
The genetic ancestry of American Creole cattle inferred from ...
Upload
independentCategory
view
0download
0
Schizophrenia Research 120 (2010) 87ndash94
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage wwwe lsev ie rcom locate schres
Substance use disorder comorbidity with schizophrenia in families ofMexican and Central American Ancestry
Lorena Jimeacutenez-Castro ab Elizabeth Hare aj Rolando Medina ac Henriette Raventos bHumberto Nicolini d Ricardo Mendoza e Alfonso Ontiveros f Alvaro Jerez g Rodrigo Muntildeoz hAlbana Dassori c Michael Escamilla aija South Texas Psychiatric Genetics Research Center Paul L Foster School of Medicine Texas Tech University Health Science Center San Antonio TX United Statesb Centro Investigacioacuten en Biologiacutea Molecular y Celular University of Costa Rica San Joseacute Costa Ricac Department of Psychiatry South Texas Veterans Health System San Antonio San Antonio TX United Statesd Grupo de Estudios Meacutedicos y Familiares Carraci SC Meacutexico DF Mexicoe Department of Psychiatry and Biobehavioral Science University of California Los Angeles Medical Center United Statesf Instituto de Informacioacuten e Investigacioacuten en Salud Mental Monterrey Mexicog Centro de Investigaciones Biomeacutedicas Guatemala City Guatemalah Department of Psychiatry University of California San Diego CA United Statesi Department of Psychiatry Paul L Foster School of Medicine Texas Tech University Health Science Center El Paso TX United Statesj Neuroscience Center of Excellence Paul L Foster School of Medicine Texas Tech University Health Science Center El Paso TX United States
a r t i c l e i n f o
Abbreviations DD dual diagnosis SC schizophreDiagnostic Interview for Genetics Studies FIGS FamiEdition PCP phenylcyclohexylpiperidine LSD lyserg Corresponding author Neuroscience Center of Exc
El Paso TX 79905 United States Tel +1 915 545 68E-mail address mescamillattuhscedu (M Escam
0920-9964$ ndash see front matter copy 2010 Published bydoi101016jschres2010021053
a b s t r a c t
Article historyReceived 14 October 2009Received in revised form 8 February 2010Accepted 15 February 2010Available online 19 March 2010
Objectives The aims of this study were to estimate the frequency and course of substances usedisorders in Latino patients with schizophrenia and to ascertain risk factors associated withsubstance use disorders in this populationMethod We studied 518 subjects with schizophrenia recruited for a genetic study from theSouthwest United States Mexico and Central America (Costa Rica and Guatemala) Subjectswere assessed using structured interviews and a best estimate consensus process Logisticregression χ2 t test Fishers exact test and Yates correction as appropriate were performedto assess the sociodemographic variables associated with dual diagnosis We defined substanceuse disorder as either alcohol or substance abuse or dependenceResults Out of 518 patients with schizophrenia 121 (234) had substance use disordersComorbid substance use disorders were associated with male gender residence in the UnitedStates immigration of Mexican men to the United States history of depressive syndrome orepisode and being unemployed The most frequent substance use disorder was alcohol abusedependence followed by marijuana abusedependence and solvent abusedependenceConclusion This study provides data suggesting that depressive episode or syndromeunemployment male gender and immigration of Mexican men to the United States werefactors associated with substance use disorder comorbidity in schizophrenia Binary logisticregression showed that country of residence was associated with substance use disorder inschizophrenic patients The percentage of subjects with comorbid substance use disorders washigher in the Latinos living in the United States compared with subjects living in CentralAmerica and Mexico
copy 2010 Published by Elsevier BV
KeywordsAlcoholDrug abuseSubstance misuseDual diagnosisSchizophreniaLatino populations
nia SUDs substance use disorders US United States NIMH National Institute of Mental Health DIGSly Interview for Genetics Studies DSM-IV The Diagnostic and Statistical Manual of Mental Disorders 4thic acid diethylamideellence Paul L Foster School of Medicine Texas Tech University Health Science Center 5001 El Paso Drive31 fax +1 210 562 5114illa)
Elsevier BV
88 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
1 Introduction
There is little data on dual diagnosis (DD) of schizophrenia(SC) and substance use disorders (SUDs) in the Latinopopulation The aims of this paper were to estimate thefrequency of comorbid alcohol and drug use disorders inLatinos with SC from Mexican and Central American ancestryand to describe the risk factors associated with SC in thispopulation
Lifetime prevalence rates of SUD have ranged from 146 to266 in the general United States (US) population (Baumeisterand Haumlrter 2007 Kessler et al 1994 Kessler et al 2005a) andfrom 99 to 187 in Europe (Bijl et al 1998 Jacobi et al2004) In studies from the US lifetime prevalence of SUD inLatinos (112 to 161) (Alegriacutea et al 2008 Breslau et al2006) is lower than in non-Latino whites (Alegria et al 2006Zhang and Snowden 1999) In Latinos living outside of the USlifetime prevalence of SUD is also lower than in the general USpopulation (Andrade et al 2000 Medina-Mora et al 2007)
Persons with SC have substantially higher lifetime risk ofhaving SUD than do persons from the general population(McCreadie 2002 Kessler et al 2005b Regier et al 1990Ringen et al 2008 Soyka et al 2001 Swartz et al 2006)ranging from 40 to 60 (Cantor-Graae et al 2001) In theUS an epidemiologic study found lifetime history of comorbidSUD was 47 for persons with SC or schizophreniformdisorder a rate 46 times higher than for the generalpopulation (Kavanagh et al 2004) In a recent nation-widestudy of SC in the US even higher rates of SUD were found603 of 1460 persons with SC reported a SUD (Rosenmanetet al 2000) Similar high rates of SUD with SC have beenfound in studies from Europe (Dervaux et al 2001 Fowleret al 1998 Kavanagh et al 2004 Menezes et al 1996Ringen et al 2008 Rosenman et al 2000 Verma et al2002)
Despite recent interest in how rates of psychiatricdisorders vary in Latinos (Breslau et al 2006 Grant et al2004 Vega and Sribney 2003) there are only a couple ofstudies which have looked specifically at comorbidity of SUDin SC as a function of ethnicity Montross et al (2005) foundthe prevalence of DD was lower in Latino Americans than inEuropean and African Americans in San Diego County (US)An epidemiologic study conducted in Mexican Americansfound the lifetime prevalence of SUD in those subjects withcomorbid psychotic symptoms was 20 for immigrants and49 for those born in the US (Vega et al 2006) Outside ofthese two studies there are no published reports of SC andSUD comorbidity rates in samples of Latino subjects and noepidemiologic studies that have investigated these comor-bidities in an international sample
The present analyses utilized the largest known sample ofsystematically assessed subjects with SC from the Latinopopulation drawn from the NIMH Genetics of Schizophreniain Latino Populations study to estimate the frequency of DDin the subjects in this study In addition the present studydescribes the clinical characteristics of subjects with comor-bid SUD in these Latino subjects and compares rates of DDacross three geographic regions (the Southwest UnitedStates Mexico and Central America) We also tested severalhypotheses regarding SUD comorbidity in SC subjects withinthis sample These hypotheses included that SUD comorbidity
would be higher in the US subjects compared to those fromMexico and Central America and that rates of comorbiditywould be in general less than previous studies of SC in non-Latino populations Based on studies conducted in othersamples (Bartels et al 1993 Menezes et al 1996 Soyka etal 2001 Swartz et al 2006 Weaver et al 1999) we alsohypothesized that gender marital status employment statusand immigration to the US from Mexico would be associatedwith comorbidity in this sample We hypothesized thatincreased lifetime history of depression and level of deteri-oration would be associated with comorbid SUD in SCsubjects from the current study Finally we investigated theages of onset of SUD and SC in comorbid cases to betterunderstand how these comorbidities develop in Latinoa menand women
2 Methods
21 Subjects
All participants were recruited in accordance with theprinciples of theDeclaration of Helsinki andwith approval fromthe Institutional Review Boards of each participating site aspart of a family based linkage study of SC and schizoaffectivedisorder Recruitment teams were located in San Antonio(Texas US) Los Angeles and San Diego (California US)Monterrey and Mexico City (Mexico) Guatemala City(Guatemala) and San Joseacute (Costa Rica) All sites participatedin group training sessions to standardize assessments using theDiagnostic Interview for Genetic Studies (DIGS) (Nurnbergeret al 1994) the Family Interview for Genetic Studies (FIGS)(Maxwell 1992) and a review of psychiatric records Familieswere eligible for study if they had at least two siblings withhospital or clinical diagnoses of SC or schizoaffective disorderSubjects included in the study were all over 18 years of agewilling to contribute a blood sample and complete a diagnosisinterview Subjects were recruited if their parents had ancestryfrom Central America or Mexico Subjects were also asked todescribe their parents ethnicity as part of the DIGS interview(see description in Results) After complete description of thestudy to the subjects written informed consent was obtained
22 Diagnosis
Subjects were diagnosed according to the DSM-IV by abest estimate consensus process using a DIGS a FIGS andreview of all available medical records this best estimateprocedure has been described in detail (Escamilla et al2007) Each best estimator was a bilingual bicultural clinician(psychiatrist or psychologist) and cases were diagnosedindependently followed by a discussion of any differencesin diagnosis and a final consensus was completed for specificdisorders syndromes and ages of onset After completion ofthe best estimate consensus process 518 subjects (from 284separate families) met DSM-IV criteria for SC Tables shown inthis article are for the entire sample of affected participantsSUD was defined as either alcohol or substance abuse ordependence by best estimate consensus Best estimators alsodetermined age of onset of each SUD as well as the age wheneach subject first met full DSM-IV criteria for SC and whetheror not each subject had ever met criteria for a full depressive
89L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
episode or syndrome using DSM-IV criteria Best estimatorsindependently rated the level of deterioration experienced bysubjects using the measure included in the Lifetime Dimen-sion of Psychosis Scale (Levinson et al 2002) and the rateraverage was used in these analyses Other demographicvariables were captured in the DIGS Best estimators were notaware of any of the specific hypotheses being tested in thispaper
23 Data analysis
Statistical analysis was carried out with the programStatistical Procedures for Science Society version 150 To testspecific hypotheses we used a subset of the full sample (onesubject with SC per family) to avoid bias that could be causedby potential correlations between relatives The singleindividual per family with SC was selected using the randomnumber generator function in Microsoft Excel Since eachhypotheses tested was a specific one based on previousanalyses we considered probability values le005 to bestatistically significant All tests were two-tailed When achi-square could not be calculated a 2times2 table was built andits significancewas determined bymeans of the Fisher test orYates correction test as appropriate
To test hypotheses that gender age living situationemployment status marital status deterioration or historyof depressive disorders are associated with SUD in thesesubjects we used a t test for age at interview years of schooland deterioration Fischers exact test was used for gender
Table 1Demographic characteristics
Characteristics Substance use disorderand schizophrenia
Demographic characteristics N
Count 121 234Male 107 315Female 14 79
Mean SD
Age at interview 382 105Years of education 91 36Deterioration a 32 08
Depressive syndromeepisode N
Yes 64 529No 57 471
Living situation b N
Alone 7 60With family or other people 102 872In residential treatment facility 3 25Other 5 43
Marital status c N
Never married 89 761Ever married 28 239
Gender Fischers exact test χ2=12116 pb0001Depression Fischers exact test χ2=6479 pb0013Age at interview years of education deterioration living situation marital status =
a 11 missingb 14 missingc 11 missing
depressive syndrome or episode marital status employmentand migration status Yates correction test was used forrelative onset of SC and SUD Binary logistic regression wasused to model the relationship between the dependentvariable SUD and predictor variable living situation Tocontrol for confounding effects of SUD and gender in socio-demographic variables such as marital status and employ-ment logistic regression methods were used for eachoutcome variable In order to test whether country ofresidence was associated with different rates of SUD logisticregression methods were utilized
3 Results
Ethnicity of the participants in this study was by selfreport Costa Rican subjects reported 100 bilineal ancestryfrom Costa Rica with two subjects reporting partial Nicar-aguan ancestry Guatemalan subjects reported 100 bilinealancestry from Guatemala with two of the subjects reportingpartial known European ancestry (Belgian and Spanishancestry) Of the 310 subjects from Mexico who reportedon their ancestry 100 reported bilineal Mexican ancestrywith four reporting partial known ancestry from WesternEurope (Spain France) 3 reporting partial known ancestryfrom Eastern Europe (Poland) and one reporting partialknown ancestry from Puerto Rico Subjects from the UnitedStates reported primarily bilineal Mexican ancestry (94 ofsubjects) with 5 reporting half Mexican ancestry (oneparent) and half non-Hispanic white ancestry (other parent
Schizophrenia only All subjects
N
397 766 518233 685 340164 921 178
Mean SD Mean SD
377 109 378 11389 38 89 3831 09 31 08
N N
161 405 225 434236 595 293 566
N N
19 49 26 51355 917 457 90710 26 13 263 08 8 16
N All subjects (adjustedby sex)
295 756 69795 244 303
pN005
Table 3Age of onset of substance use disorder SC in comorbid subject andschizophrenia only
Age Totalsubjects
Male Female Both
Age of onset Mean SD Mean SD Mean SD N
Schizophrenia(in subjectswith comorbidity)
209 60 196 58 207 59 121
Substances usedisorder (in subjectswith comorbidity)
183 52 231 83 189 58 121
Schizophrenia only 202 70 209 73 205 71 397
t test = pN005
90 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
with Anglo-Saxon or Western European ancestry) and 1person reporting Mexican ancestry from one parent andPuerto Rican ancestry from the other parent Of the subjectsfrom the United States 4 reported known partial NativeAmerican ancestry one reported Guatemalan ancestry and 3additional subjects with bilineal Mexican ancestry reportedpartial known European ancestry
Sample characteristics are described in Table 1 Out of 518SC subjects 234 had DD (SC and SUD) Of 178 femalesubjects with SC 79 had SUD comorbidity and out of 340male subjects with SC 315 had comorbid SUD Theproportion of subjects who reported a history of depressivesyndrome or episode was large among those who had SUDRegardless of history of SUD the majority of subjects hadnever married
History of marriage frequencies was essentially the samefor women with and without a history of SUD (385 of DDwomen 394 of SC only women) For men those with ahistory of DD had higher frequencies of ever having beenmarried (221 of DD men had been married versus 139 ofSC only men) The variable ldquoever marriedrdquo included thosewho were married separated divorced or widowed Rates ofever marrying were higher for women than for menregardless of SUD comorbidity history
Unemployment rates were higher for SC subjects with ahistory of DD but this was primarily due to differences inmales Only 295 of men with a DD were employedcompared to 438 of men with SC only Employment ratesfor women were 538 and 51 respectively for DD cases andSC only cases Regardless of DD history males were morefrequently unemployed than females It is important to notehowever that the variable ldquoemployedrdquo included any type ofemployment including lsquohousewifersquo which may explain thehigher employment rates for women in this sample
Table 2 shows the lifetimeprevalence of SUD by gender andcountry of residence in the total sample For both genders themost frequent substance of abusedependence was alcoholfollowed by marijuana In the whole sample one in four of themen had history of alcohol abuse or dependence and almostone in six men had history of marijuana abuse or dependenceInhalant misuse and cocainemisuse occurred in approximately4 of the men All other substances had lifetime abusedependence rates below 1 in men For women the same
Table 2Frequency of each substance misuse in the Latino schizophrenic sample by country of residence and gender (N=518)
US(N=111)
Mexico(N=310)
Costa Rica(N=65)
Guatemala(N=32)
All sample
Gender MaleN=78
FemaleN=33
MaleN=193
FemaleN=117
MaleN=48
FemaleN=17
MaleN=21
FemaleN=11
MaleN=340
FemaleN=118
Type of SUD N N N N N N N N N N
Alcohol 30 385 5 152 36 187 2 17 13 271 1 59 6 286 0 0 85 250 8 45Marijuana 23 295 3 91 25 130 4 34 4 83 0 0 1 48 0 0 53 156 7 39Inhalantsolvent 6 77 1 30 8 41 1 09 1 21 0 0 0 0 0 0 15 44 2 11Cocaine 7 90 2 61 6 31 0 0 1 21 0 0 0 0 0 0 14 41 2 11Amphetamine 3 38 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 09 0 0Opioid 1 13 1 30 1 05 0 0 0 0 0 0 0 0 0 0 2 06 1 06LSD 1 13 1 30 0 0 0 0 0 0 0 0 0 0 0 0 1 03 1 06Other drugs 1 13 0 0 1 05 1 09 0 0 0 0 0 0 0 0 2 06 1 06
US United States SUD substance use disorder PCP phenylcyclohexylpiperidine LSD lysergic acid diethylamide None of the subjects were diagnosed withabusedependence of ecstasy heroin or PCP
four substances were the substances with lifetimemisuse ratesgreater than 1 although the rates were much less than theequivalent rates in men
As shown in Table 3 for men with DD histories the meanage of onset of SUDwas 26 years earlier than the mean age ofonset of SC For females with DD history the mean onset ofSUD was 35 years after the onset of SC
Among men and women with DD each gender had caseswhere either SUD or SC occurred first but there were cleardifferences in these patterns between genders (Table 4)
There were clear differences in SUD comorbidity betweenthe different geographic regions in this collaborative study(Table 5) All sites showed higher rates of comorbid SUD inmen than in women For men SUD comorbidity was highestin Latinos living in the US (51) lowest in Latinos fromMexico (233) and intermediate in Latinos from CentralAmerica (319) For women SUD comorbidity was 273 inLatinas from the US and very low in both Latinas fromMexicoand Central America (34 and 35 respectively)
Regarding migration status in the whole sample 36subjects migrated from their original countries Out of those36 subjects 34 migrated from Mexico to the US 1 fromGuatemala to the US and 1 from the US to Costa Rica
Out of 36 subjects whomigrated 15 met criteria for DD ofthose 15 subjects 13 migrated from Mexico to the US onemigrated from Guatemala to the US and another one from USto Costa Rica
Table 4Relative onset of schizophrenia and substance misuse by gender
Gender
Male Female Both
Relative Onset N N N
Onset of substance misuse camefirst
74 692 5 357 79 653
Onset of schizophrenia came first 23 215 7 500 30 248Equal age onset SC and substancemisuse
10 93 2 143 12 99
Total 107 1000 14 1000 121 1000
χ2=5657 Yates correction=3850 p=005
91L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
Table 6 shows that out of 34 Mexican-born subjects whomigrated to the US 13 (382) met lifetime criteria for SUDwhereas out of 293 Mexican-born subjects who did notmigrate and reside in their own country (Mexico) 45 (154)had a lifetime history of SUD For individuals whose countryof residence was the US 47 (N=31) of the US-born subjectshad lifetime SUD while 40 (N=14) of the immigrants metcriteria for lifetime SUD
Specific hypotheses were tested using one subject perfamily We found that male gender was significantlyassociated with comorbid SUD (Fischers exact testχ2=2116 pb0001) and that history of depression wassignificantly associated with SUD (Fischers exact testχ2=6479 p=0013) Furthermore individuals with SUD
Table 5Frequency of dual diagnosis in 518 schizophrenic subjects by country of residence
Gender US (N=111) Mexico (N=310)
SC+SUD SC only SC+SUD
N N N
Male 40 513 38 487 45 233Female 9 273 24 727 4 34Total sample 49 441 62 558 49 158
Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ratios=0263Central American B=minus0818 Wald χ2=4444 df=1 p=0035 odd ratios=04 Fishers exact test χ2=18349 p=0001
Table 6Characteristics of migration status in the schizophrenic sample by dual diagnosis an
Gender Male
Diagnosis Dual diagnosis SC only
Mexican-born subjectsa c N N
Migrated to US 12 444 15 55Residing in Mexico 41 224 142 77
US residentsb d N N
Immigrants 13 e 464 15 53US-born 24 558 19 44
US = United Statesa Mexican-born men by Dual Diagnosis or Schizophrenia only Fischers exact tesb US residents by Dual Diagnosis or Schizophrenia only = pN005c 17 missing it was unknown where 17 of the subjects residing in Meacutexico wered 10 missing it was unknown where 10 subjects residing in US where borne Subjects migrated from Meacutexicof Subjects migrated from Guatemala
had a higher rate of unemployment than individuals with SConly (Fischers exact test χ2=6773 p=0010) Binarylogistic regression showed that SUD was a significantpredictor of unemployment (SUD B=0746 Wald=5774df=1 p=0016 odd ratio=2159) Gender was not relatedto unemployment In this procedure we used the variableemployment as a dependent variable and predictors wereSUD and gender
The three countrieswere significantlydifferent in their ratesof DD (χ2=18349 pb0001) When binary logistic regressionwas used to analyze country of residence Mexico and CentralAmerican schizophrenic patients were less likely to bediagnosed with SUD than subjects from the US (Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ra-tios=0263 Central American B=minus0818 Wald χ2=4444df=1 p=0035 odd ratios=0441) therefore country ofresidence was a significant predictor of SUD
Mexican-born men who migrated to the US had asignificantly higher rate of DD than those who did notemigrate (Fischers exact test χ2=6057 df=1 p=002)
Deterioration current living situation and marital statuswere not associated with comorbid diagnoses For maritalstatus binary logistic regression showed that gender was asignificant predictor of marital status because femalescompared with males were more likely to be married (B=minus1104 Wald χ2=12278 pb0001 exp (B)=0331) andSUD was not associated with marital status (p=0198) Inthis model marital status was the dependent variable and
and gender
Central America (N=97) Total
SC only SC+SUD SC only
N N N
148 767 22 319 47 681 340113 966 1 36 27 964 178261 842 23 237 74 763 518
41
d gender
Female Total
Dual diagnosis SC only
N N N
6 1 143 6 857 34
6 4 36 106 964 293
N N N
6 1 f 143 6 857 35
2 7 304 16 696 66
t χ2=6057 df=1 p=002
born
92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146

88 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
1 Introduction
There is little data on dual diagnosis (DD) of schizophrenia(SC) and substance use disorders (SUDs) in the Latinopopulation The aims of this paper were to estimate thefrequency of comorbid alcohol and drug use disorders inLatinos with SC from Mexican and Central American ancestryand to describe the risk factors associated with SC in thispopulation
Lifetime prevalence rates of SUD have ranged from 146 to266 in the general United States (US) population (Baumeisterand Haumlrter 2007 Kessler et al 1994 Kessler et al 2005a) andfrom 99 to 187 in Europe (Bijl et al 1998 Jacobi et al2004) In studies from the US lifetime prevalence of SUD inLatinos (112 to 161) (Alegriacutea et al 2008 Breslau et al2006) is lower than in non-Latino whites (Alegria et al 2006Zhang and Snowden 1999) In Latinos living outside of the USlifetime prevalence of SUD is also lower than in the general USpopulation (Andrade et al 2000 Medina-Mora et al 2007)
Persons with SC have substantially higher lifetime risk ofhaving SUD than do persons from the general population(McCreadie 2002 Kessler et al 2005b Regier et al 1990Ringen et al 2008 Soyka et al 2001 Swartz et al 2006)ranging from 40 to 60 (Cantor-Graae et al 2001) In theUS an epidemiologic study found lifetime history of comorbidSUD was 47 for persons with SC or schizophreniformdisorder a rate 46 times higher than for the generalpopulation (Kavanagh et al 2004) In a recent nation-widestudy of SC in the US even higher rates of SUD were found603 of 1460 persons with SC reported a SUD (Rosenmanetet al 2000) Similar high rates of SUD with SC have beenfound in studies from Europe (Dervaux et al 2001 Fowleret al 1998 Kavanagh et al 2004 Menezes et al 1996Ringen et al 2008 Rosenman et al 2000 Verma et al2002)
Despite recent interest in how rates of psychiatricdisorders vary in Latinos (Breslau et al 2006 Grant et al2004 Vega and Sribney 2003) there are only a couple ofstudies which have looked specifically at comorbidity of SUDin SC as a function of ethnicity Montross et al (2005) foundthe prevalence of DD was lower in Latino Americans than inEuropean and African Americans in San Diego County (US)An epidemiologic study conducted in Mexican Americansfound the lifetime prevalence of SUD in those subjects withcomorbid psychotic symptoms was 20 for immigrants and49 for those born in the US (Vega et al 2006) Outside ofthese two studies there are no published reports of SC andSUD comorbidity rates in samples of Latino subjects and noepidemiologic studies that have investigated these comor-bidities in an international sample
The present analyses utilized the largest known sample ofsystematically assessed subjects with SC from the Latinopopulation drawn from the NIMH Genetics of Schizophreniain Latino Populations study to estimate the frequency of DDin the subjects in this study In addition the present studydescribes the clinical characteristics of subjects with comor-bid SUD in these Latino subjects and compares rates of DDacross three geographic regions (the Southwest UnitedStates Mexico and Central America) We also tested severalhypotheses regarding SUD comorbidity in SC subjects withinthis sample These hypotheses included that SUD comorbidity
would be higher in the US subjects compared to those fromMexico and Central America and that rates of comorbiditywould be in general less than previous studies of SC in non-Latino populations Based on studies conducted in othersamples (Bartels et al 1993 Menezes et al 1996 Soyka etal 2001 Swartz et al 2006 Weaver et al 1999) we alsohypothesized that gender marital status employment statusand immigration to the US from Mexico would be associatedwith comorbidity in this sample We hypothesized thatincreased lifetime history of depression and level of deteri-oration would be associated with comorbid SUD in SCsubjects from the current study Finally we investigated theages of onset of SUD and SC in comorbid cases to betterunderstand how these comorbidities develop in Latinoa menand women
2 Methods
21 Subjects
All participants were recruited in accordance with theprinciples of theDeclaration of Helsinki andwith approval fromthe Institutional Review Boards of each participating site aspart of a family based linkage study of SC and schizoaffectivedisorder Recruitment teams were located in San Antonio(Texas US) Los Angeles and San Diego (California US)Monterrey and Mexico City (Mexico) Guatemala City(Guatemala) and San Joseacute (Costa Rica) All sites participatedin group training sessions to standardize assessments using theDiagnostic Interview for Genetic Studies (DIGS) (Nurnbergeret al 1994) the Family Interview for Genetic Studies (FIGS)(Maxwell 1992) and a review of psychiatric records Familieswere eligible for study if they had at least two siblings withhospital or clinical diagnoses of SC or schizoaffective disorderSubjects included in the study were all over 18 years of agewilling to contribute a blood sample and complete a diagnosisinterview Subjects were recruited if their parents had ancestryfrom Central America or Mexico Subjects were also asked todescribe their parents ethnicity as part of the DIGS interview(see description in Results) After complete description of thestudy to the subjects written informed consent was obtained
22 Diagnosis
Subjects were diagnosed according to the DSM-IV by abest estimate consensus process using a DIGS a FIGS andreview of all available medical records this best estimateprocedure has been described in detail (Escamilla et al2007) Each best estimator was a bilingual bicultural clinician(psychiatrist or psychologist) and cases were diagnosedindependently followed by a discussion of any differencesin diagnosis and a final consensus was completed for specificdisorders syndromes and ages of onset After completion ofthe best estimate consensus process 518 subjects (from 284separate families) met DSM-IV criteria for SC Tables shown inthis article are for the entire sample of affected participantsSUD was defined as either alcohol or substance abuse ordependence by best estimate consensus Best estimators alsodetermined age of onset of each SUD as well as the age wheneach subject first met full DSM-IV criteria for SC and whetheror not each subject had ever met criteria for a full depressive
89L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
episode or syndrome using DSM-IV criteria Best estimatorsindependently rated the level of deterioration experienced bysubjects using the measure included in the Lifetime Dimen-sion of Psychosis Scale (Levinson et al 2002) and the rateraverage was used in these analyses Other demographicvariables were captured in the DIGS Best estimators were notaware of any of the specific hypotheses being tested in thispaper
23 Data analysis
Statistical analysis was carried out with the programStatistical Procedures for Science Society version 150 To testspecific hypotheses we used a subset of the full sample (onesubject with SC per family) to avoid bias that could be causedby potential correlations between relatives The singleindividual per family with SC was selected using the randomnumber generator function in Microsoft Excel Since eachhypotheses tested was a specific one based on previousanalyses we considered probability values le005 to bestatistically significant All tests were two-tailed When achi-square could not be calculated a 2times2 table was built andits significancewas determined bymeans of the Fisher test orYates correction test as appropriate
To test hypotheses that gender age living situationemployment status marital status deterioration or historyof depressive disorders are associated with SUD in thesesubjects we used a t test for age at interview years of schooland deterioration Fischers exact test was used for gender
Table 1Demographic characteristics
Characteristics Substance use disorderand schizophrenia
Demographic characteristics N
Count 121 234Male 107 315Female 14 79
Mean SD
Age at interview 382 105Years of education 91 36Deterioration a 32 08
Depressive syndromeepisode N
Yes 64 529No 57 471
Living situation b N
Alone 7 60With family or other people 102 872In residential treatment facility 3 25Other 5 43
Marital status c N
Never married 89 761Ever married 28 239
Gender Fischers exact test χ2=12116 pb0001Depression Fischers exact test χ2=6479 pb0013Age at interview years of education deterioration living situation marital status =
a 11 missingb 14 missingc 11 missing
depressive syndrome or episode marital status employmentand migration status Yates correction test was used forrelative onset of SC and SUD Binary logistic regression wasused to model the relationship between the dependentvariable SUD and predictor variable living situation Tocontrol for confounding effects of SUD and gender in socio-demographic variables such as marital status and employ-ment logistic regression methods were used for eachoutcome variable In order to test whether country ofresidence was associated with different rates of SUD logisticregression methods were utilized
3 Results
Ethnicity of the participants in this study was by selfreport Costa Rican subjects reported 100 bilineal ancestryfrom Costa Rica with two subjects reporting partial Nicar-aguan ancestry Guatemalan subjects reported 100 bilinealancestry from Guatemala with two of the subjects reportingpartial known European ancestry (Belgian and Spanishancestry) Of the 310 subjects from Mexico who reportedon their ancestry 100 reported bilineal Mexican ancestrywith four reporting partial known ancestry from WesternEurope (Spain France) 3 reporting partial known ancestryfrom Eastern Europe (Poland) and one reporting partialknown ancestry from Puerto Rico Subjects from the UnitedStates reported primarily bilineal Mexican ancestry (94 ofsubjects) with 5 reporting half Mexican ancestry (oneparent) and half non-Hispanic white ancestry (other parent
Schizophrenia only All subjects
N
397 766 518233 685 340164 921 178
Mean SD Mean SD
377 109 378 11389 38 89 3831 09 31 08
N N
161 405 225 434236 595 293 566
N N
19 49 26 51355 917 457 90710 26 13 263 08 8 16
N All subjects (adjustedby sex)
295 756 69795 244 303
pN005
Table 3Age of onset of substance use disorder SC in comorbid subject andschizophrenia only
Age Totalsubjects
Male Female Both
Age of onset Mean SD Mean SD Mean SD N
Schizophrenia(in subjectswith comorbidity)
209 60 196 58 207 59 121
Substances usedisorder (in subjectswith comorbidity)
183 52 231 83 189 58 121
Schizophrenia only 202 70 209 73 205 71 397
t test = pN005
90 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
with Anglo-Saxon or Western European ancestry) and 1person reporting Mexican ancestry from one parent andPuerto Rican ancestry from the other parent Of the subjectsfrom the United States 4 reported known partial NativeAmerican ancestry one reported Guatemalan ancestry and 3additional subjects with bilineal Mexican ancestry reportedpartial known European ancestry
Sample characteristics are described in Table 1 Out of 518SC subjects 234 had DD (SC and SUD) Of 178 femalesubjects with SC 79 had SUD comorbidity and out of 340male subjects with SC 315 had comorbid SUD Theproportion of subjects who reported a history of depressivesyndrome or episode was large among those who had SUDRegardless of history of SUD the majority of subjects hadnever married
History of marriage frequencies was essentially the samefor women with and without a history of SUD (385 of DDwomen 394 of SC only women) For men those with ahistory of DD had higher frequencies of ever having beenmarried (221 of DD men had been married versus 139 ofSC only men) The variable ldquoever marriedrdquo included thosewho were married separated divorced or widowed Rates ofever marrying were higher for women than for menregardless of SUD comorbidity history
Unemployment rates were higher for SC subjects with ahistory of DD but this was primarily due to differences inmales Only 295 of men with a DD were employedcompared to 438 of men with SC only Employment ratesfor women were 538 and 51 respectively for DD cases andSC only cases Regardless of DD history males were morefrequently unemployed than females It is important to notehowever that the variable ldquoemployedrdquo included any type ofemployment including lsquohousewifersquo which may explain thehigher employment rates for women in this sample
Table 2 shows the lifetimeprevalence of SUD by gender andcountry of residence in the total sample For both genders themost frequent substance of abusedependence was alcoholfollowed by marijuana In the whole sample one in four of themen had history of alcohol abuse or dependence and almostone in six men had history of marijuana abuse or dependenceInhalant misuse and cocainemisuse occurred in approximately4 of the men All other substances had lifetime abusedependence rates below 1 in men For women the same
Table 2Frequency of each substance misuse in the Latino schizophrenic sample by country of residence and gender (N=518)
US(N=111)
Mexico(N=310)
Costa Rica(N=65)
Guatemala(N=32)
All sample
Gender MaleN=78
FemaleN=33
MaleN=193
FemaleN=117
MaleN=48
FemaleN=17
MaleN=21
FemaleN=11
MaleN=340
FemaleN=118
Type of SUD N N N N N N N N N N
Alcohol 30 385 5 152 36 187 2 17 13 271 1 59 6 286 0 0 85 250 8 45Marijuana 23 295 3 91 25 130 4 34 4 83 0 0 1 48 0 0 53 156 7 39Inhalantsolvent 6 77 1 30 8 41 1 09 1 21 0 0 0 0 0 0 15 44 2 11Cocaine 7 90 2 61 6 31 0 0 1 21 0 0 0 0 0 0 14 41 2 11Amphetamine 3 38 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 09 0 0Opioid 1 13 1 30 1 05 0 0 0 0 0 0 0 0 0 0 2 06 1 06LSD 1 13 1 30 0 0 0 0 0 0 0 0 0 0 0 0 1 03 1 06Other drugs 1 13 0 0 1 05 1 09 0 0 0 0 0 0 0 0 2 06 1 06
US United States SUD substance use disorder PCP phenylcyclohexylpiperidine LSD lysergic acid diethylamide None of the subjects were diagnosed withabusedependence of ecstasy heroin or PCP
four substances were the substances with lifetimemisuse ratesgreater than 1 although the rates were much less than theequivalent rates in men
As shown in Table 3 for men with DD histories the meanage of onset of SUDwas 26 years earlier than the mean age ofonset of SC For females with DD history the mean onset ofSUD was 35 years after the onset of SC
Among men and women with DD each gender had caseswhere either SUD or SC occurred first but there were cleardifferences in these patterns between genders (Table 4)
There were clear differences in SUD comorbidity betweenthe different geographic regions in this collaborative study(Table 5) All sites showed higher rates of comorbid SUD inmen than in women For men SUD comorbidity was highestin Latinos living in the US (51) lowest in Latinos fromMexico (233) and intermediate in Latinos from CentralAmerica (319) For women SUD comorbidity was 273 inLatinas from the US and very low in both Latinas fromMexicoand Central America (34 and 35 respectively)
Regarding migration status in the whole sample 36subjects migrated from their original countries Out of those36 subjects 34 migrated from Mexico to the US 1 fromGuatemala to the US and 1 from the US to Costa Rica
Out of 36 subjects whomigrated 15 met criteria for DD ofthose 15 subjects 13 migrated from Mexico to the US onemigrated from Guatemala to the US and another one from USto Costa Rica
Table 4Relative onset of schizophrenia and substance misuse by gender
Gender
Male Female Both
Relative Onset N N N
Onset of substance misuse camefirst
74 692 5 357 79 653
Onset of schizophrenia came first 23 215 7 500 30 248Equal age onset SC and substancemisuse
10 93 2 143 12 99
Total 107 1000 14 1000 121 1000
χ2=5657 Yates correction=3850 p=005
91L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
Table 6 shows that out of 34 Mexican-born subjects whomigrated to the US 13 (382) met lifetime criteria for SUDwhereas out of 293 Mexican-born subjects who did notmigrate and reside in their own country (Mexico) 45 (154)had a lifetime history of SUD For individuals whose countryof residence was the US 47 (N=31) of the US-born subjectshad lifetime SUD while 40 (N=14) of the immigrants metcriteria for lifetime SUD
Specific hypotheses were tested using one subject perfamily We found that male gender was significantlyassociated with comorbid SUD (Fischers exact testχ2=2116 pb0001) and that history of depression wassignificantly associated with SUD (Fischers exact testχ2=6479 p=0013) Furthermore individuals with SUD
Table 5Frequency of dual diagnosis in 518 schizophrenic subjects by country of residence
Gender US (N=111) Mexico (N=310)
SC+SUD SC only SC+SUD
N N N
Male 40 513 38 487 45 233Female 9 273 24 727 4 34Total sample 49 441 62 558 49 158
Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ratios=0263Central American B=minus0818 Wald χ2=4444 df=1 p=0035 odd ratios=04 Fishers exact test χ2=18349 p=0001
Table 6Characteristics of migration status in the schizophrenic sample by dual diagnosis an
Gender Male
Diagnosis Dual diagnosis SC only
Mexican-born subjectsa c N N
Migrated to US 12 444 15 55Residing in Mexico 41 224 142 77
US residentsb d N N
Immigrants 13 e 464 15 53US-born 24 558 19 44
US = United Statesa Mexican-born men by Dual Diagnosis or Schizophrenia only Fischers exact tesb US residents by Dual Diagnosis or Schizophrenia only = pN005c 17 missing it was unknown where 17 of the subjects residing in Meacutexico wered 10 missing it was unknown where 10 subjects residing in US where borne Subjects migrated from Meacutexicof Subjects migrated from Guatemala
had a higher rate of unemployment than individuals with SConly (Fischers exact test χ2=6773 p=0010) Binarylogistic regression showed that SUD was a significantpredictor of unemployment (SUD B=0746 Wald=5774df=1 p=0016 odd ratio=2159) Gender was not relatedto unemployment In this procedure we used the variableemployment as a dependent variable and predictors wereSUD and gender
The three countrieswere significantlydifferent in their ratesof DD (χ2=18349 pb0001) When binary logistic regressionwas used to analyze country of residence Mexico and CentralAmerican schizophrenic patients were less likely to bediagnosed with SUD than subjects from the US (Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ra-tios=0263 Central American B=minus0818 Wald χ2=4444df=1 p=0035 odd ratios=0441) therefore country ofresidence was a significant predictor of SUD
Mexican-born men who migrated to the US had asignificantly higher rate of DD than those who did notemigrate (Fischers exact test χ2=6057 df=1 p=002)
Deterioration current living situation and marital statuswere not associated with comorbid diagnoses For maritalstatus binary logistic regression showed that gender was asignificant predictor of marital status because femalescompared with males were more likely to be married (B=minus1104 Wald χ2=12278 pb0001 exp (B)=0331) andSUD was not associated with marital status (p=0198) Inthis model marital status was the dependent variable and
and gender
Central America (N=97) Total
SC only SC+SUD SC only
N N N
148 767 22 319 47 681 340113 966 1 36 27 964 178261 842 23 237 74 763 518
41
d gender
Female Total
Dual diagnosis SC only
N N N
6 1 143 6 857 34
6 4 36 106 964 293
N N N
6 1 f 143 6 857 35
2 7 304 16 696 66
t χ2=6057 df=1 p=002
born
92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146

89L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
episode or syndrome using DSM-IV criteria Best estimatorsindependently rated the level of deterioration experienced bysubjects using the measure included in the Lifetime Dimen-sion of Psychosis Scale (Levinson et al 2002) and the rateraverage was used in these analyses Other demographicvariables were captured in the DIGS Best estimators were notaware of any of the specific hypotheses being tested in thispaper
23 Data analysis
Statistical analysis was carried out with the programStatistical Procedures for Science Society version 150 To testspecific hypotheses we used a subset of the full sample (onesubject with SC per family) to avoid bias that could be causedby potential correlations between relatives The singleindividual per family with SC was selected using the randomnumber generator function in Microsoft Excel Since eachhypotheses tested was a specific one based on previousanalyses we considered probability values le005 to bestatistically significant All tests were two-tailed When achi-square could not be calculated a 2times2 table was built andits significancewas determined bymeans of the Fisher test orYates correction test as appropriate
To test hypotheses that gender age living situationemployment status marital status deterioration or historyof depressive disorders are associated with SUD in thesesubjects we used a t test for age at interview years of schooland deterioration Fischers exact test was used for gender
Table 1Demographic characteristics
Characteristics Substance use disorderand schizophrenia
Demographic characteristics N
Count 121 234Male 107 315Female 14 79
Mean SD
Age at interview 382 105Years of education 91 36Deterioration a 32 08
Depressive syndromeepisode N
Yes 64 529No 57 471
Living situation b N
Alone 7 60With family or other people 102 872In residential treatment facility 3 25Other 5 43
Marital status c N
Never married 89 761Ever married 28 239
Gender Fischers exact test χ2=12116 pb0001Depression Fischers exact test χ2=6479 pb0013Age at interview years of education deterioration living situation marital status =
a 11 missingb 14 missingc 11 missing
depressive syndrome or episode marital status employmentand migration status Yates correction test was used forrelative onset of SC and SUD Binary logistic regression wasused to model the relationship between the dependentvariable SUD and predictor variable living situation Tocontrol for confounding effects of SUD and gender in socio-demographic variables such as marital status and employ-ment logistic regression methods were used for eachoutcome variable In order to test whether country ofresidence was associated with different rates of SUD logisticregression methods were utilized
3 Results
Ethnicity of the participants in this study was by selfreport Costa Rican subjects reported 100 bilineal ancestryfrom Costa Rica with two subjects reporting partial Nicar-aguan ancestry Guatemalan subjects reported 100 bilinealancestry from Guatemala with two of the subjects reportingpartial known European ancestry (Belgian and Spanishancestry) Of the 310 subjects from Mexico who reportedon their ancestry 100 reported bilineal Mexican ancestrywith four reporting partial known ancestry from WesternEurope (Spain France) 3 reporting partial known ancestryfrom Eastern Europe (Poland) and one reporting partialknown ancestry from Puerto Rico Subjects from the UnitedStates reported primarily bilineal Mexican ancestry (94 ofsubjects) with 5 reporting half Mexican ancestry (oneparent) and half non-Hispanic white ancestry (other parent
Schizophrenia only All subjects
N
397 766 518233 685 340164 921 178
Mean SD Mean SD
377 109 378 11389 38 89 3831 09 31 08
N N
161 405 225 434236 595 293 566
N N
19 49 26 51355 917 457 90710 26 13 263 08 8 16
N All subjects (adjustedby sex)
295 756 69795 244 303
pN005
Table 3Age of onset of substance use disorder SC in comorbid subject andschizophrenia only
Age Totalsubjects
Male Female Both
Age of onset Mean SD Mean SD Mean SD N
Schizophrenia(in subjectswith comorbidity)
209 60 196 58 207 59 121
Substances usedisorder (in subjectswith comorbidity)
183 52 231 83 189 58 121
Schizophrenia only 202 70 209 73 205 71 397
t test = pN005
90 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
with Anglo-Saxon or Western European ancestry) and 1person reporting Mexican ancestry from one parent andPuerto Rican ancestry from the other parent Of the subjectsfrom the United States 4 reported known partial NativeAmerican ancestry one reported Guatemalan ancestry and 3additional subjects with bilineal Mexican ancestry reportedpartial known European ancestry
Sample characteristics are described in Table 1 Out of 518SC subjects 234 had DD (SC and SUD) Of 178 femalesubjects with SC 79 had SUD comorbidity and out of 340male subjects with SC 315 had comorbid SUD Theproportion of subjects who reported a history of depressivesyndrome or episode was large among those who had SUDRegardless of history of SUD the majority of subjects hadnever married
History of marriage frequencies was essentially the samefor women with and without a history of SUD (385 of DDwomen 394 of SC only women) For men those with ahistory of DD had higher frequencies of ever having beenmarried (221 of DD men had been married versus 139 ofSC only men) The variable ldquoever marriedrdquo included thosewho were married separated divorced or widowed Rates ofever marrying were higher for women than for menregardless of SUD comorbidity history
Unemployment rates were higher for SC subjects with ahistory of DD but this was primarily due to differences inmales Only 295 of men with a DD were employedcompared to 438 of men with SC only Employment ratesfor women were 538 and 51 respectively for DD cases andSC only cases Regardless of DD history males were morefrequently unemployed than females It is important to notehowever that the variable ldquoemployedrdquo included any type ofemployment including lsquohousewifersquo which may explain thehigher employment rates for women in this sample
Table 2 shows the lifetimeprevalence of SUD by gender andcountry of residence in the total sample For both genders themost frequent substance of abusedependence was alcoholfollowed by marijuana In the whole sample one in four of themen had history of alcohol abuse or dependence and almostone in six men had history of marijuana abuse or dependenceInhalant misuse and cocainemisuse occurred in approximately4 of the men All other substances had lifetime abusedependence rates below 1 in men For women the same
Table 2Frequency of each substance misuse in the Latino schizophrenic sample by country of residence and gender (N=518)
US(N=111)
Mexico(N=310)
Costa Rica(N=65)
Guatemala(N=32)
All sample
Gender MaleN=78
FemaleN=33
MaleN=193
FemaleN=117
MaleN=48
FemaleN=17
MaleN=21
FemaleN=11
MaleN=340
FemaleN=118
Type of SUD N N N N N N N N N N
Alcohol 30 385 5 152 36 187 2 17 13 271 1 59 6 286 0 0 85 250 8 45Marijuana 23 295 3 91 25 130 4 34 4 83 0 0 1 48 0 0 53 156 7 39Inhalantsolvent 6 77 1 30 8 41 1 09 1 21 0 0 0 0 0 0 15 44 2 11Cocaine 7 90 2 61 6 31 0 0 1 21 0 0 0 0 0 0 14 41 2 11Amphetamine 3 38 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 09 0 0Opioid 1 13 1 30 1 05 0 0 0 0 0 0 0 0 0 0 2 06 1 06LSD 1 13 1 30 0 0 0 0 0 0 0 0 0 0 0 0 1 03 1 06Other drugs 1 13 0 0 1 05 1 09 0 0 0 0 0 0 0 0 2 06 1 06
US United States SUD substance use disorder PCP phenylcyclohexylpiperidine LSD lysergic acid diethylamide None of the subjects were diagnosed withabusedependence of ecstasy heroin or PCP
four substances were the substances with lifetimemisuse ratesgreater than 1 although the rates were much less than theequivalent rates in men
As shown in Table 3 for men with DD histories the meanage of onset of SUDwas 26 years earlier than the mean age ofonset of SC For females with DD history the mean onset ofSUD was 35 years after the onset of SC
Among men and women with DD each gender had caseswhere either SUD or SC occurred first but there were cleardifferences in these patterns between genders (Table 4)
There were clear differences in SUD comorbidity betweenthe different geographic regions in this collaborative study(Table 5) All sites showed higher rates of comorbid SUD inmen than in women For men SUD comorbidity was highestin Latinos living in the US (51) lowest in Latinos fromMexico (233) and intermediate in Latinos from CentralAmerica (319) For women SUD comorbidity was 273 inLatinas from the US and very low in both Latinas fromMexicoand Central America (34 and 35 respectively)
Regarding migration status in the whole sample 36subjects migrated from their original countries Out of those36 subjects 34 migrated from Mexico to the US 1 fromGuatemala to the US and 1 from the US to Costa Rica
Out of 36 subjects whomigrated 15 met criteria for DD ofthose 15 subjects 13 migrated from Mexico to the US onemigrated from Guatemala to the US and another one from USto Costa Rica
Table 4Relative onset of schizophrenia and substance misuse by gender
Gender
Male Female Both
Relative Onset N N N
Onset of substance misuse camefirst
74 692 5 357 79 653
Onset of schizophrenia came first 23 215 7 500 30 248Equal age onset SC and substancemisuse
10 93 2 143 12 99
Total 107 1000 14 1000 121 1000
χ2=5657 Yates correction=3850 p=005
91L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
Table 6 shows that out of 34 Mexican-born subjects whomigrated to the US 13 (382) met lifetime criteria for SUDwhereas out of 293 Mexican-born subjects who did notmigrate and reside in their own country (Mexico) 45 (154)had a lifetime history of SUD For individuals whose countryof residence was the US 47 (N=31) of the US-born subjectshad lifetime SUD while 40 (N=14) of the immigrants metcriteria for lifetime SUD
Specific hypotheses were tested using one subject perfamily We found that male gender was significantlyassociated with comorbid SUD (Fischers exact testχ2=2116 pb0001) and that history of depression wassignificantly associated with SUD (Fischers exact testχ2=6479 p=0013) Furthermore individuals with SUD
Table 5Frequency of dual diagnosis in 518 schizophrenic subjects by country of residence
Gender US (N=111) Mexico (N=310)
SC+SUD SC only SC+SUD
N N N
Male 40 513 38 487 45 233Female 9 273 24 727 4 34Total sample 49 441 62 558 49 158
Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ratios=0263Central American B=minus0818 Wald χ2=4444 df=1 p=0035 odd ratios=04 Fishers exact test χ2=18349 p=0001
Table 6Characteristics of migration status in the schizophrenic sample by dual diagnosis an
Gender Male
Diagnosis Dual diagnosis SC only
Mexican-born subjectsa c N N
Migrated to US 12 444 15 55Residing in Mexico 41 224 142 77
US residentsb d N N
Immigrants 13 e 464 15 53US-born 24 558 19 44
US = United Statesa Mexican-born men by Dual Diagnosis or Schizophrenia only Fischers exact tesb US residents by Dual Diagnosis or Schizophrenia only = pN005c 17 missing it was unknown where 17 of the subjects residing in Meacutexico wered 10 missing it was unknown where 10 subjects residing in US where borne Subjects migrated from Meacutexicof Subjects migrated from Guatemala
had a higher rate of unemployment than individuals with SConly (Fischers exact test χ2=6773 p=0010) Binarylogistic regression showed that SUD was a significantpredictor of unemployment (SUD B=0746 Wald=5774df=1 p=0016 odd ratio=2159) Gender was not relatedto unemployment In this procedure we used the variableemployment as a dependent variable and predictors wereSUD and gender
The three countrieswere significantlydifferent in their ratesof DD (χ2=18349 pb0001) When binary logistic regressionwas used to analyze country of residence Mexico and CentralAmerican schizophrenic patients were less likely to bediagnosed with SUD than subjects from the US (Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ra-tios=0263 Central American B=minus0818 Wald χ2=4444df=1 p=0035 odd ratios=0441) therefore country ofresidence was a significant predictor of SUD
Mexican-born men who migrated to the US had asignificantly higher rate of DD than those who did notemigrate (Fischers exact test χ2=6057 df=1 p=002)
Deterioration current living situation and marital statuswere not associated with comorbid diagnoses For maritalstatus binary logistic regression showed that gender was asignificant predictor of marital status because femalescompared with males were more likely to be married (B=minus1104 Wald χ2=12278 pb0001 exp (B)=0331) andSUD was not associated with marital status (p=0198) Inthis model marital status was the dependent variable and
and gender
Central America (N=97) Total
SC only SC+SUD SC only
N N N
148 767 22 319 47 681 340113 966 1 36 27 964 178261 842 23 237 74 763 518
41
d gender
Female Total
Dual diagnosis SC only
N N N
6 1 143 6 857 34
6 4 36 106 964 293
N N N
6 1 f 143 6 857 35
2 7 304 16 696 66
t χ2=6057 df=1 p=002
born
92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146
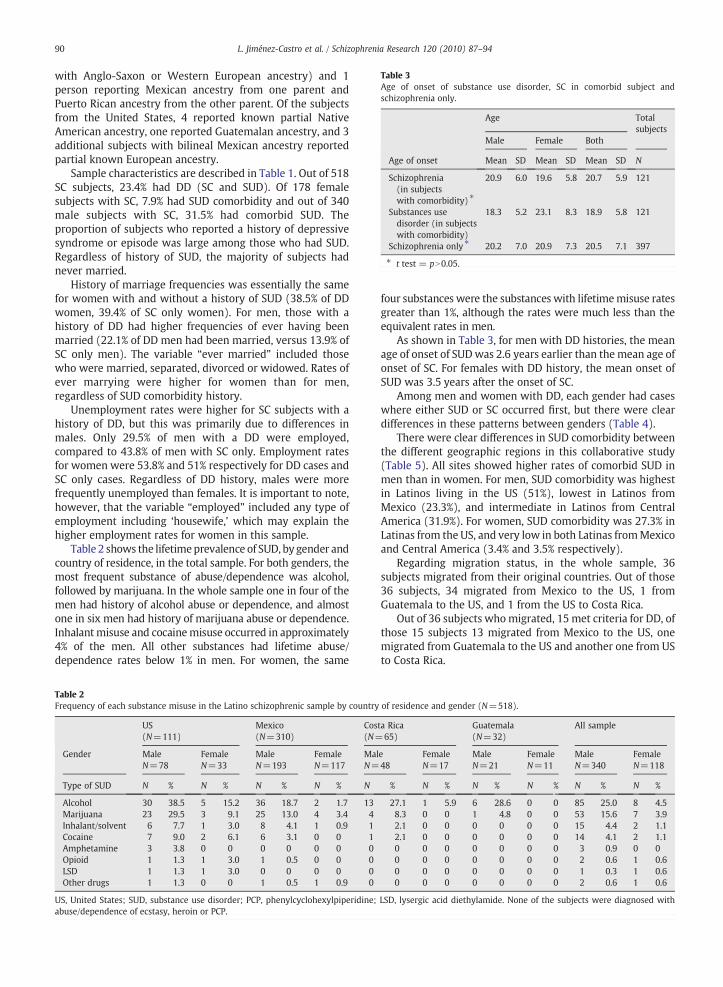
Table 3Age of onset of substance use disorder SC in comorbid subject andschizophrenia only
Age Totalsubjects
Male Female Both
Age of onset Mean SD Mean SD Mean SD N
Schizophrenia(in subjectswith comorbidity)
209 60 196 58 207 59 121
Substances usedisorder (in subjectswith comorbidity)
183 52 231 83 189 58 121
Schizophrenia only 202 70 209 73 205 71 397
t test = pN005
90 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
with Anglo-Saxon or Western European ancestry) and 1person reporting Mexican ancestry from one parent andPuerto Rican ancestry from the other parent Of the subjectsfrom the United States 4 reported known partial NativeAmerican ancestry one reported Guatemalan ancestry and 3additional subjects with bilineal Mexican ancestry reportedpartial known European ancestry
Sample characteristics are described in Table 1 Out of 518SC subjects 234 had DD (SC and SUD) Of 178 femalesubjects with SC 79 had SUD comorbidity and out of 340male subjects with SC 315 had comorbid SUD Theproportion of subjects who reported a history of depressivesyndrome or episode was large among those who had SUDRegardless of history of SUD the majority of subjects hadnever married
History of marriage frequencies was essentially the samefor women with and without a history of SUD (385 of DDwomen 394 of SC only women) For men those with ahistory of DD had higher frequencies of ever having beenmarried (221 of DD men had been married versus 139 ofSC only men) The variable ldquoever marriedrdquo included thosewho were married separated divorced or widowed Rates ofever marrying were higher for women than for menregardless of SUD comorbidity history
Unemployment rates were higher for SC subjects with ahistory of DD but this was primarily due to differences inmales Only 295 of men with a DD were employedcompared to 438 of men with SC only Employment ratesfor women were 538 and 51 respectively for DD cases andSC only cases Regardless of DD history males were morefrequently unemployed than females It is important to notehowever that the variable ldquoemployedrdquo included any type ofemployment including lsquohousewifersquo which may explain thehigher employment rates for women in this sample
Table 2 shows the lifetimeprevalence of SUD by gender andcountry of residence in the total sample For both genders themost frequent substance of abusedependence was alcoholfollowed by marijuana In the whole sample one in four of themen had history of alcohol abuse or dependence and almostone in six men had history of marijuana abuse or dependenceInhalant misuse and cocainemisuse occurred in approximately4 of the men All other substances had lifetime abusedependence rates below 1 in men For women the same
Table 2Frequency of each substance misuse in the Latino schizophrenic sample by country of residence and gender (N=518)
US(N=111)
Mexico(N=310)
Costa Rica(N=65)
Guatemala(N=32)
All sample
Gender MaleN=78
FemaleN=33
MaleN=193
FemaleN=117
MaleN=48
FemaleN=17
MaleN=21
FemaleN=11
MaleN=340
FemaleN=118
Type of SUD N N N N N N N N N N
Alcohol 30 385 5 152 36 187 2 17 13 271 1 59 6 286 0 0 85 250 8 45Marijuana 23 295 3 91 25 130 4 34 4 83 0 0 1 48 0 0 53 156 7 39Inhalantsolvent 6 77 1 30 8 41 1 09 1 21 0 0 0 0 0 0 15 44 2 11Cocaine 7 90 2 61 6 31 0 0 1 21 0 0 0 0 0 0 14 41 2 11Amphetamine 3 38 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 09 0 0Opioid 1 13 1 30 1 05 0 0 0 0 0 0 0 0 0 0 2 06 1 06LSD 1 13 1 30 0 0 0 0 0 0 0 0 0 0 0 0 1 03 1 06Other drugs 1 13 0 0 1 05 1 09 0 0 0 0 0 0 0 0 2 06 1 06
US United States SUD substance use disorder PCP phenylcyclohexylpiperidine LSD lysergic acid diethylamide None of the subjects were diagnosed withabusedependence of ecstasy heroin or PCP
four substances were the substances with lifetimemisuse ratesgreater than 1 although the rates were much less than theequivalent rates in men
As shown in Table 3 for men with DD histories the meanage of onset of SUDwas 26 years earlier than the mean age ofonset of SC For females with DD history the mean onset ofSUD was 35 years after the onset of SC
Among men and women with DD each gender had caseswhere either SUD or SC occurred first but there were cleardifferences in these patterns between genders (Table 4)
There were clear differences in SUD comorbidity betweenthe different geographic regions in this collaborative study(Table 5) All sites showed higher rates of comorbid SUD inmen than in women For men SUD comorbidity was highestin Latinos living in the US (51) lowest in Latinos fromMexico (233) and intermediate in Latinos from CentralAmerica (319) For women SUD comorbidity was 273 inLatinas from the US and very low in both Latinas fromMexicoand Central America (34 and 35 respectively)
Regarding migration status in the whole sample 36subjects migrated from their original countries Out of those36 subjects 34 migrated from Mexico to the US 1 fromGuatemala to the US and 1 from the US to Costa Rica
Out of 36 subjects whomigrated 15 met criteria for DD ofthose 15 subjects 13 migrated from Mexico to the US onemigrated from Guatemala to the US and another one from USto Costa Rica
Table 4Relative onset of schizophrenia and substance misuse by gender
Gender
Male Female Both
Relative Onset N N N
Onset of substance misuse camefirst
74 692 5 357 79 653
Onset of schizophrenia came first 23 215 7 500 30 248Equal age onset SC and substancemisuse
10 93 2 143 12 99
Total 107 1000 14 1000 121 1000
χ2=5657 Yates correction=3850 p=005
91L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
Table 6 shows that out of 34 Mexican-born subjects whomigrated to the US 13 (382) met lifetime criteria for SUDwhereas out of 293 Mexican-born subjects who did notmigrate and reside in their own country (Mexico) 45 (154)had a lifetime history of SUD For individuals whose countryof residence was the US 47 (N=31) of the US-born subjectshad lifetime SUD while 40 (N=14) of the immigrants metcriteria for lifetime SUD
Specific hypotheses were tested using one subject perfamily We found that male gender was significantlyassociated with comorbid SUD (Fischers exact testχ2=2116 pb0001) and that history of depression wassignificantly associated with SUD (Fischers exact testχ2=6479 p=0013) Furthermore individuals with SUD
Table 5Frequency of dual diagnosis in 518 schizophrenic subjects by country of residence
Gender US (N=111) Mexico (N=310)
SC+SUD SC only SC+SUD
N N N
Male 40 513 38 487 45 233Female 9 273 24 727 4 34Total sample 49 441 62 558 49 158
Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ratios=0263Central American B=minus0818 Wald χ2=4444 df=1 p=0035 odd ratios=04 Fishers exact test χ2=18349 p=0001
Table 6Characteristics of migration status in the schizophrenic sample by dual diagnosis an
Gender Male
Diagnosis Dual diagnosis SC only
Mexican-born subjectsa c N N
Migrated to US 12 444 15 55Residing in Mexico 41 224 142 77
US residentsb d N N
Immigrants 13 e 464 15 53US-born 24 558 19 44
US = United Statesa Mexican-born men by Dual Diagnosis or Schizophrenia only Fischers exact tesb US residents by Dual Diagnosis or Schizophrenia only = pN005c 17 missing it was unknown where 17 of the subjects residing in Meacutexico wered 10 missing it was unknown where 10 subjects residing in US where borne Subjects migrated from Meacutexicof Subjects migrated from Guatemala
had a higher rate of unemployment than individuals with SConly (Fischers exact test χ2=6773 p=0010) Binarylogistic regression showed that SUD was a significantpredictor of unemployment (SUD B=0746 Wald=5774df=1 p=0016 odd ratio=2159) Gender was not relatedto unemployment In this procedure we used the variableemployment as a dependent variable and predictors wereSUD and gender
The three countrieswere significantlydifferent in their ratesof DD (χ2=18349 pb0001) When binary logistic regressionwas used to analyze country of residence Mexico and CentralAmerican schizophrenic patients were less likely to bediagnosed with SUD than subjects from the US (Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ra-tios=0263 Central American B=minus0818 Wald χ2=4444df=1 p=0035 odd ratios=0441) therefore country ofresidence was a significant predictor of SUD
Mexican-born men who migrated to the US had asignificantly higher rate of DD than those who did notemigrate (Fischers exact test χ2=6057 df=1 p=002)
Deterioration current living situation and marital statuswere not associated with comorbid diagnoses For maritalstatus binary logistic regression showed that gender was asignificant predictor of marital status because femalescompared with males were more likely to be married (B=minus1104 Wald χ2=12278 pb0001 exp (B)=0331) andSUD was not associated with marital status (p=0198) Inthis model marital status was the dependent variable and
and gender
Central America (N=97) Total
SC only SC+SUD SC only
N N N
148 767 22 319 47 681 340113 966 1 36 27 964 178261 842 23 237 74 763 518
41
d gender
Female Total
Dual diagnosis SC only
N N N
6 1 143 6 857 34
6 4 36 106 964 293
N N N
6 1 f 143 6 857 35
2 7 304 16 696 66
t χ2=6057 df=1 p=002
born
92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146
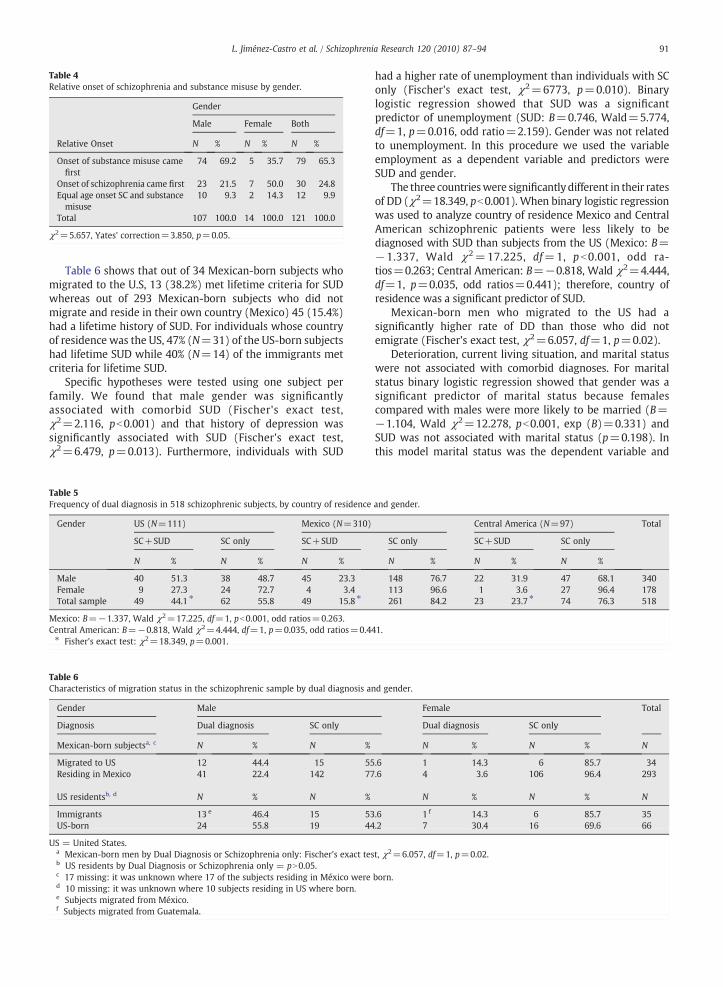
Table 4Relative onset of schizophrenia and substance misuse by gender
Gender
Male Female Both
Relative Onset N N N
Onset of substance misuse camefirst
74 692 5 357 79 653
Onset of schizophrenia came first 23 215 7 500 30 248Equal age onset SC and substancemisuse
10 93 2 143 12 99
Total 107 1000 14 1000 121 1000
χ2=5657 Yates correction=3850 p=005
91L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
Table 6 shows that out of 34 Mexican-born subjects whomigrated to the US 13 (382) met lifetime criteria for SUDwhereas out of 293 Mexican-born subjects who did notmigrate and reside in their own country (Mexico) 45 (154)had a lifetime history of SUD For individuals whose countryof residence was the US 47 (N=31) of the US-born subjectshad lifetime SUD while 40 (N=14) of the immigrants metcriteria for lifetime SUD
Specific hypotheses were tested using one subject perfamily We found that male gender was significantlyassociated with comorbid SUD (Fischers exact testχ2=2116 pb0001) and that history of depression wassignificantly associated with SUD (Fischers exact testχ2=6479 p=0013) Furthermore individuals with SUD
Table 5Frequency of dual diagnosis in 518 schizophrenic subjects by country of residence
Gender US (N=111) Mexico (N=310)
SC+SUD SC only SC+SUD
N N N
Male 40 513 38 487 45 233Female 9 273 24 727 4 34Total sample 49 441 62 558 49 158
Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ratios=0263Central American B=minus0818 Wald χ2=4444 df=1 p=0035 odd ratios=04 Fishers exact test χ2=18349 p=0001
Table 6Characteristics of migration status in the schizophrenic sample by dual diagnosis an
Gender Male
Diagnosis Dual diagnosis SC only
Mexican-born subjectsa c N N
Migrated to US 12 444 15 55Residing in Mexico 41 224 142 77
US residentsb d N N
Immigrants 13 e 464 15 53US-born 24 558 19 44
US = United Statesa Mexican-born men by Dual Diagnosis or Schizophrenia only Fischers exact tesb US residents by Dual Diagnosis or Schizophrenia only = pN005c 17 missing it was unknown where 17 of the subjects residing in Meacutexico wered 10 missing it was unknown where 10 subjects residing in US where borne Subjects migrated from Meacutexicof Subjects migrated from Guatemala
had a higher rate of unemployment than individuals with SConly (Fischers exact test χ2=6773 p=0010) Binarylogistic regression showed that SUD was a significantpredictor of unemployment (SUD B=0746 Wald=5774df=1 p=0016 odd ratio=2159) Gender was not relatedto unemployment In this procedure we used the variableemployment as a dependent variable and predictors wereSUD and gender
The three countrieswere significantlydifferent in their ratesof DD (χ2=18349 pb0001) When binary logistic regressionwas used to analyze country of residence Mexico and CentralAmerican schizophrenic patients were less likely to bediagnosed with SUD than subjects from the US (Mexico B=minus1337 Wald χ2=17225 df=1 pb0001 odd ra-tios=0263 Central American B=minus0818 Wald χ2=4444df=1 p=0035 odd ratios=0441) therefore country ofresidence was a significant predictor of SUD
Mexican-born men who migrated to the US had asignificantly higher rate of DD than those who did notemigrate (Fischers exact test χ2=6057 df=1 p=002)
Deterioration current living situation and marital statuswere not associated with comorbid diagnoses For maritalstatus binary logistic regression showed that gender was asignificant predictor of marital status because femalescompared with males were more likely to be married (B=minus1104 Wald χ2=12278 pb0001 exp (B)=0331) andSUD was not associated with marital status (p=0198) Inthis model marital status was the dependent variable and
and gender
Central America (N=97) Total
SC only SC+SUD SC only
N N N
148 767 22 319 47 681 340113 966 1 36 27 964 178261 842 23 237 74 763 518
41
d gender
Female Total
Dual diagnosis SC only
N N N
6 1 143 6 857 34
6 4 36 106 964 293
N N N
6 1 f 143 6 857 35
2 7 304 16 696 66
t χ2=6057 df=1 p=002
born
92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146

92 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
ldquonever marriedrdquo was selected as the reference category withcovariables being SUD and gender with any SUD and male aspredictor variables
Comorbid SUD did not contribute to earlier onset of SCThe difference in the means of age of onset of SC inparticipants with and without SUD was not statisticallysignificant when the t test was used (t=0853 df=282p=0394) In participants with comorbid SC and SUDsubjects were more likely to have the SUD occur before orat the same time as the SC rather than after onset of SC(χ2=5657 Yates correction=3850 p=0050) althoughthis was driven largely by men in this sample
4 Discussion
The lifetime prevalence of comorbid SUD in this Latinosample of subjects with SC was on the low end compared torates documented in previous studies from Europe and non-Latino US populations (Cantor-Graae et al 2001) Howeverthe prevalence rates of comorbidity varied among Latinosbased on the country they were living in Latinos living in theUS had lifetime rates of DD similar to what has described forSC subjects in the US (Cantor-Graae et al 2001 Kessler et al2005b Regier et al 1990) In contrast Latinos living inCentral America and Mexico had much lower rates ofcomorbid SUD which were comparable with studies of withDD in Latino populations (Montross et al 2005 Vega et al2006)
The country of residence with the highest frequency of DDwas the US followed by Central America and finally Mexicoand these differences were statistically significant Immigra-tion fromMexico to the US was significant associated with anincrease in the diagnosis of SUD These increased rates of SUDin US residents and in Mexican subjects that immigrated tothe US compared to subjects living in Mexico is consistentwith the data of Vega (Vega and Sribney 2003) and otherswho suggest that acculturation to the US might be associatedwith increased psychiatric comorbidity for both genders aswell as a risk factor for SUD in non-psychiatric samples(Buchanan and Smokowski 2009 Prado et al 2009) It hasbeen suggested that the more typical interconnectedness oflarge families and other cultural factors among Latinos mayrepresent protective dynamics contributing to lower rates ofDD among Latinos and that these factors may begin to breakdown or have less effect once Latinos are exposed to adifferent culture through residence in the US (Alegria et al2006 Montross et al 2005 Vega et al 2009) Since thisstudy was done uniformly across sites our findings suggestthat environment (country of residence) indeed plays asignificant role in development of SUD in schizophrenicindividuals among LatinosLatinas
In the current study male gender and unemployed statuswere significantly associated risk factors for DD as has beenreported in previous investigations in other cultures (Ringenet al 2008 Swartz et al 2006 Verma et al 2002) Althoughour sample of DD women was small the finding that womenwere older compared to men at the outset of SUD is also inagreement with the literature (Cantor-Graae et al 2001Gearon et al 2003) For men our results suggest that the vastmajority will have the onset of SUD prior to or in the sameyear as they develop the full diagnosis of SC In women there
is a smaller prevalence of SUD and when it occurs the SUD isas likely to occur after the onset of full SC as before Thissuggests that for men SUD may be more likely to act as aldquotriggerrdquo for onset of SC whereas for women it is equallylikely that SUD may occur after SC has already started
In the Latino populations from the present study alcoholwas themost frequently abused substance which is similar towhat has been found in previous studies conducted in the USand other countries (Cantor-Graae et al 2001 Regier et al1990 Rossi Menezes and Ratto 2004 Verma et al 2002)Thesecond most frequently described SUD in this sample wasmarijuana Given recent findings on possible involvement ofthe cannabinoid receptor in SC (Chavarriacutea-Siles et al 2008) itis intriguing to note the prominence of this SUD in the DDcases studied here The thirdmost common type of SUD in ourstudy was for solvent abuse or dependence a problem thatothers have suggested is a particular problem in Latinopopulations (Padilla et al 1979) Cocaine SUD occurred in arelatively small number of subjects contrary to what ispresented in the literature for other populations which havereported cocaine abuse as one of the most frequent SUDs(Lammertink et al 2001 Mueser et al 2000 Soyka et al2001) Newer drugs (ie ecstasy) and drugs thought to play arole in SC risk in previous eras or different cultures (ielysergic acid hallucinogens PCP) were negligible in thecurrent study sample
We found in this research that depression was correlatedwith SUD in SC clients in accord with previous studies thathave showed that depressive symptoms may be a risk factorfor SUD in patients with SC (Addington and Duchak 1997Dixon et al 1990) The association of depression and SUD inour sample could represent use of SUD to self-medicatedepressive mood or alternately depressogenic effects of SUDLongitudinal studies would be necessary to better tease outthe reason for this interesting association
The strengths of this research include that this study wasconducted in a sample of Latino subjects with SC from threedifferent geographic areas in the same time period usingstandardized interviews conducted by psychiatrists the samediagnostic system across sites and a consensus process fordiagnosis Few international studies using large well diag-nosis samples have been carried out since WHOs Interna-tional Study took place decades ago (Sartorious et al 1972)
The limitations in this study are several First the studysample is not representative of all SC subjects from thesepopulations but represents a sample of SC subjects fromfamilies where there are multiple SC cases Whether SC inmultiplex families is different from SC observed in sporadiccases is not known The current sample is also notrepresentative of all Latinos as it does not include SouthAmericans Puerto Ricans or other Caribbean ancestry LatinosFurther studies about the relationship of SC and SUD inadditional Latino populations and in more randomly ascer-tained subjects would be necessary to have data representa-tive of the larger Latin American population
In conclusion the present study finds that there is highcomorbidity of SUD in Latinos (particularly men)with SC andthat this varies across countries Male gender and history ofdepression are important risk factors for comorbidity in theseLatino populations The substances of abusedependence thataremost frequent are alcohol cannabis solvents and cocaine
93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146

93L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
The sequence of onset of SUD in comorbid cases also suggestthat potential preventative strategies may be of use in men(prior to onset of SC) and that SUD prevention in womenmaybe especially important after the development of SC Furtherexploration and study of the ldquoprotectiverdquo aspects of Latinoculture in Latino countries and the increased risk associatedwith Latinos living in the US will be valuable in treating andpreventing SUD in subjects with SC
Role of funding sourceThis research was supported by the following grants from the National
Institute of Mental Health MH60881 and MH60875 Dr Jimenez-Castro wassupported by a fellowship of grant D43 TW06152-01 from the NationalInstitute of Mental Health the National Institute of Drug Abuse and theFogarty Institute These institutions had no further role in the study design inthe collection analysis and interpretation of data in writing of the reportand in the decision to submit the paper for publication
ContributorsAll authors have contributed to and approved the final manuscript
Conflict of interestThe current study was not supported by any pharmaceutical funding
The investigators report no competing interest
AcknowledgmentsThe authors thank the many families who participated in this research
project as well as clinicians and hospitals throughout the Southwest UnitedStates Mexico Costa Rica and Guatemala We also thank Erasmo Cano GaryBurk and Joseph Peters for research support activities and Drs Regina ArmasMercedes Ramirez Salvador Contreras Alec Miller and Douglas Levinson fortheir assistance as part of the best estimate diagnostic team Data andbiomaterials used in this research report were collected by the InternationalNeuro-Genetics Association of Spanish America and the United States(INGASU)
Appendix A Supplementary data
Supplementary data associatedwith this article can be foundin the online version at doi101016jschres2010021053
References
Addington J Duchak V 1997 Reasons for substance use in schizophreniaActa Psychiatr Scand 96 (5) 329ndash333
AlegriacuteaM CaninoG Shrout PEWooMDuanN Vila D TorresM Chen CN Meng XL 2008 Prevalence of mental illness in immigrant and non-immigrant US Latino groups Am J Psychiatry 165 (3) 359ndash569
Alegria M Canino G Stinson FS Grant BF 2006 Nativity and DSM-IVpsychiatric disorders among Puerto Ricans Cuban Americans and non-Latinowhites in the United States results from the National EpidemiologicSurvey on Alcohol and Related Conditions J Clin Psychiatry 67 (1) 56ndash65
Andrade L Caraveo-Anduaja JJ Berglund P Bijl RV Kessler RC DemlerO Walters EE Kyacutelyacutec C Offord D Uumlstuumln TB 2000 Cross-nationalcomparisons of the prevalences and correlates of mental disorders WHOInternational Consortium in Psychiatric Epidemiology Bull WorldHealth Organ 78 (4) 413ndash426
Bartels SJ Teague GB Drake RE Clark RE Bush PW Noordsy DL1993 Substance abuse in schizophrenia service utilization and costsJ Nerv Ment Dis 181 (4) 227ndash232
Baumeister H Haumlrter M 2007 Prevalence of mental disorders based ongeneral population surveys Soc Psychiatry Psychiatr Epidemiol 42 (7)537ndash546
Bijl RV Ravelli A van Zessen G 1998 Prevalence of psychiatric disorder in thegeneral population results of The Netherlands Mental Health Survey andIncidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol 33 (12)587ndash595
Breslau J Aguilar-Gaxiola S Kendler KS Su M Williams D Kessler RC2006 Specifying race-ethnic differences in risk for psychiatric disorder ina USA national sample Psychol Med 36 (1) 57ndash68
Buchanan RL Smokowski PR 2009 Pathways from acculturation stress tosubstance use among Latino adolescents Subst UseMisuse 44 (5) 740ndash762
Cantor-Graae E Nordstroumlm LG McNeil TF 2001 Substance abuse inschizophrenia a review of the literature and a study of correlates inSweden Schizophr Res 48 (1) 69ndash82
Chavarriacutea-Siles I Contreras-Rojas J Hare E Walss-Bass C Quezada PDassori A Contreras S Medina R Ramiacuterez M Salazar R Raventos HEscamilla MA 2008 Cannabinoid receptor 1 gene (CNR1) andsusceptibility to a quantitative phenotype for hebephrenic schizophre-nia Am J Med Genet B Neuropsychiatr Genet 147 (3) 279ndash284
Dervaux A Bayleacute FJ Laqueille X Bourdel MC Le BorgneMH Olieacute JP KrebsMO 2001 Is substance abuse in schizophrenia related to impulsivitysensation seeking or anhedonia Am J Psychiatry 158 (3) 492ndash494
Dixon L Haas G Weiden P Sweeney J Frances A 1990 Acute effects ofdrug abuse in schizophrenic patients clinical observations and patientsself-reports Schizophr Bull 16 (1) 69ndash79
Escamilla MA Ontiveros A Nicolini H Raventos H Mendoza R MedinaR Munoz R Levinson D Peralta JM Dassori A Almasy L 2007 Agenome-wide scan for schizophrenia and psychosis susceptibility loci infamilies of Mexican and Central American ancestry Am J Med Genet BNeuropsychiatr Genet 144 (2) 193ndash199
Fowler IL Carr VJ Carter NT Lewin TJ 1998 Patterns of current andlifetime substance use in schizophrenia Schizophr Bull 24 (3) 443ndash455
Gearon JS Nidecker M Bellack A Bennett M 2003 Gender differences indrug use behavior in people with serious mental illnesses Am J Addict12 (3) 229ndash241
Grant BF Stinson FS Hasin DS Dawson DA Chou SP Anderson K2004 Immigration and lifetime prevalence of DSM-IV psychiatricdisorders among Mexican Americans and non-Hispanic whites in theUnited States results from the National Epidemiologic Survey on Alcoholand Related Conditions Arch Gen Psychiatry 61 (12) 1226ndash1233
Jacobi F Wittchen HU Holting C Houmlfler M Pfister H Muumlller N Lieb R2004 Prevalence co-morbidity and correlates of mental disorders in thegeneral population results from the German Health Interview andExamination Survey (GHS) Psychol Med 34 (4) 597ndash611
Kavanagh DJ Waghorn G Jenner L Chant DC Carr V Evans MHemnan H Jablensky A McGrath JJ 2004 Demographic and clinicalcorrelates of comorbid substance use disorders in psychosis multivar-iate analyses from an epidemiological sample Schizophr Res 66 (2ndash3)115ndash124
Kessler RC Berglund P Demler O Jin R Merikangas KR Walters EE2005a Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication Arch GenPsychiatry 62 (6) 593ndash602
Kessler RC Birnbaum H Demler O Falloon IR Gagnon E Guyer MHowes MJ Kendler KS Shi L Walters E Wu EQ 2005b Theprevalence and correlates of nonaffective psychosis in the NationalComorbidity Survey Replication (NCS-R) Biol Psychiatry 58 (8) 668ndash676
Kessler RC McGonagle KA Zhao S Nelson CB Hughes M Eshleman SWittchen HU Kendler KS 1994 Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States Results from theNational Comorbidity Survey Arch Gen Psychiatry 5 (1) 8ndash19
Lammertink M Loumlhrer F Kaiser R Hambrecht M Pukrop R 2001Differences in substance abuse patterns multiple drug abuse aloneversus schizophrenia with multiple drug abuse Acta Psychiatr Scand104 (5) 361ndash366
Levinson DF Mowry BJ Escamilla MA Faraone SV 2002 The LifetimeDimensions of Psychosis Scale (LDPS) description and interraterreliability Schizophr Bull 2 (4) 683ndash695
Maxwell ME 1992 The Family Interview for Genetic Studies Manual InClinical Neurogenetics Branch IRP National Institute of Mental HealthWashington DC
McCreadie RG 2002 Use of drugs alcohol and tobacco by people withschizophrenia casendashcontrol study Br J Psychiatry 181 (4) 321ndash325
Medina-Mora ME Borges G Benjet C Lara C Berglund P 2007Psychiatric disorders in Mexico lifetime prevalence in a nationallyrepresentative sample Br J Psychiatry 190 (6) 521ndash528
Menezes PR Johnson S Thornicroft GMarshall J ProsserD Bebbington PKuipers E 1996 Drug and alcohol problems among individuals withsevere mental illness in south London Br J Psychiatry 168 (5) 612ndash619
Montross LP Barrio C Yamada AM Lindamer L Golshan S Garcia PFuentes D Daly RE Hough RL Jeste DV 2005 Tri-ethnic variationsof co-morbid substance and alcohol use disorders in schizophreniaSchizophr Res 79 (2ndash3) 297ndash305
Mueser KT Yarnold PR Rosenberg SD Swett C Miles KM Hill D2000 Substance use disorder in hospitalized severely mentally illpsychiatric patients prevalence correlates and subgroups SchizophrBull 26 (1) 179ndash192
Nurnberger Jr JI Blehar MC Kaufmann CA York-Cooler C Simpson SGHarkavy-Friedman J Severe JB Malaspina D Reich T 1994 Diagnostic
94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146

94 L Jimeacutenez-Castro et al Schizophrenia Research 120 (2010) 87ndash94
interview for genetic studies Rationale unique features and trainingNIMH Genetics Initiative Arch Gen Psychiatry 51 (11) 849ndash859
Padilla E Padilla A Morales A Olmedo E 1979 Inhalant marijuana andalcohol abuse among barrio children and adolescents Int J Addict 14 (7)945ndash964
PradoG Huang S Schwartz SJMaldonado-MolinaMM Bandiera FC de laRosa M Patin H 2009 What accounts for differences in substance useamong US-born and immigrant Hispanic adolescents results from alongitudinal prospective cohort study J Adolesc Health 45 (2) 118ndash125
Regier DA Farmer ME Rae DS Locke BZ Keith SJ Judd LL GoodwinFK 1990 Comorbidity of mental disorders with alcohol and other drugabuse Results from the Epidemiologic Catchment Area (ECA) StudyJAMA 264 (19) 2511ndash2518
Ringen PA Melle I Birkenaes AB Engh JA Faerden A Joacutensdoacutettir HNesvaringg R Vaskinn A Friis S Larsen F Opjordsmoen S Sundet KAndreassen OA 2008 Illicit drug use in patients with psychotic disorderscomparedwith that in the general population a cross-sectional study ActaPsychiatr Scand 117 (2) 133ndash138
Rosenman S Korten A Medway J Evans M 2000 Characterisingpsychosis in the Australian National Survey of Mental Health andWellbeing Study on Low Prevalence (psychotic) Disorders Aust N Z JPsychiatry 34 (5) 792ndash800
Rossi Menezes P Ratto LR 2004 Prevalence of substance misuse amongindividuals with severe mental illness in Satildeo Paulo Soc PsychiatryPsychiatr Epidemiol 39 (3) 212ndash217
Sartorious N Shapiro R Kimura M Barrett K 1972 WHO internationalpilot study of schizophrenia Psychol Med 2 (4) 422ndash425
Soyka M Albus M Immler B Kathmann N Hippius H 2001 Psychopa-thology in dual diagnosis and non-addicted schizophrenicsmdashare theredifferences Eur Arch Psychiatry Clin Neurosci 251 (5) 232ndash238
SwartzMSWagner HR Swanson JW Stroup TS McEvoy JP Canive JMMiller DD Reimherr FMcGeeM Khan A VanDorn R Rosenheck RALieberman JA 2006 Substance use in persons with schizophreniabaseline prevalence and correlates from the NIMH CATIE study J NervMent Dis 194 (3) 164ndash172
Vega WA Canino G Cao Z Alegria M 2009 Prevalence and correlates ofdual diagnoses in US Latinos Drug and Alcohol Dependence 100 (1ndash2)32ndash38
Vega WA Sribney WM 2003 Achara-Abrahams I Co-occurring alcoholdrug and other psychiatric disorders among Mexican-origin people inthe United States Am J Public Health 93 (7) 1057ndash1064
Vega WA Sribney WM Miskimen TM Escobar JI Aguilar-Gaxiola S2006 Putative psychotic symptoms in the Mexican American popula-tion prevalence and co-occurrence with psychiatric disorders J NervMent Dis 194 (7) 471ndash477
Verma SK Subramaniam M Chong SA Kua EH 2002 Substance abusein schizophrenia A Singapore perspective Soc Psychiatry PsychiatrEpidemiol 37 (7) 326ndash328
Weaver T Renton A Stimson G Tyrer P 1999 Severe mental illness andsubstance misuse BMJ 318 (7177) 137ndash138
Zhang AY Snowden LR 1999 Ethnic characteristics ofmental disorders in fiveUS communities Cultur Divers Ethnic Minor Psychol 5 (2) 134ndash146
Copyright © 2022 FDOKUMEN




















