Expectations and Perceptions of Healthcare Professionals for ...

Cogniţie, Creier, Comportament / Cognition, Brain, Behavior
Copyright © 2012Romanian Association for Cognitive Science. All rights reserved.
ISSN: 1224-8398 Volume X, No. 3 (September), 423-452
SYSTEMATIC REVIEW OF BURNOUT RISK
FACTORS AMONG EUROPEAN HEALTHCARE
PROFESSIONALS
Mara BRIA* 1 , Adriana BĂBAN 1 , Dan L. DUMITRAŞCU 2
1Department of Psychology, Babeş-Bolyai University, Cluj-Napoca, Romania
2University of Medicine and Pharmacy “Iuliu Haţieganu”, Cluj-Napoca,
Romania
ABSTRACT
Healthcare professionals‟ burnout is a response to the prolonged
exposure to occupational stress and affects negatively both the employee
and the organization. The aim of the present review is to discuss the
relevant burnout risk factors for European healthcare professionals
working in hospitals and clinics. A systematic search of articles
published between January 2000 and December 2011 was conducted in
several databases (ISI Web of Knowledge, PsychArticles, SagePub,
PubMed and Cochrane database of systematic reviews). After the
analysis of the 4335 articles found, 53 met the inclusion criteria and were
included in the review. Results confirm the main role of occupational and
organizational risk factors while pointing out that psychosocial factors
have a small yet statistically significant influence on burnout
development. Socio-demographic factors, although included in the
majority of studies, seem to have little impact on burnout. In conclusion,
the review pointed out that although the healthcare systems across
Europe are fundamentally different, healthcare professionals present
similar risk factors concerning burnout.
KEYWORDS: burnout, risk factors, healthcare professionals, systematic review
Healthcare professionals are frequently exposed to occupational
stress, especially due to overwhelming emotional and interpersonal
* Corresponding author:
E-mail: [email protected]
interactions. This kind of long term job strain can lead to burnout symptoms
such as emotional exhaustion, depersonalization, and reduced professional
efficacy (Maslach, Schaufeli, & Leiter, 2001), and may have negative
consequences for both the individual and the organization. Burnout among
healthcare professionals has often been associated with depression (Ahola &
Hakanen, 2007), insomnia (Vela-Bueno et. al., 2008), or alcohol abuse
(Moustou, Montgomery, Panagopoulou, & Benos, 2010). Professional stress
affects doctors‟ and nurses‟ health. Studies indicate that professional stress
is associated with inflammatory markers among physicians (Poantă,
Crăciun, & Dumitraşcu, 2010) or with increased risk of cardiovascular
diseases (Melamed, Shirom, Toker, Berliner, & Shapira, 2006). Burnout
also jeopardizes organizational performance in medical settings. Healthcare
professionals‟ burnout has been related to low performance (Keijsers,
Schaufeli, Le Blanc, Zwerts, & Miranda, 1995), high turnover intentions
(Leiter & Maslach, 2009), suboptimal care (Shanafelt, Bradley, Wipf, &
Black, 2002), and medical errors.
A recent survey shows that high levels of burnout are strongly
correlated with major medical errors among American surgeons. Burnout
was demonstrated to be an independent predictor of reporting medical
errors, even when controlling for occupational factors like the number of
overnight shifts, compensation practices, or number of working hours. More
than 70% of them blamed the individual factors, and not the organization or
the medical system factors (Shanafelt, et. al., 2010). The relationship
between burnout and perceived medical errors is even stronger among
residents. According to a longitudinal study conducted among junior
doctors, all three dimensions of burnout, exhaustion, depersonalization, and
reduced professional efficacy are strong predictors of perceived medical
error rates reported three months later (West et al., 2006). In a meta-analysis
on the link between burnout and objective performance, Taris (2006)
concludes that emotional exhaustion and depersonalization have a stronger
impact on reporting medical errors than on personal accomplishment.
Similar results were reported by Prins et al. (2009) in a study conducted
among Dutch residents from different specialties. The study also shows that
perceived errors due to lack of time are more strongly linked to burnout than
perceived errors due to inexperience or errors in judgment.
The literature has systematically linked workload to burnout (Lee &
Ashforth, 1996) and medical errors. Studies have highlighted that extended
work shifts expose medical professionals to burnout (Iskera-Golec, Folkard,
& Morek, 1996) and serious medical errors (Rogers, Hwang, Scott, Aiken,
& Dinges, 2004). Motivated by the desire to reduce medical errors, the
Accreditation Council for Graduate Medical Education limited in 2003 the
working hours for American junior doctors to 80 hours a week (ACGME,
2003). Studies confirm the positive impact of these regulations. Residents
were more likely to be involved in serious medical errors when they worked
24-hour shifts while the number of errors was reduced by 36% under the
new regulations (Landrigan et. al., 2004).
Since 1993, similar, but more restrictive, regulations were imposed
by the European Commission through the European Working Time
Directive (93/104/EC). The intention was to improve patient and doctor-
safety by limiting progressively the maximum weekly work hours of junior
doctors to 56 since 2003 and to 48 since 2009 (2003/88/EC). Studies
confirm the efficiency of European Working Time Directive (EWTD) for
doctors in training. Tucker and collaborators‟ study (2010) highlight that
designing work schedules according to EWTD reduces doctors‟ fatigue and
work – life interference. The main concerns about the implementation of
EWTD were that they will be detrimental to the training of junior doctors
and to the continuity of care for patients (Paice & Reid, 2004). Although
there are no studies to confirm the reduced educational opportunities of
junior doctors when working according to the EWTD, studies prove that
working 48 hours a week does not affect patient safety (Cappuccio,
Bakewell, Taggart, Ward, Ji, & Sullivan, 2009).
Negative consequences of burnout on both the employee and the
organization call for preventive measures in order to reduce the impact of
the risk factors. Burnout prevention strategies, either addressing to the
general working population (primary prevention) or the occupational groups
which are more vulnerable (secondary prevention), are focused on reducing
the impact of risk factors. Reviews of healthcare professionals‟ burnout
focusing on identifying risk factors have been conducted previously. For
example, Prins and collaborators‟ review (2007) focused on correlates of
burnout among junior doctors, while other reviews focused on specific
medical specialties, like palliative care (Carvalho, Pereira, & Fonseca,
2011), mental health workforce (Paris & Hoge, 2009), community mental
health nursing (Edwards, Burnard, Coyle, Fothergill, & Hannigan, 2000),
and cancer professionals (Trufelli et al., 2008).
There are many studies about burnout risk factors among samples of
European nurses (Hansen, Sverke, & Naswall, 2008; Kowalski et al., 2010)
and doctors (Graham, Potts, & Ramirez, 2002; Visser, Smets, Oort, & de
Haes, 2003) regardless of their medical specialties. Overview of research
studies among other professional roles, such as European teachers‟ stress
and burnout has been conducted previously (Rudow, 1999). But there are no

studies which integrates studies about burnout risk factors among European
healthcare professionals.
The objective of the present review is to discuss the relevant burnout
risk factors for European healthcare professionals which share the same
work setting. To our knowledge, this is the first study which gathers studies
of burnout risk factors among healthcare professionals working in European
hospitals, regardless of their specialty or professional role.
METHODS
A systematic search of articles published between January 2000 and
December 2011 was conducted in several databases (ISI Web of
Knowledge, PsychArticles, SagePub, PubMed and Cochrane database of
systematic reviews) and in the reference lists of all selected journals. The
focus was to identify peer reviewed journal articles which studied the risk
factors of burnout in samples of European healthcare professionals working
in hospitals. The search terms used were “burnout” along with each of the
following: “risk factors”, “predictors”, “causes”, “antecedents”, “medical
professionals”, “doctors”, “residents”, and “nurses”, respectively. A total
of 4343 abstracts resulted. After removing all the duplicates 4262 abstracts
were analyzed according with the inclusion/exclusion criteria described
below. When a decision could not be made based on the abstract analysis,
the full text article was reviewed when available. One hundred and sixty
nine full text articles were screened and in the end 53 articles matched all
the inclusion criteria. The article selection steps are presented in Figure 1
and Table 1 offers a summary of the articles included in the review.
The selected studies had to meet several criteria in order to be
included in the analysis. Research articles which operationalized a measure
of burnout or burnout dimensions were discussed. Studies had to include: 1)
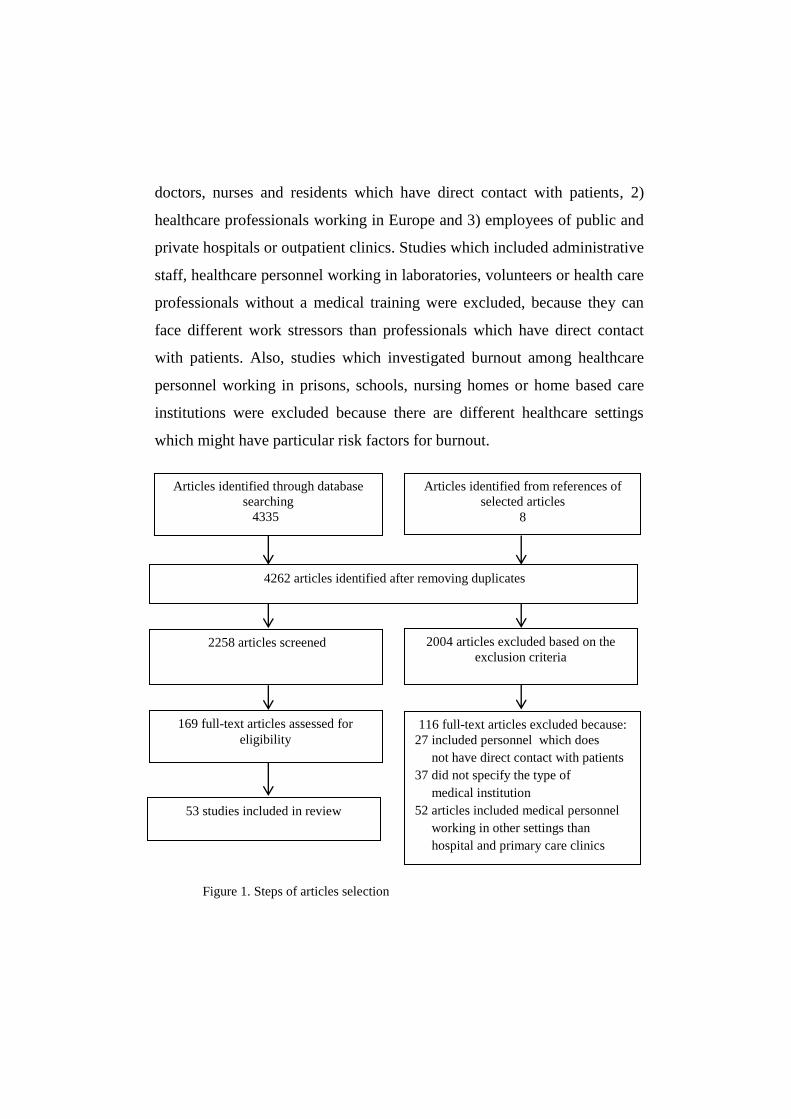
doctors, nurses and residents which have direct contact with patients, 2)
healthcare professionals working in Europe and 3) employees of public and
private hospitals or outpatient clinics. Studies which included administrative
staff, healthcare personnel working in laboratories, volunteers or health care
professionals without a medical training were excluded, because they can
face different work stressors than professionals which have direct contact
with patients. Also, studies which investigated burnout among healthcare
personnel working in prisons, schools, nursing homes or home based care
institutions were excluded because there are different healthcare settings
which might have particular risk factors for burnout.
Figure 1. Steps of articles selection
Articles identified through database
searching
4335
Articles identified from references of
selected articles
8
4262 articles identified after removing duplicates
2258 articles screened
2004 articles excluded based on the
exclusion criteria
169 full-text articles assessed for
eligibility 116 full-text articles excluded because:
27 included personnel which does
not have direct contact with patients
37 did not specify the type of
medical institution
52 articles included medical personnel
working in other settings than
hospital and primary care clinics
53 studies included in review
RESULTS
The majority of studies included in the review adopted a cross-
sectional design and only three studies opted for a longitudinal design. This
suggests that the majority of the European studies on burnout are focused
more on describing than on explaining this phenomenon. Maslach Burnout
Inventory was the most commonly used instrument, although there are
many instruments designed for the evaluation of burnout (e.g., Oldenburg
Burnout Inventory, the Burnout Measure, Shirom-Melamed Burnout
Questionnaire, etc.). From these articles, 47 opted for Maslach Burnout
Inventory – Human Services Survey (MBI-HSS) and included all three
subscales in their research, while 6 applied only the emotional exhaustion
scale and 3 applied both emotional exhaustion and depersonalization scales.
More than half of the studies addressed healthcare professionals
working in West European countries, followed by countries from the
Central and Eastern Europe and by the North European countries,
respectively. The majority of researches included only nurses, while about
one fifth of them addressed nurses and doctors together or only doctors and
residents.
Socio-demographic factors
The majority of the studies analyzed the role of socio-demographic
variables in burnout development, e.g. country, medical specialty, hospital
type, gender, age, or marital status.
Although burnout rates seem to vary from country to country, about
one third of the participants from the studies included in the review scored
high on the burnout scales. Healthcare professionals from South - Eastern
Europe shared the highest burnout rates. Almost half of the Serbian primary

healthcare physicians (49% of women and 41% of men) and more than one
third of Greek orthopedic nurses (38, 3 %) had high emotional exhaustion
scores (Kiekkas, Spyratos, Lampa, Aretha, & Sakellaropoulos, 2010; Putnik
& Houkes, 2011). Studies from the Scandinavian countries suggested that
healthcare professionals are most protected from burnout, as they reported
the lowest burnout rates: only 25% of Swedish nurses obtained high
exhaustion and 6, 9% scored high for depersonalization (Glasberg, Eriksson,
& Norberg, 2007; Gunnarsdottir, Clarke, Rafferty, & Nutbeam, 2009).
These results are descriptive as few studies compared if burnout
differences across countries were statistically significant. One study for
example compared burnout levels between Italian and Dutch healthcare
professionals and concluded that Italian healthcare professionals
experienced higher burnout scores (Pisanti, van der Doef, Maes, Lazzari, &
Bertini, 2011). The authors explained those differences as a consequence of
unfavorable job characteristics, like high work and time pressure or high
physical demands.
Studies comparing burnout among specialties converged on the
conclusion that healthcare professionals working in surgical areas had a
higher risk of developing burnout than other medical specialties (Upton et
al., 2012). Oncology personnel are more exposed to burnout in comparison
to other medical specialists. Ksiazek and colleagues‟ study (2011)
concluded that Polish surgical oncology nurses experienced higher burnout
rates compared with general surgery nurses, while another study showed
that burnout was more frequent among Italian oncology physicians and
nurses than among healthcare professionals working with AIDS patients
(Dorz, Novara, Sica, & Sanavio, 2003). Still, a research among UK
colorectal healthcare professionals brought interesting results and pointed
out that burnout was unrelated with cancer workload (Sharma, Sharp,
Walker, & Monson, 2007). Looking at healthcare staff, a study pointed out
that Italian dermatology nurses had a lower risk for burnout development
than nurses working in general hospitals (Renzi, Tabolli, Ianni, Pietro, &
Puddu, 2005).
Studies focused on identifying if burnout scores varied among
different hospital types offer divergent results: two Turkish studies found
higher burnout rates among healthcare professionals working in public
hospitals (Demir, Ulusoy, & Ulusoy, 2003; Ersoy-Kart, 2009) while a
Finnish study concluded that nurses working in the university hospital
experienced slightly higher burnout rates than those working in public
hospital (Koivula, Paunonen, & Laippala, 2000). Two other studies
analyzed burnout rates from private and public hospitals and found also
divergent results. One study indicated that Swedish nurses from private
hospitals experienced significantly higher burnout levels than nurses in
public hospitals (Hansen, Sverke, & Naswall, 2009), while another study
indicated that Turkish physicians working in private hospitals experienced
the lowest burnout rates, compared to public hospitals (Ozyurt, Hayran, &
Sur, 2006). Those differences may be explained by particularities of the
medical systems of each country and not by hospital type.
Although some studies suggested that women tend to report higher
emotional exhaustion scores (Chiron, Michinov, & Olivier-Chiron, 2010),
while men tend to report higher depersonalization (Klersy et al., 2007) and
personal accomplishment scores (Grassi & Magnani, 2000), the majority of
studies concluded that gender does not influence burnout development,
neither among UK doctors (Sharma, Sharp, Walker, & Monson, 2008), nor
Spanish residents (Castelo-Branco et al., 2006) or Spanish and UK nurses
(Garrosa, Moreno-Jimenez, Rodrigues-Munoz, & Rodiguez-Carvajal, 2011;
Losa Iglesias, de Bengoa Vallejo, & Paloma Salvadores Fuentes, 2010;
Sundin, Hochwalder, Bildt, & Lisspers, 2007).
The majority of studies investigating the relationship between
burnout and age of healthcare professionals included age as a control
variable. Results of those studies are inconclusive, as half of them found no
burnout differences comparing young and senior healthcare professionals
and the other half found higher depersonalization rates among young
healthcare professionals (e.g., Castelo-Branco et al., 2006; Sharma et al.,
2008).
Marital status and burnout seems unrelated, as studies do not offer
congruent results. Seven studies underlined that having a partner is a
protective factor (e.g., Alacacioglu, Yavuzsen, Dirioz, Oztop, & Yilmaz,
2009) while another seven studies found no differences in burnout scores
based on the marital status of participants (e.g., Panagopoulou,
Montgomery, & Benos, 2006).
Psychosocial factors
Studies investigating the role of psychosocial factors in burnout
development offered a more coherent picture than the demographical factors
and highlighted that stress, personality variables, and coping mechanisms all
favor burnout development.
About a quarter of the studies included in the review supported the
hypothesis that stress is an important predictor of burnout. While the cross-
sectional studies concluded that stress is associated with the development of
burnout (Ahola & Hakanen, 2007; Hudek-Knezevic, Maglica, & Krapic,
2011; Sharma et al., 2007; Sharma et al., 2008), results of a longitudinal
study (McManus, Winder, & Gordon, 2002) brought evidence about the
causality of this relationship. Physicians‟ stress and burnout were measured
at three year interval and the results pointed out that there is a reciprocal
causality relationship between stress and burnout, meaning that higher stress
levels cause higher burnout and higher burnout increases stress.
Studies associated different coping mechanisms with burnout and
highlighted that healthcare professionals who experience burnout use more
emotion focused coping (e.g., substance misuse, unhealthy eating habits) or
defensive coping strategies (e.g., isolating from friends and family, denying
the problem or the use of humor) (Demir et al., 2003; Sharma et al., 2007;
Sharma et al., 2008). For example, a study among Italian HIV/AIDS and
oncology health care workers revealed that denying the problem predicted
lower personal accomplishment while using humor as a coping strategy
explained higher emotional exhaustion (Dorz et al., 2010).
Personality variables like extraversion, optimism and neuroticism
seemed to be significant but weak burnout predictors, especially for
personal accomplishment dimension (Buhler & Land, 2003; Hudek-
Knezevic et al., 2011). Hardiness as personality characteristic predicted all
burnout dimensions, according to a study among a sample of Spanish nurses
(Garrosa et al., 2011).
Occupational factors
High workload, emotional demands, work – family interference and
role stress proved to be the most relevant occupational risk factors for
burnout.
Workload was one of the most studied occupational factors in
relation to burnout defined either as quantitative demands (number of

working hours, of shifts or of attended patients) or as perceived workload.
The studies included in the present review indicated that the number of
working hours or shifts per month contribute to burnout development.
Greek residents, for example experienced higher depersonalization as
working hours increased (Panagopoulou et. al., 2006), while another study
indicated that emotional exhaustion in a sample of Italian dialysis healthcare
professionals was affected by the number of working hours (Klersy et al.,
2007). The more shifts in a month the higher the probability to experience
emotional exhaustion, depersonalization, and lower personal
accomplishment, according to a study among Turkish physicians (Ozyurt et
al., 2006). Nurses were also affected by the weekly work duration and shifts
(Ilhan, Durukan, Taner, Maral, & Bumin, 2007). Number of patient
interactions per day proved to be a strong predictor for all burnout
dimensions only among Spanish junior doctors (Castelo-Branco, et al.,
2006). This relationship was not validated among Spanish nurses (Garrosa
et al., 2011).
Perceived workload might be a stronger burnout predictor than
objective quantitative demands. Studies included in the review offered
results to support the direct relationship between perceived high workload
and burnout in nurses (Hansen et al., 2009; Kiekkas et al., 2010; Tummers,
Janssen, Landeweerd, & Houkes, 2001; Tummers, Landeweerd, & van
Merode, 2002), doctors (Panagopoulou et al., 2006), and both nurses and
doctors (Leiter, Gascon, & Martinez-Jarreta, 2010). Panagopoulou and
collaborators‟ study (2005) underlined that the evaluation of one's work is
what counts most. The study highlighted that perceived workload predicted
burnout after controlling the number of working hours.
Emotional job demands represent emotionally overtaxing job
situations like dealing with social cases, aggressive patients or facing death.
Although only a few studies tested the role of emotional demands in burnout
development, the results were congruent and supported its predictive role.
Studies pointed out that having demanding patients increased emotional
exhaustion (Escriba-Aguir & Martin-Baena, 2006) and decreased personal
accomplishment (Bressi et al., 2008). A study among Swedish nurses
concluded that emotional demands were a strong predictor for all burnout
dimensions (Sundin et al., 2007).
Emotion work is a type of emotional job demands specific to
professions in which the interpersonal dimension is especially important,
like health, sales or teaching. Usually, healthcare staff is encouraged to
inhibit both the experience and the expression of feelings in relations to
their patients but in the long run this proved to be detrimental to their well-
being (Zapf, 2002). One study from those included in the review brought
strong evidence for the role of emotion work in burnout development
among a sample of Greek residents and specialists. More precisely, emotion
work predicted emotional exhaustion among residents and depersonalization
among specialists (Panagopoulou et al., 2006).
Although work-home interference was present in only some of the
studies from the current review, results pointed out that having difficulties
balancing professional role with personal life fueled burnout development
(Sharma et al., 2007; Sharma et al., 2008; Verdon, Merlani, Perneger, &
Ricou, 2008). Some studies highlighted that work – family interference was
not only a predictor for burnout but that it also mediated the relationship
between job demands and burnout (Panagopolou et al., 2006).

Role conflict and role ambiguity proved their predictive role for
burnout. Some cross-sectional studies showed that while role ambiguity
seems to account for all burnout dimensions among Turkish healthcare
professionals (Tunc & Kutanis, 2009) role conflict was related only to
emotional exhaustion and depersonalization (Hansen et al., 2009; Tummers
et al., 2002). Nurses seemed to experience higher levels of role conflict and
role ambiguity compared to physicians, at least according to a Turkish study
(Tunc & Kutanis, 2009).
Organizational factors
Perceived job control, values incongruence, organizational justice,
social support at work, effort-reward imbalance, perceived burnout
complaints among colleagues and hospital organizational characteristics
were all confirmed as burnout risk factors by the studies included in the
present review.
Perceived job control has gained attention as a burnout risk factor
mainly through the Demand – Control model (Karasek, 1979; Karasek &
Theorell, 1990), which promoted the concept as a key work stressor. Studies
stressed that perceived control was both a proximal risk factor (Escriba-
Aguir & Perez-Hoyos, 2007; Hansen et al., 2009; Pisanti et al., 2011;
Sundin et al., 2007) or a distal burnout risk factor (Hochwalder, 2007;
Tummers et al., 2002). Leiter and collaborators‟ study (2010) brought
evidence to support the pivotal role of perceived job control in employees‟
work experience. More precisely, the results of their study among a sample
of Spanish healthcare professionals pointed out that perceived job control is
directly related to work characteristics like supervision, workload and
fairness and indirectly to all three burnout dimensions. Research also
highlighted that perceived values incongruence was another significant
proximal risk factor for all burnout dimensions, while perceived
organizational justice contributed to burnout indirectly, through perceived
values. The research confirmed the mediation model of job burnout (Leiter
& Maslach, 2005; Maslach & Leiter, 1997) which conceptualized burnout
as a consequence of the incongruence between the employee and
organization in major aspects like values, communication or fairness.
The hypothesis of effort – reward imbalance model (Siegrist, 1996),
according to which burnout is a consequence of the disproportion between
sustained effort (extrinsic job demands and intrinsic motivation to meet
those job demands) and rewards received (like salary, career opportunities,
etc.) was confirmed by one study of the present review. The research
pointed out that effort – reward imbalance was predictive for high emotional
exhaustion and depersonalization but not for personal accomplishment
among a sample of German healthcare professionals (Bakker, Killmer,
Siegrist, & Schaufeli, 2000).
One of the organizational factors that studies have systematically
linked to the development of burnout was low social support at work, both
from colleagues and supervisors. Studies pointed out that low social support
from colleagues was associated especially with higher emotional exhaustion
among doctors (Tummers et al., 2001), nurses (Hochwalder, 2007; Jenkins
& Elliott, 2004; Sundin et al., 2007), and both doctors and nurses (Escriba-
Aguir et al., 2006).
While supervisors‟ support proved to predict burnout among
healthcare professionals (Pisanti et al., 2011, Prins et al., 2007), some
studies could not find any relationship between the two variables (Hansen et
al., 2009). Leadership style seemed to favor burnout development, as one
study suggested that transactional leadership predisposed Belgian nurses to
burnout (Stordeur, D‟hoore, & Vandenberghe, 2001).
Bakker and collaborators (2005) offered an interesting perspective
showing that organizational social factors explain burnout development
more than occupational factors. Results of their study demonstrated that
burnout was more frequent among members of the same team work. As
burnout was shared by the members of the same team work the authors
concluded that it was somehow “contagious”. Their results pointed out that
perceived burnout complaints among colleagues was the most important
predictor for higher emotional exhaustion and depersonalization, even after
controlling the impact of the occupational factors like job demands and
decision latitude.
There are also studies which highlight the role of hospital
organizational characteristics such as hospital management or nurse staffing
in burnout development. Emotional exhaustion among nurses was affected
by doctor-nurse relationship, hospital management and organizational
support, while personal accomplishment was explained only by the latter
(Van Bogaert, Meulemans, Clarke, Vermeyen, & Van de Heyning, 2009).
Nurse staffing also favored burnout development, as studies concluded that
nurses working in Icelandic and UK hospitals with the heaviest nurse-
patient ratio were more likely to experience higher emotional exhaustion
(Gunnarsdottir et al., 2009; Rafferty et al., 2007).
DISCUSSIONS
Burnout affects diverse professional categories, such as teachers
(Simbula, Guglielmi & Schaufeli, 2011), police officers (Martinussen,
Richardsen, & Burke, 2007), software developers (Singh, Suar, & Leiter,
2011), coaches (Hjalm, Kentta, Hassmenan, & Gustafsson, 2007) or lawyers
(Tsai, Huang, & Chang, 2009). Still, burnout is the most studied among
healthcare professionals. Early research suggested that healthcare
professionals report higher burnout rates than other occupations. Recent
studies provide information according to which there are rather different
burnout patterns than occupational differences. For example, a study which
compared burnout scores among five professional categories (teaching,
social services, medicine, mental health and police officers) from United
States and The Netherlands found no major differences in burnout levels
(Schaufeli & Enzmann, 1998). Still, different burnout patterns have been
identified: emotional exhaustion was higher among teachers and lower
among healthcare professionals, while cynicism seems higher among police
officers and lower among American mental health workers. Studies do
report however burnout differences among countries, suggesting that
burnout is more prevalent among North American employees than among
European (Schaufeli & Buunk, 2003). Literature suggests that those
differences might be attributable to cultural values; North American
employees might be less reluctant to give unfavorable answers while
European employees might be less likely to respond at the extremes to self-
report questionnaires (Maslach, Schaufeli, & Leiter, 2001; Schaufeli &
Buunk, 2003).
Although healthcare professionals‟ burnout has been extensively
studied, there are only a few reviews on burnout risk factors among
European professionals. Given this, the present research aims to discuss the
relevant socio-demographic, psycho-social, occupational and organizational
burnout risk factors among European healthcare personnel.
The majority of studies investigate socio-demographic correlates of
burnout, but results are not consistent and offer little support to these
variables. Gender, for example, did not prove to be a risk factor for
burnout, as studies included in the present review bring inconclusive results.
Although there are minor gender differences in exhaustion and
depersonalization scores, meta-analytic research draw a similar conclusion
ruling out the role of gender in burnout development (Purvanova & Muros,
2010). Schaufeli and Buunk (2003) points out that gender differences in
burnout found by some studies might be due to occupational differences.
The same hypothesis may be drawn for burnout differences based on
hospital type or medical specialty.
Differences in burnout scores across countries highlighted by the
present review are congruent with other studies. For example, a study
among European family physicians pointed out that those medical
professionals from South European countries obtained significantly higher
burnout scores when compared to other European countries (Soler et al.,
2008).
Infirming the role of socio-demographic variables in burnout
development offers support for models which conceptualize burnout as a
consequence of occupational and organizational aspects, like The Job
Demands-Resources Model (Demerouti, Nachreiner, Bakker, & Schaufeli,
2001) or The Mediation Model of Burnout (Leiter & Maslach, 2005;
Maslach & Leiter, 1997). For example, differences in burnout rates across
countries can be accounted by the job–demands resources model which
conceptualizes burnout as a consequence of the imbalance between job
pressure and available resources. Healthcare professionals working in
Scandinavia (known for the lowest burnout rates across Europeans), have
lower occupational pressure and more resources than those working in
South – Eastern Europe. Norway has the second highest rate of nurses per
1000 population (15.47 nurses per 1000 population), while Greece has one
of the lowest (with 3.27 nurses per 1000 population). Moreover, Norway
has the highest rate of health expenditure per capita, with $4520, while
Croatia has one of the lowest, with $358 (Schafer et al., 2010).
In conclusion, as differences between burnout rates based on socio-
demographic factors might be confounded with occupational or
organizational differences, socio-demographic variables might best be
included in future studies as control variables.
Studies analyzing the role of psycho-social correlates of burnout
development offer support for factors like stress, coping mechanisms and
personality variables. Stress has been extensively studied in relation to
burnout. Researches strongly confirm that it is a significant burnout
predictor. These studies usually draw on the idea that burnout is a
consequence of long-term exposure to chronic work stress. The
Conservation of Resources model (Hobfoll & Shirom, 2001), The Demand
Control Model (Karasek, 1979; Karasek & Theorell, 1990) or The Job-
Demands Resources model (Demerouti, et al., 2001) all conceptualize
burnout as a strain reaction. Different but complementary approaches point
out that although stress and burnout are both responses to the occupational
stress, they have different antecedents and causes. Pines and Keinan (2005)
propose that burnout is a consequence of questioning the importance of
one‟s job. The mediation model of job burnout (Maslach & Leiter, 1997;
2005) defines burnout as an erosion of work engagement after the person
experiences work dissonance between him and the organization.
Although less studied, personality variables proved to be significant,
but modest predictors of burnout. The results of the present review are in
line with meta-analytic studies, concluding that persons high in neuroticism
and low in extraversion, conscientiousness, and agreeableness are more
likely to experience burnout (Alarcon, Eschleman, & Bowling, 2009;
Swider & Zimmerman, 2010).
Occupational factors are central antecedents and the most robust
predictors of burnout in the studies included in the review. Occupational
characteristics are best presented as burnout risk factors through the Job –
Demands Resources model (Demerouti et al., 2001) which conceptualize
burnout as a result of the imbalance between job pressures and available
resources. The model was developed as a response to the simplistic (Bakker,
Veldhoven, & Xanthopoulou, 2010; Jansen, Bakker, & De Jong, 2001)
Demand-Control Model (Karasek, 1979; Karasek & Theorell, 1990), which
defined stress as a response to a demanding job doubled by perceived low
control. The Job Demands – Resources model offers a more complex and
comprehensive understanding of burnout. It proposes a broader category of
job demands and resources than the previous mentioned model. Workload,
emotional demands and negative work-home interference are the most
relevant burnout antecedents according to this model (Bakker, Demerouti,
& Verbeke, 2004; Schaufeli & Bakker, 2004). De Jonge and collaborators
(1999) presents results which demonstrate that the Demand-Control Model
does not offer a comprehensive operationalization of job demands,
especially for healthcare professional roles. The authors recommend the
introduction of emotional job demands in the evaluation of health care work
environment. Studies tested and confirmed the role of emotional job
demands as burnout risk factors (Le Blanc, Bakker, Peeters, van Heesch, &
Schaufeli, 2001; Xanthopoulou et al., 2007) and also of emotion work (de
Jonge, le Blanc, Peeters, & Noordam, 2008; Zapf, Seifert, Schmutte,
Mertini, & Holz, 2001).
Workload proved to be the strongest predictor for emotional
exhaustion (Duquette, Kerouac, Sandhu, & Beaudet, 1994; Lee & Ashforth,
1996). Literature offers support for both quantitative demands (like number
of working hours or shifts) and perceived workload as burnout risk factors.
Still, accumulated evidence support the subjective job experience as a
strong burnout antecedent (Lee & Ashforth, 1996; Montgomery,
Panagopoulos, Kehoe, & Valkanos, 2011; Schaufeli & Enzmann, 1998).
Shirom and collaborators (2010) make an interesting clarification, pointing
out that in burnout development perceived workload is the main
determinant, while case load and work time contribute indirectly to burnout,
through perceived workload.
Another concept that received support as a burnout risk factor is role
stress. Studies confirmed the causal effect of both role conflict and role
ambiguity on burnout (Schaufeli, Bakker, van der Heijden, & Prins, 2009).
Longitudinal studies highlighted that role conflict and role ambiguity
explain increasing emotional exhaustion over time, while role conflict
predicts depersonalization and role ambiguity predicts lower personal
accomplishment (Peiro, Gonzalez-Roma, Tordera, & Manas, 2001).
Perceived job control is a key concept in both the job demand -
control model (Karasek, 1979; Karasek & Theorell, 1990) and the mediation
model of job burnout (Leiter & Maslach, 2005; Maslach & Leiter, 1997).
Although the demand – control model has received support for both the role
of high job demands and low perceived control in burnout development
(Jonge, Janseen, & Van Breukelen, 1996), critics point out that there are few
studies to confirm the interaction effect between job demands and perceived
control (Bakker, Le Blanc, & Schaufeli, 2005; Demerouti, Bakker, de
Jonge, Janssen, & Schaufeli, 2001; Rijk, Le Blanc, Schaufeli, & de Jonge,
1998; Taris, 2006).
A complementary argument for the role of perceived job control in
burnout development is brought forward by the mediation model of job
burnout (Leiter & Maslach, 2005; Maslach & Leiter, 1997). More popular in
US than in Europe, the model states that burnout develops as the employee
perceives a mismatch between him and the organization. Burnout is,
therefore, a result of the perceived incongruence between the employee and
the organization in six major aspects: workload, values, community, reward,
control and fairness. The model has been validated across different
countries and professional roles like administrative and business services
(Maslach & Leiter, 2008), health care professionals (Leiter & Maslach,
2009) or university staff (Siegal & McDonald, 2004). The model
incorporates the most relevant organizational risk burnout factors: perceived
job control, value congruence, supervision and social support. To
summarize, studies bring consistent results to support the predictive role of
perceived job control in burnout development.
CONCLUSIONS
The present review offers an analysis of the salient burnout risk
factors for healthcare personnel working in European hospitals and clinics.
In line with previous researches it confirms the main role of occupational
and organizational risk factors while pointing out that psychosocial factors
have a small yet statistically significant influence on burnout development.
Socio-demographic factors, although included in the majority of studies,
seems to have little impact on burnout.
The present review has several limitations. First, as the analysis
included only English-published articles, others found matching the search
criteria were excluded as they had been published in other languages.
Second, the majorities of studies included in the review were descriptive
and focused more on describing burnout than on explaining the
development processes. Third, because of the samples‟ heterogeneity it was
not possible to analyze the burnout risk factors separate for nurses and
doctors.
Some suggestions can be made after analyzing the studies of the
present review. The inconclusive results for some factors (e.g., socio-
demographic) illustrate the need for more systematic designs. Longitudinal
studies are needed to gather relevant data about the relation between risk
factors and burnout.
Factors that literature has highlighted as important burnout
predictors, such as negative work – home interaction, received little
attention throughout the articles included in the review. Emotion work has
been widely studied in relation to burnout (Montgomery, Panagopoulou, de
Wildt, & Meenks, 2006; Zapf et al., 2001) but still only one study from the
present review tested this relation. Studies operationalized the job demands
only through physical or emotional demands, while other job pressures were
ignored. For example, there are studies which indicated cognitive demands
as important burnout predictors (Peeters, Montgomery, Bakker, &
Schaufeli, 2005). Organizational demands are not included either, although
studies confirmed them as burnout antecedents (Bakker, Demerouti, de
Boer, & Schaufeli, 2003; Xanthopoulou et al., 2007).
In conclusion, the present review offers a systematic investigation of
socio-demographic, psycho-social, occupational and organizational
correlates of burnout and confirms the primary role of occupational factors.
Although the healthcare systems across Europe are fundamentally different,
the review showed that occupational factors (such as perceived job demands
or job stress) and organizational characteristics (such as perceived job
control or social support) are robust predictors of the burnout syndrome
among different professional roles and specialties.
ACKNOWLEDGEMENTS
This paper was supported by THE SECTORAL OPERATIONAL PROGRAM FOR
HUMAN RESOURCES DEVELOPMENT via the POSDRU contract 88/1.5/S/56949 –
“Reform project of the doctoral studies in medical sciences: an integrative vision from
financing and organization to scientific performance and impact.
This paper was partly supported by the European Union Framework Seven (EU-FP7
Health) via the project “Improving quality and safety in the hospital: The link between
organisational culture, burnout and quality of care”.
REFERENCES
*articles included in the review
ACGME (2003). ACGME-Approved Specialty Specific Duty Hour Language, page
available at http://www.acgme.org/acWebsite/dutyHours/dh_specificDutyHours.pdf
*Ahola, K. & Hakanen, J. (2007) Job strain, burnout and depressive symptoms: A
prospective study among dentists. Journal of Affective Disorders; 104:103–110. Doi:
10.1016/j.jad.2007.03.004.
*Alacacioglu, A., Yavuzsen, T., Dirioz, M., Oztop, I., & Yilmaz, U. (2009). Burnout in
nurses and physicians working at an oncology department. Psycho-Oncology, 18,
543-548. Doi: 10.1002/pon.1432.
Alarcon, G., Eschleman, K. J., & Bowling, N. A. (2009). Relationships between personality
variables and burnout: A meta-analysis. Work & Stress, 23 (3), 244-263.
Doi:10.1080/02678370903282600.
*Alimoglu, M. K. & Donmez, L. (2005). Daylight exposure and the other predictors of
burnout among nurses in a University Hospital. International Journal of Nursing
Studies, 42, 549-555. Doi: 10.1016/j.ijnurstu.2004.09.001.
Bakker, A. B., Demerouti, E., de Boer, E., & Schaufeli, W. B. (2003). Job demands and job
resources as predictors of absence duration and frequency. Journal of Vocational
Behaviour, 62, 341-356.
Bakker, A. B., Demerouti, E., & Verbeke, W. (2004). Using the Job Demands Resources
Model to Predict Burnout and Performance, Human Resources Management, 43, 1,
83-104.
*Bakker, A. B., Killmer, C. H., Siegrist, J., & Schaufeli, W. B. (2000). Effort-reward
imbalance and burnout among nurses. Journal of Advanced Nursing, 31, 4, 884-891.
*Bakker, A. B., Le Blanc, P. M., & Schaufeli, W. B. (2005). Burnout contagion among
intensive care nurses. Journal of Advanced Nursing, 51, 3, 276-287.
Bakker, A. B., Veldhoven, M. V., & Xanthopoulou, D. (2010). Beyond the Demand-
Control Model: Thriving oh High Job Demands and Resources. Journal of
Personnel Psychology, 9, 1, 3-16. Doi:10.1027/1866-5888/a000006.
*Bressi, C., Manenti, S., Porcellana, M., Cevales, D., Farina, L., Felicioni, I., Meloni, G.,
Milone, G., Miccolis, I. R., Pavanetto, M., Pescador, L., Poddique, M., Scotti, L.,
Zambon, A., Corrao, G., Lambertenghi-Deliliers, G., & Invernizzi, G. (2008).
Haemato-oncology and burnout: an Italian survey. British Journal of Cancer, 98,
1046-1052. Doi: 10.1038/sj.bjc.6604270.
*Buhler, K.-E. & Land, T. (2003). Burnout and Personality in Intensive Care: An Empirical
Study. Hospital Topics, 81, 4, 5-12.
*Buunk, B. P., Ybema, J. F., Van Der Zee, K., Schaufeli, W. B., & Gibbons, F. X. (2001).
Affect Generated by Social Comparisons among Nurses High and Low in Burnout.
Journal of Applied Social Psychology, 31, 7, 1500-1520.
Cappuccio, F. P., Bakewell, A., Taggart, F. M., Ward, G., Ji, C., Sullivan, J. P., Edmunds,
M., Pounder, R., Landrigan, C. P., Lockley, S. W., & Peile, P. (2009). Implementing
a 48 h EWTD-compliant rota for junior doctors in the UK does not compromise
patients safety: assessor-blind pilot comparison. Q J M: An international Journal of
Medicine. 102, 4, 271–82.
*Castelo-Branco, C., Figueras, F., Eixarch, E., Quereda, F., Cancelo, M., Gonzalez, S., &
Balasch, J. (2006). Stress symptoms and burnout in obstetric and gynaecology
residents. BJOG An international Journal of Obstetrics and Gynaecology, 114, 94-
98. Doi: 10.1111/j.1471-0528.2006.01155.x.
*Chiron, B., Michinov, E., Olivier-Chiron, E., Laffon, M., & Rusch, E. (2010). Job
Satisfaction, Life Satisfaction and Burnout in French Anaesthetists. Journal of
Health Psychology, 15, 6, 948-958. Doi: 10.1177/1359105309360072.
Council Directive 93/104/EC of 23 November 1993 concerning certain aspects of the
organization of working time. Available from: http://eur-
lex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:31993L0104:EN:NOT
Council Directive 2003/88/EC of the European Parliament and of the Council of 4
November 2003 concerning certain aspects of the organization of working time.
Available from: http://eur-
lex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:32003L0088:EN:NOT
Demerouti, E., Bakker, A. B., Jonge, J. De, Janssen, P. P. M., & Schaufeli, W. B. (2001).
Burnout and engagement at work as a function of demands and control.
Scandinavian Journal for Work Environment and Health, 27, 279-286.
Demerouti, E., Nachreiner, F., Bakker, A., & Schaufeli, W. (2001). The Job Demands-
Resources Model of Burnout, Journal of Applied Psychology, 86, 3, pp. 499-512.
*Demir, A., Ulusoy, M., & Ulusoy, M. F. (2003). Investigation of factors influencing
burnout levels in the professional and private lives of nurses. International Journal
of Nursing Studies, 40, 807-827. Doi: 10.1016/S0020-7489(03)00077-4.
*Diez-Pinol, M., Dolan, S. L., Sierra, V., & Cannings, K. (2008). Personal and
organisational determinants of well-being at work: The case of Swedish physicians.
International Journal of Health Care Quality Assurance, 21, 6, 598-610.
*Dorz, S., Novara, C., Sica, C., & Sanavio, E. (2003). Predicting Burnout among
HIV/AIDS and Oncology Health Care Workers. Psychology & Health, 18, 5, 677-
684. Doi: 10.1080/0887044031000141180.
Duquette, A., Kerouac, S., Sandhu, B. K., & Beaudet, L. (1994). Factors related to nursing
burnout: A review of empirical knowledge. Issues in Mental Health Nursing, 15,
337-358.
Edwards, D, Burnard, P. Coyle, D., Fothergill, A., & Hannigan, B. (2000). Stress and
burnout in community mental health nursing: A review of the literature. Journal of
Psychiatric and Mental Health Nursing, 7, 1, 7-14. Doi: 10.1046/j.1365-
2850.2000.00258.x.
*Ersoy-Kart, M. (2009). Relations among Social Support, Burnout, and Experiences of
Anger: An Investigation among Emergency Nurses. Nurses Forum, 44, 3, 165-174.
*Escriba-Aguir, V., Martin-Baena, D., & Perez-Hoyos, S. (2006). Psychosocial work
environment and burnout among emergency medical and nursing staff. International
Archives of Occupational and Environmental Health, 80, 127-133.
*Escriba-Aguir, V. & Perez-Hoyos, S. (2007). Psychological well-being and psychosocial
work environment characteristics among emergency medical and nursing staff.
Stress and health, 23, 153-160. Doi:10.1002/smi.1131.
*Garrosa, E., Moreno-Jimenez, B., Rodriquez-Munoz, B., & Rodriguez-Carvajal, R.
(2011). Role stress and personal resources in nursing: A cross-sectional study of
burnout and engagement. International Journal of Nursing Studies, 48, 479-489.
Doi: 10.1016/j.ijnurstu.2010.08.004.
*Gilibert, D. & Daloz, L. (2008). Disorders associated with burnout and causal attributions
of stress among health care professionals in psychiatry. Revue européenne de
psychologie appliqué, 58, 263-274.
*Glasberg, A. L., Eriksson, S., & Norberg, A. (2007). Burnout and „stress of conscience‟
among healthcare personnel. Journal of Advanced Nursing, 57, 4, 392-403. Doi:
10.1111/j.1365-2648.2006.04111.x
Graham, J., Potts, H. W. W., & Ramirez, A. J. (2002). Stress and burnout in doctors. The
Lancet, 360, 9349, 1975-1976. doi:10.1016/S0140-6736(02)11871-X
*Grassi, L. & Magnani, K. (2000). Psychiatric Morbidity and Burnout in the Medical
Profession: An Italian Study of General Practitioners and Hospital Physicians.
Psychotherapy and Psychosomatics, 69, 6, 329-334.
*Gunnarsdottir, S., Clarke, S. P., Rafferty, A. M., & Nutbeam, D. (2009). Front-line
management, staffing and nurse - doctor relationships as predictors of nurse and
patient outcomes. A survey of Icelandic hospital nurses. International Journal of
Nursing Studies, 46, 920-927. Doi: 10.1016/j.ijnurstu.2006.11.007.
*Hansen, N., Sverke, M., & Naswall, K. (2009). Predicting nurse burnout from demands
and resources in three acute care hospitals under different forms of ownership: A
cross-sectional questionnaire survey. International Journal of Nursing Studies, 46,
96-107. Doi: 10.1016/j.ijnurstu.2008.08.002
*Hochwalder, J. (2007). The psychosocial work environment and burnout among Swedish
registered and assistant nurses: The main, mediating, and moderating role of
empowerment. Nursing and Health Sciences, 9, 205-211. Doi: 10.1111/j.1442-
2018.2007.00323.x.
*Hudek-Knezevic, J., Maglica, B. K., & Krapic, N. (2011). Personality, organizational
stress, and attitudes toward work as prospective predictors of professional burnout in
hospital nurses. Croatian Medical Journal, 52, 538-549.
*Ilhan, M. N., Durukan, E., Taner, E., Maral, I., & Ali Bumin, M. (2007). Burnout and its
correlates among nursing staff: a questionnaire survey. Journal of Advanced
Nursing, 61, 1, 100-106. Doi: 10.1111/j.1365-2648.2007.04476.x
Iskera-Golec, I., Folkard, S., & Marek, T. (1996). Health, well-being and burnout of ICU-
nurses on 12- and 8-h shifts. Work & Stress, 10, 3, 251-256.
Janssen, P. P. M., Bakker, A. B., & de Jong, A. (2001). A Test and Refinement of the
Demand-Control-Support Model in the Construction Industry. International Journal
of Stress Management, 8, 4, 315-322.
*Jaworek, M., Marek, T., Karwowski, W., Andrzejczak, C., & Genaidy, A. M. (2010).
Burnout syndrome as a mediator for the effect of work-related factors on
musculoskeletal complaints among hospital nurses. International Journal of
Industrial Ergonomics, 40, 368-375. Doi: 10.1016/j.ergon.2010.01.006.
*Jenkins, R. & Elliott, P. (2004). Stressors, burnout and social support: nurses in acute
mental health settings. Journal of Advanced Nursing, 48, 6, 622-631.
Jonge, J. de, Janseen, P. P. M., & Van Breukelen, G. J. P. (1996). Testing the demand-
control-support model among health-care professionals: a structural equation model.
Work & Stress, 10, 3.
Jonge, J. de, Le Blanc, P. M., Peeters, M. C. W., & Noordam, H. (2008). Emotional job
demands and the role of matching job resources: A cross-sectional survey among
health care workers. International Journal of Nursing Studies, 45, 10, 1460-1469.
Doi: 10.1016/j.ijnurstu.2007.11.002.
Jonge, J. de, Mulder, M. J. G. P., & Nijhuis, F. J. N. (1999). The incorporation of different
demand concepts in the Job Demand-Control Model: Effects on health care
professionals. Social Sciences and Medicine, 48, 9, 1149-1160.
Karasek, R. A. Jr. (1979). Job Demands, Job Decision Latitude and Mental Strain:
Implications for Job Redesign. Administrative Science Quarterly, 24, 2, 285-308.
Karasek & Theorell (1990). Healthy Work: Stress, Productivity, and the Reconstruction of
Working Life. New York: Basic Books.
Keijsers, G. J., Schaufeli, W. B., Le Blanc, P. M., Zwerts, C., & Miranda, D. R. (1995).
Performance and burnout in intensive care units. Work & Stress, 9, 4:513-527.
*Kiekkas, P., Spyratos, F., Lampa, E., Aretha, D., & Sakellaropoulos, G. C. (2010). Level
and Correlates of Burnout Among Orthopaedic Nurses in Greece. Orthopaedic
Nursing, 29, 3, 203-209.
Kilfedder, C. J., Power, K. G., & Wells, J. J. (2001) Burnout in psychiatric nursing. Journal
of Advanced Nursing, 34, 3, 385-396.
*Klersy, C., Callegari, A., Martinelli, V., Vizzardi, V., Navino, V., Malberti, F., Tarchini,
V., Montagna, G., Guastoni, C., Bellazzi, R., Rampino, T., David, S., Barbieri, C.,
Dal Canton, A., & Polizi, P. (2007). Burnout in health care providers of dialysis
service in Northern Italy – a multicentre study. Nephrology Dialysis
Transplantation, 22, 2283-2290. Doi: 10.1093/ndt/gfm111.
*Koivula, M., Paunonen, M., & Laippala, P. (2000). Burnout among nursing staff in two
Finnish hospitals. Journal of Nursing Management, 8, 149-158.
Kowalski, C., Ommen, O., Driller, E., Ernstmann, N., Wirtz, M. A., Kohler, T., & Pfaff, H.
(2010). Burnout in nurses – the relationship between social capital in hospital and
emotional exhaustion. Journal of Clinical Nursing, 19, 1654-1663. Doi:
10.1111/j.1365-2702.2009.02989.x

*Ksiazek, I., Stefaniak, T. J., Stadnyk, M., & Ksiazek, J. (2011). Burnout syndrome in
surgical oncology and general surgery nurses: A cross-sectional study. European
Journal of Oncology Nursing, 15, 347-350. Doi: 10.1016/j.ejon.2010.09.002.
Hjalm, S., Kentta, G., Hassmenan, P., & Gustafsson, H. (2007). Burnout among Elite
Soccer Coaches; Journal of Sport Behavior, 30, 4:415.
Hobfoll, S. E. & Shirom, A. (2001). Conservation of Resources Theory. In R.
Golembiewski (Ed.), Handbook of Organizational Behavior (pp. 57-80). New York,
NY:Dekker.
Landrigan, C. P., Rothschild, J. M., Cronin, J. W., Kaushal, R.., Burdick, E., Katz, J. T.,
Lilly, C. M., Stone, P. H., Lockley, S. W., Bates, D. W., & Czeisler, C.A. (2004).
Effects of Reducing Interns‟ Work Hours on Serious Medical Errors in Intensive
Care Units. The New England Journal of Medicine, 351, 1838-1848.
Le Blanc, P. M., Bakker, A. B., Peeters, M. C. W., van Heesch, N. C. A., & Schaufeli, W.
B. (2001). Emotional Job Demands and Burnout among Oncology Care Providers.
Anxiety, Stress and Coping, 14, 243-263.
Lee, R. T. & Ashforth, B. E. (1996). A Meta-Analytic Examination of the Correlates of the
Three Dimensions of Job Burnout. Journal of Applied Psychology, 81, 123 - 136.
*Leiter, M. P., Gascon, S., & Martinez-Jareta, B. (2010). Making Sense of Work Life: A
Structural Model of Burnout. Journal of Applied Social Psychology, 40, 1, 57-75.
Leiter, M. P. & Maslach, C. (2005). A mediation model of job burnout. in A.-S. G. Antoniu
& C. L. Cooper (Eds.) Research Companion to Organizational Health Psychology.
New Horizons in Management; 2005:544-564.
Leiter, M. P. & Maslach, C. (2009). Nurse turnover: the mediating role of burnout. Journal
of Nursing Management, 17, 3; 331-339.
*Losa Iglesias, M. E., de Bengoa Vallejo, R. B., & Salvadores Fuentes, P. (2010). The
relationship between experiential avoidance and burnout syndrome in critical care
nurses: A cross-sectional questionnaire survey. International Journal of Nursing
Studies, 47, 30-37. Doi: 10.1016/j.ijnurstu.2009.06.104.
Maslach, C. & Leiter, M. (1997). The Truth about Burnout, Jossey-Bass, San Francisco.
Maslach, C & Leiter, P. M. (2008). Early Predictors of Job Burnout and Engagement,
Journal of Applied Psychology, 93, 3, pp. 498-512.
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job Burnout. Annual Review of
Psychology; 52:397-422.
Martinussen, M., Richardsen, A. M., & Burke, R. J. (2007). Job demands, job resources
and burnout among police officers; Journal of Criminal Justice, 35, 3:239-249.
*McManus, I., Winder, B. C., & Gordon, D. (2002). The causal links between stress and
burnout in a longitudinal study of UK doctors. The Lancet, 359, 2089-2090.
Melamed, S., Shirom, A. Toker, S., Berliner, S., & Shapira, I. (2006). Burnout and Risk of
Cardiovascular Disease: Evidence, Possible Causal Path, and promising Research
Directions. Psychological Bulletin, 132, 3, 327-353. Doi: 10.1037/0033-
2909.132.3.327.
Montgomery, A., Panagopoulou, E., & Benos, A. (2006) Work-family interference as a
mediator between job demands and job burnout among doctors. Stress and Health,
22, 203 - 212. Doi: 10.1002/smi.1104.
Montgomery, A., Panagopoulou, E., de Wildt, & Meenks, (2006). Work-Family
Interference, Emotional Labor and Burnout. Journal of Managerial Psychology, 21,
36-51.
Montgomery, A., Panagopoulos, E., Kehoe I., & Valkanos, E. (2011). Connecting
organisational culture and quality of care in the hospital: is job burnout the missing
link?, Journal of Health Organization and Management, 25, 1, 108-123.
Moustou, I., Montgomery, A., Panagopoulou E., & Benos, A. (2010). Burnout Predicts
Health Behaviors in Ambulance Workers; The Open Occupational Health & Safety
Journal, 2:16-18.
Hansen, N., Sverke, M., & Naswall, K. (2008). Predicting nurse burnout from demands and
resources in three acute care hospitals under different forms of ownership.
International Journal of Nursing Studies, 46, 96-107. Doi:
10.1016/j.ijnurstu.2008.08.002
*Ozyurt, A., Hayran, O., & Sur, H. (2006). Predictors of burnout and job satisfaction
among Turkish physicians. QJM An international Journal of Medicine, 99, 161-169.
Doi: 10.1093/qjmed/hcl019.
Paice, E. & Reid, W. (2004) Can training and service survive the European Working Time
Directive?. Medical Education; 38:336–339.
*Panagopoulou, E., Montgomery, A., & Benos, A. (2006). Burnout in internal medicine
physicians: Differences between residents and specialists. European Journal of
Internal Medicine, 17, 195-200.
Paris, Jr. M. & Hoge, M. A. (2009). Burnout in the Mental Health Workforce: A Review.
The Journal of Behavioral Health Services and Research, 37, 4, 519-528.
Peeters, M. C. W., Montgomery, A. J., Bakker, A. B., & Schaufeli, W. B. (2005).
Balancing Work and Hone: How Job and Home Demands are Related to Burnout.
International Journal of Stress Management, 12, 1: 43-61.
Peiro, J. M., Gonzalez-Roma, V., Tordera, N., & Manas, M. A. (2001). Does role stress
predict burnout over time among health care professionals?. Psychology & Health,
16, 511-525.
Pines, A. M. & Keinan, G. (2005). Stress and burnout: The significant difference.
Personality and Individual Differences, 39, 3, 625-635.
*Pisanti, R., van der Doef, M., Maes, S., Lazzari, D., & Bertini, M. (2011). Job
characteristics, organizational conditions, and distress/well-being among Italian and
Dutch nurses: A cross-sectional comparison. International Journal of Nursing
Studies, 48, 829-837. Doi: 10.1016/j.ijnurstu.2010.12.006.
Poantă, L., Crăciun, A., & Dumitraşcu, D. L. (2010). Professional Stress and Inflammatory
Markers in Physicians. Romanian Journal of Internal Medicine, 48, 1, 57-63.
*Popa, F., Arafat, R., Purcărea, V. L., Lală, A., Popa-Velea, O., & Bobirnac, G. (2010).
Occupational Burnout levels in Emergency Medicine – a stage 2 nationwide study
and analysis. Journal of Medicine and Life, 3, 4, 445 – 453.
Prins, J.T., van der Heijden, F.M.M.A., Hoekstra-Weebers, J.E.H.M., Bakker, A. B., van de
Wiel, H.B.M., Jacobs, B., & Gazendam-Donofrio, S.M. (2009). Burnout,
engagement, and resident physicians‟ self-reported errors. Psychology, Health &
Medicine, 14, 6, 654-666.
*Prins, J.T., Hoekstra-Weebers, J.E.H.M., Gazendam-Donofrio, S.M., van de Wiel,
H.B.M., Sprangers, F., & van der Heijden, F.M.M.A. (2007). The role of social
support in burnout among Dutch medical residents. Psychology, Health and
Medicine, 12, 1, 1-6. http://dx.doi.org/10.1080/13548500600782214.
Purvanova, R. K. & Muros, J. P. (2010). Gender differences in burnout: A meta-analysis.
Journal of Vocational Behavior, 77, 168-185.
*Putnik, K. & Houkes, I. (2011). Work related characteristics, work-home and home-work
interference and burnout among primary healthcare physicians: A gender perspective
in a Serbian context. BMC Public Health, 11, 716. Doi: 10.1186/1471-2458-11-716.
*Quattrin, R., Zanini, A., Nascig, E., Annunziata, M. A., Calligaris, L., & Brusaferro, S.
(2006). Level of Burnout Among Nurses Working in Oncology in an Italian Region.
Oncology Nursing Forum, 33, 4, 815-820.
*Rafferty, A. M., Clarke, S. P., Coles, J., Ball, J., James, P., McKee, M., & Aiken, L. H.
(2007). Outcomes of variation in hospital nurse staffing in English hospitals: Cross-
sectional analysis of survey data and discharge records. International Journal of
Nursing Studies, 44, 175-182. Doi: 10.1016/j.ijnurstu.2006.08.003.
*Renzi, C., Tabolli, S., Ianni, A., Di Pietro, C., & Puddu, P. (2005). Burnout and job
satisfaction comparing healthcare staff of a dermatological hospital and a general
hospital. Journal of European Academy of Dermatology and Venereology, 19, 153-
157. Doi: 10.1111/j.1468-3083.2005.01029.x.
Rijk, A. E., Le Blanc, P., Jonge, J. de, & Schaufeli, W. B. (1998). Active coping and need
for control as moderators of the job demand-control model: Effects on burnout.
Journal of Occupational and Organizational Psychology, 71, 1-18.
Rogers, A. E., Hwang, W.-T., Scott, L.-D., Aiken, L. H., & Dinges, D. F. (2004). The
Working Hours of Hospital Staff Nurses and Patient Safety. Health Affairs, 23, 4:
202-212.
Rudow, B. (1999). Stress and burnout in the teaching profession: European studies, issues
and research perspectives. In Vandenberghe, R. & Huberman, A. M. (Eds).
Understanding and preventing teacher burnout: A sourcebook of international
research and practice, (pp. 38-58). New York, NY, US: Cambridge University
Press. Doi: 10.1017/CBO9780511527784.004
Schafer, W., Kroneman, M., Boerma, W., Van Der Berg, M., Wester, W., Deville, W., &
Van Ginneken, E. (2010). The Netherlands. Health System Review. Health Systems
in Transition, 12, 1. European Observatory on Health Systems and Policies.
Schaufeli, W. & Bakker, A. (2004). Job demands, job resources and their relationship with
burnout and engagement: a multi-sample study. Journal of Organiza-tional
Behavior, 25, 293-315.
Schaufeli, W. B., Bakker, A. B., van der Heijden, F. M. M. A., & Prins, J. T. (2009).
Workaholism, burnout and well-being among junior doctors: The mediating role of
role conflict. Work & Stress, 23, 2, 155 – 172.
Schaufeli, W. B. & Buunk, B. P. (2003). Burnout: An Overview of 25 Years of Research
and Theorising, in M.J. Schabracq, J.A.M. Winnubst and C.L. Cooper (Eds.) The
Handbook of Work and Health Psychology, John Wiley & Suns.
Schaufeli, W. B. & Enzmann, D. (1998). The Burnout Companion to Study & Practice: A
Critical Analysis. Philadelphia: Taylor & Francis.
*Sharma, A., Sharp, D. M., Walker, L. G., & Monson, J. R. T. (2007). Stress and burnout
among colorectal surgeons and colorectal nurse specialists working in the National
Health Service. Colorectal Disease, 10, 397-406.
*Sharma, A., Sharp, D. M., Walker, L. G., & Monson, J. R. T. (2008). Stress and burnout
in colorectal and vascular surgical consultants working in the UK National Health
Service. Psycho-Oncology, 17, 570-576.
Siegal, M. & McDonald, T. (2004). Person – organization value congruence, burnout and
diversion of resources. Personnel Review, 33, 3, 291-301.
Siegrist, J. (1996). Adverse health effects of high effort-low reward conditions. Journal of
Occupational Health Psychology, 1, 27-41.
Simbula, S., Guglielmi, D., & Schaufeli, W. B. (2011). A three wave study on job
resources, self-efficacy and work engagement among Italian school teachers.
European Journal of Work and Organizational Psychology, 20, 285-305. Doi:
10.1080/13594320903513916.
Singh, P., Suar, D., & Leiter, M. (2010). Antecedents, Work-Related Consequences, and
Buffers of Job Burnout Among Indian Software Developers; Journal of Leadership
and Organisational Studies, 19, 1:83-104.
Shanafelt, T. D., Blach, C. M., Bechamps, G., Russell, T., Dyrbye, L., Satele, D., Collicott,
P., Novotny, P. J., Sloan, J., & Freischlag, J. (2010). Burnout and Medical Errors
among American Surgeons; Annals of Surgery, 251: 995-1000.
Shanafelt, T. D., Bradley, K. A., Wipf, J. E., & Black, A. L. (2002). Burnout and Self-
reported Patient Error in an Internal Medicine Residency Program; Annals of
Internal Medicine; 136,5: 358-367.
Shirom, A., Nirel N., & Vinokur, A. D. (2010). Work Hours and Caseload as Predictors of
Physician Burnout: The Mediating Effects by Perceived Workload and by
Autonomy. Applied Psychology. An international Review, 59, 4, 539-565.
Sofia Carvalho, A., Martins Pereira, S., & Fonseca, A. M. (2011). Burnout in palliative
care: A systematic review. Nursing Ethics, 18, 3, 317-326. Doi:
10.1177/0969733011398092.
Solera, J. K., Yamanb, H., Estevac, M., Dobbsd, F., Asenovae, R. S., Katićf, M., Ožvačićf,
Z., Desgrangesg, J. P., Moreauh, A., Lionisi, C., Kotányij, P., Carellik, F., Nowakl,
P. R., Azeredom, Z. A., Marklundn, E., Churchillo, D., & Ungan, E. (2008). Burnout
in European family doctors: the EGPRN Study. Family Practice, 25, 4, 245-265.
Doi: 10.1093/fampra/cmn038.
*Stordeur, S., D‟hoore, W., & Vandenberghe, C. (2001). Leadership, organizational stress,
and emotional exhaustion among hospital nursing staff. Journal of Advances
Nursing, 35, 4, 533-542.
*Sundin, L., Hochwalder, J., Bildt, C., & Lisspers, J. (2007). The relationship between
different work-related sources of social support and burnout among registered and
assistant nurses in Sweden: A questionnaire survey. International Journal of Nursing
Studies, 44, 758-769. Doi: 10.1016/j.ijnurstu.2006.01.004.
Swider, B, W. & Zimmerman, R. D. (2010). Born to burnout: A meta-analytic path model
of personality, job burnout and work outcomes. Journal of Vocational Behavior, 76,
3, 487-506.
Taris, T. W. (2006). Bricks without clay: On urban myths in occupational health
psychology. Work & Stress: An International Journal of Work, Health &
Organisations. 20, 2, 99-104.
Trufelli, D. C., Bensi, C. G., Garcia, J. B., Narahara, J. L., Abrao, M. N., Diniz, R. W., Da
Costa Miranda, V., Soares, H. P., & Del Giglio, A. (2008). Burnout in cancer
professionals: a systematic review and meta-analysis. European Journal of Cancer
Care, 17, 6, 524-531. Doi: 10.1111/j.1365-2354.2008.00927.x.
Tsai, F. J., Huang, W. L., & Chang, C. C. (2009). Occupational Stress and Burnout of
Lawyers. Journal of Occupational Health, 51: 443-450.
*Tselebis, A., Moulou, A., & Ilias, I. (2001). Burnout versus depression and sense of
coherence: Study of Greek nursing staff. Nursing and Health Sciences, 3, 69-71.
*Tummers, G. E. R., Janssen, P. P. M., Landeweerd, A., & Houkes, I. (2001). A
comparative study of work characteristics and reactions between general and mental
health nurses: a multi-sample analysis. Journal of Advanced Nursing, 36, 1, 151-
162.
*Tummers, G. E. R., Landeweerd, J. A., & van Merode, G. G. (2002). Work Organization,
Work Characteristics, and Their Psychological Effects on Nurses in the Netherlands.
International Journal of Stress Management, 9, 3, 183-206.
*Tunc, T. & Kutanis, R. O. (2009). Role conflict, role ambiguity, and burnout in nurses and
physicians at a university hospital in Turkey. Nursing and Health Sciences, 11, 410-
416.
Upton, D., Mason, V., Doran, B., Solowiej, K., Shiralkar, U., & Shiralkar, S. (2012). The
experience of burnout across different surgical specialties in the United Kingdom: A
cross-sectional survey. Surgery, 151, 4, 453-501. Doi: 10.1016/j.surg.2011.09.035
*Van Bogaert, P., Meulemans, H., Clarke, S., Vermeyen, K., & Van de Heyning, P. (2009).
Hospital nurse practice environment, burnout, job outcomes and quality of care: test
of a structural equation mode. Journal of Advanced Nursing, 65, 10, 2175-2185.
Doi: 10.1111/j.1365-2648.2009.05082.x.
Vela-Bueno, A., Moreno-Jiménez, B., Rodríguez-Muño, A., Olavarrieta-Bernardino, S.,
Fernández-Mendoza, J., De la Cruz-Troca, J. J., Bixier, E. O., & Vgontzas, A. N.
(2008). Insomnia and sleep quality among primary care physicians with low and
high burnout levels. Journal of Psychosomatic Research; 64:435-442.
*Verdon, M., Merlani, P., Perneger, T., & Ricou, B. (2008). Burnout in a surgical ICU
team. Intensive Care Medicine, 34, 152-156. Doi: 10.1007/s00134-007-0907-5.
Visser, M. R. M., Smets, E. M. A., Oort, F. J., & de Haes, H. C. J. M. (2003). Stress,
satisfaction and burnout among a Dutch medical specialists. Canadian Medical
Association Journal, 168, 3, 271-275.
West, C. P., Huschka, M. M., Novotny, P. J., Sloan, J. A., Kolars, J. C., Habermann, T. M.,
& Shanafelt, T. D. (2006). Association of perceived medical errors with resident
distress and empathy – A prospective longitudinal study. Journal of the American
Medical Association, 296, 9, 1071-1078.
Xanthopoulou, D., Bakker, A. B., Dollard, M. F., Demerouti, E., Schaufeli, W. B., Taris, T.
W., & Schreurs, P. J. G. (2007). When do job demands particularly predict burnout?
The moderating role of job resources. Journal of Managerial Psychology, 22, 8, 766
– 786.
Zapf, D. (2002). Emotion work and psychological wellbeing: A review of the literature and
some conceptual consideration. Human Resources Management Review, 12, 2, 237-
268.
Zapf, D., Seifert, C., Schmutte, B., Mertini, H., & Holz, M. (2001). Emotion work and job
stressors and their effects on burnout. Psychology & Health, 16, 5, 527-545.

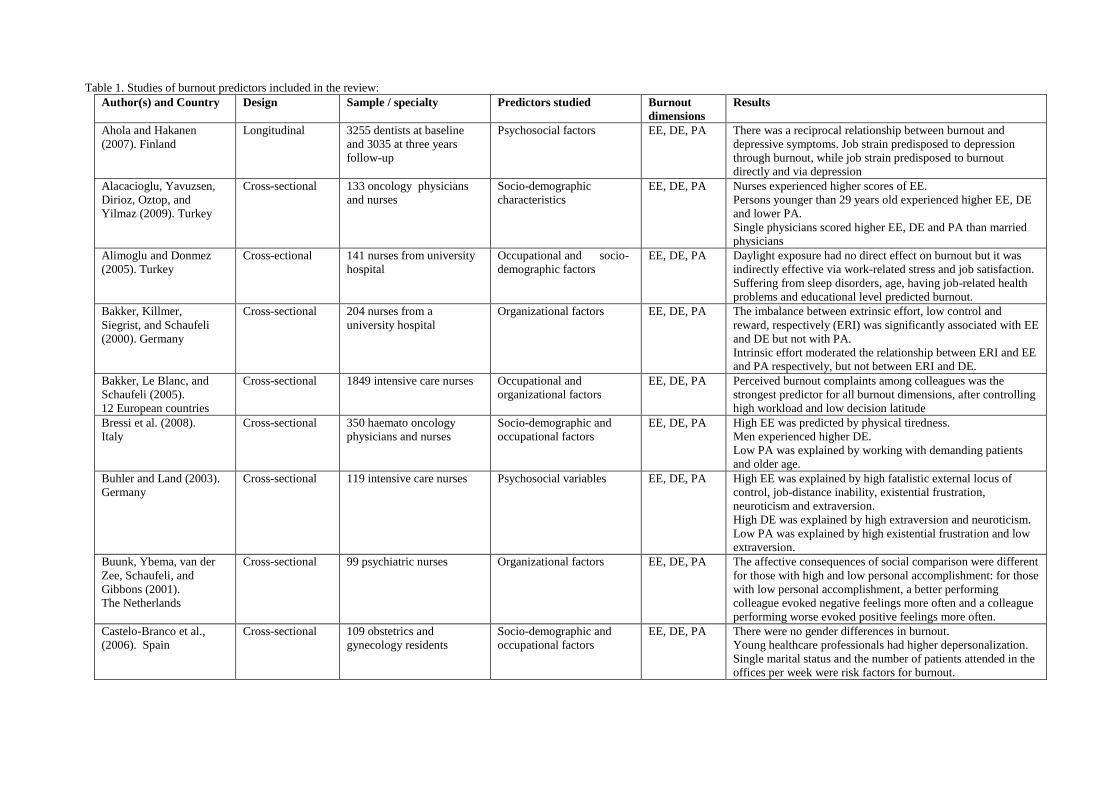
Table 1. Studies of burnout predictors included in the review:
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Ahola and Hakanen
(2007). Finland
Longitudinal 3255 dentists at baseline
and 3035 at three years
follow-up
Psychosocial factors EE, DE, PA There was a reciprocal relationship between burnout and
depressive symptoms. Job strain predisposed to depression
through burnout, while job strain predisposed to burnout
directly and via depression
Alacacioglu, Yavuzsen,
Dirioz, Oztop, and
Yilmaz (2009). Turkey
Cross-sectional 133 oncology physicians
and nurses
Socio-demographic
characteristics
EE, DE, PA Nurses experienced higher scores of EE.
Persons younger than 29 years old experienced higher EE, DE
and lower PA.
Single physicians scored higher EE, DE and PA than married
physicians
Alimoglu and Donmez
(2005). Turkey
Cross-ectional 141 nurses from university
hospital
Occupational and socio-
demographic factors
EE, DE, PA Daylight exposure had no direct effect on burnout but it was
indirectly effective via work-related stress and job satisfaction.
Suffering from sleep disorders, age, having job-related health
problems and educational level predicted burnout.
Bakker, Killmer,
Siegrist, and Schaufeli
(2000). Germany
Cross-sectional 204 nurses from a
university hospital
Organizational factors EE, DE, PA The imbalance between extrinsic effort, low control and
reward, respectively (ERI) was significantly associated with EE
and DE but not with PA.
Intrinsic effort moderated the relationship between ERI and EE
and PA respectively, but not between ERI and DE.
Bakker, Le Blanc, and
Schaufeli (2005).
12 European countries
Cross-sectional 1849 intensive care nurses Occupational and
organizational factors
EE, DE, PA Perceived burnout complaints among colleagues was the
strongest predictor for all burnout dimensions, after controlling
high workload and low decision latitude
Bressi et al. (2008).
Italy
Cross-sectional 350 haemato oncology
physicians and nurses
Socio-demographic and
occupational factors
EE, DE, PA High EE was predicted by physical tiredness.
Men experienced higher DE.
Low PA was explained by working with demanding patients
and older age.
Buhler and Land (2003).
Germany
Cross-sectional 119 intensive care nurses Psychosocial variables EE, DE, PA High EE was explained by high fatalistic external locus of
control, job-distance inability, existential frustration,
neuroticism and extraversion.
High DE was explained by high extraversion and neuroticism.
Low PA was explained by high existential frustration and low
extraversion.
Buunk, Ybema, van der
Zee, Schaufeli, and
Gibbons (2001).
The Netherlands
Cross-sectional 99 psychiatric nurses Organizational factors EE, DE, PA The affective consequences of social comparison were different
for those with high and low personal accomplishment: for those
with low personal accomplishment, a better performing
colleague evoked negative feelings more often and a colleague
performing worse evoked positive feelings more often.
Castelo-Branco et al.,
(2006). Spain
Cross-sectional 109 obstetrics and
gynecology residents
Socio-demographic and
occupational factors
EE, DE, PA There were no gender differences in burnout.
Young healthcare professionals had higher depersonalization.
Single marital status and the number of patients attended in the
offices per week were risk factors for burnout.
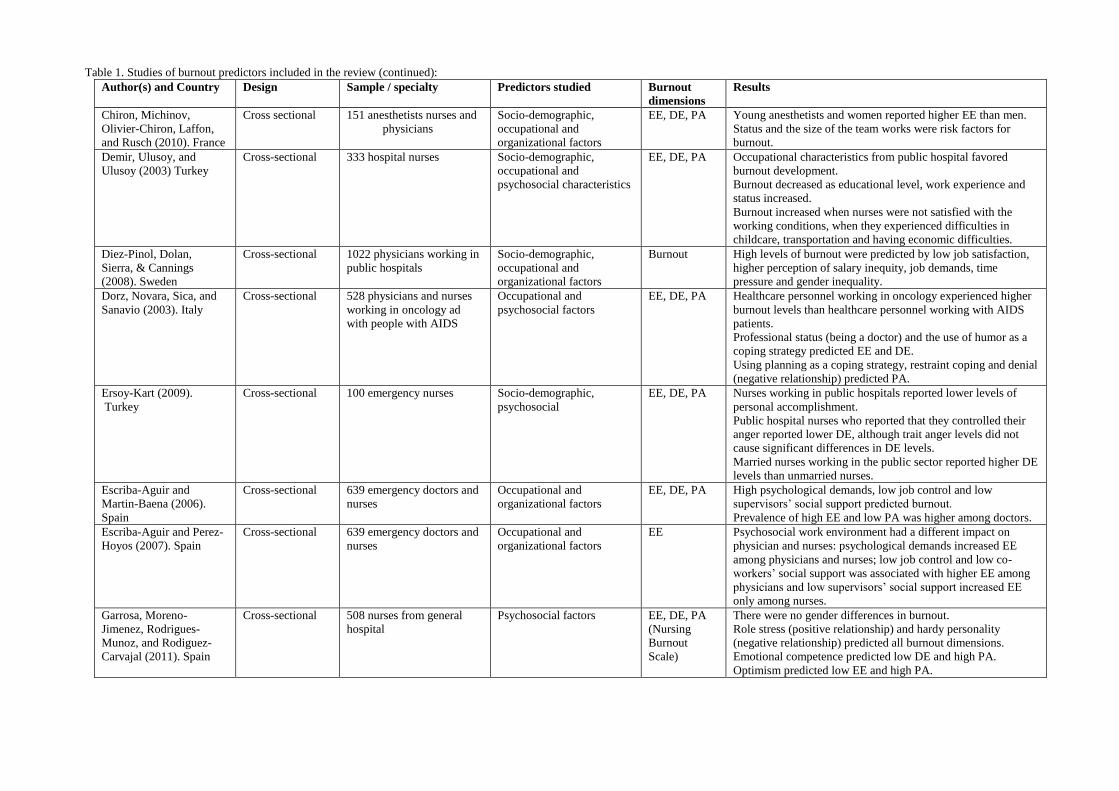
Table 1. Studies of burnout predictors included in the review (continued):
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Chiron, Michinov,
Olivier-Chiron, Laffon,
and Rusch (2010). France
Cross sectional 151 anesthetists nurses and
physicians
Socio-demographic,
occupational and
organizational factors
EE, DE, PA Young anesthetists and women reported higher EE than men.
Status and the size of the team works were risk factors for
burnout.
Demir, Ulusoy, and
Ulusoy (2003) Turkey
Cross-sectional 333 hospital nurses Socio-demographic,
occupational and
psychosocial characteristics
EE, DE, PA Occupational characteristics from public hospital favored
burnout development.
Burnout decreased as educational level, work experience and
status increased.
Burnout increased when nurses were not satisfied with the
working conditions, when they experienced difficulties in
childcare, transportation and having economic difficulties.
Diez-Pinol, Dolan,
Sierra, & Cannings
(2008). Sweden
Cross-sectional 1022 physicians working in
public hospitals
Socio-demographic,
occupational and
organizational factors
Burnout High levels of burnout were predicted by low job satisfaction,
higher perception of salary inequity, job demands, time
pressure and gender inequality.
Dorz, Novara, Sica, and
Sanavio (2003). Italy
Cross-sectional 528 physicians and nurses
working in oncology ad
with people with AIDS
Occupational and
psychosocial factors
EE, DE, PA Healthcare personnel working in oncology experienced higher
burnout levels than healthcare personnel working with AIDS
patients.
Professional status (being a doctor) and the use of humor as a
coping strategy predicted EE and DE.
Using planning as a coping strategy, restraint coping and denial
(negative relationship) predicted PA.
Ersoy-Kart (2009).
Turkey
Cross-sectional 100 emergency nurses Socio-demographic,
psychosocial
EE, DE, PA Nurses working in public hospitals reported lower levels of
personal accomplishment.
Public hospital nurses who reported that they controlled their
anger reported lower DE, although trait anger levels did not
cause significant differences in DE levels.
Married nurses working in the public sector reported higher DE
levels than unmarried nurses.
Escriba-Aguir and
Martin-Baena (2006).
Spain
Cross-sectional 639 emergency doctors and
nurses
Occupational and
organizational factors
EE, DE, PA High psychological demands, low job control and low
supervisors‟ social support predicted burnout.
Prevalence of high EE and low PA was higher among doctors.
Escriba-Aguir and Perez-
Hoyos (2007). Spain
Cross-sectional 639 emergency doctors and
nurses
Occupational and
organizational factors
EE Psychosocial work environment had a different impact on
physician and nurses: psychological demands increased EE
among physicians and nurses; low job control and low co-
workers‟ social support was associated with higher EE among
physicians and low supervisors‟ social support increased EE
only among nurses.
Garrosa, Moreno-
Jimenez, Rodrigues-
Munoz, and Rodiguez-
Carvajal (2011). Spain
Cross-sectional 508 nurses from general
hospital
Psychosocial factors EE, DE, PA
(Nursing
Burnout
Scale)
There were no gender differences in burnout.
Role stress (positive relationship) and hardy personality
(negative relationship) predicted all burnout dimensions.
Emotional competence predicted low DE and high PA.
Optimism predicted low EE and high PA.
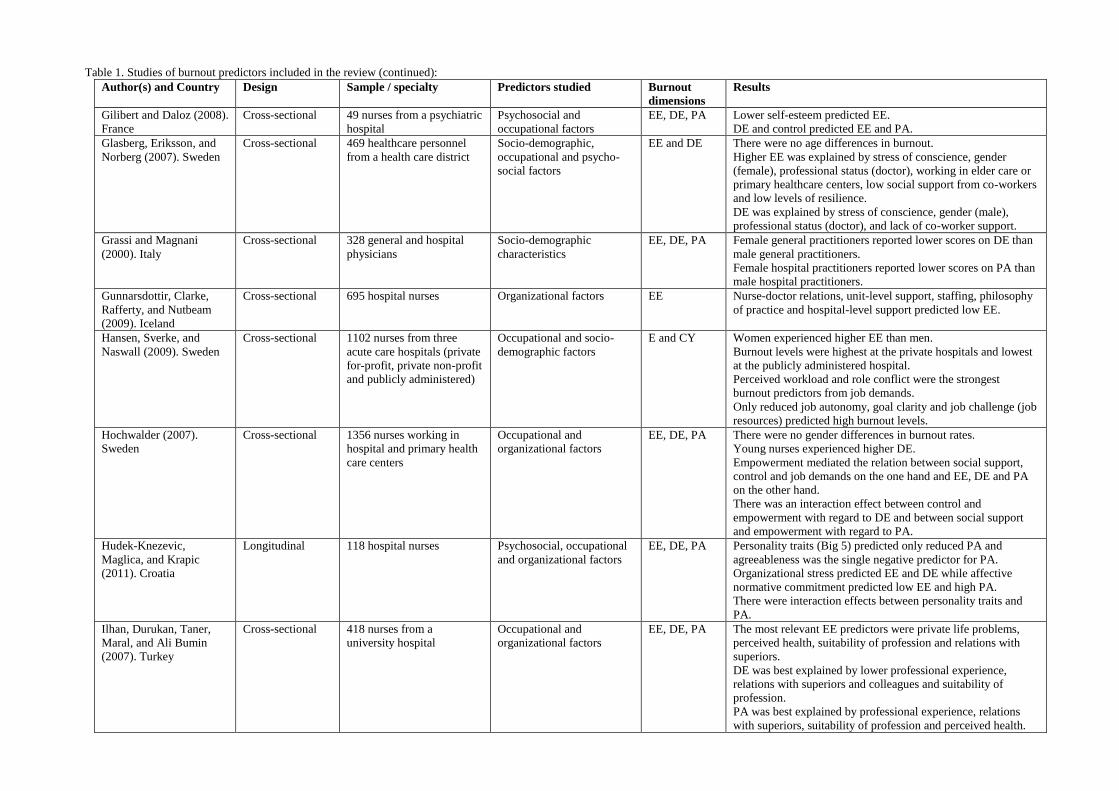
Table 1. Studies of burnout predictors included in the review (continued):
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Gilibert and Daloz (2008).
France
Cross-sectional 49 nurses from a psychiatric
hospital
Psychosocial and
occupational factors
EE, DE, PA Lower self-esteem predicted EE.
DE and control predicted EE and PA.
Glasberg, Eriksson, and
Norberg (2007). Sweden
Cross-sectional 469 healthcare personnel
from a health care district
Socio-demographic,
occupational and psycho-
social factors
EE and DE There were no age differences in burnout.
Higher EE was explained by stress of conscience, gender
(female), professional status (doctor), working in elder care or
primary healthcare centers, low social support from co-workers
and low levels of resilience.
DE was explained by stress of conscience, gender (male),
professional status (doctor), and lack of co-worker support.
Grassi and Magnani
(2000). Italy
Cross-sectional 328 general and hospital
physicians
Socio-demographic
characteristics
EE, DE, PA Female general practitioners reported lower scores on DE than
male general practitioners.
Female hospital practitioners reported lower scores on PA than
male hospital practitioners.
Gunnarsdottir, Clarke,
Rafferty, and Nutbeam
(2009). Iceland
Cross-sectional 695 hospital nurses Organizational factors EE Nurse-doctor relations, unit-level support, staffing, philosophy
of practice and hospital-level support predicted low EE.
Hansen, Sverke, and
Naswall (2009). Sweden
Cross-sectional 1102 nurses from three
acute care hospitals (private
for-profit, private non-profit
and publicly administered)
Occupational and socio-
demographic factors
E and CY Women experienced higher EE than men.
Burnout levels were highest at the private hospitals and lowest
at the publicly administered hospital.
Perceived workload and role conflict were the strongest
burnout predictors from job demands.
Only reduced job autonomy, goal clarity and job challenge (job
resources) predicted high burnout levels.
Hochwalder (2007).
Sweden
Cross-sectional 1356 nurses working in
hospital and primary health
care centers
Occupational and
organizational factors
EE, DE, PA There were no gender differences in burnout rates.
Young nurses experienced higher DE.
Empowerment mediated the relation between social support,
control and job demands on the one hand and EE, DE and PA
on the other hand.
There was an interaction effect between control and
empowerment with regard to DE and between social support
and empowerment with regard to PA.
Hudek-Knezevic,
Maglica, and Krapic
(2011). Croatia
Longitudinal 118 hospital nurses Psychosocial, occupational
and organizational factors
EE, DE, PA Personality traits (Big 5) predicted only reduced PA and
agreeableness was the single negative predictor for PA.
Organizational stress predicted EE and DE while affective
normative commitment predicted low EE and high PA.
There were interaction effects between personality traits and
PA.
Ilhan, Durukan, Taner,
Maral, and Ali Bumin
(2007). Turkey
Cross-sectional 418 nurses from a
university hospital
Occupational and
organizational factors
EE, DE, PA The most relevant EE predictors were private life problems,
perceived health, suitability of profession and relations with
superiors.
DE was best explained by lower professional experience,
relations with superiors and colleagues and suitability of
profession.
PA was best explained by professional experience, relations
with superiors, suitability of profession and perceived health.
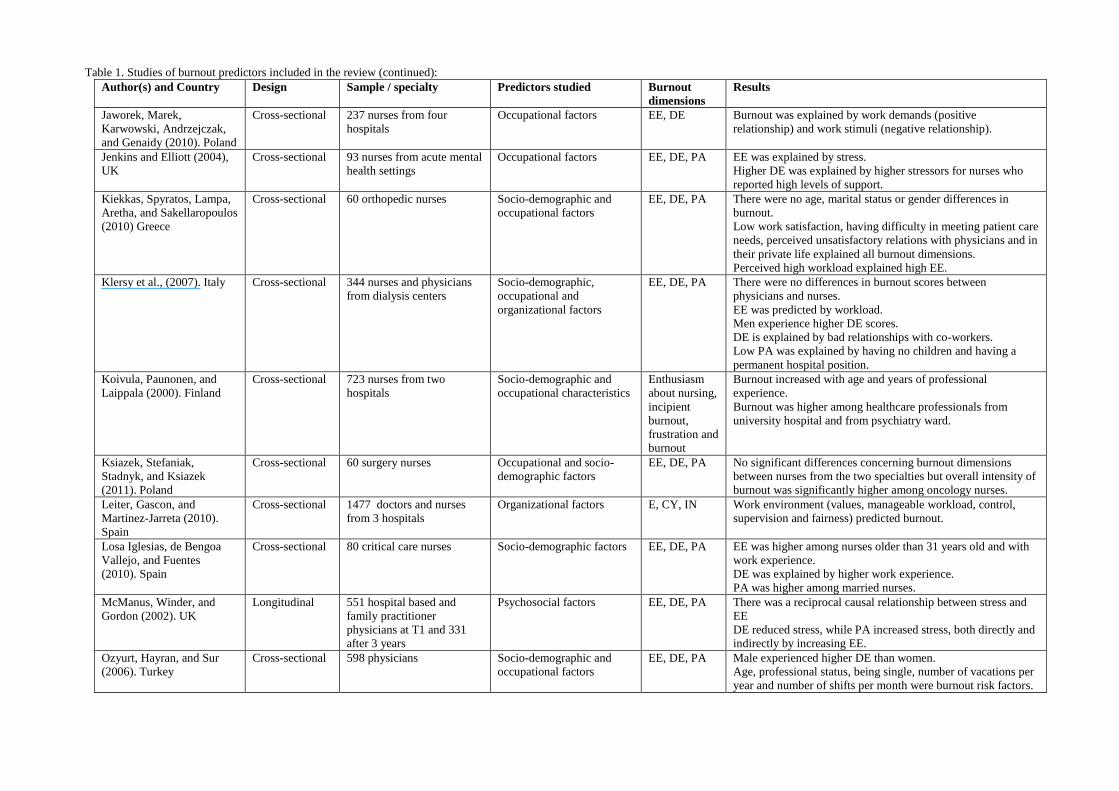
Table 1. Studies of burnout predictors included in the review (continued):
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Jaworek, Marek,
Karwowski, Andrzejczak,
and Genaidy (2010). Poland
Cross-sectional 237 nurses from four
hospitals
Occupational factors EE, DE Burnout was explained by work demands (positive
relationship) and work stimuli (negative relationship).
Jenkins and Elliott (2004),
UK
Cross-sectional 93 nurses from acute mental
health settings
Occupational factors EE, DE, PA EE was explained by stress.
Higher DE was explained by higher stressors for nurses who
reported high levels of support.
Kiekkas, Spyratos, Lampa,
Aretha, and Sakellaropoulos
(2010) Greece
Cross-sectional 60 orthopedic nurses Socio-demographic and
occupational factors
EE, DE, PA There were no age, marital status or gender differences in
burnout.
Low work satisfaction, having difficulty in meeting patient care
needs, perceived unsatisfactory relations with physicians and in
their private life explained all burnout dimensions.
Perceived high workload explained high EE.
Klersy et al., (2007). Italy Cross-sectional 344 nurses and physicians
from dialysis centers
Socio-demographic,
occupational and
organizational factors
EE, DE, PA There were no differences in burnout scores between
physicians and nurses.
EE was predicted by workload.
Men experience higher DE scores.
DE is explained by bad relationships with co-workers.
Low PA was explained by having no children and having a
permanent hospital position.
Koivula, Paunonen, and
Laippala (2000). Finland
Cross-sectional 723 nurses from two
hospitals
Socio-demographic and
occupational characteristics
Enthusiasm
about nursing,
incipient
burnout,
frustration and
burnout
Burnout increased with age and years of professional
experience.
Burnout was higher among healthcare professionals from
university hospital and from psychiatry ward.
Ksiazek, Stefaniak,
Stadnyk, and Ksiazek
(2011). Poland
Cross-sectional 60 surgery nurses Occupational and socio-
demographic factors
EE, DE, PA No significant differences concerning burnout dimensions
between nurses from the two specialties but overall intensity of
burnout was significantly higher among oncology nurses.
Leiter, Gascon, and
Martinez-Jarreta (2010).
Spain
Cross-sectional 1477 doctors and nurses
from 3 hospitals
Organizational factors E, CY, IN Work environment (values, manageable workload, control,
supervision and fairness) predicted burnout.
Losa Iglesias, de Bengoa
Vallejo, and Fuentes
(2010). Spain
Cross-sectional 80 critical care nurses Socio-demographic factors EE, DE, PA EE was higher among nurses older than 31 years old and with
work experience.
DE was explained by higher work experience.
PA was higher among married nurses.
McManus, Winder, and
Gordon (2002). UK
Longitudinal 551 hospital based and
family practitioner
physicians at T1 and 331
after 3 years
Psychosocial factors EE, DE, PA There was a reciprocal causal relationship between stress and
EE
DE reduced stress, while PA increased stress, both directly and
indirectly by increasing EE.
Ozyurt, Hayran, and Sur
(2006). Turkey
Cross-sectional 598 physicians Socio-demographic and
occupational factors
EE, DE, PA Male experienced higher DE than women.
Age, professional status, being single, number of vacations per
year and number of shifts per month were burnout risk factors.
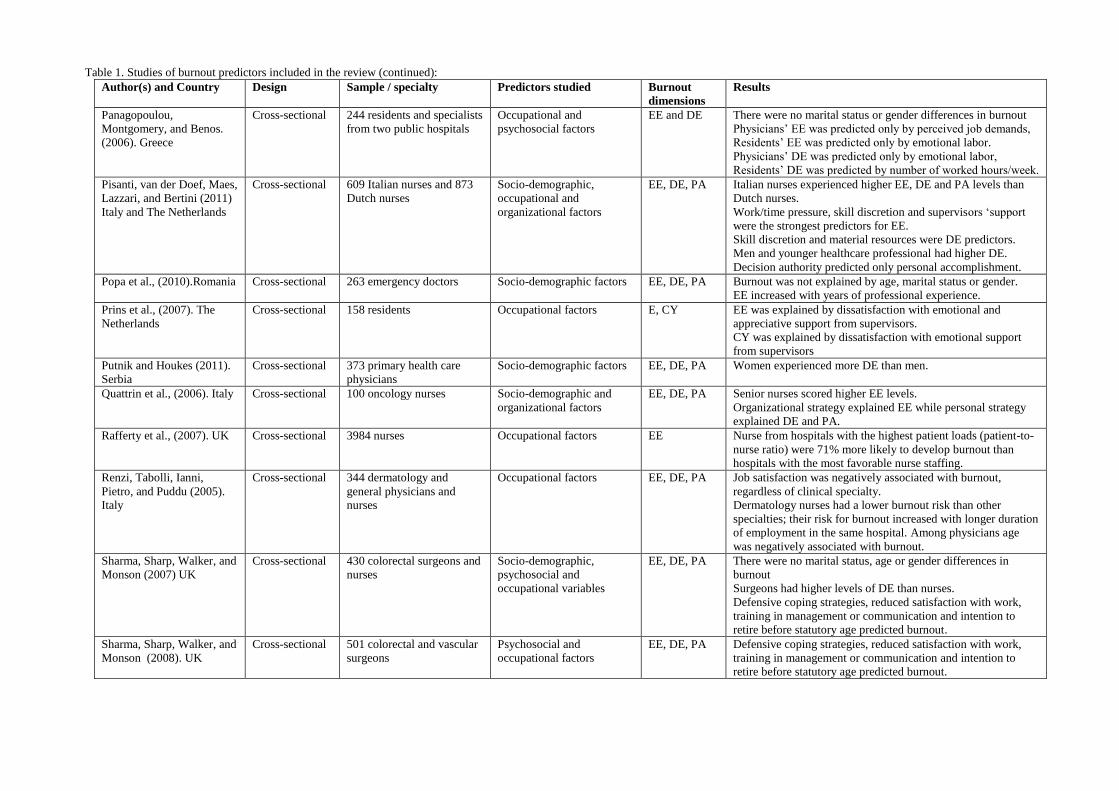
Table 1. Studies of burnout predictors included in the review (continued):
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Panagopoulou,
Montgomery, and Benos.
(2006). Greece
Cross-sectional 244 residents and specialists
from two public hospitals
Occupational and
psychosocial factors
EE and DE There were no marital status or gender differences in burnout
Physicians‟ EE was predicted only by perceived job demands,
Residents‟ EE was predicted only by emotional labor.
Physicians‟ DE was predicted only by emotional labor,
Residents‟ DE was predicted by number of worked hours/week.
Pisanti, van der Doef, Maes,
Lazzari, and Bertini (2011)
Italy and The Netherlands
Cross-sectional 609 Italian nurses and 873
Dutch nurses
Socio-demographic,
occupational and
organizational factors
EE, DE, PA Italian nurses experienced higher EE, DE and PA levels than
Dutch nurses.
Work/time pressure, skill discretion and supervisors „support
were the strongest predictors for EE.
Skill discretion and material resources were DE predictors.
Men and younger healthcare professional had higher DE.
Decision authority predicted only personal accomplishment.
Popa et al., (2010).Romania Cross-sectional 263 emergency doctors Socio-demographic factors EE, DE, PA Burnout was not explained by age, marital status or gender.
EE increased with years of professional experience.
Prins et al., (2007). The
Netherlands
Cross-sectional 158 residents Occupational factors E, CY EE was explained by dissatisfaction with emotional and
appreciative support from supervisors.
CY was explained by dissatisfaction with emotional support
from supervisors
Putnik and Houkes (2011).
Serbia
Cross-sectional 373 primary health care
physicians
Socio-demographic factors EE, DE, PA Women experienced more DE than men.
Quattrin et al., (2006). Italy Cross-sectional 100 oncology nurses Socio-demographic and
organizational factors
EE, DE, PA Senior nurses scored higher EE levels.
Organizational strategy explained EE while personal strategy
explained DE and PA.
Rafferty et al., (2007). UK Cross-sectional 3984 nurses Occupational factors EE Nurse from hospitals with the highest patient loads (patient-to-
nurse ratio) were 71% more likely to develop burnout than
hospitals with the most favorable nurse staffing.
Renzi, Tabolli, Ianni,
Pietro, and Puddu (2005).
Italy
Cross-sectional 344 dermatology and
general physicians and
nurses
Occupational factors EE, DE, PA Job satisfaction was negatively associated with burnout,
regardless of clinical specialty.
Dermatology nurses had a lower burnout risk than other
specialties; their risk for burnout increased with longer duration
of employment in the same hospital. Among physicians age
was negatively associated with burnout.
Sharma, Sharp, Walker, and
Monson (2007) UK
Cross-sectional 430 colorectal surgeons and
nurses
Socio-demographic,
psychosocial and
occupational variables
EE, DE, PA There were no marital status, age or gender differences in
burnout
Surgeons had higher levels of DE than nurses.
Defensive coping strategies, reduced satisfaction with work,
training in management or communication and intention to
retire before statutory age predicted burnout.
Sharma, Sharp, Walker, and
Monson (2008). UK
Cross-sectional 501 colorectal and vascular
surgeons
Psychosocial and
occupational factors
EE, DE, PA Defensive coping strategies, reduced satisfaction with work,
training in management or communication and intention to
retire before statutory age predicted burnout.
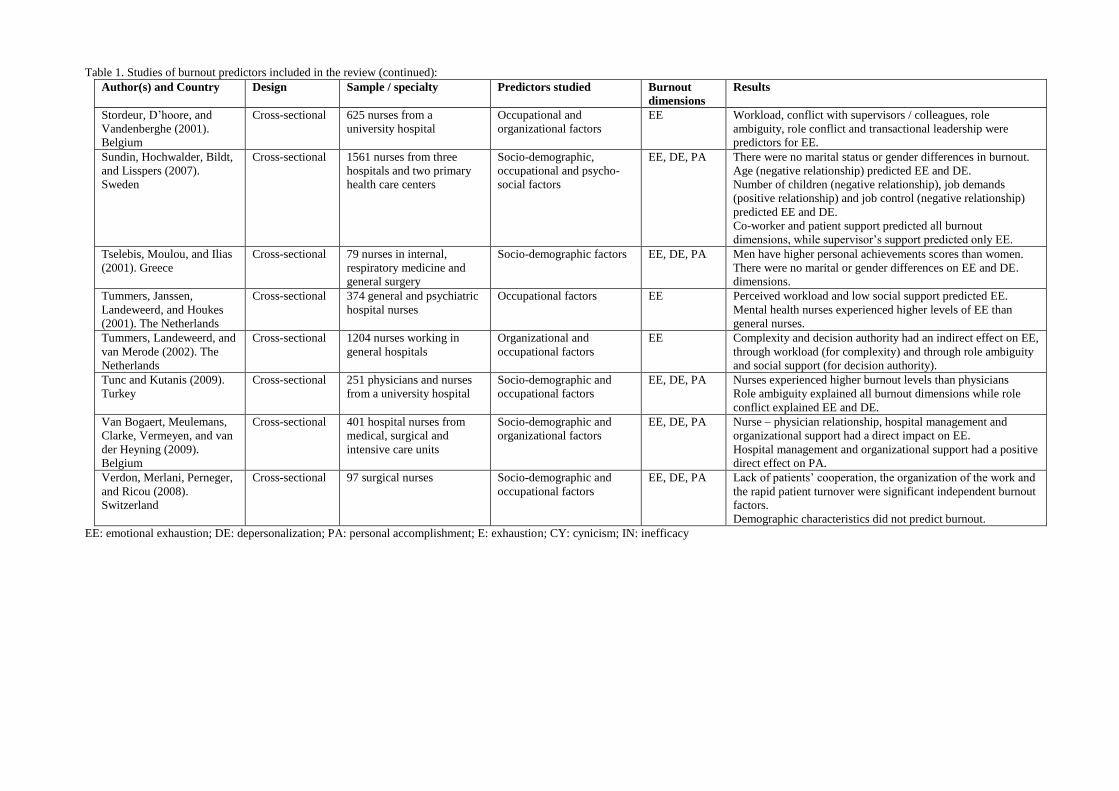
Table 1. Studies of burnout predictors included in the review (continued):
Author(s) and Country Design Sample / specialty Predictors studied Burnout
dimensions
Results
Stordeur, D‟hoore, and
Vandenberghe (2001).
Belgium
Cross-sectional 625 nurses from a
university hospital
Occupational and
organizational factors
EE Workload, conflict with supervisors / colleagues, role
ambiguity, role conflict and transactional leadership were
predictors for EE.
Sundin, Hochwalder, Bildt,
and Lisspers (2007).
Sweden
Cross-sectional 1561 nurses from three
hospitals and two primary
health care centers
Socio-demographic,
occupational and psycho-
social factors
EE, DE, PA There were no marital status or gender differences in burnout.
Age (negative relationship) predicted EE and DE.
Number of children (negative relationship), job demands
(positive relationship) and job control (negative relationship)
predicted EE and DE.
Co-worker and patient support predicted all burnout
dimensions, while supervisor‟s support predicted only EE.
Tselebis, Moulou, and Ilias
(2001). Greece
Cross-sectional 79 nurses in internal,
respiratory medicine and
general surgery
Socio-demographic factors EE, DE, PA Men have higher personal achievements scores than women.
There were no marital or gender differences on EE and DE.
dimensions.
Tummers, Janssen,
Landeweerd, and Houkes
(2001). The Netherlands
Cross-sectional 374 general and psychiatric
hospital nurses
Occupational factors EE Perceived workload and low social support predicted EE.
Mental health nurses experienced higher levels of EE than
general nurses.
Tummers, Landeweerd, and
van Merode (2002). The
Netherlands
Cross-sectional 1204 nurses working in
general hospitals
Organizational and
occupational factors
EE Complexity and decision authority had an indirect effect on EE,
through workload (for complexity) and through role ambiguity
and social support (for decision authority).
Tunc and Kutanis (2009).
Turkey
Cross-sectional 251 physicians and nurses
from a university hospital
Socio-demographic and
occupational factors
EE, DE, PA Nurses experienced higher burnout levels than physicians
Role ambiguity explained all burnout dimensions while role
conflict explained EE and DE.
Van Bogaert, Meulemans,
Clarke, Vermeyen, and van
der Heyning (2009).
Belgium
Cross-sectional 401 hospital nurses from
medical, surgical and
intensive care units
Socio-demographic and
organizational factors
EE, DE, PA Nurse – physician relationship, hospital management and
organizational support had a direct impact on EE.
Hospital management and organizational support had a positive
direct effect on PA.
Verdon, Merlani, Perneger,
and Ricou (2008).
Switzerland
Cross-sectional 97 surgical nurses Socio-demographic and
occupational factors
EE, DE, PA Lack of patients‟ cooperation, the organization of the work and
the rapid patient turnover were significant independent burnout
factors.
Demographic characteristics did not predict burnout.
EE: emotional exhaustion; DE: depersonalization; PA: personal accomplishment; E: exhaustion; CY: cynicism; IN: inefficacy

Copyright © 2022 FDOKUMEN