Surgical Critical Care Residency Program - Baylor College of ...
Upload
hms-harvardCategory
view
0download
0
Journal ofmedical ethics, 1988, 14, 91-96
Teaching medical ethics
Teaching clinical medical ethics: a modelprogramme for primary care residencyRobert M Arnold, Lachlan Forrow, Steven A Wartman, Joan Teno Division of General Internal Medicine,Brown University Program in Medicine, USA
Authors' abstractFew residency training programmes explicitly requiresubstantive exposure to issues in medical ethics andfewerstill have a formal curriculum in this area. Traditionalundergraduate medical ethics courses teach preclinicalstudents to identify ethical issues and analyse them at atheoretical level. Residency training, however, is the idealtime to establish the critical behavioural link which makesethics truly useful in clinical medicine. The GeneralInternalMedicine Residency TrainingProgram atRhodeIsland Hospital has developed an integrated, three-yearcuriculum with the goals ofhelping residents to perceiveethical issues in clinical practice, to utilise basicphilosophical principles in resolving ethical dilemmas andto communicate these issues clearly and sensitively topatients. The currculum has been well received byresidents and has had a hospital-wide impact. We believethat training residents in medical ethics and communicationskills is an effective approach to developing physicians'humane qualities.
IntroductionPerhaps in response to increasing complaints about thetechnological bias of medical education, the number ofmedical schools with course offerings in medical ethicsin the humanities grew from 12 pilot programmes in1972 to 89 in 1980 (1). These traditional undergraduatemedical ethics programmes teach preclinical studentsto identify ethical issues and analyse them on atheoretical level. Too often, however, the theoreticalinformation taught in these courses is not utilised whenthese students become clinical clerks and residents.Without frequent reinforcement, a student's attentionto these critical issues declines after medical school (2).If training in the ethical dimensions of medicine isabsent in the formative years of residency training(when young clinicians develop enduring practicestyles), physicians are likely to conclude that ethicalanalysis is peripheral to the real work of medicine.
Key words
More importantly, they will use only their intuition toconfront difficult ethical issues in clinical practice,when more powerful and reliable tools exist.
Although internal medicine residency programmesrarely require formal training in medical ethics or inthe communication skills necessary for a properdoctor-patient relationship, residency trainingprovides a unique opportunity to demonstrate thepractical contributions of medical ethics to clinicalpractice (3). Faced with direct patient careresponsibility for the first time, residents are usuallyquite receptive to learning how to manage ethicalproblems. Moreover, residents have acquired theexpertise necessary to place ethical issues in properperspective as well as to appreciate fully theirdiagnostic and therapeutic implications. Yet it is stillearly enough in their careers for ethics programmes tohave a profound and lasting impact. Formal training inclinical ethics during the residency years is thus likelyto offer the best opportunity to ensure that futurepractising physicians will understand and be able toincorporate the concepts and analytic methods ofmedical ethics into clinical care.To give internal medicine residents the cognitive
skills necessary to deal with ethical dilemmas, theGeneral Internal Medicine Residency TrainingProgram at Rhode Island Hospital has designed athree-year curriculum in medical ethics. Theprogramme features a unique integration of ethicaltheory and communication skills (4). We report herethe first four years of our experience to assist otherresidency programmes in developing similar curricula.
Curricular goalsThe authors designed a clinical ethics curriculum tohelp residents in the General Internal MedicineResidency Training Program at Rhode Island Hospitaladdress the ethical issues that arise in primary careinternal medicine. The programme's goal was not todevelop moral philosophers, but to help cliniciansapply the principles of medical ethics to their dailyclinical practice. To accomplish this goal, all residentsare required to meet the following objectives:
Medical ethics; medical education; residency training; 1. Recognise the ethical implications of both inpatientcommunication skills. and outpatient clinical cases. This requires that
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from
92 RobertM Arnold, Lachlan Forrow, Steven A Wartman andJoan Teno
residents be attentive to the moral dimensions of aclinical situation and that they have a basicunderstanding of ethical concepts.2. Apply ethical concepts and decision-makingprocedures to arrive at a well-rounded clinical strategy.3. Communicate sensitively with patients and otherhealth professionals about these ethical concepts andproposed management plans.
Accomplishing these objectives requires training inboth medical ethics and communication skills. Thediscipline of medical ethics offers the cognitiveframework necessary to help residents systematicallyanalyse ethical problems (objectives 1 and 2).However, for training in ethical theory to be useful itmust help clinicians solve the ethical problems thatarise in clinical care. Ethical theory is best taught, notfor its own sake, but as an analytical tool to help resolveclinical problems (5). Moreover, cognitive training inmedical ethics alone is not sufficient to producehumane physicians. While able to foster awareness,impart factual knowledge, and encourage criticalanalysis, training in medical ethics may not by itselfchange behaviour (6). Even the clearest understandingof an ethical concept, such as informed consent, haslittle clinical value without the behavioural skillsrequired to converse clearly and sensitively withpatients (objective 3). Teaching communication skillsis directed towards improving these humanebehaviours. While ethics helps one decide what to say,communication skills are necessary in order to learnhow to express one's thoughts clearly and in a sensitivemanner. Together, medical ethics and communicationskills provide the necessary foundation for managingmedicine's ethical dimensions.CurriculumThe General Internal Medicine Residency Program atRhode Island Hospital has developed a three-year,multidisciplinary programme in medical ethicsdesigned to fulfil the above objectives. The curriculumis divided into two overlapping components:
A. GENERAL CONCEPTS
This phase of our curriculum has been in place since1984. A core of ten structured sessions in the first twoyears of residency training were developed to giveresidents the necessary observational, cognitive, andbehavioural skills. The sessions take place during theresidents' month-long ambulatory (outpatient) block.Separated from the exhausting schedule of inpatientmedical care, the ambulatory block is a period duringwhich residents focus exclusively on ambulatorymedicine and the psychosocial aspects of health care.Scheduling these sessions when residents are neithersleep-deprived nor distracted by the demands ofhospitalised patients allows residents to read,concentrate, and thoughtfully reflect on ethical issues.
Behaviourally defined objectives that applycurricular goals to common ethical situations are
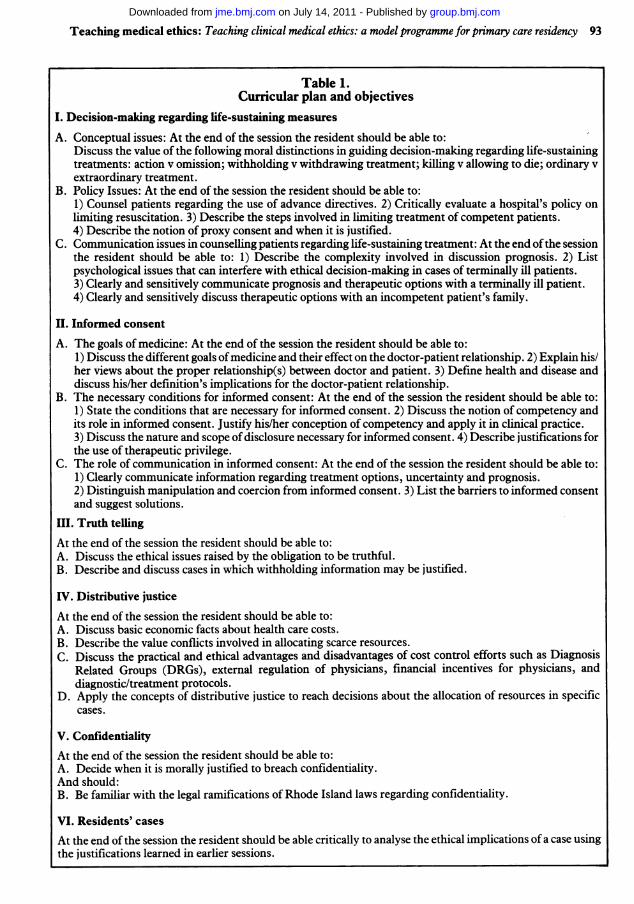
distributed prior to each session. These objectives,modified from recommendations of the DecampConference on the Teaching of Medical Ethics, covermajor ethical issues in internal medicine such as thegoals of medicine, informed consent, care of theterminally ill, confidentiality, truth telling, anddistribution of health care (7) (Table 1). Many of theobjectives may seem to imply there are non-controversial, 'correct' answers to all major moralconflicts in medicine. That interpretation, ofcourse, isnot the case. Throughout the curriculum, an effort ismade to deepen residents' understanding of thesources of ethical disagreement to help them deal moreeffectively with value conflicts.
1. Seminars in medical ethicsThe format of these sessions emphasises groupdiscussions and role-playing rather than didacticlectures, to encourage residents' participation.Individual sessions are taught by a team that incudes aphysician, a philosopher with special expertise inmedical ethics and a medical communicationsspecialist. Background readings which summarise thesalient ethical and clinical points are distributed priorto the session. A philosopher opens each session with abrief overview of the ethical issues raised in thereadings. A specific case, drawn from either medicalliterature or a resident's own caseload, is thenpresented and discussed. For example, during thesession on confidentiality the following case is used:
William M, a 37-year-old man, comes to you for a pre-employment physical (medical examination) that isrequired as part of the company's health insuranceprogramme. He brings you a form which you are to fillout documenting his physical problems and any knownmedical problems. During the history you find out heis a homosexual and that he recently gave blood but waslater called by the blood bank and told his blood cannotbe used and that he should not give blood in the future.What should you do?
Residents are asked to choose, and then justify, aparticular course of action to other sessionparticipants. Often, residents request extra infor-mation. They are asked to explain why suchinformation is necessary and how it might change one'sbehaviour. For example, some residents point out theimportance of knowing why the blood was rejected.They may try to justify reporting chronic hepatitis butnot reporting a positive HIV test (or vice versa). Toemphasise the role of uncertainty in clinical decision-making, residents may be asked to make choices basedupon incomplete information, for example, if thepatient refuses to authorise a phone call to the bloodbank. The goal of the discussion is not for the residentsto arrive at a 'correct' decision, but to improve theresidents' ability to identify the value conflict involved,to propose and justify possible solutions to theseconflicts, and to explain how any solution might be
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from
Teaching medical ethics: Teaching clinical medical ethics: a model programme for primary care residency 93
Table 1.Curricular plan and objectives
I. Decision-making regarding life-sustaining measures
A. Conceptual issues: At the end of the session the resident should be able to:Discuss the value of the following moral distinctions in guiding decision-making regarding life-sustainingtreatments: action v omission; withholding v withdrawing treatment; killing v allowing to die; ordinary vextraordinary treatment.
B. Policy Issues: At the end of the session the resident should be able to:1) Counsel patients regarding the use of advance directives. 2) Critically evaluate a hospital's policy onlimiting resuscitation. 3) Describe the steps involved in limiting treatment of competent patients.4) Describe the notion of proxy consent and when it is justified.
C. Communication issues in counselling patients regarding life-sustaining treatment: At the end ofthe sessionthe resident should be able to: 1) Describe the complexity involved in discussion prognosis. 2) Listpsychological issues that can interfere with ethical decision-making in cases of terminally ill patients.3) Clearly and sensitively communicate prognosis and therapeutic options with a terminally ill patient.4) Clearly and sensitively discuss therapeutic options with an incompetent patient's family.
II. Informed consent
A. The goals of medicine: At the end of the session the resident should be able to:1) Discuss the different goals ofmedicine and their effect on the doctor-patient relationship. 2) Explain his/her views about the proper relationship(s) between doctor and patient. 3) Define health and disease anddiscuss his/her definition's implications for the doctor-patient relationship.
B. The necessary conditions for informed consent: At the end of the session the resident should be able to:1) State the conditions that are necessary for informed consent. 2) Discuss the notion of competency andits role in informed consent. Justify his/her conception of competency and apply it in clinical practice.3) Discuss the nature and scope of disclosure necessary for informed consent. 4) Describe justifications forthe use of therapeutic privilege.
C. The role of communication in informed consent: At the end of the session the resident should be able to:1) Clearly communicate information regarding treatment options, uncertainty and prognosis.2) Distinguish manipulation and coercion from informed consent. 3) List the barriers to informed consentand suggest solutions.
III. Truth tellingAt the end of the session the resident should be able to:A. Discuss the ethical issues raised by the obligation to be truthful.B. Describe and discuss cases in which withholding information may be justified.
IV. Distributive justiceAt the end of the session the resident should be able to:A. Discuss basic economic facts about health care costs.B. Describe the value conflicts involved in allocating scarce resources.C. Discuss the practical and ethical advantages and disadvantages of cost control efforts such as Diagnosis
Related Groups (DRGs), external regulation of physicians, financial incentives for physicians, anddiagnostic/treatment protocols.
D. Apply the concepts of distributive justice to reach decisions about the allocation of resources in specificcases.
V. ConfidentialityAt the end of the session the resident should be able to:A. Decide when it is morally justified to breach confidentiality.And should:B. Be familiar with the legal ramifications of Rhode Island laws regarding confidentiality.
VI. Residents' cases
At the end of the session the resident should be able critically to analyse the ethical implications of a case usingthe justifications learned in earlier sessions.
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from
94 RobertM Arnold, Lachlan Forrow, Steven A Wartman and oan Teno
discussed or negotiated with the patient or otherrelevant parties.An attending physician (roughly speaking, an
independent practitioner with admitting privileges tothe hospital concerned), either from the academic staffor a private practitioner, attends each session. Thisphysician is asked to comment on each case's relevanceto daily practice, on the practical obstacles to fulfillingethical ideals and on the way he deals with ethicalissues. The involvement of attending physicians helpsto ensure that discussions are clinically based andpractically orientated. Furthermore, because thesephysicians are role models for house staff, theirparticipation underscores the importance of the ethicaland other humane dimensions of clinical practice.Finally, these physicians themselves learn from theirparticipation in the course, and may thereby becomemore aware of ethical problems that arise in their ownpractice and more skilled in the resolution of theseproblems.
2. Doctor-patient communication
A behavioural scientist with special training in doctor-patient communication attends many sessions to teachand to observe how effectively residents discussdifficult ethical issues with patients. There are alsothree sessions which deal exclusively with thebehavioural aspects of clinical ethics. Residentsdevelop their behavioural skills in managing ethicallycharged situations through video-taped role playing,and observing video-tapes of faculty interacting withstandardised actor-patients.These communication sessions are integral to our
ethics curriculum. They illustrate both the behaviouralconsequences of ethical theory and the challenges oftranslating theory into clinical practice. Furthermore,the sessions give residents a chance to practisecommunicating about difficult issues.
3. Ethical issues in ambulatory (outpatient) medicine
Traditionally, medical ethics has concentrated on lifeand death issues which arise in the hospital care ofpatients. However, philosophers have recently begunto stress the important ethical issues which occur in theoutpatient setting (8). To increase residents' awarenessof ethical issues in ambulatory care, a philosopher hasbeen leading case-orientated conferences in clinic on aregular basis. The cases often come from residentexperiences. A more formal curriculum is beingdeveloped to ensure that residents are exposed to thecommon ethical issues which arise in outpatientmedicine.
B. RESIDENTS' APPLICATION OF ETHICAL PRINCIPLES
The second phase of the curriculum allows residents tointegrate the skills and knowledge obtained in the firsttwo years into their clinical practice. This phase, whichconsists of two components, was first offered in 1986.
Each resident is required to present a patient whosecase raises ethical issues to fellow residents and faculty.The resident is responsible for presenting the medicaland social facts, analysing the value conflicts in thecase, reviewing the pertinent literature and justifyingthe proposed management plan.
Finally, third-year residents participate in threemultidisciplinary sessions, each one involving a case inoccupational health, geriatrics or adolescent health (9).The aim of these sessions is to help residents integratetheir knowledge ofmedical ethics into common clinicalsituations. A case with a bibliography is distributed tothe residents prior to the sessions and a faculty resourceperson identified. Each resident is charged withinstructing the other residents about different aspectsof the case (for example, the disability law in RhodeIsland or issues concerning society's moral obligationto injured workers). After residents present theirinformation, the group attempts to resolve thedifficulties in the case. A multidisciplinary panel isavailable to guide the residents and to ask and answerquestions. This experience allows residents tointegrate clinical medical ethics with other disciplinesin order to solve common but complex clinicalproblems.
EvaluationAlthough evaluation is an important part of everyeducational programme, the goals and methods ofevaluation in clinical medical ethics training arecontroversial (10). It is difficult to demonstrate theeffectiveness of any single component of medicaleducation in producing skilled clinicians. We do notexpect our biochemistry faculty be able to prove thatthe ability to describe gluconeogenesis improves one'smanagement of diabetic ketoacidosis. Similarly,programmes in medical ethics cannot be expected todemonstrate an immediate effect on residentbehaviour. Evaluation of any new curriculum isextremely important for at least two reasons. First,feedback from programme participants can be animportant measure of whether stated curricular goalswere achieved. Second, this same feedback can be usedto modify the curriculum for each subsequent year.
For evaluation of our programme, we have reliedheavily on the judgements of the residents themselves,who completed detailed questionnaires about eachsession at the end of their ambulatory blocks. Forboth educational and evaluative purposes, eachsession, therefore, has had explicit, narrowlydefined objectives that were stated and distributed inadvance. Residents were asked several questionsregarding the clarity of the stated objectives and theeffectiveness of the individual aspects of each session(for example, readings, discussions, role-playing) inachieving those objectives. Whenever possible,residents were asked to respond by circling onenumber on a 1-5 scale.
Because the responses of each group of residentsabout a session were used to alter the structure or
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from

Teaching medical ethics: Teaching clinical medical ethics: a model programme for primary care residency 95
content of that session for future residents, it is notstrictly possible to present aggregate evaluations formost questions. Two particularly important findingsfrom these evaluations bear emphasis. First, residentsin our programme have been extremely receptive to theclinical ethics curriculum and report that this trainingis useful and improves their perceived ability tomanage ethical problems. For example, many of theresidents reported that prior to the course they oftenasked families of acutely ill patients 'What do you wantme to do for your mother/father?' However, afterlearning about the principles of proxy consent anddiscussing the issue with the communication specialistand chaplain who teach how to talk with families in theintensive care units, residents changed theirbehaviour. They now ask families 'What would yourparent want if he or she were able to talk with us?',believing that this question is both ethically moreappropriate and emotionally less distressing. Becauseof its positive contribution to clinical practice, theresidents felt strongly that the curriculum should be arequired part of internal medicine training.
Second, residents insist that readings, casediscussions, and in fact, every aspect of the curriculumshould be closely tied to the practical issues of patientcare. Long theoretical readings, or long discussionsabout moral philosophy were criticised. Although thefaculty evaluations also reported satisfaction with theprogramme, one difficulty in teaching becameapparent early in the programme. Integrating theclinical, ethical and behavioural components of eachcase into a single session turned out to be unwieldy andunduly labour-intensive. A practical solution has beento make the primary focus of each individual sessioneither ethical theory and principles (including casediscussions) or communication skills training(including role-playing and video-tapes).An important measure of any ethics programme's
success is its effect on the frequency of explicitdiscussions of ethical issues in day-to-day clinical care.By this criterion the Rhode Island Hospitalprogramme in clinical ethics has proved to be verysuccessful. The curriculum legitimated the role ofethical analysis in patient care. Since the curriculumbegan, primary care residents have brought up ethicalconcerns more frequently in other clinical settings. Anongoing bi-monthly noon conference has beenorganised to allow residents on the inpatient service todiscuss difficult cases in their clinical practices.Residents have also become involved in a variety ofother projects which deal with ethical issues in clinicalpractice, such as serving on the hospital's new ethicscommittee, assisting in the re-writing of the hospital'spolicy on resuscitation, and developing researchprotocols to study this revised policy.
Following the initiation of the formal residencycurriculum in ethics, the programme's philosopherwas awarded a grant to serve half time for nine monthsas the hospital's philosopher-in-residence. This oppor-tunity was an important addition to his formal work
within the curriculum, allowing him to raise ethicalissues with residents during their daily work on thewards and in intensive care units.The Departments of Medicine and Nursing have
also devoted much greater explicit attention to ethicalissues during this period. In addition to sponsoring agrowing number of grand rounds, other conferencesand day-long symposia on ethical issues, an ethicscommittee has been formed within the Department ofMedicine through which physicians, nurses, families,and others can obtain assistance in making difficultethical decisions in patient care.
DiscussionIn the last few years there has been increasing interestin the ethical and interpersonal dimensions ofresidency training (11,12). The American Board ofInternal Medicine, for example, has begun to includeevaluations of residents' interpersonal andcommunication skills as a prerequisite for boardcertification (13). However, few internal medicineresidency programmes require formal training in bothmedical ethics and communication skills. RhodeIsland Hospital's General Internal Medicine ResidencyTraining Program has put into place a three-yearcurriculum to help residents deal with the ethicaldimensions of clinical care. Our programme's specialemphasis on improving residents' actual clinicalpractice has lead to the integration of training in bothmedical ethics and in communication skills.
Residents have responded enthusiastically to thiseffort and have reported that the curriculum has had apositive impact on their clinical practice. Theprogramme also has increased residents' sensitivity toethical issues and has legitimated the inclusion ofmedical ethics into other aspects ofresidency training.We believe that our experience can assist other
residency training programmes to institute similarformal curricula in medical ethics. Such programmes,presented to physicians in their formative years, mayprovide the best chance of producing physicians whoexemplify 'integrity, respect and compassion' in theircare of patients (13).
AcknowledgementsThe authors thank Drs Dan Brock and Pam Rowland-Morin for their help in structuring and teaching thecourse; Drs Julie Nissen and Sankey Williams for theirinsightful comments, and Amy Laub and MaryO'Brien for secretarial assistance.
At the time of the study Drs Arnold and Forrow wereresidents at Rhode Island Hospital. Dr Arnold is currentlya Veterans Administration Robert Wood3Johnson ClinicalScholar, Division of General Internal Medicine,University ofPennsylvania. Dr Forrow is a Fellow in theDivision of General Medicine, Beth Israel Hospital,Harvard School of Medicine. Dr Wartman is AssociateProfessor of Medicine and Community Health, Brown
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from

96 RobertM Arnold, Lachlan Forrow, Steven A Wartman andJoan Teno
University Program in Medicine, and Director, DivisionofGeneral Internal Medicine, Rhode Island Hospital. DrTeno was a Clinical Instructor in Medicine at RhodeIsland Hospital, and is currently a Fellow in Geriatrics atRoger Williams Hospital, Providence, Rhode Island, inthe United States ofAmerica.
Requests for reprints should be addressed to: Steven AWartman, MD PhD, Division of General InternalMedicine, Rhode Island Hospital, 593 Eddy Street,Providence, RI 02903.
Papers invitedCritical or philosophical medical ethics teaching is justbeginning to take off in Britain and also in othercountries in Europe and the Commonwealth. Muchcareful experiment and mutual learning will be neededto develop successful approaches. One source ofimportant information in this area is the United Statesand much could be learned both from its successes andits failures in the very extensive experience of medicalethics teaching now available across the Atlantic. Thisjournal will welcome short submissions for its newintermittent series on the teaching of medical ethics;the intention is to provide a national and internationalexchange of ideas about which ways of teachingmedical ethics work well - and which do not.
Papers should be sent to: The Editor, Journal ofMedical Ethics, IME Publications, 151 Great PortlandStreet, London WIN 5FB. See also Notes onsubmitting manuscripts for publication at thebeginning of the journal.
References(1) Pellegrino E D, McElhinney T K. Teaching ethics, the
humanities and human values in medical school: A ten-yearoverview. Washington, D C: Institute of Human Values
in Medicine, 1981.(2) Carlton W. In our professional opinion: The primacy of
clinicaljudgement over moral choice. South Bend, Indiana:University of Notre Dame Press, 1978.
(3) Seigler M. The legacy of Osler: Teaching clinical ethicsat the bedside. Journal of the American MedicalAssociation 1978; 239: 951-955.
(4) Arnold R M, Povar G J, Howel J D. The humanities,humanistic behavior, and the humane physician: Acautionary note. Annals of Internal Medicine. 1987; 2:313-318.
(5) Agich G J. Evaluating medical ethics teaching. Society ofHealth and Human Values (notes). 1985; Sept: 3-4.
(6) Goodpaster K E. Is teaching ethics 'making' or 'doing'?Hastings Center Report 1982; 12: 36-39.
(7) Culver C, Clouser K D, Gert B, Brody H, Fletcher J, etal. Basic curricular goals in medical ethics. New EnglandJournal ofMedicine 1985; 312: 253-256.
(8) Barnard D. Unsung questions of medical ethics. Socialscience and medicine 1985; 21: 243-249.
(9) Colby K K, Almy T P, Zubkoff M. Problem basedlearning of social sciences and humanities by fourth yearmedical students. Journal ofmedical education 1986; 61:413-416.
(10) Ruddick W. What should we teach and test? HastingsCenter report 1983; 13: 20-22.
(11) Povar G J, Keith K J. The teaching of liberal arts ininternal medicine residency training. Journal ofmedicaleducation 1984; 59: 714-721.
(12) Boufford J I, Carson R A, eds. The teaching ofhumanitiesand human values in primary care training. McLean,Virginia: Society for Health and Human Values, 1984.(Available from the Society for Health and HumanValues, 1311A Dolley Madison Boulevard, McLean,VA 22101.)
(13) Subcommittee on Evaluation of Humanistic Qualities inthe Internist. A guide to awareness and evaluation ofhumanistic qualities in the internist. Portland, Oregon:American Board of Internal Medicine, 1985. (Availablefrom the American Board of Internal Medicine, 200 SWMarket Street, Portland, OR 97201).
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from

doi: 10.1136/jme.14.2.91 1988 14: 91-96J Med Ethics
R M Arnold, L Forrow, S A Wartman, et al. for primary care residency.ethics: a model programme Teaching clinical medical
http://jme.bmj.com/content/14/2/91found at: Updated information and services can be
These include:
References http://jme.bmj.com/content/14/2/91#related-urls
Article cited in:
serviceEmail alerting
right corner of the online article.cite this article. Sign up in the box at the top Receive free email alerts when new articles
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 14, 2011 - Published by jme.bmj.comDownloaded from
Copyright © 2022 FDOKUMEN