SYED MAHBOOB AHMAD.pdf
128
i “A STUDY ON ANTI-ULCER AND ANTI-INFLAMMATORY ACTIVITIES OF TUBER EXTRACTS OF SOLANUM TUBEROSUM (SOLANACEAE) IN RATS” By SYED MAHBOOB AHMAD B. Pharm. Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru In partial fulfillment of the requirements for the degree of MASTER OF PHARMACY IN PHARMACOLOGY Under the Guidance of Dr. T. SHIVARAJ GOUDA Associate Professor Department of Pharmacology V. L. College of Pharmacy Raichur- 584103 2011
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of SYED MAHBOOB AHMAD.pdf

i
“A STUDY ON ANTI-ULCER AND ANTI-INFLAMMATORY
ACTIVITIES OF TUBER EXTRACTS OF SOLANUM TUBEROSUM
(SOLANACEAE) IN RATS”
By
SYED MAHBOOB AHMAD
B. Pharm.
Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru
In partial fulfillment of the requirements for the degree of
MASTER OF PHARMACY
IN
PHARMACOLOGY
Under the Guidance of
Dr. T. SHIVARAJ GOUDA Associate Professor
Department of Pharmacology
V. L. College of Pharmacy Raichur- 584103
2011

ii
Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled “A STUDY ON ANTI-ULCER
AND ANTI-INFLAMMATORY ACTIVITIES OF TUBER EXTRACTS OF SOLANUM
TUBEROSUM (SOLANACEAE) IN RATS” is a bonafide and genuine research work
carried out by me under the guidance of Dr. T. Shivaraj Gouda, Associate Professor,
V.L. College of Pharmacy, Raichur.
Date: Place: Raichur (Syed Mahboob Ahmad)

iii
Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru. Dr. T.Shivaraj Gouda Dept of Pharmacology M.Pharm., Ph. D. V.L. College of Pharmacy Associate Professor Raichur – 584 103.
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A STUDY ON ANTI-ULCER AND
ANTI-INFLAMMATORY ACTIVITIES OF TUBER EXTRACTS OF SOLANUM
TUBEROSUM (SOLANACEAE) IN RATS” is a bonafide research work done by
Syed Mahboob Ahmad in partial fulfillment of the requirement for the degree of Master
of Pharmacy in Pharmacology.
Date: Signature of the Guide Place: Raichur

iv
Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru.
Dr. N. Venkat Rao Dr. S.M. Shantha Kumar M.Pharm., Ph D. M.Pharm., Ph. D, F.I.C Professor & HOD Principal Dept. of Pharmacology V.L. College of Pharmacy V.L. College of Pharmacy Raichur – 584 103. Raichur – 584 103.
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE
INSTITUTION
This is to certify that the dissertation entitled “A STUDY ON ANTI-ULCER AND
ANTI-INFLAMMATORY ACTIVITIES OF TUBER EXTRACTS OF SOLANUM
TUBEROSUM (SOLANACEAE) IN RATS” is a bonafide research work done by
Syed Mahboob Ahmad under the guidance of Dr. T. Shivaraj Gouda, Associate
Professor, V.L. College of Pharmacy, Raichur.
Dr. N. Venkat Rao Dr. S.M. Shantha Kumar M. Pharm., Ph. D. M.Pharm., Ph. D, F.I.C
Date: Date:
Place: Raichur Place: Raichur

v
COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this dissertation in print or
electronic format for academic / research purpose.
Date:
Place: Raichur (Syed Mahboob Ahmad)
© Rajiv Gandhi University of Health Sciences, Karnataka.

vi
Dedicated To My Beloved Family
Members

vii
Acknowledgement
First of all, I am grateful to the omnipresent, omniscient
and omnipotent, the Almighty ALLAH without whose grace I
could never have done the work and to whom I am
accountable for my every act done in this mundane world.
This thesis is the end of my journey in obtaining my
postgraduate degree in Pharmacology. I have not travelled in
a vacuum in this journey and some people who made this
journey easier with words of encouragement to expand my
thoughts and ideas.
It is an exciting, unforgettable and memorable moment
of my life, to express my profound and heartful thanks to my
beloved research guide Dr. T. SHIVARAJ GOUDA, Associate
Professor, Department of Pharmacology, V.L. College of
Pharmacy , Raichur, Karnataka, who has provided excellent
guidance. I am highly indebted to him for his valuable
presence, which helped me to complete this work successfully.

viii
I express my sincere gratitude, thanks and respect to
Dr. N.VENKAT RAO, Professor and Head Department of
Pharmacology, V.L. College of Pharmacy, Raichur, excellent
guidance during thesis work.
With pride and pleasure, I wish to express my thanks to
Dr. S.M SHANTHA KUMAR, Principal, V.L. College of Pharmacy,
Raichur, for his valuable help to carry out this work with great
ease and precision.
I express my heartful thanks to Dr. D. JEEVAN MANI BABU,
Asst. Professor, Dept. of Pharmacology for his help during the
work.
I wish to offer my respectable thanks to Dr. V. Hemanth
Kumar, Vice principal, V.L. College of Pharmacy, Raichur for
his support and kind cooperation.
I wish to offer my respectable thanks to Dr. K. M. SWAMY,
Dr. MD SALAHUDDIN, Dr. SREENIVAS, Dr. AYESHA, Mrs. HAFSA
MOHAMMADI, Dr. SHALAM, Sri MD SHAMSUDDIN V.L.College of
Pharmacy, Raichur for their encouragement during the course
of study.

ix
I express my sincere and heartful thanks to my seniors
Mr. BASHA, Mr. YASAR, Mr. NAZEER, Mr. HASNUDDIN,
Mr. RAJESH, Mr. NISHANT, Mr. VENU and Ms. MINHAZ. I thank
them all for their timely support and words of encouragement.
I would like to place on record the constant
encouragement and moral support to my batch mates
Mr. RAJESH, Mr. FASIH, Mr. BASHEER, Mr. MANOJ, Mr. RIZWAN,
Mr. SHIV, PETRICEA, RADHIKA and SWOMYA for completing this
task.
I express my thanks to all my juniors Mr. Vinod,
Mr. Karthik, Mr. Snehal, Mr. Riyaz, Mr. Promod, Mr. Lakshmi
Kanth, Mr. Maruthi, Ms. Manisha, Ms. Aruna, Ms. Sunanda,
Ms. Regina and Ms. Soumya for their constant, affectionate,
encouragement throughout my project work.
I express my sincere and heartful thanks to my Dy. Sales,
RSM and Dy. RSM of Macleod Pharmaceutical Ltd.
Mr. Sandeep Nayyar, Mr. Vivek Shael Mishra, and Mr. Omesh
Bhat, Delhi. I thank them all for their timely support and
words of encouragement.

x
I thank Smt Vasundhra, Sri Satyanarayan, Sri RK Patil,
Smt Vijaylakshmi, Sri Kantacharya, Sri Shekhar, Sri Gopal Rao
and Mareppa, for their cooperation and help throughout the
project work.
I extend my profound respect and heartful gratitude to
my beloved father JB SYED MAHMOOD AHMAD who always
covered me under the shade of love, affection and blessings
and my warmest of warm and the most important
acknowledgement, by far, is to my mother UMME HABIBA who is
the constant source of love, care, support, encouragement and
blessing. I am indebted for them for whole of my life.
I also thank my brothers JB HABIB AHMAD, SYED ZAFAR
ALI and SYED IMRAN SHAHID, my loving sisters GULRANA
PARVEEN, GUFRANA PARVEEN & ZEENAT FATIMA, Brother-In-
Law MD IDREES SIDDIQUE, SUHAIL SIDDIQUE and MASROOR
HUSSAIN my nephew AMAN & UMAR neice ZOYA and MAHIRA.
Whose moral and mental support, encouragement and prayers
have been the driving force behind my efforts and are
responsible for whatever I am today.

xi
Finally, I thank all those people who directly or indirectly
helped me and encouraged me during each and every step of
my life.
Date:
Place: Raichur (SYED MAHBOOB AHMAD)

xii
LIST OF ABBREVIATIONS
1. OC - Degree centigrade
2. ANOVA - Analysis of variance
3. Kg - Kilogram
4. LD50 - Lethal dose
5. mg - milligram
6. ml - millilitre
7. µg - microgram
8. Min - minutes
9. OECD - Organization for Economic Co-operation and Development
10. p.o. - Per Oral
11. S - Seconds
12. SEM - Standard Error Mean
13. i.p - Intra peritoneal
14. ED50 - Effective dose50
15. AOT - Acute Oral Toxicity
16. Fig. - Figure
17. IAEC - Institutional Animal Ethical Committee
18. NSAID’s - Nonsteroidal anti-inflammatory drugs
19. NaOH - Sodium hydroxide
20. %ROV - Percentage reduction in oedema volume
21. SD - Standard Deviation
22. vs - Versus

xiii
23. WHO - World Health Organization
24. Vol - Volume
25. S. tuberosum - Solanum tuberosum
26. NaCl - Sodium Chloride
27. H. pylori - Helicobacter pylori
28. AETST - Alcoholic Extract of Tubers of Solanum tuberosum
29. AQETST - Aqueous Extract of Tubers of Solanum tuberosum

xiv
ABSTRACT
Objectives:
To evaluate the anti-ulcer and anti-inflammatory activities of tubers extracts of
S. tuberosum in rats.
Background:
In Ayurvedic texts it was reported that tubers of S. tuberosum are used for anti-
ulcer, anti-gout, anti-inflammatory, anti-arthritic, diuretic, anti-scurvy and to increase
milk in lactating mothers. For external use, the grated raw S. tuberosum is applied
locally in cases of arthritis, itching, neuralgia and in mild burns. Since no scientific data
is available on anti-ulcer and anti-inflammatory activities of tubers extracts (alcoholic
and aqueous) of this plant, hence the present work is planned to evaluate the above
mentioned activities in experimental animal, rats.
Materials and methods:
For assessing anti-ulcer and anti-inflammatory activities, ulcer models like
pylorus ligation induced ulcer and stress induced ulcers by cold water immersion
models and carrageenan, histamine and formalin induced inflammatory models are
used. Standard reference compounds like Ranitidine and Ibuprofen respectively are
used in the above mentioned two models.
Resuts:
When AETST and AQETST are subjected for LD50 study none of them produced
behavior abnormalities or mortality even at the dose level of 2000 mg/kg body weight.
Preliminary phytochemical investigation reveals the presence of tannins, carbohydrate,
sterols, flavonoids, glycosides, alkaloid and triterpines in both the extracts.

xv
In pylorus ligation induced ulcer model, selected doses like low (100 mg/kg),
medium (200 mg/kg) and high (400 mg/kg) doses (AETST and AQETST) of both the
extracts significantly reduced the ulcers (P < 0.05*, 0.01** and 0.001***). In stress
induced ulcers by cold water immersion model also both the extracts with the doses
mentioned above significantly reduced the ulcers (P < 0.05*, 0.01** and 0.001***).
In carrageenan, histamine and formalin induced paw oedema inflammatory
models both the extracts with the 3 selected doses mentioned above significantly
reduced inflammation.
Conclusion:
The present study reveals that both the AETST and AQETST possessed both anti-
ulcer and anti-inflammatory activities. Phytochemical constituent like tannins,
flavonoids and triterpines are already reported for their anti-ulcer and anti-inflammatory
activities. These phytochemical constituents are present in both the extracts, hence
responsible for the observed activities.
Key words:
S. tuberosum, tubers, alcoholic and aqueous extracts, anti-ulcer activity, pylorus
ligation, stress, anti-inflammatory activity, carrageenan, histamine and formalin.

xvi
TABLE OF CONTENTS
S. No.
Contents
Page No.
1
Introduction
1-3
2
Objectives of the study
4
3
Review of Literature
5-47
4
Methodology
48-62
5
Results
63-88
6
Discussion
89-91
7
Conclusion 92
8
Summary
93
9
Bibliography 94-103
10
Annexures
104-107

xvii
LIST OF TABLES
S. No. Tables Page No.
1 Table No: 3.1 Name of the plants reported for anti-ulcer activity. 28
2 Table No: 3.2 Summary of the principal substances released in inflammation. 35
3 Table No: 3.3 Name of the plants reported for anti-inflammatory activity. 45
4 Table No: 3.4 Name of the plants reported for anti-ulcer and anti-inflammatory activities. 47
5 Table No: 4.1 List of materials and equipments used during experiment. 48
6 Table No: 4.2 Nature and Percentage yield of the extracts. 50
7 Table No: 4.3 Details of qualitative phytochemical tests. 51
8 Table No: 4.4 Ulcer scores. 56 9 Table No: 5.1 Antiulcer effects of AETST and AQETST in
pylorus ligation model in rats.
66
10 Table No: 5.2 Antiulcer effects of AETST and AQETST in pylorus ligation model in rats.
67
11 Table No: 5.3 Antiulcer effects of AETST and AQETST in stress induced ulcer model in rats.
68
12 Table No: 5.4 Antiulcer effects of AETST and AQETST in stress induced ulcer model in rats. 69
13 Table No: 5.5 Antiulcer effects of AETST and AQETST in different ulcer models in rats. 70
14 Table No: 5.6 Anti-inflammatory effects of AETST and AQETST in Carrageenan induced paw oedema in rats. 77
15 Table No: 5.7 Anti-inflammatory effects of AETST and AQETST in Carrageenan induced paw oedema in rats at different time intervals.
78
16 Table No: 5.8 Anti-inflammatory effects of AETST and AQETST in Histamine induced paw oedema in rats.
81

xviii
17 Table No: 5.9 Anti-inflammatory effects of AETST and AQETST in Histamine induced paw oedema in rats at different time intervals.
82
18 Table No: 5.10 Anti-inflammatory effects of AETST and AQETST in Formalin induced paw oedema model in rats.
85
19 Table No: 5.11 Anti-inflammatory effects of AETST and
AQETST in Formalin induced paw oedema model in rats at different time intervals.
86

xix
LIST OF FIGURES
S. No. Figures Page No.
1 Fig No.3.1 Gastric acid secretion. 17
2 Fig No.3.2 Events in Acute and Chronic Inflammation. 34
3 Fig No.3.3 Mechanism of action of NSAIDs. 42
4 Fig No.5.1 Anti-ulcer activity of AETST and AQETST in pylorus ligation induced ulcer model in rats.
71
5 Fig No.5.2 Anti-ulcer activity of AETST and AQETST on free acidity in pylorus ligation induced ulcers in rats.
71
6 Fig No.5.3 Anti-ulcer activity of AETST and AQETST on total acidity in pylorus ligation induced ulcers in rats.
72
7 Fig No.5.4 Anti-ulcer activity of AETST and AQETST in stress induced ulcer model in rats.
73
8 Fig No.5.5 Anti-ulcer activity of AETST and AQETST on free acidity in stress induced ulcers in rats.
73
9 Fig No.5.6 Anti-ulcer activity of AETST and AQETST on total acidity in stress induced ulcers in rats.
74
10 Fig No.5.7 Anti-inflammatory activity of AETST and AQETST in Carrageenan induced paw oedema model in rats.
87
11 Fig No.5.8 Anti-inflammatory activity of AETST and AQETST in Histamine induced paw oedema model in rats.
87
12
Fig No.5.9 Anti-inflammatory activity of AETST and AQETST in Formalin induced paw oedema model in rats.
88

Dept. of Pharmacology, V.L.C.P Raichur Page 1
1. INTRODUCTION
Plants have been one of the important sources of medicine since dawn of human
civilization. These are the gifts of nature to mankind for treating different types of diseases.
Almost from prehistoric period herbal medicine are used for alleviation of suffering caused
by different diseases in human. Further they are well documented in India and other
countries: even today they are in great use in these countries. There are several beliefs or
claims regarding the therapeutic utility of herbs and herbal formulation i.e;
• Herbal medicines exhibit fewer side effects and are safe.
• Herbs and herbal formulations are cheaper and easily available.
• For certain disease like hepatitis, herbs and herbal drugs are the only remedies.
• Certain chemical constituents from the herbs are serving as prototype molecules for
the discovery of more effective drugs than existing ones.
Medicinal plants are treated as a subject of serious study and undergoing intense
research all over the World to identify the lead molecules. The immense surge of scientific
interest in natural products as a potential source of drugs has contributed to the
development of phytopharmacology research. In many developing countries, phyto-
pharmaceuticals form the main base of National Health Care Programmed e.g. the use of
herbal extracts in the treatment of various diseases in different countries and they are also
known to possess a rich traditional medicine. In South Africa it is estimated that 80% of
the black population consults traditional practitioners, perhaps this is not one and only
reason for the developing countries to invest in plant based pharmaceuticals but also has
been a global resurgence of interest in plant based drugs.

Dept. of Pharmacology, V.L.C.P Raichur Page 2
Herbal therapy provides rational means for the treatment of many diseases which are
considered to be obstinate and incurable in other system of medicine. It lays a great deal of
emphasis upon the maintenance of positive health of an individual and thus aims at both
the prevention and cure of diseases.
Hyperacidity / Ulcers which require the treatment for chronic period of time and the
usage of such drugs may cause various side effects, sometimes with permanent damage of
vital organs. The ulcer is one of chronic disease which is normally treated with H2-receptor
blockers (Cimetidine, Ranitidine) and proton pump inhibitors (Omeprazole, Pentaprazole).
These drugs are known to effect microsomal enzyme system of the liver resulting in the
pharmacokinetic type of drug- drug interaction with other drugs. But in herbal / traditional
medicines, there are several preparations prescribed to treat hyperacidity and ulcers.
Inflammation is a normal protective response to tissue injury caused by physical
trauma, noxious chemical or microbiological agents. It is body’s response for tissue repair
and is triggered by the release of chemical mediators from injured tissue and migrating
cells. The mechanism of anti-inflammatory drugs is considered to be inhibition of
prostaglandins synthesis at the site of injury. The anti-inflammatory potency of different
compounds roughly corresponds with their ability to inhibit cyclooxygenase enzyme
(COX).
The traditional medicine is largely gaining popularity over allopathic medicine
because of the following reasons.
• Rising cost of medical care.
• Natural products are free from side effects.

Dept. of Pharmacology, V.L.C.P Raichur Page 3
• No reoccurrence after the treatment.
• Easy availability of the drugs from natural sources especially in Developing
countries.
• Cure of disease by the changes in life style and social pathology.
• Renewable sources.
In the present study, we have chosen a plant S. tuberosum (Solanaceae) for which
different pharmacological activities are reported with different parts of the plant. From the
literature Ayurvedic texts we found that tubers of S. tuberosum have been traditionally
indicated for the treatments of anti-ulcer and anti-inflammatory condition. However anti-
ulcer and anti-inflammatory activities of this plant are not reported. But for its medicinal
properties reported in the Ayurvedic texts prompted us to select tubers extracts of this plant
for the study of anti-ulcer and anti-inflammatory activities in different experimental animal
models1-6.

Dept. of Pharmacology, V.L.C.P Raichur Page 4
2. OBJECTIVES OF THE STUDY
Since the plant S. tuberosum has not explored to significant extent and on the
background of available information of the plant, the present work was planned with the
following objectives.
1. To prepare various extracts (alcoholic and aqueous) with tubers of S. tuberosum, family
Solanaceae, by successive extraction technique and to analyze the extracts for the
phytochemical constituents.
2. To establish the pharmacological profile of the extracts of tubers of S. tuberosum.
• To assess the acute toxicity (LD50) of the two extracts.
• To screen for the anti-ulcer and anti-inflammatory activities in rats.
o To evaluate anti-ulcer activity of the tubers extracts in various
experimental animal models like-
a) Pylorus ligation induced ulcers in rats (SHAY) with the
estimation of parameters like volume of gastric juice, pH, free and
total acidity and ulcer index.
b) Stress induced ulcers (cold-water immersion induced ulcers).
o To evaluate anti-inflammatory activity of the tubers extracts in various
experimental animal models like-
a) Carrageenan induced paw oedema model in rats.
b) Histamine induced paw oedema model in rats.
c) Formalin induced paw oedema model in rats.

Dept. of Pharmacology, V.L.C.P Raichur Page 5
3. REVIEW OF LITERATURE
Plant name: S. tuberosum Family: Solanaceae
S. tuberosum plant

Dept. of Pharmacology, V.L.C.P Raichur Page 6
S. tuberosum tuber
3.1 Description of the Plant:
Family : Solanaceae
Genus : Solanum
Species : S. tuberosum
Synonym : Hindi – Alu
Sanskrit– Golakandah
Kannada – Batate
Marathi – Batata
Distribution: It grows throughout India and World.
The Plant: The S. tuberosum is a starchy, tuberous crop from the perennial S. tuberosum
of the Solanaceae family (also known as the nightshades).
Leaves: Leaves are very variable 2-6 in a whorl and green in colour.
Flowers: They bear white, pink, red, blue or purple flowers with yellow stamens.
Tubers: The tubers of varieties with white flowers have white skins, while those of
varieties with colored flowers tend to have pinkish skins.
Roots: Roots are reddish brown.

Dept. of Pharmacology, V.L.C.P Raichur Page 7
Major chemical constituents:
S. tuberosum contains starch, sugar (glucose, sucrose and fructose), cellulose (10-
20%), crude fiber, pectin substances (0.7-1.5% of dry wt), hemicelluloses (1%), fat (1.1%)
and vitamin C. The proteins of S. tuberosum tuber are comprised of about 60-70% globulin
and 20-40% glutelin with no albumin. 21 amino acids have been identified as normal
constituents of the alcohol - soluble nitrogen of S. tuberosum tuber tissue which is cystine,
aspartic, glutamic acids, serine, glycine, asparagine, theonine, alanine, glutamine, alpha
amino n-butyric acid, histidine, arginine, lysine, proline, methionine sulfoxide, valine,
isoleucine, phenylalanine, trylophane and tyrosine. Citric, isocitric, ascorbic, lactic, malic,
tartaric, succinic, oxalic, hydroxymalonic, aconitic, phytic, alpha ketoglutaric, guinic,
caffeic and chlorogenic organic acids are present in S. tuberosum.
The inorganic constituents or mineral content of S. tuberosum vary with variety.
Medicinal uses:
S. tuberosum tubers are used as anti-ulcer, anti-gout, anti-inflammatory, anti-arthritic,
diuretic, anti-scurvy and to increase milk in lactating mothers. For external use, the grated
raw S. tuberosum is applied locally in cases of arthritis, itching, neuralgia and in mild
burns7-8.

Dept. of Pharmacology, V.L.C.P Raichur Page 8
3.2 ULCER
Ulcer is defined as the erosion in the lining of the stomach or duodenum and is
caused by the disruptions of the gastric mucosal defense and repair systems. Ulcer in the
stomach is called gastric ulcer and in the duodenum is called duodenal ulcer and together
peptic ulcer. In clinical practice, peptic ulcer is one of the most prevalent gastrointestinal
disorders, commonly occurs in developed countries (Gregory M et al, 2009) 9.
Peptic ulcer, also known as PUD or peptic ulcer disease is a break in the lining
(mucosa) of the digestive tract produced by digestion of the mucosa by pepsin and acid,
occurs when pepsin and acid are present in high concentration or when some other
mechanism reduces the normal protective mechanism of the mucosa; bile salts may play a
part, especially in stomach ulcer10.
It was once commonly thought that stress, smoking and diet were the principal causes
of stomach ulcers. However, the Helicobacter pylori (H. pylori) bacterium is now known
to be responsible for most duodenal ulcers and 60 per cent of stomach ulcers. The H. pylori
a gram -ve bacterium also produce many symptoms of dyspepsia or indigestion. Treatment
for stomach ulcers includes acid-suppressing drugs and the use of antibiotics to kill the
infection.
3.2.1 Symptoms:
Symptoms of a peptic ulcer are
• Abdominal pain, classically epigastric with severity relating to mealtimes, after
around 3 hours of taking a meal (duodenal ulcers are classically relieved by food,
while gastric ulcers are exacerbated by it).

Dept. of Pharmacology, V.L.C.P Raichur Page 9
• Bloating.
• Water brash (rush of saliva after an episode of regurgitation to dilute the acid in
esophagus)
• Nausea and copious vomiting.
• Loss of appetite and weight.
• Hematemesis (vomiting of blood); this can occur due to bleeding directly from a
gastric ulcers or from damage to the esophagus from severe/continuing vomiting.
• Melena (tarry, foul-smelling feces due to oxidized iron from hemoglobin).
• Rarely, an ulcer can lead to a gastric or duodenal perforation, which leads to acute
peritonitis. This is extremely painful and requires immediate surgery.
3.2.2 Complications:
• Gastrointestinal bleeding is the most common complication and sudden large
bleeding can be life-threatening, occurs when the ulcer erodes one of the blood
vessels.
• Perforation (a hole in the wall) often leads to catastrophic consequences. Erosion of
the gastro-intestinal wall by the ulcers leads to spillage of stomach or intestinal
content into the abdominal cavity. Perforation at the anterior surface of the stomach
leads to acute peritonitis, initially chemical and later bacterial peritonitis. The first
sign is often sudden intense abdominal pain. Posterior wall perforation leads to
pancreatitis; pain in this situation often radiates to the back.
• Penetration is when the ulcer continues into adjacent organs such as the liver and
pancreas.

Dept. of Pharmacology, V.L.C.P Raichur Page 10
• Scarring and swelling due to ulcers causes narrowing in the duodenum and gastric
outlet obstruction. Patient often presents with severe vomiting.
• Cancer is included in the differential diagnosis (elucidated by biopsy), H pylori as
the etiological factor making it 3 to 6 times more likely to develop stomach cancer
from the ulcers11.
3.2.3 Classification of peptic ulcer:
Peptic ulcer may arise at various locations:
a) Stomach (called gastric ulcer)
b) Duodenum (called duodenal ulcer)
c) Esophagus (called esophageal ulcer) and
d) Meckel's diverticulum12.
a) Stomach Ulcer (Gastric Ulcer):
A stomach ulcer is small erosion (hole) in the stomach are called gastric ulcers. An
ulcer is contagious or cancerous. Duodenal ulcers are almost always benign, while stomach
ulcers may become malignant.
Stomach ulcer disease is common, affecting millions of peoples yearly. The size of a
stomach ulcer can range between 1/8 to 3/4 of an inch. Children too develop stomach
ulcers.
Stomach ulcers may be a symptom of another disease or condition and are often
common in mastocytosis. Bleeding from stomach ulcers may cause iron deficiency anemia.

Dept. of Pharmacology, V.L.C.P Raichur Page 11
The direct cause of peptic ulcers is the destruction of either gastric or intestinal
mucosal lining of the stomach/ intestine by hydrochloric acid, normally present in the
digestive juices of the stomach. Infection with the bacterium H. pylori is thought to play an
important role in causing both gastric and duodenal ulcers, may be transmitted from person
to person through contaminated food and water. Antibiotics are the most effective
treatment for H. pylori induced peptic ulcers13.
Causes of Stomach Ulcers:
• Family history of ulcers, smoking, excess alcohol consumption, improper diet,
skipped meals and Zollinger-Ellison syndrome.
• Use of nonsteroidal anti-inflammatory medications or corticosteroids.
• Type O blood (for duodenal ulcers).
• Stress does not cause an ulcer, but may be a contributing factor.
• Chronic disorders such as liver disease, emphysema, rheumatoid arthritis may
increase vulnerability to ulcers13.
Symptoms of ulcers in stomach:
The major symptom of an ulcer is a burning or gnawing feeling in the stomach area
that lasts between 30 min to 3 h. This pain is often interpreted as heartburn, indigestion or
hunger usually occurs in the upper abdomen, but sometimes it may occur below the
breastbone. In some individuals the pain occurs immediately after eating. In other
individuals, the pain may not occur until hours after eating and frequently awakens the
person at night13.
b) Duodenal ulcer:

Dept. of Pharmacology, V.L.C.P Raichur Page 12
Stomach normally produces acid to help the digestion of food and to kill bacteria and
is corrosive and some cells on the inside lining of the stomach and duodenum produce a
natural mucus barrier which protects the lining of both the stomach and duodenum. There
is normally a balance between the amount of acid and the mucus defense barrier. An ulcer
may develop with an alteration in this balance allowing the acid to damage the lining of the
stomach or duodenum14.
Causes Duodenal Ulcer:
• Infection with H. pylori.
• Anti-inflammatory drugs - including aspirin, ibuprofen, diclofenac etc.
• Zollinger-Ellison syndrome.
• Other factors such as smoking, stress and drinking heavily may possibly increase
the risk of having a duodenal ulcer14.
Symptoms of Duodenal Ulcer:
• Pain in the upper abdomen just below the sternum (breastbone) is the common
symptom. On and off occurs most before meals or in hunger conditions. It may be
eased with food or antacid tablets.
• Other symptoms which may occur include: bloating, retching and a feeling of
sick. Sometimes food makes the pain worse.
• Complications occur in some cases and can be serious. These include:
Bleeding ulcer. This can range from a 'trickle' to a life-threatening
bleed.

Dept. of Pharmacology, V.L.C.P Raichur Page 13
Perforation. This is where the ulcer goes right through (perforates)
the wall of the duodenum. Food and acid in the duodenum then leak
into the abdominal cavity. This usually causes severe pain and is a
medical emergency14.
c) Esophageal ulcer:
Esophageal Ulcers are defined as open sores or lesions in the lining of the esophagus,
usually cause pain felt behind or just below breastbone, similar to heartburn symptoms.
Healing is slow, chronic and severe recurrences can result in a narrowing of esophagus
after healing15.
Causes:
The direct cause of esophageal ulcers is the destruction of the lining of the esophagus
H. pylori bacteria usually found in the stomach.
Other common causes of esophageal ulcers are: Chronic use of anti-inflammatory
medications, smoking cigarettes, chewing tobacco, Gastro Esophagal Reflux Disorder
(GERD) and bulimia15.
Symptoms of Esophageal Ulcers:
Heartburn, inflammation of the esophagus.
A slight bleeding, blood vomiting bright red in colour and coffee ground black or
dark tarry stools.
Include nausea, abdominal indigestion and cramping15.
d) Meckel's Diverticulum:

Dept. of Pharmacology, V.L.C.P Raichur Page 14
It was first described by Fabricius Hildanus in the 16th century and later named after
Johann Friedrich Meckel, who described the embryological origin of this type of
diverticulum in 1809.
Meckel's diverticulum a true congenital diverticulum is a small bulge in the small
intestine present at birth. It is a vestigial remnant of the omphalomesenteric duct (also
called the vitelline duct) and is the most frequent malformation of the gastrointestinal tract.
It is present in approximately 2% of the population, with males more frequently
experiencing the symptoms.
Presentation:
Meckel's diverticulum is located in the distal ileum, usually about 60-100 cm of the
ileocecal valve. It is typically 3-5 cm long, runs antimesenterically and has its own blood
supply. It is a remnant of the connection from the umbilical cord to the small intestine
present during embryonic development. It can also present as an indirect hernia, where it is
known as a "Hernia of Littre". Furthermore, it can be attached to the umbilical region by
the vitelline ligament with the possibility of vitelline cysts, or even a patent vitelline canal
forming a vitelline fistula when the umbilical cord is cut. Torsions of intestine around the
intestinal stalk may also occur, leading to obstruction, ischemia and necrosis.
Symptoms:
Approximately 98% of people affected with Meckel's diverticulum are
asymptomatic. If symptoms do occur, they typically appear before the age of two.
The most common presenting symptom is painless rectal bleeding, followed by
intestinal obstruction, volvulus and intususception. Occasionally, Meckel's diverticulitis
may present with all the features of acute appendicitis. Also, severe pain in the upper

Dept. of Pharmacology, V.L.C.P Raichur Page 15
abdomen is experienced by the patient along with bloating of the stomach region. At times,
the symptoms are so painful such that they may cause sleepless nights with extreme pain in
the abdominal area16.
3.2.4 Gastrointestinal Tract:
In order to digest food, absorb nutrients and excrete unabsorbed waste products, the
gastrointestinal tract has to perform a number of coordinated activities and to provide the
whole body with a continual supply of water, electrolytes and nutrients. In order to achieve
these objectives, several organs have to integrate with each other and regulated by nervous
and hormonal system, as well as the central nervous system17.
3.2.5 Control and Co-ordination of GI Tract:
The blood vessels and the glands (exocrine, endocrine and paracrine) that comprise
the gastrointestinal tract are under the control of both neuronal and hormonal
mechanisms.
a) Neuronal Control:
There are two principal intramural plexuses in the tract: the myenteric plexus
(Auerbach's plexus) between the outer, longitudinal and the middle, circular muscle layers
and the submucous plexus (Meissner's plexus) on the luminal side of the circular muscle
layer. These plexuses are interconnected and their ganglion cells receive preganglionic
parasympathetic fibres from the vagus, which are mostly cholinergic and excitatory,
although a few are inhibitory. Incoming sympathetic fibres are largely postganglionic and
these in addition to innervating blood vessels, smooth muscle and some glandular cells
directly may terminate in these plexuses, where they inhibit acetylcholine secretion. The
neurons within the plexuses constitute the enteric nervous system and secrete not only

Dept. of Pharmacology, V.L.C.P Raichur Page 16
acetylcholine and noradrenaline (norepinephrine), but also 5-hydroxytryptamine, purines,
nitric oxide and a variety of pharmacologically active peptides. The enteric plexus also
contains sensory neurons, which respond to mechanical and chemical stimuli.
B) Hormonal Control:
The hormones of the gastrointestinal tract include both endocrine and paracrine
secretions. The endocrine secretions (i.e. substances released into the bloodstream) are
mainly peptide in nature and are synthesised by endocrine cells in the mucosa. Important
examples include gastrin and cholecystokinin. The paracrine secretions include many
regulatory peptides released from special cells found throughout the wall of the tract.
These hormones act on nearby cells, and in the stomach the most important of these is
histamine. Some of these paracrine factors also function as neurotransmitters18.
3.2.6 Physiology of Gastric Secretion:
The parietal cell contains receptors for gastrin, histamine (H2) and acetylcholine
(muscarinic, M3). When acetylcholine or gastrin bind to the parietal cell receptors, they
cause an increase in cytosolic calcium, which in turn stimulates protein kinases that
stimulate acid secretion from a H+/K+ ATPase (the proton pump) on the canalicular
surface.
In close proximity to the parietal cells are gut endocrine cells called enterochromaffin-like
(ECL) cells. ECL cells have receptors for gastrin and acetylcholine and are the major
source for histamine release. Histamine binds to the H2 receptor on the parietal cell,
resulting in activation of adenylylcyclase, which increases intracellular cyclic adenosine
monophosphate (cAMP). cAMP activates protein kinases that stimulate acid secretion by
the H+/K+ ATPase. In humans, it is believed that the major effect of gastrin upon acid

Dept. of Pharmacology, V.L.C.P Raichur Page 17
secretion is mediated indirectly through the release of histamine from ECL cells rather than
through direct parietal cell stimulation19.
Fig No.3.1 Gastric acid secretion
3.2.7 Pathophysiology:
Peptic ulcers are defects in the gastric or duodenal mucosa that extend through the
muscularis mucosa. H. pylori infection and NSAID use are the most common etiologic
factors. Other, less common causes are hypersecretory states such as Zollinger-Ellison
syndrome.

Dept. of Pharmacology, V.L.C.P Raichur Page 18
Under normal conditions, a physiologic balance exists between peptic acid secretion
and gastroduodenal mucosal defense. Peptic ulcer occurs when the balance between the
aggressive factors and the defensive mechanisms is disrupted. Aggressive factors, such as
NSAIDs, H. pylori, alcohol, bile salts, acid and pepsin can alter the mucosal defense
mechanisms19.
3.2.8 H. pylori in the pathogenesis of peptic ulcer disease:
H. pylori are a spiral shaped Gram -ve bacterium with flagella that has a urease
enzyme which hydrolyzes urea into ammonia and bicarbonate. The alkaline
microenvironment produced by this action protects the organism from gastric acid. Active
motility of the organism by virtue of its flagella allows it to penetrate the mucus layer of
the gastric mucosa. Pathogenesis of gastroduodenal injury due to H. pylori infection is
explained by ‘leaking roof hypothesis’. H. pylori infection is believed to injure submucosal
tissue by causing a 'leak' in its protective coating of mucin gel and epithelial cells (the roof)
thereby making it susceptible to gastric acid (the rain). Secretion of urease, specific
adhesion receptor interaction, cytotoxins (including hemolysin), superoxide dismutase,
heat shock proteins, mucinase, lipase and phospholipase are some of bacterial virulence
determinants. H. pylori strains collected from patients ulcers with are genetically different
from those isolated from asymptomatic individuals20, 21.
Clinical manifestations of H. pylori:
H. pylori, are the primary cause for gastric inflammation, resides exclusively in
gastric mucosa, but can be found in remote areas that have undergone metaplastic changes
in which gastric epithelial cells are present such as esophagus, duodenum or Meckel's

Dept. of Pharmacology, V.L.C.P Raichur Page 19
diverticulum. A higher concentration of bacteria is found in the antral area and the major
risk factors for bleeding are H. pylori infection NSAID’s use and stress22, 23.
3.2.9 Pathologic changes in peptic ulcers:
Peptic ulcers are solitary (80%), small (1-2.5 cm in diameter) and round to oval. The
mucosal folds converge towards the ulcer and vary in depth from superficial (confined to
mucosa) to deep ulcers (penetrating into the muscular layer). Chronic duodenal ulcer never
turns malignant, while chronic gastric ulcer turns to carcinoma. Malignant gastric ulcers
are larger, bowl-shaped with elevated and indurate mucosa of the margin24.
Macroscopical appearance:
Gastric ulcers are most often localized on the lesser curvature of the stomach, round
to oval parietal defect (hole) 2 to 4 cm diameter, with a smooth base and perpendicular
borders. These borders are not elevated or irregular in the acute form of peptic ulcer,
regular but with elevated borders and inflammatory surrounding in the chronic form. In the
ulcerative form of gastric cancer the borders are irregular. Surrounding mucosa may
present radial folds, as a consequence of the parietal scarring25.
Microscopical appearance:
Gastric / peptic ulcer is a mucosal defect which penetrates the muscularis mucosa and
muscularis propria, produced by acid-pepsin aggression. Ulcer margins are perpendicular
and present with chronic gastritis. Microscopically, chronic peptic ulcers have 4
histological zones, from outside to inside are-
i) Necrotic zone- It lies in the floor of the ulcer and is composed of fibrous exudates
containing necrotic debris and a few leucocytes.

Dept. of Pharmacology, V.L.C.P Raichur Page 20
ii) Superficial exudative zone- It lies underneath the necrotic zone. The tissue elements
show coagulative necrosis giving eosinophilic, smudgy appearance with nuclear debris.
iii) Granulation tissue zone- It is seen merging into the necrotic zone, composed of non-
specific inflammatory infiltrate and proliferating capillaries.
iv) Zone of cicatrisation- It is seen merging into thick layer of granulation tissue,
composed of dense fibro-collagenic scar tissue over which granulation tissue rests.
Thrombosis or sclerotic arteries cross the ulcer, which on erosion results in hemorrhage26.
3.2.10 Clinical features:
1. Pain- In gastric ulcer, epigastric pain occurs immediately or within 2 h after food
and never occurs at night. In duodenal ulcer, pain is severe, occurs late night
(hunger pain) and is usually relieved by food.
2. Age- The peak incidence of duodenal ulcer is in 5th decade while that for gastric
ulcer is a decade later.
3. Periodicity- The attacks in gastric ulcer last from 2-6 weeks, with interval of
freedom from 1-6 months. The attacks of duodenal ulcer are classically worsened
by ‘work, worry and weather’.
4. Vomiting- Vomiting which relieves the pain is a conspicuous feature in patients of
gastric ulcer. Duodenal ulcer patients rarely have vomiting but instead get heart-
burn (retrosternal pain) and water brash (burning fluid into the mouth).
5. Hematemesis and melaena - Hematemesis and melaena occur in gastric ulcers in
gastric ulcers in the ratio of 60:40, while in duodenal ulcers in the ratio of 40:60.

Dept. of Pharmacology, V.L.C.P Raichur Page 21
Both may occur together more commonly in duodenal ulcer than in gastric ulcer
patients.
6. Appetite- The gastric ulcers patients, though have good appetite but are afraid to
eat, while duodenal ulcer patients have very good appetite.
7. Diet- Patients of gastric ulcer commonly get used to a bland diet consisting of milk,
eggs etc and avoid taking fried foods, curries and heavily spiced foods. In contrast,
duodenal ulcer patients usually take all kinds of diet.
8. Weight- Loss of weight is a common finding in gastric ulcer patients while patients
of duodenal ulcer tend to gain weight due to frequent ingestion of milk to avoid
pain.
9. Deep tenderness- Deep tenderness is present in both types of peptic ulcers. In the
case of gastric ulcer it is in the midline of the epigastrium, while in the duodenal
ulcer it is in the right hypochondrium26, 27.
3.2.11 Complications:
If ulcers remain untreated they may lead to:
Gastrointestinal bleeding: It is the most common complication and sudden large bleeding
can be life threatening, occurs when the ulcer erodes one of the blood vessels.
Perforation (hole in the wall): It often leads to catastrophic consequences. Erosion of the
gastro-intestinal wall by the ulcer leads to spillage of stomach or intestinal content into
abdominal cavity. Perforation at the anterior surface of stomach leads to acute peritonitis,
initially chemical and later bacterial peritonitis. Often first sign is sudden intense

Dept. of Pharmacology, V.L.C.P Raichur Page 22
abdominal pain. Posterior wall perforation leads to pancreatitis; pain in this situation often
radiates to back.
Penetration: It occurs when the ulcer continues into adjacent organs such as liver and
pancreas.
Obstruction: Scarring and swelling due to ulcers causes narrowing in the duodenum and
gastric outlet obstruction. Patient often presents with severe vomiting26,27.
3.2.12 Treatment of Peptic Ulcers:
Classification of Antiulcer Drugs:
A. Reduction of gastric acid secretion -
1. H2 receptor antagonist -
Ex. - Cimetidine, Ranitidine, Famotidine.
2. Proton pump inhibitors -
Ex. – Omeprazole, Pantoprazole, Lansoprazole, Rabeprazole.
3. Anticholinergics -
Ex. – Pirenzepine.
4. Prostaglandins analogue -
Ex. – Mesoprostol.
B. Neutralizing of gastric acid -
1. Systemic antacid -

Dept. of Pharmacology, V.L.C.P Raichur Page 23
Ex. – Sodium bicarbonate, Sodium citrate.
2. Non systemic antacid-
Ex. – Alluminium hydroxide, Magnesium hydroxide, Magaldrate, Calcium carbonate.
C. Ulcer protective -
Ex. – Sucralfate.
D. Anti- H. Pylori drugs -
Ex. - Amoxicillin, Clarithromycin, Metronidazole, Tinidazole.
A. Reduction of gastric acid secretion:
1. H2 receptor antagonists:
Mechanism of action - Drugs like cimetidine, ranitidine, famotidine are act on the H2
receptors and they inhibit the gastric acid secretion.
H2 receptor antagonists competitively blocking the binding of histamine to H2
receptors and reduce intracellular concentration of cyclic AMP and there by secretion of
gastric acid.
Pharmacokinetic-
Cimetidine - It is given orally, distribute throughout the body, excreted mainly in the
urine, bioavailability is 60-80% due to first pass metabolism. About 2/3rd of dose is
excreted unchanged in the urine and bile. The elimination t ½ is 2-3 h.

Dept. of Pharmacology, V.L.C.P Raichur Page 24
Ranitidine - Compared to cimetidine, ranitidine is 5 to 10 times more potent and minimal
side effects and the elimination t ½ is 2-3 h.
Famotidine- Famotidine is 20-160 time more potent than ranitidine and the oral
bioavailability is 40-50%, excreted through kidney; elimination t ½ is 2.5 to 3.5 h.
Adverse effects - The most common side effect is headache, dizziness, diarrhoea and
muscular pain. CNS side effects are confusion, hallucination, reduce of sperm count and
also inhibit cytochrome P-450 which can slow the metabolism of several drugs.
Dose – Cimetidine 400 mg BD, Ranitidine 150 mg BD, Famotidine 20 mg BD.
2. Proton pump inhibitors:
Mechanism of action - (Omeprazole, Pantoprazole, Lansoprazole, Rabeprazole) These
drugs bind to the H+ / K+ ATPase enzyme system (Proton pump) of parietal cells
suppressing the secretion of hydrogen ions into the gastric lumen. The membrane bound
proton pump is the final step in the secretion of gastric acid.
Omeprazole, Pantoprazole, Lansoprazole and Rabeprazole inhibit the basal and
stimulated gastric acid secretion (more than 90% acid suppression) begins within 1-2 h
after first dose.
Pharmacokinetic - Plasma t ½ is 1-2 h and metabolites of these agents are excreted in
urine and faeces.

Dept. of Pharmacology, V.L.C.P Raichur Page 25
Adverse effects - These drugs are generally well tolerated. Minimal side effects are
nausea, vomiting, loose stool, headache, abdominal pain, muscle and joint pains and
dizziness are complained by 3-5% of patients.
Dose- Omeprazole 20 mg daily, Pantoprazole 40 mg daily, Lansoprazole 15-30 mg daily,
Rabeprazole 20 mg daily.
3. Anticholinergics - (Pirenzepine) Muscaranic receptor stimulation increases
gastrointestinal motility and secretory activity. Cholinergic antagonist such as pirenzepine
is used in the management of peptic ulcer, which reduces the volume of gastric juice
without raising the gastric pH but is reduced by 40-50% without producing intolerable side
effects.
4. Prostaglandin analogues - (Mesoprostol) Prostaglandins produced by the gastric
mucosa, inhibit secretion of Hcl and stimulate secretion of mucus and bicarbonate.
Deficiency of PG involved in the pathogenesis of peptic ulcer. Mesoprostol, an
analogue of PG E is the only agent approved for prevention of gastric ulcer induced by
NSAIDs.
It is less effective than H2 antagonist for acute treatment of peptic ulcers and
clinically effective only at higher doses that diminish gastric acid secretion.
Adverse effects - Diarrhoea, abdominal cramps, uterine bleeding are the adverse effect and
it is contraindicated in pregnancy.
Dose - 400 μg 4 times a day.
B. Neutralizing of gastric acid (Antacids):

Dept. of Pharmacology, V.L.C.P Raichur Page 26
Antacids are weak bases that react with gastric acid to form salts and water there by
diminishing gastric acidity. Since pepsin is inactivated at pH > 4.0 antacids also reduce
gastric acidity. Antacids are of two types –
a) Systemic Antacids.
b) Non systemic antacids.
a) Systemic Antacids –
Sodium bicarbonate is an example of systemic antacid, act rapidly and raises the pH
to 7.4. On neutralizing of gastric acid it form NaCl and CO2. NaCl remain unchanged and
is unable to neutralize the bicarbonate in the intestine therefore later absorbed causing
systemic alkalosis. Formation of CO2 can dangerous if the ulcers is near perforation.
b) Non systemic antacids –
They are of two types-
i) Buffer type.
ii) Non buffer type.
i) Buffer type –
Alluminium hydroxide - They have a slow onset of action but longer duration of action
and raise the pH 3.5- 4.0. It has astringent and demulcent properties by which it forms a
protective coating over the ulcer crater.
Adverse effects - Constipation is only major side effect because of formation of an
Alluminium phosphate and mucosal astringent action of Alluminium salt.

Dept. of Pharmacology, V.L.C.P Raichur Page 27
Magnesium trisilicate - They have also a slow onset of action but longer duration of
action. Hydrated silicon dioxide has adsorbent properties similar to those of Alluminium
hydroxide.
Adverse effects - It may cause mild diarrhoea because of formation of Magnesium salt.
ii) Non buffer type –
Calcium carbonate - This is a very powerful antacid with fast onset of action and raise the
pH >7.
Adverse effects - Excessive doses of calcium carbonate if given along with milk can lead
to hypercalcaemia. It causes constipation due to formation of calcium stearate in intestine.
Magnesium hydroxide - It is a quick acting antacid and the action is prolonged.
Adverse effects - Magnesium hydroxide has a mild cathartic action which can be
countered by combining with alluminium based antacid. Small amount of magnesium is
absorbed into the blood; it produces toxicity only in the presence of impaired renal
function.
C. Ulcer protective drugs–
Sucralfate – It is a complex of an Octa-alluminium sulphate of sucrose. At low pH it
forms a sticky paste in the stomach and forms a barrier for acid and also binds to pepsin
and bile salts to reduce peptic activity.
Dose- 1 g tablet before a meal and at bed time.
D. Anti-H. Pylori drugs -

Dept. of Pharmacology, V.L.C.P Raichur Page 28
(Amoxicillin, Clarithromycin, Metronidazole, Tinidazole) H. pylori are a gram –ve
bacteria found in the stomach, which attach to the surface of epithelium beneath the mucus
has high urease activity can form a microenvironment around the bacteria.
It has accepted that it is the main contribution to the causation of chronic gastritis,
dyspepsia and peptic ulcer. Anti-H. pylori therapy is recommended for those patients
whose test are positive for H. pylori26,27.
Table No: 3.1 Name of the plants reported for anti-ulcer activity
S. No. Name of Plants Family Chemical constituents References
01 Tectona grandis (Trunk Bark and wood chips)
Verbenaceae Phenolic acids, β-sitosterol
& triterpenoids.
02. Wedelia calendulacea (Leaves)
Compositae Saponin, phytosterol &
isoflavonoids.
03. Glycyrrhiza glabra (Root)
Papilionaceae Glycyrrhizin, triterpene,
saponin & isoflavonoids.
Goel and Sairam28,
2002.

Dept. of Pharmacology, V.L.C.P Raichur Page 29
04. Ficus religiosa (Bark)
Moraceae β-sitosteryl-D-glucoside,
Vitamin K & Lanosterol,
stigmasterol.
05. Bacopa monniera (Whole plant)
Scrophulariaceae Saponins, monnierin,
hersaponin, bacosides A
and B,brahmine &
herpestine
06. Convolvulus pluricaulis (Whole plant)
Papilionaceae N-methylconiene, flavone
glycoside, diosmin &
chlorogenic acid.
07. Emblica
officinalis (Leaves)
Euphorbiaceae Vitamin C, minerals &
amino acids.
Sairam et al29, 2002.
08. Asparagus racemosus (Root)
Liliaceae Neoprazerigenin A-3-O- β-
lycotetraoside, steroidal
saponins & sibiricoside A
and B.
Sairam et al30, 2003.
09. Centella asiatica (Whole plant)
Umbelliferae Saponins, monnierin,
hersaponin & bacosides A
and B.
Sairam et al31, 2001.
10. Ocimum sanctum (Leaves)
Labiatae Camphor, pinene,
limonene, terpinolene,
myrcene, linalool &
borneol.
Dharmani et al32,
2006.
11. Allophylus serratus (Leaves)
Sapindaceae saponin & isoflavonoids Dharmani et al33,
2005.
12. Desmodium gangeticum (Leaves)
Leguminosae Pterocarpanoids—
gangetin, gangetinin,
desmodin & several
alkaloids.
Dharmani et al 34,
2005.

Dept. of Pharmacology, V.L.C.P Raichur Page 30
13. Terminalia pallida (Leaves)
Combretaceae Glycosides, flavones,
tannins, oligomeric &
proanthocyanidins.
Gupta et al 35, 2005.
14. Musa sapientum (Leaves)
Scitaminaceae Acylsterylglycoside &
sitoindoside IV.
Sanyal et al 36, 1998.
15 Bidens pilosa (Hole plant)
Compostiae Phenylheptatriyne. Alvarez et al 37,
1999. 16. Hemidesmus
indicus (Hole plant)
Asclepiadaceae Coumarino-lignoids,
hemidesmine, hemidesmin-
1, 2 & pregnane glycosides.
Anoop and Jegadees
38, 2003.
17. Maytenus ilicifolia (Leaves)
Celastraceae Alkaloids, tannins &
flavones.
Martins et al 39,
2003.
18. Phyllanthus niruri (Aerial part)
Euphorbiaceae Niuride. Okoli et al 40, 2009.
3.3 INFLAMMATION
Inflammation (Latin, inflammare, to set on fire) is part of the complex biological
response of vascular tissues to harmful stimuli, such as pathogens, damaged cells or
irritants. Inflammation is a protective attempt by the organism to remove the injurious
stimuli and to initiate the healing process. Inflammation is not a synonym for infection,
even in cases where inflammation is caused by infection. Infection is caused by an
exogenous pathogen, while inflammation is one of the responses of the organism to the
pathogen41.
Causes of inflammation:

Dept. of Pharmacology, V.L.C.P Raichur Page 31
The numerous causes of inflammation may be classified as follows:
• Microbes, e.g. bacteria, viruses, protozoa and fungi.
• Physical agents, e.g. heat, cold, mechanical injury, ultraviolet and ionising
radiation.
• Chemical agents: organic, e.g. microbial toxins and organic poisons such as weed
killers. Inorganic, e.g. acids, alkalis.
• Antigens that stimulate immunological responses.
Inflammation can be classified as:
1. Acute Inflammation.
2. Chronic Inflammation.
3.3.1 Acute Inflammation:
Episodes of acute inflammation are usually of short duration e.g. days to a few weeks
and may range from mild to very severe. The cardinal signs of inflammation are: redness,
heat, pain, swelling and loss of function.
The acute inflammatory response is described in a series of overlapping stages:
A. Increased blood flow
B. Increased formation of tissue fluid
C. Increased permeability of small blood vessel walls

Dept. of Pharmacology, V.L.C.P Raichur Page 32
D. Increased hydrostatic pressure
E. Migration of leukocytes
F. Chemotaxis
A. Increased blood flow:
Following injury, both the arterioles supplying the damaged area and the local
capillaries dilate, increasing blood flow to the site. This is caused mainly by the local
release of a number of chemical mediators from damaged cells e.g. histamine and
serotonin. Increased blood flow to the area of tissue damage provides more oxygen and
nutrients for the increased cellular activity that accompanies inflammation. Increased blood
flow causes the increased temperature and reddening of an inflamed area.
B. Increased formation of tissue fluid:
One of the cardinal signs of inflammation is swelling (oedema) of the tissues
involved, which is caused by fluid leaving local blood vessels and entering the interstitial
spaces.
C. Increased permeability of small blood vessel walls:
This is caused by inflammatory mediators, e.g. prostaglandins, histamine and
serotonin, which are released by injured cells and cause the cells that form the single
layered venule wall to pull apart from one another. This opens channels that allow the
movement of:
• Excess fluid, which leaves the blood and enters the tissues and
• Plasma proteins, which are normally retained within the bloodstream and contribute
to the osmotic pressure of the blood. When plasma proteins leave the blood, as in

Dept. of Pharmacology, V.L.C.P Raichur Page 33
inflammation, the osmotic pressure of the blood falls and water moves from the
bloodstream into the tissues.
D. Increased hydrostatic pressure:
The increased blood flow into the capillary bed forces fluid out of the vessels and
into the tissues. Some interstitial fluid returns to the capillaries but most of the
inflammatory exudate, phagocytes and cell debris are removed in lymph vessels because
the pores of lymph vessels are larger and the pressure inside is lower than in blood
capillaries.
E. Migration of leukocytes:
Loss of fluid from the blood thickens it, slowing flow and allowing the normally fast-
flowing white blood cells to make contact with and adhere to the vessel wall. In the acute
stages, the most important leukocyte is the neutrophil, which adheres to the blood vessel
lining, squeezes between the endothelial cells and enters the tissues, where its main
function is in phagocytosis of antigens.
Later in the inflammatory response, after about 24 h, macrophages become the
predominant cell type at the inflammed site and they persist in the tissues if the situation is
not resolved, leading to chronic inflammation. Macrophages are larger and longer lived
than the neutrophils. They phagocytose dead/dying tissue, microbes and other antigenic
material and dead/dying neutrophils.
F. Chemotaxis:
This is the chemical attraction of leukocytes to an area of inflammation. The role of
chemoattractants and the way in which they work is not fully understood.
It may be that chemoattractants act to retain passing leukocytes in the inflammed
area, rather than actively attracting them from distant areas of the body. Known

Dept. of Pharmacology, V.L.C.P Raichur Page 34
chemoattractants include microbial toxins, chemicals released from leukocytes,
prostaglandins from damaged cells and complement proteins42.

Dept. of Pharmacology, V.L.C.P Raichur Page 35
Fig No.3.2 Events in Acute and Chronic Inflammation
Table No: 3.2 Summary of the principal substances released in inflammation

Dept. of Pharmacology, V.L.C.P Raichur Page 36
Substances Made by Trigger for release Main pro-inflammatory
actions
Histamine Mast cells (in most
tissues), basophils
(blood); stored in
cytoplasmic granules.
Binding of antibody
to mast cells and
basophils.
Vasodilatation, itching,
vascular permeability,
degranulation, smooth
muscle contraction (e.g.
bronchoconstriction).
Serotonin (5-HT) Platelets, Mast cells
and basophils (stored
in granules). Also in
CNS (acts as
neurotransmitter).
When platelets are
activated, and when
mast cells/basophils
degranulate.
Vasoconstriction,
vascular permeability.
Prostaglandins (PGs) Nearly all cells; not
stored, but made from
cell membranes as
required.
Many different
stimuli,e.g. drugs,
toxins, other
inflammatory
mediators,
hormones, trauma.
Diverse, sometimes
opposing, e.g. fever,
pain, vasodilatation or
vasoconstriction,
vascular permeability.
Heparin Liver, mast cells,
basophils (stored in
cytoplasmic granules).
Released when cells
degranulate.
Anticoagulant (prevents
blood clotting), which
maintains blood supply
(nutrients, O2) to injured
tissue and washes away
microbes and wastes.
Bradykinin Tissues and blood. When blood clots, in
trauma and
inflammation.
Pain, Vasodilatation.

Dept. of Pharmacology, V.L.C.P Raichur Page 37
Outcomes of acute inflammation:
Resolution:
When the injury is limited or short-lived, when there has been no or minimal tissue
damage and when the tissue is capable of replacing any irreversibly injured cells, the usual
outcome is restoration to histologic and functional normalization. This involves
neutralization or removal of the various chemical mediators, normalization of vascular
permeability and cessation of leukocyte emigration with subsequent death (by apoptosis)
of extravasated neutrophils. Eventually, the combined efforts of lymphatic drainage and
macrophage ingestion of necrotic debris lead to the clearance of the edema fluid,
inflammatory cells and detritus from the battlefield.
Scarring or fibrosis:
Scarring or fibrosis results after substantial tissue destruction or when inflammation
occurs in tissues that do not regenerate. In addition, extensive fibrinous exudates (due to
increased vascular permeability) may not be completely absorbed and are organized by in
growth of connective tissue with resultant fibrosis. Abscess formation may occur in the
setting of extensive neutrophilic infiltrates or in certain bacterial or fungal infections (these
organisms are then said to be pyogenic or "pus forming"). Due to the extensive underlying
tissue destruction (including the extracellular matrix), the only outcome of abscess
formation is scarring.
Development of chronic inflammation:
Progression to chronic inflammation may follow acute inflammation, although signs
of chronic inflammation may be present at the onset of injury (e.g., in viral infections or

Dept. of Pharmacology, V.L.C.P Raichur Page 38
immune responses to self-antigens). Depending on the extent of the initial and ongoing
tissue injury, as well as the capacity of the affected tissues to re-grow, chronic
inflammation may be followed by regeneration of normal structure and function
(regeneration) or may lead to scarring.
3.3.2 Chronic Inflammation:
Chronic inflammation can be considered to be inflammation of prolonged duration
(weeks to months to years) in which active inflammation, tissue injury and healing proceed
simultaneously. In contrast to acute inflammation, which is distinguished by vascular
changes, edema and a largely neutrophilic infiltrate, chronic inflammation is characterized
by the following:
• Infiltration with mononuclear (chronic inflammatory) cells, including macrophages,
lymphocytes and plasma cells.
• Tissue destruction is largely directed by the inflammatory cells.
• Repair, involving new vessel proliferation (angiogenesis) and fibrosis.
Chronic inflammation arises in the following settings:
• Viral infections, intracellular infections of any kind typically require lymphocytes
(and macrophages) to identify and eradicate infected cells.
• Persistent microbial infections, most characteristically by a selected set of
microorganisms including mycobacteria (Tubercle bacilli), Treponema pallidum
(causative organism of syphilis) and certain fungi. These organisms are of low
direct pathogenicity, but typically they evoke an immune response called delayed
hypersensitivity, which may culminate in a granulomatous reaction.

Dept. of Pharmacology, V.L.C.P Raichur Page 39
• Prolonged exposure to potentially toxic agents. Examples include nondegradable
exogenous material such as inhaled particulate silica, which can induce a chronic
inflammatory response in the lungs (silicosis and endogenous agents such as
chronically elevated plasma lipid components, which may contribute to
atherosclerosis).
• Autoimmune diseases, in which an individual develops an immune response to
self-antigens and tissues. Because the responsible antigens are in most instances
constantly renewed, a self-perpetuating immune reaction results (e.g., Rheumatoid
arthritis or Multiple sclerosis).
Mediators of chronic inflammation:
Macrophages:
They constitute the critical mainstay and heart of chronic inflammation. Macrophages
secrete a wide variety of biologically active products that if unchecked, can result in the
tissue injury and characteristic of chronic inflammation.
Complement components and coagulation factors:
Activated macrophages may release significant amounts of these proteins locally into
the extracellular matrix. These include complement proteins C1 to C5, properdin,
coagulation factors V and VIII.
Arachidonic acid metabolites.
Cytokines, such as IL-1 and TNF, as well as a variety of growth factors that influence
the proliferation of smooth muscle cells and fibroblasts and the production of extracellular
matrix. At the sites of acute inflammation when the process is resolved, macrophages

Dept. of Pharmacology, V.L.C.P Raichur Page 40
eventually die or wander off into lymphatic. In chronic inflammatory sites, however
macrophage accumulation persists and macrophages can proliferate. Other types of cell
present in chronic inflammation are lymphocytes, plasma, cells, eosinophils and mast cells.
Granulomatus Inflammation:
Granulomatus inflammation is a distinctive pattern of chronic inflammation
characterized by aggregates of activated macrophages that assume a squamous cell like
(epitheloids) appearance43.
3.3.3 Non-Steroidal Anti-Inflammatory Drugs:
Nonsteroidal anti-inflammatory drugs, usually abbreviated to NSAIDs, but also
referred to as nonsteroidal anti-inflammatory agents/analgesics (NSAIAs), are drugs with
analgesic and antipyretic (fever-reducing) effects and which have in higher doses, anti-
inflammatory effects.
The term "nonsteroidal" is used to distinguish these drugs from steroids, which,
among a broad range of other effects, have a similar eicosanoid-depressing, anti-
inflammatory action. As analgesics, NSAIDs are unusual in that they are non-narcotic.
The most prominent members of this group of drugs are aspirin, ibuprofen and
naproxen all of which are available over the counter in many areas44.

Dept. of Pharmacology, V.L.C.P Raichur Page 41
Classification of NSAIDs:
NSAIDs can be classified based on their chemical structure or mechanism of action.
1. Salicylates:
Aspirin (acetylsalicylic acid), Diflunisal, Salsalate.
2. Propionic acid derivatives:
Ibuprofen, Naproxen, Fenoprofen, Ketoprofen, Flurbiprofen.
3. Acetic acid derivatives:
Indomethacin, Sulindac, Etodolac, Ketorolac, Diclofenac, Nabumetone.
4. Enolic acid (Oxicam) derivatives:
Piroxicam, Meloxicam, Tenoxicam, Droxicam, Lornoxicam, Isoxicam.
5. Fenamic acid derivatives:
Mefenamic acid, Meclofenamic acid, Flufenamic acid, Tolfenamic acid.
6. Selective COX-2 inhibitors:
Celecoxib, Rofecoxib, Valdecoxib, Parecoxib, Lumiracoxib, Etoricoxib, Firocoxib.
7. Sulphonanilides:
Nimesulide (systemic preparations are banned by several countries for the potential
risk of hepatotoxicity)
8. Others:
Licofelone, acts by inhibiting LOX (lipooxygenase) & COX and hence known as 5-
LOX/COX inhibitors.

Dept. of Pharmacology, V.L.C.P Raichur Page 42
Mechanism of action:
Most NSAIDs act as nonselective inhibitors of the enzyme cyclooxygenase (COX),
inhibiting both the cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2)
isoenzymes. COX catalyzes the formation of prostaglandins and thromboxane from
arachidonic acid (itself derived from the cellular phospholipid bilayer by phospholipase
A2)45.
NSAIDs have antipyretic activity and can be used to treat fever, caused by elevated
levels of prostaglandin E2, which alters the firing rate of neurons within the hypothalamus
that control thermoregulation. Antipyretics work by inhibiting the enzyme COX, which
causes the general inhibition of prostanoid biosynthesis (PGE2) within the hypothalamus.
PGE2 signals to the hypothalamus to increase the body's thermal set point. Ibuprofen has
been shown to be more effective as an antipyretic than acetaminophen. Arachidonic acid is
the precursor substrate for cyclooxygenase leading to the production of prostaglandins F, D
& E46,47.
Pharmacokinetics:
Most nonsteroidal anti-inflammatory drugs are weak acids, with a pKa of 3-5,
absorbed well from the stomach and intestinal mucosa. They are highly protein-bound in
plasma (typically >95%), usually to albumin, so that their volume of distribution typically
approximates to plasma volume. Most NSAIDs are metabolised in the liver by oxidation
and conjugation to inactive metabolites which are typically excreted in the urine, although
some drugs are partially excreted in bile. Metabolism may be abnormal in certain disease
states and accumulation may occur even with normal dosage.

Dept. of Pharmacology, V.L.C.P Raichur Page 43
Ibuprofen and diclofenac have short half-lives (2–3 h). Some NSAIDs (typically
oxicams) have very long half-lives (e.g. 20–60 h).
Fig No.3.3 Mechanism of action of NSAIDs48
Adverse effects:
1. Cardiovascular –
A recent meta-analysis of all trials comparing NSAIDs found an 80% increase in the
risk of myocardial infarction with both newer COX-2 antagonists and high dose traditional
anti-inflammatories compared with placebo49.

Dept. of Pharmacology, V.L.C.P Raichur Page 44
2. Gastrointestinal –
The main adverse drug reactions (ADRs) associated with use of NSAIDs relate to direct
and indirect irritation of the gastrointestinal (GI) tract. NSAIDs cause a dual insult on the
GI tract: the acidic molecules directly irritate the gastric mucosa and inhibition of COX-1
and COX-2 reduces the levels of protective prostaglandins. Inhibition of prostaglandin
synthesis in the GI tract causes increased gastric acid secretion, diminished bicarbonate
secretion, diminished mucus secretion and diminished trophic effects on epithelial mucosa.
Common gastrointestinal ADRs include:
Nausea/vomiting, dyspepsia, gastric ulceration/bleeding50 and diarrhea.
3. Inflammatory bowel disease (IBD) –
NSAIDs are never to be used in individuals with inflammatory bowel disease (e.g.
Crohn's disease or ulcerative colitis) due to their tendency to cause gastric bleeding and
form ulceration in the gastric lining. Pain reliever drug such as codeine (which slows down
bowel activity) are safer medications for pain relief in IBD.
4. Renal –
NSAIDs are also associated with a relatively high incidence of renal adverse drug
reactions (ADRs). The mechanism of these renal ADRs is due to changes in renal
haemodynamics (blood flow), ordinarily mediated by prostaglandins, which are affected by
NSAIDs. Prostaglandins normally cause vasodilation of the afferent arterioles of the
glomeruli. This helps maintain normal glomerular perfusion and glomerular filtration rate
(GFR), an indicator of renal function. This is particularly important in renal failure where
the kidney is trying to maintain renal perfusion pressure by elevated angiotensin II levels.
At these elevated levels, angiotensin II also constricts the afferent arteriole into the
glomerulus in addition to the efferent arteriole one it normally constricts. Prostaglandins

Dept. of Pharmacology, V.L.C.P Raichur Page 45
serve to dilate the afferent arteriole; by blocking this prostaglandin-mediated effect,
particularly in renal failure, NSAIDs cause unopposed constriction of the afferent arteriole
and decreased renal perfusion pressure.
5. Other –
Common adverse drug reactions (ADR) include: raised liver enzymes, headache,
dizziness and photosensitivity. Uncommon ADRs include: hyperkalaemia, confusion,
bronchospasm, rash, rapid and severe swelling of the face and body. Ibuprofen may also
rarely cause symptoms of irritable bowel syndrome.
Uses:
NSAIDs are generally indicated for the symptomatic relief of the following conditions:
• Rheumatoid arthritis, osteoarthritis, acute gout, metastatic bone pain, headache,
migraine, postoperative pain and dysmenorrhoea (menstrual pain).
• Inflammatory arthropathies (e.g. ankylosing spondylitis, psoriatic arthritis, Reiter's
syndrome).
• Mild-to-moderate pain due to inflammation and tissue injury.
• They are also given to neonate infants whose ductus arteriosus is not closed within
24 h of birth51.
Selective COX-2 inhibitors:
The discovery of COX-2 in 1991 by Daniel L. Simmons at Brigham Young
University raised the hope of developing an effective NSAID without the gastric problems
characteristic of these agents. It was thought that selective inhibition of COX-2 would
result in anti-inflammatory action without disrupting gastroprotective prostaglandins.

Dept. of Pharmacology, V.L.C.P Raichur Page 46
Table No: 3.3 Name of the plants reported for anti-inflammatory activity
S. No. Plant Family Chemical constituent Reference
1. Cassia fistula Caesalpinaceae Flavone glycoside,
oxyanthraquinones,
chrysophanol &
chrysophanein.
Ilavarasan et al52,
2005.
2. Margaritaria
discoidea
Euphorbiaceae Phylochrysine &
Securinine.
Adeolu et al53,
2009.
3. Eclipta prostrata Astearaceae Triterpenoid saponins.
Arunachalam et
al54
2009.
4. Curcuma amada Zingiberaceae Hydroxyl, ester, carbonyl
& olefinic groups.
Mujumdar et al55,
2000.
5. Borassus
flabellifer
Arecaceae Alkaloids, terpenoids,
saponins & phenolic
compounds.
Paschapur et al56,
2006.
6. Vitex negundo Verbenaceae Alkaloids, saponins &
tannins.
Dharmasiri et
al57, 2003.
7. Securidaca
longipedunculata
Polygalaceae Elymoclavine,
dehydroelymoclavine,
ergoline, cinnamonic
acid, flavonoids &
xanthones.
Okoli et al58,
2005.
8. Gongronema
latifolium
Asclepiadaceae Alkaloids, saponins,
tannins & flavanoids.
Akuodor et al59,
2010.

Dept. of Pharmacology, V.L.C.P Raichur Page 47
9. Teucrium
buxifolium
Lamiaceae Sugars, phenolic
compound, flavones,
saponins, steroids &
resins.
Puntero et al60,
1997.
10. Arecastrum
romanzoffianum
Arecaceae Galactomannoglucan. Silva et al61,
2010.
11. Stachytarpheta
cayennensis
Verbenaceae
Iridoid ipolamide &
phenylethanoid glycoside
aceteoside.
Schapoval et al62,
1998.
12. Zizyphus lotus Verbenaceae Cyclopeptide alkaloids,
dammarane saponins &
flavonods.
Borgi et al63,
2007.
13. Solanum nigrum Solanaceae
Flavones, saponins,
steroids & alkaloids.
Ravi et al64,
2009.
14. Anthurium
cerrocampanense
Arecaceae Terpenoids, saponins and
alkaloids.
Segura et al65,
1998.
15. Byrsocarpus
coccineus
Connaraceae Alkaloids, saponins,
tannins, phlobatannins,
anthraquinones,
glycosides & simple
sugars.
Akindele et al66,
2007.

Dept. of Pharmacology, V.L.C.P Raichur Page 48
Table No: 3.4 Name of the plants reported for anti-ulcer and anti-inflammatory
activities
S. No. Plant Family Chemical constituent Reference
1. Bryophyllum
pinnata
Crassulaceae glycosides - quercetin
and kaempferol &
fumaric acid.
Pal et al67, 1991.
2. Calligonum
comosum
Verbenaceae Flavonoids, alkaloids
and saponins.
Liu et al68, 2001.
3. Calotropis
procera
Asclepiadaceae Alkaloids & glycosides Basu et al69 1997.
4. Psidium guajava Myrtaceae linoleic acid & Vitamin
C.
Kulkarni et al70,
1999.
5. Mikania cordata Compositae Stigmasterol, β-
sitosterol, sesquiterpene
& scandenolide
Bhattacharya et
al71, 1988.
6. Rhamnus
procumbers
Rhamnaceae kaempferol, kaempferol
-7-O-methyl ether
kaempferol-4-O-methyl
ether & flavones.
Goel et al72,
1988.
7. Rhamnus
triquerta
Rhamnaceae Emodin, kaempferol &
8 β-D-glucoside.
Goel et al73,
1991.

Dept. of Pharmacology, V.L.C.P Raichur Page 49
4. METHODOLOGY
Table No: 4.1 List of materials and equipments used during experiment
S. No. Name of the materials and equipment
1 Anaesthetic ether (Sigma Solvents and Pharmaceuticals, Mumbai)
2 Ibuprofen (Cipla, Mumbai)
3 Carrageenan (Hi-Media Laboratory, Mumbai.)
4 Ethanol (Nice-Cochin)
5 Formalin (Nice-Cochin)
6 Ranitidine (Glaxo Smithkline Ltd, Mumbai)
7 Absolute alcohol (Nice-cochin)
8 Distilled water (Mysore Petro Chemicals, Raichur, India)
9 Microscope (R-motion Opik – India)
10 Evans blue (S.D. Fine chemicals, Mumbai)
11 Lead Mercury (S.D. Fine chemicals, Mumbai)
12 Histamine (S.D. Fine chemicals, Mumbai)
13 Restraint cages (Shri. Venkateswara Enterprises, Bangalore)
14 Chloroform (Nice-Cochin)
15 Refrigerator (Whirlpool-Kelvinator India Ltd, India)
16 Sodium Hydroxide (Nice-Cochin)

Dept. of Pharmacology, V.L.C.P Raichur Page 50
EXPERIMENTAL
4.1 Preparation of Different Extracts74:
A. Preparation of alcoholic extract:
Tubers of S. tuberosum were collected in the month of August from the Hind
Pharmacy, Sultanpur (U.P) and dried in shade at room temperature then subjected to size
reduction to a fine powder with the help of mixer grinder.
The tubers powder was packed in a soxhlet apparatus and extracted with 95% alcohol
for 18 h. Appearance of colourless solvent in the siphon tube was taken as the termination
of extraction. The extract was then transferred into the previously weighed empty beaker
and evaporated to a thick paste on the water bath, maintained at 50oC to get alcoholic
(AETST) extract. The extract was finally air dried thoroughly to remove all traces of the
solvent and the percentage yield was calculated.
B. Preparation of aqueous extract:
About 100 g of tubers powder was taken in a round bottom flask (2000 ml) and
macerated with 500 ml of distilled water with 10 ml of chloroform (preservative) for 24 h
with shaking for every hour in a closed vessel. Then the marc was removed by filtering the
extract (AQETST) and then it was concentrated on a water bath maintained at 50oC.
These two extracts were stored in airtight containers in a refrigerator below 10oC.
The two extracts were examined for their colour and consistency. Their percentage yield
was calculated with reference to air-dried powder sample used for the extraction.

Dept. of Pharmacology, V.L.C.P Raichur Page 51
Table No: 4.2 Nature and Percentage yield of the extracts
Both the AETST and AQETST were subjected to the following investigations:
1. Preliminary phytochemical screening.
2. Pharmacological activities
a. Toxicity studies (LD50).
b. Anti-ulcer activity.
c. Anti-inflammatory activity.
4.2 Preliminary phytochemical investigations:
The preliminary phytochemical investigations were carried out with AETST and
AQETST for qualitative identification of phytochemical constituents present with each
extract and test were carried out by following standard methods74,75,76. All the chemicals
and reagents used were of analytical grade.
S. No. Name of the Extract Nature Colour %Yield
( w/w) g
1. Alcohol
(AETST) Sticky Reddish Brown 12.50
2. Aqueous
(AQETST) Solid Dark brown 12.00

Dept. of Pharmacology, V.L.C.P Raichur Page 52
Table No: 4.3 Details of qualitative phytochemical tests
Test AETST AQETST
I. Tests for sterols
1. Test solution + Conc H2SO4 + +
2. Salkowski’s test + +
3. Test solution + sulphur + +
4. Libermann Burchard’s test + +
II. Tests for Glycosides
1. Baljet’s test + +
2. Keller – killiani test + +
3. Bromine water test. + +
4. Legal’s test + +
III. Test for Saponins
1. Foam test _ _
IV. Tests for Carbohydrates
1. Molisch’s test + +
2. Barfoed’s test + +
3. Benedict’s test + +
4. Fehling test + +
V. Tests for Alkaloids
1. Mayer’s test. + +
2. Wagner’s test. + +
3. Hager’s test + +
4. Dragendorff’s test + +
VI. Test for Ascorbic acid
1. Dichlorophenolindophenol test _ _

Dept. of Pharmacology, V.L.C.P Raichur Page 53
VII. Tests for Flavonoids
1. Ferric chloride test + +
2. Shinoda test _ _
3. Zn-Hcl reduction test + +
4. Sodium hydroxide test + +
5. Lead acetate test. + +
VIII. Tests for Tannins
1. Ferric chloride test. + +
2. Gelatin test _ _
IX. Tests for Proteins 1. Million’s test _ _
2. Biuret’s test _ _
3. Ninhydrin test _ _
X. Test for fixed oils and fats
1. Spot test _ _
XI. Tests for triterpines
1. Salkowski’s test + +
2. Libermann- Burchard test + +
(+) Indicates positive result and (–) Indicates negative result.

Dept. of Pharmacology, V.L.C.P Raichur Page 54
4.3 Pharmacological activities:
Experimental animals:
Albino rats (Wistar strain) of either sex weighing between 120-200 g and Albino
mice 18-22 g were procured from National Centre for Laboratory Animal sciences, C/0
Shri. Venkateswara Enterprises, Bengaluru for experimental purpose and the animals were
acclimatized for 7 days under standard husbandry condition as:
Room temperature - 26 ± 20 C
Relative humidity - 45-55%
Light/ dark cycle - 12:12 h
The animals were fed with synthetic standard pellet diet purchased from Amrut
Laboratories & Pranav Agro industries Ltd. Sangli (MS) and water was allowed ad libitum
under strict hygienic conditions. All animal studies were performed in accordance to
CPCSEA Guidelines No. 425 and Institutional Animal Ethical Committee (IAEC) of V.L.
College of Pharmacy, Raichur (Karnataka) with CPCSEA Registration Number
557/02/e/CPCSEA. The procedures were followed as per rules and regulations.
4.3.1 Determination of acute toxicity (LD50)77
Method:
The acute toxicity of AETST and AQETST was determined in albino mice of either
sex weighing between 18-22 g those maintained under standard husbandry conditions. The
animals were fasted 3 h prior to the experiment and “up and down” (OECD Guideline No.
425) method of CPCSEA was adopted for toxicity studies. Animals were administered

Dept. of Pharmacology, V.L.C.P Raichur Page 55
with single dose of extracts and observed for its mortality during 48 h study period (short
term) toxicity. Based on the short-term toxicity profile of the extracts the doses of the next
animals were determined as per as OECD Guidelines No: 425. All the animals were
observed for long term toxicity (7 days) and then 1/5th, 1/10th and 1/20th of the maximum
dose tested for LD50 of the individual extract was taken as effective dose ED50 and were
used throughout the experimental studies.
4.3.2 Determination of Anti-ulcer Activity:
1. Pylorus Ligation Model78-81:
Albino rats weighing between 150-200 g and each group containing 6 animals were
divided into 8 groups.
Group A: Normal animals treated with vehicle only
Group B: Standard Ranitidine (30 mg/kg i.p)
Group C: AETST (100 mg/kg p.o)
Group D: AETST (200 mg/kg p.o)
Group E: AETST (400 mg/kg p.o)
Group F: AQETST (100 mg/kg p.o)
Group G: AQETST (200 mg/kg p.o)
Group H: AQETST (400 mg/kg p.o)

Dept. of Pharmacology, V.L.C.P Raichur Page 56
Experimental Procedure:
Albino rats weighing between 150-200 g were divided into 8 groups of 6 rats in
each. They were fasted in individual cages for 24 h prior to the experiment with free
access to water with measures to avoid coprophagy. Group A served as normal control,
which was given with vehicle only. Group B with standard drug, groups C, D, E and F,
G, H treated with low, medium and high doses of AETST and AQETST respectively.
The various groups were treated with vehicle/extracts 30 min prior to pylorus ligation.
Under light ether anesthesia, the abdomen was opened and the pylorus was ligated
and sutured. 4 h after ligation all the animals were sacrificed with excess of anaesthetic
ether and the stomach were dissected out. Gastric juice was collected into tubes and
centrifuged at 1000 rpm for 10 min and volume was noted. The pH of the gastric juice will
be recorded by pH meter. The gastric content was subjected for analysis of free and total
acidity. The glandular portion of the stomach was opened along the greater curvature and
the severity of hemorrhagic erosions in the acid secreting mucosa was assessed on a scale
of 0 to 3, i.e. ulcer index was determined by the following formula,
Ui = UN+US+UP×10-1
Where Ui is Ulcer index
UN = average of number of ulcers per animal
US = average of severity score
UP = percentage of animals with ulcers
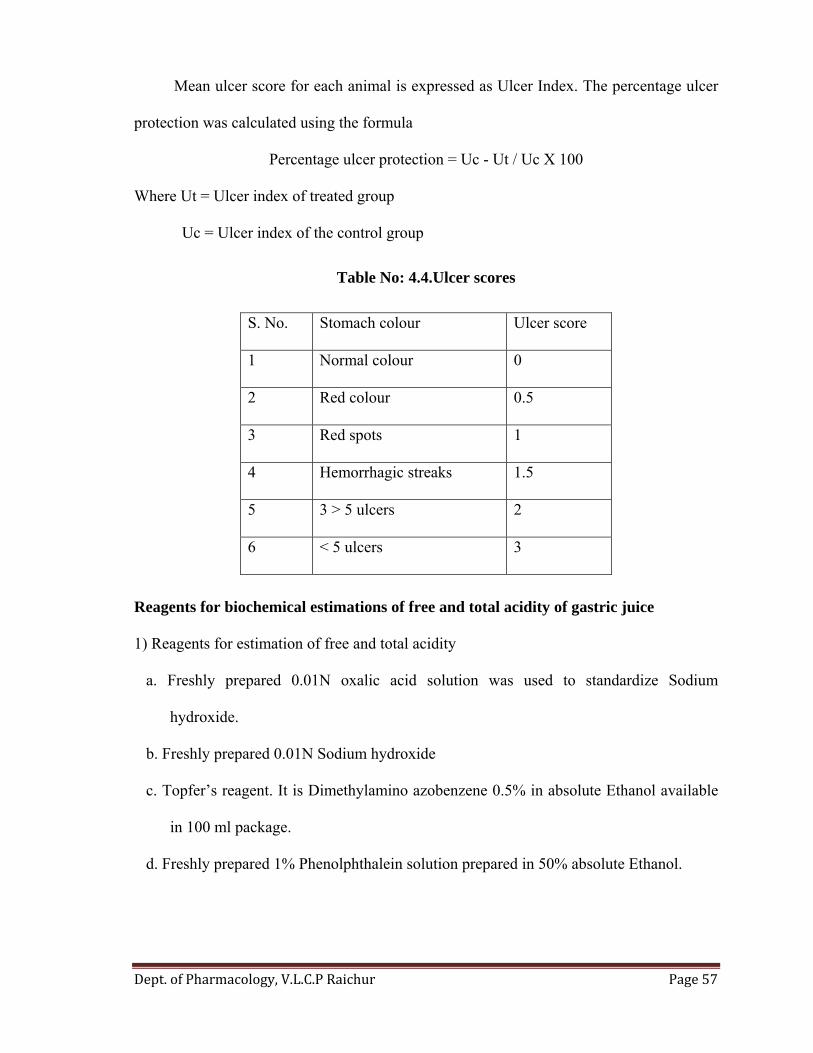
Dept. of Pharmacology, V.L.C.P Raichur Page 57
Mean ulcer score for each animal is expressed as Ulcer Index. The percentage ulcer
protection was calculated using the formula
Percentage ulcer protection = Uc - Ut / Uc X 100
Where Ut = Ulcer index of treated group
Uc = Ulcer index of the control group
Table No: 4.4.Ulcer scores
Reagents for biochemical estimations of free and total acidity of gastric juice
1) Reagents for estimation of free and total acidity
a. Freshly prepared 0.01N oxalic acid solution was used to standardize Sodium
hydroxide.
b. Freshly prepared 0.01N Sodium hydroxide
c. Topfer’s reagent. It is Dimethylamino azobenzene 0.5% in absolute Ethanol available
in 100 ml package.
d. Freshly prepared 1% Phenolphthalein solution prepared in 50% absolute Ethanol.
S. No. Stomach colour Ulcer score
1 Normal colour 0
2 Red colour 0.5
3 Red spots 1
4 Hemorrhagic streaks 1.5
5 3 > 5 ulcers 2
6 < 5 ulcers 3

Dept. of Pharmacology, V.L.C.P Raichur Page 58
Methods for biochemical estimation of free and total acidity:
Collection of gastric juice82,83
Gastric content collected from pylorus ligated rats was centrifuged and the volumes
of gastric juice as well as pH of gastric juice were noted. Further the gastric juice was
subjected to biochemical estimations as follows:
Determination of free and total acidity
1 ml of gastric juice was pipetted into a 100 ml conical flask, 2 or 3 drops of Topfer’s
reagent was added and titrated with 0.01N Sodium hydroxide until all traces of red colour
disappears and the colour of the solution was yellowish orange. The volume of alkali
added was noted. This volume corresponds to free acidity. Then 2 or 3 drops of
Phenolphthalein solution was added and titration was continued until a definite red tinge
appears. Again the total volume of alkali added was noted now this volume corresponds to
total acidity.
Acidity was calculated by using the formula
Volume of NaOH × Normality of NaOH × 100
Acidity = --------------------------------------------------------------------- m eq/lt/100 g
0.1

Dept. of Pharmacology, V.L.C.P Raichur Page 59
2. Stress induced ulcers by cold water immersion84:
Albino rats weighing between 150-200 g and each group containing 6 animals were
divided into 8 groups.
Group A: Normal control treated with vehicle only
Group B: Standard Ranitidine (30 mg/kg i.p)
Group C: AETST (100 mg/kg p.o)
Group D: AETST (200 mg/kg p.o)
Group E: AETST (400 mg/kg p.o)
Group F: AQETST (100 mg/kg p.o)
Group G: AQETST (200 mg/kg p.o)
Group H: AQETST (400 mg/kg p.o)
Experimental Procedure:
Albino rats of either sex weighing between 150-200 g were divided into 8 groups
of 6 rats in each. Group A served as normal control, which was given with vehicle only.
Group B with standard drug. Groups C, D, E and F, G, H treated with low, medium and
high doses of AETST and AQETST respectively. After 30 min of oral administration of
the vehicle/Std/extracts, rats were placed vertically in individual restraint cages in cold
water maintained at 220C for 1 h. Then, they were taken out, dried and injected with 30
mg/kg Evans blue i.v. via the tail vein. 10 min later, sacrificed with ether and their
stomachs were removed. Formol-saline (2%v/v) is then injected into the totally ligated
stomachs for overnight storage. The next day, the stomachs were opened along the
greater curvature, washed in warm water and examined for ulcers microscopically with
the help of hand lens (10x). Mean ulcer score for each animal is expressed as ulcer index.

Dept. of Pharmacology, V.L.C.P Raichur Page 60
4.3.3 Determination of anti-inflammatory activity:
1. Carrageenan induced paw edema85-87:
Group A: Toxicant control (0.1 ml of 1% w/v Carrageenan, hind paw)
Group B: Standard (Ibuprofen 40 mg/ kg, p.o)
Group C: AETST (100 mg/kg p.o)
Group D: AETST (200 mg/kg p.o)
Group E: AETST (400 mg/kg p.o)
Group F: AQETST (100 mg/kg p.o)
Group G: AQETST (200 mg/kg p.o)
Group H: AQETST (400 mg/kg p.o)
Experimental Procedure:
Male albino rats (125-150 g) of 8 groups were housed as groups of six, fasted
overnight prior to and during the experiment but have free access to water. Group A was
served as normal toxicant control treated with toxicant carrageenan, group B with Ibuprofen
(40 mg/kg p.o.) served as standard, groups C, D and E administered with AETST and
groups F, G and H with AQETST (low, medium and high doses p.o) respectively. The rats
in Groups B, C, D, E, F, G and H were administered with 0.1 ml of 1% w/v of carrageenan
into sub plantar region of right hind paw of rats 1 h after the administration of
Ibuprofen/extracts. Immediately thereafter the oedema volumes of the injected paws were
measured plethysmographically at prefixed time intervals.

Dept. of Pharmacology, V.L.C.P Raichur Page 61
2. Histamine induced paw edema85-87:
Group A: Toxicant control (0.1 ml of 1% w/v histamine, hind paw)
Group B: Standard (Ibuprofen 40 mg/ kg)
Group C: AETST (100 mg/kg p.o)
Group D: AETST (200 mg/kg p.o)
Group E: AETST (400 mg/kg p.o)
Group F: AQETST (100 mg/kg p.o)
Group G: AQETST (200 mg/kg p.o)
Group H: AQETST (400 mg/kg p.o)
Experimental Procedure:
Male albino rats (125-150 g) of 8 groups were housed as groups of 6, fasted overnight
prior to and during the experiment but have free access to water. Group A was served as
toxicant control treated with inflammogen histamine, group B with Ibuprofen (40 mg/kg
p.o.) that served as standard. Groups C, D, E and F, G, H will administered with AETST and
AQETST (low, medium and high dose p.o) respectively. The rats of groups B, C, D, E, F, G
and H were administered with 1% w/v of histamine into sub plantar region of right hind paw
of rats 1 h after administration of Ibuprofen/extracts. Immediately thereafter the oedema
volumes of the injected paws were measured plethysmographically at prefixed time
intervals.

Dept. of Pharmacology, V.L.C.P Raichur Page 62
3. Formalin Induced Paw Oedema84-87:
Group A: Toxicant control (Formalin 1%, hind paw)
Group B: Standard (Ibuprofen 40 mg/ kg)
Group C: AETST (100 mg/kg p.o)
Group D: AETST (200 mg/kg p.o)
Group E: AETST (400 mg/kg p.o)
Group F: AQETST (100 mg/kg p.o)
Group G: AQETST (200 mg/kg p.o)
Group H: AQETST (400 mg/kg p.o)
Experimental Procedure:
Male albino rats (125-150 g) of 8 groups were housed as groups of 6, fasted overnight
prior to and during the experiment but have free access to water. Group A was served as
toxicant control treated with toxicant Formalin, group B with Ibuprofen (40 mg/kg p.o.) that
served as standard. Groups C, D, E and F, G, H were administered with AETST and
AQETST (low, medium and high dose p.o) respectively. The rats of groups B, C, D, E, F, G
and H were administered with 1% of Formalin into sub plantar region of right hind paw of
rats 1 h after administration of Ibuprofen/extracts. Immediately thereafter the oedema
volumes of the injected paws were measured plethysmographically at prefixed time
intervals.

Dept. of Pharmacology, V.L.C.P Raichur Page 63
For comparison purpose, the volume of oedema was measured at prefixed time
intervals. The difference between paw volumes of the treated animals was measured and the
mean oedema volume was calculated. Percentage reduction in oedema volume was
calculated by using the formula,
Vo - Vt
Percentage reduction = x 100
Vo
Where, Vo = Volume of the paw of control at time‘t’.
Vt = Volume of the paw of drug treated at time‘t’.
Statistical analysis:
All results will be expressed as mean ± SEM from 6 animals. Statistical difference in
mean will be analyzed using one-way ANOVA (analysis of variance) followed by Post hoc
test (Dunnett‘s‘t’ test). P< 0.05*, 0.01** and 0.001*** will be considered as statistically
significant.

Dept. of Pharmacology, V.L.C.P Raichur Page 64
5. RESULTS
5.1 Preliminary Phytochemical studies
Preliminary phytochemical screening:
AETST and AQETST were subjected for phytochemical screening and found to
contain tannins, carbohydrate, sterols, flavonoids, glycosides, alkaloid and triterpines both
in alcoholic and aqueous extracts.
5.2 Pharmacological activities
5.2.1 Acute oral toxicity study:
The mice treated with AETST and AQETST at a dose of 2000 mg/kg, p.o.
exhibited normal behaviour, without any signs of passivity, stereotypy and vocalization.
Their motor activity and secretory signs were also normal and no sign of depression.
AETST and AQETST even up to the dose level of 2000 mg/kg body weight did not
produce any behavioural symptoms or mortality. So 1/5th, 1/10th and 1/20th doses of LD50
(maximum dose tested for each extract) was selected as low, medium and high doses and
were used in the present study to explore anti-ulcer and anti-inflammatory activities.
5.2.2 Anti-ulcer activity:
1. Pylorus ligation induced ulcer model in rats:
In pylorus ligation induced ulcer model in rats (positive control) a significant
increase in ulcer number (5.00 ± 0.51), ulcer score (2.41 ± 0.27) and ulcer index (10.74)
are noted. In the same model a significant increase in volume of gastric juice (6.70 ± 0.10
ml), free acidity (31.33 ± 1.15 m eq/L) and total acidity (82.33 ± 1.89 m eq/L) are noted.

Dept. of Pharmacology, V.L.C.P Raichur Page 65
In the group of rats treated with standard drug ranitidine (30 mg/kg) has
significantly reduced ulcer number (0.33 ± 0.21), ulcer score (0.50 ± 0.12), ulcer index
(3.41), volume of gastric juice (4.28 ± 0.13 ml), free acidity (17.33 ± 0.66 m eq/L), total
acidity (43.50 ± 1.17 m eq/L) and the ulcers are inhibited by 68.24 %.
AETST with low, medium and high dose treatment showed a significant decrease
in ulcer number (3.66 ± 0.42, 1.33 ± 0.33 and 0.83 ± 0.16), ulcer score (2.33 ± 0.21, 1.58 ±
0.08 and 0.83 ± 0.10), ulcer index (10.59, 10.29 and 8.49), volume of gastric juice (6.03 ±
0.07 ml, 5.01 ± 0.07 ml and 4.75 ± 0.07 ml), free acidity (25.00 ± 0.85, 22.33 ± 0.66 and
20.83 ± 1.01 m eq/L), total acidity (59.67 ± 1.05, 47.33 ± 2.01and 46.67 ± 0.80 m eq/L)
and the ulcers are inhibited by 1.39, 4.18 and 20.94 % respectively.
AQETST with low, medium and high dose treatment showed a significant decrease
in ulcer number (3.33 ± 0.21, 1.16 ± 0.16 and 0.66 ± 0.21), ulcer score (2.08 ± 0.20, 1.33 ±
0.10 and 0.75 ± 0.11), ulcer index (10.54, 10.24 and 6.80), volume of gastric juice (5.71 ±
0.11 ml, 4.85 ± 0.05 ml and 4.56 ± 0.12 ml), free acidity (23.83 ± 1.35, 21.83 ± 0.65 and
20.00 ± 0.73 m eq/L), total acidity (58.00 ± 1.39, 46.67 ± 1.99 and 46.00 ± 0.96 m eq/L)
and the ulcers are inhibited by 1.86, 4.65 and 36.68 % respectively.
The order of potency in antiulcer activity is Ranitidine >AQETST > AETST.
The results are shown in Table Nos.5.1 and 5.2 and represented graphically in Fig Nos.
5.1, 5.2 and 5.3.
2. Stress induced ulcer model in rats:
In stress induced ulcer model in rats (positive control) a significant increase in
ulcer number (4.67 ± 0.33), ulcer score (2.67±0.21), ulcer index (10.73), volume of gastric

Dept. of Pharmacology, V.L.C.P Raichur Page 66
juice (6.77 ± 0.09 ml), free acidity (33.33 ± 0.66 m eq/L) and total acidity (84.83 ± 1.19 m
eq/L) are noted.
In the group of rats treated with standard drug ranitidine (30 mg/kg) has significantly
reduced ulcer number (0.50 ± 0.22), ulcer score (0.75 ± 0.11), ulcer index (5.12), volume
of gastric juice (4.38 ± 0.10 ml), free acidity (19.00 ± 0.68 m eq/L), total acidity (45.67 ±
0.91 m eq/L) and the ulcers are inhibited by 52.28 % .
AETST with low, medium and high dose treatment showed a significant decrease in
ulcer number (3.50 ± 0.22, 1.67 ± 0.21 and 0.83 ± 0.16), ulcer score (2.50 ± 0.22, 1.83 ±
0.10 and 1.08 ± 0.08), ulcer index (10.60, 10.35 and 8.52), volume of gastric juice (6.20 ±
0.05 ml, 5.15 ± 0.04 ml and 4.88 ± 0.06 ml), free acidity (26.83 ± 0.60, 24.50 ± 0.88 and
22.67 ± 0.71 m eq/L), total acidity (61.67 ± 0.95, 49.00 ± 1.15 and 48.67 ± 0.61 m eq/L)
and the ulcers are inhibited by 1.21, 3.54 and 20.59 % respectively.
AQETST with low, medium and high dose treatment showed a significant decrease
in ulcer number (3.17 ± 0.16, 1.50 ± 0.22 and 0.83 ± 0.16), ulcer score (2.50 ± 0.22, 1.67 ±
0.10 and 0.91 ± 0.08), ulcer index (10.56, 10.31 and 8.50), volume of gastric juice (6.02 ±
0.07 ml, 4.95 ± 0.07 ml and 4.77 ± 0.07 ml), free acidity (25.67 ± 0.84, 23.33 ± 0.76 and
21.50 ± 0.76 m eq/L), total acidity (60.33 ± 0.55, 47.83 ± 1.57 and 47.17 ± 0.94 m eq/L)
and the ulcers are inhibited by 1.58, 3.91 and 20.78 % respectively.
The order of potency in antiulcer activity is Ranitidine >AQETST > AETST.
The results are shown in Table Nos.5.3 and 5.4 and represented graphically in Fig Nos.
5.4, 5.5 and 5.6.

Dept. of Pharmacology, V.L.C.P Raichur Page 66
Table No: 5.1 Antiulcer effects of AETST and AQETST in pylorus ligation induced ulcer model in rats
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum.
Ulcer number
Animals Control Ranitidine 30 mg/kg
AETST 100 mg/kg
AETST 200 mg/kg
AETST 400 mg/kg
AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 5 0 3 1 0 4 1 0 B 4 0 3 1 1 4 1 1 T 6 0 3 3 1 3 1 1
HB 7 1 5 1 1 3 2 0 HT 4 0 3 1 1 3 1 1 BT 4 1 5 1 1 3 1 1
mean±SEM 5.00±0.51 0.33±0.21*** 3.66±0.42* 1.33±0.33*** 0.83±0.16*** 3.33±0.21** 1.16±0.16*** 0.66±0.21***
Ulcer Score H 3.0 0.0 2 1.5 0.5 3.0 1.5 0.5 B 2.0 0.5 2 1.5 0.5 2.0 1.5 0.5 T 3.0 0.5 2 2.0 1.0 2.0 1.5 1.0
HB 3.0 1.0 3 1.5 1.0 2.0 1.5 0.5 HT 2.0 0.5 2 1.5 1.0 1.5 1.0 1.0 BT 1.5 0.5 3 1.5 1.0 2.0 1.0 1.0
mean±SEM 2.41±0.27 0.50±0.12*** 2.33±0.21ns 1.58±0.08** 0.83±0.10*** 2.08±0.20ns 1.33±0.10*** 0.75±0.11***

Dept. of Pharmacology, V.L.C.P Raichur Page 67
Table No: 5.2 Antiulcer effects of AETST and AQETST in pylorus ligation induced ulcer model in rats
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum.
VOLUME OF GASTRIC JUICE (ml)
Animals Control Ranitidine 30 mg/kg
AETST 100 mg/kg
AETST 200 mg/kg
AETST 400 mg/kg
AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 6.5 4.5 5.9 5.0 5.0 6.2 5.1 4.3 B 6.5 4.8 6.0 4.8 4.5 5.5 4.8 4.2 T 7.0 4.0 5.8 5.2 4.7 5.4 4.8 5.0
HB 6.4 3.9 6.2 4.9 4.9 5.9 4.9 4.5 HT 6.8 4.3 6.0 5.3 4.8 5.7 4.7 4.8 BT 7.0 4.2 6.3 4.9 4.6 5.6 4.8 4.6
mean±SEM 6.70±0.10 4.28±0.13*** 6.03±0.07*** 5.01±0.07*** 4.75±0.07*** 5.71±0.11*** 4.85±0.05*** 4.56±0.12*** FREE ACIDITY (m eq/L)
H 35 16 27 20 22 27 20 19 B 30 15 25 22 21 25 22 21 T 28 19 23 24 18 20 24 18
HB 32 18 28 23 20 28 23 20 HT 34 17 23 24 19 21 22 19 BT 29 19 24 21 25 22 20 23
mean±SEM 31.33±1.15 17.33±0.66*** 25.00±0.85*** 22.33±0.66*** 20.83±1.01*** 23.83±1.35*** 21.83±0.65*** 20.00±0.73*** TOTAL ACIDITY (m eq/L)
H 76 41 56 53 46 55 52 43 B 82 44 58 50 48 54 50 47 T 88 48 59 42 44 56 42 44
HB 86 40 60 41 49 60 41 49 HT 78 45 62 47 45 62 44 45 BT 84 43 63 51 48 61 51 48
mean±SEM 82.33±1.89 43.50±1.17*** 59.67±1.05*** 47.33±2.01*** 46.67±0.80*** 58.00±1.39*** 46.67±1.99*** 46.00±0.96***

Dept. of Pharmacology, V.L.C.P Raichur Page 68
Table No: 5.3 Antiulcer effects of AETST and AQETST in stress induced ulcer model in rats
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum.
Ulcer number
Animals Control Ranitidine 30 mg/kg
AETST 100 mg/kg
AETST 200 mg/kg
AETST 400 mg/kg
AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 4 1 4 2 1 4 2 1 B 4 0 3 2 1 3 1 1 T 6 0 3 1 0 3 2 1
HB 5 1 3 1 1 3 1 1 HT 5 0 4 2 1 3 2 0 BT 4 1 4 2 1 3 1 1
mean±SEM 4.67±0.33 0.50±0.22*** 3.50±0.22** 1.67±0.21*** 0.83±0.16*** 3.17±0.16*** 1.50±0.22*** 0.83±0.16***
Ulcer score H 2.0 1.0 3.0 2.0 1.0 3.0 2.0 1.0 B 3.0 0.5 2.0 2.0 1.5 2.0 1.5 1.0 T 3.0 0.5 2.0 1.5 1.0 3.0 1.5 1.0
HB 3.0 1.0 2.0 1.5 1.0 2.0 1.5 0.5 HT 3.0 0.5 3.0 2.0 1.0 2.0 2.0 1.0 BT 2.0 1.0 3.0 2.0 1.0 3.0 1.5 1.0
mean±SEM 2.67±0.21 0.75±0.11*** 2.50±0.22 ns 1.83±0.10** 1.08±0.08*** 2.50±0.22 ns 1.67±0.10*** 0.91±0.08***

Dept. of Pharmacology, V.L.C.P Raichur Page 69
Table No: 5.4 Antiulcer effects of AETST and AQETST in stress induced ulcer model in rats
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum.
VOLUME OF GASTRIC JUICE (ml)
Animals Control Ranitidine 30 mg/kg
AETST 100 mg/kg
AETST 200 mg/kg
AETST 400 mg/kg
AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 6.8 4.6 6.2 5.2 5.1 6.2 5.1 4.6 B 6.6 4.8 6.0 5.0 4.7 5.9 4.9 4.8 T 7.0 4.1 6.1 5.1 4.8 5.8 4.8 5.0
HB 6.4 4.2 6.2 5.2 5.0 6.2 5.1 4.5 HT 6.8 4.3 6.4 5.3 4.9 5.9 4.7 4.8 BT 7.0 4.3 6.3 5.1 4.8 6.1 5.1 4.9
mean±SEM 6.77±0.09 4.38±0.10*** 6.20±0.05*** 5.15±0.04*** 4.88±0.06*** 6.02±0.07*** 4.95±0.07*** 4.77±0.07*** FREE ACIDITY (m eq/L)
H 31 20 25 24 23 26 20 21 B 33 17 26 22 24 28 24 24 T 32 21 27 28 20 24 23 22
HB 34 20 29 23 22 28 25 19 HT 35 19 26 26 22 23 23 20 BT 35 17 28 24 25 25 25 23
mean±SEM 33.33±0.66 19.00±0.68*** 26.83±0.60*** 24.50±0.88*** 22.67±0.71*** 25.67±0.84*** 23.33±0.76*** 21.50±0.76*** TOTAL ACIDITY (m eq/L)
H 80 44 58 50 48 60 52 45 B 83 43 62 52 50 60 51 50 T 86 48 60 48 48 58 44 44
HB 88 48 64 45 51 61 45 49 HT 87 47 62 47 47 62 44 48 BT 85 44 64 52 48 61 51 47
mean±SEM 84.83±1.19 45.67±0.91*** 61.67±0.95*** 49.00±1.15*** 48.67±0.61*** 60.33±0.55*** 47.83±1.57*** 47.17±0.94***

Dept. of Pharmacology, V.L.C.P Raichur Page 70
Table No: 5.5 Antiulcer effects of AETST and AQETST in different ulcers models in rats
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum
Pylorus ligation model Stress induced ulcer model
Groups Treatment Ulcer
Number Ulcer Score
Incidence of Ulcers
(%)
Ulcer Index
Inhibition of Ulcers
(%)
Ulcer Number
Ulcer score
Incidence of Ulcers
(%)
Ulcer Index
Inhibition of Ulcers
(%)
Control vehicle
10 ml/kg p.o 5.00
±0.51 2.41
±0.27 100 10.74 - 4.67
±0.33 2.67
±0.21 100 10.73 --
Standard Ranitidine 30 mg/kg
0.33 ±0.21***
0.50 ±0.12***
33.33 3.41 68.24 0.50 ±0.22***
0.75 ±0.11***
50 5.12 52.28
AETST 100 mg/kg
p.o 3.66
±0.42* 2.33
±0.21ns 100 10.59 1.39 3.50 ±0.22**
2.50 ±0.22 ns
100 10.60 1.21
AETST 200 mg/kg
p.o 1.33
±0.33*** 1.58
±0.08** 100 10.29 4.18 1.67
±0.21*** 1.83
±0.10** 100 10.35 3.54
AETST 400 mg/kg
p.o 0.83
±0.16*** 0.83
±0.10*** 83.33 8.49 20.94 0.83
±0.16*** 1.08
±0.08*** 83.33 8.52 20.59
AQETST 100 mg/kg
p.o 3.33
±0.21** 2.08
±0.20ns 100 10.54 1.86 3.17 ±0.16***
2.50 ±0.22 ns 100 10.56 1.58
AQETST 200 mg/kg
p.o 1.16
±0.16*** 1.33
±0.10*** 100 10.24 4.65 1.50
±0.22*** 1.67
±0.10*** 100 10.31 3.91
AQETST 400 mg/kg
p.o 0.66
±0.21*** 0.75
±0.11*** 66.66 6.80 36.68 0.83
±0.16*** 0.91
±0.08*** 83.33 8.50 20.78

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.1
Fig No.5.2

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.3

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.4
Fig No.5.5

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.6

Dept. of Pharmacology, V.L.C.P Raichur
5.2.3 Anti-inflammatory activity:
1. Anti-inflammatory activity of AETST and AQETST in Carrageenan induced paw
oedema model in rats:
The AETST and AQETST with three selected doses i.e. 100, 200 and 400 mg/kg
have exhibited a significant reduction in paw oedema volume in carrageenan induced paw
oedema in rats at different time intervals. Results are tabulated in Table No. 5.7. Ibuprofen
(40 mg/kg) was used as standard reference and it has significantly reduced paw oedema
volume by 42.85% at 1st h, 61.43% at 2nd h, 79.29% at 3rd h and 85.33% at 4th h, thus
standard drug has exhibited time dependent reduction in oedema volume.
During 1st h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 4.85%, 14.28%, 24.00% and 9.71%, 19.14%,
28.57% respectively, which was found to be a time dependent effect.
During 2nd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 7.62%, 23.09%, 30.71% and 11.44%, 26.78%,
38.33% respectively a time dependent effect.
During 3rd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 13.66%, 27.53%, 37.88% and 17.14%, 31.05%,
44.72% respectively a time dependent effect was noted.
During 4th h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 22.22%, 33.33%, 59.25% and 29.55%, 40.66%,
66.66% respectively a time dependent effect was noted and result are graphically
represented in Fig No.5.7.

Dept. of Pharmacology, V.L.C.P Raichur
ANOVA indicates a significant difference among the AETST and AQETST treated
groups. Dunnett’s‘t’ test confirms a significant anti-inflammatory activity with both the
extracts, but more with AQETST than AETST.

Dept. of Pharmacology, V.L.C.P Raichur Page 77
Table No: 5.6 Anti-inflammatory effects of AETST and AQETST in Carrageenan induced paw oedema model in rats
Time after Paw oedema volume (ml) Treatment Animals Toxicant Standard AETST
100 mg/kg AETST
200 mg/kg AETST
400 mg/kg AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 0.35 0.20 0.35 0.25 0.25 0.30 0.25 0.30 B 0.40 0.25 0.40 0.30 0.30 0.30 0.30 0.25 T 0.30 0.10 0.25 0.30 0.25 0.35 0.20 0.20
HB 0.35 0.30 0.35 0.35 0.30 0.30 0.30 0.30 BT 0.35 0.20 0.30 0.30 0.30 0.35 0.35 0.25
1 h
HT 0.35 0.15 0.35 0.30 0.20 0.30 0.30 0.20 mean±SEM 0.350±0.012 0.200±0.028*** 0.333±0.021ns 0.300±0.012ns 0.266±0.016* 0.316±0.010ns 0.283±0.021ns 0.250±0.018**
H 0.50 0.15 0.35 0.25 0.25 0.35 0.30 0.20 B 0.40 0.25 0.40 0.40 0.30 0.40 0.30 0.25 T 0.45 0.10 0.35 0.35 0.35 0.40 0.25 0.30
HB 0.40 0.25 0.45 0.40 0.30 0.35 0.40 0.30 BT 0.45 0.15 0.45 0.30 0.25 0.45 0.30 0.25
2 h
HT 0.40 0.10 0.40 0.30 0.35 0.35 0.35 0.30 mean±SEM 0.433±0.016 0.167±0.027*** 0.400±0.018ns 0.333±0.024** 0.300±0.018*** 0.383±0.016ns 0.317±0.021** 0.267±0.016***
H 0.50 0.10 0.40 0.30 0.30 0.40 0.40 0.20 B 0.45 0.15 0.45 0.40 0.30 0.40 0.35 0.25 T 0.50 0.00 0.40 0.35 0.35 0.40 0.30 0.30
HB 0.50 0.15 0.45 0.40 0.25 0.35 0.30 0.30 BT 0.45 0.10 0.40 0.35 0.30 0.45 0.35 0.35
3 h
HT 0.50 0.10 0.40 0.30 0.30 0.40 0.30 0.20 mean±SEM 0.483±0.010 0.100±0.022*** 0.417±0.010* 0.350±0.018*** 0.300±0.012*** 0.400±0.012** 0.333±0.016*** 0.267±0.024***
H 0.50 0.10 0.30 0.30 0.20 0.30 0.30 0.15 B 0.45 0.00 0.40 0.35 0.15 0.35 0.30 0.10 T 0.40 0.15 0.35 0.30 0.30 0.30 0.25 0.20
HB 0.50 0.10 0.40 0.25 0.10 0.25 0.30 0.15 BT 0.40 0.05 0.35 0.35 0.15 0.40 0.25 0.20
4 h
HT 0.45 0.00 0.30 0.25 0.20 0.30 0.20 0.10 mean±SEM 0.450±0.018 0.066±0.024*** 0.350±0.018** 0.300±0.018*** 0.183±0.027*** 0.317±0.021*** 0.267±0.016*** 0.150±0.018***
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum .

Dept. of Pharmacology, V.L.C.P Raichur Page 78
Table No: 5.7 Anti-inflammatory effects of AETST and AQETST in Carrageenan induced paw oedema model in rats at different time intervals
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant. ROV- Reduction of Oedema Volume.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum .
S.No. Groups Treatment 1 h %
ROV 2 h % ROV 3 h % ROV 4 h % ROV
A Toxicant Carrageenan
(1% w/v) 0.350 ±0.012
-- 0.433 ±0.016
-- 0.483 ±0.010
-- 0.450 ±0.018
--
B Standard Ibuprofen 40 mg/kg
0.200 ±0.028***
42.85
0.167 ±0.027***
61.43 0.100 ±0.022***
79.29 0.066 ±0.024***
85.33
C AETST 100 mg/kg 0.333 ±0.021ns
4.85 0.400 ±0.018ns
7.62 0.417 ±0.010*
13.66 0.350 ±0.018**
22.22
D AETST 200 mg/kg 0.300 ±0.012ns
14.28
0.333 ±0.024**
23.09 0.350 ±0.018***
27.53 0.300 ±0.018***
33.33
E AETST 400 mg/kg 0.266 ±0.016*
24.00
0.300 ±0.018***
30.71 0.300 ±0.012***
37.88 0.183 ±0.027***
59.25
F AQETST 100 mg/kg 0.316 ±0.010ns
9.71
0.383 ±0.016ns
11.44 0.400 ±0.012**
17.14 0.317 ±0.021***
29.55
G AQETST 200 mg/kg 0.283 ±0.021ns
19.14
0.317 ±0.021**
26.78 0.333 ±0.016***
31.05 0.267 ±0.016***
40.66
H AQETST 400 mg/kg 0.250 ±0.018**
28.57
0.267 ±0.016***
38.33 0.267
±0.024*** 44.72 0.150 ±0.018***
66.66

Dept. of Pharmacology, V.L.C.P Raichur Page 79
2. Anti-inflammatory activity of AETST and AQETST in Histamine induced paw
oedema model in rats:
The AETST and AQETST with three selected doses i.e. 100, 200 and 400 mg/kg
have exhibited a significant reduction in paw oedema volume in histamine induced paw
oedema in rats at different time intervals. Results are tabulated in Table No. 5.9. Ibuprofen
(40 mg/kg) was used as standard reference and it has significantly reduced paw oedema
volume by 56.39% at 1st h, 70.44% at 2nd h, 86.80% at 3rd h and 92.93% at 4th h, thus
exhibited a time dependent reduction in oedema volume.
During 1st h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 4.17%, 17.23%, 39.16% and 8.61%, 26.10%,
47.78% respectively, which was found to be a time dependent effect.
During 2nd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 11.11%, 26.00%, 44.44% and 18.44%, 29.55%,
51.77% respectively noted a time dependent effect.
During 3rd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 16.60%, 36.66%, 56.66% and 26.60%, 43.40%,
63.40% respectively a time dependent effect was noted.
During 4th h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 25.05%, 46.46%, 67.88% and 35.76%, 53.53%,
74.94% respectively a time dependent effect was noted and result are graphically
represented in Fig No.5.8.

Dept. of Pharmacology, V.L.C.P Raichur Page 80
ANOVA indicates a significant difference among the AETST and AQETST treated
groups. Dunnett’s‘t’ test confirms a significant anti-inflammatory activity with both the
extracts, but more with AQETST than AETST.

Dept. of Pharmacology, V.L.C.P Raichur Page 81
Table No: 5.8 Anti-inflammatory effects of AETST and AQETST in Histamine induced paw oedema model in rats
Time after Paw oedema volume (ml) Treatment Animals Toxicant Standard AETST
100 mg/kg AETST
200 mg/kg AETST
400 mg/kg AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 0.35 0.15 0.40 0.25 0.20 0.30 0.25 0.20 B 0.40 0.10 0.35 0.25 0.25 0.40 0.30 0.15 T 0.40 0.20 0.30 0.35 0.30 0.40 0.35 0.20
HB 0.40 0.20 0.40 0.40 0.20 0.35 0.30 0.20 BT 0.40 0.20 0.35 0.30 0.25 0.30 0.25 0.25
1 h
HT 0.35 0.15 0.40 0.35 0.20 0.35 0.25 0.20 mean±SEM 0.383±0.010 0.167±0.016*** 0.367±0.016ns 0.317±0.024* 0.233±0.016*** 0.350±0.018ns 0.283±0.016** 0.200±0.012***
H 0.45 0.20 0.45 0.30 0.20 0.35 0.35 0.25 B 0.50 0.15 0.30 0.30 0.25 0.40 0.30 0.20 T 0.40 0.10 0.30 0.35 0.30 0.40 0.35 0.25
HB 0.50 0.15 0.50 0.35 0.20 0.30 0.30 0.20 BT 0.45 0.10 0.45 0.35 0.25 0.35 0.30 0.15
2 h
HT 0.40 0.10 0.40 0.35 0.30 0.40 0.30 0.25 mean±SEM 0.450±0.018 0.133±0.016*** 0.400±0.034ns 0.333±0.010*** 0.250±0.018*** 0.367±0.016* 0.317±0.010*** 0.217±0.016***
H 0.45 0.10 0.45 0.30 0.20 0.30 0.30 0.15 B 0.50 0.15 0.40 0.30 0.20 0.35 0.30 0.15 T 0.50 0.00 0.40 0.35 0.25 0.40 0.25 0.20
HB 0.55 0.00 0.40 0.30 0.20 0.35 0.30 0.20 BT 0.50 0.05 0.45 0.35 0.25 0.40 0.25 0.15
3 h
HT 0.50 0.10 0.40 0.30 0.20 0.40 0.30 0.25 mean±SEM 0.500±0.012 0.066±0.024*** 0.417±0.010** 0.317±0.010*** 0.217±0.010*** 0.367±0.016*** 0.283±0.010*** 0.183±0.016***
H 0.45 0.00 0.40 0.20 0.15 0.25 0.20 0.10 B 0.40 0.10 0.35 0.25 0.15 0.30 0.20 0.10 T 0.50 0.00 0.30 0.30 0.20 0.30 0.15 0.15
HB 0.50 0.00 0.30 0.25 0.10 0.30 0.25 0.10 BT 0.50 0.00 0.40 0.30 0.15 0.30 0.20 0.10
4 h
HT 0.45 0.10 0.35 0.20 0.15 0.35 0.30 0.15 mean±SEM 0.467±0.016 0.033±0.021*** 0.350±0.018*** 0.250±0.018*** 0.150±0.012*** 0.300±0.012*** 0.217±0.021*** 0.117±0.010***
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum .

Dept. of Pharmacology, V.L.C.P Raichur Page 82
Table No: 5.9 Anti-inflammatory effects of AETST and AQETST in Histamine induced paw oedema model in rats at different
time intervals
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant. ROV- Reduction of Oedema Volume.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum .
S.No. Groups Treatment 1 h % ROV 2 h % ROV 3 h % ROV 4 h % ROV
A Toxicant Histamine (1% w/v)
0.383 ±0.010
-- 0.450 ±0.018
-- 0.500 ±0.012
-- 0.467 ±0.016
--
B Standard Ibuprofen 40 mg/kg
0.167 ±0.016***
56.39 0.133 ±0.016*** 70.44 0.066
±0.024*** 86.80 0.033
±0.021*** 92.93
C AETST 100 mg/kg 0.367 ±0.016ns
4.17 0.400 ±0.034ns
11.11 0.417 ±0.010**
16.60 0.350 ±0.018*** 25.05
D AETST 200 mg/kg 0.317 ±0.024*
17.23 0.333 ±0.010*** 26.00 0.317
±0.010*** 36.66 0.250
±0.018*** 46.46
E AETST 400 mg/kg 0.233 ±0.016***
39.16 0.250
±0.018**
*
44.44 0.217 ±0.010***
56.66 0.150 ±0.012*** 67.88
F AQETST 100 mg/kg 0.350 ±0.018ns
8.61 0.367 ±0.016*
18.44 0.367 ±0.016***
26.60 0.300 ±0.012*** 35.76
G AQETST 200 mg/kg 0.283 ±0.016**
26.10 0.317 ±0.010*** 29.55 0.283
±0.010*** 43.40 0.217
±0.021*** 53.53
H AQETST 400 mg/kg 0.200 ±0.012***
47.78 0.217 ±0.016*** 51.77 0.183
±0.016*** 63.40 0.117
±0.010*** 74.94

Dept. of Pharmacology, V.L.C.P Raichur
3. Anti-inflammatory activity of AETST and AQETST in Formalin induced paw
oedema model in rats:
The AETST and AQETST with three selected doses i.e. 100, 200 and 400 mg/kg
have exhibited a significant reduction in paw oedema volume in Formalin induced paw
oedema in rats at different time intervals. Results are tabulated in Table No. 5.11.
Ibuprofen (40 mg/kg) was used as standard reference and it has significantly reduced paw
oedema volume by 54.25% at 1st h, 64.23% at 2nd h, 83.90% at 3rd h and 89.64% at 4th h,
which was found to be a time dependent effect.
During 1st h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 4.25%, 16.75%, 37.50% and 8.25%, 20.75%,
41.75% respectively noted as time dependent effect.
During 2nd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 7.28%, 21.41%, 42.82% and 10.70%, 28.69%,
50.10% respectively noted as time dependent effect.
During 3rd h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 12.95%, 32.30%, 54.92% and 19.34%, 38.68%,
61.31% respectively recorded as time dependent effect.
During 4th h of study AETST and AQETST with low, medium and high doses have
significantly reduced oedema volume by 24.01%, 44.72%, 65.42% and 34.36%, 51.75%,
72.46% respectively which was recorded as time dependent effect and result are
graphically represented in Fig No.5.9.

Dept. of Pharmacology, V.L.C.P Raichur
ANOVA indicates a significant difference among the AETST and AQETST treated
groups. Dunnett’s‘t’ test confirms a significant anti-inflammatory activity with both the
extracts, but more with AQETST than AETST.

Dept. of Pharmacology, V.L.C.P Raichur Page 85
Table No: 5.10 Anti-inflammatory effects of AETST and AQETST in Formalin induced paw edema model in rats
Time after Paw oedema volume (ml) Treatment Animals Toxicant Standard AETST
100 mg/kg AETST
200 mg/kg AETST
400 mg/kg AQETST 100 mg/kg
AQETST 200 mg/kg
AQETST 400 mg/kg
H 0.40 0.20 0.40 0.30 0.25 0.40 0.35 0.25 B 0.40 0.20 0.40 0.35 0.30 0.35 0.35 0.20 T 0.45 0.15 0.25 0.30 0.20 0.40 0.25 0.20
HB 0.40 0.25 0.40 0.40 0.25 0.35 0.30 0.25 BT 0.35 0.20 0.45 0.30 0.30 0.30 0.30 0.30
1 h
HT 0.40 0.10 0.40 0.35 0.20 0.40 0.35 0.20 mean±SEM 0.400±0.012 0.183±0.021*** 0.383±0.027ns 0.333±0.016ns 0.250±0.018*** 0.367±0.016ns 0.317±0.016* 0.233±0.016***
H 0.50 0.20 0.50 0.30 0.30 0.50 0.30 0.20 B 0.45 0.15 0.40 0.40 0.25 0.35 0.35 0.25 T 0.50 0.20 0.45 0.35 0.30 0.40 0.30 0.20
HB 0.45 0.20 0.40 0.40 0.20 0.35 0.35 0.30 BT 0.40 0.15 0.45 0.40 0.25 0.40 0.30 0.20
2 h
HT 0.50 0.10 0.40 0.35 0.30 0.50 0.40 0.25 mean±SEM 0.467±0.016 0.167±0.016*** 0.433±0.016ns 0.367±0.016** 0.267±0.016*** 0.417±0.027ns 0.333±0.016*** ±0.233±0.016***
H 0.55 0.10 0.45 0.40 0.30 0.5 0.25 0.15 B 0.50 0.05 0.50 0.35 0.25 0.45 0.30 0.20 T 0.50 0.10 0.40 0.30 0.20 0.40 0.35 0.20
HB 0.50 0.10 0.45 0.30 0.25 0.30 0.35 0.25 BT 0.50 0.10 0.40 0.35 0.20 0.45 0.35 0.20
3 h
HT 0.55 0.05 0.50 0.40 0.20 0.40 0.30 0.20 mean±SEM 0.517±0.010 0.083±0.010*** 0.450±0.018ns 0.350±0.018*** 0.233±0.016*** 0.417±0.027** 0.317±0.016*** 0.200±0.012***
H 0.50 0.10 0.35 0.30 0.20 0.40 0.20 0.10 B 0.45 0.00 0.40 0.25 0.20 0.30 0.20 0.15 T 0.50 0.00 0.30 0.20 0.15 0.30 0.30 0.10
HB 0.45 0.10 0.40 0.25 0.20 0.25 0.20 0.20 BT 0.50 0.10 0.35 0.30 0.10 0.35 0.25 0.10
4 h
HT 0.50 0.00 0.40 0.30 0.15 0.30 0.25 0.15 mean±SEM 0.483±0.010 0.050±0.022*** 0.367±0.016** 0.267±0.016*** 0.167±0.016*** 0.317±0.021*** 0.233±0.016*** 0.133±0.016***
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum .

Dept. of Pharmacology, V.L.C.P Raichur Page 86
Table No: 5.11 Anti-inflammatory effects of AETST and AQETST in Formalin induced paw oedema model in rats at different
time intervals
n = 6, Significant at P < 0.05*, 0.01** and 0.001***, ns = not significant. ROV- Reduction of Oedema Volume.
AETST- Alcoholic Extract of Tuber of S. tuberosum, AQETST- Aqueous Extract of Tuber of S. tuberosum.
S.No. Groups Treatment 1 h % ROV 2 h % ROV 3 h % ROV 4 h % ROV
A Toxicant Formalin (1% w/v)
0.400 ±0.012
-- 0.467 ±0.016
-- 0.517 ±0.010
-- 0.483 ±0.010
--
B Standard Ibuprofen 40mg/kg
0.183 ±0.021***
54.25 0.167 ±0.016***
64.23 0.083 ±0.010***
83.90 0.050 ±0.022***
89.64
C AETST 100 mg/kg 0.383 ±0.027ns
4.25 0.433 ±0.016ns
7.28 0.450 ±0.018ns
12.95 0.367 ±0.016**
24.01
D AETST 200 mg/kg 0.333 ±0.016ns
16.75 0.367 ±0.016**
21.41 0.350 ±0.018***
32.30 0.267 ±0.016***
44.72
E AETST 400 mg/kg 0.250 ±0.018***
37.50 0.267 ±0.016***
42.82 0.233 ±0.016***
54.92 0.167 ±0.016***
65.42
F AQETST 100 mg/kg 0.367 ±0.016ns
8.25 0.417 ±0.027ns
10.70 0.417 ±0.027**
19.34 0.317 ±0.021***
34.36
G AQETST 200 mg/kg 0.317 ±0.016*
20.75 0.333 ±0.016***
28.69 0.317 ±0.016***
38.68 0.233 ±0.016***
51.75
H AQETST 400 mg/kg 0.233 ±0.016***
41.75 ±0.233 ±0.016***
50.10 0.200 ±0.012***
61.31 0.133 ±0.016***
72.46

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.7
Fig No.5.8

Dept. of Pharmacology, V.L.C.P Raichur
Fig No.5.9

Dept. of Pharmacology, V.L.C.P Raichur
6. DISCUSSION
Peptic ulcer is a conglomerate of most common heterogenous disorders, present as a
crater in the lining of the GIT mucosa due to acid, pepsin, bile acid, pancreatic enzyme and
bacteria. It is due to an imbalance between aggressive (acid and pepsin) and defensive
(bicarbonates, mucin, PG etc) factors. Peptic ulcer disease also occurs due to
administration of NSAIDs, stress, H. pylori or pathological condition like Zollinger –
Ellison syndrome. NSAIDs causes erosions, petechiae, type C gastritis,
ulceration/combination with interference of ulcer healing. Further they also induce damage
of the mucosa with imbalance between aggressive and defensive factors. Though a very
good numbers of anti-ulcers drugs like antisecretory drugs, H2 receptor antagonists, proton
pump inhibitors, antimuscaranic, cytoprotectants and Prostaglandins analogues are
available, the side effects associated with these drugs limit their use. Many herbal drugs
from Ayurveda of Indian traditional system of medicine are advocated for the management
of peptic ulcer. Herbal medicines used as whole plant powders/extracts from different parts
are now a days consider as safe medication for the treatment of a numbers of diseases as it
is a general notion that plant based drugs are safer without any side effects28,79,88.
Though the presently available anti-ulcer drugs have remarkable effects in ulcer
therapy the efficacy is still incomplete as there are many a number of incidences of relapse
with adverse effects and drug-drug interaction are reported with the therapy. Hence there is
a need for ideal anti-ulcer drugs with extended action from herbal source with a calibre of
better protection and low incidence of relapse of ulcers89,90.
In Indian system of medicine a very good numbers of herbs are reported to produce
antiulcer and anti-inflammatory activities. Hence in the present study a plant by name

Dept. of Pharmacology, V.L.C.P Raichur
S. tuberosum has considered to evaluate its antiulcer and anti-inflammatory activities
scientifically. For this alcohol and aqueous extracts prepared from the tubers of the plant
were tested against different ulcer models in rats and inflammatory models also in rats8.
In pylorus ligation induced ulcer model, ulcers are produced due to accumulation of
acid at the pyloric end that causes ulcers. Both the extracts AETST and AQETST
significantly reduced ulcers by decreasing gastric volume and increasing the pH, thereby
reducing the severity of ulcers i.e. ulcers numbers and ulcers index91.
Stress induced ulcer are due to release of histamine with an increase in acid secretion
and reduction in mucus production. Stress stimulate adenohypophysial axis and causes
release of endogenous opiates and also produces severe gastric erosion by the activation of
central vagal discharge which release endogenous opiates that cause mucosal congestion
by peripheral mechanism to develop gastric ulcers. Both the extracts have significantly
reduced gastric secretion thus prevented gastric mucosa from the development of ulcers.
Several studies reported that gastroduodenal protection by prostaglandins is due to increase
in mucosal resistant and decrease in aggressive factors like acid and pepsin92.
Tannins89, carbohydrate93, flavonoids94, glycosides95 and triterpines96 are reported for
their anti-ulcers activity. Both AETST and AQETST contained all the above mentioned
phytoconstituents and hence these might have contributed for the anti-ulcer activity. The
anti-ulcerogenic effect of AETST and AQETST may be related to their antisecretory action
since acid is a major factor in the development of peptic ulcers.
Carrageenan induced paw oedema model is used for screening of NSAIDs and
inflammation produced by its biphasic in nature with the release of serotonin, bradykinin
and histamine at I Phase followed by release of prostaglandins in II Phase.

Dept. of Pharmacology, V.L.C.P Raichur
Histamine being an important mediator of inflammation and also a potent vasodilator
that causes increase in vascular permeability. In both phases due to release of these
mediators cause pain and fever and both the extracts significantly reduced paw oedema in
II Phase of the inflammation indicating there effect on prostaglandins97.
Formalin induced paw oedema model consist of two phases too with nociception in
neurogenic and inflammatory phases. Drugs that primarily act on central nervous system
are capable to inhibit both phases equally and by inhibiting the late phase, peripherally
acting drugs produce there anti-inflammatory activity. The neurogenic and inflammatory
phases are due to release of substance P, serotonin, histamine, prostaglandins and
leukotrienes respectively. Both the extracts significantly reduced both phases of
inflammation in formalin induced paw oedema model in rats87.
Tannins, sterols, flavonoids, alkaloids and triterpines are reported for their anti-
inflammatory activity. Both AETST and AQETST contained all the above mentioned
phytoconstituents and hence these might have contributed for the anti-inflammatory
activity54,98.

Dept. of Pharmacology, V.L.C.P Raichur
7. CONCLUSION
Preliminary phytochemical evaluation of both AETST and AQETST revealed the
presence of tannins, carbohydrate, sterols, flavonoids, glycosides, alkaloids and
triterpines in both the extracts. Acute oral toxicity studies no mortality recorded with
either of the extracts even at the dose level of 2000 mg/kg body weight.
Anti-ulcer and anti-inflammatory activities confirmed with both the extracts in
experimental animals, rats with different ulcer and inflammatory models. In both ulcer
and inflammatory models both the extracts at low, medium and high doses produced a
significant anti-ulcer and anti-inflammatory activities (P < 0.05*, 0.01** and 0.001***).
Phytochemical constituents like tannins, flavonoids and triterpines are already
reported for their anti-ulcer and anti-inflammatory activities and both the extracts
contained the above mentioned constituents. Hence these can be accounted for the
observed anti-ulcer and anti-inflammatory activities in rats.

Dept. of Pharmacology, V.L.C.P Raichur
8. SUMMARY
S. tuberosum is mentioned for its anti-ulcer and anti-inflammatory activities in
Ayurvedic texts without an available scientific data. Hence the present study is planned to
explore anti-ulcer and anti-inflammatory activities of AETST and AQETST.
Preliminary phytochemical investigations identified with tannins, carbohydrate,
sterols, flavonoids, glycosides, alkaloid and triterpines in both extracts. Acute oral
toxicity studies revealed that there is no mortality with both the extracts even upto the
dose level of 2000 mg/kg.
In pylorus ligation induced ulcer model, selected doses like low (100 mg/kg),
medium (200 mg/kg) and high (400 mg/kg) doses (AETST and AQETST) of both the
extracts significantly reduced the ulcers (P < 0.05*, 0.01** and 0.001***). In stress
induced ulcers by cold water immersion model also both the extracts with the doses
mentioned above significantly reduced the ulcers (P < 0.05*, 0.01** and 0.001***).
In carrageenan, histamine and formalin induced inflammatory models both the
extracts significantly reduced inflammation (P < 0.05*, 0.01** and 0.001***).

Dept. of Pharmacology, V.L.C.P Raichur
9. BIBLIOGRAPHY
1. http://web1.msue.msu.edu/msue/imp/modzz/masterzz.html. Access file 25/09/10.
2. Ahmed MKK, Rana AC, Dixit VK, Shivananda BG. Internet-implications for the
future of phytopharmacological research. Indian J Exp Biol 2003; 41: 1233-38.
3. WHO, 2002. World Health Organization fact sheet No.271. World Health
Organization, Geneva.
4. Farnsworth NR, Soejarto DD. Global importance of medicinal plants. 1st ed.
Cambridge University Press, New York, USA 1991: 25-51.
5. Mwale M, Bhebhe E, Chimonyo M, Halimani E. Use of herbal plants in poultry
health management in the Mushagashe small-scale commercial farming area in
Zimbabwe. Intern J Appl Res Vet Med 2005; 3(2): 163-170.
6. Khare CP. Indian medicinal plants. 1st ed. Springer Science+Business Media Spring
Street, New York, USA 2007: 614-615.
7. hppt://www.ikisan.com/links/ap_potatochemicalcomposition.shtml. Access
date 25/09/10.
8. Kurian JC. Plants that heal. 7th ed. Oriental Watchman Publishing House, Pune
2007: 130.
9. Gregory M, Vithalrao KP, Franklin G, Kalaichelavan V. Anti-ulcer (ulcer-
preventive) activity of Ficus arnottiana Miq. (Moraceae) leaf methanolic extract.
Ame J Pharmacol Toxicol 2009; 4(3): 89-93.
10. Khandare RA, Gulecha VS, Mahajan MS, Mundada AS, Gangurde HH. Evaluation
of antiulcer activity polyherbal formulation. Intern J Pharmaceut Res Dev 2009; 10:
0974 – 9446.
11. http://en.wikipedia.org/wiki/Peptic_ulcer. Access file 18/10/10.

Dept. of Pharmacology, V.L.C.P Raichur
12. Satoskar RS, Bhandarkar SD, Ainapure SS. Pharmacology and
pharmacotherapeutics, 16 th ed. Popular Prakashan Pvt Ltd, Mumbai 1999: 609-
623.
13. http://www.mamashealth.com/stomach.asp. Access file 18/10/10.
14. http://www.patient.co.uk/health/Duodenal-Ulcer.htm. Access file 25/10/10.
15. http://www.articlesbase.com/diseases-and-conditions-articles/what-is-an-esophageal-ulcer-
433370.html. Access file 25/10/10.
16. http://en.wikipedia.org/wiki/Meckel's_diverticulum. Access file – 18/11/10.
17. Ganong WF. Regulation of gastrointestinal function In: Review of medical
physiology. 14th ed. Practice-Hall Englewood Cliffs, New Jersey, USA 2001: 448-
466.
18. Rang HP, Dale MM, Ritter JM, Moore PK. Pharmacology. 5th ed. Churchill
Livingstone, New Delhi 2000: 385.
19. Mycek MJ, Harvey RA, Champe PC. Lippincotts illustrated reviews:
Pharmacology. 3rd ed. Cooper Graphics Hampton, New Jersey 2006: 329- 35.
20. Editorial. Helicobacter pylori infection. Indian Pediatrics 1996; 33: 899-903.
21. Sotoudehmanesh R, Asgari AA, Fakheri HT, Nouraie M, Khatibian M, Shirazian
N. Peptic ulcer bleeding: Is Helicobacter pylorus a risk factor in an endemic area?.
Indian J Gastroenterol 2005; 24: 59-61.
22. Laine L, Schoenfeld P, Fennerty MB. Therapy for H. pylori in patients with
nonulcer dyspepsia. Annals Internal Med 2001; 134(5): 361-369.

Dept. of Pharmacology, V.L.C.P Raichur
23. Majumdar D, Bebb J, Atherton J. Helicobacter pylori infection and peptic ulcers.
Medicine 2007; 35(4): 204-209.
24. Szasz TS. Factors in the pathogenesis of peptic ulcer. A Symposium Psychoanalyt
1949; 11(5): 300-304.
25. http://www.news-medical.net/health/Peptic-Ulcer-Diagnosis.aspx. Access file
20/11/10.
26. Tripathi KD. Essentials of medical pharmacology. 5th ed. Jaypee Brothers Medical
Publishers, New Delhi 2003: 627-638.
27. Kalyanakrishnan R, Robert CS. Peptic ulcer disease. J Ethnopharmacol 2007;
76(7): 1005-1012.
28. Goel RK, Sairam K. Anti-ulcer drugs from indigenous sources with emphasis on
Musa sapientum, Tamrabhasma, Asparagus racemosus and Zingiber officinale.
Indian J Pharmacol 2002; 34: 100-110.
29. Sairam K, Rao CV, Babu MD, Kumar VK, Agarwal VK, Goel RK.
Antiulcerogenic effect of ethanolic extract of Emblica officinalis: an experimental
study. J Ethnopharmacol 2002; 82: 1-9.
30. Sairam K, Priyambada S, Arya NC, Goel RK. Gastroduodenal ulcer protective
activity of Asparagus racemosus: an experimental biochemical and histological
study. J Ethnopharmacol 2003; 86: 1-10.
31. Sairam K, Rao CV, Goel RK. Effect of Centella asiatica Linn on physical and
chemical factors induced gastric ulceration and secretion in rats. Ind J Exp Biol
2001; 39: 137-42.
32. Dharmani P, Palit G. Exploring Indian medicinal plants for anti-ulcer activity.
Indian J Pharmacol 2006; 32(2): 95-99.

Dept. of Pharmacology, V.L.C.P Raichur
33. Dharmani P, Mishra PK, Maurya R, Chauhan VS, Palit G. Allophylus serratus: a
plant with potential anti-ulcerogenic activity. J Ethnopharmacol 2005; 99: 361-63.
34. Dharmani P, Mishra PK, Maurya R, Chauhan VS, Palit G. Desmodium gangeticum:
a plant with potent anti-ulcer effect. Indian J Exp Biol 2005; 43: 517-21.
35. Gupta M, Mazumder UK, Manikandan L, Bhattacharya S, Senthikumar GP, Suresh
R. Anti-ulcer activity of ethanol extract of Terminalia pallida Brandis in Swiss
albino rats. J Ethnopharmacol 2005; 97: 405-8.
36. Sanyal AK, Gupta KK, Chowdhury NK. Banana and experimental peptic ulcer.
Indian J Pharmacol 1963; 15: 283-4.
37. Alvarez A, Pomar F, Sevilla MA, Montero MJ. Gastric antisecretory and antiulcer
activities of an ethanolic extract of Bidens pilosa L var radiata Schult. J
Ethnopharmacol 1999; 67: 333-40.
38. Anoop A, Jegadeesan M. Biochemical studies on the anti-ulcerogenic potential of
Hemidesmus indicus. J Ethnopharmacol 2003; 84: 149-56.
39. Martins AG, Guterres SS, Ortega GG. Anti-ulcer activity of spray-dried powders
prepared from leaf extracts of Maytenus ilicifolia Martius ex Reiss. Am J Pharm
2003; 22 (1): 39-44.
40. Okoli CO, Ezike AC, Akah PA, Udegbunam OS, Okoye TC, E. Ugwu. Studies on
wound healing and antiulcer activities of extract of aerial parts of Phyllanthus
niruri L. (Euphorbiaceae). Am J Pharmacol Toxicol 2009; 4 (4): 118-26.
41. Ferrero ML, Nielsen OH, Andersen PS, Girardin SE. Chronic inflammation:
importance of NOD2 and NALP3 in interleukin-1beta generation. Clin Exp
Immunol 2001; 147 (2): 227–35.

Dept. of Pharmacology, V.L.C.P Raichur
42. Waugh A, Grant A. Ross and Wilson Anatomy and physiology in health and
illness. 9th ed. Churchill Livingstone Elsevier science, New Delhi 2001: 375-377.
43. Kumar V, Cotran RS, Robbins SL. Robbin’s Basic pathology.7th ed. Harcourt
(India) Pvt Ltd, New Delhi 2003: 52-56.
44. Warden SJ. Prophylactic Use of NSAIDs by athletes: a risk/benefit assessment. The
Physician and Sports Medicine 2010; 38 (1): 132–138.
45. Hinz B, Cheremina O, Brune, K. Acetaminophen (paracetamol) is a selective
cyclooxygenase-2 inhibitor in man. Feder Am Soci Exper Biol 2008; 22 (2): 383–
90.
46. David MA, Eric GH. Antipyretics: mechanisms of action and clinical use in fever
suppression. Afr J Med 2001; 111(4): 110-12.
47. Coceani F, Bishai I, Lees J, Sirko S. Prostaglandin-E2 and fever: a continuing
debate. Yale J Biol Med 1986; 59(2): 169–74.
48. Michael MJ. Medical pharmacology at a glance. 4th ed. Blackwell Science Ltd,
Germany 2002: 70.
49. Kearney PM, Baigent C, Godwin J, Halls H, Emberson J, Patrono C. Do selective
cyclo-oxygenase-2 inhibitors and traditional nonsteroidal anti-inflammatory drugs
increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ
2006; 33 (7): 1-8.
50. Traversa G, Walker AM, Ippolito F, Maggini M, Alegiani S, Raschetti R et al.
Gastroduodenal toxicity of different nonsteroidal antiinflammatory drugs.
Epidemiol 1995; 6 (1): 49–54.

Dept. of Pharmacology, V.L.C.P Raichur
51. Rossi S. Australian medicines handbook, 3rd ed. Australian Medicines Handbook
Pvt Ltd Adelaide, South Australia 2006; 220-24.
52. Ilavarasan R, Mallik M, Venkataraman S. Anti-inflammatory and antioxidant
activities of Cassia fistula linn bark extracts. Afr J Trad CAM 2005; 2 (1): 70 – 85.
53. Adedapo AA, Sofidiya MO, Afolayan AJ. Anti-inflammatory and analgesic
activities of the aqueous extracts of Margaritaria discoidea (Euphorbiaceae) stem
bark in experimental animal models. Rev Biol Trop (Int J Trop Biol) 2009; 57 (4):
1193-1200.
54. Arunachalam G, Subramanian N, Pazhani G, Ravichandran V. Anti-inflammatory
activity of methanolic extract of Eclipta prostrata L (Astearaceae). Afr J Pharm
Pharmacol 2009; 3(3): 97-100.
55. Mujumdar AM. Naik DJ, Dandge CN, Puntambekar HM. Antiinflammatory
activity of Curcuma amada in albino rats. Indian J Pharmacol 2000; 32: 375-377.
56. Paschapur MS, Patil MB, Kumar R, Patil SR. Evaluation of anti-inflammatory
activity of ethanolic extract of Borassus flabellifer L male flowers (inflorescences)
in experimental animals. J Medic Plants Res 2009; 3(2): 49-54.
57. Dharmasiri MG, Jayakody JRAC, Galhena G, Liyanage SSP, Ratnasooriya WD.
Anti-inflammatory and analgesic activities of mature fresh leaves of Vitex negundo.
J Ethnopharmacol 2003; 87: 199-06.
58. Okoli CO, Akah PA, Ezugworie U. Anti-inflammatory activity of extracts of root
bark of Securidaca longipedunculata Fres (Polygalaceae). Afr J Trad CAM 2005;
2(3): 54-63.

Dept. of Pharmacology, V.L.C.P Raichur
59. Akuodor GC, Idris-Usman MS, Mbah CC, Megwas UA, Akpan JL, Ugwu TC.
Studies on anti-ulcer, analgesic and antipyretic properties of the ethanolic leaf
extract of Gongronema latifolium in rodents. Afr J Biotech 2010; 9 (5): 2316-21.
60. Puntero BF, Peinado II, Fresno AMVD. Anti-inflammatory and antiulcer activities
of Teucrium buxifolium. J Ethanopharmacol 1997; 55: 93-98.
61. Silva BPD, Parente JP. Chemical properties and anti-inflammatory activity of a
galactomannoglucan from Arecastrum romanzoffianum. J Ethnopharmacol 2010; 3:
109-12.
62. Schapoval EES, Vargas MRW, Chaves CG, Bridi R, Zuanazzi JA, Henriques AT.
Antiinflammatory and antinociceptive activities of extracts and isolated compounds
from Stachytarpheta cayennensis. J Ethnopharmacol 1998; 60: 53–59.
63. Borgi W, Ghedira K, Chouchane N. Antiinflammatory and analgesic activities of
Zizyphus lotus root bark. Fitoterapia 2007; 78: 16–19.
64. Ravi V, Saleem TSM, Patel SS, Ramamurthy J, Gauthaman K. Anti-Inflammatory
effect of methanolic extract of Solanum nigrum Linn Berries. Intern J Appl Res Nat
Prod 2009; 2(2): 33-36.
65. Segura L, Vila R, Gupta MP, Avella ME, Adzet T, Canigueral A.
Antiinflammatory activity of Anthurium cerrocampanense Croat in rats and mice. J
Ethnopharmacol 1998; 61: 243–248.
66. Akindele AJ, Adeyem OO. Antiinflammatory activity of the aqueous leaf extracts
of Byrsocarpus coccineus. Fitoterapia 2007; 78: 25–28.
67. Pal S, Chaudhuri AK. Studies on the ant-ulcer activity of a Bryophyllum pinnatum
leaf extract in experimental animal. J Ethnopharmacol 1991; 33: 97-102.

Dept. of Pharmacology, V.L.C.P Raichur
68. Liu XM, Zakaria MNM, Islam MW, Radhakrishnan R, Imail A, Chen HB. Anti-
inflammatory and anti-ulcer activity of Calligonum comosum in rats. Fitoterapia
2001; 72: 487-491.
69. Basu A, Sen T, Pal S, Nag Chaudhuri AK, Mascolo N, Capass F. Studies on the
anti-ulcer activity of the chloroform fraction of Calotropis procera root extract.
Phytother Res 1997; 11: 163-165.
70. Kulkarni AR, Kulkarni VH, Shastry CS, Sateesh B, Hukkeri VI, Marihal SC.
Sceening of guava leaves extracts of analgesic, anti-inflammatory and anti-ulcer
activity in albino rats. Indian Drugs 1999; 36(6): 363-67.
71. Bhattacharya S, Pal S, Nag Chaudhuri AK. The effects of Mikania cordata (Burm)
B. L. Robbinson root extract on gastro-duodenal ulcer models in rats and
guineapigs. Phytother Res 1988; 2: 180-182.
72. Goel RK, Pandey VB, Dwivedi SPD, Rao YV. Anti-inflammatory and anti-ulcer
effects of Kaempferol, flavones isolated from Rhamnus procumbers. Ind J Exp Biol
1988; 26: 121-124.
73. Goel RK, Das Gupta G. Antiulcerogenic and anti-inflammatory effect of emodin
isolated from Rhamnus triquerta wall. Ind J Exp Biol 1991; 29: 230-232.
74. Kokate CK. Practical pharmacognosy. 14th ed. Vallabh Prakashan, New Delhi
1994: 110-111.
75. Khandelwal KR. Practical pharmacognosy-techniques and experiments, 2nd ed.
Nirali Prakashan, Pune 2000: 25.
76. Trease GE, Evans MC. Text book of pharmacognosy. 2nd ed. Elseveir Science Ltd,
London 2000: 193, 336.

Dept. of Pharmacology, V.L.C.P Raichur
77. OECD 2001-guidelines on acute oral toxicity (AOT) Environmental health and
safety monograph series on testing and adjustment No. 425.
78. Brodie DA. Experimental peptic ulcer. Gastroenterol 1968; 55(1): 125-133.
79. Bhatnagar M, Jain CP, Sisodia SS. Anti-ulcer activity of Withania somnifera in
stress plus pyloric ligation induced gastric ulcer in rats. J Cell Tis Res 2005; 5(1):
287-292.
80. Singh S, Majumdar DK. Evaluation of the gastric antiulcer activity of fixed oil of
Ocimum sanctum (Holy Basil). J Ethnopharmacol 1999; 65: 13–19.
81. Umamaheswari M, Asokkumar K, Rathidevi R, Sivashanmugam AT, Subhadradevi
V, Ravi TK. Antiulcer and in vitro antioxidant activities of Jasminum grandiflorum
L. J Ethnopharmacol 2007; 110: 464–70.
82. Deshpande SS, Shah GB, Parmar NS. Antiulcer activity of Tephrosia purpurea in
rats. Indian J Pharmacol 2003; 38:168-172.
83. Rajkapoor B, Anandan R, Jayakar B. Antiulcer effect of Nigella sativa Linn.
against gastric ulcers in rats. Cur Sci 2002; 82(2):177-179.
84. Vogel HG, Vogel WH. Drug discovery and evaluation of pharmacological assays.
2nd ed. Springer-verlag Berlin Heidelberg, Germany 2002: 759,760, 869.
85. Kasture SB, A Handbook of experiments in pre-clinical pharmacology. 3rd ed.
Career Publication Nashik, Maharashtra 2006: 156.
86. Gupta M, Mazumder UK, Kumar RS, Kumar TS. Studies on anti-inflammatory,
analgesic and antipyretic properties of methanol extract of Caesalpinia bonducella
leaves in experimental animal models. Iran J Pharmaco therap 2003: 30-34.

Dept. of Pharmacology, V.L.C.P Raichur
87. Sharma A, Bhatia S, Kharya MD, Gajbhiye V, Ganesh N, Namdeo AG et al. Anti-
inflammatory and analgesic activity of different fractions of Boswellia serrata.
Intern J Phytomed 2010; 2: 94-99.
88. Patidar DK. Anti-ulcer activity of aqueous extract of Murraya koenigii in albino
rats. Inter J Pharm and Bio Sci 2011; 2(1): 524-529.
89. Thirunavukkarasu P, Ramkumar L, Ramanathan T. Anti-ulcer activity of
Excoecaria agallocha bark on NSAID-induced gastric ulcer in Albino rats. Global
J Pharmacol 2009; 3 (3): 123-126.
90. Gupta AK, Gowda SKP, Mahesh CM. Antiulcer effect of aqueous extract of
Physalis minima in ethanol induced acute gastric ulcer in rats. J Pharmacy Res
2010; 3(4): 671-674.
91. Raju D, Ilango K, Chitra V, Ashish K. Evaluation of anti-ulcer activity of
methanolic extract of Terminalia chebula fruits in experimental rats. J Pharm Sci
Res 2009; 1(3): 101‐107.
92. Yelken B, Dorman T, Erkasap S, Dundar E, Tanriverdi B. Clonidine Pretreatment
Inhibits Stress-Induced Gastric Ulcer in Rats. Anesth Analg 1999; 89(1): 159-62.
93. Mahendran P, Vanisree AJ, Devi CSS. The antiulcer activity of Garcinia cambogia
extract against indomethacin induced gastric ulcer in rats. Phytother Res 2002; 16:
80–83.

Dept. of Pharmacology, V.L.C.P Raichur
94. Mota KSDL, Dias GEN, Pinto MEF, Ferreira AL, Souza-Brito ARM and Hiruma-
Lima CA et al. Flavonoids with gastroprotective activity. Molecules 2000; 14: 979-
1012.
95. Jain AS, Surana J. Antiulcerogenic effects of Spathodea falcata against different
experimental models. Afr J Pharmceut Clin Res 2009: 2: 54-59.
96. Devaraj VC, Asad M, Prasad S. Effect of leaves and fruits of Moringa oleifera on
gastric and duodenal ulcers. Pharmaceut Biol 2007; 45 (4): 332–338.
97. Pendota SC, Yakubu MT, Grierson DS, Afolayan AJ. Anti-inflammatory, analgesic
and antipyretic activities of the aqueous extract of Hippobromus pauciflorus (Lf)
Radlk leaves in male Wistar rats. Afr J Biotech 2009; 8 (10): 2036-2041.
98. Hemamalini KK, Naik OP, Ashok A. Anti-inflammatory and analgesic effect of
methanolic extract of Anogeissus acuminata leaf. Int J Pharm Biomed Res 2010;
1(3): 98-100.
INSTITUTIONAL ETHICAL COMMITTEE
V.L.COLLEGE OF PHARMACY, RAICHUR-584103
KARNATAKA, INDIA.
Institutional ethical committee of V.L. College of Pharmacy, Raichur met on 16-11-
2009 to discuss about the details of animal experiments required to be carried out by PG
students of different Departments during their project work of 2010-2011. The following
members were present.
1. Dr. S.M. SHANTA KUMAR CHAIRMAN
2. Dr. N.VENKAT RAO CONVENER
3. Dr. LAKSHMAYYA MEMBER
4. Dr. SOMASHEKAR SHYALE MEMBER

Dept. of Pharmacology, V.L.C.P Raichur
5. Dr. Y.C.MAYUR MEMBER
6. Dr. T.SHIVARAJ GOUDA MEMBER
7. Dr. SRINIVAS MEMBER
The requirement for different experiments of each PG student were discussed in
detail. After thorough discussion the experiments to be carried out by the students of
individual Department were approved. The details are as follows.
1) Department of Pharmaceutics
S. No. Name Title of the work Type of work Animals required
Number
1. Shashikala
Development and characterization of
transdermal films of flurbiprofen
In-vitro Permeation studies Rats 24
2. Prashant Development and evaluation
of TTS containing few antihypertensive agents
Skin permeation Rats 20
3. Azhar
Development and evaluation of mucoadhesive buccal drug delivery systems of few Anti-
emetic drugs
Mucosal permeation Bovine mucosa
20
2) Department of Pharmacology
S. No. Name Title of the work Type of work Animals required Number
1. Radhika
A study on drug-drug interaction between
Candesartan and Glimepiride in rats
Drug-Drug interaction Rats 100
2. Syed Mahboob Ahmad
A study on antiulcer and antinflammatory activities of
tuber extracts of Solanum tuberosum (Solanaceae) in
rats
Antiulcer and antinflammatory activities
Rats 180
3. C.Yasar Ahmaed A study on anti-arthritic and antiulcer activities of Saraca
indica in rats/mice
Anti-arthritic and antiulcer activities
Rats/mice 150/40
4. Sowmya U.
A study on drug-drug interaction between
Carvedilol and Gliclazide in rats
Drug-Drug interaction Rats 100
5. J.Manoj Antiobesity activity of
Citrullus vulgaris (Cucurbitaceae) seed
Antiobesity activity Rats 160

Dept. of Pharmacology, V.L.C.P Raichur
extracts in rats.
6. Petricia Regina Irene
A study on Nootropic activity of fruit extracts of
Litchi chinensis Sonn(Sapindaceae) in mice
and rats
Nootropic activity Rats/mice 50/200
7. Patel Shivabhai
A Study on Nootropic activity of root extracts of
Vanda tessallata(Orchidaceae) in
mice and rats
Nootropic activity Rats/mice 150/150
8. Md. Basheer
Food-drug interactions between Capsicum
frutescens L.(Solanaceae)fruit extract and glimepiride in diabetic
rats
Food-drug interaction Rats 200
9. Venu Kola
Evaluation of anti arthritic and antiulcer activity of
root etracts of Momordia charantia in rats and mice
Anti-arthritic and antiulcer activities
Rats /mice 220/40
10. Rajesh Kumar
Calcium channel blockers as hepatoprotective agents
in different hepatotoxic models in rats
Hepatoprotective activity Rats 260
11. Rizwan A. Sheikh A study on hepatoprotective activity of bark extracts of Bassia latifolia roxb.in rats
Hepatoprotective activity Rats 260
12. Md. Fasih Ahmad
A study of herb-drug interaction between
Ocimum sanctum and Glimepiride in diabetic rats
Drug-Drug interaction Rats 240

Dept. of Pharmacology, V.L.C.P Raichur

Dept. of Pharmacology, V.L.C.P Raichur