) clockwise CTI dependent atrial flutter and one (6%) example of intra-isthmus re-entry. Two (11%) cases of upper loop re-entry were observed. Two (11%) circuits were consistent with left atrial flutter. Maps had a mean of 24,202±9,939 points acquired in a mean of 21±14 minutes. Activation maps showed marked regional variability in conduction velocity. Notably however, no patients demonstrated conduction slowing within the CTI and this correlated with this region having preserved voltage. Regions of slow conduction (SC) and con-duction block (CB) were observed in the following regions: crista terminalis (SC 3; CB 6); septal RA at anatomic region of fossa ovalis (SC 6; CB 2); posterior RA (SC 1, CB 0) superior RA (SC 4, CB 0) and lateral RA (SC 1, CB 0). In all cases the region of SC with isochronal crowd-ing corresponded to an arc or region of lower voltage (Figure). There was no fixed pattern to the regions of abnormal substrate demon-strated with marked variability observed even in patients with CTI dependent flutter.
Conclusions: During MAT, there is a close correlation between regions of abnormal atrial substrate and regions of conduction slowing. There is considerable individual substrate variation even for an apparently stereotypic arrhythmia such as CTI dependent flutter. HD 3D electroanatomical mapping systems provide new insights into the nature of arrhythmia substrate in patients with MAT.
HIGH DENSITY MAPPING OF ATRIAL MACRO-REENTRY. NEW INSIGHTS INTO THE RELATIONSHIP BETWEEN ACTIVATION PATTERNS AND SUBSTRATEBhupesh Pathik1, Geoff Lee1, Matthew Bates1, Jonathan Lipton1, Sandeep Prabhu1, Chrishan Nalliah1, Joseph Morton1, Paul Sparks1, Peter Kistler2, Jonathan Kalman1 1Royal Melbourne Hospital, Melbourne, Australia; 2Alfred and Baker IDI, Melbourne, Australia
CLINICAL ELECTROPHYSIOLOGY OP 4-01

22
Introduction: The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) score was recently developed and validated for stroke risk stratification for atrial fibrillation (AF). This study compared predictive ability of the ATRIA, CHA2DS2-VASc, CHADS2, and R2CHADS2 scores and their implications for anticoagulant treatment in AF patients.
Methods: Patients with non-valvular AF not prescribed oral anticoagulants (OACs) were included from 506,806 adults in prospective co-hort data collected by the Korean National Health Insurance Service. Patients were followed from AF diagnosis until occurrence of isch-emic stroke, prescription of OAC, death, or the study’s end. Independent predictors of ischemic stroke were identified and the c-index and net reclassification improvement were calculated.
Results: During 14,430 person-years of follow-up, we observed 188 ischemic strokes. Annualized stroke rate was 1.3%. The C statistics for the full-range ATRIA score was 0.77 (95% confidence interval [CI]: 0.74 to 0.80), significantly better than the CHA2DS2-VASc of 0.74 (95% CI: 0.70 to 0.77), the CHADS2 of 0.74 (95% CI: 0.71 to 0.78), and the R2CHADS2 of 0.74 (95% CI: 0.70 to 0.78). The ATRIA score also improved the net reclassification index by 34% compared with the CHA22DS2-VASc score, 17% compared with the CHADS2 score, and 27% com-pared with the R2CHADS2 score. Patients with an ATRIA score of 0 to 5 were substratified as low, moderate, and high-risk on the basis of CHA2DS2-VASc score, and annual stroke rates ranged from 0.13% to 0.56%.
Conclusions: The ATRIA score performed best in the Korean national cohort. It more accurately identified low risk patients than the CHA2DS2-VASc score, which categorized those patients as higher risk. Reclassification of stroke risk based on the ATRIA score could di-minish anticoagulant overuse in AF patients with very low stroke risk.
COMPARISON OF STROKE PREDICTION PERFORMANCE OF ATRIA, CHADS2, R2CHADS2, AND CHA2DS2-VASC RISK SCORES IN PATIENTS WITH ATRIAL FIBRILLATION: A NATIONWIDE COHORT STUDY IN KOREADaehoon Kim, Pil-Sung Yang, Tae-Hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY OP 4-03

23
Introduction: One demonstrated mechanism of persistent and long-standing persistent (LSP) atrial fibrillation (AF) is that due to activa-tion emanating from multiple foci (sustained and/or intermittent) and nonrandom breakthrough sites of different cycle lengths (CLs) which activate the atria, maintaining AF. The purpose of this study was to quantify characteristics of sustained and intermittent focal, and nonrandom breakthrough activation identified during high density mapping of AF in patients with persistent and LSP AF.
Methods: We recorded the atrial activation sequence during AF in 12 patients with persistent and LSP AF (1 month-9 years duration) at open heart surgery. During AF, electrograms were simultaneously recorded from both atria for 1-5 minutes from 510-512 epicardial elec-trodes, arranged in bipolar pairs, along with ECG lead II. From each patient, analysis of consecutive 32 secs of identified multiple focal (sustained and/or intermittent) and nonrandom breakthrough sites was performed.
Results: During persistent and LSP AF, multiple foci (sustained [1-2 sites] and/or intermittent [1-3 sites]) of different CLs were present in both atria in 11/12 patients. 8 sustained foci (mean CL 170±19 ms; range 142-200 ms; duration 32 s) and 21 intermittent foci (mean CL 176±18 ms; range 143-211 ms) were identified in 11 patients. Temporal CL behavior of sustained foci varied (6/8, maximum change of mean CL: 20 ms). Periods of no focal activation were due to either a spontaneous pause (16/21) or activation of the focal site by wave fronts originating from another focus or a breakthrough site (9/21). 10 nonrandom breakthrough sites (mean CL 166±20 ms; range 136-195 ms) were identified in 7 patients. Periods of no nonrandom breakthrough activation were due to a spontaneous pause (8/12), activa-tion of the site by another wave front (3/12), or uncertain (5/12). No reentry was found.
Conclusions: During persistent and LSP AF, 1) each sustained focus manifested variable CLs over time; 2) intermittent foci and nonran-dom breakthrough sites manifested variability in both CLs and periods of activity; 3) spontaneous pauses or activation from other wave fronts explained the intermittency of the intermittent foci and nonrandom breakthrough; 4) no reentry was found.
CHARACTERIZATION OF FOCI AND NONRANDOM BREAKTHROUGH DURING PERSISTENT AND LONG-STANDING PERSISTENT ATRIAL FIBRILLATION IN PATIENTS-STUDIES USING HIGH DENSITY (510-512 ELECTRODES) BI-ATRIAL EPICARDIAL MAPPINGSeungyup Lee, Jayakumar Sahadevan, Celeen Khrestian, Albert Waldo
Case Western Reserve University, Cleveland, United States
CLINICAL ELECTROPHYSIOLOGY OP 4-04

24
Introduction: Ventricular premature complex (VPC) causes impaired heart contractility and enlarged ventricular size, so-called VPC in-duced cardiomyopathy. According to previous works, the lower limit of VPC burden causing cardiomyopathy was 10% to 20% of day total heart beats. Systolic blood pressure response (SBPR) is a measure of the difference of systolic blood pressure between during peak exer-cise and during rest. It was recently identified as a prognostic factor of heart failure. Lower SBPR predicts worse outcome of chronic heart failure. However, there is no literature addressing the relationship between VPC burden and SBPR.
Methods: From 2015.01 to 2015.12, all patients with 24 hours electrocardiography recordings and treadmill exercise test in our hospital were enrolled. Patients with atrial fibrillation or with ischemic result of treadmill test were excluded. The VPC burden was counted with the 24 hours electrocardiograpy recordings and the SBPR was measured during the treadmill test. The basic characteristic, disease his-tory, medication history and echocardiographic findings were collected.
Results: According to the VPC burden, all patients (n=153) were classified into three groups: group 1: VPC<1,000/24 hours (n=78), group 2: VPC 1,000-10,000/24 hours (n=54), group 3: VPC>10,000/24 hours (n=21). Patients in group 1 were associated with significant higher SBPR than patients in group 2 and group 3 (53.8±16.4 vs. 33±17 and 26.5±9.8, P<0.05, Figure A). In all patients, lower VPC burden was associated with higher SBPR (Figure B). Setting SBPR<40 as a cut-off point, the receiver operating characteristic curve of VPC burden was created. The area under the curve was 0.85 and the best predicting value of VPC burden was 1,055/24 hours (Figure C). The echocar-diographic finding showed lower left ventricular ejection fraction, larger left ventricular internal diameters in group 3. The other parame-ters were not significantly different among the three groups.
Conclusions: Higher VPC burden was associated with lower SBPR. Because SBPR is a prognostic factor for heart failure, VPC burden for VPC induced cardiomyopathy may be lowered to 1,055/24 hours. Although the conventional parameters were unchanged, VPC may im-pact heart function, even as less as 1,055/24 hours.
HIGHER VENTRICULAR PREMATURE COMPLEX BURDEN, LOWER SYSTOLIC BLOOD PRESSURE RESPONSEWeita Chen1, Jia En Chi2, Jing Wei Kang2, Wei Hsiang Yang2 1Graduate Institute of Clinical Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan; 2School of Medicine, Taipei Medical University, Taipei, Taiwan
CLINICAL ELECTROPHYSIOLOGY OP 4-05

25
Introduction: Current gold-standard for imaging follow-up is known to be a trans-esophageal echocardiogram (TEE) after percutaneous left atrial appendage (LAA) occlusion procedure (LAAO). However, there is no human data for the appropriate duration for complete seal-off of LAA after LAAO. We retrospectively evaluated LAA contrast-filling rate in follow-up heart CT after LAAO.
Methods: Among 51 patients (67.8±10.5 years old, CHA2DS2-VASc 4.3±1.6, HAS-BLED 3.7±1.4) who underwent LAAO (23 WATCHMAN [W] and 28 Amplatzer Cardiac Plug [ACP]), follow-up heart CTs have been conducted in 38 patients (74.5%). We retrospectively evaluated contrast-filling rates in LAA and compared them with TEE findings.
Results: 1) The Proportions of the patients with LAA contrast-filling in CT after LAAO were 53.3% (16/30) at 2 months, 46.1% (6/13) at 2-12 months, and 40% (6/15) after 12 months. 2) Among 26 patients who showed no peri-device leak at 2 months in TEE, LAA contrast-fillings were found in 9 patients (34.6%, 7 W, 2 ACP), and 7 out of 9 patients who showed peri-device leak <5 mm at 2 months in TEE revealed LAA contrast-fillings at 6.2±8.1 month follow-up CT (77%). 3) LAA contrast fillings in heart CT and no peri-device leak in TEE were found in 60% (6/10) in W and 40% (4/10) in ACP. 4) Among 8 patients with serial follow-up CT images, partial reductions of LAA contrast filling were found in 3 patients [2 W, 1 ACP], but no complete LAA seal-off was observed after 19.0±11.3 months follow-up. 5) During 27.8±15.2 months follow-up, delayed strokes occurred in 5 patients (9.8%, 2 W and 3 ACP; one major stroke) and LAA contrast-fillings (heart CT) were observed in 4 patients (80%) in spite of none of them showed peri-device leak ≥5 mm (TEE).
Conclusions: LAA contrast-filling is a common finding after LAAO with considerable discrepancy between heart CT and TEE evaluation. Although clinical significance of LAA contrast-filling is unclear, 2 months seems to be not enough for complete LAA seal-off after LAAO.
LEFT ATRIAL APPENDAGE CONTRAST-FILLING IN HEART COMPUTED TOMOGRAMS AFTER PERCUTANEOUS LEFT ATRIAL APPENDAGE OCCLUSION PROCEDUREYeong-Min Lim, Jung-Sun Kim, Tae-Hoon Kim, Jae-Sun Uhm, Chi Young Shim, Boyoung Joung, Geu-Ru Hong, Moon-Hyoung Lee, Yang-Soo Jang, Hui-Nam Pak
Yonsei University Health System, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY OP 4-06

ORAL PRESENTATION 05(14 October)

27
Introduction: Primary prevention implantable cardioverter-defibrillators (ICD) reduce mortality in selected patients with severe systolic dysfunction. Current guidelines suggest a 3-6 months waiting period before implantation.
Methods: We retrospectively studied 29 consecutive patients with newly-diagnosed non-ischemic cardiomyopathy (NICM) who underwent primary prevention ICD implantation within six months of diagnosis between 1/2008 and 4/2014. Cardiac MRI (CMR) evaluated left ventric-ular ejection fraction (LVEF) and regional fibrosis pre-implant. The primary endpoint was ‘failure to qualify for an ICD at 12 months post implant’, either due to LVEF≥35% or deterioration necessitating mechanical support or transplantation, without appropriate ICD therapy. Secondary endpoints were appropriate and inappropriate ICD therapy.
Results: Baseline mean age was 44.2±14.8 years and median LVEF 16.4%. Median time from diagnosis to implant was 32 days. At 12 months, 17 patients (58.6%) no longer qualified for an ICD, mainly due to LVEF improvement (Figure 1). At follow-up (mean 32.0±20.6 months), three patients received appropriate therapy (one for ventricular fibrillation). All three had CMR late Gadolinium enhancement (LGE) and non-sustained ventricular tachycardia (NSVT) pre-implant. Cardiac resynchronisation at implant predicted LVEF improvement.
Conclusions: Early appropriate therapy, particularly for VF, is infrequent for patients with very severe NICM who have ICDs implanted within six months of diagnosis. The majority of these patients would not qualify for an ICD at 12 months post-insertion. In the absence of a multi-modality risk score, early ICD insertion should only be considered in selected cases (presence of LGE and NSVT). Wearable cardio-verter-defibrillators may have a role as a bridge to ICD decision.
EARLY IMPLANTATION OF PRIMARY PREVENTION IMPLANTABLE CARDIOVERTER-DEFIBRILLATORS FOR PATIENTS WITH NEWLY DIAGNOSED SEVERE NON-ISCHEMIC CARDIOMYOPATHYAleksandr Voskoboinik, Jason Bloom, Andrew Taylor, Justin Mariani
Alfred Hospital, Melbourne, Australia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 5-01

28
Introduction: Prolongation of the Tpeak-Tend (TpTe) interval, as a measurement of transmural dispersion of repolarization (TDR), is an in-dependent risk factor for chronic heart failure mortality. However, the cardiac resynchronization therapy (CRT)’s effect on TDR is contro-versial. Therefore, this study aimed to evaluate CRT’s acute and chronic effects on repolarization dispersion. Furthermore, we aimed to investigate the relationship between TpTe changes and ventricular arrhythmia.
Methods: The study group consisted of 101 patients treated with CRT-D. TpTe was measured at baseline, immediately and 1 year post CRT implantation. CRT responders defined by LV reverse remodeling that the LV end-diastolic dimeter (LVEDd) decreased by at least 10% after 6 months follow-up. Incidence of appropriate ICD therapy was determined based on routing and directed device interrogations. Ob-served the evolution of TpTe after CRT implantation in overall patients and responders as well as non-responders. According to whether TpTe was shortened at immediate and 1-year post-CRT, patients were grouped at acute changes and chronic changes. The echocardio-gram index and ventricular arrhythmia were observed and analyzed in these subgroups.
Results: For all patients, TpTe slightly increased immediately after CRT-D implantation, and then decreased at the 1-year follow-up (from 107±23 to 110±21 ms within 24 hours, to 94±24 ms at 1-year follow-up, F=19.366, P<0.001). Responders (n=59) had a significant reduc-tion of TpTe at 1 year after CRT implantation (92±20 ms at 1-year follow-up vs. 112±21 ms within 24 hours, t=20.349, P=0.010), rather than non-responders (n=42). At the 1-year follow-up, 22 patients (22%) experienced appropriate therapy because of ventricular tachycar-dia and ventricular fibrillation (VT/VF) episodes. No significant difference in left ventricular reverse remodeling (56% vs. 60%, χ2=0.209, P=0.648) and VT/VF episodes (log-rank test, χ2=0.574, P=0.449) between the TpTe immediately shortened and TpTe immediately non-shortened groups. However, patients in the TpTe at 1 year shorten had a higher rate of LV reverse remodeling (65% vs. 44%, χ2=4.495, P=0.038) and less VT/VF episodes (log-rank test, χ2=10.207, P=0.001) compared with TpTe 1-year non-shortened group. On multivariate Cox regression analysis, TpTe immediately after CRT-D independently predicted VT/VF episodes at 1-year follow-up (hazard ratio [HR], 1.03; P=0.001].
Conclusions: Patients with TpTe shortened at 1 year after CRT had a higher rate of LV reverse remodeling and less VT/VF episodes. Elec-trical remodeling play a role in mechanical remodeling post CRT implantation. TpTe immediately after CRT-D independently predicted VT/VF episodes at 1-year follow-up.
ACUTE AND CHRONIC CHANGES AND PREDICTIVE VALUE OF TPTE FOR VENTRICULAR ARRHYTHMIA RISK IN CARDIAC RESYNCHRONIZATION THERAPY PATIENTS Cong Xue, Wei Hua, Chi Cai, Li-Gang Ding, Zhi-Min Liu, Xiao-Han Fan, Yun-Zi Zhao, Shu Zhang
Fuwai Hospital, Beijing, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 5-02

29
Introduction: Multipoint pacing (MPP) and RV synchronized LV pacing have been shown to reduce QRSd and enhance some of the effects of CRT. Utilizing a device based Negative Hysteresis algorithm (NH), this analysis studied and compared the effects of the NH algorithm and multipoint LV pacing in CRT patients.
Methods: Consecutive patients implanted with a SJM quadripolar lead and MPP programmable device were screened. Those patients with preserved AV function (PR interval <350 ms) were enrolled. 12 lead ECG’s were performed in intrinsic rhythm and in device derived best biventricular pacing mode (BiV). MPP was performed from the most anatomically separate electrodes with successful LV capture with an intra LV delay of 5 ms and a total LV to RV delay identical to that in best BiV mode. The NH was performed in both best BiV mode and MPP mode with NH delays from -10 to -80 ms.
Results: Both MPP and NH were feasible in all patients. The mean QRSd reduced with both MPP and NH. Best BiV 150±15 ms, best MPP 142.5±13 ms and best NH 130.7±17 ms. The mean best NH was with an interval of-40 ms (range -10 to -70 ms). The combination of MPP and NH improved QRSd further with a mean of 123.3±16 ms. 70% of patients had the shortest QRSd in combined NH and MPP mode. Patients with an intrinsic QRSd >150 ms had a greater improvement in QRSd with combined NH and MPP 13±11 ms compared with 6±13 ms in patients with an intrinsic QRSd <150 ms.
Conclusions: Combining MPP and NH in a single device, results in the best acute electrical measures of resynchronization.
NEGATIVE AV HYSTERESIS AND MPPDavid O’Donnell1, Juliette Young1, Taylah Smart2, Ryan Spencer1, Hui-Chen Han1, Lisa Odgers3, Tina Lin2 1Austin Hospital, Heidelberg, Australia; 2Genesis Care, Heidelberg, Australia; 3St. Jude Medical, Heidelberg, Australia
HEART FAILURE OP 5-03

30
Introduction: Implantable cardioverter defibrillators (ICD) offer potential life-saving therapy for patients with heart failure (HF). However, current utilization rates and determinants of ICD uptake within Asia are unclear.
Methods: We studied 5,276 patients with HF and ejection fraction (EF) <40% from 11 Asian regions in the prospective Asian Sudden Car-diac Death in Heart Failure Registry. ICD-eligible patients were: EF≤35% and New York Heart Association class II-III. In addition to so-cio-demographics and clinical characteristics, patients’ perceptions on device use were gathered through an interviewer-administered questionnaire.
Results: Of 5,276 patients, 3240 (61%) were ICD-eligible and only 389 (21%) of these received the device. ICD utilization rates varied widely across Asia (Figure). ICD recipients were older (63±11 vs. 58±11 years; P<0.001), and more likely to be male (83.5% vs. 78.5%; P=0.021), have a history of atrial fibrillation (OR 1.44; 95% CI 1.03-2.01), and have a higher Charlson Comorbidity Index (≥3 vs. <3; OR 1.60; 95% CI 1.05-2.42) compared to non-recipients. ICD recipients were also more likely to have received tertiary (vs primary or lower) education (OR 5.12; 95% CI 3.33-7.87) and to be residing in a higher income region (Singapore, Hong Kong, Taiwan, South Korea, Japan) (OR 5.38; 95% CI 3.58-8.08) vs. lower income region (Indonesia, Philippines, India). Among non-recipients, 33% of respondents were willing to receive and ICD while 44% were unfamiliar with the benefits of ICD. Of those who provided suggestions on how to facilitate patients’ decision-making, 26% preferred more information from a healthcare provider.
Conclusions: Our study highlights the under-utilization of ICD in Asia, striking disparity across different regions and socioeconomic sta-tus, and the urgent need for better patient education.
DISPARITY IN UTILIZATION OF IMPLANTABLE CARDIOVERTER DEFIBRILLATORS IN ASIAN PATIENTS WITH HEART FAILUREEugene S.J. Tan1, Yvonne Chia2, Tiew-Hwa Katherine Teng3, Wan Ting Tay3, A. Mark Richards1, Calvin Woon Loong Chin3, Wataru Shimizu4, Sang Weon Park5, Chung-Lieh Hung6, Lieng Hsi Ling1, Tachapong Ngarmukos7, Razali Omar8, Bambang S. Siswanto9, Calambur Narasimhan10, Shu Zhang11, Eugene B. Reyes12, Cheuk-Man Yu13, Inder Anand14, Eric A. Finkelstein15, Carolyn S.P. Lam3 1National University Heart Centre Singapore, Singapore; 2Duke-NUS Medical School, Singapore; 3National Heart Centre Singapore, Singapore; 4Nippon Medical School, Tokyo, Japan; 5Korea University Hospital, Seoul, Republic of Korea; 6Mackay Memorial Hospital, Taipei, Taiwan; 7Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 8Institut Jantung Negara, Kuala Lumpur, Malaysia; 9National Cardiovascular Center Universitas Indonesia, Jarkata, Indonesia; 10CARE Hospital, Hyderabad, India; 11Fuwai Hospital, Beijing, China; 12Manila Doctors Hospital, Manila, Philippines; 13Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong; 14VA Medical Center, University of Minnesota, Minneapolis, United States; 15Duke-NUS, Health Services and Systems Research, Singapore
HEART FAILURE OP 5-04

31
Introduction: AF ablation improves symptoms and systolic function in patients with comorbid persistent AF (PeAF) and idiopathic dilated cardiomyopathy (IDCM). Whether regression of associated diffuse ventricular fibrosis accompanies LVEF recovery, has not previously been explored.
Methods: Patients with IDCM and PeAF were recruited between January 2014 and January 2016 from 3 Australian centres. Patients were included if they had a LVEF≤45%, PeAF, and no contraindication to cardiac MRI (CMR). All patients underwent baseline CMR with native ventricular T1 mapping, a histologically validated index of diffuse ventricular fibrosis, followed by randomisation to either AF ablation, or ongoing medical rate control. CMR was repeated at 6 months.
Results: 23 patients met the inclusion criteria and were randomised to catheter ablation (CA group, n=14) or to ongoing medical rate control (MRC group, n=9). There was no significant difference in baseline characteristics between the groups with respect to age (MRC vs. CA: 63±4.9 vs. 61±12 years, P=0.51), gender (100% vs. 81% male, P=0.41), LVEF (32±8.2% vs. 338.0%, P=0.76), AF duration (15±6.1 vs. 12±6.5 months, P=0.17), average baseline NYHA class (2.3±0.5 vs. 2.4±0.5, P=0.67), baseline heart rate (80±13 vs. 83±10 bpm, P=0.51), LA size (35±1.9 vs. 33±4.6 cm2, P=0.17) or baseline native T1 times (1,212±106 vs. 1,268±112 ms, P=0.25). All patients in the CA group maintained SR at 6 months follow up. The CA group showed significant improvement in LVEF (baseline vs. 6 months: 33±8.0 vs. 49±11%, P<0.001), and BNP (baseline vs. 6 months: 361 vs. 105 ng/L, P=0.003), compared to the MRC group (baseline vs. 6 months: LVEF: 32±8.1% vs. 33±6.6%, P=0.83; BNP: 293 vs. 292 ng/L, P=0.99). Average native T1 times were significantly reduced in the CA group at fol-low-up (baseline vs. 6 months: 1,268±112 vs. 1186±76 ms, P=0.03) but not the MRC group (1,212±106 vs. 1,200±182 ms, P=0.82).
Conclusions: LVEF improvement in patients with PeAF and IDCM undergoing AF ablation is associated with a shortening of native T1 times consistent with regression ventricular fibrosis. The restoration of SR with AF ablation may promote reverse ventricular structural remodelling in patients with IDCM and PeAF.
REVERSE VENTRICULAR REMODELLING FOLLWING AF ABLATION IN PATIENTS WITH PERSISTENT AF AND SYSTOLIC DYSFUNCTION -A PROSPECTIVE RANDOMISED STUDYSandeep Prabhu1,2, Ben Costello1,2, Sarah Gutman1, Alexandr Voskoboinik1,2, Liang-Han Ling1,2, Alex Mclellan1,2, Kah Peck1, Bupesh Pathik3, Chrishan Nalliah3, Geoff Wong3, Sonia Azzopardi1,2, Justin Mariani1,2, Siobhan Lockwood5, Geoff Lee3, Jonathan Kalman3, Andrew Taylor1,2, Peter Kistler1,2 1Alfred Health, Melbourne, Australia; 2Baker IDI, Melbourne, Australia; 3Royal Melbourne Hospital, Melbourne, Australia; 4Royal Melbourne Hospital, Melbourne, Australia; 5Monash Heart, Melbourne, Australia
HEART FAILURE OP 5-05

32
Introduction: Modern implantable cardioverter defibrillators (ICDs) use biphasic waveforms, which reduce the energy required for inter-nal defibrillation of the heart. A superior performance of a tuned waveform over a standard 65/65% tilt waveform has been documented before. However, there is no consensus on the optimal pulse widths or waveform tilt (percentage of initial voltage drawn from a capacitor) for defibrillation. This study compared DFTs for 65/65% tilt waveforms and the fixed pulse width tuned biphasic wave forms.
Methods: Nine closed chest pigs with heart failure were studied. These pigs weighing between 42 and 47 kg were anesthetized. High volt-age lead impedance was measured and used to select the pulse widths for tuned and 65/65% tilt defibrillation waveforms. Optimal pulse durations have been tabulated for various resistances and ICD capacitances for membrane time constants of 2.0 and 3.5. Fixed pulse width tuned waveforms may reduce delivered energy and voltage defibrillation thresholds in pigs with heart failure.
Results: Table summarizes the DFT data for tuned and 65/65% tilt waveforms. In 5 pigs (71%), delivered energy and delivered voltage were lower for the tuned than for the 65/65% tilt waveform.
Conclusions: Energy and voltage DFTs are lowered with an ICD that uses a tuned waveform compared to a standard 65/65% tilt biphasic waveform in pigs with heart failure. Fixed pulse width tuned waveforms may reduce delivered energy and voltage defibrillation thresholds in pigs with heart failure.
FIXED PULSE WIDTH TUNED WAVEFORMS REDUCE DELIVERED ENERGY AND VOLTAGE DEFIBRILLATION THRESHOLDS IN PIGS WITH HEART FAILUREYusuke Kondo, Marehiko Ueda, Masahiro Nakano, Kazuo Miyazawa, MIyo Nakano, Tomohiko Hayashi, Yoshio Kobayashi
Chiba University Graduate School of Medicine, Chiba, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES OP 5-06
ORAL PRESENTATION 06(14 October)

34
Introduction: Mechanisms of human AF are debated but may mainly reflect mapping technique. Localized AF drivers are detected rarely by traditional activation mapping, yet often by phase mapping. We hypothesized that factors such as non-uniform conduction slowing and difficulty in electrogram annotation may explain discrepancies and reflect advanced substrate.
Methods: We recruited 60 patients at 5 international centers in whom persistent AF terminated by local ablation (area <3 cm2) targeted by phase mapping. We performed traditional activation annotation for 4s of AF from 64 pole baskets using -dv/dt or peak amplitude criteria (A) and visualized the results on isochronal maps (B). As indicators for Remodeling BMI, CHADSVASc and LA area were documented.
Results: All patients (n=60, age 62±10 years, LA area 75.8 mm2, AF history 5.95±4.49 years, 100% persistent) had AF termination by lo-calized ablation prior to PVI (50% to sinus). We found rotational sources by traditional mapping at sites of AF termination in 15/60 (25%) cases. In remaining cases, traditional maps did not explain AF termination and showed partial rotations (45%) or transient foci (30%). This divergence from phase maps related to higher BMI and CHADSVASc>3 (P<0.05).
Conclusions: For the first time, we reveal rotational drivers of persistent AF by traditional mapping, whose ablation led to termination. These maps agreed with phase mapping. However, with increased substrate complexity, activation maps were more challenging to inter-pret and no longer detected AF drivers, shown by phase mapping. These data may help to reconcile AF mechanisms and suggest future directions for mapping.
ATRIAL REMODELING EXPLAINS DISCREPANCIES BETWEEN ACTIVATION MAPPING AND PHASE MAPPINGChristopher Kowalewski1, Junaid A. B. Zaman1, Mahmood Alhusseini1, Tina Baykaner1, Ryan T. Borne2, Nicholas S. Peters3, Wouter J. Rappel4, William H. Sauer2, Johannes Brachmann5, David Krummen6, John M. Miller7, Sanjiv M. Narayan1 1Stanford University, Palo Alto, United States; 2U C Denver, Aurora, United States; 3Imperial College, London, United Kingdom; 4UCSD, La Jolla, United States; 5Klinikum Coburg, Coburg, Germany; 6VA Medical Center, San Diego, United States; 7Indiana University, Indianapolis, United States
CATHETER ABLATION OP 6-01

35
Introduction: Type of atrial fibrillation (AF) can change depending on the condition and time, and some of patients with initially presented persistent AF (PeAF) changed to paroxysmal AF (PAF) after anti-arrhythmic drug (AAD) medication and/or cardioversion (CV). We hypoth-esized that CPVI alone is an effective rhythm control strategy for radiofrequency catheter ablation (RFCA) in patients with PeAF to PAF.
Methods: We prospectively enrolled consecutive 113 patients with PeAF to PAF (male 75.2%, 60.4±10.1 years old) and randomly assigned them to either CPVI alone group (n=58) or the CPVI plus linear ablation group (posterior box + anterior line; Dallas lesion set; n=55). The primary outcome was freedom from clinical recurrence of AF after RFCA.
Results: 1) Compare to CPVI+linear ablation group, CPVI alone group required shorter procedure (185.8±57.5 minutes vs. 212.2±63.7 minutes, P=0.025) and ablation times (4,917.7±1,119.9 seconds vs. 6,186.9±1,418.7 seconds, P<0.001) without significant difference in procedure related major complication rate (3.4%, vs. 1.8%, P=0.590). 2) During the 18.6±11.4 months of follow-up, the clinical recurrence rates were not significantly different between CPVI alone group (19.0%) and CPVI+linear ablation group (29.1%, P=0.271). 3) AAD utility rates after RFCA were not significantly different between two groups (27.6% vs. 38.2%, P=0.316). 4) AAD free AF recurrence was not sig-nificantly different between two groups (Log-rank, P=0.208).
Conclusions: CPVI alone is an effective rhythm control strategy with shorter procedure time for PeAF who were converted as PAF with AADs after external electrical cardioversion, compared to CPVI with additional linear ablation.
PULMONARY VEIN ISOLATION ALONE IS AN EFFECTIVE RHYTHM CONTROL STRATEGY IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATION THOSE CHANGED TO PAROXYSMAL TYPE WITH ANTIARRHYTHMIC DRUG THERAPY: A MULTI-CENTER PROSPECTIVE RANDOMIZED STUDYHee Tae Yu1, Jaemin Shim2, Junbeom Park3, In-Soo Kim1, Tae-Hoon Kim1, Jae-Sun Uhm1, Boyoung Joung1, Moon-Hyoung Lee1, Young-Hoon Kim2, Hui-Nam Pak1 1Yonsei University Health System, Seoul, Republic of Korea; 2Korea University Cardiovascular Center, Seoul, Republic of Korea; 3Ewha Womans University, Seoul, Republic of Korea
CATHETER ABLATION OP 6-02

36
Introduction: Collateral damage to periesophageal vagal plexus (PNI) with symptomatic gastric hypomotility is not uncommon after cath-eter ablation of AF, especially using cryo-energy. The study aimed to investigate whether PNI is reversible and its relationship to long-term outcome after AF cryoablation (CA).
Methods: Of consecutive 24 patients (54±9 y/o, male 18) admitted for catheter ablation using 2nd generation cryoballoon, a validated questionnaire suggested by the Rome Committee for the Investigation of functional GI disorders was evaluated before, immediately after and 3 months after AF CA. The association of GI symptoms and AF recurrence was evaluated.
Results: Before CA, 7 (29%) patients had dyspepsia symptoms. Higher incidence of GI symptoms were complained in 16 (67%, P=0.02, compared to before CA) patients immediately after CA. Three months after CA, only 6 (29%, P=1.00, compared to before CA; P=0.008, compared to immediate after CA) patients had dyspepsia symptoms. The detailed GI symptoms were described in Table 1. During a mean follow-up of 8±5 months, AF recurrence was noted in 3 (13%) patients. Those with newly developed dyspepsia symptoms immediately af-ter CA had a lower incidence of AF recurrence during follow-ups, compared to those without symptoms immediately after CA (P=0.04).
Conclusions: The PNI associated dyspepsia symptoms is not uncommon after CA of AF. Newly developed dyspepsia symptoms immedi-ately after CA are reversible and associated with a better long term outcome, suggesting the transmural ablation lesions during CA pro-cedures.
REVERSIBLE PERIESOPHAGEAL VAGAL NERVE INJURY IS COMMON AFTER AF CRYOABLATION AND PREDICTS A FAVORABLE OUTCOMEShin Huei Liu, Li-Wei Lo, Hung-Yu Chang, Yenn-Jiang Lin, Shih-Lin Chang, Yu-Feng Hu, Fa-Po Chung, Yu-Hui Chou, Wei-Lun Lin, Ching-Liang Lu, Shih-Ann Chen
Taipei Veteran General Hospital, Taipei, Taiwan
CATHETER ABLATION OP 6-03
Table 1. Questionnaire Survey for Dyspepsia Symptoms Before, Immediate After and 3 Months After CA
Symptoms Before CA (n=24)
Immediate After CA (n=24)
3 Months After CA (n=24)
P value
Upper GI symptoms 7 (29) 16 (67) 6 (25) 0.005
(1) Chest pain, heart burn or acid regurgitation (n, %) 6 (25) 14 (58) 6 (25) 0.02
(2) Postprandial abdominal fullness, bloating or swelling (n, %) 6 (25) 8 (33) 6 (25) 0.76
(3) Early satiety (n, %) 4 (17) 9 (38) 3 (13) 0.08
Lower GI symptoms 2 (8) 0 (0) 1 (4) 0.35
(1) Abdominal pain or fullness, relieved after a bowel movement (n, %) 0 (0) 0 (0) 1 (4) 0.36
(2) Hard or lumpy stools, loss of mushy stools (n, %) 1 (4) 0 (0) 1 (4) 0.60
(3) Straining during a bowel movement (n, %) 1 (4) 0 (0) 1 (4) 0.60
(4) Feeling of incomplete emptying after a bowel movement (n, %) 2 (8) 0 (0) 1 (4) 0.35

37
Introduction: Left atrial appendage flow velocity (LAAFV) and spontaneous echo contrast (SEC) in transesophageal echocardiography (TEE) are associated with left atrial function. However, the relationship between such TEE parameters and the long-term outcomes after catheter ablation for non-paroxysmal atrial fibrillation (AF) is unclear.
Methods: We retrospectively evaluated consecutive 357 patients underwent radiofrequency catheter ablation for non-paroxysmal AF from 2005 to 2015.
Results: The average age was 63.6±8.8 years and mean AF duration was 1.85±3.43 years. Mean CHADS2 score was 1.1±1.0 and left atri-al (LA) dimension was 44.4±6.5 mm. Within 48 hours before the ablation procedure, patients were evaluated by TEE to exclude the LA thrombus, and LAAFV and SEC were measured. SEC was scaled in four grades. The average LAAFV and SEC grade were 45.1±19.5 cm/sec and 0.95±1.1, respectively. All patients underwent extensive encircling pulmonary vein isolation. Additional ablations including com-plex fractionated atrial electrograms ablation, LA linear ablation, cavotricuspid isthmus ablation, and superior vena cava isolation were performed whenever necessary. During the average follow up of 3.74±2.47 years, the rate of SR maintenance was 47.6% after 1st session and 57.5% after multiple sessions without antiarrhythmic drugs. We divided the patients into 2 groups according to TEE parameters; those with and without preserved LA function (LAF). Preserved LAF was defined as LAAFV>=45 cm/sec and SEC grade 0. A total of 79 pa-tients (26.2%) had preserved LAF. The rates of SR maintenance after 1st session and multiple sessions were significantly higher among those with preserved LAF as compared to those with decreased LAF (64.6% vs. 44.6%, P=0.0022, and 78.5% vs. 52.0%, P<0.001, respec-tively).
Conclusions: LAAFV and SEC in TEE before AF ablation were strong predictors of long-term success in patients undergoing non-paroxys-mal AF ablation.
LEFT ATRIAL APPENDAGE FLOW VELOCITY AND SPONTANEOUS ECHO CONTRAST IN TRANSESOPHAGEAL ECHOCARDIOGRAPHY ARE PREDICTORS OF LONG-TERM SUCCESS AFTER CATHETER ABLATION FOR NON-PAROXYSMAL ATRIAL FIBRILLATIONTakashi Yoshizawa, Satoshi Shizuta, Takeshi Kimura
Kyoto University Hospital, Kyoto, Japan
CATHETER ABLATION OP 6-04

38
Introduction: During ablation of persistent atrial fibrillation, analysis of wave propagation for signals with wide temporal and spatial dis-parities was difficult. Phase mapping of highly fractionated and non-stationary electrograms could provide additional insights into AF mechanism. We studied the feasibility of rotors quantification using phase mapping methodology in a computer simulation model.
Methods: Cellular automation method was applied to simulate electrical wave propagation in the 2-dimensional atrial substrate. The vector field (Figure A) showing as averaged waveform propagation was used to quantify rotors in high-similarity electrogram region. The quantifying physical parameters were divergence and curvature force (Curl). Rotor identification index (RI) was mathematically defined as the product of divergence and curl.
Results: The curl, divergence, and maximum RI values were dependent on the integrating path radius and distance to rotor center (Figure B). The RI reached maximal value at rotor boundaries. The divergence force became constant and curvature force decreased when in-ter-electrode distance of spiral catheter exceeded that of rotor radius. A focal source could be identified with a very small reentry source. The regional distribution of RI was integrated into an automatic algorithm to define rotors in a demonstrative model (Figure C). Range of deviation distance between catheter and rotor center are represented by curves in (Figure D).
Conclusions: By using our model, AF rotors can be more precisely identified via quantification of curvature and divergence forces derived from wave dynamics during phase mapping. Rotor size can be quantified. Rotor identification was enhanced with optimal size matching between recording catheter and rotor.
A NOVEL COMPUTER SIMULATION MODEL FOR PRECISE ROTOR QUANTIFICATION EMPLOYING PHASE MAPPING METHODOLOGY FOR PATIENTS WITH PERSISTENT ATRIAL FIBRILLATIONYenn-Jiang Lin1, Men-Tzung Lo2, Chen Lin2, Shih-Lin Chang1, Li-Wei Lo1, Shih-Ann Chen1 1Taipei Veterans General Hospital, Taipei, Taiwan; 2National Central University, Jhong-Li, Taiwan
CATHETER ABLATION OP 6-05

39
Introduction: In patients with persistent atrial fibrillation (AF), sinus rhythm (SR) restoration by only antiarrhythmic drugs (AADs) is un-commonly observed and may occur in patients with less chronic and less remodeled atria. We sought to determine whether the patients with a history of cardioversion by only AAD have better outcome after catheter ablation of persistent AF.
Methods: A total of 356 consecutive patients with persistent AF who underwent catheter ablation were enrolled (mean 56±10 years old, 16.9% female). We divided them into two groups according to history of SR conversion by AAD: group 1 (32 patients with history of chemi-cal cardioversion (CCV) before ablation) and group 2 (324 patients without history of CCV). Clinical, imaging parameters, ablation findings and outcomes were compared between two groups. Late gadolinium enhancement (LGE) in cardiac magnetic resonance image (MRI) were also assessed.
Results: There were no significant differences in baseline characteristics including gender (P=0.846), hypertension (P=0.561), diabetes mellitus (P=0.158) and rate of use of AADs (P=0.479). Procedure time was significantly shorter in group 1 than those in group 2 (P<0.001). The need of biatrial ablation in addition to pulmonary-vein isolation was significantly lower in group 1 as compared with group 2 (9.4% vs. 37.7%, P<0.001 for LA ablation; 15.6% vs. 53.1% for bi-atrial ablation, P<0.001). During 50±28 months follow-up, 26 (81.3%) patients in group 1 were free from AF recurrence compared with group 2 (152 (46.9%)) (P<0.001). LGE-MRI scar burden in group 1 were lower than group 2, but there was no statistical significance (26.3±22.4% vs. 38.5±23.4%, P=0.085). In the multivariate analysis, a history of CCV (HR 0.128, 95% CI 0.128-3.103, P<0.001) and LA size (HR 5.531, 95% CI 1.877-16.297, P=0.002) were significantly associated with AF recur-rence after catheter ablation.
Conclusions: Following AF ablation in persistent AF patients who had CCV to SR, procedural time was significantly shorter and AF recur-rence rate was significantly lower than in those who failed to do so. This study suggested that a history of SR restoration by only AADs as-sociates with a less chronically remodeled atria and then is a valuable predictor of better outcome following catheter ablation in patients with persistent AF.
PROCEDURAL AND CLINICAL OUTCOME OF PATIENTS WITH CHEMICALLY CARDIOVERTED PERSISTENT ATRIAL FIBRILLATION Yong-Soo Baek, Anupam Jena, Hee-Soon Park, Kwang-No Lee, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CATHETER ABLATION OP 6-06

ORAL PRESENTATION 07(15 October)

41
Introduction: Electrical storm is a life-threatening syndrome that is defined by 3 or more sustained episodes of VT, VF, or appropriate shocks from an ICD within 24 hours. Such episodes are common post myocardial infarction. The conventional antiarrhythmic therapy comprising class I and III drugs do not salvage a large fraction of such patients. Increased sympathetic activity is known to contribute to the development of ischemic VT/VF. It was hence postulated that sympathetic blockade in the form of esmolol infusion would prevent re-currence of such episodes. The importance of targeting the mechanism of dysrhythmia is further conveyed through this case series.
Methods: Fifteen patients who had electrical storm associated with a recent MI were selected (group 1). Two patients with past history of MI (scar VT) and one patient with ARVC who had electrical storm were also selected (group 2). All these patients were treated with con-ventional agents resulting in either recurrence or non- resolution of the arrhythmia. Esmolol infusion was started for all such patients with a bolus followed by maintenance. Class I and III drugs were stopped and esmolol infusion was overlapped with oral beta blockade.
Results: Thirteen patients in group 1 had no recurrence of the arrhythmia, two patients died. All patients who survived the electrical storm did well till last scheduled follow up and remained arrhythmia free throughout. Two patients underwent successful cardiac trans-plant. Both the patients with scar VT in group 2 did not survive, the patient with ARVC responded only to anti-tachycardia pacing.
Conclusions: Sympathetic blockade was superior to conventional therapy in treating patients with electrical storm. It is highlighted here that increased sympathetic activity underlies the genesis of electrical storm. Sympathetic blockade in the form of beta blockers should be the first choice of management in patients with electrical storm with history of recent MI. Esmolol, an ultra-short acting beta blocker with rapid onset of action and minimal hemodynamic compromise forms the choice of sympathetic blockade. Further large scale studies are needed to establish this as part of practice guidelines.
ARE YOU HITTING THE BULLS EYE? ROLE OF ESMOLOL IN ELECTRICAL STORM: A CASE SERIESAbhinay Tibdewal, V S Prakash, Nagamalesh U.M, Anupama Hegde, Sarthak Sahoo
MS Ramaiah Medical College, Bangalore, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-01

42
Introduction: The impact of Late Gadolinium Enhancement (LGE) in cardiovascular magnetic resonance (CMR) on mortality and overall clinical outcomes remains an area of uncertainty. We conducted a systematic review and meta-analysis evaluating the prognostic impor-tance of the presence and burden of LGE in Ischemic and nonischemic cardiomyopathy (ICM/NICM).
Methods: The study was prospectively registered in PROPSERO. (CRD 42016039034) Electronic databases and reference lists were searched for studies evaluating the impact of LGE-CMR on clinical outcomes. Data were extracted from 26 studies including n=5,095 pa-tients.
Results: In included studies, the presence of LGE was strongly associated with the study endpoints of all-cause mortality HR 2.60 (95% CI:2.14, 3.17, P<0.001), cardiovascular mortality 2.79 (95% CI:1.71,4.54, P<0.001), ventricular arrhythmia and sudden cardiac death HR 3.73 (95% CI: 3.01, 4.62, P<0.001), and major adverse cardiovascular events HR 3.38 (95% CI:2.27, 5.04, P<0.001). In subgroup analyses, LGE was associated with all-cause mortality and cardiovascular mortality in both LVEF≤35% and LVEF>35% patients (P<0.01 all endpoints), as well as in nonischemic and ischemic cardiomyopathy.
Conclusions: The presence of Late Gadolinium Enhancement (LGE) in CMR predicts all-cause mortality, cardiovascular mortality, ventric-ular arrhythmia and sudden death, and major adverse cardiovascular events, independent of LVEF. Consideration should be given to these data in defining recommendations for the utilisation of LGE-CMR in contemporary appropriate use criteria for cardiovascular imaging.
IMPACT OF LATE GADOLINIUM ENHANCEMENT ON PATIENT OUTCOMES IN ISCHEMIC AND NONISCHEMIC CARDIOMYOPATHY: A SYSTEMATIC REVIEW AND META-ANALYSISAnand Ganesan, James Gunton, Andrew McGavigan, Joseph Selvanayagam
Flinders Medical Centre, Bedford Park, Australia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-02

43
Introduction: Risk stratification in Brugada syndrome remains a controversial and unresolved clinical problem, especially in asymptom-atic patients with a type 1 ECG pattern. The purpose of this study is to derive and validate a prediction model based on simple clinical and ECG parameters to effectively identify patients with a type 1 ECG pattern who are at high risk of arrhythmic events during follow up.
Methods: This study analyzed data from 74 consecutive patients (82.4% male, median age of 47 years) with Brugada Type 1 ECG pattern. The prediction model was derived using logistic regression with major arrhythmic events (MAE) as the primary outcome, and patient de-mographic and electrocardiographic parameters as potential predictor variables. We externally validated the model in an independent co-hort of 21 patients with a Type 1 ECG pattern.
Results: During follow up (median 74.6 months, IQR 34.6-89.4 months), 11 patients had major arrhythmic events (9 resuscitated ventricu-lar tachycardia (VT)/ventricular fibrillation (VF), 2 sudden cardiac death). The final prediction model (FAST score) consisted of 4 indepen-dent predictors (1 point each) of MAE : aborted cardiac arrest, QRS fragments in inferior leads >3, S wave upslope ratio >0.8, and T peak-T end>100 ms. The FAST score (area under the curve=0.97, 95% CI 0.0.95-0.99) stratifies patients with a type 1 ECG pattern into low (FAST score<2) and high (FAST score>3) risk classes, with a class specific risk of MAE of 1.6-5.3% and 90.9-100% across the derivation and vali-dation cohorts, respectively. Considering survival free of MAE, kaplan- meier analysis showed that patients with high risk FAST scores had worse long term outcomes (Figure, log-rank test, P<0.0001).
Conclusions: The FAST score is a simple bed-side tool with high predictive accuracy, for risk stratification of patients with a Brugada Type 1 ECG pattern. Prospective validation of our prediction model is necessary before this score can be implemented in clinical practice.
A NOVEL PREDICTION MODEL FOR RISK STRATIFICATION OF PATIENTS WITH TYPE 1 BRUGADA ECG PATTERNMuthiah Subramanian, Natarajan Kumaraswamy, Mukund Prabhu, M.S. Harikrishnan, Praveen G. Pai, Saritha Sekhar
Amrita Institute of Medical Sciences, Kochi, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-03

44
Introduction: It has been indicated in case reports that electrocardiogram (ECG) is occasionally transferred to Brugada type ECG (BTE) due to acute myocardial ischemia of right ventricle outflow tract (RVOT). However, no studies have explored the association of inducible ventricular tachyarrhythmia with development of BTE due to acute ischemia of RVOT in humans.
Methods: We studied 13 consecutive patients with acute ischemia of RVOT during coronary catheterization. Patients were divided into two groups with or without ECG transferred to BTE and compared about clinical characteristics. Moreover in group BTE, inducibility of ventric-ular tachyarrhythmia was assessed.
Results: The incidence of male was significantly higher in patients with than without ECG transferred to BTE (100% vs. 25%; P=0.006), however there was no significant difference in other parameters including age, comorbidity, medication, cardiac function between two groups. All polymorphic ventricular tachycardia (VT) or ventricular fibrillation (VF) events were developed together with augmentation of ST elevation in the only patients with BTE. Furthermore, among patients with BTE, VT/VF were significantly observed in patients without preexisting organic change in conus or right ventricular (RV) branches (0% vs. 80%; P=0.033), perfusing RVOT, and with shorter elapsed time for acute ischemia of RVOT.
Conclusions: Acute myocardial ischemia in conus branch and/or RV branch is involved in depolarization/repolarization abnormalities de-generating into BTE, especially in males. Moreover, acute exposure to regional ischemia without precondition may predispose to develop-ment of VT/VF.
LIFE-THREATENING VENTRICULAR ARRHYTHMIA ASSOCIATED WITH BRUGADA-TYPE ST-SEGMENT ELEVATION DUE TO ACUTE ISCHEMIA OF RIGHT VENTRICULAR OUTFLOW TRACTRena Nakamura, Noriyoshi Yamawake, Yuta Taomoto, Miki Amemiya, Yosuke Yamakami, Munehiro Iya, Yoshikazu Sato, Kuniaki Nakano, Hiroshi Shimada, Masato Shimizu, Hiroyuki Fujii, Mitsuhiro Nishizaki, Harumizu Sakurada, Masayasu Hiraoka
Yokohama Minami Kyosai Hospital, Yokohama, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-04
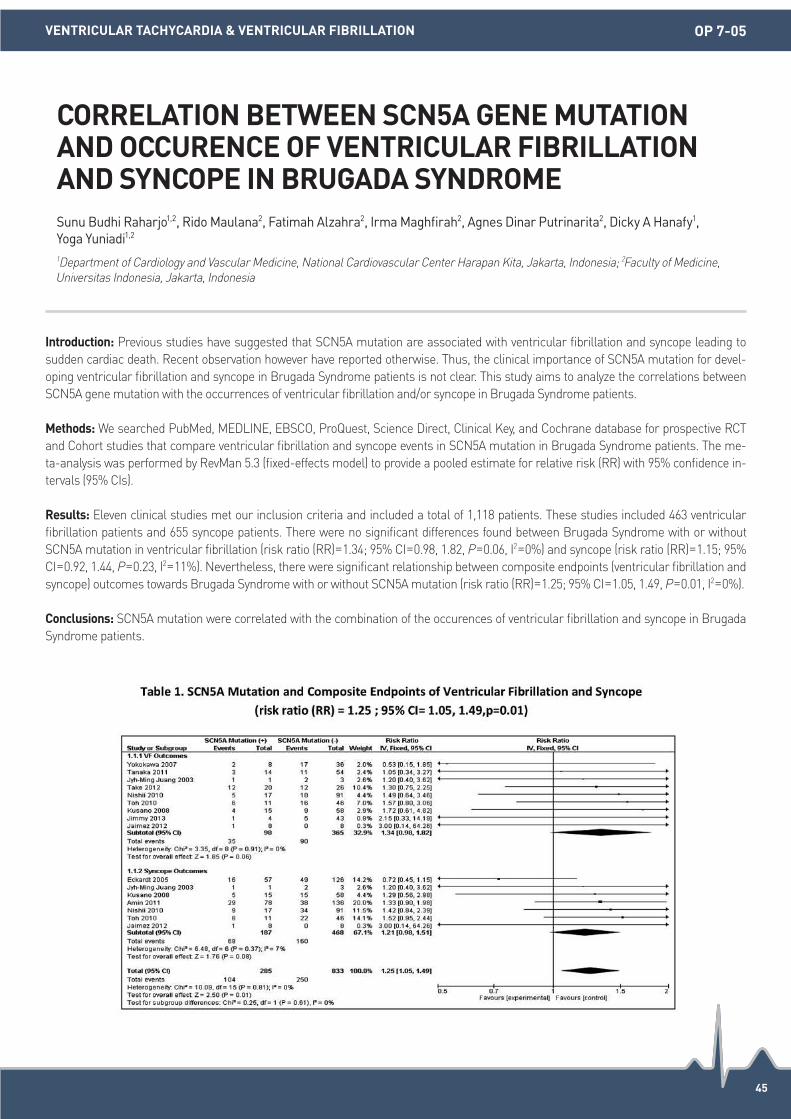
45
Introduction: Previous studies have suggested that SCN5A mutation are associated with ventricular fibrillation and syncope leading to sudden cardiac death. Recent observation however have reported otherwise. Thus, the clinical importance of SCN5A mutation for devel-oping ventricular fibrillation and syncope in Brugada Syndrome patients is not clear. This study aims to analyze the correlations between SCN5A gene mutation with the occurrences of ventricular fibrillation and/or syncope in Brugada Syndrome patients.
Methods: We searched PubMed, MEDLINE, EBSCO, ProQuest, Science Direct, Clinical Key, and Cochrane database for prospective RCT and Cohort studies that compare ventricular fibrillation and syncope events in SCN5A mutation in Brugada Syndrome patients. The me-ta-analysis was performed by RevMan 5.3 (fixed-effects model) to provide a pooled estimate for relative risk (RR) with 95% confidence in-tervals (95% CIs).
Results: Eleven clinical studies met our inclusion criteria and included a total of 1,118 patients. These studies included 463 ventricular fibrillation patients and 655 syncope patients. There were no significant differences found between Brugada Syndrome with or without SCN5A mutation in ventricular fibrillation (risk ratio (RR)=1.34; 95% CI=0.98, 1.82, P=0.06, I2=0%) and syncope (risk ratio (RR)=1.15; 95% CI=0.92, 1.44, P=0.23, I2=11%). Nevertheless, there were significant relationship between composite endpoints (ventricular fibrillation and syncope) outcomes towards Brugada Syndrome with or without SCN5A mutation (risk ratio (RR)=1.25; 95% CI=1.05, 1.49, P=0.01, I2=0%).
Conclusions: SCN5A mutation were correlated with the combination of the occurences of ventricular fibrillation and syncope in Brugada Syndrome patients.
CORRELATION BETWEEN SCN5A GENE MUTATION AND OCCURENCE OF VENTRICULAR FIBRILLATION AND SYNCOPE IN BRUGADA SYNDROMESunu Budhi Raharjo1,2, Rido Maulana2, Fatimah Alzahra2, Irma Maghfirah2, Agnes Dinar Putrinarita2, Dicky A Hanafy1, Yoga Yuniadi1,2 1Department of Cardiology and Vascular Medicine, National Cardiovascular Center Harapan Kita, Jakarta, Indonesia; 2Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-05

46
Introduction: It is widely accepted that exercise is associated with decreased cardiovascular events and mortality. Previous studies report-ed the relationship between sudden cardiac arrest (SCA) and exercise in specific populations, but the impact of exercise in general popu-lations in real world are still unclear.
Methods: Among 506,805 individuals (253,825 men and 252,980 women) of sample cohort in Korean National Health Insurance Service between 2003 through 2013, we searched the individuals with SCA (ICD-10 code I46). Based on the questionnaires regarding general health status in medical screening program, the degree and frequency of exercise was evaluated. The intensity of physical activity was classified according to the WHO guideline.
Results: During 46.2±15.1 months of follow up, 1,019 SCA events were occurred, and the age and sex standardized incidence of SCA was 56.7 events per 100,000 person-year. Compared with individuals without exercise, those who exercised more than 30 minutes, more than 3 times a week were associated with decreased age and sex adjusted risk of all-cause mortality (HR 0.691, 95% CI 0.657-0.726, P<0.001), cardiovascular death (HR 0.590, 95% CI 0.524-0.664, P<0.001) and SCA (HR 0.695, 95% CI 0.613-0.787, P<0.001). Multivariate Cox-regres-sion analysis with the known risk factor of SCA revealed that the 25.7%, 40.6% and 33.9% risk reduction of SCA by walking, moderate to vigorous intensity exercise, respectively. Subgroup analysis revealed that the middle aged individuals (HR 0.952, 95% CI 0.761-1.190, P=0.663) showed no statistically significant risk reduction of SCA with exercise. Exercise seems to be most beneficial to older aged female group (HR 0.468, 95% CI 0.362-0.604, P<0.001).
Conclusions: Regular exercise is associated with decreased SCA events, especially in older aged and female gender group, whereas in middle aged group, no significant association was seen between exercise and SCA events.
THE IMPACT OF EXERCISE INTENSITY IN SUDDEN CARDIAC ARREST: A NATIONWIDE COHORT STUDYYoung-Ah Park1, Pil-Sung Yang1, Hancheol Lee2, Tae-Hoon Kim1, Jae-Sun Uhm1, Hui-Nam Pak1, Moon-Hyoung Lee1, Boyoung Joung1 1Severance Hospital, Seoul, Republic of Korea; 2National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION OP 7-06

ORAL PRESENTATION 08(15 October)

48
Introduction: An 35-year-old women with sick-sinus-syndrom and patent foramen ovale (PFO) received in 2008 an two chamber-pace-maker (PM) with wrongfully placed ventricular lead through PFO in the left ventricle. In 2003, 2008 und 2013 recurring cerebral infarctions happens, triggered by paradox embolism from PFO. Since 2008 the patient received phenprocoumon for oral anticoagulation. She was send in our hospital for minimally invasive operativ extraction of PM-leads and closure of PFO.
Methods: N/A.
Results: After reviewing diagnostic findings we decided, with prior consultation of the patient,a two-sided therapy. In first step the ex-traction and re-implantation of PM-system (to be used for MRI), in the second step closure of the PFO by an occluder should be per-formed, The first operation was done in the operation theatre. For extraction of the ventricular lead in the left ventricle we needed an 14CH- laser-sheet, because of multiple adhesions of the lead. We do this under control of fluoroscopy and transesophageal echocardiog-raphy. At end of operation new two-chamber-pacemaker was successfully placed. 3 months afterwards we implanted an 25 mm Am-platzer- occluder via inguinal venous approach. In all postinterventional echocardiography controls an sufficient closure of the PFO could be demonstrated. Because of sinus rhythm and sufficient closure of PFO we stopped therapy with phenprocoumon immediately. Acetyl-salicylic acid 300 mg was prescribed for 3 months and 100 mg following 3 months, in addition clopidogrel 75 mg for 3 months.
Conclusions: With this case we showed, that it is possible to treat sufficient and safe, with an combination of transcutaneous interven-tions, wrongly placed leads and closure of PFO without use of heart-lung machine as it has been necessary in past.
WRONG PLACED VENTRICULAR LEAD AND PATENT FORAMEN OVALE-REASON FOR HEART-LUNG MACHINE?Gerhard Goebel, Heiko Burger, Christoph Liebertrau, Thomas Walther
Kerckhoff-Klinik gGmbH, Bad Nauheim, Germany
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-01

49
Introduction: Percutaneous Transluminal Septal Myocardial Ablation (PTSMA) is an effective treatment for selected patients with symp-tomatic HOCM but may be associated with conduction disturbances & arrhythmias. We analysed their incidence in patients undergoing PTSMA in a single tertiary centre.
Methods: Consecutive patients undergoing PTSMA from 2000-2016 were included in a retrospective analysis. All procedures were per-formed by a single experienced operator, under general anesthesia with transesophageal myocardial contrast echocardiographic guid-ance for anatomical selection of appropriate sub-branches of septal perforators. A temporary pacing wire remained in-situ for 24-48 hours & patients were monitored in hospital for 5 days post-procedure. 12-lead ECGs were recorded at baseline & daily thereafter until discharge, & were systematically analyzed for conduction disturbances.
Results: 76 patients (mean age 60±15 years, 50% male) underwent successful PTSMA. Baseline & post-procedural ECG changes are shown in Table 1. Intra-procedural ventricular arrhythmias necessitating DC cardioversion occurred in 3/76 patients (3.9%)-1 of these oc-curred during septal wiring & 2 during injection of the echo contrast agent. Post-procedure, 14/64 patients (21.9%) developed complete heart block (CHB) & required PPM implantation. CHB was not associated with volume of alcohol infused (2.1±0.8 vs. 2.0±0.8 mL, P=0.44) or number of septal perforators injected (1.1±0.3 vs. 1.1±0.4, P=0.77), but was more likely in patients with pre-existing LBBB (21.4 vs. 4.0%; P=0.06). In patients not requiring a PPM (n=50), the most common new conduction abnormalities were RBBB (n=15, 30%), 1st de-gree AV block (n=9, 18%) & LBBB (n=5, 10%).
Conclusions: Conduction disturbances (but not ventricular arrhythmias) are common after PTSMA for selected patients with symptomat-ic HOCM. Pre-existing LBBB is a predictor for the development of CHB & the need for a PPM.
RESTING ELECTROCARDIOGRAPHIC CHANGES AND THE NEED FOR PERMANENT PACEMAKER INSERTION AFTER PERCUTANEOUS TRANSLUMINAL SEPTAL MYOCARDIAL ABLATION FOR HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY: A 16 YEAR AUSTRALIAN EXPERIENCEJason Nogic, Youlin Koh, Liam McCormick, Marek Bak, Robert Gooley, Ian Meredith
Monash Heart, Monash Health, Clayton, Victoria, Australia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-02
ECG findings pre procedure and at discharge
Pre Procedure At Discharge
Sinus Rhythm, n (%) 61/76 (80) 47/76 (62)
Atrial Fibrilation/Flutter, n (%) 3/76 (4) 3/76 (4)
Total Paced Rhythm, n (%) 12/76 (16) 26/76 (34)
Left Bundle Branch, n (%) 5/64 (8) 7/50 (14)
Right Bundle Branch, n (%) 8/64 (13) 19/50 (38)
First Degree AV Block, n (%) 11/64 (17) 14/50 (28)
Left Anterior Fasicular Block, n (%) 3/64 (5) 5/50 (10)
Left Posterior Fasicular Block, n (%) 1/64 (2) 3/50 (6)

50
Introduction: A 60-year-old gentleman with end stage renal failure presented with symptoms of giddiness and inability to tolerate hemo-dialysis via left arm arteriovenous fistula (AVF). Electrocardiogram (ECG) showed second-degree atrioventricular (AV) block and was planned for permanent pacemaker insertion. He was deemed unsuitable for conventional pacemaker insertion due to thin body habitus and need for preservation of vascular access for hemodialysis. A decision was made for leadless pacemaker insertion.
Methods: N/A.
Results: MicraTM Transcatheter Pacing System was used and pacemaker delivery was uneventful with optimal parameters. However, during the removal of the tether, we accidentally displaced the implanted pacemaker and it flipped towards the tricuspid valve. We postu-late that this happened due to the continuous pulling force applied during removal of the tether. We proceeded with retrieval of pacemaker using EV3 snare kit with 7 mm loop but we failed as the orientation of pacemaker was not coaxial with the delivery system. We changed to an AgilisTM NxT Steerable Introducer and an EV3 snare kit with 15 mm loop. At this point, we were only able to catch hold of the device body. As such, we found it difficult to straighten and retrieve it via the delivery system. After multiple manoeuvres, we were able to straighten and retrieve the pacemaker. There are several learning points from this case. Firstly, to avoid displacing implanted leadless pacemakers, the cup needs to be mated as close as possible to the device. Secondly, when flossing the tether, identify the side with most resistance. Thirdly, cut the floss at the side where resistance is highest and only then pull the tether out. Fourthly, ensure that delivery sys-tem is coaxial during retrieval and use gentle extraction force. As we had to use a third party device for retrieval of pacemaker we were unable to reimplant the same device. We reimplanted a new Micra device and the procedure was uneventful. Pacing parameters were within range. The patient was discharged well and is currently asymptomatic on regular hemodialysis with marked improvement in his quality of life.
Conclusions: This case demonstrates the need for correct patient selection for leadless pacemaker, anticipating difficulties that can be encountered during implantation and methods used to overcome arising complications.
ALL SAVIORS COME IN PAIRSKantha Rao Narasamuloo, Ahmad Faiz Mohd Ezanee, Wan Faizal Wan Rahimi Shah, Gerard Jason Mathews, Ahmad Shukri Saad, Yi Zhi Cheng, Kai Soon Liew, Chian Hui Yeoh, Muhammad Khairul Taufiq Rosli, Azrina Abdul Kadir, Ryan Khoo Song Weng, Dharmaraj Karthikesan, Saravanan Krishinan
Hospital Sultanah Bahiyah, Alor Setar, Malaysia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-03
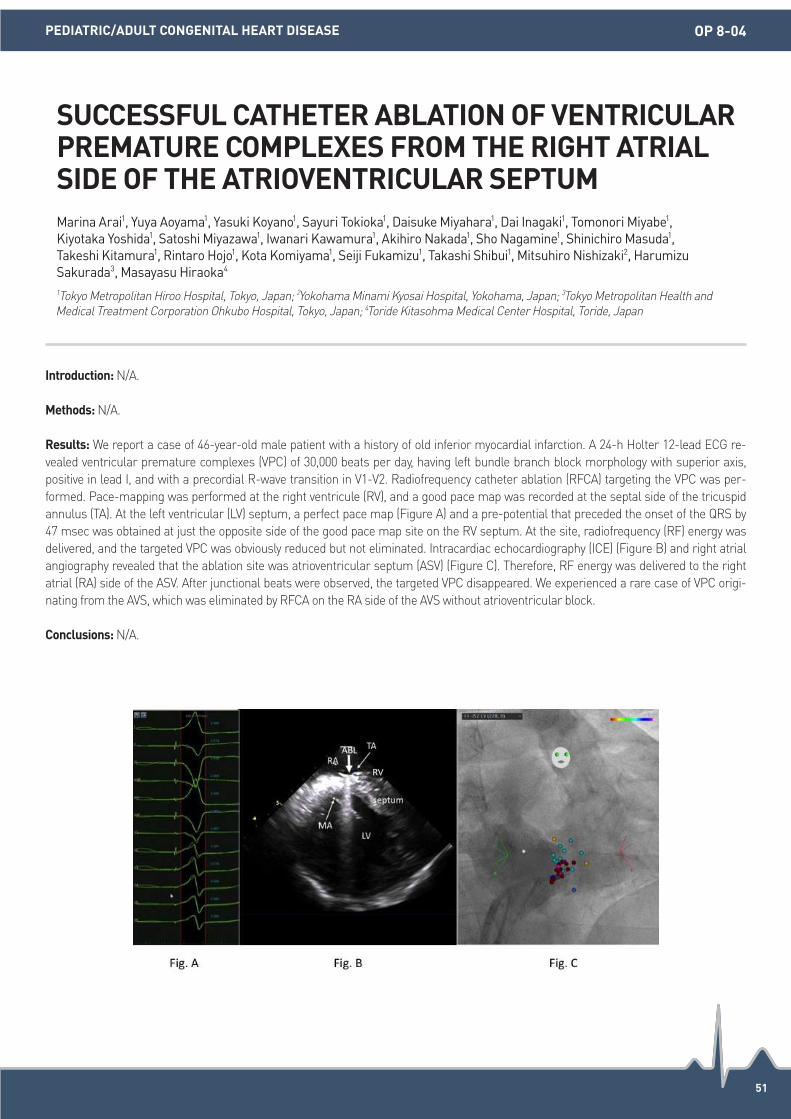
51
Introduction: N/A.
Methods: N/A.
Results: We report a case of 46-year-old male patient with a history of old inferior myocardial infarction. A 24-h Holter 12-lead ECG re-vealed ventricular premature complexes (VPC) of 30,000 beats per day, having left bundle branch block morphology with superior axis, positive in lead I, and with a precordial R-wave transition in V1-V2. Radiofrequency catheter ablation (RFCA) targeting the VPC was per-formed. Pace-mapping was performed at the right ventricule (RV), and a good pace map was recorded at the septal side of the tricuspid annulus (TA). At the left ventricular (LV) septum, a perfect pace map (Figure A) and a pre-potential that preceded the onset of the QRS by 47 msec was obtained at just the opposite side of the good pace map site on the RV septum. At the site, radiofrequency (RF) energy was delivered, and the targeted VPC was obviously reduced but not eliminated. Intracardiac echocardiography (ICE) (Figure B) and right atrial angiography revealed that the ablation site was atrioventricular septum (ASV) (Figure C). Therefore, RF energy was delivered to the right atrial (RA) side of the ASV. After junctional beats were observed, the targeted VPC disappeared. We experienced a rare case of VPC origi-nating from the AVS, which was eliminated by RFCA on the RA side of the AVS without atrioventricular block.
Conclusions: N/A.
SUCCESSFUL CATHETER ABLATION OF VENTRICULAR PREMATURE COMPLEXES FROM THE RIGHT ATRIAL SIDE OF THE ATRIOVENTRICULAR SEPTUMMarina Arai1, Yuya Aoyama1, Yasuki Koyano1, Sayuri Tokioka1, Daisuke Miyahara1, Dai Inagaki1, Tomonori Miyabe1, Kiyotaka Yoshida1, Satoshi Miyazawa1, Iwanari Kawamura1, Akihiro Nakada1, Sho Nagamine1, Shinichiro Masuda1, Takeshi Kitamura1, Rintaro Hojo1, Kota Komiyama1, Seiji Fukamizu1, Takashi Shibui1, Mitsuhiro Nishizaki2, Harumizu Sakurada3, Masayasu Hiraoka4 1Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan; 2Yokohama Minami Kyosai Hospital, Yokohama, Japan; 3Tokyo Metropolitan Health and Medical Treatment Corporation Ohkubo Hospital, Tokyo, Japan; 4Toride Kitasohma Medical Center Hospital, Toride, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-04

52
Introduction: The term upper common pathway refers to AV nodal tissue that connects the tachycardia circuit to the atria. The existence and concept of the upper and lower common pathways is uncommon and not well established yet. Whether slow and fast pathways con-nect directly with the atria or via upper common pathways is still debatable. Several studies report that atrial myocardium is essential for atrioventricular nodal reentry tachycardia (AVNRT), when the others are not. We report a case of AVNRT with persistent complete VA dis-sociation that mimick others tachycardia and it may supporting the existence of an AV node of upper common pathway.
Methods: A 32 yo male was referred for ablation of recurrent palpitation since 1 year ago. He had documented tachycardia with narrow and wide QRS complexes with RBBB pattern. Resting ECG showed sinus rhythm with incomplete RBBB. The results of physical examina-tion, chest X-ray and echocardiography were normal.
Results: Tachycardia with constant HV interval of 53 msec and H-H cycle length of 270 msec was induced with AEST 500/340 msec from CS ostium, following decremental AH interval. Tachycardia showed complete VA dissociation. During narrow QRS tachycardia, QRS spon-taneously change to wide QRS tachycardia with LBBB and RBBB pattern. HV intervals during RBBB and LBBB pattern were 60 msec and 65 msec. H-H cycle lengths during narrow and wide QRS tachycardia either RBBB or LBBB, were constant as 275 msec. Changes in the QRS duration and pattern did not alter H-H cyle length. During tachycardia, ventricular entrainment could not be demonstrated due to failure of RV pacing to capture A. Several ventricle premature extrastimuli from RV apex and close to the His site during His-bundle re-fractoriness failed to interrupt the tachycardia or did not advance the next His potential. The tachycardia was thus considered AVNRT rath-er than concealed nodoventricular or nodofascicular, ventricular tachycardia or automatic junctional tachycardia. Ablation of slow pathway during tachycardia succeed to terminate tachycardia. Tachycardia could not be induced after ablation.
Conclusions: Continuing AVNRT despite complete VA dissociation may support the existence of upper common pathway. Careful diag-nostic approach to such case is very important to differentiate it from others tachycardia.
COMPLETE VA DISSOCIATION IN NARROW QRS TACHYCARDIA: ATRIOVENTRICULAR NODAL REENTRY TACHYCARDIA WITH UPPER COMMON PATHWAYMohammad Iqbal, Anupam Jena, Hee-Soon Park, Yong-Soo Baek, Kwang-No Lee, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-05

53
Introduction: Azygos continuation of the inferior vena cava (IVC) is a rare congenital anomaly, that however, can occur in catheter ablation practice of atrial fibrillation. Some laboratories reported up to 0.8% prevalence among atrial flutter ablation patients. As azygos continua-tion of the IVC significantly complicates the femoral technique, limited but there are case reports of successful ablation of atrial fibrilla-tion/atrial flutter through azygos continuation. This report is to present ablation of persistent atrial fibrillation (AF) via trans-jugular and trans-azygos vein access in patient with azygos continuation of the IVC with multidetector CT imaging and 3D reconstruction.
Methods: N/A.
Results: A 60 year old male with persistent AF with CHADS2 score equal to 3 (hypertension and prior stroke) was symptomatic and refrac-tory to propafenone. After having 2 years of follow up he was referred and scheduled for ablation. On echocardiography examination, the left atrium diameter was 45 mm and the left ventricular ejection fraction was 43%. Transesophageal echocardiography excluded left atrial thrombus. Multidetector CT scanning was performed for image intergration of 3D mapping system. The patient had engorged azygos vein and interruption of IVC. Coronary sinus catheterization was performed via femoral approach using SR-0 catheter and the transseptal nee-dle (BRK 90o) was introduced via right internal jugular vein using SL-3 long sheath. Circumferential pulmonary vein isolation and linear ablation was performed via azygos continuation of the IVC. The 3D reconstruction was constructed by 3D CT and merged. Pulmonary vein ablation and atrial substrate modification were successfully performed and AF was terminated (Figure 1).
Conclusions: Multidetector CT scanning and 3D image integration can assess the mediastinal structure and vessel anomaly before cath-eter ablation. In patients with complete interruption of IVC, catheter ablation of AF via trans-azygos vein is a feasible alternative technique.
CATHETER ABLATION OF PERSISTENT ATRIAL FIBRILLATION IN A PATIENT WITH INTERRUPTED INFERIOR VENA CAVAMungun-Ulzii Khurelbaatar1,2, Yenn-Jiang Lin2, Shih-Ann Chen2 1Shastin Third State Central Hospital, Ulaanbaatar, Mongolia; 2Taipei Veteran’s General Hospital, Taipei, Taiwan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE OP 8-06

ORAL PRESENTATION 09(15 October)
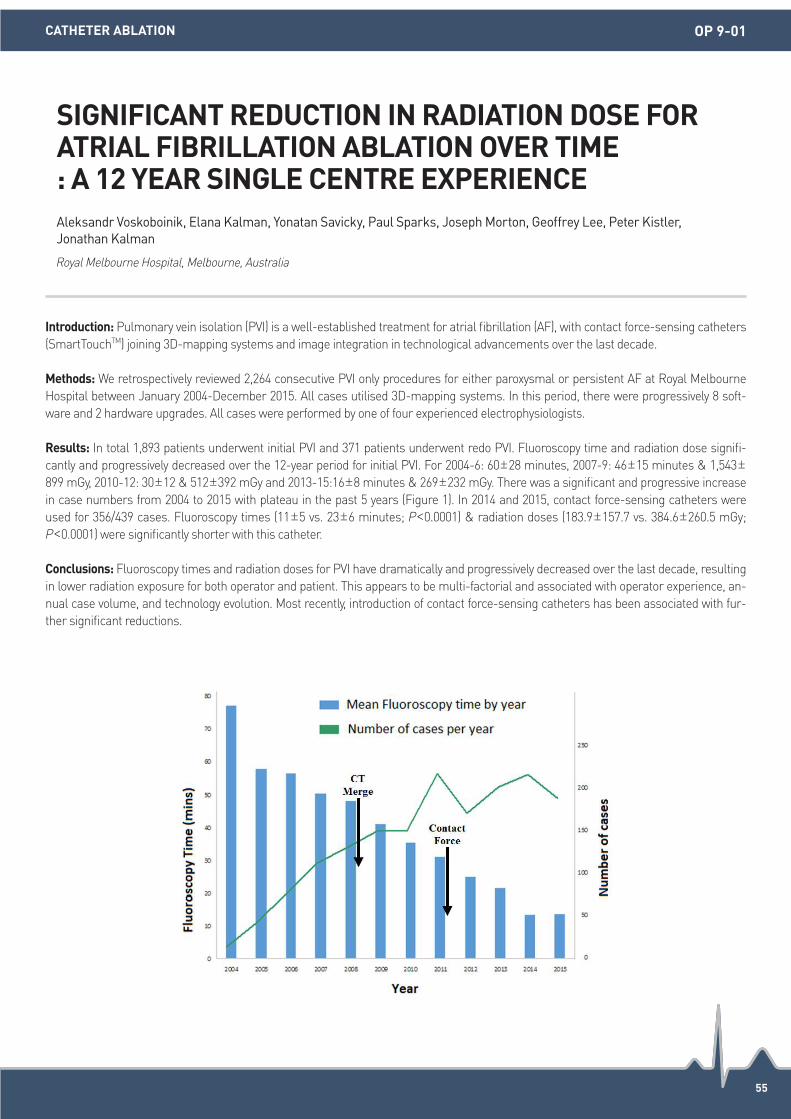
55
Introduction: Pulmonary vein isolation (PVI) is a well-established treatment for atrial fibrillation (AF), with contact force-sensing catheters (SmartTouchTM) joining 3D-mapping systems and image integration in technological advancements over the last decade.
Methods: We retrospectively reviewed 2,264 consecutive PVI only procedures for either paroxysmal or persistent AF at Royal Melbourne Hospital between January 2004-December 2015. All cases utilised 3D-mapping systems. In this period, there were progressively 8 soft-ware and 2 hardware upgrades. All cases were performed by one of four experienced electrophysiologists.
Results: In total 1,893 patients underwent initial PVI and 371 patients underwent redo PVI. Fluoroscopy time and radiation dose signifi-cantly and progressively decreased over the 12-year period for initial PVI. For 2004-6: 60±28 minutes, 2007-9: 46±15 minutes & 1,543±899 mGy, 2010-12: 30±12 & 512±392 mGy and 2013-15:16±8 minutes & 269±232 mGy. There was a significant and progressive increase in case numbers from 2004 to 2015 with plateau in the past 5 years (Figure 1). In 2014 and 2015, contact force-sensing catheters were used for 356/439 cases. Fluoroscopy times (11±5 vs. 23±6 minutes; P<0.0001) & radiation doses (183.9±157.7 vs. 384.6±260.5 mGy; P<0.0001) were significantly shorter with this catheter.
Conclusions: Fluoroscopy times and radiation doses for PVI have dramatically and progressively decreased over the last decade, resulting in lower radiation exposure for both operator and patient. This appears to be multi-factorial and associated with operator experience, an-nual case volume, and technology evolution. Most recently, introduction of contact force-sensing catheters has been associated with fur-ther significant reductions.
SIGNIFICANT REDUCTION IN RADIATION DOSE FOR ATRIAL FIBRILLATION ABLATION OVER TIME : A 12 YEAR SINGLE CENTRE EXPERIENCEAleksandr Voskoboinik, Elana Kalman, Yonatan Savicky, Paul Sparks, Joseph Morton, Geoffrey Lee, Peter Kistler, Jonathan Kalman
Royal Melbourne Hospital, Melbourne, Australia
CATHETER ABLATION OP 9-01

56
Introduction: Pulmonary vein isolation (PVI) is an established treatment for paroxysmal atrial fibrillation (PAF) however recurrence can occur despite pulmonary vein (PV) Isolation because of abnormal left atrial substrate which requires further ablation. The P wave trig-gered signal averaged ECG (SAECG) has been shown to demonstrate longer P wave duration and higher P wave energies in patients with paroxysmal atrial fibrillation (PAF) compared to controls. We postulated that this technique might be used to identify patients with signifi-cant atrial substrate change who may require additional ablation beyond PVI to avoid recurrence.
Methods: We recruited 119 consecutive patients with PAF in the study undergoing either PVI alone, PVI with cavotriscupid isthmus (CTI) ablation(if in flutter), PVI with additional left atrial ablation lines and PVI with DC cardioversion (if in AF at the end of PVI). Ethical approval has been obtained prior to the study. Signal averaged ECG data was recorded using the Spider view high resolution ECG recording system (Sorin), which records both time domain analysis (Pdur, root mean squared velocities RMS10, 20, 30 mSec) and frequency domain analysis (energies at various band frequencies, 20 Hz-150 Hz). Patients were followed up for 12 months. Data was analysed using unpaired t-tests and one way ANOVA analysis.
Results: There was a statistically significant difference in pre ablation P wave duration (Pdur) of patients who were in sinus rhythm at the end of procedure (ie had PVI only or PVI+CTI ablation) vs. patients who were still in AF (ie required additional left atrial ablation or DCCV) (143.1±1.32 vs. 157.5±6.6 ms, P=0.001) (Figure 1). One-way Anova analysis has demonstrated differences in Pdur in various ablation groups. Time domain and frequency domain analysis of the signal averaged P waves did not show any significant differences in the pre ablation parameters (Table 2).
Conclusions: The pre ablation P wave SAECG showed a longer P wave duration in pts with PAF who were not in sinus rhythm at the end of PVI. This may reflect the presence of more extreme atrial substrate change and act as a guide to individuals who will do well with PVI alone compared to those in whom additional ablation will be required.
P WAVE DURATION & SPECTRAL ANALYSIS OF SIGNAL AVERAGED P WAVE: CAN THIS GUIDE US IN DECIDING EXTENT OF ABLATION TO BE PERFORMED DURING PULMONARY VEIN ISOLATION? A PROSPECTIVE STUDYSubrahmanya Srinivas Varanasi, Gavin S Chu, Shoaib Siddiqui, Sharon Man, Riyaz Somani, Alastair Sandilands, Peter Stafford, G Andre Ng
Glenfield Hospital, Leicester, United Kingdom
CLINICAL ELECTROPHYSIOLOGY OP 9-02

57
Introduction: During atrial ablation of atrial fibrillation (AF) embolism (AE) is rare complication but it can be life threatening and may af-fect clinical and procedural outcome.
Methods: We reviewed manifestations, management and outcomes of accompanied by air embolism occurred during atrial catheteriza-tion for ablation of AF.
Results: Between January 1 2006 and April 30 2016, 2,614 patients underwent AF ablation and 7 cases of AE were reported. Most (6/7) of AE occurred immediate after trans-septal puncture. All cases presented ST elevation (STE) of inferior and/or lateral precordial leads. 3 cases showed only ST change and 2 cases showed transient AV block as well as ST change without hemodynamic instability, followed cor-onary angiography showed no blood flow interference or overt air embolism. The remaining 2 cases eventually progressed to ventricular fibrillation. One patient recovered to sinus rhythm by defibrillation and elimination of air in right coronary artery (RCA) and left atrial ap-pendage (LAA), other patient needed extracorporeal membrane oxygenation until recovering from ventricular arrhythmia. After manage-ment of AE, all patient performed atrial ablation without interruption and recovered completely. Recurrence of atrial tachy-arrhythmia (ATA) occurred in 1 of 5 cases presenting only ST elevation and in 1 of 2 cases presenting shock related ventricular arrhythmia, respective-ly.
Conclusions: Trans-septal puncture performed in the supine position accumulate air to RCA and/or LAA by anatomical location, which can cause fatal AV block or ventricular arrhythmia and affect procedural outcome. Left atrial catheterization and ablation should be con-ducted carefully.
CASES OF AIR EMBOLISM DURING ATRIAL ABLATION OF ATRIAL FIBRILLATIONHee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-young Roh, Jaemin Shim, Jong Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CATHETER ABLATION OP 9-03
Table 1. Patient characteristics and the clinical manifestation with air embolism
Sex/ Age
AF Type
LAD (mm)/LVEF (%)
Location of STE
Rhythm Change
Coronary Angiogram
Management of AE
Management of rhythm change
Hospitaliza-tion duration
(days)
Recur-rence of ATA
M/53 PAF 24/55 Inferior leads
- Normal Spontaneously recovered
- 3 36 months
M/53 PAF 43/52 Inferior leads
2:1 AVB, NSVT
Normal Spontaneously recovered
- 7 No recur
M/75 PAF, redo
41/55 Inferior leads
CAVB, VF
AE in RCA Saline injection Defibrillation 8 14 months
M/73 PeAF 49/35 Inferior leads
- Normal Spontaneously recovered
- 3 No recur
M/58 LPeAF 47/45 Inferior leads, V5-6
VF AE in RCA Aspiration and saline injection
Defibrillation, ECMO
3 No recur
M/58 PeAF 45/55 Inferior leads, V5-6
- - Spontaneously recovered
- 4 No recur
M/65 PAF 34/55 Inferior leads, V5-6
High grade AVB
Normal Spontaneously recovered
- 7 No recur
58
Introduction: Adequate contact force (CF) with the atrial tissues is a critical component of lesion formation during radiofrequency (RF) ab-lation of atrial fibrillation (AF). Late gadolinium enhancement magnetic resonance imaging (LGE-MRI) is a unique tool for the evaluation of lesion formation and detection of acute esophageal injury.
Methods: LGE-MRIs were obtained prior, within 24 hours of, and at 3 months after first AF ablation in 34 patients. AF ablation was per-formed with a CF sensing ablation catheter. The Visitag module of CARTO3 was used to collect ablation parameters (force, duration, force-time integral (FTI)) for each registered ablation point on the LGE-MRIs rendering of LA. The minimum CF resulting in permanent lesions by LGE-MRI was determined. Esophageal enhancement was classified as mild, moderate and severe. The mean CF threshold resulting in esophageal enhancement was determined.
Results: A total of 7680 registered ablation points were analyzed for powers used 25, 35, and 50 W. For 50 W, a A CF greater than 11.5 grams was more likely to create a permanent lesion than forces less than 11.5 grams (11.5±5.4 g vs. 10.7±5.4 g, P<0.001). Similarly, an FTI greater than 67.4 gs was more likely to create permanent lesions (67.4±55.7 gs vs. 60.4±48 gs, P<0.001). Higher CF was needed to create lesions when power was reduced (35 W, 16.3±9.6 g vs. 13.0±7.2 g, P<0.001; 25 W 15.7±8.5 g vs. 14.1±8.5 g, P<0.01). Ablation ear-lier in the procedure was more likely to result in permanent lesion formation (50 W, 308±775 s vs. 540±1,513 s, P<0.001). The mean CF in areas of esophageal enhancement was greater than areas without (50 W, 14.1±6.5 g vs. 11.8±4.7 g, P=0.002, n=9 patients).
Conclusions: CF needs to be adjusted based on the power use to create adequate lesions. A minimum CF of 11-12 for 50 W and 15-16 grams for 25-35 W and earlier time during the procedure predicts permanent RF lesion formation. The latter suggest that edema forma-tion may interfere with the ability to create permanent lesions later in the procedure. CF greater than 14 g at 50 W over esophagus may lead to esophageal injury however without long term clinical consequences (mild and moderate esophageal injury).
ASSESSMENT OF LESION FORMATION AND ESOPHAGEAL INJURY BY LGE-MRI IN ATRIAL FIBRILLATION ABLATION WITH A FORCE SENSING CATHETERMihail Chelu, Alan Morris, Eugene Kholmovski, Gagandeep Kaur, Nassir Marrouche
University of Utah, Salt Lake City, United States
CATHETER ABLATION OP 9-04

59
Introduction: Left atrial (LA) reverse remodeling does not always occur even if sinus rhythm is maintained after catheter ablation for atrial fibrillation (AF). The purpose of this study is to investigate the predictors of no reverse remodeling after AF ablation.
Methods: This study consisted of 55 patients (paroxysmal AF: 28) with enlarged LA (LA volume>40 mL: calculated by using the Prolate el-lipsoid method in preprocedural echocardiography) who maintained sinus rhythm at least three years after the procedure. The responder of reverse remodeling was defined as the patient who had ≥15% reduction of LA volume at long-term follow-up.
Results: A mean of 63±14 months after the procedure, 23/55 (42%) patients (paroxysmal AF: 14) were classified as non-responders. In univariate analysis, hypertension was more frequently observed and left ventricular ejection fraction was significantly lower in non-re-sponders compared to responders (61% (14/23) vs. 22% (7/32), P=0.005 and 61.5±8.6% vs. 66.2±7.5%, P=0.03, respectively). In multivari-able analysis, the history of hypertension was the only independent predictor of non-responder (odds ratio 3.82, 95% CI 1.06 to 13.82, P=0.04).
Conclusions: AF patients with hypertension are likely to be non-responder of LA reverse remodeling following successful AF ablation.
PREDICTOR OF NO ATRIAL REVERSE REMODELING AFTER SUCCESSFUL CATHETER ABLATION FOR ATRIAL FIBRILLATIONRyohsuke Narui, Michifumi Tokuda, Ryota Isogai, Kenichi Tokutake, Kenichi Yokoyama, Mika Kato, Seigo Yamashita, Keiichi Inada, Kenri Shibayama, Seiichiro Matsuo, Kenichi Sugimoto, Teiichi Yamane
The Jikei University of Medicine, Tokyo, Japan
CATHETER ABLATION OP 9-05
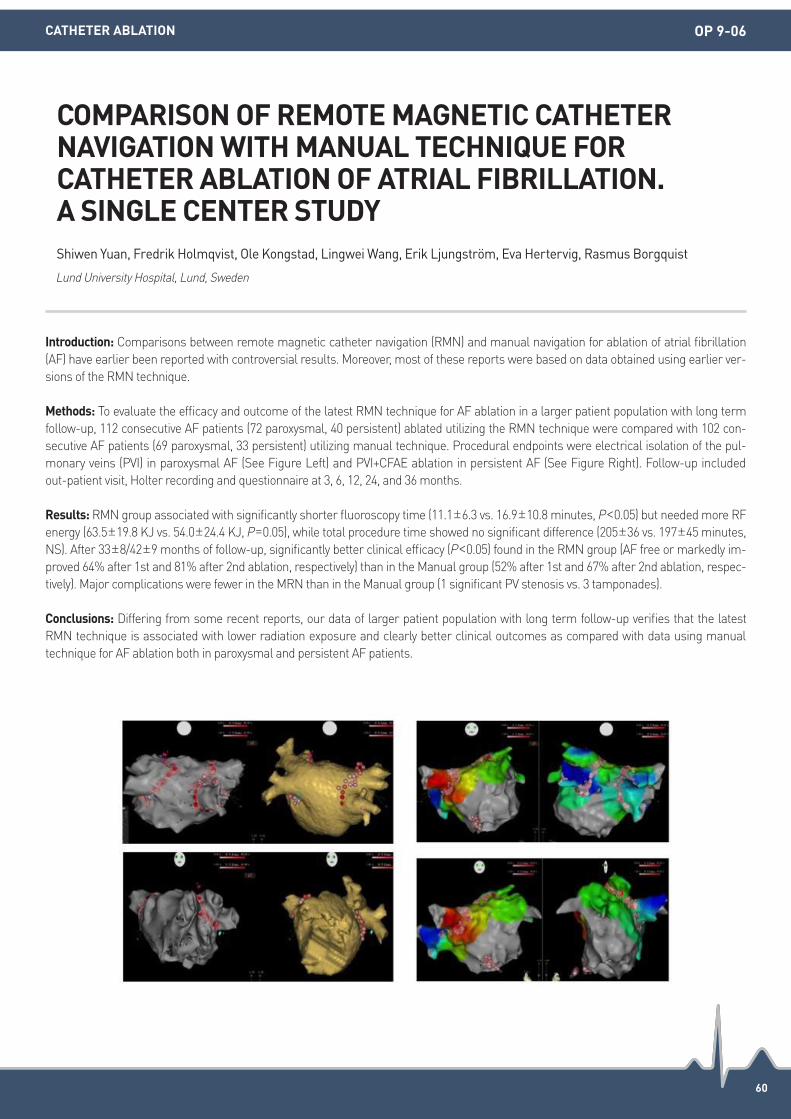
60
Introduction: Comparisons between remote magnetic catheter navigation (RMN) and manual navigation for ablation of atrial fibrillation (AF) have earlier been reported with controversial results. Moreover, most of these reports were based on data obtained using earlier ver-sions of the RMN technique.
Methods: To evaluate the efficacy and outcome of the latest RMN technique for AF ablation in a larger patient population with long term follow-up, 112 consecutive AF patients (72 paroxysmal, 40 persistent) ablated utilizing the RMN technique were compared with 102 con-secutive AF patients (69 paroxysmal, 33 persistent) utilizing manual technique. Procedural endpoints were electrical isolation of the pul-monary veins (PVI) in paroxysmal AF (See Figure Left) and PVI+CFAE ablation in persistent AF (See Figure Right). Follow-up included out-patient visit, Holter recording and questionnaire at 3, 6, 12, 24, and 36 months.
Results: RMN group associated with significantly shorter fluoroscopy time (11.1±6.3 vs. 16.9±10.8 minutes, P<0.05) but needed more RF energy (63.5±19.8 KJ vs. 54.0±24.4 KJ, P=0.05), while total procedure time showed no significant difference (205±36 vs. 197±45 minutes, NS). After 33±8/42±9 months of follow-up, significantly better clinical efficacy (P<0.05) found in the RMN group (AF free or markedly im-proved 64% after 1st and 81% after 2nd ablation, respectively) than in the Manual group (52% after 1st and 67% after 2nd ablation, respec-tively). Major complications were fewer in the MRN than in the Manual group (1 significant PV stenosis vs. 3 tamponades).
Conclusions: Differing from some recent reports, our data of larger patient population with long term follow-up verifies that the latest RMN technique is associated with lower radiation exposure and clearly better clinical outcomes as compared with data using manual technique for AF ablation both in paroxysmal and persistent AF patients.
COMPARISON OF REMOTE MAGNETIC CATHETER NAVIGATION WITH MANUAL TECHNIQUE FOR CATHETER ABLATION OF ATRIAL FIBRILLATION. A SINGLE CENTER STUDYShiwen Yuan, Fredrik Holmqvist, Ole Kongstad, Lingwei Wang, Erik Ljungström, Eva Hertervig, Rasmus Borgquist
Lund University Hospital, Lund, Sweden
CATHETER ABLATION OP 9-06

MINI ORAL SESSION 01(13 October)

62
Introduction: Patient-activated ambulatory ECG monitors have been widely used in the outpatient setting for patients with infrequent symptoms. The optimal duration for diagnosis and the predictors of detection remain unclear.
Methods: Patients with palpitations or dizziness received a patient activated handheld ECG monitor which records 30 seconds single lead ECG strips. Patients were monitored in an ambulatory setting for a range of 1-4 weeks and rhythm strips were interpreted by 5 indepen-dent electrophysiologists. Event pick-up rates and clinical covariates were then analysed.
Results: Of the 335 adults (age 50±16 years, 58% female) with palpitations (90%) and dizziness (25%) who were monitored, 288 patients (86%) reported events, with 73 (25%) patients having clinically significant events detected (Figure). 7% of patients had ≥2 significant events and 75% of patients had events detected in the first 3 days. No significant events were detected after 12 days. The most common ECG ab-normalities detected were premature ventricular ectopics (39%), premature atrial ectopics (38%) and atrial fibrillation/flutter (33%). Pre-dictors of a clinically significant event included age, irregular rhythm, known AF or arrhythmia and previous abnormal ambulatory moni-toring (all P<0.05). Patients older than 50 years were 84% more likely to have a clinically significant event (P=0.02).
Conclusions: Patient-activated ambulatory ECG monitoring for 2 weeks was optimal in the diagnosis of patients with palpitations as sig-nificant events first detected beyond 10 days were rare. Patients older than 50 years were more likely to have a clinically significant event.
OPTIMAL DURATION AND PREDICTORS OF DIAGNOSTIC UTILITY OF PATIENT -ACTIVATED AMBULATORY ECG MONITORINGEugene S.J. Tan, Swee Chong Seow, Pipin Kojodjojo, Devinder Singh, Wee Tiong Yeo, Toon Wei Lim
National University Heart Centre Singapore, Singapore
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION MO 1-01

63
Introduction: Idiopathic ventricular arrhythmias (Vas) are commonly originated from right coronary cusp (RCC) and left coronary cusp (LCC). Several previous studies have revealed differences in the electrocardiographic characteristics of VAs originating from RCC and LCC. However, the electrocardiographic criterion for distinguishing these arrhythmias is still to be elucidated and the utility of aVL/aVR ratio is unknown.
Methods: We studied 21 consecutive patients (mean age 56±16 years, 5 male) who underwent successful catheter ablation for idiopathic VAs originated from RCC (n=6) and LCC (n=15). QRS waveform, duration and amplitude from standard 12-lead ECG were measured.
Results: All patients with RCC VAs presented with R morphology in lead I, whereas for patients with LCC VAs, 4 presented with QS mor-phology, 10 with RS or rs morphology and 1 with R morphology (χ2=16.80, P<0.01). All patients demonstrated with R morphology in inferi-or leads and QS morphology in aVR. 2 patients demonstrated QS morphology and 4 with rS morphology in lead V1 for patients with RCC VAs, while for patients with LCC VAs, 4 present QS morphology, 7 with rS morphology, 3 with qrS morphology and 1 with R morphology. The QRS duration in lead aVL was significant longer in patients with LCC VAs than in patients with RCC VAs (129±18 ms vs. 102±22 ms, P<0.01) and the QRS amplitude in lead III, aVL and aVF was significant higher in patients with LCC VAs compared to patients with RCC VAs (1.85±0.43 mv vs. 1.70± 0.38 mv, P<0.01; 1.19±0.24 mv vs. 0.61±0.21 mv, P<0.01; 1.98±0.36 mv vs. 1.51±0.36 mv, P<0.05). Com-pared to patients with RCC VAs, III/II ratio and aVL/aVR ratio were significant higher in patients with LCC VAs (1.09±0.12 vs. 0.79±0.11; 1.31±0.35 vs. 0.61±0.22, all P<0.001). The ability of aVL/aVR ratio to distigush LCC VAs was assessed by using an ROC curve. The area under the curve for the ROC curve of aVL/aVR ratio was 0.967 [95% confidential interval 0.892-1.000]. An aVL/aVR ratio of more than 1.01 had 80% sensitivity and 100% specificity for detecting patients with LCC VAs.
Conclusions: A relatively large R wave in lead I is seen in RCC VAs. Patients with LCC VAs showed longer QRS duration in lead aVL and higher QRS amplitude in lead III, aVL and aVF than patients with RCC VAs. The ratio of aVL/aVR >1 is a simple and reliable index in distin-guishing VAs from LCC and RCC.
THE RATIO OF AVL/AVR IS SIMPLE IN DISTINGUISHING VENTRICULAR ARRHYTHMIAS ORIGINATED FROM THE RIGHT AND THE LEFT CORONARY CUSPHong-wei Tan, Xu-min Zhang, Yu Zou, Jian Zhou, Jian Zhou
Shanghai East Hospital Affiliated to Tongji University, Shanghai, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION MO 1-02

64
Introduction: Recent research has shown that sympathectomy and pharmacological sympathetic blockades are effective treatments for fatal arrhythmia. The cholinergic anti-inflammatory pathway (CAIP) is a complex immune mechanism that regulates peripheral inflam-matory responses and can be triggered by the central nervous system. This study evaluated the antiarrhythmic effect of sympathectomy is related with the activation of CAIP using experimental autoimmune myocarditis (EAM).
Methods: Experimental autoimmune myocarditis (EAM) was produced by injecting 2 mg of porcine cardiac myosin into footpads. Fifty-two rats were assigned to the normal control group (control, n=10), the EAM group (Myo, n=15), the sympathectomy plus EAM group (MyoSB, n=15), the β-blocker pus EAM group (MyoBB, n=9), and the only sympathectomy group (SB, n=8). Relevant signaling pathways were stud-ied to compare their effects on myocarditis, survival rate, histopathological changes, ultrastructural changes, electrophysiological chang-es, and cytokine levels.
Results: In the Myo group, 4 (27%) rats died suddenly at 14±4 days after acute myocarditis and 7 (47%) surviving rats had arrhythmia. However, no rat died and had arrhythmia in the control or MyoSB groups (all P=0.02). Compared with control, left ventricular dysfunction and higher levels of inflammation such as Cox2, iNOS, TNF-α, IL-6, and HMGB1 increase (P<0.05 vs. control) and increased fibrosis with slower conduction velocity (CV; P<0.01 vs. control) were observed in Myo, but not in MyoSB. Compared with control (100%), the Myo group showed reduced phosphate/total STAT3 (0.5±0.1 times, P=0.001) and JAK2 (0.5±0.0 times, P=0.01). However, compared with Myo, MyoSB showed significantly enhanced JAK2 activation (2.2±0.1 times, P<0.001) followed by STAT3 phosphorylation (2.2±0.2 times, P<0.001) with the increased secretion of acetylcholine (105±1%, P=0.03). In addition, the same trends in levels of protein expression were observed in the lungs, liver and spleen containing innate immune cells.
Conclusions: Sympathectomy increased survival and showed antiarrhythmic effects along with the reduction of inflammation in EAM models via activation of the JAK2-STAT3-mediated signaling cascade. It represents an exciting opportunity to develop new and novel ther-apeutics to attenuate cardiac inflammation.
SYMPATHETIC NERVE BLOCK ATTENUATES INFLAMMATION-INDUCED ARRHYTHMIA VIA A CHOLINERGIC ANTI-INFLAMMATORY PATHWAYHyelim Park1, Hyewon Park1, Hyo-Eun Kim1, Seung-Hyun Lee1, Michael Kim2, Hui-Nam Pak1, Moon-Hyoung Lee1, Boyoung Joung1 1Yonsei University Health System, Yonsei University College of Medicine, Seoul, Republic of Korea; 2Duke University, Durham, United States
BASIC/TRANSLATIONAL SCIENCE MO 1-03

65
Introduction: We investigated the comparison and association of clinical characteristics including medication and intervention between survival and non-survival on the return of spontaneous circulation (ROSC) of the Out-of Hospital Cardiac Arrest (OHCA) for 6 years.
Methods: Retrospective analysis of data from consecutive 229 OHCA occurring from 2010 to 2016 in which patients aged 19 years or older had an OHCA after arrival of emergency room, were treated in the Emergency Room and admitted into cardiology in Eulji University Hos-pital, Deajeon, Republic of Korea. All patients have undertaken emergent or elective coronary angiogram and echocardiogram to evaluate the cause of OHCA and divided into two groups; survival vs. non-survival.
Results: All consecutive 229 patients with ROSC were compared between survival (n=102) and non-survival (n=127) who admitted to car-diac intensive care unit (ICU). The mean age of survival was younger than non-survival (60±16 vs. 70±15, P<0.001). However, the propor-tion of gender, hypertension and diabetes were similar between two groups. The proportion of ventricular tachycardia or fibrillation on the ECG before ROSC was significantly higher in the survival than non-survival (64% vs. 19%, P<0.001) while the proportion of amiodarone in-fusion was similar between two group (33.3% vs. 23.6%, P=0104). However, the etiology proportion of acute myocardial infarction con-firmed by emergent intervention was similar between two groups (44% vs. 50%, P=0.345). In addition, the ejection fraction, hemoglobin and arterial pH were significantly higher in the survival than non-survival (43±16% vs. 23±27%, P<0.001; 13±2 g/dL vs. 12±2 g/dL, P<0.001; 7.1±0.1 vs. 7.0±0.1, P<0.001). Multivariate logistic regression showed that hemoglobin level and arterial pH were odd ratio 0.78 (0.67-0.90) with P=0.003 and 0.07 (0.01-0.40) with P=0.001. ROC analysis showed that hemoglobin >13 (sensitivity 75% and specificity 61%) and arterial pH >7.0 (sensitivity 62% and specificity 62%) were predictable for survival after ROSC.
Conclusions: Among the patients on the ROSC with OHCA, survival was significantly associated with hemoglobin and arterial pH among the characteristics and treatment including amiodarone and emergent intervention. Multicenter randomized prospective study was need-ed to confirm this result.
ARTERIAL PH AND HEMOGLOBIN REGARDLESS OF AMIODARONE AND EMERGENT INTERVENTION ARE DETERMINANTS FOR SURVIVAL ON THE RETURN OF SPONTANEOUS CIRCULATION OF THE OUT-OF HOSPITAL CARDIAC ARRESTKi-Woon Kang, Won Hyung Sung, Sang Won Seo, Yu Jeong Choi, San Hyun Park, Jung Yeon Chin, Won Ho Kim, Won Suk Lee, Jang Young Lee
Eulji University Hospital, Deajeon, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION MO 1-04

66
Introduction: The Lead Extraction Difficulty (LED) score was developed on a derivation sample to predict complex procedures of transve-nous lead extraction (TLE), LED>10 criterion was estimated to be associated with a 78.3% sensitivity and 76.3% specificity. The aim of this study was to validate the LED index on an independent validation sample.
Methods: Consecutive patients undergoing TLE between January 2014 and January 2016 were included in this analysis. Procedures were classified as complex if the cumulative fluoroscopy time was >90th percentile at the end of the procedure. LED score is equal to the num-ber of leads to be extracted + years from implant of the oldest target lead + 1 (if a dual-coil ICD lead must be removed)-1 (if vegetation is confirmed along the lead body). We tested whether LED ≥10 predicts complex procedures.
Results: In total, 446 permanent leads (232 pacemaker, 143 ICD, and 71 sinus coronary leads) were removed during 233 TLE procedures. Complete procedural success was achieved in 232 (99.1%) patients with no major complications. The figure reports the complete set of classification probabilities of the LED index on this validation sample. Over the 23 cases with high fluoroscopy time, 20 had LED score>10 and were corrected classified. Only 3 procedures resulted false negative cases, leading to a 86.9% sensitivity and 98.0% negative predictive value.
Conclusions: The validation of the estimation model based on the LED index >10 confirmed a good sensitivity and an excellent negative predictive value proving reliable specially in detecting simple cases. The LED score may allow less experienced centres to more easily de-cide whether or not to refer to expert centres reducing overall patient risks.
PREDICTING THE DIFFICULTY OF A TRANSVENOUS LEAD EXTRACTION PROCEDURE : VALIDATION OF THE LED INDEXLuca Bontempi1, Francesca Vassanelli1, Manuel Cerini1, Lorenza Inama1, Francesca Salghetti1, Nicolò Dasseni1, Clara Villa1, Daria Liberto2, Daniele Giacopelli3, Alessio Gargaro3, Abdallah Raweh4, Antonio Curnis1 1Spedali Civili-University of Brescia, Brescia, Italy; 2University of Catania, Catania, Italy; 3Biotronik Italia, Milano, Italy; 4L.U.de.S. University, Lugano, Switzerland
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES MO 1-05

67
Introduction: There are few reports about the clinical predictive factor which the appropriate implantable cardioverter defibrillator (ICD) therapies produces, and in regard to the adaptation of the ICD, there is a difference in Japan and European and American guidelines, and it is the present conditions in that is controversial. The aim of this study is to assess the validity of risk stratification for indication of ICD in Japanese patients with hypertrophic cardiomyopathy (HCM) by the 2014 ESC guideline. Hypothesis: The risk stratification for sudden car-diac death by the 2014 ESC guideline is valid in the Japanese patients with HCM.
Methods: We analyzed the characteristics of and outcomes for Japanese HCM patients with ICD. All patients were followed-up at our center.
Results: A total of consequence 51 HCM Japanese patients with ICD were enrolled in this study. All the patients meet class I or IIa in the guideline in Japan and the U.S. Over a mean follow-up period of 43±27 months, 7 patients (14%) received appropriate ICD therapies. The characteristics and outcomes of the patients were shown in the table and the figure, respectively. In patients with an ICD shock therapy during this follow up period, the 2014 ESC guideline would have recommended ICD implantation in 86% (6/7).
Conclusions: The risk stratification for sudden cardiac death by the 2014 ESC guideline seems to be valid in the Japanese patients with HCM.
RISK STRATIFICATION FOR SUDDEN CARDIAC DEATH IN JAPANESE HYPERTROPHIC CARDIOMYOPATHY PATIENTS WITH IMPLANTABLE CARDIOVERTER-DEFIBRILLATORMiyo Nakano1, Yusuke Kondo2, Marehiko Ueda1, Masahiro Nakano1, Kazuo Miyazawa1, Tomohiko Hayashi1, Yoshio Kobayashi1 1Chiba University Graduate School of Medicine, Department of Cardiovascular Medicine, Chiba, Japan; 2Chiba University Graduate School of Medicine, Department of Advanced Cardiovascular Therapeutics, Chiba, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES MO 1-06

68
Introduction: Abnormal calcium release from sarcoplasmic reticulum (SR) is considered an important mechanism of atrial fibrillation (AF). Dysfunction of type-2 ryanodine receptor channels (RyR2) promote ectopic activity, conduction abnormalities, facilitating reentry, and AF-related remodeling. Because decreased LA voltage is one of important markers reflecting atrial fibrosis, we investigated the associa-tion between genetic polymorphisms of RyR2 and left atrial (LA) voltage among AF patients who underwent catheter ablation.
Methods: Mean LA voltage was obtained from individual LA voltage mapping in 469 patients (mean age 50.6±7.9 years, 82% male, 72% paroxysmal AF) who underwent AF catheter ablation. Total 292 single nucleotide polymorphisms in RyR2 were analyzed.
Results: In multivariate linear regression analysis adjusted by age, sex, and AF type, two single-nucleotide polymorphisms (SNPs) (rs1337797, rs2490372) in RyR2 were independently associated with mean LA voltage after Bonferroni adjustment (rs1337797: beta -0.182, 95% confidence interval [CI] -0.261 to -0.102, P=9.64×10-6, P=0.004 with Bonferroni adjustment; rs2490372: beta -0.164, 95% CI -0.243 to -0.083, P=7.13×10-5, P=0.028 with Bonferroni adjustment). In rs1337797, the heterozygous haplotype (n=221) demonstrated a 14% lower mean LA voltage (1.20 mV) and the homozygous risk allele carriers (n=73) demonstrated a 22% lower mean LA voltage (1.09 mV) com-pared with wild type (n=175, 1.40 mV) (P=0.0004).
Conclusions: Two risk alleles in RyR2, rs1337797 and rs2490372, are independently associated with decreased mean LA voltage in AF pa-tients. Our findings suggest that common genetic variations in RyR2 also related to atrial structural remodeling.
GENETIC POLYMORPHISM OF RYANODINE RECEPTOR 2 AND LEFT ATRIAL VOLTAGE IN PATIENTS WITH ATRIAL FIBRILLATIONPil-Sung Yang, Ji-Young Lee, Tae-Hoon Kim, Jae-Sun Uhm, Boyoung Joung, Moon-Hyoung Lee, Hui-Nam Pak
Yonsei University Health System, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE MO 1-07

69
Introduction: Sustained Ventricular Tachycardia (VT) is common in patients with arryhthmogenic right ventricular cardiomyopathy (ARVC/D), and associated with frequent ICD interventions, hospitalizations and reduced quality of life. Antiarryhtmic drugs are not always effec-tive in suppressing ventricular arrhythmias and frequently associated with side effects. We assessed short term outcomes of radio fre-quency catheter ablation (RFA) for VT in a single -center cohort of patients with ARVC/D.
Methods: All RFA procedures addressing VT performed in our center between 1998 and 2015 in 40 patients (49.2±15.8 years; 83% male) with definite (n=32) or borderline (n=8) ARVC/D were analyzed. Procedural data and short-term success were determined.
Results: 71 RFA procedures using a three-dimensional mapping system were performed (mean 1.8 procedures/patient), of these 55% (n=39) using an endocardial approach, 34% (n=24) using a combined endo-epicardial approach, and 11% (n=8) using an epicardial ap-proach. VT was inducible in 86% of patients referred for RFA of VT. In 44% of ablations >1 sustained VT was inducible and multiple VT morphologies (1.5±1.0) were common (38%). The mean cycle length of induced VT was 351±78 ms. Most VT had a LBBB morphology and superior axis, correlating with the subtricuspid area as the most frequent VT exit site. Although fibro-fatty infiltration typically begins sub-epicardially, an endocardial substrate with low voltage (bipolar <1.5 mV) and fragmented/late potentials was found in the majority patients (55%). Procedural data are shown in the table. RFA was successful (defined as abolishment of all inducible VTs) in 86%, and partially suc-cessful (defined as abolishment of all clinical VTs) in 10%. 3 procedures on two different patients were not successful. The reason was the close proximity of the target substrate and ICD lead (combined endo-/epicardial approach) in the first case, and hemodynamically not tol-erable VT in the second patient. VT ablation was generally safe with 1 (1.4%) pericardial tamponade occurring after epicardial puncture, and 9 minor complications (pericardial effusion n=2, mild pericarditis n=4, mild femoral hematoma n=3). The majority of patients had an ICD (76%). The number of sustained VT significantly decreased after RFA compared to before (27±38 vs. 4±12, P<0.05). The number of patients on anti arrhythmic drugs did not significantly change before and after RFA (93% vs. 90%, P=ns).
Conclusions: RFA is an effective strategy to reduce the sustained VT burden in patients with ARVC/D. Although the pathologic process be-gins in the subepicardium, the majority of patients referred for VT ablation has rather advanced disease stages, and thus presents with an endocardial substrate amenable to endocardial RFA. Endocardial RFA has a high acute success rate, potentially obviating the need for a more invasive epicardial approach in some of these patients.
CATHETER ABLATION OF VENTRICULAR TACHYCARDIA IN ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY-EXPERIENCE OF A TERTIARY CARE CENTERShibu Mathew, Ardan Saguner, Niklas Schenker, Andreas Metzner, Christine Lemes, Tilmann Maurer, Christan Heeger, Francesco Santoro, Karl-Heinz Kuck, Feifan Ouyang
Asklepios St. Georg, Hamburg, Germany
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION MO 1-08

70
Introduction: Traditionally epicardial pacing systems have been routinely used for cardiac pacing in children weighing ≤12 kg. Transve-nous pacemaker implantation in this subgroup presents unique challenges in terms of venous access, size of the veins, pacemaker pock-et, and the hardware available. The disadvantages of smaller pulse generators available for children are, shorter battery life, and non-availability in many parts of the world. We describe a technique of transvenous lead implantation in children between ≤12 kg using conventional adult pacemaker and leads.
Methods: This is an analysis of pediatric patients <12 kg who underwent permanent pacemaker implantation from January 2008 to May 2016 for standard Class I indication using a standard technique. All patients underwent PPI using a standard technique. An extra thoracic axillary vein puncture was performed using a 20-gauge needle, and wired using 0.025” guide wire. The 0.025” guide wire was exchanged for a 0.038” guide wire through a 4 F angiographic sheath. Sequential dilatation was performed using 5, 6 and 7 F dilators to introduce a 7F PLI. An active fixation 52 cms 6F lead was positioned in the RV, connected to the adult pulse generator. The pulse generator was placed in a subpectoral pocket.
Results: A total of 13 patients underwent PPI of whom 9 (62%) were males and 4 (38%) were females, mean age (2.46±0.8 years), mean body weight (9.69±1.45 kg). Indication for pacing was surgical AV block in 8 (61.6%) patients, and congenital AV block in 5 (38.4%). A single chamber VVIR pacemaker with a bipolar active fixation lead was implanted in all patients. Implant parameters were, mean R wave 11.19±4.54 (6.65 to 15.73) mV, mean impedance 652.46±136.6 (515.86 to 789.72) ohms, mean threshold 0.81±0.39 (.42 to 1.42) volts at 0.4 ms pulse width. The mean length of hospital stay was 5.3± 0.63 (4.67 to 5.93) days. Over a follow up of 96 months a mean R wave 10.5±3.9 (6.6 to 14.4) mV, mean impedance 688.23±160.7 (527.53 to 848.93) ohms, threshold 0.98±0.36 (.62 to 1.34) volts at 0.4 ms pulse width was. There were no complications at implant and follow up.
Conclusions: Transvenous pacemaker implantation in children ≤12 kg weight is feasible, safe, has short hospital stay with good medium term follow up results.
TRANSVENOUS PACING USING CONVENTIONAL PACEMAKER IN PEDIATRIC PATIENTS ≤12 KGS : TECHNIQUE AND MIDTERM RESULTSVivek Pillai, Vidhyakar Balasubramaniam, Sivasankara Chakali, Jayaprakash Shenthar
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, India
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES MO 1-09

71
Introduction: Low-level electrical stimulation (LL-ES) of automomic nerve was reported to suppress atrial fibrillation (AF) by inhibiting the intrinsic cardiac autonomic nervous system and bring both anti- arrhythmia and anti-inflammation effect. However, it was still unknown whether LL-ES could reverse the structural remodeling of myocardial fibrosis and atrial enlargement following heart failure (HF) Aim: This study was designed to investigate the anti-cardiac remodeling effect of LL-ES of the aortic root ventricular GP.
Methods: Twenty dogs were randomly divided into control group and LL-ES group after rapid right ventricle pacing was performed to es-tablish heart failure model. Following a week of LL-ES of the aortic root ventricular GP, bioactive factors for HF including angiotensin II, TGF-β,mitogen-activated protein kinase (MAPK), matrix metalloproteinase (MMP) was assessed. Furthermore, ventricle size, cardiac fi-brosis as well as left ventricular ejection fraction were also determined.
Results: Compared by control group, expression of angiotensin II, TGF-β, MAPK, and MMP were significantly down-regulated in LL-ES group (P<0.05). Moreover, the volume of left ventricle and cardiac fibrosis were markedly decreased, and LVEF in LL-ES group was signifi-cantly increased compared with those in control group (P<0.05).
Conclusions: Long term LL-ES of the aortic root ventricular GP improved rapid pacing induced cardiac structural and functional remod-eling by attenuating the sympathetic tone.
EFFECT OF LOW-LEVEL ELECTRICAL STIMULATION OF THE AROTIC ROOT VENTRICULAR GANGLIONATED PLEXI ON STRUCTURAL REMODLING IN DOGS WITH HEART FAILUREHong-Tao Wang, Qiang-Sun Zheng
Tangdu Hospital, Xi’an, China
BASIC/TRANSLATIONAL SCIENCE MO 1-10

72
Introduction: Permanent His bundle pacing (HBP) has been pioneered recently while concern of HBP safety remains. This study assessed safety and feasibility of permanent HBP in heart failure patients with atrioventricular node (AVN) ablation for atrial fibrillation.
Methods: Fifty-two connective heart failure patients who received HBP and AVN ablation attempts were enrolled. In each patient, acute HBP was attempted in the AV septum superior to tricuspid valve with a Select Site sheath (C304 or C315) and the Select Secure 3830 pac-ing lead. Once HBP was achieved, AVN ablation was conducted. Success of AVN ablation produced a complete atrioventricular block with-out an injury to the HBP site and its distal part. Then, permanent HBP was applied with backup right ventricular pacing or bi-ventricular pacing. Follow-up was conducted to assess BHP.
Results: Acute HBP was achieved in 50 of 52 enrolled patients (96%), of whom, 42 patients (84%) received permanent HBP while remain-ing 8 patients (16%) did not receive permanent HBP due to His bundle injury by successful AVN ablation (N=2), incomplete AVN ablation (N=2) and later resumption of AV conduction following successful AVN ablation (N=4). After permanent HBP in 42 patients with follow-up of a median 20 months, there was no lead dislodgement; implant-related hospitalization occurred in two patients (1 for device replace-ment and 1 for minor device pocket infection); HBP threshold was stable with the percent change of 6.2±53.1% (median: 0%) in HBP thresholds at the last follow-up over baseline HBP thresholds (1.4±0.9 volts); and the percentage of HBP remained at 99.2±1.3%. After permanent HBP, LVEF increased to 60.1±8.8% from the baseline 44.9±14.4% (P<0.001) and NYHA classification reduced to 1.4±0.5 from the baseline 2.8±0.6 (P<0.001). All 42 patients had at least one hospitalization for heart failure within one year prior to HBP while only 2 patients (4.8%) had heart failure-related hospitalization after HBP (P<0.001 vs. baseline).
Conclusions: Permanent HBP with backup right ventricular or bi-ventricular pacing is safe and stable with improved clinical outcomes in a population of heart failure patients who underwent AVN ablation for atrial fibrillation.
SAFETY AND STABILITY OF PERMANENT HIS BUNDLE PACINGWeijian Huang1, Lan Su1, Shengjie Wu1, Lei Xu1, Zhenyu Dai1, Xiaohong Zhou2, Xiaohong Zhou2, Shungang Yang3 1The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China; 2CRHF Division, Medtronic, plc, Mounds View, United States;
3Medtronic Shanghai Innovation Center, Shanghai, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES MO 1-11

MINI ORAL SESSION 02(14 October)

74
Introduction: In patients with persistent atrial fibrillation (AF), extensive biatrial ablation is known to have better outcomes than left atrial (LA) ablation. Altered interatrial connections after biatrial ablation may provide an arrhythmogenic substrate for biatrial macro-reentrant atrial tachycardia (MRAT).
Methods: Patients with biatrial MRAT underwent a repeat procedure for recurrent atrial tachyarrhythmias after persistent AF ablation. All patients underwent extensive ablation at the LA, including at the Bachmann’s bundle (BB).
Results: Two patients showed biatrial septal MRAT (tachycardia cycle length=270-330 ms); As shown in representative figure, the other 2 patients showed biatrial MRAT rotating along the right atrial free wall (tachycardia cycle length=410-470 ms). Electroanatomic mapping clarified the wavefront of biatrial MRAT propagating through the upper and lower interatrial connections. Ablation at the right atrial sep-tum around the upper interatrial groove successfully terminated the biatrial MRAT (repsentative Figure C).
Conclusions: Extensive biatrial ablation at BB resulted in altered interatrial conduction, providing a substrate for biatrial MRAT. Ablation of the right atrial upper septum near the interatrial groove effectively terminated the biatrial MRAT.
BIATRIAL MACRRENTRANT ATRIAL TACHYCARDIA AFTER ABLATION AT BACHMANN’S BUNDLE IN PATIENTS WITH ATRIAL FIBRILLATIONDae In Lee, Iqbal Mohammad, Kwang-No Lee, Seung Young Roh, Jinhee Ahn, Dong-Hyeok Kim, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE MO 2-01

75
Introduction: Recently, it was suggested that lowering the age threshold for stroke risk estimation help identify truly low stroke risk in Tai-wan atrial fibrillation (AF) patients. This study hypothesized that lowering the cutoff age in current risk stratification scores (CHA2DS2-VASc, CHADS2, and R2CHADS2) might provide better stroke prediction.
Methods: We included non-valvular AF patients not using oral anticoagulants (OACs) from 506,805 adults in prospective cohort data col-lected by the National Health Insurance Service in Korea. The younger age groups of the current risk scores were divided into 2 subgroups by a cutoff of 55 years. We assigned -1 point to the younger subgroup (<55 years of age) and did not change the points assigned to other groups. The modified risk scores were compared with each original score by calculating the c-statistics and net reclassification improve-ment (NRI).
Results: During 14,430 person-years of follow-up, we observed 188 ischemic strokes. Annualized stroke rate was 1.3%. C-statistics for the full point scores improved after modifying the age criteria in all the risk scores (CHA2DS2-VASc: from 0.74 to 0.75; CHADS2: from 0.74 to 0.76; R2CHADS2: from 0.74 to 0.75). In the primary prevention subset (3,286 patients with no history of prior stroke), there were similar improvements of c-statistics (CHA2DS2-VASc: from 0.68 to 0.70; CHADS2: from 0.67 to 0.70; R2CHADS2: from 0.67 to 0.70). The NRIs were positive comparing the modified score with each original score (CHA2DS2-VASc: 27.1%; CHADS2: 4.7%; R2CHADS2: 2.2%).
Conclusions: By using the lowered cutoff age (55 years of age), refining the age criteria of current risk scores provided improved stroke prediction in atrial fibrillation patients.
AGE CRITERIA MODIFICATION OF CURRENT RISK SCORES PREDICTING STROKE IN PATIENTS WITH ATRIAL FIBRILLATION: A NATIONWIDE COHORT STUDY IN KOREADaehoon Kim, Pil-Sung Yang, Tae-Hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY MO 2-02
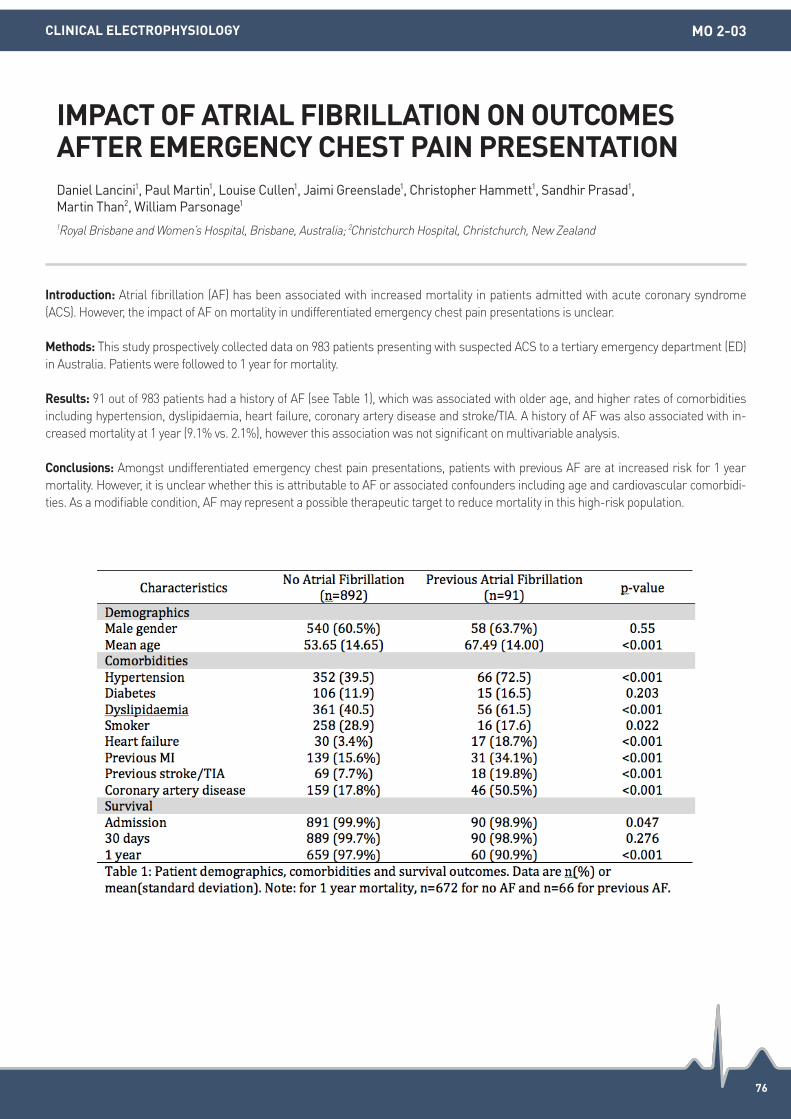
76
Introduction: Atrial fibrillation (AF) has been associated with increased mortality in patients admitted with acute coronary syndrome (ACS). However, the impact of AF on mortality in undifferentiated emergency chest pain presentations is unclear.
Methods: This study prospectively collected data on 983 patients presenting with suspected ACS to a tertiary emergency department (ED) in Australia. Patients were followed to 1 year for mortality.
Results: 91 out of 983 patients had a history of AF (see Table 1), which was associated with older age, and higher rates of comorbidities including hypertension, dyslipidaemia, heart failure, coronary artery disease and stroke/TIA. A history of AF was also associated with in-creased mortality at 1 year (9.1% vs. 2.1%), however this association was not significant on multivariable analysis.
Conclusions: Amongst undifferentiated emergency chest pain presentations, patients with previous AF are at increased risk for 1 year mortality. However, it is unclear whether this is attributable to AF or associated confounders including age and cardiovascular comorbidi-ties. As a modifiable condition, AF may represent a possible therapeutic target to reduce mortality in this high-risk population.
IMPACT OF ATRIAL FIBRILLATION ON OUTCOMES AFTER EMERGENCY CHEST PAIN PRESENTATIONDaniel Lancini1, Paul Martin1, Louise Cullen1, Jaimi Greenslade1, Christopher Hammett1, Sandhir Prasad1, Martin Than2, William Parsonage1 1Royal Brisbane and Women’s Hospital, Brisbane, Australia; 2Christchurch Hospital, Christchurch, New Zealand
CLINICAL ELECTROPHYSIOLOGY MO 2-03

77
Introduction: This observational study aims to describe the clinical manifestation, diagnostic criterion and management of a cohort of pa-tients with frequent accelerated ventricular rhythm (FAVR) and to investigate the underlying electrophysiological mechanism of FAVR as well as its impact on the prognosis.
Methods: 20 patients (15 males) suspected with FAVR were consecutively enrolled in our study. ECG, 24-hour Holter monitoring and transthoracic echocardiogram were performed during hospitalization. Drug sensitivity test, treadmill test, electrophysiological study and catheter ablation would be applied after informed consent obtained. The patients were followed 5 months to 12 years after discharge.
Results: The average age of the patients was 31.8±14.7 years. None of them were accompanied with structural heart disease except that two of them were diagnosed with dilated cardiomyopathy and mirror-image dextrocardia, respectively. FAVR was exhibited on the surface ECG and 24-hour Holter at admission. There was significant differences between FAVR arising from working ventricular myocytes and His-Purkinje system in terms of QRS complex duration (175±17.7 ms vs. 118.2±11.6 ms, P<0.001). There were significant negative cor-relations between left ventricular ejection fraction (LVEF) and FAVR burden (2-tailed, R2=0.66, P<0.01), as well as LVEF and average heart rate (2-tailed, R2=0.45, P<0.05). FAVR would be easily accelerated during isoproterenol intravenous administration and treadmill test. But when the heart rate climbed over 130 bpm, sinus rhythm would be dominant on the surface ECG. A centrifugal pattern was exhibited during electrophysiological study. Sensitive drugs were diverse from each other, whereas metoprolol could be chosen if the drug sensitivi-ty test was not accepted by the patients because most of FAVRs were sensitive to it (87.5%, 7/8). During follow-up period, two of them de-ceased (case 3, case 9). Most of the patients with impaired LVEF got complete recovery (5/6). Nevertheless, one of them only got partial recovery. The rest had no discomfort complaints and got FAVR burden reduced.
Conclusions: Palpitation and symptoms associated with heart failure are considered to be the major discomforts for patients with FAVR. Although most of them are free of structural heart disease, but the FAVR itself has the possibility to impact LVEF. FAVR could be well con-trolled by catheter ablation and sensitive drug administration. Catheter ablation should be considered as first-line therapy for patients with high risks. Enhancement of focal automaticity and imbalance of autonomic nervous system are suspected to be the electrophysio-logical mechanisms of FAVR.
FREQUENT ACCELERATED VENTRICULAR RHYTHMHailei Liu, Minglong Chen
The First Affliated Hospital of Nanjing Medical University, Nanjing, China
CLINICAL ELECTROPHYSIOLOGY MO 2-04

78
Introduction: Sudden cardiac death (SCD) among military recruits is rare but devastating. The underlying causes of SCD in young soldiers have not been studied in Korea.
Methods: We reviewed 21 patients (mean age of 21 years, 20 males) who were referred for the evaluation and management of aborted SCD or syncope due to life threatening ventricular tachycardia (VT) from 2012 to 2015.
Results: The underlying heart diseases and treatment modalities were summarized in Figure. Ventricular fibrillation (VF) was document-ed on automated external defibrillator (AED) in 16 patients. Among them, 13 patients received implantable cardioverter-defibrillator (ICD). Two patients with Wolff-Parkinson-White syndrome underwent radiofrequency catheter ablation for accessary pathway. One with coro-nary artery spasm was treated with medications. Four patients with long QT syndrome and syncope due to nonsustained fast polymorphic VT were found to have genetic mutation (KCNH2) and managed with beta blocker. In one soldier with asymptomatic Brugada syndrome, ICD was implanted for primary prevention because he was a sibling of the soldier proband, and also had SCN5A mutation with easily in-ducible fast polymorphic VT degenerating to VF during electrophysiology study.
Conclusions: Most life threatening ventricular tachyarrhythmias were caused by electrical heart diseases. Channelopathies accouted for nearly half of them. Therefore, an initial approach in this population should be focused on evaluation for the electrical heart disease. Above all, basic life support training and AED disposition should be emphasized for the successful resuscitation of SCD in young healthy sol-diers.
ABORTED SUDDEN CARDIAC DEATH OR SYNCOPE DUE TO LIFE THREATENING VENTRICULAR TACHYARRHYTHMIA IN YOUNG KOREAN SOLDIERSHee Sun Mun1, Jung Myung Lee2, Kyung Ho Kim1, Jinyoung Park1, Sung Soon Kim1 1Korean Armed Forces Capital Hospital, Seongnam, Republic of Korea; 2Kyung Hee University, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY MO 2-05

79
Introduction: The sympathetic nervous system has long been associated with the genesis and maintenance of many life threatening ven-tricular arrhythmias. The standard of care in patients with ventricular tachycardia storm representing a clinical situation of acute electri-cal stability has long been antiarrhythmic therapies and catheter ablation. In this case series we have presented five patients who under-went cardiac sympathetic denervation as a last resort to treat their recurring ventricular arrhythmias.
Methods: All patients (Table) presented with several episodes of ventricular tachycardia (VT) refractory to medical therapy. All the patients (except case 4 which was not performed due to proximity of foci to the coronary artery) underwent endocardial and/or epicardial radiofre-quency catheter ablation procedure which failed to prevent recurrences. As a next step, video assisted thoracoscopic sympathectomy pro-cedure was performed under general anesthesia from the lower half of stellate ganglion to T4.
Results: During the follow-up all patients were free of VT episodes. Patient 1 received a heart transplant after one year. Patient 3 who had the sympathectomy procedure after surgical replacement of mitral valve did not experience further VT episodes but died of sepsis in the hospital after 2 months. Patient 4 did not have further VTs but was found to have similar premature ventricular contractions with up to 40% burden. Two of our patients underwent bilateral cardiac sympathetic denervation (case 5 had prior left sympathectomy), however the other patients were not amenable for bilateral denervation. Though it is still a debate to remove unilateral or bilateral portion of the sym-pathetic chain (lower half of stellate ganglion and T2-T4), bilateral CSD is the preferred procedure in our center whenever possible from surgical standpoint.
Conclusions: The presented case series, despite disparate causes responded to cardiac sympathetic denervation in all of the patients without any further clinical VTs. Cardiac sympathectomy is an emerging effective alternative therapy for those patients who deemed unre-sponsive to standard treatment with medical therapy and catheter ablation.
CARDIAC SYMPATHETIC DENERVATION AFTER FAILED RADIOFREQUENCY ABLATIONIlknur Can1, Jian Ming Li2, Rosemary F Kelly3, Venkatakrishna Tholakanahalli2 1Necmettin Erbakan University, Konya, Turkey; 2University of Minnesota VA Medical Center Cardiology, Minneapolis, United States; 3University of Minnesota VA Medical Center Cardiothoracic Surgery, Minneapolis, United States
ALLIED PROFESSIONALS MO 2-06
Patient Age-sex Heart disease EF (%) ICD VT ablation Sympathectomy Follow-up (months) Recurrence
1 64 M NICM 20 + Endo Bilateral 12 None
2 66 M ICM 45 + Endo+Epi Left 24 None
3 73 M MVR 40 - Endo Left 2 Died (sepsis)
4 42 M Idiopathic 55 - - Bilateral 24 No VT, but PVCs
5 61 M NICM 40 + Endo+Epi Right 1 None

80
Introduction: It is sometimes difficult to complete the block line at mitral isthmus because of instability of ablation catheter.
Methods: N/A.
Results: The 1st case is 70-year-old man with atrial tachycardia (AT). He developed AT during a follow-up period after pulmonary vein iso-lation (PVI). Although mitral flutter was induced in the 2nd session, but a complete block line could not be achieved. In the 3rd session, af-ter ablation with cryoballoon to Left pulmonary vein, mitral flutter (MF) was induced. MF was terminated by 6th cryoenergy delivery with Freezer max (FM) to mitral isthmus (Figure). The 2nd case is a 39-year-old male with Atrial fibrillation (AF) and AT. After PVI with cryobal-loon, MF was induced. MF was terminated by 3rd cryoenergy delivery with FM. The 3rd case is a 73-year-old male with AF. During PVI with cryoballoon, AF appeared spontaneously and changed to MF. After PVI was completed with cryoballoon, MF was terminated by 2nd cryoenergy delivery with FM to mitral isthmus. A total of 9, 4, 8 times of cryoenergy per each patient was delivered and a bidirectional block was completed in all patients. During the mean follow-up of 223 days, no AF or AT did not recur in all patients.
Conclusions: Freezer Max can be a powerful tool to complete a block line at mitral isthmus due to its property of freezing and sticking onto atrial muscle.
THE EFFICACY OF FREEZER MAX TO MITRAL ISTHMUS ABLATION: THREE CASE REPORTSKenji Kuroki, Akihiko Nogami, Tomoaki Hasegawa, Fumi Yamagami, Yasutoshi Shinoda, Satoshi Aita, Eiko Sai, Ai Hattori, Toru Adachi, Yuki Komatsu, Keita Masuda, Takeshi Machino, Hiro Yamasaki, Yukio Sekiguchi, Nobuyuki Murakoshi, Keisuke Kuga, Kazutaka Aonuma
University of Tsukuba, Tsukuba, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE MO 2-07

81
Introduction: Over the past 15 years (2002-2016), 750,960 people participated in the Hong Kong Standard Chartered Marathon, which is one of the largest marathon event in Asian Pacific Region. We aim to study the prevalence of non-fatal myocardial injury among the mara-thon runners.
Methods: All the Standard Chartered Marathon related hospital admissions over the past 15 years (2002-2016) were retrieved from Acci-dent and Emergency Department admission record. We reviewed the prevalence, epidemiological profile and clinical outcome of mara-thon runners admitted for non-fatal myocardial injury.
Results: The past 15 years, among the 750,960 marathon participants, there were 33 runners admitted for non-fatal myocardial injury (Mean age 41.8±12 years old. 28 Males. Eleven 10 km runners, 12 half-marathon runners and 8 full marathon runner. Race distance was unknown in 2 runners). Among the 33 runners, only 5 (15.2%) complained of chest pain. Twenty-one (63.6%) developed syncope. ST-seg-ment changes greater than 1 mm were observed in 12 (36%) patients. One patient had Wolff-Parkinson-White Syndrome and received successful radiofrequency ablation of accessory pathway. One patient developed atrial fibrillation. The mean left ventricular ejection frac-tion was 58±4%. Four patients underwent exercise treadmill tests, which were all negative for ischemia. Coronary angiograms were per-formed in 8 (24%) patients, revealing mild coronary artery disease, single vessel disease and triple vessels disease in 3, 1 and 4 patients respectively. Computed tomography coronary angiogram done in 2 (6%) patients revealed normal coronary arteries. Angiogram was not performed in 70% of patients because of low pre-test likelihood of coronary artery disease. Percutaneous coronary angioplasty and coro-nary artery bypass surgery were performed in 3 and 2 patients respectively.
Conclusions: The prevalence of non-fatal myocardial injury among Standard Chartered Marathon runners was 4.4 per 100,000 (33 pa-tients) over past 15 years. Syncope and chest pain occurred in 63.6% and 15.2% of patients respectively. Significant ST segment changes occurred in only 1/3 of patients. Coronary artery intervention was required only in a minority of patients.
NON-FATAL MYOCARDIAL INJURIES AMONG MARATHON RUNNERS-A 15-YEARS EXPERIENCE OF HONG KONG STANDARD CHARTERED MARATHONKit Chan1, Kuang An Wan1, Sai Chau Leung1, Ngai Shing Mok2, Natalie Leung3, Jessica, Wai Ling Poon1, Yuk Kong Lau1 1Ruttonjee and Tang Shiu Kin Hospitals, Wan Chai, Hong Kong; 2Princess Margaret Hospital, Lai Chi Kok, Hong Kong; 3Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong
CLINICAL ELECTROPHYSIOLOGY MO 2-08

82
Introduction: Usual causes of left ventricular tachycardia include coronary artery disease, cardiac sarcoidosis, left ventricular tumor, cha-gas disease and idiopathic left ventricular tachycardia.
Methods: N/A.
Results: A 40 years male patient presented with incessant left ventricular tachycardia which was controlled with combination of antiar-rhythmic therapy. Contrast enhanced cardiac MRI showed abnormal sub-endocardial and mural late gadolinium enhancement within apical inferior and apical septal wall of left ventricle. CECT chest, cardiac PET-CT and coronary angiography were normal. Mantoux test was positive and The QuantiFERON-TB Gold test (QFT-G) was within normal range. Endomyocardial biopsy showed myocyte loss and fatty replacement. A diagnosis of left dominant arrhythmogenic cardiomyopathy (LDAC) was made. Genetic analysis using Next Generation se-quencing technique and targeting genes associated with arrhythmogenic cardiomyopathy showed that individual harboured a variation (p.Thr277Ser) caused by a substitution (c.829A>T) in exon 10 of the TMEM43 gene. His mother did not have this variation by mutation analysis study and father was not available for gene testing. Although concurrent left ventricular involvement along with right ventricle oc-curs in 75% cases of advanced arrhythmogenic right cardiomyopathy (ARVC), isolated LV involvement is rare. In a study of 200 patients 5% patients had isolated left ventricular involvement. About 75% of LDAC present with ventricular arrhythmia from left ventricle. TMEM43 is a highly conserved inner nuclear membrane (INM) protein. Mutation of TMEM43 may cause arrhythmogenic cardiomyopathy by altering the structure and function of desmosomal proteins. Significance of p.Thr277Ser substitution is unclear. Till date this variation is considered as variant of unknown significance (VUS).
Conclusions: we report a case of incessant left ventricular tachycardia due to unusual form of arrhythmogenic cardiomyopathy (LDAC) associated with variation in TMEM43 gene.
INCESSANT LEFT VENTRICULAR TACHYCARDIA OF UNUSUAL ETIOLOGY Praloy Chakraborty1, H S Isser1, Sudheer Arava2, Kausik Mandal3 1VMMC and Safdarjung Hospital, Delhi, India; 2All India Institute of Medical Science, Delhi, India; 3Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE MO 2-09

83
Introduction: Electrical storm is a life-threatening medical emergency and a challenging problem for physician. Refractory electrical storm could happen even through high arrhythmic medical control and deep sedation and mechanical support. We introduce a case about catheter ablation of ventricular premature contraction triggered ventricular fibrillation under extracorporeal membrane oxygen-ation and intra-aortic balloon pumping support.
Methods: Catheter ablation was performed under ensite 3D mapping system under ECMO and IABP and ventilator support. Clinical VPC showed left axis deviation and right bundle branch block, which was suspected left ventricular origin. One 4 Fr. decapolar catheter were introduced percutaneously into the right femoral vein, which was positioned in the right atrium with cross tricuspid valve, and the tip was in the apex of right ventricle. Geometry creation and voltage mapping (setting 0.2-0.8 mV) were performed with the 7 Fr. quadripolar irri-gation ablation catheter. Posterior view of voltage map presented left posterior fasicular site at border zone. Right anterior oblique view of voltage map presented large scar area at inferior and anteroseptal site. The ablation catheter detect the Purkinje-like potential at border zone. During ablation over left posterior fascicular site, VF and short-run ventricular tachycardia were induced. The morphology of VT was similar to clinical VPC. Pacing mapping also showed 12/12 matching. Raiofrequency energy 50 Watts (at target of 48 Celcius) for 30 secs at each points was appiled from inferior posterioseptal (fascicular site) to anterioseptal border zone region. Substrate modification of the border zone was performed ablation till no Purkinje potentials with voltage less than 0.1 mV. No more VT/VF could be induced till triple extrastimuli pacing (right ventricular pacing: 400/280/270/260 ms) under control. A total ablation area was 6.1 cm2.
Results: ICD record did not detect any episode of ventricular arrhythmia at three-month follow-up period.
Conclusions: Catheter ablation is an efficacy method to deal with electrical storm even if ECMO and IABP use.
CATHETER ABLATION FOR A VENTRICULAR PREMATURE CONTRACTION TRIGGER REFRACTORY ELECTRICAL STORM AND VENTRICULAR FIBRILLATIONWeichieh Lee, Huang-Chung Chen, Yung-Lung Chen, Mien-Cheng Chen
Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE MO 2-10

84
Introduction: Risks with exposure to radiation especially in young patients undergoing electrophysiology procedures and medical staff en-gaged in are a serious concern. We studied whether the use of a novel fluoroscopy image integrated 3-dimensional electroanatomical mapping system (CARTO3 with UNIVU module) could reduce radiation exposure during ablation for various pediatric arrhythmias.
Methods: This study was a retrospective, single-centere study. The primary endpoints of this study was the change of fluoroscopy time and fluoroscopy dose using flouroscopy integreted 3D mapping (UNIVU) compared with the conventional 3D mapping system (CARTO3). Eligible subjects were consecutive patients <20 years of age who performed radiofrequency catheter ablation for various arrhythmias us-ing CARTO3 system. In the first 4 months before UNIVU became available in our hospital on October 2015, the control group used conven-tional CARTO3 system was enrolled. In the following 4 months UNIVU group was enrolled. Results of categorical variables are expressed as number and percentage of patients. Statistical analyses of categorical variables were done using Pearson’s chi-square test. Continu-ous variables are expressed as median and IQR. Statistical analyses were done using Wilcoxon signed-rank test. Significance level was set at P<0.05.
Results: In this retrospective study, in total 46 consecutive patients were included (UNIVU group: N=18, CARTO3 group: N=28). The age, body weight and the incidence of patients with congenital heart disease did not differ between the two groups: 10.1 (7.2-14.0) years vs. 11.1 (7.28-14.6) years (P=0.761); 31.3 (20.5-43.1) kg vs. 35.6 (19.8-28.8) kg (P=0.919); 4 (22.2%) vs. 7.1% (P=0.138). The target arrhythmias of the two groups were: WPW syndrome (11 vs. 17), ventricular arrhythmias originated from outflow (2 vs. 6), others (5 vs. 5). The incidence of procedures using retrograde approach and using trans-septal puncture were not differ between the two groups: 1(8.7%) vs. 3 (10.7%) (P=0.545); 5 (27.8%) vs. 8 (28.6%) (P=0.954). Four different operators performed ablation procedures. The median years of experience of operators was shorter in UNIVU group than CARTO3 group: 0.67 (0.58-0.57) years vs. 12.2 (4.17-12.3) years. In total, the UNIVU allowed a reduction in fluoroscopy time: 2.6 (0.38-5.22) minutes vs. 18.4 (14.7-27.8) minutes (P<0.001), and fluoroscopy dose (Air Kirm): 17.5 (6.00-35.8) mGy vs. 78.5 (33.5-307) mGy (P<0.001). The number of ablation points, procedure time, acute success rate and incidence of adverse events did not differ.
Conclusions: The image integrated 3-dimensional electroanatomical mapping system contributed to significant reduction of radiation ex-posure to pediatric patients and staff during electrophysiological procedures.
FLUOROSCOPY IMAGE INTEGRATED 3D MAPPING SYSTEM REDUCES RADIATION EXPOSURE DURING ABLATION FOR PEDIATRIC CARDIAC ARRHYTHMIASYoko Yoshida1, Shigeo Watanabe1, Shuichiro Yoshida1, Tsugutoshi Suauki1, Yoshihide Nakamura2 1Osaka City General Hospital, Osaka, Japan; 2Kinki University, Osaka, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE MO 2-11
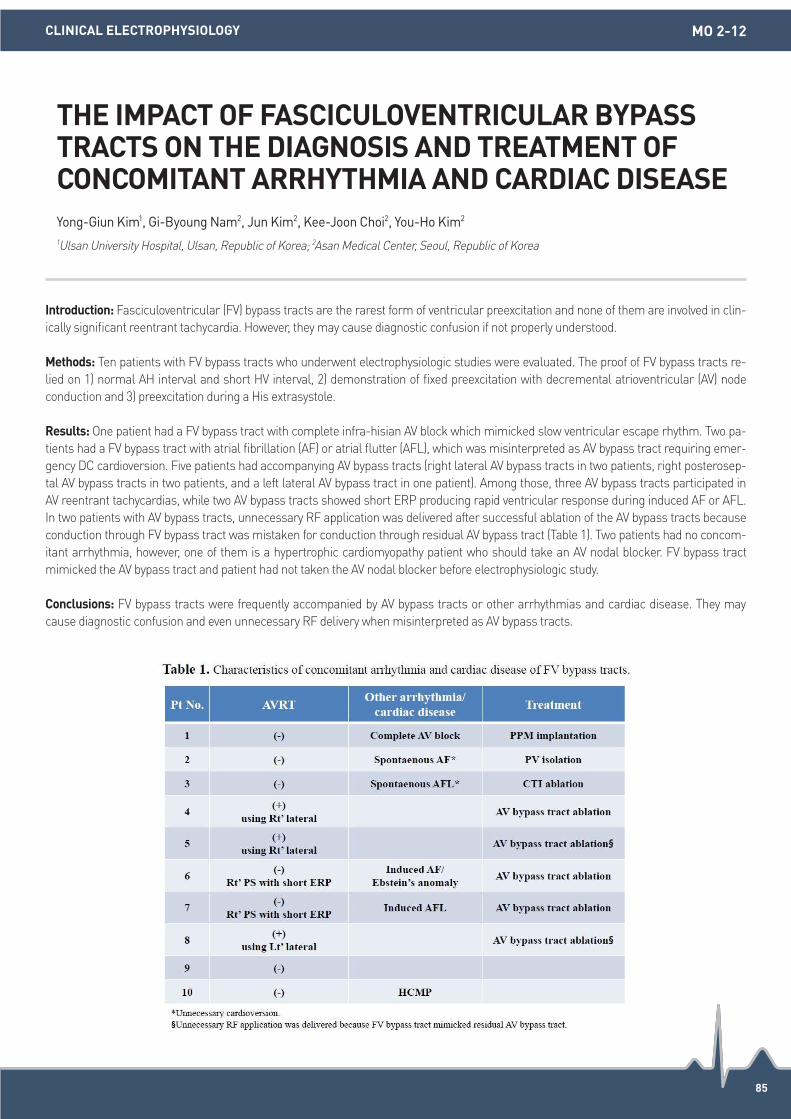
85
Introduction: Fasciculoventricular (FV) bypass tracts are the rarest form of ventricular preexcitation and none of them are involved in clin-ically significant reentrant tachycardia. However, they may cause diagnostic confusion if not properly understood.
Methods: Ten patients with FV bypass tracts who underwent electrophysiologic studies were evaluated. The proof of FV bypass tracts re-lied on 1) normal AH interval and short HV interval, 2) demonstration of fixed preexcitation with decremental atrioventricular (AV) node conduction and 3) preexcitation during a His extrasystole.
Results: One patient had a FV bypass tract with complete infra-hisian AV block which mimicked slow ventricular escape rhythm. Two pa-tients had a FV bypass tract with atrial fibrillation (AF) or atrial flutter (AFL), which was misinterpreted as AV bypass tract requiring emer-gency DC cardioversion. Five patients had accompanying AV bypass tracts (right lateral AV bypass tracts in two patients, right posterosep-tal AV bypass tracts in two patients, and a left lateral AV bypass tract in one patient). Among those, three AV bypass tracts participated in AV reentrant tachycardias, while two AV bypass tracts showed short ERP producing rapid ventricular response during induced AF or AFL. In two patients with AV bypass tracts, unnecessary RF application was delivered after successful ablation of the AV bypass tracts because conduction through FV bypass tract was mistaken for conduction through residual AV bypass tract (Table 1). Two patients had no concom-itant arrhythmia, however, one of them is a hypertrophic cardiomyopathy patient who should take an AV nodal blocker. FV bypass tract mimicked the AV bypass tract and patient had not taken the AV nodal blocker before electrophysiologic study.
Conclusions: FV bypass tracts were frequently accompanied by AV bypass tracts or other arrhythmias and cardiac disease. They may cause diagnostic confusion and even unnecessary RF delivery when misinterpreted as AV bypass tracts.
THE IMPACT OF FASCICULOVENTRICULAR BYPASS TRACTS ON THE DIAGNOSIS AND TREATMENT OF CONCOMITANT ARRHYTHMIA AND CARDIAC DISEASEYong-Giun Kim1, Gi-Byoung Nam2, Jun Kim2, Kee-Joon Choi2, You-Ho Kim2 1Ulsan University Hospital, Ulsan, Republic of Korea; 2Asan Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY MO 2-12

MINI ORAL SESSION 03(15 October)

87
Introduction: Some posteroseptal accessory pathways have an epicardial course within the middle cardiac vein (MCV) and require abla-tion within the MCV. Failure to recognize this is one of the causes of unsuccessful ablation. The electrocardiographic, electrophysiologic features of manifest posteroseptal pathways requiring ablation within middle cardiac vein (MCV) have not been well described.
Methods: All patients who underwent ablation of manifest posteroseptal accessory pathway from 2008 to May 2016 were included in the study. All patients underwent coronary sinus venogram during the study. Patients who had coronary sinus diverticulum on venogram were excluded from the analysis and the rest were classified as Group I (pathway ablated within the MCV), and group II (pathway ablated in the posteroseptal region). The clinical, electrocardiographic, and electrophysiological, features were analysed retrospectively.
Results: There were 168 patients with mean age of 38±13 years (12-68 years), of whom 98 were males and 70 females. Twenty eight pa-tients had coronary sinus diverticulum and were excluded from the study. Of the remaining 140, there were 26 (18.6%) patients in Group I (MCV) and 114 (81.4%) Group II. The ECG feature suggestive of Group I were, QS in lead III with notching of the descending limb of S wave (sensitivity 74%, specificity 90%), positive delta wave in lead aVR (sensitivity 73%, specificity 90%), negative delta wave in lead II (sensitivity 72%, specificity 89%), deep S in V6 (sensitivity 63%, specificity 88%). The local VA time on IEGM was longer in Group I compared to Group II (90±20 ms vs. 74±15 ms [P=0.001]). A discrete potential was seen near the ostium of MCV at the site of successful ablation.
Conclusions: The posteroseptal accessory pathways requiring ablation inside the MCV specific features. They are a) QS in lead III with notching of descending limb of S wave, b) negative delta in lead II, c) positive delta wave in lead aVR, and d) a deep S wave in lead V6. The presence of these findings are useful for anticipating and planning the ablation strategy.
ELECTROCARDIOGRAPHIC ELECTROPHYSIOLOGICAL FEATURES OF EPICARDIAL ACCESSORY PATHWAYS ABLATED WITHIN THE MIDDLE CARDIAC VEINBalasubramanian Vidhyakar, Pillai Vivek, Sivasankara Chikalli, Shenthar Jayaprakash
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, India
CATHETER ABLATION MO 3-01

88
Introduction: AF can be initiated by triggers near pulmonary veins (PV), yet it is unproven if AF can actually be sustained by focal atrial tachycardias (sources) in the atria. We hypothesized that panoramic mapping may reveal organized AF sources which meet classical mechanistic criteria for organized tachycardia.
Methods: We performed basket mapping of AF ablation at 3 centers. We selected cases in whom AF terminated abruptly by ablation at localized sources, defined as centrifugal activation from an origin during AF, with electrograms on global atrial mapping spanned <50% of AF cycle length.
Results: Sixteen patients (age 64.6±8.4 years, LA vol. index 2.1±0.1 mL/m2, LVEF 55.3±6.3%) met a priori criteria for focal AF sources. Figure A shows AF in a 56 year old woman, in whom 4 sequential maps (B) showed repetitive anisotropic centrifugal activation from an origin, (C) with electrograms spanning <50% AF CL (blue arrow). This AF-driving focal tachycardia lay within a 2-3 cm2 area. Targeted ab-lation terminated AF to sinus rhythm. Neither AF nor AT were inducible afterwards. In both the left and right atria 75% of Focal drivers lay in the atria and away from the PVs.
Conclusions: This study demonstrates that focal atrial tachycardias away from the PVs may sustain human persistent AF, meeting classi-cal mechanistic criteria for focal sources and producing fibrillatory conduction, where targeted ablation eliminated AF. Future studies should determine how focal sources relate to rotational circuits and their relationship to AF triggers.
MECHANISTIC PROOF THAT HUMAN AF CAN BE DRIVEN BY ATRIAL TACHYCARDIAS OUTSIDE THE PULMONARY VEINSChristopher Kowalewski1, Junaid A. B. Zaman1, Ryan T. Borne2, Tina Baykaner1, Shirley Park1, Mohan Viswanathan1, Paul J. Wang1, David Krummen3, William H. Sauer2, Sanjiv M. Narayan1 1Stanford University, Palo Alto, United States; 2UC Denver, Aurora, United States; 3VA Medical Center, San Diego, United States
CATHETER ABLATION MO 3-02

89
Introduction: Right ventricular (RV) synchronized left ventricular (LV) pacing has been shown to reduce QRSd and enhance some of the effects of cardiac resynchronisation therapy (CRT). Additionally an R wave in V1 on the surface ECG is useful for guiding programming and predicting response to CRT. Utilizing a device based Negative Hysteresis (NH) algorithm, this study compared the ECG effects of increas-ing NH delays with increasing LV pre-excitation in chronically implanted CRT patients.
Methods: Consecutive patients implanted with a SJM quadripolar lead and SJM device were screened. Those patients with PR interval <350 ms were enrolled. All RV leads were midseptal with a Q-RV duration <15 ms (mean 7.4±6 ms), the LV lead had a mean Q-LV duration of 134 ±21 ms and QLV% of 87%±7. 12 lead ECGs were performed in intrinsic rhythm and in best biventricular pacing mode (BiV). NH was per-formed with NH delays from -10 to -80 ms, and with both simultaneous RV and LV activation (Sim) and with LV 40 ms ahead of RV (LV+40 ms). The QRSd was recorded. The relative contribution of R wave vector in V1 was measured as % of total QRS vector in V1.
Results: 17 patients were evaluated, the mean QRSd was reduced with the best NH mode (130.7±17 ms) compared to the best BiV mode (150±15 ms). A NH between -10 and -50ms resulted in the lowest QRSd in 90% of patients. The QRSd did not change significantly be-tween Sim (130.7±17 ms) and LV+40 (133.4±18 ms). Relative contribution of R wave vector in V1 was significantly greater in LV+40 (34±21%) compared to Sim mode (15±11%).
Conclusions: The NH algorithm can reduce QRSd compared with best BiV settings. Manipulation of LV pre-excitation can increase the R wave in V1 suggesting increased LV contribution to the ECG without prolonging QRSd.
OPTIMIZING CRT WITH NEGATIVE HYSTERESIS AND LV PRE-EXCITATIONDavid O’Donnell1,2, Taylah Smart2, Juliette Young1, Ryan Spencer1, Hui Chen Han1, Lisa Odgers3, Tina Lin1,2 1Austin Hospital, Melbourne, Australia; 2Genesis Care, Melbourne, Australia; 3St. Jude Medical, Melbourne, Australia
HEART FAILURE MO 3-03

90
Introduction: It remains unclear whether the upgrade cardiac resynchronization therapy (CRT) would show better outcomes than the de-novo CRT. We compared the efficacy of CRT between the de-novo and upgrade groups, especially focused on the effect of upgrade CRT in patients with pacing-induced cardiomyopathy (PiCM).
Methods: The PiCM was defined by the new-onset dilated cardiomyopathy following pacemaker implantation in patients with baseline normal ejection fraction (>50%). Electrico-mechanical reverse remodeling and clinical outcomes were compared among the de-novo (n=62), PiCM upgrade (n=7), and non-PiCM upgrade (n=8) CRT groups.
Results: The PiCM upgrade group showed a significantly greater electrico-mechanical reverse remodeling compared to the de-novo CRT or non-PiCM upgrade groups at 6-month follow-up. The rate of super-responder was significantly higher in the PiCM upgrade than the other CRT groups. The group factor of the PiCM upgrade was identified as an independent predictor of super-responder in multivariate analysis (odds ratio, 13.03; 95% CI, 1.32-129.1; P=0.03). During the median follow-up of 15.8 months, the PiCM upgrade group showed the lowest rate in composite clinical outcome including cardiac death, heart transplantation, and heart failure-related rehospitalization (P=0.17).
Conclusions: The upgrade CRT for PiCM patients showed a better performance in terms of electrico-mechanical reverse remodeling and composite clinical outcomes, compared to de-novo implantation or upgrade for non-PiCM patients.
COMPARISON OF DE-NOVO vs. UPGRADE CARDIAC RESYNCHRONIZATION THERAPY; FOCUSED ON THE UPGRADE FOR PACING-INDUCED CARDIOMYOPATHYHye Bin Gwag, Jin Kyoung Hwang, Kyoung-Min Park, Young Keun On, June Soo Kim, Seung-Jung Park
Samsung Medical Center, Seoul, Republic of Korea
HEART FAILURE MO 3-04

91
Introduction: Radiofrequency catheter ablation (RFA) for Wolff-Parkinson-White (WPW) Syndrome is successful in the majority of pa-tients. However, failure does occur in a small percentage of this population. This study aims to describe the WPW patients who underwent RFA and to report factors associated with acute failure of the procedure.
Methods: This is a retrospective study of all cases of WPW patients, including those with concealed pathways and pre-excited, who under-went RFA from June 2008 until April 2016.
Results: A total of five hundred WPW patients underwent RFA during the specified time period. Seventy-two percent (72%, n=360) of the patients were males, and eighty percent (80%, n=402) were Chinese. Patients’ ages ranged from 9 years to 80 years, with the mean age of 35±10 years. Of the 500 cases reported, 25 patients (5%) had failure of initial RFA. Eighty percent (80%, n=20) of these failed cases were males. Seventy six percent (76%, n=19) were Chinese. The age of these patients ranged from 11-80 years. Among those with failed RFAs, 64% (n=16) had right-sided pathways and 36% (N=9) had left sided pathways. For those with right-sided pathways, five were found in the posteroseptal region, four in the parahisian region, and six in the right free wall. One patient had multiple right-sided accessory pathways. For those with left-sided pathways, two were in the left posteroseptal region and seven were in the left free wall site. Associated congeni-tal heart disease, due to Ebstein anomaly, was seen in two patients with failed initial RFA.
Conclusions: Among patients with failed RFA, it was found that the majority of the patients were males. The most common site for failure are right-sided pathways, mostly in the right free wall. Presence of congenital and structural abnormalities, such as Ebstein anomaly, also contributed to failure of initial RFA in two subjects.
FAILURES IN RADIOFREQUENCY CATHETER ABLATION OF PATIENTS WITH WOLFF-PARKINSON-WHITE SYNDROME: AN 8-YEAR RETROSPECTIVE STUDY OF FACTORS RELATED TO FAILURE OF INITIAL RFAMaria Blanca De Guzman, Htoo Lwin Kaung, Paul Lin, Daniel Chong, Boon Yew Tan, Kah Leng Ho, Chi Keong Ching, Wee Siong Teo
National Heart Centre Singapore, Singapore
CATHETER ABLATION MO 3-05
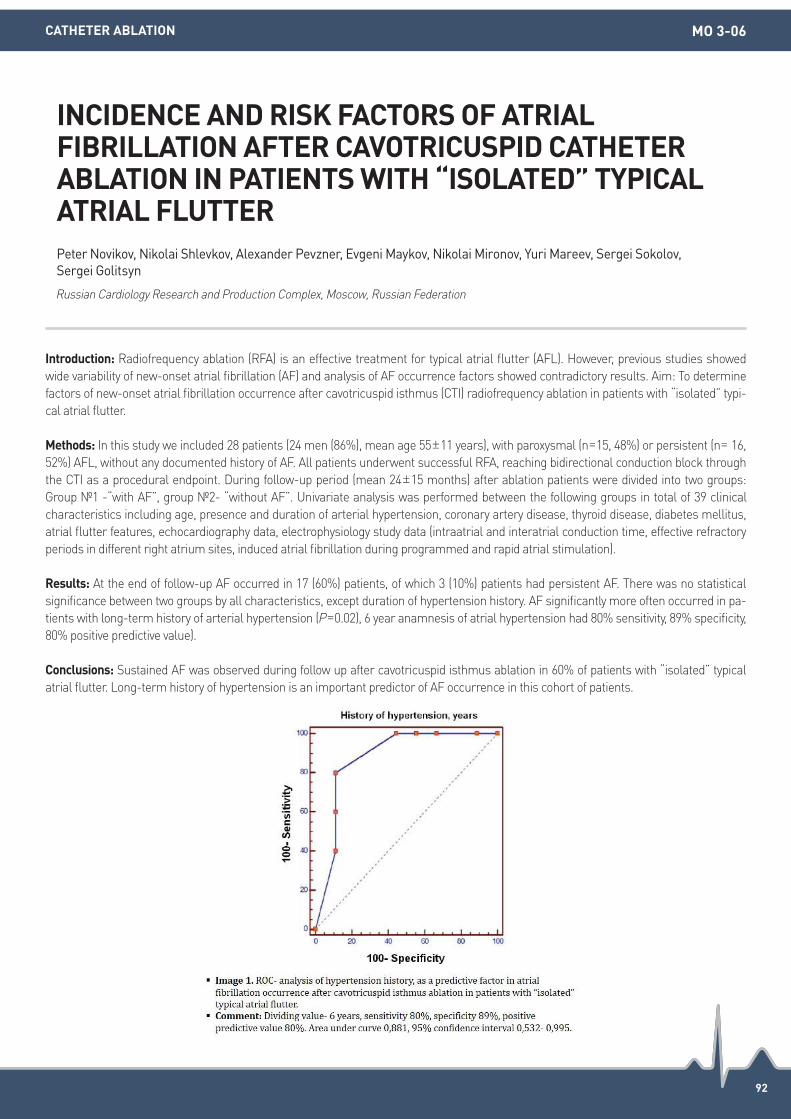
92
Introduction: Radiofrequency ablation (RFA) is an effective treatment for typical atrial flutter (AFL). However, previous studies showed wide variability of new-onset atrial fibrillation (AF) and analysis of AF occurrence factors showed contradictory results. Aim: To determine factors of new-onset atrial fibrillation occurrence after cavotricuspid isthmus (CTI) radiofrequency ablation in patients with “isolated” typi-cal atrial flutter.
Methods: In this study we included 28 patients (24 men (86%), mean age 55±11 years), with paroxysmal (n=15, 48%) or persistent (n= 16, 52%) AFL, without any documented history of AF. All patients underwent successful RFA, reaching bidirectional conduction block through the CTI as a procedural endpoint. During follow-up period (mean 24±15 months) after ablation patients were divided into two groups: Group 1 -“with AF”, group 2- “without AF”. Univariate analysis was performed between the following groups in total of 39 clinical characteristics including age, presence and duration of arterial hypertension, coronary artery disease, thyroid disease, diabetes mellitus, atrial flutter features, echocardiography data, electrophysiology study data (intraatrial and interatrial conduction time, effective refractory periods in different right atrium sites, induced atrial fibrillation during programmed and rapid atrial stimulation).
Results: At the end of follow-up AF occurred in 17 (60%) patients, of which 3 (10%) patients had persistent AF. There was no statistical significance between two groups by all characteristics, except duration of hypertension history. AF significantly more often occurred in pa-tients with long-term history of arterial hypertension (P=0.02), 6 year anamnesis of atrial hypertension had 80% sensitivity, 89% specificity, 80% positive predictive value).
Conclusions: Sustained AF was observed during follow up after cavotricuspid isthmus ablation in 60% of patients with “isolated” typical atrial flutter. Long-term history of hypertension is an important predictor of AF occurrence in this cohort of patients.
INCIDENCE AND RISK FACTORS OF ATRIAL FIBRILLATION AFTER CAVOTRICUSPID CATHETER ABLATION IN PATIENTS WITH “ISOLATED” TYPICAL ATRIAL FLUTTERPeter Novikov, Nikolai Shlevkov, Alexander Pevzner, Evgeni Maykov, Nikolai Mironov, Yuri Mareev, Sergei Sokolov, Sergei Golitsyn
Russian Cardiology Research and Production Complex, Moscow, Russian Federation
CATHETER ABLATION MO 3-06

93
Introduction: Heart failure (HF) is associated with increased recurrence of AF following interventional or other rhythm control strategies. We performed detailed electrophysiologic and electroanatomic mapping of the PV antrum in patients with and without HF.
Methods: Consecutive patients undergoing AF ablation with PeAF and LVEF<45% (HF group) were compared to LVEF>55% (Normal LV (NLV) group). In AF, PVCL was recorded via a multipolar catheter in each PV and the left atrial appendage (LAA) for 100 consecutive cycles. The average PV cycle length (PVCL) of all 4 veins (PV4Vaverage), the fastest PV average (PVFVaverage) and the overall fastest CL of any PV (PVfast) relative to the average LAA cycle length (LAAaverage), was determined. Following DCR, high density mapping of the LA including the PV an-trum using a contact force catheter (points>10 g) was performed to determine voltage, scar, fractionation and conduction velocity (CV).
Results: 28 patients (age 58±8, AF duration 11±8.6 months) were enrolled (HF=13, NLV=15). The HF group had significantly higher PV4Vav-
erage/LAAaverage, PVFVaverage/LAAaverage and PVfast/LAAaverage ratios, compared to NLV group. The PV antrum in HF had more fractionation, scar, and reduced tissue voltage, without difference in CV. In the HF group, reduced tissue voltage was more pronounced in the PV antrum than non-antral regions (Bipolar: 1.36±0.5 vs. 1.95±0.8 mV, P=0.016) and fractionation (37 vs. 23%, P=0.009), but not in NLV group.
Conclusions: HF is associated with reduced relative PVCL and increased antral structural remodelling compared to NLV. This may in part explain an increased propensity to AF in HF with implications for ablation strategy.
THE PULMONARY VENOUS ANTRUM IN PATIENTS WITH PERSISTENT AF AND HEART FAILURE-ELECTROPHYSIOLOGIC AND ELECTRO-ANATOMICAL ASSESSMENTSandeep Prabhu1,2, Alex Voskoboinik1,2, Kah Peck1, Alex Mclellan1,2, Liang-han Ling1,2, Bupesh Pathik3, Chrishan Nalliah3, Geoff Wong3, Siobhan Lockwood4, Geoff Lee3, Sonia Azzopardi1,2, Justin Mariani1,2,Andrew Taylor1,2, Jonathan Kalman3, Peter Kistler1,2 1Alfred Health, Melbourne, Australia; 2Baker IDI, Melbourne, Australia; 3Royal Melbourne Hospital, Melbourne, Australia; 4Monash Health, Melbourne, Australia
CATHETER ABLATION MO 3-07

94
Introduction: Atrial fibrillation (AF) is associated with left ventricular diastolic dysfunction and atrial remodeling. We hypothesized that left atrial (LA) pressure change as heart rate reflects functional remodeling of LA in the patient with AF.
Methods: We measured peak LA pressure (LAPp) response as heart rate (HR) change by incremental dual chamber pacing during sinus rhythm in patients who underwent catheter ablation (CA) needs LA assess. The degree of late gadolinium enhancement (LGE) of LA in cardiac MR (CMR) was checked in patient with AF. LAPp response was compared between 4 groups: group 1 AF patients with LGE <25 (n=120), group 2 25≤LGE<50 (n=50), group 3 LGE≥≥50, control) patients without AF (n=34).
Results: AF was induced by pacing to older (58 vs. 53 years) patients with longer baseline cycle length (BCL) (1,072 vs. 940 ms) (both P=0.02). Baseline LAP in group 3 was significantly increased compared to group 1, 2 and control (30±11 vs. 21±6, 24±7 and 19±5, P<0.001). LAPp was gradually increased as HR change in all groups (P<0.001). An increment of LAPp at pacing of 300ms was significantly different in all 4 groups (77±37, 65±30, 42±21, and 92±20, % in each group, P=0.01). The LGE in CMR was significantly associated with baseline LAPp (r=0.497), response of LAPp (r=-0.266) (all P<0.05). LGE in CMR ([B]=0.082; 95% CI 1.024-1.150; P=0.006) and LVEF ([B]=0.072; 95% CI 0.780-0.993; P=0.038) were independent predictors of low LAPp response (<10 mmHg).
Conclusions: The response of LAPp during incremental pacing in AF patients was lower than in control group. It is associated with LGE degree in CMR among patients with AF. The clinical implication of this association warrant further investigation.
LEFT ATRIAL PRESSURE RESPONSE DURING INCREMENTAL DUAL CHAMBER PACING IN THE PATIENTS WITH ATRIAL FIBRILLATION : THE CONCEPT OF ADAPTATION AND STIFFNESSSeung-Young Roh, Hee-Soon Park, Kwang No Lee, Yong-Soo Baek, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION MO 3-08

95
Introduction: Atrial fibrillation (AF) is associated with impaired cognitive function (CogF) and/or dementia, but it is unclear whether rhythm control of AF recovers CogF. We explored whether radiofrequency catheter ablation (RFCA) improved CogF, and evaluated several predictive biomarkers.
Methods: This observational cohort study included 290 patients (73.4% male, 60.0±10.8 years of age, 31.8% with persistent AF) who un-derwent RFCA for AF and 15 controls who receiving no rhythm control drugs or RFCA, and measured the Montreal Cognitive Assessment (MoCA) score one day before, 3 months after and 1-year after the procedure. We defined impaired CogF as a MoCA<23, and multiple cir-culating biomarkers were evaluated for the prediction of CogF improvement.
Results: 1) Pre-RFCA CogF impairment was detected in 67 out of 290 (23.4%) patients who undergoing RFCA, and found to be associated with old age (P<0.001), being female (P<0.001), hypertension (P=0.005), stroke/TIA (transient ischemic attack) history (P=0.001), larger LA volume index (P=0.001) and higher circulating leptin levels (P<0.001). 2) MoCA scores improved 3 months after RFCA (24.37±3.52 to 25.67±3.18, P<0.001), particularly in the visuoexecutive, attention, language, abstraction, and delayed recall function subdomains. 3) MoCA scores also improved in controls (23.87±4.97 to 24.67±4.59, P=0.028), and showed no significant difference between 290 patients who underwent RFCA and 15 controls (post 3 month-pre-RFCA MoCA score; 1.32±2.13 vs. 0.80±1.26, P=0.352). 4) These improvements after RFCA were maintained 1-year after the RFCA (25.82±2.94 to 26.31±2.72). 5) Low pre-RFCA MoCA scores (odds radio [OR] 0.73; 95%CI 0.66 to 0.81), larger LA volume index (OR 1.01; 95%CI 1.00 to 1.02), and high plasma levels of leptin (OR 1.22; 95%CI 1.06 to 1.39) were associated with post-AF ablation improvements in CogF.
Conclusions: About a quarter of the patients who underwent AF catheter ablation had underlying impaired CogF, but reducing the AF burden by RFCA significantly improved CogF. Our results suggest the important role of RFCA and potential involvement of metabolic hor-mone (leptin) in cognitive protection in patients with AF.
CIRCULATING LEPTIN PREDICTS IMPROVEMENT IN COGNITIVE FUNCTION AFTER CATHETER ABLATION FOR ATRIAL FIBRILLATION : 1-YEAR FOLLOW-UP DATATae-Hoon Kim1, Ki-Woon Kang2, Jae-Sun Uhm1, Boyoung Joung1, Moon-Hyoung Lee1, Eosu Kim1, Hui-Nam Pak1 1Yonsei University Severance Hospital, Seoul, Republic of Korea; 2Eulji University Hospital, Daejeon, Republic of Korea
CATHETER ABLATION MO 3-09

96
Introduction: Mitral isthmus (MI) is accepted for ablation target of peri-mitral atrial flutter. However, it is sometimes difficult to create complete conduction block at MI. Marshall Vein (MV) always anatomically courses across MI. Therefore, ethanol injection into MV (EIMV) has a profound influence on construction of MI block. In this study, we analyzed the extent of ablated area produced by EIMV, and evaluat-ed clinical impact of EIMV on construction of complete MI block.
Methods: 38 patients with atrial fibrillation (AF) who underwent EIMV concomitant with cryoballoon (CB) guided pulmonary vein (PV) iso-lation were involved. EIMV was done first prior to PV isolation. After PV isolation, we developed a voltage map around MI using merged CT image reconstructed by 3D-mapping system. We analyzed the extent of low voltage area (LVA), which was defined as less than 0.5 mV, es-pecially around MI. Then, we ablated survived endocardial sites of other than LVA on the MI line with maximum radiofrequency (RF) ener-gy of 35 W in order to create complete MI block. If endocardial RF ablation failed to create MI block, we performed coronary sinus (CS) ab-lation with maximum RF energy of 25 W.
Results: Total amount of ethanol was 4.4±0.8 mL (2-6 mL). In all patients, LVA was always present at PV ridge site. Total length of MI line was 38.8±7 mm (25-54 mm). Length of LVA on MI line was 21.9±7 mm (10-36 mm), which accounted for 56±14% (25-80%), and LVA area was 5.7±3.4 cm2 (0.7-13.8 cm2). The distance between left inferior PV and the ostium of MV was 23.4±7.9 mm (7-40 mm). Length of LVA within left atrial appendage was 17.2±8.9 mm (2-36 mm). The size and shape of LVA was vastly different in each patient, and had no sig-nificant relationship to total amount of ethanol. Complete MI block was achieved in 36 of 38 (95%) patients. In all patients, LVA was always present at PV ridge site. In successful 36 patients, the average number of endocardial RF application was 6.8±4.4, and intra-CS ablation was needed in 17 (47%) patients to create complete MI block. No complications occurred.
Conclusions: LVA was always created at PV ridge site by EIMV, and LVA on MI line accounted for more than half of total length of MI. EIMV can safely and dramatically improve achievement of complete MI block, although intra-CS ablation is required in about half of patients.
IMPACT OF CHEMICAL ABLATION OF THE MARSHALL VEIN ON CREATION OF MITRAL ISTHMUS BLOCKYasuteru Yamauchi
Yokohama City Minato Redcross Hospital, Yokohama, Japan
CATHETER ABLATION MO 3-10

97
Introduction: Usually atrial fibrillation (AF) ablation is performed under fluoroscopic guide and the image integration onto pre-made three dimensional computed tomography (3DCT) of left atrium (LA) in electro-anatomical mapping system. The recent major topic is how the operator can reduce fluoroscopic time. We have already invented the High-Resolution Sound Map using an intra cardiac echo catheter (ICE) equipped with a magnetic sensor, SOUNDSTAR® for CARTOSOUND module of CARTO±3. We assess that AF ablation with this Sound Map may reduce the fluoroscopic time.
Methods: High-resolution sound map was created using the SoundMap function of CARTO SOUND± module. The 3D LA image is reconstructed by multiple 2D LA contours drawn with ultrasound fans. These LA contour were obtained by manipulation of the ICE not only from right atrium, but from LA by navigation of this ICE to LA via atrial septal puncture hole. Clear echo contour of the left pulmonary vein (PV), left atrial appendage, anterior ridge area of left PVs and right PVs were easily drawn especially from LA. AF ablation was per-formed with this map as a optimal LA geometry in total 468 cases from February 2013 to June 2016. We assessed the feasibility and clini-cal usefulness of this method for AF ablation in these cases. We extract first 50 cases as group F and latest 50 cases as group L to com-pare, creating sound map time, procedure time and fluoroscopic time between them.
Results: Among these cases, there were 48 cases AF ablation without any image information of LA excluding Sound Map. In total, proce-dure time is 67 ± 15, fluoroscopic time is 28 ± 15, making sound map time is 23 ± 6 (min). The comparison data be-tween group F and L is shown in the table below.
Conclusions: This study showed that there is a reduction of procedure time and fluoroscopic time with Sound Map and the more experi-ence gained, the more Sound Map time can be reduced. This Sound Map provides precise anatomical information of LA as a reliable and real time geometry for AF ablation. Circumferential PV isolation was safely and successfully performed without 3DCT of LA. In conclusion, High-Resolution Sound Map is useful for the AF ablation.
FEASIBILITY AND CLINICAL USEFULNESS OF HIGH-RESOLUTION LEFT ATRIAL SOUND MAP AS A RELIABLE GEOMETRYYeongHwa (Eiwa) Chun (Zen)
Takeda Hospital, Kyoto, Japan
CATHETER ABLATION MO 3-11
Comparison Data
Procedure time Creating sound map Fluoroscopic time
group F 72 ±28 26 ±8 36 ±17
group L 36 ±17 12 ±5 8 ±3

98
Introduction: Catheter ablation of atrial fibrillation (AF) has been an established therapeutic modality for the treatment of patients with symptomatic AF. However, data regarding the long-term outcomes of AF ablation are still lacking. We sought to investigate the long-term outcomes over 10-year after catheter ablation in patients with AF.
Methods: From 2004 to January 2016, a total 2,221 consecutive patients who underwent catheter ablation, including circumferential pul-monary vein isolation (CPVI) were studied (mean 55±11 years old, 20.3% female, 59.0% paroxysmal AF). Additional ablations were per-formed according to AF type and the physicians’ discretion. Clinical characteristics, imaging parameters, ablation findings and outcomes were analyzed in all patients. Late gadolinium enhancement (LGE) in cardiac magnetic resonance image (MRI) were also assessed.
Results: CPVI with or without ablation of cavo-tricuspid isthmus was accomplished in 49.2% of the patients. More extensive ablation pre-vailed in persistent AF types (P<0.001). Repeated ablations were performed in 480 patients (2nd procedure=418, 3rd procedure=56, and 4th procedure=6, respectively). Patients with persistent AF underwent significantly more repeat procedures than those with paroxysmal AF (26.6% vs. 13.4%, P<0.001). The patients with multiple procedure had higher proportions of atrial tachycardia or atrial flutter than those with index procedure (42.8% vs. 59%, P<0.001). After the index procedure, sinus rhythm (SR) was present in 1,490 of 2,221 (67.1%) during a median follow-up period of 54 months. After redo procedures of 448 patients, 83.3% of the patients remained in SR. In sub-anal-ysis, LGE-MRI scar burden in patients with CR were higher than those without CR (21.8±13.7% vs. 36.2±23.9, P<0.001). In the multivari-ate analysis, persistent AF (HR 2.203, 95% CI 1.396-3.477, P<0.001) and MR LGE ≥25% (HR 1.944, 95% CI 1.224-3.087, P=0.005) were sig-nificantly associated with AF recurrence after catheter ablation.
Conclusions: In patients with AF, repeat procedures of catheter ablation showed a similar long-term outcome to single procedure during 10 years follow-up. And, this study supports that AF substrate that was represented by persistent AF and MR-LGE is associated with re-currence after catheter ablation
LONG-TERM OUTCOMES OF CATHETER ABLATION OF ATRIAL FIBRILLATION: A MORE THAN 10 YEARS OF EXPERIENCEYong-Soo Baek, Jong-Il Choi, Hee-Soon Park, Anupam Jena, Kwang-No Lee, Seung-Young Roh, Jinhee Ahn, Dong-Hyeok Kim, Jaemin Shim, Jin Seok Kim, Hong Euy Lim, Sang-Weon Park, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CATHETER ABLATION MO 3-12

YIA SESSION [BASIC](13 October)
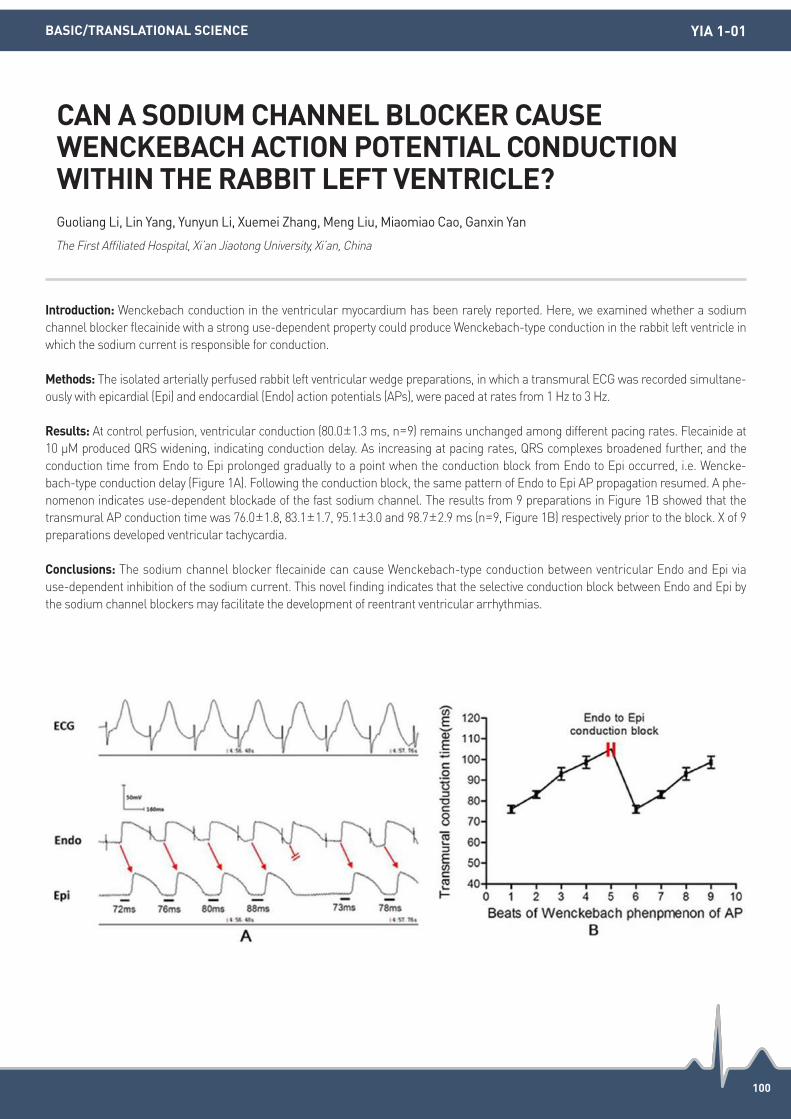
100
Introduction: Wenckebach conduction in the ventricular myocardium has been rarely reported. Here, we examined whether a sodium channel blocker flecainide with a strong use-dependent property could produce Wenckebach-type conduction in the rabbit left ventricle in which the sodium current is responsible for conduction.
Methods: The isolated arterially perfused rabbit left ventricular wedge preparations, in which a transmural ECG was recorded simultane-ously with epicardial (Epi) and endocardial (Endo) action potentials (APs), were paced at rates from 1 Hz to 3 Hz.
Results: At control perfusion, ventricular conduction (80.0±1.3 ms, n=9) remains unchanged among different pacing rates. Flecainide at 10 μM produced QRS widening, indicating conduction delay. As increasing at pacing rates, QRS complexes broadened further, and the conduction time from Endo to Epi prolonged gradually to a point when the conduction block from Endo to Epi occurred, i.e. Wencke-bach-type conduction delay (Figure 1A). Following the conduction block, the same pattern of Endo to Epi AP propagation resumed. A phe-nomenon indicates use-dependent blockade of the fast sodium channel. The results from 9 preparations in Figure 1B showed that the transmural AP conduction time was 76.0±1.8, 83.1±1.7, 95.1±3.0 and 98.7±2.9 ms (n=9, Figure 1B) respectively prior to the block. X of 9 preparations developed ventricular tachycardia.
Conclusions: The sodium channel blocker flecainide can cause Wenckebach-type conduction between ventricular Endo and Epi via use-dependent inhibition of the sodium current. This novel finding indicates that the selective conduction block between Endo and Epi by the sodium channel blockers may facilitate the development of reentrant ventricular arrhythmias.
CAN A SODIUM CHANNEL BLOCKER CAUSE WENCKEBACH ACTION POTENTIAL CONDUCTION WITHIN THE RABBIT LEFT VENTRICLE?Guoliang Li, Lin Yang, Yunyun Li, Xuemei Zhang, Meng Liu, Miaomiao Cao, Ganxin Yan
The First Affiliated Hospital, Xi’an Jiaotong University, Xi’an, China
BASIC/TRANSLATIONAL SCIENCE YIA 1-01

101
Introduction: Premature ventricular contractions (PVCs) are implicated in development of cardiomyopathy. A potential mechanism is au-tonomic dysregulation. However, the autonomic changes in a PVC-induced cardiomyopathy are poorly understood.
Methods: We developed a canine model of PVC-induced cardiomyopathy. We implanted a pacemaker and delivered bigeminal right ven-tricular PVCs at a coupling interval of 220-250 ms in 6 canines over 3 months. Data Sciences International radiotelemetry devices were implanted for continuous ambulatory recordings of left stellate ganglion (SGNA) and left cardiac vagal nerve activity (VNA) (n=6). In-vivo left ventricular systolic pressure (LVSP) (n=2/6) and ambulatory systolic blood pressure (SBP) was recorded (n=3/6).
Results: Acute PVC initiation immediately (<1 minute) increased LVSP (N=4) from 78±8 to 101±6 mmHg (P=0.006), and ambulatory SABP (N=3) from 102±4 to 128±7 mmHg (P=0.06), and reduced 2-min averaged SGNA from 33.2±8.7 to 21.3±7.1 uV-s (N=6, P=0.008) and VNA from 24.1±5.1 to 12.4±6.2 uV-s (P=0.008). Elimination of PVCs reversed all the above findings. After 24-hours of PVCs, there was a decline in averaged daily SGNA 33.2±8.7 to 18.3±11.7 uV-s (P=0.01) but not VNA (from 23.1±17.8 to 21.7±16.2 uV-s) (P=0.21). More chronic (3-month) PVC exposure reduced averaged daily SGNA from 86.7±60 to 78±58 uV-s (P=0.02) without change in VNA (from 26.1±25.1 to 25.1±13.4 uV-s (P=0.47). There was a loss in circadian variability (daily standard deviation) of SGNA from 87.1±58.6 to 73±57.4 uV-s (P=0.014), and peak daily SGNA response to activity declined from 547.5±277.7 to 384.3±252.1 uV-s (P=0.038).
Conclusions: Acute and chronic bigeminal PVCs are associated with a significant reduction and loss of circadian variability of cardiac sympathetic nerve activity but not vagal nerve activity. The mechanism may be a baroreflex mediated suppression of sympathetic outflow. The suppression and loss of circadian variability of cardiac sympathetic nerve activity may have implications for the development of PVC induced cardiomyopathy.
ACUTE AND CHRONIC SUPPRESSION AND LOSS OF CIRCADIAN VARIABILITY OF CARDIAC SYMPATHETIC NERVE ACTIVITY IN A CANINE MODEL OF PREMATURE VENTRICULAR CONTRACTION-INDUCED CARDIOMYOPATHYRicardo Cardona Guarache1, Karoly Kaszala1, Anthony Minisi1, Shien-Fong Lin2, Kenneth Ellenbogen1, Jose Huizar1, Alex Tan1 1Virginia Commonwealth University, Richmond, United States; 2Indiana University School of Medicine, Indianapolis, United States
BASIC/TRANSLATIONAL SCIENCE YIA 1-02

102
Introduction: Elevated maternal serotonin (5-hydroxytryptamine, 5-HT) production is an important determinant of normal fetal develop-ment. However, what roles the elevated serotonin plays in the electrophysiology of the mother’s heart has not been studied. In the present study, we therefore assessed the relationship between QTc duration and serotonin and studied underlying mechanisms.
Methods: Patch clamp; Immunoprecipitation; Immunostaining; Western blotting.
Results: During pregnancy, 5-HT and tryptophan hydroxylase 1, a rate-limiting enzyme of serotonin synthesis, were markedly increased in hearts and serum. We measured QT intervals and ventricular potassium outward currents in wild-type (WT) and 5-HT3a receptor knock-out (Htr3a-/-) mice at non-pregnant (NP) and late-pregnant (LP) state. The 5-HT as well as m-CPBG, an Htr3 agonist, increased Ipeak and Ito,f densities with the shortening of QTc duration in WT NP, but not in WT LP and Htr3a-/- mice. Additionally an Htr3a antagonist, on-dansetron (5 μM) decreased Ipeak and Ito,f only in WT LP, but not in WT NP mice. In contrast, Ipeak and Ito,f densities were unchanged upon 5-HT and m-CPBG application in left ventricular myocytes freshly-isolated from the Htr3a-/--LP mice. Kv4.3 protein and Htr3a is co-local-ization in the membrane and t-tubule of cardiomyocytes. Co-immunoprecipitation showed that Kv4.3 protein directly interacts with 5-HT3a receptor. Moreover, the binding between 5-HT3a receptor and Kv4.3 was facilitated by 5-HT. This increase was mediated by 5-HT3a receptor dependent promotion of Kv4.3 channel trafficking to the cell membrane. However, these findings were not observed in WT LP mice. The heat-shock protein-90 (Hsp90) inhibitor geldanamycin abolished 5-HT-induced increase of Ipeak and Ito,f densities. Finally, we evaluated and found that serotonin could shorten QTc interval by increasing potassium outward currents in rat and rabbit.
Conclusions: Elevated 5-HT levels were associated shorter QTc intervals by acceleration of Ipeak and Ito,f densities in mouse, rat and rabbit. 5-HT acts on Kv4.3 channels via enhanced 5-HT3a-receptor-medicated Hsp90 interaction, augments membrane trafficking and thereby increases repolarizing current. These results provide mechanistic insights into hormonal control of ventricular repolarization.
SEROTONIN REGULATES QT-INTERVAL: ACCELERATION OF CARDIAC REPOLARIZATION BY ENHANCED KV4.3 MEMBRANE TRAFFICKINGShanyu Cui, Boyoung Joung
Division of Cardiology, Yonsei University College of Medicine, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE YIA 1-03

103
Introduction: Tranilast has been shown to be beneficial in preventing atrial remodelling in animal models of atrial tachypacing and hyper-tension (HTN). However, it remains unknown whether anti-fibrotic agent has a role in reversing the abnormal changes seen with estab-lished atrial substrate.
Methods: Twelve months old spontaneously hypertensive rats (SHR, n=32) and normotensive Wistar-Kyoto controls (WKY, n=8) were studied. The SHR group was divided into HTN controls (n=8) and treatment groups: Perindopril (PRD-0.5 mg/kg/day, n=8); Tranilast (Tran-600 mg/kg bid, n=8); PRD+Tran combination (n=8) for 4 weeks. Electrophysiological studies of superfused atria were performed using a custom multi-electrode array to assess effective refractory period (ERP), conduction and AF inducibility followed by detailed histological and immunohistochemistry analysis.
Results: Hypertension resulted in significant atrial electro-structural and molecular abnormalities leading to increased AF inducibility (HTN vs. WKY normotensive controls, Table). PRD, TRAN and PRD+TRAN treatments improved atrial conduction, interstitial fibrosis, myo-cyte hypertrophy and various signalling molecules expressions leading to reduced AF vulnerability. PRD+TRAN treatment resulted in pro-nounced beneficial reverse remodelling compared to single agent therapy.
Conclusions: Tranilast has similar reverse remodelling effects in hypertensive atria as compared to Perindopril despite not affecting blood pressure levels. Additional beneficial effects were evident with the use of anti-fibrotic agent in combination with anti-hypertensive therapy.
ROLE OF ADJUNCTIVE ANTI-FIBROTIC THERAPY WITH TRANILAST IN REVERSING ATRIAL REMODELLING IN SPONTANEOUSLY HYPERTENSIVE RATSShivshankar Thanigaimani1, Do Yeon Kim1, Jim Manavis1, Darren Kelly2, Pawel Kuklik1, Prashanthan Sanders1, Dennis Lau1 1University of Adelaide, Adelaide, Australia; 2University of Melbourne, Melbourne, Australia
BASIC/TRANSLATIONAL SCIENCE YIA 1-04

104
Introduction: Plasma microvesicles (MV) from mesenchymal stem cells (MSC) has known as cell to cell messengers. However, the role of MV which regulate molecular interactions in atrial fibrillation (AF) remain unfortunately much unknown. This study investigated that MV derived from hypoxic conditioned MSCs help to prevent calcium overloading in atrial myocytes during tachycardia.
Methods: MVs were isolated from plasma by differential centrifugation and microfiltration. The HL-1 atrial cardiomyocytes were prepared with normal paced (1 Hz) or tachy-paced (5 Hz). Before pacing, HL-1 cell were treated with the MVs. The effects of MV on paced HL-1 cell were examed using a patch clamp, a confocal Ca2+ imaging, western blot analysis and imunofluorescent staining.
Results: Tachypacing induced shortening of APD, Ca2+ overload, activation of Histone Deacetylase-6 (HDAC-6) and depolymerization of microtubules in the HL-1 myocyte. However, MV inhibited the transient Ca2+ reductions in tachy-paced (TP) HL-1 myoctes and L-type Ca2+
current were also preserved with MV. Depolymerization of microtubues by tachypacing were also prevented by MV via HDAC-6 pathway.
Conclusions: MV successfully preserved calcium regulation and de-activation of HDAC-6 in TP HL-1 cell model. This results suggest that MVs would be a therapeutic option for control of atrial tachyarrhythmia.
MICROVESICLES FROM MESENCHYMAL STEM CELLS IMPROVES CALCIUM REGULATION BY HISTONE DEACETYLASE-6 INHIBITION IN TACHYCARDIA MODEL OF HL-1 MYOCYTEYoo Ri Kim1, Hyo-Eun Kim2, Hyewon Park2, Hyelim Park2, Sanyou Chui2, Seung-Hyun Lee2, Nam Kyun Kim2, Hui-Nam Pak2, Moon-Hyoung Lee2, Michael Kim1, Boyoung Joung2 1The Catholic University of Korea, Incheon, Republic of Korea; 2Yonsei University College of Medicine, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE YIA 1-05

105
Introduction: The aim of the present study was to determine whether spinal cord stimulation (SCS) could inhibit atrial fibrillation (AF) in-ducibility in paroxysmal AF dog model and to explore its underlying mechanism.
Methods: First, all the dogs were implanted pacemakers for long-term intermittent right atrial pacing (RAP) at 400 b.p.m. for 8 hours a day. Then the dogs were divided into four groups: control group (n=6), vagus nerve stimulation group (VNS, n=8), SCS group 1 (n=8), SCS group 2 (n=8). 8 weeks later, control group dogs were given no stimulation; VNS group dogs experienced low-level VNS for 30 minutes; SCS group 1 dogs experienced low-level SCS for 30 minutes, while SCS group 2 dogs underwent bilateral vagotomy and simultaneously received low-level SCS for 30 minutes. Effective refractory period (ERP), ERP dispersion and AF vulnerability were measured at pacing 8 weeks and SCS 30 minutes later. Five millilitres of venous blood were collected in thylenediaminetetraacetic acid vacutainers at the base-line, pacing 8 weeks, and after SCS.
Results: Compared with pacing 8 weeks later, VNS and SCS both induced a significant increase in ERP at left and right atrium and four pulmonary veins and ERP dispersion was decreased, along with the decrease in AF inducibility. After bilateral vagotomy, these electrical physiological parameters had no changes before and after SCS. VNS suppressed the increasing trend of tumor necrosis factor α (TNF-α) and interleukin 6 (IL-6) in the atrial tissue and circulating blood by prolonged RAP. Correspondingly, the level of acetylcholine (ACH) and α7 subunit of the nicotinic acetylcholine receptor (α7nAchR) expression significantly increased. VNS also inhibited the phosphorylation of nu-clear factor κB (NF-κB) signaling pathway related protein. SCS had the similar effects, but were eliminated by bilateral vagotomy.
Conclusions: SCS suppresses prolonged RAP-induced AF, which might related to the immunosuppressing function of VN. VN through its nerve endings release ACH activated CAP, thereby inhibit its downstream NF-kB signaling pathway and suppress the release of TNF-α and IL-6.
SPINAL CORD STIMULATION SUPPRESSES ATRIAL FIBRILLATION BY ACTIVATING CHOLINERGIC ANTI-INFLAMMATORY PATHWAYZixuan Dai
Renmin Hospital of Wuhan University, Wuhan, China
BASIC/TRANSLATIONAL SCIENCE YIA 1-06

YIA SESSION [CLINICAL](13 October)

107
Introduction: Activation mapping guided catheter ablation (CA) of ventricular arrhythmias (VAs) is known to be effective, however, is limit-ed in some cases when it is only relied on bipolar electrogram (EGM). We hypothesized that activation mapping with use of combined bi-polar and unipolar EGM facilitates to identify the focal origin of VAs and results in reduction of recurrence rate of CA of VAs.
Methods: We retrospectively analyzed the data of patients who underwent CA of premature ventricular contractions (PVC) and ventricular tachycardia (VT). From 2001 to 2016 a total of 500 patients underwent ablation for PVC and VT. Out of those cases 56 patients underwent repeat ablation for recurrence of PVC and focal, non-reentrant VT. The EGM of the initial ablation and repeat ablations were compared for earliest local activation time, presence of discrete potentials, and polarity reversal. Where unipolar recordings were available they were analyzed for unipolar potential morphology (QS or non-QS), potential amplitude and activation slope. Unipolar activation slope was defined as the ratio of voltage and time interval from onset of QS to the nadir of S wave.
Results: The EGMs were compared between the initial and repeat ablations in 37 patients. The earliest local activation time prior to QRS onset was significantly less in the initial ablation procedure as compared to the repeat procedure (31.85 msec vs. 36.90 msec, P<0.01). The incidence of discrete potentials and polarity reversal were similar in both procedures (51% vs. 57%, P=0.8 and 62% in both the occa-sions, respectively). The unipolar voltage was similar in both occasions (6.94 mV in first ablations vs. 7.22 mV in repeat ablations, P=0.7). The unipolar activation slope was also similar in the initial and repeat ablations (0.156 mV/msec vs. 0.171 mV/msec, P=0.2). We started recording unipolar EGMs from 2011 in all cases of PVC and VT ablations. The recurrence rate (15 out of 261 patients, 5.7%) was signifi-cantly lower with routine use of combined unipolar and bipolar EGMs, as compared to the use of bipolar EGM alone (40 out of 239 pa-tients, 16.7%).
Conclusions: Use of both bipolar and unipolar electrograms helps in better delineation of the sites of earliest activation for effective abla-tion of VAs. Use of unipolar electrograms in addition to bipolar electrograms is associated with lower long term recurrence rate.
UNIPOLAR AND BIPOLAR ELECTROGRAM CHARACTERISTICS OF RECURRENT CASES OF VENTRICULAR ARRHYTHMIAS UNDERGOING CATHETER ABLATIONAnupam Jena, Mohammad Iqbal, Hee-Soon Park, Yong-Soo Baek, Kwang-No Lee, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION YIA 2-01

108
Introduction: The significance of adenosine induced dormant pulmonary vein (PV) conduction in AF ablation remains controversial. The optimal dose of adenosine to determine dormant PV conduction is yet to be systematically explored
Methods: Consecutive patients undergoing index AF ablation were prospectively enrolled. Each received 3 adenosine doses (12 mg, 18mg, 24 mg) in a randomized blinded order, immediately after PVI. Electrophysiological (PR prolongation, AV block (AVB) and PV reconnection) and hemodynamic (BP) parameters were measured.
Results: 339 doses (113/dose) assessed 191 PVs in 50 patients (66% male, 72% PAF, 52% hypertensive). Dormant PV conduction occurred in 28% of patients (16.5% (32) of PVs). All cases were associated with AVB (AVB: PV reconnection vs. no PV reconnection 100% vs. 83%, P=0.007). AVB occurred more frequently at 24 mg vs. 12 mg (92% vs. 82%, P=0.019) but not vs. 18 mg (91%, P=0.62). AVB duration pro-gressed between 12 mg (12.0±8.9s), 18 mg (16.1±9.1s, P=0.001) and 24 mg (19.0±9.3s, P<0.001) doses. MBP fell further at 24 mg (MBP: 27±12 mmHg) and 18 mg (26±13 mmHg) dose compared to 12 mg (22±10 mmHg vs., P<0.001). A significant reduction in AVB in patients >110 kg (65% vs. 91% in 70-110 kg group, P<0.001) in response to adenosine was seen (see figure).
Conclusions: An adenosine dose producing AVB is required to unmask dormant PV conduction. AVB is significantly reduced in patients >110 kg. Weight and dosing variability may in part explain the conflicting results of studies evaluating the clinical utility of adenosine in PVI.
DETERMINING THE OPTIMAL DOSE OF ADENOSINE FOR UNMASKING DORMANT PULMONARY VEIN CONDUCTION FOLLOWING ATRIAL FIBRILLATION ABLATION: ELECTROPHYSIOLOGICAL AND HEMODYNAMIC ASSESSMENT. DORMANT-AF STUDYSandeep Prabhu1, VIncent Mackin2, Alex Mclellan1, Tuong Phan2, Desmond McGlade2, Kah Peck3, Alexandr Voskoboinik1, Bupesh Pathik4, Chrishan Nalliah4, Geoff Wong4, Sonia Azzopardi1, Geoff Lee4, Justin Mariani1, Andrew Taylor1, Jonathan Kalman4, Peter Kistler1 1Alfred Health and Baker IDI, Melbourne, Australia; 2Cabrini Health, Melbourne, Australia; 3Alfred Health, Melbourne, Australia; 4Royal Melbourne Hospital, Melbourne, Australia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION YIA 2-02

109
Introduction: The clinical importance of early recurrence is increasingly reinforced for atrial fibrillation ablation as it is found to be a pow-erful independent predictor of late recurrence. It is of great significance to search for predictors of early recurrence. The study is designed to assess the association and the predictive value of plasma homocysteine (Hcy) with early recurrence in persistent atrial fibrillation pa-tients after a single ablation procedure.
Methods: Two hundred and fifty-seven consecutive patients with persistent atrial fibrillation who underwent successful catheter ablation were enrolled. Early recurrence of atrial tachyarrhythmia was documented within 3 months after ablation. The logistic regression analysis and Kaplan-Meier curve analysis were used to evaluate the association of Hcy with early recurrence.
Results: During the 3-month follow-up, 75 (29.2%) patients experienced recurrence. Patients with early recurrence were older, more like-ly to have larger left atrial diameter and higher CHA2DS2-VASc score (all P<0.001). Plasma homocysteine (Hcy) levels were significantly el-evated in patients with early recurrence compared with those without early recurrence (15.1±4.1 μmol/L vs. 12.4±3.7 μmol/L, P<0.001). In multivariate analysis, Hcy was significantly associated with early recurrence (OR 1.188, 95% CI 1.097-1.286, P<0.001). Hcy demonstrated a predictive value with AUC of 0.688 (95% CI 0.623-0.753, P<0.001). The optimal cut-off value was 14 μmol/L for Hcy (sensitivity 69%, speci-ficity 59%). Patients with Hcy ≥14 μmol/L had higher early recurrence rate compared with those with Hcy <14 μmol/L (41% vs. 22%, P=0.006).
Conclusions: Plasma Hcy levels are associated with early recurrence of atrial tachyarrhythmia after catheter ablation in persistent atrial fibrillation patients, thus it should be taken into account in prediction of early recurrence.
PLASMA HOMOCYSTEINE LEVELS PREDICT EARLY RECURRENCE AFTER CATHETER ABLATION OF PERSISTENT ATRIAL FIBRILLATIONYan Yao, Xin Du, Jianzeng Dong, Changsheng Ma
Beijing Anzhen Hospital, Beijing, China
CATHETER ABLATION YIA 2-03

110
Introduction: Papillary muscle ventricular arrhythmia (PM-VA) and fascicular ventricular arrhythmia (FVA) are characterized by different mechanism but similar morphology. Using electrocardiographic pattern for differential diagnosis may be suboptimal due to the close proximity of papillary muscle and conduction system.
Methods: The FVT is in mechanism and only single beat of long CI should be observed after a preceding ectopy or capture beat. The high-er morphology dispersion should be observed in PM-VT due to the presence of multiple exits. We aimed at evaluating the feasibility of two novel criteria, including (1) the high dispersion of arrhythmia morphology and (2) the presence of consecutive 2 beats of long coupling in-terval (CI).The morphology deviation was evaluated using all beats of ventricular arrhythmia before introducing any catheter inside left ventricles. An objective method of morphology-variability measurement was used that the first beat of VPC was selected as the template for matching algorithms based on the ECG average correlation algorithms (ECG-AC) embedded in the LabSystem Pro workstation. The presence of consecutive 2 beats of long CI was evaluated by using all the ventricular tachycardia during electrophysiology study and 24-hour Holter monitoring. The difference between the CI0-1 and the CIave3 (ΔCI0-1-CIave3) were measured in the presence of a CI1-2 greater than CIave3. The presence of consecutive 2 beats of long CI was defined as Δ (CI0-1-CIave3) >0.
Results: Total 39 patients with FVA and PM-VT were admitted for catheter ablation and were enrolled consecutively in the present study. Frequent ventricular ectopy but no sustained ventricular tachycardia were observed in all the patients with PM-VT but not FVT. The mor-phology dispersion is higher in patients with PM-VT than FVT (ECG-AC 3.0±1.8 vs. 1.6±1.0). The presence of consecutive 2 beats of long CI was observed in patients with PM-VT but never in FVT (44% vs. 0%).
Conclusions: The combination of novel criteria based on morphology dispersion and the characteristics of CI may well differentiate be-tween FVA and PM-VT.
DIFFERENTIATION BETWEEN PAPILLARY MUSCLE AND FASCICULAR VENTRICULAR ARRHYTHMIA USING NOVEL ELECTROCARDIOGRAPHIC INDICESYao Ting Chang, Yenn-Jiang Lin, Fa-Po Chung, Li-Wei Lo, Yu-Feng Hu, Shih-Lin Chang, Jo-nan Liao, Tze-Fan Chao, Ta-Chuan Tuan, Chin-Yu Lin, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION YIA 2-04
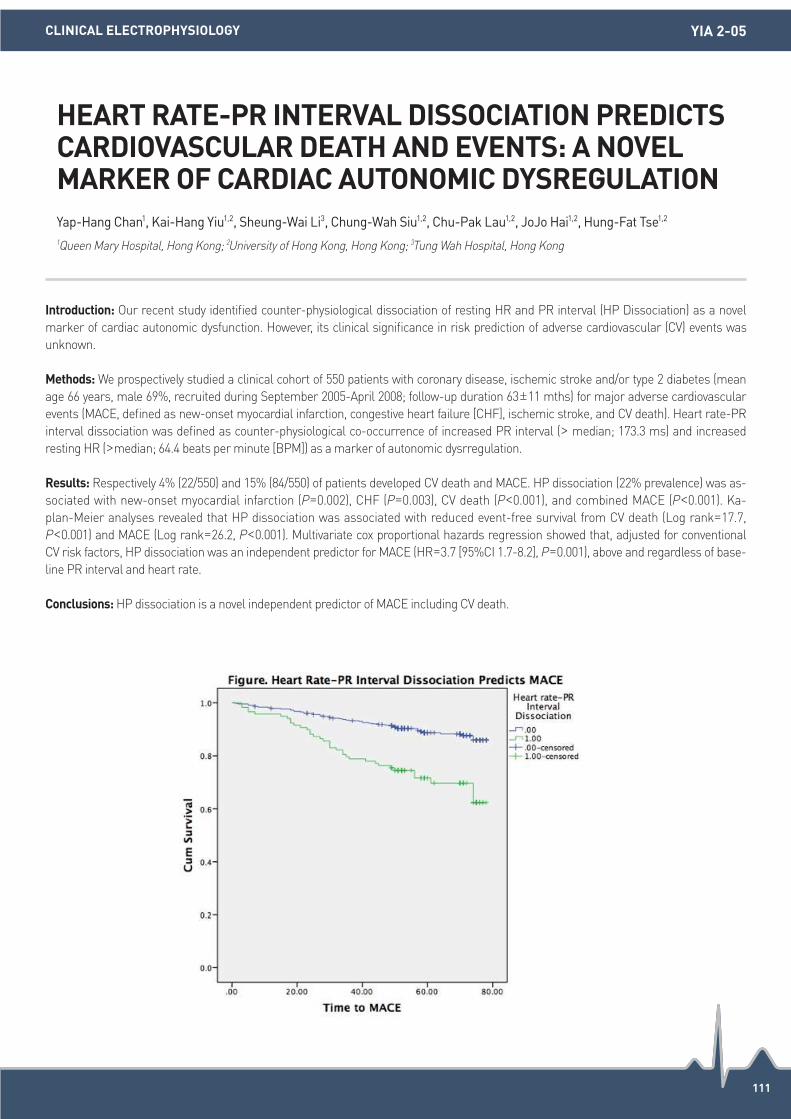
111
Introduction: Our recent study identified counter-physiological dissociation of resting HR and PR interval (HP Dissociation) as a novel marker of cardiac autonomic dysfunction. However, its clinical significance in risk prediction of adverse cardiovascular (CV) events was unknown.
Methods: We prospectively studied a clinical cohort of 550 patients with coronary disease, ischemic stroke and/or type 2 diabetes (mean age 66 years, male 69%, recruited during September 2005-April 2008; follow-up duration 63±11 mths) for major adverse cardiovascular events (MACE, defined as new-onset myocardial infarction, congestive heart failure [CHF], ischemic stroke, and CV death). Heart rate-PR interval dissociation was defined as counter-physiological co-occurrence of increased PR interval (> median; 173.3 ms) and increased resting HR (>median; 64.4 beats per minute [BPM]) as a marker of autonomic dysrregulation.
Results: Respectively 4% (22/550) and 15% (84/550) of patients developed CV death and MACE. HP dissociation (22% prevalence) was as-sociated with new-onset myocardial infarction (P=0.002), CHF (P=0.003), CV death (P<0.001), and combined MACE (P<0.001). Ka-plan-Meier analyses revealed that HP dissociation was associated with reduced event-free survival from CV death (Log rank=17.7, P<0.001) and MACE (Log rank=26.2, P<0.001). Multivariate cox proportional hazards regression showed that, adjusted for conventional CV risk factors, HP dissociation was an independent predictor for MACE (HR=3.7 [95%CI 1.7-8.2], P=0.001), above and regardless of base-line PR interval and heart rate.
Conclusions: HP dissociation is a novel independent predictor of MACE including CV death.
HEART RATE-PR INTERVAL DISSOCIATION PREDICTS CARDIOVASCULAR DEATH AND EVENTS: A NOVEL MARKER OF CARDIAC AUTONOMIC DYSREGULATIONYap-Hang Chan1, Kai-Hang Yiu1,2, Sheung-Wai Li3, Chung-Wah Siu1,2, Chu-Pak Lau1,2, JoJo Hai1,2, Hung-Fat Tse1,2 1Queen Mary Hospital, Hong Kong; 2University of Hong Kong, Hong Kong; 3Tung Wah Hospital, Hong Kong
CLINICAL ELECTROPHYSIOLOGY YIA 2-05

112
Introduction: The main purpose of performing radiofrequency catheter ablation (RFCA) in atrial fibrillation (AF) patients is to improve the quality of life (QoL) and alleviate AF-related symptoms. We aimed to determine the qualitative and quantitative effects of RFCA on the QoL in AF patients.
Methods: We performed a systemic review and meta-analysis using a random effects model. We searched for the studies that reported the physical component summary score (PCS) and mental component summary score (MCS) of the short form-36, a validated system to assess and quantify the QoL in AF patients, before and after RFCA in AF patients. PCS and MCS are T-scores with a mean of 50 and stan-dard deviation of 10.
Results: Of the 470 studies identified, we included 13 studies for pre-RFCA vs. the post-RFCA analysis and 5 studies for treatment suc-cess vs. AF recurrence analyses. In the pre-RFCA vs. post-RFCA analysis, RFCA was associated with a significant increase in both the PCS (weighted mean difference [WMD]=6.33 [4.81-7.84]; P<0.001; Figure 1A) and MCS (WMD=7.80 [6.15-9.44]; P<0.001; Figure 1B). The ∆PCS (post-RFCA PCS-pre-RFCA PCS) and ∆MCS values were used for the treatment success vs. AF recurrence analysis. Patients with successful treatment had a higher ∆PCS (WMD=7.46 [4.44-10.49]; P<0.001; Figure 2A) and ∆MCS (WMD=7.59 [4.94-10.24]; P<0.001; Fig-ure 2B).
Conclusions: RFCA is associated with a significant increase in the PCS and MCS in AF patients. Patients without AF recurrence after RFCA had a better improvement in the PCS and MCS than the patients who had AF recurrence.
RADIOFREQUENCY CATHETER ABLATION IMPROVES THE QUALITY OF LIFE MEASURED WITH A SHORT FORM-36 QUESTIONNAIRE IN ATRIAL FIBRILLATION PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSISYun Gi Kim, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION YIA 2-06

113
CATHETER ABLATION YIA 2-06

LATE-BREAKING TRIAL(13 October)

115
Introduction: Radiofrequency catheter ablation (RFCA) for persistent AF (PeAF) still has a substantial recurrence rate. We recently devel-oped an in-silico 3D AF model with clinically acceptable computing speed, and validated 86% match of the best virtual ablation lesion set and empirical ablation lesion set in retrospective study. We conducted prospective study to test feasibility, efficacy, and safety of virtual ab-lation guided RFCA (V-ABL), comparing with empirical ablation (Em-ABL) in patients with PeAF.
Methods: We included 108 patients with antiarrhythmic drug (AAD) resistant PeAF (77.8% male, 60.8±9.9 years old) who underwent RFCA, and randomly assigned to V-ABL (n=53) and Em-ABL (n=55). For V-ABL, we tested 5 different ablation lesion sets (circumferential pulmonary vein isolation (CPVI), CPVI+posterior box (PostBox) lesion, CPVI+PostBox+anterior line (AL), CPVI+roof line (RL) +left lateral isthmus line (LLI), and CPVI+complex fractional atrial electrogram (CFAE) ablation) at LA-CT image integrated in-silico AF modeling. We compared procedure related factors and clinical outcome between V-ABL and Em-ABL strategies.
Results: 1) In overall patients, pre-procedural computing time for 5 different ablation strategy was about 3 hours, and CPVI+PostBox+AntL most commonly showed the earliest termination rate (52.8%). 2) Among Em-ABL group, the earliest terminating in-silico ablation strate-gy match with empirical ablation in 21.9%. 3) V-ABL was not inferior to Em-ABL in terms of procedure time (256.2±69.0 vs. 271.5±104.7 minutes, P=0.403), ablation time (4,954.7±2,804.0 vs. 5,272.8±2,368.2 seconds, P=0.510), and major complication rate (4.4% vs. 4.0%, P=0.900). 4) During 12.6±3.8 months follow-up, clinical recurrence rate after 3 month of ablation were 14.0% in V-ABL group and 18.9% in Emp-ABL group (P=0.538). 5) After excluding the patients matching the best virtual ablation strategy and empirical ablation strategy in Emp-ABL group, clinical recurrence rates were 14.0% in V-ABL group and 22.0% in Emp-ABL group, respectively (P=0.355).
Conclusions: V-ABL was feasible in clinical practice with non-inferiority to Em-ABL in terms of procedure time, ablation time, complica-tion rate, and short-term clinical recurrence rate in patients with PeAF.
VIRTUAL IN-SILICO MODELING GUIDED CATHETER ABLATION VS. EMPIRICAL ABLATION FOR LONGSTANDING PERSISTENT ATRIAL FIBRILLATION : MULTICENTER PROSPECTIVE RANDOMIZED STUDYHui-Nam Pak1, Jaemin Shim2, Young-Seog Oh3, Gi-Byung Nam4, Young Keun On5, Tae-Hoon Kim1, Seil Oh6, Byung-Hyun Lim1, Minki Hwang1, Eun-Bo Shim7 1Yonsei University Severance Hospital, Seoul, Republic of Korea; 2Korea University Cardiovascular Center, Seoul, Republic of Korea; 3Catholic University, Seoul, Republic of Korea; 4Asan Medical Center, Seoul, Republic of Korea; 5Samsung Medical Center, Seoul, Republic of Korea;
6Seoul National University, Seoul, Republic of Korea; 7Kangwon National University, Chuncheon, Republic of Korea
CATHETER ABLATION LBT 1-01

116
Introduction: In the largest multicenter, multinational, randomized trial of catheter ablation for atrial fibrillation, we compared clinical outcomes after subgroup analyses by baseline patient demographics and examined costs associated with catheter ablation by either cryoballoon or radiofrequency current (RFC) technology.
Methods: Regression models were used to examine the association between baseline patient demographics and cardiovascular (CV) re-hospitalizations, including the evaluation of patient cohorts that respond more favorable to either catheter technology. Also, a trial-based economic analysis of healthcare costs was conducted from the payer perspective. Analyses were based on rehospitalizations during the trial, with unit costs based on national tariffs (Germany €, UK £, and US $). Total healthcare costs were calculated and differences were analyzed using non-parametric methods.
Results: Subjects (N=750) were randomized 1:1 to cryoballoon or RFC ablation (max follow-up =3 years; mean=1.5 years). Significant baseline demographics associated with CV rehospitalizations were age, BMI, CHA2DS2-VASc score, sex, HATCH score, hypertension, DC cardioversion, and systolic BP. Cryoballoon treated patients had a lower CV rehospitalization rate (P<0.001) and significantly lower than RFC patients in the following subgroups: CHA2DS2-VASc score 0-1 (P=0.01), no heart failure (P=0.07), and prior DC cardioversion (P=0.01). No subgroup analysis favored RFC therapy. The differences in mean total costs of healthcare (per patient) during follow-up were €640, £364, and $925 in favor of the cryoballoon group (P=0.012, 0.013, and 0.016, respectively).
Conclusions: There were demographic characteristics that favored a reduction in CV rehospitalizations for the cryoballoon group, and an economic analysis demonstrated a reduction in costs that persisted across multiple healthcare systems. These important clinical and economic implications should be considered in clinical practice and by health technology assessments.
THE FIRE AND ICE TRIAL: IMPACT OF CATHETER ABLATION TECHNOLOGIES ON PATIENT DEMOGRAPHIC-BASED CLINICAL OUTCOME AND HEALTHCARE COSTSKarl-Heinz Kuck1, Josep Brugada2, Claudio Tondo3, Jean-Paul Albenque4 1Asklepios Klinik St. Georg, Hamburg, Germany; 2Hospital Clinic, Barcelona, Spain; 3Centro Cardiologico Monzino, Milan, Italy; 4Clinique Pasteur, Toulouse, France
CATHETER ABLATION LBT 1-02

117
Introduction: The presence of thrombus in the left ventricle indicates anticoagulation for the potential life threatening of embolic compli-cations, Vitamin K antagonists were the anticoagulants of choice. With the release of new oral anticoagulants (NOAC) and their advantag-es over vitamin K antagonists, the NOAC have replaced the warfarin in many indications. Rivaroxaban is approved for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation (AF), as well as prevention and treatment of venous throm-boembolism.
Methods: N/A.
Results: Ten adult patients (≥ 18 years old) were reported by the echocardiography to have LV thrombus in 2016 at PSMMC cardiac cen-ter. The 9 patients have documented congestive heart failure with systolic dysfunction and normal lab parameters. Four of patients’ have diabetes mellitus, five have hypertension and two have diastolic dysfunction. Patients were initiated on Rivaroxaban with the absence of any contraindications. Response to rivaroxaban was monitored by serial ECHOs at 2, 4, 8 and 12 weeks of Rivaroxaban initiation. In addi-tion the Treatment safety monitored by periodic follow up CBCs & U/E, any signs of bleeding, hemoglobin and INR at clinical visits. Fol-lowing the initiation of Rivaroxaban the LV thrombus sizes have been reduced for all patients; and have disappeared in 7 patients, without any reporting of bleeding or side effects. Only one Patient had ischemic stroke because of missing some doses of rivaroxaban for a period of two weeks, which has been confirmed by the pharmacy records of patients’ medication refill.
Discussion and Conclusions: A case report described the growth of a left atrial appendage thrombus despite well-conducted treatment with a VKA, which then disappeared during treatment with rivaroxaban 15 mg/d. Another recent Japanese team published three cases of left atrial appendage thrombus resolution using rivaroxaban 10 mg/d. To the best of our knowledge the current case series is the first in-cluding 9 patients have successful reduction of LV thrombus and complete dissolution in 6 patients with rivaroxaban in relatively short time compared to VKA.
RIVAROXABAN FOR TREATMENT OF LEFT VENTRICLE THROMBOSISMonirah Albabtain1, Yahya Alhebaishi1, Adel Othman1, Ola Al-Yafi2, Hatim Kheirallah1, Ahmed Alfagih1 1Prince Sultan Cardiac Center, Riyadh, Saudi Arabia; 2Al Maarefa Colleges, Riyadh, Saudi Arabia
HEART FAILURE LBT 1-03

118
Introduction: The majority of patients with non-ischemic cardiomyopathy (NICM) do not have macroscopic scar at autopsy. Presence of CMR-identified late gadolinium enhancement (LGE), representing regional fibrosis, can predict sustained monomorphic VT (SMVT) on ICD follow-up. We characterised CMR findings of ventricular LGE in cardiac arrest (CA) survivors with ventricular fibrillation (VF).
Methods: We examined consecutive VF patients with resuscitated CA undergoing contrast-enhanced 1.5-T CMR between 9/2007-7/2016. We excluded SMVT, hypertrophic cardiomyopathy, amyloid/sarcoid, ARVC, channelopathy, coronary artery disease. VF patients were divid-ed into three groups: (i) NICM, (ii) LV dilatation with normal LVEF, (iii) Normal LV size and LVEF. Two control groups of NICM patients with and without SMVT were also examined.
Results: We analysed 87 VF patients, and found that LGE was seen in 8/22 (36%) with NICM (LVEF 38±11%, LVEDVI 134±68 mL/BSA), 11/40 (28%) with LV dilatation and normal LVEF (LVEDVI 103±17 mL/BSA), 4/25 (16%) with normal LV size and LVEF. The incidence of LGE in all VF groups was less than both control groups (P<0.01), with 117/277 (42%) NICM patients without prior VT/VF (LVEF 36±12%, LVEDVI 141±46 mL/BSA) and 22/37 (59%) NICM patients with SMVT (LVEF 42±11%, LVEDVI 123±48 mL/BSA) being LGE-positive.
Conclusions: The majority of patients presenting with VF do not have LGE on CMR, including those with NICM and LV dilatation. Most failed to meet primary prevention ICD criteria based on LVEF. While LGE predicts increased risk of ventricular arrhythmias (esp. SMVT), its absence does not signify a low risk of VF. Novel risk-stratification tools are needed in NICM.
ABSENCE OF REGIONAL FIBROSIS ON CARDIAC MRI IN VENTRICULAR FIBRILLATION AND NON-ISCHEMIC CARDIOMYOPATHYAleksandr Voskoboinik1, Michael Wong2, Jessica Elliott3, Ben Costello3, Sandeep Prabhu1, Jonathan Kalman4, Peter Kistler5, Andrew Taylor5, Joseph Morton4 1Alfred & Royal Melbourne Hospitals, Baker IDI, Melbourne, Australia; 2Western Health / Eastern Health, Melbourne, Australia; 3Alfred Hospital, Melbourne, Australia; 4Royal Melbourne Hospital, Melbourne, Australia; 5Alfred Hospital & Baker IDI, Melbourne, Australia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION LBT 1-04

THURSDAY POSTER PRESENTATION
(13 October)
120
Introduction: Brugada syndrome is characterized by ST-segment elevation in the right precordial lead of standard electrocardiogram and associated with an increased risk of SCD because of ventricular fibrillation, and is responsible for 4 to 12% of sudden cardiac death in the general population. The frequency is higher in Southeast Asia including Japan compared with Western countries. To date, 20 genes have been associated with Brugada syndrome, but pathogenic mutations in the genes are identified in only about 30% of patients. We have found a novel mutation in CACNA1C gene from a patient with Brugada syndrome who has experienced syncope. The purpose of this study is to identify the electrophysiology mechanisms of a mutation fund inα1 subunit of LTCC (Cav1.2) of a proband with Brugada syndrome.
Methods: The candidate genes were screening by direct sequencing (including: KCNQ1, KCNH2, SCN5A, ANK2, KCNE1, KCNE2, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP9, SNTA1; SCN5A, CACNA1C, CACNB2, GPD1L, SCN1B, KCNE3, SCN3B, HCN4, RYR2 and CASQ2). Whole cell patch clamp analysis of the HEK293 cell with express the mutant channel was used to investigate the molecular and electro-physiology mechanism.
Results: Sequence analysis of the coding region of the CACNA1C gene, identified a G to A heterozygous missense mutation at nucleotide site 5,849 that resulted in an amino acid substitution of arginine to lysine at amino acid site 1950 (R1950K) [Figure 1]. Patch clamp analysis showed that the R1950K significantly reduce the current density of LTCC in transfected HEK293 cell (R1950K: -9.80±2.90 pA/pF; vs. WT: -26.64±3.17 mV; P<0.001). The reduction rate was almost 36.79%. The half-maximal activation (V1/2) and slope value (k) were not different between R1950K and WT (V1/2: 12.22±0.41 mV; vs. 12.23±0.28 mV, P=0.786; K: 6.82±0.26; vs. 6.11±0.38; P=0.194).
Conclusions: This is the first CACNA1C mutation related to Brugada syndrome in Chinese population, and the electrophysiology mecha-nism was reduced function of LTCC.
THE ELECTROPHYSIOLOGY MECHANISM OF CACNA1C (R1950K) CAUSE L TYPE CALDIUM CHANNEL DYSFUNCTION WITH BRUGADA SYNDROMELi Feng, Ke-juan Ma, Xin Li, Changsheng Ma
Beijing Anzhen Hospital, Beijing, China
BASIC/TRANSLATIONAL SCIENCE P 1-001

121
Introduction: Long QT syndrome (LQTS) is characterized by prolonged QT intervals on the electrocardiogram, and ventricular arrhyth-mias. Mutations in genes encoding cardiac ion channels result in ion channel dysfunction and cause LQTS. KCNH2 encodes Kv11.1 chan-nel which produces rapid component of delayed rectifier potassium current and its mutations cause LQTS type 2. This study aimed to identify mutations in LQTS related genes and perform functional analysis of mutant channel which remains to be elucidated.
Methods: The genetic screening for LQTS related genes was performed in two unrelated LQTS probands. KCNH2-Wild-type (WT) and/or T826I were expressed in Chinese hamster ovary cells, and currents were recorded using the patch clamp technique. Immunostaining was performed using Human embryonic kidney cells transfected with WT and/or T826I. Cells were permeabilized, incubated with anti-Kv11.1 antibody, labeled with secondary antibody, and studied by a confocal microscope.
Results: We identified a heterozygous mutation, KCNH2-T826I (c.2477 c>t), in the probands. Figure shows Kv11.1 current traces of WT and/or T826I, the current-voltage relations and normalized activation curves. Compared with WT, WT+T826I decreased Kv11.1 currents, and no currents were observed in T826I alone. In cells expressing WT alone and WT+T826I, we could detect fluorescence on the cell membrane, while in cells expressing T826I alone, it was mostly distributed in cytosol.
Conclusions: KCNH2-T826I disrupted the intracellular transport of Kv11.1 to the cell membrane and exerted loss-of-function type of ef-fects on Kv11.1, which may explain the clinical phenotypes of the probands.
KCNH2 MUTATION IN PATIENTS WITH LONG QT SYNDROME TYPE 2Daisuke Fukumoto, Seiko Ohno, Yuko Wada, Yusuke Fujii, Mari Ichikawa, Hideki Ito, Wei-Guang Ding, Hiroshi Matsuura, Minoru Horie
Shiga University of Medical Science, Otsu, Japan
BASIC/TRANSLATIONAL SCIENCE P 1-002

122
Introduction: Short leukocyte telomere length (LTL) is related to aging disease. However, the impact of LTL in atrial substrate remodeling and outcome after catheter ablation of paroxysmal atrial fibrillation (AF) has not been evaluated. This study aims to correlate LTL with atrial substrate and test the role of LTL as a new biologic aging marker to predict the recurrence after AF ablation.
Methods: A total of 78 participants including 26 healthy individuals and 52 symptomatic paroxysmal AF patients received catheter ablation were enrolled. Peripheral blood mononuclear cells of all the participants were collected to measure leukocyte telomere length (LTL). Par-oxysmal AF patients received catheter ablation were divided into two group: recurrent AF post catheter ablation (n=11) and no recurrent AF post catheter ablation (n=41). All of paroxysmal AF patients received atrial eletroanatomic voltage mapping during eletrophysiologic study.
Results: LTL in healthy individuals (n=17) is longer than that in paroxysmal AF patients (n=12) with age under 50 years old. Using ROC curve analysis, the length of LTL <7.12 kbp can discriminate paroxysmal AF from normal subjects at age under 50 years old with sensitiv-ity of 83%; specificity of 68%. In paroxysmal AF patients group, LTL was positive correlated with left atrial bipolar voltage (R=0.839, P<0.001) and was negative correlated with bipolar scar area (R=-0.353, P=0.01). LTL was shorter in the patient with recurrent AF post catheter ablation in patients without recurrent AF post catheter ablation (6.53±0.25 kbp vs. 6.95±0.5 kbp P=0.01). Using ROC curve analy-sis, cutoff value of <6.54 kbp with a specificity of 0.636, a sensitivity of 0.805 to predict the recurrent AF post catheter ablation in young pa-tient diagnosed with symptomatic paroxysmal AF.
Conclusions: Paroxysmal AF patients had shorter LTL compared to normal subjects at the age under 50 years old. Shorter LTL with de-generative atrial substrate also can predicts recurrent AF post catheter ablation in young paroxysmal AF patients.
SHORTER LEUKOCYTE TELOMERE LENGTH IS ASSOCIATED WITH ATRIAL REMODELING AND PREDICTS THE RECURRENCE OF ATRIAL FIBRILLATION AFTER RADIO FREQUENCY ABLATION THERAPYKuo Li Pan
Division of Cardiology, Chang Gung Memorial Hospital, Chiayi, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 1-003

123
Introduction: Lamins are fibrous proteins providing structural function and transcriptional regulation in the cell nucleus. Nuclear lamina lies on the inner nuclear membrane, which serves to maintain nuclear stability and connection to the cytoskeleton and bind nuclear pore complex, envelope proteins, and transcription factors. Lamin A/C is encoded by the LMNA gene which is the most common A-type lamins, predominantly expressing in differentiated cells. LMNA mutations can lead to various diseases such as cardiomyopathy, congenital mus-cular dystrophy, lipodystrophy syndromes, peripheral neuropathy, mandibuloacral dysplasia, and progeria. LMNA-related cardiomyopathy is associated with familial dilated cardiomyopathy (DCM) with cardiac conduction system disease (CCD). Patients exhibit cardiac pheno-types with advancing age. However, the crucial disease causing mechanism is still unexplained. Human Induced pluripotent stem cells (hiPSCs) offer an opportunity to model human diseases in relevant cell types. We aimed to recapitulate the phenotype of LMNA-related cardiomyopathy using hiPSCs derived cardiomyocytes (hiPSC-CMs). CRISPR-Cas9 system using the RNA-guided DNase Cas9 has proven to be an efficient genome-editing tool even in hiPSCs. Cas9 nickase was reported to enable to mutate genes with minimizing off-target effects.
Methods: Two sets of Guide RNA were designed for LMNA knock-out process which target the exon 1 or exon 2 of LMNA gene. We evalu-ated the activity of the CRISPR-Cas9 nickase vectors in HEK293 cells using pCAG-EGxxFP validation plasmid which is incorporating target region. Then, the designed guides have been transfected into wild type hiPSCs. Off target candidates were PCR amplified and sequenced.
Results: Approximately, 70% of HEK cells have been transfected, and 20% of them showed EGFP fluorescence 48 hrs after transfection while the cells which were transfected without target plasmid did not revealed any fluorescence. Wild type hiPSCs were successfully ge-nome edited by CRISPR-Cas9 nickase, and LMNA-KO hiPSCs has been obtained. Two sets of Guide RNA has edited LMNA exon 1 or exon 2. Interestingly, no homozygous editing has been produced in exon 1, while three variants of homozygously edited clones were detected in exon 2. We obtained 43% (13/30 clones) LMNA genome edited clones in picked up clones, and homozygous knock out clones were only 23% (3/13 clones).
Conclusions: Our data demonstrate that hiPSCs gene can be differentiated into cardiomyocytes even under the LMNA deficiency. Since homozygous LMNA deficiency human is unable to survive, homozygous LMNA deficiency hiPSCs may reveal severe phenotype, which is very useful for understanding the disease causing mechanism of laminopathies.
GENERATION OF LMNA KNOCK OUT HUMAN INDUCED PLURIPOTENT STEM CELLS USING THE CRISPR-CAS9 NICKASE SYSTEMYimin Wuriyanghai1, Takeru Makiyama2, Suguru Nishiuchi2, Fumika Yokoi2, Mamoru Hayano2, Yuta Yamamoto2, Takeshi Harita2, Hirohiko Kohjitani2, Ayako Hirose2, Seiko Ohno3, Yoshinori Yoshida4, Minoru Horie3, Takeshi Kimura2
1Shiga University of Medical Science, Otsu, Japan; 2Department of Cardiovascular Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan; 3Department of Cardiovascular and Respiratory Medicine, Shiga University of Medical Science, Otsu, Japan; 4Center for iPS Cell Research and Application, Kyoto University, Kyoto, Japan
BASIC/TRANSLATIONAL SCIENCE P 1-004
124
Introduction: Aging is a very important factor to increase the incidence of atrial fibrillation (AF) and to confer the risk of thromboembo-lism, however, the pathogenesis of aged atrial fibrillation remains poorly understood.
Methods: Samples of right atrial appendage were collected from patients undergoing aortic valve replacement. Patiens with mitral valve diseases, rheumatic valve diseases, left atrial dimension >50 mm were not included. Patients were divided into six groups: aged 40 in si-nus rhythm (SR-40), aged 50 in sinus rhythm (SR-50), aged 60 in sinus rhythm (SR-60), aged 70 in sinus rhythm (SR-70), aged 60 in AF (AF-60) and aged 70 in AF (AF-70). Genome-wide transcriptomic profiling was performed.
Results: Among four SR groups, we found 257 genes accociated with atrial aging were significantly up-regulated and 304 genes were sig-nificantly down-regulated. Among SR-60, SR-70, AF-60 and AF-70, 62 genes accociated with atrial fibrillation were significantly up-regu-lated and 56 genes were significantly down-regulated. 10 genes were identified with both atrial aging and atrial fibrillation. Functional classification based on Gene Ontology Database were conducted and demonstrated these genes were strikingly accociated with immuno-modulatory regulation and electrophysiological remodeling.
Conclusions: Our study first revealed 10 genes and several signaling pathways significantly involved in aged AF-related transcriptional expression, which may yield novel insight into aged AF pathogenesis.
TRANSCRIPTIONAL PROFILE AND FUNCTIONAL ANALYSIS OF AGED ATRIAL FIBRILLATIONYan Yao, Xin Du, Jianzeng Dong, Changsheng Ma
Beijing Anzhen Hospital, Beijing, China
BASIC/TRANSLATIONAL SCIENCE P 1-005

125
Introduction: PITX2 encodes paired-like homeodomain transcription factor-2 and its genetic variants are associated with atrial fibrillation (AF).We aimed to assess the associations between single nucleotide polymorphisms (SNPs) of PITX2 and the risk of AF in a Chinese Han Population.
Methods: We genotyped five SNPs including four tagging SNPs and one previously reported SNP using the improved multiplex ligation detection reaction (iMLDR) technique. To confirm the observed effects of rs2200733 on AF, genotyping was performed again using the TaqMan allelic discrimination assay. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated in logistic regression models.
Results: We recruited a total of 2,300 Chinese Han origin individuals in this study, including 1,150 AF patients and 1,150 AF-free controls. Among the five SNPs analyzed in the study, the T allele of rs1982361 in PITX2 was found to be significantly associated with a decreased risk of AF (crude OR=0.75, 95% CI: 0.67-0.85, P=2.840×10−6; adjusted OR=0.75, 95% CI: 0.66-0.85, P=2.75×101). While the T allele of rs2200733 was associated with an increased risk of AF (crude OR=2.13, 95% CI: 1.88-2.41, P=8.13×10−34; adjusted OR=2.10, 95% CI: 1.85-2.40, P=2.53×10−29). To confirm the observed effects of rs2200733 on AF, genotyping was performed again using the TaqMan allelic dis-crimination assay. Finally, theassociation between rs2200733 and AF risk was consistently (adjusted OR =2.10, 95% CI: 1.84-2.40, P=6.59×10-29, call rate=99.7%). Stratification analyses indicated that there were no significant differences of association between the SNPs and AF risk on age, gender, diabetes and hypertension.
Conclusions: Our findings suggest that two SNPs rs1982361 (C>T) and rs2200733 (T>C) of PITX2 may contribute to the risk of AF in Chi-nese Han populations. However, future biological function analyses and pharmacological investigation are warranted to confirm our find-ings.
GENETIC POLYMORPHISMS IN PITX2 ARE ASSOCIATED WITH ATRIAL FIBRILLATION IN A CHINESE HAN POPULATIONFengxiang Zhang, Liyan Zhao, Zhen Fang, Yan Xu
The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
BASIC/TRANSLATIONAL SCIENCE P 1-006

126
Introduction: Recent studies identified nine new susceptibility single nucleotide polymorphisms (SNPs) for atrial fibrillation (AF) in individ-uals of the European ancestry. We aimed to replicate the associations between these SNPs and the risk of AF in a Chinese Han popula-tion.
Methods: We genotyped eight SNPs (rs6584555, rs10507248, rs13216675, rs6490029, rs9388451, rs10428132, rs251253 and rs11047543) using the improved multiplex ligation detection reaction (iMLDR) technique. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated in logistic regression models.
Results: We enrolled a total of 2,300 Chinese Han origin individuals in this study, including 1,150 AF patients and 1,150 AF-free controls. Logistic regression analyses in additive genetic model revealed that 4 SNPs (rs6584555, rs10507248, rs13216675 and rs11047543) were associated with an increased risk of AF (OR=1.51, 95% CI: 1.27-1.78, Padd=1.95×10-6; OR=1.16, 95% CI: 1.02-1.31,Padd=0.022; OR=1.16, 95% CI=1.02-1.31, Padd=0.025; OR=1.25, 95% CI: 1.03-1.52, Padd=0.025, respectively). After multiple comparisons, the SNP rs6584555 re-mained significant association with the risk of AF (OR=1.51, 95% CI: 1.27-1.78, Padd=1.95×10-6, PFDR =1.56×10-5). Stratification analyses in-dicated that there were no significant differences of association between the SNPs and AF risk on age, gender, diabetes and hypertension.
Conclusions: Our findings suggest that SNPs rs6584555 C allele may contribute to the risk of AF in Chinese Han populations. However, future biological function analyses and pharmacological investigation are warranted to confirm our findings.
THE RS6584555 PLYMORPHISM IN NEURL IS ASSOCIATED WITH THE RISK OF ATRIAL FIBRILLATION IN CHINESE HAN POPULATIONFengxiang Zhang, Liyan Zhao, Zhen Fang, Yan Xu
The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
BASIC/TRANSLATIONAL SCIENCE P 1-007

127
Introduction: A recent genome-wide association study (GWAS) identified a single nucleotide polymorphism (SNP) in SCN10A associated with atrial fibrillation (AF) risk in European descent populations. The aim of this study was to evaluate whether SCN10A polymorphisms are associated with AF risk in the Chinese Han population.
Methods: A total of 2,300 Chinese Han origin individuals were recruited in this study. We genotyped three potentially functional SNPs in a Chinese Han population. Logistic regression models were utilized to calculate odds ratios (ORs) and 95% confidence intervals (CIs).
Results: Logistic regression analyses in an additive genetic model revealed that one SNP in SCN10A (rs6771157) was associated with an increased risk of AF (adjusted OR=1.20, 95% CI: 1.06-1.36, P=0.003). Stratification analysis of several main AF risk factors indicated that the risk associations with rs6771157 were not statistically different among different subgroups.
Conclusions: In summary, our study suggests the possible involvement of the SCN10A variant in AF development in Chinese Han popula-tions. Further biological function analyses are required to confirm our finding.
THE RS6771157 C/G POLYMORPHISM IN SCN10A IS ASSOCIATED WITH THE RISK OF ATRIAL FIBRILLATION IN A CHINESE HAN POPULATIONFengxiang Zhang1, Zhen Fang1, Yaowu Liu2, Liyan Zhao2, Yan Xu2 1The First Affiliated Hospital of Nanjing Medical University, Nanjing, China; 2Zhongda Hospital of Southeast University, Nanjing, China
BASIC/TRANSLATIONAL SCIENCE P 1-008

128
Introduction: Cardiac Channelopathy affecting sodium channel mutation may have multiple clinical manifestations.
Methods: N/A
Results: A 50 year old female presented with sustained monomorphic ventricular tachycardia requiring DC cardioversion. Post cardiover-sion she developed bradycardia with irregular ventricular rate and no visible P wave. Echocardiography showed dilatation of right atrium (RA) and right ventricle (RV). Invasive electrophysiological testing showed presence atrial electrogram but despite highest output pacing, right atrium could not be captured. Son of the proband (30 year, male) presented with history of syncope. Surface ECG revealed absent P wave. Echocardiography showed dilatation of RA and RV. Invasive electrophysiological testing was suggestive of atrial standstill. A histo-logical specimen from the right ventricular endocardium was normal. Sister of proband (38 year female) presented with intermittent atrial fibrillation and incomplete RBBB. 24 hours monitoring showed long sinus pauses. Echocardiography showed dilated RA and RV. Invasive electrophysiological testing showed electrically active right atrium. Son of the proband was subjected to genetic analysis by Next Genera-tion sequencing (NGS) technique, which showed that the individual harbours variation in SCN5A (p.Asp1275Asn) and BRCA1 (p.Ser1503T-er) gene. Mutation analysis study showed that proband and her sister harbour the same variation in SCN5A and BRCA1. Apart from LQTS3 and Brugada syndrome, SCN5A mutation can cause inherited progressive cardiac conduction defect (PCCD), sick sinus syndrome, atrial fibrillation, dilated cardiomyopathy and atrial standstill. Overlap syndromes of cardiac sodium Channelopathy consisting of multiple rhythm disturbances within one family, as in our case have also been reported. Concurrent role of BRCA1 mutation is not clear. BRCA1 mutation has been reported to be associated with increased cardiac apoptosis. Whether it is implicated with the disease manifestations (direct or as genetic modifier) or it is an incidental polymorphism, requires further research.
Conclusions: We report a family presenting with various arrhythmias associated with SCN5A and BRCA1.
PLEOMORPHIC MANIFESTATIONS OF SODIUM CHANNELOPATHY IN A FAMILYPraloy Chakraborty1, H S Isser1, Sudheer Arava2, Kausik Mandal3 1VMMC and Safdarjung Hospital, Delhi, India; 2All India Institute of Medical Science, Delhi, India; 3Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India
BASIC/TRANSLATIONAL SCIENCE P 1-009

129
Introduction: Low-density lipoprotein receptor-related protein 6 (LRP6) is a coreceptor for the Wnt signaling cascade and plays a critical role in regulating Wnt signaling. Dysregulated Wnt signaling contributed to a high incidence of arrhythmias. Thus, it was suggested the possible relationship between genetic variations of LRP6 and sudden cardiac death (SCD). We explored the associations between LRP6 polymorphisms and prognosis of patients with chronic heart failure (CHF).
Methods: From July 2005 to December 2009, patients with CHF referred from 10 hospitals and participants without structural heart dis-ease in China were undergone a prospective study. Based on the result of pre-test, the single-nucleotide polymorphism (SNP) rs2302684 was selected to evaluate the effect of LRP6 polymorphisms on the survival of the patients by cox proportional hazards models.
Results: A total of 1,887 patients were finally enrolled for the analysis, including 1,437 patients with CHF and 450 patients in the control group. During a median follow-up of 61 months (range 0.4 to 129 months), a total of 546 (38.00%) patients died, including 201 (36.81%) cases with SCD and 345 (63.19%) cases with non-SCD. No end point event occurred in the control group. Patients carrying A allele of rs2302684 had increased risks of all-cause death (HR 1.396, 95% CI 1.167-1.670; P<0.001) and SCD (HR 1.832, 95% CI 1.378-2.435; P<0.001). After adjusted for the other risk factors, the associations remained significant in all-cause death (HR 1.370, 95% CI 1.143-1.643; P=0.001) and SCD (HR 1.763, 95% CI 1.321-2.353; P<0.001).
Conclusions: The SNP rs2302684 T>A in LRP6 indicated a higher risk of all-cause death and SCD in patients with CHF.
RELATIONSHIP BETWEEN LRP6 POLYMORPHISMS AND SUDDEN CARDIAC DEATH IN PATIENTS WITH CHRONIC HEART FAILUREQi Guo, Jielin Pu, Jianmin Chu, Shu Zhang
Fuwai Hospital, Beijing, China
BASIC/TRANSLATIONAL SCIENCE P 1-010

130
Introduction: Mutations in ANK2 have been reported to cause various arrhythmia phenotypes. However, prevalence of ANK2 mutation carriers in inherited primary arrhythmia syndromes (IPAS) in Japanese is still unclear. Using next generation sequencers, we aimed to identify ANK2 mutations in our cohort of IPAS in whom had no pathogenic mutations in major causative genes, and assess the clinical characteristics of ANK2 mutation carriers.
Methods: We screened 535 probands with IPAS: 341 LQTS, 58 Brugada syndrome (BrS), 40 idiopathic ventricular fibrillation (IVF), 27 cate-cholaminergic polymorphic ventricular tachycardia (CPVT), 22 sick sinus syndrome (SSS)/atrial fibrillation (AF), 16 sudden cardiac death (SCD) (molecular autopsy), 11 short-coupled variant of torsade des points (SCTdP), seven ventricular tachycardia (VT), seven short QT syn-drome (SQTS), and six complete AV block (CAVB). We analyzed 45 genes including whole ANK2 exons using a bench-top next generation sequencer (MiSeq, Illumina), or performed whole-exome-sequencing using HiSeq2000 (Illumina).
Results: Twelve of 535 probands (2.2%, aged from 0 to 61, six males) were found to carry seven different heterozygous ANK2 mutations. ANK2-W1535R was identified in five LQTS patients and one symptomatic BrS and was predicted as damaging by multiple prediction soft-wares. In total, there were eight LQTS, two BrS, one IVF, and one SSS/AF. Seven of 12 patients were documented malignant ventricular tachyarrhythmias. Surprisingly, seven of eight probands showing LQTS phenotype (87.5%) were concealed type of LQTS. Additional factors disclosed their QT prolongation and provoked torsades de pointes, and after removal of these modifiers, the QTc interval was nearly nor-malized (443±37 ms). Furthermore, their mean age of first diagnosis (39±17 years old) was older than that in typical congenital LQTS. They are also consistent with acquired type of LQTS.
Conclusions: We identified multiple ANK2 mutations in IPAS patients using NGS. Various ANK2 mutations are associated with a wide range of phenotypes, and Ankyrin-B syndrome would be of primary importance for the differential diagnosis of IPAS, especially those with malignant ventricular tachycarrhythmias and/or aLQTS phenotype.
VARIOUS ANK2 MUTATIONS IN PATIENTS WITH INHERITED PRIMARY ARRHYTHMIA SYNDROMESMari Ichikawa1, Takeshi Aiba2, Seiko ohno1, Daichi Shigemizu3, Junichi Ozawa1, Keiko Sonoda1, Megumi Fukuyama1, Hideki Itoh1, Yoshihiro Miyamoto2, Tatsuhiko Tsunoda3, Takeru Makiyama4, Toshihiro Tanaka5, Wataru Shimizu6, Minoru Horie1 1Shiga University of Medical Science, Shiga, Japan; 2National Cerebral and Cardiovascular Center, Suita, Japan; 3Tokyo Medical and Dental University, RIKEN Center for Integrative Medical Sciences, Tokyo, Yokohama, Japan; 4Kyoto University Graduate School of Medicine, Kyoto, Japan; 5Tokyo Medical and Dental University, Tokyo, Japan; 6Nippon Medical School, Tokyo, Japan
BASIC/TRANSLATIONAL SCIENCE P 1-011

131
Introduction: LQTS 10 is among the very rare forms of LQTS described sparingly. Phenotypically it is supposed to mimic LQTS 3 and is as-sociated with sodium channel dysfunction due to defective gene SCN4B. We present a case of a 2 year old boy and his mother having SCN4B mutation with the child having congenital complete heart block (CCHB) and documented LQTS.
Methods: N/A
Results: A 2 year old child presented to us with recurrent “seizures” on crying and immune mediated congenital complete heart block in 2009. The child had bradycardia related polymorphic Ventricular Tachycardia and a prolonged QT. An ECG of 2008 showed QT of 480 and QTC of 537 ms. His mother apart from being positive for anti Ro and anti La antibodies had history of documented seizures with an MRI showing demyelinating lesions in the brain. She, her husband and paternal grandmother had a normal ECG. The child was given an en-docardial VVIR pacemaker and put on beta-blockers after which he stopped having “seizures”. However, after being on paced rhythm he rarely showed an obvious LQTS and never had a documented tachycardia. Neither did the pacemaker ever show ventricular high rates. We were no longer certain about the diagnosis over the years till we got the opportunity to get the exome analysis. Our whole exome anal-ysis revealed a heterozygous frameshift deletion (c.110delG; p.G37fs) in exon 2 of SCN4B gene, which is predicted to be deleterious by SIFT Indel tool. This variant is found to be present in affected child and mother but absent in unaffected father and paternal grandmother. The present variation is not present in 1,000 genome, ExAC, and internal database suggesting that the mutation is novel. The child is now nearly 11 years old and is on extended release Propranolol 480 mg/day.
Conclusions: Facilities for in house genetic testing that have become available to us in India only recently, unraveled a rather remarkable association. The only rather faded initial ECG of 2008 showed a pattern similar to LQTS 3. Though prolonged QTc is considered an indica-tion to pace in immune mediated CCHB there are hardly any reports documenting this association and its genetics. It would be interesting to evaluate all such patients and identify the underlying putative mutations.
LQTS 10 IN A CHILD WITH CONGENITAL COMPLETE HEART BLOCKRajnish Juneja1, Ankit Verma2, Neeraj Parakh1, Rijith Jayarajan2, Rowmika Ravi2, Shamsudeen Karuthedath Vellarikkal2, Gautam Sharma1, Nitish Naik1, Vinod Scaria2, Sridhar Sivasubbu2 1All India Institute of Medical Sciences, New Delhi, India; 2Institute of Genomics & Integrative Biology, New Delhi, India
BASIC/TRANSLATIONAL SCIENCE P 1-012

132
Introduction: Recently, we identified 6 common genetic susceptibility loci for the risk of early onset atrial fibrillation (AF) before 60 years old by genome-wide association studies (GWAS) in Korean AF network. The purpose of this study was to validate those early onset-AF as-sociated genetic loci by genetic risk score (GRS) using longitudinal data of independent Korean community based cohort.
Methods: Counted GRS were constructed from 6 SNPs related to early onset AF proven in the previous Korean AF GWAS and replication studies. We conducted a population based case-control study consisting men and women, aged 40-69 years recruiting between June 2001 and January 2003. We examined new and prevalent cases of AF, which were ascertained by electrocardiogram using follow-up data, and conducted logistic regression analyses considering GRS and potential risk factors collected from a baseline questionnaire.
Results: 1) During median follow-up duration of 9.9 years, 127 cases of AF were examined (25 cases prevalent and 102 cases of new on-set AF). 2) The mean age, body mass index (BMI), CHA2DS2-VASc score, and GRS were significantly higher in AF cases compare to those of controls in comparisons of baseline values. 3) In multivariable analysis, GRS was independently associated with AF risk (OR 1.20 [1.08-1.34], P<0.001) after adjusting confounding risk factors, such as age, BMI, CHA2DS2-VASc score, cigarette smoking status and alcohol drinking. 4) In the age-dependent tertile analysis, GRS had a significant association with early-onset AF cases (≤60 years old, OR 1.22 [1.02-1.47], P=0.031), but not with new onset AF at the age over 60. 5) GRS predicted higher greater risk of AF in men (OR 1.32 [1.16-1.50], P<0.001), but not associated with AF risk of women.
Conclusions: Korean AF network identified GRS for early onset AF predicts AF risk in the independent community-based cohort, espe-cially among the patients young than 60 years old and male gender.
VALIDATION OF KOREAN AF NETWORK GENETIC RISK SCORE FOR EARLY ONSET ATRIAL FIBRILLATION IN THE INDEPENDENT COMMUNITY-BASED COHORJi-Young Lee1, Hong-Euy Lim2, Eui-Keun Choi3, Jaemin Shim4, Tae-Hoon Kim1, Eunsoon Shin5, Jae-Sun Uhm1, Jin-Seok Kim2, Boyoung Joung1, Seil Oh3, Moon-Hyoung Lee1, Young-Hoon Kim4, Hui-Nam Pak1 1Yonsei University College of Medicine, Seoul, Republic of Korea; 2Korea University Guro Hospital, Seoul, Republic of Korea; 3Seoul National University Hospital, Seoul, Republic of Korea; 4Korea University Anam Hospital, Seoul, Republic of Korea; 5DNA Link Incorporaton, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 1-013

133
Introduction: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is mainly associated with desmosomal gene mutations. Some other gene mutations, such as desmin gene (DES) or catenin alpha 3 gene (CTNNA3), were reported to be related with ARVC from West-ern countries. Desmin is an intermediate-filament protein of muscle cells. Catenin constitutes the area composita enhancing cell-cell adhesion. However, non-desmosomal gene mutations and their phenotype have been rarely reported in Japanese patients.
Methods: We analyzed three patients without desmosomal gene mutations by cardiomyopathy panel for next generation sequencer (NGS), and studied the phenotypical characteristics.
Results: The first patient was a 53-year-old man, who resuscitated from sudden ventricular fibrillation by automated external defibrillator and was admitted urgently. Electrocardiogram (ECG) showed epsilon waves in the V1 lead. Echocardiogram (UCG) represented dilatation and dysfunction in bi-ventricle. Fatty replacement of RV muscle was revealed by CT. According to ARVC diagnostic criteria 2010, he was clinically diagnosed as borderline ARVC. We identified a missense mutation in DES (c.129G>T, p.K43N). Next patient was a 45-year-old man, who was affected with skeletal myopathy. In the V1-V4 leads of ECG, there were incomplete right bundle brock (IRBBB) and epsilon waves. UCG, MRI and right ventriculography indicated RV dilatation and an aneurism at the base of RV. He was diagnosed as definite ARVC. We identified DES splice error (c.639-1G>C). The last patient was a 70-year-old man, who visited our hospital to treat paroxys-mal atrial fibrillation. ECG showed IRBBB. Late potentials by signal-averaged ECG were positive. UCG revealed RV dilatation and apical asynergy. He was diagnosed as borderline ARVC. We detected a missense mutation in CTNNA3 (c.1382T>C, p.N462S).
Conclusions: Although the frequency of ARVC patients caused by mutations in DES or CTNNA3 is low, the genetic screening for these genes is indispensable to elucidate the genetic background of the patients. To detect the mutations in rare genes, cardiomyopathy panel for NGS would be useful.
NON DESMOSOMAL MUTATIONS DETECTED IN JAPANESE PATIENTS WITH ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHYKoichiro Takayama, Seiko Ohno, Yuko Wada, Minoru Horie
Shiga University of Medical Science, Otsu, Shiga, Japan
BASIC/TRANSLATIONAL SCIENCE P 1-014

134
Introduction: Recent evidence has demonstrated that specialised multidisciplinary care, in addition to software support to facilitate guide-line adherence, was associated with enhanced patient outcomes in the AF population. This study aimed to examine the difference be-tween adherence to guideline recommended care in the specialist EP managed arrhythmia clinic (AC) and general cardiologist managed cardiac clinic (CC).
Methods: A retrospective audit was undertaken for AF patients managed in the specialist arrhythmia and general cardiac clinics of a large tertiary referral centre from January to December 2014. Four aspects of AF care were evaluated: 1) Appropriate anticoagulation ac-cording to the CHA2DS2-VASc score; 2) Appropriate use of anti-arrhythmic medications (not used in those with permanent AF) and appro-priate utilization of investigations in the preceding two years: 3) Transthoracic echocardiogram and 4) Thyroid function testing.
Results: A total of 304 AF (111 AC and 193 CC) patients were included for analysis (see Table). Patients were age and gender matched, however, the mean CHA2DS2-VASc score was lower and valvular and permanent AF was less prevalent in the arrhythmia clinic group. Ap-propriate anticoagulation occurred more frequently in those attending the AC as compared with the CC. There was no significant differ-ence in adherence to appropriate use of antiarrhythmic therapy, transthoracic echocardiography and thyroid function testing.
Conclusions: Specialist EP management is associated with greater guideline adherence to appropriate anticoagulation that may translate to improved patient outcomes. Further prospective studies are needed to demonstrate the advantages of integrated multidisciplinary AF care with EP input.
SPECIALISED AF MANAGEMENT IS ASSOCIATED WITH GREATER ADHERENCE TO GUIDELINE RECOMMENDED CARECeline Gallagher1, Geoffrey R Wong2, Geetanjali Rangnekar1, Simon Rocheleau2, Anthony Brooks1, Jeroen Hendriks1, Melissa Middeldorp1, Rajiv Mahajan1, Prashanthan Sanders1, Dennis Lau1 1University of Adelaide, South Australian Health and Medical Research Institute, Adelaide, Australia; 2Royal Adelaide Hospital, Adelaide, Australia
ALLIED PROFESSIONALS P 1-015

135
Introduction: Radiofrequency catheter ablation (RFA) for Wolff-Parkinson-White (WPW) Syndrome is successful in the majority of pa-tients. However, failure occurs in a small percentage of patients. This study aims to determine factors and techniques that may help over-come failure of initial RFA procedures.
Methods: This is a retrospective study of all cases of WPW patients who underwent RFA from June 2008 until April 2016. The factors as-sociated with successful repeat ablation were studied.
Results: A total of five hundred WPW patients underwent RFA during the specified time period. Of these reported, 25 patients (5%) had failure of initial RFA. Eighty percent (n=20) of these failed cases were males. Seventy six percent (n=19) were Chinese. The age of these patients ranged from 11-80 years. Among the subjects with initial failed RFAs, 15 (60%) underwent a re-do RFA procedure. The repeat ab-lation was successful in 12 (80%) of the re-do cases, while 3 (20%) still had failed RFA procedures. Subjects with successful redo RFAs had the following pathway sites: 25% (n=3) at right posteroseptal, 25% (n=3) at right parahisian, 25% (n=3) at left free wall, 17% (n=2) at right free wall, and 8% (n=1) at right sided multiple accessory pathway with Ebstein anomaly. For those who have successful redo RFAs, long sheaths were used in 40% (n=6) of patients, 3D mapping system was used in 40% (n=6) of patients, cool flow irrigation system was used in 47% (n=7) of patients; and stereotaxis remote magnetic navigation system (MNS) was used in 13% (n=2) of patients.
Conclusions: The use of long sheaths, irrigated catheters together with 3D mapping systems and remote MNS may be useful to deal with cases with previous failed RF ablation of accessory pathways.
HOW TO OVERCOME FAILURES OF INITIAL RADIOFREQUENCY CATHETER ABLATION OF PATIENTS WITH WOLFF-PARKINSON-WHITE SYNDROME: AN 8-YEAR RETROSPECTIVE STUDYKaung Htoo Lwin, Maria Blanca De Guzman, Paul Chun Yih Lim, Daniel Thuan Tee Chong, Tan Boon Yew, Ho Kah Leng, Ching Chi Keong, Teo Wee Siong
National Heart Centre of Singapore, Singapore
ALLIED PROFESSIONALS P 1-016

136
Introduction: Right ventricular outflow tract (RVOT) septal pacing was thought to be superior to apical pacing in the prevention of cardiac dyssynchrony in early stage, however, there have been no reports on the contribution of long term high percentage RVOT septal pacing to left ventricular (LV) function. This study aims to evaluate the effect of long term high percentage RVOT septal pacing on LV function com-pared with long term low percentage RVOT septal pacing.
Methods: A total of 100 patients diagnosed with sick sinus syndrome or complete AV block who received pacemaker implantation therapy were enrolled and divided into 2 groups: RVOT septal pacing >90% (n=49), and RVOT septal pacing <10% (n=51). Patients underwent a comprehensive Doppler echocardiography examination to evaluate LV volume, systolic and diastolic function and interventricular, intra-ventricular dyssynchrony.
Results: Clinical follow-up periods were not significantly different in RVOT septal pacing >90% group and RVOT septal pacing <10% group (3.69±2.68 years vs. 2.99±2.34 years, P=0.16). However, the RVOT septal pacing >90% group had significant lower LV ejection fraction (58.52±13.82% vs. 69.74±6.83%, P<0.001); higher Tei index (0.66±0.26 vs. 0.36±0.12), longer septal to posterior wall motion delay (SPW-MD) (137.70±57.44 ms vs. 80.93±31.89 ms), and longer interventricular mechanical delay (IVMD) (24.57±14.95 ms vs. 11.89±9.85 ms).
Conclusions: Long term high percentage (ventricular pacing >90%) RVOT septal pacing impaired LV systolic and diastolic function and made LV intracentricular dyssyncrony and interventricular dyssynchrony.
LONG TERM HIGH PERCENTAGE RIGHT VENTRICULAR OUTFLOW TRACT SEPTAL PACING CONTRIBUTES TO LEFT VENTRICULAR FUNCTIONAL REMODELINGKuo Li Pan
Division of Cardiology, Chang Gung Memorial Hospital, Chiayi, Taiwan
ALLIED PROFESSIONALS P 1-017
137
Introduction: In order to study clinical outcomes of using thrombolytic agent (alteplase) as primary reperfusion in patients with acute ST-segment elevation myocardial infarction in The Ha Tinh General Hospital.
Methods: Data on demographics, medications, in-hospital outcomes were collected from a prospective registry of acute ST-segment ele-vation myocardial infarction patients (age≤75) admitted from August, 2013 to February, 2016.
Results: During the 2.5-year period, 32 consecutive patients with acute ST-segment elevation myocardial infarction who received al-teplase were enrolled. The mean age was 62.4 year and 84.3% were male. There were 12 patients (37.5%) which the time from symptom onset to hospital presentation ≤180 minutes and 20 others (62.5%) from >180 to 360 minutes. Median time door to needle was 50 min-utes. ST-segment resolution was found in 93.7% of patients (10 of them (31.2%) had ST-segment renormalization). In the earlier hospital presentation patient group, the ST-segment renormalization was better than the other group. There was no bleeding complication in this study. In-hospital mortality was 3.1%. Revascularization was performed in 62.5% at Hanoi hospitals.
Conclusions: Our data, alteplase in acute STEMI provided very good clinical reperfusion with no bleeding complication in 32 patients. Most of our patients needed secondary angioplasty intervention to fix their coronary artery disease.
RESULTS OF REPERFUSION THERAPY FOR ACUTE ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION WITH THROMBOLYTIC AGENTAnh X. Pham1, Dung V. Le2, Tri S. Dao3 1Hoan My Vinh Hospital, Nghe An, Viet Nam; 2Ha Tinh Gereral Hospital, Ha Tinh, Viet Nam; 3Dong Nai Hospital, Dong Nai, Viet Nam
ALLIED PROFESSIONALS P 1-018

138
Introduction: Patients with heart failure meeting guideline criteria for cardiac resynchronization therapy (CRT) may also meet criteria for placement of an implantable-cardioverter defibrillator (ICD). The present study aims to investigate factors determining the selection of CRT with ICD (CRT-D) compared with CRT pacemaker (CRT-P) in a multicenter cohort of Chinese patients with heart failure.
Methods: This cross-sectional study was conducted in 22 hospitals from 15 provinces in China. All patients more than 18 years old were enrolled if they received a CRT device with or without ICD during a hospitalization between January 1, 2014 and November 16, 2015. We collected patients’ demographic and clinical factors, and geographic regions. Cardiac diagnoses of clinical relevance included ischemic heart disease, non-ischemic cardiomyopathy, history of ventricular arrhythmia or syncope, atrial fibrillation, QRS duration, and atrio-ven-tricular block. Multivariable logistic regression was used to identify determinants of CRT-D use vs. CRT-P use.
Results: After excluding patients with missing or invalid data and those requiring device replacement, a total of 454 patients receiving new implant of CRT were included in our analysis. About over half of patients received CRT-D implantation (52.2%). The hospital-level variation in the use of CRT-D mainly attributed to the inter-hospital differences in CRT implantation volumes. Compared with CRT-P, CRT-D im-plant was more common in patients with history of ventricular arrhythmias (29.7% vs. 4.1%, P<0.001) or syncope (16.0% vs. 9.5%, P=0.046), but less frequent in patients more than 70 years old (20.7% vs. 30%, P=0.023), and in those with atrio-ventricular block (8.9% vs. 23%, P<0.001). Factors that were not associated with selection of CRT-D included ischemic heart disease, male gender, left ventricular eject fraction≤25%, atrial fibrillation, QRS duration≥150 ms, and geographic regions. After multivariable logistic regression analysis, CRT-D implant was associated with prior ventricular arrhythmia (OR, 6.75; 95% CI, 2.99-15.28), atrio-ventricular block (OR, 0.32; 95% CI, 0.15-0.69), left ventricular end diastolic diameter≥70 ms (OR, 2.45; 95% CI, 1.03-5.85), Digoxin (OR, 2.05; 95% CI: 1.20-3.49), and provinces with high GDP (OR, 7.62; 95% CI, 2.17-25.6).
Conclusions: Over half of heart failure patients in this contemporary China cohort underwent implantation of CRT-D. Determinants of CRT-D implant included demographic, clinical and economic factors. Understanding of these determinants may help to improve optimal device selection in clinical practice.
DETERMINANTS OF UTILIZATION OF CARDIAC RESYNCHRONIZATION THERAPY WITH OR WITHOUT DEFIBRILLATOR IN CHINAXiaohan Fan1, Keping Chen1, Ji Yan2, Yangang Su3, Jiangang Zou4, Jingfeng Wang5, Wei Hua1, Shu Zhang1 1Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China; 2Department of Cardiology, Anhui Provincial Hospital, Hefei, Anhui, Hefei, China; 3Department of Cardiology, Zhongshan Hospital, Fudan University, Shanghai Institute of Cardiovascular Diseases, Shanghai, China; 4Department of Cardiology, First Affiliated Hospital, Nanjing Medical University, Nanjing, Nangjing, China; 5Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-019

139
Introduction: Atrioventricular block (AVB) occurs occasionally after Transcatheter aortic valve implantation (TAVI), and permanent pace-maker (PPM) implantation is often required. The aim of this study was to investigate the rate and factors for recovery of AVB in patients who have developed AVB after TAVI.
Methods: Electrocardiographic data were reviewed retrospectively in patients who had developed AVB following TAVI procedure. PM de-pendency was reviewed by PPM interrogation data in patients who received permanent pacemaker after TAVI.
Results: Total 70 consecutive patients included in this analysis (mean age 78.4±7.1, male 38.6%). Twelve patients (17.1%) had developed high-degree AVB after TAVI. Among these, seven (58.3%) patients recovered from AVB, range of 1 to 10 days. Preexisting right bundle branch block increases the risk of AVB (OR 6.11 [95% CI 1.1-35.1]). Five patients received PPM (5 to 9 days after TAVI), 3 (60%) displayed PM dependency during long term follow up. The ratio of A/V rate more than 2:1 in the immediate post-procedural period was associated with persistent AV block (60% vs. 0%, P=0.04). Other factors including QRS duration, development of LBBB or RBBB were not associated with recovery from AVB.
Conclusions: Immediate high degree AV block more than 2:1 was predictors for persistent AVB. PPM implantation can be deferred until over 10 days after TAVI in patients with A/V rate 2:1 or less to discriminate recovering from AVB.
PREDICTORS AND DURATION OF RECOVERY FROM ATRIOVENTRICULAR CONDUCTION DISORDERS AFTER TRANSCATHETER AORTIC VALVE IMPLANTATIONJu-Youn Kim1, Young Choi1, Youngsu Lee1, Yoo Ri Kim2, Tae-Seok Kim3, Sung-Hwan Kim1, Yoon-Seok Koh1, Ji-Hoon Kim4, Sung-Won Jang5, Kiyuk Chang1, Man-Young Lee6, Tai-Ho Rho5, Yong-Seog Oh1 1Seoul St. Mary’s Hospital, Seoul, Republic of Korea; 2Incheon St. Mary Hospital, Incheon, Republic of Korea; 3Daejeon St. Mary’s Hospital, Daejeon, Republic of Korea; 4St. Vincent Hospital, Suwon, Republic of Korea; 5St. Paul’s Hospital, Seoul, Republic of Korea; 6Yeouido St. Mary’s Hospital, Seoul, Republic of Korea
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-020

140
Introduction: A novel miniaturized leadless transcatheter pacing system (TPS) was approved in Europe and America as alternative to tra-dition transvenous pacing system. This new system eliminated complication related to pacing lead and pocket. However the delivery of large transfemoral catheter delivery system introducer (27 French outer diameter) in small body sized Chinese may be challenging. The purpose of this study was to report initial experience of leadless pacemakers implantation for Chinese in two centers.
Methods: This is a prospective cohort study from two medical centers. TPS (MICRA, Medtronic, MN, USA) was implanted percuatanously without sedation. Pre-procedural venogram was not performed in all patients and all implants were done over right femoral vein. All pa-tients who underwent procedure had guideline-based Class I or II indication for single chamber ventricular demand pacing. The primary efficacy end point was the percentage of patients with low and stable pacing capture thresholds (<2 V at a pulse width of 0.24 msec and an increased of <1.5 V from the time of implantation) at the latest follow up. The safety end point was freedom from procedure and system related complications.
Results: TPS were successfully implanted in consecutive 16 patients (Age 77.5±13.3, Male=8) and the mean follow up was 4.7±2.9 months. One patient has bioprosthetic tricuspid valve, three patients underwent hemodialysis, two patients had body weight below 40kg and 1 patient has absence of superior vena cava after surgical resection for locally advanced chrondrosacroma over right clavicle before procedure. The primary indications were sick sinus syndrome (37.5%) and atrioventricular block (62.5%). The mean body weight was 59.5±12.1 kg (The lowest one was 34 kg). Procedure time was 44.3±10.6 min and fluoroscopy time was 7.3±2.3 minutes. First attempt successful rate was 10/16 and 2 patients required 7 attempts. Two patients received implant at right ventricular outflow tract and 14 re-ceived implant at right ventricular apex. Safety endpoint was 87.5%. Two patients suffered from groin hematoma and treated conserva-tively. Neither device dislodgement nor perforation was found. There was also no pericardial effusion after procedure. The rate of the pri-mary efficacy end point was 100%. The mean pacing capture threshold was 0.72 V at a pulse width of 0.24 msec. The mean R wave ampli-tude was 8.3 mV and the mean pacing impedance was 616 ohms.
Conclusions: TPS has high successful rate of implantation in Chinese. It is safe and achieving low and stable pacing threshold in our pop-ulation. Delivery of large introducer sheath without pre-procedural venogram is feasible in small body sized Chinese. The performance of TPS implantation in Chinese was comparable to other reported series.
INITIAL EXPERIENCE OF LEADLESS PACEMAKER IMPLANTATION IN CHINESEChin Pang Chan1, Yun Qian Niu2, Kun Chong Tam2, Joseph Yat Sun Chan1 1The Chinese University of Hong Kong, Hong Kong; 2Kiang Wu Hospital, Macau, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-021

141
Introduction: Previous reports have shown a high prevalence of sleep disordered breathing (SDB) in patients implanted with cardiac pace-maker. A minute ventilation sensor (based on thoracic impedance (TI) measurements), normally used to activate a heart rate response function, has a potential to detect SDB. Thus, we investigated the usefulness of this device function to evaluate SDB.
Methods: Thirty-two patients (9 male, 77±6 years old) who had cardiac pacemakers implanted (REPLY200TM, Sorin Group) were enrolled in this study. All patients underwent Epworth Sleepiness Scale (ESS) assessment and sleep study with a portable polygraph monitor. SDB was defined as respiratory disturbance index (apnea+hypopnea events/hour) evaluated by portable polygraph monitor (RDI-PG) ≥20 events/h in this study. Minute Ventilation sensor with TI was also used to measure apnea and hypopnea events during sleep periods. RDI counted by the pacemaker TI sensor (RDI-PM) was compared with RDI-PG during the same night. Furthermore, the ability of the RDI-PM to identify SDB was analyzed by receiver operating characteristics (ROC) analysis.
Results: Twenty-three of 32 patients (72%) had SDB diagnosed by portable polygraph monitor. Mean ESS score was in the normal range (5.1±3.6) and there was only two patients who had an abnormal score (ESS≥12). RDI-PM was correlated with RDI-PG (r=0.484, P=0.005). The ROC for RDI-PM showed an area under the curve of 0.829. When the cutoff RDI-PM value was 15.5, RDI-PM predicted SDB with a sensitivity of 87% and a specificity of 78%.
Conclusions: Minute ventilation sensor with TI showed an acceptable degree of correlation with portable polygraph monitor. This function could be useful to detect SDB in patients implanted with cardiac pacemaker.
SCREENING OF SLEEP DISORDERED BREATHING BY USING A TRANSTHORACIC IMPEDANCE SENSOR IN PATIENTS IMPLANTED WITH CARDIAC PACEMAKER Kensuke Fujiwara
Saitama Cardiovascular and Respiratory Center, Kumagaya, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-022

142
Introduction: Right ventricular (RV) apical pacing is the most commonly used site for permanent ventricular pacing. Sustained RV apical pacing has been associated with histological and structural changes that causes left ventricular function to deteriorate. RV outflow tract and septal pacing has been evaluated as an alternative to RV apical pacing without proven clinical benefit. Both direct His bundle pacing (HBP) and parahisian pacing have gained prominence as they preserve a near-to-normal electrical activation of the left ventricle.
Methods: A comprehensive structured literature search was performed using MEDLINE for studies that report on His-bundle pacing, para Hisian pacing, cardiac pacing.
Results: Direct HBP remains more technically challenging than parahisian pacing and is associated with high pacing thresholds. Due to the high pacing thresholds, direct HBP entails greater energetic consumptive and reduced device longevity. Parahisian pacing seems to guarantee an early invasion of the His-Purkinje conduction system and hence a shift towards parahisian pacing. The electrical parame-ters are also superior in those of parahisian pacing. Previous studies involved an additional safety lead inserted at the RV apex or outflow tract especially in patients with pure direct HBP. Studies on permanent HBP in patients with atrioventricular block (AVB) included only pa-tients with preserved His-Purkinje conduction (narrow QRS). Recent observations suggest that permanent HBP without a backup RV lead can be achieved in up to 80% of unselected patients, including patients with advanced AVB. Parahisian pacing is preferred in patients with infranodal AVB to ensure local RV myocardial capture in addition to his bundle capture. Success rates for permanent HBP varied from 52% to 84% and complication rate is low. It is feasible to normalize the QRS in patients with bundle branch block with direct HBP. Direct HBP may be an alternative treatment for cardiac resynchronization therapy especially for populations with right bundle branch block and heart failure, CRT non-responders and in whom left ventricular stimulation via the coronary sinus was not achievable.
Conclusions: Permanent HBP is feasible in unselected patients. Large randomized controlled trial and long term follow up is necessary to assess the efficacy and safety of HBP. Due to higher pacing thresholds of permanent HBP compared to standard RV lead, improvement in lead designs, delivery sheaths, and new devices with longer battery life may be necessary.
PERMANENT DIRECT HIS BUNDLE AND PARAHISIAN PACING: A SYSTEMATIC REVIEWChiw Yeh Lim, Kelvin Cheok Keng Wong
Changi General Hospital, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-023

143
Introduction: Before implanting new device, venography is recommended to confirm cephalic and subclavian venous locations and run-ning conditions. However contrast medium is unsuited for patients with reduced renal function or allergy. Therefore we use guide wire in-stead of contrast medium to confirm subclavian vein.
Methods: We identified 14 consecutive patients with the indication for new pacemaker. Four patients had reduced renal function. No pa-tient had allergy for contrast medium. Before implantation we inserted a 0.025 inch guide wire from forearm vein instead of venography. After leads insertion the wire was removed from peripheral.
Results: Only 2 patients had tortuous vessel and guide wire could not passed. Of the remaining 12, we successfully inserted guide wires into subclavian vein (7 patients via cephalic and 5 patients via axillary vein). We accessed to veins by cutdown for 8 patients and puncture for 6 patient. All patients had no perioperative complication. No infection had happened to the present time.
Conclusions: This guide wire technique is simple and safe. We can avoid using contrast medium which have risk of renal damage and al-lergy. Since guide wire is constantly visible under fluoroscopy, we can confirm venous running during procedure. We can easily find ce-phalic vein because the vessel containing black color wire is distinguished from other vessels visually. Instead of venography, this guide wire technique should be used for a de novo device implantation.
NEW WIRE TECHNIQUE FOR VENOUS ACCESS OF DEVICE IMPLANTATIONNarutaka Ohashi, Yasuo Kurita, Hiroya Iwahori, Masato Goto, Asuka Furukawa, Yuichi Tamura, Yukiko Karube, Teruo Okabe, Takao Kato, Satoshi Ogawa
International University of Health and Welfare, Mita Hospital, Tokyo, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-024

144
Introduction: The number of patients treated with a dual chamber (DDD) pacemaker is continually increasing each year, The Optimal AV synchrony will not only maximize cardiac output by increasing ventricular preload, thus lowering mean atrial pressure, but also minimize the diastolic mitral regurgitation. However, individualized optimization of the AVI is not performed in clinical routine. This is mainly because of the time-consuming process of manual optimization and the lack of guideline recommendations.
Methods: After approval of Local Ethics Committee and obtaining an informed consent, a prospective, comparative randomized study was conducted on 56 patients with symptomatic bradyarrhythmia requiring a dual chamber pacemaker implantation. All patients were as-sessed by thorough history taking, clinical examination, 12 lead surface ECG, and Echocardiography, They were randomly divided into two groups. Group A (28 patients): where their AVD was set at the default values, while in group B the AVD was optimized with guidance of the transmitral Doppler waves on echocardiography. Then echocardiography follow up was done after 12 months.
Results: Statistically significant increase was found in the LVEF in group B from 67.71±4.58 to 73.43±4.74 (P<0.0001) while it was found to decrease in group A from 72.21±6.28 to 69.43±5.41 after 12 months of device implantation (P<0.0001). Similar results were observed as regard the RVEF which decreased not significantly in group A after 12 months from 49.0±5.82 to 48.07±5.13 (p: 0.07), while in group B a significant increase from 48.57±5.1 to 53.14±7.31 was observed (P<0.0001). Confirming these results again by analyzing the total change in LVEF and RVEF after one year and comparing the two groups directly. Both LVEF and RVEF show a highly significant increase in group B in comparison with group A (P<0.0001).
Conclusions: Optimizing the AVD for all patients of DDD pacemakers may lead to long term beneficial effects mainly on the systolic func-tions.
OPTIMIZING THE ATRIOVENTRICULAR DELAY PACEMAKERSJane Aboulenein1, Mazen Tawfik2 1Mansoura University, Mansoura, Egypt; 2Ain Shams University, Cairo, Egypt
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-025

145
Introduction: The risk factor of pacing-induced cardiomyopathy (PICMP) was still controversial in the complete AV block (CAVB) who un-dertaken with permanent pacemaker (PPM). Our objective was to investigate a clinical risk factor for PICMP in the PPM with CAVB during 15 years follow-up.
Methods: We reviewed retrospectively cohort of consecutive patients with PPM who had CAVB in Chung-Nam National and Eulji Universi-ty Hospital, Deajeon-Chungcheong Province, South Korea from December 2001 to August 2015. Total 130 CAVB patients with PPM (>90% chronic pacing) who undertook ECG, echocardiogram, medication and laboratory data in the before and after PPM implant were analyzed. The data including cardiac events were collected and compared between non-PICMP and PICMP group from index pacemaker implant during follow-up 15 years.
Results: Total 15.3% (n=20) PICMP among all patients was found. The average age (74±11 vs. 76±11), the proportion of sex (35.5% vs. 30.0%), hypertension (54.5% vs. 75.0%), diabetic mellitus (27.3% vs. 15.0%), ischemic heart disease (10.9% vs. 15.0%), alcohol consump-tion (11.8% vs. 15.0%), pre-implant ejection fraction (66±9% vs. 66±8%), septal pacing (38.8% vs. 40.7) and post-implant p-QRS axis (2±78° vs. -3±90°) were similar between two groups. Pre-implant QRS duration (123±34 ms vs. 147±32 ms) and post-implant p-QRS dura-tion (138±29 ms vs. 164±27 ms) were significantly different between two groups. ROC curve showed that above p-QRS duration 146 ms is cut-off value for associated PICMP with the sensitivity of 85% and specificity of 52%. Cox Regression analysis showed that p-QRS duration was significantly associated with PICMP (HR)=1.04, confidence interval (CI)=1.02-1.06, P<0.001.
Conclusions: Our long-term retrospective analysis found that post-implant p-QRS duration regardless of pacing-site was associated with greater risk for PICMP. Large, prospective, multicenter and randomized controlled trials are needed to clarify this result.
PACING-QRS DURATION REGARDLESS OF PACING-SITE IS A MAJOR DETERMINANT FOR OCCURRENCE OF PACING-INDUCED CARDIOMYOPATHY IN THE COMPLETE AV BLOCK FOR 15 YEARS FOLLOW-UPKi-Woon Kang1, Jin Kyung Oh2, Jung Yeon Chin1, Jae-Hyeong Park2, Yu Jeong Choi1, Kyung Tae Jung1, Jun Hyung Kim2 1Eulji University Hospital, Deajeon, Republic of Korea; 2Chung-Nam National University Hospital, Deajeon, Republic of Korea
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-026

146
Introduction: Paroxysmal atrioventricular block (AVB) is a known cause of syncope and sudden cardiac death, because it could lead to torsades de pointes and/or ventricular fibrillation. It was first described in 1933, but the details of clinical course of paroxysmal AVB are still not well known.
Methods: We retrospectively studied 490 patients (pts) with permanent pacemaker implantation (PMI) for AVB since 2007 to 2016. Thir-ty-six cases (average age 65.7 ± 12.8 y.o, 20 men/16 women) were implanted due to paroxysmal AVB. Chronological changes of per-cent ventricular pacing (% Vp) were studied (mean follow-up period 1490 ± 729 day) and clinical characteristics/echocardiographic findings were also analized.
Results: All subjects in this study were divided into two group, i.e. high % Vp group (H group; more than 50%, 14 pts) and low % Vp group (L group; less than 50%, 22 pts) at the last follow up (f/u) day. In 8 pts of H group, % Vp at the first f/u day was less than 50%. While, in 5 pts of L group, % Vp was more than 50% initially. Only BNP level before the PMI and age showed significant statistical differences in the compar-ison of patients’ characteristics, laboratory findings and echocardiographic findings between the 2 groups. According to the ROC curve, cut off value of BNP level for the prediction of H group was the 35 pg/mL. Although no pts died during f/u, two cases of H group experi-enced upgrade operation from pacemaker to ICD and CRTD during f/u period.
Conclusions: About 40% of paroxysmal AVB pts showed marked change of % Vp during the f/u period. In general, prognosis of these pts was good, however, some of the high % Vp pts showed deterioration into heart failure and ventricular tachyarrhythmias. High BNP could predict future high % Vp even in the pts with initially low % Vp. Careful observation should be recommended in the elderly pts and the pts with high BNP level.
BRAIN NATRIURETIC PEPTIDE CAN PREDICT THE CLINICAL COURSE OF PAROXYSMAL ATRIOVENTRICULAR BLOCKHitoshi Mori, Ritsushi Kato, Sou Asano, Sayaka Tanaka, Kouji Goto, Yoshifumi Ikeda, Yuichirou Siki, Shigeyuki Nishimura, Shirou Iwanaga, Toshihiro Muramatsu, Kazuo Matsumoto
Saitama Medical University International Medical Center, Saitama, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-027

147
Introduction: Trans venous right ventricular endocardial lead placement is the routine practice in clinical pacing. Inaccessibility of right ventricle mandates search for other sites in certain clinical situations. Epicardial pacemaker lead implantation is usually associated with development of high threshold and requires limited thoracotomy. Left ventricular lead implantation via coronary sinus is applied to cardiac resynchronization therapy (CRT) to correct heart desynchronization. The method resolves the high threshold and requires limited thora-cotomy caused by epicardial pacing. We reported CS pacing in 5 patients with inaccessibility of right ventricle pacing and assessed the availability and reliability of CS pacing.
Methods: Five patients with rheumatic heart disease and bradycardias, who already accepted mechanical prosthetic tricuspid valve re-placement or tricuspid valvoplasty, were involved the present research. The left ventricular leads were implanted into anterior-lateral vein of CS and all parameters were programmed after operation.
Results: In all the procedures of the five cases, there were no dissections of CS, and the parameters were fine. During the follow-up of 2 months to 6 years separately, no threshold increase and lead dislocation occurred.
Conclusions: Left ventricular lead implantation through coronary sinus is a safe and useful access in patients with inaccessibility of right ventricle pacing.
CLINICAL INVESTIGATION OF LEFT VENTRICULAR PACING USING CORONARY SINUS IN PATIENTS WITH MECHANICAL PROSTHETIC TRICUSPID VALVE REPLACEMENTKelan Zha1, Kaijun Cui2, Kaijun Cui2, Xingbin Liu2, Yuan Fang2 1Southwest Medical University, Luzhou, China; 2West China hospital of Sichuan University, Chengdu, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-029

148
Introduction: Primary prevention implantable cardioverter-defibrillator devices (ICD) improve mortality in patients with heart failure (HF) and reduced ejection fraction (EF). Studies in Western populations showed general under-utilisation of ICDs in eligible patients, particu-larly among women. We aim to assess ICD implantation rates in women versus men with HF from a multi-ethnic Southeast Asian popu-lation.
Methods: Patients with HF were enrolled in a prospective nation-wide multi-centre registry and followed up for 2 years. Eligibility for pri-mary prevention ICD was defined as left ventricular EF ≤35% without prior ventricular tachyarrhythmias. We analysed ICD implantation rates in this cohort and factors that may influence implantation rates and survival.
Results: Of a total of 1,100 patients, 607 (55.2%) were eligible for ICD, but only 36 (5.9%) had ICD implanted. Eligible women were as likely to receive ICD as men (5 of 79 [6.3%] women vs. 31 of 528 [5.9%] men; P=0.87). ICD implantation was related to ethnicity (Malays 3.1%, Chinese 5.9%, Indians 13.4%; P=0.003) but not age, HF aetiology, NYHA class or co-morbidities. Over 2 years of follow-up, there was a high mortality rate in the overall cohort (105 of 629 [17.5%]), but this was not significantly different between ICD eligible patients with (6 of 36 [16.7%]) or without (99 out of 571 [17.3%]) ICD. There were no significant differences in mortality between women and men (14.9% vs. 17.7% respectively, AOR: 0.68; 95% CI: 0.32-1.48; P=0.338), after adjusting for age, ethnicity, HF aetiology, ICD implantation, co-morbidities and serum NTproBNP.
Conclusions: Primary prevention ICD implantation rates in the Asian population was low in both men and women. More men than wom-en fulfil criteria for ICD, reflecting the predominance of heart failure with reduced ejection in men compared to women. Mortality rates were comparable to that seen in the control arms of previous primary prevention ICD clinical trials, suggesting benefit from a higher rate of ICD implantation. The reasons for this low implantation rate is not clear and further study of barriers to their use is needed.
PRIMARY PREVENTION IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR DEVICES IN MEN AND WOMEN IN A MULTI-ETHNIC SOUTHEAST ASIAN POPULATION WITH HEART FAILURE-FINDINGS FROM SHOPElaine Boey1, Siew Pang Chan1, David Sim2, Poh Shuan Daniel Yeo3, Fazlur Jaufeerally4, Gerard Leong5, Hean Yee Ong6, Mark Richards1, Lieng Hsi Ling1, Su Ping Carolyn Lam2, Toon Wei Lim1 1National University of Singapore, Singapore; 2National Heart Centre Singapore, Singapore; 3Tan Tock Seng Hospital, Singapore; 4Duke-NUS Graduate Medical School Singapore, Singapore; 5Changi General Hospital, Singapore; 6Khoo Teck Puat Hospital, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-030

149
Introduction: Wearable Cardioverter Defibrillator (WCD) is considered suitable for temporal and intensive observation of patients under considerable risk for life-threatening arrhythmia. Although its cost is partly reimbursable in Japan, its clinical use and experience are still limited.
Methods: We have experienced 15 cases with WCD use in outpatient setting. The benefits and issues in WCD use through our initial expe-riences are discussed.
Results: The 15 patients were out of 16 total patients with WCD use in outpatient setting in our institute. One patient was prescribed WCD under hospital admission during waiting for ICD implantation. The age of 15 patients was 50±19 years, 14 male, the left ventricular ejec-tion fraction (LVEF) was 48±13%. The underlying heart disease was ischemic heart disease in 6, cardiomyopathy in 3, Brugada syndrome in 4 and idiopathic VF in 2 patients. One patient was waiting for scheduled lead extraction. In total, WCD was prescribed for the examina-tion for primary prevention of VT/VF in 3, and for secondary prevention in 14 patients. The mean observation period under outpatients set-ting was 45±15 days, and 1 appropriate and 1 inappropriate shock were observed during this period. As a result, 2 patients were not indi-cated for ICD because of successful catheter ablation; howerver, the remaining 13 patients were indicated for ICD implantation. During the observation period, mean wearing time in day was 23±0.9 hours, and the acceptance of ICD therapy was good in all patients.
Conclusions: WCD is safe and feasible in outpatient setting. WCD may improve the acceptance of device implantation therapy.
INITIAL EXPERIENCES OF WEARABLE CARDIOVERTER DEFIBRILLATOR IN OUTPATIENT SETTINGTamami Fujiishi, Jun Kishihara, Shinichi Niwano, Hidehira Fukaya, Ryo Nishinarita, Ai Horiguchi, Hironori Nakamura, Tazuru Igarashi, Naruya Ishizue, Tomoharu Yoshizawa, Jun Oikawa, Akira Satoh, Masami Murakami, Junya Ako
Department of Cardiovascular Medicine, Kitasato University School of Medicine, Sagamihara, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-031

150
Introduction: Drug resistant symptomatic hypertrophic obstructive cardiomyopathy (HOCM) patients should be considered surgical my-ectomy. In selected HOCM patients. implantable cardioverter defibrillators (ICDs) are important device to prevent sudden cardiac death (SCD). But it is unclear about appropriate selection of high risk SCD after surgical myectomy. The aim of this study was to assess the ne-cessity of prevention of SCD after surgical myectomy.
Methods: Between March 2008 and Augast 2015 in our institute, we identified 11 patients who underwent implantation of ICDs and surgi-cal myectomy. We checked the episode of ICD interventions (anti-tachycardia pacing and shocks). Of the ICD interventions, we also partic-ularly investigated inappropriate ICD interventions.
Results: No patient who underwent surgical myectomy received ICD interventions including inappropriate ICD interventions (mean fol-low-up 1.3 years). Study limitations were small sample size, short time follow-up.
Conclusions: Further investigation is necessary, surgical myectomy may reduce arrhythmia risk.
ARRHYTHMIA RISK OF HOCM PATIENTS AFTER SURGICAL MYECTOMYKei Mabuchi
Sakakibara Heart Institute, Tokyo, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-032

151
Introduction: Most of the patients with Brugada syndrome who need implantable cardioverter-defibrillator (ICD) have a good indication for subcutaneous ICD (S-ICD), for their younger age and less necessity of bradycardia pacing. However the eligibility for S-ICD in Brugada syndrome patients is not well known. We aimed to clarify the suitability of S-ICD for patients with Brugada syndrome.
Methods: We enrolled consecutive 105 patients with Brugada syndrome who visited our hospital from December 2015 to May 2016. They were assessed by standing and supine ECG limb lead recording to simulate the three S-ICD sensing vectors. S-ICD eligibility required one lead to satisfy the S-ICD screening template in both standing and supine positions. We also assessed the participant’s clinical data and standard 12-lead ECG parameters (QRS duration, QT interval, presence of a negative T wave, complete right bundle branch block (CRBBB), incomplete right bundle branch block (IRBBB), and QRS-T discordance in leadsI, II, and III). QRS-T discordance was defined as the case that the vectors of QRS and T wave are oppositely-oriented. The patients with a paced QRS complex were excluded.
Results: The mean age of study patients was 54.2 (±12.7) years and 103 (98%) were men. A total of 84 (80%) were satisfied with S-ICD screening template. The S-ICD screening template matched more often by alternate vector (82%) and secondary vector (61%) compared to primary vector (33%). Twenty patients have CRBBB. The CRBBB was a significant predictor of ineligibility of S-ICD screening ECG adaptive criteria in surface 12-lead ECG (odds ratio 6.72, P<0.01, 95% confidence interval 2.28-19.83).
Conclusions: CRBBB was a predictive factor for ineligibility for S-ICD in patients with Brugada syndrome.
FACTORS FOR INELIGIBILITY OF CANDIDATES FOR S-ICDS IN PATIENTS WITH BRUGADA SYNDROMEYu Nagano1, Motomi Tachibana2, Nobuhiro Nishii2, Shuko Naito2, Yoshimasa Morimoto2, Satoshi Kawada2, Hiroyasu Sugiyama2, Akihito Miyoshi2, Koji Nakagawa2, Atsuyuki Watanabe2, Naoki Mukouhara1, Hiroshi Morita2, Hiroshi Ito2 1Himeji Red Cross Hospital, Department of Cardilogy, Himeji, Japan; 2Okayama University, Department of Cardiovascular Medicine, Okayama, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-033

152
Introduction: The infective endocarditis and lead injury are the major serious complication of transvenous ICD. On the other hand, subcu-taneous ICD (S-ICD) isn’t suitable for the patients who need bradycardia pacing. Along with a reduction in the risk of lead replacement, the number of combination therapy of leadless pacemaker with S-ICD is expected to increase in the future. However the eligibility for S-ICD in patients with ventricular pacing is not well known. We aimed to clarify the suitability of S-ICD in patients with ventricular pacing.
Methods: We enrolled consecutive 444 of patients with heart disease with and without ventricular pacing. All patients were assessed the eligibility of S-ICD screening ECG criteria using standing and supine ECG limb lead recording to simulate the three S-ICD sensing vectors. S-ICD eligibility required one lead to satisfy the S-ICD screening template in both standing and supine positions. We also assessed the clinical data (age, sex, and body mass index) and standard 12-lead ECG parameters (QRS duration, QT interval, morphology of QRS-T wave, the presence of a negative T wave and atrial fibrillation) in the patients with ventricular pacing, and compare the differences be-tween S-ICD eligible and ineligible patients.
Results: The mean age of study patients was 51 (±21) years and 307 (69%) were men. Seventy patients were with ventricular pacing. A to-tal of 344 (77%) were satisfied S-ICD screening template. In the patients with ventricular pacing, 26 out of 70 patients were not suitable for S-ICD. The ventricular pacing was a significant predictor for the ineligibility of S-ICD screening ECG criteria (19% vs. 37%, P<0.01), where-as no predictive factor for S-ICD ineligibility was observed among baseline clinical data and standard 12-lead ECG parameters.
Conclusions: The ventricular pacing was a predictive factor for the ineligibility of S-ICD in patients. For the patients whom both leadless pacemaker and S-ICD are applied to, this study could suggest the eligibility for the S-ICD screening ECG criteria should be assessed in advance by temporarily using right ventricular pacing before leadless pacemaker is permanently implanted.
THE ADAPTATION OF SICD SHOULD BE EVALUATED IN THE S-ICD SCREENING ECG BEFORE LEADLESS PACEMAKER IMPLANTATIONMotomi Tachibana1, Nobuhiro Nishii1, Shuko Naito1, Yu Nagano2, Yoshimasa Morimoto1, Satoshi Kawada1, Hiroyasu Sugiyama1, Akihito Miyoshi1, Koji Nakagawa1, Atsuyuki Watanabe1, Hiroshi Morita1, Hiroshi Ito1 1Department of Cardiology, Okayama University Hospital, Okayama, Japan; 2Department of Cardiology, Himeji Red Cross Hospital, Himeji, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-034

153
Introduction: Implantable-cardioverter defibrillator (ICD) shock is the most effective way to terminate lethal ventricular tachyarrhythm (VTVF). The burden of ICD shocks has recently been observed to associate with increase in cardiac morbidity and mortality. This study in-vestigated the feasibility of using a weighted score algorithm to predict, days in advance, VTVF events that required ICD shocks.
Methods: Twenty-five patients who received ICD were prospectively enrolled and followed for 6 months. Appropriate VTVF events were de-termined and classified into shock- and ATP terminated events. Directional variation in multiple device-derived parameters in Carelink Cardiac Compass were assessed by an algorithm that created a baseline weighted score over a 15-day moving window. VTVF prediction was conducted in a prospective fashion based on the comparison between the weighted score one day before an event vs. the score calcu-lated for immediately prior 15-day window. ICD-shock related hospitalization was counted.
Results: The study pool consisted of 20 (80%) patients with a history of sustained VT or VF and 5 in the primary prevention population. The patients had LVEF 45.0±15.4% and NYHA class 1.4±0.6. Eleven (44%) had coronary heart disease and 14 (56%) had ischemic or non-isch-emic cardiomyopathy. Of 25 patients, 10 (40%) developed a total of 123 appropriate ICD-terminated VTVF episodes (12.4±13.2, median 5 per patient). Of these 123 episodes, 23 episodes in 5 patients were terminated by ICD shocks while the remaining 100 episodes in 9 pa-tients were terminated by ATP. When the weighted-score algorithm was tested in all 25 patients, the prediction of VTVF events one day be-fore the occurrence had a 100% sensitivity and 74% specificity. For the patients with episodes terminated by ICD shocks, the algorithm predicted all shock-terminated episodes one day before the events. All five patients who experienced ICD shocks were hospitalized fol-lowing shocks.
Conclusions: VTVF events that required ICD shocks can be predicted one day in advance by a weighted score algorithm based on device monitoring parameters, which provides a time window for taking appropriate measures to prevent impending VTVF and hence avoid ICD shocks and shock-related hospitalization.
PREDICTION OF VENTRICULAR TACHYARRHYTHMIAS TERMINATED BY IMPLANTABLE-CARDIOVERTER- DEFIBRILLATOR SHOCKSNgai-Yin Chan1, Lok-Yan Tam2, Xiaohong Zhou3, Tina Ling4, Hongyang Lu5 1Princess Margaret Hospital, Kowloon, Hong Kong; 2Queen Elizabeth Hospital, Kowloon, Hong Kong; 3Medtronic Inc, Minneapolis, United States; 4Medtronic Inc, Kowloon, Hong Kong; 5Medtronic Inc, Shanghai, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-035

154
Introduction: Over the past 20 years, defibrillation threshold (DFT) testing has been an integral part of defibrillator implantation. With the development of increasingly reliable defibrillators, and lack of survival benefit with increased risk of testing-associated complications, routine peri-implant testing is now less commonly practiced. The primary aim of our study was to determine the efficacy of current devic-es in DFT and DFT related complication rates.
Methods: We conducted a retrospective study on all patients undergoing DFT at the time of left pectoral defibrillator implant at our centre from 2009 to 2014. Standard axillary or subclavian vein access was obtained and defibrillation leads placed at the right ventricular apex. Post implant, defibrillation testing was performed utilizing a single shock step up protocol starting at 10J energy, with progressively higher shock energy settings if initial shocks were unsuccessful. Patients were sedated with intravenous midazolam or propofol, based on physi-cian preference. External rescue defibrillation was performed if ICD shocks failed to terminate VF. We examined the safety margin for de-fibrillation success in comparison to the maximum output of the implants. A safety margin of <10J was defined as a high defibrillation threshold.
Results: 174 patients underwent DFT at the time of device implant. 82.2% of patients had primary prevention indications for device im-plant. The mean±SD LVEF was 27.7±11.6% and BMI of 24.9±4.94. 79.3% of patients had ischemic heart disease and 8% with hypertro-phic cardiomyopathy. The mean safety margin from the maximum device output was 24.4±3.9J. 1 patient (0.6%) had a high defibrillation threshold initially at implant for which DFT was repeated post implant with >10J safety margin on repeat testing. There were no DFT re-lated complications. With the lack of reproducibility and probabilistic nature of DFT testing, together with highly reliable modern devices and lack of survival benefit, there has been a recent trend towards not perfoming routine DFT on conventional left sided pectoral implants. Our study demonstrates a high level of defibrillation efficacy in modern day devices. With progressively higher energy devices, the mean safety margin for our cohort was close to 25J. However, this may not apply to non-left pectoral implants where shock vectors potentially capture less myocardium.
Conclusions: Modern day defibrillators are highly efficacious for left pectoral implants. Less than 1% of our patients had high defibrilla-tion thresholds on initial testing. The mean safety margin achieved was close to 25J.
HIGH DEFIBRILLATION EFFICACY OF PERI-IMPLANT DEFIBRILLATION TESTINGNewman Sze Yan Cheng1, Paul Chun Yih Lim2, Daniel Thuan Tee Chong2, Boon Yew Tan2, Kah Leng Ho2 1Singapore General Hospital, Singapore; 2National Heart Centre, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-036

155
Introduction: Prevention of SCD using ICDs is recommended in high-risk patients, but there is no consensus on the best lead and device in routine ICD implants. Trends on device and coil used across Asia are unknown. It is expected that single coil leads’ use will be more widespread, as dual coil leads are more difficult and riskier to extract because of fibrotic adherences.
Methods: The Improve SCA Clinical Trial is a worldwide, prospective study with centers in Asia, Latin America, the Middle East, Africa, and Central and Eastern Europe. Data on the first 2005 enrolled patients is available. For this analysis, only implanted patients with known RV lead models are included.
Results: The analysis includes 688 ICD-implanted patients. 70% of patients from Asia (compared to 57% in the rest of the world, P=0.03) were implanted with a single chamber ICD, and 61% (compared to 39% in the rest of the world, P=0.0003) were implanted with a single coil RV lead. Within Asia, single chamber ICD patients were more likely (P=0.04) to get a single coil lead than dual chamber patients. There is a wide disparity in use of single chamber ICDs and in use of single coil leads. There were an additional 302 patients from Asia who received a CRT-D, with 44% having a single coil lead. This is a lower percentage of single coil leads (P<0.0001) compared to ICDs.
Conclusions: Single chamber ICD use and single coil RV lead use is higher in Asia than in other countries, though use varies by country. While centers are willing to implant both single and dual chamber devices, most demonstrate a preference for only single or only dual coil RV leads.
DEVICE AND COIL TYPE USED ACROSS ASIA DIFFERS IN THE IMPROVE SCA TRIALDiego A. Rodriguez1, Balbir Singh2, Azlan Hussin3, Dejia Huang4, Chi-Keong Ching5, Yen-Bin Liu6, Young-Hoon Kim7, Alexandr Robertovich Chasnoits8, Boyoung Joung9, Jeffrey Cerkvenik10, Katy Muckala10, Shu Zhang11 1Fundación Cardioinfantil, Bogota, Colombia; 2Medanta, The Medicity Hospital, Gurgaon, Gurgaon, Haryana, India; 3Institut Jantung Negara, Kuala Lumpur, Malaysia; 4West China Hospital, Sichuan University, Chengdu, China; 5National Heart Centre of Singapore, Singapore; 6Korea University Medical Center, Seoul, Republic of Korea; 7National Taiwan University Hospital, Taipei, Taiwan; 8Republican Scientific Practical Centre Cardiology, Minsk, Belarus; 9Severence Hospital, Seoul, Republic of Korea; 10Medtronic, Minneapolis, United States; 11Fuwai Cardiovascular Hospital, Beijing, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-037

156
Introduction: Subcutaneous (SQ) ICDs provide alternatives to transvenous systems when intravascular placement is not desired or not possible, yet SQ lead placement requires higher shock outputs without option of anti-tachycardia pacing. The SPACE study evaluated the feasibility of cardiac pacing from an extravascular substernal location.
Methods: The SPACE study was a prospective study with a primary objective to evaluate the feasibility of pacing from a decapolar EP cath-eter (Marinr, 7 Fr, Medtronic) acutely implanted in the anterior mediastinum (substernal space) at or adjacent to the sternal midline. The decapolar catheter was introduced into the substernal tissues via minimally invasive subxiphoid access, using fluoroscopic guidance. The middle electrodes of the EP catheter were centered over the RV surface of the cardiac silhouette. Pacing data were collected in ≥7 vectors (≥3 bipolar and ≥4 unipolar) using constant current stimulation up to 20 mA and pulse width (PW) up to 10 ms.
Results: Twenty-six pts (21 males; age 64.4±10.0 years) indicated for cardiac surgery (25) or SQ ICD (1) underwent the study procedure at 8 sites in the US and Canada. Catheter placement was successful in all 26 pts, with a mean placement time of 11.7±10.1 minutes. Suc-cessful ventricular capture in ≥ 1 tested vector was observed in 18 of 26 pts (69%). The pacing configuration with lowest threshold was bi-polar for 10 pts and unipolar for 7 pts (no difference for 1 pt). Failed ventricular capture in 8 pts was generally associated with sub-optimal catheter placement. Mean pacing thresholds at PW 10 ms, 3 ms, 1 ms were 7.3±4.2 mA (18 pts), 9.0±4.7 mA (13 pts), 11.8±4.5 mA (7pts), respectively. Among subjects with bipolar capture, widely spaced electrode pairs were consistently associated with the lowest thresholds: mean pacing threshold of 7.2±5.5 mA (5.5±6.0 volts) using an electrode spacing of 19 mm and 10 ms PW.
Conclusions: These data demonstrate that pacing is feasible from the novel extravascular substernal location. A substernal electrode configuration has the potential to provide pacing in a future extravascular defibrillator using a simple, single implant procedure.
RESULTS OF THE SUBSTERNAL PACING ACUTE CLINICAL EVALUATION (SPACE) STUDY: FEASIBILITY OF EXTRAVASCULAR SUBSTERNAL PACINGPeter Leong-Sit1, Darius Sholevar2, Stanley Tung3, Vikas Kuriachan4, Henri Roukoz5, Gregory Engel6, Steven Kutalek7, Devender Akula2, Melissa Christie8, Marina Ostanniy8, Amy Thompson8, Franck Molin9 1London Health Sciences Centre, London, Canada; 2Our Lady of Lourdes Medical Center, Camden, United States; 3Royal Columbian Hospital, New Westminster, Canada; 4Foothills Hospital, Calgary, Canada; 5University of Minnesota Medical Center, Minneapolis, United States;
6Sequoia Hospital, Redwood City, United States; 7Hahnemann University Hospital, Philadelphia, United States; 8Medtronic, Mounds View, United States; 9Institut Universitaire de Cardiologie et de Pneumologie de Québec, Quebec, Canada
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-038

157
Introduction: Cardiac implantable electronic device (CIED) longevity is an important clinical and economic factor when considering device selection. Registries on “real” device longevity are naturally limited by the fact that they compile data on “outdated” models at time of pub-lication. We sought to assess device longevity in contemporary devices from different manufacturers using standardized pacing and re-mote monitoring settings.
Methods: Data were derived from manuals and communication with research and development departments of device manufacturers. All longevities estimations were based on the following: output of 2.5 V, 0.40 ms, 500 Ω and standardized pacing loads of 50 or 100% at 60 bpm [ventricular (V) channel in single chamber (SR) devices; atrial (A) and V channel in dual chamber (DR) low-voltage (LV) devices]; 0% or 15% in ICDs; and 15% or 100% biventricular (BiV) pacing in CRT-Ds. All high voltage (HV) longevities were assessed at the conditions of zero clinical shock with minimum number of charges required for capacitor reform and all pre-IEGM, wireless transmissions and home monitoring turned ON.
Results: The mean predicted longevity of LV devices at 50% pacing load was 11.3 years (Range between 8.9 years [Boston Advantio DR] and 15.3 years [St. Jude Assurity SR]. Overall longevity was reduced by a mean of 1 year with activation of remote monitoring, pre-IEGMs or blended rate response sensors. Similarly, increased pacing load to 100% reduced overall longevity by 1.2 years. Under monitoring con-ditions only (zero percentage pacing), the mean longevity of HV devices (ICD and CRT-D) was 12 years (Range between 7.8 years [Medtron-ic DR] to 18 years [Sorin VR]). At nominal pacing load (A 15%; BiV 100%) the average longevity of CRT-D devices was 8.4 years, ranging from 5.7 years (Medtronic) to 12.7 years (Sorin).
Conclusions: This study shows that with identical pacing settings, there are substantial variations in the operating lifespans of CIEDs. This has significant implications for clinical practice with potential differences in economic burden and morbidities associated with future gen-erator replacements.
COMPARATIVE ANALYSIS OF PREDICTED LONGEVITIES OF CARDIAC IMPLANTABLE ELECTRONIC DEVICES: IMPLICATIONS FOR CLINICAL PRACTICEDian Munawar, Geoffrey R. Wong, Rajiv Mahajan, Sharath Kumar, Kashif Khokhar, Anand Thiyagarajah, Melissa E. Middledorp, Prashanthan Sanders, Dennis H. Lau
University of Adelaide, Adelaide, Australia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-039

158
Introduction: Traditional ICD (T-ICD) system induce myocardial injury with high output shock deliver, but subcutaneous ICD (S-ICD) stan-derd defibrillation shock output energy is approximately 4 times that of the T-ICD system.The objective of this study was to evalulate myo-cardial injury with defibrillation test (DT) after implanting S-ICD by clinical investigation and computer simulation test model.
Methods: In computer simulation, we created human torso model using SCIRun software and human voltage gradient >30 V/cm in this model. In clinical investigation, a total of 4 patients for S-ICD implantation were performed (mean age 39.66 years ; males 4 (100%), idio-pathic VF4 (100%)). Serum levels of high sense troponin T (TpT) and creatine kinase muscle isoenzyme (CK-MB) were measured at base-line plus 3, 6, and 24 hours after implanting S-ICD with DT.
Results: The proportions with myocardial injury were 0.7% and 0% for right and left ventricles in computer model, on the other hand, in clinical research, VF terminated by delivered 65J in three patients, but one patient need 2 time shock deliver 80J and 65J due to sensing failure, serum TpT was slightly elevated after procedure at 6 hours (0.015±0.008 ng/mL, baseline 0.006±0.004 ng/mL).
Conclusions: TpT data indicate significantly less cardiac injury from 65J S-ICD shocks, the computer simulation could be a new noninva-sive procedure for predicting myocardial injury.
THE INVESTIGATION OF MYOCARDIAL INJURY AFTER SUBCUTANEOUS ICD IMPLANTATION WITH DEFIBRILLATION TEST IN COMPUTER SIMULATION MODEL AND CLINICAL CASESTakayuki Shimizu1, Keijiro Nakamura1, Rina Ishii1, Yasutake Toyoda1, Naohiko Sahara1, Masako Asami1, Takahito Takagi1, Yuriko Narabayashi1, Hikari Hashimoto1, Takao Sakata1, Masato Nakamura1, Xin Zhu2, Mahito Noro3, Kaoru Sugi4 1Toho University Ohasi Medical Center, Tokyo, Japan; 2University of Aizu, Fukushima, Japan; 3Toho University Sakura Medical Center, Tiba, Japan; 4Odawara Cardiovascular Hospital, Kanagawa, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-040

159
Introduction: Defibrillation testing (DFT) in patients undergoing implantable cardioverter defibrillators (ICD) implantation has been rou-tine, until recent data argue against such testing. However, the need to perform DFT is controversial recently.
Methods: All patients who were implanted with de novo ICD at Chonnam University Hospital were enrolled in this study between 2012 September to 2015 February. Total 67 patients (51.5±16.9 years old, 50 males) were treated with ICD. Patients were implanted with ICD due to several causes (14 idiopathic ventricular fibrillation, 6 Brugada syndrome, 7 long QT syndrome, 1 ARVD, 9 dilated cardiomyopathy, 9 hypertrophic cardiomyopathy, 20 ischemic cardiomyopathy, 3 early repolarization syndrome). Among them, 31 patients underwent DFT testing intraoperatively. Primary outcomes were all cause mortality, composite end point of ICD efficacy (arrhythmic deaths and ineffective shocks) and composite safety endpoint (the sum of complications recorded at 30 days). Chest X-ray (CXR), 12 lead ECG, interrogation pa-rameter was checked immediately post implantation and at 6 months intervals.
Results: No significance difference was observed in the baseline clinical characteristics between two groups. Total 23 shocks (19 appro-priate shocks, 4 inappropriate shocks) was happened during 2.31±0.83 years. First shock success was 95% (22/23). During follow up peri-od, there was 2 cardiac deaths and 0 failed appropriate shock.
Conclusions: No significant differences in the incidence of mortality, malignant ventricular arrhythmias, or appropriate ICD discharges were observed between patients who underwent DFT testing compared to those who did not. Our results may support avoiding routine DFT testing.
DEFIBRILLATION THRESHOLD TESTING DURING IMPLANTABLE CARDIOVERTER DEFIBRILLATOR PLACEMENT: SINGLE CENTER EXPERIENCESung Soo Kim1, Hyung Wook Park2, Ki Hong Lee2, Nam Sik Yoon2, Jeong Gwan Cho2, Dong Goo Kang1, Seung Wook Lee1, Sang Ki Cho1 1Kwangju Christian Hospital, Gwangju, Republic of Korea; 2Chonnam University Hospital, Gwangju, Republic of Korea
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-041

160
Introduction: Transvenous (TV) ICD systems represent the device-based standard of care for treatment of arrhythmia, yet TV lead implan-tation is often not possible. Subcutaneous (SQ) ICDs have emerged as a non-TV option, but energy requirements for defibrillation through the chest wall have resulted in larger, heavier SQ ICDs with high defibrillation thresholds (DFTs). Described here are the results of pre-clinical animal research evaluating the DFT of a novel substernal-lateral electrode vector, as compared to both TV and SQ DFTs.
Methods: Each animal was implanted with three leads. A 5.7 cm coil was implanted in the right ventricle, an 8 cm coil was tunneled SQ and positioned parasternally (right side) and an 8 cm coil was introduced into the substernal (SS) space at or adjacent the sternal midline via minimally invasive subxiphoid access. An active can emulator (ACE) was placed in a pocket on the left lateral thorax at the level of the heart. DFT testing was performed using a step-up, step-down DFT search protocol, with DFTs calculated via logistic regression.
Results: DFT testing was completed in n=11 pigs (39.3±9.5 kg). Average DFTs (see graph) expressed in Joules (J) were 15±6 J (TV), 22±6 J (SS) and 99±29 J (SQ). Average shock impedances were 38.9±3.3 Ω (TV), 37.7±5.4 Ω (SS) and 43.2±8.8 Ω (SQ).
Conclusions: The novel SS-lateral configuration produced DFTs that were markedly lower than SQ DFTs and closer in value to TV DFTs. Substernal therapy delivery may represent a clinically meaningful solution for treating cardiac arrhythmia, overcoming the high energy requirements and increased device size of SQ ICDs.
RESULTS OF DEFIBRILLATION THRESHOLD TESTING COMPARING TRANSVENOUS, SUBCUTANEOUS AND NOVEL SUBSTERNAL ELECTRODE CONFIGURATIONS IN SWINEAmy Thompson, Vladimir Nikolski, Jian Cao, Melissa Christie, Paul DeGroot
Medtronic, Mounds View, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-042

161
Introduction: Electrical storm (ES) is associated with poor prognosis in ICD patients. However, the difference between the characteristics of ES-related events and the other isolated events is unknown.
Methods: 104 patients (98 are secondary prevention, and 60 are ischemic cardiomyopathy) underwent ICD implantation, including single lead, dual lead ICD and CRT-D, in the past 10 years in our center. Totally 669 episodes of sustained ventricular tachyarrhythmia, including 521 ES-related events (Group 1) and 148 isolated events (Group 2) were analyzed retrospectively.
Results: The etiologies of ES-related events were different from the isolated events. Their tachycardia cycle lengths were similar. However the ES-related events received fewer ATP therapies (1.64±1.50 vs. 1.94±1.91, P=0.019) but more shocks (0.39±0.96 vs. 0.33±0.7, P=0.043) per event than the isolated events. Regarding the therapeutic efficacy, ES-related events were more easily terminated by one ATP (56% vs. 42%, P=0.007) or first therapy (ATP or shock) (58% vs. 45%, P=0.013). Overall, the ES-related events were more likely terminated suc-cessfully by the device (92% vs. 84%, P=0.041).
Conclusions: In conclusion, ICD therapies on ES-related events are highly effective. Electrical storm is a status of provoking arrhythmia initiation; their termination remains similar to isolated events.
EFFICACY OF ICD THERAPY ON ELECTRICAL STORMYing Chieh Liao, Tsu-Juey Wu
Taichung Veterans General Hospital, Taichung, Taiwan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-043
Characteristics of ES Related Event and Isolated Events
ES related-events (N=521) isolated events (N=148) p
Cycle length (ms) 380.50±66.72 366.82±62.83 0.092
No. of ATP per events 1.64±1.50 1.94±1.91 0.019
No. of CV per events 0.39±0.96 0.33±0.7 0.043
Ishcemic CM/DCM 159/362 62/86 0.013
VT 382 (73%) 108 (73%) NS
VF and FVT 138 (27%) 40 (27%) NS
Successful Therapy 470 (92%) 124 (84%) 0.041
Successful first ATP 286 (56%) 62 (42%) 0.007
Successful first therapy (ATP or CV) 298 (58%) 67 (45%) 0.013

162
Introduction: Post MI patients with LV dysfunction and symptomatic VT (more than 48 Hours after MI) are at an increased risk for SCD. They benefit by Coronary revascularisation followed by Antiarrhythmic therapy (AAD) and AICD implantation. However in developing na-tions, many such patients cannot afford AICD due to financial constraints. We compared the clinical events between patients with AIE im-plantation plus Antiarrhythmic medications and those with only Antiarrhythmic medications during follow-up period.
Methods: Patients admitted in our hospital from 2010-2015 were enrolled. All patients had Post MI LV Dysfunction with LVEF less than 35% with evidence of secondary VT with or without Cardiac arrest. After coronary revascularisation they were divided into 2 groups.Group 1-Underwent AICD Implantation+AADGroup 2-Only on AAD-Both groups were followed up for a mean of 3 years.
Results: Total 68 patients were enrolled & followed up. 45 (66%) belonged to Group 1 & 23 (34%) belonged to Group 2. Patient character-istics & risk profile of both groups were matched. All patients received standard antianginal & antiarrhythmic drugs. During follow up in Group 1, 43 (95%) patients had shocks (both appropriate & inappropriate). 2 patients had lead dislodgement & 2 had pocket infection needing repeat procedure. 6 (13%) patients died (2 had CCF, 3 had noncardiac cause & 1 unknown cause) In Group 2, 18 (78%) had SCD during follow up, most deaths were arrhythmic. Remaining 5 (22%) patients had multiple hospitalisation due to arrhythmias.
Conclusions: AICD Implantation in post MI LV dysfunction patients with symptomatic VT definitely improves survival. However it has asso-ciated minor incidence of Device related complications.
A COMPARATIVE STUDY OF POST MI LV DYSFUNCTION PATIENTS WITH SECONDARY VT-AAD + AICD VERSUS AADPraveen Pai
AIMS, Kochi, India
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-044

163
Introduction: Improve SCA aims to find a group of primary prevention (PP) ICD patients that have VT/VF treatment rates similar to sec-ondary prevention (SP) patients. The study evaluates the benefits of therapy for high-risk patients in countries where ICD therapy for PP of SCA is underutilized. The study intends to enroll 3,725 subjects in Asia, Latin America, Africa, and Eastern Europe.
Methods: Patients were identified as PP or SP. PP patients who met at least one of four risk criteria (syncope, NSVT, frequent PVCs, or LVEF<25%) were identified as 1.5 patients. The decision to implant an ICD was made by the patient. Only subjects at Asian sites are in-cluded in this analysis.
Results: Through 20 months of study enrollment, there were 1,673 patients at Asian sites with an average age of 59.0, 76% male, 29% were SP. Of the PP patients, 73% were in the 1.5 category. As expected, the rate of implant varied depending on the indication. Overall, 87% of SP, 50% of 1.5, and 36% of 1.0 patients chose implant, which differs from the assumed 57%, 45% and 22% for SP, 1.5 and 1.0 pa-tients, respectively. There were also differences in implant refusal rate within the enrolling countries (figure), most commonly due to in-ability to pay.
Conclusions: Initial enrollment in the Improve SCA study, conducted in emerging countries, has seen higher ICD implant than what was expected prior to the study. The implant refusal rate varies by country. 1.5 patients were less likely to decline implant than those who were PP, suggesting use of these risk markers may influence a patient’s perception of risk and the need for an ICD.
STUDYING ICD THERAPY WHERE ICDS ARE UNDERUTILIZED: IMPLANT RATES HIGHER THAN EXPECTED IN THE IMPROVE SCA TRIALBalbir Singh1, Azlan Hussin2, Dejia Huang3, Chi-Keong Ching4, Diego A. Rodriguez5, Young-Hoon Kim6, Yen-Bin Liu7, Alexandr Robertovich Chasnoits8, Joao Monteiro9, Katy Muckala9, Shu Zhang10 1Medanta, The Medicity Hospital, Haryana, India; 2Institut Jantung Negara, Kuala Lumpur, Malaysia; 3West China Hospital, Sichuan University, Chengdu, China; 4National Heart Centre of Singapore, Singapore; 5Instituto de Cardiologia - Fundacion Cardioinfantil, Bogota, Colombia;
6Korea University Medical Center, Seoul, Republic of Korea; 7National Taiwan University Hospital, Taipei, Taiwan; 8Republican Scientific Practical Centre Cardiology, Minsk, Belarus; 9Medtronic, Minneapolis, United States; 10Fuwai Cardiovascular Hospital, Beijing, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 1-045

164
Introduction: AF is a common cardiac arrhythmia, with increasing incidence due to ageing population. Catheter ablation of AF is a Class I indication in drug refractory paroxysmal forms & a Class IIA in Persistent AF. The Hansen® is a robotic catheter system allowing mapping & ablation by remote navigation utilising a robotically steerable sheath which may be useful in the ablation of AF due to improved tissue contact & reduction in radiation exposure. However, concerns remain regarding higher complications rate due to the rigidity of the robotic sheath & lack of tactile feedback. We present the largest series in the Asia Pacific region of AF ablation utilising the Hansen® system, re-porting efficacy & safety data.
Methods: The series consists of 238 consecutive procedures using the Hansen® system performed from March 2010 to December 2014. Majority of the data was collected prospectively with retrospective case notes review of Holter monitor, ECG, correspondence letters, im-planted cardiac device checks & medical records where necessary. Primary efficacy endpoint was drug-free freedom from atrial arrhyth-mia at 1year, defined as recurrence of AF, occurrence of A. Flutter or A. tachycardia, use of antiarrhythmic drugs, or repeat ablation fol-lowing a 90 day period after the index ablation. Secondary efficacy endpoints included single procedure, drug free freedom from AF at 1 year for patients undergoing de-novo AF ablation with the Hansen® system & drug free freedom from AF at 1 year following multiple pro-cedures. The primary safety end point was a composite of death, cerebrovascular events, or serious treatment-related adverse events at 6 months.
Results: A total of 238 procedures were performed using the Hansen® system on 220 patients. 7 procedures were performed for condi-tions other than AF & excluded from analysis. Mean age was 63±10.1 years & majority of patients were male (64%). Mean BMI was 29±4.9. 90% of the patients had a CHADS2 score of ≤1.39 patients (16%) had incomplete data. They were included in efficacy data if had docu-mented recurrence of AF, but were otherwise excluded in the primary efficacy endpoint. All satisfied inclusion for the purpose of safety endpoint. Of the 174 patients, almost 80% (139/174) satisfied the primary efficacy endpoint of drug free freedom from AF at 1 year follow up. 21% (45/213) patients had index procedure prior to Hansen® programme, leaving 79% (168/213) patients for secondary efficacy analy-sis. Single procedure drug free success was 77%, rising to 85.5% with a mean of 1.24 procedures. Safety data was complete for 231 pro-cedures. Rate of major complications was 4.3% (10/231). Atrio-oesophageal fistula/death-1 (0.4%). CVA-2 (0.8%). Pulmonary vein steno-sis-2 (0.8%). Cardiac tamponade-4 (1.7%).
Conclusions: The Hansen® robotic system provides an effective approach for AF ablation with similar complications rate to those reported in series using manual ablation.
SAFETY AND EFFICACY OF AF ABLATION USING HANSEN® MEDICAL SENSEI® ROBOTIC CATHETER SYSTEM: LARGEST SERIES IN ASIA PACIFIC REGIONWaheed Ahmad, Anand Ganesan, John Bowyer, Cameron Singleton, Fahd Chahadi, Andrew D McGavigan
Flinders Medical Centre, Adelaide, Australia
CATHETER ABLATION P 1-047
165
Introduction: Superior transseptal approach is often used in mitral repair to provide a better exposure of the mitral valve. Superior trans-septal approach has a high risk of atrial tachycardia (AT) than the left atrial approach. We report a case of a patient who received catheter ablation of AT and atrial fibrillation (AF) after mitral valve repair by superior transseptal approach.
Methods: N/A
Results: A 66-year-old woman presented to our hospital for catheter ablation of AT and AF. She had undergone mitral valve repair for mi-tral valve regurgitation due to prolapse 9 years ago. She had atrial fibrillation after open-heart surgery. She developed heart failure due to AT a year ago. Antiarrhythmic drug therapy failed to suppress the tachycardia, catheter ablation was performed. Circumferential pulmo-nary vein isolation was performed using a 3D electroanatomical mapping system (CARTO3, Biosense Webster Inc., Diamond Bar, CA). The clinical AT was induced by atrial burst pacing. The tachycardia cycle length was 213 msec and the coronary sinus activation was proximal to distal. Post pacing intervals after entrainment pacing from coronary sinus ostium, low lateral right atrium, and cavotricuspid isthmus were 100-130 msec longer than the tachycardia cycle length, therefore we performed left atrial mapping. The left atrial ablation at inci-sional scar of interatrial septum and anterior wall did not influence the AT. We performed right atrial ablation at incisional scar of inter-atrial septum and right lateral free wall and then repeat prolongations of AT cycle length were observed. AT finally changed common atrial flutter and cavotricuspid isthmus ablation resulted in direct termination of tachycardia to sinus rhythm. AT and AF was no more induced by any stimuli after the procedure.
Conclusions: We successfully performed a catheter ablation of AF and AT after mitral valve repair by superior transseptal approach.
SUCCESSFUL CATHETER ABLATION OF ATRIAL TACHYCARDIA AFTER MITRAL VALVE REPAIR BY SUPERIOR TRANSSEPTAL APPROACHMadoka Akashi, Ken Kato, Makiko Suzuki, Wataru Yamagata, Akihisa Kimura, Ayano Yoshida, Yuta Okabe, Kansuke Ito, Syogo Hari, Mutsuhiro Nishimura, Hiroaki Morinaga, Masataka Ogiso, Yuya Mitsuhashi, Kenichiro Nagata, Toshiaki Isogai, Hiroyuki Tanaka, Tamotsu Teshima
Tokyo Metropolitan Tama Medical Center, Tokyo, Japan
CATHETER ABLATION P 1-048

166
Introduction: Catheter ablation is an established treatment option for patients with symptomatic paroxysmal atrial fibrillation (PAF). How-ever, it has not been widely adopted in the elderly population. They were initially excluded from many cathter ablation trials due to con-cerns about procedural complications and the rate of recurrence. The aim of the present study was to investigate retrospectively the safe-ty and clinical efficacy of PAF ablation in patients ≥75 years compared with younger patients <75 years.
Methods: From July 2009 to June 2014, a total of 1,037 PAF patients received a stepwise catheter ablation. In our series, 131 patients (12.6%) were ≥75 years (mean age 77.5 years, range 75-85 years), and 906 patients (87.4%) were <75 years (mean age 60.8 years, range 18-74 years). We evaluated procedural major complications and recurrence of AF after 3 years follow-up. The major complications were included any bleeding complications requiring blood transfusion or surgical intervention, pericardial effusion treated with dranage, atri-al-esophageal fistula and cerebral infarction.
Results: Procedural major complications were not significantly different with both study groups, 4 elderly patients versus 23 younger pa-tients (3.05% vs. 2.54% P=0.735). Also there were no significant difference in arrhythmia recurrence for 3 years among two groups, 34 el-derly patients compared with 235 younger patients (26.0% vs. 26.0% P=0.8666).
Conclusions: The catheter ablation of PAF in the elderly patients could be safely performed and results are comparable to a younger pop-ulation.
SAFETY AND EFFICACY OF ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION IN OLDER ADULTSKengo Ando
Kokura Memorial Hospital, Fukuoka, Japan
CATHETER ABLATION P 1-049

167
Introduction: Catheter ablation (CA) is effective and curative therapy for atrial fibrillation (AF) and the number of CA for AF has increased. Among the complications of AF ablation, cardiac tamponade may cause a fetal result. Recently we can use the ablation catheter with measuring contact force, and this tool is useful to make adequate ablation region and to prevent perforation.In this study, we evaluate the safely of the ablation catheter with contact force compared with the ablation catheter without contact force retrospectively.
Methods: We perfumed CA in AF cases with the ablation catheter with contact force in 264 cases (Group A), and with the ablation catheter without contact force 240 cases (Group B). When we use the ablation catheter with contact force, we performed CA with contact force 10-20 g.
Results: Although there were 5 cardiac tamponade cases (1.9%) in Group A, there was no cardiac tamponade case (0%) in Group B.
Conclusions: Measuring of contact force is useful to prevent cardiac tamponade.
SAFETY OF CATHETER ABLATION WITH CONTACT FORCEManabu Fujimoto, Tatsunori Ikeda, Masaru Kiyama, Kazuyasu Okeie, Masakazu Yamamoto
Kouseiren Takaoka Hospital, Takaoka, Japan
CATHETER ABLATION P 1-051

168
Introduction: Pulmonary vein isolation (PVI) is the established lesion set for paroxysmal atrial fibrillation (PAF). Additional ablation, either linear (roof and mitral isthmus) or CFAE guided, has not been shown to improve results in persistent (PsAF) where outcomes remain infe-rior to PAF. We describe our experience of left atrial posterior wall isolation (LAPWI)-the “box set lesion pattern”.
Methods: Patients with symptomatic PsAF, or recurrent PAF after PVI refractory to anti-arrhythmic drugs (AAD) are offered LAPWI. This is either via catheter alone or a hybrid ablation where a surgical ablation is performed via a right VATS approach and then two months lat-er a catheter ablation is performed. The decision on technique is determined by multi-disciplinary team discussion. Patients with long-standing PsAF (LsPsAF) and those with large left atria are favoured for the hybrid approach. Follow-up is with clinical review at 4, 12 and 24 months with 7-day monitoring at 12 and 24 months. Further review and monitoring is guided by symptoms.
Results: Fifty-eight patients have undergone LAPWI (25 catheter, 33 hybrid). In the catheter group 5/25 had PAF but all were redo cases (median 2 prior ablations), 4/25 LsPsAF and 16/25 had PsAF. In the hybrid group all had PsAF with 28/33 LsPsAF. Median CHADSVASc score was 1 in the catheter group and 2 in the hybrid group. There have been no acute complications with catheter ablation in either group but one patient had a fatal CVA after surgery. LAPWI with entrance and exit block was achieved in 19/25 of the catheter group and 32/33 of the hybrid group. Forty-five patients have more than 3 months follow-up (19 catheter, 26 Hybrid). At a median 12 months follow-up (IQR 7-22) 76% (34/45) remain arrhythmia free (7/45 on AAD). In the catheter group after a follow-up of 16 months (IQR 10-23) 74% are free of arrhythmia recur-rence (2/19 on AAD). In the hybrid group after 11 months follow-up (IQR 11-20) 77% are free of arrhythmia recurrence (5/26 on AAD).
Conclusions: LAPWI appears to give greater freedom from atrial arrhythmia than the STAR AF II lesion sets. Outcomes were equivalent with both the catheter and hybrid methods however the hybrid group was primarily LsPsAF. No evidence of oesophageal complications was seen in either group.
LEFT ATRIAL POSTERIOR WALL ISOLATION (THE “BOX LESION PATTERN”) IN THE TREATMENT OF ATRIAL FIBRILLATION: A SINGLE CENTRE EXPERIENCEGuy Furniss, Dimitrios Panagopoulos, David Tomlinson, Malcolm Dalrymple-Hay, Guy Haywood
South West Cardiothoracic Centre, Plymouth, United Kingdom
CATHETER ABLATION P 1-052

169
Introduction: The 28 mm-cryoballoon system demonstrates wide circumferential lesions. However, the excessive range of the cryoabla-tion lesion, especially in physically small Asian patients remains unknown. The purpose of this study was to determine the impact of both the lesions extending into the left atrial (LA) body and the ablation related arrhythmia inducibility after cryoballoon ablation.
Methods: Seventy-four paroxysmal AF patients underwent a 28 mm-cryoballoon ablation and high-density LA mapping was performed before and after the ablation. A cryoablation lesion in the LA body was determined by any low-voltage areas (LVA <0.5 mV), and an overlap of the LVAs was evaluated as a local conduction block. The arrhythmia inducibility was checked in all patients.
Results: A wide range of the cryoablation lesion was observed in the posterior (46 [28-62]%) and roof (44 [31-70]%) regions. Unintentional roof conduction block occurred in 8 (10.4%) patients and roof-dependent atrial flutter (AFL) was induced in 2 (3%) patients. In the patients with unintentional roof conduction block, no regular atrial tachycardia was documented within the 6 months follow up. The patients with unintentional roof conduction block had a significantly lower-body surface area (1.54±0.17 vs. 1.70±0.17 cm2, P=0.029) and shorter dis-tance between the left and right pulmonary vein (PV) carinas (34±5 vs. 46±7 mm, P<0.001).
Conclusions: In our patient series, the excessive range of the cryoablation lesions resulted in the occurrence of unintentional roof con-duction block and roof-dependent AFL. The clinical implication in the long term follow up is unknown, but the physical constitution and LA anatomical factors were involved in those events.
INCIDENCE OF A NON-INTENTIONAL BLOCK LINE AT THE LEFT ATRIAL ROOF DUE TO SECOND-GENERATION CRYOABLATION: OCCURRENCE OF A ROOF-DEPENDENT ATRIAL FLUTTERYuichi Hori, Shiro Nakahara, Naofumi Anjou, Naoki Nishiyama, Akiko Hayashi, Takaaki Komatsu, Sayuki Kobayashi, Yoshihiko Sakai, Isao Taguchi
Dokkyo Medical University Koshigaya Hospital, Saitama, Japan
CATHETER ABLATION P 1-053

170
Introduction: SMART CHINA registry evaluates safety and effectiveness of AF ablation with THERMOCOOL® SMARTTOUCHTM catheter in Chinese patients.
Methods: This ongoing prospective, multicenter study aims to enroll 200 patients from 15 sites with follow-up at 3, 6, 9, and 12 M. CARTO VISITAGTM module identified sites of stable contact. We present acute safety, effectiveness, procedural data, contact force (CF), and short term success.
Results: As of April 15, 2016, 108 patients were enrolled (safety cohort: age, 62.2±8.9 years; 60.2% men; 99.1% Han); 104 met I/E criteria (ITT cohort). PVs were targeted in all patients without acute reconnections in 91.6% (98/107) patients. Seventeen patients (15.7%) received additional linear ablations (cavotricuspid isthmus ablation: 10/17 [58.8%]). Acute success (entrance block confirmation) was high (99.1% [107/108] patients). Most investigators selected CF working ranges between 5-30 g (32%) and 5-40 g (34%). Mean CF, 14.4±3.9 g, was similar to previous reports (Figure). Median (Q1, Q3) procedure, ablation, and fluoroscopy time was 141.5 (120, 180), 55 (41.5, 95), and 15 (9.8, 19.9) minutes. Of 7 SAEs reported in 6 (5.6%) patients, 2 (1.9%) were device/procedure related (cardiac tamponade, pericardial effu-sion); no deaths were reported. At 3 M, 100% (47/47) of ITT patients with available data had no AF/AT/AFL recurrence.
Conclusions: In interim analysis, AF ablation with CF sensing catheter was safe in Chinese patients, with 3 M success rate of 100%. Pro-cedural/CF results were similar to western patients.
SMART CHINA REGISTRY: INTERIM SAFETY AND EFFECTIVENESS OF PAROXYSMAL AF ABLATION USING THERMOCOOL® SMARTTOUCH™ CATHETER IN CHINESE PATIENTSCongxin Huang1, Jingquan Zhong2, Heng Cai3, Lianjun Gao4, Xiaoshu Cheng5, Zulu Wang6, Xi Su7, Xinchun Yang8, Yan Yao9, Lee Ming Boo10, Ling Tian11, Minglong Chen12 1Renmin Hospital of Wuhan University, Wuhan, China; 2Qi Lu Hospital of Shandong University, Ji’nan, China; 3Tian Jin Medical University General hospital, Tianjin, China; 4The First Affiliated Hospital of Dalian Medical University, Dalian, China; 5The Second Affiliated Hospital to Nanchang University, Nanchang, China; 6The General Hospital of Shenyang Military Region, Shenyang, China; 7Wu Han Asia Heart Hospital, Wuhan, China; 8Beijing Chao-Yang Hospital, Beijing, China; 9Fu Wai Hospital CAMS & PUMC, Beijing, China; 10Biosense Webster, Inc., Diamond Bar, United States; 11Johnson & Johnson Medical China, Beijing, China; 12The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
CATHETER ABLATION P 1-054

171
Introduction: Hybrid procedure, minimally invasive video-assisted thoracoscopic surgical ablation in conjunction with endocardial radiof-requency catheter ablation (RFCA), is supposed to be an alternative option of RFCA but the treatment efficacy is still unclear. We com-pared arrhythmic outcomes after hybrid procedure and RFCA in patients with atrial fibrillation (AF).
Methods: Between January 2010 and April 2015, a total of 335 ablation naïve patients were enrolled and performed either hybrid proce-dure (n=90) or RFCA (n=245) for drug-refractory AF. Using propensity score matching method, 65 patients of hybrid group were matched with 102 patients of RFCA group. The primary outcome was recurrence rate of AF after 3 months of window period.
Results: Median follow-up period was 2.1 (interquartile range: 1.2 to 3.1) years. Mean age was 52.7±9.80 years and 84.8% was male. Pa-tients with long standing persistent AF, history of congestive heart failure, and stroke were more performed hybrid than RFCA. Left atrial volume index (LAVI) was more increased in hybrid group than RFCA group (47.86±14.31 vs. 38.07±11.87, P <0.01). After 3 months of win-dow period, AF recurred in 24.3% of hybrid (19 patients) and 33.7% of RFCA (62 patients). In multivariate analysis, recurrence of AF was improved in hybrid procedure compared with RFCA (adjusted hazard ratio [HR]: 0.49, 95% confidence interval [CI]: 0.28 to 0.87, P =0.02). After propensity score-matching analysis, AF recurrence rate was lower in hybrid procedure than those of RFCA (20.4% versus 41.3%, HR: 0.50, 95% CI: 0.26 to 0.97, P =0.04). In subgroup analysis, benefit of hybrid procedure for reduction of AF recurrence was prominent in pa-tients who had persistent AF irrespective of LAVI (Log Rank P =0.03).
Conclusions: A hybrid procedure reduced recurrence rate of AF compared with RFCA alone in patients with AF. The treatment benefit was prominent in persistent AF. Our data suggest that hybrid procedure may improve long-term arrhythmic outcome in patients with drug-re-fractory persistent AF.
COMPARISON OF TREATMENT EFFICACY BETWEEN HYBRID TREATMENT AND REDIOFREQUENCY CATHETER ABLATION FOR ATRIAL FIBRILLATIONJin Kyung Hwang, Dong Seop Jeong, Seung-Jung Park, Kyuong-min Park, June Soo Kim, Young Keun On
Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 1-055

172
Introduction: Pulmonary vein isolation (PVI) is an established treatment in patients with symptomatic and drug-refractory atrial fibrilla-tion (AF). More and more elderly patients with AF is getting eligible to this procedure, but feasibility or efficacy in such patients is remained to be elucidated. The purpose of this study is to evaluate the efficacy and safety of PVI in AF patients over 80 years.
Methods: Symptomatic and drug-refractory AF patients without frailty who underwent PVI, 1,982 patients, from May, 2012 to May, 2016, were included in this study.
Results: The number of patients over 80 years was 48 [27 men, age 81.8±1.9 years, paroxysmal AF 38 (79%), persistent AF 8 (17%), and long-standing persistent AF 2 (4%)]. There were no difference in left atrium diameter (38.1±7.6 mm vs. 37.0±7.1 mm, P=0.32), ejection fraction (64.5±13.6% vs. 65.0±10.9%, P=0.73) and chronic heart failure (18.8% vs. 12.4%, P=0.19) between over 80 group and younger group. CHADS2 score (2.6±1.8 vs. 1.2±1.4, P<0.001) and HASBLED score (2.3±1.2 vs. 1.3±1.0, P<0.001) were significantly higher in over 80 group. The rate of recurrence (35.4% vs. 37.3%, P=0.88) and complications (16.7% vs. 10.9%, P=0.237) after a single procedure were not significantly different between both groups.
Conclusions: In this study, efficacy and safety of pulmonary vein isolation in patients with atrial fibrillation over 80 years, who were eligible for catheter ablation, were similar compared to younger group, regardless of the severities of CHADS2 score or HASBLED score.
EFFICACY AND SAFETY OF PULMONARY VEIN ISOLATION IN PATIENTS WITH ATRIAL FIBRILLATION OVER 80 YEARSTakashi Ikenouchi1, Junichi Nitta1, Tsukasa Iwasaki1, Yousuke Hayashi1, Kazuya Murata1, Kiko Lee1, Keita Watanabe1, Tatsuhiko Hirao1, Tomomasa Takamiya1, Nobutaka Kato1, Yukihiro Inamura1, Masashiko Goya2, Kenzo Hirao2 1Saitama Red Cross Hospital, Saitama, Japan; 2Tokyo Medical and Dental University, Heart Rhythm Center, Tokyo, Japan
CATHETER ABLATION P 1-056

173
Introduction: We already know less effectiveness of additional substrate modification for persistent atrial fibrillation (AF) patients from some study. But it is unclear about effectiveness of additional substrate modification for recurrent AF patients. The purpose of this study was to evaluate effectiveness of additional substrate modification for recurrent AF patients with chronic pulmonary vein (PV) reconnection.
Methods: We enrolled 366 consecutive recurrent AF patients who underwent second procedure from July 2009 to December 2015. We retrospectively extracted patients with chronic PV reconnection from the database. These patients were divided into two groups; pulmo-nary vein isolation (PVI) alone group and PVI plus additional substrate modification group at second procedure. Outcome measure was freedom from AF recurrence rate at 1, 2, 3 years after second procedure. We also evaluated patient characteristics.
Results: The number of PVI alone group was 97 [mean age 58.2±10.1 years, male 78 (81.3%)] and PVI plus substrate modification group was 269 [(60.9±10.2 years, male 199 (74.0%)].Mean follow up period was 901.1±591.0 days. At 1, 2, 3 years after second procedure, there was significant difference in freedom from recurrence rate (90.8% vs. 85.3%, 83.9% vs. 72.6%, 76.8% vs. 60.7%, respectively; P=0.0336). In persistent AF patients at the time of first procedure, compared to paroxysmal AF patients, there was significantly more patients who un-derwent PVI plus substrate modification in second procedure [95 (90.5%) vs. 174 (66.7%), respectively; P<0.0001].
Conclusions: Recurrence rate of PVI plus additional substrate modification group is significantly higher than PVI alone group.
EFFECTIVENESS OF ADDITIONAL SUBSTRATE MODIFICATION IN RECURRENT ATRIAL FIBRILLATION PATIENTSTakahiro iseda, Kenichi Hiroshima, Michio Nagashima, Jyunji Morita, Shouta Tohoku, Kengo Ando, Kenji Ando
Kokura Memorial Hospital, Kitakyushu, Japan
CATHETER ABLATION P 1-057

174
Introduction: Pulmonary vein isolation (PVI) with radiofrequency (RF) energy is a well-established treatment for patients with paroxysmal atrial fibrillation (PAF), but requires difficult, lengthy and operator-dependent procedure. Cryoballoon ablation with non-selective and con-tinuous stable contact has been proved to be safe and effective, though freezing areas and lesion depths might be limited due to atrial an-atomical variables. We presume that combined energy of cryoballoon and RF ablation is feasible, safe and might achieve more continu-ous, transmural and long-lasting lesions during PVI, resulting in elevated success rate for PAF patients.
Methods: We continuously enrolled 69 patients with documented symptomatic PAF. All patients underwent PVI with first generation 28 mm cryoballoon followed by RF ablation to reassure left atrium-pulmonary vein bi-directional block. For each pulmonary vein (PV), cryoablation was conducted twice mostly with 240 seconds each time. PV isolation rate was identified and analyzed. All patients were fol-lowed up by 7-day holter monitor and a 90-day blanking period was considered.
Results: There were 69 patients enrolled in our study, 47 (68.1%) of them were male. The average age was 64.0±10.8 years and average time from PAF diagnosis to procedure was 60.1±7.1 months. Patients had average CHA2DS2-VASc score of 2.0±1.4. Cryoablation pro-duced acute isolation in 123 (44.6%) PVs, while only 5 (7.2%) patients achieved isolation in all four PVs with balloon catheter alone. After RF ablation, all PVs were confirmed isolated. After average follow-up of 9.65±3.49 months, 59 patients (85.5%) remain in sinus rhythm. 1 patient experienced tamponade during procedure and recovered by pericardiocentesis and drainage. 2 patients suffered from phrenic nerve impairment and 1 recovered after procedure. No patients developed atrioesophageal fistula or other sever contradiction.
Conclusions: The strategy of combining cryoballoon technique and RF ablation in pulmonary vein isolation procedure is feasible, safe and associate with elevated success rate in paroxysmal atrial fibrillation patients.
COMBINED ABLATION OF CRYOBALLOON AND RADIOFREQUENCY FOR PAROXYSMAL ATRIAL FIBRILLATIONChenyang Jiang, Jun Zhu, Lu Yu, Xia Sheng, Ruhong Jiang
Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China
CATHETER ABLATION P 1-058

175
Introduction: Cryoballoon-based ablation (CBA) and remote magnetic navigation-guided (RMN) ablation are two novel means to treat paroxysmal atrial fibrillation (PAf), however, no controlled data have been reported in China. This prospective, controlled study was to as-sess the safety and efficacy of these two techniques and compare the procedure-related outcome.
Methods: A total of 80 patients with PAf were enrolled and divided into two groups (CBA group, n=40; RMN group, n=40). The primary endpoint was acute success of complete pulmonary vein antrum isolation (PVAI). The secondary endpoints were procedural parameters including complications, procedure time, ablation time, and fluoroscopy time. Freedom from AF recurrence was evaluated at 3 months follow-up.
Results: Complete PVAI were achieved during the first ablation procedure in CBA group. Acute success rate of PVAI was 97.5% patients in RMN group. No major complication including cardiac temponade and atrial-esophageal fistulae occurred in RMN group. Phrenic nerve palsy occurred in one patient of CBA group. The complication rate was not different. Compared to RMN group, procedure time of CBA group was significantly reduced (138±35 minutes vs. 110±31 minutes, P<0.01); However, fluoroscopy time was significantly increased (6.4±2.6 minutes vs. 16.6±4.5 minutes, P<0.001). Freedom from AF recurrence was similar between these two groups (RMN vs. CRYO: 87.5% vs. 82.5%, P>0.05) within 3 months (blanking period).
Conclusions: Both CBA and RMN are safe and effective to complete PVAI in patients with PAf. Our data indicated that RMN-guided PAf ablation can markedly reduce the fluoroscopy time, and CBA can shorten the procedure time.
CRYOBALLOON ABLATION VERSUS REMOTE MAGNETIC NAVIGATION ABLATION IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION: A PROSPECTIVE, CONTROLLED STUDYQi Jin, Ning Zhang, Qingzhi Luo, Yanxin Han, Tianyou Ling, Kang Chen, Wenqi Pan, Liqun Wu
Shanghai Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
CATHETER ABLATION P 1-059
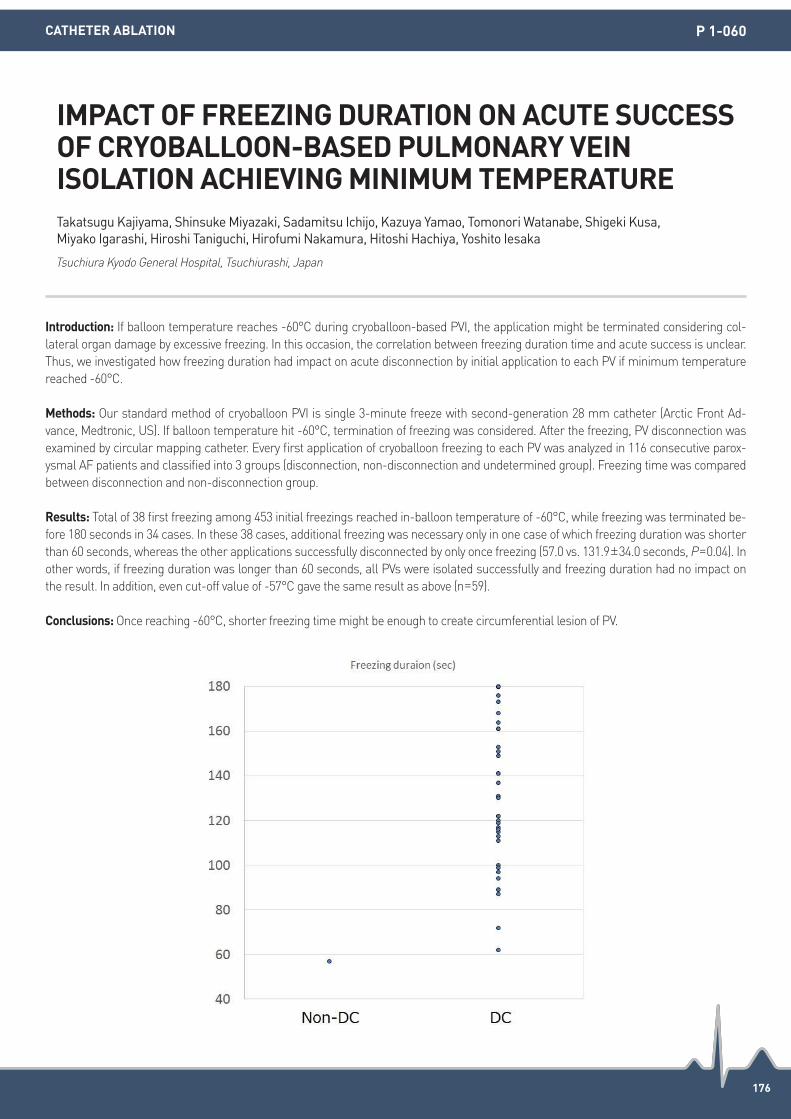
176
Introduction: If balloon temperature reaches -60°C during cryoballoon-based PVI, the application might be terminated considering col-lateral organ damage by excessive freezing. In this occasion, the correlation between freezing duration time and acute success is unclear. Thus, we investigated how freezing duration had impact on acute disconnection by initial application to each PV if minimum temperature reached -60°C.
Methods: Our standard method of cryoballoon PVI is single 3-minute freeze with second-generation 28 mm catheter (Arctic Front Ad-vance, Medtronic, US). If balloon temperature hit -60°C, termination of freezing was considered. After the freezing, PV disconnection was examined by circular mapping catheter. Every first application of cryoballoon freezing to each PV was analyzed in 116 consecutive parox-ysmal AF patients and classified into 3 groups (disconnection, non-disconnection and undetermined group). Freezing time was compared between disconnection and non-disconnection group.
Results: Total of 38 first freezing among 453 initial freezings reached in-balloon temperature of -60°C, while freezing was terminated be-fore 180 seconds in 34 cases. In these 38 cases, additional freezing was necessary only in one case of which freezing duration was shorter than 60 seconds, whereas the other applications successfully disconnected by only once freezing (57.0 vs. 131.9±34.0 seconds, P=0.04). In other words, if freezing duration was longer than 60 seconds, all PVs were isolated successfully and freezing duration had no impact on the result. In addition, even cut-off value of -57°C gave the same result as above (n=59).
Conclusions: Once reaching -60°C, shorter freezing time might be enough to create circumferential lesion of PV.
IMPACT OF FREEZING DURATION ON ACUTE SUCCESS OF CRYOBALLOON-BASED PULMONARY VEIN ISOLATION ACHIEVING MINIMUM TEMPERATURETakatsugu Kajiyama, Shinsuke Miyazaki, Sadamitsu Ichijo, Kazuya Yamao, Tomonori Watanabe, Shigeki Kusa, Miyako Igarashi, Hiroshi Taniguchi, Hirofumi Nakamura, Hitoshi Hachiya, Yoshito Iesaka
Tsuchiura Kyodo General Hospital, Tsuchiurashi, Japan
CATHETER ABLATION P 1-060

177
Introduction: The STAR AF II trial demonstrated that there was no reduction in the rate of recurrent atrial fibrillation (AF) when either lin-ear ablation or complex fractionated atrial electrogram (CFAE) ablation in addition to pulmonary vein isolation (PVI). However, whether combination of all three methods of ablation improves outcomes remains unclear.
Methods: Total 448 consecutive patients with persistent AF were divided by 3 groups: PVI with linear ablation (n=191), PVI with ablation of CFAE (n=189), and PVI with linear ablation plus ablation of CFAE (n=68).
Results: Mean age was 56±10 years old, 85.2% were male, mean AF duration was 53±58 months and mean LA size was 44±6 mm. Ab-lation times were not significantly different among the three groups (P=0.544), although total procedure times were significantly longer in two groups who received ablation of CFAE (373±107 and 369±97 minutes, respectively) compared to patients who underwent PVI with lin-ear ablation alone (vs. 319±89, P<0.001). During the mean 55±25 months, there was no significant difference in the rate of recurrence of atrial tachyarrhythmias between patients who received PVI with ablation of CFAE and those who underwent PVI with linear ablation (29.6% vs. 36.6%, P=0.330). However, the rate of recurrence of atrial tachyarrhythmias was significantly reduced in patients who received ablation of CFAE in addition to PVI with linear ablation compared to those who underwent PVI with linear ablation alone (22.1% vs. 36.6%, P=0.041).
Conclusions: This long-term follow-up data suggests that combination of all methods with additional substrate modification improves the efficacy of PVI with linear ablation in patients with persistent AF.
COMBINATION STRATEGY OF SUBSTRATE MODIFICATION IN ADDITION TO PULMONARY VEIN ISOLATION WITH LINEAR ABLATION IMPROVES THE EFFICACY IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATIONDong-Hyeok Kim1, Jong-Il Choi2, Sang-Weon Park1, Young-Hoon Kim2, Jaemin Shim2, Kwang-No Lee2, Seung-Young Roh2, Hong Euy Lim3, Jin Seok Kim4 1Sejong General Hospital, Bucheon, Republic of Korea; 2Korea University Medical Center, Seoul, Republic of Korea; 3Korea University Guro Hospital, Seoul, Republic of Korea; 4Korea University Ansan Hospital, Ansan, Republic of Korea
CATHETER ABLATION P 1-061

178
Introduction: We recently reported low left atrial (LA) compliance estimated by LA pulse pressure (LApp) contributes to clinical recurrence after catheter ablation for atrial fibrillation (AF). Catheter ablation is one of destructive procedure and more touch makes more scar. We hypothesized that extensive AF ablation reduces LA compliance and LA endocardial voltage in patients who underwent repeat procedure.
Methods: This observational cohort study included 75 patients (78.7% male, 55.5±10.9 years old, 62.7% paroxysmal AF) who underwent a second ablation procedure for anti-arrhythmic resistant recurred AF. We compared LApp and LA voltage measured at the beginning of the procedures, and compared those parameters measured at de novo procedure.
Results: 1) Second procedures were conducted 18.7±14.2 months after de novo procedure, and LApp increased from 8.94±5.11 to 11.07±5.19 (P=0.022) and LA voltage decreased from 0.97±0.44 to 0.84±0.41 (P<0.001). 2) AF type (PeAF at de novo procedure, P=0.002), addi-tional linear ablation (P=0.028), ablation time (P=0.025) were significantly associated with LApp increase at redo procedure in univariate linear regression analysis, and persistent AF at de novo procedure was independently associated with LApp increase (β= 4.44, 95% CI 0.19 to 8.69, P=0.041). In sub-analysis among patients with PAF, ablation time showed independent association with LApp increase (min, β= 0.11, 95% CI 0.01 to 0.21, P=0.035). 3) Hypertension was independently associated with reduction of mean LA voltage (β=-0.30, 95% CI -0.56 to -0.03, P=0.029).
Conclusions: LApp is increased even after single ablation procedure, especially in PeAF patients who undergoing additional linear abla-tion with prolonged ablation time.
REDUCED LEFT ATRIAL COMPLIANCE AND ENDOCARDIAL VOLTAGE AFTER CATHETER ABLATION FOR ATRIAL FIBRILLATIONTae-Hoon Kim, Jae-Sun Uhm, Jong-Youn Kim, Boyoung Joung, Moon-Hyoung Lee, Hui-Nam Pak
Severance Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 1-062

179
Introduction: It is not clear whether bidirectional block (BDB) of linear ablations reduces AF recurrence after RFCA. We hypothesized that BDB of linear ablation has prognostic significance after RFCA for persistent AF (PeAF).
Methods: Among 1,793 consecutive patients in Yonsei AF ablation Cohort, we included 398 patients with PeAF (75.6% male, 59.8±10.3 years old) who underwent catheter ablation with consistent ablation protocol of Dallas lesion set: CPVI, cavotricuspid isthmus ablation (CTI), roof line (RL), postero-inferior line (PIL), and anterior line (AL).
Results: BDB rates of de novo ablation lines were 100% in CPVI, 100% in CTI, 84.7% in RL, 44.7% in PIL, and 63.6% in AL. During the 29.0±18.4 months of follow-up, 31.7% (126/398) showed clinical recurrence. Left atrial posterior wall (LAPW) isolation (BDBs of RL and PIL) was independently associated with lower clinical recurrence (HR 0.68, 95% CI 0.47-0.98, P=0.041, Log-rank P=0.017), whereas those with BDB of RL or AL were not (Log-rank P=0.178 for RL, P=0.764 for AL). Among 52 patients who underwent repeat procedures (23.0±16.1 months after de novo procedure), maintenance rate of LAPW isolation was 75% (18/24), and BDB maintenance rates for CTI, RL, and AL were 94.2% (49/52), 75% (33/44), and 72.4% (21/29), respectively.
Conclusions: Although PIL crosses esophageal contact area, LAPW isolation is important for the better clinical outcome in catheter abla-tion with linear ablation strategy for the patients with PeAF.
DURABILITY OF LEFT ATRIAL LINEAR ABLATION AND CLINICAL OUTCOME AFTER CATHETER ABLATION FOR PERSISTENT ATRIAL FIBRILLATIONTae-Hoon Kim1, Junbeom Park2, Jae-Sun Uhm1, Jong-Youn Kim1, Boyoung Joung1, Moon-Hyoung Lee1, Hui-Nam Pak1 1Severance Hospital, Seoul, Republic of Korea; 2Ewha Womans University, Seoul, Republic of Korea
CATHETER ABLATION P 1-063

180
Introduction: Adiponectin has anti-diabetic, anti-atherogenic and anti-inflammatory properties, but, many studies exploring the predictive value of adiponectin in cardiovascular disease have yielded opposite results, known as the “adiponectin paradox”. Recently, we reported that overweight and metabolic syndrome have relation with clinical recurrence of atrial fibrillation (AF) 2-years after catheter ablation. We hypothesized that the pre-procedural plasma level of adiponectin has a prognostic value in patients who underwent AF catheter ablation.
Methods: This study included 874 patients (73.0% male, 57.6±11.2 years of age) who underwent RFCA for paroxysmal AF, and conducted quartile analyses for pre-procedural plasma levels of adiponectin to determine AF-related clinical factors.
Results: 1) The highest quartile of plasma adiponectin were more likely to be older (P<0.001), and had higher proportions of females (P<0.001) and higher CHA2DS2-VASc scores (P<0.001) than others. 2) Plasma level of adiponectin was independently associated with fe-male gender (B 2.92, 95% CI 1.84 to 4.00, P<0.001), older age (B 0.06, 95% CI 0.03 to 0.10, P<0.001), lower body mass index (B -0.22, 95% CI -0.42 to -0.03, P=0.025), and greater LA volume index (B 0.05, 95% CI 0.01 to 0.08, P=0.005). 3) During the 29.9±18.0 months of fol-low-up, patients in the highest quartile of plasma adiponectin showed higher clinical recurrence rate than other groups (Kaplan-Meier analysis, log rank P=0.029), and the plasma adiponectin level (HR 1.17, 95% CI 1.02-1.35, P=0.022) was independently associated with clinical recurrence of AF after catheter ablation for paroxysmal AF.
Conclusions: High circulating adiponectin is independently associated with recurrence of AF after catheter ablation for paroxysmal AF.
HIGH CIRCULATING ADIPONECTIN IS ASSOCIATED WITH POOR LONG-TERM CLINICAL OUTCOME AFTER CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATIONTae-Hoon Kim, Jae-Sun Uhm, Jong-Youn Kim, Boyoung Joung, Moon-Hyoung Lee, Hui-Nam Pak
Severance Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 1-064

181
Introduction: Focal impulse and rotor mapping (FIRM) is increasingly used to treat persistent atrial fibrillation. Good positioning of basket catheters is vital for optimal FIRM maps. Until now, the basket catheter reconstruction and navigation can only be supported by electro-anatomic mapping systems. We present the first X-ray based software tool for basket catheter visualization and navigation during AF ab-lation procedures.
Methods: The new software was utilised in 10 patients with AF undergoing ablation using FIRM. A 3D image of the left atrium (LA) was segmented out of a pre-procedural magnetic resonance angiogram (MRA) of the left atrium. The LA image was superimposed onto fluo-roscopic images and registered to the patient’s anatomy using the new software. Based on a biplane fluoroscopic image a basket catheter model was generated and added to the composite image (Figure). Physicians underwent a questionnaire based on saved images.
Results: The software was able to reconstruct the basket catheter in 100% of applications (10 AF ablation procedures with 35 basket po-sitions). The mean time for basket reconstruction was 268±45 seconds. In 33/35 (94%) basket images, physician surveys confirmed that the overlaid 3D left atrial anatomy and the reconstructed basket catheters would significantly aid intra-procedural orientation (P<0.05).
Conclusions: We present a new imaging software supporting basket placement, able to reconstruct catheters and support procedural navigation. The new software does not require additional equipment or new hardware. Instead, it uses and combines the existing devices and data in the EP lab using X-ray images only.
EVALUATION OF NEW IMAGING SOFTWARE FOR FOCAL IMPULSE AND ROTOR MAPPING IN ATRIAL FIBRILLATION ABLATION PROCEDURESChristopher Kowalewski, Junaid A. B. Zaman, Tina Baykaner, Mahmood Alhousseini, Fatemah Shenasa, Mohan Viswanathan, Paul J. Wang, Sanjiv M. Narayan
Stanford University, Palo Alto, United States
CATHETER ABLATION P 1-065

182
Introduction: The ligament of Marshall may hinder the creation of mitral isthmus (MI) block or pulmonary vein (PV) isolation (PVI) in ra-diofrequency (RF) catheter ablation of atrial fibrillation (AF). We aimed to assess the benefit of RF ablation targeting the vein of Marshall (VOM) in failed cases of MI block or PVI.
Methods: We reviewed the medical records of patients who underwent RF ablation targeting the VOM after failed MI ablation or left PVI using the conventional method, which included circumferential point-by-point ablation around the PV antrum and carina, or endocardial MI and epicardial distal coronary sinus (CS) ablation for MI block. The VOM was identified by using selective VOM venography with an ex-ternal irrigation RF ablation catheter. RF ablation targeting the VOM was performed with RF application at the ostium of the VOM inside the CS or at the endocardial region facing the VOM course.
Results: CS venography was performed in 42 patients after failure of left PVI (n=5) or MI block (n=37). Under CS venography, the VOM was visualised in 22 of 42 patients (MI=19, PVI=3). During selective venography of the VOM, no procedure-related complication was observed. RF application targeting the VOM successfully achieved MI block in 13 patients (68.4%) and PVI in 2 (66.7%).
Conclusions: Selective VOM venography using an irrigated ablation catheter is feasible and safe. RF ablation targeting the VOM may pro-vide additional benefit in failed cases of MI block or PVI.
RADIOFREQUENCY CATHETER ABLATION TARGETING THE VEIN OF MARSHALL IN DIFFICULT MITRAL ISTHMUS ABLATION OR PULMONARY VEIN ISOLATIONJi Hyun Lee, Minsu Kim, You Mi Hwang, Jongmin Hwang, Jun Kim, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim
Asan Medical Center, Seoul, Republic of Korea
CATHETER ABLATION P 1-067

183
Introduction: Mitral isthmus (MI) ablation has been shown to be effective for management of perimitral atrial flutter (AFL). However, achieving bidirectional block across the MI is technically challenging. We evaluated the clinical and procedural characteristics between patients with successful peri-mitral block [PMB] and those without.
Methods: We retrospectively reviewed the patients who had undergone mitral isthmus ablation during catheter ablation of AF in our insti-tute, from January 2010 to May 2015. And we also investigated the ablation combinations for achieving PMB.
Results: MI ablation was performed in 268 patients during the set period. Successful bidirectional PMB was accomplished in 193 (72%) patients. Single endocardial MI ablation achieved PMB in 41 patients only. Additional distal coronary sinus (CS) ablation led to PMB in 120 patients. In failed PMB cases with distal CS and MI ablation, additional ablations of double separate endocardial MI line (n=17), anterior line (n=10) or RF application targeting the vein of Marshall (VOM, n=5) were required to achieve PMB. The success rates of PMB were 59% (17/29) with double separate MI ablation, 48% (10/21) with anterior line ablation and 50% (5/10) with VOM ablation. The patients who had successful MI block showed shorter left atrium (LA) diameter (42.3±6.0 mm vs. 44.3±5.5 mm, P=0.009) and lower left ventricle mass (165.1±41.6 g vs. 185.0±43.5 g, P=0.001). In univariable binary logistic regression model, the LA diameter (odds ratio [OR]: 0.941, 95% confidence interval [CI]: 0.898-0.986, P=0.010) and left ventricle mass (OR: 0.898, 95%CI: 0.893-0.996, P=0.001) were significantly associ-ated with achieving bidirectional MI block.
Conclusions: The success rate of mitral isthmus block was about 72% in our institute. Single endocardial MI ablation alone was not enough to achieve PMB. Additional RF application including distal CS ablation, double MI ablation, VOM ablation and anterior line ablation were required for PMB. Smaller LA diameter and LV mass were significantly associated with achieving successful bidirectional block in MI ablation.
MANAGEMENT OF DIFFICULT MITRAL ISTHMUS ABLATIONSJi Hyun Lee, Minsu Kim, You Mi Hwang, Jongmin Hwang, Jun Kim, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim
Asan Medical Center, Seoul, Republic of Korea
CATHETER ABLATION P 1-068
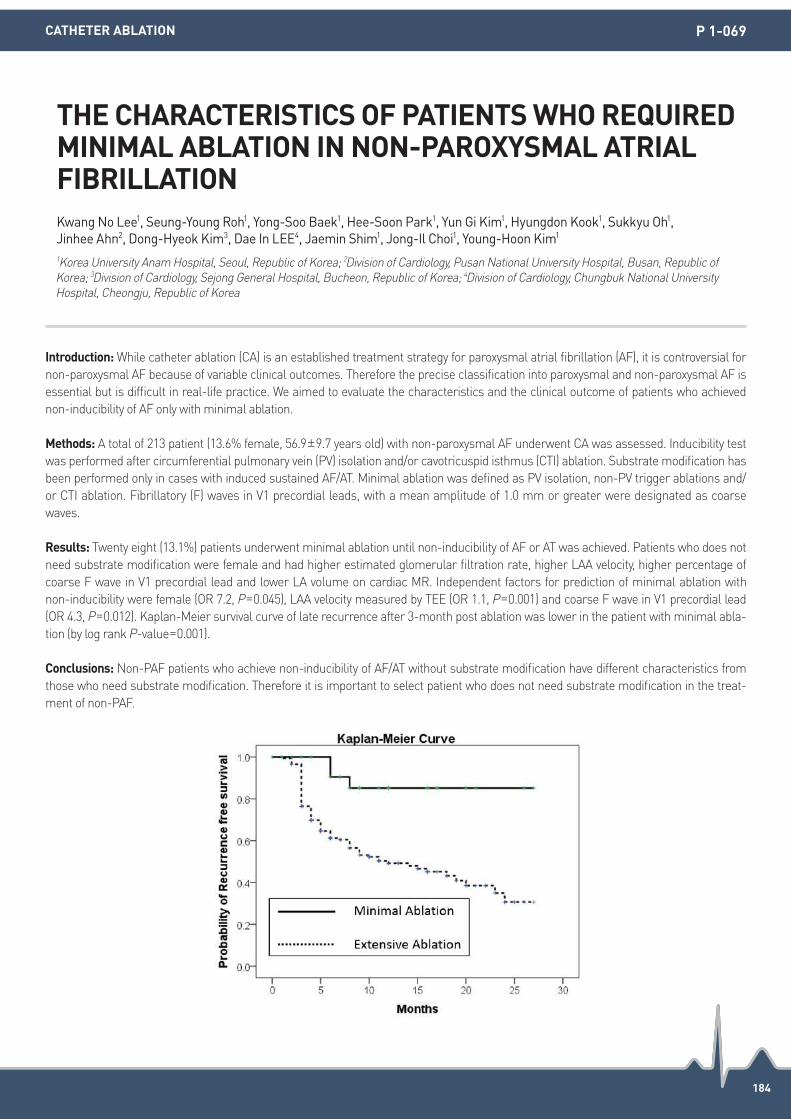
184
Introduction: While catheter ablation (CA) is an established treatment strategy for paroxysmal atrial fibrillation (AF), it is controversial for non-paroxysmal AF because of variable clinical outcomes. Therefore the precise classification into paroxysmal and non-paroxysmal AF is essential but is difficult in real-life practice. We aimed to evaluate the characteristics and the clinical outcome of patients who achieved non-inducibility of AF only with minimal ablation.
Methods: A total of 213 patient (13.6% female, 56.9±9.7 years old) with non-paroxysmal AF underwent CA was assessed. Inducibility test was performed after circumferential pulmonary vein (PV) isolation and/or cavotricuspid isthmus (CTI) ablation. Substrate modification has been performed only in cases with induced sustained AF/AT. Minimal ablation was defined as PV isolation, non-PV trigger ablations and/or CTI ablation. Fibrillatory (F) waves in V1 precordial leads, with a mean amplitude of 1.0 mm or greater were designated as coarse waves.
Results: Twenty eight (13.1%) patients underwent minimal ablation until non-inducibility of AF or AT was achieved. Patients who does not need substrate modification were female and had higher estimated glomerular filtration rate, higher LAA velocity, higher percentage of coarse F wave in V1 precordial lead and lower LA volume on cardiac MR. Independent factors for prediction of minimal ablation with non-inducibility were female (OR 7.2, P=0.045), LAA velocity measured by TEE (OR 1.1, P=0.001) and coarse F wave in V1 precordial lead (OR 4.3, P=0.012). Kaplan-Meier survival curve of late recurrence after 3-month post ablation was lower in the patient with minimal abla-tion (by log rank P-value=0.001).
Conclusions: Non-PAF patients who achieve non-inducibility of AF/AT without substrate modification have different characteristics from those who need substrate modification. Therefore it is important to select patient who does not need substrate modification in the treat-ment of non-PAF.
THE CHARACTERISTICS OF PATIENTS WHO REQUIRED MINIMAL ABLATION IN NON-PAROXYSMAL ATRIAL FIBRILLATIONKwang No Lee1, Seung-Young Roh1, Yong-Soo Baek1, Hee-Soon Park1, Yun Gi Kim1, Hyungdon Kook1, Sukkyu Oh1, Jinhee Ahn2, Dong-Hyeok Kim3, Dae In LEE4, Jaemin Shim1, Jong-Il Choi1, Young-Hoon Kim1 1Korea University Anam Hospital, Seoul, Republic of Korea; 2Division of Cardiology, Pusan National University Hospital, Busan, Republic of Korea; 3Division of Cardiology, Sejong General Hospital, Bucheon, Republic of Korea; 4Division of Cardiology, Chungbuk National University Hospital, Cheongju, Republic of Korea
CATHETER ABLATION P 1-069

185
Introduction: Obstructive sleep apnea has been known to be a risk factor of atrial fibrillation (AF) recurrence after radiofrequency cathe-ter ablation (RFCA), but snoring events during procedure can affect the catheter stability and technical failure. We hypothesized snoring events during AF ablation procedure increase procedure time and recurrence rate.
Methods: We prospectively included 216 consecutive patients (71.3% male, 60.7±10.5 years old, 69.9% paroxysmal AF) who underwent RFCA for AF under conscious sedation (remifentanil and midazolam). Respiratory patterns were monitored by single channel nasal pres-sure (SCNP) device (Apnealink, Resmed) during the procedure, and analyzed respiratory amplitude, rate, kurtosis and skewness of fre-quency, apnea-hypopnea index (AHI), and snoring event (number of episodes with pressure wave subtracted filtered signal 0-60 Hz) per min (SEPM). We evaluated the relationship between respiratory parameters and clinical parameters including ablation time, procedure time, complication rate, and AF recurrence rate.
Results: 1) SEPM during procedure was significantly associated procedure time (β=3.11 [0.31-5.91], P=0.030) and longer ablation time (β=2.76 [0.94-4.57], P=0.003). Kurtosis of respiratory frequency was associated with longer ablation time (β=-1.50 [-2.70--0.31], P=0.013). However, any respiratory parameters did not increase procedure related complication rate. 2) Among 93 patients with linear ablation, bidi-rectional block (BDB) rate was significantly lower in patients with high SEPM (based on median value) than those with low SEPM (37.8% vs. 60.4%, P=0.029). SEPM was independently associated with lower BDB rate of linear ablation (OR 0.743 [0.566 to 0.976]; P=0.033). 3) SEPM was an independent risk factor of clinical recurrence of AF among the patients with persistent AF (Adjusted by age, gender; HR 1.337 [1.027 to 1.740], P=0.031), but not in paroxysmal AF. 4) Over-night polysomnogram (PSG) was conducted in 114 patients one day be-fore the procedure, and PSG measured AHIs were weak correlation with SCNP device measured AHI (r=0.210, P=0.026).
Conclusions: Snoring events per minute during AF ablation procedure prolong the ablation time and procedure time, and hamper the completeness of linear ablation. Respiratory parameters may affect AF ablation outcome by technical factors in patients with persistent AF.
SNORING EVENTS DURING THE CATHETER ABLATION INCREASE TOTAL PROCEDURE TIME AND CLINICAL RECURRENCE RATE IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATIONYeong-Min Lim, Tae-Hoon Kim, Jae-Sun Uhm, Jong-Youn Kim, Boyoung Joung, Moon-Hyoung Lee, Hui-Nam Pak
Yonsei University Health System, Seoul, Republic of Korea
CATHETER ABLATION P 1-070

186
Introduction: Stepwise ablation strategy is effective for persistent atrial fibrillation (AF). Previous study revealed that most patients con-verted to sinus rhythm via atrial tachycardias (ATs) during the ablation procedure. We sought to investigate clinical characteristics associ-ated with types of AT occurring after termination of AF during the ablation procedure.
Methods: Patients undergoing catheter ablation of persistent AF were studied. Catheter ablation was performed during AF from pulmo-nary vein isolation followed by electrogram-based substrate modification until termination of AF. Left atrial linear ablation was subse-quently performed if AF converted to macro-reentrant ATs. The mechanism of AT occurring AF termination during the ablation procedure was assessed. All patients were followed without anti-arrhythmic drugs, and atrial tachyarrhythmias occurring after a 2-month blanking period were assessed.
Results: 174 patients (65±9 years old, male 74%, longstanding persistent AF 25%), were studied. During a median of 558 days of fol-low-up, 61 patients (35%) were free from atrial tachyarrhythmias. AF was terminated by ablation in 123 patients (70%). AF was converted to sinus rhythm directly in 25 patients (14%, SR group), while 98 patients (56%) had conversion of AF into ATs. The mechanism of AT oc-curring after AF termination was focal ATs in 42 patients (24%, focal group), macro-reentrant AT in 49 patients (28%, macro-reentrant group), and AT with unknown mechanism in 7 patients (4%). There were no difference in age, duration of continuous AF, left atrial diame-ter, and left ventricular ejection fraction between groups. Age was associated with the mechanism of AT occurring after AF termination. Patients younger than 65 years were more likely to have focal AT rather than macro-reentrant AT (focal vs. macro-reentrant, 22% vs. 16%) compared to patients older than or equal to 65 years (14% vs. 26%, P=0.04). Long term outcome after single procedure was not different between SR, focal and macro-reentrant groups (P=0.14), while after multiple procedures, long-term arrhythmia-free rate was the best in SR group, and the worst in focal group (P=0.04).
Conclusions: In persistent AF, conversion of AF into macro-reentrant AT during the ablation procedure was more commonly observed in elderly patients. AF conversion to focal AT during the index procedure was predictive of poor outcome after multiple procedures.
CLINICAL CHARACTERISTICS AND TYPES OF ATRIAL TACHYCARDIA OCCURRING AFTER TERMINATION OF AF DURING STEPWISE ABLATION FOR PERSISTENT AFMayumi Masumura1, Yoshihide Takahashi1, Shu Yamashita1, Masahito Suzuki1, Kenzo Hirao2, Mitsuaki Isobe2 1National Disaster Medical Center, Tokyo, Japan; 2Tokyo Medical and Dental University, Tokyo, Japan
CATHETER ABLATION P 1-072

187
Introduction: Termination of atrial fibrillation (AF) is often used as the procedural endpoint for persistent AF. We sought to investigate as-sociation between duration of radiofrequency (RF) energy delivery and long-term clinical outcome after single- and multiple-procedures.
Methods: Patients undergoing catheter ablation of persistent AF were studied. Catheter ablation was performed during AF with endpoint of termination of AF by ablation. Isolation of the pulmonary veins was performed followed by electrogram-based substrate modification or linear ablation until termination of AF. All patients were followed without anti-arrhythmic drugs, and occurrence of atrial tachyarrhyth-mias after a 2-month blanking period was assessed.
Results: 174 patients (65±9 years old, male 74%, longstanding persistent AF 25%), were studied. Median RF duration was 4,432 (IQR 3,505-5,336) seconds. AF was terminated by ablation in 123 patients (69%). During a median of 558 days of follow-up, 61 patients (35%) were free from atrial tachyarrhythmias. RF duration was associated with AF termination during the procedure (4,185 seconds vs. 4,749 seconds, P=0.02), while left atrial diameter (LAD) and duration of continuous AF were not associated with AF termination (P=0.08, 0.14, respectively). After adjustment of LAD, duration of AF, and termination of AF by ablation, RF duration was independently predictive of bet-ter outcome (P=0.015). In the subgroup of AF termination, from ROC curve analysis, the best cut-off value of RF duration of index proce-dure for predicting maintenance of sinus rhythm for 1 year after single-procedure was 4,257 sec (AUC 0.65, sensitivity 0.66, specificity 0.63). Arrhythmia-free rate after multiple-procedures was not associated with RF duration of index procedure (RF duration less than or equal to 4,257 vs. more than 4,257 seconds, 95% vs. 87%, P=0.1). In the subgroup of no AF termination, long-term outcome was not dif-ferent according to RF duration after single- and multiple-procedures (P=0.4, 0.3, respectively). Arrhythmia-free rate was lower even after multiple procedures compared to patients with AF termination (70% vs. 90%, P=0.002).
Conclusions: In patients with persistent AF, less RF duration was predictive of freedom from atrial tachyarrhythmia after single-proce-dure.
DURATION OF RADIOFREQUENCY ENERGY DELIVERY IS PREDICTIVE OF ARRHYTHMIA RECURRENCE AFTER STEPWISE ABLATION FOR PERSISTENT ATRIAL FIBRILLATIONMayumi Masumura1, Yoshihide Takahashi1, Shu Yamashita1, Masahito Suzuki1, Kenzo Hirao2, Mitsuaki Isobe2 1National Disaster Medical Center, Tokyo, Japan; 2Tokyo Medical and Dental University, Tokyo, Japan
CATHETER ABLATION P 1-073

188
Introduction: Catheter ablation is less successful for persistent atrial fibrillation (PersAF) than for paroxysmal atrial fibrillation. Guidelines suggest adjuvant substrate modification in addition to pulmonary-vein isolation (PVI) in PersAF. Yet, the optimal ablation strategy remains unclear. Mapping and ablation of electrical rotors or focal sources that sustain atrial fibrillation has been suggested to improve procedural success rates of PersAF ablation
Methods: Mapping of focal sources and rotors was performed using the novel FIRM-Software (RhythmView, Topera, Menlo Park, CA, USA). For this purpose a basket catheter was placed within the right atrium (RA) then left atrium (LA). First, identified rotors were targeted for radiofrequency ablation (RFA). Repeat mapping was performed until all sources and rotors were eliminated before PVI was performed.
Results: Nineteen patients (7 woman, 66±8 years) presenting for interventional treatment of symptomatic PersAF were included in the study. Furthermore, all included patients presented in continuous AF and no patient had a prior ablation.3.0±1.0 rotors were identified per patient. 2/13 right-sided rotors were located in the His region and 1/32 left-sided rotors was located within the left pulmonary vein. The re-maining 42/45 were eliminated by RFA. Subsequent PVI was successfully performed in all patients. Interestingly, PersAF terminated in no patient after FIRM-guided ablation, while cycle length (CL) prolongation of ≥10% after rotor ablation was observed in 5/19 patients (26.3%). Procedure duration was 270±68 minutes and fluoroscopy time was 22.1±7 minutes.
Conclusions: FIRM-mapping in patients with PersAF can identify focal sources and rotors which can be eliminated by RFA. The impact of FIRM-guided ablation on long-term results of catheter ablation in patients presenting in PersAF remains to be elucidated.
CATHETER ABLATION OF PERSISTENT ATRIAL FIBRILLATION ENHANCED BY FIRM GUIDED ABLATION-PROCEDURAL EXPERIENCEShibu Mathew, Tilmann Maurer, Johannes Riedl, Christine Lemes, Christian Heeger, Bruno Reissmann, Francesco Santoro, Andreas Metzner, Christan Sohns, Feifan Ouyang, Karl-Heinz Kuck
Asklepios St. Georg, Hamburg, Germany
CATHETER ABLATION P 1-074

189
Introduction: Although extensive pulmonary vein isolation (EPVI) can be performed using a variety of irrigation catheters, 8 mm-tip cathe-ter (Ablaze) is often used as it is easy to use. The aim of this study was to evaluate whether non-contact force irrigation catheter (FlexAbili-ty) was useful or not for Ablaze users.
Methods: We studied 40 patients consecutively who underwent catheter ablation using EnSite Navix for paroxysmal AF and persistent AF (of less than one year) were studied. All patients underwent EPVI and additional focal ablation of non-PV foci initiating AF if present. Ablaze was used with the first 20 patients (A-group: PAF 75%), and FlexAbility was used with the last 20 patients (F-group: PAF 65%). We retro-spectively analyzed the time required for PVI (Isolation times). We also analyzed whether there were existence of dormant conductions or not.
Results: There were no differences in clinical characteristics between A-group and F-group except for EF ( 63±7 vs. 56±8, P<0.05). Isola-tion times (excluding additional applications) were significantly shorter in F-group than that of A-group (1,327±400 seconds vs. 1,861±594 seconds, P<0.05). However, the appearances of dormant conduction during isoproterenol and adenosine triphosphate administration were more frequent in F-group than that of A-group in the both PV (Left-PV: 55% vs. 10%, P<0.05, Right-PV: 45% vs. 5%, P<0.05).
Conclusions: This study showed FlexAbility may be simple to use and can be expected to achieve better success rate similar to Ablaze. This is possible if there are adequate additional applications in PVI procedures by Ablaze users.
IS FLEXABILITY SIMPLE TO USE FOR 8MM-TIP ABLATION CATHETER USERS IN PULMONARY VEIN ISOLATION?Mutsuki Miyagawa, Yuji Watari, Mina Hatsuno, Shuji Otsuki, Taiji Furukawa, Ken Kozuma
Teikyo University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 1-075
190
Introduction: Surgical ablation can be done in patients with chronic atrial fibrillation (AF) concomitant with mitral valve surgery. This study was design to identify the relationship between pre-operative and post operative left atrial volume indices (LAVi) and short term success of restoration sinus rhythm after surgical AF ablation concomitant with mitral valve surgery.
Methods: Data were collected retrospectively from our hospital medical record. These included electrocardiograms, laboratory, echocar-diography before and after surgical ablation in all patients. Each patient was evaluated at the outpatient hospital clinic. The AF recurrence was evaluated from the ECG recording within 1 month after surgery. Left atrial volume was calculated using modified Simpson’s method. Volume was corrected by surface area.
Results: From March 2012 through January 2015, there were 46 patients who underwent surgical AF ablation concomitant with mitral valve surgery. The mean age was 42.7±9.6 year-old (males were 19 (41.3%) and females were 27 (58.7)). Early mortality was found in 5 pa-tients (8.7%). Sinus rhythm was restored and maintained within first month in 30 patients (65.2%) of the 46 patients. The pre-operative LAVi was smaller in patients who was restored in sinus rhythm (SR) compared with those who was unsuccessfully restored in SR, but sta-tistically insignificant (156.83±84.3 vs. 189.4±92 mL/m2, P=0.256). However, post-operative LAVi was smaller and statistically significant in those patients who was successfully restored in SR compared with those who was unsuccessfully restored in SR (95.2±55,4 vs. 126±43.9 mL/m2, P=0.029). Multivariate analysis using logistic regression analysis showed post-operative LAVi (OR was 1.02 (CI 95% 1.001-1.04, P= 0.043) and beta blocker usage early post hospitalisation [OR was 0.02 (CI 95% 0.001-0.364, P=0,008)] were independent predictor of main-taining SR after surgical AF ablation concomitant with mitral valve surgery.
Conclusions: Short term success rate of the surgical AF ablation in patients with chronic AF and concomitant mitral valve surgery was 65.2%. Post operative LAVi and post operative beta blocker therapy was independent predictor of maintaining SR after surgical AF abla-tion concomitant with mitral valve surgery.
THE ROLE OF POST-OPERATIVE LEFT ATRIAL VOLUME INDEX IN MAINTAINING SINUS RHYTHM AFTER SURGICAL ABLATION IN PATIENTS WITH CHRONIC ATRIAL FIBRILATION AND CONCOMITAN MITRAL SURGERYLarasati Munawar1, Amiliana Soesanto1, Dicky Hanafy1, Muhammad Munawar2 1University of Indonesia, Jakarta, Indonesia; 2Binawaluya Cardiac Center, Jakarta, Indonesia
CATHETER ABLATION P 1-076
191
Introduction: Both radiofrequency (RF) catheter and cryoballoon ablation can achieve a pulmonary vein isolation. We aimed to elucidate the characteristics of the atrial fibrillation (AF) burden after each procedure utilizing a telemonitoring electrocardiogram (ECG).
Methods: A consecutive series of 167 paroxysmal AF patients (age: 59±11 years, male: 141, CHADS: 0.6±0.9) who underwent a PVI since 2014 was evaluated. Out of them, 114 patients underwent an RF catheter PVI (RF group) and 53 received a cryoballoon PVI (Cryo group). No substrate modification was performed besides a cavotricuspid isthmus ablation. The patients recorded their telemonitoring ECG twice daily and upon symptoms and were followed-up for 10.5±6.2 months. The AF burden was defined by the proportion of patients with AF lasting more than 30 seconds on the telemonitoring ECG.
Results: The patient background, such as the CHADS2 score, age, serum BNP level, and appendage flow velocity measured using transe-sophageal echocardiography did not differ between the groups. The mean LA size was significantly larger (RF vs. Cryo: 3.7±0.5 vs. 3.9±0.6 cm, P=0.025) in the Cryo group. The AF burden of the Cryo group was 45.5% the first month after the procedure, 24.4% the second month, and 25.6% the third month, respectively, which were higher compared to the RF group of 27.1% (P=0.032), 11.8% (P=0.069), and 8.9% (P=0.015), respectively. The Kaplan Meier curve of the AF-free survival rate during the first 4.3±2.0 months was significantly better in the RF group (70.8% vs. 53.3%, P=0.032), which became insignificant when setting a 3-month blanking period (90.6% vs. 84.4%, P=0.099). The LA-size adjusted logistic regression analysis revealed that cryoablation was not an independent factor for the AF burden (P=0.086). The prevalence of AF at the last clinic visit did not differ between the groups (RF vs. Cryo: 1.8% vs. 7.5%, P=0.061).
Conclusions: The AF burden during the blanking period might be higher after cryoablation compared to RF ablation.
A COMPARISON OF THE ATRIAL FIBRILLATION BURDEN BETWEEN RADIOFREQUENCY ABLATION AND CRYOABLATIONKazuaki Nakajima
Keio University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 1-077

192
Introduction: A recent randomized controlled trial showed no reduction in the recurrence rate of atrial fibrillation (AF) by applying linear ablation or ablation of complex fractionated electrograms (CFE) in addition to pulmonary vein (PV) isolation among patients with per-sistent AF. However, these techniques may be complementary and in clinical practice, some patients requires linear ablation after CFE ablation and vice versa. Then the purpose of this study is to elucidate how many patients need to receive both CFE and linear ablation af-ter PV isolation.
Methods: We retrospectively analyzed patients with persistent AF who underwent catheter ablation in our hospital. Patients with AF dura-tion over 5 years were excluded. Applied ablation strategies and the order of them were reviewed.
Results: A total of 43 patients (29 males, 66.7±9.7 years of age) were included in this study. Median AF duration was 5 months (IQR: 2.5 to 13 months, max 46 months. All patients underwent successful PV isolation and all but 1 patients also had successful isolation of the pos-terior wall of left atrium (box isolation). Fifteen patients finished the procedure after the box isolation alone, however, 27 patients under-went further ablation for refractory AF. Among 19 patients who underwent CFE ablation, 13 of them (68.4%) needed to undergo linear ab-lation of the mitral isthmus (MI) between left PV and mitral annulus (4 for perimitral atrial tachycardia and 9 for AF supression). On the other hand, 4 out of 8 patients (50%) who underwent MI ablation after box isolation needed to apply CFE ablation for AF termination. Even-tually, 14 out of 17 patients (82.3%) who needed both linear and CFE ablation resulted in AF termination without cardioversion. All 14 pa-tients (32.5%) with recurrence of atrial tachyarrhythmia underwent the second procedure and 1 patient had three procedures, then 19 pa-tients (44.2%) underwent both CFE and MI ablation. After all, 38 patients (88.3%) were free from any atrial tachyarrhythmia without an-ti-arrhythmic drug after a median of 12-months follow-up (IQR: 0.6 to 1.4 months).
Conclusions: In patients with persistent AF, a significant part of patients needs to undergo both CFE and mitral isthmus ablation after box isolation.
BOTH LINEAR AND COMPLEX FRACTIONATED ELECTROGRAMS ABLATION IS NECESSARY IN SIGNIFICANT PART OF PATIENTS WITH PERSISTENT ATRIAL FIBRILLATIONTaku Nishida, Akihiro Takitsume, Tomoya Ueda, Tunenari Soeda, Satoshi Okayama, Makoto Watanabe, Hiroyuki Kawata, Rika Kawakami, Hiroyuki Okura, Yoshihiko Saito
Nara Medical University, Nara, Japan
CATHETER ABLATION P 1-078

193
Introduction: Atrial fibrillation (AF) is the most common arrhythmia in the clinical settings and its incidence increases with age. Contact force (CF) guided catheter ablation for AF in the younger patients has been widely accepted as a treatment option for drug refractory symptomatic AF. However, there is little data about efficacy and safety of CF guided AF ablation in the elderly patients.
Methods: The total of 376 patients (mean age 61.2 years, 259 men, 272 paroxysmal AF [PAF]) undergoing first-ever contact force guided catheter ablation for AF from October 2012 to June 2015 was studied. Patients ≥75 years were categorized into Group 1 (n=33, age 78±2, 16 men, 30 PAF, left atrial diameter [LAD] 41±5 mm) and the others were in Group 2 (n=343, age 60±11, 243 men, 242 PAF, LAD 39±7 mm). All patients took oral anticoagulants (32.5% warfarin, 67.5% direct oral anticoagulants) for at least 4 weeks before AF ablation. Pre-procedural transthoracic and transesophageal echocardiography were performed in all patients to assess cardiac function and to confirm the absence of left atrial thrombi. The primary endpoints were incidence of periprocedural complications, long-term adverse events and freedom from AF beyond the blanking period.
Results: The mean follow-up period was 14.1±6.4 months. CHA2DS2-VASc score was significantly higher in Group 1 than in Group 2 (4.0±1.3 vs. 1.8±1.3, P<0.001). AF recurrence free rate after the index procedure was 81.8% (27/33: PAF 80.0% [24/30] vs. persistent AF 100% [3/3]) and 82.2% (282/343: PAF 86.0% [208/242] vs. persistent AF 73.3% [74/101]), that after latest procedure was 81.8% (27/33) and 84.0% (288/343), in Groups 1 and 2, respectively (P=NS between groups by log-rank test). During the follow-up period, 7 (1.9%) periprocedural complications (0 in Group 1 and 7 in Group 2, P=NS) and 12 (3.3%) adverse events (1 in Group 1 and 11 in Group 2, P=NS) were occurred.
Conclusions: The efficacy and safety of CF-guided AF ablation in the elderly patients are similar to those in the younger patients.
EFFICACY AND SAFETY OF CONTACT FORCE GUIDED CATHETER ABLATION FOR ATRIAL FIBRILLATION IN THE ELDERLY PATIENTSKimitaka Nishizaki1, Masaomi Kimura1, Shingo Sasaki1, Daisuke Horiuchi1, Kenichi Sasaki1, Taihei Itoh1, Yuji Ishida1, Takahiko Kinjo1, Yoshihiro Shoji1, Yuichi Tshushima1, Ken Okumura2 1University of Hirosaki Department of Cardiology, Hirosaki, Japan; 2Kumamoto Saiseikai Hospital, Kumamoto, Japan
CATHETER ABLATION P 1-079
194
Introduction: Usefulness of cryoballon ablation has been reported in previous papers. However the comparison between cryoballoon and radiofrequency ablation is limited. We evaluate the difference of procedure details and recurrent rate.
Methods: Subjects were 280 paroxysmal atrial fibrillation (AF) patients. RF group and Cryo group were defined as each consecutive 140 patients which were performed radiofrequency and cryoballoon pulmonary vein isolation (PVI) just before and after introduction of cryoab-lation. Non-pulmonary vein foci were investigated using high-dose isoproterenol and treated in induced patients. Blanking period was de-fined as within three month after procedure.
Results: There was no significant difference in basic characteristics in the groups. Operation time was significantly longer in RF group (P<0.001). 46 patients had recurrent AF within the blanking period of follow-up. In this period, Cryo group was significantly higher recur-rent rate than RF group (Cryo 21.4% vs. RF 11.4% P=0.035). But after blanking period, half of the recurrent patients in Cryo group were free from AF. Recurrent free rate at six month was no different in each group (Cryo 87.9% vs. RF 89.3% P=0.851).
Conclusions: Early recurrence in blanking period was significantly higher in Cryo group. But recurrent free rate after the period showed no significant difference at six month follow-up. Cryoballoon ablation might achieve equivalent long term outcome with short operation time compared with radiofrequency ablation.
CRYOBALLOON ABLATION ACHIEVES EQUAL SUCCESS RATE COMPARED WITH RADIOFREQUENCY ABLATION REGARDLESS OF FREQUENT RECURRENCE IN BLANKING PERIODJunichi Nitta, Keita Watanabe, Akira Sato
Saitama Red Cross Hospital, Saitama, Japan
CATHETER ABLATION P 1-080

195
Introduction: Today, both Cryoballoon Ablation (CBA) and Radiofrequency Ablation (RFA) are widely used for Pulmonary Vein Isolation (PVI) to treat paroxysmal Atrial Fibrillation (pAF). Numerous studies have compared the two modalities on procedure times, safety, efficacies, and complications. However, few have carefully investigated the fluoroscopy use between the two. This study aims to compare CBA and RFA specifically on the fluoroscopy use during PVI.
Methods: A single-center cohort study evaluated continuous patients who underwent PVI for pAF using CBA or RFA. Patients with prior PVIs were excluded. Detailed fluoroscopy use, including time, dose, and imaging mode (CINE or exposure), were recorded for every major step of the ablation procedures. The fluoroscopy settings (resolution, frame rate, etc.) for each case are exactly the same. Procedure times, acute success rates, and complications were also recorded.
Results: A total of 43 patients (CBA=22, RFA=21) were included. Procedure times were similar with CBA and RFA (Figure 1). Fluoroscopy times were slightly longer (but significant) with CBA. Most importantly, the fluoroscopy doses were substantially higher in CBA compared with RFA (218% higher for total procedure, 330% higher for procedure in left atrium). The higher fluoroscopy dose in CBA was due to the need to confirm occlusion for every PV under CINE as required by the standard CBA protocol.
Conclusions: In our study, the fluoroscopy doses were significantly higher in CBA compared with RFA due to PV occlusion requirement. Physicians should be reminded that the commonly reported fluoroscopy times do not fairly represent the actual radiation doses during CBA vs. RFA.
COMPARISON OF FLUOROSCOPY USE BETWEEN CRYOBALLOON AND RADIOFREQUENCY CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATIONGuodong Niu1, Ni Suo1, Hongtao Chu2, Yali Di3, Jinxuan Lin1, Tianjie Feng1, Gang Chen1, Ligang Ding1, Zhimin Liu1, Lihui Zheng1, Xiaohan Fan1, Yan Yao1, Shu Zhang1 1Fuwai Hospital, Beijng, China; 2Zaozhuang Municipal Hospital, Zaozhuang,Shandong, China; 3Division of Cardiology,Tangshan Woker’s Hospital, Tangshan, Hebei, China
CATHETER ABLATION P 1-081

196
Introduction: Complete conduction block of cavotricuspid isthmus (CTI) is the gold standard of typical Atrial Flutter (AFL) ablation. Various ways of confirming CTI block have been proposed, including prolongation of the trans-isthmus conduction (TIC) time, double potentials along the ablation line, right atrium activation pattern, etc. An empirical approach adopted by some physicians is to use bidirectional TIC time > 130 ms as a method for ascertaining CTI block. The aim of this study was to evaluate the accuracy of using this method alone to predict complete CTI block during AFL ablation.
Methods: Data from 11 patients who underwent radiofrequency ablation of AFL at our center were retrospectively analyzed. TIC times were measured by pacing from either the coronary sinus ostium (CSO) or low lateral right atrial (LRA) and sensing from the other end. Bi-directional TIC was defined as the shorter time of the two TIC times. Complete CTI block was determined by high density mapping (HDM) of the right atrial activation. The sensitivity, specificity, positive and negative predictive values were calculated for the criterion of using bidi-rectional TIC time > 130ms to predict complete CTI block.
Results: After the initial CTI ablation, conduction gaps in the ablation line were found in 4 of the 5 patients with TIC time ≥130 ms and 5 of the 6 patients with TIC time <130 ms. The criterion of using bidirectional TIC time > 130 ms predicted complete CTI block with 50% sensitivity and 55.6% specificity. The positive and negative predictive values were 20% and 83.3%, respectively. Of the 9 cases with conduc-tion gaps post ablation, 7 were found on the inferior vena cava (IVC) end of the CTI and 1 were found on the tricuspid valve end.
Conclusions: Our results suggest that bidirectional TIC time > 130 ms alone cannot predict complete CTI block reliably in typical AFL ablation. IVC end of the CTI is the most common site for conduction gaps.
TRANS-ISTHMUS CONDUCTION TIME ALONE IS INSUFFICIENT FOR PREDICTING COMPLETE CONDUCTION BLOCK OF CAVOTRICUSPID ISTHMUS IN TYPICAL ATRIAL FLUTTER ABLATIONGuodong Niu1, Jinxuan Lin1, Ni Suo1, Tianjie Feng1, Yali Di2, Hongtao Chu3, Ligang Ding1, Gang Chen1, Zhimin Liu1, Lihui Zheng1, Xiaohan Fan1, Yan Yao1, Shu Zhang1 1Division of Clinical Electrophysiology, Fuwai Hospital and Cardiovascular Institute, CAMS and PUMC, Beijing, China; 2Division of Cardiology, Tangshan Worker’s Hospital, Tangshan, Hebei, China; 3Zaozhuang Municipal Hospital, Zaozhuang, Shandong, China
CATHETER ABLATION P 1-082

197
Introduction: Treatment of long-standing persistent Atrial Fibrillation (LsPsAF) remains challenging, with the optimal ablative approach unclear. Non-concomitant hybrid AF ablation is a novel, but increasingly popular technique for the treatment of LsPsAF patients. We de-scribe our findings during the EP study stage of the procedure.
Methods: LsPsAF patients with unfavourable characteristics for catheter ablation alone (continuous AF duration >1 year, enlarged left atrium (LA), previous failed catheter ablation) are chosen for the procedure. The first stage is a right, video-assisted thoracoscopic (VATS) approach. The Cobra Fusion RF system (Atricure Inc, West Chester, OH) is used to deliver epicardial RF ablation forming a “box lesion” to isolate the LA Posterior Wall (LAPW). All patients then return for a staged catheter procedure approximately 60 days later, with, if required, additional lesions to complete LAPW isolation.
Results: Twenty-seven patients have been through both stages of the procedure (all LsPsAF, median age 67 years, average AF duration 37 months, median BMI 30, 23 males, 4 females). Fourteen patients (52%) had bidirectional block confirmed on epicardial pacing on com-pletion of the first stage. On second stage, the LAPW was isolated at baseline in 6 patients (22%). In the remaining 21 patients, 60 gaps were identified, which required further endocardial lesions to isolate the PVs and LAPW. Frequent location of gaps were at the roof line (15 gaps), anterior to the RSPV (12 gaps), anterior to the LSPV (9 gaps) and in the ridge anterior to RPVs (8 gaps).
Conclusions: In our series the most frequent areas of reconnection were along the superior line of the “box” lesion set. This could be ex-plained by the sharp angulation of the superior pulmonary veins, curvature of the device or, as has been previously hypothesized, in-creased pericardial fat thickness in this area. It is clear from the high reconnection rate (57% of those with initial bidirectional epicardial block) and the number of isolated LAPW at baseline (22%), that a 2 stage approach is necessary to ensure durable lesions.
DESCRIPTION OF EP FINDINGS AT SECOND STAGE OF NON-CONCOMITANT HYBRID AF ABLATION WITH THE COBRA FUSION DEVICEPanagopoulos Dimitrios, Furniss Guy, Dalrymple-Hay Malcolm, Haywood Guy
Plymouth University Hospital, Plymouth, United Kingdom
CATHETER ABLATION P 1-083

198
Introduction: This study evaluated the status of common variants of single nucleotide polymorphisms (SNPs) in young patients (<40 years old) with lone atrial fibrillation (AF) and effects on the results after catheter ablation.
Methods: A total of 43 consecutive patients (mean age 36.3±3.5 years, 41 males) with drug-refractory paroxysmal (55.8%) or persistent (44.2%) AF who underwent catheter ablation were included. Sixteen SNPs including rs13376333, rs10465885, rs10033464, rs2200733, rs17042171, rs6843082, rs7193343, rs2106261, rs17570669, rs853445, rs11708996, rs6800541, rs251253, rs3807989, rs11047543 and rs3825214 were genotyped using real-time polymerase chain reaction and fluorescence resonance energy transfer. Serial 48-day Holter electrocardiographic recordings were acquired to detect AF recurrences during long-term follow up.
Results: Twenty eight patients (65%) were free from AF after mean follow up duration of 32.5±14 months and overall success rate after repeated ablation was 84%. We defined risk allele for each SNP which showed higher recurrence rate. No single risk allele increased sig-nificant risk for AF recurrence during long-term follow up. However, the recurrence rate increased significantly as the sum of risk allele increases [N of risk allele: 2-3 (3/13, 18.8%) vs. 4-6 (7/14, 33.3%) vs. 7-8 (6/7, 85.7%), P=0.008] (Figure 1).
Conclusions: The sum of risk allele was associated with long-term success after catheter ablation in Korean patients with early onset lone AF (<40 years old).
THE EFFECTS OF COMMON VARIANTS OF SINGLE NUCLEOTIDE POLYMORPHISMS IN YOUNG PATIENTS WITH LONE ATRIAL FIBRILLATION AFTER CATHETER ABLATIONYae Min Park1, Seung Young Roh2, Dae In Lee2, Jaemin Shim2, Jong-Il Choi2, Sang Weon Park2, Young-Hoon Kim2 1Gachon University Gil Medical Center, Incheon, Republic of Korea; 2Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 1-084

199
Introduction: Epicardial (EPI) catheter approach is considered as an accessory to endocardial ablation for persistent atrial fibrillation (PeAF). We evaluated the effect of EPI ablation as first option to the patients who had multiple failed endocardial ablation for PeAF.
Methods: Sixteen patients (57±7 years old, 15 male) who had undergone failed conventional endocardial (ENDO) ablation for PeAF more than two times were prospectively enrolled. These patients were randomized to epicardial ablation first (EPI group, n=8) or conventional ENDO ablation with EPI mapping (ENDO group, n=8). Procedural endpoint was non-inducibility of sustained AF/atrial tachycardia (AT). Procedural characteristics and freedom from AF/AT recurrence was compared between both groups.
Results: Recurred clinical arrhythmias were fourteen AT and two AF. Total 29 AT and 3 AF was terminated by ablation. Procedural end-point was achieved in all patients. AF/AT were terminated at septum (n=9), left atrial anterior wall (n=5), peri-mitral isthmus (n=4), lateral ridge (n=4), coronary sinus (n=3), Bachmann’s bundle area (n=2), and left atrial roof, crista terminalis, sinus venosus (each n=1) by abla-tion. Potential in LAA was delayed in 10 patients and isolated in 5 patients at the end of procedure. Complete transmural (TM) lesion was achieved at all termination sites in EPI group but failed to achieve at 2 termination sites in ENDO group. EPI mapping showed ENDO-EPI dissociation and sequence of tachycardia in left atrial wall. EPI ablation can achieve block to find gap in EPI side. However septal AT was substantial portion and EPI ablation was not helpful to patient with septal AT.
Conclusions: EPI mapping and ablation was effective to find gap and achieve TM lesion except septal AT. To compare long-term clinical outcome between both groups was required.
EPICARDIAL CATHETER ABLATION IN REPEATED CATHETER ABLATION FOR PERSISTENT ATRIAL FIBRILLATION: A PRELIMINARY RESULT OF PROSPECTIVE RANDOMIZED CONTROLLED TRIALSeung-Young Roh, Yong-Soo Baek, Hee-Soon Park, Kwang no Lee, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 1-085

200
Introduction: Combination of ganglionated plexi (GP) ablation and pulmonary vein antral isolation (PVAI) is one of the effective procedure for atrial fibrillation (AF). However, detection of GP point by high-frequency-stimulation (HFS) has several limitations.
Methods: Eleven patients undergoing AF ablation were investigated. Inferior GP points located outside of antral were detected by HFS (30 mA, 20 Hz, 5 seconds). PVAI with HFS guided-GP ablation on the antral was performed. HFS was delivered to inferior GP points again.
Results: The total of 92 inferior GP points located outside of antral was detected by HFS initially. After PVAI with HFS guided-GP ablation on the antral, vagal response to HFS at the inferior GP points outside of antral was significantly reduced than base line in each patient (8.4±2.9 points vs. 3.8±3.1 points, P<0.0001). In 3 patients, this phenomenon was observed in more than 75% of inferior GP points.
Conclusions: The part of inferior right GP, playing a role of final common input to AV node, is modified by PVAI with GP ablation on the an-tral. After that, the sensitivity of HFS at inferior GP located outside of antral becomes much lower than base line. To avoid the underesti-mation of GP points, the order of ablation is important in combination of GP ablation and pulmonary vein antral isolation.
IMPORTANCE OF THE ORDER OF ABLATION IN COMBINATION OF GANGLIONATED PLEXI ABLATION AND PULMONARY VEIN ANTRAL ISOLATIONYuichiro Sakamoto, Daisuke Yoshimoto, Sachiko Bando, Kazuto Kujira, Takahiko Suzuki
Cardiovascular Medicine, Toyohashi Heart Center, Toyohashi, Japan
CATHETER ABLATION P 1-086
201
Introduction: Left atrial appendage (LAA) has been reported to play an important role in initiation and maintenance of atrial fibrillation (AF). Electrical isolation of LAA (EIA) can occur inadvertently or intentionally during catheter ablation (CA) of AF. However, there are limited data on clinical outcomes of patients with EIA.
Methods: A total of 34 consecutive patients (mean age 59±9 years, 91% male, mean CHA2DS2-VASc score =1.2±1.3) in whom EIA oc-curred during CA of AF were enrolled. Ablation strategies included pulmonary vein isolation, biatrial ablation of complex fractionated elec-trograms (CFE), and linear lesions using stepwise approach. Transesophageal echocardiography (TEE) was performed during follow-up.
Results: The initial diagnosis was paroxysmal, persistent, or longstanding persistent AF in 3 (8.8%), 7 (20.6%), and 24 (70.6%) patients, re-spectively. The EIA occurred after a mean of 2.3±0.8 prior procedures (range, 1 to 5) and was performed intentionally in 18 (52.9%) pa-tients due to atrial tachycardia (AT) originating from the LAA. In the remaining patients, EIA occurred inadvertently during generation of both anterior and perimitral isthmus line, or extensive CFE ablation. Mean LAA flow velocity measured by TEE significantly decreased (from 42.0±19.7 cm/s to 33.5±18.8 cm/s, P=0.034) and LAA thrombus was detected in 2 (5.9%) patients after EIA. During a mean fol-low-up of 15±12 months, stroke occurred in 4 patients (11.7%). Two ischemic and 1 hemorrhagic stroke occurred in 3 patients who were taking warfarin, 1 ischemic stroke in a patient on aspirin. LAA occlusion was performed in 3 patients (8.8%) who experienced ischemic stroke. Freedom from recurrence of AF/AT was observed in 27 patients (79.4%) while 14 (41%) patients on antiarrhythmic drug.
Conclusions: Even though patients with EIA showed favorable rhythm outcome, there is a substantial increase in stroke and LAA throm-bus formation.
CLINICAL OUTCOMES OF ELECTRICAL ISOLATION OF LEFT ATRIAL APPENDAGE DURING CATHETER ABLATION OF ATRIAL FIBRILLATIONJaemin Shim, Hee-Soon Park, Kwang-No Lee, Yong-Soo Baek, Seung-Young Roh, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 1-087

202
Introduction: Typical right atrial cavo tricuspid isthmus- dependent flutters have been well described. But few data are available about left atrial (LA) flutters. This study describes the electrophysiological characteristics, results of ablation and recurrence in a series of 21 pa-tients presenting with spontaneous LA flutter.The goal of this study was to find out the recurrence rate of Left Atrial flutter post ablation and its correlation to probable etiological variables.
Methods: We performed conventional and 3D mapping of the LA for 21 patients between August 2013 and March 2016 (13 males, 8 fe-males with mean age of 61.1 years). They had been suffering from persistent atrial flutter despite the use of antiarrhythmic drugs. The patients were followed-up over a period of 12 months. Reappearance of flutter after this period defined recurrence.The mapping was based on identifying the narrow isthmus using activation and entrainment mapping techniques.
Results: Eight of the 21 patients (38%) had structural heart disease mainly in the form of Rheumatic valvular heart disease of which 4 had undergone mitral valve replacement. 2 (9.5%) patients had coronary artery disease and had undergone PTCA and CABG respectively. Oth-er co-morbidities included Hypothyroidism (28.5%), Hypertension (71.4%), Diabetes Mellitus (38%) and Obstructive sleep apnoea (14.2%).The mean LVEF was 47.9% and mean LA size was 4.4. Out of 21 patients, four (19.04%) had recurrence of Left atrial flutter 3 months or more after the ablation procedure. Recurrence was seen among patients with Hypertension, Hypothyroidism. 2 patients were those who had mitral valve replacement for a Rheumatic valve disease.
Conclusions: Left atrial flutter ablation is effective in varied settings and is associated with good long term results and marked improve-ment in symptomatic status.
MAPPING AND ABLATION OF LEFT ATRIAL FLUTTERS AND ITS RECURRENCEBalbir Singh, Bhavani Shanker, Brajesh Mishra
Medanta, The Medicity Hospital, Gurgaon, India
CATHETER ABLATION P 1-088

203
Introduction: Percutaneous transcatheter radiofrequency ablation of atrial fibrillation is a technically challenging procedure requiring complex catheter manipulation, long procedural times and significant radiation exposure to both patient and physician. Remote controlled magnetic navigation (RMN) allows unrestricted multiplanar navigation of the ablation catheter to aid accurate electroanatomic mapping, precise intracardiac catheter movements and facilitates radiofrequency ablation of difficult to reach anatomic regions. The atraumatic catheter tip design combined with a 3 dimensional electroanatomic mapping plateform also significantly reduces fluoroscopy use. Select-ed case reports have shown its superiority to conventional manual (MAN) ablation techniques. We compared acute success rates, safety profile and fluoroscopy times between patients undergoing MAN versus RMN ablation of atrial fibrillation.
Methods: We reviewed consecutive patients undergoing pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. They consisted of 2 cohorts: a RMN group and a MAN ablation group. All patients underwent pulmonary vein antral isolation with further abla-tions performed as necessary. Procedural success was defined as complete electrical isolation of all 4 pulmonary veins. Procedure time was taken as onset of first puncture to complete sheath removal.
Results: A total of 443 patients were included in this analysis-the RMN group consisted of 214 patients and the MAN group of 229 pa-tients. Both groups had similar mean age, CHA2DS2-VASc scores, and had comparable proportion of first vs. repeat ablations and atrial flutter ablations. The RMN cohort had a greater proportion of patients undergoing additional atrial flutter ablation compared to the MAN group (RMN 50.5% vs. MAN 35.4%. P<0.01). Acute procedural success was comparable between the RMN group and the MAN group (RMN 98.6% vs. MAN 95.6% P=0.07). Overall complications were lower in the RMN group compared to the MAN group (RMN 1.9% vs. MAN 4.6% P=<0.01) but catheter related complications were similar with 2.3% in the RMN group vs. 4.8% in the MAN group (P=0.164). Fluoroscopic use was significantly lower in the RMN cohort with mean±SD times of 53.5±30.1 minutes compared to 68.1±27.6 in the MAN cohort (P≤0.001). The total procedural times however were longer in the RMN group with mean 276.9±75.0 minutes vs. 208.3±61.6 in the MAN group (P≤0.001).
Conclusions: RMN ablation is associated with significantly reduced radiation exposure to the patient and even more so for the operator. This however comes at a cost of longer total procedural times. Acute success rates and safety profile are comparable.
REDUCED FLUOROSCOPY USE WITH REMOTE MAGNETIC CATHETER NAVIGATION COMPARED TO CONVENTIONAL ABLATION IN ATRIAL FIBRILLATION ABLATIONHooi Khee Teo
National Heart Centre, Singapore
CATHETER ABLATION P 1-089

204
Introduction: Radiofrequency ablation for atrial fibrillation (AF) is superior to antiarrhythmic therapy in the maintenance of sinus rhythm but entails complex catheter manipulation, long procedural times, considerable radiation exposure and risk of complications. This study aims to (1) evaluate acute success and complication rates of AF ablation, (2) assess the efficacy of ablation at 1 year follow up for a subset of patients, (3) compare remote controlled magnetic navigation (RMN) assisted ablation versus manual conventional (MAN) ablation of atrial fibrillation.
Methods: We performed an analysis of patients at National Heart Centre Singapore who underwent initial radio-frequency ablation of atrial fibrillation spanning July 2009 to May 2015. Electro anatomic mapping systems were utilised. Remote navigation and intra-cardiac echocardiogram were used depending on physician preferences. Standard catheters were used with double transeptal punctures to allow for left atrial access with circular mapping catheters and ablation catheters. Power delivery was limited to 40 watts and temperature at 40 degrees Celsius. Intra-procedural anticoagulation was achieved with intravenous unfractionated heparin with target APTT of 300 to 400. Atrial fibrillation ablation success was defined as successful pulmonary vein isolation. Patients were followed up for 1 year as per normal clinic schedules. Surveillance of atrial fibrillation recurrence was done in office with 12 lead electrocardiograms and Holter studies within a year post ablation. Additional Holters or transtelephonic monitors were performed if necessary, depending on patient’s symptoms and physician preferences.
Results: 391 patients underwent initial atrial fibrillation ablation at our centre between 2009 and 2015 with acute procedural success achieved in 98.0% and a complication rate of 3.6% including 4 patients with hemopericaridum and 2 with thromboembolic complications. 205 patients were followed up for 1 year and 72.7% were arrhythmia free. Success at 1 year correlated with left atrial anteroposterior di-ameter on transthoracic echocardiogram. A comparison between patients undergoing RMN vs. MAN ablation showed similar efficacy and complication rates. There was significant reduction in fluoroscopy in RMN (45.3±22.7 minutes) compared to MAN (64.6±23.7 minutes) cohorts (P=<0.01) but this came at a cost of longer procedural times with RMN (258.4±68.0 minutes) compared to MAN (196.6±54.6 min-utes) ablations (P=<0.01).
Conclusions: We report a 72.7% freedom from arrhythmia recurrence in our patients undergoing RFA for AF at 1 year, noting a significant correlation with echographic LA diameter as a predictor of arrhythmia recurrence. In comparison to MAN ablation of AF, RMN ablation reduces radiation exposure to both patient and physician at the expense of longer procedural times, with comparable success and com-plication rates.
CATHETER ABLATION OF ATRIAL FIBRILLATION: A SINGLE CENTRE EXPERIENCE AND COMPARISON BETWEEN REMOTE MAGNETIC NAVIGATION VERSUS CONVENTIONAL ABLATIONJoseph Jia Hong Toh, Paul Chun Yih Lim, Daniel Thuan Tee Chong, Boon Yew Tan, Kah Leng Ho, Wee Siong Teo, Chi Keong Ching
National Heart Centre Singapore, Singapore
CATHETER ABLATION P 1-090

205
Introduction: The infusion of adenosine triphosphate (ATP) after radiofrequency (RF) pulmonary vein isolation (PVI), which may result in in acute transient PV-atrium reconnection, can unmask dormant conduction. The purpose of this study is to compare the incidence and characteristics of dormant conduction following cryoballoon (CB) and RF ablation for atrial fibrillation (AF).
Methods: Of 414 consecutive patients undergoing initial catheter ablation for paroxysmal AF, 246 propensity score-matched patients (123 CB-PVI and 123 RF-PVI) were included.
Results: Dormant conduction was less frequently observed in patients who underwent CB-PVI than it was in those who underwent RF-PVI (4.5% vs. 12.8% of all PVs, P<0.0001, Figure). The site of dormant conduction was mainly located around the bottom of both inferior PVs after CB-PVI. A multivariable analysis revealed that a longer time to the elimination of the PV potential (OR=1.018, 95% CI 1.001-1.036, P=0.04) and the necessity of touch-up ablation (OR=3.242, 95% CI 2.761-7.111, P<0.0001) were independently associated the presence of dormant conduction after CB-PVI. After the elimination of dormant conduction by additional ablation, AF-free rate was similar between with and without dormant conduction both after CB-PVI and RF-PVI (P=0.28 and P=0.73, respectively).
Conclusions: The results of the propensity score matched-analysis showed that dormant PV conduction was less frequent after CB abla-tion than after RF ablation and was not associated with the ablation outcomes.
ADENOSINE TESTING DURING CRYOBALLOON ABLATION AND RADIOFREQUENCY ABLATION FOR ATRIAL FIBRILLATION: A PROPENSITY SCORE MATCHED ANALYSISMichifumi Tokuda, Seiichiro Matsuo, Ryota Isogai, Kenichi Tokutake, Kenichi Yokoyama, Mika Katoh, Ryohsuke Narui, Shinichi Tanigawa, Seigo Yamashita, Keiichi Inada, Michihiro Yoshimura, Teiichi Yamane
The Jikei University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 1-091

206
Introduction: Pulmonary vein isolation (PVI) using 2nd-generation cryoballoon (CB) for paroxysmal atrial fibrillation (PAF) has emerged as an alternative treatment to PVI with radiofrequency energy. However, suppression effect of AF with CB remains undetermined.
Methods: This study comprised of 66 patients who admitted to our hospital to treat PAF (52 male, 64±9 y/o). All the patients underwent PVI with CB and then were followed-up for at least 6 months including a 3-month blanking period. In addition, electrical isolation of supe-rior vena cava (N=6, Group-SVC) and defragmentation in the right atrium (N=3, Group-DRA) were needed to suppress PAF because of higher activation of local electrograms, which could interfere with PAF termination even after PVI with CB in cases who exhibited PAF during the ablation session. Radiofrequency energy was used for additional ablation.
Results: During mean follow-up of 376±102 days, overall recurrence rate of PAF using CB was 12.1%. Out of them, 2 patients in Group-SVC (33%) and one patient in Group-DRA (33%) developed PAF recurrence. Compared to those who needed additional ablation (Group-SVC/DRA), Group-CB had higher freedom of PAF recurrence (P<0.05).
Conclusions: This study may suggest that PVI with CB in PAF patients provides similar or even better outcome compared to that with ra-diofrequency energy. This technology may limit PAF suppression in patients who may have extra-PV foci triggering PAF and substrates initiating PAF. In some of the patients who will plan to undergo PVI with CB, additional radiofrequency ablation may be needed to suppress AF recurrence, and further study should be considered for selecting and predicting such patients to obtain better outcome in PAF.
ONE-YEAR OUTCOMES OF ABLATION WITH CRYOBALLOON FOR PAROXYSMAL ATRIAL FIBRILLATION: NEED OF ADDITIONAL ABLATION FOR EXTRA FOCUS AND SUBSTRATEAkira Ueno, Norishige Morita, Takayuki Iida, Yoshinori Kobayashi
Division of Cardiology, Tokai University Hachioji Hospital, Tokyo, Japan
CATHETER ABLATION P 1-092
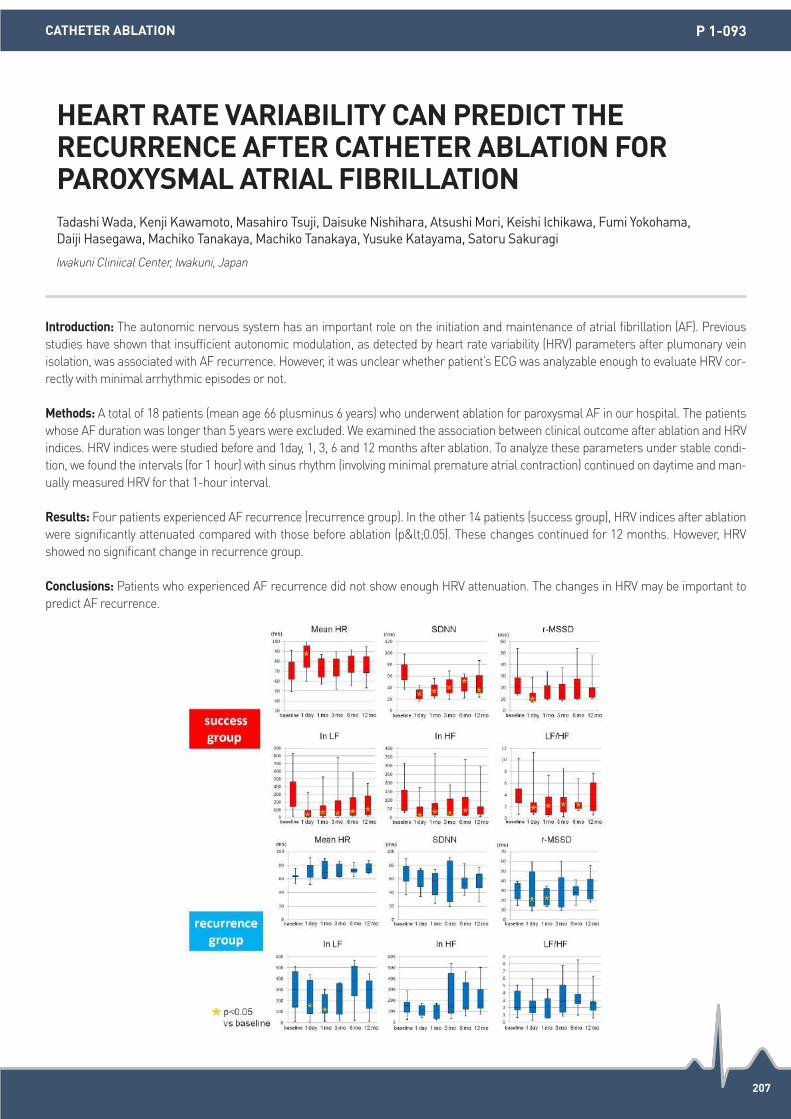
207
Introduction: The autonomic nervous system has an important role on the initiation and maintenance of atrial fibrillation (AF). Previous studies have shown that insufficient autonomic modulation, as detected by heart rate variability (HRV) parameters after plumonary vein isolation, was associated with AF recurrence. However, it was unclear whether patient’s ECG was analyzable enough to evaluate HRV cor-rectly with minimal arrhythmic episodes or not.
Methods: A total of 18 patients (mean age 66 plusminus 6 years) who underwent ablation for paroxysmal AF in our hospital. The patients whose AF duration was longer than 5 years were excluded. We examined the association between clinical outcome after ablation and HRV indices. HRV indices were studied before and 1day, 1, 3, 6 and 12 months after ablation. To analyze these parameters under stable condi-tion, we found the intervals (for 1 hour) with sinus rhythm (involving minimal premature atrial contraction) continued on daytime and man-ually measured HRV for that 1-hour interval.
Results: Four patients experienced AF recurrence (recurrence group). In the other 14 patients (success group), HRV indices after ablation were significantly attenuated compared with those before ablation (p<0.05). These changes continued for 12 months. However, HRV showed no significant change in recurrence group.
Conclusions: Patients who experienced AF recurrence did not show enough HRV attenuation. The changes in HRV may be important to predict AF recurrence.
HEART RATE VARIABILITY CAN PREDICT THE RECURRENCE AFTER CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATIONTadashi Wada, Kenji Kawamoto, Masahiro Tsuji, Daisuke Nishihara, Atsushi Mori, Keishi Ichikawa, Fumi Yokohama, Daiji Hasegawa, Machiko Tanakaya, Machiko Tanakaya, Yusuke Katayama, Satoru Sakuragi
Iwakuni Cliniical Center, Iwakuni, Japan
CATHETER ABLATION P 1-093

208
Introduction: Low voltage zone (LVZ) in the left atrium (LA) plays an important role as atrial fibrillation (AF) substrates and macroreen-trant atrial tachycardias (AT). Recently, the efficacy of LVZ ablation in addition to pulmonary vein isolation for patients with LVZ has been reported. However, it is not well known whether LVZ works as an origin of focal firings in patients with AF.
Methods: We examined the characteristics of focal firings originated from LVZs in the LA among 514 patients (paroxysmal AF=370, non-paroxysmal AF=144) who underwent AF ablation and voltage mapping during sinus rhythm using NavX. LVZ was defined as an area with bipolar voltage of <0.5 mV.
Results: LVZs were identified in 118 patients, among which focal firings were originated from the LVZs in 9 patients (8%), including AF triggers in 3 (Figure), focal AT in 4, and frequent PACs in 2. The distribution of the focal firing was in the LA anterior wall in 5 patients, pos-terior wall in 2, base of the LA appendage in 1, and LA septum in 1. In 5 patients, the focal firings were identified in the second session. Regional LVZ ablation including the origins eliminated the focal firings in all patients. Seven patients had no atrial tachyarrhythmia recur-rences during 12±12 months follow-up.
Conclusions: LVZ in the LA could be a source of focal firing, which also suggests the significance of LVZ ablation in patients with LVZs in the LA.
SIGNIFICANCE OF LOW VOLTAGE ZONES IN LEFT ATRIUM AS A SOURCE OF FOCAL FIRINGSTakanori Yamaguchi1, Takeshi Tsuchiya2, Akira Fukui2, Kenichi Eshima1, Naohiko Takahashi3 1Saga-Ken Medical Centre Koseikan, Saga, Japan; 2EP Expert Doctors-Team Tsuchiya, Kumamoto, Japan; 3Department of Cardiology and Clinical Examination, Faculty of Medicine, Oita University, Yufu, Japan
CATHETER ABLATION P 1-094

209
Introduction: Mini electrodes located at the distal tip of the ablation electrode can provide more near-field signals excluding far-field sig-nals. We sought to investigate the utility of mini electrodes on the 8 mm-tip to identify critical lesion on the cavotricuspid isthmus (CTI) for the establishment of bidirectional block.
Methods: A total of 15 patients (age: 63±8 years, male: 15) who underwent CTI ablation was studied. CTI geometry was created and the local atrial signals were mapped with mini-electrode (ME) of non-irrigated ablation catheter (Intella Tip Micro Fidelity; Boston Scientific, MA, USA) using 3D-electroanatomical mapping system (NavX; St. Jude Medical Inc., St. Paul, MN, USA), thereafter the same map with 8mm-tip electrode (8 mmE) was acquired on the off-line analysis. The length of CTI was defined as the shortest distance between the right ventricular (RV) and inferior vena cava where the atrial signals were recorded on the mapping electrode and measured on the NavX system. CTI ablation was performed with targeting the atrial signals recorded on the ME at first and the additional radiofrequency (RF) applications for the extended area were applied if necessary. CTI length measured by the different mapping electrodes and ablation re-sults were assessed.
Results: A total of 192±72 and 114±55 mapping points on the CTI using ME and 8 mmE were acquired with 272±94 seconds of mapping time. The CTI length with ME was significantly shorter than that with 8 mmE (28.2±9.0 mm vs. 33.9±8.8 mm, P<0.001). The difference of the CTI distance between ME and 8 mmE was observed on the RV side in all patients. The bidirectional block of the CTI line could be es-tablished in all cases with 182±149 seconds of mean RF time. Moreover, any additional RF applications for the lesion demonstrating atrial signals on the 8 mmE but ME were not necessary for the establishment of CTI block in all patients. No complication including steam pop and cardiac tamponade occurred during the procedure.
Conclusions: ME guide ablation for CTI block was feasible and safe, which can provide more critical CTI lesion than 8 mmE due to exclu-sion of atrial far-field signals especially on the RV side, and may reduce RF time for the establishment of bidirectional block.
UTILITY OF MINI ELECTRODES ON THE 8MM-TIP FOR CAVOTRICUSPID ISTHMUS ABLATIONSeigo Yamashita, Seiichiro Matsuo, Kenichi Tokutake, Kenichi Yokoyama, Ryohsuke Narui, Mika Kato, Shinichi Tanigawa, Michifumi Tokuda, Keiichi Inada, Kenri Shibayama, Satoru Miyanaga, Kenichi Sugimoto, Michihiro Yoshimura, Teiichi Yamane
The Jikei University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 1-095
210
Introduction: Some studies reported that the appearance of adenosine-induced dormant pulmonary vein (PV) re-conduction itself could be associated with atrial fibrillation (AF) recurrence following PV isolation even after elimination of dormant PV re-conduction. On the oth-er hand, repeated provocation and elimination of dormant PV has been shown to further improve clinical outcome of AF ablation.
Methods: 224 paroxysmal AF patients who underwent repeat elimination of dormant PV conduction during the initial segmental PV isola-tion were included in the present study. Dormant PV conduction was induced by the administration of ATP and eliminated by supplemen-tal radiofrequency application at least twice in each PV. All patients were divided into two groups according to the presence or absence of dormant conduction and clinical outcome was compared between two groups.
Results: Dormant PV conduction was induced in 114 (51%) of patients and was successfully eliminated in 90.3% (103/114) of those follow-ing PV isolation. After the procedure, 87% of patients with dormant conduction remained sinus rhythm, while 84% of those without dor-mant conduction was in sinus rhythm (P=0.40).
Conclusions: Clinical outcome was comparable between patients with and without the appearance of dormant PV conduction. Repeat evaluation and elimination of dormant conduction should be performed to improve clinical outcome in patients with paroxysmal AF.
DOSE THE APPEARANCE OF DORMANT PULMONARY VEIN CONDUCTION PREDICT RECURRENCE OF ATRIAL FIBRILLATION AFTER CATHETER ABLATION?Kenichi Yokoyama
The Jikei University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 1-096

211
Introduction: Effective catheter ablation strategy beyond pulmonary vein isolation (PVI) for persistent atrial fibrillation (AF) is desired. On the other hand, recovered left atrium-PV conduction also causes recurrent atrial tachyarrhythmia after PVI for persistent AF. The aim of this study is to clarify the effect and limitation of PVI alone strategy with multiple procedure, and additional effect of superior vena cava isolation (SVCI) for persistent AF.
Methods: Consecutive 70 patients with persistent AF underwent strict sequential catheter ablation strategy targeting PV and SVC were included in this study. Initial ablation strategy was circumferential PVI. Segmental SVCI was only applied at repeat ablation procedures when patients demonstrated no PV reconnection.
Results: After the first ablation procedure, sinus rhythm was documented in 39 of 70 (55.7%) patients during follow-up of 32 months (range 12 to 57 months). After multiple procedure, sinus rhythm was maintained in 46 (65.7%) and 52 (74.3%) patients by PVI alone and PV plus SVC isolation strategy. Persistent AF duration (HR: 1.017 [95% confidence interval: 1.009 to 1.024]; P<0.0001) independently predicted persistent AF recurrences. Patients with persistent AF duration of <2 years had a significantly higher ablation success rate than patients whose persistent AF duration was > 2 years (65.1% vs. 40.7% at the initial procedure to 80.5% vs. 41.4% and 90.0% vs. 53.3%, respectively; P=0.048, P=0.001 and P<0.001) after PV alone and PV plus SVC isolation strategy with multiple procedure.
Conclusions: The outcomes of catheter ablation targeting PV were favorable for patients with persistent AF duration of <2 years. Initial SVCI had additional effect to maintain sinus rhythm in 9% of patients with persistent AF.
STRICT SEQUENTIAL CATHETER ABLATION STRATEGY TARGETING PULMONARY VEIN AND SUPERIOR VENA CAVA FOR PERSISTENT ATRIAL FIBRILLATIONYasuhiro Yoshiga, Akihiko Shimizu, Takeshi Ueyama, Makoto Ono, Hironori Ishiguchi, Masafumi Yano
Yamaguchi University Graduate School of Medicine, Ube, Japan
CATHETER ABLATION P 1-097

212
Introduction: Recurrence of paroxysmal atrial fibrillation (PAF) after radiofrequency catheter ablation (RFCA) is related to the reconnec-tion of circumferential pulmonary vein isolation (CPVI). We hypothesized that endurance ablation with moderately increased radiofrequen-cy (RF) power would facilitate long-lasting CPVI and better clinical outcomes in patients with PAF.
Methods: We included 508 PAF patients (76.0% male, 56.2±9.5 years old) who underwent CPVI without additional left atrial (LA) ablation. We compared endurance ablation (ENDU-abl; n=254, 30 sec ablation at each point with 35W on anterior PV antrum and 25-30W on pos-terior LA) group with an age-, sex-, and follow up duration-matched conventional ablation (CONV-abl; n=254, just elimination of PV poten-tial [PVP] with 25W) group.
Results: 1) Total procedure time (P<0.001) and ablation time (P<0.001) were longer, and complication rate was higher (6.3% vs. 1.6%, P=0.006) in ENDU-abl group than in CONV-abl group. 2) HF domain (P=0.010) and LF/HF ratio (P<0.001) were significantly lower at 3rd month follow-up heart rate variability, and the degree of LA reverse remodeling was more significant at 1-year follow-up echocardiogram (ΔLAVI; -6.0±8.3 vs. -3.5±9.5 mL/m2, P=0.031) in ENDU-abl group than in CONV-abl group. 3) During 37.2±17.5 months of follow-up, the clinical recurrence of AF was significantly lower in ENDU-abl group than in CONV-abl group (log-rank, P<0.001). 4) Among 38 patients who underwent redo-ablation at 15.1±12.1 months, reconnected PVPs were found in 4/11 patients (36.4%) in ENDU-abl group and 26/27 patients (96.3%) in the CONV-abl group (P<0.001).
Conclusions: In spite of longer procedure time and higher complication risk, ENDU-abl with moderately increased RF power facilitated long-lasting CPVI, more significant autonomic neural remodeling and LA reverse remodeling, and better clinical outcome than CONV-abl in PAF patients.
ENDURANCE ABLATION WITH MODERATELY INCREASED RADIOFREQUENCY POWER FACILITATES LONG-LASTING CIRCUMFERENTIAL PULMONARY VEIN ISOLATION AND BETTER CLINICAL OUTCOMES IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATIONHee Tae Yu1, Junbeom Park2, Tae-Hoon Kim1, Jae-Sun Uhm1, Jong-Youn Kim1, Boyoung Joung1, Moon-Hyoung Lee1, Hui-Nam Pak1 1Yonsei University Health System, Seoul, Republic of Korea; 2Ewha Womans University, Seoul, Republic of Korea
CATHETER ABLATION P 1-098

213
Introduction: Limited data are available on hemodynamic factors associated with ventricular premature complex (VPC)-related symptom. This study aims to investigate the association of hemodynamic parameters assessed by transthoracic echocardiography (TTE) with VPC-related subjective symptom.
Methods: We prospectively enrolled a total of 23 patients with VPCs (>1% burden per 24 hours) during TTE examinations and no structur-al heart disease. The patients were categorized into two groups according to the VPC-related subjective symptom of dropped beats (n=12, without subjective symptom; n=11, with subjective symptom). TTE parameters including left ventricular volumes, mitral inflow velocity, mitral and tricuspid tissue Doppler imaging, and aortic time-velocity integral were measured during a VPC and sinus beat right before and after the VPC.
Results: The median stroke volume (SV) in a sinus beat before VPC (SVSinus) was similar in both groups (81.2 vs. 75.5 mL, P=0.16), while SV during a VPC (SVVPC) and a sinus beat after VPC (SVpost) were significantly smaller in symptomatic patients (45.4 vs. 33.4 mL, P=0.03; 77.0 vs. 63.1 mL, P=0.04). A sum of SVVPC and SVpost and a sum adjusted with SV in sinus rhythm ([SVVPC+SVpost]/SVSinus) was also smaller in symptomatic patients (P=0.002 and 0.01, respectively).
Conclusions: VPC-related symptom might be associated with decreased stroke volume during and/or after a VPC.
DECREASED STROKE VOLUME DURING AND AFTER A VENTRICULAR PREMATURE COMPLEX IS ASSOCIATED WITH VENTRICULAR PREMATURE COMPLEX-RELATED SYMPTOMHye Bin Gwag, Jin Kyung Hwang, Young Keun On, June Soo Kim, Seung-Jung Park, Kyoung-Min Park
Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-099

214
Introduction: The incidence, time course, and presentation of drug-induced Torsades de Pointes (TdP) with intravenous (IV) amiodarone are not well defined.
Methods: The present study is an analysis of drug-induced TdP with intravenous amiodarone from January 2015 to December 2015. Re-cords of patients, who received intravenous (IV) amiodarone, for acute control of a ventricular rate of atrial arrhythmias or prevention of recurrent ventricular tachycardia, were reviewed. The institutional protocol for infusion of IV amiodarone was as recommended.
Results: A total of 134 patients received IV amiodarone (71 for ventricular tachycardia, 52 for atrial flutter/fibrillation, and 11 for incessant atrial tachycardia). Four of the 134 (2.99%) developed torsades de pointes (Atrial flutter/fibrillation 3; Ventricular tachycardia 1)after a mean dose of 690+176.63 mg, infused over a period of 12+5.88 hours. There were 3 females and 1 male (rheumatic mitral stenosis 1; sick sinus syndrome with VVI pacemaker 1; dilated cardiomyopathy 1; hypertensive heart disease 1) with a mean age of 51.25+9.17 years. The QTc was 505+9.02 ms with pause dependent TdP degenerating to ventricular fibrillation requiring cardioversion. Treatment involved stop-ping amiodarone, IV magnesium, IV lignocaine in all, isoprenaline in 1, and pacing in 3 patients. There was no mortality, and QTc normal-ized to 433.75+6.13 ms 4-72 hours after stopping amiodarone.
Conclusions: The incidence of drug-induced TdP with IV amiodarone is about 2.9%, and occurs during first 24 hours. It is associated with QTc prolongation, is pause dependent and can occur with normal baseline QTc in patients without genetic predisposition. QTc normalizes 48-72 hours after stopping therapy. Risk factors include female sex, left ventricular dysfunction, electrolyte abnormalities, baseline pro-longed QTc, concomitant beta-blocker, and digoxin therapy. Patients who develop TdP with IV amiodarone should not be treated with amiodarone in the future.
THE UNDER-RECOGNIZED RISK OF DRUG INDUCED TORSADES DE POINTES WITH INTRAVENOUS AMIODARONE: RECOGNITION AND MANAGEMENTVivek Pillai, Mukund Aravind Prabhu, Jayasheelan Mambally Rachaiah, Vidhyakar Balasubramaniam, Sivasankara Chakali, Jayaprakash Shenthar
Sri Jayadeva Institute of Cardiovascular Sciences and Research,Bangalore, Bangalore, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-100

215
Introduction: Ventricular arrhythmias secondary to Takayasu’s arteritis have yet to be described.
Methods: N/A
Results: A 41 year old Chinese lady without any cardiovascular risk factors presented to the Emergency Department with heart failure. Physical examination revealed low oxygen saturations, basal lung crepitations and asymmetrical pulses. ECG and echocardiography showed LBBB and moderately impaired LV (EF 38%). She consented to coronary angiography. Femoral arterial access was achieved but passage of the coronary catheters to the ascending aorta was difficult due to extensive, severe stenosis within the femoral, iliac arteries and distal aorta. Eventually coronary angiography via the right radial artery was performed to reveal ostial stenoses in the left anterior and right coronary arteries, requiring percutaneous coronary intervention(PCI). 2 days later, she developed a transitory left 6th cranial nerve palsy which resolved after 2 days. Vascular imaging confirmed multiple ulcers within the aorta and plaques within the carotid arteries, es-tablishing a diagnosis of Takayasu’s arteritis. She was commenced on high-dose prednisolone therapy but within the next 5 months, she was hospitalized for mesenteric ischaemia which resolved with conservative management, followed by another heart failure hospitaliza-tion due to monomorphic ventricular tachycardia. Repeat coronary angiography showed a de novo lesion distal to the previous bio-ab-sorbable scaffold, necessitating further PCI. Prior to discharge, a dual chamber defibrillator was implanted and over the next 3 months, she continued to have more than 20 episodes of symptomatic VT, all terminated with ATP. She was counselled about VT ablation. Concur-rently, due to rapid progression of vascular disease, she was commenced on infliximab infusions which resulted in immediate cessation of VT.
Conclusions: We present an unusual case of ischaemic VT secondary to Takayasu’s arteritis which was suppressed with anti-TNF alpha therapy.
VENTRICULAR TACHYCARDIA SECONDARY TO TAKAYASU’S ARTERITIS SUPPRESSED WITH ANTI-TNF-ALPHA THERAPYNaveen Velaga1, Adrian Low2, Manjari Lahiri2, Pipin Kojodjojo2 1Ng Teng Fong General Hospital, Singapore; 2National University Hospital, Singapore
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-101

216
Introduction: The long-term clinical impact of low frequency of premature ventricular complexes (PVCs) on the risks of mortality and morbidity has not been fully studies. This study aimed to investigate the association between the low frequency of PVCs and adverse clini-cal outcomes.
Methods: We analyzed 5,778 baseline pacemaker-free and ventricular tachycardia-free individuals receiving 24-hour electrocardiography monitoring examination between January 1, 2002, and December 31, 2004. Multivariate Cox hazards regression models and propensi-ty-score matching were applied to assess associations between premature contractions and adverse clinical outcome.
Results: Average follow-up time was 10±1 years. In all, 1,403 participants expired, 1,301 participants hospitalized to cardiovascular (CV)-related ward, 3,384 hospitalized for any reason, and 631 participants developed new-onset heart failure (HF). The optimal cut-off of PVC frequency for predicting mortality was 12 beats per day, with a sensitivity of 58.4% and specificity of 59.8%. In multivariate analysis, a PVC frequency >12 beats per day was an independent predictor for all mortality (HR: 1.429, 95% CI: 1.284-1.590), CV hospitalization (HR: 1.127, 95% CI: 1.008-1.260), all-cause hospitalization (HR 1.094, 95% CI: 1.021-1.173), and new-onset HF (HR: 1.411, 95% CI: 1.203-1.655). Patients with PVC frequency >12 beats per day had increased risk of cardiac death attributable to heart failure and sudden cardiac death.
Conclusions: PVC frequency >12 beats per day was associated with a higher incidence of all mortality, CV hospitalization, all-cause hos-pitalization, and new-onset HF independent of other clinical risk factors.
IMPACT OF LOW FREQUENCY PREMATURE VENTRICULAR COMPLEXES ON LONG-TERM CLINICAL OUTCOMETing-Yung Chang, Chin-Yu Lin
Taipei Veterans General Hospital, Taipei, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-102

217
Introduction: The early repolarization (ER) pattern was regarded as a benign ECG variant but increasing studies showed it might be relat-ed to sudden cardiac arrest and idiopathic ventricular fibrillation. However, the prognostic information of ER pattern on RFCA of idiopathic VT remains unknown.
Methods: A total of 350 patients (age 41±14 years, 154 males) with idiopathic VT (227 RVOT, 66 FAS, 23 LVOT, 19 PAP, 4 AMC, 3 GCV and 8 others) undergoing catheter ablation were consecutively enrolled. Baseline ECG was obtained and ER pattern was evaluated by 2 inde-pendent observers. Patients were categorized into 2 groups regarding the presence of ER pattern.
Results: ER pattern was identified in 36 patients (10%; group 1; others without ER: group 2). There were higher incidences of HTN and DM in group 1 than group 2 (44.4% vs. 28.0%, P=0.041 and 13.9% vs. 5.1%, P=0.035, Table 1). During a mean follow-up period of 51±49 months, VA recurrences were recognized in 81 patients (23%). Patients in group 1 had higher VA recurrences than those in group 2 (Figure 1). In multi-variant analysis, the independent predictors of VA recurrence in idiopathic VT was ER pattern (P=0.011, Odds ratio 2.125, 95% CI 1.191-3.791, Table 2). In spite of the higher recurrences, there was no significant mortality difference in mortality between 2 groups.
Conclusions: Patients with ER pattern had higher incidence of VA recurrences after successful RFCA of idiopathic VT. However, the long-term prognosis was similar regardless the recurrences of VA.
THE IMPACT OF EARLY REPOLARIZATION PATTERN ON THE OUTCOME OF CATHETER ABLATION OF IDIOPATHIC VENTRICULAR TACHYCARDIAYuan Hung1, Fa-Po Chung2, Shih-Ann Chen2 1Tri-Service General Hospital, Taipei, Taiwan; 2Taipei Veteran General Hospital, Taipei, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-103
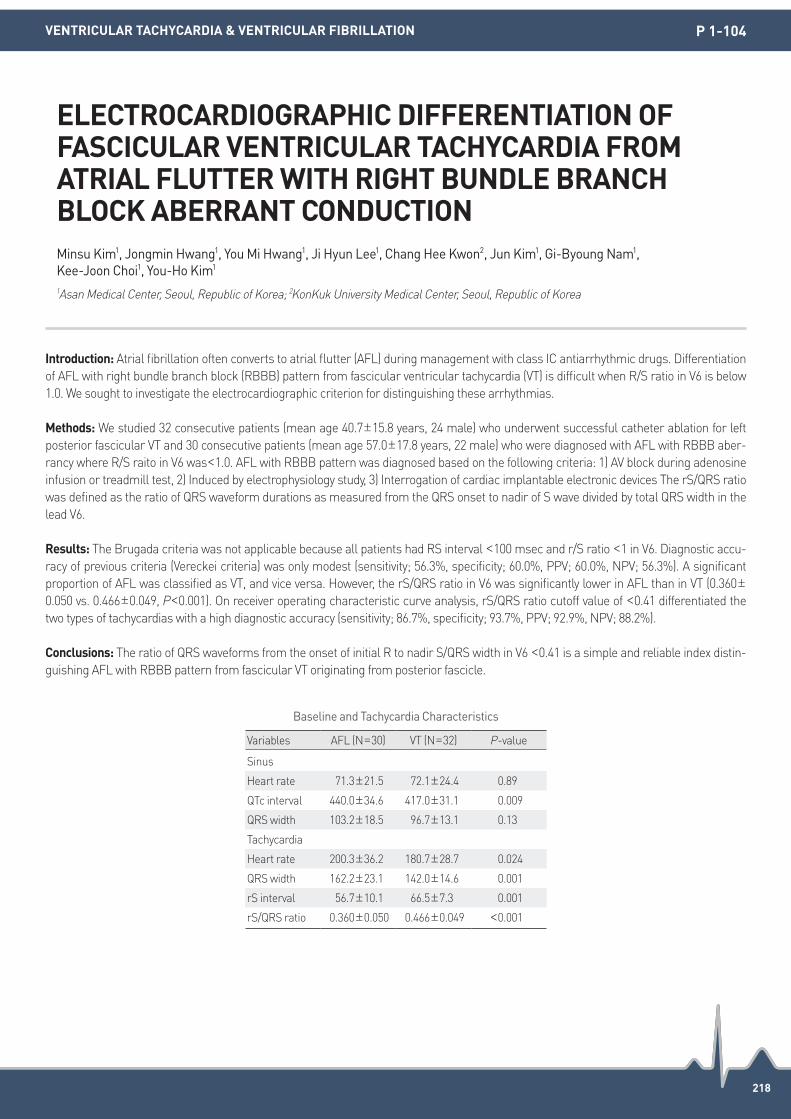
218
Introduction: Atrial fibrillation often converts to atrial flutter (AFL) during management with class IC antiarrhythmic drugs. Differentiation of AFL with right bundle branch block (RBBB) pattern from fascicular ventricular tachycardia (VT) is difficult when R/S ratio in V6 is below 1.0. We sought to investigate the electrocardiographic criterion for distinguishing these arrhythmias.
Methods: We studied 32 consecutive patients (mean age 40.7±15.8 years, 24 male) who underwent successful catheter ablation for left posterior fascicular VT and 30 consecutive patients (mean age 57.0±17.8 years, 22 male) who were diagnosed with AFL with RBBB aber-rancy where R/S raito in V6 was<1.0. AFL with RBBB pattern was diagnosed based on the following criteria: 1) AV block during adenosine infusion or treadmill test, 2) Induced by electrophysiology study, 3) Interrogation of cardiac implantable electronic devices The rS/QRS ratio was defined as the ratio of QRS waveform durations as measured from the QRS onset to nadir of S wave divided by total QRS width in the lead V6.
Results: The Brugada criteria was not applicable because all patients had RS interval <100 msec and r/S ratio <1 in V6. Diagnostic accu-racy of previous criteria (Vereckei criteria) was only modest (sensitivity; 56.3%, specificity; 60.0%, PPV; 60.0%, NPV; 56.3%). A significant proportion of AFL was classified as VT, and vice versa. However, the rS/QRS ratio in V6 was significantly lower in AFL than in VT (0.360±0.050 vs. 0.466±0.049, P<0.001). On receiver operating characteristic curve analysis, rS/QRS ratio cutoff value of <0.41 differentiated the two types of tachycardias with a high diagnostic accuracy (sensitivity; 86.7%, specificity; 93.7%, PPV; 92.9%, NPV; 88.2%).
Conclusions: The ratio of QRS waveforms from the onset of initial R to nadir S/QRS width in V6 <0.41 is a simple and reliable index distin-guishing AFL with RBBB pattern from fascicular VT originating from posterior fascicle.
ELECTROCARDIOGRAPHIC DIFFERENTIATION OF FASCICULAR VENTRICULAR TACHYCARDIA FROM ATRIAL FLUTTER WITH RIGHT BUNDLE BRANCH BLOCK ABERRANT CONDUCTIONMinsu Kim1, Jongmin Hwang1, You Mi Hwang1, Ji Hyun Lee1, Chang Hee Kwon2, Jun Kim1, Gi-Byoung Nam1, Kee-Joon Choi1, You-Ho Kim1 1Asan Medical Center, Seoul, Republic of Korea; 2KonKuk University Medical Center, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-104
Baseline and Tachycardia Characteristics
Variables AFL (N=30) VT (N=32) P-value
Sinus
Heart rate 71.3±21.5 72.1±24.4 0.89
QTc interval 440.0±34.6 417.0±31.1 0.009
QRS width 103.2±18.5 96.7±13.1 0.13
Tachycardia
Heart rate 200.3±36.2 180.7±28.7 0.024
QRS width 162.2±23.1 142.0±14.6 0.001
rS interval 56.7±10.1 66.5±7.3 0.001
rS/QRS ratio 0.360±0.050 0.466±0.049 <0.001

219
Introduction: Idiopathic ventrilcular fibrillation (IVF) is a cause of sudden cardiac death. Previous studies have demonstrated its potential arrhythmogenicity and an association between J wave and sudden cardiac death. Previous studies also have described that fragmented QRS complexes (f-QRS) also is a predictor of cardiac events and mortality in patients with structural heart disease. We evaluate the preva-lence and clinical significance of J wave and fragmented QRS complexes in patients with idiopathic ventricular fibrillation.
Methods: We retrospectively studied 81 patients who have received the implantation of Implantable cardioverter defibrillator (ICD) due to idiopathic ventricular tachyarrhythmia between October 1999 and June 2015 from a single cardiology center. We assessed the prevalence of J wave and f-QRS in resting 12-lead electrocardiogram (ECG). All patients were classified among three groups based on the electrocar-diographic morphology: group I (J wave group, n=35), group II (f-QRS group, n=20), group III (neither J wave nor f-QRS group, n=26). The control group comprised 81 subjects without heart disease who were matched for age, sex, races. We evaluated baseline characteristics, history of syncope, sudden cardiac arrest and appropriate ICD shock among three groups. We also evaluate the prevalence of J wave and f-QRS compared to control group.
Results: The median follow-up duration was 4.1 years. J wave and f-QRS were more frequent in patients with idiopathic ventricular fibril-lation than in control subjects (43.2%, 21% vs. 24.7%, 19.7%, P<0.001). The incidence of MACE were more frequent in f-QRS group among three group, but not significantly different between J wave and f-QRS group (50% vs. 45.7% vs.11.5%, P=0.028). Comparing between J wave group plus f-QRS group and Normal ECG group, J wave group plus f-QRS group were more frequent than Normal ECG group in MACE (47.3% vs. 11.5%, P=0.009).
Conclusions: In a single-center retrospective study, this study suggests that the IVF patients have more increased prevalence of J wave or f-QRS and IVF patients with J wave or f-QRS have more increased risk of recurrent cardiac events.
PREVALENCE AND CLINICAL SIGNIFICANCE OF FRAGMENTED QRS COMPLEX OR J WAVE IN PATIENTS WITH IDIOPATHIC VENTRICULAR FIBRILLATIONChoong-Sil Seong, Jin Kyung Hwang, Seung Jung Park, Kyoung-Min Park, June Soo Kim, Young Keun On
Samsung Medical Center, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-105

220
Introduction: Outflow tract premature ventricular contractions (PVCs) are a very common arrhythmia. The analysis of circadian pattern and affecting factors could provide information to evaluate occurrence and the optimal treatment. Yet the relation between PVCs overload and heart rate (HR) and the circadian distribution still remain unknown. The present study is to investigate the effect of PVCs overload, through examining the association with heart rate (HR) and the circadian pattern grouped by the sum of outflow tract PVCs.
Methods: One hundred and thirty five outflow tract PVCs patients were enrolled. The 24h Holter ECG was used to evaluate PVCs occur-rence. The outflow tract PVCs were divided into Group I (<5,000/24 hours), Group II (5,000-10,000/24 hours), Group III (10,000-20,000/24 hours), Group IV (20,000-30,000/24 hours) and Group V (>30,000/24 hours) based on the sum of the PVCs. The relationship between mean HR and the sum of PVCs in each group was analyzed. The distribution of PVCs was assessed by grouping the events into four time peri-ods: 7 AM to 12 AM, 1 PM to 6 PM, 7 PM to 0 AM, and 1 AM to 6 AM.
Results: In 135 subjects, there were 25 Group I, 24 Group II, 30 Group III, 28 Group IV, and 28 Group V. PVCs were positively associated with mean HR, especially in Group III (r=0.446, P=0.013). The occurrence of PVCs had a trend of circadian variation. Only in group 3 and group 4, the occurrence of PVCs showed an apparent circadian variation with a nadir about at midnight (P<0.05).
Conclusions: In certain overload of outflow tract PVCs (10,000-30,000/24 hours), an apparent circadian variation and positive correlations between PVCs and mean HR were found.
CIRCADIAN DISTRIBUTION AND RELATION WITH HEART RATE IN THE DIFFERENT OVERLOAD OF OUTFLOW TRACT PREMATURE VENTRICULAR CONTRACTIONSLiang Shan, Min Tang
Department of Cardiology, State Key Laboratory of Cardiovascular Disease, Cardiovascular Institute, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-106

221
Introduction: Implantable cardioverter defibrillator (ICD) is an effective treatment for secondary prevention of ventricular tachycardia/ven-tricular fibrillation (VT/VF). Left ventricular (LV) remodeling may develop before ICD implant and over time. However, it remains unclear how LV remodeling affects subsequent risk for recurrence VT/VF in secondary prevention ICD recipients.
Methods: From May of 2004 to June of 2015, 144 patients received ICD implantation for secondary prevention were enrolled in this study. All information interrogated from ICD devices during follow-up or shock events were reviewed and validated the occurrences of VT/VF.
Results: At a mean follow-up of 1,110.5±860.6 days, 53 patients (36.8%) had recurrence of VT/VF episodes and 91 patients had no recur-rence of VT/VF episode after ICD implant. Left ventricular end-diastolic volume (LVEDV) >163.5 mL had significant predictive value for VT/VF recurrence (area under the curve: 0.602, P=0.041). Moreover, the percentage of patients with LVEDV >163.5 mL was significantly high-er in patients with recurrent VT/VF than patients without recurrent VT/VF (62.3 vs. 40.0%, P=0.010). Left ventricular ejection fraction ≤30% (P=0.031) and LVEDV >163.5 mL (P=0.012) were significant predictors for VT/VF recurrence by univariate Cox regression analysis. Howev-er, only LVEDV >163.5 mL (hazard ratio: 2.018, 95% confidence interval: 1.156-3.521, P=0.013) was an independent predictor for recur-rence of VT/VF after multivariable adjustment.
Conclusions: Left ventricular remodeling is an independent predictor for VT/VF recurrence during follow-up in secondary prevention ICD recipients under optimal medical therapy, independent of LV ejection fraction.
LEFT VENTRICULAR REMODELING PREDICT VENTRICULAR ARRHYTHMIA IN THE PATIENTS WITH ICDWeichieh Lee, Mien-Cheng Chen
Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-108

222
Introduction: The present study aimed to determine whether the combination of clinical factors at admission may improve the long term sudden cardiac death (SCD) risk prediction in dilated non-ischemic cardiomyopathy (NICM) patients with LVEF≤35%.
Methods: We prospectively enrolled a set of NICM patients with echocardiogram LVEF<35% from December 2010 to April 2013.Patients with known SCD events history, valvar heart disease and hypertensive heart disease were exculed. Baseline clinical characteristics, lab test and echocardiogram results at admission were collected. All Patients were followed up for 3 years by phone and clinical visits. The primary endpoint was defined as SCD events composite of SCD, aborted cardiac arrest and documented appropriate ICD therapy for sus-tained ventricular tachycardia or ventricular fibrillation.
Results: A total of 154 NICM patients were finally included, 79.7% were male, the mean age was 36.86±11.84 years and 81.8% patients had NYHA heart function class III and IV. 20 patients were implanted with ICD during follow up. After 3 years’ follow up, SCD events oc-curred in 24 patients (14 for SCD, 3 for aborted cardiac arrest and 7 for appropriate ICD therapy). After adjusted age, sex, QRS duration, LVEF and premature ventricular beats burden by multivariate COX analysis, the increased risk of clinical events were independently asso-ciated with low body mass index(BMI, <18.25 kg/m2,Hazard ratio [HR] 7.43, 95% confidential interval [CI]: 2.70-20.46) and relative lower hemoglobin level (HGB level, <155 g/L, HR 6.32, 95% CI 1.80-22.13). Kaplan-Meier curves showed that individuals with both relative lower HGB and BMI suffered higher 3-year cumulative SCD risk than those with 1 or without them (80.0% vs. 16.1% vs. 2.9%, P<0.0001, Figure B).
Conclusions: Relative reduced hemoglobin level and lower BMI might be predictors for SCD events in dilated NICM patients with LVEF≤35%, and patients with both of them may experience increased risk for 3-year cumulative SCD events.
COMBINATION OF ADMISSION HEMOGLOBIN LEVEL AND BMI PREDICTS 3-YEAR CUMULATIVE SUDDEN CARDIAC RISK IN DILATED NON-ISCHEMIC CARDIOMYOPATHY PATIENTS WITH SEVERE HEART FAILUREXiaofei Li, Wei Sun, Yan Yao, Minjie Lu, Wei Hua, Shu Zhang, Xiaohan Fan
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-109

223
Introduction: Left posterior fascicular ventricular tachycardia (LPF-ILVT) is a common form of sustained ventricular tachycardia. This study aims to retrospectively investigate long-term clinical outcomes of patients undergoing ablation of LPF-ILVT with development left posterior fascicular block and characteristics of repeat procedures.
Methods: 195 Patients (mean age, 29.76±1.03 years,16.4%female)underwent catheter ablation for left posterior fascicular ILVT(LPF-ILVT) in Fuwai Hospital from January 2000 to June 2013 were consecutively enrolled. These patients were divided into two groups by inducible IVLT or non-induicle ILVT by programmed stimulation. Programmed stimulation with and without isoproterenol was performed to induce ventricular tachycardia. While Electroanatomical mapping was performed to map and ablate for recurrent ILVT. The early retrograde fas-cicular potential was mapped at the posterior pukinje fiber network along the posterior mid-septal left ventricle during sinus rhythm. The endpoint of ablation LPF-ILVT is noninducible of ventricular tachycardia and development a new-onset left posterior fascicular (LPF) block. Follow-up with clinic visits, ECG, or Holter monitoring was performed at least 6 months after procedure.
Results: 142 of 195 (72.82%) patients was inducible of Clinical LPF-ILVT. 190 patients underwent successfully ablation developed left pos-terior fascicular block (LPF block) and 5 patients had no LPF block but noninducible after procedure. With a median follow-up of 85.61 (18-181) months, 172/195 (88.21%) patients undergoing first procedure had long freedom of ILVT. There are no statistics difference be-tween two groups during the outcome of catheter ablation LPF-ILVT (P=0.142). 23 patients were recurrent ILVT, and 21 undergone repeat procedure. A ECG morphology of ILVT with incomplete LPF block and without LPF block recurred in 16 patients, repeat procedure with the endpoint of LPF block and no induction of tachycardia. 7 patients developed new-onset upper septal ILVT that was successfully ablated. With a median follow-up of 83.35 (12-136) months, These patients undergone repeat procedure were long freedom of ventricular tachy-cardia. No patients had atrioventricular block, but1 patient had incomplete left bundle branch block and 1 patient were LAF block in the repeat procedure.
Conclusions: Ablation of ILVT with development LPF block is associated with a single procedural success rate without the use of antiar-rhythmic drugs of 88.21%. There are no difference between inducible and non- inducible patients with use of this procedure of long out-come freedom ILVT. Recurrent ILVT trended to be no left posterior fascicle block and incomplete LPF block and a new type of upper septal ILVT recurrence.
LONG-TERM OUTCOME OF CATHETER ABLATION FOR LEFT POSTERIOR FASCICULAR VENTRICULAR TACHYCARDIA WITH DEVELOPMENT OF LEFT POSTERIOR FASCICULAR BLOCK AND CHARACTERISTICS OF REPEAT PROCEDURESBin Luo, Gongbu Zhou, Xiaogang Guo, Xu Liu, Jiandu Yang, Qi Sun, Jian Ma
Beijing Fuwai Hospital, Beijing, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-110

224
Introduction: Cardiac resynchronization therapy (CRT) has been established for heart failure patients with intraventricular conduction de-lay. Although there are various reports about ventricular arrhythmia (VA) after CRT therapy, it is not clear which patients have the risk of VA after CRT implantation. Then, we investigated the VA events in patients with CRT in our hospital, retrospectively.
Methods: We evaluated the VA events and predictive factor for VA events in 115 patients with CRT implantation in our hospital, from 2002 to 2015. VA events were defined as appropriate implantable cardioverter-defibrillator (ICD) therapy, documented sustained VA and sudden death. Patients who had the history of sustained VA were in secondary prevention group (S group), and patients who did not have the his-tory of sustained VA were in primary prevention group (P group).
Results: In all 115 patients, mean age was 63.8±12.0 years old, 68 out of 115 (59.1%) patients were male, mean ejection fraction was 28.1±8.6%, mean New York Heart Association class was 2.9±0.4. Eighty out of 115 (69.5%) patients were responder after CRT implanta-tion. Fourteen out of 115 patients were CRT without ICD (CRT-P), 101 out of 115 patients were CRT with ICD (CRT-D). Thirty patients were in S group, and 85 patients were in P group. During mean follow-up periods of 44.2±28.5 months, there were 17 (56.7%) VA events in S group, and 26 (30.6%) VA events in P group (P=0.016). In Kaplan-Meier analysis, VA events in P group were insignificantly lower than that in S group (P=0.16). In all patients, male and history of VA were predictive factor for VA in univariate and multi variate analysis. In only P group, male was predictive factor of VA in univariate analysis. However, there was no predictive factor for AE in multivariate analysis.
Conclusions: Male and history of VA were predictive factor for VA in all patients. However, there was not obvious predictive factor of AE in P group. Then, more extended investigations will be needed to decide which patients should be implanted CRT-D.
VENTRICULAR ARRHYTHMIC EVENT AFTER CRT IMPLANTATIONHiroyasu Sugiyama, Nobuhiro Nishii, Yoshimasa Morimoto, Satoshi Kawata, Motomi Tachibana, Atsuyuki Watanabe, Hiroshi Morita, Hiroshi Ito
Okayama University, Okayama, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-112

225
Introduction: N/A
Methods: N/A
Results: A 54-year-old male with idiopathic premature ventricular contraction (PVC) was admitted for the treatment. His past medical history was bronchial asthma and sarcoidosis. A 12-lead ECG revealed frequent repetitive PVC, which showed right bundle branch block pattern and superior axis morphology. A total of 61,373/136688 monofocal PVCs (44.9%) were detected all through day by ambulatory Holter ECG monitoring. An echocardiography showed normal LV contraction without abnormal thickening of LV wall. Endocardial pace mapping was performed under the guidance of CARTOSOUND. A perfect pace map was obtained at the left ventricular septum. The po-tential inscribed at the site proceeded the onset of QRS complex by 14 msec during PVC. The image of CARTOSOUND corresponded to the basal portion of left ventricular papillary muscle. Radiofrequency energy application (35W with temperature limit set at 45C°for 60 seconds) completely abolished the PVC.
Conclusions: N/A
RADIOFREQUENCY CATHETER ABLATION UTILIZING CARTOSOUND WAS EFFECTIVE FOR A CASE OF IDIOPATHIC PREMATURE VENTRICULAR CONTRACTION ARISING FROM THE LEFT VENTRICULAR PAPILLARY MUSCLEHideshi Aoyagi, Yasuteru Yamauchi, Tokuhiko Ito, Takatoshi Shigeta, Yusuke Tsuchiya, Mitsumi Yamashita, Tomofumi Nakamura, Mitsutoshi Asano, Hidetoshi Suzuki, Tsukasa Shimura, Manabu Kurabayashi, Kaoru Okishige
Yokohama City Minato Red Cross Hospital, Yokohama, Kanagawa, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-113

226
Introduction: Arrhythmogenic right ventricular cardiomyopathy (ARVC) originates from fatty change and fibrosis of right ventricular myo-cardium. Delayed enhancement of contrast cardiac MRI can detect the arrythmogenic substrate. However, in many patients, MRI is con-traindicated due to non-MRI conditional implantable cardioverter defibrillator (ICD). Komatsu et al. reported that fat tissue detected with MDCT was associated with low voltage zone and local abnormal ventricular activity (LAVA) in the epicardium. We experienced a case that low voltage zone of unipolar voltage map matched fat tissue found by MDCT in ARVC patient with non-MRI conditional ICD. It is reason-able to expect low voltage zone and existence of LAVA with MDCT before radiofrequency catheter ablation (RFCA) for VT in patients of ARVC.
Methods: N/A
Results: A 78 year-old-female with ARVC and sustained VT had received non-MRI conditional ICD implantation. Anti-tachycardia pacing and defibrillation due to sustained VT were observed repeatedly thereafter. Remaining capacity of battery was decreased and she was ad-mitted for ICD generator exchange and RFCA for sustained VT. Contrast MDCT was obtained before RFCA. Multiple VTs were induced, and activation mapping with entrainment was performed for mappable VT, and substrate based ablation for elimination of delayed potentials were performed for the non-mappable VTs, which led to non-inducibility of all the VTs. Bipolar voltage map showed localized low voltage area in the RV free wall near the tricuspid annulus. However, Unipolar voltage map showed much larger low voltage area extending to the RVOT and apex. The unipolar low voltage zone showed great correlation with fat tissue detected with MDCT, suggesting much larger sub-strate in the RV epicardium, and potential use in assessment of arrythmogenic substrate in patients with ARVC.
Conclusions: The fat tissue detected by MDCT matched the unipolar low voltage zone in a patient undergoing RFCA for ARVC, suggesting the usefulness of this technique in substrate-based ablation of ARVC.
EFFICACY OF MYOCARDIAL FAT DETECTION WITH MDCT FOR SUBSTRATE-BASED ABLATION OF ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY PATIENT WITH NON-MRI CONDITIONAL ICDHirofumi Arai, Akira Mizukami, Shunsuke Kuroda, Maki Ono, Makoto Suzuki, Akihiko Matsumura
Kameda Medical Center, Kamogawa, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-114

227
Introduction: In arrhythmogenic right ventricular cardiomyopathy (ARVC), cardiac magnetic resonance (CMR) has an excellent correlation with histopathology and predicted inducible VT on programmed electrical stimulation, suggesting a possible role in diagnosis and progno-sis of these patients. Increasing age-related right ventricular (RV) dilatation is possibly a marker of disease progression as a basis for right heart failure. The aim of the study was to evaluate the relationship between the presence of RV abnormalities detected by cardiac mag-netic resonance (CMR) and the aging, a strong predictor of sudden death in ARVC.
Methods: A consecutive series of five patients from a single institution were recruited with a clinical diagnosis of ARVC based on the diag-nostic criteria. All patients underwent systematic clinical evaluation, including history and examination, electrocardiography, 24-hour Holter monitor, chest radiography, echocardiography and CMR examination and were divided into two groups according to the age: group I, age of ≥ 60 years old; group II, age of<60 yo. The relationship between the characteristic parameters of CMR image and age were ana-lyzed in two groups.
Results: This study showed that the mean age of presentation in our population was relatively late (52.4±21.03 yo), and patients with age of ≥60 yo have more enlargement of RV end diastolic volume (63.3±25.2 mL vs. 214.55±68.8 mL; P<0.05), lower RV ejection fraction (38.6±4.2% vs. 23.7±4.6%; P<0.05), and worst RV wall motion abnormality (akynesia vs. diskinesia).
Conclusions: We conclude that increasing age-related right ventricular abnormality is possibly a marker of disease progression as a ba-sis for right heart failure.
AGE RELATED RIGHT VENTRICULAR ABNORMALITY IN ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHYHaryadi Haryadi1, Sunu Budhi Raharjo2, Dicky Armein Hanafy2, Ardian Rizal3, Yoga Yuniadi2 1National Cardiovascular Center Harapan Kita, Pekanbaru, Indonesia; 2National Cardiovascular Center Harapan Kita, Jakarta, Indonesia;
3National Cardiovascular Center Harapan Kita, Malang, Indonesia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-115
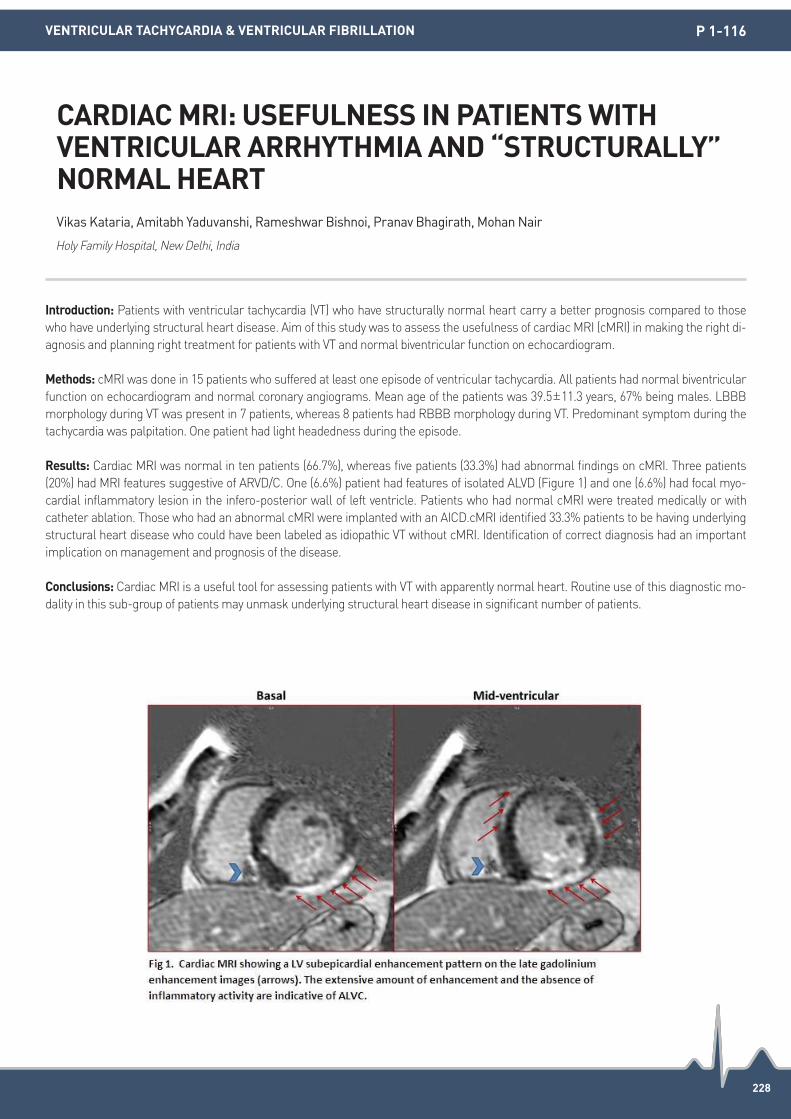
228
Introduction: Patients with ventricular tachycardia (VT) who have structurally normal heart carry a better prognosis compared to those who have underlying structural heart disease. Aim of this study was to assess the usefulness of cardiac MRI (cMRI) in making the right di-agnosis and planning right treatment for patients with VT and normal biventricular function on echocardiogram.
Methods: cMRI was done in 15 patients who suffered at least one episode of ventricular tachycardia. All patients had normal biventricular function on echocardiogram and normal coronary angiograms. Mean age of the patients was 39.5±11.3 years, 67% being males. LBBB morphology during VT was present in 7 patients, whereas 8 patients had RBBB morphology during VT. Predominant symptom during the tachycardia was palpitation. One patient had light headedness during the episode.
Results: Cardiac MRI was normal in ten patients (66.7%), whereas five patients (33.3%) had abnormal findings on cMRI. Three patients (20%) had MRI features suggestive of ARVD/C. One (6.6%) patient had features of isolated ALVD (Figure 1) and one (6.6%) had focal myo-cardial inflammatory lesion in the infero-posterior wall of left ventricle. Patients who had normal cMRI were treated medically or with catheter ablation. Those who had an abnormal cMRI were implanted with an AICD.cMRI identified 33.3% patients to be having underlying structural heart disease who could have been labeled as idiopathic VT without cMRI. Identification of correct diagnosis had an important implication on management and prognosis of the disease.
Conclusions: Cardiac MRI is a useful tool for assessing patients with VT with apparently normal heart. Routine use of this diagnostic mo-dality in this sub-group of patients may unmask underlying structural heart disease in significant number of patients.
CARDIAC MRI: USEFULNESS IN PATIENTS WITH VENTRICULAR ARRHYTHMIA AND “STRUCTURALLY” NORMAL HEARTVikas Kataria, Amitabh Yaduvanshi, Rameshwar Bishnoi, Pranav Bhagirath, Mohan Nair
Holy Family Hospital, New Delhi, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-116

229
Introduction: The optimal ablation strategy or endpoint for ventricular tachycardias (VT) in noninducible patients remains to be elucidated. We report a non-inducible case with successful catheter ablation for VT.
Methods: N/A
Results: A 49 years-old woman with non-ischemic cardiomyopathy suffered from VT storm. Left ventricular (LV) ejection fraction was 30% and delayed enhancement was detected at the base of posterior LV by contrast-enhanced MRI. During VT, mapping at both the endo- and epicardium showed a centrifugal pattern with the earliest activation at the epicardium of the postero-lateral LV. VT was not terminated by ablation at the earliest activated site. 11 days later, the repeat procedure was performed due to the recurrence of VT storm. VT was not in-duced by ventricular programmed electric stimulation at multiple sites with or without isoproterenol. Mapping during sinus rhythm demonstrated the low voltage area with late potentials (LPs) at the epicardium of the postero-inferior LV, 2 cm distant from the ablation site of the prior procedure. The duration of QRS-LPs gradually increased in the low voltage area from lateral to inferior wall of the LV. In this area, good pacemap was obtained, and stimulus-QRS time correlated with the duration of QRS-LPs. These findings indicated the LPs were critical substrate for VT and VT exit site was at the lateral LV. Ablation at the lateral LV, where shorter QRS-LPs was shown, success-fully isolated all of LPs in this area. The patient was free from VTs after the repeat ablation procedure.
Conclusions: Pacemapping was helpful for localization of the critical substrate and exit site of VT. Isolation of critical substrate was feasi-ble and effective in non-inducible patient.
ISOLATION OF LATE POTENTIALS FOR VENTRICULAR TACHYCARDIA IN A NON-INDUCIBLE PATIENTMasahito Suzuki1, Yoshihide Takahashi1, Ryo Nagasawa1, Mayumi Masumura1, Shu Yamashita1, Yasuhiro Sato1, Kenzo Hirao2, Mitsuaki Isobe3 1National Hospital Organization Disaster Medical Center, Tokyo, Japan; 2Heart Rhythm Center, Tokyo Medical and Dental University, Tokyo, Japan; 3Department of Cardiology, Tokyo Medical and Dental University, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-118

230
Introduction: Patients with hypertension are often complicated with electrocardiogram (ECG) abnormality and enlarged left atrium (LA) or/and left ventricular hypertrophy (LVH). However, few data demonstrate the association between PR interval and abnormality in heart structure. The present study aimed to investigate the association of PR interval with enlarged LA or LVH in patients with hypertension.
Methods: We retrospectively analyzed a community-based cohort of hypertensive patients enrolled from a rural area in China between 2004 and 2005 who had both available data of ECG and echocardiogram. LVH was diagnosed by the criteria of LV mass >49.2 g/m2.7 for men and 46.7 g/m2.7 for women. LV geometric patterns (normal, concentric remodeling, concentric or eccentric hypertrophy) were calcu-lated according to LV hypertrophy and relative wall thickness. Enlarged LA was defined as LA anteroposterior diameter >37 mm for men and 35 mm for women. Prolonged PR interval was defined as PR >200 ms.
Results: Of all the 2,865 patients with hypertension, 69.1% (1,979/2,865) were female, the mean age was 57.6±8.1 years old. The mean PR interval of all hypertensive patients was 155.3±41.7 ms and 1.6% had prolonged PR. The mean PR interval was longer in patients with LVH than those without LVH (158.0±50.5 ms vs. 153.7±35.5 ms, P=0.008). However, there was no significant difference between patients with and without enlarged LA (153.6±21.3 vs. 155.4±42.5, P=0.6). The PR intervals were also significant different among patients with normal, concentric remodeling, eccentric or concentric hypertrophy (153.0±35.9 ms vs. 154.7±35.1 ms vs. 156.8±49.2 ms vs. 159.0±51.6 ms, P=0.037). After adjusted for age, sex, BMI, systolic blood pressure and diastolic blood pressure, prolonged PR was independently as-sociated with LVH (OR=2.24, 95% CI 1.21-4.15) and concentric hypertrophy (OR=2.47, 95% CI 1.06-5.77).
Conclusions: Prolonged PR interval might be associated with LVH instead of enlarged left atrium in the Chinese community-based hyper-tensive patients.
PR INTERVAL IS ASSOCIATED WITH LEFT VENTRICULAR HYPERTROPHY INSTEAD OF ENLARGED LEFT ATRIUM IN PATIENTS WITH HYPERTENSIONSiyang Fan, Xiaofei Li, Jingzhou Chen, Kai Sun, Yan Yao, Rutai Hui, Xiaohan Fan
Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-119

231
Introduction: We hypothesize that the duration required for the diagnosis of syncope using an implantable loop recorder (ILR) may differ depending upon the underlying etiology. To test this hypothesis, we analyzed the relationship between the duration of ILR use and the final diagnosis.
Methods: In 61 of 86 patients (71%) with implanted ILR for evaluation of syncope of unknown etiology, diagnoses were made after ILR im-plantation for a mean follow-up period of 215 days (range, 2-1,352 days). Of these, 40 patients (66%) were diagnosed with cardiogenic syn-cope and 14 (23%) were diagnosed with non-cardiogenic syncope. These 54 patients were divided into two groups: those diagnosed within four months and those diagnosed five months or greater after ILR implantation.
Results: Twenty-nine of 54 patients (54%; mean age, 65±20 years; 21 males; mean follow-up period, 40±36 days) were diagnosed within four months after ILR implantation. Of these, 25 (86%) were diagnosed with cardiogenic syncope. The remaining 25 patients (46%; mean age, 69±16 years; 15 males; mean follow-up period, 460±315 days) were diagnosed five months or more after ILR implantation. Fifteen (60%) of these patients were diagnosed with cardiogenic syncope. Cardiogenic event detection by ILR was significantly greater within four months of ILR implantation. Non-cardiogenic syncope event detection more commonly occurred five months or more after ILR implanta-tion (P=0.035). Interestingly, in 26 of 40 patients (65%), cardiogenic events were diagnosed by ILR without any symptoms of syncope.
Conclusions: The duration of ILR implantation in syncope patients correlated with the underlying cause of syncope. Cardiogenic events were detected relatively early, with or without a syncopal event.
CHARACTERISTICS FOR DETECTED DURATION AND ETIOLOGIES IN THE CAUSE OF SYNCOPE USING IMPLANTABLE LOOP RECORDERRitsuko Kohno, Yasushi Oginosawa, Hisaharu Ohe, Masao Takahashi, Haruhiko Abe
University of Occupational and Environmental Health, Kitakyushu, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-120
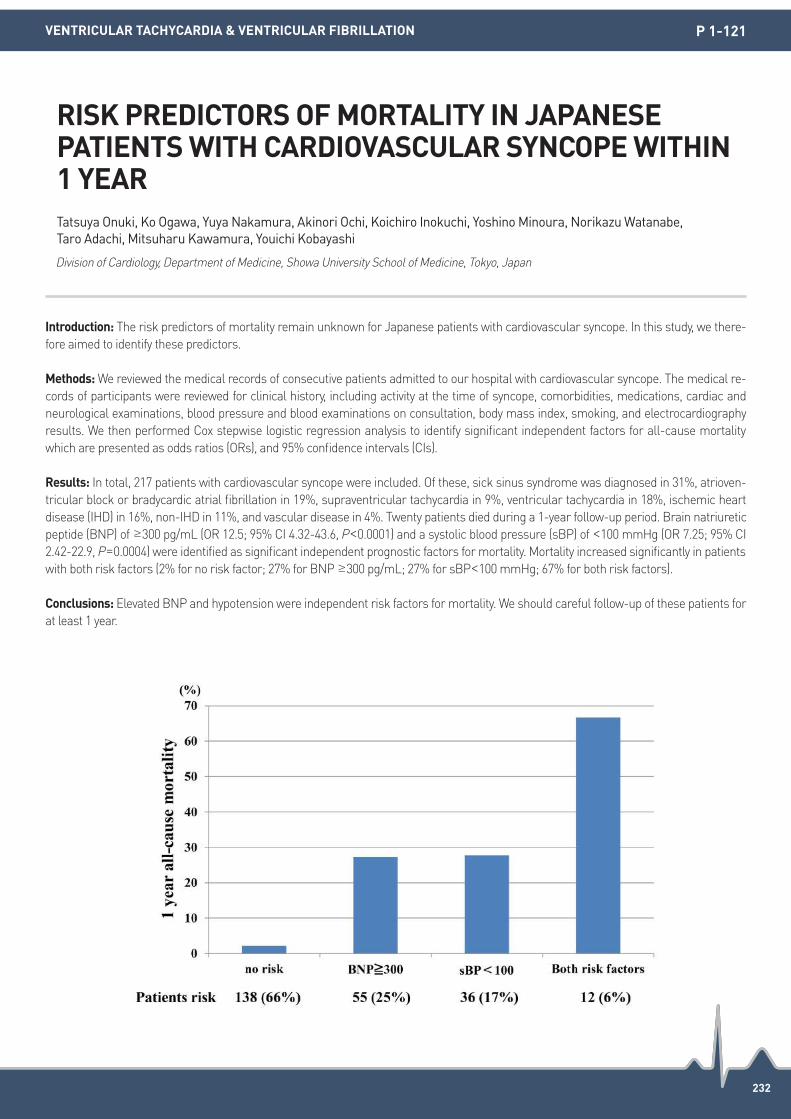
232
Introduction: The risk predictors of mortality remain unknown for Japanese patients with cardiovascular syncope. In this study, we there-fore aimed to identify these predictors.
Methods: We reviewed the medical records of consecutive patients admitted to our hospital with cardiovascular syncope. The medical re-cords of participants were reviewed for clinical history, including activity at the time of syncope, comorbidities, medications, cardiac and neurological examinations, blood pressure and blood examinations on consultation, body mass index, smoking, and electrocardiography results. We then performed Cox stepwise logistic regression analysis to identify significant independent factors for all-cause mortality which are presented as odds ratios (ORs), and 95% confidence intervals (CIs).
Results: In total, 217 patients with cardiovascular syncope were included. Of these, sick sinus syndrome was diagnosed in 31%, atrioven-tricular block or bradycardic atrial fibrillation in 19%, supraventricular tachycardia in 9%, ventricular tachycardia in 18%, ischemic heart disease (IHD) in 16%, non-IHD in 11%, and vascular disease in 4%. Twenty patients died during a 1-year follow-up period. Brain natriuretic peptide (BNP) of ≥300 pg/mL (OR 12.5; 95% CI 4.32-43.6, P<0.0001) and a systolic blood pressure (sBP) of <100 mmHg (OR 7.25; 95% CI 2.42-22.9, P=0.0004) were identified as significant independent prognostic factors for mortality. Mortality increased significantly in patients with both risk factors (2% for no risk factor; 27% for BNP ≥300 pg/mL; 27% for sBP<100 mmHg; 67% for both risk factors).
Conclusions: Elevated BNP and hypotension were independent risk factors for mortality. We should careful follow-up of these patients for at least 1 year.
RISK PREDICTORS OF MORTALITY IN JAPANESE PATIENTS WITH CARDIOVASCULAR SYNCOPE WITHIN 1 YEARTatsuya Onuki, Ko Ogawa, Yuya Nakamura, Akinori Ochi, Koichiro Inokuchi, Yoshino Minoura, Norikazu Watanabe, Taro Adachi, Mitsuharu Kawamura, Youichi Kobayashi
Division of Cardiology, Department of Medicine, Showa University School of Medicine, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-121

233
Introduction: The recurrence of vasovagal syncope (VVS) is a concerning situation that could be unpredicted, especially referred to the head up tilt-table test (HUT). We investigated a simple surrogate marker and predictor for the recurrent syncope referred to HUT.
Methods: The 150 consecutive patients with VVS (age 28±11 years, 42% male) who referred by a cardiologist or neurologist and had un-dergone an echocardiogram and a treadmill exercise test (TMT) were prospectively recruited. All patients were divided into two groups based on the result of HUT. The TMT data was analyzed and compared between VVS patients and control 150 patients without VVS who were enrolled in the same study period (age 28±5 years, 40% male).
Results: The heart rate recovery (HRR), recovery systolic blood pressure (RecSBP), diastolic BP (RecDBP), HRR/RecSBP and HRR/RecDBP were significantly different between controls and VVS. Within VVS, even if, baseline characteristics were similar between negative and positive HUT (n=96 vs. n=54). HRR (31±10 vs. 35±10), HRR/RecSBP (0.24±0.09 vs. 0.28±0.09) and HRR/RecDBP (0.49±0.18 vs. 0.58±0.19) were significantly different between negative and positive HUT results. Especially, HRR/RecSBP and HRR/RecDBP were significantly correlated with recurrent syncope with a sensitivity and specificity ([60%, 79%] cut-off 0.31; [72%, 72%] cut-off 0.63). In the age- and sex-adjusted regression, the odd ratio of HRR/RecSBP and HRR/RecDBP were 776.7 (confidence interval 2.60-12,728, P=0.010) and 29.5 (confidence interval 2.56-339.56, P=0.006).
Conclusions: HRR/RecSBP and HRR/RecDBP may be a surrogate marker and useful predictor of recurrent VVS, especially mixed pat-tern, in the reference to HUT.
HEART RATE RECOVERY AND RECOVERY OF THE BLOOD PRESSURE RATIO ON THE EXERCISE TREADMILL TEST PREDICT A RECURRENT VASOVAGAL SYNCOPE REFERRED TO THE HEAD-UP TILT TABLE TESTKi-Woon Kang, Sang Hyun Jang, Jeagook Kim, Soojoo Lee
Eulji University Hospital, Deajeon, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-122

234
Introduction: About one third of patients with structural heart disease (SHD) and history of syncope have neurally mediated syncope. Head up tilt test (HUTT) with Isoprenaline provocation is associated with significant adverse events. This study aims to assess the safety of HUTT with sublingual nitroglycerine provocation in patients with SHD and left ventricular dysfunction.
Methods: Patients with SHD and suspected neurocardiogenic syncope, and who had a negative electrophysiological study (EPS) were subjected to HUTT with sublingual NTG provocation performed using the Italian protocol.
Results: In this prospective study between January 2010 and June 2015, a total of 41 patients with SHD underwent HUTT. The mean age of the patients was 58.71±16.79 (16-85) (Median 63 IQR 51-78.5 years), with male preponderance (73.17%). There were 27 (65.85%) pa-tients with ischemic heart disease, 14 (34.15%) with dilated cardiomyopathy. The median left ventricular ejection fraction was 42% (30-49%). A positive test was seen in 25 (60.97%) patients. The most common response was the Type III response seen in 13 (52%), followed by Type I response in 6 (24%), Type 2B in 5 (20%), with the least common response being the Type 2A response seen in in 1 (4%) patient. Ar-rhythmias that occurred in 29 (70.73%) patients consisted of bradyarrhythmias in 29.27%, premature beats in 34.14% and tachyarrhyth-mias in 7.31%. Bradyarrhythmias were always a part of the positive HUTT test. The incidence of tachyarrhythmias was 7.31% and consist-ed of atrial tachycardia in 2 (4.87%) and atrial fibrillation in 1 (2.43%). There were no significant ventricular arrhythmias, and all patients tolerated the procedure well. On 16-72 months follow up there have been no deaths.
Conclusions: Neurocardiogenic syncope may be the cause of syncope in about 60% of patients with SHD, negative EPS, and no docu-mented arrhythmias. HUTT with sublingual NTG provocation is useful, safe, and should be considered in the evaluation of syncope in pa-tients with SHD.
UTILITY AND SAFETY OF HEAD UP TILT TEST WITH SUBLINGUAL NITROGLYCERINE PROVOCATION IN PATIENTS WITH STRUCTURAL HEART DISEASE AND SYNCOPEVivek Pillai, Mukund Aravind Prabhu, Vidhyakar Balasubramaniam, Sivasankara Chakali, Jayaprakash Shenthar
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 1-123
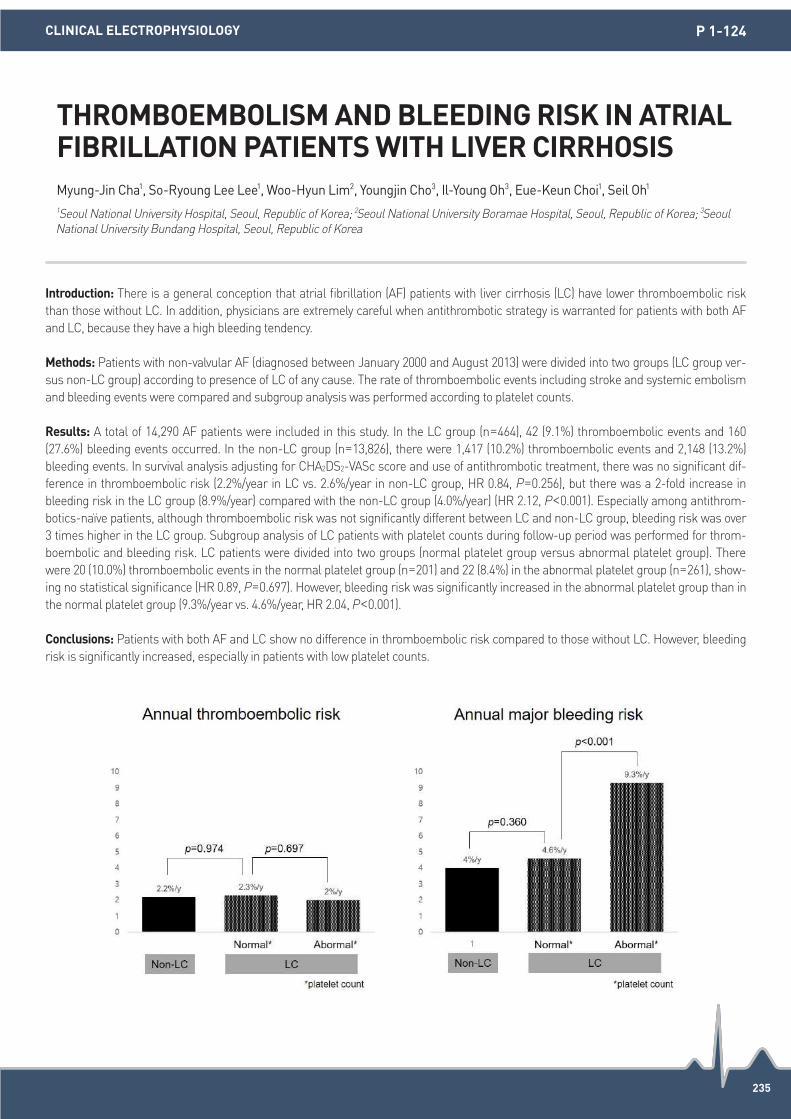
235
Introduction: There is a general conception that atrial fibrillation (AF) patients with liver cirrhosis (LC) have lower thromboembolic risk than those without LC. In addition, physicians are extremely careful when antithrombotic strategy is warranted for patients with both AF and LC, because they have a high bleeding tendency.
Methods: Patients with non-valvular AF (diagnosed between January 2000 and August 2013) were divided into two groups (LC group ver-sus non-LC group) according to presence of LC of any cause. The rate of thromboembolic events including stroke and systemic embolism and bleeding events were compared and subgroup analysis was performed according to platelet counts.
Results: A total of 14,290 AF patients were included in this study. In the LC group (n=464), 42 (9.1%) thromboembolic events and 160 (27.6%) bleeding events occurred. In the non-LC group (n=13,826), there were 1,417 (10.2%) thromboembolic events and 2,148 (13.2%) bleeding events. In survival analysis adjusting for CHA2DS2-VASc score and use of antithrombotic treatment, there was no significant dif-ference in thromboembolic risk (2.2%/year in LC vs. 2.6%/year in non-LC group, HR 0.84, P=0.256), but there was a 2-fold increase in bleeding risk in the LC group (8.9%/year) compared with the non-LC group (4.0%/year) (HR 2.12, P<0.001). Especially among antithrom-botics-naïve patients, although thromboembolic risk was not significantly different between LC and non-LC group, bleeding risk was over 3 times higher in the LC group. Subgroup analysis of LC patients with platelet counts during follow-up period was performed for throm-boembolic and bleeding risk. LC patients were divided into two groups (normal platelet group versus abnormal platelet group). There were 20 (10.0%) thromboembolic events in the normal platelet group (n=201) and 22 (8.4%) in the abnormal platelet group (n=261), show-ing no statistical significance (HR 0.89, P=0.697). However, bleeding risk was significantly increased in the abnormal platelet group than in the normal platelet group (9.3%/year vs. 4.6%/year, HR 2.04, P<0.001).
Conclusions: Patients with both AF and LC show no difference in thromboembolic risk compared to those without LC. However, bleeding risk is significantly increased, especially in patients with low platelet counts.
THROMBOEMBOLISM AND BLEEDING RISK IN ATRIAL FIBRILLATION PATIENTS WITH LIVER CIRRHOSISMyung-Jin Cha1, So-Ryoung Lee Lee1, Woo-Hyun Lim2, Youngjin Cho3, Il-Young Oh3, Eue-Keun Choi1, Seil Oh1 1Seoul National University Hospital, Seoul, Republic of Korea; 2Seoul National University Boramae Hospital, Seoul, Republic of Korea; 3Seoul National University Bundang Hospital, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-124

236
Introduction: Catheter ablation for ventricular arrhythmia originating from papillary muscle (VA-PM) is challenging due to deep located origin and multiple exits. We reported that structure heart disease might be found in refractory cases and was associated high recurrence rate.
Methods: There were total 25 patients found to have VA-PM since December, 2010. MRI or PET scan was arranged in 11 patients based on the physicians’ clinical decision. The presence of abnormal substrate was evaluated by exam the abnormal enhancement at papillary muscle and nearby myocardium.
Results: There were 3 of 14 patients in the success group received MRI study. No abnormal contrast enhancement was noted. On the contrary, 7 of 11 patients in recurrence group received MRI and PET study. Total five patients (20%) were found to have structure heart dis-ease. There was no difference in LVEF between patients with and without structure heart disease. However, a non-significant trend toward thicker ventricular wall and higher burden of VPC were noted (with vs. without structure heart disease; IVSd 12±3 mm vs. 10±2 mm; LVPWd 13±5 mm vs. 10±2 mm; Holter VPC burden 18.9±11.8% vs. 11.5±12.0%) There were 1 hypertrophic cardiomyopathy, 1 non-com-paction cardiomyopathy (figure), 1 ischemic cardiomyopathy, 1 subendocardial infarction close to junction of ventricle wall and papillary muscle, and a suspected myocarditis with enhancement under PET scan. All these cases had recurrence of VA after catheter ablation and 3 patients (60%) received redo procedure for more than 2 times.
Conclusions: In patients with refractory VA-PM, complete survey should be performed to unhide focal diseased substrate.
THE ASSOCIATION OF STRUCTURE ABNORMALITIES IN REFRACTORY VENTRICULAR ARRHYTHMIA ORIGINATING FROM PAPILLARY MUSCLEYaoTing Chang, Yenn-Jiang Lin, Shih-Lin Chang, Li-Wei Lo, Yu-Feng Hu, Fa-Po Chung, Jo-nan Liao, Tze-Fan Chao, Ta-Chuan Tuan, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 1-125

237
Introduction: Poor patient understanding of atrial fibrillation (AF) may contribute to suboptimal management and the underuse of antico-agulation. However, there are no validated instruments to measure patient knowledge in Asian cohorts. We aimed to validate a dis-ease-specific questionnaire that measures the level of understanding of AF and its treatment among patients previously diagnosed with AF in Singapore.
Methods: A 10-question interviewer-administered questionnaire was created based on previously published questionnaires. Face and content validity were first assessed. AF patients (n=165) were identified by convenience sampling in the cardiology clinics of a tertiary hos-pital. The questionnaire was administered in either English (n=53) or Mandarin (n=112). Exploratory factor analysis using the method of principal components was performed to determine the optimal number of factors. Internal consistency was evaluated using Cronbach’s alpha coefficient.
Results: Face validity was tested by surveying 10 cardiologists, all of whom could identify that the questionnaire was intended to measure the level of understanding of AF and its treatment. Mean content validity ratio across items according to Lawshe’s content validity rule was 0.9. Interview participants were 68.7±10.5 years old and 55.8% were male. Most (95.2%) were on oral anticoagulation. Exploratory factor analysis yielded a Kaiser-Meyer-Olkin measure of 0.67 and Bartlett’s test of sphericity was significant (P<0.01). Four factors were retained based on the eigenvalue >1; i.e. knowledge of disease characteristics, knowledge of disease-specific treatment, knowledge of role of treatment in symptom management and knowledge of treatment mechanisms. Internal consistency was good (Cronbach’s alpha=0.71). Participants had poor understanding of their disease beyond the symptoms that they may experience and low levels of knowledge about role of treatment.
Conclusions: An interviewer-administered questionnaire on the knowledge of AF was validated in a cohort of Asian patients in both En-glish and Mandarin. It allows us to quantify patients’ knowledge and may be useful in Asian populations to assess the efficacy of interven-tions to improve patients’ understanding of AF.
DEVELOPMENT AND VALIDATION OF A QUESTIONNAIRE MEASURING PATIENT KNOWLEDGE OF ATRIAL FIBRILLATION IN AN ASIAN COHORTRebecca Hoe1, Wanyun Lin2, Toon Wei Lim2, Mary Ann Bautista3, Hubertus Johannes Maria Vrijhoef4
1 National University of Singapore, Singapore; 2National University Hospital, Singapore; 3Duke-NUS Medical School, Singapore; 4Saw Swee Hock School of Public Health, Singapore
CLINICAL ELECTROPHYSIOLOGY P 1-126

238
Introduction: The CHADS2 and CHA2DS2-VASc scores are found to predict the occurrence of stroke, coronary arteriosclerosis, dementia, and death in patients with or without atrial fibrillation (AF). However, the relations between these scores and atherosclerotic biomarkers are unknown.
Methods: Patients with stable angina and received percutaneous coronary interventions were enrolled. Clinical data and blood samples were collected during their admission. Serum samples were analyzed for hs-CRP, monocyte chemoattractant protein 1 (MCP-1), vascular cell adhesion molecule 1 (VCAM-1), intercellular adhesion molecule 1 (ICAM-1), circulating soluble CD40 ligand (sCD40L), and P selectin. The relations between CHADS2, CHA2DS2-VASc scores and these biomarkers are analyzed.
Results: A total of 295 patients (66.5±0.6 years), 235 males and 60 females, were studied. Co-morbidities included 6% AF. Greater CHADS2 score was significantly associated with greater VCAM-1 level (p for trend=0.010) in a linear fashion, but not hs-CRP, MCP-1, ICAM-1, sCD40L, or P selectin levels (p for trend>0.1). Meanwhile, greater CHA2DS2-VASc score was significantly associated with greater VCAM-1 level (p for trend=0.001) in a linear fashion, but not hs-CRP, MCP-1, ICAM-1, sCD40L, or P selectin levels (p for trend>0.1).
Conclusions: The CHADS2 and CHA2DS2-VASc scores are associated to VCAM-1 in an incremental manner. The result implies that these scores are related to systemic endothelial damage. This finding explains previous epidemiological findings about the relations between these scores and cardiovascular adverse outcomes.
THE CHADS2 AND CHA2DS2-VASC SCORES ARE ASSOCIATED WITH VASCULAR CELL ADHESION MOLECULE 1 (VCAM-1) IN AN INCREMENTAL MANNERChen-Ying Hung1, Yu-Cheng Hsieh2, Wen-Lieng Lee2, Kae-Woei Liang2, Cheng-Hung Li2, Ying-Chieh Liao2, Jin-Long Huang2, Wayne Huey-Herng Sheu2, Tsu-Juey Wu2 1Taipei Veterans General Hospital, Hsinchu Branch, Hsinchu, Taiwan; 2Taichung Veterans General Hospital, Taichung, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 1-128

239
Introduction: Relationship between atrial conduction time and hypertension (HTN) was shown in previous studies. However, there was limited data about the association between the non-dipping status and ventricular electromechanical intervals in pre-HTN patients.
Methods: The Kosin University ambulatory blood pressure monitoring, echocardiography and electrocardiogram (ECG) database were re-viewed from 2011 to 2014 to identify patients with non-dipper pre-hypertension. ECGs recorded closest to the time of the echocardiogram were carefully reviewed and measured PR interval, QRS duration, QT and QTc intervals. All patients were evaluated by transthoracic echo-cardiography by guidelines.
Results: The pre-HTN patients with non-dipper status (n=119) showed more prolonged QT interval (non-dipper status vs. dipper status; 397.0±36.4 vs. 384.5±36.3 ms, P<0.034) and QTc intervals (429.9±28.0 vs. 420.1±22.2 ms, P=0.016) compared to those with dipper status (n=80). Left ventricular mass index (LVMI) was significantly higher in non-dipper pre-HTN patients (137.2±49.6 vs. 122.1±26.7 g/m2, P=0.039) , even though there was no difference of 24 hours mean systolic (SBP) and diastolic blood pressures (DBP) in both group (SBP, 138.5±18.1 vs. 136.2±14.6 mmHg, P=0.343; DBP, 87.3±15.6 vs. 88.2±10.9 mmHg, P=0.647).
Conclusions: The patients with non-dipper pre-HTN, even though there was no difference of 24 hr mean systolic and diastolic blood pres-sures in both group, were associated with more prolonged QT, QTc intervals and higher LVMI, suggesting closer clinical follow-up will be required.
IMPACT OF NON-DIPPING STATUS ON THE VENTRICULAR ELECTRICAL AND MECHANICAL DYSFUNCTION IN PRE-HYPERTENSIVE PATIENTSSung Il Im, Kyoung Im Cho, Hyun Su Kim, Jeong Ho Heo, Tae Joon Cha
Kosin University Gospel Hospital, Busan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-129

240
Introduction: Relationship between atrial fibrillation (AF) and inflammation was shown in previous studies. However, there was limited data about the association between the periodontitis and atrial fibrillation in the long-term follow up. The aim of this study was to evaluate the impact of periodontitis on long-term clinical outcomes in patients with AF.
Methods: The Kosin University echocardiography, electrocardiogram (ECG) and periodontitis database were reviewed from 2010 to 2015 to identify patients with AF and periodontitis. Patients were followed for a median of 2.1 years and were divided into two groups according to the absence or presence of periodontitis in patients with AF.
Results: Among 227 patients with AF, 47 (20.7%) patients had periodontitis. Total any event rates were significantly higher in patients with periodontitis compared to those without periodontitis (P<0.001). Arrhythmias including AF, atrial tachycardia, atrial premature beat, ven-tricular tachycardia, and ventricular premature beat also occurred in 36 patients, with a significantly higher incidence in patients with periodontitis than in those without periodontitis (P<0.001). In univariate analysis, age, CHA2DS2 VASc, Left atrial volume index (LAVI) and periodontitis were significantly associated with arrhythmic events and total any events including bleeding events, thromboembolic events, arrhythmic events, re-hospitalizations and mortality. In multivariate analysis, LAVI (P=0.005) and periodontitis (P<0.001) were independent risk factors for arrhythmic events and periodontitis (P<0.001) for total any events at the long-term follow-up.
Conclusions: The patients with periodontitis were associated with higher total any events and arrhythmic events, suggesting more inten-sive medical therapy with close clinical follow-up will be required.
IMPACT OF PERIODONTITIS ON LONG TERM CLINICAL OUTCOMES IN PATIENTS WITH ATRIAL FIBRILLATIONSung Il Im, Jinho Heo, Kyoung Im Cho, Hyun Su kim, Jeong Ho Heo, Tae Joon Cha
Kosin University Gospel Hospital, Busan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-130

241
Introduction: Premature atrial contraction (PAC) was well known as a predictor of atrial fibrillation (AF) and ischemic stroke. However, it is not clear whether duration of PAC until AF is associated with ischemic stroke.
Methods: Total 1,078 consecutive patients with PAC in 24 hours Holter monitoring were enrolled. They all were diagnosed with AF after 24 hours Holter monitoring. We investigated PAC burden, duration of PAC until AF, and ischemic stroke risk.
Results: Mean age was 60.3±12.9 years old, male was 56.8%, mean CHA2DS2-VASc score was 3.9±1.3, mean PAC per hour was 39.5 beats, mean PAC burden (PAC per 24 hours total beatsx 100%) was 1.0%. Of note, incidence of ischemic stroke after diagnosis with AF was 9.5%, it is unexpectedly so high. PAC burden of initial 24 hours Holter monitoring was not significantly different between patients with ischemic stroke (group A, 102 patients) and those without ischemic stroke (group B, 976 patients); respectively 1.00% vs. 0.95%, P=0.820. PAC burden was divided 3 categories; PAC<1%, 1%≤PAC<10%, PAC≥10% in each group. It was not significantly different between two groups (Table 1). However, duration of PAC until AF was longer in group A than group B (1,002 vs. 638 days, P<0.001, Figure 1).
Conclusions: This study showed PAC burden was not associated with ischemic stroke. However, results of study demonstrated that pa-tient with ischemic stroke with PAC and AF had longer duration of PAC until diagnosis with AF than those without ischemic stroke, sug-gesting that chronic PAC might make remodeling of left atrium and influence risk of ischemic stroke.
LONG DURATION OF PREMATURE ATRIAL CONTRACTIONS UNTIL DIAGNOSIS WITH ATRIAL FIBRILLATION INCREASES ISCHEMIC STROKEDong-Hyeok Kim1, Jong-Il Choi2, Sang-Weon Park1, Young-Hoon Kim2, Jaemin Shim2, Kwang-No Lee2, Seung-Young Roh2, Hong Euy Lim3, Jin Seok Kim4 1Sejong General Hospital, Bucheon, Republic of Korea; 2Korea University Medical Center, Seoul, Republic of Korea; 3Korea University Guro Hospital, Seoul, Republic of Korea; 4Korea University Ansan Hospital, Ansan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-131
Table 1. Difference of PAC according to Ischemic Stroke
group A; stroke (+) (n=102)
group B; stroke (-) (n=976)
P value
PAC<1% 81 (79.4%) 755 (77.4%) 0.709
1%≤PAC<10% 21 (20.6%) 216 (22.1%) 0.802
PAC≥10% 0 (0%) 5 (0.5%) 1.000

242
Introduction: The relationship between anemia and sudden cardiac arrest (SCA) is unclear in general population. This study assessed the effect of anemia on SCA in general population.
Methods: From the Korean National Health Insurance Database Cohort (NHID-Cohort), we studied 494,948 subjects (mean age, 47.8 [SD, 14.2] years; 245,333 men [49.6%]) with national health check-up. Hemoglobin (Hb, g/dl) was evaluated as both a continuous and a cate-gorical variable (mild anemia, 11 ≤ Hb<13 for men and 11 ≤ Hb<12 for women; moderate anemia, 8 ≤ Hb<11; and severe anemia<8).
Results: During a mean follow up period of 5.4 years, SCA occurred in 989 participants (352 women). Incidence rates for SCA increased across the 4 anemia groups in men (0.5, 2.6, 8.8, and 8.9 per 1,000 person-years) and women (0.3, 0.7, 0.9, and 1.9 per 1,000 person-years), respectively. In multivariable models adjusted for cardiovascular factors and interim myocardial infarction, a 26 and 28% increase in SCA risk per 1-unit decrease in Hb was observed in men (95% confidence interval [CI], 20-33%; P<0.001) and in women (95% CI, 19-39%; P<0.001). Adjusted hazard ratios for SCA associated with anemia and severe anemia were 2.08 (95% CI, 1.71-2.53; P<0.001) and 7.58 (95% CI, 2.82-20.35; P<0.001) for men, and 1.88 (95% CI, 1.50-2.35; P<0.001) and 7.81 (95% CI, 3.45-17.67; P<0.001) for women, respectively.
Conclusions: Anemia was associated with increased risk of SCA in general population. Therapeutic strategies aimed to correct anemia in general population should be investigated.
ANEMIA AND THE RISK OF SUDDEN CARDIAC ARREST IN GENERAL POPULATIONIn-Jung Kim, Pil-Sung Yang, Tae-Hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-132

243
Introduction: There is a paucity of information on whether liver cirrhosis (LC) is associated with atrial fibrillation (AF) development. This study aimed to investigate the impact of LC on AF development, and prognostic implication of AF development on mortality in LC patients.
Methods: Patients with LC (n=3,596, mean age 54.7±12.3 years, male 72.5%) without previous AF were selected from the National Sam-ple Cohort database derived from the Korean National Health Insurance Service between 2004 and 2008. Age- and sex-matched controls (n=17,980) were 1:5 randomly sampled from non-LC individuals in 2004. Both cohorts were followed up for incident AF and death until 2013.
Results: During 9 years follow-up, newly diagnosed AF was detected in 113 (3.1%) LC patients and 385 (2.1%) controls (incidence 3.48 and 2.16 per 1,000 person-years, respectively). The LC group showed higher risk of AF development compared to the non-LC group (hazard ratio (HR) 1.64, 95% confidence interval (CI) 1.33-2.02). After adjustment with hypertension, diabetes mellitus, dyslipidemia, and conges-tive heart failure, LC was shown to be an independent risk factor of AF development (HR 1.45, 95% CI 1.17-1.79). The LC group showed in-creased overall mortality compared to the non-LC group (HR 4.17, 95% CI 3.89-4.48), whereas there was no significant difference in car-diovascular mortality (HR 1.10, 95% CI 0.86-1.41, P=0.438). Furthermore, LC patients with new-onset AF did not show increased risk of overall and cardiovascular mortality compared to those without new-onset AF (all, P>0.10).
Conclusions: LC was shown to be an independent risk factor for AF development. However, the increased risk of overall mortality due to LC could attenuate the prognostic implication of new-onset AF on mortality in patients with LC.
LIVER CIRRHOSIS IS A RISK FACTOR FOR ATRIAL FIBRILLATION: A NATIONWIDE POPULATION-BASED STUDYHyunJung Lee, Eue-Keun Choi
Seoul National University Hospital, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-133
Incidence and Risk of AF in Cirrhotic and Non-cirrhotic Patients
LC group (n=3,596)
non-LC group (n=17,980) p-value
AF cases, n (%) 113 (3.1%) 385 (2.1%) <.001
Follow-up duration, years 9.03±1.39 9.91±0.77 <.001
AF incidence
(per 1,000 person-years) 3.48 2.16
Crude HR (95% CI) 1.64 (1.33-2.02) 1 (reference) <.001
adjusted HR (95% CI) 1.45 (1.17-1.79) 1 (reference) <.001

244
Introduction: Elevated level of circulating γ-glutamyl-transpeptidase (GGT) is associated with increased risk of metabolic and cardiovas-cular disease. There is paucity of information on the association between GGT and incident atrial fibrillation (AF). We evaluated the impact of GGT on AF incidence and the interaction between GGT and obesity on developing AF in a large population based cohort.
Methods: A total of 251,574 individuals without underlying AF, aged of 40 years or older who received health care checkups performed by the national insurance program between 2002 and 2008 were screened. We excluded individuals with liver disease (acute/chronic hepati-tis and liver cirrhosis). Subjects were categorized by GGT level in quartile (range of GGT; Q1 ≤15 U/L, Q2 16-23 U/L, Q3 24-37 U/L, and Q4 ≥38 U/L). Associations between GGT levels and AF incidence were analyzed using multivariate Cox proportional hazards regression mod-els, adjusted for age, sex, body mass index (BMI), and comorbidities.
Results: A total of 243,598 individuals were included (mean age 54±10.5 years, men 47.5%). During a median 8 years follow-up, 4,545 (1.9%) individuals were newly identified as AF. The crude AF incidence were gradually increased by GGT level (1.9, 2.5, 2.7 and 3.0 per 1,000 person-years in population with Q1, Q2, Q3 and Q4, respectively) (p for trend<0.001). Population with the highest quartile of GGT showed significant higher AF risk compared to those with the lowest quartile of GGT (adjusted HR 1.36, 95% CI 1.23-1.50, P<0.001). When the analysis was stratified by BMI, non-obese population (BMI<25 kg/m2) showed significant correlation between GGT level and risk of AF, whereas obese population (BMI≥25 kg/m2) did not (p interaction<0.001) (Figure).
Conclusions: In this large population based study, elevated level of GGT showed significant association with an increased risk of AF, espe-cially in non-obese population.
THE ASSOCIATION BETWEEN γ-GLUTAMYL-TRANSPEPTIDASE LEVEL AND RISK OF ATRIAL FIBRILLATION: A NATIONWIDE POPULATION-BASED STUDYSo-Ryoung Lee1, Eue-Keun Choi1, Tae-Min Rhee1, Hyun-Jung Lee1, Woo-Hyun Lim2, Si-Hyuck Kang3, Kyung-Do Han4, Myung-Jin Cha1, Youngjin Cho1, Il-Young Oh3, Seil Oh1 1Seoul National University Hospital, Seoul, Republic of Korea; 2Seoul National University Boramae Medical Center, Seoul, Republic of Korea;
3Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 4College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-135

245
Introduction: Fast resting heart rate (RHR) had been related to increased risk of all-cause and cardiovascular death in patients with hy-pertension. The present study aimed to investigate the clinical characteristics of hypertensive patients with fast RHR and its relationship to chronic comorbidities.
Methods: We retrospectively analyzed the clinical characteristics of hypertensive and normotensive subjects in a large cohort enrolled from Jan 2000 to Apr 2005 in Shandong, China. The demographic data, medical history, resting heart rate (RHR), body mass index (BMI), waist and hip circumference, sitting blood pressure and blood samples were collected. RHR above 85 beats per minute (bpm) were de-fined as fast RHR.
Results: Of all the 18,183 subjects, 61.6% were male, 41.7% were hypertensive patients, and the mean age was 45.2±12.7 years old. The mean RHR was significantly faster in hypertensive patients than normotensive subjects (73.5±11.6 vs. 70.6±9.6, P<0.001). Subjects with fast RHR were more common in hypertensive patients than normotensives (14.5% vs. 6.4%, P<0.001). As compared with hypertensive pa-tients with normal RHR, those with fast RHR were older (55.0±12.2 vs. 52.9±11.5, P<0.001), had lower BMI (25.7±3.7 vs. 26.3±3.5, kg/m2 P<0.001), higher fasting blood glucose (FBG, 6.0±2.4 vs. 5.6±1.5 mmol/L, P<0.001), triglyceride (TG) and LDL-C level (1.9±1.8 vs. 1.6±1.2 P<0.001; 3.2±0.9 vs. 3.1±0.8 mmol/L, P=0.001), and higher prevalence of diabetes (9.8% vs. 7.4%, P=0.007) and stroke (7.2% vs. 3.5%, P<0.001). After adjustment of conventional risk factors, fast RHR was associated with increased risk of stroke (OR 1.94, 95% CI 1.45-2.56).
Conclusions: Hypertensive patients with fast RHR seem to be older, thinner and with higher fasting blood FBG, TG and LDL-C levels. Faster RHR may increase the risk of stroke in hypertensive patients.
RELATIONSHIP BETWEEN CHRONIC COMORBIDITIES AND FAST RESTING HEART RATE IN HYPERTENSIVE PATIENTSXiaofei Li, Kai Sun, Jingzhou Chen, Rutai Hui, Yan Yao, Xiaohan Fan
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, Beijing, China
CLINICAL ELECTROPHYSIOLOGY P 1-136

246
Introduction: Proteinuria (PU) is one of well-known predictor of cardiovascular disease. However the impact of PU on the incidence of atrial fibrillation (AF) has not been well elucidated. In this study, we investigated the association between PU detected by dipstick urine test and the risk of AF development.
Methods: We analyzed 389,431 subjects (≥20 year-old, 52.1% male) without prior AF, and who had received biennial medical evaluations provided by the National Health Insurance Corporation between 2004 and 2008 in Korea. Subjects were classified according to the results of dipstick urine test (no, trace (±), 1+/2+, and 3+/4+).
Results: Trace, low-grade (1+/2+), and high-grade (3+/4+) PU were detected in 5,958 (1.5%), 6,481 (1.7%) and 397 (0.1%) subjects, respec-tively. During a mean follow-up of 7.5 years, a total of 5,105 (1.3%) developed AF (1.74 per 1,000 person-year). Old age (≥65), male gender, obesity (BMI ≥30 kg/m2), hypertension, ischemic heart disease, chronic heart failure, and PU (≥3+) were independent and strong predic-tors for AF development. The presence and severity of PU was associated with higher AF risk compared with those without PU after mul-tivariable adjustment: hazard ratios and 95% confidence intervals of AF occurrence were 1.23 (1.01-1.51), 1.36 (1.16-1.60), and 2.52 (1.70-1.87) with trace, low-grade, and high-grade PU, respectively (p for trend <0.001). Among individuals with no or trace PU initially, AF risk was additionally increased by 51% when PU had progressed (≥1+) at next medical evaluations.
Conclusions: The presence and severity of PU detected by dipstick urine test showed a significant association with the incidence of new onset AF. This study suggests that PU on dipstick test could be a useful predictor for AF development.
PROTEINURIA DETECTED BY DIPSTICK URINE TEST PREDICTS ATRIAL FIBRILLATION: A NATIONWIDE POPULATION-BASED STUDYWooHyun Lim1, Eue-Keun Choi2, So-Ryoung Lee2, Si-Hyuck Kang3, Kyung-Do Han4, Myung-Jin Cha2, Youngjin Cho3, Il-Young Oh3, Seil Oh2 1Seoul National University Boramae Medical Center, Seoul, Republic of Korea; 2Seoul National University Hospital, Seoul, Republic of Korea;
3Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 4The Catholic University of Korea, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-137

247
Introduction: Catheter ablation for is well-established to provide treatment for cardiac arrhythmias including supraventricular tachycar-dia (SVT), atrial fibrillation (AF) and ventricular arrhythmia (VA). We sought to examine temporal and regional trends in the provision of these services over the past decade in Australia.
Methods: A retrospective review of the numbers for ablation from January 2006 to December 2015 was performed on data from the Medi-care Australia database (MA) reflecting data on patients with private health insurance (approximately half of the population in Australia). Numbers for EP were collected by type of procedure and by region. Two regions (Northern Territory and Tasmania) did not have an abla-tion service available locally.
Results: In the 10 years analyzed, 32,123 SVT ablations, 19,117 AF ablations, and 2,777 VT ablations were reported. Over the 10 years there was an overall 142% increase in the number of ablation procedures. Population adjusted increase was highest for AF ablations (170%), followed by VT ablations (100%) and SVT ablations (70%) In regions without an EP service, number of ablations performed was lower (P<0.05), as demonstrated in the figure.
Conclusions: The provision of ablation procedures for privately insured patients in Australia has continued to increase over the past de-cade. Growth is greatest for AF ablation, followed by VT and SVT ablation. Incidence of ablation procedures in regions without an EP center is lower, which may be a reflection of reduced awareness and/or access to the services.
PROVISION OF CATHETER ABLATION PROCEDURES IN AUSTRALIAJonathan Lipton1, Saurabh Kumar1, Joseph Morton1, Paul Macintyre2, Jonathan Kalman1 1Royal Melbourne Hospital, Parkville, Australia; 2Royal Hobart Hospital, Hobart, Australia
CLINICAL ELECTROPHYSIOLOGY P 1-138
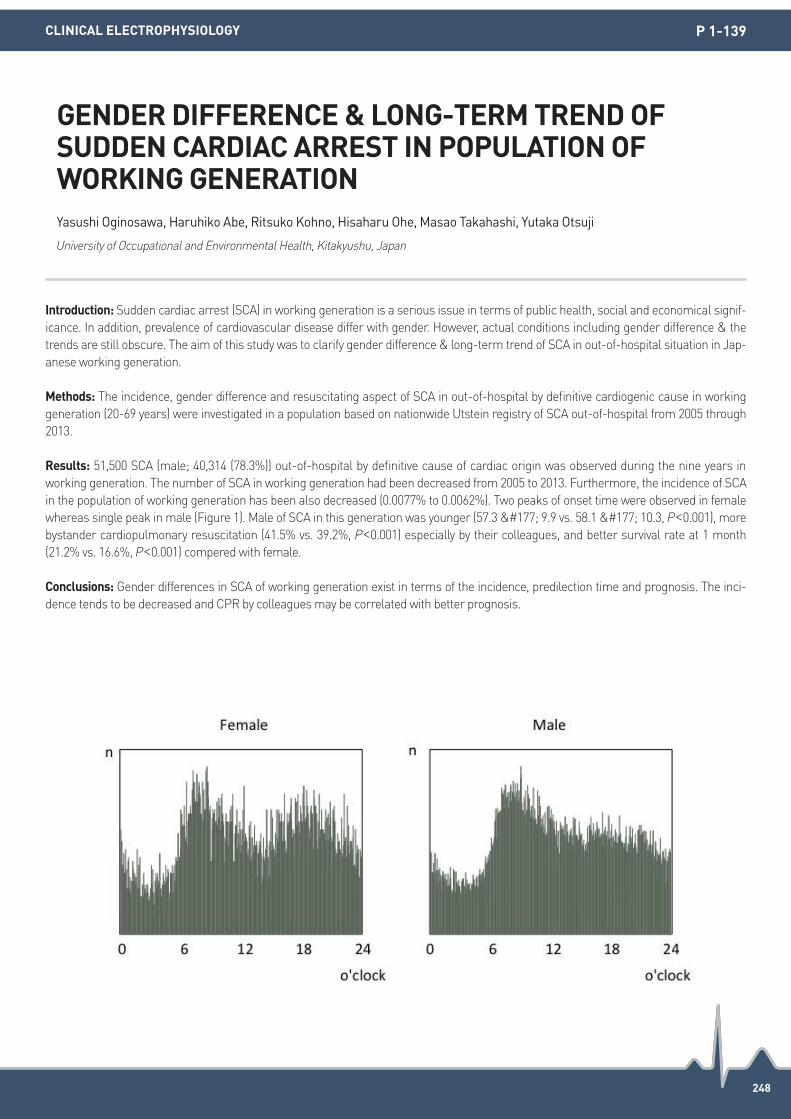
248
Introduction: Sudden cardiac arrest (SCA) in working generation is a serious issue in terms of public health, social and economical signif-icance. In addition, prevalence of cardiovascular disease differ with gender. However, actual conditions including gender difference & the trends are still obscure. The aim of this study was to clarify gender difference & long-term trend of SCA in out-of-hospital situation in Jap-anese working generation.
Methods: The incidence, gender difference and resuscitating aspect of SCA in out-of-hospital by definitive cardiogenic cause in working generation (20-69 years) were investigated in a population based on nationwide Utstein registry of SCA out-of-hospital from 2005 through 2013.
Results: 51,500 SCA (male; 40,314 (78.3%)) out-of-hospital by definitive cause of cardiac origin was observed during the nine years in working generation. The number of SCA in working generation had been decreased from 2005 to 2013. Furthermore, the incidence of SCA in the population of working generation has been also decreased (0.0077% to 0.0062%). Two peaks of onset time were observed in female whereas single peak in male (Figure 1). Male of SCA in this generation was younger (57.3 ± 9.9 vs. 58.1 ± 10.3, P<0.001), more bystander cardiopulmonary resuscitation (41.5% vs. 39.2%, P<0.001) especially by their colleagues, and better survival rate at 1 month (21.2% vs. 16.6%, P<0.001) compered with female.
Conclusions: Gender differences in SCA of working generation exist in terms of the incidence, predilection time and prognosis. The inci-dence tends to be decreased and CPR by colleagues may be correlated with better prognosis.
GENDER DIFFERENCE & LONG-TERM TREND OF SUDDEN CARDIAC ARREST IN POPULATION OF WORKING GENERATIONYasushi Oginosawa, Haruhiko Abe, Ritsuko Kohno, Hisaharu Ohe, Masao Takahashi, Yutaka Otsuji
University of Occupational and Environmental Health, Kitakyushu, Japan
CLINICAL ELECTROPHYSIOLOGY P 1-139

249
Introduction: Cancer has been known to associate with cardiovascular disorders, including heart failure or cardiotoxicity related to che-motherapy. Breast cancer, a chest wall disease, has been rapidly increasing malignancy. We sought to investigate whether breast cancer is associated with cardiac arrhythmias.
Methods: Total 668 patients who underwent sono-guided breast biopsy from 2011 to 2013 were studied. All baseline 12-lead electrocar-diogram (ECG) were assessed in 467 patients diagnosed with breast cancer (right, n=225; left, n=242) compared to 201 patients diag-nosed with benign breast disease, as a control group. ECG parameter was also analyzed according to the position of malignancy. Twen-ty-four hours Holter ECGs were conducted in symptomatic patients.
Results: All of patients were women and mean age of patients was 50.7 years. There were no difference in heart rate, QRS axis, bundle branch pattern, QRS duration, corrected QT interval, ST-segment change between two groups. PR interval was significantly prolonged in the cancer group compared to benign group (155 ms vs. 149 ms, P=0.001), however there was no significant difference in PR interval be-tween patient with right breast cancer and those with left breast cancer (155 ms vs. 154 ms, P=0.768). In ECGs, ventricular premature complex (VPC) and atrial premature complex (APC) were documented only in breast cancer group (VPC, 0.64%; APC, 0.64%). Holter was conducted in 17 patients (cancer, n=9, vs. benign disease, n=8). Occasional APCs occurred more often in cancer group (66.7%, vs. 12.5%, P=0.05).
Conclusions: This study showed that PR interval on ECGs was significantly prolonged and APCs was more prevalent in patients with breast cancer compared to those with benign breast disease, suggesting that breast cancer may increase risk of arrhythmogenesis.
ELECTROCARDIOGRAPHIC FINDINGS OF BREAST CANCER COMPARED TO BENIGN BREAST DISEASESuk-kyu Oh, Jong-Il Choi, Seung Pil Jung, Yun Gi Kim, Hyungdon Kook, Hee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-Young Roh, Jaemin Shim, Jin Seok Kim, Hong Euy Lim, Young-Hoon Kim
Korea University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-140

250
Introduction: Pectus excavatum is a known Brugada phenocopy. Brugada phenocopy is characterized by an Brugada ECG pattern without family history or clinical manifestations including syncope, arrhythmia and sudden cardiac death.
Methods: This study included a total of 97 consecutive patients (age>18) with who diagnosed pectus excavatum in the university of Korea hospital, Anam from January 2005 to Apirl 2016. We analyzed clinical manifestation, ECG and imaging study including echocardiography, Computer tomography (CT) or magnetic resonance imaging (MRI).
Results: A total of 97 consecutive patients were enrolled. The mean age of patients was 22.2±4.9 years; 13 (13.4%) of them were women. Mean QRS duration and QT interval were 98±10.3 ms and 378±25 ms, respectively. 30 (30.9%) patients showed right bundle branch block (RBBB), 4 (4.1%) patients showed Brugada ECG pattern. Imaging study showed no structural abnormality except compression of right ventricle by chest wall deformity. 14 (14.4%) patients were presented palpitation, chest discomfort or syncope. There was no patient with sudden cardiac arrest or sustained ventricular arrhythmia. 3 (3.1%) of patients presented sustained supraventricular tachycardia and un-derwent electrophysiology study and radio-frequency ablation therapy. Among patients with Haller index (maximal transverse diameter/narrowest anterior-posterior length of chest) lesser than 3.25, 1 patient showed incomplete RBBB and there was no Brugada ECG pat-tern. Patients with higher Haller index (≥3.25) showed longer corrected QT interval than lower Haller index (<3.25) (412±25 vs. 404±22, P=0.02).
Conclusions: Currently pectus excavatum is known as a BrP. But chest deformity like pectus excavatum can affect formation of normal anatomy or conduction system. Further research is needed to evaluate these preliminary findings in a larger population to evaluate the relationship between chest deformity and Brugada pattern ECG and clinical significance.
ECG AND CLINICAL MANIFESTATION OF PECTUS EXCAVATUM AS A BRUGADA PHENOCOPYHee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-141
251
Introduction: Low resting heart rate (HR) has been associated with atrial fibrillation (AF) in athletes. The objective was to examine the as-sociation of sinus bradycardia with incidence of AF in general population.
Methods: The population-based Ansung-Ansan cohort, consisting of 9,865 healthy participants aged between 40 and 70 years with no history of atrial fibrillation, were evaluated. All Subjects’ electrocardiography (ECG) was measured. Incidence of AF diagnosed by ECG was checked every 2 years. The Cox proportional hazards model was used to predict atrial fibrillation at 10 years.
Results: The mean age was 52.2±8.9 years, and 47.3% were male. 238 participants (68.6% male) showed sinus bradycardia (HR<50 bpm) using ECG. During a mean follow-up period of 10 years, 104 participants (62.5% male) were diagnosed with AF. Low resting heat rate itself (HR<50 bpm) was not significantly associated with incidence of AF in both gender (HR=2.50, 95% CI 0.92-6.78, P=0.073). However, Risk of AF independently increased with ECG-documented sinus bradycardia in women (Adjusted HR=6.82, 95% CI 1.55-30.00, P=0.011).
Conclusions: In this prospective cohort study, sinus bradycardia is independently associated with an increased risk of AF in women.
ECG-DIAGNOSED SINUS BRADYCARDIA PREDICT ATRIAL FIBRILLATION IN GENERAL POPULATION: A 10-YEAR COMMUNITY-BASED PROSPECTIVE STUDYJin-Kyu Park1, Junbeom Park2, Hwan-Cheol Park3 1Hanyang University Medical Center, Seoul, Republic of Korea; 2Ewha Womans University Medical Center, Seoul, Republic of Korea; 3Hanyang University Guri Hospital, Guri, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-142

252
Introduction: It is reported that new onset atrial fibrillation (AF) increases in patients with co-morbidity disease. However, it is unknown whether pre-hypertension and impaired fasting glucose (IFG) are associated with new onset AF in healthy populations without co-morbid-ities.
Methods: We included 367,938 subjects (≥20 years) not diagnosed with non-valvular AF from the Korean National Health Insurance Ser-vice-National Sample Cohort (NHIS-NSC) from 2003 to 2008. In all, 140,836 subjects diagnosed with all diseases related to new onset AF were excluded and finally 227,102 healthy population were followed-up until December 2013. Body mass index, blood pressure (BP) and fasting glucose (FG) level were acquired at National healthy check-ups, smoking and alcohol were recorded by detailed questionnaires. AF incidences were defined as the first date documented by a hospital visit. Pre-hypertension and impaired FG (IFG) were defined with 120≤systolic BP<140 or 80≤diastolic BP<90, and 100≤FG<126 mg/dL respectively.
Results: New onset AF occurred in 1470 (0.7%) subjects during a mean of 7.7±2.1 years. Population with pre-hypertension (HR 1.13, P=0.039) or IFG (HR 1.17, P=0.010) has higher risk on new onset AF respectively. The risk (HR 1.18, P=0.025) on AF incidence of IFG was more prominent in population with BMI<25 kg/m2. As the risk number of pre-hypertension, IFG and high BMI (25 kg/m2) increased (n=0, 1, 2 and 3), the incidence of AF increased progressive (p for trend <0.001). In even though heathy population, population with all 3 risks showed higher risk (HR 1.61, P=0.006) of AF than those without risk factors after adjusting age, gender, smoking and alcohol.
Conclusions: In even though healthy populations without comorbidities, pre-hypertension and IFG were important risk factor of AF inci-dence. And IFG was more important risk factor of AF in population with low BMI.
CLINICAL IMPLICATION OF IMPAIRED FASTING GLUCOSE AND PRE-HYPERTENSION RELATED TO NEW ONSET ATRIAL FIBRILLATION IN HEATHY POPULATION WITHOUT UNDERLYING DISEASES: A NATIONWIDE COHORT STUDY IN KOREAJunbeom Park1, Kyoung Ae Kong1, Boyoung Joung2 1Ewha Womans University Medical Center, Seoul, Republic of Korea; 2Yonsei University Health System, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-143

253
Introduction: Brugada syndrome (BrS) often lead to devastating but preventable sudden cardiac death (SCD). So far, ICD implantation still the corner stone’s management. But, low rate of appropriate shocked after ICD implantation makes the big question about which patient will get the most benefit. In addition, the value of electrophysiologic studies for predicting spontaneous VF remains controversial. The aim of this study was to investigate which characteristics of BrS that has can be used as a predictor of appropriate shock due to ventricular arrhythmia (VA).
Methods: We did a retrospective cohort study of total 13 BrS patient, from Januari 2013-December 2014. Characteristic of BrS that we analyzed were baseline characteristics (age and sex), Clinical finding (syncope, cardiac arrest), ECG finding (spontaneous type 1 or drug-induced) and electrophysiology study result (inducible VA and RV ERP). Our primary outcome are appropriate shock during ICD in-terrogation for those who have been implanted an ICD, and documented VA for those who didn’t received ICD.
Results: Independent predictor of appropriate shock and documented VA are History of syncope (P=0.049), Spontaneous type 1 Brugada ECG (0.021) and result from EP study RV ERP<190 ms (P=0.048). Another variables that proven had no correlationship with ICD event and VA are age (P=0.123); inducible VA in EP study (P=0.357).
Conclusions: The hystory of syncope, a spontaneous type 1 Brugada ECG and RV ERP<200 ms during electrophysiological study were predictors of approriate shocks in our population.
PREDICTORS OF APPROPRIATE SHOCKS AND VENTRICULAR ARRHYTHMIAS IN A INDONESIAN PATIENTS WITH BRUGADA SYNDROMEArdian Rizal, Sunu Budi Raharjo, Dicky Hanafy, Haryadi Haryadi, Yoga Yuniadi
National Cardiovascular Center Harapan Kita, Jakarta, Indonesia
CLINICAL ELECTROPHYSIOLOGY P 1-144

254
Introduction: Atrial fibrillation (AF) is a major risk factor for stroke and AF-related strokes tend to be increased mortality. This study ex-amined the incidence and risk factors for stroke in patients with AF.
Methods: The National Health Insurance Service (NHIS) database was searched AF patients aged ≥30 years without previous stroke from 2007 to 2013. The study sample comprised 5,713 men and 4,941 women. The incidence of stroke in patients with AF was calculated ac-cording to the age, sex and CHA2DS2-VASc score. Independent risk factors of stroke in patients with AF were investigated in univariate and multivariate Cox proportional hazard models.
Results: During a mean follow-up period of 3.2 years, 2,059 (19.3%) patients were diagnosed with stroke. Of these, 87.5% had CHA2DS2-VASc score of ≥2. The rate of oral anticoagulation therapy was 13.2%. The overall incidence rate was 62.1/1,000 person-years. The inci-dence rate increased with age (30-39 years: 14.9/1,000 person-years and ≥80 years: 133.4/1,000 person-years, respectively). The inci-dence rate per 1,000 person-years in men and women was 60.3 and 64.1, respectively. The incidence rate per 1,000 person-years in CHA2DS2-VASc score of 0, 1, 2, 3-4 and 5-7 was 17.3, 26.9, 49.3, 87.2 and 127.4, respectively. The incidence of stroke in patients with warfa-rin use more than 1 month was lower than non-use (HR: 0.839, 95% CI: 0.723-0.974). Increasing age, specific components of CHA2DS2-VASc score (congestive heart failure, hypertension, diabetes mellitus) and ischemic heart disease were significantly associated with in-creased risk of stroke in both univariate and multivariate analyses.
Conclusions: We found that the incidence rate of stroke in patients with AF in Korea increased with CHA2DS2-VASc score and age. The treatment rate for anticoagulation was very low in patients with AF. To prevent stroke, active programs for the detection and management of AF are needed.
RISK FOR STROKE IN KOREAN PATIENTS WITH ATRIAL FIBRILLATION: THE KOREA NATIONAL HEALTH INSURANCE SERVICE DATABASE 2007 TO 2013Mi Kyoung Son, Nam-Kyoo Lim, Hyun-Young Park
Korea National Institute of Health, Cheongju, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-145

255
Introduction: The incidence of acute myocarditis complicated with ventricular tachycardia is unknown. This study aimed to investigate the association between myocarditis and the incidence of VT and mortality.
Methods: From 2000 to 2004, 13,250 patients with a history of myocarditis were identified from the Taiwan National Health Insurance Re-search Database. The same number of healthy individuals with a matched sex and underlying diseases were selected as the control group. The long-term risks of life-threatening ventricular arrhythmias and mortality in patients with a history of myocarditis were investi-gated by an adjusted Cox proportional hazards regression.
Results: After a mean follow-up of 10.4±2.94 years (interquartile range: 12, 10.19-12), the myocarditis patients showed a higher incidence of new onset VT events compared with healthy controls (5.4% [519 per 100,000 person-year] in the myocarditis group vs, 0.47% [43 per 100,000 person-year] in the healthy controls; adjusted hazard ratio [HR]: 16.1, 95% CI: 12.4-20.9; P<0.001). A higher incidence of cardio-vascular death was noted in the myocarditis group than healthy controls (6.52% vs. 3.18%; HR: 2.42, 95% CI: 2.14-2.73; P<0.001) after ad-justing for the multivariate confounders including the sex, age, underlying comorbidities, and medications. The Kaplan-Meier curve (Fig-ure 1A-D) also demonstrated that the patients with previous history of myocarditis have increased risk for new-onset VT events, decreased survival and increased risk for ICD implantation compared with the healthy cohort.
Conclusions: The results of this study suggested there was a higher incidence of life-threatening VT and mortality during the very long-term follow-up in patients with a history of myocarditis. Future work should focus on an in-depth risk stratification of VT in myocarditis patients.
INCREASED RISK OF VENTRICULAR TACHYCARDIA AND CARDIOVASCULAR DEATH IN PATIENTS WITH MYOCARDITIS DURING THE LONG-TERM FOLLOW-UP: A NATIONAL REPRESENTATIVE COHORT FROM THE NATIONAL HEALTH INSURANCE RESEARCH DATABASEAbigail Louise Te1, Yenn-Jiang Lin1, Yun-Yu Chen1, Fa-Po Chung1, Shih-Lin Chang1, Li-Wei Lo1, Yu-Feng Hu1, Kuo Liong Chien2, Shih-Ann Chen1 1Taipei Veterans General Hospital, Taipei, Taiwan; 2Institute of Epidemiology and Preventive Medicine College of Public Health, National Taiwan University, Taipei, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 1-146

256
Introduction: The relationship between the incidence of atrial fibrillation (AF) and comorbid chronic obstructive pulmonary disease (COPD) is unclear. And the risk of stroke or mortality associated with COPD in patients with AF is not well known. We hypothesize that COPD is associated with the occurrence of new-onset AF and clinical outcomes of AF patients.
Methods: From the National Health Insurance Service-National Sample Cohort of Korea, we enrolled 506,772 subjects (≥18 years old) with health examination from 2009 through 2013. We analyzed the development of new AF in 499,392 patients without AF and the clinical outcomes in 6,817 patients with AF after excluding patient with mitral stenosis or prosthetic valve.
Results: 4.8% of non-AF patients and 18.6% of AF patients had comorbid COPD. Patients with COPD were older, more likely to be male and current or former smoker, with higher CHA2DS2-VASc score (all P<0.001). Over a follow-up period (45.5±14.9 months), the incidence of AF in COPD patients was significantly higher than that in non-COPD patients (3.6% vs. 1.0%, P<0.001). In a multivariate Cox regression, COPD predicted incidence of AF independently of other risk factors (HR 1.27, 95% CI 1.16-1.39, P<0.001). The all-cause mortality of AF patients with COPD was significantly higher than that of AF patients without COPD (16.0% vs. 5.8%, P<0.001). In a multivariate Cox re-gression, COPD was still an independent risk factor for all-cause mortality (HR 1.32, 95% CI 1.07-1.63, P=0.011), but not a risk factor for stroke (P=0.186).
Conclusions: The presence of COPD is an independent risk factor for new-onset AF. In AF patients, COPD is independently associated with all-cause mortality, but not stroke.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCREASES THE RISK OF NEW-ONSET ATRIAL FIBRILLATION AND MORTALITY OF PATIENTS WITH ATRIAL FIBRILLATIONPil-Sung Yang, Tae-Hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University Health System, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-148

257
Introduction: Both atrial fibrillation (AF) and osteoporosis are common in older adults. AF is associated with dizziness, weakness, and decreased cardiac and cerebral perfusion, and these in turn may increase the likelihood of falls. Oral anticoagulants, used to prevent stroke in AF, have also been linked to reduced bone mineral density. However, the associations of comorbid AF with the incidence and outcome of fracture in patients with osteoporosis are not well understood. The purpose of this study was to investigate whether comorbid AF was associated with facture occurrence or mortality after fracture in patients with osteoporosis.
Methods: This nationwide, population-based, propensity score-matched cohort study used data from Korean National Health Insurance Service-National Sample Cohort. We included 36,179 patients with osteoporosis who aged 50 years and older and received national health check-up between 2009 and 2013. Patients with malignant neoplasm history were excluded. Propensity scores for comorbid AF were es-timated for each of study patients and used to assemble a cohort for patients with AF (n=1,479) and matched patients without AF (n=4,437), who were balanced on 14 baseline characteristics.
Results: 4.1% (1,484 of 36,179) of osteoporotic patients had comorbid AF. Compared with the matched cohort, the incidence of fracture in AF patients was significantly higher than that in non-AF patients (38.8 vs. 32.0 per 1,000 person-year, P=0.015 in chi-square test, P=0.021 in Kaplan-Meier analysis). In a multivariate Cox regression analysis, AF was associated with incidence of fracture independently of other risk factors among propensity-matched patients with osteoporosis (HR: 1.24, 95% CI: 1.05-1.46, P=0.010). In subgroup analysis, this asso-ciation was especially pronounced in patients without heart failure (HR: 1.34, 95% CI: 1.09-1.64, P=0.006) and patients with hypertension (HR: 1.28, 95% CI: 1.08-1.53, P=0.005). The mortality after fracture event of the osteoporotic patients with AF was significantly higher than that of osteoporotic patients without AF (28.1% vs. 8.4%, during follow-up, P<0.001).
Conclusions: Comorbid AF in patients with osteoporosis is an independent risk factor for facture occurrence and increases mortality after fracture event.
THE IMPACT OF COMORBID ATRIAL FIBRILLATION ON THE INCIDENCE AND OUTCOME OF FRACTURE IN PATIENTS WITH OSTEOPOROSIS: A PROPENSITY SCORE MATCHED ANALYSISPil-Sung Yang, Daehoon Kim, Dong Geum Shin, Tae-Hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University Health System, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-149

258
Introduction: Atrial fibrillation (AF) and heart failure affect each other, contributing to increase cardiovascular morbidity and mortality. Al-though rate control has become front-line therapy in the management of AF, data on the survival benefits of rate control are still contro-versial. The aim of this study is to assess the efficacy of rate-control medications in AF patients according to concomitant heart failure.
Methods: Using Korean National Health Insurance Service-National Sample Cohort data from 2002 through 2013, we identified 11,047 AF patients over age 20 years with (n=4,047, 36.6%) or without (n=7,000, 63.4%) heart failure. There were 4,171 (37.8%), 557 (5.0%) and 1,230 (11.1%) patients enrolled in the groups receiving beta-blockers, calcium channel blockers and digoxin, respectively. The primary outcome was cardiovascular (CV) mortality.
Results: During a follow-up of 5.3±3.5 years, CV mortality occurred in 994 patients (9.0%). In the overall population, digoxin use was a risk factor for CV mortality (adjusted HR 1.42, 95% CI 1.18-1.72, P<0.001). In the subgroup analysis based on coexistence with heart failure or not, the use of beta-blockers, calcium channel blockers or digoxin was not associated with CV mortality risk in AF patients with heart fail-ure. However, digoxin use was associated with an increased risk of CV death (adjusted HR 1.90, 95% CI 1.23-2.94, P=0.004) in AF patients without heart failure.
Conclusions: Digoxin should not be used in AF patients without heart failure because it was associated with an increased risk of CV death in these populations. Considering the multiple conflicting reports about digoxin’s safety, well-designed trial of digoxin use in AF and heart failure is greatly needed.
OUTCOMES OF RATE-CONTROL TREATMENT IN PATIENTS WITH ATRIAL FIBRILLATION AND HEART FAILURE: A NATIONWIDE COHORT STUDYHee Tae Yu1, Hancheol Lee2, Tae-Hoon Kim1, Jae-Sun Uhm1, Jong-Youn Kim1, Hui-Nam Pak1, Moon-Hyoung Lee1, Boyoung Joung1 1Yonsei University College of Medicine, Seoul, Republic of Korea; 2National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 1-150

259
Introduction: Although the patients of first documented nonischemic heart failure with reduced left ventricular ejection fraction (LVEF) are often diagnosed as dilated cardiomyopathy, their cardiac function may recover after optimal medication therapy. In those patients, a predictive index of improving their cardiac function is not well known.
Methods: In 40 patients with first documented nonischemic heart failure with reduced LVEF, a signal averaged electrocardiogram was used to measure ventricular late potential (VLP) in steady state following acute heart failure therapy. They were divided into two groups according to LVEF after optimal medication, one is recovery group and another is non-recovery group. Between two groups, we compared clinical characteristics, VLP, electrocardiographic and echocardiographic parameters measured before optimal medication therapy.
Results: In acute phase, average LVEF of all 40 patients was 29.0±6.5%. After optimal medication, 25 patients showed improved LVEF (57.1±10.1%) and remaining 15 patients did not (29.3±7.6%) (P<0.001). When comparing these recovery and non-recovery group, clinical backgrounds including prescribed medication did not show any difference. Similarly, LVEF of acute phase showed no significant difference between the two groups (28.7±6.8% vs. 29.5±6.1%). In non-recovery group, positive VLP was more often than in recovery group (66.7% vs. 8.0%, P<0.001). The sensitivity of VLPs for non-recovery LVEF was 83.3% and specificity was 82.1%.
Conclusions: Although the other clinical data did not show any difference, positive VLP was more often in non-recovery group than in re-covery group in this study. In the patients with first documented non-ischemic heart failure with reduced LVEF, VLP measured in acute phase can be a feasible index to predict left ventricular reverse remodeling.
IMPACT OF VENTRICULAR LATE POTENTIAL TO PREDICT REVERSE REMODELING IN THE PATIENTS WITH FIRST DOCUMENTED NONISCHEMIC HEART FAILURE WITH REDUCED LEFT VENTRICULAR EJECTION FRACTIONYuya Aoyama1, Seiji Fukamizu1, Yasunori Koyano1, Daisuke Miyahara1, Sayuri Tokioka1, Tomonori Miyabe1, Dai Inagaki1, Marina Arai1, Kiyotaka Yoshida1, Satoshi Miyazawa1, Iwanari Kawamura1, Akihiro Nakada1, Sho Nagamine1, Shinichiro Masuda1, Takeshi Kitamura1, Rintaro Hojo1, Takaaki Tsuchiyama1, Kota Komiyama1, Takashi Shibui1, Mitsuhiro Nishizaki2, Harumizu Sakurada3, Masayasu Hiraoka4 1Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan; 2Yokohama Minami Kyosai Hospital, Yokohama, Japan; 3Tokyo Metropolitan Health and Medical Treatment Corporation Ohkubo Hospital, Tokyo, Japan; 4Toride Kitasohma Medical Center Hospital, Ibaraki, Japan
HEART FAILURE P 1-151

260
Introduction: Research on the serum bilirubin level, cardiac function and outcomes in heart failure patients with cardiac resynchroniza-tion therapy (CRT) has not yet been reported. The aim of this study was to analyze the relationship between change in serum bilirubin level and left ventricular reverse remodeling, and the impact of the change in bilirubin on clinical outcomes in heart failure patients with CRT.
Methods: We evaluated 105 consecutive patients who underwent CRT. Patients who had no data on both baseline and 3-9 months’ fol-low-up serum total-bilirubin or had died less than 3 months after CRT implantation were excluded. Accordingly, a total of 69 patients were included in the present analysis. The patients were divided into two groups; decreased bilirubin group (total-bilirubin level at follow-up was less than or equal to that of baseline; n=48) and increased bilirubin group (total-bilirubin level at follow-up was more than that of baseline; n=21).
Results: A mean follow-up period was 39.3±29.6 months. In decreased bilirubin group, the mean left ventricular end-diastolic diameter (LVEDd) decreased from 64.7±10.0 mm to 61.9±10.6 mm (P=0.002), the mean LV end-systolic diameter (LVESd) decreased from 54.5±10.9 mm to 50.2±12.5 mm (P=0.001), and the mean LV ejection fraction (LVEF) increased significantly from 29.8±10.4% to 37.0±13.2% (P=0.001). In increased bilirubin group, there was no significant difference in echocardiographic parameters from baseline to follow-up. In Kaplan-Meyer analysis, cardiac mortality combined with heart failure hospitalization in increased bilirubin group was significantly higher than that in decreased bilirubin group (log-rank P=0.018). Multivariate Cox regression analysis revealed that increased bilirubin was an independent predictor of cardiac mortality combined with heart failure hospitalization (OR=2.14, P=0.045).
Conclusions: The change in serum bilirubin predicts left ventricular reverse remodeling and outcomes in heart failure patients with CRT.
THE IMPORTANCE OF A CHANGE IN SERUM BILIRUBIN IN PREDICTING LEFT VENTRICULAR REVERSE REMODELING AND OUTCOMES IN HEART FAILURE PATIENTS WITH CARDIAC RESYNCHRONIZATION THERAPYJunya Hosoda, Toshiyuki Ishikawa, Katsumi Matsumoto, Kohei Iguchi, Hirooki Matsushita, Yutaka Ogino, Yuka Taguchi, Teruyasu Sugano, Tomoaki Ishigami, Kazuo Kimura, Satoshi Umemura
Yokohama City University Hospital, Yokohama, Japan
HEART FAILURE P 1-152

261
Introduction: In patients with acute heart failure (AHF), initial risk stratification using EKG parameters is poor validated. The present study aimed to elucidate the EKG parameter predicting clinical outcome in patients with AHF.
Methods: We evaluated the patients hospitalized for AHF in ten regionally-representative tertiary university hospitals who registered in the Korean Acute Heart Failure (KorAHF) Registry from March 2011 to February 2014. The EKG parameters including PR interval, QRS dura-tion, corrected QT interval and presence of atrial fibrillation (AF) were accessed.
Results: 5,625 patients were registered at KorAHF Registry. Mean age was 72.0±13.3 and 717 patients (40.5%) were male. Mean follow up duration was 777±408 days. AF, 1st degree AV block (PR 200 ms), QRS widening (QRS >120 ms) and QT prolongation (QTc > 500 ms) were documented in 27.6% (n=1550), 8.9% (n=500), 22.0% (n=1236) and 24.4% (n=1371), respectively. In Kaplan-Meier survival analysis, pa-tients with 1st degree AV block showed worse survivals rate than those without 1st degree AV block (P<0.01). Cox regression analysis re-vealed that presence of 1st degree AV block, age and decreased LVEF (EF<45%) were independently associated with out of hospital death.
Conclusions: 1ST degree AV block, traditionally accepted as benign finding, might be significantly associated with long-term clinical out-come in patients with acute heart failure. A combination of 1st degree AV block, age and LVEF might refine the accuracy of risk stratifica-tion in those patients.
FIRST DEGREE AV BLOCK AS A PARAMETER PREDICTING LONG-TERM PROGNOSIS IN PATIENTS WITH ACUTE HEART FAILURE_ FROM KOREAN ACUTE HEART FAILURE REGISTRY (KORAHF REGISTRY)Dae In Lee, Ju-Hee Lee, Sang-Min Kim, Jan-Whan Bae, Kyung-Kuk Hwang, Dong-Woon Kim, Myeong-Chan Cho
Chunbuk National University Hospital, Seoul, Republic of Korea
HEART FAILURE P 1-153

262
Introduction: Ebstein anomaly is frequently complicated by the supraventricular and ventricular arrhythmia. The components of the ar-rhythmic substrate are atrioventricular accessory pathways, the distended and damaged atrial or atrialized right ventricular myocardium, and atriotomy scar. The Cone procedure has been widely used for the Ebstein anomaly, in which the atrialized right ventricle (RV) was ver-tically plicated. We report an Ebstein anomaly case with early postoperative sustained ventricular tachycardia (VT) originating from the site of vertical plication.
Methods: A 13-year-old boy was diagnosed with Ebstein anomaly and he underwent the surgical correction using the Cone technique. The atrialized right ventricle was plicated vertically, and the right atrial reduction plasty was also done. The 5 days after operation, the monomorphic VT, with RBBB pattern superior axis QRS morphology, was shown while the patient having defecation, which was resistant to DC cardioversion, overdrive pacing, intravenous amiodarone and other antiarrhythmic drugs. His other vital signs were relatively stable despite of progressive cardiomegaly.
Results: The 17th day after operation, the electrophysiological study and radiofrequency (RF) catheter ablation was performed. The map-ping at the left ventricular septum showed that the earliest activation site was broad and 0 millisecond before the QRS beginning. Right ventriculography showed a recess pocket at the RV apico-septum by vertical plication of the Cone procedure. After the careful exploring RV septal area, the earliest signal was detected 26 milliseconds earlier than the QRS beginning of VT. The origin of automatic VT was found at the recess by the plication, where the VT was terminated successfully. There was no acute complication and VT-free for 6 months of follow-up.
Conclusions: We report the first case of early postoperative sustained VT following the Cone procedure. The RF ablation was safe and ef-fective, even during the very early valvuloplasty and ventriculoplasty condition of Ebstein anomaly.
SUCCESSFUL CATHETER ABLATION FOR EARLY POSTOPERATIVE VENTRICULAR TACHYCARDIA IN AN EBSTEIN ANOMALY PATIENT WITH CONE PROCEDUREKyung Jin Ahn1, Ja Kyoung Yoon1, Eun Jung Bae1, Mi Kyung Song1, Gi Beom Kim1, Chung Il Noh1, Se il Oh2, Woong Han Kim1 1Seoul National University Children’s Hospital, Seoul, Republic of Korea; 2Seoul National University Hospital, Seoul, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-155

263
Introduction: We have sometimes experienced junctional ectopic tachycardia (JET) after the surgery of congenital heart diseases. Howev-er it is hard to maintain the tachycardia in spite of various treatments. It has reported that Nifecalant (NIF), pure Ikr blocker was effective for post-operative JET. This study aimed to clarify which would be better medication for post-operative JET, amiodarone or nifecalant.
Methods: Fifteen post-operative JET patients who treated with amiodarone (AMD) or NIF in our hospital between 2011 and 2015 were in-cluded. To clarify the efficacy and the adverse events of those drugs, the patients characteristics, the efficacy, the change of JET rate, sys-tolic blood pressure (BPs), corrected QT interval (QTc) 3 hours after the initiation of medications, and the adverse events were compared between two groups: AMD and NIF, retrospectively. The effectiveness was defined by sinus conversion or more than 10% reduction of JET rate and stabilized hemodynamic status in 3 hours.
Results: In NIF in 5 and AMD in 10, the types of surgery were various from radical to palliative operation. The body weight, JET rate and catecholamine score were not significantly different between two groups [BW: NIF 3.3 kg and AMD 6.5 kg (P=0.08), JET rate NIF 190 bpm, AMD 187 bpm (P=0.73)]. The efficacy were 100% in NIF and 80% in AMD. The change of JET rate was tend to decrease in NIF than in AMD [NIF-21%, AMD-10% (P=0.057)]. BPs was not significantly different [NIF+35%, AMD+15% (P=0.35)]. The change of QTc was significantly different (NIF +24%, AMD +1%). Three patients died of non-arrhythmic reasons, NIF in one, AMD in two, respectively. NIF group had no ar-rhythmic events including torsade de points. AMD group had a case who required re-thoracotomy because of bradycardia and the other with liver dysfunction.
Conclusions: NIF could be superior to AMD in terms of the efficacy and adverse events to post-operative JET. However we should pay at-tention to torsade de points caused by the NIF induced QT prolongation.
WHICH WOULD BE BETTER MEDICATION FOR POST-OPERATIVE JUNCTIONAL ECTOPIC TACHYCARDIA, AMIODARONE OR NIFECALANT?Hisaaki Aoki, Yasuhiro Hirano, Tomohiko Tanaka, Kunihiko Takahashi, Sanae Yamauchi, Shigemitsu Iwai, Futoshi Kayatani
Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-156

264
Introduction: We experienced that the boy had heart failure by pacemaker due to complete atrioventricular block after radical operation of Fallot and the cardiac resynchronization therapy (CRT) was effective.
Methods: N/A
Results: 3 year-old-boy. He had radical operation in 2 year-old due to Fallot, pulmonary atresia and major aortopulmonary collateral ar-teries. At that time, the conduit pressed right coronary and made him complete atrioventricular block. We changed the conduit and im-planted epicardium leads at right atrium and right free wall. Pacing mode was DDD. After the operation, he suffered from heart failure and mediastinitis. The QRSduration was 131 ms. He also had dissynchrony of left ventricular by speckle tracking of echocardiography. Then, we assessed that cardiac resynchronization therapy was effective for him. However, epicardium leads were impossible for him be-cause of mediastinitis and pleural effusion. So, we tried CRT-P implantation by transvenous lead, nevertheless his body weight was still 10kg, and the therapy made him recovery. 4 months after the CRT-P implantation, we changed to epicardium leads. 1 month after the op-eration, we removed the transvenous leads without complications and venous obstruction.
Conclusions: CRT-P by transvenous leads was effective as bridging therapy even for the boy of 10 kg.
3 YEAR-OLD-BOY WITH HEART FAILURE DUE TO RIGHT VENTRICLE PACING FOR ATRIOVENTRICULAR BLOCK, CRT WITH TRANSVENOUS LEAD WAS EFFECTIVEMisugi Emi, Aoki Hisaaki
Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-157

265
Introduction: Since its introduction in 1971, the Fontan operation has consistently been the primary surgical technique used for palliation of patients with single-ventricle physiology Postoperative arrhythmias after the Fontan operation have been described since the procedure was introduced. The extracardiac conduit (ECC) Fontan procedure has been theorized to reduce the risk of sinus node dysfunction (SND) and atrial arrhythmia because of the avoidance of extensive atrial suture lines and exclusion of the atrial chamber from elevated systemic venous pressure.We aim to describe the prevalence of arrhythmia after ECC Fontan procedure in a single institution.
Methods: A retrospective study was done to evaluate the prevalence of post-operative arrhythmia in congenital heart disease patients who underwent ECC Fontan procedure in the National Cardiac Centre Harapan Kita, Jakarta, Indonesia from April 2006 to April 2016. Baseline characteristics and patients data were obtained from medical records, and post-operative arrhythmias were studied from ECG recordings.
Results: There were 63 patients who underwent ECC Fontan procedure during the time period. Median age was 5 years old (3-19 years), including 38 boys (60.3%) and 25 girls (39.7%). Post-operative arrhythmia occurred in 18 (28.6%) patients. The most frequent arrhythmias were significant sinus bradycardia in 5 patients (7.9%), sinus node dysfunction (sinus arrest or recurrent pause) in 3 patients (4.8%), total atrio-ventricular block (TAVB) in 2 patients (3.2%) and atrial rhythm in 2 patients (3.2%). All patients with TAVB underwent permanent pacemaker implantation before discharged. The duration of arrhythmia ranged from 2-24 days (median of 7 days).
Conclusions: The prevalence of arrhythmia after Fontan procedure with ECC technique in our institution was 28.6% with significant sinus bradycardia as the most frequent (7.9%).
PREVALENCE OF ARRHYTHMIA AFTER EXTRACARDIAC CONDUIT FONTAN PROCEDURE: A SINGLE INSTITUTION STUDYRahmalia Gusdina, Dicky A Hanafy, Poppy S. Roebiono, Sunu Budiraharjo, Yoga Yuniadi
Department of Cardiology and Cardiovascular Medicine Universitas Indonesia, Jakarta, Indonesia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-158

266
Introduction: Children and young adults with permanent pacemaker implantation (PPI) for complete heart block (CHB) have distinct characteristics from adults. The goal of the present study was to determine the etiology of CHB and long-term outcome for patients un-der 30 years of age who underwent PPI.
Methods: Retrospective review of 25 consecutive patients (15 girls, and 10 boys) between 11 and 30 years of age who received transvenous PPI for high grade atrioventricular block (AVB) at a tertiary centre from 1998 to 2015.
Results: Presenting symptoms were syncope or presyncope in 8 patients, effort intolerance in 7 (NYHA class 2 or 3) while 7 were asymp-tomatic. Paroxysmal third degree AVB or long pause was noted in 6 patients on Holter monitoring of which the baseline electrocardio-gram (ECG) was normal in 3 patients. Eleven (44%) patients had congenital heart disease (CHD) of which 1 was a single ventricle with chronic heart failure. A well-defined cause of AVB was seen in 15 (60%) patients [7 post-operative cardiac surgery, 2-post catheter abla-tion for supraventricular tachycardia, 5-autoimmune, 1 muscle dystrophy] rest were classified congenital or idiopathic. Five patients (20%) had definite markers of immunologic disease of which 1 had end stage lupus nephritis.Mean age at first implant was 16+8.5 years (6 months-30 years) of which 5 had prior implants (4 epicardial, 1 transvenous). Pacemakers were programmed in VVIR mode in 14, DDD in 6 and the rest VDD. Percentage of ventricular pacing was in the range 4-100. During mean follow-up period of 11.4±7.1 years, (6 months-32 years) at a median interval of 4 months, 19 patients needed generator change at elective replacement interval. Median interval for replacement was 5.25 years. There was no mortality, and most patients were asymptomatic without symptom recurrence, 3 developed nonspecific chest pain. There was significant improvement in effort tolerance as only 3 patients with chronic heart failure were in NYHA class 3 at follow-up.
Conclusions: CHB especially presenting as paroxysmal AVB is unusual in younger age, but should be considered as a possible etiology in patients presenting with recurrent episodes of syncope. Post surgical heart block is the most common cause and pacemaker implanta-tion not only resolves symptoms but also has better overall long term outcome.
CHARACTERISTICS AND LONG-TERM FOLLOW-UP OF YOUNG ADULTS FOLLOWING PERMANENT PACEMAKER PLACEMENT FOR COMPLETE HEART BLOCKAtul Prabhu, Lo Wei Lo, TC Tuan, T F Chao, J N Liao, Lee PC, SA Chen
Taipei Veterans General Hospital, Taipei, Taiwan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-159
267
Introduction: Cryoablation has been suggested as an alternative treatment for atrioventricular nodal reentrant tachycardia (AVNRT) and para-Hisian accessory pathway (AP) with low complication rate. The study reported the preliminary data about the success rate and com-plication rate in our center.
Methods: From February 2015 to June 2016, 29 patients with AVNRT and 8 patients with Para-Hisian AP were included.
Results: A total of 37 patients, 21 females and 16 males, underwent cryoablation procedure and mean age of procedure was 16.09±5.76 years. For patients with AVNRT, 23 (79.3%) was typical form, 3 was atypical form (10.3%), and another three had both typical and atypical form. The mean tachycardia cycle length (TCL) was 338.8 msec. For Para-Hisian AP, four was right mid-septal and another four was right anterior septal AP. The mean TCL was 378.8 msec for Para-Hisian AP related atrioventricular reentry tachycardia (AVRT). The median to-tal procedure time was 116 minutes (range 69-331 minutes), and the median fluoroscopy time was 26.5 minutes (range 10.2-99.5 min-utes). The Cryocatheter tip size was 4 mm for 4 patients, 6 mm for 21 patients and 8-mm in 13 patients. After median 7 try of cryomapping and 3 try of cryoablation, the arrhythmia substrate was successfully ablated in of 36 of 37 patients (97.3%). Seven developed Mobitz type II AVB, and the other one patient with Para-Hisian AP had transient 3rd degree AV block occurred, which lasted for 10 seconds, but none of them had permanent AV block or other complications. After mean follow-up of 8.8±5.1 months (range 0-16 months). There were two AVNRT recurrence (5.4%).
Conclusions: Cryoablation for AVNRT and Parra-Hisian AP in pediatric and adolescent patients is safe and effective. Whether recurrence rate is low as our result needs long term follow-up.
ACUTE OUTCOMES FOR CRYOABLATION OF PEDIATRIC PATIENTS WITH TACHYARRHYTHMIA IN TAIWAN: SINGLE CENTER REPORTKun-Lang Wu1, Shuenn-Nan Chiu2, Chun-Wei Lu2, Wei-Chieh Tseng2, Mei-Hwan Wu2 1Changhua Christian Hospital, Changhua, Taiwan; 2National Taiwan University Hospital, Taipei, Taiwan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-161

268
Introduction: Catecholaminergic polymorphic ventricular tachycardia (CPVT) and Long QT syndrome (LQTS) are a potentially lethal genet-ic arrhythmia syndrome. A syncope induced by exercise or emotional stress in a young patient with a structurally normal heart occurs in both LQTS and CPVT. This condition is associated with sudden cardiac death due to malignant ventricular arrhythmia. Ankyrin-B (ANK2) mutation is a very rare cause of Long QT syndrome (LQT4), which shows very diverse clinical manifestations such as sinus node dysfunc-tion, atrial fibrillation, catecholaminergic polymorphic ventricular tachycardia (CPVT), and torsades de pointes.
Methods: N/A
Results: We report a young patient who developed refractory exercise-related catecholaminergic polymorphic ventricular tachycardia, atrial tachycardia and resting bradycardia with a borderline QTc prolongation. The patient received implantable cardioverter-defibrillator and thoracoscopic left sympathectomy, as well as beta blocker. Nevertheless he experienced frequent ICD shock therapy for ventricular tachycardia or fibrillation provoked by emotional stress and exercise. By the comprehensive molecular genetic testing, the concurrent ANK2 and RyR2 mutation was finally confirmed.
Conclusions: We report the first genetically proven Korean LQT4, who also has concurrent RyR2 mutation.
CONCURRENT ANK2 AND RYR2 MUTATION IN A PATIENT WITH REFRACTORY TACHYCARDIAJakyoung Yoon
Seoul National University Children’s Hospital, Seoul, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-162

269
Introduction: Short QT syndrome (SQTS) is a recently-discovered inheritable arrhythmogenic disease of the heart characterized by abnor-mally short QT intervals (QTIs) on the ECG. Some studies indicate that female gender and black race have predisposition to QTI prolonga-tion. The current study therefore tries to identify SQTI in apparent healthy young African and Caucasian subjects.
Methods: 59 participants-41 Nigerians: 20 males (NM) age 20.60+3.08 years, 21 females (NF) age 19.19+2.04 years; 18 Brazilians: 8 males (BM) age 20.50+2.00 years, 10 females (BF); age 21.80+3.26 years. These were apparently healthy medical students. Pulse, blood pressure measurements, standardized ECG were made before and after 6 MWT. QTI was measured according to AHA/ACCF/HRS Recommenda-tions (2012). HR correction formulae were used: Bazett (QTcB), Fredericia (QTcF), Framingham (QTcFr). Predicted QTI by P.M. Rautaharju et al. (1992) was used: SQTI:≤88%=SQTI. Proposed “QT scale” by S.Viskin (2009) was used.
Results: NMs showed an increase in QT from 356+38.72 to 362+37.78, P=0.93; NFs also showed an increase from 345.71+30.43 to 354.29+34.14, P=0.049. In Brazilian participants QTI showed a decrease from 360±10.69 to 350+35.45 (P=0.25) and 382+30.48 to 368+36.76 (P=0.32) for males and females. QTcB: SQTI revealed in 20% of NMs and 4.8% of NFs, 30% of BFs; vSQTI-35% of NMs and 67.2% of NFs, 62.5% of BMs and 20% BFs; eSQTI-15% of NMs and 24% of NFs, 10% of BFs. QTcF: SQTI revealed in 20% of NMs and 19.2% of NFs, 37.5% of BMs and 10% BFs; vSQTI-35% of NMs and 28.8% of NFs; eSQTI-15% of NMs. QTcFr: SQTI revealed in 20% of NMs and 24% of NFs, and 37.5% of BMs and 10% BFs; vSQTI-10% of NMs and 24% of NFs. After the 6MWT, QTcB: SQTI revealed in 10% of NMs, 50% of BMs and 30% of BFs; vSQTI-20% of NMs and 43.2% of NFs, 25% of BMs and 40% BFs; eSQTI- 25% of NMs and 28.8% of NFs, 12.5% of BMs and 10% of BFs. QTcF: SQTI revealed in 50% of NMs and 19.2% of NFs, 20% of BFs; vSQTI-5% of NMs and 14.4% of NFs, 12.5% of BMs and 10% BFs; eSQTI-4.8% of NFs. QTcFr: SQTI revealed in 35% of NMs and 24% of NFs, 37.5 0f BMs and 10% of BFs; vSQTI-10% of NMs and 24% of NFs; eSQTI-4.8% of NFs. In NM 30% of showed an elongation in QTI with HR increase: QTc before vs. QTc after (P=0.004) and HR before vs. HR after (P=0.009). In NFs 57% showed prolongation of QT after HR increase: QTc before vs. QTc after (P=0.06) and HR before vs. HR after (P=0.003). In the Caucasians, 25% of males and 20% of females showed deceleration dependent SQTI. For QTI ≤88% of QTp as the upper limit, short QT was observed in 20% and 38% of NMs and NFs.
Conclusions: NFs and BMs have shorter QTI. Africans have a high prevalence of SQTI. QTp is a more appropriate method of SQTI identifi-cation.
SHORT QT INTERVAL IN YOUNG HEALHTY SUBJECTS OF AFRICAN AND CAUCASIAN RACE DURING 6-MINUTE WALK TESTTatiana Dronova, Afriyie Mintah Adu-Parkoh, Romidan Ewere Omodolor, Evangeline Ositelu
Kursk State Medical University, Kursk, Russian Federation
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-163

270
Introduction: QT prolongation has been known to increase the risk for arrhythmic events, particularly in long QT syndrome. Sudden cardi-ac death (SCD) due to ventricular arrhythmia is a main cause of mortality in hypertrophic cardiomyopathy (HCM). However, whether QT in-terval predicts SCD or cardiac events in patients with HCM remains largely unknown.
Methods: Total 129 consecutive patients with HCM was studied. Primary endpoint was SCD events, and secondary endpoints included syncope, atrial fibrillation, ventricular tachycardia/fibrillation, stroke, cardiovascular death and all-cause death. The clinical outcomes were compared between patients with QTc≥480 ms (n=32) and those with QTc <480 ms (n=97).
Results: Mean age was 63.5 years old at diagnosis and mean duration of followed-up was 119±7 months since initially diagnosed with HCM. Patients with apical HCM were 48.8%. Compared to patients with QTc<480 ms, patients who had QTc≥480 ms showed a signifi-cantly wider QRS width (106.9 vs. 97.0 ms, P=0.05), larger left atrial size (46.4 vs. 42.7 mm, P=0.036), whereas having lower rate of systolic anterior motion of mitral leaflet. Logistic-regression using a multivariate model showed QTc≥480 ms was significantly associated with cardiovascular death (OR 13.571, 95% CI 1.457-126.398, P=0.022) and marginal association with SCD (OR 9.828, 95% CI 0.984-98.125, P=0.052). Kaplan-Meier analysis showed that the rate of SCD event-free survival was significantly lower in patients with QTc≥480 ms compared to those with QTc<480 ms (91.8% vs. 98.8%, P=0.025 by log-rank) during mean 10 years of follow-up period, as well as cardio-vascular death (87.7% vs. 98.8%, P=0.007 by log-rank). There was no significant difference in incidence of syncope, stroke and all-cause mortality between two groups.
Conclusions: QTc interval ≥480 ms is associated with life-threatening cardiovascular events in patients with HCM. This study suggests that the prolongation of QTc interval can be considered a risk factor for SCD in patients with HCM, leading to change the current guideline.
PROLONGATION OF CORRECTED QT INTERVAL PREDICTS THE RISK FOR CARDIAC DEATH IN PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHYHyungdon Kook, Jong-Il Choi, Mi-Na Kim, Suk-kyu Oh, Yun Gi Kim, Hee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-Young Roh, Jaemin Shim, Jin Seok Kim, Hong Euy Lim, Young-Hoon Kim
Korea University College of Medicine and Korea University Medical Center, Seoul, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-164

271
Introduction: Congenital myopathy is a rare genetic muscle disorder. Pulmonary vein isolation (PVI) represents a valid treatment option in patients with atrial fibrillation. However, no studies have reported on PVI in patient with congenital myopathy.
Methods: N/A
Results: A 55-year-old woman with a history of congenital myopathy (Nemaline myopathy) and dilated cardiomyopathy like heart was re-ferred to our hospital for the treatment of congestive heart failure and persistent atrial fibrillation (AF) lasting less than 1 year refractory to amiodarone. Regarding her past medical history, about 40 years ago, she developed limbs weakness. She was diagnosed congenital my-opathy at 40 years old when she developed congestive heart failure due to severe left ventricular (LV) dysfunction and largely dilated LV (LV ejection fraction 25%). Then, implantable cardioverter defibrillator (ICD) was implanted as primary prevention. Three months prior to treatment of AF, inappropriate ICD shock was delivered due to AF refractory to amiodarone. Therefore, she underwent pulmonary vein isolation (PVI). PVI by radiofrequency energy was performed with an irrigated tip catheter, using double circular multipolar catheter, navi-gated by electroanatomical mapping system (CARTO3 system). Bilateral pulmonary veins were successfully isolated. No acute reconnec-tion was observed during continuous isoproterenol (ISP) administration after PVI. No dormant conduction was detected and no non-PV foci was provoked with intravenous infusion of adenosine triphosphate during continuous ISP administration after PVI. Cardiac involve-ment is not an uncommon complication of congenital myopathy. It can manifest as dilated cardiomyopathy, hypertrophic cardiomyopathy, or as restrictive cardiomyopathy. Although it has been reported that the prevalence of AF in patient with primary myopathies amounted to 6.1%, to the best of our knowledge, there was no case of congenital myopathy with AF treated by PVI in the literature.
Conclusions: We have experienced a case of AF with congenital myopathy, which was successfully treated with catheter ablation.
SUCCESSFUL CATHETER ABLATION FOR ATRIAL FIBRILLATION IN A PATIENT WITH CONGENITAL MYOPATHYYasuki Koyano, Takeshi Kitamura
Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-165

272
Introduction: Atrial fibrillation (AF) is a common complication in elderly patients with congenital heart diseases (CHDs). The purpose of this study was to examine the efficacy of the maze procedure in these patients.
Methods: Between January 2000 to December 2013, 74 patients underwent the maze procedure as a concomitant operation with congen-ital heart disease. The mean follow-up duration was 68.6±42.0 months. Electrocardiography was performed 1 month, 3 month, 6 month, and 1 year after surgery, and checked annually after that.
Results: Mean age was 45.7±17.6 and male was 33 of 74. CHDs were consisted of simple shunt disease (ASD, VSD) and complex CHDs (TOF, Ebstein’s anomaly, and single ventricle (SV)). Biatrial Maze was underwent in 48 patient, right-sided maze was 23, and left-sided maze was 3. AF persisted in 9 patients after surgery and 3 patients were not followed. When including the patients who took antiarrhyth-mic drugs, 80% were in sinus rhythm. Freedom from AF recurrence at 6 month, 1 year, 2 year, 3 year, and 5 year after surgery were 97.8±2.1, 95.7±3.0, 93.5±3.7, 91.1±4.3, and 85.8±5.4, retrospectively. There are two early mortality and one late mortality after operation. In comparison of freedom from AF recurrence according complexity of CHDs, types of Maze, and cardiac surgery experiences, there was no significant difference.
Conclusions: Concomitant treatment with the maze procedure and CHDs repair is safe and effective for restoring the sinus rhythm.
OUTCOME OF THE MAZE PROCEDURE IN PATIENTS WITH CONGENITAL HEART DISEASESSangyun Lee, Chang-Ha Lee, Seong-Ho Kim, Sang-Won Park
Sejong General Hospital, Bucheon, Republic of Korea
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 1-166

FRIDAYPOSTER PRESENTATION
(14 October)

274
Introduction: Endothelial progenitor cells (EPGs) are released in to the circulation after myocardial injury to improve tissue repair. Radiof-requency ablation (RFA) of cardiac arrhythmias particularly for atrial fibrillation has been shown to trigger the release of EPGs through in-flammatory mediators. We hypothesized that EPGs can still be detected in the circulation after non-extensive ablations like slow pathway or accessory pathway ablations which has not been studied before.
Methods: Twenty-nine patients (14 male, 54 [18-74] years old) who underwent radiofrequency ablation of slow pathway for atrioventricular nodal reentrant reentrant tachycardia (n=21) and accessory pathway ablation for atrioventricular reentrant tachycardia (n=8) were includ-ed. Peripheral blood percent change in CD34+ cell count (%ΔCD34+) and multiple serologic markers [troponin I, C-reactive protein (CRP), interleukin-6, stromal cell derived factor 1 alpha were evaluated before and after ablation (7 and 30 days).
Results: The %ΔCD34+ cells was significantly increased seven days after the ablation compared to baseline (22,6 [5-79] vs. 33 [15-133], P<0.001). Troponin-I and CRP were also significantly higher seven days after ablation which are markers of tissue injury and systemic in-flammation, respectively. SDF1-α;; , a chemokine which is a messenger for mobilization of EPGs did not differ post ablation day 7 or day 30 compared to baseline. The amount of energy applied during RFA was significantly correlated with the rise in % ΔCD34+ (r=0.4, P=0.001).
Conclusions: Peripheral blood EPGs are increased after slow pathway or accessory pathway ablations which are less extensive ablations compared to atrial fibrillation ablation. The levels return to basal levels by thirty days post-ablation. The rise in EPGs was correlated to the amount of energy delivered during RFA.
THE EFFECT OF RADIOFREQUENCY ABLATION ON STEM CELLS AND SYSTEMIC INFLAMMATION IN PATIENTS WITH SUPRAVENTRICULAR TACHYCARDIAAhmet Lutfu Sertdemir1, Ilknur Can1, Hall Ibrahim Erdogan1, Bahadir Fevzioglu1, Mehmet Tokac2 1Necmettin Erbakan University, Konya, Turkey; 2Katip Celebi University, Izmir, Turkey
BASIC/TRANSLATIONAL SCIENCE P 2-001

275
Introduction: There is evidence suggesting that heat shock proteins may protect against clinical atrial fibrillation (AF). Recently investiga-tors have been reported that the HSP inducing compound GGA prevents atrial remodeling induced by AF and attenuates the promotion of AF. An important key factor in AF promotion is that atrial cardiomyocytes have constitutively active acetylcholine-activated K+ (IKACh) current that is enhanced by the tachycardia. However, it is not clear whether GGA can regulate the IKACh. We examined the effect of GGA on IKACh current in mouse atrial cardiomyocytes and in vitro atrial cell line (HL-1) model of tachycardia remodeling.
Methods: In the present study, the IKACh current was recorded using a nystatin-perforated whole cell patch-clamp technique following acti-vation by acetylcholine (10 μM for 2 minutes). After the measurement of the baseline IKACh current, atrial cardiomyocytes were treated with GGA 10 μM for 10 minutes and the IKACh current was re-measured. HL-1 myocytes were tachypaced by stimulating at 5 Hz with square-wave 10-ms pulses. Results of paced cells were compared with non-paced cells studied in parallel.
Results: IKACh current in mouse atrial cardiomyocyte treated with acetylcholine was significantly increased, which was markedly attenuat-ed by GGA 10 μM treatment (n=5, peak; 54±11.2%, quasi-steady-state; 58±11.4%, P<0.001). In addition, GGA recovered acetylcholine-in-duced APD shortening. GGA-treated paced myocytes were significantly increased all major heat shock proteins, including HSP90, HSP70 and HSP27. Also, GGA attenuated tachypaing-induced reactive oxygen species (ROS) and nitric oxide production (NO). To evaluate the pathway of GGA on the regulation of IKACh, we co-treated with GGA and wortmannin, PI3K inhibitor, and the results indicated that WMN completely blocks GGA’s IKACh current blocking effect.
Conclusions: This study provides important evidences that the HSP inducer GGA facilitates its potent antiarrhythmic effect by inhibiting IKACh, and blocking ROS production which underlies electrical remodeling in mammalian atrial cardiomyocytes. Furthermore, the results of this study indicate possible therapeutic benefit of GGA able to boost the expression of heat shock protein in patients with AF.
HEAT SHOCK PROTEIN INDUCER GERANYLGERANYLACETONE (GGA) PROTECTS AGAINST ATRIAL FIBRILLATION VIA THE PI3K PATHWAYEun Kyoung Choi, Ga-In Yu, Bong Joon Kim, Dong Hyeon Park, Tae-joon Cha
Cardiovascular Research, Kosin University Gospel Hospital, Busan, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-002

276
Introduction: Ethanol exerts biological effects through multiple receptors, including ion channels. Receptor desensitization is a nearly universal phenomenon among these channels, and its modulation by ethanol may be a crucial aspect of alcohol pharmacology. Alcohol intoxication may induce atrial fibrillation (AF)-prone cellular electrophysiological changes and arrhythmias, primarily AF. Modifications of inward rectifier potassium currents have been implicated in the pathogenesis of AF. However, the mechanisms underlying the potential association between acute ethanol exposure and AF remain unclear. Therefore, we hypothesized that alcohol may affect acetylcholine (ACh)-activated K+ current in atrial cardiomyocytes.
Methods: In the present study, IKACh current was recorded using a nystatin-perforated whole cell patch-clamp technique following activa-tion by ACh (10 μM for 2 minutes). After the measurement of baseline IKACh current, atrial cardiomyocytes were exposed to ethanol (100 mM for 10 minutes) and IKACh current was re-measured. Current-voltage (I-V) curves were obtained from the current response induced by voltage ramps between -120 and +60 mV from the holding potential of -40 mV.
Results: Application of ACh (10 µM) to the bath solution promptly activated IKACh in mouse atrial cardiomyocytes. After switching the bath solution to an ethanol mixed solution, IKACh desensitization was attenuated and the plateau phase (quasi-steady-state) of IKACh current was prolonged. The ethanol-induced prolongation of the plateau phase was slowly decreased 4-5 minutes thereafter. The amplitude of IKACh upon second exposure to ACh was similar to that upon initial exposure. The characteristics of IKACh activation and plateau phase prolonga-tion by ethanol were further investigated using current-voltage (I-V) curves. The I-V curve in the presence of ethanol was significantly larg-er than that in the presence of ACh. In addition, tertiapin-q inhibited the activation of IKACh current as well as plateau phase prolongation by ethanol, while atropine did not.
Conclusions: Our results indicated that ethanol prolongs the duration of the plateau phase (quasi-steady-state) of ACh-activated K+ cur-rent. This is the first study demonstrating the effects of ethanol on atrial IKACh, which could explain the mechanism of AF initiation resulting from heavy alcohol drinking.
ETHANOL INDUCES PROLONGATION OF THE PLATEAU PHASE OF ACETYLCHOLINE-ACTIVATED K+ CURRENT IN MOUSE ATRIAL CARDIOMYOCYTESEun Kyoung Choi, Ga-In Yu, Bong Joon Kim, Dong Hyeon Park, Tae-joon Cha
Cardiovascular Research, Kosin University Gospel Hospital, Busan, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-003

277
Introduction: Acetylcholine-activated K+ channels are distributed in the atrium of the human heart and contribute to atrial repolarization. Recently, the upregulation of IKACh and muscarinic receptor expression has been reported in atrial fibrillation (AF) patients and in AF in-duced experimentally in dogs. Therefore blockage of IKACh could terminate AF induced by increased vagal tone. Blockade of atrial-specific K+ channels (IKur and/or IKACh) could provide an approach for the treatment of atrial arrhythmia without adverse ventricular effects. Ran-domized trials have demonstrated that β-AR blockers have beneficial long-term effects on mortality and morbidity in patients with heart failure. However, not all β-blockers have identical effects, and the use of various β-AR blockers in AF has yet to be thoroughly evaluated. Therefore, we examined the effects of carvedilol and atenolol on acetylcholine-activated K+ channels in mouse atrial cardiomyocytes.
Methods: In the present study, IKACh current was recorded using a nystatin-perforated whole cell patch-clamp technique. Mouse atrial car-diomyocytes were voltage clamped at -40 mV, and IKACh was activated by extracellular application of acetylcholine (Ach, 10 μM for 2 min-utes). After the baseline IKACh current was measured, varying concentrations of β-AR blockers were applied for 5 minutes, and a second IKACh current was recorded. Action potential duration (APD) and current-voltage (I-V) curves were recorded from isolated atrial myocytes.
Results: The application of acetylcholine (10 μM) to the bath solution activated IKACh in mouse atrial myocytes. Carvedilol inhibited acetyl-choline-activated K+ current (IKACh) in a dose-dependent manner between 0.1 and 5 μm. The concentration required for half-maximal inhi-bition (IC50) was 1.03 μm for the peak and 1.04 μm for the quasi-steady-state. In addition, carvedilol attenuated acetylcholine-induced APD shortening. We next investigated the effects of atenolol on IKACh using the same experimental protocol. Addition of atenolol to the bath solution did not alter the peak amplitude or quasi-steady-state of the IKACh currents compared to controls.
Conclusions: We found that the β blocker carvedilol suppressed acetylcholine-activated potassium current, while another β blocker, aten-olol, did not. Blockade of atrial K+ channels by carvedilol provides another potential option for the treatment of AF. These findings suggest that carvedilol may be used in AF as an atrial-specific antiarrhythmic agent.
DIFFERENTIAL EFFECTS OF CARVEDILOL AND ATENOLOL ON ACETYLCHOLINE-ACTIVATED K+ CURRENT: POSSIBLE ATRIAL-SPECIFIC ANTIARRHYTHMIC EFFECTS OF CARVEDILOL ON ATRIAL FIBRILLATIONEun Kyoung Choi, Ga-In Yu, Bong Joon Kim, Dong Hyeon Park, Tae-Joon Cha
Cardiovascular Research, Kosin University Gospel Hospital, Busan, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-004

278
Introduction: Resveratrol downregulated fibrosis in LA and regulated variation in ionic channels to reduce AF through the PI3K-AKT sig-naling pathway. The PI3K-AKT pathway is reported to activate downstream of HIPPO-YAP. The aim of this study was to testify the hypothe-sis that the resveratrol enhances HIPPO-YAP through activation PI3K/AKT pathway to down-regulate VA.
Methods: HF rabbits are created 4 weeks after undergoing coronary ligation. Group 1 (n=6) included (a) normal; (b) HF sham; (c) HF rab-bits treated for 1 week with intraperitoneal injections of resveratrol; (d) resveratrol+wortmannin, and (e) resveratrol+diphenyleneiodonium chloride (DPI). All rabbits underwent epicardial catheter stimulation. Collagen content, mRNA and protein expression in ionic channels, and PI3K/AKT and HIPPO-YAP signaling pathways are studied in LV. To investigate acute drug effects on LV electrophysiology, Groups 2 a-e (n=6) are subjected to Langendorff perfusion.
Results: The level of Yap1 protein was increased , and the espression of cleaved-caspase 3 was decreased in HF LVs after treated with resveratrol. The activity of PI3K- p85 and p-AKT were also up-regulated in HF LV after treated with resveratrol (Figure A). Compared to HF LVs, a-caspase 3 was decreased in HF LVs after treated with resveratrol (Figure B).
Conclusions: Resveratrol enhances cardiomyocyte survival and decreases apoptosis through Hippo-YAP signaling pathway.
RESVERATROL PROMOTES CARDIOMYOCYTE SURVIVAL AND DECREASES APOPTOSIS THROUGH HIPPO-YAP SIGNALING PATHWAYYu-Ting Huang
Taipei Veterans General Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 2-005
279
Introduction: Cardiac delayed rectifier potassium channel dysfunction due to hERG mutation causes congenital long QT syndrome type 2, which leads to fatal ventricular tachyarrhythmia, Torsade de Pointes and sudden cardiac death. hERG mutations are associated with con-genital cardiac disorder, fetal death and defect in cardiac development, but the mechanism of it is still unrevealed. A561V-hERG is a mis-sense mutation whose 561th amino acid alanine is substituted by valine, causing mutate protein accumulate in endoplasmic reticulum, membrane localization inefficiency and decreased IKr. Unfolded (or misfolded) protein reaction (UPR) is the most common trigger of en-doplasmic reticulum stress. Proteins failed to get properly folded accumulated in endoplasmic reticulum causes a series of downstream reaction which called UPR. When UPR occur, the endoplasmic reticulum stress can be switched on by several pathways, result in in-creased chaperone expression, decreased global translation, endoplasmic reticulum associated degradation and even apoptosis. Based on these theories did we propose a hypothesis that hERG mutation causes cardiomyocyte apoptosis via endoplasmic reticulum stress pathway.
Methods: In order to investigate the potential role of ER stress in A561V mutation caused cell apoptosis we constructed the plasmid as vector contain A561V-hERG and transient transfected to HEK293 cell to imitate patients’ cardiomyocyte with homozygous A561V-hERG mutation. The WT-hERG plasmid is also transfected to HEK293 cell as a control. The certain cells are treated with endoplasmic reticulum stress inhibitor 4-PBA 40 mmol/L for 4 hours. We detect the cell apoptosis level by Hoechst33342 staining. The ER stress associated pro-tein express level such as GRP78 is confirmed by western blotting.
Results: We found that A561V-hERG protein accumulated in the HEK293 cell endoplasmic reticulum while barely have no membrane ex-pression. Apoptosis can be observed more often in A561V-hERG cells compared with the WT cells and heterozygous A561V-WT-hERG mutation. These observations can be reversed under the ER Stress inhibitor 4-PBA treatment. The endoplasmic reticulum stress protein GRP78 is increased in A561V-hERG cells compared with WT-hERG cells (P<0.05), and can be reversed by endoplasmic reticulum stress inhibitor 4-PBA.
Conclusions: This research confirmed that hERG mutation A561V-hERG can cause cell apoptosis in transfected HEK293 cell model. The apoptosis may be caused via endoplasmic reticulum stress pathway.
MISSENSE MUTATION A561V-HERG CAUSES CARDIOMYOCYTE APOPTOSIS VIA ENDOPLASMIC RETICULUM STRESS PATHWAYShuting Ma1, Yun Zhao1, Chaofeng Sun2 1The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China; 2Xi’an Jiaotong University College of Medicine, Xi’an, China
BASIC/TRANSLATIONAL SCIENCE P 2-007
280
Introduction: Poor cell survival post transplantation heavily limits the therapeutic benefits of mesenchymal stem cells (MSCs) in myocar-dial infarction (MI). Hepatocyte growth factor (HGF) is a very important cytokine for angiogenesis, anti-inflammation and anti-apoptosis. This study aimed to evaluate the cardioprotective effects of MSCs overexpressing HGF in a mouse model of MI.
Methods: The apoptosis of umbilical cord-derived MSCs (UC-MSCs) and HGF-UC-MSCs under normoxic and hypoxic conditions was measured by TUNNEL staining. The conditioned medium (CdM) of UC-MSCs and HGF-UC-MSCs under a hypoxic condition was harvest-ed and the protective effects of CdM on Neonatal cardiomyocytes (NCMs) under a hypoxic challenge were examined. UC-MSCs and HGF-UC-MSCs were transplanted into the peri-infarct region following MI in mice. Heart function was examined at 4 weeks post cell trans-plantation.
Results: Compared with UC-MSCs, apoptosis was remarkably decreased in HGF-UC-MSCs under hypoxic challenge. The apoptosis of NCMs induced by hypoxia was significantly reduced when co-cultured with HGF-UC-MSCs hypoxic CdM (HGF-UC-MSCs-hy-CdM) com-pared with UC-MSCs hypoxic CdM (UC-MSCs-hy-CdM). ELISA showed that the concentration of some growth factors including HGF, EGF, bFGF and VEGF was dramatically increased in HGF-UC-MSCs-hy-CdM compared with UC-MSCs-hy-CdM. Transplantation of HGF-UC-MSCs significantly improved heart function, decreased infarct size, inhibited cardiomyocyte apoptosis and enhanced angiogenesis com-pared with UC-MSCs. Moreover, the survival rate of HGF-UC-MSCs in the ischemic heart was much higher than UC-MSCs.
Conclusions: Overexpression of HGF significantly improves MSCs survival in the harsh environment and increases the paracrine effects. This study might provide a novel therapeutic strategy for MSC-based therapy in cardiovascular disease.
ENHANCED CELL SURVIVAL AND PARACRINE EFFECTS OF MESENCHYMAL STEM CELLS OVEREXPRESSING HEPATOCYTE GROWTH FACTOR PROMOTE CARDIOPROTECTION IN MYOCARDIAL INFARCTION MYOCARDIAL INFARCTIONFengxiang Zhang, Liyan Zhao, Xiaolin Liu, Yan Xu, Zhen Fang
The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
BASIC/TRANSLATIONAL SCIENCE P 2-008

281
Introduction: Although it is known that autonomic nervous system (ANS) plays a significant role in atrial fibrillation (AF), its effects on the cardiac wave dynamics of AF are not fully understood. In this in silico study, we modeled the ANS in the left atrium (LA), and examined the effects of ANS on the cardiac wave dynamics of AF.
Methods: Ionic currents in the human atrial action potential model of Courtemanche et al. were adjusted and incorporated into a single cell and 3D realistic LA model. The morphology of the GP and nerves was modeled based on the “Octopus hypothesis”. A model of acetyl-choline (ACh)-activated potassium current was used to examine the effect of ACh. Complex fractionated atrial electrogram (CFAE) cycle length was calculated for the models integrated by 10 patients’ LA geometry.
Results: 1) Single cell model exhibited a late Phase 3 Early after-depolarization (EAD)-like depolarization immediately after rapid pacing with ACh stimulation (ACh-stim, 0.03 μM). 2) Spontaneous pulmonary vein (PV) tachycardia was observed at left atrial (LA)-PV junction af-ter ACh-stim on GPs and isoproterenol stimulation (5×ICa-L) in 3D model. 3) During AF state, PV triggers near GP area were shown under the ionic current conditions of sustained AF. 4) GP stimulation reduced complex fractionated atrial electrogram (CFAE) cycle length (CL; 137±18 ms to 127±14 ms, P<0.001) and maintenance duration of phase singularities (PS), (66±100 ms to 60±88 ms, P<0.001), and in-creased co-localized GP area with CFAE-CL≤120 ms area (2.9% to 25.1%, P<0.001).
Conclusions: Simultaneous GP and ICa-L stimulation induced triggered activity from LA-PV junction and PV tachycardia, changing wave-dy-namics of AF maintenance mechanism in single cell and 3D in silico octopus-GP model of the LA.
GANGLIONATED PLEXI STIMULATION INDUCES PULMONARY VEIN TRIGGERS AT LEFT ATRIUM-PULMONARY VEIN JUNCTION CHANGING WAVE-DYNAMICS: IN SILICO MODELING STUDYMinki Hwang1, Byounghyun Lim1, Jun-Seop Song1, Young-Seon Lee1, Eun-Bo Shim2, Hui-Nam Pak1 1Yonsei University Health System, Seoul, Republic of Korea; 2Kangwon National University, Chuncheon, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-009

282
Introduction: We previously reported that stable rotors were observed in in-silico human atrial fibrillation (AF) models, and well repre-sented by dominant frequency (DF). We explored spatiotemporal stability of DF sites in patients’ left atrial (LA) CT image imported 3D-AF modeling.
Methods: The 3-D homogeneous in-silico model of human LA was reconstructed by EnSite NavX® system (Endocardial Solutions, St. Jude Medical, Inc., St. Paul, MN, USA) with CT image data of 10 clinical persistent AF patients (male 80%, 61.8±13.5 years old). After in-duction, we obtained 6 seconds AF mapping for DF analyses in every 30 seconds interval (T1-T9). LA was divided by 10 sections. Spatio-temporal changes of DF and variation of temporal consistency were evaluated at each sections of LA. High DF area was defined as the area with the highest 10% DF.
Results: 1) There was no spatial consistency of high DF distribution at each LA sections during T1-T9 except for one patient (P=0.027). 2) Coefficients of variation for the high DF area were highly different among 10 LA sections (P<0.001), and it was significantly higher in 4 pul-monary vein (PV) areas, LA appendage, and peri-mitral area than other LA sections (P<0.001). 3) When we conduct virtual ablation of 10, 15, and 20% of the highest DF areas, AF was changed to atrial tachycardia (AT) at the rate of 39, 48, and 64%, respectively.
Conclusions: Spatiotemporal consistency of DF area was observed in 10% of AF patients, and high DF areas were temporally variable, es-pecially on PV, LA appendage, or peri-mitral areas. Virtual ablation of DF is effective in AF termination and changing into AT.
THE SPATIOTEMPORAL STABILITY OF DOMINANT FREQUENCY SITES IN IN-SILICO MODELING OF 3-DIMENSIONAL LEFT ATRIAL MAPPING OF ATRIAL FIBRILLATIONByounghyun Lim, Minki Hwang, Jun-Seop Song, Young-Seon Lee, Boyoung Joung, Hui-Nam Pak
Yonsei University Health System, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-010

283
Introduction: We reported that stable rotors were observed in in-silico human atrial fibrillation (AF) models, and well represented by dominant frequency (DF). We hypothesized that the effects of DF ablation at different condition of conduction velocities (CVs) in patients’ left atrial (LA) CT image imported 3D-AF modeling.
Methods: We integrated 3-D CT images of LA obtained from 10 patients with persistent AF (male 80%, 61.8±13.5 years old) into in-silico AF model and generated the conditions with CVs 0.4 m/s, 0.5 m/s, and 0.6 m/s by changing diffusion coefficient. After AF induction, we measured AF maintenance duration (max 280 seconds) and conducted DF analysis and virtual DF ablation in every 30 seconds interval at 3 different CVs. Virtual DF ablations were targeted to 10, 15, and 20% of the highest DF areas, and AF termination and conversion to atrial tachycardia (AT) were determined within 30 sec after virtual interventions.
Results: 1) AFs were induced and maintained over 280 seconds in 100% at 0.4 m/s condition. However, AFs were induced in 70% but ter-minated within 33.5±27.5 seconds at 0.5 m/s condition (P<0.001), and induced in 50% and terminated in 15.2±7.3 seconds at CV 0.6 m/s condition (P<0.001), respectively. 2) At 0.4 m/s condition, DF ablation induced AF termination rates were 1% after 10% highest DF abla-tion, 1% after 15% highest DF ablation, and 4% after 20% highest DF ablation. 3) Virtual DF ablation resulted in higher AF termination rates in CV 0.5 m/s condition (P<0.001); 20, 60, and 40% after 10, 15, and 20% highest DF ablations, respectively). 4) At 0.6 m/s condition, AF termination rates were 67, 50, and 50% after 10, 15, and 20% highest DF ablations, respectively (P<0.001). 5) In the episodes DF abla-tion followed by AF termination, baseline AF maintenance duration (without ablation) was significantly shorter than those without AF ter-mination (73.7±97.2 seconds vs. 231.5±59.8 seconds, P<0.001).
Conclusions: DF ablation terminated AF more likely under the condition with easily terminating AF, but not long-lasting sustaining AF condition.
DOMINANT FREQUENCY ABLATION TERMINATES ATRIAL FIBRILLATION DEPENDING ON CONDUCTION VELOCITY IN-SILICO 3-DIMENSIONAL MODEL OF LEFT ATRIUMByounghyun Lim, Minki Hwang, Jun-Seop Song, Young-Seon Lee, Boyoung Joung, Hui-Nam Pak
Yonsei University Health System, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 2-011

284
Introduction: Risk factor modification improves outcomes for patients with atrial fibrillation (AF). However, whether there is a difference in benefits between genders has not been characterised.
Methods: Of 1,415 consecutive patients referred for electrophysiology management of AF, 825 had BMI≥27 kg/m2 and were offered weight management. After screening for exclusion criteria, 355 were included in this analysis. Patients were divided into gender (Male: 234, Female: 121) to undertake analysis.
Results: Females were significantly older (68±10 vs. 61±10, P<0.001) with greater BMI (34.3±5.5 vs. 32.7±4.0, P=0.009) and normal-ized cardiorespiratory fitness (97±35 vs. 85±18%, P=0.001) compared to male patients. Notably, females were more likely to have parox-ysmal AF compared to males (53.5% vs. 30%, P<0.001) yet were equally symptomatic. The mean number of anti-arrhythmics was re-duced from baseline to follow-up with no significant effect of gender (P=0.092). There was no difference between genders in requirement for catheter ablation. There was similar risk factor clinic attendance between genders (Males 58.7%, Females 60%, P=0.82). Gender was not a significant predictor of weight loss or fitness gain (P>0.05). With every 1-kg weight loss, there was a significant reduction in AF re-currence for both males (HR: 0.97, 95% CI: 0.95-0.99) and females (HR 0.97, 95% CI: 0.95-1.0). Weight loss was a significant predictor of AF symptom improvement (P<0.001), with no effect of gender (P=0.88). For fitness improvement, the benefits of each 1-MET gain on AF recurrence were similar for both genders (Male: HR 0.86, 95% CI 0.77-0.95; Female: HR 0.83, 95% CI 0.71-0.96).
Conclusions: Despite gender differences at baseline with regards to AF type, age, BMI and cardiorespiratory fitness, the benefits of weight loss and fitness gain are equally favourable for both men and women. This study reinforces the need to address lifestyle risk factors to mi-nimise arrhythmia recurrence and reduce symptom severity for all individuals.
BENEFITS OF RISK FACTOR MODIFICATION ON AF RECURRENCE STRATIFIED BY GENDERMelissa Middeldorp, Adrian Elliott, Rajeev Pathak, Megan Meredith, Rajiv Mahajan, Dennis Lau, Prashanthan Sanders
Centre for Heart Rhythm Disorders, Adelaide, Australia
ALLIED PROFESSIONALS P 2-012

285
Introduction: The Riata family ICD leads have been reported of early failure from insulation defect with externalized conductors (EC). We found an up to 10% EC rate after a median time of 3.4 years post implantation. A screening program with device interrogation and fluo-roscopy has been conducted since then. Here we report the 4-year additional follow up data.
Methods: All patients implanted with Riata ICD lead who had their follow up visit at our institute were scheduled for fluoroscopy and de-vice interrogation at a 4-8 months interval. EC was classified into 5 grades, 0=normal, 1=separation of conductor, 2=one extruding exter-nal conductor, 3=two extruding external conductors and 4=fracture of conductor wire. Parameter of interest included new or progression of EC, shock failure, lead extraction, lead replacement, and death.
Results: Total of 40 patients were enrolled in this study. Mean age was 58 (range 21-86) years, and most (82.5%) were male. The preva-lence of EC was 10% (4 cases, all were grade 1 with normal electrical function) at a median duration of 3.4 years from implantation. After this early period of follow up, no new incidence or progression in previous EC, 8 patients died, 6 from non-cardiac causes included 2 EC cases, 1 from heart failure. One patient suffered sudden death which was presumed to be arrhythmic death. He recently had device inter-rogation and fluoroscopy two months prior to death which did not reveal any electrically abnormality. Fourteen patients underwent device generator change. Of these, two patients had their lead extracted and re-implanted with new ICD lead. One patient had a new ICD lead in-serted with abandon Riata lead. None of the extracted leads had any defect. There has been no additional EC case during the 4-year ex-tended period of follow up.
Conclusions: The prevalence of EC in Riata leads is significantly high (10%) early after implanted. However, with long-term follow up, the EC rate declined obviously.
LOW PREVALENCE OF EXTERNALIZED CONDUCTOR AND ELECTRICAL ABNORMALITIES IN RIATA LEAD AFTER LONG TERM FOLLOW UP: A SINGLE CENTER EXPERIENCENapawan Pornnimitthum, Arisara Suwanagool, Satchana Pumprueg, Warangkna Boonyapisit, Arjbordin Winijkul, Charn Sriratanasathavorn
Mahidol University, Bangkok, Thailand
ALLIED PROFESSIONALS P 2-013

286
Introduction: Perioperative cardiac events after non-cardiac surgery might be a serious problem among the aging population in recent years. By modifying the ACC/AHA guideline for non-cardiac surgery 2007, we developed a cardiovascular screening system as Cardiovas-cular Preparative Screening (CPS) in order to evaluate necessity of cardiology consultation before planned non-cardiac surgery. Purpose of this study was to evaluate the usefulness of this system and the incidence of the events.
Methods: A total of 8,581 male consecutive adult patients (3,831 male, age of 61±17 y/o) who underwent planned non-cardiac surgery in our hospital from August 2013 to June 2015 were included to the study. Patients were evaluated one month before surgery by being asked about the presence of active cardiac diseases, exercise capacity (measured in metabolic equivalents: METs) and clinical risk factors. They were classified into 4 categories from C4 to C1; C4 (active cardiac diseases), C3 (<4 METS and clinical risk factors >1), C2 (<4 METS and no clinical risk factors), C1 (>4 METS). In CPS, C4 and C3 groups should have cardiology consultation, and C2 and C1 groups may under-go surgery without any cardiac consults.
Results: CPS was performed in 7,220 cases (84.1%); C4: 230 cases, C3: 262, C2: 310, C1: 6,418. Out of these 7,220 cases, 1,010 cases (14.0%) were consulted to cardiologist. Among 7,220 patients, 58 (0.8%) had cardiovascular events during and/or after surgery. Out of these events, 29 cases (50%) had arrhythmic events (17 atrial fibrillation, 3 atrioventricular block [worse than 2nd degree], 3 premature atrial contraction/atrial tachycardia, 3 atrial flutter, 2 ventricular tachycardia, and 1 sick sinus syndrome), 11 (19%) ischemic events (4 va-sospastic angina, 4 acute myocardial infarction, 2 stable angina, and 1 ischemic heart failure), 11 (19%) pulmonary embolism/deep vein thrombosis, and 9 miscellaneous events.
Conclusions: The half of the cardiovascular events after non-cardiac surgery was an arrhythmic event. Our CPS system provides safety during the perioperative period of non-cardiac surgery.
CARDIAC ARRHYTHMIAS DURING PERIOPERATIVE PERIOD OF NON-CARDIAC SURGERYSeiichi Taniai, Shinsuke Takeuchi, Satoko Yamasaki, Tomoko Yorozu, Hideaki Yoshino
Kyorin University School of Medicine, Tokyo, Japan
ALLIED PROFESSIONALS P 2-015

287
Introduction: Insertable cardiac monitors (ICM) are used to detect and monitor arrhythmias in patients for up to 3 years. The newest iter-ation of the ICM is a miniaturized version of its predecessor with a minimally invasive insertion procedure. The patient home monitor as-sociated with this device offers wireless automatic daily transmissions and manual data transmissions for remote monitoring. Much has been published on the functionality of this device but little has been presented on the patient experience with the device and home moni-toring system.
Methods: The LINQTM Usability trial was a prospective, multi-center global study that enrolled 151 patients with an indication for an ICM. Patients were inserted with a miniaturized ICM device and followed for 12 months. Patient survey data was collected at 1, 6 and 12 month follow up visits. Percentages were calculated from the total responses from all patients across the 3 time periods.
Results: Of the 151 patients inserted with an ICM, 66.9% (n=101) were male, with a mean age of 56.6±12.1 years and BMI of 28.1±4.4. The response rate to the patient survey across all time points was 96.5% (437 of 453 expected). Throughout the course of the study, 96.8% patients indicated they were satisfied or very satisfied with the miniaturized ICM. The insertion procedure was considered comfortable or very comfortable by 81.8% (n=122) of patients, with 16.1% (n=24) indicating it was somewhat uncomfortable and 2.0% (n=3) uncomfort-able. Overall, 93.5% of patient responses indicated no concern about scar noticeability from the insertion procedure. The home monitor for device transmissions was considered easy or very easy to set up by 95.3% (n=141) of patients and, throughout the study, 97.8% of re-sponses indicated it was easy/very easy to use. Daily activity was not limited due to the device in 98.6% of patients and 92.7% stated they would likely or definitely recommend the miniaturized ICM to another patient.
Conclusions: The miniaturized ICM device and patient monitor is highly accepted by patients with minimal impact to daily activities.
PATIENT EXPERIENCE WITH MINIATURIZED INSERTABLE CARDIAC MONITORPrashanthan Sanders1, Lukas Dekker2, Evgeny Pokushalov3, Katherine Lindborg4, Helmut Purerfellner5 1University of Adelaide and Royal Adelaide Hospital, Adelaide, Australia; 2Catharina Hospital, Eindhoven, Netherlands; 3State Research Institute of Circulation Pathology, Novosibirsk, Russian Federation; 4Medtronic, Mounds View, United States; 5Public Hospital Elisabethinen, Academic Teaching Hospital of the University of Innsbruck, Linz, Austria
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-016

288
Introduction: Several modern implantable CRT-D and ICD devices measure intrathoracic impedance (Z) across RV-coil to can vector that can be useful in monitoring worsening heart failure (HF). Both raw Z and fluid index derived from Z (e.g. OptiVol, Medtronic Plc) have been shown to be useful. However, how Z depends on patient characteristics such as age, weight, height and body mass index (BMI) has not been well studied.
Methods: Existing device data from 109 pts (age 70±11 years, 76% male) followed for 21±10 months with adjudicated HF hospitalizations (HFHs) were used for analysis. Data from the first 6 months were excluded because Z is known to rise slowly during this period. Thereaf-ter, a 30-day segment with no HFH was used to compute mean Z, and pts were categorized into tertiles (Low Z:<61 Ω, Medium Z: 61.5-70.5 Ω, High Z: >70.5 Ω). Mean age, weight, height and BMI for all Z groups were computed, and relationships between Z and patient characteristics investigated.
Results: Table shows age, weight, height and BMI for all Z groups. Pair-wise comparisons for different Z groups revealed no statistically significant differences for age (P=0.15), weight (P=0.15) and height (P=0.78). BMI for Low Z group was statistically different from High Z group (P=0.04). Remaining two BMI comparisons (Low Z vs. Medium Z and Medium Z vs. High Z) were not statistically different.
Conclusions: Baseline intrathoracic impedance increases with increasing patient BMI likely resulting from greater resistance to current flow by adipose tissue. Accounting for BMI dependent increase in impedance could potentially enhance the performance of impedance based HF monitoring algorithms.
INFLUENCE OF PATIENT CHARACTERISTICS ON INTRATHORACIC IMPEDANCE MEASUREMENTS IN CRT-D/ICD PATIENTSVinod Sharma, Jodi Koehler
Medtronic Inc., Minneapolis, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-017
Patient Characteristics for Three Z Groups
Impedance Group # Pts Impedance (ohms) Age (yr) Weight (kg) Height (cm) BMI
Low (<61.5) 35 54.3±6.5 69±12 77±20 171±11 25.8±4.5
Medium (61.5-70.5) 35 65.0±2.3 72±11 84±23 172±12 28.1±5.5
High (>70.5) 36 75.5±6.4 67±9 85±16 172±9 28.9±5.6
289
Introduction: The Reveal LINQ is a miniaturized insertable cardiac monitor (ICM) that is inserted subcutaneously through a minimally in-vasive procedure in patients with suspected arrhythmias. The device has a lifespan of up to 3 years. While the insertion technique has been documented in previous publications, the explant procedure has yet to be characterized.
Methods: The Reveal LINQ Usability trial was a multi-center global study that enrolled 151 patients with an indication for an ICM. During follow up, 11 patients had their LINQ ICM explanted. Explant techniques and resources used were documented.
Results: Eleven explants were performed due to study end (7; 63.6%) diagnosis (3; 27.3%); or patient request (1; 9.1%) with a median fol-low up time prior to explant of 13.1 months (25-75th percentile: 7.0-13.2 months). Explants were performed in 3 countries at 4 centers (1 center in Russia (7); 2 centers in Austria (3); and 1 center in The Netherlands (1)). All the explants occurred in a catheterization lab (9, 81.8%) or an operating room (2, 18.2%) and were performed by an electrophysiologist (9, 81.8%) or cardiologist (2, 18.2%) with a nurse (11, 100%) and technician (10, 90.9%) present. One patient received general anesthesia due to a concurrent ICD implant, while the remaining patients (10, 90.9%) were given a local anesthetic. The incision site was prepared with a local antiseptic for all patients. Procedures were performed by accessing the device through an incision superior to the device. Physicians used the following tools to retrieve the device: scalpel (11, 100%) forceps (10, 90.9%) and scissors (1, 9.1%). Wound closure was accomplished with 1-2 sutures. No medications were stopped prior to the procedure and patients were not limited from activity after the explant. No serious adverse events were reported in relation to the explant procedures.
Conclusions: LINQ ICM explant is a minimally invasive procedure that can be successfully performed with currently available resources.
EXPLANT PROCEDURE FOR THE REVEAL LINQ INSERTABLE CARDIAC MONITOR: EXPERIENCES FROM THE LINQ USABILITY TRIALPrashanthan Sanders1, Helmut Purerfellner2, Evgeny Pokushalov3, Clemens Steinwender4, Kevin Vernooy5, Baerbel Maus6, Artem Strelnikov3 1University of Adelaide and Royal Adelaide Hospital, Adelaide, Australia; 2Public Hospital Elisabethinen, Academic Teaching Hospital of the University of Innsbruck, Linz, Austria; 3State Research Institute of Circulation Pathology, Novosibirsk, Russian Federation; 4Linz General Hospital, Faculty of Medicine, Johannes Kepler University Linz, Linz, Austria; 5Maastricht University Medical Center, Maastricht, Netherlands;
6Medtronic Bakken Research Center, Maastricht, Netherlands
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-018

290
Introduction: The reduction in size and simplification of the insertion procedure of the Reveal LINQ insertable cardiac monitor (ICM) has had a positive effect on procedure-related safety compared with previous iterations. In this interim analysis of the Reveal LINQ Registry, we sought to examine the impact of age on procedure characteristics and safety.
Methods: Ongoing, prospective, multi-center study evaluating real-world performance of the ICM and enrolling approximately 2300 pa-tients who will be followed for 3 years. Patients with an ICM inserted at least 30 days prior to this analysis were included. Chi-square tests and two-sample t-tests were used for categorical variables and continuous variables, respectively.
Results: A total of 488 patients (55.5% male, age 61.8±16.3 years) were grouped into 2 cohorts (<or ≥65 years). The percentage of pa-tients with adverse events (AEs) was 1.4%: 3 infections and 2 pocket erosions (both in the same patient) in the <65 group (1.6%); and 1 in-fection, 1 migration and 1 pocket erosion in the ≥65 group (1.3%). One infection (<65 group), 1 migration (<65 group) and both erosions (1 in <65 group, 1 in ≥65 group) resulted in device explant. There were no significant differences in pre-procedural antibiotics use (P=0.63) and a marginally significant difference in post-procedural antibiotics use (P=0.058), higher in the <65 group. Baseline OAC usage (P=0.0095), renal dysfunction (P=0.0129), hypertension (P<0.0001), MI (P=0.0089), and cancer (P=0.0002) were more prevalent in the ≥65 group.
Conclusions: Although the low rate of adverse events precludes formal statistical testing for differences, there is no observed increase in adverse events in the older age group despite their higher presence of co-morbidities.
IMPACT OF AGE ON THE INSERTION PROCEDURE OF THE REVEAL LINQ™ INSERTABLE CARDIAC MONITOR: RESULTS FROM A REAL-WORLD GLOBAL MULTI-CENTER REGISTRYAtul Verma1, Suneet Mittal2, Sean Beinart3, Andrea Natale4, Alpesh Amin5, Scott Kasner6, Erika Pouliot7, Hans-Cristoph Diener8 1Southlake Regional Health Centre, Newmarket, Canada; 2Electrophysiology Laboratory, The Valley Hospital Health System, Ridgewood, United States; 3Center for Cardiac and Vascular Research, Washington Adventist Hospital, Rockville, United States; 4Texas Cardiac Arrhythmia Institute, St. David’s Medical Center, Austin, United States; 5University of California, Irvine, United States; 6University of Pennsylvania Health System, Philadelphia, United States; 7Medtronic plc, Minneapolis, United States; 8University Hospital Essen, Essen, Germany
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-019

291
Introduction: Cardiac resynchronization therapy (CRT) is an effective treatment for heart failure but left ventricular lead implantation is frequently challenging. A single center experience with telescoping-support system (TSS) using Amplatz Left 2 (AL-2, 6F, Boston Scientif-ic) catheter to access the coronary sinus (CS) is reported.
Methods: We reviewed charts of consecutive patients (pts) who underwent CRT-P or CRT-D implantation between July 2005 and Novem-ber 2015. In January 2009, strategy to use AL-2 catheter as TSS was implemented. Group A (between July 2005 to December 2008) in-cluded 78 pts (mean age 66.8 years; 49 males; 54 CRT-D) who underwent CRT implant using standard CS sheaths utilizing over the wire technique or a deflectable EP catheter. Group B (between January 2009 to November 2014) included 184 pts (mean age 72.9 years; 115 males; 138 CRT-D) who underwent CRT implant using TSS utilizing AL-2 catheter. The primary outcome was success of LV lead place-ment and secondary outcome was procedural fluoroscopy time.
Results: Successful LV lead placement was significantly higher in Group B (97.8% vs. 91% P=0.017). In addition procedural fluoroscopy time was also significantly lower in Group B (17.2 vs. 30.5 minutes P=0.0001). Average fluoroscopy time was significantly reduced even in 2009 when TSS strategy was first implemented as shown in Table 1. Fluoroscopy times improved further with experience. Of the 4 pts in Group B who has failed LV lead placement-one had occluded venous access, one developed pericardial effusion and in 2 other patients CRT implant was attempted from right pectoral region. Since January 2014 CS cannulation time (time of introduction of CS sheath in vas-culature to CS cannulation) was less than 5 minutes in 89% of pts. No specific complications resulted from use of AL-2 catheter.
Conclusions: Higher success rate of CRT implant and shorter fluoroscopy times was seen using TSS utilizing AL-2 catheter without need for excess contrast or specialized tools.
SIMPLIFIED USE OF TELESCOPING-SUPPORT CATHETER SYSTEM FOR LEFT VENTRICULAR LEAD PLACEMENT IN PATIENTS UNDERGOING CARDIAC RESYNCHRONIZATION THERAPYDevender Akula
Our Lady of Lourdes, Moorestown, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-020
Table 1. Average Fluoroscopy Time (min)
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
29.2 29.6 31.9 28.5 22.6 19.9 20.3 13.5 13.5 13.7

292
Introduction: Extravascular ICD (EVICD) systems present a promising alternative to the transvenous approach in some patients. Place-ment of a lead under the sternum and closer to the heart may require less energy for defibrillation while also allowing for anti-tachycardia pacing. Implanting a lead in this space may be unfamiliar to implanting physicians. Quantification of heart and lung location relative to the sternum enables development of a safe and effective implant procedure.
Methods: Cardiovascular patient CT images were segmented using commercial software such that geometric relationships between tis-sues in the space beneath the sternum could be characterized. Polygonized surfaces representing these tissues were generated. The lo-cations of the right ventricular center of mass (RVCOM), epicardial surface, sternal margins, and lungs were assessed from the surfaces.
Results: Sixty-eight patients were successfully analyzed. The RVCOM was left of the sternal midline >92% of the time. RVCOM was within 25 mm (either above or below) of xiphisternal junction (XJ). The myocardial surface was within 10 mm of the sternum between the XJ and fifth intercostal space in ≥92% of pts (Table). In locations on the sternum where the heart was in close proximity, the lungs were found to be ≥5 mm from the sternum ≥91% of the time.
Conclusions: Despite the considerable anatomical variability in the substernal space, these results suggest that close proximity to the heart is possible while minimizing interaction with the lungs with an appropriately placed substernal lead.
FUNDAMENTAL ANATOMICAL INPUTS TO MOTIVATE SAFE IMPLANTATION OF A NOVEL EXTRAVASCULAR ICD SYSTEMRyan Lahm, Megan Harris, Varun Bhatia
Medtronic Plc, Mounds View, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-021

293
Introduction: Placing the ICD or pacemaker is mainly by utilizing a superior venous approach via the jugular or subclavian veins. While many patients with congenital heart disease have concurrent anomalous venous anatomy, then we must consider alternatives. This study explores the feasibility of percutaneous transhepatic approach in post-Glenn or Fontan patients with ICD and pacemaker implant.
Methods: Case 1: A 42-year-old man accepted a surgery operation that the superior vena cava was connected to the right pulmonary ar-tery to cure congenital heart disease seven years ago. Postoperative ECG found a IIIo AVB and paroxysmal ventricular tachycardia, in order to place pacemaker, the routine superior venous approach via the jugular or subclavian veins failed. An angiography of the accessory he-patic vein was performed via the inferior vena cava. The accessory hepatic vein was punctured and one 9F peel-away sheath was inserted in the right atrium. Along the sheath ventricular lead was placed to the right ventricular apex and the parameters was tested. The atrial lead was placed to right atrium, the pacemaker parameter was good. A capsule was made in the right lower quadrant abdominal external oblique muscle surface and perpendicular to the spine, the lead connected to the pacemaker and buried in the capsule. Case 2: A 19-year-old man who previously underwent a Glenn operation presented with repeated syncope resistant to antiarrhythmic medication. The electrocardiogram indicated ventricular tachycardia. Therefore, the patient was admitted to our hospital for implantable cardioverter defibrillator implantation.The patient with limited venous access from an inferior approach had to use percutaneous transhepatic access. The puncturing process was similiar to case 1. A screw-in ICD lead was inserted in the right ventricular apex. The lead was curved in the right atrium to ensure effective shock delivery. The ICD generator was inserted into the anterior abdominal wall in a position anterior to the rectus abdominis muscle. The ICD generator delivered a shock of 30 J successfully terminated the induced VF.
Results: In the two patients with percutaneous hepatic vein approach, the ICD and pacemaker worked normally, no obvious complications was observed. In the follow-up period, mild dislocation of lead in the atrium of the two patients was found, which owing to gravity or physi-cal activities, but there was no influence for pacing or shock. Therefore leaving a long coil or pacemaker lead in the atrium to prevent dis-location was needed.
Conclusions: In patients with limited venous access from an inferior approach and who require ICD and pacemaker implantation, percu-taneous transhepatic access offers an alternative approach. Before the procedure, complete understanding of the anatomy of the venous system is needed.
EXPERIENCE OF PERCUTANEOUS TRANSHEPATIC VENOUS ACCESS FOR ICD AND PACEMAKER IMPLANTATIONZhifu Cen, Kaijun Cui, Yuan Fang
West China Hospital, Sichuan University, Chengdu, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-022

294
Introduction: In small Right Atrium (RA) screw-in lead can be put in right inferolateral region which is well away from phrenic nerve and vital structures when it is difficult to screw the lead in appendage and upper lateral RA.
Methods: N/A
Results: Cases: 1) 26 years old pregnant lady (26th week) admitted with dyspnea on exertion & presyncope starting after 20th week of pregnancy with no history of syncope. Electrocardiogram (ECG) showed complete heart block. Echocardiogram (ECHO) showed normal LV function and no pulmonary arterial hypertension. Ultrasonography abdomen showed single live fetus with utero-placental insufficien-cy. Autoimmune profile was negative. So she was planned for permanent pacemaker implantation (PPI). Right ventricular lead was placed at RV apex easily but due to small size of RA lead couldn’t be placed inside RA appendage with multiple attempts and various size of pre-formed and manually formed U- shaped guidewire. Lead placement at superolateral right atrium (RA) caused phrenic nerve stimulation every time. So in the end we placed the lead in inferolateral portion of RA after giving a curve (S-shaped; Figure 1B) to the guidewire (help-ing the lead to track down to favourable position). 2) 36 years old lady admitted with dyspnea on exertion and giddiness since 2 months. There were 2 episodes of presyncope but no syncope. ECG showed complete heart block. ECHO showed normal LV function and normal pulmonary arterial pressure. Autoimmune profile was negative. So PPI was planned. Right ventricular lead was placed at RV apex easily but due to small size of RA lead couldn’t be placed inside RA appendage and superolateral RA lead placement had phrenic nerve stimula-tion every time. Again a S shaped guidewire was used to place RA lead into the inferolateral wall of right atrium.
Conclusions: Young patients need pacemakers for various indications. The morphology of RA is of great importance. These patients in absence of pulmonary arterial hypertension have small RA size. There can be difficulty in proper positioning of lead in this small RA and it is really problematic if superolateral lead placement is having phrenic nerve stimulation. In such situation placing the RA lead into the in-ferolateral wall of right atrium with S-shaped manual curve of guidewire can be used as a novel technique in such patients.
NOVEL TECHNIQUE FOR RIGHT ATRIAL LEAD PLACEMENT IN YOUNG PATIENTS WITH SMALL RIGHT ATRIUMDinesh Choudhary, Rakesh Mahla, Sunil Budania, Ashwini Kumar, Pinto Nahata
SP Medical College, Bikaner, India
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-023
295
Introduction: N/A
Methods: N/A
Results: The subcutaneous implantable cardioverter-defibrillator(S-ICD) is a novel technology for the treatment of sudden cardiac death. The pulse generator is implanted in the left axillary position and the single subcutaneous lead is implanted in the left parasternal, but, it comes to the question of where we should place subcutaneous lead for S-ICD implantation just after cardiac operation like mitral valve replacement (MVR) to prevent oversensing by contact with sternal wire, or anatomical evaluation using CT imaging is need to make sure the tissue infection around median sternotomy before implantation in these cases. In 6 cases, S-ICD was implanted, CT imaging was per-formed in all patients to evaluate the inflammation around subcutaneous lead after implantation, any infection was not found. And, CT imaging at pre and post implantation was performed in S-ICD implantation just after MVR, we could evaluate the location of sternal wire or the tissue around the sternum by CT imaging before implantation, and we finally avoid infection and oversensing. We will report about the clinical significance of CT imaging pre and post S-ICD implantation with clinical review.
Conclusions: N/A
THE CLINICAL SIGNIFICANCE OF ANATOMICAL EVALUATION USING 3D-CT FOR SUBCTANEOUS-ICD IMPLANTATION JUST AFTER MITRAL VALVE REPLACEMENT WITH VENTRICULAR FIBRILLATIONHikari Hashimoto1, Keijirou Nakamura1, Taito Nagai1, Rina Ishii1, Yasutake Toyoda1, Takahito Takagi1, Naohiko Sahara1, Yuriko Narabayashi1, Yoshinari Enomoto1, Shingo Kujime1, Hidehiko Hara1, Masao Moroi1, Mahito Noro2, Masato Nakamura1, Karou Sugi3 1Toho University Ohashi Medical Center, Tokyo, Japan; 2Toho University Sakura Medical Center, Tokyo, Japan; 3Odawara Cardiovascular Hospital, Odawara, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-024
296
Introduction: Prolonged pacing from the atrial appendage and the right ventricular apex has been shown to be associated with the in-creased risk of atrial fibrillation and the progressive left ventricular dysfunction, and so atrial septal pacing and high right ventricular sep-tal pacing have been proposed as alternatives to non-septal atrial pacing and ventricular apical pacing. However, there is currently no in-formation on mid-term atrial and ventricular leads (FINELINE II Sterox EZ; Boston Scientific) electrical performances from these sites in advanced age patients.
Methods: Thirty-one patients who had undergone pacemaker implantation with atrial septal pacing and high right ventricular septal pac-ing were analyzed retrospectively. Mid-term follow up (55±3 days) was obtained in all advanced aged patients (mean age 81±7 years, 12 men). Information on stimulation threshold, P and R-wave sensing, lead impedance and lead complication were collected.
Results: Lead performances at the atrial septal position and the high right ventricular septal position were stable in the mid-term. Atrial and ventricular electrical parameters were acceptable with stable mid-term stimulation thresholds, sensing and impedance. About two-month follow up demonstrated atrial and ventricular mean stimulated thresholds of (0.81±0.55, 0.56±0.33 V/0.4 msec), mean P and R waves of (3.3±1.1, 12.5±6.5 mV), and mean impedance values of (433±54, 484±67 omega). There was no case of high pacing threshold, inadequate sensing or lead dislodgement, and no episode of sustained atrial fibrillation.
Conclusions: This study confirms satisfactory mid-term performance with leads placed on the atrial septum and high right ventricular septum in advanced age patients.
ATRIAL SEPTAL AND HIGH RIGHT VENTRICULAR SEPTAL PACING IN ADVANCED AGE PATIENTS: MID-TERM FOLLOW-UP ATRIAL AND VENTRICULAR LEADS PERFORMANCESTatsuo Misawa1, Toshinori Sasaki2, Shun Szuki2 1Yamagata Prefectural Kahoku Hospital, Kahoku, Japan; 2Boston Scientific Japan K.K., Sapporo, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-025

297
Introduction: As the number of cardiac device implantations is on a rise, there is a parallel increase in the long-term complications such as device-related infections requiring lead extraction. Patients are prone to develop new-onset Pulmonary Hypertension (P. HTN) during the procedure. We sought to determine the risk of increased Pulmonary Artery Systolic Pressure (PASP) following device extraction pro-cedures.
Methods: A chart review of 113 patients who underwent cardiac devices’ lead extraction between January, 2002 to July, 2015 was carried out. Six patients had lead extraction twice, making the total number of extractions to be 119. Only 45 cases had PASP measurement via Transthoracic Echocardiography (TTE) prior to and after device extraction. A difference of 10 mmHg or more in the PASP was considered clinically significant.
Results: Median follow up of TTE after lead and device extraction was 5 months. The majority of our sample were males (68.9%). Average age was 46.5 (SD=17) years. Eleven patients (24.4%) experienced a significant increase of PASP, 9 patients (20.0%) showed improvement, and the remaining (55.6%) had no changes. Average implantation-to-extraction duration of the leads was higher among those who had no pressure difference (50.6 vs. 23.3 months). The majority of patients who developed P. HTN (72.7%) had extractions secondary to an infec-tion (wound infections and/or infective endocarditis) opposed to 3 (27.3%) who had other indications. When looking through potential pre-dictors that may increase the likelihood of developing P. HTN, there was no association with a pre-existing lead-attached vegetation (2 pa-tients only), nor the type of lead (6 high-voltage leads vs. 5 pacing leads across the tricuspid valve).
Conclusions: Our simple descriptive study showed that the risk of developing P. HTN following lead and device extraction is negligible. However, our small sample size may have influenced the results and further exploration is advised.
CHANGES IN PULMONARY ARTERY SYSTOLIC PRESSURE FOLLOWING PACEMAKER/DEFIBRILLATOR LEAD EXTRACTIONAlwaleed Aljohar1, Abdullah Aljasser1, Hind Alonazi2, Ahmed Alfagih2, Yahya Alhebaishi2, Adil Ahmed2, Khaled Dagriri2 1King Saud University, Riyadh, Saudi Arabia; 2Prince Sultan Cardiac Center, Riyadh, Saudi Arabia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-026
298
Introduction: The number of cardiac device implantations is on rise, there is a parallel increase of long-term risks such as device infec-tions and malfunctions mandating device and lead extraction. Two major extraction techniques are being practiced; Simple Traction (ST) and Advanced Extraction (AE). Risk of complications is associated with the latter. In addition, AE requires more sophisticated preparations than ST. We aimed to identify the predictors of which tool to use during lead and device extraction.
Methods: We conducted a retrospective chart review in 113 patients who underwent lead and device extraction between January 2002 and July 2015. Six patients underwent extraction twice, making the final number of extractions 119. The final number of leads was 223. Two groups were identified according to the tool of extraction; ST vs. AE, where AE includes extraction via Lead Locking Device stylet and/or High Frequency Excimer Laser Sheath.
Results: The average age in our cohort was 50 years (SD=18), with predominance of males (72.7%). ST was used for 120 leads (53.8%), while AE techniques were used for 103 leads (46.2%). Tips of 119 (53.4%) leads were located in Right Ventricle (RV), 84 (37.7%) in the RA, and 20 (9.0%) in the Coronary Sinus (CS). Average duration of implantation-to-extraction period was significantly higher in the leads ex-tracted by AE (81.2 vs. 19.4 months; P=<0.001). The majority of RA and CS leads were extracted using ST (63.1% and 65.0%, respectively), whereas almost half of the RV leads were extracted using AE (54.6%) (Combined P=0.026). There was no significant difference in the tool of extraction when correlated with the type of lead (Pacing vs. High-voltage) (P=0.616), or the indication of extraction (infection vs. non-in-fection) (P=0.450).
Conclusions: We conclude that the duration of lead within cardiac chambers, and lead tip location were the only significant predictors of extraction by AE. Our findings may promote better risk stratification and management approach in patients undergoing lead and device extraction.
THE USE OF SIMPLE TRACTION VS. ADVANCED EXTRACTION TECHNIQUES IN CARDIAC DEVICES LEAD EXTRACTION: IDENTIFICATION OF PREDICTORSAlwaleed Aljohar1, Abdullah Aljasser1, Hind Alonazi2, Ahmed Alfagih2, Yahya Alhebaishi2, Adil Ahmed2, Khaled Dagriri1 1King Saud University, Riyadh, Saudi Arabia; 2Prince Sultan Cardiac Center, Riyadh, Saudi Arabia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-027

299
Introduction: Despite advancement in sterile cardiac device implantation techniques, wound infections and/or bacteremia remain a sig-nificant problem. The presence of a vegetation in lead-induced endocarditis (LIE) is a critical factor in determining the management. Transthoracic (TTE) and Transesophageal (TEE) Echocardiography are two different cardiac imaging modalities used in such circum-stances. Our purpose of this study is to identify which of the two has the highest sensitivity in detecting lead attached vegetations. In addi-tion, we aim to correlate the existence of a vegetation with blood and wound culture results.
Methods: We conducted a chart review in 113 patients whom underwent lead extraction during the period of January, 2002 to July, 2015. Six patients underwent lead extraction twice, increasing the number to be a 119 cases. Out of the study cohort, we include 38 patients who had both TTE and TEE done prior to lead extraction. Data regarding TTE, TEE, as well as blood and wound cultures were collected from echocardiography and microbiology lab reports using a well-structured case report form.
Results: Of the study population, 21 patients (55.3%) had existing lead vegetations. Nineteen were detected by TEE, compared to 6 only when TTE was used. The sensitivity of TEE and TTE were 90.5% (CI: 69.6% to 98.8%) and 28.5% (CI: 11.3% to 52.1%), respectively. Culture results showed that in the presence of a vegetation, blood cultures were positive in 55% of the cases (P=0.036) while 44.4% of those with vegetations had a positive wound culture (P=0.347).
Conclusions: TEE has higher sensitivity in detecting vegetations compared to TTE in LIE. The presence of a vegetation is more likely to be associated with a positive blood culture than a positive wound culture. Further studies ought to measure the additive value of blood and wound cultures to the overall cardiac imaging sensitivity.
TRANSESOPHAGEAL VS. TRANSTHORACIC ECHOCARDIOGRAPHY: WHAT VISUALIZES CARDIAC DEVICE LEAD VEGETATIONS BETTER?Alwaleed Aljohar1, Abdullah Aljasser1, Hind Alonazi2, Ahmed Alfagih2, Yahya Alhebaishi2, Adil Ahmed2, Khaled Dagriri2 1King Saud University, Riyadh, Saudi Arabia; 2Prince Sultan Cardiac Center, Riyadh, Saudi Arabia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-028

300
Introduction: Despite advanced sterile techniques in cardiac device implantations, long-term complications such as wound infections and/or lead-induced endocarditis can develop mandating lead and device extraction. It has been suggested that lead extraction carries a risk of new-onset Tricuspid Regurgitation (TR), or a deterioration of a formerly known regurgitant valve. In this study we aim to explore the risk of TR following lead extraction.
Methods: We conducted a retrospective chart review in 113 patients whom underwent lead extraction during the period of January, 2002 to July, 2015. Six patients underwent lead extraction twice, making the total number of extractions to be 119. We include 52 cases who had Tricuspid valve function evaluation via Transthoracic Echocardiography (TTE) prior to and after device and lead extraction. TR severity was assessed using a grading system as the following; normal, mild, mild-to-moderate, moderate-to-severe, and severe. Worsening or im-provement by more than 1 grade was considered clinically significant.
Results: Follow up duration was examined over a median of 5 months. The majority of the cohort were males (71.2%). The average age was 46 (SD=18) years. Eleven patients (21.2%) experienced worsening of TR (3 had normal functioning valves before extraction, and 8 were known to have TR prior to extraction), 2 (3.8%) had improvement, and the majority (75.0%) did not experience any significant chang-es. Compared with those who had no change, average lead duration was higher in the worsening TR group (67.2 vs. 27.9 months). A lead-attached vegetation was detected in 4 out of the 11 patients with TR. Lead type (High-voltage vs. Pacing) was not predictive of devel-oping TR.
Conclusions: Our study could not find overwhelming evidence to support the claim that there is an elevated risk of TR following pacemak-er/defibrillator lead extraction.
PACEMAKER/DEFIBRILLATOR LEAD EXTRACTION AND THE RISK OF TRICUSPID VALVE REGURGITATIONAlwaleed Aljohar1, Abdullah Aljasser1, Hind Alonazi2, Ahmed Alfagih2, Yahya Alhebaishi2, Adil Ahmed2, Khaled Dagriri2 1King Saud University, Riyadh, Saudi Arabia; 2Prince Sultan Cardiac Center, Riyadh, Saudi Arabia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-029

301
Introduction: Transvenous lead extraction (TLE) remains a challenging procedure with inherent risks, despite general safety, surgery can be still required in elective cases and the involvement of a surgical team during TLE procedures is still debated. In this study, we report our experience with a minimally invasive “hybrid” approach, defined as a procedure performed by an electrophysiologist with the support of a cardiac surgeon in the same procedure.
Methods: From January 2013 to December 2015, we identified patients who could deserve a hybrid approach due to a conceivable com-plex TLE procedure. In these patients, a minithoracotomy or a thoracoscopic access was performed in order to have direct visualization of the involved cardiac structures during the TLE procedure.
Results: We reported 12 cases of planned hybrid lead extraction; minithoracotomy and thoracoscopy were performed in 10 (83%) and 2 (17%) patients, respectively. A total of 25 leads out of 27 (median lead age 19 years) were successfully extracted with laser, mechanical or combined transvenous sheath. In three patients the direct monitoring of vascular and myocardial integrity allowed prompt treatment of potential vascular injury during the lead extraction manoeuvres: in a case a purse-string suture was placed on a thinning of the lateral wall of the right atrium, and in two patients tapes were passed around the superior vena cava due to a minor tearing. Mean in-hospital stay was 4±2 days. There were no major intraoperative complications and no deaths occurred after 30-days follow-up.
Conclusions: The hybrid approach, with minithoracotomy or thoracoscopy, may be recommended to increase the safety in the most chal-lenging TLE procedures: the minimally-invasive surgical intervention allows continuous monitoring of the critical cardiac structures and prompt treatment of potential complications.
ENHANCED SAFETY OF TRANSVENOUS LEAD EXTRACTION IN HIGH-RISK PATIENTS: A HYBRID MINIMALLY INVASIVE APPROACHLuca Bontempi1, Francesca Vassanelli1, Manuel Cerini1, Lorenza Inama1, Francesca Salghetti1, Nicolò Dasseni1, Clara Villa1, Daria Liberto2, Daniele Giacopelli3, Alessio Gargaro3, Abdallah Raweh4, Antonio Curnis1 1Spedali Civili-University of Brescia, Brescia, Italy; 2University of Catania, Catania, Italy; 3Biotronik Italia, Milano, Italy; 4L.U.de.S. University, Lugano, Switzerland
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-030

302
Introduction: Pacemaker lead extractions described as safe and efficacious procedure. Superior approach using locking stylet plays a major role because of ability to pull the most distal part of the lead. When femoral approach is used, “Needle’s eye snare” is usually need-ed and it should be applied to as distal as possible for grasping the tip of the lead. This technique was thought for preventing abandoning the lead or incomplete lead extraction because of grasping the lead stronger. Using similar concept we report our small series of a new technique using double snare for femoral approach of pacemaker lead extraction. With holding the proximal part of the lead by the second snare, then the first snare can be moved as distal as possible using the lead as a rail. The first snare then, can pull the lead with gentle traction.
Methods: Between January 2014 and June 2015, 17 leads extraction (5 atrial, 10 ventricle and 2 coronary sinus leads) procedures were performed in 11 patients. Nine of the procedures were performed using the new technique and included in the study (from 6 patients).
Results: Eight leads (88%) were successfully extracted, and failed in 1 (12%). The age of the lead was 65±10 months (range 14 to 144 months). No incomplete extraction in our small series. No complication occurred. The failure was due to very extensive fibrosis along the vena cava superior, finally was extracted by thoracotomy and done by cardiac surgeon.
Conclusions: This technique is especially useful if the leads to be extracted were previously cut and had retracted into central circulation. Although our experience is based on a small series, we can conclude that this new technique is safe and effective. To the best our knowl-edge, this new technique is the first report.
DOUBLE SNARE TECHNIQUE: A NEW AND SIMPLE FEMORAL APPROACH FOR LEAD EXTRACTIONMohammad Iqbal, Anggia Chairuddin Lubis, Dian Andina Munawar, Beny Hartono, Muhammad Munawar
Binawaluya Cardiac Center, Jakarta, Indonesia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-031

303
Introduction: The optimal management of anticoagulation in the CIEDs (cardiac implantable electrophysiological devices) perioperative period remains unclear. We evaluated perioperative complications in patients recieving warfarin or direct oral anticoagulants (DOACs).
Methods: A total of 389 patients recieving anticoagulation therapy underwent CIEDs operation from April 2011 to December 2015. We compared major bleeding and thromboembolic complications between continued warfarin, interrupted warfarin with heparin bridging, interrupted warfarin, continued DOACs and interrupted DOACs group. Major bleeding complications were defined as bleeding requiring surgical intervention, prolongation of hospitalization, and discontinuation of the anticoagulant. Thromboembolic complications were de-fined as stroke, pulmonary embolism, deep vein thrombosis, and myocardial infarction.
Results: Of 332 patients recieving warfarin, continued-warfarin group were 83 patients, interrupted warfarin with heparin-bridging group were 97 patients and interrupted-warfarin group were 159 patients. Of 57 patients recieving DOACs, continued-DOACs group were 12 pa-tients and interrupted-DOACs group were 45 patients. Major bleeding event rates were the lowest rate in the interrupted DOACs group (18.1% vs. 13.4% vs. 3.7% vs. 16.7% vs. 0.0%, P<0.01). The rate of thromboembolic events did not significantly differ in each group (1.2% vs. 0.0% vs. 0.6% vs. 0.0% vs. 0.0%, P=0.80).
Conclusions: Interrupted DOACs group had the lowest rate of major bleeding and no thromboembolic events. Interrupted DOACs is best management of anticoagulation in the CIEDs perioperative period for patients receiving anticoagulation.
MANAGEMENT OF ANTICOAGULATION IN CARDIAC IMPLANTABLE ELECTROPHYSIOLOGICAL DEVICES PERIOPERATIVE PERIODJunji Morita, Michio Nagashima, Shota Tohoku, Kenichi Hiroshima, Kenji Ando
Kokura Central Hospital, Kitakyusyu, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-032

304
Introduction: Backgrounds: Cardiac device infections (CDIs) are a serious complication associated with the implantation of cardiac rhythm managed devices (CRMDs). The purpose of this study was to evaluate the outcome of patients undergoing transvenous lead ex-traction (TLE) of CDIs.
Methods: Between 2009 September and 2015 August, we performed TLE of 595 electrodes in 251 patients (pts). Out of these, 242 (83.1%) pts had been performed TLE because of infectious indications. The majority of pts (202 [85%]) presented with localized infection involving the device pocket. The remaining 39 pts (15%) presented with infectious endocarditis. Of the total 211 pathogens isolated, of which 85% were Staphylococcus species, and almost half of these were methicillin resistant. In-hospital mortality was 1.6% (4 pts). Only 1 deaths were extraction related. Major complications occurred to 5 pts for the perioperative period of TLE (tamponade in three, one died because of bleeding, and one hemothorax). Among the total cohort, 4 (1.6%) pts had relapsing infection. Mean periods between second TLE and re-implantation of CRMDs after initial TLE were 339±529 days. Pathogenic bacteria were detected in 3 infectious cases and were found to be originally pathogenic at initial TLE.
Results: N/A
Conclusions: CDIs are most often caused by Staphylococcus species, half of which are methicillin resistant. Percutaneous lead and de-vice removal along with antibiotic therapy are effective as primary interventions. The overall relapse rate is 1.6%, and in-hospital mortality rate is 1.6%.
CARDIAC RHYTHM MANAGED DEVICE INFECTIONSMichio Nagashima, Kenichi Hiroshima, Jyunji Morita, Takahiro Iseda, Kengo Kourai, Kenji Andou
Kokura Memorial Hospital, Kitakyushu, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-033

305
Introduction: Cardiac resynchronization therapy represents an established treatment for heart failure, yet issues related to optimal lead positioning and stability in the coronary veins contribute to complications such as phrenic nerve stimulation and lead dislodgment. Novel active fixation left ventricular (LV) leads are emerging as a means of providing precise lead placement and improved stability, warranting further consideration of LV active fixation lead extractability compared to passive fixation leads. Described here is the longest reported du-ration chronic implant experience related to extractability of LV active fixation leads.
Methods: Seventeen sheep were implanted with an LV lead (either the Medtronic active fixation Attain Stability® Model 20,066 with side helix or the Model 4,193 passive fixation control). A right ventricular lead (Medtronic Model 4,076) was also implanted in all animals to mimic lead-to-lead interaction. All leads were extracted at -26, 52 or 118 weeks. With deference to HRS guidelines regarding procedural and clinical success, extractions were conducted according to a predetermined protocol, beginning with simple traction of up to 0.9 kg (2 lbs). Sheep were monitored for 30-90 minutes after extraction, including via echocardiography. Gross pathology and histology of the heart and the lead tract were evaluated.
Results: All extractions were successful using a locking stylet and simple traction with less than 1 kg of pull force, with all leads removed in their entirety. In all cases, the active fixation side helix performed as designed, with the helix pitch opening and releasing from the tis-sue, causing no adverse effects to the local coronary vein binding site or the more proximal venous course, and without signs of venous tear or tamponade. Gross pathology and histology were remarkably normal. The fibrotic reaction at the side-helix location was not signifi-cantly different from the passive fixation LV control lead.
Conclusions: LV active fixation lead extraction from the coronary veins is safe, successful and free of complications after two years of im-plant duration in sheep. LV active fixation leads represent a clinically meaningful solution for LV lead stability and optimized positioning within the coronary veins.
PRECLINICAL RESULTS DEMONSTRATING THE TWO-YEAR EXTRACTABILITY OF A NOVEL LEFT VENTRICULAR ACTIVE FIXATION LEAD FROM THE CORONARY VEINSAmy Thompson1, Laurie Foerster2, Douglas Hine1, Kyle Marquard1, Stuart Adler3 1Medtronic, Mounds View, United States; 2Medtronic, Fridley, United States; 3HealthEast Heart Care, Saint Paul, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-034

306
Introduction: The need for ICD lead extraction (EXT) continues to increase, however, ICD leads are more difficult to extract due to in-creased fibrosis and lead complexity. There are no standard methods to quantify the amount of tension required to free bound leads, ac-cordingly we sought to characterize and quantify tension required to manually extract recent generation ICD leads.
Methods: Patient’s undergoing ICD lead extraction without evidence of infective vegitations were consented & enrolled at high volume centers (>40 cases/year). After lead prep, a strain gauge was connected to the locking stylet (LS) and direct traction force was continu-ously recorded with progressive traction forces (1, 2 and 3 kg×2 minutes each until the moment of release or physician discretion). If trac-tion was ineffective, advanced tools were used. All tools, levels of effort, & adverse events were recorded.
Results: Overall, 57 pts were enrolled at 7 centers, and 50 pts (57.9±14.3 years) underwent extraction. Leads from 4 manufacturers and 9 lead families were included. The mean implant duration was 80±29 months (range 26-150). LS traction achieved complete lead removal in 7 of 47 pts attempted (15%) with a mean force of 0.8±0.4 kg (0.3-1.4). The mean implant dwell time of the leads removed with traction was 54.1±15.6 months (range 26-77) as compared to the dwell of 84.6±28.5 months (range 38-150) (P=0.001) non-successful traction attempts. The overall extraction success rate was 98.0%. The overall major complication event rate was 4.0%, application of direct trac-tion was not related to any of these events.
Conclusions: In patients with contemporary ICD leads, manual traction alone only results in successful lead removal in 15% of cases. Short dwell times (<5 years) were associated with successful manual traction.
TRACTION ALONE IS RARELY EFFECTIVE IN REMOVING CONTEMPORARY ICD LEADS: RESULTS FROM THE ICDTEA LEAD EXTRACTION TENSILE FORCE ASSESSMENT (ICDTEA) STUDYPierce Vatterott1, Jonathan Picinni2, Dwight Reynolds3, Martin Burke4, Loren Berenbom5, Charles Gornick6, Hector Mazzetti7, Mark Marshall8 1United Heart & Vascular Clinic, St Paul, United States; 2Duke Univesity, Durham, United States; 3The University of Oklahoma College of Medicine-OU Science Center, Oklahoma City, United States; 4University of Chicago Hospitals, Chicago, United States; 5Mid-America Cardiology, Inc., University of Kansas Medical Center, Kansas City, United States; 6Minneapolis Cardiology Associates, Minneapolis, United States; 7Hospital Fernadez, Buenos Aires, Argentina; 8Medtronic, Mounds View, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 2-035

307
Introduction: Atrial fibrillation (AF) sometimes coexists with heart failure (HF) and can exacerbates HF resulting from increased atrial or ventricular rates. It is still uncertain whether rhythm or rate control strategy is more beneficial in patients with AF and HF.
Methods: We conducted a meta-analysis of randomized controlled trials (RCT) and cohort studies comparing rhythm vs. rate control in patients with AF and left ventricular ejection fraction (LVEF) equal or less than 50%. Changes in LVEF, quality of life or functional capacity, and the rate of worsening HF was investigated.
Results: Six trials (four RCTs and two cohort studies) with 1601 patients were included in this analysis. Mean age was 61.7 years, 81.9% were male and persistent AF consisted of 71.6%. A total of 791 patients (49.4%) was treated with rhythm control: medical therapy (86.2%) or catheter ablation (13.8%). Mean follow-up was 17.6 months. In random-effect model, rhythm control was associated with increased LVEF (mean difference 9.82%; 95% CI 7.13, 12.51; P<0.001) and better quality of life (mean difference in MLWHF score -11.73; 95% CI -20.29, -3.18; P=0.007) compared with rate control group. Functional capacity calculated by 6-minute walking distance was better in rhythm control group, but was not significant (mean difference 16.89; P=0.35). The rate of worsening HF was similar between two groups (risk ratio 0.9; 95% CI 0.77, 1.06; P=0.23).
Conclusions: In patients with both of AF and HF, even though functional capacity and HF exacerbation rate were similar, rhythm control strategy was superior to rate control in terms of improvement in LVEF and quality of life.
RHYTHM VS. RATE CONTROL IN PATIENTS WITH ATRIAL FIBRILLATION COMBINED WITH LEFT VENTRICULAR SYSTOLIC DYSFUNCTION: A META-ANALYSISJinhee Ahn1, Jaemin Shim2, Jong-Il Choi2, Young-Hoon Kim2 1Pusan National University Hospital, Busan, Republic of Korea; 2Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 2-036

308
Introduction: Early recurrence (ER) of atrial tachyarrhythmias after catheter ablation for atrial fibrillation (AF) is associated with higher late recurrence (LR). Earlier restoration of sinus rhythm can be achieved by cardioversion (early cardioversion, ECV), however, the impact of ECV on long-term outcomes has not been clear.
Methods: Between 2011 and 2014, a total of 286 (30.5%) experienced ER after AF ablation (mean 57.7 years old; 84.3% male; 29.3% par-oxysmal AF). Of those 186 patients (65.1%) underwent ECV, which was defined as cardioversion performed in the first 90 days and catego-rized as early (within 14 days) and late (beyond 15 days). Whether ECV affects a long-term clinical outcome was investigated.
Results: During the mean follow-up of 27.9 months, LR occurred less commonly in patients with early ECV compared to those without or late ECV (52.6% vs. 78.0% and 69.1%, P=0.031). This difference was significant in patients with persistent AF (P=0.001), but not in parox-ysmal AF (P=0.595). In multivariate analysis, early ECV (OR 0.310, 95% CI 0.116-0.831, P=0.020) and persistent AF (OR 2.022, 95% CI 1.129-3.621, P=0.018) were predictors for long-term clinical outcome.
Conclusions: ECV performed in the first 14 days after AF ablation was associated with a favorable long-term clinical outcome compared to no or late ECV. This impact depended on the AF type, favoring persistent AF.
THE CLINICAL OUTCOME OF EARLY CARDIOVERSION IN PATIENTS WITH EARLY RECURRENCE OF ATRIAL TACHYARRHYTHMIAS: THE EFFECT OF TIMING AND ATRIAL FIBRILLATION TYPEJinhee Ahn1, Kwang-No Lee2, Dong-Hyeok Kim3, Seung-Young Roh2, Dae-In Lee4, Jaemin Shim2, Jong-Il Choi2, Young-Hoon Kim2 1Pusan National University Hospital, Busan, Republic of Korea; 2Korea University Anam Hospital, Seoul, Republic of Korea; 3Cardiovascular Center, Sejong Hospital, Bucheon, Republic of Korea; 4Chungpuk National University Hospital, Chungji, Republic of Korea
CATHETER ABLATION P 2-037

309
Introduction: Statin therapy, reducing low-density lipoprotein cholesterol (LDL-C) levels, has been known to be an upstream strategy for atrial fibrillation (AF). However, whether use of statin prevents the recurrence after catheter ablation of atrial fibrillation (AF) remains de-bated. We aimed to assess the long-term effect of lipid reduction on the clinical outcomes following catheter ablation in patients with AF regardless of administration of statin.
Methods: A total of 553 consecutive patients who underwent catheter ablation were retrospectively studied (mean 57±11 years old, 20.4% female, 57.0% paroxysmal AF). Of them, three groups divided based on the degree of LDL-C reduction one year after index ablation were compared (Group 1, LDL-C reduction <10%, n=399; Group 2, 10%≤LDL-C reduction <30%, n=123; Group 3, 30%≤LDL-C reduction, n=31). Late gadolinium enhancement (LGE) in cardiac magnetic resonance image (MRI) were also assessed.
Results: Among each group, there was no significant difference in AF type (P=0.063). The proportions of heart failure (P=0.501), hyper-tension (P=0.358) and diabetes mellitus (P=0.734) were similar among each groups. Rates of use of statin after catheter ablation were similar in each groups (25.8% vs. 22.8% vs. 22.6%, P=0.754). During 58±37 months follow-up, 25 (80.6%) patients in group 3 have free-dom from AF recurrence compared with other groups [236 (59.7%) in group 1, P=0.024; 80 (68.4%) in group 2, P=0.163]. Kaplan-Meier estimates showed a significant difference in the recurrence of AF between group 1 and group 3. LGE-MRI scar burden in group 3 were lower than other groups, but there was no statistical significance (10.6±9.7% vs. 20.9±22.3%, vs. 17.8±17.2%, P=0.451). Cox-regression using a multivariate model revealed that persistent AF (HR 2.239, 95% CI 1.616-3.103, P<0.001) and LDL-C reduction≥30% (HR 0.185, 95% CI 0.046-0.745, P=0.018) were significantly associated with AF recurrence after catheter ablation.
Conclusions: Moderate to high-intensity reduction of LDL-C significantly improved the long-term success rate of catheter ablation in pa-tients with AF. This study suggests the aggressive LDL-C lowering strategy including lifestyle modification, independent of use of statin, facilitate the clinical outcomes for rhythm control.
REDUCTION OF BLOOD CHOLESTEROL ON RECURRENCE AFTER CATHETER ABLATION IN PATIENTS WITH ATRIAL FIBRILLATIONYong-Soo Baek, Jong-Il Choi, Hee-Soon Park, Kwang-No Lee, Seung-Young Roh, Jinhee Ahn, Dong-Hyeok Kim, Dae In Lee, Jaemin Shim, Jin Seok Kim, Hong Euy Lim, Sang-Weon Park, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CATHETER ABLATION P 2-038

310
Introduction: Catheter-tissue contact is one of the determinant for effective lesion formation. The purpose of the study was to determine the clinical outcomes of radiofrequency (RF) ablation using open-irrigated contact force (CF)-sensing ablation catheter compared with conventional catheter ablation in Thailand.
Methods: We retrospectively studied consecutive 601 RF ablation procedures (462 patients). The inclusion criteria was the patients who underwent catheter ablation by using electroanatomical mapping with image integration (CARTO) at Ramathibodi hospital from 2010 to 2015 (210 males, mean age 52±14 years, follow up time 39±19.5 months). The open-irrigated CF-sensing catheters, the THERMOCOOL® SMARTTOUCHTM Catheter (Biosense Webster) were applied to 95 procedures. All of the clinical outcomes were recorded. The endpoint was analyzed by x2 for nominal variables and t-test for continuous variables, P≤0.05 was considered significant.
Results: All procedures consisted of 401 atrial arrhythmias (167 AF, 135 AFL, 49 PAC, 50 AT), 194 ventricular arrhythmias (156 RVOT-PVC, 20 LV-VT 20, 18 other VT), 6 SVT (2 AVNRT, 1 AVRT, 1 JET), The CF-sensing ablation catheters were applied to atrial arrhythmia (58 proce-dures), ventricular arrhythmia (35 procedures) and SVT (4 procedures). During follow up, the total recurrence rate developed in 119 cases (19.8%). Compared with conventional catheter ablation group, the CF-sensing ablation catheter group had significantly lower recurrence rate (P=0.026), particularly focused on atrial arrhythmia RF ablation (22% and 38%, P=0.029). Most of recurrence occurred within 1 year. RF times were lower in AF cases (2,864.5±1,333 vs. 3,617.5±1,824 minutes, P=0.02). Fluoroscopic times were longer in CF-sensing ab-lation catheter group (20.8±20 minutes vs. 16.5±12.9 minutes, P=0.02). There was no mortality in all RF applications. There was no dif-ference in procedure times (230.6±107 minutes vs. 226±100 minutes, P=0.78) and serious complications (P=0.56). Contrast with ven-tricular arrhythmia cases, which were no difference of recurrence rate in CF-sensing group compared with conventional ablation group (8% vs. 10%, P=0.3), RF times (P=0.22), procedure times (P=0.06) and fluoroscopic times (P=0.38).
Conclusions: Application of open-irrigated force-sensing ablation catheter associated with lower recurrence rate, particularly in atrial ar-rhythmia and decrease RF time in AF ablation.
IMPACT OF CONTACT FORCE AS A PREDICTOR OF CLINICAL OUTCOME IN RADIOFREQUENCY ABLATIONSanisara Chandrachamnong, Tachapong Ngarmukos
Ramathibodi Hospital, Bangkok, Thailand
CATHETER ABLATION P 2-039

311
Introduction: Catheter ablation of the pulmonary veins is the firs-line therapy for drug-refractory paroxysmal atrial fibrillation (PAF). Ra-diofrequency and cryoballoon ablation are two frequently technologies, but which is better choice for PAF remains uncertain. The present systematic review and meta-analysis aims to assess safety and efficacy between radiofrequency and cryoballoon for PAF.
Methods: A systematic review was conducted in Medline, PubMed, Embase, Cochrane Library et al. All trials comparing radiofrequency and cryoballoon were screened and included if matching inclusion criteria.
Results: We identified 26 eligible studies, 10 randomized controlled trials (RCTs) and 16 non- RCTs, adding up to 9,047 patients. Pool- analyses indicated that CB ablation can bring more benefit in procedure duration (WMD=-14.17, 95% CI: -27.68 to -0.66), major complica-tions (RR=0.75, 95% CI: 0.62-0.91; I2=0%, P=0.48), and have a tendency to reduction atrial arrhythmias recrudescence (RR=0.93, 95% CI: 0.85-1.02; I2=38%, P=0.05) for PAF. Subgroup analysis, the results of non-RCTs were similar to overall trails,for RCTs, CB ablation was associated with a significantly reduction of major complications, procedure time, ablation time and atrial arrhythmias recrudescence were noninferior to RF ablation, however, longer fluoroscopy time was found in cryoballoon ablation.
Conclusions: Available overall and subgroups data suggested that cryoballoon ablation was more safer than RF ablation, and efficacy of cryoballoon ablation was noninferior to RF ablation for the treatment of PAF. Whereas, a tendency of longer fluoroscopic time should be improved in the future.
RADIOFREQUENCY OR CRYOBALLON ABLATION FOR PAROXYSMAL ATRAIL FIBRILLATION? A META-ANALYSIS AND SYSTEMATIC REVIEWChao-feng Chen, Yi-zhou Xu
Hangzhou First People Hospital, Hangzhou, China
CATHETER ABLATION P 2-040

312
Introduction: Myocardial infarction (MI) has a high risk for stroke due to thrombus formation after MI and the coexistent atherosclerosis of cerebral arteries. Atrial fibrillation (AF) is also a risk factor of stroke. We evaluate the impact of AF on stroke after MI, through a retrospec-tive analysis of data from the Taiwan National Health Insurance Research Database.
Methods: This is a nationwide, propensity score-matched case-control study of patients admitted between 2000/01 and 2012/12 with a primary diagnosis of a first acute MI. 170,472 patients were selected and 8,530 patients also had a diagnosis of AF (AF group). A propensity score, one-to-one matching on the variables of sex and age was used to match 8,530 controls without AF for analysis (control group). Stroke was defined as the following admission with a primary diagnosis of stroke after up to 13 years of follow up.
Results: AF group had more NSTEMI (66.07% vs. 62.44%, P<0.001), heart failure (29.57% vs. 19.64%, P<0.001), and COPD (7.15% vs. 6.19%, P=0.0119) but less hypertension (30.81% vs. 35.38%, P<0.001), DM (20.2% vs. 29.84%, P<0.001), dyslipidemia (8.84% vs. 14.87%, P<0.001), ESRD (1.41% vs. 1.79%, P=0.0441), and intervention (PCI/CABG) (40.47% vs. 42.39%, P=0.0108). The use of aspirin (82.91% vs. 77.95%, P<0.001), clopidogrel (64.33% vs. 59.34%, P<0.001), ACEI/ARB (66.62% vs. 59.5%, P<0.001), beta blocker (53.22% vs. 48.36%, P<0.001), warfarin (12.26% vs. 2.06%, P<0.001), Class III antiarrhythmic drugs (AAD) (37.55% vs. 8.56%, P<0.001), digoxin (27.21% vs. 8,19%, P<0.001), and non-dihydropyridine CCB (21.47% vs. 11.84%, P<0.001) were higher in AF group but the use of statin was lower (30.6% vs. 32.4%, P=0.0111). The stroke rate after a first MI was higher in AF group (6.27% vs. 3.82%, P<0.001). Subgroup analysis re-vealed that stroke was not significant higher in patients with COPD (HR 1.12; 95% CI, 0.76-1.66) and ESRD (HR 2.62; 95% CI, 0.89-7.69), and with the use of warfarin (HR 1.33; 95% CI, 0.82-2.15), Class III AAD (HR 1.15; 95% CI, 0.85-1.53), and Digoxin (HR 1.29; 95% CI, 0.98-1.71) (Figure 1).
Conclusions: In patients with AMI after up to 13 years of follow up, stroke was significant higher in AF group. Subgroup analysis revealed that stroke was not significant higher in patients with COPD, ESRD, and with the use of warfarin, Class III AAD, and Digoxin.
RISK OF STROKE AFTER MYOCARDIAL INFARCTION IN PATIENT WITH OR WITHOUT ATRIAL FIBRILLATIONCheng-Hung Chiang, Hsiao-Chin Lin, Tzu-Jung Chuang, Pei-Ling Tang, Wei-Chun Huang, Guang-Yuan Mar, Chun-Peng Liu
Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
CATHETER ABLATION P 2-041

313
CATHETER ABLATION P 2-041

314
Introduction: The STAR-AF II trial revealed the meaninglessness of additional modification of the pulmonary vein isolation (PVI) in per-sistent atrial fibrillation (AF). We aimed to elucidate the effectiveness of an intensive isolation by routinely performing PVI with a posterior wall isolation and linear ablation.
Methods: A total of 219 persistent AF patients (age: 58±9 years, CHADS2: 0.8±0.9, male: n=196 [89.5%], longstanding persistent AF: n=95 [43.4%]) who underwent radiofrequency catheter ablation were evaluated. The patients were divided into 3 groups according to the ablation protocols performed; 1) a PVI with or without cavotricuspid isthmus ablation (PVI±CTI group, n=109); 2) a PVI with a linear abla-tion of a roof, bottom, or left mitral isthmus line (PVI+Line group, n=39), and 3) a simultaneous isolation of the posterior wall and all PVs in combination with a linear ablation of both the cavotricuspid isthmus and left mitral isthmus (BOX+LMI+CTI group, n=70). Patients were followed-up for 28.0±17.6 months. A relapse was defined either by AF at the last clinic visit or by redo sessions performed during the fol-low-up period. The patient background and ablation outcomes were compared among the groups.
Results: The mean CHADS2 score, CHA2DS2-VASc score, age, body mass index, serum BNP level, and left atrial size measured using transthoracic echocardiography did not differ among the groups. The proportion of a female gender, patients with the post-procedural be-ta-blockers, or antiarrhythmic drugs did not differ among the groups. The flow velocity of the left atrial appendage measured using trans-esophageal echocardiography was significantly slower in the BOX+LMI+CTI group (49.4±18.9 [n=96] vs. 51.2±18.9 [n=31] vs. 39.2±17.8 cm/sec [n=69], P<0.001). The number of ablation applications was significantly higher in the PVI+Line group (83.4±29.8 [n=73] vs. 104.4±30.7 [n=25] vs. 89.7±23.5 [n=54], P=0.007). AF relapses were the lowest in the BOX+LMI+CTI group (37.3% [n=41] vs. 33.3% [n=13] vs. 21.4% [n=15], P=0.080), though it was not significant. The number of patients with atrial tachycardia was the highest in the PVI+Line group (4.5% [n=5] vs. 10.2% [n=4] vs. 8.6% [n=6], P=0.377).
Conclusions: The posterior wall isolation in addition to the PVI and linear ablation might yield a better prognosis in persistent AF.
THE FEASIBILITY OF A BOX ISOLATION WITH LINEAR ABLATION IN PERSISTENT ATRIAL FIBRILLATIONTaishi Fujisawa, Takehiro Kimura, Seiji Takatsuki
Keio University Hospital, Shinjuku, Tokyo, Japan
CATHETER ABLATION P 2-042

315
Introduction: To date, radiofrequency catheter ablation (RFCA) and cryoballoon-base ablation (CBA) have been used in the largest num-ber of AF patients. However, it remains unknown that the extent of inflammatory cytokines are different between RFCA and CBA. The level of inflammatory cytokines might be useful for identifying those patients likely to have better outcomes after catheter ablation.
Methods: We collected serum from paroxysmal AF patients who underwent RFCA or CBA. Thirty-one cytokines, chemokines and growth factors (TNF-a, IFN-g, G-CSF, GM-CSF, IL-1a, IL-8, IP-10, Rantes, VEGF, EGF, IL-6, Resistin, PAI-1, IL-12, IL-13, Eotaxin-3, PDGF-BB, PIGF-1, b-NGF, SCF, MCP-1, MIP-1a, IL-2, IL-4, IL-10, FGFb, Leptin, IGF-1, TGF-b, Adipo, and IL-1b) expressions were screened by en-zyme-linked immunosorbent assay.
Results: Our data indicated the level of IL-2 was increased both in RFCA and CBA patients. RFCA patients had a higher serum level of IL-2 compared to that in CBA patients. We also found the level of IL-6 and TGF-b were increased in RFCA, but decreased in CBA. In addi-tion, there are eighteen inflammatory factors lower expression in CBA than in RFCA.
Conclusions: Postoperative inflammatory reaction was stronger in RFCA group than in CBA group in our study population.
THE LEVEL OF INFLAMMATORY CYTOKINES BETWEEN RADIOFREQUENCY AND CRYOBALLOON AFTER ATRIAL FIBRILLATION ABLATIONYa-Wen Hsiao
Taipei Veterans General Hospital, Taipei, Taiwan
CATHETER ABLATION P 2-043

316
Introduction: Although radiofrequency catheter ablation (RFCA) is an effective rhythm control strategy in patients with persistent AF (PeAF), it still has a substantial recurrence rate. We recently developed patient’s heart CT-left atrial (LA) image integrated in-silico 3D AF modeling with clinically acceptable computing speed, and validated 86% match of the best virtual ablation lesion set and empirical abla-tion lesion set in retrospective study. We conducted prospective study to test feasibility, efficacy, and safety of virtual ablation guided RFCA (V-ABL), comparing with empirical ablation (Em-ABL) in patients with PeAF.
Methods: We included 108 patients with antiarrhythmic drug (AAD) resistant PeAF (77.8% male, 60.8±9.9 years old) who underwent RFCA, and randomly assigned to V-ABL (n=53) and Em-ABL (n=55). For V-ABL, we tested 5 different ablation lesion sets (circumferential pulmonary vein isolation (CPVI), CPVI+posterior box (PostBox) lesion, CPVI+PostBox+anterior line (AL), CPVI+roof line (RL)+left lateral isth-mus line (LLI), and CPVI+complex fractional atrial electrogram (CFAE) ablation) at LA-CT image integrated in-silico AF modeling, and the operator followed the ablation strategy with the shortest AF maintenance. We evaluated computing time for testing the best V-ABL strate-gy, and compared procedure related factors and clinical outcome between V-ABL and Em-ABL strategies.
Results: 1) In overall patients, pre-procedural computing time for 5 different ablation strategy was about 3 hours, and CPVI+PostBox+AntL most commonly showed the earliest termination rate (52.8%). 2) Among Em-ABL group, the earliest terminating in-silico ablation strate-gy match with empirical ablation in 21.9%. 3) V-ABL was not inferior to Em-ABL in terms of procedure time (256.2±69.0 vs. 271.5±104.7 minutes, P=0.403), ablation time (4,954.7±2,804.0 vs. 5,272.8±2,368.2 seconds, P=0.510), and major complication rate (4.4% vs. 4.0%, P=0.900). 4) During 12.6±3.8 months follow-up, clinical recurrence rate after 3 month of ablation were 14.0% in V-ABL group and 18.9% in Emp-ABL group (P=0.538). 5) After excluding the patients matching the best virtual ablation strategy and empirical ablation strategy in Emp-ABL group, clinical recurrence rates were 14.0% in V-ABL group and 22.0% in Emp-ABL group, respectively (P=0.355).
Conclusions: V-ABL was feasible in clinical practice with non-inferiority to Em-ABL in terms of procedure time, ablation time, complica-tion rate, and short-term clinical recurrence rate in patients with PeAF.
VIRTUAL IN-SILICO MODELING GUIDED CATHETER ABLATION VS. EMPIRICAL ABLATION FOR LONGSTANDING PERSISTENT ATRIAL FIBRILLATION: MULTICENTER PROSPECTIVE RANDOMIZED STUDYHui-Nam Pak1, Jaemin Shim2, Young-Seo Oh3, Gi-Byung Nam4, Young-Geun On5, Tae-Hoon Kim1, Seil Oh6, Byung-Hyun Lim1, Minki Hwang1, Eun Bo Shim7 1Severance Hospital, Seoul, Republic of Korea; 2Korea University College of Medicine, Seoul, Republic of Korea; 3The Catholic University of Korea School of Medicine, Seoul, Republic of Korea; 4Asan Medical Center, Seoul, Republic of Korea; 5Samsung Medical Center, Seoul, Republic of Korea; 6Seoul National University College of Medicine, Seoul, Republic of Korea; 7Kangwon National University College of Medicine, Chuncheon, Republic of Korea
CATHETER ABLATION P 2-045

317
Introduction: Pulmonary vein isolation (PVI) with radiofrequency energy is widely used as a strategy for catheter ablation of atrial fibrilla-tion (AF). Single-shot devices for PVI have been developed to facilitate safe and simple PVI to treat paroxysmal AF (PAF). PVAC GOLD® (Pulmonary Vein Ablation Catheter (PVAC) using gold electrode; Medtronic, Minneapolis, MN) is one of those kinds of catheters and it may have a similar safety and efficacy profile as the standard approach, but with reduced procedure and fluoroscopy time. Herein, we report our results of the acute procedural results and parameters of AF catheter ablation using PVAC GOLD®.
Methods: From December 2015 to April 2016, we consecutively enrolled 22 patients with symptomatic, drug refractory AF. All patients un-derwent PVI using PVAC GOLD®.
Results: Mean patients age was 62.4±6.4 years and mean CHA2DS2-Vasc score was 2.1±1.4. Twelve patients (50%) were male and 5 pa-tients (23%) were persistent AF. Complete PVI was achieved during procedure in 20 patients (acute PVI success rate 91%). Two patients resulted incomplete PVI and three dimensional electroanatomic mapping system was used for additional PVs isolation. Procedural pa-rameters were as follows: mean procedure time 160.6±72.5 minutes, mean fluoroscopy time 36.7±23.6 minutes, mean radiofrequency energy duration time 29.6±9.7 minutes. There were no procedure related complications.
Conclusions: The novel pulmonary vein ablation catheter PVAC GOLD® showed acceptable acute procedural outcome in terms of PVI suc-cess rate and procedural parameters. Midterm follow up results will be presented later.
ACUTE PROCEDURAL OUTCOME AND PROCEDURAL PARAMETERS OF ATRIAL FIBRILLATION CATHETER ABLATION USING THE NOVEL PULMONARY VEIN ABLATION CATHETER PVAC GOLD®
Jongmin Hwang, Jun Kim, Minsu Kim, Ji Hyun Lee, You Mi Hwang, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim
Heart Institute, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Republic of Korea
CATHETER ABLATION P 2-046

318
Introduction: Successful catheter ablation (CA) for atrial fibrillation (AF) leads to improved renal function in patients with chronic kidney disease (CKD). However, it is unclear whether multiple sessions for treating recurrent AF can improve renal function.
Methods: One hundred and eighty seven paroxysmal and persistent AF patients who underwent CA between September 2013 and August 2015 were included. Estimated glomerular filtration rate (eGFR) was calculated, and the patients were classified into two groups accord-ing to the baseline eGFR: CKD group-eGFR < 60 mL/min/1.73m², and non-CKD group-eGFR ≥ 60 mL/min/1.73m². Patients underwent electrophysiological study (EPS) and 2nd session if needed, six months apart, and were followed up for recurrence of atrial arrhythmia and changes in eGFR.
Results: A total of 167 patients were included in the study. Twenty patients were excluded for reasons such as on-going dialysis, EPS not performed at 6 months after the 1st session, and no follow-up data from blood sampling. If recurrence did not occur by 6 months after the 1st session, eGFR increased significantly compared to baseline in both, CKD (n=41, 52.31±8.08 to 59.23±11.82, p < 0.001) and non-CKD groups (n=82, 73.27±10.78 to 76.93±11.37, P=0.001). In patients with recurrence, eGFR did not increase significantly in the CKD group (n=14, 49.44±9.84 to 51.91±11.61, P=0.232) and no increase was observed in the non-CKD group (n=27, 72.20±13.36 to 71.40±12.84, P=0.703). Within the CKD group, in patients with recurrence after 1st session but free from atrial arrhythmia after 2nd, eGFR at 1 year after 1st session increased significantly compared to baseline (n=7, 48.59±10.20 to 53.77±12.75, P=0.016). However, the eGFR did not increase in patients with recurrence even after 2nd session (n=6, 51.40±10.70 to 50.07±12.02, P=0.662).
Conclusions: Successful CA in multiple sessions for recurrent AF can improve the renal function in patients with CKD.
SUCCESSFUL CATHETER ABLATION WITH MULTIPLE SESSIONS FOR RECURRENT ATRIAL FIBRILLATION IMPROVES THE RENAL FUNCTION IN PATIENTS WITH CHRONIC KIDNEY DISEASEDai Inagaki1, Seiji Fukamizu1, Yasuki Koyano1, Sayuri Tokioka1, Daisuke Miyahara1, Marina Arai1, Tomonori Miyabe1, Kiyotaka Yoshida1, Satoshi Miyazawa1, Iwanari Kawamura1, Akihiro Nakada1, Syo Nagamine1, Shinichiro Masuda1, Takeshi Kitamura1, Rintaro Hojo1, Yuya Aoyama1, Takaaki Tsuchiyama1, Kota Komiyama1, Takashi Shibui1, Mitsuhiro Nishizaki2, Harumizu Sakurada3, Masayasu Hiraoka4 1Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan; 2Yokohama Minami Kyosai Hospital, Yokohama, Japan; 3Tokyo Metropolitan Health and Medical Treatment Corporation Ohkubo Hospital, Tokyo, Japan; 4Toride Kitasohma Medical Center Hospital, Toride, Japan
CATHETER ABLATION P 2-047
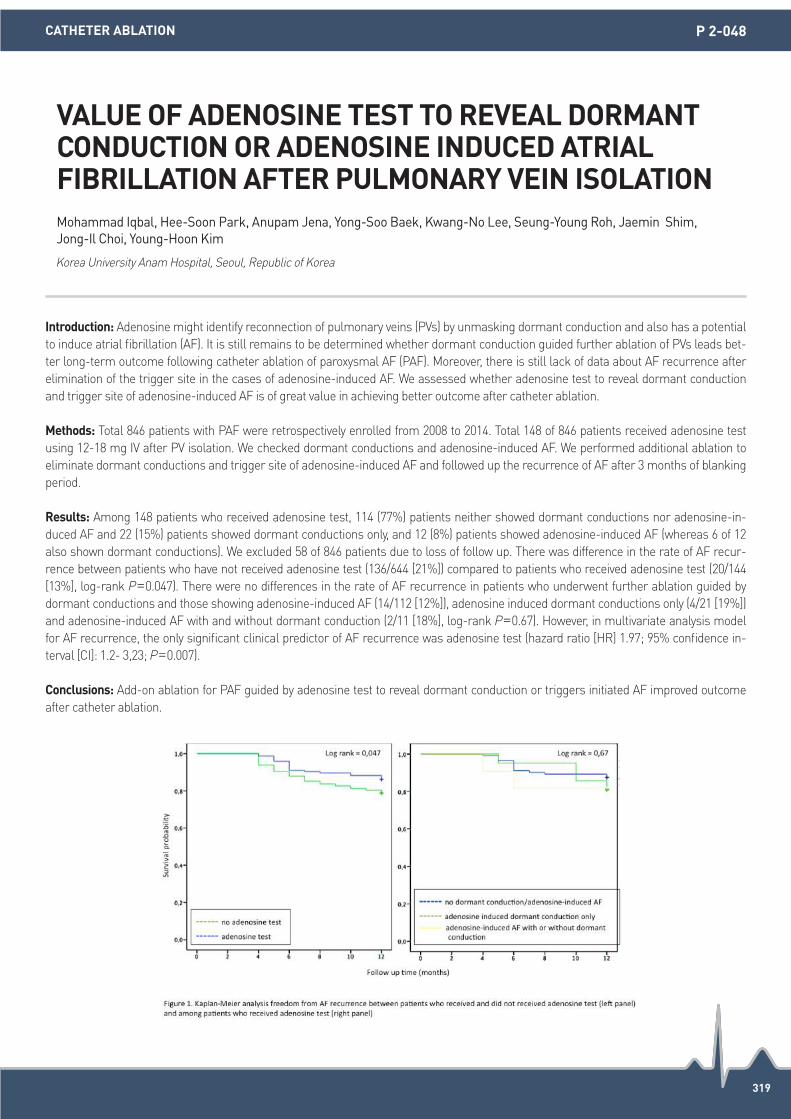
319
Introduction: Adenosine might identify reconnection of pulmonary veins (PVs) by unmasking dormant conduction and also has a potential to induce atrial fibrillation (AF). It is still remains to be determined whether dormant conduction guided further ablation of PVs leads bet-ter long-term outcome following catheter ablation of paroxysmal AF (PAF). Moreover, there is still lack of data about AF recurrence after elimination of the trigger site in the cases of adenosine-induced AF. We assessed whether adenosine test to reveal dormant conduction and trigger site of adenosine-induced AF is of great value in achieving better outcome after catheter ablation.
Methods: Total 846 patients with PAF were retrospectively enrolled from 2008 to 2014. Total 148 of 846 patients received adenosine test using 12-18 mg IV after PV isolation. We checked dormant conductions and adenosine-induced AF. We performed additional ablation to eliminate dormant conductions and trigger site of adenosine-induced AF and followed up the recurrence of AF after 3 months of blanking period.
Results: Among 148 patients who received adenosine test, 114 (77%) patients neither showed dormant conductions nor adenosine-in-duced AF and 22 (15%) patients showed dormant conductions only, and 12 (8%) patients showed adenosine-induced AF (whereas 6 of 12 also shown dormant conductions). We excluded 58 of 846 patients due to loss of follow up. There was difference in the rate of AF recur-rence between patients who have not received adenosine test (136/644 [21%]) compared to patients who received adenosine test (20/144 [13%], log-rank P=0.047). There were no differences in the rate of AF recurrence in patients who underwent further ablation guided by dormant conductions and those showing adenosine-induced AF (14/112 [12%]), adenosine induced dormant conductions only (4/21 [19%]) and adenosine-induced AF with and without dormant conduction (2/11 [18%], log-rank P=0.67). However, in multivariate analysis model for AF recurrence, the only significant clinical predictor of AF recurrence was adenosine test (hazard ratio [HR] 1.97; 95% confidence in-terval [CI]: 1.2- 3,23; P=0.007).
Conclusions: Add-on ablation for PAF guided by adenosine test to reveal dormant conduction or triggers initiated AF improved outcome after catheter ablation.
VALUE OF ADENOSINE TEST TO REVEAL DORMANT CONDUCTION OR ADENOSINE INDUCED ATRIAL FIBRILLATION AFTER PULMONARY VEIN ISOLATIONMohammad Iqbal, Hee-Soon Park, Anupam Jena, Yong-Soo Baek, Kwang-No Lee, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 2-048

320
Introduction: Arial fibrillation (AF) is known to be common in patients with hypertrophic cardiomyopathy (HCM). The clinical characteris-tics of AF in HCM patients are not well elucidated. Here, we evaluated the prevalence of HCM in AF ablation candidates and evaluated its impact on the ablation outcome.
Methods: A consecutive series of 501 paroxysmal AF (male: n=410 [81.8%], age: 61±10 years, CHADS2: 0.7±0.9) who underwent cathe-ter ablation were evaluated. The ablation protocol was limited to a pulmonary vein isolation with or without other linear ablation by ex-cluding cases with CFAE ablation and superior vena cava isolations. HCM was diagnosed by transthoracic echocardiography, performed prior to the ablation session. The patients were followed-up for 18.9±10.9 months after the procedure. AF relapses were defined either by AF at the last clinic visit or by the necessity for a redo session performed during the follow-up period. The patient characteristics and ab-lation outcome were assessed between the non-HCM group and HCM group.
Results: The prevalence of HCM was 2.4% (n=12) in the AF ablation candidates. The mean age, CHADS2 score, CHA2DS2-VASc score, body mass index, and prevalence of a female gender did not differ between the groups. The serum BNP level was significantly higher in the HCM group (65.7±124.8 [n=460] vs. 212.9±293.7 pg/mL [n=10], P=0.001), but the left ventricular ejection fraction was significantly higher in the HCM group (59.4±8.1 [n=450] vs. 65.0±6.7% [n=12], P=0.015). The deceleration time of the mitral flow was significantly longer (207.2±49.8 [n=424] vs. 240.0±35.7 msec [n=12], P=0.006) and the septal E/E’ was significantly larger (8.5±3.4 [n=310] vs. 11.7±3.7 [n=8], P=0.010) in the HCM group. The left atrial size (P=0.100), atrial kick of the mitral flow, and flow velocity of the left atrial append-age (P=0.591) did not differ between the groups. The number of patients receiving a left mitral isthmus ablation was higher in the HCM group (6.5% [n=32] vs. 25% [n=3], P=0.013, odds ratio [OR]: 4.760, 95% confidence interval [CI]: 1.228-18.453), but those with a cavotri-cuspid isthmus ablation or roof line did not differ. The post-procedural use of beta-blockers and antiarrhythmic drugs did not differ. AF re-lapses were significantly higher in the HCM group (22.3% [n=119] vs. 50% [n=6], P=0.024, OR: 3.486, 95% CI: 1.102-11.026). The incidence of atrial tachycardia was also higher in the HCM group (5.1% [n=25] vs. 25% [n=3], P=0.003, OR: 6.187, 95% CI: 1.576-24.279).
Conclusions: The ablation outcome of paroxysmal AF in HCM patients was poor, but the well-known atrial parameters did not show se-vere remodeling.
THE CHARACTERISTICS OF PAROXYSMAL ATRIAL FIBRILLATION IN HYPERTROPHIC CARDIOMYOPATHYShin Kashimura, Taishi Fujisawa, Kazuaki Nakajima, Akira Kunitomi, Yoshinori Katsumata, Takahiko Nishiyama, Takehiro Kimura, Nobuhiro Nishiyama, Yoshiyasu Aizawa, Keiichi Fukuda, Seiji Takatsuki
Keio University Hospital, Tokyo, Japan
CATHETER ABLATION P 2-049

321
Introduction: Several studies reported the risk factor of recurrence of atrial fibrillation (AF) after catheter ablation (CA). However, the dif-ference between early and late phase AF recurrence (AFR) after CA was unclear.
Methods: A total of 805 consecutive patients underwent 1st session of CA (1stCA) for AF between January 2011 to December 2013. After pulmonary vein isolation (PVI), all patients underwent high-dose isoproterenol infusion (up to 20 μg/min) for the detection of non-PV foci, and underwent CA for non-PV foci. During 23±11 months follow up period, 249 patients (61.4±10.4 years, male 174, paroxysmal AF (PAF) 145) experienced AFR, and 213 patients underwent 2nd session of CA (2ndCA). In 2ndCA, left atrium and PV reconnection was evaluated, and existence of non-PV foci was also re-evaluated using high-dose isoproterenol. We divided them into 2 groups; 196 patients with AFR within a year after 1stCA (early phase recurrence, ER-group) and 53 patients with AFR more than 1 year (late phase recurrence, LR-group), and difference between ER-group and LR-group was evaluated.
Results: There were no significant differences in preoperative values and distribution of non-PV foci in 1stCA between ER-group and LR-group. In 2ndCA, prevalence of reconnection of left-sided PVs and non-PV foci from interatrial septum (IAS) were significantly higher in ER-group (61% vs. 49% and 35% vs. 16%, P=0.02, respectively). In PAF patients, there were no significant differences in preoperative val-ues and distribution of non-PV foci in 1stCA and 2ndCA between both groups. In non-PAF patients, lower EF was significantly associated with ER-group (hazard ratio 1.09, 95% confidence interval 1.01-1.17, P=0.02) in multivariable model. In 2ndCA, the prevalence of recon-nection of left-sided PVs and non-PV foci from IAS were significantly higher in ER-group (61% vs. 28% and 42% vs. 11%, P=0.02, respec-tively).
Conclusions: Early phase AFR was more involved in reconnection of left-sided PVs and non-PV foci from IAS than late phase AFR.
IMPACT OF DIFFERENT MECHANISM BETWEEN EARLY AND LATE PHASE RECURRENCE OF ATRIAL FIBRILLATION AFTER CATHETER ABLATIONNobutaka Kato1, Junichi Nitta1, Takashi Ikenouchi1, Yousuke Hayashi1, Kazuya Murata1, Kiko Lee1, Tatsuhiko Hirao1, Tomomasa Takamiya1, Yukihiro Inamura1, Akira Sato1, Masahiko Goya2, Kenzo Hirao2 1Saitama Red Cross Hospital, Saitama, Japan; 2Heart Rhythm Center, Tokyo Medical and Dental University, Tokyo, Japan
CATHETER ABLATION P 2-050

322
Introduction: Identification of a left atrial appendage (LAA) thrombus before pulmonary vein antral isolation (PVAI) is an important pre-procedural imaging step. There was a single case report of accidental embolic episode after direct current cardioversion in a patient who did not exhibit a thrombus on pre-procedural TEE, likely because of the delay between imaging and the procedure. Therefore we in-vestigated the presence of stagnant dye staining detected via LAA angiography (LAA-AG) during PVAI. Results of real-time LAA stagnant dye staining detection via LAA-AG, TEE, cardiac MDCT and LAA voltage mapping were compared.
Methods: A total of 130 patients with AF who underwent PVAI were consecutively enrolled. During PVAI, after interatrial septal puncture, Swartz 8 F, SL 0 or 1 sheaths were inserted into the LA and pulmonary venograms and LAA-AG were performed by hand injection of 10 cc contrast agent (VISIPAQUE-iodxanol). The results of LAA-AG were divided into two groups: the LAA stagnant dye staining group (presence of stagnant LAA staining during LAA-AG, n=46) and the LAA non-staining group (absence of stagnant LAA staining during LAA-AG, n=84). LAA function was measured via TEE and LAA density was assessed by cardiac MDCT. Also, we measured LAA and LA voltage using the Carto-3 system during PVAI.
Results: At baseline, the duration of AF and PT INR did not vary between groups. The LAA stagnant dye staining group showed signifi-cantly reduced LAA function and a higher prevalence of spontaneous echo contrast (SEC) than the LAA non-staining group (LAA inflow velocity (cm/s): 32.0±16.7 vs. 48.3±18.5, P<0.001; LAA outflow velocity (cm/s): 37.7±15.9 vs. 51.1±16.3, P<0.001; SEC: 52.2% vs. 19.0%, P=0.008). There were no significant differences in LAA density during the enhancement phase (in Hounsfield units (HU): 338.2±75.4 vs. 352.9±75.0, P=0.289; mean LAA/ascending aorta HU ratio: 0.89±0.96 vs. 0.91±0.73, P=0.191) on cardiac MDCT. Also, the two groups showed no significant differences in mean LAA voltage (bipolar (mV): 3.00±1.41 vs. 3.04±1.64, P=0.932; unipolar (mV): 3.69±1.42 vs. 4.08±1.98, P=0.464) and mean LA voltage (Bipolar (mV); 1.05±0.56 vs. 1.20±0.75, P=0.462 and Unipolar (mV); 2.06±0.74 vs. 2.38±0.85, P=0.187).
Conclusions: This is the first report of real-time stagnant dye staining during PVAI. LAA stagnant dye staining detected on LAA-AG was related to decreased LAA function.
DETECTION OF REAL-TIME LEFT ATRIAL APPENDAGE STAGNANT DYE STAINING DURING PULMONARY VEIN ANTRAL ISOLATIONBong-Joon Kim, Ga-In Yu, Dong-Hyun Park, Tae-Joon Cha
Kosin University Gospel Hospital, Busan, Republic of Korea
CATHETER ABLATION P 2-051

323
Introduction: The choice of oral anticoagulants (OACs) has been broadened for atrial fibrillation (AF) catheter ablation. We aimed to eluci-date the characteristics of the use of OACs in AF ablation candidates and discriminate the risk of the procedural complications.
Methods: A consecutive series of 1,278 AF ablation sessions (male: 1,087 [85.1%]; Age: 59±10 years old; CHADS2: 0.7±0.9, CHA2DS2-VASc: 1.3±1.3, persistent AF: 463 [36.3%]) since 2010 were retrospectively evaluated. The OACs were administered either using warfarin, dabigatran, rivaroxaban, or apixaban, at least 1 month prior to the catheter ablation. The OACs were withheld within 6 hours prior to the session and resumed after the session.
Results: The number of sessions with warfarin, dabigatran, rivaroxaban, and apixaban were 656, 199, 329, and 86, respectively. The choice of OACs was changed yearly; the proportion of patients with OACs except for warfarin was 11.6% in 2011, 39.1% in 2012, 56.1% in 2013, 77.9% in 2014, 66.5% in 2015, and 83.6% in 2016. The CHADS2 score differed significantly among the OACs (warfarin: 0.9±1 vs. dabigatran: 0.7±0.9 vs. rivaroxaban 0.6±0.8 vs. apixaban 0.5±0.7, P<0.001). The mean age was the highest with apixaban (warfarin: 60±10 vs. dab-igatran: 58±10 vs. rivaroxaban 58±10 vs. apixaban 62±11 y/o, P<0.001). The creatinine clearance was the highest with dabigatran (war-farin: 72.8±23.3 vs. dabigatran: 82.6±33.6 vs. rivaroxaban 79.9±24.4 vs. apixaban 72.2±21.8 mL/min, P<0.001). The proportion of per-sistent AF did not differ among the OACs (P=0.163). The left atrial size measured using transthoracic echocardiography did not differ among the OACs (P=0.092), however, the mean flow velocity of the left atrial appendage measured using transesophageal echocardiogra-phy was the lowest with warfarin (P=0.012). The incidence of pericardial effusions did not differ among the OACs (warfarin: 8 [1.2%] vs. dabigatran: 2 [1%] vs. rivaroxaban 3 [0.9%] vs. apixaban 0 [0%], P=0.758). The incidence of femoral fistulae (P=0.433), pseudoaneurysms (P=0.922), or post procedural strokes (P=0.648) did not differ among the OACs.
Conclusions: The use of OACs except for warfarin was widely accepted in Japan and the patient background varied, the procedural com-plications did not differ among the OACs.
THE CHARACTERISTICS OF ATRIAL FIBRILLATION PATIENTS WITH PERIPROCEDURAL ORAL ANTICOAGULANTSTakehiro Kimura, Taishi Fujisawa, Kazuaki Nakajima, Shin Kashimura, Akira Kunitomi, Takahiko Nishiyama, Yoshinori Katsumata, Nobuhiro Nishiyama, Yoshiyasu Aizawa, Keiichi Fukuda, Seiji Takatsuki
Keio University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 2-052

324
Introduction: A dimension, volume and function of LA and LGE of the LA are known as a prognostic factor for the clinical outcome of AF ablation. This study aimed to compare efficiency of prediction among those parameters using echocardiography and CMR.
Methods: 88 patients (67 males; 55 years old; 45 persistent AF) underwent TTE and CMR was performed one day before AF ablation.-As-sessing LA function Phasic volumes were used to calculate LA emptying fraction (LAEF) ([maximum-minimum LAV]/maximum LAV×100). Definition of LGE and LGE stageLGE was defined as areas with thresholds of 6-SD above mean signal in unenhanced LV wall. The LGE stage was defined based on delayed enhancement (DE) volume area divided by LA volume (Stage 1: 5%, Stage 2:15%, Stage 3 25%, Stage 4: 35%).
Results: During follow-up (mean follow-up duration: 103 months), AT/AF recurred in 19/88 patients (21.5%; 3/43 in PAF; 16/45 in PeAF). Compared to patients without recurrence, those with recurrence had larger maximal/minimal LAVi (maximal: 5,421 vs. 4516, P=0.07; minimal: 4,022 vs. 2614, P=0.02) and LAD (45.56.5 vs. 40.15.8, P=0.001) and lower LAEF (2,410 vs. 4,516, P=0.001). ROC analysis for re-currence showed that LAEF had the largest area under curve (AUC=0.86, P=0.0001) compared to maximal LAVi (AUC =0.38, P=0.12), minimal LAVi (AUC=0.27, P=0.003) and LAD (AUC=0.23, P=0.0001). LGE stage was insignificantly higher in patients with recurrence (3.60.7 vs. 2.90.9, P=0.46). Cut-off value of LAEF for freedom from recurrence was 31.0% (sensitivity=0.82, specificity=0.78, P=0.001). However, in patients with PAF, those parameter was not significantly related with clinical outcome. In case of PeAF, only lower LAEF (2,311 vs. 407, P=0.001) and larger LAD (7.1 vs. 6.3, P=0.02) were significantly related with recurrence. Moreover only three (12.5%) of 24 patients with PeAF and LAEF>31.0% had recurrence during follow-up. Adjusting clinical risk factor, Cox-regression analysis showed that LAEF was only independent predictor for freedom from recurrence (HR=0.88; 95% CI; 0.82-0.95; P=0.001).
Conclusions: LAEF measured by CMR was superior to maximal/minimal LAVi, LAD and LGE stage in predicting the AT/AF recurrence af-ter AF ablation. Moreover, patients with PeAF and LAEF>31% had excellent clinical outcome.
LEFT ATRIAL EMPTYING FRACTION AS A PREDICTOR FOR CLINICAL OUTCOME IN PATIENTS WITH ATRIAL FIBRILLATION ABLATIONDae In Lee, Iqbal Mohammad, Kwang-No Lee, Seung Young Roh, Jinhee Ahn, Dong-Hyeok Kim, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 2-053

325
Introduction: Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and an independent risk factor for the development of thromboembolism leading to fatal or disabling stroke. Percutaneous LAA occlusion has the potential to change the clinical approach to stroke prevention in selected patients with AF, and several devices have been adopted to various degrees internationally. However until 2015 no peer-reviewed reports of experience with LAmbre™ are available.
Methods: A single-center, retrospective, nonrandomized study was conducted of LAA closure with the LAmbre or Watchman device in 43 patients with nonvalvular and valvular AF in 2012-2016. The primary outcome was to compare procedural: successful rate and composite procedure related event (pericardial effusion, device embolization, bail out surgery, stroke/embolism, major bleeding and death), and the secondary outcome was stroke/embolic event during follow up.
Results: LAmbre and Watchman were implanted in 17 and 26 patients, and both devices show promising implantation rate; 100% and 96% in LAmbre and Watchman group consecutively. LAmbre has lower procedural time (51.24±13.5 vs. 61.19±19.1, P=0.07), but higher composite procedure related event (11.8% vs. 0%, P=0.08). Both devices demonstrate that annualised stroke rates after LAA occlusion are favourable than expected stroke rates as predicted by CHADS-VASc score. However the median follow up in Watchman was only 12 months, in contrast to 37 months in LAmbre.
Conclusions: Our experience shows that both devices have comparable procedural successful rate, and has been shown to be efficacious strategy for stroke prevention. LAmbre can be perform faster and might be useful in high-volume laboratory, while Watchman has less composite complications. Continued investigation is required to evaluate success and complication rates in comparison with both devices.
LEFT ATRIAL APPENDAGE CLOSURE USING LAMBRE AND WATCHMAN DEVICE: CONSECUTIVE OBSERVATIONAL STUDYAnggia Lubis, Mohammad Iqbal, Emile Parapat, Dian Munawar, Beny Hartono, Muhammad Munawar
Binawaluya Cardiac Center, Jakarta Timur, Indonesia
CATHETER ABLATION P 2-054
Procedural Outcome
LAmbre Watchman P-value
Succesful Rates, % 100 96
Procedural Time, mean in minute 51.24±13.5 61.19±19.1 0.07
Composite Complication,% 11.80 0 0.08

326
Introduction: Little is known about the association between B-type natriuretic peptide (BNP) levels and catheter ablation of atrial fibrilla-tion (AF) in patients with heart failure. This study aimed to examine the impact of elimination of AF by catheter ablation on BNP levels in patients with left ventricular systolic dysfunction.
Methods: Fifty-four AF patients (mean age=59.8±12.5 years, 85% men) with left ventricular ejection fraction (LVEF) less than or equal to 50%, who underwent radiofrequency catheter ablation therapy of AF, were included. Mean LVEF was 39.7±10.2%. BNP sampling was performed at baseline, 3 days, and 1 month after ablation. The primary follow-up endpoint of this study was the recurrence of any AF or atrial tachycardia of more than 30 seconds duration, as confirmed by testing 6 months after ablation.
Results: All of the patients successfully underwent the catheter ablation procedure without development of decompensated heart failure. After a follow-up period of 6 months, the BNP levels decreased significantly in the non-recurrence group (n=35) (median 126.3 [interquar-tile 57.2-206.5] pg/mL, 63.5 [23.9-180.2] pg/mL, and 45.9 [21.9-160.3] pg/mL, P<0.001, respectively), but not in the recurrence group (n=19) (144.7 [87.1-217.3] pg/mL, 88.8 [12.9-213.2] pg/mL, and 118.5 [51.6-298.2] pg/mL, P=0.368, respectively). The patients in the non-recurrence group had a higher percentage relative reduction in BNP levels from baseline to 1 month after ablation than those in the recurrence group (56.5 [-9.0-77.4]% vs, -2.4 [-47.1-60.9]%, P=0.027). The cut-off value of relative reduction in BNP levels for freedom from recurrence of AF based on receiver operating characteristic curve was 16.8%, with a specificity of 74% and a sensitivity of 69%, respective-ly. Additionally, a relative reduction in BNP levels significantly correlated with an increase in LVEF after ablation (r=0.486, P<0.001).
Conclusions: Plasma BNP levels decreased significantly with successful catheter ablation of AF in patients with impaired LVEF. The de-crease in BNP levels might be associated with early recovery of cardiac function and subsequent maintenance of sinus rhythm at fol-low-up.
DECREASE IN B-TYPE NATRIURETIC PEPTIDE LEVELS AND SUCCESSFUL CATHETER ABLATION FOR ATRIAL FIBRILLATION IN PATIENTS WITH HEART FAILURE: A CLINICAL INDICATOR OF REVERSE REMODELINGYosuke Murase1, Yasuya Inden1, Satoshi Yanagisawa1, Aya Fujii1, Yosuke Kamikubo1, Yasunori Kanzaki1, Monami Ando1, Junya Funabiki1, Masaki Takenaka1, Noriaki Otake1, Makoto Hirai2, Toyoaki Murohara1 1Nagoya University Graduate School of Medicine, Nagoya, Japan; 2Nagoya University School of Health Sciences, Nagoya, Japan
CATHETER ABLATION P 2-055

327
Introduction: Low voltage zone (LVZ) represents fibrotic tissue and are substrates for atrial fibrillation (AF). Substrate ablation of LVZ in addition to pulmonary vein isolation (PVI) has been reported to improve the clinical outcome of persistent AF ablation. However, it is un-clear the difference of LVZ between patients with paroxysmal AF (PAF) and non-PAF for AF ablation. To clarify this issue, we analyzed the rate of LVZ and the recurrence rate during follow-up in PAF and non-PAF patients between those with and without LVZ.
Methods: One-hundred forty-five patients undergoing PVI and ganglionated plexus (GP) ablation were divided into 2 groups; patients with PAF (PAF group, n=77) and non-PAF (non-PAF group, n=68). Voltage mapping at left atrium (LA) was performed in all patients by 3-D au-tomated mapping system (NavX Velocity) during sinus rhythm before radiofrequency application. LVZ was defined as an area with bipolar peak-to-peak voltage amplitude <0.5 mV and ablated during AF ablation. Anti-arrhythmic medication was continued after AF ablation in 7 patients (PAF group, 9%) and in 27 patients (non-PAF group, 40%). The rate of LVZ and clinical outcome was compared in 2 groups be-tween patients with and without LVZ.
Results: LVZ was identified in 13 patients (17%) in PAF group and 42 patients (62%) in non-PAF group (P<0.01). The follow-up period was 10.4±2.2 months. In PAF group, AF recurred in 4 of 13 patients (31%) with LVZ and 7 of 64 patients (11%) without LVZ (P=0.16). Mean-while, in non-PAF group, AF recurrence observed in 4 of 42 patients (9%) with LVZ and 2 of 26 patients (8%) without LVZ (NS). No atrial tachycardia was identified in all patients in 2 groups.
Conclusions: LVZ is observed more in non-PAF patients. LVZ ablation in addition to PVI+GP ablation in non-PAF patients provides the similar outcome to those without LVZ. However, the clinical outcome tends to be poor in PAF patients with LVZ though additional substrate ablation at LVZ is added.
THE COMPARISON OF LEFT ATRIAL LOW VOLTAGE ZONE BETWEEN PAROXYSMAL ATRIAL FIBRILLATION (PAF) AND NON-(PAF) PATIENTS FOR ATRIAL FIBRILLATION ABLATIONYasutsugu Nagamoto, Yuji Muraoka, Yuto Fujii, Yuichi Morita, Yusuke Ueda, Kenichi Yamane, Yasuko Miyake, Mai Fujiwara, Shinji Mito, Hiromichi Tamekiyo, Tomokazu Okimoto, Yasuhiko Hayashi
Tsuchiya General Hospital, Hiroshima, Japan
CATHETER ABLATION P 2-056
328
Introduction: It is known that recurrence of atrial fibrillation (AF) during blanking period (BP) after catheter ablation (CA) is a risk of recur-rence after BP, but the relation between the pattern of sinus rhythm (SR) recovery in the cases with AF recurrence during BP and out-comes after BP is unclear. We sometimes experience the cases with recurrences of AF immediately after restoration of SR. We investigat-ed the relation between the presence of such immediate recurrences during BP and the recurrence rate after BP.
Methods: Among consecutive 133 patients who underwent first-time CA for paroxysmal AF (PAF) from January 2015 to August 2015 at our institution, we observed AF recurrence in 38 (28%) patients during BP of 3 months after procedures. The AF-free rate at 6 months af-ter CA was 44%. Then, they were divided into Group-A (patients with recurrences of AF within 10 minutes after restoration of SR by cardio-vesion electrically or pharmacologically; n=17) and Group-B (those maintained SR after cardioversion more than 10 minutes; n=21). We compared AF-free rate at 6 months between Group-A and Group-B.
Results: We found that the rate in Group-A was only 23% (n=5) and was significantly lower than that in Group-B (Group-A vs. Group-B= 18% vs. 62%, P=0.02).
Conclusions: About 40% of AF ablation patients with recurrences within BP were free from AF after BP. The phenomenon of immediately recurrence of AF during BP was a strong marker of AF recurrence afterwards.
PATTERN OF SINUS RHYTHM RECOVERY BY CARDIOVERSION AFTER RECURRENCE DURING BLANKING PERIOD IN PAROXYSMAL ATRIAL FIBRILLATION PATIENTS RECEIVING CATHETER ABLATION WAS ASSOCIATED WITH ABLATION OUTCOMERyo Nakamaru, Koichi Inoue, Koji Tanaka, Yuko Toyoshima, Takafumi Oka, Nobuaki Tanaka, Masato Okada, Hiroyuki Inoue, Katsuomi Iwakura, Kenshi Fujii
Sakurabashi Watanabe Hospital, Osaka, Japan
CATHETER ABLATION P 2-057

329
Introduction: Vitamin K Antagonist (VKA) to prevent thromboembolism in atrial fibrillation (AF) patients has limitations due to its narrow therapeutic window. Lower intensity of anticoagulation increases the risk of thromboembolism and infarction while higher intensity in-creases the risk of bleeding. We investigated current status of anticoagulation therapy with VKA and clinical bleeding event rates in Kore-an patients with AF through real-world registry.
Methods: Data were abstracted from the KORean Atrial Fibrillation Investigation II [KORAFII] registry. It was a multicenter, non-interven-tional, prospective observational study in which AF patients with CHADS2 ≥1 and newly started with VKA (started within the last 3 months) were enrolled from April 2013 to March 2014. Time in therapeutic range (TTR) >60% indicates well-controlled INR. Therapeutic target was INR of 2.0 to 3.0 in patients aged <70 years and 1.6 to 2.6 in patients aged≥70 years. 877 patients (Mean age 67, Male 60%) were en-rolled and followed up for one year.
Results: Among 852 patients who had one or more INR measurement during their follow-up period, 226 (27%) satisfied criteria for well-controlled INR and were classified as well controlled (WC), while 626 (73%) were classified as poorly controlled (PC). CHA2DS2-VASc score was higher in WC than in PC (3.2 vs. 2.9, P<0.001). The major bleeding events occurred more frequently among patients in PC than those in WC (5 cases vs. none) (P=0.16 by log-rank test), while the mean time to minor or clinically relevant non-major bleeding events were 290 days and 319 days for patients in WC and PC, respectively (P=0.07 by log-rank test). Patients in PC were younger (66 vs. 72 years, P<0.001) and had higher HAS-BLED score (1.5 vs. 1.4, P=0.03) than patient in WC.
Conclusions: In real-world practice, INR was poorly-controlled in patients with high bleeding risk, although it was relatively well-con-trolled in patients with high stroke risk than those with low risk. Repeated assessment, close monitoring of bleeding risk, and efficient treatment options to lower bleeding risk are needed during anticoagulation therapy.
QUALITY OF ANTICOAGULATION AND BLEEDING EVENT IN PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION NEWLY TREATED WITH VITAMIN K ANTAGONIST: A REVIEW OF REAL-WORLD REGISTRY [THE KORAF II]Il-Young Oh1, Jae-Seok Park2, Dae-Hee Shin3, Hyoung-Seob Park4, Jun-Hyung Kim5, Nam-Ho Kim6, Min-Soo Ahn7, Bo-Jeong Seo8, Young-Joo Kim8, Juneyoung Lee9, Young-Hoon Kim10 1Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 2Sejong General Hospital, Bucheon, Republic of Korea;
3Gangneung Asan Hospital, Gangneung, Republic of Korea; 4Dongsan Medical Center, Keimyung University, Daegu, Republic of Korea;
5Chungnam National University College of Medicine, Chungnam, Republic of Korea; 6Wonkwang University Hospital, Iksan, Republic of Korea; 7Yonsei University, Wonju Severance Christian Hospital, Wonju, Republic of Korea; 8Corporate Affairs & Health and Value, Pfizer Pharmaceuticals Korea Ltd., Seoul, Republic of Korea; 9Department of Biostatistics, College of Medicine, Korea University, Seoul, Republic of Korea; 10Korea University College of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 2-059

330
Introduction: How catheter ablation for atrial fibrillation affect patients taking dabigatran in real-world settings is unknown.
Methods: We investigated 1,252 patients prescribed dabigatran between April 2011 and February 2015, 281 (22.4%) of whom underwent catheter ablation for atrial fibrillation during the follow-up period (ABL group). Cerebral infarction, embolic events, hemorrhagic events, and all-cause death were compared between the ABL and non-ABL group (971 patients, 77.6%).
Results: The mean age was 69.1±11.4 years. Men accounted for 65.5% (820/1,252 patients). The average period of postprescription mon-itoring was 10.4±10.6 months. The mean CHADS2 score was 0.85±0.95 in the ABL group and in 1.87±1.32 in the non-ABL group. Cere-bral infraction occurred in no one in the ABL group and in 10 patients in the non-ABL group (0% vs. 1.0%, P=0.09), 9 of whom had poor adherence leading to poor anticoagulation control. The incidences (number of events) of other outcome measures compared between the ABL and non-ABL groups were as follows: embolic events, 0% (0) vs. 1.4% (14), P=0.04; hemorrhagic events, 3.6% (10) vs. 7.9% (77), P=0.01; and all-cause death, 0.4% (1) vs. 4.9% (48), P<0.01.
Conclusions: Catheter ablation for atrial fibrillation significantly reduced risk of embolic events, hemorrhagic events, and all-cause death in patients taking dabigatran. We speculate that the risk of cerebral infarction is reduced by optimal anticoagulant therapy maintained in patients undergoing catheter ablation for atrial fibrillation because they receive compliance education from cardiologists when they un-dergo periodic examinations.
IMPACT OF CATHETER ABLATION FOR ATRIAL FIBRILLATION ON PATIENTS TAKING DABIGATRANNoriyuki Ohashi, Hiroshi Tasaka, Masatomo Ozaki, Mitsuru Yoshino, Satoki Fujii, Kazushige Kadota
Kurashiki Central Hospital, Okayama, Japan
CATHETER ABLATION P 2-060
331
Introduction: Intravenous adenosine triphosphate (ATP) administration could reveal dormant conduction (DC) gaps on ablation line for pulmonary vein (PV) isolation. The objective of this study was to evaluate whether the presence of ATP-induced DC would affect the inci-dence of AF recurrence even after all DCs were eliminated, and whether the effect would differ depending on a length of time to recur-rence after the procedure.
Methods: We enrolled consecutive 376 patients who underwent first-time radiofrequency catheter ablation for AF and ATP administration to check DCs after PV isolation in our institute. They were divided into two groups based on the presence or absence of ATP-induced DC (DC-positive group; n=153 vs. DC-negative group; n=223). We eliminated all DCs by additional energy application and periodical follow-up was performed after ablation. The end point of this study was AF recurrence, which was defined as recurrent atrial tachyarrhythmia last-ing for >30 seconds with a blanking period of 3 months post ablation. The initial recurrence between 3 and 6 months, 6 and 12 months and over 12 months after ablation were defined as early recurrence (ER), late recurrence (LR), and very late recurrence (VLR), respectively. In each period, we compared the recurrence rate between the groups.
Results: At the mean follow-up period of 841±27 days after ablation, there was no significant difference in the recurrence rate between DC-positive group and the other (37% vs. 31%, hazard ratio [HR], 1.30; 95% confidence interval [CI], 0.91-1.86; P=0.14). When stratifying by the length of time to recurrence, ER was more frequent in DC-positive group than the other (23% vs. 14%, HR, 1.68; 95%CI, 1.03-2.75; P=0.03). Among patients without ER, presence of ATP-induced DC was not associated with LR (19% vs. 16%, HR, 1.17; 95%CI, 0.67-2.04; P=0.57). Among patients without recurrence in the previous periods, VLR was observed in 17 patients (8%), and there was also no statisti-cal difference in the incidence of VLR between the groups (6% vs. 9%, HR, 0.72; 95%CI, 0.27-1.94; P=0.53).
Conclusions: Even after the elimination of any ATP-induced DC, presence of DC was associated with recurrence within first 3 month after the blanking period, however it did not affect the recurrence in subsequent period.
THE IMPACT OF ADENOSINE-INDUCED DORMANT CONDUCTION ON RECURRENCE AFTER ATRIAL FIBRILLATION ABLATION; AN ANALYSIS STRATIFIED BY TIME TO RECURRENCEMasato Okada, Koichi Inoue, Koji Tanaka, Yuko Toyoshima, Takafumi Oka, Nobuaki Tanaka, Hiroyuki Inoue, Ryo Nakamaru, Katsuomi Iwakura, Kenshi Fujii
Sakurabashi Watanabe Hospital, Osaka, Japan
CATHETER ABLATION P 2-061

332
Introduction: Gender disparities in outcome after catheter ablation for atrial fibrillation (AF) have been reported in the Western countries, which should also be examined in Japanese population.
Methods: We included consecutive 574 Japanese patients (paroxysmal AF [pAF]; n=368, non-pAF; n=206) who underwent first radiofre-quency catheter ablation for AF into this single center observational study, and compared AF recurrence rate between males and females. AF recurrence was defined as recurrent atrial tachyarrhythmia lasting for >30 seconds with a blanking period of 3 months post ablation.
Results: The number of female patients was 126 (23.3%). Females were older (female vs. male, 66±8 vs. 60±11 years, P<0.001) and had paroxysmal AF more frequently (75.4% vs. 60.8%, P=0003) than males. At the median follow-up period of 687 days after ablation, AF re-currence was more frequently observed in females than males (44% vs. 35%, P=0.08). Female sex was a significant risk of recurrence af-ter adjustment for age by cox regression analysis (hazard ratio [HR]; 1.40, 95% confidence interval [CI]; 1.01-1.93, P=0.04). The same dif-ference was observed in non-pAF subgroup (58% vs. 37%, HR; 2.26, 95%CI; 1.28-3.97, P=0.005). However, there was no significant differ-ence in patients with pAF (39% vs. 34%, HR; 1.20, 95% CI; 0.81-1.79, P=0.35).
Conclusions: Female sex was a significant risk of recurrence after ablation not for pAF but for non-pAF in Japanese population. Female sex might associate with progression of AF substrate.
GENDER DIFFERENCE IN OUTCOMES OF CATHETER ABLATION FOR ATRIAL FIBRILLATION IN JAPANESE POPULATIONMasato Okada, Koichi Inoue, Koji Tanaka, Yuko Toyoshima, Takafumi Oka, Nobuaki Tanaka, Hiroyuki Inoue, Ryo Nakamaru, Katsuomi Iwakura, Kenshi Fujii
Sakurabashi Watanabe Hospital, Osaka, Japan
CATHETER ABLATION P 2-062

333
Introduction: Focal impulse and rotor modulation (FIRM) ablation offers the possibility of mechanistically guided ablation of atrial fibrilla-tion however, the acute procedural and clinical outcomes of FIRM ablation for atrial fibrillation are unclear. This study aimed to conduct a systematic review and meta-analysis to provide aggregate acute procedural and clinical outcomes of FIRM ablation.
Methods: An electronic database search was conducted for all published studies describing acute and clinical outcomes of FIRM ablation, with supplementary hand searches of published bibliographies. Two reviewers (COS, AG) independently reviewed studies and extracted data. The study was prospectively registered in PROSPERO.
Results: Data were extracted from 7 studies (6 case series, 1 randomized controlled trial), with a total of 335 patients who underwent FIRM ablation. Baseline characteristics included age 61.8 years (95% CI: 60.0, 63.4, P<0.001; LA diameter 49.3 mm (95% CI: 34.2, 55.4, P<0.001), 28.6% paroxysmal AF (95% CI: 11.2%, 56.0%, P=0.12). Per patient there was an average of 3.1 rotors identified (95% CI: 2.50, 3.70, P<0.001), procedure time 289 minutes (95% CI: 241, 337, P<0.001), fluoroscopy time 48.6 minutes (95% CI: 37.1, 59.9, P<0.001). Acute procedural success, defined as AF termination or AF cycle length slowing >10% as in the original CONFIRM study, was 50.1% (95% CI: 30.8%, 69.4%). The AF termination rate was 20.4% [95% CI: 10.9%, 30.8%, P=0.002]. Freedom from atrial arrhythmia at longest fol-low-up after FIRM ablation was 40.5% (95% CI: 24.7%, 58.6%, P=0.30; mean follow-up 9.3 months (95% CI: 4, 15.7, P=0.001). Complica-tions occurred in 6.7% (95% CI: 3.7%, 11.9%, P<0.001). Significant heterogeneity was observed for all measured acute and long-term clinical arrhythmia outcomes (I²>50% for all variables).
Conclusions: These data provide aggregate acute and long-term procedural results of FIRM ablation with significant heterogeneity in re-sults across reporting studies. The precise role of FIRM in AF ablation will require additional standardised multi-centre investigations.
IMPACT OF FOCAL IMPULSE AND ROTOR MODULATION ON PROCEDURAL AND CLINICAL OUTCOMES: A SYSTEMATIC REVIEW AND META-ANALYSISCatherine O’Shea
Flinders Medical Centre, Bedford Park, South Australia, Australia
CATHETER ABLATION P 2-063
334
Introduction: The use of VKAs has limitations such as frequent monitoring, dietary restrictions, and drug interactions for preventing storke in atrial fibrillation (AF). This study was conducted to provide an in-depth exploration of treatment satisfaction with VKA therapy in patients with AF from South Korea.
Methods: The KORAF II study was a prospective, multicenter, observational study. Patients with CHADS2 ≥1 who just initiated VKAs use or started it within the last 3 months were recruited at 20 general hospitals from April 2013 to March 2014. Treatment satisfaction was measured by two questionnaires (a simple questionnarie; The Treatment Satisfaction Questionnaire for Medication, TSQM) and at any time on or after 3 months of follow-up. As potential factors related to TSQM, the demographic factors, the clinical features including risk factors of stroke and VKA treatment status, and the treatment patterns were considered.
Results: A total of 730 patients (mean age 67.9 years old, and male 59.0%) performed the patient’s treatment satisfaction survey. More than half of patients (56.6%) had CHADS2 ≥2, 86.4% of patients had CHA2DS2-VASc ≥2, and mean of AF duration was 19.8 months. Of those patients, 91 (12.5%) patients reported dissatisfaction with the VKAs treatment in the simple questionnaire. The major reasons for dissatisfaction were restrictions on diet or alcohol intake (36.3%), frequent hospital visits for the blood test (18.7%), occurrence of side-ef-fects (16.5%) such as bleeding or bruising etc. TSQM subscale scores (mean±standard deviation) for effectiveness, side-effect, conve-nience, and global satisfaction were 57.9±12.0, 96.3±11.6, 64.0±13.5, and 55.6±14.5, respectively. In multivariable linear regression analysis, the associations with lower effectiveness score and global satisfaction score were shown in long standing persistent AF com-pared to that of first diagnosed AF (β=-5.6, P<0.05; β=-6.8, P<0.05). In addition, the presence of a comorbid mental condition compared to none was associated with lower effectiveness score (β=-4.5, P<0.05). The higher convenience score was related to the higher VKAs dose (β=1.7, P<0.01), and high level education of at least post-graduation school compared to no education (β=7.4, P<0.05). Side-effect score was not related to any of the factors.
Conclusions: The principal reasons for discontent about VKAs therapy were dietary restrictions, regular monitoring etc. Global satisfac-tion score was lower among VKAs users with non-valvular AF than those of previous studies on treatment satisfaction in other diseases (hypertension: 72.1, epilepsy: 68.4, and chronic diseases: 68.8). Alternative oral anticoagulant therapy should be considered for patients who revealed low treatment satisfaction.
SATISFACTION WITH VITAMIN K ANTAGONISTS IN PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION [THE KORAF II]Hyung-Wook Park1, June-Soo Kim2, Yong-Seog Oh3, Dong-Gu Shin4, Hui-Nam Pak5, Gyo-Seung Hwang6, Kee-Joon Choi7, Seil Oh8, Jin-Bae Kim9, Man-Young Lee10, Jae-Seok Park11, Dae-Kyeong Kim12, Eun-Sun Jin13, Il-Young Oh14, Bo-Jeong Seo15, Young-Joo Kim15, Young-Hoon Kim16 1Chonnam National University Hospital, Chonnam, Republic of Korea; 2Samsung Medical Center, Seoul, Republic of Korea; 3Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Republic of Korea; 4Yeungnam University College of Medicine, Daegu, Republic of Korea;
5Severance Hospital, Yonsei University Health System, Seoul, Republic of Korea; 6Ajou University Hospital, Suwon, Republic of Korea; 7Asan Medical Center, Seoul, Republic of Korea; 8Seoul National University Hospital, Seoul, Republic of Korea; 9Kyung Hee University Medical Center, Seoul, Republic of Korea; 10Yeoyuido St. Mary’s Hospital, The Catholic University of Korea, Seoul, Republic of Korea; 11Sejong General Hospital, Bucheon, Republic of Korea; 12Inje University Busan Paik Hospital, Busan, Republic of Korea; 13Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea; 14Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 15Corporate Affairs & Health and Value, Pfizer Pharmaceuticals Korea Ltd, Seoul, Republic of Korea, 16Korea University College of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 2-064

335
Introduction: VKA has considerable limitations due to comorbid diseases, its narrow therapeutic window and interaction with many drugs including antiplatelet or non- steroidal anti-inflammatory drugs, which may increase the risk of bleeding. To compare both the mainte-nance of optimal international normalized ratio (INR) and the occurrence of VKA associated side effects between AF patients simultane-ously taking VKA along with antiplatelets and those taking VKA only.
Methods: Nonvalvular AF patients with CHADS2≥1 who have newly started with VKA were enrolled from April 2013 to March 2014 at 20 tertiary hospitals in Republic of Korea and were followed up for one year. Treatment pattern and INR levels at every follow-up were col-lected. The achievement of optimal INR range was evaluated by Point Prevalence of patients with optimal INR range and Proportion of Tests within optimal INR Range (PTR), which was defined as well-controlled for ≥60%.
Results: Total 866 nonvalvalvular AF patients (mean age 67.7 years old, male 60.1%) without bleeding history were analyzed. 41.6% pa-tients had paroxysmal type, and 55.8% had CHADS2≥2 (CHA2DS2-VASC≥2 in 83.4%). Total patients were divided into simultaneous use of antiplatelets and VKA group (n=229) and VKA alone group (n=637) at baseline. There were no significant differences between two groups in baseline characteristics except HAS-BLED score (1.94 in simultaneous use group vs. 1.25 in VKA alone group; P<0.01). First of all, there was no difference in the proportion of patients maintaining VKA between two groups (71.2% vs. 75.8%; P=NS). Mean INR level and the proportion of patients with optimal INR range were lower in simultaneous use group than VKA alone group (1.65 vs. 1.94 with P<0.01; 18.7% vs. 26.7% with P<0.01). However, there was no difference in point prevalence of patients with optimal INR range between two groups when only INR levels after reaching optimal INR range were considered. There was also no difference in PTR of ≥60% in both groups. (33.9% in simultaneous use group vs. 35.3% in VKA alone group; P=NS). Finally, 5 patients (2.2%) in simultaneous use group and 9 patients (1.4%) in VKA alone group had stopped VKA due to side effects including major & minor bleeding without significant difference (P=NS).
Conclusions: INR levels were poorly controlled both in AF patients taking antiplatelets along with VKA and those taking VKA alone. Al-though there was no statistical difference, patients taking antiplatelets along with VKA had slightly more side effects than those taking VKA alone. These findings suggest that other antithrombotic treatment options (i.e., NOAC or non-pharmacologic therapy) are warranted in AF patients with high risk of stroke and bleeding.
INTERNATIONAL NORMALIZED RATIO CONTROL AND SIDE EFFECTS IN PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION TAKING VITAMIN K ANTAGONIST WITH OR WITHOUT ANTIPLATELET DRUGS [THE KORAF II]Jaeseok Park1, June-Soo Kim2, Yong-Seog Oh3, Dong-Gu Shin4, Hui-Nam Pak5, Gyo-Seung Hwang6, Kee-Joon Choi7, Seil Oh8, Jin-Bae Kim9, Man-Young Lee10, Hyung-Wook Park11, Dae-Kyeong Kim12, Eun-Sun Jin13, Il-Young Oh14, Young-Hoon Kim15 1Bucheon Sejong General Hospital, Bucheon, Republic of Korea; 2Samsung Medical Center, Seoul, Republic of Korea; 3Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Republic of Korea; 4Yeungnam University College of Medicine, Daegu, Republic of Korea;
5Severance Hospital, Yonsei University Health System, Seoul, Republic of Korea; 6Ajou University Hospital, Suwon, Republic of Korea; 7Asan Medical Center, Seoul, Republic of Korea; 8Seoul National University Hospital, Seoul, Republic of Korea; 9Kyung Hee University Medical Center, Seoul, Republic of Korea; 10Yeoyuido St. Mary’s Hospital, The Catholic University of Korea, Seoul, Republic of Korea; 11Chonnam National University Hospital, Gwangju, Republic of Korea; 12Inje University Busan Paik Hospital, Busan, Republic of Korea; 13Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea; 14Seoul National University Bundang Hospital, Seongnam, Republic of Korea;
15Korea University College of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 2-065

336
Introduction: Left atrial appendage closure is a non-pharmacological alternative for stroke prevention in high-risk patients with non-val-vular atrial fibrillation. The objective of the multicentre WASP registry was to obtain clinical data on WATCHMAN procedural success, complications and long-term patient outcomes during real world clinical use in patients across Asia. Here, we report on the peri-proce-dural outcomes up to 30 days.
Methods: WASP Registry was designed as an observational, prospective, non-randomized, study including 201 patients enrolled at 9 sites in Australia, Hong Kong, Indonesia, Kingdom of Saudi Arabia, Malaysia, South Korea and Thailand.
Results: Subjects in the study were at high risk of stroke (mean CHA2DS2-VASc: 3.9±1.6) and moderate-to-high risk of bleeding (mean HAS-BLED score: 2.1±1.2). The mean age of subjects was 70.8±9.4 with 67.2% males (135/201) and 32.8% females (66/201). More than one third of subjects (37.8%) had a history of TIA, ischaemic stroke, or haemorrhagic stroke; 71% of patients were deemed unsuitable for long-term oral anticoagulant by their physician. The device was successfully deployed in 98.5% of patients with no flow or minimal residu-al flow achieved in 100% of implanted patients. Post-implant 57% of patients were prescribed a short-term oral anticoagulant, 38% were prescribed single or dual antiplatelet and 5% were on no therapy. Fourteen subjects (7.0%) experienced 17 serious adverse events (SAEs) within 30 days of the procedure. The overall 30-day mortality rate was 0.5%. There were no periprocedural strokes or TIAs and no device embolizations. Significant pericardial effusion/cardiac tamponade occurred in 3 patients with 2 requiring percutaneous intervention.
Conclusions: Real world experience of left atrial appendage closure with the WATCHMAN device has demonstrated a high successful im-plant rate and low peri-procedural risk in an Asian population. Further data is awaited on long term outcomes in these patients.
IMPLANT SUCCESS AND SAFETY OF LEFT ATRIAL APPENDAGE CLOSURE WITH THE WATCHMAN DEVICE IN AN ASIAN POPULATION: PERI-PROCEDURAL OUTCOMES FROM THE WASP REGISTRYKaren Phillips1, Teguh Santoso2, Prashanthan Sanders3, Jeffrey Alison4, Jason Leung Kwai Chan5, Hui-Nam Pak6, Mann Chandavimol7, Mohamad AlGhamdi8, Kenneth Stein9, Razali Omar10 1HeartCare Partners, Greenslopes Private Hospital, Brisbane, Australia; 2Medistra Hospital, Jakarta, Indonesia; 3Royal Adelaide Hospital, Adelaide, Australia; 4Monash Medical Centre, Melbourne, Australia; 5Queen Elizabeth Hospital, Hong Kong; 6Severance Hospital, Seoul, Republic of Korea; 7Ramathibodi Hospital, Bangkok, Thailand; 8Prince Sultan Cardiac Center, Hofuf, Saudi Arabia; 9Boston Scientific Corporation, Minneapolis, United States; 10National Heart Institute, Kuala Lumpur, Malaysia
CATHETER ABLATION P 2-066

337
Introduction: Canpolat et al. reported that monocyte-to-High-Density Lipoprotein ratio (M/H ratio) was the indicator of inflammation and oxidatvie stress and related to atrial fibrillation (AF) recurrence after cryoballoon-based catheter ablation. We hypothesized that inflam-mation and oxidative stress made substrate of AF and the patients with more inducibility of AF had more substrate of AF. The aim of this study was to investigate the relationship between M/H ratio and substrate of AF.
Methods: In this retrospective case control study, we enrolled 124 patients (Male 92, mean age 64.6±9.8) underwent pulmonary vein iso-lation (PVI) with the second-generation 28 mm cryoballoon for AF from September 2014 to June 2016 and were analysed M/H ratio. We induced AF by rapid atrial continuous stimulation with stimulation cycles of 240 ms to 140 ms via left and right atrium under infusion of high dose isoproterenol after PVI. We classified 78 patients with AF into Substrate Group, and 46 patients without any atrial arrhythmia or with atrial arrhythmia except AF into No Substrate Group. We analyzed M/H ratio between Substrate group and No Substrate group.
Results: M/H ratio in Substrate group significantly increased compared with in No substrate group(4.92±2.22 vs. 6.41±3.33, P=0.008). However, M/H ratio had no relation to both non-PV trigger foci and AF recurrence in this study.
Conclusions: The patients with AF by induction after cryoballoon-based catheter ablation had more M/H ratio. M/H ratio was not associ-ated with non-PV trigger foci. This study supported M/H ratio had the role as the predictor of substrate for AF but not non-PV tirrger foci.
IMPACT OF MONOCYTE-TO-HIGH-DENSITY LIPOPROTEIN RATIO AS THE PREDICTOR FOR SUBSTRATE OF ATRIAL FIBRILLATIONAkira Sato
Saitama Red Cross Hospital, Saitama, Japan
CATHETER ABLATION P 2-067

338
Introduction: Although radiofrequency catheter ablation (RFCA) for longstanding persistent atrial fibrillation (L-PeAF) is effective in rhythm control, the predictive value of electrocardiogram (ECG) has not yet been evaluated thoroughly. We hypothesized that change of P-wave axis is associated with clinical outcome of L-PeAF ablation including anterior linear ablation.
Methods: We included 304 patients (77% male, 60±10 years) with L-PeAF who underwent RFCA with consistent strategy including cir-cumferential pulmonary vein isolation, cavotricuspid isthmus line, posterior box lesion, and anterior line. We analyzed P-wave axes of pre-and post-procedural sinus rhythm ECGs, and 1-year follow-up ECG taken from 93 patients who maintained sinus rhythm without anti-ar-rhythmic drug (AAD). We evaluated the relationships between P-wave axis and clinical characteristics and bidirectional block (BDB) of an-terior line.
Results: 1) Compared to pre-procedural ECG, P-wave axis shifted inferiorly at immediate post-procedure [49.4° (46.6-52.2°) vs. 67.6° (65.0-70.1°), P<0.001], and was independently correlated with BDB of anterior line (β=10.4, 95% CI 2.79-17.94, P=0.008). 2) During 34.4±15.0 months of follow-up of 93 patients who remained sinus rhythm without AAD for 1-year, very late recurrence rate after 1-year was 24.7% and the inferior shift of P-wave axis disappeared at 1-year post ablation ECG in the patients with recurrence than those without [-4.48° (-16.21-7.25°) vs. 16.43° (10.29-22.58°), P=0.003). 3) Inferior shift of the P-wave axis was an independent predictor of no recurrence 1-year after L-PeAF ablation (HR 0.98; 95% CI 0.97-0.99, P=0.024). 4) Among 22 patients who underwent redo-procedure, degree of P-ax-is inferior shift was more significant in patients who maintained BDB of anterior line than those with reconnected anterior line block [5.50° (-4.12-15.13°) vs. -28.88° (-0.99-56.76°), P=0.015].
Conclusions: Catheter ablation for L-PeAF including anterior line shifts P-wave axis inferiorly, and closely associated with BDB of anterior line and AF recurrence after catheter ablation.
THE INFERIOR SHIFT OF P-WAVE AXIS IS ASSOCIATED TO LINEAR ABLATION AND CLINICAL OUTCOME IN PATIENTS WITH LONGSTANDING PERSISTENT ATRIAL FIBRILLATIONDong Geum Shin, Tae-Hoon Kim, Jae-Sun Uhm, Boyoung Joung, Moon-Hyoung Lee, Hui-Nam Pak
Yonsei University College of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 2-068

339
Introduction: Catheter ablation of atrial fibrillation often involved ablation of the cavotricuspid isthmus (CTI) either as a standard part of the procedure or in response to documented typical atrial flutter. This prospective randomized controlled trial study evaluated impact of pulmonary vein isolation (PVI) with additional CTI ablation in patients with paroxysmal AF and without documented atrial flutter (AFL).
Methods: We enrolled 119 patients (56±10 years) with paroxysmal AF and randomized them to the PVI alone (n=58) or the PVI plus CTI (n=61) in 1:1 ratio at two tertiary hospitals. During follow up, clinical recurrence was evaluated with 24 hours Holter recording at 3, 6 and 12 months and event recording.
Results: All patients achieved PVI successfully and the bidirectional blocks of CTI were achieved in 100% of patients in PVI plus CTI group. The PVI alone group had shorter ablation time (2,575.0±890.2 vs. 3,312.6±1,173.5 seconds, P<0.001) and fluroscopy time (27.0±8.7 vs. 31.5±13.0 minutes, P=0.03) than the PVI plus CTI group. There were no significant difference between the two groups in terms of proce-dure-related complication rate. During 15.3±5.7 months of follow-up, 26 (22.4%) patients experienced clinical recurrence, and 1 patient from each group were excluded due to loss of follow up. The clinical recurrence rates were not significantly different between PVI alone and PVI plus CTI group (23.2% vs. 21.7%, P=0.81).
Conclusions: Among patients with paroxysmal AF and without AFL, CTI ablation in addition to PVI did not reduction in the rate of clinical recurrence.
CLINICAL OUTCOME OF ADDITIONAL CAVOTRICUSPID ISTHMUS ABLATION IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION AND WITHOUT ATRIAL FLUTTER: PROSPECTIVE RANDOMIZED STUDYDong Geum Shin1, Junbeom Park2, Tae-Hoon Kim1, Jae-Sun Uhm1, Hui-Nam Pak1, Moon-Hyoung Lee1, Boyoung Joung1 1Yonsei University College of Medicine, Seoul, Republic of Korea; 2Ewha Womans University College of Medicine, Seoul, Republic of Korea
CATHETER ABLATION P 2-069

340
Introduction: It is reported that ethanol infusion into the vein of Marshall (EIM) is one of the therapeutic options however, the efficacy and feasibility remain to be determined. many The morphology of M, which will affect the efficacy, varies among individuals, so that we might not expect the efficacy uniformly by EIM. The aim of this study was to compare the morphological characteristics of VOM among patients treated with EIM, and investigate the correlation between those with the clinical efficacy.
Methods: Seventy eight patients who underwent EIM (mean age: 65.2 years, mean left atrial diameter: 42.1 mm)were enrolled in this study. We examined the length of M, and the distance from the coronary sinus (CS) ostium to the entrance of M derived from non-selective CS venography before EIM. We also examined the length of M obtained by selective contrast medium injection into the M at the time of EIM. Furthermore, we checked whether an extravasation of contrast medium was present or not at the first time of EIM, and whether a postoperative pericardial effusion was present or not.
Results: The length of M derived from CS venography was correlated with that obtained by selective contrast medium injection into M, but there was no significant difference between them (r=0.28). Extravasations of contrast medium occurred in 21.8% (7/78) cases at the first time of selective contrast media injection into M, but a pericardial effusion had remained all through the procedure in 29.4% (5/17). On the other hand, a postoperative pericardial effusion was observed in 19.7% (12/61) even in the cases without extravasation at the first injection (P=0.4). Pericardiocentesis was required in 11.8% (2/17) cases in whom postoperative pericardial effusion was observed. The risks of pericardial effusion depended on the number of EIM (P=0.006), and the area under the receiver operating characteristic curve was high-est when the number of EIM was more than 4 times.
Conclusions: The morphology of the M derived from CS venography may be different from the actual form. We should keep in mind that we may inject ethanol within 3 times.
THE MORPHOLOGICAL CHARACTERISTICS OF THE VEIN OF MARSHALL UTILIZED ON THE CHEMICAL ABLATIONYuya Takahashi1, Kazuo Kato2, Ryosuke Kametani2 1Ichinomiya Nishi Hospital, Ichinomiya, Aichi, Japan; 2Nagoya Tokusyukai General Hospital, Kasugai, Aichi, Japan
CATHETER ABLATION P 2-070

341
Introduction: Recent study showed that successful atrial fibrillation (AF) ablation may reduce the risk of thromboembolic (TE) events. Long-term use of oral anticoagulants (OACs) after catheter ablation may increase the incidence of bleeding events. We hypothesized that stopping OACs after successful AF ablation could reduce the risk of bleeding without increasing risk of TE events.
Methods: We retrospectively studied about the use of OACs and the incidence of TE and bleeding events in the patients after AF ablation in our hospital from January 2012 to December 2015.
Results: A total of 269 patients (66±11 years of age, 197 males) were analyzed. Of those, 132 patients with no documented AF recurrence and no history of TE events discontinued OACs (No-OAC group, CHADS2 score=0.85±0.97, HAS-BLED score=1.20±1.09). One hundred thirty seven patients continued OACs (Do-OAC group, CHADS2 score=1.96±1.33, HAS-BLED score=2.16±1.17). And 3 patients were ex-cluded from this study because the state of OAC use could not be identified. In No-OAC group, there were 1 ischemic stroke and 1 tran-sient ischemic attack per 231.8 person-years while there was 1 ischemic stroke per 239.0 person-years in Do-OAC group (0.86 vs. 0.42 events per 100 person-years, P=0.581). No major bleeding events occurred in No-OAC group but 3 major bleeding events (two gastroin-testinal bleeding, one pulmonary bleeding) occurred in Do-OAC group (0 vs. 2.09 events per 100 person-years, P=0.081). The combined event rates of TE and major bleeding were not different between these two groups (0.86 vs. 1.67 events per 100 person-years, P=0.39)
Conclusions: Stopping OACs after successful AF ablation may be reasonable in patients without any history of TE events.
THE SAFETY OF STOPPING ORAL ANTICOAGULATION THERAPY AFTER SUCCESSFUL ABLATION OF ATRIAL FIBRILLATIONAkihiro Takitsume, Taku Nishida, Jin Nakagawa, Tomoya Ueda, Kenji Onoue, Tsunenari Soeda, Satoshi Okayama, Makoto Watanabe, Hiroyuki Kawata, Rika Kawakami, Hiroyuki Okura, Yoshihiko Saito
Nara Medical University First Department of Internal Medicine, Nara, Japan
CATHETER ABLATION P 2-071

342
Introduction: The purpose of this study was to evaluate the effect of vaso-vagal reaction (VVR) during cryoballoon ablation for atrial fibril-lation (AF) on immediate and long-term outcomes.
Methods: We performed pulmonary vein isolation by 2nd generation cryoballon on 46 consecutive paroxysmal AF patients between Octo-ber 2015 and December 2015. VVR was defined as sinus bradycardia (less than 40 b.p.m.), asystole, atrioventricular block, or hypotension that occurred during the phases of balloon thawing and deflation. Temporary pacing was performed or atropine was administered intra-venously when a symptomatic VVR occurred. All patients were followed up at 1, 3, and 6 months after the procedure.
Results: The mean age was 67.5±9.1 years. Men accounted for 63.0% (29/46 patients). VVR occurred in 8 patients (VVR group). Seven epi-sodes of VVR were observed during the deflation phase for the left superior pulmonary vein (LSPV). The mean freezing time for the LSPV was significantly shorter in the VVR group than in the non-VVR group (184±24 seconds vs. 271±123 seconds, P<0.01). No significant dif-ferences were noted in other three PVs. After a single procedure, 7 of 8 patients in the VVR group and 26 of 34 patients in the non-VVR group (87.5% vs. 76.5%, P=0.66) maintained sinus rhythm 6 months after the procedure (mean follow-up period: 182±9 days and 192±17 days).
Conclusions: VVR during cryoballoon ablation for AF significantly shortened the freezing time for the LSPV, but did not affect the long-term outcomes.
EFFECT OF VASO-VAGAL REACTION ON IMMEDIATE AND LONG-TERM OUTCOMES OF CRYOBALLOON ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATIONHiroshi Tasaka, Satoki Fujii, Masatomo Ozaki, Mitsuru Yoshino, Noriyuki Ohashi, Kazushige Kadota
Kurashiki Central Hospital, Kurashiki, Japan
CATHETER ABLATION P 2-072

343
Introduction: Phrenic nerve pacing is necessary to avoid phrenic nerve injury (PNI) during the right pulmonary vein cryoballoon ablation for atrial fibrillation (AF). We evaluated the stability of phrenic nerve capture during pacing from subclavian vein compared with the supe-rior vena cava (SVC).
Methods: Cryoballoon ablation was performed in consecutive 167 patients with paroxysmal AF. During right PV isolation, PN was paced from the subclavian vein or the SVC. The output of subclavian vein and SVC pacing were set at minimum pacing threshold and 20V, re-spectively. Loss of pace capture was defined as disappearance of movement of phrenic membrane (palpation or on X-ray).
Results: The PN was paced from subclavian vein and SVC in 88 and 79 patients, respectively. The median capture threshold of subclavian vein pacing was 2.8V. Although pacing output was lower in subclavian vein, loss of capture due to catheter instability was less frequently occurred during subclavian vein pacing than SVC pacing (1.1% (1/88) vs. 7.6% (6/79), P=0.04). PNI occurred in 11 patients (4.6% in subcla-vian pacing and 8.9% in SVC pacing, P=0.43).
Conclusions: Subclavian vein pacing was more favorable for the stable PN stimulation compared with the SVC pacing during cryoballoon ablation.
SUBCLAVIAN VEIN PACING FOR PHRENIC NERVE MONITORING DURING CRYOBALLOON ABLATION OF ATRIAL FIBRILLATIONKenichi Tokutake, Michifumi Tokuda, Ryota Isogai, Kenichi Yokoyama, Mika Hioki, Ryosuke Narui, Seigo Yamashita, Keiichi Inada, Kenri Shibayama, Seiichiro Matsuo, Satoru Miyanaga, Kenichi Sugimoto, Michihiro Yoshimura, Teiichi Yamane
The Jikei University School of Medicine, Tokyo, Japan
CATHETER ABLATION P 2-073

344
Introduction: Early recurrence of atrial fibrillation (ERAF) after pulmonary vein isolation (PVI) for atrial fibrillation (AF) are accepted as part of the blanking period. We evaluate the incidence and investigate some factors that may predict early recurrence of AF after radiofrequen-cy catheter ablation procedure.
Methods: This is a retrospective cohort study. A total of 29 atrial fibrillation patients who underwent radiofrequency catheter ablation for atrial fibrillation during the period of 2014-2015 and had been followed for 3 months were included in this study. Variables studied includ-ed demographic and comorbidities data, left ventricular function, left atrial dimension, type of AF (paroxysmal vs. persistent) and ablation procedure. Early recurrence of AF was defined as any documented episodes of AF during the first 3 months of follow-up.
Results: During a follow-up of 3 months, there were 9 AF recurrence (31%). There was no significant difference in the recurrence of AF with regard to gender, age, comorbidities, echocardiographic findings, oral medications, underlying disease and ablation technique. The type of AF (paroxysmal vs. non paroxysmal) [OR 3.27 (CI 95%, 1.02-10.49, P=0.043)] was the only independent predictors of early AF recur-rence.
Conclusions: The type of atrial fibrillation seems to be more important than any other parameters (hypertension, diabetes mellitus, heart failure, body mass index and left atrial diameter) in predicting the short term success of AF ablation.
EARLY RECURRENCE OF ATRIAL FIBRILLATION FOLLOWING RADIOFREQUENCY CATHETER ABLATION IN NATIONAL CARDIOVASCULAR CENTER HARAPAN KITA- A 3 MONTHS FOLLOW UPPriyandini Wulandari, Sunu Budhi Raharjo, Galuh Anggraini, Detrianae Rampay, Dicky Armein Hanafy, Yoga Yuniadi, Amiliana Mardiani Soesanto
Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Indonesia-National Cardiovascular Center Harapan Kita, Jakarta, Indonesia
CATHETER ABLATION P 2-074
345
Introduction: The right phrenic nerve (PN) function is routinely monitored during cryoballoon ablation (CBA) by stimulating right PN from superior vena cava and manually assessing the strength of diaphragmatic contraction for prevention of PN injury (PNI). However the left PN (LPN) could also be damaged during CBA.
Methods: The electrical pacing was performed from the left subclavian veins (LSV).The diaphragmatic compound motor action potentials (CMAP) were recorded during CBA for assessment of LPN function.
Results: CBA was performed in 234 patients (143 males, average age of 62±11 years old) concomitant with CMAP monitoring. Stable capture of the LPN by stimulating the LSV was achievable 225 of 234 patients (96%). Temporary LPN paralysis occurred in 7 (3%) patients, and average CMAP amplitude decreased in these patients from 1.02±0.11 to 0.26±0.08 (p< 0.01). Example case: 59-year-old male un-derwent CBA for paroxysmal atrial fibrillation using the second-generation 28 mm cryoballoon. After left inferior pulmonary vein isolation, the fluoroscopy demonstrated the weakness of left diaphragmatic contraction. His LPN paralysis continued for 8 months. All PNI patients including this, PNI resolved within a year without serious sequelae.
Conclusions: The LPN can be electrically stimulated from the LSV in the majority of patients. The monitoring the LPN function is an im-portant technique during CBA.
ELECTRICAL PACING FROM LEFT SUBCLAVIAN VEIN FOR PREVENTION OF LEFT PHRENIC NERVE INJURY DURING CRYOBALLOON ABLATION OF ATRIAL FIBRILLATIONMitsumi Yamashita, Kaoru Okishige
Yokohama Bay Red Cross Hospital, Yokohama, Japan
CATHETER ABLATION P 2-075

346
Introduction: Elevated red blood cell distribution width (RDW) predicts poor prognosis in patients with cardiovascular diseases. However, little is known about the association between RDW and outcomes after catheter ablation of atrial fibrillation (AF).
Methods: A total of 757 patients who underwent radiofrequency catheter ablation of AF for the first time between January 2009 and De-cember 2014 were divided into heart failure (HF, n=79) and non-HF (n=678) groups; RDW was assessed as a predictor after catheter ab-lation in each. Patients with HF are defined as a history of HF hospitalization or left ventricular ejection fraction ≤40% on baseline echo-cardiography.
Results: During a 22.3-month follow-up period, the baseline RDW in the HF group was greater in the recurrence group than in the non-recurrence group (14.5±2.0% vs. 13.5±0.9%, P=0.013). In contrast, no significant difference in RDW at baseline was found in the non-HF group between the recurrence and non-recurrence groups (13.3±0.8% vs. 13.2±0.8%, P=0.332, respectively). Multivariate analy-sis demonstrated that RDW (hazard ratio 1.20, 95% confidence interval 1.01-1.40, P=0.034) was an independent predictor of AF recur-rence in the HF group. The cut-off values of RDW for the recurrence of AF and major adverse events including all-cause death, HF hospi-talization, and cerebral infarction in the HF group were 13.9% and 14.8%, respectively. Kaplan-Meier curves demonstrated significant dif-ferences within the HF group both in event-free survivals for recurrence of AF (RDW ≥13.9% and <13.9%, P=0.019) and for major ad-verse events (RDW ≥14.8% and <14.8%, P<0.001). In contrast, there was no difference in events-free survival regarding AF recurrence (P=0.585) and major adverse events (P=0.874) in the non-HF group.
Conclusions: High RDW is an independent predictor for the recurrence of AF and major adverse events in patients with HF after catheter ablation. In addition to the established factors of the recurrence of AF after ablation, RDW is a potential noninvasive marker in AF patients complicated with HF.
ELEVATED RED BLOOD CELL DISTRIBUTION WIDTH PREDICTS RECURRENCE AFTER CATHETER ABLATION FOR ATRIAL FIBRILLATION IN PATIENTS WITH HEART FAILURE: COMPARISON WITH NON-HEART FAILURE PATIENTS Satoshi Yanagisawa, Yasuya Inden, Aya Fujii, Yasunori Kanzaki, Yosuke Kamikubo, Monami Ando, Yosuke Murase, Junya Funabiki, Masaki Takenaka, Noriaki Otake, Rei Shibata, Toyoaki Murohara
Nagoya University Graduate School of Medicine, Nagoya, Japan
CATHETER ABLATION P 2-076

347
Introduction: Atrial fibrillation (AF) is common in patients with hypertrophic cardiomyopathy (HCM). Catheter ablation is useful therapy for AF treatment, however it is still uncertain the efficacy of catheter ablation for HCM patients in long-term follow-up.
Methods: From 2005 to 2015, 1,234 patients were underwent AF ablation. The number of 36 patients (2.9%) was diagnosed HCM before ablation. We compared the patients with HCM (group HCM) to patients without cardiomyopathy (group NCM).
Results: In HCM group, the average age was 66.6±9.0 years, 21 patients (58.3%) were male, mean CHADS2 score was 1.35±1.1 and 21 patients (58.3%) were paroxysmal AF. In HCM group, left atrial dimension (47.9±6.2 mm) and BNP levels (306±235 pg/mL) were signifi-cantly higher than NCM group (P<0.001, P<0.001), but the other baseline characteristics was no significance between two groups. Aver-age follow up period is 3.95±2.62 year, and 2 patients were died during follow-up in HCM group. All patients underwent pulmonary vein isolation (PVI). The number of 7 patients (19.4%) was treated with additional focal ablation in the left atrium and superior vena cava isola-tion was performed 6 patients (16.7%). After multiple-procedure, the success rate was 47.2% in HCM group and 72.5% in NCM group (P=0.0017) without anti-arrhythmic drugs (AADs), and 72.2% in HCM group and 85.1% in NCM group (P=0.035) with AADs. The success rate is significant lower in HCM than NCM in long-term follow up.
Conclusions: The rate of sinus rhythm maintenance in patients with HCM after AF-ablation is significant lower than without cardiomyop-athy.
LONG-TERM OUTCOME OF CATHETER ABLATION FOR ATRIAL FIBRILLATION IN HYPERTROPHIC CARDIOMYOPATHYTakashi Yoshizawa, Satoshi Shizuta, Takeshi Kimura
Kyoto University Hospital, Kyoto, Japan
CATHETER ABLATION P 2-077

348
Introduction: Pulmonary vein isolation has become a standard treatment strategy for atrial fibrillation, however some serious complica-tions can occur.
Methods: N/A
Results: A 60-year-old man was referred to our hospital for catheter ablation for paroxysmal atrial fibrillation and atrial flutter. The sus-tained atrial flutter terminated during linear radiofrequency (RF) ablation of the cavo-tricuspid isthmus and bidirectional isthmus conduc-tion block was accomplished. Subsequently, pulmonary veins isolation for atrial fibrillation was going to be performed. After atrial trans-septal puncture and pulmonary vein angiography, an electrocardiogram (ECG) showed marked extension of QRS duration, prolonged PR interval and frequent premature ventricular contractions (PVCs), and arterial blood pressure declined from 129 mmHg to 72 mmHg, prior to application of radiofrequency energy in the left atrium. Immediately, cardiopulmonary resuscitation, right ventricular pacing and percu-taneous cardiopulmonary support were performed for rapidly progressive deterioration of circulation, electrical conduction block and ventricular fibrillation (VF). Coronary angiography showed total occlusion at the ostium of left and right coronary artery. However, both coronary arteries flow were recovered in several seconds after administration of nitrate in left and right coronary artery respectively. The hemodynamics and ECG changes improved gradually after that. We interpreted this simultaneous total occlusion of left and right coro-nary artery was due to coronary artery spasm, which caused the whole cardiac ischemia, acute circulatory collapse and electrical con-duction disturbance. Coronary artery spasm during atrial transseptal puncture or RF ablation in left atrium has rarely been reported. In most cases, ST-segment elevations were showed on ECG and were resolved immediately by intravenous administration of nitrates.
Conclusions: We report a case of severe complication that a simultaneous spasm of right and left coronary artery caused electrical ab-normality such as conduction block, PVCs and VF, but without ST-segment elevation, subsequently led to cardiopulmonary arrest during the ablation procedure for atrial fibrillation.
SEVERE COMPLICATION DURING CATHETER ABLATION FOR ATRIAL FIBRILLATION DUE TO SIMULTANEOUS SPASM OF RIGHT AND LEFT CORONARY ARTERYAkemi Aso, Toshihiro Nakamura, Koudai Shibao, Daiki Akagaki, Masahiro Araki, Yujirou Ura, Kyohei Meno, Yukimitsu Kuwabara, Emiko Ejima, Takahiro Mori, Katsuhiko Takenaka, Koutaro Numaguchi, Yoshinobu Murasato, Koji Hiyamuta
National Hospital Organization Kyushu Medical Center, Fukuoka, Japan
CATHETER ABLATION P 2-078

349
Introduction: Although pulmonary vein (PV) isolation was established treatment for patients with atrial fibrillation (AF), this procedure may be complicated by the occurrence of PV stenosis (PVS).
Methods: we assessed 1,077 patients who performed PV isolation from January 2005 to March 2014 (157 cases was treated by using non-irrigation catheter and 920 cases by using irrigation catheter) and took computerized tomography (CT) after 1 year from PV isolation, and evaluate PVS in these patients. PVS was defined as a more than 90% stenosis and total occlusion in CT analysis.
Results: There were 13 PVS in 11 patients (11 male, age: 62.0±9.7, 8 paroxysmal AF), 1 left superior (LS) PV, 9 left inferior (LI) PV, and 3 right inferior (RI) PV. 2 patients had multi PVS (LS+LI, LI+RI). 6 patients presented with pleural effusion, 2 with dyspnea at rest, and 2 with hemoptysis. Only one case was treated by using non-irrigation catheter, and irrigation catheter was used for the other 10 cases. There was only one patient in superior PVS, however he suffered from repetitive hemoptysis. On the other hand, 8 of 10 patient with inferior PVS did not complain any symptoms.
Conclusions: In our hospital, 1.02% of patients who were performed PV isolation presented PVS. The site of PVS tended to be higher in left inferior than other PV, thus we reduce radiofrequency energy to 20-25 W at LI PV ablation.
CLINICAL PRESENTATION OF PULMONARY VEIN STENOSIS COMPLICATING ABLATION FOR ATRIAL FIBRILLATIONYukihiro Inamura1, Junichi Nitta1, Takashi Ikenouchi1, Yosuke Hayashi1, Kazuya Murata1, Kikou Lee1, Tatsuhiko Hirao1, Tomomasa Takamiya1, Nobutaka Kato1, Akira Sato1, Masahiko Goya2, Kenzo Hirao2 1Saitama Red Cross Hospital, Saitama, Japan; 2Tokyo Medical and Dental University, Tokyo, Japan
CATHETER ABLATION P 2-079

350
Introduction: A tip of the long sheath (SL0, Daig) is softened in order not to damage the atrial wall or the pulmonary veins.
Methods: N/A
Results: A seventy-four-year-old female was referred to our hospital for catheter ablation of recurrent atrial fibrillation. She underwent cavo-tricuspid isthmus ablation in 2003 and Hot balloon pulmonary vein isolation in 2013. A 8.5 French SL0 long sheath was inserted from the right femoral vein to the right atrium. The subcutaneous tissue of the puncture site at the right femoral vein was hard due to the previ-ous procedures, but the sheath was inserted without difficulty. However, fluoroscopy revealed that the soft tip of the sheath was turned in-side out. The sheath was pulled out of the body without resistance. The tip of the sheath was intact. The procedure was continued and pulmonary vein reisolation and left atrial roof linear ablation were performed successfully.
Conclusions: Especially during the repeat ablation procedure, the soft tip of the SL0 long sheath can get turned inside out and the tip of the sheath becomes very hard. If an operator is unaware of this, the tip can damage the cardiac wall or the cardiac structure. Also trans-septal sheath insertion can become difficult or impossible. Thrombus formation at the tip of the sheath is possible. Knowing this, and to confirm the tip with fluoroscopy is necessary for the safety of the ablation procedure.
BE CAUTIOUS. A SOFT TIP OF THE LONG SHEATH CAN BECOME DANGEROUSRyusuke Kimura1, Takafumi Makino2, Tetsuya Ishiki2, Takako Zukeran2, Taketoshi Maeda2, Koichi Oshiro2 1Okinawa Ohama Daiichi Hospital/Kanazawa Cardiovascular Hospital, Naha/Kanazawa, Japan; 2Okinawa Ohama Daiichi Hospital, Naha, Okinawa, Japan
CATHETER ABLATION P 2-080

351
Introduction: Pulmonary vein isolation using cryoablation is undertaken with increasing frequency for the treatment of symptomatic, drug-refractory atrial fibrillation (AF). Local guidelines recommend overnight hospital admission following the procedure, but with ex-panding experience this may be unnecessary.
Methods: We performed a retrospective case note analysis of all patients who underwent cryoablation pulmonary vein isolation for AF at Waikato Hospital over a 43-month period, and calculated the 24-hour post-procedure complication rate.
Results: From November 2012 to June 2016, 157 pulmonary vein isolation procedures using cryoablation were performed. Intra-proce-dural complications (1 stroke, 1 pericardial tamponade) necessitating hospital admission occurred in 2 patients (1.3%), who were excluded from the analysis. Of the remaining 155 patients (98 (63%) males; age 57±11 years), 137 (88%) had paroxysmal AF and 18 (12%) had per-sistent AF. Mean procedure time was 130±29 minutes, 148 (95%) were anticoagulated pre-operatively, and 153 (99%) were performed without general anaesthetic. After 4 hours observation 8 patients (5%) were discharged on the day of the procedure, without complica-tions. The remaining 147 patients (95%) were admitted overnight as per local protocol. In the 24-hour post-operative period 141 (96%) pa-tients had no complications, and were safely discharged home the following day. Post-procedure complications requiring medical assess-ment±intervention occurred in 6 patients: 1 stroke, 4 femoral haematomas/bleeds (all managed non-invasively), 1 pericardial tamponade requiring drainage. These complications were all identified within 6 hours. The acute post-procedure complication rate was 3.9%. The mean length of hospital stay post-procedure was 1.02±0.53 days, and the 30-day readmission rate was 1.9%.
Conclusions: Pulmonary vein isolation using cryoablation has a low acute complication rate, and our results suggest that this procedure can be safely performed as a day-case without obligatory need for overnight hospital admission. Overnight admission in our hospital costs approximately NZ$700 per patient; our results indicate considerable savings if unnecessary hospital admission is avoided.
PULMONARY VEIN ISOLATION USING CRYOABLATION CAN BE SAFELY PERFORMED AS A DAY-CASE PROCEDUREEdwin Kooijman1, Rob Carr2, Dean Boddington3, Spencer Heald1, Martin K Stiles1, Janice Swampillai1 1Waikato District Health Board, Hamilton, New Zealand; 2Auckland University, Auckland, New Zealand; 3BoP District Health Board, Tauranga, New Zealand
CATHETER ABLATION P 2-081

352
Introduction: Cryoablation has been used in the Midland region of New Zealand to treat paroxysmal atrial fibrillation (PAF) and selected persistent AF (PeAF) cases since November 2012. We aimed to assess 6 month and 1 year efficacy of cryoablation for AF.
Methods: Until November 2015, 216 patients (male 147), aged 58±10 years; range 22 to 79 years (CHA2DS2-VASc 0-5, median 1) with par-oxysmal (N=199) or persistent AF (N=17) underwent cryoablation. Follow-up was via medical records, ambulatory monitoring and phone calls. Procedural success and recurrence were defined according to HRS guidelines.
Results: Mean procedure time was 129±31 and screening time 35±13 minutes. At 6 months follow up 117 patients (59%) with PAF were free of AF without drugs. Another 49 patients were free of AF on anti-arrhythmic therapy (84% on drug success). For PeAF, 6 patients (35%) were free of AF without drugs with an additional 3 free of AF on medication (53% on drugs success). With 12 months follow up (N=179, including 13 PeAF) 105 patients (63%) with PAF were AF free without drugs and another 22 patients were free of AF on anti-ar-rhythmic drugs (76% on-drug success). For the PeAF group (N=13), 7 (54%) were free of AF. Of patients with any recurrent AF (N=38), 18 patients had or are planned for subsequent radiofrequency ablation (8% of entire cohort). Transient phrenic nerve palsy (PNP) occurred in 26 patients (12%). PNP persisted beyond the lab in 6 patients and 1 at one year follow up. Thirty day mortality was 1; the patient died 4 weeks post ablation from a dissection of the ascending aorta.
Conclusions: Our 1 year success rate for cryoablation of PAF approximates other published data and, as expected, is less for peAF. Re-peat ablation rates are less than AF recurrence rates as some patients chose not to have a repeat procedure due to improved quality of life. Other reasons are unclear.
EFFICACY OF CRYOABLATION FOR PAROXYSMAL AND PERSISTENT AF IN THE MIDLAND REGION OF NEW ZEALANDEdwin Kooijman1, Dean Boddington2, Spencer Heald1, Janice Swampillai1, Rosemary Allen1, Irene Gray1, Martin K Stiles1 1Waikato District Health Board, Hamilton, New Zealand; 2BoP District Health Board, Tauranga, New Zealand
CATHETER ABLATION P 2-082

353
Introduction: During cavo-tricuspid isthmus (CTI) ablation, the risk of damage to the conduction system is very low. There are a few re-ports on atrio-ventricular (AV) block during radiofrequency CTI ablation, however there are none on AV block caused by right coronary ar-tery (RCA) acute stenosis, with narrowing of the RCA due to radiofrequency (RF) energy analyzed using optical frequency-domain imaging (OFDI).
Methods: N/A
Results: Case: A 67-year-old male underwent catheter ablation in our hospital for drug-resistant paroxysmal atrial fibrillation and atrial flutter. After pulmonary vein isolation, a CTI ablation was performed with a 3.5 mm-tip irrigated catheter. Eight seconds after initiating the ablation application, sudden 2:1 AV block occurred with ST segment elevation in the inferior leads. Immediately after turning off the ra-diofrequency energy delivery, the 2:1 AV block disappeared, while ST elevation continued. Then, coronary angiography (CAG) showed that the distal segment of the RCA (#4 AV branch) became 99% severely stenosed (TIMI class II). Real-time OFDI imaging revealed that the vessel wall bulged eccentrically at the narrowed site and the bulge had the same density as normal vessel walls. After five months, the CAG and OFDI showed that the stenotic RCA lesion disappeared almost to a normal degree. We speculated that the cause of coronary ar-tery stenosis was acute edema caused by heating from the RF energy, which induced severe ischemia at the AV junction region resulting in transient AV block.
Conclusions: We observed the time course of RF energy’s severe heating effects on the RCA in a patient with transient AV block, and at-tention should be paid to this during CTI ablation procedures.
2:1 ATRIO-VENTRICULAR BLOCK DURING CAVO-TRICUSPID ISTHMUS ABLATION Takuro Nishimura1, Shinya Shiohira1, Takakatsu Yoshitake1, Yasuhiro Shirai1, Shingo Maeda1, Takeshi Sasaki1, Mihoko Kawabata1, Tetsuo Sasano1, Masahiko Goya1, Takashi Ashikaga2, Kenzo Hirao1 1Heart Rhythm Center, Tokyo Medical and Dental University, Tokyo, Japan; 2Department of Cardiovascular Medicine, Tokyo Medical and Dental University, Tokyo, Japan
CATHETER ABLATION P 2-083

354
Introduction: N/A
Methods: N/A
Results: A 64-year-old man was admitted to our hospital for atrial fibrillation ablation. He had mitral valvuloplasty due to mitral valve pro-lapse with infectious endocarditis. Recently he had paroxysmal atrial fibrillation and cerebral infarction. Pulmonary vein isolation (PVI) was performed extensive anatomical antrum PVI using electroanatomical mapping system and irrigation radiofrequency (RF) catheter. Cavo-tricuspid isthmus (CTI) ablation was performed by 8mm-tip non-irrigation RF ablation catheter. After 14 times point by point ablations, complete linear isthmus block line was created. Just after CTI ablation, inferior leads showed ST elevation. Coronary angiogram showed distal right coronary artery (#4AV) was totally occluded. The occlusion site was coincidence the ablation site (Figure). However coronary vasodilator injection, the total occlusion site was unchanged. Drug-eluting stent was delivered at the total occlusion site. Coronary occlu-sion due to coronary spasm during CTI ablation was found here and there. But right coronary artery occlusion that required PCI during RF ablation of typical atrial flutter was rare. We report consideration from literatures.
Conclusions: N/A
RIGHT CORONARY ARTERY OCCLUSION AFTER CAVOTRICUSPID ISTHMUS ABLATIONErika Yamashita, Norihito Nuruki, Kazuyuki Tanoue, Masahiro Sonoda
National Hospital Organization Kagoshima Medical Center, Kagoshima, Japan
CATHETER ABLATION P 2-085

355
Introduction: Hypertrophic cardiomyopathy (HCM) is the most common of the genetic cardiovascular diseases and predominantly an ob-structive disease. Patients with severe obstruction and significant symptoms that persist despite optimal medical treatment are candi-dates for an Alcohol Septal Ablation (ASA) therapy. The result, however, has been inconsistent in each individual including complication. Therefore, we try to search the clinical predictors for ASA complication focused on total AV block (TAVB).
Methods: We studied 24 patients with severely symptomatic obstructive hypertrophic cardiomyopathy who referred for ASA from 2011 to 2015 (mean age 45.48±15.70 and 56.6% male).
Results: The mean resting LVOT gradient (105.57±45.96 mmHg), post ASA the gradient was decrease (44.18±32.3 mmHg) and also the delta gradient (61.39±27.3 mmHg). The use of absolute alcohol was varying (2.07±0.66 mL), proximal septal branch anatomy (69.6%). The procedural complication was TAVB (17.4%) and two patients required device implantation (PPM/ICD). There are no mortality, ventricu-lar arrhythmias and cardiac tamponade during and after the procedure. There are no relation between TAVB with age, anatomy of septal branch during the procedure, quantity of alcohol and gradient before and after the procedure, but the pre procedural gradient determine post procedural gradient (16.04+0.43 mmHg [P<0.0001]).
Conclusions: Based on our data, there are no significant predictors of TAVB in HOCM patients who undergo ASA. Gradient before ASA can determine the decreasing gradient after ASA and it was not related to the development of TAVB.
CLINICAL PREDICTORS OF TOTAL AV BLOCK IN HYPERTROPHY OBSTRUCTIVE CARDIOMYOPATHY UNDERGO ALCOHOL SEPTAL ABLATIONHaikal Balweel, Sunu Budi Raharjo, Dicky Armein Hanafy, Mira Fauziah, Yoga Yuniardi
National Cardiovascular Centre Harapan Kita, Jakarta, Indonesia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-086

356
Introduction: The usual method used during the mapping and ablation of ventricular arrhythmias originating from left ventricle is a retro-grade transaortic approach, which is limited in some cases. The experience of transseptal approach for ventricular aneurysm related ventricular tachycardia ablation has not been reported in China. The aim of our study was to test the feasibility and assess the safety of a transseptal approach for ventricular aneurysm related ventricular tachycardia mapping and ablation in those who had contraindication or failed to ablation via retrograde transaortic route.
Methods: Five patients with ventricular aneurysm related ventricular tachycardia were selected for mapping and ablation. After a routine retrograde transaortic LV-mapping approach was failed in all these cases, catheter ablation was performed via transseptal approach with an Agilis sheath.
Results: In these five patients, four had LV aneurysms located in the left ventricular apical area, one in the basal inferoseptum. Acute ab-lation successes were failed to achieve via a transaortic route. One is due to aortic stenosis and tortuous peripheral arteries and the oth-ers due to failed to achieve optimal target potential for VT ablation. All ablation procedures succeeded via transseptal approach with an Agilis sheath and no major complications related with the transseptal approach were reported. During the 12-month (5-22 months) fol-low-up, no VT recurrence occurred.
Conclusions: Transseptal approach is a feasible, safe and effective method of radiofrequency ablation in patients with ventricular aneu-rysm related ventricular tachycardia and may be considered as an alternative to the transaortic route.
FEASIBILITY OF THE TRANSSEPTAL APPROACH FOR VENTRICULAR ANEURYSM RELATED VENTRICULAR TACHYCARDIA MAPPING AND ABLATIONLian Chen
Fuwai Hospital, National Center for Cardiovascular Disease, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-087

357
Introduction: Pre-systolic Purkinje Potential (PPP) and Mid Diastolic Potential (MDP) in the region of the posterior fascicle is the compo-nent of reentry circuit for Idiopathic Left fascicular Tachycardia (ILVT). It may be difficult to map MDP during tachycardia. The ablation done solely based on PPP may be effective in abolishing the VT.
Methods: Of the 297 cases of Cardiac electrophysiology and radiofrequency ablations done at this centre since August 2012, there were six patients of ILVT. The electrophysiological signals on ablation catheter prior to ablation were analyzed for the success of the outcome. The PPP during the VT was identified by fragmented low voltage signals preceding the reference QRS onset. The electro-anatomic map-ping was done to confirm whether the site of earliest activation matches with the region of fragmented PPP.
Results: All six patients with the ILVT had tachycardia with RBBB and superior axis mean QRS 122+12 msec, mean cycle length of 310+34 seconds. The tachycardia was easily inducible in all with rapid ventricular pacing except with one case that required Isoprenaline induc-tion. VA dissociation was present in 4 and two patient had 1:1 VA conduction. The posterior fascicle was mapped in Left ventricular septum in the postero-inferior region of junction between distal 1/3rd and proximal 2/3 in RAO 30 degree. The PPP during the tachycardia had low voltage fragmented signals proceeding 10-26 mesc prior to the earliest reference QRS on the surface or intra-cardiac ECG. The Elec-tro-anatomic mapping using NaviX System (St. Jude Medical) showed earliest activation during tachycardia originating from the same re-gion of fractionated PPP. The MDP was either not present or was inconspicuous during tachycardia. The ablation guided by the character-istic PPP was effective in terminating the VT with no subsequent recurrence.
Conclusions: The PPP acts as a surrogate marker for diseased Purkinje network in the reentry circuit of ILVT and characteristic frag-mented potential preceding the QRS during tachycardia identified the site of ablation.
CATHETER ABLATION OF LEFT FASCICULAR VENTRICULAR TACHYCARDIA BASED ON FRACTIONATED PRESYSTOLIC PURKINJE POTENTIALPradeep Hasija1, Prashant Bhardwaj1, Rajkumar Mantravadi2 1Armed Forces Medical College, Pune, India; 2Shayadri Hospital, Pune, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-088
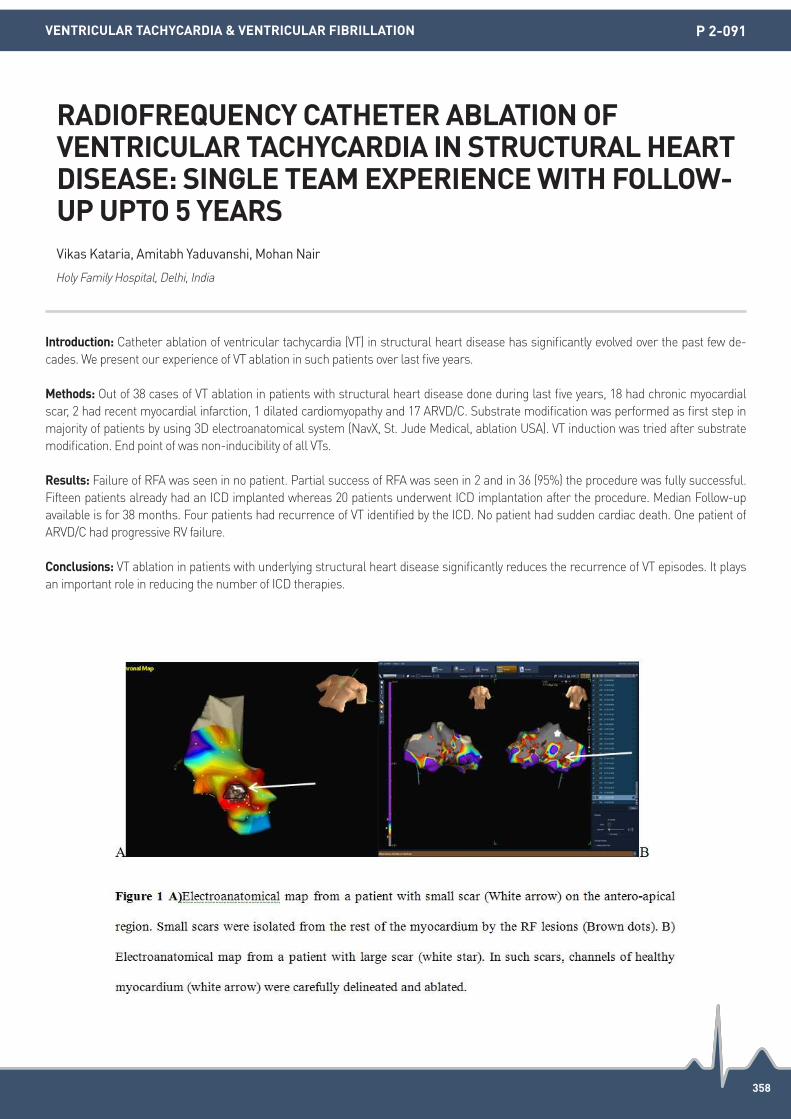
358
Introduction: Catheter ablation of ventricular tachycardia (VT) in structural heart disease has significantly evolved over the past few de-cades. We present our experience of VT ablation in such patients over last five years.
Methods: Out of 38 cases of VT ablation in patients with structural heart disease done during last five years, 18 had chronic myocardial scar, 2 had recent myocardial infarction, 1 dilated cardiomyopathy and 17 ARVD/C. Substrate modification was performed as first step in majority of patients by using 3D electroanatomical system (NavX, St. Jude Medical, ablation USA). VT induction was tried after substrate modification. End point of was non-inducibility of all VTs.
Results: Failure of RFA was seen in no patient. Partial success of RFA was seen in 2 and in 36 (95%) the procedure was fully successful. Fifteen patients already had an ICD implanted whereas 20 patients underwent ICD implantation after the procedure. Median Follow-up available is for 38 months. Four patients had recurrence of VT identified by the ICD. No patient had sudden cardiac death. One patient of ARVD/C had progressive RV failure.
Conclusions: VT ablation in patients with underlying structural heart disease significantly reduces the recurrence of VT episodes. It plays an important role in reducing the number of ICD therapies.
RADIOFREQUENCY CATHETER ABLATION OF VENTRICULAR TACHYCARDIA IN STRUCTURAL HEART DISEASE: SINGLE TEAM EXPERIENCE WITH FOLLOW-UP UPTO 5 YEARSVikas Kataria, Amitabh Yaduvanshi, Mohan Nair
Holy Family Hospital, Delhi, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-091

359
Introduction: Catheter ablation for idiopathic ventricular arrhythmia (VA) is effective and safe, but efficacy is frequently limited due to an epicardial origin and difficult anatomy. The remote magnetic navigation (RMN) catheter has a flexible catheter design allowing access to difficult anatomy. We describe the efficacy of the RMN for ablation of idiopathic-VA after failed manual-ablation.
Methods: Among 235 patients with idiopathic-VA referred for catheter ablation, we identified 51 patients who were referred for repeat-ab-lation after a failed manual-ablation. We analyzed the clinical characteristics, including the successful ablation site and findings at elec-trophysiology study, in repeat procedures conducted using RMN as compared with manual ablation.
Results: Among these patients, 22 (43%) underwent repeat-ablation with the RMN and 29 (57%) underwent repeat-ablation with a manu-al-ablation. Overall successful ablation rate was significantly higher using RMN as compared with manual-ablation (91% vs. 69%, P=0.02). Fluoroscopy time in the RMN was 17±12 minutes as compared with 43±18 minutes in the manual-ablation (P=0.009). Suc-cessful ablation rate in the posterior right ventricular outflow tract (RVOT) plus posterior-tricuspid annulus was higher with RMN as com-pared with manual-ablation (92% vs. 50%, P=0.03). Neither groups exhibited any major complications.
Conclusions: The RMN is more effective in selected patients with recurrent idiopathic VA after failed manual-ablation and is associated with less fluoroscopy time. The RMN catheters have a flexible design enabling them to access otherwise difficult anatomy including the posterior tricuspid annulus and posterior RVOT.
COMPARISON OF REMOTE MAGNETIC NAVIGATION ABLATION AND MANUAL ABLATION OF IDIOPATHIC VENTRICULAR ARRHYTHMIA AFTER FAILED MANUAL ABLATIONMitsuharu Kawamura, Yuya Nakamura, Tatsuya Onuki, Youichi Kobayashi
Division of Cardiology, Showa University of Medicine, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-092

360
Introduction: Brugada syndrome (BrS) is an inheritable disease with variable transmission that is characterised by coved ST-segment el-evation in the V1-V3 leads and an increased risk of fatal arrhythmias. Though the implantable cardiac defibrillator (ICD) is currently the standard of care for symptomatic patients, frequent ICD shocks can pose a challenge to electrophysiologists. Epicardial ablation of ar-rhythmogenic substrate in the RVOT has been documented to reduce the occurance of VT/VF in Brugada syndrome patients.
Methods: N/A
Results: We report a case of epicardial radiofrequency (RF) ablation in a 58 year old patient with BrS and inferior early repolarization pat-tern ECG who had recurrent appropriate ICD shocks for spontaneous VF. As he received 4 appropriate shocks within the year for recur-rent spontaneous VF, we attempted substrate modification to reduce recurrent episodes. Endocardial followed by epicardial mapping for arrhythmogenic substrate of the RV was performed utilising a 3-dimensional non fluoroscopic navigation system with remote magnetic navigation and a 3.5 mm irrigated magnetic mapping and ablation catheter. Electroanatomic mapping showed areas of highly fractionated electrograms extending beyond the QRS complex in the anterior RVOT region (Figure 1A). Similarly, fractionated electrograms were ob-served in the anterior-inferior aspect of the right ventricle (Figure 1B), in keeping with early repolarisation seen in inferior leads. Ablation targets were areas of low voltage (≤1 mv), fractionated electrograms or late potentials extending beyond the QRS complex. RF ablation was applied from the epicardial aspect to these 2 regions, with resolution of the coved ST appearances in V1 and V2. The ST segment in V1-V2 remained elevated immediately post ablation and the subtle early repolarisation pattern in the inferior limb leads persisted, consis-tent with myocardial injury from RF application. Our patient made an uneventful post procedure recovery. Serial ECGs performed during follow up showed abolishment of both the coved shaped ST appearances and the ST elevations in V1 and V2. Subtle ST elevations persist-ed in the inferior leads.
Conclusions: RF ablation resulted in resolution of coved ST-T changes. The patient remained arrhythmia free over a one year follow up period post procedure.
A ONE YEAR FOLLOW-UP AFTER EPICARDIAL ABLATION IN A PATIENT WITH BRUGADA SYNDROME AND INFERIOR EARLY REPOLARISATIONEdward Lee, Paul Lim, Daniel Chong, Boon Yew Tan, Kah Leng Ho, Chi Keong Ching, Wee Siong Teo
National Heart Centre Singapore, Singapore
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-094

361
Introduction: Catheter ablation has been widely performed for ventricular tachyarrhythmias, however, there is paucity for the long-term clinical outcome, and the predictor for recurrences remains debated.
Methods: A total of 498 patients (49.6% female, mean 44.9±14.8 years old) who underwent catheter ablation for ventricular tachyarrhyth-mias (VAs), including ventricular tachycardia (VT) or premature ventricular contraction (PVC), were studied retrospectively. VAs was divided by 4 groups according to the type of bundle branch block morphology (LBBB or RBBB) and the axis of QRS complex (inferior or superior). Recurrence was defined as recurred VT or less than an 80% decrease in PVC burden.
Results: Assorted patients were 26 (5.2%) with LBBB and superior axis, 319 (64.1%) with LBBB and inferior axis, 89 (17.9%) with RBBB and superior axis, and 54 (10.8%) with RBBB and inferior axis. In Kaplan-Meier curve, during 20.1±30.3 months follow-up, cumulative re-currence-free survival were significantly different in 4 groups (by log rank, P=0.013). Cox regression using multivariate models showed that the assorting by ECG morphology (P=0.034) and the left ventricular end diastolic dimension (LVEDD) measured by transthoracic echocardiography (HR 1.047, 95% CI 1.009-1.086, P=0.003) were significantly associated with the recurrences after catheter ablation.
Conclusions: This long-term follow-up data showed that the site of origin manifested by ECG patterns was a rate-limiting factor for the efficacy of catheter ablation in patients with VAs, and the LVEDD predict the recurrence after catheter ablation for VAs.
LONG-TERM CLINICAL OUTCOMES OF CATHETER ABLATION FOR VENTRICULAR TACHYARRHYTHMIAS ACCORDING TO THE SITE OF ORIGIN: LEFT VENTRICULAR END DIASTOLIC DIMENSION PREDICTS THE RECURRENCESKwang No Lee1, Choi Jong-Il1, Sukkyu Oh1, Hyungdon Kook1, Yun Gi Kim1, Seung-Young Roh1, Hee-Soon Park1, Yong-Soo Baek1, Jinhee Ahn2, Dong-Hyeok Kim3, Dae In Lee4, Jin Seok Kim5, Jaemin Shim1, Hong Euy Lim6, Young-Hoon Kim1 1Korea University Anam Hospital, Seoul, Republic of Korea; 2Division of Cardiology, Pusan National University Hospital, Busan, Republic of Korea; 3Division of Cardiology, Sejong General Hospital, Bucheon, Republic of Korea; 4Division of Cardiology, Chungbuk National University Hospital, Chungju, Republic of Korea; 5Korea University Medical Center Ansan Hospital, Ansan, Republic of Korea; 6Korea University Medical Center Guro Hospital, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-095

362
Introduction: Catheter ablation (CA) of the premature ventricular contractions (PVCs) performed in highly symptomatic patients. PVCs from the parahisian region is rare and CA has a high risk of heart block. Here, we report a case of successful CA of multiform PVCs in-cluding parahisian region by only one ablation point in the channel of myocardial infraction scar.
Methods: N/A
Results: A 73-year-old man had spontaneous PVCs with 3 QRS morphologies before procedure and had an old myocardial infraction. PVC with LBBB and inferior axis similar to QRS of sinus rhythm was designated as PVC1, and PVC with RBBB and left superior axis was des-ignated as PVC2. PVC with RBBB and left inferior axis was designated as PVC3. PVC1 was mapped in the right ventricular and the earliest ventricular activation preceding the QRS onset was recorded on a slightly remote from the maximal His potential. In the left ventricular tract, the earliest V-QRS was also recorded on parahisian region. PVC2 was mapped in the left ventricular. The earliest V-QRS of 43ms was recorded on posterior left ventricular septum with fractionated potential. Pace mapping of this point produced 2 QRS morphologies similar to PVC2 and PVC3. After radiofrequency energy was delivered to the only one point in posterior left ventricular septum, all PVCs were eliminated. Bipolar voltage map was proceeded, and revealed the scar in posterior left ventricular septum. And a channel was iden-tified by adjusting the voltage limit of bipolar maps less than 0.5 mV. Ablated point was on the exit of the channel. Therefore, we consider that PVCs had the same origin, and had each different exits. We experienced multiple PVCs were successfully ablated only one point on the channel of the scar.
Conclusions: We successfully ablated the multiple parahisian PVCs due to the changing value of low voltage area and the identification of channel.
CATHETER ABLATION OF PARAHISIAN VENTRICULAR ARRHYTHMIAS WITH THREE QRS MORPHOLOGIES ORIGINATE FROM ONE FOCUS USING IDENTIFICATION OF CHANNELYuya Nakamura, Mitsuharu Kawamura
Showa University School of Medicine, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-097

363
Introduction: Radiofrequency catheter ablation (RFCA) of ventricular tachycardia (VT) in arrhythmogenic right ventricular dysplasia (ARVD) and other nonischemic cardiomyopathy (NICM) was considered as an alternative strategy for drug refractory cases after implantable car-dioverter-defibrillator implantation. The aim of current study investigated the efficacy of RFCA in prevention of further unfavorable ar-rhythmic events in ICD-implanted patients with different etiologies of cardiomyopathy.
Methods: A total of 105 patients [mean age: 59±18; 79 (75.2%) male] with an ICD implantation were enrolled. Patients were categorized into 2 groups, including 33 patients with arrhythmogenic right ventricular dysplasia (ARVC) in group 1 and 72 patients with nonischemic cardiomyopathy (NICM) rather than ARVC in group 2. All patients underwent ICD implantation for experienced VT episodes, syncope, or aborted sudden cardiac death. RFCA was performed in 20 patients for documented electrical storm (12 in group 1; 8 in group 2). Long-term outcome was investigated and endpoints composited of all cause mortality and recurrent ICD therapy.
Results: The baseline characteristics were shown in Table 1. Patients in group 2 had higher incidence of congestive heart failure than those in group 1 (45% vs. 21%, P=0.03). There were no significant differences between patients with vs. without RFCA. During a mean fol-low-up of 35 months, events were identified in 56 patients, including 20 (19%; 2 in group 1 and 18 in group 2) with mortality and 36 (34%, 17 in group 1 and 19 in group 2) with recurrent ICD therapies (5 with anti-tachycardia pacing; 31 with ICD shock). After multivariable Cox regression analysis, only left ventricular systolic dysfunction significant predicted further unfavorable events (P<0.001, HR: 4.34, 95% CI: 2.33-8.11) in overall NICM patients (Table 2). Kaplan-Merier curves demonstrated survival benefit for patients undergoing RFCA in group 1 (P=0.03), but not for patients in group 2 (P=0.92, Figure 1).
Conclusions: LV systolic dysfunction significantly affected the clinical outcome in patients with NICM regarding ablation or not. RFCA in patients with NICM demonstrated divergent prognostic implication, and favorable outcome of RFVA was noted in patients with ARVC after ICD implantation during long-term follow-up.
DIVERGENT LONG-TERM OUTCOME OF CATHETER ABLATION FOR VENTRICULAR TACHYCARDIA IN CARDIOMYOPATHY WITH DIFFERENT ETIOLOGIESChing Ju Wu, Fa Po Chung, Yenn Jiang Lin, Shih Lin Chang, Li Wei Lo, Yu Feng Hu, Ta Chuan Tuan, Tze Fan Chao, Jo Nan Liao, Shih Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-098

364
Introduction: Forty one year old male underwent Aortic Valve replacement with Bileaflet tilted disc valve for severe valvular AS in 2013. He presented with recurrent palpitations for one month durations. ECG during palpitations showed RBBB with Right axis deviation VT with early transition. Baseline ECG showed First degree AV block with incomplete LBBB. Echo showed no RWMA and LVEF 55% with concen-tric LVH. CAG showed normal coronaries.
Methods: Baseline AH nterval was 318 msec and HV interval was 57 msec with first degree heart block with LBBB. On V burst pacing two morphology of VT one with RBBB and Right axis and another one RBBB with left axis deviation with early transition in precordial lead was inducible and spontaneously terminated or terminated on overdrive pacing. The VT CL was 470 msec for RBBB and Right axis deviation with VA conduction which was concentric. Second VT was CL 511 msec and RBBB with Left axis deviation. On a pacing further dual AV nodal physiology present and AVNRT was frequently inducible even it lead to stimulation of RBBB and RAD VT.So slow pathway ablation done without increase in PR interval and AVNRT was non-inducible. Thereafter transeptal puncture done and activation mapping of RBBB and RAD VT done by using Navix 3D ensite system (St. Jude Medical). VT mapping showed focal origin from anterior papillry muscle inside the tip and centrifugal propagation. This VT was tried to ablate but catheter was unstable. Therefore encircling lesion was given and VT was non inducible but it never terminated during ablation. Thereafter second VT was mapped which was also focal arising from more basal part of posterior papillary muscle but it was not totally encircled and still inducible. In this VT also stability of catheter was problem-atic.
Results: Idiopathic Papillary VT is rare form of Idiopathic VT. In this patient it developed after AVR. This VT was arising from both papillary muscles and focal automatic in mechanism. This patient was also having AVNRT with prolonged PR interval and sometime driving VT from papillary muscle. Successful RF ablation of slow pathway done and Anterior papillary muscle was encircled by RF ablation which was non-inducible but posterior papillary VT was still inducible
Conclusions: Major problem in ablating the papillary muscle VT is due to its deeper origin in muscle and totally instability of ablation cath-eter either deviating to either side of papillary muscle. Cryo ablation might be better option due to freezing of ablation catheter to the pap-illary muscle.
IDIOPATHIC FOCAL VT FROM BOTH PAPILLARY MUSCLES AND AVNRT IN A PATIENT WITH POST AVRRamdeo Yadave
Batra Hospital, New Delhi, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-099

365
Introduction: Idiopathic VT from LV base near mitral annulus is rarely reported. Here reporting a case of VT in fourty five year old male de-veloping recurrent paroxysmal palpitaions for six months. ECG during palpitations showed regular repetitive wide QRS tachycardia with RBBB and Right Axis deviation morphology with V1 to V6 positive R wave suggestive of arising near Mitral annulus. I and aVL was positive so it is coming out from mid anterior wall of LV. MRI done showed some edema in LV mid septum. FDG PET CT was done which was nor-mal. Echo showed LVEF 50 to 55% without regional wall motion abnormality. Coronary angiography showed 30% stenosis in RCA. Took him for 3D mapping by Navix system.
Methods: VT was easily spontaneously induced and sustained on Isoprenaline infusion. Activation mapping was done by using 3D Navix from St. Jude Medical. Activation and propagation map showed focal onset of VT from Anterior Mitral annulus with centrifugal spread of electrical wavefront. RF ablation was done by single RF application in the LV base near mitral annulus. No VT was thereafter inducible even on maximum dose of Isoprenaline infusion.
Results: Successful RF ablation of VT done without any complications. Over 6 months of follow up he is VT free.
Conclusions: Idiopathic VT from LV base near anterior mitral annulus is very rare. The mechanism of this VT is increased Automaticity from focal onset. RF ablation by 3D mapping system is curative in this patient.
IDIOPATHIC VT FROM LV BASE NEAR ANTERIOR MITRAL ANNULUSRamdeo Yadave
Batra Hospital, New Delhi, India
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-100

366
Introduction: N/A
Methods: N/A
Results: The patient was 64 years old female. She had sudden onset of palpitation and Holter ECG detected frequent premature ventricu-lar contractions (PVCs) and paroxysmal supraventricular tachycardia (PSVT). In electrophysiological study, atrio-ventricular node had dual ante-grade pathway. Ante-grade slow pathway and retro-grade fast pathway showed stably 1:1 conduction. Atrioventricular reentrant tachycardia and atrial tachycardia were denied by ventricular-atrial conduction pattern and decremental conduction property, so PSVT was diagnosed to slow-fast atrio-ventricular node reentrant tachycardia (AVNRT). At the site where atrio-ventricle ratio was almost 1:10, accelerated junctional rhythm appeared during radiofrequency catheter ablation (RFCA). After RFCA, slow pathway conduction were dis-appeared. The QRS morphology of PVC showed left bundle block pattern and superior axis, but ‘rS’ type in III lead. The origin of PVC was predicted at lower site than right ventricular outflow tract (RVOT), where was near Koch’s triangle. The PVC had the earliest activation site at 5 mm below His potential, and perfect pace map was obtained the same site. The PVC was eliminated by RFCA at the good activation site without any atrio-ventricular block. Koch’s triangle generally become the target site of slow pathway ablation in AVNRT patient. How-ever sometime ventricular arrhythmias also originated from Koch’s triangle of the base of right ventricular septum, where accelerated junctional beat occurs during RFCA. The attention to atrio-ventricular block is important in RFCA of these arrhythmias.
Conclusions: N/A
A CASE OF SUCCESSFUL RADIOFREQUENCY CATHETER ABLATION OF BOTH SLOW-FAST ATRIOVENTRICULAR NODE REENTRANT TACHYCARDIA AND FREQUENT IDIOPATHIC PREMATURE VENTRICULAR CONTRACTION WITH IN KOCH’S TRIANGLEYoshiaki Yui, Kou Suzuki, Masakazu Kaneko, Tomohiko Harunari, Tooru Iwama
Tokyo Metropolitan Bokutoh Hospital, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-101

367
Introduction: Bipolar radiofrequency (RF) catheter ablation is a therapeutic option for the treatment of arrhythmias originating from deep inside of the thick myocardium, but this approach has a potential risk of serious complications including a steam-pop.
Methods: To obtain electrical parameters for safely and effectively performing the bipolar RF ablation, experimental studies were per-formed using the porcine left ventricular myocardium (17.9±2.9 mm). Two open irrigation ablation catheters were placed on opposite surfaces of the myocardium either with or without the contact force control (CFC) at 20-g, and RF current (40 or 50 W) was delivered for 60 seconds. The endocardial catheter was connected to the active channel and the epicardial catheter to the ground channel of the RF gen-erator.
Results: (1) Safety parameters to avoid steam-pop phenomena. Steam-pop was occurred 20% in 50W ablation without CFC, 12% in 50W with CFC, 8% in 40W without CFC and none in 40W with CFC. Steam-pop was associated with greater decrement of the total impedance (-26.9±12.7 vs. -17.9±6.5 ohm, P=0.0004) and time rate change of impedance (dv/dt impedance decrement) (-2.5±1.9 vs. -1.5±0.4 ohm/s, P<0.0001). Thinner wall thickness (odds: 0.305, 95% CI: 0.121-0.540, P<0.0001) and higher radiofrequency energy (odds: 32.57, 95% CI: 3.276-830.64, P=0.0013) were also related to the occurrence of steam-pop. (2) Efficacy parameters for deeper lesions. The integration of impedance decrement and RF delivering time (IIT) was correlated to total lesion depth (r=0.5949, P<0.0001). The integral value corrected by wall thickness showed a stronger correlation coefficient (r=0.6433, P<0.0001).
Conclusions: As well as contact force monitoring, new electrical parameters (dv/dt and IIT) would be useful to create sufficiently deeper lesions in avoiding the steam-pop during bipolar RF ablation. In addition, measurement of the thickness of the target myocardium using 3-D mapping system would be helpful in programing the appropriate RF energy for each site.
ESTABLISHMENT OF ADDITIONAL ELECTRICAL PARAMETERS FOR SAFELY AND EFFECTIVELY PERFORMING BIPOLAR RADIO-FREQUENCY ABLATION: OBSERVATIONS FROM AN EXPERIMENTAL STUDYOsamu Saitoh1, Junya Watanabe1, Ayari Sugai1, Katsuya Suzuki2, Minoru Tagawa3, Hiroshi Furushima4, Masaomi Chinushi1 1Graduate School of Health Sciences, Niigata University, Niigata, Japan; 2Kido Hospital, Niigata, Japan; 3Nagaoka Chuo General Hospital, Niigata, Japan; 4Furushima Clinic, Niigata, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-103

368
Introduction: Catheter ablation has become an established treatment strategy for ventricular tachycardia (VT). However, steam pop is an important complication, since it can make severe myocardial injury.
Methods: N/A
Results: A 55-year-old man with dilated cardiomyopathy and implantable cardio-defibrillator was admitted for cathter ablation due to symptomatic monomorphic VT. The hear rate of VT was 119 bpm and the morphology was inferior axis and right bundle branch block (RBBB). The left ventricular (LV) activation mapping of the three-dimensional mapping system Carto 3 (Biosense Webster) demonstrat-edthat the mechanism of this VT was a re-entry, localized at the border zone between the scar and the lateral LV normal wall. Linear ab-lation was performed to the border zone. PVC short run remained after the linier ablation, therefore we add to bonus ablation to the oppo-site endocardial side. RF ablation was performed using 4 mm irrigation catheter with contact force monitoring. After RF energy was deliv-ered for 21 seconds (38W, 40°C, mean contact force14g), it was interrupted due to steam pop. The patient was asymptomatic and no peri-cardial effusion was seen on ICE. However coronary angiography showed the fistula between the distal portion of the circumflex artery and left ventricule and ICE confirmed the air bubble flowing into LV.
Conclusions: This case is, to the best our knowledge, the first report on the coronary artery-LV fistula induced by a steam pop that hap-pened during ablation to VT.
CORONARY ARTERY-LEFT VENTRICULE FISTULA FOLLOWING VENTRICULAR TACHYCARDIA ABLATIONChihiro Ota, Yukio Sekiguchi, Kenji Kuroki, Fumi Yamagami, Yasutoshi Shinoda, Satoshi Aita, Eikou Sai, Tomoaki Hasegawa, Takeshi Machino, Hiro Yamasaki, Nobuyuki Murakoshi, Akihiko Nogami, Kazutaka Aonuma
University of Tsukuba, Tsukuba, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-104

369
Introduction: Early repolarization of surface ECG is associated with ventricular tachycardia/fibrillation (VT/VF). However, the characteristic of early repolarization (ER) in patient with acute myocardial infarction (AMI) and subsequent VT/VF has not been well evaluated.
Methods: We enrolled 26 patients who had myocardial infarction. We trace the EKG from the time of initial presentation of myocardial in-farction to the acute episode subsiding, and noticed the EKG morphology was dynamic just as the previous study had mentioned.
Results: The baseline characteristics of study patients is shown in Table 1. The J wave would appeared at initial presentation and disap-peared in the following in those patient who had subsequent VT/VF. Eight patients (61.5%) had J wave at inferior lead (II, III, aVF), three pa-tients (23.1%) at left precordial leads (V4, V5, V6), four patient (30.7%) at lateral leads (I, aVL), 3 patients (23.1%) at right precordial leads (V1, V2, V3). The duration from initial J wave presentation to VT/Vf was 0-90 days (median 16 days).
Conclusions: ER in the inferior leads is associated with the occurrence of VT/VF in patients with AMI, suggesting that ER might be a sign of increased vulnerability for ventricular tachyarrhythmias after acute ischemia.
THE CHARACTERISTIC OF EARLY REPOLARIZATION IN PATIENT WITH ACUTE MYOCARDIAL INFARCTION AND SUBSEQUENT VENTRICULAR ARRHYTHMIACheng-I Wu, Shih-Lin Chang, Li-Wei Lo, Fa-Po Chung, Tze-Fan Chao, Jo-nan Liao, Yu-Feng Hu, Ta-Chuan Tuan
Taipei Veterans General Hospital, Taipei, Taiwan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 2-105

370
Introduction: Anticoagulation is recommended to continue at least 2 months after radiofrequency catheter ablation (RFCA) of atrial fibril-lation (AF). NEW REDUCIBLE STUDY was a multicenter, prospective, randomized clinical trial testing the hypothesis that Novel Oral Anti-coagulants (NOAC) use for the first 1 month after the RFCA for patients with paroxysmal AF and low thromboembolic risk would be suffi-cient for efficacy and safety compared to conventional NOAC use for 2 months.
Methods: We enrolled 130 paroxysmal AF patients who underwent RFCA (mean age 53±10 years, 27 (20.8%) female) with randomized short group (1 month use of NOAC) versus conventional group (2 month use of NOAC). Clinical variables were compared between two groups. The primary efficacy and safety end points including any kind of thromboembolic complications and bleeding events were as-sessed.
Results: 1) Total 130 patients were enrolled 70 patients (52±10 years, 14 [20.0%] female) with short group and 60 patients (55±10 years, 13 [21.7%] female) with conventional group. There were no differences in the CHA2DS2-VASc (P=0.726) and HAS-BLED scores (P=0.688) between the groups. 2) There was no thromboembolic event including ischemic stroke, myocardial infarction, pulmonary embolism, vas-cular site thrombotic occlusion and other organ thrombotic event. One case of periprocedural cardiac tamponade occurred in convention-al group. There was no signifi-cant difference minor bleeding events between the two groups (2 cases vs. 4 cases, P=0.459). Conventional group tended to have more gastrointestinal trouble such as dyspepsia or reflux symptom, but it did not show statistical significance (3 cases vs. 6 cases, P=0.145). 3) During 8±5 months follow-up, 68 (97.1%) patients in short group were free from AF recurrence compared with 59 (98.3%) for conventional group (P=0.478).
Conclusions: NOAC use for the first 1 month after the RFCA for patients with paroxysmal AF and low thromboembolic risk would be suf-ficient for efficacy and safety compared to conventional NOAC use for 2 months. These data support larger clinical evaluations of this therapy strategy.
INTERIM RESULTS FROM NEW REDUCIBLE STUDY: A MULTICENTER, PROSPECTIVE, RANDOMIZED CLINICAL TRIAL OF INVESTIGATION ON APPROPRIATE DURATION OF NOVEL ORAL ANTICOAGULANTS USE AFTER CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATION IN PATIENTS WITH LOW THROMBOEMBOLIC RISKYong-Soo Baek, Anupam Jena, Hee-Soon Park, Kwang-No Lee, Seung-Young Roh, Jinhee Ahn, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-106

371
Introduction: Atrial fibrillation (AF) is the most common tachyarrhythmia and its prevalence is 0.77% in China. Pharmacologic therapy is the basis of all strategies. However, drug side effects are the common barriers for AF management. There is little report about the ad-verse reactions of both beta blocker and amiodarone responsible for cutaneous damages in AF patients. Here, we report a rare case that the administration of metoprolol and amiodarone intended to manage AF combined with heart failure were both hindered by psoriasis.
Methods: N/A
Results: A 49-year-old male patient was diagnosed as atrial fibrillation after a repairing operation of atrial septum defects, mitral and tri-cuspid valvuloplasty. He refused a standardized treatment until admitted in hospital because of dyspnea, chest discomfort and facial ede-ma. He had a 20 years history of psoriasis. His physical examination and laboratory examination supported the diagnosis of persistent atrial fibrillation, heart failure and psoriasis. On admission, he was treated with digoxin 0.125 mg qd and metoprolol 50 mg qd to control ventricular rate. After one week, the patient complained the aggravation of his original psoriatic lesions. After discontinue of digoxin and metoprolol, amiodaroe as an alternative was prescribed. However, the psoriatic lesions still further developed. Then we start metoprolol 12.5 mg bid and topical treatment with corticosteroid. The psoriatic lesions gradually improved and showed no progress during the subse-quent follow-up weeks.
Conclusions: Dermatologic side effects of cardiovascular pharmaceutical therapy is rarely fatal, however, their influence on quality of life and mental state will restrict the medication administrating and further exacerbate original heart disease. Consequently, this case aims to promote the clinicians keep caution when they charge AF patients with a history of dermatologic diseases or cutaneous damage.
TREATMENT OF ATRIAL FIBRILLATION PATIENT WITH METOPROLOL AND AMIODARONE COMPLICATED BY PSORIASISMiaomiao Cao, Yanrong Yin, Ling Cao, Xiaolin Xue, Chaofeng Sun, Guoliang Li
Department of Cardiovascular Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China
CLINICAL ELECTROPHYSIOLOGY P 2-107

372
Introduction: Currently, the use of CHA2DS2-VASc score is taken as a prediction tool for the stroke risk in individual patients. The purpose of this study is finding out the incidence, the risk factor of stroke and the appropriateness of CHA2DS2-VASc score to predict stroke in Thai patients.
Methods: We retrospectively enrolled non-valvular AF patients who have not been treated with anticoagulant from January 1st, 2006 to December 31st, 2013. Stroke risk factors were collected and patients were monitored for a period of 3 years.
Results: A total of 257 patients (136 men, 53%; median age 69 years, range 34 to 93 years) were enrolled. During a median follow-up of 3 years, 39 patients (15%) developed ischemic stroke. This represents an incidence rate of 6.6 cases per 100 patient-years. Diabetes melli-tus is the only risk factor that significantly affect to the ischemic stroke (P=0.005). At CHA2DS2-VASc score 0 and 1, our study demonstrate ischemic stroke rate per 100 patient-years at 2.94 and 2.73 respectively. The ischemic stroke rate of CHA2DS2-VASc score 2-6 is between 4.39-13.33 per 100 patient- years which is higher than those of score 0-1 significantly (P=0.04).
Conclusions: The incidence of ischemic stroke in this population was 6.6 cases per 100 patient-years. The significant risk factor for devel-oping thromboembolic event was diabetes mellitus. At CHA2DS2-VASc score between 0 and 1, our study cannot demonstrate the low thromboembolic event rate, but it clearly shows different thromboembolic event rate in CHA2DS2-VASc 0-1 and CHA2DS2-VASc ≥ 2 at 2.78 and 7.80 respectively.
INCIDENCE AND RISK FACTORS OF ISCHEMIC STROKE AMONG NON-VALVULAR ATRIAL FIBRILLATION IN THAILANDThunyarat Chaipruckmalakarn, Warangkna Boonyapisit
Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
CLINICAL ELECTROPHYSIOLOGY P 2-108

373
Introduction: To describe the baseline characteristics and antithrombotic treatment of patients with non-valvular atrial fibrillation in the Macau.
Methods: A total of 472 patients (mean age: (73.0±10.9) years old, 41.7% female (n=197) diagnosed with non-valvular atrial fibrillation were recruited between January 2014 and December 2014 in the Centro Hospitalar Conde de São Januário (CHCSJ). Baseline data in-cluded demographics, medical history, nature of atrial fibrillation, and medical treatment. Calculated CHA2DS2-VASc score, score≥2 means high risk of stroke; calculated HAS-BLED score, score≥3 means high risk of hemorrhage.
Results: There were 244 (51.7%) patients with age above 75 years old, 97 (21.6%) patients had history of stroke or TIA, 288 (61.0%) patients were hypertension, 116 (24.6%) patients were diabetes mellitus. Mean CHA2DS2-VASc score was (3.4±1.8), 389 (82.4%) patients CHA2DS2-VASc score≥2. Mean HAS-BLED score was (1.96±1.03), 132 (28.0%) patients HAS-BLED score≥3.55, 4% (n=257) patients received ei-ther warfarin (n=101, 21.6%) or new oral anticoagulants (NOAC) (n=156, 33.8%); 38.9% (n=184) patients received antiplatelet therapy and 11.2% (n=53) patients received no anti-thrombosis treatment. Among patients with CHA2DS2-VASc≥2 (n=389), 55.3% (n=215) patients receive anticoagulant therapy, and more patient received NOVC than received Warfarin.
Conclusions: Stroke prevention according to risk scores and current guidelines is very well carrying out in NVAF patients in Macau, the increasing risk of hemorrhage affects the usage of anticoagulation therapy in the patients with very high risk of stroke.
THE ANTICOGULATION THERAPY OF PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION IN MACAURuohan Chen1, KePing Chen1, Toi-Meng MOK2, Evora Mario2, Shu Zhang1 1Fuwai Hospital, Beijing, China; 2The Centro Hospitalar Conde de São Januário, Macau, China
CLINICAL ELECTROPHYSIOLOGY P 2-109
CHA2DS2-VASc Score and Anticogulation Therapy
CHA2DS2-VASc sore No Warfarin NOVA anti-platelet None HAS-BLED
0 28 3 (10.7%) 10 (35.7%) 9 (32.1%) 6 (21.4%) 0.2
1 55 10 (18.2%) 19 (34.5%) 20 (36.4%) 8 (14.5%) 0.9
2 72 14 (19.4%) 32 (44.4%) 21 (29.2%) 6 (8.3%) 0.9
3 99 25 (25.2%) 41 (41.4%) 31 (31.3%) 9 (9%) 2.0
4 93 21 (22.6%) 35 (37.6%) 32 (34.4%) 10 (10.7%) 2.3
5 60 14 (23.3%) 19 (31.6%) 26 (43.3%) 5 (8.3%) 2.6
>6 65 14 (21.5%) 10 (15.4%) 35 (53.8%) 9 (13.8%) 3.1

374
Introduction: Apixaban is an oral factor Xa inhibitor used to prevent stroke and systemic embolism (SE) in patients with nonvalvular atrial fibrillation (NVAF). In these interim analyses, we assessed the baseline characteristics of enrolled patients in the apixaban postmarketing surveillance (PMS).
Methods: Patients diagnosed with NVAF, in need of anticoagulation therapy for stroke/SE prevention and receiving apixaban 2.5 or 5 mg twice daily for the first time were enrolled. Patient registration is on-going in Korea and is completed in Japan. Descriptive analyses were used to assess the baseline characteristics of the pooled Korean and Japanese populations.
Results: From PMS in Japan (until May 17, 2015) and Korea (until December 31, 2015), a total of 7,426 patients (41.6% women) 73.4±10.3 years old were enrolled. CHA2DS2-VASc score was 3.5±1.8 and HAS-BLED score was 1.9±1.2 (Table). In this pooled population, 87.6% patients had comorbidity (renal disorder: 23.4%, heart failure: 21.1%, hypertension: 62.6%, stroke or TIA: 20.6%) and 63.1% were pre-scribed apixaban 5 mg twice daily. Most (97.5%) of the eligible patients were prescribed with a reduced dose, while 15.7% of the non-eligi-ble patients received a lower dose than recommended. The 2,370 Korean patients (42.5% women) were aged 71.1±10.0 years with CHA2DS2-VASc score of 3.6±1.7 and HAS-BLED score of 2.4±1.2. In this population, 74.8% were prescribed apixaban 5 mg BD and 94.7% had comorbidity (renal disorder: 44.4%, heart failure: 3.1%, hypertension: 67.3%, stroke or TIA: 41.8%).
Conclusions: The data on the characteristics of the eligible patients were comparable across the study populations. The reason for the use of reduced dose of apixaban should be further assessed.
APIXABAN POSTMARKETING SURVEILLANCE OF KOREAN AND JAPANESE PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION: BASELINE CHARACTERISTICS OF THE POOLED STUDY POPULATIONSeongwook Han1, Hiroshi Inoue2, Masahiro Yasaka3, Youngja lee4, Hiroyuki Hashimoto5, Michiaki Umeyama6, Moon-Hyoung Lee7, Jong S. Kim8 1Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Republic of Korea; 2Saiseikai Toyama Hospital, Toyama, Japan; 3Department of Cerebrovascular Medicine and Neurology, National Hospital Organization, Kyushu Medical Center, Fukuoka, Japan; 4Bristol-Myers Squibb Korea, Seoul, Republic of Korea; 5Pfizer Japan Inc., Tokyo, Japan; 6Bristol-Myers Squibb K.K., Tokyo, Japan; 7Division of Cardiology, Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea; 8Department of Neurology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-111
Patient Characteristics across Pooled Data
Entire population (N=7,426)
Apixaban 5 mg BD (n=4,688)
Apixaban 2.5 mg BD (n=2,728)
Other doses of apixaban (n=10)
Women, n (%) 3,092 (41.64) 1,584 (33.79) 1,505 (55.17) 3 (30.00)
Age (year), mean±SD 73.40±10.26 68.86±9.10 81.20±6.92 76.00±5.56
Weight (kg), mean±SD 60.89±12.57 65.35±11.72 53.45±10.21 59.67±10.59
Serum Creatinine ≥ 1.5 mg/dL, n (%) 316 (4.26) 55 (1.17) 260 (9.53) 1 (10.00)
Comorbidity, n (%) 6,502 (87.56) 4,029 (85.94) 2,645 (90.36) 8 (80.00)
Prior medication (anticoagulants), n (%) 4,435 (59.72) 2,813 (60.00) 1,616 (59.24) 6 (60.00)
CHADS2 score, mean±SD 2.14±1.38 1.86±1.35 2.61±1.30 2.00±1.70
CHA2DS2-VASc score, mean±SD 3.46±1.70 3.01±1.65 4.24±1.49 3.40±1.84
HAS-BLED score, mean±SD 1.89±1.17 1.75±1.19 2.13±1.09 2.30±1.70

375
Introduction: Digoxin-associated mortality was recently reported in atrial fibrillation (AF). Our objective was to investigate a clinical risk factor for digoxin-associated mortality during 10 years follow-up.
Methods: We reviewed retrospective cohort of AF patient in Eulji University Hospital, Deajeon, South Korea from May 2004 to July 2015. The continuous digoxin uses in consecutive 402 AF patients that undertaken ECG, echocardiogram, medication and laboratory data were analyzed. The cardiac including cerebral events were collected and analyzed from index prescription for digoxin during follow-up 10 years.
Results: The duration of QRS, QTc interval and ejection fraction were similar between two groups. The mean age was 68±11 and propor-tion of male was 40% at index period. Total cardiac mortality including sudden cardiac death (n=15), recurrent ischemic heart disease (IHD) (n=19) and heart failure aggravation (n=17) was found during the 10 years. Cox Regression Univariate analysis showed that diabetes mellitus was hazard ratio (HR) =2.0, confidence interval (CI) =1.08-3.72, P=0.027, serum digoxin concentration (SDC) was HR=1.35, CI=1.02-1.80, P=0.034, CHA2DS2-VASc score was HR=1.30, CI=1.00-1.70, P=0.049, previous ischemic heart disease (IHD) was HR=4.45, CI=1.62-12.20, P=0.002. Multivariate analysis showed that previous IHD was HR=4.27, CI=1.54-11.82, P=0.005. In addition, Age (78±11 vs. 77±14, P=0.769), Ejection fraction (51±15% vs. 50±17%, P=0.759) and SDC (0.9±0.8 ng/mL vs. 1.2±1.0 ng/mL, P=0.201) were simi-lar between previous IHD and non-IHD. Previous IHD group have higher proportion of male (39.1% vs. 63.2%, P=0.037), hypertension (64.6% vs. 94.7%, P=0.007), diabetes (22.6% vs. 52.6%, P=0.003), CHA2DS2-VASc (2.8±1.1 vs. 4.4±0.7, P<0.001), anti-platelet therapy (51.2% vs. 84.2%, P=0.005), beta blocker therapy (29.7% vs. 57.9%, P=0.009).
Conclusions: Our retrospective analysis found that continuous digoxin use in AF with previous IHD was associated with greater risk for cardiac mortality. Large, prospective, multicenter, randomized controlled trials are needed to clarify this result.
PRE-EXISTING ISCHEMIC HEART DISEASE IS A RISK FACTOR FOR CARDIAC MORTALITY IN ATRIAL FIBRILLATION WITH CONTINUOUS DIGOXIN USE FOR 10-YEAR FOLLOW-UPKi-Woon Kang, Sangil Kim, Yu Jeong Choi, Kyung Tae Jung, Sang Hyun Park, Jeong Yun Chin, Won Ho Kim
Eulji University Hospital, Deajeon, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-112

376
Introduction: Previous randomized studies have shown a decreased risk of intracranial hemorrhage (ICH) with use of novel oral anticoag-ulants. However, the effect of oral anticoagulation therapy (OAT) in atrial fibrillation (AF) patients with history of intracranial hemorrhage (ICH) is poorly defined. This study evaluated the efficacy and safety of OAT in AF patients with an ICH history.
Methods: In 547 consecutive non-valvular AF patients with previous ICH history, we compared the composite endpoint, including throm-boembolic and major bleeding events, between AF patients with previous ICHs who were taking NOAC (n=119), warfarin (n=254) and no oral anticoagulation therapy (no-OAT) (n=174).
Results: In NOAC group, 38 (31.9%), 42 (35.3%) and 39 (32.8%) patients was prescribed dabigatran, apixaban and ribaroxaban, respective-ly. During the follow up period of 30.1±29.1 months, 3.1 and 5.5 major bleeding events/100 patient-years were observed in the non-OAT and warfarin groups. However, there is no bleeding event in patient with NOAC. Thromboembolic events occurred in 0, 2.4 and 8.3 events/100 patient-years in NOAC, warfarin and no-OAT, respectively. Composite endpoints occurred in 0, 6.9 and 7.6/100 patient-years in NOAC, warfarin and no-OAT, respectively. Compared with patients with non-OAT or warfarin, patients with NOAC had a better cumulative survival free of major bleeding (P=0.028) and composite endpoints (P=0.001).
Conclusions: In AF patients who require anticoagulation and have previous ICH, NOAC can improve clinical events including composite endpoints. This result suggests that NOAC should be preferred as an anticoagulation method in AF patients with history of ICH.
SAFETY AND EFFICACY OF NOVEL ORAL ANTICOAGULATION IN PATIENT WITH ATRIAL FIBRILLATION AND PRIOR INTRACEREBRAL HEMORRHAGEKyu Kim, Young-Ah Park, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-113

377
Introduction: The effect of anticoagulation is controversial in atrial fibrillation (AF) patients with newly diagnosed cancer. The effect of war-farin was poor in these patients, because of poor INR control caused by cancer treatment. However, the effect of novel oral anticoagulant (NOAC) has not been fully elucidated. This study evaluated the effect of NOAC and warfarin in AF patients with cancer.
Methods: In 1,651 consecutive non-valvular AF patients with newly diagnosed cancer, we analyzed the composite endpoints including ma-jor adverse cardiac events (MACEs) and major bleeding. Based on a propensity score matching, 2 groups with 476 matched pairs were created.
Results: Patient baseline characteristics were comparable among the matched groups. During a follow-up period of 1.8±1.9 years, 4 (0.98%/year) and 41 (1.86%/year) patients had MACEs in the propensity score-matched NOAC and warfarin groups, respectively (P=0.046). The incidence of major bleeding was significantly lower in NOAC than warfarin groups (1.46 vs. 4.31%/year, P<0.001). The incidence of composite outcome was also significantly lower in NOAC than warfarin group (2.48 vs. 8.59%/year, P<0.001). Compared with warfarin, the patients with NOAC had a decreased hazard ratio of MACE (0.33, 95% confidence interval [CI] 0.11-0.98), major bleeding (0.23, 95% CI 0.11-0.55), and composite endpoints (0.22, 95% CI 0.11-0.44).
Conclusions: Compared warfarin, NOAC showed significantly improved composite endpoints by reducing both MACE and major bleeding. This result suggests that NOAC should be preferred as anticoagulation method in AF patient with newly diagnosed cancer.
FAVORABLE EFFECT OF NOVEL ORAL ANTICOAGULATION IN ATRIAL FIBRILLATION PATIENTS WITH NEWLY DIAGNOSED CANCERKyu Kim, Yong-Joon Lee, Tae-hoon Kim, Jae-Sun Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-114

378
Introduction: The phase III ROCKET AF trial and the subsequent East Asia subgroup analysis showed that rivaroxaban was effective for the prevention of stroke in patients with non-valvular AF, and form the basis of its recommendation by the APHRS. The prospective, non-interventional XANTUS study showed low rates of bleeding and stroke/systemic embolism (SE) with rivaroxaban for patients with AF in routine clinical practice. XANAP is a sister study to XANTUS and focused on patients in the Asia Pacific region.
Methods: Like XANTUS, XANAP was a prospective, observational study in unselected patients with non-valvular AF newly starting rivarox-aban. Patients were followed for 1 year, at approximately 3-month intervals, or for at least 30 days after permanent discontinuation. The primary outcomes were major bleeding events, safety events and all-cause mortality. Major outcomes (recorded as adverse events [AEs] or serious AEs [SAEs]) were adjudicated by a central committee.
Results: In total, 2,273 patients were enrolled from January 2013 to September 2015. 49.8% received the 20 mg once daily dose of rivarox-aban; the majority of the remaining 50.2% received a dose of 15 mg once daily. 63.7% had prior antithrombotic therapy. The mean treat-ment duration (±SD) was 295.9 days (129.35), age was 70.5 years (10.57; 36.3% >75 years) and weight was 66.1 kg (12.78); 58.1% of pa-tients were male; 22.2% had newly diagnosed AF and 30.5% had paroxysmal AF. Co-morbidities included hypertension (73.6%), diabetes mellitus (26.6%), congestive heart failure (20.1%), prior stroke/non-CNS SE/TIA (32.8%) and prior myocardial infarction (MI [3.8%]).Mean CHADS2 and CHA2DS2-VASc score were 2.3 and 3.7, respectively; mean HAS-BLED score was 2.1. Clinical outcomes are shown in the Ta-ble. Treatment persistence was 66.2%.
Conclusions: In the XANAP real-world study of stroke prevention in AF in the Asia Pacific region, event rates were low and consistent with XANTUS, and with findings from the phase III ROCKET AF trial and its East Asian subanalysis.
XANAP: REAL-WORLD, PROSPECTIVE, OBSERVATIONAL STUDY OF PATIENTS TREATED WITH RIVAROXABAN FOR STROKE PREVENTION IN ATRIAL FIBRILLATIONYoung-Hoon Kim1, Thititat Thanachartwet2, John Camm3 1Korea University Medical Center, Seoul, Republic of Korea; 2Bayer (South East Asia) Pte Ltd, Singapore; 3St. George’s, University of London, and Imperial College, London, United Kingdom
CLINICAL ELECTROPHYSIOLOGY P 2-116

379
Introduction: Atrial fibrillation (AF) burden defined as the amount of time spent in AF is associated with increased risk of stroke and it is ideal to be monitored by a cardiac implantable electronic devices (CIED). The timing of prescribing an anti-arrhythmic drug (AAD) to re-duce AF burden remains controversial. This study was to investigate the effect of AAD in patients with different AF burden via CEID moni-toring.
Methods: This multi-center retrospective study screened all non-permanent AF patients with a dual-chamber CIED, and only enrolled those receiving a naïve AAD within 2009/9 to 2014/12. AF burden and maximum time of the longest episode was calculated by CIED at 0 and 3-6 months after starting AAD. The classic of AAD was prescribed by physician’s decision, including propafenone, sotalol, amiodarone, and dronedarone. Patients’ characteristics, risk factors and echocardiographic parameters were reviewed. All enrolled were divided into four groups: AF Burden <1%, 1-4%, 4-18%, and ≧18%. The changes in AF burden were observed via CIED monitoring. Pre-dictors for change in AF burden were identified using univariate and multivariate generalized linear regression analyses.
Results: Among 1,222 patients with a dual-chamber CIED and non-permanent AF, 145 eligible subjects received a naïve ADD. Mean change of AF burden in four groups (AF Burden <1%, 1-4%, 4-18%, and ≧18%) was -65.3%, -46.4%, -34.7% and -27.9%, respectively (P=0.005). Mean change in maximum time of the longest episode was -26.8%, -12.4%, +4.2% and +6.0% (P=0.006). Moreover, there was no difference of effect between various AADs. Low baseline AF burden, female, absence of mitral regurgitation, and non-diabetes were in-dependent predictors for greater reduction of AF burden in the multivariate regression model.
Conclusions: The lower baseline AF burden was associated with the greater AF reduction by any AAD, which was suggestive of early rhythm control.
EFFICACY OF RHYTHM CONTROL AND ITS RESPONSE PREDICTORS IN PATIENTS WITH CARDIAC IMPLANTABLE ELECTRONIC DEVICES & ATRIAL FIBRILLATIONPo-Lin Lin1, Chun-Che Huang2, Ying-Hsiang Lee3 1MacKay Memorial Hospital, Hsinchu, Taiwan; 2Health Policy and Management, National Taiwan University, Taipei, Taiwan; 3MacKay Memorial Hospital, Taipei, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 2-117

380
Introduction: Effects of statin in preventing new-onset AF among patients with chronic kidney disease (CKD) remains incompletely stud-ied. We aimed to determine whether statin use is associated lower risk of incident AF in CKD patients in comparison with non-CKD pa-tients.
Methods: A national insurance claim dataset of 1,000,000 enrollees was used to identify 3,528 patients with CKD and 39,045 randomly se-lected age- and gender-matched controls between January 1, 1996 and December 31, 2001. Both groups were followed up from January 1, 2002 through December 31, 2011 for comparing the risk and incidence of new-onset AF in relation to statin use. Statin user was defined as those who had been taking statin ≥30 days within 6 months before the start of 2002, whereas the non-user cohort did not receive sta-tin throughout the entire observation period. The study endpoint was the first date of occurrence of the following events: the diagnosis of AF, death, withdrawal from the Taiwan National Health Insurance program or the end of 2011. The analysis of the AF risk was performed using Cox proportional hazards regression model.
Results: During the observation period, the incidence rate and risk of new-onset AF between statin users and non-users was similar among CKD patients (5.50 vs. 7.11 per 1,000 person-years, adjusted hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.39-1.52, P=0.45). Whereas, the incidence rate and risk of newly diagnosed AF was significantly lower in statin users in non-CKD group (4.18 vs. 4.30 per 1,000 person-years, HR 0.54, 95% CI 0.38-0.76, P=0.0005) (Figure). In non-CKD group, stain users with a CHA2DS2-VASc score of ≥2, or use of high-potency statins was associated with a lower risk of new-onset AF.
Conclusions: Use of statin was associated with a lower risk for developing new-onset AF in non-CKD patients particularly in those with a CHA2DS2-VASc score of ≥2, or receiving high-potency statins, but this beneficial effect of statin was not seen in CKD patients.
DIFFERENTIAL EFFECTS OF STATIN IN PREVENTING NEWLY ONSET ATRIAL FIBRILLATION BETWEEN PATIENTS WITH AND WITHOUT CHRONIC KIDNEY DISEASEYen-Nien Lin, Yin-Huei Chen, Hung-Pin Wu, Kuo-Hung Lin, Jan-Yow Chen, Kuan-Cheng Chang
China Medical University Hospital, Taichung, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 2-118

381
Introduction: Perception of stroke risk and stroke knowledge may affect oral anticoagulant (OAC) preferences of atrial fibrillation (AF) pa-tients. Purpose: To assess patient perceptions of stroke, stroke knowledge and factors determining OAC treatment.
Methods: Cross-sectional, prospective survey of 937 AF patients receiving an OAC (recruited from 5 countries). Three groups were includ-ed: recent onset-AF (≤6 m [≤12 m in Japan]) & no stroke (36.5%), established AF (7-24 m [1-3y in Japan]) & no stroke (42.8%), and AF & recent stroke (≤6 m; 20.7%). Open-ended questions determined stroke knowledge, assessed according to a pre-defined scoring system.
Results: Patients perceived AF as serious and were concerned about stroke, particularly those with recent stroke, but less in patients with established AF diagnosis. A total of 47% of patients had good/moderate stroke knowledge; 53% low/no knowledge. More than half the pa-tients (55%) preferred to be involved in OAC-treatment choices. Stroke prevention was the most important factor when choosing an OAC, followed by bleeding risk, particularly for patients with established AF without recent stroke. All groups rated dosing frequency as signifi-cantly less important than stroke prevention (P<0.001).
Conclusions: The majority of patients perceive AF as serious and rate stroke prevention as the most important factor when choosing an OAC.
AN INTERNATIONAL SURVEY OF PATIENT PERCEPTIONS OF ATRIAL FIBRILLATION, STROKE RISK, AND ORAL ANTICOAGULATION TREATMENTGregory YH Lip1, Juliane Meyerhoff2, Ute Rohner2, Deirdre Lane3 1University of Birmingham, Birmingham, United Kingdom; 2Boehringer Ingelheim Corporation, Ingelheim, Germany; 3University of Birmingham Institute of Cardiovascular Sciences, Birmingham, United Kingdom
CLINICAL ELECTROPHYSIOLOGY P 2-119
Overall (n=937)
Recent AF, no stroke (1) (n=342)
Established AF, no stroke (2) (n=401)
AF, recent stroke
(n=194)
Patient characteristics Mean (SD) age, years 54.3 (16.6) 55.1 (15.7) 56.8 (16.0)* 47.6 (17.5)*
Female 37.1% 41.5% 35.4% 33.0%
CHA2DS2-VASc ≥2 (female) ; ≥1 (male)
85.0% 78.1%* 83.5% 100%*
Perception of seriousness Extremely/Very serious 39.4 38.9 32.2* 55.2*
of AF (%) Somewhat serious 41.6 40.1 44.9 37.6
Not at all/Not serious 19.0 21.1 22.9* 7.2*
Concern about stroke (%) Often/Always 43.4 39.5 34.9* 68.0*
Occasionally 45.4 46.8 52.4* 28.4*
Never/Don’t know 11.2 13.7 12.7 3.6*
Most important factor for Stroke prevention 47.4 49.1 52.6* 33.5*
choice of OAC (%) Risk of major bleeding 14.7 15.5 14.7 13.4
Other side effects 10.0 10.2 10.0 9.8
Dosing frequency 8.2 7.6 7.2 11.3
Antidote availability 7.8 6.4 7.2 11.3
Dietary restrictions 7.0 6.1 5.0 12.9*
Take with/without food 4.8 5.0 3.2 7.7
*p<0.001 vs. other 2 groups pooled; (1) Canada, USA, Germany, France: ≤6 months; Japan ≤12 months; (2) Canada, USA, Germany, France: 7 months-2 years; Japan 1-3 years.

382
Introduction: This international prospective study assessed differences in atrial fibrillation (AF) patients’ stroke knowledge, self-perceived adherence, oral anticoagulant (OAC)-treatment decision preferences and OAC attributes affecting treatment choice, in Asia (represented by Japan), North America (USA, Canada) and Europe (France, Germany).
Methods: Cross-sectional survey of 937 AF patients on OAC in 5 countries; 36.5% of patients had recent onset-AF (≤6 m [≤12 m in Ja-pan]) & no stroke; 42.8% had established AF (7-24 m [1-3 y in Japan]) & no stroke; 20.7% had AF & recent stroke (≤6 m).
Results: Stroke knowledge was similar across countries; about half of patients had good/moderate vs. low/no knowledge. Stroke preven-tion was stated as the reason for OAC prescription more frequently by Asians (59%; P<0.001 vs. rest of the world). Self-perceived OAC ad-herence was lowest in Asians with certain reasons stated significantly more often than in other countries (Table). A total of 60% and 58% of French and Japanese patients, respectively, preferred their physicians to choose an OAC; 62% of Americans/59% of Canadians/66% of Germans preferred shared decision-making or patient choice. Stroke prevention was the most important factor for all patients when choosing OAC, followed by bleeding risk in all countries except Japan, where side effects other than major bleeding risk were rated more important.
Conclusions: Country-specific differences exist in AF patients’ perceptions about OAC therapy with stroke prevention rated the most im-portant factor by all patients.
ATRIAL FIBRILLATION PATIENTS’ PERCEPTIONS OF ANTICOAGULATION THERAPY: COMPARING ASIA WITH THE REST OF THE WORLDGregory YH Lip1, Juliane Meyerhoff2, Ute Rohner2, Deirdre Lane3 1University of Birmingham, Birmingham, United Kingdom; 2Boehringer Ingelheim Corporation, Ingelheim, Germany; 3University of Birmingham Institute of Cardiovascular Sciences, Birmingham, United Kingdom
CLINICAL ELECTROPHYSIOLOGY P 2-120
Overall (n=937)
Japan (n=139)
USA (n=322)
Canada (n=145)
France (n=171)
Germany (n=160)
Mean (SD) age, years 54.3 (16.6) 59.1 (11.8)** 56.0 (16.9)* 52.8 (17.4) 49.6 (18.8)** 53.0 (14.6)CHA2DS2-VASc ≥2 (female); ≥1 (male) (%)
85.0 88.5 87.0 89.0 76.0** 83.8
Knowledge of stroke (%) Good/moderate 47.4 48.2 45.3 49.7 42.7 53.8Low/none 52.6 51.8 54.7 50.3 57.3 46.3
Reason for OAC given by prescriber was stroke prevention
46.5 59.4** 50.8 36.6** 33.9** 49.4
Self-reported adherence (%) I always take OAC as prescribed
79.9 67.4** 83.5* 84.8 80.1 78.8
Reason for non-adherence (%) Side-effects 21.8 53.3** 22.6 9.1 2.9** 5.9*Effective enough to skip a dose
21.8 37.8** 15.1 18.2 11.8 23.5
Not easy to take 11.7 31.1** 1.9 9.1 5.9 8.8Too many medications 17.6 33.3** 13.2 13.6 5.9* 17.6
Most important factor for Stroke prevention 47.4 30.9** 49.4 48.3 48.5 55.6* choice of OAC (%) Risk of major bleeding 14.7 15.8 17.7 11.7 13.5 11.9
Other side effects1 10.0 18.0** 7.1* 11.0 6.4 11.9Dosing frequency 8.2 12.9* 7.8 9.0 7.0 5.6Antidote availability 7.8 8.6 6.5 8.3 9.9 6.9Dietary restrictions 7.0 9.4 6.2 5.5 9.9 5.0Take with/without food 4.8 4.3 5.3 6.2 4.7 3.1
*p<0.05; **p<0.001 vs. other countries pooled; 1side effects other than major bleeding.

383
Introduction: Warfarin is currently used to prevent the ischemic stroke in patients with atrial fibrillation (AF), but the labile international normalized ratio (INR) in these patients is problematic leading to the occurrence of ischemic stroke or bleeding complication. Previous study used SAMeTT2R2 score to predict the labile INR in these patients, but lack of data in Thai AF patients. This study was conducted to determine the proportion of Thai AF patients used warfarin with labile INR in each SAMeTT2R2 score.
Methods: This study was the retrospective observational study in Thai AF patients in Central Chest Institute of Thailand. They took the warfarin for at least 3 months before enrollment. The patients discontinued the warfarin during INR monitoring because of surgery or in-vasive procedure or hospitalization or any etiologies were excluded. Each AF patients was measured the INR to determine the proportion of patients with labile INR in each SAMeTT2R2 score.
Results: A total of 40 AF patients were enrolled. The mean age was 64.35±10.69 years old. Most patients were paroxysmal AF. The aver-age CHA2DS2-VASc score was 3.20±1.56. A half of these patients had hypertension and dyslipidemia. Almost one-fifth of these patients had the history of ischemic stroke. This study showed the increased proportion of AF patients with labile INR according to the increased SAMeTT2R2 score. The AF patients with SAMeTT2R2 score of 3 or more had the proportion of patients with labile INR more than the ones with SAMeTT2R2 score of 2 or less with borderline significance (p value=0.056).
Conclusions: The Thai AF patients used warfarin had the increased proportion of these patients with labile INR according to the increased SAMeTT2R2 score. However, the larger study is needed to use SAMeTT2R2 score for predicting the Thai AF patients with labile INR in the future.
PROPORTION OF THAI PATIENTS WITH ATRIAL FIBRILLATION RECEIVING WARFARIN WITH LABILE INR IN EACH GROUP OF SAMeTT2R2 SCOREKomsing Methavigul
Central Chest Institute of Thailand, Nonthaburi, Thailand
CLINICAL ELECTROPHYSIOLOGY P 2-121

384
Introduction: The safety and efficacy of left atrial appendage occluder device using Warfarin during the initial 45 days period is well estab-lished. The value of new oral anticoagulants (NOACs) in place of warfarin has not been reported previously. We sought to evaluate the safety and efficacy outcomes of the NOACs post Watchman device implantation as compare to standard warfarin therapy.
Methods: Patients with atrial fibrillation and CHA2DS2-VASc score of at least 2 were screened for suitability of Watchman implant. Inclu-sion criteria for implantation were: high bleeding risk, erratic INR, and poor compliance with medication. Patients were divided into a standard per protocol Warfarin therapy and the NOACs groups. Their safety and efficacy outcomes were compare at each follow-up peri-od at 45 days, 180 days and 360 days respectively.
Results: A total of 93 patients had successful implantation of the LAA occluder device. 52 (55.9%) patients received Warfarin and 41 (44.1%) received NOACs immediately post procedure. At baseline comparing the warfarin vs. NOAC groups, the mean age was 65.7+11.4 years in both groups, ejection fraction was 57.5+9.7% vs. 53.2+14.6%, less female (50% vs. 68.3%, p value=0.051) and 1.9% vs. 7.3% (p val-ue=0.203) had prior stroke respectively. Majority of patients were implanted a size 24 or 27 mm device (73.1% vs. 48.8%, p value=0.016). There was a 1.9% reported case of pericardial effusion in warfarin vs. none in NOAC (p value=0.366). At 45 days follow up, there was 1 (1.1%) case of device related thrombus in each groups. 1 patient in NOAC group (1.1%) showed a 6 mm peri-device leak as compare to none in warfarin group. No cases of cerebrovascular events reported at 6 months and 1 year follow-up. 95.7% vs. 81.6% (p value=0.035), 97.4% vs. 94.1% (p value=0.491), and 100% vs. 91.3% (p value=0.085) of patients were able to come off oral anticoagulants at 45 days, 140 days and 365 days respectively. At 12+3 months follow-up, one patient (0.46%) had a thromboembolic cerebral stroke, 2 had systemic em-bolism (0.92%) and total overall mortality of 7 patients (6.95% per patient year).
Conclusions: This is the largest single center registry data for Watchman implant in the Asia Pacific region. The use of new oral anticoag-ulants in place of warfarin results in comparatively similar safety and efficacy benefit post watchman implant.
ROLE OF NEW ORAL ANTICOAGULANTS (NOACs) IN LEFT ATRIAL OCCLUDER DEVICE-WATCHMAN IMPLANTZulkeflee Muhammad, Razali Omar, Surinder Kaur Khelae
National Heart Institute of Malaysia (IJN), Kuala Lumpur, Malaysia
CLINICAL ELECTROPHYSIOLOGY P 2-122

385
Introduction: The management of oral anticoagulant (OAC) after atrial fibrillation (AF) ablation remains at issue. This systematic review evaluates the outcome of anticoagulant therapy beyond 3 months after AF ablation.
Methods: English scientific literature was searched using Pubmed/Embase with keywords of “anticoagulant”, “atrial fibrillation”, “cathe-ter ablation”. 919 references were reviewed. After exclusions, 5 studies with a total of 10,258 participants reporting the outcome of throm-boembolism (TE) and bleeding events were analyzed.
Results: There was no difference in the risk of TE between the group with OAC-ON and OAC-OFF (1.1% vs. 0.7%, Odd ratio [OR] 1.49, Con-fidence Interval [CI] 0.64-3.46, i2 47%, P<0.35). In addition, two of the studies analyzing both groups based on CHADS score showed no significant difference in TE between OAC-ON and OAC-OFF, in the subgroup of CHADS 0, CHADS 1, and CHADS more than 2 (See table). Nevertheless, continuation of OAC was related with a higher incidence of bleeding events as compared to discontinuation of OAC (OR 11.33 [CI 2.01-64.01], i2 77%, P<0.01).
Conclusions: Discontinuation of oral anticoagulant therapy after successful AF ablation is safe. Serious bleeding risk associated with con-tinuation of OAC outweighed the advantages of thromboembolic reduction.
LONG-TERM SAFETY OF ORAL ANTICOAGULANT DISCONTINUATION AFTER ATRIAL FIBRILLATION RADIOFREQUENCY ABLATION: SYSTEMATIC REVIEW AND META-ANALYSISDian Munawar, Rajiv Mahajan, Thomas Agbaedeng, Sharath Kumar, Kashif Khokhar, Dennis Lau, Prashanthan Sanders
University of Adelaide, Adelaide, Australia
CLINICAL ELECTROPHYSIOLOGY P 2-123
Comparison of Outcomes Based on CHADS Score
Sub-Groups Thromboembolic events
Odd ratio [Confidence interval]; p value; i2
CHADS score 0 0% vs. 0.28%
OR 0.71 (0.03-16.75); P 0.83; i2 53%
CHADS score 1 0.74% vs. 0.18%
OR 0.39 (0.60-18.71); P 0.17; i2 0%
CHADS score >2 1.2% vs. 0.45%
OR 1.65 (0.21-12.86); P 0.63; i2 36%

386
Introduction: The management of anticoagulation in patients undergoing atrial fibrillation (AF) ablation is controversial. This systematic review evaluates the outcome of different peri-procedural anticoagulant protocols in AF ablation.
Methods: English scientific literature was searched using Pubmed/Embase with keywords of “anticoagulant”, “atrial fibrillation”, “cathe-ter ablation”. 914 references were reviewed. After exclusions, 32 studies with a total of 25,860 participants reporting the outcome of thromboembolism (TE) and bleeding events were analyzed.
Results: See Table. There was no difference in TE between continuous VKA and interrupted NOAC (0.9% vs. 0.9%, P<0.17), or uninter-rupted NOAC (0.1% vs. 0.3%, P<0.29). Major bleeding were also similar for continuous VKA vs. interrupted NOAC (1.5% vs. 2.2%, P<0.35), or uninterrupted NOAC (1.0% vs. 1.2%, P<0.53). However, interruption of VKA with heparin bridging was related with higher incidence of TE, compared to interrupted NOAC (2.3% vs. 1.1%, P<0.05), or continuous VKA (2.1% vs. 0.6%, P<0.0007). Similarly, major bleeding is sig-nificantly higher in the group of interrupted VKA with heparin bridging versus interrupted NOAC (0.9% vs. 0.5%, P<0.01).
Conclusions: This meta-analysis demonstrates that either NOAC (interrupted or uninterrupted) or continual VKA are safe for AF ablation. Interruption of VKA with heparin bridging is associated with an increased risk of peri-ablation TE and major bleeding.
NEW ORAL ANTICOAGULANT AND VITAMIN K ANTAGONIST MANAGEMENT IN PERI-PROCEDURAL ATRIAL FIBRILLATION RADIOFREQUENCY ABLATION: SYSTEMATIC REVIEW AND META-ANALYSISDian Munawar1, Rajiv Mahajan1, Thomas Agbaedeng1, Darragh Twomey1, Sharath Kumar1, Kashif Khokhar1, Dennis Lau1, Muhammad Munawar2, Prashanthan Sanders1 1University of Adelaide, Adelaide, Australia; 2University of Indonesia, Jakarta, Indonesia
CLINICAL ELECTROPHYSIOLOGY P 2-124
Comparison of Outcomes between Groups
Groups Absolute incidence (Confidence intervals) Odd ratio [Confidence interval]; p value; i2
Thromboembolic events Major bleeding
Interrupted NOAC vs. Continuous VKA 0.9% (CI 0.3-1.8) vs. 0.9% (CI 0.3-1.8%) 1.5% (CI 0.7-2.7%) vs. 2.2% (CI 1.7-3.0%)
OR 1.59 (0.82-3.09); P 0.17; i2 3% OR 0.66 [0.28-1.57]; P 0.35; i2 61%
Uninterrupted NOAC vs. Continuous VKA 0.1% (CI 0.02-0.3%) vs. 0.3% (CI 0.08-0.6%) 1.0% (CI 0.6-1.6%) vs. 1.2% (0.8-1.8%)
OR 0.39 (0.07-2.22); P 0.29; i2 0% OR 0.81[0.41-1.58]; P 0.53; i2 0%
Interrupted NOAC vs. Interrupted VKA 1.1% (CI 0.7-1.7%) vs. 2.3% (CI 1.3-3.6%) 0.5% (CI 0.2-0.9%) vs. 0.9% (CI 0.4-1.7%)
with Heparin bridging OR 0.44 (0.19-1.01); P 0.05; i2 0% OR 0.47 [0.28-0.78]; P 0.004; i2 0%
Continuous VKA vs. Interrupted VKA 0.6% (0.3-1.0%) vs. 2.1% (CI 0.7-4.1%) 3.0% (CI 1.4-5.3%) vs. 3.6% (1.3-6.9%)
with Heparin bridging OR 0.25 (0.11-0.56); P 0.0007; i2 57% OR 0.78[0.51-1.19]; P 0.25; i2 40%

387
Introduction: Atrial fibrillation (AF) is the most common arrhythmia. AF-related stroke tends to be more severe, and mortality rate is higher compared with stroke without AF. Cardiac implantable electronic devices (CIEDs) are useful to detect AF. However, little is known about incidence of AF and stroke events in patients with CIED. The purpose of this study was to identify the incidence of stroke events in Japanese patients with and without AF detected by CIED.
Methods: We analyzed retrospectively the database of our CIED clinic. AF burden was checked every 6 months.
Results: A total of consecutive 310 patients (age 68±14 years, male 64%, defibrillator 57%, follow-up period of 67±27 months) were en-rolled in this study. One hundred thirty-four patients (43%) were prescribed anti-coagulation therapies. One hundred thirty-eight patients (45%) had AF detected by CIEDs, including 56 patients (18%) with subclinical AF. The mean of CHADS2 score and CHA2DS2-VASc score were 1.8±1.2 points and 3.0±1.5 points (congestive heart failure 68%, hypertension 40%, age≧75 years 40%, diabetes mellitus 20%, ischemic stroke 11%, vascular disease 20%, 65≦age≦74 years 18%, female 33%), repectively. The mean of HAS-BLED score was 1.7±1.2 points (abnormal renal/liver function 34%, stroke 3.4%, bleeding 1.7%, labile INR 0.6%, age≧65 years 33%, Drugs 19%). Thirty three pa-tients (12%) and 16 patients (5.7%) had ischemic stroke events with and without AF, respectively. Five patients (1.8%) and 4 patients (1.4%) had bleeding stroke events with and without AF, respectively. The incidence of ischemic and bleeding stroke events were 2.1 and 1.4 times higher in patients with than without AF in this population, respectively (P=0.013 vs. P=0.88).
Conclusions: Stroke events were common in patients with CIED. The incidence of ischemic stroke event was significantly higher in pa-tients with than without AF in this population. The strict rhythm control, as well as optimal anticoagulation therapy, should be considered to reduce any stroke events.
IMPACT OF STROKE EVENTS IN JAPANESE PATIENTS WITH ATRIAL FIBRILLATION DETECTED BY CARDIAC IMPLANTABLE ELECTRONIC DEVICEMiyo Nakano1, Yusuke Kondo2, Marehiko Ueda1, Masahiro Nakano1, Kazuo Miyazawa1, Tomohiko Hayashi1, Yoshio Kobayashi1 1Chiba University Graduate School of Medicine, Chiba, Japan; 2Chiba University Graduate School of Medicine, Department of Advanced Cardiovascular Therapeutics, Chiba, Japan
CLINICAL ELECTROPHYSIOLOGY P 2-125

388
Introduction: The clinical characteristics and cardiovascular prognosis of asymptomatic atrial fibrillation (AF) patients have not been elu-cidated completely.
Methods: We evaluated the efficacy of antiarrhythmic drug therapy (AAD) and long-term cardiovascular prognosis in patients with asymp-tomatic paroxysmal AF in comparison to those with symptomatic paroxysmal AF. This retrospective study included 334 patients (229 men and 105 women, mean age 69±11 years, mean follow-up 60±35 months) who were divided into two groups; patients with symptomatic AF (group I, N=289) and those with asymptomatic AF (group II, N=45) on the basis of subjective symptoms.
Results: 1) CHADS2 score was significantly greater in group II (1.63±1.27) than in Group I (1.14±1.18) (P<0.05). 2) Actuarial rates of pa-tients without AF recurrence, those with AF recurrence and with electrical/pharmacological cardioversion to restore sinus rhythm, and those with conversion to permanent AF despite AAD after rhythm control therapy were 40%, 41% and 19% respectively in group I, and 22%, 24% and 54% respectively in group II at the end of follow up period. At 60 months, the percentage of patients with conversion to the permanent form of AF was significantly greater in group II than in group I (P<0.05, group I vs. group II). 3) Survival rates free from symp-tomatic thromboembolism at 36, 60 and 120 months were 96%, 93% and 88% respectively in group I, and 82%, 76% and 71% respectively in group II (P<0.05, group I vs. group II). In patients not undergoing anticoagulant therapy, the annual rate of symptomatic thromboembo-lism was significantly greater in group II (5.3%) than in group I (2.3%) (P<0.05), while in patients undergoing anticoagulant therapy there was no significant difference in the annual rate of symptomatic thromboembolism between group I (0.9%) and group II (1.8%).
Conclusions: The clinical course of asymptomatic paroxysmal AF is refractory to AAD when compared to symptomatic AF, meaning that anticoagulant therapy is required to prevent symptomatic thromboembolism in the asymptomatic paroxysmal AF group.
EFFICACY OF ANTIARRHYTHMIC DRUGS THERAPY IN PREVENTING AF RECURRENCE AND LONG-TERM CARDIOVASCULAR PROGNOSIS IN PATIENTS WITH ASYMPTOMATIC PAROXYSMAL ATRIAL FIBRILLATIONShingen Owada, Takashi Komatsu, Reisuke Yoshizawa, Fusanori Kunugita, Mahito Ozawa, Yoshihiro Sato, Yoshihiro Morino, Motoyuki Nakamura
Iwate Medical University, Morioka, Japan
CLINICAL ELECTROPHYSIOLOGY P 2-126

389
Introduction: The choice of new oral anticoagulants (NOAC) and dosing would be considered based on co-medication, age, renal function, and weight. There is few data regarding the efficacy and safety of NOAC in patients with underweight (UW) patients. We sought to compare the risk of stroke, thromboembolism (TE) and bleeding in patients with underweight in real-word population.
Methods: We had retrospectively recruited 1,993 AF patients prescribed NOAC between 2012 and 2016. Of these, 1,355 patients were ana-lyzed in this study whose anthropometric data were available. Stroke, TE, and bleeding events were collected during follow-up period. We compared these clinical events between underweight (Underweight group, <18.5 kg/m2) and normal or overweight (non-UW group, ≥18.5 kg/m2).
Results: Patients with UW group showed older age, more heart failure and less hypertension history compared to non-UW group. CHA2DS2-Vasc score, previous history of stroke and diabetes mellitus were comparable between groups. Dabigatran, rivaroxaban and apixaban were prescribed in 46%, 36% and 18% of patients, respectively. Standard dosage of NOAC was prescribed in 24% of the UW group and 37% of the non-UW group (P=0.041). There were 11 thromboembolic (TE) events (1 in UW and 10 in non-UW group). The annu-al TE risk was not significantly different between groups (1.6%/year in UW group vs. 0.4%/year in non-UW group, P=0.155). There were 53 bleeding events (6 in UW and 47 in non-UW group), and the annual bleeding risk was significantly higher in the UW group 12.9%/year compared to non-UW group 3.0%/year (P<0.001). Most of patient in UW group were prescribed with reduced dose (76%). Bleeding more frequently occurred in UW group, when using standard-dose of NOAC (HR 6.589, P=0.014) but not reduced-dose (HR 1.737, P=0.299). In multivariable analysis, underweight was significantly associated with bleeding when full-dose NOAC was prescribed (HR 6.931, P=0.025), but no significant association was observed when reduced-dose was taken (HR 1.156, P=0.806). There was no significant difference in stroke and TE events according to dosage of NOAC.
Conclusions: Subjects who were underweight showed higher risk of bleeding. When multivariate analysis was performed stratified by NOAC dosage, bleeding was significantly associated with UW in the standard-dose group, but not in the reduced-dose group.
IMPACT OF NOVEL ORAL ANTICOAGULANTS ACCORDING TO DOSAGE ON CLINICAL OUTCOMES IN ATRIAL FIBRILLATION PATIENTS WITH UNDERWEIGHTChan Soon Park, Eue-Keun Choi, Hyue Mee Kim, Myung-Jin Cha, Seil Oh
Seoul National University Hospital, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-127

390
Introduction: After radiofrequency catheter ablation (RFCA) of atrial fibrillation (AF), oral anticoagulation for ≥2 months post-procedure are recommended currently. But benefit and risks of short term OAC for patient with low thromboembolic risk are uncertain.
Methods: Patients with symptomatic paroxysmal AF refractory to ≥1 antiarrhythmic medication and low CHA2DS2-VASc score (0 or 1) were enrolled after planning of RFCA. After RFCA, patients were randomly assigned to receive warfarin therapy for 1 or 2 months. The pri-mary end point was incidence of thromboembolic and bleeding events.
Results: A total of 96 patients were randomly assigned to continue warfarin therapy for 1 month (n=40) or 2 months (n=31) from Novem-ber 2013 to March 2016. During follow-up (median follow-up 14.4 months) there was no stroke, systemic embolism and major bleeding. Minor bleeding was not significantly different between two groups (7.5% vs. 6.5%, P=0.35). The rate of recurrence of atrial tachyarrhyth-mia (ATA) (15.0% vs. 19.3%, P=0.13) and any hospitalization (15.0% vs. 9.7%, P=0.09) were similar between two groups.
Conclusions: Low thromboembolic risk patients with 1 month warfarin therapy after RFCA of AF, compared with 2 months warfarin ther-apy, showed similar rate of bleeding and procedural outcome. Further research is needed to evaluate these preliminary findings in a larg-er study population to determine the optimal duration of OAC therapy after RFCA of AF.
1 OR 2 MONTHS WARFARIN THERAPY WITH LOW THROMBOEMBOLIC RISK PATIENTS AFTER RADIOFREQUENCY CATHETER ABLATION OF ATRIAL FIBRILLATION: INTERIM RESULTS OF SINGLE CENTER PROSPECTIVE RANDOMIZED STUDYHee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-128
Table 1. Incidence of adverse event and procedural outcome
1 month (n=40) 2 months (n=31) P value
Stroke or Systemic embolism 0 0 -
Major bleeding 0 0 -
Minor bleeding 3 (7.5%) 2 (6.5%) 0.35
Any hospitalization 6 (15.0%) 3 (9.7%) 0.09
Early recurrence of ATA (<3 months) 3 (7.5%) 3 (9.7%) 0.24
Recurrence of ATA (≥3 months) 6 (15.0%) 6 (19.3%) 0.13
Redo RFCA 4 (10.0%) 3 (9.7%) 0.87

391
Introduction: Despite increased usage of novel anticoagulants (NOACs) for stroke prevention worldwide, there have not been any real world studies on its efficacy and safety in the Malaysian government hospital setting.
Methods: This is a retrospective study evaluating all patients with atrial fibrillation who were prescribed Dabigatran, Rivaroxaban or Apix-aban for stroke prevention in Hospital Kuala Lumpur between 2014 and 2016. Basic characteristics, laboratory data and complications were computed and analysed.
Results: A total of 71 patients (38 males and 33 females) were included in the study. Median age was 71 years (range 39-87). Half of them (52.1%, n=37) was prescribed Dabigatran 110 mg BD, followed by a third being given 150 mg BD strength (31%, n=22). There were 7 pa-tients on Rivaroxaban and 5 patients on Apixaban. Median CHA2DS2-VASc score was 3 and median HAS-BLED score was 1. Whilst 90% (n=64) had hypertension, only 45% (n=32) had diabetes mellitus and 21% (n=15) had history of previous stroke. Echocardiographic data was available in 52 (73%) patients; of whom, 4 had reduced ejection fraction of<40%. NOACs were discontinued in 2 patients as one had difficulty adhering to treatment whilst another had worsening renal function limiting use of NOAC. None developed stroke post com-mencement of NOACs. Four patients (5.6%) had adverse effects of bleeding (two had gastrointestinal bleed, followed by one each for hae-maturia and retinal haemorrhage). All four were on Dabigatran.
Conclusions: This study provides real world insight into the usage of NOACs in Malaysian government hospital. With low adverse event rates, NOACs serve as excellent alternatives to conventional warfarin, even in the elderly population.
NOAC EXPERIENCE FROM A TERTIARY GOVERNMENT HOSPITAL IN MALAYSIANoel Ross, Min Hui Tan, Glendon Seng Kiong Lau, Winn Hui Han, Lai Teck Gew, Marina Taufik Ismail Taufid, Philip Thomas, Kim Fong Ng, Pravindh Arumugam, Yen Yew Ngau
Kuala Lumpur General Hospital, Kuala Lumpur, Malaysia
CLINICAL ELECTROPHYSIOLOGY P 2-129

392
Introduction: Non-vitamin K antagonist oral anticoagulants (NOACs) is increasingly used for stroke prevention in patients with non-valvu-lar atrial fibrillation (NVAF) showing a good efficacy and safety compared with warfarin. But it is not well-known about rates or reasons of discontinuations in daily care. The aim of this study is to compare the persistence and the safety among apixaban (A), rivaroxaban (R) and dabigatran (D).
Methods: We retrospectively studied 1,619 patients with NVAF who had newly started NOACs between January 2012 and September 2015 from a single cardiology center (320 apixaban, 783 rivaroxaban, 516 dabigatran).
Results: The median follow-up duration was 316 days. The discontinuation rates were similar in rivaroxaban group (41%) and dabigatran group (41%) but higher in apixaban group (45%). The major causes of discontinuation were adverse events including all bleeding and gas-trointestinal symptoms, maintenance of sinus rhythm, patient desire and the patient’s own decision. The discontinuation rate by adverse event were lower in both apixaban and rivaroxaban group than dabigatran group. No significant differences were in thromboembolic and major bleeding events among three groups.
Conclusions: In a single-center retrospective study, NOACs showed significantly different discontinuation rates and adverse event rates when compared to each other. But thromboembolic and major bleeding events were not significantly different in patients with NVAF.
THE PERSISTENCE AND SAFETY OF NON VITAMIN K ANTAGONIST ORAL ANTICOAGULATION IM KOREA PATIENTS WITH ATRIAL FIBRILLATIONChoong-Sil Seong, Jin Kyung Hwang, Seung Jung Park, Kyoung-Min Park, June Soo Kim, Young Keun On
Samsung Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 2-130

393
Introduction: Cardiogenic cerebral infarction has been reported despite taking appropriate oral anticoagulation (OAC) in patients with non-valvular atrial fibrillation (AF). They might need additional therapy such as percutaneous left atrial appendage closure. We examined the risk factors for left atrial appendage thrombus (LAAT) in patients during taking appropriate OAC with non-valvular AF.
Methods: We retrospectively studied 703 consecutive patients (age 67±11, 488 men, 306 with paroxysmal AF) who take oral anticoagula-tion (OAC) therapy (392 with warfarin and 311 with direct oral anticoagulants; DOACs) more than one month who underwent transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) prior to cardioversion or catheter ablation for AF. Clinical data, CHADS2, CHA2DS2-VASc and TTE parameters were evaluated.
Results: LAAT were detected in 57/703 patients (8%) using TEE. Patients with LAAT showed a high rate of warfarin taking [43/392 (11%) with warfarin vs. 14 /311 (5%) with DOACs, P=0.002], a high prevalence of persistent AF (n=347, 13% vs. 3%, P<0.0001), larger left atrial dilatation (LAD, n=57, 48 mm vs. 42 mm, P<0.0001), lower left ventricular ejection fraction (n=57, 51% vs. 60%, P=0.0007), left ventricu-lar hypertrophy (LVH) (n=84, 19% vs. 6%, P<0.0001), higher rate of congestive heart failure (n=147, CHF) (17% vs. 5%, P<0.0001), hyper-tension (n=369, 12% vs. 3%, P<0.0001) and vascular disease (n=331, 11% vs. 5%, P=0.0049). Meanwhile, age, diabetes mellitus, prior stroke/TIA, sex, type of AF, and taking period of OAC were not related with LAAT. On multivariate analysis, persistent AF (P=0.0002, harard ratio: 4.4, 95%CI 1.9 to 11.9), large LAD (>40 mm) (P=0.0020, harard ratio: 4.9, 95%CI 1.7 to 20.6), LVH (P=0.0062, harard ratio: 2.5, 95%CI 1.3 to 4.8), history of CHF (P=0.0169, harard ratio: 2.2, 95%CI 1.2 to 4.1) and hypertension (P=0.0132, hazard ratio: 2.5, 95%CI 1.2 to 5.7) were independently associated with LAAT.
Conclusions: Persistent AF, large LAD, LVH, history of CHF and hypertension might provide additional risk stratification for LAAT in pa-tients during taking appropriate OAC with non-valvular AF.
RISK FACTORS FOR THE LEFT ATRIAL APPENDAGE THROMBUS IN PATIENTS TAKING APPROPRIATE ORAL ANTICOAGULATION WITH ATRIAL FIBRILLATIONSatoshi Takahashi, Takanao Mine, Kenki Ashida, Hideyuki Kishima, Masaharu Ishihara, Tohru Masuyama
Hyogo College of Medicine, Nishinomiya, Japan
CLINICAL ELECTROPHYSIOLOGY P 2-131

394
Introduction: Amiodarone, an iodinated benzofuran derivative, a class III antiarrhythmic is used across the spectrum of ventricular and supraventricular tachyarrhythmias. This drug with a long half-life tends to accumulate in several organs in the course of treatment in-cluding the lungs. Owing to the wide use of this drug the clinician should be vigilant. Through this series, we want to highlight the com-monly encountered adverse effects and the importance of serial monitoring of patients on this drug and their effective titration.
Methods: Ten patients on amiodarone were randomly selected from those presenting at our centre to either OPD or ER who were receiv-ing the drug for at least two years or more. Data regarding dose, duration and indication were collected and a complete assessment of adverse effects was done with respect to ten parameters ranging from blood pressure to pulmonary involvement.
Results: All patients were receiving at least 100 mg/day of amiodarone for at least six months. Two patients were receiving the drug for 5 years. 25% patients presented with acute pulmonary toxicity and were effectively treated with cessation of drug and pulse steroid therapy. 45% had thyroid abnormalities out of which 2 developed hypothyroidism and 3 had features of thyroiditis, 50% had visual disturbances/corneal deposits. 40% had LFT abnormalities and 33% presented with hypotension. 50%, 40%, 40%, 16% and 16% patients reported fa-tigue, sleep disturbances, headache, loss of appetite and memory loss respectively.
Conclusions: No relationship was seen regarding the dose of drug and duration to the incidence of APT. Thyroid abnormalities are com-mon and need regular monitoring and thyroxine replacement as required. LFT abnormalities were transient and rarely needed a dose ad-justment. Visual disturbances were not disabling but almost all patients developed corneal microdeposits. Hypotension was addressed with down titration of the drug. Other side effects although not dose or duration dependent interfered with drug compliance but were not disabling. Excessive caution is desired when initiating this drug, ‘a double-edged sword’.
AMIODARONE, A DOUBLE EDGED SWORD: A CASE SERIES ON THE TOXIC EFFECTS OF THE DRUGAbhinay Tibdewal, V S PRAKASH, Nagamalesh U M, Anupama Hegde, Karthik Naidu, Sarthak Sahoo
MS Ramaiah Medical College, Bangalore, India
CLINICAL ELECTROPHYSIOLOGY P 2-132

395
Introduction: AF increases the risk of embolic stroke; hence, anticoagulation is recommended to substantially reduce this risk. Based on the ESC Guidelines, CHA2DS2-VASc score can be used for embolic stroke prediction in atrial fibrillation patients and HAS-BLED score to assess bleeding risk. This study was to evaluate anticoagulant usage for AF patients in a local secondary institution in Tangerang, a highly populated city with population of 1.79 million assumed to represent urban community in Indonesia.
Methods: We performed a cross-sectional consecutive study for a one-year period of 2015 on patient diagnosed with AF included in Atrial Fibrillation Registry in Tangerang, Indonesia. From a total of 167 patients, 52 patients were excluded from the study due to valvular etiolo-gy.
Results: There were 66 (57.4%) female. Age, CHA2DS2-VASc and HAS-BLED score: 58.66±13.04, 2.40±1.45, 1.44±1.19 respectively. Sev-enty nine (68.7%) patients had a CHA2DS2-VASc score of ≥2 and were considered as high risk for embolic stroke which 28 (35.4%) patients received oral anticoagulant (OAC). The anticoagulant that was used was 100% VKA, 25 (31.6%) did not receive any anticoagulant or anti-platelet, 2 (2.5%) received clopidogrel, 13 (16.5%) received aspirin, 6 (7.6%) received DAPT, 3 (3.8%) received a combination VKA and aspi-rin, and 2 (2.5%) received a combination VKA and DAPT. Twenty two (19.1%) patients had HAS-BLED score of ≥3 and were considered as high risk for bleeding. Among those, 4 (18.2%) received VKA, 11 (50%) did not receive any anticoagulant or antiplatelet, 4 (18.2%) received aspirin, 1 (4.5%) received DAPT, 2 (9.1%) received a combination VKA and aspirin and no patients received either clopidogrel or combina-tion between VKA and DAPT. There are 26.6% patients that are high risk in both scoring.
Conclusions: Our registry shows a unique presentation that in contrast to western countries where the preference of anticoagulant has shifted to NOAC as in the new guideline, we still use VKA as the choice of anticoagulant. We also face similar problem namely low rate us-age of anticoagulant despite high CHA2DS2-VASc score.
TREATMENT ADHERENCE FOR ANTICOAGULANT THERAPY IN PATIENTS WITH ATRIAL FIBRILLATIONSteven Alviano Yuwono1, Marwali K2, Wibowo ANM1, Hadi D1, Vatvani A1, Soetjipto AS1, Ng S1,2
1Faculty of Medicine, University of Pelita Harapan, Banten, Indonesia; 2Siloam Hospital Lippo Village, Banten, Indonesia
CLINICAL ELECTROPHYSIOLOGY P 2-133

396
Introduction: Response to cardiac resynchronization therapy (CRT) is commonly assessed at 6 or 12 months after implantation. However, clinical characteristics of patients showing later responses to CRT are not well established. We evaluated clinical outcomes and subse-quent change of QRS duration in patients responding after one year of CRT implantation.
Methods: We performed a retrospective, single center analysis in patients who survived one year after CRT implantation. Positive CRT re-sponse was defined as ≥15% reduction in LVESV or ≥10% increase in left ventricular ejection fraction (LVEF) on any follow up echocar-diogram. We defined patients responding before 12 months as early responders, and patients responding after 12 months as late re-sponders. Patients not responding on any follow up echocardiogram were defined as non-responders. Subsequent change in QRS dura-tion, echocardiographic parameters and clinical outcomes were compared in three groups.
Results: Among inclusion, there were 17/32 (53.1%) early responders, 9/32 (28.1%) late responders and 6/32 (18.7%) non-responders. Compared to early responders, the late responder group had trends toward lower baseline LVESV [158.0 (109.8-194.0) mL vs. 134.0 (100.7-182.0) mL, P=0.396 in early and late responders], higher baseline LVEF [24.0 (18.0-29.0)% vs. 27.5 (22.4-29.0)%, P=0.312] and shorter pre-implant QRS duration [174 (156-192) ms vs. 157 (137-171) ms, P=0.025]. QRS duration was continuously decreased after 6 months in the late responder group whereas shortening of QRS duration was not maintained in the non-responder group (Figure 1). The late re-sponder group showed intermediate long term clinical outcome assessed by all-cause death (5.9% vs. 11.1% vs. 33.3% in early, late and non-responders, P=0.215) and the number of heart failure events requiring hospitalization per year [0 (0-0.06) vs. 0 (0-0.19) vs. 0.67 (0-0.81), P=0.022].
Conclusions: Patients responding to CRT after one year show intermediate clinical outcome compared to early responders and non-re-sponders. Long term maintenance of QRS duration shortening is an important feature of CRT response.
CLINICAL CHARACTERISTICS OF PATIENTS RESPONDING ONE YEAR AFTER CARDIAC RESYNCHRONIZATION THERAPYYoung Choi1, Ju Youn Kim1, Sung-Hwan Kim1, Ho-Joong Youn1, Tae-Suk Kim2, Ji-Hoon Kim3, Yoo Ri Kim4, Sung-Won Jang5, Tai-Ho Rho5, Man-Young Lee6, Yong-Seog Oh1 1Seoul St. Mary’s Hospital, Seoul, Republic of Korea; 2Daejeon St. Mary’s Hospital, Daejeon, Republic of Korea; 3St. Vincent’s Hospital, Suwon, Republic of Korea; 4Incheon St. Mary’s Hospital, Incheon, Republic of Korea; 5St. Paul’s Hospital, Seoul, Republic of Korea; 6Yeouido St. Mary’s Hospital, Seoul, Republic of Korea
HEART FAILURE P 2-134
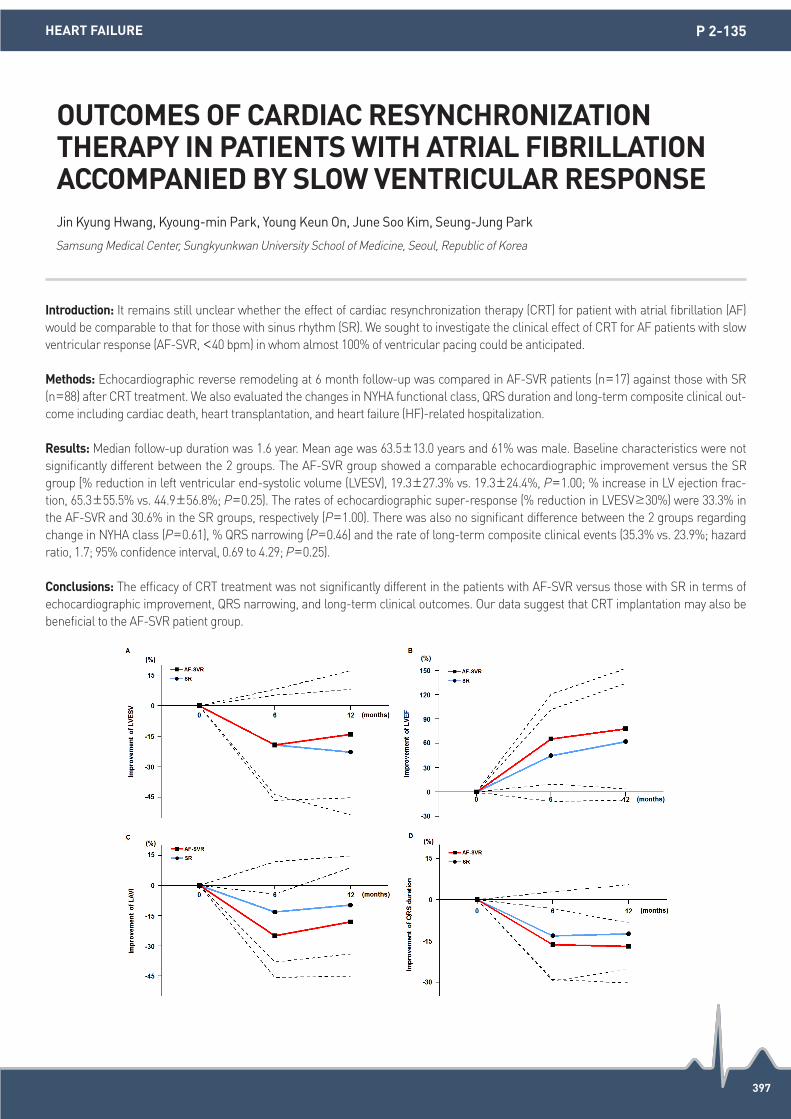
397
Introduction: It remains still unclear whether the effect of cardiac resynchronization therapy (CRT) for patient with atrial fibrillation (AF) would be comparable to that for those with sinus rhythm (SR). We sought to investigate the clinical effect of CRT for AF patients with slow ventricular response (AF-SVR, <40 bpm) in whom almost 100% of ventricular pacing could be anticipated.
Methods: Echocardiographic reverse remodeling at 6 month follow-up was compared in AF-SVR patients (n=17) against those with SR (n=88) after CRT treatment. We also evaluated the changes in NYHA functional class, QRS duration and long-term composite clinical out-come including cardiac death, heart transplantation, and heart failure (HF)-related hospitalization.
Results: Median follow-up duration was 1.6 year. Mean age was 63.5±13.0 years and 61% was male. Baseline characteristics were not significantly different between the 2 groups. The AF-SVR group showed a comparable echocardiographic improvement versus the SR group [% reduction in left ventricular end-systolic volume (LVESV), 19.3±27.3% vs. 19.3±24.4%, P=1.00; % increase in LV ejection frac-tion, 65.3±55.5% vs. 44.9±56.8%; P=0.25). The rates of echocardiographic super-response (% reduction in LVESV≥30%) were 33.3% in the AF-SVR and 30.6% in the SR groups, respectively (P=1.00). There was also no significant difference between the 2 groups regarding change in NYHA class (P=0.61), % QRS narrowing (P=0.46) and the rate of long-term composite clinical events (35.3% vs. 23.9%; hazard ratio, 1.7; 95% confidence interval, 0.69 to 4.29; P=0.25).
Conclusions: The efficacy of CRT treatment was not significantly different in the patients with AF-SVR versus those with SR in terms of echocardiographic improvement, QRS narrowing, and long-term clinical outcomes. Our data suggest that CRT implantation may also be beneficial to the AF-SVR patient group.
OUTCOMES OF CARDIAC RESYNCHRONIZATION THERAPY IN PATIENTS WITH ATRIAL FIBRILLATION ACCOMPANIED BY SLOW VENTRICULAR RESPONSEJin Kyung Hwang, Kyoung-min Park, Young Keun On, June Soo Kim, Seung-Jung Park
Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
HEART FAILURE P 2-135

398
Introduction: Cardiac resynchronization therapy (CRT) has been demonstrated as a beneficial therapy option in certain subgroups of chronic heart failure (HF) patients by improving left ventricular (LV) function, survival, and symptoms. Some group of patient show such important clinical improvement and reverse remodelling after CRT. These patients have been so-called super-responders. Therefore our main objective is to identify predictors of super-responder after CRT in advanced HF.
Methods: This is a retrospective, single center study. Patients advanced HF during period of January 2008 until December 2015 were as-signed to CRT with paired echocardiograms at baseline and up to 12 months after implantation (n =55) are enrolled in this study. Patients with a two-fold or more increase of left ventricular ejection fraction (LVEF), or >15% increase of LVEF, or a final LVEF 45% were identified as super-responders. Bivariate and multivariate analysis using logistic regression analysis were used in this study.
Results: In the periods of the study, there were 76 patients advanced heart failure (HF) underwent CRT implantation, and 55 patient were eligible for this study. The male/female ratio was 4.5 and their average age was 54.3±2.7 years. Fifty one of them were still alive at the end of the study. Eight of them were underwent epicardial implantation of the left ventricular lead (14.5%). There were 19 super-responders patients (34.5%). Bivariate analysis demonstrated that 3 predictors were associated with super-responder to CRT therapy: non-ischemic etiology (odds Ratio [OR] was 11.55 and 95% CI was 3.05 and 43.79, P=<0.001); QRS duration (OR was 1.05 and 95% CI was 1.02 and 1.08, P=0.001); and left bundle branch block (OR was 8.4 and 95% CI was 2.36 and 29.89, P=0.001). Multivariate analysis showed non-ischemic etiology (OR was 7.28 and 95% CI was 1.77 and 30.05, P=0.006) and left bundle branch block (OR was 6.14 and 95% CI was 1.54 and 24.55, P=0.010) were associated with super-responder to CRT therapy.
Conclusions: Non-ischemic etiology and left bundle branch block may predict super-responder group of advanced heart failure patients who undergo CRT implantation.
PREDICTORS OF SUPER-RESPONDER TO CARDIAC RESYNCHRONIZATION THERAPY IN ADVANCED HEART FAILURE PATIENTSA. Hafiedz A. Kartamihardja1, Anggia Lubis2, Irlandi M. Suseno1, Riesma V. Sari1, Fonny M. Tedjo2, Vekky Sariowan2, Dian Munawar2, Beny Hartono2, Muhammad Munawar2, Augustine Purnomowati1, Toni M. Aprami1 1Hasan Sadikin General Hospital/Medical Faculty of Padjajaran University, Bandung, Indonesia; 2Binawaluya Cardiac Center, Jakarta Timur, Indonesia
HEART FAILURE P 2-136

399
Introduction: Left bundle branch block (LBBB) is a well-known predictor for good response to cardiac resynchronization therapy (CRT). Recently, the presence of typical LBBB was reported to be associated with improved long-term clinical outcomes after CRT. Therefore, we hypothesized that typical LBBB will be helpful to predict CRT response rather than non-typical LBBB.
Methods: We retrospectively analyzed 51 LBBB patients with CRT implantation from January 2010 to October 2015 with follow-up (median 555 days). CRT responders were defined as decreased LV end systolic volume >15%. Typical LBBB was defined as 1) QRS duration of ≥140 ms in men or ≥130 ms in women & 2) QS or rS in leads V1 and V2 & 3) mid-QRS complex slowing or notching in ≥2 contiguous leads of V1, V2, V5, V6, I, and aVL.
Results: Mean age, baseline LVEF and QRS duration were 67±10 years, 24.3±6.1% and 166±19 ms, respectively. The prevalence of men and ischemic origin HF were 45.1% and 9.8%, respectively. There were 45 (88.2%) typical LBBB patients including notching in V1-2 (5.9%), V5-6 (51.0%), I & aVL (68.6%) leads. The CRT response rate in typical LBBB group was significantly higher (60.0% vs. 0%, P=0.017) com-pared to non-typical LBBB group. Especially, mid-QRS notching in V5-6 was significantly related to CRT response (odd ratio: 10.23, 95% confidence interval: 1.91-54.96, P=0.007) after adjusting other confounders. The LBBB patients with typical LBBB had significantly lower mortality rate (8.9% vs. 66.7%, P=0.004) and tended to readmit less for HF aggravation (15.6% vs. 33.3%, P=0.284).
Conclusions: Typical LBBB, especially mid-QRS notching in V5-6 was related to more favorable CRT response and clinical outcomes com-pared to non-typical LBBB. The identification of typical LBBB may be helpful to select good responder to CRT, even in LBBB patients.
TYPICAL LEFT BUNDLE BRANCH BLOCK IS ASSOCIATED WITH MORE FAVORABLE RESPONSE TO CARDIAC RESYNCHRONIZATION THERAPY IN HEART FAILURE PATIENTSJaewon Oh, Jae-Sun Uhm, In-Cheol Kim, Tae-Hoon Kim, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung, Seok-Min Kang
Yonsei University College of Medicine, Seoul, Republic of Korea
HEART FAILURE P 2-138

400
Introduction: Recent studies have demonstrated an association between a high body mass index (BMI) and a better prognosis in patients with heart failure. However, little is known about the association between body weight and prognosis in heart failure patients after cardiac resynchronization therapy-defibrillator (CRT-D) implantation. This study aimed to examine the effect of CRT-D therapy on the association between BMI and mortality among heart failure patients.
Methods: We retrospectively investigated 125 patients (33 overweight patients [BMI ≥25 kg/m2], 75 normal weight patients [BMI 18.5-24.9 kg/m2], and 17 underweight patients [BMI< 18.5 kg/m2]) who underwent CRT-D implantation. The clinical outcome endpoints were all-cause death and appropriate shock therapy.
Results: During the follow-up period (mean 3.1±1.8 years), 23 patients died (1 [3.0%] overweight, 17 [22.7%] normal weight, and 5 [29.4%] underweight patients), and appropriate shock events were observed in 14 patients (2 [6.1%] overweight, 10 [13.3%] normal weight, and 2 [11.8%] underweight patients). All patients survived shock therapy. After adjusting for confounding factors, the overweight group had sig-nificantly fewer outcomes relating to all-cause death and appropriate shock events (hazard ratio 0.27, 95% confidence interval 0.08-0.91, P=0.034) than the normal weight group. However, the prognostic difference between the overweight and normal weight patients could be somewhat diminished as a result of the successful appropriate shock therapies (P=0.067). Additionally, prognosis did not differ between the overweight and normal weight patients among the responders, but did differ among the non-responders.
Conclusions: Although high BMI was associated with better outcomes among heart failure patients with CRT-D implantations, CRT-D therapy as a therapeutic option might have an impact on the association between BMI and prognosis in heart failure patients.
IMPACT OF CARDIAC RESYNCHRONIZATION THERAPY-DEFIBRILLATOR IMPLANTATION ON THE ASSOCIATION BETWEEN BODY MASS INDEX AND PROGNOSIS IN PATIENTS WITH HEART FAILURE Masaki Takenaka, Hunabiki Junya, Murase Yosuke, Otake Noriaki, Monami Ando, Kamikubo Yosuke, Kanzaki Yasunori, Yanagisawa Satoshi, Inden yasuya, Murohara Toyoaki
Nagoya University, Nagoya, Japan
HEART FAILURE P 2-140

401
Introduction: Cardiac resynchronization therapy (CRT) improve survival and life quality among advanced heart failure patients with pro-longed QRS duration. The purpose of this study was to assess the prognostic value of baseline pre-implant plasma level of big endothe-lin-1 (ET-1) among CRT recipients.
Methods: A total of 367 consecutive single-center patients with CRT between January 2010 and December 2015 were retrospectively en-rolled, and categorized into two groups based on the baseline big ET-1 cutoff value that predicted all-cause mortality (including heart transplantation) by receiver operating characteristic (ROC) analysis. Survival curves free from all-cause mortality or heart failure hospital-izations (HFH) were assessed. Big ET-1 was evaluated in a multivariate Cox regression model as an independent prognostic factor.
Results: Over a median follow-up of 21 months, 48 (13.1%) patients died, 6 (1.6%) underwent heart transplantation and 100 (27.2%) had HFH. Patients were stratified into Group A (the big ET-1 ≥0.645 pmol/L) and Group B (the big ET-1 <0.645 pmol/L ) based on the ROC de-termined cutoff. A significant difference in event free survival between the two groups, with high level of big ET-1 having worse survival than low (log-rank test, P<0.001). In the multivariate model, big ET-1 ≥0.645 pmol/L was an independent predictor for all-cause mortali-ty (HR: 2.272 [95% CI 1.398-3.693]).
Conclusions: In CRT patients, baseline big ET-1 ≥0.645 pmol/L was independently associated with higher all-cause mortality.
ASSOCIATION OF BASELINE BIG ENDOTHELIN -1 LEVEL WITH LONG-TERM CLINICAL OUTCOMES AMONG CARDIAC RESYNCHRONIZATION THERAPY RECIPIENTSShengwen Yang, Zhimin Liu, Jiarui Mi, Shangyu Liu, Ligang Ding, Wei Hua, Shu Zhang
State Key Laboratory of Cardiovascular Disease, Department of Cardiology, Cardiovascular Institute, Fuwai Hospital, Beijing, China
HEART FAILURE P 2-142

402
Introduction: Cardiac resynchronization therapy (CRT) has become an accepted therapy in patients with drug-refractory heart failure. It is important to identify the intraventricular dyssynchrony in the left ventricle for predicting CRT response, though opinions are divergent on selection criteria. We investigated whether assessment of mechanical interventricular dyssynchrony evaluated by Quantitative Blood-pool SPECT (QBS) coincides with CRT response.
Methods: 8 patients with heart failure in NYHA class IIm-IV implanted CRT from February to December 2015 underwent QBS before and after CRT, variables analyzed were LV systolic function (LV ejection fraction [EF], LV end-diastolic [EDV] and end-systolic volume [ESV]), phase analysis LV intraventricular dyssynchrony (entropy, LV septum-lateral delay) and QRS duration. Patients were divided into two groups according to improvement in NYHA class: responder (n=6) with NYHAI-IIs after CRT, and non-responder (n=2) without a signifi-cant change. There was no significant difference in base NYHA class, QRS duration in ECG and LV systolic function in echocardiogram be-tween two groups.
Results: Both groups showed improvement of the degree of dyssynchrony (P<0.05). Only mean LV septum-lateral delay before CRT was significant deference. It was longer in responder than non-responder (responder:179 ± 143 msec, non-responder:-26.2 ± 56 msec P=0.033), whereas LV septum-lateral delay was no significant difference between two groups (responder:92.7 ± 95.0 msec, non-responder:-144 ± 60 msec P=0.43) after CRT. No significant difference was observed in QRS duration, improvement of entropy, EF, EDV and ESV before and after CRT.
Conclusions: LV septum-lateral delay in QBS make it possible to identify the intraventricular dyssynchrony in the left ventricle, which may play a role in predicting CRT response.
LEFT VENTRICULAR DYSSYNCHRONY ASSESSMENT BY QUANTITATIVE BLOOD POOL SPECT FOR PREDICTION OF CRT RESPONSEYuriko Yoshida
Sakakibara Heart Institute, Tokyo, Japan
HEART FAILURE P 2-143

403
Introduction: N/A
Methods: N/A
Results: We report a 67-year-old female suffering from persistent atrial fibrillation (AF) with left atrial dilatation and high atrial defibrilla-tion threshold. Anti-arrhythmic drug was not effective for AF, so we performed catheter ablation. To investigate arrhythmogenic sites in-volved in maintaining AF, we firstly evaluated the continuous wavelet transform (CWT) during AF in both atrium bofore ablation. In CWT analysis, we hypotesized that the high pseudo-frequency site (>6 Hz) was related to AF maintenance mechanism such as micro-reentry or other arrhythmogenic substrate. We also evaluated complex fractionated electrograms (CFE) mean by NavX Ensite system (sense>0.04 mV, fractionated index 0 to 50 ms, and refractory 20 ms). Left superior pulmonary vein (LSPV) was the highest pseudo-fre-quency site, where pseudo-frequency of 6.54 Hz was detected. There was also an temporally and spatially stable high frequency site in left posterior wall. Abnormal CFE mean was detected at left inferior atrium. We performed extensive pulmonary vein isolation (PVI) during AF. Internal cardioversion was delivered up to 30 J after PVI, but it was not effective, so AF was terminated by external cardioversion with 150 J. Sinus rhythm was kept without antiarrhythmic drug after catheter ablation. LSPV and left posterior wall were identified as the main source of AF in this case. We thought that defibrillation electrodes in coronary sinus and right atrium did not surround LSPV or left poste-rior wall because of atrial dilatation, which might be a cause of high atrial defibrillation threshold with internal cardioversion.
Conclusions: N/A
HIGH ATRIAL DEFIBRILLATION THRESHOLD WITH INTERNAL CARDIOVERSION CAUSED BY LEFT ATRIAL DILATATION IN PERSISTENT ATRIAL FIBRILLATION CASE Satoshi Aita, Akira Kimata, Yasuhiro Yokoyama
St. Luke’s International Hospital, Tokyo, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-144

404
Introduction: Any level of atrioventricular blocks may lead to profound bradycardia and can be potentially life-threatening. Arrhythmia such as atrioventricular blocks might be the only clinical presentation in patients with acute myocarditis, which is a rare event. The unique manifestation of varying arrhythmia in the setting of acute myocarditis have made it a challenge to diagnose in cardiology.
Methods: N/A
Results: This is a case of a 35 year-old male filipino, no known cardiovascular risk factors, who came in due to syncope. A history of flu-like symptoms the previous week was elicited. On admission, electrocardiogram showed sinus rhythm, ST-segment elevation in leads V1-V4 with left bundle-branch block pattern. Troponin-T and creatinine kinase-MB were elevated. Transthoracic echocardiogram revealed normal left ventricular dimension and systolic function. Cardiac magnetic resonance imaging (CMRI) showed increased T2 signal of the myocardium matched with hyperemia and sub-epicardial delayed hyper-enhancement of the lateral wall consistent with acute myocardi-tis (image). Cardiac monitoring showed paroxysmal third-degree atrioventricular block with ventricular rate of 37 bpm and episode of si-nus pauses with junctional escape. Hence, temporary pacemaker was placed.During his hospital stay, cardiac rhythm converted high-grade atrioventricular blocks and eventually first-degree atrioventricular block with narrow complex QRS. He was discharged and im-proved with normal electrocardiogram on follow up. Varying atrioventricular blocks in young adult is uncommon clinical presentation of patients with acute myocarditis. Higher-degree AV block is correlated with greater myocardial injury with a potential life-threatening con-sequence. However, in the majority of cases this rhythm disturbance is transient and does not require permanent pacemaker placement.
Conclusions: Varying atrioventricular blocks associated with acute myocarditis can be life-threatening, but the overall prognosis is good in previously healthy young adult and if diagnosed early and proper management advocated.
VARYING ATRIOVENTRICULAR BLOCKS IN A YOUNG ADULT WITH ACUTE MYOCARDITIS: A CASE REPORTAndre Awaloei, Helga Santa Maria, Helen Ong Garcia
St. Luke’s Medical Center, Quezon City, Philippines
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-145

405
Introduction: The cardiac resynchronization therapy (CRT) has been reported to have an effect on children. The endo-cardial leads were commonly used in adult, but they were avoided because of venous obstruction, difficulty of extraction of the leads, or right-to-left shunt. We reported a three-year-old boy who had CRT with endo-cardial leads as a bridging therapy to CRT with epi-cardial leads.
Methods: N/A
Results: Three-year-old boy with tetralogy of Fallot, pulmonary atresia, and major systemic-pulmonary collateral arteries had right ven-tricular (RV) infarction and complete atrioventricular block following severe right ventricular dysfunction after radical operation: right ven-tricular outflow tract reconstruction (RVOTR) and closure of ventricular septal defect. After re-RVOTR and dual chamber pacing with epi-cardial leads at the site of right atrial appendage and the basement of right ventricle, he had been having severe biventricular dys-function with left ventricular dyssynchrony and bilateral pleural effusion requiring the continuous drainage. The CRT with endo-cardial leads which were 4.8 Fr screw-in leads at right atrium and right ventricular septum and 4 Fr coronary sinus lead, was performed in body weight of 10 kg. He had dramatically improved and the CRT was exchanged to CRT with epi-cardial leads after four months because of the possibility of venous obstruction. The extraction of the endocardial CRT was safely processed.
Conclusions: Endocardial CRT was effective to 10-kg-boy as bridging therapy.
ENDOCARDIAL CARDIAC RESYNCHRONIZATION THERAPY IN SMALL CHILDREN WITH BIVENTRICULAR DYSFUNCTION AND COMPLETE ATRIOVENTRICULAR BLOCKMisugi Emi, Hisaaki Aoki, Futoshi Kayatani
Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-146

406
Introduction: Sarcoidosis is a systemic granulomatous disease which may involve heart and cause ventricular arrhythmia (VA). Because VA in patients with cardiac sarcoidosis (CS) are sometimes uncontrollable by medication, catheter ablation (CA) is another option to sup-press VA. We experienced three CS cases who underwent endocardial CA for drug-refractory ventricular arrhythmias.
Methods: N/A
Results: Case 1 was 68 year-old female with apparent inflammatory findings in ventricular septum by MRI and PET examinations but without reduced LV function. She had two types of VT, one with RBBB configuration, inferior axis, relatively narrow QRS, S wave in V6 and precordial transition zone in V5 (LV septum), and another with left bundle branch block (LBBB) configuration, inferior axis (R>S in II and aVf, R<S in III), RR’ pattern in I and precordial transition zone in V5 (postero-lateral tricuspid annulus). Local abnormal ventricular activi-ties (LAVAs) were seen in RV septum and CS distal. After elimination of LAVAs in RV septum, VTs disappeared during six months fol-low-up. Case 2 was 69 year-old female with reduced LV function (LVDd/Ds 64/60 mm, EF 14%). She experienced repetitive appropriate ICD shocks for VT. There were two VT morphologies, one with RBBB configuration, inferior axis (RII<RIII), QS pattern in V5-6 (antero-lat-eral LV), and another with LBBB configuration, inferior axis (RII<RIII), relatively narrow QRS, precordial transition zone in V5, QS pattern in I and aVL (septum). We found a large low voltage area with LAVAs in antero-lateral LV and ablation of all the area with LAVAs suppressed VTs. Case 3 was 64 year-old female with reduced left ventricular (LV) function (LVDd/Ds 61/56 mm, EF 18%), frequent non-sustained VT (NSVT). Wall thinning and akinesis were seen in basal inferior wall and severe hypokinesis in the other area. Endocardial CA failed to elim-inate all of the substrates for VTs because there were multiple origins including epicardial lesions.
Conclusions: Endocardial origins of VTs were found in all patients with CS. Substrate-based endocardial CA, guided by voltage and LAVA mapping, was effective to suppress in some patients with CS.
THE CHARACTERISTICS OF THREE CARDIAC SARCOIDOSIS CASES WHO UNDERWENT CATHETER ABLATION FOR VENTRICULAR TACHYCARDIANaotaka Hashiguchi, Takashi Kurita, Yasuhito Kotake, Ryobun Yasuoka, Koichiro Motoki, Yoshitaka Iwanaga, Shunichi Miyazaki
Kindai University, Osakasayama, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-147

407
Introduction: The previous studies have demonstrated that cryoballoon ablation is a safe and effective alternative to anti-arrhythmic treatment of paroxysmal atrial fibrillation (AF). However, femoral vascular complications remain a significant complication as a result of relatively large vascular sheath sizes and peri-procedural anti-coagulation protocols.
Methods: N/A
Results: We experienced a case with right femoral hematoma 2 days after cryoballoon ablation in a 64-year-old female with symptomatic AF. By using a right femoral venous access site, a double transseptal puncture was performed. Steerable (FlexCath Advance 15Fr, Medtronic CryoCath) and nonsteerable (8Fr) sheaths were placed into the left atrium. The cryoballoon ablation procedure for a 4-pulmo-nary vein isolation was successfully performed (Arctic Front Advance 28 mm, 10.5Fr). Her PT-INR level before the procedure was 2.22 with oral coumadin (2.25 mg/day). The activated clotting time was maintained at more than 300 seconds through whole procedure. Two days later, an enlargement of the right femoral hematoma was noticed. The hematoma was scanned and an active bleeding from the superfi-cial branch of the femoral artery was detected by color Doppler echocardiography (Figure). Ultrasound guided compression successfully controlled the arterial bleeding without any invasive treatment.
Conclusions: We experienced a case with right femoral hematoma after cryoballoon ablation caused by an active bleeding from the su-perficial branch of the femoral artery.
EARLY DETECTION OF ACTIVE BLEEDING FROM THE SUPERFICIAL BRANCH OF THE FEMORAL ARTERY AFTER CRYOBALLOON ABLATION IN A PATIENT WITH PAROXYSMAL ATRIAL FIBRILLATIONSatoshi Higa1, Sugako Ishigaki1, Akira Maesato1, Nobumori Yagi2 1Cardiac Electrophysiology and Pacing Laboratory, Division of Cardiovascular Medicine, Makiminato Central Hospital, Okinawa, Japan;
2Division of Cardiovascular Medicine, Nakagami Hospital, Okinawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-148

408
Introduction: Cardiac resynchronization therapy (CRT) is often used to prevent and treat asynchronous ventricular activation. Studies have shown that CRT pacing can improve functional status in subgroups of patient with systolic congestive heart failure (CHF) and intrinsic or iatrogenic intraventricular conduction delay. Although optimal ventricular lead positioning in CRT has not been fully elucidated, standard lead positions are the RV apex and a posterolateral coronary vein via the coronary sinus.
Methods: N/A
Results: An 83 year-old male with chronic systolic heart failure (NYHA class III, LVEF 40%) and prior implant of a dual-chamber pace-maker for AV block presented with worsening dyspnea. ECG showed intermittent AV sequential pacing. His pacemaker was interrogated and showed 96% ventricular pacing. Due to his worsening symptoms he was scheduled for upgrade to a CRT device. During the proce-dure it was noted that the prior RV lead had been positioned high in the septal wall. Advancing the LV lead posterolaterally into the only available lateral branch showed insufficient separation between the ventricular leads. The LV lead was repositioned through the middle cardiac vein into an apicolateral position. In addition to an acceptable threshold value and absence of diaphragmatic stimulation, this posi-tion yielded significantly greater separation between the RV and LV leads. The patient endorsed an improvement in his symptoms after-wards.
Conclusions: Separation between ventricular leads is an important factor in improving outcomes from CRT. Novel lead locations may be necessary for effective CRT depending on venous anatomy and positions of previously placed RV leads.
UNUSUAL LEFT VENTRICULAR LEAD PLACEMENT FOR IMPROVED RESPONSE TO CARDIAC RESYNCHRONIZATION THERAPYYong Ji1, Tahmina Samad1, Brandon Woodbury1, Ronald Lo2 1Loma Linda University Medical Center, Loma Linda, United States; 2VA Loma Linda Healthcare System, Loma Linda, United States
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-149

409
Introduction: Pulmonary vein isolation (PVI) with radiofrequency (RF) ablation is one of the treatment modalities for drug-refractory par-oxysmal atrial fibrillation (AF). Bradycardia and asystole during catheter ablation (CA) has been reported as related to ablation around the ganglionic plexus. We report on a case where multiple bradycardia and asystolic episodes occurred during CA, and required atrial pacing during CA for completion of pulmonary vein isolation.
Methods: N/A
Results: A 65 year old female with history of MI, symptomatic paroxysmal atrial fibrillation with multiple cardioversions was referred for RF ablation after failing three anti-arrhythmic medications. She has tried dofetilide and dronedarone in the past, currently on sotalol, with breakthrough episodes. Her past medical history was also significant for prior successful ablation for atrial flutter several years ago. She complained of being in palpitations, shortness of breath, and fatigue. She was taken to the electrophysiology laboratory and CA was per-formed using RF ablation. During ablation in the carina of left superior and inferior pulmonary vein, it provoked significant bradycardia and subsequent pauses and hypotension present for up to 15 seconds which recovered with time. This occurred multiple times and limit-ed further ablation. She required atrial pacing during ablation to complete full pulmonary vein isolation. She remained asymptomatic and in sinus rhythm following the PVI.
Conclusions: The proposed mechanism for asystole and bradycardia during CA is vagal denervation from ganglionic plexus. These pro-longed asystole events during RF ablation usually resolve spontaneously, and has been associated with improved outcomes in AF ablation. Episodes of bradycardia and asystole may be mitigated with atrial pacing.
A RARE CASE OF PULMONARY VEIN ISOLATION INDUCED ASYSTOLEYong Ji1, Deepika Narasimha1, Mary Bato2, Ronald Lo2 1Loma Linda University Medical Center, Loma Linda, United States; 2VA Loma Linda Healthcare System, Loma Linda, United States
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-150

410
Introduction: Swallowing-induced atrial fibrillation (AF) is a rare clinical entity generally assumed to be caused by abnormal parasympa-thetic nervous reflexes. This report describes a successful therapy for cold water swallowing-induced paroxysmal AF by performing pul-monary vein isolation (PVI) and non pulmonary vein (PV) foci ablation.
Methods: N/A
Results: A 39-year-old man presented to our hospital for catheter ablation of paroxysmal AF. He felt palpitations when he drank cold wa-ter during exercise about 20 years ago. He had been diagnosed with paroxysmal AF about 8 years ago by electrocardiogram. Because he had drug resistant AF and highly symptomatic AF, we decided to perform catheter ablation using a 3D electroanatomical mapping system (CARTO3, Biosense Webster Inc., Diamond Bar, CA). AF was not induced by cold water injection in esophagus under a 20 µg bolus admin-istration of isoproterenol, but atrial ectopic beats from the coronary sinus (CS) ostium were observed reproducibly. We tried to map the ectopic beats, but inducibility decreased by repeat cold water injection. Then, we performed circumferential pulmonary vein isolation and superior vena cava isolation. A 20-mg bolus of adenosine triphosphate (ATP) was rapidly injected intravenously to induce the reconnection of the pulmonary veins under a 5 µg bolus infection of isoproterenol. No dormant PV conduction was observed, but AF was induced by ec-topic beat originating from CS ostium. AF was not induced after ablation at the foci. AF was also induced by another ectopic beat originat-ing from lateral right atrium. During radiofrequency (RF) ablation at the foci, atrial tachycardia (AT) was induced spontaneously. RF appli-cation at postero-inferior right atrium resulted in direct termination of the AT. AT and AF was no more induced by any stimuli and ATP ad-ministration after the procedure.
Conclusions: We successfully performed a catheter ablation for swallowing-induced paroxysmal AF by ectopic beats originating from the right atrium.
CATHETER ABLATION FOR SWALLOWING-INDUCED PAROXYSMAL ATRIAL FIBRILLATION BY ECTOPIC BEATS ORIGINATING FROM THE RIGHT ATRIUMKen Kato, Masataka Ogiso, Makiko Suzuki, Wataru Yamagata, Akihisa Kimura, Ayano Yoshida, Yuta Okabe, Kansuke Ito, Shogo Hari, Yoshihiro Nishimura, Hiroaki Morinaga, Madoka Akashi, Yuya Mitsuhashi, Kenichiro Nagata, Toshiaki Isogai, Hiroyuki Tanaka, Tamotsu Tejima
Tokyo Metropolitan Tama Medical Center, Tokyo, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-151

411
Introduction: The knowledge of cardiac anatomy and anomaly is critical in performing catheter ablation of arrhythmias. We report a rare vascular anomaly which hinders the catheter ablation procedure.
Methods: N/A
Results: A sixty-seven-year-old male was referred to our hospital for atrial fibrillation ablation. Preoperative echocardiography and cardi-ac CT revealed no abnormality of the heart. During the procedure, the wire was inserted from the right femoral vein to the superior vena cava (SVC), but right atriography revealed that the tip of this wire was not in the SVC. The wire from the right jugular vein was inserted into the right atrium, the right ventricle and the hepatic veins but not in the inferior vena cava (IVC). Contrast injection revealed that the hepatic segment of the IVC was absent. The catheter was inserted through the azygos vein to the SVC and the right atrium. However, the manipu-lation of the catheter was not possible through this approach and the procedure was suspended. Azygos continuation of the inferior vena cava is an uncommon anatomical abnormality. The hepatic segment of the IVC is absent and blood flow drains through the azygos vein to the SVC. It is reported to associate with polysplenia, asplenia and other congenital heart diseases. But recent advance in CT imaging dis-covered many asymptomatic cases without other anatomical abnormalities.
Conclusions: Azygos continuation of the inferior vena cava is a rare anomaly. Preoperative knowledge of this anatomical abnormality is important for catheter ablation procedure and cardiac surgery.
A CASE OF ATRIAL FIBRILLATION WITH AZYGOS CONTINUATION OF THE INFERIOR VENA CAVARyusuke Kimura, Chikara Fujita, Yohei Yakuta, Daisuke Tsujimoto, Tadatsugu Gamou, Hidenobu Terai, Yuki Horita, Masatoshi Ikeda, Masanobu Namura
Kanazawa Cardiovascular Hospital, Kanazawa, Ishikawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-152

412
Introduction: The gradient magnetic field and radiofrequency energy generated during MRI scan can affect pacmaker leadsensing, pac-ing thresholds, and impedances, causing inappropriate pacing acceleration or inhibition.
Methods: N/A
Results: We present case report of 69 years old hypertensive male implanted with non-MRI pacing system of St. Jude Medical, VerityTM ADx XL DR 5356 and Tendril® ST Model 1888 Right Atrium (RA) & Right Ventricular (RV) leads with RA/RV lead capture threshold (CT) & lead impedance (LI) of [email protected] ms & 400Ω/[email protected] ms & 710Ω on 06/05/2015 at our Hospital Fortis Escorts Heart Institute & Research Center, New Delhi, India. Later patient reported at our center on 09/03/2016 with recurrent episodes of syncope diagnosed as “Stokes Ad-ams syndrome” due to ventricular non-capture (RA/RV CT & LI were [email protected] ms & 436Ω/[email protected] ms & 344Ω), 12-lead ECG confirmed no RV pacing (Figure 1). Patient was shifted to Cath Lab and both RA & RV leads were replaced (Tendril ST 1,888TC). The post-implant RA/RV CT and LI were [email protected] ms & 480 Ω/[email protected] ms & 710Ω. Earlier leads not extracted for further evaluation due to anatomical rea-sons. Patient’s family informed about brain MRI scan (0.3 Tesla Hitachi) on 07/02/2016 for head injury at Tier-II Radiology Center without any evaluation/changes (asynchronous mode) in pacemaker parameters. On 08/02/2016 patient fainted at home,transferred to secondary care hospital with multiple episodes of syncope and unresponsiveness later discharged on 18/02/2016 without any resolution.
Conclusions: It was implied that MRI scan caused lead parameter changes. We recommend only MRI labelled devices should be subject-ed to MRI scan.
CASE REPORT OF PACEMAKER LEAD COMPLICATION DUE TO BRAIN MAGNETIC RESONANCE IMAGING (MRI) SCANTarlochan Kler, Viney Jetley, Avinash Verma
Fortis Escorts Heart Institute & Research Center, Delhi, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-153

413
Introduction: Brugada syndrome is known to overlap with ARVC particularly when monomorphic VT occurs. Brugada pattern resolution post ablation is a potential prognostic procedural endpoint based on previous reports.
Methods: N/A
Results: A 46 year old male presented with palpitations and presyncope with classic type I Brugada pattern. During his investigations he was found to overlap with ARVC with 1 major criteria of Epsilon wave in V2 and 2 minor criteria of a negative T wave in V1, V2 plus NSVT with LBBB pattern with unknown axis on loop recorder. He also had right ventricular wall fibrofatty infiltration with dyskinesia and mi-croaneurysms but normal chamber size on cardiac MRI. Genetic testing found a SCN5A variant (p.GIn646fs). The patient had a loop re-corder implanted and by 3 months had 3 episodes of monomorphic VT, the longest 46 seconds at 261 bpm. Ventricular stimulation in-duced ventricular flutter and he proceeded to ICD implantation. At 1 year the device check revealed 2 episodes of ATP for monomorphic VT. The patient underwent mapping and endocardial ablation to the high anterior RVOT. The Brugada pattern resolved and this has per-sisted for 21 months with no further episodes of NSVT on subsequent device interrogations.
Conclusions: Persistent resolution of Brugada pattern with endocardial ablation in this case of SCN5A variant Brugada has correlated with resolution of arrhythmia. This adds to the growing body of literature suggesting post ablation Brugada pattern resolution be consid-ered a potentially important endpoint. It also emphasises the importance of SCN5A testing in these BRS ARVC overlap patients.
BRUGADA PATTERN RESOLUTION AFTER ENDOCARDIAL ABLATION IN A PATIENT WITH BRUGADA ARVC OVERLAP. A CASE REPORT IN SCN5A VARIANT BRUGADA SYNDROMESimon Binny, John Atherton, Julie McGaughran, Kate Noonan, Daniel Lancini, Paul Martin
Royal Brisbane Hospital, Brisbane, Australia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-154
Figure 1. Left: Baseline ECG; Centre: ECG 21 months post ablation; Right: Mapping and ablation focus (brown lesions; lower voltage areas in blue/yellow).

414
Introduction: We present a case of atrioventricular nodal non-reentrant tachycardia (AVNNRT or “double fire tachycardia”) that presented as a severe cardiomyopathy following a two year period of misdiagnosis as atrial fibrillation (AF).
Methods: N/A
Results: A 58 year old man presented with 3 years of palpitations and the recent onset of clinical heart failure. Transthoracic echocardio-gram revealed a severe dilated cardiomyopathy (LVEF=27%). Two years prior he was diagnosed with ‘AF’ and commenced on aspirin and atenolol. His LVEF at that time was normal (65%). Closer inspection of his presenting ECG (Figure 1A) revealed a regularly irregular rhythm with a sinus P-wave followed by two QRS complexes. This phenomenon was incessant and persisted despite variation in sinus rates with ventricular rates up to 190 bpm. This was consistent with AVNNRT with each sinus impulse propagating to the ventricle via both the fast and slow pathways. An electrophysiology study confirmed this diagnosis with 2 sets of His and ventricular electrograms fol-lowing each sinus impulse (Figure 1B). Slow pathway ablation abolished the 2nd QRS complex, resulting in sinus rhythm with 1:1 AV con-duction (Figures 1C, D). At 3 month follow up, his LVEF had improved to 50% and his heart failure symptoms had resolved. Retrospective analysis of all his old ECGs revealed only AVNNRT which had been misdiagnosed as AF.
Conclusions: “Double fire tachycardia” or AVNNRT is a rare manifestation of dual AV nodal physiology that is often misdiagnosed as AF. An accurate appreciation of the rhythm is paramount as a delay in diagnosis can result in inappropriate therapy and the development of a tachy-cardiomyopathy.
PROVOCATIVE CASES-INCESSANT DOUBLE FIRE CARDIOMYOPATHYAdam Lee, Srikanth Adusumalli, Robert Gluer, Daniel Wright, Russell Denman
The Prince Charles Hospital, Chermside, Australia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-155

415
Introduction: Entrainment pacing is major method to identify tachycardia circuit and a critical site of ablation. Atrial tachycardia after car-diac surgery can have complex tachycardia circuit including scar or cavotricuspid isthmus.
Methods: N/A
Results: The patient was 56-year-old man. He underwent mitral valve and annulus plasty with transseptal approach when he was 44 years old. He was diagnosed with atrial tachycardia when he was 53 years old and catheter ablation was scheduled. P wave polarity of the tachycardia was negative in II, III and aVF leads. Its tachycardia cycle length was 290 ms. We arranged an electrode catheter with 20 elec-trodes around the tricuspid valve annulus and an electrode catheter with 10 electrodes into the coronary sinus. When we performed en-trainment pacing at right atrial free wall, it fulfilled concealed entrainment criteria and the post pacing interval was 15 ms. When entrain-ment pacing at the cavotricuspid isthmus, it also fulfilled concealed entrainment criteria and the post pacing interval was 15ms. We diag-nosed it as cavotricuspid isthmus dependent atrial tachycardia. We performed activation mapping with CARTO system because he under-went mitral surgery. It revealed that the tachycardia was scar related atrial tachycardia which turned around the incisional line of trans-septal approach. We delivered RF applications at the site of fractionated potential beside incisional line, but the tachycardia didn’t termi-nate. We performed linear ablation from incisional line to tricuspid annulus at right atrial anterior wall, and then this tachycardia termi-nated.
Conclusions: We experienced an unusual case with atrial tachycardia that was shown to be cavotricuspid isthmus dependent atrial tachy-cardia by entrainment pacing but 3D mapping revealed it was scar related atrial tachycardia turning around the incisional line of trans-septal approach.
A CASE OF SCAR RELATED ATRIAL TACHYCARDIA AFTER THE SURGERY OF MITRAL VALVE PLASTY WHOSE CIRCUIT COULD NOT BE IDENTIFIED WITHOUT USING 3D MAPPINGTomoaki Nakano, Akio Hirata, Ryohei Amiya, Masao Koide, Kazunori Kashiwase, Yoshiharu Higuchi, Yoshio Yasumura
Osaka Police Hospital, Osaka, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-156

416
Introduction: A 63 years old lady with underlying diabetes mellitus and hypertension was diagnosed with complete heart block. Perma-nent pacemaker (PPM) bipolar (VVI) was inserted in 10th August 2010 on the left anterior chest wall with paced-rate 60 bpm, threshold 0.5V and lead model number: 507658, screw-in lead. She was on regular follow-up under cardiology unit since 2010. During follow-up in March 2016, we noted the battery approaching End of Life (EOL).
Methods: N/A
Results: A decision was made to upgrade to dual chamber pacemaker. During the interrogation of the device, we noted a high threshold in the right ventricular lead, ranging 2.75V/0.4 msec-3.0V/0.4 msec. This clearly indicates the reason for the short lifespan of the battery. During implantation of the new device, we planned for lead retraction of the old lead. Before the old lead retraction was done, new leads were placed in mid septum of the right ventricle and right atrial appendage. A skin incision was made over the old scar till the old device was visible. The previous device was identified and removed from the well-encapsulated pocket. We unlocked the old lead from the pace-maker. The old lead was identified and adhesions released using artery forceps and scalpel. Sutures over the sleeve were released and free mobility of the lead checked. A stylet was inserted through the old lead and proceeded to unscrew the lead with fluoroscopy guidance. Traction was applied with controlled counter traction while slowly retracting the lead. Once the old lead was removed, we observed for bleeding from the exit site. The new device is then placed within the pocket and closed in the usual manner. Finally, we performed an echocardiogram to look pericardial effusion, in view of a high risk for venous dissection during lead extraction. An essential learning point from this case is the strict adherence of proper steps using the conventional method which can ensure safety and successful extraction.
Conclusions: This case demonstrates the need for a proper technique and correct patient selection for lead extraction using the conven-tional method.
ANCIENT TECHNIQUE STILL FEASIBLE?Kantha Rao Narasamuloo, Dharmaraj Karthikesan, Azrina Abdul Kadir, Liew Kai Soon, Ryan Khoo Song Weng, Gerard Jason Mathews, Wan Faizal Wan Rahimi Shah, Muhammad Khairul Taufiq Rosli, Ahmad Faiz Mohd Ezanee, Yeoh Chian Hui, Cheng Yi Zhi, Ahmad Shukri Saad, Saravanan Krishinan
Hospital Sultanah Bahiyah, Alor Setar, Malaysia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-157

417
Introduction: It is known that premature ventricular contractions (PVCs) originating in the vicinity of the His bundle show the narrow QRS. Radiofrequency (RF) application at the His bundle region has a risk of inadvertent atrioventricular block. We report a case of idiopathic PVCs with narrow QRS duration originating from the middle portion of the left ventricular septum, and we show this mechanism.
Methods: N/A
Results: A 65-year-old man with highly symptomatic PVCs was referred for ablation. Holter monitoring demonstrated frequent mono-morphic PVCs with 20,722 per day. The ECG of the clinical PVCs showed similar sinus rhythm pattern in the precordial leads, narrow QRS duration (110 msec) and an inferior axis. Thus, these PVCs might be originating in the vicinity of the His bundle. The sharp pre-potentials (Potential of His bundle, Potential of left anterior fascicle, Potential of right bundle branch, Purkinje potential) preceding the potential of ventricle were recorded in the area of the cardiac conduction system during sinus rhythm. Further, these sharp pre-potentials preceding the potential of ventricle were recorded in the same sites when the PVCs occurred. During activation mapping, the earliest activation of PVCs was identified at the middle portion of the left ventricular septum, preceding the QRS onset by 28 m seconds and pace mapping pro-vided an identical match with the spontaneous PVCs. The sharp pre-potentials were ascending from the earliest activation site to the His bundle, and descending to the right ventricle through the right bundle branch. This conduction property can elucidate the mechanism that the ECG of PVCs showed narrow QRS duration. Application of RF energy (35 w) to earliest activation site abolished the PVCs within 5 sec-onds, and applied a left anterior fascicular block.
Conclusions: This finding can be helpful for planning catheter ablation of the PVCs with narrow QRS duration.
A CASE OF IDIOPATHIC PREMATURE VENTRICULAR CONTRACTIONS WITH NARROW QRS DURATION ORIGINATING FROM THE MIDDLE PORTION OF THE LEFT VENTRICULAR SEPTUMYoshimi Onishi1, Taku Asano2, Yuya Nakamura2, Mitsuharu Kawamura2, Youichi Kobayashi2 1Koyama Memorial Hospital, Ibaraki, Japan; 2Showa University School of Medicine, Tokyo, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-158

418
Introduction: The usefulness of manifest entrainment to determine the tachycardia circuit of ATP-sensitive atrial tachycardia originating from the atrioventricular annulus has been shown recently.
Methods: N/A
Results: Case: A 65-year-old Japanese male who was diagnosed as tachycardia-induced cardiomyopathy was admitted to the hospital for the radiofrequency catheter ablation of the Long RP’ tachycardia. There was only fast pathway with conduction delay in response to in-crease in the rate for atrioventricular conduction and there was no ventriculoatrial conduction. After the isoproterenol administration, the tachycardia with the cycle length of 380 ms was induced by atrial extrastimulus pacing. Ventricular rapid pacing during the tachycardia showed VA dissociation, and differential atrial overdrive pacing showed no VA relationship. Inverse relation between pacing cycle length and the return cycle of the tachycardia was shown by rapid pacing from coronary sinus during tachycardia. The tachycardia was reproduc-ibly terminated by ATP 2 mg. By the methods stated above, this tachycardia was diagnosed as re-entrant ATP-sensitive atrial tachycardia. The earliest atrial activation site, or the exit point from the area of the slow conduction area of the reentry circuit, was in the 8-o’clock po-sition of the tricuspid annulus. Manifest entrainment with orthodromic capture of the earliest atrial activation site was demonstrated by pacing from the anterior right atrium, where is considered to be proximal to slow conduction area of the reentry circuit. Radiofrequency energy was delivered to a site 3 cm away from the earliest atrial activation site in the direction of the anterior pacing site. First application of the energy terminated the tachycardia and no inducibility of the tachycardia was confirmed. Discussion: According to Yamabe et al., the distance between the earliest atrial activation site and the successful energy application site was 10.4±2.4 mm. They started the deliver-ing energy at a site 2 cm away from the earliest atrial activation site in the direction of entrainment pacing site. In our case the successful site was 3 cm away which demonstrated the possibility of longer slow conduction zone in the case of ATP-sensitive atrial tachycardia orig-inating from the atrioventricular annulus. When the tachycardia circuit is close to the atrioventricular node, we may consider delivering the energy starting at longer distance from the node.
Conclusions: We experienced a case of ATP-sensitive atrial tachycardia with possible longer slow conduction zone.
A CASE OF LONGER SLOW CONDUCTION ZONE IN ATP-SENSITIVE ATRIAL TACHYCARDIA ORIGINATING FROM THE ATRIOVENTRICULAR ANNULUS Maki Ono, Akira Mizukami, Hirofumi Arai, Shunsuke Kuroda, Shunsuke Kuroda, Makoto Suzuki
Kameda Medical Center, Kamogawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-159

419
Introduction: Unexplained dyspnea after invasive procedures for atrial fibrillation should raise suspicion for stiff left atrial (LA) syndrome.
Methods: N/A
Results: A 74 year old man presented four years after mitral valve (MV) replacement with a one year history of worsening dyspnea on ex-ertion, orthopnea, paroxysmal nocturnal dyspnea, and abdominal distension. History was notable for rheumatic fever, severe mitral regur-gitation (MR) status post MV repair in 1995 with subsequent redo MV replacement and maze procedure with PFO closure in 2004, and persistent atrial fibrillation on anticoagulation. Physical exam demonstrated irregular rhythm, variable prosthetic S1, normal S2, no gal-lops, jugular venous distention to angle of jaw with a large V wave, markedly distended abdomen with a fluid wave, and 1+ pitting edema bilaterally. Echocardiogram demonstrated moderate right ventricle (RV) enlargement, right ventricular systolic pressure (RVSP) of 45 mmHg, severe tricuspid valve regurgitation, MV prosthesis diastolic gradient of 6 mmHg, and dilated inferior vena cava with reduced in-spiratory collapse without evidence of pericardial constriction or restriction. Cardiac catheterization demonstrated elevated LA pressure at 19 mmHg with a large V wave of 29 mmHg. Other measurements were notable for mean pulmonary artery pressure of 30 mmHg, RVSP 43 mmHg, right atrial pressure of 15 mmHg, and cardiac index of 2.97 L/min/m2. These findings contrasted with his pre-operative echocardiogram four years prior with RVSP of 39 mmHg. A diagnosis of LA diastolic dysfunction or a stiff LA with resultant mild pulmo-nary hypertension and right heart failure was made. He was diuresed aggressively with symptomatic improvement. Despite aggressive medical management, he ultimately required tricuspid valve repair for worsening right heart failure.
Conclusions: LA diastolic dysfunction (stiff LA syndrome) should be considered in patients with history of invasive atrial fibrillation proce-dures presenting with unexplained dyspnea. Invasive hemodynamic evaluation demonstrating large V waves and pulmonary hypertension in absence of MR is diagnostic.
DYSPNEA FOLLOWING MAZE PROCEDUREJae Yoon Park, Sudhir S. Kushwaha
Mayo Clinic, Rochester, United States
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-160

420
Introduction: Sudden cardiac death (SCD) risk-stratification in Brugada syndrome (BS) is controversial and depends on its phenotypic ex-pression. Electrophysiology study (EPS) with programmed ventricular stimulation (PES) is a class IIB recommendation by current interna-tional guidelines due to protocols low reproducibility and high variability. Ajmaline has a key-role in BS diagnosis. Epicardial ablation of the right ventricular outflow tract (RVOT) to reduce ICD discharges confirmed a sectorial vulnerability. We report a BS patient who experi-enced different ventricular arrhythmias (VAs) inducibility depending on RVOT PES timing with or without type 1 BS ECG unmasked by ajmaline, in order to better understand the dynamic mechanisms responsible for the existing controversies between centers, and for the wide spectrum of clinical presentations, including occasional fatal events.
Methods: N/A
Results: A 68-year-old man with prior syncope, episodes of persistent atrial fibrillation treated by successful electrical cardioversion, and family history of SCD had a J-wave and a convex upwards ST-segment elevation >2 mm in V1-V3 at peak ECG cycle ergometer stress test. Baseline ECG showed incomplete right bundle branch block (RBBB) QRS 105 ms, J-point and ST-segment elevation of 0.14 mV in V1 and 0.18 mV in V2 concave upwards compatible with type 2 BS ECG. Ajmaline (1 mg/kg iv in 10 min) unmasked “coved” type 1 BS ECG (QRS 150 ms, complete RBBB with J-point and ST-segment elevation of 0.38 mV convex upwards and negative T-waves in V1-V2; J-point and ST-segment elevation of 0.14 mV in aVL, 0.1 mV in D1). After 40 minutes, type 2 BS ECG was restored. PES was perfomed from the right ventricular apex (RVA) and RVOT by double extrastimuli up to ventricular effective refractory period (VERP) without VAs induction. PES was repeated after restoration of type 1 BS ECG by ajmaline (0.5 mg/kg iv in 10 min), from the RVA and the RVOT up to VERP of 500-300-210 ms and 400-350-200 ms. RVA PES induced ventricular couples, and RVOT PES induced a reproducible self-terminated symptom-atic ventricular fibrillation, CL 260 ms, HR 230 bpm. An ICD was implanted, per international guidelines, after informed consent was ob-tained.
Conclusions: PES of the vulnerable RVOT during BS channelopathy maximization induces VAs. Fatal events in BS happen when 2 factors are combined: ventricular extrastimuli or ectopies, and the greatest expression of the channelopathy depending on multiple factors. EPS poor reproducibility and non-proper SCD risk-stratification are due to different protocols used in various centers. BS phenotypic hetero-geneity and wide spectrum of clinical presentations are due to the underlying mechanisms and require standardized SCD risk-stratifica-tion protocols, that may improve patient selection and timing for ICD implantation when no history of cardiac arrest is present, and may return EPS its deserved prognostic value.
VENTRICULAR ARRHYTHMIAS INDUCTION BY PROGRAMMED ELECTRICAL STIMULATION OF THE RIGHT VENTRICULAR OUTFLOW TRACT ONLY DURING TYPE 1 BRUGADA ECG MAXIMIZATIONBich Lien Nguyen, Roberta Sergiacomi, Fabrizio Tufano, Flavia Tersigni, Alessandro Persi, Ilaria Maraschi, Nicola Alessandri
Sapienza University of Rome, Rome, Italy
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-161

421
Introduction: Catheter ablation of AV node reentrant tachycardia (AVNRT) is regarded as first-line therapy for treatment of symptomatic AVNRT. It is potentially curative, and chronic pharmacological therapy is usually not needed after the procedure. Slow- pathway ablation (also called modification) is the preferred target during ablation of AVNRT.The success rates of slow-pathway ablation is >95%, with <1% risk of AV block. The options for patients who fail slow pathway modification are usually repeat procedure or antiarrhythmic drug therapy. We report a patient with typical AVNRT who had refractory, recurrent, drug resistant, AVNRT in whom slow pathway modification was un-successful after repeat procedures both from the right and left side. He underwent a successful fast pathway modification.
Methods: N/A
Results: A 44 years male radiographic technician, had history of recurrent PSVT resistant to verapamil, metoprolol, flecanaide singly and in combination. He had failed slow pathway modification for AVNRT 3 month’s prior, and had developed recurrences, and hyperthyroidism on amiodarone. EP study revealed easily inducible AVNRT but attempt at slow pathway modification failed. Slow pathway modification was attempted inside the CS, and from the left side through transseptal approach but was unsuccessful. He subsequently underwent a fast pathway modification which was successful, ECG reveals first degree AV block, and on treadmill test he has normal effort tolerance with 1:1 conduction up HR of 150 bpm. He has no higher degree of AV block and has been free of symptoms for >4 years.
Conclusions: Fast pathway ablation can be considered in patients who have failed slow pathway modification and have drug resistant AVNRT with no risk of complete AV block on medium term follow up.
AN UNCOMMON PROCEDURE FOR A COMMON ARRHYTHMIA: FAST PATHWAY ABLATION AFTER FAILED SLOW PATHWAY MODIFICATION FOR TYPICAL AV NODE REENTRANT TACHYCARDIAVivek Pillai, Vidhyakar Balasubramaniam, Sivasankara Chakali, Jayaprakash Shenthar
Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-162

422
Introduction: Here we report two cases of persistent atrial fibrillation who become sinus tachycardia after pulmonary vein isolation and dominant frequency ablation.
Methods: N/A
Results: Case 1: 56-year-old male. Radiofrequency catheter ablation (RFCA) was performed to atrial fibrillation (AF) persisted for 3 months. First, pulmonary vein isolation (PVI) was performed. Next, frequency analysis was done, and ablation was performed to high dominant frequency (DF) area which was located at upper anterior region. There was no recurrence of AF after the session. Heart rate (HR) in electrocardiogram (ECG) was 96 beats per minute (bpm) at a day after session and more increased to 106 bpm at 3 weeks later. HR maintained more than 100 bpm after that, so oral administration of atenolol was started and HR decreased to around 80 bpm stably. Case 2: 50-year-old male. RFCA was performed to AF persisted for 2 years. First, PVI was performed. Next, frequency analysis was done, and ablation was performed to high DF area which was located at upper anterior region and roof. There was no recurrence of AF after the session. HR in ECG was 92 bpm at a day after session and more increased to 102 bpm at 4 weeks later. HR maintained more than 100 bpm after that, so oral administration of atenolol was started and HR decreased to around 80 bpm stably.
Conclusions: It seemed that the ablation site of upper anterior region in right superior pulmonary vein was at relatively deeper site of pul-monary vein in both cases. Also, this lesion was close to right atrium-SVC junction. It may implied that the ablation lowered the activity of vagal ganglion plexus. Also, it may implied that ablation stimulate the activity of sinus node lesion positively.
TWO CASES OF PERSISTENT ATRIAL FIBRILLATION WHO BECOME SINUS TACHYCARDIA AFTER PULMONARY VEIN ISOLATION AND DOMINANT FREQUENCY ABLATIONYoshinao Sugai, Koji Kumagai, Kentaro Minami, Yoshiyuki Kitagawa, Hiroyuki Motoda, Yoshimitsu Otsuka, Michiharu Senga, Yutaka Take, Toshiaki Yano, Takehito Sasaki, Kohki Nakamura, Shigeto Naito, Shigeru Oshima
Gunma Prefectural Cardiovascular Center, Maebashi, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-164
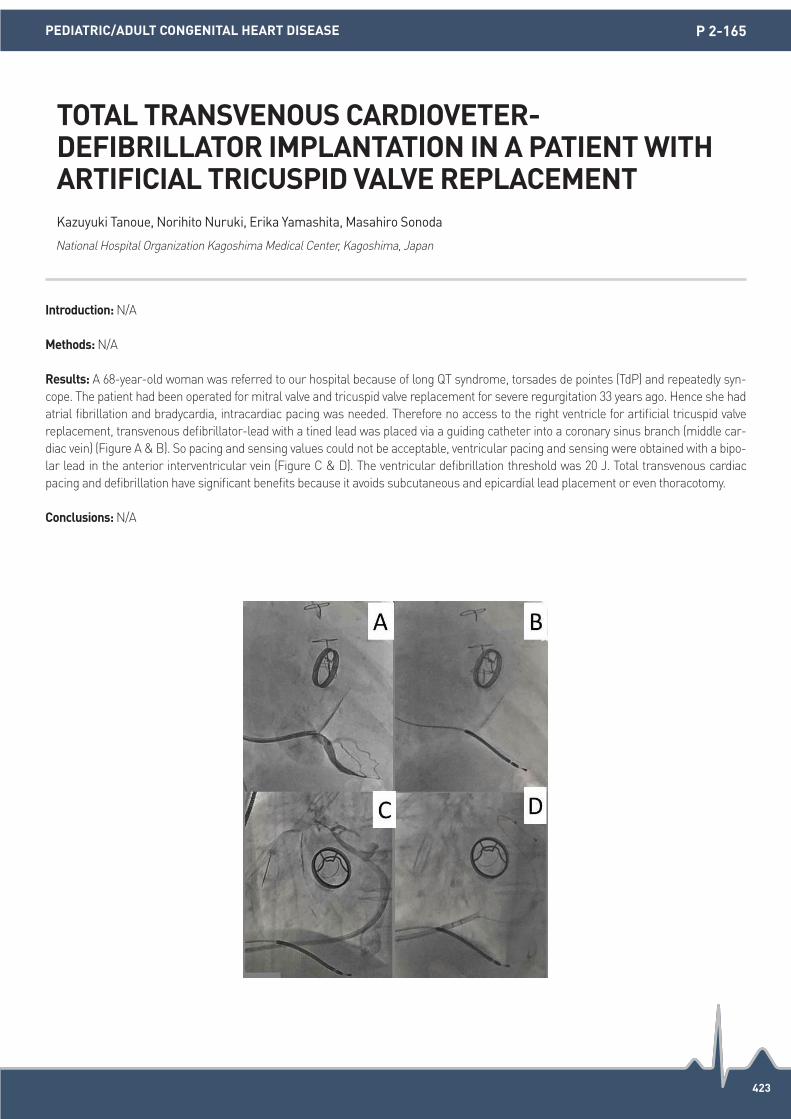
423
Introduction: N/A
Methods: N/A
Results: A 68-year-old woman was referred to our hospital because of long QT syndrome, torsades de pointes (TdP) and repeatedly syn-cope. The patient had been operated for mitral valve and tricuspid valve replacement for severe regurgitation 33 years ago. Hence she had atrial fibrillation and bradycardia, intracardiac pacing was needed. Therefore no access to the right ventricle for artificial tricuspid valve replacement, transvenous defibrillator-lead with a tined lead was placed via a guiding catheter into a coronary sinus branch (middle car-diac vein) (Figure A & B). So pacing and sensing values could not be acceptable, ventricular pacing and sensing were obtained with a bipo-lar lead in the anterior interventricular vein (Figure C & D). The ventricular defibrillation threshold was 20 J. Total transvenous cardiac pacing and defibrillation have significant benefits because it avoids subcutaneous and epicardial lead placement or even thoracotomy.
Conclusions: N/A
TOTAL TRANSVENOUS CARDIOVETER-DEFIBRILLATOR IMPLANTATION IN A PATIENT WITH ARTIFICIAL TRICUSPID VALVE REPLACEMENTKazuyuki Tanoue, Norihito Nuruki, Erika Yamashita, Masahiro Sonoda
National Hospital Organization Kagoshima Medical Center, Kagoshima, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-165

424
Introduction: Tachycardias like AF and VT are seen in patients with PPM implantations. A 20 year old girl underwent PPM for CHB 3 years back. She presented with palpitations and multiple high rate episodes with a heart rate of 160-180 bpm. Device interrogation showed si-multaneous atrial (A) and ventricular (V) activation during tachycardia suggestive of AVNRT. An EP study was done to study the tachycar-dia.
Methods: N/A
Results: A 20 years old lady presented with 3 episodes of syncope in 2013. Her ECG showed CHB and a dual chamber PPM was done. She was symptomatically better with no episodes of syncope. However in the last one year she has been complaining of severe palpita-tions, which are triggered by exertion. However no ECG during tachycardia could be recorded. Device interrogation showed multiple high rate episodes lasting for few seconds to an hour (Figure 1). The device recorded EGM showed rate of 160-180 bpm with simultaneous atri-al (A) and ventricular (V) activation, similar to AVNRT (Figure 2). An EP study was carried out. The AV conduction wenckebached at 100 bpm while the VA was dissociated, thereby ruling out AVNRT and AVRT. However, with isoprenaline, she developed sinus tachycardia of 160-180 bpm with a prolonged PR of 300-320 ms with 1:1 AV conduction (Figure 3 & 4). This was recorded by the device as high rate epi-sodes depicting them as simultaneous A and V activation. The upper tracking rate was then increased to 160 bpm with a short PR inter-val. The patient has been asymptomatic since then.
Conclusions: Narrow QRS tachycardias with 1:1 AV conduction are rare in patients with PPM for complete heart block. Our patient had si-nus tachycardia with a very prolonged PR giving an impression of AVNRT (simultaneous A and V) on device interrogation. Beta-blockers and increasing the upper tracking rate cured the patient of her symptoms.
NARROW QRS TACHYCARDIA WITH SIMULTANEOUS ATRIAL AND VENTRICULAR ACTIVATION IN A PATIENT WITH COMPLETE HEART BLOCK (CHB) WITH PERMANENT PACEMAKER (PPM) IMPLANTATIONAmeya Udyavar
P.D. Hinduja National Hospital, Mumbai, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-166

425
Introduction: It is still not clear whether treatment of obstructive sleep apnea syndrome (OSA) has a significant impact on premature ven-tricular contractions/ventricular tachycardias (PVCs/VTs).
Methods: N/A
Results: We experienced an incessant form of PVCs/VTs originating from the left sinus of Valsalva in a 47-year-old man. He has experi-enced mild palpitations, dizziness, and syncope from 22-years old. He was also diagnosed with severe obstructive sleep apnea syndrome (apnea hypopnea index: 61.9/h; average O2 saturation during polysomnography: 74.5%). The 24h-Holter monitoring demonstrated an in-cessant form of PVCs/VTs (total PVCs 50,924 beats, 39% of the total heart beats, runs 1930). After C-PAP treatment (apnea hypopnea in-dex: 2.9/h), incidence of his incessant PVCs/VTs was significantly improved (total PVCs 16,116 beats, 14% of the total heart beats, runs 710). The electrophysiological study demonstrated a spontaneous onset of incessant PVCs/VTs without any pacing maneuvers and VT rates accelerations during an isoproterenol infusion. Isochronal mapping demonstrated the earliest activation site during PVCs/VTs at left sinus of Valsalva, and temperature-controlled RF energy (4 mm-tip non-irrigation <35W) successfully eliminated his PVCs/VTs. We con-firmed the elimination of the PVCs/VTs under a high dose isoproterenol infusion after ablation without any complications or recurrences during a follow-up period of 54 months.
Conclusions: We experienced a significant impact of OSA in a patient with an incessant form of PVCs/VTs originating from the left sinus of Valsalva.
SIGNIFICANT IMPACT OF OBSTRUCTIVE SLEEP APNEA IN A PATIENT WITH AN INCESSANT FORM OF VENTRICULAR TACHYCARDIA ORIGINATING FROM THE LEFT SINUS OF VALSALVANobumori Yagi1, Satoshi Higa2 1Division of Cardiovascular Medicine, Nakagami Hospital, Okinawa, Japan; 2Cardiac Electrophysiology and Pacing Laboratory, Division of Cardiovascular Medicine, Makiminato Central Hospital, Okinawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 2-167

SATURDAYPOSTER PRESENTATION
(15 October)

427
Introduction: Therapeutic hypothermia (TH, 30°C) increases the susceptibility to ventricular fibrillation (VF) by decreasing ventricular con-duction velocity (CV). Enhancing ventricular CV by rotigaptide, which is a gap junction enhancer, protects the hearts from VF during TH. Di-vergence is a parameter used to quantify the beat-to-beat morphological variation among a series of electrical signals. We hypothesize that divergence is a robust parameter to predict the occurrence of pacing-induced VF during TH.
Methods: Six Langendorff-perfused isolated rabbit hearts were subjected to 30-minutes TH (30°C) followed by 20-minutes treatment with rotigaptide (300 nM) to enhance CV during TH. VF inducibility test was done at TH and after rotigaptide treatment by burst ventricular pac-ing at the shortest pacing cycle length (PCL) that achieves 1:1 ventricular capture. During burst ventricular pacing to induce VF, the pseu-do-ECGs were recorded for divergence analysis.
Results: A total of 46 pseudo-ECG recordings of VF induction tests during TH were analyzed (22 were before, and 24 after rotigaptide). Rotigaptide decreased the percentage of pacing-induced VF episodes from 50% (11/22) to 16.7% (4/24) (P=0.027). The divergence was sig-nificantly higher in the pacing-induced VF episodes (0.07±0.01, n=15) than those pacing failed to induce VF (0.03±0.02, n=31) (P<0.001) after the 3rd pacing beat during TH. Rotigaptide decrease the divergence from 0.05±0.03 to 0.03±0.02 during TH (P=0.03) (see Figure).
Conclusions: Rotigaptide decreased divergence during burst pacing and prevented the hearts from VF during TH. Divergence is a robust parameter to early detect the risk of VF when patients receive anti-bradycardia pacing during TH.
ROTIGAPTIDE DECREASES THE SUSCEPTIBILITY TO VENTRICULAR FIBRILLATION BY DECREASING DIVERGENCE DURING THERAPEUTIC HYPOTHERMIAYu-Cheng Hsieh1, Wan-Hsin Hsieh2, Yenn-Jiang Lin3, Men-Tzung Lo4, Chen-Ying Hung1, Cheng-Hung Li1, Jiunn-Cherng Lin1, Ying-Chieh Liao1, Ketil Haugan5, Bjarne D. Larsen5, Shien-Fong Lin6, Tsu-Juey Wu7, Shih-Ann Chen3 1Cardiovascular Center, Taichung Veterans General Hospital and Chiayi Branch, Taichung, Taiwan; 2St. Jude Medical, Sylmar, United States;
3Division of Cardiology, Taipei Veterans General Hospital, Taipei, Taiwan; 4Research Center for Adaptive Data Analysis, Analysis and Center for Dynamical Biomarkers and Translational Medicine, National Central University, Jhongli, Taiwan; 5Zealand Pharma A/S, Glostrup and Department of Cardiology, Roskilde University Hospital, Roskilde, Denmark; 6Institute of Biomedical Engineering, National Chiao Tung University, Hsinchu, Taiwan; 7Institute of Clinical Medicine and Cardiovascular Research Center, National Yang-Ming University School of Medicine, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-001
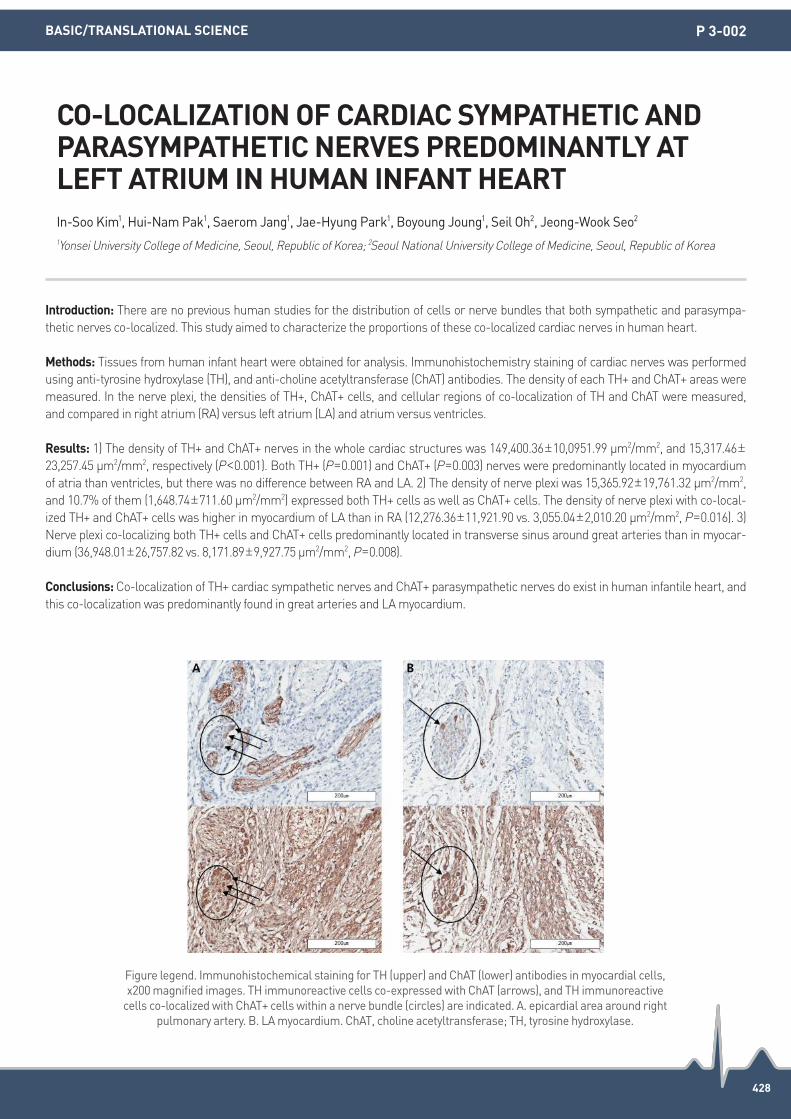
428
Introduction: There are no previous human studies for the distribution of cells or nerve bundles that both sympathetic and parasympa-thetic nerves co-localized. This study aimed to characterize the proportions of these co-localized cardiac nerves in human heart.
Methods: Tissues from human infant heart were obtained for analysis. Immunohistochemistry staining of cardiac nerves was performed using anti-tyrosine hydroxylase (TH), and anti-choline acetyltransferase (ChAT) antibodies. The density of each TH+ and ChAT+ areas were measured. In the nerve plexi, the densities of TH+, ChAT+ cells, and cellular regions of co-localization of TH and ChAT were measured, and compared in right atrium (RA) versus left atrium (LA) and atrium versus ventricles.
Results: 1) The density of TH+ and ChAT+ nerves in the whole cardiac structures was 149,400.36±10,0951.99 μm2/mm2, and 15,317.46±23,257.45 μm2/mm2, respectively (P<0.001). Both TH+ (P=0.001) and ChAT+ (P=0.003) nerves were predominantly located in myocardium of atria than ventricles, but there was no difference between RA and LA. 2) The density of nerve plexi was 15,365.92±19,761.32 μm2/mm2, and 10.7% of them (1,648.74±711.60 μm2/mm2) expressed both TH+ cells as well as ChAT+ cells. The density of nerve plexi with co-local-ized TH+ and ChAT+ cells was higher in myocardium of LA than in RA (12,276.36±11,921.90 vs. 3,055.04±2,010.20 μm2/mm2, P=0.016). 3) Nerve plexi co-localizing both TH+ cells and ChAT+ cells predominantly located in transverse sinus around great arteries than in myocar-dium (36,948.01±26,757.82 vs. 8,171.89±9,927.75 μm2/mm2, P=0.008).
Conclusions: Co-localization of TH+ cardiac sympathetic nerves and ChAT+ parasympathetic nerves do exist in human infantile heart, and this co-localization was predominantly found in great arteries and LA myocardium.
CO-LOCALIZATION OF CARDIAC SYMPATHETIC AND PARASYMPATHETIC NERVES PREDOMINANTLY AT LEFT ATRIUM IN HUMAN INFANT HEARTIn-Soo Kim1, Hui-Nam Pak1, Saerom Jang1, Jae-Hyung Park1, Boyoung Joung1, Seil Oh2, Jeong-Wook Seo2 1Yonsei University College of Medicine, Seoul, Republic of Korea; 2Seoul National University College of Medicine, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 3-002
Figure legend. Immunohistochemical staining for TH (upper) and ChAT (lower) antibodies in myocardial cells, x200 magnified images. TH immunoreactive cells co-expressed with ChAT (arrows), and TH immunoreactive
cells co-localized with ChAT+ cells within a nerve bundle (circles) are indicated. A. epicardial area around right pulmonary artery. B. LA myocardium. ChAT, choline acetyltransferase; TH, tyrosine hydroxylase.

429
Introduction: Ventricular fibrillation (VF) is the main cause of out-of-hospital cardiac arrest (OHCA). In survivors of OHCA, therapeutic hy-pothermia (TH) retards hypoxic injury of the central nervous system. However, TH using severe hypothermia (SH, 30°C) might decrease ventricular conduction velocity (CV) and facilitated spatial CV heterogeneity, leading to the increased susceptibility of ventricular arrhyth-mias. Rotigaptide is a gap junction enhancer, which might increase ventricular CV during TH. Whether rotigaptide also abolishes spatial CV heterogeneity and decreases VF vulnerability remains unclear. We hypothesize that rotigaptide can increase ventricular CV and de-crease CV heterogeneity, and decrease the susceptibility to pacing-induced ventricular fibrillation (PIVF) during TH at SH and moderate hypothermia (MH, 33°C).
Methods: Langendorff-perfused isolated rabbit hearts were subjected to 30-minutes MH followed by 20-minutes treatment with rotigap-tide (300 nM, n=8) or vehicle (n=5). The same protocol was also performed at SH (n=8 for rotigaptide, n=5 for vehicle). With an optical mapping system, epicardial CV was evaluated by S1 pacing. VF inducibility was tested by burst pacing for 30 s at the shortest pacing cycle length (PCL) that achieved 1:1 ventricular capture.
Results: Rotigaptide increased ventricular CV during MH (PCL 300 ms, from 76±6 cm/s to 84±7 cm/s, P=0.039) and SH (PCL 300 ms, from 62±6 cm/s to 68±4 cm/s, P=0.008). The spatial heterogeneities of CV among anterior/posterior (A/P) aspects of both ventricles (RV/LV) were significantly increased during MH (14±7, 18±7, 14±4, and 28±8 cm/s, for RVA, RVP, LVA, and LVP, respectively, P<0.01) and SH (11±5, 25±4, 10±2, 29±8 cm/s, for 4 sites, respectively, P<0.01). Treatment with rotigaptide abolished these heterogeneities during MH (14±8, 18±7, 15±6, 21±8 cm/s, for 4 sites, respectively, P=0.21) and SH (13±6, 17±6, 12±4, 17±4 cm/s, for 4 sites, respectively, P=0.126). PIVF inducibility was decreased by rotigaptide at MH (P=0.039) and SH (P=0.042).
Conclusions: In addition to improve ventricular CV, rotigaptide protects the hearts against ventricular arrhythmias by facilitating conduc-tion homogeneity during TH. Enhancing cell-to-cell coupling by rotigaptide might be a novel approach to prevent ventricular arrhythmias during TH.
ROTIGAPTIDE DECREASES THE INDUCIBILITY OF VENTRICULAR FIBRILLATION BY REDUCING SPATIAL CONDUCTION VELOCITY HETEROGENEITY DURING THERAPEUTIC HYPOTHERMIA IN ISOLATED RABBIT HEARTSJiunncherng Lin1, Yu-Chieh Hsieh1, Ying-Chieh Liao2, Cheng-Hung Li3, Chen-Ying Hung2, Tsu-Juey Wu3 1Chiayi branch, Taichung Veterans General Hospital and National Yang-Ming University School of Medicine, Chiayi and Taipei, Taiwan;
2Taichung Veterans General Hospital, Taichung, Taiwan; 3Taichung Veterans General Hospital and National Yang-Ming University School of Medicine, Taichung and Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-003

430
Introduction: Ischemic heart disease is the leading cause of death worldwide. Contemporary research has identified delivery of mesen-chymal stem cells (MSC) to the heart as a possible therapy. Microvesicles (MVs) contain bioactive molecules critical to intracellular signal-ing and have cardioprotective effects in ischemia/reperfusion (IR) injury hearts. Whether MVs derived from hypoxia preconditioned human MSCs are effective in other species has not been evaluated. This study investigated the cardioprotective utility of human-derived MVs in mouse, rat, and rabbit IR injury hearts and studied the principal mechanism by determining the expression levels of connexin 43 (Cx43).
Methods: MVs were isolated from hypoxia-preconditioned human MSCs. Mouse, rat, and rabbit IR injury models were treated with MV solution (0.4 μg/μL) via leg vein. Langendorff perfusion and dual optical mapping were performed on IR model hearts to analyze action potential duration (APD), to produce activation maps, and to test for VF vulnerability. The intracellular calcium dynamic was measured in mouse HL-1 cells and neonatal rat and adult rat cardiomyocytes treated with MVs after hypoxic injury. The impact of MV injection on the Wnt signaling pathway activation and Cx43 expression were analyzed by western blot.
Results: Detection of PKH26 staining in IR+MV hearts confirmed successful MV delivery. The MV treatment significantly improved electri-cal conduction, diminished infarct size (24±2 vs. 8±1%, P<0.001), and reduced arrhythmias in all three animal models. In murine models, Ca2+ wave frequency and amplitude were increased in hypoxia/reoxygenation (HR) cells and reduced in HR+MV cells. MV treatment pre-vented Ca2+ overloading typically induced by HR injury in mouse HL-1 cells and rat and rabbit cardiomyocytes. In rat tissue analyzed by western blot, IR injury reduced Wnt1, β-catenin, and Cx43 expression. However, MV injection boosted Wnt1, β-catenin, and Cx43 levels while downregulating GSK 3β (P<0.05).
Conclusions: Human-derived MVs universally improved electrical conduction, diminished the infract size, and reduced the incidence of arrhythmias in three mammalian IR injury models via activation of the Wnt signaling pathway and upregulation of Cx43. These results suggest that hypoxia-preconditioned human MSCs might be used as a therapeutic tool in case of IR injury.
MITIGATING ISCHEMIA/REPERFUSION INJURY: MICROVESICLES DERIVED FROM HYPOXIC HUMAN MESENCHYMAL STEM CELLS IMPROVE ELECTRICAL CONDUCTION IN MOUSE, RAT, AND RABBIT MODELSHyewon Park1, Hyelim Park1, Hyo-Eun Kim1, Seung-Hyun Lee1, Michael Kim2, Shanyu Cui1, Dasom Mun1, Hui-Nam Pak1, Moon-Hyoung Lee1, Boyoung Joung1 1Yonsei University College of Medicine, Seoul, Republic of Korea; 2Duke University, Durham, United States
BASIC/TRANSLATIONAL SCIENCE P 3-004

431
Introduction: Transmural dispersion and increased variability of repolarization are associated with ventricular arrhythmias (VAs). Left ventricular (LV) transmural repolarization gradient has been demonstrated in animal models with a longer endocardial action potential duration (APD) compared to the epicardial. Such gradient has not been demonstrated in vivo in humans. We aimed to record in vivo endo-cardial and epicardial QT intervals in patients undergoing a percutaneous left-sided atrial ablation procedure.
Methods: A total of 12 patients (7 men, mean age 56.4±18.9 years-old) were enrolled in the study. All patients underwent an ablation pro-cedure (8 atrial fibrillation, 4 atrio-ventricular reentrant tachycardia). Data were obtained using a standard electrophysiology recording system. Endocardial and epicardial LV electrograms (EGMs) were recorded using a standard bipolar ablation catheter. LV endocardial EGMs were obtained by the ablation catheter positioned at the posterior-lateral basal LV; LV epicardial EGMs of the same segment were obtained by the ablation catheter positioned in the left inferior pulmonary vein.
Results: Mean EF was 58.4±18.9%. Mean LV dimensions were: VTD 96.1±7.7 mL, DTD 49.8±4.6 mm, PWD 9.7±1.9 mm, IVSD 10.3±2. 1 mm. Mean ECG intervals were: RR 752.8±247.7 ms, QRS 98.3±27.8 ms, QTc 438.4±36.9 ms. Unlike the animal setting, the epicardial QT interval was longer (309.7±38.1 ms), and the endocardial QT interval was shorter (231.8±42.6 ms), with a LV repolarization gradient of 77.8±37.0 ms. Significant relationships between QTc and repolarization gradient (r=0.032, 95% CI -0.01-0.086, P<0.05) and between en-docardial QT and repolarization gradient (r=0.3, 95% CI -0.85-0.04, P<0.05) were present.
Conclusions: A LV transmural repolarization gradient has been demonstrated also in humans, however, unlike animal models, the epi-cardial APD was longer compared to the endocardial APD. LV transmural repolarization gradient relates to QTc. Analysis of the transmu-ral ventricular repolarization gradient variability could be helpful in finding new markers of VAs and in stratifying the risk for sudden cardi-ac death regardless of EF.
LEFT VENTRICULAR TRANSMURAL REPOLARIZATION GRADIENT IN HUMANSBich Lien Nguyen, Loredana Iannetta, Alessandro Persi, Gianfranco Piccirillo, Ilaria Maraschi, Nicola Alessandri, Elisa Rauseo, Eleonora Indolfi, Carlo Gaudio, Paolo Emilio Puddu
Sapienza University of Rome, Rome, Italy
BASIC/TRANSLATIONAL SCIENCE P 3-005

432
Introduction: Heart failure (HF) causes atrial remodeling and increases the incidence of atrial fibrillation (AF). Renal denervation (RDN) has been shown to decrease the development of AF. The aim of the study was to identify the effects of RDN on the atrial arrhythmogenic substrates in the HF.
Methods: Rabbits were classified into four groups: control (n=9), RDN (n=10), HF (n=6) and HF-RDN (n=9). Surgical and chemical RDN was approached through bilateral retroperitoneal flank incisions in RDN and HF-RDN. Rapid ventricular pacing of 400 bpm for 4 weeks was applied in the HF and HF-RDN. After 4 weeks, the rabbits were sacrificed and the atrial myocardium were obtained for immunoblot study for ionic channel protein and Trichrome staining for fibrosis evaluation.
Results: The left atrial effective refractory period (ERP) of HF (95.8±4.8 msec) was significantly longer compared with that of control (65.2±4.0 msec, P<0.05) and RDN (78.0±6.0 msec, P<0.05), but there was no difference in left atrial ERP between HF and HF-RDN (90.5±3.2 msec). Ionic channel protein expressions of CaV1.2, NaV1.5, Kir2.1, SERCA2 and NCX were similar among 4 groups. The degree of left atrial fibrosis was extensive in HF (17.8±2.8%), when compared to that of control (6.4±1.4%, P<0.01), RDN (9.4±0.4%, P<0.05) and HF-RDN (8.3±1.4%, P<0.05), respectively.
Conclusions: The left atrial ERP prolongation of HF and HF-RDN are noted compared with that of control and RDN. There are no differ-ences ionic channel protein expressions in atria among all groups. The degree of atrial fibrosis is severe in HF, but not in HF-RDN, sug-gesting that RDN might regulate the atrial arrhythmogenic substrates in HF mostly through reverse structural remodeling.
RENAL DENERVATION REGULATES THE ATRIAL ARRHYTHMOGENIC SUBSTRATES THROUGH REVERSE STRUCTURAL REMODELING IN HEART FAILURE RABBIT MODELLing-Hui Chiang, Yamada Shinya, Li-Wei Lo, Shih-Huei Liu, Yu-Hui Chou, Wei-Lun Lin, Tsung-Ying Tsai, Wen-Han Cheng, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-006

433
Introduction: Despite its dramatic effects of blood pressure reduction in early trials, the utility of catheter based radiofrequency ablation of renal sympathetic nerves has not been firmly established in patients with resistant hypertension. There might still be a role for renal denervation, which needs refined treatment strategy with detailed technical and anatomical considerations. We sought to investigate the detailed anatomic conformation of peri-renal arterial sympathetic nerve fibers with living human specimens.
Methods: Peri-renal arterial tissues were harvested from subjects undergoing elective radical nephrectomy. Each artery with surround-ing soft tissue was fixed under physiologic pressure with formalin, and sectioned at 2 mm intervals from the distal bifurcation. To obtain accurate sympathetic nerve contour, digital images of each section were obtained after immunohistochemical staining with anti-tyrosine hydroxylase antibodies. The number and individual size of nerve fibers, distance of each nerve fibers from the luminal surface of renal ar-teries were measured.
Results: A total of 2,431 nerve fibers were identified from 45 sections of peri-renal arterial tissue of 15 patients (mean age 59±9 years, male 53%). The mean number of nerve fibers per section was 20.1±12.4 (6 mm proximal to the bifurcation), 19.6±12.5 (4 mm proximal), 18.5±12.0 (2 mm proximal), and 23.0±15.3 (at bifurcation). The median diameter of nerve fiber was 61 μm (range 11-629 μm). The median distance from the arterial lumen to the nerve fibers was 1.50 mm (range 0.33-11.39 mm), and mean distance per section was 2.12±1.69 mm (6 mm proximal), 2.03±1.51 mm (4 mm proximal), 1.94±1.57 mm (2 mm proximal), and 2.00±1.41 mm (at bifurcation), respectively. There was no significant trend in the number or distance of nerve fibers among the segments according to their proximity to aorta.
Conclusions: The distribution of renal nerve around renal artery was diverse in human living tissue. Correct understanding of anatomic conformation of peri-renal arterial sympathetic nerve fibers is essential for device development and technical refinement of renal dener-vation procedure.
ANATOMIC CONFORMATION OF RENAL SYMPATHETIC NERVE FIBERS IN LIVING HUMAN SPECIMENSWon-Seok Choe1, Eue-Keun Choi1, So-Ryoung Lee1, Myung-Jin Cha1, Chang Wook Jeong2, Seil Oh1 1Division of Cardiology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 2Department of Urology, Seoul National University Hospital, Seoul, Republic of Korea
BASIC/TRANSLATIONAL SCIENCE P 3-007

434
Introduction: Excess weight gain and obesity have been linked with increased prevalence for arrhythmia and sudden death. We aimed to study the electrophysiological characteristics, ventricular remodelings and arrrhythmogenecity in rabbits fed with high fat diet (HFD).
Methods: Twelve rabbits, randomized to control and HFD groups. After feeding for 3 months, all rabbits received electrophysiologic study and VT/VF inducibility test (Max output with shortest 1:1 cycle length pacing) with a high-density contact multielectrode plaque mapping after induction of sustained VT/VF. Ventricular myocardium was harvested for Western blot and Trichrome stain.
Results: Body weight was higher in HFD group compared to control group (3.84±0.11 vs. 2.35±0.04 kg, P<0.001). In HFD group, the ven-tricular effective refractory periods were longer in LV (188±17 vs. 152±11 ms, P<0.05) and RV (174±16 vs. 148±3 msec, P<0.05), the VF inducibility was higher (61±11 vs. 13±2%, P<0.01), when compared to those in control group, respectively. The dominant frequency (DF) during VF was similar between 2 groups. Western blot study of ventricular calcium channel protein expressions revealed increased CaV 1.2, NCX and SERCA 2 proteins in HFD group, compared to control group, respectively (Figure A). Advanced fibrosis was noted in HFD group, but not control group (Figure B and C).
Conclusions: Obesity causes ventricular remodeling with up-regulated calcium handling proteins and advances fibrosis, leading to in-creased ventricular arrhythmogenecity and risk of sudden cardiac death.
OBESITY CAUSES VENTRICULAR IONIC AND STRUCTURAL REMODELING AND INCREASES ARRHYTHMOGENECITY IN RABBIT MODELYu-Hui Chou, Li-Wei Lo, Wei-Lun Lin, Shih-Lin Chang, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-008

435
Introduction: Atrial fibrillation (AF) is the most common arrhythmia in a clinical practice, however, the optimal treatment for keeping si-nus rhythm remains elusive. This difficulty lead us to develop a novel therapeutic approach for AF targeting to the atrial specific modifica-tion by adeno-associated viral gene transfer of connexin proteins.
Methods: Ten rats were randomized into 2 groups, control and connexin (Cx) 43 gene delivered rats. Animals underwent open chest sur-gery that included electrophysiological study, atrial gene painting and transverse aortic banding. In gene delivered group, we painted Cx43 encoding adeno-associated virus serotype1 onto the rat atria from the epicardium surface. Two months later, rats underwent terminal electrophysiological study.
Results: We found that conduction time from sinus node to left atrial appendage was significantly shortened in Cx43 delivered rats com-pared to control rats (68.2±2.1 msec vs. 91.4±5.3 msec, P<0.05). The number of rats with inducible AF was significantly less in the Cx43 groups compared to control rats (20% vs. 80%). However, there was no difference between gene delivered and control rats for atrial re-fractory periods (50.6±4.8 msec vs. 50.3±2.4 msec, P=NS) and monophasic action potential durations (56.0±3.2 msec vs. 58.0±4.7 msec, P=NS). We also observed that the expression of Cx43 in intercalated disk of atrial cardiomyocytes was significantly increased in gene de-livered rats (1.41±0.23 AU, P<0.05).
Conclusions: Gene therapy of Cx43 preserved atrial conduction time and prevented AF for a long-term period.
LONG-TERM GENE EXPRESSION OF CONNEXIN43 PRESERVED CONDUCTION TIME AND PREVENTED ATRIAL FIBRILLATION IN RATSTomonori Igarashi1, Yasushi Oginosawa1, Ritsuko Kohno1, Susumu Ueno1, J. Kevin Donahue2 1University of Occupational and Environmental Health, Kitakyushu, Japan; 2University of Massachusetts Medical School, Worcester, United States
BASIC/TRANSLATIONAL SCIENCE P 3-009

436
Introduction: Myocardial infarction (MI) is a common cardiovascular disease. Autonomic imbalance with increased sympathetic and de-creased parasympathetic activities is observed in patients after MI.
Methods: Wireless transmission of polysomnographic recording was performed in sham and left coronary artery (LCA) ligation male rats during normal daytime sleep with and without atenolol treatment. Spectral analyses of the electroencephalogram (EEG) and electromyo-gram (EMG) were evaluated to define active waking (AW), quiet and paradoxical sleeps (QS, PS). Cardiac autonomic activities were mea-sured by analyzing the power spectrum of heart rate variability (HRV). EEG, EMG and HRV were recorded 24 hours for consecutive 3 days in all groups (see Fig.).
Results: In LCA ligation group, there were higher LF and LF/HF ratio on QS phase, but not AW and PS phases, compared to atenolol treated sham and LCA ligation group, respectively (Figure A, B). The HF component was not significantly change on all groups in both sleep and awake phases (Figure C). Sleep interruption was more frequent in LCA ligation rats compared to sham, and it was not found in LCA ligation with atenolol treatment group (Figure E). Increased PS time was noted in LCA ligation group, compared to sham and it was restored to baseline in LCA ligation with atenolol treatment group (Figure F).
Conclusions: Our results demonstrate significant sleep fragmentation with sympathetic hyperactivity during QS stages after MI, and atenolol could restore the autonomic dysfunction and sleep disturbance. The finding explains the cause of sleep-related fetal arrhythmia and sudden cardiac death after MI.
FRAGMENTATION AND PROLONGATION OF PARADOXICAL SLEEP PHASE WITH SYMPATHETIC HYPERACTIVITY IN LEFT CORONARY ARTERY LIGATION RATS FACILITATES FETAL ARRHYTHMIA AND SUDDEN DEATH AFTER MYOCARDIAL INFARCTIONWei-Lun Lin1, Li-Wei Lo1, Chun-Ting Lai2, Terry B.J. Kuo2, Shih-Ann Chen1 1Taipei Veterans General Hospital, Taipei, Taiwan; 2National Yang-Ming University, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-010

437
Introduction: The strong relationship between sympathetic nerve and afferent nerve following Myocardial Infarction (MI). It is known that MI induce Stellate Ganglion (SG) and Doral Root Ganglion (DRG) remodeling from our study. The aim of our study is to investigate the re-lationship sympathetic and afferent nerve remodeling in MI model and to evaluate the effect of activation recovery interval (ARI) dispersion or these neuro remodeling for the inducibility of ventricular arrhythmia.
Methods: The total of 15 myocardial infarction pigs were studied. The MI is induced by LAD occlusion. Six weeks after MI creation, we per-formed electrophysiological studies for measuring ARI by using sock type electrode that was put on whole heart and for evaluating ven-tricular arrhythmia inducibility by programmed ventricular stimulation in EP lab, and then two extracardiac cardiac ganglionated plexus-es, SG and DRG were collected after dissection, and nerve area and density were also quantified to evaluate morphological and neuro-chemical changes.
Results: Ventricular arrhythmia (VA) was induced in 8 pigs by extrastimuli pacing study, we divided two group; VA group (n=8) and non-VA group (n=7). No significant differences in ARI and ARI dispersion were present between these two groups, and there was no significant difference in the number of neurons counted in two groups. In the SG and DRG of VA group, neuronal size was increased compared to non-VA group (517.0±69 μm2 vs. 454.8±31 μm2, P<0.05; for SG, and 1,743.7±303 μm2 vs. 1,432.3±208 μm2, P<0.05 for DRG, respectively), but increased expression of alcitonin-gene related peptide (CGRP), a marker of sensory afferent, was not difference in two groups (2.49±1.2% vs. 1.81±1.0%, P=NS for SG, and 45.9±13% vs. 36.4±12%, P=NS; for DRG, respectively).
Conclusions: There is an association between ventricular arrhythmia inducibility and the enlargement in neurons within the SG and DRG in MI model. These findings suggest that abnormally cardiac afferent and efferent signaling post MI may be in part responsible for the oc-currence of ventricular arrhythmia and sudden cardiac death post MI.
THE IMPACT OF NEURAL REMODELING FOLLOWING MYOCARDIAL INFARCTION ON INDUCIBILITY OF VENTRICULAR ARRHYTHMIA IN PORCINE MODEL Keijiro Nakamura, Olujimi Ajijola, Marmar Vaseghi, Jeffrey Ardell, Kalyanam Shivkumar
UCLA Cardiac Arrhythmia Center, Los Angeles, United States
BASIC/TRANSLATIONAL SCIENCE P 3-011

438
Introduction: The impact of myocardial infarction (MI) on neuronal nitric oxide synthase (nNOS), an important mediator of cardiac neuro-transmission is poorly understood.
Methods: Yorkshire pigs (n=10) underwent anterior MI by LAD occlusion. After 6-8 weeks, bilateral stellate ganglia (SG), T1 dorsal root ganglia (DRG), right atrial (RAGP) and ventral inter-ventricular ganglionated plexi (VIVGP) were extracted, formalin-fixed, paraffin-embed-ded, and sectioned. Immno-staining for nNOS was performed on representative slides through the middle of the ganglia, and for calci-tonin-gene related peptide (CGRP), a marker of sensory afferent neurons. The percentage of immunoreactive (IR) neurons was quantified.
Results: An average of 63.1±40.7, 169.7±55.5, and 448.1±204.5 neurons were counted in the GPs, DRG, and SG respectively. There was no significant difference in the number of neurons counted in controls vs. MIs. In the GPs, nNOS was differentially altered by MI, with sig-nificant upregulation in VIVGP but not RAGP of MI (13.8±2.8% vs. 46.6±5.3%, P<0.001; and 12.1±3.6% vs. 12.5±2.9%, P=NS, respectively) compared to control animals. In the DRG, IR of both CGRP and nNOS was increased (36.3±6.2% vs. 65.3±4.8%, P<0,001 for nNOS; and 64.1±6.2% vs. 85.2±5.6%, P<0.001 for CGRP), with increased co-expression of both CGRP and nNOS in approximately 20% of DRG neu-rons. In the SG, the number of neurons demonstrating strong IR for nNOS was approximately 0.4% in control animals. After MI, this in-creased 8-fold to 3.12% (P<0.01).
Conclusions: nNOS expression is upregulated differentially following MI in the GPs, with increased expression in the ventricular GP inner-vating the region of MI, but not in the RAGP. Both cardiac sympathetic afferent (DRG) neurons, and efferent (SG) neurons increase expres-sion of nNOS following MI. The impact of nNOS in these different sites warrants further investigation.
NEURONAL ISOFORM OF NITRIC OXIDE SYNTHASE IS UPREGULATED IN CARDIAC INTRINSIC AND EXTRINSIC SYMPATHETIC AFFERENT AND EFFERENT GANGLIA FOLLOWING MYOCARDIAL INFARCTIONKeijiro Nakamura, Olujimi Ajijola, Marmar Vaseghi, Jeffrey Ardell, Kalyanam Shivkumar
UCLA Cardiac Arrhythmia Center, Los Angeles, United States
BASIC/TRANSLATIONAL SCIENCE P 3-012

439
Introduction: Patients with rheumatoid arthritis (RA) are twice likely to experience sudden cardiac death than general population. The ob-jective of this study was to find the mechanism of arrhythmia caused by rheumatoid arthritis and the role of sympathetic nerve activity in the RA.
Methods: Arthritis was induced in Lewis rats by intradermal injection of emulsion of type II collagen at days 0 and 7. Single lead electro-cardiogram (ECG) recordings were made weekly in CIA rats and controls. We assessed the autonomic activity by heart rate variability (HRV), the intrinsic heart rate (IHR) and direct sympathetic nerve measurement in a rat collagen-induce arthritis (CIA) model.
Results: Rats were divided into 3 groups, normal rats (CON; n=3), collagen-induced arthritis (CIA; n=3) and collagen-induced arthritis treated with propranolol (CIA-PRO; n=3). At the beginning of inflammation reflex, LF/HF of CIA group was significant higher than controls (1st week: 2.41±0.7 vs. 1.76±0.6, P<0.05; 2nd week: 2.24±0.5 vs. 1.58±0.5, P<0.05). The deceleration capacity appeared progressive low-er and acceleration capacity value was increasing despite of no significant increase of the LF/HF compared with controls since 4th week. The sensitivity of the sympathetic tone was higher in CIA than CON. The propranolol was effective to alleviate the sympathetic over-activa-tion. The action potential durations (APDs) and the conduction velocity (CV) were not significantly difference in this three groups, but the maximal slope of CIA (slope=1.01±0.3) was higher than CON (slope=0.43±0.1). Unexpectedly, after treated with propranolol, the maximal slope of CIA-PRO (slope=0.46±0.1) was much lower than CIA.
Conclusions: The maximal slopes of APD restitution of CIA was higher than CON and CIA-PRO. Propranolol was effective to flatten the APD restitution which is close to CON. Compared with CON, arrhythmias was easily induced in CIA rats, but reduced the chance of ar-rhythmias was observed after treated with propranolol. In conclusion, the arrhythmia caused by RA is less associated with the regulation of ion channel in heart, and the sympathetic plays a major role causing arrhythmogenesis in RA.
AUTONOMIC MECHANISM OF ARRHYTHMOGENESIS IN RHEUMATOID ARTHRITIS RATSYen-Ling Sung1, Ting-Tse Lin2, Chi-En Wu1, Yen-Bin Liu2, Shien-Fong Lin1 1National Chiao-Tung University, Hsinchu, Taiwan; 2National Taiwan University Hospital, Hsinchu Branch, Hsinchu, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-013

440
Introduction: The right ventricular outflow tract (RVOT) related ventricular arrhythmia has gained much attention in recent years. The electrophysiological characteristics in the RVOT have not been well characterized.
Methods: Eight dogs, aged 1 to 2 years, were used as study animals. We harvested the RVOT with right coronary artery pedicle for Lang-erdoff perfusion. High-resolution dual-voltage and calcium optical mapping were then performed to record action potentials and calcium transients in both epicardium and endocardium.
Results: The action potential duration (APD) was similar between RVOT endocardium and epicardium. The maximal APD restitution slope was also similar between endocardium and epicardium (1.23±0.12 vs. 1.11±0.17). The onset pacing cycle length (PCL) of temporal APD alternans (ALT) was also similar between RVOT endocardium and epicardium (352±22.7 ms vs. 380±14.1 ms). However, the magnitude of APD-ALT was larger in the epicardium than the endocardium, and a repolarization gradient between epicardium and endocardium was noted at shorter PCLs. A biphasic phenomenon of the relationship between APD-ALT and PCLs with contradictory decreased APD-ALT at shorter PCL was noted in both epicardium and endocardium. The onset PCL of calcium transient alternans was also similar between RVOT endocardium and epicardium (322.5.7±13.3 ms vs. 310±5.8 ms). However, the occurrences of APD-ALT and Ca-ALT were not close-ly coupled.
Conclusions: The RVOT cardiomyocytes have unique electrophysiological features including biphasic phenomenon in the relationship be-tween PCL and APD-ALT magnitude, phase 1 alternans and uncoupling of APD-ALT and Ca-ALT. Normal RVOT may already be suscepti-ble to re-entrant arrhythmia at higher heart rates because of a repolarization gradient between epicardium and endocardium and large APD-ALT magnitude in epicardium.
DISTINCT ELECTROPHYSIOLOGICAL CHARACTERISTICS OF RIGHT VENTRICULAR OUTFLOW TRACT-A CANINE MODEL STUDYWei-Chieh Tseng, Shuenn-Nan Chiu, Lian-Yu Lin, Mei-Hwan Wu, Shu-Chien Huang, Yih-Sharng Chen, Jou-Kou Wang, Ling-Ping Lai, Jiunn-Lee Lin, Chia-Ti Tsai
National Taiwan University Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-014

441
Introduction: The aged spontaneously hypertensive rat (SHR) model is recognized for human cardiovascular pathology and is a high risk group for sudden cardiac death caused by ventricular arrhythmia. The autonomic nervous system plays an important role in blood pres-sure regulation and in the development of hypertension. We hypothesized that the susceptibility to aged and hypertension-induced ven-tricular tachycardia (VT) and ventricular fibrillation (VF) is improved by exercise.
Methods: 80 weeks old SHR were randomly divided into two groups, the aged hypertension rats (HPT) and aged hypertension rats living with exercise wheel (HPT-EW). Hypertension was spontaneous in Wistar Kyoto (WKY) Rat, on wheel for 8 weeks. Single-lead electrocar-diogram (ECG) was recorded. We measured heart rate variability (HRV) parameters, heart rate deceleration capacity (DC), acceleration capacity (AC), in vivo VF inducibility in hypertensive rat model. Optical mapping was also performed in isolated hearts. Action potential du-ration (APD) was measured at 70% repolarization (APD70), APD70 and conduction velocity (CV) were measured by high-resolution optical mapping in ventricular anterior wall. Linear and non-linear HRV were analyzed.
Results: Compared to HPT, the incidence of VT and VF were decreased in HPT-EW (VT: 15.18±21.47 ms vs. 5.26±4.85 ms, VF: 62.95±69.68 ms vs. 3.63±3.83 ms), APD70 were shortened in HPT-EW (P<0.05, at pacing cycle length [PCL] 200 ms), unexpectedly, CVs are de-creased in HPT-EW (P<0.05, at PCL 120, 140, 180, 200 and 250 ms). The maximal of APD restitution curve slope of HPT-EW (slope=0.14) was more flatten than HPT (slope=2.31). In the non-linear HRV parameters, the AC and LF of HPT-EW was significantly lower than HPT (-8.6±0.2 vs. -7.0±0.3, P<0.05; 39.1±5.0 vs. 69.5±8.0, P<0.05); the DC and HF of HPT-EW was significantly higher than HPT (9.6±0.4 vs. 8.1±0.0, P<0.05; 60.4±4.9 vs. 30.5±8.0, P<0.05).
Conclusions: These results indicated that exercise shorten APD and flatten the APD restitution can alleviate the incidence of VF and pre-vent degeneration of VT into a fibrillation-like state in aged hypertension rats. Although CVs are decreased in HPT-EW, the CV heteroge-neity of HPT is high. This issue needs to be explored further. In summary, exercise is beneficial to prevent severe arrhythmia in aged spon-taneously hypertensive rat model.
EFFECTS OF EXERCISE ON ARRHYTHMOGENESIS IN SPONTANEOUSLY HYPERTENSION RAT MODELChih-En Wu1, Yen-Ling Sung1, Bo-Jau Kuo2, Jai-Yi Li2, shin-Ann Chen3, Yu-Feng Hu3, Chieh-Wen Chen2, Ching-Hui Weng3, Wen-shiuan Shia3, Wei-hsuan Hsu3, Shien-Fong Lin1 1National Chiao-Tung University, Hsinchu, Taiwan; 2National Yang-Ming University, Taipei, Taiwan; 3Taipei Veteran General Hospital, Taipei, Taiwan
BASIC/TRANSLATIONAL SCIENCE P 3-015
442
Introduction: Nurses play an important role of measuring vital signs including pulse palpation in clinical practice or epidemiologic study. The poor pulmonary function is associated with cardiac arrhythmia. Pulse palpation is useful screening method for early detection of car-diac arrhythmia. This study is to investigate the correlation between poor pulmonary function and irregular pulse.
Methods: Data was from a representative sample of commUniversity-dwelling South Koreans using the fifth Korean National Health and Nutrition Examination Survey. We analyzed 2,347 subjects ≥65 years who completed the health examination survey and performed spi-rometry. Pulse palpation was initially performed for 15 seconds and again for 60 seconds to confirm the findings.
Results: We identified 474 (20.2%) subjects with predicted forced vital capacity (FVCp) <80%, and 669 (28.5%) subjects had a 1-second forced expiratory volume/forced vital capacity ratio (FEV1/FVC) <0.7. The prevalence of irregular pulse was 2.6%. After adjustment for tra-ditional cardiovascular risk factors, FVC P<80% remained a significant risk factor for irregular pulse (adjusted OR=2.477, 95% CI 1.223-5.016, P=0.012). FEV1 was inversely associated with the incidence rate of irregular pulse (adjusted OR=5.504, 95% CI 1.431-21.174, P=0.013). A restrictive or obstructive pulmonary pattern was a risk factor for irregular pulse (adjusted OR=2.123, 95% CI 1.012-4.455, P=0.047).
Conclusions: This study demonstrated that the pulmonary function influence irregular pulse on routine palpation. It implies how import-ant taking a careful and exact measurement of pulse palpation by nurses in subjects with reduced pulmonary function for screening of arrhythmia.
PULSE PALPATION ON SUBJECTS WITH POOR PULMONARY FUNCTION FOR SCREENING OF CARDIAC ARRHYTHMIASun Hwa Kim1, Jinho Shin1, Seon Young Hwang2, Jin Kyu Park1 1Hanyang University Medical Center, Seoul, Republic of Korea; 2College of Nursing, Hanyang University, Seoul, Republic of Korea
ALLIED PROFESSIONALS P 3-016

443
Introduction: Spontaneous echo-contrast (SEC) on transesophageal echocardiography (TEE) is known to be a surrogate marker for the risk of ischemic stroke in patients with atrial fibrillation (AF) or atrial flutter (AFL). The efficacy of non-vitamin K antagonist anticoagulants (NOAC) to prevent SEC as compared to warfarin in patients with AF or AFL is not known.
Methods: We included AF or AFL patients who underwent cardioversion and pre-cardioversion TEE evaluation based on our cardioversion registry. We compared the incidence of SEC between patients who received NOAC and those who took warfarin. The NOAC included direct thrombin inhibitor and factor Xa inhibitors.
Results: Of the 918 patients who were considered to undergo cardioversion, 345 patients prescribed with anticoagulants and underwent TEE before cardioversion for AF or AFL were included (155 NOAC user vs. 190 warfarin users). Fifteen patients were deferred due to thrombus in left atrium (LA) or left atrial appendage (LAA) observed in TEE. The incidence of SEC in patients taking NOAC showed a nu-merically lower percentage compared to those who received warfarin, but there was no statistical significance (40.6% vs. 47.4; P=0.211; Figure 1). Compared to warfarin users, patients taking NOAC had no significant difference in the incidence of moderate to severe SEC (12.9% vs. 14.7%; P=0.624; Figure 2) and overt thrombus (3.9% vs. 4.2%; P=0.874).
Conclusions: This study demonstrated that NOAC have a similar efficacy compared to warfarin in preventing SEC and LA and LAA throm-bus in patients with AF or AFL undergoing cardioversion.
NON-VIT K ANTAGONIST ANTICOAGULANTS VERSUS WARFARIN FOR THE INCIDENCE OF SPONTANEOUS ECHO-CONTRAST IN PATIENTS WITH ATRIAL FIBRILLATIONYun Gi Kim, Jong-Il Choi, Mi-Na Kim, Dong-Hyuk Cho, Suk-Kyu Oh, Hyungdon Kook, Hee-Soon Park, Kwang No Lee, Yong-Soo Baek, Seung-Young Roh, Jaemin Shim, Seong-Mi Park, Wan Joo Shim, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
ALLIED PROFESSIONALS P 3-017

444
Introduction: The long QT syndrome is a disorder of ventricular myocardial repolarization characterized by a prolonged QT interval on the electrocardiogram that can lead to symptomatic ventricular arrhythmias and can lead to an increased risk of sudden cardiac death.
Methods: N/A
Results: A 24 year-old woman admitted to emergency room with chief compliant of syncope and seizure. Three days before admitted, pa-tient had two episodes of syncope and general seizure. The patient was taken to other Hospital and diagnosed as refracter VT. She had no risk factors for coronary artery disease, but her sister was suffered from sudden cardiac death in young age. The patient was referred to our Hospital for further management. In our emergency department, she was intubated with GCS E4M6V. Her vital signs and laboratory test were unremarkable. ECG show prolonged QT (QTc: 0.52 seconds). The echocardiogram showed: normal ejection fraction (56%) with-out wallmotion abnormality, TAPSE 24 mm and normal valve function. First day in ICU, her heart rate decrease around 40-50 bpm, and the ECG monitor show early after depolarization (EADs) follow by TdP, serial ECG done in the ICU did reveal a prolonged QTc. We gave MgSO4 2 mg and then temporally pacemaker was inserted with setting lower rate 80 bpm, output 5 V, threshold 3 V. The scoring result based on Schwartz score is 7 point which mean high probability to have LQTS. Based on those data, we did not perform the additional testing. We also exclude acquired LQTS such as abnormal electrolyte test, myocardial infarction, atrioventricular block or drugs induced. In this case, we did not use beta blocker, because of frequent bradycardia and as we paid attention that the development of EADs is poten-tiated by bradycardia. Therefore, we implant temporary pace maker (TPM) in order to control heart rate. After TPM implantation no epi-sode of TdP were noted. We decided to implant ICD since she has a high risk of sudden cardiac death.
Conclusions: Early diagnosis and preventive treatment are instrumental in preventing sudden cardiac death in patients with the congeni-tal LQTS. Schwartz score can be used to the diagnosis of congenital LQTS. ICD implantation can prevent sudden cardiac death caused by TdP in LQTS.
TORSADES DE POINTES IN LONG QT SYNDROME: A CASE REPORTHengky Hengky, Daniel Tanubudi, M. Yamin, Reza Octavianus, Ade Widyastuti, Stefanus Andy Wiyono, Emanoel Oepangat
Eka Hospital BSD, Jakarta, Indonesia
ALLIED PROFESSIONALS P 3-020

445
Introduction: Creation of conduction block of the lateral mitral isthmus (LMI) by the cryoballoon (CB) has never been reported.
Methods: N/A
Results: A 66-year-old female suffered from palpitations due to paroxysmal atrial fibrillation (AF). She underwent AF ablation using a second-generation CB (28 mm diameter, Arctic Front AdvanceTM, Medtronic) under 3D mapping system guidance (EnSite VelocityTM, St. Jude Medical). After selective pulmonary vein (PV) venographies was obtained, the CB was navigated with a steerable sheath (FlexCathTM, Medtronic) and multipolar circumferential mapping catheter (AchieveTM, Medtronic). First, the left superior PV (LSPV) isolation was at-tempted. After inflation, the CB was advanced to the LSPV but venography to confirm optimal PV occlusion revealed a slight leak at the roof. After a 3-minute freeze, the AchieveTM’s intracardiac electrograms exhibited no sequence change or delay. Another 3-minute freeze was applied to the LSPV without convincingly isolating the PV because the AchieveTM’s PV potentials were too small during the CB abla-tion. After pulling back the AchieveTM to the LSPV ostium, electrical stimulation from the coronary sinus (CS) was applied, and revealed an LSPV isolation as well as counter-clockwise conduction block at the LMI. When pacing was applied from the left atrial appendage (LAA), clockwise conduction block of the LMI was revealed. Retrospective analyses of the venography, fluoroscopy, and 3D mapping revealed the first LSPV freeze was delivered at the LAA ostium. Creating cryothermal lesions at the lower part of the LAA and LSPV ostia led to con-duction block at the LMI.
Conclusions: Incidental cryothermal applications by the CB at both the LAA and LSPV created complete conduction block at the LMI, for-tunately without accompanied electrical isolation of the LAA.
INADVERTENTLY ACHIEVED BIDIRECTIONAL CONDUCTION BLOCK OF THE LATERAL MITRAL ISTHMUS BY CRYOBALLOON APPLICATIONS APPLIED AT THE LEFT ATRIAL APPENDAGE AND LEFT SUPERIOR PULMONARY VEINNobuhiro Nishiyama, Seiji Takatsuki, Kazuaki Nakajima, Shin Kashimura, Akira KUniversityomi, Yoshinori Katsumata, Takahiko Nishiyama, Takehiro Kimura, Kotaro Fukumoto, Yoshiyasu Aizawa, Keiichi Fukuda
Keio University School of Medicine, Tokyo, Japan
ALLIED PROFESSIONALS P 3-021
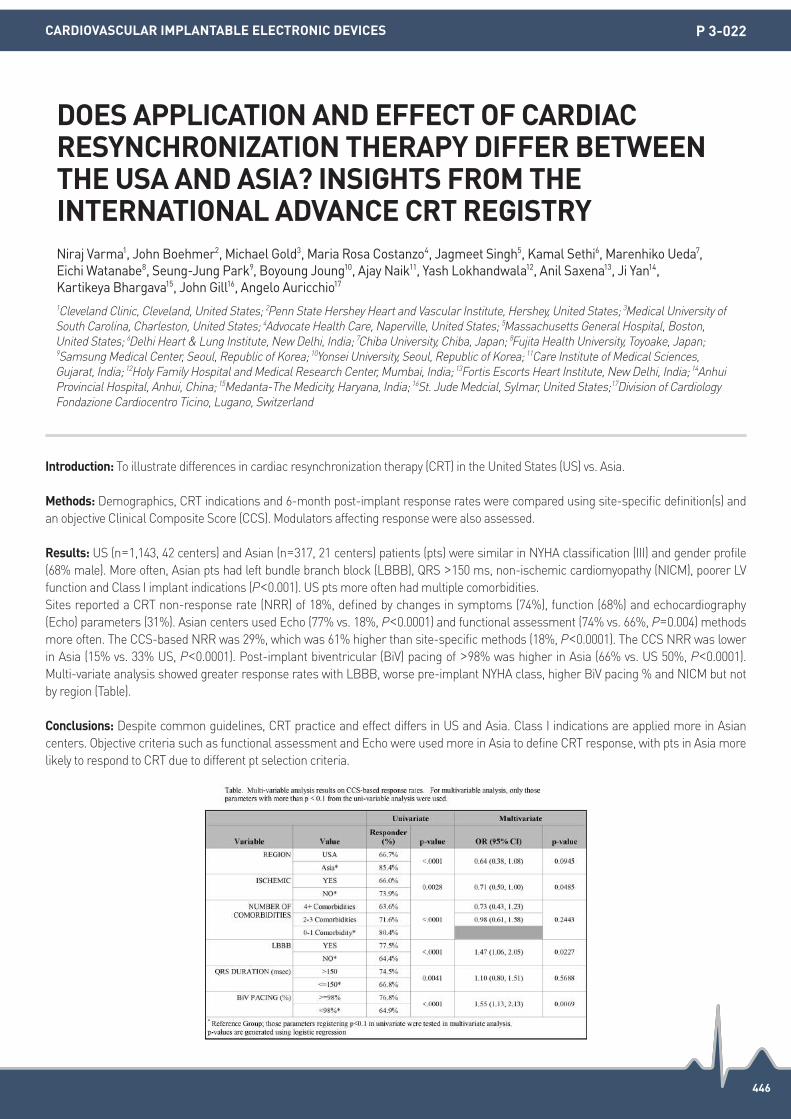
446
Introduction: To illustrate differences in cardiac resynchronization therapy (CRT) in the United States (US) vs. Asia.
Methods: Demographics, CRT indications and 6-month post-implant response rates were compared using site-specific definition(s) and an objective Clinical Composite Score (CCS). Modulators affecting response were also assessed.
Results: US (n=1,143, 42 centers) and Asian (n=317, 21 centers) patients (pts) were similar in NYHA classification (III) and gender profile (68% male). More often, Asian pts had left bundle branch block (LBBB), QRS >150 ms, non-ischemic cardiomyopathy (NICM), poorer LV function and Class I implant indications (P<0.001). US pts more often had multiple comorbidities.Sites reported a CRT non-response rate (NRR) of 18%, defined by changes in symptoms (74%), function (68%) and echocardiography (Echo) parameters (31%). Asian centers used Echo (77% vs. 18%, P<0.0001) and functional assessment (74% vs. 66%, P=0.004) methods more often. The CCS-based NRR was 29%, which was 61% higher than site-specific methods (18%, P<0.0001). The CCS NRR was lower in Asia (15% vs. 33% US, P<0.0001). Post-implant biventricular (BiV) pacing of >98% was higher in Asia (66% vs. US 50%, P<0.0001). Multi-variate analysis showed greater response rates with LBBB, worse pre-implant NYHA class, higher BiV pacing % and NICM but not by region (Table).
Conclusions: Despite common guidelines, CRT practice and effect differs in US and Asia. Class I indications are applied more in Asian centers. Objective criteria such as functional assessment and Echo were used more in Asia to define CRT response, with pts in Asia more likely to respond to CRT due to different pt selection criteria.
DOES APPLICATION AND EFFECT OF CARDIAC RESYNCHRONIZATION THERAPY DIFFER BETWEEN THE USA AND ASIA? INSIGHTS FROM THE INTERNATIONAL ADVANCE CRT REGISTRYNiraj Varma1, John Boehmer2, Michael Gold3, Maria Rosa Costanzo4, Jagmeet Singh5, Kamal Sethi6, Marenhiko Ueda7, Eichi Watanabe8, Seung-Jung Park9, Boyoung Joung10, Ajay Naik11, Yash Lokhandwala12, Anil Saxena13, Ji Yan14, Kartikeya Bhargava15, John Gill16, Angelo Auricchio17 1Cleveland Clinic, Cleveland, United States; 2Penn State Hershey Heart and Vascular Institute, Hershey, United States; 3Medical University of South Carolina, Charleston, United States; 4Advocate Health Care, Naperville, United States; 5Massachusetts General Hospital, Boston, United States; 6Delhi Heart & Lung Institute, New Delhi, India; 7Chiba University, Chiba, Japan; 8Fujita Health University, Toyoake, Japan;
9Samsung Medical Center, Seoul, Republic of Korea; 10Yonsei University, Seoul, Republic of Korea; 11Care Institute of Medical Sciences, Gujarat, India; 12Holy Family Hospital and Medical Research Center, Mumbai, India; 13Fortis Escorts Heart Institute, New Delhi, India; 14Anhui Provincial Hospital, Anhui, China; 15Medanta-The Medicity, Haryana, India; 16St. Jude Medcial, Sylmar, United States;17Division of Cardiology Fondazione Cardiocentro Ticino, Lugano, Switzerland
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-022

447
Introduction: Remote monitoring (RM) allows the transmission of device checks and alerts from home via a secured server. This has shown to improve patient safety by notifying the physician earlier of alerts as compared to routine in-office (RIO) checks, hence allowing timely intervention. We compared the time from event occurrence to its identification, defined as actionable alert (AA) between patients with RM as compared to patients only on RIO checks.
Methods: We performed a retrospective analysis for all patients with cardiac implantable electronic devices (CIED) over a 12 month peri-od. Clinical demographics, RM and in-office device check data was collected. Actionable device checks were defined as: VT/VF episodes, battery ERI, lead impedance or threshold variation compared to previous check. Comparisons were performed using a two-tailed chi-squared test.
Results: 2,730 patients were enrolled. The RM systems used were: Carelink (Medtronic, Minneapolis, MN, USA) (42%), Biotronik home monitoring (Biotronik, Berlin, Germany) (27%) and Merlin (St. Jude Medical, Inc., St. Paul, MN, USA) (31%). 939 Implantable cardiac de-fibrillator (ICD)/ Cardiac resynchronisation therapy- defibrillators (CRT-D) patients and 1,791 permanent pacemaker (PPM) patients had a total of 9,304 device checks over a period of twelve months. 7,722 device checks were performed in the RIO group (59% PPMs, 41% ICDs/CRT-Ds) versus 1,582 device checks in the RM group (31% PPMs, 69% ICDs/ CRT-Ds). The RIO group had 2.2% AA- 56 battery depletion, 8 lead alerts and 707 VT/VF episodes. The RM group had 2.4% AA-2 battery depletion, 52 VT/VF episodes and 5 lead alert. The time taken from event occurrence to its identification via AA was significantly shorter in the RM group: 5 days±11 days (RM) vs. 60 days±84 days (RIO) (P< 0.05).
Conclusions: The time of event occurrence to its identification was significantly shorter in the RM group vs. the RIO group. This allows early intervention and improves patient safety.
REMOTE MONITORING ENABLES SIGNIFICANTLY EARLIER DETECTION OF CARDIAC IMPLANTABLE ELECTRONIC DEVICE ALERTS COMPARED TO CONVENTIONAL IN-OFFICE DEVICE CHECKSHui Min Chong, Kwei Koon Lim, Jie Ying Hazel Huang, Su Yi Ho, Boon Yew Tan, Daniel Thuan Tee Chong, Kah Leng Ho, Wee Siong Teo, Chi Keong Ching
National Heart Centre Singapore, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-023

448
Introduction: Even though the sensitivity of modern ICD devices is very high in detecting life-threatening arrhythmias, the incidence of in-appropriate shocks remains as high as 30% in previous reports. In our institution, we applied the strategic programming protocols based on ADVANCE III, MADIT-RIT and PROVE since January 2014. In this retrospective study, we sought to examine the efficacy of strategic pro-gramming in reducing inappropriate shock in patients with ICD or CRT-D.
Methods: This is a single tertiary center retrospective study, evaluating the clinical outcomes, especially regarding inappropriate therapy in patients with ICD or CRT-D. Enrolled patients underwent ICD or CRT-D implantation from January 2014 to May 2016. Clinical informa-tion was attained by thorough chart review. The patient related data included baseline and clinical characteristics of the patients. In addi-tion, the device related parameters including programming parameters, and follow up information whether appropriate/inappropriate therapy was delivered.
Results: We analyzed 103 patients during January 2014 to May 2016. Mean age of the patients was 55.6±14.3 years, device implanted for primary prevention in 34 patients (33%) and secondary prevention for the 69 patients (67%). 81 patients had ICD (78.6%) and 22 CRT-D (21.4%), mean follow up after device implantation was 373.7±233.5 days. Overall, total delivered therapy including anti-tachycardia pacing was 37 episodes in 20 patients. Appropriate therapy including anti-tachycardia pacing delivered in 19 patients (36 episodes) and inappro-priate shock in a single patient (1 episode). With long detection interval, there was no adverse clinical event related to delayed ventricular arrhythmia detection.
Conclusions: Clinical application of long detection interval of ventricular arrhythmia according to ADVANCE III, MADIT-RIT and PROVE tri-als showed markedly low incidence of inappropriate therapy in both primary and secondary prevention patients. Even in secondary pre-vention patients, long detection setting program was safe and effective in reducing inappropriate shock.
EFFECTIVE REDUCTION OF INAPPROPRIATE SHOCK AFTER APPLYING LONG DETECTION INTERVAL OF VENTRICULAR ARRHYTHMIAYou-Mi Hwang, Jun Kim, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim, Ji Hyun Lee, Minsu Kim, Jongmin Hwang
Asan Medical Center, Seoul, Republic of Korea
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-024

449
Introduction: The Wearable cardioverter-defibrillator (WCD; Life Vest 4000, Zoll, PA, USA) plays a role not only as a cardioverter-defibrilla-tor but as an arrhythmic event monitor and symptomatic event ECG recorder. Detection of non-sustained asymptomatic tachyarrhyth-mias, however, is not equipped algorithmically, and its usefulness remains unclear.
Methods: We studied 62 patients at high risk of ventricular tachyarrhythmias who were prescribed WCD (9 for out of hospital use; 46 for secondary prevention) from April 2014 to April 2016. We analyzed transmitted events via Lifevest network, which consisted of automatic detection (AD) and patient-initiated detection (PD) by holding the response button for >3 seconds. In the former 20 patients, a single tachycardia detection for tachycardia ≥200 beats/minute (bpm) was programmed (SD mode), while in the latter 42, dual tachycardia de-tection (ventricular tachycardia (VT) for ≥130 and ventricular fibrillation (VF) for ≥200 bpm) was programmed (DD mode).
Results: During a median wearing duration of 13 (IQR 7-25) days, 663 events were transmitted. Of these, 580 were detected by AD and the other 83 by PD. Most of the transmissions in AD (n=562, 97%) were caused by noise detection, and most of transmissions in PD (n=77, 93%) were by frequent interruption of gong alarm for dislocated electrodes. Twenty-three (3.5%) true arrhythmic events were transmitted (sustained VT, 6; non-sustained VT, 6; asystole, 4; intermittent 2:1 atrioventricular block, 2; atrial fibrillation, 2; premature contractions, 3). In AD, true ventricular tachyarrhythmic event occurred in 12 episodes (SD mode, 1; DD mode, 11). After adjusting the number of patients and wearing duration, transmitted events were 3.7 and 4.3, and true ventricular tachyarrhythmia events were 0.02 and 0.11. The ratio of true ventricular tachyarrhythmia event to all of the transmitted events were 0.6% in SD mode, and 2.6% in DD mode. True arrhythmic event was detected more in DD mode than in SD mode, but noise detection was higher in DD mode.
Conclusions: Monitoring function of WCD is limited because of false events, and seems to be insufficient in judging the necessity of im-plantable cardioverter-defibrillator by itself.
EVALUATION OF ARRHYTHMIC EVENT MONITORING FUNCTION OF WEARABLE CARDIOVERTER-DEFIBRILLATOR IN PATIENT AT HIGH RISK OF SUDDEN CARDIAC DEATHYuji Ishida1, Shingo Sasaki1, Kimitaka Nishizaki1, Yoshihiro Shoji1, Kenichi Sasaki1, Daisuke Horiuchi1, Masaomi Kimura1, Ken Okumura2 1Department of Cardiology, Hirosaki University School of Medicine, Hirosaki, Japan; 2Department of Cardiology, Saiseikai Kumamoto Hospital, Kumamoto, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-025

450
Introduction: Atrial fibrillation (AF) is one of most common cardiac arrhythmia which affected quality of life, mortality and stroke rate re-gardless of paroxysmal or persistent. To identify one who have paroxysmal AF is a challenge. Currently, with an advanced cardiac investi-gation and treatment technology, permanent pacemaker as a treatment for patient’s with bradycardia, can provided an information about intracardiac electrogram for both atrium and ventricle. Any tachyarrhythmia occur in atrial chambers at a certain rate will be report as atrial high rate events (AHRE). This could lead to a detection of subclinical AF, even though asymptomatic. However, there is still no data about prevalence of AHRE in Thai population, and stroke correlation. The primary and secondary outcome of this study were to evaluate the prevalence of AHRE in patients who underwent CIED implantation in Thai population and its correlation to stroke in these populations, respectively.
Methods: We conducted a retrospective cohort descriptive study in patients who underwent a dual chamber CIED implantation over 7 years period, each of them was follow up for at least 2 years. Exclusion criteria include patients with previously diagnose AF or currently on oral anticoagulant.
Results: A total of 207 patients who underwent a dual chamber CIED implantation and have been followed up for at least 2 years were retrospectively reviewed. According to the primary outcome, AHRE were detected in 142 of 207 dual chamber CIED implantation patients (68.6%) which stroke occurred in 4 out of 142 patients of AHRE group (2.8%) but in contrast there was no experienced stroke in non AHRE group. However, there was no statistically significant (P=0.31) between group. From all 4 patients with stroke, 3 were ischemic and 1 was subdural hematoma (SDH). Mortality rate was also more prevalent in AHRE group when compare to non AHRE (11/142, (7.7%) vs. 2/65 (3.1%), P=0.35).
Conclusions: This study presents an AHRE which assumed to be subclinical AF and was found in majority (68.6%) of Thai population who were implanted with dual chamber CIED. Unfortunately, this study has showed no statistically significant association between AHRE and stroke, even though all stroke occurred in AHRE group.
PREVALENCE OF SUBCLINICAL ATRIAL FIBRILLATION PATIENTS DETECTED BY CARDIAC IMPLANTABLE ELECTRICAL DEVICE AND ASSOCIATION WITH ISCHEMIC STROKE, A SINGLE CENTER STUDYSirichai Jamnongprasatporn, Arisara Suwanagool, Napawan Pornnimitthum
Siriraj Hospital, Bangkok, Thailand
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-026

451
Introduction: Cardiovascular implantable electronic devices (CIEDs) have expanded in number and complexity. Standard ambulatory fol-low-up is time-consuming and not able to detect asymptomatic CIEDs malfunction. Previous studies have shown that remote monitoring (RM) could reduce the number of ambulatory visits and facilitates the early detection of arrhythmic events and CIEDs malfunctions. Lead failure often could be notified by RM earlier, but CIEDs sometimes have diagnosed lead failure as just arrhythmic events without any warning. We sought to examine what is the major first notification of lead failure in CIEDs patients followed by RM.
Methods: From 2009 to 2015, we have followed patients with CIEDs by RM. We usually have made one report for one transmitted data by RM. Now, we have followed 1,398 patients, including 832 pacemaker, 351 implantable cardioverter defibrillator (ICD), 191 cardiac resyn-chronization therapy with ICD (CRT-D), and 7 CRT without ICD (CRT-P). And we have made 12,236 reports for transmitted data by RM. We retrospectively analyzed how lead failure was notified by RM.
Results: During follow-up periods of 5 years, there were 29 events of lead failure. Nine was implantable cardioverter defibrillator (ICD) lead, 13 was atrial lead, and 6 was ventricular lead. There was no clinical adverse event, including inappropriate ICD therapy in all 29 events. In 18 of 29 (62.1%) events, the first notification of lead failure was only arrhythmic events. In 12 of 18 arrhythmic events, CIEDs did not send any warning. In these events, it was very difficult to detect lead failure without analysis of arrhythmic events. In 6 of 29 (20.7%) events, the first notification of lead failure was only lead impedance abnormality. In 5 of 29 (17.2%) events, the first notification of lead fail-ure was both arrhythmic events and lead impedance abnormality.
Conclusions: RM can detect lead failure earlier before clinical adverse events. However, CIEDs often diagnose lead failure as just arrhyth-mic events without any warning. Then, to detect lead failure earlier, careful analysis of arrhythmic events may be necessary.
FIRST NOTIFICATION OF LEAD FAILURE IS ARRHYTHMIC EVENTS IN PATIENTS FOLLOWED BY REMOTE MONITORINGNobuhiro Nishii, Akihito Miyoshi, Yoshimasa Morimoto, Satoshi Kawata, Hiroyasu Sugiyama, Motomi Tachibana, Koji Nakagawa, Atsuyuki Watanabe, Hiroshi Morita, Hiroshi Ito
Okayama University, Okayama, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-027

452
Introduction: Atrial Fibrillation (AF) has grown to global epidemic proportions as the most common arrhythmia of clinical significance. However, evidence suggests that there may be considerable regional heterogeneity in the prevalence of AF, with differing rates in the de-veloped and developing world. Part of this difference may be accounted for by differing medical care facilities in these countries. We hy-pothesized that comparison of prevalence rate of AF between different populations as detected on Cardiac Implantable Electronic Devices (CIEDs) may provide a more realistic assessment of the true prevalence rate of asymptomatic AF in patients with HF.
Methods: The study was performed in the Department of Cardiac Electrophysiology, Medanta-The Medicity, India on 93 consecutive chronic stable HF patients with CIEDs implanted for an appropriate clinical indication. The primary objective of the study was to ascertain the burden of asymptomatic AF in our select study population and compare it with that in other populations using CIED reported preva-lence rates of asymptomatic AF.
Results: As compared to patients with no device detected AF, those with AF were significantly (P=0.026) older, had CIEDs implanted for a longer (P=0.633) duration, had higher (P<0.001) CHA2DS2-VASc scores, and were more likely to be hypertensive (P=0.002), have coronary artery/other vascular atherosclerotic disease (P=0.008), and less likely to have non-ischemic cardiomyopathy (P=0.033). No significant difference was found when our calculated AF incidence was compared to three large cohorts (the TRENDS and PANORAMA studies, and the Italian Clinical Service Registry Project).
Conclusions: AF incidence rates obtained in our study did not deviate significantly from global values for device-detected AF in heart fail-ure patients. These, including under-detection due to inadequate health care access, underreporting of manifest disease and lack of elec-trocardiographic documentation, may have contributed to the lower incidence rates reported in previous studies. Our study thus suggests that, contrary to prior research, ethnicity may not be the causal factor affecting AF prevalence but may be incidental to the ‘developing’ status of these nations.
DEVICE-DETECTED ASYMPTOMATIC ATRIAL TACHYARRHYTHMIAS IN INDIAN HEART FAILURE PATIENTS: THE ATTEND STUDYNayani Makkar1, Balbir Singh2, Inder Anand3 1Mayo Clinic, Rochester, United States; 2Medanta, The Medicity Hospital, Gurgaonn, India; 3VA medical Centre, San Diego, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-028

453
Introduction: MR conditional pacing systems have not been systematically studied in China. This study aimed to observe the safety and efficacy of the ImageReadyTM MR conditional pacing system in Chinese subjects.
Methods: 10 patients from 2 centers were enrolled in this prospective, single-arm study. All patients (male 5, age 69.4±9.9 years, sick si-nus syndrome 7) were implanted with an ImageReady pacing system (Vitalio MRI pulse generator and Ingevity MRI lead(s), Boston Scien-tific, USA) successfully. 7 patients were implanted with dual chamber pacemakers. All patients underwent a non-indicated 1.5T MR scan covering both thoracic and lumbar spines 6-9 weeks after implantation. The primary efficacy endpoints included increase of pacing threshold (at 0.5 ms pulse width) greater than 0.5 V, and decrease of sensed amplitude greater than 50% one month post-MR scan com-pared to pre-MR scan. The primary safety endpoint was MR scan related complications.
Results: There were no primary endpoint events in the study. The atrial pacing thresholds pre- and post-MR scan were 0.66±0.22 V and 0.63±0.28 V, respectively (P=0.837); and the ventricular pacing thresholds were 0.64±0.08 V and 0.60±0.11 V, respectively (P=0.362). The atrial sensed amplitudes pre- and post-MR scan were 3.09±1.54 mV and 3.83±2.62 mV, respectively (P=0.537); and the ventricular sensed amplitudes were 17.32±6.55 mV and 18.60±6.50 mV, respectively (P=0.665, see figure). There were no MR scan or pacing system related complications during the study period.
Conclusions: The ImageReadyTM MR Conditional Pacing System appeared to be safe and effective in Chinese subjects.
OBSERVATION OF IMAGEREADYTM MR CONDITIONAL PACING SYSTEM IN CHINAYangang Su1, Kejiang Cao2, Xiaofeng Hou2, Wei Wang1, Chun Chen2, Minglong Chen2, Kai Gu2, Xueying Chen1, Jin Bai1, Shu Zhang3 1Department of Cardiology, Zhongshan Hospital, Fudan University, Shanghai Institute of Cardiovascular Diseases, Shanghai, China; 2Division of Cardiology, First Affiliated Hospital of Nanjing Medical University, Nanjing, China; 3State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Disease, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-029
Figure: lead measurement change pre- and post-MR Scan

454
Introduction: Previous studies have demonstrated patient activity (PA) could predict all-cause mortality. However, the underlying mecha-nism and association of PA are unclear. The aim of this study is to evaluate if PA could predict cardiac death and what’s the cut-off of PA to discriminate cardiac death, and the relationship between PA and heart rate variability in patients with home monitoring.
Methods: This study retrospectively analyzed the clinical and implantable cardioverter-defibrillator (ICD)/cardiac resynchronization thera-py defibrillator (CRT-D) device data in 845 patients. Data of PA and PP variability during the first 30-60 days recording by home monitoring were collected and calculated an average in each patients. The primary endpoint was cardiac death and the second endpoint was all-cause mortality. Spearman correlation coefficient was conducted between PA and PP variabiltiy.
Results: The mean PA was 11±5.8%. Based on the receiver operating characteristic curve, the cut-off value of PA=7.84% (113 minutes) was identified to predict cardiac death. During a mean follow-up period of 31.1±12.9 months (range from 3 to 60 months), PA≤7.84% was associated with increased risk of cardiac death (HR=4.13, 95% CI=2.813-6.064, P<0.001) and all-cause mortality (HR=4.091, 95% CI=2.884-5.8, P<0.001) in an unadjusted analysis, after adjusting in a multivariate Cox model, these relationships remained significant be-tween PA≤7.84% and cardiac death (HR=3.639, 95% CI=2.42-5.471, P<0.001) or PA≤7.84% and all-cause mortality (HR=3.677, 95% CI=2.535-5.334, P<0.001). The average 30-day average PP variability was 86.7±27.6 ms. PA was significant correlation with PP variability (r=0.6012, P<0.001).
Conclusions: Baseline PA≤7.84% has a higher risk of cardiac death and all-cause mortality. There is a significant correlation between PA and HRV. These results will be helpful for doctors make clinical proper decision.
PHYSICAL ACTIVITY COULD PREDICT CARDIAC DEATH IN IMPLANTABLE CARDIOVERTER-DEFIBRRILATOR AND CARDIAC RESYNCHRONIZATION THERAPY-DEFIBRILLATOR PATIENTSShuang Zhao1, Keping Chen1, Yangang Su2, Wei Hua1, Tengyong Jiang3, Jiefu Yang4, Wei Jin5, Silin Chen6, Yansheng Ding7, Zhaoguang Liang8, Wei Xu9, Shu Zhang1 1State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, Beijing, China; 2Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University, Shanghai, China; 3Beijing Anzhen Hospital, Capital Medical University, Beijing, China; 4Beijing Hospital, Beijing, China; 5First People’s Hospital Affiliated to Shanghai Jiao Tong University, Shanghai, China; 6Guangdong Cardiovascular Institute, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China; 7First Hospital Beijing Medical University, Beijing, China;
8First Affiliated Hospital of Harbin Medical University, Harbin, China; 9Nanjing Drum Tower Hospital, Nanjing, China
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-030
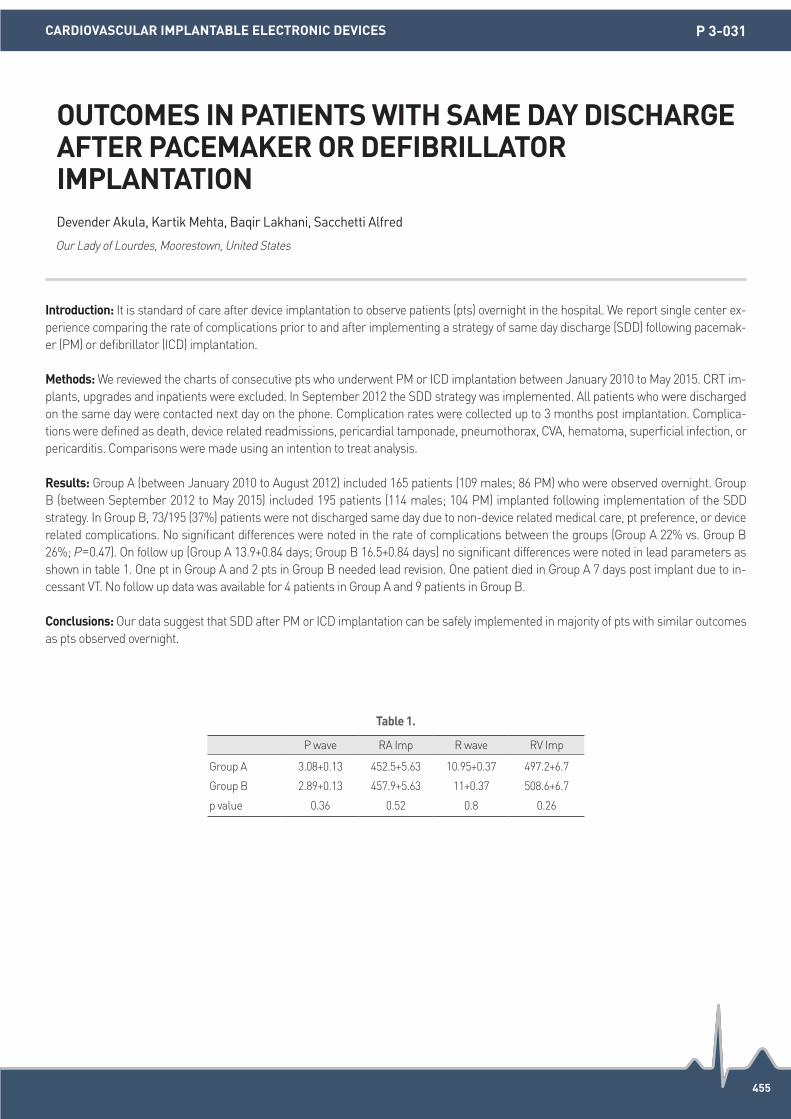
455
Introduction: It is standard of care after device implantation to observe patients (pts) overnight in the hospital. We report single center ex-perience comparing the rate of complications prior to and after implementing a strategy of same day discharge (SDD) following pacemak-er (PM) or defibrillator (ICD) implantation.
Methods: We reviewed the charts of consecutive pts who underwent PM or ICD implantation between January 2010 to May 2015. CRT im-plants, upgrades and inpatients were excluded. In September 2012 the SDD strategy was implemented. All patients who were discharged on the same day were contacted next day on the phone. Complication rates were collected up to 3 months post implantation. Complica-tions were defined as death, device related readmissions, pericardial tamponade, pneumothorax, CVA, hematoma, superficial infection, or pericarditis. Comparisons were made using an intention to treat analysis.
Results: Group A (between January 2010 to August 2012) included 165 patients (109 males; 86 PM) who were observed overnight. Group B (between September 2012 to May 2015) included 195 patients (114 males; 104 PM) implanted following implementation of the SDD strategy. In Group B, 73/195 (37%) patients were not discharged same day due to non-device related medical care, pt preference, or device related complications. No significant differences were noted in the rate of complications between the groups (Group A 22% vs. Group B 26%; P=0.47). On follow up (Group A 13.9+0.84 days; Group B 16.5+0.84 days) no significant differences were noted in lead parameters as shown in table 1. One pt in Group A and 2 pts in Group B needed lead revision. One patient died in Group A 7 days post implant due to in-cessant VT. No follow up data was available for 4 patients in Group A and 9 patients in Group B.
Conclusions: Our data suggest that SDD after PM or ICD implantation can be safely implemented in majority of pts with similar outcomes as pts observed overnight.
OUTCOMES IN PATIENTS WITH SAME DAY DISCHARGE AFTER PACEMAKER OR DEFIBRILLATOR IMPLANTATIONDevender Akula, Kartik Mehta, Baqir Lakhani, Sacchetti Alfred
Our Lady of Lourdes, Moorestown, United States
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-031
Table 1.
P wave RA Imp R wave RV Imp
Group A 3.08+0.13 452.5+5.63 10.95+0.37 497.2+6.7
Group B 2.89+0.13 457.9+5.63 11+0.37 508.6+6.7
p value 0.36 0.52 0.8 0.26

456
Introduction: The progressive increase of cardiovascular implantable electronic devices (CIED) recipients has led to an amplified CIED in-fection. Implantable device procedures are performed in not only dedicated electrophysiology laboratory (DEL) but also shared cardiac catheterization laboratory (SCL) in most medical centers. Recently, we observed increased CIED infection rate in our hospital, and there-fore sought to investigate whether the type of laboratory affect the incidence of infection.
Methods: 538 patients (mean age 71±13 years, 52.2% male) who underwent CIED implantation at a single center from 2011 to 2015 were enrolled. The patients were divided into two groups according to the laboratory where the procedure was performed: 377 patients in DEL and 161 patients in SCL. Data on all patients diagnosed with CIED infection were reviewed and compared. Variables were assessed for in-dependent association with CIED infection by multivariate model.
Results: CIED infection was diagnosed in 23 patients (mean age 63±20 years, 82.6% male) of our study population. 16 of 377 (4.2%) and 7 of 161 (4.3%) patients with CIED infection occurred in DEL and SCL, respectively (P=0.957). Among them, 10 patients (43.5%) had pace-makers, 10 (43.5%) ICDs, and 3 (13.0%) CRTs. Regarding the reasons for first device implantation, there were also no differences between the two groups (P=0.945 for sinus node dysfunction or AV block, P=0.856 for sudden cardiac arrest (SCA), P=0.675 for dilated cardiomy-opathy, hypertrophic cardiomyopathy, and idiopathic ventricular tachycardia or fibrillation). In the multivariate analysis, male (odds ratio [OR] 3.762, 95% confidence interval [CI] 1.214-11.664, P=0.022), diabetes (OR 2.591, 95% CI 1.048-6.403, P=0.039), renal failure (OR 5.831, 95% CI 2.333-14.576, P<0.001), and SCA (OR 3.763, 95% CI 1.214-11.664, P=0.035) were independently associated with CIED infection, but SCL did not show a significant risk (OR 0.762, 95% CI 0.279-2.078, P=0.595).
Conclusions: There was no difference in the incidence of CIED infection between DEL and SCL in our study. Regardless of the type of lab-oratory, male sex, diabetes, renal failure, and SCA were associated with an increased risk of CIED infection.
THE INCIDENCE OF INFECTION AFTER CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICE: DEDICATED ELECTROPHYSIOLOGY LABORATORY VERSUS SHARED CARDIAC CATHETERIZATION LABORATORYYong-Soo Baek, Anupam Jena, Hee-Soon Park, Kwang-No Lee, Seung-Young Roh, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Medical Center, Seoul, Republic of Korea
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-032
457
Introduction: Contrast venography is a safe and a reliable method of identifying blood vessels prior to device lead insertion. The purpose of this study was to evaluate the safety and efficacy of performing contrast venography versus the blind anatomical approach.
Methods: This is a retrospective/prospective chart review done at the The Medical City from January 2013 to December 2015. A total of 88 patients were included in the study however 8 patients were excluded due to poor data collection. The control group, comprised of 28 pa-tients, underwent blind insertion while 52 patients underwent a venogram prior to lead insertion. Six patients subsequently converted to contrast venography due to difficulty of access. The blind and venogram groups were compared based on the following parameters; Total dye load (mL), Fluoroscopic time (minute), Total procedure time (minutes), Time to access (minute), Intraoperative blood loss, hematoma formation, post operative bleeding, creatinine before and after procedure, total hospital stay (days), hospital stay after the procedure (days) and major and minor complications. Major complications comprised of surgical site infection/sepsis, cardiac perforation, pneumothorax >10%, pleural effusion requiring drainage, wound dehiscence, lead dislodgement bleeding >50 cc and hematoma formation requiring in-tervention. Minor complications include surgical site pain, pneumothorax <10%, minimal pleural effusion not requiring drainage and pal-pitations.
Results: Independent Samples t-test at 5% level of significance was used to compare the data and results showed that mean differences in fluoroscopic time (P=0.180), time to access (P=0.222), blood loss (P=0.602), total hospital stay (P=0.117), and post procedure hospital stay (P=0.103) were not significantly different between the two groups. Mean procedure time however, was found to be significantly short-er in the study group compared to the control group (P=0.006). Using the Fisher Exact Test, existence of minor complications was found to be significantly different between the groups, while those in the study group had fewer complications (P=0.017). The existence of major complications, was not significantly different between the 2 groups (P=0.125).
Conclusions: Contrast venography prior to pacemaker/ICD/CRT-D lead insertion is safe and associated with significantly lower rate of minor complications and lower total procedure time.
CONTRAST VENOGRAPHY BEFORE PACEMAKER AND IMPLANTABLE CARDIOVERTER DEFIBRILLATOR LEAD INSERTION IMPROVES PATIENT OUTCOMES VERSUS BLIND LEAD INSERTION USING ANATOMICAL LANDMARKSRaymond Bayaua
The Medical City, Marikina, Philippines
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-033

458
Introduction: Cardiac pacemakers, defibrillators and Cardiac resynchronization therapies are very common. These devices are suscepti-ble to erosion, exposure, or infection and plastic surgeons are consulted when salvage is required.
Methods: We report turn over pectoral muscle flap approach to effectively and safely relocate the device into the subcutaneous position. Eight patients required repositioning of cardiac devices over period of three years for exposure, erosion, infection, and fat necrosis. All pa-tients were treated with turn over pectoral muscle flap in subcutaneous pocket with capsule remaining intact over the device.
Results: Seven of 8 patients (87.5%) achieved successful long-term repositioning in the same pocket with turn over muscle flap without recurrent exposure or hematoma and with good cosmetic results. One patient required pacemaker explantation and re-implant from the opposite side due to underlying infection.
Conclusions: The turn over pectoral muscle flap technique proposed by the authors for defibrillator or pacemaker salvage is a feasible technique with promising results. Plastic surgeons should be aware of this simple and effective approach.
TURN OVER PECTORAL MUSCLE FLAP TO SALVAGE IMPLANTABLE DEVICES. IS IT FEASIBLE!Anoop Gupta, Niraj Yadav, Vijay Bhatia
Sterling Hospital, Ahmedabad, India
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-034

459
Introduction: Some report shows steroid therapy is effective for pericardial effusion following device implantation. However, the patients with pericardial effusion following device implantation who treated with only colchicine were rare.
Methods: N/A
Results: Eighty seven years old man with idiopathic dilated cardiomyopathy with left bundle branch block was admitted with heart failure. Cardiac echocardiography showed that left ventricular dysfunction. After heart failure was subsided by medication, cardiac resynchroniza-tion therapy (CRT) was performed for heart failure without any complication. The patient clinically improved heart failure. Therefore, 1 week after CRT implantation, he was discharged with no significant laboratory data, chest X-ray and echocardiography data. However, he visited outpatient clinic with dyspnea and low grade fever after 1 month from discharge. The chest X-ray showed dilation of cardiac silhou-ette. Furthermore, moderate pericardial effusion was observed by echocardiography. There was no sign of cardiac chamber collapse. The pericardial effusion was not enough to drainage. Although chest computed tomography suggested that atrial lead injured pericardium, laboratory data showed no sign of anemia and bleeding. Electrocardiogarm showed atrial fibrillation with tachycardia. After oral be-ta-blocker administration as rate control started, the dyspnea was diminished. However, pericardial effusion gradually increased. Labora-tory data showed elevation of inflammatory marker and still no sign of anemia. From the above, we speculated the pericardial effusion was due to the inflammation by post-cardiac injury syndrome. Therefore, treatment by colchicine was started. After three days, the in-flammation marker decreased. Furthermore, the pericardial effusion was diminished after 1 month from colchicine therapy was started.
Conclusions: Not only steroid therapy but also colchicine therapy is effective for pericardial effusion following device implantation as an-ti-inflammation effect. Therefore, we reported this case as case report.
COLCHICINE REDUCED PERICARDIAL EFFUSION FOLLOWING CARDIAC RESYNCHRONIZATION THERAPY IMPLANTATION: CASE REPORTTadashi Hoshiyama, Keiichi Ashikaga, Yoshisato Shibata
Miyazaki Medical Association Hospital, Miyazaki, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-035

460
Introduction: Inappropriate shocks are common and significant problems in patients with implantable cardioverter defibrillator (ICD). It is well known that patients who experienced inappropriate and unnecessary shocks due to ICD lead fracture or atrial fibrillation have ad-verse psychological morbidity compared with control patients. However, little is known about the relationship between physical activities and inappropriate shocks in patients with ICD. Physical activity data are collected automatically by ICDs. This study was designed to deter-mine the change of physical activities after and the predictors of inappropriate shock therapies in Japanese patients with ICD.
Methods: We examined the database of remote monitoring systems of ICD patients at a single center in Japan. The physical activities one month before and after inappropriate shocks due to atrial fibrillation (AF) were analyzed. Fisher’s exact test were used for discrete vari-ables. Multivariate Cox regression analysis with the forward selection method was used to find predictors for inappropriate shocks.
Results: A total of 172 Japanese patients were enrolled in this study (age 61±13 years, male 74%). Sixty seven patients (39%) received an ICD for secondary prevention of sudden cardiac death. Fifty patients (29%) had atrial fibrillation (AF). After a mean of 22±15 months, 11 patients (6.4%) experienced an inappropriate shock. Causes of inappropriate shocks were AF (9) and supraventricular tachycardia (2). In-appropriate shocks reduced the physical activities by forty percent. AF (82% vs. 25%, P<0.001), ventricular pacing (VP)<5% (91% vs. 62%, P=0.047) and single chamber ICD (36% vs. 5.6%, P=0.0049) were more prevalent in these patients. AF (Hazard ratio: 16.88, 95% Confi-dence interval: 2.99-94.19, P=0.0014) and VP<5% (Hazard ratio: 10.01, 95% Confidence interval: 1.06-94.71, P=0.045) were the indepen-dent predictors of inappropriate shocks.
Conclusions: In appropriate shock therapies reduced the physical activities of ICD patients. AF and very low ventricular pacing percentiles strongly predict inappropriate shock therapies. The strict rate-control of AF using remote monitoring systems should be considered to keep the physical activities and reduce the incidence of inappropriate ICD shock therapies in this population.
CHANGE OF PHYSICAL ACTIVITY AFTER INAPPROPRIATE SHOCK THERAPIES IN JAPANESE PATIENTS WITH IMPLANTABLE CARDIOVERTER DEFIBRILLATOR Yusuke Kondo, Marehiko Ueda, Masahiro Nakano, Kazuo Miyazawa, MIyo Nakano, Tomohiko Hayashi, Yoshio Kobayashi
Chiba University Graduate School of Medicine, Chiba, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-036

461
Introduction: Implantable cardiac defibrillators (ICD) are recommended as secondary prevention for malignant ventricular arrhythmias and resuscitated sudden cardiac death. They are also indicated as primary prevention for patients with severe cardiomyopathy and inher-ited disorders predisposing to ventricular arrhythmia. Previous studies have shown that patients with ICDs have comparable quality of life (QOL) to those without devices. However, several risk factors negatively impact QOL in these patients, including young age, shock experi-ence, psychiatric disorders and lack of device understanding. We aim to assess patients’ device understanding and impact on QOL.
Methods: A questionnaire was designed with two main arms. The first was to assess patients’ understanding of their device function and limitations. The second assessed patients’ QOL, with questions based on depression and anxiety. The latter included a question regarding activity avoidance due to fear of shocks. The final question assessed symptoms using the New York Heart Association classification. Questionnaires were completed by patients attending the device clinic during routine follow up. Ethics approval was obtained prior to the commencement of study.
Results: A total of 37 questionnaires were completed between January-May 2016. The mean patient age was 66 years (±10) with 89% be-ing male and 11% being female. 60% of patients reported a good QOL, whereas 10.8% of patients reported a significantly reduced QOL. There was a higher rate of decreased QOL in secondary vs. primary prevention patients (50 vs. 33%). 73% of patients answered incorrectly regarding their device function and limitations, including 56.8% not recalling being informed about the possibility of inappropriate shocks prior to ICD implantation. There was no difference in device understanding between patients with and without reduced QOL (73 vs. 72.7% answering incorrectly regarding device function respectively). There was a higher proportion of impaired QOL in patients who reported shocks from their ICD (42.9%) compared to those who had not received prior shocks.
Conclusions: The majority of patients with ICDs in this study enjoy a good quality of life. Our findings suggest that patient understanding of devices is generally poor, but this does not appear to impact on QOL. Factors associated with impaired QOL were secondary prevention devices and experience of prior shocks. This is consistent with current literature on QOL predictors. This study highlights the role of physi-cians and heart failure nurses in the adequate education of patients prior to implantation both regarding their disease and the benefits/limitations of devices.
A PROSPECTIVE OBSERVATIONAL COHORT STUDY: ASSESSING ICD RECIPIENTS’ DEVICE UNDERSTANDING AND QUALITY OF LIFEPaul Maggiore1, David Chieng2, Primero Ng1, Paul Stobie1, Justin Ng1 1Sir Charles Gairdner Hospital, Perth, Australia; 2Royal Perth Hospital, Perth, Australia
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-037

462
Introduction: Automatic implantable defibrillator (AD) i.e., implantable cardioverter-defibrillator (ICD) and cardiac resynchronization ther-apy with defibrillator (CRTD) has been thought to be the one of the therapeutic options for patients with high risks of sudden cardiac death. However, the implantation criteria of those devices made by the western countries remain controversial in Japan.
Methods: We examined the clinical course in 60 patients implanted AD since 2009, (26 in ICD, 34 in CRTD). They consisted of 28 cases with ischemic background, 3 cases with vasospasm (VS) induced fatal tachyarrhythmia (FA), and 29 cases with non-ischemic cardiomyop-athy, mean age and ejection fraction (EF) were 41.4 and 63.1, respectively. Twenty seven cases who had been implanted AD for primary prevention satisfied criteria of MADIT-II, DEFINIT, and SCD-HeFT. Thirty three cases for secondary prevention had history of documented FA or unknown syncope with low EF. We analyzed if cases had experienced the following events; appropriate shock, inappropriate shock, anti-tachycardia pacing (ATP), cardiac death, and non-cardiac death, and compared them with their background.
Results: Patients for primary prevention received appropriate shocks and/or ATP less frequently than those for secondary prevention. However, those did inappropriate shocks more frequently (not significant) than those for secondary prevention. There was no appropriate shock delivered in patients for secondary prevention of VS induced FA. One died of systemic device infection after replacement of former device which had been implanted for primary prevention, and had not delivered any shock.
Conclusions: AD might be effective for secondary prevention of sudden cardiac death likewise in Japan. However, patients for primary prevention and secondary prevention for VS induced FA received appropriate shock less frequently, and a few of them experienced adverse events other than appropriate operations of the AD, which may suggest prophylactic medical managements would be effective in Japa-nese patients. Further investigations will be needed to determine who will require AD for primary prevention.
CLINICAL COURSE OF PATIENTS WITH AUTOMATIC IMPLANTABLE DEFIBRILLATORS IN JAPAN -RETROSPECTIVE SINGLE CENTER STUDY-Naomi Miki, Kazuo Kato, Masayuki Nakamura, Hirotaka Ootake, Shingo Yoshioka, Akimitsu Tanaka, Miyuki Andou, Takashi Shimozato, Hidekazu Aoyama, Ryousuke Kametani, Kenta Murakami, Norihisa Shibata, Hideki Wada
Nagoya Tokushukai General Hospital, Kasugai, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-038

463
Introduction: Takotsubo cardiomyopathy (TCM), also called stress cardiomyopathy, is a transient cardiac syndrome that’s often brought on by stressful situations such as intense emotional and/or physical stress.
Methods: To clarify the TCM shortly after pacemaker implantation (PMI), we investigated among 247 consecutive patients who underwent PMI from 2011 to 2015 in our hospital.
Results: Among 247 consecutive patients who underwent PMI from 2011 to 2015 in our hospital, 3 patients (1.2%, median age 83 years) suffered TCM until postoperative day 3. They had no symptoms, however, 12-lead ECG showed deeply inverted T-wave with QT prolonga-tion under ventricular pacing and laboratory result was elevated BNP level and troponin I or T. Echocardiogram showed LV basal hyper-contraction and severe apical akinesis despite normal LV wall motion before PMI. Emergency coronary angiography was performed in 2 patients and showed no significant coronary artery disease. Left ventriculography confirmed the same findings as echocardiogram. No harmful event associated with TCM occurred. Serial ECG and LV wall motion using echocardiography in these 3 patients under ventricular pacing showed same findings for TCM in patient with spontaneous R waves.
Conclusions: We should pay attention to this finding that asymptomatic TCM occurred in 1.2% of patients shortly after PMI. ECG findings despite ventricular pacing may be helpful to make us diagnose Takotsubo cardiomyopathy.
TAKOTSUBO CARDIOMYOPATHY ASSOCIATED WITH PACEMAKER IMPLANTATIONYuko Miki1, Satoru Shimizu1, Mai Azuma1, Midori Takakura1, Naoki Iinuma1, Tatsuya Nakachi1, Kazuki Fukui1, Toshiyuki Ishikawa2 1Kanagawa Cardiovascular and Respiratory Center, Yokohama, Japan; 2Yokohama City University Hospital, Yokohama, Japan
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-039

464
Introduction: Primary prevention Implantable Cardioverter Defibrillator (ICD) has been shown to improve prognosis in the Caucasian population. We evaluated the impact of ICD implantation on the outcomes of heart failure patients and identify barriers to the uptake of ICD in a multi-racial cohort.
Methods: Total 389 patients who fulfilled Class 1 indication for primary prevention ICD were followed up in the heart failure clinic over 2 years (2012 & 2013) were studied retrospectively. Case notes and electronic patient records were used for data collection.
Results: The baseline clinical characteristics of this cohort was as follows: mean age 67±13 years old, 73% (284) male, 51% (198) Chi-nese, 31% (120) Malay, 9% (37) Indian, 9% (34) others, 82% (319) IHD, 68% (266) hypertension, 56% (217) diabetes mellitus 20% (78) cardio-vascular accident, 14% (56) Atrial fibrillation and median NYHA class was 2 and mean left ventricular function 22±8. Of the 389 patients, only 16% (61) were counselled by the Cardiac Rhythm Management team, 28% (111) were counselled by the cardiologists and 44% (171) patients were not counselled for ICD insertion. Only 67 patients (17%) had ICD implantation. The most common reasons for not implant-ing ICD were unsuitable as deemed by the physician 65 (20.1%), patient feeling well 81 (25.2%), social reasons such as social and finical 71 (22.0%). Cultural reasons 1 (1.0%) only accounted for a minority of cases. After a mean follow up of 37±7 months, the overall mortality was 30%, CV death accounted for 48 (12.3%); arrhythmia death 18 (4.6%), non-arrhythmia death 30 (14.1%) and non CV death was 59 (17.7%). On Univariate analysis, ICD did not improve outcomes (13.4% vs. 13.3%, P=1.0). On multi-variate analysis, high NT-ProBNP (OR 1.10, P=0.021), high urea (OR 1.29, P=0.007), hyponatremia (OR 0.64, P=0.008) hypokalemia (OR 0.08, P=0.001) and ICD implantation (OR 6.34, P=0.008) were independent predictors of cardiovascular death.
Conclusions: In this multi-racial, predominantly non-Caucasian cohort, ICD uptake was low at 17%. However, there was no significant dif-ference in mortality between patients with or without ICD. In fact, ICD implantation and Biomarkers such as Na, K, NTProBNP and urea were independent predictors for CV deaths. The main barriers to ICD implantation were physician factors and patients’ sense of well-be-ing and not understanding the rationale of primary prevention.
BARRIERS TO THE UPTAKE OF PRIMARY PREVENTION INTERNAL CARDIOVERTER DEFIBRILLATOR (ICD) & OUTCOMES IN A MULTI-RACIAL COHORT FOLLOWED UP IN HEART FAILURE CLINIC: SINGLE CENTRE EXPERIENCEAye Aye Mon1, Ai Ling Him2, Zaw Min Tun1, Carmen Jia Wen Kam2, Michael Macdonald2, Tan Vern Hsen2, Tong Khim Leng2, Gerard Leong2, Kelvin C K Wong2 1MOHH, Singapore; 2Changi General Hospital, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-040

465
Introduction: Cardiac resynchronization therapy defibrillators (CRT) have shown to reduce mortality and morbidity in patients with broad QRS complexes and heart failure. Current guidelines indicate that patients who have a LVEF of <35% or less with 40% ventricular pacing requirement should receive cardiac resynchronization therapy. The aim of this study was to determine the incidence of patients with pre-existing implantable cardiac defibrillators (ICD) who subsequently develop need for >40% ventricular pacing.
Methods: A retrospective review was performed among patients with ICDs that were on active follow up. ICD implantation was for stan-dard indications. We reviewed these patients for significant ventricular pacing requirements (>40%) due to new onset atrioventricular node dysfunction was determined.
Results: Our cohort consisted of 298 patients with single or dual chamber ICDs. Patients were followed up for a mean±SD of 48.0±27.7 months. The mean left ventricular ejection fraction was 24.2±7.4%. 4.0% (12 out of 298) of patients developed ventricular pacing of >40%. The onset of frequent pacing occurred over a mean duration of 35.3±20.4 months. The development of frequent ventricular pacing was 1% per year.
Conclusions: Development of frequent ventricular pacing can lead to detrimental effects on cardiac hemodynamics and patient out-comes. Based on our results, the mean incidence of atrioventricular node dysfunction leading to ventricular pacing of >40% was 1% per year. This group of patients may be considered for upgrade to cardiac resynchronization therapy.
DEVELOPMENT OF FREQUENT VENTRICULAR PACING IN PATIENTS WITH IMPLANTABLE CARDIAC DEFIBRILLATORSDawn Oh, Paul Chun Yih Lim, Daniel Thuan Tee Chong, Boon Yew Tan, Kah Leng Ho, Wee Siong Teo, Chi Keong Ching
National Heart Center, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-041
466
Introduction: Implantable cardioverter defibrillator (ICD) has been proven as an effective therapy for primary and secondary prevention of sudden cardiac death in appropriately selected patients with established risk. However, up to 50% of ICD therapies are inappropriate. Dual or triple chamber (DTC) ICD offer potential advantages over single-chamber (SC) in reducing inappropriate therapies (IT). However, stud-ies have shown conflicting results. Hence, this systematic review and meta-analysis sought to determine any advantage of DTC over SC ICD in reducing IT.
Methods: MEDLINE, EMBASE and clinicaltrials.gov databases were searched to identify relevant studies. Studies that compare DTC vs. SC ICD on IT reduction were included. The primary outcome was IT reduction. Secondary outcomes included mortality as well as proce-dural complications. Both randomized and non-randomized studies were included. Data were pooled and analyzed using Stata (v12) sta-tistical software using randomized effects models. The effect size is presented as the relative risk reduction (RR) and 95% confidence in-terval (CI). Statistical heterogeneity was evaluated using I2 statistic.
Results: 15 studies met the inclusion criteria including 7 randomized trials. The 15 studies included 9,505 (4,001 SC ICD and 5,504 DTC ICD) patients. Most (79%) participants were male, had history of ischemic heart disease (62%) and were prescribed beta-blockers (80%). Average follow-up duration was 23 months. There was no difference in IT reduction comparing SC vs. DTC ICD (RR: 1.16; 95% CI: 0.94-1.42; P=0.16; I2: 51%). Similar observation (no difference in IT reduction) when randomized (RR: 1.20; 95% CI: 0.82-1.76; P=0.36; I2: 60%) and non-randomized studies (RR: 1.16; 95% CI: 0.89-1.51; P=0.27; I2: 45%) were analyzed separately. There were also no differences in mortality rates (RR: 1.07; 95% CI: 0.46-2.45; P=0.88; I2: 76%) or procedural complication rates (RR: 0.58; 95% CI: 0.29-1.16; P=0.12; I2: 47%) observed in SC versus DTC ICD group.
Conclusions: DTC ICD showed no significant advantage in IT reduction over SC ICD.
REDUCTION OF INAPPROPRIATE THERAPY IN SINGLE CHAMBER VERSUS DUAL/TRIPLE CHAMBERS IMPLANTABLE CARDIOVERTER DEFIBRILLATORS: A SYSTEMATIC REVIEW AND META-ANALYSISVern Hsen Tan, Kelvin Cheok Keng Wong, Khim Leng Tong
Changi General Hospital, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-042

467
Introduction: Dual chamber pacemakers have the advantage over single chamber in reducing the risk of developing atrial fibrillation. They also provide atrioventricular synchrony, improving the hemodynamics and cardiac output, hence reducing admissions for congestive cardiac failure. However, literature has demonstrated conflicting reports on survival effect of single versus dual chamber pacemakers. We compared our patients’ survival at 2 years post implant between single and dual chamber pacemakers at our centre.
Methods: A retrospective review of 1,669 patients who underwent single and dual chamber pacemaker implantation between 2000 and 2012 at the National Heart Centre, Singapore was performed. Device implants were for standard indications. These patients were then followed up for 1 year post implant. The primary end point was all-cause mortality between patients with single and dual chamber pace-makers.
Results: 840 (50.3%) patients had single chamber pacemakers implanted and 820 (49.7%) dual chamber pacemakers. Patients with sin-gle chamber pacemakers were significantly older (Single 73.2±10.2 vs. Dual 67.4±12.6 years old, P<0.01), and had more atrial fibrillation (Single 17.0% vs. Dual 9.0%, P<0.01) compared to dual chamber pacemakers. A greater proportion of patients with dual chamber pace-makers had hypertension (P<0.01), diabetes mellitus (P=0.02) and ischemic heart disease (P<0.01). Rates of renal impairment and com-plication rates were comparable. Variables that correlated with survival included age (OR 1.03 CI 1.01-1.05, P<0.01) and the presence of renal impairment (OR 0.27 CI 0.15-0.51 P<0.01). There was no significant association seen with hypertension, diabetes, ischemic heart disease, atrial fibrillation, and com-plications during implant. Cox regression survival curves, after adjustment for covariates, showed significantly greater survival of patients at 1 year in patients with dual chamber pacemakers implanted (OR 4.04 CI 2.45-6.56 P<0.01).
Conclusions: Survival superiority in dual chamber pacemakers could be attributed to better hemodynamics and hence reduced clinically significant cardiac failure. However, single chamber pacemakers are often implanted in patients who are older and with more co-morbid-ities.
SURVIVAL SUPERIORITY IN PATIENTS WITH DUAL CHAMBER PACEMAKER VS. SINGLE CHAMBER PACEMAKER: A SINGLE CENTRE REVIEWHooi Khee Teo
National Heart Centre, Singapore
CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES P 3-043

468
Introduction: The EASTAR (ElectroAnatomic SoluTion for All aRrhythmias) principle was firstly advocated by our center since 2009. The purpose of this study was to investigate the feasibility of this principle in the catheter ablation of supraventricular tachycardia (SVT) with the analysis of six-year single center’s data.
Methods: Data of consecutive patients with SVT (including atrioventricular nodal reentrant tachycardia [AVNRT] and atrioventricular reen-trant tachycardia [AVRT]) underwent initial catheter ablation therapy in our center from January 2009 to December 2014 were retrospec-tively analyzed based on the guidance of three-dimensional electroanatomic mapping systems (Carto and NavX). The feasibility of the EASTAR principle was illustrated with the variations of annual procedure times, fluoroscopy times and radiation doses which then com-pared with non-EASTAR cases. The “learning curve” was reflected by the growth of a single operator.
Results: A total of 790 patients with SVT (386 [31.9% male] AVNRT and 404 [55.9% male] AVRT) were enrolled for this study. The mean age was 51.4±15.6 and 46.5±15.5 years, respectively. The use of electroanatomic mapping systems increased significantly annually (from 0 in 2009 to 100% in 2014) under the guidance of EASTAR principle. The average procedure times (from 91.8±19.4 minutes in 2009 to 59.6±19.1 minutes in 2014), fluoroscopy exposure times (from 11.3±2.3 minutes in 2009 to 2.9±2.4 minutes in 2014) and doses (from 42.0 mGy in 2009 to 6.8±5.7 mGy in 2014) declined correspondingly despite variant tachycardia substrates. The advantages existed when compared with 122 non-EASTAR cases (55 [47.3% male] AVNRT and 67 [59.7% male] AVRT patients). The average procedure times (AVNRT: 78.5±26.5 minutes vs. 87.7±27.7 minutes, P=0.017; AVRT: 71.5±29.2 minutes vs. 93.5±53.5 minutes, P<0.001), fluoroscopy exposure times (AVNRT: 5.7±3.6 minutes vs. 12.7±6.8 minutes, P<0.001; AVRT: 8.1±6.0 minutes vs. 11.6±6.6 minutes, P<0.001) and radiation doses (AVNRT: 19.5±15.2 mGy vs. 88.5±54.1 mGy, P<0.001; AVRT: 30.4±20.8 mGy vs. 59.7±44.0 mGy, P<0.001) were significantly lower in EASTAR cases. The success rate was much higher in the EASTAR cases (97.6% [771/790] vs. 94.3% [115/122], P=0.040) with similar safety endpoints during the follow-up compared with the non-EASTAR cases. The “learning curve” could be optimized under this principle.
Conclusions: Advantages in the decrement of procedure times and fluoroscopy exposure in the catheter ablation therapy of supraventric-ular tachycardia with the guidance of the EASTAR principle are confirmed based on the six-year single center’s data analysis.
CATHETER ABLATION OF SUPRAVENTRICULAR TACHYCARDIA UNDER THE GUIDANCE OF THE EASTAR PRINCIPLE: SIX-YEAR DATA ANALYSIS OF SINGLE CENTERXianfeng Du
Ningbo First Hospital, Ningbo, China
CATHETER ABLATION P 3-044

469
Introduction: The study was to investigate the feasibility and safety of the application of positional reference catheter (PRC) in pulmonary artery (PA) in radiofrequency ablation of atrial fibrillation (AF) by the NavX electroanatomic system compared with the conventional PRC in the coronary sinus (CS).
Methods: A total of 304 consecutive patients with AF who underwent the first catheter ablation from January 2012 to December 2013 in our hospital were randomized into group A (n=152, PRC in PA) or group B (n=152, PRC in CS). Circumferential pulmonary vein isolation were deployed in all subjects while additional complex fractionated electrogram ablation and linear ablation in the roof of LA, mitral isth-mus, cavo-tricuspid isthmus as well as superior vena cava or CS if necessary in patients with persistent AF.
Results: The reconstructive frequency ([1-2, 1.09±0.28] vs. [1-3, 1.18±0.44], P<0.05) and the fluoroscopy time ([3.00-23.26, 9.32±3.77] minutes vs. [2.53-39.37, 11.22±6.83] minutes, P<0.01) were obviously lower in group A than those in group B. The success rates of total patients (77.63% vs. 68.42%, P>0.05) and paroxysmal AF cases (80.95% vs. 77.94%, P>0.05) were similar between two groups during the follow-up. But the success rate of persistent AF cases in group A is higher compared with that in group B (75.28% vs. 60.71%, P<0.05). No significant differences existed in complication rates.
Conclusions: The novel reference technique with catheter in pulmonary artery may reduce the possibility of model drift and reconstruc-tion as well as the fluoroscopy exposure and improve the success rate in persistent cases in the radiofrequency ablation of atrial fibrilla-tion guided by the NavX electroanatomic system.
THE APPLICATION OF POSITIONAL REFERENCE CATHETER IN PULMONARY ARTERY IN RADIOFREQUENCY ABLATION OF ATRIAL FIBRILLATION BY NAVX SYSTEMXianfeng Du
Ningbo First Hospital, Ningbo, China
CATHETER ABLATION P 3-045

470
Introduction: Pace mapping studies historically have utilised semi-quantitative methods to compute distances. The objective of the cur-rent study was to develop new approaches based on computational geometric tools to improve the spatial accuracy of pace mapping uti-lizing the 3-dimensional exported meshes in CARTO.
Methods: Clinical mapping data was acquired in SVT patients mapped during the waiting period after electrophysiology study, utilising CARTO. A paced template was acquired in a single cardiac chamber e.g. right ventricular outflow tract, and compared to n=50 pace maps acquired serially in different regions of the same chamber. Quantitative correlation to surface ECG template was assessed with the CAR-TO PaSo module. The 3D geometry was exported in CARTO, along with the triangulated mesh view. The spatial accuracy of pace-mapping was quantified with two methods, in custom software developed in Matlab: (i) the geodesic distance across the CARTO 3D mesh was computed with a novel greedy algorithm based on Dijkstra’s theorem of the shortest geodesic path across the 3D mesh; (ii) the spatial volume occupied by the convex hull of the 3D point cloud of pace maps.
Results: The mapping study was performed in a pilot study of n=8 patients (778 points). The relationship between Cartesian and geodesic distance, and PaSo correlation coefficient was analysed with multi-level linear models. Decreasing PaSo correlation coefficient showed a linear inverse relationship with distance from the primary template, with 0.1 University decrease in PaSo correlation coefficient associated with 4.7 mm increased Cartesian distance from the template point, 95% CI 5.3,4.2, P<0.001) and 9.2 mm increased geodesic distance from the template 95% CI, 7.8,10.4, P<0.001. Similarly, PaSo correlation coefficient showed a strong linear inverse relationship with con-vex hull point cloud volume (0.01 University increase in Paso correlation coefficient associated with 334 mm3 decrease in volume, 95% CI 284,386, P<0.0001).
Conclusions: These data demonstrate the capacity of novel investigative measures based on computational surface geometric principles to be utilised for the assessment of spatial accuracy of pace mapping. Future investigations will be required to understand the relationship between computational pace mapping assessment and traditional human 12-lead ECG matching.
QUANTITATIVE PACE MAPPING-DEVELOPMENT OF NEW METHODS TO DETERMINE SPATIAL ACCURACYAnand Ganesan, Dhani I Gusti Ayu Agung, Waheed Ahmad, Andrew McGavigan
Flinders University, Adelaide, Australia
CATHETER ABLATION P 3-046
471
Introduction: The advent of 3-dimensional electroanatomical mapping systems have made possible zero fluoroscopy use during electro-physiological procedures. Routine zero fluoroscopy use could significantly reduce risks of radiation for patients and medical personnel. In this pilot study, we explore the feasibility of zero fluoroscopy use in two low volume centres in Southeast Asia.
Methods: 45 consecutive patients undergoing electrophysiological procedures were recruited, with the aim of using zero fluoroscopy. Pa-tients who required trans-septal approach were excluded. 4 operators used the EnSite NavXTM, CARTO 3® or CARTO 3® system with ste-reotaxis. Each had less than 5 years electrophysiological experience. Data including fluoroscopy, radiofrequency (RF), procedure times and complications were collected. Further subgroup analysis was performed on patients who received supraventricular tachycardia/ca-vo-tricuspid isthmus (CTI) ablation procedures, in comparison with matched controls in whom electroanatomical systems had not been used.
Results: In the zero fluoroscopy group, 18 (40%) received AVNRT ablation, 11 (24%) accessory pathway ablation, 7 (16%) CTI ablation, 5 VT ablations (11%), 1 (2%) atrial tachycardia ablation and 3 (7%) diagnostic studies. In 42 out of the 45 cases (93%), the operators were able to achieve zero fluoroscopy. Of the 3 unsuccessful cases, 1 case of RVOT VT ablation required 1s of fluoroscopy for registration of the stereo-taxis system; another was a redo ablation of mid-coronary sinus (CS) AT, requiring fluoroscopy to help guide wire and sheath across a CS stenosis; the last was a right free wall accessory pathway in which ablation was unsuccessful in spite of both electroanatomical mapping and fluoroscopic guidance. In the SVT/CTI subgroup, zero fluoroscopy was used for 35 out of 36 patients. As a result, the average fluoros-copy time (0.2±1.2 vs. 25.3±17.4 minutes), dose area product (180 vs. 21,855 mGy/cm2) and air kerma (2 vs. 191 mGy) were significantly different as compared to the 30 patients in the matched control group. The total procedural time (91.9.±40.0 vs. 101.6±42.3 minutes, P=0.34), time required for positioning of the catheter (19.8±12.2 vs. 15.8±7.8 minutes, P=0.16) and RF time (5.5±6.8 vs. 9.4±9.8 minutes, P=0.07) were not significantly different. The total ablation times (25.5±25.7 vs. 60.5±43.1 minutes, P<0.01) and number of RF lesions tar-getted (8.6±7.4 vs. 18.0±16.3, P<0.01) were significantly less in the zero fluoroscopy group. All but one procedures were acutely success-ful.
Conclusions: Even in low volume centres, zero fluoroscopy is feasible, even for complex ablations such as scar, fascicular and RVOT VT. The use of zero fluoroscopy and electroanatomical mapping in the subgroup of SVT/CTI ablations did not increase procedure time, and in fact reduced total ablation time. Further study to establish safety with zero fluoroscopy is needed.
USE OF ZERO FLUOROSCOPY FOR ELECTROPHYSIOLOGICAL INTERVENTION: THE ZEROX PILOT STUDYAudry Lee1, S. Liang1, K. Saravanan2, C.K. Ching3, V.H. Tan1, K. Wong1 1Changi General Hospital, Singapore; 2Hospital Sultanah Bahiyah, Alor Setar, Malaysia; 3National Heart Centre, Singapore
CATHETER ABLATION P 3-047

472
Introduction: A specialized automated 3D electroanatomic reconstruction tool has recently been introduced; the system automatically configures a geometric model of heart chamber from contact mapping and performs electrogram activity analysis including bipolar and unipolar signal of these structures. The aim of this study was to compare the measurements of low voltage area, activation time, in the same mapping density by the new model to that obtained by manual mapping right ventricle and to assess the reproducibility and accura-cy of this new method compared to manual detection.
Methods: We included 14 patients who underwent EP study and RFCA. The substrate data and area were evaluated by the manual 3D electroanatomic mapping (CARTO 3) method and by the automatic software (CARTO 3 CONFIDENSETM module).
Results: We showed an excellent correlation between the measurements obtained by both intra-class correlation coefficient (ICC): 0.806 (0.494-0.936), Cronbach’s alpha: 0.901 for unipolar mean voltage, ICC: 0.652 (0.202-0.878) Cronbach’s alpha: 0.772 for bipolar mean volt-age, ICC: 0.914 (0.753-0.973), Cronbach’s alpha: 0.967 for total activation time, ICC 0.897 (0.707-0.967), Cronbach’s alpha 0.951 for unipolar low voltage zone, and ICC: 0.905 (0.728-0.970), Crobach’s alpha 0.953 for bipolar low voltage zone, with no significant differences regard-less of the method used. There are more inaccurate points (%) and longer post-possessing time while using manual detection in compar-ison to auto-mapping (15.3±6.8 vs. 2.3±0.8%, P<0.001 and 3.6±1.1 vs. 0.6±0.4 minutes, P<0.001 respectively).
Conclusions: The CONFIDENSETM module software allows modeling and quantifying the ventricle from 3D data. There are less inaccurate annotation and less post-possessing time while using CONFIDENCE system.
ACCURACY AND REPRODUCIBILITY OF NOVEL ELECTROANATOMIC THREE-DIMENSIONAL AUTOMATED MAPPING SOFTWARE (CARTO 3 SYSTEM CONFIDENSETM MODULE) FOR THE ASSESSMENT OF THE RIGHT VENTRICULAR SUBSTRATE IN VENTRICULAR ARRHYTHMIAChin-Yu Lin, Yenn-Jiang Lin, Fa-Po Chung, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
CATHETER ABLATION P 3-048

473
Introduction: Novel methods of mapping the human atrium in atrial fibrillation (AF) include the multi-electrode basket catheter which al-lows simultaneous electrogram acquisition of the left atrium. However, the efficacy of this catheter in providing adequate electrode con-tact and electrogram recordings of the entire left atrium is unclear.
Methods: Global left atrial mapping was performed in 12 patients using the 56 bipolar electrode Boston Scientific Constellation basket catheter. Appropriate basket size was chosen based on pre-procedural cardiac CT imaging and intra-procedural transesophageal echo-cardiography. We analyzed specific spatial characteristics of the basket catheter and in particular its ability to provide global LA mapping for AF mapping including 1. Number of electrodes within 2 mm of the endocardial surface 2. Number of electrodes with suitable signal quality 3. Percentage of LA mapped 4. Interspline distance (distance between adjacent splines as shown by the white arrow in Figure, panel A).
Results: 12 patients were studied. 60 mm basket catheters were used in 3 (25%) patients, 48 mm catheters in 8 (67%) and the 38 mm catheter in 1 patient. In 50% of patients, the Agilis sheath was used for basket catheter positioning. The mean number of electrodes within 2 mm of the endocardial surface was 29±3 (45%). Of the 56 bipolar electrograms, mean of 28±7 (48%) had suitable signal quality to allow annotation for activation times. The mean percentage of LA mapped was 20.3%. There was marked variability in the inter-spline distance. The greatest inter-spline distance was at the equator (19.3±1.2 mm) with the least inter-spline distance at the distal pole (12.4±0.9 mm) (Figure, panel B).
Conclusions: The constellation multipolar basket catheter provide limited coverage of the left atrium with poor signal quality and contact with the endocardial surface. Improved catheter technology is necessary to facilitate global mapping of the left atrium.
THE EFFICACY OF MULTIPOLAR BASKET CATHETERS IN MAPPING THE ENTIRE LEFT ATRIUM IN HUMAN PERSISTENT ATRIAL FIBRILLATIONBhupesh Pathik1, Tomos Walters1, Pawel Kuklik2, Jichao Zhao3, Andrew Madry1, Sandeep Prabhu1, Chrishan Nalliah1, Jonathan Lipton1, Joseph Morton1, Paul Sparks1, Peter Kistler4, Jonathan Kalman1, Geoff Lee1 1Royal Melbourne Hospital, Melbourne, Australia; 2Maastricht University Medical Center, Maastricht, Netherlands; 3University of Auckland, Auckland, New Zealand; 4Alfred and Baker IDI, Melbourne, Australia
CATHETER ABLATION P 3-049
474
Introduction: The objective of the present study was to determine the effects of preexcitation on left ventricular wall motion in patients with Wolff-Parkinson-White (WPW) syndrome.
Methods: We consecutively included 230 patients who underwent pre-procedural echocardiography and catheter ablation for WPW syn-drome. Among them, 54 patients underwent post-procedural echocardiography. We analyzed QRS duration, the location of the accessory pathway (AP), left ventricular wall motion abnormality and ejection fraction.
Results: APs were located in the left, septal, right wall in 122, 63, and 45 patients, respectively. Wall motion abnormality at the AP location was more frequent in patients with septal and right AP than patients with left AP (63.5%, 46.7%, and 23.0%, respectively, P<0.001). QRS duration was significantly longer in patients with wall motion abnormality at the AP location than in patients without wall motion abnor-mality (141.1±23.0 and 124.6±20.6, respectively, P=0.013). There was no significant difference in left ventricular ejection fraction among three groups (60.3±10.8, 61.6±9.5, and 64.2±6.3%, respectively, P=0.451). In 87.9% of the patients with wall motion abnormality, wall mo-tion abnormality improved after catheter ablation.
Conclusions: Wall motion abnormality related to the septal AP is frequent in patients with WPW syndrome. Wall motion abnormality im-proves in the most patients with AP.
ACCESSORY PATHWAY-RELATED WALL MOTION ABNORMALITY AND LEFT VENTRICULAR DYSFUNCTION IN PATIENTS WITH WOLFF-PARKINSON-WHITE SYNDROMEJae-Sun Uhm, Tae-Hoon Kim, Boyoung Joung, Hui-Nam Pak, Moon-Hyoun Lee
Severance Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 3-050

475
Introduction: Non-Pulmonary Vein (NPV) foci are implicated as initiators of Atrial Fibrillation (AF), focal drivers of AF, and originator of Atrial Tachycardia (AT). Atrial tachycardia from NPV are relatively uncommon and being of shorter cycle length than Pulmonary vein tachy-cardia often go unrecognized and have unusual presentations. We report two cases of incessant left atrial tachycardia with varied presen-tation who had successful ablation using different electro-anatomic mapping techniques.
Methods: N/A
Results: Case 1: A 23-year-old male, with progressive dyspnea had incessant atrial tachycardia causing tachy-cardiomyopathy. The CS activation pattern, VAAV response and VA dissociation suggested AT originating from Left atrium (LA). After trans-septal puncture with standard Brokenborough technique, 9 F Multielectrode Array balloon (St. Jude Medical) for Non-contact mapping was introduced in the LA through the cook sheath and 7F ablation catheter through Agilis sheath (St. Jude). The AT terminated after trans-septal puncture and the virtual activation map identified the focus of atrial ectopics below the left upper pulmonary vein. Focal ablation at this site was suc-cessful. Follow up at 6 months showed significant improvement of LV function. Case 2: A 46-year old male, had vague symptoms of un-easiness resulting in anxiety, insomnia and depression. He was detected to have incessant AT and borderline LV systolic function. He un-derwent Electrophysiological study with NavX system. After transeptal puncture 7 F 20-pole circular mapping catheter (Optima; St. Jude Medical) was introduced through Agilis sheath and electro-anatomical map of left atrium was created. The focus of atrial tachycardia was located between left atrial appendage and left lower pulmonary vein. Focal ablation with 7 F ablation catheter at this location was suc-cessful. There has been no recurrence over two months of follow up.
Conclusions: Incessant left atrial tachycardia from NPV may present with unusual symptoms rather than palpitations. Electro-anatomic mapping is useful in guiding ablation of unpredictable atrial ectopics and focal tachycardia originating at locations outside the pulmonary veins.
CATHETER ABLATION OF INCESSANT ATRIAL TACHYCARDIA FROM NON-PULMONARY VEIN FOCIPradeep Hasija1, Rajkumar Mantravadi2, Prashant Bharadwaj1 1Armed Forces Medical College, Pune, India; 2Shayadri Hospital, Pune, India
CATHETER ABLATION P 3-051

476
Introduction: Ablation of para-Hisian accessory pathway is challenging due to risk of heart block. We hypothesized that insufficient ener-gy-delivery during catheter ablation at para-Hisian area leads to reconnection of the accessory pathway.
Methods: Among total 275 consecutive patients with accessory pathway, catheter ablation was performed in 86 patients at para-Hisian (near His- or septal region) area and in 189 patients rat non-septal areas. The ablation sites at para-Hisian area were mid septum (20.9%), anteroseptum (11.6%) and posteroseptum (67.4%). Non-septal areas included lateral (71.8%), anterolateral (13.2%) and posterolateral (14.8%) area. We compared the clinical outcomes of catheter ablation between para-Hisian and non-septal accessory pathway.
Results: The baseline characteristics were similar between two groups; age (38.8±40.4 vs. 61.1±10.4 years, P=0.511), male (70.2% vs. 58.1%, P=0.465), hypertension (17.5% vs. 16.3%, P=0.864), diabetes (3.7% vs. 3.5%, P=0.930), vascular disease (6.9% vs. 5.8%, P=0.741), coexisting arrhythmias (5.8% vs. 5.8%, P=0.785). Proportion of preexcitation was greater in para-Hisian group than in non-septal group (54.7% vs. 36.0%, P=0.005). Compared to non-septal group, para-Hisian group showed longer total ablation time (382±34 vs. 281±19 sec-onds, P=0.006), greater number of energy-delivery each procedure (10.6±1.1 vs. 5.7±0.4 times, P<0.001), and less contact time per ener-gy-delivery (51.3±32.9 vs. 61.5±42.1 seconds, P=0.048). Retrograde ventriculo-atrial dissociation after catheter ablation was not signifi-cant different (43.9% vs. 57.0%, P=0.051). However, rates of recurrence were greater in the para-Hisian area group compared to non-sep-tal group (19.7% vs. 3.7%, P<0.001). The number of energy-delivery each procedure is associated with reconnection of bypass tract (OR 1.046, 95% CI 1.005-1.088, P=0.026).
Conclusions: This study demonstrated that, compared to non-septal group, incomplete and repetitive contact at para-Hisian accessory pathway is the main cause of the reconnection, leading to the recurrence.
CATHETER ABLATION OF PARA-HISIAN VERSUS NON-SEPTAL ACCESSORY PATHWAY: IMPACT OF CONTACT NUMBER AND TIME DURING ENERGY-DELIVERY ON RECONNECTIONDong-Hyeok Kim1, Jong-Il Choi2, Jaemin Shim2, Sang-Weon Park1, Young-Hoon Kim2, Kwang-No Lee2, Seung-Young Roh2, Hong Euy Lim3, Jin Seok Kim4 1Sejong General Hospital, Bucheon, Republic of Korea; 2Korea University Medical Center, Seoul, Republic of Korea; 3Korea University Guro Hospital, Seoul, Republic of Korea; 4Korea University Ansan Hospital, Ansan, Republic of Korea
CATHETER ABLATION P 3-052

477
Introduction: There are few reports about biatrial tachycardia in patients with no history of catheter ablation or cardiac surgery.
Methods: N/A
Results: A 64-year-old woman with no history of cardiac disease had palpitations and was referred to our hospital for ablation. Her clini-cal diagnosis was common atrial flutter (AFL). Activation mapping of the right atrium (RA) was first performed during ablation and re-vealed this tachycardia to be circling counter-clockwise around the tricuspid valve. The post-pacing interval (PPI) was consistent with the tachycardia cycle length (CL) (360 msec) both at the lateral RA and the cavotricuspid isthmus (CTI); therefore, we suspected this tachycar-dia was common AFL. However, the PPI at the distal coronary sinus (CS) was also equal to the tachycardia CL, which was only 239 msec in the activation map and did not cover the overall CL (360 msec). Involvement of the left atrium (LA) was strongly suspected, and we made an additional activation map of the LA via a transseptal approach. The map of both atria covered the overall CL and revealed that the tachycardia circuit largely traveled around both atria (Figure). Furthermore, a low-voltage area was widely distributed around the CTI, and the excitement could conduct from the lateral RA only to the CS, not to the septum, via the CTI. Just one radiofrequency application to the residual myocardium in the CTI stopped the tachycardia and formed a bidirectional conduction block. To date, there has been no post-ab-lation recurrence.
Conclusions: We experienced a rare case of biatrial tachycardia mimicking common AFL. Additional mapping of the LA was useful to identify the complete circuit.
A CASE OF BIATRIAL TACHYCARDIA MIMICKING COMMON ATRIAL FLUTTERKeita Masuda, Kenji Kuroki, Hiro Yamasaki, Yukio Sekiguchi, Akihiko Nogami, Kazutaka Aonuma
University of Tsukuba, Tsukuba, Japan
CATHETER ABLATION P 3-054

478
Introduction: In Taiwan, RFCA is the first-line treatment for AVNRT and no data about cryoablation for AVNRT has been reported. The purpose of this study was to compare the short term outcome and complications of cryoablation and RFCA for AVNRT in children and ad-olescents.
Methods: All patients receiving transcatheter ablations for AVNRT in children and adolescents in NTUCH from February 2000 to June 2016 were retrospectively reviewed.
Results: Totally, 153 consecutive patients were enrolled. RFCA was arranged in 123 patients (from January 2000 to January 2015) and cryoablation was arranged in 30 patients (from February 2015 to June 2016). Among them, 31 (25.2%) in RFCA group didn’t receive abla-tion due to risk of atrioventricular (AV) block, and one (0.33%) didn’t receive cryoablation due to no antegrade fast pathway was document-ed. Therefore, 122 ablation procedures (92 RFCA and 30 cryoablation) were performed in 114 patients. There were 52 males and 62 fe-males, and all of them presented with palpitations. The basic demographic characteristics were similar between two groups including gender (P=0.55), using anti-arrhythmic drug (P=0.67), and associated congenital heart disease (P=0.95). The mean age was 16.9±5.8 years in cryoablation group and 13.2±4.7 years in RFCA group (P<0.001), and the mean body weight was 57.4±12.9 kg in cryoablation group and 47.7±12 kg in RFCA group (P=0.001). Acute procedural success rate was 96.5% in cryoablation group and 97.6% in RFCA group (P=0.72). Eight patients in RFCA group had recurrence of AVNRT (9.52%) with median duration of recurrence as 12 months. There were two recurrences (6.89%) in cryoablation group (P=0.86). No permanent atrioventricular block was found in both groups. The fluoroscopy time was similar between the two group (28.9±18.7 vs. 28.6±14.8 minutes; P=0.698). The follow-up time was significantly longer in RFCA group than cryoablation group (P<0.001).
Conclusions: Cryoablation for AVNRT in children and adolescents is as effective but with lower recurrence rate than RFCA at short term follow-up. No AV block occurred in both group but more patients in RFCA group chose not to receive ablation due to risk of AV block. Whether the recurrence rate is as low as our result needs long term follow-up.
TRANSCATHETER ABLATION OF ATRIOVENTRICULAR NODAL REENTRANT TACHYCARDIA IN CHILDREN AND ADOLESCENTS IN TAIWAN: COMPARISON OF CRYOABLATION WITH RADIOFREQUENCY ABLATIONKun-Lang Wu1, Shuenn-Nan Chiu2, Chun-Wei Lu2, Wei-Chieh Tseng2, Mei-Hwan Wu2 1Changhua Christian Hospital, Changhua, Taiwan; 2National Taiwan University Hospital, Taipei, Taiwan
CATHETER ABLATION P 3-056

479
Introduction: Thirty one year old female presented with recurrent paroxysmal palpitations. ECG during tachycardia showed regular nar-row QRS tachycardia with CL 260 msec. ECG in Sinus rhythm showed no preexcitation. Referred for EPS and RF ablation.
Methods: Induction of Tachycardia by Atrial premature beat due atrial Extrastimuli may be reentry beat with eccentric retrograde atrial activationEP Study: Intracardiac Electrogram during Tachycarda with CL 260 msec with earliest A at distal CS. Differential Diagnosis of Regular narrow QRS tachycardia with earliest A at dsistal CS: Left Lateral concealed AP mediated circus movement ORT. Atrial Tachycar-dia from lateral Mitral Annulus. Left sided circuit in AVNRT fast-slow type. Burst Pacing of RV septum with concentric retrograde conduc-tion Electrophysiological Maneuvers to distinguish these three tachycardia: Pacing LV with concentric conduction. Pacing of LV lateral wall during tachycardia with VAVA response on stopping Pacing excludes left mitral annular Atrial Tachycardia A on V tachycardia was fre-quently inducible with VA interval <70 msec indicates Slow-Fast AVNRTA on V tachycardia was frequently inducible with VA interval <70 msec indicates Slow-Fast AVNRT.
Results: Successful slow pathway ablation done by Electrogram and anatomical guided near the upper lip of CS with frequent junctional beats. Transeptal Puncture was done but on LV pacing there was no conduction through AP (no eccentric atrial activation) therefore not ablated. No tachycardia was inducible by any means. Resetting from three slow pathway region by giving delayed atrial extramuli during tachycardia and demonstrating His preexcitation (resetting) confirms part of circuit and ablation should be done there.
Conclusions: This narrow QRS tachycardia with Eccentric and Concentric atrial conduction could be due to left sided (Fast-Slow type) and right sided (Slow-Fast type) circuit of AVNRT but fusion beat terminates tachycardia proves AP mediated ORT. Although episodic bypass conduction can cause orthodromic circus movement tachycardia. Over eight months of follow up no recurrence of any tachycardia.
IS IT LEFT SIDED CIRCUIT IN AVNRT?Ramdeo Yadave
Batra Hospital, New Delhi, India
CATHETER ABLATION P 3-057

480
Introduction: Mr. S.N. fifty two year man presented with recurrent paroxysmal palpitations since 2003. In some of the episodes he had syncope. Consulting cardiologist diagnosed NSR with LBBB and thought syncope is due to Infra-Hisian conduction defect. He put the pa-tient on PPI-VVI at 70 ppm of Shree Pacetronic India. After pacemaker implantation his incidence of palpitation increased in frequency and syncope still used to occurred.
Methods: Baseline ECG showed pre-excitation with LBBB with LAD. X ray chest normal size heart and lung parenchyma and vascularity. Echo showed structurally and functionally normal heart.
Results: Baseline ECG showed pre-excitation with HV interval 20 mesc suggestive of right antero-septal accessory pathway. On V pacing VA conduction was concentric and nondecremental suggestive of retrograde conduction was through anteroseptal accessory pathway. On A pacing pre-excitation was further increased. On A pacing regular wide QRS tachycardia was induced with earliest A at His bundle. His EGM started after ventricular electrogram with negative HV interval suggestive of pre-excited tachycardia with LBBB with LAD with late transition in V5. Atrial extra during HIS refractory failed to pre- excite next V and A suggestive of no antedromic pathway mediated tachy-cardia. On ventricular pacing during tachycardia and on stopping cPPI was less than 110 mesc suggest ORT due to Anteroseptal AP wich was ablated during tachycardia with termination of tachycardia without A suggests termination due to block in retrograde conduction in the accessory pathway. The prexcitation remain present which was not increasing with atrial pacing and HV interval remain short and fixed at 20 mesc. On A pacing on adenosine showed blocked paced A suggestive of Fasciculoventricular pathway.
Conclusions: This patient is having both antegrade and retrograde conducting anteroseptal accessory pathway which lead to orthodromic tachycardia and after its ablation during tachycardia pre-excitation remain present suggest fasciculoventricular pathway. No further tachycardia was induced. Fasciculoventricular AP does not need RF ablation as it is not involved in tachycardia mechanism.
REGULAR WIDE QRS TACHYCARDIA WITH BASELINE PRE-EXCITATION: WHAT IS THE MECHANISM?Ramdeo Yadave
Batra Hospital, New Delhi, India
CATHETER ABLATION P 3-058

481
Introduction: Forty three year old male presented with recurrent paroxysmal palpitations with giddiness. ECG during sinus rhythm showed pre-excitation with Right lateral wall Accessory pathway. ECG during tachycardia was SVT suggestive of ORT. Echo was normal study. Taken up for EP study and RF ablation.
Methods: I tried to map the preexcitation and found earliest V than delta in sinus rhythm is equally earlier at Anteroseptal region and right lateral area but on RF delta did not disappeared so thought of mapping in Right atrial appendage area where ventricular and atrial signals are closest and was mapped from Right internal jugular route with loss of delta with single RF applications with VA block through path-way.
Results: Successful RF ablation of RAA to RV Accessory pathway was ablated without complications. One may confuse and might ablate at anteroseptal region with risk of heart block.
Conclusions: WPW syndrome with Right lateral wall AP may be located between RAA and RV junction and can be successfully ablated from internal jugular route. Suspicion of such pathway is possible beforehand if earliest AV EGM present equally at both Antero-septal re-gion and Right free wall region.
WPW SYNDROME WITH RIGHT ATRIAL APPENDAGE TO RV ACCESSARY PATHWAYRamdeo Yadave
Batra Hospital, New Delhi, India
CATHETER ABLATION P 3-059

482
Introduction: We describe a case of postero-septal accessory pathway (AP) that required radiofrequency (RF) energy applications at both the right and left sided postero-septum.
Methods: N/A
Results: An 11-year-old boy who suffered from recurrent palpitations was referred to our institution. During sinus rhythm, 12-lead ECG showed the ventricular pre-excitation with the negative delta wave in leads III and V1, and the positive delta wave in lead V2, indicating a postero-septal AP (Figure A). Mapping at the right sided postero-septum revealed that the earliest ventricular activation was at the bottom of the CS ostium preceding 42 ms from the onset of the delta wave. Ablation at this site changed the delta wave from negative to positive in lead V1 (Figure B), suggesting that the AP remained on the left side. Mapping was then performed at the mitral annulus, demonstrating the earliest ventricular activation at the left postero-septum. RF energy application at this site successfully eliminated the AP conduction.
Conclusions: RF energy applications at both the CS ostium and postero-septal mitral annulus were effective for elimination of the poste-ro-septal AP. This suggests that this case had the broad AP extending from the left endocardium to the right epicardium.
POSTERO-SEPTAL ACCESSORY PATHWAY REQUIRING ABLATIONS AT BOTH THE RIGHT AND LEFT SIDED POSTERO-SEPTUM; A CASE REPORTShu Yamashita1, Yoshihide Takahashi1, Masahito Suzuki1, Rho Nagasawa1, Mayumi Masumura1, Yasuhiro Sato1, Kenzo Hirao2, Mitsuaki Isobe1 1National Hospital Organization Disaster Medical Center, Tachikawa, Japan; 2Heart Rhythm Center, Tokyo Medical and Dental University, Bunkyo, Japan
CATHETER ABLATION P 3-060

483
Introduction: Transseptal puncture is a common approach of left-sided accessory pathway (AP) ablation with risk of cardiac perforation and extra cost of ICE using. In some circumstances, the probe-patent foramen ovale (PFO) could be a potential access of left atrial cathe-terization. In this study, we aimed to examine the incidence and feasibility of transseptal approach via Probe-PFO without atrial septal puncture in Left AP ablation.
Methods: Ninty-six consecutive patients (64 men; mean age: 42.5±14.2 years) with diagnosis of Left AP by EP study from January 2015 to December 2015 were enrolled. All patients had no structural heart disease and PFOs were detected by trans-thoracic echocardiography (TTE). Under the guidance of fluoroscopy, transspetal access via Probe-PFO were directly attempted by a 7F mapping catheter. If the transseptal approach via Probe-PFO was unsuccessful after 180s, the Left AP was ablated by transaortic or standard atrial septal punc-ture access.
Results: All cases of Left AP were successfully ablated without complications. 36 patients (37.5%) were performed by transseptal access via Probe-PFO without atrial septal puncture; 49 (51.0%) by transaortic approach and 11 (11.5%) by standard atrial septal puncture ap-proach. The average fluoroscopy duration of transseptal attempting via Probe-PFO were 45.8±18.4s (27.3-75.8s). No recurrence of tachy-cardia in 6-18 months of follow-ups.
Conclusions: Left AP ablation by transseptal access via Probe-PFO without atrial septal puncture is a feasible approach in patient with normal heart structure and no PFO detection in TTE. In this study, there are about one third of the Left AP cases can be successfully ablat-ed using this technique.
TRANSSEPTAL CATHETER ABLATION OF LEFT SIDED ACCESSORY PATHWAY VIA PROBE-PATENT FORAMEN OVALE WITHOUT ATRIAL SEPTAL PUNCTUREXu Zhou, XueFeng Guang, XiaoYong Zhang
Kunming Yanan Hospital, Kuming, China
CATHETER ABLATION P 3-061
484
Introduction: Non compliance in patients is a worldwide problem and is multifactorial. Travel distance, age, gender and other clinical fac-tors have been showed to be related to patient compliance to treatment. Our study aimed to examine the demographic and clinical factor to patient compliance in management of atrial fibrillation.
Methods: The study was designed as a cross-sectional observational study with consecutive sampling done from January to December 2015. One hundred fifty seven patients that were diagnosed with atrial fibrillation were included, their sex and age determined, CHA2DS-2VASC and HASBLED score were calculated along with the distance between the patient’s home and the medical centre while also factor-ing in patient’s symptoms. Compliance is defined on whether or not the patient came for the first follow up after their admission.
Results: The result was obtained on 157 samples and presented as follow [Median, [min-max)]: There were 91 females (57%), distance to medical centres are [13, (1, 3-257)], CHA2DS2VASC [2, (0-7)] and HASBLED [1, (0-5)]. Among 157 samples only 59 came back for their fol-low up. Of those 59 samples coming back for their follow up, 37 were females and 22 were males, age [59, (20-84)], CHA2DS2VASC [2, (0-6)], HASBLED [1, (0-5)], distance results [13, (2-257)]. Additionally, 44 samples of those 59 came back for the second follow up visit. The correlations between age, CHADVASC, HASBLED, and distance to compliance related to initial follow up was insignificant, Interestingly the correlation of the initial follow up visit to the second follow up visit were vastly significant with correlation coefficients of 0,719 and (p value<0.05). In addition, the correlation between symptoms to compliance related to initial follow up was mostly insignificant except for feeling of bloatedness which is associated significantly with correlation coefficients of -0,264 and (p value<0.05).
Conclusions: There were no significant correlations between the demographic and clinical factors to compliance regarding the first follow up visit but there were significant correlation found between the initial follow up visit with the second follow up visit and symptoms of bloatedness with initial follow up visit.
CORRELATION OF DEMOGRAPHIC FACTORS AND PATIENT SYMPTOMS WITH PATIENT COMPLIANCE IN FOLLOWING UP ONE MONTH AFTER ADMISSION IN AF PATIENTS IN A LOCAL SECONDARY HOSPITALDylan Hadi1, K Marwali2, Wibowo ANM1, SA Yuwono1, Vatvani A1, Soetjipto AS1, Ng S1,2
1Faculty of Medicine, Universitas Pelita Harapan, Tangerang, Indonesia; 2Siloam General Hospital, Tangerang, Indonesia
CATHETER ABLATION P 3-062
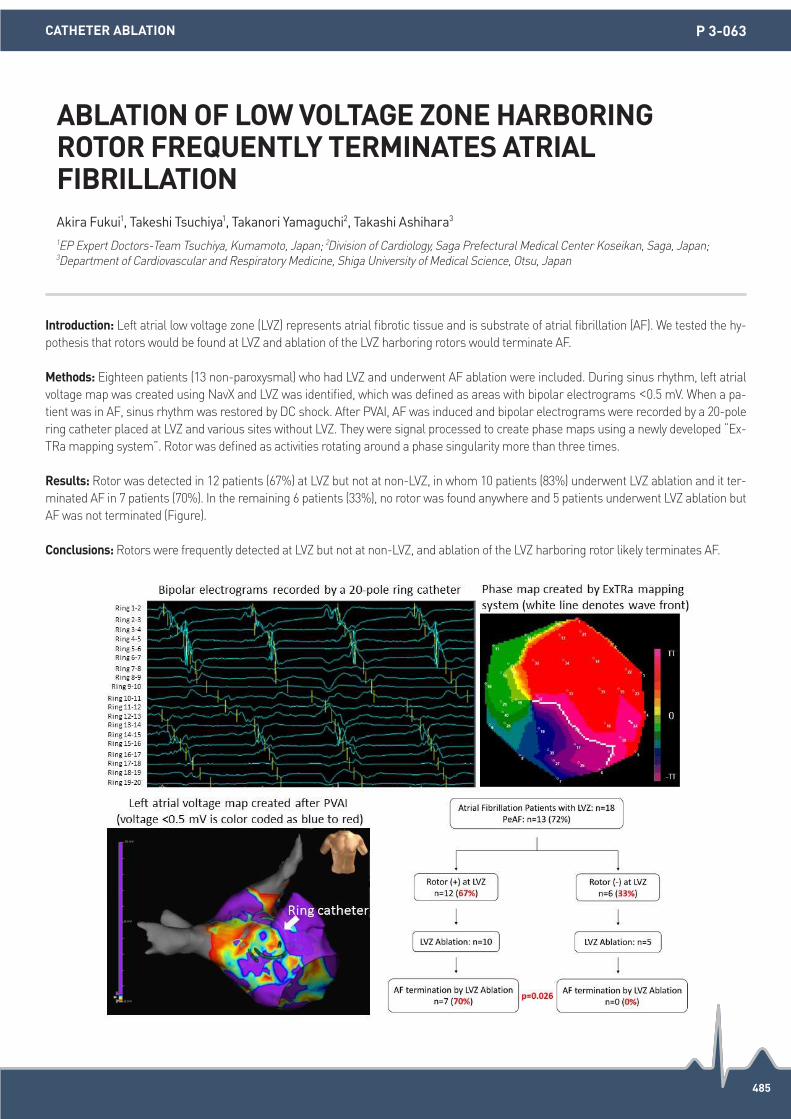
485
Introduction: Left atrial low voltage zone (LVZ) represents atrial fibrotic tissue and is substrate of atrial fibrillation (AF). We tested the hy-pothesis that rotors would be found at LVZ and ablation of the LVZ harboring rotors would terminate AF.
Methods: Eighteen patients (13 non-paroxysmal) who had LVZ and underwent AF ablation were included. During sinus rhythm, left atrial voltage map was created using NavX and LVZ was identified, which was defined as areas with bipolar electrograms <0.5 mV. When a pa-tient was in AF, sinus rhythm was restored by DC shock. After PVAI, AF was induced and bipolar electrograms were recorded by a 20-pole ring catheter placed at LVZ and various sites without LVZ. They were signal processed to create phase maps using a newly developed “Ex-TRa mapping system”. Rotor was defined as activities rotating around a phase singularity more than three times.
Results: Rotor was detected in 12 patients (67%) at LVZ but not at non-LVZ, in whom 10 patients (83%) underwent LVZ ablation and it ter-minated AF in 7 patients (70%). In the remaining 6 patients (33%), no rotor was found anywhere and 5 patients underwent LVZ ablation but AF was not terminated (Figure).
Conclusions: Rotors were frequently detected at LVZ but not at non-LVZ, and ablation of the LVZ harboring rotor likely terminates AF.
ABLATION OF LOW VOLTAGE ZONE HARBORING ROTOR FREQUENTLY TERMINATES ATRIAL FIBRILLATIONAkira Fukui1, Takeshi Tsuchiya1, Takanori Yamaguchi2, Takashi Ashihara3 1EP Expert Doctors-Team Tsuchiya, Kumamoto, Japan; 2Division of Cardiology, Saga Prefectural Medical Center Koseikan, Saga, Japan;
3Department of Cardiovascular and Respiratory Medicine, Shiga University of Medical Science, Otsu, Japan
CATHETER ABLATION P 3-063
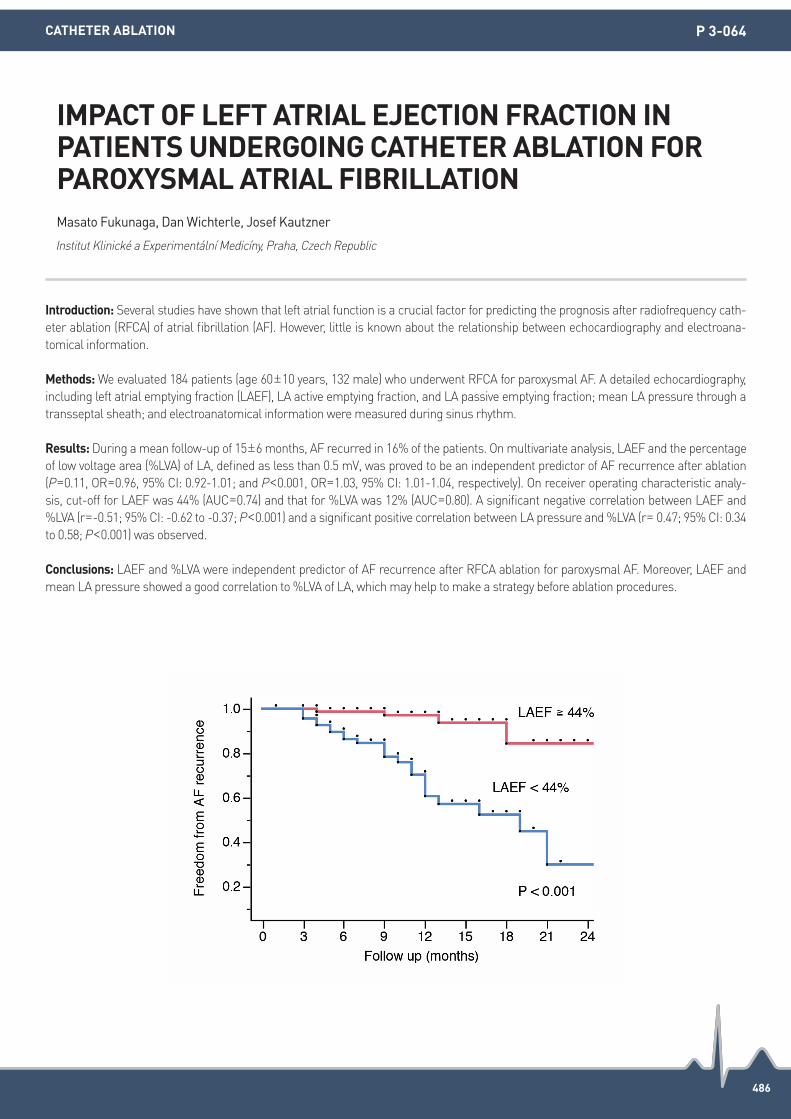
486
Introduction: Several studies have shown that left atrial function is a crucial factor for predicting the prognosis after radiofrequency cath-eter ablation (RFCA) of atrial fibrillation (AF). However, little is known about the relationship between echocardiography and electroana-tomical information.
Methods: We evaluated 184 patients (age 60±10 years, 132 male) who underwent RFCA for paroxysmal AF. A detailed echocardiography, including left atrial emptying fraction (LAEF), LA active emptying fraction, and LA passive emptying fraction; mean LA pressure through a transseptal sheath; and electroanatomical information were measured during sinus rhythm.
Results: During a mean follow-up of 15±6 months, AF recurred in 16% of the patients. On multivariate analysis, LAEF and the percentage of low voltage area (%LVA) of LA, defined as less than 0.5 mV, was proved to be an independent predictor of AF recurrence after ablation (P=0.11, OR=0.96, 95% CI: 0.92-1.01; and P<0.001, OR=1.03, 95% CI: 1.01-1.04, respectively). On receiver operating characteristic analy-sis, cut-off for LAEF was 44% (AUC=0.74) and that for %LVA was 12% (AUC=0.80). A significant negative correlation between LAEF and %LVA (r=-0.51; 95% CI: -0.62 to -0.37; P<0.001) and a significant positive correlation between LA pressure and %LVA (r= 0.47; 95% CI: 0.34 to 0.58; P<0.001) was observed.
Conclusions: LAEF and %LVA were independent predictor of AF recurrence after RFCA ablation for paroxysmal AF. Moreover, LAEF and mean LA pressure showed a good correlation to %LVA of LA, which may help to make a strategy before ablation procedures.
IMPACT OF LEFT ATRIAL EJECTION FRACTION IN PATIENTS UNDERGOING CATHETER ABLATION FOR PAROXYSMAL ATRIAL FIBRILLATIONMasato Fukunaga, Dan Wichterle, Josef Kautzner
Institut Klinické a Experimentální Medicíny, Praha, Czech Republic
CATHETER ABLATION P 3-064

487
Introduction: As catheter ablation of atrial fibrillation (AF) is performed under fluoroscopic guidance, it carries the risk of radiation expo-sure for both the patient and the electrophysiology (EP) lab staff. Non-fluoroscopic mapping systems and technologies (to allow non-fluo-roscopic catheter visualization) together with intracardiac echo (ICE) have reduced but not replaced fluoroscopy exposure. We follow the ALARA principle (as low as reasonably achievable) and demonstrate the feasibility and the safety of catheter ablation for AF (without the radiation exposure).
Methods: From August 2015 to May 2016, 100 patients (35 females; mean age, 67 years) with AF (62 paroxysmal, 28 persistent) underwent zero fluoroscopy catheter ablation for AF using the non-fluoroscopic mapping system (CARTO3 system). Insertion of two sheaths (8.5Fr Agiris, and 9Fr or 10Fr), ICE and catheter placement, trans-septal puncture, mapping, and ablation were all performed without fluorosco-py using ICE and CARTO3 mapping. In all cases, the catheter ablation endpoint was confirmation of pulmonary vein isolation. In patients with persistent AF, supra vena cava isolation and left atrial linear ablation were also performed.
Results: In all patients, zero fluoroscopy catheter ablation was performed successfully and no procedure-related complications were re-corded. Mean recorded times, with the fluoroscopy time being 0 minutes, were EP lab occupancy (patient-in to patient-out) 223 ± 47.6 minutes, skin-to-skin procedure time 166 ± 38.8 minutes.
Conclusions: Zero fluoroscopy catheter ablation of AF using CARTO3 system was safely performed and it conformed to the ALARA princi-ple.
ZERO FLUOROSCOPY ABLATION OF ATRIAL FIBRILLATION USING THE CARTO3 SYSTEMTohru Kawakami
Ichinomiya Nishi Hospital, Ichinomiya, Japan
CATHETER ABLATION P 3-065
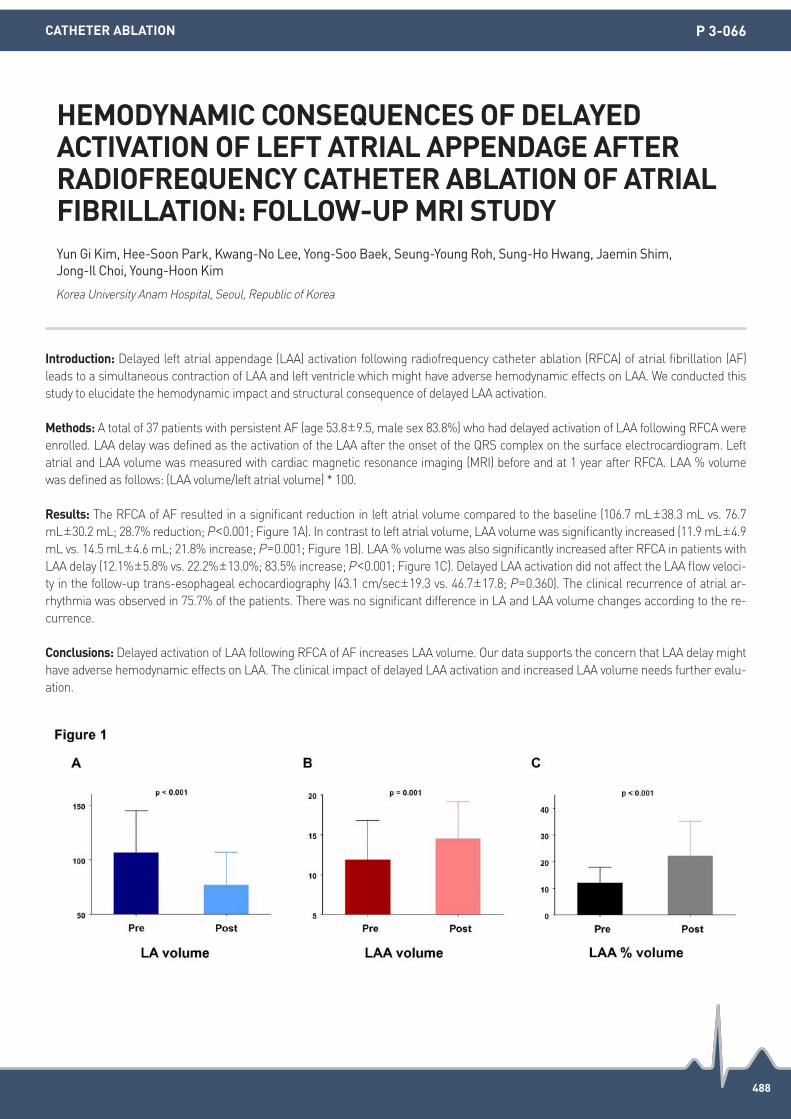
488
Introduction: Delayed left atrial appendage (LAA) activation following radiofrequency catheter ablation (RFCA) of atrial fibrillation (AF) leads to a simultaneous contraction of LAA and left ventricle which might have adverse hemodynamic effects on LAA. We conducted this study to elucidate the hemodynamic impact and structural consequence of delayed LAA activation.
Methods: A total of 37 patients with persistent AF (age 53.8±9.5, male sex 83.8%) who had delayed activation of LAA following RFCA were enrolled. LAA delay was defined as the activation of the LAA after the onset of the QRS complex on the surface electrocardiogram. Left atrial and LAA volume was measured with cardiac magnetic resonance imaging (MRI) before and at 1 year after RFCA. LAA % volume was defined as follows: (LAA volume/left atrial volume) * 100.
Results: The RFCA of AF resulted in a significant reduction in left atrial volume compared to the baseline (106.7 mL±38.3 mL vs. 76.7 mL±30.2 mL; 28.7% reduction; P<0.001; Figure 1A). In contrast to left atrial volume, LAA volume was significantly increased (11.9 mL±4.9 mL vs. 14.5 mL±4.6 mL; 21.8% increase; P=0.001; Figure 1B). LAA % volume was also significantly increased after RFCA in patients with LAA delay (12.1%±5.8% vs. 22.2%±13.0%; 83.5% increase; P<0.001; Figure 1C). Delayed LAA activation did not affect the LAA flow veloci-ty in the follow-up trans-esophageal echocardiography (43.1 cm/sec±19.3 vs. 46.7±17.8; P=0.360). The clinical recurrence of atrial ar-rhythmia was observed in 75.7% of the patients. There was no significant difference in LA and LAA volume changes according to the re-currence.
Conclusions: Delayed activation of LAA following RFCA of AF increases LAA volume. Our data supports the concern that LAA delay might have adverse hemodynamic effects on LAA. The clinical impact of delayed LAA activation and increased LAA volume needs further evalu-ation.
HEMODYNAMIC CONSEQUENCES OF DELAYED ACTIVATION OF LEFT ATRIAL APPENDAGE AFTER RADIOFREQUENCY CATHETER ABLATION OF ATRIAL FIBRILLATION: FOLLOW-UP MRI STUDYYun Gi Kim, Hee-Soon Park, Kwang-No Lee, Yong-Soo Baek, Seung-Young Roh, Sung-Ho Hwang, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 3-066

489
Introduction: Cardiac magnetic resonance (CMR) is known to be useful to predict procedural and clinical outcomes in patients with atrial fibrillation (AF). Late gadolinium enhancement (LGE) of the atrium has been used for measurement of myocardial fibrosis or scar. We hy-pothesized that the difference in the extent of pre- and 1 year post-ablation LGE of the left atrium (LA-LGE) is increased by transmural ab-lation lesion and has associations with clinical recurrence of AF/atrial tachycardia (AT) after AF ablation.
Methods: A total of 65 patients (50.7% paroxysmal, 72.5% female, 54.4±10.4 years old) underwent post-ablation CMR after 1 year or be-fore redo-ablation. LA-LGE in CMR was defined as signal intensities equal to or greater than the 6-standard deviation from the signal in-tensity of left ventricular myocardium.
Results: The differences between mean extent of pre- and post-ablation LA-LGE were 31.7±25.8% in all patients, 26.7±23.1% in PAF and 36.7±27.8% in non-PAF. The difference in extent of LA-LGE after ablation had no significant relationship with number of ablation lesion (P=0.04). Area under the ROC curve to predict clinical recurrence after ablation with extent of LA-LGE was 0.53 (P=0.68). Similar results were observed in the subgroup analyses by AF type (PAF and non-PAF). In Cox regression analysis, age (HR 0.91, 95% CI 0.82-0.99, P=0.04) and extent of LA-LGE (HR 1.11, 95% CI 1.03-1.20, P=0.009) before ablation were independent predictors for clinical recurrence.
Conclusions: The LGE area in the LA at baseline is associated with clinical outcome after CA, however, the difference between pre- and post-ablation LA-LGE is not related to the number of ablation lesions and clinical recurrence of AF/AT.
IS THE DIFFERENCE OF LATE GADOLINIUM ENHANCEMENT IN THE LEFT ATRIUM BETWEEN PRE- AND 1 YEAR POST-ABLATION ASSOCIATED WITH RECURRENCE OF ATRIAL FIBRILLATION/TACHYCARDIA?Kwang No Lee, Sung Ho Hwang, Seung-Young Roh, Hee-Soon Park, Yong-Soo Baek, Jaemin Shim, Jong-Il Choi, Young-Hoon Kim
Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 3-067

490
Introduction: The use of 3D mapping system achieved significant reduction of radiation exposure during catheter ablation procedures. We aimed to compare the efficacy of non-fluoroscopic 3D mapping system on reducing fluoroscopy time in patients undergoing radiofre-quency catheter ablation (RFCA) for cavo-tricuspid isthmus (CTI)-dependent atrial flutter (AFL), especially in patients with structural heart disease (SHD).
Methods: We retrospectively analyzed 130 patients (mean age 60.4±13.4 years, men 83.1%) who underwent RFCA for CTI-dependent AFL consecutively enrolled in two tertiary referral center between 2007 and 2016. Patients with non-CTI dependent atrial tachycardia or previ-ous CTI ablation were excluded. Fifteen (11.5%) patients had used 3D non-fluoroscopic mapping for ablation procedure because of having prior cardiac surgery or cardiomyopathy. We compared these patients with conventional fluoroscopy ablation (CONV, n=115). Further-more, patients were compared among 3 groups: conventional fluoroscopy group without structural heart disease (SHD) (CONV-NL, n=82), conventional fluoroscopy group with structural heart disease (SHD) (CONV-SHD, n=33) and 3D non-fluoroscopic mapping group with SHD (3D-SHD, n=15). Total procedure, ablation time and overall fluoroscopy times were compared among groups.
Results: The overall fluoroscopy time was shorter in the 3D-SHD group compared to the CONV group (32.1±24.6 vs. 64.9±38.6 minutes, P=0.002). The procedure time and ablation time did not show significant difference in both groups (procedure time, 138.2±49.1 vs. 126.1±58.6 minutes; ablation time, 24.6±18.2 vs. 29.6±18.2 minutes, all, P>0.05). The 3D-SHD group showed shorter overall fluoroscopy time compared to the CONV-SHD group (32.1±24.6 vs. 65.9±44.5, P=0.008). The procedure time and ablation time did not show significant dif-ference in both groups (procedure time, 138.2±49.1 vs. 125.7±64.4; ablation time, 24.6±11.2 vs. 29.6±21.2, all, P>0.05). Acute success rate was similar in CONV-NL, CONV-SHD and 3D-SHD group (95.1% vs. 93.9% vs. 86.7%, respectively, P=0.341).
Conclusions: Non-fluoroscopic 3D mapping system could help reducing fluoroscopy time in patients undergoing RFCA for CTI-dependent AFL, especially in those with SHD.
EFFICACY OF A NON-FLUOROSCOPIC THREE-DIMENSIONAL MAPPING SYSTEM ON REDUCING FLUOROSCOPY TIME IN ATRIAL FLUTTER ABLATION IN PATIENTS WITH OR WITHOUT STRUCTURAL HEART DISEASESo-Ryoung Lee1, Eue-Keun Choi1, Woo-Hyun Lim2, Myung-Jin Cha1, Youngjin Cho3, Il-Young Oh1, Seil Oh1 1Seoul National University Hospital, Seoul, Republic of Korea; 2Seoul National University Boramae Medical Center, Seoul, Republic of Korea;
3Seoul National University Bundang Hospital, Seongnam, Republic of Korea
CATHETER ABLATION P 3-068

491
Introduction: Computed Tomography (CT) can visualize left atrium (LA) in detail easily, however in some patients such as allergy, asthma and renal dysfunction it cannot perform without a contrast medium. LA 3D mapping using intracardiac echocardiography (ICE) can also draw similar with CT and is very useful. We speculated ICE mapping from intra LA could be more clearly than from right atrium (RA).
Methods: Thirty nine atrial fibrillation patients (21 men; 63.5±10.2 years; 25 paroximal, 6 persistent, 7 long-standing) underwent pulmo-nary vein (PV) isolation. LA 3D image was created using 64-slice CT 1-3 days before ablation. CT scan was performed during a single breath-hold at the end-expiratory phase. During the scan, the electrocardiogram was recorded. A transseptal access guided by ICE was obtained. Ablation performed with 3.5 mm-tip irrigated catheter to create a single circular line around 2 ipsilateral PVs and complete block between PV and LA. In 14 of 39 patients (35.9%) ICE carried to LA through foramen ovale, and LA 3D echo map was created using ICE from LA directly (LA-group). On the other hands, ICE did not insert to LA in remaining 25 patients, and LA map drew with ablation catheter and ICE which positioned in RA (RA-group). We compared 1) distances between CT map and 3D echo map 2) difference mapping time between groups.
Results: Mean distance between CT map and 3D echo map was closer LA-group than RA-group (1.86±0.89 vs. 2.90±1.00 mm, P<0.01), and maximum distance was obviously longer RA-group than LA-group (10.18±2.98 vs. 6.41±2.32 mm, P<0.01). In both groups, the dis-tance reached maximum at around mitral valve. This is considered to be influenced by motion of the mitral valve. Furthermore, a mapping time was shorter LA-group compared with RA-group (12.9±4.3 vs. 20.0±12.1 minutes, P<0.01).
Conclusions: LA 3D mapping using ICE from intra LA can detect accurate LA anatomy than from RA. When patients cannot be adminis-trated contrast medium, it may be as useful as CT.
INTRACARDIAC ECHOCARDIOGRAPHY FROM INTRA LEFT ATRIUM CAN DETECT ACCURATE LEFT ATRIUM ANATOMICAL INFORMATION FOR PULMONARY VEIN ISOLATIONEmi Nakano1, Hisao Matsuda1, kazuto omiya1, Tomoo Harada2, Yoshihiro Akashi2 1St. Marianna University Yokohama City Seibu Hospital, Yokohama, Japan; 2St. Marianna University School of Medicine, Kawasaki, Japan
CATHETER ABLATION P 3-069

492
Introduction: The left atrial appendage (LAA) is well known as the major source of thromboembolism. Transient ischemic attack (TIA) is reversible episode of neurologic deficit of ischemic origin that resolved completely within 24 hours. We investigated this study to compare the LAA morphology and clinical variables between stroke and TIA in patients with atrial fibrillation (AF).
Methods: We enrolled 238 patients who diagnosed with AF and ischemic stroke or TIA caused by thromboembolic event. All patients un-derwent multi-detected cardiac computed tomography and transesophageal echocardiography (TEE) for evaluation of LAA morphology and volume.
Results: The mean age of the total patients was 69.1±7.1 years (145 males, 61%). 123 patients were enrolled in stroke group and 115 pa-tients in TIA group. The patients in TIA group were younger than those of stroke group (68.2±6.9 vs. 69.9±7.1, P=0.056) and the mean of LAA flow velocity in TIA group was faster than that of stroke group (46.1±3.8 m/sec vs. 39.5±3.9 m/sec, P<0.001). CHADS2 score was not different between the two groups. In comparison of LAA morphology, the most common type is cauliflower (45%) in stroke group and Cac-tus (30%) in TIA group. In a multivariate regression analysis, LAA flow velocity (odds ratio 1.57; 95% CI 1.40-1.74; P<0.001) and Windsock morphologic type (odds ratio 0.16; 95% CI 0.05-0.52; P=0.002) were independent predictors of TIA.
Conclusions: In patients with cardioembolic stroke, high LAA flow velocity and Windsock LAA morphology are independent predictors of TIA.
THE RELATIONSHIP BETWEEN LEFT ATRIAL APPENDAGE MORPHOLOGY AND TRANSIENT ISCHEMIC ATTACK IN PATIENTS WITH ATRIAL FIBRILLATIONHwan-Cheol Park1, Yaemin Park2, Jaemin Shim3, Jong-Il Choi3, Young-Hoon Kim3 1Hanyang University Guri Hospital, Guri, Republic of Korea; 2Gachon University Hospital, Incheon, Republic of Korea; 3Korea University Anam Hospital, Seoul, Republic of Korea
CATHETER ABLATION P 3-071

493
Introduction: The mechanism of persistent atrial fibrillation (AF) remains uncertain. We sought to determine the prevalence of focal driv-ers and rotors during human persistent AF using a novel 3D Wavemapping technique that projects local activation onto a patient specific 3D geometry.
Methods: Global left atrial mapping was performed during spontaneous AF in 12 patients using the multi-electrode basket catheter and analyzed offline using novel 3D wavemapping software. Continuous one-minute AF recordings were analyzed offline using customized signal processing software (CEPAS, Curotech). The local activation at each electrode site was determined using automatic annotation with manual correction to the peak of the bipolar electrogram. Activation data was then projected onto the 3D surface geometry using custom-ized software. Activation patterns were classified into i) Wavefronts (single or multiple), ii) Rotational circuits (≥2 rotations of 360° iii) or fo-cal sources with radial spread. In addition, the spatial distribution and origin of wavefronts was determined.
Results: Over 5,000 activation patterns were analyzed. Mean AF cycle length per AF segment analyzed was 185±107 ms. Activation pat-terns observed were highly dynamic and heterogeneous. The most common patterns were i. single wavefronts (75.9%), ii two simultane-ous wavefronts 6.4%, iii. transient focal activations in 17.7%. No sustained focal activity or rotors were seen. In the majority of maps (54.2%), the wavefronts appeared to originate from the anterior wall of the left atrium. Focal activity most commonly arose from the pos-terior wall adjacent to the left superior pulmonary veins. No wavefronts or focal activity was seen to originate from the left atrial append-age.
Conclusions: Activation patterns in persistent atrial fibrillation are highly heterogeneous with single wavefronts appearing to be dominant subtype. No rotors or sustained focal activity were observed.
THREE-DIMENSIONAL WAVEMAPPING OF HUMAN PERSISTENT ATRIAL FIBRILLATIONBhupesh Pathik1, Tomos Walters1, Pawel Kuklik2, Jichao Zhao3, Andrew Madry1, Sandeep Prabhu1, Chrishan Nalliah1, Jonathan Lipton1, Joseph Morton1, Paul Sparks1, Peter Kistler4, Jonathan Kalman1, Geoff Lee1 1Royal Melbourne Hospital, Melbourne, Australia; 2Maastricht University Medical Center, Maastricht, Netherlands; 3University of Auckland, Auckland, New Zealand; 4Alfred and Baker IDI, Melbourne, Australia
CATHETER ABLATION P 3-072

494
Introduction: High density basket catheter and Rhythmia system (Boston scientific) are new technology for mapping and understanding complex arrhythmia. However, few cases underwent mapping had been reported. Our case series was conducted to examine feasibility and advantage of this system.
Methods: A case series included 8 patients, 4 of atrial and 4 of ventricular arrhythmia. There were typical AFL, post AF ablation atypical AFL, AT and PAC induce AF in atrial arrhythmia group. In ventricular arrhythmia group, there were RVOT VT, PVC from RVOT, PVC from LV and LV VT in DCM patient. All patients were mapped with high density basket catheter and Rhythmia mapping system. Ablation was done with 4mm, non-pressure gated,open irrigated tip catheter base on local activation time mapping and EGMs.
Results: All chambers and epicardial space can be map with basket catheter. Our procedure time and fluoroscopic time were 349±123 and 38.7±14 minutes. Acquired EGMs, ablation points and RF times were 19,703±15,848 EGMs, 30±16 points, 20.9±10.7 minutes per case, respectively. Two complete map in atriums were CTI dependent AFL and post AF ablation atypical AFL. In atypical AFL, circuit prop-agation was around low voltage area, probably scar from previous ablation. In ventricular arrhythmia, we can completely mapped in RVOT VT, PVC from LV and VT from LV in DCM patients. One of RVOT VT patient was inadequate PVC or VT for mapping, ablation was done by pace mapping. All cases were successfully done without immediate complication. We appreciate high resolution mapping, auto annota-tion and template matching for PVC.
Conclusions: High density mapping basket catheter and Rhythmia mapping system are feasible and safe for electroanatomical mapping in all cardiac chambers and in epicardial space.
EXPERIENCE OF ATRIAL AND VENTRICULAR TACHYARRHYTHMIAS MAPPING WITH HIGH DENSITY BASKET CATHETER IN RAMATHIBODI HOSPITAL, THAILANDAsadayudh Phoolpithayadhorn, Tachapong Ngarmukos
Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
CATHETER ABLATION P 3-073

495
Introduction: The right atrium (RA) is readily and safely accessible and considered representative of the substrate responsible for AF how-ever catheter ablation (CA) is largely focused on the LA. We performed detailed bi-atrial electroanatomic mapping in patients with PeAF prior to CA.
Methods: Consecutive patients with PeAF underwent DCR prior to AF ablation. Bi-atrial electro-anatomical mapping (CARTO) with a con-tact force catheter with points >10 g force was performed. Points were analysed offline for complex electrograms, low voltage (<0.5 mV), scarring (<0.05 mV), global and regional conduction velocity (CV) and bipolar voltage.
Results: (See Table): 30 patients (mean age 58.5±8 years, AF duration 11.5±8.8 months, 67% long standing, LA area: 28±5.7 mm2, RA area: 24±5.6 mm2, LVEF: 45±16%) underwent biatrial mapping (number of points: LA 207±67 vs. RA 209±52, P=0.92). There was no dif-ference in global bipolar voltage (LA 2.05±0.72 vs. RA 1.89±0.65 mV, P=0.36); complex electrograms (LA 20% vs. RA 19%, P=0.99), low voltage (LA 13% vs. RA 14%, P=0.19) or proportion of scar (LA 0.5% vs. RA 0.9%, P=0.47). Significantly lower regional bipolar voltage was noted in the posterior atrium (RA 1.25±0.49 mV vs. LA 1.89±0.75 mV, P<0.001) however good correlation was seen in other regions. Glob-al CV was significantly slower in RA 0.93±0.16 ms-1 vs. LA 1.08±0.15, P<0.001) with no difference in regional CV.
Conclusions: There were no significant differences in global bipolar voltage, low voltage or fractionation between RA and LA, despite some regional variation. CV was significantly slower in the RA. These findings should be considered when interpreting RA mapping stud-ies purporting to represent the LA.
BI-ATRIAL ELECTROANATOMIC MAPPING IN PERSISTENT AF: DOES THE RIGHT ATRIUM REPRESENT THE LEFT?Sandeep Prabhu1, Alexandr Voskoboinik1, Alex Mclellan1, Liang-han Ling1, Bupesh Pathik2, Chrishan Nalliah2, Geoff Wong2, Kah Peck3, Sonia Azzopardi1, Geoff Lee2, Justin Mariani1, Andrew Taylor1, Jonathan Kalman2, Peter Kistler1 1Alfred Health and Baker IDI, Melbourne, Australia; 2Royal Melbourne Hospital, Melbourne, Australia; 3Alfred Health, Melbourne, Australia
CATHETER ABLATION P 3-074

496
Introduction: AF and heart failure (HF) frequently coexist however, the contribution of HF on the biatrial substrate in patients with per-sistent AF (PeAF) is unknown.
Methods: Consecutive patients with PeAF and either normal LV (NLV) function (LVEF>55%) or HF (LVEF≤45%) for AF ablation were en-rolled. High-density biatrial electroanatomical mapping was performed during CS pacing with a contact force enabled catheter (CARTO). Complex electrograms, voltage, scarring and conduction velocity were assessed.
Results: (See Table) 32 patients met inclusion criteria (HF: n=16, NLV: n=16). Patients were well matched regarding AF duration (NLV vs. HF: 11±7 vs. 12±11 months, P=0.78), LA area (27±5.1 vs. 29±6 cm2, P=0.27) and other comorbidities. Bi-atrial tissue voltage was signifi-cantly lower and more variable (co-efficient of variation [CV] SD/mean) in the HF group (LA: NLV vs. HF: unipolar: 3.7±0.9 vs. 2.6±0.9 mV, P=0.002, CV: 0.48 vs. 0.59, P=0.004; bipolar: 2.2±0.7 vs. 1.6±0.4 mV, P=0.003, CV: 0.67 vs. 0.79, P=0.003). The HF group had significantly more fractionation (LA: 29% vs. 9.5%, P<0.001; RA: 27% vs. 10%, P<0.001), low voltage (<0.5 mV) (LA: 19% vs. 8%, P=0.002; RA: 18% vs. 9%, P=0.008) and presence of scar (LA: 75% vs. 18% of patients, P<0.001; RA: 44% vs. 0%, P=0.006). There was a trend to reduced global con-duction velocity in the RA (73±13 vs. 83±6 cm/s, P=0.051).
Conclusions: HF is associated with significant bi-atrial structural remodelling over and above that attributable to PeAF alone. Such re-modelling may impact post ablation outcomes in patients with HF.
BI-ATRIAL ELECTRICAL AND STRUCTURAL REMODELLING IN HEART FAILURE: ELECTROANATOMIC MAPPING IN PERSISTENT ATRIAL FIBRILLATION IN HUMANSSandeep Prabhu1, Alexandr Voskoboinik1, Alex Mclellan1, Kah Peck2, Bupesh Pathik3, Chrishan Nalliah3, Geoff Wong3, Siobhan Lockwood4, Justin Mariani1, Liang-han Ling1, Andrew Taylor1, Jonathan Kalman1, Peter Kistler1, Geoff Lee3 1Alfred Health and Baker IDI, Melbourne, Australia; 2Alfred Health, Melbourne, Australia; 3Royal Melbourne Hospital, Melbourne, Australia;
4Monash Health, Melbourne, Australia
CATHETER ABLATION P 3-075

497
Introduction: Creating a line of block at mitral isthmus can sometimes be challenging due to anatomical variance, epicardial conduction and poor manipulation of catheter. Conventional methods for confirmation of line of block is usually done by differential pacing from prox-imal and distal coronary sinus (CS). However, this method fails to confirm endocardial line of block in certain cases.
Methods: We reported a case of 55 year-old male who presented with tachycardia-induced caridomyopathy and reduced EF due to long-stainding AF. During the first session PV isolation alone was done but the patient had a recurrence as early as one week later. Sec-ond session was performed 3 months later during which detailed left atrial mapping shows recurrence of LIPV conduction and low-volat-ge are at mitral isthmus. Additional ablation line was performed at the mitral isthmus using steerable Agilis sheath and irrigated catheter. However, conventional method of left atrial appendage (LAA) and CS pacing fails to show a complete line of block. We then peformed high-resolution automated mapping of the mitral isthmus area in order to localize conduction gap.
Results: Due to high resolution mapping, we were able to locate residual gap at the very ventricular end of mitral isthmus line. Additional ablation of the site provides complete line of block confirmed by delay conduction on Ensite mapping. LAA pacing however fails to show proximal-to-distal CS sequence probably due to isolated epicardial musculature.
Conclusions: Automated high-resolution mapping provides a rapid and reliable way to localize conduction gap in mitral isthmus even in low-voltage area after repated ablation.
LOCALIZATION OF MITRAL ISTHMUS GAP USING NOVEL HIGH-DENSITY ENSITE AUTOMATED MAPPING SYSTEMTeerawut Ruedeejaroonrung
Ayase Heart Hosptial, Tokyo, Japan
CATHETER ABLATION P 3-076

498
Introduction: X-ray radiation may suppress and damage human tissue cells, causing immUniversityy declining and even cancer. But medical workers who engage in first-line interventional diagnosis and treatment work have to expose themselves to X-ray radiation long time and frequently. To protect medical workers health, it is high time to reduce radiation dose. So this paper aim at evaluating the utility of a new imagefusionmodule (Carto-UNIVU system) in reducing X-ray exposure time and radiation dose, improving procedure success rate and safety and shortening procedure time.
Methods: In this retrospective survey conducted at West China Hospital of Sichuan University in 2016, there were 30 patients with AF un-derwent radiofrequency catheter ablation guided by Carto-UNIVU system (study group) and 30 patients with AF underwent radiofrequency catheter ablation guided by Carto 3 system (control group). The parameters in two groups, such as procedure duration, X-ray exposure time, radiation dose (total radiation dose/effective radiation dose/cumulative air kerma), procedure success rate, complications and re-currence rate of 6 months after procedure were compared.
Results: Comparing procedure duration of two groups, Carto-UNIVU group’s time was shorter (119±31 minutes vs. 131±35 minutes), the difference was statistically significant. Carto-UNIVU system reduced X-ray exposure time [(6.4±0.9) minutes vs. (16.0±1.3) minutes, P<0.001] and radiation dose significantly (3,726±552 cGy/cm2 vs. 6,369±568 cGy/cm2, P<0.001). Carto-UNIVU group’s success rate was 100%. No complications occurred in Carto-UNIVU group and 1 patient AT relapsed in 6 months after procedure. Carto 3 group’s success rate was 100%. 1 patient occured cardiac tamponade in Carto-Merge group and 1 patient replased AF in 6 months after operation.
Conclusions: Both fixed fluoroscopic images and cines can be integrated with 3D EAMS based on Carto-UNIVU system. This combination of different images indicates the anatomy of heart completely (e.g. coronary artery, abnormal anatomy of congenital heart disease). It is helpful to determine ablation target and understand the establishing and maintaining mechanisms for arrhythmia. It also help making the ablation procedure safer and more effective. Carto-UNIVU system can minimize procedure time, X-ray exposure time and radiation dose, improve ablation success rate and safety, reduce complications risk.
THE UTILITY OF RADIOFREQUENCY CATHETER ABLATION OF ATRIA FIBRILLATION GUIDED BY CARTO-UNIVU SYSTEMZhonghui Xie, Kaijun Cui
West China Hospital Sichuan University, Chengdu, China
CATHETER ABLATION P 3-077

499
Introduction: Recently, a sensor based electromagnetic non fluoroscopic catheter tracking system (MediGuideTM) has been introduced. However, the accuracy and clinical applicability of this technology have not been evaluated. We aimed to investigate the anatomical accu-racy between electromagnetic (MediGuideTM) and impedance (EnSite VelocityTM) based mapping systems.
Methods: The study subjects consisted of 5 patients (4 males, mean age 54±10 years) underwent pulmonary veins (PV) isolation for par-oxysmal AF. Contrast-enhanced CT image of LA was acquired just before catheter ablation. 3D geometry of LA was constructed using both electromagenetic and impedance mappings (EM, IM) during catheter ablation. We measured the 4 PV angles between the main trunk of each PV and the LA (Figure 1A, ①-④). The longitudinal axis of the LA was defined as the line between the center points of the ip-silateral PVs. Additionally, the posterior LA surface area was measured (Figure 1A, ⑤). We compared the absolute difference and the rela-tive difference of 4 PV angles and the posterior LA surface area in EM, and IM, compared to that of CT LA geometry.
Results: The differences (both absolute and relative) of the PV angles to LA were smaller between EM to CT than IM to CT geometries (Figure 1B). The posterior LA surface area from the EM mapping was significantly closed to that in CT image, when compared to that in IM (Figure 1C).
Conclusions: Image integration with EM enables high accurate visualization of cardiacanatomy compared to IM. Thus, this technology can facilitate the determination of the arrhythmogenic substrate for successful catheter ablation and increase procedural safety.
THE ACCURACY AND CLINICAL APPLICABILITY OF A SENSOR BASED ELECTROMAGNETIC NON FLUOROSCOPIC CATHETER TRACKING SYSTEMShinya Yamada, Li-wei Lo, Yenn-Jiang Lin, Shih-Lin Chang, Yu-Feng Hu, Fa-Po Chung, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
CATHETER ABLATION P 3-078

500
Introduction: A 66-year-old woman diagnosed with light-chain amyloidosis had symptoms of palpitation. Electrocardiography revealed a sustained atrial flutter with cycle length of 210 ms, negative in inferior leads, negative in V1 and radiofrequency catheter ablation was per-formed.
Methods: An activation map using three-dimensional electro-anatomical mapping system suggested a circuit going from anterior to lat-eral right atrial lateral wall. A fragmented potential was detected on the lateral wall of the right atrium. The post pacing interval of the ca-votricuspid isthmus (CTI) was more 70 ms longer than the tachycardia cycle length. There was no possibility of a circuit that went through the CTI. The post pacing interval at the fragmented potential was tachycardia cycle length plus 10 ms.
Results: RF energy delivered at the fragmented potential terminated the tachycardia. During tachyarrhythmia, there was a wide range low voltage zone (LVZ) at the bottom from the anterior to the lateral right atrium, including the ablation area. Ablation for border of the LVZ rendered the tachycardia non-inducible.
Conclusions: Cardiac amyloidosis has LVZ in the atrium, and intracardiac conductions are sometimes disturbed. In this case, there was LVZ in the right atrium. It is preferable to use electro-anatomical mapping in the presence of LVZ, keeping in mind the right atrium ar-rhythmia of primary cardiac amyloidosis.
A CASE OF PRIMARY CARDIAC AMYLOIDOSIS WITH CATHETER ABLATION FOR PERSISTENT ATRIAL FLUTTERKiyotaka Yoshida
Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan
CATHETER ABLATION P 3-079

501
Introduction: Ethanol injection into the Vein of Marshall (VOM) has been performed when attempting catheter ablation of atrial fibrillation (AF) and atrial tachycardia (AT) which were associated with atrial tissue embedding VOM area. We hereby present two informative cases which reinforces the utility of this therapeutic technique.
Methods: N/A
Results: Case 1. A 71-year-old woman was referred to our institution because of the intractable AF/AT. She had undergone catheter abla-tion for 3 times at other hospital but still suffering from AF/AT. The electroanatomical mapping revealed the sustained tachycardia to be a peri-mitral flutter which rotating around the mitral annulus in counter-clockwise fashion. This finding indicated that mitral isthmus (MI) block line was not successfully constructed even with meticulous radiofrequency (RF) ablation in prior sessions. It seemed that MI block line construction might be difficult only by endocardial RF application, therefore, chemical ablation for VOM was attempted. Small amount of ethanol (0.5 mL) slow injection into the VOM immediately terminated the AT. After total of 4 mL injection of ethanol, any tachycardia be-came non-inducible at all and she has been free from any symptoms after the final ablation procedure.Case 2. A 72-year-old man has undergone pulmonary vein (PV) isolation for persistent AF. He began to feel palpitation due to AF/AT 1 month after the first ablation session. In the second session, the electrical isolation of PVs were preserved and AF was triggered by ecto-pic beats arising from left atrial (LA) posterior wall. It implied that posterior wall isolation was mandatory, but construction of LA roof and bottom block line was very challenging because of easy AF inducibility: the conductive gaps were unable to be detected during AF. The chemical ablation for VOM was performed. His heart rhythm restored to sinus rhythm spontaneously during ethanol injection and it was maintained afterwards. The MI block line was also constructed by chemical ablation. The posterior wall isolation was accomplished and he has been free from any symptoms after the ablation procedure.
Conclusions: Chemical ablation into the VOM can be a mighty blow for intractable AF/AT.
CLINICAL USEFULNESS OF CHEMICAL ABLATION IN TERMS OF TREATING ATRIAL FIBRILLATION; REPRESENTATIVE TWO COMPLICATED CASESTomofumi Nakamura, Kaoru Okishige, Tokuhiko Itou, Takatoshi Shigeta, Yusuke Tsuchiya, Mitsumi Yamashita, Mitsutoshi Asano, Tsukasa Shimura, Hidetoshi Suzuki, Hideshi Aoyagi, Manabu Kurabayashi, Yasuteru Yamauchi
Yokohama City Bay Red Cross Hospital, Yokohama, Japan
CATHETER ABLATION P 3-080

502
Introduction: The ventricular ganglionated plexi (GP) is interconnected with atrial GP to govern heart function, although the effect of ven-tricular GP modification on AF vulnerability remains elusive. Therefore, This study investigated the effect of electrical stimulation of aortic root ventricular GP on AF inducibility.
Methods: Effective refractory periods (ERP) of a trial PVs were measured at the baseline, during high-level (HL-ES) and low-level (LL-ES) electrical stimulation of aortic root GP. Arrhythmogenic threshold of acetylcholine and isoproterenol was determined at baseline, during HL-ES and LL-ES. Moreover, AF was induced at PV by programmed electrical stimulation following HL-ES or LL-ES. Immunohistochem-istry staining was performed to examine the autonomic activity from aortic root GP to the PVs.
Results: Compared with baseline group, HL-ES of aortic root GP significantly shortened AERP (95±13 vs.122±9 ms) and PVERP (104±11 vs. 131±12 ms); decreased the threshold concentration of AF by both acetylcholine (1.3±0.2 vs. 3.2±0.3 μmol/L) and isoproterenol (0.3±0.1 vs. 1.3±0.2 μmol/L), and increased AF inducing rate from PVs (90% vs.30%). In contrast, LL-ES of this GP prevented the shortening of ERP and PVERP to 125±10 ms and 133±11 ms, respectively; increased threshold levels of acetylcholine and isoproterenol to 5.7±0.4 μmol/L and 3.2±0.3 μmol/L, respectively, and decreased AF inducing rate to 5%. Our findings also revealed that the biotinylated dextran amine-containing varicose fibers projected directly from aortic root GP to the left PVs.
Conclusions: These findings suggested that autonomic innervations of left PVs were partly originated from aortic root ventricular GP. Moreover, LL-ES of aortic root ventricular GP suppressed AF inducibility arose from PVs mediated by the autonomic nervous system.
EFFECT OF LOW-LEVEL ELECTRICAL STIMULATION OF AORTIC ROOT VENTRICULAR GANGLIONATED PLEXI ON AUTONOMIC NERVOUS SYSTEM-MEDIATED ATRIAL FIBRILLATIONHong-Tao Wang, Qiang-Sun Zheng
Tangdu Hospital, Division of Cardiology, Xi’an, China
CATHETER ABLATION P 3-081

503
Introduction: Recent studies show a positive correlation of the transmural dispersion of repolarization (TDR) with ischemia. The study aims to determine the correlation of TDR to coronary artery disease in patients with Non-ST elevation Myocardial Infarction (NSTEMI).
Methods: A retrospective analysis of patients who had coronary angiography between May 2014 and January 2015 was done. 71 patients were included in the study group and 75 patients with normal coronaries were assigned to the control group. The electrocardiographic parameters (Heart Rate, QT interval, Corrected QT (Bazette), Tpeak-end (Tpe) and the Tpe/QTc.), were measured from the precordial leads of the 12L ECG and measurements done using a manually operated digital caliper. The Tpeak-end/Corrected QT was measured in the precordial leads and the overall computed TDR as the median of the highest and lowest values.
Results: The Independent Sample T-test was used to determine the difference in the mean TDR of control vs. study groups. The study group had a mean TDR of 0.2464 (TDR Max 0.2822 and TDR Min 0.2106) and the control group had a mean TDR of 0.1882 (TDR Max 0.2249 and TDR Min 0.1516). The difference between the two groups was statistically significant (P=0.000145) and the study group had signifi-cantly higher TDR than Control Group. Male subjects in both groups had a higher mean TDR but the results were not statistically signifi-cant (P=0.051). Age had a low correlation with TDR (P=0.6948).
Conclusions: TDR (Tpe/QTc) is increased in patients with Non-ST elevation MI and significant coronary artery disease.
ELECTROCARDIOGRAPHIC TRANSMURAL DISPERSION OF REPOLARIZATION AS A MARKER OF CORONARY ARTERY DISEASE IN PATIENTS WITH NON ST ELEVATION ACUTE CORONARY SYNDROMERaymond Bayaua
The Medical City, Marikina, Philippines
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-083

504
Introduction: Patients with serious mental illness (SMI) are known to have higher incidences of sudden death compared to the general population. Higher rates of abnormal late potentials (LP) on signal-averaged electrocardiogram (SAECG), which may be a predictor of sudden death risk, have been shown in patients with schizophrenia. We sought to assess the prevalence and predictors of LP in a mixed SMI population.
Methods: As part of a study of medical comorbidity in SMI, patients had SAECG recorded in addition to data collection on mental health diagnoses, other health conditions, medication prescriptions and doses. Standard criteria for abnormal SAECG were used (filtered QRS duration ≥114 ms, late potential duration ≥38 ms, root mean square voltage of terminal 40 ms ≤20 microV). Baseline 12-lead electrocar-diograms (ECGs) were also analysed. Univariate and multivariate logistic regression analyses were performed with predictors tested in-cluding gender, age, QRS duration, QTc, Tpeak -Tend interval, QRS fragmentation, early repolarisation pattern (ERP), parietal block, and SMI clinical diagnosis categorised as either psychosis (any cause), schizophrenia/schizoaffective disorder, or other.
Results: Eighty patients, 49% male, mean age 39±17 years were enrolled. Twenty-seven (34%) patients had abnormal SAECG, with 1, 2 or 3 criteria being displayed by 19, 3 and 5 patients respectively. In the final multivariate model, SAECG was significantly associated with male gender (OR 6.7; 95% CI 1.9-23.7), QRS fragmentation (OR 4.7; 95% CI 1.2-18.0), ERP (OR 4.4; 95% CI 1.1-18.1) and schizophrenia/schizoaffective disorder diagnosis (OR 9.0; 95% CI 1.9-42.2).
Conclusions: In the mixed SMI population studied, there was a substantially increased rate of abnormal SAECG-detected LP (34%), com-pared to background population rates of up to 6%. The presence of LP was best predicted by male gender, QRS fragmentation, ERP and, most strongly, by a diagnosis of schizophrenia/schizoaffective disorder. Further study of this population is warranted in order to define the mechanisms and prognostic implications of these observations.
LATE POTENTIAL PREVALENCE AND PREDICTORS IN PATIENTS WITH SERIOUS MENTAL ILLNESSJohn Fitzgerald1, Karen Hay2, Judith Sheridan3, Alex Chadwick3, Andrew Burke1, Haris Haqqani1 1University of Queensland, St. Lucia, Brisbane, Queensland, Australia; 2Queensland Institute of Medical Research Berghofer Medical Research Institute, Herston, Brisbane, Queensland, Australia; 3The Prince Charles Hospital, Chermside, Brisbane, Queensland, Australia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-084

505
Introduction: The heart rate variability (HRV) analysis is an important clinical tool for characterizing the cardiac autonomic status. Most HRV studies, especially on non-linear techniques, are based on 24 h ambulatory recordings. However, the necessity of a short-term (<10 min) HRV analysis for various applications is increasing. The purpose of this study was to define the clinical role of HRV parameters de-rived from short-term period for predicting mortality in Koreans.
Methods: A total of 1,828 consecutive patients (range 20-84 years [median 48 years], men 64.8%) who received a medical check-up from January to December 2004 were recruited. The patients with atrial fibrillation (n=7) and inappropriate data (n=3) were excluded. The RR intervals extracted from 10 minutes ECGs were used for the computation of the following HRV parameters: conventional measurements (time- and frequency-domain), Shannon Entropy (ShanEn), approximate entropy (ApEn), and sample entropy (SampEn) as non-linear pre-dictors. The detrended fluctuations (DFA) a1 and DFAa2 were measured as fractal measures. All-cause mortality and cardiac mortality were the endpoints of this study.
Results: The natural logarithmic values of the low frequency power (lnLF) and high frequency power (lnHF) decreased in sequence ac-cording to the age. Almost all time domain parameter values (lnLF and the lnHF) were higher in the male group. Sixty-seven patients (in-cluding 13 deaths by suicide or accidents) died during a 10-year follow-up period. Among them, 54 patients (including 14 deaths by cardi-ac causes), excluding deaths by suicide or accidents, were included in the mortality analysis. The patients with mortality were older (64±11 vs. 48±12 years, P<0.001), but the mean heart rate did not differ (66±11 vs. 64±10 years, P=0.404) at baseline. Among the HRV pa-rameters, the predictive factors for all-cause mortality were the LF/HF ratio (OR 0.876, 95% CI 0.780-0.983, P=0.025), ShanEn (OR 0.372, 95% CI 0.154-0.900, P=0.028), and ApEn (OR 0.093, 95% CI 0.011-0.794, P=0.030) in the multivariate logistic regression analysis. The age was also a powerful risk factor for all-cause mortality (OR=1.141, 95% CI 1.106-1.178, P<0.001). However, there were no predictive factors of cardiac mortality among the HRV parameters.
Conclusions: These results suggest that the short-term HRV, especially the non-linear heart rate dynamics, would be further adjunctive parameters to predict mortality in the general population.
CLINICAL VALUE OF SHORT-TERM HEART RATE VARIABILITY FOR PREDICTION OF MORTALITY IN KOREANS: EFFICACY OF NONLINEAR HEART RATE DYNAMICSChan-Hee Lee1, Kang-Un Choi1, Jong-Ho Nam1, Kyu-Hwan Park1, Jeon Lee2, Dong-Gu Shin1 1Yeungnam University Medical Center, Daegu, Republic of Korea; 2Yonsei University, Wonju, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-085

506
Introduction: A decreased HRV is associated with an increased mortality in post myocardial infarction (MI) patients. There are, however, few reports about the very low frequency (VLF) component of HRV that may be linked to the prognosis of them.
Methods: Forty post MI patients who underwent implantable cardiac defibrillator (ICD) implantation and Holter electrocardiogram at ap-proximately the same time were enrolled. 6 patients who had at least one episode of appropriate therapy or cardiac death within one year after Holter electrocardiogram were assigned to cardiac event group, and the other 34 patients to control group. Time domain and fre-quency analysis (including VLF) of Holter electrocardiogram were carried out.
Results: In univariate analysis, LF, HF and VLF were decreased significantly in cardiac event group. In multivariate analysis, VLF power predicted cardiac events independently of LF, HF (Odds Ratio 0.21, 95% confidence interval: 0.054-0.818, P=0.025).
Conclusions: VLF was a notable predictor of fatal ventricular tachyarrhythmia risk and cardiac death within one year.
THE IMPACT OF VLF COMPONENT IN HOLTER ELECTROCARDIOGRAMS ON FATAL VENTRICULAR ARRHYTHMIA AND CARDIAC DEATH IN POST MI PATIENTSYoshikazu Sato1, Noriyoshi Yamawake1, Yuuta Taomoto1, Miki Amemiya1, Munehiro Iiya1, Yousuke Yamakami1, Rena Nakamura1, Kuniaki Nakano1, Hiroshi Shimada1, Masato Shimizu1, Hiroyuki Fujii1, Mitsuhiro Nishizaki1, Harumizu Sakurada2, Masayasu Hiraoka3 1Yokohama Minami Kyosai Hospital, Yokohama, Japan; 2Tokyo Metropolitan Health and Medical Treatment Corporation Ohkubo Hospital, Tokyo, Japan; 3Toride-Kitasoma Medical Association Hospital, Ibaraki, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-086

507
Introduction: Although atrial fibrillation (AF) is one of the major causes of embolic stroke with unknown source (ESUS), the diagnosis or prediction of AF is not easy in daily clinical practice. Prior studies demonstrated that P wave signal averaged ECG (P-SAECG) could predict AF in patients who underwent cardiac surgery. Therefore, we evaluated the predictive value of P-SAECG in patients with ESUS.
Methods: Patients diagnosed as ESUS, control subjects without AF, and paroxysmal AF patients without stroke were enrolled. P-SAECG and 24 hour-Holter ECG were performed at baseline. In ESUS group, standard 12-lead ECG and 24-hour Holter ECG were taken at 1-3 months and 6-12 months after index event and diagnosis of AF was followed.
Results: ESUS group (n=29, 67.5±12.7 years-old), control group (n=58, 49.1±18.7 years-old), and AF group (n=21, 62.3±14.8 years-old) were enrolled. At baseline, standard P wave duration (PWD) and total PWD were significantly longer in ESUS group than control group (131.6±23.9 ms vs. 114.5±14.0 ms, P=0.001). PWD was similar in ESUS group and AF group (131.6±23.9 ms vs. 124.5±31.4 ms, P=0.383). AF detection rate was 25% at 4.4±1.7 months of mean follow-up.
Conclusions: Using P-SAECG, we might predict AF in ESUS patients. Further follow-up and investigation may be required.
CAN P WAVE SIGNAL AVERAGED ECG PREDICT ATRIAL FIBRILLATION IN PATIENTS WITH EMBOLIC STROKE WITH UNKNOWN SOURCE?Seung Yong Shin
Chung-Ang University Hospital, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-087

508
Introduction: ST elevation Myocardial Infarction is clinical syndrome characterized with symptoms suggesting myocardial ischemia in the presence of ST segment elevation and rise of cardiac biomarker values. In acute event, there is pathological electrolytes shifting leading to abnormal repolarization. Repolarization inhomogeneity occurred transmurally contributed diastolic and systolic dysfunction lead to acute heart failure and cardiogenic shock, and also arrhythmia. Those ultimately can progress to death. Electrocardiogram is a simple and widely used tool that can reflect this repolarization dispersion. Tpeak reflects end of epicardium repolarization whereas Tend reflects end of M cell repolarization. The interval between Tpeak and Tend was suggested as dispersion of repolarization.
Methods: We performed cross sectional study of STEMI patients from March to June 2016 with onset less than 12 hours and underwent revascularization either fibrinolytic or percutaneous coronary intervention. In hospital mayor cardiac events (MACE) comprises acute heart failure, cardiogenic shock, ventricular arrhythmia, and death were noted. We analyze statistically Tpeak-Tend interval and Tpeak-Tend/QT ratio in MACE and No-MACE group.
Results: We enrolled 50 patients with STEMI whose onset less than 12 hours and underwent revascularization. There were 10 patients suffered from MACE. Tpeak-Tend interval in MACE group is longer than No-MACE group (147.21+107 msec vs. 114.16+18 msec, P=0.641). Tpeak-Tend/QT ratio is also higher in MACE group (0.27+0.04 vs. 0.26+0.05, P=0.081).
Conclusions: Both Tpeak-Tend interval and Tpeak-Tend/QT ratio were higher in MACE group but unsignificant statistically.
REPOLARIZATION DISPERSION PARAMETER FOR PREDICTING INHOSPITAL MAJOR ADVERSE CARDIAC EVENT IN ST ELEVATION MYOCARDIAL INFARCTION: TPEAK-TEND OR TPEAK-TEND/QT RATIO?Erdiansyah Zulyadaini, Mahbubi Mustika, Dwijanarko Windhi, Maharani Erika
Faculty of Medicine, Universitas Gadjah Mada, Yogyakarta, Indonesia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-088

509
Introduction: Regional perfusion disturbance cause transmural myocardial repolarization dispersion in ST elevation myocardial infarc-tion. This can be seen as a prolongation of Tpeak-Tend (Tp-Te) from electrocardiography. Previous studies had revealed that prolonged Tp-Te interval as a predisposing factor for ventricular arrhythmia. Primary PCI or successful fibrinolytic therapy allows the improvement of coronary artery patency in order to increase myocardial perfusion. This process might improve repolarization dispersion marked by Tp-Te interval shortening. Coronary arterial blood flow patency is better after primary PCI compared to successful fibrinolytic therapy alone. This might be reflected by the Tp-Te interval reduction differences between primary PCI and fibrinolytic therapy.
Methods: We performed a cross-sectional study of STEMI patients from January 2016-July 2016 hospitalized in Dr Sardjito Hospital with onset of<12 hours and underwent revascularization either primary PCI or successful fibrinolytic therapy. We analyze Tp-Te interval before, soon after, and 24 hours after reperfusion therapy. T-test analysis used to compare Tp-Te interval changes differences after revasculariza-tion between two groups.
Results: Among 87 patients, 45 patients underwent primary PCI while 42 patients underwent successful fibrinolytic therapy. Both groups had prolonged Tp-Te interval before reperfusion (117,03±15,57 ms vs. 119,95±13,23 ms in primary PCI group and fibrinolytic therapy group respectively). The reduction of Tp-Te interval (∆Tp-Te) in primary PCI group were 20,16±15,84 soon after intervention and 30,04±24,14 ms in 24 hours after intervention, while in fibrinolytic group were 17,14±13,97 ms 30 minutes after intervention and 19,99±15,96 ms in 24 hours after intervention. There was no significant reduction differences of Tp-Te (∆Tp-Te) soon after intervention (P= 0.35). But there was a significant reduction differences of ∆Tp-Te in 24 hours after intervention (P=0.026).
Conclusions: This study showed a significantly larger reduction in Tp-Te interval after primary PCI compared to successful fibrinolytic therapy in 24 hours after intervention in patient with STEMI.
COMPARISON OF INTERVAL TPEAK-TEND REDUCTION IN PRIMARY PERCUTANEUS CORONARY INTERVENTION VS. FIBRINOLYTIC THERAPY IN ST ELEVATION MYOCARDIAL INFARCTIONErdiansyah Zulyadaini, Mustika Mahbubi, Windhi Dwijanarko, Hasanah Mumpuni, Erika Maharani
Faculty of Medicine Universitas Gadjah Mada, Yogyakarta, Indonesia
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-089

510
Introduction: Chronic obstructive pulmonary disease (COPD) is a major health problem that globally contributes to substantial morbidity and mortality. The incidence of sudden cardiac arrest (SCA) increases dramatically with age (especially ≥65 years old) and with underlying cardiac disease. Our aim was to investigate whether there is an association between COPD and SCA in total population under 65 years.
Methods: In Korean National Health Insurance Database Cohort (NHIS-cohort), we studied 429,204 subjects (mean age, 47.8 [SD, 14.2] years; 217,618 men [50.7%]) with national health check-up, who received national health check-up after 2009 were enrolled, and follow up until 2013.
Results: COPD was diagnosed in 12,598 patients (2.94%). During the mean follow-up period of 45.5±14.9 months, SCA occurred 426 sub-jects (113 women). Incidence rates for SCA increased in COPD group, in non-COPD (0.4548 per 1,000 person-years), in COPD (1.7778 per 1,000 person-years) respectively. In under 65 years population crude mortality risk of COPD was hazard ratio 3.37 (95% CI: 2.42 to 4.68, P<0.001). After adjusted with age and sex, increasing tendency of SCA continued (HR 1.82, 95% CI 1.30-2.54, P<0.001). Chronic obstruc-tive pulmonary disease was associated with an increased risk of sudden death under 65 years (age, sex, hypertension, diabetes mellitus, heart failure, chronic kidney disease, previous myocardial infarction, and smoking status-adjusted hazard ratio, HR: 1.56, 95% CI 1.11-2.18, P=0.01). The risk particularly increased in the male under 65 years with COPD (HR 1.58, 95% CI 1.07-2.33, P<0.022), but there was no significant difference of the sudden arrest risk in women under 65 years (HR 1.53, 95% CI 0.79-2.98, P=0.208).
Conclusions: COPD is associated with an increased risk for SCA especially in male under 65 years old. This result suggests that COPD should be considered as a useful prognosticator, and therapeutic strategies aimed to treat COPD in mild age male should be investigated.
INCREASED SUDDEN ARREST WITH CHRONIC OBSTURCTIVE PULMONARY DISEASE IN GENERAL POPULATION; THE EFFECT OF AGEShinjeong Song, Pil-Sung Yang, Tae-Hoon Kim, Jae-Sum Uhm, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung
Yonsei University College of Medicine, Seoul, Republic of Korea
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-090

511
Introduction: Brugada syndrome (BrS) is an inherited channelopathy. Mutations in at least 12 genes encoding the sodium, calcium and potassium channels have been associated with BrS. SCN5A mutations account for 30% of BrS. We aim to look at the genotype-phenotype characteristics of BrS in our local patients.
Methods: Probands with Type 1 ECG (spontaneous or drug-induced) were included. Probands with type 2 or 3 ECGs had provocative test-ing with up to 400 mg of oral flecainide. For genetic testing, 1 mL of saliva was collected via self-collection kit (Oragene-DNA: OG-500) af-ter fasting for 30 minutes. Informed consents were obtained. All salivary specimens were sent to National Heart Centre, Singapore for ge-netic sequencing.
Results: 16 probands having BrS were recruited for genetic study between October 2014 and April 2015 (mean age: 44.81±14.18 years, 57% males). 8 probands (50%; 5 males) were genotype positive for pathogenic variants. 3 had variants in genes associated with BrS (SC-N5A n=1, CACNA1c n=2). 4 had variants in MYH17, DSC2, MYBPC3 and MYH7 respectively. 1 had MYH6 and HFE. 1 proband (Chinese; male) had a novel SCN5A variant (DNA coding c.5103G>C; variant p.M1701I; missense) and MYL2. He had recurrent palpitations, spon-taneous type I ECG and reproducibly inducible ventricular fibrillation (VF) leading to primary prevention implantable cardioverter defibrilla-tor (ICD) implant aged 33 years. 6 years later, he had inappropriate shocks for sinus tachycardia due to partial fracture of the right ventric-ular shocking lead which was extracted and replaced. 2 apparently unrelated Malay probands had the same CACNA1C variant (DNA cod-ing c.5731G>C; variant p.G1911R; missense). This variant had been associated with increased arrhythmogenesis and sudden unex-plained infant death. The male had syncope, family history of premature sudden death, fever-induced type I ECG and reproducibly induc-ible VF aged 19 years. An ICD was recommended but patient did not proceed due to financial constraints. The female had a fever-induced type I ECG, was asymptomatic, and had a negative VT stimulation aged 58 years but has a son who had an incidental spontaneous type 1 ECG picked up aged 40 years. At follow-up, all are alive.
Conclusions: In our small cohort, variants in genes associated with BrS were observed in 19% of our patients. Given the low genetic yield for SCN5A (6%), it was unclear whether genetic screening should be offered to family members.
THE GENOTYPE-PHENOTYPE TRAITS OF BRUGADA SYNDROME IN BRUNEI DARUSSALAMBee Lau1, Nazar Luqman1, Chi Keong Ching2, Boon Yew Tan2, Kah Leng Ho2, Wee Siong Teo2, Sofian Johar1 1Ripas Hospital, Bandar Seri Begawan, Brunei Darussalam; 2National Heart Centre Singapore, Singapore
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-091

512
Introduction: Because sudden cardiac death (SCD) prevalently occurs in the general population, additional predictors are needed to iden-tify patients at high-risk for SCD. Ventricular arrhythmias (VAs) are associated with increased cardiac repolarization variability. Malignant early repolarization (ER) can lead to SCD. Several markers to identify malignant ER patients have been proposed, but an effective SCD prevention is still lacking. Speckle-tracking echocardiography (STE) showed to be a promising tool to help assess SCD in several patient subsets. To date, the role of STE in SCD risk assessment in ER patients has never been investigated. We aimed to compare STE indices in ER patients with and without VAs.
Methods: We enrolled 30 ER patients (26 without VAs, 4 with VAs and ICD). STE was performed in all patients using QLAB software 10.5 version by Philips Medical System (Eindhoven, the Netherlands). Segmental 2D speckle-tracking analysis was performed by manually tracing the endocardial border at an end-systolic frame.
Results: Mean age was greater in the VAs group compared to the non-VAs group (54.7±16.7 vs. 35.0±9.7, respectively, P=0.006). LVEF and QTc did not differ between groups. Several systolic and diastolic radial and longitudinal segmental and global STE variables were sta-tistically significant between groups. ROC curves identified cutoff values with 100% sensitivity and 80% specificity in predicting VAs.
Conclusions: Radial and longitudinal STE are markers of VAs in ER patients. STE analysis could be helpful in stratifying SCD risk. These novel parameters may add important information about the susceptibility for VAs and SCD in this otherwise undertreated population. Fur-ther prospective larger studies are needed to impact clinical practice.
MALIGNANT EARLY REPOLARIZATION ASSESSMENT BY 2D SPECKLE-TRACKING ECHOCARDIOGRAPHYBich Lien Nguyen, Ilaria Maraschi, Alessandro Persi, Raffaele Quaglione, Elisa Rauseo, Eleonora Indolfi, Gianfranco Piccirillo, Nicola Alessandri, Luciano Agati, Carlo Gaudio
Sapienza University of Rome, Rome, Italy
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-092

513
Introduction: Magnetcardiograms (MCGs) are noninvasively acquired maps that measure the cardiac magnetic fields on the body surface. Previous studies associated with MCGs have been using a superconducting quantum interference device (SQUID) system. Although SQUID system is the most sensitive of all instruments for measuring a magnetic field at low frequencies, it requires liquid helium for cooling the system and the running cost is expensive. Magnetoresistance (MR) magnetometers use a change in resistance caused by an external magnetic field, and are attractive for low cost applications. This study was aimed to acquire MCGs by using MR sensors.
Methods: We recorded MCGs of five healthy subjects by using MR sensors array which were developed for measuring picoTesla-level magnetic field and for reducing noise level (TDK, Japan). A 30-channel MR sensors array (sensor interval: 4.0 cm, sensor arrangement: 6 by 5 matrix) was placed in a magnetically shield room, and cardiac magnetic fields were recorded in the anterior chest. We performed chest X-ray before recording MCGs confirming that the sensor array covered the whole heart, and ECG was simultaneously recorded. We measured the normal components of the cardiac magnetic fields. All the five subjects underwent MCGs recording by SQUID system after measurement by MR sensor array, and the results were compared.
Results: In all the five subjects, MCGs are successfully recorded by MR sensors. Cardiac magnetic fields corresponding P, QRS and T wave on ECG were detectable by signal-averaging of 300 beats. Comparing with MCGs acquired by SQUID system, MR sensors array ac-complished comparable wave form at each site of the heart which was confirmed by chest X-ray.
Conclusions: MR sensors array was applicable for measuring cardiac magnetic fields. Our results can contribute the development of low-cost device for recording MCGs, which enables the progression of non-invasive diagnostic modality in the cardiovascular field.
MEASUREMENT OF MAGNETOCARDIOGRAM USING MAGNETORESISTIVE SENSORYasuhiro Shirai1, Kenzo Hirao1, Tomohiko Shibuya2, Shuta Ushio1, Kensuke Sekihara1, Shigenori Kawabata1 1Tokyo Medical and Dental University, Tokyo, Japan; 2TDK Corporation, Tokyo, Japan
VENTRICULAR TACHYCARDIA & VENTRICULAR FIBRILLATION P 3-093

514
Introduction: Right free wall atrioventricular accessory pathway originating from the small cardiac vein with right atrial orifice is very rare. We reported a successful case of catheter ablation for the rare accessory pathway using fluoroscopy integrated 3D mapping system.
Methods: A 46-year-old male was referred to our hospital with chief complaint of palpitations for 12 years. The resting ECG indicated pre-excited right bypass tract, and the patient had the PSVT and atrial fibrillation. The patient received catheter ablation in 12 and 8 years ago, but it was failed to abolish the antegrade and retrograde conduction of accessory pathway. The patient had more severe symptom re-cently, we prepared to perform catheter ablation again using fluoroscopy integrated 3D mapping system (CARTO-UNIVU system).
Results: The earliest ventricular activity in sinus rhythm was documented with large A wave and small V wave at the atrial side of the tri-cuspid annulus. Radiofrequency energy delivery with an irrigated ablation catheter eliminate antegrade and retrograde AV conduction over the bypass tract, but impedance was rised immediately. Angiography was performed through the distal port of the ablation catheter indicated catheter placement into a small cardiac vein. The application of radiofrequency energy with an irrigated ablation catheter, suc-cessfully abolished the antegrade and retrograde conduction of the accessory pathway.
Conclusions: Fluoroscopy integrated 3D mapping system (CARTO-UNIVU system) is helpful to ablate the complicated accessory pathway including rare accessory pathway originating from the small cardiac vein with right atrial orifice.
ATRIOVENTRICULAR ACCESSORY PATHWAY ORIGINATING FROM THE SMALL CARDIAC VEIN WITH RIGHT ATRIAL ORIFICE USING FLUOROSCOPY INTEGRATED 3D MAPPING SYSTEMKaijun Cui, Yuhua Chen
West China Hospital Sichuan University, Chengdu, China
CLINICAL ELECTROPHYSIOLOGY P 3-095

515
Introduction: Preexcitation may be overt, intermittent or inapparent. We report the onset of a new left antero-lateral preexcitation pattern in a patient successfully ablated 3 months earlier of a left posterior overt accessory pathway (AP).
Methods: N/A
Results: An asymptomatic 40 y/o man underwent electrophysiological study (EPS) for overt preexcitation. At sinus cycle length of 950 ms, HV was 28 ms. Atrial pacing induced maximal preexcitation which was compatible with a left posterior AP (negative delta waves in inferior leads). Orthodromic reentrant tachycardia at 320 ms cycle length was reproducibly induced. Atrial fibrillation (AF) occurred with a shortest preexcited RR at 190 ms and spontaneously degenerated in ventricular fibrillation which necessitated 3 electrical cardioversions to stop. Radiofrequency catheter ablation was performed by a transeptal approach and the AP was successfully ablated on the mitral annulus at a 6 o’-clock position. Post ablation EPS showed no residual preexcitation. At 3 months, the clinical course was uneventful but ECG showed new large R waves in V1-V2 (Figure 1) compatible with reappearance of a left preexcitation. At EPS, atrial pacing revealed a pattern of a new left antero-lateral preexcitation (Figure 2). The AP effective refractory period was 400 ms. No ablation was attempted. Five years later the patient is asymptomatic and still presenting with the same permanent left antero-lateral preexcitation.
Conclusions: The left anterior preexcitation was not apparent either during AF nor during EPS after ablation of the posterior preexcitation. There is no reason for this anterior preexcitation to be acquired. So it must have been present before but in a latent status. To the best of our knowledge, we are not aware of such a behavior for an AP as they conduct in an all-or-none fashion.
SECONDARY ONSET OF A NEW LEFT ANTERIOR PREEXCITATION AFTER SUCCESFUL ABLATION OF A LEFT POSTERIOR ACCESSORY PATHWAY-LATENT PREEXCITATION: A CASE REPORTChristophe d’Ivernois1, Najmeddine Echahidi2 1Service de Rythmologie, Centre Hospitalier Côte Basque, Bayonne, France; 2Centre Hospitalier Universitaire Dupuytren, Limoges, France
CLINICAL ELECTROPHYSIOLOGY P 3-096

516
Introduction: The electrocardiography of trained athletes show a broad range of abnormal patterns. T wave inversion (TWI), which com-monly appears in healthy athlete that can indicated a pathologic condition such as hypertrophic cardiomyopathy (HCM) or arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D). Published data shows that the prevalence of TWI is ethnically related, with African/Caribbean (black) athletes showing a higher rate of TWI compared to Caucasians (white). However, there is limited published data on the prevalence of TWI in East Asia populations. This study aimed to surmise the ECG repolarization characteristics and investigate the preva-lence of TWI in Chinese young athletes.
Methods: This study evaluated 490 healthy young Chinese athletes (mean age 21.4±2.5 years old), including 175 highly trained athletes and 315 collegiate athletes, and 214 healthy controls of a similar age (21.7±1.8 years old). A medical history, physical examination, 12-lead ECG, and 2-dimensional echocardiography were collected. Detailed ECG analysis was performed to evaluate the repolarization patterns.
Results: The overall prevalence of TWI was 1.4%. In highly trained athletes and collegiate athletes, it was 1.7% and 1.3% respectively. None of the control showed TWI. Athlete’s ECGs showed higher prevalence of terminal activation duration (TAD) than controls, and cor-related with training intense.
Conclusions: In young Chinese athletes, the overall prevalence of TWI was similar with Caucasian athletes, at 1.4%. Besides TWI, TAD was also relatively common in athlete’s ECGs.
PREVALENCE OF T-WAVE INVERSION IN RIGHT PRECORDIAL LEADS OF A 12-LEAD ELECTROCARDIOGRAM IN CHINESE YOUNG ATHLETESLi Feng, Xin Li
Beijing Anzhen Hospital, Beijing, China
CLINICAL ELECTROPHYSIOLOGY P 3-097

517
Introduction: Hypertrophic cardiomhyopathy (HCM) is a main cause of sudden cardiac death (SCD) in any age group. Effective risk stratifi-cation to identify patients at risk of SCD is important. There have been some attempts to identify HCM patients at high risk of SCD using heart rate variability (HRV) obtained from the RR series of ECG data. In recent years, deceleration capacity (DC) and deceleration runs (DRs), were proved to be significant predictors of mortality after myocardial infarction. However, the study about correlation between DC or DRs and SCD caused by HCM has not been reported.
Methods: 24-hour dynamic electrocardiogram (ECG) recordings of 28 healthy persons (control group) and 28 patients with HCM were evaluated using DC, acceleration capacity (AC), DRs and several typical HRV measures in time and frequency domains. There were no statistical differences in age and sex between the control group and the HCM group. Additionally, all patients in the HCM group did not take any drugs at last 7 days before ECG recording. The time domain HRV methods included SDNN, normal-to-normal RR intervals in all 5-minute segments (SDANN), standard deviation of differences between adjacent normal-to-normal RR intervals (SDSD), root mean square successive difference (RMSSD), proportion derived by dividing the number of interval differences of normal-to-normal RR intervals greater than 50 ms by the total number of normal-to-normal intervals (pNN50), and HRV triangular index (HRVTI). The frequency domain HRV methods comprised low frequency power in normalized Universitys (LF norm), high frequency power in normalized Universitys (HF norm), and ratio of LF to HF (LF/HF). DC, AC and DRs are measures of cardiac vagal modulation.
Results: DC (4.807±1.382 vs. 7.287±2.036, P<0.001), absolute of AC (5.396±1.505 vs. 8.320±2.276, P<0.001), and DR4 (0.487±0.209 vs. 0.888±0.391, P<0.001) significantly decreased in the HCM group compared with the control group. Only one HRV measure, HF norm (43.412±12.637 vs. 35.393±11.026, P=0.014), showed significant difference between the HCM group and the control group. However, there was no significant difference of other measures between the HCM group and the control group (all P>0.05). Additionally, risk stratification based on DC value presented significant difference between the HCM group and the control group (2.538±0.573 vs. 2.929±0.262, P=0.005). However, risk stratification based on DRs showed no statistical difference.
Conclusions: For this observation, clear differences of DC, AC and DR4 were obtained between the HCM and the control groups, although the subjects studied here was small. Measures such as DC, AC and DR4 may be used as predictor of SCD of HCM. In the future, risk stratification criteria and mortality endpoint event analysis for HCM patients based on DC and DRs need be developed using large data.
OBSERVATIONS OF DECELERATION CAPACITY AND DECELERATION RUNS ON HYPERTROPHIC CARDIOMHYOPATHY PATIENTSHouyuan Hu, Mi He, Yongqin Li
Southwest Hospital, Third Military Medical University, Chongqing, China
CLINICAL ELECTROPHYSIOLOGY P 3-098

518
Introduction: A short atrioventricular decrementally conducting accessory pathway is a common Mahaim fiber preexcitation in Chinese patient. Available data suggest that wide QRS tachycardia of these patients might be the first reason to see doctor in outpatient.
Methods: We compared clinical, electrocardiographic and electrophysiologic parameters in two groups of patients in sinus rhythm and tachycardia: 26 patients with a short A-V Mahaim pathway (Group A), and 20 patients with atriofascicular pathways (Group B). Radiofre-quency catheter ablation was carried out guided by mapping early ventricular activition at the annulus in Group A patients and targeting the “M” potential in Group B patients.
Results: All patients had a pre-excited atrioventricular tachycardia with anterograde conduction over anterograde decrementally conduct-ing fiber. 31 of 46 patients (67.39%) are no preexcitation and 10 of 46 patients (21.73%) are visibly late excitation during sinus rhythm. 12 of 46 patinets has rS in III lead.During radiofrequency catheter ablation an automatic rhythm occurred in 16 of 26 patients in group A. During sinus rhythm it has an rS pattern in 7 of 26 patients in group A. Intravenous adenosine caused conduction a block in the Mahaim fiber in 14 of the 26 patients tested. In group B, no patient showed clear preexcitation (P<0.01) .while 60% has a minimal preexcitation pattern. During radiofrequency catheter ablation 18 of 20 patients showed accessory pathway automaticity. During sinus rhythm it has an rS pat-tern in 5 of 20 patients in group B. Adenosine caused transient block at the atriofascicular pathway in 18 (90%).
Conclusions: Short decrementally atrioventri accessory pathways pattern are more often than atriofascicular pathways,there are different from each other in electrophysiologic properties. Those pathways can be successfully blocked by catheter ablation.
SHORT ATRIOVENTRICULAR MAHAIM FIBERS IN CHINESE PATIENTS: OBSERVATIONS ON THEIR CLINICAL, ELECTROCARDIOGRAPHIC, AND ELECTROPHYSIOLOGIC PROFILEBin Luo, Xiaogang Guo, Xu Liu, Gongbu Zhou, Jiandu Yang, Qi Sun, Jian Ma, Shu Zhang
Beijing Fuwai Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, China
CLINICAL ELECTROPHYSIOLOGY P 3-099

519
Introduction: The term linking or concealed retrograde invasion is used to describe the mechanism for perpetuation of functional ante-grade bundle branch block during supraventricular tachycardia. The occurrence of atrioventricular block during SVT rules out atrioven-tricular reciprocating tachycardia.
Methods: N/A
Results: A 55 years male with history of recurrent palpitations was referred for electrophysiology study. Baseline ECG showed normal si-nus rhythm, no evidence of preexcitation, baseline intervals were normal. On Programmed stimulation retrograde nodal conduction. Atri-al pacing showed dual AV nodal physiology and easily inducible narrow QRS regular tachycardia of tachycardia cycle length (TCL) 390 ms. During tachycardia VA interval was 20 ms, concentric retrograde atrial activation, and earliest A recorded on HIS catheter. HIS refractory VPC did not advance A. Entrainment of atrium from ventricle demonstrated, same atrial activation sequence as during tachycardia,VAV response, these features were suggestive of slow fast AVNRT. There was spontaneously initiated RBBB morphology regular tachycardia of TCL 368 ms, with VA interval of 20 ms, concentric retrograde atrial activation, earliest A recorded on HIS catheter, which converted to nar-row QRS regular tachycardia of same TCL by spontaneous VPC. There was no change in atrial activation sequence and VA interval. Tran-sition from RBBB morphology to narrow QRS tachycardia by critically timed VPC, without changing TCL, VA interval and atrial activation sequence explained by termination of transseptal concealed conduction by VPC and peeling back of refractory period of right bundle. During slow pathway RF ablation narrow QRS tachycardia with 2:1 AV block induced which resolved to 1:1 AV conduction with LBBB pat-tern by single APC. This indicates functional nature of AV block. Further RF ablation at slow pathway region leads to termination of tachy-cardia. Post RF ablation there was no evidence of dual AV nodal physiology and no inducible tachycardia.
Conclusions: Atrioventricular block is reported in about 10% cases of AVNRT. It is infranodal and functional in nature. These patients shows relatively high incidence of associated bundle branch block aberrancy.
SUPRAVENTRICULAR TACHYCARDIA WITH BUNDLE BRANCH BLOCK AND ATRIOVENTRICULAR BLOCKAmit Malik1, Chi Keong Ching2, Wee Siong Teo2 1Max Super Speciality Hospital, Delhi, India; 2National Heart Centre, Singapore
CLINICAL ELECTROPHYSIOLOGY P 3-100

520
Introduction: Increased atrial premature complexes (APC) increases the risk of atrial fibrillation (AF). But little scientific attention has been given to the association between frequent APCs and incidence of stroke.
Methods: Databases including MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials through June 2016 were searched for relevant studies that reported the incidence of stroke in patients with or without frequent APCs whether AF is preceding or not. By conducting a meta-analysis of these studies, we calculated the pooled risk ratios (RR) with a 95% confidence intervals (CI) for isch-emic stroke related events including stroke death and all-cause mortality.
Results: Six clinical trials (all observational studies) representing a total of 86,890 patients, with or without frequent APCs (n=4,922, 5.7% vs. n=81,968, 94.3%) were followed up for a mean duration of 12 years. Ischemic stroke including stroke death occurred in 186 (3.8%) pa-tients with frequent APCs, 1,180 (1.4%) patients without frequent APCs. Pooled analysis revealed that ischemic stroke related events in-cluding stroke death (RR: 2.21; 95% CI: 1.61 to 3.04; P<0.001) and all-cause mortality (RR: 9.43; 95% CI: 4.62 to 19.28; P<0.001) were meaningfully higher in patients with frequent APCs compared to patients without frequent APCs. Multivariate adjusted risk estimates for the risk of stroke were significantly greater in patients with frequent APCs (OR: 4.38; 95% CI: 3.37 to 5.69; P<0.001).
Conclusions: Frequent APCs was associated with an increased risk of ischemic stroke related events including stroke death and all-cause death regardless of the presence of preceding AF.
FREQUENT ATRIAL PREMATURE COMPLEXES AND ITS ASSOCIATION WITH RISK OF STROKE: A META-ANALYSISHo-Cheol Shin, Jae-Sik Jang, Han-Young Jin, Jeong-Sook Seo, Tae-Hyun Yang, Dae-Kyeong Kim, Dong-Soo Kim
Pusan Paik Hospital, Busan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-101

521
Introduction: The occurrence of J wave (Osborn wave) with hypothermia is well known, but the relationship of J waves and torsade de points (Tdp) with hypothermia has not been clarified.
Methods: In this study, 31 consecutive patients (13 men; mean age, 73±15 years) were admitted to our hospital with accidental hypother-mia, and were classified into 3 groups according to rectal temperature on admission (group A: 33-35°C, group B: 30-33°C, and group C: under 30°C). ECG was recorded on admission. The ECG parameters including J-waves were compared with the clinical data and coursed. Special attention was paid to the ECG characteristics of the patients who had Tdp.
Results: Consciousness disorders were observed in 4 of 9 patients in group A, in 4 of 6 patients in group B, and in 15 of 16 patients in group C (P=0.0191). Heart rate was slower in group C than in group A and B (group A: 85.8±28.2/minutes, group B: 64.3±22.2/minutes, and group C: 42.8±3.9/minutes). Although ECGs showed sinus rhythm in 8 of the 9 patients in group A, bradycardia atrial fibrillation or junctional rhythm was observed in 11 of 15 patients in group C. J waves (slurs or notches ≧0.1 mV in amplitude) were observed in a lll patients in group C and in 5 of 6 patients in group B, but in none of 9 patients in group A. PQ interval, QRS duration, and QT interval were longer in group C than in group B and C (PQ interval; group A: 145.7±29.9 ms, group B: 170.0±34.6 ms, and group C: 256.7±110.5 ms [P=0.0347]; QRS duration; group A: 101.2±8.9 ms, group B: 107.0±6.8 ms, and group C: 142.8±23.5 ms [P<0.0001]; QT interval; group A: 424.4±72.5 ms, group B: 506.2±81.2 ms, and group C: 567.8±87.0 ms [P=0.0012]). No significant differences in laboratory blood results were found among the three groups. Tdp was observed in 3 patients in group C. The ECGs of the 3 patients showed atrial fibrillation with bradycardia, and rate-dependent changes in the J-wave amplitude. Whereas J waves in other patients did not show such rate-dependen-cy of the J-wave amplitude.
Conclusions: ECG characteristics including J waves were affected by rectal temperature in the patients with accidental hypothermia. Tdp developed in 3/31 (9.7%) and they had J waves showing heart rate dependent variation and atrial fibrillation with slow ventricular rates.
THE RELATIONSHIP OF ELECTROCARDIOGRAPHIC CHARACTERISTICS, PRESENCE OF J-WAVES AND TORSADE DE POINTES WITH HYPOTHERMIAMinoru Tagawa1, Yuichi Nakamura1, Yukie Ochiai1, Masaomi Chinushi2, Yoshifusa Aizawa3 1Department of Cardiology, Nagaoka Chuo General Hospital, Nagaoka, Japan; 2Department of Cardiovascular Biology and Medicine, Niigata University School of Medicine, Niigata, Japan; 3Department of Cardiology, Tachikawa Medical Center, Nagaoka, Japan
CLINICAL ELECTROPHYSIOLOGY P 3-102

522
Introduction: To describe the baseline characteristics and treatment of atrial fibrillation (AF) patients in Macau and contribute to further studies on AF in future.
Methods: This retrospective study enroll all the atrial fibrillation patient consulted at cardiology clinic in the Centro Hospitalar Conde de São Januário (CHCSJ), the only one public hospital in Macau. Baseline data included demographics, clinical characteristics and treat-ments.
Results: A total of 652 AF patients (mean age: (72.1±11.5) years old, 49% female (n=320) were recruited between January 2014 and De-cember 2014. There were 211 patients (32.3%) with age above 80 years old, 135 patients (20.7%) had history of thromboembolism event, 410 patients (62.9%) had hypertension. Valvular, non-valvular and lone AF were 27.6%, 42.1% and 30.4%, respectively. Mean CHA2DS2-VASc score was 3.2, and 519 patients (79.6%) had a CHA2DS2-VASc score≥2. 257 patients (54.4%) received either warfarin (n=101, 21.4%) or new oral anticoagulants (n=156, 33.0%).
Conclusions: The AF patient in Macau is more older, the percentage of valvular AF is higher. Due to more than half part patients accept anticoagulation therapy, the percentage of stroke is low.
THE ATRIAL FIBRILLATION IN MACAURuohan Chen1, Keping Chen1, Toi-Meng MOK2, Evora Mario2, Shu Zhang1 1Fuwai Hospital, Beijing, China; 2Centro Hospitalar Conde de Sao Januario, Macau, China
CLINICAL ELECTROPHYSIOLOGY P 3-103
The Characteristics of Atrial Fibrillation Patients
Age 72.1Femal 320 (49%)Hypertension 410 (62.9%)CAD 78 (12.0%)Heart failure 129 (19.8%)DM 155 (23.8%)Kidney failure 74 (11.3%)Paroxysmal AF 86 (13.2%)Persistent AF 23 (4.0%)Chronic AF 543 (82.8%)

523
Introduction: Aortic stiffness as a surrogate of central hypertension is increasingly recognised for its adjunctive value over and above the traditional cardiovascular risk factors. A meta-analysis was performed for corroborative enumeration of publish data in order to provide additional ground to integrate the “novelty” of aortic stiffness in clinical risk stratification of cardiovascular diseases. In addition, quantita-tive evaluation of evidence to summarise the predictive role of pulse pressure in new onset of atrial fibrillation (AF), was delineated.
Methods: Data sources: Literature search was carried out by exploring PubMed for studies published in English until 14th August 2015. Data Extraction; Quality of each study was assessed by two independent reviewers and divergent views were resolved by developing a con-sensus.
Results: Meta-analysis was performed on 22 longitudinal studies out of which 19 reported aortic stiffness indices as an independent pre-dictor of mortality and the rest of the three had described all-embracing association between pulse pressure and atrial fibrillation onset in 25,987 participants followed up for 7.83±4.4 years with a mean age of 59.7±10.3 years and 17,582 individuals with mean age of 61±4 years followed up for 8.3±3.5 years respectively. In high versus low PWV group the calculated pooled odd ratio (OR) for cardiovascular (CV) and all cause mortality was 2.34 (95% CI 1.81-3.02, 10 studies) and 1.57 (95% CI 1.2-2.1, 6 studies) correspondingly. Adjusted 1m/s in-crease in PWV imposed 26% (95% CI 17-36%, 11 studies) and 16% (95% CI 8-25%, 5 studies) risk escalation for CV and all cause mortality respectively. Each 10 mmHg increase in peripheral pulse pressure adjusted for age, BMI and conventional CV risk factors, incurred a pooled hazard ratio (HR) of 1.12 (95% CI 1.07-1.17) in onset of new AF.
Conclusions: Increasing aortic stiffness as a marker of reduced conduit arterial tree compliance is an independent predictor of CV and all cause mortality. With every 10mmHg increase in pulse pressure there was an adjusted 12% (95% CI 7-17%) escalated risk of developing atrial fibrillation.
A SYSTEMIC REVIEW AND META- ANALYSIS TO APPRAISE AORTIC STIFFNESS AS A PREDICTIVE TOOL FOR CARDIOVASCULAR AND ALL CAUSE MORTALITY WITH EVIDENTIAL INSIGHT INTO ADDENDUM ROLE OF PULSE PRESSURE IN AFKashif Khokhar1,2, Adrian Elliot2, Dennis Lau1,2, Rajiv Mahajan1,2, Dian Andien Munawar1,2, Sharath Kumar1,2, Anand Thiyagarajah1,2, Martin Stiles3, Celine Gallaghar1,2, Prashanthan Sanders1,2 1Royal Adelaide Hospital, Adelaide, Australia; 2University of Adelaide, Adelaide, Australia; 3Waikato Hospital, Hamilton Waikato, Hamilton, New Zealand
CLINICAL ELECTROPHYSIOLOGY P 3-104
Cardiovascular Mortality: High v Low Groups

524
CLINICAL ELECTROPHYSIOLOGY P 3-104
All-cause Mortality: High vs Low Groups
Cardiovascular Mortality: Per 1 m/s increase
All-cause Mortality: Per 1 m/s increase
Pulse pressure and AF

525
Introduction: Direct-current cardioversion (DCC) in patients with persistent atrial fibrillation (AF) is known to have high acute success rate and low complication rate, but 50% of those with acute success showed recurrence. There is paucity of information whether the energy amount used in DCC has prognostic implication after successful cardioversion in patients with persistent AF.
Methods: Consecutive patients with AF who underwent elective cardioversion between 2010 and 2016 were included. DCC was started with initial low energy, 100 J, and if failed to be defibrillated, gradual higher energy, 150 J and 200 J were delivered sequentially. After 3rd shock, 200 J was delivered again using adhesive patch. Clinical, echocardiographic, cardioversion characteristics were evaluated. Primary outcome was 1-month recurrence of AF. According to the energy amount delivered at final successful cardioversion, patients were classi-fied into low energy (<200 J) and high energy (≥200 J) groups.
Results: In total of 458 patients who underwent successful cardioversion (age, 62.2±9.3 years; 70.5% male; left atrium (LA) size, 49.2±6.4 mm), 266 patients (58.1%) showed 1-month recurrence. Compared to patients remained in sinus rhythm (no recurrence), patients with AF recurrence were male predominant (74.1% vs. 65.4%, P=0.046), have longer AF duration (52.0 vs. 37.3 months, P=0.001), and were deliv-ered higher total energy for DCC (186.2 vs. 153.1 J, P=0.013). Age (62.0 vs. 62.4 years, P=0.613) and LA size (49.1 vs. 49.3 mm, P=0.725) was not significantly different in both groups. One-month recurrence rate was lower in patients successfully defibrillated with lower ener-gy (55.6% vs. 58.6% vs. 74.5% in 100, 150 and 200J respectively, p for trend=0.020). In multivariable analysis, long AF duration (≥48 months) (odds ratio [OR], 2.1; 95% confidence interval [CI], 1.42-3.14; P<0.001), cardioversion by high energy (OR, 2.3; 95% CI, 1.2-4.4; P=0.011) were independent predictors of AF recurrence.
Conclusions: Successful electrical cardioversion with low energy showed less early recurrence than high energy group in patients with persistent AF. Necessity for high energy for cardioversion is presumed to have vulnerable feature for AF recurrence.
SUCCESSFUL ELECTRICAL CARDIOVERSION WITH LOW ENERGY SHOWED LESS RECURRENCE RATE IN PATIENTS WITH PERSISTENT ATRIAL FIBRILLATIONChee Hae Kim
Seoul National University Hospital, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-105

526
Introduction: New-onset atrial fibrillation (NOAF) is a common type of tachyarrhythmia in patients with severe sepsis or septic shock and associated with increased in-hospital mortality. However, the association of NOAF and future mortality in such patients remains unclear.
Methods: A total of 503 consecutive patients with severe sepsis or septic shock, who were admitted to a medical intensive care University (ICU) between 2011 and 2014 were screened. Of these, 135 patients died during hospitalization and 55 patients had no follow-up data after discharge. Finally, 313 patients with severe sepsis or septic shock with survival discharge were included into the study. NOAF was detect-ed by continuous electrocardiographic monitoring. Patients were categorized by the presence of NOAF or not. The interest endpoint of this study was all-cause mortality.
Results: During a follow-up of 21.7±17.4 months, 69 patients experienced all-cause death, including 20 of cardiovascular (CV) death and 29 of non-CV death. Patients with NOAF were older than those without NOAF. Moreover, patients with NOAF had higher prevalence of cor-onary artery disease (CAD), congestive heart failure (CHF), and prior stroke. Although septic patients with NOAF were associated with an increased risk of mortality during follow-up, the multivariate Cox regression analysis could not demonstrated the NOAF predicted future mortality after adjusting the underlying comorbidities (hazard ratio: 1.29; 95% CI: 0.791-2.106, P=0.306).
Conclusions: NOAF in patients with severe sepsis or septic shock could not independently predict future mortality. We need larger study to clarify the association between NOAF and long-term mortality in such patients.
COULD NEW-ONSET ATRIAL FIBRILLATION IN PATIENTS WITH SEVERE SEPSIS OR SEPTIC SHOCK PREDICT FUTURE MORTALITY?Wen-Yu Lin
Tri-Service General Hospital, Taipei, Taiwan
CLINICAL ELECTROPHYSIOLOGY P 3-106
Univariate and Multivariate Cox Regression Analysis for Predictors of All-cause Mortality
VariablesUnivariate analysis Multivariate analysis
Harzard ratio 95% CI P value Hazardratio 95% CI P value
NOAF 1.710 1.066-2.745 0.026 1.291 0.791-2.106 0.306Age 1.033 1.012-1.054 0.002 1.027 1.005-1.049 0.015CAD 1.990 1.237-3.200 0.005 1.795 1.113-2.894 0.016CHF 1.330 0.696-2.542 0.388Prior Stroke 1.782 1.070-2.967 0.026 1.472 0.879-2.462 0.141

527
Introduction: Hyperthyroidism is an important cause of atrial fibrillation (AF). However, the prevalence of thyroid-related antibodies in a normal thyroid function state has not yet been thoroughly documented. Therefore, we aim to identify the relationship between thyroid-re-lated antibodies and AF in euthyroid AF patients compared with age-matched control patients.
Methods: A cross-sectional survey of 1,294 patients (mean age 57.09±14.27 years, 476 males, 818 females) who were euthyroid without anti-thyroid medication was performed. Serum TSH receptor antibodies, anti-microsomal antibodies and anti-thyroglobulin antibody level were measured in 844 non-AF control patients and 450 AF patients using a radioimmunoassay kit.
Results: TSH receptor antibodies were significantly increased in euthyroid AF patients. TSH receptor antibodies were present at 4.23±21.85 μ/L and 10.15±45.07 μ/L (control vs. AF, respectively; P=0.029). Anti-thyroglobulin antibody levels were 64.31±105.59 μ/mL and 71.53±114.51 μ/mL (control vs. AF, respectively; P=0.282). Anti-microsomal antibodies were present at 155.53±352.35 μ/mL and 198.67±404.50 μ/mL (P=0.068, control vs. AF, respectively). Seropositivity was defined as a TSH receptor antibody level exceeding 10 μ/L and sero-positivity was compared between groups using the chi-square test. In total, 26/569 (4.6%) of control patients and 35/278 (11.2%) of AF pa-tients were seropositive, representing a significant difference (odds ratio, 2.629; P<0.001).
Conclusions: Patients seropositive for TSH receptor antibody were at high risk of AF even when in the euthyroid state.
THE RELATIONSHIP BETWEEN THYROID-RELATED ANTIBODIES AND ATRIAL FIBRILLATION IN EUTHYROID PATIENTSDong Hyun Park, Bong Joon Kim, Ga In You, Tae Joon Cha
Kosin University Gospel Hospital, Busan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-107

528
Introduction: Left atrium of patients with atrial fibrillation (AF) has a unique flow dynamics compared to normal sinus rhythm. Under-standing and investigating hemorrheologic parameters including erythrocyte deformability can give us meaningful information for treat-ment approaches of AF. But little is known about association between erythrocyte deformability and AF. The aim of this study is to evaluate the association between AF and erythrocyte deformability.
Methods: From August 2014 to July 2015, we recruited 155 patients visiting Yeungnam University Medical Center. They consisted of 77 AF patients and 78 control patients who had atypical chest pain. Erythrocyte deformability, expressed as elongation index (EI) of erythrocyte, was measured at 3 Pa by using microfluidic ektacytometer (Rheoscan-D®, Rheo-Meditech, Seoul, Korea), and other hemorrheologic pa-rameters including critical shear stress were also compared between two groups.
Results: Baseline characteristics showed large proportion of male patients, history of stroke and vitamin K antagonist in AF group. EI was significantly lower in AF group (0.309626±0.019471 vs. 0.316274±0.018726, P=0.032) but critical shear stress did not show any difference between two groups. In subgroup analysis, persistent AF showed a lower tendency of EI compared to paroxysmal AF (0.306796±0.0.017400 vs. 0.315176±0.022330, P=0.074). CHA2DS2-VASc score had significant negative correlation with EI (R2=0.141, P<0.001).
Conclusions: We demonstrated erythrocyte deformability and features of other hemorrheologic parameters in a condition of AF. Under-standing hemorrheologic characteristics including erythrocyte deformability may provide valuable supplementary information for man-agement of patients with AF.
ANALYSES OF ASSOCIATION BETWEEN ATRIAL FIBRILLATION AND ERYTHROCYTE DEFORMABILITY USING MICROFLUIDIC EKTACYTOMETERKyu-Hwan Park, Kang-Un Choi, Jong-Ho Nam, Chan-Hee Lee, Dong-Gu Shin
Yeungnam University Medical Center, Daegu, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-108

529
Introduction: Entrainment mapping is an established electrophysiological technique to identify arrhythmia mechanism and define com-ponents of the reentrant circuit. With the recent advent of high resolution 3D electroanatomical mapping that allows automated electro-gram annotation and rapid acquisition of activation points, the ongoing utility of entrainment to define reentrant circuits is uncertain. We sought to determine whether all apparent reentrant loops seen on high density 3D electroanatomical maps are active circuits when using entrainment mapping.
Methods: 16 patients with macro reentrant atrial tachycardia undergoing catheter ablation were studied. High density (HD) 3D electro-anatomical mapping was performed using a novel basket catheter with 64 electrodes and automated electrogram annotation. Entrain-ment mapping was performed at multiple sites in the atria considered to be part of the active circuit on the propagation map.
Results: In the 16 patients studied, 18 atrial flutter circuits were observed. 11 (61%) re-entry circuits were consistent with counterclock-wise CTI dependent atrial flutter, 2 (11%) clockwise CTI dependent atrial flutter and one (6%) example of intra-isthmus re-entry. 2 (11%) cases of upper loop re-entry were observed. Two (11%) circuits were consistent with left atrial flutter. Maps had a mean of 24,202±9,939 points acquired in a mean of 21±14 minutes. In 9 of 11 patients with counterclockwise CTI dependent flutter (diagnosed on activation and entrainment mapping), lower loop reentry appeared to be present with a wavefront crossing the crista terminalis posteriorly. However in 6/9 pts (67%), entrainment mapping demonstrated that this location was not part of the active circuit (Figure 1). A passive ascending wave front meeting a passive descending wavefront created the visual appearance of break across the CT which was not actually present.
Conclusions: HD 3D electroanatomical mapping systems can rapidly produce highly accurate and dense maps of atrial activation pat-terns during a variety of atrial macro-reentry circuits. However, circuitous propagation not involved in the arrhythmia mechanism can mimic the appearance of a critical reentrant circuit. Simple entrainment mapping remains an important adjunctive tool when using latest generation HD mapping systems.
CAN WE ALWAYS BELIEVE WHAT WE SEE? ENTRAINMENT REMAINS IMPORTANT FOR DIAGNOSIS OF ATRIAL MACRO-REENTRY IN THE ERA OF HIGH DENSITY 3D MAPPINGBhupesh Pathik1, Geoff Lee1, Matthew Bates1, Jonathan Lipton1, Sandeep Prabhu1, Chrishan Nalliah1, Joseph Morton1, Paul Sparks1, Peter Kistler2, Jonathan Kalman1 1Royal Melbourne Hospital, Melbourne, Australia; 2Alfred and Baker IDI, Melbourne, Australia
CLINICAL ELECTROPHYSIOLOGY P 3-109
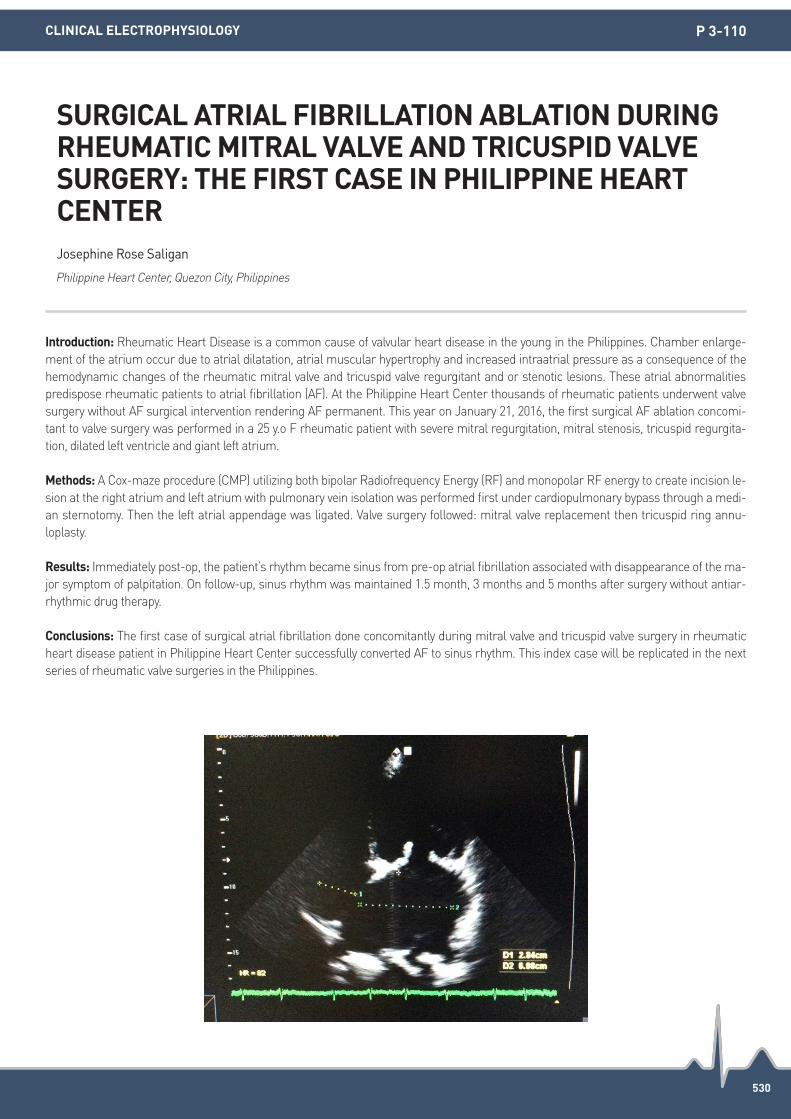
530
Introduction: Rheumatic Heart Disease is a common cause of valvular heart disease in the young in the Philippines. Chamber enlarge-ment of the atrium occur due to atrial dilatation, atrial muscular hypertrophy and increased intraatrial pressure as a consequence of the hemodynamic changes of the rheumatic mitral valve and tricuspid valve regurgitant and or stenotic lesions. These atrial abnormalities predispose rheumatic patients to atrial fibrillation (AF). At the Philippine Heart Center thousands of rheumatic patients underwent valve surgery without AF surgical intervention rendering AF permanent. This year on January 21, 2016, the first surgical AF ablation concomi-tant to valve surgery was performed in a 25 y.o F rheumatic patient with severe mitral regurgitation, mitral stenosis, tricuspid regurgita-tion, dilated left ventricle and giant left atrium.
Methods: A Cox-maze procedure (CMP) utilizing both bipolar Radiofrequency Energy (RF) and monopolar RF energy to create incision le-sion at the right atrium and left atrium with pulmonary vein isolation was performed first under cardiopulmonary bypass through a medi-an sternotomy. Then the left atrial appendage was ligated. Valve surgery followed: mitral valve replacement then tricuspid ring annu-loplasty.
Results: Immediately post-op, the patient’s rhythm became sinus from pre-op atrial fibrillation associated with disappearance of the ma-jor symptom of palpitation. On follow-up, sinus rhythm was maintained 1.5 month, 3 months and 5 months after surgery without antiar-rhythmic drug therapy.
Conclusions: The first case of surgical atrial fibrillation done concomitantly during mitral valve and tricuspid valve surgery in rheumatic heart disease patient in Philippine Heart Center successfully converted AF to sinus rhythm. This index case will be replicated in the next series of rheumatic valve surgeries in the Philippines.
SURGICAL ATRIAL FIBRILLATION ABLATION DURING RHEUMATIC MITRAL VALVE AND TRICUSPID VALVE SURGERY: THE FIRST CASE IN PHILIPPINE HEART CENTERJosephine Rose Saligan
Philippine Heart Center, Quezon City, Philippines
CLINICAL ELECTROPHYSIOLOGY P 3-110

531
Introduction: Most patients requires internal cardioversion (CV) during catheter ablation (CA) for atrial fibrillation (AF). Some patients show high atrial defibrillation threshold (A-DFT) or CV-resistant AF. We investigated whether A-DFT predicts the outcome of CA for AF.
Methods: We studied 87 patients (57 men, 66±8 years, 28 with non-paroxysmal AF) who underwent CA for AF. Clinical and echocardio-graphic data were evaluated before CA. A-DFT was measured after AF was induced by atrial high rate pacing in patients with sinus rhythm. The CV protocol was started at 5J and was increased incrementally in 5J steps until successful CV and to a maximum of 30 J.
Results: Recurrent AF was detected in 29/87 patients (32%) during the follow-up period (11±5 months). Univariate analysis revealed high-er A-DFT (12.9±9.0 J vs. 8.0±4.8 J, P=0.0013), larger left atrial diameter (43±7 mm vs. 39±7 mm, P=0.0245), and the higher prevalence of non-paroxysmal AF (48% vs. 24%, P=0.0231) as significant variables. On multivariate analysis, higher A-DFT (P=0.0207, OR 1.567 for each 5 J increase in A-DFT, 95%CI 1.014-1.180) was only independently associated with recurrent AF. Patients with high A-DFT (>10 J) had a higher risk of recurrent AF (log rank P=0.0082).
Conclusions: High atrial defibrillation threshold associated with poor outcome after catheter ablation for atrial fibrillation. Patients with high atrial defibrillation threshold might need additional ablation procedures.
ATRIAL DEFIBRILLATION THRESHOLD PREDICTS THE OUTCOME OF CATHETER ABLATION FOR ATRIAL FIBRILLATIONSatoshi Takahashi, Takanao Mine, Kenki Ashida, Hideyuki Kishima, Masaharu Ishihara, Tohru Masuyama
Hyogo College of Medicine, Nishinomiya, Japan
CLINICAL ELECTROPHYSIOLOGY P 3-111

532
Introduction: Long-standing Atrial Fibrillation (LS-AF) is hard to keep sinus rhythm after catheter ablation (PVI). The steerable sheath is powerful tool for catheter ablation of afib. We examined the effect of a steerable sheath for ablation of atrial fibrillation at patient with LS-AF.
Methods: Ninety nine patients ware underwent PVI at 2014 in our institute, involved the thirteen LS-AF patient (62.8±11.8 y/o, ten male) who diagnosed as LS-AF by the duration of afib ware more than twelve month. Our ablation method is the steerable sheath steer ablation use the Agilis steerable transseptal sheath (St. Jude Medical), and when PVI does not complete, using pace-and-ablate technique. End point of procedure is no inducibility of afib, and performed step wise approach to get the ablation end point.
Results: These patients character was as follow; CHADS2 score 0.69, EF 56.3±14.4%, LAD 34.3±6.9 mm, LA volume194.2±43.5 mL. Av-erage procedure was 1.23 sessions and an observation period was 217.6 day. We performed full line ablation (PVI+CTI+MVI+roof line) in 69.3% patients. 84.6% of patients got the ablation end point. (no inducibility of afib) 69.2% of patient was keep sinus rhythm at one year.
Conclusions: Steerable sheath is powerful tool for ablation of atrial fibrillation at patient with LS-AF.
EFFICACY OF ABLATION TO LONG-STANDING ATRIAL FIBRILLATION USING STEERABLE SHEATH STEER ABLATION METHODTaku Asano, Yuya Nakamura, Akinori Ochi, Yoshimi Onishi, Tatsuya Onuki, Norikazu Watanabe, Youichi Kobayashi
Division of Cardiology, Department of Medicine, Showa University School of Medicine, Tokyo, Japan
CLINICAL ELECTROPHYSIOLOGY P 3-113

533
Introduction: Previously reported P wave indices are associated with atrial fibrillation (AF) development, progression of AF, AF recurrence after pulmonary vein isolation (PVI), or atrial substrate remodeling. We hypothesized that an inhomogenous slow atrial depolarization would be more likely related to AF recurrence, and a potential reduction in atrial depolarization time after PVI could be related to a favor-able clinical outcome. The aim of this study was to pursue this new ECG-based criterion of the P wave, P wave deflection, and to investi-gate the relationship between the P wave deflection and the clinical outcomes after PVI in paroxysmal AF.
Methods: A total of 143 patients with paroxysmal AF who underwent PVI were analyzed retrospectively. The independent measurements of various P wave indices including the new ECG variable of P wave deflection defined as the interval measured from the onset of the P wave to the peak of the P wave depolarization time in any of the 12-leads were undertaken using the CardioLab/Prucka recording system prior to ablation and immediately after PVI. We categorized the study patients according their clinical outcome as either the sinus rhythm (SR) maintenance group (n=103) or AF recurrence group (n=41).
Results: In our analysis of P wave deflection pre- and post-ablation, the maximum P wave deflection (79.2±14.3 ms vs. 63.5±14.9 ms, P<0.001) and P wave deflection dispersion (41.6±13.1 ms vs. 28.1±14.8 ms, P<0.001) were significantly decreased immediately after PVI in SR maintenance group. However, there were no significant differences in P wave deflection and other indices in the AF recurrence group. In addition, there was a significant reduction in time to maximum P wave deflection (15.9±10.7 ms vs. 8.3±9.2 ms, P<0.001) and P wave deflection dispersion (13.6±9.4 ms vs. 7.1±9.3 ms, P=0.001) in the SR maintenance group as compared to the AF recurrence group.
Conclusions: The significant reductions in P wave deflection and dispersion following PVI were associated with maintenance of SR, thus suggesting new ECG prognostic parameters after PVI that may be helpful in patients with paroxysmal AF.
USEFULNESS OF P-WAVE DEFLECTION IN PREDICTING CLINICAL RECURRENCE AFTER PULMONARY VEIN ISOLATION IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATIONJi-Eun Ban, Dong-Jin Oh
Hallym University Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-114

534
Introduction: A reduction in surface ECG P wave duration has been associated with improved clinical outcomes in both paroxysmal and persistent atrial fibrillation ablation. We investigated the effects of different ablation strategies on P wave duration, hypothesising that ex-tensive LA ablation with left atrial posterior wall isolation via catheter or hybrid approaches would give a greater reduction in P wave dura-tion than more limited ablation techniques.
Methods: A retrospective analysis of ECG’s from patients who have undergone AF ablation was performed. Pre-procedural sinus rhythm ECG’s were compared with the post procedure ECG’s. ECG’s were identified and measured by one investigator then anonymised, ran-domised and re-measured by two further investigators. Maximal P wave duration was measured in the limb leads I or II and a mean value calculated for each patient. The left atrial dimensions and medications at the time of ECG were also documented. Ablation strategies compared were; pulmonary vein isolation (PVI) for paroxysmal atrial fibrillation (PAF) and the persistent AF (PsAF) ablation strategies of pulmonary vein isolation plus additional linear or CFAE ablation (PVI.Lines), left atrial posterior wall isolation via catheter (PWI) and left atrial posterior wall isolation via non-concomitant surgical and catheter ablation (hybrid).
Results: Seventy-five patients ECG’s were analysed: 20 PVI, 21 PVI. Lines, 15 PWI, 19 Hybrid. Only a weak positive correlation was seen between pre-procedure left atrial size and P wave duration (r=0.2475) but LA size and P wave duration was larger in PsAF patients. Medi-an LA AP diameter: PVI-35 mm (IQR 35-40.75), PVI.Lines-40 mm (34-52), PWI-41 mm (35-43), Hybrid-46.5 mm (44-47.75). Median P wave pre: PVI-120 ms (IQR 100-128), PVI.Lines-135 ms (120-140), PWI-120 ms (120-140, Hybrid -130 ms (120-146) Antiarrhythmic medication varied between patients but in only 10/75 was there a change between ECG recordings. There was no significant difference in P wave change between PVI, PVI.Lines or PWI (Figure 1) but Hybrid AF ablation produced a significant reduction in P wave duration compared to the other approaches (vs PVI P=0.0014, vs. PVI.Lines P=0.014, vs. PWI P=0.014). Median P wave reduction: PVI-3.75 ms (IQR -20.6-8.1), PVI.lines-12.5 ms (-7.5-20), PWI-0 ms (0-10), Hybrid-30 ms (2.5-55).
Conclusions: Hybrid AF ablation via a combined surgical and catheter ablation significantly reduced P wave duration compared to other ablation strategies including posterior wall isolation via catheter. Further study is necessary to investigate if this is due to a more durable lesion set or an alternative mechanism such as modulation of the autonomic nervous system in surgical epicardial ablation.
THE EFFECT OF DIFFERENT ATRIAL FIBRILLATION ABLATION STRATEGIES ON P WAVE DURATIONGuy Furniss, Dimitrios Panagopoulos, Edward Davies, David Tomlinson, Guy Haywood
South West Cardiothoracic Centre, Plymouth, United Kingdom
CLINICAL ELECTROPHYSIOLOGY P 3-115

535
Introduction: Patients with degenerative aortic stenosis (AS) are known to be prone to conduction disturbance compared to healthy popu-lation of same age. However, incidence of atrial arrhythmic events that requires medical attention are not investigated in isolated aortic valve replacement with degenerative AS. We sought to evaluate the incidence and prognosis of atrial arrhythmia during long term follow up after AVR.
Methods: This is a single tertiary center retrospective study, evaluating the clinical outcomes, especially regarding conduction disturbance development in patients who underwent isolated surgical aortic valve replacement due to aortic stenosis. Enrolled patients underwent ei-ther surgical isolated aortic valve replacement from January 2005 to May 2015. Clinical information were examined by thorough chart re-view. We reviewed pre-operative electrocardiogram (ECG) and described as baseline rhythm. Perioperative, postoperative and most recent obtainable ECGs including Holter data were all thoroughly reviewed. The patient related data included baseline and clinical characteristics of the patients and the surgical data included valve type, size and cardiopulmonary bypass time during AVR. In addition, any adverse clini-cal event during follow up period was gathered.
Results: We analyzed 665 patients, pathologically proven degenerative AS with obtainable ECGs. Mean age of the patients was 67.8±2.3 years, 224 patients had bicuspid aortic valve (32.7%), mean follow up after AVR was 1,026±357 days. Immediate postoperative atrial ar-rhythmias were observed in 106 patients (15.5%, among them, 66 patients were atrial fibrillation). Most of the patients with immediate postoperative atrial arrhythmias (83 patients, 81.1%) had transient arrhythmia documented only during index hospitalization. From dis-charge day to final follow up day (follow up period), 63 patients (9.4%) developed de novo atrial arrhythmias. Most of the newly developed atrial arrhythmia was atrial fibrillation (n=44, 69.8%) which required further medical intervention.
Conclusions: Isolated AVR in degenerative AS patients carry relatively high incidence of atrial arrhythmic event during follow up. In con-clusion, atrial arrhythmia is not so rare following AVR and needs medical attention as it carries further necessity of anticoagulation, anti-arrhythmic drugs, catheter ablation and maybe pacemaker. However, further studies are needed to investigate the predictors and clinical implication of atrial arrhythmia after isolated AVR.
PREVALENCE OF DE NOVO ATRIAL FIBRILLATION AFTER ISOLATED SURGICAL AORTIC VALVE REPLACEMENT IN SEVERE AORTIC STENOSISYou-Mi Hwang, Jun Kim, Minsu Kim, Ji Hyun Lee, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim
Asan Medical Center, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-116

536
Introduction: Ergonovine is ergoline-derivatives that act at alpha-adrenergic, dopaminergic and serotonin receptors (5-HT2 receptor). In-fluence of serotonin and 5-HT2 receptor agonist on cardiomyocytes has been known. However, there was limited data about the associa-tion between QRS duration changes during ergonovine provocation test and arrhythmic complications.
Methods: A total of 182 patients who underwent coronary angiography (CAG) with ergonovine provocation test were consecutively enrolled (mean age; 53.9±10.4 years, 59.3% male) at Kosin university gospel hospital from September, 2014 to May, 2015. ECGs recorded closest to the time of CAG were carefully reviewed and measured PR interval, QRS duration, QT and QTc intervals.
Results: Total 41 (22.5%) patients had arrhythmic events including atrial fibrillation, atrial tachycardia, atrial premature beat, ventricular tachycardia, and ventricular premature beat during follow-up. The patients with QRS prolongations had higher incidences of arrhythmic events compared with those without QRS changes (P=0.025). In univariate analysis, diabetes mellitus (P=0.05), coronary artery spasm (P=0.031) and QRS prolongations (P=0.036) were significantly associated with arrhythmic events. In multivariate analysis, QRS prolonga-tions [OR 2.496 (1.077-5.784), P=0.033] was independent risk factors for arrhythmic events at the long-term follow-up.
Conclusions: The patients with QRS duration prolongations during Ergonovine provocation test were associated with higher incidence of arrhythmic events, suggesting more intensive medical therapy with close clinical follow-up will be required.
IMPACT OF QRS DURATION CHANGES DURING ERGONOVINE PROVOCATION TEST ON ARRHYTHMIC COMPLICATIONSSung Il Im, Kyoung Im Cho, Hyun Su Kim, Jeong Ho Heo, Tae Joon Cha
Kosin University Gospel Hospital, Busan, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-117
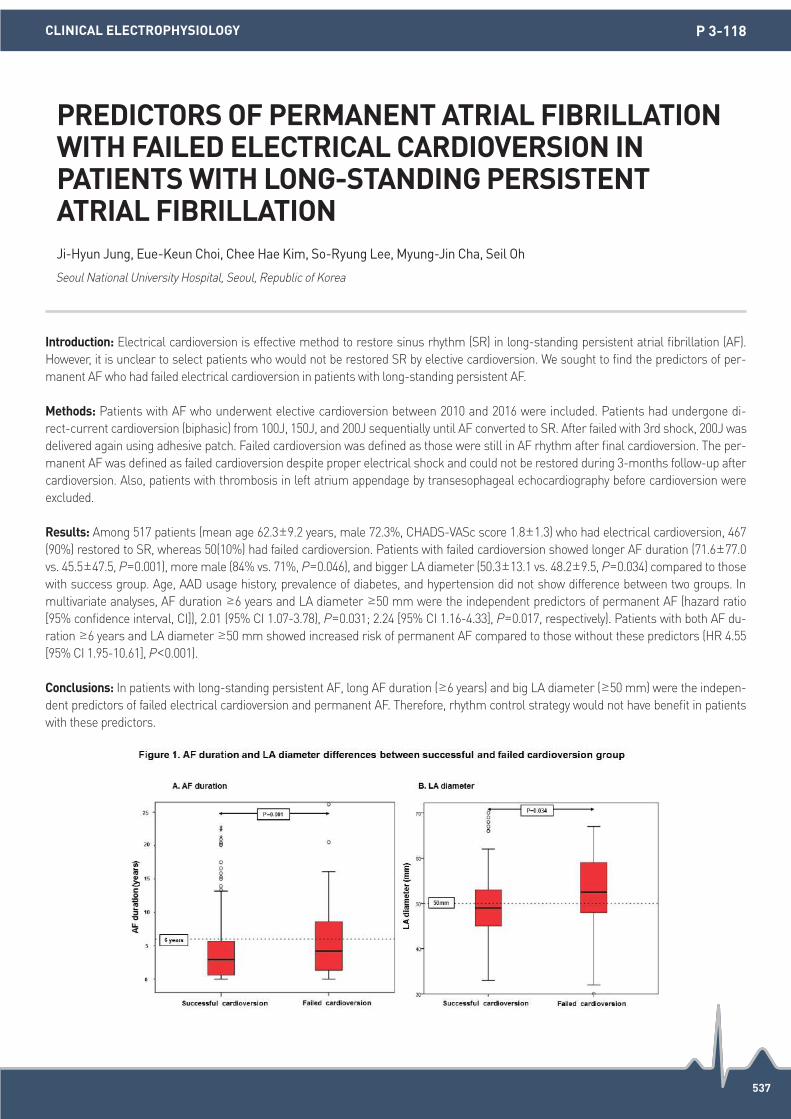
537
Introduction: Electrical cardioversion is effective method to restore sinus rhythm (SR) in long-standing persistent atrial fibrillation (AF). However, it is unclear to select patients who would not be restored SR by elective cardioversion. We sought to find the predictors of per-manent AF who had failed electrical cardioversion in patients with long-standing persistent AF.
Methods: Patients with AF who underwent elective cardioversion between 2010 and 2016 were included. Patients had undergone di-rect-current cardioversion (biphasic) from 100J, 150J, and 200J sequentially until AF converted to SR. After failed with 3rd shock, 200J was delivered again using adhesive patch. Failed cardioversion was defined as those were still in AF rhythm after final cardioversion. The per-manent AF was defined as failed cardioversion despite proper electrical shock and could not be restored during 3-months follow-up after cardioversion. Also, patients with thrombosis in left atrium appendage by transesophageal echocardiography before cardioversion were excluded.
Results: Among 517 patients (mean age 62.3±9.2 years, male 72.3%, CHADS-VASc score 1.8±1.3) who had electrical cardioversion, 467 (90%) restored to SR, whereas 50(10%) had failed cardioversion. Patients with failed cardioversion showed longer AF duration (71.6±77.0 vs. 45.5±47.5, P=0.001), more male (84% vs. 71%, P=0.046), and bigger LA diameter (50.3±13.1 vs. 48.2±9.5, P=0.034) compared to those with success group. Age, AAD usage history, prevalence of diabetes, and hypertension did not show difference between two groups. In multivariate analyses, AF duration ≥6 years and LA diameter ≥50 mm were the independent predictors of permanent AF (hazard ratio [95% confidence interval, CI]), 2.01 (95% CI 1.07-3.78), P=0.031; 2.24 [95% CI 1.16-4.33], P=0.017, respectively). Patients with both AF du-ration ≥6 years and LA diameter ≥50 mm showed increased risk of permanent AF compared to those without these predictors (HR 4.55 [95% CI 1.95-10.61], P<0.001).
Conclusions: In patients with long-standing persistent AF, long AF duration (≥6 years) and big LA diameter (≥50 mm) were the indepen-dent predictors of failed electrical cardioversion and permanent AF. Therefore, rhythm control strategy would not have benefit in patients with these predictors.
PREDICTORS OF PERMANENT ATRIAL FIBRILLATION WITH FAILED ELECTRICAL CARDIOVERSION IN PATIENTS WITH LONG-STANDING PERSISTENT ATRIAL FIBRILLATIONJi-Hyun Jung, Eue-Keun Choi, Chee Hae Kim, So-Ryung Lee, Myung-Jin Cha, Seil Oh
Seoul National University Hospital, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-118

538
Introduction: Atrial arrhythmias (AAs) after lung transplantation (LT) are common and often associated with increased hospital stay and mortality. However, clinical implications of postoperative AA are not fully determined. Our aim was to investigate the incidence, predispos-ing factors and clinical outcomes of AAs after lung transplantation in adults.
Methods: Total 113 consecutive patients who underwent lung transplantation from May 2011 to December 2015 were evaluated retro-spectively. All patients were performed post-operative electrocardiographic monitoring. An arrhythmia episode is defined as documented atrial fibrillation (AF), atrial flutter (AFL) or atrial tachycardia (AT) lasting >30 minutes on 12-lead ECG or telemetry monitoring. Uni- and multivariate logistic regression models were constructed to identify predictors of AAs.
Results: Mean follow-up period was 15.7±15.5 months. Postoperative AAs occurred in 33 of 113 patients (29.2%), of whom 24 patients (21.2%) had AF, 16 (14.1%) had AFL, and 10 (8.8%) had AT. The mean time to onset after LT was 9.1±7.5 days for AF, 12.4±8.2 days for AFL and 28.0±25.2 days for AT, respectively. AAs were more likely to occur in patients with older age (56.4±11.1 arrhythmia vs. no arrhythmia group 47.3±14.2; P=0.001), combined HTN (33.3% vs. 15.0%; P=0.028), coronary artery disease (15.2% vs. 2.5%; P=0.022), history of AF before transplant (12.1% vs. 1.3%; P=0.025) and postoperative tracheostomy (75.8% vs. 43%; P=0.002) which means longer period of me-chanical ventilation. Advanced age (hazard ratio [HR] 1.05, P=0.013) and postoperative tracheostomy (HR 4.02, P=0.004) were found to be independent risk factors for AAs after surgery. Although most of AAs were paroxysmal, and well controlled with rate control strategy, in-hospital mortality (42.4% vs. 20%; P=0.014) and 1 year overall mortality (60.6% vs. 31.3%; P=0.004) were significantly higher in patients who had postoperative AAs.
Conclusions: Incidence of AAs after LT was 29.2% in this study. Advanced age and postoperative tracheostomy, which indicates longer du-ration of mechanical ventilation increase the risk of AAs after lung transplantation. AAs were relatively transient after LT, but significantly related with increased mortality.
INCIDENCE, RISK FACTORS AND CLINICAL IMPACT OF ATRIAL ARRHYTHMIAS AFTER LUNG TRANSPLANTATIONByung Gyu Kim1, Dong Geum Shin1, Young Ah Park1, Yeong Min Lim1, Pil Sung Yang1, Hee Tae Yu1, Tae Hoon Kim1, Bo Young Joung1, Hui Nam Park1, Jae Sun Uhm1, Song-Yee Kim2, Moo Suk Park2, Jin Gu Lee3, Hyo Chae Paik3, Moon Hyoung Lee1 1Department of Cardiology, Yonsei Cardiovascular Center, Yonsei University College of Medicine, Seoul, Republic of Korea; 2Department of Pulmonology, Yonsei Health Care Center, Yonsei University College of Medicine, Seoul, Republic of Korea; 3Department of Thoracic and Cardiovascular Surgery, Yonsei Cardiovascular Center, Yonsei University College of Medicine, Seoul, Republic of Korea
CLINICAL ELECTROPHYSIOLOGY P 3-119

539
Introduction: We investigated the electrocardiographic and electrophysiological parameters of macroreentrant atrial tachycardias (ATs) to discriminate whether macroreentrant circuits are mitral isthmus or left atrial roof dependent after atrial fibrillation (AF) ablation.
Methods: Thirty three continuous patients with macroreentrant AT related with catheter ablation for AF. We divided into 2 groups by the location of the successful ablation line (success-line) and entrainment mapping findings. We defined 2 groups as followed, in the mitral isthmus (MI)-group (n=21), the success-line was at the MI and the success-line was at the roof in roof-group (n=11). We compared the patient characteristics and P wave deflection during AT in the 12-lead ECG between them.
Results: The basic characteristics and echocardiographic findings including left atrial volume and left ventricular function showed no sig-nificant differences between 2 groups. The ratio of aVR/aVL in the P wave deflection during the AT was significantly larger in the roof-group than that in the MI-group (1.41±0.50 vs. 1.02±0.42, P=0.030). The cutoff value of aVR/aVL ratio for predicting of roof dependent AT was 1.22 with sensitivity of 81.8% and specificity of 66.7% (the area under the receiver operating characteristic curve =0.742 (95% confi-dence interval: 0.568-0.917).
Conclusions: The larger value in aVR/aVL ratio may suggest a roof dependent AT.
ELECTROCARDIOGRAPHIC PARAMETERS FOR DIFFERENTIATING BETWEEN LEFT ATRIAL ROOF DEPENDENT AND MITRAL ISTHMUS DEPENDENT MACROREENTRANT ATRIAL TACHYCARDIASTomonori Watanabe, Hitoshi Hachiya, Sadamitsu Ichijo, Kazuya Yamao, Takatsugu Kajiyama, Shigeki Kusa, Miyako Igarashi, Hiroaki Nakamura, Shinsuke Miyazaki, Yoshito Iesaka
Tsuchiura Kyodo General Hospital, Tsuchiura, Japan
CLINICAL ELECTROPHYSIOLOGY P 3-120

540
Introduction: Heart failure (HF) is associated with changes in cardiac substrate utilization and energy metabolism, including a decline in high-energy phosphate content, mitochondrial dysfunction, and phosphotransfer enzyme deficiency.
Methods: A review was conducted in Medline, PubMed, Embase, Cochrane Library et al. All articles about modulating effects of cardiac resynchronization therapy on myocardial metabolism in heart failure were included.
Results: A shift toward glucose metabolism was noted in the end stage of HF in animals, although HF in humans may not be associated with a shift toward predominant glucose utilization. Deficiencies of micronutrients are well-established causes of cardiomyopathy. Cor-rection of these deficits can improve heart function. The genes governing the energy metabolism were predominantly underexpressed in nonischemic cardiomyopathy and hypertrophic cardiomyopathy but were overexpressed in ischemic cardiomyopathy.
Conclusions: Cardiac resynchronization therapy has been proven to increase cardiac efficiency without increasing myocardial oxygen consumption. Altered myocardial metabolism is normalized by cardiac resynchronization therapy to improve ventricular function.
THE MODULATING EFFECTS OF CARDIAC RESYNCHRONIZATION THERAPY ON MYOCARDIAL METABOLISM IN HEART FAILURE Chao-feng Chen, Xiao-fei Gao
Hangzhou First People Hospital, Hangzhou, China
HEART FAILURE P 3-122

541
Introduction: Cardiac resynchronization therapy (CRT) can improve cardiac function through reverse left ventricular (LV) remodeling in heart failure (HF) patients with wide QRS duration. Recently, ‘super-response’ to CRT is known to be associated with improved survival. We assessed clinical characteristics, predictors and outcomes of super-responder in CRT.
Methods: We retrospectively enrolled 76 patients with CRT implantation from January 2010 to October 2015. Pre-defined CRT responders were: responders (decreased LV end systolic volume, LVESV 15-29%), and super-responders (decreased LVESV ≥30%). The response timing before or after 6 months was defined as early or late response, respectively. Clinical outcomes including all-cause mortality and rehospitalizations were assessed during follow-up period (median 555 days).
Results: Mean age, baseline LVEF and QRS duration were 66±11 years, 24.8±6.3% and 164±24 ms, respectively. The prevalence of men, LBBB and ischemic origin HF were 46.1%, 69.7% and 14.5%, respectively. At early period, there were 7 (9.2%) responders and 8 (10.5%) super-responders, while 9 (14.3%) responders and 22 (34.9%) supper-responders at late period. There were no mortality cases in early and late overall responders and fewer HF rehospitalization (4.5% vs. 22.2% for responders, P=0.055) in super-responders. There were not any significant differences between responders and super-responders in terms of the prevalence of men, ischemic origin HF and age, baseline LVEF, QRS duration. However, the follow up QRS duration was significantly narrower (150±20 ms vs. 169±21 ms, P=0.037) and the prevalence of LBBB was higher (90.9% vs. 44.4%, P=0.012) in super-responders than that in responders.
Conclusions: Super-responders of CRT showed favorable clinical outcomes compared to nonresponders or even to responders. The de-crease of QRS duration after CRT implantation can be a clinical predictor for super-response to CRT.
CLINICAL CHARACTERISTICS, PREDICTORS, AND OUTCOMES OF EARLY OR LATE SUPER-RESPONDER IN CARDIAC RESYNCHRONIZATION THERAPY OF PATIENTS WITH HEART FAILUREJaewon Oh, Jae-Sun Uhm, In-Cheol Kim, Tae-Hoon Kim, Hui-Nam Pak, Moon-Hyoung Lee, Boyoung Joung, Seok-Min Kang
Yonsei University College of Medicine, Seoul, Republic of Korea
HEART FAILURE P 3-124

542
Introduction: Electrical characteristics e.g. left ventricular (LV) activation delay (qLV), LV conduction barriers (esp. in ischemic cardiomy-opathy (ICM)), and slow propagation of LV paced wavefronts affect CRT efficacy.
Methods: In CRT patients with LBBB (age 69±11 years, EF 26±8%, QRSd 159±20 ms) and quadripolar leads, timing was measured in proximal vs. distal LV bipoles during intrinsic conduction (IC [qLV]), RV pacing, and from LV pacing (either bipole) to RV activation. Results in ICM were contrasted to non-ischemic (NICM) patients.
Results: During IC, maximal qLV/QRSd was >0.77 (i.e. the LV lead marked terminal LV activation) but qLV was<95 ms in >20% of patients in ICM and NICM. Distal bipoles were later in 35%. An inter-bipole gradient of >20 m occurred equally in ICM and NICM (-25% patients) indicating NICM did not prevent conduction barriers. Although RV-sense to LV-sense time was similar during intrinsic conduction, RV-pace to LV-sense time was greater in proximal vs. distal bipoles in both ICM and NICM. These were significantly shorter than the LV-pace to RV-sense times (i.e. anisotropic index). LV-paced propagation was longer in ICM vs. NICM patients in both distal and proximal bipoles, and exceeded 200 ms in 27% ICM vs. 3% NICM (P<0.05).
Conclusions: LV conduction delays during IC as well as LV and RV pacing occur in typical CRT patients with LBBB. Basal LV sites are not always activated later. LV pacing generated large conduction barriers in >25% of ICM but not NICM. These barriers are unpredictable from RV pacing effects and are due to anisotropic ventricular conduction. Quadripolar LV leads reveal conduction characteristics import-ant to individualized CRT programming.
ELECTRICAL SUBSTRATE IN LBBB-ISCHEMIC VS. NON-ISCHEMIC-ASSESSED BY QUADRIPOLAR LV LEADSBrian Wisnoskey1, Niraj Varma2 1St. Jude Medical, Cleveland, United States; 2Cleveland Clinic-Cardiovascular Medicine, Cleveland, United States
HEART FAILURE P 3-125

543
Introduction: Cardiac resynchronization therapy (CRT) is used to synchronize contraction in heart failure patients by pacing both ventri-cles. However, pacemaker inappropriate setting sometimes identified during ECG monitoring. Sensing abnormalities, such as lack of or inappropriate pacemaker artifacts, are the most common device setting problems. This condition may have serious consequences.
Methods: N/A
Results: A 53-year-old man with CHF NYHA class III (LVEF 19%) underwent CRT-D implantation. His ECG showed non-LBBB with QRS >0.12 msec. He underwent implant procedure via left axillary vein. Pacing parameters (threshold, impedance, sensitivity) in all leads were good. Right ventricular (RV) sensitivity was set at 0.3 mV. One week after implantation, this patient came to follow up his condition. He had no symptom despite of his electrocardiogram showed the device could not achieve 100% biventricular pacing. Paced ventricular activity is absent in every after T wave post pacing. This pacing oversensed T wave as QRS complex. The generator labeled it as VS. Lack of pace-maker artifact or failure to deliver output might happen due to component failure, total battery depletion, lead fracture or disconnection, and over sensing. In our patient, pacemaker inappropriate setting happened due to oversensing T wave. T wave was sensed by the ven-tricular sensing and resulted failure to deliver output. The consequence of pacemaker failure to deliver output can be harmful for pace-maker-dependent patients. Oversensing can be corrected by reprogramming the sensitivity. In our case, this oversensing disappeared af-ter we changed RV lead sensitivity to 0.6 mV and followed by appropriate RV pacing.
Conclusions: CRT implantation is used to treat advanced heart failure. The implant is just a first step in the whole management. However, prudent follow up and device programming is also essential in the continuum of treatment.
NON PACING AFTER CARDIAC RESYNCHRONIZATION THERAPY IMPLANTATION: A CASE REPORTMuhammad Yamin, Simon Salim
Cipto Mangunkusumo Hospital, Jakarta, Indonesia
HEART FAILURE P 3-126

544
Introduction: Symptomatic advanced heart failure patients (CHF NYHA functional class III and IV), with LVEF 35% or less and an intraven-tricular conduction delay of >120 msec, are indicated to undergo cardiac resynchronization therapy (CRT). Medtronic, as one of the big-gest supplier in CRT devices, produce “Attain Select” catheter system to facilitate transvenous pacing leads delivery to the coronary sinus. This system includes a delivery catheter and a soft inner catheter. A case of a catheter fragment embolization is presented.
Methods: N/A
Results: A 34-year old man with CHF NYHA Class III (LVEF 12%) and QRS duration of 0.12 msec underwent CRT-D implantation. During the coronary sinus cannulation, the tip of the inner catheter inadvertently sheared off and several attempts to retrieve the broken catheter tip by endovascular technique using a snare were unsuccessful due to the fragility of the material. The catheter fragment was further split to smaller fragments during snaring attempts. Pulmonary arteriogram was conducted and confirmed the embolized material at the very distal part of the artery. This man was observed in cardiac ward for 1 day and developed no symptoms from catheter fragment. His CRT-D was also functioned well and he was permitted to discharge. Clinical follow up after 3 months was uneventful. In our patient, the tip of in-ner catheter was sheared off due to friction with outer catheter during manipulation. During retrieval process, the fragment was split into smaller fragments and embolized to distal pulmonary arteries. No complication during follow up was observed. Smaller size of the frag-ments and lodgment to distal pulmonary arteries might lower the risk of complication in our patient.
Conclusions: Our attempts of retrieval inadvertently splits the fragment into smaller fragments might eventually help protect the patients from complication. The decision to retrieve the catheter fragments however, should be individualized, depends on its location and possible complication.
INNER CATHETER FRAGMENTS EMBOLIZATION IN CRT IMPLANT: A CASE REPORTMuhammad Yamin, Simon Salim
Cipto Mangunkusumo Hospital, Jakarta, Indonesia
HEART FAILURE P 3-127

545
Introduction: Recently, a quadripolar LV pacing lead (QuartetTM, St. Jude Medical) was introduced in China. Pacing with quadripolar LV lead not only provides more options to manage complications (e.g. phrenic nerve stimulation (PNS) and high pacing thresholds) but also helps physicians to pace from an optimal site for improved CRT response. The aim of this study was to evaluate whether the QuartetTM LV lead offers more viable LV pacing site (LVPS) options than its bipolar equivalent in our clinical practice.
Methods: Patients implanted with QuartetTM LV pacing lead underwent pacing threshold measurement and PNS test at pre-discharge. A viable LVPS was defined as an anatomical location at where the electrode on the LV lead had at least one pacing configuration (0.5ms pulse width) with pacing threshold ≤2.5 V and freedom from PNS at twice the pacing threshold. Bipolar lead configurations were modeled by eliminating the two proximal electrodes on the QuartetTM LV lead in this analysis.
Results: A total of 24 patients were included. QuartetTM LV lead provided more viable LVPSs compared with the bipolar equivalents (medi-an 3 [IQR 2-4] vs. median 2 [IQR 1-2] (P<0.001) (Figure 1A). The percentage of patients with at least 1, 2, 3, and 4 viable LVPSs were 100% (24/24), 91.7% (22/24), 58.3% (14/24) and 33.3% (8/24) for QuartetTM and 91.7% (22/24), 70.8% (17/24), 0% (0/24) and 0% (0/24) for the bipo-lar equivalent, respectively (Figure 1B).
Conclusions: Compared with the bipolar equivalent, QuartetTM LV lead provides more viable LVPSs and opportUniversityies for CRT opti-mization and potentially multipoint LV pacing. More than half of the patients had 3 or 4 viable LVPSs, which cannot be achieved with the bipolar equivalent.
QUADRIPOLAR LEFT VENTRICULAR LEADS PROVIDE MORE VIABLE PACING SITES THAN BIPOLAR EQUIVALENTSMin Gu, Wei Hua, Xiaohan Fan, Ligang Ding, Cong Xue, Han Jin, Shu Zhang
Cardiac Arrhythmia Centre, Fuwai Hospital, Beijing, China
HEART FAILURE P 3-128

546
Introduction: Quadripolar left ventricular (LV) pacing has been widely used in North America and Europe since the introduction of the first quadripolar LV lead-QuartetTM (St. Jude Medical). The present study aims to demonstrate the safety and efficacy of the QuartetTM lead im-plantation in Chinese patients.
Methods: From September 2013 to September 2015, a consecutive series of heart failure patients underwent de novo CRT implantation with a QuartetTM LV lead were enrolled to this study at the National Centre of Cardiovascular Disease, China. Demographic, clinical, and device characteristics were collected at the time of implantation, pre-discharge, and 6-month follow-up.
Results: A total of 24 patients (70.8% men; age 55±9 years; LV ejection fraction 27.5±4.5%; QRS duration 164±24 ms) were studied. The implantation was successful in all 24 patients with one LV lead dislodgement and one pocket hematoma found shortly after the proce-dure. Four clinical PNS and two high pacing threshold were reported during follow-up, all of which were eliminated by reprogramming the device to a different pacing configuration without surgical intervention. At 6-month follow-up, LVEF increased significantly from 27.5±4.5% to 38.1±11.0% (P<0.001). Among the 24 patients, 17 patients (70.8%) were CRT responders based on echocardiographic assess-ment (>15% reduction in end-systolic volume at 6-month follow-up relative to baseline) and 16 patients (66.7%) improved by at least one class on the New York Heart Association scale (Figure 1).
Conclusions: Implantation of the QuartetTM LV lead was highly successful in Chinese patients with a low complication rate and high CRT response rate at 6-month follow-up.
IMPLANTATION EXPERIENCE WITH THE QUARTETTM
QUADRIPOLAR LEFT VENTRICLE LEAD IN CHINESE PATIENTS WITH HEART FAILUREMin Gu, Wei Hua, Ligang Ding, Jing Wang, Xiaohan Fan, Shu Zhang
Cardiac Arrhythmia Centre, Fuwai Hospital, Beijing, China
HEART FAILURE P 3-129

547
Introduction: The ability to pacing at one or more optimal sites in the left ventricle has been increasingly recognized as a key factor for op-timizing cardiac resynchronization therapy (CRT) response in individual patients. The aim of this study was to evaluate the acute and long-term availability of viable left ventricular pacing sites (LVPSs) provided by a quadripolar LV pacing lead in the Chinese population.
Methods: A single-center cohort study evaluated consecutive patients who underwent a CRT implant with the QuartetTM LV lead (St. Jude Medical, Sylmar, USA) under local guidelines. A viable LVPS was defined as an anatomical location at where the electrode on the LV lead had at least one pacing configuration (0.5 ms pulse width) with pacing threshold ≤2.5 V and freedom from PNS at twice the pacing threshold. The availability of viable LVPSs was assessed at the pre-discharge and 3-month follow-up visit.
Results: A total of 24 patients with complete 3-month follow-up were included in the study. The median and IQR values of viable LVPSs provided by the QuartetTM LV lead remained the same (3 [IQR 2-4]) between pre-discharge and 3-month follow-up (P=0.45) (Figure 1A). The percentage of leads offering at least 1, 2, 3, and 4 viable LVPSs were 100% (24/24), 91.7% (22/24), 58.3% (14/24) and 33.3% (8/24) at pre-discharge, and 95.8% (23/24), 87.5% (21/24), 58.3% (14/24) and 29.2% (7/24) at 3-month follow-up, respectively (Figure 1B).
Conclusions: These results demonstrate that the QuartetTM LV lead provides two or more viable LVPSs in 91.7% of patients at pre-dis-charge and 87.5% at 3-month follow-up, enabling LVPS optimization and multipoint pacing.
ACUTE AND THREE-MONTH AVAILABILITY OF VIABLE LEFT VENTRICULAR PACING SITES WITH QUARTETTM LEADS IN THE CHINESE POPULATIONMin Gu, Wei Hua, Ligang Ding, Jing Wang, Xiaohan Fan
Cardiac Arrhythmia Centre, Fuwai Hospital, Beijing, China
HEART FAILURE P 3-130

548
Introduction: While quadripolar leads enable more pacing sites and vectors to avoid phrenic nerve stimulation (PNS), pacing in a larger caliber proximal coronary vein (CV) location often requires a higher pacing capture threshold (PCT). Acuity X4 leads were evaluated in a series of animal and human studies to optimize the lead design to conform to the patients’ anatomy and achieve a predefined GOAL (PCT less than or equal to 2.5V at least 75% of the time) in mid-basal region of the left ventricle (LV).
Methods: During the concept development, 90 prototype leads with a straight distal tip followed by a 3-D spiral with 3 electrodes were evaluated in 20 swine. The spiral electrode location was identified by clock position. Implantable coronary vein lengths (CVL) defined as the distance from CV OS to 4F diameter vein were measured from 50 patients’ rotational venograms during CRT implants. 3 prototypes were evaluated acutely in 50 patients prior to CRT implantation in LILAC study for final design confirmation. In the final premarket clinical trial, 485 Acuity X4 Spiral leads were evaluated in NAVIGATE X4 trial for three months.
Results: Acute swine studies demonstrated that no single clock electrode position could reach the GOAL. However, the combination of 3 electrodes ranging from 4:30-10:00 o’clock found at least 1 of 3 did reach the GOAL. From CVL data, the predicted fit in a posterior or lat-eral CV was 88% for a 60 mm required CV implantable length and 64% for 75 mm. Therefore two tip lengths and two clock electrode posi-tions were evaluated in the LILAC study where 60 mm tip fit 92% of 50 patients and 75 mm tip fit all 22 tested patients. The best spiral electrode PCT median 1.0V and 0.9V at the mid-basal location in LILAC and NAVIGATE X4 accordingly. The success rate is summarized in the figure.
Conclusions: Acute and chronic human trial results demonstrate Acuity X4 lead well exceeded its design goal. The three electrodes locat-ed on the 3-D spiral from 4:30 to 10:00 counter clockwise and two implantable tip lengths (60 mm and 75 mm) fit CV anatomy, keep low PCT at the LV mid-basal location, and provide two-zone pacing in CRT patients.
ACUITY X4 QUADRIPOLAR LEAD-FROM CONCEPT TO CLINICALLili Liu, Eric Hammill, Ronald Kunkel, Kimberly Miklos, Andrew De Kock, Sean Coe, Kyle Hoecke, Matt Miller
Boston Scientific, St. Paul, United States
HEART FAILURE P 3-131

549
Introduction: The nonresponder rate following cardiac resynchronization therapy is greater than 30 percent. Various improvisations in-cluding multipoint pacing have been incorporated in improving the responder rate. However there is limited data on the responder rate following epicardial left ventricular (LV) lead placement. We set out to compare the responder rates in these two groups.
Methods: Of 120 patients who met the criteria for cardiac resynchronization therapy (CRT), 90 underwent left ventricular (LV) lead place-ment by the endocardial route in group 1 while 30 had an epicardial LV lead placement through a lateral thoracotomy in group 2.
Results: Table 1 (please refer to image 1).
Conclusions: Epicardial LV lead placement significantly increases the responder rate of patients undergoing CRT. The threshold to switch to epicardial LV lead placement when optimal LV lead positioning is not feasible by endocardial route should be low. The major limiting factor is the requirement for general anaesthesia and extended hospital stay.
CARDIAC RESYNCHRONIZATION THERAPY EPICARDIAL LEFT VENTRICULAR LEAD PLACEMENT A MAJOR FACTOR TO IMPROVE RESPONDER RATEAbhinay Tibdewal, V S Prakash, Nagamalesh U M, Anupama Hegde, Karthik Naidu
MS Ramaiah Medical College, Bangalore, India
HEART FAILURE P 3-132

550
Introduction: Paroxysmal atrial fibrillation (AF) is most often triggered by the sources inside the pulmonary veins. On the other hand, it was reported that there may be a trigger-based mechanism of AF persistence in some of the persistent AF patients. Confined pulmonary vein (PV) fibrillation is a rare finding in patients with persistent AF.
Methods: N/A
Results: A 58-year-old man with decreased left ventricular function underwent second catheter ablation procedure for recurrent per-sistent AF. Bilateral upper PV reconnection was identified. Following the re-isolation of right superior PV during AF, PV fibrillation reiniti-ated spontaneously in right superior PV. Following the antrum ablation of left superior PV, AF continued. A 30-J internal cardioversion ter-minated AF and restored sinus rhythm in the left atrium but induced a fast and irregular tachycardia confined within the bilateral superior PV spontaneously. A second 20-J internal cardioversion during sinus rhythm terminated the tachycardia confined within the bilateral su-perior PV. Soon after the cardioversion, PV fibrillation reinitiated spontaneously in bilateral superior PV. Confined PV fibrillation was termi-nated by additional radiofrequency application inside an isolated area after the achievement of vein isolation.
Conclusions: Bilateral confined PV fibrillation might be associated with the mechanism of sustaining AF in this case.
REPRODUCIBLE BILATERAL CONFINED PULMONARY VEIN FIBRILLATION IN A PATIENT WITH PERSISTENT ATRIAL FIBRILLATIONKeiichi Ashikaga
Miyazaki Medical Association Hospital, Miyazaki, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-133

551
Introduction: Ventricular Tachycardia is one of the ominous arrhythmias detected during cardiac arrest.
Methods: N/A
Results: This is a case of a 51 year old male who presented with ventricular tachycardia. Conversion to sinus rhythm revealed T wave in-versions with an epsilon wave. Echocardiogram revealed dilation of the right sided chambers and right ventricular outflow tract and right ventricle hypokinesia. Magnetic resonance imaging revealed right ventricle aneurysms, dyskinesia.
Conclusions: Imaging may diagnose arrhythmogenic cardiomyopathy.
MULTIMODALITY DIAGNOSIS OF ARRHYTHMOGENIC CARDIOMYOPATHYAriston Bautista, Paolo Nocom
Philippine Heart Center, Manila, Philippines
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-134

552
Introduction: The effects of radiation therapy (RT) on cardiac implantable electronic devices (CIEDs) are well reported. These changes may be acute or long term, and often depends on the cumulative radiation dose. These effects range from mild corruption to complete device failure, and even the potentially fatal “runaway pacemaker” phenomenon. We present a 68-year-old gentleman who had a leadless Medtronic Micra® pacemaker implanted for symptomatic Sick Sinus Syndrome. He was subsequently diagnosed with rectal cancer and required 28 fractions of radiotherapy.
Methods: The Medtronic Micra® leadless pacemaker presents several novel challenges during RT: 1) Fixation involves four extendable/re-tractable nitinol tines and it is not designed to be explanted even in end-of-service (EOS). 2) Implantation is via a 23Fr trans-femoral intro-ducer sheath, and device positioned in the right ventricle. There are no surface markers/scars to determine location, and no quick percu-taneous access even if explantation is attempted. 3) Flash memory is used in the Medtronic Micra® due to its non-volatility, fast read ac-cess times, mechanical shock resistance and durability. Ionizing radiation may affect a whole range of parameters, which are not as well characterized compared to complementary metal oxide semiconductor (CMOS) circuits in standard pacemakers. The Medtronic Micra® device was interrogated before the initiation of RT and the pacing requirement was low at 8%. Battery status, pacing and sensing thresh-olds were satisfactory. The anticipated dose received by the device was<2 Gy. In the unlikely event of a “runaway pacemaker”, the device has a runaway protect circuit rate of 195 bpm. As the patient was not pacemaker dependent, the device was programmed to “OFF to OOO mode” before each RT fraction. It was felt that should RT result in Flash memory damage and non-programmability, it would probably be safer being in a permanent “OFF to OOO mode” rather than the runaway circuit rate of 195 bpm. The patient was monitored closely during RT with resuscitation facilities on standby. Radiation dose was measured with two optically stimulated luminescence dosimeters (OSLD), which were placed on the precordium near the apex of the heart. Radiation beam energy was limited to <10 MV. After each RT fraction, the device was interrogated and reprogrammed. The cumulative radiation dose was calculated after each fraction, and all the device pa-rameters were documented.
Results: The battery status, sensing and pacing thresholds, as well as the programmability of the device remained stable during RT.
Conclusions: We present the first patient with a Medtronic Micra® pacemaker to have successfully completed RT. We recommend a mul-tidisciplinary approach, consideration of the “OFF to OOO” mode in non-pacemaker dependent patients, as well as the application of cen-tre specific algorithm for patients with CIED undergoing RT.
RADIATION THERAPY IN MEDTRONIC MICRA® LEADLESS PACEMAKERKenneth Chew1, Phong Teck Lee1, Michael Wang2, Wee Siong Teo1, Chi Keong Ching1, Boon Yew Tan1 1National Heart Centre Singapore, Singapore; 2Singapore General Hospital, Singapore
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-135
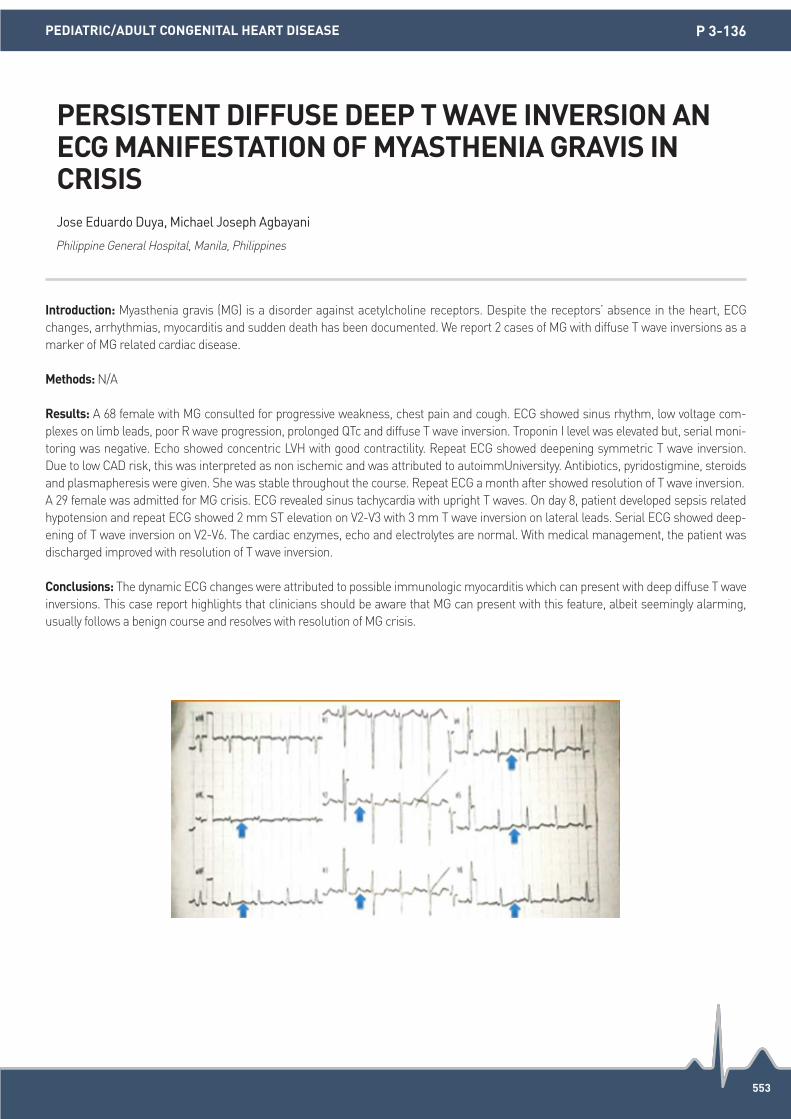
553
Introduction: Myasthenia gravis (MG) is a disorder against acetylcholine receptors. Despite the receptors’ absence in the heart, ECG changes, arrhythmias, myocarditis and sudden death has been documented. We report 2 cases of MG with diffuse T wave inversions as a marker of MG related cardiac disease.
Methods: N/A
Results: A 68 female with MG consulted for progressive weakness, chest pain and cough. ECG showed sinus rhythm, low voltage com-plexes on limb leads, poor R wave progression, prolonged QTc and diffuse T wave inversion. Troponin I level was elevated but, serial moni-toring was negative. Echo showed concentric LVH with good contractility. Repeat ECG showed deepening symmetric T wave inversion. Due to low CAD risk, this was interpreted as non ischemic and was attributed to autoimmUniversityy. Antibiotics, pyridostigmine, steroids and plasmapheresis were given. She was stable throughout the course. Repeat ECG a month after showed resolution of T wave inversion.A 29 female was admitted for MG crisis. ECG revealed sinus tachycardia with upright T waves. On day 8, patient developed sepsis related hypotension and repeat ECG showed 2 mm ST elevation on V2-V3 with 3 mm T wave inversion on lateral leads. Serial ECG showed deep-ening of T wave inversion on V2-V6. The cardiac enzymes, echo and electrolytes are normal. With medical management, the patient was discharged improved with resolution of T wave inversion.
Conclusions: The dynamic ECG changes were attributed to possible immunologic myocarditis which can present with deep diffuse T wave inversions. This case report highlights that clinicians should be aware that MG can present with this feature, albeit seemingly alarming, usually follows a benign course and resolves with resolution of MG crisis.
PERSISTENT DIFFUSE DEEP T WAVE INVERSION AN ECG MANIFESTATION OF MYASTHENIA GRAVIS IN CRISISJose Eduardo Duya, Michael Joseph Agbayani
Philippine General Hospital, Manila, Philippines
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-136

554
Introduction: N/A
Methods: N/A
Results: Complication of contralateral pneumothorax due to the right atrial lead is rare. The concomitant steroid use was known as a risk factor for pacemaker lead perforation. We report a case of subacute contralateral pneumothorax after dual-chamber pacemaker implant, with using steroid, resulting from screw-in atrial lead perforation. A 67-years-old man, who was on long-term steroid use for pemphigoid, was hospitalized for the treatment of syncope due to 2:1 atrioventricular block. He underwent dual-chamber pacemaker implantation (St. Jude Medical® Assurity MRITM) via puncture of the left subclavian vein. The right ventricular (RV) bipolar screw-in lead (St. Jude Medical® Tendril MRITM) was positioned in the RV apex. The right atrial (RA) bipolar screw-in lead (St. Jude Medical® Tendril MRITM) was positioned in the RA appendage. Four days after pace maker implantation, the chest X-ray examination showed right-sided asymptomatic pneumo-thorax. CT scan of the chest revealed right anterior pneumothorax and perforation of RA wall by the helix of atrial screw-in lead. The sig-nificant pericardial effusion was not showed via transthoracic echocardiography. Interrogation of the pacemaker showed no change in measurements lead parameters. The pneumothorax was gradually improved with conservative therapy.
Conclusions: N/A
SUBACUTE CONTRALATERAL PNEUMOTHORAX ASSOCIATED WITH ATRIAL LEAD PERFORATION IN A PATIENT WITH ON CORTICOSTEROID THERAPYNaruya Ishizue, Jun Kishihara, Shinichi Niwano, Hidehira Fukaya, Hironori Nakamura, Tazuru Igarashi, Tamami Fujiishi, Tomoharu Yoshizawa, Akira Satoh, Masami Murakami, Junya Ako
Kitasato University, Sagamihara,Kanagawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-137
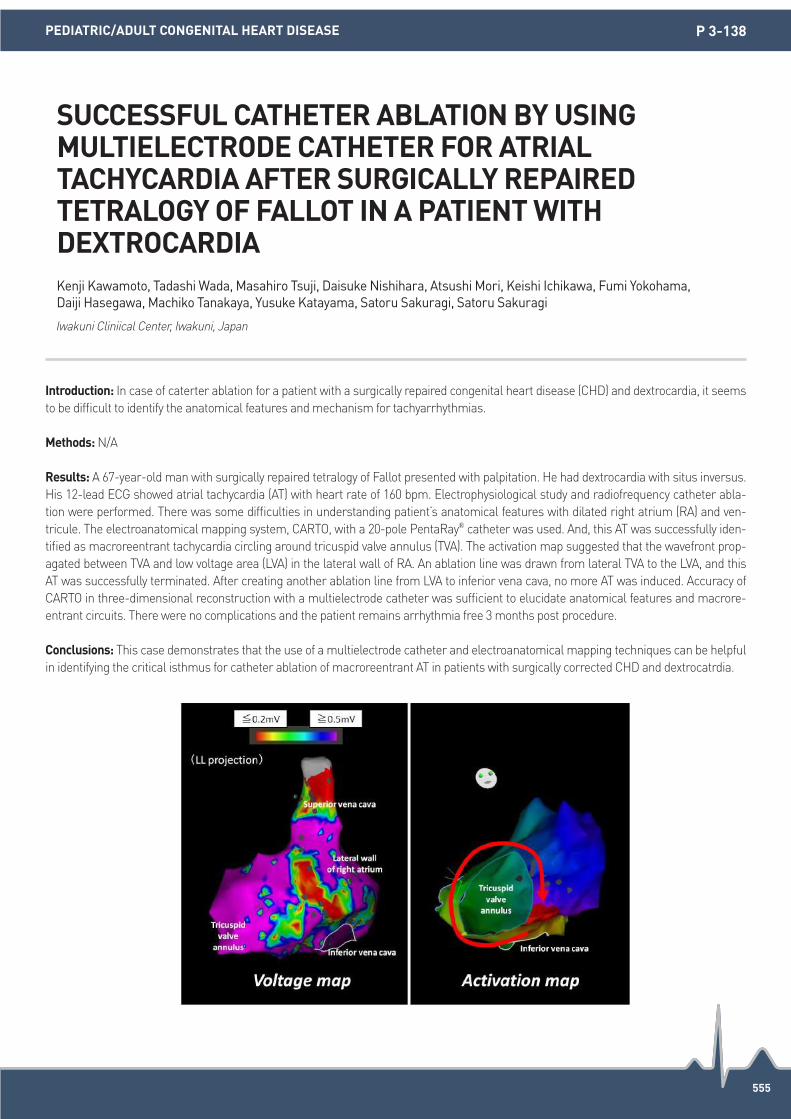
555
Introduction: In case of caterter ablation for a patient with a surgically repaired congenital heart disease (CHD) and dextrocardia, it seems to be difficult to identify the anatomical features and mechanism for tachyarrhythmias.
Methods: N/A
Results: A 67-year-old man with surgically repaired tetralogy of Fallot presented with palpitation. He had dextrocardia with situs inversus. His 12-lead ECG showed atrial tachycardia (AT) with heart rate of 160 bpm. Electrophysiological study and radiofrequency catheter abla-tion were performed. There was some difficulties in understanding patient’s anatomical features with dilated right atrium (RA) and ven-tricule. The electroanatomical mapping system, CARTO, with a 20-pole PentaRay® catheter was used. And, this AT was successfully iden-tified as macroreentrant tachycardia circling around tricuspid valve annulus (TVA). The activation map suggested that the wavefront prop-agated between TVA and low voltage area (LVA) in the lateral wall of RA. An ablation line was drawn from lateral TVA to the LVA, and this AT was successfully terminated. After creating another ablation line from LVA to inferior vena cava, no more AT was induced. Accuracy of CARTO in three-dimensional reconstruction with a multielectrode catheter was sufficient to elucidate anatomical features and macrore-entrant circuits. There were no complications and the patient remains arrhythmia free 3 months post procedure.
Conclusions: This case demonstrates that the use of a multielectrode catheter and electroanatomical mapping techniques can be helpful in identifying the critical isthmus for catheter ablation of macroreentrant AT in patients with surgically corrected CHD and dextrocatrdia.
SUCCESSFUL CATHETER ABLATION BY USING MULTIELECTRODE CATHETER FOR ATRIAL TACHYCARDIA AFTER SURGICALLY REPAIRED TETRALOGY OF FALLOT IN A PATIENT WITH DEXTROCARDIAKenji Kawamoto, Tadashi Wada, Masahiro Tsuji, Daisuke Nishihara, Atsushi Mori, Keishi Ichikawa, Fumi Yokohama, Daiji Hasegawa, Machiko Tanakaya, Yusuke Katayama, Satoru Sakuragi, Satoru Sakuragi
Iwakuni Cliniical Center, Iwakuni, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-138

556
Introduction: In Brudaga syndrome (BrS), type 1 electrocardiogram is sometimes intermittent, and fever is one of possible triggers. We encountered a case with electric storm, while only occurring during a febrile state.
Methods: N/A
Results: A 72-year-old man has been followed at our hospital because of myelodysplastic syndromes (MDS) for six years. He developed ventricular fibrillation (VF) during hospitalization with febrile neutropenia, and received the diagnosis of BrS on the basis of Brugada type 1 ECG pattern after resuscitation. He did not have history of prior syncope nor family history of sudden cardiac death. The type 1 ECG was gradually disappeared with antipyretic therapy. The patient was discharged after implantable cardioverter-defibrillator (ICD) implantation. He was free of arrhythmic events for six months despite repeated events of fever of unknown origin.Six months after implantation, he was admitted at our hospital again for electric storm with multiple appropriate ICD shocks resulting from recurrent ventricular fibrillation. He had a fever and type 1 ECG pattern again. He was treated with isoproterenol and antipyretic agent infusion, leading to electric storm sup-pression. But it was repeated a similar VF storm with fever in the two weeks after. Although ICD was removed and switched to wearable cardioverter-defibrillator, repeated fever events could not be suppressed. Finally, MDS turned into leukemia, and he passed away by the progression of leukemia. ECG changes with BrS are dynamic, often hidden, and may reveal themselves in the presence of triggers like fe-ver, intoxication, vagal stimulation, electrolyte imbalance, anesthetics, psychotropic agents, and sodium channel blockers. The prognosis of fever-induced BrS is unclear. In this patient, fever was a very critical risk factor of ECG changes and VF storm.
Conclusions: Patients with BrS who develop type 1 ECG with fever are at risk of arrhythmic events. Although it is difficult to make a diag-nosis of these type of BrS, it is important to consider the possibility of BrS in the differential diagnosis of patients presenting with fever and episodes of syncope.
A CASE OF FEVER-INDUCED BRUGADA SYNDROME WITH VENTRICULAR FIBRILLATION STORM COMBINED WITH MYELODYSPLASTIC SYNDROMESAkira Kimata1, Satoshi Aita1, Yasuhiro Yokoyama1, Takakazu Higuchi1, Akihiko Nogami2, Kazutaka Aonuma2 1St. Luke’s International Hospital, Tokyo, Japan; 2University of Tsukuba, Ibaraki, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-139

557
Introduction: Pacing induced cardiomyopathy (PiCMP) is associated with increased rates of morbidity and mortality. In children, the prev-alence of PiCMP PiCMP has been reported at 13.4% within 10 years of pacemaker (PPM) implantation. Cardiac resynchronisation therapy (CRT) is a promising treatment in PiCMP in adults, but its benefit in the paediatric population remains unproven. Here, we describe two cases of PiCMP in young patients that improved following CRT.
Methods: N/A
Results: Case 1 is a male patient with symptomatic congenital complete heart block who underwent implantation of an epicardial dual chamber PPM system aged 10. Transthoracic echocardiogram (TTE) then showed normal left ventricular ejection fraction (LVEF). At age 18, he developed significant effort intolerance, NYHA III, with a repeat LVEF of 15% and a dilated left ventricle (LV). PPM interrogation re-vealed 99.8% dependence on ventricular pacing (AsVp). He underwent an upgrade to a transvenous CRT-defibrillator system. 10 months later, he reported significant improvement in effort tolerance to NYHA I, with repeat TTE showing LVEF of 45% and a reduction in LV size. Case 2 is a male patient who developed viral myocarditis aged 8, causing high grade atrioventricular block necessitating implantation of an epicardial dual chamber PPM. He was referred to adult service at age 17 for ongoing management, at which point he described NYHA II effort intolerance. TTE showed LVEF of 35%. PPM check revealed 99.8% AsVpa and the battery elective replacement indicator suggested replacement was due within a year. He underwent an elective upgrade to a transvenous CRT-pacemaker (CRT-P) system. His symptoms improved at 4 months post CRT-P, with an increase in LVEF to 44%. Both patients have maintained their clinical improvement up to 5 years post CRT implantation.
Conclusions: Despite the disparate underlying aetiologies necessitating PPM implantation in these patients, our case series adds to the growing literature that suggests favourable long term functional and haemodynamic outcomes with CRT in a small but unique population of young adults with PiCMP. More robust prospective randomized studies are required to establish appropriate guidelines for patient se-lection in this heterogenous group of individuals.
CARDIAC RESYNCHRONISATION THERAPY FOR THE TREATMENT OF PACING INDUCED CARDIOMYOPATHY IN YOUNG PATIENTSSL Kui, CY Chin, O Goh, D Chong, KL Ho, BY Tan, WS Teo, CK Ching
National Heart Centre Singapore (NHCS), Singapore
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-140

558
Introduction: Tachycardia-induced cardiomyopathy (TIC) is one of the causes of heart failure and dilated cardiomyopathy. TIC is a rare but important disease because it is treatable. We report two cases of extreme tachycardia induced cardiomyopathy.
Methods: N/A
Results: Case 1. A 12 -year old boy presented to a local hospital with dyspnea. Echocardiogram demonstrated a severely decreased left ventricular systolic function (EF 10%). He was diagnosed with idiopathic dilated cardiomyopathy. 2 months of anti-heart failure treatment failed to improve his clinical status and the patient was referred to our institution for heart transplant assessment. The initial ECG showed ectopic atrial tachycardia with heart rate 150bpm and was thought to have developed severe left ventricular dysfunction due to incessant tachycardia. He was treated with amiodarone and beta-blockers with successful rate control. In contrast to his improved clinical status, the ventricular dysfunction remained unchanged after 3 months of adequate rate control. Case 2. A 5-month old infant presented with poor feeding. Echocardiogram demonstrated a dilated left ventricle with an EF of 20%, and she was transferred to our hospital for sus-pected myocarditis. The initial ECG demonstrated atrial flutter with 2:1 AV conduction with a heart rate of 200 bpm. She was commenced on amiodarone with successful cardioversion. However, her clinical status rapidly deteriorated and she was placed on mechanical sup-port. Her cardiac function improved dramatically on mechanical support and she was successfully decannulated after one month of ther-apy. After decannulation, she developed bursts of ectopic atrial tachycardia with multiple foci and was diagnosed with chaotic atrial tachy-cardia. The tachycardia is well controlled with oral beta-blockers and sotalol and echocardiogram continues to show normal ventricular function.
Conclusions: The diagnosis of tachycardia-induced cardiomyopathy can be a challenge, as the culprit tachyarrhythmia may not always be apparent. TIC is generally reversible following control of the underlying arrhythmia, therefore prompt diagnosis and treatment is import-ant. The extent and time to recovery of ventricular function varies, as did in our two cases.
TACHYCARDIA-INDUCED CARDIOMYOPATHY- IS IT TRULY BENIGN?Takashi Kuze, Hiroko Asakai, Kazuhiro Shiraga, Takahiro Shindo, Yoichiro Hirata, Ryo Inuzuka, Akira Oka
The University of Tokyo Hospital, Tokyo, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-141

559
Introduction: N/A
Methods: N/A
Results: The Stress cardiomyopathy induces transient ventricular dysfunction, resulting from catecholamine mediated myocardial injury, could be associated with tirades de points (TdP) caused by severe QT prolongation. We experienced a interesting case of stress cardiomy-opathy with frequent TdP caused by the recurrence of heart failure. This case was diagnosed tachycardia cardiomyopathy caused by atrial fibrillation at admission, so rate control therapy was performed, because his QT interval was normal. But at 1 day after admission, TdP with QT prolongation occurred, intra-aortic balloon pumping and respiration therapy were needed after electrical cardioversion because of low output syndrome. However, he had recurrence of TdP with QT prolongation caused by heart failure even though improving ventricu-lar ejection fraction. Thus, increasing β-blocker was started, QT interval was normalized. Sympathetic activity on stress cardiomyopathy is closely related with QT prolongation. The clinical significance of β-blocker on stress cardiomyopathy was highly suggested for prevention of TdP with QT prolongation from this case report.
Conclusions: N/A
THE CLINICAL SIGNIFICANCE OF β-BLOCKER ON STRESS CARDIOMYOPATHY FOR PREVENTION OF TORSADES DE POINTES WITH QT PROLONGATION FROM CASE REPORT STUDY Taito Nagai1, Keijiro Nakamura1, Hikari Hashimoto1, Hiroki Niikura1, Hidehiko Hara1, Masao Moroi1, Masato Nakamura1, Mahito Noro2, Kaoru Sugi3 1Toho University Ohashi Medical Center, Tokyo, Japan; 2Toho University Sakura Medical Center, Chiba, Japan; 3Odawara Cardiovascular Hospital, Kanagawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-143

560
Introduction: The adaptive cardiac resyncronization therapy (CRT) algorithm is a novel pacing algorithm to provide optimal CRT by mea-suring intracardiac conduction parameters. We reported a super responder case after device upgrade to adaptive CRT.
Methods: N/A
Results: A case was 60’s year old male with chronic heart failure. Electrocardiograhy revealed left bundle branch block (QRS 182 msec). Echocardiography revealed diffuse hypokinesis (ejection fraction 21.6%) with mechanical dyssynchrony and severe mitral regurgitation. After CRT-D implant, QRS duration shorted 132 msec and ejection fraction improved 27.0%. Four years after CRT-D implant, ventricular fibrillation storm happened suddenly and CRT-D worked 32 times defibrillation. Treatment by CRT-D succeeded in lifesaving, so a battery remaining amount even consumed a little. We replaced a CRT-D device with an adaptive CRT-D device. Seven months after working adap-tive CRT, cardiomegaly improved dramatically (Figure). Left ventricular pacing rate was average 77% (57-94%). When increasing Optivol values, this meant getting worse heart failure, left ventricular pacing rate was increased in more than 90%.
Conclusions: Despite this case was CRT responder, the device upgrade to adaptive CRT was more effective to condition of heart failure. Left ventricular pacing rate was adjusted by the heart failure condition. This case suggested that adjusting automatically left ventricular pacing to right ventricular activation was more effectiveness than standard bi-ventricular pacing.
A SUPER RESPONDER CASE AFTER DEVICE UPGRADE TO ADAPTIVE CARDIAC RESYNCHRONIZATION THERAPYYoshiki Nagata, Yoichiro Nakagawa, Yusuke Takeda, Masaki Kinoshita, Takashi Kusayama, Akio Chikata, Michiro Maruyama, Kazuo Usuda
Toyama Prefectural Central Hospital, Toyama, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-144

561
Introduction: Systemic involvement of sarcoidosis could lead to devastating sequelae, especially if heart is involved. However, its rarity and paucity of definitive studies and imagings have precluded early detection and intervention. In Malaysia, the reported cases were way back in 1964 and 1970, which further emphasize its scarcity. Cardiac involvement worldwide is only up to 25%.
Methods: N/A
Results: We reported a case of a 72-year-old Pakistani Malaysian with a background history of longstanding lung sarcoidosis who was admitted electively for pacemaker change. During this time she experienced intermittent palpitations of one-year duration with ECG evi-dence of recurrent trifascicular block. She was first diagnosed with pulmonary sarcoidosis at the age of 56 while presenting with chronic non-productive cough of 5-month duration. Subsequent biopsies from hilar nodes (both bronchoscopic and CT guided) confirmed the di-agnosis. Five years later, she had acute myocardial infarction with systolic dysfunction (ejection fraction of 34%). Coronary angiography was normal and pacemaker was subsequently inserted for trifascicular block likely secondary to cardiac sarcoidosis. Her lung disease has never in remission as she became steroid dependent. She developed long-term steroid complications of diabetes, cataract and oste-oporosis. No lupus pernio or skin involvement.Pakistan immigrant with sarcoidosis has first been reported early this year in Europe. To our knowledge, this will be the first reported Pakistani case from Southeast Asia. The difference between the two is that the first one came with severe respiratory distress, while our case was rather atypical in the sense that both lung and heart were severe. This case de-viate from normal belief that patients with heart sarcoid tend not to have severe extracardiac sarcoidosis.
Conclusions: Aforementioned case highlights the importance of appraising differential diagnosis of cardiac sarcoidosis in this Southeast Asian region, particularly in those with background of such systemic infiltrative disorder. Many of which could have been overshadowed by tuberculosis due to the fact that tuberculous infection is endemic in this region. However, long term outcome despite treatment remains unknown.
HEART BLOCK ! HEART BLOCK !-A DISEASE OF GREAT MIMICRY (SARCOIDOSIS) WITH CARDIAC AND PULMONARY INFILTRATIONSChoon Seong Ng, Shawal Mohamad, Chee Ken Choor, Hamat Hamdi, Shathiskumar Govindaraju, Oteh Maskon
Cardiology University, Department of Internal Medicine, Hospital Canselor Tuanku Muhriz, University Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-145
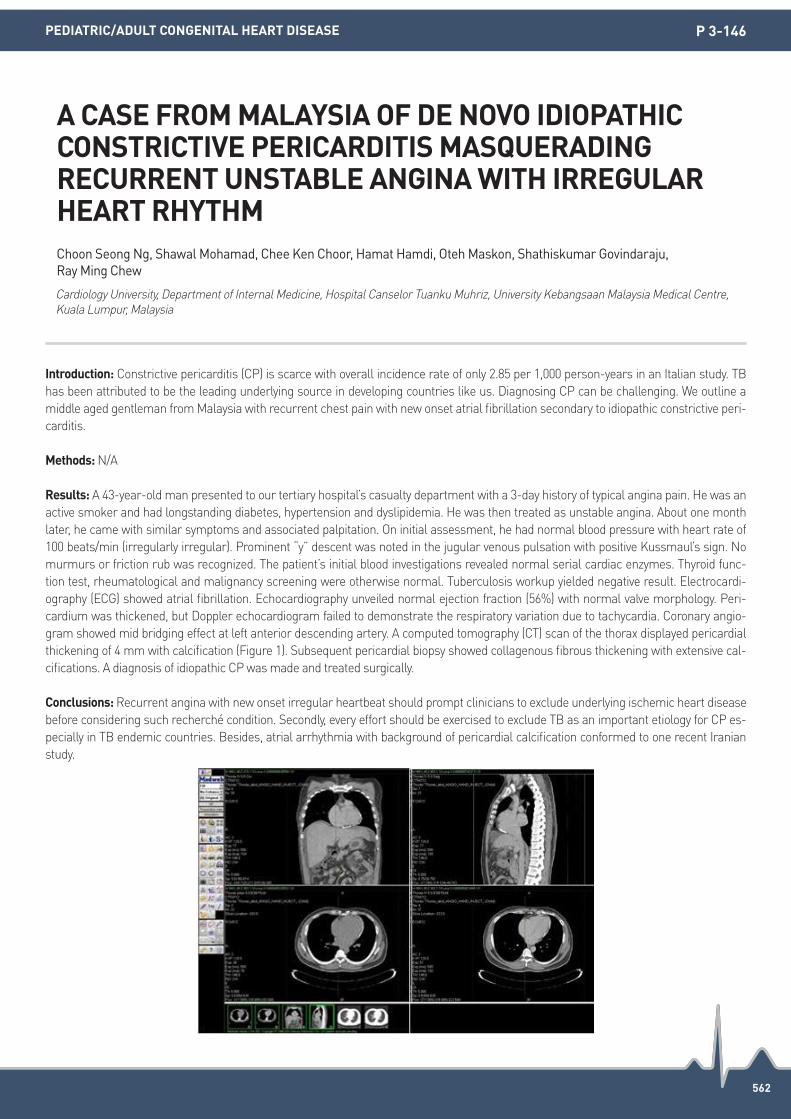
562
Introduction: Constrictive pericarditis (CP) is scarce with overall incidence rate of only 2.85 per 1,000 person-years in an Italian study. TB has been attributed to be the leading underlying source in developing countries like us. Diagnosing CP can be challenging. We outline a middle aged gentleman from Malaysia with recurrent chest pain with new onset atrial fibrillation secondary to idiopathic constrictive peri-carditis.
Methods: N/A
Results: A 43-year-old man presented to our tertiary hospital’s casualty department with a 3-day history of typical angina pain. He was an active smoker and had longstanding diabetes, hypertension and dyslipidemia. He was then treated as unstable angina. About one month later, he came with similar symptoms and associated palpitation. On initial assessment, he had normal blood pressure with heart rate of 100 beats/min (irregularly irregular). Prominent “y” descent was noted in the jugular venous pulsation with positive Kussmaul’s sign. No murmurs or friction rub was recognized. The patient’s initial blood investigations revealed normal serial cardiac enzymes. Thyroid func-tion test, rheumatological and malignancy screening were otherwise normal. Tuberculosis workup yielded negative result. Electrocardi-ography (ECG) showed atrial fibrillation. Echocardiography unveiled normal ejection fraction (56%) with normal valve morphology. Peri-cardium was thickened, but Doppler echocardiogram failed to demonstrate the respiratory variation due to tachycardia. Coronary angio-gram showed mid bridging effect at left anterior descending artery. A computed tomography (CT) scan of the thorax displayed pericardial thickening of 4 mm with calcification (Figure 1). Subsequent pericardial biopsy showed collagenous fibrous thickening with extensive cal-cifications. A diagnosis of idiopathic CP was made and treated surgically.
Conclusions: Recurrent angina with new onset irregular heartbeat should prompt clinicians to exclude underlying ischemic heart disease before considering such recherché condition. Secondly, every effort should be exercised to exclude TB as an important etiology for CP es-pecially in TB endemic countries. Besides, atrial arrhythmia with background of pericardial calcification conformed to one recent Iranian study.
A CASE FROM MALAYSIA OF DE NOVO IDIOPATHIC CONSTRICTIVE PERICARDITIS MASQUERADING RECURRENT UNSTABLE ANGINA WITH IRREGULAR HEART RHYTHMChoon Seong Ng, Shawal Mohamad, Chee Ken Choor, Hamat Hamdi, Oteh Maskon, Shathiskumar Govindaraju, Ray Ming Chew
Cardiology University, Department of Internal Medicine, Hospital Canselor Tuanku Muhriz, University Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-146

563
Introduction: N/A
Methods: N/A
Results: Case Report-A young male patient came with history of repeated episodes of palpitations. ECG showed short PR interval with delta wave with small r wave predominant negative QRS in V1 with transition at V2 suggestive of septal accessory pathway (AP). Patient was taken up for EP study with a plan to perform RF ablation of AP. Intracardiac electrograms activation pattern in coronary sinus (CS) suggestive of right sided AP. Incremental ventricular pacing induced orthodromic AVRT using the septal AP. Tricuspid annulus was mapped during sinus rhythm with 6F 4 mm tip non irrigated RFablation catheter for close AV signal. At 4 o’clock position just above the CS ostium (Figure A) fused AV signal obtained and started RF energy delivery and with in 5 seconds, the AP conduction disappeared (Figure A) and the energy delivery continued for 60 seconds. It was noted that the AP conduction returned immediately after stoppage of RF energy delivery. Inspite of good fused AV electrograms repeated RF energy delivery even with a long supporting sheath, AP conduction continued to recurr. At this juncture, it was decided to map the mitral annular septum. Through retroaortic route the mitral annulus mapped and a reasonably short AV signal obtained at 5 o’clock position of mitral annulus (Figure B) and RF energy delivery resulted in total disappear-ance of AP conduction (Figure B). Post RFA no tachycardia or AP conduction even on isoprenaline and adenosine challenge was noted. Discussion-A QS wave in lead V1 will identify AP connections at the postero septal tricuspid annulus (PSTA), while an isoelectric initial QRS complex with rSR’ pattern in lead V1 identifies AP connections closer to the mitral annulus; however, an ECG pattern with an initial slightly positive or isoelectric vector in lead II as noted in our case will be found in AP connections at both the PSTA and mitral annuli. Depending on the orientation, depth, or width of the AP, ablation at the PSTA region may not be able to produce a sufficient lesion to completely elimi-nate AP conduction. A left-sided approach or ablation at both PSTA and mitral annular regions may be necessary, and a significantly earli-er activation time at the PSMA region during sinus rhythm may not be necessary as noted in our patient for successful ablation at this site.
Conclusions: N/A
A DIFFICULT POSTERO SEPTAL ACCESSORY PATHWAY -SUCCESSFUL RADIO FREQUENCY ABLATION BY BIVENTRICULAR APPROACHOruganti Sai Satish
Nizam’s Institute of Medical Sciences, Hyderabad, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-147

564
Introduction: Few cases of ventricular tachycardia in pheochromocytoma have been described so far. Here, we report a case of pheochro-mocytoma-induced cardiomyopathy presenting with recurrent episodes of VT and the effectiveness of the elimination of VT by radiofre-quency catheter ablation (RFCA).
Methods: N/A
Results: A 52-year-old female was diagnosed with pheochromocytoma-induced cardiomyopathy and underwent adrenalectomy in 2006. In 2010, she underwent ICD implantation due to recurrent VT. Recently, she presented with recurrent VT and heart failure symptoms with frequent episodes of ICD therapy noted during follow-up in the outpatient department, hence, referral for radiofrequency ablation of VT. The coronary angiography was normal and 2D echocardiography revealed biventricular systolic dysfunction. Pleomorphic VT was induced with 2 dominant sustained VTs observed (Figure 1A) during programmed electrical stimulation. The 3D electroanatomic map and voltage map were created using Carto 3 Confidence Module version 4.3 system (Biosense Webster, Inc., USA) and a high-density mapping cathe-ter (Pentaray, Biosense Webster, Inc., USA), which showed extensive low voltage zones (<1.5 mV) around the mitral annulus. In the low voltage regions, pace mapping showed prolonged S-QRS intervals (54±6 ms) (Figure 1B). Local abnormal ventricular activities (LAVA) and late potentials were also observed. Critical conduction isthmuses were identified during entrainment and pace mapping yielded 12/12 leads matched QRS morphology (Figure 1C and D). We performed scar dechanneling and elimination of LAVA and late potentials with RF energy delivered in a temperature-controlled mode at 30-35 Watts targeting for an impedance drop of 10 Ohms. This successfully termi-nated the VT and inducibility test post-ablation were negative. The patient’s follow-up at 3 months and 6 months were uneventful.
Conclusions: The present case demonstrated the substrate property of pheochromocytoma-induced cardiomyopathy. Radiofrequency catheter ablation of VT was feasible and current strategies in substrate modification can be employed to reduce the burden of VT episodes and appropriate shock therapy.
RADIOFREQUENCY ABLATION OF PLEOMORPHIC VENTRICULAR TACHYCARDIA IN PHEOCHROMOCYTOMA-INDUCED CARDIOMYOPATHYAbigail Louise Te, Shih-Lin Chang, Yenn-Jiang Lin, Shih-Ann Chen
Taipei Veterans General Hospital, Taipei, Taiwan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-148

565
Introduction: A 76-year-old woman was admitted to our hospital with syncope. She was implanted a dual chamber pacemaker with the ventricular lead placed in the septum for complete atrioventricular (AV) block at age 73. A whole-body computed tomography scan showed the enlarged lymph nodes in multiple organs, including lung, and blood chemistry showed an increase in the serum level of solu-ble interleukin-2 receptor. These findings and axillary lymph node biopsy showing the presence of non-caseating granulomas revealed that she was suffering from cardiac sarcoidosis (CS) which led to complete AV block. She had been well until one week before admission, and the pacemaker interrogation revealed a normal threshold value for the ventricular pacing (0.5 volts at a pulse width of 0.4 ms). On ad-mission, a 12-lead electrocardiogram showed the failure of ventricular pacing with complete AV block. The ventricular lead impedance and lead position were unchanged, however, a marked rise in the ventricular threshold was observed (4.75 volts at a pulse width of 0.7 ms). 99m Technetium myocardial scintigraphy showed the hypoperfusion in the anteroseptal wall, whereas 18F-Fluorodeoxyglucose Pos-itron Emission Tomography showed increased uptakes in the anteroseptal and inferior wall of the left ventricle. Thus, an increased activity in CS was suspected and treatment with oral prednisolone 30 mg/day was instituted. After the commencement of prednisolone, the pac-ing threshold reverted to normal and became stable in 0.75 volts at a pulse width of 0.4 ms. Prednisolone was reduced gradually to 15 mg/day in 6 weeks by reduction of the daily dosage of 5 mg once every other week without worsening of ventricular pacing threshold.
Methods: N/A
Results: N/A
Conclusions: This is a case of sudden marked deterioration of ventricular pacing threshold resulting in pacemaker failure 3 years after a ventricular septal lead implantation for complete AV block. Our case suggests that the sudden increased threshold might be reversible by early treatment with prednisolone in CS patients.
A SUDDEN DETERIORATION OF VENTRICULAR PACING THRESHOLD VOLTAGE IN A PATIENT WITH CARDIAC SARCOIDOSIS-A CASE REPORTYosuke Terui, Hideaki Endo, Takahide Kadosaka, Takashi Nakata, Tasuku Watanabe, Kenjiro Sato, Masanori Kanazawa, Kazuki Noda, Masateru Kondo, Toru Takahashi, Akihiro Nakamura, Eiji Nozaki
Iwate Central Prefectural Hospital, Morioka, Iwate, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-149

566
Introduction: Junctional ectopic tachycardia (JET) has been commonly described in pediatric, but very rarely in the adult population. The incidence is sporadic, and previously reported to be associated with both congenital heart disease and structurally normal heart. Albeit highly symptomatic, this form of tachyarrhytmia is usually not responding effectively to pharmacological treatment. Catheter ablation has offered an alternative solution for refractory cases.
Methods: We report a case of JET in an adult who underwent successful radiofrequency catheter ablation of the automatic focus, while preserving the normal AV node function.
Results: A 46-year-old nun came to the National Cardiovascular Center Harapan Kita, Jakarta, Indonesia with history of frequent syncope two years ago. Holter monitoring revealed intermittent junctional rhyhtm, and structural heart disease excluded by other examinations. Subsequent electrophysiology study demonstrated episodes of atrial standstill with junctional escape rhythm, despite normal sinus node refractory time (SNRT). A decision to implant an AAIR pacemaker was made and the patient was discharged with beta blocker and amiodarone. However, the patient returned twenty months later, complaining of bothersome palpitation with increasing intensity. Pace-maker interrogation showed accelerated junctional rhythm with AV dissociation. Attempts to overdrive the abnormal rhythm by modifying the pacemaker setting was in vain. During her second electrophysiology study, we induced JET, alternating with sinus tachycardia during isoproterenol infusion. We were able to map the earliest H potential during junctional beats (-22 ms) with a standard 4-mm 7F radiofre-quency catheter. Multiple short 10-15 second ablations at 30W were performed at anterior septum, between the typical fast pathway and slow pathway area. Successful ablation site was just inferior to the reference his catheter. No sign of AV block was observed after the pro-cedure.
Conclusions: At centers where safer cryoablation equipment is unavailable, a careful radiofrequency ablation may be performed safely for retractable JET. Nevertheless, the associated risk of AV block should always be communicated to the patient.
RADIOFREQUENCY ABLATION OF AUTOMATIC JUNCTIONAL ECTOPIC TACHYCARDIA IN ADULT WITH PRESERVATION OF AV NODE FUNCTIONAlexander Edo Tondas1, Dicky Armein Hanafy2 1Mohammad Hoesin General Hospital, Palembang, Indonesia; 2National Cardiovascular Center Harapan Kita, Jakarta Barat, Indonesia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-150

567
Introduction: The leadless ECG on single coil defibrillator (ICD) have superior vena cava (SVC coil)-can configuration as its default config-uration. However, in the absence of the SVC coil, the leadless ECG may record erroneous signals from outside the heart or from the de-vice.
Methods: N/A
Results: Three patients underwent single chamber ICD implantation (SJM) for pimary prevention of cardiac arrest due to left ventricular dysfunction. During follow-up, regular signals with a cycle length of 1,000 ms were detected on the leadless ECG in all 3 patients. These signals had no relation with the patient’s atrial or ventricular activity (Panel A) & masked the normal QRS (Panel C) in some patients. In single chamber ICDs, the default leadless ECG configuration is between SVC coil and can. In a single-coil lead with no SVC coil, there may be signals seen on the Leadless ECG, which are not heart signals. The signals recorded in our patients are caused by the protection field effect transistors (FETs) being refreshed once every second. They have a very minor effect on a loaded sense line but it will be pronounced in an unloaded lead. The leadless ECG configuration can be changed to RV coil-can configuration to get rid of these signals (Panel B). These signals may not have any therapy implications as the leadless ECG is not used for interpretation by the device, however they may cause confusion while interpreting leadless ECG.
Conclusions: Field effect transistor signals are detected in single coil ICD leads which could lead to confusion while interpreting leadless ECG. The leadless ECG configuration would need to be changed to RV coil-can to get rid of these signals.
PROTECTION FIELD-EFFECT TRANSISTORS SIGNALS DETECTED ON THE LEADLESS ECG IN PATIENTS WITH SINGLE COIL DEFIBRILLATORS Ameya Udyavar
P. D. Hinduja National Hospital, Mumbai, India
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-151

568
Introduction: Ventricular tachycardia (VT) is frequent long term complications in grown up congenital heart disease patients. They are of-ten poorly tolerated and medical treatment is frequently inadequate. One of the main mechanism of this is presence of previous ventricu-lar surgical scars or patching material, which predispose to macro re-entrant VT. However ablation still remains a challenge especially when the nature of the patient’s corrective surgery is unknown.
Methods: We present a case of a 40 years old male with an unknown congenital heart disease, who had undergone corrective surgery during childhood. There were no available records. Postulation of a prior Ventricular Septal Defect was made from patient’s vague history. Serial Transthoracic Echocardiography failed to show neither residual lesions nor defects. He was relatively well till he developed recur-rent bouts of VT since December 2015. The arrhythmias were unresponsive to medical treatment. He was referred to us after his latest episode, which reverted only with cardioversion. We took our patient in with 3D Ensite mapping system. Map of the RVOT & RV was creat-ed in sinus rhythm. Breakthrough VT of 2 different morphologies was found. VT of LBBB with inferior axis and another one of RBBB with superior axis. Substrate mapping was done and low voltage scars were noted at a patch site, in which mapping suggested previous cor-rected Atrioventricular Canal Defect. Figure of 8 paths of entry and exit were found. Ablation upon a single point at earliest breakthrough site, located at Right Ventricular anterior wall at the isthmus causes VT acceleration and termination of tachycardia. Further consolidation lesions were delivered along the scar border. No further VT was inducible with aggressive programmed electrical stimulation.
Results: Patient was discharged well post procedure with no recurrence. He had no more readmissions for palpitations or any further documented tachycardia.
Conclusions: Radiofrequency ablation for still remains a challenge for corrected patients Congenital Heart Disease. However this treat-ment modality will likely remain the best therapeutic option for these arrhythmias.
BUTTERFLY IN THE BROKEN HEART-A CASE OF 2 VENTRICULAR TACHYCARDIAS IN A CORRECTED CONGENITAL HEART DISEASEWan Faizal Wan Rahimi Shah, Kantha Rao Narasamuloo, Saravanan Krishinan
Hospital Sultanah Bahiyah, Alor Star, Kedah, Malaysia
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-152

569
Introduction: Interfascicular Ventricular Tachycardia (VT) is an uncommon arrhythmia among the left sided ventricular tachycarrhyth-mias. Almost all publications on it were case reports. Even in the largest series of Bundle Branch Block Reentry VT ablation experience, only 2 patients had this arrhythmia.
Methods: We present a case of a young 27 years old lady, who was initially diagnosed of having Left Fascicular Ventricular Tachycardia in 2009. She had undergone ablation procedure then at another centre, in which from documentation showed ablation was delivered at api-cal posterior septum area. She was discharged from follow up as the symptoms did not recur. However the palpitation episodes returned back in 2014. Initial ECG showed narrow complex tachycardia with RBBB pattern & negative QRS in leads II, III, aVF. Our initial diagnosis was recurrence of her previous arrhythmia. We proceed to on 2 back to back ablation attempts in September 2014. Despite adequate mapping with 3D CARTO system and ablating pre-Purkinje potentials at posterior/posterior inferior septum, it refused to go away with re-currences almost immediately upon completion of procedure. We elected to perform a Cardiac MRI which did not show any left ventricu-lar structural abnormality. In our final attempt in March 2015, we encountered more difficulty. An initial mapping on the left side with ret-rograde approach showed all signals were late. We turned over to the right side, which initially showed what seems to be the earliest breakout site. Entrainment was good and ablation was performed here. Again the tachycardia was only transiently terminated, before re-curring again on table. Another exhausting mapping was repeated in which a transient change in morphology ticks us towards diagnosis of Interfascicular VT. Early Purkinje signals were found and ablated then and the VT is at last terminated. Subsequently P1 & P2 signals were seen, with reversal of P2 with PVC. No further VT was induced.
Results: After her latest ablation, she remained asymptomatic on regular follow up. She had no more readmissions for palpitations or any further documented tachycardia.
Conclusions: Radiofrequency ablation for Interfascicular VT is challenging as it is less commonly encountered. Presentation of RBBB morphology also easily confuses the diagnosis with typical Left Fascicular VT.
INTERFASCICULAR VENTRICULAR TACHYCARDIA-THE ONE WHICH REFUSED TO GO AWAYWan Faizal Wan Rahimi Shah1, Saravanan Krishinan1, Kelvin Wong Cheok Keng2 1Hospital Sultanah Bahiyah, Alor Star, Kedah, Malaysia; 2Changi General Hospital, Singapore
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-153

570
Introduction: Accelerated idioventricular rhythm (AIVR) is described as an ectopic rhythm with >3 consecutive ventricular premature beats with 50-100 beats per minute. AIVR gradually emerges and terminates. In adults, it is often transiently encountered in patients with acute myocardial infarction, digitalis intoxication, and valvular disease. In rare cases, AIVR can occur in patients with structurally normal hearts without any identifiable reasons. We experienced a case with long-lasting AIVR in a patient without organic heart disease.
Methods: N/A
Results: A 23-year-old woman with long-lasting AIVR exhibited palpitation and dyspnea on exertion. Electrocardiogram (ECG) abnormali-ties were showed intermitted AIVR (heart rate 102 bpm) after a physical examination at age 12. Holter ECG revealed that the AIVR was in-termitted throughout the day (total heart beat 109,160/day, AIVR 40,244/day). Transthoracic echocardiography showed almost normal con-struction, left ventricular ejection fraction (LVEF) of 60% and left ventricular end-systolic diameter (LVDd) of 53 mm. Cardiac magnetic resonance imaging (CMRI) was not showed organic cardiac abnormalities. Pharmacology therapy was ineffective. She was referred to un-dergo catheter ablation for drug-refractory AIVR. The electrophysiological study and catheter ablation were performed. Multipolar elec-trode catheters were positioned at the high right atrium (HRA), His bundle recording area, and the right ventricular apex (RVA), via the right femoral vein. One 4 mm tip deflectable 8Fr catheter (Flex Ability®; St. Jude Medical, St. Paul, Minnesota) was inserted via the right femoral artery for mapping and ablation. The activation map of the right and left ventricle during AIVR using an electroanatomical map-ping system (EnSite NavX® System; St. Jude Medical, St. Paul, Minnesota) revealed the focus of the AIVR at the anteroseptal site of the LV. In the bipolar recording, the potential at the earliest site was existed with prepotential and preceded the surface QRS wave by 37 ms. The unipolar recording exhibited QS pattern. Radiofrequency energy application (power of 30W with a target temperature of 50°C) at the site of the earliest activation was successful in terminating the AIVR. The patient was maintained sinus rhythm immediately, and tachycardia was not inducible at the end of the study. Holter ECG was performed for 6 and 12 months after catheter ablation. The patient had no recur-rence of AIVR during following up to 12 months.
Conclusions: The patient had no recurrence of AIVR during following up to 12 months.
SUCCESSFUL CATHETER ABLATION OF LONG LASTING ACCELERATED IDIOVENTRICULAR RHYTHM IN A PATIENT WITHOUT ORGANIC HEART DISEASEMarie Yoshikawa, Tadashi Hashida, Tomihisa Nanao, Susumu Sakama, Daisuke Fujibayashi, Shigetaka Kanda, Mari Amino, Koichiro Yoshioka, Yuji Ikari
Department of Cardiovascular Medicine, Tokai University School of Medicine, Isehara, Kanagawa, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-154

571
Introduction: N/A
Methods: N/A
Results: An 80-year old woman presented with dyspnea and admission to another hospital. She was diagnosed with congestive heart fail-ure due to severe aortic valve stenosis and was referred to our hospital for transcatheter aortic valve implantation (TAVI) intervention. TAVI was performed through a retrograde transfemoral approach with local anesthesia. Although the preoperative electrocardiogram (ECG) showed sinus rhythm with a normal QRS width, the ECG after TAVI demonstrated sinus rhythm with first degree AV block and left bundle branch block. Two days after TAVI, supraventricular tachycardia (SVT) suddenly occurred and sustained. Adenosine triphosphate rapid in-jection let the tachycardia terminate transiently but SVT occurred repeatedly, so diltiazem was injected continuously via peripheral injec-tion. When diltiazem was decreased, however, SVT recurred and the patient felt palpitation and chest pain. We performed electrophysiolo-gy study and catheter ablation. AH and HV intervals measured 156 ms and 62 ms, respectively. The earliest retrograde atrial activation site during right ventricular apex (RVA) pacing was the left posterolateral region of the mitral annulus without decremental conduction prop-erties. The response of para-Hisian pacing indicated retrograde conduction occurring exclusively over an accessory pathway. SVT was in-duced by atrial extra-stimulus without jump up. We diagnosed SVT as atrioventricular reentrant tachycardia (AVRT), and mapped mitral annulus during RVA pacing using a 4-mm non-irrigated ablation catheter access to the left atrium via the transseptal approach. The site of earliest retrograde atrial activation during RVA pacing was found to be posterolateral region. Radio frequency energy was delivered and 2.9 seconds later the retrograde conduction was lost. Electrical storm of AVRT associated with TAVI had never been reported before. Par-tial damage to the conduction system during TAVI resulted in antegrade conduction delay, which might allow left-side accessory pathway to conduct retrograde to the atrium easily. Catheter ablation by an anterograde transseptal approach was effective and safety in achieving permanent loss of left-side accessory pathway conduction in spite of acute phase of TAVI.
Conclusions: N/A
A CASE WITH ELECTRICAL STORM OF ATRIOVENTRICULAR REENTRANT TACHYCARIDIA AFTER TAVI, WHICH MIGHT RESULT FROM PARTIAL DAMAGE TO THE CONDUCTION SYSTEM DURING TAVIDaisuke Yoshimoto, Yuichiro Sakamoto, Sachiko Bandou, Kazuto Kujira, Takahiko Suzuki
Toyohashi Heart Center, Toyohashi, Japan
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-155

572
Introduction: It is very safe to routinely use a circular mapping catheter (CMC) (St. Jude Medical, Inc., St. Paul, MN) to assess for pulmo-nary venous isolation in patients with atrial fibrillation (AF) at the end of the ablation procedure. However, we report a case where a metal-lic electrode displaced from a CMC was seen free floating in the right atrium on fluoroscopy. Luckily, the electrode inconceivably travelled retrogradely and became lodged in a terminal branch of the right inferior pulmonary vein (PV).
Methods: A 66-year-old Chinese gentleman with paroxysmal AF underwent successful isolation of all 4 pulmonary veins using a cryoab-lation balloon. A CMC was used to assess for pulmonary venous isolation at the end of the procedure.
Results: Upon removal of the CMC from the left atrium, a free floating metallic electrode that has displaced from the CMC was seen on fluoroscopy free floating within the left atrium (Figure 1A-D). Utmost concern was the potential for embolization particularly to the brain. The patient was counseled about the complication and plans for urgent cardiac surgery to retrieve the electrode was made. Whilst waiting for the operating theatre to be ready, the electrode inconceivably travelled retrogradely and became lodged in a terminal branch of the right inferior pulmonary vein, as seen on fluoroscopy (Figure 1E, F) and computed tomography angiography where it remained during fol-low-up 6 month later (Figure 1G, H).
Conclusions: We considered this incident a near miss with the potential of systemic embolization and the appropriate regulatory authori-ties have been notified. Yet, inconceivably, the electrode managed to float retrogradely and lodge within a terminal branch of the pulmo-nary veins.
DISLODGEMENT OF CIRCULAR MAPPING CATHETER ELECTRODE IN THE LEFT ATRIUM: A NEAR MISSFengxiang Zhang, Lijun Tang, Bing Yang, Gang Yang, Minglong Chen
The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-156

573
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-157
Introduction: Congenitally corrected transposition of the great arteries is a rare condition representing approximately 0.5% of all Congen-ital heart Diseases. Young adults may present with symptoms related to systemic right ventricular dysfunction or cardiac conduction de-fects. The anatomy of the conduction system in such patients is altered in the form of a second AV node positioned anteriorly which gives rise to an elongated AV bundle. We put forward two atypical presentations at our center.
Methods: N/A
Results: A nineteen year male presented with recurrent seizures of acute onset and treated with anti-epileptic drugs, continued to have recurrent symptoms. The CT brain was normal and the patient had no other neurological deficits. On cardiac evaluation the patient was found to have an advanced AV block with CCTGA and treated with a VVI pacemaker. The patient subsequently had no symptoms and the AEDs were withdrawn. A thirty year male presented with epigastric pain and vomiting, was diagnosed as having acute pancreatitis and medically managed for the same. The patient’s symptoms did not subside. On further evaluation the 2DECHO showed CCTGA and the EKG was suggestive of advanced AV block. The patient was treated with a DDD pacemaker with complete resolution of symptoms subse-quently.
Conclusions: Both the patients have been on regular follow up without recurrence of symptoms. Young adults with CCTGA with no other cardiac defects may remain asymptomatic till the second or third decade of life. The age related risk of development of complete heart block is about 2% per year. A high index of suspicion is paramount in such cases with atypical presentations. A permanent pacemaker is the treatment of choice leading to complete cessation of symptoms associated with cardiac conduction defects. A baseline cardiac evalu-ation for all such patients is emphasized.
SEIZURES? PANCREATITIS? JACK IN THE BOX!-ATYPICAL PRESENTATIONS OF A RARE CONGENITAL HEART DISEASEAbhinay Tibdewal, Anupama Hegde, V S Prakash, Sarthak Sahoo
MS Ramaiah Medical College, Bangalore, India

574
PEDIATRIC/ADULT CONGENITAL HEART DISEASE P 3-158
Introduction: Electrophysiological procedures are challenging in patients who underwent lateral tunnel and extracardiac conduit Fontan operation, because the caval veins are not connected to the atria and ventricles.
Methods: We consecutively included 10 patients [median age (interquartile range), 23.0 (16.0-27.8) years; 6 men] who underwent catheter ablation or pacemaker implantation via Fontan conduit puncture. In 6 and 4 patients, lateral tunnel and extracardiac conduit Fontan oper-ation have been performed, respectively.
Results: In 9 of 10 patients, Fontan conduit puncture via the right femoral vein and the inferior vena cava was successfully performed without complications under intracardiac echocardiographic guidance. In 5 patients with the Fontan conduit made of the pericardium, a Bronckenbrough transseptal needle or a radiofrequency transseptal needle with a snare was used. In 4 patients with the Fontan conduit made of Gore-tex, a radiofrequency transseptal needle with a snare, and percutaneous transluminal angioplasty balloon were used. In 1 patient with extracardiac conduit made of the pericardium, conduit puncture was failed due to interruption of the both femoral veins. Fon-tan conduit puncture time was significantly longer in patients with the conduit made of Gore-tex than in patients with the conduit made of the pericardium [91.0 (59.8-130.5) and 9.5 (8.0-18.3) minutes, respectively; P=0.018].
Conclusions: Conduit puncture is feasible and safe in patients with lateral tunnel and extracardiac Fontan circulation. Puncture of the Go-re-tex conduit is more difficult than the pericardium conduit.
CONDUIT PUNCTURE FOR ELECTROPHYSIOLOGICAL PROCEDURES IN PATIENTS WITH FONTAN CIRCULATIONJae-Sun Uhm, Nam Kyun Kim, Tae-Hoon Kim, Boyoung Joung, Hui-Nam Pak, Moon-Hyoung Lee
Severance Hospital, Seoul, Republic of Korea







![10 11 Session HR Session Seri Management[1]](https://static.fdokumen.com/doc/165x107/6314ba61fc260b71020fb0ee/10-11-session-hr-session-seri-management1.jpg)











