
Taking Less Than Prescribed: Medication Nonadherence and Provider-Patient Relationships in...
12
Taking Less Than Prescribed: Medication Nonadherence and Provider-Patient Relationships in Lower-Income, Rural Minority Adults With Hypertension Michelle Y. Martin, PhD 1 , Connie Kohler, DrPH 2 , Young-il Kim, PhD 1 , Polly Kratt, PhD 1 , Yu- Mei Schoenberger, PhD 2 , Mark S. Litaker, PhD 3 , Heather M. Prayor-Patterson, MS 1 , Stephen J. Clarke, PhD 1 , Shiquina Andrews, MS 1 , and Maria Pisu, PhD 1 1 Department of Medicine, Division of Preventive Medicine, University of Alabama at Birmingham, Birmingham, AL 2 School of Public Health, Health Behavior, University of Alabama at Birmingham, Birmingham, AL 3 Dental Diagnostic Sciences, University of Alabama at Birmingham, Birmingham, AL Abstract Control of hypertension remains poor, and lack of adherence to medication is considered a primary reason. Few studies have examined the reasons for medication nonadherence in African American, lower-income, rural adults receiving medications at no personal cost. Moreover, our understanding of how the provider-patient relationship influences adherence in this population is limited. In this study, the authors (1) examined reasons for taking less medication than prescribed and (2) examined the association between provider-patient variables and medication adherence. A total of 434 participants (94.8% African American) were included. The most frequently endorsed reasons for taking less medication than prescribed were not having blood pressure medicine when it was time to take a dose (36%), running out of medicine (35%), bothered by side effects (29%), and a change in one’s daily routine (27%). Nonadherent individuals were significantly more likely to report discomfort with asking the health provider questions (74% vs 63%), were more likely to report that health care visits were stressful (25% vs 16%), and exhibited more depressive symptoms (58% vs 45%). Adherent patients had lower blood pressure (systolic: 133±15.8 mm Hg vs 138±17.6 mm Hg, P value=.002; diastolic: 80±9.8 mm Hg vs 83±11 mm Hg, P value=.003) than individuals who were less adherent. Clinicians providing care to rural, poor hypertensive patients should routinely assess self-management behaviors, logistical barriers, and emotional health. Creating clinical encounters that minimize the stressful nature of the visit and encourage patient question-asking behavior may also be important for the optimal management of hypertension. Hypertension is the most common modifiable cardiovascular risk factor. With an estimated 73 million hypertensive Americans, 1 the clinical management of hypertension is central to the practice of many physicians. Despite the efficacy of pharmacologic treatment, control of hypertension in the United States is inadequate. 2 Medication nonadherence is one factor contributing to poor blood pressure (BP) control. 3 Patient-related factors associated with medication nonadherence may be unintentional (eg, forgetting to take medications, running out of medication, lack of knowledge) 4,5 or © 2010 Wiley Periodicals, Inc. Address for correspondence: Michelle Y. Martin, PhD, University of Alabama at Birmingham, Department of Medicine/Division of Preventive Medicine, 1717 11th Avenue South, 1503 3rd Avenue South, MT617, Birmingham, AL 35294-4410 [email protected]. NIH Public Access Author Manuscript J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16. Published in final edited form as: J Clin Hypertens (Greenwich). 2010 September ; 12(9): 706–713. doi:10.1111/j.1751-7176.2010.00321.x. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Taking Less Than Prescribed: Medication Nonadherence and Provider-Patient Relationships in...

Taking Less Than Prescribed: Medication Nonadherence andProvider-Patient Relationships in Lower-Income, Rural MinorityAdults With Hypertension
Michelle Y. Martin, PhD1, Connie Kohler, DrPH2, Young-il Kim, PhD1, Polly Kratt, PhD1, Yu-Mei Schoenberger, PhD2, Mark S. Litaker, PhD3, Heather M. Prayor-Patterson, MS1,Stephen J. Clarke, PhD1, Shiquina Andrews, MS1, and Maria Pisu, PhD1
1Department of Medicine, Division of Preventive Medicine, University of Alabama at Birmingham,Birmingham, AL2School of Public Health, Health Behavior, University of Alabama at Birmingham, Birmingham, AL3Dental Diagnostic Sciences, University of Alabama at Birmingham, Birmingham, AL
AbstractControl of hypertension remains poor, and lack of adherence to medication is considered aprimary reason. Few studies have examined the reasons for medication nonadherence in AfricanAmerican, lower-income, rural adults receiving medications at no personal cost. Moreover, ourunderstanding of how the provider-patient relationship influences adherence in this population islimited. In this study, the authors (1) examined reasons for taking less medication than prescribedand (2) examined the association between provider-patient variables and medication adherence. Atotal of 434 participants (94.8% African American) were included. The most frequently endorsedreasons for taking less medication than prescribed were not having blood pressure medicine whenit was time to take a dose (36%), running out of medicine (35%), bothered by side effects (29%),and a change in one’s daily routine (27%). Nonadherent individuals were significantly more likelyto report discomfort with asking the health provider questions (74% vs 63%), were more likely toreport that health care visits were stressful (25% vs 16%), and exhibited more depressivesymptoms (58% vs 45%). Adherent patients had lower blood pressure (systolic: 133±15.8 mm Hgvs 138±17.6 mm Hg, P value=.002; diastolic: 80±9.8 mm Hg vs 83±11 mm Hg, P value=.003)than individuals who were less adherent. Clinicians providing care to rural, poor hypertensivepatients should routinely assess self-management behaviors, logistical barriers, and emotionalhealth. Creating clinical encounters that minimize the stressful nature of the visit and encouragepatient question-asking behavior may also be important for the optimal management ofhypertension.
Hypertension is the most common modifiable cardiovascular risk factor. With an estimated73 million hypertensive Americans,1 the clinical management of hypertension is central tothe practice of many physicians. Despite the efficacy of pharmacologic treatment, control ofhypertension in the United States is inadequate.2 Medication nonadherence is one factorcontributing to poor blood pressure (BP) control.3
Patient-related factors associated with medication nonadherence may be unintentional (eg,forgetting to take medications, running out of medication, lack of knowledge)4,5 or
© 2010 Wiley Periodicals, Inc.Address for correspondence: Michelle Y. Martin, PhD, University of Alabama at Birmingham, Department of Medicine/Division ofPreventive Medicine, 1717 11th Avenue South, 1503 3rd Avenue South, MT617, Birmingham, AL 35294-4410 [email protected].
NIH Public AccessAuthor ManuscriptJ Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
Published in final edited form as:J Clin Hypertens (Greenwich). 2010 September ; 12(9): 706–713. doi:10.1111/j.1751-7176.2010.00321.x.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

intentional (eg, concern over perceived side effects, general dislike of medication, absenceof symptoms, negative attitudes toward medication).4,6 Recent studies suggest that thequality of the relationship with the physician may also play a role. In one study, adherentpatients cited “faith in the physician” as influencing their adherence to antihypertensivemedication.6 In an urban, primarily black female population, poor adherence toantihypertensive medications was associated with a perceived need to have longer visitswith the physician and lack of comfort in asking the physician questions.7 In a more recentstudy of urban, primarily lower income African Americans, adherent hypertensive patientsdescribed their physician as possessing a collaborative communication style.8
In the present study, we examined the association between aspects of the provider-patientrelationship and medication adherence among Southern, rural, low-income, AfricanAmerican hypertensive adults. It is well documented that place of residence is associatedwith cardiovascular health outcomes. For example, the stroke mortality rate is highest in theSoutheast, an area known as the “Stroke Belt.”9 In a recent study, socioeconomic status,chronic diseases (including hypertension), race/ethnicity, and stroke risk factors accountedfor 72% of the excess stroke risk in the Stroke Belt.10 This finding highlights the importanceof conducting studies in this region and conducting those studies among a demographic athigh risk for poor hypertension-related outcomes.
METHODSThe data described in this study are baseline data for participants of a randomized trial of anintervention to reduce hypertension in a rural low-income population in Alabama. The studywas approved by the University of Alabama at Birmingham institutional review board.
Hypertensive adults were recruited from rural community clinics that provided hypertensionmedications free of charge to residents who met poverty guidelines. One clinic partner, theAlabama Department of Public Health, offered a limited number of medications at no cost toresidents of Wilcox and Lowndes counties whose doctors prescribed a regimen fromavailable medications. A second clinic partner, also in Wilcox County, was a FederallyQualified Health Center. This clinic obtained hypertension medications for indigent patientsthrough the pharmaceutical companies’ Patient Assistance Plans. The study eligibilitycriteria included: (1) a diagnosis of hypertension, (2) age 19 years or older, and (3)engagement with a health care provider. There were no exclusion criteria.
The data for this study were collected using a computer-assisted telephone interview after aninitial clinic visit where the informed consent form was discussed and signed. Participantswere compensated with a $10 payment for completing the baseline telephone survey. Forstudy participants without a telephone, arrangements were made to have the phone callcompleted at a relative’s or friend’s home.
MeasuresSelf-Reported Medication-Taking Behavior—Medication-taking behavior wasmeasured by 10 questions assessing how frequently patients took less than the prescribedamount of medication under a range of circumstances. Items on this measure include itemssimilar to the medication adherence questions used in the National Institute of Allergy andInfectious Diseases (NIAID) Adult AIDS Clinical Trials Group, a multicenter nationwidestudy, and the Steps to Maximize Adherence to Antiretroviral Therapy (SMAART) projectfunded by the NIAID. Items were scored on a 4-point scale from 1 (never) to 4 (all thetime). Items were reverse scored and summed to yield a total score. Higher scores reflected agreater degree of medication adherence. Internal consistency of this scale in our sample, asmeasured by Cronbach’s α, was 0.92. Because 40% of the individuals in the sample reported
Martin et al. Page 2
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

that they never took less than the prescribed amount of medication, medication-takingbehavior was conceptualized as a dichotomous variable (ie, individuals who reported thatthey never took less medication than prescribed [adherent] vs all others [nonadherent]).
Provider-Patient Relationship—Eight independent questions assessed dimensions ofthe provider-patient relationship. These reflected aspects of the relationship that werespecific to high BP (eg, “Has your health care provider ever told you about the side effectsof your BP?”) and questions that assessed aspects that were more general and suggested bythe literature to be associated with medication adherence (eg, “Do you feel uncomfortableasking your health care provider questions about your health?”). Participants responded“yes,” “no,” or “don’t know” to each of these questions.
Barriers—Barriers reflect challenges to medication adherence reported in the literature. Toassess barriers to medication adherence, participants reported the frequency of: (1)forgetting to take their medications, (2) being too busy to take medication, (3) difficulty intaking their medication at the same time every day, and (4) occasions when it was difficultto travel to the clinic to fill their prescription.
Depression—Depression has been shown to be a factor in past medication adherencestudies.11 To examine this in our population, the 10-item Center for Epidemiologic StudiesDepression Scale (CES-D) short-form (SF) was used to provide a measure of depressivesymptoms, with the responses for each item: 1 (rarely or none of the time), 2 (some or alittle of the time), 3 (occasionally or a moderate amount of time); or 4 (all of the time).Following reverse scoring as appropriate, responses were summed. A scale score of 10 orabove is indicative of significant depressive symptoms.12
Demographics and General Health—Sociodemographic data included sex, age,education, income, marital status, and employment. The standard health status question fromthe SF-12 “In general would you say your health is: excellent, very good, good, fair, andpoor” was also posed to study participants.13
Blood Pressure—BP was taken at the baseline clinic visit by a clinic nurse or technicalstaff. Because of large patient loads, the clinics agreed to take only one BP reading. In caseswhere two readings were taken, the readings were averaged. BP was measured in all clinicswith a sphygmomanometer.
Statistical AnalysisSAS version 9.1 (SAS Institute, Cary, NC) was used to conduct the statistical analyses. Wecalculated descriptive statistics to characterize our study sample. To determine whetheradherent vs nonadherent individuals differed on sociodemographic and clinical variables,chi-square tests were used for categoric variables and t tests for continuous variables. Toexamine the reasons for medication nonadherence, frequency counts were calculated foritems on the Self-Reported Medication-Taking Behavior scale and for the 4 general barriers.To assess whether adherent and nonadherent individuals differed on the provider-physicianrelationship variables, we conducted chi-square analyses.
RESULTSA total of 434 adults (94.8% African American) participated in the study. The mean age ofparticipants was 56.1±13.1 years. The majority of the sample were women (67%) who hadan income of <$15,000, and just over 50% reported fair or poor health. Just over 50% alsoindicated significant symptoms of depression. Comparing sociodemographic and clinical
Martin et al. Page 3
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
characteristics in adherent and nonadherent adults revealed that many variables were similarin the two groups (P>.05). Adherent and nonadherent individuals did differ on levels ofdepression (P<.01). In particular, 66% of respondents with CES-D score ≥10 werenonadherent, compared with 54% of respondents scoring <10. Adherent individuals had BPvalues significantly lower than nonadherent patients. These values were 133±15.8 vs138±17.6 for systolic BP (P=.002) and 80±9.8 vs 83±11 for diastolic BP (P=.003) (Table I).
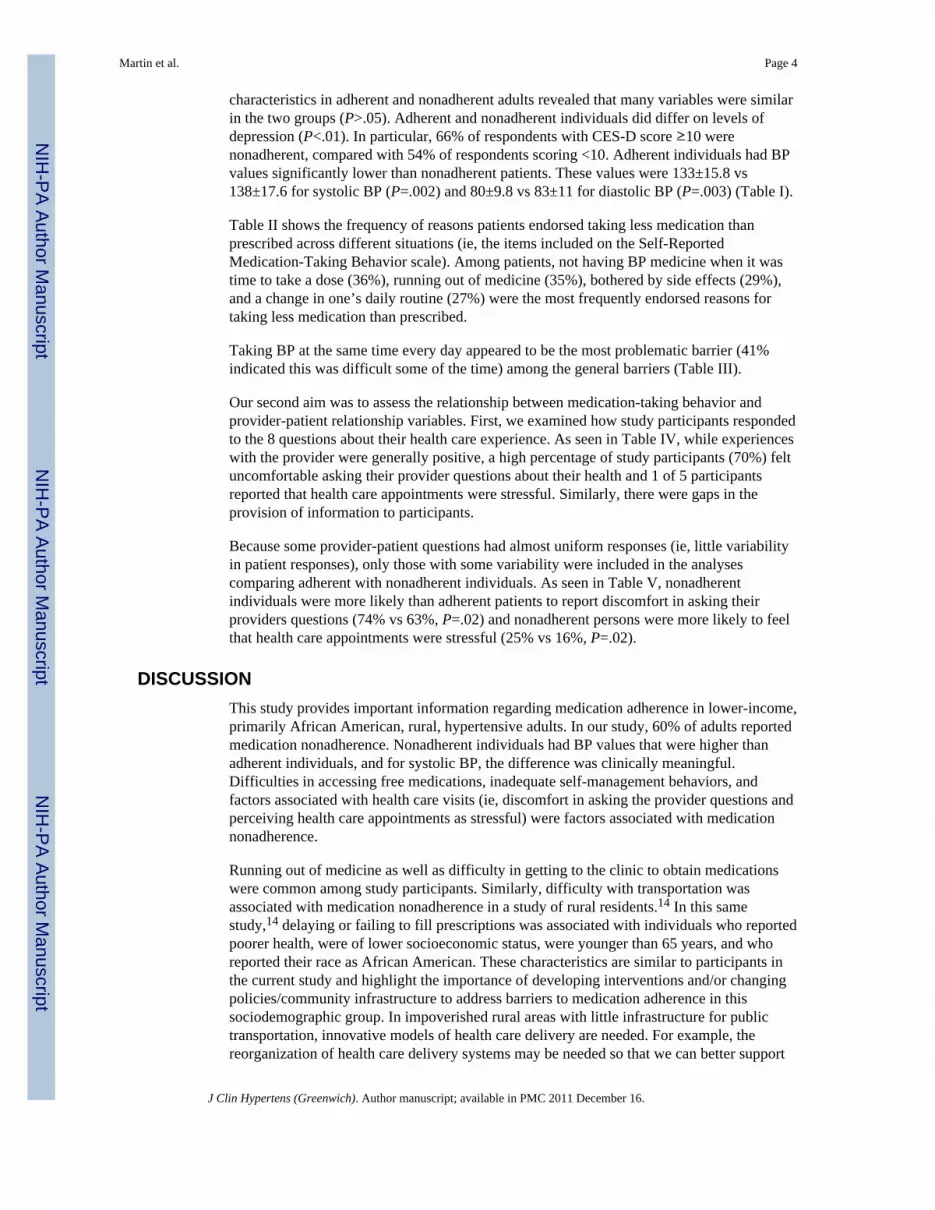
Table II shows the frequency of reasons patients endorsed taking less medication thanprescribed across different situations (ie, the items included on the Self-ReportedMedication-Taking Behavior scale). Among patients, not having BP medicine when it wastime to take a dose (36%), running out of medicine (35%), bothered by side effects (29%),and a change in one’s daily routine (27%) were the most frequently endorsed reasons fortaking less medication than prescribed.
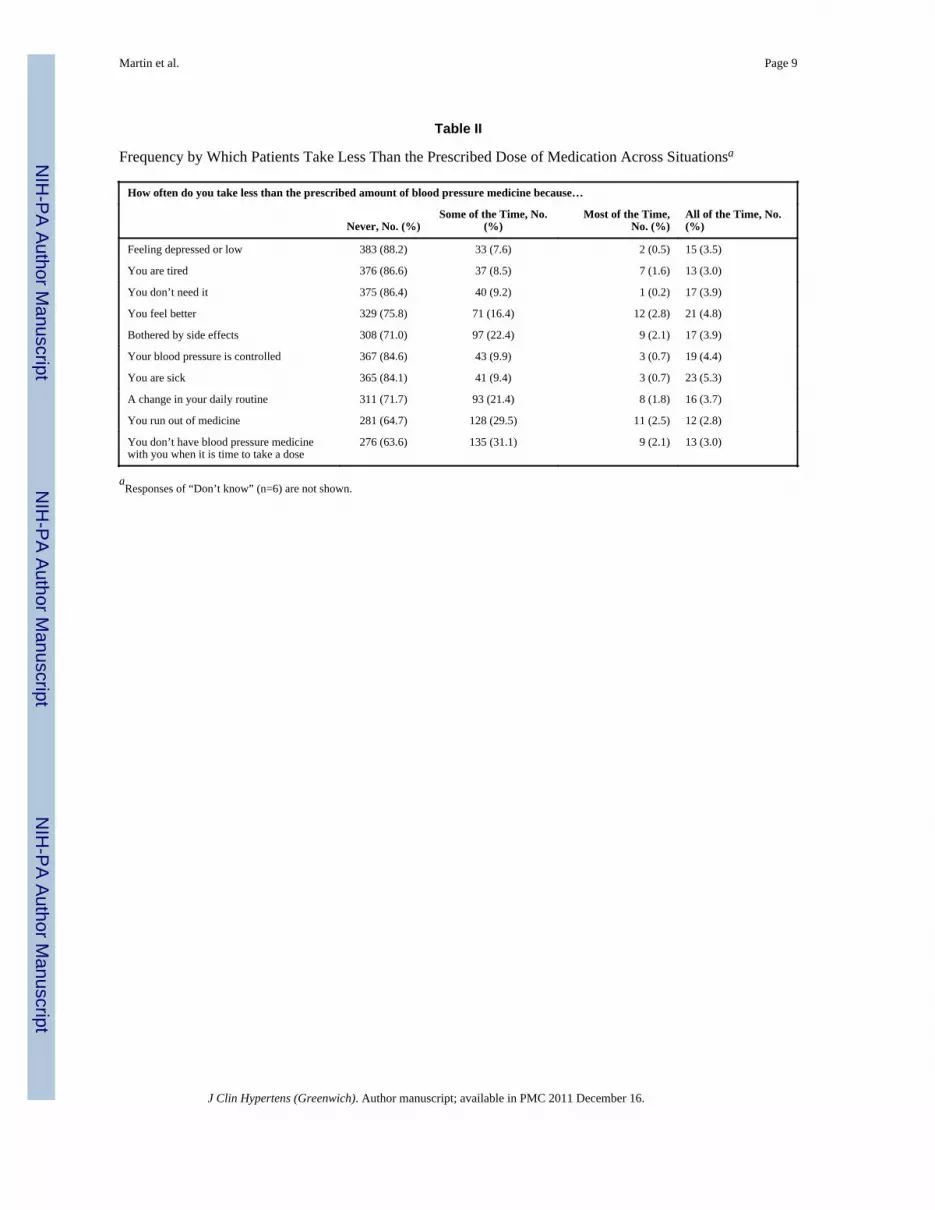
Taking BP at the same time every day appeared to be the most problematic barrier (41%indicated this was difficult some of the time) among the general barriers (Table III).
Our second aim was to assess the relationship between medication-taking behavior andprovider-patient relationship variables. First, we examined how study participants respondedto the 8 questions about their health care experience. As seen in Table IV, while experienceswith the provider were generally positive, a high percentage of study participants (70%) feltuncomfortable asking their provider questions about their health and 1 of 5 participantsreported that health care appointments were stressful. Similarly, there were gaps in theprovision of information to participants.
Because some provider-patient questions had almost uniform responses (ie, little variabilityin patient responses), only those with some variability were included in the analysescomparing adherent with nonadherent individuals. As seen in Table V, nonadherentindividuals were more likely than adherent patients to report discomfort in asking theirproviders questions (74% vs 63%, P=.02) and nonadherent persons were more likely to feelthat health care appointments were stressful (25% vs 16%, P=.02).
DISCUSSIONThis study provides important information regarding medication adherence in lower-income,primarily African American, rural, hypertensive adults. In our study, 60% of adults reportedmedication nonadherence. Nonadherent individuals had BP values that were higher thanadherent individuals, and for systolic BP, the difference was clinically meaningful.Difficulties in accessing free medications, inadequate self-management behaviors, andfactors associated with health care visits (ie, discomfort in asking the provider questions andperceiving health care appointments as stressful) were factors associated with medicationnonadherence.
Running out of medicine as well as difficulty in getting to the clinic to obtain medicationswere common among study participants. Similarly, difficulty with transportation wasassociated with medication nonadherence in a study of rural residents.14 In this samestudy,14 delaying or failing to fill prescriptions was associated with individuals who reportedpoorer health, were of lower socioeconomic status, were younger than 65 years, and whoreported their race as African American. These characteristics are similar to participants inthe current study and highlight the importance of developing interventions and/or changingpolicies/community infrastructure to address barriers to medication adherence in thissociodemographic group. In impoverished rural areas with little infrastructure for publictransportation, innovative models of health care delivery are needed. For example, thereorganization of health care delivery systems may be needed so that we can better support
Martin et al. Page 4
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

patients with economic and geographic barriers. As technology improves, health caredelivery systems in which home BP monitoring data is transmitted to the physician’s officemay permit medication refills remotely for patients with controlled BP.
In the present study, not having medications when it was time to take them and the findingthat 36% indicated that they forget to take their medications suggests that individual-levelinterventions are still needed to promote medication adherence. Reminding patients to taketheir medications has been an important component of medication adherenceinterventions.15 This type of intervention may be especially important in helping patientsmanage a chronic illness without overt symptoms.
Our results also suggests a need for rural care providers, especially those serving low-socioeconomic communities, to take depression symptoms into account when counselinghypertensive patients about medication adherence strategies. In our study, participantsclassified as exhibiting symptoms of depression were more likely to be nonadherent to theirmedication regimens than those with lower CES-D scores. The association betweendepression and adherence suggests that developing strategies for coping with depression-related internal and external triggers may improve adherence in this vulnerable population.Identifying resources to deliver mental health care in a medically underserved community,however, remains a persistent challenge.
In our study, the provider-physician relationship also played an important role inmedication-taking behavior. Nonadherent patients reported that health care appointmentswere stressful and that they were uncomfortable asking questions. These findings should bethe catalyst for future research. For example, what factors contribute to being uncomfortablewith asking questions? Patient-related factors may include not knowing what questions toask, a general level of discomfort with authority figures, or concerns about a physician’sbusy schedule. Alternatively, aspects of the clinical encounter and the physician’sdisposition may make it uncomfortable for patients to pose questions. In a study of ruralpatients, researchers found that medication nonadherence (defined as delaying or not fillingprescriptions during the past 12 months) was associated with patients who reported that theywere not satisfied with how they were treated by office staff, lack of confidence in theirphysician’s ability to help them, and dissatisfaction with the level of concern they perceivedwas shown to them by their physician.14 An ongoing study that focuses on enhancing theinterpersonal relationship between physicians and patients in an effort to improve patientadherence and BP control may specifically elucidate the aspects of the relationship that aremost important in improving patient outcomes.16 Similarly, we need to more fullyunderstand what factors contribute to patients viewing health care appointments as stressful.Answers to these questions will inform the type of intervention needed to improvemedication adherence.
LimitationsThe present study is not without limitations. Our assessment of medication-taking behaviorrelies on self-report. While this method has its limitations, all measures of adherence (eg,medication event monitoring systems, pill count, biological assays, prescription refills) havetheir respective strengths and limitations.17 Self-report provides an inexpensive andrelatively straightforward method of obtaining information regarding medication-takingbehavior barriers and could stimulate discussions with physicians during clinical visits. Infact, physician recognition of patient-related barriers to medication adherence is animportant physician role.18 Moreover, studies suggest that self-report is associated withimportant outcomes. For example, in one study, a single question, “In the past month, howoften did you take your medications as the doctor prescribed,” with response choices similarto the ones used in the present study, predicted future cardiovascular events.19 Finally, the
Martin et al. Page 5
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

concern with self-report medication measures is that they may overestimate the degree ofadherence. Our findings, however, are in line with the findings of a study using the Moriskyscale, and, in fact, 55% were classified as nonadherent in their study while 60% receivedthat designation in our study.8 Nonetheless, researchers should consider additional self-report assessment tools that were developed with careful attention to the principles of testdevelopment and psychometric analysis.20
CONCLUSIONSIn our study of low-income, rural, primarily African American hypertensive adults, severalimportant practice implications emerge. First, health care providers should routinely explorebarriers to medication adherence, including reasons that are primarily logistical oremotional. Second, creating clinical encounters and clinical environments that minimize thestressful aspect of appointments and is conducive to patients having information needs met(eg, asking questions) may impact medication adherence and ultimately patient outcomes.Probably the most interesting finding in our study was, despite the fact that almost allpatients believed their providers cared about them as individuals and found it easy to talkwith their providers, almost 70% were uncomfortable asking questions. Simple interventionsthat ensure that clinic visits include allocating time in the appointment for patient questionsmay be helpful. A low-cost intervention that may improve hypertension management mayinvolve the use of question prompt sheets designed to ensure that patients have theirinformational needs met during the clinical encounter. These prompt sheets are beingdesigned and evaluated in other chronic disease populations.21,22 Finally, in our study,adherent and nonadherent hypertensive adults were similar with regard to socioeconomicstatus, perceived health, education, and other sociodemographic indicators. As we strive toimprove clinical outcomes for all patients, we should also take the time to acknowledgepatients who successfully manage their medication-taking behavior and high BP in spite ofdifficult life circumstances. Oftentimes the answer to pressing public health problems lieswith those most affected by the disease.
AcknowledgmentsAcknowledgements and disclosures: The authors would like to thank Diane Williams for assistance in formattingthe manuscript; Drs Karen Matthews, Keith Whitfield, and Lloyd Edwards for serving as our data, safety, andmonitoring committee; and Dr Dale Williams for his many contributions. Funding was provided by the NationalHeart Lung and Blood Institute (RO1 HL 69375).
References1. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics – 2009 update: a
report from the American Heart Association Statistics Committee and Stroke StatisticsSubcommittee. Circulation. 2009; 119:480–486. [PubMed: 19171871]
2. Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertensionamong United States adults 1999–2004. Hypertension. 2007; 49:69–75. [PubMed: 17159087]
3. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee onPrevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA.2003; 289:2560–2572. [PubMed: 12748199]
4. Ogedegbe G, Harrison M, Robbins L, et al. Barriers and facilitators of medication adherence inhypertensive African Americans: a qualitative study. Ethn Dis. 2004; 14:3–12. [PubMed:15002917]
5. Turner BJ, Hollenbeak C, Weiner MG, et al. Barriers to adherence and hypertension control in aracially diverse representative sample of elderly primary care patients. Pharmacoepidemiol DrugSaf. 2009; 18:672–681. [PubMed: 19479901]
Martin et al. Page 6
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

6. Svensson S, Kjellgren KI, Ahlner J, et al. Reasons for adherence with antihypertensive medication.Int J Cardiol. 2000; 3:157–163. [PubMed: 11104870]
7. Hyre AD, Krousel-Wood MA, Muntner P, et al. Prevalence and predictors of poor antihypertensivemedication adherence in an urban health clinic setting. J Clin Hypertens (Greenwich). 2007; 9:179–186. [PubMed: 17344769]
8. Schoenthaler A, Chaplin WF, Allegrante JP, et al. Provider communication effects medicationadherence in hypertensive African Americans. Patient Educ Couns. 2009; 75:185–191. [PubMed:19013740]
9. Perry HM, Roccella EJ. Conference report on stroke mortality in the southeastern United States.Hypertension. 1998; 31:1206–1215. [PubMed: 9622131]
10. Liao Y, Greenlund KJ, Croft JB, et al. Factors explaining excess stroke prevalence in the USStroke Belt. Stroke. 2009; 40:3336–3341. [PubMed: 19679841]
11. Wang PS, Bohn RL, Knight E, et al. Noncompliance with antihypertensive medications: the impactof depressive symptoms and psychosocial factors. J Gen Intern Med. 2002; 17:504–511. [PubMed:12133140]
12. Andresen EM, Malmgren JA, Carter WB, et al. Screening for depression in well older adults:evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). AmJ Prev Med. 1994; 10:77–84. [PubMed: 8037935]
13. Ware, JE.; Kosinski, M. How to Score Version 2 of the SF-12 Health Survey. Lincoln, RI:QualityMetric, Inc; 2005.
14. Wroth TH, Pathman DE. Primary medication adherence in a rural population: the role of thepatient-physician relationship and satisfaction with care. J Am Board Fam Med. 2006; 19:478–486. [PubMed: 16951297]
15. Haynes RB, Yao X, Degani A, et al. Interventions to enhance medication adherence. CochraneDatabase Syst Rev. 2005; 4:CD000011. [PubMed: 16235271]
16. Cooper LA, Roter DL, Bone LR, et al. A randomized controlled trial of interventions to enhancepatient-physician partnership, patient adherence and high blood pressure control among ethnicminorities and poor persons: study protocol NCT00123045. Implement Sci. 2009; 4:7. [PubMed:19228414]
17. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005; 353:487–497. [PubMed:16079372]
18. Harmon G, Lefante J, Krousel-Wood M. Overcoming barriers: the role of providers in improvingpatient adherence to antihypertensive medications. Curr Opin Cardiol. 2006; 21:310–315.[PubMed: 16755199]
19. Gehi AK, Ali S, Na B, et al. Self-reported medication adherence and cardiovascular events inpatients with stable coronary heart disease: the heart and soul study. Arch Intern Med. 2007;167:1798–1803. [PubMed: 17846400]
20. Morisky DE, Ang A, Krousel-Wood M, et al. Predictive validity of a medication adherencemeasure in an outpatient setting. J Clin Hypertens (Greenwich). 2008; 10:348–354. [PubMed:18453793]
21. Glynne-Jones R, Ostler P, Lumley-Graybow S, et al. Can I look at my list? An evaluation of a‘prompt sheet’ within an oncology outpatient clinic. Clin Oncol (R Coll Radiol). 2006; 18:395–400. [PubMed: 16817331]
22. Hebert RS, Schulz R, Copeland VC, et al. Pilot testing of a question prompt sheet to encouragefamily caregivers of cancer patients and physicians to discuss end-of-life issues. Am J Hosp PalliatCare. 2009; 26:24–32. [PubMed: 18843134]
Martin et al. Page 7
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 8
Tabl
e I
Bas
elin
e So
ciod
emog
raph
ic a
nd C
linic
al C
hara
cter
istic
s of H
AR
P St
udy
Parti
cipa
nts i
n W
ilcox
and
Low
ndes
Cou
nty,
Ala
bam
a
Var
iabl
e
Tot
al S
ampl
e (N
=434
)A
dher
ent (
N=1
73)
Non
adhe
rent
(N=2
61)
P V
alue
Freq
uenc
y%
Freq
uenc
y%
Freq
uenc
y%
Mar
ital s
tatu
s
M
arrie
d/pa
rtner
152
35.0
5934
.193
35.6
.74
Sex
Fe
mal
e29
367
.511
465
.917
968
.6.5
6
Educ
atio
n
<H
igh
scho
ol21
950
.584
48.6
135
51.7
.58
=H
igh
scho
ol16
337
.670
40.5
9335
.6
>H
igh
scho
ol52
12.0
1911
.033
12.6
Inco
me,
$
<1
5,00
035
581
.814
181
.521
482
.0.9
0
Empl
oym
ent
Em
ploy
ed11
225
.842
24.3
7026
.8.1
8
U
nem
ploy
ed11
927
.441
23.7
7829
.9
O
ther
203
46.8
9052
.011
343
.3
Sour
ce o
f car
e
A
DPH
297
68.4
124
71.7
173
66.3
.24
FQ
HC
137
31.6
4928
.388
33.7
Hea
lth st
atus
Ex
celle
nt/v
ery
good
4510
.424
13.9
218.
0.1
5
G
ood
170
39.2
6437
106
40.6
Fa
ir/po
or21
950
.585
49.1
134
51.3
Dep
ress
ive
sym
ptom
s
≥
10 sc
ore
229
52.8
7845
.115
157
.9.0
09
Blo
od p
ress
ure,
mm
Hg
Sy
stol
ic13
6±17
.113
3±15
.813
8±17
.6.0
02
D
iast
olic
82±1
0.7
80±9
.883
±11
.003
Abb
revi
atio
ns: A
DPH
, Ala
bam
a D
epar
tmen
t of P
ublic
Hea
lth; F
QH
C, F
eder
ally
Qua
lifie
d H
ealth
Cen
ter;
HA
RP,
Hyp
erte
nsio
n an
d A
dher
ence
in R
ural
Pra
ctic
e
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 9
Table II
Frequency by Which Patients Take Less Than the Prescribed Dose of Medication Across Situationsa
How often do you take less than the prescribed amount of blood pressure medicine because…
Never, No. (%)Some of the Time, No.
(%)Most of the Time,
No. (%)All of the Time, No.(%)
Feeling depressed or low 383 (88.2) 33 (7.6) 2 (0.5) 15 (3.5)
You are tired 376 (86.6) 37 (8.5) 7 (1.6) 13 (3.0)
You don’t need it 375 (86.4) 40 (9.2) 1 (0.2) 17 (3.9)
You feel better 329 (75.8) 71 (16.4) 12 (2.8) 21 (4.8)
Bothered by side effects 308 (71.0) 97 (22.4) 9 (2.1) 17 (3.9)
Your blood pressure is controlled 367 (84.6) 43 (9.9) 3 (0.7) 19 (4.4)
You are sick 365 (84.1) 41 (9.4) 3 (0.7) 23 (5.3)
A change in your daily routine 311 (71.7) 93 (21.4) 8 (1.8) 16 (3.7)
You run out of medicine 281 (64.7) 128 (29.5) 11 (2.5) 12 (2.8)
You don’t have blood pressure medicinewith you when it is time to take a dose
276 (63.6) 135 (31.1) 9 (2.1) 13 (3.0)
aResponses of “Don’t know” (n=6) are not shown.
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 10
Table III
Frequency of Barriers to Medication Adherencea
How often …
Never, No. (%)Some of the Time,
No. (%)Most of the
Time, No. (%)All of the Time,
No. (%)
Do you forget to take a dose of your blood pressuremedicine?
276 (63.6) 144 (33.2) 6 (1.4) 7 (1.6)
Are you too busy to take your blood pressure medicines? 368 (84.8) 56 (12.9) 2 (0.5) 7 (1.6)
Is it difficult to take your blood pressure at about the sametime every day?
205 (47.2) 177 (40.8) 23 (5.3) 28 (6.5)
Is it hard to get to the clinic or drug store to fill yourprescription?
286 (65.9) 114 (26.3) 15 (3.5) 17 (3.9)
aResponses of “Don’t know” (n=2) are not shown.
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 11
Table IV
Patient-Provider Relationships: Affirmative Responses From Participants
Percentagea
Do you find it easy to talk with your health care provider? 97
Do you feel that your healthcare provider cares about you as a person? 97
Do you find it hard to understand instructions about how to take your blood pressure medicine? 7
Do you get as much information as you want about your high blood pressure from your health care provider? 85
Do you feel uncomfortable asking your health care provider questions about your health? 70
Has your health care provider ever told you about the side effects your blood pressure medicine may have? 63
Has your health care provider ever explained what to do if you’re bothered by side effects of your blood pressure medicine? 50
In general, do you feel that health care appointments are stressful? 21
aPercentage of participants responding “Yes” to the question.
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 12
Tabl
e V
Patie
nt-P
rovi
der Q
uest
ions
End
orse
d by
Med
icat
ion
Adh
eren
t vs N
onad
here
nt In
divi
dual
s
Adh
eren
t (N
=173
)N
onad
here
nt (N
=261
)
P V
alue
Freq
uenc
y%
Freq
uenc
y%
Do
you
get a
s muc
h in
form
atio
n as
you
wan
t abo
ut y
our h
igh
bloo
d pr
essu
re fr
om y
our h
ealth
car
e pr
ovid
er?
152
87.9
218
84.5
.33
Do
you
feel
unc
omfo
rtabl
e as
king
you
r hea
lth c
are
prov
ider
que
stio
ns a
bout
you
r hea
lth?
109
63.0
192
73.9
.02
Has
you
r hea
lth c
are
prov
ider
eve
r tol
d yo
u ab
out t
he si
de e
ffec
ts y
our b
lood
pre
ssur
e m
edic
ine
may
hav
e?11
266
.716
162
.0.3
4
Has
you
r hea
lth c
are
prov
ider
eve
r exp
lain
ed w
hat t
o do
if y
ou’r
e bo
ther
ed b
y si
de e
ffec
ts o
f you
r blo
od p
ress
ure
med
icin
e?88
51.4
131
52.7
.79
In g
ener
al, d
o yo
u fe
el th
at h
ealth
car
e ap
poin
tmen
ts a
re st
ress
ful?
2816
.265
25.4
.02
J Clin Hypertens (Greenwich). Author manuscript; available in PMC 2011 December 16.




















